Drugs, Health Technologies, Health Systems
Health Technology Review
Disease-Modifying Therapies for Metabolic Dysfunction–Associated Steatohepatitis
Metabolic dysfunction–associated steatohepatitis (MASH) is an increasingly prevalent liver disease in Canada. While MASH is traditionally managed with lifestyle modifications, the conditional regulatory approval of the first disease-modifying therapy in December 2025 marks a potential change in the treatment landscape. This development creates opportunities to assess the readiness of health systems for the potential adoption of disease-modifying therapies. This report outlines how the potential introduction of disease-modifying therapies into clinical care creates a timely opportunity to enhance coordinated screening, standardized care pathways, education, and equitable access.
Key Messages
What Is the Issue?
Metabolic dysfunction–associated steatohepatitis (MASH), an advanced stage of metabolic dysfunction–associated steatotic liver disease (MASLD), is emerging as a leading cause of liver cancer and transplant in Canada, with prevalence projected to rise.
Management of MASH traditionally relies on lifestyle modifications, including diet and exercise. New disease-modifying therapies (DMTs) may target underlying disease mechanisms and promote fibrosis (liver scarring) regression from moderate disease stages.
In Canada, the first DMT for MASH — a glucagon-like peptide-1 receptor agonist — received conditional regulatory approval in December 2025. In other countries, a glucagon-like peptide-1 receptor agonist and/or a thyroid hormone receptor–beta agonist (liver-directed thyroid hormone receptor therapy) have received conditional regulatory approval.
In 2020, the annual cost of managing MASH and MASLD in Canada was an estimated $3.76 billion, largely driven by other medical conditions such as diabetes and cardiovascular disease.
What Did We Do?
Canada’s Drug Agency sought to assess the readiness of health care systems in Canada for the potential introduction of DMTs for MASH. We summarized evidence and experiences along the current patient pathway for MASH, including specific system-level challenges and opportunities to improve care.
We applied a mixed-evidence approach, combining targeted literature searches on health system readiness and diagnostic accuracy of noninvasive tests. Evidence was supplemented through consultations with clinical experts and engagement with patients, carers, and Indigenous people to capture contextual insights on care pathways, equity, and cultural considerations in anticipation of the potential introduction of DMTs in Canada.
What Did Canada’s Drug Agency Find?
The introduction of DMTs into clinical care for MASH in Canada may increase pressure on existing health care systems. Evidence and insights shared from clinical providers and patients on the MASH care pathway highlight areas that may constrain care integration and the uptake of DMTs.
MASH is a progressive, multisystem disease that often involves complex care needs and interconnected comorbidities.
As awareness and treatment options for MASH expand, there may be a need to strengthen diagnostic capacity and improve access to specialists who typically treat advanced MASH across jurisdictions.
Clinical guidance is evolving to support earlier risk identification and management across the disease spectrum, reflecting a shift from a historical focus on late-stage disease toward earlier intervention.
People with low-risk MASH may be monitored. Earlier and more proactive care may help prevent or slow MASH progression.
Emerging MASH care pathways emphasize coordinated, multidisciplinary care to support patients with complex needs across specialties.
What Does This Mean?
The report highlights system-level opportunities to improve how MASH is identified and managed in Canada as new DMTs emerge. Strengthening MASH care would require greater coordination. Processes could be standardized and consolidated to prepare for rising demand. Evidence and engagement feedback point to a few high-level priorities, including:
strengthening awareness and education about MASH and its multisystemic nature to support early identification and reduce stigma
increasing diagnostic testing capacity to enable earlier and timely identification
expanding and standardizing multidisciplinary care models to improve coordination and continuity and to support patients with complex metabolic and liver needs
embedding equity considerations across the care pathway.
Abbreviations
AASLD
American Association for the Study of Liver Diseases
AI
artificial intelligence
BMI
body mass index
CDA-AMC
Canada’s Drug Agency
CPG
clinical practice guideline
CVD
cardiovascular disease
DMT
disease-modifying therapy
EASD
European Association for the Study of Diabetes
EASL
European Association for the Study of the Liver
EASO
European Association for the Study of Obesity
ELF
Enhanced Liver Fibrosis
FIB-4
Fibrosis-4
GLP-1
glucagon-like peptide-1
MASH
metabolic dysfunction–associated steatohepatitis
MASLD
metabolic dysfunction–associated steatotic liver disease
MRE
magnetic resonance elastography
NIT
noninvasive test
PCP
primary care provider
PDFF
proton density fat fraction
RA
receptor agonist
SWE
shear wave elastography
T2DM
type 2 diabetes mellitus
THR-beta
thyroid hormone receptor–beta
VCTE
vibration-controlled transient elastography
Approach
Context
Defining Metabolic Dysfunction–Associated Steatohepatitis and Metabolic Dysfunction–Associated Steatotic Liver Disease
Metabolic dysfunction–associated steatohepatitis (MASH) is an advanced stage of metabolic dysfunction–associated steatotic liver disease (MASLD). It is characterized by cellular-level tissue changes, including hepatocellular ballooning (swollen, damaged liver cells) and lobular inflammation (cellular damage within specific liver structures).1
MASLD, the broader condition, is defined by fat accumulation on the liver (steatosis) in combination with 1 or more cardiometabolic risk factors (i.e., obesity, type 2 diabetes mellitus [T2DM], dyslipidemia, or hypertension) and the absence of harmful alcohol intake.2,3 MASLD can progress to advanced stages without ever developing into MASH.
The terms MASH and MASLD were recently introduced to replace nonalcoholic steatohepatitis (NASH) and nonalcoholic fatty liver disease (NAFLD) to better reflect the underlying role of metabolic dysfunction, avoid stigmatizing language, and provide clearer, more clinically meaningful definitions.4 A detailed overview of the updated nomenclature and diagnostic criteria is provided in Appendix 1, Table 4. The term lean is added to MASH and MASLD when these conditions occur in individuals with healthy body weights who develop the disease.5,6 Excess weight is not required for diagnosis, but patients without excess weight may represent a distinct population.7
If left untreated, MASH and MASLD can progress to fibrosis (liver scarring), cirrhosis (advanced liver scarring), portal hypertension (elevated pressure in the portal vein), decompensated cirrhosis (advanced cirrhosis), and hepatocellular carcinoma (liver cancer), each associated with progressively worse outcomes and higher mortality risk. This progression is illustrated in Figure 1.8-10
Figure 1: The Progressive Nature of MASLD — Liver Changes and the Potential Development of MASH, Cirrhosis, and Liver Cancer
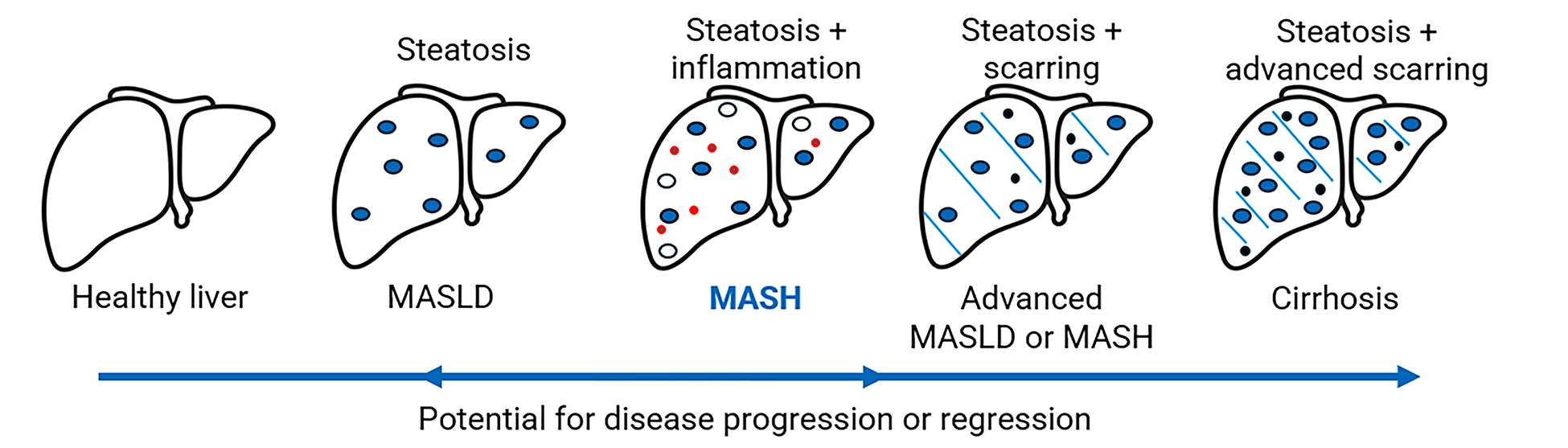
MASH = metabolic dysfunction–associated steatohepatitis; MASLD = metabolic dysfunction–associated steatotic liver disease.
Source of icon: Icon Vectors by Vecteezy (https://www.vecteezy.com/free-vector/icons).
Scope and Impact of Disease
MASH increases liver cancer risk and is a primary reason for adult liver transplant worldwide.2,11-13 In Canada, it represents approximately 25.5% of MASLD cases, affecting an estimated 6.0% of the population.14,15 MASLD is the most common liver disease in Canada, affecting more than 1 in 5 people (about 22.2% of the population) and its prevalence is projected to increase by 20% (to approximately 26.6%) between 2019 and 2030.14,15
Populations at Risk for MASH
MASH is a multisystemic disease linked to metabolic dysfunctions such as insulin resistance, impaired glucose regulation, abnormal lipid metabolism, and inflammation.16 It frequently co-occurs with other metabolic conditions such as obesity and T2DM.2,11,17 Of all individuals who have T2DM, who represent almost 10% of the population, up to 70% also have MASLD.12,18-20
Several clinical factors are associated with a higher risk of developing MASH and MASLD, as illustrated in Figure 2, including:21-25
dysglycemia (e.g., T2DM)
elevated body mass index (BMI) or obesity
presence of 1 or more cardiometabolic risk factors (e.g., dyslipidemia, high blood pressure).
Figure 2: Common Clinical Risk Factors for MASH and MASLD
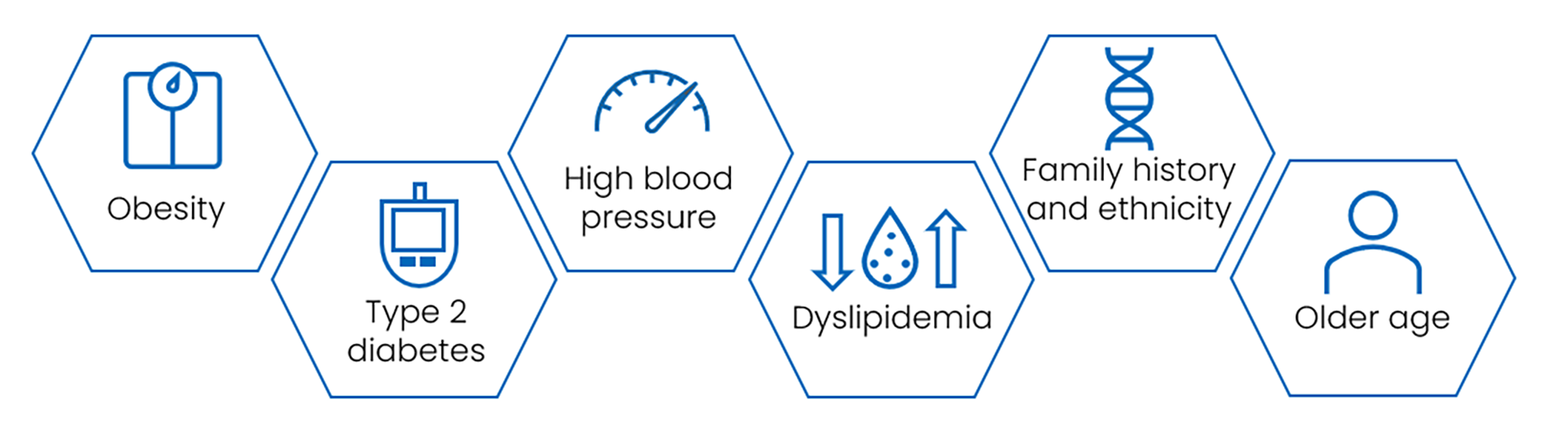
MASH = metabolic dysfunction–associated steatohepatitis; MASLD = metabolic dysfunction–associated steatotic liver disease.
Beyond these metabolic risk factors,2,17 several systemic conditions have also been linked with MASH, including cardiovascular disease (CVD), chronic kidney disease, cognitive impairment, and colorectal, breast, and pancreatic cancers.16,26 Figure 3 depicts the interconnected multisystemic spectrum of MASH.
Figure 3: High-Level Multisystemic Connections in MASH — Metabolic, Inflammatory, and Endocrine Interactions
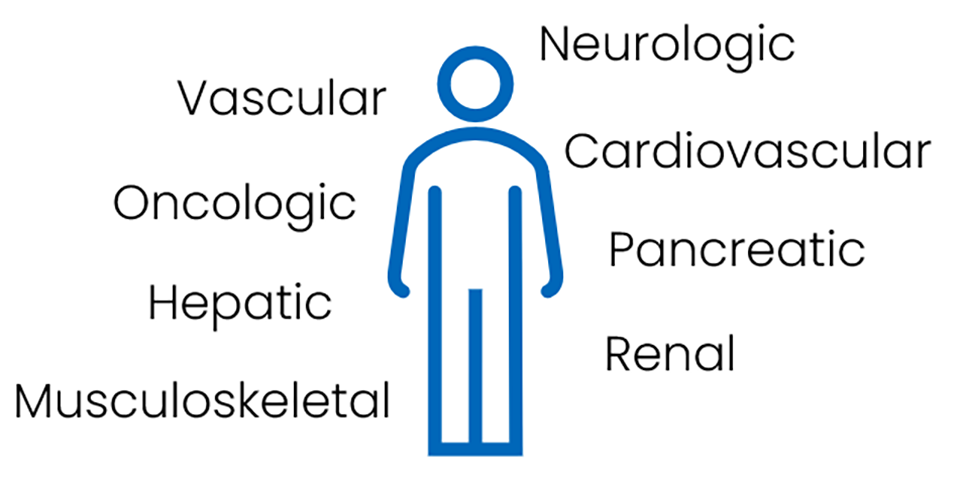
MASH = metabolic dysfunction–associated steatohepatitis.
The burden of MASH and MASLD varies across populations. Global and national evidence shows higher prevalence among Hispanic, Latino, and some Asian populations, including individuals at risk for lean MASLD and lean MASH.27,28 MASH is reported to disproportionately affect communities with higher rates of poverty and food insecurity.29-34 These structural barriers may also leave people with lower incomes, immigrant populations, and racialized groups at greater risk of undetected disease.34,35 Further details on risk factors are outlined in Appendix 2. This underscores the diversity of clinical presentation relevant to system-level identification and response in Canada.
The annual cost of managing MASH and MASLD in Canada was estimated at $3.76 billion in 2020.36 Costs were largely driven by the treatment of comorbid conditions.36 Costs climb as liver damage worsens, and with obesity and T2DM increasing, health spending is expected to increase unless early detection and prevention efforts expand.36
Available Treatments for MASH
Current management of MASH focuses on lifestyle modifications, weight loss, and pharmacologic treatment of associated comorbidities. In advanced stages, surgical options may include bariatric surgery (because it has been associated with sustained weight loss and potential improvements in steatohepatitis and fibrosis) and liver transplant for end-stage disease. Figure 4 illustrates the current spectrum of treatment approaches for MASH. Emerging disease-modifying therapies (DMTs), including glucagon-like peptide-1 (GLP-1) receptor agonists (RAs) and thyroid hormone receptor (THR)–beta agonists, aim to target underlying disease mechanisms and promote fibrosis regression in people with MASH or MASLD.37,38 In December 2025, Health Canada approved the first pharmacologic therapy for patients with MASH, a GLP-1 RA.39
Figure 4: Current Treatment Options for MASH in Canada
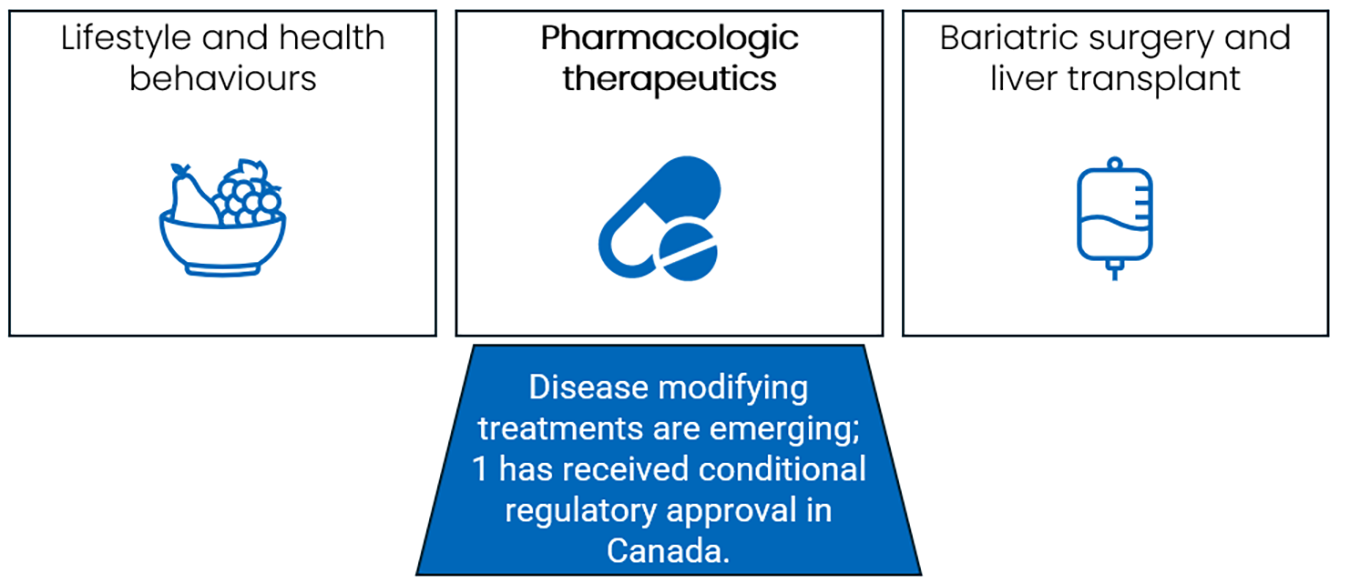
MASH = metabolic dysfunction–associated steatohepatitis.
The introduction of DMTs into clinical care could have important implications for health systems, as DMTs may require expanded capacity for diagnosis, monitoring, and coordinated clinical follow-up to support their appropriate and equitable use. Considerations related to access and coverage would also influence how these therapies would be integrated into care.
MASH and Health System Readiness
MASH is progressive, common, and increasingly treatable. The potential introduction of DMTs into clinical care presents an opportunity to assess the readiness of health systems for their adoption. This report presents evidence along the patient care pathway and identifies system-level opportunities to support earlier detection, coordinated care, and sustainable integration of emerging therapies.
Objectives
This report assesses the readiness of health care systems in Canada for the introduction of pharmacologic DMTs for MASH.
We summarize the current patient pathway for MASH to:
describe the underlying care infrastructure and processes across the clinical pathway
identify the incremental capabilities required to enable the adoption of DMTs.
Methods
A mixed-evidence approach was used to inform this assessment, drawing on systematic searches of the literature, targeted consultations with clinical experts, engagement with people with lived and living experience of MASH, and contextual knowledge shared by members of Indigenous communities.
Literature Search
An information specialist conducted targeted literature searches, balancing comprehensiveness with relevance, of multiple sources (including grey literature). Two searches were completed for:
the diagnostic accuracy of noninvasive tests, conducted on July 4, 2025
health system readiness, conducted on July 10, 2025.
Health system readiness literature was reviewed for relevance and used to describe current care pathways, disease risk factors, available and emerging treatments, and equity considerations. Regular alerts updated the database literature searches until the final draft of the report. Detailed methods are provided in Appendix 3.
Evidence on the diagnostic accuracy of noninvasive tests was sought to inform a broad understanding of existing and recommended tools and their ability to detect MASH. Rapid review methods were used to identify, review, and extract information from systematic reviews considered by the team from Canada’s Drug Agency (CDA-AMC) to be of moderate to high methodological quality. The results were supplemented with input from clinical experts on tools currently used in Canada. Detailed methods for the rapid review are provided in Appendix 4, with full results provided in Appendix 5.
Engagement With Clinicians, Patients, Carers, and Indigenous Communities
To complement published literature, CDA-AMC engaged clinical experts, individuals living with MASH, carers, patient group representatives, and Indigenous people. These participants provided contextual insights in the following areas:
diagnostic processes
patient needs and priorities
treatment practices
therapeutic readiness
health system use
ethics and equity considerations.
Clinician Engagement
Consultations with clinicians were conducted between August and October 2025 with 6 clinicians from the specialties of gastroenterology and hepatology (2), diagnostic pathology (1), endocrinology (1), radiology (1), and primary care (1). The clinicians were from Nova Scotia (1), Ontario (2), Alberta (1), and British Columbia (2).
Patient Engagement
We engaged people living with MASH and patient group representatives to capture lived experiences with MASH care, including perspectives on current and future patient pathways, treatment acceptability, accessibility, and equity considerations. Outreach activities included:
a statement of interest published on the CDA-AMC website
outreach to patient groups and clinical societies
social media promotion.
A total of 6 individuals participated in this engagement activity: 4 people with lived experience of MASH and 2 patient group representatives (1 of whom also had lived experience). Participants lived in Newfoundland and Labrador (1), Ontario (3), and Alberta (2). Engagement questions explored participants’ experiences with accessing health care providers, diagnostic services, and currently available treatments as well as care pathway and treatment expectations for the potential adoption of DMTs in MASH care.
Engagement With Indigenous Communities
Historical and ongoing colonial policies underpin inequities in infrastructure and resource distribution and availability, which may contribute to a disproportionate impact of MASH in First Nations, Inuit, and Métis populations. Confirming the prevalence of MASH and the impact on communities through published scientific studies may not be feasible or appropriate.40 The lived experience and insights of individuals in Indigenous communities provides contextualized knowledge that reaches beyond colonial scientific measures.41 This knowledge is highly important and can help inform decisions and actions.42 Research involving Indigenous Peoples must be guided by relevant frameworks such as:43-45
First Nations Ownership, Control, Access, and Possession (OCAP) principles
Métis Ownership, Control, Access, and Stewardship (OCAS) principles
Inuit Qaujimajatuqangit.
Recognizing these considerations, CDA-AMC contracted an external consultant to engage patients living with MASH and report on findings with an Indigenous lens. The consultant contacted participants, developed questions, and organized and facilitated the sessions. A member of the team at CDA-AMC attended the sessions and provided context based on an overview of MASH and the organization’s work.
CDA-AMC and Indigenous-led engagement approaches are reported according to the Guidance for Reporting Involvement of Patient and the Public (version 2) short-form (GRIPP2-SF) check list46 available in Table 13, Appendix 6. The summary of inputs from both engagement activities are available on the project web page.
Dashboard Using Real-World Evidence
Purpose
CDA-AMC created the interactive Metabolic Dysfunction–Associated Steatohepatitis (MASH) System Readiness dashboard to complement this report and provide detailed, up-to-date decision support information for health system planning. This dashboard allows users to explore trends and visualize insights to inform planning, prioritization, and resource allocation.
Scope
The dashboard consolidates publicly available, real-world data on factors relevant to readiness for the potential introduction of MASH DMTs, including:
diagnostic imaging capacity
liver clinic distribution
population health characteristics
clinician workforce distribution at jurisdictional and national levels.
Additionally, at an international level, it provides data on DMT availability, ongoing clinical trials for DMTs for MASH, and consensus-based and evidence-based guidelines that support earlier risk identification and management across the disease spectrum. These data were gathered via literature searches and were supplemented with information from web-based sources.
Health System Readiness
Awareness of MASH is limited and associated stigma may affect access to care.
MASH is often identified after it has progressed beyond the earliest treatable stage.
Early intervention, including lifestyle modifications and emerging DMTs, has the potential to prevent or slow disease progression and reduce costs.
Diagnostic and care infrastructure may need adaptation to meet growing demand.
Coverage for testing and tailored lifestyle treatment plans vary across jurisdictions, which may affect equitable access.
People living in rural, remote, and northern areas; younger adults; people with lower incomes; immigrants and newcomers; and Indigenous people may experience additional barriers to accessing testing and treatments.
Preparing Canada’s Health Systems for MASH DMTs
The recent conditional regulatory approval of a MASH DMT in Canada39 provides an opportunity to review the current patient care pathway and assess readiness should MASH DMTs be adopted as part of clinical care. By outlining the steps for diagnosing and treating MASH, this report uses clinical evidence to inform system-level insights. Examining the full care pathway also highlights opportunities to strengthen the health system, including:
optimizing resources across disease stages
expanding diagnostic capacity
streamlining referral pathways
enhancing multidisciplinary care models
strengthening treatment monitoring structures.
This report presents evidence on existing processes and care practices from diagnosis to treatment monitoring. It assesses system readiness by examining the capacity to integrate MASH DMTs into the care pathway, with the potential to improve patient care and potentially prevent or slow disease progression. A visual representation of the pathway is presented in Figure 5 and includes insights from evidence, clinical consultations, and proposed treatment steps from international clinical guidelines.
Implementation Considerations
There are several crosscutting considerations that may support efficient, patient-centred care, including with DMTs, should they become adopted in clinical practice along the care pathway, as outlined in the following points.
Disease Awareness
There is limited awareness of MASH. A survey of physicians in Canada found that 58% of primary care providers (PCPs) were somewhat familiar — or unfamiliar — with the condition.47 Insights from CDA-AMC–led engagement with people living with MASH reinforced this finding. Targeted awareness initiatives for both providers and patients, particularly in settings with patient at high risk (e.g., diabetes and obesity clinics), may prompt patient inquiries, support clinician screening, and promote early disease detection.
“I had to explain what NASH [now referred to as MASH] was to a walk-in doctor… They’d never heard of it.”
– Participant in the CDA-AMC–led engagement who lives with MASH, describing the need for education
Stigma
MASH can be a highly stigmatized disease due to links with weight and use of the term fatty liver, as well as misconceptions that the disease is caused by excessive alcohol use, even though the disease develops independently of alcohol consumption.48-52 In health care settings, stigma can undermine trust between patients and health care providers and is associated with delayed care seeking, reduced engagement with health services, and lower treatment uptake and adherence.48,53 Education for physicians with accurate, nonstigmatizing information may help ensure people living with MASH are treated respectfully and receive timely, appropriate care without needing to self-advocate.
Treatment Information
First-line interventions focused on diet and exercise can improve liver outcomes and slow disease progression.2,54-59 People living with MASH who contributed to this report described the importance of access to clear guidance from experts on recommended lifestyle adjustments that are aligned with dietary needs, cultural practices, and existing mobility or economic restrictions.
Figure 5: Potential Model of Care With DMTs for Patients With MASH
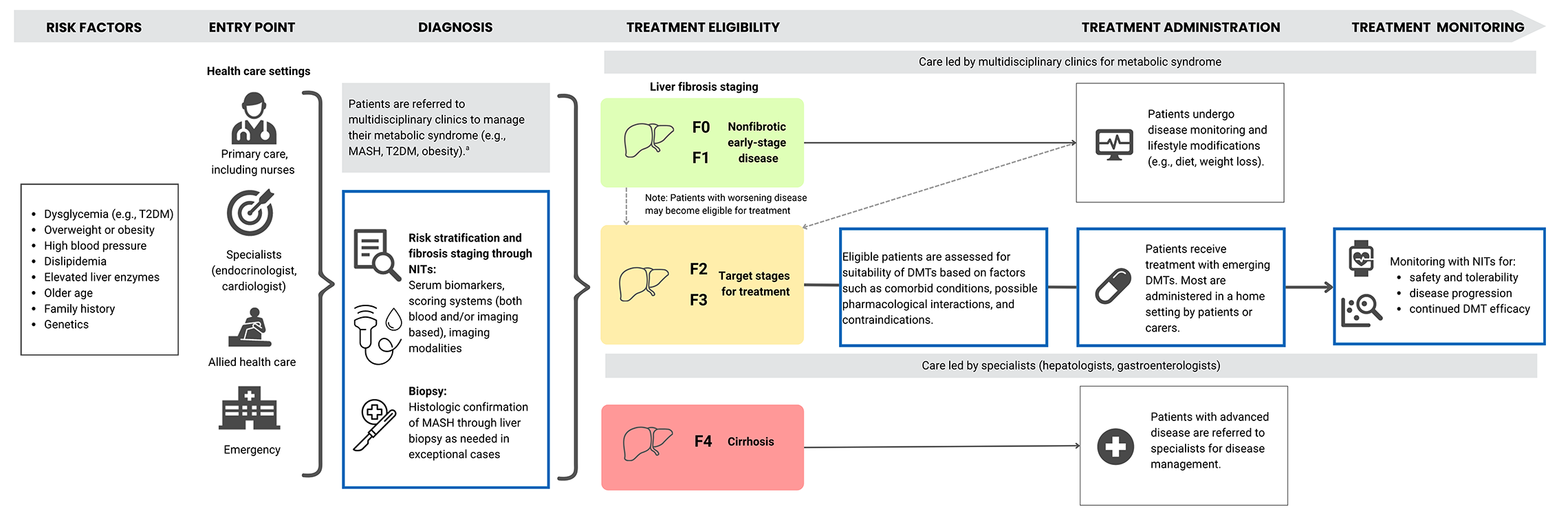
DMT = disease-modifying therapy; MASH = metabolic dysfunction–associated steatohepatitis; NIT = noninvasive test; T2DM = type 2 diabetes mellitus.
aHealth care practitioners who could be implicated in the multidisciplinary care model to assess, manage, and treat patients with metabolic syndrome would include, but are not limited to: registered nurses and nurse practitioners, primary care physicians, internists, endocrinologists, cardiologists, dietitians, psychotherapists, pharmacists, social workers, and addiction counsellors.
Provider Training
Many health care providers have reported having limited knowledge or training on MASH or MASLD,60,61 including how to communicate effectively with patients about liver fibrosis. This may contribute to the inconsistent use of guideline-recommended tools and may hinder timely diagnosis and optimal patient management.49,62-70 Expanding specialist and primary care training may support accurate and early diagnosis and effective patient management as liver disease prevalence rises.71-73
Access to Primary Care
An estimated 17% of adults living in Canada lack a regular PCP, although access varies within and across jurisdictions.74 Access tends to be lowest among younger adults, people with lower incomes, immigrants and newcomers to Canada, people living in northern communities, people living in rural and remote areas, and Indigenous adults (around 30% of whom report unmet primary health care needs).75,76 Opportunities to strengthen access to primary care reported in the literature include:
expanding provider access
reducing wait times for appointments and services77
enhancing local care availability to minimize travel, including in remote and northern communities
promoting culturally safe and inclusive care
increasing resources and support for rural, remote, and northern areas.78
These factors highlight opportunities to strengthen care coordination and continuity.79-82 Across all engagement sessions, people living with MASH consistently identified delayed access to primary care as a key challenge, with many reporting having to wait several months or, in some cases, more than a year before receiving care.
Access to Specialist Care
Opportunities exist to strengthen access to specialist care and to ensure timely support for people living with MASH. Hepatologists and gastroenterologists currently focus on patients with advanced or complex cases, highlighting the potential to expand capacity and coordination across the care pathway. Improving referral systems, reducing travel requirements, and addressing socioeconomic and racial inequities could enhance timely access to and continuity of care.79-84 Important areas for development identified in the literature and through clinical expert consultation include:
expanding liver-focused training beyond a single pathology fellowship program currently available in Canada (based on the clinical expert consultation)
increasing the number of radiologists and pathologists practising in Canada73
reducing geographic disparities in specialist availability.83
Access to Diagnostic Testing
Improving availability and public coverage of serum-based tests (e.g., the Enhanced Liver Fibrosis [ELF] test and the Fibrosis-4 [FIB-4] test), imaging (e.g., magnetic resonance elastography [MRE], shear wave elastography [SWE] and vibration-controlled transient elastography [VCTE]), and pathology diagnostic tests (e.g., liver biopsy) could enhance consistent and equitable access across jurisdictions.83,85-87 Such efforts should specifically consider capacity outside urban centres, especially for rural, remote, northern, and Indigenous communities.73,83,87-94 Information on jurisdiction-specific diagnostic testing practices is provided in Appendix 1, Table 5.
Coordinated Care
Canada may be well-positioned to adopt multidisciplinary pathways that are reported to be effective internationally.95 These approaches could support earlier intervention and may enhance continuity of care for individuals with, or at risk for, MASH. Key enablers reported in the literature include:96,97
standardized protocols
clearly defined team roles
reimbursement pathways that support diagnostic tests and treatments
culturally safe care options.
Sustainable implementation of potential DMTs for MASH in local contexts may be supported by tailored processes and guidance that consider local infrastructures, workforce availability, and funding models. Considerations for public drug coverage may focus specifically on the need for health technology assessment (HTA) evaluation and agreement(s) on pricing.94
Estimation of the Population With Treatable MASH
An estimated 2,415,796 people in Canada are living with MASH. An estimated 168,449 of those adults currently meet the criteria for treatable MASH (staged at moderate to advanced fibrosis).
By 2030, the number of patients with treatable MASH is projected to grow, reaching 198,731 adults.
These estimates reflect published estimates of the number of people with MASLD who have moderate to advanced fibrosis (stages F2 to F3) and the proportion of those with MASH.
Estimation of the Patient Population With Treatable MASH and Future Demand
As the first DMT for MASH has received conditional regulatory approval in Canada, understanding the size of the population who may be eligible for treatment can help system-level planning. Estimating the number of adults with moderate to advanced fibrosis (stages F2 to F3) provides an early indication of the potential demand for diagnostic services, specialist input, monitoring capacity, and coverage considerations. These estimates help demonstrate the current burden and the potential for growing demand as prevalence rises and more patients are diagnosed over time.
An estimated 2,415,796 people in Canada are living with MASH, of whom approximately 168,449 adults currently meet criteria for treatable disease (stages F2 to F3). This highlights a substantial overall disease burden, with a smaller but sizable subgroup driving near-term demand for treatment and specialized care.15
A progressive, stepwise approach was used to estimate the population with MASH at disease stages potentially eligible for treatment (full methodology and limitations can be found in Appendix 7). Estimates were based on Canadian sources when available. Clinical experts reviewed and provided feedback on the approach and parameters; however, results should be interpreted with consideration of underlying uncertainties.
The model begins with the total population in Canada and sequentially applies estimates for MASH prevalence, fibrosis staging distribution, and adult population adjustments to arrive at an estimate of the population with treatable MASH. Using this approach, approximately 168,449 adults were estimated to be eligible for treatment in 2025, increasing to 198,731 adults by 2030, reflecting projected demographic growth and disease progression (Table 1). These estimates should be interpreted as indicative rather than definitive and likely represent a lower-bound estimate of the true eligible population.
Table 1: Summary of the Estimated Population With Treatable MASH in Canada
Population of interest | Approach | Estimated N |
|---|---|---|
Adult population with treatable MASH, estimate for 2025 in Canada | Stepwise approach: starting from the total population and applying MASH prevalence, proportion of the population with relevant stages of fibrosis, and age adjustment (full details are provided in Appendix 7) | 168,449 |
Adult population with treatable MASH, estimate for 2030 in Canada | Stepwise approach as described in the previous row with projected estimates used (full details are provided in Appendix 7) | 198,731 |
MASH = metabolic dysfunction–associated steatohepatitis.
Clinical experts consulted for this report indicated that the estimated population with treatable MASH is likely underestimated. This potential underestimation may reflect:
limited early identification and diagnosis of disease
reliance on historical obesity trends, which may not capture recent trends
not fully accounting for the high prevalence of related conditions, including diabetes and CVD24,25,98,99
incomplete accounting for individuals with lean MASH, who are estimated to compose about 20% to 50% of all MASLD cases98,99
a large undiagnosed population.
Taken together, these factors suggest the true number of patients who may be eligible for treatment could be meaningfully higher than modelled estimates, particularly as awareness, screening, and diagnostic capacity improve over time.
Describing the Care Pathway for MASH in Canada
Assessment and Diagnosis
MASH is shaped by both clinical factors (e.g., obesity, T2DM) and social determinants of health (e.g., income, access to care), underscoring the importance of equity-focused strategies that address structural barriers to care and upstream drivers of disease.
Limited awareness and understanding of MASH across the health system highlight the need for education, standardized guidance, and coordinated care pathways.
The current diagnostic and care infrastructure targets patients with high-risk disease after progression beyond the earliest treatable stages and may not be able to meet the growing prevalence of disease.
Social Factors That Affect the Care Pathway
Population groups experiencing multiple, intersecting structural and social determinants of health appear to experience a higher burden of MASH. These patterns can be understood through a framework of intersectionality, which outlines how social determinants of health categories such as race, class, and gender interact with broader social and institutional structures to shape differential outcomes, in this case disparities in MASH risk.100 Evidence suggests that disease progression to advanced fibrosis, cirrhosis, and cardiovascular complications are more common among groups facing overlapping structural and social disadvantages. Specific examples of how MASH burden and progression vary across populations due to interacting demographic, clinical, behavioural, and structural risk factors are described in Appendix 2.
Insights from individuals living with MASH who participated in the Indigenous-led and CDA-AMC–led engagement activities described experiences of inequity across the care pathway. Across engagement sessions, participants highlighted several system-level considerations, including:
low awareness of MASH in standard care practices throughout the system
stigma and assumptions about alcohol use and body weight
limited access to local testing in rural and remote areas.
Participants in the Indigenous-led engagement activities additionally emphasized:
frequent diagnostic delays attributed to racism and misattributed symptoms.
Entry Point Into the Care Pathway
Early-stage disease is often asymptomatic. People living with MASH may present with nonspecific symptoms such as fatigue, weakness, abdominal discomfort, and bloating.101 Because of the multisystem nature of MASH and lack of clear early indicators, identifying MASH early can be challenging.
Participants in the Indigenous-led and CDA-AMC–led engagement activities described a lack of disease awareness. They emphasized the need for self-directed education and advocacy with health care providers to receive testing for a diagnosis. Participants reported that delays in accessing testing and diagnosis contributed to worsening symptoms as well as to heightened anxiety and stress, negatively affecting both physical and emotional well-being.
“If I don’t take charge of this, then I am going to be in trouble.”
– Participant in the CDA-AMC–led engagement who lives with MASH, describing a need to advocate for themselves
Liver disease may be identified through multiple entry points in the health system, including:
primary care assessment in which routine blood work may reveal elevated liver enzymes or incidental imaging findings suggest steatosis (fat accumulation) or fibrosis (scarring)
screening programs for MASH that often target patients managing comorbid conditions with increased liver disease risk14
emergency department visits in which individuals seek care for complications of advanced disease or decompensated cirrhosis
specialist care referral for which individuals are referred for liver assessment by a specialist in another discipline, such as cardiology, endocrinology, or internal medicine
recognition by allied health professionals who are increasingly positioned to identify patients at risk and initiate referral for further screening.
Improving disease awareness in Canada may help improve MASH care by equipping health care providers with training on early identification and effective communication, particularly at the entry point of the health care pathway.
Participants in the Indigenous-led and CDA-AMC–led engagement activities reported experiencing vague symptoms, limited access to primary care, long wait times for imaging and specialist follow-up, minimal diagnostic communication with care providers, confusion about their diagnosis, and substantial travel and cost burdens for testing, especially for those living in remote regions.
“Pain… A lot of pain and suffering.”
– Participant in the Indigenous-led engagement, describing when their MASH was first identified in a late disease stage
Additionally, competing health priorities and stigma may hinder early identification of MASH or timely engagement with the health care pathway.
Competing Health Priorities
Patients with MASH often manage multiple comorbid conditions, which may take precedence over liver disease, particularly when MASH is asymptomatic.102 Clinicians may also underrecognize or underprioritize MASH amid competing health demands and limited time for complex care decisions.101,103
Participants in the Indigenous-led and CDA-AMC–led engagement activities noted that MASH risks, symptoms, and management were often not discussed while they were being monitored for associated comorbidities like obesity and T2DM. They also described receiving information about their condition only when it became clinically necessary. Together, these factors may contribute to delayed identification of MASH, particularly among populations at high risk.
“They told me it’s nothing to worry about.”
– Participant in the CDA-AMC–led engagement who lives with MASH, describing when their mild liver fibrosis was first identified
Stigma
MASH-related stigma can arise from multiple sources, including outdated disease terminology, risk factors such as body weight and alcohol use, and social determinants of health categories such as race, gender, and age.48 This stigma can contribute to moral judgment, misattribution of symptoms, and reduced care seeking.49-52 Although efforts to reduce stigma — such as replacing terms like nonalcoholic and fatty liver disease— have been made, some patients continue to identify the condition as fatty liver disease, which can perpetuate feelings of shame and disengagement.4
All participants in the Indigenous-led and CDA-AMC–led engagement activities highlighted stigma around liver disease. Many noted that people, including health providers, often assumed their liver issues were caused by alcohol. One Indigenous participant shared that clinicians immediately questioned their alcohol history, even after clarifying their condition was metabolic. Other Indigenous participants echoed that community members asked if they “used to drink a lot.”
Clinical Practice Guidelines for MASH
Several clinical practice guidelines (CPGs) have been developed for MASLD and MASH. Recent Canadian evidence-based and consensus-based guidelines provide national guidance.104-106 As well, health organizations within certain jurisdictions have developed management pathways tailored to local contexts, including Kingston Health Sciences Centre in Ontario, Shared Health in Manitoba, and Alberta Health Services.107-109
Many physicians in Canada also refer to guidance from international groups. These international guidelines are briefly described in Appendix 2. Canadian and international guidelines are consistent in several key areas. They recommend assessing MASH in individuals with T2DM or abdominal obesity plus 1 additional metabolic risk factor, or when liver function test results are abnormal.2,3,14,105 They also suggest that potential alternative causes of liver disease should be evaluated alongside MASLD. These conditions can co-occur, mimic, or mask MASH on imaging and laboratory testing, adding diagnostic and treatment uncertainty or complexity.2,3,14,105 These may include:
alcohol consumption patterns
drug-induced liver disease
viral hepatitis
extrahepatic and hepatic autoimmune diseases
certain genetic conditions
endocrine disorders
environmental toxins
nutritional-related causes.
Guidelines are also aligned on the populations at risk of developing MASH, how to assess fibrosis risk, and the use of dietary and behavioural interventions as first-line treatments. However, they differ on the specific techniques used for fibrosis staging, current recommendations for pharmacologic treatment, and their integration of DMTs. Details on the alignment of Canadian and international guidelines are provided in Appendix 1, Table 6 and Table 7. Additional information on available guidelines is also presented in the dashboard under the Guidelines tab.
Baseline Fibrosis Staging and Assessment in the Care Pathway
Fibrosis Staging System
Fibrosis severity is a key marker of MASH progression and a strong predictor of mortality. Given that emerging DMTs target specific fibrosis stages (F2 to F3), these stages are often grouped into 3 clinically relevant categories, from F0 to F4:38
F0 to F1 — early-state disease
F2 to F3 — moderate to advanced fibrosis
F4 — cirrhosis.
Liver Biopsy
MASH is characterized by specific histological features that can only be definitively diagnosed through liver biopsy, a procedure in which tissue samples are collected for microscopic assessment.110 Although biopsy is the definitive test for MASH and MASLD, its use is limited because it is invasive, costly, time consuming to perform, and carries the risk for potential complications. These factors make routine biopsy impractical for large patient populations, particularly given the high prevalence of MASH and MASLD. As a result, noninvasive tests (NITs) are increasingly relied on for disease staging and risk stratification.110-112
The types of invasive and noninvasive tests are illustrated in Figure 6.
Figure 6: Diagnostic Tools for Detecting MASH and MASLD
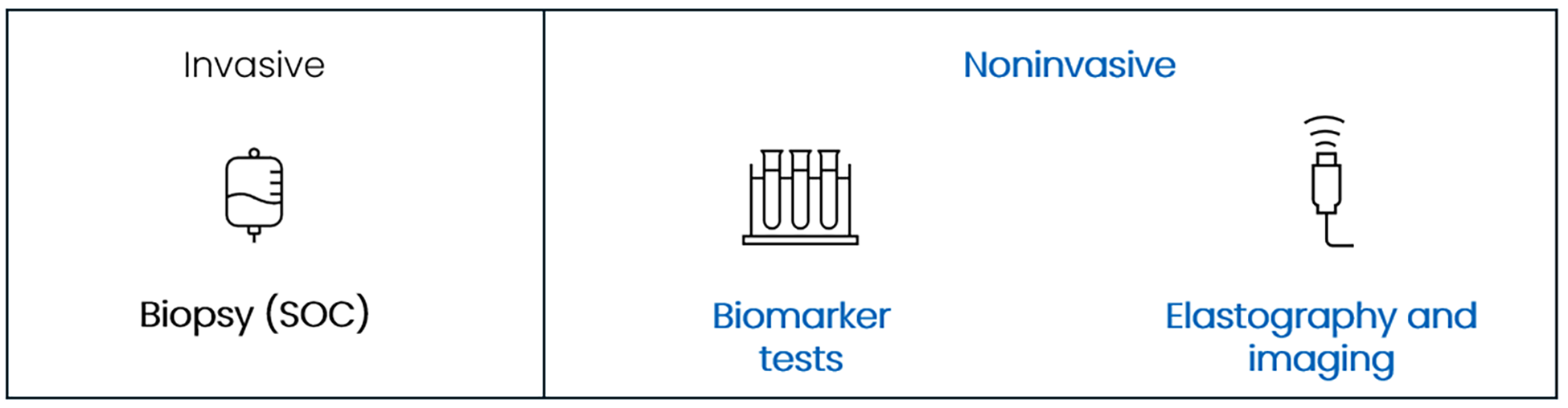
MASH = metabolic dysfunction–associated steatohepatitis, MASLD = metabolic dysfunction–associated steatotic liver disease; SOC = standard of care.
NITs for Fibrosis Assessment
NITs have been developed as practical alternatives to biopsy to help with the staging and detection of fibrosis.104,105,113 These tests allow clinicians to align results with the fibrosis staging system and stratify patients’ disease into low-, intermediate-, and high-risk categories for fibrosis and high-risk MASLD or MASH.105,114
All evidence- and consensus-based CPGs mentioned previously recommend a stepwise approach to fibrosis assessment using NITs. Figure 7 illustrates this pathway, with recommendations to begin with simple, low-cost tools for initial risk stratification and progress to more advanced imaging for confirmation when needed.
Initial risk stratification uses the FIB-4 index.
Secondary staging tests include the ELF score, VCTE, or SWE.14,104-106
Figure 7: Current Recommended Pathway for Assessment of Fibrosis in Patients
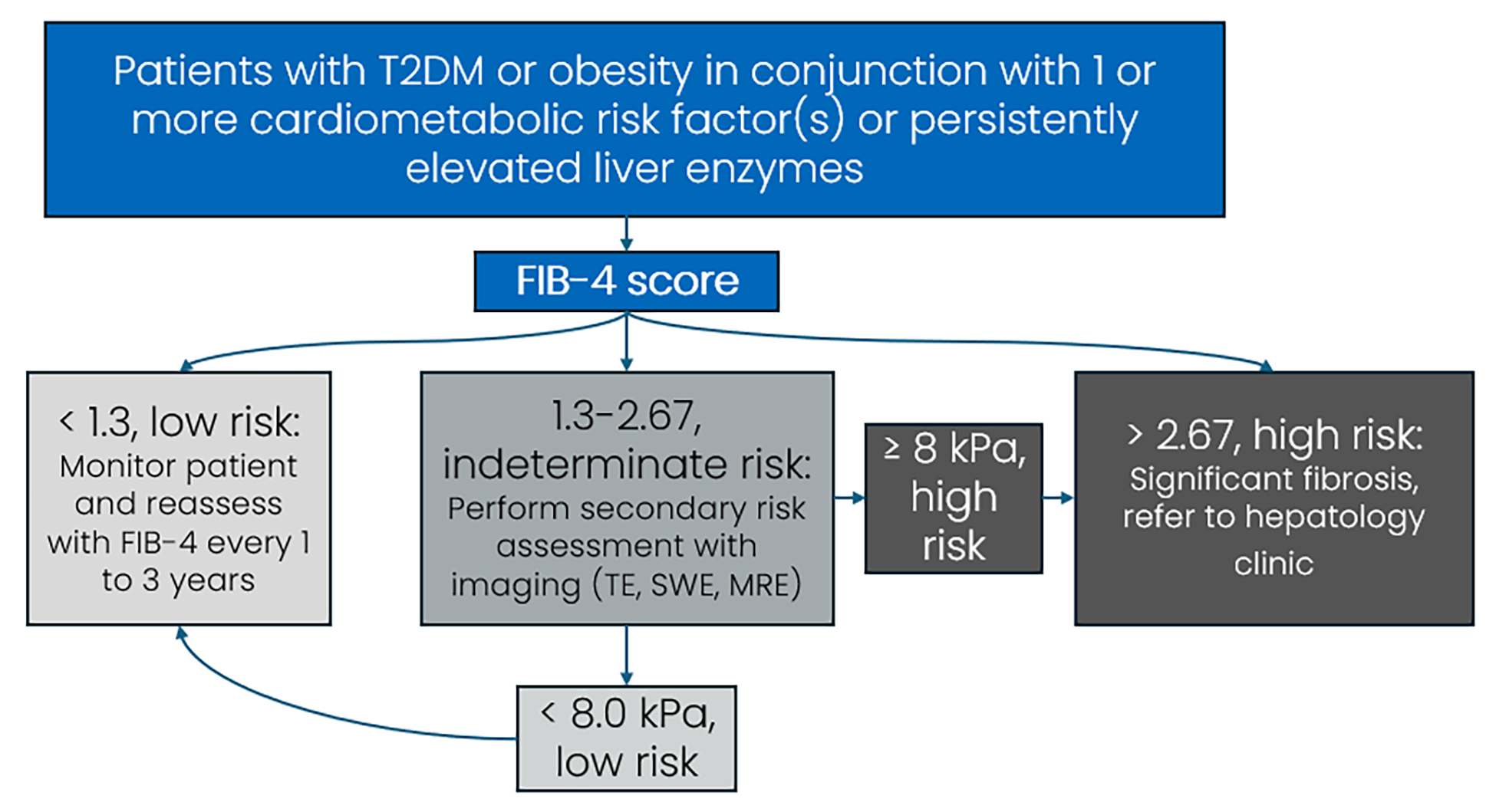
ELF = Enhanced Liver Fibrosis; FIB-4 = Fibrosis-4; MRE = magnetic resonance elastography; NIT = noninvasive test; SWE = shear wave elastography; T2DM = type 2 diabetes mellitus; TE = transient elastography.
Notes: For adults aged older than 65 years, an indeterminate FIB-4 threshold is between 2.0 and 2.67. Thresholds presented in Figure 7 are for patients aged between 35 years and 65 years.
Thresholds for secondary NITs (e.g., kPa levels) are for VCTE measurements. Alternative tests (e.g., SWE, MRE, ELF) may have adapted or alternative thresholds.
Sources: European Association for the Study of the Liver, European Association for the Study of Diabetes, European Association for the Study of Obesity;2 Sebastiani and Cinque;59 and Wilson et al.105
Reviewing Evidence on NITs for Accuracy and Reliability
NITs are increasingly used to support the assessment and staging of MASH. While NITs reduce reliance on biopsy, evidence shows variation in diagnostic performance across settings, disease stages, and patient populations. Because current diagnostic pathways were largely developed to identify high-risk advanced disease, earlier stages may be underdetected. As a result, diagnostic pathways may inadvertently limit detection of patients with early and moderate fibrosis who could benefit from emerging therapies. Reviewing the evidence on NIT performance provides context for understanding the current testing landscape and identifying gaps that may affect early patient identification.
Scope of the Rapid Review
CDA-AMC conducted a rapid review of recent systematic reviews and meta-analyses investigating the diagnostic accuracy of NITs. Six reviews considered to be of moderate or high methodological quality were included (full methods are available in Appendix 3 and results are available in Appendix 4).
To ensure practical relevance, the synthesis focused on the most commonly used tools referenced in CPGs (refer to Table 2). While this overview cannot fully resolve all remaining uncertainties in the diagnostic evidence, it provides critical context on:
how these tools are currently applied
where evidence gaps remain
what considerations may influence future diagnostic pathways.
Key Findings From the Rapid Review
The rapid review found few large-scale (adequately powered) studies and noted inconsistencies (heterogeneity) across available evidence. Further, no NIT — or combination of NITs — demonstrated sensitivity and specificity (reflecting how well they correctly detect people who have the disease while accurately excluding those who do not) higher than 0.80 across multiple studies for detecting MASH.
No single definitive test: More than 100 NITs exist, but none of the common tests demonstrated similar diagnostic accuracy (sensitivity and specificity) across all studies, populations, disease stages, or settings. Evidence remains limited to support using any existing NIT as a stand-alone screening tool or biopsy replacement.
Diagnostic accuracy: The included evidence suggested MRE had the highest diagnostic accuracy followed by SWE and VCTE; however, cut-off thresholds and diagnostic definitions differed across studies (more details are provided in Appendix 5, Table 11).
Risk of bias: Across included systematic reviews, most studies were at high or unclear risk of bias, as appraised by the systematic review authors (refer to Appendix 5, Table 10 for more details).
Generalizability: Across the included systematic reviews, no subgroup analyses were conducted to determine whether test accuracy differed based on characteristics such as age, sex, or race. This limits our ability to assess whether these diagnostic tools perform consistently across diverse populations. The lack of evidence-based information on race is a challenge, as evidence shows that some populations are at higher risk for developing MASH.
Summary of NITs: Strengths, Limitations, and Key Characteristics
The NITs referenced here reflect those most frequently cited in Canadian CPGs and current care pathways. Practical considerations — such as accessibility, cost, and technical requirements — that influence their use in clinical settings are outlined in Table 2. Further details on each tool’s main characteristics are provided in Appendix 2, and Table 11 in Appendix 5 provides reported sensitivity and specificity from evidence included in the rapid review.
Table 2: Summary of Strengths and Limitations of Common NITs
Tool | Strengths | Limitations | Recommended in Canadian guidelines? |
|---|---|---|---|
Scores with biomarkers and patient characteristics | |||
FIB-4 score |
|
| |
ELF score |
|
| |
Imaging-based tools | |||
VCTE |
|
| |
SWE — point or 2D |
| ||
MRE |
|
| Yes — secondary NIT105,a |
MRI-PDFF |
|
| Yes — secondary NITa preferred technique for liver steatosis grading104 |
CAP = controlled attenuation parameter; CSPH = clinically significant portal hypertension; ELF = Enhanced Liver Fibrosis; FIB-4 = Fibrosis-4; MASH = metabolic dysfunction–associated steatohepatitis; MRE = magnetic resonance elastography; NIT = noninvasive test; PDFF = proton density fat fraction SWE = shear wave elastography; VCTE = vibration-controlled transient elastography.
aSecondary NIT is a confirmatory test for patients with high-risk results on initial screening (e.g., high FIB-4 scores).
Implications for Practice
The rapid review shows substantial variability in the accuracy and performance of NITs across populations, settings, and disease stages. These findings suggest that guideline approaches that emphasize risk stratification for advanced disease may limit detection of earlier stages. These findings suggest a need for clearer diagnostic pathways and broader validation of NITs in diverse populations.
System-Level Considerations for MASH Assessment
Diagnostic capacity is variable in Canada, with the greatest disparities in rural, remote, and northern communities.
Clinical readiness of health care providers is needed for appropriate screening and testing and for the diagnosis of MASH in Canada.
Access to NITs varies across jurisdictions, with many patients facing out-of-pocket costs for testing.
The most cost-effective screening approach is unclear, but using multiple tools consecutively is likely to accurately identify late-stage disease.
There are system-level considerations for assessing and diagnosing MASH with NITs, which are increasingly relevant with the recent conditional regulatory approval of a DMT in Canada. Earlier sections of this report, along with insights from clinical experts and patient engagement, point to challenges in diagnostic infrastructure, workforce capacity, provider readiness, reimbursement variation, and equity. The following subsections outline these considerations in detail and describe how they may affect the ability to scale timely and equitable diagnostic pathways, should DMTs become available and integrated into clinical practice.
Diagnostic Testing Infrastructure
Considerations for diagnostic capacity include the need for equipment (i.e., imaging devices, elastography systems, and blood sample processing), skilled operators, MRI procurement requirements, and, in some cases, patent-restricted technologies.83,88,89 Supporting appropriate access to testing — particularly in rural, remote, and northern areas — could help minimize travel burdens for patients and families who typically need to visit large urban centres for testing.
Access to Testing
Noninvasive imaging tools, including VCTE, SWE, and MRI-based modalities, are concentrated in urban areas in Canada, while 30% of the population lives in rural or remote regions.92 Wait times may also pose challenges; in 2024, the median wait time for an MRI in Canada was 16.2 weeks,73 with the longest delays in smaller provinces and northern regions.83 Clinical experts and engagement participants similarly reported limited access to elastography, ELF testing, and MRI outside major centres, contributing to delays in screening and diagnosis.
For patients in rural and remote communities, long travel distances and extended wait times may delay disease staging. Participants in Indigenous-led and CDA-AMC–led engagement activities noted long wait times led to worsening physical and emotional well-being, including worsening severity of MASH and heightened stress and anxiety. Refer to the dashboard under the Liver Clinics and Diagnostic Units for Liver Fibrosis tab for more information on the known distribution of diagnostic tools in Canada. Refer to Appendix 1, Table 5 for further diagnostic differences across specific jurisdictions.
Human Resources
Demand for imaging and other diagnostic professionals continues to rise, while workforce growth has not kept pace with demand across Canada.73 Training, upskilling, and retaining staff require time and resources and may affect service capacity. Demand for radiologists and technologists is high, particularly in rural regions where recruitment and retention rates are lower than in urban centres.73,92 These disparities may affect wait times and reduce timely access to diagnostic services for patients outside major centres.
Canada also has limited numbers of diagnostic and molecular pathologists (3 per 100,000 population in 2024), which may affect turnaround times for results and the availability of specialized interpretation.84 Additional information on provider distribution is available in the dashboard under the tab Number of Physicians.
Clinical Readiness and Testing Coverage
Increasing disease awareness and use of consensus pathways and CPGs, including embedding the FIB-4 calculation into standard laboratory test requisitions, have been suggested to strengthen risk stratification in primary care and reduce unnecessary specialist referrals.94,132 However, the uptake of these approaches may vary across jurisdictions. Coverage for AST testing and VCTE varies, and in some areas availability may be limited to urban centres or require out-of-pocket costs.14
Cost-Effectiveness
Evidence indicates that noninvasive screening is cost-effective, particularly for populations living with obesity or T2DM. A Canadian study on the cost-effectiveness of risk stratification strategies in the community setting (i.e., FIB-4 assessment followed by SWE or VCTE) found that the most cost-effective strategy for identifying patients with substantial fibrosis (stages F2 higher) was using SWE alone.133
Additionally, a study from the UK on the use of noninvasive liver fibrosis tests in primary care found that VCTE alone was the most effective for identifying patients with severe disease, while a sequential approach using the FIB-4 index followed by ELF testing offered the greatest cost savings.134 These differences highlight how population characteristics and system structure influence optimal screening pathways.
Equitable Assessments Using NITs
Global studies have shown that standard screening thresholds, such as BMI, waist circumference, and fibrosis indices, were developed mainly in populations of white males in Western countries. As a result, these thresholds may underestimate risk in Indigenous populations, racialized communities, and females. These limitations in the data may affect the accuracy of assessments in diverse population groups and potentially lead to misclassification of liver disease status in diverse population groups.28,135,136 Additionally, factors such as sex and age influence liver stiffness and fat distribution, affecting test sensitivity and specificity.137
Comorbidities such as obesity and T2DM alter biomarker levels and disease progression, requiring tailored interpretation.138 A standardized core outcome set of NITs, inclusive of diverse population characteristics, may help ensure more accurate diagnosis and risk stratification across all patient groups, including Indigenous Peoples and racialized populations.139-141
The potential introduction of DMTs may also increase demand for liver biopsy as a confirmatory tool, even with expanded use of NITs. Eligibility for treatment may require definitive confirmation of fibrosis stage or steatohepatitis, and NITs may be insufficient in patients with borderline or discordant cases.110-112 This could place additional strain on already limited specialist capacity, including pathologists.73,84
Treatment
The December 2025 conditional regulatory approval of the first DMT for MASH, a GLP-1 RA, by Health Canada,39 as well as emerging THR-beta agonists, may shift treatment approaches in Canada. This report draws on international clinical guidance that incorporates DMTs to outline emerging drug treatment procedures (also visualized in Figure 5) and provides system-level context for how these therapies may potentially be integrated into care pathways in Canada.
Current management in Canada relies on dietary and lifestyle interventions.
Drugs in each of 2 drug classes — GLP-1 RAs and THR-beta agonists — have received regulatory approval internationally; in December 2025, Health Canada conditionally approved a GLP-1 RA for patients with MASH. No drugs have been submitted for reimbursement review in Canada.
Several additional therapies are in clinical development.
Clinical and system-level considerations for determining treatment eligibility and the choice of treatment for patients include:
standardization of fibrosis staging using NITs
updated prescribing infrastructures and clinical guidance
coverage considerations that support consistent and equitable access
continuity of care supported by multidisciplinary teams
patient engagement strategies to address acceptance and safety concerns.
First-Line Approach
Lifestyle modification remains the cornerstone of MASH management in Canada. Diet and physical activity aimed at weight loss — typically 7% to 10% of body weight — are associated with improved liver fibrosis, while even modest reductions can benefit lean individuals (those with BMI < 25 kg/m2 or < 23 kg/m2 if Asian).142,143 Eligibility for these interventions does not require a confirmed MASH diagnosis. Dietary and lifestyle changes that may be considered include:
DMTs are intended to build on existing lifestyle-based strategies, forming 1 part of a layered approach to MASH management rather than replacing foundational interventions.
Education and Support for Lifestyle Change
Effective lifestyle modification depends on supports that reflect individuals’ cultural, linguistic, and personal needs. A range of supportive tools may facilitate communication and engagement with health care providers, including:
culturally and linguistically appropriate education28,147,148
peer and community-based navigation programs149
digital tools to support adherence (e.g., mobile apps, reminders, and telehealth follow-ups).150,151
However, these supports are not consistently available across Canada. Rural and northern communities, in particular, have infrastructure limitations, connectivity challenges, and workforce constraints that reduce access to digital and culturally grounded resources.75,152,153 When integrated into practice effectively, these support tools can promote shared decision-making by enabling culturally and linguistically aligned communication; supporting patient understanding of treatment options; facilitating ongoing monitoring of symptoms and treatment adherence; and helping patients address individual needs, navigate real-life challenges, and maintain sustained engagement and treatment consistency.144-146,150,151
Lifestyle and Behavioural Support
Sustaining lifestyle changes may require addressing systemic barriers such as limited access to healthy food, safe spaces for physical activity, childcare, or flexible work hours. Evidence suggests that personalized and culturally aligned approaches — often supported through eHealth tools like online programs, smartwatch tracking, or reminder systems — can improve engagement and behaviour change.154,155 These considerations highlight that lifestyle-based management is not solely a clinical issue but also a structural one, underscoring the need for context-appropriate supports as part of comprehensive MASH care.
Insights From People With Lived Experience
Participants in the Indigenous-led and CDA-AMC–led engagement activities described the need for more information and guidance about MASH. They noted it was difficult to understand which lifestyle modifications and therapies were appropriate for their stages of disease or comorbid conditions.
“I felt like I was wandering in the dark.”
– Participant in the CDA-AMC–led engagement who lives with MASH, reflecting on the limited information on treatment options
Participants reported having to research information about the disease and its treatments from other sources (e.g., internet searches, community support groups), and some later shared this information with their health care providers. Those who received lifestyle advice commented that it was not tailored to their culture or dietary preferences, and many sought alternative private services with added financial cost.
Indigenous participants reported the need for:
plain-language information on MASLD and MASH
workshops delivered within communities
resources available in Indigenous languages
culturally grounded teaching.
One participant expressed a desire for sessions specifically for female patients. Further, Indigenous participants emphasized that culturally safe liver care requires acknowledging and integrating Indigenous approaches.
“[Health systems could] access the traditional Healers and get their contributions.”
– Participant in the Indigenous-led engagement who lives with MASH, reflecting on how to improve the system
These perspectives reinforce the importance of culturally informed, accessible, and community-centred approaches as DMTs for MASH may become more integrated and available in Canada.
Recent Developments in DMTs for MASH
Internationally, 2 drug classes — GLP-1 RAs and THR-beta agonists — have approved therapies for MASH (refer to Table 3). More detailed descriptions of both GLP-1 RAs and THR-beta agonists, including their mechanisms and clinical roles, as well as evidence on existing and emerging DMTs in clinical development, are included in Appendix 2, Table 8.
Table 3: Regulatory Status and Health Technology Assessment Status of DMTs for MASH in Canada and Internationally as of March 2026
Jurisdiction | Drug class | |
|---|---|---|
GLP-1 RA | THR-beta agonist | |
Canada | One GLP-1 RA has received conditional regulatory approval by Health Canada for the treatment of MASH.39 It has not been submitted for reimbursement review. | No THR-beta agonists have yet been submitted for regulatory or reimbursement review. |
International | One GLP-1 RA has received regulatory approval in the US.156,157 No health technology assessments on the clinical or cost-effectiveness of this treatment for MASH have been conducted. | One THR-beta agonist has received regulatory approval in the US and in Europe.158-161 In Europe, no health technology assessments have been published, although some are currently in development.162,163 In the US, a health technology assessment on the clinical and cost-effectiveness of this drug concluded it demonstrates a net health benefit and is cost-effective.164 |
DMT = disease-modifying therapy; GLP-1 = glucagon-like peptide-1; MASH = metabolic dysfunction–associated steatohepatitis; RA = receptor agonist; THR = thyroid hormone receptor.
Eligibility for MASH DMTs
Determining Eligibility and Prescribing DMTs
Emerging DMTs are indicated for people with moderate to advanced fibrosis (stages F2 to F3). In Canada, treatment with the Health Canada–approved GLP-1 RA is indicated for noncirrhotic MASH with F2 to F3 fibrosis, alongside diet and exercise.165 Eligibility is therefore contingent on accurate fibrosis staging, which is typically assessed using NITs. Screening tools such as FIB-4 assist with risk stratification but do not provide the level of precision needed to confirm fibrosis stage.2,166,167
Current Practice and Opportunities
Clinicians frequently manage MASH indirectly through cardiometabolic therapies.63,168-178 Opportunities to strengthen the treatment pathway have been identified and include:
standardizing fibrosis staging protocols and thresholds167,179-181
tailoring care to address structural barriers influencing access and treatment adherence.28,135,190-192
Refer to Appendix 2, for detailed information on indirect prescribing practices; fibrosis staging and related equity considerations; and provider roles and scope in MASH care. Appendix 2 also provides additional context on patient perspectives, including treatment stigma, perceptions of DMTs, and structural barriers, that influence engagement with care.
Treatment Administration
GLP-1 RAs are typically administered as subcutaneous injections, while THR-beta agonists are administered orally.
Access to a pharmacy and cold chain management may limit treatment options for some people, especially those in rural and remote communities.
Treatment administration requires planning and customized support for health behaviours and lifestyle factors that complement pharmacologic mechanisms.
Administration of DMTs may raise multiple implementation considerations including clinical protocol, patient support and accessibility, infrastructure, and care coordination. Addressing these considerations could help ensure equitable availability and use of emerging MASH DMTs, should they become widely integrated in Canada.
Practice guidance from the US provides approaches for patient eligibility assessment, noninvasive fibrosis assessment, structured monitoring, and coordinated care.167,180,193 Clinical experts engaged for this review noted that similar guidance could help support consistent, equitable implementation in Canada.
“I don't think we should have to beg.”
– Participant in the Indigenous-led engagement activity who lives with MASH, reflecting on the need for affordable medicine
Participants from Indigenous-led and CDA-AMC–led engagement sessions shared concerns about the potential introduction of emerging DMTs in Canada, especially related to cost and coverage. Indigenous participants highlighted concerns around Non‑Insured Health Benefits coverage and related administrative processes. Participants noted uncertainty about whether the drugs would be accessible, including coverage by provincial , or federal programs; affordability concerns for people on fixed incomes; potential Non‑Insured Health Benefits delays or denials; and lack of clarity about who would ultimately qualify for treatment.
Treatment Monitoring and Life Cycle Management
Experts engaged for this review noted that effective management of patients who initiate treatment with DMTs such as GLP-1 RAs or THR-beta agonists may benefit from a structured life cycle approach. This approach could support safety, tolerability, and sustained treatment effectiveness.
While monitoring protocols are still evolving, international expert consensus and updated practice guidance provide early direction for clinical practice.167,180,193 A structured life cycle typically includes early follow-up (within the first 3 months) to assess treatment adherence and tolerability; an effectiveness assessment at 6 to 12 months using NITs and laboratory test markers; and ongoing periodic monitoring according to disease severity and comorbidities, followed by continuation or discontinuation based on response, safety, and patient preference.167,180,193 Clinical responses that may result in discontinuation of treatment include improvement in liver fibrosis, normalization or reductions in liver enzymes and other cardiometabolic markers, or weight loss and metabolic improvement.
A brief overview of the life cycle is visualized in Figure 8 and additional details on life cycle monitoring steps are outlined in Appendix 2.
Figure 8: Treatment Monitoring and Life Cycle Management for MASH DMTs
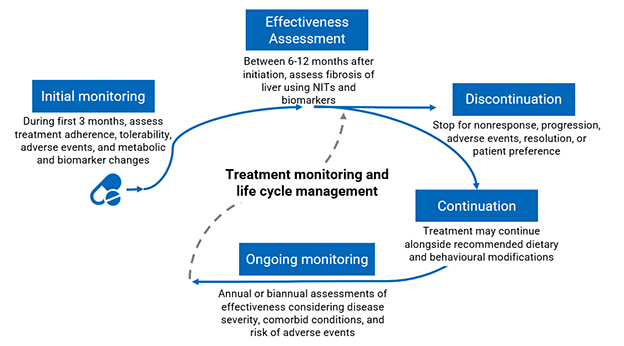
NIT = noninvasive test.
Sources: Bansal et al.193 and Chen et al.180
System enablers to support monitoring may include remote follow-up,194,195 integrated clinical decision support, risk-adapted monitoring, shared care models involving nurses and pharmacists,196,197 and multidisciplinary approaches encompassing both liver and cardiometabolic care.198-201 Sustained access to laboratory testing and imaging is essential for repeat assessments, but capacity may be limited — particularly in Indigenous, rural, remote, and northern communities.95,167,180,193,202-205 Appendix 2 provides additional details on multidisciplinary monitoring approaches, coordinated access to testing, and support for treatment adherence.
Coordinating Care Pathways
Early identification and management of MASH may help prevent or slow disease progression, avoid costly complications (e.g., cirrhosis, decompensated cirrhosis, liver cancer, transplant), and improve quality of life. Canadian14,107,108 and international181,206 clinical practice guidance emphasize the central role of primary care in early detection and the need for coordinated care.
However, there is no standardized MASH care pathway in Canada and no clear standard regarding which health care providers or specialists should coordinate care.207 As a result, patients often consult multiple providers before receiving a diagnosis.24 According to clinical experts consulted for this review, these unclear referral responsibilities and fragmented care processes contribute to delays in identification and treatment.
Multidisciplinary Team Roles
Advanced disease is typically managed by hepatologists; however, growing evidence supports the adoption of multidisciplinary and nurse-led collaborative models across all stages of care.95,202 Without such coordination, patients may remain undiagnosed until advanced stages of disease, leading to higher system costs as well as higher rates of morbidity and mortality.208
Experts consulted for this review suggested that effective management of MASH may be achieved through collaboration models that include multiple providers:
primary care (physicians and nurse practitioners for early detection and ongoing management)
specialists (hepatologists, endocrinologists, gastroenterologists, and transplant teams for advanced disease)
allied health care providers (dietitians, diabetes educators, mental health professionals, and obesity or weight management specialists)
laboratory medicine and imaging specialists (for disease staging and monitoring)
social workers, care coordinators, and system navigators (to address social determinants of health and connect patients to resources)
pharmacists (for medication management and adherence).
System-Level Challenges for Integrating Care
Some system-level challenges may limit integrated care for MASH in Canada, particularly in anticipation of potential DMTs, including limited access to PCPs, specialist physicians, and coordinated care models. Additional considerations for coordinated care include integrated pathways and jurisdictional capacity.
Integrated Pathways
Currently, there are limited or no standardized referral pathways or secure digital information sharing platforms, which may limit collaboration, delay early intervention, and create workflow challenges, especially if demand for services increases.95,209-211 According to a gastroenterologist consulted for this review, fragmentation of the health care delivery system and unclear referral responsibilities can hinder timely care, particularly when PCPs require additional knowledge or guidance in managing metabolic liver disease. Indigenous individuals living with MASH who contributed insights to this report recommended that liver assessments be integrated into existing chronic disease management (e.g., diabetes care) to support earlier detection and reduce burdens experienced by patients.
Jurisdictional Capacity
According to a pathologist consulted for this review, in smaller provinces, such as those in Atlantic Canada, limited hepatology capacity and reliance on out-of-province pathology services can delay diagnosis and disrupt care coordination. Rural areas may have limited diagnostic infrastructure as well as licensure and recruitment challenges, which have been shown to result in hepatology consultation wait times of up to a year — often longer than those experienced by people living with MASH in urban areas.83,212 For more detailed information on capacity and staffing resources, use the dashboard to access detailed information: select the Liver Clinics and Diagnostic Units for Liver Fibrosis tab for more information on the distribution of diagnostic tools in jurisdictions in Canada and the Number of Physicians tab for information on the distribution of physicians across Canada.
Clear responsibilities and standardized MASH care pathways — supported by interoperable data systems, coordinated referral structures, multidisciplinary models, and culturally safe care approaches — could improve equity, efficiency, and outcomes across the MASH care continuum. Additional detailed findings on equity considerations, referral processes, and system navigation challenges are provided in Appendix 2.
Technologies for Integrated MASH Care
A range of technologies could support efficient, coordinated care with attention paid to building on existing infrastructure and ensuring equitable access across diverse populations.
Insights from a DocuStory film co-created with First Nations and Métis Knowledge Keepers, community advocates, and Elders highlighted the importance of understanding liver health within community and cultural contexts, reinforcing that collective well-being depends on both system and relational balance.213 This emphasis on balance can guide how care is designed and how technologies are selected for integrated MASH care.
System-Level Technologies
Health care organizations and authorities are increasingly adopting digital records and supporting mobile health and telehealth programs for more efficient care delivery in Canada.214,215 As individuals with MASH often consult multiple health care providers for metabolic, hepatic, and cardiovascular care, there may be value in coordinated care and interoperable systems.
There is an opportunity to strengthen coordination by building digital infrastructure with interoperable records, which could improve timely access, enable effective data sharing, and support patient-centred service delivery.216,217 Such infrastructure could also facilitate rapid, consent-based information access across communities, institutions, and jurisdictions218 to reduce redundancy, strengthen integration, and thereby help ensure that care is both efficient and responsive to patient needs.
Some technologies and strategies may offer opportunities to enhance system capacity and improve coordination of care, including:
decentralized blockchain-based systems, which provide shared, tamperproof records managed collectively rather than by a single authority (these are being explored in the modernization of health systems in Canada, particularly for consent management, data security, and audit trails; their adoption remains exploratory and would require governance frameworks, technical standards, and phased pilot testing)219,220
mobile health clinics (these are used in Australia and the UK for liver disease screening and staging and could support MASH point-of-care assessment and management in Canada;221 mobile programs in Canada currently offer services such as screening and vaccinations, but liver-specific care remains limited)221-223
telehealth (or telemedicine) to support MASH care through live video consultation, storage and forwarding of messages, and remote monitoring for both patient–provider and provider–provider communication (while used in Canada, broader adoption requires interoperable electronic records, interjurisdictional licensing, and strategies to address privacy and security risks associated with digitized health records)224-227
immersive training technologies (virtual reality simulations can enhance practitioners’ training through hands-on experience performing technical procedures such as percutaneous liver biopsy;228 these technologies could improve access to standardized education across the system).
Emerging MASH-Specific Technologies
Building on system-level infrastructure, targeted tools for MASH may improve access to and efficiency of diagnosis, staging, and patient-centred management.229
Emerging technologies to consider for enhancing system capacity and MASH care include the following options.
Artificial Intelligence and Machine Learning Models
Artificial intelligence (AI) and machine learning models are increasingly being applied to imaging modalities (e.g., ultrasound, MRI) for detecting, quantifying, and staging steatosis, fibrosis, and related changes.230-232 While these tools are not currently integrated in routine clinical practice, they have the potential to improve diagnostic accuracy and efficiency.
However, AI tools trained using homogenous datasets that underrepresent diverse populations risk introducing bias.233-235 Fair implementation requires diverse data, bias auditing, strong governance and oversight,236 secure data management,237 and coordinated infrastructure and implementation readiness.237-239 Transparent use of AI may support, not replace, clinical interactions to build trust and meaningful care provision.240
Digital Pathology and Spatial Omics
Digital pathology and spatial omics allow detailed visualization of liver inflammation and fibrosis patterns in MASH. Digital pathology uses high-resolution scans of liver biopsy slides, while spatial omics maps how genes and proteins are expressed within specific areas of the tissue. Readily available digitized images may improve access, reduce turnaround times, and decrease costs.
Emerging AI-based tools include:
PathAI’s AIM-MASH, which uses deep learning to automatically score biopsy features like ballooning and fibrosis
HistoIndex’s qFibrosis, which quantifies tissue architecture without traditional chemical stains.241-243
These tools may support novel biomarker discovery and improved diagnostic precision but are still in development and may require advanced equipment and standardized methods.244,245
Multiomics and Biomarker Approaches
Multiomics and biomarker approaches (i.e., genomics, transcriptomics, proteomics, and metabolomics) provide high-throughput profiles of disease mechanisms, offer noninvasive biomarkers for diagnosis and staging, and may identify novel therapeutic targets in MASH.246-248 Successful clinical translation will require validation in diverse populations, robust computational frameworks, and workflow integrated adoption.249
Decision Support Tools
Decision support tools and automatic risk flagging embedded in electronic medical record decision support tools can automatically flag patients at high risk, prompt screening (e.g., FIB-4 score calculations), and support clinician decision-making.250-252 These tools can reduce gaps in care but depend on communication between data systems, clinician workflow integration, and equitable access.253
Endoscopic Biopsies
Endoscopic biopsies can combine multiple diagnostic procedures into a single session, reducing patient burden and improving efficiency. Ultrasound-guided endoscopic liver biopsies are conducted in some places in Canada.254 However, tissue samples collected using ultrasound-guided endoscopic biopsies are often smaller or fragmented, which can make it harder to accurately assess fibrosis stage or may result in diagnosing milder stages of fibrosis when the disease is, in fact, advanced.255,256
Limitations
This report aims to provide a high-level overview of health system readiness and related considerations for the potential introduction of emerging DMTs in Canada. It does not assess the clinical effectiveness of these treatments. As of the timing of the publication of this report, 1 pharmacologic therapy for MASH has received conditional regulatory approval in Canada, a GLP-1 receptor agonist. No other treatments, including THR‑beta agonists, are currently approved or under regulatory or reimbursement review in Canada. Additional DMTs in earlier stages of development, which may involve distinct considerations, are outside the scope of this report.
This report is also limited to information publicly available online and accessible through database or manual literature searches. Given the complex nature of health care systems in Canada and of MASH care, it is possible that not all jurisdictional perspectives were captured through our expert consultations. Some of the challenges and considerations discussed in this report may only apply to certain provinces or territories, or their effects may differ in magnitude across provinces and territories. Access to provincial and territorial health systems data could provide important information around the demographic profile and clinical profiles of patients with MASH. This information, in conjunction with knowledge about the current care pathways, could be used to project MASH demographic characteristics and plan for care optimization. Similarly, not all perspectives were captured by the Indigenous-led and CDA-AMC–led engagement activities. The lack of certain perspectives (including racialized communities, individuals from 2SLGBTQ+ communities, and individuals with low incomes) may limit the breadth of considerations, especially related to equity and experiences with existing MASH care pathways. Limitations of the rapid review are detailed in Appendix 4.
Future Considerations and System Readiness for MASH Treatments
The conditional regulatory approval of the first DMT in Canada signals an opportunity to assess how MASH is identified and managed, including potential pressure points and opportunities for system change. Early identification of MASH remains critical.
When diagnosis and treatment are delayed, disease progression can lead to substantially higher burden for both individuals and the health system.257 Globally, more than 10% of individuals with cirrhosis are estimated to experience decompensated cirrhosis each year.258 Decompensated cirrhosis may cause complications such as ascites (fluid build-up in the abdomen), variceal bleeding (bleeding from veins in the esophagus), and hepatic encephalopathy (change in mental state), which are associated with high health care use and patient burden.259
Emerging DMTs target specific disease stages (typically F2 to F3) and therefore are intended to reduce disease progression and downstream system effects by intervening earlier in the disease course. Lifestyle modifications may also effectively slow or prevent MASH progression. Realizing these benefits, however, depends on timely, reliable, and coordinated pathways to screen for, diagnose, and treat MASH.
Indigenous participants identified specific barriers that require attention — such as travel burdens, limited availability of culturally safe care, and experiences of misattributed symptoms. Improving access to Indigenous care navigators may help strengthen trust and support more equitable navigation of MASH diagnostic and treatment pathways.
System Priorities to Strengthen the MASH Care Pathway
This assessment highlights that changes within the patient care pathway may strengthen readiness for the potential introduction of DMTs into clinical care. To support existing care while avoiding widening inequities, health systems may consider the following efforts.
Improve Early Detection and Diagnostic Infrastructure
Launch education and awareness initiatives with destigmatized MASH information.
Integrate screening into mobile or telehealth programs and chronic disease programs for diabetes, obesity, and cardiovascular care.
Build capacity for noninvasive diagnostic tests, including blood tests and elastography.
Enhance provider training for new biomarkers and NITs.
Develop diagnostic pathways for early disease detection.
Expand screening and staging capacity to support diagnostic efficiency.
Ensure access to standardized blood tests for early fibrosis detection.
Support Care Coordination and Multidisciplinary Models
Integrate multidisciplinary care providers (nurses, pharmacists, allied health care providers) with standardized approaches to reduce fragmentation.
Workforce planning to ensure hepatologist, radiologist, and pathologist capacity can meet demand.
Provide tailored treatment plans; culturally safe and linguistically appropriate education; and peer and community-based navigation programs.
Develop multidisciplinary models with interoperable data systems and clear protocols.
Embed equity considerations across diagnostic pathways and strengthen navigation and shared care models to improve continuity of care for patients from populations disproportionately affected by fragmented services and geographic barriers.
Build Capacity for Monitoring, Integrated Digital Health, and Emerging DMTs
Build digital infrastructure with governance models for remote diagnostic and monitoring capabilities.
Explore digital adherence tools to support shared decision-making, lifestyle changes, and treatment consistency.
Standardize and align processes for equitable access to diagnostic tests and therapies.
Expand culturally safe care approaches with options that consider underserved populations, including Indigenous Peoples, racialized populations, immigrants and newcomers to Canada, and people living in rural, remote, northern, and low-income settings.
Explore future technologies, including AI-driven tools, to improve diagnostic consistency and access.
This report highlights that specific groups of people in Canada may face challenges in accessing clinicians with the knowledge to identify and diagnose MASH. The technologies and services needed to diagnose the presence and severity of the disease may be difficult to access. Some populations — including Indigenous Peoples; people living in rural, remote, and northern areas; people in low-income settings; racialized populations; and immigrants — often face obstacles when attempting to access health care systems, which can undermine efforts to achieve health equity.
Alignment in disease identification, severity assessment, and treatment protocols, along with patient and caregiver engagement, could support a patient-centred approach to the management of MASH. Such changes would require consideration of human resources, clinical training, and infrastructure needs to support sustainable, equitable care delivery. Strategies may differ among provincial and territorial health care systems, given existing local structures and population needs.
References
1.Leow WQ, Chan AW, Mendoza PGL, Lo R, Yap K, Kim H. Non-alcoholic fatty liver disease: the pathologist's perspective. Clin Mol Hepatol. 2023;29(Suppl):S302-S318. doi:10.3350/cmh.2022.0329 PubMed
2.European Association for the Study of the Liver, European Association for the Study of Diabetes, European Association for the Study of Obesity. EASL-EASD-EASO Clinical Practice Guidelines on the management of metabolic dysfunction-associated steatotic liver disease (MASLD). J Hepatol. 2024;81(3):492-542. doi:10.1016/j.jhep.2024.04.031 PubMed
3.Rinella ME, Neuschwander-Tetri BA, Siddiqui MS, et al. AASLD Practice Guidance on the clinical assessment and management of nonalcoholic fatty liver disease. Hepatology. 2023;77(5):1797-1835. doi:10.1097/hep.0000000000000323 PubMed
4.Rinella ME, Lazarus JV, Ratziu V, et al. A multisociety Delphi consensus statement on new fatty liver disease nomenclature. J Hepatol. 2023;79(6):1542-1556. doi:10.1016/j.jhep.2023.06.003 PubMed
5.Sato-Espinoza K, Chotiprasidhi P, Huaman MR, Díaz-Ferrer J. Update in lean metabolic dysfunction-associated steatotic liver disease. World J Hepatol. 2024;16(3):452-464. doi:10.4254/wjh.v16.i3.452 PubMed
6.Albhaisi S, Chowdhury A, Sanyal AJ. Non-alcoholic fatty liver disease in lean individuals. JHEP Rep. 2019;1(4):329-341. doi:10.1016/j.jhepr.2019.08.002 PubMed
7.Njei B, Ameyaw P, Al-Ajlouni Y, Njei LP, Boateng S. Diagnosis and Management of Lean Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD): A Systematic Review. Cureus. 2024;16(10):e71451. doi:10.7759/cureus.71451 PubMed
8.Vilar-Gomez E, Calzadilla-Bertot L, Wai-Sun Wong V, et al. Fibrosis Severity as a Determinant of Cause-Specific Mortality in Patients With Advanced Nonalcoholic Fatty Liver Disease: A Multi-National Cohort Study. Gastroenterology. 2018;155(2):443-457.e17. doi:10.1053/j.gastro.2018.04.034 PubMed
9.Angulo P, Kleiner DE, Dam-Larsen S, et al. Liver Fibrosis, but No Other Histologic Features, Is Associated With Long-term Outcomes of Patients With Nonalcoholic Fatty Liver Disease. Gastroenterology. 2015;149(2):389-397.e10. doi:10.1053/j.gastro.2015.04.043 PubMed
10.Ng CH, Lim WH, Hui Lim GE, et al. Mortality Outcomes by Fibrosis Stage in Nonalcoholic Fatty Liver Disease: A Systematic Review and Meta-analysis. Clin Gastroenterol Hepatol. 2023;21(4):931-939.e5. doi:10.1016/j.cgh.2022.04.014 PubMed
11.Chan WK, Chuah KH, Rajaram RB, Lim LL, Ratnasingam J, Vethakkan SR. Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD): A State-of-the-Art Review. J Obes Metab Syndr. 2023;32(3):197-213. doi:10.7570/jomes23052 PubMed
12.Younossi ZM, Golabi P, Paik JM, Henry A, Van Dongen C, Henry L. The global epidemiology of nonalcoholic fatty liver disease (NAFLD) and nonalcoholic steatohepatitis (NASH): a systematic review. Hepatology. 2023;77(4):1335-1347. doi:10.1097/hep.0000000000000004 PubMed
13.Paklar N, Mijic M, Filipec-Kanizaj T. The Outcomes of Liver Transplantation in Severe Metabolic Dysfunction-Associated Steatotic Liver Disease Patients. Biomedicines. 2023;11(11):3096. doi:10.3390/biomedicines11113096 PubMed
14.Kim J, Bajaj HS, Ramji A, Bemeur C, Sebastiani G. Diabetes and Metabolic Dysfunction-associated Steatotic Liver Disease in Adults: A Clinical Practice Guideline. Can J Diabetes. 2025;49(4):222-236. doi:10.1016/j.jcjd.2025.04.003 PubMed
15.Swain MG, Ramji A, Patel K, et al. Burden of nonalcoholic fatty liver disease in Canada, 2019-2030: a modelling study. CMAJ Open. 2020;8(2):E429-E436. doi:10.9778/cmajo.20190212 PubMed
16.Tantu MT, Farhana FZ, Haque F, et al. Pathophysiology, noninvasive diagnostics and emerging personalized treatments for metabolic associated liver diseases. npj Gut Liver. 2025;2:18. doi:10.1038/s44355-025-00030-2
17.Younossi ZM, Razavi H, Sherman M, et al. Addressing the High and Rising Global Burden of Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD) and Metabolic Dysfunction-Associated Steatohepatitis (MASH): From the Growing Prevalence to Payors' Perspective. Aliment Pharmacol Ther. 2025;61(9):1467-1478. doi:10.1111/apt.70020 PubMed
18.Yeh ML, Huang JF, Dai CY, Huang CF, Yu ML, Chuang WL. Metabolic dysfunction-associated steatotic liver disease and diabetes: the cross-talk between hepatologist and diabetologist. Expert Rev Gastroenterol Hepatol. 2024;18(8):431-439. doi:10.1080/17474124.2024.2388790 PubMed
19.Ma J, Ma Y, Wan X, et al. Metabolic and genetic mechanisms of metabolic dysfunction-associated steatotic liver disease: an integrative perspective from molecular pathways to clinical challenges. Front Endocrinol (Lausanne). 2025;16:1639064. doi:10.3389/fendo.2025.1639064 PubMed
20.Government of Canada. Diabetes in Canada: An interactive report on key statistics. Accessed April 9, 2026. https://health-infobase.canada.ca/diabetes/
21.Cusi K, Abdelmalek MF, Apovian CM, et al. Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD) in People With Diabetes: The Need for Screening and Early Intervention. A Consensus Report of the American Diabetes Association. Diabetes Care. 2025;48(7):1057-1082. doi:10.2337/dci24-0094 PubMed
22.Koufakis T, Popovic DS, Papadopoulos C, Giouleme O, Doumas M. Effectively addressing cardiovascular risk in people with metabolic-dysfunction associated fatty liver disease: not yet ready for prime time! Expert Opin Pharmacother. 2024;25(2):123-126. doi:10.1080/14656566.2024.2312239 PubMed
23.Quek J, Chan KE, Wong ZY, et al. Global prevalence of non-alcoholic fatty liver disease and non-alcoholic steatohepatitis in the overweight and obese population: a systematic review and meta-analysis. Lancet Gastroenterol Hepatol. 2023;8(1):20-30. doi:10.1016/s2468-1253(22)00317-x PubMed
24.Rodriguez-Araujo G. Nonalcoholic fatty liver disease: implications for endocrinologists and cardiologists. Cardiovasc Endocrinol Metab. 2020;9(3):96-100. doi:10.1097/xce.0000000000000197 PubMed
25.En Li Cho E, Ang CZ, Quek J, et al. Global prevalence of non-alcoholic fatty liver disease in type 2 diabetes mellitus: an updated systematic review and meta-analysis. Gut. 2023;72(11):2138-2148. doi:10.1136/gutjnl-2023-330110 PubMed
26.Medina-Julio D, Ramírez-Mejía MM, Cordova-Gallardo J, Peniche-Luna E, Cantú-Brito C, Mendez-Sanchez N. From Liver to Brain: How MAFLD/MASLD Impacts Cognitive Function. Med Sci Monit. 2024;30:e943417. doi:10.12659/msm.943417 PubMed
27.Fu CE, Teng M, Tung D, et al. Sex and Race-Ethnic Disparities in Metabolic Dysfunction-Associated Steatotic Liver Disease: An Analysis of 40,166 Individuals. Dig Dis Sci. 2024;69(9):3195-3205. doi:10.1007/s10620-024-08540-4 PubMed
28.Tsuchiyose E, Salimi A, Magee C, Khalili M. Culturally tailored steatotic liver disease management: Latino and Asian community partner perspectives and recommendations. Hepatol Commun. 2025;9(7):e0749. doi:10.1097/hc9.0000000000000749 PubMed
29.Kehm RD, Vilfranc CL, McDonald JA, Wu HC. County-Level Food Insecurity and Hepatocellular Carcinoma Risk: A Cross-Sectional Analysis. Int J Environ Res Public Health. 2025;22(1):120. doi:10.3390/ijerph22010120 PubMed
30.Zelber-Sagi S, Carrieri P, Pericas JM, Ivancovsky-Wajcman D, Younossi ZM, Lazarus JV. Food inequity and insecurity and MASLD: burden, challenges, and interventions. Nat Rev Gastroenterol Hepatol. 2024;21(10):668-686. doi:10.1038/s41575-024-00959-4 PubMed
31.Paik JM, Duong S, Zelber-Sagi S, Lazarus JV, Henry L, Younossi ZM. Food Insecurity, Low Household Income, and Low Education Level Increase the Risk of Having Metabolic Dysfunction-Associated Fatty Liver Disease Among Adolescents in the United States. Am J Gastroenterol. 2024;119(6):1089-1101. doi:10.14309/ajg.0000000000002749 PubMed
32.Golovaty I, Tien PC, Price JC, Sheira L, Seligman H, Weiser SD. Food Insecurity May Be an Independent Risk Factor Associated with Nonalcoholic Fatty Liver Disease among Low-Income Adults in the United States. J Nutr. 2020;150(1):91-98. doi:10.1093/jn/nxz212 PubMed
33.Tamargo JA, Sherman KE, Campa A, et al. Food insecurity is associated with magnetic resonance-determined nonalcoholic fatty liver and liver fibrosis in low-income, middle-aged adults with and without HIV. Am J Clin Nutr. 2021;113(3):593-601. doi:10.1093/ajcn/nqaa362 PubMed
34.Abu-Rumaileh M, Dhoop S, Pace J, et al. Social Determinants of Health Associated With Metabolic Dysfunction-Associated Steatotic Liver Disease Prevalence and Severity: A Systematic Review and Meta-Analysis. Am J Gastroenterol. 2025;120(12):2810-2830. doi:10.14309/ajg.0000000000003421 PubMed
35.Bruce SG, Riediger ND, Lix LM. Chronic disease and chronic disease risk factors among First Nations, Inuit and Métis populations of northern Canada. Chronic Dis Inj Can. 2014;34(4):210-217. doi:10.24095/hpcdp.34.4.04 PubMed
36.Memedovich KA, Shaheen AA, Swain MG, Clement FM. Projected Healthcare System Cost Burden of Metabolic Dysfunction-Associated Steatotic Liver Disease in Canada. Gastro Hep Adv. 2024;3(7):965-972. doi:10.1016/j.gastha.2024.05.010 PubMed
37.Harrison SA, Bedossa P, Guy CD, et al. A Phase 3, Randomized, Controlled Trial of Resmetirom in NASH with Liver Fibrosis. N Engl J Med. 2024;390(6):497-509. doi:10.1056/NEJMoa2309000 PubMed
38.Sanyal AJ, Newsome PN, Kliers I, et al. Phase 3 Trial of Semaglutide in Metabolic Dysfunction-Associated Steatohepatitis. N Engl J Med. 2025;392(21):2089-2099. doi:10.1056/NEJMoa2413258 PubMed
39.Novo Nordisk A/S. Wegovy® (semaglutide injection) Receives Conditional Marketing Authorization from Health Canada as the First and Only Treatment for Adults with Non-Cirrhotic MASH, a Serious Liver Disease Novo Nordisk A/S; 2025. Accessed January 7, 2026. https://www.novonordisk.ca/content/dam/nncorp/ca/en/press-releases/2025/wegovy-mash-authorization-press-release-en-dec-15.pdf
40.Smith PLT. Decolonizing Methodologies: Research and Indigenous Peoples. Zed Books; 2021.
41.Tassell-Matamua N. Indigenous knowledges. What they are and why they matter. Explore (NY). 2025;21(3):103144. doi:10.1016/j.explore.2025.103144 PubMed
42.Melro CM, MacDonald K, Cowan T, et al. Integrating Indigenous Ways of Knowing Into Learning Health Systems: Moving From Learning Health Systems to Learning Communities. The Canadian Journal of Psychiatry. 2026;71(4):257-262. doi:10.1177/07067437251380734 PubMed
43.First Nations Information Governance Centre. Welcome to The Fundamentals of OCAP®. Accessed September 10, 2025. https://fnigc.ca/ocap-training/take-the-course/
44.National Aboriginal Health Organization. Principles of Ethical Métis Research. NAHO Métis Centre; 2011. Accessed September 10, 2025. https://achh.ca/wp-content/uploads/2018/07/Guide_Ethics_NAHOMetisCentre.pdf
45.Nunavut Impact Review Board. Inuit Qaujimajatuqangit. Accessed September 10, 2025. https://www.nirb.ca/inuit-qaujimajatuqangit
46.Staniszewska S, Brett J, Simera I, et al. GRIPP2 reporting checklists: tools to improve reporting of patient and public involvement in research. BMJ. 2017;358:j3453. doi:10.1136/bmj.j3453 PubMed
47.Sebastiani G, Ramji A, Swain MG, Patel K. A Canadian survey on knowledge of non-alcoholic fatty liver disease among physicians. Can Liver J. 2021;4(2):82-92. doi:10.3138/canlivj-2020-0033 PubMed
48.Logie CH, Nyblade L. Recognizing and responding to stigma-related barriers in health care. Nature Reviews Disease Primers. 2024;10(1):70. doi:10.1038/s41572-024-00554-6 PubMed
49.Younossi ZM, Alqahtani SA, Alswat K, et al. Global survey of stigma among physicians and patients with nonalcoholic fatty liver disease. J Hepatol. 2024;80(3):419-430. doi:10.1016/j.jhep.2023.11.004 PubMed
50.Åström H, Takami Lageborn C, Hagstrom H. Psychosocial risks in metabolic dysfunction-associated steatotic liver disease. Expert Rev Gastroenterol Hepatol. 2025;19(3):273-290. doi:10.1080/17474124.2025.2468297 PubMed
51.Alqahtani SA, Alswat K, Mawardi M, et al. Stigma in steatotic liver disease: A survey of patients from Saudi Arabia. Saudi J Gastroenterol. 2024;30(5):335-341. doi:10.4103/sjg.sjg_122_24 PubMed
52.Carol M, Pérez-Guasch M, Solà E, et al. Stigmatization is common in patients with non-alcoholic fatty liver disease and correlates with quality of life. PLoS One. 2022;17(4):e0265153. doi:10.1371/journal.pone.0265153 PubMed
53.Nyblade L, Stockton MA, Giger K, et al. Stigma in health facilities: why it matters and how we can change it. BMC Med. 2019;17(1):25. doi:10.1186/s12916-019-1256-2 PubMed
54.Koutoukidis DA, Koshiaris C, Henry JA, et al. The effect of the magnitude of weight loss on non-alcoholic fatty liver disease: A systematic review and meta-analysis. Metabolism. 2021;115:154455. doi:10.1016/j.metabol.2020.154455 PubMed
55.Zelber-Sagi S, Moore JB. Practical Lifestyle Management of Nonalcoholic Fatty Liver Disease for Busy Clinicians. Diabetes Spectr. 2024;37(1):39-47. doi:10.2337/dsi23-0009 PubMed
56.Del Bo’ C, Perna S, Allehdan S, et al. Does the Mediterranean Diet Have Any Effect on Lipid Profile, Central Obesity and Liver Enzymes in Non-Alcoholic Fatty Liver Disease (NAFLD) Subjects? A Systematic Review and Meta-Analysis of Randomized Control Trials. Nutrients. 2023;15(10):2250. doi:10.3390/nu15102250 PubMed
57.Zhang S, Liu Z, Yang Q, et al. Impact of smoking cessation on non-alcoholic fatty liver disease prevalence: a systematic review and meta-analysis. BMJ Open. 2023;13(12):e074216. doi:10.1136/bmjopen-2023-074216 PubMed
58.Kim D, Vazquez-Montesino LM, Li AA, Cholankeril G, Ahmed A. Inadequate Physical Activity and Sedentary Behavior Are Independent Predictors of Nonalcoholic Fatty Liver Disease. Hepatology. 2020;72(5):1556-1568. doi:10.1002/hep.31158 PubMed
59.Sebastiani G, Cinque F. Navigating the Maze: A Mini-Guide for the Management and Therapy of Metabolic Dysfunction-associated Steatotic Liver Disease. Can Prim Care Today. 2024;2(2):34–40. doi:10.58931/cpct.2024.2232
60.Lazarus JV, Mark HE, Anstee QM, et al. Advancing the global public health agenda for NAFLD: a consensus statement. Nat Rev Gastroenterol Hepatol. 2022;19(1):60-78. doi:10.1038/s41575-021-00523-4 PubMed
61.Alemany-Pagès M, Moura-Ramos M, Araújo S, et al. Insights from qualitative research on NAFLD awareness with a cohort of T2DM patients: time to go public with insulin resistance? BMC Public Health. 2020;20(1):1142. doi:10.1186/s12889-020-09249-5 PubMed
62.Kanwal F, Shubrook JH, Younossi Z, et al. Preparing for the NASH Epidemic: A Call to Action. Gastroenterology. 2021;161(3):1030-1042.e8. doi:10.1053/j.gastro.2021.04.074 PubMed
63.Anstee QM, Hallsworth K, Lynch N, et al. Real-world management of non-alcoholic steatohepatitis differs from clinical practice guideline recommendations and across regions. JHEP Rep. 2021;4(1):100411. doi:10.1016/j.jhepr.2021.100411 PubMed
64.Burnside J, Djerboua M, Flemming J, et al. O004 Significant decline in liver fibrosis screening among people living with diabetes in Ontario: A population-based study. In: The Annual Canadian Liver Meeting 2025 of the Canadian Association for the Study of the Liver (CASL), the Canadian Network on Hepatitis C (CanHepC) and CanMASLD. Can Liver J. 2025;8(1):102-103. doi:10.3138/canlivj-8.1-abst
65.Chami N, Li Y, Weir S, Wright JG, Kantarevic J. Effect of Strict and Soft Policy Interventions on Laboratory Diagnostic Testing in Ontario, Canada: A Bayesian Structural Time Series Analysis. Health Policy. 2021;125(2):254-260. doi:10.1016/j.healthpol.2020.10.007 PubMed
66.Canadian Society of Clinical Chemists. Clinical Biochemistry Recommendations. Choosing Wisely Canada. 2025. Accessed September 23, 2025. https://choosingwiselycanada.org/recommendation/clinical-biochemistry/
67.Mohammed-Ali Z, Bhandarkar S, Tahir S, et al. Implementing effective test utilization via team-based evaluation and revision of a family medicine laboratory test requisition. BMJ Open Qual. 2021;10(1):e001219. doi:10.1136/bmjoq-2020-001219 PubMed
68.Strauss R, Cressman A, Cheung M, et al. Major reductions in unnecessary aspartate aminotransferase and blood urea nitrogen tests with a quality improvement initiative. BMJ Qual Saf. 2019;28(10):809. doi:10.1136/bmjqs-2018-008991 PubMed
69.Boughrassa F, Framarin A. Usage judicieux de 14 analyses biomédicales [Wise use of 14 biomedical tests]. INESSS; 2014. Accessed May 21, 2026. https://www.bibliotheque.assnat.qc.ca/DepotNumerique_v2/AffichageFichier.aspx?idf=141645
70.Alberta Medical Association. FIB-4: New test in Alberta to risk stratify patients of developing liver fibrosis. Alberta Medical Association. 2024. Accessed September 23, 2025. https://cd-secureweb.albertadoctors.org/albertadoctorsorg-a2s9c/pages/2de52671d3bbee11a88a000c29ee8689.html
71.Canadian Association of Pathologists. Fellowships. Accessed October 06, 2025. https://cap-acp.org/general/custom.asp?page=fellowships
72.Dalhousie University. Liver/Gastrointestinal Pathology Fellowship. Accessed October 06, 2025. https://medicine.dal.ca/departments/department-sites/pathology/education/liver-gastrointestinal-fellowship.html
73.Canada's Drug Agency. Health Technology Review: Canadian Medical Imaging Inventory 2022-2023: The Medical Imaging Team. Can J Health Technol. 2024;4(8):1-40. doi:10.51731/cjht.2024.953
74.Canadian Institute for Health Information. Better access to primary care key to improving health of Canadians. 2024. Accessed September 25, 2025. https://www.cihi.ca/en/taking-the-pulse-measuring-shared-priorities-for-canadian-health-care-2024/better-access-to-primary-care-key-to-improving-health-of-canadians
75.Canadian Institute for Health Information. Access to primary care: Many Canadians face challenges. 2024. Accessed October 22, 2025. https://www.cihi.ca/en/primary-and-virtual-care-access-emergency-department-visits-for-primary-care-conditions/access-to-primary-care-many-canadians-face-challenges
76.Kiran T, Daneshvarfard M, Wang R, et al. Public experiences and perspectives of primary care in Canada: results from a cross-sectional survey. CMAJ. 2024;196(19):e646-e656. doi:10.1503/cmaj.231372 PubMed
77.Canadian Institute for Health Information. Canadians are not getting appointments quickly when they need them. 2025. https://www.cihi.ca/en/taking-the-pulse-measuring-shared-priorities-for-canadian-health-care-2025/primary-health-care-2025/canadians-are-not-getting-appointments-quickly-when-they
78.Wilson CR, Rourke J, Oandasan IF, Bosco C. Progress made on access to rural healthcare in Canada. Canadian Journal of Rural Medicine. 2020;25(1):14-19. doi:10.4103/cjrm.Cjrm_84_19 PubMed
79.Mathews M, Ryan D, Deslauriers V, et al. Care-seeking experiences of unattached patients in the Canadian health care system: Qualitative study. Can Fam Physician. 2024;70(6):396-403. doi:10.46747/cfp.7006396 PubMed
80.Rush KL, Seaton CL, Burton L, Smith MA, Li EPH. The healthcare experiences of rural-living Canadians with and without a primary care provider: a qualitative analysis of open-ended cross-sectional survey responses. Prim Health Care Res Dev. 2025;26:e1. doi:10.1017/s1463423624000677 PubMed
81.Statistics Canada. Health care access and experiences among Indigenous people, 2024. Government of Canada; 2024. Accessed October 22, 2025. https://www150.statcan.gc.ca/n1/daily-quotidien/241104/dq241104a-eng.htm
82.Srugo SA, Ricci C, Leason J, Jiang Y, Luo W, Nelson C. Disparities in primary and emergency health care among “off-reserve” Indigenous females compared with non-Indigenous females aged 15-55 years in Canada. CMAJ. 2023;195(33):E1097-E1111. doi:10.1503/cmaj.221407 PubMed
83.Burnside J, Thomas T, Sebastiani G, Saeed S. Geographical disparities in gastroenterologists and transient elastography across Canada. Can Liver J. 2023;6(4):417-424. doi:10.3138/canlivj-2023-0010 PubMed
84.Canadian Institute for Health Information. Supply, Distribution and Migration of Physicians in Canada, 2024 - Data Tables. 2024. Accessed November 12, 2025. https://www.cihi.ca/sites/default/files/document/supply-distribution-migration-physicians-in-canada-2024-data-tables-en.xlsx
85.MacKay J. Listowel Liver screening clinics may expand. CKNX News. April 11, 2024. Accessed October 21, 2025. https://cknxnewstoday.ca/midwestern/news/2024/04/11/listowel-liver-screening-clinics-may-expand
86.Gastrointestinal Society. Early Detection of Liver Disease With FibroScan®. Gastrointestinal Society & Canadian Society of Intestinal Research; 2024. Accessed October 21, 2025. https://badgut.org/information-centre/product-reviews/fibroscan/
87.Castagneto-Gissey L, Bornstein SR, Mingrone G. Can liquid biopsies for MASH help increase the penetration of metabolic surgery? A narrative review. Metabolism - Clinical and Experimental. 2024;151:155721. doi:10.1016/j.metabol.2023.155721 PubMed
88.Woodard JS, Velji-Ibrahim J, Abrams GA. Significant Within-Individual Variability in VCTE Liver Stiffness Measurements at Two Intercostal Spaces in Subjects with MASLD: Implications for Evaluating Improvement in Liver Fibrosis After Weight-Loss or Liver-Directed Therapy. Diseases. 2024;12(11):288. doi:10.3390/diseases12110288 PubMed
89.Li G, Zhang X, Lin H, Liang LY, Wong GL, Wong VW. Non-invasive tests of non-alcoholic fatty liver disease. Chin Med J (Engl). 2022;135(5):532-546. doi:10.1097/cm9.0000000000002027 PubMed
90.Ozercan AM, Ozkan H. Vibration-controlled Transient Elastography in NAFLD: Review Study. Euroasian J Hepatogastroenterol. 2022;12(Suppl 1):S41-S45. doi:10.5005/jp-journals-10018-1365 PubMed
91.Zhang S, Mak LY, Yuen MF, Seto WK. Screening strategy for non-alcoholic fatty liver disease. Clin Mol Hepatol. 2023;29(Suppl):S103-S122. doi:10.3350/cmh.2022.0336 PubMed
92.Davidson M, Kielar A, Tonseth RP, Seland K, Harvie S, Hanneman K. The Landscape of Rural and Remote Radiology in Canada: Opportunities and Challenges. Can Assoc Radiol J. 2024;75(2):304-312. doi:10.1177/08465371231197953 PubMed
93.Canada's Drug Agency. Health Technology Review: Planning for the Introduction of New CT Services in Rural and Remote Communities in Canada. Can J Health Technol. 2025;5(2):1-13. doi:10.51731/cjht.2025.1090
94.Kim J, Raggi P, Carreau AM, Wharton S, Cheng AYY, Swain MG. A review of multidisciplinary care in metabolic dysfunction-associated steatohepatitis and cardiometabolic disease, with a focus on Canada. Diabetes Obes Metab. 2025;27:6831-6846. doi:10.1111/dom.70117 PubMed
95.Stine JG, Bradley D, McCall-Hosenfeld J, et al. Multidisciplinary clinic model enhances liver and metabolic health outcomes in adults with MASH. Hepatol Commun. 2025;9(2):e0649. doi:10.1097/hc9.0000000000000649 PubMed
96.Brown BB, Patel C, McInnes E, Mays N, Young J, Haines M. The effectiveness of clinical networks in improving quality of care and patient outcomes: a systematic review of quantitative and qualitative studies. BMC Health Serv Res. 2016;16(1):360. doi:10.1186/s12913-016-1615-z PubMed
97.Sedgewick JR, Ali A, Badea A, Carr T, Groot G. Service providers’ perceptions of support needs for Indigenous cancer patients in Saskatchewan: a needs assessment. BMC Health Serv Res. 2021;21(1):848. doi:10.1186/s12913-021-06821-6 PubMed
98.Young S, Tariq R, Provenza J, et al. Prevalence and Profile of Nonalcoholic Fatty Liver Disease in Lean Adults: Systematic Review and Meta-Analysis. Hepatol Commun. 2020;4(7):953-972. doi:10.1002/hep4.1519 PubMed
99.Wang AY, Dhaliwal J, Mouzaki M. Lean non-alcoholic fatty liver disease. Clin Nutr. 2019;38(3):975-981. doi:10.1016/j.clnu.2018.08.008 PubMed
100.Crenshaw K. Mapping the Margins: Intersectionality, Identity Politics, and Violence against Women of Color. Stanford Law Rev. 1991;43(6):1241-1299. doi:10.2307/1229039
101.Flavin B. Nonalcoholic steatohepatitis/metabolic dysfunction-associated steatohepatitis emerging market: Preparing managed care for early intervention, equitable access, and integrating the patient perspective. J Manag Care Spec Pharm. 2024;30(9-a Suppl):S1-S13. doi:10.18553/jmcp.2024.30.9-a.s1
102.Tincopa MA, Wong J, Fetters M, Lok AS. Patient disease knowledge, attitudes and behaviours related to non-alcoholic fatty liver disease: a qualitative study. BMJ Open Gastroenterol. 2021;8(1):e000634. doi:10.1136/bmjgast-2021-000634 PubMed
103.Grønkjær LL, Lauridsen MM. Quality of life and unmet needs in patients with chronic liver disease: A mixed-method systematic review. JHEP Rep. 2021;3(6):100370. doi:10.1016/j.jhepr.2021.100370 PubMed
104.Wilson MP, Tang A, Low G, et al. Part 1: CAR Metabolic Dysfunction-Associated Steatotic Liver Disease Working Group Guidance Statements for Detecting and Grading Hepatic Steatosis Using Ultrasound, CT, or MRI. Can Assoc Radiol J. 2025;77(1):58-72. doi:10.1177/08465371251357444 PubMed
105.Wilson MP, Low G, Shaheen AA, et al. Part 2: CAR Metabolic Dysfunction-Associated Steatotic Liver Disease Working Group Recommendations for Risk Stratifying Patients With MASLD. Can Assoc Radiol J. 2025;77(1):73-84. doi:10.1177/08465371251357447 PubMed
106.Wilson MP, Low G, Medellin A, et al. Part 3: CAR Dysfunction-Associated Steatotic Liver Disease Working Group Recommendations for Ultrasound Shear Wave Elastography and MR Elastography Program Implementation, Funding, and Quality Assurance. Can Assoc Radiol J. 2025;77(1):85-97. doi:10.1177/08465371251357446 PubMed
107.Alberta Health Services. Non-Alcoholic Fatty Liver Disease (NAFLD) Primary Care Pathway. 2021. Accessed September 10, 2025. https://www.albertahealthservices.ca/assets/about/scn/ahs-scn-dh-pathway-nafld.pdf
108.Shared Health Manitoba. Management of Metabolic Dysfunction Associated Steatotic Liver Disease (MASLD). Shared Health Manitoba; 2024. Accessed October 09, 2025. https://healthproviders.sharedhealthmb.ca/files/provincial-clinical-guideline-masld.pdf
109.Kingston Health Sciences Centre. Primary Care Management Pathway: Metabolic-Associated Steatotic Liver Disease. 2025. Accessed September 22, 2025. https://kingstonhsc.ca/media/15943/download?attachment
110.Frączek J, Sowa A, Agopsowicz P, Migacz M, Dylińska-Kala K, Holecki M. Non-Invasive Tests as a Replacement for Liver Biopsy in the Assessment of MASLD. Medicina (Kaunas). 2025;61(4):736. doi:10.3390/medicina61040736 PubMed
111.Thomaides-Brears HB, Alkhouri N, Allende D, et al. Incidence of Complications from Percutaneous Biopsy in Chronic Liver Disease: A Systematic Review and Meta-Analysis. Dig Dis Sci. 2022;67(7):3366-3394. doi:10.1007/s10620-021-07089-w PubMed
112.Myers RP, Fong A, Shaheen AA. Utilization rates, complications and costs of percutaneous liver biopsy: a population-based study including 4275 biopsies. Liver Int. 2008;28(5):705-712. doi:10.1111/j.1478-3231.2008.01691.x PubMed
113.Aljawad M, Yoshida EM, Uhanova J, Marotta P, Chandok N. Percutaneous liver biopsy practice patterns among Canadian hepatologists. Can J Gastroenterol. 2013;27(11):e31-e34. doi:10.1155/2013/429834 PubMed
114.Hudson D, Afzaal T, Bualbanat H, et al. Modernizing metabolic dysfunction-associated steatotic liver disease diagnostics: the progressive shift from liver biopsy to noninvasive techniques. Ther Adv Gastroenterol. 2024;17:17562848241276334. doi:10.1177/17562848241276334 PubMed
115.Siddiqui MS, Yamada G, Vuppalanchi R, et al. Diagnostic Accuracy of Noninvasive Fibrosis Models to Detect Change in Fibrosis Stage. Clin Gastroenterol Hepatol. 2019;17(9):1877-1885.e5. doi:10.1016/j.cgh.2018.12.031 PubMed
116.Kim BK, Kim DY, Park JY, et al. Validation of FIB-4 and comparison with other simple noninvasive indices for predicting liver fibrosis and cirrhosis in hepatitis B virus-infected patients. Liver Int. 2010;30(4):546-553. doi:10.1111/j.1478-3231.2009.02192.x PubMed
117.Nouso K, Kawanaka M, Fujii H, et al. Validation study of age-independent fibrosis score (Fibrosis-3 index) in patients with metabolic dysfunction-associated steatotic liver disease. Hepatol Res. 2024;54(10):912-920. doi:10.1111/hepr.14039 PubMed
118.van Kleef LA, Sonneveld MJ, de Man RA, de Knegt RJ. Poor performance of FIB-4 in elderly individuals at risk for chronic liver disease - implications for the clinical utility of the EASL NIT guideline. J Hepatol. 2022;76(1):245-246. doi:10.1016/j.jhep.2021.08.017 PubMed
119.Hamelius L, Nordin G, Bjellerup P, Larsson A. Age- and sex-specific reference values for FIB-4 derived from the Nordic Reference Interval Project (NORIP). Scand J Clin Lab Invest. 2025;85(6):462-467. doi:10.1080/00365513.2025.2559352 PubMed
120.Thiele M, Madsen BS, Hansen JF, Detlefsen S, Antonsen S, Krag A. Accuracy of the Enhanced Liver Fibrosis Test vs FibroTest, Elastography, and Indirect Markers in Detection of Advanced Fibrosis in Patients With Alcoholic Liver Disease. Gastroenterology. 2018;154(5):1369-1379. doi:10.1053/j.gastro.2018.01.005 PubMed
121.Younossi ZM, Felix S, Jeffers T, et al. Performance of the Enhanced Liver Fibrosis Test to Estimate Advanced Fibrosis Among Patients With Nonalcoholic Fatty Liver Disease. JAMA Netw Open. 2021;4(9):e2123923. doi:10.1001/jamanetworkopen.2021.23923 PubMed
122.Siddiqui MS, Vuppalanchi R, Van Natta ML, et al. Vibration-Controlled Transient Elastography to Assess Fibrosis and Steatosis in Patients With Nonalcoholic Fatty Liver Disease. Clin Gastroenterol Hepatol. 2019;17(1):156-163.e2. doi:10.1016/j.cgh.2018.04.043 PubMed
123.Jalil S, Pagadala M, Dunn N, et al. Transient Elastography and Fibroscan: Stethoscope of a Hepatologist in Today’s World. Curr Hepatol Reps. 2025;24(1):41. doi:10.1007/s11901-025-00713-7 PubMed
124.Aljawad M, Sirpal S, Yoshida EM, Chandok N. Transient Elastography in Canada: Current State and Future Directions. Can J Gastroenterol Hepatol. 2015;29(7):373-376. doi:10.1155/2015/672853 PubMed
125.Castéra L, Foucher J, Bernard P-H, et al. Pitfalls of Liver Stiffness Measurement: A 5-Year Prospective Study of 13,369 Examinations. Hepatology. 2010;51(3):828-835. doi:10.1002/hep.23425 PubMed
126.Perazzo H, Veloso VG, Grinsztejn B, Hyde C, Castro R. Factors That Could Impact on Liver Fibrosis Staging by Transient Elastography. Int J Hepatol. 2015;2015(1):624596. doi:10.1155/2015/624596 PubMed
127.Moini M, Onofrio F, Hansen BE, Adeyi O, Khalili K, Patel K. Combination of FIB-4 with ultrasound surface nodularity or elastography as predictors of histologic advanced liver fibrosis in chronic liver disease. Sci Rep. 2021;11(1):19275. doi:10.1038/s41598-021-98776-1 PubMed
128.Frulio N, Trillaud H. Ultrasound elastography in liver. Diagn Interv Imaging. 2013;94(5):515-534. doi:10.1016/j.diii.2013.02.005 PubMed
129.Chimoriya R, Piya MK, Simmons D, Ahlenstiel G, Ho V. The Use of Two-Dimensional Shear Wave Elastography in People with Obesity for the Assessment of Liver Fibrosis in Non-Alcoholic Fatty Liver Disease. J. 2021;10(1):95. doi:10.3390/jcm10010095
130.Vuorenmaa AS, Siitama EMK, Mäkelä KS. Inter-operator and inter-device reproducibility of shear wave elastography in healthy muscle tissues. J Appl Clin Med Phys. 2022;23(9):e13717. doi:10.1002/acm2.13717 PubMed
131.Byenfeldt M, Elvin A, Fransson P. Influence of Probe Pressure on Ultrasound-Based Shear Wave Elastography of the Liver Using Comb-Push 2-D Technology. Ultrasound Med Biol. 2019;45(2):411-428. doi:10.1016/j.ultrasmedbio.2018.09.023 PubMed
132.Davyduke T, Tandon P, Al‐Karaghouli M, Abraldes JG, Ma MM. Impact of Implementing a “FIB‐4 First” Strategy on a Pathway for Patients With NAFLD Referred From Primary Care. Hepatol Commun. 2019;3(10):1322-1333. doi:10.1002/hep4.1411 PubMed
133.Congly SE, Shaheen AA, Swain MG. Modelling the cost effectiveness of non-alcoholic fatty liver disease risk stratification strategies in the community setting. PLoS One. 2021;16(5):e0251741. doi:10.1371/journal.pone.0251741 PubMed
134.Srivastava A, Jong S, Gola A, et al. Cost-comparison analysis of FIB-4, ELF and fibroscan in community pathways for non-alcoholic fatty liver disease. BMC Gastroenterol. 2019;19(1):122. doi:10.1186/s12876-019-1039-4 PubMed
135.Zaiou M, Joubert O. Racial and Ethnic Disparities in NAFLD: Harnessing Epigenetic and Gut Microbiota Pathways for Targeted Therapeutic Approaches. Biomolecules. 2025;15(5):669. doi:10.3390/biom15050669 PubMed
136.Pericàs JM, Anstee QM, Augustin S, et al. A roadmap for clinical trials in MASH-related compensated cirrhosis. Nat Rev Gastroenterol Hepatol. 2024;21(11):809-823. doi:10.1038/s41575-024-00955-8 PubMed
137.Lallukka S, Sädevirta S, Kallio MT, et al. Predictors of Liver Fat and Stiffness in Non-Alcoholic Fatty Liver Disease (NAFLD) - an 11-Year Prospective Study. Sci Rep. 2017;7(1):14561. doi:10.1038/s41598-017-14706-0 PubMed
138.L’homme L, Sermikli BP, Haas JT, et al. Adipose tissue macrophage infiltration and hepatocyte stress increase GDF-15 throughout development of obesity to MASH. Nature Communications. 2024;15(1):7173. doi:10.1038/s41467-024-51078-2 PubMed
139.Lavergne MR, Bodner A, Peterson S, et al. Do changes in primary care service use over time differ by neighbourhood income? Population-based longitudinal study in British Columbia, Canada. Int J Equity Health. 2022;21(1):80. doi:10.1186/s12939-022-01679-4 PubMed
140.Barbo G, Alam S. Indigenous people's experiences of primary health care in Canada: a qualitative systematic review. Health Promot Chronic Dis Prev Can. 2024;44(4):131-151. doi:10.24095/hpcdp.44.4.01 PubMed
141.Martin D, Miller AP, Quesnel-Vallée A, Caron NR, Vissandjée B, Marchildon GP. Canada's universal health-care system: achieving its potential. Lancet. 2018;391(10131):1718-1735. doi:10.1016/s0140-6736(18)30181-8 PubMed
142.Vilar-Gomez E, Martinez-Perez Y, Calzadilla-Bertot L, et al. Weight Loss Through Lifestyle Modification Significantly Reduces Features of Nonalcoholic Steatohepatitis. Gastroenterology. 2015;149(2):367-378.e5. doi:10.1053/j.gastro.2015.04.005 PubMed
143.Alam S, Jahid Hasan M, Khan MAS, Alam M, Hasan N. Effect of Weight Reduction on Histological Activity and Fibrosis of Lean Nonalcoholic Steatohepatitis Patient. J Transl Int Med. 2019;7(3):106-114. doi:10.2478/jtim-2019-0023 PubMed
144.Murdan S, Wei L, van Riet-Nales DA, et al. Association between culture and the preference for, and perceptions of, 11 routes of medicine administration: A survey in 21 countries and regions. Explor Res Clin Soc Pharm. 2023;12:100378. doi:10.1016/j.rcsop.2023.100378 PubMed
145.Drumond N, van Riet-Nales DA, Karapinar-Çarkit F, Stegemann S. Patients' appropriateness, acceptability, usability and preferences for pharmaceutical preparations: Results from a literature review on clinical evidence. Int J Pharm. 2017;521(1-2):294-305. doi:10.1016/j.ijpharm.2017.02.029 PubMed
146.Huynh TK, Ostergaard A, Egsmose C, Madsen OR. Preferences of patients and health professionals for route and frequency of administration of biologic agents in the treatment of rheumatoid arthritis. Patient Prefer Adherence. 2014;8:93-99. doi:10.2147/ppa.S55156 PubMed
147.Jull J, Giles A, Boyer Y, Stacey D, Minwaashin Lodge TAWsSC. Cultural adaptation of a shared decision making tool with Aboriginal women: a qualitative study. BMC Med Inform Decis Mak. 2015;15(1):1. doi:10.1186/s12911-015-0129-7 PubMed
148.Patel S, Partida D, Magee C, et al. Steatotic Liver Disease Education Enhances Knowledge and Confidence to Adhere to Provider Recommendations in Diverse and Vulnerable Populations. Gastro Hep Adv. 2025;4(3):100589. doi:10.1016/j.gastha.2024.11.005 PubMed
149.Dalal N, Catalli L, Miller SA, et al. BRIDGE to liver health: implementation of a group telehealth psychoeducational program through shared medical appointments for MASLD management. BMC Public Health. 2024;24(1):1546. doi:10.1186/s12889-024-18865-4 PubMed
150.Belete AM, Gemeda BN, Akalu TY, Aynalem YA, Shiferaw WS. What is the effect of mobile phone text message reminders on medication adherence among adult type 2 diabetes mellitus patients: a systematic review and meta-analysis of randomized controlled trials. BMC Endocr Disord. 2023;23(1):18. doi:10.1186/s12902-023-01268-8 PubMed
151.Kwon OY, Lee MK, Lee HW, Kim H, Lee JS, Jang Y. Mobile App-Based Lifestyle Coaching Intervention for Patients With Nonalcoholic Fatty Liver Disease: Randomized Controlled Trial. J Med Internet Res. 2024;26:e49839. doi:10.2196/49839 PubMed
152.Jongebloed H, Anderson K, Winter N, et al. The digital divide in rural and regional communities: a survey on the use of digital health technology and implications for supporting technology use. BMC Res Notes. 2024;17(1):90. doi:10.1186/s13104-024-06687-x PubMed
153.Maita KC, Maniaci MJ, Haider CR, et al. The Impact of Digital Health Solutions on Bridging the Health Care Gap in Rural Areas: A Scoping Review. Perm J. 2024;28(3):130-143. doi:10.7812/tpp/23.134 PubMed
154.Chen MJ, Chen Y, Lin JQ, et al. Evidence summary of lifestyle interventions in adults with metabolic dysfunction-associated steatotic liver disease. Front Nutr. 2025;11:1421386. doi:10.3389/fnut.2024.1421386 PubMed
155.Zafar Y, Sohail MU, Saad M, et al. eHealth interventions and patients with metabolic dysfunction-associated steatotic liver disease: a systematic review and meta-analysis. BMJ Open Gastroenterology. 2025;12(1):e001670. doi:10.1136/bmjgast-2024-001670 PubMed
156.Novo Nordisk A/S. Prescribing information: Wegovy (semaglutide), for subcutaneous use. U.S. Food and Drug Administration; 2025. Accessed 2025 October 03. https://www.accessdata.fda.gov/drugsatfda_docs/label/2025/215256s024lbl.pdf
157.U.S. Food and Drug Administration. FDA Approves Treatment for Serious Liver Disease Known as 'MASH'. Accessed October 27, 2025. https://www.fda.gov/drugs/news-events-human-drugs/fda-approves-treatment-serious-liver-disease-known-mash
158.Madrigal Pharmaceuticals Inc. Prescribing information: Rezdiffra (resmetirom) tablets, for oral use. U.S. Food and Drug Administration; 2024. Accessed October 03, 2025. https://www.accessdata.fda.gov/drugsatfda_docs/label/2024/217785s000lbl.pdf
159.U.S. Food and Drug Administration. FDA Approves First Treatment for Patients with Liver Scarring Due to Fatty Liver Disease. Accessed September 22, 2025. https://www.fda.gov/news-events/press-announcements/fda-approves-first-treatment-patients-liver-scarring-due-fatty-liver-disease
160.European Medicines Agency. Committee for Medicinal Products for Human Use (CHMP) summary of positive opinion for Rezdiffra. European Medicines Agency; 2025. Accessed October 03, 2025. https://www.ema.europa.eu/en/documents/smop-initial/chmp-summary-positive-opinion-rezdiffra_en.pdf
161.Madrigal Pharmaceuticals Inc. Madrigal Receives European Commission Approval for Rezdiffra™ (resmetirom) for the Treatment of MASH with Moderate to Advanced Liver Fibrosis. Accessed October 27, 2025. https://www.biospace.com/press-releases/madrigal-receives-european-commission-approval-for-rezdiffra-resmetirom-for-the-treatment-of-mash-with-moderate-to-advanced-liver-fibrosis
162.National Institute for Health and Care Excellence (NICE). Semaglutide for treating moderate to advanced liver fibrosis (without cirrhosis) caused by metabolic dysfunction-associated steatohepatitis [ID6458]. Accessed November 27, 2025. https://www.nice.org.uk/guidance/indevelopment/gid-ta11477
163.National Institute for Health and Care Excellence (NICE). Resmetirom for treating non-alcoholic steatohepatitis and liver fibrosis [TSID11905] [ID6529]. Accessed November 27, 2025. https://www.nice.org.uk/guidance/awaiting-development/gid-ta11414
164.Tice J, Suh K, Fahim S, et al. Resmetirom and Obeticholic Acid for Non-Alcoholic Steatohepatitis (NASH); Final Evidence Report & Meeting Summary. ICER; 2023. Accessed November 13, 2025. https://icer.org/wp-content/uploads/2025/01/NASH-Final-Report_Updated_011025.pdf
165.Novo Nordisk Canada Inc. Wegovy (semaglutide injection) Product Monograph. Health Canada; 2025. Accessed January 7, 2026. https://pdf.hres.ca/dpd_pm/00082777.PDF
166.Allen AM, Younossi ZM, Diehl AM, Charlton MR, Lazarus JV. Envisioning how to advance the MASH field. Nature Reviews Gastroenterology & Hepatology. 2024;21(10):726-738. doi:10.1038/s41575-024-00938-9 PubMed
167.Noureddin M, Charlton MR, Harrison SA, et al. Expert Panel Recommendations: Practical Clinical Applications for Initiating and Monitoring Resmetirom in Patients With MASH/NASH and Moderate to Noncirrhotic Advanced Fibrosis. Clin Gastroenterol Hepatol. 2024;22(12):2367-2377. doi:10.1016/j.cgh.2024.07.003 PubMed
168.Chee NM, Sinnanaidu RP, Chan WK. Vitamin E improves serum markers and histology in adults with metabolic dysfunction-associated steatotic liver disease: Systematic review and meta-analysis. J Gastroenterol Hepatol. 2024;39(12):2545-2554. doi:10.1111/jgh.16723 PubMed
169.Sanyal AJ, Chalasani N, Kowdley KV, et al. Pioglitazone, Vitamin E, or Placebo for Nonalcoholic Steatohepatitis. N Engl J Med. 2010;362(18):1675-1685. doi:10.1056/NEJMoa0907929 PubMed
170.Ndakotsu A, Vivekanandan G. The Role of Thiazolidinediones in the Amelioration of Nonalcoholic Fatty Liver Disease: A Systematic Review. Cureus. 2022;14(5):e25380. doi:10.7759/cureus.25380 PubMed
171.Zhao Y, Zhao W, Wang H, Zhao Y, Bu H, Takahashi H. Pioglitazone on nonalcoholic steatohepatitis: A systematic review and meta-analysis of 15 RCTs. Medicine (Baltimore). 2022;101(46):e31508. doi:10.1097/md.0000000000031508 PubMed
172.Zhang S, Ren X, Zhang B, Lan T, Liu B. A Systematic Review of Statins for the Treatment of Nonalcoholic Steatohepatitis: Safety, Efficacy, and Mechanism of Action. Molecules. 2024;29(8):1859. doi:10.3390/molecules29081859 PubMed
173.Arai T, Atsukawa M, Tsubota A, et al. Efficacy and safety of oral semaglutide in patients with non-alcoholic fatty liver disease complicated by type 2 diabetes mellitus: A pilot study. JGH open. 2022;6(7):503-511. doi:10.1002/jgh3.12780 PubMed
174.Zhu K, Kakkar R, Chahal D, Yoshida EM, Hussaini T. Efficacy and safety of semaglutide in non-alcoholic fatty liver disease. World J Gastroenterol. 2023;29(37):5327-5338. doi:10.3748/wjg.v29.i37.5327 PubMed
175.Alkhouri N, Charlton M, Gray M, Noureddin M. The pleiotropic effects of glucagon-like peptide-1 receptor agonists in patients with metabolic dysfunction-associated steatohepatitis: a review for gastroenterologists. Expert Opin Investig Drugs. 2025;34(3):169-195. doi:10.1080/13543784.2025.2473062 PubMed
176.Wang Y, Zhou Y, Wang Z, Ni Y, Prud'homme GJ, Wang Q. Efficacy of GLP-1-based Therapies on Metabolic Dysfunction-Associated Steatotic Liver Disease and Metabolic Dysfunction-Associated Steatohepatitis: A Systematic Review and Meta-Analysis. J Clin Endocrinol Metab. 2025;110(10):2964-2979. doi:10.1210/clinem/dgaf336 PubMed
177.Mo M, Huang Z, Liang Y, Liao Y, Xia N. The safety and efficacy evaluation of sodium-glucose co-transporter 2 inhibitors for patients with non-alcoholic fatty liver disease: An updated meta-analysis. Dig Liver Dis. 2022;54(4):461-468. doi:10.1016/j.dld.2021.08.017 PubMed
178.Zhou P, Tan Y, Hao Z, Xu W, Zhou X, Yu J. Effects of SGLT2 inhibitors on hepatic fibrosis and steatosis: A systematic review and meta-analysis. Front Endocrinol (Lausanne). 2023;14:1144838. doi:10.3389/fendo.2023.1144838 PubMed
179.Foundation for the National Institutes of Health. NCT07122700: Evaluation of Non-Invasive Tests for Metabolic Liver Disease (NIMBLE). ClinicalTrials.gov. Accessed September 22, 2025. https://clinicaltrials.gov/study/NCT07122700
180.Chen VL, Morgan TR, Rotman Y, et al. Resmetirom therapy for metabolic dysfunction-associated steatotic liver disease: October 2024 updates to AASLD Practice Guidance. Hepatology. 2025;81(1):312-320. doi:10.1097/HEP.0000000000001112 PubMed
181.Younossi ZM, Zelber-Sagi S, Lazarus JV, et al. Global Consensus Recommendations for Metabolic Dysfunction-Associated Steatotic Liver Disease and Steatohepatitis. Gastroenterology. 2025;169(5):1017-1032.e2. doi:10.1053/j.gastro.2025.02.044 PubMed
182.Nephew LD, Aitcheson G, Iyengar M. The Impact of Racial Disparities on Liver Disease Access and Outcomes. Curr Treat Options Gastroenterol. 2022;20(3):279-294. doi:10.1007/s11938-022-00390-1
183.Farahvash A, Lee MCM, Jain R, Jaakkimainen L. Pattern of semaglutide prescription in a real-world Canadian patient cohort. Prim Care Diabetes. 2025;19(5):512-516. doi:10.1016/j.pcd.2025.06.006 PubMed
184.Simacek KF, Ko JJ, Moreton D, Varga S, Johnson K, Katic BJ. The Impact of Disease-Modifying Therapy Access Barriers on People With Multiple Sclerosis: Mixed-Methods Study. J Med Internet Res. 2018;20(10):e11168. doi:10.2196/11168 PubMed
185.Kruja K, Mestre-Ferrandiz J, Hopkins MM, Ryll B, Kalo Z, Moon S. Policies to promote affordability and access across the life cycle of costly new drugs. BMJ. 2025;391:e086516. doi:10.1136/bmj-2025-086516 PubMed
186.Freund T, Everett C, Griffiths P, Hudon C, Naccarella L, Laurant M. Skill mix, roles and remuneration in the primary care workforce: who are the healthcare professionals in the primary care teams across the world? Int J Nurs Stud. 2015;52(3):727-743. doi:10.1016/j.ijnurstu.2014.11.014 PubMed
187.Casler K, Trees K, Bosak K. Providing Care for Fatty Liver Disease Patients: Primary Care Nurse Practitioners' Knowledge, Actions, and Preparedness. Gastroenterol Nurs. 2020;43(5):E184-E189. doi:10.1097/SGA.0000000000000487 PubMed
188.Lazarus JV, Kakalou C, Palayew A, et al. A Twitter discourse analysis of negative feelings and stigma related to NAFLD, NASH and obesity. Liver Int. 2021;41(10):2295-2307. doi:10.1111/liv.14969 PubMed
189.Younossi ZM, AlQahtani SA, Funuyet-Salas J, et al. The impact of stigma on quality of life and liver disease burden among patients with nonalcoholic fatty liver disease. JHEP Reports. 2024;6(7):101066. doi:10.1016/j.jhepr.2024.101066 PubMed
190.Thomas MK, Lammert LJ, Beverly EA. Food Insecurity and its Impact on Body Weight, Type 2 Diabetes, Cardiovascular Disease, and Mental Health. Curr Cardiovasc Risk Rep. 2021;15(9):15. doi:10.1007/s12170-021-00679-3 PubMed
191.Gyawali B, Mkoma GF, Harsch S. Social Determinants Influencing Nutrition Behaviors and Cardiometabolic Health in Indigenous Populations: A Scoping Review of the Literature. Nutrients. 2024;16(16):2750. doi:10.3390/nu16162750 PubMed
192.Montesanti S, Fleming E, Furlano J, et al. Navigating policy and infrastructure inequities in Indigenous primary health care: A qualitative comparative policy analysis of Alberta and Ontario. SSM - Health Systems. 2025;5:100109. doi:10.1016/j.ssmhs.2025.100109
193.Bansal MB, Patton H, Morgan TR, Carr RM, Dranoff JA, Allen AM. Semaglutide therapy for metabolic dysfunction-associated steatohepatitis: November 2025 updates to AASLD Practice Guidance. Hepatology. 2026;83(5):1326-1340. doi:10.1097/HEP.0000000000001608 PubMed
194.Fouad Y, Mostafa AM, Pan Z, et al. Evaluation of Stigma Toward Fatty Liver Disease. Endocr Metab Immune Disord Drug Targets. 2025:1-8. doi:10.2174/0118715303359141250420070406 PubMed
195.Wiedmeyer ML, Pedersen JS, Wakil Z, Hedden L. Equity in practice: Integrating cross cultural health brokers for culturally safe primary care for immigrants and refugees in British Columbia. Healthc Manage Forum. 2024;37(1_suppl):23s-27s. doi:10.1177/08404704241264426 PubMed
196.Allen AM, Charlton M, Cusi K, et al. Guideline-based management of metabolic dysfunction-associated steatotic liver disease in the primary care setting. Postgrad Med. 2024;136(3):229-245. doi:10.1080/00325481.2024.2325332 PubMed
197.Berardinelli D, Conti A, Hasnaoui A, et al. Nurse-Led Interventions for Improving Medication Adherence in Chronic Diseases: A Systematic Review. Healthcare (Basel). 2024;12(23):2337. doi:10.3390/healthcare12232337 PubMed
198.Abejirinde IO, Kishimoto V, Pfisterer KJ, et al. An equity analysis of remote patient monitoring programs unveils assumptions on digital health equity. NPJ Digit Med. 2025;8(1):320. doi:10.1038/s41746-025-01731-x PubMed
199.Thomas EE, Taylor ML, Banbury A, et al. Factors influencing the effectiveness of remote patient monitoring interventions: a realist review. BMJ Open. 2021;11(8):e051844. doi:10.1136/bmjopen-2021-051844 PubMed
200.Turer CB, Park JJ, Gupta OT, et al. Electronic phenotypes to distinguish clinician attention to high body mass index, hypertension, lipid disorders, fatty liver and diabetes in pediatric primary care: Diagnostic accuracy of electronic phenotypes compared to masked comprehensive chart review. Pediatr Obes. 2023;18(10):e13066. doi:10.1111/ijpo.13066 PubMed
201.Zhang X, Yip TC, Wong GL, et al. Clinical care pathway to detect advanced liver disease in patients with type 2 diabetes through automated fibrosis score calculation and electronic reminder messages: a randomised controlled trial. Gut. 2023;72(12):2364-2371. doi:10.1136/gutjnl-2023-330269 PubMed
202.Lionis C, Papadakis S, Anastasaki M, et al. Practice Recommendations for the Management of MASLD in Primary Care: Consensus Results. Diseases. 2024;12(8):180. doi:10.3390/diseases12080180 PubMed
203.Garattini L, Badinella Martini M, Mannucci PM. Integrated care: easy in theory, harder in practice? Intern Emerg Med. 2022;17(1):3-6. doi:10.1007/s11739-021-02830-9 PubMed
204.Martens M, Danhieux K, Van Belle S, et al. Integration or Fragmentation of Health Care? Examining Policies and Politics in a Belgian Case Study. Int J Health Policy Manag. 2022;11(9):1668-1681. doi:10.34172/ijhpm.2021.58 PubMed
205.Smeets M, Baldewijns K, Vaes B, Vandenhoudt H. Integration of Chronic Care in a Fragmented Healthcare System Comment on “Integration or Fragmentation of Health Care? Examining Policies and Politics in a Belgian Case Study.” Int J Health Policy Manag. 2023;12:7143. doi:10.34172/ijhpm.2022.7143 PubMed
206.Basu R, Noureddin M, Clark JM. Nonalcoholic Fatty Liver Disease: Review of Management for Primary Care Providers. Mayo Clin Proc. 2022;97(9):1700-1716. doi:10.1016/j.mayocp.2022.04.005 PubMed
207.Castera L, Alazawi W, Bugianesi E, et al. A European Survey to Identify Challenges in the Management of Metabolic Dysfunction-Associated Steatotic Liver Disease. Liver Int. 2025;45(2):e16224. doi:10.1111/liv.16224 PubMed
208.Allen AM, Lazarus JV, Younossi ZM. Healthcare and socioeconomic costs of NAFLD: A global framework to navigate the uncertainties. J Hepatol. 2023;79(1):209-217. doi:10.1016/j.jhep.2023.01.026 PubMed
209.Kumar S, Mohanty A, Mantry P, et al. Deploying a metabolic dysfunction-associated steatohepatitis consensus care pathway: findings from an educational pilot in three health systems. BMC Prim Care. 2024;25(1):265. doi:10.1186/s12875-024-02517-y PubMed
210.Moolla A, Motohashi K, Marjot T, et al. A multidisciplinary approach to the management of NAFLD is associated with improvement in markers of liver and cardio-metabolic health. Frontline Gastroenterol. 2019;10(4):337. doi:10.1136/flgastro-2018-101155 PubMed
211.Cobbold JFL, Raveendran S, Peake CM, Anstee QM, Yee MS, Thursz MR. Piloting a multidisciplinary clinic for the management of non-alcoholic fatty liver disease: initial 5-year experience. Frontline Gastroenterol. 2013;4(4):263. doi:10.1136/flgastro-2013-100319 PubMed
212.Bain VG, Wong WW, Greig PD, Yoshida EM. Hepatology and the Canadian gastroenterologist: interest, attitudes and patterns of practice: results of a national survey from the Canadian Association of Gastroenterology. Can J Gastroenterol. 2003;17(1):25-29. doi:10.1155/2003/709303 PubMed
213.Liver Canada. Wholistic Conversations on Liver Wellness: An Indigenous Perspective. Accessed October 10, 2025. https://liver.ca/resource/wholistic-conversations-on-liver-wellness-an-indigenous-perspective/
214.Maillet L, Thiebaut GC, Goudet A, Marchand JS. Promoting Coevolution Between Healthcare Organizations and Communities as Part of Social and Health Pathways Management in Quebec: Contributions of the Complex Adaptive Systems Approach. Health Serv Insights. 2025;18:11786329251332797. doi:10.1177/11786329251332797 PubMed
215.Allana A, Kuluski K, Tavares W, Pinto AD. Building integrated, adaptive and responsive healthcare systems – lessons from paramedicine in Ontario, Canada. BMC Health Serv Res. 2022;22(1):595. doi:10.1186/s12913-022-07856-z PubMed
216.Health Canada. Caring for Canadians: Canada's Future Health Workforce: The Canadian Health Workforce Education, Training and Distribution Study Executive Summary. Government of Canada; 2025. Accessed October 22, 2025. https://www.canada.ca/en/health-canada/services/health-care-system/health-human-resources/workforce-education-training-distribution-study.html
217.Moecke DP, Holyk T, Beckett M, et al. Scoping review of telehealth use by Indigenous populations from Australia, Canada, New Zealand, and the United States. J Telemed Telecare. 2024;30(9):1398-1416. doi:10.1177/1357633x231158835 PubMed
218.Cordes A, Bak M, Lyndon M, et al. Competing interests: digital health and indigenous data sovereignty. NPJ Digit Med. 2024;7(1):178. doi:10.1038/s41746-024-01171-z PubMed
219.Al-Khasawneh MA, Faheem M, Alarood AA, Habibullah S, Alzahrani A. A secure blockchain framework for healthcare records management systems. Healthc Technol Lett. 2024;11(6):461-470. doi:10.1049/htl2.12092 PubMed
220.Bayle A, Koscina M, Manset D, Perez-Kempner O. When Blockchain Meets the Right to Be Forgotten: Technology versus Law in the Healthcare Industry. Proc IEEE WIC ACM Int Conf Web Intell Intell Agent Technol. 2018:788-792. doi:10.1109/WI.2018.00133
221.Nguyen AXL, Kevorkov A, Li P, Benkelfat R. 93 Mapping Mobile Health Clinics in Canada: Delivering Equitable Primary Care to Children and Vulnerable Populations. Paediatr Child Health. 2022;27(Supplement_3):e43-e44. doi:10.1093/pch/pxac100.092
222.TELUS. TELUS Mobile Health Clinics. Accessed May 26, 2026. https://www.telus.com/en/social-impact/innovating-healthcare/health-for-good#Mobile-Health-Clinics
223.Pathways to Recovery. Mobile Health Clinics. Accessed January 9, 2026. https://pathwaystorecovery.ca/mobile-health-clinics/
224.Canada's Drug Agency. Policy Brief: Inter-jurisdictional Medical Licensing to Support Telemedicine. CDA-AMC; 2020. Accessed October 10, 2025. https://www.cda-amc.ca/sites/default/files/hta-he/cadth-policy-brief-interjurisdictional-licensing-final.pdf
225.Ige AB, Chukwurah N, Idemudia C, et al. Ethical Considerations in Data Governance: Balancing Privacy, Security, and Transparency in Data Management. IJERD. 2024;20:462-468.
226.Kuziemsky C, Hunter I, Udayasankaran JG, et al. Telehealth as a Means of Enabling Health Equity. Yearb Med Inform. 2022;31(1):60-66. doi:10.1055/s-0042-1742500 PubMed
227.Mustafa D, Al-Kfairy M. Editorial: Ethical considerations in electronic data in healthcare. Front Public Health. 2024;12:1454323. doi:10.3389/fpubh.2024.1454323 PubMed
228.Mangalote IAC, Aboumarzouk O, Al-Ansari AA, Dakua SP. A comprehensive study to learn the impact of augmented reality and haptic interaction in ultrasound-guided percutaneous liver biopsy training and education. Artif Intell Rev. 2024;57(7):186. doi:10.1007/s10462-024-10791-6
229.Pugliese N, Bertazzoni A, Hassan C, Schattenberg JM, Aghemo A. Revolutionizing MASLD: How Artificial Intelligence Is Shaping the Future of Liver Care. Cancers (Basel). 2025;17(5):722. doi:10.3390/cancers17050722 PubMed
230.Malik S, Das R, Thongtan T, Thompson K, Dbouk N. AI in Hepatology: Revolutionizing the Diagnosis and Management of Liver Disease. J Clin Med. 2024;13(24):7833. doi:10.3390/jcm13247833 PubMed
231.Yin C, Zhang H, Du J, Zhu Y, Zhu H, Yue H. Artificial intelligence in imaging for liver disease diagnosis. Front Med (Lausanne). 2025;12:1591523. doi:10.3389/fmed.2025.1591523 PubMed
232.Zhao Q, Lan Y, Yin X, Wang K. Image-based AI diagnostic performance for fatty liver: a systematic review and meta-analysis. BMC Med Imaging. 2023;23(1):208. doi:10.1186/s12880-023-01172-6 PubMed
233.Koçak B, Ponsiglione A, Stanzione A, et al. Bias in artificial intelligence for medical imaging: fundamentals, detection, avoidance, mitigation, challenges, ethics, and prospects. Diagn Interv Radiol. 2025;31(2):75-88. doi:10.4274/dir.2024.242854 PubMed
234.Ricci Lara MA, Echeveste R, Ferrante E. Addressing fairness in artificial intelligence for medical imaging. Nat Commun. 2022;13(1):4581. doi:10.1038/s41467-022-32186-3 PubMed
235.Schattenberg JM, Chalasani N, Alkhouri N. Artificial Intelligence Applications in Hepatology. Clin Gastroenterol Hepatol. 2023;21(8):2015-2025. doi:10.1016/j.cgh.2023.04.007 PubMed
236.Ueda D, Kakinuma T, Fujita S, et al. Fairness of artificial intelligence in healthcare: review and recommendations. Jpn J Radiol. 2024;42(1):3-15. doi:10.1007/s11604-023-01474-3 PubMed
237.World Health Organization. Ethics and governance of artificial intelligence for health. Guidance on large multi-modal models. World Health Organization; 2024. Accessed January 27, 2026. https://ieea.ch/wp-content/uploads/2025/04/WHO_Ethics-and-governance-of-AI-for-health.pdf
238.Government of Canada. Pan-Canadian AI for Health (AI4H) Guiding Principles. Accessed January 27, 2026. https://www.canada.ca/en/health-canada/corporate/transparency/health-agreements/pan-canadian-ai-guiding-principles.html
239.Yousefi Nooraie R, Lyons PG, Baumann AA, Saboury B. Equitable Implementation of Artificial Intelligence in Medical Imaging: What Can be Learned from Implementation Science? PET Clin. 2021;16(4):643-653. doi:10.1016/j.cpet.2021.07.002 PubMed
240.Glenning J, Gualtieri L. Patient Perspectives on Artificial Intelligence in Medical Imaging. J Particip Med. 2025;17:e67816. doi:10.2196/67816 PubMed
241.Pulaski H, Harrison SA, Mehta SS, et al. Clinical validation of an AI-based pathology tool for scoring of metabolic dysfunction-associated steatohepatitis. Nat Med. 2025;31(1):315-322. doi:10.1038/s41591-024-03301-2 PubMed
242.Abdurrachim D, Lek S, Ong CZL, et al. Utility of AI digital pathology as an aid for pathologists scoring fibrosis in MASH. J Hepatol. 2025;82(5):898-908. doi:10.1016/j.jhep.2024.11.032 PubMed
243.Akbary K, Noureddin M, Yayun R, Tai D, Boudes P. Development of AI Based Fibrosis Detection Algorithm by SHG/TPEF Microscopy for Fully Quantified Liver Fibrosis Assessment in MASH. Liver Int. 2025;45(9):e70258. doi:10.1111/liv.70258 PubMed
244.Meroueh C, Warasnhe K, Tizhoosh HR, Shah VH, Ibrahim SH. Digital pathology and spatial omics in steatohepatitis: Clinical applications and discovery potentials. Hepatology. 2025;82(6):1619-1644. doi:10.1097/hep.0000000000000866 PubMed
245.Colella F, Henderson NC, Ramachandran P. Dissecting the mechanisms of MASLD fibrosis in the era of single-cell and spatial omics. J Clin Invest. 2025;135(18):e186421. doi:10.1172/JCI186421 PubMed
246.Castañé H, Jiménez-Franco A, Hernández-Aguilera A, et al. Multi-omics profiling reveals altered mitochondrial metabolism in adipose tissue from patients with metabolic dysfunction-associated steatohepatitis. eBioMedicine. 2025;111:105532. doi:10.1016/j.ebiom.2024.105532 PubMed
247.Pirola CJ, Sookoian S. Multiomics biomarkers for the prediction of nonalcoholic fatty liver disease severity. World J Gastroenterol. 2018;24(15):1601-1615. doi:10.3748/wjg.v24.i15.1601 PubMed
248.Bourganou MV, Chondrogianni ME, Kyrou I, et al. Unraveling Metabolic Dysfunction-Associated Steatotic Liver Disease Through the Use of Omics Technologies. Int J Mol Sci. 2025;26(4):1589. doi:10.3390/ijms26041589 PubMed
249.Thiele M, Villesen IF, Niu L, et al. Opportunities and barriers in omics-based biomarker discovery for steatotic liver diseases. J Hepatol. 2024;81(2):345-359. doi:10.1016/j.jhep.2024.03.035 PubMed
250.Fishman J, Alexander T, Kim Y, Kindt I, Mendez P. A clinical decision support tool for metabolic dysfunction-associated steatohepatitis in real-world clinical settings: a mixed-method implementation research study protocol. J Comp Eff Res. 2024;13(10):e240085. doi:10.57264/cer-2024-0085 PubMed
251.Docherty M, Regnier SA, Capkun G, et al. Development of a novel machine learning model to predict presence of nonalcoholic steatohepatitis. J Am Med Inform Assoc. 2021;28(6):1235-1241. doi:10.1093/jamia/ocab003 PubMed
252.Douali N, Abdennour M, Sasso M, et al. Noninvasive diagnosis of nonalcoholic steatohepatitis disease based on clinical decision support system. Stud Health Technol Inform. 2013;192:1178. doi:10.3233/978-1-61499-289-9-1178 PubMed
253.Spann A, Bishop KM, Weitkamp AO, Stenner SP, Nelson SD, Izzy M. Clinical decision support automates care gap detection among primary care patients with nonalcoholic fatty liver disease. Hepatol Commun. 2023;7(3):e0035. doi:10.1097/hc9.0000000000000035 PubMed
254.Benmassaoud A, Bessissow A, Samoukovic G, et al. EUS-Guided Liver Biopsy and Portal Pressure Measurement Compared With a Transjugular Approach: A Randomized Controlled Trial. Clin Gastroenterol Hepatol. 2025:S1542-3565(25)00850-X. doi:10.1016/j.cgh.2025.09.025 PubMed
255.Lariño-Noia J, Fernández-Castroagudín J, de la Iglesia-García D, et al. Quality of Tissue Samples Obtained by Endoscopic Ultrasound-Guided Liver Biopsy: A Randomized, Controlled Clinical Trial. Am J Gastroenterol. 2023;118(10):1821-1828. doi:10.14309/ajg.0000000000002375 PubMed
256.Colloredo G, Guido M, Sonzogni A, Leandro G. Impact of liver biopsy size on histological evaluation of chronic viral hepatitis: the smaller the sample, the milder the disease. J Hepatol. 2003;39(2):239-244. doi:10.1016/S0168-8278(03)00191-0 PubMed
257.Ames JB, Djerboua M, Terrault NA, Booth CM, Flemming JA. Rising Healthcare Costs and Utilization among Young Adults with Cirrhosis in Ontario: A Population-Based Study. Canadian Journal of Gastroenterology and Hepatology. 2022;2022:6175913. doi:10.1155/2022/6175913 PubMed
258.Lee S, Saffo S. Evolution of care in cirrhosis: Preventing hepatic decompensation through pharmacotherapy. World J Gastroenterol. 2023;29(1):61-74. doi:10.3748/wjg.v29.i1.61 PubMed
259.Premkumar M, Anand AC. Overview of Complications in Cirrhosis. J Clin Exp Hepatol. 2022;12(4):1150-1174. doi:10.1016/j.jceh.2022.04.021 PubMed
260.LifeLabs. LifeLabs Brings New Liver Health Test to Ontario and British Columbia, Empowering Better Health Decisions. 2024. Accessed September 22, 2025. https://www.lifelabs.com/lifelabs-brings-new-liver-health-test-to-ontario-and-british-columbia-empowering-better-health-decisions/
261.Newfoundland and Labrador Health Services. Initial investigation of liver disease using Clinical Chemistry tests. Newfoundland and Labrador Health Services; 2014. Accessed November 24, 2025. https://www.gov.nl.ca/labformulary/files/Initial-Investigation-of-Liver-Disease-using-Clinical-Chemistry-Tests.pdf
262.Newfoundland and Labrador Health Services. Aspartate Aminotransferase. Accessed November 24, 2025. https://www.gov.nl.ca/labformulary/formulary/aspartate-aminotransferase/
263.Nova Scotia Health. Metabolic Dysfunction Associated Steatotic Liver Disease (MASLD) Pathway. Accessed November 24, 2025. https://www.hepatology.clinic/uploads/1/0/4/4/104488225/masld_2023_pathway.pdf
264.Ontario Ministry of Health. Schedule of Benefits for Laboratory Services. Government of Ontario; 2025. Accessed May 21, 2026. https://www.ontario.ca/files/2026-04/moh-ohip-schedule-of-benefits-laboratory-services-2026-04-01.pdf
265.LifeLabs. Liver Fibrosis Testing. Accessed November 24, 2025. https://www.lifelabs.com/test/liver-fibrosis-testing/
266.LifeLabs. LifeLabs introduces new Enhanced Liver Fibrosis Score in Ontario. 2023. Accessed September 22, 2025. https://www.lifelabs.com/notification/lifelabs-introduces-new-enhanced-liver-fibrosis-score-in-ontario/
267.King City Imaging. Shear Wave Liver Elastography (SWE). Accessed November 24, 2025. https://kingcityimaging.ca/shear-wave-liver-elastography-swe/
268.Wattacheril JJ, Abdelmalek MF, Lim JK, Sanyal AJ. AGA Clinical Practice Update on the Role of Noninvasive Biomarkers in the Evaluation and Management of Nonalcoholic Fatty Liver Disease: Expert Review. Gastroenterology. 2023;165(4):1080-1088. doi:10.1053/j.gastro.2023.06.013 PubMed
269.Cusi K, Isaacs S, Barb D, et al. American Association of Clinical Endocrinology Clinical Practice Guideline for the Diagnosis and Management of Nonalcoholic Fatty Liver Disease in Primary Care and Endocrinology Clinical Settings: Co-Sponsored by the American Association for the Study of Liver Diseases (AASLD). Endocr Pract. 2022;28(5):528-562. doi:10.1016/j.eprac.2022.03.010 PubMed
270.American Diabetes Association Professional Practice Committee. 4. Comprehensive Medical Evaluation and Assessment of Comorbidities: Standards of Care in Diabetes—2025. Diabetes Care. 2025;48(Supplement 1):S59-S85. doi:10.2337/dc25-S004 PubMed
271.de Groot JM, Geurtsen ML, Santos S, Jaddoe VWV. Ethnic disparities in liver fat accumulation in school-aged children. Obesity (Silver Spring). 2022;30(7):1472-1482. doi:10.1002/oby.23478 PubMed
272.Charlton M, Tonnu-Mihara I, Teng CC, et al. Evaluating the burden of illness of metabolic dysfunction-associated steatohepatitis in a large managed care population: The ETHEREAL Study. J Manag Care Spec Pharm. 2024;30(12):1414-1430. doi:10.18553/jmcp.2024.24106 PubMed
273.Asfari MM, Niyazi F, Lopez R, Dasarathy S, McCullough AJ. The association of nonalcoholic steatohepatitis and obstructive sleep apnea. Eur J Gastroenterol Hepatol. 2017;29(12):1380-1384. doi:10.1097/MEG.0000000000000973 PubMed
274.Aron-Wisnewsky J, Minville C, Tordjman J, et al. Chronic intermittent hypoxia is a major trigger for non-alcoholic fatty liver disease in morbid obese. J Hepatol. 2012;56(1):225-233. doi:10.1016/j.jhep.2011.04.022 PubMed
275.Sarkar M, Terrault N, Chan W, et al. Polycystic ovary syndrome (PCOS) is associated with NASH severity and advanced fibrosis. Liver Int. 2020;40(2):355-359. doi:10.1111/liv.14279 PubMed
276.Mantovani A, Petracca G, Beatrice G, et al. Non-alcoholic fatty liver disease and increased risk of incident extrahepatic cancers: a meta-analysis of observational cohort studies. Gut. 2022;71(4):778-788. doi:10.1136/gutjnl-2021-324191 PubMed
277.Muhamad NA, Maamor NH, Leman FN, et al. The Global Prevalence of Nonalcoholic Fatty Liver Disease and its Association With Cancers: Systematic Review and Meta-Analysis. Interact J Med Res. 2023;12:e40653. doi:10.2196/40653 PubMed
278.Zelber-Sagi S, Ivancovsky-Wajcman D, Fliss Isakov N, et al. High red and processed meat consumption is associated with non-alcoholic fatty liver disease and insulin resistance. J Hepatol. 2018;68(6):1239-1246. doi:10.1016/j.jhep.2018.01.015 PubMed
279.Balakrishnan M, Patel P, Dunn-Valadez S, et al. Women Have a Lower Risk of Nonalcoholic Fatty Liver Disease but a Higher Risk of Progression vs Men: A Systematic Review and Meta-analysis. Clin Gastroenterol Hepatol. 2021;19(1):61-71.e15. doi:10.1016/j.cgh.2020.04.067 PubMed
280.Gulati R, Moylan CA, Wilder J, et al. Racial and ethnic disparities in metabolic dysfunction-associated steatotic liver disease. Metab Target Organ Damage. 2024;4(2):9. doi:10.20517/mtod.2023.45
281.Siemens Healthineers Canada. Enhanced Liver Fibrosis (ELFTM) Test. Accessed September 22, 2025. https://www.siemens-healthineers.com/en-ca/laboratory-diagnostics/assays-by-diseases-conditions/liver-disease/elf-test
282.Siemens Healthineers Canada. Literature Compendium Volume I: The Enhanced Liver Fibrosis (ELFTM) Blood Test. Siemens Healthcare Diagnostics Inc.; 2021. https://marketing.webassets.siemens-healthineers.com/8f5cdbb2d5ed0014/54c771b687e8/ES-ELF-Literature_Compendium_Vol1
283.Health Canada. Medical Devices Active Licence Listing: Atellica IM Enhanced Liver Fibrosis (ELF). Government of Canada. 2024. Accessed September 22, 2025. https://health-products.canada.ca/mdall-limh/information?deviceId=1078427&deviceName=ATELLICA%20IM%20ENHANCED%20LIVER%20FIBROSIS%20(ELF)&licenceId=108758&type=active&lang=eng
284.Rosenberg WM, Voelker M, Thiel R, et al. Serum markers detect the presence of liver fibrosis: a cohort study. Gastroenterology. 2004;127(6):1704-1713. doi:10.1053/j.gastro.2004.08.052 PubMed
285.Avcu A, Kaya E, Yilmaz Y. Feasibility of Fibroscan in Assessment of Hepatic Steatosis and Fibrosis in Obese Patients: Report From a General Internal Medicine Clinic. Turk J Gastroenterol. 2021;32(5):466-472. doi:10.5152/tjg.2021.20498 PubMed
286.Sarkar Das T, Meng X, Abdallah M, Bilal M, Sarwar R, Shaukat A. An Assessment of the Feasibility, Patient Acceptance, and Performance of Point-of-Care Transient Elastography for Metabolic-Dysfunction-Associated Steatotic Liver Disease (MASLD): A Systematic Review and Meta-Analysis. Diagnostics (Basel). 2024;14(22):2478. doi:10.3390/diagnostics14222478 PubMed
287.Reinson T, Byrne CD, Patel J, El-Gohary M, Moore M. Transient elastography in patients at risk of liver fibrosis in primary care: a follow-up study over 54 months. BJGP Open. 2021;5(6):BJGPO.2021.0145. doi:10.3399/bjgpo.2021.0145
288.Kataria S, Juneja D, Singh O. Transient elastography (FibroScan) in critical care: Applications and limitations. World J Meta-Anal. 2023;11(7):340-350. doi:10.13105/wjma.v11.i7.340
289.Kumari S, George M. Diagnostic Accuracy of a Nurse-Led Transient Elastography: A Study of a Tertiary Hospital Experience. Gastroenterol Nurs. 2023;46(2):118-127. doi:10.1097/sga.0000000000000707 PubMed
290.Singh Y, Gogtay M, Gurung S, Trivedi N, Abraham GM. Assessment of Predictive Factors of Hepatic Steatosis Diagnosed by Vibration Controlled Transient Elastography (VCTE) in Chronic Hepatitis C Virus-Infected Patients. J Community Hosp Intern Med Perspect. 2022;12(4):58-65. doi:10.55729/2000-9666.1071 PubMed
291.Zenovia S, Stanciu C, Sfarti C, et al. Vibration-Controlled Transient Elastography and Controlled Attenuation Parameter for the Diagnosis of Liver Steatosis and Fibrosis in Patients with Nonalcoholic Fatty Liver Disease. Diagnostics (Basel). 2021;11(5):787. doi:10.3390/diagnostics11050787 PubMed
292.Zhou XD, Yip TC, Huang DQ, Muthiah MD, Noureddin M, Zheng MH. Vibration-controlled transient elastography in shaping the epidemiology and management of steatotic liver disease: Editorial on “Current burden of steatotic liver disease and fibrosis among adults in the United States, 2017-2023.” Clin Mol Hepatol. 2025;31(2):620-624. doi:10.3350/cmh.2024.1131 PubMed
293.Indre MG, Leucuta DC, Lupsor-Platon M, et al. Diagnostic accuracy of 2D-SWE ultrasound for liver fibrosis assessment in MASLD: A multilevel random effects model meta-analysis. Hepatology. 2025;82(2):454-469. doi:10.1097/hep.0000000000001190 PubMed
294.Dawod S, Brown K. Non-invasive testing in metabolic dysfunction-associated steatotic liver disease. Front Med (Lausanne). 2024;11:1499013. doi:10.3389/fmed.2024.1499013 PubMed
295.Cathcart J, Barrett R, Bowness JS, Mukhopadhya A, Lynch R, Dillon JF. Accuracy of Non-Invasive Imaging Techniques for the Diagnosis of MASH in Patients With MASLD: A Systematic Review. Liver Int. 2025;45(4):e16127. doi:10.1111/liv.16127 PubMed
296.Bresnahan R, Duarte R, Mahon J, et al. Diagnostic accuracy and clinical impact of MRI-based technologies for patients with non-alcoholic fatty liver disease: systematic review and economic evaluation. Health Technol Assess. 2023;27(10):1-115. doi:10.3310/kgju3398 PubMed
297.Zhang YX, Feng YP, You CL, Zhang LY. The diagnostic value of MRI-PDFF in hepatic steatosis of patients with metabolic dysfunction-associated steatotic liver disease: a systematic review and meta-analysis. BMC Gastroenterol. 2025;25(1):451. doi:10.1186/s12876-025-04017-4 PubMed
298.Sebastiani G, Patel K, Ratziu V, et al. Current considerations for clinical management and care of non-alcoholic fatty liver disease: Insights from the 1st International Workshop of the Canadian NASH Network (CanNASH). Can Liver J. 2022;5(1):61-90. doi:10.3138/canlivj-2021-0030 PubMed
299.Midia M, Odedra D, Shuster A, Midia R, Muir J. Predictors of bleeding complications following percutaneous image-guided liver biopsy: a scoping review. Diagn Interv Radiol. 2019;25(1):71-80. doi:10.5152/dir.2018.17525 PubMed
300.Mohan BP, Shakhatreh M, Garg R, Ponnada S, Adler DG. Efficacy and safety of EUS-guided liver biopsy: a systematic review and meta-analysis. Gastrointest Endosc. 2019;89(2):238-246.e3. doi:10.1016/j.gie.2018.10.018 PubMed
301.Zhou F, Stueck A, McLeod M. Liver biopsy complication rates in patients with non-alcoholic fatty liver disease. Can Liver J. 2022;5(2):106-112. doi:10.3138/canlivj-2021-0019 PubMed
302.Davison BA, Harrison SA, Cotter G, et al. Suboptimal reliability of liver biopsy evaluation has implications for randomized clinical trials. J Hepatol. 2020;73(6):1322-1332. doi:10.1016/j.jhep.2020.06.025 PubMed
303.Merck Sharp & Dohme LLC. NCT06465186: A Clinical Study of Efinopegdutide in People With Compensated Cirrhosis Due to Steatohepatitis (MK-6024-017). ClinicalTrials.gov. Accessed September 23, 2025. https://clinicaltrials.gov/study/NCT06465186
304.Zhejiang Doer Biologics Co. Ltd. NCT07024212: Phase II Study Evaluating the Efficacy and Safety of DR10624 Injection in MASLD and MetALD Subjects. ClinicalTrials.gov. Accessed September 23, 2025. https://clinicaltrials.gov/study/NCT07024212
305.Aligos Therapeutics. NCT05090111: A Study of ALG-055009 in Healthy Volunteers and Subjects With Hyperlipidemia. ClinicalTrials.gov. Accessed September 23, 2025. https://clinicaltrials.gov/study/NCT05090111
306.Corcept Therapeutics. NCT06108219: A Phase 2b, Study Evaluating Miricorilant in Adult Patients With Nonalcoholic Steatohepatitis/Metabolic Dysfunction-Associated Steatohepatitis (MONARCH). ClinicalTrials.gov. Accessed September 23, 2025. https://clinicaltrials.gov/study/NCT06108219
307.GlaxoSmithKline. NCT05583344: Phase 2b Study of GSK4532990 in Adults With NASH (HORIZON). ClinicalTrials.gov. Accessed April 27, 2026. https://clinicaltrials.gov/study/NCT05583344
308.Boehringer Ingelheim. NCT06309992: A Study to Test Whether Survodutide Helps People Living With Obesity or Overweight and With a Confirmed or Presumed Liver Disease Called Non-alcoholic Steatohepatitis (NASH) to Reduce Liver Fat and to Lose Weight. ClinicalTrials.gov. Accessed September 23, 2025. https://clinicaltrials.gov/study/NCT06309992
309.Boehringer Ingelheim. NCT06632457: LIVERAGE™ - Cirrhosis: A Study to Test Whether Survodutide Helps People With a Liver Disease Called NASH/MASH Who Have Cirrhosis. ClinicalTrials.gov. Accessed September 23, 2025. https://clinicaltrials.gov/study/NCT06632457
310.Boehringer Ingelheim. Boehringer receives U.S. FDA Breakthrough Therapy designation and initiates two phase III trials in MASH for survodutide. Boehringer Ingelheim; 2024. Accessed September 23, 2025. https://www.boehringer-ingelheim.com/human-health/metabolic-diseases/survodutide-us-fda-breakthrough-therapy-phase-3-trials-mash
311.89bio Inc. NCT06419374: A Study to Evaluate the Efficacy and Safety of Pegozafermin in Participants With Compensated Cirrhosis Due to MASH. ClinicalTrials.gov. Accessed September 23, 2025. https://clinicaltrials.gov/study/NCT06419374
312.89bio Inc. NCT06318169: A Study Evaluating the Efficacy and Safety of Pegozafermin in Participants With MASH and Fibrosis (ENLIGHTEN-Fibrosis). ClinicalTrials.gov. Accessed September 23, 2025. https://clinicaltrials.gov/study/NCT06318169
313.Akero Therapeutics Inc. NCT06161571: A Study Evaluating Efruxifermin in Subjects With Non-invasively Diagnosed Nonalcoholic Steatohepatitis (NASH)/Metabolic Dysfunction-Associated Steatohepatitis (MASH) and Nonalcoholic Fatty Liver Disease (NAFLD)/Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD). ClinicalTrials.gov. Accessed September 23, 2025. https://clinicaltrials.gov/study/NCT06161571
314.GlaxoSmithKline. NCT07221227: A Pivotal Clinical Study to Investigate Efimosfermin Alfa in Participants With Biopsy-confirmed F2- or F3-stage MASH (ZENITH-1). ClinicalTrials.gov. Accessed April 27, 2026. https://clinicaltrials.gov/study/NCT07221227
315.Inventiva Pharma. NCT04849728: A Phase 3 Study Evaluating Efficacy and Safety of Lanifibranor Followed by an Active Treatment Extension in Adult Patients With (NASH) and Fibrosis Stages F2 and F3 (NATiV3). ClinicalTrials.gov. Accessed September 23, 2025. https://clinicaltrials.gov/study/NCT04849728
316.Novo Nordisk A/S. Health Canada accepts semaglutide 2.4 mg, a GLP-1RA treatment for MASH, as a supplemental New Drug Submission under the Priority Review Policy. Novo Nordisk A/S; 2025. Accessed September 22, 2025. https://www.novonordisk.ca/content/dam/nncorp/ca/en/press-releases/2025/mash-health-canada-priority-review-press-release-english.pdf?utm_source=chatgpt.com
317.Wilson R, Rourke J. Report card on access to rural health care in Canada. Rural Remote Health. 2023;23(1):8108. doi:10.22605/rrh8108 PubMed
318.Eii MN, Walpole S, Aldridge C. Sustainable practice: Prescribing oral over intravenous medications. BMJ. 2023;383:e075297. doi:10.1136/bmj-2023-075297 PubMed
319.Lazure P, Tomlinson JW, Kowdley KV, et al. Clinical practice gaps and challenges in non-alcoholic steatohepatitis care: An international physician needs assessment. Liver Int. 2022;42(8):1772-1782. doi:10.1111/liv.15324 PubMed
320.Medina SP, Kim RG, Magee C, Stapper N, Khalili M. Cross-sectional study on stigma and motivation to adhere to lifestyle modification among vulnerable populations with fatty liver disease. Obes Sci Pract. 2023;9(6):581-589. doi:10.1002/osp4.688 PubMed
321.Sundareswaran M, Martignetti L, Purkey E. Barriers to primary care among immigrants and refugees in Peterborough, Ontario: a qualitative study of provider perspectives. BMC Prim Care. 2024;25(1):199. doi:10.1186/s12875-024-02453-x PubMed
322.Ayesh H, Beran A, Suhail S, Ayesh S, Niswender K. Efficacy and safety of resmetirom in MASLD and MASH: network meta-analysis of randomized clinical trials. J Basic Clin Physiol Pharmacol. 2025;36(1):3-11. doi:10.1515/jbcpp-2024-0140 PubMed
323.Targher G, Byrne CD, Tilg H. NAFLD and increased risk of cardiovascular disease: clinical associations, pathophysiological mechanisms and pharmacological implications. Gut. 2020;69(9):1691. doi:10.1136/gutjnl-2020-320622 PubMed
324.Fan J-G, Xu X-Y, Yang R-X, et al. Guideline for the Prevention and Treatment of Metabolic Dysfunction-associated Fatty Liver Disease (Version 2024). J Clin Transl Hepatol. 2024;12(11):955-974. doi:10.14218/JCTH.2024.00311 PubMed
325.Olukotun M, Olanlesi-Aliu A, Idi Y, et al. Institutional and systemic barriers and facilitators affecting healthcare access for Black women in Alberta. SSM Qual Res Health. 2024;6:100485. doi:10.1016/j.ssmqr.2024.100485
326.Indigenous Primary Health Care Advisory Panel. Honouring our roots: growing together towards a culturally safe, wholistic primary health care system for Indigenous peoples. Government of Alberta; 2023. Accessed May 21, 2026. https://open.alberta.ca/publications/maps-indigenous-primary-health-care-advisory-panel-final-report
327.Karam M, Chouinard M-C, Kevork M, Fleming R, Arnaud D. Nurses’ and Patients’ Perspectives on Care Coordination Across Health Care and Social Services Sectors: A Qualitative Study. Can J Nurs Res. 2026;58(1):48-57. doi:10.1177/08445621251395347 PubMed
328.Manns BJ, Hastings S, Marchildon G, Noseworthy T. Health system structure and its influence on outcomes: The Canadian experience. Healthc Manage Forum. 2024;37(5):340-350. doi:10.1177/08404704241248559 PubMed
329.Hiscock EC, Stutz S, Mashford-Pringle A, et al. An environmental scan of Indigenous Patient Navigator programs in Ontario. Healthc Manage Forum. 2022;35(2):99-104. doi:10.1177/08404704211067659 PubMed
330.Rabi S, Santana M, Dimitropoulos G, et al. Exploring Patient Understandings of Navigation Services Within Alberta's Healthcare System: A Qualitative Study. Health Expect. 2025;28(4):e70383. doi:10.1111/hex.70383 PubMed
331.Green M. Action still needed on health disparities affecting rural and remote communities. Can Fam Physician. 2024;70(9):597. doi:10.46747/cfp.7009597 PubMed
332.Xu X, Zhang Y, Zhu Q, et al. Diagnostic accuracy of two-dimensional shear wave elastography and point shear wave elastography in identifying different stages of liver fibrosis in patients with metabolic dysfunction-associated steatotic liver disease: A meta-analysis. Biomol Biomed. 2025;25(4):810-821. doi:10.17305/bb.2024.11577 PubMed
333.Decharatanachart P, Chaiteerakij R, Tiyarattanachai T, Treeprasertsuk S. Application of artificial intelligence in chronic liver diseases: a systematic review and meta-analysis. BMC Gastroenterol. 2021;21(1):10. doi:10.1186/s12876-020-01585-5 PubMed
334.Zamanian H, Shalbaf A, Zali MR, et al. Application of artificial intelligence techniques for non-alcoholic fatty liver disease diagnosis: A systematic review (2005-2023). Comput Methods Programs Biomed. 2024;244:107932. doi:10.1016/j.cmpb.2023.107932 PubMed
335.Sun Y, Hu D, Yu M, et al. Diagnostic Accuracy of Non-Invasive Diagnostic Tests for Nonalcoholic Fatty Liver Disease: A Systematic Review and Network Meta-Analysis. Clin Epidemiol. 2025;17:53-71. doi:10.2147/clep.S501445 PubMed
336.Castellana M, Donghia R, Guerra V, et al. Fibrosis-4 Index vs Nonalcoholic Fatty Liver Disease Fibrosis Score in Identifying Advanced Fibrosis in Subjects With Nonalcoholic Fatty Liver Disease: A Meta-Analysis. Am J Gastroenterol. 2021;116(9):1833-1841. doi:10.14309/ajg.0000000000001337 PubMed
337.Pennisi G, Enea M, Falco V, et al. Noninvasive assessment of liver disease severity in patients with nonalcoholic fatty liver disease (NAFLD) and type 2 diabetes. Hepatology. 2023;78(1):195-211. doi:10.1097/hep.0000000000000351 PubMed
338.Ismaiel A, Leucuta DC, Popa SL, et al. Noninvasive biomarkers in predicting nonalcoholic steatohepatitis and assessing liver fibrosis: systematic review and meta-analysis. Panminerva Med. 2021;63(4):508-518. doi:10.23736/s0031-0808.20.04171-3 PubMed
339.Gosalia D, Ratziu V, Stanicic F, et al. Accuracy of Noninvasive Diagnostic Tests for the Detection of Significant and Advanced Fibrosis Stages in Nonalcoholic Fatty Liver Disease: A Systematic Literature Review of the US Studies. Diagnostics (Basel). 2022;12(11):2608. doi:10.3390/diagnostics12112608 PubMed
340.Eguchi Y, Wong G, Akhtar O, Sumida Y. Non-invasive diagnosis of non-alcoholic steatohepatitis and advanced fibrosis in Japan: A targeted literature review. Hepatol Res. 2020;50(6):645-655. doi:10.1111/hepr.13502 PubMed
341.Ravaioli F, Dajti E, Mantovani A, Newsome PN, Targher G, Colecchia A. Diagnostic accuracy of FibroScan-AST (FAST) score for the non-invasive identification of patients with fibrotic non-alcoholic steatohepatitis: a systematic review and meta-analysis. Gut. 2023;72(7):1399-1409. doi:10.1136/gutjnl-2022-328689 PubMed
342.Vali Y, Lee J, Boursier J, et al. FibroTest for Evaluating Fibrosis in Non-Alcoholic Fatty Liver Disease Patients: A Systematic Review and Meta-Analysis. J Clin Med. 2021;10(11):2415. doi:10.3390/jcm10112415 PubMed
343.Contreras D, Gonzalez-Rocha A, Clark P, Barquera S, Denova-Gutierrez E. Diagnostic accuracy of blood biomarkers and non-invasive scores for the diagnosis of NAFLD and NASH: Systematic review and meta-analysis. Ann Hepatol. 2023;28(1):100873. doi:10.1016/j.aohep.2022.100873 PubMed
344.Malandris K, Arampidis D, Mainou M, et al. FibroScan-AST score for diagnosing fibrotic MASH: A systematic review and meta-analysis of diagnostic test accuracy studies. J Gastroenterol Hepatol. 2024;39(12):2582-2591. doi:10.1111/jgh.16770 PubMed
345.Selvaraj EA, Mózes FE, Jayaswal ANA, et al. Diagnostic accuracy of elastography and magnetic resonance imaging in patients with NAFLD: A systematic review and meta-analysis. J Hepatol. 2021;75(4):770-785. doi:10.1016/j.jhep.2021.04.044 PubMed
346.Mózes FE, Lee JA, Vali Y, et al. Diagnostic accuracy of non-invasive tests to screen for at-risk MASH-An individual participant data meta-analysis. Liver Int. 2024;44(8):1872-1885. doi:10.1111/liv.15914 PubMed
347.Garg S, Varghese M, Shaik F, et al. Efficacy of Non-invasive Biomarkers in Diagnosing Non-alcoholic Fatty Liver Disease (NAFLD) and Predicting Disease Progression: A Systematic Review. Cureus. 2025;17(2):e78421. doi:10.7759/cureus.78421 PubMed
348.Statistics Canada. Table 17-10-0005-01: Population estimates on July 1, by age and gender. Accessed December 15, 2025. https://doi.org/10.25318/1710000501-eng
349.Statistics Canada. Table 17-10-0058-01: Components of projected population growth, by projection scenario (x 1,000). Accessed December 15, 2025. https://doi.org/10.25318/1710005801-eng
Appendix 1: Nomenclature and Jurisdictional Diagnostic Pathways
Please note that this appendix has not been copy-edited.
Table 4: Changes in Nomenclature and Diagnostic Criteria Introduced by the 2023 Multisociety Delphi Consensus Redefining NAFLD as MASLD
Previously: NALFD | Updated: MASLD |
|---|---|
Hepatic steatosis with all 3:
| Hepatic steatosis with ≥ 1 of the following cardiometabolic factors:
|
MASLD = metabolic dysfunction–associated steatotic liver disease; NAFLD = nonalcoholic fatty liver disease.
Table 5: Jurisdictional Overview of MASH Care Pathways and Diagnostic Tools in Canada
Jurisdiction | Care pathwaya | Diagnostic tools and reimbursementa |
|---|---|---|
Newfoundland and Labrador | No provincial or regional clinical pathways were identified, although internal pathways may exist. | Although there are provincial laboratory formulary guidelines which specify that AST is a secondary test following ALT, there are no restrictions on ordering or reimbursement of AST testing in Newfoundland and Labrador.261,262 VCTE is available in Newfoundland and Labrador, but an online and literature search did not identify any SWE units in this jurisdiction. |
Prince Edward Island | No provincial or regional clinical pathways were identified, although we were informed of an unpublished regional clinical pathway. | AST and ELF testing are available in Prince Edward Island. VCTE is available in Prince Edward Island, but an online and literature search did not identify any SWE units in this jurisdiction. |
Nova Scotia | A provincial clinical pathway for MASLD and MASH developed by Nova Scotia Health exists.263 | No jurisdiction-specific information on laboratory diagnostics (e.g., AST, FIB-4, ELF) were identified. VCTE is available in Nova Scotia. Although an online and literature search did not identify any SWE units in this jurisdiction. It is highlighted in the provincial clinical pathway as a viable option for imaging assessments. |
New Brunswick | No provincial or regional clinical pathways were identified, although internal pathways may exist. | No jurisdiction-specific information on laboratory diagnostics (e.g., AST, FIB-4, ELF) were identified. VCTE is available in New Brunswick, but an online search and literature search did not identify any SWE units in this jurisdiction. |
Quebec | No provincial or regional clinical pathways were identified, although internal pathways may exist. | First-time AST requisitions for liver-related investigations are automatically converted to ALT. Only if ALT levels are elevated is AST added by the algorithm.69 Both VCTE and SWE are available in Quebec. Quebec is the only jurisdiction where VCTE is publicly funded; elsewhere patients typically pay out of pocket or access it through select specialty clinics.83,85,86 |
Ontario | Regional pathways have been developed, particularly to provide localized solutions for AST testing coverage. An online search identified a regional pathway from Kingston Health Science Centre.109 | In 2007, AST testing was replaced by ALT on the Ontario laboratory requisition form. This reduced unnecessary testing but also decreased the use of FIB-4 in Canada despite CPG recommendations.63-69 Currently, AST testing (required for FIB-4 calculations) is only publicly reimbursed when ordered by liver specialists or emergency physicians; otherwise patients pay out of pocket.67,68,264 Automated FIB‑4 calculations (paid out of pocket) are available at some community laboratories.265 The ELF score is available through some community laboratories, but patients pay out of pocket.260,266 Both VCTE and SWE are available in Ontario. Neither is covered by the Ontario Health Insurance Plan (OHIP).267 |
Manitoba | A provincial clinical pathway for MASLD and MASH management from Shared Health Services exists.108 | No jurisdiction-specific information on laboratory diagnostics (e.g., AST, FIB-4, ELF) were identified. Both VCTE and SWE are available in Manitoba. |
Saskatchewan | No provincial or regional clinical pathways were identified, although internal pathways may exist. | No jurisdiction-specific information on laboratory diagnostics (e.g., AST, FIB-4, ELF) were identified. Both VCTE and SWE are available in Saskatchewan. |
Alberta | Calgary pathway — A provincial clinical pathway for MASLD and MASH developed by Alberta Health Services exists, known as the Calgary Pathway.107 | Although AST is not included on provincial laboratory requisition forms, the FIB-4 index calculation was added to standard requisition forms to simplify ordering and automate the calculation for physicians.70 According to a primary care physician practising in Alberta and consulted for this review, the ELF score is available to patients through community laboratories. Both VCTE and SWE are available in Alberta. According to a primary care physician practising in Alberta and consulted for this review, in Calgary, SWE is preferred over VCTE for the assessment of liver fibrosis stage. SWE is reimbursed by Alberta Health. |
British Columbia | No provincial or regional clinical pathways were identified, although internal pathways may exist. | Although AST is not included on provincial laboratory requisition forms as ALT is the preferred enzyme for evaluating liver function, there are no restrictions on ordering or reimbursement of AST testing in British Columbia. The ELF score is available through some community laboratories, but patients pay out of pocket.260 Both VCTE and SWE are available in British Columbia. |
Yukon | No provincial or regional clinical pathways were identified, although internal pathways may exist. | No jurisdiction-specific information on laboratory diagnostics (e.g., AST, FIB-4, ELF) were identified. Diagnostic imaging units (e.g., VCTE, MRI) and a liver clinic are only available in Whitehorse. An online and literature search did not identify any SWE units in this jurisdiction. |
Northwest Territories | No provincial or regional clinical pathways were identified, although internal pathways may exist. | No jurisdiction-specific information on laboratory diagnostics (e.g., AST, FIB-4, ELF) were identified. According to information submitted by manufacturers and imaging centres, there are no VCTE or MRI units in the Northwest Territories. An online and literature search did not identify any SWE units in this jurisdiction. |
Nunavut | No provincial or regional clinical pathways were identified, although internal pathways may exist. | No jurisdiction-specific information on laboratory diagnostics (e.g., AST, FIB-4, ELF) were identified. According to information submitted by manufacturers and imaging centres, there are no VCTE or MRI units in Nunavut. An online and literature search did not identify any liver clinics or SWE units in this jurisdiction. |
ALT = alanine aminotransferase; AST = aspartate aminotransferase; CPG = clinical practice guideline; ELF = enhanced liver fibrosis; FIB-4 = Fibrosis-4; MASLD = metabolic dysfunction–associated steatotic liver disease; MASH = metabolic dysfunction–associated steatohepatitis; VCTE = vibration-controlled transient elastography.
aInformation presented in this table is based on available information from targeted online searches and interviews with content experts in Canada. Content experts consulted were from British Columbia, Alberta, Ontario, and Nova Scotia. Additional jurisdictional activities or considerations may exist that are not capture herein. Additional information on the distribution of diagnostic units and liver clinics is available in the dashboard.
Table 6: Alignment of Canadian Guidelines and Pathways for MASH
Guideline (evidence- or consensus-based) | Year | Recommendations | Key differences from other guidelines and limitations |
|---|---|---|---|
Diabetes Canada (evidence-based)14 | 2025 | Population
Assessment methods
Treatment
|
|
Canadian Association of Radiologists (consensus-based)104-106,a | 2025 |
|
|
Alberta Health Services (provincial clinical pathway)107 | 2021 | Population
Assessment methods
Treatment
|
|
Shared Health Manitoba (provincial clinical pathway)108 | 2024 | Population
Assessment methods
Treatment
|
|
Nova Scotia Health (provincial clinical pathway)263 | 2023 | Assessment methods
Treatment
|
|
Kingston Health Sciences Centre (regional clinical pathway)109 | 2025 | Population
Assessment methods
Treatment
Ongoing disease monitoring should also happen for low-risk patients. Recalculate FIB-4 every 2 to 3 years (order ALT, AST, platelets). If FIB-4 continues to be < 1.30, continue care within a primary care setting. |
|
ALT = alanine aminotransferase; AST = aspartate aminotransferase; ELF = Enhanced Liver Fibrosis; FIB-4 = Fibrosis-4; MASH = metabolic dysfunction–associated steatohepatitis; MASLD = metabolic dysfunction–associated steatotic liver disease; MRE = magnetic resonance elastography; SWE = shear wave elastography; T2DM = type 2 diabetes mellitus; VCTE = vibration-controlled transient elastography.
aGiven the focus of this report and other guidelines are on the use of the FIB-4, ELF, SWE, and VCTE for MASH diagnostics, only recommendations related to these NITs have been included in this table. Additional recommendations from the Canadian Association of Radiologists are available for the use of other diagnostic tests.
Table 7: Alignment of International Guidelines and Pathways
Guideline (evidence- or consensus-based) | Year | Recommendations | Key differences from other guidelines and limitations |
|---|---|---|---|
European Association for the Study of the Liver, European Association for the Study of Obesity, European Association for the Study of Diabetes (evidence-based)2 | 2024 | Population
Assessment Methods
Monitoring and Management
Treatment
|
|
American Association for the Study of Liver Diseases (evidence-based)3,180,193 | 2023 | Population
Assessment methods
Monitoring and Management
Treatment
|
|
American Gastroenterological Association (consensus-based)268 | 2023 | Assessment methods
|
|
American Association of Clinical Endocrinology (evidence-based)269 | 2022 | Population
Assessment methods
|
|
American Diabetes Association (evidence-based)270 | 2025 | Population
Assessment methods
|
|
ALT = alanine aminotransferase; AST = aspartate aminotransferase; ELF = enhanced liver fibroses; FIB-4 = fibrosis-4; GLP-1 RA = glucagon-like peptide 1 receptor agonist; HCC = hepatocellular carcinoma; MASH = metabolic dysfunction–associated steatohepatitis; MASLD = metabolic dysfunction–associated steatotic liver disease; MRE = magnetic resonance elastography; NIT = noninvasive test; SGLT2 = sodium-glucose cotransporter-2; SWE = shear wave elastography; T2DM = type 2 diabetes mellitus; VCTE = vibration-controlled transient elastography.
Appendix 2: Evidence From the Clinical Pathway
Please note that this appendix has not been copy-edited.
Risk Factors and Groups at Risk
Differences in Disease Burden Across Populations
Observational studies show that MASH and MASLD do not affect all populations equally. Compared to the general population, certain groups experience higher prevalence or more severe outcomes:
Hispanic, Latino, and some Asian populations experience higher prevalence of MASLD and MASH, including higher risk of lean disease in certain Asian populations.27,28
Mexican American individuals, and females of all ethnicities experience higher comorbidity rates.18,27
non-Hispanic Black individuals may have a lower overall prevalence but experience higher cardiovascular morbidity and mortality when MASH is present.18,27
children from racialized communities may have higher rates of liver fat accumulation, suggesting inequities in MASH risk may begin early and persist into adulthood.271
Clinical and Behavioural Contributors to Risk and Progression
Clinical characteristics and coexisting conditions further influence the course of disease. In a large US cohort of more than 18,500 patients with MASH, 43% had T2D, 58% were living with overweight or obesity, and 17% had CVD.272 MASH is strongly associated with T2D, and has also been linked to conditions such as obstructive sleep apnea, polycystic ovary syndrome (also known as polyendocrine metabolic ovarian syndrome), and hepatic and extrahepatic cancers.273-277 Additional information on health behaviours related to MASH throughout Canada is available in the dashboard.
Individual-level behavioural factors reported in the literature to be associated with MASH and MASLD include, sedentary behaviour, diet quality, and consumption of red and processed meats.58,278 However, these individual choices may also be influenced by broader structural inequities as will be discussed in the next section. Risk factors differ between MASH and MASLD: males are more likely to develop MASLD, while females — particularly those older than age 50 and those with T2D — have a higher risk of progression to advanced fibrosis once diagnosed with MASLD.279
Structural Inequities and Intersecting Risk Factors
Health inequities are shaped by structural barriers to health including the social determinants of health such as income, education, housing, and access to primary care and by food insecurity, cultural and language barriers, geographic access, and transportation issues. Individuals with limited access to primary and specialist care, lower income, or unstable insurance coverage may be more likely to present with advanced disease and experience poorer cardiometabolic outcomes.280 MASH is reported to disproportionately impact communities with higher rates of poverty and food insecurity.29-34 These structural barriers may also leave people with lower incomes, immigrant populations, and racialized groups at greater risk of undetected disease.34,35
A recent global survey found that 20% of patients had not scheduled or had missed an appointment for MASLD or MASH due to stigma and discrimination.49 Stigma linked to weight, alcohol use, and the term “fatty liver” may discourage patients from seeking care.50-52 Despite recent efforts to reduce stigma by removing terms like “nonalcoholic” and “fatty,” some patients still identify with “fatty liver disease,” perpetuating feelings of shame and disengagement.4
Clinical Guidelines
Several American guidelines exist, including evidence-based guidelines from the American Association for the Study of Liver Diseases (AASLD), the American Association of Clinical Endocrinology co-sponsored with the AASLD, and the American Diabetes Association, as well as an expert review from the American Gastroenterological Association.3,268-270
In Europe, a CPG on the management of MASLD was jointly updated and published in 2024 by the European Association for the Study of the Liver (EASL), European Association for the Study of Diabetes (EASD) and European Association for the Study of Obesity (EASO).2 Several of these guidelines have integrated suggestions for the use of DMTs following regulatory approval in their jurisdictions.2,180,193
Diagnostic Tools
Noninvasive Blood-Based Techniques
Blood-based techniques are widely used to assess liver fibrosis and identify patients who may be eligible for DMTs in countries where these have been approved. These tools are generally more accessible than imaging modalities and play a key role in risk stratification and early detection.
Fibrosis-4 Index: The FIB-4 index is a composite algorithm calculated using age and 3 blood-based biomarkers — aspartate aminotransferase (AST), alanine aminotransferase (ALT), and platelet count — to assess liver cell stress and predict substantial fibrosis.14 It is recommended by Diabetes Canada as a first-line stratification tool to identify patients at risk of advanced fibrosis or cirrhosis (stages F3 to F4).14,105 Refer to Table 2 for information on its strengths and limitations, and Appendix 5, Table 11 for details on its diagnostic accuracy.
Enhanced Liver Fibrosis Score: The ELF score is a patented blood-based NIT that is available in some parts of Canada, though it is not routinely used in clinical practice.281-283 The ELF test is a score that can establish fibrosis stage with a single blood draw by measuring 3 direct biomarkers of fibrosis: hyaluronic acid, tissue inhibitor of metalloproteinase 1, and amino-terminal propeptide of procollagen III.282,284
Unlike the FIB-4 index, the ELF score may capture patients with early disease and can provide estimates for the stage of disease. It could potentially play a growing role in identifying patients with moderate to advanced disease (F2 to F3). Refer to Table 2 for information on its strengths and limitations, and Appendix 5, Table 11 for details on its diagnostic accuracy.
Noninvasive Imaging Techniques
Noninvasive imaging techniques are essential for staging liver fibrosis and monitoring disease progression in patients with MASLD and MASH. Compared with blood-based tests, these modalities provide direct, quantitative measures of liver stiffness and in some instances fat content, enabling more accurate risk stratification and treatment planning.
Vibration-Controlled Transient Elastography (FibroScan®): VCTE is a widely used ultrasound-based tool that assesses the stiffness of the liver. VCTE measures fibrosis from a fixed, relatively small target area of the liver without generating an anatomic image.
It can be performed at the point-of-care in primary, outpatient, inpatient, or community settings.285-290 It is a rapid and painless technique that does not require administration by a medical professional, although training is required. Canadian guidelines recommend VCTE for evaluating fibrosis in patients with an indeterminate risk of MASLD and MASH.14,105
Since 2013, VCTE devices have incorporated controlled attenuation parameter technology, which enables the simultaneous assessment of liver fat.291 This dual capability — measuring the severity of liver scarring and fat content — supports earlier identification of liver disease in patients at risk of MASH.292 Refer to Table 2 for information on its strengths and limitations, and Appendix 5, Table 11 for details on its diagnostic accuracy.
Shear Wave Elastography: SWE is an ultrasound-based tool that also measures fibrosis through liver stiffness. Unlike VCTE, SWE provides real-time imaging of a larger region of interest and can be added as a module to existing ultrasound equipment.293 Most new standard ultrasound machines come equipped with SWE capabilities, enabling use in primary, secondary, and tertiary care settings for patients at risk of MASH.293
Canadian consensus-based guidelines recommend SWE for evaluating fibrosis in patients with indeterminate risk of MASLD and MASH.14,105 Refer to Table 2 for information on its strengths and limitations, and Appendix 5, Table 11 for details on its diagnostic accuracy.
Magnetic Resonance Elastography: MRE is an MRI-based imaging technique that quantitatively measures liver stiffness while also providing high-resolution anatomic images.294,295 It is considered the most accurate available test for noninvasive imaging as it outperforms VCTE and SWE in detecting early fibrosis and fibrosis in patients with obesity or inflammation.294 MRE requires specialized hardware and software that can be added to existing MRI equipment from select manufacturers.296
Canadian consensus-based guidelines recommend MRE as a second-line imaging option in cases when laboratory testing is inconclusive.105 Refer to Table 2 for information on its strengths and limitations, and Appendix 5, Table 11 for details on its diagnostic accuracy.
MRI – Proton Density Fat Fraction: MRI-proton density fat fraction (MRI-PDFF) is another MRI-based imaging technique that quantifies liver fat content, which is a key early marker of MASH and the initial stage of liver disease.295-297 MRI-PDFF can be integrated into existing abdominal MRI protocols on select scanners and does not require additional hardware, although specialized training is required by the technologist to administer the exam protocol.296 Refer to Table 2 for information on its strengths and limitations, and Appendix 5, Table 11 for details on its diagnostic accuracy.
Invasive Diagnostic Approach
Liver Biopsy
The histological features which characterize MASH, hepatocellular ballooning (swollen damaged liver cells) and lobular inflammation (cellular damage within specific liver structures), can only be identified through liver biopsy.1,298 Based on the presence, location, and degree of ballooning, inflammation, and steatosis, specialists trained in liver and gastroenterologic pathology use biopsy samples to diagnose steatohepatitis, as well as to evaluate (stage) fibrosis and, when considered in conjunction with clinical history, diagnose MASH as the underlying cause of liver disease.1
Liver biopsy is typically used conservatively to confirm advanced fibrosis, clarify inconclusive results from NITs, or when investigating alternative or competing causes of liver disease that may require different management (e.g., autoimmune liver disease).113,114
A Canadian study found that serious complications from liver biopsy such as major bleeding, severe pain, and hospitalization are rare, occurring in approximately 1.4% of cases.111,299-301 Minor complications associated with the procedure, including bleeding at the biopsy site, transient hypotension, pain, and fever are more common.111,300 Technical failure (e.g., insufficient specimen, inability to retrieve sample) can also occur, leading to repeat procedures increasing risk and patient burden.111,300,302
DMTs in the Clinical Pipeline
A range of DMTs for MASH are in development, spanning multiple drug classes. These are outlined in Table 8: MASH Agents Currently in Phase II and Phase III Clinical Development. These therapies target different stages of disease and through distinct mechanisms of action.
Table 8: MASH Agents Currently in Phase II and Phase III Clinical Development
Clinical development phase | Drug class examples | Target liver stage | Mechanism of action |
|---|---|---|---|
Phase IIa | Dual agonist: Glucagon/GLP-1 (e.g., Efinopegdutide)303 | Cirrhosis (F4) | Activates glucagon and GLP-1 receptors to enhance energy expenditure, insulin secretion, and lipid metabolism, reducing hepatic fat accumulation and improving glycemic control. |
Tri-agonist: Glucagon/GLP‑1/FGF-21 (e.g., DR10624)304 | Noncirrhotic fibrosis | Stimulates insulin secretion, decreases glucagon secretion, and suppresses appetite leading to weight loss and decreased liver fat. | |
Selective THR-beta agonist (e.g., ALG-055009)305 | Noncirrhotic fibrosis | Activates thyroid hormone receptor–beta found in liver to regulate lipid metabolism, decrease steatosis, and improve hepatic function. | |
Dual selective glucocorticoid modulator/mineralocorticoid antagonist (e.g., Miricorilant)306 | Noncirrhotic fibrosis | Modulates glucocorticoid and mineralocorticoid receptors to normalize cortisol and aldosterone signalling, counteracting metabolic dysfunction, hepatic steatosis, and fibrosis. | |
siRNA therapy (e.g., gatuzosiran)307 | Moderate to advanced fibrosis (F3-F4) | Targets specific genetic risk factors in hepatocytes (liver cells) to break down mRNA and reduce production of HSD17B13 protein. | |
Phase IIIb | Advanced disease (F3) and cirrhosis (F4) | Activates glucagon and GLP-1 receptors to increase energy expenditure, improve glucose and lipid metabolism, and reduce hepatic fat content and fibrotic progression in advanced liver disease. | |
FGF-21 receptor analogues (e.g., Pegozafermin, Efruxifermin, efimosfermin alfa)311-314 | Moderate to advanced fibrosis, including Cirrhosis (F4) | Activates FGF-21 receptors to inhibit hepatic stellate cell activation, suppress inflammation, and reduce liver fat synthesis and deposition. | |
PPAR agonist (e.g., lanifibranor)315 | Noncirrhotic MASH | Activates PPAR-alpha, delta, and gamma pathways to inhibit hepatic stellate cell proliferation and activation, preventing fibrosis development and progression. |
FGF-21 = fibroblast growth factor 21; GLP-1 = glucagon-like peptide-1; PPAR = pan-peroxisome proliferator-activated receptor; siRNA = Small interfering RNA;THR- beta = thyroid hormone receptor-beta.
aPhase II clinical trials focus on establishing proof of concept, determining optimal dosing, and monitoring short-term side effects.
bPhase III clinical trials confirm effectiveness and safety in large, diverse populations.
Treatment Administration
Treatment Options Approved for MASH
GLP-1 RAs are intended to support broad cardiometabolic benefits including improvements in BMI, glycemic control, and cardiovascular and renal outcomes.316 By addressing early-stage metabolic dysfunction, the underlying driver of MASH, GLP-1 therapies have the potential to play a role in disease management and could reduce reliance on MASH-specific treatments that do not provide other metabolic benefits.38 A GLP-1 RA was approved by Health Canada in December 2025 and by the US FDA in August 2025 for the treatment of MASH.39,156,157
THR-beta agonists target receptors in the liver and are designed to affect liver-specific pathways. A THR-beta agonist was approved by the US FDA in March 2024 and received conditional approval from the European Commission in August 2025.157,159,160 However, no THR-beta agonists have been submitted for regulatory review in Canada.
Indirect Prescribing for MASH Management
Many clinicians manage MASH indirectly by addressing associated metabolic comorbidities, such as diabetes or dyslipidemia. While the emergence of DMTs may bring change, clinicians also commonly prescribe other medications — such as statins, metformin, vitamin E, and pioglitazone — to manage cardiometabolic comorbidities63 and indirectly support liver health by reducing inflammation, liver fat accumulation, and fibrosis.168-178 This variation reflects both limited available therapies and gaps in awareness, training, and standardized care pathways across primary and specialty settings.154,155
There may be opportunities to strengthen the care pathway by standardizing treatment eligibility criteria, integrating care across chronic disease management, destigmatizing treatment, and providing individualized care.
Route of Administration
GLP-1 RAs are typically administered as subcutaneous injections, while THR-beta agonists are administered orally. Some injectable therapies, such as GLP-1s, require strict cold chain management and storage protocols to maintain drug stability and effectiveness, which must be considered during distribution, administration, and home use. This may be challenging in rural and remote settings where consistent refrigeration, pharmacy access, and follow-up care may be limited.317
Oral administration may be preferred in some instances to lower infection risk, reduce nursing workload, support adherence, or for a potentially lower carbon footprint.146,318
Protocols for Clinicians
Prescribers are responsible for determining appropriate dosing and titration schedules, monitoring treatment response and safety, and setting stopping rules for adverse events or lack of effectiveness. However, primary care providers internationally and in Canada report limited familiarity with MASH pharmacotherapy or decision support tools, which may increase dependence on specialist centres.47,319 Effective management may be supported by:
familiarity with CPGs
availability of safety monitoring protocols
coordinated care pathways for referral.
Fibrosis Staging and Equity Considerations
As DMTs emerge, NITs increasingly guide treatment eligibility. Evidence shows that current NIT thresholds may miss patients who otherwise qualify for therapy, highlighting the need for improved staging protocols.167,180
Many commonly used indices were validated predominantly in white, Western populations, which may underestimate disease severity in racialized communities, Indigenous Peoples, women, and individuals with lean MASLD/MASH.28,135,192
Novel NIT thresholds have been proposed to better guide treatment decisions. Standardized staging processes could reduce access barriers, especially in rural, remote, and northern regions where provider shortages can delay assessment.167,179,181
Provider Roles and Prescribe Scope
Under all indications for GLP-1 RAs approved in Canada, including for diabetes and weight management, prescribing authority extends to a wide range of health care practitioners. Prescribers include PCPs, endocrinologists, internists, cardiologists, nephrologists, gastroenterologists, neurologists, and psychiatrists.183 Clarifying roles of providers in monitoring, patient support, and coordination could improve patient outcomes,186,187 especially in primary care settings where many patients are seen first.182,184,185
Enhanced role clarity may also help reduce fragmentation, streamline referrals, and support shared care approaches between primary care and specialists as treatment options expand.
Destigmatizing Treatment and Patient Perceptions
Patient perceptions of treatment options may influence acceptance and adherence. Stigma related to obesity and weight loss may discourage engagement.49,188,189 For example:
THR-Beta agonists are liver specific and may be perceived as “liver drugs”
GLP-1 RAs are primarily indicated for T2D and obesity and may be viewed as “weight loss drugs.”
Additionally, patients may prioritize management of comorbid conditions (e.g., T2D, CVD) over MASH.101-103 This can limit patient engagement with liver-focused care and impact treatment uptake, especially when lifestyle interventions such as diet and exercise are emphasized as the primary management strategy. If lifestyle and diet modifications are required for eligibility criteria in Canada, as is the case in the US and Europe, this may be a barrier to treatment eligibility.156,158,160
Structural Inequities, Access Barriers, and Engagement-Informed Supports
Adherence to diet and lifestyle interventions is influenced by not only behavioural factors but by structural factors. Indigenous Peoples, people living in rural, remote, and northern areas, and people with low incomes who are living with MASH may experience additional barriers to DMTs despite clinical eligibility, as they are disproportionately impacted by food insecurity, limited access to healthy food, and physical impairments.190,191 Participants engaged for this report also emphasized that acceptance of new therapies to patients from different backgrounds depends on culturally safe communication, trust, and care approaches that acknowledge Indigenous experience and healing practices.
Participants from Indigenous-led and CDA-AMC-led engagement activities described challenges with attending frequent follow-up appointments due to travel, cost, and mobility issues, noting that integrated care pathways make ongoing management easier. They suggested mobile clinics could improve testing access and Indigenous navigators would support care.
Treatment Monitoring and Life Cycle
Initial Monitoring
Early monitoring is critical to ensure safe and effective treatment initiation. During the first 3 months, clinicians may focus on the following:167,180,193
confirm patient adherence to the prescribed regimen
assess treatment tolerability
identify and address any adverse effects
monitor baseline changes in metabolic and liver-related biomarkers.
These initial evaluations lay the foundation for long-term care and help identify patients who may need additional support.167,180,193
Effectiveness Assessment
As treatment continues, improvements in liver health typically take time to emerge — often between 6 and 12 months after initiation.167 At this time, monitoring should incorporate NITs, including:167,180,193
fibrosis staging using methods such as VCTE, MRE, or ELF scores
liver function tests and metabolic panels.
These assessments provide insight into treatment response and inform decisions about ongoing therapy. Over time, meaningful improvements — such as fibrosis regression and resolution of steatohepatitis — may be observed.
Ongoing Monitoring
Beyond the first year, monitoring should continue on an annual or biannual basis,167 depending on:
disease severity and fibrosis stage
presence of comorbid conditions (e.g., T2D, CVD)
risk of progression or adverse events.
Adherence to monitoring for patients diagnosed with MASH can be hindered by informational, psychosocial, and socioeconomic barriers, such as:
limited awareness among both the public and clinicians, which may lead to decreased engagement with ongoing care — particularly among immigrants and newcomers to Canada and individuals with low health literacy who may face additional challenges to navigating the health systems and advocating for care.194,195
psychosocial challenges, including anxiety and depression, which can reduce adherence to scheduled assessments.195,320,321
out-of-pocket costs for noninvasive tests and laboratory services which may disproportionately affect individuals with lower incomes or without private insurance and may challenge continuity of care for people receiving DMTs.
Continuation of Treatment
Evidence on the long-term use of these treatments would help inform decisions around treatment continuation and discontinuation.2,180,193
In the US and in Europe, regulatory authorities recommend patient monitoring of disease progression and treatment effectiveness through NITs.2,180,193 Indications of clinical response may include:
regression of disease and improvement in liver fibrosis
normalization or reduction in liver enzymes and other cardiometabolic markers
weight loss and metabolic improvement.
Discontinuation of Treatment
Specific criteria for discontinuation of treatment would be required if DMTs become available. According to the clinical experts engaged for this review, these may include lack of therapeutic response, disease progression, patient safety, or patient preference. If DMTs for MASH were discontinued, patients may still require regular follow-up at multidisciplinary clinics to reassess alternative treatment options (e.g., lifestyle therapy, clinical trials, combination or adjunctive therapies). There are several considerations around the discontinuation of treatment.
Safety monitoring: Adverse events reported for people using DMTs include mild to moderate gastrointestinal disorders, including nausea and diarrhea.173,174,322 Because MASH is a multisystemic condition, safety monitoring may also need to extend beyond liver outcomes to include cardiovascular, cancer, renal function, and glycemic control risks.323,324 People with multiple comorbidities may require additional safety monitoring.
Multidisciplinary Coordination
Integrating nurse- or pharmacist-led monitoring, shared care models, and community-based programs may help distribute follow-up responsibilities.196,197 Multidisciplinary care teams may support optimal patient management, with monitoring that encompasses both liver health and broader cardiometabolic conditions.198-201
Coordinating Access to Testing
Repeat eligibility assessments may require additional laboratory testing and imaging to assess ongoing treatment effectiveness, underscoring the need for sustained access to these services and specialist follow-up.
As emerging NITs and blood-based biomarkers may refine monitoring protocols and inform treatment decisions, their integration into practice may require coordinated alignment across laboratory services, imaging capacity, and clinical workflows.167,180,193 Ongoing challenges include limited hepatology capacity, care coordination, and access to these resources in rural, remote, and northern regions and in Indigenous communities, resulting in the need for distant travel.95,202-205
Supporting Treatment Adherence
Monitoring practices adapted to population specific needs could be considered, including:
providing culturally appropriate education
offering navigation support
implementing digital tools that promote continuity of care and empower patients to remain engaged throughout treatment
continued access to dietary and behavioural therapies.
Existing Inequities in Access to Care
Low-income and racialized populations have been reported to receive fewer specialist referrals, rely more heavily on emergency departments, and experience additional barriers linked to racism, out-of-pocket expenses, and transportation.139,325 Limited specialist availability, combined with structural and racial inequities, can delay interventions and compromise ongoing management. These challenges are further compounded for Indigenous communities, where access to culturally safe care is limited, and historical mistreatment within colonial health systems continues to influence trust and engagement.326 Referral processes themselves are often fragmented, with unclear responsibilities, limited standardized pathways, and inconsistent communication between primary care and specialists, contributing to delays in assessment and treatment.
Indigenous and CDA-AMC-led engagement participants noted that limited primary care access, high travel and financial demands, and mobility or social constraints disproportionately affect rural, northern, and other underserved populations. These factors may contribute to delays in diagnosis and treatment, reinforcing systemic inequities.
System Navigation
People living with MASH and their providers must often navigate multiple entry points and disconnected providers leading to fragmented care experiences. Care navigators can mitigate these challenges by helping to coordinate services, facilitate referrals, and improve care continuity across settings; however, access to care navigation supports is uneven across Canada.327-329 In some jurisdictions, formal systems of care navigation are limited or unavailable, and existing navigator roles may be restricted to specific diseases or settings.328,330 These challenges are amplified for rural communities, immigrants, and newcomers, who may face long travel distances, language barriers, and limited access to care navigators.321,331 Without navigation support, individuals may experience delayed diagnosis, inconsistent follow-up, and suboptimal outcomes.328,330 Indigenous patient participants highlighted the need for increased access to Indigenous primary care providers and navigators.
“There should be Indigenous navigators around the clock.”
– Participant living with MASH in the Indigenous-led engagement activity, describing the need for Indigenous-specific support
Clear responsibilities and standardized MASH care pathway can lead to earlier diagnosis, treatment opportunities, and reduced costs. Coordinated, multidisciplinary models — supported by clear referral protocols, interoperable data systems, and culturally safe care — are approaches that could improve equity, efficiency, and outcomes across the continuum of care.95,202
Appendix 3: Methodology for the Review of Health System Readiness
Please note that this appendix has not been copy-edited.
We conducted exploratory literature searches to inform topic refinement and question development. Targeted internet searches were conducted to identify documents both nationally and internationally. Results of the searches were used in project planning and in guiding consultations with decision-makers and collaborators.
Subsequently, we conducted a review of relevant literature to summarize and synthesize information on the health system readiness for potential DMTs for MASH in Canada. Each section of the evidence review was informed by guiding questions developed through internal discussions and refined during the discovery and consultation phases. These guiding questions help ensure the evidence we gather is directly relevant to system-level decision-making across domains such as diagnostics, treatment, policy, and implementation. Throughout the review, equity considerations were integrated for each question.
Overview Questions
The health system readiness search supported findings on system readiness related considerations for the potential introduction of DMTs for MASH. These analyses were also informed by input from clinical experts. We identified and synthesized available evidence on system readiness to supplement findings from both the literature review and engagement activities. Research questions for the review included:
What are the clinical pathways for a person with suspected MASH in Canada, including primary care initiation and processes for specialist referral?
What is the landscape of clinical management of MASH in Canada, including multidisciplinary care, barriers, and facilitators?
What biomarkers are used to diagnose MASH and determine treatment eligibility for DMTs?
What imaging modalities are used to diagnose MASH and determine treatment eligibility for DMTs?
What are the new and emerging technologies that may support system readiness for the introduction of DMTs for MASH?
What equity considerations are raised by the diagnosis and treatment of MASH?
Search
An information specialist conducted a targeted literature search on MEDLINE, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of health technology assessment agencies in Canada and major international HTA agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concepts were MASH and system readiness. The search was completed on July 11, 2025, and limited to English-language documents published since January 1, 2020. Additional searches, with the same limits, were conducted using the search concepts MASH and relevant concerns related to system readiness, including but not limited to access and availability, novel drugs, safety, ethics and equity, specific tests, and population size. Search filters were applied to these additional searches to limit retrieval to health technology assessments, systematic reviews, meta-analyses, indirect treatment comparisons, or guidelines. For certain concepts, search terms for reviews of any type were also included. Regular alerts updated the database literature searches until the publication of the final report.
Screening and Extraction
Two reviewers screened articles in Covidence at the title and abstract stage in 2 phases. During the first phase, each reviewer performed a single-level review of half of all included studies References were tagged according to a predefined list of terms relevant to the health system readiness component of the report. References that met the exclusion criteria were omitted. A second-pass screening at the title and abstract level was then conducted on references tagged with “MASH.” Both reviewers independently reviewed all articles based on the inclusion criteria. Any conflicts were resolved during a follow-up consensus meeting. If saturation was reached in any topic area, the following criteria for including studies were applied:
Sample size of population or number of studies included in analysis
Relevance to practice in Canada (e.g., OECD)
Studies that contain large data points (global studies)
Robustness of methods or comprehensiveness of report
Date of publication
Overall relevance
For all included studies addressing health system readiness and emerging technologies, a narrative/summative approach to data extraction was undertaken to capture the key information. Data extraction focused on the current state of health care systems in Canada regarding diagnosing and treating MASH and enablers or barriers to the introduction of DMTs for MASH in health care systems in Canada.
Synthesis
Data were synthesized into a health system readiness report, highlighting the health system readiness for potential introduction of DMTs for MASH. We summarized available information (including from experts in Canada) within each domain, noting practical considerations and system-level implications for implementation in health care contexts in Canada.
Appendix 4: Methodology for the Review of the Diagnostic Accuracy of Noninvasive Tools
Please note that this appendix has not been copy-edited.
We conducted a rapid review to identify literature on diagnostic tools to identify MASH, their clinical characteristics, and diagnostic accuracy.
The rapid review method was chosen to support timely health system planning. By focusing on recent systematic reviews, this report provides a broad, evidence-informed understanding of the current diagnostic landscape, prioritizing evidence from reviews with moderate-high reporting standards supports transparency. While acknowledging that some relevant studies may have been excluded, this review was meant to provide an overview of the noninvasive tools landscape instead of a detailed comparative analysis. Rather than a comprehensive synthesis, this targeted review aimed to help decision-makers understand the diagnostic accuracy and key considerations of noninvasive tools and identify which tools may show higher sensitivity and specificity for detecting MASH.
Based on scoping activities, we developed the preliminary review questions and selection criteria, as well as developing related questions for clinical experts’ engagement consultations. An internal project plan for the rapid review was developed before undertaking the searches. The plan is available on request. The plan did not prespecify cut-offs or all possible outcomes that would be collected beyond sensitivity, specificity, and area under the curve if applicable. It also outlined extracted data would include key findings, strengths, and limitations from each included systematic review to identify areas for decision-making consideration across sources.
Overview Questions
The rapid review of diagnostic tools provided information about noninvasive ways to diagnose MASH. These analyses were also informed by input from clinical experts and clinical practice guidelines — for example, insights on which tools are currently in use across Canada. We identified, synthesized, and appraised available evidence on diagnostic tools and combined findings from both the literature review and engagement activities. Initial research questions for the rapid review included:
What measures (e.g., quantitative liver stiffness measure, quantitative estimate of accumulation of fat on liver, blood serum biomarkers, imaging parameters, risk score) for NITs are used for the screening or diagnosis of MASH?
What is the diagnostic accuracy of NITs with liver biopsy as the reference standard?
What are the strengths and limitations of existing NITs? (Answering this was supplemented by other literature outside the rapid response search)
Search
An information specialist conducted a literature search on MEDLINE, the Cochrane Database of Systematic Reviews, the International Health Technology Assessment (HTA) Database, the websites of health technology assessment agencies in Canada and major international HTA agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concepts were MASH and imaging or scoring systems. Search filters were applied to limit retrieval to health technology assessments, systematic reviews, meta-analyses, or indirect treatment comparisons. The search was completed on July 4, 2025, and limited to English-language documents published since January 1, 2020, to ensure the review captured the most recent evidence in this rapidly evolving area, as MASH research, guidelines, and treatments have advanced significantly in recent years. Regular alerts updated the database literature searches until the publication of the final report.
Screening and Data Extraction
One reviewer screened records retrieved by the searches in 2 steps; first by titles and abstracts, then by full text. Selected studies that met the eligibility criteria were based on study type (systematic reviews that defined themselves as such), population (adults aged 18 years older who were biopsied for MASH, excluding pediatric populations), interventions (noninvasive diagnostic and screening tests for MASH), reference standard (liver biopsy), and outcomes (diagnostic accuracy of noninvasive tests).
One reviewer extracted summary study information from included studies, including first author and year, country, review type, study objective, included populations, number of studies, tests evaluated, outcomes assessed, main conclusions, limitations, and strengths. Further 1 reviewer assessed the methodological quality according to the AMSTAR 2 tool for systematic reviews. Systematic reviews judged to be of moderate to high methodological quality by this assessment were included in the rapid response; relevant systematic reviews considered to be of low or very low methodological quality were excluded. For each included study, additional data were extracted including index test, tool type, number of studies contributing data, diagnosis as defined by reference standard, test cut-offs or thresholds, prevalence of MASH (when reported), measure of fibrosis or steatosis, sensitivity and specificity with 95% confidence intervals, and the reported area under the curve, where applicable. Risk of bias assessments from the included studies was extracted as reported by respective study authors. Some characteristics commonly reported in systematic reviews (e.g., date of last search, number of included studies and patients, prevalence of MASH, population characteristics, and heterogeneity measures) were captured during data extraction but not fully reported in the summary table because these details were not consistently available across all included studies. To avoid selectively presenting information, we chose to summarize only those elements that were consistently reported in all reviews.
Although not all items were directly applicable, using AMSTAR 2 allowed us to systematically capture methodological features of the included reviews, providing a rapid overview of the quality of the study reporting.
Limitations
To meet timelines, single-reviewer screening, data extraction, and quality assessment were used. These methods increase the risk of error and bias compared with full systematic review processes. The use of AMSTAR 2, which is not specifically designed for diagnostic test accuracy reviews, also limits the precision of methodological quality assessments. Another team using different tools may reach different conclusions regarding the quality of the included systematic reviews.
As a rapid review, this review is not comprehensive. Excluding lower-quality systematic reviews may omit evidence for certain noninvasive tests, and the included reviews may not represent the optimal balance of quality, recency, relevance, and comprehensiveness. Thus, results should be interpreted as a high-level overview rather than a complete synthesis of all available evidence.
Only systematic reviews rated as moderate or high methodological quality were included. No additional screening was conducted for recency, relevance, comprehensiveness, or alignment with the population, intervention, comparison, and outcome framework, and primary study overlaps across systematic reviews were not assessed. As a result, the included reviews may not provide a comprehensive or fully current synthesis of the diagnostic accuracy literature, and the rapid review should be interpreted as a high-level overview, not an exhaustive summary of all evidence.
Because we relied exclusively on eligible systematic reviews, supplemental primary studies were not searched for or included, except in 1 case where no MASH-specific accuracy data existed for a commonly used tool; in that instance, a MASLD accuracy study was added to provide at least some evidence.
The primary studies included within the systematic reviews were frequently assessed by review authors as high risk of bias, limiting the certainty of the diagnostic accuracy estimates. Other factors that reduce confidence in the evidence include:
indirectness, where populations or thresholds differed across studies
inconsistency, with sensitivity and specificity varying widely across primary studies
imprecision, particularly for tools assessed in small samples
potential publication bias, which could not be assessed within this rapid review.
Deviations from the plan occurred during literature searching, screening, and data extraction due to the high volume of evidence, but they were made in consultation with the study team and advisors and did not compromise the review’s aim to inform decision-makers of relevant tools.
The initial search for literature on MASH diagnostic accuracy yielded approximately 2,500 articles, which was not feasible to screen within the rapid review time frame. The review was therefore refocused on systematic reviews to provide an overview of evidence on noninvasive diagnostic tools.
During screening, studies were further excluded if they did not report sensitivity and specificity for MASH specifically, but only for MASLD (Figure 9; n = 30).
During extraction, more than 100 tools were identified in systematic reviews after reviewing basic information from just 5 studies. To maintain feasibility, we narrowed the focus to “commonly used” tools — those mentioned in clinical practice guidelines or reported to be used in Canada by clinical experts. One tool initially excluded had to be added; because no MASH-specific accuracy data existed in the included reviews, a MASLD diagnostic accuracy study was subsequently included from previously excluded literature to provide at least some evidence for that tool. Similarly, we only reported the sensitivity and specificity of the tools as reported by the systematic reviews.
During synthesis, key characteristics of several commonly used tools were not available in the systematic reviews. Clinical experts were consulted and targeted handsearching was conducted to obtain essential details.
Overall Interpretation
These limitations mean that the review does not provide a comprehensive synthesis of all available diagnostic accuracy evidence for all noninvasive tests. Instead, it offers a decision-focused snapshot of the tools most commonly used in practice and whether any appear suitable as potential biopsy replacements.
Appendix 5: Results of the Review of the Diagnostic Accuracy of Noninvasive Tools
Please note that this appendix has not been copy-edited.
After screening 189 articles, 17 systematic reviews met the inclusion criteria. Basic study information was extracted, and methodological quality was assessed using AMSTAR-2. As described in the methods and protocol deviations, the synthesis focused only on commonly used or recommended tools. To ensure coverage of these tools, 1 additional review evaluating the diagnostic accuracy of ShearWave Elastography (SWE) for MASLD — rather than MASH specifically — was included, bringing the total to 18 reviews.332
Although 6 reviews were rated as moderate to high quality, limiting reporting to commonly used and recommended tools further narrowed the pool of relevant evidence; 4 of these 6 reviews contained applicable data on those specific tools (Table 11).
Key Evidence Findings on NITs
No single definitive test: More than 100 NITs exist, but none of the common tests demonstrated the same diagnostic accuracy (sensitivity and specificity) across all reported studies, populations, disease stages, or settings. Evidence remains limited to support using any existing NIT as a stand-alone screening tool for early-stage disease or as a biopsy replacement.
Diagnostic accuracy: The included evidence suggested MRE had the highest diagnostic accuracy followed by SWE and VCTE, however cut-off thresholds and diagnostic definitions differed across studies (More details in Appendix 5, Table 11).
Risk of bias: Across included systematic reviews, most studies were at high or unclear risk of bias, as appraised by the systematic review authors (refer to Appendix 5, Table 10 for more details).
Generalizability: Across the included systematic reviews, no subgroup analyses were conducted to determine whether test accuracy differed based on characteristics such as age, sex, or race. This limits our ability to assess whether these diagnostic tools perform consistently across diverse populations. The lack of evidence-based information on race is concerning as evidence shows that some populations are at higher risk of developing MASH.
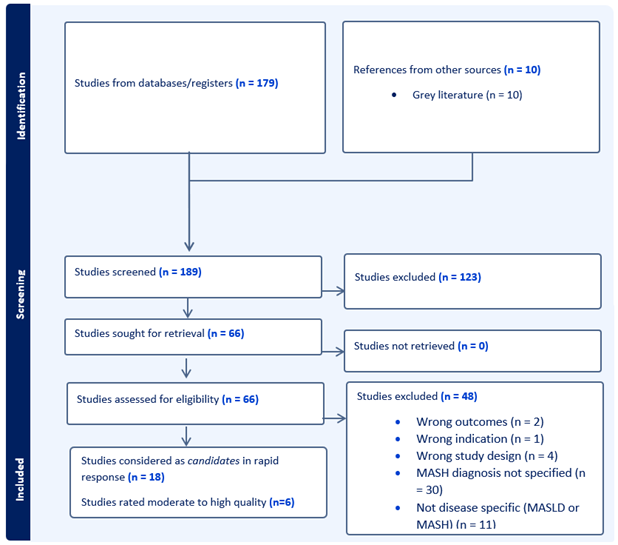
Table 9: AMSTAR 2 Ratings of Systematic Reviews on Noninvasive Tools for MASH Diagnosis
Study | AMSTAR 2 domains | Overall confidenceb | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
1 | 2a | 3a | 4a | 5 | 6 | 7 | 8 | 9a | 10 | 11a | 12 | 13a | 14 | 15a | 16 | ||
Decharatanachart et al.333 | Yes | Yes | Yes — inferred | Yes | Yes | Yes | Yes | No | Yes | No | No meta-analysis | No meta-analysis | Yes | Yes | Yes | Yes | Moderate |
Zamanian et al.334 | No | No | Yes — inferred | Partial Yes | No | No | Yes | No | No | No | No meta-analysis | No meta-analysis | No | No | No | Yes | Critically low |
Sun et al.335 | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | High |
Bresnahan et al.296 | Yes | Yes | Yes — inferred | Yes | Yes | No | Yes | Yes | Yes | No | Yes | Yes | Yes | No | No | Yes | Moderate |
Cathcart et al.295 | Yes | Yes | Yes — inferred | Yes | No | No | Yes | No | Yes | No | No meta-analysis | No meta-analysis | No | Yes | No | Yes | Critically low |
Castellana et al.336 | Yes | Yes | Yes — inferred | No | Yes | Yes | Yes | Yes | Yes | No | No MASH meta-analysis | Yes | Yes | Yes | No | Yes | Critically low |
Pennisi et al.337 | Yes | Yes | Yes | Yes | No | No | Yes | Yes | Yes | No | Yes | Yes | Yes | No | No | Yes | Low |
Ismaiel et al.338 | Yes | No | Yes — inferred | Partial Yes | No | Yes | Yes | Partial Yes | Yes | Yes | Yes | No | Yes | Yes | No | Yes | Critically low |
Gosalia et al.339 | Yes | No | Yes — inferred | No | Yes | No | No | Partial Yes | No | No | No meta-analysis | No meta-analysis | No | No | No | Yes | Critically low |
Eguchi et al.340 | Yes | No | Yes | Yes | No | No | No | Partial Yes | No | No | No meta-analysis | No meta-analysis | No | No | No | Yes | Critically low |
Ravaioli et al.341 | Yes | Yes | Yes — inferred | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | No | Yes | Low |
Vali et al.342 | Yes | Yes | Yes | Yes | No | No | Yes | Partial Yes | Yes | No | No MASH meta-analysis | No | No | Yes | No | Yes | Low |
Contreras et al.343 | Yes | Yes | Yes — inferred | Yes | Yes | Yes | Yes | No | Yes | No | Yes | No | Yes | Yes | Yes | Yes | Moderate |
Malandris et al.344 | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | No | Yes | Yes | Yes | Yes | High |
Selvaraj et al.345 | Yes | Yes | Yes — inferred | Yes | Yes | Yes | Yes | Partial Yes | Yes | No | Yes | Yes | Yes | Yes | No | Yes | Low |
Mózes et al.346 | Yes | Yes | Yes | Yes | No | No | Yes | Partial Yes | Yes | No | Yes | Yes | Yes | No | No | Yes | Low |
Garg et al.347 | Yes | No | Yes — inferred | Yes | Yes | No | Yes | Partial Yes | Yes | No | No meta-analysis | No meta-analysis | Yes | Yes | No | Yes | Critically low |
Xu et al.332 | Yes | Yes | Yes — inferred | Yes | Yes | Yes | Yes | Partial Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | High |
Note: The checklist with full details is available at: https://www.bmj.com/content/bmj/suppl/2017/09/21/bmj.j4008.DC1/sheb036104.wf1.pdf.
aCritical domains for the AMSTAR 2 assessment.
bOverall: based on https://amstar.ca/Amstar-2.php, only bolded studies with moderate-high confidence in quality were included for reporting diagnostic accuracy of noninvasive tools.
Source: Shea BJ, Reeves BC, Wells G, Thuku M, Hamel C, Moran J, Moher D, Tugwell P, Welch V, Kristjansson E, Henry DA. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomized or nonrandomized studies of health care interventions, or both. BMJ. 2017 Sep 21;358:j4
Table 10: QUADAS-2 Reported in Systematic Reviews on Noninvasive Tools for MASH Diagnosis of Moderate-High Reporting Quality Based on AMSTAR 2
ID | Study author, (year), and reference | Overall confidence AMSTAR-2 (Table 9)a | QUADAS-2 overview | Specific QUADAS -2 reporting |
|---|---|---|---|---|
1 | Decharatanachart, P., et al. (2021)333 | Moderate | Low ROB in 4 of 5 | Four of 5 MASH-related studies had low risk of bias; 1 had uncertain risk due to using ultrasonography with liver function tests as the reference standard. All 5 had no applicability concerns. |
3 | Sun Y., et al. (2025)335 | High | High ROB in 2 domains | Of 180 studies, applicability was generally low concern (97% to 100% across domains). However, risk of bias was high: 75% lacked clear reporting for patient selection and reference standard, and 81% for the index test. |
4 | Bresnahan, R. et al. (2023)296 | Moderate | High ROB in at least 1 domain 12 of 13 of studies | Only 1 of 13 studies had low risk of bias across all domains. Most studies (11 of 13) had bias or uncertainty in the index test (no prespecified thresholds), 4 of 13 in the reference standard (unclear blinding), and 2 of 13 in flow/timing (delayed or incomplete biopsy). Only 1 study had no applicability concerns; 12 of 13 had either uncertainty (6 of 13 – NAFLD patients with prior NIT indicating advanced disease) or high-risk concerns (6 of 13 – mixed liver populations or unreported NAFLD subgroups). Three studies had high-risk concerns for index test applicability due to noncommercial MRE designs or analyses not reflecting clinical practice. |
13 | Contreras, D. et al. (2023)343 | Moderate | High ROB in 2 domains 50% or more of studies | Many studies (more than 75%) had high or uncertain risk of bias in the flow and timing domain, 50% in the index text domain and only about 30% had concerns in the patient selection, reference standard, and applicability domains. |
14 | Malandris, K. et al. (2024)344 | High | High ROB in 2 domains of more than 50% or more studies | High risk of bias due to patient selection and/or suboptimal reporting of blinding of reference standard for index score (12 of 16), uncertain risk of bias due to inadequate description of reference standard (biopsy specimens' quality criteria) 9 of 16. One study raised applicability concerns because of population selection from a MASH clinical trial. |
18 | Xu, X. et al. (2025)332 | High | High ROB in 1 domain more than 50% of studies | Most studies had low overall risk of bias, though 30% had unclear patient selection, 40% unclear and 45% high risk in index test, 2 studies high and 1 unclear risk in reference standard, and 55.6% high and 30% unclear risk in flow/timing. Applicability concerns were minimal across all domains. |
ROB = risk of bias.
aOverall: Based on https://amstar.ca/Amstar-2.php, only bolded studies with moderate-high confidence in quality were included for reporting diagnostic accuracy of noninvasive tools.
Table 11: Diagnostic Accuracy of Common Noninvasive Diagnostic Tools
Tool | Hepatic pathology | Diagnostic definition used | Cut-off(s) | Sensitivity (95% CIs) | Specificity (95% CIs) | Reference |
|---|---|---|---|---|---|---|
Scores with biomarkers + patient characteristics | ||||||
FIB-4 index | Fibrosis | High-risk NASHa (NAS ≥ 4, ≥ F2) | NR | 0.62 (0.48, 0.74) | 0.68 (0.52, 0.8) | Sun et al. (2025)335 |
NASHa – criteria not stated | ≥ 3.25 (ruling in¥) | 0.57 (0.39, 0.74) | 0.89 (0.77, 0.95) | Contreras et al. (2023)343 | ||
ELF score | Fibrosis | Diagnosing NASHa vs. NAFLD | NR | 0.68 (0.29, 0.94) | 0.68 (0.24, 0.95) | Sun et al. (2025)335 |
High-risk NASHa (NAS ≥ 4, ≥ F2) | NR | 0.99 (0.96, 1) | 0.07 (0.01, 0.2) | Sun et al. (2025)335 | ||
NFS (NAFLD score) | Fibrosis | High-risk NASHa (NAS ≥ 4, ≥ F2) | NR | 0.7 (0.56, 0.83) | 0.52 (0.32, 0.69) | Sun et al. (2025)335 |
Fibrosis | NASHa – criteria not stated | ≥ 0.676 | 0.3 (0.27, 0.33) | 0.96 (0.95, 0.96) | Contreras et al. (2023)343 | |
Imaging-based methods | ||||||
VCTE | Fibrosis | Diagnosing NASHa vs NAFLDa | NR | 0.81 (0.69, 0.9) | 0.66 (0.49, 0.8) | Sun et al. (2025)335 |
High-risk NASHa (NAS ≥ 4, ≥ F2) | NR | 0.86 (0.74, 0.94) | 0.45 (0.25, 0.64) | Sun et al. (2025)335 | ||
Shear wave elastography | ||||||
2D SWE | Fibrosis | MASLD with significant fibrosis (F ≥ 2) | NR | 0.71 (0.63, 0.78) | 0.83 (0.76, 0.88) | Xu, X., et al. (2025)347 |
Point SWE | Fibrosis | MASLD with significant fibrosis (F ≥ 2) | NR | 0.77 (0.68, 0.84) | 0.76 (0.66, 0.84) | Xu, X., et al. (2025)347 |
MRI | ||||||
MRE | Fibrosis and steatosis | NASH:a NAS ≥ 4 with ≥ 1 ballooning/inflammation | 3.3kPa (ruling in¥) | 0.79 (0.69, 0.87) | 0.34 (0.22, 0.47) | Bresnahan et al. (2023)296 |
NASH:a ≥ 1 steatosis, ≥ 1 hepatocyte ballooning and ≥ 1 lobular inflammation | 0.88kPa (ruling in)b | 0.45 (0.23, 0.68) | 1 (0.78, 1.00) | Bresnahan et al. (2023)296 | ||
NASH:a ≥ 1 steatosis, ≥ 1 hepatocyte ballooning and ≥ 1 lobular inflammation | 2.27kPa (ruling in)b | 0.7 (0.46, 0.88) | 0.87 (0.60, 0.98) | Bresnahan et al. (2023)296 | ||
Advanced NASH:a NAS ≥ 4, ≥ F2 | 3.5kPa (ruling in)b | 0.69 (0.57, 0.80) | 0.49 (0.37, 0.60) | Bresnahan et al. (2023)296 | ||
MRI - PDFF | Steatosis | NASH:a NAS ≥ 4 with ≥ 1 ballooning/inflammation | 10% (ruling in)b | 58 (35.3, 77.8) | 67.8 (56.3, 77.4) | Bresnahan et al. (2023)296 |
Advanced NASH:a NAS ≥ 4, ≥ F2 | 10% (ruling in)b | 49.4 (19.1, 80.1) | 60.5 (50.1, 70.0) | Bresnahan et al. (2023)296 | ||
ALT = alanine aminotransferase; AST = aspartate aminotransferase; CAP = controlled attenuation parameter; CI = confidence interval; cT1 = corrected T1; ELF = Enhanced Liver Fibrosis; FIB-4 = Fibrosis-4; kPA = kilopascal; MASLD = metabolic dysfunction–associated steatotic liver disease; MRE = magnetic resonance elastography; NAFLD = nonalcoholic fatty liver disease; NAS = NAFLD activity score; NASH = nonalcoholic steatohepatitis; NR = not reported; PDFF = proton density fat fraction; VCTE, vibration-controlled transient elastography.
aNASH/NAFLD was used as nomenclature in some research despite the internationally recognized recent nomenclature change to MASH/MASLD.
bRuling out excludes advanced fibrosis with high confidence; ruling in confirms advanced fibrosis with high confidence.
Table 12: Summary of Additional Noninvasive Diagnostic Tools
Tool | Hepatic pathology | Tool components |
|---|---|---|
Serum-based biomarkers | ||
CK-18 | Liver cell damage | Protein detected in serum-based test |
CK18-M30 | Liver cell damage — hepatocyte apoptosis | Protein detected in serum-based test |
AST/ALT ratio | Fibrosis | AST, ALT |
APRI | Fibrosis | AST, platelet count |
ELF score335 | Fibrosis | Hyaluronic acid, tissue inhibitor of metalloproteinase 1, and amino-terminal propeptide of procollagen III |
Scores with biomarkers + patient characteristics | ||
Fibrosis | Age, AST, ALT, and platelet count | |
NFS (NAFLD score) | Fibrosis | Age, BMI, fasting glucose/T2D, AST, ALT, platelet count, albumin |
BARD score | Fibrosis | BMI (≥ 28), AST/ALT ratio, T2D |
Scores with imaging or elastography | ||
FAST score | Fibrosis and steatosis | Controlled attenuation parameter, liver stiffness measurements by vibration-controlled transient elastography, and AST levels |
Imaging-based methods | ||
Transient Elastography335 | Fibrosis | Ultrasound-based measure of the velocity of shear waves generated through the liver |
MRI - PDFF296 | Steatosis | MRI-based measure of liver fat content calculated as the fat-to-water signal ratio |
MRI - cT1 | Fibrosis | MRI-based measure of water signal relaxation time post-excitation, corrected for iron content and scanner variability |
Magnetic resonance elastography296 | Fibrosis and steatosis | MRI-based measure of the propagation of mechanical waves through soft tissue |
Shear wave elastography – point or 2D347 | Fibrosis | Ultrasound-based quantitative measure of stiffness (can include imaging components for fat accumulation) |
ALT = alanine aminotransferase; APRI = AST to platelet ratio index; AST = aspartate aminotransferase; BARD = BMI, AST/ALT Ratio, and Diabetes; BMI = body mass index; CK-18 = cytokeratin 18; cT1 = corrected T1; ELF = Enhanced Liver Fibrosis; FAST = FibroScan-AST; FIB-4 = Fibrosis-4; MRI = MRI; NFS = NAFLD fibrosis score; PDFF = proton density fat fraction; T2D = type 2 diabetes.
Note: Equity considerations in diagnostic tools: Across the reviews assessing the accuracy of the diagnostic tools for MASH, none explicitly incorporated an equity framework such as PROGRESS-Plus or conducted equity-stratified analyses. Demographic reporting was largely limited to characteristics such as age and sex. While these variables were commonly described, no subgroup analyses were conducted to determine whether test accuracy differed by age or sex. There were also no subgroup analyses based on other PROGRESS-Plus factors such as race/ethnicity, socioeconomic status, geography, disability, education, or social capital. This lack of evidence limits our ability to assess whether these diagnostic tools perform consistently across diverse patient populations. We would not anticipate the accuracy of the diagnostic tools to vary based on factors such as socioeconomic characteristics, education, geography, or social capital. However, the lack of evidence-based information on PROGRESS-Plus factors is concerning, as evidence shows that some populations are at higher risk for developing MASH.
Appendix 6: Guidance for Reporting the Involvement of Patients and the Public (Version 2) Short-Form Reporting Checklist
Please note that this appendix has not been copy-edited.
Table 13: GRIPP2-SF46 of Indigenous-Led and CDA-AMC–Led Engagement Activities
GRIPP2 | Summary |
|---|---|
1. Aim | To gather lived experience and community perspectives on MASH/fatty liver disease to help contextualize clinical and health system evidence, fill in gaps not reflected in the literature, and help inform ethics and equity considerations for this report. Engagement activities focused on diagnostic and treatment experiences and the related equity considerations. |
2. Methods | Two distinct engagement activities were conducted, 1 led by CDA-AMC and 1 by the Indigenous consulting firm Sage Solutions. CDA-AMC-led engagement methods: Total participants: 6 4 people living with MASH with lived experience of MASH 2 patient group representatives (1 also living with MASLD and 1 as Policy Lead) Place of residence: Alberta (2), Ontario (3), Newfoundland and Labrador (1) Missing perspectives: Caregivers; members of racialized communities; 2SLGBTQ+ participants; individuals with low incomes; people who speak languages other than English; rural/remote residents. Participants took part in 5 engagement sessions in October and November 2025. Semistructured interviews and facilitated discussion questions explored symptom onset, diagnosis, treatment experiences, system navigation, access barriers, and awareness of disease-modifying therapies. Insights were qualitatively analyzed and grouped into descriptive themes. Insights were reported in the “What We Heard” summary and integrated into the overall project findings. Indigenous-led engagement methods: Total participants: 4 First Nations living with MASH, of which 1 also a caregiver of a person living with MASH Place of residence: Alberta, Ontario, British Columbia. Participants chose from 3 online engagement sessions scheduled in October 2025, or the option for an individual interview online. Each virtual engagement was grounded in respectful dialogue and guided by a facilitation approach that centred Indigenous knowledge systems and lived experience. Insights were reported in the “What We Heard” summary and integrated into the overall project findings. |
3. Results | Participants across CDA-AMC and Indigenous-led sessions identified diagnostic delays, limited information sharing, structural barriers to diagnosis and treatment, including anti-Indigenous racism, stigma, high travel and cost burdens (particularly for northern people living with MASH), and availability of health care providers. They emphasized the need for improved provider education, peer support, and equitable access to diagnostics and treatments, especially considering the potential introduction of DMTs for MASH in Canada. |
4. Discussion | Engagement participants’ insights helped contextualize report findings by identifying current diagnostic and treatment needs, and the implications of health systems gaps and structural barriers to accessing and benefiting from MASH diagnosis and treatment. |
5. Reflections and Critical Perspective | The contributions of people with lived experience helped identify important diagnostic and treatment considerations, needs, and health system limitations relevant to the assessment of health system readiness outlined in this report. However, specifically in the CDA-AMC-led engagement sessions, individuals from structurally marginalized groups were not included, limiting breadth of insight. Future engagement activities should proactively seek to include individuals with diverse ethnic/racial backgrounds, living with low-income, and living in rural/remote locations. |
Appendix 7: Methodology for Estimation of the Population With Treatable MASH
Please note that this appendix has not been copy-edited.
First, the total population in Canada was obtained from Statistics Canada 2025 estimates. Second, published Canadian and international epidemiological studies were reviewed to identify the prevalence and incidence of MASH, previously observed or estimated. Third, eligibility criteria were applied based on disease stage (e.g., fibrosis stages F2 and F3) as reported in the literature. Finally, an age restriction was applied to only include adult population (≥ 18 years) as the emerging DMTs are only approved for adult populations.
Limitations
These estimates are based on projected numbers of individuals living with MASH according to estimates of NASH (the previous nomenclature and definition) using historical trends in obesity that modelled future disease burden. These estimates are not based on confirmed diagnoses and do not account for individuals with lean MASH, who may also be eligible. Another limitation is the unknown proportion of individuals with MASH who have fibrosis staged at F2–F3 and are therefore eligible for DMTs. These estimates assume that the proportion of F2–F3 fibrosis is equivalent between NAFLD and NASH. Further, the assumed proportion is based on modelling data, not confirmed fibrosis staging. Additionally, with the introduction and increasing use of GLP-1 therapies to support weight loss and metabolic improvements, the future impact on population-level weight trends and MASH development in Canada (or internationally) remains uncertain.
Table 14: Estimated Population With Treatable MASH as of 2025
Population and step | Approach | Rationale | N | Percentage of population |
|---|---|---|---|---|
All ages (2025 estimates)348 | Estimated population in Canada | Provides the total population denominator for all subsequent prevalence estimates | 41,651,653 | — |
Modelled MASH prevalence (estimated for 2025 based on historical obesity trends)15 | Age-adjusted modelled prevalence of MASH from historical obesity trends; 5.80% of all ages | Establishes the baseline MASH population in Canada using estimated prevalence data | 2,415,796 | 5.80% |
Estimated MASH patients with fibrosis F2–F315 | NAFLD F2+F3 proportion = (F2 + F3)/total NAFLD = (451,000 + 293,000)/8,712,000 ≈ 8.54% Applied to MASH: 2,415,796 × 0.085399 = 206,307 | Identifies subset of MASH patients with F2-F3 fibrosis staging - emerging DMTs only indicated for these stages | 206,307 | 8.54% |
Proportion who are adults (18+ years)348 | Adjusted for age < 18 | Focuses on the adult population who would be eligible for emerging DMTs (children not eligible) | 168,449 | 81.65% |
Treatable MASH population estimate for 2025 | Stepwise approach: starting from total population, applying MASH prevalence, fibrosis proportion, and adult adjustment | Final estimate of target population | 168,449 | 0.40% |
Table 15: Estimated Population With Treatable MASH in 2030
Population step | Approach | Rationale | N | Percentage of total population |
|---|---|---|---|---|
All ages 2030349 | Estimate population in Canada in 2030 | Provides the total population denominator for all subsequent prevalence estimates | 42,447,500.00 | — |
Modelled MASH prevalence estimate for 203015 | All ages modelled prevalence of MASH from historical obesity trend; 6.1% in 2030 | Establishes the baseline MASH population in Canada using estimated prevalence data | 2,589,297.50 | 6.10% |
Estimated MASH patients with fibrosis F2–F315 | Staged F2-F3/ total NAFLD (518,000 + 357,000)/9,305,000 | Identifies subset of MASH patients with F2-F3 fibrosis staging - emerging DMTs only indicated for these stages | 243,393.97 | 9.40% |
Proportion who are adults (18+)348 | Same proportion as in 2025, which may change by 2030 | Focuses on the adult population who would be eligible for emerging DMTs (children not eligible) | 198,731.17 | 81.65% |
Treatable MASH population estimate for 2030 | Stepwise approach: Starting from total population, applying MASH prevalence, fibrosis proportion, and adult adjustment | Final estimate of target population | 198,731.17 | 0.47% |
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.