Drugs, Health Technologies, Health Systems
Health Technology Review
Injectable Opioid Agonist Treatment for Patients With Opioid Use Disorder: An Updated Review of Clinical and Cost-Effectiveness
Summary
Main Take-Away
Injectable opioid agonist treatment (iOAT) may be a promising option for individuals with opioid use disorder (OUD), particularly those whose disease has not responded to oral treatment. The evidence suggests benefits in treatment retention, reductions in illicit opioid and cocaine use, fewer interactions with the criminal justice system, and a potentially acceptable safety profile.
Key Messages
What Is the Issue?
OUD is a chronic, relapsing medical condition defined by a problematic pattern of opioid use over a 12-month period that leads to substantial impairment or distress. This disorder is characterized by symptoms such as a loss of control over use, craving, tolerance, withdrawal, and continued use of opioids despite negative social, occupational, or health consequences.
Decision-makers are interested in understanding the clinical effectiveness, safety, and cost-effectiveness of iOAT for patients with OUD.
What Did We Do?
We searched key resources, including journal citation databases, and conducted a focused internet search for relevant evidence published since 2020.
What Did We Find?
iOAT with or without an oral opioid agonist may be more effective than other therapies (e.g., oral opioid agonist alone) or no therapy in improving treatment retention, reducing illicit opioid and cocaine use, and decreasing interactions with the criminal justice system.
Injectable hydromorphone administered under medical supervision showed a good safety profile, with only mild adverse events reported and no significant differences compared to placebo.
An economic evaluation from Australia found that a model prioritizing unsupervised iOAT with a smaller proportion of patients receiving supervised iOAT may be cost-effective. Scenarios focused more heavily on supervised iOAT were not cost-effective in that context.
What Does This Mean?
iOAT may be a promising treatment option for individuals with OUD, particularly for those whose disease has not responded to oral opioid agonist treatment.
The evidence suggests benefits in treatment retention, reductions in illicit opioid and cocaine drug use, less involvement with the criminal justice system, and a potentially acceptable safety profile.
Policy-makers may consider models of care that incorporate unsupervised or take-home iOAT to expand access to clinically effective and cost-effective care.
Limitations in the evidence — such as incomplete outcome reporting, small sample sizes, lack of formal certainty assessments, and limited generalizability to health care systems in Canada — should be considered when making decisions.
Abbreviations
AE
adverse event
CDA-AMC
Canada’s Drug Agency
CI
confidence interval
Crl
credible interval
GRADE
Grading of Recommendations Assessment, Development and Evaluations
iOAT
injectable opioid agonist treatment
MD
mean difference
NMA
network meta-analysis
OAT
opioid agonist treatment
OR
odds ratio
OUD
opioid use disorder
RCT
randomized controlled trial
Context and Policy Issues
What Is Opioid Use Disorder?
Opioid use disorder (OUD) is a chronic and relapsing medical condition defined by a problematic pattern of opioid use that causes substantial impairment or distress.1 According to the Diagnostic and Statistical Manual of Mental Disorders (Fifth Edition) (DSM-5), a diagnosis requires at least 2 of 11 specific symptoms to be present within a 12-month period.1,2 These symptoms include a loss of control over opioid use, craving, tolerance, and withdrawal, as well as continued use despite negative social, occupational, or health consequences.1,2 In North America, the term OUD is often used interchangeably with opioid dependence.3,4
The global burden of opioid dependence or OUD is substantial.4 The Global Burden of Diseases, Injuries, and Risk Factors study estimated that 40.5 million people were dependent on opioids worldwide in 2017.4 Opioid dependence or OUD leads to considerable morbidity and premature mortality, ranking as the third most important substance use disorder globally (after tobacco and alcohol). In 2017, an estimated 109,500 people died from opioid overdoses globally.4
The current opioid crisis in high-income countries, particularly Canada and the US, was initially driven by increased prescribing of opioids for patients with chronic noncancer pain, resulting in iatrogenic dependence and subsequent increases in illicit opioid use.4 The increasingly toxic and unpredictable unregulated drug supply has been a primary driver of opioid-related mortality.5 Since approximately 2013, a third wave of extramedical opioid use has involved the influx of highly potent synthetic opioids, such as illicitly manufactured fentanyl.4
In Canada, both illicit and prescription opioids are contributing to the growing crisis.6 Between 2019 and 2021, the annual number of deaths related to opioid use rose from 3,007 to 6,222, and the number of years of life lost increased from 126,115 to 256,336 (or from 3.5 to 7.0 years of life lost per 1,000 people).7 The crisis disproportionately affects males, who accounted for 74% of these deaths.6 Furthermore, adults aged between 30 and 39 years were the most affected age group, representing 28% of all deaths and accounting for the greatest number of years of life lost in 2021.6,7
What Are the Current Treatments for OUD?
Opioid agonist treatment (OAT), typically involving methadone or buprenorphine (as monoproducts or as the combination of buprenorphine-naloxone), is the most effective treatment for patients with OUD, and the pharmacologic therapies used are listed as WHO essential medicines.1,4 The traditional treatment process for patients with OUD involves 3 main stages: stabilization (maintenance), withdrawal, and relapse prevention.3 OAT is effective in reducing overall mortality and key causes of death, including overdose, suicide, accidental injuries, HIV, and hepatitis C virus infection.4,8 OAT could help people adhere to treatment programs, reduce illicit opioid use, and have fewer interactions with the criminal justice system.3,4 Other pharmacologic options include naltrexone (an opioid antagonist) for relapse prevention. Lofexidine and clonidine are primarily used to help patients manage symptoms during withdrawal. Despite the evidence for OAT's effectiveness, coverage is typically low globally, even in high-income countries, and treatment quality is often suboptimal.4
What Is Injectable OAT?
Injectable OAT (iOAT) involves the supervised administration of injectable opioid agonists, which have a rapid onset of action and shorter duration to reach peak values compared to oral forms.9 iOAT is a resource-intensive option within the OUD continuum of care and is typically provided in specialized clinics with integrated psychosocial supports and counselling aimed at improving health, reducing the risk of overdose and harm, and engaging individuals who may not have achieved treatment goals while receiving oral opioid agonists.9,10
In Canada, the main medications used in iOAT include diacetylmorphine (medical heroin) and hydromorphone.10 Health Canada has approved injectable opioid agonists for urgent public health needs and for severe OUD.10 However, service gaps persist and access remains limited, particularly for diacetylmorphine, due to regulatory issues concerning importation and supply chain operations.9
Why Is it Important to Do This Review?
The severity of the ongoing opioid overdose crisis, particularly in North America, underscores the need for a comprehensive public health response.4 Conventional OAT is the standard of care, but it may not be effective for all patients with OUD.1,11 In 2020, CADTH reviewed the evidence regarding iOAT and found that iOAT is clinically effective for individuals with OUD who have not benefited from conventional therapies.12 iOAT was associated with improved treatment retention, less illicit drug use, and fewer interactions with the criminal justice system.12 However, people receiving iOAT reported more adverse events (AEs).12 Economic evaluations included in this review indicated that iOAT provided greater health benefits at lower costs compared to methadone for individuals who had previously used other treatment options.12
Given that iOAT is an emerging treatment option, monitoring of the evidence base is necessary to inform rapidly evolving policy and practice.10 This updated review by Canada’s Drug Agency (CDA-AMC) may inform policy decisions regarding iOAT by summarizing evidence on its clinical effectiveness, safety, and cost-effectiveness.
Objective
To support decision-making regarding the provision and funding of iOAT, CDA-AMC updated a Rapid Review to summarize available evidence published since 2020 on the clinical effectiveness, safety, and cost-effectiveness of iOAT for treating adults with OUD.
Research Questions
What are the clinical effectiveness and safety of iOAT compared with alternative pharmacologic treatments or no treatment for patients with OUD?
What is the cost-effectiveness of iOAT compared with alternative pharmacologic treatments or no treatment for patients with OUD?
Methods
Literature Search Methods
An information specialist conducted a customized literature search of multiple sources and grey literature on September 8, 2025.
The literature search strategy used in this report is an update of 1 developed for a previous CADTH report.12 For the current report, an information specialist conducted a literature search on key resources including MEDLINE, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of health technology assessment agencies in Canada and of major international health technology assessment agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevance. The initial search was limited to English-language documents published between January 1, 2010, and April 24, 2020. For the current report, database searches were rerun on September 8, 2025, to capture any articles published or made available since the initial search date. The grey literature search was performed to retrieve documents published since April 2020. The search strategy is available on request.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Adults (aged 18 years or older) with opioid use disorder |
Interventions |
|
Comparators | Alternative pharmacologic treatment, any formulation (e.g., alternative iOAT, buprenorphine-naloxone, injectable buprenorphine, methadone); no treatment |
Outcomes | Question 1:
Question 2:
|
Study designs | Systematic reviews, randomized controlled trials, nonrandomized studies,a health technology assessments, and economic evaluations |
AE = adverse event; iOAT = injectable opioid agonist treatment; QALY = quality-adjusted life-year.
aThe reviewer used a hierarchical approach to identify primary studies. If nonrandomized studies with comparative evidence were identified, single-arm (noncomparative) studies were excluded.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1 or if they were published before 2020. We excluded meeting abstracts or duplicate publications. We also excluded studies that did not clearly specify whether the OAT was injectable or oral.
Critical Appraisal of Individual Studies
One reviewer critically appraised the included publications using the following tools as a guide: A Measurement Tool to Assess Systematic Reviews 2 (AMSTAR 2)13 for systematic reviews; a questionnaire to assess the relevance and credibility of a network meta-analysis14 for systematic reviews and network meta-analyses (NMA); the Downs and Black checklist15 for primary studies; and the Drummond checklist16 for economic evaluations. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
A total of 559 citations were identified in the literature search. Following the screening of titles and abstracts, 543 citations were excluded and 16 potentially relevant reports from the electronic search were retrieved for full-text review. Eight potentially relevant publications were found in the grey literature search. Of these potentially relevant articles, 20 publications were excluded for various reasons and 4 publications met the inclusion criteria and were included in this report. These publications include 1 systematic review and network meta-analysis of randomized controlled trials ,17 1 observational study,18 1 within-subject RCT,19 and 1 health economic evaluation.20 Appendix 1 presents the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA)21 flow chart of the study selection.
Summary of Study Characteristics
Appendix 2 provides details regarding the characteristics of the included studies (Table 2).
Study Design
Bansback and colleagues conducted a systematic literature review and NMA of 24 RCTs, with the search conducted on October 25, 2024.17 The included studies had follow-up periods ranging from 3 to 12 months, with most reporting outcomes at 6 months. Dobischok and colleagues conducted a secondary analysis of police record data from a clinical trial (SALOME), transforming the clinical trial into an observational study.18 Participants in this cohort received 6 months of iOAT and were observed over a 3-year period, beginning 1 year before randomization and ending 2 years after. Agin-Liebes and colleagues used a randomized, double-blind, placebo-controlled, within-subject crossover trial design to assess the dose efficacy of hydromorphone compared to placebo in reducing acute pain responses in patients receiving maintenance therapy of moderate to high doses of oral methadone (80 to 100 mg/day).19 After each experimental session, participants were monitored overnight, with assessments conducted the following day. Tse and colleagues conducted health economic evaluations that used a decision tree model to simulate different public health scenarios, each with a 1-year time horizon.20
Country of Origin
The systematic review and NMA conducted by Bansback et al. had an international scope, including trials from Australia, Canada, the US, and various European countries.17 The observational study by Dobischok et al. was conducted in Vancouver, Canada.18 The within-subject RCT by Agin-Liebes et al. took place in the US.19 The health economic model developed by Tse et al. was specifically designed for the Australian context.20
Patient Population
The systematic review and NMA by Bansback et al. focused broadly on people with OUD who use street opioids (i.e., opioids manufactured outside the regulated supply that are often of unpredictable doses) and whose disease had not responded to conventional treatments.17 The observational study by Dobischok et al. included 192 clinical trial participants with severe, chronic OUD and a history of injection drug use.18 The RCT by Agin-Liebes et al. had the most specific population, consisting of 8 individuals without chronic pain whose conditions were stabilized with high-dose oral methadone.19 The health economic model by Tse et al. was based on a hypothetical cohort of 10,000 people who inject opioids.20
Interventions and Comparators
The systematic review and NMA by Bansback et al. compared iOAT, such as diacetylmorphine (medical heroin) and hydromorphone, against conventional oral treatments such as methadone and sublingual buprenorphine.17 Most included trials of diacetylmorphine were conducted with injectable diacetylmorphine; only 1 trial included in the systematic review gave participants the option of an injectable or inhalable form. Buprenorphine was consistently administered sublingually across all included trials. Methadone was primarily administered orally. However, 2 trials investigated both oral and injectable routes, and 1 trial did not specify the route of administration. Given the predominance of the oral form, this report will refer to methadone without specifying the route, assuming the oral formulation.
The observational study by Dobischok et al. compared criminal justice system involvement during periods of iOAT, periods of other treatments like oral methadone, and periods of no treatment for the same individuals.18 In the RCT by Agin-Liebes et al.,19 each participant served as their own control, receiving both an escalating IV dose of hydromorphone and an IV placebo. iOAT can be delivered through supervised and unsupervised models. For supervised iOAT, patients self-inject prescribed opioids under direct medical observation in a clinical setting, typically 2 to 3 times per day. This approach maximizes safety, but it also demands substantial infrastructure and requires patients to adhere to a rigid schedule of clinic attendance. Unsupervised iOAT allows patients greater flexibility and autonomy. It enables them to self-administer prescribed opioids outside clinics, often through take-home doses or specialized dispensing machines. However, this convenience comes with greater safety risks than supervised iOAT. The economic model by Tse et al. compared various scenarios, adding different types of iOAT (supervised or unsupervised) to the existing treatment (oral OAT).20
Outcomes
The systematic review and NMA by Bansback and colleagues focused on treatment retention, days of illicit drug use (opioid and cocaine use), and involvement in criminalized activities, as reported by the study authors.17 Treatment retention was often defined by included clinical trials as either attending the final trial follow-up visit or completing the planned treatments.17
The primary outcomes of the observational study by Dobischok and colleagues were the rates of criminal charges, obtained from the Vancouver Police Department and other local police jurisdictions, spanning a period of 1 year before randomization to 2 years afterward.18
The within-subject RCT by Agin-Liebes and colleagues measured the analgesic response (e.g., quantitative sensory testing, cold pressor test, pressure pain, thermal pain), outcomes reported by the authors as abuse liability (e.g., visual analogue scale, money versus drug questionnaire, next-day questionnaire, AEs), and other physiological measures (e.g., vital signs, pupil diameter).19 Of these outcomes, only AEs were relevant to our review and are summarized in this report.
The health economic model by Tse and colleagues estimated the number of fatal and nonfatal overdoses, total treatment costs, and the cost per life saved based on the Australian government perspective.20 The time horizon of modelled scenarios was 1 year.20
Summary of Critical Appraisal
Reporting
Bansback and colleagues registered the protocol for their systematic review and NMA17 in the International Prospective Register of Systematic Reviews (PROSPERO) and followed the PRISMA guidelines. Agin-Liebes and colleagues presented a Consolidated Standards of Reporting Trails (CONSORT) diagram in their RCT report.19 Tse and colleagues adhered to the Consolidated Health Economic Evaluation Reporting Standards (CHEERS) checklist in their economic model study.20 A limitation of the systematic review's reporting was that detailed outcome measures for illicit drug use (opioid and cocaine use) and criminalized activities from the included studies were not fully presented.17 The systematic review17 and the included observational study18 by Dobischok and colleagues did not report on AEs or safety outcomes, which limits a full understanding of the risk-benefit profile of the intervention. For the economic model study,20 specific details on currency adjustments for inflation and statistical measures, such as confidence intervals (CIs) for stochastic data, were not thoroughly reported.
Internal Validity
The systematic review and NMA17 that Bansback et al. conducted included a comprehensive search, had dual independent reviewers, and used Bayesian methods with sensitivity analyses. The review reported low to moderate heterogeneity across the main networks. The authors employed random-effects models, which are a suitable statistical approach for accounting for heterogeneity between studies in most cases. However, for outcomes with sparse data (e.g., criminalized activity), random-effects models may yield unstable results with wide credible intervals (CrIs). The authors used a node-splitting method to assess discrepancies between direct and indirect evidence and did not identify any substantial inconsistencies, suggesting the consistency assumption was likely met.
The review noted several potential differences or effect modifiers across the included trials, such as patients' prior treatment experience, variations in dosing strategies, and differing follow-up durations.17 The researchers conducted several sensitivity and subgroup analyses, noting that the study's main conclusions were robust, which indicates that the transitivity assumption was likely met.
However, several limitations could affect its conclusions. The analysis had to address inconsistencies in definitions and timing of outcomes across the included primary studies.17 Studies with missing outcomes were excluded from analyses rather than being addressed through imputation.17 The review also did not include a formal certainty of evidence assessment, such as using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) system.17
The Dobischok et al. study,18 being an observational analysis, cannot be used to infer causality. A key limitation is that the posttrial treatment states were not randomized; participants self-selected into different paths, introducing potential confounding.18 Adherence to these posttrial treatments was not monitored,18 which could have influenced the outcomes.
The Agin-Liebes et al. within-subject RCT19 used a design that minimizes bias between the intervention and placebo. However, it had an important limitation in its sample size of only 8 participants, which was lower than its planned enrolment (N = 15) and likely left the study underpowered to detect true differences (type II error).19 The administration of fixed hydromorphone doses without adjustment for patient weight or methadone blood levels19 may have influenced the results.
The Tse et al. health economic evaluation20 managed uncertainty through probabilistic and univariate sensitivity analyses. A limitation inherent to the modelling study is its reliance on effectiveness estimates and assumptions drawn from existing literature,20 particularly given the scarcity of data for certain parameters, such as unsupervised iOAT.
External Validity
The Bansback et al. systematic review and NMA17 synthesized evidence from multiple countries and regions, including Australia, Canada, Europe, and the US. The findings of the review may be broadly applicable to people with OUD in Canada. However, its generalizability may be limited by its focus on English-language publications and its specific population of individuals who use injectable street opioids, which may not represent all people with OUD.
The Dobischok et al. observational study18 was conducted in a single site in Vancouver and may not be directly applicable to other geographical or health care contexts across Canada. The Agin-Liebes et al. RCT19 has limited generalizability due to its small, demographically homogeneous sample from a single site in the US and its focus on a highly specific clinical population (patients receiving stable, high doses of methadone without chronic pain).
The Tse et al. economic models20 were specifically designed for the Australian context, and their conclusions on cost-effectiveness may not be applicable to other countries, including Canada. The model’s 1-year time horizon also limits its ability to predict the longer-term economic and health effects of implementing iOAT programs.20
Additional details regarding the strengths and limitations of the included studies are provided in Appendix 3.
Summary of Findings
Based on 1 systematic review and NMA,17 1 observational study,18 1 within-subject and crossover RCT,19 and 1 health economic modelling study,20 we have summarized the clinical effectiveness, safety, and cost-effectiveness of iOAT for adults with OUD. Appendix 4 presents the main study findings, which are summarized by outcome.
Effectiveness
Treatment Retention (1 Systematic Review and NMA)
The evidence indicates that iOAT with or without oral OAT may be associated with greater odds of treatment retention compared to most oral therapies alone. The NMA17 findings indicated:
patients receiving injectable diacetylmorphine (heroin) with or without methadone had higher odds of completing treatment compared to those receiving methadone alone (odds ratio [OR] = 2.01; 95% CrI, 1.07 to 3.71) or buprenorphine plus naloxone alone (OR = 4.45; 95% CrI, 1.39 to 13.19)
patients receiving injectable hydromorphone plus low-dose oral methadone had higher odds of completing treatment compared to those receiving low- or medium-dose buprenorphine, medium-dose buprenorphine plus naloxone alone, low- or high-dose methadone alone, or depot formulations of injectable naltrexone
in nearly all comparisons that did not reach statistical significance, the ORs consistently favoured treatment with iOAT over treatments without iOAT.
Days of Opioid Use in the Past Month (1 Systematic Review)
The evidence indicates that iOAT with or without oral OAT may lead to significant reductions in the use of opioids in the past month compared to methadone alone. The NMA17 findings indicated:
injectable hydromorphone with or without methadone may result in fewer days of opioid use in the past month compared to methadone alone (mean difference [MD] = −5.20 days; 95% CrI, −7.89 days to −2.55 days) or buprenorphine alone (MD = −9.77 days; 95% CrI, −14.00 days to −5.54 days)
injectable diacetylmorphine with or without methadone may result in fewer days of opioid use per month compared to methadone alone (MD = −6.11 days; 95% Crl, −7.08 days to −5.07 days) or buprenorphine alone (MD = −10.63 days; 95% CrI, −14.11 days to −7.25 days)
for comparisons that did not reach statistical significance, treatment with iOAT appeared to result in fewer days of opioid use than treatment without iOAT.
Days of Cocaine Use in the Past Month (1 Systematic Review)
The evidence indicates that iOAT plus methadone may lead to a significant reduction in the use of cocaine in the past month compared to methadone alone. The NMA17 found that:
compared to high-dose methadone alone, patients receiving injectable diacetylmorphine plus low-dose methadone may have fewer days of cocaine use in the past month (MD = −4.32 days; 95% CI, −7.86 days to −0.70 days)
days of cocaine use in the past month did not differ significantly across treatments in the network defined at the medication level.
Interactions With the Criminal Justice System, Reported in Studies as Criminalized Activities (1 Systematic Review and 1 Observational Study)
The evidence from 2 studies17,18 demonstrates that iOAT with or without oral OAT may reduce patients’ involvement with the criminal justice system.
The NMA17 found that patients receiving injectable diacetylmorphine with or without methadone may have lower odds of participating in criminalized activity (as reported by study authors) compared to patients receiving oral methadone alone (OR = 0.74; 95% CI, 0.58 to 0.95).
One observational study18 found that participants were more likely to be charged with a crime (as reported by study authors) during periods of no treatment before the trial compared to when they were receiving iOAT (adjusted rate ratio = 2.61; 95% CI, 1.64 to 4.14).
The observational study18 found that the rate of criminal charges (as reported by study authors) during periods while patients received other treatment (e.g., oral OAT) was higher than during periods while they received iOAT, but the difference was not statistically significant.
Safety
Adverse Events (1 RCT With 8 Participants)
A within-subject clinical trial19 compared the AEs associated with injectable hydromorphone use (administered under medical supervision) versus those associated with placebo and found injectable hydromorphone to be safe and well-tolerated.
There were no reports of any serious AEs.
All AEs reported were rated as mild in severity.
More AEs occurred during placebo sessions than during hydromorphone sessions of the trial. The most common AEs included:
nausea (20%), infusion site pain (20%), pruritus (20%), headache (20%), and hives or rash (20%) with hydromorphone
headache (25%), nausea (25%), somnolence (12.5%), hypoesthesia (12.5%), and hives or rash (12.5%) with placebo.
No significant differences were found in AE frequency between the hydromorphone and placebo sessions.
Health Economic Evaluation (1 Modelling Study)
One modelling study20 evaluated the cost-effectiveness of introducing different scenarios of supervised and unsupervised iOAT compared to the status quo (oral OAT) in Australia.
Scenario 4 of the study, implementing oral OAT with 1.2% of patients receiving supervised iOAT and 10% receiving unsupervised iOAT, was found to be the most cost-effective approach.
Scenario 4 yielded a cost per death averted of AU$3,723,340 (95% uncertainty interval, AU$3,385,878 to AU$3,894,379) and a cost per overdose averted of AU$56,598 (95% uncertainty interval, AU$50,655 to AU$59,637).
The models indicated that scenario 4 was cost-effective because the cost was lower than the Australian government's willingness-to-pay threshold.
Scenarios that focused more on supervised iOAT (oral OAT with 5% of patients receiving supervised iOAT; oral OAT with 5% of patients receiving supervised iOAT and 5.69% of patients receiving unsupervised iOAT) were not found to be cost-effective.
The authors concluded that incorporating iOAT for individuals whose disease does not respond to conventional oral OAT may reduce overdoses and overdose deaths compared to oral OAT only. The study model indicates that using more unsupervised iOAT relative to supervised iOAT could deliver these benefits at a lower cost.
Limitations
The body of evidence supporting this review has several important limitations that need to be considered when interpreting the findings. There were some evidence gaps in reporting across the included studies. Neither the systematic review17 by Bansback et al. nor the observational study18 by Dobischok et al. reported AEs or safety outcomes, which prevents a full assessment of the risk-benefit profile of iOAT from this evidence. The economic model by Tse et al. lacked thorough details on currency adjustments and only reported results for a 1-year horizon.20
There are some methodological limitations within the evidence base, which are outlined in the Summary of Critical Appraisal section. For example, in their network meta-analysis, Bansback et al. had to manage inconsistent outcome definitions and timings across studies but did not include a formal certainty of evidence assessment (e.g., GRADE).17 The observational nature of the Dobischok et al. study18 suggests causality cannot be inferred; participant self-selection into posttrial treatment states introduces a high risk of confounding. The within-subject RCT19 by Agin-Liebes et al. was likely underpowered due to its very small sample size (N = 8), limiting its ability to detect true differences in safety outcomes (type II error).
The generalizability of the findings to the broader context in Canada varies. The systematic review and NMA17 synthesized international evidence and may be applicable to settings in Canada. The findings from the observational study18 by Dobischok et al. (based on a single site in Vancouver) and the RCT19 by Agin-Liebes et al. (based on a small, homogeneous sample at a single US site) have limited generalizability. The economic models20 were specifically designed for the Australian context; their conclusions on cost-effectiveness are not directly transferable to other health care systems, such as those in Canada. The 1-year time horizon also limits the prediction of longer-term effects.20
Conclusions and Implications for Decision- or Policy-Making
CDA-AMC conducted this review to summarize evidence on the clinical effectiveness, safety, and cost-effectiveness of iOAT compared to no treatment or other treatments. We included 1 systematic review and NMA,17 1 observational study,18 1 within-subject RCT,19 and 1 health economic modelling study.20 Despite the limitations of the body of evidence, the findings provide evidence that iOAT may be an effective and safe treatment option for adults with OUD.
Effectiveness
Based on 1 systematic review and NMA,17 iOAT alone or in combination with other treatments may be more effective than other treatments (e.g., oral OAT) for improving treatment retention and reducing opioid use and cocaine use in the past month. For example, patients receiving injectable hydromorphone may have higher odds of being retained in treatment compared to those receiving oral methadone. iOAT was associated with fewer days of illicit opioid use in the past month compared to buprenorphine. Evidence from 1 systematic review and NMA17 and 1 observational study18 also showed that iOAT may reduce involvement in criminalized activities compared to both oral OAT and periods of no treatment.
The effectiveness of iOAT aligns with the findings of the 2020 CADTH review12 regarding improvements in treatment retention, reductions in illicit drug use, and reductions in criminalized activities. However, we did not identify any studies that reported the effects of iOAT on rates of convictions, imprisonment, or mortality in this review.
Safety
Based on 1 small RCT (N = 8),19 injectable hydromorphone (administered under medical supervision) appears to have a good safety profile. No serious AEs were reported and all AEs were mild. There were no significant differences in AE frequency between the groups receiving hydromorphone or placebo. The results indicate that injectable hydromorphone (administered under medical supervision) had little or no difference in safety profile compared to placebo. Due to the low confidence in the findings regarding safety, we suggest considering the findings of the 2020 CADTH review for a better understanding of the safety profile of iOAT.12
Cost-Effectiveness
Based on 1 economic modelling study from Australia,20 the cost-effectiveness of iOAT depends on the model of implementation. A scenario prioritizing unsupervised iOAT (received by 10% of the patient population) alongside a smaller component of supervised iOAT (1.2%) was found to be cost-effective, with a cost per death averted of AU$3,723,340.20 Scenarios focusing primarily on supervised iOAT were not found to be cost-effective within the Australian context.20 We did not identify any cost-effectiveness studies of iOAT compared to other treatments within the Canadian context.
Considerations for Future Research
To address the identified evidence gaps, future primary studies should use robust designs with adequate sample sizes and ensure comprehensive reporting of all outcomes, including AEs. Future systematic reviews should include a formal certainty of evidence assessment (e.g., GRADE) and investigate sources of heterogeneity by exploring the potential subgroup effects. High-quality research on the implementation of unsupervised iOAT may be needed. To inform policy decisions in Canada, cost-effectiveness analyses specific to health care contexts in Canada are required.
Implications for Clinical Practice and Policy-Making
Despite the limitations, the body of evidence suggests that iOAT may be an effective intervention with a good safety profile that reduces illicit opioid and cocaine use and interactions with the criminal justice system. iOAT should be considered an option in the continuum of care for individuals with OUD, particularly for patients whose disease has not responded to oral OAT. The findings on cost-effectiveness suggest that policy-makers should consider models of care that incorporate unsupervised or take-home iOAT, because this may offer a more cost-effective approach to expanding treatment access and averting overdose deaths.
References
1.Yakovenko I, Mukaneza Y, Germé K, et al. Management of opioid use disorder: 2024 update to the national clinical practice guideline. CMAJ. 2024;196(38):E1280-e1290. PubMed
2.Schuckit Marc A. Treatment of Opioid-Use Disorders. N Engl J Med. 2016;375(4):357-368. PubMed
3.Praveen KT, Law F, O'Shea J, Melichar J. Opioid dependence. BMJ Clin Evid. 2011;2011.
4.Degenhardt L, Grebely J, Stone J, et al. Global patterns of opioid use and dependence: harms to populations, interventions, and future action. Lancet. 2019;394(10208):1560-1579. PubMed
5.Holland A, Brothers TD, Lewer D, Maynard OM, Southwell M. “Safer supply” alternatives to toxic unregulated drug markets. BMJ. 2024;384:q6. PubMed
6.Belzak L, Halverson J. The opioid crisis in Canada: a national perspective. Health Promot Chronic Dis Prev Can. 2018;38(6):224-233. PubMed
7.Ledlie S, Juurlink DN, Tadrous M, Mamdani M, Paterson JM, Gomes T. Opioid-related deaths between 2019 and 2021 across 9 Canadian provinces and territories. CMAJ. 2024;196(14):E469-e476. PubMed
8.Santo T, Jr., Clark B, Hickman M, et al. Association of Opioid Agonist Treatment With All-Cause Mortality and Specific Causes of Death Among People With Opioid Dependence: A Systematic Review and Meta-analysis. JAMA psychiatry. 2021;78(9):979-993. PubMed
9.Schwarz T, Akartuna D, Busch M, Krausz RM, Uhl A. Challenges for the implementation of injectable opioid agonist treatment: a scoping review. Harm reduction journal. 2024;21(1):217. PubMed
10.Eydt E, Glegg S, Sutherland C, et al. Service delivery models for injectable opioid agonist treatment in Canada: 2 sequential environmental scans. CMAJ Open. 2021;9(1):E115-e124. PubMed
11.Fairbairn N, Ross J, Trew M, et al. Injectable opioid agonist treatment for opioid use disorder: a national clinical guideline. CMAJ. 2019;191(38):E1049-e1056. PubMed
12.Banerjee S, Wright MD. CADTH Rapid Response Reports. Injectable Opioid Agonist Treatment for Patients with Opioid Dependence: A Review of Clinical and Cost-Effectiveness. Ottawa (ON): Canadian Agency for Drugs and Technologies in Health.Copyright © 2020 Canadian Agency for Drugs and Technologies in Health.; 2020.
13.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
14.Jansen JP, Trikalinos T, Cappelleri JC, et al. Indirect treatment comparison/network meta-analysis study questionnaire to assess relevance and credibility to inform health care decision making: an ISPOR-AMCP-NPC Good Practice Task Force report. Value Health. 2014;17(2):157-173. PubMed
15.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
16.Higgins JPT, Green S, editors. Figure 15.5.a: Drummond checklist (Drummond 1996). Cochrane handbook for systematic reviews of interventions. London (GB): The Cochrane Collaboration; 2011: http://handbook-5-1.cochrane.org/chapter_15/figure_15_5_a_drummond_checklist_drummond_1996.htm. Accessed 2025 Sep 22.
17.Bansback N, Tam ACT, Palis H, et al. Oral and injectable opioid agonist treatments for people who use street opioids: a systematic literature review and network meta-analysis. BMC Public Health. 2025;25(1):2974. PubMed
18.Dobischok S, Guh D, Marchand K, et al. The Impact of Injectable Opioid Agonist Treatment (iOAT) on Involvement in Criminalized Activities: A Secondary Analysis from a Clinical Trial in Vancouver, BC. Subst Abuse Rehabil. 2023;14:147-156. PubMed
19.Agin-Liebes G, Huhn AS, Strain EC, et al. Methadone maintenance patients lack analgesic response to a cumulative intravenous dose of 32 mg of hydromorphone. Drug Alcohol Depend. 2021;226:108869. PubMed
20.Tse WC, Scott N, Dietze P, Nielsen S. Modeling the cost and impact of injectable opioid agonist therapy on overdose and overdose deaths. J Subst Abuse Treat. 2022;143:108871. PubMed
21.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
Appendix 1: Selection of Included Studies
Figure 1: PRISMA Flow Chart of Study Selection
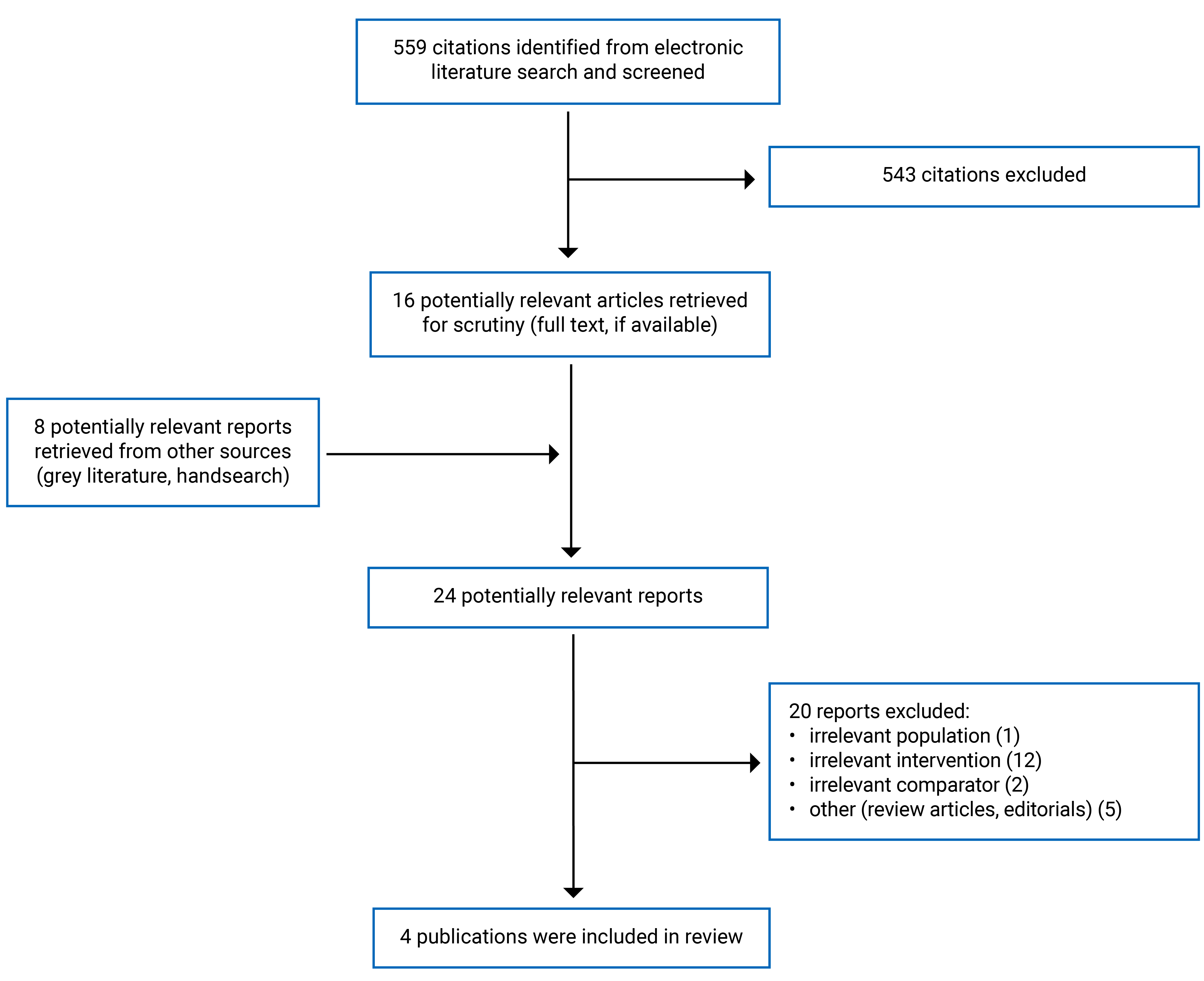
PRISMA = Preferred Reporting Items for Systematic reviews and Meta-Analyses.21
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of Included Systematic Reviews
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Bansback et al. (2025)17 Canada Funding source: CIHR | Study design: Systematic review and Bayesian network meta-analysis of RCTs Number of included studies: 24 trials (28 articles) Country: Canada, US, UK, Germany, Netherlands, Spain, Belgium, Austria, Italy, Norway, Switzerland, and Australia Included studies: published from January 2013 to October 2024 | Population: Non-incarcerated, non-pregnant individuals with OUD Number of participants: over 4,000 overall, individual trial size ranged from 27 to 740 Mean age: NR Sex: NR Disease duration: NR | Intervention and comparators:
| Outcomes:
Follow-up: from 3 to 12 months, with most trials reporting outcomes at 6 months (0.5 months) |
CIHR = Canadian Institutes of Health Research; NMA = network meta-analysis; NR = not reported; OAT = opioid agonist treatment; OUD = opioid use disorder; RCT = randomized controlled trial.
Note: This table has not been copy-edited.
Table 3: Characteristics of Included Primary Clinical Studies
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, Treatment period |
|---|---|---|---|---|
Dobischok et al. (2023)18 Canada (Vancouver, British Columbia) Funding source: CIHR and other programs | Design: Secondary analysis of a Phase III, double-blind, non-inferiority RCT (SALOME). Focus: Examined police record data over a 3-year period to assess the impact of iOAT on criminal charges. | Adult patients (≥ 18 years) with long-term opioid use disorder enrolled in the SALOME trial Gender, %:
Mean age (SD), years: 44.5 (NR) Ethnicity, %:
Housing status, %:
Substance use history:
| Intervention iOAT using:
Comparator:
| Number and type of criminal charges during different treatment states. Treatment Duration: 6 months of iOAT Follow-Up: Each participant was followed from 1 year before randomization to 2 years after (3-year observation period). |
Agin-Liebes et al. (2021)19 US Funding Source:
| Design: within-subject double-blind RCT Focus: Assessed analgesic and abuse liability effects of escalating IV hydromorphone doses in methadone-maintained individuals Setting: Residential research unit at Johns Hopkins Bayview Medical Center | Population Characteristics Sample Size: 8 participants (originally planned for 15) Age: Mean 43.5 years (SD = 9.7, range 31 to 58) Gender: 63% male Ethnicity: 88% white Methadone Maintenance Duration: Mean 17.8 months (SD = 26.5; range 1 to 71) Inclusion Criteria: Adults aged 18 to 60 on stable methadone dose (80 to 100 mg/day), no chronic pain Exclusion Criteria: Alcohol dependence, illicit drug use, medical/psychiatric conditions affecting QST, pregnancy/lactation, analgesic use, hydromorphone allergy | Intervention: IV hydromorphone administered in escalating doses (4 mg + 4 mg + 8 mg + 16 mg = 32 mg total) Comparator: IV placebo (saline) Within-subject crossover; each participant received both the intervention and the comparator in separate sessions | Primary Outcomes:
Treatment Duration: Single-day sessions for each condition, spaced at least 1 week apart. Follow-Up: Participants monitored overnight after each session; next-day assessments conducted |
CIHR = Canadian Institutes of Health Research; iOAT = injectable opioid agonist treatment; NMA = network meta-analysis; NR = not reported; OAT = opioid agonist treatment; RCT = randomized controlled trial, VAS = visual analogue scale.
Note: This table has not been copy-edited.
Table 4: Characteristics of Included Economic Evaluation
Study citation country, funding source | Type of analysis, time horizon, perspective | Population characteristics | Intervention and comparator(s) | Approach | Source of clinical, cost, and utility data used in analysis | Main assumptions |
|---|---|---|---|---|---|---|
Tse et al. (2023)20 Australia (modelling based on Australian parameters) Funding source: National Health and Medical Research Council of Australia a | Type of Analysis:
Time horizon: 1-year per modelled scenario Perspective: Government perspective, focusing on direct treatment costs (excluding societal costs like hospitalizations or criminal justice) | Inclusion Criteria:
| Intervention: iOAT Comparator: Current opioid agonist therapy (OAT) only (methadone and buprenorphine) Scenarios: 1. OAT only 2. OAT + 5% supervised iOAT 3. OAT + 5% supervised + 5.69% unsupervised iOAT 4. OAT + 1.2% supervised + 10% unsupervised iOAT | Decision tree modelling with probabilistic sensitivity analysis Outcomes modelled include:
Parameters derived from literature, expert input, and Australian cohort data | Clinical data: Systematic reviews, cohort studies, targeted PubMed searches (up to June 20, 2020) Cost data:
Utility data: Not explicitly modelled, the focus was on overdose and death outcomes. | 1. Equal overdose risk for supervised and unsupervised iOAT (same drug/dose) 2. Fatal overdose risk assumed equal for witnessed and unwitnessed events without naloxone 3. Cost of unsupervised iOAT estimated by subtracting clinic costs from supervised iOAT |
iOAT = injectable opioid agonist therapy; OAT = opioid agonist therapy.
aAuthors received unrelated funding from Indivior, Seqirus, Gilead Sciences, and Reckitt Benckiser.
Note: This table has not been copy-edited.
Appendix 3: Critical Appraisal of Included Publications
Please note that this appendix has not been copy-edited.
Table 5: Strengths and Limitations of Systematic Reviews Using AMSTAR 2 and the ISPOR Questionnaire
Strengths | Limitations |
|---|---|
Bansback et al. (2025)17 | |
|
|
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; Bayesian NMA = Bayesian network meta-analysis; CENTRAL = Cochrane Central Register of Controlled Trials; CIHR = Canadian Institutes of Health Research; CINAHL = Cumulative Index to Nursing and Allied Health Literature; CRD = Centre for Reviews and Dissemination (used in PROSPERO registration number); Embase = Excerpta Medica Database; GRADE = Grading of Recommendations Assessment, Development and Evaluation; ISPOR = International Society for Pharmacoeconomics and Outcomes Research (used here to refer to their questionnaire for assessing network meta-analysis credibility); OAT = opioid agonist treatment; OUD = opioid use disorder; PICOS = population, intervention, comparison, outcomes, and study design; PRISMA = Preferred Reporting Items for Systematic Reviews and Meta-Analyses; PROSPERO = International Prospective Register of Systematic Reviews; PubMed = Public/Publisher MEDLINE; RCT = randomized controlled trial.
Table 6: Strengths and Limitations of Clinical Studies Using the Downs and Black Checklist
Strengths | Limitations |
|---|---|
Dobischok et al. (2023)18 | |
Reporting:
Internal validity:
External validity:
|
|
Agin-Liebes et al. (2021)19 | |
Reporting:
Internal Validity:
External Validity:
|
|
iOAT = injectable opioid agonist treatment; RCT = randomized controlled trial.
Table 7: Strengths and Limitations of Economic Evaluation Using the Drummond Checklist
Strengths | Limitations |
|---|---|
Tse et al. (2023)20 | |
Study design:
Data collection:
Analysis and interpretation
|
|
iOAT = injectable opioid agonist treatment; OAT = opioid agonist treatment; RCT = randomized controlled trial.
Appendix 4: Main Study Findings
Please note that this appendix has not been copy-edited.
Table 8: Summary of Findings by Outcome — Retention by Medication
Study citation and study design | Intervention | Comparator | Point estimate (OR) | 95% credible interval |
|---|---|---|---|---|
Bansback et al. (2025)17 Systematic review and NMA of RCTs | Heroin | Methadone | 2.17 | (0.76, 6.43) |
Buprenorphine | 2.8 | (0.75, 10.29) | ||
Buprenorphine + naloxonea | 4.84 | (1.16, 19.73) | ||
Naltrexone | 4.45 | (0.81, 23.08) | ||
Heroin + methadone | Methadonea | 2.01 | (1.07, 3.71) | |
Buprenorphine | 2.59 | (0.95, 6.61) | ||
Buprenorphine + naloxonea | 4.45 | (1.39, 13.19) | ||
Naltrexone | 4.09 | (0.93, 16.17) | ||
Hydromorphone | Methadonea | 8.19 | (1.58, 53.29) | |
Buprenorphinea | 10.58 | (1.74, 77.57) | ||
Buprenorphine + naloxonea | 18.18 | (2.72, 144.83) | ||
Naltrexonea | 16.77 | (1.98, 155.77) | ||
Hydromorphone + methadone | Methadone | 2.1 | (0.46, 9.31) | |
Buprenorphine | 2.71 | (0.50, 14.01) | ||
Buprenorphine + naloxone | 4.69 | (0.77, 26.39) | ||
Naltrexone | 4.31 | (0.58, 29.63) |
NMA = network meta-analysis; OR = odds ratio; RCT = randomized controlled trial.
aStatistically significant at P < 0.05
Table 9: Summary of Findings by Outcome — Retention by Dosage Strength
Study citation and study design | Intervention | Comparator | Point estimate (OR) | 95% credible interval |
|---|---|---|---|---|
Bansback et al. (2025)17 Systematic review and NMA of RCTs | Heroin | High-dose methadone | 1.86 | (0.68, 5.02) |
Medium-dose methadone | 1.84 | (0.51, 5.92) | ||
Low-dose methadone | 2.99 | (0.84, 9.90) | ||
High-dose buprenorphine | 1.1 | (0.08, 11.32) | ||
Medium-dose buprenorphine | 2.55 | (0.68, 8.29) | ||
Low-dose buprenorphinea | 6.85 | (1.67, 25.58) | ||
Buprenorphine + naloxonea | 4.44 | (1.18, 14.16) | ||
Naltrexone | 4.32 | (0.92, 16.42) | ||
Heroin + low-dose methadone | High-dose methadonea | 3.67 | (1.83, 8.35) | |
Medium-dose methadonea | 3.66 | (1.57, 8.82) | ||
Low-dose methadonea | 5.88 | (2.34, 16.33) | ||
High-dose buprenorphine | 2.21 | (0.18, 21.54) | ||
Medium-dose buprenorphinea | 5.07 | (2.03, 12.47) | ||
Low-dose buprenorphinea | 13.55 | (4.51, 42.52) | ||
Buprenorphine + naloxonea | 8.8 | (3.11, 23.96) | ||
Naltrexonea | 8.54 | (2.30, 27.93) | ||
Heroin + medium-dose methadone | High-dose methadone | 1.08 | (0.50, 2.49) | |
Medium-dose methadone | 1.06 | (0.50, 2.34) | ||
Low-dose methadone | 1.72 | (0.70, 4.48) | ||
High-dose buprenorphine | 0.64 | (0.05, 6.57) | ||
Medium-dose buprenorphine | 1.46 | (0.64, 3.42) | ||
Low-dose buprenorphinea | 3.94 | (1.41, 11.36) | ||
Buprenorphine + naloxone | 2.55 | (0.91, 7.02) | ||
Naltrexone | 2.47 | (0.67, 8.26) | ||
Hydromorphone | High-dose methadonea | 7.5 | (1.77, 42.23) | |
Medium-dose methadonea | 7.38 | (1.46, 46.84) | ||
Low-dose methadonea | 12.17 | (2.35, 77.24) | ||
High-dose buprenorphine | 4.5 | (0.28, 67.28) | ||
Medium-dose buprenorphinea | 10.21 | (1.95, 64.72) | ||
Low-dose buprenorphinea | 27.52 | (4.82, 192.48) | ||
Buprenorphine + naloxonea | 17.86 | (3.32, 109.66) | ||
Naltrexonea | 17.17 | (2.67, 118.22) | ||
Hydromorphone + low-dose methadone | High-dose methadonea | 3.88 | (1.05, 15.59) | |
Medium-dose methadone | 3.83 | (0.95, 15.70) | ||
Low-dose methadonea | 6.25 | (1.49, 27.50) | ||
High-dose buprenorphine | 2.32 | (0.16, 29.92) | ||
Medium-dose buprenorphinea | 5.3 | (1.26, 22.28) | ||
Low-dose buprenorphinea | 14.21 | (2.98, 69.52) | ||
Buprenorphine + naloxonea | 9.23 | (2.04, 41.05) | ||
Naltrexonea | 8.98 | (1.62, 43.95) |
NMA = network meta-analysis; OR = odds ratio; RCT = randomized controlled trial.
aStatistically significant at P < 0.05
Table 10: Summary of Findings by Outcome — Retention by Dosing Variability
Study citation and study design | Intervention | Comparator | Point estimate (OR) | 95% credible interval |
|---|---|---|---|---|
Bansback et al. (2025)17 Systematic review and NMA of RCTs | Heroin | Methadone (variable) | 1.86 | (0.50, 7.12) |
Buprenorphine (fixed) | 8.18 | (0.42, 170.50) | ||
Buprenorphine (variable) | 3.43 | (0.56, 19.61) | ||
Buprenorphine (variable) + naloxone | 4.63 | (0.83, 24.75) | ||
Methadone (fixed) | 5.77 | (0.30, 116.87) | ||
Naltrexone | 4.22 | (0.58, 28.60) | ||
Heroin + methadone (variable) | Methadone (variable)a | 2 | (1.03, 3.85) | |
Buprenorphine (fixed) | 8.61 | (0.55, 152.04) | ||
Buprenorphine (variable) | 3.67 | (0.91, 14.30) | ||
Buprenorphine (variable) + naloxonea | 4.96 | (1.38, 16.94) | ||
Methadone (fixed) | 6.1 | (0.40, 103.10) | ||
Naltrexone | 4.59 | (0.88, 20.76) | ||
Hydromorphone | Methadone (variable)a | 7.47 | (1.39, 53.14) | |
Buprenorphine (fixed)a | 33.01 | (1.33, 934.86) | ||
Buprenorphine (variable)a | 13.74 | (1.70, 132.55) | ||
Buprenorphine (variable) + naloxonea | 18.63 | (2.50, 166.31) | ||
Methadone (fixed)a | 23.42 | (1.01, 618.74) | ||
Naltrexonea | 17.27 | (1.80, 183.14) | ||
Hydromorphone + methadone (variable) | Methadone (variable) | 2.12 | (0.44, 9.66) | |
Buprenorphine (fixed) | 9.08 | (0.42, 220.03) | ||
Buprenorphine (variable) | 3.9 | (0.51, 26.43) | ||
Buprenorphine (variable) + naloxone | 5.22 | (0.75, 33.09) | ||
Methadone (fixed) | 6.42 | (0.30, 150.80) | ||
Naltrexone | 4.83 | (0.53, 37.37) |
NMA = network meta-analysis; OR = odds ratio; RCT = randomized controlled trial.
aStatistically significant at P < 0.05
Table 11: Summary of Findings by Outcome — Days of Opioid Use by Medication
Study citation and study design | Intervention | Comparator | Point estimate (MD) | 95% credible interval |
|---|---|---|---|---|
Bansback et al. (2025)17 Systematic review and NMA of RCTs | Heroin | Methadonea | −6.71 | (−9.61, −3.94) |
Buprenorphinea | −11.29 | (−15.68, −6.92) | ||
Heroin + methadone | Methadonea | −6.11 | (−7.08, −5.07) | |
Buprenorphinea | −10.63 | (−14.11, −7.25) | ||
Hydromorphone | Methadonea | −12.03 | (−16.41, −7.82) | |
Buprenorphinea | −16.59 | (−22.02, −11.15) | ||
Hydromorphone + methadone | Methadonea | −5.2 | (−7.89, −2.55) | |
Buprenorphinea | −9.77 | (−14.00, −5.54) |
MD = mean difference; NMA = network meta-analysis; RCT = randomized controlled trial.
aStatistically significant at P < 0.05
Table 12: Summary of Findings by Outcome — Days of Opioid Use by Dosage Strength
Study citation and study design | Intervention | Comparator | Point estimate (MD) | 95% credible interval |
|---|---|---|---|---|
Bansback et al. (2025)17 Systematic review and NMA of RCTs | Heroin | High-dose methadonea | −6.7 | (−9.51, −3.86) |
Buprenorphine (low)a | −12.06 | (−17.57, −6.72) | ||
Low-dose methadonea | −7.08 | (−12.75, −1.10) | ||
Medium-dose methadonea | −8.04 | (−11.72, −4.40) | ||
Heroin + low-dose methadone | High-dose methadonea | −6.14 | (−7.27, −4.97) | |
Buprenorphine (low)a | −11.43 | (−16.31, −6.78) | ||
Low-dose methadonea | −6.43 | (−11.51, −1.34) | ||
Medium-dose methadonea | −7.46 | (−9.89, −5.17) | ||
Heroin + medium-dose methadone | High-dose methadonea | −3.44 | (−6.84, −0.03) | |
Buprenorphine (low)a | −8.76 | (−14.12, −3.56) | ||
Low-dose methadone | −3.77 | (−9.44, 1.98) | ||
Medium-dose methadonea | −4.81 | (−8.26, −1.21) | ||
Hydromorphone | High-dose methadonea | −12.05 | (−16.53, −7.71) | |
Buprenorphine (low)a | −17.34 | (−24.05, −11.02) | ||
Low-dose methadonea | −12.4 | (−19.31, −5.74) | ||
Medium-dose methadonea | −13.35 | (−18.57, −8.40) | ||
Hydromorphone + low-dose methadone | High-dose methadonea | −5.27 | (−8.08, −2.61) | |
Buprenorphine (low)a | −10.54 | (−16.18, −5.35) | ||
Low-dose methadone | −5.59 | (−11.31, 0.08) | ||
Medium-dose methadonea | −6.57 | (−10.09, −3.31) |
MD = mean difference; NMA = network meta-analysis; RCT = randomized controlled trial.
aStatistically significant at P < 0.05
Table 13: Summary of Findings by Outcome — Days of Opioid Use by Dosing Variability
Study citation and study design | Intervention | Comparator | Point estimate (MD) | 95% credible interval |
|---|---|---|---|---|
Bansback et al. (2025)17 Systematic review and NMA of RCTs | Heroin | Methadone (variable)a | −6.7 | (−9.52, −3.92) |
Heroin + methadone (variable) | Methadone (variable)a | −6.11 | (−7.12, −5.07) | |
Hydromorphone | Methadone (variable)a | −11.95 | (−16.25, −7.75) | |
Hydromorphone + methadone (variable) | Methadone (variable)a | −5.28 | (−7.98, −2.69) |
MD = mean difference; NMA = network meta-analysis; RCT = randomized controlled trial.
aStatistically significant at P < 0.05
Table 14: Summary of Findings by Outcome — Days of Cocaine Use by Medication
Study citation and study design | Intervention | Comparator | Point estimate (MD) | 95% credible interval |
|---|---|---|---|---|
Bansback et al. (2025)17 Systematic review and NMA of RCTs | Heroin | Methadone | 1.68 | (−1.92, 5.18) |
Heroin + methadone | Methadone | −1.04 | (−2.33, 0.21) | |
Hydromorphone + methadone | Methadone | 2.57 | (−0.83, 5.85) |
MD = mean difference; NMA = network meta-analysis; RCT = randomized controlled trial.
Table 15: Summary of Findings by Outcome — Days of Cocaine Use by Dosage Strength
Study citation and study design | Intervention | Comparator | Point estimate (MD) | 95% credible interval |
|---|---|---|---|---|
Bansback et al. (2025)17 Systematic review and NMA of RCTs | Heroin | High-dose methadone | 1.77 | (−1.80, 5.22) |
Medium-dose methadone | 2.18 | (−2.83, 7.31) | ||
Heroin + low-dose methadone | High-dose methadone | −0.51 | (−1.76, 0.78) | |
Medium-dose methadone | −0.05 | (−4.12, 3.94) | ||
Heroin + medium-dose methadone | High-dose methadonea | −4.32 | (−7.86, −0.70) | |
Medium-dose methadonea | −3.88 | (−7.10, −0.58) | ||
Hydromorphone + low-dose methadone | High-dose methadone | 3.06 | (−0.24, 6.28) | |
Medium-dose methadone | 3.57 | (−1.68, 8.72) |
MD = mean difference; NMA = network meta-analysis; RCT = randomized controlled trial.
aStatistically significant at P < 0.05
Table 16: Summary of Findings by Outcome — Days of Cocaine Use by Dosing Variability
Study citation and study design | Intervention | Comparator | Point estimate (MD) | 95% credible interval |
|---|---|---|---|---|
Bansback et al. (2025)17 Systematic review and NMA of RCTs | Heroin + methadone (variable) | Methadone (variable) | −1.05 | (−2.35, 0.23) |
Hydromorphone + methadone (variable) | Methadone (variable) | 2.54 | (−0.86, 5.99) |
MD = mean difference; NMA = network meta-analysis; RCT = randomized controlled trial.
Table 17: Summary of Findings by Outcome — Participating in Illegal Activity
Study citation and study design | Intervention | Comparator | Point estimate (MD) | 95% credible interval |
|---|---|---|---|---|
Bansback et al. (2025)17 Systematic review and NMA of RCTs | Heroin | Methadone | 0.72 | (0.28, 1.88) |
Heroin + methadone | Methadonea | 0.74 | (0.58, 0.95) |
MD = mean difference; NMA = network meta-analysis; RCT = randomized controlled trial.
aStatistically significant at P < 0.05
Table 18: Summary of Findings by Outcome — Criminal Charge Rate
Study citation and study design | Intervention | Comparator | Unadjusted rate ratio (95% CI) | Adjusted rate ratio (95% CI) |
|---|---|---|---|---|
Dobischok et al. (2023)18 Observational study | Diacetylmorphine or hydromorphone | Other treatment | 1.27 (0.73 to 2.21) | 1.25 (0.64 to 2.47) |
Methadonea | 0.74 | (0.58, 0.95) | ||
No treatment – post SALOME trial | 2.08 (1.41 to 3.05) | 1.72 (0.99 to 2.97) | ||
No treatment – prior SALOME trial | 2.73 (1.96 to 3.80) | 2.61 (1.64 to 4.14) |
CI = confidence interval; MD = mean difference.
aStatistically significant at P < 0.05
Table 19: Summary of Findings by Outcome — Safety
Study citation and study design | Adverse events | Placebo | Hydromorphone |
|---|---|---|---|
Agin-Liebes et al. (2021)19 RCT | Nausea | 2 (25%) | 1 (20%) |
Hypoesthesia | 1 (12.5%) | 0 | |
Infusion site pain | 0 | 1 (20%) | |
Pruritus | 0 | 1 (20%) | |
Headache | 2 (25%) | 1 (20%) | |
Hives/rash | 1 (12.5%) | 1 (20%) | |
Somnolence | 1 (12.5%) | 0 |
RCT = randomized controlled trial.
Note: There were no significant differences between groups.
Table 20: Summary of Findings of Included Economic Evaluation
Main study findings | Authors’ conclusion |
|---|---|
Tse et al. (2023)20 | |
| “Modeling the provision of a mix of OAT, supervised iOAT, and unsupervised iOAT suggests that the incorporation of iOAT for people who do not respond to conventional OAT treatment may decrease the number of overdoses and overdose deaths compared to maintaining the status quo in treatment provision. Our model suggests that benefits could be achieved with lower costs if a greater proportion of unsupervised iOAT is used relative to supervised iOAT, without increased overall harm.” (p. 9) |
iOAT = injectable opioid agonist treatment; OAT = opioid agonist treatment; UI = uncertainty interval.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@cda-amc.ca.