Drugs, Health Technologies, Health Systems
Health Technology Review
Alternate Level of Care in Canada: Evidence Assessment Report
Key Messages
What Is Alternate Level of Care?
Alternate level of care (ALC) is a designation used and applied by clinical staff to the portion of a patient’s hospital stay when the patient is occupying a bed in a facility (e.g., acute care; mental health; rehabilitation; and chronic, intermediate, or complex continuing care settings) but they no longer require the intensity of resources or services provided in that care setting.
What Are the Challenges?
In 2022–2023, an estimated 6.2% of hospitalizations in Canada had an ALC component, with a provincial and territorial range of 1.0% to 8.3%. An estimated 17.0% of hospital days were for patients in ALC, with a provincial and territorial range of 6.8% to 26.1%.
Patients with an ALC designation may be more at risk of adverse events, hospital-acquired infections, mental and physical deterioration, and mortality. ALC bed days also contribute to higher hospital costs and system flow issues, including overcapacity, emergency department (ED) and hospital overcrowding, and prolonged wait times.
Patients of any age and any health condition may remain in hospital after their acute care needs have been met; however, the most common group of patients who are in ALC are older adults.
Determining whether a patient’s stay receives an ALC designation requires the application of the ALC definition while considering the individual patient’s context. There are many factors that influence whether a hospital stay will result in an ALC designation, including variations in patients, settings, and circumstances.
The ALC indicator was originally meant to capture unmet needs of patients. It is now predominantly a designation placed on a portion of patients’ hospital stays, and often patients are unaware of their ALC status and what it means.
The variation in ALC definitions and their application, as well as situational contexts such as the demographics of patients, ALC rates, and interventions, make it difficult to compare ALC between jurisdictions.
What Did We Do?
To inform policy and decision-making in support of evidence-informed strategies to reduce the time people spend in ALC, we assess:
ALC definitions in Canada and how they are applied across jurisdictions
reasons for ALC designation, including the reasons people with unmet needs receive ALC designation and remain in ALC in acute inpatient care settings and the relevant, related ethical considerations
effectiveness and harms of published interventions to alleviate the ALC burden
other interventions implemented in Canada and internationally that exist to help alleviate the ALC burden
economic and resource considerations associated with ALC interventions to health systems and patients
implementation considerations to identify facilitators of, and barriers to, implementation of ALC interventions.
Interventions were aligned with 3 categories: ALC avoidance (upstream), ALC patient flow (midstream), and ALC patient discharge (downstream).
To supplement findings from the evidence, review and to help describe the ALC landscape across Canada, we also conducted an analysis of real-world data. We developed an interactive dashboard that includes figures that describe ALC data by different provinces and territories in Canada, over time.
To support this work, we engaged people with personal and/or professional experience with ALC, caring for older adults as they age, or health care decision-making in Canada. We searched key information and data sources — including journal databases, trial registers, and websites — and conducted focused internet searches for relevant evidence on initiatives to reduce ALC.
What Did We Find?
Across the jurisdictions, ALC is defined in alignment with the Canadian Institute for Health Information (CIHI) definition as patients occupying a bed while no longer requiring the services provided by their admitting acute care facility or department as they wait for transfer to more appropriate care settings. Slight differences arise from the designation criteria and the code assignments for patients.
ALC designation involves assigning specific codes or criteria to reflect the change in a patient’s status and reasons for the designation.
ALC days are widely used as a performance indicator across jurisdictions to assess ALC, along with other metrics such as the percentage of hospitalized patients designated as ALC and the number of ALC beds occupied per day.
We found that individual sociodemographic and clinical factors, process and practice factors within and across acute and nonacute care settings, and structural factors contribute to ALC designations. We also found that multiple, intersecting factors that contribute to ALC can raise ethical considerations and present ethical dilemmas for patients, care partners, families, health care providers, and health systems in the context of ALC designations.
We examined evidence on the effectiveness of 6 multicomponent interventions that have been described in comparative studies in the published literature intended to alleviate the ALC burden in acute care hospital settings. Overall, there was very low–certainty evidence of the clinical benefits of these interventions:
The Humber River Health’s Humber’s Elderly Assess and Restore Team (HEART) program (a midstream-downstream intervention) and a step-down intermediate care unit for older patients who are hospitalized plus a 72-hour discharge target (a downstream intervention) may reduce ALC rates compared with usual care, but the evidence is very uncertain due to critical or serious risk of bias and indirectness.
The Sub-Acute Care for Frail Elderly (SAFE) Unit located in a long-term care [LTC] home in Ontario (a downstream intervention), vertical integration of care (a system-level intervention), and urgent and emergency care vanguards (a system-level intervention) may reduce ALC lengths of stay compared with usual care or no intervention, but the evidence is very uncertain due to critical risk of bias and indirectness.
Coordinated care planning based on the Health Links model (a system-level intervention) may make little to no difference on ALC lengths of stay compared to no intervention, but the evidence is very uncertain due to serious risk of bias and serious imprecision.
We also identified 11 noncomparative studies (that were not critically appraised) of the following:
six midstream interventions — increased step-down beds, specialized acute care space or service, and enhanced discharge planning
two downstream interventions — transitional care units
three system-level interventions — integrated care for older people and home-first strategies.
From the literature, we identified a total of 19 new and emerging interventions in Canada, 10 international interventions, and 2 international case studies. Interventions intended to help reduce ALC designation of patients, improve patient flow, facilitate patient discharge, and provide educational and practical guidance about ways to alleviate the ALC burden.
Findings from a survey conducted as part of our environmental scanning activities suggested that although most jurisdictions use the CIHI definition of ALC, there is variation in the type of staff who assign ALC codes, the uses of ALC data, and fees associated with ALC designation. Strategies to alleviate the ALC burden most often aim to reduce ALC length of stay, are typically set in hospitals, involve a wide range of clinical and nonclinical staff, and are frequently targeted toward older adults, people awaiting discharge to residential care, and people with complex needs.
Resource impacts should be considered with respect to the implementation of any strategies to alleviate the ALC burden, including those pertaining to set-up, management, and delivery of care, alongside careful consideration of coordination, flow between different strategies, and redistribution implications. We identified 1 Canadian economic evaluation on the cost-effectiveness of the SAFE Unit (a downstream intervention) compared with usual care to alleviate the ALC burden. The overall literature suggests that this and other strategies for alleviating ALC may be less costly, resulting in the opportunity to treat more patients at the required level of care and thus increase efficiency in the use of health care resources.
Key participants in the implementation of ALC interventions include patients, care partners, clinicians, support staff, government, administrators, and communities, suggesting everyone involved plays a role in the successful implementation of these interventions.
Care providers should consider the use of cross-sector integration, enhanced communication, and multidisciplinary collaboration, supported by high-quality data that are integrated with the flow of the patient through their health journey to inform decision-making to aid in successfully implementing of ALC interventions.
Implementation should be approached as a continuum where approaches are tailored to the needs and complexities of the individual patient while assessing the requirements to transition between each step of care.
Next Steps
Our Health Technology Expert Review Panel will use the findings of this report to support deliberations that will result in the development of guidance to inform decisions around evidence-informed strategies and initiatives that could be considered to reduce the time patients spend with an ALC designation.
Introduction
What Is Alternate Level of Care?
ALC is a designation used and applied by clinical staff to the portion of a patient’s hospital stay when the patient is occupying a bed in a facility (e.g., acute care, mental health, rehabilitation, and chronic, intermediate, or complex continuing care settings) but they no longer require the intensity of resources or services provided in the setting where they are currently receiving care.2 This designation is documented in their medical record. The ALC designation may apply when a patient continues to have an unmet need for care; for example, they may require more time to recover or arrange for supports in their home. Other times, ALC may apply when a patient is waiting for transfer to another unit in the same facility or to another facility. Recognizing that the definition of ALC varies across jurisdictions and health care centres, we have adopted the ALC definition most commonly used and developed by CIHI for this report: patients “who no longer need acute care services but continue to occupy an acute care bed or use acute care resources while waiting to be discharged to a more appropriate care setting.” Note ALC is not meant to a be a label applied to patient themselves.
The variation in ALC definitions and their application across jurisdictions in Canada will be further explored in the ALC Definitions in Canada section.
Background and Context
When a patient presents to the hospital requiring care, the ideal trajectory would be for their acute issue to be resolved, allowing the patient to leave the hospital and return to the community. That acute care bed can then be occupied by the next person who needs that level of care. With ALC, this flow is blocked or stalled as the patient remains in the acute care setting even though they no longer need acute care services. As in most health systems worldwide (where it is often referred to as delayed discharge), ALC is a current challenge in Canada. In 2022–2023, an estimated 6.2% of hospitalizations had ALC, with a provincial and territorial range of 1.0% to 8.3%;1 an estimated 17.0% of hospital days were for patients in ALC, with a provincial and territorial range of 6.8% to 26.1%.1
Patients who have an ALC component to their stay may be at risk of more adverse events and hospital-acquired infections, mental and physical deterioration (loss of function), and mortality.3-8 Patients, family, and care partners have reported poor experiences with ALC, including confusion, stress, uncertainty, and frustration.6,8,9
ALC also impacts hospitals as well as the entire health care system and thus all other patients indirectly.10 ALC bed days significantly contribute to system flow issues, including overcapacity, which in turn impacts ED and hospital overcrowding as well as wait times because these spaces in acute care remain unavailable to new patients who need them.11 It can be an inefficient use of finite and costly hospital resources and restricts acute care capacity.12 Higher hospital costs can be attributed to a variety of factors. These may include the cost of patients occupying beds after they are medically fit for discharge and the associated delays in hospital admissions that may occur when beds are still occupied by those that with an ALC designation. Backlogs in ED and patient flow, deferred surgeries, hospital staff time, and administration costs may also contribute.3 Patients remain in those acute care beds due to their needs that remain unmet due to challenges accessing intermediate, community, and primary care resources.
The costs associated with ALC have been noted in multiple reports, with Canadian estimates ranging from $273 per ALC designate bed per day on mixed ALC and acute medical wards in British Columbia (2014 values)13 to $450 for an average ALC bed-day in Ontario (2010 value)14 to $842 per patient per day for an acute care facility in Ontario (2017 value).15
The CIHI guidelines to support ALC designation in acute inpatient care recommend ALC assessment takes place for patients in acute care as part of daily assessment by clinical staff.2 The assessment of ALC status is based on a variety of factors, including patient characteristics (e.g., clinical or functional status, safety risk, activity tolerance, and clinical practices and process), clinical interventions required (e.g., medication and fluids, diagnostics, and therapeutics), and need for specialized care or other scenarios (e.g., palliative care, mental health, respiratory care). It is important to recognize that the patient is not responsible for their ALC designation, and they are often unaware of their ALC status. They should not be blamed for “bed blocking” or using hospital resources. Many factors contribute to ALC designation that are often systemic and beyond a patient’s control. The ALC portion of a patient’s stay should only be reported to CIHI if it occurs for at least 24 hours.2
Designating a patient to ALC is not as simple as applying the definition without context.16 There is variation in patient factors, settings, clinician factors, and circumstances that contribute to the decision-making process.16 The variation in ALC definitions and their application, as well as situational context, make it difficult to compare ALC rates and characteristics of patients designated as ALC between jurisdictions.16
For this report, we used a modified version of the categorization by Durante et al. (2023),16 whereby opportunities for ALC reduction and optimization are organized by the point of interaction in the health system: ALC avoidance (upstream), ALC patient flow (midstream), and ALC patient discharge (downstream). The upstream category refers to strategies to reduce the number and length of ALC stays and avoid unnecessary hospital admissions; midstream refers to patient flow and efficiency, especially as it contributes to the length of ALC stays; and downstream refers to leaving the hospital.16
Figure 1: Categorization of ALC Patient Flow
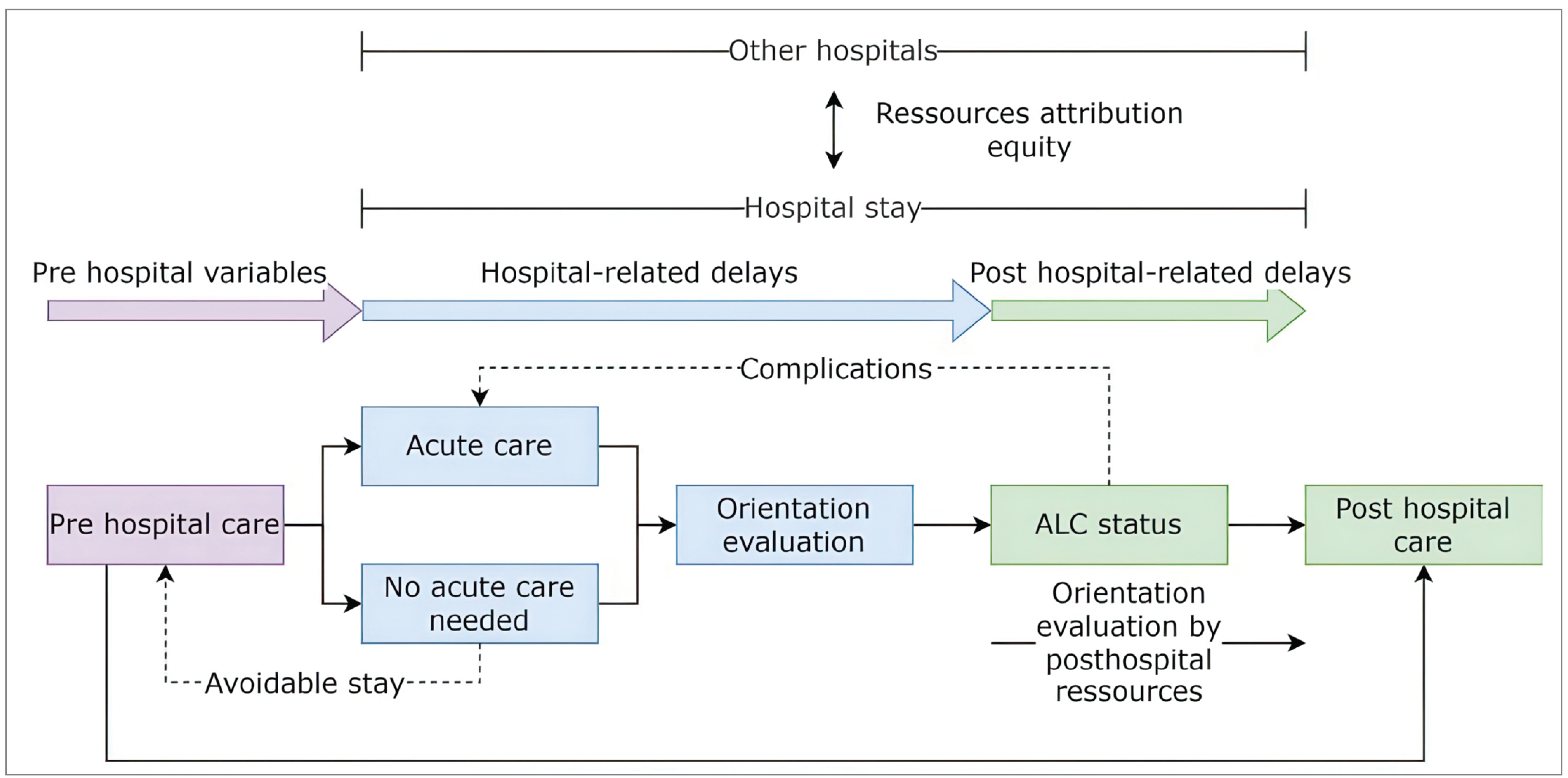
ALC = alternate level of care.
Source: Lamarre M, Daignault M, Cheung VW, Forget MF, Nguyen QD. Factors Associated with Alternate Level of Care Status Designation: a Case-Control Study and Model to Optimize Care Trajectories. Can Geriatr J. 2024;27(2):152-158. Available from: https://cgjonline.ca/index.php/cgj/article/view/697.17 This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License: https://creativecommons.org/licenses/by-nc-nd/4.0/
There are several reasons that patients continue to occupy a hospital care bed or use hospital resources after their acute care needs have been met and subsequently receive an ALC designation. People may present to a hospital ED with nonacute medical reasons due to a real, or perceived, lack of access to more appropriate services (e.g., primary care, LTC, community supports), which then leads to hospitalization and ALC.6,18,19 Patients who have received an ALC designation during their stay may remain in hospital while waiting for availability of new or additionally required services outside of the hospital, such as home care or specialized care, or may be waiting to be transferred to a different area within the same hospital, or to an alternative facility (e.g., rehabilitation centre).12,20 Other factors contributing to ALC include the underestimation of the potential for patient independence, deconditioning of patients as a consequence of inactivity and bedrest while in hospital, and lack of hospital staff awareness about available resources for patients to receive care at home and in the community.6,8
Trends and Sociodemographic Characteristics of People at Risk of ALC Designation
Patients of any age and with any health condition may be designated as ALC; however, adults aged 65 years and older make up most of this group. People who require a place in residential care make up a significant proportion of the patient population with ALC designation, with estimates ranging from 42% to 90%.21-25 These numbers will vary depending on the ALC designation criteria and how they are applied. In 2019, there were 6.6 million older adults aged 65 years and older and 838,200 people aged 85 years and older living in Canada.26 By 2040, one-quarter (10.7 million people) of people in Canada will be older adults, with the number aged 85 years and older expected to triple to more than 2 million by 2050.26,27
People may experience health challenges and the need for care and support during their years lived at older age.26 Rates of chronic disease and neurodegenerative disorders are also increasing in Canada.28 People are also living longer, accumulating multiple chronic diseases and are at increased risk of frailty.
These factors lead to increased demands for support along the continuum of care including acute episodic care at the hospital level and within the community for residential care, which includes LTC homes or facilities, private care homes, and special care homes.28 Unless these demands can be supported in alternate settings, such as community-based care settings, ALC rates are expected to increase.29
A number of risk factors associated with an ALC designation for patients of all ages have been identified in the literature, including advanced age (e.g., older than 80 years), female sex, a diagnosis of dementia, history of falls, social vulnerability, and need for residential care.7,30-33 A CADTH report on Strategies to Reduce ALC34 completed in June 2024 analyzed CIHI data related to ALC and average length of ALC in older adults awaiting LTC in Canada, and specifically found the following:
The mean age of patients in Canada aged 55 years and older with ALC designation and awaiting admission to adequate facility elsewhere was 80 years, and more than 55% were female.
At least 70% of ALC days across jurisdictions were from patients aged 75 years and older. Patients who lived in rural areas had longer lengths of stay in ALC than patients who lived in urban areas in most jurisdictions (19 days [interquartile range, 7 to 46 days] versus 10 days [interquartile range, 4 to 24 days]).34
Most patients (86%) designated as ALC were initially admitted in an unplanned hospital admission. Dementia was identified in 23% of patients in ALC but data limitations may have underestimated the true prevalence; patients with dementia had a median length of stay in ALC almost twice as long as the median length of stay in ALC calculated for all patients.
Patients with lower incomes had a larger contribution to ALC days in hospitals compared to patients with higher incomes.34
Objectives
This report was undertaken to support efforts across jurisdictions in Canada to implement interventions to reduce ALC rates in acute care settings. The findings from this report will be used by the Canada’s Drug Agency (CDA-AMC) multidisciplinary expert panel, the Health Technology Expert Review Panel (HTERP), to develop trusted guidance for health care decision-makers to support identification and implementation of evidence-informed strategies and initiatives to reduce the length of time people spend in ALC.
To inform policy- and decision-making, we address the following in this report:
What are the reasons patients who may benefit from alternative social and/or health care enter and/or remain in ALC in acute inpatient care settings in Canada?
For individuals of any age who are designated as ALC or at risk of becoming designated as ALC in acute care hospital settings, what are the benefits and harms of interventions to alleviate the ALC burden?
What policy, funding, and other systemic barriers may challenge the implementation of promising ALC interventions in Canada? How have jurisdictions in Canada or internationally overcome these implementation barriers?
Evidence Assessment Methods
To facilitate decision-making, we assessed:
ALC definitions in Canada — A scan of the definitions of ALC and their applications in jurisdictions across Canada.
Reasons for ALC designation — A review of the literature to identify and descriptively summarize the reasons people with unmet needs receive ALC designation and remain in ALC in acute inpatient care settings as well as the relevant related ethical considerations.
Effectiveness and harms of published interventions — A rapid review of systematic reviews and primary studies to evaluate the effectiveness and harms of interventions to alleviate the ALC burden.
Other interventions for ALC in place in Canada and internationally — An Environmental Scan to identify interventions implemented in Canada and international interventions that exist to help alleviate the ALC burden.
Economic and resource considerations — A review of the literature to identify economic and resource considerations associated with ALC interventions.
Implementation considerations — A review of the implementation literature to identify facilitators of, and barriers to, implementation of ALC interventions.
Details on the methodology, including the literature searches and inclusion criteria, can be found in the Supplemental Material.
ALC Data Dashboard
To supplement findings from the evidence assessment and to help describe the ALC landscape across Canada, we conducted an analysis of real-world hospitalization data from Canada. An interactive dashboard was developed that includes figures describing ALC data by different provinces and territories in Canada over time. Details on the methodology can be found in the Supplemental Material.
Engagement
To enhance the quality and relevance of this work, we engaged people with extensive personal and/or professional experience with ALC, caring for older adults as they navigate time spent with an ALC designation, or health care decision-making in Canada.
In October 2024, we held 3 virtual round table sessions with care partners, health care providers, and clinicians from across Canada. These sessions were intended to validate our approach in studying the issues and to obtain input to ensure that our evidence product is relevant and reflects the needs of patients, families, and clinicians.
In October 2024, we also held 2 round table sessions with jurisdictional decision-makers to validate our planned approach and help ensure that our evidence product would be relevant and meet the needs of the health systems. The sessions included an overview of our proposed approach to this work followed by a facilitated discussion.
In December 2024, we held 2 engagement sessions with health policy, services, and technology researchers; policy analysts; and implementation scientists with knowledge and expertise on this topic to discuss possible barriers to action in this area.
In December 2024, we presented to Healthcare Excellence Canada’s Federal, Provincial, and Territorial Government Quality and Patient Safety Network members. The purpose was to supplement the decision-maker round tables from October and collect feedback to better understand the decision-making needs and pressure points in jurisdictions across Canada.
What Did We Hear?
Our engagement sessions with care partners and clinicians highlighted the desire to understand the factors that contribute to why people remain in hospital (e.g., infrastructure and staff capacity, in-hospital information and communication, care partners and housing, cost). Participants also highlighted the emotional, physical, and financial impact of ALC.
During our engagement sessions with decision-makers, we heard there was a desire to learn about ALC policies and strategies that have been successful, a need to address education for providers and operational staff (e.g., accurate coding and improving data quality), and a desire to discuss considerations for priority populations and impacts of ALC designation and patient flow. There were also conversations about risk and returning home.
Finally, health policy researchers, administrators, and implementation specialists emphasized the importance of an integrated approach to ALC, with a focus on interdisciplinary teams and connection to community services. They also highlighted how a better understanding of why people are designated ALC could allow for better meeting their individual needs for their personal care but also can be used for strategic planning in a broader sense. Much of the discussion focused on the needs of older adults and people with frailty.
Findings from our engagement sessions are detailed throughout this report alongside those identified in the literature. The Engagement Summary document details the approach to and full summaries of these sessions.
ALC Definitions in Canada
To inform our understanding of how ALC is conceptualized across the country, we performed a scan (including a literature review and survey of jurisdictional contacts) to identify the various definitions and applications of ALC used across jurisdictions in Canada. Details of the definitions, application of the definitions, and ALC designation criteria are outlined in Table 1 and Table 2. Methodological details are provided in the Supplemental Material.
Across jurisdictions, ALC is defined in alignment with the CIHI definition as patients occupying a bed while no longer requiring the intensity of services provided by their admitting acute care facility or department as they await transfer to more appropriate care settings. Nearly all respondents from the survey we conducted reported using the standard CIHI definition, and one noted that they use a modified version with additional information on intensity and resources as instructed by a provincial committee. The purpose of using this modified definition was reported to improve the usability of ALC data. Three respondents reported that although they use the CIHI definition, in their jurisdictions, there is inconsistent interpretation of the definition between hospital sites and varied application by practitioners. This varied application can impact the usefulness of these data.
Table 1: Alternate Level of Care Designations, Definitions, and Performance Indicators Across Jurisdictions in Canada
Jurisdiction | ALC definition | ALC “designator” (if available) | Performance indicator(s) and measurement (s) | Measurement definition (if available) |
|---|---|---|---|---|
Newfoundland and Labrador | “Clinical designation to identify patients occupying hospital beds who do not need the intensity of resources or services provided with acute care.”46 | NA | Number of ALC days for acute inpatient care as a percentage of total patient days46 | NA |
Prince Edward Island | “Patients using a hospital bed and are waiting for a bed or service which betters meets their care needs.”41 | Most responsible physician and a discharge planner or clinical lead41 | Percentage of ALC days | “Proportion of days when patient is assigned to the ALC patient service.”48 |
ALC patient-days48 | NA | |||
Average ALC beds as a percentage of total medical beds48 | NA | |||
Number of individuals in ALC59 | NA | |||
Nova Scotia | “Patients who do not require inpatient acute care services at the health care facility they are being held at.”37 | The most responsible health care provider37 | ALC days | “Measure of total nonacute days of stay for patients awaiting discharge from acute care hospitals.”47 |
New Brunswick | Patients who remain at the hospital after receiving acute care but cannot leave without putting their health and safety at risk.54 | NA | Percentage of patients designated ALC hospitalized in acute care beds | “Percentage of acute care beds occupied by patients who would be able to receive care outside the hospital.”55 |
Total length of stay (ALC only) and percent ALC days | “Average length of stay designated as ALC as a proportion of the total length of hospital stays.”45 | |||
Average number of ALC beds per day | “Average number of hospital beds occupied by patients designated as ALC daily over the fiscal year.”45 | |||
Number of ALC stays56 | NA | |||
Average ALC days (per site)56 | NA | |||
ALC days and percentage of ALC days | “Percentage of ALC days as a proportion of total adult patient days.”57 | |||
Ontario | “Patient occupying a bed in hospital who does not require the intensity of resources and services provided in the care setting.”35 | By the physician or the patient’s delegate35 | ALC rate | Percentage of inpatient days that beds were occupied by patients designated as ALC patients (patients who could have been receiving care elsewhere). Indicator measures the total number of ALC days; the unit of measurement is rate per 100 inpatient days.58 |
Manitoba | “Patient occupying an acute care hospital bed but not acutely ill or does not require the intensity of resources or services provided in a hospital setting” (i.e., treatment and hospital care).”40 | By their attending physician or an authorized delegate40 | Hospital days for ALC stays | “Number of hospital days coded as ALC per 1,000 residents.”53 |
ALC days | “Inpatient days in which a patient no longer requires the level of care their care setting provides and where the patient is awaiting discharge to a more appropriate nonacute care setting.”44 | |||
Percentage of ALC hospitalizations | Percentage of residents who were designated as ALC.44 | |||
Saskatchewan | “Patient occupying a bed in a facility and does not require the intensity of resources and/or services provided in that care settings.”36 | The physician or any health care team member36 | ALC days49 | NA |
Alberta | “Any inpatient who does not need the intensity of care or level of service provided by their admitting acute care facility.” Patients are clinically stable and at low risk of health decline or needing new diagnoses.38 | Most appropriate care team member, including but not limited to physician, long-term care assessor, patient care manager, or discharge planner or other care team member.38 | Percentage of ALC42 patient daysa | Percentage of acute care days occupied by patients designated as ALC (waiting for discharge to more appropriate care setting).42 |
British Columbia | Patients occupying a bed in a facility but do not need the services provided in that care facility because their condition has stabilized and/or they are waiting to be placed in other types of care, such as assisted living or mental health services.39,50-52 | Designated by the most appropriate care team member: physician, patient care coordinator, transition liaison, most responsible clinician, clinical operations manager, or other care team member39 | ALC daysb and ALC percentage | Comparison of the actual date patients were discharged from the hospital with the date the patient was expected to leave the hospital. The difference is the extra ALC days. The ALC percentage is this number divided by the total number of patient-days.43 |
ALC rate | Percentage of total patient-days by patients designated as ALC. Patient-days are the number of patients who are in hospital multiplied by the number of days they spent in hospital.52 | |||
Yukon | “Patients who no longer require hospital care and may require another type of care, such as continuing care or home care.”62 | NA | Number of patients designated as ALC62 | NA |
Northwest Territories | Status of patients who no longer require inpatient care but still occupy an acute care hospital. The discharge is not possible because alternative care is needed.60 | NA | Median number of days for ALC stay | “Halfway point where 50% of patients have stayed less than and 50% of patient stayed more than; length of ALC stay.”60 |
Proportion of hospitalizations by length of ALC stay60 | NA | |||
Nunavut | Patients who could be discharged from hospital because they no longer require acute care services but do require ALC.61 | NA | NA | NA |
ALC = alternate level of care; NA = not available.
aAlso referred to as percentage of time a hospital’s beds are occupied by patients who require an alternate level of care according to Health Quality Council of Alberta.63
bAlso referred to as ALC stay days as a proportion of total stay days in some health authorities according to Vancouver Coastal Health.64
Some jurisdictions have a standardized provincial definition, namely Nova Scotia, Ontario, and Saskatchewan, with distinct designation criteria.35-37 The role of health care providers is central to this process, with physicians or designated personnel (e.g., discharge planners or transition liaison officers) typically responsible for assigning the ALC status.35,37-40 Certain regions also incorporate LTC assessors or clinical operations managers.38,39 This information was verified through the survey we conducted, from which we learned that the type of staff that assign ALC codes varies across jurisdictions. Other staff identified as assigning ALC codes included registered nurses, nurse practitioners, patient flow managers, social workers, therapists, program directors, and other clinical members of an interprofessional team. One respondent noted that they have an ALC authorizer, who is a regulated health professional (e.g., physician, nurse, LTC assessor) as part of the clinical care team.
Common discharge destinations include LTC homes, assisted-living services, or community services. In Alberta, Ontario, and Saskatchewan, a known discharge destination is not required for ALC designation.35,36,38 To be designated as ALC, vital signs, clinical status, and the condition must stabilize to baseline or a new baseline.35,37,38 Likewise, a patient is designated ALC after their medication adjustments are complete and their assessments and laboratory tests have been reduced to the minimum necessary for their care. It is specified that medication titration and change must be complete, as well as assessments and laboratory tests drop to a minimum.37,38
ALC designation involves assigning specific codes or criteria to reflect a change in the patient’s status and reasons for the designation. For instance, Manitoba specifies that patients should have at least 1 reason code, 1 International Classification of Disease, Tenth Revision, Canada (ICD-10-CA) diagnosis Z-code that indicates the reason for ALC designation, and a main patient service code.40 Prince Edward Island uses 2 distinct designations: 1 used when patients are waiting for admission to LTC after being accepted by the Long-Term Care Admission Committee and 1 used when patients are not waiting for LTC admission.41
ALC days are used as a performance indicator across jurisdictions to assess ALC rates and efficiency in health systems.42-49 ALC days are often expressed as a percentage of total inpatient days. Some jurisdictions also use metrics such as the average number of ALC beds occupied per day or as a proportion of total medical beds.45,48
There was limited information available from the territories, particularly Nunavut and Yukon. No information was identified regarding ALC processes in Quebec.
Table 2: Summary of ALC Designation Criteria and Notes Across Jurisdictions in Canada
Jurisdiction | Designation criteria |
|---|---|
Nova Scotia | For a patient to be designated as ALC, all the following criteria must be met:
On the ALC Status Form, the ALC Support Required and the date of ALC designation must be documented. |
New Brunswick | The patient remains in the hospital and does not require hospital care and is usually awaiting other services, such as a special care home, long-term care home, or home care.54 |
Prince Edward Island | Two ALC designations:
|
Ontario | The patient’s care goals must have been met and progress reached a plateau, the patient reached their potential program or level of care, or an admission for supportive care occurred because services were not accessible in the community. Discharge destination includes home, rehabilitation, complex continuing care, transitional care bed, long-term care home, group home, convalescent care bed, palliative care bed, retirement home, shelter, supportive housing.35 |
Manitoba | Patients usually require placement into personal care homes, home care, or other services. Patients designated as ALC should have at least 1 ALC reason code, at least 1 ICD-10-CA diagnosis Z-code that indicates the reason for ALC designation, and a main patient service code or a Service Transfer code = 99 (ALC). Another form of identifying patients designated as ALC includes identifying patients with hospitalizations categorized as possible ALC hospitalizations. For this, patients do not have an ALC reason code included on their hospital abstract and are not designated as ALC, but there may be a nonacute stay for a portion of their acute care stay.40 |
Saskatchewan | During the ALC designation process, there must be a main reason identified for why the patient is in ALC as well as an applicable ICD-10-CA code for all reasons why a patient is assigned ALC (main and secondary reasons) Main reasons include waiting for assessment to determine ALC care needs; approved and waiting for admission to facility or bed; waiting for community service, helping agency, or home services arrangement; or other waiting period for investigation and treatment. Secondary reasons include:
It is not necessary to know the discharge destination before an ALC designation. Patients must meet the criteria to be designated ALC for a minimum of 24 hours before they can be designated as ALC. Exceptions: Patient admitted as ALC when an appropriate alternate level of care is not available (i.e., admission for respite care).36 |
Alberta | The most appropriate care team member changes the patient status to ALC. Discharge destination does not have to be known at the time of ALC designation. The decision to assign ALC is a clinical responsibility. Patient’s assessments can decrease to weekly and vital signs decrease to Connect Care minimum use norms. Routine laboratory tests should be minimized. All major medical interventions should be complete and admitting problems be resolved or stabilized, as well as comorbidities return to baseline status. A clear discharge plan should be documented. When initiating the ALC order, designators put the order as ALC-TBD. After that, transition coordinators and/or nursing staff select a Z-code when details about the discharge destination become clearer.38 |
ALC = alternate level of care; ICD-10-CA = International Classification of Disease, Tenth Revision, Canada; TBD = to be determined; LTC = long-term care.
Use of ALC Coding and Data
Respondents to our survey reported that ALC coding is often part of a policy. These policies are typically established by provinces and territories and are centred around general ALC management, bed management, discharge planning, patient flow and access standards, and data reporting to CIHI. Less frequently, coding was reported as being part of interventions, including patient flow projects, patient chart reviews, and patient care planning, or part of programs, such as patient flow programs.
Most respondents indicated that ALC coding is used for data collection and monitoring purposes. This information is reported to be used for a variety of purposes, including informing wait times, performance measurement and quality improvement, discharge planning, matching patients to appropriate services, and general ALC data collection purposes. It is also used to help identify barriers to discharge so that teams can focus their efforts on addressing these barriers.
ALC Fees
According to survey respondents, some jurisdictions charge patients in ALC a daily fee. The fees reported range is from $59.95 per day to $250 per day. The amount that patients are charged depends on factors such as income sources, the types of LTC homes that patients are waiting for, and the reason patients remain in hospital. For example, those who are waiting to leave the hospital (e.g., waiting for LTC) may be charged less than those who remain in acute care after refusing a placement or discharge plan.
Reasons for ALC Designation and Remaining in ALC
Key Take-Aways
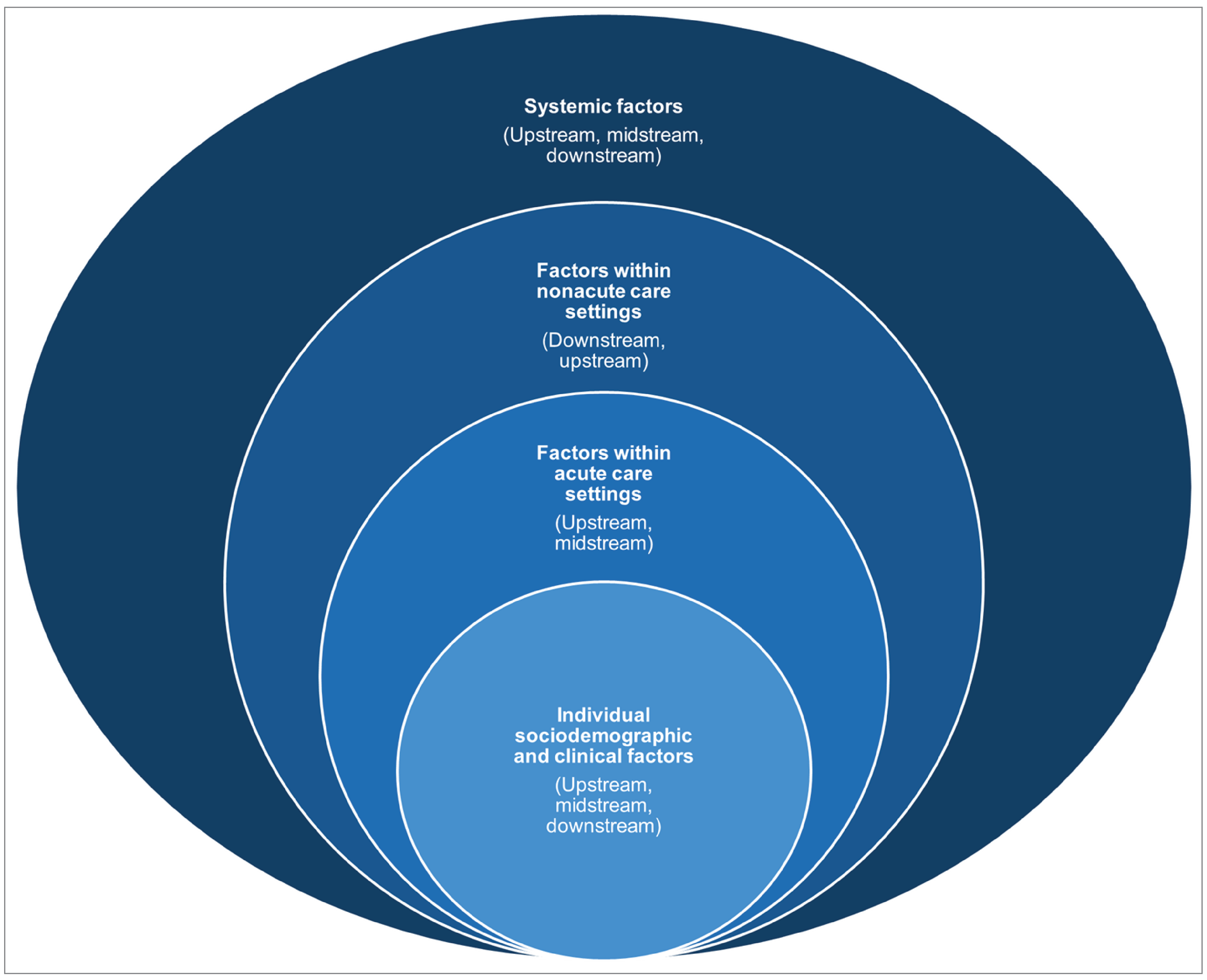
We identified 4 interrelated categories of reasons that people with unmet needs receive an ALC designation and remain in ALC in acute inpatient care settings:
Individual sociodemographic and clinical factors, including but not limited to, age, sex, frailty, comorbidities, lower income, and social isolation.
Processes and practices in acute care settings, including ALC designation practices, deconditioning and hospital-related complications, and discharge and discharge planning practices.
Processes and practices in nonacute care settings, including the limited availability of and access to home and community care and supports, acceptable housing, and publicly funded LTC homes as well as the fragmented coordination of care.
Systemic factors, including fragmented and complex health and social care regulations and policies; beliefs and values regarding patient-centred care, resource stewardship, and health system efficiency; and social and built environments. Structural determinations of ALC designations intersect with other identified factors and may also deepen disparities among some individuals with unmet needs, such as older adults; younger people; racialized and/or ethnic groups; those with dementia, mental health conditions, or intellectual or developmental disabilities (IDDs); people who require bariatric care or specialized interventions; and those living in social isolation and with low and middle incomes.
This review also describes how factors contributing to ALC designations raise ethical considerations and dilemmas regarding:
The ability to preserve patients’ human dignity and to prevent avoidable harm in the context of potentially inconsistent and low-quality acute care and deprioritized ALC care.
The ability of patients, care partners, and families to exercise autonomy in the context of systemic pressures for timely discharges that do not align with patients’ physical, psychosocial, and cultural needs.
Competing priorities for acute care staff between person-centred care for patients in ALC and resource stewardship and health systems efficiency to ensure that care is available for future patients.
Lack of procedural fairness and the inequitable allocation of limited resources in nonacute care settings.
Methods
The purpose of this review is to identify and descriptively summarize information on reasons people with unmet needs receive ALC designation and remain in ALC in Canada and the relevant related ethical considerations. We adopted a content analysis approach65 to sort, select, and descriptively categorize information from the literature, including government and nongovernment documents, such as policy briefs and practice guides, and other relevant grey literature. Additionally, we included findings from our round tables with jurisdictional decision-makers (e.g., those working in ministries or departments of health, or health service delivery organizations [e.g., regional health authorities]), and with care partners and health care providers (herein referred to as the “engagement sessions”). Readers can find a detailed description of our methods and included literature in the Supplemental Material.
Findings
The literature and inputs from our engagement sessions identified several reasons why people with unmet needs receive ALC designation and remain in acute inpatient care settings (herein referred to as “ALC”). These reasons (outlined in Table 3 and detailed in the following sections) involve individual sociodemographic and clinical factors, process and practice factors within and across acute and nonacute care settings, and structural factors. Structural factors (e.g., persistent and stable historical, sociocultural, and environmental practices and norms) are factors that systemically benefit some groups while disadvantaging others and, thus, contribute to disparities in health or social care opportunities and outcomes.66,67 In this review, we integrated systemic structural factors with the other identified factors. Structural factors include legislative and regulatory systems, policies, shared practices, and beliefs and values (i.e., ideas) of various interested and impacted parties. This review also identifies how the multiple intersecting factors that contribute to ALC raise ethical considerations and present ethical dilemmas for patients, care partners, families, health care providers, and health systems in the context of ALC admissions, stays, and discharges.
Figure 2 shows the interconnected categories of reasons why people who may benefit from alternative social or health care services enter or remain in ALC in acute inpatient care settings and categorizes them according to the stages of interaction with the health system. Factors are organized according to whether they lead to receiving ALC designations and/or indirectly to inpatient acute care admissions that will likely result in ALC designations (i.e., upstream factors), whether they are inpatient acute care patient flow factors that contribute to an increased length of ALC stay (i.e., midstream factors), or factors that hinder effective, timely, and long-lasting discharges from inpatient acute care settings (i.e., downstream factors).16
Individual Sociodemographic and Clinical Factors
Broadly, individual factors highlighted in the literature were those associated with adverse health and social outcomes leading to potential dependence on others for activities of daily living (ADLs) or instrumental ADLs and/or complex care needs.8,15-17,31,68 These sociodemographic and clinical factors often intersect and may contribute to an individual’s increased susceptibility to ALC. For example, Mah et al.69 conducted a secondary analysis of a single-centre cohort study set in a large tertiary care centre in Halifax, Nova Scotia, to examine how social vulnerability contributes to hospital outcomes for older adults presenting to the ED. In this study, the authors reported that social vulnerability (i.e., the degree to which an individual’s overall social circumstances leave them susceptible to adverse health or social outcomes) contributed to ALC status and prolonged length of stay in ALC.69 Individual adverse health or social outcomes may lead a person to require continued care or support following their acute care stay. Within the literature, it was reported that discharge destinations other than home without support, and especially to a LTC home, were associated with ALC admissions and prolonged length of stay in ALC.15,16,18,67,70-75
Table 3: List of Individual Factors
Factor type | Individual factors |
|---|---|
Sociodemographic |
|
Clinical | |
Health conditions |
|
Admissions and care during acute care admissions |
|
ED = emergency department; IDD = intellectual or development disability.
Individual Sociodemographic Factors
Sociodemographic factors commonly reported in the literature and engagement sessions are reported in this section.
Age, Sex, and Gender
Generally, within the literature, older age8,16,17,30,31,70,75-78 and female sex16,30,70,75,76 were reported as being associated with admissions to or prolonged length of stay in ALC.
The findings from the literature align with the CDA-AMC analysis of data on hospitalizations in Canada showing that, in the 2023–2024 fiscal year, 92% of patients in Canada (excluding Quebec) designated as ALC were aged 55 years or older at admission and 54% were female (CDA-AMC Alternate Level of Care Dashboard).
This analysis also showed that patients designated as ALC had a median age of 80 years. Older adults, particularly those aged 80 years and older, are more likely to experience additional factors related to ALC, such as frailty, comorbidities, lower income, and social isolation.8,16
Due to their longer life expectancies, females also have greater representation in the older population.16
However, Stock et al. (2016),71 in their population-based cohort study of survivors of hypoxic-ischemic brain injury, reported that being younger was a significant predictor of having more ALC days relative to overall length of stay during an acute care episode. The authors noted there may be fewer LTC options available for younger people with complex needs.71 Additionally, Carfagnini et al. (2023),73 in their retrospective cohort study based on data collected at a multisite large community hospital in Ontario, examined factors that increase the odds of long-stay delayed discharges (i.e., 30 days or more), and reported that males were significantly more likely to have long ALC stays. The authors acknowledged the finding related to sex “[diverged] from the majority of literature identifying female patients most often associated with delayed discharge.”73 Sourial et al. (2020),79 in their repeated cohort study comparing primary care and health service use indicators for newly identified men and women with dementia in Ontario, similarly reported that men experienced longer discharge delays. Little et al. (2015)78 and Little et al. (2019)77 also reported that being male was significantly associated with experiencing ALC and long ALC stays in inpatient mental health settings in Ontario.
Of note, the CDA-AMC analysis of data on hospitalizations in Canada (excluding Quebec) showed the same median length of stay in ALC for males and females, although there was variation among jurisdictions (CDA-AMC Alternate Level of Care Dashboard).
The included literature did not report findings regarding gender-nonconforming persons.
Other Sociodemographic Factors
Other factors reported as being associated with ALC included:
living alone
being unmarried (category used in the included literature)
experiencing social isolation
not having completed a high school degree17
being exposed to neglect or abuse.31
Of note, the CDA-AMC analysis of hospitalizations designated as ALC found that, in general (with some variation across jurisdictions), a high proportion of patients designated as ALC resided in neighbourhoods with low incomes (CDA-AMC Alternate Level of Care Dashboard).
Within the literature, it was also reported that residents of assisted-living facilities or retirement homes (i.e., privately owned and operated facilities that provide residents with housing and communal activities) may have higher ALC days than people living in LTC homes, receiving home care, or described as “community dwelling.”83,84 When discussing these findings, Manis et al.(2022)84 suggested that high costs associated with living in these privately funded facilities may limit residents’ ability to afford additional necessary care or support.
With 1 exception,70 it was generally reported in the literature that living in an urban area was associated with ALC admissions or that persons living in rural areas had lower rates of delayed discharges.15,75,76,85
The CDA-AMC analysis of hospitalizations indicated that, while 84% of patients admitted to ALC resided in urban areas, people from urban areas had shorter median stays compared with those from rural areas (8 versus 13 days, respectively), although there was variation among jurisdictions (CDA-AMC Alternate Level of Care Dashboard).
One participant from our engagement sessions also highlighted that resource allocation and capacity limitations, combined with increasing demands of a growing urban population, are factors contributing to ALC admissions and stays in rural areas. However, as detailed subsequently, there may be fewer postacute care and support resources in rural areas, which may contribute to longer lengths of stay in ALC for patients living in these settings. Reported findings regarding the association between ALC and speaking a primary language other than English or French varied.31,77,80
Individual Clinical Factors
Clinical factors highlighted in the literature as being associated with ALC included conditions associated with vulnerability to adverse health or social outcomes and the nature of acute care admissions.
Health Conditions
Within the literature, the following health conditions were reported as being associated with ALC admissions and prolonged ALC stays:
frailty, comorbidities, and multimorbidites8,16,18,31,32,69,70,72,75,76,82,86
dementia (especially when diagnosed during one’s hospital admission) and other neurocognitive or neurodegenerative conditions (e.g., Parkinson disease, multiple sclerosis, and brain injuries)8,18,30-32,72,74,76,78,82,87
the CDA-AMC analysis of hospitalizations (which excluded data from Quebec) found that, in the 2023–2024 fiscal year, 19% of patients designated as ALC had dementia and they contributed approximately 32% of ALC days
psychiatric conditions (although findings regarding specific conditions varied), substance use, behavioural disorders, and IDDs18,31,70,71,73,76-78,80,88-92
diabetes with complications73
obesity requiring bariatric care73
infection requiring isolation.73
Admissions and Care During Acute Care Admissions
In the literature, the identifying factors associated with ALC admissions generally described patients receiving ALC designation as those having emergent or complex health conditions. Emergent and complex health conditions may potentially lead to continued functional impairment and resulting care needs after becoming medically stable. These factors include the following:15,32,70,72,76
being admitted to inpatient units through the ED
arriving by ambulance
being triaged in the ED as requiring resuscitation, emergent care, or urgent care
being admitted for emergency (i.e., nonelective) surgery.
The CDA-AMC analysis of hospitalizations in Canada (excluding Quebec) found that, in the 2023–2024 fiscal year, an estimated 86% of hospitalizations were coded as urgent admissions (CDA-AMC Alternate Level of Care Dashboard) and 70% of hospitalizations were admitted by ambulance.93 However, Carfagnini et al. (2023)73 reported that patients admitted to acute care via transfer had the highest likelihood of experiencing discharge delays over 30 days compared with direct admissions and admissions through the ED. The CDA-AMC analysis of hospitalization data in Canada also found that that an estimated 15% of patients designated as ALC were transfers from inpatient units (compared with only 1% admitted from LTC).
Factors related to care during acute care admissions also included:
being admitted for conditions or procedures that could lead to prolonged functional impairment, including dementia, traumatic injuries, or falls (16% of patients in Canada [excluding Quebec] designated as ALC were admitted to hospital with a fall-related diagnosis code in the 2023–2024 fiscal year [CDA-AMC Alternate Level of Care Dashboard])
general illnesses, such as infections, neurosurgery, or procedures for peripheral arterial disease75,76
having more investigative technologies or health care providers involved in care (indicative of medical complexity)76,78
being referred to allied health professionals (i.e., physiotherapists, occupational therapists, and speech language pathologists) with expertise in assessing and offering interventions to support ADLs and instrumental ADLs.30
Within the literature, it was also reported that having longer acute care stays or complications during these stays were associated with ALC admissions.70,76
Factors Within Acute Care Settings
The literature and engagement sessions provided insight into how challenges within acute care settings can lead patients to receive designation and remain in acute inpatient care settings. These challenges related to:
varied and inappropriate ALC designations
deconditioning and hospital-related complications
processes and practices related to discharge planning
inaccurate assessment of patients’ postacute care and support needs
timing of discharge planning and discharge
factors influencing decision-making and consent practices.
Factors Underpinning Varied and Inappropriate ALC Designations
ALC designation practices are enacted at the hospital level and vary within and across health organizations and jurisdictions. Variations may arise from complex or limited organizational or jurisdictional regulations or procedures, variations in support systems for staff, and health care organizational pressures to meet funding-related performance targets. Complex or limited organizational or jurisdictional regulations or standardized coding procedures may result in misunderstandings and inconsistent designation practices among staff, potentially contributing to inappropriate designations. For example, admissions to hospitals of individuals with unmet clinical needs and reduced access to social and community supports (i.e., “social admissions”) often raise questions of compliance with regulations and may contribute to diverse designation practices. Additionally, it was reported within the literature and by participants in the engagement sessions that acute care staff may lack the tools (e.g., operational definitions, guidelines, or prompts) and training necessary to consistently make ALC designations and re-evaluate the appropriateness as patients’ needs evolve.16 However, even when such tools exist, staff may feel pressured to assign earlier ALC designations to improve health system efficiencies and meet funding-related performance measures, such as length of stay targets. Inappropriately or inconsistently designating patients with acute care needs as ALC creates inaccuracies in data that inform decisions on funding and implementing interventions aimed at mitigating the phenomenon.16 As detailed subsequently, inappropriate ALC designations, such as premature designations, may also lead patients to experience preventable harms, which raises ethical concerns and leads to prolonged lengths of stay in ALC.
Deconditioning and Hospital-Related Complications
Deconditioning and other complications related to hospitalizations contribute to and are, at times, the result of ALC designations.7,9,16,30,72,86,92,94 It was reported in the literature and by participants in the engagement sessions that acute care settings that do not meet patients’ complex needs may impart risk of hospital-related harms and deterioration once there is an ALC designation.9,30,86 Resulting long-term health and social needs may complicate discharge planning, which can prolong length of stay in ALC and create confusion for patients and their care partners.9 Limited practices to prevent deconditioning and other hospital-related harms may stem from limited staff with expertise to care for vulnerable groups (e.g., slow communication strategies with patients living with dementia to enhance collaboration and reduce behavioural issues), challenges collecting data necessary to gain organizational support for these practices, and global rather than activity-based funding in hospitals.16,90,95
Patients and their care partners have reported feeling their care was deprioritized after an ALC designation, leading to confusion and frustration.9,92 As one care partner noted: “things just got different, and I didn’t know why.”92 Patients designated as ALC and their care partners have reported unmet needs for daily activities such as ambulation, dressing, bathing, meal support, and recreation.9,92 To receive such care, patients relied on their informal care partners, who may experience increased emotional, financial, and time-related burdens associated with travelling to hospitals and witnessing and compensating for their care recipients’ deprioritized care.9,94 However, the availability of informal care partners is limited by cultural shifts away from intergenerational caregiving and reduced care partner capacity.9 Reduced capacity may stem from an aging caregiving population with its own health needs as well as care partner stress and burnout.16,82 Care partners’ stress may increase alongside the complexity of a care recipient’s needs and is underpinned by inadequate care partner supports, including financial supports and respite services.16,68,82,96 Participants in the care partner and health care provider engagement sessions noted that respite services are often cut during budget restrictions. As previously noted, it was reported within the literature that care partner stress or burnout are factors associated with patients entering and remaining in ALC.
The potential for inconsistent, low-quality, and deprioritized ALC care in acute care inpatient settings raises ethical concerns regarding the ability to preserve human dignity (e.g., attending to personal care needs such as personal hygiene), maintain autonomy (e.g., having the ability to ambulate freely as opposed to being restrained to preserve safety and protect from a fall), and prevent avoidable harm (e.g., due to deconditioning and other complications).9 Those with frailty, dementia, behavioural disorders, and IDDs may be at an increased risk of deconditioning and hospital-related harms, such as infections, falls, and delirium, which can cause lasting impairments necessitating ALC.16,90,91,95
Processes and Practices Related to Discharge Planning
Discharge planning processes and practices that have been reported to contribute to prolonged ALC stays or prevent long-lasting discharges include those underpinning:
the inaccurate assessment of a patients’ postacute care and support needs
planning and/or discharges that occur too early or too late
decision-making and consent processes that do not appropriately involve patients and their care partners.
Inaccurate Assessment of Patients’ Postacute Care and Support Needs
Inaccurate assessment of patients’ physical, psychosocial, and cultural postacute care needs can lead to ALC admissions, prolonged ALC stays, or discharges that are not long-lasting (e.g., when a person is discharged into an inappropriate context).68,90,91,97 Reasons underpinning inaccurate assessments includes entering or remaining in ALC while waiting for a higher level of postacute care than necessary. In these instances, health care providers would assess patients’ needs before reablement or trialling discharge with lower levels of support.68,91,97 A lack of sufficient acute care staff with expertise in evaluating the needs of certain groups, including those with dementia, IDD, or dual diagnoses, was also reported within the literature and by participants in the engagement sessions.88,90 Barriers to interprofessional collaboration may further hinder accurate needs assessments.98
Excluding patients and families from discharge planning has also been reported to hinder accurate need assessments because patients and families have vital insights regarding their preferences, goals, and needs.92 Excluding patients and their families from discharge planning may also lead them to experience uncertainty related to discharge planning. This raises ethical concerns because it can limit patients’ and families’ autonomy in planning discharge according to their preferences and goals.9,68,92 Reported reasons why patients and families might be excluded include:68,88,90,92
organizational policies that exclude patients and care partners from interprofessional discussions
providers feeling they would be unable to answer questions from patients and their families in the context of uncertainty
acute care staff’s perceived lack of time to focus on psychosocial care
ageist or ableist assumptions embedded in our social and cultural systems that shape understandings and practices regarding the decision-making capacity of older adults or those with disabilities.
Factors Impacting the Timing of Discharge Planning and Discharge
Because identifying and coordinating appropriate postacute care and supports can take time, it is important for discharge planning to occur early in a patient’s acute care stay.90 Factors impacting the timing of discharge planning and discharge include complex, unclear, and fragmented regulations, funding models, and policies within and between acute and nonacute care settings. These factors also include pressures to expedite discharge as well as beliefs and values regarding patient-centred care, resource stewardship, and the desirability of LTC.
Regulations related to hospital care, consent related to acute care services, and LTC home applications, wait-list management, and prioritization are complex, sometimes lacking or lacking clarity in their applications for health care organizational leaders and providers, and vary by jurisdiction.68,91,96,97 As a result, acute care staff may misunderstand their accountabilities and roles in discharge planning and resource stewardship.68,91,96,97 Misunderstandings regarding, for example, who has authority to decide when a patient without acute care needs leaves the hospital can impede planning and lead to delayed discharge.97
The fragmentation and siloing of health care and social care laws, regulations, funding models, and policies within and across acute and nonacute care settings further hinders timely discharge planning.18,68,88,98 Such fragmentation can lead to unclear accountabilities for staff across sectors, little incentive for staff to communicate and collaborate, and misalignments in processes and procedures between sectors.68,96 It is possible then to observe poor communication, a lack of agreement regarding a patient’s anticipated safety, and prolonged wait times for assessments for discharge destinations, which can hinder timely and effective discharge planning and delay discharge.17,80,90,98
Pressures to quickly discharge patients from acute care settings can also lead to discharge plans that do not address patients’ physical, psychosocial, and cultural needs.100 These pressures may be underpinned by hospital funding models that rely on metrics such as overall acute care length of stay.100 Pressures may also derive from acute care staff’s competing priorities between providing person-centred care and ensuring patient throughput to maintain reasonable access to acute care for future patients.99 Acute care staff may experience moral distress when faced with the ethical dilemma of balancing the provision of patient-centred care for those in ALC with supporting resource stewardship and health systems efficiency to ensure that care is available for future patients.68,99,100 How providers prioritize these dual obligations (to present and future patients) varies, but prioritizing patient-centred care for patients who are currently hospitalized over those awaiting hospitalization may contribute to patients entering and remaining in ALC.16
However, patients and care partners report valuing patient-centred approaches and choice when planning discharge.9,68 Patients and their care partners expect postacute care and supports to be affordable, geographically close to their support networks, and aligned with their physical, psychosocial, and cultural needs.9,68 Most older adults and some care partners prefer aging in place due to negative perceptions of LTC homes (especially following the COVID-19 pandemic).101 However, the engagement sessions highlighted how patients and care partners with negative experiences with alternatives such as home care may still prefer discharge to a LTC home. When given the option, they may reject discharge plans that do not align with their needs, which may prolong stays in ALC.80 Within the literature, it was also reported that patients with care partners or providers who had social or political connections or the ability to advocate for them may receive LTC home placements before others in the context of regulations that are nonexistent or difficult to interpret.9,90 These findings raise ethical concerns regarding procedural fairness in LTC home prioritization, which may contribute to inequities in opportunities to exit ALC in a timely manner.99 Providers’ beliefs about LTC homes as the ideal or desirable location, especially for older adults with medical or social complexity, are also reported to influence discharge.16,91 Acute care staff may prefer LTC homes due to risk aversion and a perceived lack of alternatives.16,92
Factors Influencing Decision-Making and Consent Practices
Within the literature, it was reported that some patients and care partners perceived being coerced or pressured to accept discharge plans not aligned with their needs.9,90 Pressures to accept discharge plans can derive from policy tools (e.g., per diem fees), provider and care partner decision-making practices, and misalignment across complex consent regulatory frameworks and practice.
Per diem fees to patients designated as ALC who remain in acute care settings are a policy tool used to incentivize people to limit their stay.16,68,102 However, although intended to expedite discharge, these fees may not incentivize people to leave when acute care setting costs are lower than costs associated with available care alternatives.16,68,102 Additionally, participants in the engagement sessions highlighted that per diem fees disproportionately affect patients and care partners with low and middle incomes who cannot afford postacute care options. Higher per diem fees raise considerations regarding equity in health outcomes because patients may be pressured to leave acute care settings into contexts that do not align with their needs.99
Prioritizing patient safety, especially when understood as the complete absence of risk, can lead providers or care partners to be risk averse and make discharge decisions that overlook a patient’s goals, values, and risk tolerance.16,97-99 Providers may be risk averse due to fear of legal repercussions following adverse outcomes postdischarge.16,98 Participants in the engagement sessions also perceived that providers may have higher risk aversion in the context of discharge planning for older adults. Although this practice may stem from ageist assumptions regarding older adults’ decision-making capacity, an engagement session participant also perceived this practice as common within cultures where older adults are highly valued and deemed worthy of protection.
Within the literature examining consent processes in the context of ALC, it was also reported that policies and practices within acute care settings may not always align with complex regulatory frameworks concerning acute care services, consent for those services, and LTC home admissions.97,99 In the context of complex regulatory frameworks, acute care staff may engage in practices such as seeking consent in circumstances when doing so is not required, disregarding patients’ known prior expressed wishes regarding alternate levels of postacute care, taking directions from a patients’ family when a patient is capable, or taking directions from someone other than a substitute decision-maker when a patient is incapable.97 These practices may contribute to patients remaining in ALC.97 Following pressure for hospitals to discharge patients and for patients to accept discharges into settings not aligned with their needs, patients and their care partners may experience psychological distress, trauma, and rehospitalizations (potentially leading to another ALC admission).90 This raises potential ethical considerations regarding free and informed consent, equity considerations, and harms associated with inappropriate discharges in the context of paternalistic decision-making practices and systemic pressures to promote timely discharges.99 Additional ethical considerations include questions about whose interests (e.g., patients currently in acute care settings, their care partners, or other patients awaiting acute care) are prioritized in consent and shared decision-making processes.99
Factors Within Nonacute Care and Support Settings
Nonacute care settings include those within hospitals (e.g., rehabilitation and transitional care units), within the community (e.g., primary and specialist care clinics, personal residences, assisted living and supportive housing, hospices, and shelters), and LTC facilities. Challenges within these settings can prevent people from accessing necessary care and support, leading to acute care (and potentially ALC) admissions and hindering timely, long-lasting discharges.68,88 Available home and community care and support services, care coordination services, housing, and publicly funded LTC homes may not be sufficient to address the increasingly complex and diverse needs of the population in Canada.16,18,68,72,80,88,90,91,96,100,102 Overarching factors that have been reported to underpin limitations and disparities include past legislative and policy decisions that impact funding, service and support eligibility, and the availability and retention of trained care and support providers.
The CDA-AMC Aging in Place Evidence Report101 provides further details on factors identified in this section relevant specifically to older adults and postacute care and support services, including
the lack of availability and accessibility of home and community care and support services
limitations in availability and access to acceptable housing
the importance of trauma-informed and culturally informed LTC
care provider and care partner challenges.
Home and Community Care and Support Services
The Canada Health Act provides a national legislative framework exclusively for the provision of publicly funded acute care and physician services.16,99 In practice, implementation of the framework has led to observations of some variations in the types and volumes of publicly funded nonacute care services across jurisdictions.90,101 Differences in services and programs perpetuate ethically concerning inequities in accessing and benefiting from home and community health and social care services and supports (hereafter, indicated only as home and community services) across Canada, including the following:
In the absence of publicly funded home and community care services, people with health or social needs must rely on private alternatives.8,16,68,90 However, available publicly funded home and community services have been reported as insufficient at times (e.g., regarding maximum allotted hours) and unreliable yet private services may be unaffordable for those with low or middle incomes.16,68,72,80,91,96,102
Funding and eligibility requirements may also create unequal or inequitable access to these services. For example, people without a fixed address or with incomes above certain thresholds may not qualify for publicly funded home care services, limiting access for those who are unhoused or have middle incomes.100 Time-consuming and administratively burdensome funding applications for these services may also result in people losing access.90 Certain groups lack available home and community care services, including those with IDD, psychiatric conditions, dual diagnoses, and substance use disorders who agencies may be reluctant to accept due to stigma, fear, and a lack of training (the latter of which is discussed subsequently).88,90
Ageism and ableism, as highlighted during the engagement sessions, may also hinder the implementation of care and supports for older adults and people with disabilities, respectively. Relatedly, available care and supports may be physically challenging to access for older people with disabilities or living in rural communities with limited transportation options.101
Challenges concerning care providers also affect the availability and quality of home and community services. There is a reported need for more providers, especially in rural areas, who are trained to recognize and address complex health and social needs.16,18,68,88,90,91,94,96,102 Provider shortages may affect service availability, leading to potentially longer wait-lists for — or a lack of — available services, especially for those with complex physical and mental health needs.68,88,90 Policies preventing acute care staff from following and supporting patients and their nonacute care providers after hospital discharge may also hinder long-lasting discharges.68,88 Participants in the engagement sessions and findings from 1 qualitative study68 attributed shortages in home and community care and support providers to concerns regarding compensation. An organizational leader, for example, reported that people who could provide home care for close to or at minimum wage may prefer working less demanding jobs for the same pay.68 Additionally, although high frequency and continuity of primary care was reported within the literature as being associated with decreased delayed discharges from acute care, Canada spends less on primary care services than comparable countries.16,18,74,90,91,102
Acceptable Housing
Acceptable housing includes assisted and supportive housing that integrates health and social care allowing individuals the opportunity to access and address their needs.16,82,88,90,91,100 However, housing-related policy changes influence the overall availability of acceptable housing and may disproportionately disadvantage certain groups (e.g., people who are racialized or have disabilities).88,90,100 For example, group homes and shelters often operate over capacity and may be staffed by people who are not health care providers.100 These settings may set limits on care needs they can accommodate.90,100 Additionally, strict rules on substance use and curfews in social housing limit autonomy and equitable access for those with substance use disorders or irregular work hours.100 It was reported within the literature and by participants in the engagement sessions that privately owned assisted living or retirement homes may similarly lack resources to address complex care needs and may be unaffordable for individuals with low or middle incomes.68
Publicly Funded LTC Home Availability and Access
Reporting within the literature suggests that the number of LTC homes in Canada is insufficient to meet demand, resulting in long wait-lists.16,68,91,99 LTC homes may have stringent eligibility criteria and may not meet the needs of younger people; racialized and/or ethnic groups; those with dementia, mental health conditions, or IDDs; and people who require bariatric care or specialized interventions such as dialysis or ventilation assistance.8,68,90,91 These groups may be unfairly disadvantaged in accessing LTC that can address their needs, raising ethical concerns related to the lack of procedural fairness and the inequitable allocation of limited resources.99 Available beds may also be located far from patients’ communities, loved ones, and informal care partners, which may cause ethically concerning preventable harms associated with care not aligned with a patients’ best interests, particularly for people in rural or remote communities with fewer LTC home beds.99 Although bed availability is one of the components contributing to ALC designations and prolonged stays, increasing LTC home beds alone may be ineffective or counterproductive in addressing ALC designations without increasing other types of supports and challenging assumptions that LTC is the best option for people with complex health or social needs.70,91
Care Coordination and Navigation Services
Some participants in the engagement sessions, including care partners with experience working in the health system, reported experiencing challenges with navigating complex and fragmented services. The qualitative literature provided insight into how people who are unaware of available supports and believe that providers would inform them of their needs may perceive their living situation and unmet needs as “normal.”94 This perception may prevent them from advocating for additional services, leading to declining health and the need for acute care.94 Of note, the lack of care coordinators knowledgeable about community services working within acute care settings has been reported to further hinder timely discharge because acute care staff may have limited awareness of available services and supports.92,98
Effectiveness and Harms of Published Interventions
Key Take-Aways
We included 6 primary comparative studies in our review of the clinical effectiveness on interventions aiming to alleviate the ALC burden.
Overall, there was very low–certainty evidence of the clinical benefits of the midstream-downstream, downstream, and system-level interventions included in our review.
The Humber River HEART program103 and step-down intermediate care may reduce ALC rates compared with usual care, but the evidence is very uncertain due to critical or serious risk of bias and indirectness.
The SAFE Unit, vertical integration of care, and urgent and emergency care vanguards may reduce lengths of stay in ALC compared with usual care or no intervention, but the evidence is very uncertain due to critical risk of bias and indirectness.
Coordinated care planning may make little to no difference on length of stay in ALC compared with no intervention, but the evidence is very uncertain due to serious risk of bias and serious imprecision.
We also identified 11 noncomparative studies of 6 midstream interventions (increased step-down beds, specialized acute care space or service, and enhanced discharge planning), 2 downstream interventions (transitional care units), and 3 system-level interventions (integrated care for older people and home-first strategies).
Our review points to an important gap in the evidence base given the scarcity and very low quality of the available published evidence.
Review Question
For individuals of any age who are designated as ALC or at risk of becoming designated as ALC in acute care hospital settings, what are the benefits and harms of interventions to alleviate the ALC burden?
Methods
The purpose of this review was to identify and describe relevant interventions to address the factors contributing to ALC. We conducted a rapid review of systematic reviews and primary studies, informed by Interim Guidance from the Cochrane Rapid Reviews Methods Group, including a literature search performed by an Information Specialist.104,105 A full description of the methods, which were decided before undertaking the review, are in the Supplemental Material document and described briefly herein.
Selection Criteria
To be eligible, studies needed to include patients who were designated as ALC or at risk of ALC (according to study authors). If only patients at risk of ALC were included, the study needed to report ALC rate or days of ALC as an outcome. Therefore, we excluded generalized studies of patient flow that were not focused directly on ALC. This was necessary to ensure that the review remained focused and with a reasonable scope. The selection criteria included:
population — patients designated as ALC or at risk of being designated as ALC in acute care hospital settings (according to study authors) and we also considered equity-focused subgroups for the potential to explore how interventions might impact health inequities106
interventions — upstream, midstream, downstream, and system-level interventions
comparators — usual care, no intervention, other active intervention, and no comparator
outcomes — ALC designation rates, length of stay in ALC, hospital length of stay, discharge destination, hospital readmission and ED visits, patient harms, or quality of life.
Study Selection, Data Extraction, and Risk of Bias Appraisal
Risk of bias appraisal was by a single reviewer using the Risk of Bias In Non-randomised Studies – of Interventions (ROBINS-I) tool (and an adapted version for interrupted time series), with verification by another reviewer. The noncomparative studies were not appraised because they were not within the focus.
We considered the following as relevant confounding domains: age group, presence of health conditions or comorbidities, socioeconomic status, and sex. We considered system-level exposures as relevant co-interventions (e.g., hospital discharge policies, levels of capacity, organizational dynamics).
Certainty of Evidence
One reviewer performed the appraisal according to the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach107 for 3 outcomes (ALC rate, length of stay in ALC, harms), with verification by a second reviewer. The GRADE domains were considered in drawing conclusions for other outcomes, but we did not produce a Summary of Findings table formally documenting the appraisal.
We use GRADE informative statements to describe the findings.108 We use results in for evidence of high certainty, likely for moderate certainty, and may for low certainty. When the evidence is very uncertain, we describe it as such.
Study Selection
The flow diagram depicting the selection of studies for the review is in the Supplemental Material document. Of 3,034 records identified by the search, we included 6 comparative primary studies and 11 noncomparative studies. No high-quality systematic reviews were identified.
Findings
Six comparative studies published between 2018 and 2023 met our inclusion criteria. All interventions were multicomponent; the most common components were cross-sector integration (e.g., collaboration between acute care, primary care, social care, and/or community services),103,109-112 multidisciplinary team or providers,103,109-111,113 and enhanced discharge planning.103,110,112,113
Table 4 presents intervention comparisons organized by the categories of factors identified in the review of relevant reasons people remain in ALC in acute inpatient care settings. For simplicity, we have listed each intervention category beside a single theme of factors. However, some interventions may target multiple themes or multiple individual factors within the themes. Table 4 also presents the direction of effect and certainty of evidence for each intervention comparison. Full details regarding the characteristics and results of the included studies and the GRADE Summary of Findings tables for ALC rate and length of stay in ALC are provided in the Supplemental Material document.
Clinical Effectiveness of Upstream Interventions Versus Usual Care
We did not identify any primarily upstream interventions.
Clinical Effectiveness of Upstream-Midstream Interventions Versus Usual Care
We did not identify any primarily upstream-midstream interventions.
Clinical Effectiveness of Midstream-Downstream Intervention Versus Usual Care
One retrospective cohort study evaluated a midstream-downstream intervention.103
Assess and Restore Program
The Humber River Health HEART program103 is based on an assess and restore model of treatment, which provides short-term inpatient and outpatient restorative care to prevent functional decline in older adults who are hospitalized in urban areas of Ontario.103 The HEART program is a patient-centred or people-focused intervention (considers the needs of specific demographics, populations, or chronic conditions and provides appropriate services or supports).
Edelstein et al. (2022)103 reported on the HEART program compared with usual care among hospitalized adults aged 65 years and older (mean age = 84 years). More than 50% of participants were at high risk of falls and 56% had a medical condition other than heart failure, pneumonia, or lower urinary tract infection. Before hospital admission, 90% of participants lived in private home residences and 10% lived in “retirement homes.”103
A single critical outcome of interest was reported (ALC rate), which we formally appraised. Results from this study suggest that the HEART program103 may result in a reduction in the proportion of patients designated as ALC. However, certainty in the evidence is very low due to critical risk of bias and indirectness (reduced generalizability).
Table 4: Interventions With Outcomes, Organized by Contributing Factors
Factor theme | Intervention | Comparator | Study population Sample size | Outcome(s) | Difference (95% CI)a | Certaintyb | What happens |
|---|---|---|---|---|---|---|---|
Upstream | |||||||
Individual sociodemographic and clinical factors | No primarily upstream intervention comparison for which we found evidence of effectiveness | ||||||
Upstream-midstream | |||||||
Processes and practices within acute care settings | No primarily upstream-midstream intervention comparison for which we found evidence of effectiveness | ||||||
Midstream-downstream | |||||||
Processes and practices between acute and nonacute care settings | Humber River Health’s Humber’s Elderly Assess and Restore Team (HEART) program103 | Usual care | Patients aged ≥ 65 years N = 1,094 | ALC rate | Relative: OR = 0.3 (0.13 to 0.69) | Very lowc | The HEART program may reduce the odds of being designated as ALC compared with usual care, but the evidence is very uncertain |
Hospital length of stay | Absolute: Median = 0 days (NR) | NA | NA | ||||
Discharge to home | Relative: OR = 2.85 (2.03 to 3.99)d | ||||||
Hospital readmission at 30 days | Relative: HR = 0.86 (0.56 to 1.32) | ||||||
ED visits at 30 days | Relative: HR = 1.16 (0.63 to 2.15) | ||||||
Downstream | |||||||
Limited availability of health and social care and supports to meet the diverse and evolving physical, psychosocial, and cultural needs of people after discharge from acute care settings | Subacute Care for Frail Elderly (SAFE) Unit113 | Usual care | Patients with frailty, aged ≥ 60 years N = 1,926 | ALC length of stay | Absolute: Median = −5 days (NR) | Very lowe | The SAFE Unit may reduce ALC length of stay compared to usual care, but the evidence is very uncertain |
Hospital length of stay | Absolute: Median = −2 days (NR) | NA | NA | ||||
Discharge to home | Absolute: + 17.8% (NR) | ||||||
Hospital readmission at 30 days | Relative: OR = 1.41 (0.86 to 2.31) | ||||||
ED visits at 30 days | Relative: OR = 1.13 (0.74 to 1.73) | ||||||
Step-down intermediate care and 72-hour discharge rate112 | Usual care | Patients aged ≥ 75 years 3 local authorities | ALC length of stay | Relative: −35% (NR) Absolute (days per 1,000 population per month): −16.04 (NR) | Very lowf | Step-down intermediate care may reduce the ALC rate compared with usual care, but the evidence is very uncertain | |
System level | |||||||
Overarching systemic factors | Full vertical integration of health and social care organizations109 | No intervention | General population NR | ALC length of stay | Relative (annual ALC bed days, averaged per day): −23.6% (−44.3% to −2.9%) | Very lowf | Vertical integration of health and social care may reduce ALC days compared with no intervention, but the evidence is very uncertain |
Urgent and emergency care vanguards110 | Usual care | General population NR | ALC length of stay | Relative (ALC days): −23.7% (NR) Absolute (ALC days per quarter per local authority): Mean = −491 (NR) | Very lowc | Urgent and emergency care vanguards may reduce ALC days compared with usual care, but the evidence is very uncertain | |
Coordinated care planning111 | No intervention | Patients aged ≥ 16 years (mean = 68 years) with 5 or more ED visits in past year N = 1,022 | ALC length of stay | Relative: IRR = 0.94 (0.49 to 1.80) | Very lowg | Coordinated care planning may make little to no difference on ALC length of stay compared to no intervention, but the evidence is very uncertain | |
Hospital length of stay | Relative: IRR = 0.97 (0.74 to 1.26) | NA | NA | ||||
Hospital readmission at 12 months | Relative: IRR = 0.96 (0.82 to 1.13) | ||||||
ED visits at 12 months | Relative: IRR = 0.88 (0.79 to 0.99) | ||||||
ALC = alternate level of care; CI = confidence interval; ED = emergency department; HR = hazard ratio; IRR = incident rate ratio; NA = not applicable; NR = not reported; OR = odds ratio.
Notes: Upstream category refers to the need for ALC admissions; and interventions focus on ALC avoidance.
Midstream category refers to refers to patient flow and efficiency, especially as it contributes to the length of ALC stays and interventions focus on improving ALC patient flow.
Downstream category refers to leaving the hospital; and interventions focus on ALC patient discharge.
System-level category combines 2 or more upstream, midstream, and/or downstream categories.
aAbsolute and relative effects are provided as available in the contributing studies (i.e., when an absolute or relative effect is not mentioned herein, it is because it was not reported in the contributing study). Relative values < 1 favour the intervention unless stated otherwise.
bWe formally assessed certainty of evidence using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach for ALC (or delayed discharge) rate and ALC length of stay only.
cDue to serious risk of bias, indirectness, and imprecision.
dValues > 1 favour the intervention.
eDue to critical risk of bias.
fDue to serious or critical risk of bias and indirectness.
gDue to serious risk or bias and imprecision.
We informally appraised the evidence for the other reported outcomes. Results suggest that the HEART program103 may reduce hospital length of stay and excessive lengths of stay. This evidence is very uncertain due to risk of bias and indirectness. No between-group differences were provided to interpret the findings beyond statistical significance.
Results of the study also suggested that the HEART program103 may increase the odds of returning home or to community living, reduce the hazard of readmission to hospital, and increase the hazard of ED visits within 30 days. This evidence is very uncertain due to the previously mentioned limitations. Additionally, the confidence intervals were wide for hospital readmission and ED admission outcomes, including the possibility of both important benefit and harm of the intervention.
The HEART program study stratified study findings by male or female, falls risk, and ambulatory status. Subgroup effects were reported but had low credibility. Analyses focused solely on statistical significance within subgroups, and the authors did not report between-group differences, which limited the potential for interpretation.103
Clinical Effectiveness of Downstream Interventions (Transitional Care) Versus Usual Care
Two studies assessed downstream interventions.112,113 These were transitional or intermediate level of care, which focus on transition of care from hospital to a posthospital destination by anticipating the future needs of patients after discharge and coordinating the different levels of the health system to facilitate continual care.114,115
SAFE Unit
The SAFE Unit is a 20-bed program in Ontario that has a strong emphasis on a restorative, collaborative, and integrated approach.113 Robert et al. (2021)113 conducted a retrospective cohort study of the SAFE Unit compared with usual care among adults aged 60 years and older with frailty who were hospitalized. Common comorbidities were hypertension, osteoarthritis, chronic coronary syndrome, diabetes, and multiple chronic conditions. Approximately 15% of the SAFE Unit study population had mood and anxiety disorders, and 10% had dementia. Approximately 42% of SAFE Unit participants had 1 or more previous acute care admissions in the previous 6 months and 26% of patients in the comparison group had 1 or more acute care admissions in the past 6 months.113
A single critical outcome of interest was reported (length of stay in ALC), which we formally appraised. Results suggested that the SAFE Unit113 may reduce median ALC days compared with usual care in older patients with frailty, but this evidence is very uncertain due to critical risk of bias (due to confounding). The authors reported statistical significance for this outcome, but did not report the between-group difference.
We informally appraised the evidence (i.e., we considered the GRADE domains when drawing conclusions but did not create the GRADE Summary of Findings tables to formally document the appraisal) for other reported outcomes. Compared with usual care, participation in the SAFE Unit was reported to have reduced hospital length of stay (median = 13 versus 15 = days) and increased discharges to home (64% versus 46%).113 However, this evidence is very uncertain due to critical risk of bias. Also, the study authors113 did not report between-group differences or the statistical significance for these outcomes.
Participation in the SAFE Unit113 may increase the odds of readmission to hospital and have little to no effect on ED visits within 30 days. However, certainty in the evidence is very low due to serious risk of bias and imprecision. The effects were not statistically significant, and the 95% confidence intervals included the potential for both benefit and harm of the intervention. No absolute between-group differences were reported.
Step-Down Intermediate Care
Step-down intermediate care for older hospitalized patients is a service tested as a part of the Reshaping Care for older People Change Fund in Glasgow City, Scotland. The intervention was a short-term care environment in a care home for a maximum of 4 weeks for older people who would otherwise have unnecessarily prolonged hospital stays or be inappropriately admitted to hospital or residential care. A 72-hour discharge target (after being deemed fit for discharge) was a separate intervention implemented several months after the implementation of step-down intermediate care.112 Levin and Crighton (2019)112 reported on step-down intermediate care plus a 72-hour discharge target compared with usual care in the 3 local authorities in Scotland. Population data for people aged 75 years and older were included (mean age = 82 years). Using the Scottish Index of Multiple Deprivation, 48% of the study population were in the lowest quintile (i.e., “most underprivileged”).112
We formally appraised ALC length of stay, the only relevant (and critical) outcome reported. The results suggested that step-down intermediate care112 may reduce ALC days compared with usual care, but this evidence is very uncertain due to serious risk of bias and indirectness.
Clinical Effectiveness of System-Level Interventions (Integrated Care) Versus Usual Care or No Intervention
Three studies evaluated system-level interventions.109-111 These were integrated care strategies based on an organizing principle for health care delivery that aims to improve patient care through better coordination of services provided.
Vertical Integration
Scotland created integration authorities to consolidate the planning, funding, and governance of adult social care, primary care, community health, and unscheduled hospital care across the country.109 The controlled interrupted time series by Alonso et al. (2022)109 assessed full vertical integration of health and social care organizations in 32 local authorities in Scotland and 47 unitary authorities and metropolitan districts in the northern regions of England compared with no intervention . Approximately 80% of the study population considered themselves to have “good” or “very good health”; 10% stated that their day-to-day activities were limited “a lot.” Approximately 16% of the study population was older than 65 years, and 60% were considered “underprivileged” on at least 1 of the following 4 dimensions: employment, education, health, and disability.109
We formally appraised ALC length of stay, the only relevant (and critical) outcome reported. The results suggested vertical integration109 may reduce the number of absolute delayed bed days per 1,000 population per month over approximately 3 years and with a relative reduction of 35% compared with no intervention. However, this evidence is very uncertain due to serious risk of bias and indirectness.
Urgent and Emergency Care Vanguards
National urgent and emergency care vanguards are local health and social care partnerships with the aim of improving integration of health and social care.110 In a controlled comparative interrupted time series, Malisauskaite et al. (2022)110 assessed urgent and emergency care vanguards in 29 local authorities in England compared with a synthetic control created from 121 English local authorities not participating in the intervention. Approximately 18% of their study population was older than 65 years, and 4% were receiving jobseeker’s allowance; 6% of participants aged 65 years and older were receiving disability living allowance.110 The included local authorities were mostly urban (i.e., 16% were rural in the intervention group and 22% in the comparison group).110
We formally appraised ALC length of stay, the only relevant (and critical) outcome reported. Urgent and emergency care vanguards110 may result in a relative reduction in ALC days compared with usual care over 6 years. However, this is very uncertain due to serious risk of bias and indirectness. Also, the study authors did not report confidence intervals around the effect estimate and so precision is unknown.
Coordinated Care Planning
A coordinated care plan based on the Health Links model (described as such in the publication but to our knowledge no longer exists under this name), which encourages greater collaboration and coordination between a patient's different health care providers as well as the development of personalized care plans, was implemented in a local health integration network in Ontario. In a retrospective cohort study. Bielska et al. (2018)111 reported on coordinated care planning compared with no intervention in patients aged 16 years and older (mean age = 68 years) with high ED use (i.e., 5 or more ED visits within the past year; mean = 7.5 visits). More than 40% of the patients in the study on coordinated care planning had arthritis, chronic obstructive pulmonary disease, or diabetes; 39% had a psychiatric condition and 22% of patients had a substance-related disorder.
A single critical outcome of interest was reported (ALC length of stay), which we formally appraised. The effect estimate was presented as an incidence rate ratio, suggesting that the study authors were considering ALC length of stay as a rate (days per unit of time) rather than a continuous variable. The appropriateness of this method was not clear because length of stay days were unlikely to be independent. The results suggested that coordinated care planning111 may have little to no effect on the number of ALC days at 6 months and 1 year. However, certainty in this evidence is very low due to serious risk of bias and serious imprecision. The 95% confidence interval included the potential for both benefit and harm of the intervention.
We informally appraised the evidence for other outcomes. The results suggested that coordinated care planning111 may have little to no effect on hospital length of stay and hospital readmissions at 6 months and 1 year. However, these effects are very uncertain, based on serious risk of bias and imprecision. The results also suggest that coordinated care plans may decrease ED visits at 6 months and 1 year, when compared with no intervention. However, certainty in this evidence is also very low due to the limitations listed previously.
Information From Noncomparative Studies
The interventions and study findings of the noncomparative studies are presented in Table 5. Full details regarding the characteristics and findings of 11 noncomparative studies are provided in the Supplemental Material document. We did not report these studies in our main synthesis because their reduced internal validity generally means that it is not possible to determine effectiveness of interventions from these study designs.116
Midstream interventions in the noncomparative studies were increased step-down beds,117 specialized acute care space118 or service,119 and enhanced discharge planning.120-122 Downstream interventions were transitional care units.13,123 System-level interventions were integrated care for older people124 and home-first strategies.15,125
Table 5: Summary of Information in Noncomparative Studies
Study author (year) Intervention name Intervention type | Setting(s) Country | Population | Brief intervention description | Study design Study findings |
|---|---|---|---|---|
Midstream interventions | ||||
Diouf et al. (2024)120 Digital matching solution Enhance discharge planning | Major metropolitan hospital in Victoria Australia | Patients who had their ACAS assessment after hospital admission but before discharge | Implementation of a digital software tool (DailyCare) that, in real time, matches patient’s information to select a residential aged care facility: geographical proximity, availability of specific services, vacancy, and capability for clinical and personal requirements. | Before-and-after evaluation ALC length of stay
Complete length of stay
|
Burke et al. (2023)117 More step-down beds Increased intermediate beds | Teaching hospital in Dublin Ireland | NR | Availability of additional step-down beds. | Pre-post medical audit Delayed discharges
|
Ibrahim et al. (2022)121 Multidisciplinary discharge coordination team Enhanced discharge planning | General medical service in largest government tertiary care hospital in Abu Dhabi United Arab Emirates | Patients with delayed discharges | Team made up of hospitalists, case managers, social workers, hospital finance representatives, and patient representatives, that meets weekly to proactively address medical delays, disposition issues, discharge delays, and patient and family concerns. | Retrospective, observational, pre-post study Length of stay
30-day hospital readmission:
|
Appel et al. (2015)118 Neurovascular unit Specialized acute care space | Acute care academic hospital in Toronto, Ontario Canada | Patients with stroke and other acute neurovascular conditions | Specialized stroke unit that is interprofessionally staffed and has a dedicated team including neurologists with expertise in stroke care, vascular neurosurgeons, nurse practitioners, nurses, and allied health professionals. | Retrospective, patient-level, pre-post study ALC days per visit (for visits with ALC > 0 days), mean
ALC days per visit (for all visits), mean (SD)
Change in ALC length of stay per visit:
Proportion of visits with acute days only (ALC = 0 days)
Total days, mean (SD) per visit
Change in total length of stay per visit
|
Bowen et al. (2013)122 Nurse-led discharge Enhance discharge planning | Academic hospital in Manchester UK | Adult patients having routine, elective, short-stay ear, nose, and throat surgery | Formal protocol for nurse-led discharge based on specific criteria and a pathway document to record the process within the patient notes and guide nursing staff. | Pre-post medical audit Rate of delayed discharge
Observed reduction in both rounds, P < 0.001 Hospital readmission
|
Mahto et al. (2009)119 Diabetes outreach service Specialized acute care resources | Hospital in Wolverhampton with approximately 700-bed capacity that provides several tertiary specialist services including renal, cardiac, and oncology services in addition to those services provided by a district general hospital UK | Inpatients with diabetes | The service aimed to prevent admissions by developing rapid and open-access services; to effectively manage diabetes of those admitted by addressing glycemic control, complication screening, and risk factor management; to manage their other medical problems or support other teams providing specialist care; to reduce delayed discharge by early formulation of an effective discharge plan and to organize appropriate follow-up to ensure continuity of diabetes care. | Pre-post medical audit Delayed discharge
|
Downstream interventions | ||||
O’Brien et al. (2017)123 Restorative care unit Transitional care unit | Urban LTC home in Corner Brook, Newfoundland and Labrador Canada | Patients ≥ 65 years with acute care length of stay ≥ 10 days; BRASS score > 9 but < 25; medically stable; sitting tolerance of 1 to 2 hours, 2 to 3 times per day; able to tolerable 30 minutes of low to moderate intensity therapy 5 days per week; waiting for alternate services or for nursing home placement; not eligible for intensive inpatient rehabilitation | A 14-bed inpatient unit providing restorative care to support the transition from hospital to community for older adults. | Single group, pre-post study. ALC cases
Length of stay in ALC (days)
Inpatient days designated as ALC
|
Manville et al. (2014)13 Transitional care unit Transitional care unit | Urban hospital in Comox, British Columbia Canada | Patients on acute medical, surgical, or psychiatric wards with ALC designation ≥ 70 years | A 22-bed inpatient unit designed to provide an age-friendly, geriatric rehabilitation–style environment. | Before-and-after structured retrospective chart audit Length of stay in ALC (days):
Total length of stay (days)
|
System-level interventions | ||||
Ahmed (2019)15 Home First Home-first strategy | 14 Local Health Integration Networks in Ontario Canada | Ontario citizens aged ≥ 65 years admitted to an Ontario acute care facility identified as at risk of being designated as ALC | A transition management strategy that focuses on providing patients with the support needed to facilitate their discharge to home with or without receiving community services. | Uncontrolled, before-and-after study using deidentified data from the ICES Data Repository ALC hospitalizations
ALC days (all patients):
Discharge home without support services
Discharge home with support services
Discharge to LTC
|
Sheaff et al. (2014)124 Improving the Future for Older People initiative Integrated care | 8 acute care hospitals UK | Inpatients aged ≥ 65 years | Local interorganizational networks (involving staff from secondary, primary, and tertiary health care; adult social care, private domiciliary services, residential and nursing homes, and third-sector organizations) with the aim of enhancing older people’s quality of life by reducing bed usage and admissions without compromising continuity of care or positive experiences of discharge Project types:
| Mixed methods case study using realistic case evaluation Percentage change in number of delayed transfers of care per 100,000 population from 2003–2004 to 2004–2005, 2004–2005 to 2005–2006, and 2005–2006 to 2006–2007:
|
Starr-Hemburrow et al. (2011)125 Home First Home-first strategy | Hospital in Mississauga Halton Local Health Integration Networks Canada | NR | Philosophical and cultural shift within acute care to change the focus through partnerships to ensure older adults can age outside of acute care to minimize the number of postacute care transitioning to LTC form in the hospitals, and to develop a comprehensive, integrated plan for appropriate interorganizational care and placement. | Uncontrolled before-and-after study ALC cases (N):
ALC days (N):
Time in gridlock:
|
ACAS = Aged Care Assessment Services; ALC = alternate level of care; BRASS = Blaylock Risk Screening Assessment; GIM = general internal medicine; ICES = Institute for Clinical Evaluative Sciences; LOS = length of stay; LTC = long-term care; NR = not reported; RR = rate ratio; SD = standard deviation; SE = standard error.
aAdjusted for age and major diagnostic category.
Other Interventions for ALC in Place in Canada and Internationally
Key Take-Aways
Both in Canada and internationally, a range of the approaches (i.e., upstream, midstream, downstream, and system level) and types of interventions (i.e., practice changes, tools and guidelines, infrastructure, and finance. and information sharing) have been used to alleviate the ALC burden. The multitude of approaches and interventions helps illustrate the complex nature of ALC and the various aspects that need to be considered.
International case studies that have demonstrated success in reducing the rates of patients designated as ALC — referred to as delayed discharge — took multisectoral, multicomponent approaches. This suggests that ALC cannot be solved by a single intervention or sector alone, but rather requires a coordinated, system-wide effort.
Methods
To help meet our objective of identifying and describing interventions that exist to help alleviate the ALC burden, we performed multiple scanning activities. We sought to identify literature that was outside the scope of the preceding work on clinical effectiveness and harms and that may still provide valuable information on interventions addressing ALC both in Canada and around the world. To do so, we took a multipronged approach, which consisted of the following:
We conducted web-based searches to compile a list of strategies, programs, and policies that address ALC across Canada.
We conducted a review of the literature to identify interventions in Canada and internationally.
We used the survey that we conducted to identify existing strategies to alleviate the ALC burden that may not be available in the literature.
When taken together, this approach allowed us to paint a more fulsome picture of the interventions that exist to address ALC.
List of Strategies, Programs, and Policies for ALC Across Canada
From the web-based search, we developed a list of interventions to provide more understanding of the programs and initiatives in place to alleviate the ALC burden in Canada. Details on how we created this list is available in the Supplemental Material. Because this area is broad and developing, we recognize that this list may not be complete. Interventions and initiatives to alleviate the ALC burden were identified in all jurisdictions, except Nunavut. More than 60% of the interventions identified were downstream and midstream, addressing solutions in improving patient discharge and patient flow to reduce ALC days or number of patients designated as ALC.
Most of the interventions identified were implemented to alleviate the ALC burden in adult patients, notably older adults, while 3 programs were implemented at a pediatric hospital.
Six interventions were implemented to alleviate the ALC burden in people who are unhoused by providing assisted-living services as well as convalescent care and medical respite to help transitions from the hospital.
Thirteen interventions were identified to reduce ALC rates for people with mental health conditions.
The findings were used to create a resource that users can access to view and navigate available strategies, programs, and policies for ALC across Canada: List of ALC Strategies and Interventions.93
Interventions in Canada
Literature-Based Findings
The interventions included in this section were described in reports published in 2020 or later and are not captured in the review of effectiveness and harms of interventions. Some of the interventions included in this section may not yet be evaluated because they have been implemented relatively recently, or they may have been evaluated and the associated data are not yet published. We included 19 identified interventions from the published and grey literature.12,16,81,82,88,95,126-139 We identified interventions that are based in Alberta, Newfoundland and Labrador, Ontario, and Saskatchewan as well as pan-Canadian.12,16,81,82,88,95,126-139
We identified 5 upstream interventions.126-130 We categorized 2 interventions as practice changes, 1 as information sharing: recommended initiatives, 1 as infrastructure and finance, and 1 as tools and guidelines.126-130 These interventions are intended to promote ALC avoidance through approaches such as hospital-at-home services, LTC at home and community services, specialized residential accommodations, and informational support.126-130
We identified 6 midstream interventions.95,132-137 We categorized 3 interventions as information sharing: recommended initiatives and 3 as infrastructure and finance.95,132-137 These interventions are intended to help improve patient flow through approaches including transitional care sites, rehabilitation services, and tailored supports in private homes and hospitals.95,132-137
We identified 3 downstream interventions.88,138,139 We categorized 1 intervention as a practice change, 1 as information sharing: recommended initiatives, and 1 as tools and guidelines.88,138,139 These interventions are intended to help facilitate and optimize the ways that patients transition out of the hospital through components including software and information technology, guiding principles, and integrated care.88,138,139
We identified 5 system-level interventions.12,16,81,82,131 We categorized 2 interventions as information sharing: recommended initiatives, 2 as tools and guidelines, and 1 as information sharing: live initiatives.12,16,81,82,131 These interventions provided educational support and practical guidance about approaches to alleviating ALC broadly.12,16,81,82,131
Survey Findings
To help ensure we were able to identify as many interventions to alleviate the ALC burden in Canada as possible, we also looked beyond the literature. As part of the survey we conducted, we asked respondents to provide information about strategies to alleviate the ALC burden that exist in their jurisdiction. We received responses about interventions from British Columbia, Manitoba, Ontario, New Brunswick, Newfoundland and Labrador, Northwest Territories, and Saskatchewan. We present a narrative summary of the findings subsequently. Detailed findings of the strategies shared by respondents are available in the Supplemental Material.
Aims and Components
All the strategies reported in this survey aim to reduce ALC length of stay. Many of these strategies have additional aims of increasing the capacity of destinations for patients designated as ALC (e.g., LTC, transitional care), and about half have a third aim of reducing the number of people who become designated as ALC.
The specific initiatives that were most common among the reported strategies to alleviate the ALC burden included interdisciplinary rounds, mobilizing patients, early discharge planning, and dedicated flow coordinators. Interventions that were identified in approximately half of the strategies included increasing transitional care capacity, rehabilitation capacity, and LTC capacity, as well as delirium protocols. Four respondents reported that their strategy included a 100 km to 150 km first-long-term-bed-available policy, and 1 reported including a discharge to assess initiative. Additional initiatives reported included ED admission avoidance teams and efficiency improvements for assessing LTC eligibility.
Setting
The setting for most strategies was the hospital only. Some strategies are implemented in other settings in addition to the hospital, including 1 that is also set in the community, 1 set in personal homes and the community, and 1 that is set in personal homes, the community, and transitional care. Another strategy is implemented in a licensed personal care home only.
Staff
Typically, the health care staff involved in these strategies include social workers, registered nurses, registered or licensed practical nurses, discharge planners, occupational therapists, and physicians (both general practitioners and specialists). Additional health care staff involved in strategies to alleviate the ALC burden include physiotherapists, exercise therapists, LTC navigators, home care coordinators, Indigenous patient navigators, activity directors, and utilization specialists. The nonclinical staff involved in strategies to alleviate the ALC burden primarily include directors and administrators. Some strategies also include information technology professionals and researchers. Additional nonclinical staff identified as involved in strategies include managers, business consultants, clinical change and professional leads, housing resources, and health economists.
Some strategies had dedicated teams. For strategies with dedicated teams, the number of known full-time equivalent health care staff ranged from 3.0 to 16.0. The number of known full-time equivalent nonclinical staff ranged from 3.0 to 6.0. One respondent also noted that the strategy is province-wide and, although exact figures are not known, a large number of both clinical and nonclinical staff are involved in the work.
Target Population
Although all reported strategies are intended for patients who have an ALC designation, some also have specific target subpopulations. These subpopulations included older adults (aged 65 years and older), people awaiting discharge to residential care, and people awaiting discharge to their own home. Some strategies are also intended for people with complex needs, such as dual dementia, acquired brain injuries, mental health or addiction issues, high physical care needs, lack of social and housing supports, and limited health care supports due to geographic location.
Evaluation
Approximately half the strategies are being or will be evaluated, and all plan to evaluate ALC length of stay as an outcome. Most also plan to evaluate ALC hospitalizations, hospital length of stay, discharge to home, and discharge to residential care. Two strategies will also evaluate ALC capacity, and 1 will evaluate total occupancy as well.
For both the literature-based and survey findings, some interventions may fit into more than 1 stream and category. For simplicity, we have categorized them into 1 stream and category that best aligned with the strategy components and objective. The identified interventions are listed in Table 6. A more detailed description of these interventions is available in the Supplemental Material.
Table 6: Descriptions of Interventions to Alleviate ALC in Canada Identified in the Environmental Scan
Intervention name | Jurisdiction | Description |
|---|---|---|
Upstream | ||
Complex Care Hub128 | Alberta | A program that provides hospital-at-home services to older adults, bridging acute care and the community. |
Virtual LTC @ Home130 | Ontario | A proposed program that would provide LTC services at home via the creation of highly coordinated and integrated care teams. |
Seniors’ housing complex127 | Ontario | A multistory building with residential units and onsite staff that will provide long-term care services and general health care services to older adults. |
Supporting OHTs to influence ALC126 | Ontario | Information to assist OHTs pursue services in community settings, including early identification and assessment, care plan development and ongoing reassessment, delivery of interventions and care tailored to older adults, and proactive transitions. |
Community paramedicine for LTC129 | Ontario | A pilot program that increases the numbers of paramedics and expands the scope of their role, offering 24/7 access to health services and ongoing monitoring of the individuals considered to be at the highest risk. |
Registered nurse navigatora | Saskatchewan | Pilot project to implement a registered nurse “navigator” in the emergency department. The purpose of this role is to create a discharge plan from the emergency department and avoid admitting consultant patients. |
Midstream | ||
Harbour Light Integrated Transitional Care Program137 | Ontario | Transitional care program in a community setting intended to support acute hospital patients designated for LTC placement return to the community. |
Ontario | A site where patients designated as ALC can be transferred that provide specialized supportive care, therapeutic recreation, case management, and assistance with personal care. | |
Acute Care Dementia Strategy95 | All provinces | A resource that proposes elements for an in-hospital comprehensive acute care dementia strategy. |
Personal support homes132 | Ontario | A resource that proposes a policy concept that allows people to leverage their empty bedrooms to temporarily house patients awaiting hospital discharge by renumerating homeowners. |
ALC and Delayed Discharge: Lessons Learned from Abroad136 | Ontario | A resources that provides promising practices to address ALC, noting that they should be multicomponent, tailored to the local context, and employ high-level policy implementation. |
Reactivation centres133 | Ontario | A collaborative and innovative approach that specializes in activation therapies. The intent of this approach is to deliver patient care in the most appropriate setting where patient privacy, dignity, and safety are a top priority. |
Reducing ALC Panela | Manitoba | The implementation of a standard LTC panelling process, consultation, tracking, and ALC flagging. This intervention is currently in process. |
Patient flow initiativea | New Brunswick | A review of patient lists to ensure each person is coded correctly. This is to allow for both proper reporting and finding alternatives to hospitalization. |
Patient flow committeea | Northwest Territories | A monthly meeting to discuss the status of individuals who have been designated as ALC, including whether an LTC application has been completed, and subsequent steps. |
Downstream | ||
DischargeHUB138 | Newfoundland and Labrador | Pilot project to develop and pilot a software and process solution which aims to streamline and coordinate the discharge of patients designated as ALC. |
Addressing Delayed Hospital Discharges for Patients with Intellectual and Developmental Disabilities and a Mental Illness88 | Ontario | Practice guidance consisting of 10 core components, intended to help facilitate the timely transition out of hospital for patients with intellectual and developmental disabilities and a mental illness. |
Co-Designing an Integrated Transitional Care Model to Address Alternate Level of Care and Promote Aging in Place139 | Ontario | Researchers proposed a qualitative study that allows individuals from various groups to help co-design appropriate care pathways for older patients designated as ALC to be discharged from hospital to home. |
STEPS Program at Diamond House Personal Care Homea | Saskatchewan | In partnership with Saskatchewan Health Authority, Golden Healthcare Management Inc. is piloting the STEPS program within Diamond House in Warman, Saskatchewan. It offers 30 ALC beds designed to support patients as they transition from acute care environments to more suitable, long-term living arrangements. STEPS provides a supportive, lower-intensity care setting that allows patients to recover, regain abilities, and plan their next steps. The program aims to improve transition outcomes, foster independence, enhance care partner engagement, and support cultural sensitivity. |
System level | ||
Implementing Alternative Levels of Care Leading Practices131 | Ontario | A report summarizing activities and discussions from a 2024 workshop on roles in the system, inner and outer setting factors affecting change, and 7 recommendations to support the implementation of ALC leading practices. |
Scenarios for Seniors’ Care: Future Challenges, Current Gaps and Strategies to Address Them12 | All provinces | Proposed opportunities to reduce ALC patient-days in the hospital setting, community and support services, care spaces for older adults, home care, primary care access; proposed policy changes, and key recommendations for provinces. |
Confronting the ALC Crisis with a Multifaceted Policy Lens16 | Aberta; Ontario; Saskatchewan | Proposed upstream interventions, midstream interventions, and downstream interventions for alleviating ALC. |
Essential Role of Caregivers in Improving Transitions and Addressing ALC82 | Ontario | Practical guide that provides information, tools, and resources for OHTs to help address ALC through integrating care partners and implementing care partner-focused strategies. |
The Alternate Level of Care Leading Practices Guide: Preventing Hospitalization and Extended Stays for Older Adults81 | Ontario | Practice guide for the care and proactive management of older adults who are hospitalized and at risk of delayed transition to an appropriate setting that can be implemented in the emergency department, acute care, and postacute care setting. |
Implementation Example of Ontario Health’s ALC Leading Practice Guidea | Ontario | Adopting a home-first philosophy for discharge planning, which is focused on early intervention and an integrated Ontario Health at Home discharge planning model. There are also length-of-stay reduction strategies in hospital (i.e., MOVE, Senior Friendly Care). |
ALC Partnership Tablea | British Columbia | NR |
General ALC strategya | New Brunswick | A multicomponent strategy that includes discharge planners having access to patient charts as soon as admission is requested, early mobilization of patients who are identified as frail, and increasing available transition beds. |
Patient flow roundsa | Newfoundland and Labrador | Conducting weekly patient flow rounds to review all patients designated as ALC as well as other patients who are at risk of becoming complex cases. |
Collaborative effort to reduce ALC in acute carea | Northwest Territories | The Department of Health and Social Services in the Northwest Territories has increased LTC beds and hired more discharge planners to help move patients designated as LTC. |
General ALC strategya | Saskatchewan | A strategy is to bring visibility to the individuals who are designated as ALC and the reason for their designation. This is followed by steps to move these individuals to a location that best suits their unique needs (e.g., home, transitional care, LTC). |
ALC = alternate level of care; LTC = long-term care; MOVE = Mobilization of Vulnerable Elders; NR = not reported; OHT = Ontario Health Team; STEPS = Short-term Enablement and Planning Suites.
aThis intervention was reported in the survey.
International Findings
To capture information about interventions to alleviate the ALC burden from outside of Canada, we searched the literature for international approaches to addressing ALC. These findings may help provide lessons for future work to alleviate the ALC burden in Canada.
We included 10 interventions identified in the published and grey literature.140-149 We identified interventions from Australia, Japan, Scotland, the UK, and the US.140-149
We identified 4 midstream interventions, all of which we categorized as practice changes.141-143,149 These interventions intend to help improve patient flow through approaches that include optimizing the number of care providers per patient, early and regularly scheduled discharge planning, and interdisciplinary care.141-143,149
We identified 2 downstream interventions.145,146 We categorized 1 intervention as a practice change and the other as a tool or guideline.145,146 These interventions intended to help facilitate the discharge of patients from the hospital though guidance about discharge pathways dependent on level of need, and dedicated areas for individuals waiting to leave the hospital.145,146
We identified 4 system-level interventions.140,144,147,148 We categorized 2 interventions as infrastructure and finance, 1 as tools and guidelines, and 1 as information sharing: recommended initiatives.140,144,147,148 Two of these interventions focused on financial support to support patient discharge from the hospital, bolster the care workforce, and expand the availability of health care infrastructure and services.144,148 One intervention specifically focused on helping reduce out-of-area residential placements and unnecessary hospital stays.147 The final intervention was intended to help facilitate timely care in hospitals during periods of high use (i.e., winter months).140
We did not identify any upstream interventions.
Some interventions may fit into more than 1 stream and category. For simplicity, we have categorized them into 1 stream and category that best aligned with the intervention’s components and objective. The included interventions are presented in Table 7. A more detailed description of these interventions is available in the Supplemental Material.
We also included 2 case studies from the UK and Scotland.150,151 These case studies discuss the successes of approaches to alleviating ALC and reducing patient length of stay.150,151 One case study described the implementation of a multiagency, decision-making team and discharge hub.151 The other case study described a complex, multi-initiative, system-wide approach.150 A more detailed description of these case studies is available in the Supplemental Material.
Table 7: Descriptions of International Interventions and Case Studies to Alleviate ALC Identified in the Literature
Intervention name | Description |
|---|---|
Midstream | |
Single-Handed Care142 | An assessment of, and approach to, an individual’s moving and handling needs. Its intent is to safely reduce the number of carers that a task requires from 2 carers to 1 carer. |
Early screening tool for discharge planning149 | A study to investigate whether early screening for risk factors for delayed discharge could improve the quality of discharge planning. |
Integrated daily discharge flow huddle and patient tracker143 | Multiagency discharge flow meeting that was chaired by a senior manager who determined actions and timescales for the team and supports the team in unlocking barriers to discharge. |
Social work-led model of care141 | Model of care that aims to address psychological and organizational factors hindering discharge. |
Downstream | |
Discharge to Assess146 | A model of hospital discharge based on the principal of conducting full health and social care assessments after (rather than before) discharge from hospital. |
Discharge lounge145 | A hospital in Illinois created a discharge lounge that was a space dedicated to handling patients ready for discharge from an inpatient unit. It moved inpatients out of the hospital faster and freed-up beds to admit patients from the ED into inpatient units. |
System level | |
Adult Social Care Discharge Fund148 | Funding provided to improve discharge from hospital into social care, support more people to work in care, and free-up time to allow carers to care. |
Funding to block-buy home beds152 | Funding provided to buy thousands of additional beds in care homes and other settings and to upgrade and expand hospitals. |
Coming Home Implementation Framework, Dynamic Support Register, and Community Living Change Fund147 | A framework for a strategy and recommendations to reduce the delayed discharges and inappropriate out-of-area residential placements for individuals with complex care needs, including learning disabilities. |
Winter Planning140 | An initiative to help facilitate care provision during winter months when there is additional pressure placed on local systems from seasonal influenza, norovirus, COVID-19, severe weather, and public holidays. It was made up of multiple projects to support the Home First pathway. |
Case studies | |
Implementing a discharge hub at Sussex Community NHS Foundation Trust151 | The Sussex Community NHS Foundation Trust implemented a multiagency decision-making team and discharge hub, with 1 hub at each of the 3 main acute hospitals in the trust’s domain. The trust also improved internal data management systems to provide real-time data updates from community intermediate care units to operational managers to support decision-making. |
East Ayrshire Health and Social Care Partnership150 | East Ayrshire Health and Social Care Partnership reduced the total time that patients spent in hospital to a rate that was well below the national average in Scotland. They attributed their success to 5 key initiatives, including early referral to a social work team, dedicated mental health officers, discharge to assess, intermediate care and enablement, and a “home from hospital” service. They also outlined multiple enabling factors spanning leadership, accountability, political and financial considerations, system integration and coordination, and openness to ideas. |
ALC = alternate level of care; ED = emergency department; NHS = National Health Service.
Economic and Resource Considerations
Key Take-Aways
We identified 1 Canadian cost-effectiveness study conducted alongside the implementation of the SAFE Unit to alleviate the ALC burden (a downstream intervention) and a Canadian costing study on the implementation of a reintegration unit (i.e., also a downstream intervention). Both initiatives reported estimated cost savings associated with the use of their respective transitional care units relative to patients remaining in their initial hospital space.
Although the literature suggests that these and other strategies for alleviating ALC may be less costly, resulting in the opportunity to treat more patients at the level of care required and thus increase efficiency in the use of health care resources relative to patients remaining in ALC, there are resource needs, coordination, and redistribution implications to consider with respect to the implementation of any strategy that are not fully captured in identified economic evaluations.
Methods
We conducted a literature review to identify economic and resource considerations associated with the implementation of ALC interventions. Our focus was to summarize relevant Canadian studies pertaining to costs, resource use, and economic implications of initiatives identified previously within the Effectiveness and Harms of Published Interventions section of this report. The high-level summary of resource considerations relevant to the introduction of interventions to help alleviate the ALC burden was further informed by round table discussions described in the Engagement section of this report and, when relevant, non-Canadian studies. All the following costs reflect the original source values. For standardized costs based on 2024 Canadian dollars and details on the category of resources included within the cost figures, please refer to Table 28 in Supplemental Material.
Findings
Costs of Interventions to Help Alleviate ALC
Compared to occupying an ALC bed, studies report lower daily costs associated with occupying a bed in a transitional care unit ($155 per patient13), in a LTC facility ($126 to $144 per patient14,15), or at home with support ($42 per patient per day for home care,15 $118 per patient for home-based palliative care14). A costing study conducted on the introduction of a reintegration unit (i.e., downstream intervention) in a Toronto hospital estimated that the direct cost of care for 102 patients with more than 12,470 patient-days was $2.4 million (2019 values).135If the same patients had spent the same time in the hospital with ALC designation, the authors’ of the study estimated that it would have theoretically cost $3.2 million. It was concluded that the reintegration unit may have resulted in an estimated savings of $861,000.135 Of note, the authors of this study did not report what cost categories were considered within this analysis.135
Cost-Effectiveness of a Downstream Intervention (SAFE Unit) Versus Usual Care
We identified 1 Canadian cost-effectiveness study153 of a downstream intervention identified within the Effectiveness and Harms of Published Interventions section of this report, the SAFE Unit study.113 The SAFE Unit is a 20-bed transitional level of care unit implemented within a larger LTC facility in Ottawa, Ontario, with care provided by an interdisciplinary team of nurses, internists, geriatricians, physiotherapists, and social workers intended to enable patients to recover and return to their place of residence. More detail on the SAFE Unit is described in the section on Clinical Effectiveness of Downstream Interventions. Eligible patients in the SAFE Unit (n = 154) were medically complex adults aged 60 years or older at risk of deconditioning in hospital but expected to return home or to a retirement home; matched patients in usual care (n = 154) were those who had been designated ALC for at least 1 day in a hospital in the same health region as the SAFE Unit. The cost-effectiveness analysis included patients in the SAFE Unit who received care between March 2018 and June 2019153(compared to the clinical publication of the SAFE Unit intervention, which included patients in the SAFE Unit who received care between March 2018 and February 2019113 and only included patients who survived a full 180 days postdischarge to ensure all included patients were eligible to achieve the primary outcome: institution-free days in the 180 days after discharge (i.e., 180 days minus days spent in acute care hospitals, mental health hospitals, rehabilitation facilities, complex continuing care facilities, or LTC facilities). The cohorts included within the cost-effectiveness study153 are therefore not identical to those described within the clinical study.113 The perspective is from a public health care payer with costs estimates included if incurred by Ontario Health during the index hospitalization through to discharge from the SAFE Unit for the patients in the SAFE Unit and during the index hospitalization through to discharge for patients in usual care.
Results for the cohorts included in the study-based cost-effectiveness analysis153 indicated that patients who were in the SAFE Unit spent an average of 162.0 institution-free days in the community within 180 days postdischarge, while patients who received usual care had an average of 140.6 institution-free days. Patients who were in the SAFE Unit spent a mean 15.6 days in hospital during their index hospitalization, of which 3.4 days were ALC, and an additional 21.8 days in the SAFE Unit. Patients who received usual care spent a mean 28.6 days in hospital, 11.3 of which were ALC.153 Mean total cost of care for the SAFE Unit group was $23,188 per patient, while usual care costs were $24,294 per patient. Because the patients who were in the SAFE Unit group had more institution-free days and incurred a lower total cost of care than those who received usual care, SAFE was deemed to be dominant (more effective, less costly) over usual care for this outcome.153 Probabilistic analyses conducted to explore uncertainty in relative costs and effectiveness reported that SAFE would be the cost-effective option more than 55% of the time when the willingness to pay per institution-free day is $0, reaching a cost-effectiveness probability of 100% if the willingness to pay is greater than $941 per institution-free day. In a scenario analysis considering “institution-free days without service” (which incorporated days with an ED, a primary care, or a home care visit as days spent in institutional facilities as described previously), patients who were in the SAFE group also had, on average, 5.9 fewer home care days and 5.2 fewer primary care days within 180 days postdischarge compared with the usual care group, although ED days were similar.153
The main limitation reported within the cost-effectiveness study153 was the potential inclusion of patients not eligible for the SAFE Unit in the usual care group due to the use of administrative data rather than screening by a program coordinator as done for patients in the SAFE Unit. As a result, patients in usual care may not have had the same rehabilitative potential as those selected for the SAFE Unit. No information was provided regarding cost or savings per incremental quality-adjusted life-year for the implementation of the SAFE Unit or for other more direct quality-of-life outcomes, such as functional status and patient preferences, or length-of-life–related outcomes. Of note, the analysis time horizon was only up to 6 months postdischarge, and any long-term impacts were not captured.
Resource Considerations for Introducing Strategies to Alleviate ALC
Successful ALC-alleviating interventions may free-up acute hospital bed space and thus have the potential to improve outcomes for patients in need of such spaces. This could reduce health care costs and improve outcomes for otherwise patients designated as ALC and delay admission to or decrease the time patients spend in LTC at least in the short term; however, some resources may need to be increased or redistributed to achieve these outcomes. To fully identify and prioritize the need for ALC interventions, consistent coding (reporting) of the health and social needs of patients designated as ALC (e.g., LTC, awaiting housing, awaiting rehabilitation services) is needed. For home care–related interventions, either those intended to pre-emptively avoid ALC (i.e., upstream) or expedite discharge for patients designated as ALC (i.e., downstream), this likely involves increasing the number of available home care providers (e.g., nurses, palliative nurses, personal support workers, cleaners), increasing needs assessment services (e.g., in-hospital assessments, social workers), increasing administrative support, and increasing the availability of community services (e.g., Meals on Wheels, transportation). For introducing or increasing the availability of transitional care units (i.e., downstream ALC-discharge interventions), facility space as stand-alone units or within hospitals or LTC facilities would be needed, along with related equipment, nursing and therapeutic staff (e.g., occupational therapists, physiotherapists, speech language pathologists, rehabilitation specialists), staff supporting daily living (e.g., personal support workers, activity coordinators, janitorial and kitchen staff), and administrative staff. Integrated care–related interventions (which could be at any stream point, including system level) may require increased planning and coordinating staff, additional coordination technology (e.g., integrated records, decision support software), increased home and community care services, and potentially partially or fully integrated budgets between health care, LTC, and social service public payers.
Studies in the UK have noted that an increased availability of home care providers is associated with reduced downstream discharge delays.135 An increased availability of LTC beds is also associated with reduced discharge delays, particularly in areas with affordable LTC beds, because patients and their families spend less time searching for care options in markets with lower LTC costs.154
Implementation Considerations
Key Take-Aways
Successful implementation of ALC interventions requires involvement from everyone involved in the process. These participants may include the patients and care partners who benefit from the changes associated with implementation, the clinicians and care providers required to make the changes, the government officials and policy-makers who approve the changes, and the evaluators who monitor the success of the changes.
Access to high-quality and complete information across the care continuum is a key facilitator to implementation of ALC interventions. Other facilitators include good communication across the care pathway; positive relationships among patients, care partners, and clinicians; and standardization of protocols for discharge, communication, and follow-up.
Misalignment of available LTC spaces and community resources may act as barriers to implementation. Additional barriers may be present when care partners determine they have limited capacity and availability to provide care and are unable to access the community supports they feel are required to provide safe and appropriate care for the patient.
Methods
We conducted a review of the implementation literature to identify facilitators of, and barriers to, the implementation of ALC interventions. The literature was reviewed by 1 author, and the relevant findings were narratively summarized. The findings also include information gathered through the implementation engagement sessions and the survey conducted by CDA-AMC.
Findings
In 2024, the Provincial Geriatrics Leadership Ontario (PGLO) and The Center for Implementation developed recommendations for implementing ALC leading practices.131 These recommendations were developed by using the interactive systems framework (ISF) for dissemination and implementation155 to identify key implementation roles in ALC. They identified the following roles in ALC implementation:
beneficiaries of the change (e.g., patients, clients, care partners, communities)
recipients who need to make the change (e.g., care providers, clinicians, nurses, front-line staff)
a behaviour change system of people working locally to make the change happen (e.g., health teams, hospital leadership, quality improvement leads, champions, implementation teams)
a support system to support the local behaviour change system (e.g., provincial or territorial health administrations, health care leadership groups, professional organizations)
a synthesis and translation system to contextualize findings (e.g., health care leadership groups, hospital leadership)
policy and government (e.g., provincial and territorial ministries of health or LTC, provincial and territorial health administration)
evaluators (e.g., health care leadership groups, academic researchers, local and community partners, provincial and territorial health administration)
secondary implementation supports with specific implementation expertise (e.g., health care leadership groups, provincial and territorial health administrations, other parts of the health system).131
As part of the recommendation development exercise, PGLO also modified The Center for Implementation’s Consolidated Framework for Implementation Research 2.0 to identify inner and outer factors affecting change and highlight those that affect implementation.131 Common responses in the exercise are summarized in Table 8.
Table 8: Inner and Outer Setting Factors Affecting Implementation and Change
Factors | Examples |
|---|---|
Inner setting factors | |
Structural characteristics |
|
Communications |
|
Culture |
|
Tension for change |
|
Relative priority |
|
Available resources |
|
Outer setting factors | |
Values and beliefs |
|
Systemic conditions |
|
Policies and laws |
|
Partnerships and connections |
|
Financing |
|
EMR = electronic medical record; LTC = long-term care.
PGLO developed 7 recommendations related to the implementation of ALC. Three of the 7 recommendations were categorized as “quick wins” (i.e., changes that could have immediate impact) or as a “lever for change” (i.e., significant system level changes that impact multiple challenges in the system).131
The first recommendation for a quick win was to enable the sharing of information, tools, and documents through a centralized organization to facilitate implementation. This could include having a single organization responsible for maintaining a central repository of tools, knowledge, and documents and making it clear how the individuals responsible for implementation can access this repository.131 Sharing information about patients was labelled as both a quick win and a lever for change. In the near term, it was suggested that partners who have the flexibility in their work flow and organization could modify their records systems to plan for strategic alignment of electronic medical records by migrating to the same or compatible vendors.131 It was also suggested they could work together to troubleshoot any data-sharing or privacy issues they encounter in the process. In the longer term, it was suggested the province could work toward a consistent electronic medical records system to facilitate sharing patient information easily and securely between different clinicians and care settings.131
A recommendation to address ageism was identified as a lever for change.131 PGLO suggested this may be one of the more difficult challenges related to the implementation of interventions for ALC but could also prove to be the most effective mode of change. Ageism was identified as a challenge across every part of the health system. Common problems observed across health systems that were suggested could be improved by tackling ageism included older adults not being considered a high-priority patient group and physicians not wanting to take on older patients.131 Individual behaviours reported to facilitate implementation and change included having leaders support the change and using clinician and administrator champions to encourage their colleagues. Reported organizational strategies included involving older adults in planning care options for their population, getting people on board with a shared vision, and identifying and engaging early adopters of change.131
The PGLO recommendations 4 through 6 were reported as topics for consideration regarding different roles in the system to facilitate implementation and change. It was suggested there must be local roles in the implementation system and the infrastructure to support implementation should be defined at the local level.131 It should be clear to participants who is a part of the implementation team at the local level and what their roles are in the implementation process. Chains of support to reach people at the individual level could facilitate change. For example, a regional support team can be put in place to provide support to implementation teams in individual hospitals or care settings. A mapping exercise may be helpful to determine which roles and supports are needed to facilitate successful implementation. The sixth PGLO recommendation was specific to the Ontario context and defining the role of PGLO in provincial implementation of ALC leading practices. The final recommendation was to strategically consider a wide variety of sources of change when attempting to implement change across a health system.131
Additional factors related to the implementation of policies and interventions to reduce ALC rates and regarding transitional care of older adults were identified from the published literature and through the CDA-AMC engagement sessions and survey for this project. Many of these factors corresponded with those previously outlined in the work by PGLO and The Center for Implementation.131
The framework used to facilitate the recommendation from PGLO was developed by Wandersman and colleagues (2008).155 They developed the ISF in an effort to bridge the gap between research science and clinical practice. The ISF was developed to aid the dissemination of innovations in prevention research, but its principles can be applied to the dissemination and implementation of all research to practice. Contextual factors should be considered when applying the framework, but context is not the focus. The framework focuses on 3 systems:
A system of synthesis and translation in which information about the intervention is translated into user-friendly formats to support uptake.
The results produced by effectiveness trials are generally not presented in a way that can be immediately used by the people responsible for delivering or supporting the intervention in clinical practice.155 Effectiveness results are not often presented in sufficient detail and contain a lot of scientific terminology that may make them difficult to interpret in a way that can be easily applied in a clinical setting. They also may not provide all of the information needed to implement the intervention, such as cost and fiscal considerations or contextual elements related to the setting of interest that may be considered within the totality of the evidence available about the intervention.155 Effectiveness findings often require further synthesis to identify the key characteristics of programs, processes, and policies before they can be appropriately applied for implementation of the intervention. Both the developers of an intervention and the researchers who evaluate its effectiveness play a key role in this synthesis to help ensure the end-user is provided with the appropriate information to make the intervention as useful as possible.155
A support system to provide training and technical assistance to the people responsible for implementing the intervention.
The support system exists to provide both innovation-specific and general support and capacity building.155 Innovation-specific support includes general information provided to an organization before deciding to implement an intervention, training before implementation that is specific to the new intervention, and providing technical assistance once the intervention is in place.155 General capacity building is intended to enhance and support the organization as a whole and does not focus on a specific intervention. These activities are not necessarily associated with the implementation of an intervention but support the health of an organization as a whole.155
A delivery system responsible for implementing the intervention in practice.155
The delivery system is responsible for the activities necessary to implement the intervention. Implementation will draw on people’s general capacities, such as activities required to maintain the organization and connect with other organizations and the community.155 People’s intervention-specific capacities will also be utilized. These include activities such as information gathering, choosing interventions, and determining the steps required to implement and maintain the use of the intervention. Overall, the elements of the framework highlight the need for partners across the system (e.g., researchers, trainers, practitioners, funders) to communicate to facilitate successful implementation of a new intervention.155
Facilitators and Barriers of Implementation of ALC Interventions
Factors that facilitate the implementation of interventions to reduce ALC, and those that act as barriers to implementation, were identified through the published literature, our implementation consultations, and survey. These factors we categorized according to the part of the health care system they most apply to. A summary of these factors is provided here.
Facilitators to Implementation of ALC Interventions
General
General facilitators include:
Access to high-quality patient information across sectors and levels of care through connected electronic medical records systems.136
Enhanced communication between all participants in a patient’s care pathway, including the patient, clinicians, hospital personnel, patient navigators and social workers, and care partners regarding in-hospital care, discharge, and future planning156,157 and relationship building across sectors (e.g., with governments, community services, and interdisciplinary care teams).
Positive relationships between the patient, their health care team, and care partners.157
Implementation considered as a continuum, tailoring approaches to the needs and complexities of the individual patient while keeping in mind the needs required to transition between each step of care and identify people most at risk at the beginning and keep them on the pathway.
Policy (System Level)
Policy (system-level) facilitators include:
High-level policy implementation at the jurisdictional level, with interventions tailored to the local context.136
Establishing networks of care with shared patient accountability across different sectors of the health system.136
Expand the supply and use of ambulatory and community care settings as alternatives to ED and in-hospital acute care.136
Creation of alternative locations outside of the acute care hospital ward where patients designated as ALC can be supported while they wait for their return to the community or to LTC.96
Integration of health and social services to enhance continuity of care.158
Providing adequate funding for new approaches.156
Hospital (Midstream)
Hospital (midstream) facilitators include:
Discharge assessment protocols that go beyond medical needs and are applied by trained and specialized discharge personnel.136
Proactive discharge planning that involves the patient, clinicians, and care partners.96,157
Standardization of protocols for communication, discharge planning, and follow-up.156
Community (Upstream and Downstream)
Community (upstream and downstream) facilitators include:
Improve access to short-term respite care or home care to support people while waiting for a transfer to LTC from their home rather than from a hospital.96
Some of these facilitating factors are mirrored in the programs and interventions identified in the clinical effectiveness review in this report. All the interventions identified were made up of multiple components. The most reported components of these interventions were:
cross-sector integration (e.g., collaboration between acute care, primary care, social care, and/or community services)103,109-112
Barriers to Implementation of ALC Interventions
General
General barriers include:
Ineffective or disrespectful communication between clinicians and care partners.157
A lack of trust between patients and care partners and clinicians.157
Hospital (Midstream)
Hospital (midstream) barriers include:
Inadequate staffing levels (e.g., hospital staff do not have the time to coordinate and conduct assessments and other steps required before successful discharge).
Poor communication while in the hospital (e.g., communication regarding care in hospital, risk assessment and expectations for care at home, as well as consistent, open communication between staff and patients and care partners).
Perceived administrative burden that gets in the way of person-centred care required for the appropriate care of older adults in hospital.
Perceived rushed hospital discharge that does not allow the patient or care partners sufficient time to plan a safe return to the community.157
Community (Upstream and Downstream)
Community (upstream and downstream) barriers include:
A lack of availability of appropriate spaces for people in LTC (e.g., close to support systems, provides the appropriate level of care for their current health status).
A lack of knowledge about what resources are available to the patient and carers after discharge.
Limited capacity and availability of adequate intermediate care, such as rehabilitation and reablement following hospital discharge.
Limited capacity and ability of care partners to provide the level of care required when the patient returns to the community (e.g., they do not have time, they do not feel comfortable, they feel a sense of responsibility for keeping the patient at home and not in LTC).
A lack of necessary social supports in the community including access to safe, culturally appropriate primary health care, health and social care at home, and home supports.
The cost of LTC may be too high for the individual or their family to manage. Due to the costs involved, they may be unable to situate themselves in their preferred type of LTC or in a location that is convenient to their family or existing community supports.
Limitations
There are limitations that should be noted when interpreting the findings in this report. These include the rapid timelines and exploratory, broad scope of the review of relevant reasons people with unmet needs receive ALC designation and that the included literature was not critically appraised. Only literature published in English was included, so some relevant studies published in French or other language may not have been captured. We also did not quantify or assess the relative impact of identified factors because this was beyond the aim of this work. Additionally, a single reviewer (with support of a second) screened, selected, and analyzed included sources within a rapid time frame and aimed to produce a succinct description of findings. Given these methods and timelines, we may have missed relevant sources and factors. Finally, the purpose of this work was to describe ethical considerations identified during the review of factors. Therefore, we did not conduct a dedicated ethics review nor a dedicated ethics literature search, and there may be additional ethical considerations not captured.
In the review of the effectiveness and harms of interventions to alleviate the ALC burden, we included all comparative and noncomparative study designs because we recognize that the feasibility of undertaking randomized controlled trials to evaluate many interventions to alleviate the ALC burden is likely to be limited (particularly those at the population level). We did not find evidence on the effectiveness of solely upstream interventions. We did not identify any randomized controlled trials or systematic reviews that met our inclusion criteria. No included studies reported data about patient harms (e.g., adverse effects) or clinician, patient, or care partner quality of life; therefore, we can form no conclusions on the impact of interventions to alleviate the ALC burden on these outcomes. A rapid approach was used for feasibility reasons. Abbreviated methods can increase the risk of error in the review (e.g., missed studies, data extraction errors), but we adhered to relevant guidance to ensure methodological robustness. We focused our appraisal on key outcomes of interest and on studies published in the past 15 years. Older studies would not be represented; however, it is likely that these would be less relevant to the present health system. For each of the included studies, we did not calculate our own effect estimates of the interventions and accompanying 95% confidence intervals using the reported dichotomous data (e.g., relative risk or odds ratio for ALC rate, discharge to home, hospital readmission, and ED visits) and continuous data (e.g., mean standardized difference for length of stay in ALC and hospital length of stay). Rather, we extracted the absolute and/or relative between-group differences as reported by the study authors for the relevant outcomes. We did not verify the accuracy of each study’s data analyses nor did we calculate between-group differences and 95% intervals when not reported in the included study reports.
We found a lack of information about equity-deserving group characteristics. Race, ethnicity or country of origin, language, gender or gender identity, newcomer status, or sexual orientation were not reported in any of the included studies. Relevant subgroup analyses were either unreported or of low credibility to inform any differences in effectiveness among equity-deserving groups. Therefore, we do not know whether equity-deserving groups were represented in these studies.
While we strived to capture as much information as possible in our environmental scans of interventions to address ALC in Canada and internationally, it is likely that we did not identify all interventions that exist. As such, the findings of this scan should not be interpreted as a comprehensive list. Additionally, we were not able to identify published outcome data for most of the interventions and therefore could not appraise or comment on the effectiveness of these interventions.
Final Thoughts
This evidence assessment report described the current challenges faced in Canada regarding ALC. Through engagement with decision-makers, researchers, administrators, clinicians, and care partners, and by searching key information and data sources, we identified reasons people remain in ALC in acute inpatient care settings as well as strategies and interventions intended to decrease the length of time people spend in ALC. We described ALC interventions that are in place across Canada and internationally and new interventions on the horizon. Economic and implementation considerations were also outlined.
We found that the factors contributing to why people enter or remain in ALC in acute inpatient care settings can be related to 3 broad categories: individual sociodemographic and clinical factors, process and practice factors within and across acute and nonacute care settings, and structural factors (e.g., legislative and regulatory systems, policies, shared practices, and beliefs and values). We also found that multiple, intersecting factors that contribute to ALC can raise ethical considerations and present ethical dilemmas for patients, care partners, families, health care providers, and health systems in the context of ALC admissions, stays, and discharges.
The effectiveness of 6 multicomponent interventions with outcomes reported in the published literature was assessed. The number of relevant studies included in the review suggests that there is only a small body of published comparative evidence available on the benefits and harms of interventions to alleviate the ALC burden, which highlights an important gap in the evidence base for ALC. The interventions identified in the review are intended to alleviate the ALC burden; however, there was very low certainty in the evidence of the benefits of all interventions examined. Additional studies of interventions to reduce ALC performed in health systems similar to those in Canada may help to provide more evidence of effectiveness and ensure the results are generalizable to the Canadian context.
Some health care resources may need to be increased or redistributed to facilitate successful implementation of ALC-alleviating interventions that can, in turn, free-up bed space in acute care or reduce treatment costs. These changes could include an increase in available home care providers, needs assessment services, administrative support, and availability of community services. The introduction of alternative treatment settings (e.g., transitional care units) would require additional facility space, related equipment, and clinical and support staff.
Key participants in the implementation of ALC interventions include patients, care partners, clinicians, support staff, government, administrators, and communities suggesting everyone involved has a part to play in the process. Successful implementation of interventions for ALC can be facilitated through enhanced communication between all participants in a patient’s care pathway and by providing them with high-quality data to inform decision-making. Cross-sector integration and multidisciplinary collaboration contribute to the success of implementation initiatives. A positive relationship between patients, families, and clinicians will enable better information sharing. Implementation should be approached as a continuum where approaches are tailored to the needs and complexities of the individual patient while assessing the requirements to transition between each step of care.
References
1.Canadian Institute for Health Information. Inpatient hospitalization, surgery and newborn statistics, 2022–2023. Ottawa (ON): CIHI; 2024: https://www.cihi.ca/en/hospital-stays-in-canada-2022-2023. Accessed 2024 Jun 12.
2.Canadian Institute for Health Information. Definitions and guidelines to support ALC designation in acute inpatient care. Ottawa (ON): CIHI; 2016: https://www.cihi.ca/sites/default/files/document/acuteinpatientalc-definitionsandguidelines_en.pdf. Accessed 2024 May 15.
3.Rojas-Garcia A, Turner S, Pizzo E, Hudson E, Thomas J, Raine R. Impact and experiences of delayed discharge: A mixed-studies systematic review. Health Expect. 2018;21(1):41-56. PubMed
4.Everall AC, Guilcher SJT, Cadel L, Asif M, Li J, Kuluski K. Patient and caregiver experience with delayed discharge from a hospital setting: A scoping review. Health Expect. 2019;22(5):863-873. PubMed
5.Jones A, Lapointe-Shaw L, Brown K, et al. Short-term mortality and palliative care use after delayed hospital discharge: a population-based retrospective cohort study. BMJ Support Palliat Care. 2024;14(e3):e2836-e2842. PubMed
6.Bender D, Holyoke P. Why some patients who do not need hospitalization cannot leave: a case study of reviews in 6 Canadian hospitals. Healthc Manage Forum. 2018;31(4):121-125. PubMed
7.Lim Fat GJ, Gopaul A, Pananos AD, Taabazuing MM. Healthcare-Associated Adverse Events in Alternate Level of Care Patients Awaiting Long-Term Care in Hospital. Geriatr. 2022;7(4):08.
8.Abdelhalim A, Zargoush M, Archer N, Roham M. Decoding the persistence of delayed hospital discharge: An in-depth scoping review and insights from two decades. Health Expect. 2024;27(2):e14050. PubMed
9.Kuluski K, Im J, McGeown M. “It's a waiting game” a qualitative study of the experience of carers of patients who require an alternate level of care. BMC Health Serv Res. 2017;17(1):318. PubMed
10.Chuang YT, Zargoush M, Ghazalbash S, Samiedaluie S, Kuluski K, Guilcher S. From prediction to decision: optimizing long‐term care placements among older delayed discharge patients. Prod Oper Manag. 2023;32(4):1041-1058.
11.Haas R, Brundisini F, Barbara A, et al. Emergency department overcrowding: an environmental scan of contributing factors and a summary of systematic review evidence on interventions. Can J Health Technol. 2023;3(11).
12.Wyonch R. Scenarios for seniors’ care: future challenges, current gaps and strategies to address them. Health Policy. Toronto (ON): C.D. Howe Institute; 2024: https://www.cdhowe.org/public-policy-research/scenarios-seniors-care-future-challenges-current-gaps-and-strategies-address. Accessed 2024 Jun 12.
13.Manville M, Klein MC, Bainbridge L. Improved outcomes for elderly patients who received care on a transitional care unit. Can Fam Physician. 2014;60(5):e263-271. PubMed
14.Klinger CA, Howell D, Marshall D, Zakus D, Brazil K, Deber RB. Resource utilization and cost analyses of home-based palliative care service provision: the Niagara West End-of-Life Shared-Care Project. Palliat Med. 2013;27(2):115-122. PubMed
15.Ahmed D. The challenge of alternate level of care (ALC) facing older adults in Ontario: Implications for government and policy makers using a descriptive data analytics approach [thesis]. Hamilton (ON): McMaster University; 2019: https://macsphere.mcmaster.ca/bitstream/11375/24951/2/Ahmed_Didi_MH_201909_MSc.eHealth.pdf. Accessed 2024 Nov 21.
16.Durante S, Fyie K, Zwicker J, Carpenter T. Confronting the alternate level of care (ALC) crisis with a multifaceted policy lens. The School of Public Policy Publications. 2023;16(1).
17.Lamarre M, Daignault M, Cheung VW, Forget MF, Nguyen QD. Factors Associated with Alternate Level of Care Status Designation: a Case-Control Study and Model to Optimize Care Trajectories. Can Geriatr J. 2024;27(2):152-158. PubMed
18.Bobrowski D, Elfassy MD, Bobrowski A. Hallway Healthcare: Solving Acute Care Overflow from the Community. Univ Toronto Med J. 2018;95(3):50-53.
19.Cadel L, Guilcher SJT, Kokorelias KM, et al. Initiatives for improving delayed discharge from a hospital setting: a scoping review. BMJ Open. 2021;11(2):e044291. PubMed
20.Canadian Institute for Health Information. Patient days in alternate level of care (percentage). Ottawa (ON): CIHI; 2023: https://www.cihi.ca/en/indicators/patient-days-in-alternate-level-of-care-percentage. Accessed 2024 May 15.
21.Canadian Institute for Health Information. Seniors in transition: exploring pathways across the care continuum. Ottawa (ON): CIHI; 2017: https://www.cihi.ca/sites/default/files/document/seniors-in-transition-report-2017-en.pdf. Accessed 2024 May 15.
22.Costa AP, Hirdes JP. Clinical Characteristics and Service Needs of Alternate-Level-of-Care Patients Waiting for Long-Term Care in Ontario Hospitals. Healthc Policy. 2010;6(1):32-46. PubMed
23.Costa AP, Poss JW, Peirce T, Hirdes JP. Acute care inpatients with long-term delayed-discharge: evidence from a Canadian health region. BMC Health Serv Res. 2012;12(1):172. PubMed
24.Fransoo R, Martens P, Prior H, Burchill CA, Koseva I, Rajotte L. Who is in our hospitals--and why? Winnipeg (MB): Manitoba Centre for Health Policy; 2013: http://mchp-appserv.cpe.umanitoba.ca/reference/ALC_4page_summary_web_version.pdf. Accessed 2024 Nov 29.
25.Nuernberger K, Atkinson S, MacDonald G. Seniors in Transition: Exploring Pathways Across the Care Continuum. Healthc Q. 2018;21(1):10-12. PubMed
26.Aging and chronic diseases: a profile of Canadian seniors. Ottawa (ON): Public Health Agency of Canada; 2020: https://www.canada.ca/content/dam/hc-sc/documents/services/publications/diseases-and-conditions/aging-chronic-diseases/canadian-seniors-report_2021-eng.pdf. Accessed 2024 Jun 5.
27.Iciaszczyk N, Arulnamby A, Brydges M, et al. Ageing in the right place: supporting older Canadians to live where they want. Toronto (ON): National Institute of Ageing; 2022: https://www.niageing.ca/airp. Accessed 2024 Jun 12.
28.Durante S. The demography and policies of alternate levels of care: a selection of Canadian case studies [thesis]. Calgary (AB): University of Calgary; 2021: https://prism.ucalgary.ca/server/api/core/bitstreams/a40f0bb5-e775-482b-be2d-4f62b01c7578/content. Accessed 2024 Jun 12.
29.Jutan N, Langlois L, Damiano N. Seniors and alternative level of care: building on our knowledge. Healthcare Quarterly. 2013;16(3):7-10. PubMed
30.Bai AD, Dai C, Srivastava S, Smith CA, Gill SS. Risk factors, costs and complications of delayed hospital discharge from internal medicine wards at a Canadian academic medical centre: retrospective cohort study. BMC Health Serv Res. 2019;19(1):935. PubMed
31.Arthur SA, Hirdes JP, Heckman G, Morinville A, Costa AP, Hebert PC. Do premorbid characteristics of home care clients predict delayed discharges in acute care hospitals: a retrospective cohort study in Ontario and British Columbia, Canada. BMJ Open. 2021;11(2):e038484. PubMed
32.Barnable A, Welsh D, Lundrigan E, Davis C. Analysis of the Influencing Factors Associated With Being Designated Alternate Level of Care. Home Health Care Manag Pract. 2015;27(1):3-12.
33.Canadian Institute for Health Information. Dementia in hospitals. Ottawa (ON): CIHI; 2024: https://www.cihi.ca/en/dementia-in-canada/dementia-care-across-the-health-system/dementia-in-hospitals. Accessed 2024 Dec 18.
34.Strategies to Reduce Alternate Level of Care. Can J Health Technol. 2024;4(7). https://www.cadth.ca/sites/default/files/pdf/htis/2024/EH0126_ALC.pdf. Accessed 2024 Dec 18.
35.Ontario Health. About Alternate Levels of Care. Toronto (ON): Government of Ontario; 2024: https://help.accesstocare.on.ca/helpfiles/WTISHelp/Working_with_Waitlist_Entries/ALC/Working_with_ALC_Waitlist_Entries.htm. Accessed 2024 Nov 5.
36.Saskatchewan Health Quality Council. Patient Flow Toolkit: Module 2: Alternate Level of Care. Saskatoon (SK): Government of Saskatchewan; 2016: https://www.saskhealthquality.ca/wp-content/uploads/2021/08/Alternate-Level-of-Care-Module-v-Apr2016.pdf. Accessed 2024 Nov 5.
37.Integrated Access and Flow Network. Provincial Alternate Level of Care (ALC) Designation Project Overview. Halifax (NS): Nova Scotia Health; 2024: https://library.nshealth.ca/ld.php?content_id=37093143. Accessed 2024 Nov 5.
38.Connect Care Manual. Edmonton (AB): Alberta Health Services: https://manual.connect-care.ca/workflows/patient-movement/alternate-level-of-care. Accessed 2024 Nov 4.
39.Interior Health Administrative Policy Manual: AP0200 – Client Rates for Alternate Level of Care Patients Awaiting Long-term Care Access. Kelowna (BC): Interior Health; 2023: https://www.interiorhealth.ca/sites/default/files/PDFS/ap0200-client-rates-for-long-stay-patients-awaiting-placement.pdf. Accessed 2024 Nov 4.
40.Max Rady College of Medicine. Concept: Alternate Level of Care (ALC) Patients - Method of Identification. Winnipeg (MB): University of Manitoba; 2024: http://mchp-appserv.cpe.umanitoba.ca/viewConcept.php?conceptID=1416. Accessed 2024 Nov 4.
41.Clinical Information Systems Monthly Bulletin. Charlottetown (PE): HealthPEI; 2019: https://src.healthpei.ca/sites/src.healthpei.ca/files/CIS/Bulletins/CIS_Updates_Week_of_November_25_2019.pdf. Accessed 2024 Nov 4.
42.2021-22 Alberta Health Services Annual Report Supplementary Information. Edmonton (AB): Alberta Health Services; 2022: https://www.albertahealthservices.ca/assets/about/publications/ahs-pub-pr-2021-22-q4-objective-01-alc.pdf. Accessed 2024 Nov 4.
43.Centre for Advanced Analytics Data Science and Innovation. Our Health Care Report Card. Surrey (BC): Fraser Health Authority; 2023: https://www.fraserhealth.ca/-/media/Project/FraserHealth/FraserHealth/About-Us/Accountability/Report-Cards/202309_ReportCards/FH-Public-Report-Card.pdf. Accessed 2024 Nov 4.
44.Manitoba Health, Seniors and Active Living. Information Management and Analytics. Annual Statistics 2018-2019. Winnipeg (MB): Government of Manitoba; 2019: https://www.gov.mb.ca/health/annstats/as1819.pdf. Accessed 2024 Nov 4.
45.New Brunswick Facility Profiles (Acute Care) 2022-2023: Five-Year Trend Analysis. Fredericton (NB): Government of New Brunswick; 2024: https://www2.gnb.ca/content/dam/gnb/Departments/h-s/pdf/en/Publications/Profiles/acute-care-facility-profiles-2022-2023.pdf. Accessed 2024 Nov 4.
46.Annual Performance Report 2023-2024. St. John's (NL): Newfoundland and Labrador Health Services; 2024: https://nlhealthservices.ca/wp-content/uploads/2024/09/NLHS_APR_2023-24_Final.pdf Accessed 2024 Nov 4.
47.Clinical Services Stering Committee. Making Better Health Care Decisions for Nova Scotia: A Report by the Clinical Services Steering Committee. Halifax (NS): Nova Scotia Department of Health; 2001: https://novascotia.ca/dhw/publications/CSSC_Report.pdf. Accessed 2024 Nov 5.
48.Health PEI Annual Report 2022-2023. Charlottetown (PE): HealthPEI; 2023: https://www.princeedwardisland.ca/sites/default/files/publications/hpei_annual_report_2022-2023.pdf. Accessed 2024 Nov 4.
49.Saskatchewan Health Authority Public Board Meeting Minutes. Date of Meeting: May 27, 2022. Saskatoon (SK): Saskatchewan Health Authority; 2022: https://www.saskhealthauthority.ca/sites/default/files/2022-10/2022-05-27-Public-Board-Meeting-Minutes.pdf. Accessed 2024 Nov 5.
50.Alternate Level of Care (ALC) Order Management Workflow Overview CST Cerner Interface. Victoria (BC): HealthCareBC; 2023: https://cstcernerhelp.healthcarebc.ca/index.htm#t=Patient_Chart%2FOrders%2FALC%2FAlternate_Level_of_Care_(ALC)_Order_Management_Workflow_Overview.htm Accessed 2024 Nov 4.
51.Healthy Aging in the North: Action Plan (2015/16- 2020/21). Prince George (BC): Northern Health; 2015: https://www.northernhealth.ca/sites/northern_health/files/health-information/seniors/documents/healthy-aging-in-the-north-action-plan-2015.pdf. Accessed 2024 Nov 4.
52.Island Health Performance Measures: Alternate Level of Care. Victoria (BC): Island Health; 2024: https://www.islandhealth.ca/sites/default/files/performance-measures/documents/alternate-level-of-care.pdf. Accessed 2024 Nov 4.
53.Manitoba Centre for Health Policy. The 2019 RHA Indicators Atlas. Winnipeg (MB): University of Manitoba; 2019: http://mchp-appserv.cpe.umanitoba.ca/reference/RHA_Report_web.pdf. Accessed 2024 Nov 4.
54.New Brunswick Health Council. The ABCs of ALCs. https://nbhc.ca/abcs-alcs. Accessed 2024 Nov 4.
55.Network's Performance Reports- Detailed. Bathurst (NB): Vitalite Health Network; 2024: https://vitalitenb.ca/en/health-network/communications/publications/networks-performance-reports-detailed. Accessed 2024 Nov 4.
56.Health Canada. Canada-Newfoundland and Labrador Home and Community Care and Mental Health and Addictions Services Funding Agreement. Ottawa (ON): Government of Canada; 2023: https://www.canada.ca/en/health-canada/corporate/transparency/health-agreements/shared-health-priorities/newfoundland-labrador.html. Accessed 2024 Nov 4.
57.Eastern Health Annual Performance Report 2019-2020. St John's (NL): Eastern Health; 2020: https://www.gov.nl.ca/hcs/files/Eastern-Regional-Health-Authority-Annual-Report-2019-20.pdf. Accessed 2024 Nov 4.
58.Ontario Health. Indicator name: alternate level of care (ALC) rate. Toronto (ON): Government of Ontario; 2019: https://indicatorlibrary.hqontario.ca/Indicator/Summary/Alternate-level-care-rate/EN. Accessed 2024 Nov 4.
59.HealthHR Group. Caring For Our Seniors: PEI Review of the Continuum of Care for Island Seniors. Charlottetown (PE): Government of Prince Edward Island; 2016: https://www.princeedwardisland.ca/sites/default/files/publications/dhw_caring_for_our_seniors.pdf. Accessed 2024 Nov 4.
60.Northwest Territories Health and Social Services System: 2018-19 Annual Report. Yellowknife (NT): Government of Northwest Territories: https://www.hss.gov.nt.ca/sites/hss/files/resources/hss-annual-report-2018-19.pdf. Accessed 2024 Nov 5.
61.Continuing Care in Nunavut: 2015 to 2035. Iqaluit (NU): Legislative Assembly of Nunavut; 2015: https://assembly.nu.ca/sites/default/files/TD%2078-4(3)%20EN%20Continuing%20Care%20in%20Nunavvut,%202015%20to%202035_0.pdf. Accessed 2024 Nov 5.
62.Chief of Medical Staff. Annual Report 2019-2020. Whitehorse (YT): Yukon Hospitals; 2020: https://yukonhospitals.ca/sites/default/files/2022-09/cos_annual_report_-_september_2020.pdf Accessed 2024 Nov 4.
63.Hospital patients who require an alternate level of care. Edmonton (AB): Health Quality Council of Alberta: https://focus.hqca.ca/charts/hospital-patients-who-require-an-alternate-level-of-care/. Accessed 2024 Nov 5.
64.Centre for Advanced Analytics Data Science and Innovation. Our Health Care Report Card. Vancouver (BC): Vancouver Costal Health; 2024: https://www.vch.ca/en/media/25996. Accessed 2024 Nov 4.
65.Forman J, Damschroder L. Qualitative Content Analysis. In: Jacoby L, Siminoff LA, eds. Empirical Methods for Bioethics: A Primer. Vol 11: Emerald Group Publishing Limited; 2007:39-62.
66.Braveman PA, Arkin E, Proctor D, Kauh T, Holm N. Systemic And Structural Racism: Definitions, Examples, Health Damages, And Approaches To Dismantling. Health Aff (Millwood). 2022;41(2):171-178. PubMed
67.Heller JC, Givens ML, Johnson SP, Kindig DA. Keeping It Political and Powerful: Defining the Structural Determinants of Health. Milbank Q. 2024;102(2):351-366. PubMed
68.Kuluski K, Cadel L, Marcinow M, Sandercock J, Guilcher SJ. Expanding our understanding of factors impacting delayed hospital discharge: Insights from patients, caregivers, providers and organizational leaders in Ontario, Canada. Health Policy. 2022;126(4):310-317. PubMed
69.Mah JC, Godin J, Stevens SJ, Keefe JM, Rockwood K, Andrew MK. Social Vulnerability and Frailty in Hospitalized Older Adults. Can Geriatr J. 2023;26(3):390-399. PubMed
70.Yung TKS. Individual and system-level factors associated with alternate level of care (ALC) in British Columbia [thesis]. Vancouver (BC): University of British Columbia; 2022: https://open.library.ubc.ca/soa/cIRcle/collections/ubctheses/24/items/1.0406234. Accessed 2024 Nov 21.
71.Stock D, Cowie C, Chan V, et al. Determinants of alternate-level-of-care delayed discharge among acute care survivors of hypoxic-ischemic brain injury: a population-based cohort study. CMAJ Open. 2016;4(4):E689-E697. PubMed
72.McCloskey R, Jarrett P, Stewart C, Nicholson P. Alternate level of care patients in hospitals: what does dementia have to do with this? Can Geriatr J. 2014;17(3):88-94. PubMed
73.Carfagnini QA, Ayanso A, Law MP, Orlando E, Faught BE. What Factors Increase Odds of Long-Stay Delayed Discharge in Alternate Level of Care Patients? J Am Med Dir Assoc. 2023;24(9):1327-1333. PubMed
74.Aaltonen M, El Adam S, Martin-Matthews A, Sakamoto M, Strumpf E, McGrail K. Dementia and Poor Continuity of Primary Care Delay Hospital Discharge in Older Adults: A Population-Based Study From 2001 to 2016. J Am Med Dir Assoc. 2021;22(7):1484-1492 e1483. PubMed
75.Jerath A, Sutherland J, Austin PC, et al. Delayed discharge after major surgical procedures in Ontario, Canada: a population-based cohort study. CMAJ. 2020;192(46):E1440-E1452. PubMed
76.Ahmadi F. Machine Learning Predictions of Alternate Level of Care (ALC) in Canada: From Emergency Department to the in-Hospital Stage [thesis]. Hamilton (ON): McMaster University; 2021. Accessed 2024 Nov 21.
77.Little J, Hirdes JP, Perlman CM, Meyer SB. Clinical Predictors of Delayed Discharges in Inpatient Mental Health Settings Across Ontario. Adm Policy Ment Health. 2019;46(1):105-114. PubMed
78.Little J, Hirdes JP, Daniel I. ALC status in in-patient mental health settings: Evidence based on the Ontario Mental Health Reporting System. Healthc Manage Forum. 2015;28(4):146-149. PubMed
79.Sourial N, Vedel I, Godard-Sebillotte C, Etches J, Arsenault-Lapierre G, Bronskill SE. Sex Differences in Dementia Primary Care Performance and Health Service Use: A Population-Based Study. J Am Geriatr Soc. 2020;68(5):1056-1063. PubMed
80.Teale AL, Morgan C, Jenkins TA, Jacobsen P. Delayed discharge in inpatient psychiatric care: a systematic review. Int J Ment Health Syst. 2024;18(1):14. PubMed
81.The Alternate Level of Care (ALC) Leading Practices Guide: Preventing Hospitalization and Extended Stays for Older Adults. Toronto (ON): Ontario Health; 2021: https://quorum.hqontario.ca/Portals/0/Indicators-and-change-ideas/ALC%20Leading%20Practices%20Guide%20v1%202021%20(2).pdf?ver=2022-03-30-133617-273. Accessed 2024 Apr 22; 2024 Nov 21.
82.Essential role of caregivers in improving transitions and addressing alternate level of care. Toronto (ON): The Ontario Caregiver Organization; 2023: https://ontariocaregiver.ca/wp-content/uploads/2023/12/6.-Essential-Role-of-Cgs-in-Improving-Transitions-and-Addressing-Alternate-Level-of-Care-EN-2.pdf. Accessed 2024 May 15; Nov 21.
83.Manis DR, Katz P, Lane NE, et al. Rates of Hospital-Based Care among Older Adults in the Community and Residential Care Facilities: A Repeated Cross-Sectional Study. J Am Med Dir Assoc. 2023;24(9):1341-1348. PubMed
84.Manis DR, Poss JW, Jones A, et al. Rates of health services use among residents of retirement homes in Ontario: a population-based cohort study. CMAJ. 2022;194(21):E730-E738. PubMed
85.Arsenault-Lapierre G, Godard-Sebillotte C, Bui T, et al. Rural-Urban Differences in Healthcare Use in Persons With Dementia Between 2000 and 2019: A Quebec Population-Based Study. Healthc Policy. 2024;19(3):78-95. PubMed
86.Guilcher SJT, Everall AC, Cadel L, Li J, Kuluski K. A qualitative study exploring the lived experiences of deconditioning in hospital in Ontario, Canada. BMC Geriatr. 2021;21(1):169. PubMed
87.Bronskill SE, Maclagan LC, Walker JD, et al. Trajectories of health system use and survival for community-dwelling persons with dementia: a cohort study. BMJ Open. 2020;10(7):e037485. PubMed
88.Selick A, Volpe T, Morris S, Lunsky Y. Addressing Delayed Hospital Discharges for Patients With Intellectual and Developmental Disabilities and a Mental Illness. Psychiatr Serv. 2025;76(2):207-209. PubMed
89.Lunsky Y, Balogh R, Chung H, et al. Repeated use of hospital-based services and delayed hospital discharges in a population-based cohort of autistic adults in Canada. Autism. 2024:13623613241299285. PubMed
90.Supporting alternate level of care (ALC) patients with a dual diagnosis to transition from hospital to home Toronto (ON): CAMH; 2023: https://www.camh.ca/-/media/files/professionals/hcardd/hcardd-supporting-alc-patients-dd-transition-hospital-practice-guidance-2023-pdf.pdf Accessed 2024 Nov 21.
91.Walker D. Caring for Our Aging Population and Addressing Alternative Level of Care Niagara (ON): Niagara Knowledge Exchange; 2011: https://www.niagaraknowledgeexchange.com/wp-content/uploads/sites/2/2014/05/Caring_for_Our_Aging_Population.pdf. Accessed 2024 Nov 29.
92.Kuluski K, Ho JW, Cadel L, et al. An alternate level of care plan: Co-designing components of an intervention with patients, caregivers and providers to address delayed hospital discharge challenges. Health Expect. 2020;23(5):1155-1165. PubMed
93.Canada's Drug Agency. Alternate level of care strategies and interventions report dashboard. Ottawa (ON): CDA-AMC; 2025: http://bit.ly/3T9sQiA. Accessed 2025 Feb 25.
94.McCloskey R, Jarrett P, Stewart C. The Untold Story of Being Designated an Alternate Level of Care Patient. Healthc Policy. 2015;11(1):76-89. PubMed
95.Molnar FJ. Hospitals “Failing To Plan For Dementia Is Planning To Fail”: All Canadian Hospitals Must Launch Acute Care Dementia Strategies If They Are Serious About Decreasing Hospital Overcrowding, Decreasing Alternate Level Of Care (ALC), And Thereby Increasing Hospital Capacity To Permit Pandemic Recovery And To Meet Future Escalating Needs. Canadian Geriatrics Society Journal of CME. 2021;Special Issue:1-8.
96.Alternate Level of Care (ALC) Capacity Challenges and Long-Term Care Placement: A Roundtable Discussion: Key Messages and Suggested Actions. Ontario Hospital Association. Toronto (ON): Ontario Hospital Association; 2012: https://www.oha.com/Documents/Alternate%20Level%20of%20Care%20(ALC)%20Capacity%20Challenges%20A%20Round%20Table%20Discussion.pdf. Accessed 2024 Dec 18.
97.Chidwick P, Oliver J, Ball D, et al. Six Change Ideas that Significantly Minimize Alternate Level of Care (ALC) Days in Acute Care Hospitals. Healthc Q. 2017;20(2):37-43. PubMed
98.Cadel L, Sandercock J, Marcinow M, Guilcher SJT, Kuluski K. A qualitative study exploring hospital-based team dynamics in discharge planning for patients experiencing delayed care transitions in Ontario, Canada. BMC Health Serv Res. 2022;22(1):1472. PubMed
99.Bean S, Kelecevic J. How Clinical Ethics Consultants Navigate Complex Acute Care Discharge Cases in Ontario. Thorny Issues in Clinical Ethics Consultation. Vol 1432022:117-124.
100.Jenkinson JIR, Strike C, Hwang SW, Di Ruggiero E. Nowhere to go: exploring the social and economic influences on discharging people experiencing homelessness to appropriate destinations in Toronto, Canada. Can J Public Health. 2021;112(6):992-1001. PubMed
101.Canada's Drug Agency. Aging in Place: Evidence Report. Ottawa (ON): CDA-AMC; 2024: https://www.cda-amc.ca/sites/default/files/hta-he/OP0555_Aging_in_Place_Report.pdf. Accessed 2024 Dec 10.
102.Rosalie Wyonch - Fixing the ALC Patient Problem is a Triple Win for Canadians. Toronto (ON): CH Howe Institute; 2024: https://www.cdhowe.org/intelligence-memos/rosalie-wyonch-fixing-alc-patient-problem-triple-win-canadians Accessed 2024 Nov 21.
103.Edelstein B, Scandiffio J. Effectiveness of an assess and restore program in treating older adults with physiological and functional decline: The HEART program. Arch Gerontol Geriatr. 2022;99:104609. PubMed
104.Garritty C, Gartlehner G, Nussbaumer-Streit B, et al. Cochrane Rapid Reviews Methods Group offers evidence-informed guidance to conduct rapid reviews. J Clin Epidemiol. 2021;130:13-22. PubMed
105.Garritty C, Hamel C, Trivella M, et al. Updated recommendations for the Cochrane rapid review methods guidance for rapid reviews of effectiveness. BMJ. 2024;384:e076335. PubMed
106.O'Neill J, Tabish H, Welch V, et al. Applying an equity lens to interventions: using PROGRESS ensures consideration of socially stratifying factors to illuminate inequities in health. J Clin Epidemiol. 2014;67(1):56-64. PubMed
107.Schünemann H, Brożek J, Guyatt G, Oxman A. Handbook for grading the quality of evidence and the strength of recommendations using the GRADE approach [updated October 2013]. Hamilton (ON): McMaster University; 2024: https://gdt.gradepro.org/app/handbook/handbook.html. Accessed 2024 Sept 13.
108.Santesso N, Glenton C, Dahm P, et al. GRADE guidelines 26: informative statements to communicate the findings of systematic reviews of interventions. J Clin Epidemiol. 2020;119:126-135. PubMed
109.Alonso JM, Andrews R. Does vertical integration of health and social care organizations work? Evidence from Scotland. Soc Sci Med. 2022;307:115188. PubMed
110.Malisauskaite G, Jones K, Allan S, et al. How local partnerships to improve urgent and emergency care have impacted delayed transfers of care from hospitals in England: an analysis based on a synthetic control estimation method. BMJ Open. 2022;12(2):e054568. PubMed
111.Bielska IA, Cimek K, Guenter D, et al. Change in health care use after coordinated care planning: a quasi-experimental study. CMAJ Open. 2018;6(2):E218-E226. PubMed
112.Levin KA, Crighton E. Measuring the impact of step down intermediate care on delayed discharge: an interrupted time series analysis. J Epidemiol Community Health. 2019;73(7):674-679. PubMed
113.Robert B, Sun AH, Sinden D, Spruin S, Hsu AT. A Case-Control Study of the Sub-Acute Care for Frail Elderly (SAFE) Unit on Hospital Readmission, Emergency Department Visits and Continuity of Post-Discharge Care. J Am Med Dir Assoc. 2021;22(3):544-550.e542. PubMed
114.Coffey A, Leahy-Warren P, Savage E, et al. Interventions to Promote Early Discharge and Avoid Inappropriate Hospital (Re)Admission: A Systematic Review. Int J Environ Res Public Health. 2019;16(14):10. PubMed
115.Roson Rodriguez P, Chen X, Arancibia M, et al. Transitional discharge interventions for people with schizophrenia. Cochrane Database Syst Rev. 2024;8(8):CD009788. PubMed
116.Cochrane Effective Practice and Organisation of Care. EPOC Resources for review authors. London (GB): The Cochrane Collaboration; 2017: https://epoc.cochrane.org/resources/epoc-resources-review-authors. Accessed 2024 Nov 29.
117.Burke C, Dolan E, Faul J, et al. Delayed hospital discharges and the trolley crisis. Ir J Med Sci. 2023;192(1):11-14. PubMed
118.Appel E, Hahn-Goldberg S, Chow E, Casaubon LK, Abrams HB. The Operational and Economic Impact of a Neurovascular Unit in an Acute Care Academic Hospital. Can J Neurol Sci. 2015;42(5):292-298. PubMed
119.Mahto R, Venugopal H, Vibhuti VS, et al. The effectiveness of a hospital diabetes outreach service in supporting care for acutely admitted patients with diabetes. QJM. 2009;102(3):203-207. PubMed
120.Diouf I, Lim WK, Jayasena R, Khanna S. Improving Residential Aged Care Placement from Hospital Through the Implementation of a Digital Matching Solution - A Before-After Evaluation. Stud Health Technol Inform. 2024;318:120-125. PubMed
121.Ibrahim H, Harhara T, Athar S, Nair SC, Kamour AM. Multi-Disciplinary Discharge Coordination Team to Overcome Discharge Barriers and Address the Risk of Delayed Discharges. Risk Manag Healthc Policy. 2022;15:141-149. PubMed
122.Bowen A, Kumar R, Howard J, E. Camilleri A. Nurse led discharge: improving efficiency, safely. Clin Gov. 2014;19(2):110-116.
123.O’Brien K, Welsh D, Barnable A, Wiseman G, Colbourne A. The impact of introducing restorative care on client outcomes and health system effectiveness in an integrated health authority. Home Health Care Manag Pract. 2017;29(1):13-19.
124.Sheaff R, Windle K, Wistow G, et al. Reducing emergency bed-days for older people? Network governance lessons from the 'Improving the Future for Older People' programme. Soc Sci Med. 2014;106:59-66. PubMed
125.Starr-Hemburrow L, Parks JM, Bisaillon S. Home First: reducing ALC and achieving better outcomes for seniors through inter-organizational collaboration. Healthc Q. 2011;14(1):70-76. PubMed
126.Supporting Ontario health teams to influence alternate level of care. Toronto (ON): Provincial Geriatrics Leadership Ontario; 2022: https://geriatricsontario.ca/wp-content/uploads/2023/06/2022-April-1-ALC-Community-_-FINAL.pdf. Accessed 2024 Jun 12.
127.Ontario Newsroom. News release: Ontario building new seniors' housing complex in Kenora. Toronto (ON): Government of Ontario; 2022: https://news.ontario.ca/en/release/1002387/ontario-building-new-seniors-housing-complex-in-kenora Accessed 2024 May 21.
128.Complex care hub: enhancing care in the community. Edmonton (AB): Alberta Health Services; 2024: https://www.albertahealthservices.ca/about/Page13602.aspx. Accessed 2024 May 24.
129.Payne E. Community paramedics will be deployed to deal with Ottawa's growing long-term care wait lists. Ottawa Citizen. 2020: https://ottawacitizen.com/news/local-news/community-paramedics-will-be-deployed-to-deal-with-ottawas-growing-long-term-care-wait-lists. Accessed 2024 May 21.
130.Kokorelias K, Flanagan A. Bringing long-term care home. Toronto (ON): The Hub; 2023: https://thehub.ca/wp-content/uploads/2023/09/HunterPrize_Kokerelias_BringingLongtermCareHome_v1.pdf. Accessed 2024 May 24.
131.Implementing Alternative Levels of Care Leading Practices. Toronto (ON): The Center for Implementation; 2024: https://geriatricsontario.ca/wp-content/uploads/2024/05/PGLO-Report-March-2024-V12.04.2024.pdf. Accessed 2024 May 15; Dec 18.
132.Nauenberg E. Personal Support Homes: An Innovative Approach to Reduce the Alternative Level of Care Population in Ontario Hospitals. Healthc Policy. 2021;17(1):91-103. PubMed
133.Central LHIN Hospitals Collaborative. Reactivation care centre. 2024; https://www.reactivationcarecentre.ca/. Accessed 2024 May 24.
134.Cheng I, Baker GR, Carew D, et al. Improving the use of healthcare resources in Canadian hospitals: the impact of a reintegration unit in expanding acute care capacity and resource use in Sunnybrook Health Sciences Centre. V1. Research Square. 2020.
135.Cheng I, Atzema CL, Carew D, et al. Using Case Costing to Evaluate the Potential Impact of a Reintegration Unit on an Acute-Care Hospital's Capacity and Resources. Healthc Q. 2022;24(4):27-33. PubMed
136.Bhatia D, Peckham A, Abdelhalim R, et al. Alternate level of care and delayed discharge: lessons learned from abroad. NAO Rapid Review No. 22. Toronto (ON): North American Observatory of Health Systems and Policies; 2020: https://naohealthobservatory.ca/wp-content/uploads/2020/03/NAO-Rapid-Review-22_EN.pdf. Accessed 2024 Nov 29.
137.Egbujie BA, Tran J, Hirdes JP. Multistate competing risk analysis of transition back to the community among long-term care home (LTC) destined patients: a brief report. J Prim Care Community Health. 2023;14:21501319231220742. PubMed
138.NL Health Services. NL Health Services Partnership Pilots Discharge Planning Solution. St John's (NL): Newfoundland and Labrador Health Services; 2024: https://nlhealthservices.ca/news/post/nl-health-services-partnership-pilots-discharge-planning-solution/. Accessed 2024 Sep 19.
139.Tran J, Woo K. Co-Designing An Integrated Transitional Care Model To Address Alternate Level Of Care And Promote Aging In Place An Experienced Based Co-Design. Int J Integr Care. 2022;22(S3):1-2.
140.Evaluation of Winter Planning 2020/2021. Edinburgh (UK): Integration Joint Board; 2021: https://democracy.edinburgh.gov.uk/documents/s34932/8.2%20Evaluation%20of%20Winter%20Planning%202020-21.pdf. Accessed 2024 Sep 23.
141.Harrison G, O’Malia A, Napier S. Addressing Psychosocial Barriers to Hospital Discharge: A Social Work Led Model of Care. Aust Soc Work. 2019;72(3):366-374.
142.Brackstone H, Bambrick K. Single-handed care in acute settings to facilitate discharge and improve patient quality of life. J Comm Nursing. 2023;37(6):43-47.
143.Wilson F. West Lothian Health and Social Care Partnership Integrated Daily Discharge Flow Huddle. Int J Integr Care. 2022;22.
144.Up to £250 million to speed up hospital discharge. London (GB): Government of the United Kingdom; 2023: https://www.gov.uk/government/news/up-to-250-million-to-speed-up-hospital-discharge?utm_medium=email&utm_campaign=govuk-notifications-topic&utm_source=30604a7c-ee7d-45df-9964-477d5590f375&utm_content=daily. Accessed 2024 Sep 23.
145.To Alleviate Boarding, Consider Creating Discharge Lounge. ED Manag. 2023;35(9):1-16.
146.Department of Health & Social Care. Hospital discharge and community support guidance. London (GB): Government of the United Kingdom; 2024: https://www.gov.uk/government/publications/hospital-discharge-and-community-support-guidance/hospital-discharge-and-community-support-guidance. Accessed 2024 Sep 23.
147.Coming Home Implementation: Report from the Working Group on Complex Care and Delayed Discharge. Edinburgh (UK): Scottish Government; 2022: https://www.gov.scot/publications/coming-home-implementation-report-working-group-complex-care-delayed-discharge/pages/12/. Accessed 2024 Sep 20.
148.Department of Health & Social Care. Our plan for patients. London (GB): Government of the United Kingdom; 2022: https://www.gov.uk/government/publications/our-plan-for-patients/our-plan-for-patients#care/. Accessed 2024 Sep 20.
149.Chen H, Hara Y, Horita N, Saigusa Y, Kaneko T. An Early Screening Tool for Discharge Planning Shortened Length of Hospital Stay for Elderly Patients with Community-Acquired Pneumonia. Clin Interv Aging. 2021;16:443-450. PubMed
150.A case study about reducing delayed discharge from hospital. Edinburgh (UK): Healthcare Improvement Scotland; 2019: https://ihub.scot/media/6261/east-ayrshire-reducing-delayed-hospital-discharge-case-study-summary.pdf. Accessed 2024 Sep 24.
151.Implementing a discharge hub: Sussex Community NHS Foundation Trust. London (GB): NHS Confederation; 2021: https://www.nhsconfed.org/case-studies/implementing-discharge-hub#:~:text=Sussex%20Community%20NHS%20Foundation%20Trust%20worked%20with%20system,decision-making%20team%20and%20discharge%20hub%20in%20April%2FMay%202020. Accessed 2024 Sep 24.
152.Department of Health & Social Care. Press release: Up to £250 million to speed up hospital discharge. London (GB): Government of the United Kingdom; 2023: https://www.gov.uk/government/news/up-to-250-million-to-speed-up-hospital-discharge?utm_medium=email&utm_campaign=govuk-notifications-topic&utm_source=30604a7c-ee7d-45df-9964-477d5590f375&utm_content=daily. Accessed 2024 Sep 23.
153.Murmann M, Sinden D, Hsu AT, et al. The cost-effectiveness of a nursing home-based transitional care unit for increasing the potential for independent living in the community among hospitalized older adults. J Med Econ. 2023;26(1):61-69. PubMed
154.Allan S, Roland D, Malisauskaite G, et al. The influence of home care supply on delayed discharges from hospital in England. BMC Health Serv Res. 2021;21(1):1297. PubMed
155.Wandersman A, Duffy J, Flaspohler P, et al. Bridging the gap between prevention research and practice: the interactive systems framework for dissemination and implementation. Am J Community Psychol. 2008;41(3-4):171-181. PubMed
156.Gagnon J, Kremer B, Arsenault-Lapierre G, Gonzalez-Reyes A, Ladores M, Vedel I. The family medicine based virtual ward: Qualitative description of the implementation process. McGill J Med. 2020;18(1):64-73.
157.Allen J, Woolford M, Livingston PM, Lobchuk M, Muldowney A, Hutchinson AM. Informal carer support needs, facilitators and barriers in transitional care for older adults from hospital to home: A scoping review. J Clin Nurs. 2023;32(19-20):6773-6795. PubMed
158.Cheng SM, Bisanz C, Catallo C. Core principles of integration of healthcare and social services that support continuity of care for vulnerable seniors with Canadian case study: home-at-last. Int J Integr Care. 2019;19(4):1-2. PubMed
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.