Drugs, Health Technologies, Health Systems
Health Technology Review Recommendation
Appropriate Use of Antipsychotics in Long-Term Care: Expert Panel Guidance
Guidance Report
Summary
The evidence-informed consensus statements were developed by a panel of experts and knowledgeable individuals, through a consensus-building process from June 2024 to January 2025.
The target for long-term care (LTC) homes in Canada reflects a level of excellence for the “potentially inappropriate use of antipsychotics in long-term care” quality indicator to which LTC homes can aspire, and represents acceptable practice in Canada. The annual improvement goal supports collective action toward the target by giving LTC homes something to strive for each year regardless of their proximity to the target rate for Canada.
The target for LTC homes in Canada and the annual improvement goal are meant to inspire change to improve the health and safety of people living in LTC by setting clear expectations of where Canada should be regarding the appropriate use of antipsychotics in LTC. They are intended to be ambitious, realistic, and encouraging for LTC homes, but they are not mandatory for LTC homes.
Consensus Statement 1: The Target for LTC Homes in Canada
The panel recommends 15% as the target for LTC homes in Canada for the “potentially inappropriate use of antipsychotics in long-term care” quality indicator.
Note: The target sets a standard for the overall risk-adjusted rate for Canada. It is a level of excellence for the quality indicator to which LTC homes can aspire. There is no time frame associated with the target.
This means that the proportion of people living in LTC homes across Canada receiving antipsychotic drugs without a diagnosis of psychosis should ideally be 15% or less. All LTC homes can contribute to reaching the target for the country through quality improvement initiatives that reduce potentially inappropriate antipsychotic use in their setting to 15% or lower.
Consensus Statement 2: Annual Improvement Goal
For LTC homes that are not meeting the target for LTC homes in Canada, the panel recommends a 15% relative reduction as the annual improvement goal for the “potentially inappropriate use of antipsychotics in long-term care” quality indicator.
This means that these LTC homes should aim to reduce the proportion of people living there who are receiving antipsychotic drugs without a diagnosis of psychosis by 15%, relative to the proportion from the previous year.
For example, if an LTC home with a rate of 20% for the quality indicator were to achieve the 15% relative reduction over 1 year, it would mean that their new rate would be 17%.
Executive Summary
What Is the Issue?
Antipsychotic medications are the main class of drugs used to treat schizophrenia or symptoms of psychosis. The use of antipsychotics in people without psychosis is considered potentially inappropriate. Potentially inappropriate use of medications can mean that the drugs are not indicated, that the risk of harms outweighs potential benefits, or that nonpharmacological approaches are more appropriate. In LTC homes, antipsychotics are sometimes used to manage responsive behaviours associated with dementia (e.g., aggression, agitation); however, the use of antipsychotics for dementia is considered “off-label” for most antipsychotics in Canada and may not be aligned with Canadian clinical practice guidelines. Using antipsychotics inappropriately can be a safety concern, as these medications are associated with higher risk of falls, fractures, stroke, and death in older adults in LTC.
In Canada, the percentage of people who may be inappropriately receiving an antipsychotic medication in LTC homes is monitored using the “potentially inappropriate use of antipsychotics in long-term care” quality indicator (refer to Appendix 1 for more details). The quality indicator excludes people with a diagnosis of psychosis, schizophrenia, or Huntington chorea; those experiencing hallucinations or delusions; people with end-stage disease; people receiving hospice or palliative care; and people who were admitted to LTC within 3 months of assessment. A lower percentage for this quality indicator means there are fewer people on antipsychotics without a diagnosis of psychosis. To enable fairer comparisons across LTC homes, the quality indicator is risk-adjusted to account for factors beyond the control of the LTC homes.
Canada’s rate for the quality indicator increased to 24.5% in 2023–2024 from 20.2% in 2019–2020. Rising rates indicate a reversal of substantial progress made by the LTC sector since 2015 to address the behavioural and psychological symptoms of dementia (BPSD) by other nondrug means. There is currently no established target for the quality indicator that would suggest acceptable practice for the LTC sector in Canada. High rates of potentially inappropriate use of antipsychotic medications in LTC in Canada will remain or continue to rise without action.
What Did We Do?
In 2023, a group of pan-Canadian health care organizations came together as the Appropriate Use Coalition to improve patient outcomes and reduce risks through appropriate use of medications in Canada. One of their first priorities was to streamline and coordinate an approach to address the appropriate use of antipsychotics in LTC homes. To support this work, Canada’s Drug Agency (CDA-AMC) and Choosing Wisely Canada (CWC) convened a multidisciplinary panel to develop evidence-informed consensus statements on the appropriate use of antipsychotics in LTC. The panel was composed of 17 experts across Canada with diverse professional and personal experience in the LTC sector. Using a modified Delphi process, the panel deliberated on a target for LTC homes across Canada and an annual improvement goal for the “potentially inappropriate use of antipsychotics in long-term care” quality indicator.
To develop consensus statements on a target and an annual improvement goal, the panel considered input from an engagement survey of interested parties, evidence from a literature-based Environmental Scan (including performance data from the Canadian Institute of Health Information [CIHI] and interRAI), and the panel’s relevant expertise in LTC throughout the consensus-building process. This report outlines that process and its outcomes, including key themes and clinical considerations when adopting the target for LTC homes in Canada and the annual improvement goal, for quality improvement and clinical care.
What Are the Consensus Statements?
Consensus statement 1: The panel recommends 15% as the target for LTC homes in Canada for the “potentially inappropriate use of antipsychotics in long-term care” quality indicator.
This means that the proportion of people in LTC homes receiving antipsychotic drugs without a diagnosis of psychosis should ideally be 15% or less for Canada. All LTC homes can contribute to reaching the target for the country through quality improvement initiatives that reduce potentially inappropriate antipsychotic use in their setting to 15% or lower.
This value is risk-adjusted, which refers to a statistical technique used to control for population differences between LTC homes. By adjusting the quality indicator for factors at the individual level (e.g., age, long-term memory problems, cognitive performance) and at the LTC home level (e.g., resource utilization), the risk-adjustment process enables a fairer comparison of the rate of potentially inappropriate antipsychotic use between LTC homes.
Consensus statement 2: For LTC homes that are not meeting the target for LTC homes in Canada, the panel recommends a 15% relative reduction as the annual improvement goal for the “potentially inappropriate use of antipsychotics in long-term care” quality indicator.
This means that these LTC homes should aim to reduce the proportion of people living there who are receiving antipsychotic drugs without a diagnosis of psychosis by 15%, relative to the proportion from the previous year.
The target for LTC homes in Canada and the annual improvement goal are not mandatory for LTC homes to implement, and there is no time limit to reach the target. The annual improvement goal complements the target for LTC homes in Canada by recommending a safe and achievable rate of change for LTC homes striving to consistently improve their performance on the quality indicator each year.
During their deliberations, the panel considered that the quality indicator categorizes some approved indications for antipsychotic use, and some off-label but perhaps clinically reasonable uses of antipsychotics, as “potentially inappropriate.” The panel discussed whether and how these indications might impact the quality indicator’s performance, which precluded striving for the target rate to be zero. Other factors discussed to inform the selection of the target and annual improvement goal values included data for the current and previous quality indicator performance across the country, results of previous Canadian quality improvement efforts, the current context of the LTC sector in Canada (e.g., available resources), and the potential risks associated with selecting a target that is too low.
What Else Do You Need to Know?
The panel highlighted the importance of safe, systematic, and sustainable approaches to achieve the target for LTC homes in Canada and annual improvement goal that focus on the appropriate use of antipsychotics. The panel acknowledged that what is “appropriate” can differ between individuals and may change over time. Person-centred care facilitates the appropriate use of antipsychotics by ensuring care plans reflect and respect the unique needs and preferences of people living in LTC homes.
The panel cautioned against prioritizing reaching the target without providing the proper resources and training to enable appropriate, person-centred care for people living in LTC. This may inadvertently lead to changes in practice that artificially lower the quality indicator rate without reducing harms or improving care and health outcomes. LTC homes may consider monitoring other quality indicators (e.g., physical restraint use, worsening behavioural symptoms) as balancing measures and monitoring for potential unintended consequences (e.g., admission refusals, inappropriate medication substitutions, changes in diagnostic patterns) to ensure efforts are headed in the right direction.
What Is the Potential Impact?
These consensus statements will serve as a starting point to inform the Appropriate Use Coalition’s future efforts, such as the alignment and development of quality improvement programs with tools and resources for LTC homes. The purpose of the target and the annual improvement goal is to inform, motivate, and monitor change that will improve the safety and quality of care for those living in LTC. Importantly, the target is a not a limit; LTC homes that are already at a 15% rate for the quality indicator are encouraged to continue their quality improvement efforts.
Recent analyses of Canada’s LTC sector show that there were no differences between high-performing and lower-performing homes in terms of size (i.e., small, medium, or large), urban or rural location, and income level (quintile). In addition, top-performing homes could be found in all provinces. This suggests that a variety of LTC homes in Canada have the potential to improve their performance on the quality indicator, regardless of home size, location, and income.
Achieving the 15% target for LTC homes in Canada through safe and sustainable quality improvement efforts is estimated to result in 21,000 fewer people receiving potentially inappropriate antipsychotics across the country, compared to the 2023–2024 national rate for Canada. This could mean fewer side effects, falls, hospitalizations, deaths, or other harms because of inappropriate antipsychotic use for up to 21,000 people in LTC homes.
Pagebreak
Setting the Context
Rising Potentially Inappropriate Antipsychotic Use in Long-Term Care
Antipsychotic medications are the main class of drug used to treat people with schizophrenia and symptoms of psychosis, including delusions and hallucinations.4 However, they are sometimes used for behaviours or conditions that may be difficult for care providers to manage in LTC, such as BPSD (e.g., responsive behaviours such as aggression, anxiety, and agitation).5 While the use of antipsychotics may be reasonable in some cases, such as severe agitation, aggression, acute delirium, or psychosis, there is concern that antipsychotics are sometimes prescribed inappropriately, such as when they are not indicated (i.e., not all antipsychotics are approved for use in people with dementia), when other nonpharmacological approaches are more appropriate, or when harms outweigh potential benefits.
Before 2020, quality improvement efforts resulted in steady progress in reducing this potentially inappropriate use of antipsychotics in LTC homes across Canada.5 In 2019–2020, potentially inappropriate use was reported to be at its lowest in the last decade at 20.2%, which was a substantial decrease from 27.2% reported for 2014–2015.5 However, rates have increased since the start of the COVID-19 pandemic and continue at an undesirable rate, reversing the progress made in the past decade.5-7 It has been suggested that the downstream impacts of the pandemic (e.g., staff shortages, social isolation, and disruption of services) may have exacerbated the conditions that can lead to inappropriate antipsychotic medication use.5,7,8 In 2023–2024, CIHI reported that the rate of potentially inappropriate use of antipsychotics in Canada was 24.5%, with most provinces well above this national average.5
Why Is This an Issue?
The number of people living with dementia in Canada is expected to reach 1 million by 2030,9 which will likely impact LTC systems and populations. With this expected rise in the prevalence of dementia, rates of potentially inappropriate antipsychotic use may continue to rise without action. Inappropriate use of antipsychotics is concerning given that the potential for harms may outweigh the potential benefits.10-12 The effectiveness of antipsychotics to manage BPSD may be limited and varies by the type of antipsychotic.13 Additionally, antipsychotic use may increase the risk of stroke, falls, fractures, fall-related hospitalizations, and mortality among people living in LTC.10,11 Most antipsychotics include a safety warning indicating that older adults with dementia treated with antipsychotics have an increased risk of death compared to placebo.14-28
Canadian clinical practice guidelines recommend against the use of antipsychotics in people with dementia living in LTC in most circumstances.13,29,30 The literature suggests that using antipsychotic medications to manage BPSD is likely an ineffective and harmful approach in the long term,10,11,29,31 especially when nondrug approaches allow LTC staff to assess and address the root cause of responsive behaviours and contributing factors that are unique to individuals and their context.32,33 BPSD can be caused by a variety of factors, such as an individual’s physical environment, pre-existing illnesses, and unmet need (e.g., pain, hunger).34
Inappropriate antipsychotic use also conflicts with an individual’s right to autonomy and dignified care. Autonomy is an individual’s right to self-govern and act in a way that is aligned to their desires and preferences. While autonomy is often compromised in advanced stages of dementia,35,36 sedative effects due to antipsychotics (often referred to as chemical restraints in the literature when used to manage behaviours) can further reduce their ability to exercise autonomy, including participating in their care. Providing dignified care involves respecting and upholding an individual’s personhood and autonomy by recognizing their capacity and goals.36,37
How Is “Potentially Inappropriate Use of Antipsychotics” Measured?
Figure 1: “Potentially Inappropriate Use of Antipsychotics in Long-Term Care” Quality Indicator2,38

LTC = long-term care.
In Canada, CIHI has been using the “potentially inappropriate use of antipsychotics in LTC” quality indicator for more than a decade to monitor the percentage of people living in LTC receiving antipsychotics without a diagnosis of psychosis.2,5 Refer to Figure 1 for an explanation of how the indicator is calculated. The quality indicator excludes people with a diagnosis of psychosis, schizophrenia, or Huntington chorea; those with hallucinations or delusions during the relevant assessment period; people with end-stage disease (with 6 months or less to live); people receiving hospice or palliative care; and people who were recently admitted to LTC (i.e., within the previous 3 months).
While a lower number is better, it is likely that performance rates on the quality indicator will never reach zero for the following reasons:
The quality indicator interprets certain approved indications for antipsychotic medications as potentially inappropriate, specifically bipolar disorder and major depressive disorder without hallucinations or delusions.
It includes a proportion of individuals who are receiving antipsychotics appropriately in LTC, such as short-term use for severe aggression.
This quality indicator is risk-adjusted to control for differences in factors that are beyond the control of LTC homes but may affect the people living in these homes, such as increased complexity of care needs (e.g., combined Alzheimer disease and other dementia) as well as younger age (patients younger than 65 years).2 Risk adjustment enables a fair comparison of the level of potentially inappropriate antipsychotic use between LTC homes across Canada.
For the LTC case-mix, CIHI uses Resource Utilization Groups version III (RUG-III) grouping methodologies to categorize people living in LTC into statistically and clinically homogeneous groups based on clinical and resource use similarities.3
This quality indicator and the methods to calculate it were developed by interRAI, a network of international experts who develop tools to facilitate evidence-based clinical practice and policy decision-making. LTC homes collect the data needed to calculate the quality indicator rates using standardized clinical assessment tools, specifically Minimum Data Set 2.0 or the interRAI Long-Term Care Facilities tool.2 The quality indicator is currently based on data from both assessment tools, but some jurisdictions have either transitioned or are in the process of transitioning to the newer interRAI Long-Term Care Facilities.2 Statistical analyses indicate that these 2 assessment tools result in comparable rates for the quality indicator, which suggests that both tools can be used without affecting rates during the transition period.2
Refer to Appendix 1 or CIHI’s website for more information about the methods used to calculate the quality indicator.
Rationale and Objectives for the Guidance
Scope of the Guidance
This report outlines the process and results of the process to create a target for LTC homes in Canada and an annual improvement goal to support the appropriate use of antipsychotics in LTC, and includes key themes and clinical considerations when using the target and annual improvement goal for quality improvement and clinical care. It is not intended as a comprehensive overview of available resources, implementation strategies, or quality improvement programs.
Why Is This Guidance Needed?
There is currently no target for LTC homes in Canada for the “potentially inappropriate antipsychotics in LTC” quality indicator. By setting a standard for an overall quality indicator rate for Canada, a target for all LTC homes can motivate change and deprescribing efforts, and also increase awareness about antipsychotic use in LTC.
In 2023, 11 pan-Canadian health care organizations came together as the Appropriate Use Coalition to improve patient outcomes and reduce risks through appropriate use of medications in Canada.39 Their focus includes sharing information and evidence, and streamlining and collaborating on appropriate use efforts across Canada. The coalition includes 2 subgroups: 1 focused on appropriate use in primary care, and another focused on LTC. As its first priority, the latter agreed to focus on the appropriate use of antipsychotics in LTC homes, including conducting an analysis of potentially inappropriate antipsychotic use rates in Canada, as well as developing quality improvement programs, critical tools, resources, and consensus-based guidance on the appropriate use of antipsychotics in LTC.5
Primary Objective
In support of the coalition’s priority in the appropriate use of antipsychotics, CDA-AMC partnered with CWC to host a multidisciplinary panel tasked with developing 2 evidence-informed consensus statements for a target for LTC homes in Canada and a complementary annual improvement goal for the “potentially inappropriate use of antipsychotics in long-term care” quality indicator. These consensus statements are intended to serve as a starting point to support future coalition initiatives to improve the safety and quality of care by reducing potentially inappropriate antipsychotic use in LTC homes.
The target for the “potentially inappropriate use of antipsychotics in LTC” quality indicator is presented as a risk-adjusted rate (expressed as a percentage) that reflects acceptable practice in LTC homes in Canada.
The target does not include a specific time frame to reach the value, as the time required to reach the target will depend in part on each LTC home’s current performance on the quality indicator.
Secondary Objective
CDA-AMC identified considerations for clinical and care practice to reduce inappropriate antipsychotic use in LTC homes. These considerations were informed by the literature, an engagement survey of interested parties, and panel input during the consensus-building process. The purpose was not to reach consensus on these considerations, but rather to offer insights for the panel to consider in their deliberations and discussions toward reaching consensus.
Key Concepts to Inform the Objectives
To inform and guide their decision-making when developing the target and the annual improvement goal, the panel was asked to consider that the target and annual improvement goal are intended to be used together, and that these values should be ambitious and inspiring for the LTC sector, be encouraging to LTC homes, and also be realistic to the current context of LTC.
The target represents acceptable practice for LTC homes across Canada. It refers to an acceptable proportion of people taking antipsychotics unrelated to a diagnosis of psychosis in LTC homes across the country. Recognizing that it takes time to safely implement meaningful change, the target was designed without a time limit. The purpose of the annual improvement goal is to support collective action toward the target and motivate LTC homes to continue quality improvement efforts by giving them something to strive for each year, regardless of their proximity to the target rate for Canada.
To support the choice of the target and annual improvement goal values, as well as inform the considerations for clinical and care practice, the panel was also asked to consider the safety of people living in LTC (e.g., avoid setting numerical values that would unintentionally promote drastic change or encourage behaviours that may cause more harm than benefit, such as medication substitution34) and Canadian clinical practice guidelines (e.g., recommendations about the appropriate use of antipsychotics in people with dementia living in LTC), and to reflect on issues that disproportionately impact people from equity-deserving groups as well as ethical considerations (e.g., autonomy and dignity in care).
Pagebreak
Modified Delphi Process
We followed an online modified Delphi process to reach consensus on a single numeric value for the target for LTC homes in Canada and a single numeric value for the annual improvement goal. An overview of the approach used to develop the consensus statements and the guidance report is provided in Figure 2. The process started in June 2024 and ended in January 2025, and adheres to the ACcurate COnsensus Reporting Document (ACCORD) recommendations for reporting consensus-based studies.40 A detailed description of the methods (including the limitations to the process) is published separately on the CDA-AMC website.
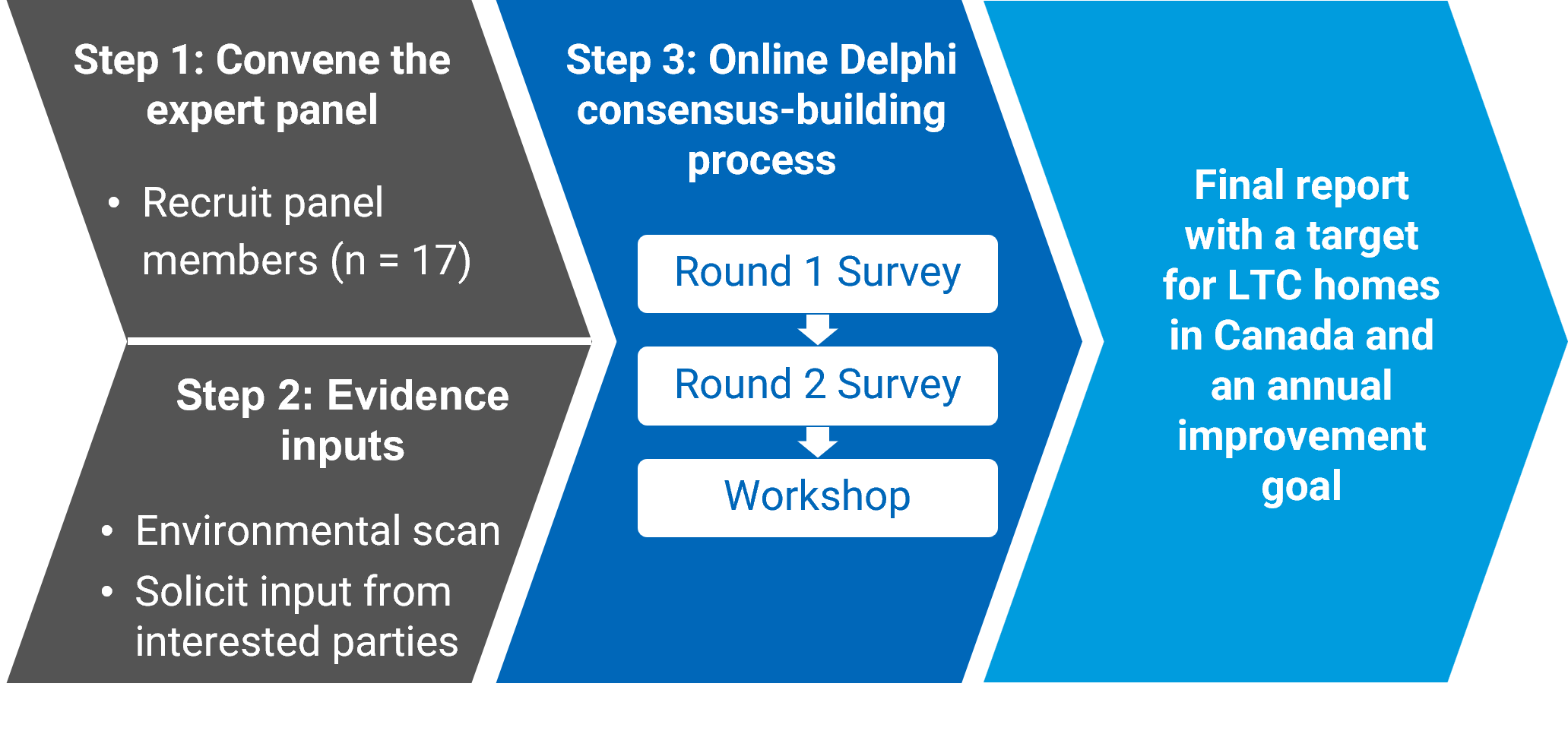
The Expert Panel
We recruited an independent, time-limited multidisciplinary panel of 17 individuals selected for their experience and expertise related to the issue of antipsychotic use in LTC settings in Canada, and their ability to contribute to the modified Delphi process on this topic. Most panel members had more than 10 years of experience in the LTC sector in Canada through a variety of roles, including health care professionals (e.g., in medicine, nursing, pharmacy) and executives, quality improvement and deprescribing experts, academics, and persons with lived experience. Some panellists held multiple perspectives. There was representation from the LTC systems of most of the provinces and territories of Canada (excluding Yukon and Nunavut). Most panel members self-identified as women (70.6%) for their gender identity, and 29.4% identified as men. The panel had representation from a diverse range of ethnicities or races, including individuals who self-identified as Black, Jewish, Mohawk, white, and/or having Caribbean or West Indies, Southeast Asian, Southern African, Western Europe, or Eastern Europe ancestry.
Refer to Appendix 2 for more details about the panel demographics.
Evidence Inputs
Concurrent with panel member identification and recruitment, we gathered the following information to inform the consensus-building process:
a literature-based Environmental Scan summarizing relevant information about potentially inappropriate use of antipsychotics in LTC in Canada and internationally (e.g., existing benchmarks or targets, performance data from CIHI and interRAI, quality improvement initiatives, guidelines, and implementation considerations)
a summary of engagement input via an online survey from interested parties (e.g., resident and caregiver associations, appropriate prescribing groups, and health organizations).
The information in the Environmental Scan was used to generate the potential options for the target and the annual improvement goal in the round 1 survey, and supported relevant sections in this guidance report (e.g., barriers and facilitators to reducing antipsychotic use from the Environmental Scan were integrated into the considerations for clinical and care practice). The engagement input allowed the panel to consider a diverse range of perspectives and views and have a more comprehensive understanding of antipsychotic use in LTC homes in Canada. Panellists were asked to consider this information and their relevant expertise when completing the surveys and in their discussions and deliberations throughout the Delphi process.
The Environmental Scan and the engagement input are published separately as supporting documents on the CDA-AMC website.
Online Consensus-Building Process
The modified online consensus-building process consisted of 3 rounds, including 2 online surveys (round 1 and round 2) and 1 online workshop with structured discussions and live ranking and voting (round 3). We defined the consensus threshold as 80% or higher agreement among panellists. Figure 3 illustrates a summary of the results of the modified online consensus-building process, including the survey options, the options added (round 1 only), and the options removed after each round.
The results from the online consensus-building process are summarized in Appendix 3, as follows:
Round 1:
Figure 6 presents the round 1 voting results for the proposed values for the target for LTC homes in Canada.
Figure 7 presents the round 1 voting results for the proposed values for the annual improvement goal.
Table 3 summarizes the potential barriers and facilitators to reducing potentially inappropriate antipsychotic use in LTC, as described by the panellists in round 1.
These themes have been incorporated into the considerations for clinical care and practice section of this report.
Round 2:
Figure 8 presents the round 2 voting results for the proposed values for the target for LTC homes in Canada.
Figure 9 presents the round 2 voting results for the proposed values for the annual improvement goal.
Round 3:
Table 4 presents the results of the round 3 ranking exercises for the target for LTC homes in Canada.
Table 5 presents the results of the round 3 ranking exercises for the annual improvement goal.
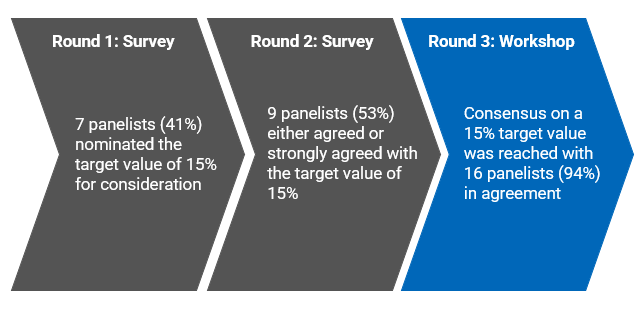
After the discussion and ranking exercises, live voting confirmed that the panel had reached consensus on 15% as the target for LTC homes in Canada, with 16 out of 17 of panel members (i.e., 94%) agreeing with this value. The panel also reached consensus on an annual improvement goal of 15% (relative reduction per year), with 17 out of 17 of panel members (i.e., 100%) agreeing with this value.

Consensus-Based Target and Annual Improvement Goal
During the consensus-building process, the panel members discussed many different ideas and considerations, which informed the selection of the numerical values of 15% for the target and 15% for the annual improvement goal. A key theme throughout the deliberations was the need to find balance between a target value that is seen as ambitious enough (i.e., a level of excellence for the quality indicator) without being unattainable (i.e., still achievable and sustainable given what was previously achieved in Canada). Other recurring themes included consideration of the current context of LTC (e.g., staffing levels, availability of resources), the desire to improve the safety and quality of care in LTC, and the need to avoid potential unintended consequences.
Consensus Statement 1: The Target for LTC Homes in Canada
The panel reached consensus with 16 of 17 panellists (94%) agreeing that 15% should be the value for the target.
Rationale for the Selection of 15% for the Target
Figure 4 provides an overview of the selection process for the 15% target value.
While 15% was not 1 of the initial options for the target, 7 panellists nominated this value for consideration in the round 1 survey. Panellists suggested 15% given that it was a middle value between 2 survey options for which there was a large gap (i.e., between 12% and 18%), and it was a good balance between a desire to improve from the current rates while still being relevant to the reality of LTC homes. In the round 2 survey, 53% of panellists either agreed or strongly agreed with the value of 15% for the target.
During the workshop, the panel members discussed and deliberated on many different ideas and considerations, which informed the selection of 15% as the target for LTC homes in Canada for the “potentially inappropriate use of antipsychotics in LTC” quality indicator.
When selecting the value for the target, panellists were concerned that an extremely high target could demotivate homes that would be starting at lower rates (or already meeting the target) from making further improvements to reduce potentially inappropriate use of antipsychotics in LTC. Conversely, other panellists suggested that extremely low values may discourage or demotivate homes that would be starting at higher rates.
The panel reflected on the importance of understanding the quality indicator (i.e., what is and is not measured by the indicator) and how it is calculated (e.g., applying the exclusion criteria, using data that are risk adjusted so that performance is comparable between homes). They discussed the challenge of differentiating potentially appropriate from potentially inappropriate antipsychotic medication use within the quality indicator, and considered some of the appropriate indications for antipsychotics that are not excluded from the indicator (e.g., bipolar disorder, major depressive disorder, short-term treatment of aggression in severe dementia) and the concern that a low target might lead to inappropriate withdrawal of medications.
While the panel noted how challenging it was to find this balance, they carefully considered and discussed the available evidence on current and past performance rates, potential unintended consequences of an extremely low target, and the availability of resources across LTC homes in Canada.
Alignment With Performance Rates in LTC Homes in Canada
Panel members described 15% as a value for the target that was both ambitious and achievable, and consistent with the evidence in the Environmental Scan. They raised the following points in their discussion:
Performance rates from the best 20th percentile of LTC homes in Canada are around 15%.
Some LTC homes are already achieving rates that are below 15%.
Fifteen percent would be a significant improvement over the current median rate in LTC homes in Canada (i.e., 23.5% in 2023–2024).
Between 2014 and 2019, the percentage of potentially inappropriate use of antipsychotics in LTC decreased from 27.2% to 20.2% in Canada due to substantial efforts to address this issue, demonstrating that reducing rates at the national level is possible over time.
Initially, some panellists preferred even more ambitious values for the target (e.g., 10% or 12%), given that homes in the 10th percentile have achieved rates below 10%, which demonstrates that this rate is achievable. They also considered that a target of 10% would be comparable to the current median rate in the US. Conversely, some panellists initially preferred a higher value for the target (e.g., 17% or 18%) that would be considered “not too aggressive,” given the current national median rate in Canada (i.e., 23.5% in 2023–2024), and the desire to set a target that was reasonably achievable for LTC homes in Canada with much higher rates on the quality indicator (e.g., 40%, 60%). However, given the other perspectives shared in the workshop and considering the target from a pan-Canadian lens, most panellists shifted their position and were in favour of 15% as the target.
Resources to Support Achieving the Target
Throughout the Delphi process, panellists regularly acknowledged the many challenges in the LTC sector, particularly regarding the availability of resources in LTC homes. The panel noted that while different LTC homes experience different barriers, and that they do not all have the same resources or facilitators for change currently available to them, it was still important to establish a target that the homes could work toward.
Panel members shared their experiences from their jurisdictions with successful quality improvement initiatives, including the following:
LTC homes that have achieved improvements in the quality indicator rates have had programs focused on minimizing reliance on antipsychotics with additional resources in place to support their efforts (e.g., external funding, educational training, one-on-one interventions).
Well-resourced LTC homes (e.g., those that are well funded, have dedicated programs, or offer music therapy and other recreation activities) have achieved rates below 10%.
The panel acknowledged that this type of initiative can be very expensive and, given the variation across LTC homes, they felt that 15% was a reasonable value for the target.
Given the current staffing levels and staffing challenges experienced in LTC homes (e.g., staff turnover, rotation of staff), panellists felt that:
15% is a value that is aspirational (i.e., a target that LTC homes can work toward in the long term) but realistic and achievable, given the current context of the LTC sector (e.g., limited resources)
it may take a substantial investment of resources and ongoing support for health care professionals to help LTC homes reduce rates of potentially inappropriate use of antipsychotics and to help sustain any progress toward the target (e.g., investment in staffing, process improvements, funding, focused programs).
Risk of Unintended Consequences
While “lower is better” when considering the definition and interpretation of the “potentially inappropriate use of antipsychotics in LTC”2 quality indicator, the panel discussed the potential implications of having a lower target for a quality indicator in practice.
When selecting the value for the target, the panel considered that if the target is too low, then it may indirectly cause LTC homes to focus on strategies to artificially lower the quality indicator rate (e.g., coding people in the data collection instruments with specific conditions so that they are excluded from the indicator), rather than focusing their efforts on providing appropriate care for the people living in LTC homes. Avoiding the potential risk for unintended consequences due to setting a target that was perceived as being “too low” contributed to the panel’s selection of 15% as the value for the target.
Panellists noted the following potential unintended consequences that could occur from trying to achieve a lower target without the proper resources and training:
admission refusals or undertreatment of people with conditions that are not excluded from the quality indicator but for which antipsychotic medication use may be clinically appropriate (e.g., people with severe major psychiatric disorders such as major depressive disorder, people with intellectual disabilities, people with severe responsive behaviours)
medication substitution to another class of medication with sedative properties (e.g., benzodiazepines) that may do little to effectively manage the responsive behaviours of dementia, and may cause harms
changes in diagnostic patterns and increased coding of conditions that are excluded from the quality indicator (e.g., increased coding of psychosis, schizophrenia, delusions, hallucinations, end-stage disease) to influence performance on the quality indicator without actually reducing inappropriate antipsychotic use.
Panellists also felt that 15% balanced being ambitious enough as a long-term target for the sector with being realistic about what is feasible in the LTC sector given the currently available resources at LTC homes across the country (e.g., challenges with staffing levels and continuity), while also minimizing the risk of unintended consequences.
Areas of Disagreement: Panellists in Favour of a Lower Target
At the workshop, 1 panellist with the perspective of a health care professional in LTC did not agree with the value of 15% as the target for LTC homes in Canada, and voted against 15% as the final value. This panellist expressed a preference for a lower, more ambitious value for the target, given that:
many LTC homes in Canada are already achieving quality indicator rates below 15%
other countries have lower rates of potentially inappropriate antipsychotic use
they were concerned that, for homes that are already at or below 15%, a target of 15% would not encourage these homes to continue to make further improvements to reduce potentially inappropriate use of antipsychotics in LTC
they considered that the target is intended to be applicable for a long time with no established revision date, and wanted to set a target that would remain relevant for an extended period.
The panel’s recommended target of 15% means that the proportion of people living in LTC homes across Canada receiving antipsychotic drugs without a diagnosis of psychosis should ideally be 15% or less. There is no time frame associated with the target, and it is not mandatory for LTC homes.
The target sets a standard for the overall risk-adjusted quality indicator rate for Canada. Risk adjustment enables a fairer comparison between LTC homes.
The panel concluded that a 15% target is both ambitious and attainable. They selected this number by considering Canadian data for the quality indicator and how rates are calculated, the current context of the LTC sector, the potential risk of harms if the target was perceived as being too low, and the need for resources to support homes to reach a target.
Consensus on the target value was reached with 94% agreement. One panellist would have preferred a lower, more ambitious value for the target, and voted against 15% as the final value.
Consensus Statement 2: Annual Improvement Goal
The panel reached consensus with 17 of 17 panellists (100%) agreeing that 15% should be the value for the annual improvement goal.
Rationale for the Selection of 15% Relative Reduction as the Annual Improvement Goal
An overview of the selection process for the 15% annual improvement goal value is provided in Figure 5.
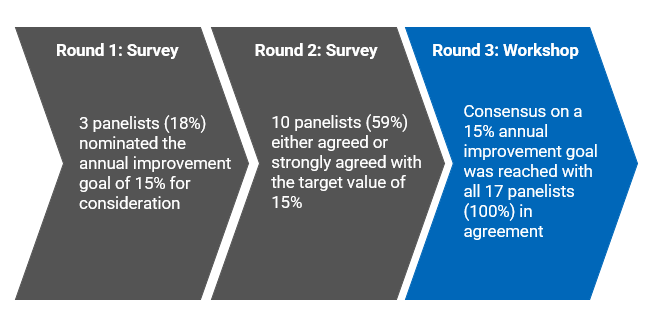
While 15% was not part of the initial options for the annual improvement goal, 3 panel members nominated it for consideration in round 1. It was suggested to be a sufficiently ambitious value while also being achievable for many LTC homes.
In the round 2 survey, 59% of panellists either agreed or strongly agreed with the value of 15% for the annual improvement goal. Panellists considered that a 15% relative reduction per year:
aligned with the results of previous Canadian quality improvement initiatives identified in the Environmental Scan
is a realistic value that would support buy-in from LTC homes
would allow for sustainable progress while accommodating the variability in resources and challenges in LTC homes.
During the workshop, the panel members discussed many different ideas when selecting a 15% relative reduction as the annual improvement goal for the “potentially inappropriate use of antipsychotics in long-term care” quality indicator.
Alignment with Quality Improvement Initiatives in Canada
Panel members described a 15% relative reduction per year as a “feasible,” “reasonable,” and “attainable” value for the annual improvement goal.
The panellists referred to evidence from previous quality improvement initiatives in Canada that were identified in the Environmental Scan, including that:
15% was aligned with the results from previous initiatives, which achieved relative reductions on this quality indicator of approximately 16% and 17% in 1 year
some homes achieved rates ranging from 20% to 40% relative reduction in 1 year, but the panel considered whether these rates would be sustainable year over year.
After the initial ranking exercise in the workshop, the top 3 ranked choices for the goal were 15%, 16%, and 17%. The panel discussed how the annual improvement goal expressed as a relative reduction meant that mathematically, from the perspective of the individual LTC homes, there would be little difference between the values of 15%, 16%, and 17%, in particular for smaller homes. For this reason, any of these values would be acceptable.
Panellists also considered that:
of the top 3 values, a goal of 15% relative reduction annually would be easier to remember and would allow for more LTC homes to aim for and achieve the annual improvement goal on a yearly basis
LTC homes that achieved the 15% relative reduction annually over the course of multiple years would contribute to a substantial reduction in the national rate.
The Need for Systematic, Sustainable, and Safe Progress
A common theme throughout the workshop discussions was selecting a value for the annual improvement goal that would allow for safe and sustainable progress toward the target. The panel reflected that the goal should promote systematic changes– that is, increasing supports so that providers can safely deprescribe antipsychotics (e.g., changing care practices, training staff, modifying spaces), and not simply stop prescribing medications.
The panel reflected on the Canadian quality improvement initiatives reported in the Environmental Scan, and discussed:
whether the relative reductions observed in these initiatives were sustained year to year, or whether the larger relative reductions only occurred in the first year, followed by a tapering of the effect
that the homes in these published initiatives had focused quality improvement programs and dedicated resources to support deprescribing efforts (i.e., the planned process of dose reduction or stopping of medications that might cause harm or may no longer be of benefit).
Based on some panel members’ experiences in their jurisdictions, the LTC homes that were able to achieve relative reductions of 16% to 17% per year were extremely motivated and had external funding and dedicated programs. However, once the additional funding or resources were gone, LTC homes limited their focus on reducing potentially inappropriate antipsychotics.
The panel acknowledged that achieving a higher relative reduction on quality indicator rates in the first year might be easier, but that as the LTC homes’ absolute rate decreases, sustaining the same degree of relative reduction could become more challenging. For example, an initial reduction could result from some “easy wins” that require fewer resources, such as chart reviews to identify opportunities for deprescribing (e.g., antipsychotics that were intended as an interim measure to help the person adjust to living in LTC but were never deprescribed; antipsychotics prescribed in the community but then continued indefinitely). However, as the absolute rate decreases, the opportunities for deprescribing may require more resources due to the complex needs of the people taking antipsychotics in LTC (e.g., additional recreational therapy).
The panellists also discussed that, given the current context of LTC in Canada, a goal that is too ambitious could:
potentially lead to unintended consequences (e.g., increased distress, risk of those living in LTC harming themselves or others) if homes deprescribe antipsychotics too quickly to meet the annual improvement goal
discourage LTC homes if they do not feel that they have the resources to achieve the annual improvement goal.
The panel considered that an annual improvement goal of 15% would:
allow all LTC homes to make measurable and manageable progress toward the target, without discouraging homes over time
require sustained resources and sustained effort for the LTC homes to achieve the goal yearly.
Panellists considered lower values for the annual improvement goal, such as 10%, to be too low as they wouldn’t provide enough motivation for LTC homes to make noticeable changes in providing appropriate care for people living in the homes. One panellist initially preferred a lower value for the annual improvement goal (i.e., 10%), as they wanted to set realistic expectations for homes with fewer resources to be able to make slow improvements; however, after hearing the other perspectives at the workshop, they shifted their thinking and agreed with 15% as the top choice for the annual improvement goal.
The panel recommends that LTC homes that are not meeting the target should aim to reduce the proportion of people without psychosis receiving antipsychotic drugs by 15% relative to the proportion from the previous year.
The annual improvement goal complements the target by recommending a safe and achievable rate of change that allows for sustainable progress toward the target. The annual improvement goal is not mandatory for LTC homes.
The panel concluded that a 15% annual improvement goal is aligned with the results of previous Canadian quality improvement initiatives, and is realistic, encouraging, and sustainable enough to promote meaningful change while minimizing the potential for unintended consequences.
The panel selected a 15% annual improvement goal with an understanding of the importance of implementing systematic changes that increase resources and supports to help care providers safely deprescribe antipsychotics over time.
The panel reached 100% agreement that a 15% relative reduction should be the value for the annual improvement goal.
Pairing the Target and Annual Improvement Goal: 15 and 15
The target and the annual improvement goal were designed to be used together to support quality improvement initiatives to reduce potentially inappropriate use of antipsychotics in LTC homes. By considering them together, an ambitious target can be set for the LTC sector in Canada (i.e., the overall percentage of people living in LTC homes in Canada who are taking antipsychotics without a diagnosis of psychosis), while offering an annual improvement goal that all LTC homes can realistically strive for, regardless of where they stand relative to the target (i.e., an interim goal that LTC homes can use to compare their progress to the previous year).
Before the workshop, panellists were asked to reflect on the evidence inputs and survey results to rank their top 3 potential values for the target and the annual improvement goal with their rationale to prepare for discussion. Many panellists ranked 15% as 1 of their top choices for the target and annual improvement goal going into the workshop. During 1 of the small group discussions, 1 panellist initially reflected on the idea of pairing a 15% value for the target with a 15% value for the annual improvement goal (i.e., 15% relative reduction annually to reach a target of 15%). This concept was well received by the other panellists and was further discussed in the subsequent workshop rounds.
Panellists further discussed the advantages of this “15 and 15” pairing of the target and goal, emphasizing how “15 and 15” are evidence-informed numbers for the target and annual improvement goal that are easy to communicate and remember. In particular, highlighting how “15 and 15” are:
simple numbers that can promote acceptance among LTC providers, and support uptake and implementation by reducing cognitive burden on providers in operationalizing the target and annual improvement goal while removing ambiguity between the value for the target and goal.
numbers that staff in LTC homes could see as achievable at the home level, and as such, promote staff engagement that can help ensure sustainable change over time.
Panel members discussed how the time frame for implementing the annual improvements and reaching the target could help inform their deliberation. During their discussions, panellists noted how a long time frame would allow them to consider a more ambitious target, whereas a short time frame (e.g., 3 to 5 years) would require a less ambitious, higher value for the target. They also noted how the time to reach the target would vary across LTC homes and depend in part on each LTC home’s current performance on the quality indicator. The panel reflected that, given that the target is intended for the long term and the annual improvement goal is intended to support homes in reaching the target over time, the pairing of “15 and 15” provides a balanced approach to promoting ambitious changes in the long term and achievable progress on an annual basis.
Pagebreak
Considerations for Clinical and Care Practice
Beyond reaching consensus on the target and annual improvement goal, this project aimed to identify key considerations for clinical and care practice that can help reduce potentially inappropriate use of antipsychotics in LTC homes in Canada. Considerations outlined in this section summarize and highlight the interrelated concepts identified in the Environmental Scan, the engagement input summary, and the panel’s inputs that can help reduce inappropriate antipsychotic use in LTC homes. Refer to Table 3 in Appendix 3 for a summary of the panel members’ input from the round 1 survey regarding barriers and facilitators to reducing inappropriate antipsychotic use.
In alignment with Canadian clinical practice guidelines identified in the Environmental Scan,13,41-44 the inputs from the engagement survey of interest holders in the LTC sector (e.g., resident and caregiver associations, appropriate prescribing groups, and health organizations) indicated that there is a limited or no role for antipsychotic use for people living in LTC homes without a diagnosis of psychosis. As 1 respondent to the engagement survey emphasized, “While medications can be part of the care plan, it should not be the whole plan.” Thoughtful deliberation of the risks and benefits of antipsychotics, underlying causes of responsive behaviours, and of other treatment options (i.e., nonpharmacological approaches) by LTC staff and caregivers may help prevent inappropriate use of antipsychotics, facilitate appropriate use, and avoid undertreatment of people living in LTC homes who may benefit from antipsychotics. The Canadian Clinical Practice Guidelines for Assessing and Managing Behavioural and Psychological Symptoms of Dementia, published in 2024, provide guidance on appropriate treatment options for specific symptoms and behaviours.13
During the workshop, panel members described scenarios of meaningful reductions in inappropriate use and successful deprescribing of antipsychotics in LTC homes. In general, as highlighted in the following sections, examples of success came from highly motivated LTC homes with engaged staff and dedicated and sustained resources for targeted interventions focused on person-centred care. This aligns with literature that suggests that adequate staffing allows for more time to implement person-centred and safer care.45 Panellists also noted that an ambitious target could potentially help guide resource planning and allocation in LTC homes.
The panel emphasized the importance of avoiding changes in care that influence the antipsychotic quality indicator rates without improving the health and safety for people in LTC homes (e.g., changes in coding or diagnostic patterns, medication substitution). Efforts are under way to reduce potentially inappropriate antipsychotic use, including the work led by the Appropriate Use Coalition. Using the target for LTC homes in Canada and annual improvement goal, the coalition plans to align and develop quality improvement initiatives and provide the resources and tools to make headway across the LTC systems in Canada.
Tailoring Resources and Processes
The interRAI analysis comparing homes in the 20th and 80th percentiles included in the Environmental Scan suggests that there was no difference between high-performing and lower-performing homes in terms of size (i.e., small, medium, or large), urban or rural location, and income quintile, and that top-performing homes could be found in all provinces (Dr. John Hirdes, interRAI Canada, University of Waterloo: unpublished data, Jan 15, 2025). While this suggests that it is possible for homes of any size, location, or income quintile to improve their performance on the quality indicator, having dedicated resources and programs for reducing inappropriate antipsychotics is likely required to achieve success.
The panel acknowledged that resources and efforts to reach the target and achieve the annual improvement goal will need to be tailored to the local context of each LTC home.
LTC homes can prioritize and sustain appropriate use efforts and person-centred care with support and adequate resources aligned with the needs of people living in LTC homes, such as appropriate staffing levels, materials or equipment for high-quality care (e.g., supplies for nonpharmacological approaches or recreational activities, education resources for staff), and a physical environment conducive to reducing inappropriate use (e.g., environments without safety concerns, spaces for recreational activities).
Beyond staffing levels, panel members highlighted the importance of staff consistency and collaboration to better address the needs of people in LTC homes and reduce inappropriate use of antipsychotics. Supportive and proactive leadership can facilitate staff retention. Strong collaboration and communication in engaged and empowered care teams can also better implement and execute the changes that encourage appropriate use of antipsychotics in LTC homes. For example, leadership and staff stability over time can provide staff the opportunity to build trusting and positive relationships with people in LTC homes, learn their triggers, and identify the most effective nondrug approach to responsive behaviours instead of using antipsychotics. The panel, as well as the literature, acknowledged staffing shortages and staff retention as a systemic challenge for the LTC sector, especially for rural LTC homes.46
Aligning LTC homes’ internal processes, tools, and policies relative to their inappropriate antipsychotic use rates with their needs can also help inform meaningful change in their context. The panel and literature provided potential process improvements that LTC homes might consider to facilitate reductions in inappropriate use, such as adopting medication review or a systematic monitoring process (e.g., for side effects) for individuals receiving antipsychotics,47-50 using care algorithms (e.g., Describe-Investigate-Create-Evaluate [DICE]34) and toolkits (e.g., Alberta’s Appropriate Use Toolkit51), and developing comprehensive treatment plans with clear timelines for reassessment and deprescribing.
Care algorithms, such as the DICE approach, provide a holistic framework for the management of BPSD that avoids superficial attempts to reduce antipsychotic use by merely shifting to use of other medications with potential harms and even less evidence of benefit.34
Toolkits provide resources and guidance that care teams may reference in practice to improve care. For example, Alberta’s Appropriate Use Toolkit51 offers guidance and tools for care providers to assess and manage responsive behaviours and facilitate appropriate use of antipsychotics.
Person-Centred Care
Initiatives aiming to support efforts to reach the target for LTC homes in Canada and the annual improvement goal should consider implementing a person-centred approach,13 in which care plans and treatment reflect the unique needs, individuality, and preferences of people in LTC homes. For example, implementing personalized schedules may avoid the potential for responsive behaviour triggered by set meal or bath times that misalign with the preferences and needs of people in LTC homes.
Person-centred care also supports autonomy by involving individuals receiving care, as well as their family or caregivers in decision-making.52-54 The panel acknowledged and underscored family or caregivers as an important part of the care team, as they can advocate for and facilitate person-centred care by sharing their knowledge of the individual’s preferences, behaviours, and background.36 The panel emphasized the role of resident and family councils in elevating the perspectives and concerns of people living in LTC homes and their families and caregivers as a collective.55 These councils’ insights can help build positive relationships with people in LTC homes and their families or caregivers, improve quality of life and care, and create community within LTC homes. Successful and robust family and resident councils have been described to have ongoing and transparent communication (between the councils and LTC leadership, people in LTC homes, and their families or caregivers), clear structure and processes, effective and knowledgeable leadership, a culture of trust and respect, continuous recruitment for new members, and resources (e.g., spaces for meetings, tables and chairs).56
Person-centred care considers various aspects of personhood, such as an individual’s cultural background, gender, ethnicity, religion, and language.13,53,57 While it is unclear whether there are racial and ethnic disparities in potentially inappropriate antipsychotic use in Canada, research from the US suggests that LTC settings with a higher proportion of racialized older adults have high rates of potentially inappropriate antipsychotic use.58 The Landmark Study by the Alzheimer Society of Canada projects an increase in the proportion of people of African, Asian, and Caribbean ethnic origin, as well as Indigenous individuals, living with dementia by 2050.59 The increase in cultural diversity in people living with dementia in Canada highlights the value of integrating inclusive practices that facilitate culturally safe and trauma informed care in LTC homes. A literature review suggests that care that respects cultural and linguistic diversity can help prevent responsive behaviour,60 and thus may minimize potentially inappropriate antipsychotic use. The results of nonrandomized studies suggest that language discordance between LTC staff and people living in LTC homes can negatively impact care and increases the risk of potentially inappropriate antipsychotic use.61,62 Language discordance can make it challenging for LTC staff to get to know people in LTC homes.61,62
The panel and the engagement survey also identified the following groups that may be more likely to be provided inappropriate antipsychotics or disproportionately harmed by antipsychotics in LTC homes:
people with experience of significant trauma who may resist care due to distrust stemming from previous experiences, such as sexual abuse, racism, and discrimination in the health care system
immigrants and newcomers who disproportionately experience mental health inequities and lack options for culturally informed and safe care
“younger” older adults who are less likely to be given access to geriatric care
individuals without advocates, family, or caregivers to push for safer and high-quality care
people with intellectual disabilities and brain injuries who may respond to medications differently.
Collecting sociodemographic data can help identify gaps and disparities in care specific to the LTC homes in Canada. Sociodemographic data can inform targeted efforts for LTC homes and quality improvement initiatives led by health systems.
Training
Panel members described successful reductions of inappropriate medication use from initiatives that provided opportunities for LTC staff training and skills development through various platforms (e.g., websites, toolkits, and guidelines). Through training, staff can better understand dementia and BPSD, antipsychotics, other pharmaceutical agents, side effects of medications, person-centred care, and nonpharmacological approaches. The panel also highlighted the value of supporting LTC staff to apply what they learned from training into practice. Families or caregivers of people in LTC homes may also benefit from increasing their knowledge in these topic areas.63 Increased knowledge empowers LTC staff and families or caregivers to challenge the status quo and implement or advocate for positive change.64,65 Additionally, the panel spoke to the benefits of trained and certified staff in LTC homes in providing high-quality care.
Access to Specialized Care
The panel also emphasized the value of specialized care, especially as LTC homes see increasingly complex cases. For example, the panel noticed a rapid increase of individuals with severe mental health disorders being admitted into LTC homes. Some LTC homes benefit from behavioural support units, which have the resources and geriatric psychiatry expertise to manage responsive behaviours appropriately. Additionally, conducting psychiatric assessments upon admission may help facilitate deprescribing inappropriate antipsychotic use and direct people to appropriate care. People in LTC homes may also benefit from access to pharmacists, family physicians with expertise in dementia, and recreation workers. Of note, rural LTC homes face longer wait times for specialized care compared to urban areas, considering the distance and time needed to reach these homes.66
Deprescribing Antipsychotics Initiated Before LTC Admission
Short-term antipsychotic use is sometimes initiated in the community or in acute care before LTC admission. In these cases, care providers in LTC homes may feel less inclined to stop antipsychotic use during admissions, especially when they feel it may help people acclimate to their new environment. However, the panel identified these circumstances as key areas of focus to start deprescribing efforts and to encourage appropriate use of antipsychotics. A retrospective study in LTC homes in Ontario suggested that adults aged 66 to 84 years are less likely to discontinue potentially inappropriate antipsychotic use within 180 days of admission compared to adults aged 85 years or older.67 This finding aligns with observations from the engagement survey about increased antipsychotic use in “younger” older adults living in LTC homes. There is also evidence to suggest that discontinuing long-term antipsychotic use is possible without exacerbating challenging behaviour,68 despite the fears and concerns expressed by health professionals and LTC staff in the literature.48-50,63,69
LTC staff sometimes lack the necessary information to make an informed and person-centred decision about deprescribing antipsychotics that were initiated before LTC admission (e.g., reasons for initiating antipsychotics, symptoms, previous courses of antipsychotic use, reasons for stopping, and effective nondrug approaches).70 Having these data may enable LTC staff to better identify side effects or avoid long-term use after admission when initiation dates for medications are available. “Accessible data” means that LTC staff can use 1 system to access all needed health information from the health continuum, inclusive of treatments received before entering LTC.70
Monitoring Balancing Measures and Unintended Consequences
The panel emphasized the importance of avoiding superficial decreases in quality indicator rates that do not improve safety and health outcomes for people in LTC homes or that limit access for people who may benefit from clinically appropriate antipsychotic use. The literature, engagement input summary, and panel discussions highlighted how monitoring the following practices may reveal whether efforts to reduce potentially inappropriate use of antipsychotics in LTC homes lead to unintended consequences:
balancing measures (i.e., quality indicators that determine whether changes designed to improve performance on 1 quality indicator are causing new problems in other quality indicators)
examples of balancing measures (many of which have been used in previous quality improvement initiatives from the Environmental Scan) include use of physical restraints, worsening behavioural symptoms, aggressive behaviour, falls, pain, delirium, worsened mood symptoms of depression, and level of independence in performing activities of daily living
use of other medications to detect any potential compensatory increases in other medications (e.g., substitutions to another class of medication with sedative effects) that may have limited evidence of benefit and may cause harm34
changes in diagnostic patterns (e.g., increased coding of psychosis, schizophrenia, or other exclusion criteria) to influence performance on the quality indicator without actually reducing inappropriate antipsychotic use
changes in populations admitted into LTC homes to detect whether LTC homes are not admitting individuals with complex needs or conditions that are not excluded from the quality indicator but for which antipsychotic medication use may be clinically appropriate (e.g., people with severe major psychiatric disorders such as major depressive disorder, people with intellectual disabilities who exhibit aggression or agitation).
The Need to Understand the Quality Indicator
Throughout the Delphi process, the panel discussion reinforced that those working in LTC homes need to understand what the quality indicator is measuring and how it is calculated to properly support interpretation and uptake of the target and the annual improvement goal. Discussions during the workshop revealed some of the nuances of the quality indicator that may be misunderstood or misinterpreted.
The Quality Indicator Is Comparable Between Homes
Quality indicator performance is comparable across LTC homes, as the data are risk-adjusted to control for population differences between LTC homes. While the panel discussed some concerns about the variation in populations between homes and the changing demographics of those admitted to LTC in relation to their potential impact on the quality indicator performance, risk adjustment of the data accounts for these variations and changes.
Table 1 provides examples of some population considerations that the panel discussed and the corresponding covariates that adjust for these factors.
Table 1: Population Considerations Discussed by the Panel and Corresponding Covariates Used in Risk Adjustment for the Quality Indicator
Population consideration | Corresponding covariate(s) used in risk adjustment at the individual level |
|---|---|
Increased number of younger people | Age younger than 65 years |
Increased number of people with brain injuries or intellectual disabilities | Moderate or impaired decision-making problem Long-term memory problem CPS |
People admitted with more advanced dementia | Alzheimer disease or other dementia |
CPS = Cognitive Performance Scale.
The Quality Indicator Captures Some Potentially Appropriate Indications
It is likely (and expected) that a proportion of individuals who are receiving antipsychotics appropriately will be included in the quality indicator because the quality indicator is only designed to measure potentially inappropriate antipsychotic use in LTC, not inappropriate use of antipsychotics.
Some of the approved indications for antipsychotics that are not excluded from the quality indicator include bipolar disorder, major depressive disorder, and the short-term treatment of aggression in people with severe dementia (refer to the Environmental Scan for details on approved indications). The indicator would categorize the off-label, yet perhaps clinically reasonable, use of antipsychotics as potentially inappropriate use (e.g., off-label use of atypical antipsychotics to treat obsessive-compulsive disorder, posttraumatic stress disorder, or generalized anxiety disorder).71 While risk adjustment can adjust performance rates to account for these situations, antipsychotic use in these potentially appropriate conditions and circumstances precludes striving for the quality indicator rate to be zero.
The panel discussed that it is important to understand whether and how these potentially appropriate indications for antipsychotic use in LTC may impact quality indicator performance:
Bipolar disorder: The contribution to the quality indicator from people with bipolar disorder is expected to be minimal, given that:
bipolar disorder is not very common in LTC (in 2023–2024, 2.7% of people living in LTC in Canada had a diagnosis of bipolar disorder)72
if a person with bipolar disorder experienced delusions or hallucinations, they would be excluded from the indicator.
Short-term treatment of aggression or agitation in people with severe dementia: While this may contribute to the quality indicator (depending on the length of treatment and timing of the assessment), the intent of the target is not to penalize LTC homes for using antipsychotics in these potentially appropriate cases. It is about ensuring that the appropriate care is provided and that clinical practice guidelines are followed (e.g., opportunities to deprescribe antipsychotics where appropriate).
People admitted to LTC after being prescribed antipsychotics in the acute care setting: If antipsychotics are continued for more than 3 months after admission, then there is the potential for this to contribute to the quality indicator. However, for an assessment to be valid (and used to calculate the quality indicator), it must be conducted more than 92 days after admission, and it cannot be the first assessment or the admission assessment. This situation represents an opportunity to deprescribe antipsychotics (when appropriate), rather than continuing them indefinitely after admission.
The Quality Indicator Excludes Antipsychotic Use for Certain Conditions
Engagement input revealed that antipsychotics may have a role in symptom management for people in end-of-life care. The quality indicator excludes individuals with an end-stage disease (with 6 months or less to live) or people receiving hospice or palliative care in LTC homes. Other indications excluded from the quality indicator are people with a diagnosis of schizophrenia or Huntington chorea, as well as people experiencing hallucinations or delusions in LTC homes. Hence, antipsychotic use for any of the excluded conditions does not impact performance on the quality indicator, and the target and goal do not preclude LTC homes from using antipsychotics in these situations.
The panel underscored the value of targeted interventions to reduce potentially inappropriate antipsychotic use in LTC homes that focus on a person-centred approach and are supported by engaged LTC staff and dedicated and sustained resources. Other factors for success discussed by the panel include providing relevant training for care teams and access to specialized care for people in LTC homes.
Top-performing LTC homes can be found in all provinces and income quintiles, which suggests that a variety of LTC homes have potential to improve their quality indicator performance. The panel discussed that tailoring resources and process changes to the needs of the LTC home may support efforts to reduce potentially inappropriate antipsychotic use in specific contexts.
The panel identified short-term antipsychotic use initiated before LTC admission as a potential starting point for deprescribing efforts with enhanced information-sharing practices (e.g., medical history) across the care continuum.
To support proper uptake of the consensus statements, the panel reinforced the need to ensure LTC providers understand the nuances of what the quality indicator measures and how it is calculated, specifically what indications the quality indicator excludes, how it captures some “potentially appropriate use,” and how and why it is risk-adjusted.
Monitoring unintended consequences and balancing measures can help identify whether efforts to achieve the target and the annual improvement goal are inadvertently causing harm.
Family and caregivers play an integral role in care teams as facilitators of person-centred care.
Pagebreak
Final Thoughts
The inappropriate use of antipsychotics is likely an ineffective and harmful approach to manage behaviours or conditions in LTC homes (e.g., BPSD), especially when used and continued without careful consideration of the risks and benefits and exhausting nonpharmacological approaches. With its sedative effect, antipsychotic use can affect quality of life and also undermine autonomy and an individual’s right to participate in their care, which may already be compromised in individuals with dementia.36
In 2023–2024, CIHI reported an average of 24.5% of potentially inappropriate antipsychotic use in Canada, with many provinces above the national average.5 The rising rate indicates a reversal of steady progress made by efforts to curb inappropriate antipsychotic use before 2020.5
Aligned with Appropriate Use Coalition priorities, CDA-AMC partnered with CWC to convene an expert panel to reach consensus on a target for LTC homes in Canada and an annual improvement goal (relative reduction per year) for the “potentially inappropriate use of antipsychotics in long-term care” quality indicator. The consensus statements will be used to inform quality improvement efforts aiming to reduce inappropriate antipsychotic use in LTC homes in Canada.
The expert panel achieved consensus on 15% as the target for LTC homes across Canada and 15% for the annual improvement goal (relative reduction per year). The target for reducing potentially inappropriate antipsychotic use in LTC homes in Canada is ambitious but feasible with steady annual improvements. It is estimated that achieving the 15% target for LTC homes in Canada would result in more than 21,000 fewer people receiving these potentially inappropriate medications across the country, compared to the 2023–2024 national rate for Canada (Dr. John Hirdes, interRAI Canada, University of Waterloo: personal communication, Feb 27, 2025). Aiming for this target for LTC homes in Canada may also help prevent more people from receiving potentially inappropriate antipsychotics in light of future changes to the LTC population and the increasing prevalence of dementia in Canada.
To support LTC homes’ efforts to reduce potentially inappropriate use of antipsychotics in LTC in Canada, the following considerations provide key insights for the successful implementation of the target and annual improvement goal.
The Target Is Not a Limit
LTC homes that have already reached the target are encouraged to continue decreasing inappropriate antipsychotic use if continuing efforts enhance safety and quality of life for those living in LTC homes without triggering unintended consequences. Top-performing homes in 2023–2024 have achieved 15% or lower rates for the “potentially inappropriate use of antipsychotics in long-term care” quality indicator, and LTC homes should feel inspired to reach or exceed the target, regardless of their size, location, or income.
The Target and the Annual Improvement Goal Are Not Mandatory
The consensus statements provide evidence-informed guidance from a panel of experts and knowledgeable individuals, but they will not be mandatory for LTC homes. Setting a target for LTC Homes in Canada and annual improvement goal is meant to support quality improvement initiatives to inform, motivate, and monitor change in the LTC sector. The Appropriate Use Coalition plans to use the consensus statements as a starting point for their efforts, such as aligning and developing quality improvement programs, tools, and resources.
The target reflects a level of excellence for the quality indicator that is intended to inspire changes in clinical practice in LTC homes. It represents a level of potentially inappropriate antipsychotic use that minimizes potential harms for people living in LTC (i.e., the proportion of people living in LTC homes across Canada receiving antipsychotic drugs without a diagnosis of psychosis should ideally be 15% or less). The target and annual improvement goal were designed to be used together to support safe and sustainable quality improvement initiatives in LTC homes.
Establishing the target for LTC homes in Canada and the related annual improvement goal was an initiative of the Appropriate Use Coalition (a grassroots group of organizations working collectively to improve health outcomes and reduce risks through appropriate prescribing and use of medications in Canada) and was supported by an engagement survey of respondents who recognized the need for a target for antipsychotic use rates in LTC homes in Canada.
Focus on Appropriate Use of Antipsychotics Through Person-Centred Care
The key objective of developing the consensus statements is to promote the appropriate use of antipsychotics and ensure people in LTC homes are provided high-quality care that prioritizes their safety and quality of life. Appropriate use means that “people are taking medications best suited for their needs in order to provide the greatest possible benefit and avoid potential harm (p. 14).”73 What is appropriate for 1 person at 1 time may not be appropriate for the same person at another time or for other people. Implementing person-centred care facilitates appropriate use of antipsychotics by ensuring care plans and treatment reflect and respect the unique needs and preferences of people living in LTC homes. Additionally, person-centred care reflects an individual’s right to dignified care that respects an individual’s personhood and autonomy, as well as recognizing their capacity and goals.36,37 The panel acknowledged the role of family or caregivers in care teams as facilitators of person-centred care.
Gaps in the literature remain about which groups or individuals may be more likely to be provided antipsychotics or disproportionately harmed by antipsychotic use. Through this work, panel members and interest holders had the opportunity to highlight groups among the LTC population who may require special consideration for these reasons, such as immigrants and newcomers, and “younger” older adults. Improving data collection in LTC by including sociodemographic data can address this gap and better identify disparities in care to inform targeted, person-centred care efforts and quality improvement initiatives led by the LTC sector.
The panel described success related to antipsychotic use in LTC homes as “having people appropriately on these medications and appropriately taken off these medications when they are no longer required.” They emphasized that focusing too much on lowering rates for the quality indicator without considering whether care is appropriate may lead to unintended consequences (e.g., increased coding of exclusions, undertreatment of people who many benefit from antipsychotics). Likewise, reductions in the quality indicator rates should reflect improvements in care (e.g., personalized schedules, access to recreation activities, appropriate opportunities for deprescribing) and health outcomes (e.g., improved quality of life, increased engagement with activities of daily living or recreational activities) versus changes in practice that may compromise care.
Emphasize Safety and Reduce Harm
A driving factor for reducing potentially inappropriate use of antipsychotics in LTC is to increase safety and decrease the risk of harm for people living in LTC homes. Antipsychotic medications have well-documented risks of adverse events for older adults with dementia,10-12,14-28,74 and there is limited evidence of their effectiveness to manage specific symptoms of dementia.10,11 Canadian clinical practice guidelines therefore recommend nonpharmacological approaches to manage BPSD instead.13,43,75-77 A 15% target for LTC homes in Canada to reduce potentially inappropriate antipsychotic use provides LTC homes with a tangible objective for quality improvement initiatives aiming to decrease these associated harms. The pairing of the target with the 15% annual improvement goal is intended to further support safety for those living in LTC by guiding sustainable progress toward the target at a reasonable pace. Monitoring balancing measures and unintended consequences can also help ensure that efforts to achieve the target and annual improvement goal are not inadvertently causing harm.
Champion Change
To reach the target, the panel recognized the need for change in LTC homes. They noted that it will require creative ideas and novel solutions (e.g., organizing LTC homes differently) to support this shift toward working differently (e.g., implementing personalized schedules, offering nonpharmacological therapies). However, the panel acknowledged the challenge of balancing the needs of the people living in LTC with the needs of the staff and the needs of the LTC home. Regularly engaging people living in LTC homes and their families or caregivers, including through resident and family councils, can help ensure change is in the right direction.
Canada’s LTC sector has previously shown its capability to implement changes and reduce inappropriate antipsychotic use, and the interRAI analysis suggests that it is possible for homes of all sizes, locations, and incomes to be top-performing homes. Without action, high rates of potentially inappropriate use of antipsychotic in LTC in Canada will remain or may continue to rise. The 15% target for LTC homes in Canada and 15% annual improvement goal set clear expectations of where Canada should be regarding appropriate use of antipsychotics, and achieving the target for Canada requires collective action from the LTC sector.
Through a coordinated response, the members of the Appropriate Use Coalition and the LTC homes can play a role in shaping this change to improve the quality of care for people living in LTC. For more information about the Appropriate Use Coalition and their efforts, visit ltcmeds.ca. This website serves as a resource for LTC homes seeking additional information on the target and annual improvement goal, available programs, and ways to stay connected for future updates.
Pagebreak
About the Expert Panel
The biographies of the 17 panel members are on the CDA-AMC website. Declarations of conflicts of interest can be found in Appendix 4.
Panel Members
Marie-Andrée Bruneau, MD, MSc
University of Montreal, Canadian Coalition for Seniors’ Mental Health
Ian DaSilva, Chief Operating Officer
Canadian Support Workers Association, Ontario Personal Support Workers Association
Lisa Dawson
Independent Long-Term Care Councils Association of British Columbia
Vivian Ewa, MD, MMEd
Alberta Health Services, University of Calgary, College of Family Physicians of Canada
Sid Feldman, MD
Baycrest Health Sciences, University of Toronto, College of Family Physicians of Canada, Choosing Wisely Canada Long-Term Care program
Carole A. Goodine, PharmD
Canadian Pharmacists Association
Aswathy Jayasree, BN, RN, GNC(C)
Canadian Nurses Association
Ashley King, BA, MBA
Loch Lomond Villa Inc., Canadian Association for Long-Term Care
Geneviève Lemay, MD, MSc, BScN
Department of Medicine, Division of Geriatrics, University of Ottawa, Canadian Geriatrics Society
Andrea Luva Moser, MD
Institute for Safe Medication Practice Canada, Canadian Society for Long-Term Care Medicine, Ontario Long-Term Care Clinicians, City of Toronto Senior Services and Long-Term Care Division
Dallas Seitz, MD, PhD
University of Calgary, Canadian Psychiatric Association
Cynthia Sinclair, RN
Healthcare Excellence Canada
Wade Thompson, PharmD, PhD
University of British Columbia, deprescribing.org
Shanna C. Trenaman BScH, BScPharm, MAHSR, ACPR, PhD
Dalhousie University
Ahmed Vanker, MD
Extendicare, Canadian Association for Long-Term Care
Shirin Vellani, NP, PhD, CDE, GNC(c)
Nurse Practitioner Association of Canada
Julie Weir, RN, BN, MN, PhD student, ICP, LTC-CIP
University of New Brunswick, Faculty of Nursing, Choosing Wisely Canada
In Partnership
CWC is the national voice for reducing unnecessary tests and treatments in Canada.
CDA-AMC is a not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs and medical devices in the health care system.
CDA-AMC and CWC have partnered to convene the expert panel tasked with developing the target for LTC homes in Canada and the annual improvement goal for the “potentially inappropriate use of antipsychotics in long-term care” quality indicator in support of the Appropriate Use Coalition.
Pagebreak
Acknowledgements
We would like to thank the clinicians, researchers, families, and community members affiliated with the following groups or institutions for their time and insights when completing the engagement survey. Their individual perspectives provided important considerations for the panel to reflect upon during their deliberations.
Alberta Health Services
Alzheimer Society of Canada
Choosing Wisely Long-Term Care Steering Committee
Government of Newfoundland and Labrador
Government of the Northwest Territories
Health Prince Edward Island
Health Quality British Columbia
Maple Ridge Senior Village
Northwest Territories Health and Social Services Authority
Ontario Health
Patient Advisory Committee, Interior Health
Sherbrooke Community Centre
University of Calgary
University of Toronto and deprescribing.org
Vancouver Island Health Authority
We appreciate the teams from CIHI and InterRAI for providing quality indicator data and related analyses for the Environmental Scan to inform panel deliberations. We also thank them for their time and expertise to establish key definitions and concepts related to the quality indicator and associated data, as well as providing advisory support for panel questions about the data during the round 3 workshop.
We are grateful to the panel members who shared their time and expertise to develop these consensus statements to support the appropriate use of antipsychotics in LTC, thereby contributing to the quality of care in LTC in Canada.
We also wish to thank the following individuals for their time and expertise in pilot testing the survey for the first round of the Delphi process.
Dr. Margaret Manville, MD FCFP
Care of the Elderly
Medical Director, Long-Term Care, Island Health
Clinical Associate Professor, UBC Faculty of Medicine, Department of Family Practice British Columbia
Dr. Elizabeth Rhynold, MD FRCPC
Geriatrician, Saskatchewan Health Authority
Assistant Professor Division of Geriatric Medicine, University of Saskatchewan
References
1.CCRS Quality Indicators Risk Adjustment Methodology. Ottawa (ON): Canadian Institute for Health Information (CIHI); 2013: https://www.cihi.ca/sites/default/files/document/ccrs_qi_risk_adj_meth_2013_en_0.pdf. Accessed 2024 Aug 9.
2.Canadian Institute for Health Information (CIHI). Potentially Inappropriate Use of Antipsychotics in Long-Term Care. Indicator Library 2023; https://www.cihi.ca/en/indicators/potentially-inappropriate-use-of-antipsychotics-in-long-term-care. Accessed 2024 Jul 17.
3.Canadian Institute for Health Information (CIHI). Case mix. 2024: https://www.cihi.ca/en/submit-data-and-view-standards/methodologies-and-decision-support-tools/case-mix. Accessed 2024 Aug 21.
4.CAMH. Antipsychotic medications. [2024]; https://www.camh.ca/en/health-info/mental-illness-and-addiction-index/antipsychotic-medication. Accessed 2024 Aug 6.
5.Choosing Wisely Canada on behalf of the Appropriate Use Coalition - LTC Subgroup. Rising Rates: Antipsychotic Use in Canada's LTC homes. [2024]; https://ltcmeds.ca/. Accessed 2024 Dec 6.
6.Winter JD, Petterson S, Qato DM, et al. Quality Gap in Long-Stay Antipsychotic Quality Measure Performance Widens Over the Pandemic, Reversing Past Gains. Gerontol Geriatr Med. 2024;10:23337214241262914. PubMed
7.Campitelli MA, Bronskill SE, Maclagan LC, et al. Comparison of Medication Prescribing Before and After the COVID-19 Pandemic Among Nursing Home Residents in Ontario, Canada. JAMA Netw Open. 2021;4(8):e2118441. PubMed
8.Yan D, Temkin-Greener H, Cai S. Did the COVID-19 Pandemic Affect the Use of Antipsychotics Among Nursing Home Residents With ADRD? Am J Geriatr Psychiatry. 2023;31(2):124-140. PubMed
9.Alzheimer Society of Canada. Navigating the path forward for dementia in Canada. The Landmark Study: Path. Toronto (ON): Alzheimer Society of Canada; 2022: https://alzheimer.ca/sites/default/files/documents/Landmark-Study-Report-1-Path_Alzheimer-Society-Canada_0.pdf. Accessed 2024 Aug 20.
10.Muhlbauer V, Mohler R, Dichter MN, Zuidema SU, Kopke S, Luijendijk HJ. Antipsychotics for agitation and psychosis in people with Alzheimer's disease and vascular dementia. Cochrane Database Syst Rev. 2021;12(12):CD013304. PubMed
11.Wells GA, Kelly S, Johnston A, et al. Atypical antipsychotics for the behavioural and psychological symptoms of dementia in the elderly. Toronto (ON): Ontario Drug Policy Research Network; 2015: https://odprn.ca/wp-content/uploads/2015/06/Antipsychotics-_-systematic-review-Final-Report_1.pdf. Accessed 2024 Aug 5.
12.By the American Geriatrics Society Beers Criteria Update Expert Panel. American Geriatrics Society 2023 updated AGS Beers Criteria(R) for potentially inappropriate medication use in older adults. J Am Geriatr Soc. 2023;71(7):2052-2081. PubMed
13.Canadian Clinical Practice Guidelines for Assessing and Managing Behavioural and Psychological Symptoms of Dementia (BPSD). Toronto (ON): Canadian Coalition for Seniors' Mental Health; 2024: https://ccsmh.ca/areas-of-focus/dementia/clinical-guidelines/. Accessed 2024 Jul 18.
14.Teva-chlorpromazine (chlorpromazine hydrochloride): 25 mg, 50 mg and 100 mg tablets [product monograph]. Toronto (ON): Teva Canada Limited; 2012 Dec 11: https://pdf.hres.ca/dpd_pm/00018580.PDF. Accessed 2024 Aug 12.
15.Perphenazine: 2 mg, 4 mg, 8 mg, and 16 mg tablets [product monograph]. Vaughan (ON): AA Pharma Inc.; 2012 Jun 6: https://pdf.hres.ca/dpd_pm/00017267.PDF. Accessed 2024 Aug 12.
16.Clopixol (zuclopenthixol as zuclopenthixol hydrochloride): 10 mg and 25 mg tablets; Clopixol-Acuphase (45.25 mg/mL zuclopenthixol as zuclopenthixol acetate): 50 mg/mL intramuscular injection; Clopixol Depot (144.4 mg/mL zuclopenthixol as zuclopenthixol decanoate): 200 mg/mL intramuscular injection [product monograph]. Montreal (QC): Lundbeck Canada Inc.; 2014 Apr 8: https://pdf.hres.ca/dpd_pm/00024771.PDF. Accessed 2024 Aug 12.
17.Pimozide: 2 mg and 4 mg tablets [product monograph]. Vaughan (ON): AA Pharma Inc.; 2014 Mar 11: https://pdf.hres.ca/dpd_pm/00024494.PDF. Accessed 2024 Aug 12.
18.Trifluoperazine (trifluoperazine hydrochloride): 1, 2, 5, 10 and 20 mg tablets [product monograph]. AA Pharma Inc.; 2014 Oct 9: https://pdf.hres.ca/dpd_pm/00027772.PDF. Accessed 2024 Aug 12.
19.Mylan-Olanzapine (olanzapine): 2.5 mg, 5 mg, 7.5 mg, 10 mg, 15 mg and 20 mg tablets; Mylan-Olanzapine ODT (olanzapine): 5 mg, 10 mg, 15 mg, 20 mg orally disintegrating tablets [product monograph]. Etobicoke (ON): Mylan Pharmaceuticals ULC; 2017 Feb 17: https://pdf.hres.ca/dpd_pm/00038283.PDF. Accessed 2024 Jul 31.
20.Auro-Clozapine (clozapine): 25 mg, 50 mg, 100 mg and 200 mg tablets [product monograph]. Woodbridge (ON): Auro Pharma Inc.; 2017 Nov 30: https://pdf.hres.ca/dpd_pm/00042421.PDF. Accessed 2024 Aug 06.
21.pms-aripiprazole (aripiprazole): 2 mg, 5 mg, 10 mg, 15 mg, 20 mg and 30 mg tablets [product monograph]. Montreal (QC): Pharmascience Inc.; 2018 Feb 14: https://pdf.hres.ca/dpd_pm/00046328.PDF. Accessed 2024 Jul 31.
22.Rexulti (brexpiprazole): 0.25 mg, 0.5 mg, 1 mg, 2 mg, 3 mg and 4 mg tablets [product monograph]. Saint-Laurent (QC): Otsuka Canada Pharmaceutical Inc.; 2019 Feb 21: https://pdf.hres.ca/dpd_pm/00049750.PDF. Accessed 2024 Jul 31.
23.AG-risperidone (risperidone): 0.25mg, 0.5mg, 1mg, 2mg, 3mg and 4 mg tablets [product monograph]. Boucherville (QC): Angita Pharma Inc.; 2019 Jan 11: https://pdf.hres.ca/dpd_pm/00049156.PDF. Accessed 2024 Jul 31.
24.Seroquel (quetiapine fumarate): 25, 100, 200 and 300 mg, immediate-release tablets, oral use [product monograph]. Mississauga (ON): AstraZeneca Canada Inc.; 2021 Nov 29: https://www.astrazeneca.ca/content/dam/az-ca/downloads/productinformation/seroquel-product-monograph-en.pdf. Accessed 2024 Jul 31.
25.Quetiapine fumarate extended-release tablets: 50 mg, 150 mg, 200 mg, 300 mg and 400 mg quetiapine (as quetiapine fumarate), oral use [product monograph]. Kirkland (QC): Accord Healthcare Inc.; 2022: https://pdf.hres.ca/dpd_pm/00064667.PDF. Accessed 2024 Dec 18.
26.Auro-ziprasidone (ziprasidone as ziprasidone hydrochloride monohydrate): 20, 40, 60, and 80 mg capsules [product monograph]. Woodbridge (ON): Auro Pharma Inc.; 2022 Oct 19: https://pdf.hres.ca/dpd_pm/00067827.PDF. Accessed 2024 Aug 12.
27.Haloperidol: 5 mg / mL, 1 mL vial for injection [product monograph]. Montreal (QC): Omega Laboratories Limited; 2023 Dec 20: https://pdf.hres.ca/dpd_pm/00073891.PDF. Accessed 2024 Aug 12.
28.Fluphenazine (fluphenazine hydrochloride): 1 mg, 2 mg, and 5 mg, oral tablets [product monograph]. Vaughan (ON): AA Pharma Inc.; 2023 Feb 21: https://pdf.hres.ca/dpd_pm/00069653.PDF. Accessed 2024 Aug 12.
29.Institut national d'excellence en santé et en services sociaux. Appropriate use of antipsychotics in residents of residential and long-term care centres (CHSLDs) with behavioural and psychological symptoms of dementia (BPSD). Montreal (QC): INESSS; 2014: https://www.inesss.qc.ca/fileadmin/doc/INESSS/Rapports/Medicaments/Outil_Amorce_EN.pdf. Accessed 2024 Jul 24.
30.Bjerre LM, Farrell B, Hogel M, et al. Deprescribing antipsychotics for behavioural and psychological symptoms of dementia and insomnia: Evidence-based clinical practice guideline. Can Fam Physician. 2018;64(1):17-27. PubMed
31.Leme DEC, Mathias K, Mofina A, Liperoti R, Betini GS, Hirdes JP. A Longitudinal Treatment Effect Analysis of Antipsychotics on Behavior of Residents in Long-Term Care. J Am Med Dir Assoc. 2024;25(11):105255. PubMed
32.Alzheimer Society of Canada. Using restraints. [2024]; https://alzheimer.ca/en/help-support/im-caring-person-living-dementia/ensuring-safety-security/using-restraints. Accessed 2024 Aug 11.
33.O'Donnell E, Holland C, Swarbrick C. Strategies used by care home staff to manage behaviour that challenges in dementia: A systematic review of qualitative studies. Int J Nurs Stud. 2022;133:104260. PubMed
34.Kales HC, Gitlin LN, Lyketsos CG. When Less is More, but Still Not Enough: Why Focusing on Limiting Antipsychotics in People With Dementia Is the Wrong Policy Imperative. J Am Med Dir Assoc. 2019;20(9):1074-1079. PubMed
35.Alzheimer's Society. Aggressive behaviour and dementia. 2021; https://www.alzheimers.org.uk/about-dementia/symptoms-and-diagnosis/symptoms/aggressive-behaviour-and-dementia. Accessed 2024 Aug 11.
36.Vaughan J. Ethical decision-making in the administration of 'as required' antipsychotics to people with dementia in care homes. Nurs Older People. 2023;35(4):36-41. PubMed
37.Social Care Institute for Excellence. Defining dignity in care. [date unknown]; https://www.scie.org.uk/providing-care/dignity-in-care/defining/. Accessed 2024 Aug 26.
38.Canadian Institute for Health Information (CIHI). Potentially inappropriate use of antipsychotics in long-term care. Your Health System [2024]; https://yourhealthsystem.cihi.ca/hsp/inbrief?lang=en#!/indicators/008/potentially-inappropriate-use-of-antipsychotics-in-long-term-care/;mapC1;mapLevel2;/. Accessed 2024 Aug 6.
39.Canada's Drug Agency. Organizations Unite to Increase the Appropriate Use of Medications in Canada. 2024 Dec 2; https://www.cda-amc.ca/news/organizations-unite-increase-appropriate-use-medications-canada. Accessed 2024 Dec 09.
40.Gattrell WT, Logullo P, van Zuuren EJ, et al. ACCORD (ACcurate COnsensus Reporting Document): A reporting guideline for consensus methods in biomedicine developed via a modified Delphi. PLoS Med. 2024;21(1):e1004326. PubMed
41.CAN/HSO 21001:2023 - Long-Term Care Services. Ottawa (ON): Health Standards Organization; 2023: https://healthstandards.org/standard/long-term-care-services-can-hso21001-2023-e/. Accessed 2024 Sep 10.
42.Canadian Geriatrics Society. Geriatrics - Eight Tests and Treatments to Question. Choosing Wisely Canada 2022; https://choosingwiselycanada.org/recommendation/geriatrics/. Accessed 2024 Jul 23.
43.Toward Optimized Practice (TOP) Cognitive Impairment CPG Committee. Cognitive impairment: diagnosis to treatment clinical practice guideline. Edmonton (AB): Toward Optimized Practice; 2017: https://www.albertadoctors.org/media/d5oox102/cognitive-impairment-guideline-part2.pdf. Accessed 2024 Jul 23.
44.Position Statement: Use of antipsychotic medications to treat people with dementia in long-term care homes. Toronto (ON): Alzheimer Society of Canada; 2017: https://alzheimer.ca/sites/default/files/documents/ASC-statement_use-of-antipsychotic-medications.pdf. Accessed 2024 Jul 25.
45.Travers JL, Hade EM, Friedman S, Raval A, Hadson K, Falvey JR. Staffing and Antipsychotic Medication Use in Nursing Homes and Neighborhood Deprivation. JAMA Netw Open. 2024;7(4):e248322. PubMed
46.Long-Term Care Staffing Study Advisory Group. Long-Term Care Staffing Study. Toronto (ON): Ontario Ministry of Long-Term Care; 2020: https://files.ontario.ca/mltc-long-term-care-staffing-study-en-2020-07-31.pdf. Accessed 2024 Aug 7.
47.Langford AV, Ngo GT, Chen TF, Roberts C, Schneider CR. Nurses', Pharmacists' and Family Physicians' Perceptions of Psychotropic Medication Monitoring in Australian Long-Term Care Facilities: A Qualitative Framework Analysis. Drugs Aging. 2021;38(2):169-179. PubMed
48.Raza A, Piekarz H, Jawad S, Langran T, Donyai P. A systematic review of quantitative studies exploring staff views on antipsychotic use in residents with dementia in care homes. Int J Clin Pharm. 2023;45(5):1050-1061. PubMed
49.Jorgensen SM, Lech LVJ, Vermehren C, et al. Healthcare professionals' experiences with the use of antipsychotics in dementia. Explor Res Clin Soc Pharm. 2024;14:100446. PubMed
50.Walsh KA, Sinnott C, Fleming A, et al. Exploring Antipsychotic Prescribing Behaviors for Nursing Home Residents With Dementia: A Qualitative Study. J Am Med Dir Assoc. 2018;19(11):948-958.e912. PubMed
51.Alberta Health Services. Appropriate Use of Antipsychotics (AUA) Toolkit. [2024]; https://www.albertahealthservices.ca/scns/auatoolkit.aspx. Accessed 2024 Jul 22.
52.Chenoweth L, Jessop T, Harrison F, Cations M, Cook J, Brodaty H. Critical Contextual Elements in Facilitating and Achieving Success with a Person-Centred Care Intervention to Support Antipsychotic Deprescribing for Older People in Long-Term Care. Biomed Res Int. 2018;2018:7148515. PubMed
53.Alzheimer Society of Canada. Providing person-centred care. [2024]; https://alzheimer.ca/en/help-support/im-healthcare-provider/providing-person-centred-care. Accessed 2024 Aug 8.
54.Cole M. Patient and Family Involvement – experience from the Appropriate use of antipsychotics (AUA) project in LTC [presentation slides]. [Calgary (AB)]: Institute for Continuing Care Education and Research (ICCER); 2016 Sep 26. Accessed 2024 Aug 8.
55.Havaei F, Novek S. How resident and family councils improve the quality of life for people living in long-term care facilities (part 1). 2025; https://www.canadian-nurse.com/blogs/cn-content/2025/03/03/resident-and-family-councils-part-1. Accessed 2025 Mar 25.
56.Staempfli S, Havaei F, Dawson L, et al. Raise Your Voice: How to Increase the Effectiveness of Resident and Family Councils in Long-Term Care Homes. Canadian journal on aging = La revue canadienne du vieillissement. 2025:1-10.
57.Seniors Health Strategic Clinical Network. Person-Centered Dementia Care. Edmonton (AB): Alberta Health Services; 2016: https://albertahealthservices.ca/assets/about/scn/ahs-scn-srs-aua-person-centred.pdf. Accessed 2024 Aug 8.
58.Lipori JP, Tu E, Shireman TI, Gerlach L, Coe AB, Ryskina KL. Factors Associated with Potentially Harmful Medication Prescribing in Nursing Homes: A Scoping Review. J Am Med Dir Assoc. 2022;23(9):1589.e1581-1589.e1510.
59.Alzheimer Society of Canada. The many faces of dementia in Canada. The Landmark Study: People. Toronto (ON): Alzheimer Society of Canada; 2024: https://alzheimer.ca/sites/default/files/documents/ASC_The%20Many%20Faces%20of%20Dementia%20In%20Canada_Landmark%20Study_Vol2.pdf. Accessed 2024 Aug 6.
60.Cabote C, Salamonson Y, Trajkovski S, Maneze D, Montayre J. The needs of older people with dementia from culturally and linguistically diverse backgrounds living in residential aged care: An integrative review. J Clin Nurs. 2023;32(17-18):5430-5444. PubMed
61.Batista R, Prud'homme D, Rhodes E, et al. Quality and Safety in Long-Term Care in Ontario: The Impact of Language Discordance. J Am Med Dir Assoc. 2021;22(10):2147-2153.e2143. PubMed
62.Reaume M, Peixoto C, Pugliese M, et al. The impact of patient-facility language discordance on potentially inappropriate prescribing of antipsychotics in long-term care home in Ontario, Canada: a retrospective population health cohort study. BMC Geriatr. 2024;24(1):889. PubMed
63.Moth AE, Holmkjaer P, Holm A, Rozing MP, Overbeck G. What Makes Deprescription of Psychotropic Drugs in Nursing Home Residents with Dementia so Challenging? A Qualitative Systematic Review of Barriers and Facilitators. Drugs Aging. 2021;38(8):671-685. PubMed
64.Harrison SL, Cations M, Jessop T, Hilmer SN, Sawan M, Brodaty H. Approaches to Deprescribing Psychotropic Medications for Changed Behaviours in Long-Term Care Residents Living with Dementia. Drugs Aging. 2019;36(2):125-136. PubMed
65.Wilson LS, Devitt P, Hally O. Standards of prescription writing in a long-term psychogeriatric unit: a series of clinical audits. Ir J Psychol Med. 2015;32(2):197-204. PubMed
66.Brassolotto J, Caspar S, Spenceley S, Haney C-A. Long-Term Care in Rural Alberta: Exploring Autonomy and Capacity for Action. Journal of Long Term Care. 2020:80-90.
67.Maclagan LC, Maxwell CJ, Harris DA, et al. Sex Differences in Antipsychotic and Benzodiazepine Prescribing Patterns: A Cohort Study of Newly Admitted Nursing Home Residents with Dementia in Ontario, Canada. Drugs Aging. 2020;37(11):817-827. PubMed
68.Van Leeuwen E, Petrovic M, van Driel ML, et al. Withdrawal versus continuation of long-term antipsychotic drug use for behavioural and psychological symptoms in older people with dementia. Cochrane Database Syst Rev. 2018;3(3):CD007726. PubMed
69.Bednarczyk E, Cook S, Brauer R, Garfield S. Stakeholders' views on the use of psychotropic medication in older people: a systematic review. Age Ageing. 2022;51(3):01.
70.Call for Less Antipsychotics in Residential Care (CLeAR). CLeAR Wave 2 Final Evaluation Report. Vancouver (BC): BC Patient Safety & Quality Council; 2017: https://healthqualitybc.ca/wp-content/uploads/2017-CLeAR-Wave-2-Evaluation-Report-Aug-3-2017_FINAL.pdf. Accessed 2024 Jul 24.
71.Anderson A. Is Health Quality Ontario (HQO) providing misleading information to the public at large? Canadian Nursing Home. 2020;31(1):11-13.
72.Canadian Institute for Health Information (CIHI). Quick Stats. 2024: https://www.cihi.ca/en/quick-stats. Accessed 2024 Nov 12.
73.A path to improving medication appropriateness in Canada: A final report from the appropriate use advisory committee. Ottawa (ON): Health Canada; 2024: https://www.canada.ca/content/dam/hc-sc/documents/corporate/about-health-canada/activities-responsibilities/canadian-drug-agency-transition-office/path-improving-medication-appropriateness-canada/path-improving-medication-appropriateness-canada.pdf. Accessed 2024 Aug 20.
74.Trenaman SC, von Maltzahn M, Sketris I, Tamim H, Wang Y, Stewart SA. Patterns of Antipsychotic Dispensation to Long-Term Care Residents. J Am Med Dir Assoc. 2023;24(2):185-191 e186. PubMed
75.Behavioural Symptoms of Dementia: Care for People in Hospitals and Long-Term Care Homes. (Quality Standard). Toronto (ON): Ontario Health; 2016 [updated 2024]: https://www.hqontario.ca/Portals/0/documents/evidence/quality-standards/qs-behavioural-symptoms-of-dementia-quality-standard-2024-en.pdf. Accessed 2024 Jul 23.
76.Centre for Effective Practice. Use of Antipsychotics in Behavioural and Psychological Symptoms of Dementia (BPSD) Discussion Guide: Long-Term Care (LTC 2nd Edition). 2016; https://tools.cep.health/tool/use-of-antipsychotics-in-behavioural-andpsychological-symptoms-of-dementia-bpsd/. Accessed 2024 Jul 23.
77.Jensen B, Jin M. Management of behavioural & psychological symptoms of dementia (BPSD). RxFiles. Saskatoon (SK): RxFiles Academic Detailing; 2024: https://www.rxfiles.ca/rxfiles/. Accessed 2024 Jul 23.
Appendix 1: “Potentially Inappropriate Use of Antipsychotics in Long-Term Care” Quality Indicator
Please note that this appendix has not been copy-edited.
Data Definition
Name: Potentially Inappropriate Use of Antipsychotics in Long-Term Care
Other name: Percentage of Residents on Antipsychotics Without a Diagnosis of Psychosis (DRG01)
Description: “This indicator looks at how many long-term care residents are taking antipsychotic drugs without a diagnosis of psychosis. These drugs are sometimes used to manage behaviours in residents who have dementia. Careful monitoring is required, as such use raises concerns about safety and quality of care.” The result on the quality indicator is expressed as a percentage (i.e., numerator/denominator), and is reported as an unadjusted and an adjusted rate.
Numerator: People living in LTC who received antipsychotic medication on at least 1 day in the week before their valid target assessment
Denominator: People living in LTC with valid assessments
Inclusions in the measurement of the quality indicator:
Residents with valid assessments. To be considered valid, the target assessment must:
be the latest assessment in the quarter
be carried out more than 92 days after the Admission Date
not be an Admission Full Assessment or First Assessment
Exclusions from the measurement of the quality indicator:
Residents who have end-stage disease (with 6 months or less to live) or who are receiving hospice or palliative care
Residents who have a diagnosis of schizophrenia or Huntington chorea, or those experiencing hallucinations or delusions
Method of adjustment: Stratification, direct standardization, indirect standardization
Covariates used in risk adjustment:
Individual covariates: Motor agitation, moderate or impaired decision-making problem, long-term memory problem, CPS, combination Alzheimer disease and other dementia, age younger than 65 years
Facility-level stratification: case-mix index
Appendix 2: Panel Demographics
Table 2: Results From Survey 1 Questions About Panel Member Demographics
Demographic characteristic | Responses | Number of panellists (%) |
|---|---|---|
Role in the health care or LTC system in Canada (Respondents could select all responses that applied) | Physician – specialty in family medicine | 3 (17.6%) |
Physician – specialty in geriatrics or gerontology | 2 (11.8%) | |
Physician – specialty in dementia and/or mental health | 3 (17.6%) | |
Pharmacist | 3 (17.6%) | |
Nurse practitioner | 1 (5.9%) | |
Registered nurse | 3 (17.6%) | |
Personal support workera | 0 | |
LTC home senior executive/administrator/manager | 1 (5.9%) | |
Quality improvement practitioner, champion, or adviser | 3 (17.6%) | |
Deprescribing practitioner, champion, or adviser | 6 (35.3%) | |
Researcher | 4 (23.5%) | |
Academic professor | 4 (23.5%) | |
Person living in a LTC home or their caregiver/family member | 2 (11.8%) | |
Otherb | 5 (29.4%) | |
Years of personal or professional experience working or interacting with the LTC setting in Canada | 0 to 5 years | 2 (11.8%) |
6 to 10 years | 2 (11.8%) | |
Over 10 years | 13 (76.5%) | |
Province(s) or Territory(ies) of Professional or Personal Experience involved in the LTC system or have personal experience with LTC (Respondents could select all responses that applied) | Newfoundland and Labrador | 2 (11.8%) |
Prince Edward Island | 2 (11.8%) | |
Nova Scotia | 3 (17.6%) | |
New Brunswick | 4 (23.5%) | |
Quebec | 2 (11.8%) | |
Ontario | 9 (52.5%) | |
Manitoba | 2 (11.8%) | |
Saskatchewan | 2 (11.8%) | |
Alberta | 4 (23.5%) | |
British Columbia | 3 (17.6%) | |
Yukon | 0 | |
Northwest Territories | 1 (5.9%) | |
Nunavut | 0 | |
All provinces and territories | 1 (5.9%) | |
Indigenous | Yesc | 1 (5.9%) |
No | 16 (94.1%) | |
Main ethnic origin(s) or race (Respondents could select all responses that applied) | Black | 1 (5.9%) |
Caribbean/West Indies | 1 (5.9%) | |
East Asia | 0 | |
Southeast Asia | 3 (17.6%) | |
Eastern Africa | 0 | |
Northern Africa | 0 | |
Southern Africa | 1 (5.9%) | |
Western Africa | 0 | |
Hispanic | 0 | |
Middle East | 0 | |
Pacific Islands | 0 | |
Western Europe | 2 (11.8%) | |
Eastern Europe | 2 (11.8%) | |
White | 9 (52.9%) | |
Prefer not to answer | 0 | |
Prefer to self-described | 2 (11.8%) | |
Persons with a disability | No | 17 (100%) |
Yes | 0 | |
Gender identity (Respondents could select all responses that applied) | Men | 5 (29.4%) |
Women | 12 (70.6%) | |
Non-binary/gender fluid | 0 | |
Transgender | 0 | |
Two-spirit | 0 | |
Queer | 0 | |
Prefer to self-describe | 0 | |
Prefer not to answer | 0 |
LTC = long-term care.
Note: In the round 1 survey, we gathered data about the demographics of panel members to better understand and describe the diversity and perspectives represented in the panel.
aWhile none of the panellists self-identified as having a personal support worker role within the health care or LTC system in Canada, 1 panellist is a representative of a provincial and a national association for personal support workers.
bRespondents self-described as a physician trained outside of Canada, coach for quality improvement programs, retired nurse or nurse manager, association executive, advocate for people in LTC, and a physician with expertise in elderly care, dementia and BPSD management.
cThe respondent self-described as mixed white and Mohawk.
dOf the 2 respondents, 1 self-described as “Jewish” and 1 as “Mohawk.”
Note that this table has not been copy-edited.
Appendix 3: Summary of the Online Consensus-Building Process
Please note that this appendix has not been copy-edited.
The modified online consensus-building process consisted of 3 rounds, including 2 online surveys (round 1 and round 2), and 1 online workshop with structured discussions and live ranking and voting (round 3).
In the surveys, panellists were asked to rate their level of agreement with proposed items on a 5-point Likert scale and to provide the rationales for their rating in open-ended responses. After round 1 and round 2, panellists were provided with a quantitative summary of their personal and group ratings (e.g., median and bar charts with the percentage for each rating) and a narrative summary of the open-ended responses.
Round 1: Survey 1 Results
We received completed responses from all 17 panellists.
Target for LTC Homes in Canada: Round 1 Results
None of the 7 potential values for the target reached the consensus threshold for disagreement.
Eight panel members suggested new potential values for consideration for the target, and 4 of these values (i.e., 13%, 15%, 17%, 20%) were included in the round 2 survey.
A total of 11 values for the target proceeded to round 2 (Survey 2).
Annual Improvement Goal: Round 1 Results
One of the 5 potential values for the annual improvement goal (i.e., 9%) reached consensus for disagreement (i.e., at least 80% of panel members rated the value with “strongly disagree” or “disagree”) and was removed from the round 2 survey.
Four of 5 potential values did not reach the threshold for consensus.
Five panel members suggested new potential values for consideration for the goal, and 3 of these values (i.e., 10%, 15%, 20%) were included in the round 2 survey.
A total of 7 values for the annual improvement goal proceeded to round 2 (Survey 2).
Figure 6 and Figure 7 present the overall round 1 survey results for the target for LTC homes in Canada and the annual improvement goal, respectively.
Figure 6: Summary of the Level of Agreement for the Proposed Values for the Target for LTC Homes in Canada — Results From Round 1
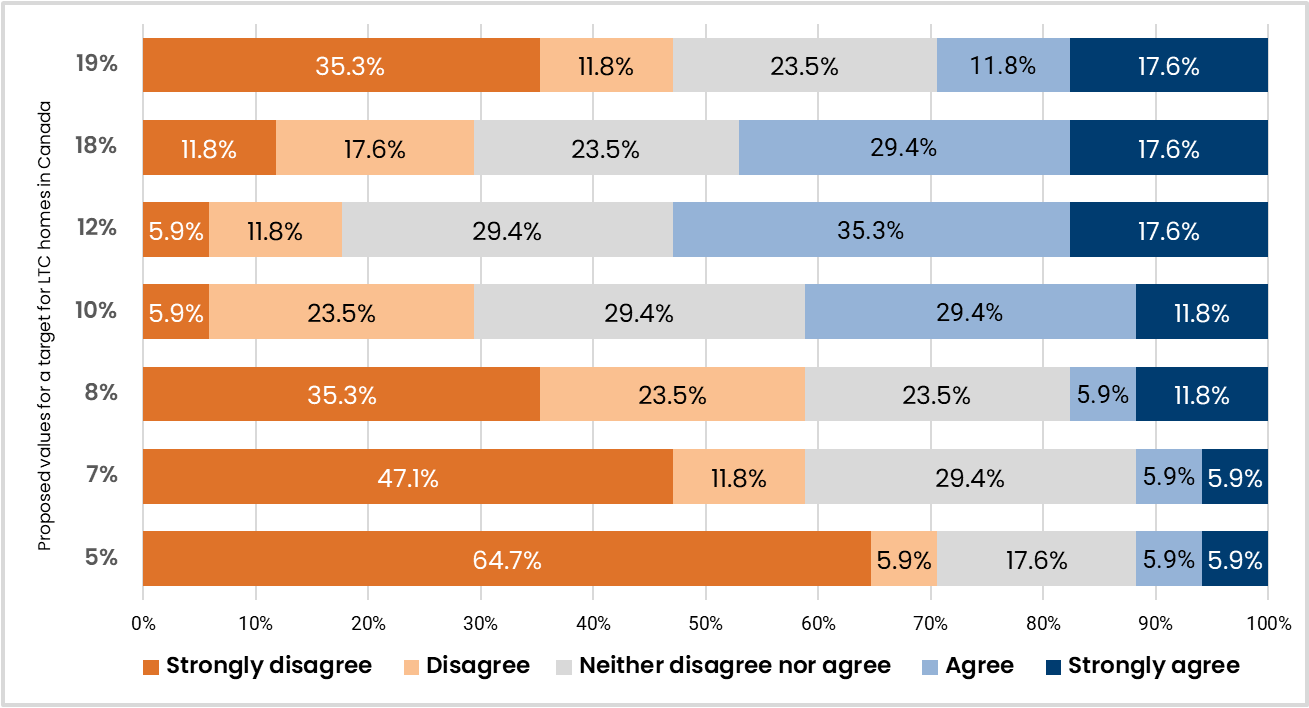
LTC = long-term care.
Note: The percentages on the bars indicate the proportion of panel members that selected each option for their level of agreement with the proposed value for the target. The consensus threshold was set at 80% for agreement (i.e., agree and strongly agree) and for disagreement (i.e., disagree and strongly disagree).
Figure 7: Summary of the Level of Agreement for the Proposed Values for the Annual Improvement Goal — Results From Round 1
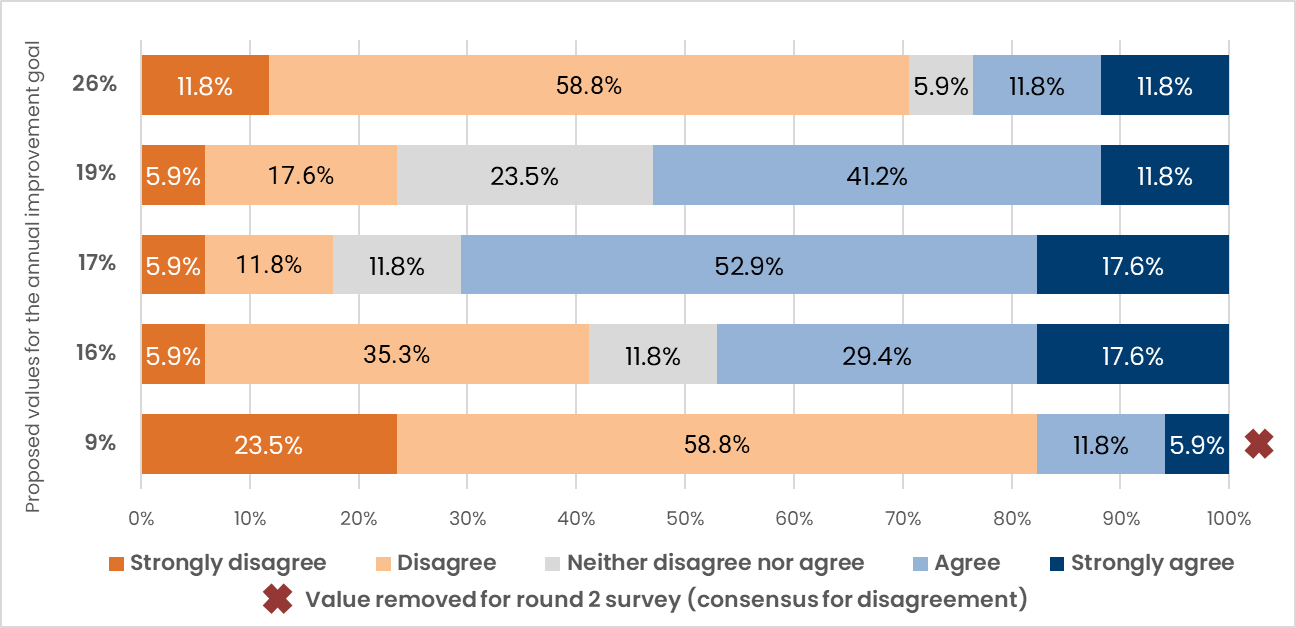
Note: The values for the annual improvement goal are expressed as a percent relative reduction, annually. The percentages on the bars indicate the proportion of panel members that selected each option for their level of agreement with the proposed value for the annual improvement goal. The consensus threshold was set at 80% for agreement (i.e., agree and strongly agree) and for disagreement (i.e., disagree and strongly disagree).
Table 3: Round 1 Summary of Potential Barriers and Facilitators to Reducing Potentially Inappropriate Antipsychotic Use in LTC Homes
Themes | Barriers to reducing potentially inappropriate use | Facilitators to reducing potentially inappropriate use |
|---|---|---|
Staff and continuity of care | Staff shortages and high staff turnover hinders the reduction of antipsychotics in LTC homes because it results in:
High management turnover can also derail improvement efforts. During transitions in leadership, unformalized policies, systems, and guidelines that reduce inappropriate use can be easily lost and deprioritized. LTC homes also struggle to understand how reducing inappropriate use can help with capacity issues as it reduces the support people in LTC homes need (e.g., support during meals). | Adequate number of staff and staff consistency allows continuity of care and provides the capacity to ensure meaningful long-term success of appropriate use efforts. Increasing capacity in LTC homes can be achieved by:
|
Resources | Lack of funding for LTC homes. | Providing care partners with resources and funding opportunities (e.g., Health care Excellence Canada) to develop and implement innovative programs. |
Skill development for staff and health care professionals | Limited access to educational resources and training leads to a lack of knowledge among LTC staff to reduce inappropriate use, specifically in the following areas:
Like staff, unsupported management could benefit from receiving training to better support appropriate use efforts and balance their overwhelming workloads. | Training empowers LTC staff and management to reduce inappropriate use by:
|
LTC work culture, care coordination, and communication | Work culture, fragmented care, and communication can hinder the reduction of antipsychotics. The contributing factors include:
| Work culture, coordinated care, and communication facilitate antipsychotic reduction when:
|
Access to specialized care for people living in LTC | Lack of access to care can hinder the reduction of antipsychotic use, specifically care from:
LTC homes in rural areas can experience greater challenges accessing specialized care. | Using technologies for virtual care can facilitate access to specialized care that can help promote appropriate use. |
Deprescribing incentive and disincentives | Challenges in identifying eligible individuals for deprescribing can hinder reductions in inappropriate use given:
Fear of worsening behaviours from deprescribing can discourage participation in reduction efforts. In Ontario, LTC homes fear potential monetary penalties and compliance orders (related to their duty to protect) when reducing antipsychotics results in worsening aggression and results in safety issues for people in LTC. | Medication review and treatment plans can support deprescribing of antipsychotics. These processes can be supported by:
|
Health care system alignment and collaboration | A misaligned and fragmented health care system can hinder reductions in inappropriate antipsychotic use, specifically discrepancies between:
| Health care system collaboration and coordination can support appropriate use efforts and can be encouraged by:
|
Demographic shifts and LTC home population | The LTC population is experiencing demographic shifts, including an increase in:
The CIHI/InterRAI indicator was designed as a tool to support the reduction of potentially inappropriate use. It is not a direct barrier to reducing inappropriate use. However, the quality indicator might position LTC homes at a disadvantage in quality improvement initiatives, specifically LTC homes:
| NA |
BPSD = behavioural psychological symptoms of dementia; CIHI = Canadian Institute of Health Information; LTC = long-term care; MDS = Minimum Data Set; NA = not applicable.
Note: This table summarizes panel members’ input regarding the barriers and facilitators to reducing potentially inappropriate antipsychotic use in LTC homes from the round 1 survey. This table was included as part of survey 1 results provided to the panel.
Round 2: Survey 2 Results
We received completed responses from all 17 panellists.
Target for LTC Homes in Canada: Round 2 Results
Four of the 11 proposed values for the target for LTC homes in Canada that panellists rated in round 2 (i.e., 20%, 19%, 7%, and 5%) reached consensus for disagreement (i.e., at least 80% of panel members rated the value with “disagree” or “strongly disagree”) and were removed and not included in the round 3 workshop.
Seven of the 11 proposed values for the target did not reach the threshold for consensus and proceeded to the round 3 workshop.
For the target, in general the panellist ratings shifted toward agreeing with central values (i.e., 12%, 13%, 15%, and 17%) and disagreeing with the values at the higher and lower ends of the options (i.e., 20% and 5%). This included 3 of the values that had been suggested by panellists in round 1 (i.e., between 12% and 18%).
Annual Improvement Goal: Round 2 Results
One of the 7 proposed values for the annual improvement goal (i.e., 26%) reached consensus for disagreement (i.e., at least 80% of panel members rated the value with “disagree” or “strongly disagree”) and was removed and not included in the round 3 workshop.
Six of 7 proposed values for the annual improvement goal did not reach the threshold for consensus and proceeded to the round 3 workshop.
For the annual improvement goal, the panellists’ ratings generally remained consistent compared to the previous round, with panellists agreeing with central values (i.e., 15%, 16%, 17%, and 19%), which included 1 of the values suggested by panellists in round 1 (i.e., 15%), and panellists disagreeing with the higher and lower options for the annual improvement goal (i.e., 26%, 10%).
Overall Trends in Round 2
For both the target and the annual improvement goal, the panellist ratings and rationales suggest that the panel aimed to identify a level of excellence for clinical practice and an achievable rate of change based on the evidence of what has been achieved previously in Canada (e.g., quality indicator data, results from quality improvement initiatives), their own experience of the current context of LTC (e.g., staffing and resource levels), and a desire to avoid risks and unintended consequences associated with a suboptimal target or annual improvement goal. They were also influenced by the positions of other panellists and considered the overall panel objective to reach consensus on a single value for the target and a single value for the annual improvement goal, which was ultimately reflected in a shift toward central tendency in round 2.
Figure 8 and Figure 9 present the overall round 2 survey results for the target for LTC homes in Canada and the annual improvement goal, respectively.
Figure 8: Summary of the Level of Agreement for the Proposed Values for the Target for LTC Homes in Canada — Results From Round 2
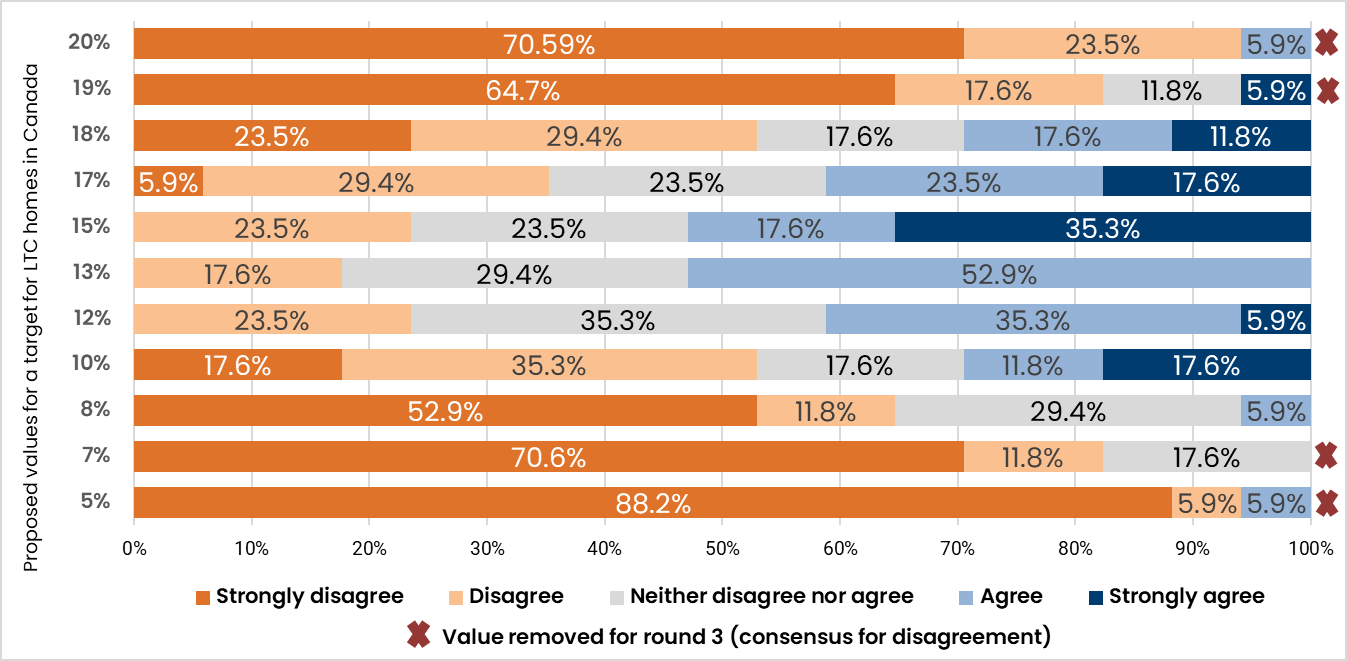
LTC = long-term care.
Note: The percentages on the bars indicate the proportion of panel members that selected each option for their level of agreement with the proposed value for the target. The consensus threshold was set at 80% for agreement (i.e., agree and strongly agree) and for disagreement (i.e., disagree and strongly disagree) The following values were added to the round 2 survey based on suggestions by panellists: 20%, 17%, 15%, 13%.
Figure 9: Summary of the Level of Agreement for the Proposed Values for the Annual Improvement Goal — Results From Round 2

Note: The values for the annual improvement goal are expressed as a percent relative reduction, annually. The percentages on the bars indicate the proportion of panel members that selected each option for their level of agreement with the proposed values for the annual improvement goal. The consensus statement threshold was set at 80% for agreement (i.e., agree and strongly agree) and for disagreement (i.e., disagree and strongly disagree). The following values were added to the round 2 survey based on suggestions by panellists: 20%, 15%, 10%.
Round 3: Workshop Results
All 17 panellists attended the online workshop and completed the ranking and voting exercises.
The online workshop included 2 sets of discussions and live ranking, followed by live voting to confirm consensus on agreement with the top ranked value for the target and the annual improvement goal, and to confirm the final consensus statements. During the discussions, panellists were asked to share their perspectives and why they agreed or disagreed with the proposed values for the target and the goal. We used Slido to conduct the ranking and live voting.
Target for LTC Homes in Canada: Round 3 Results
After the first round of discussions (which focused on the remaining items after the round 2 survey), panellists independently ranked the potential values for the target from 1 to 7, where 1 represented the top choice. After the initial ranking, the bottom 3 values based on overall panel rankings were dropped and not considered further. After a second round of discussion, panellists individually ranked the remaining values for the target from 1 to 4, where 1 represented the top choice. Table 4 presents the overall panel results for both ranking exercises for the target.
Table 4: Results of the Round 3 Ranking Exercises for the Proposed Values for the Target for LTC Homes in Canada
First ranking exercise | Second ranking exercise | ||
|---|---|---|---|
Rank | Value (%) | Rank | Value (%) |
1 | 15 | 1 | 15 |
2 | 13 | 2 | 13 |
3 | 12 | 3 | 12 |
4 | 17 | 4 | 17 |
5 | 18 | — | — |
6 | 10 | — | — |
7 | 8 | — | — |
LTC = long-term care.
Annual Improvement Goal: Round 3 Results
After the first round of discussions (which focused on the remaining items after the round 2 survey), panellists independently ranked the potential values for the goal from 1 to 6, where 1 represented the top choice. After the initial ranking, the bottom 3 values based on overall panel rankings were dropped and not considered further. After a second round of discussion, panellists individually ranked the remaining values for the target from 1 to 3, where 1 represented the top choice. Table 5 presents the overall panel results for both ranking exercises for the annual improvement goal.
Table 5: Results of the Round 3 Ranking Exercises for the Proposed Values for the Annual Improvement Goal
First ranking exercise | Second ranking exercise | ||
|---|---|---|---|
Rank | Value (% relative reduction) | Rank | Value (% relative reduction) |
1 | 15 | 1 | 15 |
2 | 16 | 2 | 16 |
3 | 17 | 3 | 17 |
4 | 19 | — | — |
5 | 20 | — | — |
6 | 10 | — | — |
Appendix 4: Expert Panel Members’ Declarations of Conflicts of Interest
Please note that this appendix has not been copy-edited.
The following are the disclosures from each of the expert panel members as per the CDA-AMC Conflict of Interest Policy:
Aswathy Jayashree, Ashley King, Dr. Geneviève Lemay, and Shirin Vellani reported no conflicts of interest.
Dre. Marie-Andrée Bruneau received funding or honorariums for speaking engagements from Janssen, Lifespeak Inc., Canadian Coalition for Seniors' Mental Health, Baycrest, Fédération des médecins omnipraticiens du Québec, Médecins francophones du Canada, and Congrès Québécois sur la maladie d’Alzheimer. In addition, Dre. Bruneau received travel or other expense payments from Otsuka/Lundbeck and Congrès Québécois sur la maladie d’Alzheimer. Dre. Bruneau received payment as an advisor or consultant from Ostuka/Lundbeck. Dre. Bruneau is the Co-Director of the Behavioural and Psychological Symptoms of Dementia committee at the Quebec Ministry of Health and participates as a consultant for ‘Optimizing Practices, Use, Care, and Services-Antipsychotics’ (OPUS-AP) in Long-Term Care Centres in Quebec.
Ian DaSilva is the COO of the Canadian Support Workers Association.
Lisa Dawson is a volunteer and board member of the Independent Long-Term Care Councils Association of BC (ILTCCABC). Lisa also serves as a chair at the Vancouver Coastal Family Councils.
Dr. Vivian Ewa is a current employee at Alberta Health Services and the University of Calgary. Dr. Ewa received payment for being a guideline development panel member at the Canadian Coalition for Seniors' Mental Health and receives research funding from CIHR for various projects.
Dr. Sid Feldman is currently employed at both Baycrest Health Sciences and the University of Toronto. Dr. Feldman receives payments for advising or consulting positions at Baycrest Global Solutions, McMaster University, Ontario College of Family Physicians, and Choosing Wisely Canada. In addition, Dr. Feldman receives travel or other expense payments as a conference invited speaker for Ontario Long-term Care Clinicians.
Dr. Carole A Goodine is employed by Horizon Health Network and Dalhousie University. Carole Goodine has received research funding or grants paid to her institution from the Public Health Agency of Canada and the Government of New Brunswick Health Seniors’ Pilot Project, AGE-WELL and ResearchNB for research on deprescribing in LTC using the electronic decision support tool MedSafer.
Dr. Andrea Luva Moser receives payments for consulting at the Institute for Safe Medication Practices Canada. Dr. Moser previously served as the interim course director at Ontario Long-term Care Clinicians. Dr. Moser currently receives payments for speaking and curriculum development at Ontario Long-term Care Clinicians.
Dr. Dallas Seitz receives research funding or grants at the University Health Foundation. Dr. Seitz is also the co-chair at the Canadian Coalition for Senior's Mental Health and a board member at the Alzheimer Society of Alberta and Northwest Territories.
Cynthia Sinclair receives payment as a coach and consultant at Health care Excellence Canada.
Dr. Wade Thompson receives funding or honorariums for writing articles or editorials for Pharmacy Practice Plus. Dr. Thompson serves as the co-lead of the website Deprescribing.org.
Dr. Shanna C. Trenaman receives funding or grants from the Drug Evaluation Alliance of Nova Scotia. Dr. Trenaman also has a nonfinancial affiliation with the Drug Evaluation Alliance of Nova Scotia to work on a descriptive study. Dr. Trenaman received payments for consulting at the Canadian Coalition for Seniors' Mental Health as well as a grant from CIHR to hold a patient engagement session. Dr. Trenaman also reviewed treatments for anxiety, 1 of which was antipsychotics, as a guideline development consultant for the Canadian Coalition for Seniors' Mental Health.
Dr. Ahmed Vanker is currently employed at Extendicare Inc. In addition, Dr. Vanker’s manuscript on strategies to reducing inappropriate use of antipsychotics was accepted and will be published by the Journal of the American Medical Directors Association.
Julie Weir received an honorarium from Choosing Wisely Canada to provide advice and leadership to the long-term care group in a co-lead capacity. Julie also receives payments from Health care Excellence Canada for coaching activities related to aging in place, nursing homes without walls, and the appropriate use of antipsychotics initiatives.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.