Drugs, Health Technologies, Health Systems
Health Technology Review
Asynchronous Teleultrasound and In-Person Ultrasound: Comparing Diagnostic Accuracy
Key Messages
What Is the Issue?
Access to ultrasound services remains limited in many parts of Canada, with fewer than 28% of rural hospitals having in-house ultrasound, often resulting in patients being transferred to urban centres.4
Ultrasound imaging requires highly trained professionals,1,2 typically sonographers, for accurate diagnostic exams and interpretation. However, Canada and many other countries are facing a shortage of trained sonographers, which can impact access to timely care.5,6
As a portable and radiation-free modality, ultrasound is ideal for real-time soft-tissue imaging, though CT, MRI, and PET-CT may be preferred for more complex cases.3
Teleultrasound (TUS) has emerged to support an increase in ultrasound demand, particularly in resource-limited environments.2,7
TUS can be delivered in real time with remote guidance from a sonographic expert, or images can be sent asynchronously for expert interpretation.1,2
TUS can be used by a variety of health care professionals with minimal ultrasound training, but as asynchronous models expand, their comparability to standard in-person ultrasound requires further evaluation.
What Did We Do?
We received a request related to the use of asynchronous TUS to support policy decision-making. In response, we prepared this rapid review to summarize and critically appraise the available studies on the quality of health care provided with asynchronous TUS (unsupervised ultrasound with remote exam interpretation by an expert) as compared to the traditional service model of ultrasound.
A literature search was conducted, limited to English-language reports published since 2019, to identify relevant studies and evidence-based guidelines. A single reviewer screened records for inclusion based on predefined criteria, critically appraised the included studies, extracted relevant data, and summarized the findings.
What Did We Find?
We found 11 cohort selection cross-sectional studies that examined health care quality (diagnostic accuracy, image quality, and acceptability) across various target conditions.
Overall, asynchronous TUS was found to be an alternative method to the standard in-person model of ultrasound for identifying certain targeted conditions, when assessing diagnostic accuracy and exam image quality.
Asynchronous TUS was accepted by patients and clinicians, based on a limited number of studies that examined this outcome.
Asynchronous TUS was studied in a wide range of clinical indications in various settings, highlighting its growing role and potential for expanded application in clinical practice.
There is uncertainty regarding the acceptable balance of sensitivity and specificity for each target condition. The heterogeneity of study results, potential bias, and a limited volume of recent evidence impacts the overall interpretability of findings.
What Does This Mean?
Asynchronous teleultrasound TUS could improve access to diagnostic imaging, particularly in underserved or low-resource settings where in-person ultrasound services are limited.
Wider clinical adoption would depend on establishing standardized training, procedural protocols, and supportive regulatory frameworks to ensure quality, consistency, and patient safety across settings.
The evidence shows potential for asynchronous TUS use in clinical practice, but variation in study quality and unclear diagnostic standards mean it should be used cautiously and evaluated carefully within specific clinical contexts.
Further research is needed to enhance understanding of patient outcomes, define condition-specific diagnostic accuracy thresholds (i.e., acceptable balance of sensitivity and specificity), and explore the impact on health system performance.
Background
Ultrasonography is a portable and noninvasive imaging method that uses sound waves to visualize internal organs, structures, and systems within the body in real time. Ultrasound examinations are primarily conducted by sonographers and interpreted by physicians specializing in medical imaging.
Ultrasound imaging is a highly operator-dependent imaging modality that requires well-trained operators to perform the scan, adjust the protocol based on clinical judgment, take appropriate images, and provide accurate technical impressions for the interpreting physician. Therefore, the accuracy of the final report depends on the expertise of the interpreting physician and the skill of the sonographer.2,3
The quality of an ultrasound exam varies depending on the sonographer’s experience with operating the equipment, whereas the image quality of CT or MRI exams is less dependent on the operator’s performance.2 As well, ultrasound is much more affordable and portable than CT and MRI, and unlike CT, it does not expose patients to radiation.4 As a result, ultrasound is the preferred method for soft-tissue imaging in cases where the higher image quality of CT and MRI is not needed.4
Access to ultrasound services in rural or underserved regions is often limited by the number of qualified professionals, available equipment, and infrastructure or resources.3,5,6 In Canada, less than 28% of rural emergency departments have in-house access to ultrasound, requiring patient transfers from rural communities to facilities with ultrasound capacity.7
Ultrasound exams are conducted by imaging professionals, a shortage of which have been reported in Canada and in many other countries worldwide.8,910 Recruitment and retention challenges have also exacerbated existing staff shortages and contribute to longer wait times for diagnostics exams.8,9
Teleultrasound (TUS) is an imaging technique that uses advances in information technology and ultrasound to support ultrasound delivery and remote clinical decision-making.1,2 TUS involves performing an ultrasound exam at 1 location and then electronically transmitting the images to another location where they are interpreted by an imaging expert.2,6,10 TUS systems support decision-making across a wide range of clinical settings, and examinations may be conducted at the point-of-care or in emergency settings, community settings, or dedicated imaging facilities.
TUS is intended to enhance patient care by offering access to specialized expertise either to complement existing services or to provide care in resource-limited settings. By expanding access to these services, TUS has the potential to improve time to diagnosis, reduce costs for both patients and the health care system, and decrease patient transfers and travel time.3,11-13
How Is Teleultrasound Delivered?
TUS can be conducted using either real-time (synchronous) or asynchronous (“store-and-forward”) video or image transmission.5,10,14
Real-time “supervised” transmission: The ultrasound exam occurs with real-time supervision by an imaging expert, often a sonographer or radiologist. The imaging expert is located in a remote location and provides guidance to an onsite ultrasound operator.2,15 Canada's Drug Agency published a report examining the comparative effectiveness of real-time teleultrasound versus in-person ultrasound.
Asynchronous transmission: The ultrasound images are captured locally, stored, and later sent to the remote expert for review and interpretation. This approach enables individuals with limited or no imaging experience (e.g., medical students, health care professionals without an imaging background) to use basic scanning protocols to obtain images, which can then be transmitted for expert review without degradation of image quality.2,5,14,16
With rapid advances in diagnostic imaging technology, asynchronous TUS has gained greater use as a tool to support the delivery of patient care, particularly in resource-limited settings.2,13,17,18 One such development in asynchronous TUS is the growing use of volume sweep imaging (VSI), which is a standardized technique that involves sweeping the ultrasound probe over a target area using simple, predefined movements to capture images. These images are then later transmitted to an expert for review.5 VSI is a method that enables individuals with little or no prior ultrasound experience to perform scans, which suggests it has potential value in settings with limited access to resources or trained imaging professionals.10
Purpose of This Review
As asynchronous TUS (i.e., unsupervised ultrasound with remote exam interpretation by an expert) continues to expand to different clinical areas, its comparability with traditional in-person ultrasound in terms of health care quality remains uncertain.1,19 This report aims to compare the diagnostic accuracy, patient care quality, and service quality provided by asynchronous TUS with that of traditional in-person ultrasound. This report also aims to summarize the recommendations from evidence-based guidelines regarding the use of TUS in clinical practice for supporting the diagnosis of various medical conditions.
Objectives
We prepared this rapid review to address the following questions:
What is the diagnostic accuracy and agreement of asynchronous TUS compared to the traditional service model of ultrasound with an in-person imaging specialist?
How do asynchronous TUS and the traditional in-person US service model compare in terms of patient care quality and service quality?
What are the evidence-based guidelines regarding the use of TUS in clinical practice for supporting the diagnosis of various medical conditions?
Methods
Literature Search Methods
The literature search strategy used in this report is an updated version of a strategy developed for a previous report published by Canada's Drug Agency on the comparative effectiveness of real-time teleultrasound versus in-person ultrasound. For the current report, an information specialist conducted a literature search using key resources, including MEDLINE, the Cumulative Index to Nursing and Allied Health Literature (CINAHL), the Cochrane Database of Systematic Reviews, and the International HTA Database. The search also included a review of websites of health technology assessment agencies in Canada and major international health technology assessment agencies, as well as a focused internet search to capture grey literature.
The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevance. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were ultrasound and telemedicine or remote supervision. The initial search was limited to English-language documents published between January 1, 2019, and August 27, 2024. For the current report, database searches were rerun on March 6, 2025, to capture any articles published or made available since the initial search date. The search of the grey literature was also updated to include documents published since August 2024.
Eligibility Criteria and Study Selection Methods
One reviewer screened records and selected studies based on the eligibility criteria presented in Table 1. In the first level of screening, the titles and abstracts were reviewed, and potentially relevant articles were retrieved for full-text review. In the second level of screening, 1 reviewer assessed potentially relevant full texts for inclusion. Articles published before 2019 were excluded from this report due to the focus on recent evidence and emerging TUS developments.
Criteria | Description |
|---|---|
Population | Patients of any age seeking ultrasound exams for any health condition |
Index test | Asynchronous TUS (i.e., unsupervised ultrasound with remote exam interpretation by an expert, “store-and-forward” method) |
Reference standard | Traditional ultrasound service model (standard in-person ultrasound delivered and interpreted by an onsite imaging specialist) |
Outcomes | Q1: Diagnostic accuracy (sensitivity, specificity, diagnostic agreement) Q2:
Q3: Recommendations regarding TUS use in clinical practice for diagnostic purposes |
Study designs | Health technology assessments, systematic reviews, single-group designs, nonrandomized studies, evidence-based guidelines |
Exclusion criteria |
|
TUS = teleultrasonography.
Data Extraction
Relevant articles underwent data extraction by 1 reviewer using a standardized form. Information extracted included study design, population characteristics, ultrasound characteristics, ultrasound operator and remote expert profile (i.e., role and experience), study inclusion and exclusion criteria, and relevant results.
Critical Appraisal of Individual Studies
One reviewer assessed the risk of bias of the included studies using Quality Assessment of Diagnostic Accuracy Studies 2 (QUADAS-2).20 The risk of bias of each included study was described narratively and summarized by the following 4 QUADAS-2 domains: patient selection, index test, reference standard, and flow and timing.
Summary of Evidence
Quantity of Research Available
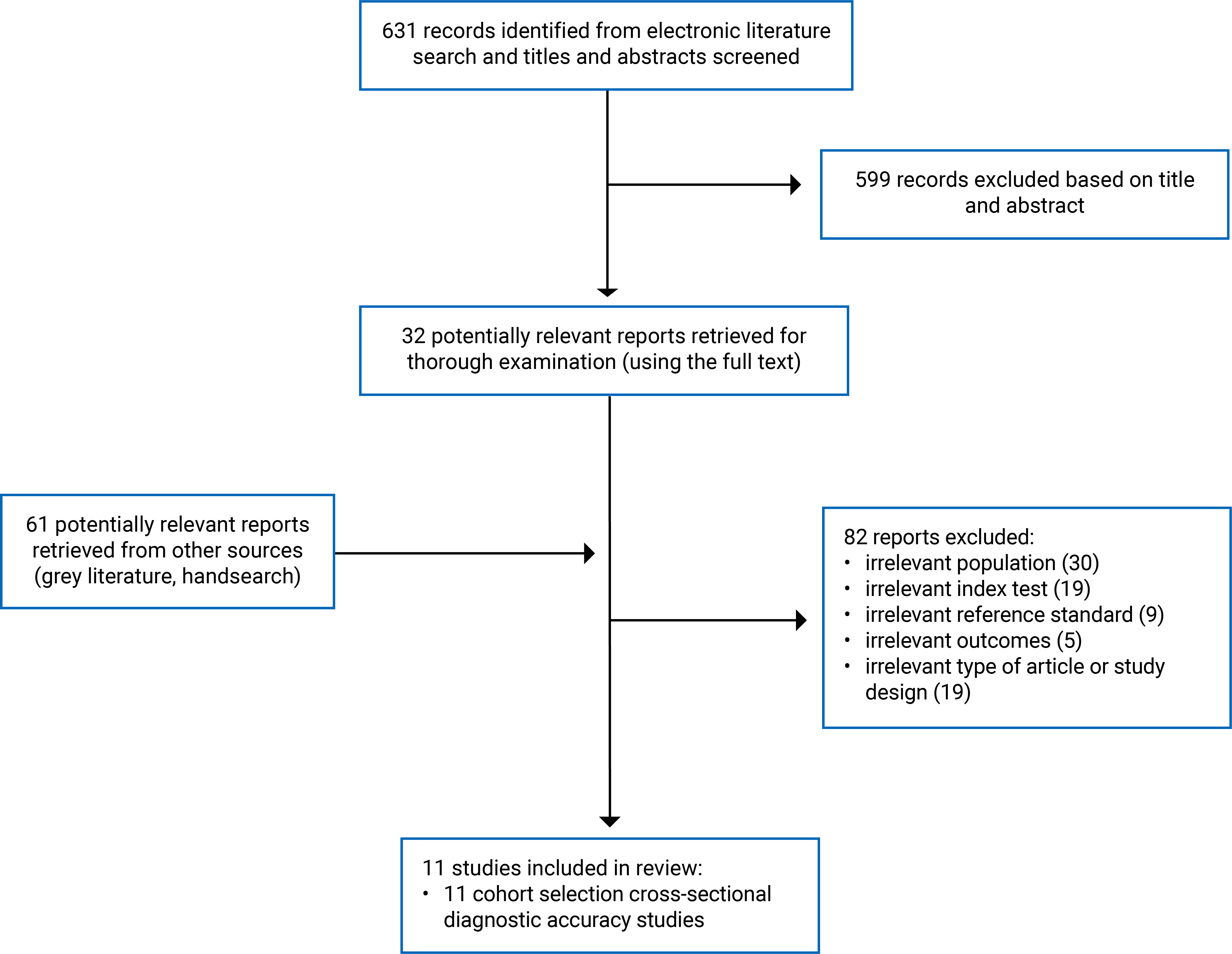
A total of 692 records from the literature search were identified, including 61 potentially relevant records from the grey literature. Following screening of titles and abstracts, 660 records were excluded, and 32 potentially relevant reports were retrieved for full-text review.
Overall, 11 unique studies met the inclusion criteria.21-31 No evidence-based guidelines for TUS were identified. Refer to Appendix 1, Figure 1 for the PRISMA32 flow chart of study selection.
Eleven primary studies across 8 countries were included in this report, totalling 976 patients who underwent either asynchronous TUS, traditional in-person ultrasound, or both.
A total of 35 remote imaging experts located in 14 countries reviewed the TUS images. Detailed characteristics of the 11 included studies are presented in Appendix 2, Table 2.
Study Design
Eleven prospective studies examining diagnostic agreement and accuracy were published between 2019 and 2024. These included 11 cohort selection cross-diagnostic accuracy studies21-31
Country of Origin
The included studies enrolled patients from 9 countries who underwent standard in-person ultrasound: Brazil,28,29 China,24 Colombia,30 France,27 Indonesia,30 Norway,23 Peru,25,26,31 Spain,21 and the US.22
The remotely located imaging experts who reviewed the TUS exams were located in 14 countries: Argentina,30 Brazil,28-30 China,24 Colombia,30 Egypt,30 England,30 France,27 Ghana,30 Ireland,30 Italy,30 Norway,23 Spain,21 Taiwan,30 and the US.22,25,26,28-31
Patient Population
A summary of the patient populations and clinical settings for each included study is presented in Appendix 2, Table 2. The 11 primary studies included 976 adult, pediatric, and pregnant individuals.
Index Test and Reference Standard
The index test used in all studies was delivered through various scanning methods:
The use of general ultrasound was reported in 5 studies,22,25,26,30,31 of which 4 used a standardized VSI protocol.22,25,26,31
The use of a hand-held electrocardiogram (ECG) device was reported in 2 studies.28,29
The use of the following imaging techniques was reported in 1 study each: 3D ultrasound,27 dermatological ultrasound,21 bedside transthoracic echocardiogram,24 and echocardiogram.23
In all cases, the reference standard was standard in-person delivered and interpreted ultrasound by a trained sonologist or medical professional with imaging expertise.
A summary of the index test, reference standard, and characteristics of the ultrasound operator and expert TUS interpreter are provided in Appendix 2, Table 2.
Outcomes
Diagnostic accuracy (sensitivity, specificity, agreement) was reported on in 11 studies.21-31
Clinical utility and acceptance (patient or health care professional) were reported on in 2 studies.27,30
Summary of Findings
Asynchronous TUS was found to be an alternative method to the standard in-person model of ultrasound for identifying certain targeted conditions when evaluating diagnostic accuracy. However, results varied across individual studies depending on the target condition.
Asynchronous TUS showed substantial diagnostic agreement with standard in-person ultrasound across most studies, although several studies showed variable findings.
In most studies, the image quality of ultrasound images transmitted to the offsite expert for interpretation was reported to be acceptable or excellent, although some studies showed mixed results.
Asynchronous TUS was reported to have high utility and acceptance by clinicians and patients, based on 2 studies that examined these outcomes.
Diagnostic Accuracy
The diagnostic accuracy of asynchronous TUS interpretation was evaluated across several key diagnostic test accuracy metrics (including sensitivity, specificity, and agreement). Notably, acceptable thresholds for these metrics may differ depending on the target condition being evaluated.
Sensitivity and Specificity
The reported sensitivity and specificity of asynchronous TUS interpretation varied within the individual studies and by target condition. In a total of 621-23,25,27,31 of the 11 included studies, the authors reported on the sensitivity and specificity of asynchronously interpreted TUS compared to standard-of-care interpreted ultrasound (Appendix 3, Table 3).
Alfageme et al. (2021)21 reported that asynchronous TUS interpretation demonstrated 100% sensitivity and 97.8% specificity for detecting malignant dermatological tumours.
Hjorth-Hansen et al. (2020)23 reported that asynchronous TUS interpretation demonstrated 100% sensitivity and 95% or higher specificity for detecting moderate mitral stenosis, mitral regurgitation, and tricuspid regurgitation. In contrast, for detecting moderate aortic stenosis, asynchronous TUS interpretation showed a sensitivity of 43% and a specificity of 97% for a subgroup analysis.
Toscano et al. (2021)31reported that asynchronous TUS interpretation demonstrated 100% sensitivity and specificity for all targeted fetal variables (i.e., fetal number, fetal presentation, placental location, amniotic fluid volume).
Marini et al. (2021)25 found that for all exams, regardless of image quality, the index test demonstrated 84.2% sensitivity (95% confidence interval [CI], 60.4 to 96.6%) and 97.7% specificity (95% CI, 91.9 to 99.7%) for identifying cholelithiasis. For exams that were considered to be of “acceptable” or “excellent” imaging quality, the index test demonstrated 93% sensitivity (95% CI, 68.1% to 99.8%) and 97% specificity (95% CI, 89.5% to 99.6%).
Morel et al. (2022)27 reported that compared to standard ultrasound, asynchronous TUS interpretation by a senior radiologist and medical resident demonstrated sensitivities of 86% and 84%, and specificities of 95% and 92%, respectively.
Dougherty et al. (2020)22 reported that the sensitivity and specificity varied widely across target variables of interest. For fetal number, the sensitivity ranged from 83% to 100%, and the specificity ranged from 99% to 100%. For placental location, sensitivity ranged from 33% to 100%, and specificity ranged from 35% to 99%.
Diagnostic Agreement
Overall, asynchronous TUS interpretation showed substantial diagnostic agreement with standard in-person ultrasound across most of the 11 included studies,21-27,29,31 although some studies showed variable findings22,26,28-30 (Appendix 3, Table 3). For studies reporting diagnostic agreement using the kappa statistic, the following classification scale was used for interpretation: “poor” (0.0), “slight” (0.01 to 0.2), “fair” (0.21 to 0.4), “moderate” (0.41 to 0.6), “substantial” (0.61 to 0.80), and “almost perfect” (0.81 to 1).33 Of note, these classifications do not account for the clinical significance of agreement levels in real-world practice.
Morel et al. (2022)27 reported almost perfect agreement between 3D ultrasound and standard abdominal ultrasound (kappa = 0.82; range, 0.72 to 0.92) when evaluated by an expert radiologist, and substantial agreement (kappa = 0.71; range, 0.58 to 0.82) when evaluated by a radiology resident.
Hjorth-Hansen et al. (2020)23 reported substantial agreement between tele-ECG and standard in-person ECG for classifying heart failure (weighted kappa = 0.73).
Marini et al. (2021)25 highlighted agreement between the abdominal VSI protocol and standard-of-care abdominal ultrasound for exams of “acceptable” or “excellent” image quality. The authors reported almost perfect agreement (86% to 100%) between the index test and reference standard for whether the exam was abnormal (94.5%) or showed liver echogenicity (100%), pancreas abnormalities (100%), liver abnormalities (98.9%), gallbladder abnormalities (86.8%), or right kidney abnormalities (86.2%).
Toscano et al. (2021)31 reported substantial to perfect agreement (85.6% to 100%) between the obstetric VSI ultrasound protocol and the standard-of-care ultrasound for several fetal variables: number of fetuses (100%), fetal presentation (95.8%; kappa = 0.78), placental location (85.6%; kappa = 0.74), and live fetus status (76.2%). Overall, exams were interpreted as normal or abnormal with almost perfect agreement (95.2% to 100%).
Lu et al. (2021)24 reported that the diagnostic agreement of onsite bedside transthoracic echocardiogram was fair (63.3%) when compared to the diagnoses provided through asynchronous TUS (kappa = 0.3 to 0.6). The authors concluded that asynchronous interpreted TUS exams had superior accuracy.
Alfageme et al. (2021)21 reported 95.7% overall concordance between the TUS and in-person diagnosis for dermatological lesions.
Marini et al. (2021)26 reported almost perfect agreement (98.3%) on the presence of a nodule between the thyroid VSI protocol and standard ultrasound (kappa = 0.91; 95% CI, 0.78 to 1) but reported lower agreement for thyroid size measurements (intraclass correlation coefficient = 0.37 to 0.58).
Dougherty et al. (2020)22 reported almost perfect agreement for the anterior and posterior variables relating to the location of the placenta (kappa = 0.81 to 0.9) and number of fetuses (kappa = 0.82 to 1) but reported slight or fair (i.e., kappa = 0 to 0.39) agreement for variables relating to the location where the placenta attaches to the uterus (left, right, fundal, low).
Nascimento et al. (2021)29 reported 80.4% and 82.2% agreement between hand-held ECG and standard ECG for identifying major heart disease and mitral valve disease, respectively, and noted 40% agreement for aortic valve disease.
Nascimento et al. (2019)28 reported substantial agreement (78.8%) between the screening ECG and standard-of-care ECG for significant heart disease.
Nieto-Calvache et al. (2024)30 reported substantial agreement (71.7%) between evaluations made by the teleconsultants and the local care team for placenta accreta spectrum.
Exam Image Quality
Overall, the quality of ultrasound images transmitted to remote experts for asynchronous interpretation was generally reported to be acceptable to excellent, though findings varied across studies (Appendix 3, Table 3). Of the 11 included studies, the authors of 621,25-27,30,31 reported on this outcome:
Toscano et al. (2021)31 reported excellent or acceptable quality in 99% of exams, whereas Marini et al. (2021)26 reported excellent quality in 88% of exams.
Alfageme et al. (2021)21 and Nieto-Calvache et al. (2024)30 reported that 4.2% and 16.7% of exams, respectively, were of insufficient quality and not included for interpretation.
Morel et al. (2021)27 reported that 84% of images were considered to be of good to excellent quality when evaluated by an expert radiologist. The authors reported that 70% of the images were considered to be of good to excellent quality when evaluated by a radiology resident.
Marini et al. (2021)25 reported that 63.2% of images were classified by offsite radiologists as being of excellent or acceptable quality.
Utility and Patient Acceptance
Overall, asynchronous TUS was reported to have high utility and acceptance. This outcome was evaluated in 27,30 of the 11 included studies (Appendix 3, Table 3):
Nieto-Calvache et al. (2024)30 reported that 100% of teleconsultants believed that telemedicine could support disease management. The authors reported that 84.6% of teleconsultants considered the TUS protocol useful for surgical treatment planning and 75% did not find remote image evaluation any more difficult than evaluating images in person.
Morel et al. (2022)27 found that the TUS images were obtained without objections from patients, parents, or the operators in more than 95% of exams.
Summary of Critical Appraisal
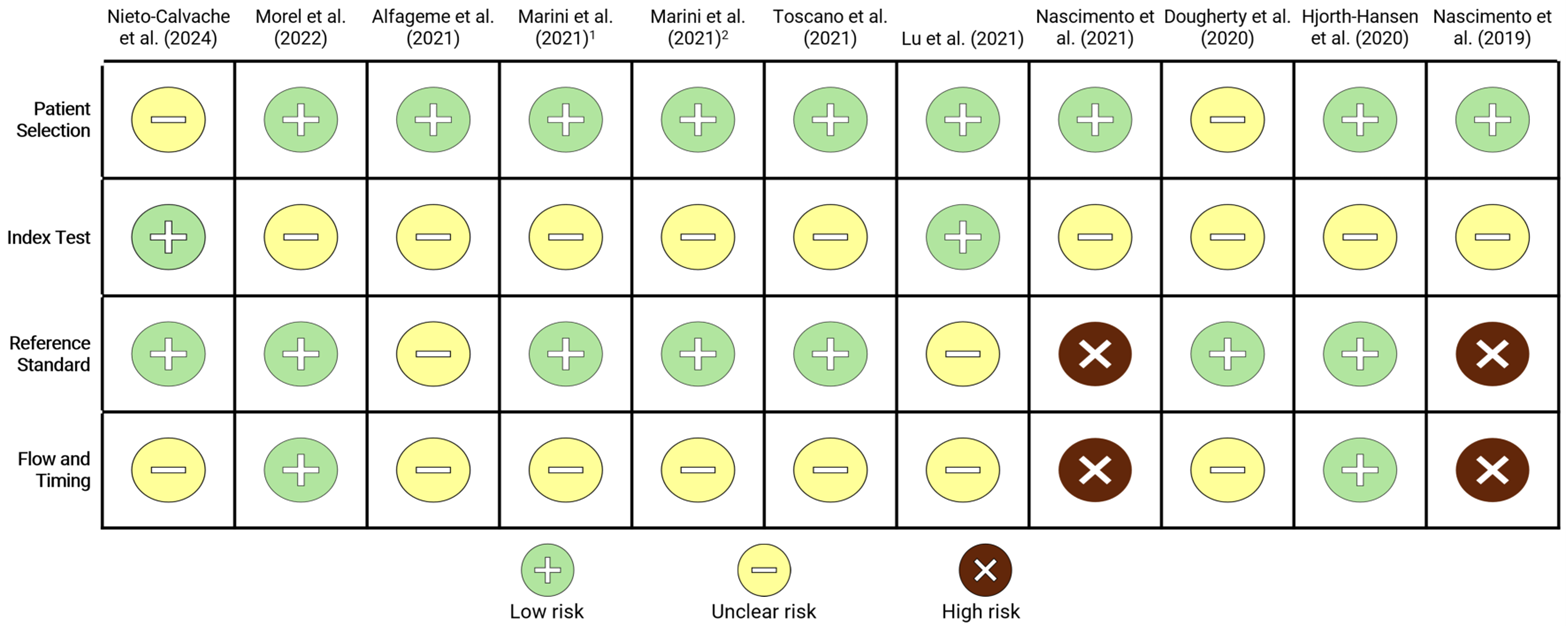
The risk of bias of the included studies was assessed using the QUADAS-2 tool. Appendix 4, Figure 2 presents a summary of the QUADAS-2 results by domain, while Appendix 4, Table 4 contains details about the strengths and limitations of the included studies.21-31
Overall, the included studies were judged to be at a low or unclear risk of bias in the domain of patient selection, with most studies using appropriate and representative recruitment methods. The index test domain was generally judged to have an unclear or high risk of bias. The reference standard domain showed a high risk of bias across studies, with several introducing potential bias through unclear blinding procedures. The flow and timing domain raised the most concern, with several studies having a high or unclear risk of bias due to variable intervals between tests and incomplete application of the reference standard (partial verification). These domain-level concerns may affect the overall internal validity and reliability of the evidence and introduce risk of bias. While the authors of most studies blinded interpretation, some included operators with limited training or lacked detail on test conduct.
Primary Studies
Patient Selection
The 11 studies21-31 comparing asynchronous TUS with standard in-person ultrasound mostly used appropriate methods for patient selection. However, 2 studies22,30 provided limited or no information about patient characteristics and sampling methods, which may have introduced an uncertain risk of bias and limits our understanding of the generalizability of the findings. The patients included in each study correspond to the population of interest in this report.
Index Test
In all 11 studies, the choice of index test (i.e., TUS with asynchronous review) aligned with those targeted by this review. In 10 studies,21-26,28-31 the index test results were interpreted without knowledge of the reference standard results, minimizing potential bias from prior knowledge. It was unclear if this was the case in the other study.27
Seven studies included ultrasound-naive operators who underwent a training protocol to administer the TUS exam.22,23,25,26,28,29,31 It is unclear whether their limited training and experience may have affected the applicability of the index test. Additionally, for 1 multicentre study,21 it was unclear whether all patients received the same index test due to variability in ultrasound equipment across participating sites. Overall, the included studies showed a high risk of bias for the index test.
Reference Standard
In 10 of the 11 studies, the reference standard (i.e., in-person delivered and interpreted ultrasound) matched those targeted by this review.21-23,25-31 In 1 of the studies, a consensus vote approach was used to establish the reference standard.24 In 8 of the 11 studies,21-23,25-27,30,31 the reference standard results were interpreted without knowledge of the results of the index test, reducing potential bias. In all studies, a reference standard likely to correctly classify the target outcomes was used, except for 1 study24 in which the authors reported operator and environmental (i.e., COVID-19) factors that may have impacted the classification accuracy of the reference standard. Overall, across all included studies, there was a high risk of bias related to the reference standard.
Flow and Timing
In 722,24-26,29-31 of the 11 studies, the time frame between interpretation of the index tests and reference standards was unclear. The unknown length of time between the index test and reference standard could lead to different results, potentially reflecting changes in a patient’s condition during that time rather than inaccuracies in the index test. In these 7 studies, the appropriateness of the time frame between the index test and reference standard could not be assessed. The authors of 1 study reported an average time frame of 2 days21 for interpretation of the index test, whereas the authors of 2 other studies reported a time frame of up to 2 months27,28 for both collection and interpretation of the reference standard. The definition of an appropriate time frame may vary by target condition and requires clinical input, which was not available. In 921-27,30,31 of the 11 studies, all patients received the reference standard. In the other 2 studies, only patients who screened positive on the index test (TUS protocol) underwent a confirmatory in-person ultrasound, which may have introduced bias.28,29 In 1 of these 2 studies,29 56% of patients who screened positive attended the follow-up in-person ultrasound, which may have introduced bias due to potential differences in the population lost to follow-up. Overall, across all included studies, there was a high risk of bias related to the flow and timing of the study.
Limitations
This report is limited in part by the quality of the primary studies, several of which are at risk of bias due to important limitations outlined in the critical appraisal section. Most notable, the exact time interval between the interpretation of the TUS and in-person ultrasound exams was unclear in most of the studies reviewed in this report. Overall, 9 studies were judged to have unclear risk of bias in at least 1 domain of the QUADAS-2, whereas 2 were assessed as having a high risk of bias.
For the included studies, clinical experts for each target condition were not consulted to confirm the appropriateness of the reference standard used. Additionally, there was a lack of clarity regarding what is considered an acceptable balance of sensitivity and specificity for these conditions. There is additional uncertainty in the QUADAS-2 appraisal about items requiring clinical expertise to determine whether the reference standard was likely to correctly classify the target condition. In the absence of clinical input, it was assumed that traditional ultrasound was an appropriate reference standard (i.e., likely to correctly classify the target condition) in all cases.
All the studies included in this review compared the image quality and the agreement and accuracy between diagnoses obtained using asynchronous TUS and standard in-person ultrasound. Our search did not identify any studies, or a very limited number of studies, within the inclusion time frame that explored outcomes relating to patient care quality, such as direct patient outcomes. These include outcomes outside of diagnostic results, such as the quality and safety of care, access to care, and how the index test performs in real-world health care settings. Notably, no studies used survey or interview tools to capture patient and ultrasound-naive operator experiences with TUS.
A further limitation of this review is the variability in image acquisition methods used across the included studies. Four studies employed VSI to standardize scan protocols, whereas the others used varied techniques. Differences in imaging methods as well as in the expertise of operators and interpreting physicians across studies may impact the comparability of results and limit conclusions about the diagnostic accuracy, agreement, and service quality of asynchronous TUS when implemented at scale. The use of different imaging methods may have led to varying goals and expectations for those involved in the studies (e.g., ultrasound operator, interpreting physician). Furthermore, the studies reviewed in this report varied in both purpose and the model of care, which may not accurately reflect and be generalizable to practice models in Canada.
The literature search was limited to English-language articles and articles published within the past 5 years. Therefore, the results and conclusions are not comprehensive of all available evidence answering the review questions. The results may have differed if all available evidence had been reviewed. Additionally, this report used a single-reviewer approach for study selection, data extraction, and risk of bias appraisal. This may have increased the risk for bias and error in these processes.
Conclusions and Implications for Decision- or Policy-Making
We reviewed the clinical evidence from 11 primary studies comparing asynchronous remote interpretation of TUS with standard in-person administered and interpreted ultrasound for various target conditions. Based on the literature search conducted for this review, we identified evidence about diagnostic accuracy, image quality, clinical utility, and acceptance. We did not identify any evidence about patient care quality that met our inclusion criteria. Additionally, although several position statements relevant to the use of TUS have been released, we did not identify any evidence-based guidelines to inform clinical practice.34-36
The role and scope of ultrasound imaging specialists and operators vary worldwide. The studies in our report included a range of imaging professionals who interpreted the TUS and in-person exams, including radiologists, specialty physicians, and family physicians with ultrasound experience. TUS and standard in-person ultrasound operators included sonologists, radiologists, physicians with and without ultrasound experience, medical trainees, and specialty physicians. The range of professionals included in this review reflects the variable exam protocols, expectations, and goals relevant to each study’s context, which may not be generalizable to the context in Canada.
Several studies identified in this report showed unclear or high risk of bias relating to patient selection, index test, reference standard, and flow and timing, which reduced the confidence in the studies’ conclusions.
Overall, asynchronous TUS was found to be a diagnostically accurate alternative to the standard in-person model of ultrasound for identifying certain targeted conditions. Asynchronous TUS was accepted by patients and clinicians in the 2 studies that examined these outcomes.27,30 Notably, the included studies performed a wide range of exam types (i.e., abdominal, thyroid, obstetrics, dermatological, and cardiac exams) and included both comprehensive and point-of-care exams, highlighting the growing role and expanding application of TUS in clinical practice.
High levels of diagnostic accuracy (e.g., sensitivity and specificity), diagnostic agreement, and exam image quality were reported across several, but not all, studies. The quality of evidence and conclusions are impacted by bias concerns, the risk of poor image quality, heterogeneity in results, and limited volume of evidence.
Notably, while 622,25,26,28,29,31 of the 11 included studies assessed TUS in low-resource settings, there was a lack of information on the experiences of patients, operators, and teleconsultants regarding factors like acceptability, accessibility, and comfort.
Considering the current limitations in the recent body of evidence, future well-designed and larger-scale studies may be needed to evaluate the quality of care provided by asynchronous TUS beyond feasibility and diagnostic outcomes. This includes exploring patient perspectives on accessibility (equitable access to services, financial burden) and personal preference and expectations, and incorporating surveys and qualitative methods into study designs to examine the impact on outcomes important to patients.
Beyond the current evidence, researchers may consider collecting equity-relevant population characteristics (e.g., gender, education, socioeconomic status, place of residence) to assess potential health disparities related to accessing ultrasound services. Researchers may also consider that equity-deserving populations, such as Indigenous communities, racialized groups, and newcomers to Canada, may face unique barriers to accessing ultrasound services. Therefore, researchers may consider efforts to recruit individuals from diverse groups in future studies. Studies that examine the real-world community, unmet clinical need, and health system impact of asynchronous TUS would also support a better understanding of the role of TUS for increasing access to services and providing timely and accurate diagnoses, particularly in resource-limited settings.3,11
Decision-makers may consider how closely the training, scope of practice, and roles of personnel in their local setting align with those in the reviewed studies. The diagnostic accuracy of asynchronous TUS may depend on the skill level of both image acquirers and interpreters. Therefore, policy or implementation decisions may benefit from being accompanied by clear protocols for training, credentialing, and oversight to ensure diagnostic accuracy, patient safety, and risk management.
References
1.Dearing E, Boniface K. Tele-Ultrasound. In: Sikka N, ed. A Practical Guide to Emergency Telehealth. Oxford University Press; 2021:chap 23.
2.Pian L, Gillman LM, McBeth PB, et al. Potential Use of Remote Telesonography as a Transformational Technology in Underresourced and/or Remote Settings. Emerg Med Int. 2013;2013(1):986160. doi:10.1155/2013/986160 PubMed
3.Adams SJ, Burbridge B, Obaid H, Stoneham G, Babyn P, Mendez I. Telerobotic Sonography for Remote Diagnostic Imaging: Narrative Review of Current Developments and Clinical Applications. Review. J Ultrasound Med. Jul 2021;40(7):1287-1306. doi:https://dx.doi.org/10.1002/jum.15525 PubMed
4.Bhide A, Datar S, Stebbins K. Ultrasound Imaging - Cheap, Versatile, and Safe (Working Paper 20-003). Harvard Business School; 2020. Accessed 2024 Oct 17. https://www.hbs.edu/ris/Publication%20Files/20-003_8157a0c0-71c9-4f6a-88c7-98cba5294123.pdf
5.Dowdy DL, Harris RD. Tele-Ultrasound: Meeting Global Imaging Challenges. Applied Radiology. 2024;53(1):38-41. doi:10.37549/ar2949
6.Duarte ML, Dos Santos LR, Iared W, Peccin MS. Telementored ultrasonography: a narrative review. Review. Sao Paulo Med J. 2022;140(2):310-319. doi:https://dx.doi.org/10.1590/1516-3180.2020.0607.R2.15092021 PubMed
7.Micks T, Sue K, Rogers P. Barriers to point-of-care ultrasound use in rural emergency departments. CJEM. Nov 2016;18(6):475-479. doi:10.1017/cem.2016.337 PubMed
8.Executive Summary. Health Sciences Association of British Columbia; 2016. Accessed 2024 Oct 8. https://www.hsabc.org/sites/default/files/uploads/Executive%20Summary_1.pdf
9.Strategic Plan 2023-2025. Sonography Canada; 2022. Accessed 2024 Oct 8. https://sonographycanada.ca/app/uploads/2022/11/Sonography-Canada-Strategic-Plan-2023-2025-Member-version.pdf
10.Britton N, Miller MA, Safadi S, Siegel A, Levine AR, McCurdy MT. Tele-Ultrasound in Resource-Limited Settings: A Systematic Review. Systematic Review. Front. 2019;7:244. doi:https://dx.doi.org/10.3389/fpubh.2019.00244 PubMed
11.Barberato SH, Lopes M. Echoes of Telecardiology Guideline. Arq Bras Cardiol. 01 2020;114(1):130-132. doi:https://dx.doi.org/10.36660/abc.20190720
12.Hanna TN, Steenburg SD, Rosenkrantz AB, Pyatt RS, Jr., Duszak R, Jr., Friedberg EB. Emerging Challenges and Opportunities in the Evolution of Teleradiology. AJR Am J Roentgenol. Dec 2020;215(6):1411-1416. doi:10.2214/ajr.20.23007 PubMed
13.Uschnig C, Recker F, Blaivas M, Dong Y, Dietrich CF. Tele-ultrasound in the Era of COVID-19: A Practical Guide. Review Research Support, Non-U.S. Gov't. Ultrasound Med Biol. 06 2022;48(6):965-974. doi:https://dx.doi.org/10.1016/j.ultrasmedbio.2022.01.001
14.Chen RJ. Teleultrasound in Remote and Austere Environments. Journal of Mobile Technology in Medicine. 2023;9(1):43-47. doi:10.7309/jmtm.9.1.5
15.Marsh-Feiley G, Eadie L, Wilson P. Telesonography in emergency medicine: A systematic review. PLoS ONE. 2018;13(5):e0194840. doi:10.1371/journal.pone.0194840 PubMed
16.Salerno A, Tupchong K, Verceles AC, McCurdy MT. Point-of-Care Teleultrasound: A Systematic Review. Systematic Review. Telemed J E Health. 11 2020;26(11):1314-1321. doi:https://dx.doi.org/10.1089/tmj.2019.0177
17.Constantinescu EC, Nicolau C, Săftoiu A. Recent Developments in Tele-Ultrasonography. Curr Health Sci J. Apr-Jun 2018;44(2):101-106. doi:10.12865/chsj.44.02.01 PubMed
18.Tenajas R, Miraut D, Illana CI, Alonso-Gonzalez R, Arias-Valcayo F, Herraiz JL. Recent Advances in Artificial Intelligence-Assisted Ultrasound Scanning. Applied Sciences. 2023;13(6):3693.
19.Li XL, Sun YK, Wang Q, et al. Synchronous tele-ultrasonography is helpful for a naive operator to perform high-quality thyroid ultrasound examinations. Ultrasonography. Oct 2022;41(4):650-660. doi:https://dx.doi.org/10.14366/usg.21204 PubMed
20.Whiting PF, Rutjes AW, Westwood ME, et al. QUADAS-2: a revised tool for the quality assessment of diagnostic accuracy studies. Ann Intern Med. Oct 18 2011;155(8):529-36. doi:10.7326/0003-4819-155-8-201110180-00009 PubMed
21.Alfageme F, Minguela E, Martinez C, et al. Dermatologic Ultrasound in Primary Care: A New Modality of Teledermatology: A Prospective Multicenter Validation Study. Multicenter Study. J Ultrasound Med. Feb 2021;40(2):351-356. doi:https://dx.doi.org/10.1002/jum.15409 PubMed
22.Dougherty A, Kasten M, DeSarno M, et al. Validation of a Telemedicine Quality Assurance Method for Point-of-Care Obstetric Ultrasound Used in Low-Resource Settings. J Ultrasound Med. Mar 2021;40(3):529-540. doi:https://dx.doi.org/10.1002/jum.15429 PubMed
23.Hjorth-Hansen AK, Andersen GN, Graven T, et al. Feasibility and Accuracy of Tele-Echocardiography, With Examinations by Nurses and Interpretation by an Expert via Telemedicine, in an Outpatient Heart Failure Clinic. J Ultrasound Med. Dec 2020;39(12):2313-2323. doi:https://dx.doi.org/10.1002/jum.15341 PubMed
24.Lu J, Lin J, Yin L, et al. Using remote consultation to enhance diagnostic accuracy of bedside transthoracic echocardiography during COVID-19 pandemic. Echocardiography. 08 2021;38(8):1245-1253. doi:https://dx.doi.org/10.1111/echo.15124
25.Marini TJ, Oppenheimer DC, Baran TM, et al. Testing telediagnostic right upper quadrant abdominal ultrasound in Peru: A new horizon in expanding access to imaging in rural and underserved areas. Research Support, Non-U.S. Gov't. PLoS ONE. 2021;16(8):e0255919. doi:https://dx.doi.org/10.1371/journal.pone.0255919 PubMed
26.Marini TJ, Weiss SL, Gupta A, et al. Testing telediagnostic thyroid ultrasound in Peru: a new horizon in expanding access to imaging in rural and underserved areas. J Endocrinol Invest. Dec 2021;44(12):2699-2708. doi:https://dx.doi.org/10.1007/s40618-021-01584-7 PubMed
27.Morel B, Hellec C, Fievet A, et al. Reliability of 3-D Virtual Abdominal Tele-ultrasonography in Pediatric Emergency: Comparison with Standard-of-Care Ultrasound Examination. Ultrasound Med Biol. Nov 2022;48(11):2310-2321. doi:10.1016/j.ultrasmedbio.2022.07.004 PubMed
28.Nascimento BR, Beaton AZ, Nunes MCP, et al. Integration of echocardiographic screening by non-physicians with remote reading in primary care. Research Support, Non-U.S. Gov't. Heart. 02 2019;105(4):283-290. doi:https://dx.doi.org/10.1136/heartjnl-2018-313593
29.Nascimento BR, Sable C, Nunes MCP, et al. Echocardiographic screening of pregnant women by non-physicians with remote interpretation in primary care. Research Support, Non-U.S. Gov't. Fam Pract. 06 17 2021;38(3):225-230. doi:https://dx.doi.org/10.1093/fampra/cmaa115
30.Nieto-Calvache AJ, Benavides-Calvache JP, Aryananda R, et al. Telemedicine ultrasound assessment for placenta accreta spectrum: Utility and interobserver reliability of asynchronous remote imaging review. Int J Gynaecol Obstet. Mar 2025;168(3):1191-1203. doi:10.1002/ijgo.15991 PubMed
31.Toscano M, Marini TJ, Drennan K, et al. Testing telediagnostic obstetric ultrasound in Peru: a new horizon in expanding access to prenatal ultrasound. BMC Pregnancy Childbirth. Apr 26 2021;21(1):328. doi:https://dx.doi.org/10.1186/s12884-021-03720-w PubMed
32.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
33.Hartling L HM, Milne A, et al. Validity and Inter-Rater Reliability Testing of Quality Assessment Instruments. Agency for Healthcare Research and Quality; 2012. Accessed 19 Sep 2025. https://www.ncbi.nlm.nih.gov/books/NBK92287/
34.Radiologist CAo. CAR Position Statement on Remote Reporting. 2025 Apr 29, https://car.ca/wp-content/uploads/2021/12/RR-Position-Statement_forPDF-1.pdf
35.Wei P-F. Chinese recommendations for the implementation of bedside echocardiography and remote consultation in patients with coronavirus disease 2019. Chin Med J (Engl). Dec 5 2020;133(23):2847-2849. doi:10.1097/cm9.0000000000001222 PubMed
36.Radiology ACo. ACR PRACTICE PARAMETER FOR RADIOLOGIST COVERAGE OF IMAGING PERFORMED IN HOSPITAL EMERGENCY DEPARTMENTS. 2023. https://gravitas.acr.org/PPTS/DownloadPreviewDocument?DocId=22
Appendix 1: Selection of Included Studies
Please note that this appendix has not been copy-edited.
Appendix 2: Characteristics of Included Studies
Please note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Studies
Study citation, country, funding source | Study design, outcomes | Population characteristics | Index test and reference standard |
|---|---|---|---|
Nieto-Calvache et al. (2024)30 Country of publication: Colombia Funding source: None | Cross-sectional cohort agreement study Type of ultrasound: Generala Patient sample size: 5 Relevant outcomes:
| Patients from Colombia and Indonesia treated for placenta accreta spectrum (PAS) requiring transabdominal and transvaginal ultrasound for prenatal staging | Index test: Asynchronous TUS interpretation with simulated consultation by 12 experts located in 11 countries: Argentina, Brazil, Colombia, Egypt, England, Ghana, Ireland, Italy (2), Taiwan, US (2) Teleultrasound interpreter: Imaging medical expert with experience in PAS Reference standard: Standard in-person ultrasound interpretation Standard ultrasound interpreter: Onsite physician sonologist |
Morel et al. (2022)27 Country of publication: France Funding source: NR | Cross-sectional cohort diagnostic accuracy study Type of ultrasound: 3D Ultrasound Aplio i800 (Canon Medical System) Patient sample size: 103 Relevant outcomes:
| Children undergoing ultrasound for abdominal pain in 2 hospitals in France (1 university and 1 regional hospital) Mean age, months ± SD:
Sex, n (%):
| Index test: Asynchronous 3D TUS interpretation Teleultrasound interpreter: 1 senior radiologist with 7 years of experience and 1 senior resident located at a university hospital Reference standard: Standard in-person ultrasound and interpretation Traditional ultrasound interpreter: Senior pediatric radiologist |
Alfageme et al. (2021)21 Country of publication: Spain Funding source: None reported | Cross-sectional cohort diagnostic accuracy study Type of ultrasound: Dermatological ultrasound Patient sample size: 143 Relevant outcomes:
| Adult patients in Spain aged from 18 to 70 years with palpable nodular skin lesions Mean age, years ± SD:
Sex, n (%):
| Index test: Asynchronous TUS interpretation of images obtained from 6 primary care centres by family physicians with a minimum of 5 years of ultrasound experience Teleultrasound interpreter: 4 dermatologists with at least 5 years of dermatological ultrasound experience located at a tertiary centre Reference standard: Standard in-person ultrasound interpretation Traditional ultrasound interpreter: Dermatologists at a tertiary centre |
Marini et al. (2021)25 Country of publication: Peru Funding source: Various | Cross-sectional cohort diagnostic accuracy study Type of ultrasound: Generala (Mindray DP-10 ultrasound machine) Sample size: 144 Relevant outcomes:
| Adult patients located at a health centre in Peru requiring ultrasound examination of the right upper abdominal quadrant Mean age, years (range):
Sex, n (%):
| Index test: Asynchronous TUS interpretation of VSI abdominal exam clips obtained by 2 ultrasound-naive operators (nurse and care technician) in Peru Teleultrasound interpreter: 2 board-certified abdominal fellowship-trained radiologists in the US Reference standard: Standard in-person ultrasound and interpretation by radiologist Traditional ultrasound interpreter: Radiologist in Peru with more than 10 years of experience |
Marini et al. (2021)26 Country of publication: Peru Funding source: Various | Cross-sectional cohort diagnostic accuracy study Type of ultrasound: Generala (Mindray DP-10 ultrasound machine) Patient sample size: 121 Relevant outcomes:
| Adult patients visiting a health centre in Peru for various reasons Mean age, years ± SD:
Sex, n (%):
| Index test: Asynchronous TUS interpretation of VSI thyroid exam clips obtained by 2 ultrasound-naive operators (nurse and care technician) in Peru Teleultrasound interpreter: 2 board-certified fellowship-trained radiologists in the US with 7 and 40 years of experience, respectively Reference standard: Standard in-person ultrasound and interpretation by radiologist Traditional ultrasound interpreter: Experienced radiologist in Peru |
Toscano et al. (2021)31 Country: Peru Funding source: Various | Cross-sectional cohort diagnostic accuracy study Type of ultrasound: Generala (Mindray DP-10 ultrasound machine) Sample size: 126 Relevant outcomes:
| Second or third trimester patients visiting a health centre in Peru for an obstetric ultrasound exam Mean age, years:
Trimester:
| Index test: Asynchronous TUS interpretation of obstetric VSI exam clips obtained by 2 ultrasound-naive operators (nurse and care technician) in Peru Teleultrasound Interpreter: An experienced maternal-fetal medicine fellow in the US Reference standard: Standard in-person ultrasound and interpretation by radiologist Traditional ultrasound interpreter: Experienced radiologist in Peru |
Lu et al. (2021)24 Country of publication: China Funding source: Medical Research Council | Cross-sectional cohort diagnostic accuracy study (consensus reference standard) Type of ultrasound: B-TTE Patient sample size: 30 Relevant outcomes:
| Patients admitted and treated for COVID-19 at a health centre in China requiring B-TTE Mean age, years ± SD (range):
Sex, n (%):
| Index test: Asynchronous interpretation of B-TTE exams obtained by 5 frontline ECG physicians Teleultrasound interpreter: 2 ECG remote consultants with specialized ultrasound training (associate chief physician and chief physician) Reference standard: In-person B-TTE and interpretation (consensus reference standard) Traditional ultrasound interpreter: Ultrasound-qualified physicians with more than 5 years of experience |
Nascimento et al. (2021)29 Country of publication: Brazil Funding source: Various | Cross-sectional cohort diagnostic accuracy study with partial verification Type of ultrasound: Hand-held (GE-VSCAN) Patient sample size: 56b of 1,112 Relevant outcomes:
| Pregnant patients undergoing screening ECG for heart disease at 22 primary care centres located in Brazil
Mean gestational age, weeks ± SD:
| Index test: Asynchronous remote interpretation of ECG exams obtained by ultrasound-naive health care workers in Brazil Teleultrasound interpreter: 3 experts (1 in Brazil and 2 in the US) Reference standard: In-person ECG exam and interpretation by expert (in cases of positive significant screening results) Traditional ultrasound interpreter: Imaging experts (physicians) located at primary care centres |
Dougherty et al. (2020)22 Country of publication: US Funding source: NR | Cross-sectional cohort diagnostic accuracy study Type of ultrasound: Voluson E8 system (GE HealthCare) and GE LOGIQ Patient sample size: 113 Relevant outcomes:
| Second trimester (14 to 16 weeks) outpatients at a university medical centre in the US requiring an obstetric ultrasound exam | Index test: Asynchronous TUS interpretation of obstetric VSI exam clips obtained by 2 ultrasound-naive operators with training (fourth-year medical students) Teleultrasound interpreter: 3 physicians with specialized training in obstetric ultrasound with between 3 and 25 years of experience Reference standard: Standard in-person ultrasound by trained sonographer Traditional ultrasound interpreter: Maternal-fetal medicine specialist or radiologist |
Hjorth-Hansen et al. (2020)23 Country of publication: Norway Funding source: NR | Cross-sectional cohort diagnostic accuracy study Type of ultrasound: Vivid 7 scanner (GE HealthCare) Patient sample size: 50 Relevant Outcomes:
| Adult patients located at an outpatient heart failure clinic in Norway requiring ECG Mean age, years (range):
Sex, n (%):
| Index test: Asynchronous TUS interpretation of images obtained by 3 specialized nurses with 6 to 12 years of heart failure experienced trained to use ECG Teleultrasound interpreter: Out-of-hospital cardiologist Reference standard: Standard in-person ultrasound immediately after teleultrasound scan Traditional ultrasound interpreter: 3 cardiologists and 1 experienced resident |
Nascimento et al. (2019)28 Country of publication: Brazil Funding source: Various | Cohort diagnostic accuracy study with partial verification Type of ultrasound: Hand-held (GE-VSCAN) Sample size: 85 of 1,004c Relevant outcomes:
| Pregnant patients undergoing screening ECG for heart disease at 16 primary care centres located in Brazil | Index test: Asynchronous remote interpretation of ECG exams obtained by 20 ultrasound-naive health care workers in Brazil (12 technicians, 4 nurses, 4 physicians) Teleultrasound Interpreter: 3 experts (1 in Brazil and 2 in the US) Reference standard: In-person portable ECG exam and interpretation by expert (within 60 days, in cases of positive significant screening results) Traditional ultrasound interpreter: Imaging experts located at primary care centres |
B-TTE = bedside transthoracic echocardiographic examination; ECG = electrocardiogram; NPV = negative predictive value; NR = not reported; PAS = placenta accreta spectrum; PPV = positive predictive value; SD = standard deviation; TUS = teleultrasonography; VSI = volume sweep imaging.
aGeneral ultrasound refers to the use of ultrasound in a broad range of clinical applications, including organ-specific exams.
bA total of 56 of 1,112 patients screened with the TUS protocol underwent a follow-up confirmatory in-person ultrasound.
cA total of 85 of 1,004 patients screened with the TUS protocol underwent a follow-up confirmatory in-person ultrasound.
Appendix 3: Main Study Findings
Please note that this appendix has not been copy-edited.
Primary study | TUS diagnostic accuracy and agreement | TUS image quality | Clinical experience |
|---|---|---|---|
Nieto-Calvache et al. (2024)30 |
|
|
|
Morel et al. (2022)27 |
|
|
|
Alfageme et al. (2021)21 |
|
| — |
Marini et al. (2021)25 |
| Image qualityd of exams rating (%):
| — |
Marini et al. (2021)26 |
|
| — |
Toscano et al. (2021)31 |
|
| — |
Lu et al. (2021)24 |
| — | — |
Nascimento et al. (2021)29 |
| — | — |
Dougherty et al. (2020)22 | The agreements among remote readers and the in-person readers varied according to placental location and fetal numbers:
| — | — |
Hjorth-Hansen et al. (2020)23 |
| — | — |
Nascimento et al. (2019)28 |
| — | — |
B-TTE = bedside transthoracic echocardiographic examination; CI = confidence interval; ICC = intraclass correlation coefficient; NPV = negative predictive value; P = P value, PAS = placenta accreta spectrum; PPV = positive predictive value; TUS = teleultrasonography; VSI = volume sweep imaging; .
aFleiss' Kappa coefficient: the strength of agreement was classified as “poor” (0.0), “slight” (0.01 to 0.2), “fair” (0.21 to 0.4), “moderate” (0.41 to 0.6), “substantial” (0.61 to 0.80), and “almost perfect” (0.81 to 1).
bThe quality of the 3D acquisitions was qualitatively assessed on a 4-point Likert scale (“technical issue,” “poor,” “good,” or “excellent”).
cThe technical quality of the images was classed as being of sufficient or insufficient quality for the teleultrasound evaluation.
dThe overall image quality was rated as “excellent,” “acceptable,” or “poor.” “Excellent” examinations showed complete or nearly complete visualization of the liver and gallbladder with appropriate imaging quality. “Acceptable” examinations showed nearly complete or partial visualization of the liver and gallbladder with appropriate imaging quality. “Poor” examinations showed only partial or inadequate visualization of the liver and gallbladder with image quality limiting evaluation.
eImage quality was rated as “excellent,” “acceptable,” or “poor.” Excellent examinations visualized the entire or nearly entire thyroid gland with good brightness and resolution. Acceptable examinations visualized > 80% of the thyroid or had slightly limited brightness/resolution but still allowed for adequate gland or nodule assessment. Poor examinations visualized less than 80% of the total thyroid or were nondiagnostic.
fImage quality was assigned using 3-point Likert scale (1 = “excellent,” 2 = “acceptable,” or 3 = “poor”) as was reader confidence in imaging findings (1 = “confident,” 2 = “intermediate,” 3 = “not confident”).
Appendix 4: Critical Appraisal of Included Studies
Please note that this appendix has not been copy-edited.
Figure 2: Results of the QUADAS-2 Risk of Bias Assessment by Domain
QUADAS-2 = Quality Assessment of Diagnostic Accuracy Studies 2.
1Marini et al. (2021)25
2Marini et al. (2021)26
Table 4: Risk of Bias Assessment of Included Studies
Study citation | Strengths | Limitations |
|---|---|---|
Nieto-Calvache et al. (2024)30 |
|
|
Morel et al. (2022)27 |
|
|
Alfageme et al. (2021)21 |
|
|
Marini et al. (2021)25 |
|
|
Marini et al. (2021)26 |
|
|
Toscano et al. (2021)31 |
|
|
Lu et al. (2021)24 |
|
|
Nascimento et al. (2021)29 |
|
|
Dougherty et al. (2020)22 |
|
|
Hjorth-Hansen et al. (2020)23 |
|
|
Nascimento et al. (2019)28 |
|
|
ECG = electrocardiogram.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.