CADTH Reimbursement Review
Pembrolizumab (Keytruda)
Sponsor: Merck Canada Inc.
Therapeutic area: Persistent, recurrent, or metastatic cervical cancer
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Stakeholder Input
Clinical Review
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Item | Description |
|---|---|
Drug product | Pembrolizumab (Keytruda), 200 mg, IV infusion |
Indication | For the treatment of adult patients with persistent, recurrent, or metastatic cervical cancer whose tumours express PD‐L1 (CPS ≥ 1) as determined by a validated test, in combination with chemotherapy with or without bevacizumab |
Reimbursement request | As per indication |
Health Canada approval status | NOC |
Health Canada review pathway | Priority review |
NOC date | April 7, 2022 |
Sponsor | Merck Canada Inc. |
CPS = combined positive score; NOC = Notice of Compliance; PD-L1 = programmed cell death 1 ligand 1.
Introduction
Cervical cancer is commonly grouped into histologic categories of epithelial tumours: squamous, adenocarcinoma, mixed adenosquamous, and other epithelial histologies.1,2 The majority of cervical cancers are associated with persistent high-risk oncologic HPV type infections.1 The organized cervical cytology screening programs across Canada and recent widespread vaccination campaigns against HPV are expected to continue to lower the incidence and mortality well into the future; however, cervical cancer is still a public health concern. According to the 2021 Canadian Cervical Cancer Statistics, approximately 1,450 Canadian women are diagnosed with cervical cancer annually, 12% of which are in stage IV, with 380 Canadian deaths annually.3 Primary treatment with surgery, radiation, or a combination of both are indicated. Between 10% to 20% of patients will have persistent, recurrent, or metastatic cervical disease after primary treatment. This can have a very high burden on patients and their family, impacting the daily life of patients, work life, sexual relationships, physical activity, and sleep patterns.1,4 The current standard of care (SOC) therapy for persistent, recurrent, or metastatic cervical after primary therapy with surgery and radiation is chemotherapy with or without the addition of bevacizumab depending on patient contraindications.
The majority of cervical cancers express programmed cell death 1 ligand 1 (PD-L1), which forms the basis for studying the use of checkpoint inhibitors in this disease. Pembrolizumab is a programmed cell death 1 protein (PD-1) inhibitor (administered as an IV infusion over 30 minutes) and has been studied in combination with SOC chemotherapy, with or without bevacizumab. The recommended dosage is either 200 mg every 3 weeks or 400 mg every 6 weeks until disease progression, unacceptable toxicity, or for a maximum of up to either 24 months or thirty-five 200 mg doses or eighteen 400 mg doses, whichever is longer.
The objective of this report is to perform a systematic review of the beneficial and harmful effects of pembrolizumab (200 mg IV every 3 weeks or 400 mg IV every 6 weeks), in combination with chemotherapy, with or without bevacizumab for adult patients with persistent, recurrent, or metastatic cervical cancer whose tumours express PD-L1 (combined positive score [CPS] ≥ 1), as determined by a validated test.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient groups who responded to CADTH’s call for patient input and from clinical experts consulted by CADTH for the purpose of this review.
Patient Input
One patient advocacy group, HPV Global Action, in collaboration with the Canadian Cancer Survivor Network, provided a joint input for the treatment of adult patients with persistent, recurrent, or metastatic cervical cancer whose tumours express PD-L1 (CPS ≥ 1) as determined by a validated test. Information was gathered from March to May 2022 through Blue Ribbon Project Inc., who reached out to 24 clinicians via email as well as 5 international organizations online seeking help to identify patients with advanced cervical cancer. Data were collected from 8 patients/caregivers through an online patient/caregiver survey, among whom 5 were from Canada and 3 from the US. Among the 8 responders, 6 had been diagnosed with metastatic disease and 1 with stage III disease. Moreover, 3 patients had first-hand experience with the therapy under review.
Fatigue, pain in the pelvic area or lower back, and abnormal vaginal bleeding after menopause were the top 3 physical symptoms identified by the patients; whereas, living with uncertainty, anxiety, panic attacks/depression, and feeling isolated or lonely were the top psychosocial problems for the responders.
In response to the survey question on side effects of the current treatments, patients described pain during sexual intercourse, difficulty urinating, difficulty having a bowel movement, and leaking of urine or feces from the vagina as having impacts on their daily lives. When asked about their considerations for outcomes while evaluating novel therapies, all patients with metastatic cervical cancer had chosen “maintain quality of life” and “access to a new treatment option” as their preferred outcomes, with “reduce side effects from current medications or treatments” and “delay onset of symptoms” as the second and third preferences. While describing their experiences with the drug under review, 2 among the 3 patients accessing pembrolizumab achieved a “no evidence of disease” (NED) status after therapy and identified it as a “positive effect.” The other patient mentioned having minimal side effects from the drug under review. While describing any negative effects from pembrolizumab, patients mentioned facing grade 2 interstitial nephritis, nausea, feeling unusually tired or weak, diarrhea, rash, joint pain, fever, dry skin, and nail breakage as some of the adverse effects. However, all 3 respondents mentioned that they were able to manage disease progression, ease of use, and more control of symptoms more effectively while being on the therapy under review. While responding to what side effects from the therapy under treatment would be acceptable for the patients, 2 patients who responded had chosen itching, rash, low levels of thyroid hormone, feeling less hungry, and patches of skin which have lost colour (vitiligo) as acceptable side effects.
Clinician Input
Input From the Clinical Experts Consulted by CADTH
Two clinical experts with experience treating cervical cancer highlighted the current significant unmet need for further effective options to treat persistent, recurrent, or metastatic cervical cancer. The clinical experts agreed that standard outcome measures of treatment response, duration of response (DOR), survival statistics, toxicities, and quality of life measures are aligned with the outcomes used in the current KEYNOTE-826 clinical trial. The clinical experts agreed that pembrolizumab should be given in a clinical setting where patients can be monitored closely for early detection and management of immune-related toxicities with appropriate patient education.
Clinician Group Input
One clinician group called Ontario Health (Cancer Care Ontario) Gynecology Cancer Drug Advisory Committee provided input for the treatment of adult patients with persistent, recurrent, or metastatic cervical cancer whose tumours express PD-L1 (CPS ≥ 1) as determined by a validated test. The clinician group commented that pembrolizumab would improve the efficacy for patients treated within the submitted indication and meet unmet needs as no curative treatment is available for this patient population. It was also highlighted that there are very limited second-line options available for patients with persistent, recurrent, or metastatic cervical cancer. The clinical group considered pembrolizumab as a first-line treatment option for persistent, recurrent, or metastatic cervical cancer in patients whose tumours express PD-L1, whereas indicated patients with contraindications to pembrolizumab and patients who do not express PD-L1 are considered to be least suitable for this treatment. The clinician group noted that they would consider disease progression or toxicity as indications to discontinue treatment with the drug under review.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may impact their ability to implement a recommendation. The drug plans identified implementation issues related to relevant comparators, considerations for initiation, prescribing, and discontinuation of therapy, generalizability, care provision, system issues, and economic considerations. The clinical experts consulted by CADTH for this review weighed evidence from the included study and other clinical considerations to provide responses to the drug plans’ implementation questions.
Clinical Evidence
Pivotal Studies and Protocol-Selected Studies
Description of Studies
The KEYNOTE-826 study is an ongoing phase III, randomized, placebo-controlled clinical trial investigating pembrolizumab in combination with SOC compared to placebo plus SOC in the treatment of patients with histologically confirmed persistent, recurrent, or metastatic cervical cancer not treated with prior systemic chemotherapy. Patients were randomized 1:1 to receive pembrolizumab 200 mg plus SOC or a placebo plus SOC. SOC was defined as paclitaxel 175 mg/m2 plus either cisplatin 50 mg/m2 or carboplatin with an area under the curve (AUC) of 5, with the addition of bevacizumab 15 mg/kg if there were no contraindications to bevacizumab. The KEYNOTE-826 trial randomization was stratified according to metastasis at initial diagnosis, bevacizumab use (according to investigators choice before randomization), and PD-L1 status (CPS < 1, 1 to < 10, and ≥ 10). There were 6 primary objectives of the study; these were to compare the progression-free survival (PFS) and overall survival (OS) of pembrolizumab plus SOC against placebo plus SOC in patients with PD-L1 with a CPS of 1 or higher, CPS of 10 or higher, and all-comers patients. Secondary objectives included determining overall response rate (ORR), DOR, 12-month PFS rate, safety and tolerability, and health-related quality of life (HRQoL). There were fewer White patients in the pembrolizumab plus SOC arm than the placebo plus SOC arm (56% versus 62.5%) and more patients from the Asia Pacific region in the pembrolizumab plus SOC arm than the placebo plus SOC arm (19.8% versus 13.8%). There were no meaningful differences in baseline characteristics in patients with PD-L1 with a CPS of 10 or higher.
Efficacy Results
HRQoL
The mean (standard deviation [SD]) baseline |||||||||| measure for patients with PD-L1 with a CPS of 1 or higher in the pembrolizumab plus SOC arm was |||||||||| and in the placebo plus SOC arm it was ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||, respectively. ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
In the pembrolizumab plus SOC arm, the proportion of patients (95% confidence interval [CI]) that deteriorated according to the |||||||||| |||||||||| |||||||||| |||||||||| |||||||||| while the proportion of patients (95% CI) that deteriorated in the placebo plus SOC arm was ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. The percent difference for pembrolizumab plus SOC compared to placebo plus SOC for ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
In the pembrolizumab plus SOC arm |||||||||| |||||||||| |||||||||| |||||||||| the proportion of patients (95% CI) that deteriorated according to the ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||, while the proportion of patients (95% CI) that deteriorated in the placebo plus SOC arm |||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. The percent difference for pembrolizumab plus SOC compared to placebo plus SOC for ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
Overall Survival
The median OS for patients with PD-L1 with a CPS of 1 or higher was not reached (NR) (95% CI, 19.8 to NR) in the pembrolizumab plus SOC arm and 16.3 months (95% CI, 14.5 to 19.4) in the placebo plus SOC arm. The hazard ratio (HR) for OS comparing pembrolizumab plus SOC and placebo plus SOC was 0.65 (95% CI, 0.50 to 0.81) with a P value of 0.0001 (multiplicity adjusted, 1-sided nominal alpha level = 0.0054906). The OS rate at 12 months was 75.5% (95% CI, 69.7% to 80%) in the pembrolizumab plus SOC arm and 63.1% (95% CI, 57% to 68.5%) in the placebo plus SOC arm.
Progression-Free Survival
The median PFS for patients with PD-L1 with a CPS of 1 or higher was 10.4 months (95% CI, 9.7 to 12.3) in the pembrolizumab plus SOC arm and 8.2 months (95% CI, 6.3 to 8.5) in the placebo plus SOC arm. The HR for PFS comparing pembrolizumab plus SOC and placebo plus SOC was 0.62 (95% CI, 0.50 to 0.77) with a P value of less than 0.0001 (multiplicity adjusted, 1-sided nominal alpha level = 0.0014426). The PFS rate at 12 months was 45.5% (95% CI, 39.2% to 51.5%) in the pembrolizumab plus SOC arm and 34.1% (95% CI, 28.3% to 40%) in the placebo plus SOC arm.
Overall Response Rate
The ORR for patients with PD-L1 with a CPS of 1 or higher in the pembrolizumab plus SOC arm was 68.1% (95% CI, 62.2% to 73.6%), including 22.7% of patients who achieved a complete response (CR). The ORR in the placebo plus SOC arm was 50.2% (95% CI, 44.1% to 56.2%), including 13.1% of patients who achieved a CR. The difference estimate for pembrolizumab plus SOC compared with placebo plus SOC was 18.0% (95% CI, 10.1% to 25.7%).
Duration of Response
For the 186 patients with PD-L1 with a CPS of 1 or higher in the pembrolizumab plus SOC arm who recorded a response, the median time to response was 2.1 months (range, 1.7 to 20.6). Of the 138 patients in the placebo plus SOC arm who recorded a response, the median time to response was 2.1 months (range, 1.3 to 7.1). The median DOR in patients in the pembrolizumab plus SOC arm was 18.0 months (range, 1.3+ to 24.2+) while the median DOR in patients in the placebo plus SOC arm was 10.4 months (range, 1.5+ to 22.0+), where “+” indicates there is no progressive disease by the time of last disease assessment.
Harms Results
In the safety analysis set at the time of data cut-off, 99.3% of patients with PD-L1 with a CPS of 1 or higher in the pembrolizumab plus SOC arm and 99.4% of the patients in the placebo plus SOC arm reported treatment-emergent adverse events (AEs). The most common AEs in the pembrolizumab plus SOC arm were anemia (61.2%), alopecia (56.4%), nausea (39.7%), and diarrhea (35.5%). The most common AEs in the placebo plus SOC arm were alopecia (57.9%), anemia (53.4%), nausea (43.7%), and constipation (33%).
The identified notable harms included in the CADTH systematic review with summary data available from the KEYNOTE-826 trial were immune-mediated AEs and infusion reactions. In the pembrolizumab plus SOC arm, immune-mediated AEs occurred in 33.9% of patients with 11.4% of patients reporting grade 3 or higher AEs. In the placebo plus SOC arm, immune-mediated AEs occurred in 15.2% of patients with 2.9% of patients reporting grade 3 or higher AEs. Infusion reactions occurred in 13.4% of patients in the pembrolizumab plus SOC arm with 2.3% reporting grade 3 or higher infusion reactions. In the placebo plus SOC arm, infusion reactions occurred in 12.6% of patients, with 2.3% reporting grade 3 or higher infusion reactions.
Table 2: Summary of Key Results From Pivotal and Protocol-Selected Studies
Key results | KEYNOTE-826 (PD-L1 CPS ≥ 1 only) | |
|---|---|---|
Pembrolizumab plus SOC (n = 273) | SOC (n = 275) | |
|||||||||||||||||||||||||||||| | ||
|||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||| |
|||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||| |
|||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||| |
|||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||| |
|||||||||||||||||||||||||||||| | ||
|||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||| |
|||||||||||||||||||||||||||||| | ||
|||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||| |
|||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||| |
OS (co-primary end point) | ||
Median OS, months (95% CI)d | NR (19.8 to NR) | 16.3 (14.5 to 19.4) |
HR (95% CI)e | 0.64 (0.50 to 0.81) | Reference |
P valuef | 0.0001 | Reference |
PFS (co-primary end point) | ||
Median PFS, months (95% CI) | 10.4 (9.7 to 12.3) | 8.2 (6.3 to 8.5) |
HR (95% CI) | 0.62 (0.50 to 0.77) | Reference |
P valueg | < 0.0001 | Reference |
ORR | ||
ORR, n (%) | 186 (68.1) | 138 (50.2) |
95% CI | (62.2 to 73.6) | (44.1 to 56.2) |
Difference estimate,h % (95% CI) | 18.0 (10.1 to 25.7) | Reference |
DOR | ||
Median DOR,c months (95% CI), n | 18.0 (1.3+ to 24.2+), 186 | 10.4 (1.5+ to 22.0+), 138 |
Harms, n (%) | n = 307 | n = 309 |
AEs | 305 (99.3) | 307 (99.4) |
SAEs | 153 (49.8) | 131 (42.4) |
WDAE (from study treatment) | 115 (37.5) | 82 (26.5) |
Deaths | 14 (4.6) | 14 (4.5) |
Notable harms, n (%) | n = 307 | n = 309 |
Immune-mediated AE | 104 (33.9) | 47 (15.2) |
Infusion reaction | 41 (13.4) | 39 (12.6) |
AE = adverse event; CI = confidence interval; CPS = combined positive score; DOR = duration of response; FIGO = Fédération Internationale de Gynécologie et d’Obstétrique; HR = hazard ratio; ORR = overall response rate; OS = overall survival; NR = not reached; PD-L1 = programmed cell death 1 ligand 1; PFS = progression-free survival; SAE = serious adverse event; SOC = standard of care; WDAE = withdrawal due to adverse event.
Note: “+” indicates there is no progressive disease by the time of last disease assessment.
aBased on a constrained longitudinal data analysis model with the patient-reported outcome scores as the response variable with covariates for treatment by study visit interaction, stratification factors metastatic at diagnosis (FIGO stage IVB) (yes or no), bevacizumab use (yes or no), and PD-L1 status (CPS < 1, CPS 1 to < 10, or CPS ≥ 10).
bDeterioration is classified as a 10 or greater point decrease at any point throughout the trial.
cBased on binomial exact CI method.
dFrom product-limit (Kaplan-Meier) method for censored data.
eBased on Cox regression model with the Efron method of tie handling with treatment as a covariate stratified by metastatic at initial diagnosis (FIGO [2009] stage IVB) (yes or no), bevacizumab use (yes or no), and PD-L1 status (CPS < 1, CPS 1 to < 10, or CPS ≥ 10).
fOne-sided P value based on log-rank test stratified by metastatic at initial diagnosis (FIGO stage IVB) (yes or no), bevacizumab use (yes or no), and PD-L1 status (CPS < 1, CPS 1 to < 10, or CPS ≥ 10). Multiplicity adjusted, 1-sided nominal alpha level of 0.0054906.
gOne-sided P value based on log-rank test stratified by metastatic at initial diagnosis (FIGO stage IVB) (yes or no), bevacizumab use (yes or no), and PD-L1 status (CPS < 1, CPS 1 to < 10, or CPS ≥ 10). Multiplicity adjusted, 1-sided nominal alpha level of 0.0014426.
hBased on the Miettinen-Nurminen method stratified by metastatic at initial diagnosis (FIGO [2009] stage IVB) (yes or no), bevacizumab use (yes or no), and PD-L1 status (CPS < 1, CPS 1 to < 10, or CPS ≥ 10).
Source: KEYNOTE-826 Clinical Study Report.5
Critical Appraisal
The KEYNOTE-826 trial was a phase III, randomized, double-blind, placebo control trial. Randomization utilized appropriate stratification factors and baseline characteristics were well balanced between the treatment groups. End points were appropriate and important to patients. The co-primary end points were PFS and OS with formal hypothesis testing conducted in 3 separate PD-L1 status population groups, all of which were randomized through stratification. An alpha of 0.05 was adequately allocated to each tested hypothesis and therefore control of multiplicity was appropriate for the co-primary end points. There was no control of multiplicity for the secondary outcomes or subgroup analyses and therefore conclusions cannot be drawn. As this review includes interim analyses of data from the KEYNOTE-826 trial, there is the possibility of bias from multiples analyses; however, the prespecified protocol adequately identified the requirements for triggering the interim analysis as well as an allocation of alpha across the analysis time points. The protocol amendment to change the measurement of the co-primary end point PFS from blinded independent committee review (BICR) to investigator assessed potentially introduced bias to the results; however, the clinical experts consulted did not anticipate this change would have an impact on the overall conclusions from the data. The short duration of follow-up and immaturity of the OS data increased the uncertainty of the results.
The KEYNOTE-826 study population was considered by the clinical experts consulted to be representative and generalizable to the expected Canadian population. The chemotherapy combination used in the trial was carboplatin or cisplatin in combination with paclitaxel. It was noted that while this does not represent all available treatment options available to patients, the majority of patients receiving chemotherapy for persistent, recurrent, or metastatic cervical cancer receive the options included in the KEYNOTE-826 study. There are generalizability concerns when considering patients with European Cooperative Oncology Group Performance Status (ECOG PS) of 2, patients with active central nervous system (CNS) metastases, and patients who receive re-treatment with pembrolizumab, as there was no reported evidence for these populations in the KEYNOTE-826 trial.
Conclusions
Evidence from the KEYNOTE-826 trial showed statistically significant and clinically meaningful benefit in PFS and OS with pembrolizumab 200 mg every 3 weeks added to SOC compared to placebo plus SOC in patients with persistent, recurrent, or metastatic cervical cancer with PD-L1 with a CPS of 1 or higher. In the opinion of the clinical experts consulted, the addition of pembrolizumab to chemotherapy (paclitaxel in combination with carboplatin or cisplatin) resulted in additional clinically relevant survival benefit and would likely become the new SOC treatment in this patient population. The secondary end points of ORR and DOR were consistent with the primary analysis. HRQoL was identified from patient input as a key end point important to patients. The KEYNOTE-826 study showed no deterioration in in overall HRQoL with the addition of pembrolizumab, and nominal improvements in some HRQoL measures; however, this is highly uncertain given the lack of power to detect differences between treatments and the reduced number of patients at advanced time points. The main evidence gaps are related to the immaturity of the OS data. The clinical experts consulted viewed the safety profile of pembrolizumab as manageable and in line with their expectations based on the extensive experience with pembrolizumab in other oncology indications.
Introduction
Disease Background
Cervical cancer is grouped into 4 major histologic types consisting of: squamous, adenocarcinoma, adenosquamous, and other rarer histologies.1,2 The majority of cervical cases (70% to 80%) are squamous cell carcinomas.1,2 Almost all cervical cancers are associated with persistent high-risk oncogenic HPV infections, with subtypes HPV 16 and 18 of particular importance.1 Cervical cancers are staged according to the Fédération Internationale de Gynécologie et d’Obstétrique (FIGO) and the Union for International Cancer Control TNM staging classifications (8th edition).1
Cervical cytology (Papanicolaou test) screening programs across Canada and the recent widespread vaccination programs against HPV will lower the incidence and mortality of cervical cancer well into the future; however, cervical cancer still occurs in Canada at the present time. Approximately 60% of current cases identified occur in women who do not participate in screening programs; the other 40% of cases occur in women who are screened but whose disease is not detected, in part due to less common histologies like adenocarcinomas and improper follow-up and treatment of abnormal screening tests. According to the 2021 Canadian Cervical Cancer Statistics, approximately 1,450 Canadian women are diagnosed with cervical cancer annually, 12% of which are in stage IV.3 This correlates to an incidence rate of 7.5 cases per 100,000.3 As many cervical cancer cases are diagnosed in early stages of disease, the 5-year survival probability is 74%3 Patients diagnosed with extrapelvic metastatic disease have a poorer prognosis with 5-year survival probability of 18% and median survival from 7 months to 12 months, and an estimated 380 Canadian deaths annually.3,6,7
Persistent, recurrent, or metastatic cervical cancer can have a very high burden on patients, impacting the daily life of patients, work life, sexual relationships, physical activity, and sleep patterns.1,4 Cervical cancer as well as its treatment can result in anxiety, mood changes, and work disruption in the prime of the patient’s life, given that approximately 40% of cervical deaths occur in women younger than 55 years.4 Common symptoms reported by patients as the most bothersome include fatigue, bowel problems, aching joints, neuropathy, nausea and vomiting, bladder problems, and loss of fertility.4
Standards of Therapy
Patients diagnosed with early clinical stage cervical cancer (cancer limited to the cervix only—stage I disease) are often treated with radical surgery to remove the central disease and to evaluate for metastatic disease. If not deemed completely resectable or with more locally advanced disease (typically stage IB and higher), patients are offered curative-intent radical chemoradiation therapy. Patients diagnosed with persistent or recurrent cervical cancer after failure of primary radical chemo-radiotherapy are sometimes offered radical exenterative surgery (i.e., resection of the female reproductive organs, lower urinary tract, and a portion of the rectosigmoid) if the disease is still confined to the central pelvis and can be resected with a clear margin with curative intent. However, most patients are considered to at this time to have non-curative disease. Radical chemoradiation to the pelvis would be recommended if the disease was treated initially only with surgery, has recurred loco-regionally, and is amenable to radiation treatment. Systemic chemotherapy, usually consisting of a combination of a platinum agent and a taxane, is commonly used if there is evidence of disease recurrence. The GOG-240 study7 showed that the addition of bevacizumab to SOC chemotherapy doublet improved OS and has been widely adopted as the preferred first-line therapy for persistent, recurrent, or metastatic cervical cancer with good performance status and no contraindications to bevacizumab.1,8 For patients with contraindications to bevacizumab, standard chemotherapy alone is recommended.1,8
Drug
Pembrolizumab belongs in the class of immune checkpoint inhibitors.9 Pembrolizumab is an antibody with high affinity against anti-PD-1. PD-1 is an immune checkpoint receptor that limits the activity of T lymphocytes in peripheral tissues (active T-cell immune surveillance). Tumour cells may engage the PD-1 pathway and inhibit active T-cell immune surveillance. Pembrolizumab binds to PD-1 thereby preventing it from binding to its ligands (PD-L1 and programmed death ligand 2) expressed on tumour cells, which results in the reactivation of tumour-specific cytotoxic T-lymphocyte activities in the tumour microenvironment.9
Pembrolizumab is approved by Health Canada for the treatment of adult patients with persistent, recurrent, or metastatic cervical cancer whose tumours express PD-L1 (CPS ≥ 1), as determined by a validated test. Pembrolizumab is administered as an IV infusion over 30 minutes in combination with SOC chemotherapy, with or without bevacizumab. The recommended dosage is either 200 mg every 3 weeks or 400 mg every 6 weeks until disease progression, unacceptable toxicity, or for a maximum of up to either 24 months or thirty-five 200 mg doses or eighteen 400 mg doses, whichever is longer.
Table 3: Key Characteristics of Pembrolizumab
Characteristic | Pembrolizumab |
|---|---|
Mechanism of action | Pembrolizumab binds to PD-1 thereby preventing it from binding to its ligands PD-L1 and PD-L2, which results in the reactivation of tumour-specific cytotoxic T lymphocytes in the tumour microenvironment |
Indicationa | For the treatment of adult patients with persistent, recurrent, or metastatic cervical cancer whose tumours express PD-L1 (CPS ≥ 1), as determined by a validated test |
Route of administration | IV |
Recommended dose | 200 mg every 3 weeks or 400 mg every 6 weeks |
Serious adverse effects or safety issues | NA |
CPS = combined positive score; NA = not applicable; PD-1 = programmed cell death 1 protein; PD-L1 = programmed cell death 1 ligand 1; PD-L2 = programmed death 1 ligand 2.
aHealth Canada–approved indication.
Source: Keytruda product monograph.9
The sponsor has requested that pembrolizumab is reimbursed as per the Health Canada indication. The Health Canada Notice of Compliance for this indication was issued on April 7, 2022.10 In October 2021, the FDA approved pembrolizumab in combination with chemotherapy, with or without bevacizumab, for the treatment of persistent, recurrent, or metastatic cervical cancer whose tumours express PD-L1 (CPS ≥ 1), as determined by an FDA–approved test.11
Pembrolizumab is indicated in Canada for classical Hodgkin lymphoma, mediastinal B-cell lymphoma, adult urothelial carcinoma, endometrial cancer, melanoma, non–small cell lung carcinoma, renal cell carcinoma, and head and neck squamous cell carcinoma. At the time of preparing this report, pembrolizumab was most recently reviewed by CADTH for first-line treatment of adult patients with unresectable or metastatic microsatellite instability-high or mismatch repair deficient colorectal cancer, and received a recommendation for reimbursement with conditions.12 Pembrolizumab is also currently under review for early stage triple-negative breast cancer, adjuvant treatment of advanced or metastatic renal cell carcinoma, and adjuvant treatment of melanoma.
Stakeholder Perspectives
Patient Group Input
This section was prepared by CADTH staff based on the input provided by patient groups. The full original patient input(s) received by CADTH have been included in the stakeholder section at the end of this report.
One patient advocacy group, HPV Global Action, in collaboration with the Canadian Cancer Survivor Network, provided a joint input for the treatment of adult patients with persistent, recurrent, or metastatic cervical cancer whose tumours express PD-L1 (CPS ≥ 1) as determined by a validated test. Information was gathered from March to May 2022 through Blue Ribbon Project Inc., who reached out to 24 clinicians via email as well as 5 international organizations online seeking help to identify patients with advanced cervical cancer. Data were collected from 8 patients/caregivers through an online patient/caregiver survey, among whom 5 were from Canada and 3 from the US.
Among the 8 responders, 6 had been diagnosed with metastatic disease and 1 with stage III disease. Moreover, 3 patients had first-hand experience with the therapy under review. Fatigue, pain in the pelvic area or lower back that may go down 1 or both legs, and abnormal vaginal bleeding after menopause were the top 3 physical symptoms identified by the patients, whereas living with uncertainty, anxiety, panic attacks/depression, and feeling isolated or lonely were the top psychosocial problems for the responders. Patients also reported that fatigue and living with uncertainty were the most difficult ones to control. One patient provided a detailed experience of dealing with cervical cancer, where she described her struggle with uncontrolled vaginal bleeding and the constant blood loss due to this issue, compromising her quality of life. The patient also shared the struggles of her immediate family members who had to make significant sacrifices as her caregiver, pointing to the overall psychosocial problems often encountered by caregivers of patients with metastatic cervical cancer.
Respondents identified cisplatin, carbotaxol-bevacizumab, carboplatin, and palliative care as currently available treatments. However, while describing the effectiveness of these treatments at controlling cancer, patients pointed those as either “somewhat effective” or “not very effective at all.” One patient identified radiotherapy and stereotactic body radiation therapy as being very effective at controlling cancer. In response to the side effects due to the current treatments, patients described pain during sexual intercourse, difficulty urinating, difficulty having a bowel movement, and leaking of urine or feces from the vagina as having impacts on their daily lives. One patient described facing side effects that included significant dehydration; digestive problems/dysfunction of the bowel such as nausea, vomiting, diarrhea, constipation, fecal urge or incontinence, gas, and lack of appetite; neuropathy and extreme fatigue from chemoradiation; brachytherapy boost; and external beam radiation therapy. She further mentioned the cisplatin-induced side effects as “horrific and a patient’s worst nightmare” and brachytherapy as “inhumane,” adding that she got post-traumatic stress disorder from brachytherapy.
While identifying issues related to current therapies, patients pointed out supply issues with administration, travel costs associated with getting therapy/treatment, and limited availability in community as the major challenges. In addition, patients identified controlling lymphedema and accessing genomic testing, similar to what is offered by Foundation Medicine, as the unmet needs regarding current therapies. When asked about their considerations for outcomes while evaluating novel therapies, all patients with metastatic cervical cancer chose maintaining quality of life and access to a new treatment option as the most important outcomes, followed by reducing side effects from current medications or treatments, and “delaying onset of symptoms.” Patients also responded that they would be willing to tolerate side effects like “hair loss, weakness, fatigue” for the new drug to help treat their cancer.
While describing their experiences with the drug under review, 2 of the 3 patients accessing the therapy reported that they had achieved a NED status from the therapy and identified it as a “positive effect.” The other patient mentioned having minimal side effects from the drug under review. When asked to describe any negative effects from the drug under review, patients reported grade 2 interstitial nephritis, nausea, feeling unusually tired or weak, diarrhea, rash, joint pain, fever, dry skin, and nail breakage as adverse effects associated with the use of pembrolizumab. All 3 respondents mentioned that the therapy under review resulted in a better management of disease progression, was easy to use, and provided more control of symptoms. When asked about side effects from the therapy under review that would be acceptable for patients, 2 patients participants selected itching, rash, low levels of thyroid hormone, feeling less hungry, and patches of skin which have lost colour (vitiligo) as acceptable AEs.
Clinician Input
Input From the Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of cervical cancer.
Unmet Needs
The clinical experts noted that no current curative treatment exists for persistent, recurrent, or metastatic cervical cancer that is not amenable to curative surgery or radiation therapy. The expected response rate to current SOC therapies is in the range of 50% to 60%, depending on the location of the recurrent or persistent disease, with an expected progression-free interval between 6 months to 8 months in responders. The clinical experts highlighted that there is significant unmet need for better and more effective treatment and DOR in the clinical setting.
Place in Therapy
The clinical experts agreed that pembrolizumab would likely be added to the existing SOC as a first-line regimen with a platinum agent plus a taxane, with or without bevacizumab depending on tolerability. The clinical experts highlighted that pembrolizumab would be the first treatment approved for first-line management of persistent, recurrent, or metastatic cervical cancers that will further address the underlying disease process in combination with standard cytotoxic therapy and antiangiogenic agents, rather than solely as a symptomatic management therapy, in appropriately selected patients who are not amenable to curative surgery or radiation therapy and can tolerate triple modality therapies.
Patient Population
The clinical experts noted that patients with persistent, recurrent, or metastatic cervical cancers who have PD-L1 with a CPS of 1 or higher on validated companion diagnostic testing who are not amenable to curative surgery or radiation therapy who can tolerate triple therapies would be most likely to benefit from the incorporation of pembrolizumab into the current SOC. These patients would represent the group with the greatest urgent unmet needs. The experts agreed that PD-L1 CPS is a reliable biomarker that can be used to predict response to pembrolizumab in this clinical scenario.
Assessing Response to Treatment
The clinical experts agreed that standard outcome measures of response, DOR, survival statistics, and quality of life measures are aligned with the outcomes used in current KEYNOTE-826 clinical trial. The clinical experts suggested that most patients would consider a prolongation of OS of at least 2 months to 3 months to be clinically meaningful. It was also noted that it is important to appreciate the prolonged DOR in those who do respond to immunotherapy compared to standard chemotherapy. The experts noted that it is unlikely that the assessment of responses will vary across physicians in term of survival or improvement in symptoms. Tumour response is expected to significantly improve patients’ symptoms especially in term of bleeding, pain, obstructive symptoms, and overall quality of life.
Discontinuing Treatment
The clinical experts agreed that treatment should be continued until disease progression, intolerable toxicities (e.g., grade 4 immune-related toxicities), or maximum number of pembrolizumab cycles as per the KEYNOTE-826 protocol (up to 35 cycles in approximately 2 years). Patients with a confirmed CR could discontinue treatment if they had received at least 8 cycles of pembrolizumab, including at least 2 cycles beyond a CR as per the KEYNOTE-826 protocol. The clinical experts also highlighted that treatment may be continued following radiographic progression if the patient is still doing well clinically and reassessed at the following radiographic imaging visit (treatment beyond progression, which is permitted in the KEYNOTE-826 trial protocol).
Prescribing Conditions
The clinical experts agreed that pembrolizumab should be given in a clinical setting where patients can be monitored closely for early detection and management of immune-related toxicities with appropriate patient education. A multidisciplinary team of specialists including a general internist, endocrinologist, gastroenterologist, pulmonologist, and dermatologist should be available to assist in management of commonly encountered toxicities associated with pembrolizumab during and after discontinuation of therapy.
Additional Considerations
The clinical experts reiterated that recurrent cervical cancer is very difficult to treat at the time of recurrence, representing a significant unmet need in Canadian population. The clinical experts noted that immunotherapies represent a significant step forward in the management of this disease with promising long DOR and a very manageable non-overlapping toxicity profile when combined with other current existing SOC therapies.
Clinician Group Input
This section was prepared by CADTH staff based on the input provided by clinician groups. The full original clinician group input(s) received by CADTH have been included in the stakeholder section at the end of this report.
One clinician group called Ontario Health (Cancer Care Ontario) Gynecology Cancer Drug Advisory Committee provided input for the treatment of adult patients with persistent, recurrent, or metastatic cervical cancer whose tumours express PD-L1 (CPS ≥ 1) as determined by a validated test. The clinician group commented that pembrolizumab would improve the efficacy for patients treated within the submitted indication and meet the unmet needs as no curative treatment is available for the patient population. It was also highlighted that there are very limited second-line options available for patients with persistent, recurrent, or metastatic cervical cancer. The clinical group considered pembrolizumab as first-line treatment option for patients with persistent, recurrent, or metastatic cervical cancer whose tumours express PD-L1, whereas indicated patients with contraindications to pembrolizumab and patients who do not express PD-L1 are considered to be least suitable for this treatment. The clinician group noted that they would consider disease progression or toxicity as indications to discontinue treatment with the drug under review.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 4.
Table 4: Summary of Drug Plan Input and Clinical Expert Response
Questions | Clinical expert response |
|---|---|
Relevant comparators | |
Comparator in the KEYNOTE-826 study was placebo plus paclitaxel 175 mg/m2 + a platinum (either cisplatin 50 mg/m2 or carboplatin AUC5) ± bevacizumab 15 mg/kg (added as per local practice) every 3 weeks. A platinum-based doublet ± bevacizumab is the current standard of practice in this setting. Other chemotherapy combinations used can include platinum + topotecan, taxane + topotecan, or single agent therapy. Are alternative chemotherapy backbones appropriate for combination with pembrolizumab (± bevacizumab) when a patient is unable to receive a platinum agent and/or a taxane? | The clinical experts consulted by CADTH noted that paclitaxel 175 mg/m2 plus carboplatin AUC5 with the addition of bevacizumab, if tolerated, is a very well-recognized standard of care and is used in ≥ 95% of patients. Other combinations are rare; however, if a patient is unable to receive either paclitaxel or carboplatin, other agents should be chosen according to patient characteristics. |
The KEYNOTE-826 study underwent a second protocol amendment which resulted in limiting the chemotherapy component of the regimen to 6 cycles of therapy, although patients with ongoing clinical benefit who were receiving chemotherapy without unacceptable side effects could continue beyond 6 cycles after consultation with the sponsor. Is there clinical evidence to support patients with ongoing clinical benefit and no intolerability continuing the chemotherapy backbone beyond 6 cycles? | The clinical experts noted that there is no clinical evidence to support chemotherapy beyond 6 cycles, but this is a common clinical practice. In the clinical trial with pembrolizumab, chemotherapy was permitted to be continued beyond 6 cycles, and clinical experts recommend that the clinical trial treatment schema be followed. |
Considerations for initiation of therapy | |
Should patients who complete 2 years of treatment and experience disease progression or recurrence off of pembrolizumab treatment be eligible for up to 1 year (17 cycles) of pembrolizumab re-treatment? | The clinical experts stated that re-treatment with pembrolizumab for patients who have completed 2 years of treatment and subsequently experience disease progression or recurrence is commonly done with pembrolizumab and expected in the cervical cancer indication as well. |
If re-treatment is permitted, would this be as pembrolizumab monotherapy or in combination with chemotherapy? | There is no evidence to suggest whether re-treatment with pembrolizumab monotherapy or pembrolizumab in combination with chemotherapy would be superior. Typically, re-treatment would be done with the full treatment regimen, in this case, pembrolizumab in combination with paclitaxel and a platinum-based chemotherapy with or without bevacizumab. |
Considerations for discontinuation of therapy | |
If a patient cannot tolerate the chemotherapy combination, are they able to continue with pembrolizumab ± bevacizumab? | The clinical experts noted this decision would be made to be in line with the conduct of the KEYNOTE-826 study. The experts noted that patients that cannot tolerate chemotherapy should continue to receive pembrolizumab with or without bevacizumab, following discontinuation of chemotherapy. |
If a patient cannot tolerate the bevacizumab, are they able to continue with pembrolizumab plus chemotherapy? | The clinical experts agreed that if a patient cannot tolerate bevacizumab, they should continue treatment with pembrolizumab plus chemotherapy, in line with the KEYNOTE-826 protocol. |
Is there a minimum number of chemotherapy cycles that must be given concurrently with pembrolizumab? | The clinical experts agreed that the KEYNOTE-826 protocol should be followed. Chemotherapy should be continued up to 6 cycles with treatment beyond 6 cycles permitted if there is clinical benefit. If chemotherapy cannot be tolerated, and is discontinued before 6 cycles, pembrolizumab should be continued with or without bevacizumab. |
Considerations for prescribing of therapy | |
Pembrolizumab was administered every 3 weeks in the KEYNOTE-826 study; however, the product monograph indicates that administration either every 3 weeks or every 6 weeks is acceptable for cervical cancer. Is a dosing interval of every 6 weeks for pembrolizumab appropriate for this indication? | The clinical experts noted that there is no clinical difference between the 2 dosing options. Although the trial used 200 mg every 3 weeks, some clinicians may choose 400 mg every 6 weeks to reduce the number of visits and chair time. |
Comments from the drug plans (response not required): If funded, to keep in line with other indications for pembrolizumab, jurisdictions would implement a weight-based dose of 2 mg/kg (up to a cap of 200 mg) every 3 weeks or 4 mg/kg (up to a cap of 400 mg) every 6 weeks. | For consideration by pERC. |
Generalizability | |
Should patients with an ECOG PS of ≥ 2 be eligible? | The clinical experts believed that the decision to treat patients with an ECOG PS of ≥ 2 will depend on the reason for the ECOG PS of 2. If it is reversible or if the score is borderline ECOG PS 1 to 2, then the patient should be offered pembrolizumab at the discretion of the treating physician, otherwise, they should not be eligible for treatment. |
There is a time-limited need to allow patients currently on platinum-based doublet chemotherapy, or alternate chemotherapy, ± bevacizumab, to add pembrolizumab. What time frame is appropriate to add pembrolizumab for patients actively on treatment (chemotherapy ± bevacizumab) or who have recently completed treatment? Should pembrolizumab be added to bevacizumab if the patient has completed the chemotherapy component? | The clinical experts agreed that it is reasonable to add pembrolizumab to patients already receiving chemotherapy with or without bevacizumab, given that there has been no disease progression. |
Care provision issues | |
Comments from the drug plans (response not required): Pembrolizumab is already prepared and administered at facilities throughout Canada. Health care professionals have extensive experience with it. Preparation and administration time for pembrolizumab are relatively reasonable and would not be expected to significantly increase health system resources. However, there is the additional cost related to drug wastage since there is only 1 vial size available. | For consideration by pERC. |
System and economic issues | |
Comments from the drug plans (response not required): Pembrolizumab use as an additional agent in this patient population would introduce a considerable impact to budget vs. chemotherapy alone, or chemotherapy plus bevacizumab | For consideration by pERC. |
AUC = area under the curve; ECOG PS = European Cooperative Oncology Group Performance Status; pERC = CADTH pan-Canadian Oncology Review Expert Committee.
Clinical Evidence
The clinical evidence included in the review of pembrolizumab is presented as follows. The systematic review includes pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those studies that were selected according to an a priori protocol.
Systematic Review (Pivotal and Protocol-Selected Studies)
Objectives
To perform a systematic review of the beneficial and harmful effects of pembrolizumab (200 mg IV every 3 weeks or 400 mg IV every 6 weeks), in combination with chemotherapy, with or without bevacizumab for adult patients with persistent, recurrent, or metastatic cervical cancer whose tumours express PD-L1 (CPS ≥ 1), as determined by a validated test.
Methods
Studies selected for inclusion in the systematic review included pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those meeting the selection criteria presented in Table 5. Outcomes included in the CADTH review protocol reflect outcomes considered to be important to patients, clinicians, and drug plans.
The literature search for clinical studies was performed by an information specialist using a peer-reviewed search strategy according to the PRESS Peer Review of Electronic Search Strategies checklist.13
Table 5: Inclusion Criteria for the Systematic Review
Criteria | Description |
|---|---|
Population | Adult patients with persistent, recurrent, or metastatic cervical cancer whose tumours express PD-L1 (CPS ≥ 1) as determined by a validated test. Subgroups:
|
Intervention | Pembrolizumab (200 mg IV every 3 weeks or 400 mg IV every 6 weeks), in combination with chemotherapy with or without bevacizumab. |
Comparator |
|
Outcomes | Efficacy outcomes:
Harms outcomes: AEs, SAEs, WDAEs, mortality, notable harms (immune-mediated AE, infusion-related reaction, fistula formation) |
Study designs | Published and unpublished phase III and IV RCTs |
AE = adverse event; CPS = combined positive score; DOR = duration of response; ECOG PS = Eastern Cooperative Oncology Group Performance Status; HRQoL = health-related quality of life; ORR = overall response rate; OS = overall survival; PD-L1 = programmed cell death 1 ligand 1; PFS = progression-free survival; RCT = randomized controlled trial; SAE = serious adverse event; WDAE = withdrawal due to adverse event.
Published literature was identified by searching the following bibliographic databases: MEDLINE All (1946–) via Ovid and Embase (1974–) via Ovid. All Ovid searches were run simultaneously as a multi-file search. Duplicates were removed using Ovid deduplication for multi-file searches, followed by manual deduplication in Endnote. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were Keytruda (pembrolizumab) and cervical cancer. Clinical trials registries were searched: the US National Institutes of Health’s clinicaltrials.gov, WHO’s International Clinical Trials Registry Platform search portal, Health Canada’s Clinical Trials Database, and the European Union Clinical Trials Register.
No filters were applied to limit the retrieval by study type. Retrieval was not limited by publication date or by language. Conference abstracts were excluded from the search results. See Appendix 1 for the detailed search strategies.
The initial search was completed on June 20, 2022. Regular alerts updated the search until the meeting of the CADTH pan-Canadian Oncology Drug Review Expert Committee (pERC) on October 12, 2022.
Grey literature (literature that is not commercially published) was identified by searching relevant websites from the Grey Matters: A Practical Tool For Searching Health-Related Grey Literature reference.14 Included in this search were the websites of regulatory agencies (FDA and European Medicines Agency). Google was used to search for additional internet-based materials. See Appendix 1 for more information on the grey literature search strategy.
Two CADTH clinical reviewers independently selected studies for inclusion in the review based on titles and abstracts, according to the predetermined protocol. Full-text articles of all citations considered potentially relevant by at least 1 reviewer were acquired. Reviewers independently made the final selection of studies to be included in the review, and differences were resolved through discussion.
A focused literature search for indirect treatment comparisons dealing with cervical cancer was run in MEDLINE All (1946–) on June 20, 2022. No limits were applied to the search.
Findings From the Literature
A total of 2 reports from 1 study were identified from the literature for inclusion in the systematic review (Figure 1). The included studies are summarized in Table 6. No indirect treatment comparison articles were identified in the literature. A list of excluded studies is presented in Appendix 2.
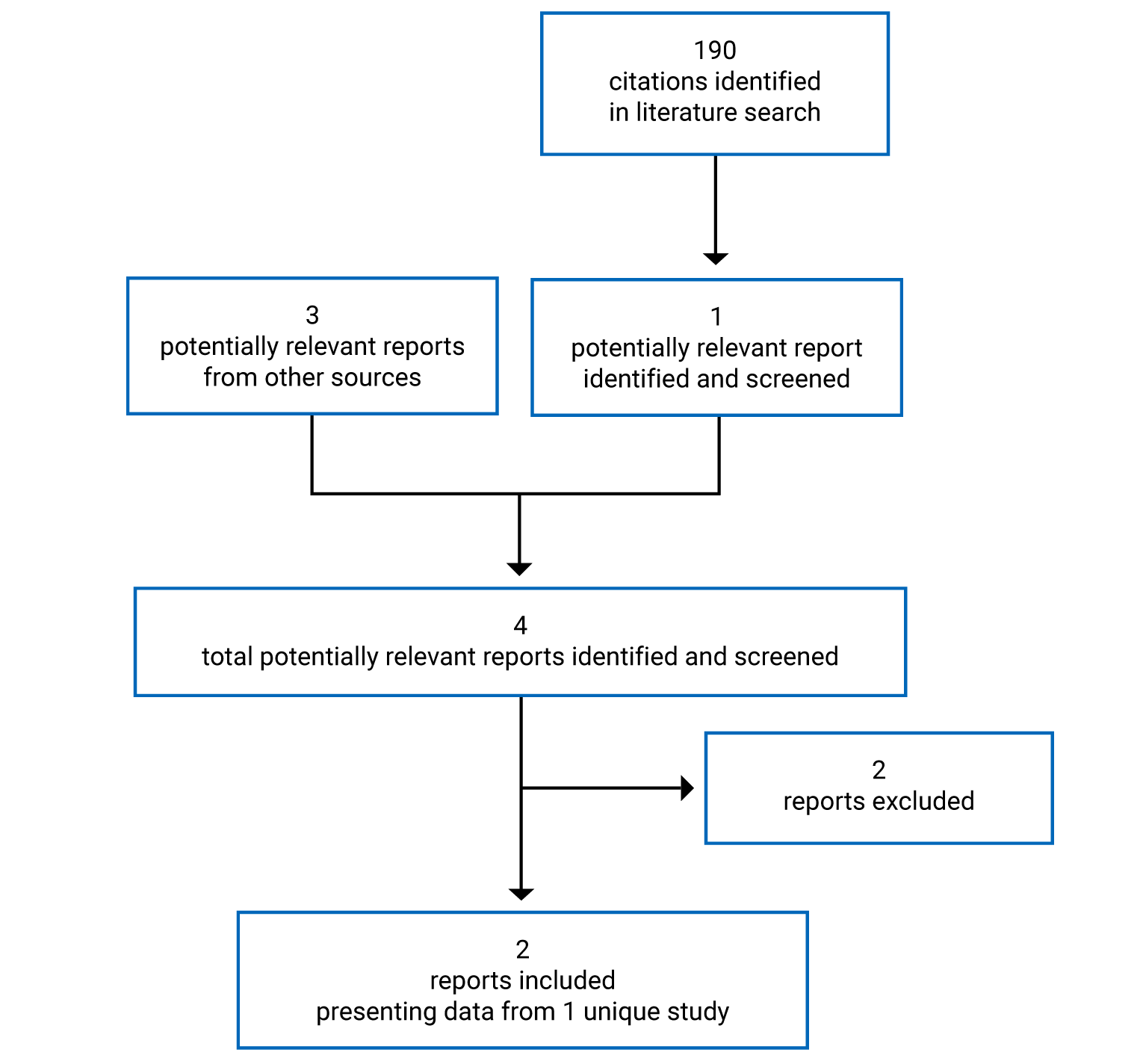
Table 6: Details of Included Studies (KEYNOTE-826)
Component | Description |
|---|---|
Designs and populations | |
Study design | Phase III, double-blind, placebo-controlled, interventional study |
Locations | Study conducted at 151 centres in 19 countries (North America [including Canada], South America, Europe, Asia, and Australia) |
Patient enrolment dates | First patient enrolled October 25, 2018 Study ongoing as of May 3, 2021, data cut-off |
Randomized (N) | 617 randomized
|
Inclusion criteria |
|
Exclusion criteria |
|
Drugs | |
Intervention | Pembrolizumab 200 mg, IV infusion once every 3 weeks for up to 35 cycles In combination with chemotherapy (paclitaxel 175 mg/m2 + carboplatin AUC5 mg/mL/min or cisplatin 50 mg/m2) IV infusion once every 3 weeks for up to 6 cycles With or without bevacizumab 15 mg/kg IV infusion once every 3 weeks continuing until disease progression or unacceptable AEs, as per local label or local practice |
Comparator(s) | Placebo IV infusion once every 3 weeks In combination with chemotherapy (paclitaxel 175 mg/m2 + carboplatin AUC5 mg/mL/min or cisplatin 50 mg/m2) IV infusion once every 3 weeks for up to 6 cycles With or without bevacizumab 15 mg/kg, IV infusion once every 3 weeks continuing until disease progression or unacceptable AEs, as per local label or local practice |
Duration | |
Phase | |
Screening | Maximum 28 days |
Double blind | Pembrolizumab administered for up to 35 cycles (approximately 2 years) |
Safety follow-up | 30 days from last dose |
Survival follow-up | Every 12 weeks until death |
Outcomes | |
Primary end point |
|
Secondary and exploratory end points | Secondary:
Exploratory:
|
Notes | |
Publications | Colombo et al. (2021)15 |
AE = adverse event; AUC = area under the curve; BICR = blinded independent central review; CNS = central nervous system; CPS = combined positive score; DOR = duration of response; ECOG PS = European Cooperative Oncology Group Performance Status; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EORTC QLQ-CX24 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire cervical cancer module; EQ-5D-5L = 5-Level EQ-5D; HRQoL = health-related quality of life; ORR = overall response rate; OS = overall survival; PD-1 = programmed cell death 1 protein; PD-L1 = programmed cell death 1 ligand 1; PD-L2 = programmed death ligand 2; PFS = progression-free survival; RECIST = Response Evaluation Criteria in Solid Tumors; WOCBP = women of childbearing potential.
Sources: KEYNOTE-826 Clinical Study Report,5 Colombo et al. (2021).15
Description of Studies
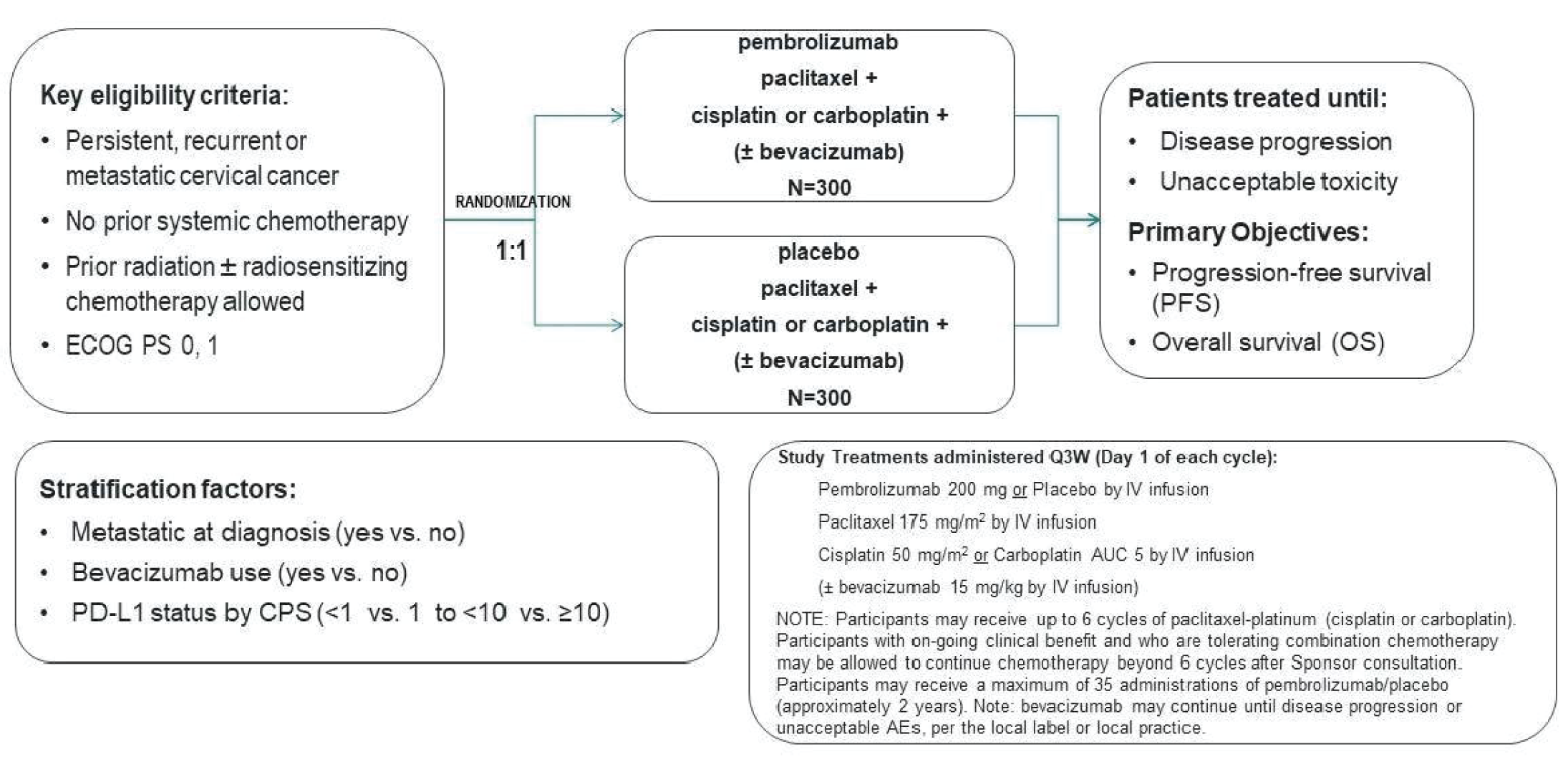
KEYNOTE-826 is an ongoing phase III, randomized, placebo-controlled clinical trial investigating pembrolizumab in combination with SOC compared to placebo plus SOC in the treatment of patients with histologically confirmed persistent, recurrent, or metastatic cervical cancer not treated with prior systemic chemotherapy. A summary of the study design and objectives is shown in Figure 2. Following a screening period of up to 28 days, patients were randomized 1:1 to receive pembrolizumab 200 mg plus SOC or a placebo plus SOC. SOC was defined as paclitaxel 175 mg/m2 plus either cisplatin 50 mg/m2 or carboplatin with an AUC of 5, with the addition of bevacizumab 15 mg/kg if there were no contraindications to bevacizumab. This combination of chemotherapy with or without the addition of bevacizumab will be referred to as SOC for the remainder of this report. Patients were treated until disease progression or unacceptable toxicity, with treatment permitted beyond progression if the treatment was deemed to be providing clinical benefit.
The KEYNOTE-826 trial randomization was stratified according to metastasis at initial diagnosis, bevacizumab use according to investigator’s choice before randomization, and PD-L1 status (CPS < 1, 1 to < 10, and ≥ 10). There were 6 primary objectives of the study and these were to compare the PFS and OS of pembrolizumab plus SOC against placebo plus SOC in patients with PD-L1 with a CPS of 1 or higher, a CPS of 10 or higher, and all-comers patients. Secondary objectives included determining ORR, DOR, 12-month PFS rate, safety and tolerability, and HRQoL. As the Health Canada–approved indication, as well as the reimbursement request, are for the population with PD-L1 with a CPS of 1 or higher, this population will be the focus of this report, with the populations with a CPS of 10 or higher and all-comers populations described in the Appendix. As the KEYNOTE-826 study is ongoing, the data presented in this report are from a planned interim analysis based on a May 3, 2021, data cut-off. There will be another interim analysis followed by a final analysis triggered by prespecified PFS events and OS events, respectively.
Key protocol amendments included a change to allow chemotherapy to be administered beyond the planned 6 cycles, if it was deemed to provide clinical benefit; this was implemented on June 25, 2019. An additional protocol amendment of note was implemented on October 30, 2020, to change the primary PFS end point and secondary ORR and DOR end points from being analyzed according to BICR to being assessed according to investigators. This was done to avoid a loss of events to censoring, as under the original primary end point using BICR, patients were censored at last disease assessment if they experienced a PFS event after initiation of a new anti-cancer therapy. The number of censored patients threatened the ability of the trial to reach the required number of events for final analysis. With investigator-assessed progression, these progression events were identified before the start of new anti-cancer therapy, reducing the number of events lost to censoring.
Figure 2: KEYNOTE-826 Study Diagram
AE = adverse event; AUC = area under the curve; CPS = combined positive score; ECOG PS = European Cooperative Oncology Group Performance Status; OS = overall survival; PD-L1 = programmed cell death 1 ligand 1; PFS = progression-free survival; Q3W = every 3 weeks.
Source: KEYNOTE-826 Clinical Study Report.5
Populations
Inclusion and Exclusion Criteria
A summary of the inclusion and exclusion criteria for the KEYNOTE-826 study is presented in Table 6. Patients with persistent, recurrent, or metastatic cervical cancer were required to have measurable disease as per investigator-assessed Response Evaluation Criteria in Solid Tumors (RECIST) 1.1. Of note, patients could only enrol in the study if they had an ECOG PS of 0 or 1. Patients were excluded from enrolment in the KEYNOTE-826 study if they had CNS metastasis or if they had received prior systemic chemotherapy for cervical cancer, although prior use of radiosensitizing chemotherapy was permitted provided it was completed at least 2 weeks before randomization.
Baseline Characteristics
Baseline characteristics for patients with PD-L1 with a CPS of 1 or higher from the KEYNOTE-826 study are shown in Table 7. The median age in both the pembrolizumab plus SOC arm and the placebo plus SOC was 51 years of age. There were fewer White patients in the pembrolizumab plus SOC arm than the placebo plus SOC arm (56% versus 62.5%) and more patients from the Asia Pacific region in the pembrolizumab plus SOC arm than the placebo plus SOC arm (19.8% versus 13.8%). There were no meaningful differences in baseline characteristics in patients with PD-L1 with a CPS of 10 or higher.
A summary of disease characteristics for patients with PD-L1 with a CPS of 1 or higher from the KEYNOTE-826 study is shown in Table 8. Most patients in both arms of the study had persistent or recurrent cervical cancer with distant metastasis at study entry (62.3% and 56.7% in the pembrolizumab plus SOC and placebo plus SOC arms, respectively). More than half the patients in both treatment arms had PD-L1 with a CPS of 10 or higher (57.9% and 57.8% in the pembrolizumab plus SOC and placebo plus SOC arms, respectively). Most patients in both treatment arms had squamous cell histology (77.3% and 71.6% in the pembrolizumab plus SOC and placebo plus SOC arms, respectively).
Table 7: Summary of Baseline Characteristics for Patients With a CPS of 1 or Higher
Characteristic | Pembrolizumab plus SOC (n = 273) | SOC (n = 275) |
|---|---|---|
Sex | ||
Female | 273 (100.0) | 275 (100.0) |
Age | ||
Mean (SD) | 51.2 (12.0) | 50.7 (12.6) |
Median (range) | 51.0 (25 to 82) | 51.0 (22 to 78) |
Race | ||
American Indian or Alaska Native | 13 (4.8) | 17 (6.2) |
Asian | 57 (20.9) | 41 (14.9) |
Black or African American | 4 (1.5) | 2 (0.7) |
Multiple | 28 (10.3) | 27 (9.8) |
Not applicable | 17 (6.2) | 16 (5.8) |
White | 153 (56.0) | 172 (62.5) |
Missing | 1 (0.4) | 0 (0.0) |
Ethnicity | ||
Hispanic or Latino | 97 (35.5) | 106 (38.5) |
Not Hispanic or Latino | 170 (62.3) | 165 (60.0) |
Not reported | 5 (1.8) | 4 (1.5) |
Unknown | 1 (0.4) | 0 (0.0) |
Geographic region | ||
Asia Pacific | 54 (19.8) | 38 (13.8) |
EU/EMEA | 91 (33.3) | 98 (35.6) |
North America | 35 (12.8) | 38 (13.8) |
Latin America | 93 (34.1) | 101 (36.7) |
CPS = combined positive score; EU = European Union; EMEA = Europe, the Middle East, and Africa; SD = standard deviation; SOC = standard of care.
Note: Values are n (%) unless otherwise indicated.
Source: KEYNOTE-826 Clinical Study Report.5
Table 8: Summary of Disease Characteristics for Patients With a CPS of 1 or Higher
Characteristic | Pembrolizumab plus SOC (n = 273) | SOC (n = 275) |
|---|---|---|
ECOG PS | ||
0 | 160 (58.6) | 148 (53.8) |
1 | 111 (40.7) | 127 (46.2) |
2 | 1 (0.4) | 0 (0.0) |
Missing | 1 (0.4) | 0 (0.0) |
Stage at initial diagnosis | ||
I | 55 (20.1) | 48 (17.5) |
II | 76 (27.8) | 85 (30.9) |
III | 5 (1.8) | 7 (2.5) |
IIIA | 4 (1.5) | 7 (2.5) |
IIIB | 41 (15.0) | 37 (13.5) |
IVA | 6 (2.2) | 3 (1.1) |
IVB | 86 (31.5) | 88 (32.0) |
Disease status at study entry | ||
Metastatic | 56 (20.5) | 59 (21.5) |
Persistent or recurrent with distant metastases at study entry | 170 (62.3) | 156 (56.7) |
Persistent or recurrent without distant metastases at study entry | 47 (17.2) | 60 (21.8) |
Histology | ||
Adenocarcinoma | 47 (17.2) | 66 (24.0) |
Adenosquamous (both squamous and adenocarcinoma) | 13 (4.8) | 12 (4.4) |
Epidermoide carcinoma | 1 (0.4) | 0 (0.0) |
Undifferentiated carcinoma | 1 (0.4) | 0 (0.0) |
Squamous cell/squamous cell carcinoma | 211 (77.3) | 197 (71.6) |
PD-L1 status | ||
1 ≤ CPS < 10 | 115 (42.1) | 116 (42.2) |
CPS ≥ 10 | 158 (57.9) | 159 (57.8) |
Bevacizumab use | ||
Yes | 175 (64.1) | 171 (62.2) |
No | 98 (35.9) | 104 (37.8) |
Prior therapy | ||
CRT and surgery | 43 (15.8) | 48 (17.5) |
Radiation and surgery | 18 (6.6) | 21 (7.6) |
CRT only | 112 (41.0) | 103 (37.5) |
Radiation only | 28 (10.3) | 21 (7.6) |
Surgery only | 16 (5.9) | 23 (8.4) |
None | 56 (20.5) | 59 (21.5) |
CPS = combined positive score; CRT = chemoradiation; ECOG PS = European Cooperative Oncology Group Performance Status; PD-L1 = programmed death ligand 1; SOC = standard of care.
Source: KEYNOTE-826 Clinical Study Report.5
Interventions
Pembrolizumab was administered as an IV infusion of 200 mg on day 1 of every 3-week cycle. The SOC combination of paclitaxel 175 mg/m2, cisplatin 50 mg/m2 or carboplatin, with or without bevacizumab 15 mg/kg, was administered as an IV infusion on day 1 of every 3-week cycle. Pembrolizumab was continued until disease progression or unacceptable toxicity up to a maximum of 35 cycles. In the case of chemotherapy, treatment was administered until disease progression, unacceptable toxicity, or a maximum of 6 cycles, although patients could continue receiving chemotherapy if they continued receiving clinical benefit. Bevacizumab, if given according to investigator’s choice before randomization, was continued until disease progression or unacceptable toxicity, as per the local label and local practices. iRECIST criteria were used for treatment decision-making, permitting ongoing treatment in clinically stable patients until confirmation of disease progression. Patients who stopped treatment with stable disease or better and subsequently experienced disease progression were permitted to be retreated for up to 17 additional administrations of pembrolizumab.
Patients were permitted to interrupt or discontinue pembrolizumab, while components of the SOC regimen could be reduced, interrupted, or discontinued, according to local practice. All components of treatment could be interrupted or discontinued independently. Pembrolizumab was permitted to be interrupted for a maximum of 12 weeks, while the components of SOC could be interrupted for a maximum of 6 weeks.
Palliative radiation therapy to a symptomatic, non-target lesion was allowed following consultation with the sponsor. On study non-palliative radiation and radiation to a target lesion per RECIST 1.1 were not permitted. Palliative radiation during the screening phase (≤ 2 weeks of radiotherapy) to non-CNS disease was allowed. Cisplatin, carboplatin, paclitaxel, and bevacizumab could be interrupted due to toxicity for a maximum of 6 weeks. Restarting these treatments after an interruption of more than 6 weeks required a signed sponsor consultation form. Supportive care measures for chemotherapy (e.g., erythrocyte infusion, thrombocyte infusion, granulocyte colony-stimulating factor, and erythropoietin) were utilized before dose modification unless other reasons to modify SOC dosing for chemotherapy agents occurred.
Outcomes
A list of efficacy end points identified in the CADTH review protocol that were assessed in the clinical trials included in this review is provided in Table 9. These end points are further summarized as follows. A detailed discussion and critical appraisal of the outcome measures is provided in Appendix 4.
Table 9: Summary of Outcomes of Interest Identified in the CADTH Review Protocol
Outcome measure | KEYNOTE-826 |
|---|---|
HRQoL | Secondary (EORTC QLQ-C30 global score) Exploratory (EORTC QLQ-CX24, EQ-5D-5L) |
OS | Co-primary |
PFS as assessed by investigator | Co-primary |
PFS as assessed by BICR | Secondary |
12-month PFS rate as assessed by investigator | Secondary |
ORR as assessed by investigator | Secondary |
DOR as assessed by investigator | Secondary |
Safety | Secondary |
BICR = blinded independent central review; DOR = duration of response; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EORTC QLQ-CX24 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire cervical cancer module; EQ-5D-5L = 5-Level EQ-5D;HRQoL = health-related quality of life; ORR = overall response rate; OS = overall survival; PFS = progression-free survival.
The secondary end point of HRQoL was as measured by the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC QLQ-C30) global status score. The EORTC QLQ-C30 is composed of both multi-item scales and single-item measures. These include 5 functional scales (physical, role, cognitive, emotional, and social), 3 symptom scales (fatigue, pain, and nausea and vomiting), a global health status/HRQoL scale, and 6 single items assessing additional symptoms commonly reported by cancer patients (dyspnea, loss of appetite, insomnia, constipation, and diarrhea) as well as perceived financial impact of the disease.16 For the 2 items that form the global HRQoL scale, the response format is a 7-point Likert-type scale with anchors of 1 indicating “very poor” and 7 indicating “excellent.” Raw scores for each scale are computed as the average of the items that contribute to a particular scale. Scale sum scores are transformed such that a high score on the functional scales represents a high or healthy level of functioning, a high score on the symptom scales represents a high level of symptomatology, and a high score on the global health status/HRQoL scale represents a high HRQoL.17 A point difference of 10 or more in HRQoL scores (on a scale of 0 to 100) was identified by the CADTH literature search as being clinically relevant for evaluating HRQoL in both the EORTC QLQ-C30 and the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire cervical cancer module (EORTC QLQ-CX24).18,19 Studied confirming the validity, reliability, and responsiveness of these measures were also identified by the CADTH literature search.20,21
HRQoL was further characterized by the 5-Level EQ-5D (EQ-5D-5L) visual analogue scale (VAS) and the EORTC QLQ-CX24 as exploratory end points. The EQ-5D-5L VAS is a 20-cm VAS that has end points labelled 0 and 100, with respective anchors of “worst imaginable health state” and “best imaginable health state.” Respondents are asked to rate their health by drawing a line from an anchor box to the point on the EQ-5D-5L VAS that best represents their health on that day. “Improved” was defined as a 10-point or more improvement in score (in the positive direction) from baseline at any time during the study and confirmed by the next consecutive visit. “Stable” was defined as a 10-point or more increase in the positive direction or a less than 10-point change in score in the positive or negative direction from baseline and confirmed by a less than 10-point change in score at the next consecutive visit, or a less than 10-point change in score and a 10-point or more increase in score at the next consecutive visit. Deterioration was defined as a 10-point or more deterioration in score from baseline at any time during the trial when the criteria for improvement or stability were not met at any other time. No evidence from the literature was found to determine a minimally important clinical difference.
The EORTC QLQ-CX24 is a supplement to the EORTC QLQ-C30 core questionnaire,22 addressing relevant areas of HRQoL in patients with cervical cancer not covered by the core questionnaire, including symptom experience, body image, and sexual/vaginal functioning. Scores were linearly transformed to a scale of 0 to 100 using the standard scoring algorithm recommended by the European Organisation for Research and Treatment of Cancer. A difference of 10 points or more in HRQoL scores (on a scale of 0 to 100) was identified through the CADTH literature search to be clinically relevant for evaluating HRQoL.18,19 In another study of patients with cervical cancer, a more than 5% difference of mean score values compared to baseline was indicative of a difference of clinical interest for the EORTC QLQ-CX24 module.23
The co-primary end point of OS was defined as the time from randomization to death due to any cause.
The co-primary end point of PFS was defined as the time from randomization to the first documented disease progression per RECIST 1.1 as assessed by investigator or death due to any cause, whichever occurs first. PFS, as defined as time from randomization to the first documented disease progression per RECIST 1.1 as assessed by BICR or death due to any cause, whichever occurs first, was also included as a secondary end point.
The secondary end point of 12-month PFS rate was defined as the proportion of participants that are PFS event-free at 12 months per RECIST 1.1 as assessed by investigator.
The secondary end point of ORR was defined as the proportion of participants who had a best overall response of either confirmed CR or partial response (PR) per RECIST 1.1 as assessed by investigator.
For patients that achieved either a CR or PR, the secondary end point of DOR was defined as the time from the first documented evidence of CR or PR until the first documented disease progression assessed per RECIST 1.1 by investigator or death due to any cause, whichever occurs first.
Safety outcomes were classified according to tiered system. Safety parameters or AEs of special interest that were identified a priori were classified as “Tier 1” safety end points that were subject to inferential testing for statistical significance. Given that the safety profile of pembrolizumab is well characterized, the sponsor did not include any Tier 1 AEs in the analysis. Tier 2 AEs required that at least 10% of participants in any treatment group exhibit the event; all other AEs and predefined limits of change were categorized as Tier 3. Safety end points that are not Tier 1 or 2 events were considered Tier 3 events.
Statistical Analysis
Treatment randomization was stratified based on the following criteria: metastatic (FIGO [2009] stage IVB) at initial diagnosis (yes versus no), investigator decision to use bevacizumab (yes versus no), and PD-L1 status (CPS < 1, CPS 1 to < 10, or CPS ≥ 10). Of note, the 2009 version of FIGO included para-aortic lymph node involvement as stage IVB disease while the 2018 version of FIGO does not include para-aortic lymph node involvement as stage IVB disease. Para-aortic lymph node involvement was considered as evidence of metastatic disease for purposes of stratification of all participants at the time of randomization in the KEYNOTE-826 study.
A total of 600 all-comers patients were expected to enrol in the KEYNOTE-826 study, with 510 patients with PD-L1 with a CPS of 1 or higher and 300 patients with PD-L1 with a CPS of 10 or greater. For the control arm, a median PFS of 7.1 months and a median OS of 15.1 months were assumed, based on historical data. For PFS in the CPS of 1 or higher population, at a 1-sided alpha of 0.004, the study had 91% power to detect a PFS HR of 0.68 with approximately 370 and 435 PFS events between both arms at the 2 planned interim analyses, respectively. For OS in patients with a CPS of 1 or higher, at a 1-sided alpha of 0.016, the study had 90% power to detect an OS HR of 0.70 at the planned analysis. The expected numbers of events between both arms were approximately 246, 321, and 378, at the 2 interim and final analyses, respectively.
For PFS in the all-comers population, at a 1-sided alpha of 0.004, the study had a 91% power to detect a PFS HR of 0.70 with 432 and 508 PFS events between both arms at the 2 planned interim analyses, respectively, given the PFS null hypothesis for a CPS of 1 or higher was rejected. For OS in all-comers patients, at a 1-sided alpha of 0.016, the study had 90% power to detect an OS HR of 0.72 at the planned analysis, given the OS null hypothesis for a CPS of 1 or higher was rejected. The expected numbers of events between both arms, were approximately 289, 378, and 445, at the 2 interim and final analyses, respectively.
For PFS in the CPS of 10 or higher population, at a 1-sided alpha of 0.005, the study had 92% power to detect a PFS HR of 0.60 with 210 and 247 PFS events between both arms at the 2 planned interim analyses, respectively, given that both PFS null hypotheses for a CPS of 1 or higher and all-comers were rejected. For OS in patients with a CPS of 10 or higher, at a 1-sided alpha of 0.020, the study had 93% power to detect an OS HR of 0.60 at the planned analysis, given that both OS null hypotheses for a CPS of 1 or higher and all-comers were rejected. The expected numbers of events between both arms were approximately 127, 167, and 196, at the 2 interim and final analyses, respectively.
Two interim analyses and 1 final analysis are planned in this study, with this report including data from the first interim analysis. Comparisons between 2 treatment arms will be conducted at the interim analyses and final analysis.
Interim analysis 1: PFS and OS analysis approximately 22 months after the first participant is randomized. The analysis will be triggered when approximately 370 PFS events for the CPS of 1 or higher group have been observed.
Interim analysis 2: PFS and OS analysis approximately 30 months after the first participant is randomized. The analysis will be triggered when at least 435 PFS events for the CPS of 1 or higher group have been observed. This represents the final PFS analysis that will be conducted.
Final Analysis: Final OS analysis approximately 40 months after the first participant is randomized. The analysis will be triggered when at least 378 OS events for the CPS of 1 or higher group have been observed.
The overall type I error rate over the multiple end points was controlled at 2.5% (1-sided). A total of a 0.5% type I error rate was allocated to test PFS superiority between 2 arms for the CPS of 10 or higher group, CPS of 1 or higher group, and all-comers; a total of a 2% type I error rate was allocated to test OS superiority between 2 arms for the CPS of 10 or higher group, CPS of 1 or higher group, and all-comers. The graphical approach of Maurer and Bretz24 was applied to reallocate alpha among the hypotheses of PFS and OS. For example, if the PFS null hypothesis is rejected in the CPS of 1 or higher group, the 0.004 alpha will be reallocated to the all-comers population, and if the PFS null hypothesis is rejected in the all-comers population, the 0.004 alpha will be allocated to the CPS of 10 or higher population. Lan-DeMets and O’Brien-Fleming group sequential methods were used to allocate alpha among the interim and final analyses for the PFS and OS end points; alpha that is not spent at the first interim analyses will be reallocated to the second interim analysis and final analysis. A visual representation of the testing schema and alpha allocation is shown in Figure 3.
A full summary of the statistical analysis of end points is shown in Table 10.The statistical model chosen for both PFS and OS was the nonparametric Kaplan-Meier (KM) method. The treatment difference in PFS and OS was assessed by the stratified log-rank test. A stratified Cox proportional hazard model with the Efron method of tie handling was used to assess the magnitude of the treatment difference (i.e., the HR) between the treatment arms. The HR and its 95% CI from the stratified Cox model with the Efron method of tie handling and with a single treatment covariate were reported. The stratification factors used for randomization were applied to both the stratified log-rank test and the stratified Cox model. Median PFS and its 95% CIs will be updated post the second interim analysis; however, no formal statistical testing will be performed. Censoring rules for sensitivity analyses for PFS are summarized in Figure 4. For OS, patients without documented death at the time of analysis was censored at the date of last known contact. Missing data for HRQoL outcomes were handled according to constrained longitudinal data analysis based on the missing at random assumption.
Figure 3: Testing Schema and Alpha Allocation for KEYNOTE-826
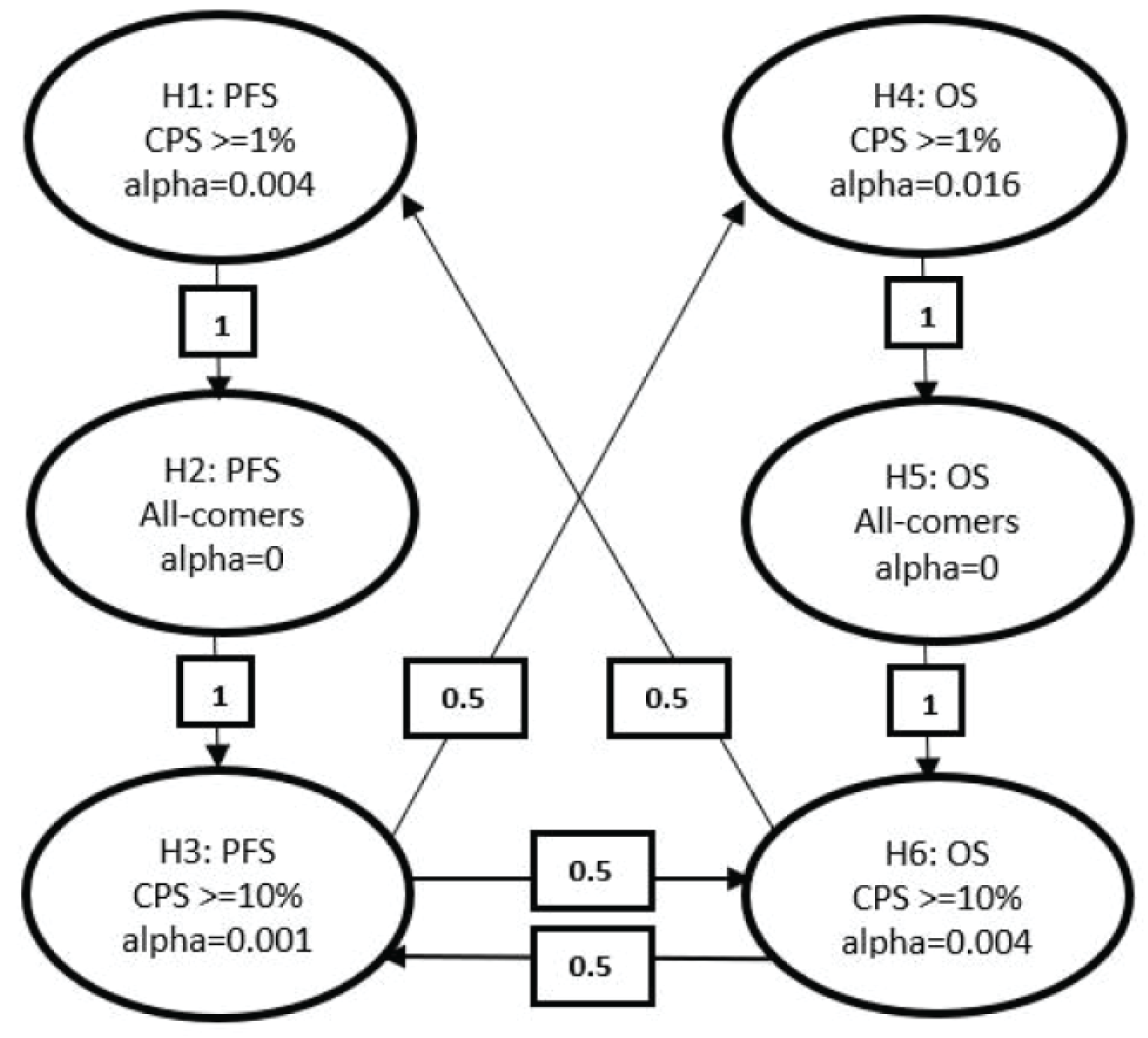
CPS = combined positive score; OS = overall survival; PFS = progression-free survival.
Note: Secondary end points were not adjusted for multiplicity.
Source: KEYNOTE-826 Clinical Study Report.5
Table 10: Statistical Analysis of Efficacy End Points
End point | Statistical model | Missing data approach |
|---|---|---|
PFS (RECIST 1.1) by investigator | Stratified log-rank test Estimation: stratified Cox model with Efron tie handling method | Censoring sensitivity analyses according to Figure 4 |
OS | Stratified log-rank test Estimation: stratified Cox model with Efron tie handling method | Censored at last known alive date |
ORR (RECIST 1.1) by investigator | Estimation: stratified Miettinen-Nurminen method | Participants with missing data are considered nonresponders |
DOR (RECIST 1.1) by investigator | Summary statistics using Kaplan-Meier method | Nonresponders are excluded from the analysis |
PFS rate at 12 months (RECIST 1.1) by investigator | Kaplan-Meier estimation with CI | Censoring sensitivity analyses according to Figure 4 |
PFS (RECIST 1.1) by BICR | Estimation: stratified Cox model with Efron tie handling method | Censoring sensitivity analyses according to Figure 4 |
HRQoL as per EORTC QLQ-C30 | Time to deterioration: Kaplan-Meier plot, stratified log-rank test and Cox proportional hazards model | Constrained longitudinal data analysis based on the missing at random assumption |
Safety and tolerability | No statistical model: safety and tolerability were assessed by clinical review of all relevant parameters including AEs, laboratory tests, vital signs, and ECG measurements | NA |
AE = adverse event; BICR = blinded independent committee review; CI = confidence interval; DOR = duration of response; ECG = electrocardiogram; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; HRQoL = health-related quality of life; NA = not applicable; ORR = overall response rate; OS = overall survival; PFS = progression-free survival; RECIST = Response Evaluation Criteria in Solid Tumors.
Source: KEYNOTE-826 Clinical Study Report.5
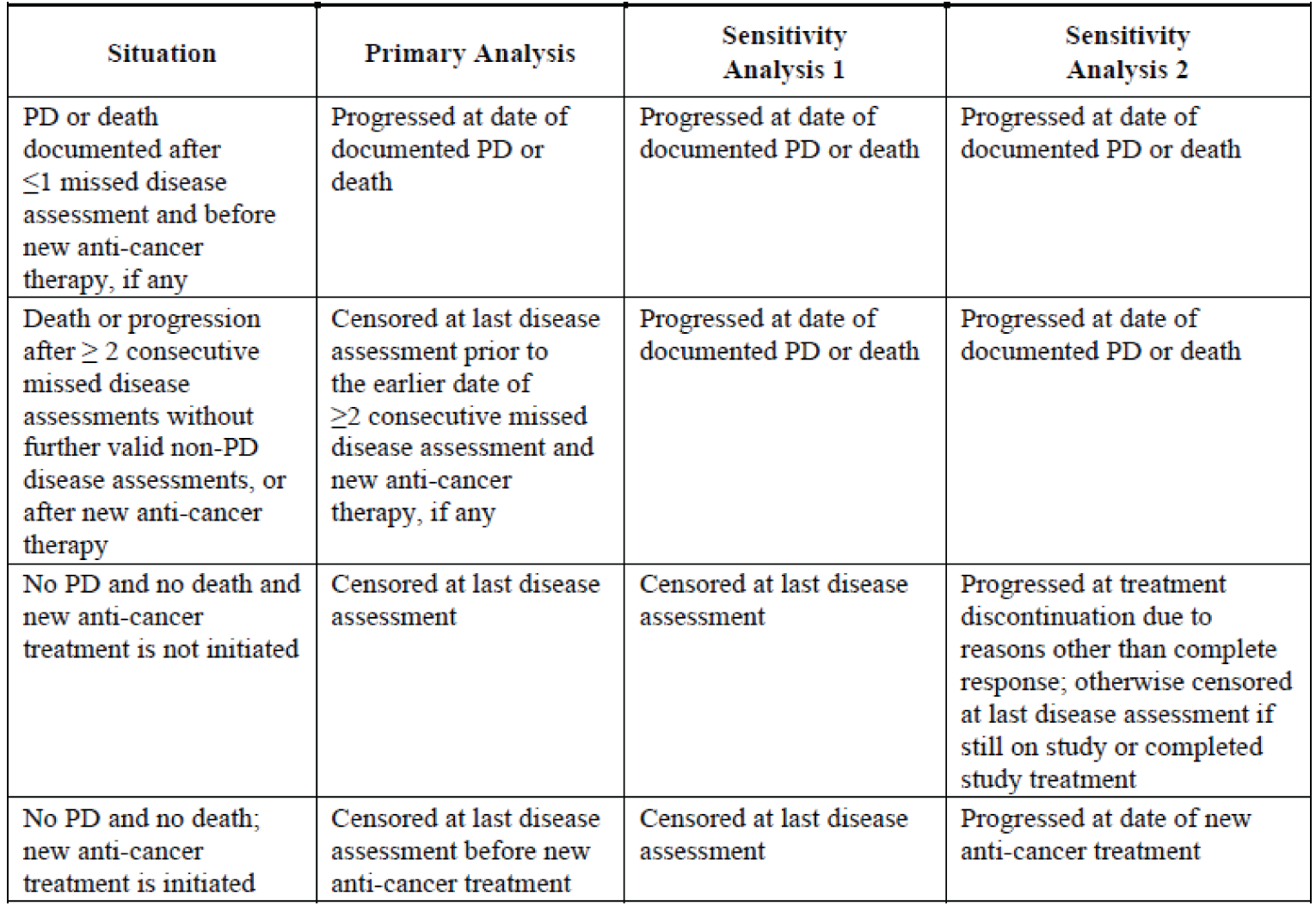
PD = progressive disease; PFS = progression-free survival.
Source: KEYNOTE-826 Clinical Study Report.5
Analysis Populations
The CPS of 1 or higher analysis set included all patients randomized who had PD-L1 with a CPS of 1 or higher.
The CPS of 10 or higher analysis set included all patients randomized who had PD-L1 with a CPS of 10 or higher.
The all-comers analysis set included all randomized patients regardless of PD-L1 status; this included patients with PD-L1 with a CPS of less than 1 as well as any with missing PD-L1 status.
The safety analysis set included all patients, regardless of PD-L1 status, who received a dose of study treatment.
Results
Patient Disposition
A summary of patient disposition for all-comers in the KEYNOTE-826 trial is shown in Table 11. Of the 883 patients screened, 30.1% did not meet screening criteria—the most common reason cited was “other”—which accounted for roughly 30% of the failed screenings. The remainder were a mix of inadequate organ function, lack of measurable disease per RECIST 1.1, lack of consent, or ECOG PS other than 0 or 1. Of the 308 all-comers patients randomized to the pembrolizumab plus SOC arm, 45.5% had discontinued from the study at the May 3, 2021, data cut-off, compared to 58.3% of the 309 patients randomized to receive placebo plus SOC. The most common reason in both arms for study discontinuation was death. At the time of data cut-off, 2.3% of patients in the pembrolizumab plus SOC arm had completed treatment; no patients in the placebo plus SOC arm had completed treatment at the time of data cut-off. For chemotherapy, patients were required to discontinue all components of the regimen to be considered as having discontinued treatment. Patients discontinued treatment due to AEs at a rate of 12.4% in the pembrolizumab plus SOC arm and 7.8% in the placebo plus SOC arm. Of the total all-comers patients randomized to receive pembrolizumab plus SOC, 88.6% were in the CPS of 1 or higher analysis set, 51.3% were in the CPS of 10 or higher analysis set, and 99.7% were in the safety set. Of the total all-comers patients randomized to receive placebo plus SOC, 89.0% were in the CPS of 1 or higher analysis set, 51.5% were in the CPS of 10 or higher analysis set, and 100% were in the safety set.
Exposure to Study Treatments
A summary of exposure to study treatments for all-comers patients in the KEYNOTE-826 trial is shown in Table 12. The median duration of treatment was 10 months (range, 0 to 26.9) in the pembrolizumab plus SOC arm and 7.7 months (0 to 27.4) in the placebo plus SOC arm. The median number of cycles of total drug were 14 (range, 1 to 39) in the pembrolizumab plus SOC arm and 11 (range, 1 to 38) in the placebo plus SOC arm.
Table 11: Patient Disposition in All-Comers in KEYNOTE-826
Patient disposition | Pembrolizumab plus SOC | SOC |
|---|---|---|
Screened, N | 883 | |
Nonrandomized, N (%) | 266 (30.1) | |
Did not meeting inclusion criteria, n | 265 | |
Inadequate organ function | 67 | |
Lack of measurable target lesion per RECIST 1.1 | 52 | |
Lack of consent | 39 | |
ECOG was not qualified | 27 | |
Other | 80 | |
Randomized, N | 308 | 309 |
Discontinued from study, n (%) | 140 (45.5) | 180 (58.3) |
Reason for discontinuation, n (%) | ||
Death | 134 (43.5) | 171 (55.3) |
Associated with COVID-19 | 0 (0.0) | 1 (0.3) |
Lost to follow-up | 0 (0.0) | 1 (0.3) |
Withdrawal by patient | 6 (1.9) | 8 (2.6) |
Study ongoing | 168 (54.5) | 129 (41.7) |
Completed treatment | 7 (2.3) | 0 (0.0) |
Discontinued treatment | 196 (63.8) | 255 (82.5) |
Adverse event | 38 (12.4) | 24 (7.8) |
Clinical progression | 12 (3.9) | 22 (7.1) |
Complete response | 2 (0.7) | 1 (0.3) |
Excluded medication | 1 (0.3) | 0 (0.0) |
Physician decision | 4 (1.3) | 4 (1.3) |
Progressive disease | 124 (40.4) | 181 (58.6) |
Protocol violation | 0 | 1 (0.3) |
Withdrawal by subject | 15 (4.9) | 22 (7.1) |
Associated with COVID-19 | 0 (0.0) | 1 (0.3) |
Participants ongoing treatment | 104 (33.9) | 54 (17.5) |
ITT all-comers, N | 308 | 309 |
Median follow-up, months (range) | 18.2 (0.5 to 28.4) | 16.3 (0.9 to 29.2) |
CPS ≥ 1, N (%) | 273 (88.6) | 275 (89.0) |
CPS ≥ 10, N (%) | 158 (51.3) | 159 (51.5) |
Safety, N (%) | 307 (99.7) | 309 (100.0) |
CPS = combined positive score; ECOG = European Cooperative Oncology Group; ITT = intention to treat; RECIST = Response Evaluation Criteria in Solid Tumors; SOC = standard of care.
Source: KEYNOTE-826 Clinical Study Report.5
Table 12: Summary of Exposure to Study Treatments for Safety Population
Characteristic | Pembrolizumab plus SOC (n = 307) | SOC (n = 309) |
|---|---|---|
Duration of therapy, months | ||
Mean (SD) | 11.8 (8.05) | 9.4 (6.79) |
Median (range) | 10.0 (0 to 26.9) | 7.7 (0 to 27.4) |
Number of cycles of total drug | ||
Mean (SD) | 16.5 (11.01) | 13.4 (9.17) |
Median (range) | 14.0 (1.0 to 39.0) | 11.0 (1.0 to 38.0) |
Number of cycles of pembrolizumab or placebo | ||
Mean (SD) | 16.0 (10.86) | 13.2 (9.10) |
Median (range) | 13.0 (1.0 to 35.0) | 11.0 (1.0 to 35.0) |
Number of cycles of chemotherapy | ||
Mean (SD) | 6.0 (10.86) | 6.4 (3.50) |
Median (range) | 6.0 (1.0 to 20.0) | 6.0 (1.0 to 33.0) |
Number of cycles of bevacizumab | ||
Mean (SD) | 15.2 (10.74) | 13.7 (10.15) |
Median (range) | 13.0 (1.0 to 38.0) | 12.0 (1.0 to 38.0) |
SD = standard deviation; SOC = standard of care.
Source: KEYNOTE-826 Clinical Study Report.5
Efficacy
Only those efficacy outcomes and analyses of subgroups identified in the review protocol are reported in the following. See Appendix 3 for detailed efficacy data.
Health-Related Quality of Life
||||||||||||||||||||||||||||||
A summary of HRQoL as measured by |||||||||||||||||||||||||||||| in patients with PD-L1 with a CPS of 1 or higher is shown in Table 13. Completion rate at baseline was |||||||||||||||| in the pembrolizumab plus SOC arm and |||||||||| in the placebo plus SOC arm |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| respectively |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| patients in the pembrolizumab plus SOC arm was |||||||||||||||||||| and in the placebo plus SOC arm it was ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||, respectively. ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
||||||||||||||||||||
A summary of time to deterioration in |||||||||||||||||||| in patients with PD-L1 with a CPS of 1 or higher is shown in Table 14. There were |||||||||||||||||||||||||||||| in the pembrolizumab plus SOC arm with a median (95% CI) time to deterioration that was ||||||||||||||||||||. In the placebo plus SOC arm there was ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. The HR (95% CI) for the comparison of pembrolizumab plus SOC to placebo plus SOC was ||||||||||||||||||||||||||||||||||||||||.
|||||||||||||||||||||||||||||| patients with PD-L1 with a CPS of 1 or higher is shown in Table 15 |||||||||||||||||||||||||||||||||||||||| in the pembrolizumab plus SOC arm and |||||||||| in the placebo plus SOC arm. ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||, respectively ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. In the pembrolizumab plus SOC arm, the proportion of patients (95% CI) that deteriorated according to |||||||||||||||||||||||||||||||||||||||||||||||||| while the proportion of patients (95% CI) that deteriorated in the placebo plus SOC arm was ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
|||||||||||||||||||||||||||||| A summary of |||||||||||||||||||| for patients with PD-L1 with a CPS of 1 or higher is shown in Table 16 |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| in the pembrolizumab plus SOC arm and |||||||||| in the placebo plus SOC arm. |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| respectively ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. In the pembrolizumab plus SOC arm |||||||||||||||||||||||||||||||||||||||||||||||||| the proportion of patients (95% CI) that deteriorated according to the |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| while the proportion of patients (95% CI) that deteriorated in the placebo plus SOC arm ||||||||||||||||||||||||||||||||||||||||||||||||||. The percent difference for pembrolizumab plus SOC compared to placebo plus SOC for ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
|||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||| | ||
|---|---|---|---|---|
|||||||||||||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
|||||||||||||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
|||||||||||||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
|||||||||||||||||||||||| | ||||
|||||||||||||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
|||||||||||||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
|||||||||||||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| | ||||||||||||| |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Note: This table was redacted at the request of the sponsor.

|||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| |
|---|---|---|
|||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| |
|||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| |
|||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| |
|||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Note: This table was redacted at the request of the sponsor.
|||||||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| | ||
|---|---|---|---|---|
|||||||||||||||||||||||| | |||||||||| | |||||||||||||||||||||||| | |||||||||| | |||||||||||||||||||||||| |
|||||||||||||||||||||||| | |||||||||| | |||||||||||||||||||||||| | |||||||||| | |||||||||||||||||||||||| |
|||||||||||||||||||||||| | |||||||||| | |||||||||||||||||||||||| | |||||||||| | |||||||||||||||||||||||| |
|||||||||||||||||||||||| | |||||||||| | |||||||||||||||||||||||| | |||||||||| | |||||||||||||||||||||||| |
|||||||||||||||||||||||| | |||||||||| | |||||||||||||||||||||||| | |||||||||| | |||||||||||||||||||||||| |
|||||||||||||||||||||||| | |||||||||| | |||||||||||||||||||||||| | |||||||||| | |||||||||||||||||||||||| |
|||||||||||||||||||||||| | |||||||||| | |||||||||||||||||||||||| | |||||||||| | |||||||||||||||||||||||| |
|||||||||||||||||||||||| | |||||||||| | |||||||||||||||||||||||| | |||||||||| | |||||||||||||||||||||||| |
|||||||||||||||||||||||| | |||||||||| | |||||||||||||||||||||||| | |||||||||| | |||||||||||||||||||||||| |
|||||||||||||||||||||||| | |||||||||| | |||||||||||||||||||||||| | |||||||||| | |||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Note: This table was redacted at the request of the sponsor.
|||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| | ||
|---|---|---|---|---|
|||||||||||||||||||||||| | |||||||||| | |||||||||||||||||||||||| | |||||||||| | |||||||||||||||||||||||| |
|||||||||||||||||||||||| | |||||||||| | |||||||||||||||||||||||| | |||||||||| | |||||||||||||||||||||||| |
|||||||||||||||||||||||| | |||||||||| | |||||||||||||||||||||||| | |||||||||| | |||||||||||||||||||||||| |
|||||||||||||||||||||||| | |||||||||| | |||||||||||||||||||||||| | |||||||||| | |||||||||||||||||||||||| |
|||||||||||||||||||||||| | |||||||||| | |||||||||||||||||||||||| | |||||||||| | |||||||||||||||||||||||| |
|||||||||||||||||||||||| | |||||||||| | |||||||||||||||||||||||| | |||||||||| | |||||||||||||||||||||||| |
|||||||||||||||||||||||| | |||||||||| | |||||||||||||||||||||||| | |||||||||| | |||||||||||||||||||||||| |
|||||||||||||||||||||||| | |||||||||| | |||||||||||||||||||||||| | |||||||||| | |||||||||||||||||||||||| |
|||||||||||||||||||||||| | |||||||||| | |||||||||||||||||||||||| | |||||||||| | |||||||||||||||||||||||| |
|||||||||||||||||||||||| | |||||||||| | |||||||||||||||||||||||| | |||||||||| | |||||||||||||||||||||||| |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Note: This table was redacted at the request of the sponsor.


Overall Survival
A summary of OS in patients with PD-L1 with a CPS of 1 or higher is shown in Table 17. At the time of data cut-off there were 118 OS events in the pembrolizumab plus SOC arm and 154 OS events in the placebo plus SOC arm. The median OS was NR (95% CI, 19.8 to NR) in the pembrolizumab plus SOC arm and 16.3 months (95% CI, 14.5 to 19.4) in the placebo plus SOC arm. The HR for OS comparing pembrolizumab plus SOC and placebo plus SOC was 0.65 (95% CI, 0.50 to 0.81) with a P value of 0.0001 (multiplicity adjusted, 1-sided nominal alpha level of 0.0054906). The OS rate at 12 months was 75.5% (95% CI, 69.7% to 80%) in the pembrolizumab plus SOC arm and 63.1% (95% CI, 57% to 68.5%) in the placebo plus SOC arm. The KM curve for OS in patients with PD-L1 with a CPS of 1 or higher is shown in Figure 8. OS results for all-comers (HR = 0.67; 95% CI, 0.54 to 0.84; P = 0.0003; multiplicity adjusted alpha level = 0.0049074) and patients with PD-L1 with a CPS of 10 or higher (HR = 0.61; 95% CI, 0.44 to 0.84; P value = 0.0013; multiplicity adjusted alpha level = 0.0114504), shown in Appendix 3, were statistically significant in favour of pembrolizumab plus SOC.
OS subgroup analysis was conducted and the results for metastasis at initial diagnosis, ECOG PS, and bevacizumab use are shown in Figure 9. For the subgroups based on ECOG PS and bevacizumab use, a benefit was shown in OS for patients receiving pembrolizumab plus SOC over placebo plus SOC regardless of ECOG PS and bevacizumab use. The HR for the comparison of pembrolizumab plus SOC and placebo plus SOC for patients with metastasis at initial diagnosis was 0.88 (95% CI, 0.58 to 1.35), showing no clear benefit, in contrast to the benefit seen in patients with no metastasis at diagnosis.
Table 17: OS in Patients With a CPS of 1 or Higher
Detail | Pembrolizumab plus SOC (n = 273) | SOC (n = 275) |
|---|---|---|
Number of events, n (%) | 118 (43.2) | 154 (56.0) |
Median follow-up, months (range) | 18.3 (0.5 to 29.4) | 16.3 (0.3 to 29.2) |
KM estimatesa | ||
Median (95% CI) | NR (19.8 to NR) | 16.3 (14.5 to 19.4) |
HR vs. control (95% CI)b | 0.64 (0.50 to 0.81) | Reference |
P valuec | 0.0001 | Reference |
OS rate, % (95% CI) | ||
6 months | 91.9 (88.0 to 94.6) | 85.5 (80.7 to 89.1) |
12 months | 75.3 (69.7 to 80.0) | 63.1 (57.0 to 68.5) |
18 months | 60.8 (54.6 to 66.4) | 47.1 (41.0 to 53.0) |
24 months | 53.0 (46.0 to 59.4) | 41.7 (34.9 to 48.2) |
CI = confidence interval; CPS = combined positive score; FIGO = Fédération Internationale de Gynécologie et d’Obstétrique; HR = hazard ratio; KM = Kaplan-Meier; OS = overall survival; NR = not reached; PD-L1 = programmed cell death 1 ligand 1; SOC = standard of care; vs. = versus.
aFrom product-limit (KM) method for censored data.
bBased on Cox regression model with Efron method of tie handling with treatment as a covariate stratified by metastatic at initial diagnosis (FIGO [2009] stage IVB) (yes or no), bevacizumab use (yes or no), and PD-L1 status (CPS < 1, CPS 1 to < 10, or CPS ≥ 10).
cOne-sided P value based on log-rank test stratified by metastatic at initial diagnosis (FIGO stage IVB) (yes or no), bevacizumab use (yes or no), and PD-L1 status (CPS < 1, CPS 1 to < 10, or CPS ≥ 10). Multiplicity adjusted, 1-sided nominal alpha level of 0.0054906.
Source: KEYNOTE-826 Clinical Study Report.5
Figure 8: OS Estimates in Patients With a CPS of 1 or Higher
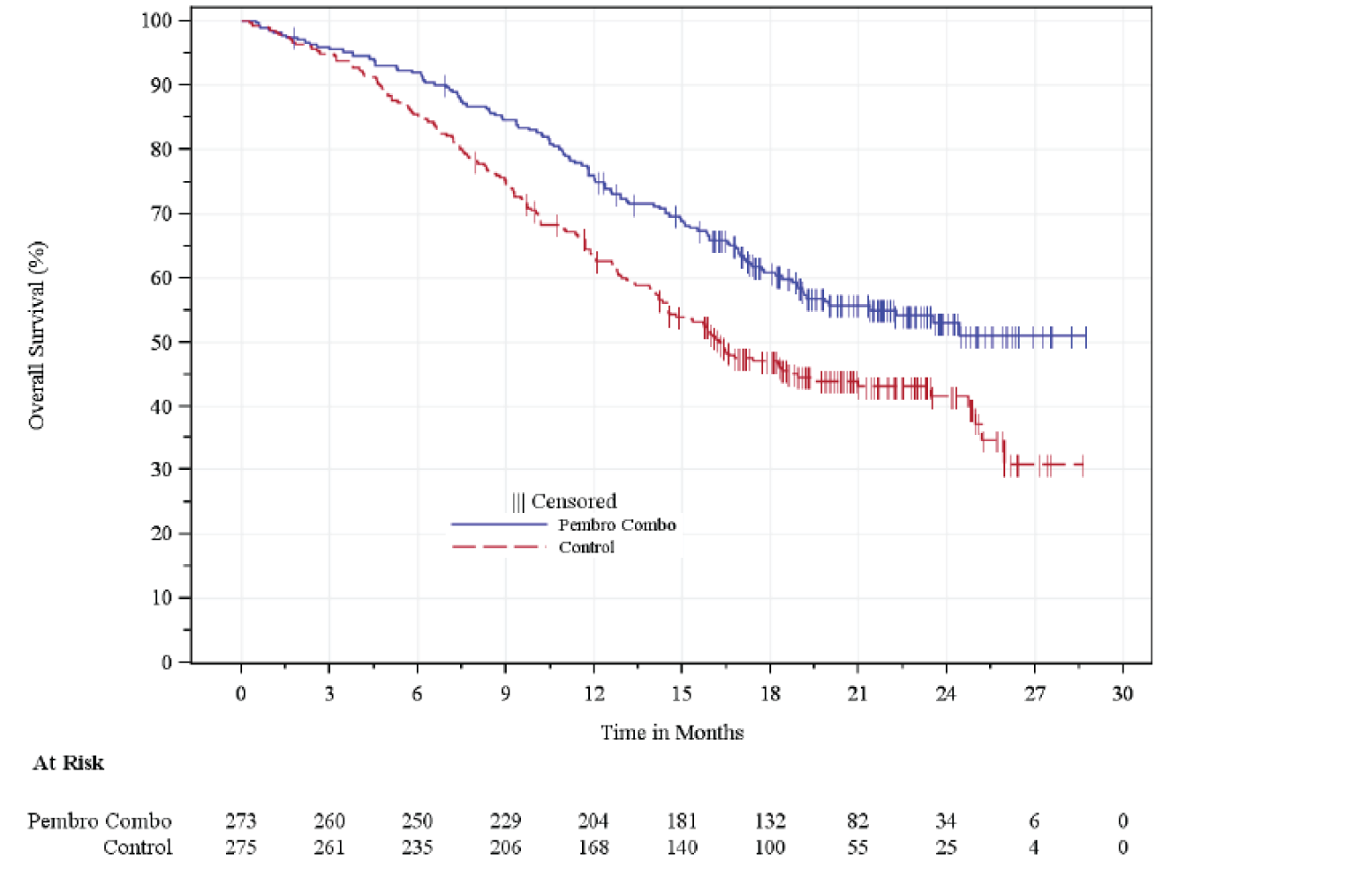
CPS = combined positive score; OS = overall survival; pembro combo = pembrolizumab in combination with SOC
Source: KEYNOTE-826 Clinical Study Report.5
Figure 9: OS in Patients With a CPS of 1 or Higher: Subgroups
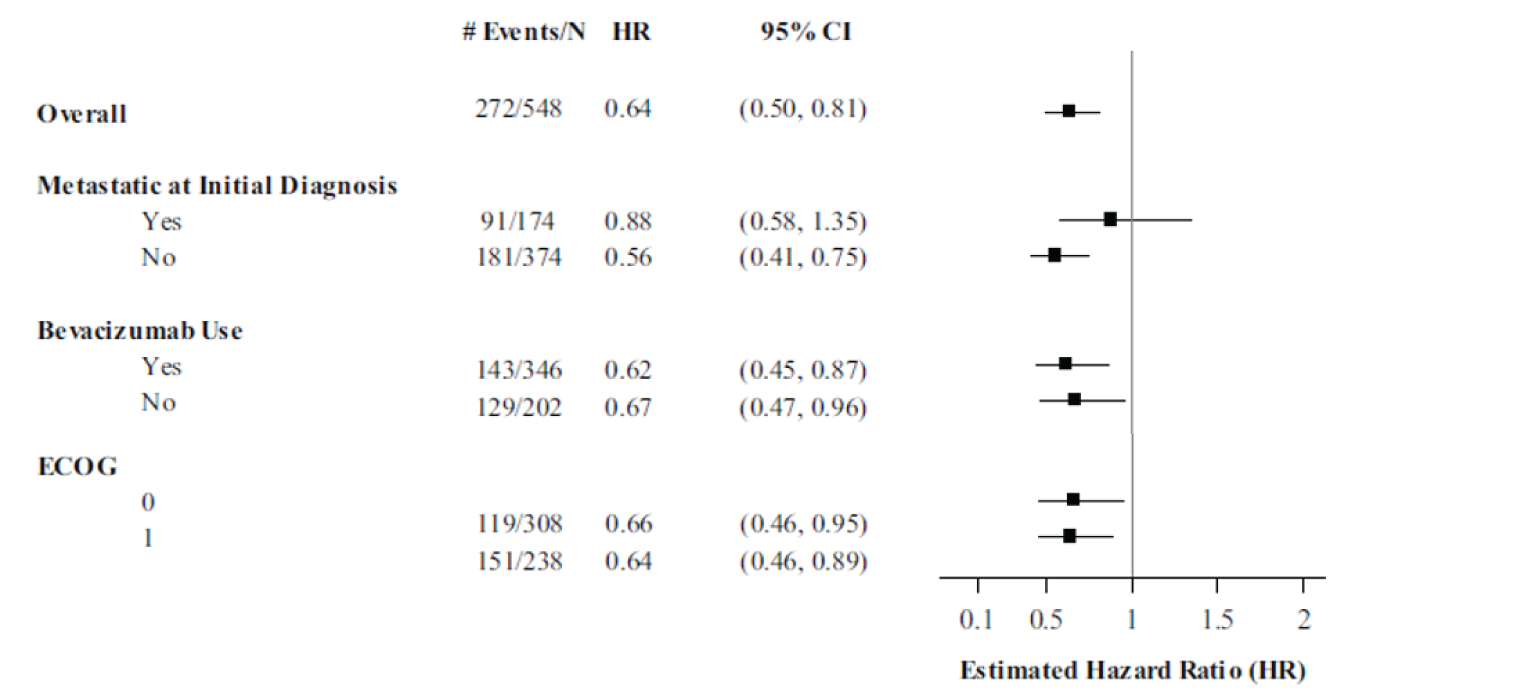
CI = confidence interval; CPS = combined positive score; ECOG = European Cooperative Oncology Group; HR = hazard ratio; OS = overall survival.
Note: Metastasis at diagnosis and bevacizumab use were used as stratification factors in the KEYNOTE-826 study.
Source: KEYNOTE-826 Clinical Study Report.5
Progression-Free Survival
A summary of investigator-assessed PFS in patients with PD-L1 with a CPS of 1 or higher is shown in Table 18. At the time of data cut-off there were 157 PFS events in the pembrolizumab plus SOC arm and 198 OS events in the placebo plus SOC arm. The median PFS was 10.4 months (95% CI, 9.7 to 12.3) in the pembrolizumab plus SOC arm and 8.2 months (95% CI, 6.3 to 8.5). The HR for PFS comparing pembrolizumab plus SOC and placebo plus SOC was 0.62 (95% CI, 0.50 to 0.77) with a P value of less than 0.0001 (multiplicity adjusted, 1-sided nominal alpha level of 0.0014426). The PFS rate at 12 months was 45.5% (95% CI, 39.2% to 51.5%) in the pembrolizumab plus SOC arm and 34.1% (95% CI, 28.3% to 40%) in the placebo plus SOC arm. The KM curve for PFS in patients with PD-L1 with a CPS of 1 or higher is shown in Figure 10. PFS results for BICR PFS in patients with PD-L1 with a CPS of 1 or higher and investigator-assessed all-comers (HR = 0.65; 95% CI, 0.53 to 0.79; P < 0.0001; multiplicity adjusted alpha level = 0.0012843) and patients with PD-L1 with a CPS of 10 or higher (HR = 0.58; 95% CI, 0.44 to 0.77; P < 0.0001; multiplicity adjusted alpha level = 0.0019593), shown in Appendix 3, were statistically significant in favour of pembrolizumab plus SOC. Sensitivity analyses based on PFS censoring rules showed results similar to the primary analysis (data not shown).
Table 18: Investigator-Assessed PFS in Patients With a CPS of 1 or Higher
Detail | Pembrolizumab plus SoC (n = 273) | SoC (n = 275) |
|---|---|---|
Number of events, n (%) | 157 (57.5) | 198 (72.0) |
Deaths | 25 (9.2) | 26 (9.5) |
Documented progression | 132 (48.4) | 172 (62.5) |
KM estimatesa | ||
Median (95% CI) | 10.4 (9.7 to 12.3) | 8.2 (6.3 to 8.5) |
HR vs. control (95% CI)b | 0.62 (0.50 to 0.77) | Reference |
P valuec | < 0.0001 | Reference |
PFS rate, % (95% CI) | ||
6 months | 81.5 (76.2 to 85.7) | 67.1 (61.0 to 72.4) |
12 months | 45.5 (39.2 to 51.5) | 34.1 (28.3 to 40.0) |
18 months | 39.3 (33.2 to 45.4) | 23.8 (18.6 to 29.4) |
24 months | 33.1 (25.7 to 40.7) | 14.0 (7.7 to 22.3) |
CI = confidence interval; CPS = combined positive score; FIGO = Fédération Internationale de Gynécologie et d’Obstétrique; HR = hazard ratio; KM = Kaplan-Meier; PD-L1 = programmed cell death 1 ligand 1; PFS = progression-free survival; SOC = standard of care; vs. = versus.
aFrom product-limit (KM) method for censored data.
bBased on Cox regression model with Efron method of tie handling with treatment as a covariate stratified by metastatic at initial diagnosis (FIGO [2009] stage IVB) (yes or no), bevacizumab use (yes or no), and PD-L1 status (CPS < 1, CPS 1 to < 10, or CPS ≥ 10).
cOne-sided P value based on log-rank test stratified by metastatic at initial diagnosis (FIGO [2009] stage IVB) (yes or no), bevacizumab use (yes or no), and PD-L1 status (CPS < 1, CPS 1 to < 10, or CPS ≥ 10). Multiplicity adjusted, 1-sided nominal alpha level of 0.0014426.
Source: KEYNOTE-826 Clinical Study Report.5
Figure 10: Investigator-Assessed KM Estimates of PFS in Patients With a CPS of 1 or Higher
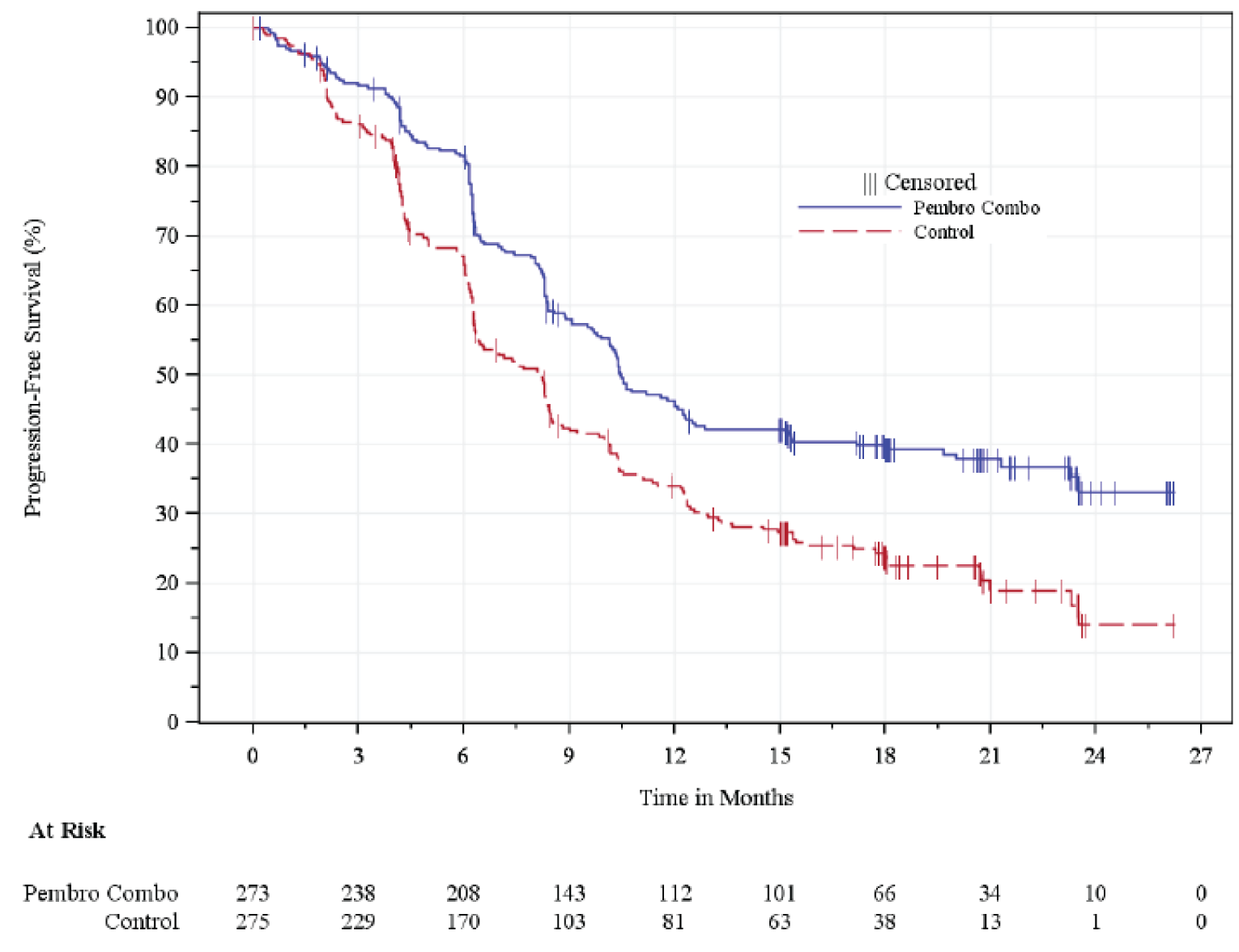
CPS = combined positive score; KM = Kaplan-Meier; pembro combo = pembrolizumab plus SOC; PFS = progression-free survival.
Source: KEYNOTE-826 Clinical Study Report.5
Figure 11: Investigator-Assessed PFS in Patients With a CPS of 1 or Higher — Subgroups
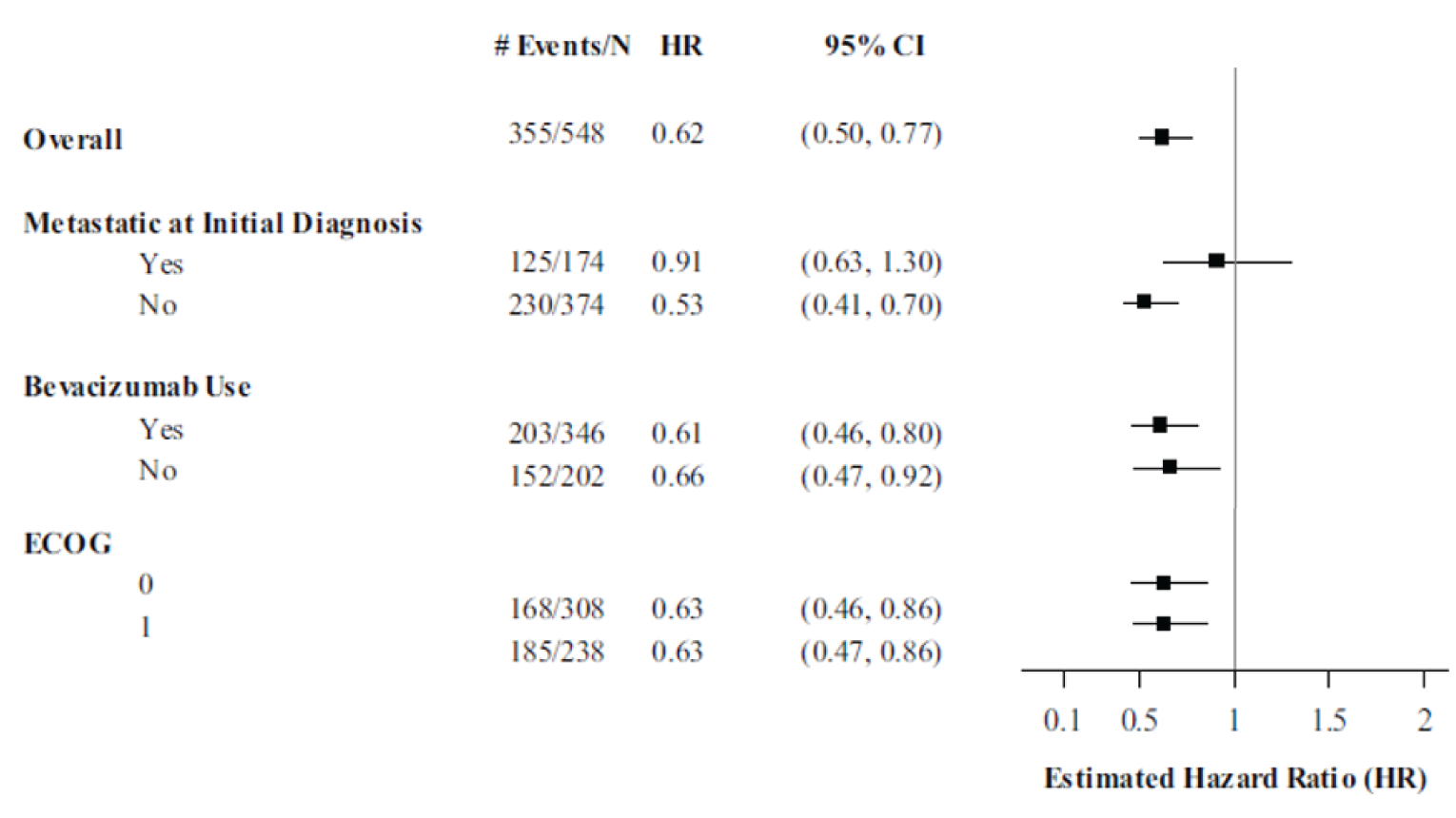
CI = confidence interval; CPS = combined positive score; ECOG = European Cooperative Oncology Group; HR = hazard ratio; PFS = progression-free survival.
Note: Metastasis at diagnosis and bevacizumab use were stratification factors in the KEYNOTE-826 study.
Source: KEYNOTE-826 Clinical Study Report.5
Post-Progression Survival
Post-progression survival was not included in the sponsors clinical submission.
Overall Response Rate
A summary of investigator-assessed ORR in patients with PD-L1 with a CPS of 1 or higher is shown in Table 19. The ORR in the pembrolizumab plus SOC arm was 68.1% (95% CI, 62.2% to 73.6%), including 22.7% of patients who achieved a CR. The ORR in the placebo plus SOC arm was 50.2% (95% CI, 44.1% to 56.2%), including 13.1% of patients who achieved a CR. The difference estimate for pembrolizumab plus SOC compared with placebo plus SOC was 18.0% (95% CI, 10.1% to 25.7%).
Duration of Response
A summary of investigator-assessed DOR in patients with PD-L1 with a CPS of 1 or higher is shown in Table 20. Of the 186 patients in the pembrolizumab plus SOC arm that recorded a response, the median time to response was 2.1 months (range, 1.7 to 20.6). Of the 138 patients in the placebo plus SOC arm that recorded a response, the median time to response was 2.1 months (range, 1.3 to 7.1). The median DOR in patients in the pembrolizumab plus SOC arm was 18.0 months (range, 1.3+ to 24.2+) while the median DOR in patients in the placebo plus SOC arm was 10.4 months (range, 1.5+ to 22.0+), where “+” indicates there is no progressive disease by the time of last disease assessment. The KM curve for investigator-assessed DOR in patients with PD-L1 with a CPS of 1 or higher is shown in Figure 12.
Table 19: Investigator-Assessed ORR in Patients With a CPS of 1 or Higher
Detail | Pembrolizumab plus SOC (n = 273) | SOC (n = 275) |
|---|---|---|
ORR, n (%) | 186 (68.1) | 138 (50.2) |
95% CI | 62.2 to 73.6 | 44.1 to 56.2 |
Difference estimate,a % (95% CI) | 18.0 (10.1 to 25.7) | Reference |
P valueb | < 0.0001 | Reference |
CR (%) | 62 (22.7) | 36 (13.1) |
PR (%) | 124 (45.4) | 102 (37.1) |
Stable disease (%) | 58 (21.2) | 88 (32.0) |
PD (%) | 9 (3.3) | 29 (10.5) |
NE (%) | 1 (0.4) | 2 (0.7) |
No assessment (%) | 19 (7.0) | 18 (6.5) |
CI = confidence interval; CPS = combined positive score; CR = complete response; FIGO = Fédération Internationale de Gynécologie et d’Obstétrique; NE = not evaluable; ORR = overall response rate; PD = progressive disease; PD-L1 = programmed cell death 1 ligand 1; PR = partial response; SOC = standard of care.
aBased on the Miettinen-Nurminen method stratified by metastatic at initial diagnosis (FIGO [2009] stage IVB) (yes or no), bevacizumab use (yes or no), and PD-L1 status (CPS < 1, CPS 1 to < 10, or CPS ≥ 10).
bOne-sided P value for testing not adjusted for multiplicity. H0: difference in percent is equal to 0 vs. H1: difference in percent is greater than 0.
Source: KEYNOTE-826 Clinical Study Report.5
Table 20: Investigator-Assessed DOR in Patients With a CPS of 1 or Higher
Detail | Pembrolizumab plus SOC (n = 273) | SOC (n = 275) |
|---|---|---|
Number of patients with a responsea | 186 | 138 |
Time to response (months) | ||
Mean (SD) | 2.8 (2.1) | 2.4 (0.9) |
Median (range) | 2.1 (1.7 to 20.6) | 2.1 (1.3 to 7.1) |
Response durationb (months) | ||
Median (range) | 18.0 (1.3+ to 24.2+) | 10.4 (1.5+ to 22.0+) |
≥ 6 months | 147 (82.7) | 105 (79.8) |
≥ 12 months | 93 (55.7) | 56 (46.0) |
≥ 18 months | 39 (49.6) | 19 (35.4) |
≥ 24 months | 4 (46.7) | 0 (0.0) |
CPS = combined positive score; DOR = duration of response; SD = standard deviation; SOC = standard of care.
aIncludes participants with best objective response with confirmation as complete response or partial response.
bFrom product-limit (Kaplan-Meier) method for censored data.
Note: “+” indicates there is no progressive disease by the time of last disease assessment.
Source: KEYNOTE-826 Clinical Study Report.5
Figure 12: KM Estimates for DOR in Patients With a CPS of 1 or Higher
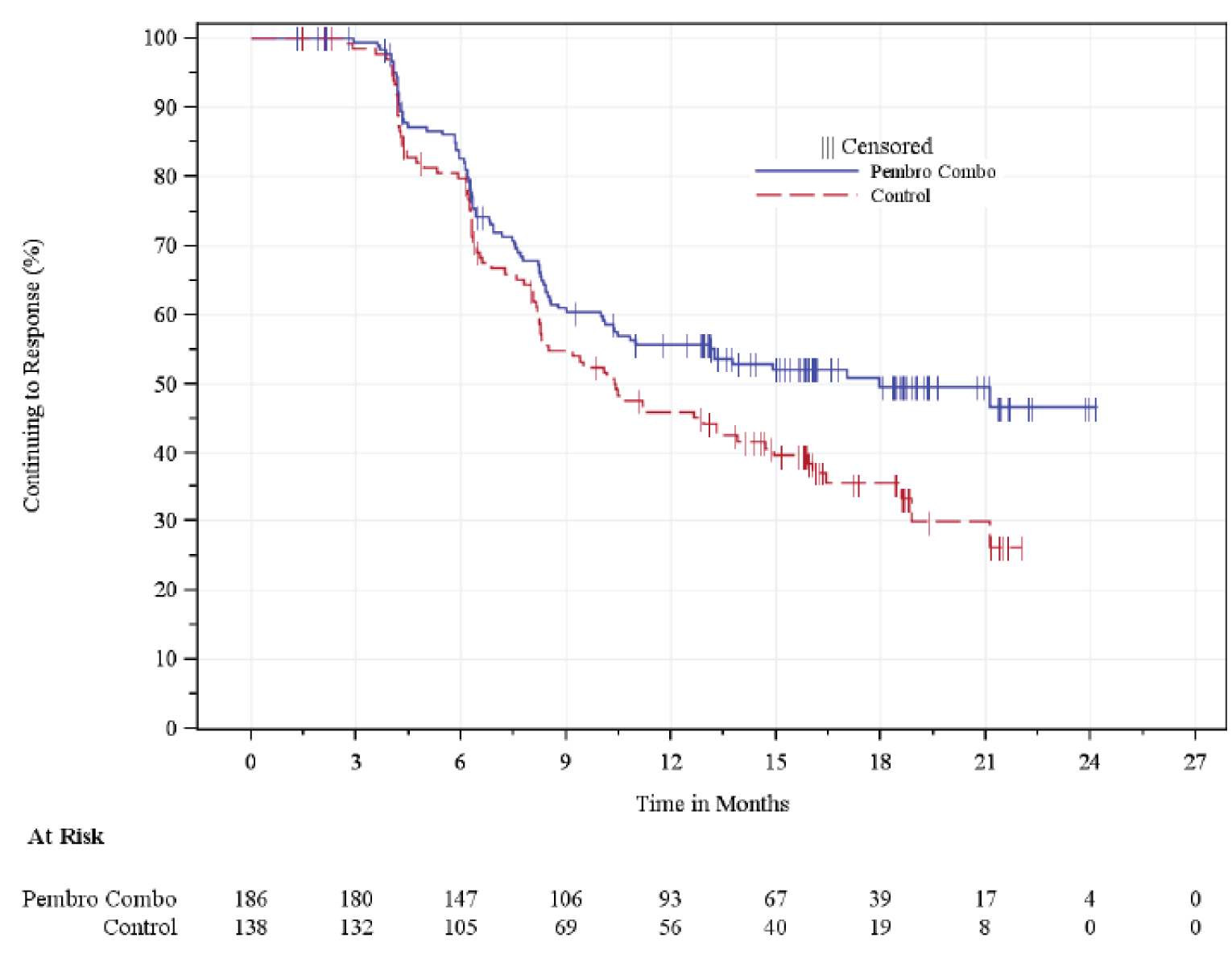
CPS = combined positive score; DOR = duration of response; KM = Kaplan-Meier; pembro combo = pembrolizumab plus SOC.
Source: KEYNOTE-826 Clinical Study Report.5
Harms
Only those harms identified in the review protocol are reported in the following. See Table 21 for detailed harms data.
Adverse Events
In the safety analysis set at the time of data cut-off, 99.3% of patients in the pembrolizumab plus SOC arm and 99.4% of the patients in the placebo plus SOC arm reported treatment-emergent AEs. The most common AEs in the pembrolizumab plus SOC arm were anemia (61.2%), alopecia (56.4%), nausea (39.7%), and diarrhea (35.5%). The most common AEs in the placebo plus SOC arm were alopecia (57.9%), anemia (53.4%), nausea (43.7%), and constipation (33%).
Serious AEs
Serious AEs occurred in 49.8% of patients in the pembrolizumab plus SOC arm and in 42.4% of patients in the placebo plus SOC arm. The most common serious AEs were febrile neutropenia (6.8% in the pembrolizumab plus SOC arm and 4.2% in the placebo plus SOC arm) and urinary tract infection (5.2% in the pembrolizumab plus SOC arm and 5.8% in the placebo plus SOC arm).
Withdrawals Due to AEs
In the pembrolizumab plus SOC arm, 37.5% of patients stopped treatment due to an AE, while 26.5% of patients in the placebo plus SOC arm stopped treatment due to an AE. The most common AEs resulting in treatment discontinuation were peripheral neuropathy (2.3% in the pembrolizumab plus SOC arm and 1.9% in the placebo plus SOC arm), peripheral sensory neuropathy (0.3% in the pembrolizumab plus SOC arm and 2.6% in the placebo plus SOC arm), and female genital tract fistula (2.0% in the pembrolizumab plus SOC arm and 2.3% in the placebo plus SOC arm).
Mortality
Deaths due to AEs occurred in 4.6% of patients in the pembrolizumab plus SOC arm and 4.5% of patients in the placebo plus SOC arm. The most common AEs responsible for patient death were sepsis (0.7% in the pembrolizumab plus SOC arm and 0.3% in the placebo plus SOC arm), and shock hemorrhage (0.7% in the pembrolizumab plus SOC arm); all of these patients had received bevacizumab as part of their treatment regimen.
Notable Harms
The identified notable harms included in the CADTH systematic review with summary data available from the KEYNOTE-826 trial were immune-mediated AEs and infusion reaction. In the pembrolizumab plus SOC arm, immune-mediated AEs occurred in 33.9% of patients with 11.4% of patients reporting grade 3 or higher AEs. In the placebo plus SOC arm, immune-mediated AEs occurred in 15.2% of patients with 2.9% of patients reporting grade 3 or higher AEs. Infusion reactions occurred in 13.4% of patients in the pembrolizumab plus SOC arm, with 2.3% reporting grade 3 or higher infusion reactions. In the placebo plus SOC arm, infusion reactions occurred in 12.6% of patients, with 2.3% reporting grade 3 or higher infusion reactions.
Detail | Pembrolizumab plus SOC (n = 307) | SOC (n = 309) |
|---|---|---|
Patients with ≥ 1 AE | ||
n (%) | 305 (99.3) | 307 (99.4) |
Most common events,a n (%) | ||
Anemia | 188 (61.2) | 165 (53.4) |
Alopecia | 173 (56.4) | 179 (57.9) |
Nausea | 122 (39.7) | 135 (43.7) |
Diarrhea | 109 (35.5) | 92 (29.8) |
Fatigue | 88 (28.7) | 84 (27.2) |
Constipation | 87 (28.3) | 102 (33.0) |
Arthralgia | 82 (26.7) | 80 (25.9) |
Neuropathy peripheral | 81 (26.4) | 79 (25.6) |
Vomiting | 81 (26.4) | 84 (27.2) |
Hypertension | 74 (24.1) | 71 (23.0) |
Urinary tract infection | 73 (23.8) | 80 (25.9) |
Neutropenia | 72 (23.5) | 60 (19.4) |
Peripheral sensory neuropathy | 71 (23.1) | 79 (25.6) |
Asthenia | 63 (20.5) | 66 (21.4) |
Decreased appetite | 61 (19.9) | 52 (16.8) |
Thrombocytopenia | 61 (19.9) | 62 (20.1) |
Myalgia | 57 (18.6) | 59 (19.1) |
Hypothyroidism | 56 (18.2) | 28 (9.1) |
Neutrophil count decreased | 56 (18.2) | 48 (15.5) |
Pyrexia | 55 (17.9) | 44 (14.2) |
Abdominal pain | 50 (16.3) | 53 (17.2) |
Platelet count decreased | 49 (16.0) | 41 (13.3) |
Headache | 48 (15.6) | 57 (18.4) |
Rash | 47 (15.3) | 35 (11.3) |
Patients with ≥ 1 SAE | ||
n (%) | 153 (49.8) | 131 (42.4) |
Most common events,b n (%) | ||
Febrile neutropenia | 21 (6.8) | 13 (4.2) |
Urinary tract infection | 16 (5.2) | 18 (5.8) |
Patients who stopped treatment due to AEs | ||
n (%) | 115 (37.5) | 82 (26.5) |
Most common events,c n (%) | ||
Neuropathy peripheral | 7 (2.3) | 6 (1.9) |
Peripheral sensory neuropathy | 1 (0.3) | 8 (2.6) |
Female genital tract fistula | 6 (2.0) | 7 (2.3) |
Deaths | ||
n (%) | 14 (4.6) | 14 (4.5) |
Most common events,d n (%) | ||
Sepsis | 2 (0.7) | 1 (0.3) |
Shock hemorrhagic | 2 (0.7) | 0 |
Notable harms | ||
Immune-mediated AE, n (%) | 104 (33.9) | 47 (15.2) |
Grade 3 to 5 | 35 (11.4) | 9 (2.9) |
Immune-mediated AE leading to discontinuation of any treatment | 16 (5.2) | 1 (0.3) |
Immune-mediated AE leading to discontinuation of all treatment | 3 (1.3) | 0 (0.0) |
Serious immune-mediated AE | 22 (7.2) | 7 (2.3) |
Deaths | 1 (0.3) | 0 (0.0) |
Infusion reactions, n (%) | 41 (13.4) | 39 (12.6) |
Grade 3 to 5 | 7 (2.3) | 7 (2.3) |
Deaths | 0 | 0 (0.0) |
AE = adverse event; SAE = serious adverse event; SOC = standard of care.
aFrequency of greater than 15%.
bFrequency of greater than 5%.
cFrequency of greater than 2%.
dFrequency of greater than 2 individual patients reporting.
Source: KEYNOTE-826 Clinical Study Report.5
Critical Appraisal
Internal Validity
The KEYNOTE-826 study was a phase III, randomized, double-blind, placebo-controlled, trial. Blinding was conducted appropriately and therefore the risk of bias both in favour and against pembrolizumab was reduced. Patients were randomly assigned to either the active treatment arm or the placebo arm, with randomization stratifications of PD-L1 status (corresponding to the indication of interest of CPS ≥ 1), presence of metastasis at initial diagnosis, and investigator’s decision to use bevacizumab. This randomization framework was appropriate, using stratification factors that the clinical experts consulted considered to be appropriate to mitigate any systematic differences between the 2 populations. The resulting baseline patients’ characteristics and disease characteristics were balanced and did not suggest that the active treatment arm and the placebo arm of the KEYNOTE-826 study would be expected to have systematically different clinical outcomes. Patient disposition did not suggest that there were important differences in study withdrawals that would be expected to bias the results either for or against pembrolizumab; there were low levels of loss to follow-up and withdrawals overall.
The end points assessed in the KEYNOTE-826 study were appropriate and important to patients. The minimally important difference (MID) used to categorize improvement and deterioration in the HRQoL end points in the trial were aligned with published literature. The validity, reliability, and responsiveness, and EORTC QLQ-C30 and EORTC QLQ-CX24 in cervical cancer were confirmed by a literature search conducted by CADTH; however, no evidence was found for EQ-5D-5L suggesting greater uncertainty in this outcome.
The KEYNOTE-826 study formally tested hypotheses for both PFS and OS outcomes in patients with PD-L1 with a CPS of 1 or higher, a CPS of 10 or higher, and all-comers. As this is 6 different hypothesis tests, there is an increased risk of type I error if multiplicity is not adjusted for. The study adequately accounted for multiplicity and the possibility of increased risk of type I error was avoided. The initial 0.05 alpha was prespecified to be allocated between the separate hypotheses for PFS and OS for each PD-L1 population within the study. The study was well powered to detect differences in the co-primary end points. Subgroup analyses were prespecified, and the chosen subgroups were relevant according to the clinical experts consulted, however, the study was not powered to assess differences between subgroups and therefore conclusions cannot be drawn from these data.
The results presented from the KEYNOTE-826 study are from the first interim analysis. While interim analyses can potentially increase the risk of type I error due to multiple analyses, the KEYNOTE-826 protocol prespecified the requirements for triggering the interim analyses and the allocation of alpha spending across the analysis time points. These considerations limit the risk of bias introduced by the interim nature of the presented results. Nevertheless, the OS results are still immature given that there is no estimate for median survival in the pembrolizumab plus SOC arm.
There were multiple protocol amendments that were implemented after patients had already been randomized. The most important protocol amendment was the decision to change the PFS, ORR, and DOR end points from BICR to investigator assessed. The sponsor indicated that this was due to discordance between the BICR assessment and the investigator assessment of these end points. This discordance resulted in a loss of patients to censoring in the BICR analysis, a systematic pattern that, if not addressed, could have impacted the power of the study to detect differences in the PFS end point. When discussed with the clinical experts consulted on this review, there was not any concern that the investigator assessment of radiographic progression would bias the results in either direction, with the clinical experts suggesting that investigator-assessed disease progression is more aligned with the clinical experience. Additionally, the sponsor provided results as per the BICR assessment and the results were consistent with that of the primary analysis.
PFS censoring sensitivity analyses were conducted to determine the robustness of the results to multiple methods of censoring with regards to PFS. Results for the investigator-assessed PFS end point were consistent when assessed according to multiple PFS censoring sensitivity analyses, suggesting that differing censoring rules had little impact on the results.
No secondary outcomes were included in the statistical hierarchy with regards to control of multiplicity concerns and therefore it is not possible to draw conclusions from specific secondary end points. HRQoL was identified as very important to patients and was included as a secondary end point for EORTC QLQ-C30 global status score and an exploratory end point for the EQ-5D-5L and the EORTC QLQ-CX24. The study, however, was not powered to determine differences and had missing data in this end point, resulting in an inability to draw conclusions.
External Validity
The KEYNOTE-826 study population was considered by the clinical experts consulted to be representative and generalizable to the expected Canadian population. The investigated dose of pembrolizumab in the KEYNOTE-826 study was 200 mg every 3 weeks, representing 1 of the options for dosing according to the product monograph, the other option being 400 mg every 6 weeks. There is no evidence from the KEYNOTE-826 study for this second option; however, the clinical experts consulted did not believe there to be a meaningful difference in safety or efficacy between these 2 doses based on extrapolation from other dosing studies.
Similarly, the KEYNOTE-826 study used multiple options for the chemotherapy backbone of the SOC combination. The treatments allowed in the trial were carboplatin or cisplatin, in combination with paclitaxel. It was noted that while this does not represent all available treatment options available to patients, and other chemotherapy options could be used in the Canadian setting, the vast majority of patients receiving chemotherapy for persistent, recurrent, or metastatic cervical cancer receive the options included in the KEYNOTE-826 study. Additionally, the clinical experts consulted did not expect there to be any difference in efficacy if a patient were to receive a chemotherapy agent not included in the KEYNOTE-826 study’s SOC combination provided that the regimen contained a platinum agent and taxane agent.
As discussed in the drug program input, patients that have not experienced disease progression while on treatment with pembrolizumab that subsequently go on to experience disease progression after stopping pembrolizumab treatment are often retreated. While this is common within Canadian jurisdictions, there is no reported evidence from the KEYNOTE-826 study that can be generalized to the use of pembrolizumab in these patients.
Similarly, there are generalizability concerns when considering patients with an ECOG PS of 2 or patients with active CNS metastases. There are no generalizability concerns with regards to background care or concomitant medication.
Discussion
Summary of Available Evidence
The pivotal trial submitted for this review, the KEYNOTE-826 study (N = 617), is a phase III, randomized, double-blind, placebo-controlled trial of pembrolizumab plus SOC compared to placebo plus SOC in patients with persistent, recurrent, or metastatic cervical cancer. The trial included patients regardless of PD-L1 status. As the Health Canada–approved indication is for patients with PD-L1 with a CPS of 1 or higher, this report focuses on the patient population with a CPS of 1 or higher (N = 548). The co-primary end points of the study were investigator-assessed PFS and OS in patients with PD-L1 with a CPS of 1 or higher, a CPS of 10 or higher, and all-comers patients. Patients in the KEYNOTE-826 study had a median age of 51 years in both treatment arms and were mostly of squamous cell histology. A limitation of the study was with regards to the need to change the co-primary end point of PFS from BICR to investigator assessed part way through the study. This was due to a power-related issue with patients systematically lost to censoring in both arms and was not expected to have a major impact on efficacy conclusions.
Interpretation of Results
Efficacy
In the KEYNOTE-826 study, pembrolizumab, when added to SOC, showed a statistically significant benefit in the co-primary end points of PFS and OS when compared to placebo plus SOC in patients with persistent, recurrent, or metastatic cervical cancer with PD-L1 with a CPS of 1 or higher. The median PFS in the pembrolizumab arm was 10.4 months (95% CI, 9.7 to 12.3) compared to 8.2 months (95% CI, 6.3 to 8.5) in the placebo plus SOC arm. This was recognized by the clinical experts as a clinically meaningful difference as well. From the patient input received, OS and HRQoL are the 2 most important outcomes highlighted by patients. OS, being the other co-primary end point, also saw statistically and clinically meaningful benefit with the addition of pembrolizumab to SOC therapy. The median OS in the pembrolizumab arm had not been reached with 43.2% of patients recording an OS event and median OS of 16.3 months (95% CI, 14.5 to 19.4) in the placebo plus SOC arm. While these results are still immature, given median OS has not been reached in the pembrolizumab arm, and with the knowledge that a final analysis of OS is planned in the future, the separation of the OS KM curves suggest that there is a benefit to adding pembrolizumab to SOC therapy with respect to OS.
HRQoL was identified by patients, alongside OS, as a key outcome that is important in the treatment of cervical cancer. The symptoms of cervical cancer can have devastating impacts on the quality of life of the patient. The KEYNOTE-826 study was not powered to detect differences in treatment in HRQoL end points, with only EORTC QLQ-C30 as a secondary end point and other measures of HRQoL included as exploratory end points. Given the lack of formal hypothesis testing and no adjustments for multiplicity, there is little that can be said regarding the impact of the addition of pembrolizumab to SOC therapy. Qualitatively, however, there does not appear to be a deterioration of HRQoL with the addition of pembrolizumab to SOC as the MID for deterioration was not met in any HRQoL end point and some end points suggested a positive change in HRQoL with the addition of pembrolizumab, though these changes are highly uncertain given the reduced number of patients reporting at advanced time points. It was noted by 1 of the clinical experts consulted that deterioration is an important signal in the assessment of pembrolizumab for patients with persistent, recurrent, or metastatic cervical cancer.
Subgroup analyses were conducted, with an ECOG PS (not included as a randomization stratification factor), use of bevacizumab, and metastasis at initial diagnosis of interest for this review. It should be noted, the trial was not powered to detect differences in the subgroups analyzed. For both co-primary end points in the study ECOG PS and the use of bevacizumab did not appear to have an impact of the efficacy of pembrolizumab. For patients that had metastatic disease at initial diagnosis, pembrolizumab appeared to have lower efficacy in PFS and OS. The clinical experts did not expect there to be any reason for pembrolizumab to have less efficacy in these patients with the difference seen in this subgroup possibly owing to the reduced patient numbers resulting in wider CIs and lower precision. Additionally, the subgroup analyzed in the KEYNOTE-826 study was metastatic disease at initial diagnosis, not metastatic disease at the time of treatment initiation, the latter being the more informative subgroup in this population.
The indication under review is for patients with PD-L1 status with a CPS of 1 or higher; however, the KEYNOTE-826 study enrolled patients irrespective of PD-L1 status. It is noted, however, that PD-L1 status (CPS ≥ 1) was a randomization stratification factor and therefore the results for the indication of interest are supported with a randomized subgroup. Prespecified analysis was conducted for PD-L1 with a CPS of 1 or higher, a CPS of 10 or higher, and all-comers, with an ad hoc analysis conducted specifically on patients with a CPS of less than 1. The positive results for the co-primary end points of PFS and OS appeared to be similar for a CPS of 1 or higher, a CPS of 10 or higher, as well as all-comers; however, the ad hoc analysis conducted in patients with a CPS of less than 1 (shown in Appendix 3) suggested a lack of activity of pembrolizumab in those patients, further supporting that pembrolizumab should only be offered to patients with PD-L1 with a CPS of 1 or higher.
Harms
In the KEYNOTE-826 study, the safety profile of pembrolizumab in addition to SOC was comparable to that of placebo plus SOC. AEs and serious AEs occurred in roughly the same proportion in both treatment arms. There were slightly more immune-mediated AEs that occurred with pembrolizumab, which is as expected given the addition of an immunotherapy to the treatment regimen. The additional immune-mediated AEs were expected by the clinical experts consulted for this review to be manageable and would not impact the ability to add pembrolizumab to the treatment regimens of patients with persistent, recurrent, or metastatic cervical cancer. Pembrolizumab has a very well-defined safety profile and is used in many indications; there does not appear to be any evidence that suggests the safety profile of pembrolizumab is any different in persistent, recurrent, or metastatic cervical cancer than other indications where pembrolizumab is recommended for reimbursement.
Conclusions
Evidence from the KEYNOTE-826 trial showed statistically significant and clinically meaningful benefit in PFS and OS with pembrolizumab 200 mg every 3 weeks added to SOC compared to placebo plus SOC in patients with persistent, recurrent, or metastatic cervical cancer with PD-L1 with a CPS of 1 or higher. In the opinion of the clinical experts consulted, the addition of pembrolizumab to chemotherapy (paclitaxel in combination with carboplatin or cisplatin) resulted in additional clinically relevant survival benefit and would likely become the new SOC treatment in this patient population. The secondary end points of ORR and DOR were consistent with the primary analysis. HRQoL was identified from patient input as a key end point important to patients. The KEYNOTE-826 study showed no deterioration in overall HRQoL with the addition of pembrolizumab, and nominal improvements in some HRQoL measures; however, this is highly uncertain given the lack of power to detect differences between treatments and the reduced number of patients at advanced time points. The main evidence gaps are related to the immaturity of the OS data. The clinical experts consulted viewed the safety profile of pembrolizumab as manageable and in line with their expectations based on the extensive experience with pembrolizumab in other oncology indications.
References
1.Marth C, Landoni F, Mahner S, McCormack M, Gonzalez-Martin A, Colombo N. Cervical cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2017;28(suppl_4):iv72-iv83. PubMed
2.Vora C, Gupta S. Targeted therapy in cervical cancer. ESMO Open. 2018;3(Suppl 1):e000462. PubMed
3.Canadian Cancer Statistics. Canadian Cancer Statistics 2021. 2021: https://cdn.cancer.ca/-/media/files/cancer-information/resources/publications/2021-canadian-cancer-statistics-special-report/0835-2976-2021-canadian-cancer-statistics-en.pdf?rev=8e016fe8c5ea4c23b05ea08bf1018ca6&hash=C5BAEC543E496EDD8460CBBF6D44A010&_ga=2.264387983.1077091045.1642544230-447695735.1612384914. Accessed 2022 Aug 3.
4.CADTH. Final Clinical Guidance Report for Bevacizumab (Avastin) for Cervical Cancer. CADTH pan-Canadian Oncology Drug Review. Ottawa: CADTH; 2015: https://www.cadth.ca/sites/default/files/pcodr/pcodr-avastin-cc-fn-cgr.pdf Accessed 2022 Aug 3.
5.Clinical Study Report: P826V01MK3475. A Phase 3 Randomized, Double-Blind, Placebo-Controlled Trial of Pembrolizumab (MK-3475) Plus Chemotherapy Versus Chemotherapy Plus Placebo for the First-Line Treatment of Persistent, Recurrent, or Metastatic Cervical Cancer (KEYNOTE-826) [internal sponsor's report]. NJ, USA: Merck Sharp & Dohme Corp., a Subsidiary of Merck & Co., Inc.; 2021.
6.National Cancer Institute. Cancer Stat Facts: Cervical Cancer (based on 2014-2018 cases and 2015-2019 deaths) https://seer.cancer.gov/statfacts/html/cervix.html Accessed August 3, 2022.
7.Tewari KS, Sill MW, Penson RT, et al. Bevacizumab for advanced cervical cancer: final overall survival and adverse event analysis of a randomised, controlled, open-label, phase 3 trial (Gynecologic Oncology Group 240). Lancet. 2017;390(10103):1654-1663. PubMed
8.NCCN. Cervical Cancer Version 1.2022 — October 26, 2021. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®). Plymouth Meeting (PA): National Comprehensive Cancer Network: https://www.nccn.org/professionals/physician_gls/pdf/cervical.pdf Accessed 2022 Aug 3.
9.Keytruda (pembrolizumab): solution for infusion 100 mg/4 mL vial [product monograph]. Kirkland (QC): Merck Canada Inc.; 2022 Apr 7.
10.Drug Reimbursement Review sponsor submission: Keytruda (pembrolizumab) [internal sponsor's package]. Kirkland (QC): Merck Canada Inc; 2022 May 20.
11.Keytruda® (pembrolizumab) injection, for intravenous use [FDA label]. Whitehouse Station (NJ): Merck Sharp & Dohme Corp.; 2021 Mar: https://www.accessdata.fda.gov/drugsatfda_docs/label/2021/125514s096lbl.pdf Accessed 2022 Aug 3.
12.CADTH. Pembrolizumab (Keytruda). CADTH Reimbursement Recommendation. Ottawa: CADTH; 2021: https://www.cadth.ca/sites/default/files/attachments/2021-07/PC0235%20Keytruda%20-%20CADTH%20Final%20Rec%20revised_1.pdf Accessed 2022 Aug 3.
13.McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 guideline statement. Journal of clinical epidemiology. 2016;75:40-46. PubMed
14.Grey matters: a practical tool for searching health-related grey literature. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/grey-matters. Accessed 2022 Jun 13.
15.Colombo N, Dubot C, Lorusso D, et al. Pembrolizumab for Persistent, Recurrent, or Metastatic Cervical Cancer. N Engl J Med. 2021;385(20):1856-1867. PubMed
16.Aaronson NK, Ahmedzai S, Bergman B, et al. The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst. 1993;85(5):365-376. PubMed
17.Fayers P, Bottomley A, Group EQoL, Quality of Life U. Quality of life research within the EORTC-the EORTC QLQ-C30. European Organisation for Research and Treatment of Cancer. Eur J Cancer. 2002;38 Suppl 4:S125-133. PubMed
18.Liu B, Li L, Wang M, et al. Health-related quality of life in locally advanced cervical cancer patients treated with neoadjuvant therapy followed by radical surgery: A single-institutional retrospective study from a prospective database. Gynecol Oncol. 2019;154(3):583-589. PubMed
19.Osoba D, Rodrigues G, Myles J, Zee B, Pater J. Interpreting the significance of changes in health-related quality-of-life scores. J Clin Oncol. 1998;16(1):139-144. PubMed
20.Paradowska D, Tomaszewski KA, Balajewicz-Nowak M, et al. Validation of the Polish version of the EORTC QLQ-CX24 module for the assessment of health-related quality of life in women with cervical cancer. Eur J Cancer Care (Engl). 2014;23(2):214-220. PubMed
21.Araya LT, Gebretekle GB, Gebremariam GT, Fenta TG. Reliability and validity of the Amharic version of European Organization for Research and Treatment of cervical Cancer module for the assessment of health related quality of life in women with cervical cancer in Addis Ababa, Ethiopia. Health Qual Life Outcomes. 2019;17(1):13. PubMed
22.Sprangers MA, Cull A, Groenvold M, Bjordal K, Blazeby J, Aaronson NK. The European Organization for Research and Treatment of Cancer approach to developing questionnaire modules: an update and overview. EORTC Quality of Life Study Group. Qual Life Res. 1998;7(4):291-300. PubMed
23.Mantegna G, Petrillo M, Fuoco G, et al. Long-term prospective longitudinal evaluation of emotional distress and quality of life in cervical cancer patients who remained disease-free 2-years from diagnosis. BMC Cancer. 2013;13:127. PubMed
24.Maurer W, Bretz F. Multiple Testing in Group Sequential Trials Using Graphical Approaches. Statistics in Biopharmaceutical Research. 2013;5(4):311-320.
25.Fayers PM. Interpreting quality of life data: population-based reference data for the EORTC QLQ-C30. Eur J Cancer. 2001;37(11):1331-1334. PubMed
26.Kim SH, Son BH, Hwang SY, et al. Fatigue and depression in disease-free breast cancer survivors: prevalence, correlates, and association with quality of life. J Pain Symptom Manage. 2008;35(6):644-655. PubMed
27.Kim SH, Kang S, Kim YM, et al. Prevalence and predictors of anxiety and depression among cervical cancer survivors in Korea. International Journal of Gynecological Cancer. 2010;20(6):1017-1024. PubMed
28.Osoba D, Bezjak A, Brundage M, Zee B, Tu D, Pater J. Analysis and interpretation of health-related quality-of-life data from clinical trials: basic approach of The National Cancer Institute of Canada Clinical Trials Group. Eur J Cancer. 2005;41(2):280-287. PubMed
29.Luckett T, King M, Butow P, Friedlander M, Paris T. Assessing health-related quality of life in gynecologic oncology: a systematic review of questionnaires and their ability to detect clinically important differences and change. International Journal of Gynecological Cancer. 2010;20(4):664-684. PubMed
30.EORTC QLC-C30 scoring manual. Brussels (BE): European Organisation for Research and Treatment of Cancer (EORTC); 2001: https://www.eortc.org/app/uploads/sites/2/2018/02/SCmanual.pdf. Accessed 2021 Apr 16.
31.Greimel ER, Kuljanic Vlasic K, Waldenstrom AC, et al. The European Organization for Research and Treatment of Cancer (EORTC) Quality-of-Life questionnaire cervical cancer module: EORTC QLQ-CX24. Cancer. 2006;107(8):1812-1822. PubMed
32.du Toit GC, Kidd M. An analysis of the psychometric properties of the translated versions of the European Organisation for the Research and Treatment of Cancer QLQ CX24 questionnaire in the two South African indigenous languages of Xhosa and Afrikaans. Eur J Cancer Care (Engl). 2016;25(5):832-838. PubMed
33.Hua CH, Guo HM, Guan XL, et al. Validation of the European Organization for Research and Treatment of Cancer cervical cancer module for Chinese patients with cervical cancer. Patient Prefer Adherence. 2013;7:1061-1066. PubMed
34.Singer S, Kuhnt S, Momenghalibaf A, et al. Patients' acceptance and psychometric properties of the EORTC QLQ-CX24 after surgery. Gynecol Oncol. 2010;116(1):82-87. PubMed
35.Du Toit GC, Nel DG. Translation and validation of the EORTC QLQ-CX24 questionnaire into the indigenous African languages of isiXhosa and Afrikaans. Southern African Journal of Gynaecological Oncology. 2012;4(2):59-62.
36.Jayasekara H, Rajapaksa LC, Greimel ER. The EORTC QLQ-CX24 cervical cancer-specific quality of life questionnaire: psychometric properties in a South Asian sample of cervical cancer patients. Psychooncology. 2008;17(10):1053-1057. PubMed
37.Ringash J, O'Sullivan B, Bezjak A, Redelmeier DA. Interpreting clinically significant changes in patient-reported outcomes. Cancer. 2007;110(1):196-202. PubMed
38.Osoba D, Aaronson N, Zee B, Sprangers M, te Velde A. Modification of the EORTC QLQ-C30 (version 2.0) based on content validity and reliability testing in large samples of patients with cancer. The Study Group on Quality of Life of the EORTC and the Symptom Control and Quality of Life Committees of the NCI of Canada Clinical Trials Group. Qual Life Res. 1997;6(2):103-108. PubMed
39.Bedard G, Zeng L, Zhang L, et al. Minimal important differences in the EORTC QLQ-C30 in patients with advanced cancer. Asia Pac J Clin Oncol. 2014;10(2):109-117. PubMed
40.Bjelic-Radisic V, Jensen PT, Vlasic KK, et al. Quality of life characteristics inpatients with cervical cancer. European journal of cancer (Oxford, England: 1990). 2012;48(16):3009-3018.
41.Shin DW, Ahn E, Kim YM, et al. Cross-cultural application of the Korean version of the European Organization for Research and Treatment of Cancer quality of life questionnaire cervical cancer module. Oncology. 2009;76(3):190-198. PubMed
42.Tounkel I, Nalubola S, Schulz A, Lakhi N. Sexual Health Screening for Gynecologic and Breast Cancer Survivors: A Review and Critical Analysis of Validated Screening Tools. Sex Med. 2022;10(2):100498. PubMed
43.Preston NJ, Wilson N, Wood NJ, Brine J, Ferreira J, Brearley SG. Patient-reported outcome measures for use in gynaecological oncology: a systematic review. Bjog. 2015;122(5):615-622. PubMed
44.Tax C, Steenbergen ME, Zusterzeel PL, Bekkers RL, Rovers MM. Measuring health-related quality of life in cervical cancer patients: a systematic review of the most used questionnaires and their validity. BMC Med Res Methodol. 2017;17(1):15. PubMed
45.Brooks R. EuroQol: the current state of play. Health policy (Amsterdam, Netherlands). 1996;37(1):53-72. PubMed
46.EuroQol Group. EuroQol--a new facility for the measurement of health-related quality of life. Health policy (Amsterdam, Netherlands). 1990;16(3):199-208. PubMed
47.Ameri H, Yousefi M, Yaseri M, Nahvijou A, Arab M, Akbari Sari A. Mapping the cancer-specific QLQ-C30 onto the generic EQ-5D-5L and SF-6D in colorectal cancer patients. Expert rev. 2019;19(1):89-96.
48.Sinnott PL, Joyce VR, Barnett PG. Guidebook: preference measurement in economic analysis. Menlo Park (CA): Health Economics Research Center; 2007: https://www.herc.research.va.gov/files/BOOK_419.pdf. Accessed 2020 Oct 13.
Appendix 1: Literature Search Strategy
Note that this appendix has not been copy-edited.
Clinical Literature Search
Overview
Interface: Ovid
Databases:
MEDLINE All (1946-present)
Embase (1974-present)
Note: Subject headings and search fields have been customized for each database. Duplicates between databases were removed in Ovid.
Date of search: June 20, 2022
Alerts: Bi-weekly search updates until project completion
Search filters applied: No filters applied
Limits:
Conference abstracts: excluded
Syntax | Description |
|---|---|
/ | At the end of a phrase, searches the phrase as a subject heading |
MeSH | Medical Subject Heading |
.fs | Floating subheading |
exp | Explode a subject heading |
* | Before a word, indicates that the marked subject heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings |
# | Truncation symbol for one character |
? | Truncation symbol for one or no characters only |
adj# | Requires terms to be adjacent to each other within # number of words (in any order) |
.ti | Title |
.ot | Original title |
.ab | Abstract |
.hw | Heading word; usually includes subject headings and controlled vocabulary |
.kf | Keyword heading word |
.dq | Candidate term word (Embase) |
.pt | Publication type |
.mp | Mapped term |
.rn | Registry number |
.nm | Name of substance word (MEDLINE) |
.yr | Publication year |
.jw | Journal title word (MEDLINE) |
.jx | Journal title word (Embase) |
freq=# | Requires terms to occur # number of times in the specified fields |
medall | Ovid database code: MEDLINE All, 1946 to present, updated daily |
oemezd | Ovid database code; Embase, 1974 to present, updated daily |
cctr | Ovid database code; Cochrane Central Register of Controlled Trials |
Multi-Database Strategy
# Searches
(Keytruda* or pembrolizumab* or lambrolizumab* or MK 3475 or MK3475 or Merck 3475 or Merck3475 or HSDB 8257 or HSDB8257 or Sch 900475 or Sch900475 or DPT0O3T46P).ti,ab,kf,ot,hw,rn,nm.
Uterine Cervical Neoplasms/
((cervic* or cervix* or endocervic* or endocervix*) and (precancer* or cancer* or neoplas* or dysplas* or dyskaryos* or tumor* or tumour* or malignan* or carcinoma* or adenocarcinoma* or lesion* or squamous or small cell or large cell or oncolog*)).ti,ab,kf.
2 or 3
1 and 4
5 use medall
*pembrolizumab/
(Keytruda* or pembrolizumab* or lambrolizumab* or MK 3475 or MK3475 or Merck 3475 or Merck3475 or HSDB 8257 or HSDB8257 or Sch 900475 or Sch900475).ti,ab,kf,dq.
7 or 8
exp uterine cervix tumor/
((cervic* or cervix* or endocervic* or endocervix*) and (precancer* or cancer* or neoplas* or dysplas* or dyskaryos* or tumor* or tumour* or malignan* or carcinoma* or adenocarcinoma* or lesion* or squamous or small cell or large cell or oncolog*)).ti,ab,kf,dq.
10 or 11
9 and 12
13 not (conference abstract or conference review).pt.
14 use oemezd
6 or 15
remove duplicates from 16
Clinical Trials Registries
ClinicalTrials.gov
Produced by the US National Library of Medicine. Targeted search used to capture registered clinical trials.
[Search -- (Keytruda* OR pembrolizumab* OR lambrolizumab* OR "MK 3475" OR MK3475 OR "Merck 3475" OR Merck3475 OR "HSDB 8257" OR HSDB8257 OR "Sch 900475" OR Sch900475) AND (cervical OR cervix OR endocervical OR endocervix) NOT "Head and Neck")]
WHO International Clinical Trials Registry Platform
International Clinical Trials Registry Platform, produced by the World Health Organization. Targeted search used to capture registered clinical trials.
[Search terms -- (Keytruda* OR pembrolizumab* OR lambrolizumab* OR "MK 3475" OR MK3475 OR "Merck 3475" OR Merck3475 OR "HSDB 8257" OR HSDB8257 OR "Sch 900475" OR Sch900475) AND (cervical OR cervix OR endocervical OR endocervix) NOT "Head and Neck")]]
Health Canada’s Clinical Trials Database
Produced by Health Canada. Targeted search used to capture registered clinical trials.
[Search terms -- Keytruda* OR pembrolizumab* OR lambrolizumab* OR "MK 3475" OR MK3475 OR "Merck 3475" OR Merck3475 OR "HSDB 8257" OR HSDB8257 OR "Sch 900475" OR Sch900475) AND (cervical OR cervix OR endocervical OR endocervix]
EU Clinical Trials Register
European Union Clinical Trials Register, produced by the European Union. Targeted search used to capture registered clinical trials.
[Search terms -- (Keytruda* OR pembrolizumab* OR lambrolizumab* OR "MK 3475" OR MK3475 OR "Merck 3475" OR Merck3475 OR "HSDB 8257" OR HSDB8257 OR "Sch 900475" OR Sch900475) AND (cervical OR cervix OR endocervical OR endocervix) NOT "head and neck"]
Grey Literature
Search dates: June 7, 2022 – June 14, 2022
Keywords: Keytruda* OR pembrolizumab* OR lambrolizumab* OR "MK 3475" OR MK3475 OR "Merck 3475" OR Merck3475 OR "HSDB 8257" OR HSDB8257 OR "Sch 900475" OR Sch900475) AND (cervical OR cervix OR endocervical OR endocervix)
Limits: None
Updated: Search updated prior to the completion of stakeholder feedback period
Relevant websites from the following sections of the CADTH grey literature checklist Grey Matters: A Practical Tool for Searching Health-Related Grey Literature were searched:
Health Technology Assessment Agencies
Health Economics
Clinical Practice Guidelines
Drug and Device Regulatory Approvals
Advisories and Warnings
Drug Class Reviews
Clinical Trials Registries
Databases (free)
Health Statistics
Internet Search
Open Access Journals
Appendix 2: Excluded Studies
Note that this appendix has not been copy-edited.
Reference | Reason for exclusion |
|---|---|
Colombo N et al. Pembrolizumab plus chemotherapy versus placebo plus chemotherapy for persistent, recurrent, or metastatic cervical cancer: randomized, double-blind, phase III KEYNOTE-826 study. ESMO Congress 2021, Abstract LBA2 | Abstract, duplicate of included study |
Colombo N, Dubot C, Lorusso D, et al. Pembrolizumab for Persistent, Recurrent, or Metastatic Cervical Cancer. N Engl J Med. 2021;385(20):1856-1867. | Duplicate of included study |
Appendix 3: Detailed Outcome Data
Note that this appendix has not been copy-edited.
HRQoL
||||||||||||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||| | ||
|---|---|---|---|---|
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Note: This table was redacted at the request of the sponsor.
||||||||||||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||| | ||
|---|---|---|---|---|
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Note: This table was redacted at the request of the sponsor.
||||||||||||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||| | ||
|---|---|---|---|---|
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | ||||
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Note: This table was redacted at the request of the sponsor.
||||||||||||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||| | ||
|---|---|---|---|---|
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | ||||
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Note: This table was redacted at the request of the sponsor.
||||||||||||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||| |
|---|---|---|
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Note: This table was redacted at the request of the sponsor.
||||||||||||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||| | ||
|---|---|---|---|---|
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Note: This table was redacted at the request of the sponsor.
||||||||||||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||| | ||
|---|---|---|---|---|
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Note: This table was redacted at the request of the sponsor.
Overall Survival
Detail | Pembrolizumab + SOC (N = 308) | SOC (N = 309) |
|---|---|---|
Number of events, n (%) | 138 (44.8) | 174 (56.3) |
KM estimatesa | ||
Median (95% CI) | 24.4 (19.2, NR) | 16.5 (14.5, 19.4) |
HR vs control (95% CI)b | 0.67 (0.54, 0.84) | Reference |
P valuec | 0.0003 | Reference |
OS rate, % (95% CI) | ||
6 months | 90.5 (86.7, 93.3) | 86.7 (82.4, 90.1) |
12 months | 74.8 (69.5, 79.3) | 63.6 (57.9, 68.7) |
18 months | 60.2 (54.3, 65.5) | 48.3 (42.6, 53.9) |
24 months | 50.4 (43.8, 56.6) | 40.4 (34.0, 46.6) |
CI = confidence interval; HR = hazard ratio; KM = Kaplan-Meier; NR = not reached; OS = overall survival.
aFrom product-limit (KM) method for censored data.
bBased on Cox regression model with the Efron method of tie handling with treatment as a covariate stratified by metastatic at initial diagnosis (FIGO [2009] stage IVB) (yes or no), bevacizumab use (yes or no) and PD-L1 status (CPS <1, CPS 1 to <10, CPS >= 10).
cOne-sided P value based on log-rank test stratified by metastatic at initial diagnosis (FIGO stage IVB) (yes or no), bevacizumab use (yes or no) and PD-L1 status (CPS <1, CPS 1 to <10, CPS >=10). Multiplicity adjusted alpha level of 0.0049074.
Source: KEYNOTE-826 CSR5
Table 32: OS in Patients With a CPS of 10 or Higher
Detail | Pembrolizumab + SOC (N = 158) | SOC (N = 159) |
|---|---|---|
Number of events, n (%) | 66 (41.8) | 88 (55.3) |
KM estimatesa | ||
Median (95% CI) | NR (19.1, NR) | 16.4 (14.0, 25.0) |
HR vs control (95% CI)b | 0.61 (0.44, 0.84) | Reference |
P valuec | 0.0013 | Reference |
OS rate, % (95% CI) | ||
6 months | 91.7 (86.2, 95.1) | 84.9 (78.3, 89.6) |
12 months | 75.7 (68.2, 81.7) | 61.5 (53.4, 68.6) |
18 months | 61.2 (52.9, 68.5) | 48.4 (40.2, 56.1) |
24 months | 54.4 (45.5, 62.4) | 44.6 (36.3, 52.5) |
CI = confidence interval; HR = hazard ratio; KM = Kaplan-Meier; NR = not reached; OS = overall survival.
aFrom product-limit (KM) method for censored data.
bBased on Cox regression model with the Efron method of tie handling with treatment as a covariate stratified by metastatic at initial diagnosis (FIGO [2009] stage IVB) (yes or no), bevacizumab use (yes or no) and PD-L1 status (CPS <1, CPS 1 to <10, CPS >=10).
cOne-sided P value based on log-rank test stratified by metastatic at initial diagnosis (FIGO stage IVB) (yes or no), bevacizumab use (yes or no) and PD-L1 status (CPS <1, CPS 1 to <10, CPS >=10). Multiplicity adjusted alpha level of 0.0114504.
Source: KEYNOTE-826 CSR5
Table 33: OS in Post Hoc of a CPS of Less Than 1 Population
Detail | Pembrolizumab + SOC (N = 35) | SOC (N = 34) |
|---|---|---|
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | ||
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
HR vs control (95% CI)b | 1.00 (0.53, 1.89) | Reference |
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | ||
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
CI = confidence interval; HR = hazard ratio; |||||||||||||||||||||||||||||||||; OS = overall survival.
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
bBased on Cox regression model with the Efron method of tie handling with treatment as a covariate stratified by metastatic at initial diagnosis (FIGO [2009] stage IVB) (yes or no), bevacizumab use (yes or no) and PD-L1 status (CPS <1, CPS 1 to <10, CPS >=10).
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Source: KEYNOTE-826 CSR5
Progression-Free Survival
Table 34: BICR-Assessed PFS in Patients With a CPS of 1 or Higher
Detail | Pembrolizumab + SOC (N = 273) | SOC (N = 275) |
|---|---|---|
Number of events, n (%) | 139 (50.9) | 178 (64.7) |
Deaths | 32 (11.7) | 33 (12.0) |
Documented progression | 107 (39.2) | 145 (52.7) |
KM estimatesa | ||
Median (95% CI) | 12.8 (10.4, 20.6) | 8.3 (7.7, 9.2) |
HR vs control (95% CI)b | 0.60 (0.48, 0.75) | Reference |
P valuec | <0.0001 | Reference |
PFS rate, % (95% CI) | ||
6 months | 81.0 (75.6, 85.3) | 71.5 (65.5, 76.7) |
12 months | 53.0 (46.5, 59.0) | 35.8 (29.6, 42.0) |
18 months | 44.5 (38.1, 50.8) | 24.7 (19.1, 30.7) |
24 months | 39.3 (32.2, 46.4) | 20.8 (14.8, 27.6) |
CI = confidence interval; HR = hazard ratio; KM = Kaplan-Meier; PFS = progression-free survival.
aFrom product-limit (KM) method for censored data.
bBased on Cox regression model with the Efron method of tie handling with treatment as a covariate stratified by metastatic at initial diagnosis (FIGO [2009] stage IVB) (yes or no), bevacizumab use (yes or no) and PD-L1 status (CPS <1, CPS 1 to <10, CPS >=10).
cOne-sided P value based on log-rank test stratified by metastatic at initial diagnosis (FIGO [2009] stage IVB) (yes or no), bevacizumab use (yes or no) and PD-L1 status (CPS <1, CPS 1 to <10, CPS >=10). Nominal, not adjusted for multiplicity.
Source: KEYNOTE-826 CSR5
Table 35: Investigator-Assessed PFS in All-Comers
Detail | Pembrolizumab + SOC (N = 308) | SOC (N = 309) |
|---|---|---|
Number of events, n (%) | 180 (58.4) | 226 (73.1) |
Deaths | 27 (8.8) | 27 (8.7) |
Documented progression | 153 (49.7) | 199 (64.4) |
KM estimatesa | ||
Median (95% CI) | 10.4 (9.1, 12.1) | 8.2 (6.4, 8.4) |
HR vs control (95% CI)b | 0.65 (0.53, 0.79) | Reference |
P valuec | <0.0001 | Reference |
PFS rate, % (95% CI) | ||
6 months | 80.5 (75.4, 84.6) | 68.5 (62.8, 73.4) |
12 months | 44.7 (38.8, 50.4) | 33.5 (28.0, 39.1) |
18 months | 38.0 (32.3, 43.7) | 21.7 (16.9, 26.9) |
24 months | 31.6 (24.7, 38.8) | 12.8 (7.0, 20.4) |
CI = confidence interval; HR = hazard ratio; KM = Kaplan-Meier; PFS = progression-free survival.
aFrom product-limit (KM) method for censored data.
bBased on Cox regression model with the Efron method of tie handling with treatment as a covariate stratified by metastatic at initial diagnosis (FIGO [2009] stage IVB) (yes or no), bevacizumab use (yes or no) and PD-L1 status (CPS <1, CPS 1 to <10, CPS >=10).
cOne-sided P value based on log-rank test stratified by metastatic at initial diagnosis (FIGO [2009] stage IVB) (yes or no), bevacizumab use (yes or no) and PD-L1 status (CPS <1, CPS 1 to <10, CPS >=10). Multiplicity adjusted alpha level of 0.0012843.
Source: KEYNOTE-826 CSR5
Table 36: Investigator-Assessed PFS in Patients With a CPS of 10 or Higher
Detail | Pembrolizumab + SOC (N = 158) | SOC (N = 159) |
|---|---|---|
Number of events, n (%) | 87 (55.1) | 116 (73.0) |
Deaths | 16 (10.1) | 16 (10.1) |
Documented progression | 71 (44.9) | 100 (62.9) |
KM estimatesa | ||
Median (95% CI) | 10.4 (8.9, 15.1) | 8.1 (6.2, 8.8) |
HR vs control (95% CI)b | 0.58 (0.44, 0.77) | Reference |
P valuec | <0.0001 | Reference |
PFS rate, % (95% CI) | ||
6 months | 84.6 (77.7, 89.5) | 64.7 (56.5, 71.8) |
12 months | 44.6 (36.3, 52.5) | 33.5 (25.9, 41.2) |
18 months | 40.6 (32.4, 48.6) | 22.2 (15.6, 29.4) |
24 months | 35.8 (26.4, 45.3) | NR (NR, NR) |
CI = confidence interval; HR = hazard ratio; KM = Kaplan-Meier; PFS = progression-free survival.
aFrom product-limit (KM) method for censored data.
bBased on Cox regression model with the Efron method of tie handling with treatment as a covariate stratified by metastatic at initial diagnosis (FIGO [2009] stage IVB) (yes or no), bevacizumab use (yes or no) and PD-L1 status (CPS <1, CPS 1 to <10, CPS >=10).
cOne-sided P value based on log-rank test stratified by metastatic at initial diagnosis (FIGO [2009] stage IVB) (yes or no), bevacizumab use (yes or no) and PD-L1 status (CPS <1, CPS 1 to <10, CPS >=10). Multiplicity adjusted alpha level of 0.0019593.
Source: KEYNOTE-826 CSR5
Table 37: Investigator-Assessed PFS in Post Hoc of a CPS of Less Than 1 Population
Detail | Pembrolizumab + SOC (N = 35) | SOC (N = 34) |
|---|---|---|
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | ||
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
HR vs control (95% CI)b | 0.94 (0.52, 1.70) | Reference |
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | ||
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||| | |||||||||| | ||||||||||||||||||||||||||||||||| |
CI = confidence interval; HR = hazard ratio; ||||||||||||||||||||||||||||||||||||||||||||||||||||||; PFS = progression-free survival.
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
bBased on Cox regression model with the Efron method of tie handling with treatment as a covariate stratified by metastatic at initial diagnosis (FIGO [2009] stage IVB) (yes or no), bevacizumab use (yes or no) and PD-L1 status (CPS <1, CPS 1 to <10, CPS >=10).
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Source: KEYNOTE-826 CSR5
Overall Response Rate
Table 38: Investigator-Assessed ORR in Patients With a CPS of 10 or Higher and All-Comers
Detail | Pembrolizumab + SO | SOC |
|---|---|---|
All-comers, N | 308 | 309 |
ORR, n (%) | 203 (65.9) | 157 (50.8) |
(95% CI) | (60.3, 71.2) | (45.1, 56.5) |
Difference estimatea, % (95% CI) | 15.3 (7.8, 22.6) | Reference |
P valueb | <0.0001 | Reference |
CPS ≥10, N | 158 | 159 |
ORR, n (%) | 110 (69.6) | 78 (49.1) |
(95% CI) | (61.8,76.7) | (41.1,57.1) |
Difference estimate, % (95% CI) | 20.5 (10.1,30.5) | Reference |
P value | 0.0001 | Reference |
CI = confidence interval; CPS = combined positive score; ORR = overall response rate.
aBased on the Miettinen-Nurminen method stratified by metastatic at initial diagnosis (FIGO [2009] stage IVB) (yes or no), bevacizumab use (yes or no) and PD-L1 status (CPS <1, CPS 1 to <10, CPS >=10).
bOne-sided P value for testing. H0: difference in % = 0 versus H1: difference in % > 0. Nominal, not adjusted for multiplicity.
Source: KEYNOTE-826 CSR5
Duration of Response
Detail | Pembrolizumab + SOC (N = 308) | SOC (N = 309) |
|---|---|---|
Number of patients with a responsea | 203 | 157 |
Time to response (months) | ||
Mean (SD) | 2.8 (2.0) | 2.4 (1.0) |
Median (Range) | 2.1 (1.7, 20.6) | 2.1 (1.3, 8.8) |
Response Durationb (Months) | ||
Median (Range) | 18.0 (1.3+, 24.2+) | 10.4 (1.5+, 22.0+) |
≥6 months | 161 (82.6) | 119 (80.7) |
≥12 months | 101 (55.0) | 63 (46.3) |
≥18 months | 43 (49.4) | 19 (31.9) |
≥24 months | 4 (45.5) | 0 |
SD = standard deviation.
aIncludes participants with best objective response with confirmation as complete response or partial response.
bFrom product-limit (Kaplan-Meier) method for censored data.
Note: “+” indicates there is no progressive disease by the time of last disease assessment.
Source: KEYNOTE-826 CSR5
Table 40: DOR in Patients With a CPS of 10 or Higher
Detail | Pembrolizumab + SOC (N = 158) | SOC (N = 159) |
|---|---|---|
Number of patients with a responsea | 110 | 78 |
Time to response (months) | ||
Mean (SD) | 2.6 (1.2) | 2.4 (1.0) |
Median (Range) | 2.2 (1.7, 8.4) | 2.1 (1.3, 7.1) |
Response Durationb (Months) | ||
Median (Range) | 21.1 (1.3+, 24.2+) | 9.4 (2.1+, 21.5+) |
≥6 months | 88 (83.8) | 58 (76.6) |
≥12 months | 56 (58.3) | 31 (43.9) |
≥18 months | 21 (53.3) | 6 (31.6) |
≥24 months | 3 (48.5) | 0 |
SD = standard deviation.
aIncludes participants with best objective response with confirmation as complete response or partial response.
bFrom product-limit (Kaplan-Meier) method for censored data.
Note: “+” indicates there is no progressive disease by the time of last disease assessment.
Source: KEYNOTE-826 CSR5
Appendix 4: Description and Appraisal of Outcome Measures
Note that this appendix has not been copy-edited.
Aim
To describe the following outcome measures and review their measurement properties (validity, reliability, responsiveness to change, and MID):
EORTC QLQ-C30
EORTC QLQ-CX24
EQ-5D-5L
Findings
Table 41: Summary of Outcome Measures and Their Measurement Properties
Outcome Measure | Type | Conclusions about Measurement Properties | MID |
|---|---|---|---|
EORTC QLQ-C30 | A 30-item, patient-reported, cancer-specific, quality of life questionnaire using 4- and 7-point Likert scales. | Validity, Reliability, and Responsiveness: The psychometric properties of EORTC QLQ-C30 have been validated among general cancer patients, demonstrating validity and reliability.16 Convergent validity, discriminant validity, internal consistency, and clinical validity have been assessed in cervical cancer patients along with its cervical cancer-specific module EORTC QLQ-CX24.20,21 Since the EORTC QLQ-CX24 addresses specific HRQoL aspects for cervical cancer patients that are not evaluated by the core EORTC QLQ-C30 scale, and the strong correlations and clinical overlapping between the EORTC QLQ-CX24 and the EORTC QLQ-C30 scales assessing similar elements (e.g., for symptom experience scale, r = -0.31-(-0.55), p <0.0001) signifies the necessity to use both questionnaires together.20,21 | On a 0-100 scale, if <34 for functioning scales, it is considered as clinically significant functional problem. If ≥66 for symptoms, it is considered as clinically significant symptoms.25-27 10% was selected as a threshold for assessing EORTC QLQ-C30’s ability to detect MCID based on the recommendation of the National Cancer Institute of Canada Clinical Trials Group,28 and based on the fact that this value is within the range of estimates for the most commonly used questionnaires for cancer patients.29 The research estimates for MCID for the EORTC QLQ-C30 ranges from 5% to 20%.29,30 A ≥ 10 points difference in HRQoL scores (on a 0–100 scale) was considered to be clinically relevant evaluating HRQoL using both EORTC QLQ-C30 along with its cervical cancer module CX-24.18,19 |
EORTC QLQ-CX24 | Generic scale that measures patient- 1-week recall | Validity, Reliability, and Responsiveness: Cronbach α: 0.72 to 0.87 (during initial development phase),31 0.81–0.88,20 0.70–0.84,21 0.73 to 0.81,32 0.73 to 0.76,32 0.71-0.82,33 0.70 to 0.87,34 showing positive internal consistency. Interclass correlation coefficient (ICC): 0.85-0.89, proving test-retest reliability.20 Adequate convergent and discriminant validity.21,31,33,35 Weak to strong correlation between EORTC QLQ-C30 subscales and EORTC QLQ-CX24 subscales, indicating concurrent validity.21 A statistically significant (r = 0.52–0.58, p < 0.0.01) inter-scale correlations indicate construct validity.36 Ability to discriminate between subgroups of patients (e.g., performance status, cancer stage and treatment status), indicating clinical validity.21,31-34,36 | In its initial development, the EORTC QLQ-CX24 symptom experience scale and the body image scale revealed significant clinical differences (> 10 points) between patients with different FIGO stages.31 On a 0-100 scale, if <34 for functioning scales, it is considered as clinically significant functional problem. If ≥66 for symptoms, it is considered as clinically significant symptoms.25-27 A ≥ 10 points difference in HRQoL scores (on a 0–100 scale) was considered to be clinically relevant evaluating HRQoL.18,19 In another study, a >5% difference of mean score values compared to baseline was indicative of a difference of clinical interest for the EORTC QLQ-CX24 module,23 which had been previously reported in other quality of life and patient-reported outcomes related studies.19,37 |
EQ-5D-5L | EQ-5D-5L is a generic, preference-based HRQoL questionnaire consisting of an index score and VAS score. The index score is based on 5 dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Score ranges from 0 (“dead”) to 1 (“perfect health”) where negative scores represent “worse than dead.” The EQ-VAS ranges from 0 (worst health imaginable) to 100 (best health imaginable). | Validity, Reliability, and Responsiveness: No evidence of validity, reliability, and responsiveness was found for cervical cancer patients. | No evidence was found for cervical cancer patients. |
EORTC QLQ-C30 = The European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EORTC QLQ-CX24 = The European Organization for Research and Treatment of Cancer Quality of Life Questionnaire cervical cancer module; EQ-5D-5L = The European Quality of Life Scale 5D-5L; FIGO = International Fédération of Gynecology and Obstetrics; HRQoL = health-related quality of life; ICC = intraclass correlation coefficient; MCID = minimal clinically important difference; MID = minimal important difference; VAS = visual analogue scale.
EORTC QLQ-C30
Description and Scoring
The EORTC QLQ-C30 is one of the most used patient-reported outcome measures in oncology clinical trials. It is a multidimensional, cancer-specific, self-administered, measure of HRQoL.16
The EORTC QLQ-C30 is composed of both multi-item scales and single-item measures. These include 5 functional scales (physical, role, cognitive, emotional, and social), 3 symptom scales (fatigue, pain, and nausea and vomiting), a global health status/HRQoL scale, and 6 single items assessing additional symptoms commonly reported by cancer patients (dyspnea, loss of appetite, insomnia, constipation and diarrhea) as well as perceived financial impact of the disease.16
The EORTC QLQ-C30 uses a 1-week recall period to assess functional status and symptoms. All scales and single-item measures are scored from 0 to 100. Most questions have 4 response options (“not at all,” “a little,” “quite a bit,” “very much”), with scores on these items ranging from one to 4. For the 2 items that form the global HRQoL scale, the response format is a 7-point Likert-type scale with anchors at 1 = “very poor” and 7 = “excellent.” Raw scores for each scale are computed as the average of the items that contribute to a particular scale. Scale sum scores are transformed such that a high score on the functional scales represents a high/healthy level of functioning, a high score on the symptom scales represents a high level of symptomatology, and a high score on the global health status/HRQoL scale represents a high HRQoL.17
According to the EORTC QLQ-C30 scoring algorithm, if there are missing items for a scale (i.e., the participant did not provide a response), the score for the scale can still be computed if there are responses for at least half of the items. The values for missing items are interpolated with the average of the respondent-completed items.17
Assessment of Validity and Reliability
In its initial development, the EORTC QLQ-C30 underwent an evaluation of its psychometric properties and demonstrated reliability and validity in cancer patients in an international field trial of 305 patients in 13 multicultural clinical research settings.16 A revision of the EORTC QLQ-C30 was undertaken to improve low internal consistency, content validity for the role functional scale, and a conceptual difficulty (undue emphasis on physical function in the global HRQoL scale).38 The original and new versions were applied in a total of 1,181 patients with cancer in Canada and the Netherlands. Internal consistency improved for the role functional scale in the new version (Cronbach alpha ranging from 0.78-0.88), and substitution of the new item for the previous version did not alter internal consistency (Cronbach alpha ranging from 0.81-0.92).38
The EORTC QLQ-C30 has been validated among cervical cancer patients along with its cervical cancer-specific module EORTC QLQ-CX24 (details are provided below).20 Since the EORTC QLQ-CX24 addresses specific HRQoL aspects for cervical cancer patients that are not evaluated by the core EORTC QLQ-C30 scale,20,21 and the strong correlations between the EORTC QLQ-CX24 and the EORTC QLQ-C30 scales assessing similar elements (e.g., for symptom experience scale, r = 0.36-0.44, p <0.01) signifies the necessity to use both questionnaires together.20
Minimal Important Difference
Change in the EORTC QLQ-C30 may be interpreted in terms of small, moderate, or large changes in HRQoL.19 A study of patients with breast cancer and small cell lung cancer estimated that a clinically relevant change in score on any of the EORTC QLQ-C30 scales to be 10 points.19 Using an anchor-based approach to estimate the MID in which patients who reported “a little” change (for better or worse) on the subjective significance questionnaire had corresponding changes on a function or symptom scale of the EORTC QLQ-C30 of approximately 5 to 10 points. Patients who reported a “moderate” change had corresponding changes in the EORTC QLQ-C30 of about 10 to 20 points, and those who reported being “very much” changed had corresponding changes of more than 20 points.
A Canadian study estimated the MID for the EORTC QLQ-C30 among 369 patients with advanced cancer, the most common cancer being breast cancer, followed by lung, prostate, gastrointestinal, renal cell, and other cancers.39 Patients completed the questionnaire at baseline and 1 month post-radiation. Using both an anchor- and distribution-based methods for improvement and deterioration, 2 anchors of overall health and overall HRQoL were used, both taken directly from the EORTC QLQ-C30 (questions 29 and 30) where patients rated their overall health and HRQoL themselves. Improvement and deterioration were categorized as an increase or decrease by 2 units to account for the natural fluctuation of patient scoring. With these 2 anchors, the estimated MIDs across all EORTC QLQ-C30 scales ranged from 9.1 units to 23.5 units for improvement, and from 7.2 units to 13.5 units for deterioration. Distribution-based estimates were closest to 0.5 SD.
The EORTC QLQ-C30 was used among 828 cervical cancer survivors to assess the prevalence and predictors of anxiety and depression in Korea.27 The scale was used to measure functioning and symptoms of patients on a linearly transformed scale of 0 to 100. If the score was <34 for functioning scales, it was considered to be a clinically significant functional problem. On the other hand, if the score was >66 for symptoms, it was considered to be a clinically significant symptoms.25-27
In a systematic review of questionnaires and their ability to detect clinically important differences and changes in gynecologic oncology (cervical, endometrial, ovarian, vulvar cancer), 10% was selected as a threshold for assessing EORTC QLQ-C30’s ability to detect minimal clinically important difference based on the recommendation of the National Cancer Institute of Canada Clinical Trials Group,28 and based on the fact that this value is within the range of estimates for the most commonly used questionnaires for cancer patients. However, the reviewers expressed concern that the review might have missed subtleties regarding the relative sensitivity and responsiveness for smaller differences due to the large threshold of 10%.29 It was pointed out that research estimates for minimal clinically important difference for the EORTC QLQ-C30 ranges from 5% to 20%.29,30
EORTC QLQ-CX24
Description and Scoring
The European Organization for Research and Treatment of Cancer Quality of Life Questionnaire cervical cancer module (EORTC QLQ-CX24) has been developed and validated specifically for cervical cancer patients, assessing disease-specific and treatment-specific components of quality of life among this patient population.31 The QLQ-CX24 is a supplement to the EORTC QLQ-C30 core questionnaire,22 addressing relevant areas of QoL not covered by the core questionnaire.
The EORTC QLQ-CX24 is composed of total 24 items including both single-item and multi-item scales. These scales can be outlined in 3 multi-item scales - symptom experience (11 items) , body image (3 items) , and sexual/vaginal functioning (4 items); and 6 single-item scales (lymphoedema, peripheral neuropathy, menopausal symptoms, sexual activity, sexual worry, sexual enjoyment).31,33 The scales and item scores are all linearly transformed to a 0-100 scale using the standard scoring algorithm recommended by the EORTC. A higher score on this scale indicates better level of functioning for 2 items (sexual activity and sexual enjoyment), and higher level of symptoms for other items and scales.33,40
Assessment of Validity and Reliability
In its initial development, the EORTC QLQ-CX24 underwent an evaluation of its psychometric properties and demonstrated reliability and validity among 346 cervical cancer patients who had radical hysterectomy and received radiotherapy and chemotherapy in a multicultural setting, which included 9 European countries, as well as Australia, Korea, Taiwan, and Brazil. The QLQ-CX24 demonstrated high internal consistencies for the subscales with Cronbach α coefficient ranging between 0.72 to 0.87 (symptom experience: 0.72; body image: 0.86; sexual/vaginal functioning: 0.87). While the symptom experience scale of the cervical cancer module was moderately correlated with the QLQ-C30 functioning scales (r = 0.40–0.48, except cognitive functioning), as well as the body image scale was moderately correlated with emotional functions (r = - 0.43) and global health/ QoL (r = - 0.41), other scales were weakly correlated (r < 0.40).
All subscales revealed good convergent validity with >0.40 item-own scale correlations, except for symptom experience (0.24–0.50). Clinical validity was tested by using Student t tests to conduct known-group comparisons (assessing the QLQ-CX24 module’s ability to discriminate between clinical subgroups), as well as using Pearson correlations for metric scales for Karnofsky performance status and the QLQ-CX24 scales. The QLQ-CX24 module showed capacity to discriminate between clinical subgroups based on their FIGO (International Fédération of Gynecology and Obstetrics) status (patients with early stage disease and with advanced-stage disease). On the other hand, a significant correlation was established between the Karnofsky PS scores and symptom experience scale (r = - 0.20; p = 0.010); the single-item scales lymphoedema (r = - 0.16; p = 0.047); and sexual worry (r = 0.16; p = 0.044). The symptom experience scale and the body image scale had shown best ability to discriminate while comparing patients with different cancer stages (FIGO stage I cancer vs FIGO stage II through IV disease). The sexual experience and sexual/vaginal functioning subscales could discriminate while comparing between patients who were on treatment and those who were off treatment. However, the scales did not exhibit any difference in patients concerning disease status (NED versus patients with recurrent disease). The scaling errors for convergent and discriminant validity below 3%.31
A study assessed the reliability and validity of the EORTC QLQ-CX24 among 134 cervical cancer patients treated with pelvic surgery in Germany. Internal consistencies for 3 multi-item scales with Cronbach α coefficient ranged between 0.70 to 0.87 for symptom experience (0.70), body image (0.87), and sexual/vaginal functioning (0.76). Scaling errors were reported to be in 6.8%, 0.0%, and 6.3% of the cases. The scales showed ability to discriminate between different subgroups of patients (e.g., disease status, stage of disease, treatment status).34 The cervical cancer module has been translated and validated in other countries as well, including Africa,32,35 China,33 Korea,41 Sri Lanka,36 Poland,20 Ethiopia.21
Based on consensus-based standards, the EORTC QLQ-CX24 has been reported to have poor internal consistency and structural validity, but excellent content and cross-cultural validity in a review report.42 In another systematic review, good evidence for reliability, construct validity and content validity, and some limited evidence for criterion validity had been reported for the EORTC QLQ-CX24.43 Another systematic review paper discussed about the uncertainty of the validity of the EORTC QLQ-CX24 questionnaire for cervical cancer patients, focusing on the fact that 5 out of 9 psychometric properties were either doubtful or not reported in current literature.44 The responsiveness was either not reported42,43 or had a doubtful design or method to get a score.44
Minimal Important Difference
In its initial development, the EORTC QLQ-CX24 symptom experience scale and the body image scale revealed significant clinical differences (> 10 points) between patients with different FIGO stages.31 The Menopausal Symptoms scale showed significant (> 10 points) between pre-menopausal and post-menopausal women (p= 0.01) as well as between patients undergoing adnexectomy and not having surgery. A > 10 points difference in HRQoL scores (on a 0–100 scale) was considered to be clinically relevant in another study evaluating HRQoL using both EORTC QLQ-C30 along with its cervical cancer module CX-24 among 275 locally advanced cervical cancer patients in China, who were treated with neoadjuvant concurrent chemoradiation or radiation alone followed by radical surgery.18,19 In this study, a clinically relevant and statistically significant improvement in physical functioning (P < 0.001) and role functioning (P = 0.002, P = 0.031) was observed in patients receiving either concurrent chemoradiation and radical surgery or radiation and radical surgery at 6 months follow-up.18
The EORTC QLQ-CX24 module was used along with the EORTC QLQ-C30 among the 828 cervical cancer survivors in Korea, and the clinically significant symptoms and functional problems were same as mentioned earlier.25-27 The EORTC QLQ-CX24 module was also used in another long-term prospective evaluation study of emotional distress and QoL among 227 early stage and locally advanced cervical cancer patients in Italy, along with the global health status scale of EORTC QLQ-C30 (version 3.0) to assess QoL.23 In this study, a >5% difference of mean score values compared to baseline was indicative of a difference of clinical interest for the EORTC QLQ-CX24 module,23 which had been previously reported in other QoL and patient-reported outcomes related studies.19,37
EQ-5D-5L
The European Quality of Life Scale (EQ-5D) is a generic HRQoL instrument that may be applied to a wide range of health conditions and treatments.45,46 The first of 2 parts of the EQ-5D is a descriptive system that classifies respondents (aged ≥ 12 years) based on the following 5 dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. The EQ-5D-5L has 5 possible levels for each domain and respondents are asked to choose the level that reflects their health state for each of the 5 domains resulting in 3,125 possible health states.47 A scoring function can be used to assign a value to self-reported health states from a set of population-based preference weights.45,46 The second part is a 20 cm VAS (EQ-VAS) that has end points labelled 0 and 100, with respective anchors of “worst imaginable health state” and “best imaginable health state.” Respondents are asked to rate their health by drawing a line from an anchor box to the point on the EQ-VAS which best represents their health on that day. Hence, the EQ-5D produces 3 types of data for each respondent:
A profile indicating the extent of problems on each of the 5 dimensions represented by a 5-digit descriptor, such as 15121, 33211, and so on.
A population preference-weighted health index score based on the descriptive system,
A self-reported assessment of health status based on the EQ-VAS.
The EQ-5D index score is generated by applying a multi-attribute utility function to the descriptive system.48 Different utility functions are available that reflect the preferences of specific populations (e.g., US or UK). Scores less than 0 represent health states that are valued by society as being worse than dead, while scores of 0 and 1.00 are assigned to the health states “dead” and “perfect health,” respectively.
Assessment of Validity and Reliability
No evidence was found for assessment of validity and reliability of EQ-5D-5L for cervical cancer patients.
Minimal Important Difference
No evidence of MID for EQ-5D-5L was found for cervical cancer patients.
Pharmacoeconomic Review
Abbreviations
AE
adverse event
BIA
budget impact analysis
CPS
combined positive score
ICER
incremental cost-effectiveness ratio
LY
life-years
OS
overall survival
PD
progressed disease
PD-L1
programmed cell death 1 ligand 1
PF
progression free
PFS
progression-free survival
PPS
post-progression survival
QALY
quality-adjusted life-year
RDI
relative dose intensity
SOC
standard of care
TTP
time to progression
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Pembrolizumab (Keytruda), 100 mg/4 mL vial of solution for IV infusion |
Submitted price | Pembrolizumab, 100 mg: $4,400.00 |
Indication | Treatment of adult patients with persistent, recurrent, or metastatic cervical cancer whose tumours express PD-L1 (CPS ≥ 1) as determined by a validated test, in combination with chemotherapy with or without bevacizumab |
Health Canada approval status | NOC |
Health Canada review pathway | Priority review |
NOC date | April 7, 2022 |
Reimbursement request | As per indication |
Sponsor | Merck Canada Inc. |
Submission history | Previously reviewed: Yes Pembrolizumab (Keytruda) has been reviewed for multiple indications at CADTH. The following indications were reviewed in 2020 and 2021: Indication: Esophageal carcinoma, gastroesophageal junction adenocarcinoma Recommendation date: December 20, 2021 Recommendation: Reimburse with clinical criteria and/or conditions Indication: Classical Hodgkin lymphoma Recommendation date: November 1, 2021 Recommendation: Reimburse with clinical criteria and/or conditions Indication: Metastatic or unresectable recurrent head and neck squamous cell carcinoma Recommendation date: December 22, 2020 Recommendation: Recommended on the condition of cost-effectiveness being improved to an acceptable level Indication: Advanced renal cell carcinoma Recommendation date: April 2, 2020 Recommendation: Recommended on the condition of cost-effectiveness being improved to an acceptable level |
CPS = combined positive score; NOC = Notice of Compliance; PD-L1 = programmed cell death 1 ligand 1.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Semi-Markov model |
Target population | Adult patients with persistent, recurrent, or metastatic cervical cancer whose tumours express PD-L1 (CPS ≥ 1) as determined by a validated test |
Treatment | Pembrolizumab plus SOC |
Comparator | SOC (cisplatin or carboplatin + paclitaxel with or without bevacizumab) |
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | Lifetime (40 years) |
Key data source | KEYNOTE-826 trial |
Submitted results | ICER = $98,849 per QALY (incremental QALYs: 1.71; incremental costs: $168,993) |
Key limitations |
|
CADTH reanalysis results |
|
CPS = combined positive score; ICER = incremental cost-effectiveness ratio; LY = life-year; PD-L1 = programmed cell death 1 ligand 1; PF = progression free; PFS = progression-free survival; QALY = quality-adjusted life-year; RDI = relative dose intensity; SOC = standard of care; TTP = time to progression.
Conclusions
Based on an appraisal of the KEYNOTE-826 trial, CADTH clinical review found that pembrolizumab in combination with chemotherapy with or without bevacizumab, may be associated with improved progression-free survival (PFS) and overall survival (OS) in adult patients with persistent, recurrent, or metastatic cervical cancer whose tumours express programmed cell death 1 ligand 1 (PD-L1) (combined positive score [CPS] ≥ 1). While OS was still immature (median OS has not been reached for patients receiving pembrolizumab plus standard of care [SOC]), the first interim analysis of Kaplan-Meier curves suggested that adding pembrolizumab to SOC therapy could result in OS benefit. The clinical experts consulted by CADTH noted that the findings appeared favourable and clinically important, while the CADTH clinical review found the KEYNOTE-826 study to be representative and generalizable to the expected Canadian population. The safety profile of pembrolizumab plus chemotherapy was comparable to that of SOC alone. However, the magnitude of effect of pembrolizumab on the health-related quality of life of patients in this setting is uncertain due to lack of formal hypothesis testing.
In addition to limitations with the clinical data, CADTH identified several key limitations with the sponsor’s economic model: overestimation of proportion of patients in the progression-free (PF) state over 40 years; an assumption of different chemotherapy regimens used among patients receiving pembrolizumab plus SOC or SOC alone; an assumption of different rates of patients undergoing subsequent treatment depending on initial treatment; and the use of relative dose intensity (RDI) to estimate treatment costs. CADTH conducted a reanalysis, which included the assumption PFS and time to progression (TTP) extrapolation curves had an exponential distribution; changing the proportion of patients receiving each treatment regimen to be equal among treatment arms; changing the proportion of patients receiving subsequent treatments to be equal among treatment arms; and setting RDI for all treatments to 100%. Based on the CADTH reanalysis, adding pembrolizumab to chemotherapy is $180,957 more costly and yields 0.66 more quality-adjusted life-years (QALYs) when compared to chemotherapy alone, resulting in an incremental cost-effectiveness ratio (ICER) of $272,958 per QALY. A price reduction of 90% would be necessary to achieve an ICER of $50,000 per QALY. Results from additional scenario analyses indicate that the cost-effectiveness of pembrolizumab is sensitive to changes from fixed to weight-based pembrolizumab dosing.
Several limitations could not be addressed by CADTH, including an implied assumption that patients in the PF state would be functionally cured (i.e., at no risk of disease progression) after approximately 10 years. This structural feature of the model was highly influential, given that nearly 100% of incremental QALYs were accumulated in the PF state over a 40-year time horizon. No clinical evidence was provided by the sponsor to support this implied assumption, and the observation period of the KEYNOTE-826 trial (median 17 months; longest observation 28.4 months) was not long enough to capture long-term effects of pembrolizumab treatment. Therefore, the long-term benefit of pembrolizumab remains unknown. Accordingly, a higher price reduction may be necessary to achieve cost-effectiveness.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, registered clinicians, and drug plans that participated in the CADTH review process.
Patient input was received from a joint submission from HPV Global Action and Canadian Cancer Survivor Network. HPV Global Action raises awareness of sexual and reproductive health. Input from these groups was based on an online survey, including 5 patients from Canada, and an interview with 1 patient. Patient input highlighted that the diagnosis of cervical cancer affected patients’ daily activities and quality of life by causing fatigue, pain in the pelvic area or lower back that may go down 1 or both legs, and abnormal vaginal bleeding after menopause. Cervical cancer also affected patients’ psychological well-being by increasing the feeling of uncertainty and isolation, and causing anxiety, panic attacks, and depression. Patients noted that current standard therapy includes platinum-based combination chemotherapy along with the biologic therapy bevacizumab. These treatments include side effects that can impact their day-to-day living, as well as their quality of life. All patients who answered the survey were seeking to maintain quality of life and access a new treatment option. Patient input also indicated that some patients were seeking to reduce side effects from current treatments and delay onset of symptoms. A total of 4 patients had experience with pembrolizumab, and most reported having a positive experience including ease of use, control of symptoms, and positive clinical response. Three patients reported having minor or mild side effects (e.g., nausea, diarrhea, rash, joint pain, dry skin, nail breakage) that were easily manageable. One patient reported having negative experience, including having interstitial nephritis as a side effect.
Clinician input was received from the Ontario Health Gynecology Cancer Drug Advisory Committee. Clinician feedback highlighted that there are few therapy options for patients with persistent, recurrent, or metastatic cervical cancer and limited second-line options, generating an unmet need for new treatments. Treatment with pembrolizumab would be appropriate to be used as first-line treatment in patients who express PD-L1. Clinicians considered that patients who have contraindications to pembrolizumab and patients who do not express PD-L1 would be less suited to receive pembrolizumab. Clinician input indicated that treatment goals include improvement in treatment efficacy.
CADTH-participating drug plans highlighted several implementation and economic considerations. The drug plans identified the following implementation considerations: whether pembrolizumab can be used in patients who cannot receive a platinum drug and/or a taxane, whether pembrolizumab’s 6-weeks dose interval was appropriate for this indication, and whether it was possible to re-treat patients with pembrolizumab after the completion of 2 years of treatment. In addition, the drug plans inquired regarding the appropriate time frame, if any, to add pembrolizumab to the treatment regimen of patients who have already started chemotherapy or just completed chemotherapy. The drug plan input highlighted implementation considerations regarding continuation of therapy with pembrolizumab when patients cannot tolerate either chemotherapy or bevacizumab. Economic considerations included the additional cost of pembrolizumab related to drug wastage since there is only 1 vial size (100 mg) available and the considerable budget impact pembrolizumab might impose when compared with chemotherapy with or without bevacizumab. Furthermore, in line with other indications for pembrolizumab, jurisdictions would implement a weight-based dose of 2 mg/kg. Finally, the drug plans considered the possibility of pembrolizumab being used in patients with Eastern Cooperative Oncology Group performance status of 2 or greater for patients with persistent, recurrent, or metastatic cervical cancer.
Several of these concerns were addressed in the sponsor’s model:
The sponsor’s submitted model accounted for quality of life and length of life by using QALYs as the primary outcome.
In addition, CADTH addressed some of these concerns as follows:
CADTH included a weight-based dose of 2 mg/kg in a scenario analysis.
CADTH was unable to address the following concerns raised from stakeholder input:
CADTH was unable to evaluate the impact of pembrolizumab being used in patients with Eastern Cooperative Oncology Group Performance Status of 2 or greater.
Economic Review
The current review is for pembrolizumab (Keytruda) in combination with chemotherapy with or without bevacizumab for adult patients with persistent, recurrent, or metastatic cervical cancer whose tumours express PD-L1 (CPS ≥ 1) as determined by a validated test.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis of pembrolizumab in patients with persistent, recurrent, or metastatic cervical cancer whose tumours express PD-L1 (CPS ≥ 1) in combination with chemotherapy with or without bevacizumab.1 The model population comprised adult patients with persistent, recurrent, or metastatic cervical cancer whose tumours express PD-L1 (CPS ≥ 1) as determined by a validated test, which was aligned with the Health Canada indication.
Pembrolizumab is available as a 100 mg/4 mL solution for infusion in a single-use vial.2 Pembrolizumab is administered intravenously for 30 minutes. The recommended dose for pembrolizumab is 200 mg every 3 weeks or 400 mg every 6 weeks until unacceptable toxicity, disease progression, or for up to 24 months (35 doses for 200 mg or 18 doses for 400 mg). At the submitted price of $4,400 per 4 mL vial, the standard cycle (28 days) cost of pembrolizumab was estimated to be $11,733, assuming 100% RDI.
In the base case, the sponsor considered SOC as the comparator which included cisplatin or carboplatin in combination with paclitaxel, with or without bevacizumab. All SOC therapies were administered intravenously. The dosage used for cisplatin was 50 mg/m2, for carboplatin was an area under the curve of 5 (assumed to be equal to 750 mg), for paclitaxel was 175 mg/m2, and for bevacizumab was 15 mg/kg. Cisplatin or carboplatin in combination with paclitaxel were administered for 6 cycles every 3 weeks, and bevacizumab was administered to a maximum of 2 years (35 doses) every 3 weeks. The treatment with cisplatin or carboplatin in combination with paclitaxel was assumed to have equal effectiveness. The 21-day cycle cost of SOC was estimated to be between $282 and $1,052 for therapeutic combinations without bevacizumab, and between $3,783 and $4,554 for therapeutic combinations with bevacizumab.
Outcomes of the model included QALYs and life-years (LYs) over a time horizon of 40 years. The base-case analysis was conducted from the perspective of the Canadian public health care system, with an annual discount rate of 1.5% applied to both costs and outcomes.
Model Structure
The sponsor submitted a semi-Markov model with 3 mutually exclusive health states including PF, progressed disease (PD), and death, to track the disease course over time, with a weekly cycle length. A figure of the sponsor’s model structure is available in Appendix 3 (Figure 1).
All patients begin in the PF health state, where they could remain PF or transition to the PD state. Patients in the PD state could only transition to death. Patients in any health state could transition to death starting in the first cycle.
Model Inputs
The model’s baseline population characteristics and clinical efficacy parameters were characterized by the KEYNOTE-826 trial, a randomized, double-blind, placebo-controlled, multicentre phase III study designed to evaluate the efficacy of pembrolizumab in combination with chemotherapy with or without bevacizumab in comparison with chemotherapy with or without bevacizumab. The sponsor assumed that the KEYNOTE-826 study population (baseline characteristics: mean age = 51.0 years; mean weight = |||||| kg; proportion with metastatic disease at diagnosis = 32%), reflected the Canadian population.
Transition probabilities from the PF health state to PD and PD to death were derived from the KEYNOTE-826 trial. To derive these probabilities, the sponsor incorporated PFS, TTP, and post-progression survival (PPS) data from the KEYNOTE-826 trial. Mortality among those in the PF and PD states was calculated for each cycle as the maximum between the transition hazard and the general Canadian population mortality.
The Kaplan-Meier curve of the KEYNOTE-826 trial was used to populate PFS and TTP data until 37 weeks. Parametric survival modelling was used to extrapolate PFS and TTP data beyond 37 weeks, with survival distributions separately fitted to KEYNOTE-826 trial data for each treatment arm. The base-case parametric functions were selected based on visual inspection of fit, clinical plausibility of long-term projections, assessment of underlying hazard functions, and statistical goodness-of-fit.
In the base-case analysis, treatment with pembrolizumab plus SOC in the PF state was assumed to have a persistent treatment effect, without waning in efficacy. Subsequent treatment lines were also assumed to have no wane of efficacy.
The drug-related grade 3 or greater adverse events (AEs) which occurred with a frequency of more than 5% (all arms) observed in the KEYNOTE-826 trial were incorporated into the model, with an associated cost and disutility. Costs were obtained from the literature and Ontario Case Costing Initiative, and disutilities associated with AEs were based on data from the KEYNOTE-826 trial.3,4 Both cost and disutilities for AEs were applied as a one-time decrement in the first model cycle. AEs observed in the post-progression setting were not included in the model.
Health state utility values were derived from the KEYNOTE-826 trial. For base-case analysis, the submitted model used a time-to-death approach, in which health utilities were applied based on distribution of patients across different categories of time-to-death (i.e., less than 30 days, 30 to 90 days, 90 to 180 days, 180 to 360 days, and more than 360 days). As a scenario analysis, a progression status approach (i.e., health utility values corresponding to each health state) was used.
Costs in the model included PD-L1 test costs, drug acquisition costs for pembrolizumab, SOC, subsequent therapies, administration costs for pembrolizumab and SOC, state-specific disease management, AEs management, and terminal care costs. PD-L1 biomarker testing cost was obtained from the literature.5 To determine the average cost required to detect 1 patient eligible for treatment with pembrolizumab, the sponsor considered that 89% of patients would have a CPS equal or greater than 1, based on data from the KEYNOTE-826 trial. The unit drug costs were obtained from CADTH reports and IQVIA Delta PA.6 The drug acquisition cost was adjusted according to the ratio of actual versus expected numbers of cycles of treatment based on data from the KEYNOTE-826 trial. In addition, costs for each treatment regimen were multiplied by the relevant proportions of patients receiving each treatment based on data from the KEYNOTE-826 trial (Table 11). The proportion of patients remaining on treatment at each scheduled infusion was based on the observed Kaplan-Meier curve for time to treatment discontinuation in the KEYNOTE-826 trial. The base-case analysis also incorporated the cost of administration of IV treatments, which was derived from the literature and considered the duration of administration for each drug.7
Treatment costs for subsequent therapies were sourced from CADTH reports. Costs of second-line therapy for cervical cancer (PD state) were included in the model. Drug acquisition costs associated with subsequent therapies were applied in the models and calculated as a function of the unit drug cost, defined dosing schedule, and duration of treatment based on data from the KEYNOTE-826 trial. In addition, in the base-case analysis, the proportion of patients receiving each subsequent therapy was based on data from the KEYNOTE-826 trial, which varied by treatment arm (Table 12). In a scenario analysis, the sponsor considered another distribution of subsequent treatment based on clinical experts’ input and literature. Administration costs of subsequent therapies were not included in the base-case analysis.
Disease management costs included routine monitoring of those in the PF and PD states and were based on 2 observational studies including data from British Columbia and Ontario.8,9 The weekly costs derived from these studies were applied in the model.
Finally, patients who transitioned to death were assumed to incur a 1-time cost associated with palliative or terminal care, which was derived from the literature.10
Summary of Sponsor’s Economic Evaluation Results
All analyses were run probabilistically (5,000 iterations for the base case). The deterministic and probabilistic results were slightly different. The probabilistic findings are presented as follows.
Base-Case Results
In the sponsor’s probabilistic base-case analysis, treatment with pembrolizumab plus SOC was associated with an ICER of $98,849 per QALY gained compared to SOC alone. Ninety-one percent of incremental QALYs were gained beyond the trial observation period of 28.4 months, indicating that most of benefit was based on extrapolation assumptions. The probability of pembrolizumab being cost-effective at a willingness-to-pay threshold of $50,000 per QALY gained was 0%. At the end of the 40-year time horizon, 2.5% of patients in the pembrolizumab arm were still alive.
The submitted analysis is based on the publicly available prices of all treatments including subsequent therapies.
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER vs. SOC ($/QALY) |
|---|---|---|---|---|---|
SOC | 88,756 | Reference | 1.76 | Reference | Reference |
Pembrolizumab plus SOC | 257,750 | 168,993 | 3.47 | 1.71 | 98,849 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; SOC = standard of care; vs. = versus.
Source: Sponsor’s pharmacoeconomic submission.
Sensitivity and Scenario Analysis Results
The sponsor conducted several sensitivity analyses and 3 scenario analyses. Scenario analyses included: change in subsequent therapies to be reflective of the Canadian clinical practice, a shorter time horizon (30 years), and a 6-cycle stopping rule for treatment with bevacizumab (instead of 35 cycles). Of note, the largest driver of the ICER was when a shorter time horizon (30 years) was applied. In this scenario the estimated ICER increased to $106,073 per QALY.
CADTH’s Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the economic analysis.
Long-term OS benefit is uncertain: The submitted model used PFS, TTP, and PPS data from the KEYNOTE-826 trial to populate patients’ transition probabilities among health states. These outcomes were used to estimate OS, which represents a composite measure of deaths occurring in the PF and PD states. Typically, trial-based models use OS data obtained directly from the trial to populate the short-term OS and estimate long-term OS. Although, the use of TTP and PPS to estimate OS was conceptually sound, CADTH’s clinical assessment highlighted that PPS and TTP were not included in the sponsor’s clinical submission and, therefore, were not critically assessed. Furthermore, as TTP and PPS were not specified as primary or secondary outcomes of the KEYNOTE-826 trial, they were not adjusted for multiplicity, resulting in increased uncertainty around those estimates.
In addition, in the sponsor’s base case, patients in the pembrolizumab plus SOC arm accumulated an additional 2.53 LYs, of which 9% were accrued within the trial period (28.4 months). Of note, the vast majority of incremental LYs and QALYs (95.6% and 96.8%, respectively) were accrued in the PF health state. Most of these incremental OS benefits (55%) were accrued between 10 and 40 years from treatment initiation. Given there is no direct comparison between groups after 28.4 months, the long-term benefit of pembrolizumab (up to 40 years) is highly uncertain.
CADTH could not address this limitation due to the absence of long-term OS data.
To explore uncertainty around the OS benefit, CADTH conducted a scenario analysis that reduced the time horizon to 10 years based on clinical feedback.
PFS benefit is overestimated and lacked face validity: The sponsor’s base case used a log-logistic distribution to extrapolate PFS and TTP data from the KEYNOTE-826 trial, which generated an implausibly high survival rate in the PF state over the 40-year time horizon. Clinical expert feedback collected by CADTH for this review suggested that this is an overestimate of expected survival in this population, and likely does not reflect patient clinical trajectory. The fact that many patients remained in the PF state for up to 40 years, particularly in the pembrolizumab plus SOC group, implied these therapies could essentially cure patients with persistent, recurrent, metastatic cervical cancer. No evidence was provided by the sponsor to support the assumption that a proportion of patients would be cured by treatment. For instance, the proportion of patients treated with pembrolizumab who remained in the PF state at 30 years after treatment initiation was 4.8%. Clinical expert feedback obtained by CADTH for this review suggested that this is an overestimate, and that this value is closer to the expected 5-year survival rate for patients receiving SOC. The sponsor’s base-case assumption therefore seems to produce a meaningful bias that favours pembrolizumab. Furthermore, as mentioned in the previous limitation, the current efficacy data available from the KEYNOTE-826 trial indicated the long-term benefit of pembrolizumab was unknown.
CADTH addressed this limitation by using the exponential distribution for PFS extrapolation function.
To explore uncertainty around the extrapolation of PFS, CADTH conducted a scenario analysis using a Weibull distribution.
Transition probabilities between PF and death states lacked face validity: Transition probabilities from the PF state to death could not be adjusted to align with baseline mortality over time. The transition probabilities from the PF state to death were modelled to be dependent on the transition probabilities of patients who remain in the PF state and patients who transition to PD. However, when using log-logistic distribution for PFS and TTP, the mortality rate for patients in the PF state was observed to be lower than the mortality rate for the general Canadian population over a large time horizon (from 9 to 40 years), which lacks face validity.
Due to structural complexity, CADTH was unable to address this limitation when keeping the log-logistic distribution for PFS and TTP. However, this limitation was not present in CADTH’s base case, which used an exponential distribution or in CADTH’s scenario analysis, which used a Weibull distribution.
Proportion of patients receiving each chemotherapy regimen was different between model arms: The sponsor assumed that the proportion of patients receiving each regimen of chemotherapy (i.e., paclitaxel + cisplatin, paclitaxel + carboplatin, paclitaxel + cisplatin + bevacizumab, paclitaxel + carboplatin + bevacizumab) would be different between treatment arms. These estimates were based on data from the KEYNOTE-826 trial. Clinical expert feedback elicited by CADTH for this review did not suggest that the chemotherapy regimen would differ based on whether a patient was also receiving pembrolizumab. The use of different proportions based on initial treatment may not reflect clinical practice and introduced a bias in cost that favoured SOC.
CADTH addressed this limitation by making the proportion of patients receiving each regimen of chemotherapy equal in both arms, based on input from clinical experts. Of note, the change made by CADTH only affected treatment costs; it did not address potential differences in efficacy between treatment regimens.
Estimates on the proportion of patients receiving subsequent treatments were inappropriately incorporated into the model: The sponsor assumed that 13.9% and 19.3% of patients in the pembrolizumab plus SOC and SOC arm would receive subsequent treatments. These estimates were based on data from the KEYNOTE-826 trial. Given the model accounts for a lifetime horizon, the use of these estimates over the extended time horizon was inappropriate. The sponsor’s approach resulted a lower cost for subsequent treatments for pembrolizumab plus SOC.
CADTH addressed this limitation by changing the proportion of patients receiving subsequent therapies to 19.3% in both arms, based on input from clinical experts. Of note, the change made by CADTH only affected treatment costs; it did not address potential differences in efficacy among distinct subsequent therapies.
RDI: The sponsor’s base case incorporated reduced or enhanced dose intensities for all therapies (expected versus observed doses). Consistent with previous reviews, given the inability to link distinct dose intensity with outcomes, the CADTH base case does not incorporate RDI. A reduction or enhancement of RDI can be derived from many factors including clinical discretion, delayed dose, a missed dose, or a reduction in dose. When considering drug wastage, each component can have a different influence on drug costs. Likewise, it is unclear how treatment discontinuation influences RDI.
In the CADTH base case, RDI calculations were excluded.
Weight-based dosing for pembrolizumab: Pembrolizumab dosing in the KEYNOTE-826 study was a fixed dose of 200 mg IV every 3 weeks or 400 mg every 6 weeks. Input from participating public drug plans indicated that jurisdictions would likely implement a weight-based dose for pembrolizumab of 2 mg/kg (up to a cap of 200 mg) every 3 weeks with the possibility of extended dosing intervals to every 6 weeks (4 mg/kg up to a 400 mg cap). The clinical experts agreed that this approach seemed reasonable, given the clear interchangeable use in dosing for other cancer sites. CADTH notes that weight-based dosing will reduce the ICER associated with pembrolizumab and give greater flexibility in dosing. However, CADTH notes that it is not possible to make the direct assumption that the use of weight-based dosing will lead to the same outcomes as the trial’s fixed dose, as patients will be exposed to a lower dose which may impact treatment efficacy.
CADTH did not address this limitation in reanalysis. To explore the uncertainty around this assumption, CADTH conducted 2 scenario analyses (drug wastage of 100% and 50%) using weight-based dosing based on an average weight of |||||| kg.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CADTH (See Table 4).
Table 4: Key Assumptions of the Submitted Economic Evaluation (Not Noted as Limitations to the Submission)
Sponsor’s key assumption | CADTH comment |
|---|---|
Costs and disutilities related to grade ≥ 3 AEs with an incidence of at least 5% in the KEYNOTE-826 trial | Inappropriate. The sponsor selected an arbitrary threshold to capture the impact of treatment-related AEs rather than selecting the most clinically meaningful AEs to include within the model. CADTH’s guidelines recommends that all AEs that have clinical or cost significance should be included in the model. Additionally, the AEs included in the sponsor’s model do not capture the range of AEs deemed to be of special interest based on clinicians’ feedback (i.e., type 1 diabetes mellitus, pancreatitis, pneumonitis, thyroiditis) received by CADTH for this review. For instance, although type 1 diabetes mellitus occurred in approximately 0.7% of patients in the pembrolizumab group, the consequences to both health-related quality of life and costs of treatment are significant and life-long. |
The benefit of pembrolizumab among subgroups in the population is uncertain | The indication assessed by CADTH, which is aligned with the Health Canada indication, included adult patients with persistent, recurrent, or metastatic cervical cancer whose tumours express PD-L1 (CPS ≥ 1). Of note, the subgroup analysis of the KEYNOTE-826 trial indicated that patients who had metastatic disease at diagnosis (n = 125 of 355; 35%) might not benefit from treatment with pembrolizumab (hazard ratio = 0.91; 95% confidence interval, 0.63 to 1.30). However, the study was not powered to assess differences between subgroups and therefore conclusions cannot be drawn from these data. |
AE = adverse event; CPS = combined positive score; PD-L1 = programmed cell death 1 ligand 1.
CADTH Reanalyses of the Economic Evaluation
Base-Case Results
CADTH’s reanalysis addressed several limitations within the economic model. The CADTH base case was derived by making changes in model parameter values and assumptions, in consultation with clinical experts.
Table 5 details each change made to derive the CADTH revised exploratory analysis, which was conducted in a stepwise approach to highlight the impact of each change. The summary of results from the stepped reanalysis are presented in Table 6 and Table 13.
The results of CADTH’s stepped analysis are presented in Table 6. The model produced small but notable differences between probabilistic and deterministic analyses. CADTH’s base-case reanalysis demonstrates that, compared with SOC alone, pembrolizumab was $180,957 more costly and yielded 0.66 more QALYs, resulting in an ICER of $272,958 per QALY. The CADTH reanalysis found that 62% of patients were still alive at 18 months (median follow-up = 78 weeks), which closely approximates the 60.8% (95% CI, 54.6 to 66.4) of patients who were still alive in the KEYNOTE-826 trial at that time point. The CADTH reanalysis was broadly aligned with the sponsor’s submission—pembrolizumab was more costly and more effective than chemotherapy.
At a $50,000 per QALY threshold there is a 0% chance that pembrolizumab is cost-effective. In the CADTH base case, 66% of predicted QALYs were generated through extrapolation beyond the period of the available KEYNOTE-826 trial data (28.4 months).
Scenario Analysis Results
CADTH undertook price reduction analyses based on the CADTH base case. These analyses demonstrated that a price reduction of 90% would be necessary to achieve cost-effectiveness at a willingness-to-pay threshold of $50,000 per QALY.
Table 5: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Changes to derive the CADTH base case | ||
1. PFS and TTP distributions | Log-logistic | Exponential |
2. Proportion of patients receiving each chemotherapy regimen | Trial-based proportions between treatment arms | Equal proportions among treatment arms |
3. Proportion of patients receiving subsequent treatment | Trial-based proportions between treatment arms | Equal proportions among treatment arms |
4. Use of RDI | Yes | No |
CADTH base case | 1 + 2 + 3 + 4 | |
PFS = progression-free survival; RDI = relative dose intensity; TTP = time to progression.
Table 6: Summary of the Stepped Analysis of the CADTH Reanalysis Results
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|---|
Sponsor’s probabilistic base case | SOC | 88,756 | 1.76 | Reference |
Pembrolizumab plus SOC | 257,750 | 3.47 | 98,849 | |
Sponsor’s deterministic base case | SOC | 90,550 | 1.83 | Reference |
Pembrolizumab plus SOC | 260,180 | 3.68 | 91,828 | |
CADTH reanalysis 1 | SOC | 88,203 | 1.43 | Reference |
Pembrolizumab plus SOC | 251,281 | 2.05 | 260,726 | |
CADTH reanalysis 2 | SOC | 90,550 | 1.83 | Reference |
Pembrolizumab plus SOC | 259,068 | 3.68 | 91,226 | |
CADTH reanalysis 3 | SOC | 90,550 | 1.83 | Reference |
Pembrolizumab plus SOC | 261,259 | 3.68 | 92,412 | |
CADTH reanalysis 4 | SOC | 95,856 | 1.83 | Reference |
Pembrolizumab plus SOC | 283,145 | 3.68 | 101,388 | |
CADTH deterministic base case (1 + 2 + 3 + 4) | SOC | 93,508 | 1.42 | Reference |
Pembrolizumab plus SOC | 273,982 | 2.05 | 288,536 | |
CADTH probabilistic base case (1 + 2 + 3 + 4) | SOC | 92,283 | 1.46 | Reference |
Pembrolizumab plus SOC | 273,240 | 2.12 | 272,958 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; SOC = standard of care.
Table 7: CADTH Price Reduction Analyses
Analysis | ICERs for pembrolizumab plus SOC vs. SOC ($/QALY) | |
|---|---|---|
Price reduction | Sponsor’s base case | CADTH reanalysis |
No price reduction | 91,826 | 288,536 |
10% | 83,595 | 261,870 |
20% | 75,363 | 235,214 |
30% | 67,132 | 208,558 |
40% | 58,900 | 181,903 |
50% | 50,669 | 155,247 |
60% | 42,437 | 128,591 |
70% | 34,206 | 101,935 |
80% | 25,974 | 75,279 |
90% | 17,743 | 48,623 |
100% | 9,511 | 21,967 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; SOC = standard of care; vs. = versus.
In addition, CADTH conducted a series of exploratory analyses to determine the impact of alternative assumptions on the cost-effectiveness of adjuvant pembrolizumab, which are outlined as follows.
Time horizon of 10 years
Weibull distribution for PFS and TTP
Weight-based dosing for pembrolizumab (100% vial sharing)
Weight-based dosing for pembrolizumab (50% vial sharing)
Results are described in Table 14. CADTH considered 2 scenario analyses to address the substantial uncertainty associated with OS benefits by reducing the time horizon of the analysis to 10 years and assuming a Weibull distribution for PFS and TTP after 37 weeks. In these scenarios, the ICER changed to $296,001 and $163,271 per QALY, respectively.
CADTH also considered 2 scenarios to address changes in pembrolizumab dose, from fixed dosing to weight-based dosing. In these scenarios, vial sharing was assumed to be 100% and 50%, resulting in an ICER of $194,437 and $241,487 per QALY, respectively.
Overall Conclusions
Based on an appraisal of the KEYNOTE-826 trial, CADTH clinical review found that pembrolizumab in combination with chemotherapy with or without bevacizumab, may be associated with improved PFS and OS in adult patients with persistent, recurrent, or metastatic cervical cancer whose tumours express PD-L1 (CPS ≥ 1). While OS was still immature (median OS has not been reached for patients receiving pembrolizumab plus SOC), the first interim analysis of Kaplan-Meier curves suggested that adding pembrolizumab to SOC therapy could result in OS benefit. The clinical experts consulted by CADTH noted that the findings appeared favourable and clinically important, while the CADTH clinical review found the KEYNOTE-826 study to be representative and generalizable to the expected Canadian population. The safety profile of pembrolizumab plus chemotherapy was comparable to that of SOC alone. However, the magnitude of effect of pembrolizumab on the health-related quality of life of patients in this setting is uncertain due to lack of formal hypothesis testing.
In addition to limitations with the clinical data, CADTH identified several key limitations with the sponsor’s economic model: overestimation of proportion of patients in the PF state over 40 years; an assumption of different chemotherapy regimens used among patients receiving pembrolizumab plus SOC or SOC alone; an assumption of different rates of patients undergoing subsequent treatment depending on initial treatment; and the use of RDI to estimate treatment costs. CADTH conducted a reanalysis, which included the assumption that PFS and TTP extrapolation curves had an exponential distribution; changing the proportion of patients receiving each treatment regimen to be equal among treatment arms; changing the proportion of patients receiving subsequent treatments to be equal among treatment arms; and setting RDI for all treatments to 100%. Based on the CADTH reanalysis, adding pembrolizumab to chemotherapy is $180,957 more costly and yields 0.66 more QALYs when compared to chemotherapy alone, resulting in an ICER of $272,958 per QALY. A price reduction of 90% would be necessary to achieve an ICER of $50,000 per QALY. Results from additional scenario analyses indicate that the cost-effectiveness of pembrolizumab is sensitive to changes from fixed to weight-based pembrolizumab dosing.
Several limitations could not be addressed by CADTH, including an implied assumption that patients in the PF state would be functionally cured (i.e., at no risk of disease progression) after approximately 10 years. This structural feature of the model was highly influential, given that nearly 100% of incremental QALYs were accumulated in the PF state over a 40-year time horizon. No clinical evidence was provided by the sponsor to support this implied assumption, and the observation period of the KEYNOTE-826 trial (median 17 months; longest observation 28.4 months) was not long enough to capture long-term effects of pembrolizumab treatment. Therefore, the long-term benefit of pembrolizumab remains unknown. Accordingly, a higher price reduction may be necessary to achieve cost-effectiveness.
References
1.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Keytruda (pembrolizumab) [internal sponsor's package]. Kirkland (QC): Merck Canada Inc; 2022 May 20.
2.Keytruda (pembrolizumab): solution for infusion 100 mg/4 mL vial [product monograph]. Kirkland (QC): Merck Canada Inc.; 2022 Apr 7.
3.Wehler E, Zhao Z, Pinar Bilir S, Munakata J, Barber B. Economic burden of toxicities associated with treating metastatic melanoma in eight countries. Eur J Health Econ. 2017;18(1):49-58. PubMed
4.Ontario Case Costing Initiative (OCCI). Toronto (ON): Ontario Health and Long-Term Care; 2017: https://data.ontario.ca/dataset/ontario-case-costing-initiative-occi. Accessed 2022 Jul.
5.Institut national d’excellence en santé et en services sociaux (INESSS). Keytruda Cancer de l’oesophage ou de la jonction gastro-oesophagienne. Québec (QC): INESSS; 2022.
6.DeltaPA. [Ottawa (ON)]: IQVIA; 2022: https://www.iqvia.com/. Accessed 2022 May 20.
7.Tam VC, Ko YJ, Mittmann N, et al. Cost-effectiveness of systemic therapies for metastatic pancreatic cancer. Curr Oncol. 2013;20(2):e90-e106. PubMed
8.De Oliveira C, Pataky R, Bremner KE, et al. Estimating the Cost of Cancer Care in British Columbia and Ontario: A Canadian Inter-Provincial Comparison. Healthc Policy. 2017;12(3):95-108. PubMed
9.Pendrith C, Thind A, Zaric GS, Sarma S. Costs of cervical cancer treatment: population-based estimates from Ontario. Curr Oncol. 2016;23(2):e109-115. PubMed
10.Rocchi A, Verma S. Anastrozole is cost-effective vs tamoxifen as initial adjuvant therapy in early breast cancer: Canadian perspectives on the ATAC completed-treatment analysis. Support Care Cancer. 2006;14(9):917-927. PubMed
11.Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Keytruda (pembrolizumab) [internal sponsor's package]. Kirkland (QC): Merck Canada Inc; 2022 May 20.
Appendix 1: Cost Comparison Table
Note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical expert(s). Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 8: CADTH Cost Comparison Table for Persistent, Recurrent, or Metastatic Cervical Cancer Whose Tumours Express PD-L1 (CPS ≥ 1)
Treatment | Strength / concentration | Form | Price ($) | Recommended dosage | Daily cost ($) | Cost per 28-day costa ($) |
|---|---|---|---|---|---|---|
Pembrolizumab (Keytruda) | 100 mg/4mL | 100 mg | 4,400.0000b | 200 mg, every 3 weeks | 419.05 | 11,733 |
400 mg, every 6 weeks | ||||||
Chemotherapy with or without bevacizumab | ||||||
Cisplatin | 1 mg/mL | 50 mg 100 mg | 135.0000 270.0000 | 50 mg/m2 on Day 1 every 3 weeks for 6 cycles | 12.86 | 360 |
Carboplatin | 10 mg/mL | 50 mg 150 mg 450 mg 600 mg | 70.0000 303.1860 881.1450 775.0000 | AUC5 on Day 1 every 3 weeks until disease progression, no evidence of further response, or unacceptable toxicity | 40.24 | 1,127 |
Paclitaxel | 6 mg/mL | 30 mg vial 96 mg vial 150 mg vial 300 mg vial | 300.0000 1,196.8000 1,870.0000 3,740.0000 | 175 mg/m2 on Day 1 every 3 weeks for 4 cycles | 192.38 | 5,387 |
Bevacizumab | 25 mg/mL | 100 mg 400 mg | 347.0000 1,391.0000 | 15 mg/kg for maximum of 35 cycles | 149.04 | 4,173 |
Cisplatin + Paclitaxel | 5,747 | |||||
Cisplatin + Paclitaxel + Bevacizumab | 8,346 | |||||
Carboplatin + Paclitaxel | 6,513 | |||||
Carboplatin + Paclitaxel + Bevacizumab | 10,686 | |||||
Note: All prices are from the Ontario Drug Benefit Formulary (accessed July 2022), unless otherwise indicated, and do not include dispensing fees.
Appendix 2: Submission Quality
Note that this appendix has not been copy-edited.
Description | Yes/No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | Yes | No comment |
Model has been adequately programmed and has sufficient face validity | No | See CADTH appraisal. The submitted model overestimated long-term PFS and OS. |
Model structure is adequate for decision problem | Yes | No comment |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | No | See CADTH appraisal. Transition probabilities between PF and death were lower than the Canadian general population mortality in several time points. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | Yes | No comment |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | No | The use of TTP, PPS, and PFS added complexity to the submission validation. |
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note that this appendix has not been copy-edited.
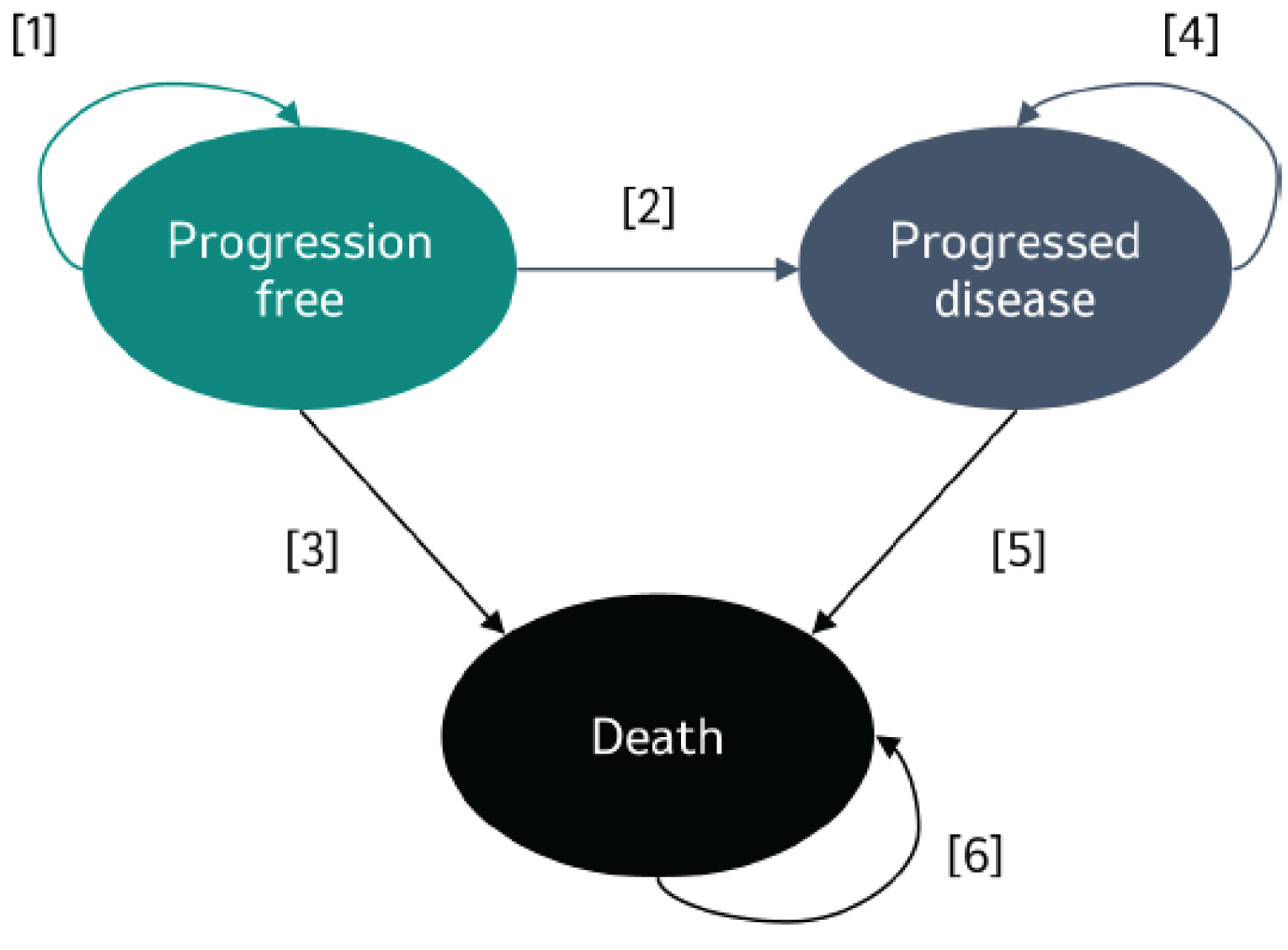
Detailed Results of the Sponsor’s Base Case
Table 10: Disaggregated Summary of Sponsor’s Economic Evaluation Results (Probabilistic)
Parameter | Pembrolizumab + SOC | SOC | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 4.93 | 2.39 | 2.53 |
Health state | |||
Pro-progression | 3.98 | 1.56 | 2.42 |
Post-progression | 0.95 | 0.84 | 0.11 |
Period | |||
On trial (28.4 months) | 1.71 | 1.46 | 0.25 |
Extrapolated results | 3.21 | 0.93 | 2.28 |
Discounted QALYs | |||
Total | 3.47 | 1.76 | 1.71 |
Time-to-death | |||
≥ 360 days | 2.88 | 1.17 | 1.71 |
180 – 360 days | 0.30 | 0.29 | 0.01 |
90-180 days | 0.16 | 0.16 | -0.01 |
30-90 days | 0.10 | 0.10 | 0.00 |
0-30 days | 0.04 | 0.04 | 0.00 |
QALY loss AEs | -0.004 | -0.003 | -0.001 |
Period | |||
On trial (28.4 months) | 1.32 | 1.11 | 0.21 |
Extrapolated results | 2.15 | 0.64 | 1.50 |
Discounted costs ($) | |||
Total | $257,750 | $88,756 | $168,993 |
Drug acquisition | $186,879 | $32,049 | $154,830 |
Pembrolizumab | $152,070 | $0 | $152,070 |
Paclitaxel | $272 | $286 | -$13 |
Cisplatin | $183 | $183 | $0 |
Carboplatin | $4,222 | $4,524 | -$302 |
Bevacizumab | $30,132 | $27,057 | $3,075 |
Administration | $8,130 | $5,899 | $2,231 |
Adverse events | $3,636 | $2,957 | $679 |
Diagnostic testing | $120 | $0 | $120 |
Subsequent treatment | $1,125 | $1,164 | -$39 |
Resource use | $34,106 | $21,874 | $12,232 |
Terminal care | $23,755 | $24,813 | -$1,059 |
ICER ($/QALY) | 98,849 | ||
ICER = incremental cost-effectiveness ratio; LY= life-year; QALY = quality-adjusted life-year; SOC = standard of care.
Table 11: Proportion of Patients Receiving Each One of the Therapeutic Regimens per Treatment Arm Based on Data From KEYNOTE-826
Regimen | Proportion of patients receiving each regimen in combination with pembrolizumab | Proportion of patients receiving each regimen in combination with placebo |
|---|---|---|
Cisplatin + Paclitaxel | 5.6% | 5.8% |
Carboplatin + Paclitaxel | 30.1% | 32.0% |
Cisplatin + Paclitaxel + Bevacizumab | 10.1% | 9.5% |
Carboplatin + Paclitaxel + Bevacizumab | 54.2% | 52.6% |
Source: Sponsor’s pharmacoeconomic report.1
Table 12: Distribution of Subsequent Treatments Observed in the KEYNOTE-826 Trial
Treatment | Pembrolizumab + SOC | SOC |
|---|---|---|
Bevacizumab | 2.2% | 5.1% |
Carboplatin | 7.7% | 5.5% |
Cisplatin | 2.9% | 4.0% |
Gemcitabine | 1.1% | 4.7% |
SOC = standard of care.
Source: Sponsor’s pharmacoeconomic report.1
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Note that this appendix has not been copy-edited.
Detailed Results of CADTH Base Case
Table 13: Disaggregated Summary of CADTH’s Economic Evaluation Results (Probabilistic)
Parameter | Pembrolizumab + SOC | SOC | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 2.81 | 1.94 | 0.87 |
Health state | |||
Pro-progression | 1.77 | 1.09 | 0.69 |
Post-progression | 1.03 | 0.86 | 0.18 |
Period | |||
On trial (28.4 months) | 1.74 | 1.48 | 0.26 |
Extrapolated results | 1.07 | 0.46 | 0.61 |
Discounted QALYs | |||
Total | 2.12 | 1.46 | 0.66 |
Time-to-death | |||
≥ 360 days | 1.51 | 0.87 | 0.64 |
180 – 360 days | 0.32 | 0.29 | 0.02 |
90-180 days | 0.17 | 0.17 | 0.00 |
30-90 days | 0.10 | 0.10 | 0.00 |
0-30 days | 0.04 | 0.04 | 0.00 |
QALY loss AEs | -0.004 | -0.003 | -0.001 |
Period | |||
On trial (28.4 months) | 1.35 | 1.13 | 0.22 |
Extrapolated results | 0.77 | 0.33 | 0.44 |
Discounted costs ($) | |||
Total | $273,240 | $92,283 | $180,957 |
Drug acquisition | $208,178 | $37,107 | $171,070 |
Pembrolizumab | $166,733 | $0 | $166,733 |
Paclitaxel | $255 | $258 | -$3 |
Cisplatin | $168 | $162 | $6 |
Carboplatin | $4,135 | $4,260 | -$125 |
Bevacizumab | $36,887 | $32,427 | $4,460 |
Administration | $8,061 | $5,894 | $2,167 |
Adverse events | $3,638 | $2,959 | $680 |
Diagnostic testing | $120 | $0 | $120 |
Subsequent treatment | $2,236 | $1,177 | $1,058 |
Resource use | $26,336 | $20,156 | $6,180 |
Terminal care | $24,672 | $24,990 | -$318 |
ICER ($/QALY) | 272,958 | ||
ICER = incremental cost-effectiveness ratio; LY= life-year; QALY = quality-adjusted life-year; SOC = standard of care.
Scenario Analyses
Table 14: Scenario Analysis (Deterministic)
Stepped analysis | Comparator | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|---|
CADTH’s base case | SOC | 93,508 | 1.42 | Ref. |
Pembrolizumab + SOC | 273,982 | 2.05 | 288,536 | |
CADTH scenario 1: Time horizon 10 years | SOC | 93,420 | 1.42 | Ref. |
Pembrolizumab + SOC | 273,360 | 2.03 | 296,001 | |
CADTH scenario 2: Weibull distribution for PFS and TTP | SOC | 93,608 | 1.44 | Ref. |
Pembrolizumab + SOC | 276,820 | 2.56 | 163,271 | |
CADTH scenario 3: Weight-based dosing for pembrolizumab (100% vial sharing) | SOC | 93,508 | 1.43 | Ref. |
Pembrolizumab + SOC | 215,125 | 2.05 | 194,437 | |
CADTH scenario 4: Weight-based dosing for pembrolizumab (50% vial sharing) | SOC | 93,508 | 1.43 | Ref. |
Pembrolizumab + SOC | 244,553 | 2.05 | 241,487 |
Appendix 5: Submitted Budget Impact Analysis and CADTH Appraisal
Note that this appendix has not been copy-edited.
Table 15: Summary of Key Take-Aways
Key take-aways of the BIA |
|---|
|
Summary of Sponsor’s Budget Impact Analysis
The sponsor submitted a budget impact analysis (BIA) estimating the budget impact of adding pembrolizumab to the treatment of adult patients with persistent, recurrent, or metastatic cervical cancer whose tumours express PD-L1 (CPS≥1) as determined by a validated test.11
The BIA base case was undertaken from a publicly funded drug plan perspective using a top-down epidemiological approach, considering drug and PD-L1 testing costs over a 3-year time horizon.
The eligible population was estimated based on data from Canada Cancer Statistics, and further limited using epidemiological estimates from various sources including published literature, experts opination, and sponsor’s internal data (Figure 2). The sponsor assumed there was no annual increase in the number of patients with persistent, recurrent, or metastatic cervical cancer over the 3-year time horizon. In the New Drug scenario, the sponsor assumed a PD-L1 testing rate would be 38% on the first year and 75% on the second and third years. The rate with a PD-L1 expression CPS ≥ 1% was based on data from KEYNOTE-826 trial.
The reference case scenario was defined as SOC therapies which included paclitaxel in combination with either carboplatin or cisplatin, with or without bevacizumab. The new reference scenario included pembrolizumab along with these comparators. The proportion of patients receiving each one of the comparators was based on sponsor’s internal research. For both reference case and New Drug scenarios, the sponsor assumed that 20% of patients would receive cisplatin and 80% would receive carboplatin.
First-line treatment costs were obtained from multiple sources including CADTH reports and Delta PA. The mean weight and body surface area to calculate paclitaxel, carboplatin, cisplatin, and bevacizumab dose were obtained from KEYNOTE-826 trial. Pembrolizumab was assumed to have a fixed dose of 200 mg every 3 weeks or 400 mg every 6 weeks. Drug costs were then multiplied by RDI. The duration of therapy was estimated from parametric distributions fitted to Kaplan-Meier time on treatment data from the KN826 trial for pembrolizumab + SOC and SOC.
Costs of subsequent therapies were included in the analysis. The subsequent treatment regimen included paclitaxel, gemcitabine, topotecan, irinotecan, and vinorelbine and the proportion of patients receiving each therapy was obtained from the EMPOWER trial and expert opinion. Finally, PD-L1 costs were sourced from literature.5
The sponsor estimated that pembrolizumab will reach a total market share of 40% after 3 years. This proportion represented 67% of the number of patients estimated to be tested for PD-L1 (75%) whose tumour expressed PD-L1 (CPS≥1) (88.8%). The sponsor also assumed that 10% of patients would be participating in clinical trials. Key inputs to the BIA are documented in Table 16.
Figure 2: Sponsor’s Estimation of the Size of the Eligible Population
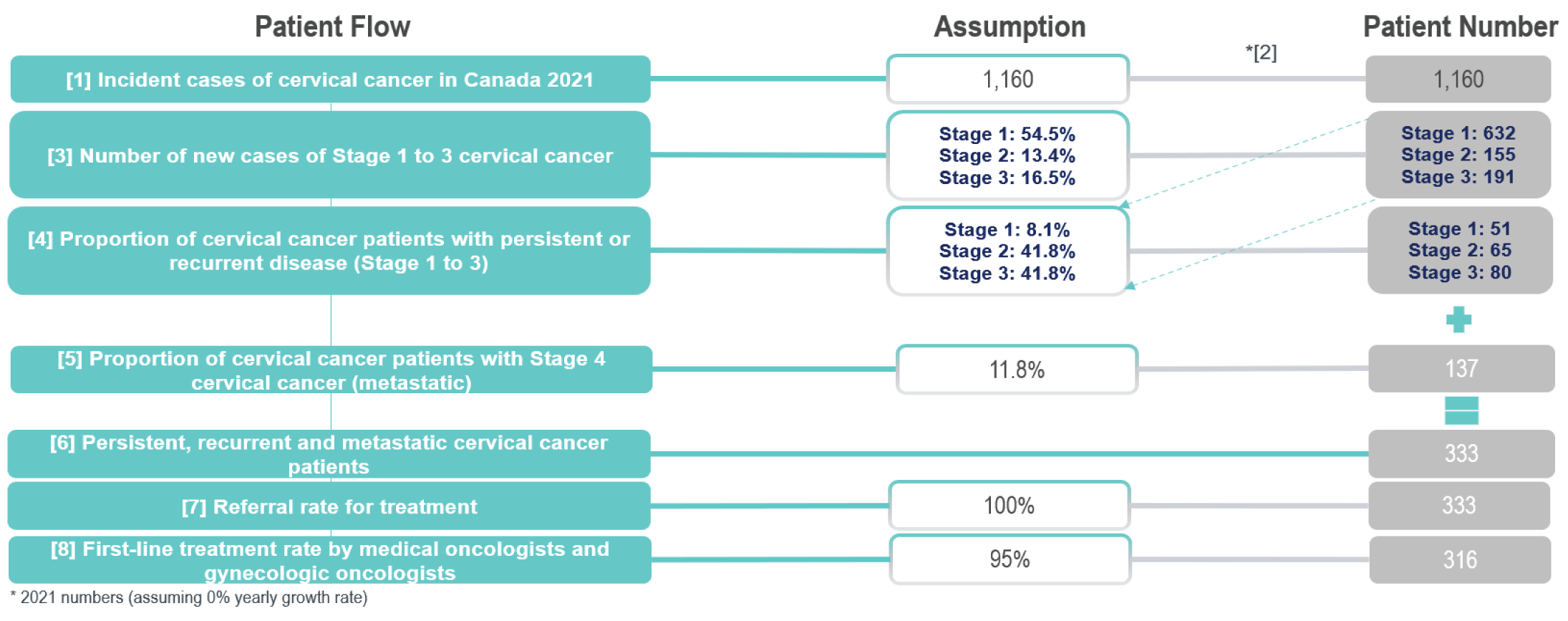
Source: Sponsor’s BIA report.11
Table 16: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as Year 1 / Year 2 / Year 3 if appropriate) |
|---|---|
Target population | |
Number of patients eligible for drug under review | 316 / 316 / 316 |
Estimated number of patients tested for PD-L1 expression | 121 / 237 / 237 |
Estimated number of patients with PD-L1 expression CPS ≥ 1 | 107 / 211 / 211 |
Market uptake (3 years) | |
Uptake (reference scenario) Paclitaxel + cisplatin or carboplatin Paclitaxel + cisplatin or carboplatin + bevacizumab Clinical trials | 36% / 36% / 36% 54% / 54% / 54% 10% / 10% / 10% |
Uptake (New Drug scenario) Pembrolizumab + paclitaxel + cisplatin or carboplatin Pembrolizumab + Paclitaxel + cisplatin or carboplatin + bevacizumab Paclitaxel + cisplatin or carboplatin Paclitaxel + cisplatin or carboplatin + bevacizumab Clinical trials | 5% / 16% / 16% 8% / 24% / 24% 31% / 20% / 20% 46% / 30% / 30% 10% / 10% / 10% |
Cost of treatment (per patient) | |
Cost of treatment over cycle Pembrolizumab + paclitaxel + cisplatin or carboplatin Pembrolizumab + paclitaxel + cisplatin or carboplatin + bevacizumab Paclitaxel + cisplatin or carboplatin Paclitaxel + cisplatin or carboplatin + bevacizumab Clinical trials | $9,405 $12,216 $1,379 $4,191 $0 |
CPS = combined positive score; PD-L1 = programmed cell death ligand 1.
Summary of the Sponsor’s BIA Results
The sponsor’s estimated budget impact of funding pembrolizumab for treatment of adult patients with persistent, recurrent, or metastatic cervical cancer whose tumours express PD-L1 (CPS≥1) as determined by a validated test from the drug plan perspective was $1,478,694, $10,905,997, $17,889,503 for years 1, 2, and 3, respectively. The 3-year total was $29,882,717.
CADTH Appraisal of the Sponsor’s BIA
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
The sponsor’s assumption regarding patient enrolment in clinical trials as a comparator is uncertain: The sponsor assumed that 10% of patients were enrolled in clinical trials and as they received trial medications, they did not incur treatment/ drug costs. For being in a time limited trial, this decreased the estimated market size and omitted potential treatment costs incurred by patients, thus underestimating the budget impact. Likewise, if pembrolizumab was approved, this may decrease clinical trial use as patients may forego a trial to be placed on a new effective therapy. Further, clinical experts consulted for this review noted that patient enrolment in clinical trials can vary significantly by province.
In the CADTH reanalysis, clinical trials were removed from the market mix; the market share of clinical trials was re-distributed over other comparators.
The market uptake for pembrolizumab may be underestimated: In their BIA, the sponsor estimated that 13% of patients would have pembrolizumab prescribed in the first year, and 40% in the second and third year. According to the clinical experts consulted for this review, there is some uncertainty regarding final uptake percentages among all clinicians in Canada, given that oncologists have experience prescribing pembrolizumab.
In the CADTH reanalysis, market uptake was changed to 90% in the first year based on clinical expert opinion.
In addition, CADTH performed a scenario analysis to explore the uncertainty in market uptake, with market uptake rates starting from 50% in the first year, reaching 75% in year 2.
The sponsor’s assumption regarding the PD-L1 testing rate may be underestimated: The sponsor assumed that, if pembrolizumab was to be funded, the PD-L1 testing rate would be 38% in the first year and 75% in the second and third years. According to clinical experts consulted by CADTH for this review, if pembrolizumab is funded, the PD-L1 testing rate would be expected to be routinely performed as part of standard practice.
In the CADTH reanalysis, the PD-L1 testing rate was changed to 95% based on clinical expert opinion.
Use of RDI is inappropriate: The sponsor’s base case incorporates relative dose intensities for pembrolizumab and SOC therapies. Consistent with previous reviews, given the inability to link RDI with outcomes, the CADTH base case does not incorporate RDI. CADTH notes RDI estimates derived from the trial apply to a fixed based dose and therefore would not be applicable to a weight-based dose.
CADTH used the functionality within the sponsor’s model to exclude RDI, assuming an RDI of 100% for all drugs.
Weight-based dosing for pembrolizumab: Pembrolizumab dosing in KEYNOTE-826 used a fixed dose of 200 mg intravenously every 21 days for adult patients. After consultation, CADTH notes that jurisdictions would likely implement a weight-based dose of 2 mg/kg (up to a cap of 200 mg) every 3 weeks with the possibility of extended dosing intervals every 6 weeks (4mg/kg up to a 400 mg cap).
In a scenario analysis, CADTH assumed pembrolizumab would be provided using a weight-based dosing based on an average weight of |||||| kg, as per KEYNOTE-826 data.
The budget impact of patients diagnosed in years 1 to 3 are not fully captured: To provide a realistic estimate over 3 years, the sponsor assumed those diagnosed with persistent, recurrent, or metastatic cervical cancer would gradually enter the BIA model over each year. Although CADTH’s base case noted that 301 patients are diagnosed in the final year of the analysis and 267 would have CPS ≥ 1, for some, full costs only reflect their first week of treatment (as costs are incurred over a year and some join at the end of the year). Although this approach hopes to represent an accurate estimate of incurred costs over a 3-year period, the analysis omits a substantial proportion of patient costs which are pushed to subsequent years not included in the BIA, thus underestimating the budget impact. Additionally, this approach makes the BIA more complex and difficult to validate.
Given complexities in the sponsor’s modelling approach, CADTH conducted a scenario analysis which estimated the full adjuvant costs for all incident patients diagnosed in years 1 to 3. To calculate this budget impact, CADTH assumed in the New Drug scenario: 267 patients would be diagnosed with persistent, recurrent, or metastatic cervical cancer CPS ≥ 1 in years 1 to 3, respectively. In all years, 90% (241 patients) would receive pembrolizumab in addition to SOC. In the reference scenario, CADTH assumed 100% of patients in all years were treated with SOC alone.
The total cost of pembrolizumab, using a fixed dose, in addition to SOC was taken from the sponsor’s cost-utility analysis. The first-year cost was estimated to be $142,175 for those receiving pembrolizumab + SOC, and $29,936 for those receiving SOC; the second-year cost was estimated to be $68,105 for those receiving pembrolizumab + SOC, and $6,238 for those receiving SOC. For simplicity, CADTH did not considered that subsequent therapy costs.
CADTH Reanalyses of the BIA
CADTH’s base case revised the proportion of patients on clinical trials, market uptake, RDI, and proportion of patients receiving PD-L1 testing.
Table 17: CADTH Revisions to the Submitted BIA
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Changes to derive the CADTH base case | ||
1. Proportion of patients on clinical trials | 10% | 0% |
2. Market uptake | 60% | 90% |
3. PD-L1 testing rate | 75% | 95% |
4. Use of RDI | Yes | No |
CADTH base case | 1 + 2 + 3 + 4 | |
BIA = budget impact analysis; RDI = relative dose intensity.
The results of the CADTH stepwise reanalysis are presented in summary format in Table 18 and a more detailed breakdown is presented in Table 19.
Based on CADTH’s base case and using a drug plan perspective, the expected budget impact for funding pembrolizumab as treatment for adult patients with persistent, recurrent, or metastatic cervical cancer whose tumours express PD-L1 (CPS≥1) as determined by a validated test is expected to be in $5,712,761 in Year 1, $25,554,791 in Year 2, and $37,973,976 in Year 3, with a 3-year budget impact of $69,241,528.
Table 18: Summary of the CADTH Reanalyses of the BIA
Stepped analysis | Three-year total |
|---|---|
Submitted base case | $29,882,717 |
CADTH reanalysis 1 | $29,882,717 |
CADTH reanalysis 2 | $49,561,917 |
CADTH reanalysis 3 | $37,851,442 |
CADTH reanalysis 4 | $32,962,317 |
CADTH base case | $69,241,528 |
BIA = budget impact analysis.
Table 19: Detailed Breakdown of the CADTH Reanalyses of the BIA
Stepped analysis | Scenario | Year 0 (current situation) | Year 1 | Year 2 | Year 3 | Three-year total |
|---|---|---|---|---|---|---|
Submitted base case | SOC | $3,432,425 | $3,993,722 | $4,003,021 | $4,004,324 | $12,001,066 |
Pembrolizumab + SOC | $3,432,425 | $5,453,295 | $14,767,992 | $21,662,497 | $41,883,783 | |
Budget impact | $0 | $1,459,573 | $10,764,971 | $17,658,173 | $29,882,717 | |
CADTH reanalysis 1 | SOC | $3,813,806 | $4,437,469 | $4,447,801 | $4,449,248 | $13,334,518 |
Pembrolizumab + SOC | $3,813,806 | $5,897,042 | $15,212,772 | $22,107,421 | $43,217,235 | |
Budget impact | $0 | $1,459,573 | $10,764,971 | $17,658,173 | $29,882,717 | |
CADTH reanalysis 2 | SOC | $3,432,425 | $3,993,722 | $4,003,021 | $4,004,324 | $12,001,066 |
Pembrolizumab + SOC | $3,432,425 | $8,059,745 | $22,280,928 | $31,222,311 | $61,562,984 | |
Budget impact | $0 | $4,066,023 | $18,277,907 | $27,217,988 | $49,561,917 | |
CADTH reanalysis 3 | SOC | $3,432,425 | $3,993,722 | $4,003,021 | $4,004,324 | $12,001,066 |
Pembrolizumab + SOC | $3,432,425 | $5,842,514 | $17,638,651 | $26,371,343 | $49,852,508 | |
Budget impact | $0 | $1,848,793 | $13,635,630 | $22,367,019 | $37,851,442 | |
CADTH reanalysis 4 | SOC | $3,788,578 | $4,406,047 | $4,415,346 | $4,416,649 | $13,238,043 |
Pembrolizumab + SOC | $3,788,578 | $6,026,291 | $16,306,069 | $23,867,999 | $46,200,359 | |
Budget impact | $0 | $1,620,244 | $11,890,722 | $19,451,350 | $32,962,317 | |
CADTH’s base case | SOC | $4,209,531 | $4,895,608 | $4,905,940 | $4,907,388 | $14,708,936 |
Pembrolizumab + SOC | $4,209,531 | $10,608,369 | $30,460,731 | $42,881,364 | $83,950,464 | |
Budget impact | $0 | $5,712,761 | $25,554,791 | $37,973,976 | $69,241,528 |
BIA = budget impact analysis; SOC = standard of care.
CADTH also conducted additional scenario analyses to address remaining uncertainty, using the CADTH base case. Results are provided in Table 20:
Price reduction of 90% in pembrolizumab cost.
Weight-based pembrolizumab.
Incident cases of metastatic cervical cancer occurred at the beginning of each year.
Results of CADTH’s scenario analyses demonstrate that both the sponsor’s analysis and CADTH’s base case do not account for a substantial budget impact that will occur in year 4. Of note, it was unclear whether this increase was due entirely to the timing of when individuals were diagnosed, due to the complexity of the sponsor’s model.
Stepped analysis | Scenario | Year 0 (current situation) | Year 1 | Year 2 | Year 3 | Three-year total |
|---|---|---|---|---|---|---|
CADTH’s base case | SOC | $4,209,531 | $4,895,608 | $4,905,940 | $4,907,388 | $14,708,936 |
Pembrolizumab + SOC | $4,209,531 | $10,608,369 | $30,460,731 | $42,881,364 | $83,950,464 | |
Budget impact | $0 | $5,712,761 | $25,554,791 | $37,973,976 | $69,241,528 | |
CADTH scenario 1: price reduction of 90% | SOC | $4,209,531 | $4,895,608 | $4,905,940 | $4,907,388 | $14,708,936 |
Pembrolizumab + SOC | $4,209,531 | $5,446,073 | $7,380,519 | $8,597,393 | $21,423,986 | |
Budget impact | $0 | $550,465 | $2,474,578 | $3,690,006 | $6,715,049 | |
CADTH scenario 2: weight-based pembrolizumab dose | SOC | $4,209,531 | $4,895,608 | $4,905,940 | $4,907,388 | $14,708,936 |
Pembrolizumab + SOC | $4,209,531 | $8,588,091 | $21,428,231 | $29,464,245 | $59,480,567 | |
Budget impact | $0 | $3,692,483 | $16,522,291 | $24,556,857 | $44,771,631 | |
CADTH scenario 3: incident cases occur at start of each year | SOC | $9,010,736 | $10,888,374 | $10,888,374 | $10,888,374 | $32,665,122 |
Pembrolizumab + SOC | $9,010,736 | $52,771,174 | $52,771,174 | $52,771,174 | $158,313,522 | |
Budget impact | $0 | $41,882,800 | $41,882,800 | $41,882,800 | $125,648,400 |
BIA = budget impact analysis; SOC = standard of care.
Stakeholder Input
Patient Input
HPV Global Action
About HPV Global Action
HPV Global Action led a collective patient input submission with the Canadian Cancer Survivor Network on pembrolizumab in combination with chemotherapy with or without bevacizumab, for the treatment of adult patients with persistent, recurrent, or metastatic cervical cancer. Both patient groups are registered with CADTH.
This is HPV Global Action’s first patient input submission to CADTH and INESSS. The group raises awareness of sex-positive inclusive sexual and reproductive health through the implementation of comprehensive programs, while emphasizing HPV and its potential consequences. They empower culturally and ideologically diverse communities across the globe through the dissemination of critical, evidence-based knowledge. They bring together provincial/territorial, federal, and global leaders to provide solutions on best practices and policies on HPV prevention, cervical screening and access to treatment. For additional information, please see www.hpvglobalaction.org.
Information Gathering
Blue Ribbon Project Inc. was contacted by HPV Global Action to assume the lead on this patient input submission, ensuring the advanced cervical cancer patient perspective was sought and captured for the therapeutic under review. The following multi-faceted outreach approach was employed:
On March 26, 2022 an online outreach was made to 7 clinicians via email who treat advanced cervical cancer patients requesting assistance identifying patients who had/have experience with the therapy under review, and willing to participate in a telephone interview to share that experience for an HTA patient input submission being made to two expert committees in Canada. That same email was followed up two weeks later (April 9, 2022).
On April 23rd, 2022, an additional 8 clinicians (Clinical Trial KEYNOTE 826 investigators) were contacted with a similar email requesting their assistance identifying advanced cervical cancer patients who might be willing to participate in a telephone interview. A second follow up email was sent one week later (April 30th, 2022). Seven U.S. based clinicians (Clinical trial 826 investigators) were also contacted at the same time with the same request.
Two additional clinicians were contacted on April 30th resulting from the kind recommendations of the HPV Global Action Board Members.
An online outreach was made to the following international organizations who provide support to cervical cancer patients on April 23-25th:
European Society of Gynaecological Oncology (esgo.org)
Jo’s Cervical Cancer Trust (jostrust.org.uk)
The Eve Appeal (eveappeal.org.uk)
Supporting Your Cancer Journey (gogirlssupport.org)
British Gynaecological Cancer Society (bgcs.org.uk)
Blue Ribbon Project Inc reached out to CCSN and kindly requested a collaborative and collective approach be assumed on this patient input submission. CCSN was in agreement for which HPV Global Action was most grateful, and CCSN, therefore, proceeded to develop an online patient and caregiver survey that was administered through Survey Monkey.
The online patient/caregiver survey was administered from April 4th – May 13th, 2022 inclusively to collect data for the submission. CCSN utilized their newsletter as well as their social media channels to promote the survey, to encourage a robust response rate. The survey spoke to the cervical cancer patient’s:
Experience with respect to the diagnosis of their cervical cancer
Experience with respect to their cervical cancer journey
Experience with respect to the drug therapies administered prior to the therapy under review
Experience with respect to the drug therapy under review
Eight respondents provided input and the results are herein attached and labelled as Appendix 2.
Three of the eight survey respondents had first-hand experience with Pembrolizumab and were able to provide input through CCSN’s online survey. The CCSN survey findings will be referenced throughout this submission to help inform the deliberations of this kind committee.
It was the clinician outreach efforts that resulted in one highly detailed and informed metastatic cervical cancer patient telephone interview. The interviewed patient (Patient A) provided firsthand compelling, relevant and high quality input regarding her:
Diagnosis of cervical cancer
Disease experience
Experience with respect to previously accessed therapies
Experience with respect to the therapy under review
Patient A is currently a 60-year-old divorcée mother of 3 adult children who resides in Ontario. The qualitative data captured from the patient’s telephone interview is summarized and represented in Appendix 1 which is attached and will also be referenced throughout this submission.
Disease Experience
The incidence of cervical cancer has certainly decreased in Canada in recent years due to widespread Human Papillomavirus (HPV) vaccination and routine cervical screenings. HPV is the necessary cause of cervical cancer, but it is difficult to predict who will develop the cancer once someone has been infected with HPV. This merely underscores the importance of promoting regular cervical screenings and HPV vaccination.
When detected in its early stages, the cancer can be treated successfully, and the prognosis may be good. Despite decreases in incidence, however, cervical cancer continues to be a highly morbid pathology in Canada and around the world. For patients diagnosed with metastatic, persistent and recurrent disease, the survival rates continue to be quite low, and prognosis remains poor due to limited and ineffective treatment options.
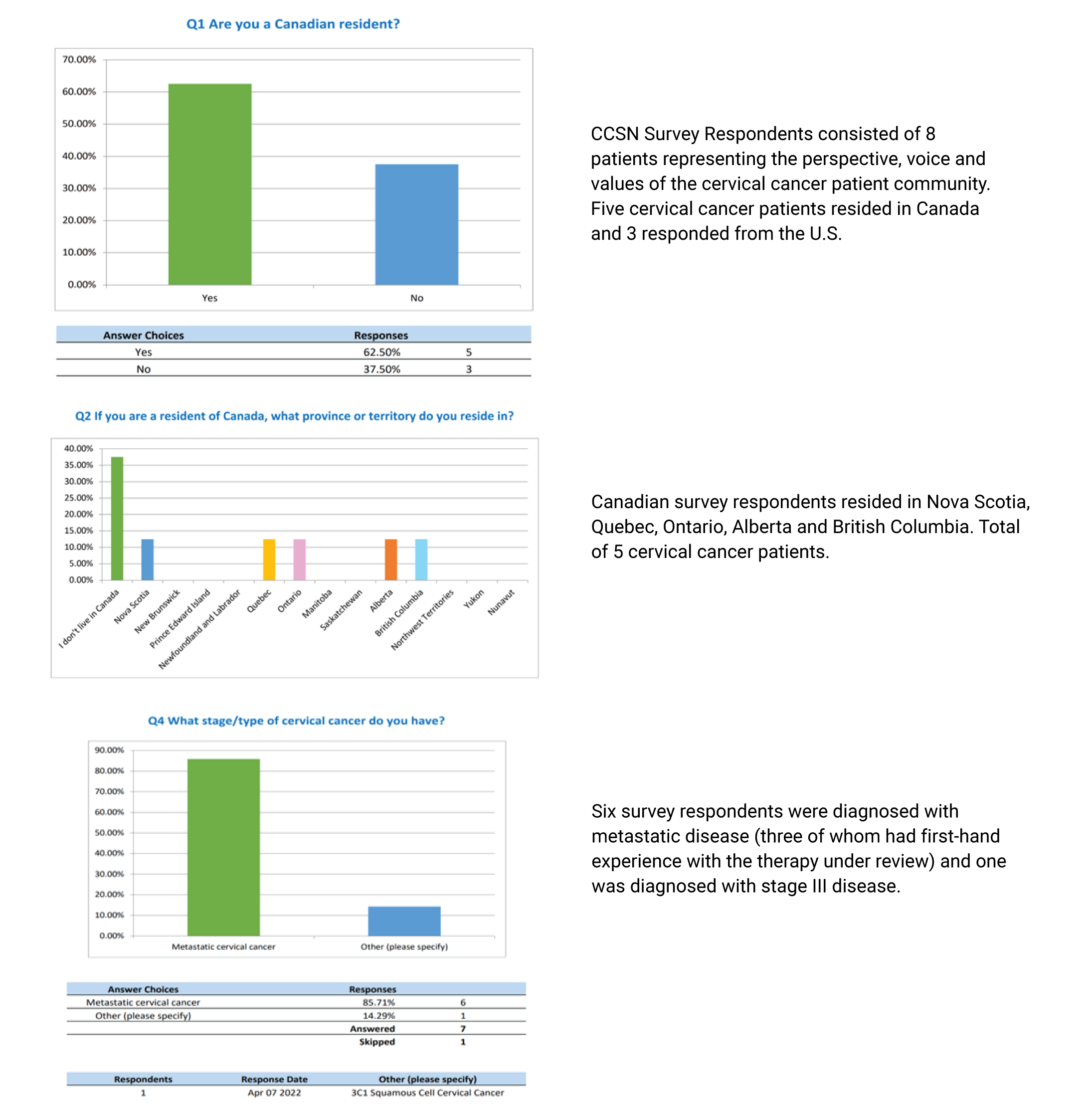
Cervical cancer typically does not produce symptoms until it is advanced. Bleeding after intercourse, bleeding after menopause onset or bleeding between menstrual periods may indicate cervical cancer, among many other symptoms. The top three symptoms (physical) experienced by survey respondents were (Q5):
Fatigue
Pain in the pelvic area or lower back that may go down one or both legs
Abnormal vaginal bleeding after menopause
And the top three problems (psychosocial) experienced were:
Living with uncertainty
Anxiety, panic attacks/depression
Feeling isolated or lonely
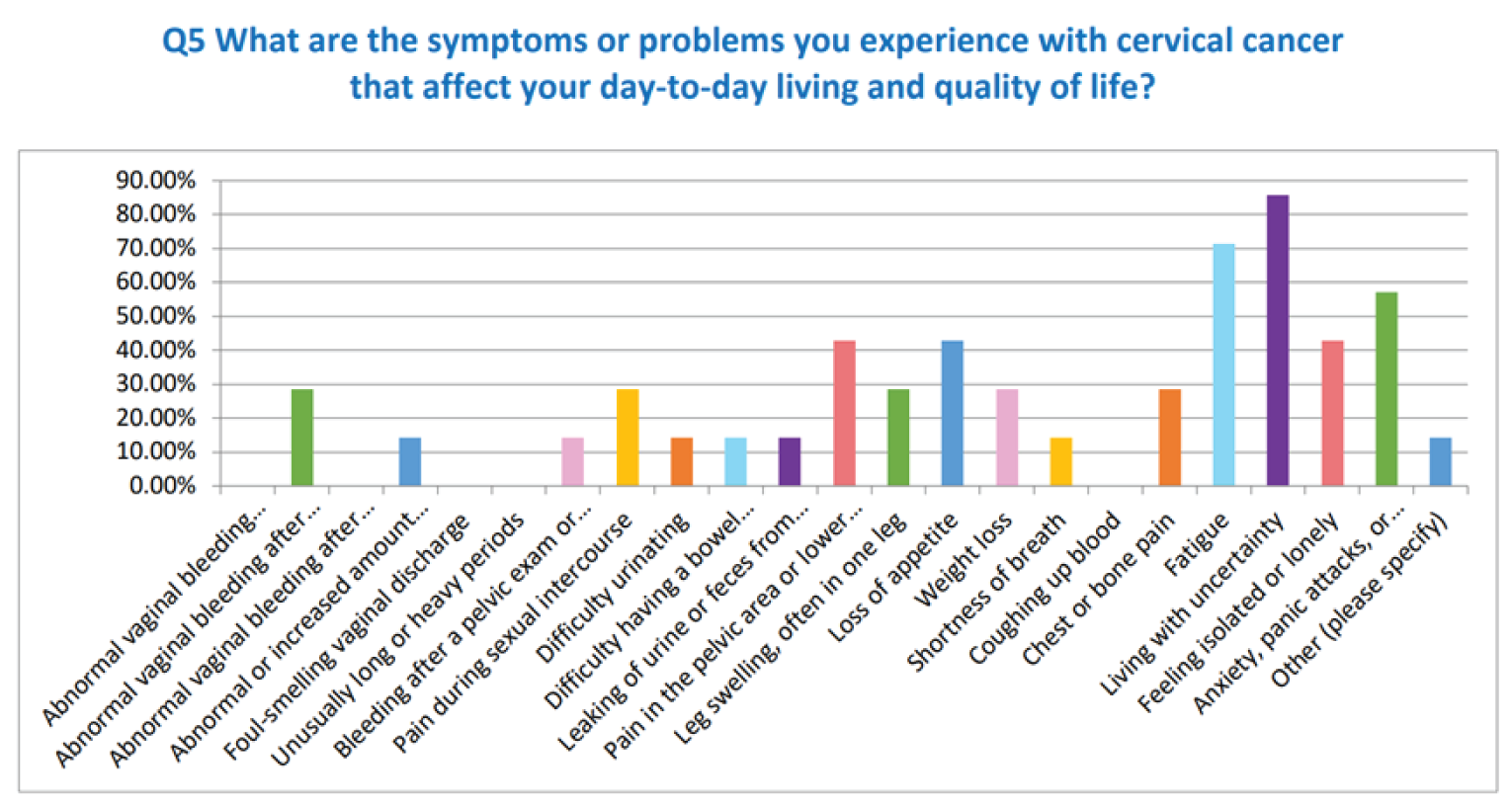
In Q6 of the CCSN survey, respondents were asked to identify their top symptom which they found most difficult to control. The majority of respondents selected Fatigue and Living with uncertainty.
Our interviewed patient, Patient A, provided thoughtful input regarding her experience with the onset of her cervical cancer symptoms experienced. In early April 2016 Patient A, a 55 year old divorcée mother of 3 was diagnosed with kidney cancer. She went on to have the kidney surgically removed in mid-May 2016 only to be subsequently diagnosed with locally advanced squamous cell cervical carcinoma around the same time of her kidney cancer surgery. Her cervical cancer diagnosis had been delayed merely because she had mistaken a number of her symptoms for the onset of menopause.
“Oh, yes, I had been symptomatic for quite some time but much like I said, I had been dismissing those symptoms because I thought some of those symptoms were due to menopause. I had been experiencing vaginal bleeding, lower abdominal pain, flue like symptoms really and that’s what prompted the testing of the pap smear and then the colposcopy because the pap smear came back abnormal. When the colposcopy came back positive, I was sent for a CT and MRI on May 30th .”
“….I could tell this journey was going to be very different from the kidney cancer journey.”
The cancer-induced symptom with which Patient A struggled most vehemently was vaginal bleeding. Despite best efforts and several different therapies, nothing could control that symptom and it prevailed. Patient A found it difficult to cope with the constant loss of blood; it impacted her daily life for an extended period of time and compromised her quality of life for she was constantly fatigued.
“Yes, the one that I had immediately before starting the trial was vaginal bleeding. I couldn’t get that one to go away. I kept losing blood all the time. My hemoglobin would be low because of it. I was tired all the time. It was a horrible symptom. It compromised my quality of life. I couldn’t go anywhere unless I was prepared to deal with that symptom.”
Patient A thoughtfully communicated the challenges and adversities imposed upon her caregivers throughout the cancer journey. Being divorced, Patient A was required to live with two of her children. She describes the journey as having been a:
“…truly horrible journey for them….Everyone had to put their lives on hold for me. My daughter had to take time off of work to take care of me before covid. It was a huge sacrifice. This was not easy for her. Imagine this young woman who was supposed to be starting her career taking time off of work to take care of her ailing mother. Not an ideal situation. My other daughter suffered in silence, and she couldn’t even turn to her mother for comfort or help because I was the sick one. My son, same…My children have had to make impossible sacrifices during covid. There has been no support system for us and the toll it has taken cannot be qualified or quantified. The toll it takes on the patient is one thing but it is an entirely different thing on the family, it is just as important and impactful.”
The above noted paragraph was just a small depiction of the painful and tearful account relayed by Patient A when describing the stressful and anxiety-stricken circumstances into which she and, just as importantly, her immediate family members were thrust after the delivery of the advanced cervical cancer diagnosis. Patient A articulately and vividly described the psychosocial toll that her metastatic cervical cancer journey imposed on her family members who cared for her in a loving, selfless and generous manner. This is a toll from which they will likely never recover because the emotional wounds inflicted were quite deep and never addressed or treated by a psychosocial professional. A diagnosis of cervical cancer can be equally frightening for the caregiver, who in this particular case is the patient’s child. They have taken on the role of true caregiver as the: housekeeper, meal preparation, psychosocial support, medical translator, online researcher and so much more. They experience fatigue, emotional drain, anxiety and worry. As is quite often the case, the caregiver’s role is overshadowed and under-valued, in large part because the focus is entirely on the patient and their journey, thus discounting the essential role played and the meaningful contribution delivered by the ever-important caregiver.
Experiences With Currently Available Treatments
Patients with recurrent, persistent and metastatic cervical cancer have limited treatment options, which accounts for the poor survival rates. If the disease is diagnosed at an early stage, however, a combination of radiation therapy and weekly chemotherapy (cisplatin) may be prescribed, with the goal of curing the cancer without surgery. All patients with locally advanced cervical cancer are potential candidates for weekly cisplatin concurrent with radiation therapy. Carboplatin may be considered in patients who are suboptimal candidates for cisplatin. And brachytherapy boost was reported to have been used post external beam radiation therapy by our interviewed patient.
Additional interventions may be administered to help bring the disease under control in the event the disease does progress on chemoradiation. Some of these interventions are discussed herein as they were accessed by patients throughout their journey, including a highly invasive surgical therapy, pelvic exenteration.
For patients whose disease is persistent, recurrent or metastatic in nature, systemic treatment is recommended and, sadly, long term survival is rare. For patients who have previously received single agent platinum therapy and now have recurrent or metastatic disease identified, platinum-based combination chemotherapy is recommended along with the biologic therapy bevacizumab, if available and appropriate. It is worth noting that the platinum-based combination therapies have significant toxicities.
The CCSN survey results identified the following therapies as the most prevalent treatments in the management of cervical cancer (Q7): Cisplatin, Carbotaxol/Bevacizumab, carboplatin and palliative care. When asked how effective each of those therapies were at controlling their cancer, patients identified the various therapies as either “somewhat effective” or “not very effective at all” (Q8). One patient provided an open-ended reply identifying “radiotherapy and SBRT as very effective at controlling her cancer”.
Patients living with the side effects of cervical cancer treatments deal with a host of physical, emotional and social issues unique to the disease. The physical side effects of locally advanced cervical cancer treatments stem largely from radiation therapy of the pelvis and include dysfunction of the bowel, bladder and sexual organs. Patients seek treatment for these symptoms aimed at identifying reversible or treatable causes of these symptoms and palliating those with irreversible causes. Not surprisingly, the following side effects were reported by survey respondents as having impacted their day to day living, as well as their quality of life:
Pain during sexual intercourse (2)
Difficulty urinating (1)
Difficulty having a bowel movement (1)
Leaking of urine or feces from the vagina (1)
As part of her cervical cancer journey, Patient A underwent chemoradiation (June 2016), followed by brachytherapy boost and then some additional external beam radiation therapy. She describes the cisplatin-induced side effects as “horrific and a patient’s worst nightmare”. Since she has one kidney, she experienced significant dehydration. She also experienced digestive problems such as nausea, vomiting, gas and lack of appetite. Additional toxicities included neuropathy, and unimaginable fatigue. The external beam radiation therapy induced severe dehydration and nausea such that she required regular hydration therapy. No effective antiemetic therapy was identified for Patient A which is why she was hospitalized on a fairly regular basis. She comments: “What kind of life is that? I didn’t feel human at all. I had lost a part of me. The part of me who was trying to achieve so much by earning my undergraduate and graduate degrees and go on to do wonderful things with my life.”
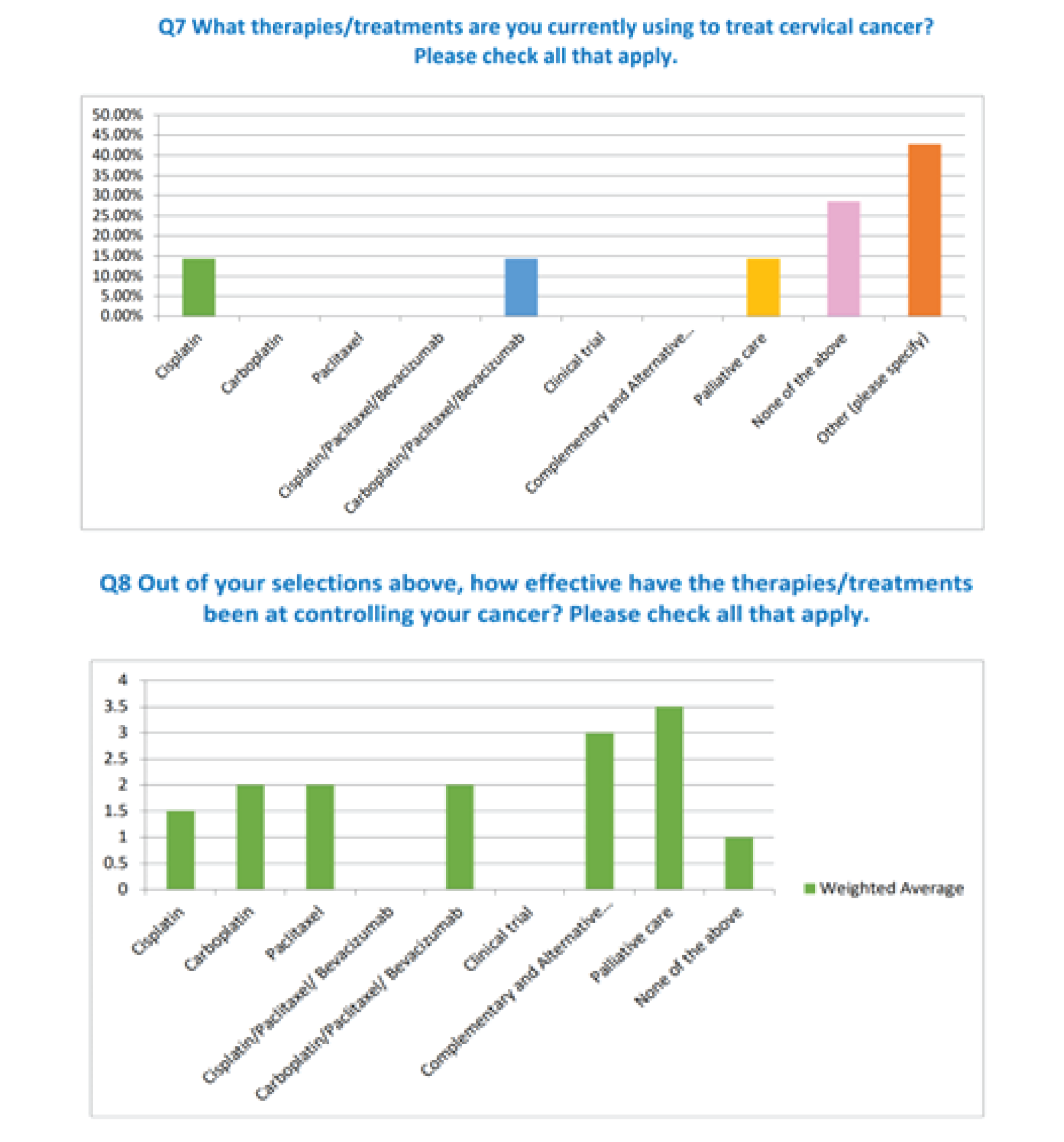
Patient A went on to access brachytherapy (August 2016) which debilitated her completely for well over two months. She then had additional radiation therapy (October 2016) because the disease was persistent. Dysfunction of the bowel is very common after pelvic irradiation, leading to symptoms that include nausea, vomiting, diarrhea, constipation and fecal urge or incontinence. Bowel symptoms, especially fecal urge and incontinence, are particularly linked to social isolation and depression. Sexual dysfunction in patients is prevalent, more pronounced in younger patients, and may be related to treatment related menopause and direct treatment effects on sexual organs. Patients may suffer in silence. After having undergone radiation therapy, brachytherapy and additional radiation therapy, Patient A shared the following regarding brachytherapy:
“I swear I got PTSD from the therapy. And just thinking about it, gives me the shakes. …..It is inhumane, totally inhumane. It was horrible, what I went through with that therapy, just brutal. I have pelvic collapse and so much sexual dysfunction. I try really hard not to think about it but it puts me into a really bad place and horrifies me. It really is not humane.”
In March 2017, Patient A underwent a pelvic exenteration, wherein her uterus, bladder, colon, vagina, rectum and cervix were removed. The surgery rendered her completely helpless for well over six months. She lost a significant amount of weight, and had to learn how to function again, and learn how to care for herself again. She learned how to drive and bathe herself again because she was unable to do the simplest of tasks while recovering from this long and invasive surgical procedure that rendered her totally incapable of living life on any meaningful level. She had no quality of life while recovering from this surgery but she does state that the surgery did manage to eradicate any visible signs of disease for approximately one year. She shared the following: “The nurse would have to come to help me change my two ostomies that resulted from the surgery. I was so weak, I couldn’t be bathed at all (by anyone). Imagine that, no bathing because I was too weak. Do you know what that does to your psyche? It really did a number on me.”
Patient A also underwent a lung resection (based on disease detected back in December 2017) in June 2018 which was quite successful. She cites no complications or difficulties from that surgical intervention and managed to heal very quickly.
In December 2019, Patient A was diagnosed with additional metastatic disease (peritoneum, maximus gluteus, outer vaginal wall) and was, therefore, referred to a medical oncologist for clinical trial consideration.
Question 9 of CCSN’s online survey identified the issues that cervical cancer patients are encountering with respect to current therapy. Some of the issues identified by patients were:
Supplies or issues with administration
Travel costs associated with getting therapy/treatment
Limited availability in my community.
When cervical cancer patients were asked if there were any needs not being met regarding their current therapies (Q10), close to half of the patients replied “yes” and offered the following open-ended replies:
Controlling lymphedema
Would like to access genomic testing like what is offered by foundation medicine
Improved Outcomes
The CCSN survey took the opportunity to ask metastatic cervical cancer patients who had not accessed the therapy under review to thoughtfully identify the outcomes which should be considered when evaluating novel therapies (Q12). All patients selected “maintain quality of life” and “access to a new treatment option” as reflected below.
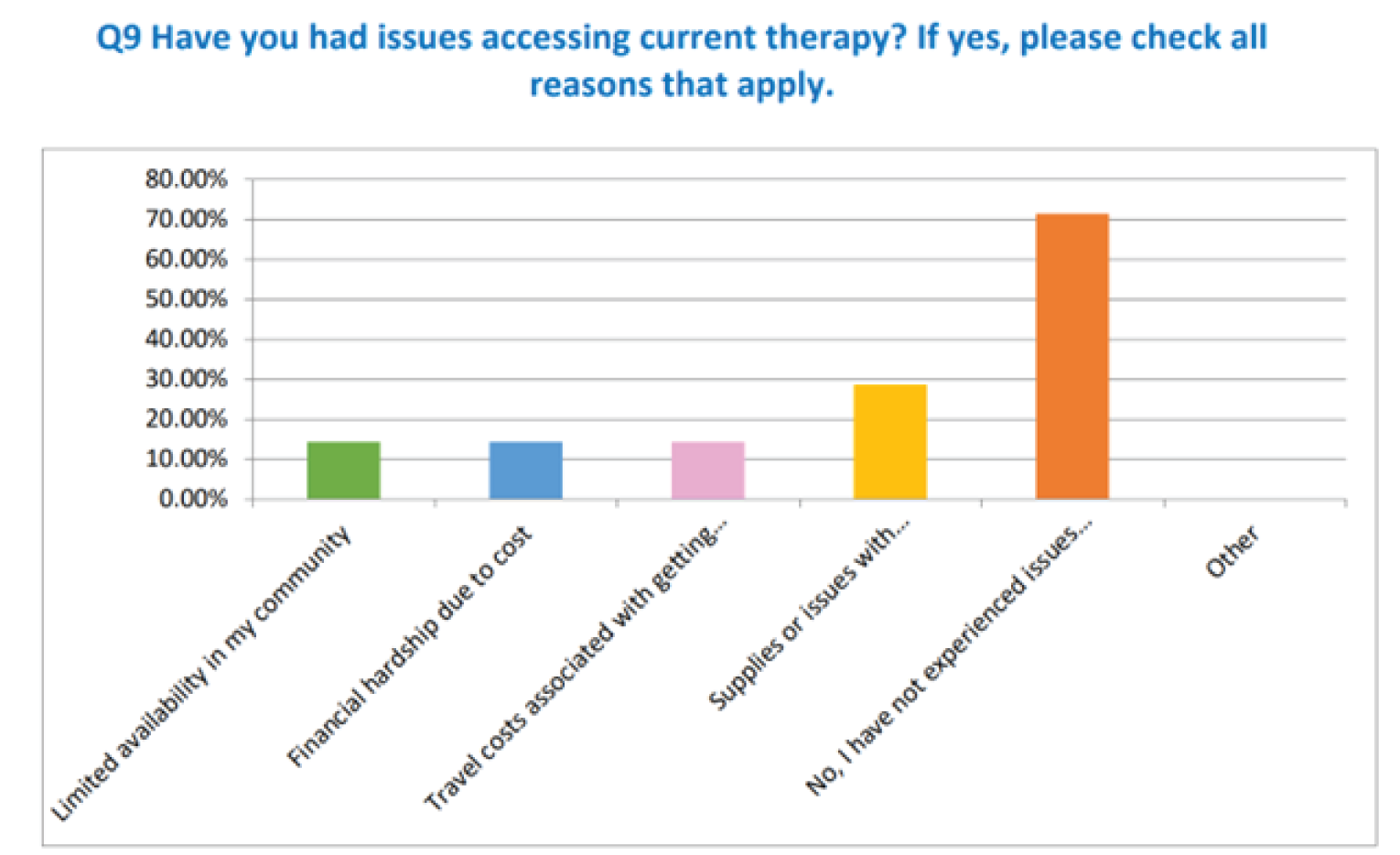
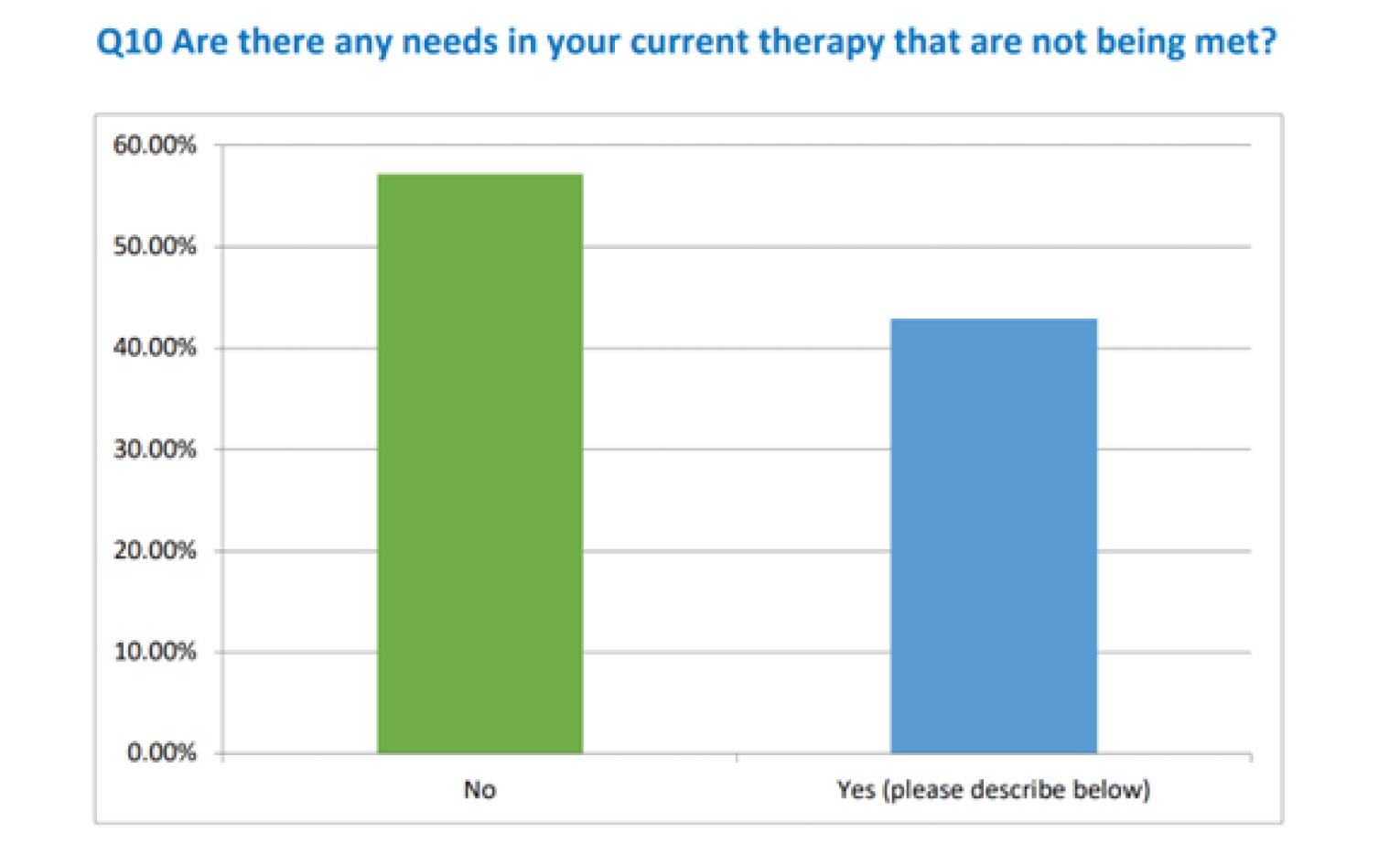
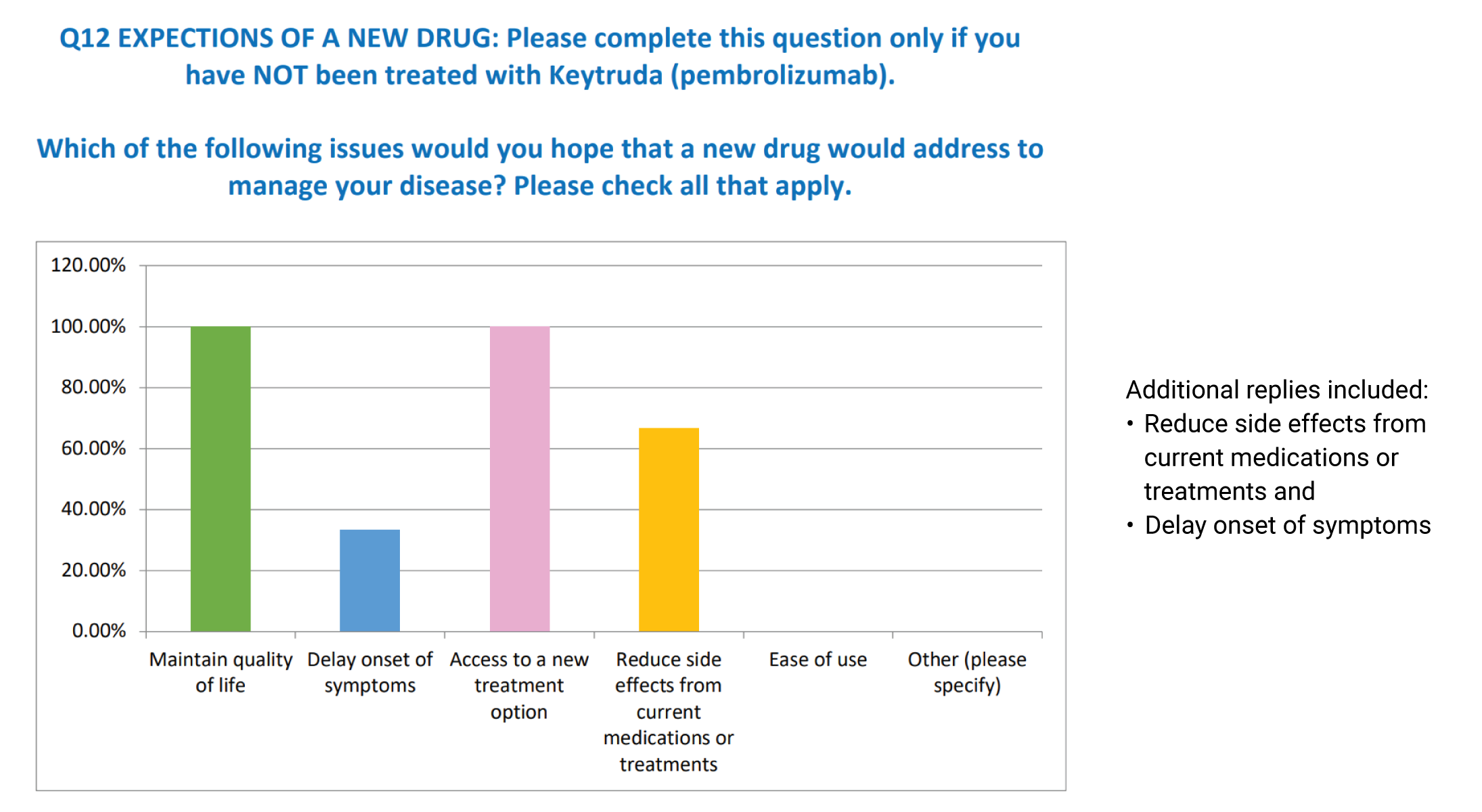
When these same patients were asked what side effects or symptoms would they be willing to tolerate in a new drug therapy to help treat their cancer (Q13), patients furnished the following open-ended replies:
“Hair loss, weakness, fatigue”
“What could be worst than chemo?”
“Honestly, anything if it were able to extend my life and help me fight”
Patient A also provided her perspective on the improvements she would wish to see associated with a new drug therapy – improvements she believes are currently not available with the standard of care therapies for the management of metastatic cervical cancer. Throughout her interview, Patient A repeatedly stressed that cervical cancer has long term effects on health-related quality of life of cancer on cancer patients after treatment. She referenced her own extensive treatment journey and the impact the treatments have had on her life. Bowel morbidity was prevalent after chemoradiotherapy as she experienced severe diarrhea, dehydration, nausea and vomiting. These are symptoms that significantly reduce quality of life. She also experienced sexual dysfunction with which she struggled and continues to experience emotional hardship. In her words:
“….I would like to see no horrific side effects for sure so that patients can lead a life with a great quality of life, hands down. And of course, a therapy that can extend life for a significant period of time, not just by a few months or a year, but a significant amount of time, such as many years. And may I say, can we consider associating adjunctive therapies to standard of care treatments much like Germany does? It may very well improve care here for patients. It can help with side effects from treatments and help the patient feel better.”
She further stressed that cervical cancer patients should not be receiving therapies from which patients derive minimal benefits at the cost of significant toxicity.
“…Up until I went on this clinical trial, I never really had that (effective and user-friendly therapies). I kept accessing toxic, ineffective and debilitating therapies that would knock me off my feet. That’s just unacceptable.”
Hence, in her opinion, the outcomes that Patient A found to be of great value were quality of life, overall survival, and disease free survival.
Experience With Drug Under Review
The therapy under review is the immune checkpoint inhibitor pembrolizumab (Keytruda) used in combination with chemotherapy, with or without bevacizumab, in people with persistent, recurrent, or metastatic cervical cancer whose tumors express the specific protein PD-L1 (CPS>1) as determined by a validated test. The CPS (combined positive score) allows clinicians to assess PD-L1 in a patient’s tumour so that candidacy for immunotherapy may be determined.
In addition to the interviewed patient, three cervical cancer patients accessed the therapy under review according to the CCSN survey results. One of those survey respondents clearly stipulated having accessed the therapy through a clinical trial. Two of the survey respondents achieved a no evidence of disease (NED) status and identified the NED status as a “positive effect” from having accessed the therapy (Q14). One of those patients states: “My tumour has reduced to being NED in 9 months”. The third patient relayed having experienced “minimal side effects. It was great. I barely felt anything at all.” We believe this patient accessed pembrolizumab monotherapy, though we cannot ascertain this without confirming this directly with the patient nor can we find any confirmatory information in the survey results.
As for any negative effects from having accessed the treatment, two patients provided the following input:
“I could only get it in a clinical trial. I can only have a set number of treatments.”
“Grade 2 interstitial nephritis, resolved.”
The three survey participants were asked if they were able to manage certain issues more effectively while on the therapy under review in comparison to previously accessed therapies (Q15). All three patients replied “yes” with respect to:
Disease progression
Ease of use
More control of symptoms
And two patients responded “yes’ with respect to “reduction in side effects from current medications or treatments”. Q16 asked “What adverse effects were caused by Pembrolizumab?”. One patient made it abundantly clear that she suffered no side effects while undergoing Pembrolizumab. Two patients selected nausea and feeling unusually tired or weak. One patient selected diarrhea, rash, joint pain and fever as pembrolizumab-induced side effects. There were additional side effects provided through the open-ended reply option which consisted of: “dry skin and nail breakage”; “interstitial nephritis”. Patients were asked to select which adverse effects would be acceptable to them and which would not (Q17). Two patients responded to this question seeing that one patient experienced no side effects while undergoing Pembrolizumab therapy. There appeared to be a consensus on five side effects wherein patients would be prepared to accept those side effects while on Pembrolizumab:
Itching
Rash
Low levels of thyroid hormone
Feeling less hungry
Patches of skin which have lost color (vitiligo)
There was no consensus among the two patients in respect of the balance of the side effects, as evidenced below (Q17).
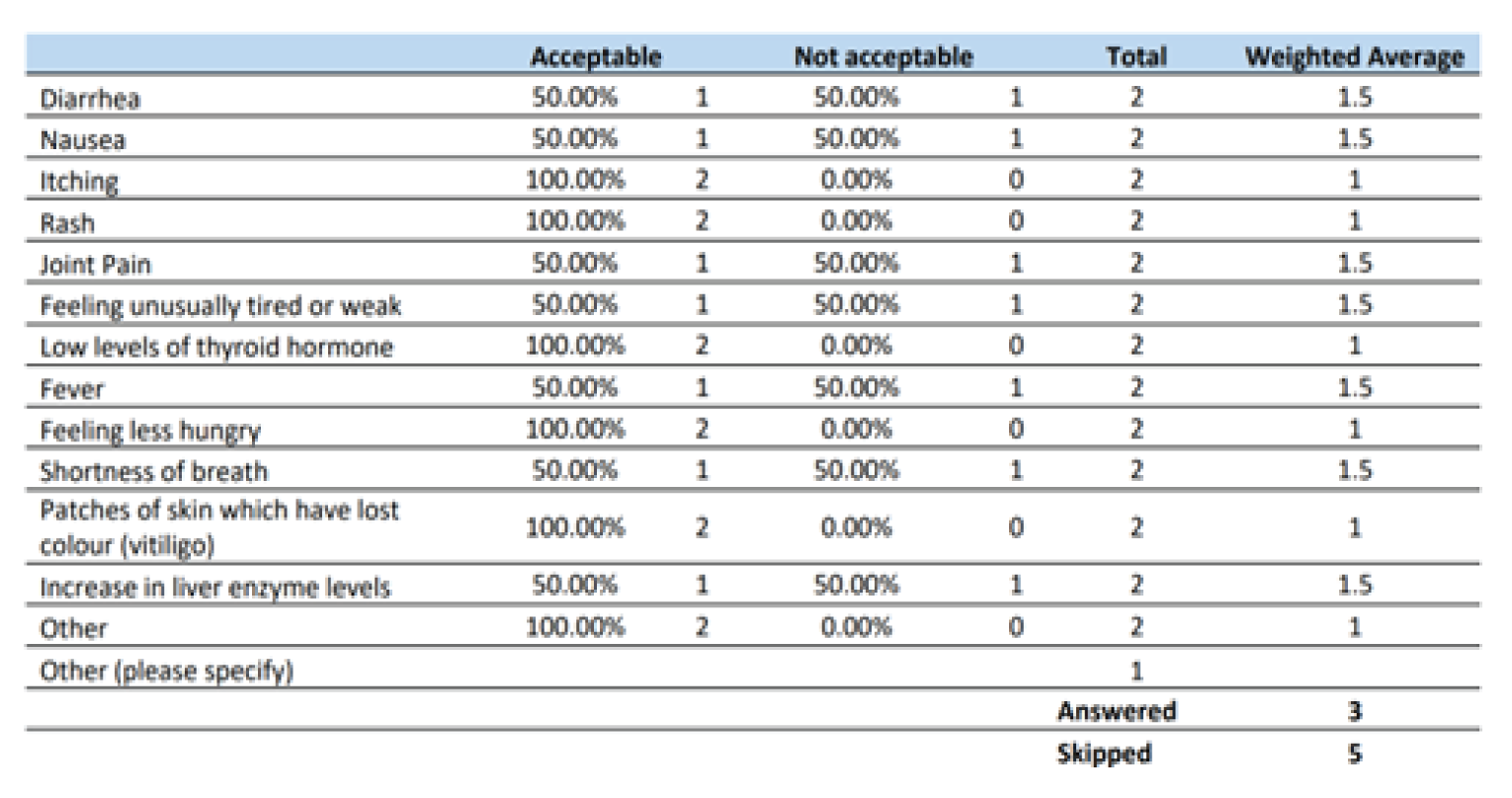
Survey participants were asked what their expectations regarding their long-term health and well-being resulting from Pembrolizumab therapy (Q18). Cervical cancer patients responded providing the following open ended replies:
“To continue to live as long as I can with good quality of life. This drug has been wonderful and easy for me. It really hasn’t been toxic or made me sick like the chemos. I hope I get to stay on it for a long time.”
“Better quality of life and not having my cancer spread.”
“No evidence of disease!”
Our interviewed patient (Patient A) accessed the therapy under review in combination with Carbotaxol and bevacizumab through a clinical trial with great anticipation and hope because she had persistent, metastatic disease that had failed to respond to multiple, previously accessed therapeutics. In June 2016, Patient A started her journey with 6 cycles of weekly cisplatin and concurrent pelvic external beam radiation therapy followed by brachytherapy for her initial diagnosis of cervical cancer. She accessed additional radiation therapy two months later for residual disease. She underwent a pelvic exenteration in March 2017 followed by a lung resection in June 2018. She accessed the KEYNOTE 826 study in January 2020 which made a profound and meaningful difference in her life and clinical outcomes.
Please note: Patient A has shared that the trial is a double blind randomized control study. As such, she has no confirmation of having received Pembrolizumab vs the placebo. However, in light of her extraordinary results – a no evidence of disease status -, she is convinced she has received the immunotherapy and as such, she has relayed the contents of her case in accordance with this heartfelt and passionate conviction. In her words:
“…I have to say this: this clinical trial is a phase III double blind clinical trial, so technically, I had no idea if I have received the Pembrolizumab or the placebo. Based on the fact that I am today no evidence of disease, I am assuming that I received the Pembrolizumab and crediting my wonderful health status to the Pembrolizumab but I have no evidence to support that, except the way I feel and CT results.”
Patient A learned of the therapy under review through a consult with a medical oncologist in December 2019 who was leading a clinical trial on that particular medication. The medical oncologist advised Patient A that she qualified for the study based on some previous molecular testing performed on her tumour twelve months prior to the consult. The results of the testing identified Patient A as a good candidate for the KEYNOTE 826 study which was randomly assigning metastatic cervical cancer patients in a 1:1 ratio to receive pembrolizumab or placebo every 3 weeks, for up to 35 cycles, plus platinum-based chemotherapy with or without bevacizumab. Patient A saw this as an opportunity and was eager to accept it and did precisely that. She claims “it was the best thing I ever did”. She expressed how overjoyed she was that she qualified for the trial based on the molecular marker – PD-L1 - a marker whose identity she was not aware of the year prior to her medical oncology consult. She experienced just a few side effects: neuropathy while she was on the Carbotaxol which is why she had to stop that treatment two months (March 2020) after initiating therapy. She also experienced some hypothyroidism and some gastrointestinal issues such as bloating and loose stools, which prohibit her from ingesting raw vegetables to date. From March 2020 to July 2021, she continued to access bevacizumab and what she believes to be pembrolizumab and experienced a much easier time on the therapy. She states:
“In comparison to the brutal side effects I have experienced with the other therapies, it has been really easy but since I have experienced some side effects on this too, because of Carbotaxol, I would have to give it an overall rating of: 7.”
Patient A accessed 24 cycles of the therapy and has, since July 2021, acquired a no evidence of disease status. She has not required or accessed any additional therapy since July 2021. Additionally, she has not only earned her master’s degree while undergoing this therapeutic but has also been accepted into a PhD Program and is working actively towards earning her doctorate. She emphatically relayed that she had great difficulty controlling a cancer-related symptom before starting this clinical trial: vaginal bleeding, but thankfully, the trial drugs have successfully managed to address this annoying symptom. Patient A maintains that the trial drugs have delivered a remarkable response, confirmed both radiographically (CT scans) and clinically (she feels wonderful and alive again). In her words:
“I had a fantastic response! According to the CT scan results (done every 3 months), I have no more disease. And I think you know that the trial experts and the hospital experts review the CT findings, so they both came to the same conclusions. No more disease for me! I am so grateful and so happy and so is my family. What a wonderful conclusion this is for me after all the suffering I went through.”
When Patient A was asked if it was worth accessing the therapy, she was quite emphatic when she replied:
“Yes, of course it has been worth it….look, I am still here today. It has to count for something. I don’t believe I would be here today if I had not accessed Pembrolizumab. I believe it is a wonder drug. I am able to still be around for my family. And guess what! I got to finish not only my undergrad degree when I got diagnosed, but my master’s degree as well and I got into a PhD program!! I want to still do so much in life and this therapy will allow me the chance to do it. Imagine, I was able to complete my master’s degree and get into a PhD program that I have been actively working on since being on this therapy. I would say that it was definitely worth accessing the therapy.”
When she was asked if she was able to fulfill or accomplish anything that she would not have otherwise been able to do had she not accessed the therapy, she provided the following heartfelt reply:
“The therapy has allowed me to get into a PhD program and work towards realizing that dream of getting my PhD. I can’t believe it is coming true. I am no evidence of disease because of that therapy and on my way towards doing wonderful things in life. I am independent, working well, active and in school. I am living my best life. I couldn’t have asked for more.”
Patient A cited how much easier the therapy under review is to use when compared to previously administered therapies resulting in a superior quality of life. She appreciated the short infusion time associated with what she believes is Pembrolizumab administered every 3 weeks, which is unlike the infusion times associated with previously administered standard of care systemic therapies for advanced cervical cancer. But more importantly, valued the much improved toxicity profile associated with pembrolizumab in combination with bevacizumab. In her own words:
“Oh, sure it has. Initially, when I started it, it was a long day but then it got so much better and everything got shorter for me, and so much easier. And the therapy is not toxic like the other therapies I was on like the brachytherapy or the chemoradiation or the pelvic exenteration. What a ride that was! The infusions, like the bevacizumab and what I believe is the pembrolizumab were short so it was all good.”
With respect to treatment cessation, Patient A cites two instances in which she had to stop therapy:
Once for a urinary tract infection and
Once wherein she was feeling poorly
Companion Diagnostic Test
Cervical cancers that express the protein programmed cell death – ligand 1 (PD-L1) may be more likely to respond to treatment with the checkpoint inhibitor immunotherapy drug, pembrolizumab. The greater the proportion of tumour cells that express PD-L1, the better the response potentially to immunotherapy. In order to assess PD-L1 in cervical tumours, a CPS (combined positive sore) metric of 1 or higher is used to help identify patients most likely to benefit from pembrolizumab. It is a ratio of the number of all PD-L1–expressing cells (tumor cells, lymphocytes, macrophages) to the number of all tumor cells multiplied by 100.
PD-L1 is indeed a biomarker for pembrolizumab in metastatic cervical cancer because it identifies patients who are likely to benefit from the therapy. And the validated test is the PD-L1 immunohistochemistry which is similar to that utilized in several sites.
Our interviewed patient expressed how grateful she was that her medical oncologist had her tumour molecularly profiled the year before she learned of and consented to the KEYNOTE 826 clinical trial. She maintains she experienced no anxiety in anticipation of the test results because she was not aware of the implications of those test results while they were being generated. The results were also being conducted at the cancer centre, at no cost to her whatsoever. It was a stress-free event from beginning to end. This patient’s experience merely serves to highlight the need to test for molecular-targeted drugs and immune modulation early on in the patient’s journey which may help to achieve improved outcomes for women with recurrent, persistent or metastatic cervical cancer.
For those patients who qualify for the immunotherapy based on CPS of 1 or higher, patients may be able to experience a life prolonging therapy. According to surveyed patients and our interviewed patient, the therapy has demonstrated great efficacy in the treatment of their recurrent/metastatic disease. Upfront testing will identify the patients who qualify for the therapy and will ultimately change the treatment paradigm and guide treatment decisions. The result, according to patient input, will be improved quality of life due to fewer treatment induced toxicities, and significant disease regression leading, potentially, to a no evidence of disease status or significant regression. Our interviewed patient passionately states:
“I just wish I had received this treatment 6 years ago so that I wouldn’t have had to go through all these body modifications and forgone these changes and horrible toxic side effects and all the suffering I went through. It has been dreadful. This therapy would have spared me that. I could have achieved a no evidence of disease a lot earlier, a lot sooner.”
For patients who are identified with the unique biomarker (PD-L1), pembrolizumab delivers on the promise of precision medicine guiding treatment decisions for the persistent, recurrent and metastatic cervical cancer patient population.
Anything Else?
There is an unmet need for novel therapies to improve clinical outcomes for patients with persistent, recurrent and metastatic cervical cancer. Most cases of cervical cancer are driven by infection with HPV which uses multiple mechanisms to avoid immune surveillance. The checkpoint inhibitor, pembrolizumab, seeks to activate the immune system in order to overcome this resistance and improve treatment outcomes. Advanced cervical cancer has a dismal prognosis and treatment options are limited for this patient population. The standard of care for patients diagnosed with metastatic disease consists of multiagent systemic chemotherapy which includes a platinum based agent in the first line setting. On its own, the therapy has low response rates and can be quite toxic creating an urgent, unmet need to provide novel therapies that can provide patients with improved outcomes. These improved outcomes may include superior quality of life, an extension in both progression free survival and overall survival. Bevacizumab has been added to first line treatment in combination with chemotherapy, but survival rates are still quite poor and additional targeted agents are required.
The patients who received pembrolizumab (surveyed patients and the interviewed patient) reported having experienced significant improvements in health status with respect to physical function and overall quality of life. The therapy itself had fewer side effects compared to previously administered therapies (surveyed patients accessed the immunotherapy as monotherapy and the interviewed patient was able to make a fair comparison because she eventually stopped the chemotherapeutic portion of the clinical trial). Patients expressed their sincere gratitude for having accessed the immunotherapy under review because according to them, it delivered a robust, durable, safe and effective response compared to previously accessed therapies. The interviewed patient and two surveyed patients managed to achieve a complete response and eradication of disease. In their words, a “no evidence of disease status” with the therapy.
Surveyed patients and our interviewed patient expressed the benefit they derived from the therapy, which was unlike any other previously accessed treatment. Our interviewed patient was able to resume a normal, active healthy lifestyle which she credits entirely to the therapy under review. She was once again engaged happily in life, enrolled in higher learning classes, spending quality time with her family and community, contributing to the world in a meaningful and productive manner, knowing that she will be able to move forward in life with hope. When Patient A was asked if she had any last thoughts to contribute during her interview, she emphatically stated:
“I guess I would have to say that it is so important that every patient who qualifies for this therapy accesses this therapy sooner rather than later. It worked for me…..Accessing the therapy sooner for patients would avoid unnecessary procedures that are painful and toxic and uncomfortable and threatens quality of life. Mostly, it avoids accessing ineffective treatments that allows for continued progression that makes the cancer more difficult to treat. Why would we want that as a cancer community? Let’s treat this type of cancer, a horrible cancer, as early as possible for women who qualify. Women have been so underserved in this type of cancer. It’s time to ensure they get a break and are treated optimally and timely. So, can you please ensure my thoughts are relayed to those who are making the decisions out there please? We need to be heard. Thank you.”
The use of the therapy helps to address the urgent, unmet need that currently exists in the management of persistent, recurrent, metastatic cervical cancer. Funding this therapy in the appropriate setting based on the identification of a unique biomarker, aligns well with the patient perspectives captured within this submission. We recognize the limitations associated with this submission: namely the small number of patients who completed the online survey and the few patients from whom we heard through telephone interviews, but we believe the perspective captured through the telephone interview to be representative of the advanced cervical cancer patient population. Our interviewed patient strongly supported the need for a positive funding recommendation be issued for pembrolizumab in combination with chemotherapy with or without bevacizumab for the treatment of persistent, recurrent and metastatic cervical cancer whose tumors express PD-L1 (CPS>1) as determined by a validated test.
The patient voice captured herein (survey and interview) underscores the need to provide a new, highly effective, and highly targeted therapeutic in the management of advanced cervical cancer, capable of delivering durable responses and improved survival. We, therefore, strongly support and urge that a positive funding recommendation be issued for pembrolizumab in combination with chemotherapy with or without bevacizumab for the treatment of persistent, recurrent and metastatic cervical cancer. We believe it aligns well with the identified patient need for a new, effective treatment option that is capable of providing a high quality of life while targeting the PD-L1 pathway in the first line setting that addresses an urgent unmet need.
Conflict of Interest Declaration — HPV Global Action
Did you receive help from outside your patient group to complete this submission? If yes, please detail the help and who provided it.
Yes, HPV Global Action commissioned the services of Filomena Servidio-Italiano from Blue Ribbon Project Inc. to author this patient input submission.
Did you receive help from outside your patient group to collect or analyze data used in this submission
Yes, HPV Global Action commissioned the services of Filomena Servidio-Italiano from Blue Ribbon Project Inc. to oversee the planning, coordination, data collection and analysis of this patient input submission.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review.
Table 1: Conflict of Interest Declaration for HPV Global Action
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Merck- direct interest | — | — | — | X |
Organon- indirect interest | — | X | — | — |
Roche | — | — | — | X |
Hologic | — | — | X | — |
BMS | X | — | — | — |
Coalition Priorité Cancer au Québec | — | — | X | |
Gilead | — | X | — | — |
Telus | — | X | — | — |
Sox-Box Accessories | X | — | — | — |
The Azrieli Foundation | X | — | — | — |
The Henry & Berenice Kaufman Foundation Grants | X | — | — | — |
Did you receive help from outside your patient group to complete this submission?
Yes, HPV Global Action commissioned the services of Blue Ribbon Project Inc. to lead and author this patient input submission.
Did you receive help from outside your patient group to collect or analyze data used in this submission?
Yes, Blue Ribbon Project Inc. oversaw the analysis of the survey findings and patient interview for this submission.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review.
Table 2: Conflict of Interest Declaration for Canadian Cancer Survivor Network
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Merck | — | — | — | X |
Clinician Input
Ontario Health Cancer Care Ontario
About Ontario Health Cancer Care Ontario
OH-CCO’s Drug Advisory Committees provide timely evidence-based clinical and health system guidance on drug-related issues in support of CCO’s mandate, including the Provincial Drug Reimbursement Programs (PDRP) and the Systemic Treatment Program.
Information Gathering
The information was gathered at a DAC meeting.
Current Treatments and Treatment Goals
Standard first-line therapy for persistent, recurrent, or metastatic cervical cancer is platinum-based chemotherapy, with a preferred regimen of a platinum compound (cisplatin or carboplatin) and paclitaxel plus bevacizumab on the basis of a balance between efficacy and safety.
Treatment goals would be delayed disease progression, prolonged life, improved health-related quality of life, reduced severity of symptoms.
Treatment Gaps (Unmet Needs)
Considering the treatment goals in Section 3, please describe goals (needs) that are not being met by currently available treatments.
Pembrolizumab would improve efficacy for persistent, recurrent, or metastatic cervical cancer. There currently is not a curative treatment for this population. There are very few options for this patient population and limited second-line options.
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
Pembrolizumab for cervical cancer would fit into first-line.
Which patients would be best suited for treatment with the drug under review? Which patients would be least suitable for treatment with the drug under review?
Patients with persistent, recurrent, or metastatic cervical cancer whose tumors express PD-L1.
Least suited patients would have contraindications to pembrolizumab and patients who do not express PD-L1
What outcomes are used to determine whether a patient is responding to treatment in clinical practice? How often should treatment response be assessed?
As per standard of care.
What factors should be considered when deciding to discontinue treatment with the drug under review?
Disease progression or toxicity.
What settings are appropriate for treatment with [drug under review]? Is a specialist required to diagnose, treat, and monitor patients who might receive [drug under review]?
Hospital (outpatient clinic) with a specialist.
Additional Information
Not applicable.
Conflict of Interest Declarations — Ontario Health Cancer Care Ontario
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please see the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission? If yes, please detail the help and who provided it.
OH-CCO provided secretariat support to the DAC in completing this input.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission? If yes, please detail the help and who provided it.
No.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician who contributed to the input — please add more tables as needed (copy and paste). It is preferred for all declarations to be included in a single document.
Declaration for Clinician 1
Name: Dr. Sarah Ferguson
Position: Gynecologic oncologist
Date: 13-06-2022
Table 3: Conflict of Interest Declaration for Ontario Health Cancer Care Ontario — Clinician 1
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
GSK — No COI | — | — | — | — |
Declaration for Clinician 2
Name: Dr. Stephen Welch
Position: Medical oncologist
Date: 13-06-2022
Table 4: Conflict of Interest Declaration for Ontario Health Cancer Care Ontario — Clinician 2
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
GSK — No COI | — | — | — | — |
Declaration for Clinician 3
Name: Dr. Orit Freedman
Position: Gynecologic oncologist
Date: 13-06-2022
Table 5: Conflict of Interest Declaration for Ontario Health Cancer Care Ontario — Clinician 3
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
GSK — No COI | — | — | — | — |
Declaration for Clinician 4
Name: Dr. Taymaa May
Position: Surgical oncologist
Date: 13-06-2022
Table 6: Conflict of Interest Declaration for Ontario Health Cancer Care Ontario — Clinician 4
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
GSK — No COI | — | — | — | — |
Declaration for Clinician 5
Name: Dr. Julie Francis
Position: Gynecologic oncologist
Date: 13-06-2022
Table 7: Conflict of Interest Declaration for Ontario Health Cancer Care Ontario — Clinician 5
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
GSK — No COI | — | — | — | — |
Declaration for Clinician 6
Name: Dr. Leah Jutzi
Position: Gynecologic oncologist
Date: 13-06-2022
Table 8: Conflict of Interest Declaration for Ontario Health Cancer Care Ontario — Clinician 6
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
GSK — No COI | — | — | — | — |
Declaration for Clinician 7
Name: Dr. Josee-Lyne Ethier
Position: Medical oncologist
Date: 13-06-2022
Table 9: Conflict of Interest Declaration for Ontario Health Cancer Care Ontario — Clinician 7
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
GSK — No COI | — | — | — | — |
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
Redactions: Confidential information in this document may be redacted at the request of the sponsor in accordance with the CADTH Drug Reimbursement Review Confidentiality Guidelines
Stakeholder Input: The views expressed in each submission are those of the submitting organization or individual; not necessarily the views of CADTH or of other organizations. As such, they are independent of CADTH and do not necessarily represent or reflect the view of CADTH. No endorsement by CADTH is intended or should be inferred. By filing with CADTH, the submitting organization or individual agrees to the full disclosure of the information. CADTH does not edit the content of the submissions.
CADTH does use reasonable care to prevent disclosure of personal information in posted material; however, it is ultimately the submitter’s responsibility to ensure no identifying personal information or personal health information is included in the submission. The name of the submitting organization or individual and all conflict of interest information are included in the submission; however, the name of the author, including the name of an individual patient or caregiver submitting the patient input, are not posted.
Accessibility: CADTH is committed to treating people with disabilities in a way that respects their dignity and independence, supports them in accessing material in a timely manner, and provides a robust feedback process to support continuous improvement. All materials prepared by CADTH are available in an accessible format. Where materials provided to CADTH by a submitting organization or individual are not available in an accessible format, CADTH will provide a summary document upon request. More details on CADTH’s accessibility policies can be found here.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.