CADTH Reimbursement Review
Nivolumab (Opdivo)
Sponsor: Bristol Myers Squibb
Therapeutic area: Non–small cell lung cancer
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Stakeholder Input
Clinical Review
Abbreviations
AE
adverse event
AJCC
American Joint Committee on Cancer
ALK
anaplastic lymphoma kinase
BICR
Blinded Independent Central Review
BIPR
Blinded Independent Pathologic Review
CCO
Cancer Care Ontario
CI
confidence interval
CrI
credible interval
DAC
Drug Advisory Committee
ECOG PS
Eastern Cooperative Oncology Group Performance Status
EFS
event-free survival
EFS2
event-free survival on the next line of therapy
EGFR
epidermal growth factor receptor
HER
electronic health record
EQ-5D-3L
3-Level EQ-5D
HR
hazard ratio
HRQoL
health-related quality of life
IA1
first interim analysis
iKM
iKnowMed
ITC
indirect treatment comparison
ITT
intention to treat
KM
Kaplan-Meier
LCC
Lung Cancer Canada
MID
minimally important difference
MPR
major pathologic response
NMA
network meta-analysis
NOC
Notice of Compliance
NSCLC
non–small cell lung cancer
OH
Ontario Health
OS
overall survival
pCR
pathologic complete response
PD-1
programmed cell death 1 protein
PD-L1
programmed cell death 1 ligand 1
PD-L2
programmed cell death 1 ligand 2
PICO
patient, intervention, comparison, outcome
PRISMA
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
RCT
randomized controlled trial
RECIST
Response Evaluation Criteria in Solid Tumours
SAE
serious adverse event
SLR
systematic literature review
TNM
tumour, node, metastasis
TTDM
time to death or distant metastases
TTLRR
time to locoregional recurrence
VAS
visual analogue scale
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Item | Description |
|---|---|
Drug product | Nivolumab (Opdivo), 360 mg intravenously, every 3 weeks for up to 3 cycles |
Indication | In combination with platinum-doublet chemotherapy for the neoadjuvant treatment of adult patients with resectable NSCLC (tumours ≥ 4 cm or node-positive) |
Reimbursement request | In combination with platinum-doublet chemotherapy for the neoadjuvant treatment of adult patients with resectable NSCLC (tumours ≥ 4 cm or node-positive) |
Health Canada approval status | Post-NOC |
Health Canada review pathway | Project Orbis |
NOC date | August 18, 2022 |
Sponsor | Bristol Myers Squibb |
NSCLC = non–small cell lung cancer; NOC = Notice of Compliance.
Introduction
Lung cancer is the most frequently diagnosed cancer in Canada, and the leading cause of cancer-related death.1 About 30,000 new diagnoses (50% in males and 50% in females)2 and 20,700 cancer-related deaths were projected in Canada in 2022,1,3 with about 98% of all cases anticipated in people 50 years and older.4 The adjusted 5-year net survival (based on 2015 to 2017 estimates) for all forms of lung cancer is only 22% (19% in males and 26% in females in Canada).1,2 Non–small cell lung cancers (NSCLCs) are the most common forms of lung cancer, accounting for more than 80% of all lung cancers in Canada.5,6 About 47.1% of all new cases of NSCLC are diagnosed at stage IV, 19.0% are diagnosed at stage III, 9.1% are diagnosed at stage II, and only 23.1% are diagnosed at stage I.7
The primary goal of treating patients with resectable NSCLC is to cure the disease, improve 5-year overall survival (OS), and prevent disease recurrence. Surgery with curative intent is the current gold standard for clinical stage I to stage IIIA NSCLC that is amenable to resection.8,9 The standard of care, according to joint guidelines from the American Society of Clinical Oncology and Ontario Health (OH) Cancer Care Ontario (CCO) for completely resectable stage IIA to IIB and stage IIIA NSCLC (American Joint Committee on Cancer [AJCC] Cancer Staging Manual, 7th edition [AJCC 7th edition]), is surgical resection followed by adjuvant cisplatin-based chemotherapy. Cisplatin-based chemotherapy is not recommended for patients with stage IA disease and not routinely recommended for patients with stage IB disease; however, postoperative evaluations are recommended.10 Stereotactic ablative radiation with curative intent is available to some patients with early-stage disease who are ineligible for surgery (e.g., because of significant comorbidities that make them a high risk for general anesthetic) or who refuse surgery, whereas patients with resectable stage III cancer may be offered chemotherapy and/or radiation in current practice before surgery.11
Neoadjuvant chemotherapy is seldom used in Canada, as it has not been shown to provide survival benefit over adjuvant therapy, and in the process of pursuing neoadjuvant chemotherapy, some patients may become ineligible for surgery (due to disease progression or treatment-related toxicity), according to the clinical experts consulted. However, neoadjuvant therapy has several advantages; for instance, it can reduce tumour size, increase resectability, and remove micrometastasis and tumour cells in more distant lymph nodes, which reduces the risk of recurrence caused by tumour cells that are not removed by surgery.12,13
Nivolumab (Opdivo) is a human immunoglobulin G4 monoclonal antibody that binds to the programmed cell death 1 protein (PD-1) receptor and blocks its interaction with programmed cell death 1 ligand 1 (PD-L1) and ligand 2 (PD-L2), releasing PD-1 pathway-mediated inhibition of the immune response, including antitumour immune response.14 Nivolumab underwent review through the Project Orbis route at Health Canada and received a notice of compliance (NOC) on August 18, 2022, for the treatment of adults with resectable NSCLC (tumours ≥ 4 cm or node-positive disease) when used in combination with platinum-doublet chemotherapy.12 The Health Canada–recommended dose of nivolumab is 360 mg administered intravenously over 30 minutes as neoadjuvant treatment in combination with platinum-doublet chemotherapy every 3 weeks for 3 cycles.14 The sponsor’s reimbursement request and patient population aligns with the Health Canada indication.
The objective of this CADTH report is to perform a systematic review of the beneficial and harmful effects of nivolumab (360 mg) in combination with platinum-doublet chemotherapy every 3 weeks for up to 3 cycles, for the neoadjuvant treatment of adults with resectable NSCLC (tumours ≥ 4 cm or node-positive disease).
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient groups who responded to CADTH’s call for patient input and from clinical experts consulted by CADTH for the purpose of this review.
Patient Input
Lung Cancer Canada (LCC), a member of Global Lung Cancer Coalition and the only national organization in Canada focused exclusively on lung cancer, engages in patient support, education, research, and advocacy. LCC submitted patient group input based on interviews conducted in Canada in September and October 2022 (1 patient with stage I to II NSCLC, 1 patient with stage III NSCLC, and 2 patients with stage IV NSCLC, and 1 caregiver for a patient with large-cell neuroendocrine carcinoma) and 1 interview with a patient who had stage IV NSCLC and had undergone an environmental scan (1 patient with stage IV NSCLC). All participants had experience with nivolumab. The LCC submitted information collected from 4 patients with stage I to IV NSCLC and from 1 patient with large-cell neuroendocrine carcinoma. The CADTH patient input summary will focus on the 2 patients with stage I to stage III NSCLC to align with the requested indication.
One patient said she used to be extremely active and was an avid runner for 10 years before her lung cancer diagnosis. The patient explained that lung cancer made exercise harder and made her feel more tired than ever, which impacted her independence. She also said that she experienced cough and some mild chest pain before her diagnosis of lung cancer. Another patient who had been diagnosed with early-stage NSCLC had two-thirds of his lung surgically removed, leaving him with 50% of his initial lung capacity. As a result, he explained, he became unable to do any vigorous exercise or activity because he tires quickly. As for improved outcomes, the input indicated that patients would value new treatment options that maintain or improve quality of life, delay the onset of symptoms, improve survivorship, improve or maintain functionality and/or mobility, and, ultimately, provide a cure. In addition, respondents said they would prefer a treatment that can be administered at a hospital located near home, or in a community clinic for those in rural settings, to minimize travel time and burden on caregivers. The input also noted that because the CheckMate 816 trial excluded patients with EGFR or ALK alterations, owing to a lack of evidence supporting neoadjuvant immunotherapy in this population, a biomarker screening (a routine practice) must be performed before neoadjuvant treatment with nivolumab.
Clinician Input
Input From Clinical Experts Consulted by CADTH
The clinical experts consulted for this review highlighted improved OS (prolonged life) and delay of disease relapse as important treatment goals in NSCLC curative settings. The clinical experts highlighted the infrequent use of neoadjuvant chemotherapy across jurisdictions in Canada because it has not been shown to provide a survival benefit over adjuvant therapy and noted that in the process of receiving neoadjuvant chemotherapy, some patients may become ineligible for surgery (due to disease progression or drug-related toxicity that may affect a patient’s performance status). The clinical experts highlighted an unmet need for patients with resectable NSCLC tumours, as some patients who undergo surgical resection and receive adjuvant chemotherapy may experience disease relapse. The clinical experts added that patients who experience relapse after surgery and/or adjuvant chemotherapy are generally incurable. Both clinical experts agreed that neoadjuvant nivolumab in combination with chemotherapy will cause a shift in the current Canadian treatment paradigm in the curative-intent setting.
The clinical experts indicated that patients with NSCLC who have tumours 4 cm or larger and/or node-positive disease, who have EGFR-negative or ALK-negative tumours, and who are eligible for upfront surgical resection (including patients with locoregional spread of the disease to lymph nodes who remain eligible for upfront surgical resection) would be eligible for treatment, provided they have no contraindications (severe and uncontrolled autoimmune disease, frailty, or poor baseline organ function). The experts explained that neoadjuvant nivolumab in combination with chemotherapy would not be appropriate for patients who are eligible for upfront surgery for borderline resectable NSCLC when the goal of neoadjuvant therapy is to downsize the tumour so the patient can become eligible for surgery. According to the clinical experts, patients are identified by a surgical and medical oncologist after appropriate review. The clinical experts added that the identification of driver mutations, like EGFR and ALK, is important but may not be routinely performed for early-stage disease at all centres.
The clinical experts added that patient response to treatment would be assessed in clinical practice using preoperative CT scans completed after neoadjuvant systemic chemotherapy, pathologic response, disease recurrence, and OS. The clinical experts emphasized that the schedule of follow-up assessments after completion of curative-intent surgery is not standardized across jurisdictions in Canada because of a lack of definitive literature suggesting the most appropriate timing for serial radiography. The clinical experts noted that nivolumab, platinum-doublet chemotherapy, or both could be discontinued at a patient’s request, in the event of disease progression during the 3 cycles of neoadjuvant therapy, or in the case of medically dangerous side effects or intolerable toxicity.
Clinician Group Input
Two clinician groups, the OH-CCO Lung Cancer Drug Advisory Committee (DAC) and LCC, each submitted inputs. The OH-CCO’s DAC provides guidance on drug-related issues, in support of CCO’s mandate, and collected information from 3 clinicians during a DAC meeting. LCC, a national charity and the only organization in Canada solely focused on lung cancer (education, advocacy, research) gathered information from published clinical data and 12 lung cancer medical oncologists across Canada.
Unmet Needs
According to the OH-CCO input, despite current treatments, a number of patients develop a recurrence quickly and do not survive. Therefore, neoadjuvant nivolumab would be an additional option for patients with resectable NSCLC. In its input, LCC cited several advantages of the neoadjuvant approach: it limits the risk of systemic dissemination of the cancer; downsizes tumours (leading to decreased postoperative complications [e.g., pain, infection], decreased performance status, improved surgical outcomes, and improved recovery times); makes the possibility of surgery easier, safer, and more efficacious; improves patient capacity to receive postoperative therapies; provides the opportunity for smoking cessation, physical therapy, and medical evaluations for surgery; helps to manage the surgical wait list; and improves the ability to provide prognosis and risk-stratification after surgery.
Place in Therapy
According to the OH-CCO clinicians, neoadjuvant nivolumab would be an additional option for patients with resectable NSCLC and could potentially replace adjuvant chemotherapy in some patients. Similarly, the LCC clinicians said that neoadjuvant nivolumab therapy would eliminate the need of postoperative, prolonged, and more expensive therapies (chemotherapy, radiation, immunotherapy). LCC clinicians noted that eligible patients might not choose neoadjuvant nivolumab therapy, such as patients with stage II, node-negative disease considered eligible for upfront surgery with optional adjuvant therapies, those at high risk of chemotherapy-associated or immunotherapy-associated complications, and those preferring upfront surgery.
Patient Population
The OH-CCO clinicians said that patients who meet the clinical trial inclusion criteria (i.e., resectable stage IIA to stage IIIB NSCLC [per AJCC 8th edition]) and/or those eligible for chemotherapy would be best suited for treatment with nivolumab. (Of note, the inclusion criterion for the CheckMate 816 trial was stage IB [tumour ≥ 4 cm] to stage IIIA NSCLC per AJCC 7th edition, which corresponds to stage IB to stage IIIB, non N3, non N2T4 per AJCC 8th edition.) LCC clinicians said that neoadjuvant therapy may be favoured for patients with stage IIIA and/or PD-L1-positive NSCLC, based on the favourable results in these strata in the CheckMate 816 study. However, the LCC group noted that a discussion with every eligible patient would be warranted and the treatment of all eligible patients with neoadjuvant therapy would be favoured to decrease the treatment burden after surgery (e.g., postoperative chemotherapy and/or atezolizumab). According to LCC clinicians, nivolumab would be least suited to patients with a contraindication to chemotherapy or immunotherapy treatments, such as those with renal failure, heart failure, severe hearing loss, severe neuropathy, an organ transplant, active and symptomatic autoimmune disease (e.g., Crohn disease being treated with immunosuppressive therapy or multiple sclerosis), and an Eastern Cooperative Oncology Group Performance Status [ECOG PS] of 2 to 4. The LCC clinicians added that a history of autoimmune disease or autoimmune disease that is clinically silent (e.g., immune thyroiditis) or well controlled without active immunosuppression is not a major contraindication. According to LCC input, the use of neoadjuvant immunotherapy in patients with EGFR, ALK, ROS1, RET, or NTRK alterations needs further investigation and/or will have to be addressed on a case-by-case basis, as these groups have not been specifically addressed in clinical trials.
Assessing Response to Treatment
The OH-CCO clinician group stated that response to nivolumab can be determined with clinical assessment of progression, the need for surgery, and pathologic assessment of a tumour. The LCC clinician group said that a CT scan would be needed after neoadjuvant therapy evaluate a patient’s eligibility for surgery. According to LCC clinicians, currently there is no clinical, biologic, or imaging tool that can be used to identify patients who will have a pathologic complete response (pCR) after neoadjuvant treatment and can be excluded from surgical treatment. At present, patients are followed with standard postoperative care, LCC clinicians reported. However, they anticipate that in the future, as more experience is gained with neoadjuvant approaches, risk-adapted follow-up strategies will be possible, based on, for example, circulating tumour DNA postoperative monitoring in combination with other clinical and pathologic features of the cancer.
Discontinuing Treatment
The OH-CCO clinicians said that intolerable toxicity and clinically obvious disease progression are factors to consider when deciding whether to discontinue nivolumab treatment. The LCC clinicians stated that clinical and biologic evaluations are performed at every cycle of therapy, as they are for patients undergoing chemotherapy and/or immunotherapy in the advanced disease setting, per standard practice in oncology.
Prescribing Conditions
The OH-CCO clinicians noted that a specialist, ideally part of a multidisciplinary team, is required in a hospital outpatient clinic to diagnose, treat, and monitor patients receiving nivolumab. The LCC clinicians also stated that, ideally, a multidisciplinary cancer tumour board, consisting of (nonexclusively) respirologists, radiologists, pathologists, thoracic surgeons, medical oncologists, and radiation oncologists, should discuss a multimodal treatment approach for patients who are usually referred to oncologic thoracic surgeons affiliated with major cancer centres. The LCC clinicians added that the delivery of care should be planned according to local structures; ideally, systemic therapies will be administered as close to a patient’s home as possible, while patients are continuously monitored by the cancer centre to coordinate neoadjuvant therapies with posttreatment imaging, preoperative evaluations, and the surgical admission itself.
Drug Program Input
Input was obtained from the drug programs that participate in the CADTH reimbursement review process. Key factors identified that could potentially impact the implementation of the CADTH recommendation for neoadjuvant nivolumab plus chemotherapy included considerations for the initiation of therapy, considerations for the discontinuation of therapy, considerations for the prescribing of therapy, and generalizability.
Clinical Evidence
Pivotal Study
Description of Study
CheckMate 816 is an ongoing, open-label, randomized, phase III trial comparing the efficacy and safety of 3 treatment regimens in patients 18 years and older with resectable (stage IB [tumours ≥ 4 cm], stage II, or stage IIIA) NSCLC: neoadjuvant nivolumab (3 mg/kg every 2 weeks for up to 3 cycles) in combination with ipilimumab (a single 1 mg/kg dose); neoadjuvant nivolumab (a 360 mg flat dose) in combination with platinum-based chemotherapy every 3 weeks for 3 cycles; and platinum-based chemotherapy alone.15 This CADTH review did not include findings from the ipilimumab plus nivolumab arm, as the indication under review is for nivolumab monotherapy in combination with platinum-based chemotherapy. Disease staging at screening was based on the AJCC/Union for International Cancer Control (UICC) TNM Classification of Malignant Tumours, 7th edition.15 After the completion of neoadjuvant treatment, all patients who remained operative candidates underwent definitive surgery for NSCLC within 6 weeks. Patients were also allowed to receive adjuvant chemotherapy with or without radiation after definitive surgery, per institutional standard at the discretion of the investigator.
pCR assessed by blinded independent pathologic review (BIPR) and event-free survival (EFS) assessed by blinded independent central review (BICR) were coprimary end points in the trial. Secondary end points included OS, time to death or distant metastases (TTDM), and major pathologic response (MPR). Safety, tolerability, and health-related quality of life (HRQoL) were exploratory outcomes.15 Radiologic tumour assessments were reviewed by a third-party vendor for BICR and BIPR. All investigator-assessed radiographic progressions and all disease recurrences were confirmed by BICR, per Response Evaluation Criteria in Solid Tumours Version (RECIST) 1.1 guidelines.
The CheckMate 816 trial was initially designed as a 2-arm trial in which patients were randomized in a 1:1 ratio to 1 of 2 treatment regimens: nivolumab plus ipilimumab (arm A); or platinum-doublet chemotherapy (arm B). An update to the protocol (protocol revision 2) introduced a third arm, nivolumab plus platinum-doublet chemotherapy (arm C) and allowed patients to be subsequently randomized in a 1:1:1 scheme to any treatment arm. A third update to the protocol (protocol revision 3) discontinued the randomization of patients to the nivolumab plus ipilimumab arm. Subsequently, patients enrolled in the study were randomized to the nivolumab plus chemotherapy arm or the chemotherapy arm in a 1:1 ratio and were stratified by 3 factors: PD-L1 expression level (1% or more versus less than 1%, not evaluable, indeterminate); disease stage (IB or II versus stage IIIA); and sex.
The primary data cut-off date for the prespecified final pCR analysis was September 16, 2020, and the data cut-off date for the first EFS interim analysis (IA1 EFS) was October 20, 2021. By the October 20, 2021, data cut-off date (IA1 EFS), ||| ||||||| |||||||| || ||| ||||| ||| ||||||||| ||||||||||| ||||| |||||||||| ||| |||| |||| || ||||||. Most patients in the nivolumab plus chemotherapy and the chemotherapy arms were male (71.5% and 70.9%, respectively), and about half were either ||||| |||||| ||| |||||| ||||||||||||| ||| ||||| |||||| ||| |||||| |||||||||||||. In total, 48.6% and 53.1% of patients in the nivolumab plus chemotherapy and chemotherapy arms, respectively, had squamous tumour histology; 63.1% and 64.2%, respectively, had stage IIIA disease, and 89.4% and 88.3%, respectively, were current or former smokers.15
Efficacy Results
Table 2 presents key efficacy end points and Table 3 presents key safety results from the CheckMate 816 trial.
Overall Survival
OS was formally tested at the IA1 EFS data cut-off date (October 20, 2021), as EFS was significant at the IA1 cut-off date. The median OS was not reached in either the nivolumab plus chemotherapy arm or the chemotherapy arm. The hazard ratio [HR] for death was 0.57 (99.67% confidence interval [CI] 0.30 to 1.07). The P value for OS (P = 0.008) did not cross the significance boundary (0.0033). A second OS testing is planned after ||| || |||||| |||| |||||||| ||| | |||| ||||| ||| ||| |||| |||||||||15
Event-Free Survival
By the October 20, 2021 cut-off date, ||| || ||| ||||||| |||||||| || ||| ||||||||| |||| |||||||||||| ||| ||| || || ||| ||||||| || ||| |||||||||||| ||| |||| |||||||| ||| ||| || ||||.15 In total, ||||| ||| || |||| EFS events had occurred in the nivolumab plus chemotherapy arm, and the median EFS was 31.57 months (95% CI, 30.16 to not available months). In the chemotherapy arm, ||||| ||| || |||| EFS events had occurred and the median EFS was 20.80 months (95% CI, 14.03 to 26.71 months). The estimated HR between nivolumab plus chemotherapy and chemotherapy was 0.63 (97.38% CI, 0.43 to 0.91), with a P value of 0.0052 from a stratified log-rank test.15 Sensitivity analyses for EFS were consistent with the primary analysis.15
Pathologic Complete Response and Major Pathologic Response
pCR and MPR analyses were conducted at the September 16, 2020, data cut-off date. The pCR rate per BIPR was 24.0% (43 of 179 patients; 95% CI, 18.0% to 31.0%) in the nivolumab plus chemotherapy arm and 2.2% (4 of 179 patients; 95% CI, 0.6% to 5.6%) in the chemotherapy arm. The stratified odds ratio between the nivolumab plus chemotherapy arm and the chemotherapy arm was 13.94 (99% CI, 3.49 to 55.75), with a P value of less than 0.0001, and the strata-adjusted difference based on the Cochran-Mantel-Haenszel method was 21.6% |||| ||| ||||| || ||||||.15 pCR sensitivity analyses were consistent with the primary analyses. In total, 36.9% of patients (95% CI, 29.8% to 44.4%) in the nivolumab plus chemotherapy arm and 8.9% (95% CI, 5.2% to 14.1%) in the chemotherapy arm were MPR responders.15
Health-Related Quality of Life
Patients completed the 3-Level EQ-5D (EQ-5D-3L) questionnaire at baseline, before on-treatment clinic visits, at postneoadjuvant visits 1 and 2, and at designated time points during the survival follow-up phase. Completion rates for the nivolumab plus chemotherapy and chemotherapy study arms were similar at baseline (EQ-5D-3L descriptive system: 94.4% versus 95.5%; EQ-5D-3L visual analogue scale [VAS]: 94.4% versus 95.0%) and did not change significantly at postneoadjuvant visit 1 (EQ-5D-3L descriptive system: 88.6% versus 83.9%; EQ-5D-3L VAS: 88.6% versus 83.9%). The EQ-5D index (based on the UK time trade-off value set) was collected for both study arms. The mean change from baseline to different time points (week 4, week 7, and postneoadjuvant visits 1 and 2) were minimal for the EQ-5D VAS and EQ-5D utility index scores of the questionnaire in the 2 treatment arms.15 Table 2 presents the change from baseline to different time points (week 4, week 7, and postneoadjuvant visits 1 and 2) in the EQ-5D VAS and EQ-5D utility index score portion of the EQ-5D-3L questionnaire.
Time to Death or Distance Metastasis
By the October 20, 2021, data cut-off date, || |||||| ||||||| ||| |||||||| || ||| ||||||||| |||| |||||||||||| ||| |||||| |||||| ||||||| || ||| |||||||||||| |||. The median time to death or distant metastasis was not reached in either study arm at the October 20, 2021, cut-off date, and the HR was 0.53 (95% CI, 0.36 to 0.77).15
EFS on Next Line of Therapy
By the October 20, 2021, data cut-off date, the median event-free survival on the next line of therapy (EFS2), per investigator assessment, was not reached in either the nivolumab plus chemotherapy or chemotherapy arm. || |||||| || |||||| ||| |||||||| || ||| ||||||||| |||| |||||||||||| ||| ||| || |||||| || ||| |||||||||||| |||. The estimated HR was 0.54 (95% CI, 0.37 to 0.80).15
Harms Results
Overall, 92.6% (n = 163) of patients in the nivolumab plus chemotherapy arm and 97.2% (n = 171) in the chemotherapy arm reported at least 1 adverse event (AE) in the CheckMate 816 trial. The most frequently reported AEs in the nivolumab plus chemotherapy arm were nausea (38.1%), constipation (33.5%), anemia (29.0%), decreased appetite (20.5%), fatigue (16.5%), and neutropenia (16.5%), and in the chemotherapy arm were nausea (44.9%), constipation (32.4%), anemia (26.7%), decreased appetite (23.3%), and neutrophil count decrease (21.0%) of any grade. AEs of grade 3 to 4 were reported in 40.9% (n = 72) and 43.8% (n = 77) of patients in the nivolumab plus chemotherapy and chemotherapy arms, respectively.15
Serious adverse events (SAEs) of any grade were reported in 30 (17.0%) patients in the nivolumab plus chemotherapy arm and 24 (13.6%) in the chemotherapy arm. SAEs of grades 3 or 4 were reported in 19 (10.8%) patients in the nivolumab plus chemotherapy arm and 17 (9.7%) patients in the chemotherapy arm.15
AEs leading to a dose delay or reduction were reported in || ||||||| ||| || ||||||| treated patients in the nivolumab plus chemotherapy and chemotherapy arms, respectively. AEs leading to discontinuation of study treatments were reported in 18 (10.2%) patients in the nivolumab plus chemotherapy arm and 20 (11.4%) in the chemotherapy arms.15
By the October 20, 2021, data cut-off date, ||||| ||| ||| || |||||||| ||| |||| || ||| ||||||||| |||| |||||||||||| ||| ||| ||||| ||| ||| patients in the chemotherapy arm.15 Notable harms reported in the nivolumab plus chemotherapy and chemotherapy arms of the CheckMate 816 trial are presented in Table 3.15
Table 2: Summary of Key Efficacy Results From the CheckMate 816 Trial
Characteristic | Nivolumab plus chemotherapy (n = 179) | Chemotherapy (n = 179) |
|---|---|---|
OS | ||
Median OS (95% CI) | NR | NR |
HR for death (99.67% CI) | 0.57 (0.30 to 1.07) | |
P value | 0.008 | |
EFS | ||
Events, n (%) | 64 (35.8) | 87 (48.6) |
Median EFS (95% CI), monthsa | 31.57 (30.16 to NA) | 20.80 (14.03 to 26.71) |
HR (97.38% CI) P valueb | 0.63 (0.43 to 0.91) P = 0.0052c | |
95% CI | 0.45 to 0.87 | — |
EFS rates, % (95% CI)a | ||
At 6 months | 85.6 (79.3 to 90.1) | 81.9 (75.1 to 87.0) |
At 12 months | 76.1 (68.8 to 81.9) | 63.4 (55.3 to 70.4) |
At 18 months | 68.3 (60.4 to 74.9) | 53.1 (44.9 to 60.7) |
At 24 months | 63.8 (55.7 to 70.9) | 45.3 (37.0 to 53.2) |
|||| || ||| |||||| |||| | ||
|||||||||||| |||||||||| |||||||| | || ||||| | || ||||| |
||||||||||||||||||||||| ||||| |||||||| | || |||||| | || |||||| |
|||||||||||||| | || |||||| | || |||||| |
||||||||| | || ||||| | || |||||| |
|||||| |||||||||||| ||| ||||||| | | ||||| | | ||||| |
|||||||||||| ||| |||||||| ||||||| |||||||| | | ||||| | | ||||| |
|||||||||||||| | | ||||| | | ||||| |
||||||||| | || ||||| | | ||||| |
|||||| |||||||||||| ||| ||||||| | || ||||| | | ||||| |
||||||| | || ||||| | || ||||| |
|||||| || |||||||| |||||||| ||| | ||| |||||| | || |||||| |
|||||||| || |||| || |||| ||||| |||||||||| | ||| |||||| | || |||||| |
pCRd (September 8, 2020, data cut-off date) | ||
Responders, n (%) | 43 (24.0) | 4 (2.2) |
95% CIf | 18.0 to 31.0 | 0.6 to 5.6 |
Difference, %f,g | 21.6 | |
99% CI | ||||| || ||||| | |
95% CI | 15.1 to 28.2 | |
Estimate of odds ratiog,h | 13.94i | |
99% CI | 3.49 to 55.75 | |
95% CI | 4.86 to 40.02 | |
MPRd (September 8, 2020, data cut-off date) | ||
Responders, n (%) | 66 (36.9) | 16 (8.9) |
95% CIe | 29.8 to 44.4 | 5.2 to 14.1 |
Difference, % (95% CI) f,g | 27.9 (19.6 to 36.1) | |
Estimate of odds ratio (95% CI)g,h | 5.70 (3.16 to 10.26) | |
TTDM | ||
Events, n (%) | || (25.1) | || (41.9) |
Median TTDM (95% CI), monthsa | Not reached (36.60 to NA) | 26.71 (22.41 to NA) |
HR (95% CI)b | 0.53 (0.36 to 0.77) | |
TTDM rates (95% CI) | ||
At 12 months | 85.7 (79.4 to 90.2) | 76.0 (68.8 to 81.8) |
At 24 months | 75.8 (68.3 to 81.7) | 57.1 (48.8 to 64.6) |
EFS2 | ||
Events, n (%) | || (23.5) | || (39.1) |
Median EFS2 (95% CI), montha | Not reached (NA to NA) | Not reached (27.40 to NA) |
HR (95% CI)b | 0.54 (0.37 to 0.80) | |
HRQoL | ||
EQ-5D utility index scores | ||
Baseline, n | 169 | 171 |
Mean (SD) | 0.89 (0.13) | 0.89 (0.16) |
Change from baseline to week 4, n | 163 | 153 |
Mean (SD) | 0.02 (0.16) | 0.00 (0.17) |
Change from baseline to week 7, n | 148 | 141 |
Mean (SD) | –0.01 (0.18) | –0.01 (0.18) |
Change from baseline to postneoadjuvant visit 1, n | 152 | 143 |
Mean (SD) | –0.01 (0.18) | –0.02 (0.21) |
Change from baseline to postneoadjuvant visit 2, n | 131 | 129 |
Mean (SD) | –0.09 (0.20) | –0.09 (0.23) |
EQ-5D VAS | ||
Baseline, n | 169 | 170 |
Mean (SD) | 83.1 (15.8) | 82.4 (14.2) |
Change from baseline to week 4, n | 163 | 153 |
Mean (SD) | –0.2 (12.1) | –1.2 (13.1) |
Change from baseline to week 7, n | 148 | 141 |
Mean (SD) | –1.3 (13.8) | –0.7 (12.6) |
Change from baseline to postneoadjuvant visit 1, n | 152 | 142 |
Mean (SD) | –0.2 (13.9) | –1.0 (15.4) |
|||||| |||| |||||||| || |||||||||||||||| ||||| || | | ||| | ||| |
Mean (SD) | –2.5 (16.5) | –2.5 (17.3) |
BICR = blinded independent central review; BIPR = blinded independent pathologic review; CI = confidence interval; CMH = Cochran-Mantel-Haenszel; EFS = event-free survival; EFS2 = event-free survival on the next line of therapy; HR = hazard ratio; HRQoL = health-related quality of life; IRT = Interactive Response Technology; MPR = major pathologic response; NA = not available; nivo = nivolumab; NR = not reported; pCR = pathologic complete response; PD-L1 = programmed cell death 1 ligand 1; SD = standard deviation; TTDM = time to death or distant metastases; VAS = visual analogue scale.
Note: The data cut-off date was October 20, 2021 (minimum follow-up was 21.0 months), except pCR and MPR were assessed at the September 2020 data cut-off date.
aBased on Kaplan-Meier estimates.
bHR of arm C to concurrent arm B from a Cox model stratified by PD-L1 expression level (≥ 1% vs. < 1%, not evaluable, or indeterminate), disease stage (IB or II vs. stage IIIA), and sex (male vs. female), as entered into the Interactive Response Technology.
cLog-rank test stratified by the same factors as in the Cox proportional hazards model. The P value threshold for statistical significance was 0.0262.
dPatients without samples for evaluation were counted as nonresponders.
eCI based on the Clopper-Pearson method.
fStrata-adjusted difference (arm C – concurrent arm B), based on the Cochran-Mantel-Haenszel method of weighting.
gStratified by PD-L1 expression level (≥ 1% vs. < 1%, not evaluable, indeterminate), disease stage (IB or II vs. stage IIIA), and sex (male vs. female), as entered into the Interactive Response Technology.
hStrata-adjusted odds ratio (arm C over concurrent arm B), the Mantel-Haenszel method.
iP < 0.0001 (2-sided P value for pCR from the stratified Cochran-Mantel-Haenszel test).
Source: Clinical Study Report.15
Table 3: Summary of Key Safety Results From the CheckMate 816 Trial
Safety parameters | Nivolumab plus chemotherapy (n = 176) | Chemotherapy (n = 176) | ||
|---|---|---|---|---|
Any grade (n, %) | Grade 3 or 4 (n, %) | Any grade (n, %) | Grade 3 or 4 (n, %) | |
All-causality AEs | 163 (92.6) | 72 (40.9) | 171 (97.2) | 77 (43.8) |
All-causality SAEs | 30 (17.0) | 19 (10.8) | 24 (13.6) | 17 (9.7) |
All-causality AEs leading to discontinuation | 18 (10.2) | 10 (5.7) | 20 (11.4) | 7 (4.0) |
AEs leading to dose delay or reduction | 53 (30.1) | 28 (15.9) | 66 (37.5) | 33 (18.8) |
|||||| | || |||||| | || |||||| | ||
Notable harms | ||||
Diarrhea or colitis | 0 | 0 | 0 | 0 |
Hepatitis | 0 | 0 | 0 | 0 |
Pneumonitis | 2 (1.1) | 0 | 1 (0.6) | 1 (0.6) |
Nephritis or renal dysfunction | 0 | 0 | 0 | 0 |
Rash | 15 (8.5) | 3 (1.7) | 1 (0.6) | 0 |
Hypersensitivity or infusion reaction | 2 (1.1) | 0 | 0 | 0 |
AE = adverse event; SAE = serious adverse event.
Note: The data cut-off date was October 20, 2021.
Source: Clinical Study Report.15
Critical Appraisal
CheckMate 816 is an ongoing, randomized, open-label, phase III trial. Randomization was conducted using an Interactive Response Technology, and treatment allocation was concealed. Patients were stratified by 3 factors: PD-L1 expression level, disease stage, and gender or sex. The methods of randomization and the stratification factors were considered appropriate by the clinical experts consulted. Baseline characteristics in the 2 arms of interest were balanced, suggesting that randomization was successful. The methods of randomization and treatment allocation were considered appropriate.
The treatment effect for EFS and pCR was estimated during a prespecified interim analysis, adjusted using the Lan-DeMets alpha spending function with O’Brien-Fleming boundaries, which accounted for the actual number of events at an overall alpha of 4% or 5%. Overall, the treatment effect of the coprimary end points was estimated during the interim analysis. There is uncertainty about the magnitude of the treatment effect, given that interim analyses have the tendency to overestimate treatment effect.
OS was statistically nonsignificant at the preplanned interim analysis stopping rule (P = 0.008 against a prespecified level of significance at the interim analysis of 0.0033). Although the results showed a promising trend toward a significant treatment effect on OS, the final analysis may be needed to confirm the findings, particularly the exact estimate of the difference in median survival, which were not estimable at the data cut-off date. A follow-up OS analysis is planned after 128 OS events have occurred in both study arms.
Performance and assessment biases due to the open-label design of the trial were considered unlikely, given that radiologic assessments of CT scans for EFS and pathologic review of tumour sections were completed by a blinded independent review team, based on prespecified, and validated (RECIST 1.1) guidelines.
Further, the proportion of patients exposed to 3 doses of chemotherapy drugs was slightly higher in the nivolumab plus chemotherapy arm than in the chemotherapy arm. There were also slight differences reported in the cumulative dose intensity, which could bias the findings in favour of nivolumab plus chemotherapy.
More patients received subsequent anticancer therapy in the chemotherapy arm than in the nivolumab plus chemotherapy arm, and a higher proportion of patients received post-surgery adjuvant therapy in the chemotherapy arm, which could bias EFS and OS. However, the potential bias from the use of subsequent anticancer and adjuvant therapies was considered low.
The sponsor’s reimbursement request aligns with the Health Canada indication. The CheckMate 816 trial enrolled only patients with an ECOG PS of 0 or 1. The magnitude of benefit of nivolumab plus chemotherapy in patients with an ECOG PS of 2 or higher is uncertain.
The baseline and demographic characteristics in the trial were considered by the clinical experts to be generalizable to the population of patients with NSCLC in Canada. The experts highlighted notable differences between the patients enrolled in the CheckMate 816 trial and the patient population in Canada (younger, more stage IIIA disease, and more expression of PD-L1); however, the impact of these differences on the generalizability of the findings was considered low.
The dosing of nivolumab in the reimbursement request aligns with the Health Canada indication. Dose adjustments were allowed for chemotherapy drugs in the trial, but not for nivolumab, which aligns with the Health Canada indication. The experts indicated that a flat-dose approach to nivolumab, as implemented in the CheckMate 816 trial, would be used in practice.
Concomitant medications administered in the trial were considered appropriate by the clinical experts, and no major discrepancies in concomitant medications administered were identified that could have had a negative impact on the findings.
Indirect Comparisons
Description of Study
The sponsor provided a network meta-analysis (NMA)16 that compared the efficacy and safety of neoadjuvant nivolumab in combination with chemotherapy with other relevant treatments, including neoadjuvant chemotherapy, neoadjuvant chemoradiotherapy, adjuvant chemotherapy, and surgery alone, in patients diagnosed with resectable nonmetastatic NSCLC. The primary efficacy end points used for NMA estimates were EFS and OS. The secondary outcomes included time to locoregional recurrence (TTLRR), TTDM, and pCR. For each outcome, base-case and sensitivity analyses were carried out whenever data were available. The base-case analysis involved patients who were deemed candidates for surgery and who had undergone third-generation platinum-based doublet chemotherapy. The sensitivity analyses expanded to include second-generation platinum-based chemotherapies, resected patient populations, data stratified by PD-L1 expression level (i.e., ≥ 1% versus < 1%), and data from the intention-to-treat (ITT) population of the CheckMate 816 trial, instead of the subpopulations of the CheckMate 816 trial (i.e., stage IB to II, stage IIIA, and stage IIIA N2) used in the base-case stage-specific networks. Furthermore, for each outcome, in addition to the stage-agnostic network, which included studies regardless of the staging of the patient population, the network was stratified by tumour staging (i.e., stage IB to II, stage IIIA, and stage IIIA N2). Eight randomized controlled trials (RCTs) were eventually included in the base-case analyses, 5 additional RCTs were included in the sensitivity analyses that involved second-generation chemotherapies, and 4 additional RCTs were included in the sensitivity analyses expanded to include resected patients.
Efficacy Results
Although both EFS and OS were selected as primary end points in the sponsor-submitted NMA, OS data from the CheckMate 816 trial were based on an immature data cut-off date. According to the base analysis of EFS, patients with stage IIIA NSCLC who received neoadjuvant nivolumab in combination with chemotherapy had a significantly lower risk of an event (i.e., EFS HR < 1, credible interval [CrI] excluding 1) than those who received neoadjuvant chemotherapy or underwent surgery alone. The risk of an event in patients with stage IIIA N2 NSCLC who received neoadjuvant nivolumab in combination with chemotherapy was also significantly lower than in those who received neoadjuvant chemoradiotherapy or neoadjuvant chemotherapy. However, in patients with stage IB to II NSCLC, EFS improvement was not significantly different between neoadjuvant nivolumab plus chemotherapy and neoadjuvant chemotherapy, adjuvant chemotherapy, or surgery alone. For stage-agnostic patients (i.e., stage IB to stage IIIA), although the EFS results showed that neoadjuvant nivolumab plus chemotherapy led to a significantly lower risk of an event than neoadjuvant chemotherapy, adjuvant chemotherapy, or surgery alone, they were considered significantly biased because of the high heterogeneity in tumour staging, supported by significant differential treatment effects observed between patients with stage IB to II NSCLC and those with stage IIIA or stage IIIA N2 NSCLC.
Harms Results
The sponsor-submitted NMA did not quantitively synthesize evidence on safety outcomes due to the sparseness of the data and the differences in treatment regimens across the base-case studies. As a result, the sponsor provided a narrative description only.
Critical Appraisal
The systematic literature review (SLR) conducted by the sponsor to identify potentially eligible studies for the NMA was methodologically sound. The sponsor used a comprehensive literature search strategy, performed study selection and data extraction in duplicate, assessed the risk of bias appropriately, and described the characteristics of the included studies and narratively summarized the results in adequate detail. However, it was unclear whether the risk-of-bias assessment was carried out by a single assessor or multiple assessors. The reporting of the sponsor-submitted NMA generally followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist.17
According to the clinical experts consulted by CADTH, the heterogeneity in tumour staging for patients with stage-agnostic NSCLC in the sponsor-submitted NMA was significant. And indeed, the effects of neoadjuvant nivolumab plus chemotherapy on EFS by stage, for example, were inconsistent between patients with stage IB to II NSCLC and those with stage IIIA or IIIA N2 NSCLC (i.e., statistically significant versus nonsignificant) compared to neoadjuvant chemotherapy in the base-case analysis. Because of the significant differential treatment effects of the 2 stage categories (IB or II versus IIIA or IIIA N2), the pooled indirect treatment comparison (ITC) results from the patients with stage-agnostic disease were deemed to be significantly biased, and the pooling to be inappropriate, methodologically, although neoadjuvant nivolumab plus chemotherapy markedly improved EFS relative to neoadjuvant chemotherapy, adjuvant chemotherapy, and surgery alone in patients with stage-agnostic NSCLC.
For each outcome examined in the NMA, both random-effects and fixed-effects models were run. The random-effects model was considered by the sponsor as the default model. However, the fixed-effects model was selected by the sponsor for all analyses in the NMA due to the sparseness of network not being able to estimate the between-study standard deviation with enough precision. Although it was considered appropriate to use the fixed-effects model instead of the random-effects model when the network is sparce, it is important to note that the fixed-effects model is not capable of capturing heterogeneity.
The misclassification of tumour stage with different versions of tumour classification criteria could have also had an impact on the ITC estimation. In the sponsor-submitted NMA, of the 8 RCTs in the base-case analysis, the CheckMate 816 trial was the only study to use TNM 7th edition to classify tumours; 2 other trials used the TNM 5th edition, 3 used the TNM 6th edition, and 2 used the 1997 International Staging System. Different staging criteria could lead to different classifications of NSCLC and would consequently result in differences in prognosis estimation and treatment selection.
Safety outcomes were only narratively described in the NMA. Without a quantitative synthesis, a balanced judgment of comparative benefits relative to comparative harms could not be made. In addition, outcomes that are important to patients, such as HRQoL, were not reported in the NMA. Furthermore, analyses comparing neoadjuvant nivolumab plus chemotherapy with adjuvant atezolizumab was determined by the sponsor to not be feasible and to be inappropriate because of significant methodological challenges. Nonetheless, feedback from the clinical experts consulted by CADTH emphasized that adjuvant atezolizumab is an appropriate treatment option for patients with resected stage IB to stage IIIA NSCLC (the 7th lung cancer TNM classification) with a PD-L1 expression level of at least 50%. Therefore, the lack of relevant analyses might have introduced uncertainty into the sponsor’s submitted analysis.
Other Relevant Evidence
Description of Study
As part of the submission for nivolumab, the sponsor submitted a systematic review and a meta-analysis that described clinical evidence in patients with nonmetastatic resectable NSCLC. The sponsor-conducted meta-analysis assessed the potential use of pathologic response (pCR or MPR) as a surrogate end point for long-term outcomes (EFS, OS) in patients with resectable NSCLC. The systematic review was informed by patient-level data from 32 studies that presented evidence of an association between OS and/or EFS and pCR and/or MPR, measured as an HR, or reported Kaplan-Meier curves for OS and/or EFS by pCR and/or MPR status, which allowed for the reconstruction of HRs.12
Efficacy Results
||||||| |||||||| || |||||||||||| |||||||| |||||||| |||||| |||| |||||| || |||||||||||||||| ||||||||||| ||||||| || ||||||||| ||| || ||| |||| |||| ||| |||| || ||||| |||||| ||| || ||||||| ||||||||| |||||||||| |||| ||||||||| ||| ||| |||||||||| |||| |||||| |||||||||||| |||||||||||| ||||||||| |||| ||||||| || ||| || || ||| |||||||| |||| |||| |||||||| ||| |||| |||| ||| |||| || ||||||
Critical Appraisal
The sponsor-submitted meta-analysis was informed by studies selected from an adequately conducted systematic review, with a clearly prespecified patient, intervention, comparison, outcome (PICO) model, in accordance with the PRISMA guidelines. The study-selection and data-extraction methods were considered appropriate. In the absence of detailed information on the baseline and study characteristics of patients enrolled in the studies included in the meta-analysis, the degree of heterogeneity between the included studies could not be assessed. Studies included had considerable variation in terms of study design (observational versus RCT) and sample size. Heterogeneity was not reported for the Bayesian analysis and, owing to the lack of baseline data on the trials included an assessment of the level of heterogeneity could not be made. The meta-analysis suggests that achievement of a pCR was associated with improved OS, based on the Bayesian and frequentist methods implemented in the analyses.
Description of Study
The sponsor submitted 1 real-world study conducted with data from electronic health records (EHRs) supplemented with chart reviews. The purpose of this retrospective, observational study was to generate real-world evidence to characterize the relationship between pathologic responses and survival and to describe patient profiles and neoadjuvant treatment patterns for patients with surgically resectable NSCLC (stage IB [tumour ≥ 4 cm] to stage IIIA) treated in the community oncology setting in the US. Neoadjuvant treatment regimens were characterized as chemotherapy or chemoradiotherapy in the study.
Efficacy Results
||| |||||| ||||||||| ||| |||| ||||||| ||| || |||||| ||||| ||||| |||||||| || ||||||| |||||||||| || |||||| |||||| || || ||||||| |||||||| |||||||| |||| ||| |||||| || || ||||||| |||||||| |||||||| || |||| ||||||||| |||||||| |||| ||| || ||||| ||||||| |||| ||| |||||||||| || || ||||||||||| ||| |||||||| ||| || ||| |||| |||| ||| |||| || |||||| |||| |||||||| ||| |||| ||||||| ||||| |||||| ||| ||||||||||| |||||||| ||| ||||||| |||||||||| |||| |||||||| || ||||||||| ||| |||| |||| ||| |||| || ||||||| |||| |||||| || ||||| |||||||| |||| |||| ||| |||| |||| ||| |||| || |||||| |||||| |||||||| || |||| |||| || |||| || ||||| |||||| ||||| |||||||| ||||||| ||||| |||| |||||||| |||| ||| |||| |||||||| || ||||| ||||||| |||| ||| |||||||||| || || ||||||||||| ||| |||||||| ||| || ||| |||| |||| ||| |||| || |||||| |||| |||||||| ||| |||| ||||||| ||||| |||||| ||||||| ||||| |||||| ||| ||||||||||| |||||||| ||| ||||||| |||||||||| |||| |||||||| || ||||||||| ||| |||| |||| ||| |||| || ||||||| ||| ||||||| ||| |||||||||||| ||||||| ||||||| ||| ||| |||||| ||||||| ||||||||| |||| |||||| || ||||| |||||||| |||| || ||| ||| |||| |||| || |||| || |||||| |||||| |||||||| || |||| |||| ||| |||| || ||||| |||||| ||||| |||||||| ||||||| || |||| ||| ||||| ||| ||||||||| |||| ||||| || || |||||| ||||||| |||||| |||| |||||||||| || ||| ||||||||| ||| |||| ||| |||| |||||||||| ||| ||||||||| ||||||||| || |||||||| ||||||||||||| |||||| ||||||||| |||||||| ||||||| || ||| || |||||||| ||||||||
Critical Appraisal
Several limitations of the study were identified: neoadjuvant treatment consisted only of chemotherapy and chemoradiotherapy, several variables had incomplete or missing data in the analyses, and sample size was reduced (and had reduced power) to assess the relationship between pCR and/or MPR and survival end points. Thus, it is difficult to conclude that this retrospective, observational study (i.e., real-world evidence), which characterizes the relationship between pathologic responses and survival, as well as patient profiles and neoadjuvant treatment patterns in patients with surgically resectable NSCLC (stage IB [tumours ≥ 4 cm] to stage IIIA) treated in the community oncology setting in the US, provides all the information required to address gaps in the evidence in support of the validity of end points in the pivotal trial.
Conclusions
Although statistically significant EFS and favourable OS outcomes were observed in the CheckMate 816 trial for nivolumab plus chemotherapy compared to chemotherapy alone for the neoadjuvant treatment of adults with resectable NSCLC (tumours ≥ 4 cm or node-positive disease), there remains uncertainty about the magnitude of the treatment effect, given that the results are based on interim analyses, OS data were immature at the October 20, 2021, cut-off date, and the HR for death was not statistically significant. Although EFS is a validated surrogate for OS, final analyses may be warranted to increase confidence in the trial findings. Prespecified EFS subgroup analyses suggested that the majority of the benefit derived from nivolumab plus chemotherapy was in subgroups of patients with stage IIIA disease and a PD-L1 expression level above 50%. However, efficacy results from these subgroup analyses should be interpreted with caution, as the study was not statistically powered to assess subgroups individually. The clinical experts indicated that patients with the highest risk of recurrence (i.e., patients with stage IIIA disease) and with a PD-L1 expression level above 50% may derive more benefit from the treatment and clinicians may be more apt to treat them with this regimen. However, regardless of the magnitude of response observed, a benefit was observed in all subgroups and in the overall study population. No detriment to quality of life was observed for patients in the trial, and the mean differences from baseline to predefined time points did not exceed minimally important differences (MIDs) for the VAS and utility score portion of the EQ-5D-3L questionnaire. Notable differences between the trial population and patients treated in Canada were related to the younger population in the trial than in the patient population in Canada, the higher proportion of patients with stage IIIA NSCLC in the trial than is seen in clinical practice, and the lack of a comparator arm with the current standard of care. However, the clinical experts noted that these differences were unlikely to affect the generalizability of the efficacy results to the patient population in Canada. The clinical experts noted that this treatment will typically be administered to patients with surgically resectable NSCLC (tumours ≥ 4 cm and or node-positive disease) and a good ECOG PS (0 and 1). The safety profile of nivolumab was consistent with the known safety profile of immunotherapies, and no new safety signals were identified. The AEs reported were considered manageable in practice by the clinical exerts consulted.
It is worth noting that the comparator in the CheckMate 816 trial (neoadjuvant chemotherapy) is not the current standard of care in Canada for patients with resectable NSCLC (which is upfront surgery with curative intent, followed by adjuvant chemotherapy), and no direct evidence was available to assess the efficacy of nivolumab plus chemotherapy relative to surgery followed by adjuvant chemotherapy. Findings from the sponsor-submitted NMA suggest an improvement in EFS in the nivolumab plus chemotherapy arm for patients with stage IIIA resectable NSCLC, compared with surgery and adjuvant chemotherapy. However, there were sources of uncertainty identified, such as the significant heterogeneity in the RCTs included, sparse networks, and immature data for OS. In addition, there were no quantitative safety data presented, so no conclusions could be drawn. The sponsor-submitted meta-analysis and real-world evidence showed favourable OS outcomes with neoadjuvant nivolumab for those who achieved a pCR compared to those who did not. However, both studies have study design limitations that preclude definitive conclusions.
Introduction
Disease Background
Lung cancer is the most frequently diagnosed cancer in Canada, and the leading cause of cancer-related death.1 About 30,000 new diagnoses (50% in males and 50% in females)2 and 20,700 cancer-related deaths were projected in Canada in 2022,1,3 with about 98% of all cases anticipated in people 50 years and older.4 The adjusted 5-year net survival (based on 2015 to 2017 estimates) for all forms of lung cancer is only 22% (19% in males and 26% in females in Canada).1,2 NSCLCs are the most common forms of lung cancer, accounting for more than 80% of all lung cancers in Canada,5,6 and adenocarcinomas are the most commonly diagnosed forms, accounting for 48% of new cases in Canada.4 The 5-year survival rate for patients with NSCLC is poor and highly dependent on disease stage at diagnosis; it is higher in patients with early-stage (stage IB) disease (66% to 68%) than in patients with stage IIA disease (52% to 60%), stage IIB disease (47% to 53%), and stage IIIA disease (36%).18
Diagnosis is based on symptoms and histology at initial presentation.19,20 Staging is key in determining disease prognosis and facilitates treatment selection.20,21 The current standard staging system recommended in Canada is the 8th edition of the AJCC/UICC staging guidelines, which involves a tumour, node, metastasis (TNM) classification of the disease based on the size and spread of the primary tumour (T), lymph node involvement (N), and occurrence of metastasis (M).22 About 47.1% of all new cases of NSCLC are diagnosed at stage IV, 19.0% at stage III, 9.1% at stage II, and only 23.1% at stage I.7 Patients with early-stage NSCLC have a higher risk of disease recurrence than patients with later-stage disease, despite curative surgery.23
General symptoms of NSCLC include worsening cough, chest pain, hemoptysis, malaise, weight loss, dyspnea, and hoarseness at clinical presentation or upon chest imaging.4,20 Patients with advanced or metastatic disease may experience additional symptoms such as trouble breathing, chronic cough and chest pain, pain in bones or the spine, yellowing of the skin or eyes, weakness or numbness of arms or legs, fatigue and unexplained weight loss, depression, insomnia, and pain.21,24 Diagnostic procedures currently recommended include imaging with CT, PET, and/or MRI scans, bronchoscopy with or without endobronchial ultrasound, and tissue biopsy.25
Available treatment options for NSCLC depend on disease stage at diagnosis, the potential for tumour resection with surgery, and eligibility of the patient for surgery (e.g., performance status, comorbidities). Treatment options include surgery, radiotherapy, and systemic therapy (with chemotherapy or immunotherapy). Patients may receive treatments before surgery (neoadjuvant setting), after surgery (adjuvant setting), before and after surgery (perioperative therapy), or after they have achieved disease control (consolidation therapy with radiation with or without chemotherapy).12 For patients with early-stage disease, eligibility for surgical resection depends on various clinical factors that determine the safety of a lung resection (e.g., overall respiratory function, tumour location, and the presence of ipsilateral vocal cord paralysis, Horner syndrome, phrenic nerve palsy, and neurologic deficits associated with Pancoast superior sulcus tumours) and on general health factors that determine eligibility for major surgery (e.g., comorbidities such as active cardiac disease).25
Standards of Therapy
The treatment goal for patients with resectable NSCLC is to cure, improve 5-year OS, and prevent disease recurrence.
Surgery with curative intent is the current gold standard for patients with clinical stage I to stage IIIA NSCLC amenable to resection.8,9 The standard of care for completely resectable stage IIA or IIB and stage IIIA NSCLC (AJCC 7th edition), according to joint guidelines from the American Society of Clinical Oncology and CCO, is surgical resection followed by adjuvant cisplatin-based chemotherapy.10 Cisplatin-based chemotherapy is not recommended for patients with stage IA disease and not routinely recommended for patients with stage IB disease; however, a postoperative evaluation is recommended.10,26 The British Colombia guidelines recommend adjuvant platinum-based therapy (cisplatin-based treatment is preferred or, if cisplatin is contraindicated, carboplatin-based treatment) as the standard of care for patients with completely resected stage II or stage IIIA (AJCC 7th edition) disease.27
Neoadjuvant chemotherapy is seldom used in Canada for resectable NSCLC, as it has not been shown to provide a survival benefit over adjuvant therapy, and in the process of pursuing neoadjuvant chemotherapy, some patients may become ineligible for surgery (owing to disease progression or treatment-related toxicity), according to the clinical experts consulted. Still, neoadjuvant therapy has several advantages: it can reduce tumour size, increase resectability, and remove micrometastasis and tumour cells in distant lymph nodes, thereby reducing the risk of recurrence from tumour cells that are not removed by surgery.12,13
Stereotactic ablative radiation with curative intent is available to some patients with early-stage disease who are ineligible for surgery (e.g., because of significant comorbidities that make them a high risk for general anesthetic) or who refuse surgery, according to the clinical experts. Patients with borderline resectable stage III cancer may be offered chemotherapy and/or radiation in current practice before surgery, whereas those with unresectable stage III NSCLC will be typically managed with combined chemoradiation followed by a year of consolidation with durvalumab if the patient has stable or responsive disease at postchemoradiation reassessment, the clinical experts explained.11 Adjuvant chemotherapy options consist of cisplatin plus vinorelbine, carboplatin plus paclitaxel for patients with a contraindication to cisplatin, gemcitabine plus carboplatin, paclitaxel plus carboplatin, pemetrexed plus cisplatin, and immune-checkpoint inhibitors (atezolizumab and durvalumab). The experts indicated that patients with node-positive NSCLC or who have tumours 4 cm or larger may receive additional postoperative treatment, such as adjuvant chemotherapy (4 cycles of cisplatin-based doublet chemotherapy with vinorelbine or pemetrexed) or adjuvant osimertinib (for 3 years, but only for patients with the common exon 19 deletion or an exon 21 insertion L858R EGFR mutation).
For patients with PD-L1 Tumour Proportion Scores above 50%, a recent Health Canada NOC for atezolizumab has recommended funding in the adjuvant setting after adjuvant chemotherapy; however, at present, it is not available outside private insurance or patient self-pay options. Postoperative adjuvant radiation is limited to use in patients with R1 resections (i.e., positive surgical margins). The experts noted that evidence from the IMPOWER010 trial supports a year of adjuvant therapy with atezolizumab after adjuvant chemotherapy. However, the Health Canada NOC limits this treatment to patients whose tumours exhibit a PD-L1 Tumour Proportion Score of 50% or more. Although this therapy has received an initial recommendation for funding by CADTH, it is not yet funded in any health jurisdiction in Canada, nor is it available through patient support programs. Adjuvant chemotherapy leads to an absolute improvement in 5-year OS of approximately 5% for all outcomes (although this is likely an underestimate in patients with higher-stage disease,28 and patients with stage IIIA disease [according to the AJCC 7th edition] have a high risk of recurrence [approximate 5-year survival in these patients is 30%]).
The clinician group input generally highlighted treatment options for resectable NSCLC similar to those described by the clinical experts consulted during this review. The clinician group input noted that adjuvant chemotherapy is not indicated for patients with stage I cancers, based on the 8th edition of the UICC staging system (tumours < 4 cm, node-negative disease).
Drug
Nivolumab is a human immunoglobulin G4 monoclonal antibody that binds to the PD-1 receptor and blocks its interaction with PD-L1 and PD-L2, releasing PD-1 pathway-mediated inhibition of the immune response, including antitumour immune response. In syngeneic mouse tumour models, blocking PD-1 activity resulted in decreased tumour growth.14 The Health Canada–recommended dose of nivolumab is 360 mg administered intravenously over 30 minutes as neoadjuvant treatment in combination with platinum-doublet chemotherapy every 3 weeks for 3 cycles.14 The key characteristics of nivolumab, carboplatin, paclitaxel, and pemetrexed are presented in Table 4.
Nivolumab underwent a review at Health Canada under Project Orbis and received a NOC on August 18, 2022, for the neoadjuvant treatment of adult patients with resectable NSCLC (tumours ≥ 4 cm or node-positive) in combination with platinum-doublet chemotherapy.12 The sponsor’s reimbursement request and population aligns with the Health Canada indication. This submission is a post-NOC request.
Table 4: Key Characteristics of Nivolumab, Carboplatin, Pemetrexed, and Paclitaxel
Characteristics | Nivolumab14 | Carboplatin29 | Pemetrexed30 | Paclitaxel31 |
|---|---|---|---|---|
Mechanism of action | Nivolumab is an IgG4 monoclonal antibody that binds to the PD-1 receptor and blocks its interaction with PD-L1 and PD-L2, releasing PD-1 pathway-mediated inhibition of the immune response, including the antitumour immune response. In syngeneic mouse tumour models, blocking PD-1 activity resulted in decreased tumour growth. | Carboplatin is a synthetic analogue of cisplatin, that, like cisplatin, interferes with DNA intrastrand and interstrand crosslinks in cells exposed to the drug. DNA reactivity has been correlated with cytotoxicity. | Pemetrexed disodium is an antifolate antineoplastic drug that exerts its action by disrupting crucial folate-dependent metabolic processes essential for cell replication. | Paclitaxel is an antimicrotubule drug that blocks cell replication in the late G2 and/or M phases of the cell cycle. Additionally, it produces unusual cytoskeletons characterized by discrete bundles or microtubules and the formation of abnormal spindle asters during mitosis. |
Indicationa | Neoadjuvant treatment of adults with resectable NSCLC (tumours ≥ 4 cm or node-positive disease) in combination with platinum-doublet chemotherapy. | The treatment of ovarian cancer of epithelial origin in first-line therapy, and in second-line therapy after other treatments have failed. | In combination with cisplatin therapy for the initial treatment of patients with a good performance status and locally advanced or metastatic nonsquamous NSCLC. For the maintenance treatment of locally advanced or metastatic nonsquamous NSCLC in patients with a good performance status and no disease progression immediately after 4 cycles of first-line platinum-doublet chemotherapy. | First-line treatment of advanced NSCLC. |
Route of administration | IV | IV | IV | IV |
Recommended dose | A flat dose of 360 mg IV infusion over 30 minutes | 400 mg/m2 as a single 15 minute to 60-minute IV infusion | In combination with cisplatin therapy, 500 mg/m2 administered as an IV infusion over 10 minutes on day 1 of each 21-day cycle | 175 mg/m2 IV infusion over 3 hours every 3 weeks, followed by cisplatin |
Serious adverse effects or safety issues | Fatal immune-mediated adverse reactions, including pneumonitis, interstitial lung disease, encephalitis, myocarditis, Stevens-Johnson syndrome, toxic epidermal necrolysis, and autoimmune hemolytic anemia | Hypersensitivity reactions Hematologic toxicity Bone marrow suppression Neurologic toxicity Fatal veno-occlusive disease Fatal hemolytic anemia Fatal hemolytic-uremic syndrome | Hepatotoxicity Contraindication to concomitant yellow fever vaccine bullous Epidermolysis Stevens-Johnson syndrome Toxic epidermal necrolysis | Severe hypersensitivity reactions (dyspnea, hypotension, angioedema, generalized urticaria) Bradycardia Peripheral neuropathy |
IgG4 = human immunoglobulin G4; NSCLC = non–small cell lung cancer; PD-1 = programmed cell death 1 protein; PD-L1 = programmed cell death 1 ligand 1; PD-L2 = programmed cell death 1 ligand 2.
aHealth Canada–approved indication.
Sources: Nivolumab PM,14 carboplatin PM,29 paclitaxel PM,31 pemetrexed PM.30
Stakeholder Perspectives
Patient Group Input
This section was prepared by CADTH staff based on the input provided by patient groups.
LCC, a member of Global Lung Cancer Coalition and the only national organization in Canada focused exclusively on lung cancer, engages in patient support, education, research, and advocacy. LCC submitted patient group input based on interviews conducted in Canada in September and October 2022 ([1 patient with stage I/II NSCLC, 1 patient with stage III NSCLC, 2 patients with stage IV NSCLC, and 1 caregiver for a patient with large-cell neuroendocrine carcinoma] and [1 interview with a patient who had stage IV NSCLC and had undergone an environmental scan]). All participants had experience with nivolumab. The patient input summary will focus on the 2 patients with stage I to stage III NSCLC to align with the requested indication.
One patient said she used to be extremely active and was an avid runner for 10 years before her lung cancer diagnosis. Lung cancer made exercise harder and made her feel more tired than before, which had an impact on her independence, she explained. She experienced cough and some mild chest pain before her diagnosis of lung cancer. Another patient who had been diagnosed with early-stage NSCLC had two-thirds of his lung surgically removed, leaving him with 50% of his initial lung capacity. As a result, he became unable to do any vigorous exercise or activity and tires quickly. The input indicated that patients value treatment options that maintain or improve quality of life, delay the onset of symptoms, improve survivorship, improve, or maintain functionality and/or mobility, and ultimately provide a cure. Also, patients prefer treatments that can be administered at a hospital located near home, or in a community clinic for those in rural settings, to minimize travel time and burden on caregivers. The input emphasized that because the CheckMate 816 trial excluded patients with EGFR or ALK alterations, owing to a lack of evidence of supporting neoadjuvant immunotherapy in this population, a biomarker screening (a routine practice) must be performed before neoadjuvant treatment with nivolumab.
Clinician Input
Input From Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise in the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of NSCLC.
Unmet Needs
The clinical experts consulted noted that the treatment goal in this setting is to cure patients (improve survival by eradicating micrometastasis) and prolong life. Secondary treatment goals include the delay of disease relapse, which will allow patients to live longer in a disease-free state.
The clinical experts noted that many patients receiving the current standard of care (surgery followed by adjuvant chemotherapy) still experience disease relapse, after which the disease generally becomes incurable. The clinical experts added that although adjuvant chemotherapy adds a survival benefit to patients in current practice, the benefit observed is modest and adjuvant treatment is associated with a toxicity burden. The clinical experts explained that many patients treated with the current standard of care decline or are ineligible for adjuvant chemotherapy because of the potential for AEs related to cisplatin doublet chemotherapy, some of which may be irreversible (e.g., kidney or nerve damage, impaired hearing). The clinical experts also mentioned that many patients are not clinically fit to undergo 4 cycles of cisplatin-based adjuvant treatment, and therefore do not receive any adjuvant therapy. Thus, there is an unmet need for new treatments for patients with resectable NSCLC.
Place in Therapy
The clinical experts explained that nivolumab would change the treatment paradigm for early-stage resectable NSCLC, as neoadjuvant therapy is not common practice in Canada. The clinical experts indicated that there might be a shift in the treatment paradigm for patients who experience disease recurrence while receiving neoadjuvant nivolumab and chemotherapy, or shortly after completion (usually within 6 months), given that the standard first-line therapy for patients diagnosed with incurable disease is based on an immunotherapy backbone with single-drug pembrolizumab or cemiplimab, or on platinum-doublet chemotherapy combined with pembrolizumab or nivolumab and ipilimumab. However, the clinical experts noted that backbone immunotherapy may not be appropriate if clinicians believe the disease is resistant to PD-1 inhibition. The clinical experts also noted that the order of therapies in the current treatment paradigm may shift, given that patients were allowed to receive additional postoperative adjuvant chemotherapy and/or radiation at the discretion of the treating physician in the CheckMate 816 trial. For the majority of patients treated with neoadjuvant chemotherapy and nivolumab in practice, this would be considered a replacement for adjuvant chemotherapy, and in most cases no further adjuvant systemic therapy would be offered.
According to the clinical experts, nivolumab plus chemotherapy would only be used in the curative-intent setting before surgery to increase the time before disease recurrence and, presumably, reduce the number of patients who will experience disease recurrence, thereby increasing cure rates and OS. The clinical experts noted that this treatment may increase the number of patients who have a complete (R0) surgical resection, and may reduce the extent of the lung removed during surgery (e.g., a patient who otherwise would have had to have a full lung removed [pneumonectomy] may be able to have a smaller surgery limited to the removal of a single lobe of the lung [lobectomy] after the downsizing effect of preoperative chemotherapy plus nivolumab). The clinical experts noted that nivolumab will be administered in practice, in addition to 3 cycles of chemotherapy, to patients with tumours 4 cm or larger or with node-positive disease.
Patient Population
The clinical experts consulted indicated that eligible patients will include those who have tumours larger than 4 cm and/or node-positive disease, who have no EGFR or ALK mutations, and who are deemed fit for upfront surgical resection, including patients with locoregional spread of disease to the lymph nodes but who remain fit for upfront resection, provided there were no contraindications (e.g., severe or uncontrolled autoimmune diseases, frailty, poor baseline organ function). The experts noted that nivolumab would not be appropriate for patients considered to have borderline resectable disease fit for upfront surgery and for whom the goal of neoadjuvant therapy would be to downsize the tumour enough to make surgical resection feasible.
The clinical experts indicated that patients with the highest risk of recurrence (i.e., patients with stage IIIA disease) and a PD-L1 expression level above 50% would likely derive benefit from the treatment, and clinicians may be apt to treat them with this regimen.
According to the clinical experts, patients will be identified by a thoracic surgeon after appropriate review. The experts noted that surgical resectability is usually determined by a thoracic surgeon, and eligibility depends on multiple factors, including a patient’s lung function (measured with pulmonary lung function tests). The clinical experts indicated that the process of determining tumour resectability for patients with early-stage NSCLC is, to a certain extent, subjective. They noted that, ideally, tumour scans are reviewed by a thoracic tumour board, but added that the process may not always be feasible. Patients should undergo baseline staging with a PET scan, MRI brain scan, and mediastinal lymph node sampling. Driver mutations (EGFR or ALK) are important but may not be routinely assessed in all centres in patients with early-stage disease; however, the experts noted that patients with unknown EGFR and ALK mutational status should not be excluded from receiving the treatment. The clinical experts added that underdiagnosis and misdiagnosis are not issues in this setting. Further, there are projections that current screening strategies in Canada may increase the number of patients with early-stage disease who are asymptomatic and are candidates for curative-intent surgery.
Assessing Response to Treatment
The clinical experts noted that patient response to treatment is assessed with preoperative CT scans done after the completion of neoadjuvant systemic therapy, pathologic response, and OS. According to the clinical experts, the interpretation of restaging results can be difficult, given that some patients who receive neoadjuvant checkpoint inhibitors tend to exhibit pseudoprogression, especially in the lymph nodes. The clinical experts noted that any areas of possible progressive disease would be verified with tissue sampling, when feasible, before it is determined that a patient is no longer eligible for surgery because of disease progression.
According to the clinical experts, follow-up after completion of curative-intent surgery is not standardized in current practice, given the lack of definitive literature suggesting the most appropriate timing interval for serial radiography. The clinical experts noted that, in practice, response assessments for patients include surveillance CT scans (typically every 6 months for 2 years, then yearly to 5 years after therapy), and that this would not change because of the use of neoadjuvant nivolumab. In addition, follow-up procedures currently in place would not be affected in patients treated with neoadjuvant chemotherapy and nivolumab; they are already in place for patients who have undergone curative-intent surgery. A clinically meaningful response would be an improvement in OS.
Discontinuing Treatment
According to the clinical experts, chemotherapy and/or nivolumab could be discontinued at a patient’s request in the event of disease progression during the 3 cycles of neoadjuvant therapy, autoimmune or medically dangerous side effects, or intolerable toxicity.
Prescribing Conditions
According to the clinical experts, nivolumab administration should be monitored by a qualified specialist medical doctor (a medical oncologist or, in very rare cases, a respirologist) with experience in the treatment of lung cancer and the use of immunotherapy checkpoint inhibitors. Hospital outpatient settings in which personnel have experience with immunotherapy checkpoint inhibitors and chemotherapy would be appropriate treatment settings.
Additional Considerations
The clinical experts highlighted the current lack of clinical evidence to support the use of adjuvant nivolumab. The experts added that there is no evidence to support the use of the Health Canada–approved atezolizumab in the adjuvant setting for patients who have received neoadjuvant chemotherapy without nivolumab.
The clinical experts advised against defining eligibility for treatment in terms of staging, as there will be further evolution of these manuals in the near future. The experts noted that in the AJCC 7th edition, T2 tumours are defined as being larger than 3 cm and up to 7 cm. On further subdivision, T2a tumours are defined as being larger than 3 cm and up to 5 cm, and T2b tumours are defined as being larger than 5 cm and up to 7 cm. If a tumour is T2aN0 (node negative), it is classified as stage IB. If a tumour is T2bN0, it is classified as stage IIA. The indication being examined for neoadjuvant nivolumab plus chemotherapy includes patients with node-negative disease and tumours 4 cm or larger, so some stage IB tumours, according to the AJCC 7th edition, would qualify for neoadjuvant nivolumab plus chemotherapy and others would not. In the AJCC 8th edition, T2a tumours have been redefined as being larger than 3 cm and up to 4 cm, T2b tumours are now larger than 4 cm and up to 5 cm, and T3 tumours are now larger than 5 cm and up to 7 cm. The overall staging for these groups has also shifted; in the AJCC 8th edition, T2aN0 tumours remain classified as stage IB, but T2bN0 tumours are now classified as stage IIA and T3N0 tumours are now classified as stage IIB. The key difference is that the cancers included in the CheckMate 816 trial, which used the AJCC 7th edition definition of stage IB (node-negative tumours from 4 cm to 5 cm), would be classified as stage IIA in the AJCC 8th edition.
Patients with N2 nodal disease limited to a single nodal station are generally considered surgical candidates, as long as there is no local invasion that would render a complete surgical resection unfeasible, according to the clinical experts. In the AJCC 7th edition, patients with T2b (> 5 cm to 7 cm), N2, or T3N2 disease were considered stage IIIA, and would have been enrolled in the CheckMate 816 trial if they were candidates for upfront resection. In the AJCC 8th edition, the clinical experts noted that patients with primary tumours larger than 5 cm and up to 7 cm are considered T3, and T3N2 tumours have been upstaged from stage IIIA to stage IIIB. Further, tumours that were classified as T3 in the AJCC 7th edition (> 7 cm or with invasion of the diaphragm) are now classified as T4 in the AJCC 8th edition, and T4N2 tumours have been upstaged from stage IIIA to stage IIIB. According to the clinical experts, this means that there are patients with stage IIIB disease who are resectable according to the AJCC 8th edition who would have been considered stage IIIA in the AJCC 7th edition and thus eligible for neoadjuvant chemotherapy plus nivolumab.
Clinician Group Input
This section was prepared by CADTH staff based on the input provided by patient groups.
Two clinician groups, the OH-CCO Lung Cancer DAC and LCC submitted 2 separate inputs. The OH-CCO’s DAC provides guidance on drug-related issues in support of CCO’s mandate and collected information from 3 clinicians during a DAC meeting. LCC, a national charity and the only organization in Canada solely focused on lung cancer (education, advocacy, research), gathered information from published clinical data and 12 lung cancer medical oncologists from across Canada.
Unmet Needs
According to the OH-CCO group, despite current treatments, a number of patients experience a recurrence quickly and do not survive. Therefore, neoadjuvant nivolumab would be an additional option for patients with resectable NSCLC. LCC cited several advantages of neoadjuvant approaches: limiting the risk of systemic dissemination of the cancer; tumour downsizing (leading to decreased postoperative complications [e.g., pain, infection], decreased performance status, improved surgical outcomes, and improved recovery times); the possibility of easier, safer, and more efficacious surgeries; improving patient capacity to receive postoperative therapies; providing the opportunity for smoking cessation, physical therapy, and medical evaluations for surgery, helping to manage the surgical wait list; and improving the ability to provide prognosis and risk-stratification after surgery.
Place in Therapy
According to the OH-CCO clinicians, neoadjuvant nivolumab would be an additional option for patients with resectable NSCLC and could potentially replace adjuvant chemotherapy in some patients. Similarly, LCC clinicians said that neoadjuvant nivolumab therapy would eliminate the need for postoperative, prolonged, and more expensive therapies (chemotherapy, radiation, immunotherapy). LCC clinicians said it is not clear whether all eligible patients would choose neoadjuvant nivolumab therapy, such as patients with stage II, node-negative disease considered for upfront surgery with optional adjuvant therapies, those at high risk of chemotherapy-associated or immunotherapy-associated complications, and those preferring upfront surgery.
Patient Population
The OH-CCO clinicians said that patients who meet the clinical trial inclusion criteria (i.e., those with resectable stage IIA to stage IIIB NSCLC [AJCC 8th edition] and/or those eligible for chemotherapy) would be best suited for treatment with nivolumab. The LCC clinicians said that neoadjuvant therapy may be favoured for patients with stage IIIA and/or PD-L1-positive disease, based on the favourable results in these strata shown in CheckMate 816 study. However, the LCC group said that a discussion with every eligible patient appears warranted, and that treating all eligible patients with a neoadjuvant would be favoured to decrease the treatment burden after surgery (e.g., postoperative chemotherapy and/or atezolizumab). According to the LCC clinicians, the least suitable patients would be those with a contraindication to chemotherapy and/or immunotherapy, such as those with renal failure, heart failure, severe hearing loss, severe neuropathy, an organ transplant, active and symptomatic autoimmune disease (e.g., patients with Crohn disease on immunosuppressive therapy or those with multiple sclerosis), and an ECOG PS of 2 to 4. The LCC group added that a history of autoimmune disease or autoimmune disease that is clinically silent (e.g., immune thyroiditis) or well controlled without active immunosuppression is not a major contraindication. Last, according to the LCC input, the use of neoadjuvant immunotherapy in patients with EGFR, ALK, ROS1, RET, or NTRK alterations needs further investigation and/or will have to be addressed on a case-by-case basis, as these groups have not been specifically addressed in clinical trials.
Assessing Response to Treatment
The OH-CCO clinician group stated that outcomes such as clinical assessment (to ensure no progression), surgery, and pathological assessment can be used to determine response to nivolumab. The LCC clinician group said that an additional CT scan would be needed after neoadjuvant therapy to evaluate a patient’s eligibility for surgery. According to LCC clinicians, currently there is no clinical, biologic, or imaging tool that can be used to identify patients who will have a pCR on pathological assessment after neoadjuvant treatment and can be excluded from surgical treatment. At present, patients are followed with standard postoperative care, the LCC clinicians reported. However, they anticipate that in the future, as more experience is gained with neoadjuvant approaches, risk-adapted follow-up strategies will be possible, based on, for example, postoperative monitoring of circulating tumour DNA in combination with other clinical and pathologic features of the cancer.
Discontinuing Treatment
The OH-CCO clinicians said that intolerable toxicity and clinically obvious disease progression are factors to consider when deciding whether to discontinue nivolumab treatment. The LCC clinicians stated that clinical and biologic evaluations are performed at every cycle of therapy, as they are for patients undergoing chemotherapy and/or immunotherapy in the advanced disease setting, per standard practice in oncology.
Prescribing Conditions
The OH-CCO clinicians noted that a specialist, ideally as part of a multidisciplinary team, is required in a hospital outpatient clinic to diagnose, treat, and monitor patients receiving nivolumab. The LCC clinicians also stated that, ideally, a multidisciplinary cancer tumour board, consisting of (nonexclusively) respirologists, radiologists, pathologists, thoracic surgeons, medical oncologists, and radiation oncologists, should discuss a multimodal treatment approach for patients who are usually referred to oncologic thoracic surgeons affiliated with major cancer centres. The LCC clinicians added that the delivery of care should be planned according to local structures; ideally, systemic therapies will be administered as close to a patient’s home as possible while patients are continuously monitored by the cancer centre to coordinate neoadjuvant therapies with posttreatment imaging, preoperative evaluations, and the surgical admission itself.
Table 5: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Relevant comparators | |
The comparator is appropriate, because if patients were to receive neoadjuvant chemotherapy, it would be platinum-doublet chemotherapy. Neoadjuvant platinum-doublet chemotherapy has an efficacy similar to that of the current standard of care in Canada (adjuvant chemotherapy). Most patients will not receive any treatment in the neoadjuvant setting. In the CheckMate 816 trial, chemotherapy with vinorelbine and cisplatin, gemcitabine and cisplatin, pemetrexed and cisplatin, or paclitaxel and carboplatin for up to 3 cycles (9 weeks) was implemented. These regimens are some of the chemotherapy options available for neoadjuvant chemotherapy. What chemotherapy regimens are appropriate for neoadjuvant use in combination with nivolumab? | The clinical experts noted that docetaxel and vinorelbine were only allowed in the chemotherapy arm of the CheckMate 816 trial but not the nivolumab arm. It would be appropriate to apply the chemotherapy drugs used in the nivolumab plus chemotherapy arm to patients in real-world practice. |
Considerations for initiation of therapy | |
In the CheckMate 816 trial, participants were excluded if they had known EGFR mutations or ALK translocation. The funding request does not reference EGFR mutation or ALK translocation status Does PD-L1 status have to be established for a patient to be eligible for nivolumab in combination with neoadjuvant chemotherapy for resectable NSCLC? | According to the clinical experts, nivolumab will be available to all patients, regardless of their PD-L1 expression level. |
There are no immunotherapy drugs currently funded in the neoadjuvant NSCLC setting at this time, and this is the first immunotherapy drug to be reviewed. In other solid tumours, patients are eligible for a downstream PD-1 or PDL-1 inhibitor, provided that disease recurrence (whether locoregional or distant) occurs 6 months or more after the last dose of the neoadjuvant PD-1 or PD-L1 inhibitor. If nivolumab is funded in this setting, will jurisdictions permit a downstream PD-1 or PDL-1 inhibitor used in a manner consistent with other tumour sites? | For pERC consideration. |
Considerations for discontinuation of therapy | |
If patients cannot tolerate chemotherapy, are they able to continue with nivolumab? Is there a minimum number of chemotherapy cycles that must be given concurrently with nivolumab? | The clinical experts explained that patients would likely go straight to surgery if they remain eligible; however, if the adverse event was attributable to chemotherapy only, then the patients may receive the remainder of the treatment with nivolumab monotherapy. A second expert noted that treatment discontinuation procedures in practice will likely follow those implemented in the CheckMate 816 trial protocol. The expert explained that in the CheckMate 816 trial, if either chemotherapy or nivolumab needed a dose delay, both were delayed until the patient met resumption criteria for both chemotherapy and nivolumab. If an adverse event could be clearly attributed to either the chemotherapy or nivolumab, which meant that that particular drug had to be discontinued, patients were allowed to continue with the other. In the event that the treating physician or patient chooses to stop both and proceed with surgery before 3 cycles are complete, it was considered appropriate, but having to stop chemotherapy should not mean that the patient cannot continue to a maximum of 3 cycles of nivolumab, or vice versa. |
Considerations for prescribing of therapy | |
PAG would like to inform pERC that jurisdictions will implement weight-based dosing up to a cap, similar to other immunotherapy policies (i.e., nivolumab 4.5 mg/kg up to 360 mg every 3 weeks). | For pERC consideration. |
Generalizability | |
Should patients with ECOG PS of 2 or greater be eligible for nivolumab in this indication? | Both clinical experts agreed that patients with an ECOG PS of 0 or 1 will benefit from the treatment. One expert noted that patients with an ECOG PS of 2 may be considered, although these patients will be few. The clinical experts emphasized the need for patients to have a robust performance status before being eligible to receive the treatment, given that patients with less clinical reserve will be susceptible to adverse events that may render them ineligible for curative-intent surgery. |
There is a time-limited need to allow patients currently on platinum-based doublet chemotherapy to add nivolumab. What time frame is appropriate to add nivolumab for patients actively on treatment (chemotherapy)? | Both experts agreed that the time-limited need to allow patients currently on platinum-based doublet chemotherapy to add nivolumab will not be an issue in current practice, given the lack of use of neoadjuvant chemotherapy in current clinical practice in Canada. In the event that patients are actively on neoadjuvant treatment with chemotherapy, the experts suggested the addition of nivolumab to any of the remaining cycles of neoadjuvant therapy. |
Care provision issues | |
Nivolumab is already prepared and administered at facilities throughout Canada. Health care professionals have extensive experience with it. Preparation and administration time for nivolumab are reasonable and would not be expected to significantly increase health system resources. | For pERC consideration. |
System and economic issues | |
Nivolumab use as an additional drug in this patient population would have a considerable impact on a budget, compared with chemotherapy alone. | For pERC consideration. |
Nivolumab is used for many other indications at this time; it is anticipated that vial sharing or dose rounding will be possible (especially in larger treatment centres). | For pERC consideration. |
ALK = anaplastic lymphoma kinase; ECOG PS = Eastern Cooperative Oncology Group Performance Status; EGFR = epidermal growth factor receptor; NSCLC = non–small cell lung cancer PD-1 = programmed cell death 1 protein; PD-L1 = programmed cell death 1 ligand 1; pERC = CADTH pan-Canadian Oncology Drug Review Expert Review Committee.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may affect their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH for nivolumab are summarized in Table 5.
Clinical Evidence
The clinical evidence included in the review of nivolumab is presented in 3 sections. The first section, the Systematic Review, includes pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as studies that were selected according to an a priori protocol. The second section includes indirect evidence from the sponsor and indirect evidence selected from the literature that met the selection criteria specified in the review. The third section includes sponsor-submitted long-term extension studies and additional relevant studies that were considered to address important gaps in the evidence included in the Systematic Review.
Systematic Review (Pivotal and Protocol-Selected Studies)
Objectives
To perform a systematic review of the beneficial and harmful effects of nivolumab (360 mg administered intravenously), in combination with platinum-doublet chemotherapy every 3 weeks for up to 3 cycles, for the neoadjuvant treatment of adults with resectable NSCLC (tumours ≥ 4 cm or node-positive disease).
Methods
Studies selected for inclusion in the Systematic Review included pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those meeting the selection criteria presented in Table 6. Outcomes included in the CADTH review protocol reflect outcomes considered to be important to patients, clinicians, and drug plans.
Two CADTH clinical reviewers independently selected studies for inclusion in the review based on titles and abstracts, according to the predetermined protocol. Full-text articles of all citations considered potentially relevant by at least 1 reviewer were acquired. Reviewers independently made the final selection of studies to be included in the review, and differences were resolved through discussion.
Table 6: Inclusion Criteria for the Systematic Review
Criteria | Description |
|---|---|
Patient population | Adults 18 years and older with resectable NSCLC (tumours ≥ 4 cm or node-positive disease) Subgroups:
|
Intervention | Nivolumab 360 mg (intravenously) in combination with platinum-doublet chemotherapy intravenously every 3 weeks for up to 3 cycles |
Comparators |
|
Outcomes | Efficacy outcomes:
Harms outcomes:
|
Study design | Published and unpublished phase III and IV RCTs |
E = adverse event; ALK = anaplastic lymphoma kinase; ECOG PS = Eastern Cooperative Group Performance Status; EFS = event-free survival; EGFR = epidermal growth factor receptor; HRQoL = health-related quality of life; MPR = major pathologic response; NSCLC = non–small cell lung cancer; OS = overall survival; pCR = pathologic complete response; PD-L1 = programmed cell death 1 ligand 1; RCT = randomized controlled trial; SAE = serious adverse event; WDAE = withdrawal due to adverse event; vs. = versus.
aIdentified by clinical experts as a relevant comparator, but not currently publicly funded in Canada
The literature search for clinical studies was performed by an information specialist using a peer-reviewed search strategy according to the PRESS Peer Review of Electronic Search Strategies checklist.32
Published literature was identified by searching the following bibliographic databases: MEDLINE All (1946–) via Ovid and Embase (1974– via Ovid. All Ovid searches were run simultaneously as a multifile search. Duplicates were removed using Ovid deduplication for multifile searches, followed by manual deduplication in Endnote. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Patient Headings) and keywords. The main search concepts were Opdivo (nivolumab) and non–small cell lung cancer. The following clinical trials registries were searched: the US National Institutes of Health’s clinicaltrials.gov, WHO’s International Clinical Trials Registry Platform (ICTRP) search portal, Health Canada’s Clinical Trials Database, and the European Union Clinical Trials Register.
CADTH-developed search filters were applied to limit retrieval to RCTS or controlled clinical trials. Retrieval was not limited by publication date or by language. Conference abstracts were excluded from the search results. Refer to Appendix 1 for the detailed search strategies.
The initial search was completed on September 29, 2022. Regular alerts updated the search until the meeting of the CADTH pan-Canadian Oncology Drug Review Expert Committee (pERC) on February 8, 2023.
Grey literature (literature that is not commercially published) was identified by searching relevant websites from the Grey Matters: A Practical Tool For Searching Health-Related Grey Literature checklist.33 Included in this search were the websites of regulatory agencies (FDA and European Medicines Agency). Google was used to search for additional internet-based materials. Refer to Appendix 1 for more information on the grey literature search strategy.
These searches were supplemented by reviewing bibliographies of key papers and through contacts with appropriate experts. In addition, the manufacturer of the drug was contacted for information regarding unpublished studies.
Findings From the Literature
A total of 640 studies were identified from the literature for inclusion in the Systematic Review (Figure 1). The included studies are summarized in Table 7. A list of excluded studies is presented in Appendix 2.
Description of Study
CheckMate 816 is an ongoing, open-label, randomized, phase III trial assessing the efficacy and safety of nivolumab (3 mg/kg every 2 weeks for up to 3 cycles) in combination with ipilimumab (single 1 mg/kg dose), nivolumab (360 mg flat dose) in combination with platinum-based chemotherapy every 3 weeks for 3 cycles, and platinum-chemotherapy alone as a neoadjuvant treatment in adults 18 years and older with resectable (stage IB [≥ 4 cm], stage II, and resectable stage IIIA) NSCLC.15 Disease staging at screening was based on the AJCC/UICC TNM 7th edition.15 After completion of neoadjuvant treatment, all patients who remained operative candidates underwent definitive surgery for NSCLC within 6 weeks. Patients were also allowed to receive adjuvant chemotherapy with or without radiation after definitive surgery, per institutional standard, at the discretion of the investigator.
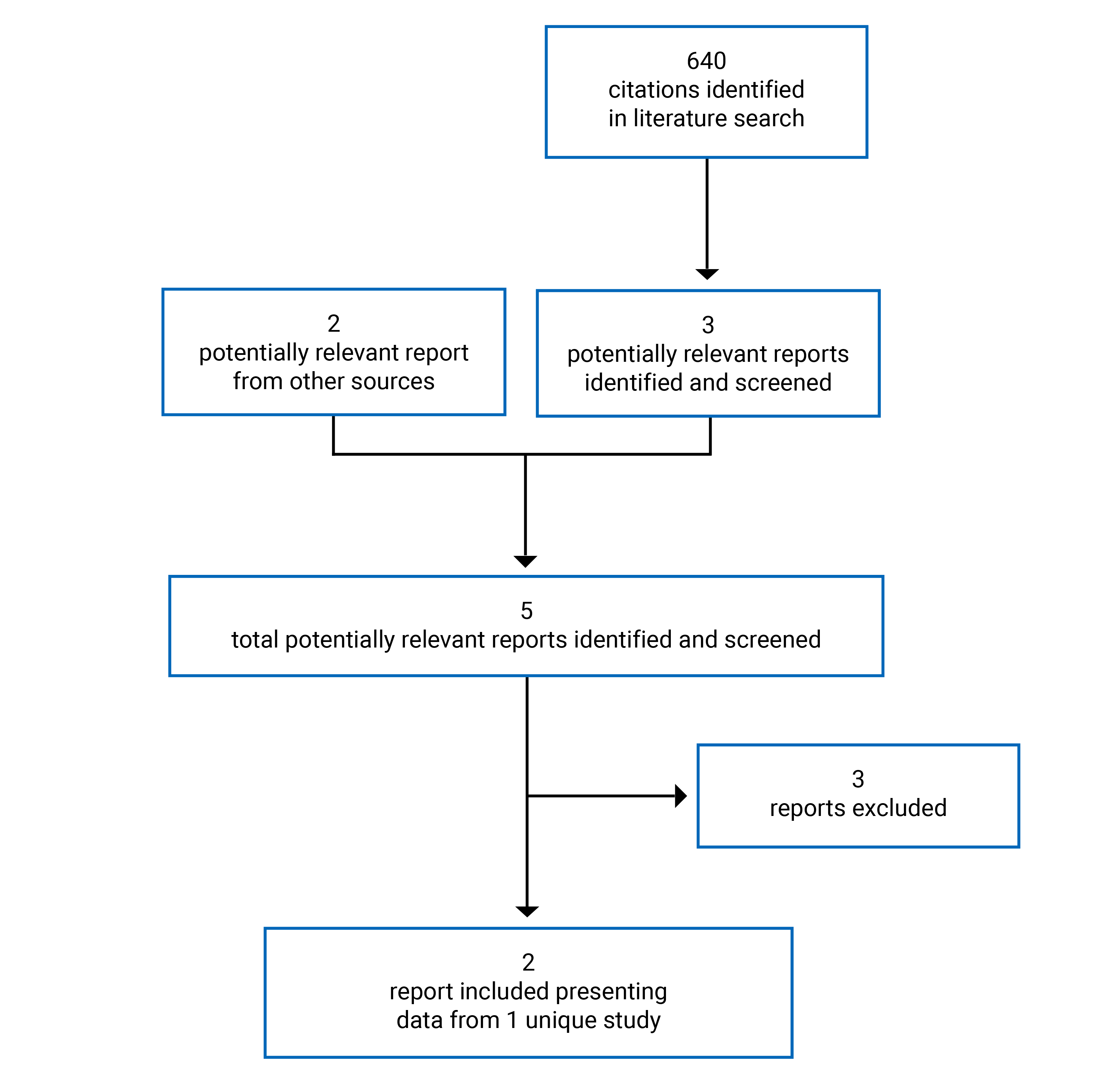
Table 7: Details of Included Study
Detail | CheckMate 816 |
|---|---|
Designs and populations | |
Study design | Ongoing, randomized, open-label, phase III trial |
Locations | 111 sites, 14 countries (North America [including Canada], Europe, Asia, and Rest of the world) |
Study duration | Ongoing |
Data cut-off date | Interim analyses:
|
Randomized (N) |
|
Inclusion criteria |
|
Exclusion criteria |
|
Drugs | |
Intervention | Nivolumab: Nivolumab 360 mg (flat dose) IV, every 3 weeks for up to 3 cycles Chemotherapy: Investigator’s choice of cisplatin (75 mg/m2 on day 1 of a 3-week cycle for up to 3 cycles) or carboplatin (AUC 5 or 6 on day 1 of a 3-week cycle for up to 3 cycles) in combination with gemcitabine (1,000 mg/m2 or 1,250 mg/m2 on days 1 and 8 of a 3-week cycle for up to 3 cycles) for squamous histology, or with pemetrexed (500 mg/m2 on day 1 of a 3-week cycle for up to 3 cycles) for nonsquamous histology, or carboplatin (AUC 5 or 6 on day 1 of a 3-week cycle for up to 3 cycles) + paclitaxel (175 mg/m2 or 200 mg/m2 on day 1 of a 3-week cycle for up to 3 cycles) for any histology. |
Comparator(s) | Chemotherapy: Investigator’s choice of cisplatin (75 mg/m2 on day 1 of a 3-week cycle for up to 3 cycles) or carboplatin (AUC 5 or 6 on day 1 of a 3-week cycle for up to 3 cycles) in combination with vinorelbine (25 mg/m2 or 30 mg/m2 on days 1 and 8 of a 3-week cycle for up to 3 cycles), docetaxel (60 mg/m2 or 75 mg/m2 on day 1 of a 3-week cycle for up to 3 cycles), gemcitabine (1,000 mg/m2 or 1,250 mg/m2 on days 1 and 8 of a 3-week cycle for up to 3 cycles) (for squamous histology only), or pemetrexed (500 mg/m2 on day 1 of a 3-week cycle for up to 3 cycles) (for nonsquamous histology only), or carboplatin (AUC 5 or 6) + paclitaxel (175 mg/m2 or 200 mg/m2) on day 1 of a 3-week cycle for up to 3 cycles) |
Duration | |
Phase | |
Screening phase | 28 days |
Open-label treatment | 3 cycles (9 weeks) |
Follow-up |
|
Outcomes | |
Primary end point |
|
Secondary and exploratory end points | Secondary:
Exploratory:
|
Publications | Forde et al. (2022)34 Provencio et al. (2022)35 |
AE = adverse event; ALK = anaplastic lymphoma kinase; AUC = area under the plasma drug concentration-time curve; BICR = blinded independent central review; BIPR = blinded independent pathologic review; CR = complete response; CTLA-4 = cytotoxic T-lymphocyte-associated protein-4; DLco = diffusing capacity; ECOG PS = Eastern Cooperative Group Performance Status; EFS = event-free survival; EFS2 = event-free survival on the next line of therapy; EGFR = epidermal growth factor receptor; EQ-5D-3L = 3-Level EQ-5D; FEV1 = forced expiratory volume in 1 second; FRC = functional residual capacity; FVC = forced vital capacity; HRQoL = health-related quality of life; IA1 = first interim analysis; IHC = immunohistochemistry; MPR = major pathologic response; N = node; NSCLC = non–small cell lung cancer; OS = overall survival; pCR = pathologic complete response; PD-1 = programmed cell death 1 protein; PD-L1 = programmed cell death 1 ligand 1; RECIST = Response Evaluation Criteria in Solid Tumours Version 1.1; SAE = serious adverse event; TTDM = time to death or distant metastases; VAS = visual analogue scale.
Source: Clinical Study Report.15
Coprimary end points investigated in the trial were pCR assessed by BIPR and EFS assessed by BICR. Secondary end points included OS, TTDM, and MPR. Safety, tolerability, and HRQoL were exploratory outcomes.15 All BICR and BIPR reviews of radiology scans and tumour and/or lymph node tissue for progression and disease recurrence were completed by a third-party vendor using prespecified guidelines (RECIST 1.1). Any investigator-assessed radiographic progression per RECIST 1.1 guidelines to confirm progression or recurrence was confirmed by BICR, per RECIST 1.1 guidelines.
The CheckMate 816 trial was initially designed as a 2-arm trial in which patients were randomized in a 1:1 ratio to 1 of 2 trial arms: nivolumab plus ipilimumab or chemotherapy. An update to the protocol (protocol revision 2) introduced a third arm, nivolumab plus chemotherapy, thereby allowing patients to be subsequently randomized in a 1:1:1 scheme to any treatment arm. A third update to the protocol (protocol revision 3) discontinued the randomization of patients to the nivolumab plus ipilimumab arm. Subsequently, patients enrolled in the study were randomized to either nivolumab plus chemotherapy or to chemotherapy in a 1:1 ratio and stratified by 3 factors:
PD-L1 expression level (≥ 1% versus < 1%, not evaluable, indeterminate)
disease stage (stage IB/ II versus stage IIIA)
gender or sex.
Patients who were already randomized to the nivolumab plus ipilimumab arm stayed in the study and continued scheduled study procedures. Study objectives in the CheckMate 816 trial were updated to focus on the comparison between nivolumab plus chemotherapy and chemotherapy for patients who were concurrently randomized. This CADTH review focuses on findings reported in the nivolumab plus chemotherapy and chemotherapy arms.
Patient enrolment began in March 2017 and the last patient was randomized on December 11, 2019. A total of 773 patients were enrolled at 111 sites in 14 countries (North America [including Canada], Europe, Asia, and the rest of the world). In total, 505 patients were randomized, 358 of whom were placed in the nivolumab plus chemotherapy arm (n = 179) or the chemotherapy arm (n = 179).15
The primary data cut-off date for the prespecified final pCR analysis was September 16, 2020, and the data cut-off date for IA1 EFS was October 20, 2021. By the October 20, 2021, data cut-off date, all treated patients had been off neoadjuvant study treatment for more than 18 months; 93.8% and 84.7% of treated patients in the nivolumab plus chemotherapy and chemotherapy arms, respectively, had completed the course of neoadjuvant therapy.15 Figure 2 presents the design flow of the CheckMate 816 trial.
At Screening
Baseline screening assessments were performed in the 28 days before randomization. PET-CT with contrast was assessed at baseline and a separate CT with contrast of the chest, abdomen, and other suspected areas (as well as the PET-CT) was required if the CT component of a PET-CT was not of sufficient diagnostic quality for RECIST 1.1 measurements. Patients with suspected brain metastases, including those with stage II disease or higher were evaluated with MRI/CT of the brain before and after contrast procedures. Tumour assessments were performed using the RECIST 1.1 guidelines.12
Figure 2: Study Design of the CheckMate 816 Trial
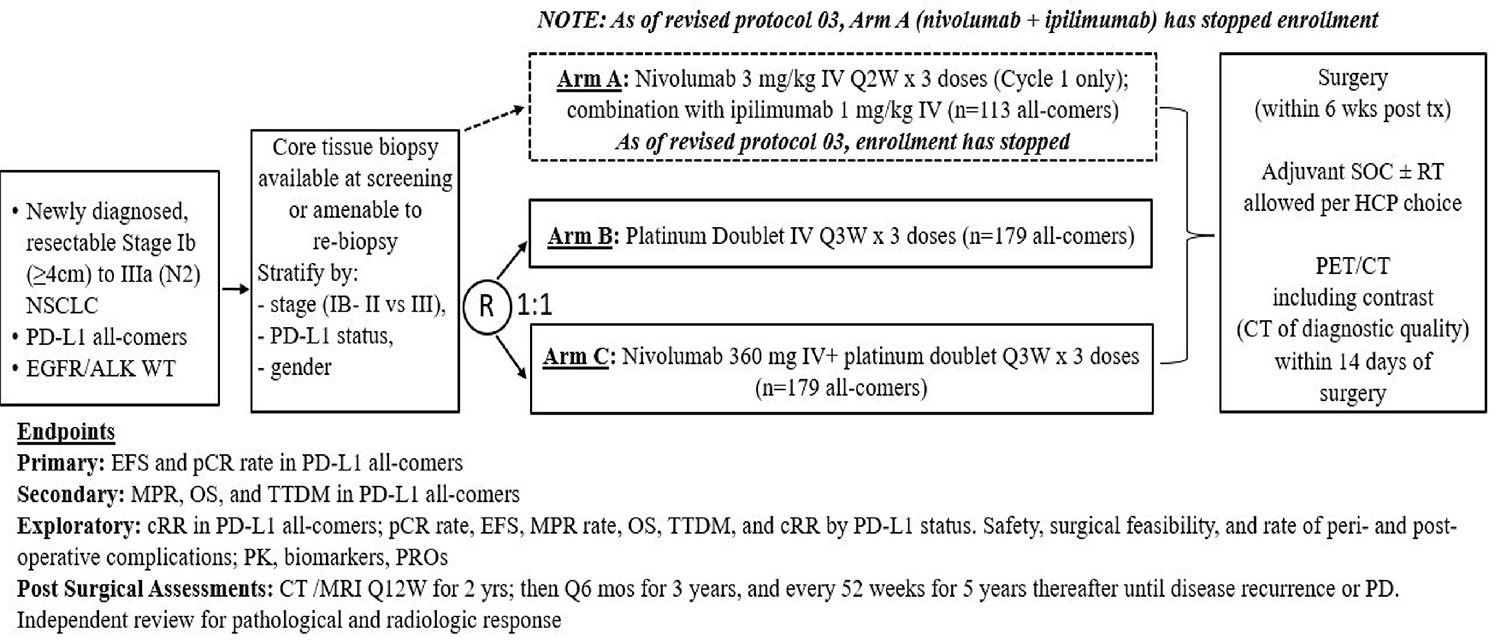
cRR = clinical response rate; EFS = event-free survival; EFS2 = event-free survival on the next line of therapy; HCP = health care provider; NSCLC = non–small cell lung cancer; OS = overall survival; pCR = pathologic complete response; PD = disease progression; PD-L1 = programmed cell death 1 ligand 1; ; PK = pharmacokinetic; PRO = patient-reported outcome; Q12W = every 12 weeks; Q2W = every 2 weeks; Q3W = every 3 weeks; Q6 mos = every 6 months; RT = radiotherapy; RT = radiotherapy; SOC = standard of care; TTDM = time to death or distant metastases; tx = treatment; WT = wild-type.
Source: Clinical Study Report.15
Postoperative Assessments
Preoperative PET-CT with contrast was obtained in the 14 days before surgery. Postoperative assessments with CT with contrast of the chest, including the adrenal glands, and CT or MRI of other additional suspected or known sites of disease were performed. The first tumour assessment took place 12 weeks (± 7 days) after definitive surgery, per RECIST 1.1, and then every 12 weeks (± 7 days) for 2 years (104 weeks), every 6 months (24 weeks ± 7 days) for 3 years, and every year (52 weeks ± 7 days) for 5 years or until disease recurrence or progression confirmed by BICR.
The same imaging methods used at baseline were recommended for postoperative procedures.12
First tumour assessments were performed 12 weeks (± 7 days) following tumour restaging in patients who did not receive definitive surgery and who had no tumour progression, as confirmed by BICR. Subsequent tumour assessments were performed for these patients using methods similar to those implemented for patients who had received definitive surgery and at the same frequency.
In the event that a planned initiation of subsequent anticancer therapy was within 12 weeks of restaging, tumour assessments were repeated before the administration of subsequent anticancer therapy.12 Postoperative radiation was administered per institutional standard of care.
The survival follow-up phase began 3 months after postneoadjuvant follow-up visit 2. Participants were followed every 3 months for survival. Survival follow-up visits could be performed with phone contact or an office visit.
Investigators at all participating sites were trained to perform radiology imaging in accordance with the study’s image acquisition guidelines before scanning the first patient.12
Loss to Follow-Up
Loss to follow-up was adequately defined in the protocol and measures were taken to account for missing data based on prespecified criteria.15
Populations
Inclusion and Exclusion Criteria
Patients 18 years and older with histologically confirmed stage IB (≥ 4 cm), stage II, or stage IIIA NSCLC (per TNM 7th edition) with resectable disease were included in the study. Patients underwent PET-CT, including contrast scans from the base of the skull to the upper thighs, to confirm disease stage. Patients were also required to undergo a CT scan with contrast of the chest, abdomen, and other suspected areas of disease (as well as the PET-CT) if the CT component of the PET-CT was not of sufficient diagnostic quality for RECIST 1.1 measurements. All suspicious mediastinal lymph nodes, including those that were pathologically enlarged or fluorodeoxyglucose avid on PET-CT required further pathologic sampling before randomization. Brain MRI or a CT of the head was required for patients with stage II or stage III disease or any patient with suspicion of brain metastases. Patients were expected to have an ECOG PS of 0 or 1 and measurable disease according to RECIST 1.1.15
Patients who had received prior chemotherapy or any other cancer therapy for early-stage NSCLC, patients with distant active brain metastases, and patients with an active, known, or suspected autoimmune disease were excluded. Patients with locally advanced, unresectable or metastatic disease and patients with known EGFR mutations or ALK translocation were also excluded.15
Baseline Characteristics
Most patients randomized to the nivolumab plus chemotherapy and chemotherapy arms were male (71.5% and 70.9%, respectively) and about half were white (49.7% and 44.7%, respectively) and about half were Asian (48.0% and 52.0%, respectively). In total, 48.6% and 53.1% of patients in the nivolumab plus chemotherapy and chemotherapy arms, respectively had squamous tumour histology; 63.1% and 64.2%, respectively, had stage IIIA disease, and 89.4% and 88.3%, respectively, were current or former smokers. PD-L1 expression in the nivolumab plus chemotherapy and chemotherapy arms was less than 1% in 43.6% and 43.0% of patients, respectively, 1% or more in 49.7% and 49.7% of patients, respectively, 1% to 49% in 28.5% and 26.3% of patients, respectively, 50% or more in 21.2% and 23.5% of patients, respectively, and not evaluable in 6.7% and 7.3% of patients, respectively. The sponsor noted that there was a small discrepancy in disease stage between the case report form and Interactive Response Technology system, which affected 8.4% of patients in the nivolumab plus chemotherapy arm and 7.8% of patients in the chemotherapy arm.15
Table 8: Summary of Baseline Characteristics — All Randomized Patients
Characteristic | Nivolumab plus chemotherapy n = 179 | Chemotherapy n = 179 |
|---|---|---|
Age (years) | ||
Mean | 64.1 | 63.6 |
Median (range) | 64.0 (41 to 82) | 65.0 (34 to 84) |
Age categorization (years), n (%) | ||
< 65 | 93 (52.0) | 83 (46.4) |
≥ 65 | 86 (48.0) | 96 (53.6) |
≥ 65 and < 75 | 75 (41.9) | 83 (46.4) |
≥ 75 and < 85 | 11 (6.1) | 13 (7.3) |
Sex, n (%) | ||
Male | 128 (71.5) | 127 (70.9) |
Female | 51 (28.5) | 52 (29.1) |
Race, n (%) | ||
White | 89 (49.7) | 80 (44.7) |
Black or African American | 4 (2.2) | 3 (1.7) |
Asian | 86 (48.0) | 93 (52.0) |
Other | 0 | 3 (1.7) |
Geographic region, n (%) | ||
North America | 41 (22.9) | 50 (27.9) |
Europe | 41 (22.9) | 25 (14.0) |
Asia | 85 (47.5) | 92 (51.4) |
Rest of the world | 12 (6.7) | 12 (6.7) |
Disease stage at study entry (CRF), n (%)a | ||
Stage IA | 0 | 1 (0.6) |
Stage IB | 10 (5.6) | 8 (4.5) |
Stage IIA | 30 (16.8) | 32 (17.9) |
Stage IIB | 25 (14.0) | 22 (12.3) |
Stage IIIA | 113 (63.1) | 115 (64.2) |
Stage IIIB | 0 | 0 |
Stage IV | 1 (0.6) | 1 (0.6) |
Cell type at study entry, n (%) | ||
Squamous cell carcinoma | 87 (48.6) | 95 (53.1) |
Nonsquamous cell carcinoma | 92 (51.4) | 84 (46.9) |
Adenocarcinoma | 86 (48.0) | 84 (46.9) |
Large-cell carcinoma | 2 (1.1) | 0 |
Other | 4 (2.2) | 0 |
Tobacco use, n (%) | ||
Never smoker | 19 (10.6) | 20 (11.2) |
Current or former | 160 (89.4) | 158 (88.3) |
Baseline ECOG PS, n (%) | ||
0 | 124 (69.3) | 117 (65.4) |
1 | 55 (30.7) | 62 (34.6) |
> 1 | 0 | 0 |
Baseline weight (kg) | ||
Mean (SD) | 71.21 (15.80) | 68.55 (13.9) |
Median (range) | 68.10 (40.4 to 147.9) | 67.20 (35.7 to 114.6) |
Time from current diagnosis to randomization (months) | ||
Mean (SD) | 1.27 (0.89) | 1.24 (0.72) |
Median (range) | 1.05 (0.0 to 9.1) | 1.08 (0.0 to 3.7) |
Time from current diagnosis to randomization, n (%) | ||
< 1 months | 85 (47.5) | 82 (45.8) |
1 to < 2 months | 68 (38.0) | 72 (40.2) |
2 to < 3 months | 23 (12.8) | 18 (10.1) |
3 to < 4 months | 2 (1.1) | 7 (3.9) |
4 to < 5 months | 0 | 0 |
≥ 5 months | 1 (0.6) | 0 |
PD-L1 expression level (clinical database), n (%) | ||
< 1% | 78 (43.6) | 77 (43.0) |
≥ 1% | 89 (49.7) | 89 (49.7) |
1% to 49% | 51 (28.5) | 47 (26.3) |
≥ 50% | 38 (21.2) | 42 (23.5) |
Not evaluable | 12 (6.7) | 13 (7.3) |
CRF = case report form; ECOG PS = Eastern Cooperative Oncology Group Performance Status; PD-L1 = programmed cell death 1 ligand 1; SD = standard deviation.
aTNM 7th edition used for classification.
Source: Clinical Study Report.15
Interventions
Nivolumab Plus Chemotherapy (Arm C)
Nivolumab: Nivolumab 360 mg (flat dose), intravenously, every 3 weeks for up to 3 cycles.
Chemotherapy: Investigator choice of platinum-based doublet chemotherapy (intravenously).
cisplatin (75 mg/m2 on day 1 of a 3-week cycle for up to 3 cycles) and 1 of the following:
gemcitabine (1,000 mg/m2 or 1,250 mg/m2 [per local prescribing information] on days 1 and 8 of a 3-week cycle for up to 3 cycles) (squamous histology)
pemetrexed (500 mg/m2 on day 1 of a 3-week cycle for up to 3 cycles) (nonsquamous histology).
carboplatin (area under the plasma drug concentration-time curve 5 or 6 on day 1 of a 3-week cycle for up to 3 cycles) and the following:
paclitaxel (175 mg/m2 or 200 mg/m2 on day 1 of a 3-week cycle for up to 3 cycles) (any histology).
Patients who were unable to tolerate cisplatin were properly documented. The investigator obtained approval from the medical monitor before using a carboplatin-containing regimen, except when the regimen was carboplatin plus paclitaxel.15
Chemotherapy (Arm B)
Investigator choice of platinum-based doublet chemotherapy (intravenously):
cisplatin (75 mg/m2 on day 1 of a 3-week cycle for up to 3 cycles) and 1 of the following:
gemcitabine (1,000 mg/m2 or 1,250 mg/m2 [per local prescribing information] on days 1 and 8 of a 3-week cycle for up to 3 cycles) (squamous histology)
pemetrexed (500 mg/m2 on day 1 of a 3-week cycle for up to 3 cycles) (nonsquamous histology)
vinorelbine (25 mg/m2 or 30 mg/m2 [per local prescribing information] on days 1 and 8 of a 3-week cycle for up to 3 cycles)
docetaxel (60 mg/m2 or 75 mg/m2 [per local prescribing information] on day 1 of a 3-week cycle for up to 3 cycles)
carboplatin (area under the plasma drug concentration-time curve 5 or 6 on day 1 of a 3-week cycle for up to 3 cycles) and the following:
paclitaxel (175 mg/m2 or 200 mg/m2 on day 1 of a 3-week cycle for up to 3 cycles).
For patients who were unable to tolerate cisplatin, the reasons were documented. The investigator obtained approval from the medical monitor before using a carboplatin-containing regimen, except when the regimen was carboplatin plus paclitaxel.15
Note that 2 chemotherapy treatments allowed in the chemotherapy arm (cisplatin plus docetaxel and cisplatin plus vinorelbine) were not allowed in the nivolumab plus chemotherapy arm because, at the time nivolumab plus chemotherapy was added to the protocol, safety data were not available for nivolumab in combination with these chemotherapy backbones. The remaining chemotherapy options were the same for the chemotherapy and nivolumab plus chemotherapy arms.15
Dose Modification: Dose reductions were permitted for platinum-doublet chemotherapy, according to the trial’s protocol. Any dose reductions implemented were permanent and were not re-escalated in subsequent cycles. Dose reductions for each drug in the chemotherapy regimen was independently adjusted in accordance with a prespecified schedule. Patients experiencing toxicity that required a dose reduction after 2 previous dose reductions for any 1 drug in the regimen were discontinued from the drug. Dose modifications were allowed for hematological toxicities due to platinum-doublet therapy, based on nadir blood counts (assessed per local standards) from the proceeding drug administration. Growth factors were permitted after cycle 1 to assist hematologic recovery. Dose reductions were not permitted for nivolumab or ipilimumab.15
Dose Delay: Dose delays were permitted for all treatments in the trial; any dose delay of more than 7 days was skipped, and treatment resumed for the patient at the next scheduled dose (provided that criteria for re-treatment were met). Nivolumab and platinum-doublet chemotherapy were delayed in the event of AEs, and patients were re-evaluated weekly and treatment was resumed if they met re-treatment criteria.15
Treatment Discontinuation: Patients were allowed to discontinue treatment for the following reasons.
At the request of the patient. Patients who chose to terminate treatments were allowed to remain in the study and receive protocol-specified follow-up procedures (unless the patient withdrew consent for further contact for all study procedures), including posttreatment study follow-up and any contact with persons previously authorized by the patient to provide follow-up information.
In the event of any clinical AE, laboratory abnormality, or intercurrent illness experienced by the patient that, in the opinion of the investigator, indicated that continued participation in the study was not in their best interest.
The study was terminated by the sponsor.
Loss of the patient’s ability to freely provide consent because of imprisonment or involuntarily incarceration for the treatment of either a psychiatric or physical (e.g., infectious disease) illness.
Treatment was also discontinued in the event that a patient became pregnant. Patients who discontinued their assigned study treatment prematurely were not allowed to receive subsequent neoadjuvant therapy and proceeded to receive surgery within the study’s indicated timelines.15
After definitive surgery, patients in each arm could receive up to 4 cycles of adjuvant chemotherapy, per institutional standard, at the discretion of the investigator. Investigators chose from the following treatments:
Treatment 1:
vinorelbine 30 mg/m2 IV push over 10 minutes on days 1 and 8
cisplatin 75 mg/m2 IV over 120 minutes on day 1, immediately following vinorelbine
Treatment 2:
docetaxel 75 mg/m2 IV over 60 minutes on day 1
cisplatin 75 mg/m2 IV over 120 minutes on day 1, immediately following docetaxel
Treatment 3 (for squamous histology):
gemcitabine 1,250 mg/m2 IV over 30 minutes on days 1 and 8
cisplatin 75 mg/m2 IV over 120 minutes on day 1, immediately following gemcitabine
Treatment 4 (nonsquamous histology only):
pemetrexed 500 mg/m2 IV over 10 minutes on day 1
cisplatin 75 mg/m2 IV over 120 minutes on day 1, immediately following pemetrexed
Concomitant Medications
Permitted Medications
Topical, ocular, intra-articular, intranasal, and inhalational corticosteroids (with minimal systemic absorption) in the absence of active autoimmune disease were permitted. Adrenal replacement steroid doses greater than 10 mg daily prednisone were also permitted. A brief (less than 3 weeks) course of corticosteroids for prophylaxis (e.g., contrast dye allergy) or for treatment of nonautoimmune conditions (e.g., delayed-type hypersensitivity reaction caused by a contact allergen) was also permitted.15
Prohibited Medications
Immunosuppressive drugs
Immunosuppressive doses of systemic corticosteroids (exception those highlighted in the protocol)
Any concurrent antineoplastic therapy (i.e., chemotherapy; hormonal therapy; immunotherapy; extensive, nonpalliative radiation therapy; or standard or investigational drugs for the treatment of NSCLC)
Discontinuation of herbal medications was encouraged before study enrolment
Live vaccines (e.g., yellow fever; measles, mumps, and rubella; nasal flu; chicken pox [varicella])
Concomitant administration of strong CYP3A4 inhibitors or inducers and docetaxel, vinorelbine, or paclitaxel
Concomitant administration of strong CYP2C8 inhibitors or inducers and paclitaxel
Concomitant administration of drugs that are also tubularly secreted (e.g., probenecid)
Outcomes
A list of efficacy end points identified in the CADTH review protocol that were assessed in the clinical trial included in this review is provided in Table 9 and subsequently summarized. A detailed discussion and critical appraisal of the outcome measures are provided in Appendix 4.
Table 9: Summary of Outcomes of Interest Identified in the CADTH Review Protocol
Outcome measure | End point | Definition | Included in the hierarchical multiple testing procedure |
|---|---|---|---|
OS | Secondary | Defined as the time between the date of randomization and the date of death from any cause. OS was censored on the last date a patient was known to be alive. | Yes |
EFS | Primary | Defined as the length of time from randomization to any of the following events:
Patients who did not undergo surgery, but for reasons other than progression, were considered to have an event at RECIST 1.1 progression (based on BICR) or death. | Yes |
pCR | Primary | Defined as the number of randomized patients with an absence of residual tumour in lung resected tissue and lymph nodes, as evaluated by BIPR, divided by the number of randomized patients in each treatment arm. Randomized patients who were no longer eligible for surgery, who received alternative anticancer therapy before surgery, who discontinued the study (e.g., withdrew consent) before surgery, or who otherwise did not have an evaluable BIPR result available were counted as nonresponders. | Yes |
HRQoL | Exploratory | Patients’ overall health status and health utility were measured with the EQ-5D-3L VAS and utility index, respectively. | No |
TTDM | Secondary | Defined as the time between the date of randomization and the first date of distant metastasis, or the date of death in the absence of distant metastasis. A distant metastasis was defined as any new lesion outside of the thorax as assessed by BICR and RECIST 1.1. Patients who had not developed distant metastasis or who had died at the time of the analysis were censored on the date of their last evaluable tumour assessment. | No |
MPR | Secondary | Defined as the number of randomized patients with residual tumour of 10% or less in lung and lymph nodes (per BIPR), divided by the number of randomized patients in each treatment arm. Viable in situ carcinomas were not included in the MPR calculation. | No |
EFS2 | Exploratory | Defined as the time from randomization to objectively documented progression, per investigator assessment, after the next line of therapy or to death from any cause, whichever occurs first. | No |
Feasibility of surgery | Exploratory | Delayed or cancelled surgery, duration of surgery, length of hospital stay, surgical approach (including completeness of surgery), incidence of AEs or SAEs associated with surgery out to 90 days after surgery. | No |
Safety | Exploratory | AE, SAEs, immune-related AEs, death, and laboratory abnormalities. | No |
AE = adverse event; BICR = blinded independent central review; BIPR = blinded independent pathologic review; EFS = event-free survival; EFS2 = event-free survival on the next line of therapy; EQ-5D-3L = 3-Level EQ-5D; HRQoL = health-related quality of life; MPR = major pathologic response; OS = overall survival; pCR = pathologic complete response; RECIST 1.1 = Response Evaluation Criteria in Solid Tumours Version 1.1; SAE = serious adverse event; TTDM = time to death or distant metastasis’ VAS = visual analogue scale.
Assessment of Outcomes
Radiologic tumour assessments were reviewed by a BICR from a third-party radiology vendor. Both the investigator and independent radiologists assessed whether each patient met RECIST 1.1 for progression or disease recurrence. All investigator-assessed radiographic progressions and all recurrences were confirmed by BICR, per RECIST 1.1 guidelines. Participants whose disease progression or recurrence was not confirmed by central review continued tumour assessments (when clinically feasible) in accordance with protocol-specified schedules. Subsequent tumour assessments were submitted to a third-party radiology vendor for subsequent review and, if applicable, patients were discontinued from the study when both the investigator and independent radiologists assessed that the participant met RECIST 1.1 for progression or recurrence.
A BIPR was implemented for the central review of tumour scans, for tumour and/or lymph node samples, and for the confirmation of end points. Personnel at participating sites were trained before enrolment of the first study participant. Sections of tumours were used for central pathology review to assess pCR and MPR. Any tumour, tumour bed, or lymph node specimens reviewed locally were submitted for central pathology review.
All participants (in either treatment arm) who remained operative candidates after completion of neoadjuvant treatment (up to 3 cycles) underwent definitive surgery for NSCLC within 6 weeks.
Lymph node levels were sampled at the time of definitive surgery:
right-sided tumour: levels 4, 7, 9R, 10R, and 11R
left-sided tumour: levels 5 and/or 6; 7, 9L, 10L, and 11L.
Tumour and lymph node samples were collected from definitive surgical resection, and sampling of fresh tumour tissue in RNAlater was mandatory for biomarker studies (as applicable, depending on the size of the residual tumour) on the day of surgery. The remainder of the specimens were processed for histopathologic analysis, performed within 72 hours of the procedure. Sections of the fresh tumour samples collected were used to assess pCR and MPR.12 Disease recurrence, change in tumour measurements, and tumour response were assessed by BICR, per RECIST 1.1. After definitive surgery, patients in each arm could receive adjuvant chemotherapy with or without radiation, per institutional standard, at the discretion of the investigator.
Health-Related Quality of Life
EQ-5D-3L is a generic preference-based HRQoL instrument that has been applied to a wide range of health conditions and treatments.36,37 One part of the EQ-5D-3L is a descriptive system that classifies respondents (12 years and older) into 1 of 243 distinct health states. The descriptive system consists of 5 dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Each dimension has 3 possible levels, with 1 indicating no problems, 2 indicating some problems, and 3 indicating extreme problems. Respondents are asked to choose 1 level that reflects their own health state for each of the 5 dimensions. A scoring function can be used to assign a value (i.e., EQ- 5D-3L index score) to each self-reported health state, based on a set of population-based preference weights.36,37 The other part of EQ-5D-3L is a vertical, calibrated EQ VAS that has end points labelled 0, indicating the worst imaginable health state, and 100, indicating the best imaginable health state. A detailed discussion and critical appraisal of the EQ-5D-3L questionnaire are available in Appendix 3.
Participants were asked to complete the EQ-5D-3L before any clinical activities were performed during on-treatment clinic visits, at postneoadjuvant visits 1 and 2, and at designated visits or during phone calls during the survival follow-up phase. A standardized script was used to facilitate telephone administration of the EQ-5D-3L.
EQ-5D-3L questionnaire completion rate (i.e., the proportion of questionnaires actually received out of the expected number of patients on treatment or in follow-up), was calculated and summarized for each assessment time point by treatment arm.
The proportion of patients reporting problems for any of the 5 EQ-5D-3L dimensions at each assessment time point was stratified by the level of problem and by treatment group. Percentages were based on the number of patients assessed at the assessment time point.
For EQ-5D-3L utility index and VAS scores, mean score and mean change from baseline at each assessment time point (baseline, week 4, week 7, postadjuvant visit 1, and postadjuvant visit 2) were stratified by treatment group using descriptive statistics (n, mean with standard deviation and 95% CI, median, first and third quartiles, minimum, maximum), and a line graph summarizing the mean changes from baseline was presented.
Harms Outcome
Safety parameters evaluated included frequency of death, SAEs, AEs leading to discontinuation or dose modification, overall AEs, AEs of special clinical interest that are potentially associated with the use of nivolumab or ipilimumab (i.e., select AEs, immune-mediated AEs), clinical laboratory assessments (hematology, serum chemistry, and liver and thyroid function tests), and vital sign measurements.12
Statistical Analysis
Sample-Size and Power Calculation: The sample size of the CheckMate 816 trial was calculated based on EFS (primary end point) and accounted for multiple primary end point comparisons (pCR and EFS), with an initial alpha allocation of 0.01 and 0.04, respectively.12
The overall type I error (alpha) was controlled using the following procedure for nivolumab plus chemotherapy versus chemotherapy (alpha and P values are 2-sided):
The primary end point of pCR rate was tested at a 1% alpha level, using a fallback method:
if the pCR rate was not significant, the primary end point EFS was tested at 4%
if the pCR rate was significant, the 1% alpha was reallocated to the EFS primary end point, which was tested at a 5% alpha level
if EFS was significant, OS was tested hierarchically at the same level as EFS.
EFS and OS were tested at a planned interim analysis, and both have a planned final analysis. Stopping boundaries were calculated for each end point individually, according to the observed number of events, using the Lan-DeMets alpha spending function with O’Brien-Fleming boundaries corresponding to an overall alpha of 4% or 5%. Given that the EFS and OS end points were tested using a group sequential approach, an overall hierarchical testing approach was used in which each end point would have its own specific Lan-DeMets alpha spending function with O’Brien-Fleming boundaries.12 The sponsor estimated that about 500 patients would be randomized in the study.12 The randomization of about 350 patients was planned for the 2 arms (175 patients each in the nivolumab plus chemotherapy and chemotherapy arms).
Primary Outcome Analyses
Pathologic Complete Response
A formal analysis for pCR took place after 350 patients who had been randomized into the nivolumab plus chemotherapy and chemotherapy arms from the start of the 1:1:1 randomization and had undergone surgery (approximately 30 months after the 1:1:1 randomization was initiated).12
The sponsor assumed that 350 patients would be needed to provide more than 90% power to detect an odds ratio of 3.857 with a 2-sided type I error rate of 1% if a pCR rate of 10% were to occur in the chemotherapy arm (arm B) and a pCR rate of 30% were to occur in the nivolumab plus chemotherapy arm (arm C).12
The pCR rate was computed for each treatment arm, along with the exact 95% CI, using the Clopper-Pearson method. The numerator was the number of randomized patients who achieved a pCR in both the tumour and the lymph nodes, as assessed by BIPR. The denominator was the number of all patients randomized to the nivolumab plus chemotherapy and chemotherapy arms. Patients who were no longer eligible for surgery, who were on an alternative anticancer therapy before surgery, who discontinued before surgery, or who did not have pCR results available were counted as nonresponders, ensuring a robust pCR definition. pCR was compared in the nivolumab plus chemotherapy and chemotherapy arms using the stratified Cochran Mantel-Haenszel test with a 2-sided 1% alpha level.12
Event-Free Survival
A formal EFS analysis took place after 148 events had occurred in the nivolumab plus chemotherapy arm and the chemotherapy arm after the start of the 1:1:1 randomization scheme (54 months after the 1:1:1 randomization scheme was initiated). The superiority hypothesis was tested in the EFS interim analysis.
In the event that pCR was significant, the 1% alpha allocated to pCR was reallocated to EFS, which was then tested at an overall 5% alpha level. The interim boundary was derived from the Lan-DeMets alpha spending function with O’Brien-Fleming boundaries.12
A stratified log-rank test, with stratification factors per Interactive Response Technology (PD-L1 expression [≥ 1% versus < 1%, not evaluable, indeterminate], disease stage [stage IB or II versus stage IIIA], and gender or sex), and a 2-sided P value was used to assess EFS between the nivolumab plus chemotherapy arms and chemotherapy. A Lan-DeMets alpha spending function with an O’Brien and Fleming type of boundary was used to determine the nominal significance levels for the interim and final analyses. The HR and the corresponding (adjusted alpha) CIs were estimated for the nivolumab plus chemotherapy and chemotherapy arms using a stratified Cox proportional hazards model with the randomized arm as a single covariate.12
The EFS curves for each randomized arm were estimated using the KM product-limit method. The median and 2-sided 95% CI for EFS in each treatment arm was computed using the log-log transformation method. In addition, EFS rates at different time points were derived from KM estimates on the EFS curve for each randomized arm. Associated 2-sided 95% CIs were calculated using the Greenwood formula (using a log-log transformation).12
The sponsor assumed that the occurrence of 185 EFS events among the 358 randomized patients would ensure that an overall 2-sided 5% significance level sequential test procedure with 2 interim analyses — after 148 events (80% of events required for final analysis) and after 167 events (90% of events required for final analysis) — would have 82% power, assuming an HR of 0.65 between the 2 arms. IA1 EFS was event driven (at least 148 events expected by data cut-off date of October 20, 2021). The stopping boundaries at the interim and final EFS analyses were derived from the exact number of events using the Lan-DeMets alpha spending function with O’Brien-Fleming boundaries.12 Figure 3 presents the schematic presentation of the planned analyses in the CheckMate 816 trial. Table 10 presents a summary of scheduled analyses in the CheckMate 816 trial.
Table 10: Scheduled Analyses, Criteria, and Projected Timelines for Formal Analyses of pCR and EFS
Scheduled analysis | Criteria and population | Projected timeline | Formal analysis |
|---|---|---|---|
pCR analysis | When patients in the nivolumab plus chemotherapy and chemotherapy arms have an opportunity for surgery | 30 months after 1:1:1 randomization (36 months from FPFV) | pCR comparison between the nivolumab plus chemotherapy and chemotherapy arms, with an alpha of 0.01 |
Interim EFS analysis First interim OS analysisa | 148 EFS events in the nivolumab plus chemotherapy and chemotherapy arms after the start of 1:1:1 randomizationb | 54 months after 1:1:1 randomization (60 months from FPFV) | The stopping boundaries were based on Lan-DeMets alpha spending function with O’Brien-Fleming boundaries EFS comparison arms: The nominal P value cut-off for the nivolumab plus chemotherapy and chemotherapy arms is 0.019 if the EFS comparison alpha is 0.04, and 0.024 if the EFS comparison alpha is 0.05 OS comparison of nivolumab plus chemotherapy and chemotherapy (if EFS is significant): The nominal P value cut-off is 0.007 if the EFS comparison alpha is 0.04, and 0.010 if the EFS comparison alpha is 0.05 |
Final EFS analysis Second interim OS analysisa | 185 EFS events in the nivolumab plus chemotherapy and chemotherapy arms after the start of 1:1:1 randomizationb | 69 months after 1:1:1 randomization (75 months from FPFV) | The stopping boundaries is based on Lan-DeMets alpha spending function with O’Brien-Fleming boundaries EFS comparison arms: The nominal P value cut-off for the nivolumab plus chemotherapy and chemotherapy arms is 0.035 if the EFS comparison alpha is 0.04, and 0.043 if the EFS comparison alpha is 0.05 OS comparison of nivolumab plus chemotherapy and chemotherapy (if EFS is significant) The nominal P value cut-off is 0.018 if the EFS comparison alpha is 0.04, and 0.023 if the EFS comparison alpha is 0.05 |
Final OS analysis | 185 OS events in the nivolumab plus chemotherapy and chemotherapy arms after the start of 1:1:1 randomization | 87 months after 1:1:1 randomization (93 months from FPFV) | OS comparison of nivolumab plus chemotherapy and chemotherapy (if EFS is significant) The stopping boundaries are based on Lan-DeMets alpha spending function with O’Brien-Fleming boundaries The nominal P value cut-off is 0.034 if the EFS comparison alpha is 0.04, and 0.042 if the EFS comparison alpha is 0.05 |
EFS = event-free survival; FPFV = first patient’s first visit; OS = overall survival; pCR = pathologic complete response.
aIf EFS reaches significance at the interim analysis of EFS but not OS, only the interim analysis of OS will be conducted; EFS will not be formally re-tested.
bIf EFS reaches significance at the interim analysis of EFS but not OS, interim OS analyses will be triggered by the number of OS events.
Source: Sponsor’s submission.12
Figure 3: Schematic Representation of the Planned Analyses Time Points
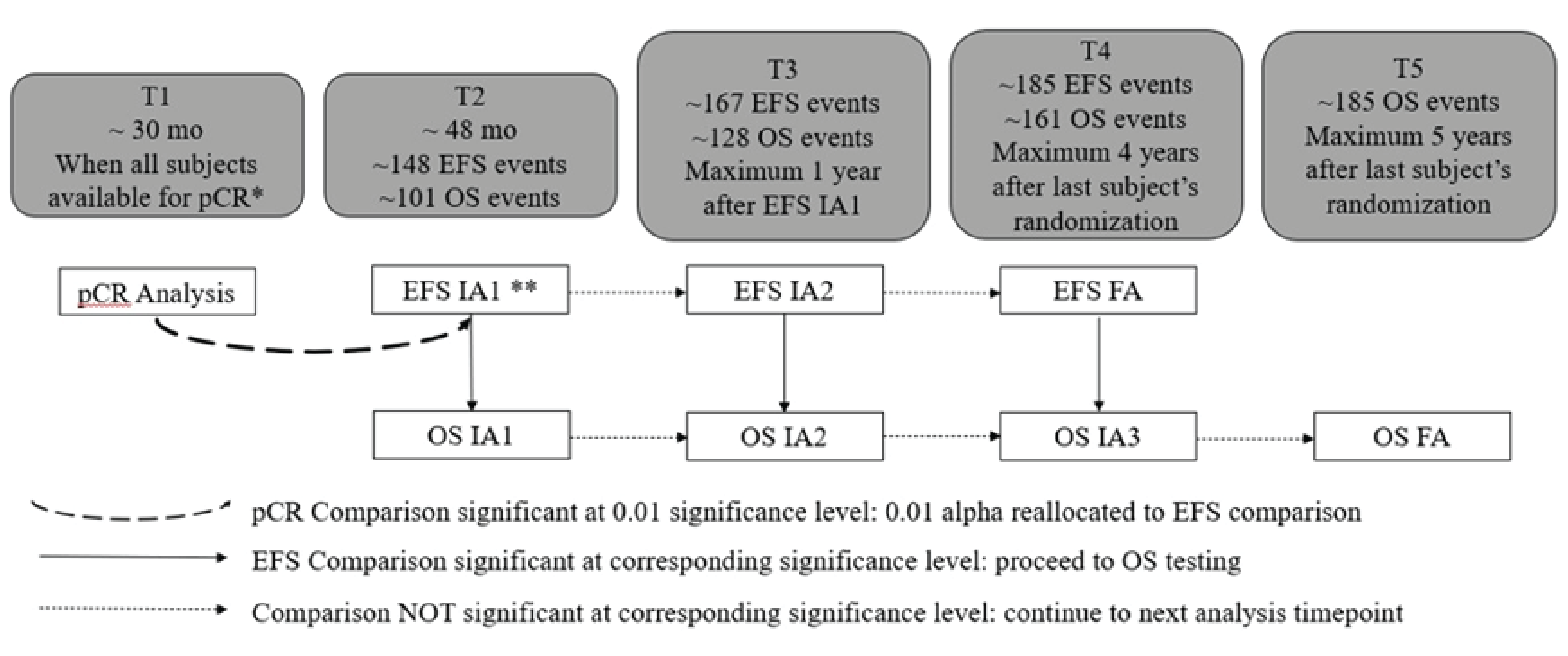
EFS = event-free survival; FA = final analysis; IA1 = first interim analysis; IA2 = second interim analysis; IA3 = third interim analysis; mo = months; OS = overall survival; pCR = pathologic complete response; t = time point.
Note: EFS and OS were tested using their own O’Brien-Fleming alpha spending functions.
* Analysis occurred at the September 16, 2020, data cut-off date.
** Analysis occurred at the October 20, 2021, data cut-off date.
Source: Sponsor submission.12
Censoring Rules for EFS (Primary Definition)
Patients who did not report progression or recurrence of disease or death will be censored on the date of their last evaluable tumour assessment.
Patients who did not have any on-study tumour assessment and did not die will be censored on the date they were randomized.
Patients who received subsequent anticancer therapy, outside of the protocol-specified adjuvant therapy, before documented progression or recurrence or death will be censored at the date of the last evaluable tumour assessment conducted on or before the date of initiation of the subsequent anticancer therapy.
Patients who did not have a documented progression or recurrence or death and who received subsequent anticancer therapy outside of the protocol-specified adjuvant therapy will be censored at the date of the last evaluable tumour assessment conducted on or before the initiation of the subsequent anticancer therapy.
Patients without a baseline scan and without surgery will be censored on the date of randomization (regardless of death).
In the case of a new primary cancer, if such lesions are present on tumour assessment at the BICR, they will be considered new lesions, because the BICR does not have access to biopsy results.
Censoring Rules for EFS (Secondary Definition)
Patients who did not report progression or recurrence of disease or death will be censored on the date of their last evaluable tumour assessment.
Patients who did not have any on-study tumour assessments and did not die will be censored on the date they were randomized.
Patients without a baseline scan and without surgery will be censored on the date of randomization (regardless of death).
Sensitivity Analyses
Sensitivity analyses were conducted in the nivolumab plus chemotherapy and chemotherapy arms for the primary end point of EFS. The P values from these sensitivity analyses were presented for descriptive purposes only and were not adjusted for multiplicity.
The following sensitivity analyses were considered:
EFS was compared between treatment groups with a 2-sided MaxCombo test.
To examine the assumption of proportional hazards in the Cox regression model, in addition to treatment, a time-dependent variable defined by a treatment by time interaction was added in the model.
A multivariate Cox regression model was used to estimate the treatment effect after adjustment for possible imbalances in known or potential prognostic factors. The factors used in the randomization were included in the model as stratification factors. All additional factors were incorporated as covariates. The additional factors, which are all measured at baseline, included:
histology (squamous, nonsquamous)
age categorization (< 65 years, ≥ 65 years)
ECOG PS (0, ≥ 1)
race (white, Black, Asian, other).
Subgroup Analyses: Subgroup analyses were conducted for pCR and EFS for the following baseline characteristics12:
age category (in years): < 65, ≥ 65 and < 75, ≥ 75 and < 85, ≥ 85, ≥ 75, ≥ 65
sex (male, female), per Interactive Response Technology and per case report form
race (white, Black, Asian, other)
region (North America, Europe, Asia, the rest of the world)
baseline ECOG PS (0, 1, > 1)
tobacco use (current/former, never smoked, unknown)
disease stage (IB or II versus stage IIIA) per Interactive Response Technology and per case report form
baseline histology (squamous, nonsquamous)
PD-L1 expression subgroups (< 1%, not evaluable, indeterminate; ≥ 1%; 1% to 49%; ≥ 50)
tumour mutational burden of tissue evaluable (≥ 12.3 mut/MB, < 12.3 mut/MB, overall)
tumour mutational burden of tissue not evaluable
type of platinum therapy (cisplatin, carboplatin, switch from cisplatin to carboplatin)
type of chemotherapy regimen in arm B (available in arm C are gemcitabine + cisplatin, pemetrexed + cisplatin, and paclitaxel + carboplatin; not available in arm C are vinorelbine + cisplatin and docetaxel + cisplatin), based on first neoadjuvant cycle.
Handling Missing Data
The sponsor outlined several methods to account for missing data for safety outcomes, missing death dates, missing data for date of progression or recurrence, missing dates for definitive surgery start date and definitive surgery end date, as follows:12
For missing and partial AE onset dates, imputation was performed using the AE domain requirements specification.
Missing and partial nonstudy medication domain dates were imputed using a derivation algorithm.
For death dates, the following conventions were used for imputing partial dates:
If only the day of the month is missing, the first of the month was used to replace the missing day. The imputed date was compared with the last known date alive, and the maximum was considered as the death date.
For a missing year, the death date was imputed as the last date the patient was known to be alive. If the date was completely missing but the reason for death was present, the death date was imputed as the last known date alive.12
Secondary Outcome Analyses
Overall Survival
The sponsor assumed that 185 OS events among the 358 randomized patients would ensure that an overall 2-sided 5% significance level sequential test procedure with 3 interim analyses — after approximately 101, 128, and 161 events (55%, 69%, and 87% of events required for final analysis, respectively) — would have 82% power, assuming an exponential distribution, with a median OS time of 54 months in the chemotherapy arm and 83 months in the nivolumab plus chemotherapy arm (corresponding to a target HR of 0.65). The sponsor anticipated that OS analyses would take place after about 48 months (IA1 EFS), 58 months (EFS interim analysis 2), 73 months (EFS final analysis), and 86 months (OS, final analysis) after the start of 1:1:1 randomization. The trigger for the timing of these interim analyses was the number of EFS events.12
In the event that EFS became significant before OS, the planned formal remaining OS analyses would be triggered by the number of OS events (approximately 128 OS events [69% information fraction] or 1 year after IA1 EFS, whichever occurred first for interim analysis 2, and 161 OS events or 4 years after last patient’s randomization, whichever occurred first for OS interim analysis 3).12
To account for a potential slowdown in event rates in the longer term, which could prevent OS analysis from being performed in a reasonable time window, the sponsor planned that in the event that the 185th event failed to occur 5 years after randomization of the last participant, the final OS analysis would be conducted at that time. The final analysis boundary would then be recalculated using the actual updated final number of events.12
Time to Death or Distant Metastases
TTDM, based on BICR assessments, was compared between the nivolumab plus chemotherapy and chemotherapy arms using the same methods as described for EFS.12
Major Pathologic Response
MPR rates were computed in each treatment group, along with the exact 95% CI, using Clopper-Pearson method. An estimate of the difference and the odds ratio in MPR rates between concurrent arms B and C and corresponding 95% CIs were calculated the using Cochran-Mantel-Haenszel methodology and adjusted by stratification factors.12
EFS on Next Line of Therapy
EFS2 was estimated using KM techniques, and graphically presented. A 2-sided 95% CI for the median in each treatment group were computed using a log-log transformation method. Events rates at fixed time points (e.g., 6 months, 12 months, depending on the minimum follow-up) were presented along with their associated 95% CIs. Estimates were derived from the KM estimate and corresponding CIs were based on the Greenwood formula for variance derivation and on log-log transformation applied to the survivor function.
Analysis Populations
Efficacy analysis population: The ITT population consisted of all randomized participants in the nivolumab plus chemotherapy and chemotherapy arms (which included all patients concurrently randomized to nivolumab plus chemotherapy or chemotherapy as of the 1:1:1 randomization and after revised protocol 2).
Safety analyses population: The primary analysis population consisted of all participants concurrently randomized to the nivolumab plus chemotherapy arm or chemotherapy arm at the 1:1:1 randomization who received at least 1 dose of any study medication in the neoadjuvant setting and was used to assess drug exposure and safety in the nivolumab plus chemotherapy and chemotherapy arms.
Protocol Amendments
Protocol revision 1 (March 3, 2017): This revision incorporated changes from amendment 2 and administrative letters 1 and 2. It clarified the use of TNM 7th edition in the study; adjusted dosing details of the chemotherapy drugs to include the dose approved by the local prescribing information and the standard-of-care infusion time for each country; clarified lymph node samples at screening and definitive surgery; clarified the tissue sample process for calculation of the primary end point; and clarified requirements for PET-CT scans and broadened the window for scans before surgery.15
Protocol revision 2 (July 6, 2017): This revision added the third arm of nivolumab plus chemotherapy; increased the sample size to 642 to accommodate the new treatment arm; changed the primary objective to dual primary objectives of pCR and EFS and changed a secondary objective to MPR based on health authority feedback; and increased the prescreening tissue requirement to 15 slides, updated contrast requirements for brain MRI scans, expanded the window for pulmonary function tests to within 6 weeks of randomization, and included updates to synopsis, rationale or background information, and study personnel.15
Protocol revision 3 (September 21, 2018): This revision stopped enrolment in the nivolumab plus ipilimumab arm, so the primary population concurrently randomized patients to the nivolumab plus chemotherapy and chemotherapy arms based on external clinical data on PD-1 expression and chemotherapy; clarified the definition of EFS, excluded patients with large-cell neuroendocrine carcinoma tumour histology, and added a platinum-doublet chemotherapy regimen (paclitaxel plus carboplatin); updated dose modification for docetaxel; added TTDM as a secondary end point; clarified tumour assessments for patients who did not proceed to definitive surgery; updated the statistical analysis plan, rationale, background information, and trial schematic; and clarified pulmonary function parameters, the time relationship between adjuvant radiotherapy and tumour imaging assessments, and the time window of cycle 1 day 1 end-of-infusion pharmacokinetic sampling.15
Protocol revision 4 (June 25, 2019): This revision updated the postsurgery collection of serum and plasma-soluble factors; added the concomitant administration of substances that are tubularly secreted (e.g., probenecid) and could potentially result in the delayed clearance of pemetrexed; added hypothesis testing for OS; and clarified the analysis population for pCR, added an exploratory end point of EFS on the next line of therapy, and added instructions for BICR.15
Protocol revision 5 (September 18, 2019): This revision made modifications to the pCR analysis population and projected timelines; updated the surgical-approach end point; updated censoring rules for TTDM; removed optional biopsy at disease progression in China; and updated the management algorithms to include myocarditis.15
Protocol revision 6 (July 14, 2020): This revision clarified an EFS event to be any progression that precluded surgery and clarified that RECIST 1.1 progression and/or recurrence, per BICR, should be applied after surgery or for patients who did not undergo surgery; corrected the number of patients; removed the first of 2 IA of EFS (60% events) and updated alpha spending based on the remaining single interim and final analyses of EFS; and clarified that the actual timing of analyses may differ from projected timing.15
Protocol revision 7 (August 18, 2021): This revision added an interim analysis of EFS and added a calendar-based rule for the final analysis of EFS, with a corresponding OS interim analysis (if EFS was significant).15
Results
Patient Disposition
Table 11 presents patient disposition data from the CheckMate 816 trial at the October 20, 2021, data cut-off date (EFS IA1). In total, 773 patients were enrolled, and 505 patients were randomized: 358 to nivolumab plus chemotherapy (n = 179) or chemotherapy (n = 179). After neoadjuvant treatment, 149 (83.2%) patients in the nivolumab plus chemotherapy arm and 135 (75.4%) in the chemotherapy arm underwent definitive surgery; 28 (15.6%) patients in the nivolumab plus chemotherapy arm and 37 (20.7%) in the chemotherapy arm did not undergo surgery for the following reasons:15
AEs, which affected 2 of 28 (7.1% of cancellations) patients in the nivolumab plus chemotherapy arm and 1 of 37 (2.7%) patient in the chemotherapy arm
disease progression, which affected 12 of 28 (42.9%) patients in the nivolumab plus chemotherapy arm and 17 of 37 (45.9%) patients in the chemotherapy arm
other (including any reason other than an AE and clinical or radiographic disease progression [e.g., unsuitable for surgery per investigator, patient refused surgery, poor lung function], which affected 14 of 28 (50.0%) patients in the nivolumab plus chemotherapy arm and 19 of 37 (51.4%) patients in the chemotherapy arm. In addition, 2 (1.1%) patients in the nivolumab plus chemotherapy arm and 7 (3.9%) in the chemotherapy arm did not complete surgery because they left the study before surgery (no longer met the study criteria, withdrawal of consent, or death).
The proportion of patients who did not complete the neoadjuvant treatment period because of study drug toxicity was similar in the nivolumab plus chemotherapy and chemotherapy arms (5.7% and 6.8%, respectively). The proportion of patients who did not complete the neoadjuvant treatment period because of disease progression was low in the nivolumab plus chemotherapy and chemotherapy arms (0.6% and 1.1%, respectively). The minimum follow-up was 21.0 months, and the median follow-up was 29.5 months.15 Table 12 presents the patients who received definitive surgery in the CheckMate 816 trial.
Disposition | Nivolumab plus chemotherapy | Chemotherapy | Total |
|---|---|---|---|
Enrolled, n | — | — | 773 |
Randomized, n (%) | 179 (100.0) | 179 (100.0) | 505 (65.2) |
Not randomized, n (%) | 0 | 0 | 268 (34.7) |
Reason for not being randomized | |||
AE | — | — | 1 (0.1) |
Withdrawal of consent | — | — | 26 (3.4) |
No longer meeting study requirement | — | — | 227 (29.4) |
Other | — | — | 14 (1.8) |
Treated | 176 (98.3) | 176 (98.3) | 495 (98.0) |
Not treateda | 3 (1.7) | 3 (1.7) | 10 (2.0) |
Reason for not being treated | |||
AE unrelated | 1 (0.6) | 0 | 1 (0.2) |
Withdrawal of consent | 0 | 2 (1.1) | 3 (0.6) |
No longer meeting study criteria | 2 (1.1) | 1 (0.6) | 6 (1.2) |
Status (%) | |||
Continuing in the neoadjuvant treatment period | 0 | 0 | 0 |
Not continuing in the neoadjuvant treatment period | 176 (100.0) | 176 (100.0) | 495 (100) |
Reason for not continuing in the neoadjuvant treatment period | |||
Completed neoadjuvant treatment | 165 (93.8) | 149 (84.7) | 443 (89.5) |
Disease progression | 1 (0.6) | 2 (1.1) | 6 (1.2) |
Study drug toxicity | 10 (5.7) | 12 (6.8) | 30 (6.1) |
Death | 0 | 0 | 1 (0.2) |
AE unrelated to study drug | 0 | 3 (1.7) | 3 (0.6) |
Patient request to discontinue study treatment | 0 | 5 (2.8) | 7 (1.4) |
Withdrawal of consent | 0 | 4 (2.3) | 4 (0.8) |
No longer meeting study criteria | 0 | 1 (0.6) | 1 (0.2) |
Continuing in the study | 175 (99.4) | 172 (97.7) | 489 (98.8) |
Not continuing in the study | 1 (0.6) | 4 (2.3) | 6 (1.2) |
Reason for not continuing in the study | |||
Death | 0 | 1 (0.6) | 2 (0.4) |
Withdrawal of consent | 1 (0.6) | 3 (1.7) | 4 (0.8) |
AE = adverse event.
aPercentages based on patients randomized.
Source: Clinical Study Report.15
Table 12: Patients Who Received Definitive Surgery — All Randomized Patients
Characteristics | Nivolumab plus chemotherapy n = 179 | Chemotherapy n = 179 |
|---|---|---|
Definitive surgery | ||
Patients with clinical downstaging,a n (%) | 55 (30.7) | 42 (23.5) |
Patients with definitive surgery, n (%) | 149 (83.2) | 135 (75.4) |
Patients with definitive surgery not reported n (%) | 2 (1.1) | 7 (3.9) |
Patients with cancelled definitive surgery, n (%) | 28 (15.6) | 37 (20.7) |
Reason for cancelled surgeryb | ||
AE | 2 (7.1) | 1 (2.7) |
Disease progression | 12 (42.9) | 17 (45.9) |
Other | 14 (50.0) | 19 (51.4) |
Patient refused surgery | 7 | 5 |
Patient not suitable for surgery | 2 | 2 |
Respiratory function not adequate | 2 | 2 |
Patient randomized but not treated | 1 | — |
Patient status did not allow neoadjuvant treatment | 1 | — |
Patient had financial difficulties | 1 | — |
Patient withdrew consent | 0 | 2 |
CR | 0 | 1 |
Patients with delayed surgery,b,c n (%) | 31 (20.8) | 24 (17.8) |
Reason for delayed surgeryd,e | ||
AE | 6 (19.4) | 9 (37.5) |
Administrative reason | 17 (54.8) | 8 (33.3) |
Other | 8 (25.8) | 7 (29.2) |
Duration of surgery (minutes) | ||
n | 122 | 120 |
Mean (SD) | 203.9 (95.9) | 221.3 (94.4) |
Median (range) | 185.0 (25 to 560) | 213.5 (46 to 486) |
Length of hospital stay (days) | ||
n | 142 | 127 |
Mean (SD) | 11.6 (8.3) | 12.8 (10.1) |
Median (range) | 10.0 (1 to 51) | 10.0 (1 to 67) |
Surgery outcome,c n (%) | ||
R0 (negative margin) | 124 (83.2) | 105 (77.8) |
R1 (microscopic positive margin) | 16 (10.7) | 21 (15.6) |
R2 (macroscopic positive margin) | 5 (3.4) | 4 (3.0) |
Unknown | 4 (2.7) | 5 (3.7) |
On-study or last assessment before subsequent anticancer therapy, n (%) | ||
Received subsequent anticancer therapyf | 12 (6.7) | 18 (10.1) |
Received subsequent systemic therapy | 6 (3.4) | 9 (5.0) |
Received subsequent radiotherapyg | 5 (2.8) | 9 (5.0) |
Received subsequent surgery | 1 (0.6) | 0 |
On study | 97 (54.2) | 66 (36.9) |
Still on neoadjuvant treatment | 0 | 0 |
Still on adjuvant treatment | 0 | 0 |
In follow-up | 97 (54.2) | 66 (36.9) |
AE = adverse event; CR = complete response; SD = standard deviation.
Notes: Patients in arm B randomized in the initial protocol are included in the total.
The data cut-off date was October 20, 2021.
aPatients with clinical downstaging have a lower disease stage before surgery than at baseline.
bDenominator based on the number of patients with cancelled surgery.
cDenominator based on the number of patients with surgery.
dDenominator based on the number of patients with delayed surgery.
eTime from last neoadjuvant dose to surgery > 6 weeks.
fIncludes patients, regardless of treatment status, who received subsequent anticancer therapy (outside of protocol-specified adjuvant therapy) without a prior reported EFS event. Those patients were censored at the last tumour assessment before or on the start date of subsequent anticancer therapy.
gRadiotherapy other than protocol-defined adjuvant radiotherapy.
Source: Clinical Study Report.15
Protocol Deviations
Important protocol deviations that were considered to potentially affect the interpretability of study results were reported in 2% of patients in the study (1.1% in the nivolumab plus chemotherapy arm and 2.2% in the chemotherapy arm). In total, 3 patients (1 in the nivolumab plus chemotherapy arm and 2 in the chemotherapy arm) received concurrent cancer therapy. Important protocol deviations in the 2 arms are presented in Table 44 in Appendix 3.
Exposure to Study Treatments
The proportion of patients who received all 3 doses of nivolumab or chemotherapy in the 2 treatment arms in the CheckMate 816 trial are presented in the Table 45 and Table 46 in Appendix 3, and are as follows:
in the nivolumab plus chemotherapy arm, the proportion was 93.2% for neoadjuvant nivolumab, 70.6% for carboplatin, 84.6% for cisplatin, 85.7% for paclitaxel, and 92.8% for pemetrexed
in the chemotherapy arm, the proportion was 66.7% for carboplatin, 79.7% for cisplatin, 89.7% for docetaxel, 81.8% for paclitaxel, and 84.1% for pemetrexed.
The proportion of all treated patients in the 2 treatment arms who received 90% or more of the planned dose intensity during the neoadjuvant period was as follows:
in the nivolumab plus chemotherapy arm, the proportion was 87.5% for nivolumab, 60.8% for carboplatin, 72.8% for cisplatin, 46.2% for gemcitabine, 60.7% for paclitaxel, and 85.5% for pemetrexed
in the chemotherapy arm, the proportion was 59.5% for carboplatin, 69.9% for cisplatin, 65.5% for docetaxel, 63.3% for gemcitabine, 81.8% for paclitaxel, 79.4% for pemetrexed, and 23.1% for vinorelbine.
Interruptions, Delays, Reductions, and Omissions of Neoadjuvant Study Therapy
Dose delays were permitted in all treated patients in the nivolumab plus chemotherapy and chemotherapy arms. Dose reductions were permitted for chemotherapy drugs only, and interruptions of infusions or infusion rate reductions were infrequent. There was a higher proportion of dose omissions for gemcitabine and vinorelbine, which are dosed twice per cycle, than for other chemotherapy drugs.15
Table 13: Interruptions, Delays, Reductions, and Omissions of Neoadjuvant Study Therapy — All Randomized Patients
Detail | Nivolumab plus chemotherapy | Chemotherapy |
|---|---|---|
Dose delays, n/N (%) | ||
Nivolumab | 44/176 (25) | NA |
Carboplatin | 7/51 (13.7) | 7/42 (16.7) |
Cisplatin | 31/136 (22.8) | 44/143 (30.8) |
Gemcitabine | 28/66 (42.4) | 22/49 (44.9) |
Paclitaxel | 5/28 (17.9) | 2/22 (9.1) |
Pemetrexed | 15/83 (18.1) | 19/63 (30.2) |
Docetaxel | — | 6/29 (20.7) |
Vinorelbine | — | 10/14 (71.4) |
Dose reductions, n/N (%) | ||
Carboplatin | 11/51 (21.6) | 13/42 (31.0) |
Cisplatin | 14/136 (10.3) | 17/143 (11.9) |
Gemcitabine | 12/66 (18.2) | 8/49 (16.3) |
Paclitaxel | 4/28 (14.3) | 7/22 (31.8) |
Pemetrexed | 1/83 (1.2) | 3/63 (4.8) |
Docetaxel | — | 5/29 (17.2) |
Vinorelbine | — | 1/14 (7.1) |
Dose omissions, n/N (%) | ||
Nivolumab | 5/176 (2.8) | NA |
Carboplatin | 1/51 (2.0) | 1/42 (2.4) |
Cisplatin | 5/136 (3.7) | 6/143 (4.2) |
Gemcitabine | 18/66 (27.3) | 8/49 (16.3) |
Paclitaxel | 1/28 (3.6) | 0/22 (0) |
Pemetrexed | 2/83 (2.4) | 3/63 (4.8) |
Docetaxel | — | 0/29 (0) |
Vinorelbine | — | 7/14 (50) |
Infusion interruptions, n/N (%) | ||
Nivolumab | 5/176 (2.8) | — |
Gemcitabine | 1/66 (1.5) | 1/49 (2.0) |
Cisplatin | 1/136 (0.7) | 1/143 (0.7) |
Carboplatin | 0/51 (0) | 1/42 (2.4) |
Paclitaxel | 4/28 (14.3) | 4/22 (18.2) |
Pemetrexed | 0/83 (0) | 0/63 (0) |
Docetaxel | — | 1/29 (3.4) |
Vinorelbine | — | 0/14 (0) |
NA = not applicable.
Source: Clinical Study Report.15
Concomitant Medications
In total, all patients in the nivolumab plus chemotherapy arm and 99.4% in the chemotherapy arm received concomitant medications during the trial.12 Table 14 presents the anatomic class of concomitant therapies permitted in the CheckMate 816 trial.
Subsequent Anticancer Therapy
Table 15 presents subsequent anticancer therapies administered to patients in the CheckMate 816 trial. In total, 38 (21.2%) patients in the nivolumab plus chemotherapy arm and 78 (43.6%) in the chemotherapy arm received subsequent cancer therapy (local and/or systemic therapy) started on or after the first study drug dose was administered (i.e., started on or after the date of randomization, if not treated) and not part of the on-protocol adjuvant study therapy (systemic and radiotherapy).12
Table 14: Concomitant Medications Permitted — All Treated Patients
Anatomic Therapeutic Chemical class generic name | Nivolumab plus chemotherapy (n = 176) | Chemotherapy (n = 176) |
|---|---|---|
Total patients using concomitant medication, n (%) | 176 (100.0) | 175 (99.4) |
Alimentary tract and metabolism, n (%) | 173 (93.3) | 172 (97.7) |
Antidiarrhea, intestinal antiinflammation, antiinfection, n (%) | 15 (8.5) | 21 (11.9) |
Antiemetic and antinauseant, n (%) | 163 (92.6) | 165 (93.8) |
Antispasmodic, anticholinergic, propulsive, n (%) | 57 (32.4) | 65 (36.9) |
Bile and liver therapy, n (%) | 7 (4.0) | 20 (11.4) |
Diabetes therapy, n (%) | 44 (25.0) | 30 (17.0) |
Digestive, including enzymes, n (%) | 7 (4.0) | 2 (1.1) |
Laxative, n (%) | 94 (53.4) | 94 (53.4) |
Mineral supplement, n (%) | 82 (46.6) | 81 (46.0) |
Other alimentary tract, metabolism product, n (%) | 11 (6.3) | 7 (4.0) |
Stomatological preparations, n (%) | 13 (7.4) | 8 (4.5) |
Vitamin, n (%) | 64 (36.4) | 76 (43.2) |
Antineoplastic and immunomodulating drug, n (%) | 37 (21.0) | 56 (31.8) |
Blood and blood forming organ, n (%) | 165 (93.8) | 158 (89.8) |
Antihemorrhagic, n (%) | 18 (10.2) | 20 (11.4) |
Antithrombic drug, n (%) | 72 (40.9) | 77 (43.8) |
Other hematological drug, n (%) | 8 (4.5) | 13 (7.4) |
Plasma substitute and perfusion solution, n (%) | 121 (68.8) | 117 (66.5) |
Serum lipid-reducing drug, n (%) | 46 (26.1) | 49 (27.8) |
Cardiovascular system, n (%) | 131 (74.4) | 128 (72.7) |
Dermatological, n (%) | 52 (29.5) | 46 (26.1) |
General antiinfective for systemic use, n (%) | 106 (60.2) | 113 (64.2) |
Genitourinary system and sex hormone, n (%) | 25 (14.2) | 22 (12.5) |
Musculoskeletal system, n (%) | 52 (29.5) | 57 (32.4) |
Sensory organ, n (%) | 9 (5.1) | 11 (6.3) |
Systemic hormonal preparation, excluding sex hormones, n (%) | 153 (86.9) | 156 (88.6) |
Various, n (%) | 80 (45.5) | 81 (46.0) |
Unassigned, n (%) | 1 (0.6) | 0 |
Source: Sponsor submission.12
Table 15: Subsequent Cancer Therapy — All Randomized Patients
Characteristic | Nivolumab plus chemotherapy (n = 179) | Chemotherapy (n = 179) |
|---|---|---|
Patients with any subsequent therapy, n (%) | 38 (21.2) | 78 (43.6) |
Patients who received subsequent radiotherapy, n (%) | 20 (11.2) | 38 (21.2) |
Patients who received subsequent surgery, n (%) | 3 (1.7) | 6 (3.4) |
Patients who received subsequent systemic therapy, n (%) | 31 (17.3) | 65 (36.3) |
Immunotherapy | 10 (5.6) | 42 (23.5) |
Anti-PD-1 | 6 (3.4) | 32 (17.9) |
Anti PD-1 | 0 | 1 (0.6) |
Nivolumab | 2 (1.1) | 8 (4.5) |
Pembrolizumab | 4 (2.2) | 22 (12.3) |
Sintilimab | 0 | 1 (0.6) |
Toripalimab | 0 | 1 (0.6) |
Anti-PD-L1 | 4 (2.2) | 14 (7.8) |
Atezolizumab | 2 (1.1) | 8 (4.5) |
Durvalumab | 2 (1.1) | 6 (3.4) |
Anti-CTLA4 | 0 | 0 |
Ipilimumab | 0 | 0 |
Targeted therapy | 13 (7.3) | 21 (11.7) |
ALK and/or EGFR tyrosine kinase inhibitors | 4 (2.2) | 9 (5.0) |
Afatinib | 0 | 1 (0.6) |
Alectinib | 0 | 2 (1.1) |
Brigatinib | 1 (0.6) | 0 |
Crizotinib | 1 (0.6) | 1 (0.6) |
Erlotinib | 1 (0.6) | 0 |
Gefitinib | 0 | 3 (1.7) |
Icotinib | 1 (0.6) | 0 |
Osimertinib | 1 (0.6) | 4 (2.2) |
VEGFR inhibitors | 10 (5.6) | 12 (6.7) |
Anlotinib | 3 (1.7) | 4 (2.2) |
Bevacizumab | 2 (1.1) | 4 (2.2) |
Endostar | 1 (0.6) | 0 |
Endostatin | 1 (0.6) | 2 (1.1) |
Ramucirumab | 3 (1.7) | 2 (1.1) |
Simvastatin | 0 | 1 (0.6) |
Other targeted therapy | 0 | 3 (1.7) |
Capmatinib | 0 | 1 (0.6) |
Entrectinib | 0 | 1 (0.6) |
Regorafenib | 0 | 1 (0.6) |
Temsirolimus | 0 | 0 |
Other systemic cancer therapy: chemotherapy, n (%) | 27 (15.1) | 40 (22.3) |
Carboplatin | 12 (6.7) | 20 (11.2) |
Cisplatin | 6 (3.4) | 10 (5.6) |
Docetaxel | 8 (4.5) | 9 (5.0) |
Etoposide | 3 (1.7) | 1 (0.6) |
Gemcitabine | 6 (3.4) | 4 (2.2) |
Tegafur, gimeracil, oteracil | 1 (0.6) | 0 |
Lobaplatin | 1 (0.6) | 0 |
Nedaplatin | 1 (0.6) | 3 (1.7) |
Paclitaxel | 14 (7.8) | 18 (10.1) |
Pemetrexed | 1 (0.6) | 7 (3.9) |
Taxane | 0 | 0 |
Tegafur | 0 | 3 (1.7) |
Vinorelbine | 6 (3.4) | 5 (2.8) |
Other systemic cancer therapy, n (%) | 0 | 6 (3.4) |
Herbs | 0 | 5 (2.8) |
MLN0128 | 0 | 0 |
Pamidronate | 0 | 1 (0.6) |
Spleen extract | 0 | 1 (0.6) |
ALK = anaplastic lymphoma kinase; CTLA-4 = cytotoxic T-lymphocyte-associated protein-4; EGFR = epidermal growth factor receptor; PD-1 = programmed cell death 1 protein; PD-L1 = programmed cell death 1 ligand 1; VEGFR = vascular endothelial growth factor receptors.
Notes: Patient may have received more than 1 type of subsequent therapy. Subsequent therapy was defined as therapy started on or after the first dosing date (randomization date if patient never treated) outside of the protocol-specified adjuvant therapy. The reported medication Avastin was coded as simvastatin by error in the locked database. It should have been bevacizumab.
The data cut-off date was October 20, 2021.
Source: Sponsor submission.12
Adjuvant Therapy
Optional adjuvant chemotherapy or radiotherapy was allowed following surgery per protocol (per the investigator’s judgment). Table 16 presents the number of patients who received adjuvant therapy in the CheckMate 816 trial.
Table 16: Adjuvant Treatment — All Treated Patients
Characteristic | Nivolumab plus chemotherapy (n = 176) | Chemotherapy (n = 176) |
|---|---|---|
Patients receiving adjuvant systemic therapy, n (%) | 26 (14.8) | 44 (25.0) |
Patients receiving adjuvant radiotherapy, n (%) | 14 (8.0) | 17 (9.7) |
Patients receiving adjuvant radiotherapy without systemic adjuvant, n (%) | 9 (5.1) | 12 (6.8) |
Patients receiving any adjuvant therapy, n (%) | 35 (19.9) | 56 (31.8) |
Source: Clinical Study Report.15
Efficacy
Only efficacy outcomes and analyses of subgroups identified in the CADTH review protocol are reported here.
Overall Survival
OS was formally tested at the October 20, 2021, data cut-off date (IA1 EFS), based on the hierarchical statistical testing rules for EFS and OS outlined in the statistical analysis plan.15
Median OS was not reached in either the nivolumab plus chemotherapy arm or the chemotherapy arm. The HR for death was 0.57 (99.67% CI, 0.30 to 1.07). The P value for OS (P = 0.008) did not cross the prespecified statistical significance boundary (0.0033). A second OS test is planned after 128 OS events have occurred (or 1 year after the IA1 EFS data cut-off date).15 Figure 4 presents the KM curves of OS at the data cut-off date.
Figure 4: OS — All Randomized Patients
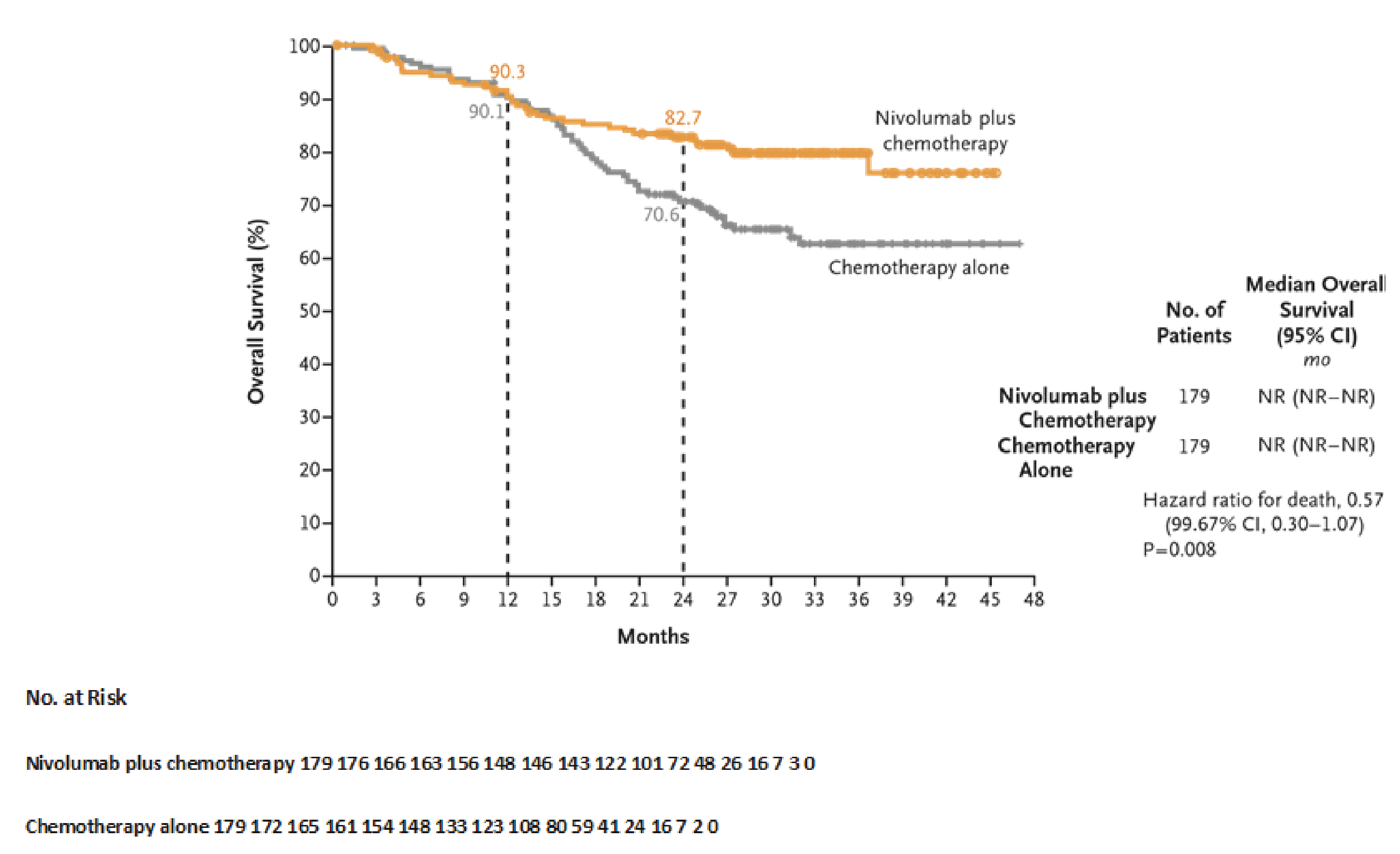
CI = confidence interval; mo = months; No. = number; NR = not reported; OS = overall survival.
Note: The data cut-off date was October 20, 2021.
Source: Forde et al. (2022).34
Event-Free Survival
Table 17 presents EFS findings at the IA1 data cut-off date (October 20, 2021) and Figure 5 presents the KM curves for the nivolumab plus chemotherapy and chemotherapy arms.
In total, 64 of 179 (35.8%) EFS events occurred in the nivolumab plus chemotherapy arm, and the median EFS was 31.57 months (95% CI, 30.16 to not available months). In the chemotherapy arm, 87 of 179 (48.6%) EFS events occurred, and the median EFS was 20.80 months (95% CI, 14.03 to 26.71 months). The estimated HR was 0.63 (97.38% CI, 0.43 to 0.91), with a P value of 0.0052 based on stratified log-rank test, which was statistically significant according to a prespecified threshold of 0.0262.15
The Cox model analyses based on baseline stratification factors (PD-L1 expression level [≥ 1% versus < 1%], disease stage [IB to II versus stage IIIA], and sex) had an HR of 0.64 (95% CI, 0.46 to 0.89); the estimated HR based on the unstratified Cox model was 0.63 (95% CI, 0.45 to 0.87). Additional sensitivity analyses that accounted for missing tumour assessments before EFS events had an estimated an HR of 0.66 (95% CI, 0.47 to 0.92).15.
Table 17: EFS per BICR — All Randomized Patients
Characteristic | Nivolumab plus chemotherapy (n = 179) | Chemotherapy (n = 179) |
|---|---|---|
Number of patients censored, n (%) | 115 (64.2) | 92 (51.4) |
Number of events (%) | 64 (35.8) | 87 (48.6) |
Median EFS (95% CI), monthsa | 31.57 (30.16 to NA) | 20.80 (14.03 to 26.71) |
HR (97.38% CI)b | 0.63 (0.43 to 0.91); P = 0.0052c | |
EFS rates (95% CI), %a | ||
At 6 months | 85.6 (79.3 to 90.1) | 81.9 (75.1 to 87.0) |
At 12 months | 76.1 (68.8 to 81.9) | 63.4 (55.3 to 70.4) |
At 18 months | 68.3 (60.4 to 74.9) | 53.1 (44.9 to 60.7) |
At 24 months | 63.8 (55.7 to 70.9) | 45.3 (37.0 to 53.2) |
Type of event n (%) | ||
Progression precluding surgeryd | 12 (6.7) | 16 (8.9) |
Progression and/or recurrence after surgerye | 39 (21.8) | 56 (31.3) |
Locoregional | 24 (13.4) | 28 (15.6) |
Distant | 14 (7.8) | 25 (14.0) |
Both locoregional and distant | 1 (0.6) | 3 (1.7) |
Progression without surgerye | 2 (1.1) | 3 (1.7) |
Locoregional | 2 (1.1) | 1 (0.6) |
Distant | 0 | 1 (0.6) |
Both locoregional and distant | 0 | 1 (0.6) |
Death | 11 (6.1) | 12 (6.7) |
BICR = blinded independent central review; CI = confidence interval; EFS = event-free survival; HR = hazard ratio; NA = not available.
Note: The data cut-off date was October 20, 2021.
aBased on KM estimates.
bHR of arm C to concurrent arm B from a Cox model stratified by PD-L1 expression level (≥ 1% vs. < 1%, not evaluable, indeterminate), disease stage (IB or II vs. stage IIIA), and sex (male vs. female) as entered into the Interactive Response Technology.
cLog-rank test stratified by the same factors as in the Cox proportional hazards model. The P value threshold for statistical significance was 0.0262.
dProgression not necessarily meeting RECIST 1.1.
eProgression and/or recurrence, per RECIST 1.1.
Source: Clinical Study Report.15
Figure 5: EFS per BICR — All Randomized Patients
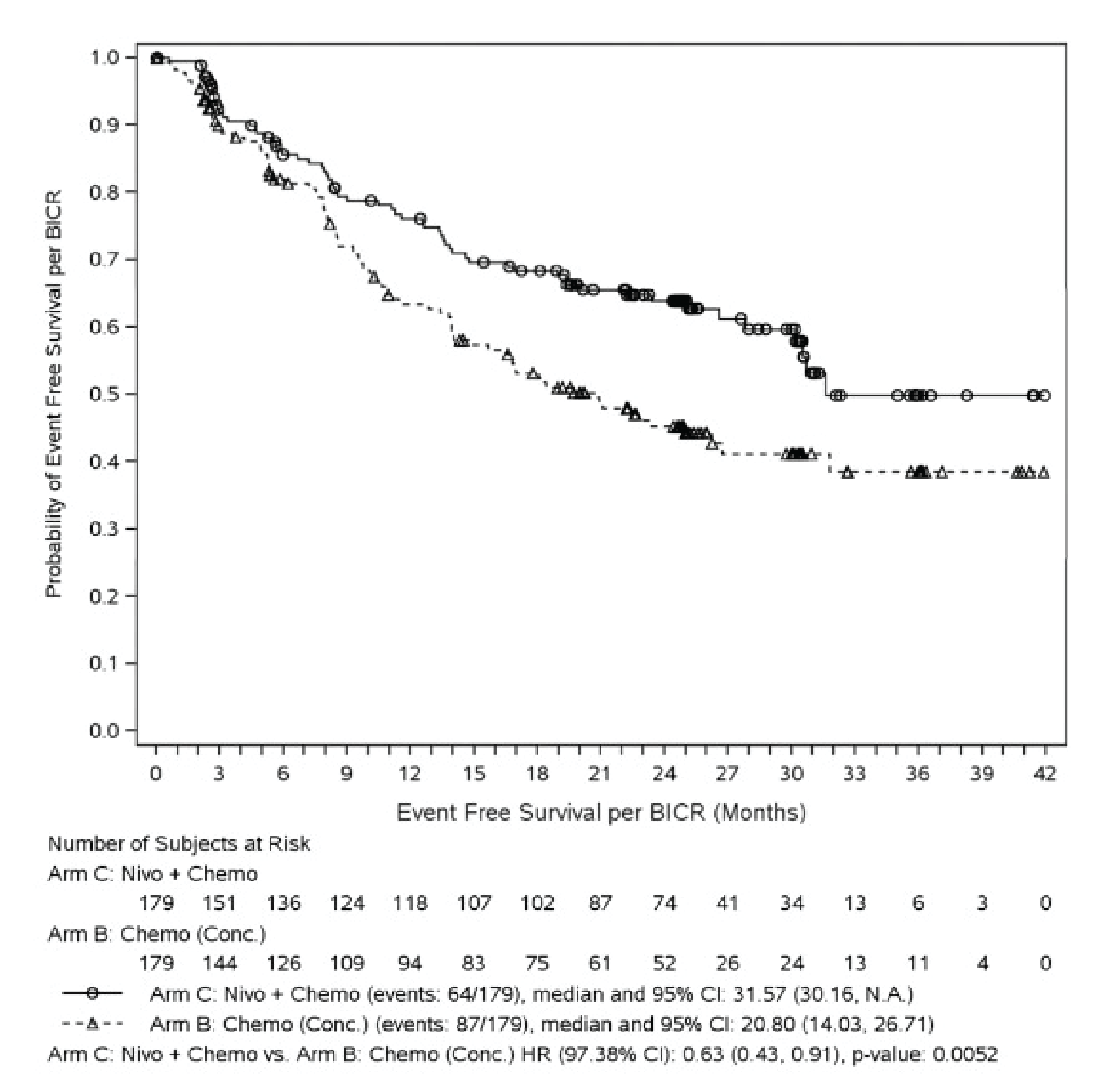
BICR = blinded independent central review; Chemo = chemotherapy; CI = confidence interval; Conc. = concurrent; EFS = event-free survival; HR = hazard ratio; KM = Kaplan-Meier; N.A. = not available; Nivo = nivolumab.
Note: The data cut-off date was October 20, 2021.
Source: Clinical Study Report.15
Subgroup Analyses
Although there were inconsistencies across identified subgroups in terms of benefit, overall, a positive EFS benefit was observed in the nivolumab plus chemotherapy arm compared with chemotherapy. Increasing benefit was reported for nivolumab plus chemotherapy over chemotherapy across the PD-L1 subgroup, with a higher magnitude of benefit reported in patients with a PD-L1 expression level of at least 50% (HR = 0.24; 95% CI, 0.10 to 0.61) than in those with a PD-L1 expression level of 1% to 49% (HR = 0.58; 95% CI, 0.30 to 1.12), of at least 1% (HR = 0.41; 95% CI, 0.24 to 0.70), and of more than 1% (HR = 0.85; 95% CI, 0.54 to 1.32). Similarly, benefit was observed in the nivolumab plus chemotherapy arm in the disease-stage subgroup, with a higher magnitude of benefit reported for patients with stage IIIA disease (HR = 0.54; 95% CI, 0.37 to 0.80) than for those with stage IB or II disease (HR = 0.87; 95% CI, 0.48 to 1.53). A benefit was also observed in the histology subgroup — the HR for patients with nonsquamous disease was 0.50 (95% CI, 0.32 to 0.79) — and in the performance-status subgroup, in which the magnitude of benefit was higher in patients with an ECOG PS of 0 (HR = 0.61, 95% CI, 0.41 to 0.91) than in those with an ECOG PS of 1 (HR = 0.71; 95% CI, 0.41 to 1.21).
A subgroup analysis conducted to evaluate EFS by pCR status showed an EFS HR for pCR versus no pCR of 0.13 (95% CI, 0.05 to 0.37) in the nivolumab plus chemotherapy arm. No results were presented for the chemotherapy arm because of the small number of patients who achieved a pCR.
Of note, multiplicity adjustments to account for a type I error were not conducted during the subgroup analyses; as such, the subgroup findings are considered exploratory. Table 47 in Appendix 4 presents EFS findings in the subgroups identified in the CADTH review protocol.
Pathologic Complete Response and Major Pathologic Response
pCR analyses were conducted at the September 16, 2020, data cut-off date. The pCR rate, per BIPR, was 24.0% (43 of 179 patients; 95% CI, 18.0% to 31.0%) in the nivolumab plus chemotherapy arm compared to 2.2% (4 of 179 patients; 95% CI, 0.6% to 5.6%) in the chemotherapy arm. The difference in MPR between the 2 arms was 27.9% (95% CI, 19.6% to 36.1%). Table 18 presents the pCR and MPR rates obtained at the September 8, 2020, data cut-off date.
The pCR rate in the sensitivity analysis was 30.5% (43 of 141 patients; 95% CI, 23.0% to 38.8%) in the nivolumab plus chemotherapy arm and 3.2% (4 of 126 patients; 95% CI, 0.9% to 7.9%) in the chemotherapy arm.
Table 18: pCR — All Randomized Patients
Characteristic | Nivolumab plus chemotherapy (n = 179) | Chemotherapy (n = 179) |
|---|---|---|
pCR | ||
Responders, n (%) | 43 (24.0) | 4 (2.2) |
95% CIa | (18.0 to 31.0) | (0.6 to 5.6) |
Difference (95% CI), %b,c | 21.6 (15.1 to 28.2) | |
MPR | ||
Responders, n (%)f | 66 (36.9) | 16 (8.9) |
95% CIa | (29.8 to 44.4) | (5.2 to 14.1) |
Difference, (95% CI), %b,c | 27.9 (19.6 to 36.1) |
CI = confidence interval; MPR = major pathologic response; pCR = pathologic complete response.
Note: The data cut-off date was September 16, 2020.
aCI based on the Clopper-Pearson method.
bStrata-adjusted difference (arm C – concurrent arm B) based on the Cochran-Mantel-Haenszel method of weighting.
cStratified by PD-L1 expression level (≥ 1% vs. < 1%, unevaluable, indeterminate), disease stage (stage IB to II vs. stage IIIA), and sex (male vs. female) as entered into the Interactive Response Technology.
Source: Clinical Study Report.15
Subgroup Analyses
The pCR rates observed in the CADTH specified-protocol subgroups favoured nivolumab plus chemotherapy over chemotherapy. A numerically higher difference between treatments was observed in the subgroup of patients with a PD-L1 expression level of at least 50% (difference = 40.0%; 95% CI, 21.7% to 55.9%) than in the other PD-L1 subgroups. Differences were also observed in the disease-stage subgroup, with a difference between treatments of 20.0% for stage IIIA disease (95% CI, 12.8% to 28.4%) and of 24.4% (95% CI, 11.6% to 36.6%) for stage IB to II disease; in the histology subgroup, with a difference between treatments of 2.1% (95% CI, 11.0% to 31.4%) for squamous cell disease and of 22.8% (95% CI, 14.2% to 32.4%) for nonsquamous cell disease; and in the performance-status subgroup, with a difference between treatments of 24.9% (16.7% to 33.4%) for an ECOG PS of 0 and of 15% (95% CI, 3.8% to 33.4%) for an ECOG PS of 1. Table 48 of Appendix 4 presents the pCR obtained in subgroups at the September 8, 2020, data cut-off date.
Time to Death or Distance Metastasis
The median TTDM was not reached in the nivolumab plus chemotherapy arm at the October 28, 2021, data cut-off date. The estimated HR was 0.53 (95% CI, 0.36 to 0.77), as presented in Table 19.
Table 19: TTDM — All Randomized Patients
Characteristic | Nivolumab plus chemotherapy (n = 179) | Chemotherapy (n = 179) |
|---|---|---|
Events, n (%) | 45 (25.1) | 75 (41.9) |
Median (95% CI), montha | Not reached (36.60 to NA) | 26.71 (22.41 to NA) |
HR (95% CI)b | 0.53 (0.36 to 0.77) | |
TDDM rates (95% CI) | ||
At 12 months | 85.7 (79.4 to 90.2) | 76.0 (68.8 to 81.8) |
At 24 months | 75.8 (68.3 to 81.7) | 57.1 (48.8 to 64.6) |
CI = confidence interval; HR = hazard ratio; NA = not available; TTDM = time to death or distance metastasis.
Note: The data cut-off date was October 20, 2021.
aBased on KM estimates.
bHR for arm C to concurrent arm B from a Cox model stratified by PD-L1 expression level (≥ 1% vs. < 1%, not evaluable, indeterminate), disease stage (IB or II vs. stage IIIA), and sex (male vs. female) as entered into the Interactive Response Technology.
Source: Clinical Study Report.15
Health-Related Quality of Life
Patients completed the EQ-5D-3L questionnaire at baseline, before on-treatment clinic visits, at postneoadjuvant visits 1 and 2, and at designated time points during the survival follow-up phase. Completion rates of questionnaires were reported for both study arms and are presented in Table 49 in Appendix 4.
EQ-5D index scores (based on the UK time trade-off value set) were collected for both study arms. Mean change from baseline in EQ-5D VAS and EQ-5D index during the neoadjuvant treatment phase were minimal and similar to baseline levels in the 2 treatment arms (Table 20 and Table 21). Figure 6 and Figure 7 presents mean changes in EQ-5D-3L utility index scores and VAS from baseline.12
Table 20: Summary of the Utility Index Score — All Randomized Patients
Nominal time point | Nivolumab plus chemotherapy (N = 179) | Chemotherapy (N = 179) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
N | Mean (SD) | 95% CI | Median | Q1, Q3 | N | Mean (SD) | 95% CI | Median | Q1, Q3 | |
Baseline | 169 | 0.89 (0.13) | 0.87 to 0.91 | 1.0 | 0.80 to 1.0 | 171 | 0.89 (0.16) | 0.86 to 0.91 | 1.0 | 0.80 to 1.0 |
Week 3 | NA | — | — | — | — | NA | — | — | — | — |
Change from baseline | NA | — | — | — | — | NA | — | — | — | — |
Week 4 | 168 | 0.91 (0.15) | 0.89 to 0.93 | 1.0 | 0.82 to 1.0 | 158 | 0.89 (0.17) | 0.86 to 0.91 | 1.0 | 0.80 to 1.0 |
Change from baseline | 163 | 0.02 (0.16) | –0.01 to 0.04 | 0.0 | 0 to 0.07 | 153 | 0.00 (0.17) | –0.02 to 0.03 | 0.0 | 0.00 to 0.05 |
Week 5 | NA | — | — | — | — | NA | — | — | — | — |
Change from baseline | NA | — | — | — | — | NA | — | — | — | — |
Week 7 | 151 | 0.89 (0.18) | 0.86 to 0.92 | 1.0 | 0.80 to1.0 | 145 | 0.89 (0.17) | 0.86 to 0.92 | 1.0 | 0.80 to 1.0 |
Change from baseline | 148 | –0.01 (0.18) | –0.04 to 0.02 | 0.0 | 0.0 to 0.04 | 141 | –0.01 (0.18) | –0.03 to 0.03 | 0.0 | 0.00 to 0.00 |
Postneoadjuvant visit 1 | 156 | 0.88 (0.18) | 0.86 to 0.91 | 1.0 | 0.80 to 1.0 | 146 | 0.86 (0.20) | 0.83 to 0.80 | 1.0 | 0.80 to 1.0 |
Change from baseline | 152 | –0.01 (0.18) | –0.04 to 0.02 | 0.0 | –0.04 to 0.02 | 143 | –0.02 (0.21) | –0.06 to 0.01 | 0.0 | –0.09 to 0.0 |
Postneoadjuvant visit 2 | 134 | 0.81 (0.25) | 0.77 to 0.85 | 0.82 | 0.73 to 1.0 | 132 | 0.80 (0.24) | 0.76 to 0.84 | 0.80 | 0.73 to 1.0 |
Change from baseline | 131 | –0.09 (0.20) | –0.12 to –0.05 | 0.0 | –0.20 to 0.0 | 129 | –0.09 (0.23) | –0.13 to –0.05 | –0.036, 0.0 | –0.20 to 0.0 |
CI = confidence interval; NA = not available; Q1 = first quartile; Q3 = third quartile; SD = standard deviation.
Note: The data cut-off date was October 20, 2021.
Source: Sponsor submission.12
Table 21: Summary of Overall Self-Rated Health Status on EQ VAS— All Randomized Patients
Nominal time point | Nivolumab plus chemotherapy N = 179 | Chemotherapy N = 179 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
N | Mean (SD) | 95% CI | Median | Q1, Q3 | N | Mean (SD) | 95% CI | Median | Q1, Q3 | |
Baseline | 169 | 83.1 (15.8) | 80.7 to 85.5 | 90.0 | 80.0 to 90.0 | 170 | 82.4 (14.2) | 80.3 to 84.6 | 85.5 | 77.0 to 90.0 |
Week 3 | NA | — | — | — | — | NA | — | — | — | — |
Change from baseline | NA | — | — | — | — | NA | — | — | — | — |
Week 4 | 168 | 83.0 (13.5) | 81.0 to 85.1 | 85.0 | 80.0 to 90.0 | 159 | 81.0 (13.4) | 78.9 to 83.1 | 80.0 | 70.0 to 90.0 |
Change from baseline | 163 | –0.2 (12.1) | –2.0 to 1.7 | 0.0 | –5.0 to 5.0 | 153 | –1.2 (13.1) | –3.3 to 0.9 | 0.0 | –10.0 to 5.0 |
Week 5 | NA | — | — | — | — | NA | NA | — | — | — |
Change from baseline | NA | — | — | — | — | NA | NA | — | — | — |
Week 7 | 152 | 81.8 (15.1) | 79.4 to 84.2 | 85.0 | 80.0 to 90.0 | 145 | 82.0 (13.2) | 79.8 to 84.2 | 84.0 | 75.0 to 90.0 |
Change from baseline | 148 | –1.3 (13.8) | –3.5 to 1.0 | 0.0 | –5.0 to 5.0 | 141 | –0.7 (12.6) | –2.8 to 1.4 | 0.0 | –5.0 to 5.0 |
Postneoadjuvant visit 1 | 156 | 83.3 (13.1) | 81.2 to 85.3 | 87.0 | 80.0 to 90.0 | 146 | 80.5 (14.9) | 78.1 to 83.0 | 80.0 | 70.0 to 90.0 |
Change from baseline | 152 | –0.2 (13.9) | –2.4 to 2.1 | 0.0 | –8.0 to 5.0 | 142 | –1.0 (15.4) | –3.5 to 1.6 | 0.0 | –10.0 to 5.0 |
Postneoadjuvant visit 2 | 134 | 81.2 (14.8) | 78.7 to 83.7 | 84.5 | 80.0 to 90.0 | 133 | 79.0 (17.1) | 76.0 to 81.9 | 80.0 | 70.0 to 90.0 |
Change from baseline | 131 | –2.5 (16.5) | –5.4 to 0.3 | 0.0 | –10.0 to 5.0 | 129 | –2.5 (17.3) | –5.5 to 0.5 | 0.0 | –10.0 to 6.0 |
CI = confidence interval; NA = not available; Q1 = first quartile; Q3 = third quartile; SD = standard deviation.
Note: The data cut-off date was October 20, 2021.
Source: Sponsor submission.12
Table 22: EFS2 — All Randomized Patients
Characteristic | Nivolumab plus chemotherapy (n = 179) | Chemotherapy (n = 179) |
|---|---|---|
Number of events (%) | 42 (23.5) | 70 (39.1) |
Median (95% CI), monthsa | Not reached (NA to NA) | Not reached (27.40 to NA) |
HR (95% CI)b | 0.54 (0.37 to 0.80) | |
Type of events (%) | ||
Disease progression after subsequent next-line systemic anticancer therapy | 15 (8.4) | 29 (16.2) |
Start of second subsequent next-line systemic anticancer therapy death | 0 | 4 (2.2) |
Death | 27 (15.1) | 37 (20.7) |
Number of patients censored (%) | 137 (76.5) | 109 (60.9) |
No subsequent next-line systemic anticancer therapy and alive | 127 (70.9) | 93 (52.0) |
Next-line systemic therapy but no progression and no second next-line therapy and alive | 10 (5.6) | 16 (8.9) |
CI = confidence interval; EFS2 = event-free survival on the next- line of therapy; HR = hazard ratio; NA = not available.
aBased on KM estimates.
bHR of arm C to concurrent arm B from a Cox Model stratified by: PD-L1 expression level (≥ 1% vs. < 1%, not evaluable, indeterminate), disease stage (IB or II vs. stage IIIA), and sex (male vs. female) as entered into the Interactive Response Technology.
Source: Clinical Study Report.15
Figure 6: Mean Change in EQ-5D-3L Utility Index Score from Baseline — All Randomized Patients
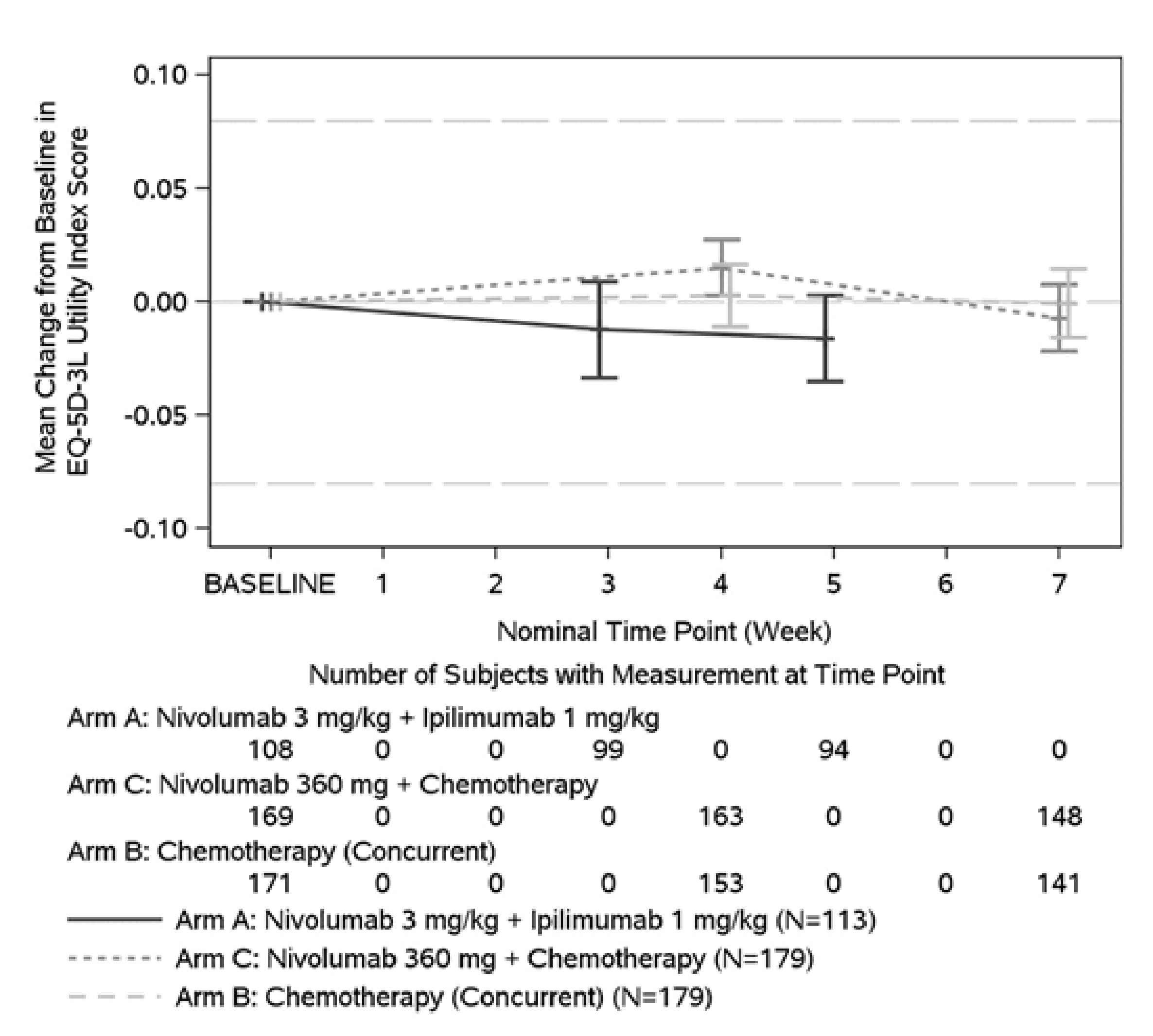
EQ-5D-3L = 3-Level EQ-5D; SD = standard deviation.
Note: The data cut-off date was October 20, 2021.
Source: Clinical Study Report.15
Figure 7: Mean Changes in Overall Self-Rated Health Status on EQ VAS From Baseline — All Randomized Patients
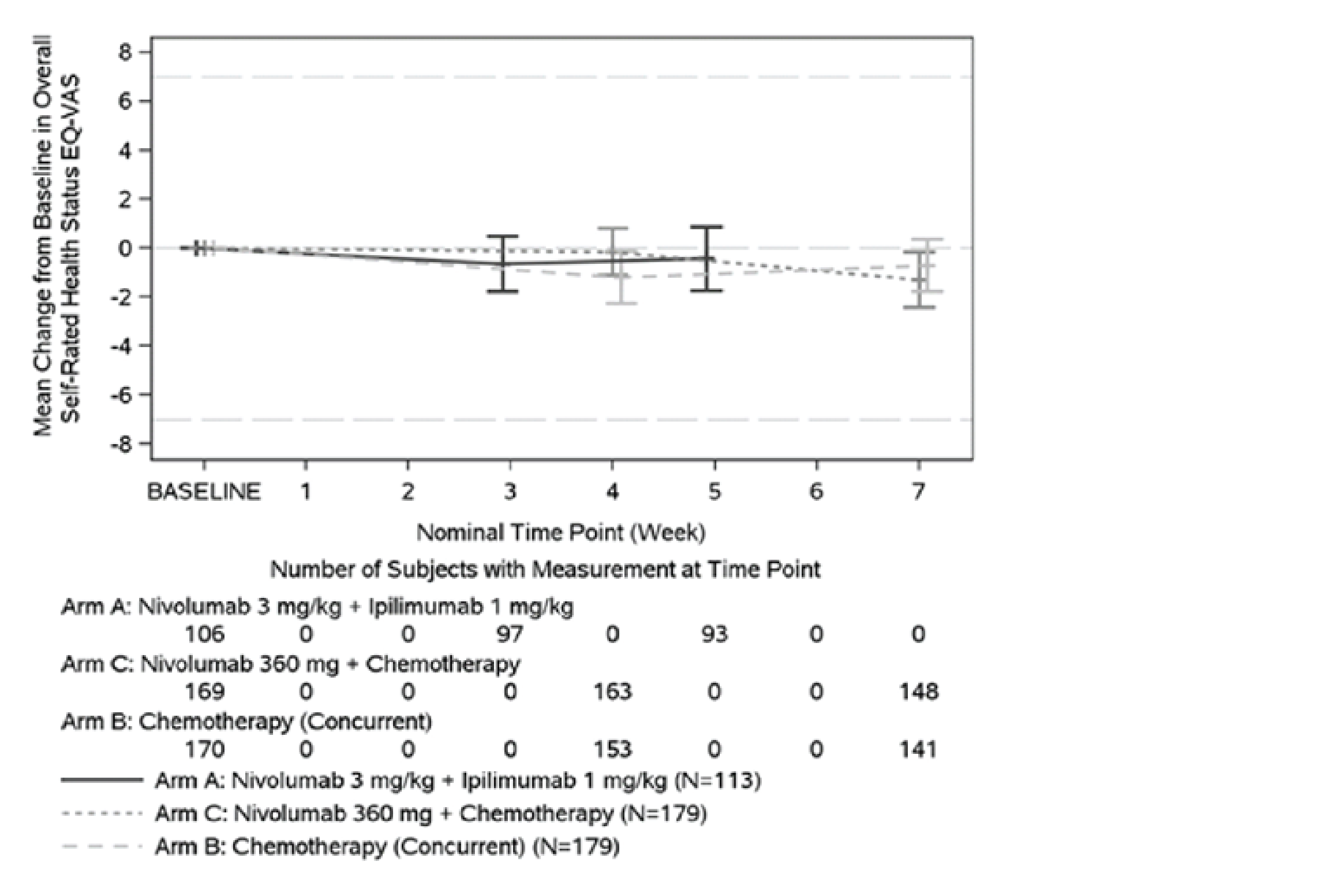
EQ VAS = EQ visual analogue scale.
Note: The data cut-off date was October 20, 2021.
Source: Clinical Study Report.15
Figure 8: EFS2 — All Randomized Patients
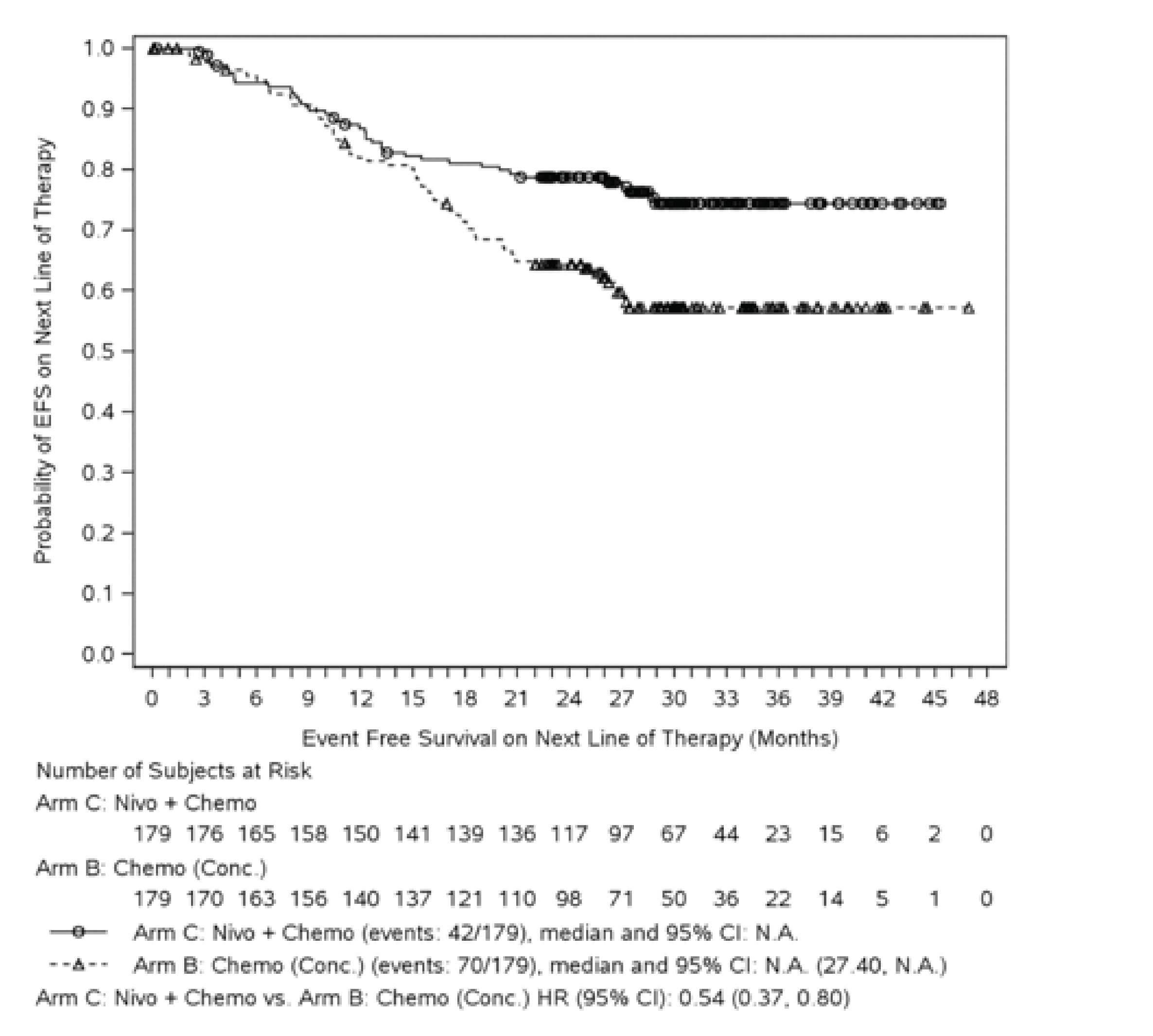
Chemo = chemotherapy; CI = confidence interval; Conc. = concurrent; EFS = event-free survival; EFS2 = event-free survival on the next line of therapy; KM = Kaplan-Meier; N.A. = not available; Nivo = nivolumab.
Note: The data cut-off date was October 20, 2021.
Source: Clinical Study Report.15
Event-Free Survival on the Next Line of Therapy
By the October 20, 2021, data cut-off date, median EFS2, per investigator, was not reached in either the nivolumab plus chemotherapy or chemotherapy arm. The estimated HR was 0.54 (95% CI, 0.37 to 0.80). Table 22 presents EFS2 data and Figure 8 presents the KM curves for the nivolumab plus chemotherapy and chemotherapy arms.
Harms
Only harms identified in the CADTH review protocol are reported here. Safety data were reported for all treated patients randomized into the nivolumab plus chemotherapy and chemotherapy arms by the October 20, 2021, data cut-off date.
Adverse Events
Overall, 163 (92.6%) patients treated in the nivolumab plus chemotherapy arm and 171 (97.2%) in the chemotherapy arm reported at least 1 AE in the CheckMate 816 trial. The most frequently reported AEs in the nivolumab plus chemotherapy arm were nausea (38.1%), constipation (33.5%), anemia (29.0%), decreased appetite (20.5%), fatigue (16.5%), and neutropenia (16.5%), and in the chemotherapy arm were nausea (44.9%), constipation (32.4%), anemia (26.7%), decreased appetite (23.3%), and decreased neutrophil count (21.0%). AEs of grade 3 or 4 were reported in 40.9% (n = 72) and 43.8% (n = 77) of patients, respectively, in the nivolumab plus chemotherapy and chemotherapy arms.15 Table 23 presents details of the most frequently reported AEs of grade 3 or 4 in the 2 study arms of the CheckMate 816 trial.
Serious Adverse Events
SAEs of any grade were reported in 30 (17.0%) patients in the nivolumab plus chemotherapy arm and 24 (13.6%) patients in the chemotherapy arm. SAEs of grades 3 or 4 were reported in 19 (10.8%) patients in the nivolumab plus chemotherapy arm and 17 (9.7%) patients in the chemotherapy arm. The most commonly reported SAEs in the nivolumab plus chemotherapy arm were vomiting (2.3%), pneumonia (2.3%), embolism (1.1%), and febrile neutropenia (1.1%), and in the chemotherapy arm were febrile neutropenia (2.8%), pneumonia (1.7%), neutropenia (1.1%), and diarrhea (1.1%).15
Dose Delay or Reduction Due to AEs
AEs leading to a dose delay or reduction were reported in 53 (30.1%) and 66 (37.5%) treated patients, respectively, in the nivolumab plus chemotherapy and chemotherapy arms.15 The most common AEs leading to a dose delay or reduction are presented in Table 23.
Discontinuations Due to AEs
AEs leading to the discontinuation of study treatments were reported in 18 (10.2%) patients in the nivolumab plus chemotherapy arm and 20 (11.4%) in the chemotherapy arm. Grade 3 or 4 AEs leading to the discontinuation of at least 1 study drug were reported in 10 (5.7%) patients in the nivolumab plus chemotherapy arm and 7 (4.0%) patients in the chemotherapy arm. The most frequently reported AEs of any grade leading to discontinuation in the nivolumab plus chemotherapy arm were anaphylactic reaction (1.7%), decreased neutrophil count (1.1%), and fatigue (1.1%), and in the chemotherapy arm were neutropenia (2.3%), decreased neutrophil count (1.1%), increased blood creatinine (1.1%), and pneumonia (1.1%).15
Mortality
By the October 20, 2021, data cut-off date, 35 (19.9%) patients had died in the nivolumab plus chemotherapy arm and 59 (33.5%) patients had died in the chemotherapy arm (Table 24). There were no deaths due to study drug toxicity (per investigator) in the nivolumab plus chemotherapy arm, but 3 deaths due to study drug toxicity (per investigator) in the chemotherapy arm (caused by pancytopenia, diarrhea, and acute kidney injury [all 3 reported in 1 patient]; enterocolitis infection; and lung infection and/or pneumonia). Among the 149 patients who underwent surgery after treatment with nivolumab plus chemotherapy, 5 (3.4%) died within 90 days of surgery, most commonly from intraoperative hemorrhage, esophageal perforation, pneumonia, cardiopulmonary arrest due to pulmonary embolism, or aortic rupture. Among the 135 patients who underwent surgery after chemotherapy, 2 (1.5%) patients died within 90 days from an AE or SAE associated with pneumonia.15
Notable Harms
AEs of special interest, specifically immune-related AEs, are presented in Table 23.
Table 23: Summary of Safety With Neoadjuvant Treatment — All Treated Patients
Safety parameters | Nivolumab plus chemotherapy (n = 176) | Chemotherapy (n = 176) | ||
|---|---|---|---|---|
Any grade | Grade 3 or 4 | Any grade | Grade 3 or 4 | |
All-causality AEs, n (%) | 163 (92.6) | 72 (40.9) | 171 (97.2) | 77 (43.8) |
≥ 10% of all treated patients in any treatment arm, by PT, n (%) | ||||
GI disorders | 102 (58.0) | 4 (2.3) | 124 (70.5) | 9 (5.1) |
Nausea | 67 (38.1) | 1 (0.6) | 79 (44.9) | 2 (1.1) |
Constipation | 59 (33.5) | 0 | 57 (32.4) | 2 (1.1) |
Vomiting | 19 (10.8) | 2 (1.1) | 22 (12.5) | 1 (0.6) |
Diarrhea | 16 (9.1) | 1 (0.6) | 24 (13.6) | 4 (2.3) |
General disorders and administration-site conditions, n (%) | 85 (48.3) | 5 (2.8) | 78 (44.3) | 4 (2.3) |
Fatigue | 29 (16.5) | 2 (1.1) | 22 (12.5) | 1 (0.6) |
Malaise | 26 (14.8) | 1 (0.6) | 25 (14.2) | 1 (0.6) |
Asthenia | 16 (9.1) | 2 (1.1) | 19 (10.8) | 1 (0.6) |
Blood and lymphatic system disorders, n (%) | 76 (43.2) | 26 (14.8) | 74 (42.0) | 36 (20.5) |
Anemia | 51 (29.0) | 7 (4.0) | 47 (26.7) | 9 (5.1) |
Neutropenia | 29 (16.5) | 16 (9.1) | 31 (17.6) | 21 (11.9) |
Investigations, n (%) | 66 (37.5) | 22 (12.5) | 77 (43.8) | 25 (14.2) |
Decreased neutrophil count | 26 (14.8) | 13 (7.4) | 37 (21.0) | 19 (10.8) |
Decreased WBC count | 13 (7.4) | 3 (1.7) | 19 (10.8) | 6 (3.4) |
Skin and subcutaneous tissue disorders, n (%) | 58 (33.0) | 4 (2.3) | 37 (21.0) | 0 |
Rash | 24 (13.6) | 1 (0.6) | 5 (2.8) | 0 |
Alopecia | 19 (10.8) | 0 | 26 (14.8) | 0 |
Metabolism and nutrition disorders, n (%) | 63 (35.8) | 9 (5.1) | 64 (36.4) | 10 (5.7) |
Decreased appetite | 36 (20.5) | 2 (1.1) | 41 (23.3) | 4 (2.3) |
Respiratory, thoracic, and mediastinal disorders, n (%) | 54 (30.7) | 1 (0.6) | 51 (29.0) | 2 (1.1) |
Hiccups | 18 (10.2) | 0 | 26 (14.8) | 0 |
≥ 20% of patients in any treatment arm, by PT, n (%) | ||||
Nausea | 67 (38.1) | 1 (0.6) | 79 (44.9) | 2 (1.1) |
Constipation | 59 (33.5) | 0 | 57 (32.4) | 2 (1.1) |
Anemia | 51 (29.0) | 7 (4.0) | 47 (26.7) | 9 (5.1) |
Decreased appetite | 36 (20.5) | 2 (1.1) | 41 (23.3) | 4 (2.3) |
Decreased neutrophil count | 26 (14.8) | 13 (7.4) | 37 (21.0) | 19 (10.8) |
All-causality select AEs, by category, n (%) | ||||
Endocrine | 11 (6.3) | 0 | 0 | 0 |
GI | 16 (9.1) | 1 (0.6) | 25 (14.2) | 4 (2.3) |
Hepatic | 15 (8.5) | 1 (0.6) | 22 (12.5) | 4 (2.3) |
Pulmonary | 2 (1.1) | 0 | 0 | 0 |
Renal | 16 (9.1) | 1 (0.6) | 21 (11.9) | 0 |
Skin | 43 (24.4) | 4 (2.3) | 20 (11.4) | 1 (0.6) |
Hypersensitivity and/or infusion reactions | 12 (6.8) | 4 (2.3) | 6 (3.4) | 2 (1.1) |
All-causality SAEs, n (%) | 30 (17.0) | 19 (10.8) | 24 (13.6) | 17 (9.7) |
≥ 1% of patients in any treatment arm, by PT | ||||
Vomiting | 4 (2.3) | 2 (1.1) | 0 | 0 |
Pneumonia | 4 (2.3) | 1 (0.6) | 3 (1.7) | 2 (1.1) |
Febrile neutropenia | 2 (1.1) | 2 (1.1) | 5 (2.8) | 5 (2.8) |
Embolism | 2 (1.1) | 1 (0.6) | 0 | 0 |
Neutropenia | 0 | 0 | 2 (1.1) | 2 (1.1) |
Diarrhea | 0 | 0 | 2 (1.1) | 2 (1.1) |
All-causality AEs leading to discontinuation, n (%) | 18 (10.2) | 10 (5.7) | 20 (11.4) | 7 (4.0) |
≥ 1% of patients in any treatment arm, by PT | ||||
Anaphylactic reaction | 3 (1.7) | 3 (1.7) | 0 | 0 |
Decreased neutrophil count | 2 (1.1) | 2 (1.1) | 2 (1.1) | 0 |
Fatigue | 2 (1.1) | 1 (0.6) | 0 | 0 |
Increased blood creatinine | 1 (0.6) | 0 | 2 (1.1) | 0 |
Neutropenia | 1 (0.6) | 0 | 4 (2.3) | 3 (1.7) |
Pneumonia | 0 | 0 | 2 (1.1) | 1 (0.6) |
Aes leading to dose delay or reduction, n (%) | 53 (30.1) | 28 (15.9) | 66 (37.5) | 33 (18.8) |
≥ 5% of patients in any treatment arm, by PT | ||||
Neutropenia | 13 (7.4) | 7 (4.0) | 17 (9.7) | 10 (5.7) |
Anemia | 11 (6.3) | 3 (1.7) | 8 (4.5) | 0 |
Decreased neutrophil count | 16 (9.1) | 8 (4.5) | 22 (12.5) | 13 (7.4) |
All-causality AEs leading to surgical delay, n (%) | 6 (3.4) | 2 (1.1) | 9 (5.1) | 4 (2.3) |
All-causality AEs leading to surgery cancellation, n (%) | 2 (1.1) | 0 | 1 (0.6) | 0 |
All-causality imAEs within 100 days of last dose, treated with immune-modulating medication, by category, n (%) | ||||
Diarrhea and/or colitis | 0 | 0 | 0 | 0 |
Hepatitis | 0 | 0 | 0 | 0 |
Pneumonitis | 2 (1.1) | 0 | 1 (0.6) | 1 (0.6) |
Nephritis and/or renal dysfunction | 0 | 0 | 0 | 0 |
Rash | 15 (8.5) | 3 (1.7) | 1 (0.6) | 0 |
Hypersensitivity and/or infusion reactions | 2 (1.1) | 0 | 0 | 0 |
All-causality endocrine imAEs within 100 days of last dose, with or without immune-modulating medication, by category, n (%) | ||||
Adrenal insufficiency | 2 (1.1) | 2 (1.1) | 0 | 0 |
Hypophysitis | 1 (0.6) | 1 (0.6) | 0 | 0 |
Hypothyroidism and/or thyroiditis | 4 (2.3) | 0 | 0 | 0 |
Hyperthyroidism | 7 (4.0) | 0 | 0 | 0 |
Diabetes mellitus | 2 (1.1) | 0 | 0 | 0 |
AE = adverse event; GI = gastrointestinal; imAE = immune-mediated adverse event; PT = preferred term, SAE = serious adverse event; WBC = white blood cell.
Note: The data cut-off date was October 20, 2021.
Source: Clinical Study Report.15
Table 24: Summary of Death — All Treated Patients
Safety parameter | Nivolumab plus chemotherapy (n = 176) | Chemotherapy (n = 176) |
|---|---|---|
Deaths, n (%) | 35 (19.9) | 59 (33.5) |
Primary reason for death, n (%) | ||
Disease | 24 (13.6) | 45 (25.6) |
Study drug toxicitya | 0 | 3 (1.7) |
Unknown | 2 (1.1) | 5 (2.8) |
Otherb | 9 (5.1) | 6 (3.4) |
Patients who died within 100 days of last neoadjuvant dose, n (%) | 9 (5.1) | 4 (2.3) |
Primary reason for death, n (%) | ||
Disease | 3 (1.7) | 1 (0.6) |
Study drug toxicity | 0 | 3 (1.7) |
Unknown | 0 | 0 |
Other | 6 (3.4) | 0 |
Notes: Only AEs that led to death within 24 hours were documented as grade 5. Events leading to death > 24 hours after onset are reported as the worst grade before death.
Data cut-off of October 20, 2021.
aThe causes of death, per investigator, in the chemotherapy arm were as follows: pancytopenia, diarrhea, and acute kidney injury (all 3 reported in 1 patient); enterocolitis infection; and lung infection and/or pneumonia.
bThe verbatim terms reported for other reasons for death and were consistent with events expected in the study population. None were considered to be related to study drug (per the investigator).
Source: Clinical Study Report.15
Critical Appraisal
Internal Validity
CheckMate 816 is an ongoing, randomized, open-label, phase III trial. Initially, patients were randomized using an Interactive Response Technology in a 1:1 ratio into 1 of 2 treatment arms, and treatment allocation was concealed. Baseline characteristics in the 2 arms of interest were balanced, suggesting that randomization was successful. The methods of randomization, treatment allocation, and stratification factors were considered appropriate. Disease stage and PD-L1 expression level were considered prognostic factors for NSCLC, and sex was considered a significant factor in the assessment of outcomes for immunotherapy.
The treatment effect for the 2 coprimary end points (EFS and pCR) was estimated during a prespecified interim analysis, adjusted using the Lan-DeMets alpha spending function with O’Brien-Fleming boundaries that accounted for the actual number of events at an overall alpha of 4% or 5%. Overall, the estimated treatment effect of the coprimary end points was based on interim analyses. There is uncertainty about the magnitude of the treatment effect, given that interim analyses have a tendency to overestimate treatment effect.38-40
OS estimated by the HR for death was statistically nonsignificant, based on the preplanned interim analysis stopping rule (P = 0.008 against a prespecified level of significance at the interim analysis of 0.0033). Although the results showed a promising trend toward a significant treatment effect for OS, the final analysis may be needed to confirm the findings, particularly the exact estimate of the difference in median survival, which was not estimable at the date cut-off date.
Performance and assessment biases due to the open-label design of the trial were considered unlikely, given that radiologic assessments of CT scans for EFS and pathologic review of tumour sections were completed by a blinded independent review team, based on prespecified and validated RECIST 1.1 guidelines. Further, an independent pathology review team assessed images and tumour or lymph node samples for pCR and MPR, which minimizes performance bias.
The proportion of patients exposed to 3 doses of chemotherapy drugs was slightly higher in the nivolumab plus chemotherapy arm than in the chemotherapy arm, which could bias the findings in favour of nivolumab plus chemotherapy (70.6% versus 66.7% for carboplatin; 84.6% versus 79.7% for cisplatin; 85.7% versus 81.8% for paclitaxel; 92.8% versus 84.1% for pemetrexed; and 72.3% versus 75.5% for gemcitabine). In addition, patients in the nivolumab plus chemotherapy arm did not receive docetaxel or vinorelbine because the safety profile of these drugs used in combination with nivolumab had not been established before the establishment of the study arm. The impact of docetaxel and vinorelbine in the estimated effect between treatment arms was considered likely to be negligible. There were also slight differences in the cumulative dose intensity (which also accounted for dose delays and reductions during the trial) in the nivolumab plus chemotherapy and chemotherapy arms for some chemotherapy drugs (46.2% versus 63.3% for gemcitabine [important]; 60.7% versus 81.8% for paclitaxel; and 85.5% versus 79.4% for pemetrexed), which may introduce bias in either direction in the nivolumab plus chemotherapy arm (it may have affected the proportion of patients that became eligible for surgery).
More patients in the chemotherapy arm than in the nivolumab plus chemotherapy arm received any subsequent therapy (n = 78 versus 38 [43.6% versus 21.2%]), received subsequent systemic anticancer therapy (n = 65 versus 31 [36.3% versus 17.3%]), and received subsequent immunotherapy (n = 42 versus 10 [23.5% versus 5.6%]). The use of subsequent anticancer therapy may bias EFS and OS outcomes in the 2 groups. Further, the proportion of patients who received subsequent adjuvant therapy (optional) after surgery was higher in the chemotherapy arm than in the nivolumab plus chemotherapy arm (n = 56 versus 35 [31.8% versus 19.9%]). The use of subsequent adjuvant therapy may bias EFS and OS findings in favour of the chemotherapy arm, which may have led to the improved OS and EFS reflected in the KM curves estimates. The sponsor-presented analyses that did not apply censoring at subsequent anticancer therapy use showed an HR of 0.63 (97.38% CI, 0.44 to 0.89), consistent with the primary analysis (HR = 0.63; 97.38% CI, 0.44 to 0.89; P = 0.0027 [descriptive]). The sponsor also performed additional analyses that adjusted for the use of adjuvant chemotherapy (as a time-dependent covariate), which favoured nivolumab plus chemotherapy over chemotherapy alone (adjusted HR = 0.65; 95% CI, 0.47 to 0.90). There is a potential risk of bias from the use of systemic anticancer therapy and adjuvant chemotherapy; however, the bias was in the outcomes was considered low.
The methods used to address missing data in the trial were considered conservative and may have had an impact on the assessment of efficacy outcomes. The extent of bias may favour of nivolumab plus chemotherapy over chemotherapy for OS and EFS outcomes, given that there were more patients in the chemotherapy arm who did not undergo definitive surgery.
All efficacy end points were adequately described in the sponsor-submitted statistical analysis plan, and censoring rules, hierarchical hypothesis testing, and stopping rules were provided for the primary outcomes, including OS, investigated in the CheckMate 816 trial. Crossing over from 1 study arm to the other was not permitted during the trial, which preserved the treatment differences observed in the randomized arms for EFS and OS. A Cox proportional hazards model, which relies on the assumption of proportional hazards in both treatment groups, was used to assess OS and EFS survival curves. Visual assessment of the KM curve for EFS did not suggest a violation of the proportional hazards assumption, as the curves did not cross; however, visual assessment of the OS curves did suggest a violation of the proportional hazards assumption. In addition, no assessment of the proportional hazards assumption was provided for EFS and OS; therefore, it is uncertain whether the sponsor addressed potential violations in their analyses.
The EQ-5D-3L questionnaire is a generic instrument that has been used to measure patient-reported outcomes and treatments across different health conditions, including cancers.36,37 However, there is limited evidence available on its validity, reliability, and responsiveness to change in patients with NSCLC. In general, the estimated MID for EQ-5D-3L index scores for patients with lung cancer was 0.06 in the US and 0.08 in the UK, using an anchor-based method.41 The MID for EQ VAS scores identified in literature was 7 to 12, and was estimated using the ECOG PS method.41 Utility index and VAS scores obtained from the EQ-5D-3L questionnaire at different time points (baseline, week 4, week 7, postadjuvant visit 1, and postadjuvant visit 2) were used to assess the general health status of patients enrolled in the trial. Missing data for HRQoL were considered missing at specific time points in the analysis. Multiplicity adjustments were not conducted to account for the type I error rate, so the findings were considered exploratory, and no conclusions could be drawn.
Several changes were made to the study protocol, which were adequately reported. These frequent amendments occurred after the study was initiated to reflect the high degree of uncertainty in the objectives when the study was designed. Sample-size calculations and other efficacy outcomes were updated in the statistical analysis plan to reflect the amendments.
All protocol deviations in the 2 study arms of the trial were adequately reported. Relevant protocol deviations were slightly higher in the chemotherapy arm than in the nivolumab plus chemotherapy arm (1.1% versus 2.2%). The most common protocol deviations were incorrect disease staging at baseline and on-treatment deviations related to concurrent cancer therapy.
There was a low risk of selective reporting, as all the outcomes prespecified in the protocol were reported. Interim analysis for pCR and EFS on the first line of therapy were prespecified in the protocol, including the trigger factors and stopping rules. The approaches used to preserve the alpha and the power in the interim analyses were outlined adequately in the statistical analysis plan and were considered to be appropriate. Efficacy analyses were conducted using the ITT population (patients randomized in the 1:1:1 randomization scheme in revised protocol 2 and in the 1:1 randomization scheme in revised protocol 3 [i.e., patients concurrently randomized in the nivolumab plus chemotherapy and chemotherapy arm]), which maintained randomization and minimized the risk of bias that could be introduced when comparing groups that differ in prognostic factors.
External Validity
The sponsor’s reimbursement request aligns with the Health Canada indication: in combination with platinum-doublet chemotherapy for the neoadjuvant treatment of adults with resectable NSCLC (tumours ≥ 4 cm or node-positive disease). The CheckMate 816 study only included patients with an ECOG PS of 0 or 1. The magnitude of benefit of nivolumab plus chemotherapy in patients with an ECOG PS of 2 or higher is uncertain. The experts highlighted the need for patients to have a robust performance status before receiving nivolumab plus chemotherapy to mitigate the risk of treatment-related toxicity, which can occur during treatment and preclude patients from receiving surgery. Thus, patients with an ECOG PS of 0 or 1 are more likely to receive the treatment than those with an ECOG PS of 2 and higher. Further, they are less likely to have other comorbidities unrelated to the cancer that would place them at higher risk for AEs.
There were differences identified in baseline characteristics between the CheckMate 816 trial population and the patient population in Canada. The mean age of patients enrolled in the CheckMate 816 trial was younger (by 10 years) than in the NSCLC population in Canada. Further, more patients with stage IIIA disease than with stage IB or stage II disease were enrolled in the trial, which, according to the experts, is uncommon in Canadian practice. As highlighted by the experts, patients eligible for surgical resection in practice are at an earlier disease stage than those eligible in the trial (the majority of patients enrolled in the trial had stage IIIA disease). The study included only patients with an ECOG PS of 0 or 1 but, according to the experts, more patients with an ECOG PS of 2 or 3 are seen in current practice than in the trial. It was also noted by the experts that a higher proportion of patients with a PD-L1 expression level of at least 50% would be expected in practice than in the CheckMate 816 trial (in practice, the proportion of patients with a PD-L1 expression level of less than 1%, 1% to 49%, and 50% or more, according to the clinical experts, is about one-third for each category. These differences were considered unlikely to affect the generalizability of the CheckMate 816 trial findings to the Canadian population, according to the clinical experts.
The dosing of nivolumab in the reimbursement request aligns with the Health Canada indication.
Dose adjustments were allowed for chemotherapy drugs but not for nivolumab in the trial, which aligns with the Health Canada indication. The experts indicated that the flat-dose approach for nivolumab, as implemented in the CheckMate 816 trial, would be used in practice because of the convenience to patients and pharmacists, and to reduce drug wastage.
The clinical experts indicated that the current standard of care in Canada for resectable NSCLC is upfront surgery with curative intent, followed by adjuvant chemotherapy. Therefore, there is uncertainty in the magnitude of benefit derived from using nivolumab plus chemotherapy in the neoadjuvant setting for patients with resectable NSCLC in the absence of a comparator arm that included surgery followed by adjuvant chemotherapy or comparative studies that evaluate the relative effects of the treatment against surgery followed by adjuvant chemotherapy. Regardless, the clinical experts noted that the magnitude of benefit in EFS for nivolumab plus chemotherapy, as estimated by the postsurgery HR, was clinically meaningful compared to current outcomes observed in patients who receive upfront surgery in current practice.
The clinical experts agreed that the chemotherapy treatments and dosing schedules implemented in the CheckMate 816 trial align with treatments used in the adjuvant setting for NSCLC in Canada. Dose delays and dose discontinuations are anticipated for chemotherapy treatments, according to the experts; however, the experts mentioned that no dose adjustments would be performed for nivolumab, and that there is currently no evidence to support the use of nivolumab in the adjuvant setting for patients with resected NSCLC.
Of note, the specific chemotherapy drugs to be used in combination with nivolumab were not specified in the indication. It is uncertain whether the addition of nivolumab to chemotherapy drugs not included in the nivolumab plus chemotherapy arm of the trial (e.g., docetaxel and vinorelbine) or in the Canadian product monograph will result in benefits similar to those seen with the chemotherapy drugs used in the CheckMate 816 trial. There is therefore uncertainty about the generalizability of the findings to real-world practice with respect to the use of chemotherapies not included in the trial.
Efficacy outcomes investigated in the CheckMate 816 trial were considered to be appropriate by the clinical experts and were considered to be important to patients and clinicians and reflective of outcomes assessed in real-world practice. There is limited evidence on the correlation of EFS as a surrogate outcome for OS with its validation for use in the neoadjuvant setting for NSCLC by regulatory agencies. The clinical experts indicated that EFS was presumably used in the CheckMate 816 trial to incorporate progression that precluded surgery and surgical mortality following neoadjuvant treatment as meaningful end points. pCR has not been validated as a surrogate outcome for OS by Health Canada. The clinical experts cited studies that have reported a correlation between pCR and MPR with OS in neoadjuvant trials for NSCLC following the use of chemotherapy; however, there is limited literature on the correlation of pCR and MPR in trials with targeted therapy or immunotherapy.11
There were more follow-up procedures implemented in the CheckMate 816 trial than would be seen in real-world practice. Patients underwent more frequent assessments in the CheckMate 816 trial than are likely reflective of real-world practice. The clinical experts noted that patients in Canada are followed according to thoracic guidelines (i.e., every 6 months in the first year and annually thereafter, which may differ by practice and may depend on how late patients are in their follow-up schedule). The diagnostic methods and efficacy measurements implemented in the CheckMate 816 trial were considered appropriate by the experts. The assessment methods implemented in the trial were considered to be more reflective of academic than practice settings by the clinical experts, which may not be reflective of current Canadian practice guidelines, as patients would not be excluded from treatment if some of the procedures applied in the trial were not conducted. The clinical experts did not identify any major deviations in the diagnostic methods or assessment procedures that might have had an impact on eligibility criteria or that might have had an influence on the generalizability of the trial findings to current patient population in Canada.
Concomitant medications administered to patients in the trial were considered appropriate by the clinical experts. No significant discrepancies were identified that would have an impact on the trial outcomes or that would deviate from medications administered in real-world practice. Subsequent anticancer therapies administered during the trial were also considered appropriate.
Indirect Evidence
Objectives and Methods for the Summary of Indirect Evidence
The objective of this section is to summarize and critically appraise available indirect evidence comparing nivolumab plus platinum-doublet chemotherapy with other relevant treatments in patients with resectable, nonmetastatic NSCLC.
A focused literature search for ITCs dealing with NSCLC was run in MEDLINE All (1946–) on September 29, 2022. No search limits were applied. Titles, abstracts, and full-text articles were screened for inclusion based on the population, intervention, comparator, and outcome criteria outlined in the protocol for the CADTH review. No eligible ITCs were identified from the CADTH literature search.
Description of Indirect Comparison
The sponsor provided an NMA16 that assessed the efficacy and safety of neoadjuvant nivolumab plus chemotherapy relative to other relevant treatments, including neoadjuvant chemotherapy, neoadjuvant chemoradiotherapy, adjuvant chemotherapy, and surgery alone in patients diagnosed with resectable, nonmetastatic NSCLC.
Methods of Sponsor-Submitted ITC
Objectives
The objective of the sponsor-submitted ITC was to evaluate the efficacy and safety of neoadjuvant nivolumab plus chemotherapy relative to other relevant treatments, including neoadjuvant chemotherapy, neoadjuvant chemoradiotherapy, adjuvant chemotherapy, and surgery alone in patients with resectable, nonmetastatic NSCLC.
Study-Selection Methods
Based on the prespecified eligibility criteria outlined in Table 25, the sponsor conducted an SLR42 to identify studies investigating the efficacy and safety of current treatments for patients diagnosed with resectable, nonmetastatic NSCLC. The literature searches, last updated on April 1, 2022, were conducted in MEDLINE, Embase, and the Cochrane Central Register of Controlled Trials. The study screening and selection process was conducted by 2 independent reviewers, and disagreement was resolved by consultation with a third reviewer. Data were extracted by 1 reviewer and verified by a second reviewer. Risk-of-bias assessment was carried out on the recommendations from the National Institute for Health and Care Excellence (NICE) Single Technology Appraisal and Highly Specialised Technologies Evaluation: User Guide for Company Evidence Submission Template.43 From the evidence base created from the SLR, the sponsor identified studies that were eligible for an ITC based on a set of additional criteria, listed in Table 25.
ITC Analysis Methods
An NMA using the Bayesian approach was conducted, and reporting of the NMA generally followed guidance for the PRISMA (Table 26).
For each outcome examined in the NMA, random-effects and fixed-effects models were run. The random-effects model was considered by the sponsor to be the default model. However, the fixed-effects model was selected by the sponsor for all analyses in the NMA because of the sparseness of the network, which was not able to estimate the between-study SD with enough precision. Deviance information criterion was also used to determine model fit, with a lower deviance information criterion indicating a relative improvement in model fit. The sponsor was not able to assess consistency between the direct and indirect evidence because of a lack of closed loops in the network. Convergence was assessed by the monitoring of plots.
The primary outcomes of interest were EFS and OS. Secondary outcomes of interest included TTLRR, TTDM, pCR, and safety outcomes. Of note, the OS data from the sponsor-conducted CheckMate 816 trial was based on an immature data cut-off date.
In addition to the stage-agnostic network, which included studies regardless of the staging of the patient population, the network for each outcome was stratified by tumour staging (i.e., stage IB or II, stage IIIA, and stage IIIA N2). The base-case analysis for each outcome in the NMA synthesized evidence from patients who were deemed candidates for surgery and received third-generation platinum-based doublet chemotherapy. Sensitivity analyses were also carried out for each outcome whenever data were available. These sensitivity analyses involved second-generation platinum-based chemotherapies, the population of resected patients, data stratified by PD-L1 expression level (i.e., ≥ 1% versus < 1%), and data from the ITT population of the CheckMate 816 trial instead the subpopulations of the CheckMate 816 trial (i.e., stage IB or II, stage IIIA, and stage IIIA N2) used in the base-case stage-specific networks.
Results of Sponsor-Submitted NMA
Summary of Included Studies
Of the 59 RCTs identified from the SLR,42 23 met the inclusion criteria (Table 25) for the sponsor-submitted NMA.16 Of those, 8 were included in the base-case analyses, 5 additional RCTs were included in the sensitivity analyses involving second-generation chemotherapies, and 4 additional RCTs were included in the sensitivity analyses expanded to capture patients who had undergone resection. With respect to the 6 RCTs that met the NMA inclusion criteria but were not analyzed in the NMA, the sponsor claimed that 2 RCTs (i.e., 1 evaluating postadjuvant atezolizumab and 1 evaluating postadjuvant pembrolizumab) would be included in exploratory analyses in a separate report. However, the sponsor confirmed later that, to date, the exploratory analyses were not available. The remaining 4 RCTs were not involved in any analysis as they included patients who had undergone complete resection and investigated a second-generation chemotherapy or the combination of tegafur plus uracil, which was relevant only to the population in Japan.
Table 27, Table 28, and Table 29 present study characteristics, patient characteristics, and tumour staging information, respectively, for the RCTs included in the base-case analyses in the sponsor-submitted NMA. Of note, the inclusion and exclusion criteria for the patient populations in the 8 included RCTs were not explicitly stated in the NMA report. In addition, according to the clinical experts consulted by CADTH, the proportion of male participants in the included RCTs was higher than would be seen in real-world clinical practice. Furthermore, no information on the modalities used to stage the tumour was provided.
Table 25: Study-Selection Criteria and Methods for SLR and ITCs
Characteristic | Sponsor-submitted SLR | Sponsor-submitted ITC |
|---|---|---|
Population |
|
|
Intervention and/or comparators |
|
|
Outcome |
|
|
Study design |
| RCTs |
Restriction |
| Same as for the SLR |
Search strategy |
| Same as for the SLR |
Selection process |
| Same as for the SLR |
Data-extraction process |
| Same as for the SLR |
Quality assessment | Assessed based on recommendations from the NICE Single Technology Appraisal and Highly Specialised Technologies Evaluation: User Guide For Company Evidence Submission Template43 | Same as for the SLR |
ALK = anaplastic lymphoma kinase; BSC = best supportive care; CR = complete response; DFS = disease-free survival; EFS = event-free survival; EGFR = epidermal growth factor receptor; HRQoL = health-related quality of life; ITC = indirect treatment comparison; MPR = major pathologic response; NICE = National Institute for Health and Care Excellence; nmNSCLC = nonmetastatic non–small cell lung cancer; OS = overall survival; pCR = pathologic complete response; PD = progressive disease; PFS = progression-free survival; PR = partial response; RCT = randomized controlled trial; RFS = recurrence-free survival; S-1 = tegafur, gimeracil, and oteracil; SLR = systematic literature review; UFT = tegafur and uracil.
aBased on study designs in which patients were enrolled before surgery with the intention of surgical resection.
bIn trials that include other stages (i.e., stage IA or stage IIIB), no more than 20% of the trial population could represent stages that were not of interest, otherwise such trials were ineligible. Of note, although the CheckMate 816 population was restricted to patients with stage IB disease and tumour sizes ≥ 4 cm, this criterion was not applied to the population, intervention, control, and outcomes study design (PICOS), as this was not consistently reported across trials.
cTo address the objectives of treatment patterns, patients receiving BSC or no treatment at all are included.
dTargeted therapies include oncogene-targeted therapies, such as tyrosine kinase inhibitors and drugs like bevacizumab.
eFirst-generation-based chemotherapies were included if they were used in the neoadjuvant setting.
fCisplatin or carboplatin in combination with gemcitabine, vinorelbine, paclitaxel, docetaxel, or pemetrexed. Note that if a trial arm included a mix of treatments (e.g., third- and second-generation platinum-based chemotherapies), at least 80% of the patients in the trial had to have received third-generation platinum-based chemotherapies for the study to be included in the base-case analysis).
gIn studies involving neoadjuvant chemotherapy or neoadjuvant chemoradiotherapy (including, for example, neoadjuvant chemotherapy and surgery), the additional administration of postsurgical chemotherapy and/or radiotherapy was permitted. Postsurgical chemotherapy and/or radiotherapy could differ across treatment arms if administered to only a subset of patients (e.g., postsurgical chemotherapy given to patients who responded to neoadjuvant chemotherapy, or chemotherapy and/or radiotherapy given to patients with an R1 or R2 resection). However, if protocol-defined chemotherapy and/or radiotherapy was administered to all patients, irrespective of surgical outcome or response to initial therapy, the same postsurgical regimen must have been used in all relevant trial arms being compared, otherwise such trials were ineligible.
hCisplatin or carboplatin in combination with the following second-generation therapies: ifosfamide, mitomycin, vindesine, vinblastine, and etoposide. Note that if a trial included a mix of treatments (e.g., second- and first-generation platinum-based chemotherapies), at least 80% of the patients in the trial had to have received second- or third-generation platinum-based chemotherapies for the study to be included in the sensitivity analysis). All other trials (e.g., trials enrolling > 20% of patients who received first-generation platinum-based chemotherapies) were excluded.
iFirst-generation chemotherapies include methotrexate, cyclophosphamide, vincristine, and doxorubicin.
jLocoregional recurrences and distant metastases were not included in the PICOS of the SLR that informed the NMA (although these data were extracted, when available); however, given their relevance to the cost-effectiveness analysis, these outcomes were included in the NMA PICOS.
Sources: Sponsor SLR and ITC report.16,42
Table 26: ITC Analysis Methods
Variable | Sponsor-submitted ITC |
|---|---|
ITC methods | |
Priors | Vague priors were used for all parameters except the prior distribution of the between-study SD in the random-effects model. An informative prior was considered if the evidence base was insufficient to estimate the vague prior’s posterior distribution with enough precision to deem the results informative. Informed priors were defined based on the posterior of the between-study SD obtained from a vague prior from the largest available network across all base-case and sensitivity analyses conducted. |
Assessment of model fit |
|
Assessment of consistency | Not performed because of a lack of closed loops in the network. |
Assessment of convergence | For each model, analyses were based on 3 chains, and a total of 100,000 simulations were run for each chain. The 20,000 of those determined to be burn-in simulations (i.e., simulations before convergence of the model) were discarded. The number of simulations was increased when the chains were slow to converge. Convergence was assessed by the monitoring of plots. |
Outcomes |
|
Base-case analysis | Analyses of patients deemed to be candidates for surgery and who received third-generation platinum-based doublet chemotherapies |
Subgroup analysis |
|
Sensitivity analysis |
|
Methods for pairwise meta-analysis | Pairwise meta-analysis was conducted using the frequentist approach with the R package “meta” which used the inverse variance approach for pooling and the DerSimonian-Laird method for estimating between-study variance |
DFS = disease-free survival; DIC = deviance information criterion; EFS = event-free survival; ITC = indirect treatment comparison; NICE = National Institute for Health and Care Excellence; NMA = network meta-analysis; OS = overall survival; pCR = pathologic complete response; PD-L1 = programmed cell death 1 ligand 1; PFS = progression-free survival; PRISMA = Preferred Reporting Items for Systematic Reviews and Meta-Analyses; RFS = relapse-free survival; SD = standard deviation; TTDM = time to death or distant metastases; TTLRR = time to locoregional recurrence.
Source: Sponsor ITC Report.16
Table 27: Study Characteristics for Base-Case Analysis in the Sponsor-Submitted NMA
Study | Total N | Intervention and/or comparator | Phase | Blinding method | Median follow-up, years (IQR) | Notes |
|---|---|---|---|---|---|---|
CheckMate 81634 | 358 | Neoadjuvant chemotherapy, neoadjuvant nivolumab in combination with chemotherapy | III | Open-label | 2.5 (NR) | — |
NATCH45 | 619 | Surgery alone, neoadjuvant chemotherapy, adjuvant chemotherapy | III | Open-label | 4.2 (NR) | — |
CHEST46 | 270 | Neoadjuvant chemotherapy, surgery alone | III | NR | 2.6 to 3.3 | Stopped early due to positive results |
SWOG S990047 | 337 | Neoadjuvant chemotherapy, surgery alone | III | Open-label | 5.3 (NR) | — |
Li (2009)48 | 56 | Neoadjuvant chemotherapy, surgery alone | III | Open-label | 3.2 (NR) | Prematurely terminated due to slow accrual |
IFCT 010149 | 46 | Neoadjuvant chemotherapy, neoadjuvant chemoradiotherapy, neoadjuvant chemoradiotherapya | II | Open-label | 2.6 (NR) | Prematurely terminated due to slow accrual |
WJTOG 990350 | 60 | Neoadjuvant chemotherapy, neoadjuvant chemoradiotherapy | III | NR | 5.1 (NR) | Prematurely terminated due to slow accrual |
SAKK 16/0051 | 232 | Neoadjuvant chemotherapy, neoadjuvant chemoradiotherapy | III | Open-label | 4.4 (NR) | — |
IQR = interquartile range; NMA = network meta-analysis; NR = not reported.
aIFCT 0101 involved 2 different regimens of induction chemoradiotherapy, which included a third cytotoxic drug (i.e., cisplatin and vinorelbine, carboplatin and paclitaxel).
Source: Sponsor ITC Report.16
Table 28: Patient Characteristics for the Studies Included in the Base-Case Analysis in the Sponsor-Submitted NMA
Study | Regimen | Sample size | Median age (years) | Male (%) | Asian (%) | ECOG PS | Histology (%) | ||
|---|---|---|---|---|---|---|---|---|---|
0 (%) | 1 (%) | SC | NSC | ||||||
CheckMate 81634 | Neoadjuvant chemotherapy | 179 | 65 | 71 | 52 | 65 | 35 | 53 | 47 |
Neoadjuvant nivolumab in combination with chemotherapy | 179 | 64 | 72 | 48 | 69 | 31 | 49 | 51 | |
NATCH45 | Surgery | 210 | 64 | 88 | NR | 49a | 50a | 50 | 50b |
Neoadjuvant chemotherapy | 199 | 65 | 88 | NR | 44a | 54a | 54 | 46b | |
Adjuvant chemotherapy | 210 | 64 | 86 | NR | 45 | 53 | 49 | 51b | |
CHEST46 | Neoadjuvant chemotherapy | 129 | 61 | 78 | NR | 74 | 26 | 37 | 63b |
Surgery | 141 | 63 | 89 | NR | 70 | 30 | 45 | 55b | |
SWOG S990047 | Neoadjuvant chemotherapy | 169 | 65 | 64 | < 1 | 66 | 34 | 34 | 66b |
Surgery | 168 | 64 | 68 | < 1 | 63 | 37 | 42 | 58b | |
Li (2009)48 | Neoadjuvant chemotherapy | 28 | 56 | 68 | 100 | 36 | 64 | 36 | 64b |
Surgery | 28 | 62 | 61 | 100 | 29 | 71 | 29 | 71b | |
IFCT 010149 | Neoadjuvant chemotherapy | 14 | 56 | 64 | NR | 71 | 29 | 57 | 43b |
Neoadjuvant chemoradiotherapy | 17 | 88 | NR | 82 | 18 | 41 | 59b | ||
Neoadjuvant chemoradiotherapy | 15 | 87 | NR | 73 | 27 | 60 | 40b | ||
WJTOG 990350 | Neoadjuvant chemotherapy | 29 | 57 | 66 | 100 | NR | NR | 28 | 72b |
Neoadjuvant chemoradiotherapy | 31 | 58 | 68 | 100 | NR | NR | 16 | 84b | |
SAKK 16/0051 | Neoadjuvant chemoradiotherapy | 117 | 60 | 67 | NR | 71 | 29 | 36 | 64b |
Neoadjuvant chemotherapy | 115 | 59 | 67 | NR | 69 | 31 | 31 | 69b | |
ECOG PS = Eastern Cooperative Oncology Group Performance Status; NMA = network meta-analysis; NR = not reported; NSC = nonsquamous cell; SC = squamous cell.
aNATCH was the only study that included patients with an ECOG PS of 2 (although the number was < 1%).
bThe sponsor inferred nonsquamous cell histology from the proportion of patients with squamous cell histology.
Source: Sponsor ITC Report.16
Table 29: Staging Information for the Studies Included in the Base-Case Analysis in the Sponsor-Submitted NMA
Study | Eligible stage | TNM staging system | Clinical stage (%)a | Nodal status (%) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
IA | IB | IIA | IIB | IIIA | N0 | N1 | N2 | |||
CheckMate 81634 | IB (TS > 4 cm) to IIIA | AJCC 7th | < 1 | 5 | 17 | 13 | 64 | NR | NR | NR |
NATCH45 | IA (TS > 2 cm) to II (T3N1) | AJCC 6th | 11 | 64 | 1 | 22 | 1 | 85 | 15 | 0 |
CHEST46 | IB to II (T3N1) | AJCC 5th | 2 | 47 | 4 | 44 | 3 | 49 | 51 | 0 |
SWOG S990047 | IB to II (T3N1) | AJCC 5th | 0 | 68 (IB to IIA) | 33 (IIB to IIIA) | NR | NR | 0 | ||
Li (2009)48 | IIIA | ISS (1997) | 0 | 0 | 0 | 0 | 100 | 0 | 23 | 77 |
IFCT 010149 | IIIA N2 | ISS (1997) | 0 | 0 | 0 | 0 | 100 | 0 | 0 | 100 |
WJTOG 990350 | IIIA N2 | AJCC 6th | 0 | 0 | 0 | 0 | 100 | 0 | 0 | 100 |
SAKK 16/0051 | IIIA N2 | AJCC 6th | 0 | 0 | 0 | 0 | 100 | 0 | 0 | 100 |
AJCC = American Joint Committee on Cancer; ISS = International Staging System; N = number of nearby lymph nodes that have cancer; NMA = network meta-analysis; NR = not reported; TMN = tumour, node, and metastasis; TS = tumour size.
aThese data may not add to 100% due to rounding.
Source: Sponsor ITC Report.16
In terms of the risk of bias in the 8 RCTs included in the base-case analysis, the sponsor reported that 2 studies46,49 had a high risk of bias in baseline similarity and all had a high risk of bias in blinding. In addition, the sponsor determined that some included studies failed to provide adequate information on the method of randomization and allocation concealment46-50 and the imbalanced drop out rates.48,49
Several potential sources of heterogeneity were noted in the 8 studies included in the base-case analysis in the sponsor-submitted NMA, including differences in the proportion of male participants (range, 61% to 89%), regimen characteristics (e.g., cisplatin-based versus carboplatin-based regimens, 2 versus 3 treatment cycles, concurrent versus sequential radiotherapy), squamous histology (range, 16% to 60%), and tumour staging (IB to IIIA).
Efficacy Results of the Sponsor-Submitted ITC
As mentioned previously, the sponsor ran both the random-effects model and the fixed-effects model for each outcome in the NMA, and considered the random-effects model to be the default. However, the fixed-effects model was selected by the sponsor for all analyses in the NMA because of the sparseness of the network, which was not able to estimate the between-study SD with enough precision.
Moreover, in this section, we present the stage-agnostic and stage-specific results from the base-case analyses (i.e., analyses of patients deemed to be candidates for surgery and who received third-generation platinum-based doublet chemotherapy) and sensitivity analyses, including analyses of patients deemed to be candidates for surgery and who received third- or second-generation chemotherapies, analyses of patients deemed to be candidates for surgery or who had already undergone tumour resection and third-generation chemotherapy, as well as analyses of patients with stage-agnostic disease deemed to be candidates for surgery who had received third-generation chemotherapies and were stratified by PD-L1 expression level (≥ 1% versus < 1%).
Event-Free Survival
The evidence networks for EFS in the base-case analyses in the sponsor-submitted NMA are displayed in Figure 9, Figure 10, Figure 11, and Figure 12.
Stage-agnostic and stage-specific network estimates for EFS HRs are shown in Table 30. In the base-case analyses, for the 1,978 patients with stage-agnostic disease, neoadjuvant nivolumab in combination with chemotherapy led to a significantly lower risk of an event (i.e., EFS HR < 1 and CrI excluding 1) than neoadjuvant chemotherapy, adjuvant chemotherapy, and surgery alone. For the 284 patients with the stage IIIA NSCLC, those who received neoadjuvant nivolumab in combination with chemotherapy had a significantly lower risk of an event than those who received neoadjuvant chemotherapy or surgery alone. For the 566 patients with stage IIIA N2 NSCLC, there was a significantly lower risk of an event in those receiving neoadjuvant nivolumab in combination with chemotherapy than in those receiving neoadjuvant chemoradiotherapy or neoadjuvant chemotherapy. However, for patients with stage IB to II NSCLC, there was no significant difference in EFS between neoadjuvant nivolumab plus chemotherapy and neoadjuvant chemotherapy, adjuvant chemotherapy, or surgery alone.
Results of stage-agnostic and stage-specific networks from the sensitivity analyses were generally consistent with those from the base-case analyses, except in the stage-agnostic network of the sensitivity analyses that involved patients with a PD-L1 expression level below 1%, there were no significant differences in EFS between neoadjuvant nivolumab plus chemotherapy and neoadjuvant chemotherapy, adjuvant chemotherapy, or surgery alone.
Figure 9: Network Diagram for the Base-Case Analysis in the Sponsor-Submitted NMA (EFS for Patients With Stage-Agnostic Disease)
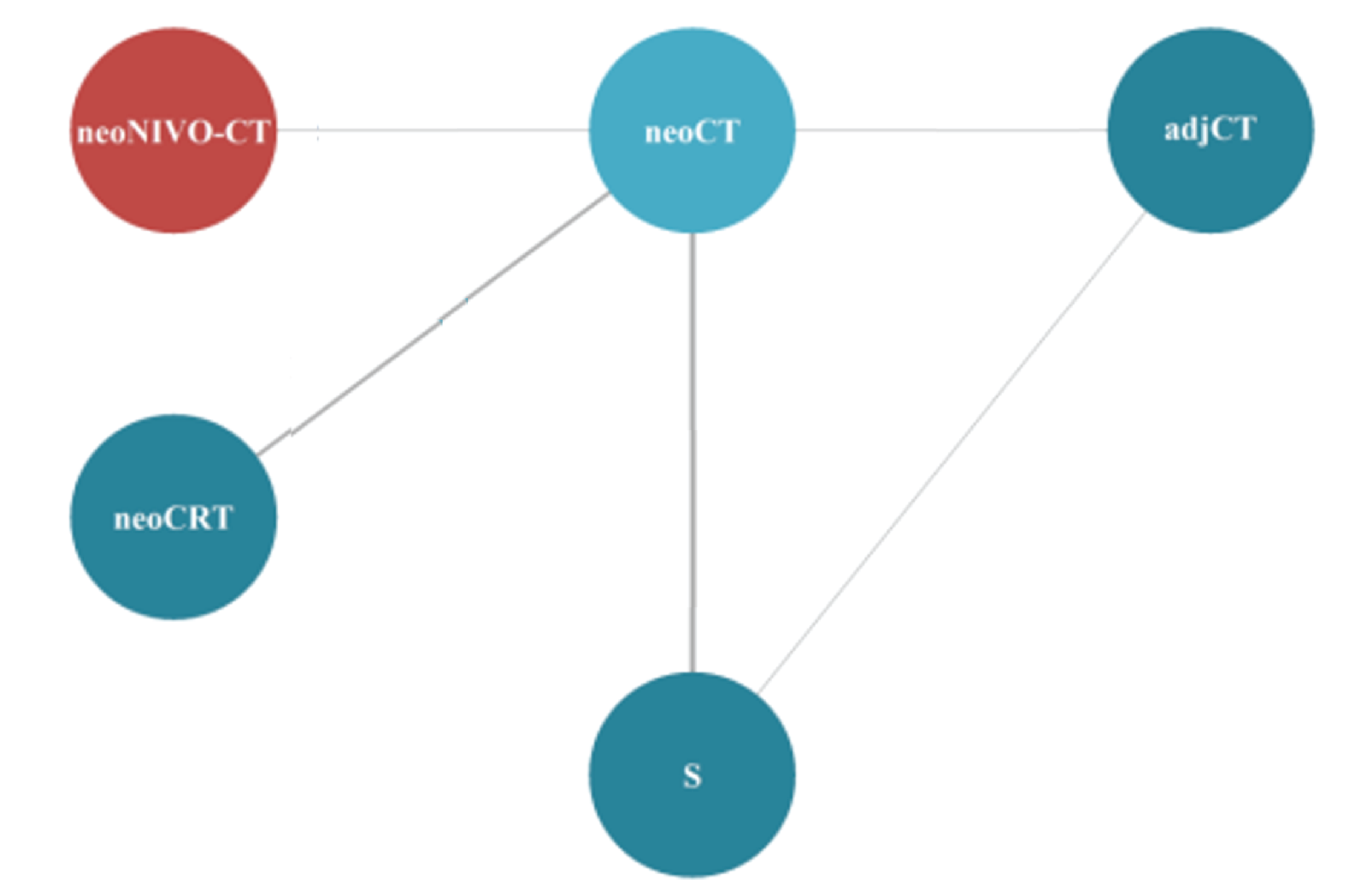
adjCT = adjuvant chemotherapy; EFS = event-free survival; neoCRT = neoadjuvant chemoradiotherapy; neoCT = neoadjuvant chemotherapy; neoNIVO-CT = neoadjuvant nivolumab in combination with chemotherapy; NMA = network meta-analysis; S = surgery.
Source: Sponsor ITC Report.16
Figure 10: Network Diagram for the Base-Case Analysis in the Sponsor-Submitted NMA (EFS for Patients With Stage IB to II Disease)
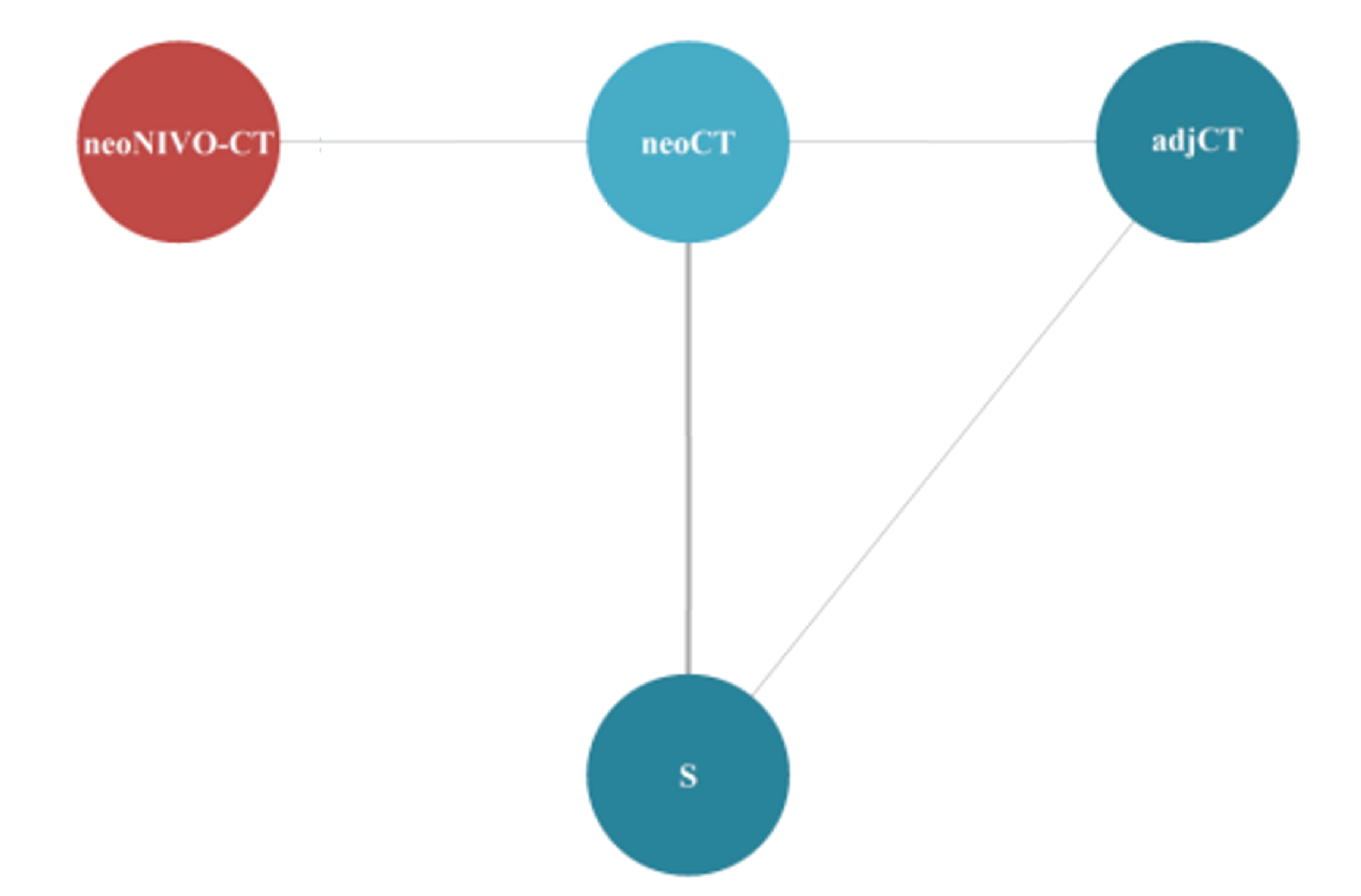
adjCT = adjuvant chemotherapy; EFS = event-free survival; neoCT = neoadjuvant chemotherapy; neoNIVO-CT = neoadjuvant nivolumab in combination with chemotherapy; NMA = network meta-analysis; S = surgery.
Source: Sponsor ITC Report.16
Figure 11: Network Diagram for the Base-Case Analysis in the Sponsor-Submitted NMA (EFS for Patients With Stage IIIA Disease)
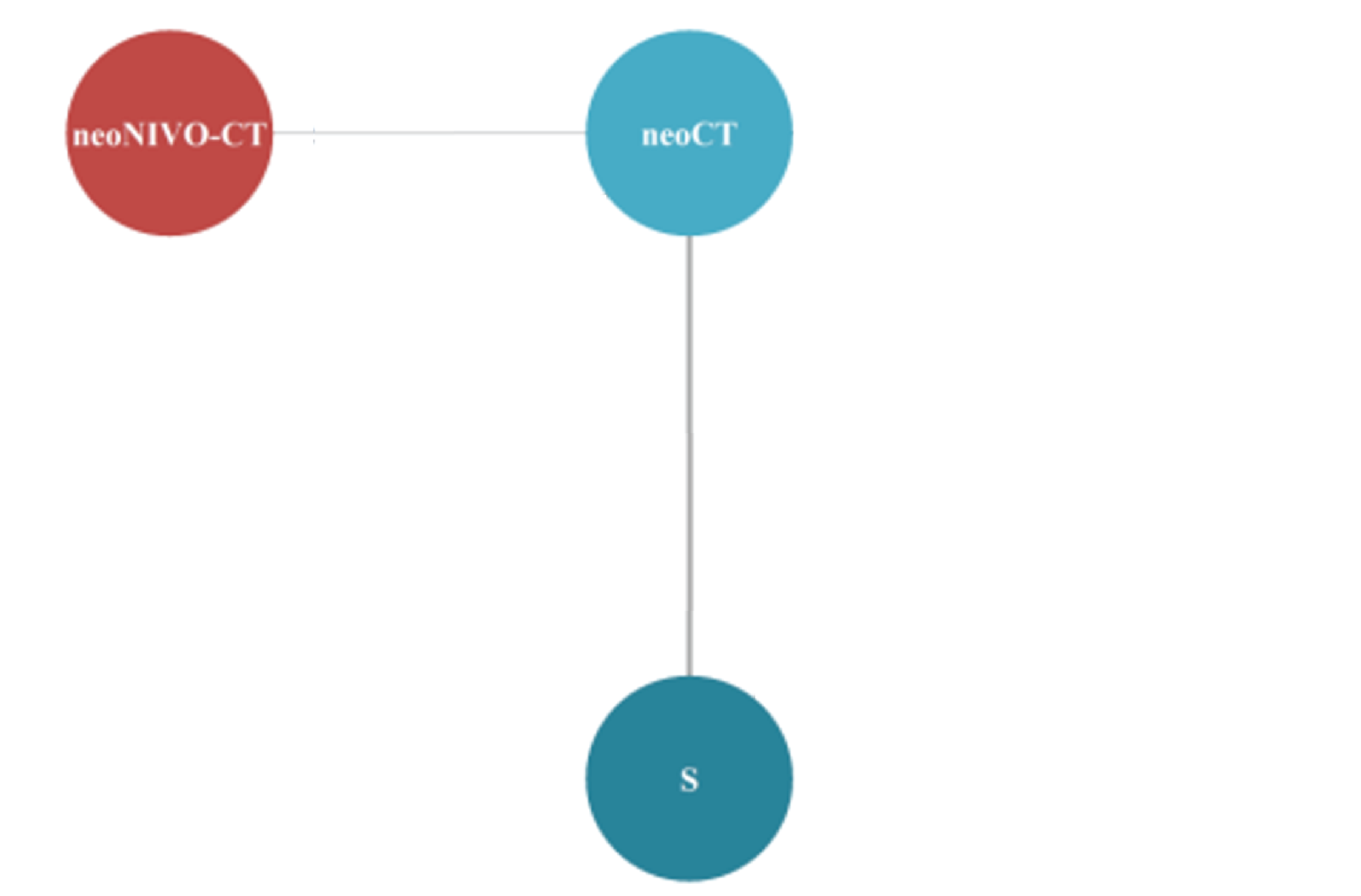
EFS = event-free survival; neoCT = neoadjuvant chemotherapy; neoNIVO-CT = neoadjuvant nivolumab in combination with chemotherapy; NMA = network meta-analysis; S = surgery.
Source: Sponsor ITC Report.16
Figure 12: Network Diagram for the Base-Case Analysis in the Sponsor-Submitted NMA (EFS for Patients With Stage IIIA N2 Disease)
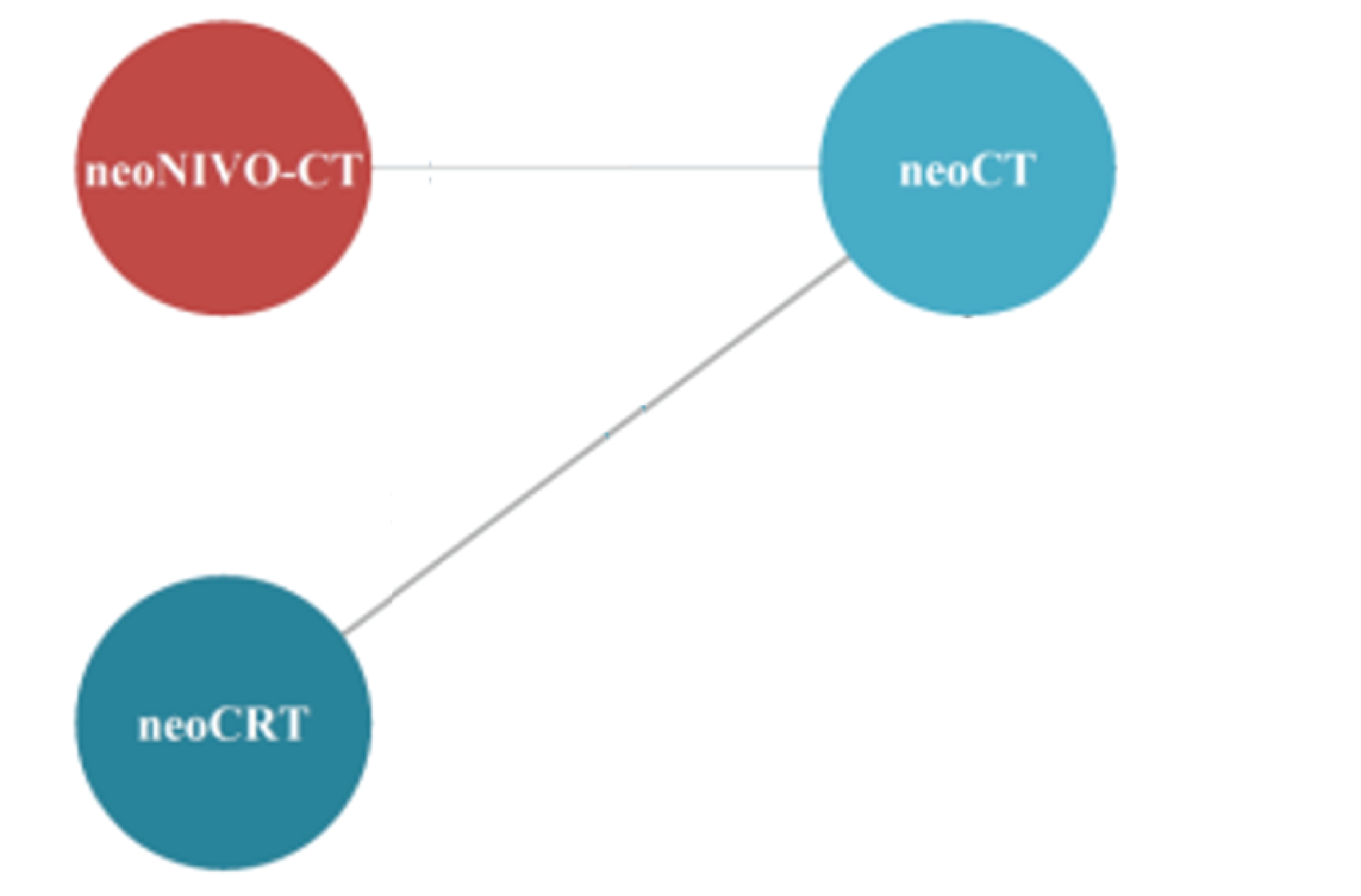
EFS = event-free survival; N = number of nearby lymph nodes that have cancer; neoCRT = neoadjuvant chemoradiotherapy; neoCT = neoadjuvant chemotherapy; neoNIVO-CT = neoadjuvant nivolumab in combination with chemotherapy; NMA = network meta-analysis.
Source: Sponsor ITC Report.16
|||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | ||||
|---|---|---|---|---|---|---|
|||| ||||||| ||||| | |||| ||||||| ||||| | |||||
|||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |||
||||| ||||||||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| |
|||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |
|||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |
|||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |
|||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |
||||| ||||| |||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| |
|||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |
|||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |
|||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |
||||| |||| |||||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| |
|||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |
|||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |
||||| |||| || |||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| |
|||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |
|||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |
|||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |||| ||||||| ||||| | |
Note: This table has been redacted at the request of the sponsor.
|||| ||||||| ||||||||| ||||||| ||||||||| ||||||| ||||||||| ||||||| ||||||||| ||||||| |||
Overall Survival
As data for OS were not mature in the sponsor-conducted CheckMate 816 trial, only the stage-agnostic network for the base-case analysis was available in the sponsor-submitted NMA (Figure 13), and the network estimates are presented in Table 31. Neoadjuvant nivolumab in combination with chemotherapy significantly reduced the risk of death, compared with neoadjuvant chemotherapy, adjuvant chemotherapy, and surgery alone. No significant difference was observed between neoadjuvant plus chemotherapy and neoadjuvant chemoradiotherapy.
Figure 13: Network Diagram for the Base-Case Analysis in the Sponsor-Submitted NMA (OS for Patients With Stage-Agnostic Disease)
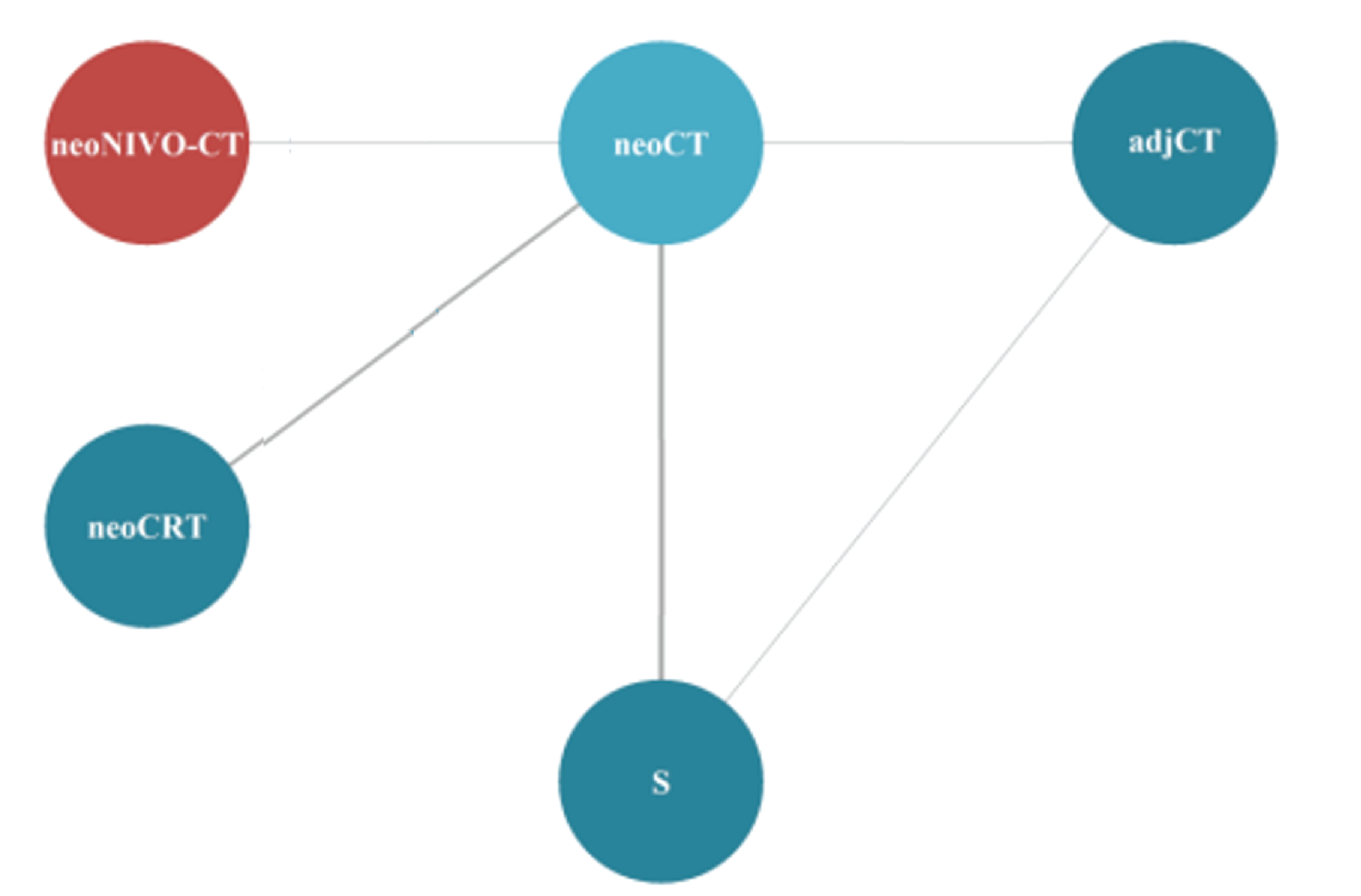
adjCT = adjuvant chemotherapy; neoCRT = neoadjuvant chemoradiotherapy; neoCT = neoadjuvant chemotherapy; neoNIVO-CT = neoadjuvant nivolumab in combination with chemotherapy; NMA = network meta-analysis; OS = overall survival; S = surgery.
Source: Sponsor ITC Report.16
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| |
|---|---|---|
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| |
||||||||||| ||||||| | ||||||||||| ||||||| | |
||||||||||| ||||||| | ||||||||||| ||||||| | |
||||||||||| ||||||| | ||||||||||| ||||||| | |
||||||||||| ||||||| | ||||||||||| ||||||| |
Note: This table has been redacted at the request of the sponsor.
Time to Locoregional Recurrence
The evidence networks for TTLRR in the base-case analyses in the sponsor-submitted NMA are presented in Figure 14, Figure 15, Figure 16, and Figure 17.
Network estimates of TTLRR HRs are presented in Table 32. Neoadjuvant nivolumab in combination with chemotherapy only had a significantly lower risk of locoregional recurrence than neoadjuvant chemotherapy in patients with stage IIIA and stage IIIA N2 disease in the base-case analyses.
Figure 14: Network Diagram for the Base-Case Analysis in the Sponsor-Submitted NMA (TTLRR for Patients With Stage-Agnostic Disease)
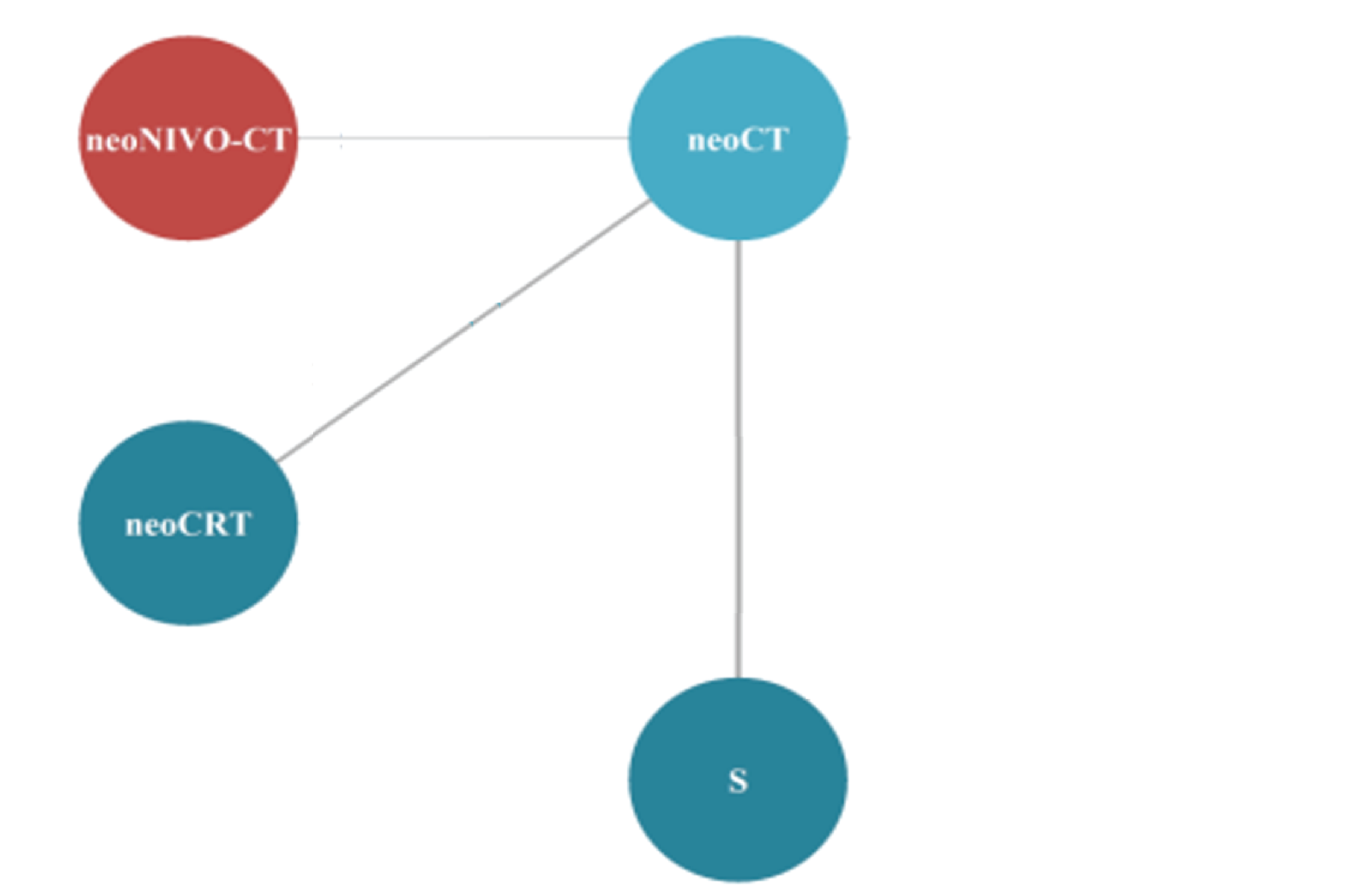
neoCRT = neoadjuvant chemoradiotherapy; neoCT = neoadjuvant chemotherapy; neoNIVO-CT = neoadjuvant nivolumab in combination with chemotherapy; NMA = network meta-analysis; S = surgery; TTLRR = time to locoregional recurrence.
Source: Sponsor ITC Report.16
Figure 15: Network Diagram for the Base-Case Analysis in the Sponsor-Submitted NMA (TTLRR for Patients With Stage IB to II Disease)
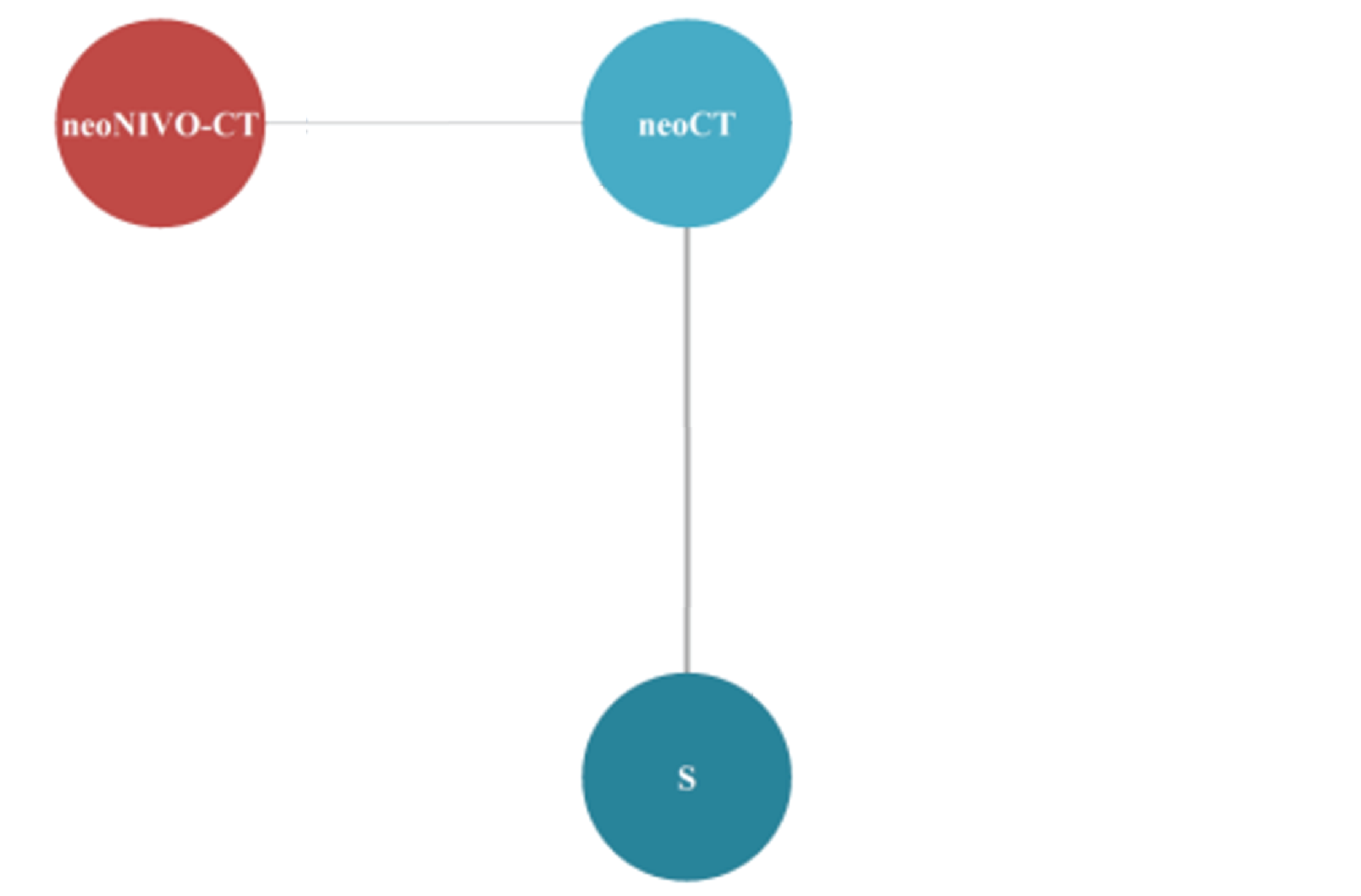
neoCT = neoadjuvant chemotherapy; neoNIVO-CT = neoadjuvant nivolumab in combination with chemotherapy; NMA = network meta-analysis; S = surgery; TTLRR = time to locoregional recurrence.
Source: Sponsor ITC Report.16
Figure 16: Network Diagram for the Base-Case Analysis in the Sponsor-Submitted NMA (TTLRR for Patients With Stage IIIA Disease)

neoCT = neoadjuvant chemotherapy; neoNIVO-CT = neoadjuvant nivolumab in combination with chemotherapy; NMA = network meta-analysis; TTLRR = time to locoregional recurrence.
Source: Sponsor ITC Report.16
Figure 17: Network Diagram for the Base-Case Analysis in the Sponsor-Submitted NMA (TTLRR for Patients With Stage IIIA N2 Disease)
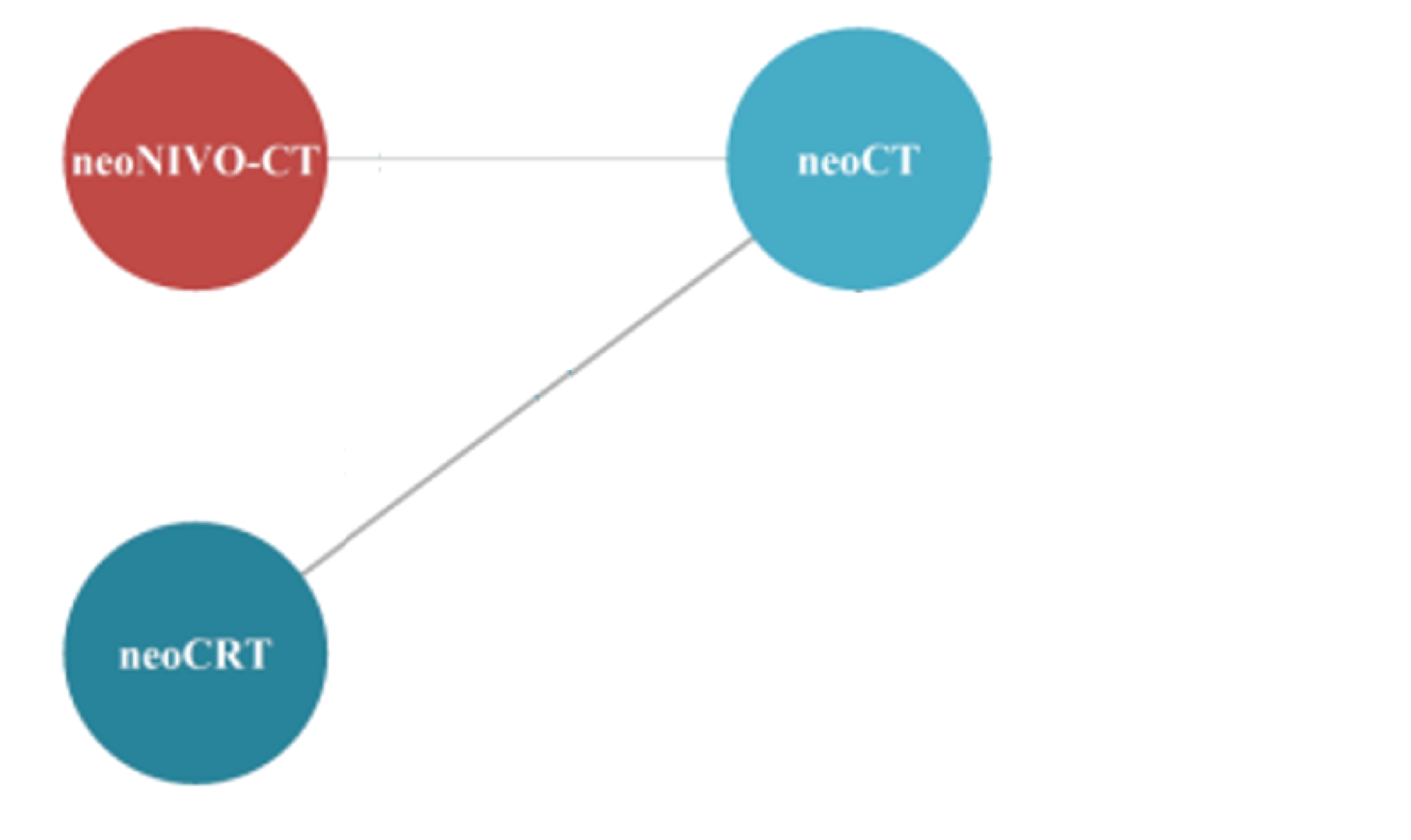
N = number of nearby lymph nodes that have cancer; neoCRT = neoadjuvant chemoradiotherapy; neoCT = neoadjuvant chemotherapy; neoNIVO-CT = neoadjuvant nivolumab in combination with chemotherapy; NMA = network meta-analysis; TTLRR = time to locoregional recurrence.
Source: Sponsor ITC Report.16
||||||||||| |||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||
|---|---|---|---|---|---|---|
||||||||||| ||||||| | ||||||||||| ||||||| | |||||
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | |||
||||||||||| |||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| |
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | |
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | |
||||||||||| |||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| |
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | |
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | |
||||||||||| |||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| |
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | |
||||||||||| |||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| |
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | |
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | |
Note: This table has been redacted at the request of the sponsor.
||||||| ||||||||| ||||||| ||||||||| ||||||| ||||||||| ||||||| ||||||||| ||||||| ||||||||| ||||||| ||||||||| ||||||| |||||16
Time to Death or Distant Metastases
The evidence networks for TTDM in the base-case analyses in the sponsor-submitted NMA are displayed in Figure 18, Figure 19, Figure 20, and Figure 21.
Network estimates for TTDM HRs are shown in Table 33. Neoadjuvant nivolumab in combination with chemotherapy significantly reduced the risk of distant metastases compared with neoadjuvant chemotherapy and surgery alone in patients with stage-agnostic disease in base-case analyses and sensitivity analyses. In addition, there were significant differences in TTDM between neoadjuvant nivolumab in combination with chemotherapy and adjuvant chemotherapy in the sensitivity analysis expanded to include patients who had undergone resection, as well as between neoadjuvant nivolumab in combination with chemotherapy and neoadjuvant chemoradiotherapy in the sensitivity analysis stratified by a PD-L1 expression level of at least 1%.
Figure 18: Network Diagram for the Base-Case Analysis in the Sponsor-Submitted NMA (TTDM for Patients With Stage-Agnostic Disease)
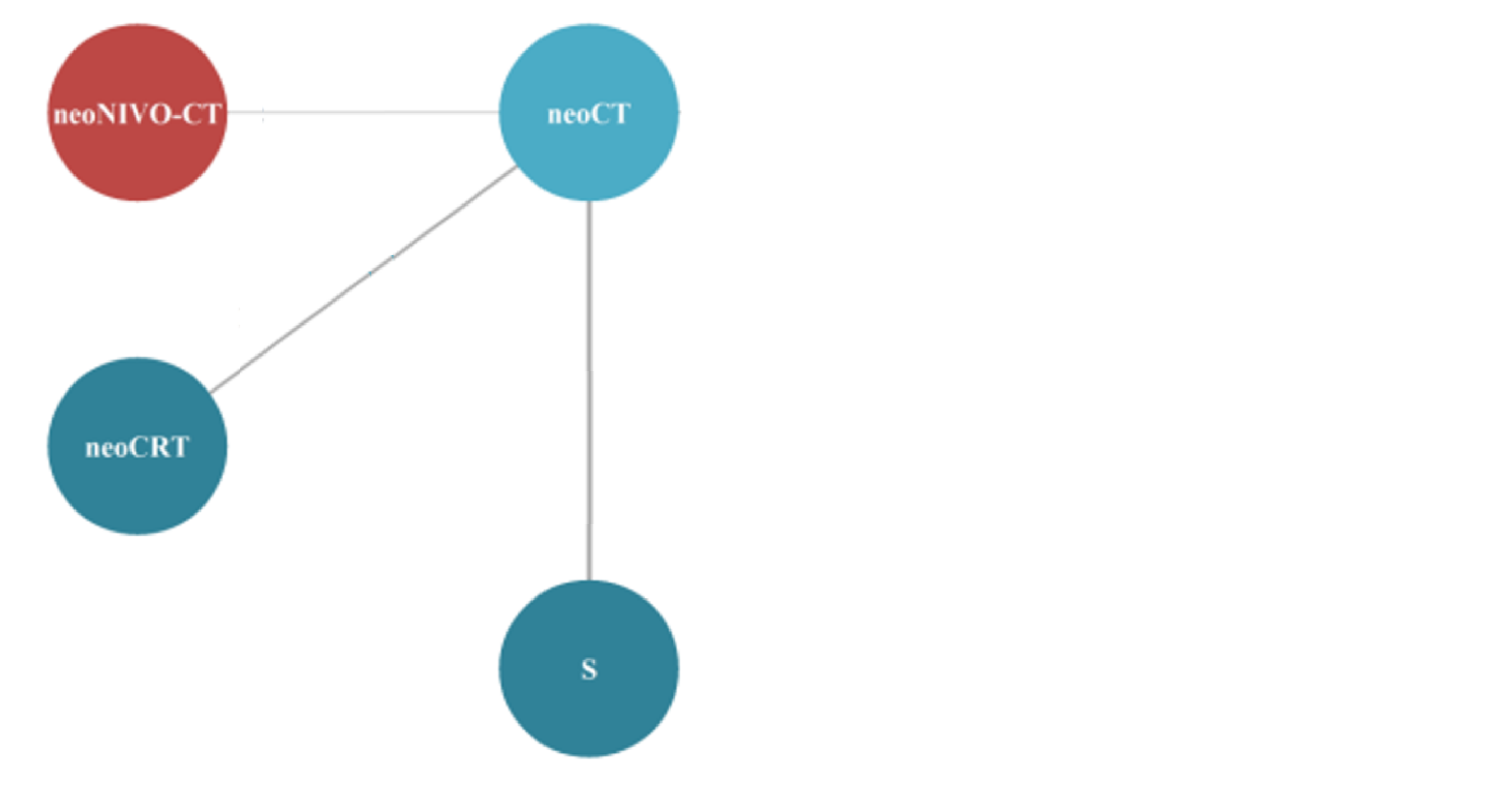
neoCRT = neoadjuvant chemoradiotherapy; neoCT = neoadjuvant chemotherapy; neoNIVO-CT = neoadjuvant nivolumab in combination with chemotherapy; NMA = network meta-analysis; S = surgery; TTDM = time to death or distant metastases.
Source: Sponsor ITC Report.16
Figure 19: Network Diagram for the Base-Case Analysis in the Sponsor-Submitted NMA (TTDM for Patients With Stage IB to II Disease)
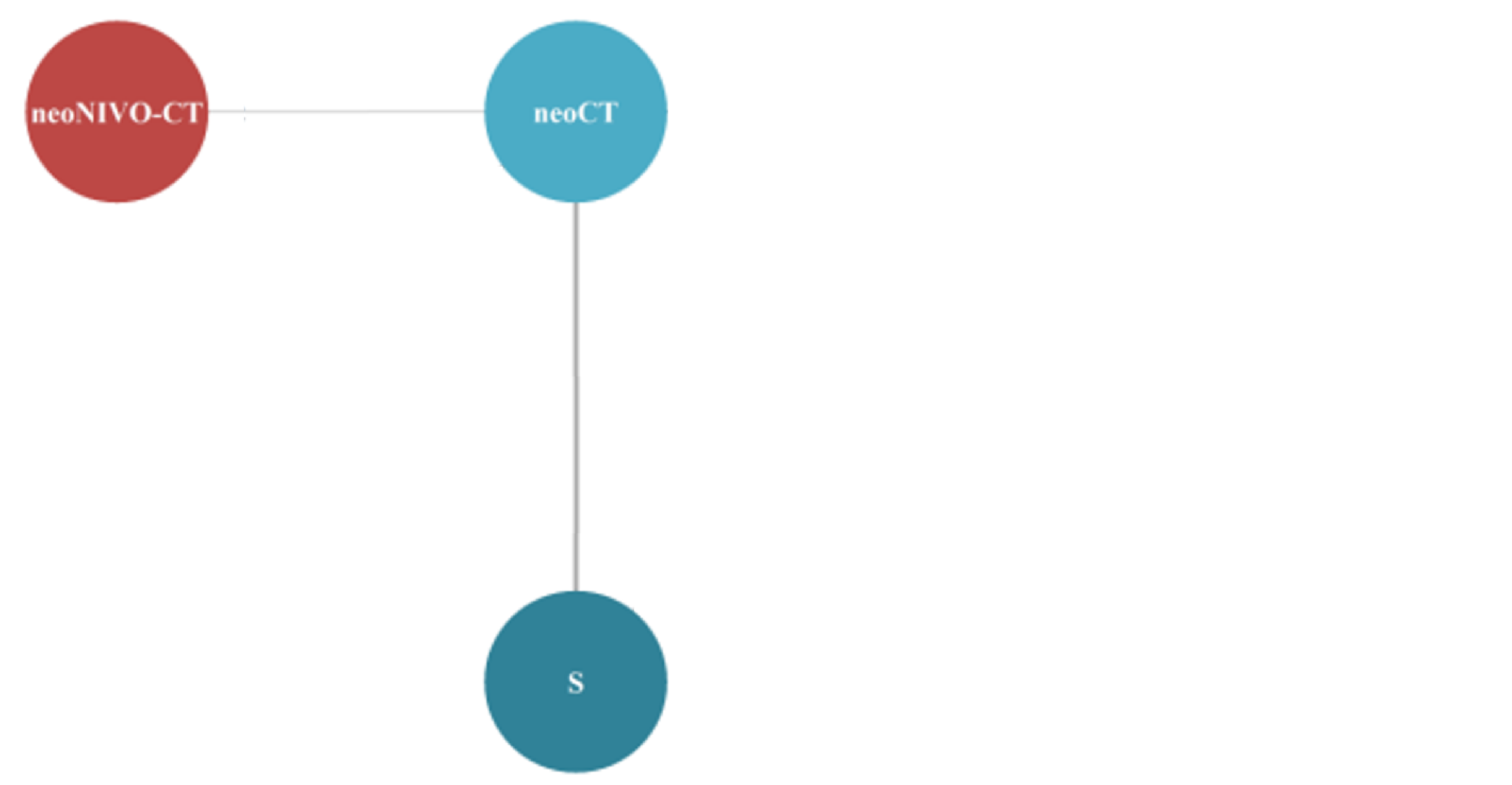
neoCT = neoadjuvant chemotherapy; neoNIVO-CT = neoadjuvant nivolumab in combination with chemotherapy; NMA = network meta-analysis; S = surgery; TTDM = time to distant death or metastases.
Source: Sponsor ITC Report.16
Figure 20: Network Diagram for the Base-Case Analysis in the Sponsor-Submitted NMA (TTDM for Patients With Stage IIIA Disease)

neoCT = neoadjuvant chemotherapy; neoNIVO-CT = neoadjuvant nivolumab in combination with chemotherapy; NMA = network meta-analysis; TTDM = time to death or distant metastases.
Source: Sponsor ITC Report.16
Figure 21: Network Diagram for the Base-Case Analysis in the Sponsor-Submitted NMA (TTDM for Patients With Stage IIIA N2 Disease)
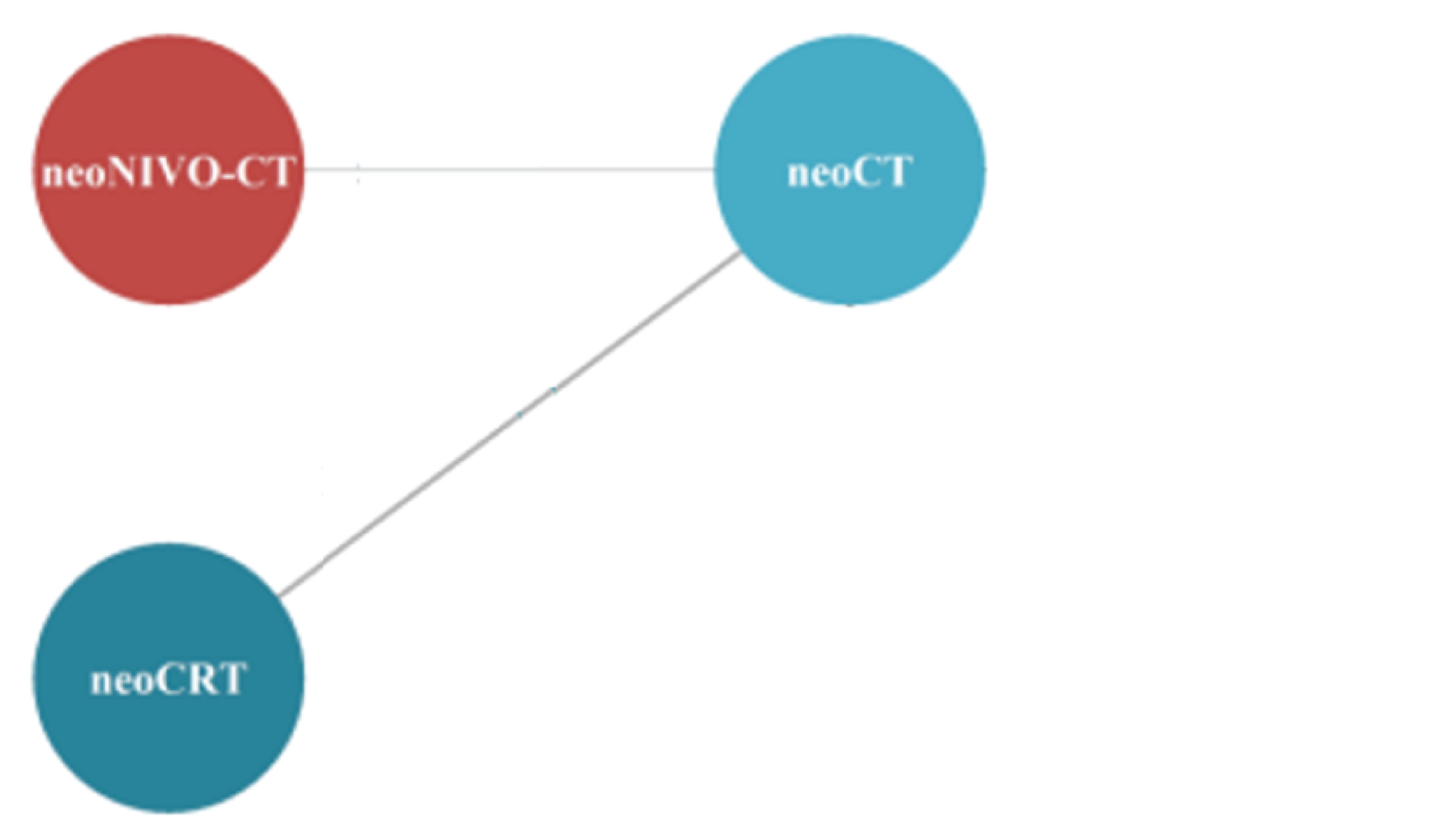
N = number of nearby lymph nodes that have cancer; neoCRT = neoadjuvant chemoradiotherapy; neoCT = neoadjuvant chemotherapy; neoNIVO-CT = neoadjuvant nivolumab in combination with chemotherapy; NMA = network meta-analysis; TTDM = time to death or distant metastases.
Source: Sponsor ITC Report.16
||||||||||| | | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||
|---|---|---|---|---|---|---|
||||||||||| ||||||| | ||||||||||| ||||||| | |||||
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | |||
||||||||||| ||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| |
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | |
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | |
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | |
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | |
||||||||||| || | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| |
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | |
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | |
||||||||||| || | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| |
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | |
||||||||||| | | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| |
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | |
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | |
Note: This table has been redacted at the request of the sponsor.
Source: ||||||| ||||||||| ||||||| ||||||||| ||||||| ||||||||| ||||||| ||||||||| ||||||| ||||||||| ||||||| |||||16
Pathologic Complete Response
The evidence networks for pCR in the base-case analyses in the sponsor-submitted NMA are displayed in Figure 22 and Figure 23.
Network estimates for pCR ORs are shown in Table 34. Patients who received neoadjuvant nivolumab in combination with chemotherapy were more likely to have a pCR of statistical significance than those who received neoadjuvant chemotherapy or neoadjuvant chemoradiotherapy in all available analyses, except in the sensitivity analysis of patients with a PD-L1 expression level below 1%, in which the effect estimate favoured neoadjuvant nivolumab in combination with chemotherapy over neoadjuvant chemoradiotherapy but without statistical significance.
Figure 22: Network Diagram for the Base-Case Analysis in the Sponsor-Submitted NMA (pCR for Patients With Stage-Agnostic and Patients With Stage IIIA N2 Disease)
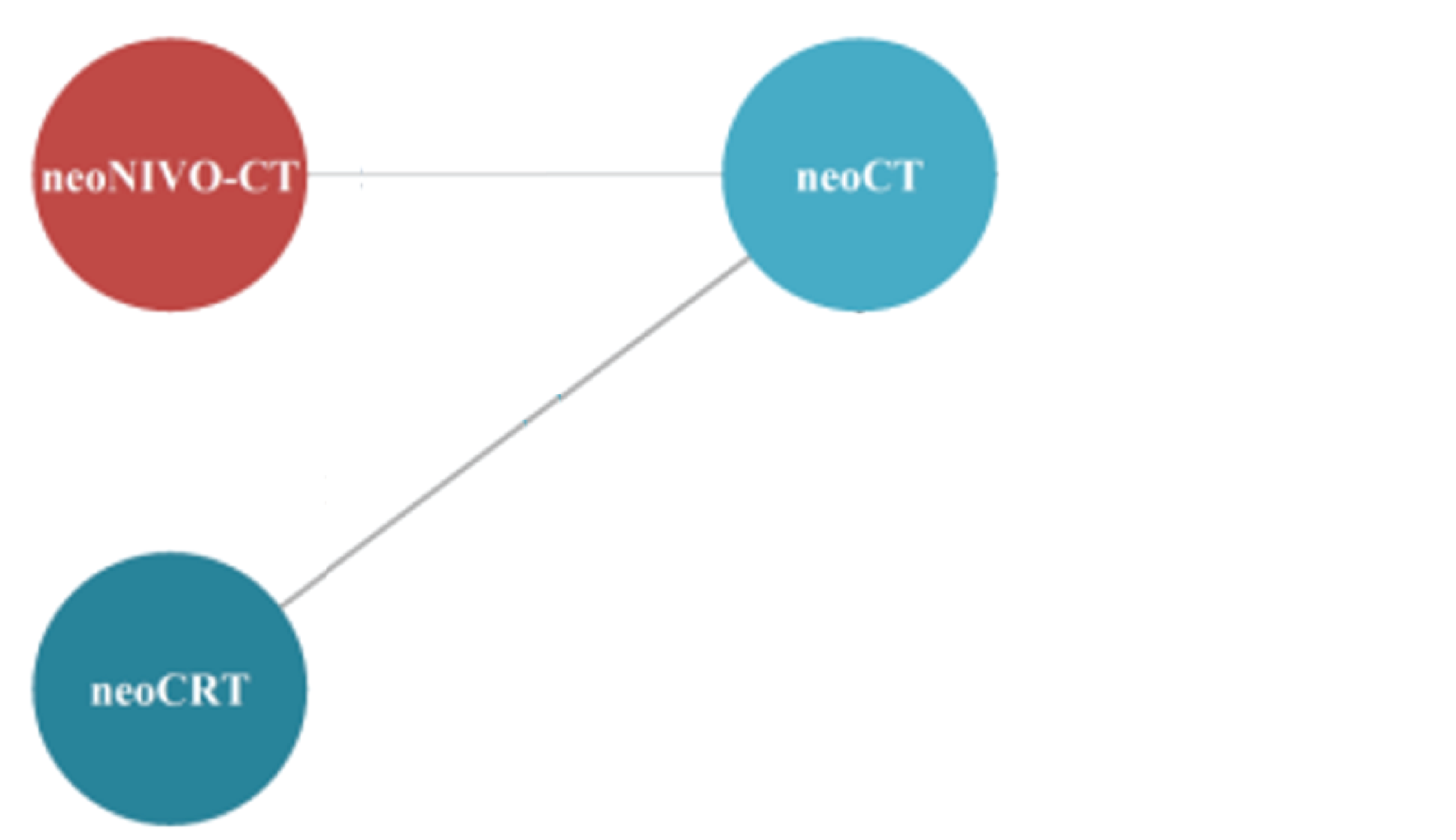
N = number of nearby lymph nodes that have cancer; neoCRT = neoadjuvant chemoradiotherapy; neoCT = neoadjuvant chemotherapy; neoNIVO-CT = neoadjuvant nivolumab in combination with chemotherapy; NMA = network meta-analysis; pCR = pathologic complete response.
Source: Sponsor ITC Report.16
Figure 23: Network Diagram for the Base-Case Analysis in the Sponsor-Submitted NMA (pCR for Patients With Stage IB to II and Patients With Stage IIIA Disease)

neoCT = neoadjuvant chemotherapy; neoNIVO-CT = neoadjuvant nivolumab in combination with chemotherapy; NMA = network meta-analysis; pCR = pathologic complete response.
Source: Sponsor ITC Report.16
||||||||||| ||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||
|---|---|---|---|---|---|---|
||||||||||| ||||||| | ||||||||||| ||||||| | |||||
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | |||
||||||||||| ||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| |
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | |
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | |
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | |
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | |
||||||||||| ||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| |
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | |
||||||||||| ||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| |
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | |
||||||||||| ||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| |
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | |
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | |
Note: This table has been redacted at the request of the sponsor.
Source: |||| ||||||| ||||||||| ||||||| ||||||||| ||||||| ||||||||| ||||||| ||||||||| ||||||| ||||||||| ||||||| ||||||||| ||||||| ||||||||| ||||||| |||||16
Harms Results of the Sponsor-Submitted ITC
The sponsor-submitted NMA34 was not able to quantitively synthesize evidence on safety outcomes, and provided a brief narrative description only. The reasons given by the sponsor were the sparseness of the data and the differences in treatment regimens across the base-case studies.
Critical Appraisal of the Sponsor-Submitted ITC
Overall, the SLR conducted by the sponsor to identify relevant studies for the NMA was methodologically sound. The sponsor used a comprehensive literature search strategy, performed study selection and data extraction in duplicate, assessed and reported the risk of bias appropriately, described the characteristics of the included studies, and narratively summarized the results in adequate detail. However, it was unclear whether the risk-of-bias assessment was carried out by a single assessor or by multiple assessors. The reporting of the sponsor-submitted NMA generally followed the PRISMA checklist.17 The sponsor explicitly stated the objectives, with reference to the participants, interventions, comparisons, outcomes, and study design of interest, and provided adequate detail in the methods, results, and discussion sections of the NMA.
Wide CrIs in the random-effects model often indicate the existence of a large degree of heterogeneity across studies and/or sparseness in the network. There are several notable sources of heterogeneity in the sponsor-submitted NMA, such as male domination (range, 61% to 89%), large variations in squamous histology (range, 16% to 60%), and tumour staging (IB to IIIA). According to the clinical experts consulted by CADTH, the heterogeneity in tumour staging for patients with stage-agnostic NSCLC was significant. And indeed, the efficacy results of neoadjuvant nivolumab in combination with chemotherapy for EFS by stage, for example, were inconsistent between patients with stage IB to II NSCLC and those with stage IIIA or stage IIIA N2 NSCLC (i.e., statistically significant versus nonsignificant), when compared with neoadjuvant chemotherapy in the base-case analysis. Given the significant differential treatment effects observed between patients with stage IB to II disease and those with stage IIIA or stage IIIA N2 NSCLC, the pooled ITC results from patients with stage-agnostic disease would be deemed significantly biased, and the pooling is inappropriate, methodologically, although neoadjuvant nivolumab in combination with chemotherapy significantly improved EFS compared with neoadjuvant chemotherapy, adjuvant chemotherapy, and surgery alone in patients with stage-agnostic NSCLC. The best practice in an ITC is, whenever possible, to apply a stratified analysis on the significant effect modifier to account for heterogeneity.
For each outcome examined in the NMA, random-effects models and fixed-effects models were run. The random-effects model was considered by the sponsor to be the default model. However, the fixed-effects model was later selected by the sponsor for all analyses in the NMA because of the sparseness of the network, which was not able to estimate between-study SDs with enough precision. Although it was considered appropriate to use the fixed-effects model instead of the random-effects model when the network was sparce, the fixed-effects model is not capable of capturing or accounting for heterogeneity because it assumes that variance is only derived from within-study variances, not from between-study variances.52 Furthermore, the fixed-effects model tends to generate a narrower CrI, which might also bias the results.
Misclassification of tumour stage using different versions of tumour classification criteria (i.e., TNM 5th edition, 6th edition, 7th edition, and the 1997 International Staging System) could have had an impact on the ITC estimation. A study53 that adopted the TNM 7th edition criteria to retrospectively reclassify 145 patients with NSCLC whose tumour stage was originally determined using the TNM 6th edition showed that the TNM 7th edition criteria for lung cancer shifted 49 of 145 patients (33.8%) to a higher or lower stage. In the sponsor-submitted NMA, of the 8 RCTs in the base-case analysis, the CheckMate 816 trial was the only study to use the TNM 7th edition classification; 2 other trials adopted the TNM 5th edition, 3 used the TNM 6th edition, and 2 used the 1997 International Staging System (Table 5). Different staging criteria could lead to the different classification of patients with NSCLC, which would consequently result in differences in prognosis estimation and treatment selection.
In the sponsor-submitted NMA, safety outcomes were only narratively described, as the sponsor considered a quantitative synthesis not feasible because of the sparseness of the data and the differences in treatment regimens across the base-case studies. However, without a quantitative synthesis, a balanced judgment of comparative benefits relative to comparative harms could not be made. In addition, outcomes that are important to patients, such as HRQoL, were not involved in the NMA. Furthermore, the sponsor claimed in correspondence with CADTH that an analysis comparing neoadjuvant nivolumab in combination with chemotherapy with adjuvant atezolizumab was not feasible and was inappropriate because of significant methodological challenges (e.g., significant heterogeneity across the patient populations). Nonetheless, feedback from the clinical experts consulted by CADTH emphasized that adjuvant atezolizumab was an appropriate treatment option for patients with resectable stage IB to stage IIIA NSCLC with a PD-L1 expression level of at least 50%. Therefore, the lack of relevant analyses might have introduced uncertainty into the sponsor’s submitted analysis.
Summary
The sponsor-submitted NMA16 evaluated the efficacy and safety of neoadjuvant nivolumab in combination with chemotherapy relative to neoadjuvant chemotherapy, neoadjuvant chemoradiotherapy, adjuvant chemotherapy, and surgery alone in patients diagnosed with resectable nonmetastatic NSCLC. The primary efficacy end points used for the NMA estimates were EFS and OS, the latter of which was based on an immature data cut-off in the sponsor-conducted CheckMate 816 trial. Secondary outcomes included TTLRR, TTDM, and pCR. For each outcome, base-case and sensitivity analyses were carried out whenever data were available. The base-case analysis involved patients who were deemed to be candidates for surgery and received third-generation platinum-based doublet chemotherapy. The sensitivity analyses expanded to second-generation platinum-based chemotherapies, patients who had undergone resection, data stratified by PD-L1 expression level (i.e., ≥ 1% versus < 1%), and data from the ITT population of the CheckMate 816 trial instead of the subpopulations from that study (i.e., stage IB to II, stage IIIA, and stage IIIA N2) that were used in the base-case stage-specific networks. Furthermore, for each outcome, in addition to the stage-agnostic network, which included studies regardless of the staging of the patient population, the network was also stratified by tumour staging (i.e., stage IB to II, stage IIIA, and stage IIIA N2). The sponsor-submitted NMA ran the random-effects model by default but selected the fixed-effects model for all analyses in the NMA because of the sparseness of network, which was not able to estimate between-study SDs with enough precision. According to the base-case analysis on EFS, patients with stage IIIA NSCLC receiving neoadjuvant nivolumab in combination with chemotherapy had a significantly lower risk of an event than those receiving neoadjuvant chemotherapy or surgery alone. For patients with stage IIIA N2 NSCLC, the risk of an event in patients receiving neoadjuvant nivolumab in combination with chemotherapy was also significantly lower than the risk of those receiving neoadjuvant chemoradiotherapy or neoadjuvant chemotherapy. However, in patients with stage IB to II NSCLC, the difference in EFS improvement was not significant between neoadjuvant nivolumab in combination with chemotherapy and neoadjuvant chemotherapy, adjuvant chemotherapy, or surgery alone. The significant differential treatment effects observed between patients with stage IB to II and patients with stage IIIA or stage IIIA N2 NSCLC suggested that the pooled ITC results from the stage-agnostic population (i.e., stage IB to stage IIIA) were significantly biased and that the pooling was inappropriate, methodologically, although neoadjuvant nivolumab in combination with chemotherapy significantly improved EFS compared with neoadjuvant chemotherapy, adjuvant chemotherapy, and surgery alone in patients with stage-agnostic NSCLC. The sponsor-submitted NMA was not able to quantitively synthesize evidence on safety outcomes, and provided a brief narrative description only, because of the sparseness of the network and the differences in treatment regimens across the base-case studies. Without a quantitative synthesis, a balanced judgment of comparative benefits relative to comparative harms could not be made.
Other Relevant Evidence
This section includes long-term extension studies and additional relevant studies included in the sponsor’s submission to CADTH that were considered to address important gaps in the evidence included in the systematic review.
Other Sponsor-Submitted Evidence
As part of the submission for nivolumab, the sponsor provided a systematic review and a meta-analysis describing clinical evidence in patients with nonmetastatic, resectable NSCLC. The objective of this section is to summarize and critically appraise the methods and findings of those submissions.
Description of Study
The sponsor conducted a systematic review and a meta-analysis of available clinical evidence presenting information on the potential of pCR and/or MPR to be used as a surrogate end point for long-term outcomes (EFS, OS) in patients with resectable NSCLC. In total, 82 studies with full text were reviewed and 32 were included in the analyses that presented evidence of an association between OS and/or EFS and pCR and/or MPR, measured as an HR, or had reported KM curves for OS and/or EFS by pCR and/or MPR status, allowing for the reconstruction of HRs.
Methods
Objectives
The objective of the sponsor-submitted meta-analysis was to investigate the potential for pCR and/or MPR as a surrogate end point for long-term outcomes (EFS, OS) in patients with resectable NSCLC. Four objectives were outlined in the sponsor-submitted meta-analysis:
to determine whether treatment effects on the potential surrogate response end points, pCR and MPR, are correlated with treatment effects on the survival-based end points of OS and EFS
to determine whether treatment effects on the composite end point of EFS are correlated with treatment effects on OS
to determine whether survival-based end points (OS and EFS) are associated with the achievement of a pathologic response (pCR or MPR)
to determine treatment effects by estimating the expected improvement in EFS and/or OS to determine the improvement in the proportion of patients who achieved a pCR.
Only results quantifying the association between pCR on OS are presented in this CADTH review report.
Study-Selection Methods
The SLR used to inform the sponsor-submitted meta-analysis was conducted using the prespecified PICO criteria outlined in Table 35 using the PRISMA guidelines. The systematic review included RCTs (which addressed the first objective [i.e., whether OS and EFS are associated with pCR and MPR]), nonrandomized studies, and cohort studies to address the second objective. ITT-derived estimates were extracted from the RCTs that informed the first 2 objectives; for objective 3, studies were restricted to retrospective, observational studies and to patients who had undergone surgery.
Online databases were searched, and a grey literature search of congress proceedings and other available grey literature sites was conducted. Articles were screened by 2 independent reviewers and a second analyst extracted data, which was validated by a second reviewer. The sponsor did not present any methods to assess the risk of bias in the included studies.
Table 35: Study-Selection Criteria and Methods for Sponsor-Submitted Meta-Analysis
Variable | Objectives 1 and 2 | Objectives 3 and 4 |
|---|---|---|
Population | Adults with resectable, early and locally advanced-stage (I to III) NSCLC | |
Intervention | Neoadjuvant or perioperative chemotherapy, targeted therapy or immunotherapy (any regimen), or surgery alonea | Neoadjuvant or perioperative chemotherapy (using third-generation chemotherapies), targeted therapy or immunotherapya |
Comparator | Neoadjuvant or perioperative chemotherapy, targeted therapy or immunotherapy (any regimen), or surgery alonea | Neoadjuvant or perioperative chemotherapy (using third-generation chemotherapy), targeted therapy or immunotherapya |
Outcome |
|
|
Study design | RCTs | RCTs, observational studies |
Publication characteristics | Database inception to March 11, 2019 | |
Exclusion criteria | Studies focusing on subsegments of the study population:
| |
Databases searched | MEDLINE (including MEDLINE in-process and e-publications ahead of print), Embase, and the Cochrane Central Register of Controlled Trials from database inception to March 11, 2019, including conference abstracts (the European Lung Cancer Congress in collaboration with the International Association for the Study of Lung Cancer and the European Society for Medical Oncology, the American Association for Cancer Research, and the American Society of Clinical Oncology). | |
Selection process | Articles were screened independently by 2 researchers A third reviewer resolved disagreements in screening | |
Data-extraction process | One reviewer extracted the data, which was independently validated by a second reviewer | |
Quality assessment | Not reported | |
ALK = anaplastic lymphoma kinase; EFS = event-free survival; EGFR = epidermal growth factor receptor; MPR = major pathologic response; NSCLC = non–small cell lung cancer; OS = overall survival; pCR = pathologic complete response; RCT = randomized controlled trial.
aAny of these therapies can be with or without radiotherapy.
Methods of Sponsor-Submitted Meta-Analysis
Table 36 presents the methods used in the sponsor-submitted meta-analysis.
Patient-level data from the 32 included trials were reconstructed from published KM curves, using the approach described by Guyot et al. (2012).54 An electronic digitizing tool was used to extract the number of patients at risk at time 0 for each group, and HRs were derived from digitized KM curves for trials that did not report HRs but reported KM curves for trial-level and frequentist analyses. Patient-level survival data were also reconstructed from the digitized KM curves for the Bayesian analyses.12
Missing data were imputed as needed. In situations where an HR was reported without an associated CI or standard error, P values were used to calculate (log) standard errors and 95% CIs, following the method described by Altman and Bland (2011).55 Funnel plots were generated and visually inspected for asymmetry to assess publication bias. Standard errors of the effect estimates were graphed against the effect estimate (i.e., HR for OS by pCR, HR for OS by MPR, HR for EFS by pCR, and HR for EFS by MPR). Table 36 presents a summary of the sponsor-submitted meta-analysis methods.12
An assessment for the risk of bias for the studies included in the meta-analysis was not presented.
Table 36: Sponsor-Submitted Meta-Analysis Methods
Variable | Meta-analysis |
|---|---|
Methods | For objectives 1 and 2 (correlation of treatment effects): A weighted linear regression model, as suggested by Cortazar et al. (2014)56 was used to capture treatment effect on a survival-based end point vs. treatment effect on response. To address objective 3 (association between survival-based end points and response, irrespective of treatment): A standard meta-analysis using Bayesian and frequentist frameworks with random effects (which assumes there is some degree of heterogeneity across studies) was performed. To address objective 4 (estimated trial-level treatment effects on survival): A Bayesian meta-analysis was conducted to predict treatment effects in survival, given the differences observed in treatment response. |
Priors | For objective 3: A noninformative inverse gamma prior distribution. The log HR for pCR was modelled assuming a noninformative normal prior distribution with θ1 ~ (0 to 102). |
Outcomes |
|
Follow-up time points |
|
Sensitivity analyses | Fixed-effect models were run as sensitivity analyses For objectives 1 and 2, sensitivity analyses were run on different time points for OS and/or EFS
|
Subgroup analysis | Bayesian hierarchical meta-analyses subgroups:
Secondary objectives
Survival-based end point definition
|
Methods for pairwise meta-analysis |
EFS and OS were modelled as piecewise exponentials.
|
CI = confidence interval; EFS = event-free survival; HR = hazard ratio; KM = Kaplan-Meier; MPR = major pathologic response; OR = odds ratio; OS = overall survival; pCR = pathologic complete response; RCT = randomized control trial.
Source: Sponsor’s submission.12
Results
Summary of Included Studies
Of the 82 studies retrieved for the patient-level analyses sets, 32 were included in the meta-analysis (Table 37) because they reported an association between OS and/or EFS and pCR and/or MPR, measured as an HR or with a KM curve for OS and/or EFS by pCR and/or MPR status, which allowed the reconstruction of HR, when needed.12
Patients received only neoadjuvant chemotherapy in 8 studies, only neoadjuvant chemotherapy plus radiotherapy in 17 studies, and a mix of chemotherapy and chemotherapy plus radiotherapy in 7 studies. Most studies retrieved were retrospective cohort studies. Most studies reported exclusively on patients who had undergone surgical resection (i.e., resected population), rather than including a mix of patients who had undergone surgical resection and who were potentially resectable but did not end up undergoing surgical resection. Table 37 presents study characteristics and characteristics of participants in the trials included in the meta-analysis. Neoadjuvant treatments included platinum-based chemotherapy with or without radiotherapy. The platinum drug used in the trials was cisplatin or carboplatin.12
A summary of specific demographic and baseline patient characteristics from the included trials was not provided, and therefore assessment of heterogeneity related to patients, outcomes, and study design was not possible.
||||||| || ||| |||||||||||||
|||| ||||||| ||| ||| ||||||||||| ||||||| |||||||| || ||| ||| ||| ||||||||| || |||| ||||| ||||||||||||||||||| ||||||||||| || ||| |||||| |||| |||||| || |||| |||||| ||||||| |||| |||||||| |||| ||| |||||||| || ||| ||| ||||||| || ||||||||| ||| || ||| |||| |||| ||| |||| || ||||| |||||| ||| || ||||||| ||||||||| |||||||||| |||| ||||||||| ||| ||| |||||||||| |||| |||||| ||||||||||||||||| |||||||| || ||| || ||||||||| ||| |||| |||||||||| |||| ||||||||||||| ||| ||| ||||||||| |||||| ||| ||||| |||||| ||||| |||| ||||||||| ||| || |||||||| ||| |||||| |||||||| || ||| |||| |||||| |||| ||||||||| ||||| ||||||| ||||||| |||||| || |||| |||||| |||||| ||||| ||||| |||||| || ||| ||||| |||| || ||||| ||||| || |||||| |||||| |||||||||| |||||||||| ||| ||||||||||| |||| ||| ||| ||||||| || |||||||| || |||| ||||| |||||||| |||||||||||||| ||| |||| || |||||| || ||||| || ||||| |||| || |||||| |||||
Table 37: Study and Patient Characteristics in the 32 Included Studies
First author (year) | Study type | Study period | Country | Stage | N | Eligible population | Neoadjuvant systemic treatment |
|---|---|---|---|---|---|---|---|
Neoadjuvant chemotherapy | |||||||
Brandt (2019) | Cohort | 2000 to 2015 | US | IB to IIIA | 184 | Resected | Platinum doublet |
Cascone (2018) | Other trial | 2007 to 2009 | US | I to III | 47 | Potentially resectable | CIS plus TXT |
Mouillet (2012) | RCT | 1991 to 2006 | France | IB to IIB | 492 | Potentially resectable | PLAT-based chemotherapya |
Pataer (2012) | Cohort | 2001 to 2006 | US | I to IV | 358 | Resected | Platinum doublet |
Qu (2019) | Cohort | 2006 to 2014 | US | II to III | 272 | Resected | Platinum doublet |
Remark (2016) | Cohort | 2008 to 2012 | France | III | 161 | Resected | Platinum doublet |
Spaggiari (2016) | Cohort | 1998 to 2013 | Italy | IIIA | 141 | Potentially resectable | CIS-based chemotherapy |
Stefani (2010) | Cohort | 2001 to 2007 | France | IIIA to IIIB | 175 | Resected | Platinum doublet |
Neoadjuvant CRT | |||||||
Appel (2017) | Cohort | 2012 to 2016 | Israel | IIB to IIIB | 52 | Resected | Platinum doublet |
Arnett (2017) | Cohort | 2004 to 2015 | US | IIIA | 44 | Resected | CARB plus TAX |
Coroller (2017) | Cohort | 2003 to 2013 | US | II to III | 85 | Resected | Not available |
Fischer (2008) | Cohort | 1999 to 2007 | Canada | IIB to IIIB | 44 | Resected | CIS plus ETO |
Haque (2019) | Cohort | 2004 to 2015 | US | III | 1,750 | Resected | Not available |
Isobe (2012) | Other trial | 2001 to 2010 | Japan | III | 30 | Potentially resectable | CARB plus TAX |
Kim (2016) | Cohort | 1997 to 2013 | Korea | IIIA to IIIB | 574 | Resected | Platinum doublet |
Kim (2011) | Cohort | 1989 to 2008 | US | IB to IIIB | 233 | Resected | PLAT-based chemotherapyb |
Lee (2012) | Cohort | 2004 to 2009 | Korea | IIIA | 205 | Resected | CIS plus ETO |
Lee (2014) | Cohort | 1997 to 2011 | Korea | IIIA | 355 | Potentially resectable | Platinum doublet |
Pöttgen (2015) | Cohort | 2000 to 2012 | Germany | III | 157 | Potentially resectable | CIS-based chemotherapy |
Shintani (2012) | Cohort | 1995 to 2008 | Japan | IIIA to IIIB | 52 | Potentially resectable | CIS-based chemotherapyc |
Shiraishi (2014) | Cohort | 1993 to 2011 | Japan | IIB to IIIB | 26 | Resected | PLAT-based chemotherapyd |
Tanaka (2018) | Other trial | 2011 to 2013 | Japan | IIIA | 40 | Potentially resectable | CARB plus TAX |
van der Meij (2011) | Cohort | 2003 to 2009 | Netherlands | III | 51 | Resected | CIS-based chemotherapy |
Yamaguchi (2013) | Cohort | 2005 to 2011 | Japan | IIIA to IIIB | 42 | Potentially resectable | CIS plus S-1 |
Yokomise (2007) | RCT | 2000 to 2006 | Japan | IIIA to IIIB | 41 | Potentially resectable | CARB plus taxane |
Neoadjuvant chemotherapy or CRT | |||||||
Couñago (2019) | Cohort | 2005 to 2014 | Spain | IIIA | 118 | Potentially resectable | Platinum doublet |
Kayawake (2019) | Cohort | 2005 to 2015 | Japan | II to III | 145 | Resected | CARB-based chemotherapy |
Krantz (2018) | Cohort | 2006 to 2012 | US | IIIA | 1,945 | Resected | Not available |
Li (2009) | Cohort | 1998 to 2004 | China | IIIA | 91 | Resected | CIS-based chemotherapy |
Martin (2002) | Cohort | 1993 to 1999 | US | IA to IV | 446 | Potentially resectable | PLAT-based chemotherapye |
Sawabata (2003) | Cohort | 1988 to 1999 | Japan | IIIA to IIIB | 131 | Resected | Not available |
Schreiner (2019) | Cohort | 2008 to 2017 | Germany | IIIA to IIIB | 55 | Resected | CIS plus ETO |
CARB = carboplatin; CIS = cisplatin; CRT = chemoradiotherapy; ETO = etoposide; PLAT = platinum; RCT = randomized controlled trial; S-1 = tegafur, gimeracil, and oteracil; TAX = paclitaxel; TXT = docetaxel.
Note: Platinum doublets consisted of carboplatin or cisplatin in combination with vinorelbine, gemcitabine, etoposide, paclitaxel, docetaxel, or pemetrexed. Chemotherapy, unless specified as old chemotherapy, consisted of vinorelbine, gemcitabine, etoposide, paclitaxel, docetaxel, or pemetrexed.
aMouillet et al. (2012) pooled results from 2 trials. In trial 1, neoadjuvant therapy consisted of cisplatin, ifosfamide, and mitomycin, whereas in trial 2, it consisted of platinum doublets (i.e., cisplatin plus gemcitabine or carboplatin plus paclitaxel).
bIn Kim et al. (2011), treatment was a mix of cisplatin, fluorouracil, plus etoposide; carboplatin, paclitaxel, and etoposide; and carboplatin plus paclitaxel.
cIn Shintani et al. (2012), treatment consisted of cisplatin in triple combination with vindesine and mitomycin, or in double combination with vindesine or vinorelbine.
dIn Shiraishi et al. (2014), treatment consisted of a mix of cisplatin alone; cisplatin in combination with docetaxel, vindesine, or fluorouracil; or carboplatin combined with docetaxel.
eIn Martin et al. (2002), treatment consisted of cisplatin in triple combination with vinblastine plus mitomycin, carboplatin plus paclitaxel, or other.
Source: Sponsor’s submission.12


Critical Appraisal
The sponsor-submitted meta-analysis was informed by studies selected from an adequately conducted systematic review with clearly prespecified PICO criteria and conducted using PRISMA guidelines. The research question for the meta-analysis was adequately reported. The search strategy and the search were conducted using several databases and were adequately reported. The study-selection and data-extraction methods were appropriate. Articles were reviewed by 2 independent reviewers and an analyst extracted data. The study-selection and data-extraction methods were considered appropriate. The outcomes included in the meta-analysis were appropriate and align with those identified as important by patients and clinical experts in the CADTH review protocol. The treatments identified in the trials are commonly used in the Canadian setting. The sponsor did not present data on the risk-of-bias assessment for the included studies.
In the absence of detailed information on the baseline and study characteristics of patients enrolled in the studies included in the meta-analysis, the degree of heterogeneity among the included studies could not be assessed. Studies included had considerable variation in terms of study design (observational versus RCT) and sample size. Allocation concealment, methods for handling missing data, and eligibility criteria for inclusion in the studies were not reported for the RCTs included. Patients’ baseline characteristics were not adequately reported across studies, especially for the key baseline characteristics important for the current reimbursement population, such as PD-L1 expression level, ECOG PS, duration of therapy, dosing regimen, age, sex distribution, race, and geographic location. It was also unclear what the average follow-up time was for patients receiving treatment. In addition, pCR and MPR definitions differed across the included studies.
The sponsor used both frequentist and Bayesian models with random effects in the meta-analysis to quantify the association between pCR and/or MPR on EFS and/or OS. Although key baseline characteristics in the included studies were not provided, the sponsor assessed clinical and methodological heterogeneity among the studies included in the analyses was assessed using I2 and Cochran’s Q heterogeneity statistics. Results and effect sizes for each outcome were presented for each study, with effect size estimated with random-effect models, which was considered appropriate. Heterogeneity assessed in the studies included in the frequentist approach was 0% for most outcomes (except OS by pCR, where I2 was 20% but less than 40% which suggested that heterogeneity was not important). Heterogeneity was not reported for the Bayesian analysis and, owing to the lack of baseline data from the trials included, an assessment of the level of heterogeneity could not be made.
The meta-analysis suggests that achievement of pCR was associated with improved OS, based on the Bayesian and frequentist methods implemented in the analyses.
Long-Term Extension Studies
This section includes a study conducted in a real-world setting submitted by the sponsor to CADTH that was considered to address important gaps (e.g., the validity of surrogate and/or intermediate end points, shortness of the duration of the studies to assess long-term OS benefit) in the evidence included in the Systematic Review.
Real-World Study
One real-world study with data from EHRs, supplemented with chart reviews, was submitted by the sponsor. The purpose of this study was to generate real-world evidence characterizing the relationship between pathologic responses and survival, and to describe profiles of patients with surgically resectable NSCLC (stage IB [tumours ≥ 4 cm] to stage IIIA) treated in the US community oncology setting and neoadjuvant treatment patterns.
Methods
This study, entitled Early End Points in Patients With Resectable NSCLC in a Real-World Setting, is retrospective and observational and uses 2 sources of data from the real-world clinical setting in the US. First, the iKnowMed (iKM) EHR database from The US Oncology Network were used to assess the study objectives. The structured data fields in the iKM EHR database were the source of data for selected variables and metrics used in end point analyses. Second, a chart review for unstructured data in the medical record was performed.
Patients diagnosed with stage IB (tumours ≥ 4 cm) to stage IIIA (AJCC 7th edition) NSCLC and initiating neoadjuvant therapy from January 1, 2008, to January 31, 2019 (the study identification period), were identified. Patients were indexed to the first date of neoadjuvant treatment. The study observation period (January 1, 2008, to July 31, 2019) comprised a 6-month preindex period (i.e., baseline period) before the index date and a postindex period (i.e., follow-up period) spanning the index date to the end of the observation period for each patient (Figure 25).
The follow-up period varied for each patient; it ended at the last encounter and/or patient record, date of death, or end of the observation period (July 31, 2019), whichever occurred first. The last visit was defined as the final physical encounter, detected with vital sign records, for a patient in The US Oncology Network, based on the records available in the study’s structured dataset. If a neoadjuvant regimen consisted of more than 1 drug and drugs were given on different dates, the date of the first administration of any drug was used as the index date. Data used to evaluate medical history extended back to July 1, 2007. The medical history period ended the day before the index date (Figure 25).
The relationship between pathologic responses (pCR and MPR) and survival outcomes (OS and EFS) was assessed as the primary objective. Clinical and demographic characteristics were measured at baseline, before the index date, as a secondary objective. Exploratory outcomes were submitted by the sponsor but not included in this report. Safety was not investigated in this study.
Populations
Identification and verification of the study population occurred in 2 phases. For phase I, patients were assessed for eligibility with structured data in the iKM database, based on the inclusion and exclusion criteria defined here. In the phase II, key eligibility criteria were confirmed by leveraging unstructured information from patients’ charts. Briefly, eligible patients from phase I were further selected for chart review. Patients were disqualified based on information in the chart that differed from what was available in the structured iKM database (i.e., a second stage of verification). Reasons for disqualification were captured and reported. Disqualified patients were excluded from the updated phase I (landscape) assessment, and the phase II (chart review) objectives were assessed for the subpopulation ultimately eligible for chart review.
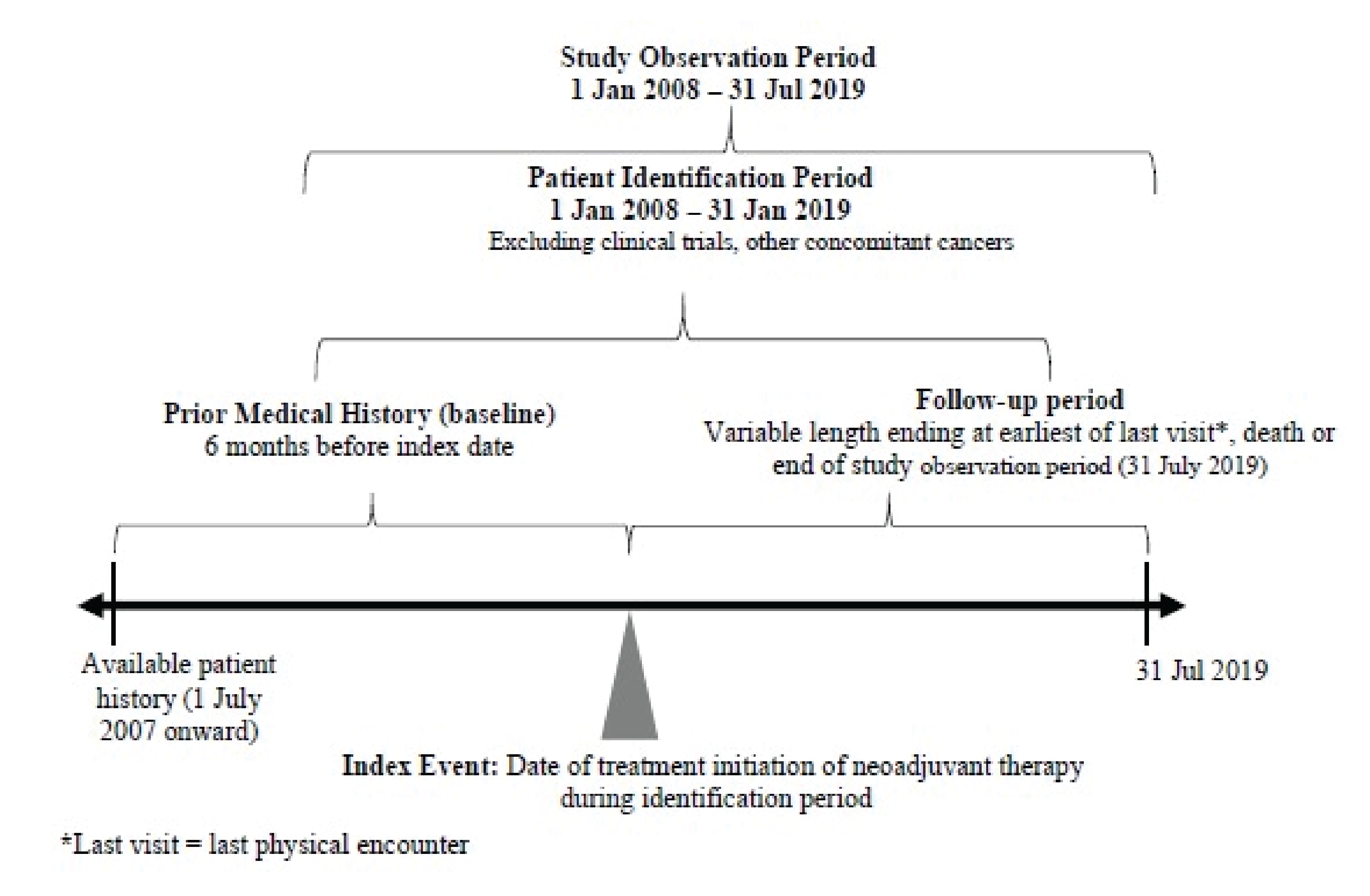
Inclusion criteria consisted of the following:
a diagnosis of stage IB (tumours ≥ 4 cm) to stage IIIA NSCLC (before January 2018, based on TNM 7th edition), or stage II to stage IIIB NSCLC (on or after January 2018, based on TNM 8th edition)
initiation of neoadjuvant therapy for stage IB (tumours ≥ 4 cm) to stage IIIA NSCLC during the study identification period (January 1, 2008, to January 31, 2019)
receipt of care at a US Oncology Network site, using the full EHR capabilities of the iKM database at the time of treatment, and having records available for research purposes
at least 2 visits with The US Oncology Network after the index date
age of at least 18 years on the index date.
Exclusion criteria consisted of the following:
enrolment in any clinical trials for nonmetastatic NSCLC at any time during the study observation period (to remove the confounding of treatment lines of therapy and outcomes with experimental therapies)
a current or prior primary diagnosis of cancer other than NSCLC that required systemic or other treatment during the patients’ baseline or follow-up period
known EGFR mutations or ALK translocation at diagnosis.
In the overall population, the median age of the 425 patients included in the analysis was 66 years (range, 27 to 89 years), and the majority of patients were male (54.6%) and white (67.3%). The majority of patients were former (61.9%) or current (6.1%) smokers. Most of the patients were diagnosed with stage III NSCLC (66%), and more than half were reported to have an ECOG PS of 1 (60.5%). The most commonly reported comorbidities were hypertension (12%), ischemic disease (6.4%), and pulmonary disease and/or asthma (6.4%). The median number of additional visits following the index date was 25 (range, 1 to 171).
The median time from diagnosis to initiation of neoadjuvant therapy was 1.3 weeks (range, 0.1 to 11.3 weeks), and paclitaxel plus carboplatin (49.2%) was the most common neoadjuvant treatment used. A total of 225 (52.9%) patients underwent a surgical resection, and 72 (32%) of those patients received adjuvant treatment with cisplatin combined with etoposide (22%), the most commonly used adjuvant treatment. Of the 200 patients who did not undergo surgery, the most common reasons were physician recommendation (36.0%), progression (27.5%), other (14.5%), patient preference (7%), and death (7%). A total of 166 (39.1%) patients received subsequent systemic treatment for NSCLC, with carboplatin plus paclitaxel (27.1%) being the most common first-line therapy reported.
Interventions
Neoadjuvant treatment regimens were characterized as chemotherapy or chemoradiotherapy. In phase I, neoadjuvant therapy was defined as the line of therapy noted by the physician. For phase II, confirmation of neoadjuvant therapy administration by chart review was required.
To be eligible, explicit documentation of neoadjuvant therapy by the physician was required. If documentation was absent, then confirmation of chemotherapy before surgery was required. If no surgery took place, the plan or intent to get surgery was required to classify treatment as having neoadjuvant intent.
Outcomes
The following primary objectives were addressed during phase I (structured data only) and phase II (structured data and chart review):
pCR and MPR in patients receiving neoadjuvant therapy for stage IB (tumours ≥ 4 cm) to stage IIIA NSCLC
the relationship between survival (EFS and/or OS) and early end points (pCR and/or MPR) in the overall population receiving neoadjuvant therapy for stage IB (tumours ≥ 4 cm) to stage IIIA NSCLC.
The following secondary objectives were addressed during phase I of the study, using structured data:
the baseline demographic, clinical, and neoadjuvant treatment characteristics of real-world patients receiving neoadjuvant therapy for stage IB (tumours ≥ 4 cm) to stage IIIA NSCLC.
Exploratory outcomes were submitted by the sponsor but are not reported in this section. Safety outcomes were not available.
The pCR and MPR for patients receiving neoadjuvant treatment and undergoing surgery were determined with a chart review of postsurgery physician notes and a pathology report of the primary lung tumour and lymph node surgical specimens following neoadjuvant treatment. pCR was defined as no viable tumour cells following surgery (pathologic stage pT0 pN0 or ypT0 ypN0). This definition indicates that involved lymph nodes are N0 after surgery. MPR was defined as residual tumour tissue in the resected lung of 10% or less.
The EFS was calculated, using KM methods, as the interval from the index date to the earliest recorded date of disease progression, precluding surgery, progression or recurrence after surgery, or death from any cause. Patients who did not undergo surgery for reasons other than progression were considered to have an event at progression or death. Relapse and/or recurrence and progression were assessed with chart review, and referred to progression recorded in physician notes only, not defined by traditional RECIST imaging (as this is affected by the frequency of imaging and may not be assessed in the same manner across groups in daily clinical practice). Patients without evidence of relapse, recurrence, progression, or death were censored on the study end date or the last visit date available in the database, whichever occurred first. OS was defined as the interval between the index date and the date of death documented in the Limited Access Death Master File or the iKM EHR database. Patients who did not die were censored on the study end date or the last visit date available in the database, whichever occurred first.
Statistical Analysis
All patients who met the inclusion criteria and none of the exclusion criteria during the specified study period were included in the final analyses. The analyses were conducted using all ascertained patient-level data, regardless of the sample size. A feasibility analysis identified 935 patients with NSCLC (stage IB [tumours ≥ 4 cm] to stage IIIA) receiving neoadjuvant therapy from January 1, 2008, to January 31, 2019. The final study population for analysis was defined after identification and review of the patient population meeting the eligibility criteria in the iKM database.
Descriptive statistics were used for continuous variables (means, SD, median, ranges), categorized continuous variables (e.g., treatment duration in weeks rather than days), and categorical variables (frequencies, counts and percentages). For percentages, the denominator was the total number of people in the study (patient count) at any point in time, and the numerator was a specific characteristic of these patients. Patients with no information available were classified as not documented.
For time-to-event end points, median times with 95% CIs were calculated. Briefly, KM methods were used to estimate time-to-event end points (e.g., OS, EFS) and generate event curves. For example, KM survival curves were generated for OS for patients who did and did not achieve pCR. With an unadjusted Cox analysis that used HRs with 95% CIs, the association between pCR and OS was obtained for the overall population. A Cox proportional hazards model was then conducted to determine the association between pCR and OS, after variables were controlled for (e.g., age, sex, disease stage, histology, site). Variables with a P value no higher than 0.20 in Cox univariate analyses were included in the multivariable analyses. The same analyses were conducted to explore the effect of pCR on EFS. The association between MPR and OS and/or EFS was explored, contingent on sample size, with a Cox proportional hazards model. Adjusted HRs and 95% CIs were estimated with a Cox proportional hazards analysis.
The follow-up period varied for each patient; it ended at the last encounter, death, or the end of the study period, whichever occurred first. However, no minimum or maximum follow-up was required for the analyses of study outcomes. A time-to-event analysis was conducted to account for differences in follow-up periods.
Patient Disposition
A total of 858 eligible NSCLC patients were identified in the structured dataset (phase I). After further inclusion and exclusion criteria were applied during the chart review (phase II), 425 patients were eligible for analysis of the overall population (Table 38).
Most patients — i.e., 28,465 (96.1%) during phase I and 291 (37.8%) owing to a lack of confirmation of neoadjuvant treatment — were excluded (Table 38).
Inclusion and exclusion criterion | Patients excluded (N) | Patients remaining (N) |
|---|---|---|
Patients with a documented diagnosis of stage IB to stage IIIB NSCLC (AJCC 7th or 8th edition) in The US Oncology Network | 29,610 | |
Provider-documented neoadjuvant therapy within The US Oncology Network during the study identification period | 28,465 | 1,145 |
Age ≥ 18 years at index date (provider-documented neoadjuvant therapy) | 0 | 1,145 |
At least 2 visits after initiation of provider-documented neoadjuvant therapy | 1 | 1,144 |
A diagnosis of stage IB to stage IIIA NSCLC (stage IB to stage IIIA before January 2018, based on AJCC 7th edition; stage II to stage IIIB on or after January 2018, based on AJCC 8th edition) | 135 | 1,009 |
Initiation of neoadjuvant therapy for stage IB to stage IIIA NSCLC (stage IB to stage IIIA before January 2018, based on the TNM 7th edition; stage II to stage IIIB on or after January 2018, based on the TNM 8th edition) during the study identification period | 121 | 888 |
A current or prior primary diagnosis of cancer other than advanced NSCLC that required systemic or other treatment during a patient’s baseline or follow-up period | 25 | 863 |
Known EGFR mutation or ALK rearrangement before the study identification period or on the index date | 5 | 858 |
Target chart review population | ||
Treatment at sites in which charts were accessible for research purposes | 89 | 769 |
Other eligibility criteria (review) during chart review | ||
Initiation of neoadjuvant therapy for stage IB to stage IIIA NSCLC during the study identification period | 291 | 478 |
Enrolment and participation in a nonmetastatic NSCLC interventional clinical trial during the study observation period | 10 | 468 |
A current or prior primary diagnosis of cancer other than advanced NSCLC that required systemic or other treatment during a patient’s baseline or follow-up period | 25 | 443 |
Stage IB NSCLC (before January 2018) with tumour size < 4 cm before the study identification period | 11 | 432 |
A confirmed EGFR mutation or ALK rearrangement before the study identification period | 7 | 425 |
Overall study population | 0 | 425 |
AJCC = American Joint Committee on Cancer; ALK = anaplastic lymphoma kinase; EGFR = epidermal growth factor receptor; NSCLC = non–small cell lung cancer; TNM = tumour, node, metastasis.
Source: Clinical Study Report (Early End Points in Patients With Resectable NSCLC in a Real-World Setting).
Exposure to Study Treatments
The median follow-up was 81.7 weeks (range, 1.9 to 589.4 weeks) for patients in the overall population. More than 42% of the patients had at least 24 months of follow-up (Table 2). The median duration of neoadjuvant chemotherapy and chemoradiotherapy was 9.1 weeks (range, 0.1 to 28.3 weeks) and 6.3 weeks (range, 1 to 32.9 weeks), respectively, in the overall population (Table 39).
Table 39: Duration of Follow-Up and Treatment
Duration | Overall population (N = 425) | |
|---|---|---|
Follow-up duration, weeks | ||
Mean (SD) | 125.9 (117.3) | |
Median (range) | 81.7 (1.9 to 589.4) | |
Follow-up duration, n (%) | ||
< 6 months | 75 (17.6) | |
6 to < 12 months | 70 (16.5) | |
12 to < 18 months | 61 (14.4) | |
18 to < 24 months | 38 (8.9) | |
24 to < 30 months | 32 (7.5) | |
30 to < 36 months | 16 (3.8) | |
36+ months | 133 (31.3) | |
Duration of neoadjuvant therapy, weeks | ||
Mean (SD) | 8.2 (4.8) | |
Median (range) | 6.4 (0.1 to 32.9) | |
Duration of neoadjuvant therapy by subgroups | ||
Neoadjuvant therapy | Chemotherapy (n = 147) | Chemoradiotherapy (n = 278) |
Mean (SD), weeks | 8.6 (4.8) | 7.9 (4.8) |
Median (range), weeks | 9.1 (0.1 to 28.3) | 6.3 (1 to 32.9) |
SD = standard deviation.
Source: Clinical Study Report (Early End Points in Patients With Resectable NSCLC in a Real-World Setting).
Efficacy
|||||||||||| ||||||| |||||| ||| ||||| ||||||||| ||| || ||||||| |||||||||| |||||||||||||| |||||||||||| ||| ||| |||||||| || ||| ||||||| ||||||||||| ||||| || || ||||||| |||||||| |||||||| |||| ||| ||| |||| || |||||||| ||||||| ||| ||| |||| ||||| ||| ||| ||||||| ||||||||||| ||| |||||||| ||||||| |||| |||||| ||| ||||||||||| ||||||| || ||||||| |||||||| ||||| ||||| |||| ||| ||| ||| ||||||| ||||| ||||| ||||||| ||| ||||| ||| |||||||||| || || ||||||||||| ||| |||||||| ||| || ||| |||| ||||||| ||||| |||||| |||| |||||||| ||| |||| ||||||| ||||| |||||| ||| ||||||||||| |||||||| ||| ||||||| |||||||||| |||| |||||||| || ||||||||| ||| |||| |||| ||| ||||| ||||||| |||||| || ||| ||| ||||| |||||||||| ||| |||| |||| || ||||| ||||| ||||||| |||| |||||| |||||||| ||||||||||| || ||||| |||| || ||||| |||||| ||| |||||| || ||||| |||||||| |||| |||| ||| |||| |||| || ||||| |||||| |||||| |||||||| || |||| |||| || ||||| ||||| |||||| ||||| |||||||| ||||||| ||||| ||| |||||| |||||||| ||||||||||||| ||||| |||||||| |||| ||| ||||||| |||| |||| ||||| |||| || ||||| ||||| ||| ||||| |||| || ||||| |||||| ||||||||||||| |||||| ||| ||||||| |||||||||| ||| ||||||||||| ||||||| |||||| || ||| |||||||| ||| || ||||| ||||||||||||||||||| |||| || ||||||| ||| ||| ||||||| |||||||| |||| ||| ||||||| |||| ||||||||||||| ||| || ||||| ||| |||||||||| || || ||||||||||| ||| |||||||| ||| ||| ||| |||| |||| ||| ||||| |||||| |||| |||||||| ||| ||||| |||||| ||| ||||||||||| |||||||| ||| ||||||| |||||||||| |||| |||||||| ||| || ||||||| |||||||||| ||||||||| ||| |||| |||| ||| ||||| ||||||| |||||| ||| ||| ||| ||||| |||||||||| ||| |||| |||| || ||||| ||||| ||||||| |||| |||||| ||| ||||||||||| || ||||| |||| || ||||| |||||| ||| |||||| ||| ||||| |||||||| |||| |||| ||| |||| |||| || ||||| ||| |||||| |||||||| || |||| |||| || ||||| ||||| |||||| ||||| |||||||| ||||||| ||||| |||||| ||| ||||||| |||
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| |
|---|---|---|---|
||||||||||| ||||||| | |||
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| |
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| |
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| |
||||||||||| ||||||| | |||
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| |
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| |
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| |
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| |
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| |
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| |
||||||||||| ||||||| | |||
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| |
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| |
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| |
||||||||||| ||||||| | |||
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| |
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| |
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| |
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| |
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| |
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| |
Note: This table has been redacted at the request of the sponsor.


||||||||||||| ||||||| |||||| ||| ||||| ||||||||| ||| || ||||||| |||||||||| |||||||||||||| |||||||||||| ||| ||| |||||||| || ||| ||||||| ||||||||||| |||||| || || ||||||| |||||||| |||||||| |||| ||| ||| |||| || |||||||| ||||||| ||| ||| |||| ||||| ||| ||| ||||||| ||||||||||| ||| ||||||| |||||||| |||| |||||| ||| ||||||||||| ||||||| || ||||||| ||| ||| ||||||| |||||||| |||| ||| ||||||| || |||| ||||||||||||| ||||| ||| |||||||||| || || ||||||||||| ||| |||||||| ||| || ||| |||| |||| ||| ||||| |||||| |||| |||||||| ||| |||| ||||||| ||||| |||||| ||||||| ||||| |||||| ||| ||||||||||| |||||||| ||| ||||||| |||||||||| |||| |||||||| || ||||||||| ||| |||| |||| ||| ||||| ||||||| |||||| || ||| ||| ||||| |||||||||| ||| |||| |||| || ||||| ||||| ||||||| |||| |||||| |||||||| ||||||||||| ||||| |||| || ||||| |||||| ||| |||||| || ||||| |||||||| |||| || ||| ||| |||| |||| || ||||| |||||| |||||| |||||||| || |||| |||| || ||||| ||||| |||||| ||||| |||||||| ||||||| || |||| ||| |||||| |||||||| ||||||||||||| ||||| |||||||| |||| ||| ||||||| || ||| |||| ||||| |||| || ||||| ||||| ||| ||||| |||| || ||||| |||||| ||||||||||||| |||||| ||| ||||||| |||||||||| ||| ||||||||||| ||||||| |||||| || ||| |||||||| ||| || ||||| |||||||||||||||||||| || ||||||| ||| ||| ||||||| |||||||| |||| ||| ||||||| |||| ||||||||||||| ||| || |||||| ||| |||||||||| || || ||||||||||| ||| |||||||| ||| ||| ||| |||| |||| ||| ||||| |||||| |||| |||||||| ||| ||||| |||||| ||| ||||||||||| |||||||| ||| ||||||| |||||||||| |||| |||||||| ||| || ||||||| |||||||||| ||||||||| ||| |||| |||| ||| ||||| ||||||| |||||| ||| ||| ||| ||||| |||||||||| ||| |||| |||| || ||||| ||||| ||||||| |||||| ||| ||||||||||| || ||||| |||| || ||||| |||||| ||| |||||| ||| ||||| |||||||| |||| |||| ||| |||| |||| ||| ||||| ||| |||||| |||||||| || |||| |||| || |||| ||||| |||||| ||||| |||||||| ||||||| ||||| |||||| ||| ||||||| ||||
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| |
|---|---|---|---|
||||||||||| ||||||| | |||
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| |
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| |
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| |
||||||||||| ||||||| | |||
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| |
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| |
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| |
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| |
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| |
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| |
||||||||||| ||||||| | |||
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| |
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| |
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| |
||||||||||| ||||||| | |||
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| |
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| |
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| |
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| |
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| |
||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| | ||||||||||| ||||||| |
Note: This table has been redacted at the request of the sponsor.


Critical Appraisal
Internal Validity
The study was conducted over a span of 10 years, had documented diagnostic, clinical, and treatment characteristics, and had outcomes data that are not easily captured in clinical trials. Also, the most widely used definition of pCR (0% viable tumour in the primary tumour and nodes, or ypT0N0) and National Comprehensive Cancer Network guidelines for treatment protocols were used to minimize heterogeneity across different clinical centres in The US Oncology Network.
However, residual heterogeneity across sites and investigators is expected to affect outcomes to various degrees in either direction. EHR data are for clinical practice purposes, not solely for research purposes. Therefore, there are limitations to the interpretation of data (e.g., incomplete data across the entire population for some variables of interest, heterogeneous analyses between pathologists and study sites). Also, no information regarding concomitant medication was provided. Even though it was generally a large population, when patients with pCR (11.3%) or MPR (18.8%) were considered in analyses of their relationship to EFS and/or OS, the size of the population starts to become limiting, especially for subgroup and/or sensitivity analyses (which were not included in this report). Without further details provided, it is unknown if the proportional hazards assumption was satisfied with Cox modelling. Last, the relationship between EFS and OS (exploratory outcome, results not included in this report) was investigated but only as an exploratory end point; therefore, the relationship between EFS and OS remains uncertain.
External Validity
This study captured the real-world experiences of patients with resectable NSCLC in the US community oncology setting, which may not be reflective of the clinical setting in Canada. However, there is a selection bias because only clinics in The US Oncology Network that use the full EHR capabilities of the iKM database are included. Practices that participate in the Network may be different from those that do not participate in areas such as the patient population seen or the prescribing practices of physicians. Also, the EHR data do not capture information about services or procedures provided outside of the practice if they are not documented in the EHR. Another source of selection bias is the fact that patients were selected after index dates.
During the 10-year study identification period, therapeutic options, such as immunotherapy and targeted therapy, for advanced NSCLC have evolved significantly, leading to improved survival rates. Therefore, further research is warranted using data comparing different treatment approaches, such as immunotherapy and targeted therapy, in the real-world setting. Because data from phase III studies of patients at earlier stages of NSCLC are still emerging in the neoadjuvant and adjuvant settings, the results from this study remain to be confirmed with clinical trial data.
Discussion
Summary of Available Evidence
This CADTH report summarizes evidence for nivolumab from 1 pivotal study (CheckMate 816), 1 ITC, 1 meta-analysis, and 1 noninterventional study submitted by the sponsor.
CheckMate 816 is an ongoing, open-label, randomized controlled, phase III trial assessing the efficacy and safety of nivolumab in combination with platinum-based chemotherapy administered every 3 weeks for 3 cycles, and platinum-chemotherapy as neoadjuvant treatment for patients with resectable (stage IB [≥ 4 cm], stage II, and resectable stage IIIA) NSCLC. pCR assessed by BIPR and EFS assessed by BICR were coprimary end points. Key secondary and exploratory end points included OS, TTDM, MPR, safety and tolerability, and HRQoL. By the October 20, 2021, data cut-off date (EFS IA1), 93.8% and 84.7% of treated patients in the nivolumab plus chemotherapy and chemotherapy arms, respectively, had completed the course of neoadjuvant therapy. Most patients randomized in the nivolumab plus chemotherapy and chemotherapy arms, respectively, were male (71.5% and 70.9%), and about half of the patients enrolled in the study were white (49.7% and 44.7%) and about half were Asian (48.0% and 52.0%). In total, 48.6% and 53.1% of patients in the nivolumab plus chemotherapy and chemotherapy arms, respectively, had NSCLC with squamous tumour histology, and 63.1% and 64.2%, respectively, had stage IIIA disease.
One sponsor-submitted ITC was summarized and critically appraised for this review. The ITC evaluated the efficacy and safety of neoadjuvant nivolumab in combination with chemotherapy relative to other relevant treatments, including neoadjuvant chemotherapy, neoadjuvant chemoradiotherapy, adjuvant chemotherapy, and surgery alone, in patients diagnosed with potentially resectable, nonmetastatic NSCLC. The primary efficacy end points investigated in the ITC were EFS and OS, the latter of which was based on an immature data cut-off date in the sponsor-conducted CheckMate 816 trial. Secondary outcomes included TTLRR, TTDM, and pCR. For each outcome, base-case and sensitivity analyses were carried out whenever data were available.
One sponsor-submitted meta-analysis describing clinical evidence of the potential for pCR or MPR as a surrogate end point for long-term outcomes (EFS, OS) in resectable NSCLC was also summarized. The systematic review used to inform the meta-analysis identified 32 studies that presented evidence of an association between OS and/or EFS and pCR and/or MPR, measured as an HR or with reported KM curves for OS and/or EFS by pCR and/or MPR status. Only results quantifying the association between pCR on OS are presented in this report.
One sponsor-submitted retrospective, observational study conducted with data from EHRs and supplemented with chart reviews was also summarized. The study characterized the relationship between pathologic response and survival, and described profiles of patients with surgically resectable NSCLC (stage IB [tumours ≥ 4 cm] to stage IIIA) treated in the US community oncology setting and neoadjuvant treatment patterns.
Interpretation of Results
Efficacy
EFS was met at the planned IA1 (October 20, 2021, data cut-off date). Median EFS was higher in patients receiving nivolumab plus chemotherapy than in those receiving chemotherapy, and the KM curves separated early and remained separated. The estimated HR suggested benefit in patients receiving nivolumab plus chemotherapy compared to chemotherapy alone. The findings were considered statistically and clinically significant. EFS was identified as an important outcome by the clinical experts, clinician groups, and patients. It is important to note that although EFS is a validated surrogate outcome for OS in some oncology trials, there is limited evidence that validates the correlation between EFS and OS in the neoadjuvant setting for patients with resectable NSCLC. Still, the clinical experts consulted considered the EFS findings clinically meaningful, and noted that, in the CheckMate 816 trial, EFS captured the surgical mortality of patients after neoadjuvant treatments.
OS, as estimated by HR, was statistically nonsignificant, based on the prespecified interim analysis stopping rule (P = 0.008 against a prespecified level of significance at the interim analysis of 0.0033). Although the results showed a promising treatment-effect benefit for OS, a final analysis is needed to strengthen confidence the findings of the trial, particularly for the exact estimate of difference in median survival, which was not estimable at the October 21, 2021, data cut-off date. A follow-up OS analysis is planned ||||| ||| || |||||| |||| |||||||| || |||| ||||| ||||. Despite the findings observed, the clinical experts considered the estimates to be convincing and clinically meaningful, suggesting better outcomes (e.g., better OS, more patients cured, fewer cases of recurrence) over time for patients treated with nivolumab plus chemotherapy in the neoadjuvant setting.
pCR was met at the September 16, 2020, data cut-off date. The pCR rate, per BIPR, was higher in the nivolumab plus chemotherapy arm than in the chemotherapy arm and was considered statistically and clinically meaningful by the clinical experts consulted. Sensitivity analyses were also consistent with the primary analysis. Although pCR is a validated surrogate outcome for OS in some oncology trials, it has not been established as a surrogate end point by Health Canada for patients with resectable NSCLC in the neoadjuvant setting. The clinical experts reported that available evidence in the neoadjuvant NSCLC setting suggests a correlation of pCR and MPR with OS after the use of chemotherapy.57,58 However, there is limited evidence to support a correlation of pCR and MPR with OS for targeted therapy or immunotherapy.11 The IONSECO study, which assessed durvalumab treatment for NSCLC in the neoadjuvant setting, showed that pCR was an independent prognostic factor for disease-free survival and OS.59 The ORs for MPR and pCR were higher in the nivolumab plus chemotherapy arm than in the chemotherapy arm.
The sponsor conducted a meta-analysis to address the potential for pCR or MPR to be a surrogate outcome for OS and EFS, pooling patient-level data from 32 studies that presented KM plots and HRs for OS by pCR in the resectable NSCLC setting. OS findings by pCR status in the frequentist and Bayesian analyses suggested a benefit across the included studies. The I2 statistic for the frequentist approach was 20%, suggesting less heterogeneity between the studies included in the analysis. However, several limitations were identified in the meta-analysis, such as variation in study design (observational versus RCT) and sample size. In addition, allocation concealment, methods for handling missing data, and eligibility criteria for inclusion in the studies were not reported for the included RCTs, and key baseline characteristics were not adequately reported across studies, such as PD-L1 expression level, ECOG PS, duration of therapy, and dosing regimen, which are important for the reimbursement population.
The EFS benefit of nivolumab plus chemotherapy over chemotherapy alone was observed across subgroups of interest in the CADTH protocol. More benefit was reported in the subgroup of patients with a PD-L1 expression level of at least 50% (HR = 0.24; 95% CI, 0.10 to 0.61) than in the subgroups with a PD-L1 expression level from 1% to 49% (HR = 0.58; 95% CI, 0.30 to 1.12), PD-L1 expression level of at least 1% (HR = 0.41; 95% CI, 0.24 to 0.70), and PD-L1 expression level of more than 1% (HR = 0.85, 95% CI, 0.54 to 1.32). Similarly, a larger benefit was observed in the subgroup with stage IIIA disease (HR = 0.54; 95% CI, 0.37 to 0.80) than in the subgroup with stage IB to II disease (HR = 0.87; 95% CI, 0.48 to 1.53), although there were fewer events reported for patients with stage IB to II disease (21 events in 65 patients) than for those with stage IIIA disease (43 events in 113 patients). Of note, randomization was stratified by disease stage and PD-L1 expression level in the CheckMate 816 trial. More benefit was observed in subgroups with non-squamous histology (HR = 0.50; 95% CI, 0.32 to 0.79) and more benefit was also observed in subgroups with an ECOG PS of 0 (HR = 0.61; 95% CI, 0.41 to 0.91) than with an ECOG PS of 1 (HR = 0.71: 95% CI, 0.41 to 1.21). The subgroup analyses also suggested that patients with stage IIIA disease derived more benefit from nivolumab plus chemotherapy than the other groups assessed in the CheckMate 816 trial (stage IB to II and other). Still, findings from the subgroup analyses should be interpretated with caution, given that the study was not statistically powered to assess subgroups individually or by type I error because multiplicity was not properly accounted for. Regardless of the magnitude of response observed, a benefit was observed in all subgroups and in the overall study population. In addition, some patients received adjuvant chemotherapy after surgery in the CheckMate 816 trial, which could have had an impact on OS and EFS.
The median TTDM was not reached in either study arm at the October 20, 2021, cut-off; however, the estimated HR suggested that patients receiving nivolumab plus chemotherapy benefited more than those receiving chemotherapy alone. The mean length of hospital stays following surgery for patients in the CheckMate 816 trial did not differ significantly in the 2 treatment arms. The clinical experts considered the findings to be in line with surgery hospital-stay data for NSCLC in current real-world practice.
HRQoL was identified as an important outcome by the clinical experts and patient groups consulted. The mean difference from baseline to week 4, week 7, postadjuvant visit 1, and post adjuvant visit 2 in EQ-5D-3L utility scores did not exceed MID values in either treatment group (0.06 in the US and 0.08 in the UK). The mean difference from baseline to week 4, week 7, postadjuvant visit 1, and postadjuvant visit 2 in the 2 groups in EQ VAS scores did not exceed the MID for VAS scores (range, 7 to 12). Caution should be taken when interpreting the findings, as the type I error rate was not accounted for during the analyses. The clinical experts noted that there was not detriment to HRQoL for patients receiving the nivolumab plus chemotherapy; the mean change from baseline to different assessment points for the VAS and the utility portion of the EQ-5D-3L did not exceed the MIDs. Nivolumab plus chemotherapy was considered tolerable to patients, which is usually desired for new treatments in current practice, according to the clinical experts and patients.
Surgery with curative intent followed by adjuvant chemotherapy was highlighted as the current standard of care in Canada by the clinical experts. Neoadjuvant chemotherapy is infrequently used for patients with resectable NSCLC in Canada because some patients can become ineligible for surgery because of disease progression or toxicity after chemotherapy. Therefore, in the absence of head-to-head trials or direct comparison studies that assess the benefit of nivolumab plus chemotherapy compared with upfront surgery followed by adjuvant chemotherapy, there is uncertainty in the magnitude of benefit derived from nivolumab plus chemotherapy in this patient population. The clinical experts noted that the magnitude of benefit in the estimated EFS HR for patients receiving nivolumab plus chemotherapy before surgery was clinically meaningful compared to current outcomes observed in patients who receive upfront surgery followed by adjuvant chemotherapy in current practice. The generalizability of the findings to patients with an ECOG PS higher than 2 is also limited, given that only patients with an ECOG PS of 0 or 1 were enrolled in the trial. The clinical experts noted that patients must have a good performance status to be eligible for the treatment, owing to the toxicity-associated risks and the potential for disease progression after treatment that can render patients ineligible for surgery. It is also uncertain whether the addition of nivolumab to chemotherapy drugs (and dosing and cycles of administration) not examined in the CheckMate 816 trial or in the Canadian product monograph will result in benefits similar to those seen with the chemotherapy drugs and doses used in that trial.
To address the lack of direct evidence comparing nivolumab plus chemotherapy with upfront surgery followed by adjuvant chemotherapy, the sponsor submitted 1 ITC. The clinical experts noted that adjuvant atezolizumab was an appropriate comparator, and that comparing nivolumab plus chemotherapy with surgery alone or with surgery plus adjuvant systematic should be adjusted for the time-lag bias. Patients with stage IIIA or stage IIIA N2 resectable NSCLC showed more improvement in EFS following neoadjuvant nivolumab in combination with chemotherapy compared to relevant comparators (i.e., neoadjuvant chemotherapy and surgery alone for stage IIIA disease, and neoadjuvant chemotherapy or neoadjuvant chemoradiotherapy for stage IIIA N2 disease). However, in patients with stage IB to II NSCLC, neoadjuvant nivolumab in combination with chemotherapy was not superior to neoadjuvant chemotherapy, adjuvant chemotherapy, or surgery alone. The treatment effects observed between patients with stage IIIA or stage IIIA N2 disease and those with stage IB to II disease (e.g., between neoadjuvant nivolumab in combination with chemotherapy and neoadjuvant chemotherapy, EFS was statistically significant in patients with stage IIIA or stage IIIA nonsquamous disease but nonsignificant in patients with stage IB to II disease) suggested that the pooled ITC results in the stage-agnostic population (i.e., stage IB to stage IIIA) were significantly biased and that pooling was inappropriate, methodologically, although neoadjuvant nivolumab in combination with chemotherapy significantly improved EFS compared with neoadjuvant chemotherapy, adjuvant chemotherapy, and surgery alone for patients with stage-agnostic NSCLC. No conclusions could be drawn about safety outcomes in the absence of a quantitative synthesis. Several sources of uncertainty were identified in the ITC, such as the significant heterogeneity in the RCTs included, sparse networks, the potential for misclassification of tumour stage when different versions of the guidelines were used, and immature data for OS, which limits the interpretability of the findings.
The sponsor-submitted retrospective study demonstrated a longer median OS for patients with a pCR than for those without. Similarly, MPR was found to be associated with improved EFS and OS, with adjusted HRs showing similar patterns. Median OS was higher in patients with an MPR than in those without. Most of the patients included in the study had stage III NSCLC, and more than half reportedly had an ECOG PS of 1. The study, conducted over 10 years, adapted the most widely used definition of pCR (ypT0N0), and National Comprehensive Cancer Network guidelines for treatment protocols were used to minimize heterogeneity across clinical centres in The US Oncology Network. There were several limitations identified in the real-world study, including the potential for missing or incomplete data for some variables in EHRs and patient charts. Further, applying definitions of pCR or MPR to the overall population reduced the sample size needed to properly assess the relationship between these end points and EFS and OS. The study also had external validity issues, such as selection bias, differences between the US community oncology setting and the clinical setting in Canada, use of the full EHR capabilities of the iKM database by specific networks that could have excluded certain populations, and patient selection after the index dates. The key limitation identified was that the study did not include immunotherapy and/or targeted therapy in neoadjuvant treatment options.
Harms
Overall, the proportion of patients reporting at least 1 AE was comparable in the 2 arms. The most frequently reported AEs in the nivolumab plus chemotherapy arm were nausea, constipation, anemia, decreased appetite, fatigue, and neutropenia. There were slightly more SAEs in the nivolumab plus chemotherapy arm than in the chemotherapy alone arm. There were slightly more dose delays or dose reductions related to AEs in the chemotherapy arm than in the nivolumab plus chemotherapy arm (37.5% versus 30.1%), but AEs leading to discontinuation did not differ significantly between the 2 arms (11.4% versus 10.2%). There were more deaths reported in the chemotherapy arm than in the nivolumab plus chemotherapy arm by the data cut-off date (October 20, 2021). Immune-related AEs reported in the nivolumab plus chemotherapy arm were consistent with the safety profile of immunotherapies.
The clinical experts consulted during the review did not identify any major concerns or new safety signals in the 2 study arms, and generally agreed that the safety of nivolumab plus chemotherapy was acceptable and manageable. The safety profile aligns with clinical expectations following the use of nivolumab or chemotherapy. The AEs reported, according to the experts, have been properly documented in literature and are manageable in clinical practice.
Conclusions
Although statistically significant EFS and favourable OS outcomes were observed in the CheckMate 816 trial for nivolumab plus chemotherapy compared to chemotherapy alone for the neoadjuvant treatment of adults with resectable NSCLC (tumours ≥ 4 cm or node-positive disease), there remains uncertainty about the magnitude of the treatment effect, given that the results are based on interim analyses, the OS data were immature at the October 20, 2021 cut-off date, and the HR for death was not statistically significant. Although EFS is a validated surrogate for OS, final analyses may be warranted to increase confidence in the trial findings. Prespecified EFS subgroup analyses suggested that the majority of the benefits derived from nivolumab plus chemotherapy were in subgroups of patients with stage IIIA disease and a PD-L1 expression level above 50%. However, efficacy results in these subgroup analyses should be interpreted with caution, as the study was not statistically powered to assess individual subgroups. The clinical experts indicated that patients with the highest risk of recurrence (i.e., patients with stage IIIA disease) and a PD-L1 expression level above 50% would be more likely to derive benefit from the treatment, and clinicians might be more apt to treat them with this regimen. However, regardless of the magnitude of response observed, a benefit was observed in all subgroups and in the overall study population. No detriment to quality of life was observed for patients in the trial, and the mean differences from baseline to predefined time points did not exceed the MIDs for the VAS and utility score portions of the EQ-5D-3L questionnaire. Notable differences between the trial population and patients in the Canadian setting were related to the younger age of the enrolled population, the higher proportion of patients enrolled with stage IIIA disease than seen in clinical practice, and the lack of a comparator arm with the current standard of care. However, the clinical experts noted that these differences are unlikely to affect the generalizability of the efficacy results to the Canadian population. The clinical experts explained that this treatment will typically be administered to patients with surgically resectable NSCLC (tumours ≥ 4 cm and/or node-positive disease) who have good a ECOG PS (0 or 1). The safety profile of nivolumab was consistent with the known safety profile of immunotherapies, and no new safety signals were identified. The AEs reported were considered manageable in practice by the clinical exerts consulted.
It is worth noting that the comparator in the CheckMate 816 trial (neoadjuvant chemotherapy) is not the current standard of care in Canada for patients with resectable NSCLC (which is upfront surgery with curative intent followed by adjuvant chemotherapy), and no direct evidence was available to assess the efficacy of nivolumab plus chemotherapy relative to surgery followed by adjuvant chemotherapy. Findings from the sponsor-submitted NMA suggest improvement in EFS with nivolumab plus chemotherapy for patients with stage IIIA, resectable NSCLC, compared with surgery and adjuvant chemotherapy. However, there were sources of uncertainty identified, such as the significant heterogeneity in the included RCTs, sparse networks, and immature data for OS. In addition, there were no quantitative safety data presented, so no conclusions could be drawn. The sponsor-submitted meta-analysis and real-world evidence showed favourable OS outcomes for patients treated with neoadjuvant nivolumab based on pCR status compared to those without pCR status. However, both studies have study design limitations that preclude definitive conclusions.
References
1.Canadian Cancer Society. Research: cancer statistics. 2022; https://cancer.ca/en/research/cancer-statistics. Accessed 2022 Oct 19.
2.Canadian Cancer Society. Cancer statistics at a glance. 2022; https://cancer.ca/en/research/cancer-statistics/cancer-statistics-at-a-glance. Accessed 2022 Oct 19.
3.Brenner DR, Poirier A, Woods RR, et al. Projected estimates of cancer in Canada in 2022. Can Med Assoc J. 2022;194(17):E601. PubMed
4.Canadian Cancer Cancer Advisory Committee. Canadian cancer statistics. 2021; https://cdn.cancer.ca/-/media/files/research/cancer-statistics/2021-statistics/2021-pdf-en-final.pdf. Accessed 2022 Jan 5.
5.Canadian Cancer Statistics Advisory Committee. Canadian cancer statistics: a 2020 special report on lung cancer. Toronto (ON): Canadian Cancer Society; 2020: https://cdn.cancer.ca/-/media/files/cancer-information/resources/publications/2020-canadian-cancer-statistics-special-report/2020-canadian-cancer-statistics-special-report-en.pdf. Accessed 2022 Mar 23.
6.Dela Cruz CS, Tanoue LT, Matthay RA. Lung cancer: epidemiology, etiology, and prevention. Clin Chest Med. 2011;32(4):605-644. PubMed
7.Canadian Cancer Statistics Advisory Committee. Canadian cancer statistics: a 2018 special report on cancer incidence by stage. Toronto, ON: Canadian Cancer Society; 2018: https://cdn.cancer.ca/-/media/files/research/cancer-statistics/2018-statistics/canadian-cancer-statistics-2018-en.pdf. Accessed 2022 Oct 19.
8.National Comprehensive Cancer Network (NCCN). Non-small cell lung cancer. Version 5.2022. (NCCN clinical practice guidelines in oncology) 2022; www.nccn.org (free registration required). Accessed 2022 Sep 26.
9.Postmus PE, Kerr KM, Oudkerk M, et al. Early and locally advanced non-small-cell lung cancer (NSCLC): ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2017;28(suppl_4):iv1-iv21. PubMed
10.Kris MG, Gaspar LE, Chaft JE, et al. Adjuvant systemic therapy and adjuvant radiation therapy for stage I to IIIA completely resected non–small-cell lung cancers: American Society of Clinical Oncology/Cancer Care Ontario clinical practice guideline update. J Clin Oncol. 2017;35(25):2960-2974. PubMed
11.Perdrizet K, Cheema PK. The evolving role of immunotherapy in stage III non-small cell lung cancer. Current Oncology. 2021;28(6):5408-5421. PubMed
12.Drug Reimbursement Review sponsor submission: Opdivo (nivolumab) 360 mg in combination with platinum-doublet chemotherapy every 3 weeks for 3 cycles; intravenous infusion [internal sponsor's package]. Montreal (QC): Bristol-Myers Squibb Canada; 2022 Sep 13.
13.Preoperative chemotherapy for non-small-cell lung cancer: a systematic review and meta-analysis of individual participant data. Lancet. 2014;383(9928):1561-1571. PubMed
14.OPDIVO® (nivolumab for injection): intravenous infusion, 10 mg nivolumab /mL, 40 mg and 100 mg single-use vials [product monograph]. Montreal (QC): Bristol-Myers Squibb Canada Co; 2022 Aug 18.
15.Clinical Study Report: CA209816. Randomized, open-label, phase 3 trial of nivolumab plus ipilimumab or nivolumab plus platinum-doublet chemotherapy versus platinum-doublet chemotherapy in early stage NSCLC (CheckMate 816: CHECKpoint pathway and nivolumab clinical trial evaluation 816) [internal sponsor's report]. Lawrenceville (NJ): Bristol-Myers Squibb Company; 2020 Jul 14.
16.Network meta-analysis of therapies for non-metastatic non-small cell lung cancer (nmNSCLC) in the neoadjuvant setting [internal sponsor's report] In: Drug Reimbursement Review sponsor submission: Opdivo (nivolumab), 360 mg, every 3 weeks for 3 cycles; intravenous infusion. Montreal (QC): Bristol Myers Squibb; 2022 Sep 13.
17.Hutton B, Salanti G, Caldwell DM, et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: checklist and explanations. Ann Intern Med. 2015;162(11):777-784. PubMed
18.Canadian Cancer Society. Survival statistics for non–small cell lung cancer. 2020; https://cancer.ca/en/cancer-information/cancer-types/lung/non-small-cell-lung-cancer-survival-statistics. Accessed 2022 Oct 19.
19.Lung Cancer Canada. Lung canacer staging in Canada. 2020; https://www.lungcancercanada.ca/Lung-Cancer/Staging.aspx. Accessed 2021 Dec 4.
20.National Cancer Institute. Non-small cell lung cancer treatment (PDQ®) – health professional version. 2021; https://www.cancer.gov/types/lung/hp/non-small-cell-lung-treatment-pdq. Accessed 2021 Dec 4.
21.National Comprehensive Cancer Network (NCCN). Non-small cell lung cancer. NCCN Clinical Practice Guidelines in Oncology. 2021; https://www.nccn.org/guidelines/guidelines-detail?category=1&id=1450 (free registration required). Accessed 2021 Dec 4.
22.Detterbeck FC, Boffa DJ, Kim AW, Tanoue LT. The Eighth Edition Lung Cancer Stage Classification. Chest. 2017;151(1):193-203.
23.Chouaid C, Danson S, Andreas S, et al. Adjuvant treatment patterns and outcomes in patients with stage IB-IIIA non-small cell lung cancer in France, Germany, and the United Kingdom based on the LuCaBIS burden of illness study. Lung Cancer. 2018;124:310-316. PubMed
24.Iyer S, Roughley A, Rider A, Taylor-Stokes G. The symptom burden of non-small cell lung cancer in the USA: a real-world cross-sectional study. Support Care Cancer. 2014;22(1):181-187. PubMed
25.BC Cancer. Lung. 2013; http://www.bccancer.bc.ca/health-professionals/clinical-resources/cancer-management-manual/lung/lung. Accessed 2021 Jun 3.
26.Pisters K, Kris MG, Gaspar LE, Ismaila N. Adjuvant systemic therapy and adjuvant radiation therapy for stage I-IIIA completely resected non–small-cell lung cancer: ASCO guideline rapid recommendation update. J Clin Oncol. 2022;40(10):1127-1129. PubMed
27.BC Cancer. Non-small cell lung cancer (NSCLC). Surgical treatment of stage I-IIIA. 2014; http://www.bccancer.bc.ca/books/lung/management/non-small-cell-lung-cancer-nsclc/surgical-treatment-of-stage-i-iiia. Accessed 2022 Dec 5.
28.Douillard JY, Tribodet H, Aubert D, et al. Adjuvant cisplatin and vinorelbine for completely resected non-small cell lung cancer: subgroup analysis of the Lung Adjuvant Cisplatin Evaluation. J Thorac Oncol. 2010;5(2):220-228. PubMed
29.Carboplatin injection BP: sterile solution, 10 mg / mL (50 mg, 150 mg, 450 mg, 600 mg of carboplatin per vial); antineoplastic agent [product monograph]. Kirkland (QC): Pfizer Canada ULC; 2022 Mar 29.
30.Pemetrexed disodium for Injection: 100 mg, 500 mg or 1000 mg pemetrexed per vial. Pemetrexed (as pemetrexed disodium hemipentahydrate) [product monograph]. Woodbridge (ON): Auro Pharma Inc.; 2021 Jun 29.
31.Long YX, Sun Y, Liu RZ, et al. Immune-related pneumonitis was decreased by addition of chemotherapy with PD-1/L1 inhibitors: systematic review and network meta-analysis of randomized controlled trials (RCTs). Current Oncology. 2022;29(1):267-282. PubMed
32.McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 guideline statement. J Clin Epidemiol. 2016;75:40-46. PubMed
33.Grey matters: a practical tool for searching health-related grey literature. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/grey-matters. Accessed 2023 Jan 16.
34.Forde PM, Spicer J, Lu S, et al. Neoadjuvant nivolumab plus chemotherapy in resectable lung cancer. N Engl J Med. 2022;386(21):1973-1985. PubMed
35.Provencio M, Serna-Blasco R, Nadal E, et al. Overall survival and biomarker analysis of neoadjuvant nivolumab plus chemotherapy in operable stage IIIA non-small-cell lung cancer (NADIM phase II trial). J Clin Oncol. 2022;71 (no pagination). PubMed
36.Brooks R. EuroQol: the current state of play. Health Policy. 1996;37(1):53-72. PubMed
37.van Reenen M, Oppe M, Secnik Boye K, et al. EQ-5D-3L user guide. 2018: https://euroqol.org/publications/user-guides/. Accessed 2022 Oct 14.
38.Wilcox RA, Djulbegovic B, Guyatt GH, Montori VM. Randomized trials in oncology stopped early for benefit. J Clin Oncol. 2008;26(1):18-19. PubMed
39.Bassler D, Briel M, Montori VM, et al. Stopping randomized trials early for benefit and estimation of treatment effects: systematic review and meta-regression analysis. JAMA. 2010;303(12):1180-1187. PubMed
40.The dangers of stopping trials early. BMJ. 2012;345. https://www.bmj.com/bmj/section-pdf/187582?path=/bmj/345/7865/Analysis.full.pdf. Accessed 2023 Jan 16.
41.Pickard AS, Neary MP, Cella D. Estimation of minimally important differences in EQ-5D utility and VAS scores in cancer. Health Qual Life Outcomes. 2007;5(1):70. PubMed
42.Paclitaxel injection (6 mg/mL), sterile; Antineoplastic agent [product monograph]. Woodbridge (ON): Auro Pharma Inc.; 2022 Jul 22. Accessed July 22, 2022.
43.Pilkington G, Boland A, Brown T, Oyee J, Bagust A, Dickson R. A systematic review of the clinical effectiveness of first-line chemotherapy for adult patients with locally advanced or metastatic non-small cell lung cancer. Thorax. 2015;70(4):359-367. PubMed
44.Dias S, Welton NJ, Sutton AJ, Ades AE. NICE DSCU technical support document 2: a generalised linear modelling framework for pairwise and network meta-analysis of randomised controlled trials. London (United Kingdom): National Institute for Health and Care Excellence (NICE); 2014.
45.Felip E, Rosell R, Maestre JA, et al. Preoperative chemotherapy plus surgery versus surgery plus adjuvant chemotherapy versus surgery alone in early-stage non-small-cell lung cancer. J Clin Oncol. 2010;28(19):3138-3145. PubMed
46.Scagliotti GV, Pastorino U, Vansteenkiste JF, et al. Randomized phase III study of surgery alone or surgery plus preoperative cisplatin and gemcitabine in stages IB to IIIA non-small-cell lung cancer. J Clin Oncol. 2012;30(2):172-178. PubMed
47.Pisters KM, Vallières E, Crowley JJ, et al. Surgery with or without preoperative paclitaxel and carboplatin in early-stage non-small-cell lung cancer: Southwest Oncology Group Trial S9900, an intergroup, randomized, phase III trial. J Clin Oncol. 2010;28(11):1843-1849. PubMed
48.Connock M, Armoiry X, Tsertsvadze A, et al. Comparative survival benefit of currently licensed second or third line treatments for epidermal growth factor receptor (EGFR) and anaplastic lymphoma kinase (ALK) negative advanced or metastatic non-small cell lung cancer: a systematic review and secondary analysis of trials. BMC Cancer. 2019;19(1):392. PubMed
49.Girard N, Mornex F, Douillard JY, et al. Is neoadjuvant chemoradiotherapy a feasible strategy for stage IIIA-N2 non-small cell lung cancer? Mature results of the randomized IFCT-0101 phase II trial. Lung Cancer. 2010;69(1):86-93. PubMed
50.Katakami N, Tada H, Mitsudomi T, et al. A phase 3 study of induction treatment with concurrent chemoradiotherapy versus chemotherapy before surgery in patients with pathologically confirmed N2 stage IIIA nonsmall cell lung cancer (WJTOG9903). Cancer. 2012;118(24):6126-6135. PubMed
51.Pless M, Stupp R, Ris HB, et al. Induction chemoradiation in stage IIIA/N2 non-small-cell lung cancer: a phase 3 randomised trial. Lancet. 2015;386(9998):1049-1056. PubMed
52.Murad MH, Montori VM, Ioannidis JPA, Prasad K, Cook DJ, Guyatt G. Fixed-effects and random-effects models. In: Guyatt G, Rennie D, Meade MO, Cook DJ, eds. Users' guides to the medical literature: a manual for evidence-based clinical practice, 3rd ed. New York (NY): McGraw-Hill Education; 2015.
53.Klikovits T, End A, Riedl G, Stiebler M, Dekan G, Klepetko W. Effects of reclassification from the TNM-6 into the TNM-7 staging system in bronchoplastic resection for non-small cell lung cancer. Interact Cardiovasc Thorac Surg. 2011;13(1):29-34. PubMed
54.Guyot P, Ades AE, Ouwens MJNM, Welton NJ. Enhanced secondary analysis of survival data: reconstructing the data from published Kaplan-Meier survival curves. BMC Med Res Methodol. 2012;12(1):9. PubMed
55.Altman DG, Bland JM. How to obtain the confidence interval from a P value. BMJ: British Medical Journal. 2011;343:d2090. PubMed
56.Cortazar P, Zhang L, Untch M, et al. Pathological complete response and long-term clinical benefit in breast cancer: the CTNeoBC pooled analysis. Lancet. 2014;384(9938):164-172. PubMed
57.Pataer A, Shao R, Correa AM, et al. Major pathologic response and RAD51 predict survival in lung cancer patients receiving neoadjuvant chemotherapy. Cancer Medicine. 2018;7(6):2405-2414. PubMed
58.Remon J, Martinez-Marti A, Carcereny Costa E, et al. Major pathological response after preoperative chemotherapy as a surrogate marker of survival in early-stage non-small cell lung cancer: cohort of NATCH phase III trial. Ann Oncol. 2017;28:v454.
59.Wislez M, Mazieres J, Lavole A, et al. 1151MO Pathological response is an independent factor of overall survival and disease-free survival after neoadjuvant durvalumab in resectable non-small cell lung cancer (NSCLC) in the IFCT-1601 IONESCO phase II trial. Ann Oncol. 2021;32:S931.
60.Duan H, Wang T, Luo Z, et al. Neoadjuvant programmed cell death protein 1 inhibitors combined with chemotherapy in resectable non-small cell lung cancer: an open-label, multicenter, single-arm study. Transl Lung Cancer Res. 2021;10(2):1020-1028. PubMed
61.Jiang J, Wang Y, Gao Y, et al. Neoadjuvant immunotherapy or chemoimmunotherapy in non-small cell lung cancer: a systematic review and meta-analysis. Transl Lung Cancer Res. 2022;11(2):277-294. PubMed
62.Cascone T, William WN, Jr., Weissferdt A, et al. Neoadjuvant nivolumab or nivolumab plus ipilimumab in operable non-small cell lung cancer: the phase 2 randomized NEOSTAR trial. Nat Med. 2021;27(3):504-514. PubMed
Appendix 1: Literature Search Strategy
Note that this appendix has not been copy-edited.
Clinical Literature Search
Overview
Interface: Ovid
Databases
MEDLINE All (1946-present)
Embase (1974-present)
Note: Patient headings and search fields have been customized for each database. Duplicates between databases were removed in Ovid.
Date of search: September 29, 2022
Alerts: Bi-weekly search updates until project completion
Search filters applied: Randomized controlled trials; controlled clinical trials.
Limits
Conference abstracts: excluded
Syntax | Description |
|---|---|
/ | At the end of a phrase, searches the phrase as a patient heading |
MeSH | Medical Patient Heading |
.fs | Floating subheading |
exp | Explode a patient heading |
* | Before a word, indicates that the marked patient heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings |
# | Truncation symbol for one character |
? | Truncation symbol for one or no characters only |
adj# | Requires terms to be adjacent to each other within # number of words (in any order) |
.ti | Title |
.ot | Original title |
.ab | Abstract |
.hw | Heading word; usually includes patient headings and controlled vocabulary |
.kf | Keyword heading word |
.dq | Candidate term word (Embase) |
.pt | Publication type |
.mp | Mapped term |
.rn | Registry number |
.nm | Name of substance word (MEDLINE) |
.yr | Publication year |
.jw | Journal title word (MEDLINE) |
.jx | Journal title word (Embase) |
freq = # | Requires terms to occur # number of times in the specified fields |
medall | Ovid database code: MEDLINE All, 1946 to present, updated daily |
oemezd | Ovid database code; Embase, 1974 to present, updated daily |
cctr | Ovid database code; Cochrane Central Register of Controlled Trials |
Multidatabase Strategy
Nivolumab/
(opdivo* or nivolumab* or nivo or bms 936558 or bms936558 or cmab 819 or cmab819 or mdx 1106 or mdx1106 or ono 4538 or ono4538 or HSDB 8256 or HSDB8256 or GTPL 7335 or GTPL7335 or 31YO63LBSN).ti,ab,kf,ot,hw,rn,nm.
1 or 2
Carcinoma, Non-Small-Cell Lung/
exp LUNG/ and Carcinoma, Large Cell/
(NSCLC* or LCLC*).ti,ab,kf.
((non small cell* or nonsmall cell* or large cell or undifferentiated) adj5 (lung* or bronch* or pulmonar*) adj5 (cancer* or tumor* or tumour* or carcinoma* or neoplas*)).ti,ab,kf.
((bronchial or pulmonary or lung) adj3 (adenocarcinoma* or adeno-carcinoma*)).ti,ab,kf.
((bronchioloalveolar or bronchiolo alveolar) adj3 (carcinoma* or cancer* or neoplas* or tumor* or tumour*)).ti,ab,kf.
or/4-9
3 and 10
11 use medall
*nivolumab/
(opdivo* or nivolumab* or nivo or bms 936558 or bms936558 or cmab 819 or cmab819 or mdx 1106 or mdx1106 or ono 4538 or ono4538 or HSDB 8256 or HSDB8256 or GTPL 7335 or GTPL7335).ti,ab,kf,dq.
13 or 14
non small cell lung cancer/ or large cell lung carcinoma/ or lung adenocarcinoma/
(NSCLC* or LCLC*).ti,ab,kf,dq.
((non small cell* or nonsmall cell* or large cell or undifferentiated) adj5 (lung* or bronch* or pulmonary*) adj5 (cancer* or tumor* or tumour* or carcinoma* or neoplas*)).ti,ab,kf,dq.
((bronchial or pulmonary or lung) adj3 (adenocarcinoma* or adeno-carcinoma*)).ti,ab,kf,dq.
((bronchioloalveolar or bronchiolo alveolar) adj3 (carcinoma* or cancer* or neoplas* or tumor* or tumour*)).ti,ab,kf,dq.
or/16-20
15 and 21
22 use oemezd
23 not (conference abstract or conference review).pt.
12 or 24
(Randomized Controlled Trial or Controlled Clinical Trial or Pragmatic Clinical Trial or Equivalence Trial or Clinical Trial, Phase III).pt.
Randomized Controlled Trial/
exp Randomized Controlled Trials as Topic/
“Randomized Controlled Trial (topic)”/
Controlled Clinical Trial/
exp Controlled Clinical Trials as Topic/
“Controlled Clinical Trial (topic)”/
Randomization/
Random Allocation/
Double-Blind Method/
Double Blind Procedure/
Double-Blind Studies/
Single-Blind Method/
Single Blind Procedure/
Single-Blind Studies/
Placebos/
Placebo/
Control Groups/
Control Group/
(random* or sham or placebo*).ti,ab,hw,kf.
((singl* or doubl*) adj (blind* or dumm* or mask*)).ti,ab,hw,kf.
((tripl* or trebl*) adj (blind* or dumm* or mask*)).ti,ab,hw,kf.
(control* adj3 (study or studies or trial* or group*)).ti,ab,kf.
(Nonrandom* or non random* or non-random* or quasi-random* or quasirandom*).ti,ab,hw,kf.
allocated.ti,ab,hw.
((open label or open-label) adj5 (study or studies or trial*)).ti,ab,hw,kf.
((equivalence or superiority or non-inferiority or noninferiority) adj3 (study or studies or trial*)).ti,ab,hw,kf.
(pragmatic study or pragmatic studies).ti,ab,hw,kf.
((pragmatic or practical) adj3 trial*).ti,ab,hw,kf.
((quasiexperimental or quasi-experimental) adj3 (study or studies or trial*)).ti,ab,hw,kf.
(phase adj3 (III or “3”) adj3 (study or studies or trial*)).ti,hw,kf.
or/26-56
25 and 57
remove duplicates from 58
Clinical Trials Registries
ClinicalTrials.gov
Produced by the US National Library of Medicine. Targeted search used to capture registered clinical trials.
[Search terms: Opdivo (nivolumab) AND non–small cell lung cancer (NSCLC)
WHO ICTRP
International Clinical Trials Registry Platform, produced by WHO. Targeted search used to capture registered clinical trials.
[Search terms: Opdivo (nivolumab) AND non–small cell lung cancer (NSCLC)
Health Canada’s Clinical Trials Database
Produced by Health Canada. Targeted search used to capture registered clinical trials.
[Search terms: Opdivo (nivolumab) AND non–small cell lung cancer (NSCLC)
EU Clinical Trials Register
European Union Clinical Trials Register, produced by the European Union. Targeted search used to capture registered clinical trials.
[Search terms: Opdivo (nivolumab) AND non–small cell lung cancer (NSCLC)
Grey Literature
Search dates: September 29, 2022 – October 3, 2022
Keywords: Opdivo (nivolumab) AND non–small cell lung cancer (NSCLC)
Limits: no limit
Relevant websites from the following sections of the CADTH grey literature checklist Grey Matters: A Practical Tool for Searching Health-Related Grey Literature were searched:
Health Technology Assessment Agencies
Health Economics
Clinical Practice Guidelines
Drug and Device Regulatory Approvals
Advisories and Warnings
Drug Class Reviews
Clinical Trials Registries
Databases (free)
Health Statistics
Internet Search
Open Access Journals
Appendix 2: Excluded Studies
Note that this appendix has not been copy-edited.
Reference | Reason for exclusion |
|---|---|
Duan et al., 202160 | Study design |
Jiang et al., 202261 | Study design |
Cascone et al., 202162 | Study design |
Appendix 3: Protocol Deviations and Treatment Exposure
Note that this appendix has not been copy-edited.
Important Protocol Deviations
Table 44: Protocol Deviations in the Nivolumab Plus Chemotherapy and Chemotherapy Arms
Status (%) | Nivolumab plus chemotherapy (N = 179) | Chemotherapy (N = 179) |
|---|---|---|
Patients with at least 1 deviation | 2 (1.1) | 4 (2.2) |
At entrance | ||
Patients with inadequate disease stage | 1 (0.6) | 2 (1.1) |
Patients with baseline ECOG PS > 1 | 0 | 0 |
On-treatment deviations | ||
Patients receiving concurrent cancer therapy | 1 (0.6) | 2 (1.1) |
Patients treated differently than as randomized | 0 | 0 |
Informed consent and/or ethics (IEC/IRB) deviations | ||
Failure to obtain written informed consent on the correct approved version and maintain in the study record | 6 | 3 |
Consistent failure to obtain ICF update from patient | 3 | 5 |
Failure to report all SAEs in accordance with the time period required by GCP, the protocol and applicable regulations | 8 | 9 |
Use of prohibited concomitant medications | 2 | 3 |
Inclusion or exclusion deviations | ||
Incorrect disease stage at baseline | 1 | 3 |
Screening procedure not done or out of window | 11 | 11 |
Patient enrolled with EGFR positive mutation | 1 | 2 |
Incorrect dosing or study treatment assignment | 1 | 5 |
Trial procedures | ||
Consistent issues with tumour assessments out of window | 3 | 6 |
Definitive pathology sample not collected per study requirements | 1 | 3 |
Presurgery scan out of window | 2 | 1 |
Protocol required biomarker labs routinely not drawn | 1 | 3 |
Safety labs not done | 8 | 5 |
ECG not performed within 28 days of randomization | 0 | 1 |
Other | ||
Misclassified stratification level [IRT vs. Clinical database] | 1 | 1 |
Follow-up visit documentation missing | 4 | 3 |
Drug accountability not completed per protocol (Receipt of study drug and unassigned kits not accounted for) | 0 | 1 |
Chemo = chemotherapy; ECOG PS = Eastern Cooperative Oncology Group Performance Status; EGFR = Epidermal growth factor receptor; GCP = Good Clinical Practice; ICF = informed consent form; IEC = independent ethics committee; IRB = institutional review board; Nivo = nivolumab; SAEs = serious adverse events; vs = versus.
Source: Clinical Study Report.15
Exposure to Study Treatments
Table 45: Cumulative Dose and Relative Dose Intensity in the Neoadjuvant Period — All Treated Patients
Nivolumab plus chemotherapy (n = 176) | |||
|---|---|---|---|
Characteristics | Nivolumab (n = 176) | Carboplatin (n = 51) | Cisplatin (n = 136) |
Number of doses received, n (%) | |||
1 | 4 (2.3) | 4 (7.8) | 10 (7.4) |
2 | 8 (4.5) | 11 (21.6) | 11 (8.1) |
3 | 164 (93.2) | 36 (70.6) | 115 (84.6) |
Cumulative dose (unit)a | |||
Mean (SD) | 1,047.3 (129.2) | 12.9 (3.5) | 203.3 (42.6) |
Median (Min-Max) | 1,080.0 (360 to 1,080) | 14.2 (4.7 to 18.4) | 223.4 (74.5 to 231.5) |
Relative dose intensity n (%) | |||
≥ 110% | 0 | 3 (5.9) | 0 |
90% to < 110% | 154 (87.5) | 28 (54.9) | 99 (72.8) |
70% to < 90% | 19 (10.8) | 18 (35.3) | 33 (24.3) |
50% to < 70% | 3 (1.7) | 1 (2.0) | 4 (2.9) |
< 50% | 0 | 0 | 0 |
Not reported | 0 | 1 (2.0) | 0 |
Characteristics | Gemcitabine (n = 65) | Paclitaxel (n = 28) | Pemetrexed (n = 83) |
Number of doses received n (%) | |||
1 | 0 | 2 (7.1) | 0 |
2 | 1 (1.5) | 2 (7.1) | 6 (7.2) |
3 | 2 (3.1) | 24 (85.7) | 77 (92.8) |
4 | 4 (6.2) | 0 | 0 |
5 | 11 (16.9) | 0 | 0 |
> 5 | 47 (72.3) | 0 | 0 |
Cumulative dose (unit)a | |||
Mean (SD) | 5,731.1 (1,096.3) | 460.428 (122.89) | 1,459.145 (132.54) |
Median (Min-Max) | 5,986.8 (2,457.7 to 7,636.3) | 518.9 (11.65 to 558.9) | 1,500.0(964.5 to 1,591.7) |
Relative dose intensity n (%) | |||
≥ 110% | 0 | 0 | 0 |
90% to < 110% | 30 (46.2) | 17 (60.7) | 71 (85.5) |
70% to < 90% | 28 (43.1) | 9 (32.1) | 12 (14.5) |
50% to < 70% | 5 (7.7) | 1 (3.6) | 0 |
< 50% | 2 (3.1) | 1 (3.6) | 0 |
Not reported | 0 | 0 | 0 |
Max = maximum; Min = minimum; SD = standard deviation
aDose in units: Nivolumab in mg (Arm C); Vinorelbine, Cisplatin, Docetaxel, Gemcitabine, Pemetrexed, and Paclitaxel, in mg/ m2, Carboplatin in AUC.
Source: Clinical Study Report.15
Table 46: Cumulative Dose and Relative Dose Intensity in the Neoadjuvant Period — All Treated Patients
Detail | Chemotherapy (N = 179) | |||
|---|---|---|---|---|
Characteristic | Carboplatin (n = 42) | Cisplatin (N = 143) | Docetaxel (N = 29) | |
Number of doses received | ||||
1 | 8 (19.0) | 13 (9.1) | 1 (3.4) | |
2 | 6 (14.3) | 16 (11.2) | 2 (6.9) | |
3 | 28 (66.7) | 114 (79.7) | 26 (89.7) | |
4 | 0 | 0 | 0 | |
5 | 0 | 0 | 0 | |
> 5 | 0 | 0 | 0 | |
Cumulative dose (unit)a | ||||
Mean (SD) | 11.929 (4.176) | 203.857 (102.392) | 196.896 (39.215) | |
Median (min - max) | 12.965 (2.90 to 18.00) | 221.883 (73.37 to 1287.65) | 218.187 (60.00 to 227.12) | |
Relative dose intensity (%) | ||||
≥ 110% | 0 | 1 (0.7) | 0 | |
90% to < 110% | 25 (59.5) | 99 (69.2) | 19 (65.5) | |
70% to < 90% | 15 (35.7) | 40 (28.0) | 10 (34.5) | |
50% to < 70% | 2 (4.8) | 3 (2.1) | 0 | |
< 50% | 0 | 0 | 0 | |
Not reported | 0 | 0 | 0 | |
Characteristic | Gemcitabine (N = 49) | Paclitaxel (N = 22) | Pemetrexed (N = 63) | Vinorelbine (N = 13) |
Number of doses received | ||||
1 | 0 | 2 (9.1) | 5 (7.9) 0 | 0 |
2 | 1 (2.0) | 2 (9.1) | 5 (7.9) | 1 (7.7) |
3 | 0 | 18 (81.8) | 53 (84.1) | 1 (7.7) |
4 | 2 (4.1) | 0 | 0 | 2 (15.4) |
5 | 9 (18.4) | 0 | 0 | 4 (30.8) |
> 5 | 37 (75.5) | 0 | 0 | 5 (38.5) |
Cumulative dose (unit)a | ||||
Mean (SD) | 5,912.493 (1,124.455) | 486.388 (123.506) | 1,362.166 (291.134) | 119.811 (33.403) |
Median (min - max) | 6,000.131 (2019.61 to 7614.90) | 516.835 (172.97 to 607.12) | 1,489.446 (491.12 to 1518.69) | 125.145 (49.85 to 153.36) |
Relative dose intensity (%) | ||||
≥ 110% | 0 | 0 | 0 | 0 |
90% to < 110% | 31 (63.3) | 18 (81.8) | 50 (79.4) | 3 (23.1) |
70% to < 90% | 11 (22.4) | 4 (18.2) | 13 (20.6) | 7 (53.8) |
50% to < 70% | 7 (14.3) | 0 | 0 | 3 (23.1) |
< 50% | 0 | 0 | 0 | 0 |
Not reported | 0 | 0 | 0 | 0 |
aDose units: Vinorelbine, Cisplatin, Docetaxel, Gemcitabine, Pemetrexed, and Paclitaxel, in mg/m2, Carboplatin in AUC.
Data cut-off: October 20, 2021
Source: Clinical Study Report.
Appendix 4: Detailed Outcome Data
Note that this appendix has not been copy-edited.
Subgroup Analyses: EFS
Table 47: EFS per BICR, Subgroup Analyses — All Randomized Patients
Subgroup | Nivolumab plus chemotherapy | Chemotherapy | Nivolumab + chemotherapy vs. chemotherapy Unstratified Hazard Ratio (95% CI) |
|---|---|---|---|
Number of events (n of patients) | Number of events (n of patients) | ||
PD-L1 Status | |||
PD-L1 < 1% | 37 (78) | 41 (77) | 0.85 (0.54 to 1.32) |
PD-L1 ≥ 1% | 21 (89) | 41 (89) | 0.41 (0.24 to 0.70) |
PD-L1 1% to 49% | 15 (51) | 21 (47) | 0.58 (0.30 to 1.12) |
PD-L1 ≥ 50% | 6 (38) | 20 (42) | 0.24 (0.10 to 0.61) |
Indeterminate/not evaluable | 6 (12) | 5 (13) | 0.92 (0.26 to 3.17) |
Disease Stage at study entry | |||
Stage IB to II | 21 (65) | 24 (62) | 0.87 (0.48 to 1.56) |
Stage IIIA | 43 (113) | 62 (115) | 0.54 (0.37 to 0.80) |
Other | 0 (1) | 1 (2) | - |
ECOG PS | |||
0 | 42 (124) | 53 (117) | 0.61 (0.41 to 0.91) |
1 | 22 (55) | 34 (62) | 0.71 (0.41 to 1.21) |
Histology at Study Entry | |||
Squamous Cell Carcinoma | 33 (87) | 43 (95) | 0.77 (0.49 to 1.22) |
Nonsquamous | 31 (92) | 44 (84) | 0.50 (0.32 to 0.79) |
CI = confidence interval; CRF = case report form; ECOG PS = Eastern Cooperative Oncology Group Performance Status; EFS = event-free survival; HR = hazard ratio; IRT = Interactive Response Technology; mEFS = median event-free survival; NA = not available; PD-L1 = programmed death ligand 1; TMB = tumour mutation burden; vs = versus.
Data cut-off: October 20, 2021
Source: Clinical Study Report.15
Subgroup Analyses: pCR
Table 48: pCR by BIPR, Subgroup Analysis — All Randomized Patients
Subgroup | Nivolumab plus chemotherapy | Chemotherapy | ||
|---|---|---|---|---|
Number of responses (n of patients) | pCR (%) (95% CI) | Number of responses (n of patients) | pCR (95% CI) | |
PD-L1 Status | ||||
PD-L1 < 1% | 13 (78) | 16.7 (9.2 to 26.8) | 2 (77) | 2.6 (0.3 to 9.1) |
PD-L1 ≥ 1% | 29 (89) | 32.6 (23 to 43.3) | 2 (89) | 2.2 (0.3 to 7.9) |
PD-L1 1% to 49% | 12 (51) | 23.5 (12.8 to 37.5) | 0 (47) | 0 (0 to 7.5) |
PD-L1 ≥ 50% | 17 (38) | 44.7 (28.6 to 61.7) | 2 (42) | 4.8 (0.6 to 16.2) |
Indeterminate/not evaluable | 1 (12) | 8.3 (0.2 to 38.5) | 0 (13) | 0 (0 to 24.7) |
Disease Stage at study entry | ||||
Stage IB to II | 17 (65) | 26.2 (16.0 to 38.5) | 3 (63) | 4.8 (1.0 to 13.3) |
Stage IIIA | 26 (113) | 23.0 (15.6 to 31.9) | 1 (115) | 0.9 (< 0.1 to 4.7) |
Other | 0 (1) | 0 (0 to 97.5) | 0 (1) | 0 (0 to 97.5) |
ECOG PS | ||||
0 | 33 (124) | 26.6 (19.1 to 35.3) | 2 (117) | 1.7 (0.2 to 6.0) |
1 | 10 (55) | 18.2 (9.1 to 30.9) | 2 (62) | 3.2 (0.4 to 11.2) |
Histology at study entry | ||||
Squamous Cell Carcinoma | 22 (87) | 25.3 (16.6 to 35.7) | 4 (95) | 4.2 (1.2 to 10.4) |
Nonsquamous | 21 (92) | 22.8 (14.7 to 32.8) | 0 (84) | 0 (0 to 4.3) |
CI = confidence interval; CRF = case report form; ECOG PS = Eastern Cooperative Oncology Group Performance Status; HR = hazard ratio; IRT = Interactive Response Technology; mEFS = median event-free survival; NA = not available; PCR = pathologic complete response; PD-L1 = programmed death ligand 1; TMB = tumour mutation burden; vs = versus.
Data cut-off: September 16, 2020
Source: Clinical Study Report.15
Table 49: Completion Rates of EQ-5D-3L Questionnaire
Nominal point | EQ-5D-3L Descriptive System | EQ-5D-3L VAS | ||
|---|---|---|---|---|
Nivolumab plus chemotherapy N = 179 | Chemotherapy N = 179 | Nivolumab plus chemotherapy N = 179 | Chemotherapy N = 179 | |
Baseline, n (%) | 169 (94.4) | 171 (95.5) | 169 (94.4) | 170 (95.0) |
On treatment | ||||
Week 3 | NA | NA | NA | NA |
Week 4 | 168/174 (96.6) | 158/166 (95.2) | 168/174 (96.6) | 159/166 (95.8) |
Week 5 | NA | NA | NA | NA |
Week 7 | 151/167 (90.4) | 145/154 (94.2) | 152/167 (91.0) | 145/154 (94.2) |
Postneoadjuvant visit 1 | 156/176 (88.6) | 146/174 (83.9) | 156/176 (88.6) | 146/174 (83.9) |
Postneoadjuvant visit 2 | 134/165 (81.2) | 132/168 (78.6) | 134/165 (81.2) | 133/168 (79.2) |
Data cut-off: October 20, 2021
Source: Sponsor submission12
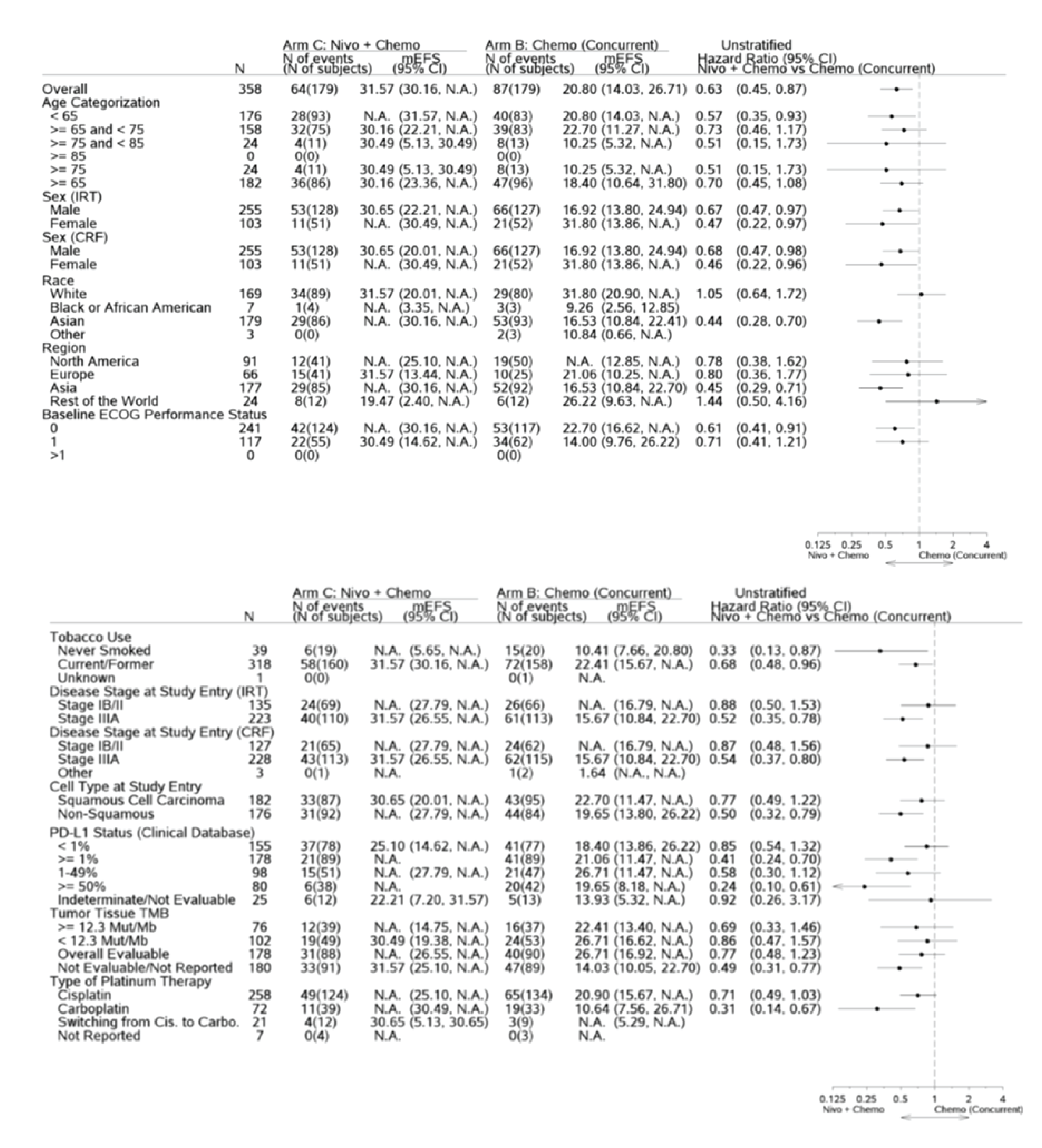
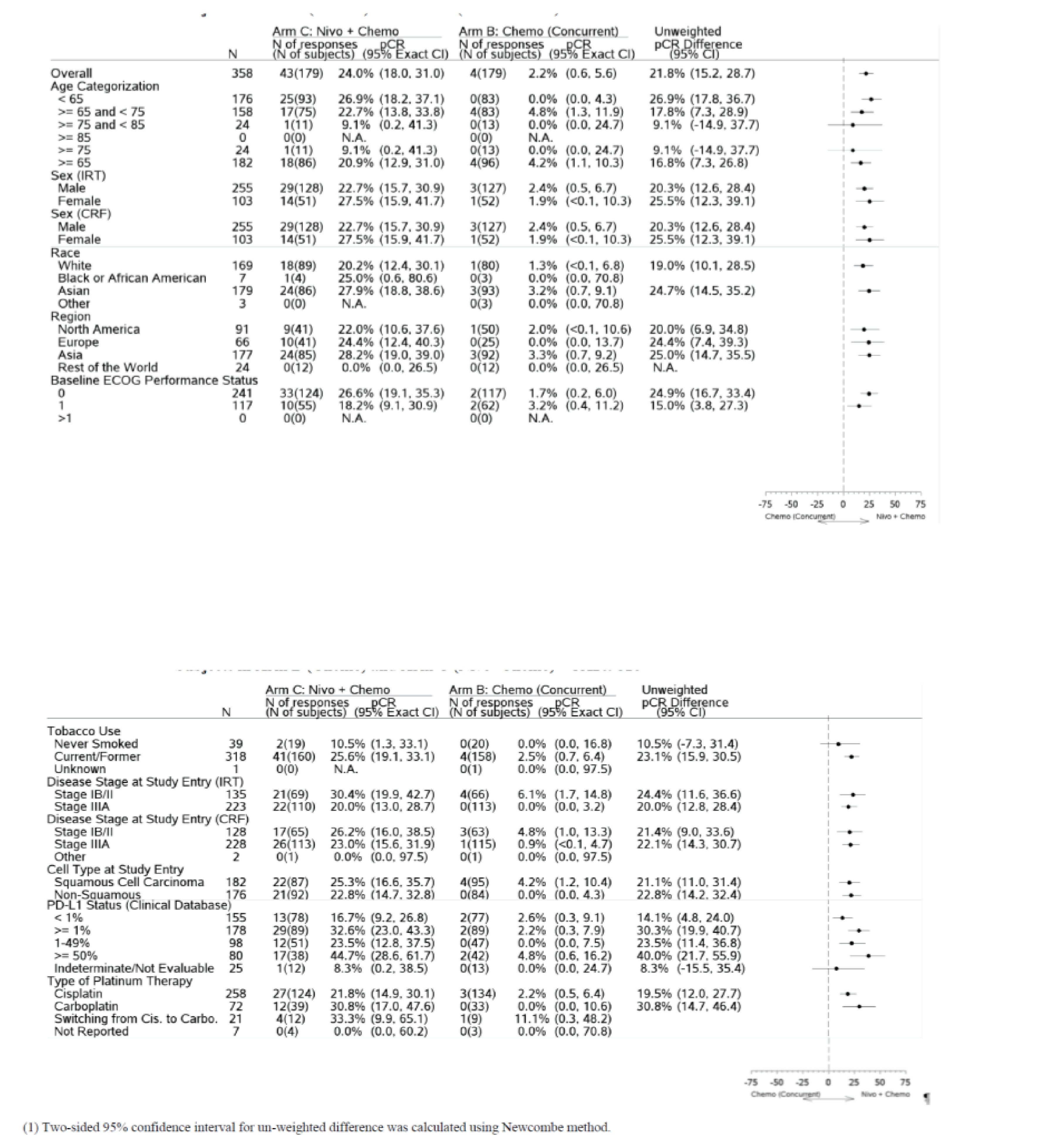
Appendix 5: Description and Appraisal of Outcome Measures
Note that this appendix has not been copy-edited.
Aim
To describe the following outcome measure and review its measurement properties (validity, reliability, responsiveness to change, and MID):
Finding
EQ-5D 3-Levels Questionnaire
EQ-5D-3L is a generic preference-based HRQoL instrument that has been applied to a wide range of health conditions and treatments.36,37 One part of the EQ-5D-3L is a descriptive system that classifies respondents (aged ≥ 12 years) into 1 of 243 distinct health states. The descriptive system consists of the following 5 dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Each dimension has 3 possible levels, 1, 2, and 3, representing ‘no problems,’ ‘some problems,’ and ‘extreme problems,’ respectively. Respondents are asked to choose 1 level that reflects their own health state for each of the 5 dimensions. A scoring function can be used to assign a value, i.e., EQ- 5D-3L index score, to each self-reported health state based on a set of population-based preference weights.36,37 The other part of EQ-5D-3L is a vertical, calibrated visual analogue scale (EQ VAS) that has end points labelled 0 and 100, with respective anchors of ‘worst imaginable health state’ and ‘best imaginable health state.’ Respondents are asked to rate their own health by drawing a line from an anchor box to the point on the EQ VAS which best represents their own health on that day. Hence, the EQ-5D-3L produces 3 types of data for each respondent:
A profile indicating the extent of problems on each of the 5 dimensions represented by a 5-digit descriptor, such as 11121, 33211.
A population preference-weighted health index score based on the descriptive system.
A self-reported current health status based on the EQ VAS that is used to assess the overall health of the respondent rather than selected dimensions of individuals’ health.
The EQ-5D-3L index score is generated by applying a multiattribute utility function to the descriptive system. Different utility functions are available that reflect the preferences of specific populations (e.g., US or UK). The lowest possible overall score (corresponding to severe problems on all 5 attributes) varies depending on the utility function that is applied to the descriptive system (e.g., −0.59 for the UK algorithm and −0.109 for the US algorithm). Scores less than 0 represent health states that are valued by society as being worse than dead, while scores of 0 and 1 are assigned to the health states ‘dead’ and ‘perfect health,’ respectively.
One limitation of the EQ-5D-3L was a significant ceiling effect and left skew of the data, therefore, EQ-5D-3L may be more useful in a population with worse overall health status.
Measurement properties
Evidence of validity, reliability, and responsiveness to change of EQ-5D-3L in patients with NSCLC has not been found through systematic literature search.
Minimally Important Difference
Pickard et al.41 estimated minimally important differences (MIDs) in 534 patients with cancer (50 of whom were patients with lung cancer) using both anchor-based (ECOG PS ratings and FACT-G total score-based quartiles) and distribution-based (SD and SEM) methods for EQ-5D-3L index-based utility (UK and US) and VAS scores. In patients with lung cancer, an estimated MID for EQ-5D-3L index score is 0.06 (US) or 0.08 (UK) using anchor-based method. An MID for VAS score estimated using ECOG grade is 7 and using FACT-G quintile subgroups is 12. MIDs estimated by distribution-method are reported as additional evidence to triangulate or confirm the anchor-based approaches (Table 50).
Table 50: MID Estimates for EQ-5D-3L in Patients With Lung Cancer
Score | Mean Difference | 0.5 SD | 0.33 SD | SEM |
|---|---|---|---|---|
EQ-5D-3L Index-based scores (estimated by FACT-G quintiles) | ||||
UK | 0.08 | 0.07 | 0.04 | 0.08 |
US | 0.06 | 0.05 | 0.03 | 0.06 |
VAS scores | ||||
Estimated by ECOG grade | 7 | 9 | 6 | 10 |
Estimated by FACT-G quintiles | 12 | 8 | 5 | 9 |
ECOG = Eastern Cooperative Oncology Group; FACT-G = Functional Assessment of Cancer Therapy – General; MID = minimally important difference; SD = standard deviation; SEM = standard error of the mean; UK = UK; US = US; VAS = visual analogue scale
This table is from an Open Access article distributed under the terms of the Creative Commons Attribution Licence (https://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Source: Pickard et al. 200741
Pharmacoeconomic Review
Abbreviations
AE
adverse event
AJCC
American Joint Committee on Cancer
BIA
budget impact analysis
DM
distant metastasis
EF
event free
EFS
event-free survival
HR
hazard ratio
ICER
incremental cost-effectiveness ratio
ITC
indirect treatment comparison
LR
locoregional recurrence
LY
life-year
NSCLC
non–small cell lung cancer
OS
overall survival
PDC
platinum-doublet chemotherapy
PD-L1
programmed cell death 1 ligand 1
QALY
quality-adjusted life-year
RCT
randomized controlled trials
TNM
tumour, node, and metastasis
TTDM
time to disease metastasis
TTLR
time to locoregional recurrence
TTP
time to any progression
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Nivolumab (Opdivo), solution for IV infusion, 40 mg and 100 mg single-use vials |
Submitted price | Nivolumab, 10 mg/mL, solution = $19.55 per mg ($782.22 per 40 mg vial; $1,955.56 per 100 mg vial) |
Indication | Nivolumab, in combination with platinum-doublet chemotherapy, is indicated for the neoadjuvant treatment of adults with resectable NSCLC (tumours ≥ 4 cm or node-positive disease) |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | August 18, 2022 |
Reimbursement request | As per indication |
Sponsor | Bristol Myers Squibb |
Submission history | Previously reviewed: Yesa Nivolumab has been reviewed and is currently under review for multiple indications at CADTH. The following indications were related to NSCLC:
|
NOC = Notice of Compliance; NSCLC = non–small cell lung cancer.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Markov model |
Target population | Adults newly diagnosed with histologically confirmed stage IB (≥ 4 cm), stage II, and stage IIIA NSCLC, based on the 7th edition of the AJCC TNM criteria, who are considered resectable |
Treatment | Nivolumab, in combination with PDC followed by surgery PDC includes cisplatin + pemetrexed, gemcitabine, vinorelbine, or docetaxel, and carboplatin + paclitaxel, pemetrexed, gemcitabine, vinorelbine, or docetaxel |
Comparators | Surgery followed by adjuvant PDC Neoadjuvant PDC followed by surgery Surgery only |
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | Lifetime (35 years) |
Key data source | CheckMate 816 trial; ITC |
Submitted results |
|
Key limitations |
|
CADTH reanalysis results |
|
AJCC = American Joint Committee on Cancer; DM = disease metastasis; ICER = incremental cost-effectiveness ratio; ITC = indirect treatment comparison; LR = locoregional recurrence; LY = life-year; NSCLC = non–small cell lung cancer; OS = overall survival; PDC = platinum-doublet chemotherapy; QALY = quality-adjusted life-year; TNM = tumour, node, and metastasis; vs. = versus.
Conclusions
Evidence from the CheckMate 816 trial demonstrated that, in the neoadjuvant setting, nivolumab (Opdivo) plus chemotherapy was associated with a statistically significant hazard ratio (HR) for event-free survival (EFS) compared to chemotherapy alone. Overall survival (OS) data were immature at the October 20, 2021, cut-off, and the HR for death was not statistically significant. Therefore, no definitive conclusions could be drawn regarding OS benefit. The comparator in the CheckMate 816 trial (neoadjuvant chemotherapy) is not the current standard of care in Canada for resectable NSCLC, and no direct evidence was available to assess the efficacy of neoadjuvant nivolumab relative to other comparators. Indirect evidence comparing neoadjuvant nivolumab plus chemotherapy to adjuvant therapy and surgery alone was limited because of the significant heterogeneity in the included randomized controlled trials (RCTs).
CADTH undertook reanalyses to address several key limitations identified in the sponsor’s model. This included applying alternative parametric extrapolations for time to progression, removing the assumption of general-population mortality for cured patients, assuming that 7.7% of patients with locoregional recurrence (LR) would transition to distant metastases (DM) annually, assuming a cure for patients with LR from year 7 onward, assuming that the efficacy of adjuvant platinum-doublet chemotherapy (PDC) and surgery alone would equal that of neoadjuvant therapy, applying weight-based dosing to nivolumab, and revising the adjuvant PDC composition to reflect Canadian clinical practice. CADTH could not resolve all outstanding limitations in the analyses and relied on scenario analyses to explore the impact of these limitations.
In the CADTH reanalysis, the incremental cost-effectiveness ratio (ICER) for the nivolumab regimen compared to surgery alone was $32,846 per quality-adjusted life-year (QALY) (incremental costs = $19,571; incremental QALYs = 0.60; incremental life-years [LYs] = 0.71) in the CheckMate 816 population. To extrapolate these results to the full Health Canada–indicated population, the assumption of equivalent treatment efficacy and long-term survival outcomes in patients with stage IB to II and stage III disease must hold. Although there is uncertainty associated with the treatment efficacy of nivolumab at different stages, evidence shows different long-term survival outcomes between patients with stage IB to II disease and those with stage IIIA disease. Given that 64% of patients in the CheckMate 816 trial had stage IIIA disease (versus 37% in the full Health Canada indication), the model results are likely not generalizable to the full Health Canada–indicated population.
If nivolumab is used predominately in patients with stage IIIA disease, as in the CheckMate 816 trial, and adjuvant chemotherapy is no better than neoadjuvant chemotherapy, no price reduction is likely required to achieve cost-effectiveness at a $50,000 per QALY threshold. If adjuvant chemotherapy is more effective than neoadjuvant chemotherapy at preventing progression to LR and DM, a price reduction may be required to ensure the cost-effectiveness of nivolumab in the neoadjuvant setting. This is because the incremental benefit of nivolumab relative to adjuvant therapy would be less than the incremental benefit relative to neoadjuvant therapy, as seen in the CheckMate 816 trial. If nivolumab is used in the full Health Canada–indicated population (only 37% of whom receive nivolumab have stage III disease), price reductions may also be required, given the uncertainty regarding cost-effectiveness in patients with stage IB to II disease.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, registered clinicians, and drug plans that participated in the CADTH review process.
One patient group, Lung Cancer Canada, provided input based on data collected during interviews, conducted in September and October 2022, with 2 patients who had stage I to stage III non–small cell lung cancer (NSCLC) and experience with nivolumab in the adjuvant setting (treatment durations were 3 months and 1 year). Both patients experienced side effects; 1 reported that these were minor, but the other reported experiencing loss of appetite leading to dramatic weight loss, nausea, and a mild skin rash enveloping one-third of their body. Overall, the patients’ disease experience was influenced by the physical symptoms associated with NSCLC (e.g., fatigue, cough, and mild chest pain) and the psychosocial effects associated with the disease. The most important outcomes for patients included delaying disease progression and achieving long-term remission, with the ultimate objective of improving survival; reducing side effects from treatment, preserving independence to minimize the burden on caregivers, and maintaining quality of life. In addition, patients emphasized the need for therapies that can be administered close to home, such as community clinics in rural settings, to minimize travel time and burden on caregivers. Last, patients noted that because the CheckMate 816 trial excluded patients with known EGFR or ALK mutations, owing to a lack of evidence supporting the use of neoadjuvant immunotherapy in this population, a biomarker screening should be performed before neoadjuvant treatment with nivolumab.
Registered clinician input was received from 2 groups: the Ontario Health-Cancer Care Ontario Lung Cancer Drug Advisory Committee and Lung Cancer Canada. According to clinician input, the current pathway of care for patients with stage IB to stage IIIA NSCLC consists of surgical resection followed by postoperative radiation, adjuvant chemotherapy, and/or adjuvant immunotherapy (including atezolizumab). Clinician input noted that neoadjuvant nivolumab in combination with PDC would be an additional option for patients with resectable stage IB to stage IIIA NSCLC that could potentially eliminate the need for prolonged adjuvant chemoimmunotherapy in some cases. The clinicians highlighted the possibility that some eligible patients may elect to forego neoadjuvant nivolumab, especially those with stage II, node-negative disease considered for upfront surgery plus optional adjuvant therapies. In fact, the clinician input noted that neoadjuvant nivolumab would be favoured for patients with stage IIIA disease and/or patients with positive programmed cell death 1 ligand 1 (PD-L1) expression, for whom CheckMate 816 the EFS findings from the CheckMate-816 trial were most encouraging. Clinician input noted that patients with an Eastern Cooperative Oncology Group Performance Status of 2 or higher would be among the least suitable for neoadjuvant nivolumab, and that the use of neoadjuvant nivolumab in patients with known EGFR, ALK, ROS1, RET, and NTRK alterations would require discussion on a case-by-case basis, given that these subgroups were not investigated in the CheckMate 816 trial. Clinicians added that, ideally, a multidisciplinary cancer tumour board that involved (nonexclusively) respirologists, radiologists, pathologists, thoracic surgeons, medical oncologists, and radiation oncologists would be required to discuss multimodal treatment approaches for patients with resectable stage IB to stage IIIA NSCLC eligible for neoadjuvant nivolumab.
The input from drug programs regarding implementation issues noted that neoadjuvant chemotherapy is rarely used in Canadian clinical practice (in only 2% to 3% of all eligible patients with resectable NSCLC).1 Participating drug plans explained that if nivolumab were funded in the neoadjuvant setting, jurisdictions would implement weight-based dosing (i.e., nivolumab 4.5mg/kg up to 360 mg, administered every 3 weeks). Moreover, drug plans indicated that vial sharing would be possible in larger treatment centres because nivolumab is commonly used for several other indications. Finally, drug programs noted that, as with to other solid tumours, patients would be eligible for re-treatment with immunotherapy (i.e., programmed cell death 1 protein [PD-1] or PD-L1 inhibitors), provided that disease recurrence occurred more than 6 months after the last dose of neoadjuvant nivolumab.
Several of these concerns were addressed in the sponsor’s model:
The model was informed by time to any progression (TTP), time to locoregional recurrence (TTLR), and time to disease metastasis (TTDM) curves, which were derived from the trial-based EFS curve, an outcome that is valued by patients.
The impact of disease and treatment on a patient’s quality of life was captured with utility values.
The model applied a re-treatment restriction, in which patients who progressed on or in the 6 months after the last dose of neoadjuvant nivolumab were not eligible for further treatment with immunotherapy.
With the exception of adjuvant atezolizumab, the comparators modelled by the sponsor reflected the current treatments available to patients with stage IA to stage IIIB NSCLC, including neoadjuvant PDC, adjuvant PDC, and surgery only.
CADTH addressed some of these concerns as follows:
Weight-based dosing and vial sharing for neoadjuvant nivolumab was incorporated in the CADTH reanalysis.
CADTH was unable to address the following concerns raised from stakeholder input:
Although clinician input noted that neoadjuvant nivolumab would be favoured for patients with stage IIIA NSCLC, CADTH was unable to explore potential differences in cost-effectiveness estimates between patients with stage IB to II NSCLC and those with stage IIIA NSCLC, given that the patient population was modelled as a single cohort.
Economic Review
The current review is for nivolumab in combination with PDC (nivolumab plus PDC) for newly diagnosed adults with histologically confirmed stage IB (≥ 4 cm), stage II, and stage IIIA NSCLC, based on the 7th edition of the American Joint Committee on Cancer (AJCC 7th edition) tumour, node, and metastasis (TNM) criteria, who are considered resectable.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis comparing nivolumab plus PDC with neoadjuvant PDC, adjuvant PDC, and surgery only. In alignment with the Health Canada–indicated population, the modelled population comprised newly diagnosed adults with histologically confirmed stage IB (≥ 4 cm), stage II, or stage IIIA NSCLC (based on AJCC 7th edition TNM criteria), who are considered resectable.2
Nivolumab is a PD-L1 inhibitor available for IV infusion as 40 mg and 100 mg concentrates in 4 mL and 10 mL single-use vials, respectively (10 mg/mL). The recommended dose of nivolumab neoadjuvant therapy is 360 mg administered intravenously over 30 minutes, in combination with PDC, every 3 weeks for 3 21-day cycles. PDC included cisplatin plus pemetrexed, gemcitabine, vinorelbine, or docetaxel, and carboplatin plus paclitaxel, pemetrexed, gemcitabine, vinorelbine, or docetaxel. Table 10 presents the dosing regimens for each PDC received in combination with neoadjuvant nivolumab. The nivolumab plus PDC neoadjuvant regimen captured in the economic model reflects the Health Canada dosing regimen. At the sponsor’s submitted price of $782.22 per 40 mg vial and $1,955.56 per 100 mg vial, the 21-day cycle cost of nivolumab would be $7,431, and the total cost $22,293 (3 cycles).2 In combination with PDC, the 21-day cycle cost of the nivolumab neoadjuvant therapy would range from $8,516 (for nivolumab plus cisplatin plus vinorelbine) to $12,277 (for nivolumab plus carboplatin plus docetaxel); whereas the total cost for all 3 cycles would range from $25,548 (nivolumab plus cisplatin plus vinorelbine) to $36,831 (nivolumab plus carboplatin plus docetaxel).
The comparators for this analysis included neoadjuvant PDC, adjuvant PDC, and surgery only.2 The dosing regimens for PDC in the neoadjuvant and adjuvant settings were based on Canadian drug monographs (Table 10), and costs were obtained from various sources, including previous CADTH reviews.3-5 These are summarized in Table 8 (Appendix 1). Neoadjuvant PDC consists of 3 cycles of PDC, whereas adjuvant PDC consists of 4 cycles of PDC. The cost for 3 cycles of neoadjuvant PDC administered every 3 weeks ranged from $3,255 (cisplatin plus vinorelbine) to $14,538 (carboplatin plus pemetrexed), based on the recommended doses. The cost for 4 cycles of adjuvant PDC administered every 3 weeks ranged from $4,340 (cisplatin plus vinorelbine) to $19,384 (carboplatin plus pemetrexed), based on the recommended doses. The sponsor’s model included drug wastage (no vial sharing).
The clinical outcomes modelled were TTP, TTLR, TTDM, mortality during the event-free (EF) health state, and mortality during LR.2 The economic evaluation was conducted over a lifetime time horizon (approximately 35 years) from the perspective of the Canadian public health care payer.2 Costs and clinical outcomes (LYs and QALYs) were discounted at 1.5% per annum.2
Model Structure
The sponsor submitted a semi-Markov model with 4 mutually exclusive health states (EF, LR, DM, and death), in which transitions between states occurred on a 21-day cycle length (Figure 1). All patients enter the model in the EF health state, from which they could experience 1 of 2 types of progression: LR or DM. Patients in the LR health state could then experience further progression, moving to the DM health state or to the death state. When patients experience DM, a lump-sum cost, QALY, and LY total is applied based on an external model developed by the sponsor for a previous submission to CADTH (the 1-off approach).6 Further outcomes thereafter are no longer tracked and the patient does not make any further state transitions. Patients in all health states, with the exception of DM, are subject to a probability of death each cycle.
Model Inputs
Baseline patient characteristics were derived from the phase III, CheckMate 816 RCT that compared nivolumab plus PDC with neoadjuvant PDC alone in patients with stage IB to stage IIIA (Union for International Cancer Control TNM Atlas, 7th edition) NSCLC. The average patient in the modelled cohort, which the sponsor assumed reflected the Canadian patient population, was 64 years old, weighed 70 kg, and was more likely to be male (71%). These characteristics were used to inform the drug dosage regimens, the age- and sex-specific distribution of the general-population mortality risk, and the length of the lifetime horizon.2
Clinical efficacy parameters used to characterize nivolumab plus PDC and neoadjuvant PDC, including the modelling of TTP, TTLR, TTDM, mortality during the EF health state, and mortality during LR, were derived from the CheckMate 816 trial, using the October 20, 2021, data cut-off date.2 Parametric survival modelling was used to extrapolate TTP, TTLR, mortality during LR, and mortality during EF transition probabilities over time, beyond the time points available in the trial. Survival distributions were selected on the basis of the clinical plausibility of long-term projections, visual inspection of fit, as well as Akaike information criterion and Bayesian information criterion. The observed TTP curves were derived from the EFS curves by censoring death events. All of the parametric distributions were deemed to fit the Kaplan-Meier data for TTP and TTLR reasonably well during the trial period. However, in the long-term, substantial differences were observed in the tails of various extrapolations. The sponsor selected joint log-normal distributions to extrapolate both the TTP and TTLR curves beyond the time points available in the trial. The sponsor indicated that the observed data for TTDM from the CheckMate 816 trial were immature, with relatively low event counts (20 and 32 DM events were observed in patients treated with nivolumab plus PDC and neoadjuvant PDC, respectively).2 Hence, instead of directly extrapolating the TTDM curve based on available data from the CheckMate 816 trial, the sponsor opted to construct the TTDM curve by calculating the difference between the extrapolated estimates from the TTP and TTLR curves.
Comparisons of nivolumab plus PDC with adjuvant PDC and surgery only required the use of a sponsor-submitted network meta-analysis. As such, the estimation of transition probabilities from the EF health state to the LR and DM health states for patients receiving adjuvant PDC or surgery only are derived from indirect treatment comparison (ITC) data. Constant HRs were applied to the TTLR curve (HR for adjuvant PDC = ||||; HR for surgery only = ||||) and to the TTDM curve (HR for adjuvant PDC = ||||; HR for surgery only = ||||) for neoadjuvant PDC (reference) to derive the long-term TTLR and TTDM for adjuvant PDC and surgery only.
Given that estimates of the probability of transition between LR and DM were not available for all patients at risk in the CheckMate 816 trial, the model assumed that 20% of patients in the LR health state would experience DM annually, based on clinical expert input.
Data characterizing mortality risks for patients who had not yet experienced a progression event (i.e., mortality during the EF health state) and for patients who had experienced LR (i.e., mortality during the LR health state) were pooled and assumed to be the same for the nivolumab plus PDC and neoadjuvant PDC interventions. Although most extrapolations of mortality during the EF health state fit the short-term data reasonably well, they diverged considerably over the long-term. As such, the extrapolated curves for mortality during the EF health state were compared to external data,7 whereby the exponential distribution was considered to offer the best fit. The extrapolated curves for mortality during LR did not provide a good fit to the Kaplan-Meier data during the observed follow-up, and differed substantially in long-term projections. The sponsor used a cumulative hazards spline model with 2 knots to fit post-LR mortality in the pooled data.8
The sponsor adopted a fixed-payoff approach to determine LYs, QALYs, and costs for patients with distant metastatic recurrence. Discounted outcomes from a prior nivolumab submission to CADTH developed by the sponsor for first-line metastatic NSCLC were selected and weighted according to their respective market shares in Canada. The sponsor applied a re-treatment restriction, in which patients who progressed on or in the 6 months after the last dose of nivolumab plus PDC (15.1%) were not eligible for further treatment with immunotherapy in the DM health state.
The sponsor applied a cure assumption to the projected TTLR, TTDM, and mortality during the EF health state curves for all comparators to reflect the proportion of patients expected to be EF during the modelled lifetime time horizon. The model assumed that, among patients receiving nivolumab plus PDC or a comparator, the proportion of patients not at risk of an NSCLC-related event increases linearly from the start of year 5, reaching a maximum of 95% at year 7, based on cure-rate estimates from clinical expert input.2 Such patients were assumed to experience no further cancer progression and to have a mortality risk equivalent to that in the general age- and sex-matched population in Canada.
Utility values were derived from an analysis of 3-Level EQ-5D index data collected in the CheckMate 816 trial. Health state–specific mean utility estimates for patients receiving nivolumab plus PDC or neoadjuvant PDC are presented in Table 11. The model assigned utility values to the EF and LR health states using pooled utility estimates across treatments. Pooled trial-based utility scores were adjusted to align estimates with scores in the general population of patients in Canada with the same age range and sex distribution as the CheckMate 816 trial. The utilities used in the model base case are summarized in Table 12. Utility in the DM health state was based on lump-sum QALY estimates derived from an external model developed by the sponsor for a previous submission to CADTH to compute outcomes for the 1-off consequence of progression to DM.6 Adverse events (AEs) of grade 3 or higher were incorporated in the model, as observed in the CheckMate 816 trial. The sponsor did not incorporate AE-specific disutilities in the model, assuming that any disutilities due to AEs would have been captured in the pooled health state trial-derived utilities. The consequences of AEs captured by the model were expressed only in terms of their management cost. Only AEs associated with initial treatment were considered; AEs associated with subsequent lines were not.
Costs captured in the model included drug-acquisition, administration, surgery, monitoring, disease management, and end-of-life. Drug-acquisition costs for nivolumab were based on the sponsor’s submitted price.2 Drug-acquisition costs for PDC were sourced from a CADTH reports database, Canada Pharmacy Online, and the literature.3-5 The dosing regimen for each PDC administered in the neoadjuvant setting was based on the dosing used in the CheckMate 816 trial, whereas dosing schedules for PDC in the adjuvant setting were based on the regimens reported in monographs from Cancer Care Ontario. The composition of neoadjuvant PDC for patients receiving nivolumab plus PDC and neoadjuvant PDC reflected what was observed in the CheckMate 816 trial, whereas the composition of adjuvant PDC was based on the sponsor’s drug-intelligence chart audit (Table 13).2
Costs of surgery for each surgical approach (i.e., minimally invasive thoracotomy [$11,589] and thoracotomy [$20,812]) were based on data from the Ontario Case Costing Initiative database for acute inpatient admissions. The distribution of patients receiving surgery after neoadjuvant therapy was informed by the CheckMate 816 trial, whereas patients receiving adjuvant PDC or surgery only were assigned surgery rates informed by the literature.9 Treatment costs for patients in the LR health state were estimated using a basket approach, which consisted of PDC (70%), radiotherapy (20%), and surgery (10%). The total weighted cost of treatment for patients in the LR health state was estimated to be $8,823 per patient. The frequency of routine medical resource use for patients in the EF and LR health states was informed by a retrospective study of patients with early-stage NSCLC conducted in Western Europe, and unit costs were extracted from Canadian costing databases. The annual cost of medical resource use was estimated to be $9,327 per year for patients in the EF health state and $11,383 per year for patients in the LR health state. End-of-life costs ($45,406) were based on a study that used data from the Ontario Cancer Registry,10 whereas treatment-specific AE costs were applied as a 1-time cost in the first model cycle (nivolumab plus PDC = $1,415; neoadjuvant and adjuvant PDC = $1,935). A lump-sum cost was applied to patients who entered the DM health state, and was calculated from an external model developed by the sponsor for a previous submission to CADTH.6
Summary of Sponsor’s Economic Evaluation Results
The sponsor conducted the base case using a probabilistic sensitivity analysis with 3,000 simulations.2 The deterministic and probabilistic results were similar. The probabilistic findings are presented here.
Base-Case Results
The sequential multiple-comparison cost-utility findings are presented in Table 3. The cost-effectiveness frontier was constituted with surgery only, neoadjuvant PDC, and nivolumab plus PDC (representing the optimal therapies). Nivolumab plus PDC was more costly but produced more QALYs than surgery only or than neoadjuvant PDC. Adjuvant PDC was extendedly dominated. Compared with neoadjuvant PDC, nivolumab plus PDC was associated with a QALY gain of 1.07 at an additional cost of $13,968, resulting in an ICER of $13,003 per QALY.
The sponsor’s analysis predicted that nivolumab plus PDC would be associated with a longer duration of life than all other comparators (incremental LYs = 1.32 versus neoadjuvant PDC; = 1.00 versus adjuvant PDC; and = 1.68 versus surgery only). Given the model’s 1-off approach for calculating DM health outcomes, the model cannot assess when health outcomes occur within the model time horizon. For example, if a patient experiences DM after 3 months in the analysis, they receive a fixed number of QALYs. If the model was run for a 3-month time horizon, all patients who did not experience DM would receive a QALY gain of 3 months, whereas those who experienced DM would receive all the QALYs they would accrue for the remainder of their life. Any analysis, based on these assumptions, that is run for less than the full lifetime horizon of the patient is, therefore, misleading. Across interventions, the 1-off cost for the DM health state was the highest cost driver; it accounted for 33% of the total costs incurred by patients receiving nivolumab plus PDC, and up to 54% of the total costs incurred by those receiving surgery only.
Nivolumab plus PDC was cost-effective at a willingness-to-pay threshold of $50,000 per QALY in 71% of the iterations. The submitted analysis was based on publicly available prices of the comparator treatments. Additional results from the sponsor-submitted economic evaluation base case are presented in Appendix 3.
Table 3: Summary of the Sponsor’s Economic Evaluation Results, Probabilistic
Drug | Total costs ($) | Total QALYs | Sequential ICER ($/QALY) |
|---|---|---|---|
Surgery only | $198,033 | 5.70 | Reference |
Neoadjuvant PDC | $200,428 | 6.00 | $7,938 vs. surgery only |
Nivolumab + PDC | $214,396 | 7.07 | $13,003 vs. neoadjuvant PDC |
ICER = incremental cost-effectiveness ratio; PDC = platinum-doublet chemotherapy; QALY = quality-adjusted life-year; vs. = versus.
Source: Sponsor’s pharmacoeconomic submission.2
Sensitivity and Scenario Analyses Results
The sponsor assessed several model parameters and assumptions in probabilistic scenario analyses, including alternate parametric extrapolations, cure assumptions, immunotherapy re-treatment rules considered in the DM health state, vial wastage, and utilities. Notably, the cost effectiveness frontier was represented by surgery only, neoadjuvant PDC, and nivolumab plus PDC in all sequential scenario analyses, with the exception of a scenario that assumed 100% ineligibility for re-treatment with immunotherapy, in which nivolumab plus PDC dominated all other interventions.
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations of the sponsor’s analysis that have notable implications for the economic analysis:
Limitations of modelling the indicated patient population as a single cohort. The sponsor modelled the indicated population of patients with newly diagnosed, resectable, stage IB, stage II, and stage IIIA (AJCC 7th edition) NSCLC as a single cohort. Although the target population modelled by the sponsor was aligned with the Health Canada indication, CADTH noted that in the modelled population (which reflected the CheckMate 816 trial sample), patients with stage IB to II disease (36%) were underrepresented and those with stage IIIA disease (64%) were overrepresented. Based on a Statistics Canada report on cancer stage at diagnosis,11 for patients with stage I to stage III NSCLC (AJCC 7th edition), the distribution of cases by stage at diagnosis was estimated to be 63% for stage I to II and 37% for stage III. Clinical expert feedback agreed that relative to the expected distribution of cases by stage at diagnosis in real-world clinical practice, the composition of the modelled cohort was skewed toward stage IIIA NSCLC.
CADTH noted that differences in EFS were observed between patients with a baseline disease stage of IB to II and those with a baseline stage of IIIA in the CheckMate 816 trial.12 The magnitude of EFS benefit was greater in patients with stage IIIA disease than in those with stage IB or II disease (Figure 2). Likewise, the EFS curves for nivolumab plus PDC and neoadjuvant PDC merged at 30 months, meaning that time to progression was only delayed, not prevented. Because stage IIIA NSCLC is overrepresented in the modelled patient cohort, the pooled EFS curves (stage IB to stage IIIA) may overestimate the expected benefit of nivolumab plus PDC in the general population in Canada, where stage IB to II NSCLC is more prevalent. The CADTH Clinical Review noted that subgroup analyses may not have been powered to detect a difference between the 2 treatment arms. Thus, the findings were considered exploratory and no definite conclusions could be made.
Beyond the potential difference in treatment efficacy between disease stages, CADTH emphasized that the core assumption of survival modelling is that the sample is taken from a common population (i.e., all individuals in the study population remaining at risk at a specific point in time have the same probability of progression).13 Clinical expert feedback indicated that the rate of progression and survival would differ between stages. For instance, the 8th edition of cancer staging from the AJCC describes 5-year NSCLC survival rates as follows: 68% for patients with stage IB disease, 60% for patients with stage IIA disease, 53% for patients with stage IIB disease, and 36% for patients with stage IIIA disease. Therefore, even if the treatment effect were equal across stages, the incremental benefit would be different, given that progression and survival rates differ across stages. As the composition of the CheckMate 816 trial population does not reflect that seen in Canada, the pooled results are highly uncertain.
CADTH asked the sponsor to provide a model that explores cost-effectiveness in 2 separate cohorts (stage IB to II and stage IIIA).
Given uncertainty about the efficacy of adjuvant therapy relative to nivolumab plus PDC (noted in a further limitation), as well as uncertainty about efficacy in the stage IB to II cohort, an additional scenario analysis was conducted that assumed an equivalent treatment effect between nivolumab plus PDC and adjuvant PDC.
Limitations of the sponsor’s 1-off modelling approach. The sponsor’s model included health states in which patients were assumed to be either EF or to have experienced a LR or a distant metastatic recurrence. For the EF and LR states, the sponsor adopted a typical Markov cohort approach, in which patients accrue costs, LYs, and QALYs based on the duration of time spent in each state. In contrast, for the DM state, the sponsor adopted a 1-off approach, in which the sponsor assigned each patient who experienced DM a fixed number of LYs, QALYs, and costs, regardless of when the patient progresses to the DM health state. CADTH equates this 1-off approach with a black-box approach to modelling, in which the resulting model structure effectively contains 2 absorbing states, given that further outcomes are no longer tracked, and patients do not make any further state transitions in the DM health state.
The external model was built to assess the cost-effectiveness of nivolumab in combination with ipilimumab for the first-line treatment of patients with metastatic or recurrent NSCLC for a previous submission to CADTH. However, CADTH noted that this analysis was informed by data from the CheckMate 9LA trial (which assessed nivolumab in combination with ipilimumab and PDC in patients with stage IV or recurrent NSCLC) and the CheckMate 227 trial (which assessed nivolumab in combination with ipilimumab in patients with stage IV or recurrent NSCLC with a PD-L1 expression level of 1% or more). There were important differences in patient populations between the CheckMate 9LA and CheckMate 227 trials and the CheckMate 816 trial, including a 20- and 23-percentage point difference in nonsquamous histological type between patients enrolled in the CheckMate 816 trial and those enrolled in the CheckMate 9LA and CheckMate 227 trials, respectively. As the external model was not provided to CADTH as part of this submission, CADTH was unable to test or explore the impact of different data and cost assumptions.
CADTH was unable to address this limitation; as such, the impact of DM on the decision problem is highly uncertain.
As a scenario analysis, CADTH explored the impact of DM on the decision problem.
Impact of nivolumab plus PDC on OS is highly uncertain. The sponsor’s base case predicts a survival advantage for nivolumab plus PDC over neoadjuvant PDC (incremental gain = 1.32 LYs). As of the first OS interim analysis (data cut of October 20, 2021), the OS data remain immature and the P value for the difference in OS between nivolumab plus PDC and neoadjuvant PDC (HR = 0.57; 99.67% confidence interval, 0.30 to 1.07; P = 0.008) did not cross the boundary for statistical significance (0.0033). In the absence of mature OS data, OS gains in the model were driven by differences in TTLR and TTDM between nivolumab plus PDC and neoadjuvant PDC. Therefore, the sponsor’s model assumed that when patients remain disease free, the probability of death is lower and patients will live longer.
There is additional uncertainty regarding the predicted LY gains associated with nivolumab plus PDC, owing to the modelling approach adopted by the sponsor. The sponsor’s model incorporates mortality data from the CheckMate 816 trial only for patients without distant recurrence, and a 1-off approach was adopted for patients with metastatic recurrence. Clinical expert feedback emphasized that prognosis for patients with stage IB to stage IIIA disease who experience distant disease metastasis is time dependent (i.e., patients who develop DM in the first 6 months after resection would be expected to have different prognoses and survival rates than patients who develop DM at a later time point). Instead, the submitted model assigned each patient who experienced DM a fixed number of LYs, regardless of the onset of metastasis. Thus, in addition to the extensive limitations of the 1-off approach (outlined previously), the modelling approach did not appropriately characterize the time dependence of prognosis and survival that is expected in patients with metastatic disease. The modelling approach also precluded CADTH from being able to generate OS curves for the entire cohort model that could be validated against real-world data.
CADTH was unable to address this limitation, owing to the structure of the sponsor’s model.
Impact of nivolumab plus PDC on long-term TTP and TTLR is uncertain. The sponsor used parametric modelling to extrapolate TTP and TTLR between nivolumab plus PDC and neoadjuvant PDC beyond the observable time points in the CheckMate 816 trial (EFS median follow-up = 29.5 months) to a lifetime horizon (35 years).
The sponsor submitted multiple extrapolation curves for TTP and TTLR and selected log-normal curves for nivolumab plus PDC and neoadjuvant PDC (single models with treatment coefficient). Based on the selected curves for TTP and TTLR, the sponsor’s model predicted that nivolumab plus PDC would continue to be more effective than neoadjuvant PDC for the remainder of the patient’s lifetime. Therefore, beyond 2 years, the probability of progression would continue to be higher for those who received neoadjuvant PDC than for those who received nivolumab. Beyond 24 months, rates of cancer progression in the trial are similar in the 2 arms. For example, at 24 months, 69.3% of the surviving cohort of patients who received nivolumab plus PDC are EF, compared with 50.8% for those who received PDC alone. At 30 months, the proportion of surviving patients who are event free decreases to 64.7% (a 4.5 percentage point reduction) and 47.9% (a 2.9 percentage point reduction) for those receiving nivolumab plus PDC versus PDC alone, respectively. Therefore, in this 6-month period, more patients experienced progression in the nivolumab arm than in the PDC alone arm. The same occurs from month 30 to month 36 and from month 36 to month 42. This may indicate a waning impact of therapy beyond 2 years, meaning that no further reductions in cancer progression are seen beyond 2 years. There is no evidence to suggest that the impact of therapy continues to increase over time.
Given that the sponsor opted to construct the TTDM curve by calculating the difference between extrapolated estimates from the TTP and TTLR curves, the clinical plausibility of the resulting TTDM curves should be judged in tandem. CADTH selected parametric distributions for TTP and TTLR based on 2 main criteria: first, the incremental effect of nivolumab plus PDC relative to neoadjuvant PDC should not extend beyond 30 months; and second, the TTDM extrapolation at 42 months should be aligned with observed data from the CheckMate 816 trial.
In light of these limitations, to address uncertainty about long-term EFS, CADTH conducted a reanalysis that incorporated alternative parametric extrapolations for TTP (log-logistic for nivolumab plus PDC and generalized-gamma for neoadjuvant PDC) and TTLR (log-logistic for nivolumab plus PDC and log-normal for neoadjuvant PDC).
Cure assumption for patients remaining in the EF health state lacks face validity. The model assumed that the proportion of patients deemed cured increases linearly from the start of year 5, reaching a maximum of 95% at year 7, based on cure-rate estimates from clinical expert input.2 Cured patients were assumed to have the same mortality outcomes as the general age- and sex-matched population in Canada (i.e., no excess cancer-related mortality). Clinical expert feedback indicated that it is unlikely that cured patients have the same long-term health outcomes as the people in general Canadian population. Although the assumption of no excess cancer-related mortality may be valid, it is not reasonable to assume no excess smoking-related mortality, for example, in a patient population that consists predominantly of current or former smokers (89% of the CheckMate 816 trial). Clinical expert feedback noted that cancer is not the only prognostic indicator of higher mortality in this patient group, given that current or former tobacco users may have significant comorbidities, including chronic obstructive pulmonary disease, and are therefore more likely to have higher mortality associated with cardiovascular and respiratory diseases. Finally, the data provided by the sponsor do not indicate a dramatic reduction in mortality for those who remain EF after 5 years, as shown in Figure 3.
CADTH conducted a reanalysis that applied no cure assumptions to the post-EF mortality extrapolations for patients remaining event free. CADTH noted that this extrapolation may still be optimistic, given that after 15 years, mortality risk is equivalent to that in the general population.
Mortality during LR was not censored by DM events. The sponsor extrapolated mortality for patients who experienced LR across interventions using Kaplan-Meier data derived from the CheckMate 816 trial. There were 76 patients in the trial who experienced LR progression. The sponsor noted that because tumour assessments were collected until disease recurrence or progression events were confirmed, no further tumour assessments were performed in patients who had a confirmed LR progression in the CheckMate 816 trial. Therefore, it is not known whether any of the 76 patients included in the post-LR mortality curve eventually developed DM after LR, although the model assumes that 20% of surviving patients develop DM annually. CADTH noted that the uncensored data, therefore, do not accurately reflect all-cause mortality during the LR health state, considering that it may have included patients for whom death was preceded by DM. Given that mortality in the DM state is assumed to be worse and all-cause mortality data in LR were not censored by DM events, the model effectively double counts mortality in patients who developed DM. Furthermore, clinical expert feedback emphasized that the prognosis for patients with stage IB to stage IIIA NSCLC who experience LR progression is time dependent (i.e., patients who develop LR in the first 6 months after resection would be expected to have different prognoses and survival rates than patients who develop LR at a later time point).
CADTH conducted a scenario analysis that assumed that patients who develop LR do not transition to DM to explore the impact that the double counting of DM mortality may have on cost-effectiveness estimates.
Progression from LR to DM is not characterized accurately. The sponsor assumed that 20% of patients with LR would experience DM annually. Data from LuCaBIS, a retrospective study of NSCLC focused on the UK, France, and Germany, estimated the rate at which patients with LR experience DM to be 7.7% annually.14 Clinical expert feedback indicated that there is no reason to believe that a greater proportion of patients in Canada would transition from LR to DM than documented in the literature. Moreover, clinical expert input noted that it is not reasonable to assume that the probability of DM remains constant over time in patients with LR. Clinical expert feedback emphasized that in Canadian clinical practice, patients who experience LR are predominantly re-treated with curative intent with several treatment modalities that may include chemo-radiotherapy, radiotherapy, and further surgical resection. Clinical experts agreed that the assumption of cure at the 5-year landmark in a proportion of patients in the LR health state is appropriate in the context of stage IB to stage IIIA NSCLC, given that the therapeutic target after re-treatment in patients with LR is a cure. Because a proportion of patients may achieve functional cure after re-treatment for LR and, therefore, no longer be considered at risk of progression if they remain in the LR health state beyond 5 years from re-treatment completion, the exponential distribution assumed by the sponsor does not accurately characterize the probability of progression from LR to DM. By assuming that the risk of progression for patients in the LR state is indefinitely constant, the sponsor predicts that, ultimately, all patients in the LR state progress to the DM state, when in reality, a proportion of patients who experience LR may achieve a cure. CADTH noted that progression from LR to DM should be represented as a time-dependent probability. As such, the model overestimates the proportion of patients who will eventually experience DM.
In line with the literature, CADTH assumed that 7.7% of patients in the LR health state would transition to DM annually. However, given the structure of the model, CADTH could not fully revise the time dependence of the risk of DM for patients who experience LR. Instead, CADTH applied an instantaneous cure assumption from year 7 onward, whereby patients would not transition from LR to DM. The 7-year landmark was selected because most patients progress from the EF to the LR health state in years 1 and 2, and clinical expert feedback agreed that the assumption of cure after re-treatment in the LR health state is clinically plausible 5 years after re-treatment completion.
Uncertainty in the comparative efficacy of nivolumab plus PDC and comparators: Head-to-head data comparing nivolumab plus PDC with neoadjuvant PDC obtained from the CheckMate 816 trial were used to assess the relative efficacy of those 2 treatment options. Comparisons of nivolumab plus PDC with adjuvant PDC and surgery only relied on indirect evidence. As such, the estimation of transition probabilities from the EF health state to the LR and DM health states for patients receiving nivolumab plus PDC or neoadjuvant PDC were derived from trial data, whereas those pertaining to patients receiving adjuvant PDC or surgery only were derived from ITC data. The CADTH Clinical Review identified several limitations of the sponsor-submitted ITC and concluded that because of significant differential treatment effects between stage categories (i.e., IB to II versus stage IIIA or stage IIIA N2), the pooled ITC results from the stage-agnostic population (i.e., stage IB to stage IIIA) would be deemed significantly biased and that the pooling is inappropriate, methodologically.
CADTH assumed that the efficacy of adjuvant PDC and surgery alone would equal that of neoadjuvant PDC.
In its scenario analyses, CADTH used estimates from the ITC and then assumed that adjuvant chemotherapy would be more effective than neoadjuvant chemotherapy (HR = 0.8 for both EF to LR and EF to DM progressions).
Dose for nivolumab does not reflect the dosing anticipated by jurisdictions. The sponsor used a fixed dose to model the required dosage for nivolumab (360 mg), which was aligned with nivolumab’s product monograph and the dose received by patients treated with nivolumab plus PDC in the CheckMate 816 trial.12,15 CADTH noted that in Canadian clinical practice, weight-based dosing is applied consistently across nivolumab indications. Participating drug plans emphasized that if nivolumab were funded in the neoadjuvant setting, jurisdictions would implement weight-based dosing (i.e., nivolumab 4.5 mg/kg up to 360 mg, administered every 3 weeks for 3 cycles). Moreover, drug plans indicated that vial sharing would be possible in larger treatment centres because nivolumab is commonly used for several other indications.
CADTH conducted a reanalysis that assumed weight-based dosing and 5% vial sharing for nivolumab.
CADTH also conducted a scenario analysis with the fixed dose modelled by the sponsor, as it reflected the dose received by patients treated with nivolumab plus PDC in the CheckMate 816 trial.
Relevant comparator not included in the analysis: The sponsor omitted adjuvant atezolizumab (administered after adjuvant chemotherapy) from the analysis because of the significant heterogeneity between patient populations in the CheckMate 816 trial and the IMpower010 trial. Although the issues related to data limitations are plausible, this comparator is relevant to this population. Clinical expert feedback noted that adjuvant atezolizumab is an appropriate treatment option for patients with resectable stage IB to stage IIIA NSCLC a PD-L1 expression level of at least 50%.
CADTH was unable to address this limitation, and noted that the cost-effectiveness relative to adjuvant atezolizumab is unknown.
PDC composition in the adjuvant setting lacks face validity. The model derived the composition of PDC regimens for patients receiving adjuvant PDC from the sponsor’s drug-intelligence chart audit. In the submitted model, 56% of patients would receive a carboplatin-based regimen and the remaining 44% would receive a cisplatin-based regimen in the adjuvant setting. Clinical expert feedback emphasized that, although there is more openness to use carboplatin-based regimens in the neoadjuvant setting, carboplatin-based regimens are not commonly prescribed in the adjuvant setting. CADTH revised the adjuvant PDC composition to exclude carboplatin-based regimens, in accordance with the treatment expectation reflected in Canadian clinical practice.
CADTH conducted a reanalysis that excluded carboplatin-based PDC regimens from the adjuvant setting. The proportions of patients who would have otherwise received these were redistributed to cisplatin-based PDC regimens.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CADTH (refer to Table 4).
Table 4: Key Assumptions of the Submitted Economic Evaluation
Sponsor’s key assumption | CADTH comment |
|---|---|
All PDC regimens administered as neoadjuvant treatment have the same efficacy. | Acceptable. Clinical expert feedback suggested that no significant difference in efficacy would be expected among PDC combinations. Data are not available to account for efficacy differences between specific PDC regimens. Adjusting the distribution of PDC in the model can affect costs but will not affect estimated survival. |
The model assumed that, for patients receiving nivolumab + PDC and comparators, the proportion of patients who achieve a functional cure and are no longer considered at risk of progression increased linearly from year 5 onward, reaching a maximum of 95% of those remaining in EFS at year 7. | Reasonable. The clinical experts consulted by CADTH for this review confirmed that the assumption of a cure in a proportion of patients in the event-free health state is appropriate in the context of NSCLC, given that the therapeutic target after surgical resection is a cure. Clinical expert feedback also confirmed that the time to establish a cure typically starts 5 years after resection in Canadian clinical practice. |
EFS = event-free survival; NSCLC = non–small cell lung cancer; PDC = platinum-doublet chemotherapy.
CADTH Reanalyses of the Economic Evaluation
Base-Case Results
CADTH’s reanalysis addressed several limitations of the economic model. The CADTH base case was derived by making changes in model parameter values and assumptions, in consultation with clinical experts. The following changes were made: applying alternative parametric extrapolations for TTP and TTLR; removing the assumption of cure from post-EF mortality to partly account for the excess smoking-related mortality in a patient population predominantly composed of current and former tobacco users; assuming that 7.7% of patients in the LR health state would transition to DM annually and applying an instantaneous cure assumption from year 7 onward to account for the curative intent of re-treatment in the LR health state; assuming that the efficacy of adjuvant PDC and surgery alone would equal that of neoadjuvant PDC for TTLR and TTDM; applying weight-based dosing and 5% vial sharing to nivolumab; and revising the adjuvant PDC composition to reflect Canadian clinical practice. These changes are summarized in Table 5.
Table 5: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
None. | — | — |
Changes to derive the CADTH reanalysis | ||
1.Impact of nivolumab + PDC on long-term TTP is highly uncertain | Parametric distribution of TTP
Parametric distribution of TTLR
| Parametric distribution of TTP
Parametric distribution of TTLR
|
2.Cure assumption among patients remaining EF lacks face validity |
| No cure assumption applied for the EF mortality |
3.Progression from LR to DM is not characterized accurately | 20% annually | 7.7% annually until year 7, 0.0% thereafter |
4.Uncertainty about the comparative efficacy of nivolumab + PDC and comparators | Indirect comparators (adjuvant PDC and surgery only) included using results from sponsor’s ITC | Clinical efficacy of adjuvant PDC and surgery only assumed to be equal to neoadjuvant PDC |
5.Dosing of nivolumab does not reflect dosing anticipated by jurisdictions |
|
|
6.PDC composition in adjuvant setting lacks face validity |
|
|
CADTH reanalysis | 1 + 2 + 3 + 4 + 5 + 6 | |
DM = disease metastasis; EF = event free; ITC = indirect treatment comparison; LR = locoregional recurrence; PDC = platinum-doublet chemotherapy; TTLR = time to locoregional recurrence; TTP = time to any progression.
In the CADTH reanalysis, nivolumab plus PDC was more costly and produced more QALYs than all comparators. Neoadjuvant PDC and adjuvant PDC were dominated by surgery alone, as equivalent efficacy was assumed for surgery, neoadjuvant therapies, and adjuvant therapies in the absence of robust evidence from the indirect comparison. Compared with surgery only, nivolumab plus PDC was associated with a QALY gain of 0.60 at an additional cost of $19,571, resulting in an ICER of $32,846 per QALY. Relative to neoadjuvant and adjuvant therapies, the ICERs for surgery only were lower, at $23,454 and $22,195 per QALY, respectively, as incremental QALYs were the same (0.60) but incremental costs were lower. The probability that nivolumab plus PDC was cost-effective at a willingness-to-pay threshold of $50,000 per QALY was 59%. The estimated ICER was higher than the sponsor’s base-case value. Across interventions, the 1-off cost in DM continued to be among the highest cost drivers, accounting for 25% of the total costs incurred by patients receiving nivolumab plus PDC and up to 36% of the total costs incurred by those receiving surgery only.
CADTH notes that given mis-sampling and the heterogeneity of the study population from which the pooled efficacy estimates were derived, the pooled cost-effectiveness results are highly uncertain and more likely to reflect the cost-effectiveness of nivolumab plus PDC for patients with stage IIIA NSCLC than of patients with stage IB to II NSCLC.
The reanalysis is based on publicly available prices of the comparator treatments. A detailed breakdown of the disaggregated results is available in Table 15.
Table 6: Summary of the Stepped Analysis of the CADTH Reanalysis Results
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|---|
Sponsor’s base case (probabilistic) | Surgery only | $198,033 | 5.70 | Reference |
Neoadjuvant PDC | $200,428 | 6.00 | $7,938 | |
Nivolumab + PDC | $214,396 | 7.07 | $13,003 | |
CADTH reanalysis 1 | Surgery only | $198,288 | 5.93 | Reference |
Neoadjuvant PDC | $200,551 | 6.19 | $8,797 | |
Nivolumab + PDC | $215,081 | 6.94 | $19,462 | |
CADTH reanalysis 2 | Surgery only | $197,248 | 5.49 | Reference |
Neoadjuvant PDC | $198,951 | 5.75 | $6,381 | |
Nivolumab + PDC | $211,423 | 6.73 | $12,741 | |
CADTH reanalysis 3 | Surgery only | $191,327 | 6.04 | Reference |
Neoadjuvant PDC | $192,173 | 6.37 | $2,506 | |
Nivolumab + PDC | $208,885 | 7.43 | $15,854 | |
CADTH reanalysis 4 | Surgery only | $196,284 | 6.00 | Reference |
Nivolumab + PDC | $215,690 | 7.10 | $17,586 | |
CADTH reanalysis 5 | Surgery only | $199,765 | 5.70 | Reference |
Neoadjuvant PDC | $201,798 | 6.00 | $6,865 | |
Nivolumab + PDC | $213,346 | 7.10 | $10,465 | |
CADTH reanalysis 6 | Surgery only | $199,765 | 5.70 | Reference |
Neoadjuvant PDC | $201,798 | 6.00 | $6,865 | |
Nivolumab + PDC | $215,690 | 7.10 | $12,589 | |
CADTH reanalysis (1 + 2 + 3 + 4 + 5 + 6) | Surgery only | $180,702 | 6.32 | Reference |
Nivolumab + PDC | $200,273 | 6.91 | $32,846 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; PDC = platinum-doublet chemotherapy.
Table 7: Summary of the CADTH Reanalysis Results
Drug | Total costs | Total QALYs | Total LYs | Sequential ICER |
|---|---|---|---|---|
CADTH reanalysis | ||||
Surgery only | $180,702 | 6.32 | 7.99 | Reference |
Nivolumab + PDC | $200,273 | 6.91 | 8.70 | $32,846 |
Dominated treatments | ||||
Neoadjuvant PDC | $186,296 | 6.32 | 7.99 | Dominated |
Adjuvant PDC | $186,992 | 6.32 | 7.99 | Dominated |
ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year; PDC = platinum-doublet chemotherapy.
Scenario Analysis Results
Although the CADTH reanalysis indicates that a price reduction may not be necessary for nivolumab plus PDC to be considered cost-effective at a threshold of $50,000 per QALY, uncertainty remains in the analysis. CADTH conducted a series of scenario analyses to determine the impact of alternative assumptions on the cost-effectiveness of neoadjuvant nivolumab plus PDC. The results of these analyses are presented in Table 16 (Appendix 4).
First, given that the EFS benefit of nivolumab plus PDC in patients with stage IB to II NSCLC is highly uncertain and no direct evidence is presented comparing nivolumab to adjuvant therapy, CADTH undertook a scenario analysis that assumed the treatment effect of nivolumab plus PDC would be indistinct from that of adjuvant PDC. In this scenario, nivolumab plus PDC resulted in a higher cost ($13,478) and lower QALYs (–0.05) relative to adjuvant therapy, resulting in dominance. This is because progression rates are equivalent but a proportion of nivolumab patients are not re-treated, resulting in poorer outcomes in the DM setting. CADTH noted that this scenario analysis only explores potential cost-effectiveness in patients with stage IB to II disease; and a more robust analysis to explore this was not provided by the sponsor.
Second, CADTH assumed that the HR for neoadjuvant versus adjuvant chemotherapy was 0.80 for both EF to LR and EF to DM progressions. Given that evidence from the network meta-analysis is limited and no direct evidence is available comparing neoadjuvant to adjuvant chemotherapy, this scenario analysis assumes that adjuvant chemotherapy is more effective than neoadjuvant chemotherapy. Given that the CheckMate 816 trial compares nivolumab to neoadjuvant therapy, this scenario analysis assumes that the incremental benefit of nivolumab would be less than that of adjuvant chemotherapy. In this scenario, nivolumab is associated with higher costs ($13,148) and higher QALYs (0.08) than adjuvant chemotherapy alone. This results in an ICER of $166,657 per QALY. In this scenario, a price reduction of 50% would be required to achieve an ICER below $50,000 per QALY.
Third, CADTH conducted a scenario analysis that assumed that patients who develop LR do not transition to the DM health state to mitigate the potential impact that double counting DM mortality may have on cost-effectiveness estimates. CADTH acknowledged that although this approach ensures that mortality is not double counted, it may underestimate the cost consequence of DM. In this scenario, the ICER increased to $37,946 per QALY.
Fourth, CADTH conducted an analysis with a fixed dose of nivolumab, as it reflected the dose received by patients treated with nivolumab plus PDC in the CheckMate 816 trial. In this scenario, the ICER increased to $36,509 per QALY.
Fifth, CADTH conducted an analysis using the sponsor-submitted ITC results. In this scenario, the frontier changes and the sequential ICER compares nivolumab to neoadjuvant PDC alone ($23,454 per QALY).
Finally, CADTH explored the impact of DM costs on the results. In the CADTH reanalysis, prevention of DM leads to $14,716 in cost savings for nivolumab relative to surgery alone. If these savings are removed from the analysis, the ICER increases to $58,113 per QALY relative to surgery alone and remains below $50,000 per QALY relative to adjuvant and neoadjuvant therapy. Therefore, although there is uncertainty related to the degree of cost savings associated with the prevention of DM, it is unlikely that this would influence the conclusion that, in patients with stage III disease at least, nivolumab plus PDC is likely cost-effective at a $50,000 per QALY threshold.
Issues for Consideration
Clinical experts indicated that, depending on the tolerability of neoadjuvant therapy, some patients with newly diagnosed, resectable, stage IB to stage IIIA NSCLC may opt to postpone or forego definitive surgery. As such, there may be a risk that offering chemotherapy in the neoadjuvant setting (relative to the adjuvant setting) may preclude patients from receiving surgical resection with curative intent. Although there is no quality of life evidence to date indicating differences between patients receiving PDC in the neoadjuvant setting and those receiving it in the adjuvant setting, the CADTH Clinical Review noted that the mean change from baseline in EQ-5D visual analogue scale and EQ-5D index during the neoadjuvant treatment phase were similar to baseline levels in patients receiving nivolumab plus PDC and neoadjuvant PDC.
Future availability of screening programs may affect the size of the indicated population for neoadjuvant nivolumab in combination with chemotherapy, as the introduction of such programs is likely to increase the proportion of diagnoses at earlier presymptomatic stages of disease (i.e., stage IB to II). CADTH reiterates that the benefit of nivolumab plus PDC in patients with stage IB to II NSCLC is highly uncertain.
Overall Conclusions
Evidence from the CheckMate 816 trial demonstrated that in the neoadjuvant setting, nivolumab plus chemotherapy was associated with a statistically significant HR for EFS compared to chemotherapy alone. OS data were immature at the October 20, 2021, cut-off, and the HR for death was not statistically significant. Therefore, no definitive conclusions could be drawn regarding OS benefit. The comparator in the CheckMate 816 trial (neoadjuvant chemotherapy) is not the current standard of care in Canada for patients with resectable NSCLC, and no direct evidence was available to assess the efficacy of neoadjuvant nivolumab relative to other comparators. Indirect evidence comparing neoadjuvant nivolumab plus chemotherapy to adjuvant therapy and surgery alone was limited, owing to significant heterogeneity in the included RCTs.
CADTH undertook reanalyses to address several key limitations identified in the sponsor’s model. These included applying alternative parametric extrapolations for time to progression; removing the assumption of general-population mortality for cured patients; assuming that 7.7% of patients in the LR health state would transition to the DM health state annually; assuming a cure for patients in the LR health state from year 7 onward; assuming that the efficacy of adjuvant PDC and surgery alone would equal that of neoadjuvant; applying weight-based dosing for nivolumab; and revising the adjuvant PDC composition to reflect Canadian clinical practice. CADTH could not resolve all outstanding limitations in the analysis and relied on scenario analyses to explore the impact of these limitations.
In the CADTH reanalysis, the ICER for the nivolumab regimen compared to surgery alone was $32,846 per QALY (incremental costs = $19,571; incremental QALYs = 0.60; incremental LYs = 0.71) in the CheckMate 816 population. To extrapolate these results to the full Health Canada population, the assumption of equivalent treatment efficacy and long-term survival outcomes in patients with stage IB to II and stage III NSCLC must hold. Although there is uncertainty associated with the treatment efficacy of nivolumab in different disease stages, evidence shows different long-term survival outcomes for those with stage IB to II disease relative to those with stage IIIA disease. Given that 64% of patients in the CheckMate 816 trial had stage IIIA NSCLC (compared with 37% in the full Health Canada–indicated population), the model results are likely not generalizable to the full Health Canada–indicated population.
If nivolumab is used predominately in patients with stage IIIA disease, per the CheckMate 816 trial, and assuming that adjuvant chemotherapy is no better than neoadjuvant chemotherapy, no price reduction is likely required to achieve cost-effectiveness at a $50,000 per QALY threshold. If adjuvant chemotherapy is more effective than neoadjuvant chemotherapy at preventing progression to the LR and DM health states, such that the HR for time to these events is less than 0.85, then nivolumab may not be cost-effective at a $50,000 per QALY threshold. There is no direct evidence comparing adjuvant chemotherapy to neoadjuvant chemotherapy, and indirect evidence is limited. Therefore, it is uncertain whether these HRs could be achieved. If nivolumab is used in the full Health Canada–indicated population (only 37% of patients who receive nivolumab have stage III disease), price reductions may be required, given the uncertainty regarding cost-effectiveness in those with stage IB to II disease. Finally, CADTH noted that cost-effectiveness is contingent on OS benefits for nivolumab relative to other comparators being achieved. Although OS data from the trial did not reach statistical significance, given the known relationship between cancer progression and mortality, patients who received nivolumab would likely have to relapse at a substantial rate 4 years after treatment for an OS benefit to not be realized. Future analyses on the OS data are planned after a prespecified number of events have occurred; these additional data on OS could be used to validate findings from the model.
References
1.Bristol Myers Squibb. Drug intelligence chart audit (2021-2022).
2.Bristol Myers Squibb. Cost-effectiveness of nivolumab as neoadjuvant treatment for resectable non-small cell lung cancer from a canadian healthcare system perspective. Technical Report. 2022.
3.CADTH. Reports database. 2022; www.cadth.ca. Accessed 2022 Apr 6.
4.Chaudhary MA, Holmberg C, Lakhdari K ea. Cost-effectiveness of nivolumab in squamous and non-squamous non-small cell lung cancer in Canada and Sweden: an update with 5-year data. . J Med Econ. 2021;24(1):607-619. PubMed
5.Canada Pharmacy Online. 2022; www.canadapharmacyonline.com. Accessed 2022 Apr 7.
6.CADTH Drug Reimbursement Review pharmacoeconomic report: nivolumab (Opdivo) in combination with ipilimumab (Yervoy). Ottawa: CADTH; 2021 Mar 4: https://www.cadth.ca/sites/default/files/pcodr/Reviews2021/10218Nivolumab-IpilimumabNSCLC_fnEGR_NOREDACT-ABBREV_Post04Mar2021_final.pdf. Accessed 2022 Oct 19.
7.Bristol Myers Squibb. Data on file: Primary non-interventional study report for study ca2097l8; meta-analysis to characterize the association between pathological response to neoadjuvant therapy and survival endpoints in patients with stage i to iii non-small cell lung cancer using patient-level data from randomized clinical trials. 2021.
8.Goldstraw P, Chansky K, Crowley J ea. The IASLC lung cancer staging project: proposals for revision of the TNM stage groupings in the forthcoming (Eighth) edition of the TNM classification for lung cancer. J Thorac Oncol. 2016;11(1):39-51. PubMed
9.Felip E, Rosell R, Maestre JA, et al. Preoperative chemotherapy plus surgery versus surgery plus adjuvant chemotherapy versus surgery alone in early-stage non-small-cell lung cancer. J Clin Oncol. 2010;28(19):3138-3145. PubMed
10.de Oliveira C, Pataky R, Bremner KE, et al. Phase-specific and lifetime costs of cancer care in Ontario, Canada. BMC Cancer. 2016;16(1):809. PubMed
11.Statistics Canada. Cancer in Canada: stage at diagnosis. 2018; https://www150.statcan.gc.ca/n1/en/pub/82-003-x/2018012/article/00003-eng.pdf?st=jO-UjdyH. Accessed 2022 Oct 19.
12.Forde PM, Spicer J, Lu S, et al. Neoadjuvant nivolumab plus chemotherapy in resectable lung cancer. N Engl J Med. 2022;386(21):1973-1985. PubMed
13.Tarride J-E, Matthew Cheung, Timothy P. Hanna, et al. CADTH Health Technology Review. Platform, basket, and umbrella trial designs: issues around health technology assessment of novel therapeutics. Canadian Journal of Health Technologies. 2022;2(7). https://canjhealthtechnol.ca/index.php/cjht/article/view/nm0002/nm0002. Accessed 2022 Oct 19.
14.Chouaid C, Danson S, Andreas S, et al. Adjuvant treatment patterns and outcomes in patients with stage IB-IIIA non-small cell lung cancer in France, Germany, and the United Kingdom based on the LuCaBIS burden of illness study. Lung Cancer. 2018;124:310-316. PubMed
15.Dinh T, Sutherland G. Understanding the gap: a pan-Canadian analysis of prescription drug insurance coverage. Ottawa (ON): The Conference Board of Canada; 2017: https://www.conferenceboard.ca/e-library/abstract.aspx?did=9326. Accessed 2022 Nov 7.
Appendix 1: Cost Comparison Table
Note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical expert(s) and drug plans. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 8: CADTH Cost Comparison Table for Resectable Stage IB to Stage IIIA NSCLC
Treatment | Strength / concentration | Form | Price | Recommended dosage | Cost per cycle or 1-time use | Cost per 28 days |
|---|---|---|---|---|---|---|
Nivolumab in combination with PDC (Neoadjuvant) | ||||||
Nivolumab | 40 mg vial 100 mg vial | 10 mg/mL IV solution | $782.2200a $1,955.5600a | 21-day cycles: 360 mg IV (fixed dose) on Day 1 | $7,431 | $9,908 |
Nivolumab + CISPPEME regimen cost (21-day cycle) | $11,697 | $15,596 | ||||
Nivolumab + CISPGEMC regimen cost (21-day cycle) | $9,134 | $12,178 | ||||
Nivolumab + CISPVINO regimen cost (21-day cycle) | $8,516 | $11,355 | ||||
Nivolumab + CISPDOCE regimen cost (21-day cycle) | $8,830 | $11,773 | ||||
Nivolumab + CRBPPACL regimen cost (21-day cycle) | $12,226 | $16,301 | ||||
Nivolumab + CRBPPEME regimen cost (21-day cycle) | $12,277 | $16,369 | ||||
Nivolumab + CRBPGEMC regimen cost (21-day cycle) | $9,714 | $12,951 | ||||
Nivolumab + CRBPVINO regimen cost (21-day cycle) | $9,096 | $12,128 | ||||
Nivolumab + CRBPDOCE regimen cost (21-day cycle) | $9,410 | $12,547 | ||||
Cisplatin-Based Regimens (Neoadjuvant, Adjuvant)b | ||||||
CISPPEME | ||||||
Cisplatin (generic) | 50 mg vial 100 mg vial | 1 mg/mL IV solution | $135.0000 $270.0000 | 21-day cycles: 75 mg/m2 IV on Day 1 | $405 | $540 |
Pemetrexed (generic) | 100 mg vial 500 mg vial 1,000 mg vial | 10 mg/mL IV solution | $2,145.00 $4,290.00 | 21-day cycles: 500 mg/m2 IV on Day 1 | $3,861 | $5,148 |
CISPPEME regimen cost (21-day cycle) | $4,266 | $5,688 | ||||
CISPGEMC | ||||||
Cisplatin (generic) | 50 mg vial 100 mg vial | 1 mg/mL IV solution | $135.0000 $270.0000 | 21-day cycles: 75 mg/m2 IV on Day 1 | $405 | $540 |
Gemcitabine (generic) | 200 mg vial 1,000 mg vial 2000 mg vial | 40 mg/mL IV solution | $54.0600 $270.3000 $540.6000 | 21-day cycles: 1000 to 1250 mg/m2 IV on Day 1 and Day 8 | $1,297 | $1,730 |
CISPGEMC regimen cost (21-day cycle) | $1,702 | $2,270 | ||||
CISPVINO | ||||||
Cisplatin (generic) | 50 mg vial 100 mg vial | 1 mg/mL IV solution | $135.0000 $270.0000 | 21-day cycles: 75 mg/m2 IV on Day 1 | $405 | $540 |
Vinorelbine (generic) | 10 mg vial 50 mg vial | 10 mg/mL IV solution | $68.0000 $340.0000 | 21-day cycles: 25 mg/m2 on Day 1 and Day 8 | $680 | $907 |
CISPVINO regimen cost (21-day cycle) | $1,085 | $1,447 | ||||
CISPDOCE | ||||||
Cisplatin (generic) | 50 mg vial 100 mg vial | 1 mg/mL IV solution | $135.0000 $270.0000 | 21-day cycles: 75 mg/m2 IV on Day 1 | $405 | $540 |
Docetaxel (generic) | 80 mg vial 160 mg vial | 20 mg/mL IV solution | $124.2500 $123.7500 | 21-day cycles: 75 mg/m2 IV on Day 1 | $994 | $1,325 |
CISPDOCE regimen cost (21-day cycle) | $1,399 | $1,865 | ||||
Carboplatin-Based Regimens (Neoadjuvant, Adjuvant)b | ||||||
CRBPPACL | ||||||
Carboplatin (generic) | 50 mg 150 mg 450 mg 600 mg | 10 mg/mL vial for injection | $70.0000 $210.0000 $599.9985 $775.0020 | 21-day cycles: Target AUC 5 to 6 on Day 1, maximum dose for AUC 5 is 750 mg, maximum dose for AUC 6 is 900 mgc | $1,195 | $1,593 |
Paclitaxel (generic) | 30 mg vial | 6 mg/mL IV solution | $300.0000 | 21-day cycles: 175 to 200 mg/m2 IV on Day 1 | $3,600 | $4,800 |
CRBPPACL regimen cost (21-day cycle) | $4,795 | $6,393 | ||||
CRBPPEME | ||||||
Carboplatin (generic) | 50 mg 150 mg 450 mg 600 mg | 10 mg/mL vial for injection | $70.0000 $210.0000 $599.9985 $775.0020 | 21-day cycles: Target AUC 5 on Day 1, maximum dose for AUC 5 is 750 mgc | $985 | $1,313 |
Pemetrexed (generic) | 100 mg vial 500 mg vial 1,000 mg vial | 10 mg/mL IV solution | $2,145.00 $4,290.00 | 21-day cycles: 500 mg/m2 IV on Day 1 | $3,861 | $5,148 |
CRBPPEME regimen cost (21-day cycle) | $4,846 | $6,461 | ||||
CRBPGEMC | ||||||
Carboplatin (generic) | 50 mg 150 mg 450 mg 600 mg | 10 mg/mL vial for injection | $70.0000 $210.0000 $599.9985 $775.0020 | 21-day cycles: Target AUC 5 on Day 1, maximum dose for AUC 5 is 750 mgc | $985 | $1,313 |
Gemcitabine (generic) | 200 mg vial 1,000 mg vial 2000 mg vial | 40 mg/mL IV solution | $54.0600 $270.3000 $540.6000 | 21-day cycles: 1000 to 1250 mg/m2 IV on Day 1 and Day 8 | $1,297 | $1,730 |
CRBPGEMC regimen cost (21-day cycle) | $2,282 | $3,043 | ||||
CRBPVINO | ||||||
Carboplatin (generic) | 50 mg 150 mg 450 mg 600 mg | 10 mg/mL vial for injection | $70.0000 $210.0000 $599.9985 $775.0020 | 21-day cycles: Target AUC 5 on Day 1, maximum dose for AUC 5 is 750 mgc | $985 | $1,313 |
Vinorelbine (generic) | 10 mg vial 50 mg vial | 10 mg/mL IV solution | $68.0000 $340.0000 | 21-day cycles: 25 mg/m2 on Day 1 and Day 8 | $680 | $907 |
CRBPVINO regimen cost (21-day cycle) | $1,665 | $2,220 | ||||
CRBPDOCE | ||||||
Carboplatin (generic) | 50 mg 150 mg 450 mg 600 mg | 10 mg/mL vial for injection | $70.0000 $210.0000 $599.9985 $775.0020 | 21-day cycles: Target AUC 5 on Day 1, maximum dose for AUC 5 is 750 mgc | $985 | $1,313 |
Docetaxel (generic) | 80 mg vial 160 mg vial | 20 mg/mL IV solution | $124.2500 $123.7500 | 21-day cycles: 75 mg/m2 IV on Day 1 | $994 | $1,325 |
CRBPDOCE regimen cost (21-day cycle) | $1,979 | $2,639 | ||||
Nondrug Intervention | ||||||
Resection Surgery | ||||||
Pneumonectomyd | Pneumonectomy may include radical mediastinal node dissection, sampling or pericardial resection requiring repair | $20,240 per patiente | NA | |||
Lobectomyd | Lobectomy may include radical mediastinal node dissection or sampling | $13,153 per patientf | NA | |||
PDC = platinum-doublet chemotherapy
Note: All prices are wholesale from IQVIA Delta PA (accessed September 2022), unless otherwise indicated, and do not include dispensing fees. Calculations assume a patient body weight of 75kg and a body surface area of 1.8 m2. Vial wastage was assumed (i.e., no vial sharing). All recommended dosages are retrieved from Cancer Care Ontario Drug Formulary Regimens.
aSponsor’s submitted price.2
bNeoadjuvant PDC consists of 3 full cycles of PDC. Adjuvant PDC consists of 4 full cycles of PDC.
cDose [mg] = Target AUC * [GFR + 25]; AUC = product of serum concentration (mg/mL) and time (min); GFR (glomerular filtration rate) expressed as measured Creatinine Clearance or estimated from Serum Creatinine (by Cockcroft and Gault method or Jelliffe method). Maximum Carboplatin Dose (mg) = Target AUC (mg/mL per min) x (125 mL/min + 25).
dOntario Case Costing Initiative (OCCI), Acute Inpatient 2017/2018 (accessed October 21, 2022). Total cost includes direct costs (costs that are directly related to the provision of care to the patient and may include nursing, diagnostic imaging, pharmacy, and labs) and indirect costs (overhead expense relating to the running of hospitals and include administration, finance, human resources, and plant operations).
eAverage cost based on 490 cases (Range: $2,427-$676,871 per case). Average length of hospital stay was 7.3 days (Range: 1 to 167 days per case).
fAverage cost based on 2,792 cases (Range: $1,922- $567,768 per case). Average length of hospital stay was 5 days (Range: 1 to 157 days per case).
Appendix 2: Submission Quality
Note that this appendix has not been copy-edited.
Description | Yes/No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | No | Population is relevant but not generalizable to the Health Canada–indicated population of patients with stage IB to IIIA NSCLC due to the under-sampling of stage IB to II and over-sampling of stage IIIA in the CheckMate 816 trial. Adjuvant atezolizumab (administered after adjuvant chemotherapy), which was no included as a comparator in the submitted model, is an appropriate treatment option for patients with resectable stage IB to IIIA NSCLC with PD-L1 ≥ 50. A subgroup analysis to explore cost-effectiveness between different cancer stages would have been appropriate. |
Model has been adequately programmed and has sufficient face validity | No | Costs and outcomes for patients in the DM health state were adopted from an external model used for prior sponsor submissions. Because the CheckMate 9LA trial, the CheckMate 227 trial and the relevant ITC were not submitted to CADTH as part of this review, the data incorporated in the external economic model from these trials (which were used to determine the “one-off” consequence of progression for patients in the DM health state) have not been appraised by CADTH as part of this submission. |
Model structure is adequate for decision problem | No | While the model structure is generally adequate (i.e., the included health states are appropriate for the indication), the sponsor adopted a “one-off” approach to modelling costs, LYs, and QALYs for the DM health state. CADTH further notes that the external model used to characterize the cost and effectiveness outcomes for the “one-off” consequence of progression to DM was a partitioned survival model, which is subject to inherent modelling limitations, and any assumptions made during the development of this external model are necessarily carried through to the current submission. Since progression from LR to DM should be represented as a time-dependent probability, the sponsor should have opted to characterize it via tunnel states. As such, the model does not accurately reflect the health consequences of preventing DM among patients for whom re-treatment with curative intent in LR may achieve a functional cure. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | Yes | No comments. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | Yes | No comments. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | No | The “one-off” approach was not transparently described. |
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note that this appendix has not been copy-edited.
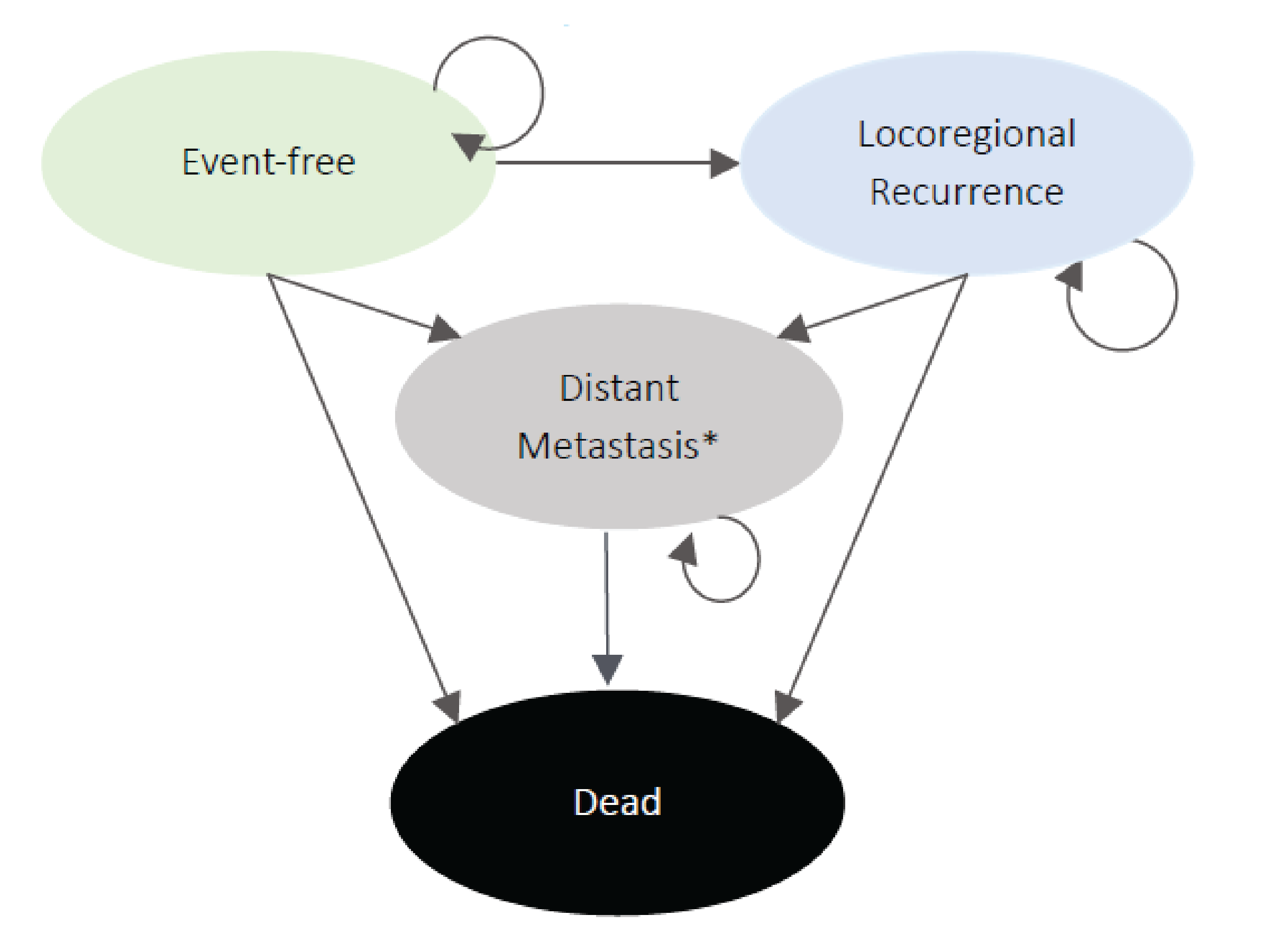
Note: A 1-off cost, life-year (LY) and quality-adjusted life-year (QALY) consequence is applied to patients entering distant metastasis (DM). The subsequent transition from DM to death is not explicitly tracked in the model.
Source: Sponsor’s pharmacoeconomic submission.2
Table 10: EQ-5D-5L Utility Index (Canada Weights), Treatment-Specific Least Squares Mean Estimates Derived From CheckMate 816 Data
Health state | Nivolumab + PDC | Neoadjuvant PDC |
|---|---|---|
Preprogression or recurrence | 0.886 (0.870, 0.902) | 0.893 (0.877, 0.908) |
Locoregional recurrence | 0.834 (0.806, 0.861) | 0.851 (0.820, 0.881) |
Distant metastases | 0.790 (0.758, 0.823) | 0.804 (0.758, 0.849) |
PDC = platinum-doublet chemotherapy.
Source: Sponsor’s pharmacoeconomic submission.2
Table 11: Pooled Utility Estimates by Health State Used in the Model
Health state | Mean Utility | Lower 95% CI | Upper 95% CI |
|---|---|---|---|
Event free | 0.842 | 0.831 | 0.853 |
Locoregional recurrence | 0.794 | 0.775 | 0.814 |
Distant metastasis | N/A | N/A | N/A |
Source: Sponsor’s pharmacoeconomic submission.2
Figure 2: EFS by Baseline Stage of Disease, CheckMate 816 Trial
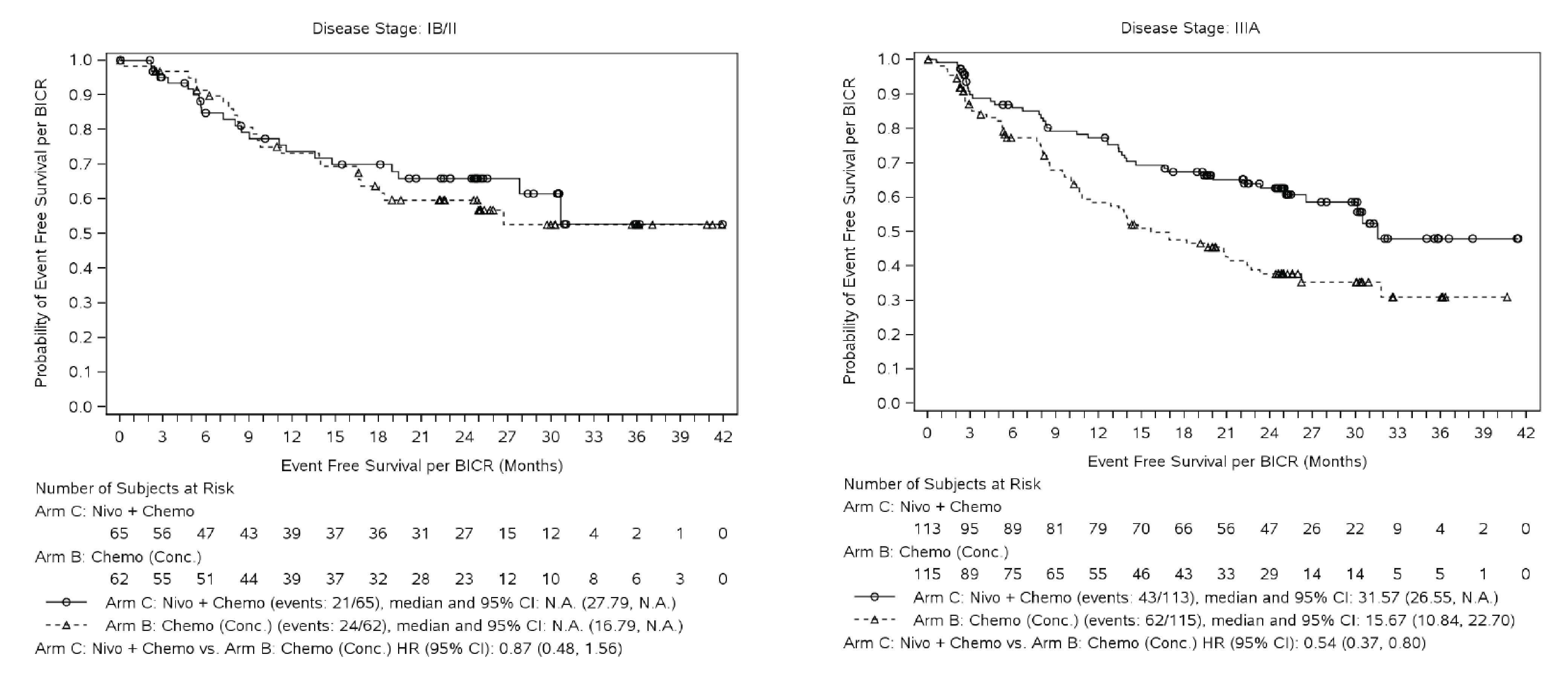
Source: Sponsor’s submitted clinical study report (Supplemental figures).
Figure 3: OS Extrapolation for Those Who Remain Event Free
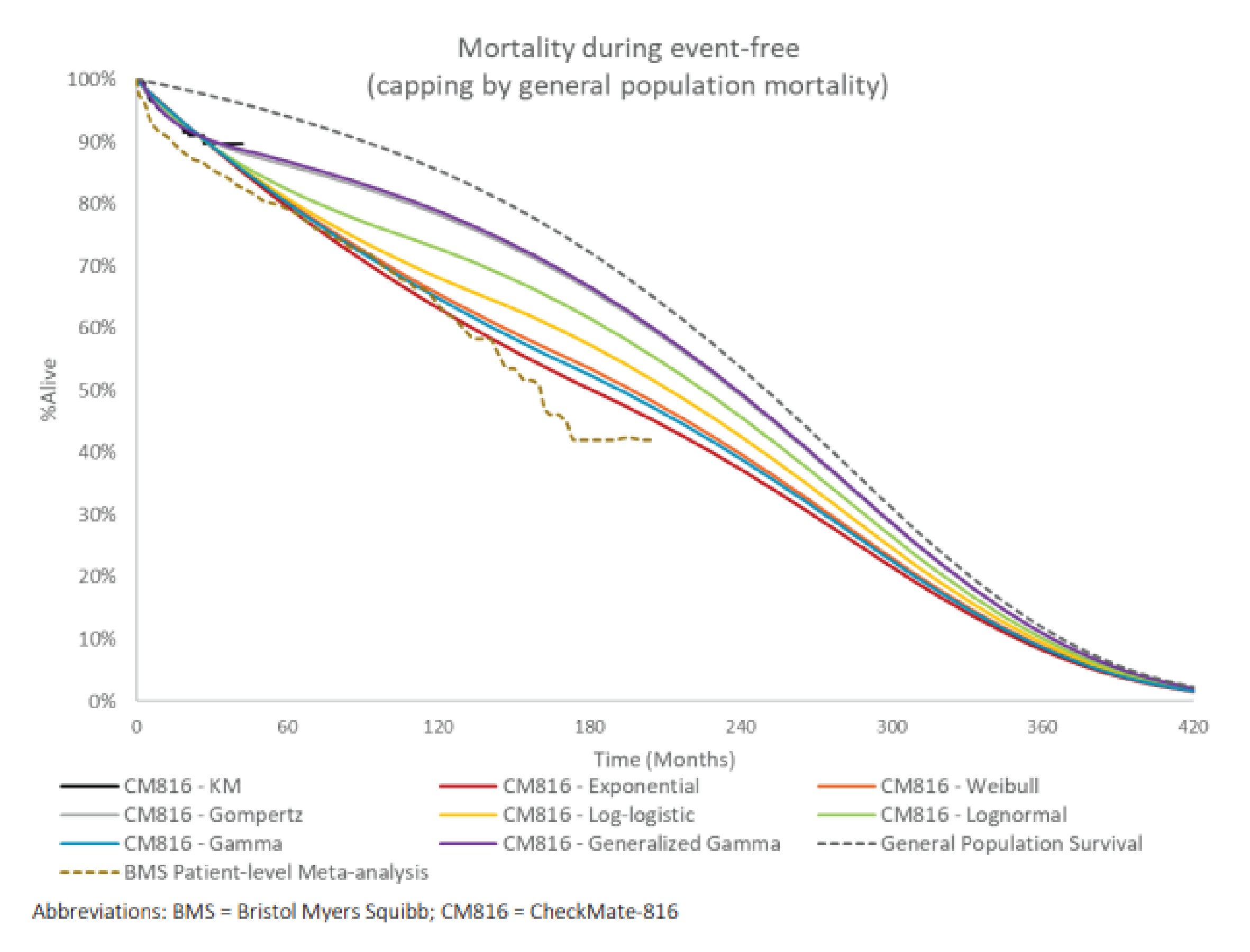
Source: Sponsor’s pharmacoeconomic submission.2
Detailed Results of the Sponsor’s Base Case
Table 12: Disaggregated Summary of CADTH’s Economic Evaluation Results
Parameter | Nivolumab + PDC | Neoadjuvant PDC | Adjuvant PDC | Surgery only |
|---|---|---|---|---|
Discounted LYs | ||||
Total | 8.88 | 7.56 | 7.88 | 7.20 |
EF | 6.92 | 5.03 | 5.50 | 4.58 |
LR | 0.76 | 0.91 | 0.72 | 0.82 |
DM | 1.19 | 1.62 | 1.66 | 1.80 |
Discounted QALYs | ||||
Total | 7.07 | 6.00 | 6.25 | 5.70 |
EF | 5.59 | 4.08 | 4.45 | 3.71 |
LR | 0.60 | 0.72 | 0.57 | 0.65 |
DM | 0.88 | 1.20 | 1.23 | 1.34 |
Discounted costs ($) | ||||
Total | $214,396 | $200,428 | $207,743 | $198,033 |
Drug acquisition | $26,338 | $4,812 | $7,284 | $0 |
Drug administration | $305 | $299 | $453 | $0 |
Surgery | $15,196 | $14,222 | $17,803 | $17,859 |
Adjuvant care after neoadjuvant | $1,574 | $2,086 | $0 | $0 |
Treatment cost in LR | $3,005 | $3,583 | $2,837 | $3,226 |
One-off cost in DM | $70,268 | $96,018 | $98,461 | $106,806 |
Disease management | $72,690 | $56,846 | $59,085 | $51,579 |
EF | $64,025 | $46,529 | $50,926 | $42,311 |
LR | $8,665 | $10,317 | $8,159 | $9,268 |
On-treatment monitoring costs | $152 | $159 | $177 | $51 |
EF | $104 | $103 | $132 | $0 |
LR | $48 | $57 | $45 | $51 |
AE management | $1,410 | $1,937 | $1,930 | $0 |
Terminal cost | $23,459 | $20,465 | $19,714 | $18,512 |
ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year.
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Note that this appendix has not been copy-edited.
Detailed Results of CADTH Reanalysis
Table 13: Disaggregated Summary of CADTH’s Economic Evaluation Results
Parameter | Nivolumab + PDC | Neoadjuvant PDC | Adjuvant PDC | Surgery only |
|---|---|---|---|---|
Discounted LYs | ||||
Total | 8.70 | 7.99 | 7.99 | 7.99 |
EF | 6.17 | 5.00 | 5.00 | 5.00 |
LR | 1.68 | 1.90 | 1.90 | 1.90 |
DM | 0.85 | 1.10 | 1.10 | 1.10 |
Discounted QALYs | ||||
Total | 6.91 | 6.32 | 6.32 | 6.32 |
EF | 5.01 | 4.06 | 4.06 | 4.06 |
LR | 1.27 | 1.44 | 1.44 | 1.44 |
DM | 0.63 | 0.81 | 0.81 | 0.81 |
Discounted costs ($) | ||||
Total | $200,273 | $186,296 | $186,992 | $180,702 |
Drug acquisition | $24,045 | $4,807 | $3,818 | $0 |
Drug administration | $303 | $299 | $468 | $0 |
Surgery | $15,196 | $14,222 | $17,803 | $17,859 |
Adjuvant care after neoadjuvant | $1,574 | $2,086 | $0 | $0 |
Treatment cost in LR | $3,213 | $3,631 | $3,631 | $3,631 |
One-off cost in DM | $50,175 | $64,891 | $64,891 | $64,891 |
Disease management | $76,159 | $67,775 | $67,775 | $67,775 |
EF | $57,076 | $46,208 | $46,208 | $46,208 |
LR | $19,082 | $21,567 | $21,567 | $21,567 |
On-treatment monitoring costs | $154 | $160 | $189 | $58 |
EF | $103 | $102 | $131 | $0 |
LR | $51 | $58 | $58 | $58 |
AE management | $1,410 | $1,937 | $1,930 | $0 |
Terminal cost | $28,043 | $26,488 | $26,488 | $26,488 |
ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year.
Scenario Analyses
Table 14: Summary of Scenario Analyses Conducted on the CADTH Base Case
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|---|
CADTH reanalysis | Surgery only | $180,702 | 6.32 | Ref. |
Nivolumab + PDC | $200,273 | 6.91 | $32,846 | |
Scenario 1: Equal efficacy between nivolumab + PDC and adjuvant PDC assumed | PDC (Adjuvant) | $187,907 | 6.99 | Reference |
Nivolumab + PDC | $201,384 | 6.94 | Dominated | |
Scenario 2: HR adjuvant vs. neoadjuvant for both event free to LR and event free to DM is 0.80. | Surgery only | $182,136 | 6.30 | Ref. |
PDC (adjuvant) | $188,236 | 6.86 | C$10,939 | |
Nivolumab + PDC | $201,384 | 6.94 | C$166,657 | |
Scenario 3: No progression from LR to DM | Surgery only | $177,520 | 6.74 | Ref. |
Nivolumab + PDC | $198,998 | 7.30 | $37,946 | |
Scenario 4: assumed fixed dosage for nivolumab | Surgery only | $180,702 | 6.32 | Ref. |
Nivolumab + PDC | $202,455 | 6.91 | $36,509 | |
Scenario 5: ITC used to estimate comparisons of nivolumab + PDC vs. adjuvant PDC and surgery only | Surgery only | $184,898 | 6.04 | Ref. |
Neoadjuvant PDC | $186,296 | 6.32 | $5,099 | |
Nivolumab + PDC | $200,273 | 6.91 | $23,454 |
ICER = incremental cost-effectiveness ratio; ITC = indirect treatment comparison; PDC = platinum-doublet chemotherapy; QALY = quality-adjusted life-year; Ref. = reference. Only comparators on the frontier are presented, adjuvant and neoadjuvant therapy are dominated in scenario analysis 2 and 3 are dominated. Adjuvant therapy is extendedly dominated in scenario analysis 5.
Appendix 5: Submitted BIA and CADTH Appraisal
Note that this appendix has not been copy-edited.
Table 15: Summary of Key Takeaways
Key Takeaways of the BIA |
|---|
|
Summary of Sponsor’s BIA
The sponsor submitted a budget impact analysis (BIA) to estimate the incremental 3-year budget impact of reimbursing neoadjuvant nivolumab + PDC for the treatment of adult patients with newly diagnosed, resectable stage IB to IIIA NSCLC. The analysis was performed from the perspective of the Canadian public drug plan formulary. The sponsor estimated the budget impact by comparing 2 scenarios: a reference scenario reflecting a market without any neoadjuvant treatment, reflecting Canadian current clinical practice, to a new scenario that included use of neoadjuvant nivolumab + PDC. The sponsor estimated the eligible population using an epidemiology-based approach, leveraging data from multiple sources in the scientific literature and assumptions based on clinical expert input. The sponsor included drug-acquisition costs associated with neoadjuvant and adjuvant preprogression therapy, as well as those associated with postprogression therapy. The dosing regimen modelled for nivolumab was 360 mg every 3 weeks for 3 cycles, as per the CheckMate 816 trial. Key inputs to the BIA are documented in Table 18.
Key model assumptions included:
Patients do not receive any neoadjuvant chemotherapy in the reference scenario.
Carboplatin- and cisplatin-based regimens are identical in terms of treatment efficacy. The model considers the weighted average of the cost per dose for cisplatin and carboplatin with the distribution of patients receiving each treatment (carboplatin: 74%; cisplatin: 26%).
The proportion of incident NSCLC that is resectable is dependent on stage at diagnosis (stage IB: 66%; stage IIA-IIB: 50%; stage IIIA: 30%).
The proportion of patients with resectable NSCLC who receive neoadjuvant treatment is dependent on stage at diagnosis (stage IB to IIA: 36%; stage IIB: 50%; stage IIIA: 60%).
Table 16: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as Year 1 / Year 2 / Year 3 if appropriate) |
|---|---|
Target Population | |
General Canadian population, sum of included CADTH jurisdictions in base year | ~29,872,595 |
Annual incidence of diagnosed NSCLC per 100,000 | Stage IB: 8.57 per 100,000 Stage IIA: 2.52 per 100,000 Stage IIB: 3.88 per 100,000 Stage IIIA: 5.87 per 100,000 |
Proportion of incident NSCLC without EGFR mutation | 85% |
Proportion of incident NSCLC that is resectable | Stage IB: 66% Stage IIA: 50% Stage IIB: 50% Stage IIIA:30% |
Proportion of patients with resectable NSCLC receiving treatment | Stage IB: 36% Stage IIA: 36% Stage IIB: 50% Stage IIIA: 60% |
Number of patients eligible for drug under review | 1,146 / 1,162 / 1,178 |
Market Uptake (3 years) | |
Uptake (reference scenario) Nivolumab + PDC No neoadjuvant therapy | 0% / 0% / 0% 100% / 100% / 100% |
Uptake (new drug scenario) Nivolumab + PDC No neoadjuvant therapy | 29% / 31% / 35% 71% / 69% / 65% |
Cost of treatment (per patient) | |
Cost of treatment per 21-day cycle Nivolumab + Platinum drug + Pemetrexed + Platinum drug + Gemcitabine + Platinum drug + Vinorelbine + Platinum drug + Docetaxel + Platinum drug + Paclitaxel | $ 8,999 $ 8,669 $ 8,013 $ 8,344 $ 8,879 |
Cost of treatment per regimen (3 cycles) Nivolumab + Platinum drug + Pemetrexed + Platinum drug + Gemcitabine + Platinum drug + Vinorelbine + Platinum drug + Docetaxel + Platinum drug + Paclitaxel | $ 26,998 $ 26,008 $ 24,040 $ 25,032 $ 26,638 |
NSCLC = non–small cell lung cancer; PDC = platinum-doublet chemotherapy.
Summary of the Sponsor’s BIA Results
Results of the sponsor’s base-case BIA suggest that the incremental expenditures associated with the reimbursement of neoadjuvant nivolumab + PDC for the Health Canada–indicated population of patients with newly diagnosed, resectable stage IA-IIIB NSCLC would be $8,089,851 in Year 1, $7,256,640 in Year 2, and $7,274,241 in Year 3, for a 3-year cumulative total of $22,620,732, under the drug plan perspective.
CADTH Appraisal of the Sponsor’s BIA
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
Dose for nivolumab does not reflect dosing anticipated by jurisdictions. The sponsor used a fixed dose to model the required dosage for nivolumab (360 mg), which was aligned with nivolumab’s product monograph, as well as the dose received by patients treated with nivolumab + PDC in the CheckMate 816 trial.12,15 CADTH notes that in Canadian clinical practice, weight-based dosing is applied consistently across nivolumab indications. Participating drug plans highlighted that if nivolumab were funded in the neoadjuvant setting, jurisdictions would implement weight-based dosing (i.e., nivolumab 4.5mg/kg up to 360 mg, administered every 3 weeks, for 3 cycles).
Based on information received from drug plans, CADTH conducted a reanalysis assuming weight-based dosing.
CADTH conducted a sensitivity analysis with the fixed dose modelled by the sponsor as it reflected the dose received by patients treated with nivolumab + PDC in the CheckMate 816 trial.
Uncertain degree of cost savings associated with cancer progression The sponsor submitted a BIA model that included a simulation of disease progression to estimate the accrual of treatment costs across 3 lines of treatment (i.e., neoadjuvant, adjuvant, and postprogression), as well as across 2 health states (i.e., event-free, and postprogression). Hence, by simulating disease progression, the BIA effectively relied upon median OS estimates originated from the sponsor-submitted pharmacoeconomic model. CADTH notes that the pharmacoeconomic model was itself subject to extensive limitations, some of which could not be adequately addressed (i.e., the “one-off” approach to model DM). The sponsor also assumes no full re-treatment with nivolumab and an exponential distribution when assuming the rate of cancer progression which differs from the assumptions used in the economic evaluation. Therefore, for this submission the sponsor provided 2 Markov models both assessing the rate of progression yet employed 2 fundamentally different approaches. Given both models are simulating the same patient cohort it is unclear why 2 separate model approaches were provided. Had the model submitted for the cost-utility analysis not used a ‘one-off’ approach for assessing the impact of DM this would have been adequate to use in the budget impact assessment.
Due to the degree of uncertainty associated with the sponsors approach of assessing postprogression costs, CADTH conducted a base-case reanalysis by excluding the treatment costs that could be accrued in the simulated postprogression health state. This analysis represents the upfront drug cost associated with using nivolumab in the neoadjuvant setting relative. CADTH acknowledges that the reanalysis excluded the potential cost savings incurred in postprogression among patients receiving neoadjuvant nivolumab + PDC however these could not be accurately assessed in the model provided by the sponsor.
CADTH conducted a sensitivity analysis that included the treatment costs that could be accrued in postprogression to present the potential cost savings that may occur among patients receiving neoadjuvant nivolumab + PDC. CADTH notes that this analysis should be interpreted with caution given the reasons outlined above.
CADTH Reanalyses of the BIA
CADTH conducted reanalyses of the BIA by assuming weight-based dosing and removing the treatment costs that could be accrued in the simulated postprogression health state.
The results of the CADTH step-wise reanalysis are presented in summary format in Table 20 and a more detailed breakdown is presented in Table 21. Based on the CADTH base case, the budget impact associated with nivolumab’s reimbursement is expected to be $8,149,659 in year 1, $8,833,668 in year 2, and $10,113,125 in year 3, with a 3-year total of $27,096,452.
CADTH conducted additional sensitivity analyses to address remaining uncertainty, using the CADTH base case. Results are provided in Table 21. Assuming a fixed dose for nivolumab in the neoadjuvant setting.
Assuming that treatment costs could be accrued in postprogression.
Table 17: CADTH Revisions to the Submitted BIA
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
None. | — | — |
Changes to derive the CADTH base case | ||
1.Dose for nivolumab does not reflect dosing anticipated by jurisdictions | Fixed dose (360 mg, administered every 3 weeks, for 3 cycles) | Weight-based dose (4.5mg/kg up to 360 mg, administered every 3 weeks, for 3 cycles) |
2.Simulation approach relied on survival estimates derived from the submitted pharmacoeconomic model | Treatment costs accrued in postprogression included | Treatment costs accrued in postprogression excluded |
CADTH base case | Combined revisions 1 + 2 | |
Table 18: Summary of the CADTH Reanalyses of the BIA
Stepped analysis | Three-year total |
|---|---|
Submitted base case | $22,620,732 |
CADTH reanalysis 1 | $20,045,997 |
CADTH reanalysis 2 | $29,671,187 |
CADTH base case | $27,096,452 |
Table 19: Detailed Breakdown of the CADTH Reanalyses of the BIA
Stepped analysis | Scenario | Year 1 | Year 2 | Year 3 | Three-year total |
|---|---|---|---|---|---|
Submitted base case | Reference | $14,957,718 | $34,723,734 | $56,120,149 | $105,801,601 |
New drug | $23,047,569 | $41,980,375 | $63,394,390 | $128,422,334 | |
Budget impact | $8,089,851 | $7,256,640 | $7,274,241 | $22,620,732 | |
CADTH base case (upfront cost of therapies only) | Reference | $6,196,768 | $6,283,523 | $6,371,492 | $18,851,784 |
New drug | $14,346,427 | $15,117,191 | $16,484,617 | $45,948,236 | |
Budget impact | $8,149,659 | $8,833,668 | $10,113,125 | $27,096,452 | |
CADTH sensitivity analysis 1: Fixed dose for nivolumab | Reference | $6,196,768 | $6,283,523 | $6,371,492 | $18,851,784 |
New drug | $15,120,817 | $15,956,576 | $17,445,578 | $48,522,971 | |
Budget impact | $8,924,048 | $9,673,053 | $11,074,086 | $29,671,187 | |
CADTH sensitivity analysis 2: Treatment costs in postprogression included | Reference | $14,957,718 | $34,723,734 | $56,120,149 | $105,801,601 |
New drug | $22,273,179 | $41,140,990 | $62,433,430 | $125,847,599 | |
Budget impact | $7,315,462 | $6,417,255 | $6,313,280 | $20,045,997 |
BIA = budget impact analysis.
Stakeholder Input
Patient Input
Lung Cancer Canada
About Lung Cancer Canada
Lung Cancer Canada is a registered national charitable organization that serves as Canada’s leading resource for lung cancer education, patient support, research, and advocacy. Lung Cancer Canada is a member of the Global Lung Cancer Coalition and is the only national organization in Canada focused exclusively on lung cancer.
Lung Cancer Canada is registered with CADTH. https://www.lungcancercanada.ca/
Information Gathering
Lung Cancer Canada interviewed 5 patients and 1 caregiver in Canada who all had experience with nivolumab. Most interviews were conducted via phone call between September to October 2022; LC’s experience was gathered through past interviews by LCC. Details of each patient and caregiver are listed in the chart below.
Table 1: Patients Interviewed About Their Experience With Nivolumab
Patient/ Caregiver | Gender of Patient | Diagnosis date | Stage & Type of Lung Cancer | Location | Source |
|---|---|---|---|---|---|
Patient | M | July 2019 | Stage 1/2 NSCLC | Quebec | Phone Interview |
Patient | F | June 2021 | Stage 3 NSCLC | Saskatchewan | Phone Interview |
Caregiver | M | October 2019 | Large cell neuroendocrine carcinoma | Ontario | Phone Interview |
Patient | F | March 2014 | Stage 4 NSCLC | Ontario | Phone Interview |
Patient | F | March 2015 | Stage 4 NSCLC | Ontario | Phone Interview |
Patient | M | Spring 2012 | Stage 4 NSCLC | Alberta | Past interviews, environmental scan |
Disease Experience
Being one of the first pharmacists in rural Saskatchewan that built up a smoking cessation program in the province, X had known about the risks and ties it had to lung cancer; however, it never crossed her mind that she’d be diagnosed one day. She was extremely active and was an avid runner since about 10 years ago. However, in June 2021, she slowly found exercise becoming harder for her and felt more tired than ever. After developing a cough and some mild chest pain one night, doctors thought she had a blood clot and followed-up with CT scans. However, the last thing they expected to find was a mass in X s lung, which was later revealed to be stage 3 non-small cell lung cancer that had already spread to multiple lymph nodes at the time - X was devastated and in shock. She had a tumour resection and 1 lymph node removed just after diagnosis and had luckily qualified for nivolumab just as it was being funded in Saskatchewan. She started on nivolumab in September 2021 and continues to be on it today.
X has had a long and unfortunate family history of lung cancer: his grandfather first died of it when X was 17, then two of his aunts, his mother, and twin brother in 2016 have all passed away from the disease. It was the diagnosis of his twin and his mother’s passing in 2012 that sparked him to get screened, and to his surprise, test results found stage 4 lung cancer with over 25 lesions that had already spread to his adrenal glands, kidneys, pancreas, and both lungs. Given 12-13 months to live, X was determined to although 1.5 years of initial chemotherapy treatments not working, he was willing to undergo any treatments available. His oncologist suggested the nivolumab clinical trial and without hesitation, X started treatment in August 2013. The results were incredible, and within 15 weeks, most of his cancer spots had shrunk down by 95%, almost immeasurable. X stopped treatment in 2017 and continues to do very well today in October 2022.
Non-small cell lung cancer (NSCLC) is the most common type of lung cancer and occurs in 80-85% of all lung cancer cases, and among those with NSCLC, about half of these patients have either early-stage or locally advanced disease (stages I to III), in which five-year survival rates plummet from 92% in stage I to 36% in stage 3 disease. With the recent advancements in lung cancer research and screening, there has been an increase in the percentage of patients diagnosed with earlier-stage disease, thus opening up the possibility of potential neo-adjuvant therapies prior to resection, including nivolumab.
The phase 3 CheckMate 816 clinical trial has shown very promising results of adding nivolumab, an immunotherapy drug, as a neoadjuvant treatment in conjunction with chemotherapy. Median event-free survival was 31.6 months in the nivolumab-chemotherapy arm compared to 20.8 months with chemotherapy alone, in addition to 24% of patients reaching complete pathological response vs 2.2% respectively (Forde et al., 2022). This marks significant clinical benefit with drastic improvements in event-free survival and higher percentage of participants having complete disease response with nivolumab. As discussed further in this document, patients with early-stage disease have found success with nivolumab and its addition will lessen the deep unmet need in this treatment paradigm.
Experiences With Currently Available Treatments
Chemotherapy
Resectable early-stage non-small cell lung cancer is typically treated with surgery alone; however, there are promising results published showing a modest benefit in disease control when paired with neoadjuvant or adjuvant chemotherapy. Chemotherapy has been a long-standing and well-documented standard of care for lung cancer patients, which has seen some benefits, though is limited as a viable long-term treatment option due to its harsh side effects. While this form of treatment has been found to work, it also creates additional burdens on patients through its harsh side effects, decreased functionality, and increased dependence on caregivers in their daily activities that have been documented in previous LCC submissions. Many of the patients interviewed for this submission consistently noted that their experiences with chemotherapy were significantly more taxing and “worse” in comparison to nivolumab in several ways: side effects, impact of treatment on mobility and functionality, and overall efficacy of the treatment to manage their disease was not worthwhile.
When X was diagnosed in 2012 with stage 4 lung cancer, radiation and surgery were both off the table because of the extent of his metastases. He was given 12-13 months to live and started palliative chemotherapy treatment in summer 2012. However, after nearly a year of treatment showed no signs of improvement, X was discouraged and didn’t think he’d be able to get past the next Christmas.
When AR was diagnosed in March 2015, X-rays showed a large mass in her lung that had already spread to her brain adrenal glands, bones and colon, and when she started treatment right away with chemotherapy, she was feeling very unwell and could barely get off the couch. Side effects of nausea and fatigue in addition to the symptoms from the cancer was very overwhelming and needed a lot of help from family and friends for help around the house. After 6 weeks of chemotherapy alongside 5 sessions of radiation, scans revealed it was only partially working. It wasn’t until she found success with nivolumab that she started to feel better.
X diagnosis only came about when she woke up one morning noticing 3 large bumps on the side of her neck, which biopsies later revealed was stage 3-4 NSCLC that had spread to all lymph nodes. She started with 12 rounds of radiation and then started chemotherapy soon after. She recalls the side effects were “brutal” – she suffered moderately severe edema in that her feet and legs were so swollen it was difficult to walk and was constantly exhausted and tired. She was unable to go about her daily life like cleaning the house or grocery shopping and relied on family for help. It was extremely tough and after oral chemotherapy showed no improvements, she switched to traditional IV chemotherapy which worked for a couple of months, but X progressed a few months later, 1.5 years after starting chemotherapy.
FM’s uncle was diagnosed with large cell neuroendocrine carcinoma in October 2019 via the provincial screening pilot program, and had an upper left lobectomy and wedge resection, while identifying additional disease in the right lung as well. He started on chemotherapy, which started off working well, but ended up hospitalized and on dialysis for 3 weeks prior to the 4th cycle due to neutropenia and renal disfunction. When biomarker tests identified the KRAS G12C mutation, he started on nivolumab in November 2020, which X continues to be on to this day.
Radiation
X s first line of treatment after being diagnosed in 2014 was radiation. She completed 12 rounds of radiation to treat the nodules that had spread to her lymph nodes in the neck, and she recalls this really was difficult for her. The implications it had on her impacted her functionality and quality of life, as because the treatment was targeted around her neck, she had a large burn in that area, leaving her having a hard time swallowing, hence eating and drinking was difficult. She remained swollen and sore; however, it was successful in shrinking the size of the tumours. When X finished treatment, she started on chemotherapy, both oral and intravenous, as described above, prior to nivolumab.
After X was diagnosed with early-stage NSCLC in July 2019, the large baseball-sized mass in his right lung led him to having a full resection of his tumour but meant two-thirds of his lung was removed in surgery, leaving him with only about 50% of his initial lung capacity left. After recovering, he underwent radiation treatments for 5-6 weeks to control any possible preliminary spread, before he was placed on the CheckMate 816 clinical trial with nivolumab in November [sic]. [Of note, Checkmate 816 only enrolled resectable patients prior to their surgery, and not patients who underwent surgery and then radiation]
Improved Outcomes
Patients with earlier stage resectable NSCLC generally have more treatable disease in comparison to advanced stage patients, where the primary goal of treatment for stage IIIC onwards is to delay disease progression and minimize symptoms. However, with early-stage I to III patients, the primary goal of treatment is the intent to cure, hence the treatment plan includes surgical resection. In these cases, patients value new treatment options that maintain or improve their quality of life, delay onset of symptoms, improve survivorship, improve or maintain functionality/mobility, and ultimately, to provide a cure. With many immunotherapies being administered at hospitals or local cancer centers, patients interviewed also noted that they preferred to undergo their treatment at a hospital closer to home, which included community clinics in the case of some rural patients to minimize travel time and relieve the burden on caregivers.
Experience With Drug Under Review
Table 2: Period and Duration on Nivolumab
Year diagnosed | Period on nivolumab | Duration on nivolumab | Currently on nivolumab? |
|---|---|---|---|
2021 | Sept 2021 – present | 1 year | Yes |
2019 | Nov 2020 – present | 23 months | Yes |
2019 | Aug – Nov 2019 | 3 months | No |
2014 | Jan 2016 – March 2022 | 6 years 2 months | No |
2015 | Aug 2015 – Sept 2017, March 2021 – May 2022 | 3 years 3 months (total) | No |
2012 | Sept 2013 – Aug 2017 | 4 years | No |
Nivolumab is durable and effective at treating patients’ disease, including patients with advanced metastases.
At diagnosis, X had already spread to her bones, adrenal glands and brain, including early signs of it being in her colon as well. After initial first line treatment with chemotherapy that proved ineffective, she started on nivolumab in August 2015. She gradually started feeling better and by next May, scans showed all of the tumours outside of her lungs were completely resolved and the primary tumour in her lung had shrunk in half from the initial 6.5cm down to only 3cm. She has continued to maintain stable disease with no signs of progression as of 2022 although she ended treatment with nivolumab in 2017.
Prior to diagnosis in Spring 2012, X felt no symptoms at all, but scans revealed he had several nodules in both his lungs, and had already spread further to his adrenal gland, kidneys, and pancreas, and was estimated to only live about 12-13 months. When chemotherapy did not yield results, he switched treatments onto nivolumab in fall 2013. Miraculously, within 9 weeks, the tumours in his lungs had already shrunk significantly, and a CT scan at 15 weeks revealed that most of the 25+ spots at diagnosis had completely resolved. X recalls, “it was just a miracle to see, and for someone facing certain death at first, I didn’t know what to say”. He ended treatment in 2017 and has since remained stable without any signs of the cancer returning.
X had metastases in all lymph nodes when she was diagnosed with stage 4 lung cancer, and initial treatments with chemotherapy and radiation were not working. She started nivolumab in January 2016 and continued to be on it for 6 years, in which overtime her tumours have shrunk by over 80%. She ended nivolumab in March 2022 and has not been receiving other courses of treatment as of October while remaining stable.
FM’s uncle started treatment with nivolumab in November 2020 after biomarker tests came back with the KRAS G12C mutation. Compared to the weeks prior to starting treatment when he was hospitalized, X started to feel better and better overtime, and ever since he started nivolumab, his disease has completely resolved and is currently NED. He continues to remain on nivolumab as of October 2022 and continues to do very well.
Side effects of nivolumab are manageable.
As per the results of the CheckMate 816 clinical trial, the most common adverse events reported include constipation, nausea, fatigue, decreased appetite, anemia, and neutropenia (Forde et al., 2022).
From the patients interviewed for this submission, 2 patients TB and FM experienced virtually no side effects at all. Similar to what was reported in the trial, HS experienced three main side effects: dramatic loss of appetite (therefore lost a lot of weight), nausea, and a mild rash that enveloped one-third of his body. However, he stresses that these are all relatively minor and has not impeded him from going about his day-to-day life in any way.
X experienced occasional muscle pain in her arm but has not impeded her mobility or functionality in any way. She mentions to Lung Cancer Canada that “she would take this side effect over what I experienced with other treatments any day”.
The main side effects X experienced were colitis, inflammatory arthritis of her joints, digestive issues, rash, and on-and-off musculoskeletal pain. She also mentioned dry eyes and dry mouth, both of which she still struggles with to this day even after she stopped treatment. The arthritic flare-ups in her knee did impact her mobility in that it hurt to walk, but once it was treated with additional medication, it has continued to be kept under control and does not impact her mobility too much anymore. Similar to X, AR stresses that all the adverse effects she has experienced with nivolumab are, by far, much more manageable than previous treatments like chemotherapy, and has allowed her to become reinvolved with life and enjoy the time she lost from feeling unwell prior to nivolumab.
Patients’ quality of life is significantly better than on other treatments. Many noted it is comparable to pre-diagnosis.
When X was on chemotherapy, she was unable to do any basic errands and live a fulfilling life because of all the impediments the side effects and symptoms of her disease had yielded, including edema that significantly impacted her mobility. Cleaning the house was an impossible task that she relied on her partner for, grocery shopping was not an option, and although she continued to work throughout the first 2 years of diagnosis, her productivity dropped because of the exhaustion. With nivolumab, a few months into treatment and her functionality and mobility improved exponentially; X says it’s “very comparable to what I had before being diagnosed with cancer”. She does tire out quicker and can’t run too long, but going shopping and cleaning the house is not an issue, and even moved homes twice to a new city while on nivolumab. She remains active and exercises in her backyard regularly, which has helped maintain her strength and mobility as well.
By the time X was about to start treatment with nivolumab, the side effects combined with the disease symptoms that were not relieved with previous treatments meant she was constantly feeling sick and nauseous, and essentially couch-ridden for the entire summer after being diagnosed in the spring. She was barely able to get up and cook and relied on her husband and friends for help with caring for her elementary-aged children. Overall, the feelings of exhaustion overtook her, and she was at a very “low and awful” point, unable to do many basic tasks. Her 2nd dose of nivolumab was interrupted as she had to have emergency surgery on a perforated bowel, delaying treatment by about a month, but she slowly started to feel better and regained her energy over the next few months. 9 months later, X felt like she was nearly back to the same lifestyle she had prior to diagnosis, albeit some side effects, but overall was feeling like herself again. When she got news that most of her cancer had disappeared and her primary tumour had shrunk by 50%, she was ecstatic and was able to become reinvolved in her life and caring for her kids. She continued with the immunotherapy for 2 years until 2017 and between then until May 2022, she had an incredible quality of life, went back to work, and just enjoyed the extra time she had gained with her family. AR briefly went back on nivolumab for a year between March 2021 to May 2022 because of increased inflammation in her lungs but has since remained stable and is doing very well.
Ever since X uncle has been on nivolumab, it seemed like a complete 180-degree change from his quality of life prior to starting. He was hospitalized and on dialysis for 3 weeks during prior treatments and because of the rarity of his type of lung cancer, it seemed like it may have been the end of the path until they found nivolumab. He has been feeling very well, has an excellent quality of life, is able to do all the activities he used to and spend lots of quality time with family and friends, and overall is “living life with joy and passion”, as FM recalls. He regularly goes for walks around the neighbourhood, which previously seemed impossible because of the pain, and is able to go about his day-to-day life running errands and requires no help around the house.
Ever since X had surgery which removed two-thirds of his right lung, he’s been working mostly on 50% lung capacity, which has not been much of an issue aside from being unable to do any vigorous exercises or activities. He notes that nivolumab has slightly improved his energy levels, he continued to drive himself to his treatments while on nivolumab about 30 mins each way, and otherwise continues to live a normal lifestyle, being able to do nearly everything he could from before his diagnosis. He does not require any additional assistance with his day-to-day, has no ability or functional limitations, and although he tires out quicker and can’t clean the house with his decreased lung capacity, it hasn’t stopped him from taking part in other errands like grocery shopping, cooking, and exercising when he can.
Similarly, X has been living her life nearly the same as she had before diagnosis – all her side effects from nivolumab are relatively minor and do not impede her mobility or functionality in any way, and because of the success she has had with nivolumab being her first line of adjuvant treatment post-surgery, she has never had any major setbacks in her disease yet. She knows that she’s very lucky to be enjoying the same quality of life, is able to perform almost all activities of daily living without assistance and has been feeling well overall. She bikes and walks 5 days a week to keep herself in shape and has been getting back into exercise over the summer before winter settles.
Patients are able to maintain their independence, return to hobbies they enjoy and make longer term plans.
As X was being interviewed by Lung Cancer Canada, she noted that nivolumab was “a miracle drug for [her]. It has given her life back in many ways, and an extra 7 years that she otherwise wouldn’t have had with her husband and young children”. With 2 kids now in middle school, AR has been passionate about becoming reinvolved with her life, diving deep into lung cancer advocacy with LCC and numerous other organizations. She has a long list of places she wants to travel to, most recently returning from a 2-week trip in Austria for the World Conference on Lung Cancer in September 2022. Thanks to nivolumab, she has been able to start initiatives of her own that otherwise would have never gotten off the ground, including a refugee sponsorship group with her neighbour. Nivolumab has given patients like AR a chance to pursue their goals and passions again.
X s uncle has continued to do extremely well even though he lives with a rare lung cancer diagnosis, all thanks to nivolumab. He repeatedly says to X, “I don’t feel like I have cancer at all. I feel as though I take these trips to the cancer center, for what? I have a therapy that lasts less than an hour, and then I’m able to go about my day. But no one would even know I have cancer. And more importantly, no one would ever know I have lung cancer, which is a death sentence for most people. I’ve been around a lot longer than I should be, and my disease is eradicated. I’m so grateful and appreciative of having access to this therapy, and able to live life in such a meaningful way. I can put one foot in front of the other and greet life well”.
Now living in a completely different part of the province from when she started, LS has quit her job since she started nivolumab and is focused on living her life one day at a time, with goals of travelling around the world and long-term commitments in the works. She has returned to doing hobbies she loves, including knitting and crocheting, and even went on several camping trips with her partner over the last 2 years. Nivolumab has managed patients like LS’s disease so well that it is no longer a “full time job being diagnosed with cancer’ and has given her the opportunity to do what she loves and return to putting herself and her happiness in first priority.
Because of his decreased lung capacity since his surgery 3 years ago, HS was not able to travel much outside of his home or exercise as much as he’d liked to, but the pandemic also played a role in limiting that as well. However as of September 2022, he has returned to work via a hybrid format, going into the office a few times per week, and his capacity for exercise has increased quite significantly. He goes swimming with his wife 3-4 times a week and takes long walks, as they were both fairly active prior to diagnosis, so HS noted that being able to return to swimming has been his main outlet for exercise and improved his mental health quite significantly as well. Nivolumab worked well for him and although he was already “cancer-free” prior to treatment, HS says that immunotherapy with nivolumab has allowed his body to learn to fight the cancer on its own while allowing him to focus on making longer-term goals because his time isn’t so limited anymore. He plans on travelling at least once a year with his wife and family, and hopefully get back to running and hiking overtime.
TB has experienced some fatigue while driving even before she was diagnosed, which has slightly impacted her independence, but shorter drives to the hospital and grocery store are not a problem. As a pharmacist, she owned her own pharmacy for a few decades and was one of the first to implement a smoking cessation program in her home province of Saskatchewan. A passionate advocate for lung cancer screening, she spoke to Lung Cancer Canada about her goals for the province to implement screening in pharmacies like hers and is already getting back to work part-time to help run the store. With a great support system with her husband and 2 daughters, TB repeatedly spoke about how fortunate she is to be living such a great quality of life thanks to nivolumab, and she continues to be doing very well on it to this day. Her access to the treatment via compassionate access is set to continue until September 2023 but is hopeful she can continue to stay on nivolumab for longer because of the great success she has had with it.
Companion Diagnostic Test
There is no diagnostic test associated with resectable NSCLC. Groups excluded from CheckMate 816 included patients with EGFR or ALK alterations, as there is a lack of data on the benefits of neoadjuvant immunochemotherapy in this population. The adoption of CheckMate 816 regimen into practice implies that the search for EGFR and ALK will need to be performed on every available patient before treatment, which are routinely tested for via biomarker testing.
Anything Else?
Nivolumab has given all these patients their independence, allowed them to spend the time they have with loved ones, many have returned to pursuing their hobbies again, all while on treatment or NED post-treatment. The success that they have found with the treatment has been a recurring theme between all of them, while side effects are minimal and manageable. We hope that pERC and CADTH are able to take these patient values and real-world experiences into consideration as the approval and reimbursement of this treatment will only be benefiting patients and their families like these at the forefront. It has seen clinical success within the CheckMate 816 trial, and its reimbursement will only generate further RWE and stories from families about its ability to treat non-small cell lung cancer, especially at this early-stage resectable indication.
Reference: Forde, P. M., Spicer, J., Lu, S., Provencio, M., Mitsudomi, T., Awad, M. M., et. al. (2022). Neoadjuvant nivolumab plus chemotherapy in resectable lung cancer. New England Journal of Medicine, 386, 1973-1985. DOI: 10.1056/NEJMoa2202170
Conflict of Interest Declaration — Lung Cancer Canada
To maintain the objectivity and credibility of the CADTH reimbursement review process, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission?
No.
Did you receive help from outside your patient group to collect or analyze data used in this submission?
No.
List any companies or organizations that have provided your group with financial payment over the past 2 years AND who may have direct or indirect interest in the drug under review.
Table 3: Financial Disclosures for Lung Cancer Canada
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Bristol-Myers Squibb | — | — | — | X |
Clinician Input
Ontario Health (Cancer Care Ontario) Lung Cancer Drug Advisory Committee
About Ontario Health (Cancer Care Ontario) Lung Cancer Drug Advisory Committee
OH-CCO’s Drug Advisory Committees provide timely evidence-based clinical and health system guidance on drug-related issues in support of CCO’s mandate, including the Provincial Drug Reimbursement Programs (PDRP) and the Systemic Treatment Program.
Information Gathering
Information was gathered during a DAC meeting.
Current Treatments and Treatment Goals
Currently, there is curative treatment for resectable NSCLC. The standard for most patients in this population is adjuvant chemotherapy after surgery, although this is dependent on stage. In Stage 1b and 2, many patients get chemotherapy in the adjuvant setting. Stage 3 patients are a heterogenous treatment population. Stage 3 treatments range from primary surgery, neoadjuvant chemotherapy, neoadjuvant chemotherapy + radiation, and definitive chemotherapy radiation followed by durvalumab. Overall, operative patients received surgery followed by 4 cycles of chemotherapy.
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
Neoadjuvant nivolumab would be an additional option for resectable NSCLC patients. The standard of care for resectable NSCLC is in a transition phase based on the funding/recommendation to use Atezolizumab. A number of patients with current treatments do recur quickly and lack survival. Nivolumab has a better survival based on the outcomes of the clinical trial.
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
Nivolumab would be given for 3 cycles with concurrent chemotherapy before surgery. It would potentially replace the use of adjuvant chemotherapy in some patient populations.
Which patients would be best suited for treatment with the drug under review? Which patients would be least suitable for treatment with the drug under review?
Patients best suited would align with the clinical trial inclusion criteria (ie, resectable NSCLC with stage IIA to IIIB (8th Edition)). Patients who would be eligible for chemotherapy would be best suited for this treatment.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice? How often should treatment response be assessed?
Outcomes used to determine whether a patient is responding are clinical assessment to make sure a patient is not progressing, surgery, and pathologic assessment of response to therapy.
What factors should be considered when deciding to discontinue treatment with the drug under review?
Intolerable toxicity and clinically obvious disease progression.
What settings are appropriate for treatment with [drug under review]? Is a specialist required to diagnose, treat, and monitor patients who might receive [drug under review]?
Specialist is required in a hospital outpatient clinic, ideally as part of a multidisciplinary team.
Additional Information
Not applicable.
Conflict of Interest Declarations — Ontario Health (Cancer Care Ontario) Lung Cancer Drug Advisory Committee
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please refer to the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission? If yes, please detail the help and who provided it.
Yes. Ontario Health provided secretariat function to the DAC.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission.
No.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician who contributed to the input — please add more tables as needed (copy and paste). It is preferred for all declarations to be included in a single document.
Declaration for Clinician 1
Name: Dr. Peter Ellis
Position: Member, Ontario Health CCO Lung Cancer Drug Advisory Committee
Date: 13/09/2022
Table 4: COI Declaration for OH-CCO Lung Cancer DAC — Clinician 1
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In excess of $50,000 |
|---|---|---|---|---|
BMS- Ad Board | X | — | — | — |
Declaration for Clinician 2
Name: Dr. Sara Kuruvilla
Position: Member, Ontario Health CCO Lung Cancer Drug Advisory Committee
Date: 13/09/2022
Table 5: COI Declaration for OH-CCO Lung Cancer DAC — Clinician 2
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Declaration for Clinician 3
Name: Dr. Donna Maziak
Position: Lead, Ontario Health CCO Lung Cancer Drug Advisory Committee
Date: 13/09/2022
Table 6: COI Declaration for OH-CCO Lung Cancer DAC — Clinician 3
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Lung Cancer Canada
About Lung Cancer Canada
Lung Cancer Canada is a national charitable organization that serves as Canada’s leading resource for lung cancer education, patient support, research and advocacy. Based in Toronto, Ontario, Lung Cancer Canada has a wide reach that includes both regional and pan-Canadian initiatives. Lung Cancer Canada is a member of the Global Lung Cancer Coalition and is the only organization in Canada focused exclusively on lung cancer.
Information Gathering
Information gathered for this submission was based on relevant published clinical data and expert evidence-based review amongst lung cancer medical oncologists across Canada. The key sources of data relevant to this new indication are below.
Current Treatments and Treatment Goals
In Canada, the treatment for Stages IB-IIIA non-small cell lung cancer (NSCLC) is stage dependent. Canadian practice is aligned with practices from around the world, as evidenced from data from both the IASLC Dataset and North American-based National Cancer Database.
For stage IB NSCLC, the primary goal is cure (i.e., to improve 5-year overall survival). To achieve this goal, the standard treatment is complete surgical resection (R0). For this stage, adjuvant platinum-doublet chemotherapy is usually not indicated considering the absence of demonstrated benefit in large studies. In a small fraction of cases, surgical resection leads to an incomplete resection, and adjuvant radiation is potentially offered in this context. In medically inoperable patients, localized radiation (external beam or stereotactic body radiation) is used as an alternative to surgery.
For stage II NSCLC, the primary goal is cure (i.e., to improve 5-year overall survival). To achieve this goal the standard treatment is complete surgical resection (R0). Thereafter, fit patients are offered adjuvant platinum-doublet chemotherapy. In a small fraction of cases, surgical resection leads to an incomplete resection, and adjuvant radiation is potentially offered in this context, which would be given sequentially to adjuvant chemotherapy when feasible.
For stage IIIA NSCLC, the primary goal is cure (i.e., to improve 5-year overall survival). To achieve this goal, the standard treatment depends on whether the primary tumour is considered resectable or not, balancing benefits and risks, including peri-operative risks, the ultimate chance of cure, the number of lobes that will be resected (e.g. lobectomy vs pneumonectomy), the number of lymph node stations involved, size of lymph nodes and the long-term residual effects of the operation (e.g. expected residual pulmonary reserve and function after a resection). If surgery is considered reasonable, the next step would depend on whether mediastinal lymph nodes are known to be involved with cancer. If not (T4N0 or T3 or T4N1), medically eligible patients will start with surgery and then proceed to adjuvant platinum-based chemotherapy. For those patients with N2 mediastinal lymph nodes involved, neoadjuvant chemotherapy, sometimes associated with concurrent radiation, followed by complete surgical resection can be offered if the nodal disease is non-bulky and limited in extent. If surgery is not considered reasonable, definitive concurrent chemo-radiation is given, followed by consideration of a year of durvalumab. In a small fraction of cases, surgical resection leads to an incomplete resection, and adjuvant radiation is potentially offered in this context, but sequentially (and not concurrent) with any adjuvant chemotherapy, when feasible.
Adjuvant platinum-doublet chemotherapy given after resection of stage IIA-IIIA NSCLC patients typically consists of four cycles of treatment, with each cycle lasting 21-28 days, for a total of 12 -16 weeks of therapy. Specific platinum-doublet chemotherapy with the best evidence of efficacy has been with the combination of cisplatin and vinorelbine. Other platinum-doublet combinations commonly used globally include cisplatin and pemetrexed or carboplatin and paclitaxel, the former restricted to non-squamous lung cancer histologies and the latter for all histologies or restricted to squamous cell tumors, based on local preferences and reimbursement issues.
The current staging system we use globally is the 8th edition of the Union of International Cancer Control (UICC) staging system. CheckMate 816 was conducted using the 7th edition of the UICC staging system. Discussion above referenced the standard practice for the 8th edition which was used in the trial. Relevant differences include stage IB cancers that are considered high risk for relapse (tumour size 4-5 cm) in this trial are now considered stage II tumors. Adjuvant chemotherapy is not required for patients with stage I cancers in the 8th edition system (< 4 cm, node negative). Stage III has now been divided into stage IIIA, IIIB and IIIC. Stage IIIC are unresectable. A subset of patients with stage IIIA and B will be resected and offered adjuvant platinum-based chemotherapy as described above. These patients previously were all typed as IIIA in the 7th edition staging.
Although adjuvant chemotherapy has been favored until now in many centers, systematic reviews have shown that neoadjuvant therapies and adjuvant therapies are associated with a similar benefit. The preference of adjuvant therapies in the past relate to the strength of data being more important in the adjuvant space and perhaps by the perception in the thoracic surgery community that the use of neoadjuvant chemotherapy may be associated in some instances with disease progression and loss of the opportunity for surgery. Absence of impact of timing of chemotherapy on overall survival (HR=0,99 – 95%CI: 0,81-1,21) in previous studies imply that a neoadjuvant approach can be used according to the clinical setting and physician judgement. Neoadjuvant chemotherapy is already being used in many centers on a case-by-case basis.
Treatment decisions have become more complex given recent results from many studies showing the benefit of immuno-chemotherapeutic options in the neoadjuvant and adjuvant spaces. The IMpower 010 study demonstrated improved survival in the PD-L1 > 50% subgroup of patients with IB-IIIA NSCLC (7th edition), HR 0,42 (0,23-0,78). On January 14, 2022, Health Canada has authorized atezolizumab as monotherapy for adjuvant treatment following complete resection and no progression after platinum-based adjuvant chemotherapy for adult patients with stage II to IIIA NSCLC whose tumors have PD-L1 expression on ≥ 50% of tumour cells (TCs). Although not currently funded by public insurance, this treatment is possible for some patients through private insurance or private pay.
Another treatment that has become recently available in the post resection setting is adjuvant osimertinib. Osimertinib is approved by Health Canada after tumor resection in patients with stage IB-IIIA non-small cell lung cancer (NSCLC) whose tumors have epidermal growth factor receptor (EGFR) exon 19 deletions or exon 21 (L858R) substitution mutations. This population is a specific subgroup of NSCLC with a sensitizing mutation in the tyrosine kinase domain of EGFR and comprises 10-15% of adenocarcinomas. The ADAURA trial results identified a reduction in the recurrence rate with a hazard ratio (HR) of 0.17 (99% CI, 0.11-0.26); p<0.001 for resected Stages II-IIIA, and HR 0.20 resected for Stages IB-IIIA. This treatment is currently variably available to Canadian patients either through public funding, private insurance, or a compassionate access program.
References
Chansky K, Detterbeck FC, Nicholson AG, Rusch VW, Vallières E, Groome P, Kennedy C, Krasnik M, Peake M, Shemanski L, Bolejack V, Crowley JJ, Asamura H, Rami-Porta R; IASLC Staging and Prognostic Factors Committee, Advisory Boards, and Participating Institutions. The IASLC Lung Cancer Staging Project: External Validation of the Revision of the TNM Stage Groupings in the Eighth Edition of the TNM Classification of Lung Cancer. J Thorac Oncol. 2017 Jul;12(7):1109-1121. doi: 10.1016/j.jtho.2017.04.011. Epub 2017 Apr 28. PMID: 28461257.
Pignon JP, Tribodet H, Scagliotti GV, Douillard JY, Shepherd FA, Stephens RJ, Dunant A, Torri V, Rosell R, Seymour L, Spiro SG, Rolland E, Fossati R, Aubert D, Ding K, Waller D, Le Chevalier T; LACE Collaborative Group. Lung adjuvant cisplatin evaluation: a pooled analysis by the LACE Collaborative Group. J Clin Oncol. 2008 Jul 20;26(21):3552-9.
Lim E, Harris G, Patel A, Adachi I, Edmonds L, Song F. Preoperative versus postoperative chemotherapy in patients with resectable non-small cell lung cancer: systematic review and indirect comparison meta-analysis of randomized trials. J Thorac Oncol. 2009 Nov;4(11):1380-8. doi: 10.1097/JTO.0b013e3181b9ecca. PMID: 19861907.
Enriqueta Felip, Heather Wakelee, Nasser Khaled Altorki, Eric Vallieres, Ihor O. Vynnychenko, Andrey Akopov, Alex Martinez-Marti, Antonio Chella, Igor Bondarenko, Sunichi Sugawara, Yun Fan, Hirotsugu Kenmotsu, Yuh-Min Chen, Yu Deng, Fan Wu, Virginia McNally, Elizabeth Bennett, Barbara Gitlitz, Caicun Zhou PL03.09 - IMpower010:Overall Survival Interim Analysis of a Phase III Study of Atezolizumab vs Best Supportive Care in Resected NSCLC. IASLC Meeting, August 2022
Yi-Long Wu, M.D., Masahiro Tsuboi, M.D., Jie He, M.D., Thomas John, Ph.D., Christian Grohe, M.D., Margarita Majem, M.D., Jonathan W. Goldman, M.D., Konstantin Laktionov, Ph.D., Sang-We Kim, M.D., Ph.D., Terufumi Kato, M.D., Huu-Vinh Vu, M.D., Ph.D., Shun Lu, M.D., et al., for the ADAURA Investigators* Osimertinib in Resected EGFR-Mutated Non–Small-Cell Lung Cancer. N Engl J Med 2020; 383:1711-1723.
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
Neoadjuvant therapies are being developed in many different tumor settings such as breast cancer, head and neck cancer, multiple digestive tract cancers and bladder cancer to name a few examples. Potential advantages to neoadjuvant approaches include the following.
Early treatment of micrometastatic disease, limiting the risk of systemic dissemination of the cancer
Tumor downstaging, limiting the extent of surgery in some patients, improving functional outcomes, decreasing complications of surgery, and decreasing the risk of margin positivity.
Treatment of patients before they suffer from complications of surgery, increasing the number of patients that can benefit from a lifesaving strategy.
Gives the opportunity to the patient for smoking cessation, physical therapy, and medical evaluations prior to the actual surgery.
Provides a window of delay to help manage surgical waiting lists.
Allows the in-vivo monitoring of drug response and improves the ability to provide prognosis and risk-stratification after surgery.
Such goals are highly relevant to lung cancer patients. Smoking cessation prior to surgery has been shown to improve surgical outcomes in an ERAS (early recovery after surgery) environment. Tumor downstaging may facilitate minimally invasive surgery and decrease the risk of extended surgeries such as pneumonectomies. Tumor downstaging may also decrease post-operative complications and recovery times. Considering that many patients must deal with post-operative pain, infections and a decreased performance status, many patients will not feel the capacity to undergo post-operative adjuvant therapies and decline optimal therapy if offered in the post-operative setting. Thus, pre-operative therapy improves the capacity of exposing a broader group of patients to useful therapies.
A potential risk of neo-adjuvant therapies is the loss of opportunity of surgery because of the delay imposed by the treatment itself. Indeed, some rare patients with rapidly progressive disease may not undergo definitive surgery after neoadjuvant therapy. These patients with have a very poor prognosis and are not the patients that are the most likely to benefit from surgery in the first place. In a sense, neoadjuvant therapies may offer the advantage limiting unnecessary surgeries in such patients.
In CheckMate 816, surgical outcomes have been evaluated as exploratory variables and show the following (nivolumab+chemo vs chemo alone):
definitive surgery rates were 83% vs 75%
minimally invasive surgery rates were 30% and 22%
conversion from minimally invasive to open surgery rates were 11% and 16%
lobectomy was performed in 77% vs 61% of pts
pneumonectomy in 17% and 25%
an R0 resection was achieved in 83% vs 78%.
there was no increase in median (Q1, Q3) duration of surgery and length of hospitalization 184 [130, 252] vs 217 [150, 283] min; and 10.0 [7, 14] vs 10.0 [7, 14] days, respectively
any-grade and grade 3–4 surgery-related AEs were reported in 41% vs 47% and 11% vs 15%
Such evaluations direct towards the possibility of easier, safer and more efficacious surgeries with the broader use of neoadjuvant immunochemotherapy. Improvement in surgical outcomes with neoadjuvant immunochemotherapy as compared to chemotherapy alone is one of the major drivers to the vast excitement of the thoracic surgeons for neoadjuvant therapies.
Reference: Spicer J, Wang C, Tanaka F, et al. Surgical outcomes from the phase 3 checkmate 816 trial: Nivolumab (NIVO) + platinum-doublet chemotherapy (chemo) vs chemo alone as neoadjuvant treatment for patients with resectable non-small cell lung cancer (NSCLC). Journal of Clinical Oncology. 2021;39(15_suppl):8503-8503. doi:10.1200/jco.2021.39.15_suppl.8503
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
Checkmate 816 is the first large, randomized trial to show many benefits of a neoadjuvant immunochemotherapeutic approach. The patients included in this trial are the typical patients that are also considered for adjuvant therapies. Patients included in this trial were evaluated to be stage IB-IIIA (per 7th TNM edition), had an ECOG performance status of 0-1 and had no EGFR mutations or ALK alterations. Stratification factors included stage (IB-II vs IIIA) and PD-L1 status ( >=1% or < 1%).
A total of 358 patients were randomized in a 1:1 ratio to receive 3 cycles of a standard platinum-doublet regimen (cisplatin-vinorelbine, docetaxel-cisplatin, gemcitabine-cisplatin for squamous only and cisplatin-pemetrexed for non-squamous only) or 3 cycles of nivolumab combined to the same chemotherapy. Patients were then reassessed radiologically and had surgery within 6 weeks of the end of therapy. Primary endpoints included pathologic complete response and event-free survival. Secondary endpoints included major pathological response, overall survival and time to death and distant metastases. This study also looked at surgical outcomes after protocol-based therapies as well as quality of life measures.
These results were presented in many meetings since the original presentation at AACR in February 2021 [sic], [Of note, AACR in April 2021] with the latest results presented at the ESMO meeting in September 2022. In summary, results of the primary and secondary endpoints favor in many aspects the combination of nivolumab and chemotherapy (nivolumab+chemo vs chemo alone):
Primary Outcomes:
There was a statistically significant improvement in the primary endpoint of pCR (OR = 13.94 [99% CI, 3.49–55.75]; P < 0.0001), and the benefit was consistent across disease stages, histologies, TMB, and PD-L1 expression levels.
There was a statistically significant improvement in EFS vs chemo (HR = 0.63 [97.38% CI, 0.43-0.91]; P = 0.0052). No significant difference was detected in this outcome according to stratification variables. EFS was improved in patients with a pCR compared with those without, suggesting pCR as an early indicator of therapeutic benefit with nivolumab + chemo.
Secondary Outcomes:
MPR and ORR were also improved.
Preliminary OS analysis showed a trend of improvement (HR = 0.57 [99.67% CI, 0.30-1.07]) while the study continues to mature.
Neoadjuvant nivolumab + chemo showed a safety profile consistent with previous reports and did not impact the feasibility of surgery vs chemo alone.
The quality-of-life measures did not detect a difference in the quality of life in both study arms and did not detect an impact on post-operative patient related outcomes.
The outcome of time to death and distant metastases has yet to be reported.
This is thus the first of many ongoing trials in this therapeutic space. The favorable outcomes observed with only 3 cycles of nivolumab and chemotherapy is driving a major shift of paradigm for the treatment of this disease. Whereas the current standard of care would favor up-front surgery followed in some patients by 4 cycles of chemotherapy, radiation and 1 year of immunotherapy. The approach proposed by Checkmate 816 facilitates the overall treatment by limiting the number of cycles of chemotherapy and offering patients the possibility of pCR in 24% of cases, providing improved surgical care and post-operative outcomes. This approach would thus eliminate the need of post-operative, prolonged and more expensive therapies. Perhaps some additional post-operative therapies would still be required for some patients that remain at high-risk of recurrence after neoadjuvant therapies and surgery and these questions need to be addressed in upcoming studies.
The randomized data from CheckMate 816 is further supported by many single arm phase II trials showing similar impressive results. At least 8 trials have evaluated monotherapy IO in the neoadjuvant setting and reported a combined major pathological response rate of 23,4% and a pCR rate of 7,5% [sic]. [Of note, these are peri-operative studies (IO pre and post-surgery)]. Another 4 studies evaluating immunotherapy combined with chemotherapy showed a MPR of 65,4% and a pCR rate of 36,6% (oral communication, Provencio et al, ESMO 2022). Likewise, a randomized phase II trial (NADIM II) has already been reported showing a pCR rate of 36,8% with carboplatin-paclitaxel-nivolumab compared to 6,9% with carboplatin-paclitaxel alone (OR=7,88, p=0,0068). A recent update from this trial with a Median follow-up time of 21.9 months showed a progression-free survival at 24 months of 67.3% (95%CI: 55.5-81.6) for patients treated with nivolumab plus chemotherapy versus 52.6% (95%CI: 36.8- 75.2) for patients treated with chemotherapy (hazard ratio: 0.56; 95%CI: 0.28-1.15; P= 0.117). Overall survival at 24 months was 85.3% (95%CI: 75.7-96.1) with nivolumab plus chemotherapy versus 64.8% (95%CI: 47.4-86.4) with chemotherapy (hazard ratio, 0.37; 95%CI, 0.14-0.93; P=0.003).
It is not yet clear if this peri-operative approach will be used for all eligible patients. Some patients with stage II, node-negative disease may still be considered for up-front surgery with the option of providing adjuvant therapies on a case-by-case basis. This may particularly be the case for patients that are felt at higher risk of chemotherapy or immunotherapy associated complications or for patients preferring upfront surgery.
References
Mariano Provencio-Pulla, Ernest Nadal, Jose Luis Gonzalez Larriba, Alex Martinez-Marti, Reyes Bernabé, Joaquim Bosch-Barrera, Joaquin Casal, Virginia Calvo, Amelia Insa, Santiago Ponce Aix, Noemi Reguart, Javier De Castro Carpeño, Joaquín Mosquera, Raquel Benitez, Carlos Aguado De La Rosa, Ramon Palmero, Florentino Hernando-Trancho, Atocha Romero, Alberto Cruz Bermudez, and Bartomeu Massuti Nivolumab plus chemotherapy versus chemotherapy as neoadjuvant treatment for resectable stage IIIA NSCLC: Primary endpoint results of pathological complete response (pCR) from phase II NADIM II trial. Journal of Clinical Oncology 2022 40:16_suppl, 8501-8501
M. Provencio1, R. Serna1, E. Nadal2, J.L. Glez Larriba3, A. Martínez-Martí4, R. Bernabé5, J. Bosch-Barrera6, C. Garcia Benito7, V. Calvo1, A. Insa8, S. Ponce9, N. Reguart10, J. De Castro11, B. Massutí12, R. Palmero2, C. Aguado de la Rosa3, J. Mosquera13, M. Cobo14, A. Aguilar15, G. López Vivanco16, C. Camps17, F. Hernando Trancho3, R. López Castro18, T. Moran19, I. Barneto20, D. Rodríguez-Abreu21, A. Romero1. PL03.12 Progression Free Survival and Overall Survival in NADIM II Study. IASLC 2022 World Conference on Lung Cancer | Vienna, Austria
Which patients would be best suited for treatment with the drug under review? Which patients would be least suitable for treatment with the drug under review?
An evaluation of the stratification factors in CheckMate 816 does not allow to distinguish for certainty who benefit best from study treatment. Nonetheless, the HR for EFS appears greater so far in the stage IIIA patients (HR=0,54) compared to stage IB-II patients (HR=0,87). Similarly, the HR in the PD-L1 > 50% expressing tumors is 0,24 compared to 0,58 and 0,85 in the 1-49% and the <1% group, respectively. There may be a clinicians’ bias towards some favoring of neoadjuvant therapy for the stage IIIA and/or PD-L1 positive patients. Nonetheless, a benefit is found in all subgroups and a discussion with every eligible patient appears warranted based on the available results presented so far. This clinical discussion will include the option of receiving post-operative chemotherapy (4 cycles instead of 3) and the further option of 1 year of atezolizumab (for patients with PD-L1 expressing > 50% only at this current time). This current reality would favor the use of a neoadjuvant in all eligible patients to decrease the treatment burden on patients that are favorable and eligible for this approach. Patients with tumors expressing PD-L1 < 50% would not be eligible for an adjuvant treatment with atezolizumab at this current time and would lose the opportunity to benefit from a checkpoint inhibitor as part of their care.
Some thoracic surgeons are more familiar with the neoadjuvant approach than others. It is to be expected that the pattern of referral of all stage II-IIIA patients to multidisciplinary tumor boards for discussion and referral to medical oncology for the assessment of neoadjuvant therapy will increase progressively. Considering that CheckMate 816 provides important data towards a change in treatment paradigm, education amongst thoracic surgeons and medical oncologists will need to be provided before widespread use of this approach is adopted, as we have witnessed for other disease settings where neoadjuvant therapies have been introduced.
Patients least suitable for treatment are those patients who have a contraindication to chemotherapy and immunotherapy treatments. Contra-indications to platinum-doublets include renal failure (GFR < 40-60 according to different experts), heart failure, severe hearing loss and severe neuropathy. Some studies have suggested that benefits of adjuvant chemotherapy appear to decline in patients aged over 70 years. Although age is not an exclusion factor for therapy, discussions of tolerance and risks of treatment are more significant with advancing age. Age was not an exclusion factor in CheckMate 816. Median age was 64, ranging from 41 to 82 years of age in the nivolumab and chemotherapy arm.
Performance status evaluated to be 2-4 is generally felt to be a contra-indication to adjuvant chemotherapy and would be also used in the clinic to exclude some patients from treatment, as was done in the clinical trial.
The strongest contra-indication to immunotherapy is the presence of an organ transplant. Patients with auto-immune disease are at higher risk of immunotherapy related complications. Risks and benefits would need to be discussed with patients who have prior or active autoimmune disease as their risk of side effects is generally higher than for those patients without such history. A history of autoimmune disease would not be considered a major contraindication, especially if the auto-immune disease is clinically silent (eg. auto-immune thyroiditis) and well controlled without active immunosuppression. On the other hand, active and symptomatic auto-immune disease (eg. Crohn’s disease on immunosuppressive therapy or multiple sclerosis) would generally be considered a contra-indication to immunotherapy, especially in a neo-adjuvant setting.
Another group excluded from CheckMate 816 was patients with EGFR mutations or ALK alterations. Patients identified with an EGFR mutation may potentially benefit from neoadjuvant immunochemotherapy although data is currently lacking in this regard. A particular additional concern is the identified risk of osimertinib use after prior immunotherapy regarding an increased risk of immune related adverse events. Considering the important benefit and the widespread clinical use of adjuvant osimertinib based on the ADAURA trial, the use of immunotherapy in the neoadjuvant space should be reserved to further investigation.
Patients with ALK translocations, and perhaps other patients with translocations, such as those involving ROS1, RET and NTRK have been previously shown to be poor responders to immunotherapy in the advanced disease setting. These patients potentially have a reduced risk of benefitting from a neoadjuvant approach with nivolumab and chemotherapy. As this group of patients has not been specifically addressed in clinical trials, treatment decisions will be left to a case by case evaluation.
The detection of biomarkers in a Canadian environment is widely variable from region to region. Since the introduction of osimertinib as an adjuvant option in patients with stage II-IIIA operated patients, the search for EGFR alterations should be standard of practice already. The adoption of CheckMate 816 regimen into practice implies that the search for EGFR and ALK will need to be performed on every available patient before treatment and after the performance of a diagnostic biopsy, since these two groups of biomarker positive patients were excluded from the trial. Therefore, ALK immunohistochemistry will have to be performed as an extra biomarker test for those patients. ALK immunohistochemistry is widely available in the country and is currently used in the advanced setting and is also already being used in high stage II-III in some centers. Considering the rarity of ROS1, RET and NTRK (<1% of NSCLC, combined) and the absence of widely available NGS screening in the early disease setting of NSCLC as well as delays to report NGS results, it does not appear feasible at this present time to mandate NGS screening in all patients before deciding on neoadjuvant therapies. In some regions of Canada, EGFR alterations are already being detected by multigene NGS panels and therefore some patients with very rare mutations may be identified in this manner. The approach for these patients will have to be addressed on a case per case setting.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice? How often should treatment response be assessed?
In Canada, PET scan evaluations and EBUS staging procedures are considered standard of care approaches for patients being investigated and staged for potential stage II-III diseases. At this present time, these patients also need to be evaluated for PD-L1 status and EGFR alterations to allow clinicians to evaluate post-operative standard adjuvant therapies. These biomarkers are currently being performed on the surgical specimen instead of the diagnostic biopsy. The emergence of neoadjuvant therapies mandates the performance of an additional CT scan assessment after neoadjuvant therapy is completed to plan the upcoming surgery and exclude patients from surgery if the disease has evolved and become too advanced.
In CheckMate 816, a pCR rate of ~ 24% was reported. A question often asked by our patients is the approach to treatment after the documentation a major radiologic response after neoadjuvant therapy. Some patients question the usefulness of surgery in these situations. At the present time, no clinical, biological, or imaging tool can be used to identify patients who will have pCR on pathological assessment, therefore it is not currently possible to exclude any patients from surgical treatment.
Standard post-operative follow up will be provided to patients treated for these types of tumors. In the future, it is possible that risk adapted follow up strategies will be developed based on pathological response to treatment and post-therapy pathological staging of the tumor. Such strategies must be developed as we gather more experience with neoadjuvant approaches. The incorporation of ctDNA post-operative monitoring is an exciting technology that may be important in the stratification of post-operative risk, in combination with other clinical and pathological features of the cancer.
What factors should be considered when deciding to discontinue treatment with the drug under review?
Clinical and biological evaluations are performed at every cycle of therapy as per standard practice in oncology. Clinicians are very familiar with the evaluation of patients undergoing chemoimmunotherapy therapies as this approach has become widespread in the advanced disease setting. In CheckMate 816, 94% of patients in the nivolumab plus chemotherapy arm were able to receive the total 3 cycles of therapy with 6% of patients discontinuing therapy for study drug toxicity and only 1 patient for disease progression.
What settings are appropriate for treatment with [drug under review]? Is a specialist required to diagnose, treat, and monitor patients who might receive [drug under review]?
Patients considered for this type of approach are usually addressed to oncologic thoracic surgeons affiliated with major cancer centers. It would appear optimal that patients eligible for a multimodal treatment approach be discussed within a multidisciplinary cancer tumor board involving (non-exclusively) respirologists, radiologists, pathologists, thoracic surgeons, medical oncologists, and radiation oncologists. The delivery of the optimal treatment for every patient will have to be discussed and planned according to local structures of delivery of care. It would appear optimal that a planning structure could be set for patients to receive systemic therapies as close to home as possible while being continuously monitored by the cancer center to coordinate neoadjuvant therapies with post treatment imaging, pre-operative evaluations, and the surgical admission itself.
Additional Information
Chronology of presentations on CheckMate 816.
2021
Patrick M. Forde; Jonathan Spicer; Shun Lu; Mariano Provencio; Tetsuya Mitsudomi; Mark M. Awad; Enriqueta Felip; Stephen Broderick; Julie Brahmer; Scott J. Swanson; Keith Kerr; Changli Wang; Gene B. Saylors; Fumihiro Tanaka; Hiroyuki Ito; Ke-Neng Chen; Cecile Dorange; Junliang Cai; Joseph Fiore; Nicholas Girard Abstract CT003: Nivolumab (NIVO) + platinum-doublet chemotherapy (chemo) vs chemo as neoadjuvant treatment (tx) for resectable (IB-IIIA) non-small cell lung cancer (NSCLC) in the phase 3 CheckMate 816 trial. Cancer Res (2021) 81 (13_Supplement): CT003. https://doi.org/10.1158/1538-7445.AM2021-CT003
Spicer J, Wang C, Tanaka F, et al. Surgical outcomes from the phase 3 checkmate 816 trial: Nivolumab (NIVO) + platinum-doublet chemotherapy (chemo) vs chemo alone as neoadjuvant treatment for patients with resectable non-small cell lung cancer (NSCLC). Journal of Clinical Oncology. 2021;39(15_suppl):8503-8503. doi:10.1200/jco.2021.39.15_suppl.8503
2022
Nicolas Girard, Jonathan Spicer, Mariano Provencio, Shun Lu, Stephen Broderick, Mark M. Awad, Tetsuya Mitsudomi, Keith Kerr, Julie Brahmer, Scott J. Swanson, Enriqueta Felip, Changli Wang, Gene B. Saylors, Ke-Neng Chen, Fumihiro Tanaka, Moishe Liberman, Cecile Dorange, Javed Mahmood, Junliang Cai, Patrick M. Forde. CT012 - Nivolumab (NIVO) + platinum-doublet chemotherapy (chemo) vs chemo as neoadjuvant treatment for resectable (IB-IIIA) non-small cell lung cancer (NSCLC): Event-free survival (EFS) results from the phase 3 CheckMate 816 trial. Proceedings of the 113th Annual Meeting of the American Association for Cancer Research; 2022 April 8-13; New Orleans LA.
Forde PM, Spicer J, Lu S, Provencio M, Mitsudomi T, Awad MM, Felip E, Broderick SR, Brahmer JR, Swanson SJ, Kerr K, Wang C, Ciuleanu TE, Saylors GB, Tanaka F, Ito H, Chen KN, Liberman M, Vokes EE, Taube JM, Dorange C, Cai J, Fiore J, Jarkowski A, Balli D, Sausen M, Pandya D, Calvet CY, Girard N; CheckMate 816 Investigators. Neoadjuvant Nivolumab plus Chemotherapy in Resectable Lung Cancer. N Engl J Med. 2022 May 26;386(21):1973-1985. doi: 10.1056/NEJMoa2202170. Epub 2022 Apr 11. PMID: 35403841.
Mariano Provencio-Pulla, Ernest Nadal, Jose Luis Gonzalez Larriba, Alex Martinez-Marti, Reyes Bernabé, Joaquim Bosch-Barrera, Joaquin Casal, Virginia Calvo, Amelia Insa, Santiago Ponce Aix, Noemi Reguart, Javier De Castro Carpeño, Joaquín Mosquera, Raquel Benitez, Carlos Aguado De La Rosa, Ramon Palmero, Florentino Hernando-Trancho, Atocha Romero, Alberto Cruz Bermudez, and Bartomeu Massuti Nivolumab plus chemotherapy versus chemotherapy as neoadjuvant treatment for resectable stage IIIA NSCLC: Primary endpoint results of pathological complete response (pCR) from phase II NADIM II trial. Journal of Clinical Oncology 2022 40:16_suppl, 8501-8501
J.S. Deutsch, A. Cimino-Mathews, E.D. Thompson, D. Wang, R.A. Anders, E. Gabrielson, P. Illei, J. Jedrych, L. Danilova, J. Spicer, M. Provencio Pulla, P.M. Forde, D. Pandya, M.P. Tran, J. Fiore, V. Devas, T.R. Cottrell, A.S. Baras, J.M. Taube LBA50 - Analysis of pathological features and efficacy outcomes with neoadjuvant nivolumab (N) plus platinum-doublet chemotherapy (C) for resectable non-small cell lung cancer (NSCLC) in CheckMate 816. Annals of Oncology (2022) 33 (suppl_7): S808-S869. DOI: 10.1016/annonc/annonc1089
E. Felip, C. Wang, T. Ciuleanu, G. Saylors, F. Tanaka, K. Chen, H. Ito, N. Girard, S. Lu, M. Provencio Pulla, T. Mitsudomi, M. Awad, P.M. Forde, R. Lawrance, F. Taylor, G. Worthy, S.I. Blum, L. Vo, J.L. Cai, J. Spicer 932MO - Nivolumab (NIVO) plus platinum-doublet chemotherapy (chemo) versus chemo as neoadjuvant treatment for resectable non-small cell lung cancer (NSCLC): Health-related quality of life (HRQoL) outcomes from CheckMate 816. Annals of Oncology (2022) 33 (suppl_7): S427-S437. DOI: 10.1016/annonc/annonc1062
Conflict of Interest Declarations — Lung Cancer Canada
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please refer to the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission?
No.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission?
No.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician who contributed to the input — please add more tables as needed (copy and paste). It is preferred for all declarations to be included in a single document.
Declaration for Clinician 1
Name: Normand Blais
Position: Medical Oncologist, CHUM Cancer Center, Montreal
Date: 29-09-2022
Table 7: COI Declaration for Lung Cancer Canada — Clinician 1
Company | Nature or description of activities or interests | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|---|
Abbvie | Advisory Board and Honoraria | X | — | — | — |
Amgen | Advisory Board and Honoraria | X | — | — | — |
Astra Zeneca | Advisory Board and Honoraria | X | — | — | — |
Beigene | Advisory Board and Honoraria | X | — | — | — |
Bristol-Myers Squibb | Advisory Board and Honoraria | X | — | — | — |
EMD Serono | Advisory Board and Honoraria | X | — | — | — |
Merck | Advisory Board and Honoraria | X | — | — | — |
Novartis | Advisory Board and Honoraria | X | — | — | — |
Pfizer | Advisory Board and Honoraria | X | — | — | — |
Roche | Advisory Board and Honoraria | X | — | — | — |
Sanofi | Advisory Board and Honoraria | X | — | — | — |
Astra Zeneca | Research Funding to institution | — | — | — | X |
Declaration for Clinician 2
Name: Silvana Spadafora
Position: Medical Oncologist, Algoma District Cancer Program
Date: 05-10-22
Table 8: COI Declaration for Lung Cancer Canada — Clinician 2
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In excess of $50,000 |
|---|---|---|---|---|
Astra Zeneca | — | X | — | — |
Merck | — | X | — | — |
Novartis | — | X | — | — |
Declaration for Clinician 3
Name: Dr. Ronald Burkes
Position: Medical oncologist, Mount Sinai Health
Date: Oct 5/2022
Table 9: COI Declaration for Lung Cancer Canada — Clinician 3
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Declaration for Clinician 4
Name: Dr. Quincy Chu
Position: Medical Oncologist, Cross Cancer Institute
Date: Oct 5/2022
Table 10: COI Declaration for Lung Cancer Canada — Clinician 4
Company | Nature or description of activities or interests | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|---|
Abbvie | Advisory Board and Honoraria | X | — | — | — |
Amgen | Advisory Board and Honoraria | X | — | — | — |
Astra Zeneca | Advisory Board and Honoraria | — | — | X | — |
Boehringer Ingeiheim | Advisory Board and Honoraria | — | X | — | — |
Bristol-Myers Squibb | Advisory Board and Honoraria | — | X | — | — |
Eisai | Advisory Board and Honoraria | X | — | — | — |
Merck | Advisory Board and Honoraria | — | — | X | — |
Novartis | Advisory Board and Honoraria | — | X | — | — |
Pfizer | Advisory Board and Honoraria | — | X | — | — |
Roche | Advisory Board and Honoraria | — | X | — | — |
Astra Zeneca | Research Funding | — | — | — | X |
Bristol-Myers Squibb | Educational Grant | X | — | — | — |
Declaration for Clinician 5
Name: Dr. Rosalyn Juergens
Position: Chair, LCC Medical Advisory Committee; Medical Oncologist, Juravinski Cancer Center
Date: Oct 5/2022
Table 11: COI Declaration for Lung Cancer Canada — Clinician 5
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In excess of $50,000 |
|---|---|---|---|---|
Bristol Myers Squibb | X | — | — | — |
Astra Zeneca | — | X | — | — |
Merck Sharp and Dohme | X | — | — | — |
Roche | X | — | — | — |
Declaration for Clinician 6
Name: Dr. Paul Wheatley-Price
Position: Medical Oncologist, The Ottawa Hospital. Associate Professor, Department of Medicine, University of Ottawa
Date: Oct 5/2022
Table 12: COI Declaration for Lung Cancer Canada — Clinician 6
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In excess of $50,000 |
|---|---|---|---|---|
Sanofi | X | — | — | — |
Astra Zeneca | X | — | — | — |
Jazz Pharmaceuticals | X | — | — | — |
Amgen | X | — | — | — |
Janssen | X | — | — | — |
Novartis | X | — | — | — |
Merck | X | — | — | — |
BMS | X | — | — | — |
Roche | X | — | — | — |
EMD Serono | X | — | — | — |
Pfizer | X | — | — | — |
Bayer | X | — | — | — |
Novartis | X | — | — | — |
Declaration for Clinician 7
Name: Dr. Barb Melosky
Position: Medical Oncologist, BC Cancer
Date: Oct 5/2022
Table 13: COI Declaration for Lung Cancer Canada — Clinician 7
Company | Nature or description of activities or interests | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|---|
Novartis | Advisory Board | X | — | — | — |
Roche | Advisory Board | X | — | — | — |
Merck | Advisory Board | X | — | — | — |
Declaration for Clinician 8
Name: Dr Jeffrey Rothenstein
Position: Medical Oncologist, Lakeridge Health
Date: Oct 5/2022
Table 14: COI Declaration for Lung Cancer Canada — Clinician 8
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In excess of $50,000 |
|---|---|---|---|---|
Roche | X | — | — | — |
Declaration for Clinician 9
Name: Dr. Kevin Jao
Position: Medical Oncologist, Hôpital Sacré-Cœur, Montreal
Date: Oct 5/2022
Table 15: COI Declaration for Lung Cancer Canada — Clinician 9
Company | Nature or description of activities or interests | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|---|
Bristol-Myers Squibb | Advisory Role | X | — | — | — |
Declaration for Clinician 10
Name: Dr Catherine Labbé
Position: Head of Respiratory Medicine Service, Université de Laval
Date: Oct 5/2022
Table 16: COI Declaration for Lung Cancer Canada — Clinician 10
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In excess of $50,000 |
|---|---|---|---|---|
Amgen | X | — | — | — |
Astra Zeneca | — | X | — | — |
Brystol-Myers Squibb | X | — | — | — |
Jazz Pharmaceuticals | X | — | — | — |
LEO Pharma | X | — | — | — |
Merck | X | — | — | — |
Pfizer | X | — | — | — |
Roche | X | — | — | — |
Sanofi Genzyme | X | — | — | — |
Declaration for Clinician 11
Name: Dorothy Lo
Position: Medical oncologist, St. Joseph's Health Centre Toronto
Date: Oct 5/2022
Table 17: COI Declaration for Lung Cancer Canada — Clinician 11
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In excess of $50,000 |
|---|---|---|---|---|
Merck | X | — | — | — |
BMS | X | — | — | — |
Sanofi | X | — | — | — |
Novartis | X | — | — | — |
Astellas | — | X | — | — |
Eisai | X | — | — | — |
Astra Zeneca | X | — | — | — |
Declaration for Clinician 12
Name: Dr Nicole Bouchard
Position: Respirologist, Sherbrooke University Hospital
Date: Oct 5/2022
Table 18: COI Declaration for Lung Cancer Canada — Clinician 12
Company | Nature or description of activities or interests | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|---|
Astra Zeneca | Advisory Role/Conference | X | — | — | — |
Bristol-Myers Squibb | Advisory Role/Research | X | — | — | — |
Merck | Advisory Role /Research/Conference | X | — | — | — |
Bayer | Advisory Role | X | — | — | — |
Pfizer | Conference/Research | X | — | — | — |
Roche | Advisory Role | X | — | — | — |
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
Redactions: Confidential information in this document may be redacted at the request of the sponsor in accordance with the CADTH Drug Reimbursement Review Confidentiality Guidelines
Stakeholder Input: The views expressed in each submission are those of the submitting organization or individual; not necessarily the views of CADTH or of other organizations. As such, they are independent of CADTH and do not necessarily represent or reflect the view of CADTH. No endorsement by CADTH is intended or should be inferred. By filing with CADTH, the submitting organization or individual agrees to the full disclosure of the information. CADTH does not edit the content of the submissions.
CADTH does use reasonable care to prevent disclosure of personal information in posted material; however, it is ultimately the submitter’s responsibility to ensure no identifying personal information or personal health information is included in the submission. The name of the submitting organization or individual and all conflict of interest information are included in the submission; however, the name of the author, including the name of an individual patient or caregiver submitting the patient input, are not posted.
Accessibility: CADTH is committed to treating people with disabilities in a way that respects their dignity and independence, supports them in accessing material in a timely manner, and provides a robust feedback process to support continuous improvement. All materials prepared by CADTH are available in an accessible format. Where materials provided to CADTH by a submitting organization or individual are not available in an accessible format, CADTH will provide a summary document upon request. More details on CADTH’s accessibility policies can be found here.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.