CADTH Reimbursement Review
Belzutifan (Welireg)
Sponsor: Merck Canada Inc.
Therapeutic area: von Hippel-Lindau disease–associated tumours
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Ethics Review
Stakeholder Input
Clinical Review
Abbreviations
AE
adverse event
BOR
best overall response
CI
confidence interval
CNS
central nervous system
CR
complete response
DCR
disease control rate
DOR
duration of response
ECOG PS
Eastern Cooperative Oncology Group Performance Status
HIF
hypoxia-inducible factor
HIF-2-alpha
hypoxia-inducible factor 2 alpha subunit
HRQoL
health-related quality of life
IQR
interquartile range
IRC
independent review committee
ITC
indirect treatment comparison
LGR
linear growth rate
MAIC
matching-adjusted indirect comparison
NCI
National Cancer Institute
ORR
objective response rate
PFS
progression-free survival
pNET
pancreatic neuroendocrine tumour
PR
partial response
RCC
renal cell carcinoma
RCT
randomized controlled trial
RECIST 1.1
Response Evaluation Criteria in Solid Tumours Version 1.1
SAE
serious adverse event
SD
standard deviation
SE
standard error
SLR
systematic literature review
TEAE
treatment-emergent adverse event
TTR
time to response
TTS
time to surgery
VHL
von Hippel-Lindau
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Table 1: Background Information of Application Submitted for Review
Item | Description |
|---|---|
Drug product | Belzutifan (Welireg), 40 mg, tablets, oral |
Sponsor | Merck Canada Inc. |
Indication | For treatment of adult patients with von Hippel-Lindau disease who require therapy for an associated nonmetastatic RCC, CNS hemangioblastoma, or nonmetastatic pNET not requiring immediate surgery |
Reimbursement request | As per indication |
Health Canada approval status | NOC |
Health Canada review pathway | Project Orbis and priority review |
NOC date | July 11, 2023 |
Recommended dosage | 120 mg (three 40 mg tablets) administered orally once daily |
CNS = central nervous system; NOC = Notice of Compliance; pNET = pancreatic neuroendocrine tumour; RCC = renal cell carcinoma.
Sources: Sponsor’s Summary of Clinical Evidence1 and product monograph.2
Introduction
Von Hippel-Lindau (VHL) disease, which is an inherited, autosomal-dominant neoplasia syndrome caused by a germline mutation and/or deletion of the VHL gene, is associated with a variety of neoplasms, such as hemangioblastomas of the central nervous system (CNS) and retina, renal cysts and clear-cell renal cell carcinomas (RCCs), pheochromocytomas, pancreatic cysts and neuroendocrine tumours (pNETs), epididymal and broad ligament cystadenomas, and endolymphatic sac tumours.3,4 VHL disease affects 1 in 36,000 live births.4,5 Approximately 20% of the cases are caused by de novo mutations and do not have a family history of VHL disease.3,6 The prevalence is estimated to be 1 in 53,000 individuals.4 In Canada, the estimated number of cases is 727.1 VHL disease is typically diagnosed through genetic testing to identify a germline-pathogenic variant in the VHL gene.7 People with VHL disease can have tumours involving multiple organs several times in their life and their symptoms will depend on the location and size of the tumours.5,8,9 CNS hemangioblastomas develop in 60% to 84% of patients, pancreatic tumour or cysts in 35% to 70% (pNETs in 11% to 17%) and renal cysts and carcinomas in 69% (RCCs in 24% to 45%) of patients with VHL during their lifetime at mean ages of 29, 36, and 39 years, respectively.3,6,10 Tumours associated with VHL disease have the potential to metastasize, and an RCC constitutes the most frequent metastasizing tumour.3
Active surveillance until treatment is indicated is currently the standard treatment for VHL disease–associated tumours. The goal of active surveillance is to find and remove tumours as early as possible before they affect the patient’s health. Surgical resection is indicated for tumours with a high symptom burden or those carrying a high risk of organ dysfunction or metastasis.10,11 Certain tumours can be treated with radiation.12 However, clinical experts consulted by CADTH for this review indicated that treatments, such as surgery and irradiation, can be morbid. Both patients and clinicians identified a need for a systemic treatment that can effectively treat VHL disease while causing less harm.
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of belzutifan (40 mg oral tablets) in the treatment of adult patients with a nonmetastatic RCC, CNS hemangioblastoma, or nonmetastatic pNET, not requiring immediate surgery.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient and clinician groups who responded to CADTH’s call for input and from clinical experts consulted by CADTH for the purpose of this review.
Patient Input
The Canadian VHL Alliance, the Canadian Organization for Rare Disorders, Kidney Cancer Canada, Pancreatic Cancer Canada, and the Canadian Neuroendocrine Tumour Society provided 1 joint input for the treatment of adult patients with VHL disease who require therapy for associated nonmetastatic RCCs, CNS hemangioblastomas, and nonmetastatic pNETs not requiring immediate surgery. Patient input was gathered from online surveys and semistructured telephone interviews among patients living with VHL and their caregivers in December 2022. In total, 123 responses were gathered (72 from patients and 51 from caregivers), and 19 of those patients had experience with belzutifan.
Patients and caregivers described ongoing physical and psychological struggles due to VHL, such as dismissal or misdiagnosis for initial symptoms; not receiving a diagnosis until they had an advanced-stage tumour affecting vision, hearing, and walking; discomfort, pain, interference with daily activities; difficulties adhering to tumour-screening guidelines, scheduling tests, and travelling for tumour screenings; and out-of-pocket payment due to noncoverage by public or private health care insurance. Surgical resection was reported as the primary treatment for symptomatic lesions. The majority of 92 respondents described undergoing multiple surgeries at multiple sites, some with life-threatening risks and side effects. Out of 98 respondents, 18 (18.4%) reported having 10 or more surgeries, and the average number of surgeries reported was 5.3.
While evaluating the importance of outcomes of new treatments, patients from the survey emphasized the need for a treatment that can improve their physical condition by decreasing or stabilizing the size of tumours (weighted average rating = 4.8 on a scale from 1 not important to 5 extremely important), improving quality of life (weighted average rating = 4.63 on a scale from 1 not important to 5 extremely important), offering long-term stability or reduction of disease (weighted average rating = 4.86 on a scale from 1 not important to 5 extremely important), and offering the opportunity to avoid surgery (weighted average rating = 4.9 on a scale from 1 not important to 5 extremely important).
The patient groups suggested providing all VHL patients with access to belzutifan based on an individual informed decision between the treating physician and the patient and their family.
Clinician Input
Input From Clinical Experts Consulted by CADTH
The clinician input was provided by a panel of 3 clinical experts with expertise in treating VHL-associated RCC, CNS hemangioblastoma, and pNET from across Canada.
The clinical experts noted that prolonging survival and improving quality of life are critical goals for patients with VHL-associated nonmetastatic RCC, CNS hemangioblastoma, and/or nonmetastatic pNET. The current treatment paradigm for VHL disease involves genetic testing for VHL at diagnosis and active surveillance until treatment is indicated for associated tumours. Reactive treatments, such as surgery and radiation, can be morbid and are usually selected to respond to the conditions or symptoms developed. The clinical experts agreed that an effective systemic treatment would minimize the morbidity associated with surgical procedures in patients with VHL-associated nonmetastatic pNET and RCC, many of whom are younger. The clinical experts noted that belzutifan, if reimbursed, would be the first systemic treatment for VHL-associated tumours and would improve the current treatment paradigm by helping patients delay or avoid the need for local therapies (e.g., surgery and radiation).
The clinical experts indicated that VHL disease is rare and that all patients with VHL disease might benefit from belzutifan. The clinical experts did not specify a subset of the patient population that is in the most need or identify any prognostic factors that might cause differential treatment effects. The clinical experts noted that, before initiating treatment with belzutifan, genetic testing for VHL should be required. The clinicians also advised that a genetic counsellor should be involved in the diagnosis of VHL disease.
The clinical experts described several situations in which belzutifan may be discontinued, including intolerable adverse events (AEs), such as becoming transfusion-dependent due to anemia or clinical disease progression (i.e., worsening of symptoms). The clinical experts indicated that strict stopping criteria based on radiographic disease progression alone would not be reasonable if a patient is still experiencing a clinical benefit. The clinical experts noted that, due to the rarity of VHL disease, it is highly likely that only specialists working in large medical centres (e.g., tertiary and specialized referral centres) in Canada may encounter patients with VHL. Prescriptions therefore may be limited to specialists (medical oncologist and neuro-oncologists) working in these large centres.
Clinician Group Input
Clinician group input was received from the Ontario Health (Cancer Care Ontario) Genitourinary Cancer Drug Advisory Committee (7 clinicians), and a group of 25 clinical subspecialists in Canada involved caring for patients with VHL disease.
The clinician groups agreed with the clinical experts consulted by CADTH that belzutifan, the first systemic therapy option for VHL disease approved in Canada, fulfills an important unmet need for the treatment of patients with VHL and represents a shift in the current treatment paradigm. They also generally agreed on treatment goals, patient populations, assessing response and treatment-discontinuation criteria, and prescribing conditions.
While the clinical experts considered genetic testing to be a prerequisite for initiating treatment with belzutifan, neither clinician group indicated whether genetic testing for a VHL mutation or deletion was required. The clinician groups indicated that belzutifan should be discontinued if the patient is pregnant.
Drug Program Input
Input was obtained from the drug programs that participate in the CADTH reimbursement review process. The following were identified as key factors that could potentially affect the implementation of a CADTH recommendation for belzutifan:
relevant comparators
consideration for initiation of therapy
consideration of discontinuation of therapy
consideration for prescribing a therapy
care provision issues
system and economic issues.
The clinical experts consulted by CADTH provided advice on the potential implementation issues raised by the drug programs (Table 4).
Clinical Evidence
Pivotal Studies and Randomized Controlled Trial Evidence
Description of Study
One sponsor-conducted, phase II, single-arm, open-label trial (LITESPARK-004, N = 61) was identified from the systematic literature review (SLR) conducted by the sponsor. The primary objective of the LITESPARK-004 trial was to evaluate the efficacy of belzutifan (oral administration at a dosage of 120 mg once daily in 3 40 mg tablets until disease progression or unacceptable toxicity for the treatment of a VHL disease–associated nonmetastatic RCC as measured by objective response rate (ORR) and assessed by an independent review committee (IRC) following Response Evaluation Criteria in Solid Tumours Version 1.1 (RECIST 1.1). Secondary objectives included evaluation of the efficacy of belzutifan for the treatment of VHL disease–associated non-RCC tumours (CNS hemangioblastoma and nonmetastatic pNET), as well as assessment of the safety and tolerability (including AEs of special interest — anemia, hypoxia, secondary primary malignancies, and hepatic safety). In terms of efficacy end points, tumour response and durability of response were assessed by ORR and duration of response (DOR), respectively. Time-to-event outcomes, such as time to surgery (TTS), progression-free survival (PFS), and time to response (TTR) were also reported. The LITESPARK-004 trial also measured end points such as disease control rate (DCR), best overall response (BOR), linear growth rate (LGR), and the number of patients who developed metastases. No inferential statistical analyses were carried out in the LITESPARK-004 trial due to the single-arm study design, and data were summarized using descriptive statistics. The LITESPARK-004 trial is ongoing, and the data submitted by the sponsor to support this reimbursement request are based on a data cut-off date of April 1, 2022, as of which the median follow-up duration was 37.7 months (range = 4.2 to 46.1).
Participants eligible to be included in the LITESPARK-004 trial were required to be at least 18 years of age, have a diagnosis of VHL disease based on a germline VHL alteration, and have had at least 1 measurable RCC. Eligible patients could have other VHL disease–associated non-RCC tumours such as CNS hemangioblastoma and pNET. Patients who had an immediate need for surgical intervention for tumour treatment or evidence of metastatic disease were excluded. Efficacy results for RCC came from the total study population (n = 61), while efficacy results for CNS hemangioblastoma (n = 50) and pNET (n = 22) were from subsets of the total study population. At baseline, for the total study population (i.e., patients with RCC), the median age was 41.0 years (range = 19.0 to 66.0), with the majority being white (90.2%; 55 of 61), and the median age at time of VHL disease diagnosis was 32.0 years (range = 4.0 to 66.0). Characteristics were similar for the subpopulations of patients with CNS hemangioblastoma and pNET.
Efficacy Results
The efficacy end points that were noted to be important to patients and clinicians based on stakeholder input are summarized in Table 2. Results are as of the April 1, 2022, data cut-off date.
Time to Surgery
Median TTS was not reached for patients with VHL disease–associated nonmetastatic RCC, CNS hemangioblastoma, or nonmetastatic pNET at the data cut-off date. Seven patients with RCC (11.5%; 7 of 61), 1 patient with CNS hemangioblastoma (2.0%; 1 of 51), and none of the patients with pNET had surgery during the follow-up period.
Progression-Free Survival
The IRC-assessed median PFS was 39.2 months (95% confidence interval [CI], 38.5 to not evaluable) for patients with a VHL disease–associated nonmetastatic RCC. The median PFS was not reached for patients with a VHL disease–associated CNS hemangioblastoma and those with a nonmetastatic pNET by the data cut-off date.
IRC-assessed results showed that, among 61 patients with RCC at baseline, 11 (18.0%) had events (i.e., progressive disease or death), and 50 (82%) were censored, mostly due to no progression at the time of data cut-off or before the end of treatment (43; 70.5%).
IRC-assessed results showed that, among 50 patients with CNS hemangioblastoma at baseline, 11 (22.0%) had events (i.e., progressive disease or death), and 39 (78%) were censored (of which 34 [68%]) were due to no progression at the time of data cut-off.
All 22 patients with pNET were censored due to no progression at the time of data cut-off.
Objective Response Rate
At a median follow-up of 37.7 months, the IRC-assessed percentage of patients who had a complete response (CR) or partial response (PR) to belzutifan was 63.9% (39 of 61) among those with a VHL-associated nonmetastatic RCC, 44% (22 of 50) among those with a VHL-associated CNS hemangioblastoma, and 90.9% (20 of 22) among those with a VHL-associated nonmetastatic pNET.
Duration of Response
IRC-assessed median DOR was not reached for responders with a VHL disease–associated nonmetastatic RCC, CNS hemangioblastoma, or nonmetastatic pNET by the data cut-off date. For patients with RCC, 74.4% of responders (29 of 39) had a DOR of 18 months or longer, 56.4% (22 of 39) had a DOR of 24 months or longer, and 25.6% (10 of 39) had a DOR of 30 months or longer. For patients with a CNS hemangioblastoma, 63.6% of responders (14 of 22) had a DOR of 18 months or longer, 59.1% (13 of 22) had a DOR of 24 months or longer, and 54.5% (12 of 22) had a DOR of 30 months or longer. For patients with a pNET, 95.0% of responders (19/20) had a DOR of 18 months or longer, 75.0% (15 of 20) had a DOR of 24 months or longer, and 40.0% (8 of 20) had a DOR of 30 months or longer.
Among 39 RCC patients with a confirmed response, 32 (82.1%) were censored due to no progression at the time of data cut-off or before the end of treatment. Out of 22 patients with CNS hemangioblastoma who showed a confirmed response, 17 were censored due to no progression at the time of data cut-off or before the end of treatment. All 20 patients with a pNET who showed a confirmed response had progression at the time of data cut-off.
Harms Results
Adverse Events
Treatment-emergent adverse events (TEAEs) were reported in all 61 patients (100%) in the LITESPARK-004 trial. The most commonly reported TEAE was anemia (90.2%), followed by fatigue (73.8%), headaches (47.5%), dizziness (45.9%), and nausea (39.3%).
Serious Adverse Events
Serious adverse events (SAEs) were reported in 18 patients (29.3%).
Withdrawal Due to Adverse Events
Treatment discontinuation due to TEAEs (i.e., dizziness or intracranial hemorrhage) was reported in 4 patients, 2 of which were drug-related.
Mortality
Two patients died during the study, 1 due to acute toxic effects of fentanyl and 1 due to suicide.
Notable Harms
As of the data cut-off, 90.2% (55 of 61) patients had 229 episodes of anemia. The average number of episodes of anemia for each patient was 4.2. One (1.6%) and 2 patients (3.3%) developed hypoxia and secondary primary malignancies, respectively. None of the participants had drug-induced liver injury.
Table 2: Summary of Key Results from Pivotal Studies and RCT Evidence
Outcome | LITESPARK-004 Belzutifan (N = 61) | |
|---|---|---|
Assessed by IRC | Assessed by investigators | |
Time to surgery for RCC | ||
Number of patients contributing to the analysis | 61 | NR |
Number of patients who underwent a surgery, n (%) | 7 (11.5) | NR |
Median, months (95% CI) | NE (NE to NE) | NR |
Progression-free survival for RCC | ||
Number of patients contributing to the analysis | 61 | 61 |
Censored patients, n (%) | 50 (82.0) | 51 (83.6) |
Median, months (95% CI) | 39.2 (38.5 to NE) | NE (NE to NE) |
Objective response rate (CR + PR) for RCC | ||
Number of patients contributing to the analysis | 61 | 61 |
n (%) [95% CI] | 39 (63.9) [50.6 to 75.8] | 37 (60.7) [47.3 to 72.9] |
Duration of response for RCC | ||
Number of patients contributing to the analysis | 39 | 37 |
Mean, months | 23.5 | 22.0 |
Median, months (95% CI) | NE (NE to NE) | NE (35.9 to NE) |
Minimum, months | 5.4+a | 2.6+ |
Maximum, months | 35.8+ | 38.7+ |
Time to surgery for CNS hemangioblastoma | ||
Number of patients contributing to the analysis | 51 | NR |
Number of patients who underwent a surgery, n (%) | 1 (2.0) | NR |
Median, months (95% CI) | NE (NE to NE) | NR |
Progression-free survival for CNS hemangioblastoma | ||
Number of patients contributing to the analysis | 50 | 51 |
Censored patients, n (%) | 39 (78.0) | 48 (94.1) |
Median, months (95% CI) | NE (38.4 to NE) | NE (NE to NE) |
Duration of response for CNS hemangioblastoma | ||
Number of patients contributing to the analysis | 22 | 18 |
Mean, months | 23.9 | 26.4 |
Median, months (95% CI) | NE (30.9 to NE) | 33.8 (33.8 to NE) |
Minimum, months | 3.7+ | 8.5+ |
Maximum, months | 38.7+ | 38.7+ |
Objective response rate (CR + PR) for CNS hemangioblastoma | ||
Number of patients contributing to the analysis | 50 | 51 |
n (%) [95% CI] | 22 (44.0) [30.0 to 58.7] | 18 (35.3) [22.4 to 49.9] |
Time to surgery for pNET | ||
Number of patients contributing to the analysis | 22 | NR |
Number of patients who underwent a surgery, n (%) | 0 (0) | NR |
Median months (95% CI) | NE (NE to NE) | NR |
Progression-free survival for pNET | ||
Number of patients contributing to the analysis | 22 | NR |
Censored patients, n (%) | 22 (100.0) | NR |
Median, months (95% CI) | NE (NE to NE) | NR |
Duration of response for pNET | ||
Number of patients contributing to the analysis | 18 | NR |
Mean, months | 27.4 | NR |
Median, months (95% CI) | NE (NE to NE) | NR |
Minimum months | 11.0+ | NR |
Maximum, months | 37.3+ | NR |
Objective response rate (CR + PR) for pNET | ||
Number of patients contributing to the analysis | 22 | NR |
n (%) [95% CI] | 20 (90.9) [70.8 to 98.9] | NR |
Harms, n (%) for overall study population (N = 61) | ||
Treatment-emergent adverse event | 61 (100.0) | |
Serious adverse event | 18 (29.5) | |
Withdrawal due to adverse event | 4 (6.6) | |
Deathb | 2 (3) | |
Notable harms for overall study population (N = 61) | ||
Anemia | ||
Number of patients who had anemia, n (%) | 55 (90.2) | |
Total number of episodes of anemia, n | 229 | |
Average number of episodes of anemia per patient | 4.2 | |
Hypoxia, n (%) | 1 (1.6) | |
Second primary malignancies, n (%) [type] | 2 (3.3) [1 vulval cancer and 1 non–small cell lung cancer] | |
Hepatic safety | ||
Participants meeting criteriac for drug-induced liver injury, n (%) | 0 (0) | |
CI = confidence interval; CNS = central nervous system; CR = complete response; IRC = independent review committee; NE = not evaluable or not estimable; NR = not reported; pNET = pancreatic neuroendocrine tumour; PR = partial response; RCC = renal cell carcinoma; RCT = randomized controlled trial.
aAccording to the sponsor’s explanation, the “+” sign indicates that the objective response in the respective participant remained ongoing, with no progressive disease or death reported at the time of data cut-off. For example, “5.4+” means that, at the data cut-off, the respective participant had been in response for 5.4 months and had not experienced disease progression or death.
bOne death was due to acute toxic effects of fentanyl, and 1 was due to suicide.
cCriteria for drug-induced liver injury: alanine transaminase or aspartate transaminase levels equal to or greater than 3 times the upper limit of normal range, and bilirubin levels equal to or twice the upper limit of normal range, and alkaline phosphatase levels of less than twice the upper limit of normal range.
Source: LITESPARK-004 Clinical Study Report.13
Critical Appraisal
Internal Validity
The LITESPARK-004 trial was a phase II, single-arm, open-label clinical trial. Given the rarity of VHL disease and that active surveillance is the current stand of care for patients with VHL-associated nonmetastatic tumours, the single-arm design and small sample size were considered appropriate from the regulatory perspective to assess the efficacy and safety of belzutifan. However, the absence of an internal comparison group in the single-arm LITESPARK-004 trial hampered the ability to establish a causal link with the efficacy or safety outcomes observed in patients.
The LITESPARK-004 trial explicitly defined the hypotheses (i.e., a null hypothesis of an ORR of 15% or lower with an alternate hypothesis of ORR of 30% or higher), which were considered clinically meaningful by the clinical experts consulted by CADTH. The selection of ORR (defined as the sum of CR and PR according to RECIST 1.1) to measure antitumour activity and DOR (in patients with CR or PR) to determine the durability of tumour response were appropriate. Additional time-to-event end points (TTS and PFS) were employed in the LITESPARK-004 trial and were considered by the clinical experts to be critical outcomes to assess the efficacy of belzutifan. However, randomized controlled trials (RCTs) are preferred over single-arm studies for time-to-event end points such as PFS due to their sensitivity to baseline differences in patient, disease, and other clinical characteristics, and interpreting results without a randomized reference could be problematic.14-16 The LITESPARK-004 trial also involved outcomes pre- and posttreatment with belzutifan (i.e., a change in LGR) to demonstrate the efficacy of belzutifan. However, without formal statistical analysis, the role of chance could not be ruled out. With respect to outcome measurement, in addition to study investigators, an IRC was used to assess radiographic outcomes and reduce the risk of bias in measuring outcomes for most of the efficacy end points in patients with a VHL-associated nonmetastatic RCC and those with a VHL-associated CNS hemangioblastoma.
Altogether, due to a lack of comparison groups and a lack of formal inferential statistical analyses, no definitive conclusions could be drawn from the LITESPARK-004 trial about the efficacy and safety of belzutifan in patients with VHL-associated nonmetastatic RCC, CNS hemangioblastoma, or nonmetastatic pNET, all of whom did not require immediate surgery.
External Validity
All participants in the LITESPARK-004 trial were required to have at least 1 RCC. The LITESPARK-004 trial therefore may not reflect results for participants with only CNS hemangioblastomas and/or pNETs. However, the clinical experts consulted by CADTH did not consider this a serious generalizability issue. According to the clinical experts, the inclusion and exclusion criteria of the LITESPARK-004 trial in general were aligned with selection criteria in the Canadian settings when identifying suitable candidates for belzutifan. However, the clinical experts noted that the requirement for patients to have an Eastern Cooperative Oncology Group Performance Status (ECOG PS) of 0 or 1 might not be necessary to initiate belzutifan in clinical practice because ECOG PS can be unstable and subjective. There were no study sites in Canada as the LITESPARK-004 trial was conducted only in Denmark, France, the UK, and the US. More than 90% of the patients in LITESPARK-004 were white, which is not representative of the racial profile of the Canadian patient population, according to the clinical experts. The dosing and administration of belzutifan in the LITESPARK-004 trial were consistent with the product monograph. The clinical experts commented that concomitant medications and procedures in the LITESPARK-004 trial were also appropriate and commonly used in the Canadian settings. The outcomes of TTS, PFS, ORR, and DOR are commonly used in clinical trials of anticancer therapy and are relevant to clinical practice, according to the clinical experts. These outcomes are also important to patients, who indicated they want treatments that offer the opportunity to avoid surgery, decrease or stabilize the size of tumours, and result in long-term stability or reduction of disease. However, LGRs have not been commonly adopted in clinical practice and may not correlate with clinical benefit. The clinical expert specializing in CNS hemangioblastoma noted that, in clinical practice, Response Assessment in Neuro-Oncology (RANO) criteria are used instead of RECIST 1.1 to assess tumour responses in patients with CNS hemangioblastomas. The LITESPARK-004 trial did not assess some outcomes that are important to patients, such as symptoms and health-related quality of life (HRQoL).
Indirect Comparisons
Description of Study
A sponsor-conducted indirect treatment comparison (ITC) was submitted to address the absence of comparative evidence of belzutifan for the treatment of adult patients with VHL disease in the LITESPARK-004 trial. The ITC compared a real-world, retrospective, noninterventional cohort study of existing medical records of VHL patients managed and treated at the National Cancer Institute (NCI) in the US or in Canada (the VHL Natural History Study) with the LITESPARK-004 trial. Patients with VHL-associated RCC from the VHL Natural History Study were reweighted to match the distribution of key baseline characteristics among patients with VHL-associated RCC in LITESPARK-004 and compared using a matching-adjusted indirect comparison (MAIC). The comparative treatment was active surveillance. The primary and only outcome assessed was time to RCC-related surgery.
Efficacy Results
The weekly exponential rate of RCC surgery was estimated at 0.00487 (standard error [SE] = 0.00034) in the matched Natural History Study sample versus 0.00071 (SE = 0.0003) in the LITESPARK-004 population.
Critical Appraisal
Findings from the sponsor-conducted ITC, which used the VHL Natural History Study as an external comparator for the LITESPARK-004 trial, were considered highly uncertain. Although the estimated decrease in the rate of surgeries in the LITESPARK-004 trial relative to the VHL Natural History Study was large, several major limitations decreased CADTH’s confidence in the results. First, the selection criteria that informed the VHL Natural History Study subcohort used in the ITC was intended to match with those from the LITESPARK-004 cohort but did not include some key criteria. Specifically, the Natural History Study cohort did not include restrictions on ECOG PS scores of 0 or 1; this difference created a risk of bias in effectiveness that may favour belzutifan. Second, it was difficult to assess the degree of heterogeneity between the included studies based on the sponsor-provided technical report because the reporting of the study design and patient characteristics were limited. It is likely that the underlying assumption of the unanchored MAIC — that all potential prognostic and effect-modifying factors were balanced across groups — was violated, which would result in a high risk of confounding. Third, the outcome definition of RCC surgery within the Natural History Study cohort is subject to potential measurement error. Specifically, the clinical experts indicated that renography and cyst removal are not definitive surgical interventions for the management of RCC, although these were considered an RCC surgery outcome in the VHL Natural History Study. The magnitude of bias due to measurement error is unknown but may overestimate the estimated relative rate of RCC surgeries in favour of belzutifan. Finally, the analysis did not provide information specific to VHL-associated CNS hemangioblastoma and pNET populations.
Studies Addressing Gaps in the Pivotal and Randomized Controlled Trial Evidence
The sponsor submitted the VHL Natural History Study17 to fill the gap in published clinical trials or observational data on the efficacy outcomes of the standard of care (active surveillance). This study provided active-surveillance efficacy data used for the ITC. The sponsor also provided a cross-sectional HRQoL survey to address the lack of HRQoL or utility values; it is summarized and critically appraised in Appendix 1. This study assessed the impact of VHL disease on HRQoL as measured by the EQ-5D questionnaire in patients with RCC, CNS hemangioblastoma, or pNET. A total of 220 patients completed the survey. Overall, patients with VHL-associated tumours had a mean EQ-5D score of 0.771. As. patients who participated in this study were not treated with belzutifan, this study does not provide information related to the effect of treatment with belzutifan on the HRQoL of patients with VHL disease.
VHL Natural History Study
Description of Study
The VHL Natural History Study,17 a retrospective real-world cohort study of growth kinetics and surgical patterns in patients with VHL disease and associated renal solid tumours, was conducted using data registered by the NCI in a hereditary database of patients with VHL syndrome. The primary study population consisted of US and Canadian patients treated at the NCI with confirmed VHL syndrome and ≥ 1 renal solid tumour with available measurement(s) during the study period (July 31, 2004, to June 30, 2020). Additional criteria were applied in an attempt to match the study population more closely to the population enrolled in the LITESPARK-004 trial.
Of 776 patients with VHL disease in the NCI hereditary database, 308 with at least 1 solid renal tumour met the eligibility criteria and were included in the primary study population. After applying additional eligibility criteria focusing on the tumour growth rate assessment, 247 patients (80.2%) were included in the trial population subgroup.
Subgroups of 131 patients and 114 patients in the primary study population and the trial population subgroup, respectively, had 3 or more serial measurements of at least 1 solid renal tumour during the study period that qualified them for inclusion in the LGR analysis subgroups to address the primary research objective.
Efficacy Results
Linear Growth Rate
The median tumour-level LGRs for the primary study population and trial population subgroup were 0.38 cm per year (interquartile range [IQR] = 0.30 to 0.49) and 0.37 cm per year (IQR = 0.29 to 0.47), respectively.
Frequency and Type of Tumour–Reduction Procedures
Of the 308 patients in the primary study population, 232 patients (75.3%) had at least 1 renal solid tumour–reduction procedure during the study period, including 225 patients (73.1%) with surgical procedures (96% of which were partial nephrectomies), 16 patients (5.2%) with ablation procedures, and 1 patient (0.3%) who received radiation. In the trial population subgroup, 184 patients (74.5%) underwent at least 1 renal solid tumour–reduction procedure. The median number of tumour-reduction procedures per patient in the trial population subgroup was 2 (range = 1 to 9).
Time to Tumour–Reduction Procedures
The 1-year, 2-year, 5-year, and 7-year intervention-free survival probabilities for the first tumour-reduction procedure were 79.0%, 69.9%, 38.3%, and 26.4%, respectively, for the trial population subgroup. The median time to first tumour-reduction procedure was 44.2 months (95% CI, 35.74 to 49.51) in the trial population subgroup.
Harm Results
Of the 217 patients (70.5%) in the primary study population with at least 1 partial nephrectomy, 413 partial nephrectomies were performed during follow-up, 124 (30.0%) of which were associated with complications. The median estimated blood loss, assessed among all surgical procedure types, was 1.5 L (IQR = 0.6 to 2.6). Two patients (0.9%) in the primary study population with at least 1 renal tumour-reduction procedure conducted at the National Institutes of Health died within 30 days of the procedure (1 nephrectomy and 1 biopsy).
Critical Appraisal
Internal Validity
This real-world retrospective cohort study did not evaluate the effect of belzutifan and did not provide evidence about the efficacy of the treatment. The presented analyses appeared to include no a priori protocol. The study was conducted using data registered by the NCI in a hereditary database of patients with VHL syndrome, but how these data were located (e.g., which search methods were used) or selected is not specified.
Some of the limitations of this study were the high level of missing data for some variables; the unavailability of longitudinal measures of tumour growth for all tumours in a systematic manner (i.e., differences may have arisen due to variation in measurement across observers) because the measures were extracted from the registry directly; incomplete documentation of metastasis; and the possibility of misclassification. There is also a possibility of loss to follow-up of patients who left the registry but for whom no relevant information was provided. Attempts were made to ensure that the trial population subgroup would be similar to the population of the LITESPARK-004 trial, based on the additional criteria that were applied. However, several criteria in the Natural History Study cohort are approximate to those of the pivotal trial due to insufficient access to information within the database. While demographics and clinical characteristics were similar for patients in the trial population and LGR analysis subgroups, many demographic characteristics (i.e., race or ethnicity and ECOG PS) were not reported in the Natural History Study report. One of the exclusion criterion was receiving systemic oncologic therapy or investigational therapy within 30 days on or before the patient-level index date. However, no specific information was given about the type of systemic or investigational therapy. Moreover, this exclusion criteria may have led to the exclusion of patients with a better prognosis, therefore affecting the results for the trial population subgroup.
External Validity
This study includes patients managed and treated at the NCI only. This may affect the overall generalizability of the study, as it may not be representative of all patients with VHL in Canada that fall within the indication. While this study presented data for renal tumours, patients included in the study also had other tumours associated with VHL. However, no additional information was provided for these tumours, which may have resulted in the exclusion of some important clinical outcomes associated with VHL syndrome. Because the indication under review includes nonmetastatic pNETs and CNS hemangioblastomas in addition to nonmetastatic RCCs, the unavailability of data related to these 2 tumours represents a gap in the evidence provided by this study. The authors of this study noted the potential risk of losing a substantial number of samples due to the eligibility criteria of recruiting patients with 3 or more serial measurements for the assessment of tumour growth rate patterns.
Conclusions
Evidence from the phase II, single-arm, open-label LITESPARK-004 trial suggests that treatment with belzutifan may have a beneficial effect in adult patients with VHL-associated nonmetastatic RCC with or without VHL-associated CNS hemangioblastoma and/or nonmetastatic pNET not requiring immediate surgery, based on the opinions of clinical experts. The clinical experts indicated that the efficacy results from the patient populations with a VHL disease–associated nonmetastatic RCC, RCC and CNS hemangioblastoma, RCC and nonmetastatic pNET, as well as an RCC, CNS hemangioblastoma, and pNET, in the LITESPARK-004 trial demonstrated a promising and durable tumour response as measured by ORR and DOR that is likely attributable to belzutifan, based on their clinical experience and expectations of the natural history of the disease. However, the absence of a comparator group in the pivotal study precluded definitive conclusions about the efficacy and safety of belzutifan, due to the potential for confounding. The findings for other supportive outcomes (e.g., TTS and PFS) are uncertain due to the lack of an internal comparator group and no inferential statistical analyses. The incidence of harms events, such as anemia and hypoxia, were acceptable, according to the clinical experts. Because VHL disease is a life-long condition and patients can receive belzutifan for an extended period, longer follow-ups would be needed to better understand the long-term benefits and harms of belzutifan, as well as the potential residual effects following discontinuation. Findings from an ITC suggest that treatment with belzutifan may have a beneficial effect on time to RCC-related surgery compared to active surveillance in patients with a VHL disease–associated nonmetastatic RCC. However, the certainty of the indirect evidence was low due to violation of the underlying assumptions of the MAIC approach that resulted in a high risk of residual confounding, and important differences in outcome definitions between the LITESPARK-004 trial and the VHL Natural History Study that would bias the findings in favour of belzutifan. Based on the evidence in the ITC analysis, the comparative efficacy of belzutifan versus active surveillance for VHL-associated CNS hemangioblastoma and nonmetastatic pNET was not assessed and is therefore unknown. The VHL Natural History Study and the VHL HRQoL survey did not provide evidence on the efficacy and safety of belzutifan as standalone studies because patients in these studies did not receive belzutifan. It is unknown whether treatment with belzutifan would improve patient quality of life.
Introduction
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of belzutifan (40 mg tablets for oral administration) in the treatment of adult patients with VHL disease who require therapy for associated nonmetastatic RCCs, CNS hemangioblastomas, or nonmetastatic pNETs not requiring immediate surgery.
Disease Background
The contents in this section were informed by materials submitted by the sponsor and clinical expert input. The following summaries of observations were validated by the CADTH review team.
VHL disease is an inherited, autosomal-dominant neoplasia syndrome caused by a germline mutation and/or deletion of the VHL gene.1 Abnormal or absent VHL tumour-suppressor function leads to dysregulation of the degradation of hypoxia-inducible factor (HIF), a key mediator of cellular adaptation to hypoxia.1 In VHL disease, HIF accumulates and its activity increases, leading to abnormal growth of both nonmalignant and malignant tumours in multiple organ systems.11 VHL disease is therefore a familial cancer-predisposition syndrome associated with a variety of neoplasms, such as hemangioblastomas of the CNS and retina, renal cysts and clear-cell RCCs, pheochromocytomas, pancreatic cysts and pNETs, epididymal and broad ligament cystadenomas, and endolymphatic sac tumours.3,4
A single mutated copy of the VHL gene is not enough to cause VHL disease, and a mutation in the other copy of the gene must occur.5 However, almost everyone born with 1 VHL mutation will eventually acquire a mutation in the second copy of the gene and develop VHL disease.5 VHL disease affects males and females and all ethnic groups equally.5 Tumours associated with VHL disease typically appear first in young adulthood but are also seen in children.5 The mean age at diagnosis is 26 years and more than 90% of patients have developed symptoms by the age of 65 years.4,10,18
VHL disease affects 1 in 36,000 live births.4,5 Approximately 20% of the cases are caused by de novo mutations and therefore do not have a family history of VHL.3,6 The prevalence is estimated to be 1 in 53,000 individuals.4 There are 200,000 cases of VHL disease worldwide and 10,000 cases in the US.4,5 In Canada, the estimated number of cases is 727.1
A diagnosis of VHL disease is typically established by identifying a germline-pathogenic variant of the VHL gene through genetic testing.7 Occasionally, VHL disease may be diagnosed based on clinical criteria, such as patients with 1 VHL-associated lesion and a family history of VHL, or patients with multiple VHL-associated tumours but who do not have access to genetic testing.7
People with VHL disease can have tumours involving multiple organs several times in their life and their symptoms will depend on the location and size of the tumours.5,8,9 CNS hemangioblastomas develop in 60% to 84% of patients, pancreatic tumours or cysts in 35% to 70% (pNET in 11% to 17%), and renal cysts and carcinomas in 69% (RCC in 24% to 45%) of patients with VHL during their lifetime at mean ages of 29, 36 and 39 years, respectively.3,6,10 The most common first manifestation of VHL disease is a retinal hemangioblastoma followed by CNS hemangioblastoma and RCC.6 An RCC is the first manifestation of VHL disease in approximately 10% of cases.18 Tumours associated with VHL disease have the potential to metastasize, and an RCC is the most frequent metastasizing tumour.3 CNS hemangioblastomas, even though nonmalignant, are a major cause of morbidity and mortality in VHL disease due to frequent and multiple recurrent and/or progressive tumours throughout the CNS, affecting vital structures by compression or as surgical sequelae.9
Standards of Therapy
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following summaries have been validated by the CADTH review team.
VHL disease has no cure and how it will progress varies by the individual. Because of the progressive, diverse nature, and high frequency of multiple neoplasms in various organ systems in patients with VHL disease, the management of a single tumour type is complicated by the presence of others.10 Active surveillance of VHL-associated tumours until treatment is the standard approach. The goal of active surveillance is to find, monitor, and remove tumours if resectable and clinically indicated before they affect the patient’s health. Surgical resection is indicated for tumours with a high symptom burden or those carrying a high risk of organ dysfunction or metastasis.10,11 Certain tumours can be treated with radiation therapy.12
Localized CNS hemangioblastoma, RCC, and pNET masses in patients with VHL are usually monitored with active surveillance until surgical resection is indicated, often when the largest tumour reaches a size of 3 cm or larger, when tumours exhibit rapid radiologic progression, or in the presence of significant symptoms, according to the literature.10,11,19 The clinical experts consulted by CADTH noted that the tumour location, the presence of symptoms, and tumour growth rate are usually more important than tumour size in determining when surgical resection is required.
Vascular endothelial growth factor receptor inhibitors (sunitinib, pazopanib, and dovitinib) were evaluated in small prospective clinical trials of patients with VHL disease to test their ability to alter the growth of tumours.20-22 However, due to TEAEs, and limited responses in non-RCC tumours such as CNS hemangioblastomas, treatment with drugs that target vascular endothelial growth factor receptors is not recommended as standard of care in VHL disease, and none of these treatments received regulatory approval for VHL disease in Canada.11 The clinical experts consulted by CADTH noted that belzutifan, if reimbursed, would be the first systemic treatment for VHL-associated tumours.
Drug Under Review
Key characteristics of belzutifan are summarized in Table 3.
Belzutifan is an inhibitor of the hypoxia-inducible factor 2 alpha subunit (HIF-2-alpha).2,23-25 Belzutifan binds to HIF-2-alpha and, in conditions of hypoxia or impairment of VHL protein function, belzutifan blocks the interaction between HIF-2-alpha and the hypoxia-inducible factor 1 beta subunit, leading to reduced transcription and expression of HIF-2-alpha downstream target genes associated with tumourigenic effects.
Belzutifan was reviewed under Project Orbis and received a Notice of Compliance from Health Canada on July 11, 2022, for the treatment of adult patients with VHL disease who require therapy for associated nonmetastatic RCC not requiring immediate surgery. On July 11, 2023, Health Canada–approved an expanded indication for belzutifan for the treatment for adult patients with VHL disease who require therapy for associated CNS hemangioblastomas or nonmetastatic pNETs not requiring immediate surgery. To date, the FDA26 and the Therapeutic Goods Administration of Australia27 have approved the use of belzutifan for the treatment of adult patients with VHL disease who require therapy for associated nonmetastatic RCCs, CNS hemangioblastomas, or nonmetastatic pNETs not requiring immediate surgery.
This is the first review of belzutifan by CADTH. The sponsor’s reimbursement request was aligned with the indication. Belzutifan is supplied as 40 mg tablets for oral administration.2 The recommended belzutifan dose is 120 mg (three 40 mg tablets) administered once daily.2 The product monograph recommends that treatment should continue until disease progression or unacceptable toxicity occurs. No dose adjustment is needed in older patients nor in the presence of renal (mild to moderate) or hepatic (mild) impairment.
Table 3: Key Characteristics of Belzutifan
Characteristic | Belzutifan |
|---|---|
Mechanism of action | Belzutifan binds to HIF-2-alpha and blocks the HIF-2-alpha–HIF-1-beta interaction in the conditions of hypoxia or impairment of VHL protein function, resulting in reduced expression of HIF-2-alpha target genes associated with tumourigenic effects |
Indication | For treatment of adult patients with VHL disease who require therapy for associated nonmetastatic RCCs, CNS hemangioblastomas, or nonmetastatic pNETs not requiring immediate surgery |
Route of administration | Oral |
Recommended dosage | 120 mg (three 40 mg tablets) administered orally once daily |
Serious adverse effects or safety Issues |
|
CNS = central nervous system; HIF-1-beta = hypoxia-inducible factor 1 beta subunit; HIF-2-alpha = hypoxia-inducible factor 2 alpha subunit; pNET = pancreatic neuroendocrine tumour; RCC = renal cell carcinoma; VHL = von Hippel-Lindau.
Source: Belzutifan (Welireg) draft product monograph.28
Stakeholder Perspectives
Patient Group Input
This section was prepared by the CADTH review team based on the input provided by patient groups. The full original patient input received by CADTH is included in the stakeholder section at the end of this report.
The Canadian VHL Alliance, Canadian Organization for Rare Disorders, Kidney Cancer Canada, Pancreatic Cancer Canada, and Canadian Neuroendocrine Tumour Society provided a single joint input for the treatment of adult patients with VHL disease who require therapy for associated nonmetastatic RCCs, CNS hemangioblastomas, and nonmetastatic pNETs not requiring immediate surgery. Patient input was gathered from online surveys and semistructured telephone interviews among patients living with VHL disease and their caregivers in December 2022. In total 123 responses were gathered (72 from patients and 51 from caregivers), and 19 patients had experience with belzutifan.
Patients and caregivers described their ongoing physical and psychological struggles due to VHL, such as dismissal or misdiagnosis of initial symptoms; not receiving a diagnosis until they had an advanced-stage tumour affecting their vision, hearing, and walking; discomfort, pain, interference with daily activities; difficulties adhering to tumour-screening guidelines, scheduling tests and travelling for tumour screenings; and paying all the expenses not covered by public or private health care insurance. Patients from the survey reported worrying about potential adverse effects of frequent screenings and the stress caused by the uncertainty of tumour activity between scans. Patients also described their experiences with VHL as “excruciatingly painful and debilitating,” diminishing their ability to care for themselves, engage in family and social activities, plan for a family, and participate in work. Patients also reported that VHL disease affected their finances, feelings of self-worth, and engagement in meaningful activities. Overall, about 45% of respondents reported a negative impact of VHL on their ability to work, travel, exercise, perform household chores, spend time with family and friends, and fulfill family obligations.
Survey respondents reported that surgical resection was the primary treatment received for symptomatic lesions. When patients and caregivers were asked about how surgeries have affected their ability to work or quality of life, 92 respondents, some of whom were taking belzutifan, provided commentary. When respondents were asked about the number of surgeries they had undergone to remove VHL cysts and tumours, 98 individuals provided a response. Of these, 18 (18.4%) reported having 10 or more surgeries, and the average number of surgeries reported was 5.3.
While evaluating the importance (on a scale of 1 [not important] to 5 [extremely important]) of outcomes of new treatments, patients from the survey emphasized the need for a treatment that can improve their physical condition by decreasing or stabilizing the size of tumours (weighted average rating = 4.8), improving quality of life (weighted average rating = 4.63), offering long-term stability or reduction of disease (weighted average rating = 4.86), and offering the opportunity to avoid surgery (weighted average rating = 4.9). Patients also expressed their willingness to tolerate moderate-to-severe side effects of a treatment that would allow them to avoid surgery to remove VHL-related cysts and tumours (weighted average rating = 3.38).
While describing their experiences with belzutifan, the patient groups suggested that all patients with VHL disease should be given access to belzutifan based on an individual informed decision between the treating physician and the patient and their family. The patient groups also emphasized that the decision to take belzutifan should consider the clinical status of the patient; the location, severity, and prognosis of the tumours; the history of surgery and outcomes; the psychological and mental health status of the patient; and other factors.
Clinician Input
Input From Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise in the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). In addition, as part of the belzutifan review, a panel of 3 clinical experts with expertise in treating VHL-associated RCCs, CNS hemangioblastomas, and pNETs from across Canada was convened to characterize unmet therapeutic needs, help identify and communicate situations in which there are gaps in the evidence that could be addressed by collecting additional data, promote the early identification of potential implementation challenges, gain further insight into the clinical management of patients living with VHL disease, and explore the potential place in therapy of belzutifan (e.g., potential reimbursement conditions). A summary of this panel discussion is presented in the sections that follow.
Unmet Needs
The clinical experts noted that prolonging survival and improving quality of life are critical goals for patients with a VHL-associated nonmetastatic RCC, CNS hemangioblastoma, and/or nonmetastatic pNET. The clinical experts also highlighted the need to improve function, preserve neurologic status, and address symptoms related to the burden of disease unique to patients with VHL-associated CNS tumours, as well as the need to delay progression to a metastatic RCC and increase the time to development of dialysis dependence for patients with VHL-associated RCC.
The clinical experts agreed that an effective systemic treatment for VHL is needed. According to the clinical experts, an effective systemic treatment would minimize the morbidity associated with surgical procedures in patients with a VHL-associated nonmetastatic pNET and RCC, many of whom are younger. An effective systemic treatment would also address neurologic disability and mortality related to growing symptomatic CNS lesions, which may be surgically inaccessible at recurrence and can only be re-resected and/or irradiated a limited number of times. The clinical experts noted that VHL disease is a multiorgan disease that is frequently highly symptomatic, requiring frequent surgical interventions, radiation, specialist review, and opioid analgesia, among other health care service interactions.
Place in Therapy
The clinical experts noted that the current treatment paradigm for VHL disease involves genetic testing for VHL at diagnosis and active surveillance until treatment is indicated for associated tumours. The clinical experts indicated that reactive treatments, such as surgery and radiation, can be morbid and are usually selected to respond to the conditions or symptoms developed. The clinical experts noted that belzutifan, if reimbursed, would be the first systemic treatment for VHL-associated tumours and would change the current treatment paradigm by helping patients delay or avoid the need for local therapies (e.g., surgery and irradiation).
Patient Population
The clinical experts indicated that VHL is a rare disease and that all patients with VHL might benefit from belzutifan. However, the clinical experts noted that the eligibility criteria of the pivotal LITESPARK-004 trial matched the patient population of the indication and reimbursement request, which is for patients with a nonmetastatic RCC, CNS hemangioblastoma, or nonmetastatic pNET not requiring immediate surgery. It was noted that all patients enrolled in the LITESPARK-004 trial would have at least 1 measurable RCC according to RECIST 1.1. The clinical experts did not specify any subset of the patient population with the greatest need or identify any prognostic factors that might cause differential treatment effects.
The clinical experts considered size to be an appropriate inclusion criterion of the LITESPARK-004 trial (i.e., no RCC tumours greater than 3 cm that necessitated immediate surgical intervention). The clinical experts advised against setting an upper limit for the size of the tumours for patients to be eligible for treatment with belzutifan, noting that a larger size is not the sole factor influencing management; tumour location, presence of symptoms, and tumour growth rate are usually equally important factors.
With respect to how VHL disease is diagnosed in Canada, the clinical experts indicated that several circumstances could trigger the need for screening and genetic testing for VHL, such as young patients with a pNET, patients with more than 1 cancer type (e.g., RCC, CNS hemangioblastoma, and pNET), and patients presenting with multiple CNS lesions. The clinical experts noted that genetic testing to confirm a VHL diagnosis should be required before initiating treatment with belzutifan. They also indicated that genetic testing for VHL is available in certain centres across Canada. The clinical experts identified multiple challenges related to genetic testing for VHL. Living in rural or remote areas may be a barrier to accessing the test, and greater awareness is needed among patients without an established family history of VHL disease so that these patients can be tested. The clinicians also noted that a genetic counsellor should be involved in the diagnosis of VHL disease.
Assessing the Response Treatment
The clinical experts noted that response assessments for CNS tumours in clinical practice typically involve the measurement of target lesions over time to determine if there is a CR, PR, stable disease, or disease progression using the RANO criteria.29 The measurement is usually performed on the brain and spine using MRI every 3 months for symptomatic patients and up to yearly for patients under surveillance. Ideally, neurologic function is also assessed. The clinical experts reported that response assessments for pNET involve CT measurements every 2 or 3 months; however, they noted that clinical response or symptoms may be difficult to assess in patients with nonmetastatic disease. For RCC, response is assessed with CT and/or MRI every 3 to 6 months, depending on patient conditions as defined by RECIST 1.1.
Discontinuing Treatment
The clinical experts referred to several situations in which belzutifan may be discontinued, including intolerable AEs (e.g., becoming transfusion-dependent due to anemia), clinical disease progression (e.g., worsening of symptoms), and radiographic disease progression. The clinical experts indicated that they might continue treatment with belzutifan in some patients who have experienced radiographic progression without clinical progression if in their opinion the patient is still deriving clinical benefit. The clinical experts noted that patients who have remained in a stable status for an extended period may base a decision to discontinue belzutifan and be actively monitored on a personal preference.
Prescribing Considerations
The clinical experts noted that, due to the rarity and complex needs of patients with VHL disease, it is highly likely that only specialists working in large medical centres (e.g., tertiary and specialized referral centres) in Canada may encounter patients with VHL. Prescription may therefore be limited to specialists (e.g., medical oncologist and neuro-oncologists) working in such centres.
Clinician Group Input
This section was prepared by the CADTH review team based on the input provided by clinician groups. The full original clinician group inputs received by CADTH are included in the stakeholder section at the end of this report.
Clinician group input was received from the 7-member Ontario Health (Cancer Care Ontario) Genitourinary Drug Advisory Committee and 25 clinical subspecialists in Canada involved in VHL care.
The clinician groups agreed with the clinical experts consulted by CADTH that belzutifan, as the first systemic therapy option for VHL disease approved in Canada, fulfills an important unmet need for the treatment of patients with VHL and represents a shift in the current treatment paradigm. They also generally agreed on treatment goals, patient populations, response treatment-discontinuation criteria, and prescribing conditions.
While the clinical experts considered genetic testing to be a prerequisite for initiating treatment with belzutifan, neither clinician group indicated whether genetic testing for a VHL mutation or deletion was required. The clinician group indicated that belzutifan should be discontinued if the patient is pregnant.
Drug Program Input
Table 4: Summary of Drug Plan Input and Clinical Expert Responses
Drug program implementation questions | Clinical expert response |
|---|---|
Relevant comparators | |
There is 1 pivotal clinical study (LITESPARK-004):
The drug plans had no issues as standard care for VHL disease is routine active surveillance. | Comment from the drug plans to inform pERC deliberations. |
The drug plans presented the following implementation issues regarding relevant comparators:
| Comment from the drug plans to inform pERC deliberations. |
Considerations for initiation of therapy | |
Should nonmetastatic status be stated in the eligibility criteria? | Nonmetastatic status should be stated in the eligibility criteria for reimbursement because the data in the LITESPARK-004 trial were from patients with VHL-associated nonmetastatic tumours (i.e., the study excluded patients with evidence of metastatic disease). However, CNS hemangioblastomas typically are not described as nonmetastatic or metastatic. |
Should pediatrics be eligible for belzutifan? | Expansion of the use of belzutifan in pediatrics is desirable, but the indication for belzutifan is for adult patients and the LITESPARK-004 trial restricted enrolment to adult patients. Expanding belzutifan in pediatrics may not be feasible due to lack of research data in this population. It may not be practical for older pediatric patients (i.e., adolescents who have a adult size and physiology) to wait until they reach 18 years of age to have access to belzutifan if they have a growing CNS tumour. If belzutifan were to be used in pediatric patients, it would be preferable to involve pediatric doctors in prescribing belzutifan. |
Should belzutifan be considered in patients with an ECOG PS > 1? | Setting requirements for ECOG PS to initiate belzutifan is not preferable because ECOG PS can be unstable and subjective. In clinical practice, a clinician may determine that a patient with an ECOG PS > 1 could benefit from belzutifan. |
Is belzutifan a life-long therapy with time off only for surgical interventions while in the nonmetastatic state? | How long patients would be on treatment with belzutifan is uncertain. The median follow-up time in the LITESPARK-004 trial at the time of this review was limited to 37.7 months. Whether belzutifan becomes a life-long therapy depends on how well and how long belzutifan can work to prevent disease progression. A time limit should not be put on the use of belzutifan, and treatment with belzutifan can continue until the patient experiences disease progression or unacceptable toxicity. |
Considerations for discontinuation of therapy | |
Should patients receive belzutifan on and off to allow for surgical interventions? | Patients may receive belzutifan on and off to allow for surgical interventions. |
What are the discontinuation criteria for belzutifan? | Belzutifan may be discontinued in the following situations:
Patients who have remained in a stable status for a long time may make a personal decision to discontinue belzutifan and be actively monitored. |
Considerations for prescribing of therapy | |
Belzutifan is taken 120 mg orally daily. | Comment from the drug plans to inform pERC deliberations. |
Care-provision issues | |
Belzutifan is provided as a 40 mg tablet (120 mg starting daily dose) in bottles of 90 tablets. Dispensing will require discussion of reproductive risk to patients (all genders), contraception, and avoidance of pregnancy throughout therapy and for at least 1 week after last dose. Based on experience during the LITESPARK-004 Study, 82% of patients experienced a dose interruption. Additionally, 18% of patients had a dose reduction to 80 mg orally daily, 6.6% of patients had a dose reduction to 40 mg orally daily, and 28% of patients discontinued therapy for reasons other than progressive disease. If reimbursed, drug wastage may occur should dose interruptions and/or discontinuations occur after a supply of belzutifan is dispensed. | Comment from the drug plans to inform pERC deliberations. |
CNS = central nervous system; ECOG PS = Eastern Cooperative Oncology Group Performance Status; pERC = CADTH pan-Canadian Oncology Review Expert Review Committee; VHL = von Hippel-Lindau.
Clinical Evidence
The objective of CADTH’s Clinical Review Report is to review and critically appraise the clinical evidence submitted by the sponsor on the beneficial and harmful effects of belzutifan (40 mg per tablet, oral administration) in the treatment of adult patients with VHL disease who require therapy for associated nonmetastatic RCC, CNS hemangioblastomas, or nonmetastatic pNET not requiring immediate surgery. The focus will be placed on comparing belzutifan to relevant comparators and identifying gaps in the current evidence.
A summary of the clinical evidence included by the sponsor in the review of belzutifan is presented in 3 sections, and CADTH’s critical appraisal of the evidence is included after each section. The first section, the systematic review, includes pivotal studies and RCTs that were selected according to the sponsor’s systematic review protocol. The second section includes indirect evidence from the sponsor. The third section includes additional studies that were considered by the sponsor to address important gaps in the pivotal and RCT evidence.
Included Studies
Clinical evidence from the following is included in the CADTH review and appraised in this document:
One pivotal phase II, single-arm, open-label trial (LITESPARK-004)
One ITC
One additional study addressing gaps in evidence (VHL Natural History Study)
In addition, a cross-sectional survey submitted by the sponsor that assessed HRQoL in patients with VHL disease who did not receive treatment with belzutifan is summarized and appraised in Appendix 1.
Pivotal Studies and Randomized Controlled Trial Evidence
Contents within this section have been informed by materials submitted by the sponsor. The following have been summarized and validated by the CADTH review team.
Description of Studies
Only 1 study (LITESPARK-004),13 which was conducted by the sponsor, met the inclusion criteria for the sponsor-submitted systematic review. Characteristics of the LITESPARK-004 trial are summarized in Table 5.
The LITESPARK-004 trial was a phase II, single-arm, open-label study of the efficacy and safety of belzutifan in 61 patients with VHL disease–associated nonmetastatic RCC across 11 centres in Denmark, France, the UK, and the US. The primary objective was to evaluate the efficacy of belzutifan for the treatment of VHL disease–associated nonmetastatic RCCs as measured by ORR. Evaluation of the efficacy of belzutifan for the treatment of VHL disease–associated nonmetastatic non-RCC tumours (e.g., CNS hemangioblastomas and pNET) as well as assessment of the safety and tolerability of belzutifan were among the secondary objectives. Evaluation of non-RCC tumours was not part of the original protocol, but was added after the completion of enrolment, using a retrospective review of existing images.
The LITESPARK-004 trial is ongoing. Data submitted by the sponsor to support this reimbursement request are based on a cut-off date of April 1, 2022. The database lock date was June 2, 2022.
Table 5: Details of Pivotal Studies and RCT Evidence Identified by the Sponsor
Detail | LITESPARK-004 |
|---|---|
Designs and populations | |
Study design | Phase II, single-arm, open-label study |
Locations | 11 centres in Denmark, France, the UK, and the US |
Patient enrolment dates | Start date: May 2, 2018 End date: Ongoing (estimated completion date: March 2026) |
Enrolled (N) | 61 patients treated with belzutifan |
Inclusion criteria |
|
Exclusion criteria |
|
Drugs | |
Intervention | Belzutifan 120 mg orally once a day |
Comparator(s) | None (single-arm study) |
Study duration | |
Screening phase | 28 days |
Run-in phase | Not applicable |
Treatment phase | Until disease progression, death, adverse event leading to discontinuation, or withdrawal of consent |
Follow-up phase | Safety follow-up: 28 days after last dose of belzutifan. Long-term follow-up: every 6 months of VHL disease–associated tumour status; any drug, surgery, or radiotherapy intervention for VHL disease–associated tumours; and survival status |
Outcomes | |
Primary end point | Objective response rate in VHL disease–associated RCC tumours defined as the proportion of patients with a best confirmed response of complete response or partial response by IRC according to RECIST 1.1. |
Secondary and exploratory end points | Secondary
Exploratorya
|
Publication status | |
Publications | Jonasch et al. (2021)30 Jonasch et al. (ASCO 2022)31 Srinivasan et al. (ESMO 2022)32 |
CNS = central nervous system; ECOG = Eastern Cooperative Oncology Group; HIF-2-alpha = hypoxia-Inducible factor 2 alpha subunit; IRC = independent review committee; pNET = pancreatic neuroendocrine tumour; RCC = renal cell carcinoma; RECIST 1.1 = Response Evaluation Criteria in Solid Tumors Version 1.1; RCT = randomized controlled trial; VEGF = vascular endothelial growth factor; VHL = von Hippel-Lindau.
Note: Details from the table have been taken from the sponsor’s Summary of Clinical Evidence.1
aEnd points including number of patients who develop a metastatic CNS hemangioblastoma or pNET, change in linear growth rate among patients with a VHL-associated nonmetastatic RCC, CNS hemangioblastoma, or pNET, and disease control rate were reported in the LITESPARK-004 Clinical Study Report but not explicitly listed as efficacy parameters in the LITESPARK-004 trial protocol. CADTH considered these exploratory end points.
Sources: LITESPARK-004 Clinical Study Report,13 LITESPARK-004 trial protocol,33 and Jonasch et al. (2021).30,34
Populations
Inclusion and Exclusion Criteria
Participants eligible to be included in the LITESPARK-004 trial were required to be at least 18 years of age and be diagnosed with VHL disease based on a germline VHL alteration, with at least 1 measurable RCC and an ECOG PS 0 or 1. Eligible patients could also have other VHL disease–associated tumours, including a CNS hemangioblastoma and pNET. Patients who had an immediate need for surgical intervention for tumour treatment or evidence of metastatic disease were excluded.
Interventions
In the single-arm, open-label LITESPARK-004 trial, belzutifan was provided centrally by the sponsor to patients and administered orally at a dosage of 120 mg (in 3 40 mg tablets) once daily until disease progression or unacceptable AEs. The tablets were taken approximately 24 hours apart. Patients who required surgery for nonrenal lesions may have had their belzutifan interrupted in the perioperative period, if necessary. Administration of belzutifan was resumed when patients could swallow and tolerate oral medications after surgery.
Patients were not allowed to receive any approved or additional investigational antineoplastic drug during the study. Pretreatment administration of prophylactic antiemetics was also not allowed but could be given if needed during study treatment. There were no constraints on the use of growth factors, including erythropoietin, during treatment. However, prophylactic use was discouraged and adherence to the American Society of Clinical Oncology or European Society for Medical Oncology guidelines was recommended. Patients should have received all necessary supportive care, including blood products, transfusions, antibiotics, pain medications, bisphosphonates, and replacement hormonal therapies (insulin, thyroid hormones, estrogen, or progesterone).
Outcomes
A list of efficacy end points assessed in this clinical review report is provided in Table 6. These end points are further summarized in the following section. Summarized end points are based on those included in the sponsor’s Summary of Clinical Evidence1 as well as any identified as important to this review by stakeholders (clinical experts, clinician groups, or patient groups). The distribution of all tumour-reduction procedures before and after treatment initiation for individual patients was also reported in the Clinical Study Report, even though this outcome was not prespecified in the study protocol.
Table 6: Outcomes Summarized From Pivotal Studies and RCT Evidence Identified by the Sponsor
Outcome measure | Time point | LITESPARK-004 |
|---|---|---|
TTS for VHL-associated nonmetastatic
| Throughout the trial | Secondary |
PFS for VHL-associated nonmetastatic
| Throughout the trial | Secondary |
ORR for VHL-associated nonmetastatic
| Throughout the trial | Primary (ORR for RCC assessed by IRC) Secondary (all other ORR) |
DOR for VHL-associated nonmetastatic
| Throughout the trial | Secondary |
DCR for VHL-associated nonmetastatic
| Throughout the trial | Exploratoryb |
BOR for VHL-associated nonmetastatic
| Throughout the trial | Exploratoryb |
TTR for VHL-associated nonmetastatic
| Throughout the trial | Secondary |
Change in LGR for VHL-associated nonmetastatic
| Before and during belzutifan treatment | Exploratoryb |
Number of patients who develop metastatic RCC | Throughout the trial | Exploratory |
Number of patients who develop metastatic pNET | Throughout the trial | Exploratoryb |
Safety and tolerability | Throughout the trial | Secondary |
BOR = best overall response; CNS = central nervous system; DCR = disease control rate; DOR = duration of response; IRC = independent review committee; LGR = linear growth rate; ORR = objective response rate; PFS = progression-free survival; pNET = pancreatic neuroendocrine tumour; RCC = renal cell carcinoma; RCT = randomized controlled trial; TTR = time to response; TTS = time to surgery; VHL = von Hippel-Lindau.
aUnless otherwise specified, outcomes assessed by investigators were not available in the LITESPARK-004 Clinical Study Report
bThese outcomes were not explicitly listed as end points in the LITESPARK-004 trial protocol, but were considered by CADTH to be exploratory end points.
Sources: LITESPARK-004 Clinical Study Report,35 LITESPARK-004 trial protocol,33,34 LITESPARK-004 statistical analysis plan,36 and Jonasch et al. (2021).30
Efficacy Outcomes
Patients were assessed radiologically about 12 weeks after initiation of treatment and every 12 weeks thereafter while continuing on belzutifan for a minimum of 3 years. After 3 years, patients were evaluated radiologically every 24 weeks, or more frequently if clinically indicated.
Patients who discontinued belzutifan for any reason underwent long-term follow-up every 6 months until the patient either withdrew consent for follow-up or died. If patients discontinued belzutifan without documented disease progression and had not met any of the discontinuation criteria for scanning (i.e., IRC-verified disease progression as defined by RECIST 1.1, the start of a new anticancer treatment, pregnancy, death, withdrawal of consent, or end of study), every effort was to be made to monitor disease status by acquiring tumour scans 6 months after the last scan and at 6-month intervals for a minimum of 2 years, or more frequently if indicated. After 2 years, scans were collected every 12 months or more frequently if clinically indicated.
Time to Surgery
TTS for VHL disease–associated nonmetastatic RCC, CNS hemangioblastomas, or pNET was defined as the interval from the start of study treatment to the date of surgery.34 Patients who did not undergo surgery were censored as of the last known alive date. Surgery was defined as any tumour-reducing intervention including partial nephrectomy, radical nephrectomy, ablative procedure (e.g., cryoablation, thermal ablation, radioablation), and tumour-debulking surgeries, but excluding radiation therapy. The data cut-off date for TTS to support this reimbursement request was April 1, 2022.
Progression-Free Survival
PFS was measured for VHL disease–associated nonmetastatic RCCs, CNS hemangioblastomas, and pNETs. PFS was defined as the interval from the start of study treatment until the earlier of the first documentation of disease progression determined by RECIST 1.1 or death from any cause.34
Several censoring rules for PFS were applied. First, if progressive disease or death was documented after no more than 1 missed disease assessment and before new anticancer therapy, PFS was considered as an event at the date of documented progressive disease or death. Second, if progressive disease or death was documented immediately after 2 or more consecutive missed disease assessments or after new anticancer therapy, the patient was censored at the last adequate disease assessment before the 2 consecutive missed disease assessments and new anticancer therapy. Third, if there was no progressive disease or death, and a new anticancer therapy was initiated, the patient was censored at the last disease assessment documented before the new anticancer therapy. Fourth, if there was no progressive disease, death, or newly initiated anticancer therapy, the patient was censored at the last adequate disease assessment. Fifth, if no adequate posttreatment tumour assessments were obtained for a patient, the patient was censored at day 1 (i.e., zero duration).36 The data cut-off date for PFS to support this reimbursement request was April 1, 2022.
Objective Response Rate
In the LITESPARK-004 trial protocol,34 ORR was defined as the proportion of patients with a best confirmed response of a CR or PR as determined by RECIST 1.1 for each VHL-associated organ system. ORR for a VHL disease–associated nonmetastatic RCC measured by IRC was the only primary end point for the LITESPARK-004 trial. All other ORR outcomes were considered secondary end points. The data cut-off date for ORR to support this reimbursement request was April 1, 2022.
Duration of Response
DOR was measured for VHL disease–associated nonmetastatic RCCs, CNS hemangioblastomas, and pNETs. DOR was defined as the interval from the first documentation of response, as determined by RECIST 1.1, to the earlier of the first documentation of disease progression or death from any cause and calculated for patients with a best confirmed response of a CR or PR.34 Start time was the first instance of a CR or PR that was subsequently confirmed, not the confirmatory date itself.
Four censoring rules for DOR were applied. First, if progressive disease or death was documented after no more than 1 missed disease assessment and before new anticancer therapy, the outcome was considered as an event and DOR was documented as progressive disease or death. Second, if progressive disease or death was documented immediately after 2 or more consecutive missed disease assessments or after new anticancer therapy, the outcome was considered a non-event and the patient was censored at the earlier date of the last adequate disease assessment before 2 or more missed adequate disease assessments and new anticancer therapy. Third, if there was no progressive disease or death, and a new anticancer therapy was initiated, the outcome was considered a nonevent and the patient was censored at the last adequate disease assessment before the new anticancer therapy. Fourth, if there was no progressive disease, death or newly initiated anticancer therapy, the outcome was considered a nonevent and the patient was censored at the last adequate disease assessment.36 The data cut-off date for DOR to support this reimbursement request was April 1, 2022.
Disease Control Rate
In the sponsor-submitted clinical evidence summary,1 DCR was defined as the proportion of patients with a best confirmed response of a CR, PR, or stable disease by an IRC as defined by RECIST 1.1. In the sponsor’s statistical analysis plan (version 3.0; February 24, 2022),36 DCR was defined as the proportion of patients who have a BOR of a CR, PR, or stable disease. However, DCR was not a predefined end point of interest in the LITESPARK-004 trial protocol (version 10.0; February 15, 2022).34 The sponsor noted that this was added post hoc to report on the proportion of patients with stable disease. The data cut-off date for DOR to support this reimbursement request was April 1, 2022.
Best Overall Response
BOR, which summarized the number of patients who had a CR, PR, stable disease, progressive disease, or a status not evaluable, was not explicitly listed as an end point and defined in the LITESPARK-004 trial protocol (version 10.0; February 15, 2022).34 The data cut-off date for BOR to support this reimbursement request was April 1, 2022.
Time to Response
TTR for VHL disease–associated nonmetastatic RCC, CNS hemangioblastomas, or pNET was defined as the interval from the start of study treatment to the first documentation of a response, as determined by RECIST 1.1, and calculated for patients with a best confirmed response of a CR or PR.34 The data cut-off date for TTR to support this reimbursement request was April 1, 2022.
Change in Linear Growth Rate
Change in LGR was not explicitly listed as an end point in the LITESPARK-004 trial protocol (version 10.0; February 15, 2022).34 According to the sponsor’s statistical analysis plan (version 3.0; February 24, 2022),36 LGRs for target tumours before and after study drug treatment were calculated for patients with at least 3 scans before treatment, including the screening scan. The data cut-off date for change in LGR to support this reimbursement request was April 1, 2022.
Number of Patients who Develop Metastases
Although not explicitly defined in the protocol, the number of patients who developed metastatic RCC and number of patients who developed metastatic pNET were reported. The number of patients who developed metastatic CNS hemangioblastomas was not applicable because CNS hemangioblastomas are nonmalignant tumours by histology and do not metastasize, according to the sponsor’s explanation, which was validated by the clinical experts consulted by CADTH.
Statistical Analysis
In the LITESPARK-004 trial, the null hypothesis was that the ORR is 15%, while the alternative hypothesis was that the ORR is 30%. The sample size was estimated at approximately 50 patients based on the following assumptions: A sample size of 50 patients would provide greater than 80% power to reject the null under the alternative hypothesis using a 1-sided test at a 0.05 level of significance.34
No inferential statistical analyses were performed as this was a single-arm trial.36 Data were summarized using descriptive statistics. For continuous variables, the number of patients with nonmissing data, mean, standard deviation (SD), median, and range were presented. For categorical data, the frequency and percent distribution were presented.
Estimates of the ORR along with the associated 95% exact binomial CIs (Clopper-Pearson method) were provided. The binomial probability that the observed RCC ORR was greater than 0.15 was calculated. BOR was summarized. Kaplan-Meier methods were used to estimate the distribution of DOR, PFS, and TTS. Quartiles including the median were estimated by the Kaplan-Meier method along with their 95% CIs (Brookmeyer-Crowley method). Kaplan-Meier cumulative estimators along with their associated 95% CIs were provided for RCC DOR rates at 26, 39, and 52 weeks. TTR was calculated and summarized descriptively. LGRs at tumour level pre- and posttreatment were calculated for tumours using at least 3 scans (including the screening scan) and linear regression was applied to the tumour size with time as a continuous variable. LGRs at the patient level pre- and posttreatment were calculated for patients with at least 3 scans (including the screening scan) and linear regression was applied to the tumour sizes with time as a continuous variable and individual tumour as a categorical variable. LGRs were derived as the coefficient of time. The number and proportion of patients developing metastatic RCC or pNET were summarized descriptively.
Tumour responses were measured by CT or MRI and assessed according to RECIST 1.1. CRs and PRs were confirmed by a second assessment at least 4 weeks after the initial response was documented. Where confirmed responses were available, the date of the first assessment was used in all analyses. If a confirmation assessment was not available, the assessment at the next scheduled time point was used for confirmation. If there were no confirmation assessments, the response was taken to be unconfirmed and considered a nonresponse. Patients who did not have a tumour assessment for any reason were considered nonresponders and included in the denominator when calculating the response rate.
AEs by maximum severity were summarized by system organ class and preferred term, according to the number and percentage of patients with at least 1 AE, SAE, death, or AE leading to drug withdrawal, or dose reduction or interruption.
Missing data were not estimated or carried forward for any of the other summaries. If only a partial date was available and was required for a calculation of whether a medication is concomitant or an AE is treatment-emergent, the start and stop dates were imputed according to a predefined standard. No other imputation of missing data was performed.
Analysis populations of the LITESPARK-004 trial are summarized in Table 7. All participants in the LITESPARK-004 trial should have had a VHL disease–associated nonmetastatic RCC to meet the eligibility criteria. Efficacy results for VHL disease–associated nonmetastatic RCCs therefore came from the efficacy analysis set, while efficacy results for VHL disease–associated CNS hemangioblastomas and nonmetastatic pNETs were from subsets of the efficacy analysis set that were defined according to the study protocol34 by the site of primary tumours other than RCCs at screening.
Protocol Amendments and Deviations
Between November 10, 2017, and February 15, 2022, 10 versions of the LITESPARK-004 trial protocol were identified. A summary of key protocol amendments implemented in the LITESPARK-004 trial is presented in Table 8.
Table 7: Analysis Populations in the LITESPARK-004 Trial
Study | Population | Definition | Application |
|---|---|---|---|
LITESPARK-004 | Efficacy analysis set | All patients who have received at least 1 dose of belzutifan and found to be radiographically eligible by the independent review committee | Primary population for efficacy analyses |
Safety analysis set | All patients who have received at least 1 dose of belzutifan | Primary population for the summaries of demographics, baseline data, safety data, and exposure |
Source: LITESPARK-004 trial protocol.33,34
Table 8: Summary of Key Protocol Amendments in LITESPARK-004
Amendment sections | Amendment details |
|---|---|
Primary objective (amendments made on December 9, 2021, in the version 9.0 study protocol) | In the version 9.0 study protocol, the primary objective was revised to “To evaluate the efficacy of PT2977 (belzutifan) for the treatment of von Hippel-Lindau (VHL) disease–associated renal cell carcinoma (RCC) as measured by overall response rate (ORR) per Response Evaluation Criteria in Solid Tumors Version 1.1 (RECIST 1.1) by an independent review committee (IRC).”a |
Exploratory objectives and end points (amendments made on February 15, 2022, in the version 10.0 study protocol) | Additional outcomes were added, including:
|
aRevisions were highlighted in bold.
Source: LITESPARK-004 trial protocol.34
As of April 1, 2022, 6 important protocol deviations were reported: 1 patient was given an unapproved drug to treat fatigue and headaches; 1 patient was administered a higher belzutifan dosage of 120 mg once a day compared with the originally prescribed dose of 80 mg once a day; 1 patient discontinued belzutifan between June 2019 and August 2019 due to abdominal pain (exceeding the 3-week off-drug interval allowed by the study protocol); 1 patient had an ECOG PS of 2, which did not meet the study eligibility criteria; 1 patient was off belzutifan for more than 3 weeks due to lack of access; 1 patient was removed from the LITESPARK-004 trial on October 22, 2020, but the date of the last dose of belzutifan was November 16, 2020.
Results
Patient Disposition
A summary of patient disposition in the LITESPARK-004 trial is provided in Table 9. Of 67 screened participants, 9.0% (6) were screen failures, all of which were due to failure to meet eligibility criteria. Because the LITESPARK-004 trial was a single-arm trial, all 61 eligible participants received the treatment of belzutifan. As of the data cut-off date of April 1, 2022, 9.8% of the study participants (5 of 61) discontinued from the study. About 37.7% of the participants (23 of 61) discontinued study treatment as of April 1, 2022, among which discontinuation due to patient decisions (n = 11; 18.0%) was the most common reason, followed by disease progression (n = 6; 9.8%). Reasons for discontinuing belzutifan due to patient decisions included: study drug side effects (i.e., 3 patients due to fatigue and 1 patient due to feeling down and disappointed), personal or logistical reasons (4 patients due to difficulty in travelling, 1 patient was not able to afford medical expenses, and 1 patient started a family), and unknown reasons (i.e., 1 patient was unable to return to the trial site and had been noncommunicative).
For this reimbursement request, efficacy data for patients with VHL disease–associated RCC were from all 61 study patients, efficacy data for patients with VHL disease–associated CNS hemangioblastoma were from 50 participants, and efficacy data for patients with VHL disease–associated pNET came from 22 patients.
Table 9: Summary of Patient Disposition From Pivotal Studies and RCT Evidence Submitted by the Sponsor
Patient disposition | LITESPARK-004 |
|---|---|
Belzutifan (N = 61) | |
Screened, N | 67 |
Reason for screening failure, N (%) | 6 (9.0) |
Eligibility criteria not met | 6 |
Allocated to study treatment, N (%) | 61 (100) |
Discontinued from study, N (%) | 6 (9.8) |
Death | 2 (3.3) |
Informed consent withdrawn | 2 (3.3) |
Other | 2 (3.3) |
Discontinued belzutifan treatment, N (%) | 23 (37.7) |
Patient decision | 11 (18.0) |
Progressive disease | 6 (9.8) |
Adverse event | 2 (3.3) |
Death | 2 (3.3) |
Lost to follow-up | 0 (0) |
Gross noncompliance with protocol | 0 (0) |
Pregnancy | 1 (1.6) |
Other | 1 (1.6) |
Treatment ongoing at data cut-off date (April 1, 2022) | 38 (62.3) |
Efficacy analysis population by tumour type, N (%) | |
Renal cell carcinoma | 61 (100) |
Central nervous system hemangioblastoma | 50 (82.0) |
Pancreatic neuroendocrine tumour | 22 (36.1) |
Safety analysis population, N | 61 |
RCT = randomized controlled trial.
Source: LITESPARK-004 Clinical Study Report.13
Baseline Characteristics
Baseline characteristics of the LITESPARK-004 trial are shown in Table 10. In the total study population (i.e., patients with RCC, N = 61), the median age was 41.0 years (range = 19.0 to 66.0), and the median age at time of VHL disease diagnosis was 32.0 years (range = 4.0 to 66.0). Approximately half of the patients were male (52.5%) and half were female (47.5%). Most patients were white (90.2%), had an ECOG PS of 0 (82.0%), and had a previous surgery or ablative procedure (96.7%). The median number of previous procedures was 5.0 (range = 1.0 to 15.0). In the total study population, 77.1% of patients had a previous surgery for an RCC, 75.4% had a previous surgery for a CNS hemangioblastoma, and 14.8% had previous pancreas surgery.
Median age was similar in the CNS hemangioblastoma and pNET subpopulations. For patients with a CNS hemangioblastoma (n = 50), the median age was 40.5 years (range = 19.0 to 65.0). For patients with a pNET (n = 22), the median age was 42.0 years (range = 19.0 to 66.0). Similar to the total study population, most patients in the CNS hemangioblastoma and pNET subpopulations were white (88.0% and 81.8%, respectively) and had an ECOG PS of 0 (78.0% and 90.9%, respectively).
Exposure to Study Treatments
At the data cut-off date of April 1, 2022, the median duration of exposure to belzutifan was 37.3 months (range = 1.9 to 46.1) and 44 patients (72%) had received treatment for at least 36 months. A total of 50 patients (82%) had a dose interruption over the course of the study; dose interruption due to AEs was reported in 26 patients (43%). Eleven patients (18%) had a dose reduction to 80 mg daily and 4 patients (7%) had a dose reduction to 40 mg daily (Table 11).
Table 10: Summary of Baseline Characteristics of Pivotal Studies and RCT Evidence Submitted by the Sponsor
Characteristics | LITESPARK-004 (as of April 1, 2022) | ||
|---|---|---|---|
Total study population (RCC population) (N = 61) | Study subpopulation (CNS population) (n = 50) | Study subpopulation (pNET population) (n = 22) | |
Age, years | |||
At baseline, mean (SD) | 41.0 (13.5) | 40.4 (12.8) | 42.4 (14.6) |
At baseline, median (range) | 41.0 (19.0 to 66.0) | 40.5 (19.0 to 65.0) | 42.0 (19.0 to 66.0) |
At time of VHL disease diagnosis, mean (SD) | 31.3 (14.3) | NR | NR |
At time of VHL disease diagnosis, median (range) | 32.0 (4.0 to 66.0) | NR | NR |
At time of RCC diagnosis, mean (SD) | 33.8 (13.1) | NR | NR |
At time of RCC diagnosis, median (range) | 32.0 (15.0 to 62.0) | NR | NR |
Sex, n (%) | |||
Male | 32 (52.5) | 30 (60.0) | 11 (50.0) |
Female | 29 (47.5) | 20 (40.0) | 11 (50.0) |
Race, n (%) | |||
American Indian or Alaska Native | 0 (0) | 0 (0) | 0 (0) |
Asian | 1 (1.6) | 1 (2.0) | 1 (4.5) |
Black or African American | 2 (3.3) | 2 (4.0) | 2 (9.1) |
Native Hawaiian or other Pacific Islander | 1 (1.6) | 1 (2.0) | 0 (0) |
White | 55 (90.2) | 44 (88.0) | 18 (81.8) |
Unknown | 2 (3.3) | 2 (4.0) | 1 (4.5) |
BMI (kg/m2) | |||
Number of patients | 59 | 48 | 22 |
Mean (SD) | 27.8 (7.4) | 28.0 (7.3) | 29.3 (9.6) |
Median (range) | 26.3 (17.2 to 52.0) | 26.7 (17.2 to 52.0) | 26.3 (17.2 to 52.0) |
ECOG Performance Status, n (%) | |||
0 | 50 (82.0) | 39 (78.0) | 20 (90.9) |
1 | 10 (16.4) | 10 (20.0) | 2 (9.1) |
2 | 1 (1.6) | 1 (2.0) | 0 (0) |
VHL disease subtype, n (%) | |||
1 | 51 (83.6) | 42 (84.0) | 17 (77.3) |
2A | 2 (3.3) | 1 (2.0) | 1 (4.5) |
2B | 6 (9.8) | 6 (12.0) | 3 (13.6) |
2C | 0 (0) | 0 (0) | 0 (0) |
Missing | 2 (3.3) | 1 (2.0) | 1 (4.5) |
Previous surgery or ablative procedure | |||
Number of patients (%) | 59 (96.7) | NR | NR |
Mean number of procedures per patient (SD) | 5.5 (3.3) | NR | NR |
Median number of procedures per patient (range) | 5.0 (1.0 to 15.0) | NR | NR |
Surgery for RCC, number of patients (%) | 47 (77.1) | NR | NR |
Partial or radical nephrectomy, n (%) | 40 (65.6) | NR | NR |
CNS hemangioblastoma surgery, n (%) | 46 (75.4) | NR | NR |
Pancreas surgery, number of patients (%) | 9 (14.8) | NR | NR |
Previous anticancer therapy | |||
Ophthalmological — bevacizumab, n (%) | 2 (3.3) | NR | NR |
Previous radiation therapy | |||
With one or more prior radiation, n (%) | 5 (8.2) | NR | NR |
CNS hemangioblastoma, n (%) | 5 (8.2) | NR | NR |
Time from genetic analysis to first dose | |||
n | 45 | 50 | 22 |
Mean (SD), months | 103.4 (96.2) | 119.0 (92.1) | 98.2 (79.0) |
Median (range), months | 77.6 (0.5, to 389.4) | 123.8 (0.0 to 326.2) | 109.0 (0.1 to 252.4) |
Time from last surgery to first dose | |||
n | 59 | NR | NR |
Mean (SD), months | 37.01 (38.5) | NR | NR |
Median (range), months | 23.49 (0.6 to 137.6) | NR | NR |
Patients with non-RCC neoplasms, IRC-determined vs. investigator-determined | |||
CNS hemangioblastomas, n (%) | 50 (82.0) vs. 51 (83.6) | NA | 17 (77.3) vs. NR |
pNET, n (%) | 22 (36.1) vs. NR | 17 (34.0) / NR | NA |
Lesion size at baseline, IRC-determined vs. investigator-determined | |||
RCC | |||
n | 114 vs. 137 | NA | NA |
Mean (SD), mm | 23.1 (7.9) vs. 20.03 (6.2) | NA | NA |
Median (range), mm | 22 (10.0 to 61.0) vs. 19.0 (10.0 to 39.4) | NA | NA |
CNS hemangioblastoma | |||
n | 64 vs. 45 | NA | NA |
Mean (SD), mm | 23.6 (16.3) vs. 9.6 (4.6) | NA | NA |
Median (range), mm | 17.0 (10.0 to 87.0) vs. 8.0 (5.0 to 26.0) | NA | NA |
pNET | |||
n | 27 vs. NR | NA | NA |
Mean (SD), mm | 21.7 (9.5) vs. NR | NA | NA |
Median (range), mm | 19.0 (10.0 to 52.0) vs. NR | NA | NA |
BMI = body mass index; CNS = central nervous system; ECOG = Eastern Cooperative Oncology Group; NA = not applicable; NR = not reported; pNET = pancreatic neuroendocrine tumour; RCC = renal cell carcinoma; SD = standard deviation; VHL = von Hippel-Lindau; vs. = versus.
Sources: LITESPARK-004 Clinical Study Report.13
Table 11: Summary of Patient Exposure from Pivotal Studies and RCT Evidence Submitted by the Sponsor
Exposure | LITESPARK-004 |
|---|---|
Belzutifan (N = 61) | |
Mean duration of therapy, months (SD) | 33.7 (10.1) |
Median duration of therapy, months (range) | 37.3 (1.9 to 46.1) |
Patients with dose interruption, n (%) | 50 (82.0) |
Patients with dose interruption due to adverse events, n (%) | 26 (42.6) |
Patients with dose reduction to 80 mg once daily, n (%) | 11 (18) |
Patients with dose reduction to 40 mg once daily, n (%) | 4 (6.6) |
RCT = randomized controlled trial; SD = standard deviation.
Source: LITESPARK-004 Clinical Study Report.35
Concomitant Medications
All concomitant medication(s) used during the study and within 28 days before the start of study drug administration were recorded. Almost all (98.4%; 60 of 61) of the participants received concomitant medications during the LITESPARK-004 trial. The most common concomitant medications (in at least 20% of total study population) included acetaminophen (39.3%), COVID-19 vaccines (36.1%), ibuprofen (23.0%), and iron (21.3%). The most frequently reported concomitant treatments were analgesics (62.3%), followed by antianemic preparations (41.0%), vaccines (39.3%), ophthalmologicals (37.7%), and psycholeptics (37.7%). One patient received radiation therapy during treatment of belzutifan for a CNS hemangioblastoma.
Efficacy
Key efficacy results are presented in Table 12. All efficacy outcomes were obtained from the data with a cut-off date of April 1, 2022. The median follow-up duration was 37.7 months (range = 4.2 to 46.1 months). IRC- and investigator-assessed efficacy outcomes were reported for most of the patients, with VHL disease–associated nonmetastatic RCC and those with CNS hemangioblastoma, whereas only IRC-assessed efficacy results were available for patients with VHL disease–associated nonmetastatic pNET. Unless otherwise specified, results described in this report were IRC-assessed.
Time to Surgery
Median TTS was not reached for patients with VHL disease–associated nonmetastatic RCCs, CNS hemangioblastomas, or nonmetastatic pNETs as of the data cut-off date (April 1, 2022). Seven (11.5%; 7 of 61) patients with an RCC, 1 patient (2.0%; 1 of 51) with a CNS hemangioblastoma, and none of the patients with a pNET had surgery during the follow-up period. (Table 12). The Kaplan-Meier plot of TTS was only presented for patients with RCC in the LITESPARK-004 trial (Figure 1).
Table 12: Summary of Key Efficacy Results from Pivotal Evidence
Efficacy outcome (as of April 1, 2022) | LITESPARK-004 Belzutifan (N = 61) | |
|---|---|---|
Assessed by IRC | Assessed by investigators | |
For patients with VHL disease–associated nonmetastatic RCC | ||
TTS for RCC | ||
Number of patients contributing to the analysis | 61 | NR |
Number of patients who underwent a surgery, n (%) | 7 (11.5) | NR |
Median, months (95% CI) | NE (NE to NE) | NR |
PFS for RCC | ||
Number of patients contributing to the analysis | 61 | 61 |
Censored patients, n (%) | 50 (82.0) | 51 (83.6) |
Median, months (95% CI) | 39.2 (38.5 to NE) | NE (NE to NE) |
ORR (CR + PR) for RCC | ||
Number of patients contributing to the analysis | 61 | 61 |
n (%) [95% CI] | 39 (63.9) [50.6 to 75.8] | 37 (60.7) [47.3 to 72.9] |
DOR for RCC | ||
Number of patients contributing to the analysis | 39 | 37 |
Mean, months | 23.5 | 22.0 |
Median, months (95% CI) | NE (NE to NE) | NE (35.9 to NE) |
Minimum, months | 5.4+a | 2.6+ |
Maximum, months | 35.8+ | 38.7+ |
DCR (CR + PR + stable disease) for RCC | ||
Number of patients contributing to the analysis | 61 | 61 |
n (%) [95% CI] | 60 (98.4) [91.2 to 100.0] | 60 (98.4) [91.2 to 100.0] |
BOR for RCC | ||
Number of patients contributing to the analysis | 61 | 61 |
CR, n (%) | 4 (6.6) | 1 (1.6) |
PR, n (%) | 35 (57.4) | 36 (59.0) |
Stable disease, n (%) | 21 (34.4) | 23 (37.7) |
Progressive disease, n (%) | 0 (0) | 0 (0) |
NE, n (%) | 1 (1.6) | 1 (1.6) |
TTR for RCC | ||
Number of patients contributing to the analysis | 39 | 37 |
Mean (SD), months | 12.4 (8.1) | 13.5 (10.3) |
Median, months | 11.1 | 8.3 |
Minimum, months | 2.7 | 2.5 |
Maximum, months | 30.5 | 35.6 |
LGR — patient level for RCC | ||
LGR (mm/year) — Linear regression model BEFORE treatment with belzutifan | ||
Median (range) [number of patients] in all contributing patients | 3.5 (−3.1 to 33.1) [n = 57] | 3.4 (−2.9 to 12.8) [n = 60] |
Median (range) [number of patients] in patients with CR | 0.96 (−1.0 to 4.9) [n = 3] | 4.7 (4.7 to 4.7) [n = 1] |
Median (range) [number of patients] in patients with PR | 3.5 (−3.1 to 33.1) [n = 32] | 2.8 (−2.9 to 12.7) [n = 35] |
Median (range) [number of patients] in patients with stable disease | 3.5 (−0.5 to 8.9) [n = 21] | 3.6 (0.0 to 12.8) [n = 23] |
LGR (mm/year) — Linear regression model AFTER treatment with belzutifan | ||
Median (range) [number of patients] in all contributing patients | −2.9 (−7.6 to 10.1) [n = 55] | −2.2 (−9.1 to 2.5) [n = 58] |
Median (range) [number of patients] in patients with CR | −4.5 (−5.0 to −3.9) [n = 4] | −3.6 (−3.6 to −3.6) [n = 1] |
Median (range) [number of patients] in patients with PR | −3.8 (−7.6 to −0.9) [n = 35] | −2.8 (−9.1 to −0.6) [n = 36] |
Median (range) [number of patients] in patients with stable disease | −0.2 (−4.3 to 10.1) [n = 20] | −0.5 (−5.3 to 2.5) [n = 22] |
LGR — lesion level for RCC | ||
Median (range) [number of lesions] in all contributing lesions, mm/year — linear regression model BEFORE treatment with belzutifan | 3.3 (−3.1 to 50.2) [n = 110] | 2.3 (−18.2 to 25.3) [n = 127] |
Median (range) [number of lesions] in all contributing lesions, mm/year — linear regression model AFTER treatment with belzutifan | −3.4 (−11.6 to 10.1) [n = 105] | −2.0 (−15.4 to 6.8) [n = 132] |
Number of participants who developed metastatic RCC | ||
Number of patients contributing to the analysis | 61 | NA |
n (%) | 1 (1.6) | NA |
For patients with VHL disease–associated CNS hemangioblastoma | ||
TTS for CNS hemangioblastoma | ||
Number of patients contributing to the analysis | 51 | NR |
Number of patients who underwent a surgery, n (%) | 1 (2.0) | NR |
Median, months (95% CI) | NE (NE to NE) | NR |
PFS for CNS hemangioblastoma | ||
Number of patients contributing to the analysis | 50 | 51 |
Censored patients, n (%) | 39 (78.0) | 48 (94.1) |
Median (95% CI), months | NE (38.4 to NE) | NE (NE to NE) |
ORR (CR + PR) for CNS hemangioblastoma | ||
Number of patients contributing to the analysis | 50 | 51 |
n (%) [95% CI] | 22 (44.0) [30.0 to 58.7] | 18 (35.3) [22.4 to 49.9] |
DOR for CNS hemangioblastoma | ||
Number of patients contributing to the analysis | 22 | 18 |
Mean, months | 23.9 | 26.4 |
Median, months (95% CI) | NE (30.9 to NE) | 33.8 (33.8 to NE) |
Minimum, months | 3.7+ | 8.5+ |
Maximum, months | 38.7+ | 38.7+ |
DCR (CR + PR + stable disease) for CNS hemangioblastoma | ||
Number of patients contributing to the analysis | 50 | 51 |
n (%) [95% CI] | 45 (90.0) [78.2 to 96.7] | 50 (98.0) [89.6 to 100.0] |
BOR for CNS hemangioblastoma | ||
Number of patients contributing to the analysis | 50 | 51 |
CR, n (%) | 4 (8.0) | 4 (7.8) |
PR, n (%) | 18 (36.0) | 14 (27.5) |
Stable disease, n (%) | 23 (46.0) | 32 (62.7) |
Progressive disease, n (%) | 3 (6.0) | 0 (0) |
NE, n (%) | 2 (4.0) | 1 (2.0) |
TTR for CNS hemangioblastoma | ||
Number of patients contributing to the analysis | 22 | 18 |
Mean, months (SD) | 10.8 (10.98) | 7.5 (7.5) |
Median, months | 5.4 | 5.3 |
Minimum, months | 2.3 | 2.5 |
Maximum, months | 33.1 | 27.4 |
LGR — patient level for CNS hemangioblastoma | ||
LGR (mm/year) — Linear regression model BEFORE treatment with belzutifan | Only LGR after treatment initiation for CNS hemangioblastomas were analyzed as no pretreatment CNS scans were collected in the clinical database | |
LGR (mm/year) — Linear regression model AFTER treatment with belzutifan | ||
Median (range) [number of patients] in all contributing patients | −1.6 (−7.0 to 3.1) [N = 27] | NR |
Median (range) [number of patients] in patients with CR | −2.7 (−2.6 to −2.6) [n = 1] | NR |
Median (range) [number of patients] in patients with PR | −1.8 (−7.0 to −0.8) [n = 18] | NR |
Median (range) [number of patients] in patients with stable disease | −0.6 (−2.3 to 3.1) [n = 6] | NR |
For patients with VHL disease–associated nonmetastatic pNET | ||
TTS for pNET | ||
Number of patients contributing to the analysis | 22 | NR |
Number of patients who underwent a surgery, n (%) | 0 (0) | NR |
Median, months (95% CI) | NE (NE to NE) | NR |
PFS for pNET | ||
Number of patients contributing to the analysis | 22 | NR |
Censored patients, n (%) | 22 (100.0) | NR |
Median, months (95% CI) | NE (NE to NE) | NR |
ORR (CR + PR) for pNET | ||
Number of patients contributing to the analysis | 22 | NR |
n (%) [95% CI] | 20 (90.9) [70.8 to 98.9] | NR |
DOR for pNET | ||
Number of patients contributing to the analysis | 18 | NR |
Mean, months | 27.4 | NR |
Median, months (95% CI) | NE (NE to NE) | NR |
Minimum, months | 11.0+ | NR |
Maximum, months | 37.3+ | NR |
DCR (CR + PR + stable disease) for pNET | ||
Number of patients contributing to the analysis | 22 | NR |
n (%) [95% CI] | 22 (100.0) [84.6 to 100.0] | NR |
BOR for pNET | ||
Number of patients contributing to the analysis | 22 | NR |
CR, n (%) | 7 (31.8) | NR |
PR, n (%) | 13 (59.1) | NR |
Stable disease, n (%) | 2 (9.1) | NR |
Progressive disease, n (%) | 0 (0) | NR |
NE, n (%) | 0 (0) | NR |
TTR for pNET | ||
Number of patients contributing to the analysis | 20 | NR |
Mean, months (SD) | 8.2 (4.3) | NR |
Median, months | 8.2 | NR |
Minimum, months | 2.5 | NR |
Maximum, months | 16.4 | NR |
LGR — patient level for pNET | ||
LGR (mm/year) — Linear regression model BEFORE treatment with belzutifan | ||
Median (range) [number of patients] in all contributing patients | 1.2 (−7.4 to 7.7) [n = 19] | NR |
Median (range) [number of patients] in patients with CR | 1.3 (0.1 to 5.9) [n = 6] | NR |
Median (range) [number of patients] in patients with PR | 1.2 (−7.4 to 7.7) [n = 11] | NR |
Median (range) [number of patients] in patients with stable disease | 1.9 (−0.8 to 4.6) [n = 2] | NR |
LGR (mm/year) – Linear regression model AFTER treatment with belzutifan | ||
Median (range) [number of patients] in all contributing patients | −4.4 (−7.6 to −0.8) [n = 19] | NR |
Median (range) [number of patients] in patients with CR | −5.1 (−7.4 to −3.0) [n = 7] | NR |
Median (range) [number of patients] in patients with PR | −5.1 (−11.0 to −1.4) [n = 13] | NR |
Median (range) [number of patients] in patients with stable disease | −1.2 (−1.5 to −0.8) [n = 2] | NR |
LGR — lesion level for pNET | ||
Median (range) [number of lesions] in all contributing lesions, mm/year — linear regression model BEFORE treatment with belzutifan | 1.3 (−14.7 to 21.3) [n = 24] | NR |
Median (range) [number of lesions] in all contributing lesions, mm/year — linear regression model AFTER treatment with belzutifan | −4.2 (−7.9 to −0.8) [n = 24] | NR |
Number of patients who developed metastatic pNET | ||
Number of patients contributing to the analysis | 61 | NA |
Patients who developed metastatic pNET, n (%) | 0 (0) | NA |
BOR = best overall response; CI = confidence interval; CNS = central nervous system; CR = complete response; DCR = disease control rate; DOR = duration of response; LGR = linear growth rate; NA = not applicable; NE = not evaluable or not estimable; NR = not reported; ORR = objective response rate; PFS = progression-free survival; pNET = pancreatic neuroendocrine tumour; PR = partial response; RCC = renal cell carcinoma; SD = standard deviation; TTR = time to response; TTS = time to surgery.
aAccording to sponsor’s explanation, the “+” sign means that the objective response in the respective participant remained ongoing no progressive disease or death was reported at the time of data cut-off. For example, “5.4+” means that, at the data cut-off, the respective participant had been in response for 5.4 months and had not experienced disease progression or death.
Source: LITESPARK-004 Clinical Study Report.13
Figure 1: Kaplan-Meier Plot of TTS for VHL Disease–Associated Nonmetastatic RCC
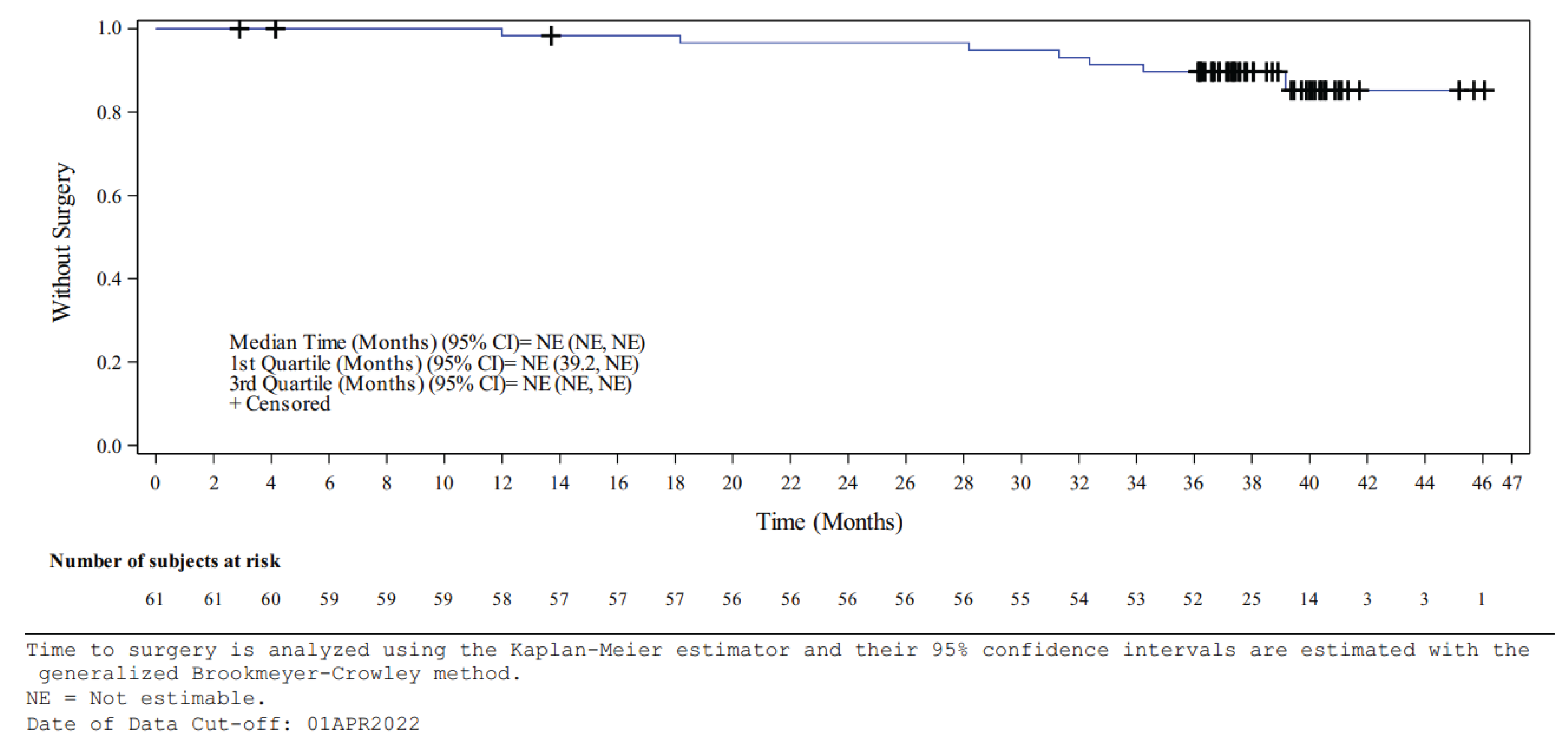
CI = confidence interval; NE = not evaluable or not estimable; RCC = renal cell carcinoma; TTS = time to surgery; VHL = von Hippel-Lindau.
Source: LITESPARK-004 Clinical Study Report.13
Progressive-Free Survival
The IRC-assessed median PFS was 39.2 months (95% CI, 38.5 to not evaluable) for patients with a VHL disease–associated nonmetastatic RCC, whereas the investigator-assessed median PFS was not reached. Median PFS was also not reached for patients with a VHL disease–associated CNS hemangioblastoma and those with a nonmetastatic pNET at the data cut-off date (April 1, 2022). Kaplan-Meier plots of PFS for patients with a VHL disease–associated nonmetastatic RCC, CNS hemangioblastoma, or nonmetastatic pNET assessed by IRC are in Figure 2, Figure 3, and Figure 4, respectively.
Details regarding the events and censoring of PFS are provided in Table 13. IRC-assessed results showed that, among 61 patients with RCC at baseline, 11 (18.0%) had PFS events (i.e., progressive disease, death), and 50 (82%) patients were censored, mostly due to no progression at the time of data cut-off or before the end of treatment (n = 43; 70.5%). Investigator-assessed results were similar to IRC-assessed results.
IRC-assessed results showed that, among 50 patients with CNS hemangioblastoma at baseline, 11 (22.0%) had PFS events (i.e., progressive disease or death), and 39 patients (78%) were censored (among which 34 [68%] were due to no progression at the time of data cut-off). However, the investigator-assessed results found that, out of 51 patients with CNS hemangioblastoma at baseline, 48 patients (94.1%) were censored, among which 46 (90.2%) were due to no progression at the time of data cut-off.
All 22 patients with pNET were censored due to no progression at the time of data cut-off.
Figure 2: Kaplan-Meier Plot of PFS for VHL-Associated Nonmetastatic RCC — IRC Assessed
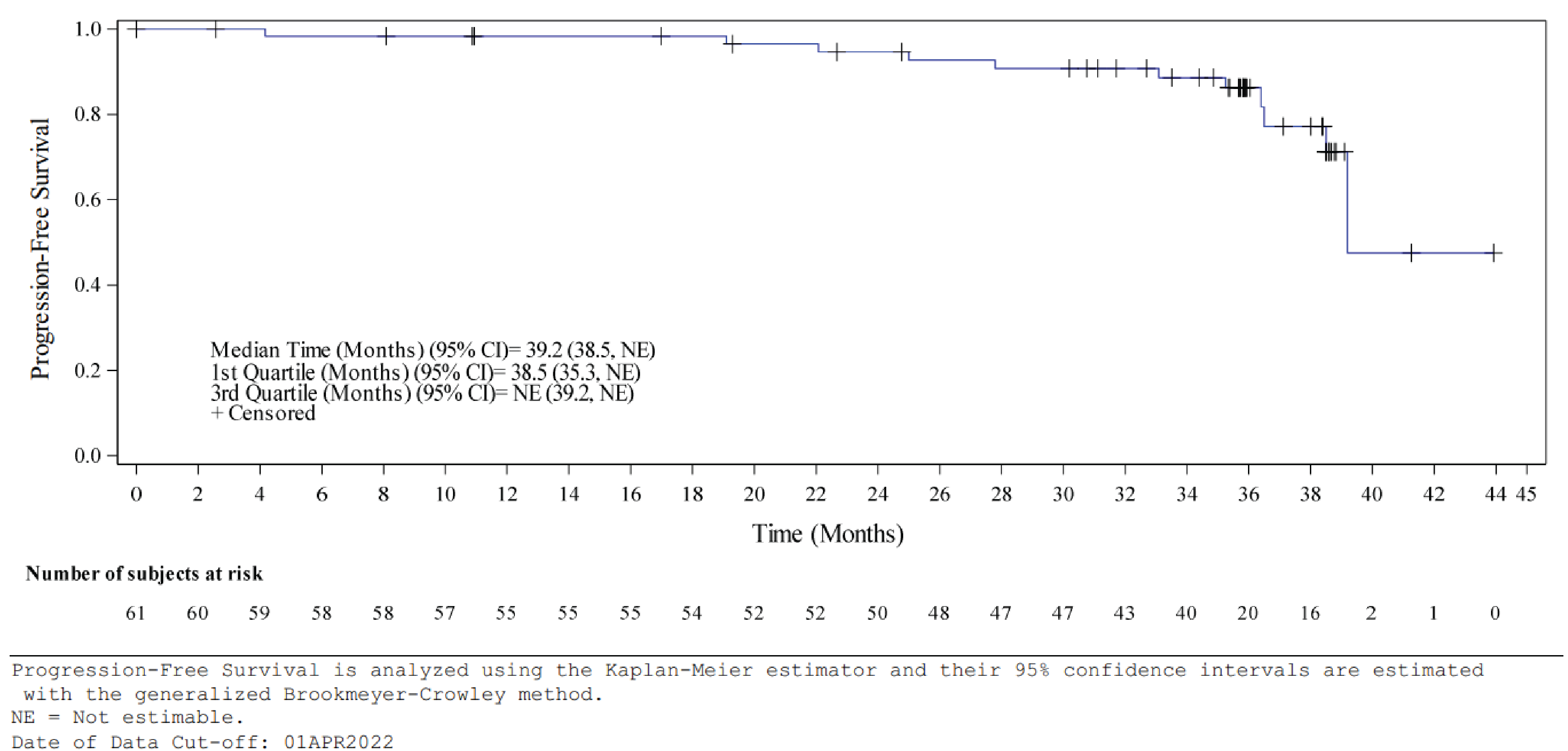
CI = confidence interval; NE = not evaluable or not estimable; IRC = independent review committee; PFS = progression-free survival; RCC = renal cell carcinoma; VHL = von Hippel-Lindau.
Source: LITESPARK-004 Clinical Study Report.13
Objective Response Rate
As of the data cut-off date of April 1, 2022, with a median follow-up of 37.7 months, the IRC-assessed percentage of patients who had a CR or PR to belzutifan was 63.9% (39 of 61) among those with a VHL-associated nonmetastatic RCC, 44% (22 of 50) among those with a VHL-associated CNS hemangioblastoma, and 90.9% (20 of 22) among those with a VHL-associated nonmetastatic pNET (Table 12). IRC- and investigator-assessed ORRs were consistent among patients with a nonmetastatic RCC or a CNS hemangioblastoma.
Figure 3: Kaplan-Meier Plot of PFS for VHL-Associated CNS Hemangioblastoma — IRC Assessed
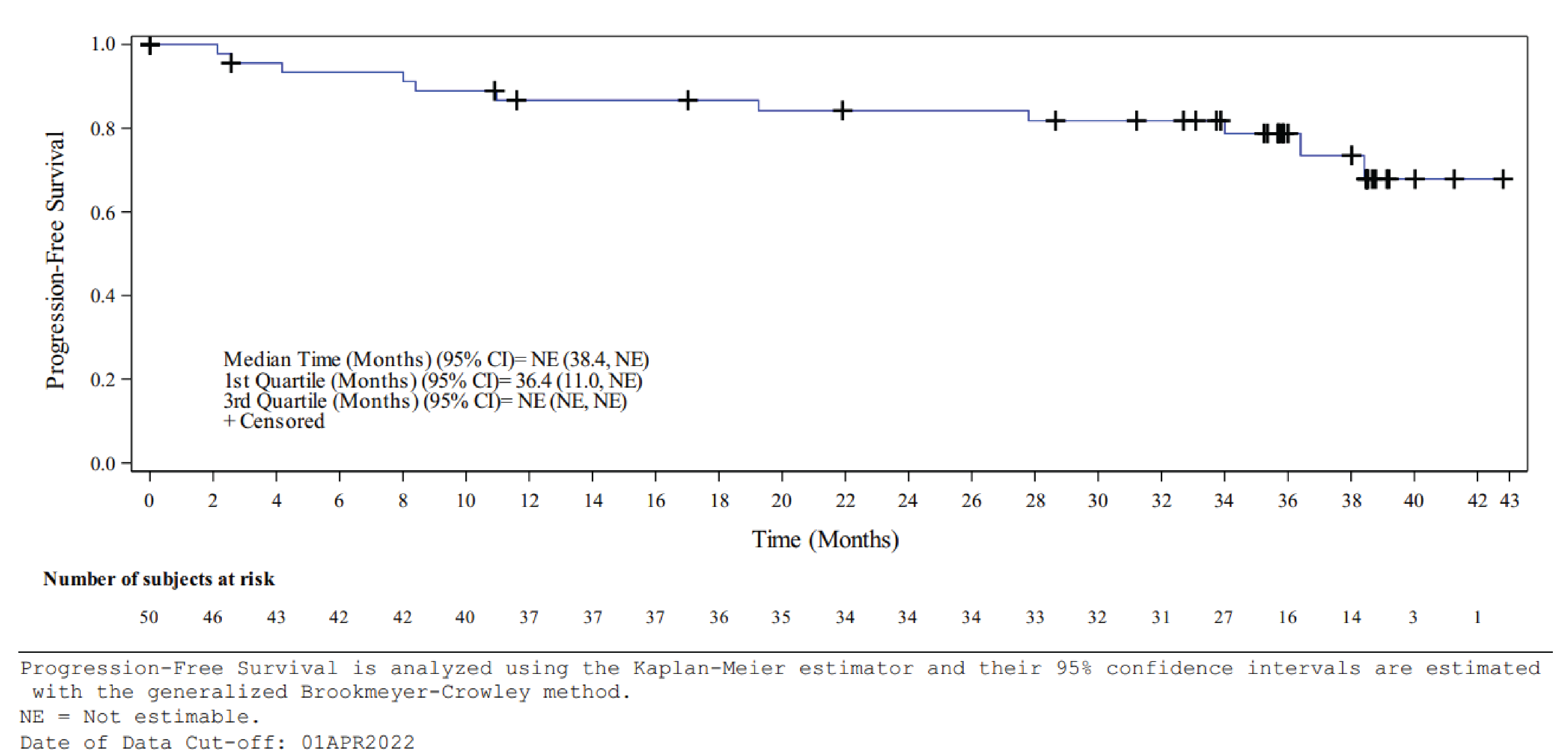
CNS = central nervous system; CI = confidence interval; NE = not evaluable or not estimable; IRC = independent review committee; PFS = progression-free survival; VHL = von Hippel-Lindau.
Source: LITESPARK-004 Clinical Study Report.13
Figure 4: Kaplan-Meier Plot of PFS for VHL-Associated Nonmetastatic pNET — IRC Assessed
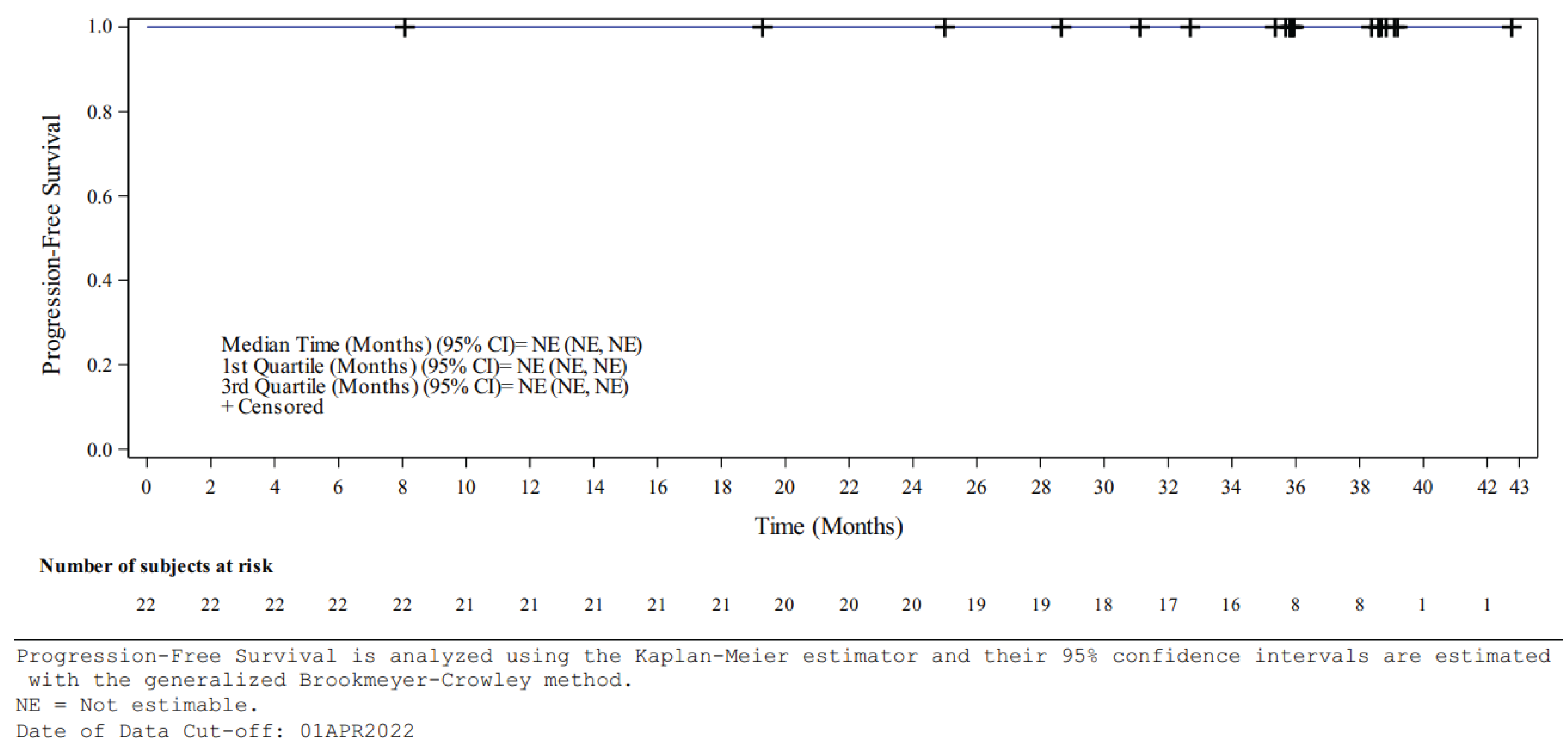
CI = confidence interval; NE = not evaluable or not estimable; IRC = independent review committee; PFS = progression-free survival; pNET = pancreatic neuroendocrine tumour; VHL = von Hippel-Lindau.
Source: LITESPARK-004 Clinical Study Report.13
Duration of Response
The investigator-assessed median DOR for patients with VHL-associated CNS hemangioblastoma (the only estimable DOR) was 33.8 months (95% CI, 33.8 to not evaluable). The IRC-assessed median DOR was not reached for responders with a VHL disease–associated nonmetastatic RCC, CNS hemangioblastoma, or nonmetastatic pNET at the data cut-off date of April 1, 2022. For patients with an RCC, 74.4% (29 of 39) of responders had a DOR of at least 18 months, 56.4% (22 of 39) had a DOR of at least 24 months, and 25.6% (10 of 39) had a DOR of at least 30 months. For patients with CNS hemangioblastoma, 63.6% (14 of 22) of responders had a DOR of at least 18 months, 59.1% (13 of 22) had a DOR of at least 24 months, and 54.5% (12 of 22) had a DOR of at least 30 months. For patients with pNET, 95.0% (19 of 20) of responders had a DOR of at least 18 months, 75.0% (15 of 20) had a DOR of at least 24 months, and 40.0% (8 of 20) had a DOR of at least 30 months.
Table 13: Details on Events and Censoring of PFS
Detail on events and censoring | LITESPARK-004 Belzutifan | |
|---|---|---|
Assessed by IRC | Assessed by investigators | |
For patients with VHL-associated nonmetastatic RCC | ||
Number of patients with RCC at baseline | 61 | 61 |
Events in patients with RCC, n (%) | 11 (18.0) | 10 (16.4) |
Progression of disease | 9 (14.8) | 8 (13.1) |
Death | 2 (3.3) | 2 (3.3) |
Censored patients with RCC, n (%) | 50 (82.0) | 51 (83.6) |
New anticancer therapy initiated | 5 (8.2) | 3 (4.9) |
No baseline or postbaseline tumour assessment | 1 (1.6) | 1 (1.6) |
Death or progression after more than 1 missed assessments | 1 (1.6) | 0 |
No progression at the time of data cut-off or before end of treatment | 43 (70.5) | 47 (77.0) |
For patients with VHL-associated CNS hemangioblastoma | ||
Number of patients with CNS hemangioblastoma at baseline | 50 | 51 |
Events in patients with CNS hemangioblastoma, n (%) | 11 (22.0) | 3 (5.9) |
Progression of disease | 9 (18.0) | 1 (2.0) |
Death | 2 (4.0) | 2 (3.9) |
Censored patients with CNS hemangioblastoma, n (%) | 39 (78.0) | 48 (94.1) |
New anticancer therapy initiated | 1 (2.0) | 1 (2.0) |
No baseline or postbaseline tumour assessment | 2 (4.0) | 1 (2.0) |
Death or progression after more than 1 missed assessments | 2 (4.0) | 0 |
No progression at the time of data cut-off or before end of treatment | 34 (68.0) | 46 (90.2) |
For patients with VHL-associated nonmetastatic pNET | ||
Number of patients with pNET at baseline | 22 | NR |
Events in patients with pNET, n (n/N%) | 0 | NR |
Progression of disease | 0 | NR |
Death | 0 | NR |
Censored patients with CNS pNET, n (%) | 22 (100.0) | NR |
New anticancer therapy initiated | 0 | NR |
No baseline or postbaseline tumour assessment | 0 | NR |
Death or progression after more than 1 missed assessments | 0 | NR |
No progression at time of data cut-off or before end of treatment | 22 (100.0) | NR |
CNS = central nervous system; NR = not reported; PFS = progression-free survival; pNET = pancreatic neuroendocrine tumour; RCC = renal cell carcinoma; VHL = von Hippel-Lindau.
Source: LITESPARK-004 Clinical Study Report.13
Kaplan-Meier plots of DOR for patients with a VHL disease–associated nonmetastatic RCC, CNS hemangioblastoma, or nonmetastatic pNET assessed by IRC are provided in Figure 5, Figure 6, and Figure 7, respectively.
Details regarding the events and censoring of DOR are provided in Table 14. Among 39 RCC patients with a confirmed response, 32 (82.1%) were censored due to no progression at the time of data cut-off or before end of treatment. Out of 22 patients with CNS hemangioblastoma who showed a confirmed response, 17 were censored due to no progression at the time of data cut-off or before the end of treatment. All 20 patients with a pNET who had a confirmed response were censored due to no progression at the time of data cut-off.
Disease Control Rate
As of the data cut-off date of April 1, 2022, the IRC-assessed percentages of patients who had a CR, PR, or stable disease were 98.4% (60 of 61) among those with a VHL-associated nonmetastatic RCC, 90% (45 of 50) among those with a VHL-associated CNS hemangioblastomas, and 100% (22 of 22) among those with a VHL-associated nonmetastatic pNET (Table 12). Similar percentages were found between IRC- and investigator-assessed DCRs among patients with a nonmetastatic RCC or a CNS hemangioblastoma.
Best Overall Response
As of the data cut-off date of April 1, 2022, the IRC-assessed percentages of patients with a VHL disease–associated nonmetastatic RCC who had a CR, PR, stable disease, progressive disease, or not evaluable while taking belzutifan were 6.6% (4 of 61), 57.4% (35 of 61), 34.4% (21 of 61), 0% (0 of 61), and 1.6% (1 of 61), respectively. IRC- and investigator-assessed BORs were consistent.
Figure 5: Kaplan-Meier Plot of DOR for VHL-Associated Nonmetastatic RCC — IRC Assessed
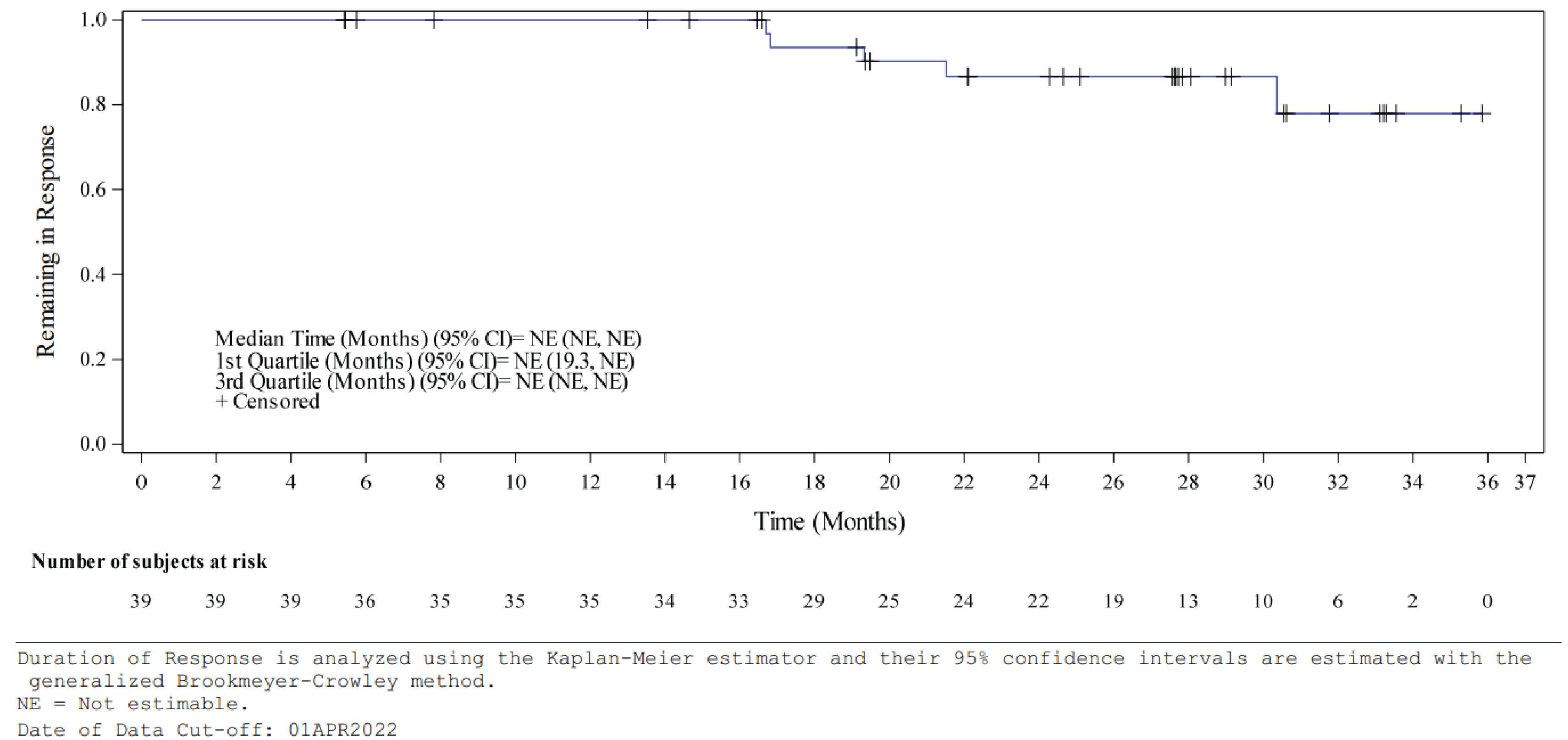
CI = confidence interval; DOR = duration of response; NE = not evaluable or not estimable; IRC = independent review committee; RCC = renal cell carcinoma; VHL = von Hippel-Lindau.
Source: LITESPARK-004 Clinical Study Report.13
Figure 6: Kaplan-Meier Plot of DOR for VHL-Associated CNS Hemangioblastoma — IRC Assessed
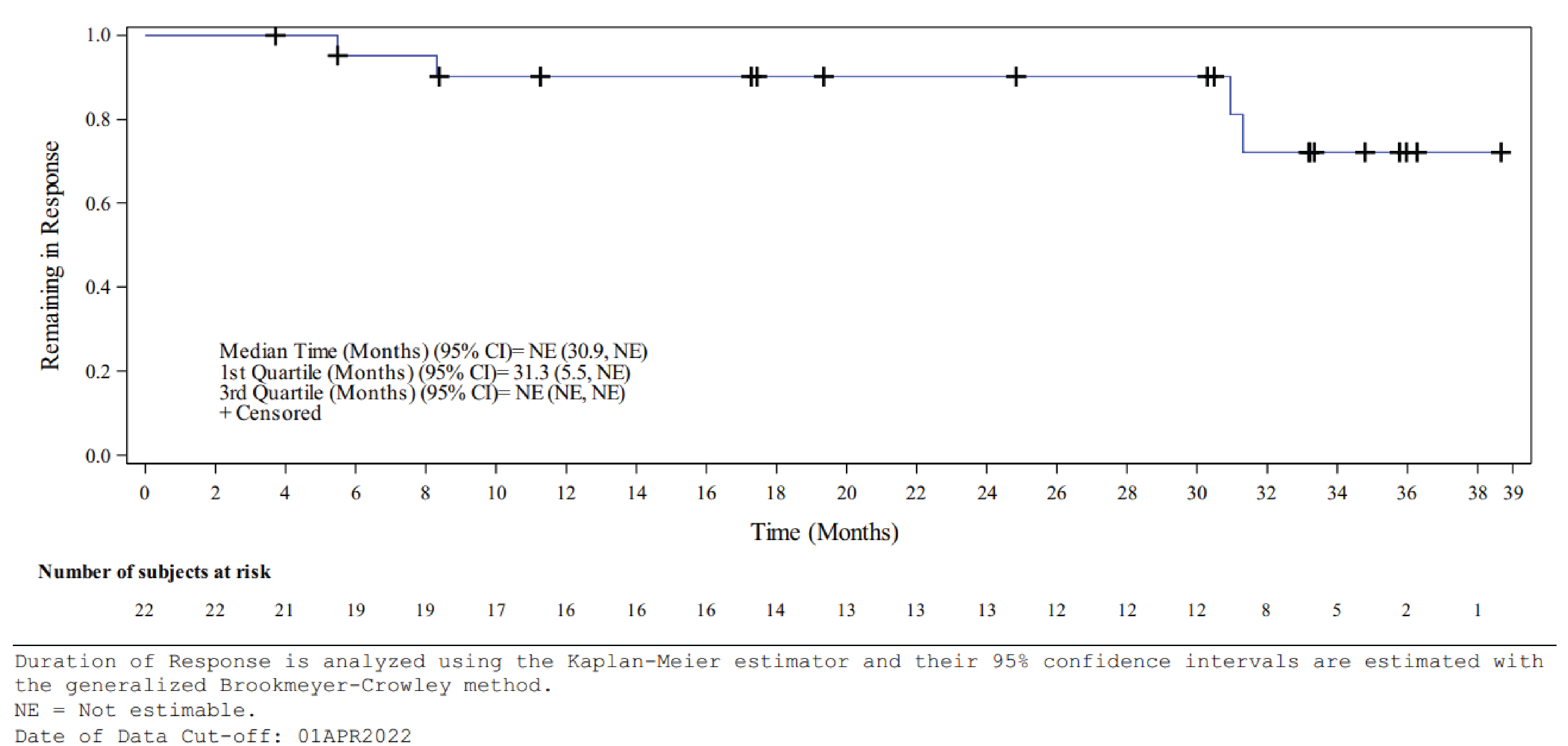
CNS = central nervous system; CI = confidence interval; DOR = duration of response; NE = not evaluable or not estimable; IRC = independent review committee; VHL = von Hippel-Lindau.
Source: LITESPARK-004 Clinical Study Report.13
Figure 7: Kaplan-Meier Plot of DOR for VHL Disease Nonmetastatic pNET — IRC Assessed
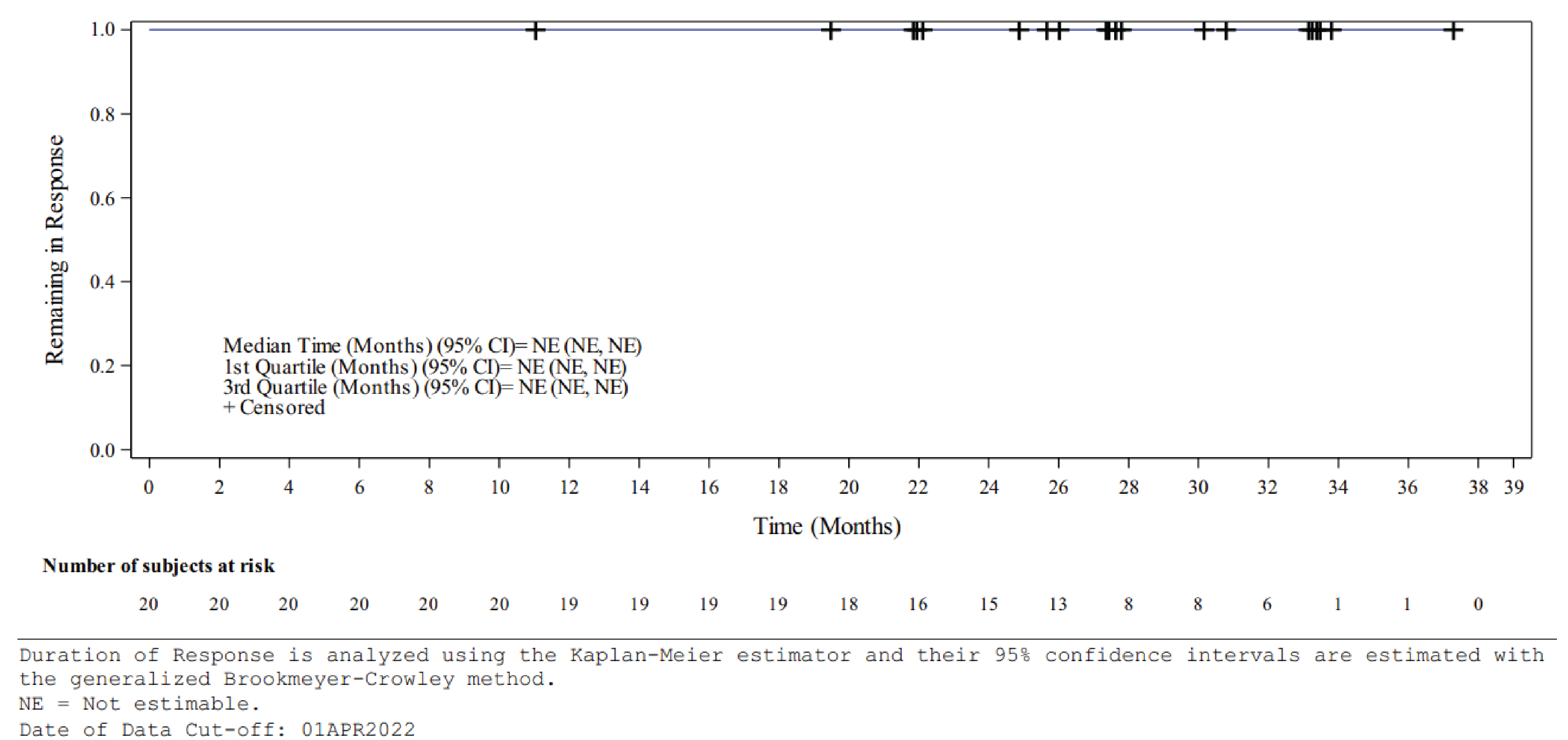
CI = confidence interval; DOR = duration of response; NE = not evaluable or not estimable; IRC = independent review committee; pNET = pancreatic neuroendocrine tumour; VHL = von Hippel-Lindau.
Source: LITESPARK-004 Clinical Study Report.13
Table 14: Details on Events and Censoring of Duration of Response
Events and censoring description of duration of response | LITESPARK-004 Belzutifan |
|---|---|
Assessed by IRC | |
For patients with VHL-associated nonmetastatic RCC | |
Number of patients with confirmed response | 39 |
Events in patients with RCC, n (%) | 5 (12.8) |
Progression of disease | 4 (10.3) |
Death | 1 (2.6) |
Censored patients with RCC, n (%) | 34 (87.2) |
New anticancer therapy initiated | 1 (2.6) |
Death or progression after more than 1 missed assessments | 1 (2.6) |
No progression at the time of data cut-off or before end of treatment | 32 (82.1) |
For patients with VHL-associated CNS hemangioblastoma | |
Number of patients with confirmed response | 22 |
Events in patients with CNS hemangioblastoma, n (%) | 4 (18.2) |
Progression of disease | 3 (13.6) |
Death | 1 (4.5) |
Censored patients with CNS hemangioblastoma, n (%) | 18 (81.8) |
Death or progression after more than 1 missed assessments | 1 (4.5) |
No progression at the time of data cut-off or before end of treatment | 17 (77.3) |
For patients with VHL-associated nonmetastatic pNET | |
Number of patients with confirmed response | 20 |
Events in patients with pNET, n (n/N%) | 0 |
Progression of disease | 0 |
Death | 0 |
Censored patients with CNS pNET, n (%) | 20 (100.0) |
No progression at the time of data cut-off or before end of treatment | 20 (100.0) |
CNS = central nervous system; DOR = duration of response; IRC = independent review committee: pNET = pancreatic neuroendocrine tumour; RCC = renal cell carcinoma; VHL = von Hippel-Lindau.
Source: LITESPARK-004 Clinical Study Report.13
The IRC-assessed percentages of patients with a VHL disease–associated CNS hemangioblastoma who had a CR, PR, stable disease, progressive disease, or not evaluable while taking belzutifan were 8% (4 of 50), 36% (18 of 50), 46% (23 of 50), 6% (3 of 50), and 4% (2 of 50), respectively. Investigator-assessed BORs were higher in patients with stable disease compared with IRC-assessed BORs (62.7% [32 of 50] versus 46% [23 of 50]).
The IRC-assessed percentages of patients with a VHL disease–associated nonmetastatic pNET who had a CR, PR, stable disease, progressive disease, or not evaluable while taking belzutifan were 31.8% (7 of 22), 59.1% (13 of 22), 9.1% (2 of 22), 0% (0 of 22), and 0% (0 of 22), respectively (Table 12).
Time to Response
As of the data cut-off date of April 1, 2022, the IRC-assessed median TTRs were 11.1 months (range = 2.7 to 30.5) among those with a VHL-associated nonmetastatic RCC, 5.4 months (range = 2.3 to 33.1) among those with a VHL-associated CNS hemangioblastomas, and 8.2 months (range = 2.5 to 16.4) among those with a VHL-associated nonmetastatic pNET (Table 12). IRC- and investigator-assessed TTRs were similar among patients with a nonmetastatic RCC or CNS hemangioblastoma.
Linear Growth Rate
The IRC-assessed LGR at both the patient and lesion levels showed a decrease in lesion LGR from before to after treatment with belzutifan in patients with a VHL-associated nonmetastatic RCC and in those with a pNET. Only LGRs after treatment with belzutifan were analyzed for patients with a VHL-associated CNS hemangioblastomas as no pretreatment CNS scans were collected in the LITESPARK-004 trial (Table 12).
Number of Patients who Developed Metastases
As of the data cut-off date of April 1, 2022, only 1 patient (1.6%) developed a metastatic RCC, while none of the patients with a VHL-associated nonmetastatic pNET developed metastatic disease.
Distribution of All Tumour–Reduction Procedures Before and After Treatment Initiation
As of the data cut-off date of April 1, 2022, fewer surgeries or tumour-reduction procedures occurred after patients received belzutifan treatment compared to the same period immediately before treatment initiation (Figure 8): 11 surgeries (7 renal, 2 CNS, and 2 retinal) were performed in 9 patients, whereas 73 surgeries in 44 patients had been performed in the 3 years before initiation of belzutifan treatment.
Figure 8: Distribution of All Tumour–Reduction Procedures Before and After Treatment Initiation for Individual Patients (Safety Analysis Set)
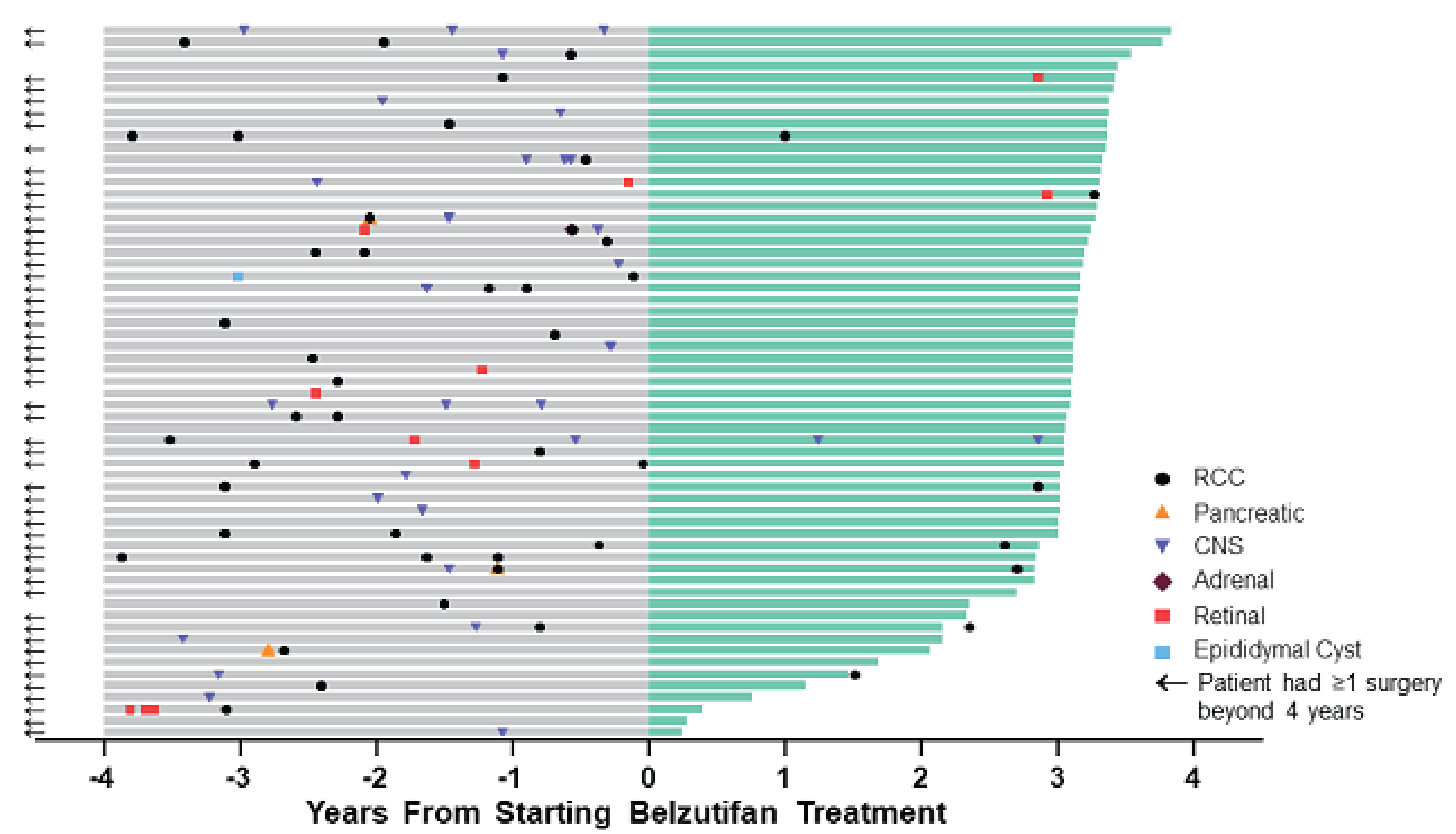
CNS = central nervous system; RCC = renal cell carcinoma.
Notes: Procedures included adrenalectomy, craniotomy, cryoablation, cryotherapy, eye removal, intradural resection, laser ablation, laser surgery, laminectomy, laser photocoagulation, pancreatectomy, partial nephrectomy, radiofrequency ablation retinal surgery, total nephrectomy, tumour enucleation, and ventriculoperitoneal shunt placement. Two patients did not undergo tumour resection procedures at any time before entering the study or while enrolled in the study. The 2 CNS surgical procedures reported after belzutifan initiation were in the same patient; 1 patient underwent radiation therapy but was not included in this figure.
Source: LITESPARK-004 Clinical Study Report.14
Harms
A summary of harms in the LITESPARK-004 trial (data cut-off date: April 1, 2022) is shown in Table 15.
Table 15: Summary of Harms — Pivotal and RCT Evidence
Adverse events | LITESPARK-004 Belzutifan |
|---|---|
Any grade (N = 61) | |
Treatment-emergent adverse event, n (%) | |
Patients with ≥ 1 treatment-emergent adverse event | 61 (100.0) |
Anemia | 55 (90.2) |
Fatigue | 45 (73.8) |
Headache | 29 (47.5) |
Dizziness | 28 (45.9) |
Nausea | 24 (39.3) |
Dyspnea | 16 (26.2) |
Myalgia | 15 (24.6) |
Constipation | 14 (23.0) |
Arthralgia | 13 (21.3) |
Vision blurred | 13 (21.3) |
Abdominal pain | 12 (19.7) |
Increased alanine transaminase | 12 (19.7) |
Back pain | 11 (18.0) |
Diarrhea | 11 (18.0) |
Upper respiratory tract infection | 11 (18.0) |
Weight increase | 10 (16.4) |
Hypertension | 9 (14.8) |
Insomnia | 9 (14.8) |
Peripheral edema | 9 (14.8) |
COVID-19 | 8 (13.1) |
Disturbance in attention | 8 (13.1) |
Urinary tract infection | 8 (13.1) |
Anxiety | 7 (11.5) |
Increased aspartate transaminase | 7 (11.5) |
Increased blood creatinine | 7 (11.5) |
Cough | 7 (11.5) |
Muscle spasms | 7 (11.5) |
Vomiting | 7 (11.5) |
Serious adverse event, n (%) | |
Patients with ≥ 1 serious adverse event | 18 (29.5) |
Embolism | 2 (3.3) |
Intracranial hemorrhage | 2 (3.3) |
Abdominal pain | 1 (1.6) |
Anemia | 1 (1.6) |
Anaphylactic reaction | 1 (1.6) |
COVID-19 | 1 (1.6) |
COVID-19 pneumonia | 1 (1.6) |
Cholecystectomy | 1 (1.6) |
Coronary artery dissection | 1 (1.6) |
Cystitis | 1 (1.6) |
Dyspnea | 1 (1.6) |
Hypertension | 1 (1.6) |
Hypotension | 1 (1.6) |
Hypoxia | 1 (1.6) |
Non–small cell lung cancer | 1 (1.6) |
Pneumonia | 1 (1.6) |
Death, n (%) | |
Patients who died | 2 (3) |
Acute toxic effects of fentanyl | 1 (1.6) |
Suicide | 1 (1.6) |
Withdrawal due to adverse events, n (%) | |
Patients who discontinued treatment due to adverse events | 4 (6.6) |
Dizziness | 1 (1.6) |
Intracranial hemorrhage | 1 (1.6) |
Toxicity to various agents | 1 (1.6) |
Suicide attempt | 1 (1.6) |
Adverse events of clinical interest | |
Anemia | |
Number of patients who had anemia, n (%) | 55 (90.2) |
Total number of episodes of anemia, n | 229 |
Average number of episodes of anemia per patient | 4.2 |
Treatment for patients who had anemia, n (%) | |
Not treated with concomitant medications/procedures | 36 (65.5) |
Erythropoiesis-stimulating drug only | 9 (16.4) |
Blood transfusion only | 1 (1.8) |
Both erythropoiesis-stimulating drug and blood transfusion | 5 (9.1) |
Iron supplement | 11 (20.0) |
Other | 2 (3.6) |
Hypoxia, n (%) | 1 (1.6) |
Second primary malignancies, n (%) [type] | 2 (3.3) [1 vulval cancer and 1 non–small cell lung cancer] |
Hepatic Safety | |
Number of participants who met the criteriaa for drug-induced liver injury, n (%) | 0 (0) |
aCriteria for drug-induced liver injury: alanine transaminase or aspartate transaminase 3 or more times the upper limit of normal range, and bilirubin 2 or more times the upper limit of normal range, and alkaline phosphatase less than twice the upper limit of normal range.
Source: LITESPARK-004 Clinical Study Report.13
Adverse Events
TEAEs were reported in all 61 patients (100%) in the LITESPARK-004 trial. The most commonly reported TEAE was anemia (90.2%), followed by fatigue (73.8%), headaches (47.5%), dizziness (45.9%), and nausea (39.3%). Other TEAEs that were reported in more than 20% of the study participants included dyspnea (26.2%), myalgia (24.6%), constipation (23.0%), arthralgia (21.3%), and blurred vision (20.3%).
Serious Adverse Events
SAEs were reported in 18 patients (29.3%). The most common SAEs were embolism (3.3%) and intracranial hemorrhage (3.3%).
Mortality
Two patients died during the study due to acute toxic effects of fentanyl (n = 1) and suicide (n = 1).
Withdrawal due to Adverse Events
Treatment discontinuation due to TEAE was reported in 4 patients, of which 2 (dizziness and intracranial hemorrhage) were considered drug-related.
Notable Harms
As of April 1, 2022, 90.2% (55 of 61) patients had 229 episodes of anemia. The average number of episodes of anemia for each patient was 4.2.
One patient (1.6%) developed hypoxia. Two patients (3.3%) developed secondary primary malignancies, 1 of whom had vulval cancer and 1 non–small cell lung cancer. None of the patients had drug-induced liver injury.
Critical Appraisal
Pivotal Evidence
Internal Validity
The LITESPARK-004 trial, the only eligible study identified from the sponsor-conducted SLR, was a phase II, single-arm, open-label clinical trial that enrolled a small number of patients (N = 61). Given the rarity of VHL disease and that active surveillance is the current standard of care for patients with VHL-associated nonmetastatic tumours, the single-arm trial design and small sample size were considered adequate from the regulatory perspective to assess the efficacy and safety of belzutifan. No serious concerns were identified in the conduct of the LITESPARK-004 trial, including protocol amendments and protocol deviations. However, the absence of an internal comparison group in the single-arm LITESPARK-004 trial is a key limitation that increases the uncertainty of the findings from the pivotal study. The lack of comparative data means that causal inferences about the efficacy and safety of belzutifan cannot be established with certainty.
As consecutive enrolment of eligible patients was not mentioned, it is unclear whether all eligible patients would have been entered into the trial, or whether selection may have been biased to include patients who were most likely to benefit. However, the clinical experts consulted by CADTH indicated that the patient population appeared to be representative of what they would expect to see in clinical practice. Almost all patients used concomitant treatments during the trial, but these were not expected to affect the reported efficacy results.
The LITESPARK-004 trial explicitly defined the hypothesis, which was a null hypothesis of an ORR of 15% or lower with an alternate hypothesis of an ORR of 30% or higher. These thresholds were considered clinically meaningful by the clinical experts consulted by CADTH. The selection of ORR (defined as sum of CR and PR as defined by RECIST 1.1) as a key efficacy end point was appropriate for the single-arm monotherapy trial design because the ORR, when defined in this manner, is generally viewed as a direct measure of antitumour activity as well as an objective and clinically relevant end point. The LITESPARK-004 trial also assessed DOR to provide evidence on the durability of tumour response (i.e., the durability of CR or PR), which is an important end point in single-arm trials in oncology.14 DCR was not a protocol-specified end point but was reported in the LITESPARK-004 Clinical Study Report, with the sponsor noting the importance of considering stable disease a potential response. However, the clinical experts consulted by CADTH also noted that tumours do not grow at a steady rate, and periods of stability might be expected as part of the natural history of the disease.
In addition to DOR, the LITESPARK-004 trial employed other time-to-event end points (TTS and PFS) to address the potential limitations of ORR (i.e., ORR does not always capture the effects of a treatment on patient survival and may not always correlate with symptoms or function).14 The clinical experts consulted by CADTH considered these the most important outcomes to assess the efficacy of belzutifan. Generally speaking, RCTs are preferred over single-arm studies for time-to-event end points such as PFS due to their sensitivity to baseline differences in patient, disease, and other clinical characteristics, and interpreting results without a randomized reference can be problematic.14-16 In the context of the LITESPARK-004 trial, medians of most of the time-to-event data were not reached, but reasons for censoring appeared to support the efficacy of belzutifan, primarily due to the lack of progression at the time of the data cut-off.
The LITESPARK-004 trial involved outcomes pre- and posttreatment with belzutifan (i.e., change in LGR) to demonstrate the efficacy of belzutifan. However, without formal statistical analysis, the role of chance could not be ruled out, despite the presence of a trend in which the growth of tumours was decreasing after treatment with belzutifan. With respect to outcome measurement, in addition to study investigators, an IRC was also involved to assess radiographic outcomes to reduce the risk of bias in measurements of the outcome for most of the efficacy end points in patients with a VHL-associated nonmetastatic RCC and those with a VHL-associated CNS hemangioblastoma.
External Validity
All participants in the LITESPARK-004 trial were required to have at least 1 RCC. The LITESPARK-004 trial therefore may not reflect results for participants with only a CNS hemangioblastoma and/or pNET. However, the clinical experts consulted by CADTH did not consider this a serious generalizability issue, and they indicated that results from the pivotal trial could still be extrapolated to VHL patients with CNS hemangioblastoma and/or nonmetastatic pNET.
According to the clinical experts consulted by CADTH, the inclusion and exclusion criteria of the LITESPARK-004 trial in general were aligned with selection criteria in the Canadian settings when identifying suitable candidates for belzutifan. However, the clinical experts noted that the requirement for patients with an ECOG PS of 0 or 1 might not be necessary in clinical practice to initiate belzutifan because ECOG PS can be unstable and subjective. The clinical experts indicated that a clinician may determine that a patient with an ECOG PS greater than 1 could benefit from belzutifan and prescribe belzutifan.
There were no study sites in Canada as the LITESPARK-004 trial was conducted in Denmark, France, the UK, and the US. More than 90% of the patients in LITESPARK-004 were white, which does not reflect the racial profile in the Canadian patient population; given the rarity of the disease, it is unclear whether this might affect the natural history or response to treatment. The dosing and administration of belzutifan in LITESPARK-004 were consistent with the product monograph. The clinical experts described the concomitant medications and procedures in the LITESPARK-004 trial as appropriate and commonly used in the Canadian settings. The outcomes of TTS, PFS, ORR, and DOR are commonly used in clinical trials of anticancer therapies and relevant to clinical practice, according to the clinical experts. However, LGR is not commonly adopted in clinical practice. The clinical expert specializing in CNS hemangioblastoma noted that, in clinical practice, RANO criteria are used instead of RECIST 1.1 to assess tumour response in patients with CNS hemangioblastoma. The LITESPARK-004 trial did not include some outcomes important to patients, such as symptoms and HRQoL.
Overall survival, which is usually viewed as the most reliable and preferred end point in oncology trials,14 was not used as an end point in the LITESPARK-004 trial. The clinical experts consulted by CADTH commented that the absence of overall survival data was acceptable given that overall survival might not be a feasible outcome in this patient population and indication because death due to VHL disease could take years to occur and that overall survival could be confounded by multiple lines of therapy. The clinical experts also pointed out that TTS and PFS are more clinically important to VHL patients with nonmetastatic disease given that delaying morbid local therapies (e.g., surgery, radiation) was a main treatment goal.
The median length of follow-up in the LITESPARK-004 trial was 37.7 months, which was adequate to observe response, but a longer follow-up would be needed to understand the full extent of the efficacy of belzutifan on time-to-event outcomes. The clinical experts consulted by CADTH noted that this length of follow-up would be adequate to capture adverse effects. However, given that the life expectancy of patients with VHL could be very long (e.g., a recent study suggested over 60 years37) and the draft product monograph recommends that treatment should continue until disease progression or unacceptable toxicity occurs, a median of 37.7 months might not be long enough to determine the long-term effects of treatment with belzutifan. In addition, the long-term effects following treatment discontinuation (e.g., due to patient preference with stable disease, need for surgery) are unknown.
Indirect Evidence
Contents within this section have been informed by materials submitted by the sponsor. The following have been summarized and validated by the CADTH review team.
Objectives for the Summary of Indirect Evidence
The pivotal evidence submitted by the sponsor was a single-arm trial38 and therefore does not provide evidence of efficacy compared to active surveillance in the Canadian health care setting. The sponsor identified no published evidence for the efficacy of the standard active surveillance therapeutic approach used in the Canadian setting that could be used for an indirect comparison with the belzutifan efficacy outcomes assessed in the LITESPARK-004 trial. The sponsor therefore conducted the VHL Natural History Study39 and submitted an ITC to supplement the lack of comparative evidence of belzutifan for the treatment of adult patients with VHL disease.40 The sponsor noted that a MAIC was chosen, rather than other potentially relevant approaches, because the external research group conducting the ITC had access to individual patient data from the comparator study but not from the LITESPARK-004 trial.
Description of Indirect Comparison — MAIC
The submitted ITC compared the VHL Natural History Study,39 a real-world, retrospective, noninterventional cohort study of existing medical records of VHL patients managed and treated at the NCI in the US or Canada, to the pivotal trial cohort from the LITESPARK-004 trial. The Studies Addressing Gaps in the Pivotal and RCT Evidence section of this report provides additional details on the VHL Natural History Study. Patients in the VHL Natural History Study cohort were reweighted to match the distribution of key baseline characteristics among patients in the LITESPARK-004 trial and compared using a MAIC.41 The comparative treatment was active surveillance, defined as enrolment into the database. The primary (and only) outcome of interest was time to RCC-related surgery.
Objectives
The objective of the ITC was to estimate the comparative treatment effect between belzutifan and active surveillance on the rate of RCC surgery in participants with VHL disease–associated tumours using a MAIC.40
Study Selection Methods
A targeted literature review conducted by the sponsor did not identify any published study that could be used to generate comparator data that would provide a benchmark against the results of the LITESPARK-004 trial in the ITC. Due to this gap in evidence, the VHL Natural History Study was conducted, and unpublished data from this study were used in the MAIC. After the initiation of the Natural History Study, an SLR with a search date of June 2022 was conducted by the sponsor. This SLR confirmed the finding of the targeted literature search conducted before the Natural History Study. There is no indication about how data were extracted for use in the MAIC, and no risk-of-bias assessment of the Natural History Study was performed.
Indirect Treatment Comparison Analysis Methods
The population considered for LITESPARK-004 was the efficacy analysis set, which included all participants who met the eligibility criteria and received at least 1 dose of the study intervention. The VHL Natural History Study cohort consisted of patients with nonmetastatic VHL disease from the US or Canada and treated at the NCI with at least 1 solid renal tumour and available measurement(s) during the study period (July 31, 2004, to June 30, 2020). The eligibility criteria described in Table 16 were applied to the VHL Natural History Study in attempt to match the selection criteria more closely to those of the LITESPARK-004 trial. Most inclusion and exclusion criteria overlapped between cohorts, namely, inclusion criteria based on age, VHL diagnosis, RCC tumour, and exclusion criteria based on prior anticancer therapy, metastatic disease progression, immediate prior surgery, or prior HIF-2-alpha inhibitor use. Several criteria in the Natural History Study cohort are approximate to those of the pivotal trial due to insufficient access to information within the database. For example, the Natural History Study cohort excluded patients who had surgery within 60 days of the index date to align with the LITESPARK-004 criteria to only include RCC tumours that do not necessitate surgery. The LITESPARK-004 cohort included additional inclusion and exclusion criteria that selected patients at low risk of AEs; these are included in Table 5.
A MAIC analysis was conducted based on individual patient data from the VHL Natural History Study and aggregate data from the LITESPARK-004 trial. The 260 patients included in the external cohort were reweighted to match the distribution of key baseline characteristics using the method-of-moment approach among patients in the LITESPARK-004 trial.40 The baseline variables used for weighting adjustment were as follows: age at patient-level index date, sex, number of renal surgeries with therapeutic intent before patient-level index date, and tumour size of the largest renal solid tumour at the patient-level index date. The variables were selected based on input from clinical experts on patient baseline characteristics that were considered prognostic of transition probabilities starting from the presurgery state, or that may modify the effect of belzutifan on these transition probabilities. The consulted experts indicated that VHL type, VHL gene alteration type, and the number of measured tumours were important effect-modifying or prognostic factors, but these were not included in the matching procedure because they were either unavailable or affected by a high proportion of missing data.
Within the Natural History Study cohort, the index date was defined as the earliest date that a measurable renal solid tumour was detected during the study period (July 31, 2004, to June 30, 2020), in contrast to the LITESPARK-004 trial, which defined the index date as the start of study treatment. In the LITESPARK-004 trial, the outcome was defined as RCC surgery from any procedure, excluding radiation, which led to a reduction in RCC tumour size. Patients who did not undergo surgery during the follow-up period were censored at the date they were last known to be alive. For the Natural History Study, the outcome was a surgical procedure defined as: complete nephrectomy (bilateral, left, right), partial nephrectomy (bilateral, left, right), ablation (not otherwise specified), microwave ablation, radiofrequency ablation, cryotherapy, renography, resection, surgery (not otherwise specified), and other-cyst removal. Patients were censored at the end of follow-up or at the time of experiencing a competing event type (metastatic disease progression or death).
The cause-specific hazard of RCC surgery for belzutifan was parametrically modelled using the observed time from the baseline visit until the first postbaseline renal surgery in the overall LITESPARK-004 trial population (N = 61). Similarly, for active surveillance, the rate of RCC surgery was estimated using patient-level time-to-event data from the VHL Natural History Study, which were reweighted to match the baseline characteristics of the LITESPARK-004 trial population. Specifically, the exponential distribution was selected due to the small number of observed events in the LITESPARK-004 trial and based on visual inspection and statistical goodness-of-fit, which was based on the minimized mean squared error for the VHL Natural History Study.
No sensitivity or subgroup analyses were conducted. No assessment of validity of method assumptions, potential unmeasured confounding, or transportability were provided. No mention was made of missing data or if any patients in the VHL study were lost to follow-up before the final calendar date.
Results of Sponsor-Submitted Matching-Adjusted Indirect Comparison
Summary of Included Studies
The distribution of baseline characteristics before and after reweighting is displayed in Table 17. After reweighting, the effective sample size from the Natural History Study decreased by 65% (from 260 to 92.2), as patients had fewer prior surgeries on average compared with their corresponding LITESPARK-004 trial samples before matching. There appear to be similarities in the balance of sex and age at time of enrolment. While the number of prior surgeries and size of tumour differed in the original sample, the reweighting balanced these covariates. Other potentially relevant baseline characteristics were not presented in the sponsor-submitted report.
Table 16: Sample Selection Process of the Natural History Study Population Used to Match LITESPARK-004
Step | Criteria | N |
|---|---|---|
1 | INCLUSION: Patients with VHL syndrome who are residents of the US or Canada | 776 |
2 | INCLUSION: Patients with ≥ 1 renal solid tumour identified and measured during the study period (July 31, 2004, to June 30, 2020) | 313 |
3 | INCLUSION: Patients with a diagnosis of VHL syndrome based on germline VHL alteration | 297 |
4 | EXCLUSION: Patients with any renal procedure in the 30 days on or before patient-level index date | 296 |
5 | EXCLUSION: Patients whose follow-up date was on or before patient-level index date | 296 |
6 | EXCLUSION: If the largest tumour at patient-level index date is ≥ 30 mm, patients with a renal surgical procedure with therapeutic intent performed within 60 days on or after the patient-level index date | 278 |
7 | EXCLUSION: Patients who received treatment with belzutifan or another HIF-2-alpha inhibitor any time before patient-level index date | 278 |
8 | EXCLUSION: Patients who received systemic oncologic or investigational therapy any time before patient-level index date | 272 |
9 | EXCLUSION: Patients with evidence of VHL disease–associated metastatic disease before the patient-level index date | 260 |
— | Natural History Study sample used to match LITESPARK-004 | 260 |
HIF-2-alpha = hypoxia-inducible factor 2 alpha; VHL = von Hippel-Lindau.
Source: Indirect Treatment Comparison Report (2022).40
Table 17: Baseline Characteristics of the Natural History Study and LITESPARK-004 Trial Populations Before and After Matching
Baseline characteristics | Natural History Study | LITESPARK-004 | |
|---|---|---|---|
Before matching (N = 260) | After matching (effective N = 92.2) | (N = 61) | |
Age at patient-level index date (years) | |||
Mean | 42.1 | 41.0 | 41.0 |
Standard deviation | 12.3 | 13.5 | 13.5 |
Sex, N (%) | |||
Female | 120 (46.2) | 43.8 (47.5) | 29 (47.5) |
Male | 140 (53.9) | 48.4 (52.5) | 32 (52.5) |
Number of renal surgeries with therapeutic intent before patient-level index date | |||
Mean | 1.4 | 2.4 | 2.4 |
Standard deviation | 1.5 | 1.6 | 1.6 |
Tumour size of the largest renal solid tumour at patient-level index date (cm) | |||
Mean | 2.1 | 2.5 | 2.5 |
Standard deviation | 1.0 | 0.9 | 0.9 |
aEffective sample size is computed as the square of the summed weights divided by the sum of the squared weights.
Source: Indirect Treatment Comparison Report (2022).40
Results
In the LITESPARK-004 cohort, 7 RCCs surgeries occurred during the follow-up; 2 patients were censored for death. In the VHL Natural History Study, 196 tumour-reduction surgeries events were observed, and the numbers of patients censored due to metastatic disease or death were 2 and 0, respectively. The weekly exponential rate of RCC surgery was estimated at 0.00487 (SE = 0.00034) in the matched Natural History Study sample versus 0.00071 (SE = 0.0003) in the LITESPARK-004 population. Figure 9 illustrates the difference in estimated time to RCC surgery distribution using the LITESPARK-004 and reweighted Natural History Study data.
Figure 9: Cause-Specific Hazard Using Exponential Distribution of RCC Surgery Based on Data From LITESPARK-004 (Belzutifan) and the VHL Natural History Study (Routine Surveillance)
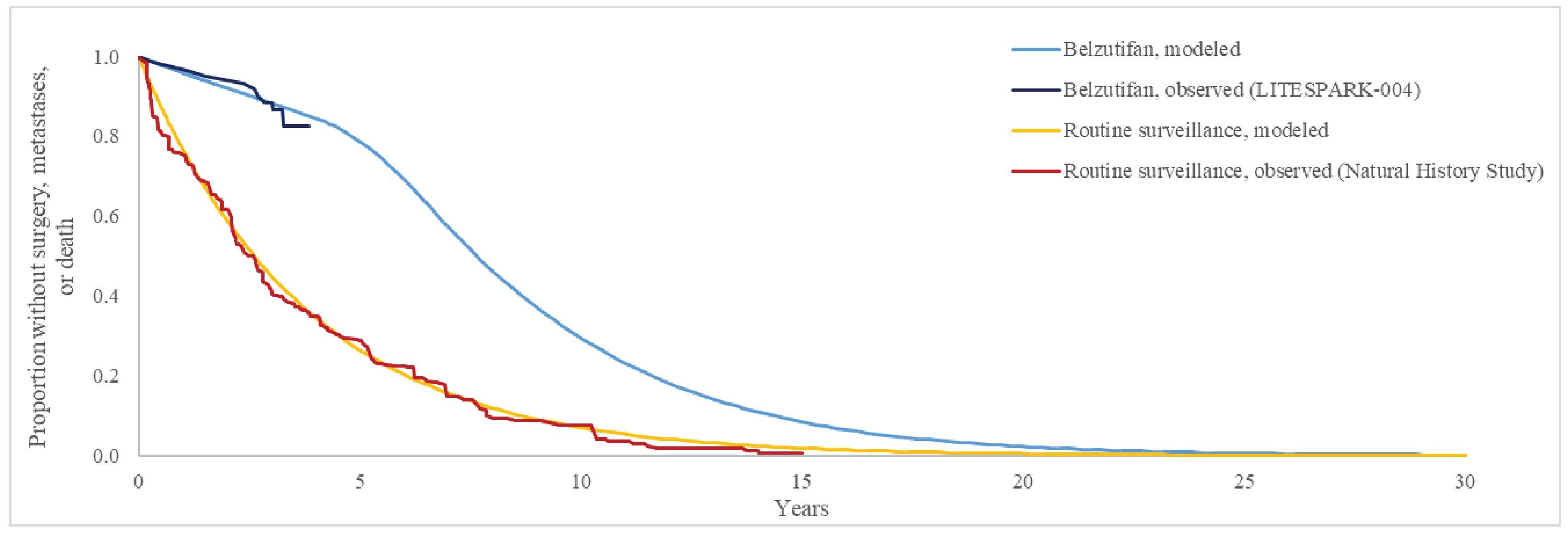
Source: Indirect Treatment Comparison Report (2022).40
Critical Appraisal of VHL Natural History Study Matching-Adjusted Indirect Comparison
Internal Validity
The sponsor-submitted MAIC was informed by patient-level data from the VHL Natural History Study and the aggregate data of the LITESPARK-004 cohort discussed in the Pivotal Studies section. There are discrepancies between the studies in the definition of outcome events and index dates. The outcome definition of RCC surgery within the Natural History Study cohort is subject to potential measurement error. Specifically, the clinical experts indicated that renography and cyst removal are not definitive surgical interventions for management of RCC, although these were considered an RCC surgery outcome in the VHL Natural History Study. The magnitude of bias due to measurement error is unknown but may overestimate the estimated relative rate of RCC surgeries in favour of belzutifan. The clinical experts noted that the definition of RCC tumour surgery used in the LITESPARK-004 trial was more restrictive compared to the Natural History Study. In the LITESPARK-004 trial the index date is treatment assignment, whereas the Natural History Study index date is the date of identification of an RCC tumour. Beyond the differences in the outcome, there is potential endogeneity in surgery event rates between populations due to unmeasured factors related to tumour identification and measurement. The clinical experts noted that the decision to perform an RCC tumour surgery is dependent on the anatomic location of resections, baseline renal function after prior surgeries, comorbidities, and other factors. In addition, 77% of the LITESPARK-004 trial population had a prior RCC surgery (Table 10), whereas the Natural History Study cohort consisted of patients at their first identifiable RCC tumour. The populations may be heterogenous, and it is unclear if the estimated rates of RCC surgery are informative of comparative efficacy.
The use of a cause-specific hazard model requires including the effect modifiers of the active treatment on each outcome. The sponsor noted that “Belzutifan is expected to improve OS mainly by preventing surgeries and distant metastases, but also by reducing the risk of transitioning directly from presurgery to death in some cases.” By only including a few potential prognostic factors of surgery events there is likely heterogeneity in the estimates of metastatic and death that result in a biased estimate of the RCC surgery event rate. Additionally, some important effect-modifying or prognostic factors were left out of the matching and reweighting because they were either unavailable or affected by a high proportion of missing data. A key underlying assumption of the unanchored MAIC approach is that all prognostic and effect-modifying factors are balanced across treatment arms. Given that this assumption was likely to have not been met and there was no information on the potential degree of residual confounding, the estimates of RCC surgery rates may be substantially biased. It is unclear why the estimated SEs are so similar (0.0003 versus 0.00034) when there is a notable difference in the number of events between groups. The LITESPARK-004 cohort had 7 events whereas the Natural History Study had 196 (Figure 9). An extrapolation from a sample of 7 events provides little reliable evidence of the treatment’s comparative efficacy on surgery rates. Because the estimated trial event rate of 7 RCC surgeries is low relative to the amount of data collected (n = 61, median follow-up 37.7 months) and the effective sample size of the VHL Natural History Study was nearly halved (n = 92.2), the robustness of the reported findings is uncertain. The choice of an exponential model was based on visual inspection and a mean squared error criteria; these are inadequate for the purpose of measuring comparative effectiveness and likely overestimate the precision and effect size within treatment groups.42
External Validity
The MAIC analysis was conducted after a literature search was unable to identify existing studies with which to contrast the efficacy of belzutifan. The cohort from the VHL Natural History Study was recruited from 2004 to 2020, and the clinical experts indicated that a diagnosis of VHL, treatment regimens for VHL, and the characteristics of patients undergoing VHL-associated RCC tumour surgeries would be similar throughout this time frame. The selection criteria that informed the Natural History Study subcohort was intended to match with those from the LITESPARK-004 cohort but did not include some key criteria. The Natural History Study cohort did not include restrictions on ECOG PS scores of 0 or 1, and this difference may have biased the effectiveness in favour of belzutifan. It was difficult to assess the degree of heterogeneity between the included studies based on the sponsor-provided technical report because reporting of study design and patient characteristics was limited. Key covariates from the pivotal trial, such as ECOG PS, were not reported, and it is therefore unclear whether these would have been balanced after the matching. For active surveillance in the VHL-associated CNS hemangioblastoma and pNET populations, an important limitation of the VHL Natural History Study data was the inability to identify patients who had CNS hemangioblastoma and pNET tumours at the patient-level index date. The ITC results therefore do not contribute to the evidence for the efficacy of belzutifan in VHL patients who had CNS hemangioblastoma and pNET tumours.
Studies Addressing Gaps in the Pivotal and Randomized Controlled Trial Evidence
Contents within this section have been informed by materials submitted by the sponsor. The following have been summarized and validated by the CADTH review team.
The sponsor submitted 1 real-world, retrospective cohort study39 to address the lack of published clinical trials or observational data on the efficacy outcomes of the standard of care (active surveillance) that could be used for an indirect comparison with the belzutifan efficacy outcomes assessed in the LITESPARK-004 trial. This study provided the active surveillance efficacy data used for the ITC discussed in the previous section (Table 18).
This section provides a summary of a real-world VHL Natural History Study39 based on a retrospective cohort of VHL patients managed and treated at NCI. The study reported on the growth kinetics and surgical patterns within these patients.
The sponsor also provided a cross-sectional HRQoL survey43 to address the lack of HRQoL or utility values, and this is summarized and appraised in Appendix 1. This study assessed the impact of VHL disease on HRQoL as measured using the EQ-5D questionnaire in patients with RCC, CNS hemangioblastoma, or pNET. A total of 220 patients completed the survey. Overall, patients with VHL-associated tumours had a mean EQ-5D score of 0.771. As patients who participated in this study did not receive belzutifan, this study does not provide information related to the effect of treatment with belzutifan on the HRQoL of patients with VHL disease.
Populations
The primary study population consisted of US and Canadian patients treated at the NCI with confirmed VHL syndrome and at least 1 renal solid tumour with available measurement(s) during the study period (July 31, 2004, to June 30, 2020). The patient-level index date was defined as the first date that a patient had a radiology report showing at least 1 measurable renal solid tumour. Additional criteria were applied in attempt to match the study population more closely to the population enrolled in the LITESPARK-004 trial (i.e., to remove patients with investigational therapy, oncologic therapy, or renal tumour-reduction procedures within 30 days before the index date). This was referred to as the “trial population subgroup.” Patients were followed until their last clinical encounter or date of death, whichever occurred first.
This was a noninterventional study with patients treated with usual care (active surveillance). No systemic therapies, including belzutifan, were allowed at study entry.
Table 18: Summary of Studies Addressing Gaps in the Evidence
Gap in pivotal and RCT evidence | Studies that address gaps | |
|---|---|---|
Study description | Summary of key results | |
No comparator in the LITESPARK-004 clinical trial (single-arm study) and no published clinical trial or natural disease history data are available to provide active surveillance efficacy data for use in an indirect treatment comparison. | The VHL Natural History Study,39 a retrospective real-world cohort study of growth kinetics and surgical patterns in patients with VHL disease and associated renal solid tumour, was conducted using data registered by the NCI in a hereditary database of patients with VHL syndrome. | The results estimated that the first renal tumour-reduction procedure has occurred in 50% of the patients within 44.2 months of active surveillance treatment. The median tumour-level LGR for the primary study population and trial population subgroup was 0.38 cm/year (IQR = 0.30 to 0.49) and 0.37 cm/year (IQR = 0.29 to 0.47), respectively. The VHL Natural History Study provided a weekly rate of undergoing a RCC surgery in patients under active surveillance to allow for the indirect treatment comparison with belzutifan described in the previous section. |
IQR = interquartile range; NCI = National Cancer Institute; RCC = renal cell carcinoma; VHL = von Hippel-Lindau.
Note: Details from the table have been taken from the sponsor’s Summary of Clinical Evidence.
Source: von Hippel-Lindau Natural History Study.39
Outcomes
The primary end point was the LGR of renal solid tumours among patients who had at least 3 serial assessments of renal tumour diameter (1 initial measurement and at least 2 subsequent measurements) for unique tumour(s) before the first of: date of death or last clinical encounter, initiation of investigational or oncologic therapy, or first renal tumour-reduction procedure affecting the tumour. Patient-level and tumour-level LGR for renal solid tumours were assessed. Tumour size metrics were collected throughout follow-ups.
Tumour size was defined as the longest diameter of the tumour in centimetres and was ascertained from the structured database. Tumour size was ascertained for all individual renal solid tumours with a serial measurement from the tumour-level index date until the end of tumour-level follow-up. The date of the renal solid tumour measurement was also collected.
Secondary end points included an assessment of the proportion of patients with tumour-reduction procedures, time from first tumour detection in the study period to first tumour-reduction procedure, frequency and type of tumour-reduction procedures, time between tumour-reduction procedures, and kidney function.
Occurrence of chronic kidney disease, anemia and patients qualifying for dialysis at key time points were also assessed as other secondary outcomes.
Statistical Analysis
In the primary analysis, LGRs for renal solid tumours were calculated using a linear mixed (multilevel) model regressing tumour size on time since the tumour-level index date, accounting for dependency of measurements within tumour and patient. The multilevel model described LGRs at 3 levels: unique patients, unique tumours nested within unique patients, and tumour measurements nested within unique tumours. LGRs were presented continuously and categorically at the patient, tumour, and population level. A secondary LGR analysis was also performed using simple linear regression models used in the LITESPARK-004 trial.
Descriptive characteristics of the number and proportion of patients with at least 1 and at least 2 tumour-reduction procedures (overall and among surgical procedures only), number of procedures during follow-up, and surgical complications (including estimated blood loss and perioperative mortality) were described. Time from the patient-level index date to first renal tumour-reduction procedure (overall and separately among surgical procedures only), and between patients’ first and second renal tumour–reduction procedures were described using Kaplan-Meier metrics and curves.
Results
Patient Disposition
Of 776 VHL patients in the NCI hereditary database, 308 patients with at least 1 solid renal tumour met the eligibility criteria and were included in the primary study population. After applying additional eligibility criteria mentioned previously (focusing on the tumour growth rate assessment), 247 patients (80.2%) were included in the trial population subgroup.
Subgroups of 131 patients and 114 patients in the primary study population and the trial population subgroup, respectively, had at least 3 serial measurements of at least 1 solid renal tumour during the study period that qualified them for inclusion in the LGR analysis subgroups to address the primary research objective.
Baseline Characteristics
Patients in the primary study population had a median age of 41 years (range = 18 to 79) at the patient-level index date, and 56% were male. The median length of follow-up was 107.2 months (approximately 9 years; range = 0.03 to 190.2 months), with 88% and 71% having at least 2 and 5 years of follow-up, respectively. At the patient-level index date, other clinical manifestations of the VHL syndrome included renal cysts (92% of patients), brain and spine hemangioblastomas (79% and 71%, respectively), pancreatic cysts (77%), retinal hemangioblastomas (57%), pancreatic solid tumours (34%), epididymal cystadenomas (26% of males), and endolymphatic sac tumours (9%). The median number of renal tumour–reduction procedures before the index date was 1 (range = 0 to 9). Demographics and clinical characteristics were similar for patients in the trial population subgroup and the subpopulation of patients eligible for the LGR analysis (i.e., with at least 3 serial measurements). However, many demographic characteristics, such as race and ethnicity and ECOG PS, were not reported in the Natural History Study report.
Efficacy
Linear Growth Rate
The median tumour-level LGRs for the primary study population and trial population subgroup were 0.38 cm per year (IQR = 0.30 to 0.49) and 0.37 cm per year (IQR = 0.29 to 0.47), respectively. In a secondary analysis using a simple linear model and multilevel modelling, median tumour-level LGRs for the primary study population and the trial population subgroup were 0.36 cm per year (IQR = 0.25 to 0.57) and 0.36 cm per year (IQR = 0.24 to 0.56), and 0.38 cm per year (IQR = 0.30 to 0.49) and 0.37 cm per year (IQR = 0.29 to 0.47), respectively.
Frequency and Type of Tumour–Reduction Procedures
Of the 308 patients in the primary study population, 232 patients (75.3%) had at least 1 renal solid tumour–reduction procedure during the study period, including 225 patients (73.1%) with surgical procedures (96% of which were partial nephrectomies), 16 patients (5.2%) with ablation procedures, and 1 patient (0.3%) who received radiation. Similar tumour resection patterns were observed in the trial population subgroup, and among the 184 patients (74.5%) who underwent at least 1 renal solid tumour–reduction procedure; 62% had at least 2 procedures during the overall follow-up, including 11 of 71 patients (15.5%) and 34 of 138 patients (24.6%) with at least 2 procedures within 2 years and 5 years of follow-up, respectively. The median number of tumour-reduction procedures per patient in the trial population subgroup was 2 (range = 1 to 9). At 2 years and 5 years of follow-up for patients in the trial population subgroup, the median numbers of procedures were 1 (range = 1 to 3) and 1 (range = 1 to 4), respectively.
Time to Tumour–Reduction Procedures
The 1-year, 2-year, 5-year, and 7-year intervention-free survival probabilities for the first tumour-reduction procedure were 79.0%, 69.9%, 38.3%, and 26.4%, respectively, for the trial population subgroup. The 25th percentile of the time to first tumour-reduction procedure was 17.5 months (95% CI, 9.13 to 24.08 months) in the trial population subgroup, with a median time-to-event of 44.2 months (95% CI, 35.74 to 49.51 months).
Harms
Of the 217 patients (70.5%) in the primary study population with at least 1 partial nephrectomy, 413 partial nephrectomies were performed during follow-up, 124 (30.0%) of which were associated with complications. The median estimated blood loss, assessed among all surgical procedure types, was 1.5 L (IQR = 0.6 to 2.6). The maximum estimated blood loss observed was 12 L in the primary study population. Two patients (0.9%) in the primary study population with at least 1 renal tumour–reduction procedure conducted at the National Institutes of Health died within 30 days of the procedure (1 nephrectomy and 1 biopsy)
Critical Appraisal
Internal Validity
The VHL Natural History Study was a real-world retrospective cohort study focusing on the natural history and progression of renal solid tumours associated with VHL syndrome. However, this study did not evaluate the effect of belzutifan and did not provide evidence about the efficacy of the treatment. No a priori protocol for the analyses appeared to be present. The study was conducted using data registered by the NCI in a hereditary database of patients with VHL syndrome, but how these data were located (e.g., which search methods were used) or selected is not specified.
Some of the limitations of this study were high levels of missing data for some variables; unavailability of longitudinal measures of tumour growth for all tumours in a systematic manner (i.e., differences may have arisen due to variation in measurement across observers), as the measures were extracted from the registry directly; incomplete documentation of metastasis; and the possibility of misclassification. There is also a possibility of loss to follow-up of patients who left the registry, but no relevant information was provided. Attempts were made to ensure that the trial population subgroup would be similar to the population of the LITESPARK-004 trial, based on the additional criteria that were applied. However, several criteria in the Natural History Study cohort approximate those of the pivotal trial due to insufficient access to information within the database. While demographics and clinical characteristics were similar for patients in the trial population subgroup and patients in the LGR analysis subgroups, many demographic characteristics (i.e., race and ethnicity and ECOG PS) were not reported in the Natural History Study report.
Receiving systemic oncologic therapy or investigational therapy within 30 days on or before the patient-level index date was part of the exclusion criteria. However, no specific information was provided about the type of systemic or investigational therapy. Moreover, this exclusion criteria may have led to the exclusion of patients with a better prognosis, which would have affected the results for the trial population subgroup.
External Validity
This study includes patients managed and treated at the NCI only. This may affect the overall generalizability of the study, as it may not be representative of all patients with VHL disease in Canada that fall within the indication. Patients selected for this study might have received a higher quality of care compared with patients treated at other centres, which might have led to lower treatment complication rates and overall morbidity associated with standard of care at the NCI compared with that generally expected at other clinical centres.
While this study presented data for renal tumours, patients included in the study also had other tumours associated with VHL disease, (e.g., renal cysts, brain, and spine hemangioblastomas, pancreatic cysts, retinal hemangioblastomas, and pancreatic solid tumours). However, no additional information was provided for these tumours, and some important clinical outcomes associated with VHL syndrome may have been excluded. As the indication under review includes patients with nonmetastatic pNETs and CNS hemangioblastomas in addition to nonmetastatic RCCs, the unavailability of data related to these 2 tumours represents a gap in the evidence provided by this study.
The authors of this study noted the potential risk of losing substantial numbers of samples due to the eligibility criteria of at least 3 serial measurements for the assessment of tumour growth rate patterns. They added that, although patients with at least 3 measurements did have longer follow-up times, on average, no substantial differences in baseline demographic and clinicopathologic characteristics were observed compared to patients with fewer than 3 measurements. Considering the substantial variation in diagnostic techniques and treatment approaches over time, the authors also raised concerns regarding whether the growth rate is generalizable to the current patient populations.
Discussion
Summary of Available Evidence
One ongoing, phase II, single-arm, open-label trial (LITESPARK-004, N = 61) was included in the SLR conducted by the sponsor. The primary objective of the LITESPARK-004 trial was an evaluation of the efficacy of belzutifan for the treatment of VHL disease–associated nonmetastatic RCC as measured by ORR. Secondary end points included ORR for patients with CNS hemangioblastoma (n = 50) and nonmetastatic pNET (n = 22); TTR, DOR, TTS, and PFS; and safety, including notable harms (i.e., anemia, hypoxia, secondary primary malignancies, and hepatic safety). The trial enrolled adults with VHL disease based on a germline VHL alteration, with at least 1 measurable RCC but without a need for immediate surgery or evidence of metastasis. Patients could have other VHL disease–associated non-RCC tumours. Efficacy analyses were conducted for the full (RCC) population, as well as for subsets of the population with a CNS hemangioblastoma or nonmetastatic pNET. Patients in the total study population (i.e., those with RCC) had a median age of 41.0 years (range = 19.0 to 66.0), and about half were male (52.5%) and half were female (47.5%). Most patients were white (90.2%), had an ECOG PS of 0 (82.0%), and had undergone a previous surgery or ablative procedure (96.7%). Reported baseline characteristics for CNS hemangioblastoma and pNET subpopulations were comparable to those of the full population.
An ITC was submitted by the sponsor to provide comparative evidence of belzutifan versus active surveillance for the treatment of adult patients with VHL disease in the LITESPARK-004 trial. The ITC compared a real-world, retrospective, noninterventional cohort study (the VHL Natural History Study) with the LITESPARK-004 trial. Patients with VHL-associated RCC from the VHL Natural History Study were reweighted in an attempt to match the distribution of key baseline characteristics among patients with VHL-associated RCC in LITESPARK-004 and compare them using an unanchored MAIC analysis. The primary and only outcome assessed in the MAIC was time to RCC-related surgery.
The VHL Natural History Study, which provided the active surveillance efficacy data used for the ITC, was also submitted by the sponsor as a standalone study addressing gaps in the pivotal and RCT evidence. In addition, the sponsor provided a cross-sectional HRQoL survey, which assessed the impact of VHL disease on HRQoL as measured by an EQ-5D questionnaire given to patients with an RCC, CNS hemangioblastoma, or pNET.
Interpretation of Results
Efficacy
Belzutifan is a first-in-class HIF inhibitor and the first systemic treatment indicated for the treatment of VHL disease. Overall, belzutifan may be a safe treatment that can provide added clinical benefit for patients with a VHL-associated nonmetastatic RCC, those with a VHL-associated CNS hemangioblastoma, and those with a VHL-associated nonmetastatic pNET, none of whom required immediate surgery. Given the rarity of VHL disease and that active surveillance is currently the standard of care for patients with VHL-associated nonmetastatic tumours, the small sample size and single-arm trial design adopted in the LITESPARK-004 trial was considered acceptable from a regulatory perspective to demonstrate the efficacy of belzutifan, but drawing definitive conclusions is challenging due to the potential for confounding. This review’s interpretation of the efficacy findings in the LITESPARK-004 trial were based on the opinions of the clinical experts consulted by CADTH and the judgment of the CADTH clinical review team. Most importantly, this interpretation should not serve as confirmation of the efficacy of belzutifan; the efficacy of belzutifan remains uncertain until a phase III RCT is conducted.
ORR and DOR observed in single-arm studies may serve as substantial evidence when there is no therapy available and presuming that major tumour regressions can be attributed to the tested treatment.14 Patients placed importance on the need for a treatment that can improve their physical condition by decreasing or stabilizing the size of tumours as well as offering long-term stability or reduction of disease. In the LITESPARK-004 trial, the magnitude of the ORR (i.e., the percentage of patients who had a CR or PR in response to belzutifan) was greater than the prespecified alternative hypothesis of 30% and considered clinically meaningful for patients with VHL-associated nonmetastatic RCC, those with VHL-associated CNS hemangioblastoma, and those with VHL-associated nonmetastatic pNET. The LITESPARK-004 trial demonstrated a greater tumour response rate when patients who had stable disease were added to those with CR and PR in the DCR end point: a DCR of 90% or greater was observed across patients with an RCC, those with a CNS hemangioblastoma, and those with a pNET. However, it is not possible to determine whether stable disease can be attributed to belzutifan or the natural history of the disease. IRC- and investigator-assessed ORR and DCR were consistent among patients with nonmetastatic RCC and those with CNS hemangioblastoma. Moreover, based on the DOR, the clinical experts consulted by CADTH considered the tumour response to be durable: among 39 patients with RCC and a confirmed response, 32 (82.1%) were censored due to no progression at the time of data cut-off or before end of treatment. Of 22 patients with a CNS hemangioblastoma who showed confirmed response, 17 were censored due to no progression at the time of data cut-off or before the end of treatment. All 20 patients with a pNET who had a confirmed response had no progression at the time of data cut-off.
In addition to ORR and DOR, the clinical experts considered TTS and PFS to be important and clinically relevant outcomes in the assessment of the efficacy of belzutifan in patients with VHL-associated nonmetastatic lesions because prolonging survival and avoiding morbid local therapies such as surgeries and radiation as much as possible are among the most critical treatment goals in clinical practice. Similarly, patients indicated that the opportunity to avoid surgery is important to them, and they expressed their willingness to tolerate moderate-to-severe side effects if a treatment would allow them to avoid surgery to remove VHL-associated cysts and tumours. In the LITESPARK-004 trial, medians of TTS and PFS were not reached, yet the efficacy of belzutifan appeared to be supported because the majority of patients were censored for PFS due to no progression during the follow-up period. The clinical experts consulted by CADTH indicated that the rates of PFS and TTS appeared to be more promising than might be expected with standard of care during the time period of follow-up (i.e., median 37.7 months). However, the follow-up time was not long enough to reveal the full extent of the efficacy of belzutifan on time-to-event outcomes. Given that the life expectancy of patients with VHL could be long (e.g., a recent study suggested > 60 years37), the length of follow-up in the trial was insufficient to determine the long-term effects of treatment with belzutifan. In addition, potential treatment effects following discontinuation (e.g., due to patient preference with stable disease and need for surgery) are unknown.
The outcome — distribution of all tumour-reduction procedures before and after treatment initiation — was not prespecified in the protocol of the LITESPARK-004 trial. Fewer tumour-reduction procedures occurred after patients received belzutifan, compared to the same period immediately before treatment initiation. This finding suggests the potential of belzutifan to delay the need for tumour-reduction procedures among patients with VHL. However, this finding, which involved VHL-associated tumours not limited to RCCs, CNS hemangioblastomas, and pNETs, was beyond the scope of the present reimbursement request.
Findings from the sponsor-conducted ITC, which used the VHL Natural History Study to provide an external comparator for the LITESPARK-004 trial, were considered highly uncertain. Although the results for the estimated number of surgeries were in favour of belzutifan compared with active surveillance and considered clinically meaningful, several major limitations decreased CADTH’s confidence in the evidence. First, the selection criteria that informed the VHL Natural History Study subcohort that was intended to match the LITESPARK-004 cohort did not include some key criteria, and the Natural History Study cohort did not include restrictions on ECOG PS scores of 0 or 1, which creates a risk of bias in effectiveness that favours belzutifan. Second, it was difficult to assess the degree of heterogeneity between the included studies based on the sponsor-provided technical report as reporting of study design and patient characteristics was limited. Third, key covariates from the pivotal trial, such as ECOG PS, were not reported, and the potential for residual confounding was not assessed and can be considered high. Fourth, the outcome definition of RCC surgery within the Natural History Study cohort is subject to potential measurement error. Specifically, the clinical experts indicated that renography and cyst removal are not definitive surgical interventions for management of a RCC, although these were considered RCC surgery outcomes in the VHL Natural History Study. The magnitude of bias due to measurement error is unknown but may overestimate the estimated relative rate of RCC surgeries in favour of belzutifan. Finally, the MAIC analysis did not report on surgeries related to CNS hemangioblastomas and pNETs at the patient-level index date.
Findings from the VHL Natural History Study and the HRQoL survey, which were submitted by the sponsor as studies addressing gaps in the pivotal and RCT evidence, did not provide information on the efficacy or safety of belzutifan as standalone studies because patients did not receive belzutifan in either of the 2 studies.
Patients placed a high value on new treatments that could improve their quality of life. HRQoL was not assessed in the LITESPARK-004 trial, the VHL Natural History Study, or the ITC. This gap in the evidence was acknowledged by the sponsor in its submission, and the sponsor submitted a cross-sectional HRQoL survey in response. Given that patients who participated in the HRQoL survey did not receive belzutifan, no information on the effects of belzutifan on HRQoL is available, and the effect of belzutifan on HRQoL in patients with VHL disease is unknown.
Harms
The challenge posed by the lack a comparator group in the LITESPARK-004 trial also applies to the interpretation of harms outcomes of belzutifan and decreases CADTH’s confidence in the findings. Almost all patients (95%) in the trial experienced anemia, and about one-third of these required treatment with either iron supplements or an erythropoiesis-stimulating drug, while blood transfusion was uncommon (2%). According to the clinical experts consulted by CADTH, the incidence of harms outcomes, including AEs of clinical interest (i.e., anemia, hypoxia, secondary primary malignancies, and hepatic events), within a median of the 37.7-month follow-up period was generally acceptable.
Regarding long-term safety, the clinical experts noted that the current follow-up time of the LITESPARK-004 trial appeared to be sufficient to observe most side effects. However, given the expectation that patients may take belzutifan for years, its long-term safety with respect to delayed toxicities or uncommon AEs is uncertain. Moreover, the harms caused by the treatments used for belzutifan-related side effects may also cause harms among patients. For example, erythropoiesis-stimulating drugs, which are used to treat anemia, may increase the risk of developing secondary malignancies.44 To further substantiate the safety of belzutifan, more data are required from the ongoing LITESPARK-004 trial (with 38 patients on the treatment of belzutifan) and other sources, such as phase III RCTs and real-world safety data.
Neither the ITC nor the studies addressing gaps in the pivotal and RCT evidence provided evidence about the safety of belzutifan. No harms outcomes were reported in the ITC, and belzutifan was not investigated in the VHL Natural History Study or the HRQoL study.
Conclusion
Based on the opinions of clinical experts, evidence from the phase II, single-arm, open-label LITESPARK-004 trial suggests that treatment with belzutifan may have a beneficial effect in adult patients with VHL-associated nonmetastatic RCC with or without a VHL-associated CNS hemangioblastoma and/or nonmetastatic pNET not requiring immediate surgery. The clinical experts indicated that the efficacy results from the patient populations with a VHL disease–associated nonmetastatic RCC, RCC and CNS hemangioblastoma, RCC and nonmetastatic pNET, as well as RCC, CNS hemangioblastoma, and pNET in the LITESPARK-004 trial indicate a promising and durable tumour response as measured by ORR and DOR, which is likely attributable to belzutifan, based on their clinical experience and expectations of the natural history of the disease. However, the absence of a comparator group in the pivotal study precluded definitive conclusions about the efficacy and safety of belzutifan, due to the potential for confounding. There was uncertainty in the findings for other supportive outcomes (e.g., TTS, PFS) due to limitations such as the lack of an internal comparator group and no inferential statistical analyses. The incidence of harms, such as anemia and hypoxia, were acceptable according to the clinical experts. Because VHL is a life-long condition and patients can receive belzutifan for an extended period, a longer follow-up would be needed to better understand the long-term benefits and harms of belzutifan, as well as the potential residual effects following discontinuation. Findings from an ITC suggest that treatment with belzutifan may have a beneficial effect on time to RCC-related surgery compared to active surveillance in patients with VHL disease–associated nonmetastatic RCC. However, the certainty of the indirect evidence was low due to a violation of the underlying assumptions of the MAIC approach that resulted in a high risk of residual confounding, and important differences in outcome definitions between the LITESPARK-004 trial and the VHL Natural History Study that would bias the findings in favour of belzutifan. In the ITC analysis, the comparative efficacy of belzutifan versus active surveillance for VHL-associated CNS hemangioblastoma and nonmetastatic pNET was not assessed and is therefore unknown. The VHL Natural History Study and the VHL HRQoL survey did not provide evidence describing the efficacy and safety of belzutifan as standalone studies because patients in these studies did not receive belzutifan. It is unknown whether treatment with belzutifan would improve patient quality of life.
References
1.Sponsor Summary of Clinical Evidence [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Belzutifan, 40 mg and oral tablet. Kirkland (QC): Merck Canada Inc.; 2023 Jan 23.
2.Welireg (belzutifan): 40 mg oral tablets [product monograph]. Kirkland (Québec): Merck Canada Inc.; 2022 Dec 13.
3.Crespigio J, Berbel LCL, Dias MA, et al. Von Hippel-Lindau disease: a single gene, several hereditary tumors. J Endocrinol Invest. 2018;41(1):21-31. PubMed
4.Orphanet. Von Hippel-Lindau Disease. 2023; https://www.orpha.net/consor/cgi-bin/OC_Exp.php?Lng=EN&Expert=892#:~:text=Disease%20definition%20Von%20Hippel-Lindau%20disease%20%28VHL%29%20is%20a,hemangioblastoma%2C%20renal%20cell%20carcinoma%20%28RCC%29%2C%20and%20pheochromocytoma.%20ORPHA%3A892. Accessed 2022 Jun 3.
5.National Organization for Rare Disorders (NORD). National Organization for Rare Disorders. Von Hippel-Lindau Disease. https://rarediseases.org/rare-diseases/von-hippel-lindau-disease/. Accessed 2022 Nov 8.
6.National Cancer Institute. Von Hippel-Lindau Disease (PDQ®)–Health Professional Version. 2023; https://www.cancer.gov/types/kidney/hp/renal-cell-carcinoma-genetics/vhl-syndrome. Accessed 2022 Jun 2.
7.Plon S, Jonasch E. Clinical features, diagnosis, and management of von Hippel-Lindau disease. In: E. A, Firth H, Perrone R, Gajjar A, Geffner M, eds. UpToDate. Waltham (MA): UpToDate; 2022.
8.National Institutes of Health. National Institute of Neurological Disorders and Stroke. Von Hippel-Lindau Disease (VHL). 2023; https://www.ninds.nih.gov/health-information/disorders/von-hippel-lindau-disease-vhl?search-term=VHL. Accessed 2022 Nov 8.
9.Takami H, Graffeo CS, Perry A, et al. Presentation, imaging, patterns of care, growth, and outcome in sporadic and von Hippel-Lindau-associated central nervous system hemangioblastomas. J Neurooncol. 2022;159(2):221-231. PubMed
10.Lonser RR, Glenn GM, Walther M, et al. von Hippel-Lindau disease. The Lancet. 2003;361(9374):2059-2067. PubMed
11.Hasanov E, Jonasch E. MK-6482 as a potential treatment for von Hippel-Lindau disease-associated clear cell renal cell carcinoma. Expert Opin Investig Drugs. 2021;30(5):495-504. PubMed
12.Louise MBM, Smerdel M, Borgwadt L, et al. von Hippel-Lindau disease: Updated guideline for diagnosis and surveillance. Eur J Med Genet. 2022;65(8):104538. PubMed
13.Clinical Study Report: P004V02MK6482. An Open Label Phase 2 Study to Evaluate PT2977 for the Treatment of von Hippel Lindau Disease-Associated Renal Cell Carcinoma [internal sponsor's report]. Toronto (Ontario): Merck Canada Inc.; 2021 Jan 7.
14.FDA. Clinical trial endpoints for the approval of cancer drugs and biologics - guidance for industry. 2018: https://www.fda.gov/media/71195/download. Accessed 2023 Mar 16.
15.European Medicines Agency. Guideline on the evaluation of anticancer medicinal products in man. 2017: https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-evaluation-anticancer-medicinal-products-man-revision-5_en.pdf. Accessed 2023 Mar 16.
16.Agrawal S, Arora S, Amiri-Kordestani L, et al. Use of Single-Arm Trials for US Food and Drug Administration Drug Approval in Oncology, 2002-2021. JAMA Oncol. 2023;9(2):266-272. PubMed
17.Natural History Report: MK6482. Von Hippel-Lindau Natural History Study [internal sponsor's report]. Kenilworth (New Jersey): Merck Sharp & Dohme Corp., a subsidiary of Merck & Co., Inc.; 2021 Jan 6.
18.Maher ER, Yates JR, Harries R, et al. Clinical features and natural history of von Hippel-Lindau disease. Q J Med. 1990;77(283):1151-1163. PubMed
19.Coco D, Leanza S. Von Hippel-Lindau Syndrome: Medical Syndrome or Surgical Syndrome? A Surgical Perspective. J Kidney Cancer VHL. 2022;9(1):27-32. PubMed
20.Jonasch E, McCutcheon IE, Gombos DS, et al. Pazopanib in patients with von Hippel-Lindau disease: a single-arm, single-centre, phase 2 trial. Lancet Oncol. 2018;19(10):1351-1359. PubMed
21.Jonasch E, McCutcheon IE, Waguespack SG, et al. Pilot trial of sunitinib therapy in patients with von Hippel-Lindau disease. Ann Oncol. 2011;22(12):2661-2666. PubMed
22.Pilié P, Hasanov E, Matin SF, et al. Pilot study of dovitinib in patients with von Hippel-Lindau disease. Oncotarget. 2018;9(34):23390-23395. PubMed
23.Merck. Welireg prescribing information. 2022; https://www.welireghcp.com/mechanism-of-action/. Accessed 2022 Nov 10.
24.American Society of Health-System Pharmacists. AHFS firstReleaseTM. Belzutifan. Am J Health-Syst Pharm. 2021;78(24):2185-2187. PubMed
25.Pelle E, Al-Toubah T, Morse B, Strosberg J. Belzutifan in a Patient With VHL-Associated Metastatic Pancreatic Neuroendocrine Tumor. J Natl Compr Canc Netw. 2022;20(12):1285-1287. PubMed
26.Food and Drug Administration. FDA approves belzutifan for cancers associated with von Hippel-Lindau disease. 2022; https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-belzutifan-cancers-associated-von-hippel-lindau-disease. Accessed 2023 Jan 25.
27.Therapeutic Goods Administration. Welireg belzutifan 40 mg film-coated tablet bottle (355338). 2022; https://www.ebs.tga.gov.au/servlet/xmlmillr6?dbid=ebs/PublicHTML/pdfStore.nsf&docid=355338&agid=%28PrintDetailsPublic%29&actionid=1. Accessed 2023 Jan 25.
28.Welireg (belzutifan): 40 mg oral tablets [proposed product monograph]. City (PROV): Merck Canada Inc.; 2023 Jul 10.
29.Lin NU, Lee EQ, Aoyama H, et al. Response assessment criteria for brain metastases: proposal from the RANO group. Lancet Oncol. 2015;16(6):e270-278. PubMed
30.Jonasch E, Donskov F, Iliopoulos O, et al. Belzutifan for Renal Cell Carcinoma in von Hippel-Lindau Disease. N Engl J Med. 2021;385(22):2036-2046. PubMed
31.Jonasch E, Iliopoulos O, Rathmell WK, et al. Abstract #4546, Poster Presentation: LITESPARK-004 (MK-6482-004) Phase 2 Study Of Belzutifan, An Oral Hypoxia-Inducible Factor 2α Inhibitor (HIF-2α), For Von Hippel-Lindau (VHL) Disease: Update With More Than Two Years Of Follow-Up Data. American Society for Clinical Oncology 2022 Annual Meeting; 2022; Chicago, IL, USA.
32.Srinivasan R, Iliopoulos O, Rathmell WK, et al. LBA69 Belzutifan, a HIF-2α Inhibitor, for von Hippel-Lindau (VHL) disease-associated neoplasms: 36 months of follow-up of the phase II LITESPARK-004 study. Annals of Oncology. 2022;33:S1433-S1434.
33.Jonasch E, Donskov F, Iliopoulos O, et al. Belzutifan for renal cell carcinoma in von Hippel–Lindau disease: Supplement. N Engl J Med. 2021;385.
34.Clinical Study Protocol: PT2977-202/MK-6482-004-16. An Open Label Phase 2 Study to Evaluate PT2977 for the Treatment of von Hippel Lindau Disease-Associated Renal Cell Carcinoma [internal sponsor's report]. Dallas (TX): Peloton Therapeutics, Inc.; 2017 Nov 10.
35.Merck Sharp & Dohme Corp. Clinical Study Report P004V02MK6482 (Data cutoff date of April 1, 2022) [internal sponsor's report]. 2022 Nov 15.
36.Statistical Analysis Plan: PT2977-202/MK-6482-004-16. An Open Label Phase 2 Study to Evaluate PT2977 for the Treatment of von Hippel Lindau Disease-Associated Renal Cell Carcinoma [internal sponsor's report]. Dallas (TX): Peloton Therapeutics, Inc.; 2020 Jul 12. Accessed Nov 10, 2022.
37.Binderup ML, Jensen AM, Budtz-Jørgensen E, Bisgaard ML. Survival and causes of death in patients with von Hippel-Lindau disease. J Med Genet. 2017;54(1):11-18. PubMed
38.Merck Sharp & Dohme Corp. Clinical Study Report P004V02MK6482 (Data cutoff date of April 1, 2022) [internal sponsor's report]. 2022 Nov 15.
39.Merck Sharp & Dohme Corp. Von Hippel-Lindau Natural History Study. Final Study Report [internal sponsor's report]. 2021.
40.Merck Canada. Von Hippel-Lindau associated non-metastaticnonmetastatic RCC, CNS hemangioblastomas or non-metastaticnonmetastatic pNET. Indirect Treatment Comparisons Natural Histry Study vs. LS-004 [internal sponsor's report]. 2022.
41.Phillippo D, Ades T, Dias S, Palmer S, Abrams KR, Welton N. NICE DSU Technical Support Document 18: Methods for population-adjusted indirect comparisons in submissions to NICE. Bristol (GB): University of Bristol; 2016: https://research-information.bris.ac.uk/ws/portalfiles/portal/94868463/Population_adjustment_TSD_FINAL.pdf. Accessed 2023 Aug 28.
42.Cawley GC, Talbot NL. On over-fitting in model selection and subsequent selection bias in performance evaluation. The Journal of Machine Learning Research. 2010;11:2079-2107.
43.Adelphi Real World. VHL-related disease impact on quality of life and work productivity in patients with renal cell carcinoma, central nervous system hemangioblastoma, or pancreatic neuroendocrine tumor manifestation. Version 1.0 ed. Rahway (NJ): Merck Sharp & Dohme Corp; 2022 Sep 23.
44.Fallah J, Brave MH, Weinstock C, et al. FDA Approval Summary: Belzutifan for von Hippel-Lindau Disease-Associated Tumors. Clin Cancer Res. 2022;28(22):4843-4848. PubMed
Appendix 1: HRQoL and VHL Disease Burden Study
Note that this appendix has not been copy-edited.
This section summarizes the HRQoL and VHL Disease Burden Study43 assessing the real-world VHL disease impact on quality of life and work productivity in patients with RCC, CNS hemangioblastoma, or pNET (both metastatic and nonmetastatic) using a noninterventional international, cross-sectional survey of 220 patients with these VHL-associated tumours. The sponsors submitted this summary to address the gap of lack of HRQoL or utility values to assess the cost-effectiveness (i.e., cost-utility) of belzutifan compared to active surveillance. However, it should be noted that it does not provide information related to the HRQoL of patients treated with belzutifan.
This study was designed to understand the patient experience and burden of disease with current management practices in the treatment of VHL disease and the treatment preferences of patients with RCC, CNS hemangioblastomas, or pNET manifestations. Specifically, the objectives were to assess the patients’ HRQoL and the patients’ work productivity loss and activity impairment. The data collected in this study included patient perceptions of the burden of VHL and their surgical experiences. The study included patient-reported outcome tools to help describe the burden (direct and indirect) of the condition, including the EQ-5D and its Visual Analogue Scale. Patient demographics, disease status (i.e., self-reported CR, PR, stable disease, progressive disease, or unknown), time since most recent surgery, current tumour type, metastatic status, prescribed medication for VHL-associated cancer and presence of key comorbidities such as chronic pain, chronic kidney disease, neurologic issues, and diabetes, were also assessed.
Data collection was conducted by Adelphi Real World through a patient advocacy group, the VHL Alliance who operates in the US, and screened online. The study sampled adult patients (age 18 years and older) from the US, Canada, UK, France, and Germany with self-reported health care professional (HCP)-diagnosed VHL disease with at least 1 kidney, brain or spinal cord, or pancreas manifestation. More than 200 patients were asked to complete an online structured survey, designed to be completed in 1 sitting between December 2021 and June 2022.
Descriptive statistics were reported depending on the type of variable being assessed:
Numeric – count, mean, standard deviation, median, 25th percentile, 75th percentile, minimum and maximum.
Categorical – frequency of responses in each category and percentage of responses in each category.
A total of 220 patients completed the survey (response rate not reported): 108 from the US, 37 from Canada, 21 from UK, 3 from France and 51 from Germany. Mean patient age was 42.5 years, 68.2% of patients were female and the majority of patients were white (88.6%). Time since diagnosis was 210.4 months, 66.4% of patients had RCC, 55.5% of patients had pNET, and 86.4% of patients had CNS hemangioblastoma and 35% had all 3 manifestations.
Overall, patients with VHL-associated tumours had a mean EQ-5D score of 0.771 (SD = 0.21). Patients with metastatic disease (n = 16) had a mean EQ-5D score of 0.667 (SD = 0.28) and patients without metastatic disease (n = 195) had a mean EQ-5D score of 0.783 (SD = 0.20). Patients with VHL-associated tumours had a mean percent overall work impairment of 30.8% (SD = 42.42). Patients with metastatic disease had a mean percent overall work impairment of 40.6% (SD: 43.97) and patients without metastatic disease had a mean percent overall work impairment of 29.3% (SD: 42.04). Patients who had their most recent surgery within the last 6 months had a mean EQ-5D of 0.727 (SD = 0.20) and patients who had their most recent surgery more than 6 months ago had a mean EQ-5D of 0.777 (SD = 0.21). Patients who underwent a surgery within the last 6 months had a mean percent overall work impairment of 53.8% (SD = 51.89) compared to 29.1% (SD = 41.71) for patients who had their most recent surgery more than 6 months ago. Patients with more than 1 tumour type had a mean EQ-5D of 0.776 (SD = 0.21) and patients with only 1 tumour type had a mean EQ-5D of 0.832 (SD = 0.09).
As this was a noninterventional study, it does not provide evidence on the effects of belzutifan on HRQoL. Because the EQ-5D is not specifically validated in VHL, the of the outcomes is uncertain for VHL population. As this was a cross-sectional study, the information captured from the patient surveys was at a single point in time and from a select group of patients who responded to the survey. It may not be representative of all patients with VHL, and it is likely that HRQoL could vary over time.
Pharmacoeconomic Review
Abbreviations
AE
adverse event
BIA
budget impact analysis
CNS
central nervous system
CUA
cost-utility analysis
HR
hazard ratio
ICER
incremental cost-effectiveness ratio
ITC
indirect treatment comparison
ORR
objective response rate
pNET
pancreatic neuroendocrine tumour
QALY
quality-adjusted life-year
PFS
progression-free survival
RCC
renal cell carcinoma
RDI
relative dose intensity
ToT
time on treatment
TTS
time to surgery
VHL
von Hippel-Lindau
WTP
willingness-to-pay
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Belzutifan (Welireg), oral tablets |
Submitted price | Belzutifan, 40 mg oral tablets: $213.33 per tablet |
Indication | For treatment of adult patients with VHL disease who require therapy for an associated nonmetastatic RCC, CNS hemangioblastoma, or nonmetastatic pNET not requiring immediate surgery |
Health Canada approval status | NOC |
Health Canada review pathway | Project Orbis and Priority Review |
NOC date | July 11, 2023 |
Reimbursement request | As per indication |
Sponsor | Merck Canada Inc. |
Submission history | Previously reviewed: No |
CNS = central nervous system; NOC = Notice of Compliance; pNET = pancreatic neuroendocrine tumour; RCC = renal cell carcinoma; VHL = von Hippel-Lindau.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Markov Model |
Target population | Adults (18 years or older) with a VHL-associated RCC, CNS hemangioblastoma, or pNET who require therapy and do not require immediate surgery; the 3 cohorts were modelled independently |
Treatment | Belzutifan |
Comparator | Active surveillance |
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, life-years |
Time horizon | Lifetime (59 years) |
Key data sources | Patient-level data from the LITESPARK-004 trial of belzutifan and a real-world natural history study of patients with VHL-associated RCC (VHL Natural History Study) |
Submitted results |
|
Key limitations |
|
CADTH reanalysis results |
|
CNS = central nervous system; ICER = incremental cost-effectiveness ratio; NOC = Notice of Compliance; pNET = pancreatic neuroendocrine tumour; QALY = quality-adjusted life-year; RCC = renal cell carcinoma; RDI = relative dose intensity; TTS = time to surgery; ToT = time on treatment; VHL = von Hippel-Lindau.
Conclusions
Evidence from the LITESPARK-004 trial and feedback from clinical experts suggest that, in adult patients with a von Hippel-Lindau (VHL) disease–associated nonmetastatic renal cell carcinoma (RCC) with or without a VHL disease–associated central nervous system (CNS) hemangioblastoma and/or nonmetastatic pancreatic neuroendocrine tumour (pNET), none of whom required immediate surgery, belzutifan demonstrated a promising and durable tumour response as measured by the objective response rate (ORR) and duration of response, which would likely not be otherwise attributable to active surveillance. However, the CADTH clinical review identified uncertainty with the LITESPARK-004 trial findings for other key supportive outcomes (e.g., time to surgery [TTS] and progression-free survival [PFS]) due to major limitations, such as the lack of an internal comparator and no inferential statistical analyses. The sponsor’s indirect treatment comparison (ITC) suggested that treatment with belzutifan may have a beneficial effect on time to RCC-related surgery compared to active surveillance in the RCC cohort; however, due to several key methodological limitations that bias the findings in favour of belzutifan, the comparative effectiveness estimates are uncertain. Given the lack of ITC evidence in the CNS hemangioblastoma and pNET cohorts, the comparative effect of belzutifan in these populations is unknown. Due to the absence of robust clinical evidence, it is unclear whether the modelled survival and quality-of-life benefits associated with belzutifan would be observed in clinical practice.
The CADTH base-case analysis resulted in an incremental cost-effectiveness ratio (ICER) of $360,193 per quality-adjusted life-year (QALY) gained (incremental costs = $975,998; incremental QALYs = 2.71) for belzutifan versus active surveillance for the VHL-RCC cohort. The CADTH base-case analysis results were similar to the sponsors’ results, where belzutifan was not considered cost-effective relative to active surveillance at a willingness-to-pay (WTP) threshold of $50,000 per QALY. A price reduction of approximately 83% is required for belzutifan to be considered cost-effective at a WTP threshold of $50,000 per QALY for the broader RCC population. Based on a price reduction of this magnitude, the cost per 28 days of treatment would be approximately $3,050 per patient. Price reductions for the CNS hemangioblastoma and pNET subgroups were similar.
The cost-effectiveness of belzutifan was sensitive to assumptions surrounding time on treatment (ToT) and residual benefit after treatment discontinuation. Specifically, the CADTH base-case analysis found no residual benefit after belzutifan treatment discontinuation beyond the maximum follow-up period of the LITESPARK-004 trial, which resulted in a smaller difference in QALYs between belzutifan and active surveillance (the sponsor reported a gain of 3.19 QALYs with belzutifan in the RCC cohort while CADTH estimated 2.71 QALYs). The majority of the incremental QALYs associated with belzutifan was driven by an assumed survival benefit. Based on the deterministic results of the CADTH base-case analysis, approximately 90% of the incremental QALYs for belzutifan accrued after the observed median follow-up period in the LITESPARK-004 trial. This benefit should be interpreted with caution given the lack of long-term survival data to confirm the modelled benefit. Uncertainty remains regarding the long-term treatment effect of belzutifan, and the relative efficacy of belzutifan compared to active surveillance in the modelled population. Furthermore, the treatment effect of belzutifan for patients with a VHL-associated CNS hemangioblastoma or pNET who do not have RCC is unknown, as the LITESPARK-004 trial population was narrower than the Health Canada–indicated population. Should RCC have no impact, the subgroup analyses conducted may be generalizable to patients with only VHL-associated CNS or pNET. As CADTH was unable to fully assess the uncertainty around long-term treatment efficacy, comparative efficacy, and missing population due to lack of data, a greater price reduction may be warranted.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, registered clinicians, and drug plans that participated in the CADTH review process.
Patient input was received from the Canadian VHL Alliance, which coordinated feedback with the Canadian Organization for Rare Disorders, Kidney Cancer Canada, Pancreatic Cancer Canada, and the Canada Neuroendocrine Tumour Society. Patient input was gathered from 123 patients and caregivers via an online survey. Patients reported that living with VHL disease is associated with ongoing physical and psychological struggles that can have a significant impact on their quality of life. When asked about the number of surgeries experienced, respondents reported having gone through many surgeries. Patients expressed a need for a treatment that would decrease or stabilize the size of tumours, reduce pain, improve breathing, offer longer-term stability or reduce disease burden, and allow them to avoid VHL-related surgery. Input was gathered from 19 patients who had experience with belzutifan for the treatment of VHL disease. These patients noted that belzutifan was moderately to extremely effective in controlling their VHL disease, with side effects being moderately tolerable to very tolerable; however, respondents acknowledged that the current evidence that belzutifan can shrink or eliminate tumours is limited, and suggested all patients receiving belzutifan should be enrolled in a patient-monitoring program to help develop treatment guidelines and protocols. The patient input noted that the use of belzutifan does not require companion diagnostic testing, although respondents pointed out that diagnostic testing is associated with a significant psychological burden, and expressed concerns regarding travel and testing costs, particularly when tests are not covered by the public health system funders. Overall feedback from patient input expressed interest in belzutifan for the treatment of patients with VHL-associated tumours.
Clinician input was received from Canadian subspecialists involved in VHL care and the Ontario Health Cancer Care Oncology Genitourinary Cancer Drug Advisory Committee. Clinicians noted that there is no definitive curative treatment options for VHL disease. Instead, the management of VHL disease involves close clinical and radiographic monitoring and appropriate timing of local strategies, with the aim of reducing the risk of further spread of disease and delaying symptomatic progression. Clinicians noted that belzutifan would fill a large unmet need, cause a shift in disease management, and allow patients to benefit from systemic therapy to address the impact of VHL disease across multiple organs. Clinicians noted that all adult patients (aged 18 years or older) with VHL disease who require treatment for VHL-associated tumours such as an RCC, CNS hemangioblastoma, or pNET without immediate need for surgery should be considered for belzutifan. Clinicians noted that belzutifan treatment should only be received under the guidance of a medical oncologist or other specialist physicians experienced in the use of systemic therapies in a cancer care centre, and that many factors may result in treatment discontinuation, including radiographic disease progression, toxicity and/or unacceptable tolerance, and pregnancy. Last, clinicians indicated that belzutifan may reduce the number of surgical interventions and hospitalizations associated with VHL disease and benefit multiple organs within VHL patients.
Drug plan input identified concerns with drug wastage due to dose interruptions or treatment discontinuation after a supply of belzutifan is dispensed, referencing the number of dose interruptions, reductions, and discontinuations observed in the LITESPARK-004 trial. It also noted that VHL disease usually appears in young adults and can be found in children, and raised the question of whether belzutifan would be considered for use in the pediatric population.
Several of these concerns were addressed in the sponsor’s model:
Severe treatment related adverse events (AEs) associated with belzutifan, health related quality of life, and surgical and hospitalization costs were included.
In addition, CADTH addressed some of these concerns as follows:
Diagnostic testing costs were considered in a scenario analysis.
CADTH was unable to address the following concerns raised from stakeholder input:
Drug wastage was not incorporated into the submitted economic model and could not be addressed by CADTH.
The use of belzutifan in patients aged less than 18 years was not incorporated into the submitted economic model and could not be addressed by CADTH due to the lack of evidence for its use in this population.
Economic Review
The current review is for belzutifan (Welireg) for the treatment of adult patients with VHL disease who require therapy for an associated nonmetastatic RCC, CNS hemangioblastoma, or nonmetastatic pNET not requiring immediate surgery.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis (CUA) to assess the cost-effectiveness of belzutifan compared with active surveillance for the treatment of adult patients with VHL disease who require therapy for associated nonmetastatic RCC, CNS, or nonmetastatic pNET not requiring immediate surgery. The model population aligns with the Health Canada indication.1 The sponsor noted that a subset of patients within each cancer cohort may have 1 or both of the other 2 tumour types, and due to varying rates of surgery that depend on the primary tumour type, it was not possible to present a single ICER combining results from 3 target populations. As a result, the sponsor modelled the 3 subgroup populations separately based on tumour location using similar model structures.2
Belzutifan is available as a 40 mg oral tablet.2 The recommended dosage of belzutifan is 120 mg (three 40 mg tablets) administrated orally once daily, with or without food, until unacceptable toxicity or disease progression.3 The submitted price of belzutifan is $213.33 per 40 mg tablet, resulting in a cost of $17,920 per 28 days.2 The comparator for this analysis was active surveillance, defined as no systemic treatments, as the sponsor noted there are no currently recommended treatments for this population in Canada.2
The analysis was conducted from the Canadian health care system perspective. Outcomes of the model included QALYs and life-years over a lifetime horizon of 59 years.2 Discounting at 1.5% per year was applied to both costs and outcomes.2 A weekly cycle length was used with a half-cycle correction applied.2
Model Structure
The sponsor submitted a Markov model consisting of the following mutually exclusive health states: presurgery, metastatic disease, first surgery, event-free after first surgery, metastatic disease after first surgery, second surgery, event-free after second surgery, metastatic disease after second surgery, 3 or more surgeries, event-free after 3 or more surgeries, metastatic disease after 3 or more surgeries, and death (the inter-relationships of these states are depicted in Figure 1).2
All patients entered the model in the presurgery health state (although they may have had an earlier surgery), informed by the baseline visit of LITESPARK-004, and remained in the presurgery state until they underwent their first tumour-reduction surgery for their primary tumour type, developed distant metastases, or died due to any cause.2 Patients who transitioned to the first-surgery health state remained in that health state for 1 cycle before either transitioning to the event-free-after-surgery health state or dying.2 After undergoing and surviving surgery, patients reside in the event-free-after-surgery state during model cycles in which they are alive, metastases-free, and not requiring immediate surgery for the primary tumour. During this time, patients are at risk of entering subsequent surgery tunnel states (modelled similarly to the first surgery health state), developing metastasis, or dying.2 Those in the metastatic-disease health states were noted to encompass RCC and pNET metastases, and patients remained in the metastatic-disease health state until death.2 Patient survival within the metastases state was expected to depend on the efficacy of the specific first-line systemic treatment received in the advanced and/or metastatic RCC or pNET setting (depending on the origin tumour).2 Each premetastatic health state included 3 different substates defined by patients ORR for their primary tumour to account for the impact of the overall response rate on patient’s health-related quality of life. In the sponsor’s base case, ToT was modelled using on/off treatment health states in which patients could transition from a given on-treatment health state to the corresponding off-treatment state. Clinical efficacy in the off-treatment health state for belzutifan were assumed to converge toward active surveillance over time.
Model Inputs
Patient baseline characteristics in the model were informed by the reported characteristics of the LITESPARK-004 trial, which enrolled adult patients with VHL-associated RCC (N = 61), many of whom also had a CNS hemangioblastoma (82%) and/or pNET (36%). As noted in the overview, the sponsor modelled 3 cohorts of patients separately based on primary tumour type.2 As a result, the RCC population includes all patients in the LITESPARK-004 trial, while the CNS hemangioblastoma and pNET populations represent subgroups of the LITESPARK-004 trial and broader RCC population. Clinical data were based on the April 1, 2022, data cut-off from the LITESPARK-004 trial.
The transition from presurgery to first surgery for belzutifan in the VHL-RCC and VHL-CNS hemangioblastoma cohorts were modelled using the exponential distribution fitted to time from baseline visit until the first postbaseline renal or CNS surgery from LITESPARK-004, respectively.2 Data informing the VHL-CNS hemangioblastoma population was based on a subset of LITESPARK-004 patients who had CNS hemangioblastoma tumours at baseline.2 The transition rate from presurgery to first surgery for belzutifan for the VHL-pNET cohort was set to equal the hazard rate (HR) of presurgery to first surgery with belzutifan versus active surveillance adjusted by (1 − ORRpNET)/(1 − ORRRCC) due to the limited number of events that occurred in patients with pNET.2 The sponsor assumed that the HR of presurgery to metastatic disease with belzutifan (versus active surveillance) was equal to the HR of presurgery to first surgery in each target population.2 In all cohorts, the sponsor assumed that belzutifan would only reduce the risk of deaths attributable to CNS hemangioblastoma progression.2 In the sponsor’s base-case analysis, the proportion of patients with deaths attributable to CNS hemangioblastoma (by tumour type) was informed by the VHL Natural History Study, in which each cohort was reweighted to match key baseline characteristics of the corresponding LITESPARK-004 trial population.2 Alternative inputs informed by the literature were explored in a scenario analysis.4,5
All transition rates from the presurgery health state for the VHL-RCC population on active surveillance were informed by the exponential function fitted to the observed data from VHL Natural History Study cohort, reweighted to match the LITESPARK-004 population.2 Due to the inability to identify CNS hemangioblastoma and pNET patients at the patient-level index date from the VHL Natural History Study, the pretreatment period of the LITESPARK-004 trial was used to inform the presurgery-to-first-surgery transitions for patients with VHL-CNS hemangioblastoma and VHL-pNET on active surveillance.2 Transitions from presurgery to metastatic disease or death for the CNS hemangioblastoma and pNET cohorts were informed using an approach analogous to that used for the VHL-RCC cohort on active surveillance. Adjustment factors were applied to HRs of surgery and metastatic disease to account for real-world standard of care.2
Transitions from any surgery tunnel state (i.e., first, second, or third or subsequent surgeries) to death were assumed to be equal between the belzutifan and active surveillance treatment arms with the perioperative mortality risk per surgery informed by published literature.2,4,6,7 The sponsor assumed that the mortality risk for all surgery tunnel states would remain the same.2
The probability of transitioning from an event-free state after surgery to the next surgery, or from event-free after surgery to metastatic disease in the VHL-RCC cohort on belzutifan was estimated by multiplying the ratio of the HR of presurgery to first surgery for belzutifan versus active surveillance to the corresponding HR of event-free after first surgery to next surgery or metastatic disease for active surveillance.2 For the VHL-CNS hemangioblastoma and VHL-pNET populations on belzutifan, it was assumed that the rates to next surgery and metastatic disease were the same as the corresponding transitions from presurgery to first-surgery and metastatic-disease health states.2 The transition probabilities from event-free after first surgery to death for belzutifan were assumed to be the same for each cohort.2
For patients on active surveillance, the transition rates from event-free after surgery to next surgery, metastatic disease, or death in the VHL-RCC population were informed by reweighted patient-level time-to-event data from the VHL Natural History Study.2 In the sponsor’s base-case analysis, exponential models were used to inform each transition.2 For the VHL-CNS hemangioblastoma and VHL-pNET cohorts, cause-specific hazards of the event-free-after-surgery to next-surgery health states were assumed to be the same as presurgery to first surgery for each respective cohort.2 The same approach was taken for the cause-specific hazards of event-free after surgery to metastatic disease and event-free after surgery to death.2
The transition from metastatic disease to death were modelled as a function of the distribution of origin tumour (i.e., RCC or pNET; informed by the VHL Natural History Study), the distribution of first-line treatments for metastatic RCC and pNET (informed by market research and clinical experts input), and the efficacy of the included first-line treatments as informed by published literature.8-10 It was assumed that the transition probabilities from metastatic disease to death were equal between belzutifan and active surveillance.2 Deaths from presurgery or event-free after surgery due to all other causes were assumed to be the same for both arms and informed by the general mortality rate from Statistics Canada.11
The sponsor’s base case included costs and disutilities of surgeries for nonprimary tumours (retinal hemangioblastoma, adrenal lesions, endolymphatic sac tumours, and epididymal cystadenomas). Incidence rates were informed by the LITESPARK-004 trial and the VHL Natural History Study for the RCC cohort on belzutifan and active surveillance, respectively.2 Incidence rates for the CNS hemangioblastoma and pNET cohorts were based on the subgroup of patients in LITESPARK-004 with CNS hemangioblastoma and pNET at baseline using data collected after treatment initiation or before treatment initiation, for belzutifan and active surveillance, respectively. The observed incidence rates of nonprimary tumour surgeries were adjusted downward to account for the fact that all patients in the CNS hemangioblastoma and pNET subgroups from the LITESPARK-004 trial also had an RCC.2
In the sponsor’s base case, the risk of AEs (those occurring in ≥ 5% of patients [all grades] and in > 0% of patients at grades 3 to 5 among belzutifan-treated patients) and mean durations were informed by the LITESPARK-004 trial (data cut-off date of April 1, 2022).2 The sponsor assumed that patients treated with active surveillance had no AEs.2 Both short-term and long-term surgical complications associated with all surgeries were incorporated in the model based on third-party claims data from the US.2 Patients who developed long-term surgical complications were assumed to have those complications for the remainder of their lifetime.2 The base-case analysis assumed that the risks of surgical complications were equal between belzutifan and active surveillance arms.2
Belzutifan ToT was informed by the Weibull parametric distribution fitted to time-to-treatment-discontinuation data from the LITESPARK-004 trial in the sponsor’s base case.2 It was assumed that, following discontinuation of belzutifan treatment, the clinical efficacy inputs for belzutifan would converge gradually over a 2.71-year period toward those of active surveillance (calculated as the amount of time required for the largest RCC tumour to grow back to baseline size assuming the pre-treatment linear growth rate) from the end of the trial.2
Health-state utility values in the model were informed by the Quality of Life Disease Burden Study and the KEYNOTE-564 trial.5,10 For the nonmetastatic states, a health-state utility value was calculated as a weighted average by objective response (complete response = 0.887, partial response = 0.814, stable disease = 0.814, progressive disease = 0.746) with the relative weights informed by the overall response rate results from the LITESPARK-004 trial for belzutifan and patient-reported responses in the Disease Burden Study for active surveillance.2 Utility values in the metastatic disease states were informed by the Disease Burden Study (preprogression metastatic disease = 0.615 and postprogression metastatic disease = 0.570).5 Disutilities associated with short- and long-term surgical complications were incorporated as a one-time or recurrent decrement following tumour-reduction surgery, respectively.5,12-19 AE disutilities were applied as one-off events upon model entry, informed by the utility data from KEYNOTE-564.20 In the sponsor’s base case, a caregiver disutility was included and informed by published literature.21-23
The sponsor’s base case included drug acquisition costs, AE management costs, surgery and surgical complication costs, disease-management costs, and terminal-care costs. Drug acquisition costs were taken from DeltaPA.24 The drug acquisition cost of belzutifan was provided by the sponsor.2 Patients on belzutifan were modelled to have a fixed dosage of 120 mg once daily with a mean relative dose intensity (RDI) of 92.5% as observed in the trial, resulting in a 28-day cost of $16,576.2 Unit cost per AE event, tumour-reduction surgery, and costs of both short- and long-term surgical complications were obtained from either the Ontario Case Costing Initiative or published literature.25-32 Unit costs used to inform health state and disease-management costs were obtained from the Ontario Schedule of Benefits, the Québec Directory and Measurement System for Medical Biology Procedures and published literature, and frequency of use was informed by clinical surveillance guidelines and clinical expert feedback.2,33-36 Terminal-care costs obtained from published literature were applied as one-off costs associated with patients who transition to death.37 All costs were expressed in 2022 Canadian dollars.
Summary of Sponsor’s Economic Evaluation Results
All analyses were run probabilistically (1,000 iterations). Submitted deterministic analyses were aligned with the probability results. The probabilistic findings are presented below.
Base-Case Results
Results were reported separately for the VHL-RCC, VHL-CNS hemangioblastoma, and VHL-pNET cohorts. The sponsor’s probabilistic base-case analysis found that belzutifan was associated with an additional 3.19 QALYs at an additional cost of $887,036 versus active surveillance for the VHL-RCC cohort. The ICER of belzutifan compared to active surveillance was therefore $278,259 per QALY gained. Similarly, belzutifan was associated with 3.10 and 3.61 more QALYs at an additional cost of $871,975 and $879,508, in the VHL-CNS hemangioblastoma and VHL-pNET cohorts, respectively. The ICERs for VHL-CNS hemangioblastoma and VHL-pNET relative to active surveillance were therefore $281,170 and $243,505 per QALY gained, respectively. Based on deterministic results, the majority (approximately 90%) of the incremental QALYs for belzutifan were found to be accrued during the extrapolation period (after the 37.8-month observed median follow-up period from the LITESPARK-004 trial).
Table 3: Summary of Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER vs. reference ($ per QALY gained) |
|---|---|---|---|---|---|
VHL-RCC cohort | |||||
Active surveillance | 461,541 | Reference | 6.72 | Reference | Reference |
Belzutifan | 1,348,577 | 887,036 | 9.91 | 3.19 | 278,259 |
VHL-CNS hemangioblastoma cohort | |||||
Active surveillance | 426,847 | Reference | 6.92 | Reference | Reference |
Belzutifan | 1,298,822 | 871,975 | 10.02 | 3.10 | 281,170 |
VHL-pNET cohort | |||||
Active surveillance | 420,860 | Reference | 4.93 | Reference | Reference |
Belzutifan | 1,300,369 | 879,508 | 8.54 | 3.61 | 243,505 |
CNS = central nervous system; ICER = incremental cost-effectiveness ratio; pNET = pancreatic neuroendocrine tumour; QALY = quality-adjusted life-year; RCC = renal cell carcinoma; VHL = von Hippel-Lindau.
Source: Sponsor’s pharmacoeconomic submission.2
Sensitivity and Scenario Analysis Results
The sponsor conducted several scenario analyses incorporating different time horizons, perspectives, efficacy and transition probabilities associated with presurgery to surgery, exclusion of adjustments for real-world standard of care, different ToT distributions for belzutifan, alternative sources to inform the proportion of patients with deaths attributed to CNS hemangioblastoma, exclusion of RDI, inclusion of vial sharing, and health-state utilities and disutilities. Results from the scenarios indicated that the ICER was most sensitive to changes associated with belzutifan ToT and efficacy: the ICER decreased in all 3 cohorts (VHL-RCC: $65,643 per QALY gained, VHL-CNS hemangioblastoma: $57,861 per QALY gained, and VHL-pNET: $52,989 per QALY gained) when no treatment-effect waning after discontinuation was assumed. The highest ICERs were associated with a scenario that did not adjust the rates of surgeries or metastases to account for suboptimal real-world surveillance practices (VHL-RCC: $358,314 per QALY gained, VHL-CNS hemangioblastoma: $378,469 per QALY gained, and VHL-pNET: $472,506 per QALY gained).
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the economic analysis:
The long-term efficacy of belzutifan for patients with VHL disease–associated nonmetastatic RCC, CNS hemangioblastoma, or nonmetastatic pNET is unknown. Treatment efficacy for belzutifan in the sponsor’s base case was primarily informed by parametric extrapolations fitted to patient-level data from the phase II, single-arm LITESPARK-004 trial. TTS was the key clinical input used to inform transitions from the presurgery health state in the economic model, in which 7 patients (11.5%) with RCC, 1 (2.0%) with CNS hemangioblastoma, and none of the patients with pNET had surgery during the follow-up period. However, as noted in the CADTH clinical report, median TTS was not reached for patients with a VHL disease–associated nonmetastatic RCC, CNS hemangioblastoma, or nonmetastatic pNET at the April 1, 2022, data cut-off date. No definitive conclusion could therefore be drawn about the long-term benefits of belzutifan on TTS. Clinical expert feedback received by CADTH noted that, while treatment with belzutifan may have an impact on TTS and the number of surgeries, the magnitude of any impact is uncertain as a result of the identified limitations with the available data. Based on the sponsor’s model structure, the assumptions around TTS resulted in a survival benefit for patients on belzutifan. As described in the CADTH clinical report, investigator-assessed median PFS was not reached for metastatic RCC, median PFS was not reached for VHL-CNS hemangioblastoma or VHL-pNET patients, and overall survival was not captured in the LITESPARK-004 trial (data cut-off of April 1, 2022). Therefore, the assumed survival benefit of belzutifan modelled by the sponsor cannot be validated based on currently available information and is associated with uncertainty.
CADTH also identified concerns regarding the generalizability of the LITESPARK-004 trial to clinical practice in Canada. As noted in the CADTH clinical report, despite the number of organs that VHL disease can affect, only a small number of patient groups (i.e., RCC only, RCC with CNS hemangioblastoma, RCC with pNET, and RCC with both CNS hemangioblastoma and pNET) were assessed in the LITESPARK-004 trial. The trial population represents a narrower population than the Health Canada–indicated population. While the clinical expert feedback received by CADTH noted that, in general, the study selection criteria were aligned with patients who may receive belzutifan in the Canadian setting, there may be limitations due to the lack of Canadian sites in the studies, and that greater than 90% of patients in the study were white, which does not reflect the racial profile in Canada.
CADTH was unable to resolve this issue due to limitations in data availability. The impact of this limitation on the cost-effectiveness of belzutifan is uncertain.
The relative efficacy of belzutifan compared with active surveillance is uncertain. In the absence of comparative clinical data, the sponsor used patient-level time-to-event data from the VHL Natural History Study (2021) cohort, reweighted to match the baseline characteristics of the LITESPARK-004 trial population, to inform the efficacy of the comparator, active surveillance. However, as noted in the CADTH clinical report, there were limitations in utilization of the VHL Natural History Study relating to the selection criteria intended to match the VHL Natural History Study’s cohort with that from the LITESPARK-004, key covariates were missing from the pivotal trial, and no adjustments were made for important effect-modifying or prognostic factors, such as VHL gene alteration type and the number of measured tumours. These made it difficult to assess the degree of heterogeneity between the populations in the LITESPARK-004 trial and VHL Natural History Study, and the potential for residual confounding was considered high. Furthermore, the sponsor was unable to identify patients who had CNS hemangioblastomas and/or pNET tumours in the VHL Natural History Study cohort. Clinical expert feedback received by CADTH noted that, despite the limitations of the available comparative evidence, belzutifan appears to have a promising tumour response compared with the experts’ experiences with the natural history of the disease. However, the clinical experts indicated that the magnitude of benefit associated with belzutifan is unknown.
CADTH was unable to resolve this issue due to limitations in data availability. As a result, the estimate of the ICER for belzutifan compared with active surveillance is associated with uncertainty.
The ToT for patients receiving belzutifan is uncertain. In the sponsor’s base case, the ToT for patients receiving belzutifan was informed by parametric curves fitted to patient-level data on the time-to-treatment-discontinuation data from LITESPARK-004. Although the Gompertz curve was the best-fitting distribution based on Akaike information criterion and Bayesian information criterion, the sponsor selected the Weibull distribution for its base-case analysis (patients received treatment for up to 14 years), stating that the longer tail was more plausible because a proportion of patients are expected to remain on treatment beyond 6 years (i.e., the point at which the Gompertz curve predicted that all patients would have discontinued). Clinical expert feedback received by CADTH noted that, given the follow-up period for the LITESPARK-004 trial (median = 37.8 months; range = 4.2 to 46.1 months), the sponsor’s ToT assumption for patients receiving belzutifan is associated with uncertainty. However, the clinical experts noted that the ToT estimates resulting from the Weibull distribution would likely overestimate the ToT for patients receiving belzutifan expected to be seen in clinical practice in Canada.
CADTH explored the impact of selecting the Gompertz curve to inform time on belzutifan treatment in a scenario analysis.
The assumption of residual benefit for belzutifan after treatment discontinuation is associated with uncertainty. In the sponsor’s submitted economic model, the ToT for patients receiving belzutifan was modelled based on Weibull distributions fitted to ToT discontinuation data from the LITESPARK-004 trial. The sponsor assumed that, at the time of discontinuing belzutifan, a patient’s largest tumour would be smaller than if the patient had not been treated with belzutifan, based on changes in RCC tumour size from the LITESPARK-004 trial. In the submitted base-case analysis, the sponsor assumed that, upon discontinuation of belzutifan treatment after the maximum trial follow-up period (46.1 months), patients’ probabilities of requiring a surgery, experiencing metastatic disease, or dying (i.e., their transition probabilities from the presurgery and event-free-after-surgery health states) would linearly converge with that of active surveillance over 2.71 years, based on the time it would take for the average size of the largest RCC tumour at belzutifan discontinuation (i.e., 15.36 mm) to grow back to the baseline size (i.e., 24.9 mm), assuming a linear growth rate equal to that of the pretreatment period of the LITESPARK-004 trial (i.e., 3.52 mm per year).
Clinical expert feedback obtained by CADTH indicated that, although there was no robust evidence to support an attenuation of benefit beyond treatment discontinuation, patients who received belzutifan may achieve some residual benefit after treatment discontinuation. However, feedback from the clinical experts considered the sponsor’s assumption of 2.71 years to be an overestimate. Clinical expert feedback noted that that tumour growth rates after treatment can vary significantly compared to the pretreatment growth rate (i.e., in some disease areas a tumour may have no growth after treatment discontinuation whereas other tumours may grow more quickly and greater in size than previously). Without post-discontinuation efficacy data there is therefore significant uncertainty in how tumours may grow after belzutifan discontinuation.
The sponsor presented a scenario analysis exploring the effects of no residual benefit. However, this scenario was inappropriate, as it reduced the ToT while maintaining the clinical efficacy of belzutifan throughout the modelled time horizon. As noted previously, there is significant uncertainty in the long term efficacy of belzutifan and therefore this method overestimates the treatment effect of belzutifan.
In the CADTH base-case analysis, patients were modelled to converge to active surveillance immediately after belzutifan treatment discontinuation after the maximum trial follow-up period.
To explore the impact of some residual benefit post-discontinuation, a scenario analysis was conducted assuming a shorter time period (1 year) to convergence.
The sponsor underestimated belzutifan drug costs. In the sponsor’s base-case analysis, the mean RDI observed in the LITESPARK-004 trial was used to derive the drug acquisition cost for belzutifan. The inclusion of RDI may underestimate the total cost of belzutifan in clinical practice as the dose received by a patient may be different from the planned dose for several reasons (e.g., missed doses or dose reductions).
Additionally, the sponsor assumed that the price of belzutifan would experience a 30% price reduction after 10 years due to the introduction of generics. Although generics for belzutifan may become available in the future, it is unknown in what capacity and at what price, and the inclusion of such a price reduction for generics in the cost-effectiveness model may therefore underestimate the total treatment cost of belzutifan to the Canadian health care system.
In the CADTH base-case reanalysis, the RDI was set to 100% (following the sponsor’s provided drop down) and price reductions associated with generics were excluded.
The inclusion of caregiver disutility in the base case was inappropriate. The sponsor noted that a patient’s health status and well-being would have a significant impact on caregivers, and it therefore included caregiver disutility in its base case. The sponsor assumed that each patient would have 1 caregiver, and disutility values were informed by published reports involving family members and caregivers of cancer patients. Although caregivers are often affected by a patient’s health status, the evidence to support the degree of impact for VHL-specific caregivers is weak and the sponsor’s incorporation of caregiver disutility is therefore uncertain. The inclusion of caregiver disutilities overestimates of the benefits associated with belzutifan in the sponsor’s base case as it increased the QALY gains received by patients in the form of caregiver benefits.
In the CADTH base-case reanalysis, caregiver disutilities were excluded. Caregiver disutilities were included in a scenario analysis with a societal perspective.
Poor modelling practices were employed. The sponsor’s submitted model included numerous IFERROR statements, which can lead to situations in which the parameter value is over-written with an alternative value without alerting the user to the automatized overwriting. The systematic use of IFERROR statements makes thorough auditing of the sponsor’s model impractical, and it remains unclear whether the model is running inappropriately by overriding errors.
CADTH was unable to address this limitation or conduct a thorough validation of the sponsor’s model.
Table 4: Key Assumptions of the Submitted Economic Evaluation (Not Noted as Limitations to the Submission)
Sponsor’s key assumption | CADTH comment |
|---|---|
VHL-RCC, VHL-CNS hemangioblastoma, and VHL-pNET were modelled as 3 separate cohorts. | Reasonable. Based on clinical expert feedback received by CADTH, the options and effectiveness of local therapies for the 3 tumour types can vary, as do prognosis and tumour-related surgery. |
The CNS and pNET cohorts were presented as distinct cohorts alongside the RCC cohort, as opposed to subgroups of a broader population. | Uncertain. Patients in the RCC cohort were duplicated in the CNS hemangioblastoma and/or pNET cohort if they had those tumours as well. The population with RCC is the overarching population in the LITESPARK-004 trial as all patients in the LITESPARK-004 trial had to have RCC to be eligible. As a result, the CNS hemangioblastoma and pNET populations represent subgroups of the RCC trial population informed by a small number of patients. The CADTH base case focuses on the RCC population, reporting the CNS hemangioblastoma and pNET populations as subgroup analyses. However, given that the clinical expert feedback received by CADTH noted that results from LITESPARK-004 may be generalizable to patients with only CNS hemangioblastoma and/or pNET, the CADTH subgroup analyses conducted may reflect patients with only VHL-associated CNS or pNET without RCC. |
Active surveillance is the most appropriate comparator. | Reasonable. Confirmed by clinical expert feedback obtained by CADTH. |
Patients with pNET on belzutifan have the same HR as presurgery to first surgery of patients with RCC on belzutifan (vs. active surveillance) adjusted by (1 − ORRpNET)/(1 − ORRRCC). | Reasonable. Clinical expert feedback received by CADTH noted that, in the absence of evidence, this was a reasonable assumption. |
The HR of presurgery to metastatic disease with belzutifan (vs. active surveillance) was equal to the HR of presurgery to first surgery in each target population. | Reasonable. Clinical expert feedback received by CADTH noted this was a reasonable assumption due to limitations in available data. |
CNS hemangioblastoma tumours are assumed to be nonmalignant. | Reasonable. Clinical expert feedback received by CADTH noted that CNS hemangioblastoma are nonmalignant tumours by histology and do not metastasize. |
Belzutifan only reduces the risk of death attributed to CNS hemangioblastoma progression in all cohorts. | Reasonable. Although CNS hemangioblastoma tumours are nonmalignant, they are major causes of morbidity and mortality in VHL disease as they can affect vital structures in the CNS by compression or as surgical sequelae. This was confirmed by clinical expert feedback obtained by CADTH. |
Proportions of patients with deaths attributable to a CNS hemangioblastoma (by tumour type) were informed by VHL Natural History Study data (reweighted to match key baseline characteristics of the corresponding LITESPARK-004 trial population). | Uncertain. There is uncertainty in the utilization of the VHL Natural History Study due to selection criteria and lack of adjusting for important effect-modifying or prognostic factors. However, results of the scenario using alternative data informed by published literature suggest that this is unlikely to have a large impact on the overall results. |
The probability of transition to death, to next surgery, and to metastatic disease after subsequent surgeries is the same as the probabilities after first surgery. | Inappropriate. Clinical expert feedback received by CADTH noted that subsequent surgeries would be associated with increased risks and other complications. While this assumption was made for both treatment arms, the sponsor’s assumption may overestimate the benefit of belzutifan in reducing subsequent surgeries. The true impact of belzutifan efficacy after subsequent surgeries is unknown. The impact of this assumption on the cost-effectiveness of belzutifan is unknown. |
Tumour response levels would affect a patient’s risk of surgery or metastatic disease and therefore affect their utility values. | Potentially reasonable. Clinical expert feedback received by CADTH noted that, while it is generally reasonable to assume that a patient’s tumour response level may affect their quality of life, some lesions, while measurable, are not symptomatic and therefore a reduction in size may not be associated with noticeable changes in quality of life. |
Genetic testing costs were excluded. | Potentially reasonable. The clinical experts consulted by CADTH did not anticipate the current landscape of VHL genetic testing would be affected greatly if belzutifan is reimbursed. However, genetic testing remains an important component of the VHL diagnostic and treatment pathway. In a scenario analysis, CADTH explored the impact of including genetic testing costs, assuming 0.75 tests per patient on active surveillance and 1 test per patient on belzutifan in the target population. |
CNS = central nervous system; HR = hazard ratio; ORR = objective response rate; pNET = pancreatic neuroendocrine tumour; RCC = renal cell carcinoma; VHL = von Hippel-Lindau.
CADTH Reanalyses of the Economic Evaluation
Base-Case Results
The CADTH base case was derived by making changes in model parameter values and assumptions, in consultation with clinical experts. These changes, summarized in Table 5, involved removal of belzutifan residual benefit after treatment discontinuation after the trial duration, removal of caregiver disutility, and correcting belzutifan costing inputs.
Table 5: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
None | — | — |
Changes to derive the CADTH base case | ||
1. Belzutifan residual benefit after treatment discontinuation | Discontinued patients would gradually converge to active surveillance efficacy after a 2.71-year period after the LITESPARK-004 trial duration | Immediate convergence to active surveillance efficacy upon belzutifan treatment discontinuation after the LITESPARK-004 trial duration |
2. Caregiver disutility | Included | Excluded |
3. Relative dose intensity | 92.5% | 100% |
4. Belzutifan price reduction following genetic entry | 30% price reduction after 10 years | 0% reduction after 10 years |
CADTH reanalysis | — | 1 + 2 + 3 + 4 |
The CADTH base-case analysis focuses on the RCC population due to duplicated patients in the CNS and/or pNET cohort. The results of the CADTH base-case analyses demonstrated that belzutifan was associated with 2.71 additional QALYs at an additional cost of $975,998 versus active surveillance for the VHL-RCC population. Therefore, the ICER of belzutifan compared to active surveillance was $360,193 per QALY gained. The probability of cost-effectiveness at a $50,000 per QALY WTP threshold was 0%. Based on the deterministic results of the CADTH base case, approximately 90% of the incremental QALYs for belzutifan were accrued during the extrapolated period (i.e., after the 37.8-month observed median follow-up period from the LITESPARK-004 trial).
CADTH conducted further subgroup analyses for the CNS hemangioblastoma and pNET populations. The results of these analyses indicated that, compared to active surveillance, belzutifan was associated with 2.61 and 3.08 more QALYs at additional costs of $961,796 and $968,488, respectively. The ICERs for VHL-CNS hemangioblastoma and VHL-pNET subgroups relative to active surveillance were therefore $368,886 per QALY gained and $314,661 per QALY gained, respectively. A summary of the CADTH base-case and subgroup-reanalysis results can be found in Table 6. Details on the stepped analysis are available in Appendix 4.
Table 6: Summary of the Stepped Analysis of the CADTH Reanalysis Results
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($ per QALY gained) |
|---|---|---|---|---|
Sponsor base case | ||||
VHL-RCC | Active surveillance | 461,541 | 6.72 | Reference |
Belzutifan | 1,348,577 | 9.91 | 278,259 | |
VHL-CNS hemangioblastoma | Active surveillance | 426,847 | 6.92 | Reference |
Belzutifan | 1,298,822 | 10.02 | 281,170 | |
VHL-pNET | Active surveillance | 420,860 | 4.93 | Reference |
Belzutifan | 1,300,369 | 8.54 | 243,505 | |
Base case: CADTH reanalysis (1 + 2 + 3 + 4) | ||||
VHL-RCC | Active surveillance | 478,842 | 8.42 | Reference |
Belzutifan | 1,454,839 | 11.13 | 360,193 | |
Key subgroups: CADTH reanalysis (1 + 2 + 3 + 4) | ||||
VHL-CNS hemangioblastoma | Active surveillance | 439,619 | 8.66 | Reference |
Belzutifan | 1,401,415 | 11.27 | 368,886 | |
VHL-pNET | Active surveillance | 433,123 | 6.64 | Reference |
Belzutifan | 1,401,611 | 9.71 | 314,661 | |
CNS = central nervous system; ICER = incremental cost-effectiveness ratio; pNET = pancreatic neuroendocrine tumour; QALY = quality-adjusted life-year; RCC = renal cell carcinoma; VHL = von Hippel-Lindau.
Note: Results were derived probabilistically.
Scenario Analysis Results
Three scenarios were conducted on the CADTH base-case analysis for the RCC population and key subgroups to investigate the impact of using the Gompertz distribution to inform belzutifan ToT, assuming convergence to active surveillance efficacy would occur gradually over 1 year after the LITESPARK-004 trial duration and including genetic testing costs. Results of scenario analyses are presented in Appendix 4.
The analysis examining the impact of using the Gompertz distribution to inform belzutifan ToT resulted in ICERs of $349,738 per QALY gained, $361,534 per QALY gained, and $304,739 per QALY gained for belzutifan compared with active surveillance for the VHL-RCC, VHL-CNS hemangioblastoma, and VHL-pNET cohorts, respectively. The analyses assuming discontinued patients would gradually converge to active surveillance efficacy over a 1-year period after the LITESPARK-004 trial duration resulted in ICERs of $344,302 per QALY gained, $352,723 per QALY gained, and $300,492 per QALY gained for belzutifan compared with active surveillance for the VHL-RCC, VHL-CNS hemangioblastoma, and VHL-pNET cohorts, respectively. Last, inclusion of genetic testing costs resulted in ICERs of $360,260 per QALY gained, $368,956 per QALY gained, and $314,720 per QALY gained for belzutifan versus active surveillance for the VHL-RCC, VHL-CNS hemangioblastoma, and VHL-pNET cohorts, respectively.
CADTH also undertook price-reduction analyses based on the sponsor’s and CADTH’s base cases. The CADTH base case suggested a price reduction of approximately 83% would be required to achieve cost-effectiveness of belzutifan at a WTP threshold of $50,000 per QALY gained in the full VHL-RCC cohort. The price reduction in the VHL-CNS hemangioblastoma, and VHL-pNET cohorts were similar (82% and 81%, respectively).
Table 7: CADTH Price-Reduction Analyses
Analysis | ICERs for belzutifan vs. active surveillance | |||||
|---|---|---|---|---|---|---|
Price reduction (unit cost in $) | Sponsor base case ($ per QALY gained) | CADTH reanalysis ($ per QALY gained) | ||||
VHL-RCC | VHL-CNS hemangioblastoma | VHL-pNET | VHL-RCC | VHL-CNS hemangioblastoma | VHL-pNET | |
None ($213.33) | 279,456 | 274,850 | 238,676 | 359,188 | 356,386 | 307,275 |
10% ($192.00) | 250,060 | 245,588 | 213,663 | 321,727 | 318,851 | 275,347 |
20% ($170.66) | 220,663 | 216,326 | 188,651 | 284,267 | 281,315 | 243,418 |
30% ($149.33) | 191,266 | 187,064 | 163,638 | 246,806 | 243,779 | 211,489 |
40% ($128.00) | 161,869 | 157,802 | 138,625 | 209,346 | 206,243 | 179,561 |
50% ($106.67) | 132,472 | 128,540 | 113,612 | 171,885 | 168,707 | 147,632 |
60% ($85.33) | 103,075 | 99,278 | 88,600 | 134,424 | 131,171 | 115,704 |
70% ($64.00) | 73,679 | 70,016 | 63,587 | 96,964 | 93,635 | 83,775 |
80% ($42.67) | 44,282 | 40,754 | 38,574 | 59,503 | 56,099 | 51,847 |
90% ($21.33) | 14,885 | 11,492 | 13,562 | 22,043 | 18,564 | 19,918 |
CNS = central nervous system; ICER = incremental cost-effectiveness ratio; pNET = pancreatic neuroendocrine tumour; QALY = quality-adjusted life-year; RCC = renal cell carcinoma; VHL = von Hippel-Lindau.
Note: All price-reduction analyses were conducted deterministically.
Issues for Consideration
Clinical expert feedback obtained by CADTH noted that the availability of belzutifan for adult patients with VHL disease who require therapy for associated nonmetastatic RCC, CNS hemangioblastoma, or nonmetastatic pNET not requiring immediate surgery is unlikely to notably increase the utilization of health care resources such as germline genetic testing as patients are expected to have already undergone genetic testing due to a family history or earlier presentation with VHL-associated morbidities, and it is not anticipated that testing will be required to confirm diagnosis for eligible patients. However, should testing frequency increase with belzutifan reimbursement, the true impact on health care resource use remains unknown. Based on a CADTH scenario analysis, the inclusion of genetic tests had minimal impact on the ICERs in all 3 of the cohorts.
Despite VHL being a multiorgan disease, only a small number of patient groups (i.e., RCC only, RCC with CNS hemangioblastoma, RCC with pNET, and RCC with both CNS hemangioblastoma and pNET) were assessed in the LITESPARK-004 trial. The trial population is therefore narrower than the Health Canada–indicated population. While the clinical expert feedback received by CADTH noted that results in the explored patient groups are likely reflective of other patient groups, the cost-effectiveness of belzutifan for patients outside of those included in the LITESPARK-004 trial is unknown.
Drug plan input obtained by CADTH considered the potential use of belzutifan in a pediatric population. At present, Health Canada has not authorized an indication for pediatric use due to the lack of data from this population. However, if a pediatric indication is authorized in the future, the cost-effectiveness and budgetary impact of using belzutifan in this population is unknown.
Overall Conclusions
Evidence from the LITESPARK-004 trial and feedback from clinical experts, suggests that, in adult patients with a VHL disease–associated nonmetastatic RCC, VHL disease–associated CNS hemangioblastoma, and VHL disease–associated nonmetastatic pNET, none of whom required immediate surgery, belzutifan demonstrated a promising and durable tumour response as measured by ORR and duration of response, which would likely not be otherwise attributable to active surveillance. However, uncertainty is associated with the LITESPARK-004 trial findings for other key supportive outcomes (e.g., TTS and PFS) due to major limitations, such as the lack of an internal comparator and no inferential statistical analyses. The sponsor’s ITC suggested that treatment with belzutifan may have a beneficial effect on time to RCC-related surgery compared to active surveillance in the RCC cohort; however, due to several key methodological limitations that bias the findings in favour of belzutifan, the comparative effectiveness estimates are uncertain. Given the lack of ITC evidence in the CNS hemangioblastoma and pNET cohorts, the comparative effects of belzutifan in these populations are unknown. Due to the absence of robust clinical evidence, it is unclear whether the modelled quality-of-life benefits associated with belzutifan would be observed in clinical practice.
CADTH identified several limitations in the sponsor’s pharmacoeconomic analysis that have notable implications on the cost-effectiveness of belzutifan. As part of the base-case analysis, CADTH revised the assumptions regarding residual benefit with belzutifan upon treatment discontinuation, removed caregiver disutilities, and removed belzutifan trial RDI and generic costing assumptions. The CADTH base-case reanalysis resulted in an ICER of $360,193 per QALY gained (incremental costs = $975,998; incremental QALYs = 2.71) for belzutifan versus active surveillance for the VHL-RCC cohort. In the VHL-CNS hemangioblastoma and VHL-pNET subgroup cohorts, the ICERs for belzutifan versus active surveillance were $368,886 per QALY gained (incremental costs = $961,796; incremental QALYs = 2.61) and $314,661 per QALY gained (incremental costs = $968,488; incremental QALYs = 3.08), respectively. The CADTH base-case results were aligned with the sponsor’s results, with belzutifan associated with a higher ICER and not considered cost-effective relative to active surveillance at a $50,000 WTP threshold. A price reduction of approximately 83% is therefore required for belzutifan to be considered cost-effectiveness at a WTP threshold of $50,000 per QALY for the broader RCC population. Based on a price reduction of this magnitude, the cost per 28 days of treatment would be approximately $3,050 per patient. Required price reductions for the CNS hemangioblastoma and pNET subgroups were similar.
The cost-effectiveness of belzutifan was sensitive to assumptions surrounding ToT and residual benefit after treatment discontinuation. Specifically, the CADTH base-case analysis considered no residual benefit after belzutifan treatment discontinuation after the maximum follow-up period of the LITESPARK-004 trial that resulted in a smaller difference in QALYs between belzutifan and active surveillance (gains in QALYs with belzutifan were 3.19 as reported by the sponsor versus 2.71 as estimated by CADTH in the RCC cohort). Although clinical expert feedback noted that belzutifan reimbursement is not expected to affect the current genetic testing landscape, CADTH undertook a scenario exploring an increase in genetic testing due to belzutifan reimbursement; the scenario analysis suggested a minimal impact on the ICER in all 3 cohorts.
The long-term treatment effect of belzutifan for the treatment of adult patients with a VHL disease–associated nonmetastatic RCC, VHL disease–associated CNS hemangioblastoma, and VHL disease–associated nonmetastatic pNET, none of whom required immediate surgery, as well as the comparative efficacy of belzutifan to active surveillance, remain uncertain. Based on the deterministic results of the CADTH base case, approximately 90% of the incremental QALYs for belzutifan accrued after the 37.8-month observed median follow-up period from the LITESPARK-004 trial. This benefit should be interpreted with caution given the lack of overall survival data to confirm this modelled benefit. Additionally, as the LITESPARK-004 trial population was narrower than the Health Canada–indicated population, there is uncertainty in the treatment effect of belzutifan for patients excluded from the analysis (i.e., patients with a VHL-associated CNS hemangioblastoma or pNET who do not have RCC). Should RCC have no effect on other tumour types, the subgroup analyses conducted may be generalized to patients with only a VHL-associated CNS or pNET. As CADTH was unable to fully assess the uncertainty around long-term treatment efficacy and comparative efficacy to active surveillance due to lack of data, a higher price reduction may be warranted.
References
1.Merck Canada response to February 17, 2023 CADTH request for additional information regarding Welireg (belzutifan) CADTH review [internal additional sponsor's information]. Kirkland (QC) Merck Canada Inc; 2023 Feb 24.
2.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Welireg (belzutifan). Kirkland (QC): Merck Canada Inc; 2023 May 1.
3.Welireg® belzutifan tablets, 40 mg, oral [product monograph]. Kirkland (QC) Merck Canada Inc; 2022 Dec 13.
4.Lonser RR, Weil RJ, Wanebo JE, DeVroom HL, Oldfield EH. Surgical management of spinal cord hemangioblastomas in patients with von Hippel-Lindau disease. J Neurosurg. 2003;98(1):106-116. PubMed
5.Adelphi Real World. VHL-Related Disease Impact on Quality of Life and Work Productivity in Patients with Renal Cell Carcinoma, Central Nervous System Hemangioblastoma, or Pancreatic Neuroendocrine Tumor Manifestation. 2022.
6.Krauss T, Ferrara AM, Links TP, et al. Preventive medicine of von Hippel-Lindau disease-associated pancreatic neuroendocrine tumors. Endocr Relat Cancer. 2018;25(9):783-793. PubMed
7.Johnson A, Sudarshan S, Liu J, Linehan WM, Pinto PA, Bratslavsky G. Feasibility and outcomes of repeat partial nephrectomy. J Urol. 2008;180(1):89-93; discussion 93. PubMed
8.Motzer R, Alekseev B, Rha SY, et al. Lenvatinib plus Pembrolizumab or Everolimus for Advanced Renal Cell Carcinoma. N Engl J Med. 2021;384(14):1289-1300. PubMed
9.Riaz IB, He H, Ryu AJ, et al. A Living, Interactive Systematic Review and Network Meta-analysis of First-line Treatment of Metastatic Renal Cell Carcinoma. Eur Urol. 2021;80(6):712-723. PubMed
10.Rini BI PE, Stus V, et al. Pembrolizumab plus axitinib versus sunitinib as first-line therapy for advanced clear cell renal cell carcinoma: Results from 42-month follow-up of KEYNOTE-426. Poster presented at the 2021 American Society of Clinical Oncology (ASCO) Annual Meeting.
11.Table: 17-10-0057-01 Projected population, by projection scenario, age and sex, as of July 1 (x 1,000). Ottawa (ON: Statistics Canada; 2022: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1710005701. Accessed 1800 Jan 1.
12.Lee AJ, Morgan CL, Conway P, Currie CJ. Characterisation and comparison of health-related quality of life for patients with renal failure. Curr Med Res Opin. 2005;21(11):1777-1783. PubMed
13.Simianu VV, Gaertner WB, Kuntz K, et al. Cost-effectiveness Evaluation of Laparoscopic Versus Robotic Minimally Invasive Colectomy. Ann Surg. 2020;272(2):334-341. PubMed
14.Gandhi SK, Jensen MM, Fox KM, Smolen L, Olsson AG, Paulsson T. Cost-effectiveness of rosuvastatin in comparison with generic atorvastatin and simvastatin in a Swedish population at high risk of cardiovascular events. Clinicoecon Outcomes Res. 2012;4:1-11. PubMed
15.Zargar M, McFarlane T, Chan KKW, Wong WWL. Cost-Effectiveness of Nivolumab in Recurrent Metastatic Head and Neck Squamous Cell Carcinoma. Oncologist. 2018;23(2):225-233. PubMed
16.Poole CD, Chambers C, Allsopp R, Currie CJ. Quality of life and health-related utility analysis of adults with moderate and severe atopic dermatitis treated with tacrolimus ointment vs. topical corticosteroids. J Eur Acad Dermatol Venereol. 2010;24(6):674-678. PubMed
17.Stevenson SM, Danzig MR, Ghandour RA, et al. Cost-effectiveness of neoadjuvant chemotherapy before radical cystectomy for muscle-invasive bladder cancer. Urol Oncol. 2014;32(8):1172-1177. PubMed
18.Wang CY, Pham PN, Kim S, et al. Predicting Cost-Effectiveness of Generic vs. Brand Dabigatran Using Pharmacometric Estimates Among Patients with Atrial Fibrillation in the United States. Clin Transl Sci. 2020;13(2):352-361. PubMed
19.Verkleij ML, Heijnsdijk EAM, Busse AML, et al. Cost-Effectiveness of Neonatal Hearing Screening Programs: A Micro-Simulation Modeling Analysis. Ear Hear. 2021;42(4):909-916. PubMed
20.National Institute for Health and Care Excellence. Pembrolizumab for adjuvant treatment of renal cell carcinoma [TA830]. 2022; https://www.nice.org.uk/guidance/ta830/documents/committee-papers. Accessed Feb 24, 2022.
21.Turner D, Adams E, Boulton M, et al. Partners and close family members of long-term cancer survivors: health status, psychosocial well-being and unmet supportive care needs. Psychooncology. 2013;22(1):12-19. PubMed
22.Sjolander C, Rolander B, Järhult J, Mårtensson J, Ahlstrom G. Health-related quality of life in family members of patients with an advanced cancer diagnosis: a one-year prospective study. Health Qual Life Outcomes. 2012;10:89. PubMed
23.Song JI, Shin DW, Choi JY, et al. Quality of life and mental health in the bereaved family members of patients with terminal cancer. Psychooncology. 2012;21(11):1158-1166. PubMed
24.Government of A. Interactive drug benefit list. 2022; https://idbl.ab.bluecross.ca/idbl/load.do. Accessed 1800 Jan 1.
25.Ontario Case Costing Initiative (OCCI). Toronto (ON): Ontario Health and Long-Term Care; 2017: https://data.ontario.ca/dataset/ontario-case-costing-initiative-occi. Accessed 1800 Jan 1.
26.Zelmer JL. The economic burden of end-stage renal disease in Canada. Kidney Int. 2007;72(9):1122-1129. PubMed
27.Manns B, Hemmelgarn B, Tonelli M, et al. The Cost of Care for People With Chronic Kidney Disease. Can J Kidney Health Dis. 2019;6:2054358119835521. PubMed
28.Spencer Netto F, Quereshy F, Camilotti BG, et al. Hospital costs associated with laparoscopic and open inguinal herniorrhaphy. JSLS. 2014;18(4). PubMed
29.Guerriere DN, Choiniere M, Dion D, et al. The Canadian STOP-PAIN project - Part 2: What is the cost of pain for patients on waitlists of multidisciplinary pain treatment facilities? Can J Anaesth. 2010;57(6):549-558. PubMed
30.Widjaja E, Guttmann A, Tomlinson G, Snead OC, 3rd, Sander B. Economic burden of epilepsy in children: A population-based matched cohort study in Canada. Epilepsia. 2021;62(1):152-162. PubMed
31.Rosella LC, Lebenbaum M, Fitzpatrick T, et al. Impact of diabetes on healthcare costs in a population-based cohort: a cost analysis. Diabet Med. 2016;33(3):395-403. PubMed
32.Bornstein SR, Allolio B, Arlt W, et al. Diagnosis and Treatment of Primary Adrenal Insufficiency: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2016;101(2):364-389. PubMed
33.Quebec Directory and Measurement System for Medical Biology Procedures. 2021-2022. https://publications.msss.gouv.qc.ca/msss/fichiers/2020/20-922-05W.pdf.
34.Schedule of benefits for physician services under the Health Insurance Act: (January 25, 2022 (effective July 1, 2022)). Toronto (ON): Ontario Ministry of Health; 2022: https://www.health.gov.on.ca/en/pro/programs/ohip/sob/physserv/sob_master.pdf. Accessed 1800 Jan 1.
35.Stellato D, Thabane ME, Chandiwana D, Park J, Delea TE. Cost Effectiveness of Ribociclib Plus a Nonsteroidal Aromatase Inhibitor in Pre-/Perimenopausal, HR+ and HER2- Advanced Breast Cancer: A Canadian Healthcare Perspective. Pharmacoeconomics. 2021;39(7):853-867. PubMed
36.Thavorn K, Wang Z, Fergusson D, van Katwyk S, Arnaout A, Clemons M. Cost implications of unwarranted imaging for distant metastasis in women with early-stage breast cancer in Ontario. Curr Oncol. 2016;23(Suppl 1):S52-55. PubMed
37.Rocchi A, Verma S. Anastrozole is cost-effective vs tamoxifen as initial adjuvant therapy in early breast cancer: Canadian perspectives on the ATAC completed-treatment analysis. Support Care Cancer. 2006;14(9):917-927. PubMed
38.Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Welireg (belzutifan). Kirkland (QC): Merck Canada Inc; 2023 Jan 23.
39.Orphanet. Von Hippel-Lindau Disease. https://www.orpha.net/consor/cgi-bin/Disease_Search.php?lng=EN&data_id=99&Disease_Disease_Search_diseaseGroup=von-hippel-lindau&Disease_Disease_Search_diseaseType=Pat&Maladie(s)/groupes%20de%20maladies=Maladie-de-von-Hippel-Lindau&title=Maladie%20de%20von%20Hippel-Lindau&search=Disease_Search_Simple. Accessed Feb 21 2023.
40.Qalcul. Qalcul Canadian drug coverage estimator. https://qalcul.com/en, 2023.
41.Understanding the gap: A pan-Canadian analysis of prescription drug insurance coverage. The Conference Board of Canada; 2018.
42.Alignment among public formularies in Canada, Part 2: Oncology medicines. Government of Canada; 2021: https://www.canada.ca/en/patented-medicine-prices-review/services/npduis/analytical-studies/formularies-part2-oncology-medicines.html
43.Phillips K. Catastrophic drug coverage in Canada. Ottawa: Library of Parliament; 2016: https://lop.parl.ca/staticfiles/PublicWebsite/Home/ResearchPublications/BackgroundPapers/PDF/2016-10-e.pdf. Accessed April 2023.
Appendix 1: Cost-Comparison Table
Note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical experts and CADTH-participating public drug plans. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 8: CADTH Cost-Comparison Table for the Treatment of Patients with von Hippel-Lindau Disease–Associated Nonmetastatic Renal Cell Carcinoma, Central Nervous System Hemangioblastoma, or Nonmetastatic Pancreatic Neuroendocrine Tumour Not Requiring Immediate Surgery
Treatment | Strength or concentration | Form | Price ($) | Recommended dosagea | Daily cost ($) | Cost per 28 days ($) |
|---|---|---|---|---|---|---|
Belzutifan | 40 mg | Oral tablet | 213.33b | 120 mg once daily | 639.99 | 17,920 |
aRecommended dosage is from the product monograph.3
bSponsor-submitted price.38
Appendix 2: Submission Quality
Note that this appendix has not been copy-edited.
Description | Yes/No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | Yes | No comment |
Model has been adequately programmed and has sufficient face validity | Yes | No comment |
Model structure is adequate for decision problem | Yes | No comment |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | No | As a result of performing analyses by tumour type, patients in one patient group may be duplicated in the CNS and/or pNET cohort if they had those tumours as well |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | Yes | No comment |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | No | Refer to CADTH critical appraisal |
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note that this appendix has not been copy-edited.
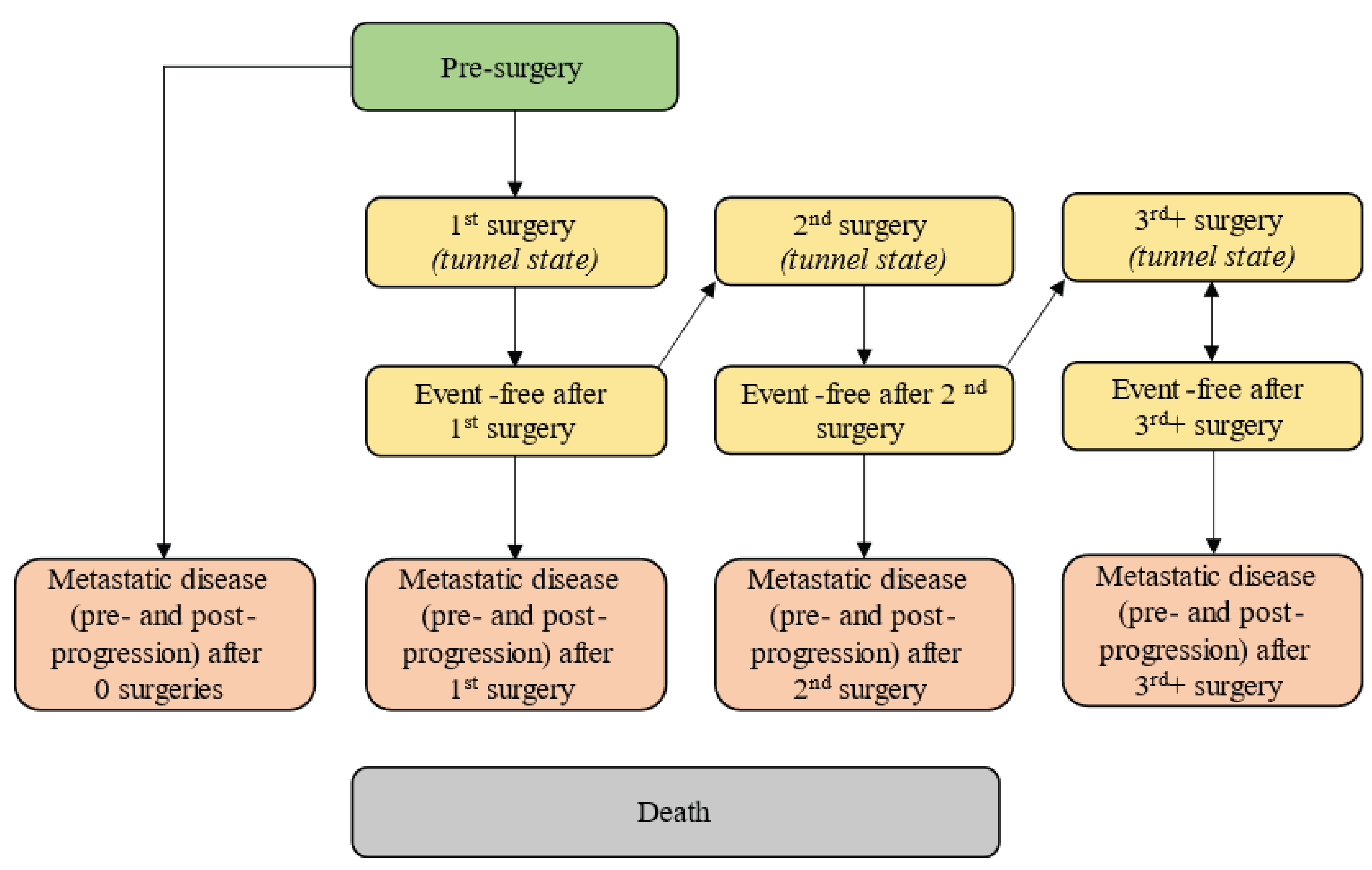
Detailed Results of the Sponsor’s Base Case
Table 10: Disaggregated Summary of Sponsor’s Base-Case Economic Evaluation Results
Parameter | VHL-RCC | VHL-CNS hemangioblastoma | VHL-pNET | |||
|---|---|---|---|---|---|---|
Belzutifan | Active surveillance | Belzutifan | Active surveillance | Belzutifan | Active surveillance | |
Discounted LYs | ||||||
Total LYs | 18.31 | 15.16 | 18.70 | 15.99 | 15.83 | 12.18 |
Presurgery | 7.73 | 3.62 | 9.94 | 5.48 | 10.84 | 6.36 |
Surgery | 0.02 | 0.02 | 0.02 | 0.02 | 0.00 | 0.00 |
Event-free after surgery | 6.96 | 7.46 | 5.65 | 6.78 | 0.40 | 0.48 |
Metastatic disease | 3.61 | 4.07 | 3.08 | 3.70 | 4.59 | 5.34 |
Discounted QALYs | ||||||
Total QALYs | 9.91 | 6.72 | 10.02 | 6.92 | 8.54 | 4.93 |
Presurgery | 6.27 | 2.87 | 8.02 | 4.35 | 8.85 | 5.06 |
Surgery | 0.01 | 0.01 | 0.02 | 0.02 | 0.00 | 0.00 |
Event-free after surgery | 5.54 | 5.93 | 4.49 | 5.39 | 0.32 | 0.38 |
Metastatic disease | 2.10 | 2.36 | 1.79 | 2.15 | 2.65 | 3.08 |
Surgical complication disutility for primary tumour | −0.88 | −0.97 | −1.93 | −2.36 | −0.01 | −0.02 |
Surgical complication disutility for other tumours | −1.53 | −1.78 | −0.79 | −0.91 | −1.70 | −1.88 |
AE-related disutility | −0.0013 | 0.0000 | −0.0013 | 0.0000 | −0.0013 | 0.0000 |
Caregiver disutility | −1.59 | −1.70 | −1.57 | −1.71 | −1.57 | −1.69 |
Discounted costs | ||||||
Total costs ($) | 1,348,577 | 461,541 | 1,298,822 | 426,847 | 1,300,369 | 420,860 |
Initial treatment costs ($) | 933,772 | 0 | 932,545 | 0 | 926,080 | 0 |
Advanced treatment costs ($) | 142,994 | 160,610 | 98,408 | 117,649 | 124,431 | 144,340 |
Adverse event costs ($) | 1,625 | 0 | 1,625 | 0 | 1,625 | 0 |
Surgery and surgical complication costs for primary tumour ($) | 106,811 | 118,230 | 89,167 | 108,443 | 1,945 | 2,290 |
Surgery and surgical complication costs for other tumours ($) | 93,399 | 107,795 | 109,371 | 125,969 | 158,311 | 177,353 |
Disease-management costs ($) | 52,161 | 55,940 | 50,051 | 56,140 | 69,250 | 76,823 |
Genetic testing costs ($) | 0 | 0 | 0 | 0 | 0 | 0 |
Terminal-care costs ($) | 17,814 | 18,966 | 17,655 | 18,647 | 18,727 | 20,054 |
Indirect costs ($) | 0 | 0 | 0 | 0 | 0 | 0 |
Incremental outcomes | ||||||
Incremental costs ($) | 887,036 | 871,975 | 879,508 | |||
Incremental QALYs | 3.19 | 3.10 | 3.61 | |||
Incremental LYs | 3.15 | 2.71 | 3.65 | |||
Incremental costs per QALY gained ($) | 278,259 | 281,170 | 243,505 | |||
CNS = central nervous system; ICER = incremental cost-effectiveness ratio; pNET = pancreatic neuroendocrine tumour, QALY = quality-adjusted life-year; RCC = renal cell carcinoma.
Source: Sponsor’s Pharmacoeconomic Evaluation.2
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Note that this appendix has not been copy-edited.
Detailed Results of CADTH Base-Case and Subgroup Analyses
Table 11: Summary of the Stepped Analysis of the CADTH Reanalysis Results
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($ per QALY gained) |
|---|---|---|---|---|
CADTH reanalysis 1 (deterministic) | ||||
VHL-RCC | Active surveillance | 461,251 | 6.71 | Reference |
Belzutifan | 1,355,901 | 9.52 | 318,415 | |
VHL-CNS hemangioblastoma | Active surveillance | 417,144 | 6.42 | Reference |
Belzutifan | 1,299,982 | 9.24 | 313,091 | |
VHL-pNET | Active surveillance | 405,745 | 4.48 | Reference |
Belzutifan | 1,304,343 | 7.78 | 272,395 | |
CADTH reanalysis 2 (deterministic) | ||||
VHL-RCC | Active surveillance | 461,251 | 8.41 | Reference |
Belzutifan | 1,350,097 | 11.48 | 289,305 | |
VHL-CNS hemangioblastoma | Active surveillance | 417,144 | 8.13 | Reference |
Belzutifan | 1,292,956 | 11.18 | 286,973 | |
VHL-pNET | Active surveillance | 405,745 | 6.18 | Reference |
Belzutifan | 1,298,228 | 9.79 | 247,196 | |
CADTH reanalysis 3 (deterministic) | ||||
VHL-RCC | Active surveillance | 476,553 | 6.71 | Reference |
Belzutifan | 1,439,531 | 9.89 | 302,763 | |
VHL-CNS hemangioblastoma | Active surveillance | 428,628 | 6.42 | Reference |
Belzutifan | 1,378,195 | 9.61 | 297,997 | |
VHL-pNET | Active surveillance | 418,408 | 4.48 | Reference |
Belzutifan | 1,384,983 | 8.22 | 258,490 | |
CADTH reanalysis 4 (deterministic) | ||||
VHL-RCC | Active surveillance | 461,251 | 6.71 | Reference |
Belzutifan | 1,355,301 | 9.89 | 281,092 | |
VHL-CNS hemangioblastoma | Active surveillance | 417,144 | 6.42 | Reference |
Belzutifan | 1,298,132 | 9.61 | 276,475 | |
VHL-pNET | Active surveillance | 405,745 | 4.48 | Reference |
Belzutifan | 1,303,466 | 8.22 | 240,077 | |
Base case: CADTH reanalysis (1 + 2 + 3 + 4; probabilistic) | ||||
VHL-RCC | Active surveillance | 478,842 | 8.42 | Reference |
Belzutifan | 1,454,839 | 11.13 | 360,193 | |
Key subgroups: CADTH reanalysis (1 + 2 + 3 + 4; probabilistic) | ||||
VHL-CNS hemangioblastoma | Active surveillance | 439,619 | 8.66 | Reference |
Belzutifan | 1,401,415 | 11.27 | 368,886 | |
VHL-pNET | Active surveillance | 433,123 | 6.64 | Reference |
Belzutifan | 1,401,611 | 9.71 | 314,661 | |
CNS = central nervous system; ICER = incremental cost-effectiveness ratio; pNET = pancreatic neuroendocrine tumour, QALY = quality-adjusted life-year; RCC = renal cell carcinoma.
Note: Discrepancies between the sponsor’s base case and CADTH stepped analysis are due to comparison of probabilistic and deterministic results, respectively.
Table 12: Disaggregated Summary of CADTH’s Base-Case Economic Evaluation Results
Parameter | VHL-RCC (base case) | VHL-CNS hemangioblastoma (subgroup) | VHL-pNET (subgroup) | |||
|---|---|---|---|---|---|---|
Belzutifan | Active surveillance | Belzutifan | Active surveillance | Belzutifan | Active surveillance | |
Discounted LYs | ||||||
Total LYs | 17.96 | 15.18 | 18.43 | 16.05 | 15.43 | 12.19 |
Presurgery | 7.27 | 3.61 | 9.44 | 5.50 | 10.33 | 6.35 |
Surgery | 0.02 | 0.02 | 0.02 | 0.02 | 0.00 | 0.00 |
Event-free after surgery | 6.99 | 7.47 | 5.81 | 6.82 | 0.39 | 0.46 |
Metastatic disease | 3.68 | 4.08 | 3.16 | 3.71 | 4.71 | 5.38 |
Discounted QALYs | ||||||
Total QALYs | 11.13 | 8.42 | 11.27 | 8.66 | 9.71 | 6.64 |
Presurgery | 5.89 | 2.86 | 7.61 | 4.37 | 8.42 | 5.05 |
Surgery | 0.01 | 0.01 | 0.02 | 0.02 | 0.00 | 0.00 |
Event-free after surgery | 5.56 | 5.94 | 4.61 | 5.42 | 0.31 | 0.36 |
Metastatic disease | 2.13 | 2.37 | 1.83 | 2.15 | 2.72 | 3.11 |
Surgical complication disutility for primary tumour | −0.89 | −0.98 | −1.99 | −2.37 | −0.01 | −0.02 |
Surgical complication disutility for other tumours | −1.58 | −1.78 | −0.81 | −0.92 | −1.72 | −1.87 |
AE-related disutility | −0.0013 | 0.0000 | −0.0013 | 0.0000 | −0.0013 | 0.0000 |
Caregiver disutility | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 |
Discounted costs | ||||||
Total costs ($) | 1,454,839 | 478,842 | 1,401,415 | 439,619 | 1,401,611 | 433,123 |
Initial treatment costs ($) | 1,018,423 | 0 | 1,016,804 | 0 | 1,010,189 | 0 |
Advanced treatment costs ($) | 159,453 | 176,564 | 109,675 | 128,270 | 138,106 | 157,439 |
Adverse event costs ($) | 1,609 | 0 | 1,609 | 0 | 1,609 | 0 |
Surgery and surgical complication costs for primary tumour ($) | 108,564 | 118,966 | 91,691 | 108,769 | 1,968 | 2,266 |
Surgery and surgical complication costs for other tumours ($) | 95,889 | 108,013 | 112,925 | 127,590 | 160,339 | 176,002 |
Disease-management costs ($) | 52,899 | 56,275 | 50,899 | 56,304 | 70,471 | 77,307 |
Genetic testing costs ($) | 0 | 0 | 0 | 0 | 0 | 0 |
Terminal-care costs ($) | 18,003 | 19,023 | 17,812 | 18,687 | 18,929 | 20,109 |
Indirect costs ($) | 0 | 0 | 0 | 0 | 0 | 0 |
Incremental outcomes | ||||||
Incremental costs ($) | 975,998 | 961,796 | 968,488 | |||
Incremental QALYs | 2.71 | 2.61 | 3.08 | |||
Incremental LYs | 2.78 | 2.38 | 3.24 | |||
Incremental costs per QALY gained ($) | 360,193 | 368,886 | 314,661 | |||
CNS = central nervous system; ICER = incremental cost-effectiveness ratio; pNET = pancreatic neuroendocrine tumour, QALY = quality-adjusted life-year; RCC = renal cell carcinoma; VHL = von Hippel-Lindau.
Scenario Analyses
Table 13: Summary of CADTH’s Economic Evaluation Results — Scenario Analyses
Cohort | Drug | Total costs ($) | Total QALYs | ICER ($ per QALY gained) |
|---|---|---|---|---|
ToT Gompertz distribution | ||||
RCC | Active surveillance | 478,842 | 8.42 | Reference |
Belzutifan | 1,269,685 | 10.68 | 349,738 | |
CNS hemangioblastoma | Active surveillance | 439,619 | 8.66 | Reference |
Belzutifan | 1,218,884 | 10.82 | 361,534 | |
pNET | Active surveillance | 433,123 | 6.64 | Reference |
Belzutifan | 1,217,274 | 9.21 | 304,739 | |
Belzutifan residual benefit convergence over 1 year post-trial period | ||||
RCC | Active surveillance | 478,842 | 8.42 | Reference |
Belzutifan | 1,452,795 | 11.25 | 344,302 | |
CNS hemangioblastoma | Active surveillance | 439,619 | 8.66 | Reference |
Belzutifan | 1,398,830 | 11.38 | 352,723 | |
pNET | Active surveillance | 433,123 | 6.64 | Reference |
Belzutifan | 1,399,272 | 9.85 | 300,492 | |
Include genetic testing | ||||
RCC | Active surveillance | 479,387 | 8.42 | Reference |
Belzutifan | 1,455,566 | 11.13 | 360,260 | |
CNS hemangioblastoma | Active surveillance | 440,164 | 8.66 | Reference |
Belzutifan | 1,402,142 | 11.27 | 368,956 | |
pNET | Active surveillance | 433,668 | 6.64 | Reference |
Belzutifan | 1,402,337 | 9.71 | 314,720 | |
CNS = central nervous system; ICER = incremental cost-effectiveness ratio, pNET = pancreatic neuroendocrine tumours, QALY = quality-adjusted life-year, RCC = renal cell carcinoma, ToT = time on treatment, VHL = von Hippel-Lindau.
Appendix 5: Submitted Budget Impact Analysis and CADTH Appraisal
Note that this appendix has not been copy-edited.
Table 14: Summary of Key Take-Aways
Key take-aways of the budget impact analysis |
|---|
|
Summary of Sponsor’s Budget Impact Analysis
The sponsor submitted a budget impact analysis (BIA) estimating the incremental budget impact of reimbursing belzutifan for patients aged 18 years and older with VHL-associated nonmetastatic RCC, CNS hemangioblastoma, or nonmetastatic pNET, not requiring immediate surgery. The reference scenario includes active surveillance as the current standard of care. The analysis was undertaken using an epidemiologic approach from the perspective of the CADTH-participating Canadian public drug plans over a 3-year time horizon (2024 to 2027). The model uses a weekly cycle length where incident patients are added to the eligible population weekly. Drug costs are estimated weekly applying treatment duration data from the LITESPARK-004 trial and number of patients on treatment each week. Key inputs to the BIA are documented in Table 16. Data informing the model were obtained from various sources including the LITESPARK-004 trial, Orphanet, clinical expert opinion, sponsor conducted market research, and the Qalcul public drug coverage estimator.2,34,39,40
The sponsor’s BIA included the following key assumptions:
The patient population is based on European reported prevalence of VHL disease and applied to Canadian adult population (excluding Québec).
ToT was derived from Kaplan-Meier data also used in the CUA.
The peak market share was assumed to be 40% and uptake is modelled using a logarithmic regression, reaching peak share at 104 weeks (the beginning of year 3).
Table 15: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1 / year 2 / year 3 if appropriate) |
|---|---|
Target population | |
Pan-Canadian population aged 18+ (excluding Québec) in year 1 | 24,647,239 |
Annual population growth rate (2017 to 2021) | 1.33% |
Prevalence of VHL disease | 1 per 53,000a |
Diagnosis rate | 50%b |
Proportion of patients covered by a public plan | 67.9%c |
Percentage of patients with VHL-associated RCC, CNS hemangioblastoma or pNET | 100% |
Percentage of patients not requiring immediate surgery | 50%b |
Number of patients eligible for drug under review | 79 / 80 / 81d |
Market Uptake (3 years) | |
Uptake (reference scenario) Active surveillance | 100% / 100% / 100% |
Uptake (new drug scenario) Belzutifan Active surveillance | 27% / 38% / 40% 73% / 62% / 60% |
Cost of treatment (per patient) | |
Cost of treatment over 28 days Belzutifan Active surveillance | $17,920 $0 |
CNS = central nervous system; pNET = pancreatic neuroendocrine tumour; RCC = renal cell carcinoma; VHL = von Hippel-Lindau.
aBased on European reported prevalence from Orphanet.39
bAssumption based on clinical expert opinion solicited by the sponsor.
cEstimated using the Qalcul estimator.40
dThe submitted model inappropriately calculated eligible patients each year which resulted in 79, 159, and 240 patients in years 1/2/3, respectively.
Summary of the Sponsor’s Budget Impact Analysis Results
The sponsor estimated the net budget impact of funding belzutifan for adults with VHL-associated RCC, CNS hemangioblastoma or pNET will be $1,880,627 in year 1, $7,274,966 in year 2, and $13,088,552 in year 3, for a 3-year total budget impact of $22,244,146.
CADTH Appraisal of the Sponsor’s Budget Impact Analysis
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
Overly complex and inaccurate modelling approach: The BIA model submitted by the sponsor incorrectly calculated eligible patients by adding the Canadian prevalent population (excluding Quebec) of adults with VHL disease annually to the model annually rather than incident cases. In the sponsor’s modelling approach, by the end of year 3 there were 240 eligible patients in the model. However, based on the sponsor’s estimates of population growth, VHL prevalence, diagnosis rate, tumour type, eligibility to start treatment (e.g., do not require immediate surgery), and public drug coverage rate the number of eligible patients by year 3 is estimated be 81 patients. This was further complicated by applying the ToT Kaplan-Meier data from the LITESPARK-004 trial which then allowed for more patients to be on treatment than the estimated eligible population which overestimated the budget impact of introducing belzutifan.
While the inappropriate addition of patients to the model overestimated the budgetary impact, the use of a weekly cycle length in the submitted model resulted in the underestimation of market share and time on treatment, thus reducing the budgetary impact. The use of a weekly cycle length in the submitted budget impact model added the cohort of eligible patients gradually every week. This method of adding patients throughout the year may underestimate drug costs given that individuals added later in the year would have less time to accrue treatment costs than if they had been added at the beginning of the year. Given that the observed treatment duration of belzutifan is multiple years (mean and median duration of treatment is 33.7 months and 37.3 months, respectively, per the LITESPARK-004 trial), the weekly change in the number of patients potentially undercounts several weeks or months of treatment for patients, and may not reflect the true budget impact in the new drug scenario. Further, the market shares were modelled weekly using a logarithmic regression which results in lower market shares at the beginning of the year which further underestimates the budget impact of belzutifan.
Given the complex manner in which the submitted model was programmed, it was not feasible to make the appropriate corrections to the addition of incident patients to the model and their time on treatment within their submitted model. Therefore, CADTH undertook a reanalysis of the estimated budgetary impact using the sponsor’s estimates of eligibility to appropriately estimate the annual number of eligible patients.
In CADTH’s approach a weekly cycle length was not used, and the median ToT from LITESPARK-004 was applied to all patients. Since the median time on treatment exceeds the time horizon of the budget impact analysis it was assumed that no patients discontinued belzutifan treatment. In the CADTH reanalysis, the maximum annual market shares reached in the sponsor’s submitted model were applied as a fixed proportion each year (i.e., 27% in year 1, 38% in year 2, and 40% in year 3).
Population size is inappropriately estimated: The sponsor narrowed the adult prevalent VHL population in a stepwise approach based on a combination of estimates from the literature, clinical expert opinion, and market research. Each step in this approach was presented to clinical experts consulted by CADTH to verify its alignment with Canadian clinical practice. The clinical experts consulted by CADTH suggested that the sponsor-assumed diagnosis rate of VHL disease of 50% was underestimated, and that they believe closer to 85% of people will be diagnosed while noting that due to the rarity of VHL disease uncertainty remained. Additionally, the experts estimated that more than 50% of patients would be eligible to start treatment, taking into account the number of patients who would not require immediate surgery.
The CADTH reanalysis assumed that 75% of adults with VHL disease would be diagnosed, and that 60% of patients would be eligible to start treatment.
The sponsor used estimates derived from an online drug coverage estimator, Qalcul, to inform their submitted model: While the sponsor provided the data inputs and assumptions that they gave Qalcul, CADTH is unable to adequately validate the background assumptions and calculations used by the third-party estimator.
The CADTH reanalysis assumed that the pan-Canadian drug coverage would be 71%, based on provincial guidelines for take-home cancer medication and estimates of public drug coverage eligibility.41,42
Given the high annual cost of belzutifan ($233,596), a scenario analysis assuming 100% drug coverage was conducted to account for the possibility that federal or provincial catastrophic drug coverage plans (e.g., Ontario’s Trillium Drug Program)43 would cover the drug cost for all eligible patients
Market share of belzutifan is underestimated: The sponsor assumed that belzutifan would reach a peak market share of 40% and uptake is modelled using a logarithmic regression, reaching peak share at 104 weeks (the beginning of year 3). As described above, the logarithmic approach to growing market shares weekly may underestimate the budgetary impact, given that at earlier time points the market share of belzutifan is lower than the anticipated market share for years 1 and 2. Clinical experts consulted by CADTH suggested that the sponsor’s market share assumptions for belzutifan were underestimated. Given that the sponsor already excluded those who required immediate surgery and without public drug coverage, the clinical experts estimated that by year 3 of the modelled time horizon at least 60% of eligible patients would be treated with belzutifan.
The CADTH reanalysis assumed that the year 1, year 2, and year 3 market shares would be 40%, 50%, and 60% respectively, applied as a fixed proportion annually.
Time on treatment for patients receiving belzutifan is uncertain: Clinical experts consulted by CADTH indicated that in their opinion, belzutifan will be a long-term treatment for patients, but that due to the short follow-up time in the LITESPARK-004 trial, uncertainty remained as to how long patients would remain on treatment. Due to the number of patients who may be expected to remain on belzutifan for longer than 3 years (the time horizon of the BIA), it is important to note that there would be a significant budgetary impact in subsequent years following the time horizon of the BIA.
The CADTH reanalysis did not incorporate a longer time horizon. However, if all patients who were receiving belzutifan in year 3 continued treatment in year 4, belzutifan would cost at least an additional $21,393,912, which does not account for incident VHL cases or the potential increase in market share.
Use of relative dose intensity to estimate drug costs is inappropriate: The sponsor assumed a 92.5% RDI for belzutifan in their base case. This assumption is inappropriate because it can be influenced by several factors. For example, the dose received by a patient may differ from the full planned dose of the drug due to dose delays, missed doses, or dose reductions to manage toxicity. Each of these reasons have differing impacts on drug costs. The CADTH reanalysis of the CUA assumes 100% RDI, and the CADTH BIA and CUA should be aligned.
In the CADTH reanalysis, 100% RDI was assumed.
CADTH Reanalyses of the Budget Impact Analysis
Given the high degree of uncertainty associated with the sponsors BIA, lack of transparency, and inflexibility of the modelling approach, CADTH does not consider the budget impact estimates provided by the sponsor’s budget impact model to be informative for decision-making. As a result, CADTH undertook a reanalysis of the estimated budgetary impact to correct issues with the addition of incident patients over the time horizon. CADTH’s reanalysis 1 incorporated the sponsor’s original epidemiologic approach to narrowing the population to estimate eligible patients (i.e., incorporated the prevalence of VHL disease, diagnosis rate, public drug coverage, and eligibility to start treatment immediately). Median ToT from the LITESPARK-004 trial was applied, and the sponsor’s market share estimates applied as a fixed value for each year, and drug cost (assuming 92.5% RDI) were used to estimate the cost of belzutifan over the time horizon to first predict the sponsor’s intended estimate of budgetary impact in CADTH reanalysis 1. Subsequent reanalyses (i.e., 2 to 6) were conducted as stepwise changes from CADTH reanalysis 1.
Table 16: CADTH Budget Impact Reanalysis
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Changes to derive the CADTH reanalysis | ||
1. Modelling of incident cases and time on treatment | Used population prevalence of VHL disease, and used time on treatment data from trial via weekly cycle length | Used incident VHL cases and applied median time on treatment via yearly approach |
2. Proportion of VHL cases diagnosed | 50% | 75% |
3. Proportion of patients eligible to start treatment | 50% | 60% |
4. Public coverage | 67.9% | 71% |
5. Market shares | 27% / 38% / 40% | 40% / 50% / 60% |
6. Relative dose intensity | 92.5% | 100% |
CADTH base case | Reanalysis 1 + 2 + 3 + 4 + 5 + 6 | |
VHL = von Hippel-Lindau.
Note: Reanalysis 1 incorporates the sponsor’s original narrowing of the population and market share assumptions. Reanalyses 2 to 6 are conducted as stepwise changes from reanalysis 1.
The results of the CADTH stepwise reanalysis are presented in summary format in Table 17 and a more detailed breakdown is presented in Table 18.
Based on CADTH’s base-case analysis, the expected budget impact for the reimbursement of belzutifan for adults with VHL-associated RCC, CNS hemangioblastoma or pNET will be $13,881,930 in year 1, $17,588,769 in year 2, and $21,393,912 in year 3, for a 3-year total budget impact of $52,864,610. As can be observed in Table 17 and Table 18, the difference between the CADTH base case and the sponsor’s base case is due to the combined impact of the individual reanalyses – there is no key driver impacting the increase in estimated budget impact of reimbursing belzutifan.
Table 17: Summary of the CADTH Reanalyses of the Budget Impact Analysis
Stepped analysis | Three-year total |
|---|---|
Submitted base case | $22,244,146 |
CADTH reanalysis 1 | $18,183,889 |
CADTH reanalysis 2 | $27,275,834 |
CADTH reanalysis 3 | $21,820,667 |
CADTH reanalysis 4 | $19,014,081 |
CADTH reanalysis 5 | $25,980,391 |
CADTH reanalysis 6 | $19,658,259 |
CADTH base case | $52,864,610 |
BIA = budget impact analysis
Note: Reanalysis 1 incorporates the sponsor’s original narrowing of the population and market share assumptions. Reanalyses 2 to 6 are conducted as stepwise changes from reanalysis 1.
Table 18: Detailed Breakdown of the CADTH Reanalyses of the Budget Impact Analysis
Stepped analysis | Scenario | Year 0 (current situation) | Year 1 | Year 2 | Year 3 | Three-year total |
|---|---|---|---|---|---|---|
Submitted base case | Reference | $0 | $0 | $0 | $0 | $0 |
New drug | $0 | $1,880,627 | $7,274,966 | $13,088,552 | $22,244,146 | |
Budget impact | $0 | $1,880,627 | $7,274,966 | $13,088,552 | $22,244,146 | |
CADTH reanalysis 1 | Reference | $0 | $0 | $0 | $0 | $0 |
New drug | $0 | $4,605,049 | $6,569,460 | $7,009,380 | $18,183,889 | |
Budget impact | $0 | $4,605,049 | $6,569,460 | $7,009,380 | $18,183,889 | |
CADTH reanalysis 2 | Reference | $0 | $0 | $0 | $0 | $0 |
New drug | $0 | $6,907,574 | $9,854,190 | $10,514,070 | $27,275,834 | |
Budget impact | $0 | $6,907,574 | $9,854,190 | $10,514,070 | $27,275,834 | |
CADTH reanalysis 3 | Reference | $0 | $0 | $0 | $0 | $0 |
New drug | $0 | $5,526,059 | $7,883,352 | $8,411,256 | $21,820,667 | |
Budget impact | $0 | $5,526,059 | $7,883,352 | $8,411,256 | $21,820,667 | |
CADTH reanalysis 4 | Reference | $0 | $0 | $0 | $0 | $0 |
New drug | $0 | $4,815,295 | $6,869,391 | $7,329,396 | $19,014,081 | |
Budget impact | $0 | $4,815,295 | $6,869,391 | $7,329,396 | $19,014,081 | |
CADTH reanalysis 5 | Reference | $0 | $0 | $0 | $0 | $0 |
New drug | $0 | $6,822,295 | $8,644,026 | $10,514,070 | $25,980,391 | |
Budget impact | $0 | $6,822,295 | $8,644,026 | $10,514,070 | $25,980,391 | |
CADTH reanalysis 6 | Reference | $0 | $0 | $0 | $0 | $0 |
New drug | $0 | $4,978,432 | $7,102,119 | $7,577,708 | $19,658,259 | |
Budget impact | $0 | $4,978,432 | $7,102,119 | $7,577,708 | $19,658,259 | |
CADTH base case | Reference | $0 | $0 | $0 | $0 | $0 |
New drug | $0 | $13,881,930 | $17,588,769 | $21,393,912 | $52,864,610 | |
Budget impact | $0 | $13,881,930 | $17,588,769 | $21,393,912 | $52,864,610 |
Note: Reanalysis 1 incorporates the sponsor’s original narrowing of the population and market share assumptions. Reanalyses 2 to 6 are conducted as stepwise changes from reanalysis 1.
CADTH also conducted additional scenario analyses to address remaining uncertainty, using the CADTH base case. Results are provided in Table 19.
Price reduction of 83% to assess the budget impact if the price of the drug under review reflected the price in which the ICER would be at $50,000 per QALY in CADTH’s base case CUA.
Inclusion of genetic testing, assuming that 100% of patients starting belzutifan are tested, and 75% of patients on active surveillance are tested, as aligned with the CUA scenario analysis.
Assume 100% public drug coverage.
Results of CADTH’s scenario analyses demonstrate that the estimated budget impact is highly sensitive to changes in drug cost (decrease of $43,877,626 from CADTH base case) and public drug coverage (increase of $21,592,588 from CADTH base case).
Table 19: Detailed Breakdown of the CADTH Scenario Analyses of the BIA
Stepped analysis | Scenario | Year 0 (current situation) | Year 1 | Year 2 | Year 3 | Three-year total |
|---|---|---|---|---|---|---|
Submitted base case | Reference | $0 | $0 | $0 | $0 | $0 |
New drug | $0 | $1,880,627 | $7,274,966 | $13,088,552 | $22,244,146 | |
Budget impact | $0 | $1,880,627 | $7,274,966 | $13,088,552 | $22,244,146 | |
CADTH base case | Reference | $0 | $0 | $0 | $0 | $0 |
New drug | $0 | $13,881,930 | $17,588,769 | $21,393,912 | $52,864,610 | |
Budget impact | $0 | $13,881,930 | $17,588,769 | $21,393,912 | $52,864,610 | |
CADTH scenario analysis: 83% price reduction | Reference | $0 | $0 | $0 | $0 | $0 |
New drug | $0 | $2,359,928 | $2,990,091 | $3,636,965 | $8,986,984 | |
Budget impact | $0 | $2,359,928 | $2,990,091 | $3,636,965 | $8,986,984 | |
CADTH scenario analysis: include genetic testing | Reference | $0 | $48,738 | $41,168 | $33,383 | $123,288 |
New drug | $0 | $13,925,253 | $17,643,659 | $21,460,677 | $53,029,589 | |
Budget impact | $0 | $13,876,515 | $17,602,491 | $21,427,294 | $52,906,300 | |
CADTH scenario analysis: 100% drug coverage | Reference | $0 | $0 | $0 | $0 | $0 |
New drug | $0 | $19,552,014 | $24,772,913 | $30,132,270 | $74,457,198 | |
Budget impact | $0 | $19,552,014 | $24,772,913 | $30,132,270 | $74,457,198 |
Ethics Review
Abbreviations
CNS
central nervous system
pNET
pancreatic neuroendocrine tumours
RCC
renal cell carcinoma
VHL
von Hippel-Lindau disease
Summary
Patient group, clinician group, clinical expert, and drug program input gathered in the course of this CADTH review, and from relevant literature, were reviewed to identify ethical considerations relevant to the use of belzutifan for the treatment of adult patients with von Hippel-Lindau (VHL) disease who require therapy for associated nonmetastatic renal cell carcinoma, central nervous system hemangioblastomas, or nonmetastatic pancreatic neuroendocrine tumours, not requiring immediate surgery.
Ethical considerations in the context of VHL disease highlighted the significant physical and psychosocial burden of the disease on patients, families, and caregivers; diagnostic and psychosocial challenges associated with hereditary nature of the disease; and the absence of systemic, disease-modifying therapies.
Clinical trial evidence indicated that there is presently evidentiary uncertainty concerning the safety and efficacy of belzutifan, particularly in the long term; this uncertainty limits assessment of clinical benefits and harms associated with treatment as well as pharmacoeconomic assessment of cost-effectiveness.
The use of belzutifan presents potential risks for patients, including common risks of anemia, hypoxia, and embryo-fetal toxicity. Patients and clinicians expressed a willingness to undertake some risks for the potential benefit of a systemic therapy that could delay disease progression given the burden associated with VHL-associated tumours and local treatments as well as the absence of alternative disease-modifying therapies. Robust informed consent processes are required to disclose risks of adverse events and evidentiary uncertainty about the long-term safety, efficacy, and tolerability of belzutifan, including the impact on fertility. Equitable access to belzutifan requires addressing potential geographic and diagnostic barriers to access, including those associated with ongoing specialist care and monitoring.
Ethical considerations for health systems related to the implementation of belzutifan highlighted the challenges of funding decisions and assessments of opportunity costs for expensive drugs for rare diseases, the need for better coordination of multidisciplinary and ongoing treatment, monitoring and care of patients with VHL disease, and improved health information systems capacity.
Objective
To identify and describe ethical considerations associated with the use of belzutifan for the treatment of adult patients with VHL disease who require therapy for an associated nonmetastatic renal cell carcinoma (RCC), central nervous system (CNS) hemangioblastoma, or nonmetastatic pancreatic neuroendocrine tumour (pNET) not requiring immediate surgery, including considerations related to the context of VHL disease, evidentiary basis, use of belzutifan, and health systems.
Research Questions
This report addresses the following research question(s):
What ethical considerations arise in the context of VHL disease, including those related to diagnosis, treatment, and outcomes?
What ethical considerations arise related to the evidence (e.g., clinical and economic data) used to evaluate belzutifan?
What ethical considerations arise in the use of belzutifan for patients, their caregivers, and clinicians?
What ethical considerations for health systems are involved in the context of belzutifan?
Methods
To identify ethical considerations relevant to the use of belzutifan for the treatment of adult patients with VHL disease who require therapy for an associated nonmetastatic RCC, CNS hemangioblastoma, or nonmetastatic pNET not requiring immediate surgery, this ethics report was driven by relevant questions identified in the EUnetHTA Core Model 3.0, Ethics Analysis Domain,1 and supplemented by relevant questions from the Equity Checklist for health technology assessment (HTA).2 These guiding questions were organized to respond to the research questions posed, and investigated ethical considerations related to:
patients living with VHL disease and their caregivers (i.e., disparities in incidence, treatment, or outcomes; challenges related to diagnosis or clinical care; factors that might prevent patients from gaining access to therapies)
evidence used to demonstrate the benefits, harms, and value of belzutifan (i.e., ethical considerations in relevant clinical trials, including their representativeness, choice of outcome measures, appropriateness of analytical methods and models to all population groups; ethical considerations related to the data or assumptions in the economic evaluation)
use of belzutifan, including considerations related to benefits and harms to patients, relatives, caregivers, clinicians or society, and considerations related to access to these therapies
uptake of belzutifan in health systems, including considerations related to the distribution of health care resources.
These were explored through a review and synthesis of project inputs and relevant literature to highlight ethical considerations across each of the domains.
Data Collection: Review of Project Inputs and Literature
Data to inform this ethics report drew from an identification of ethical considerations (e.g., values, norms, or implications related to the harms, benefits, and implications for equity, justice, resource allocation, and ethical considerations in the evidentiary basis) in the patient and clinician group, clinical expert, and drug program input collected by CADTH to inform this review, as well as a complementary search of the published literature. Ongoing collaboration and communication with CADTH reviewers working on this submission's clinical and economic reviews also helped clarify and identify the ethical considerations raised.
Review of Project Inputs
During this CADTH review, a single reviewer collected and considered input from 6 main sources to identify content related to ethical considerations relevant to addressing the research questions guiding this ethics report. In addition to published literature, this report considered the following sources:
the sponsor submission, noting relevant information and external references or sources relevant to each of the research questions driving this report
clinician group input received by CADTH from the Ontario Health (Cancer Care Ontario) Genitourinary Cancer Drug Advisory Committee and from a group of subspecialists involved in VHL disease care in Canada
patient input received by CADTH from the Canadian VHL Alliance in conjunction with the Canadian Organization for Rare Disorders, Kidney Cancer Canada, Pancreatic Cancer Canada, and the Canadian Neuroendocrine Tumour Society
drug program input received by CADTH from drug programs participating in the CADTH reimbursement review process
discussion with clinical experts (n = 3) directly engaged by CADTH over the course of this reimbursement review, including 2 consultation meetings involving 2 experts, and 1 panel discussion involving 3 experts; during each of the 3 discussions, clinical experts were asked targeted questions related to ethical considerations corresponding to the research questions driving this report; all clinical experts were practising oncologists specializing in the treatment of VHL-associated RCC, CNS hemangioblastoma, and pNET, and all had experience treating patients with VHL in Canada
engagement with CADTH clinical and economic reviewers to identify domains of ethical interest arising from their respective reviews as well as relevant questions and sources to further pursue in this report.
Literature Search Methods
An information specialist conducted 2 literature searches on key resources including MEDLINE via Ovid, Philosopher’s Index via Ovid, PsycINFO via Ovid, the Cumulative Index to Nursing and Allied Health Literature (CINAHL) via EBSCO, and Scopus. The search strategies comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The first search concept was Welireg (belzutifan) and the second search concept was VHL disease.
CADTH-developed search filters were applied to both searches to limit retrieval to citations related to ethical concepts or considerations. Duplicates were removed by manual deduplication in EndNote. The searches were completed on February 21, 2023.
A grey literature search tool was used to identify sources listed in the ethics section of the Grey Matters: A Practical Tool For Searching Health-Related Grey Literature checklist.3 The grey literature search for ethical considerations was conducted on February 16, 2023. The search concepts were Welireg (belzutifan) and VHL disease. Google was used to search for additional internet-based materials. These searches were supplemented by reviewing bibliographies of key papers, manual searching of additional key concepts, and through contacts with experts, as appropriate.
Literature Screening and Selection
Literature retrieved according to the search and selection methods detailed in the previous section was screened in 2 stages. First, retrieved titles and abstracts of citations were screened for relevance by a single reviewer. Articles were identified and retrieved for full-text review by a single reviewer if their titles or abstracts identified ethical considerations, or provided normative analysis (i.e., focusing on “what ought to be” through argumentation), or presented empirical research (i.e., focusing on “what is” through observation) of ethical considerations related to: the experiences, incidence, diagnosis, treatment, or outcomes of VHL; or the evidence on, use of, or implications of belzutifan for patients with VHL. In the second stage, full-text publications categorized as “retrieve” were reviewed by the same reviewer. Texts that included substantive information meeting the criteria described previously were included in the review, and reports that did not meet these criteria were excluded. As a parallel process, other sources drawn from relevant bibliographies, relevant key concepts, consultations with experts, or other CADTH reviewers were retrieved and reviewed using the same selection criteria.
Data Analysis
Data analysis was driven by the 4 research questions guiding this report and included the collection, coding, and thematic analysis of data drawn from the literature and project inputs. The reviewer conducted 2 iterative cycles of coding and analysis to abstract, identify, and synthesize relevant ethical considerations in the literature and from relevant project inputs.
In the initial coding phase, publications and input sources were reviewed for ethical content (e.g., claims related to potential harms, benefits, equity, justice, resource allocation and ethical issues in the evidentiary basis). Once identified, claims related to ethical content were coded using methods of qualitative description.4 In the second coding phase, major themes and subcodes were identified through repeated readings of the data,4 and summarized into thematic categories within each guiding domain or research question. Where ethical content did not fit into these categories or domains outlined in the research questions, this was noted, as were discrepancies or conflicts between ethical considerations or values identified between project sources or within thematic categories. Data analysis was iterative, and themes identified in the literature, in project inputs, and during consultation with clinical experts were used to further refine and reinterpret ethical considerations identified.
Data collected and analyzed from these sources were thematically organized and described according to the 4 research questions and domains driving this report. The results of this analysis and its limitations and conclusions are described in the following sections.
Results
Description of Included Sources
Data to inform this ethics report drew from a review of patient group input, clinician group input, drug program input, and consultation with clinical experts engaged by CADTH for this review. All clinical experts were active in relevant clinical roles as practising oncologists in Canada, and all had experience treating patients with VHL. A description and a summary of these sources are included in the Clinical Review Report.
The literature search identified 79 results and the grey literature search identified 4 additional results, for a total of 83 results. Following title and abstract screening, 57 citations were excluded and 26 potentially relevant publications from the electronic searches were retrieved for full-text review. Of the potentially relevant publications, 17 were excluded as they did not discuss ethical considerations of belzutifan or VHL disease (n = 14) or were not published in English (n = 3). Nine publications met the inclusion criteria and were included in this report. Seven additional publications were retrieved from backward searches of included publications’ reference lists or a manual search.
A total of 16 publications were used to inform this report. Of these publications, 8 discussed ethical considerations in the context of VHL disease, including those related to diagnosis and treatment; 5 discussed patient and/or family and caregiver experiences in the context of VHL disease; 1 was selected to provide a broader understanding of diversity in clinical trials; and 2 were selected to provide a broader understanding of the context of ethical considerations for drugs for rare diseases. Details regarding the characteristics of included publications are provided in Table 1.
Key Ethical Considerations
Diagnosis, Treatment, and Experiences of VHL Disease
Diagnosis, Treatment, and Care of VHL Disease
Diagnosis
VHL disease is a hereditary autosomal-dominant neoplasia syndrome caused by a germline mutation and/or deletion of the tumour-suppressor VHL gene. Patients with VHL disease are at increased risk of developing a variety of benign and malignant neoplasms, or tumours, including hemangioblastomas of the CNS and retina, renal cysts and clear cell RCC, and pNET, some of which may further metastasize.5 As a result, VHL disease is a multisystemic and multiorgan disease with a reduced life expectancy.5 VHL disease has an incidence of 1 in 36,000,5 with an estimated 727 cases in Canada.6 While most patients with VHL disease have a family of history of the disease, de novo mutations account for approximately 20% of cases.5 Onset of VHL disease ranges from childhood to late adulthood, most often occurring in early adulthood. VHL-associated phenotypic morbidities manifest heterogeneously across patients and families, which makes diagnosis, surveillance, and treatment challenging from both clinical and health systems perspectives.5,7-9
VHL disease diagnosis is typically confirmed through genetic testing to identify a germline mutation of the VHL gene. Testing is usually initiated as a result of a family history and/or clinical presentation of VHL-associated manifestations and tumours.5,10 Clinical experts noted that genetic testing for VHL disease is readily available in tertiary centres in Canada, but that timely diagnosis requires referring clinicians to be familiar with the disease. As a result, patients residing in rural or remote areas could face delays or barriers to timely genetic testing and diagnosis as primary care and specialists familiar with VHL disease may be less readily accessible in these areas. The rarity of VHL disease can present challenges for timely diagnosis in de novo cases.8 Clinician group input noted that patients with VHL disease have often already developed life-altering organ damage at the time of diagnosis.
Prognosis for patients with VHL disease has improved with the availability of genetic testing for asymptomatic individuals with a family history of VHL, as early diagnosis facilitates prophylactic surveillance and early intervention.5,9,10 Presymptomatic genetic testing of individuals with hereditary disease, including VHL, can have multiple ethical, social, psychological, and economic implications for patients, families, and health systems.5,10-12 However, the availability of disease-modifying therapy may alter the balance of benefits and harms associated with pursuing presymptomatic testing, including potentially altering patients’ and families’ decisions.10,13 As noted by clinical experts and reported in published literature, given the hereditary nature of VHL disease, access to geneticists and genetic counsellors is particularly important for patients with VHL disease. Geneticists and genetic counsellors can help inform patient care and treatment, genetic testing decisions for patients and family members (including presymptomatic testing of potentially affected children before the age of consent), interpretation of testing, genotyping, and family planning decisions.5,8,10,13-15 Additionally, they can help patients develop strategies to cope with their diagnosis and communicate sensitive information with at-risk family members, including communicating in an age-appropriate manner as may be required with children, or where identification of de novo cases initiates family-wide testing.10
Current Treatment Landscape
No disease-modifying, systemic treatment is currently available for VHL disease in Canada, including for nonmetastatic RCC, CNS hemangioblastoma, and nonmetastatic pNET not requiring immediate surgery. Instead, management and treatment of VHL centres on life-long, active surveillance paired with local treatments through primarily surgical or radiological means.5,7 Active surveillance for VHL-associated tumours begins in early childhood and involves annual screening, which can include a combination of blood pressure monitoring, urinary catecholamine, ultrasound, CT or MRI, and audiological and ophthalmological evaluations.5,7 As reported in published literature and in clinician and patient group input, active surveillance presents both a risk of adverse events for patients (e.g., due to high exposure to radiation) as well as psychological distress and psychosocial burdens for patients, caregivers, and families.8,16-18 Psychosocial burdens include distress associated with uncertainty about disease progression, heightened distress preceding screening appointments, and distress related to scheduling and accessing screening and testing, which may require travel to a tertiary centre and out-of-pocket costs for patients and families for travel, accommodations, or services not covered by public or private insurance.8,16-18 Psychological distress associated with screening may even affect patients’ decisions to continue with recommended surveillance.16
As noted by clinical experts, treatment for VHL-associated tumours most often involves surgical resection (and sometimes radiation or laser treatment) of tumours that are greater than 3 cm in size or present with a high symptom burden or a risk of organ dysfunction or metastasis.5 However, clinical experts and clinician and patient group input emphasized that treatment itself presents risks for patients. Treatment also affects patients’ quality of life and can be psychosocially and financially burdensome for patients and their families. Given the complexity and severity of VHL disease and the associated psychosocial burden, psychological support is an essential part of care for patients with VHL as well as their family members;5,8,16,17 however, only a fraction of patients and family members may receive the psychosocial support they need.8,17 Moreover, there is reportedly an absence of data concerning the experiences of patients with VHL disease from minority ethnic or racial groups, which could impair the provision of culturally appropriate psychological support for patients with VHL disease as they navigate complex decisions that raise ethical considerations associated with genetic testing, treatment, and family planning.8,13
As emphasized by clinical experts and clinician and patient group input, there is a great unmet need for a systemic, disease-modifying treatment for VHL-associated tumours. In particular, patient and clinician group input and clinical experts reported that important treatment goals of VHL disease include delaying progression, preserving organ function (e.g., renal, neurologic, vision, pulmonary), delaying time to surgery and reducing the number of surgeries required in a patient’s lifetime (reducing morbidity), and improving health-related quality of life (e.g., maintaining independence and employment and reducing psychological distress).
The Context of Care
Due to the multisystemic nature of the disease, the surveillance and management of patients with VHL disease involves multiple health care professionals and medical specialists, including geneticists, oncologists, endocrinologists, ophthalmologists, neurosurgeons, urologists, nephrologists, neurologists, otolaryngologists, and pathologists, and requires monitoring and treatment at specialized, tertiary care centres.5,7,9,18 However, clinical experts described the diagnosis and management of patients with VHL disease as not well coordinated in the health care system in Canada, and this has also been reported in published literature in the Canadian context andelsewhere.7-9,18 The lack of coordinated care for patients with VHL disease presents challenges for timely diagnosis, surveillance, and treatment, which can impair patient care and outcomes5,7 and transfer the burden of coordinating care onto patients and their families. A lack of continuity of care can present further challenges for patients when transitioning from pediatric to adult care settings.8
Patient, Family, and Caregiver Experiences of VHL Disease
Patient and clinician group input, clinical experts, and published literature reported that VHL disease is physically and psychosocially burdensome for patients.5,8,16 VHL disease is burdensome due to both the physical manifestations of the disease (e.g., pain, neurologic burden, morbidity of tumours, functional impairment, including neurologic impairment due to CNS pathologies) and associated treatments (i.e., multiple surgeries over a patients’ lifetime). As reported in the patient group input, VHL disease also imposes significant psychological burdens on patients for multiple reasons, including persistent uncertainty about disease progression due to the heterogeneity of the disease; psychological stress associated with life-long surveillance and multiple invasive treatments; challenging decisions around communicating diagnosis and family planning decisions; and negative impacts on patients’ abilities to work, travel, exercise, conduct regular household chores, spend time with family and friends, and fulfill family obligations.8,9,13,16
As a hereditary condition, VHL disease is additionally burdensome for patients and entire families who have multiple affected members.8,10,13,16,17 Members of families with a history of VHL disease face practical challenges (e.g., caregiver burden, financial burden due costs of treatment and care not covered by public or private insurance, as well as disruptions or limitations to employment) and psychological burdens associated with their own and/or other family members’ diagnosis, morbidity or passing due to VHL disease, uncertainty about disease progression, and feelings of lack of control.8,13,16-18 Clinical experts noted that, as patients’ diseases progressed, they could require greater caregiver support; caregiver burden is further complicated by the multigenerational nature of the disease in which multiple family members could be affected by VHL disease and require support at the same time. Clinical experts also noted that community-based support for patients, including those experiencing neurologic impartment and functional decline, may be heterogenous across Canada. This raises equity-related concerns about the disproportionate burden on patients and families without independent caregiver support or of limited financial means. Published literature and patient group input reported that patients with VHL disease also face psychological burdens associated with family planning decisions due to concerns about passing on the condition to children.8,10,13,16 Patients with VHL disease may also face challenges with dating and disclosing VHL diagnosis to romantic partners, and this can be exacerbated by partners’ unfamiliarity with the disease and perceptions of its severity.15
Ethics of Evidence and Evaluation of Belzutifan
As described in the CADTH Clinical Review Report for this reimbursement review, belzutifan was evaluated in a pivotal, phase II, single-arm, open-label trial, LITESPARK-004. The trial had a primary objective of evaluating the efficacy of belzutifan for the treatment of VHL-associated nonmetastatic RCC, and secondary objectives of evaluating the efficacy of belzutifan for the treatment of VHL-associated non-RCC tumours, (i.e., CNS hemangioblastoma and nonmetastatic pNET) as well as belzutifan’s safety and tolerability.
Data submitted to CADTH by the sponsor from the LITESPARK-004 trial included a median follow-up duration of 37.7 months. Efficacy results for RCC were determined from the total study population (n = 61), while the efficacy results for CNS hemangioblastoma (n = 50) and pNET (n = 22) were determined from subsets of the total study population. As all participants were required to have at least 1 RCC tumour, the trial did not reflect results for participants with only a CNS hemangioblastoma and/or pNET. However, according to the clinical experts, this did not present a serious generalizability concern, and results from the pivotal trial could still be extrapolated to VHL patients with a CNS hemangioblastoma and/or nonmetastatic pNET. Of the trial’s participants, 37.7% discontinued treatment during the trial due to side effects or personal or logistical reasons. As described in detail in the CADTH Clinical Review Report, and based on the opinions of the clinical experts, efficacy results from the LITESPARK-004 trial demonstrated a durable tumour response as measured by an objective response rate and duration of response in the study populations. However, as detailed further in the CADTH Clinical Review Report, the absence of an internal comparator group precluded definitive conclusions about the efficacy and safety of belzutifan due to the potential for confounding. Median time to surgery was not reached due to the limited duration of follow-up, and the trial did not capture patient-important outcomes, such as impact on symptoms and health-related quality of life. Findings from an indirect treatment comparison, which was the only comparative evidence available at the time of this reimbursement review, suggested that treatment with belzutifan may have a beneficial effect on time to RCC-related surgery compared to active surveillance in patients with VHL disease–associated nonmetastatic RCC. However, the certainty of the indirect evidence was very low due to methodological limitations (e.g., violation of the underlying assumptions of the matching-adjusted indirect comparison approach, which resulted in a high risk of residual confounding, and important differences in outcome definitions between the LITESPARK-004 trial and the VHL Natural History Study that would bias the findings in favour of belzutifan).
Clinical experts noted that it was preferable to have a higher level of certainty in the evidence to inform clinical decision-making for the use of belzutifan, including for each tumour subtype. However, they acknowledged that such evidentiary limitations were not outside the norm in the areas in which they practised given the rarity of VHL disease and specific tumour manifestations paired with the absence of alternative systemic treatment options. Clinician group input noted that data from a phase II, single-arm trial were suitable for a younger, rare-patient population of patients, such as those with VHL disease. Clinical experts emphasized the importance of collecting long-term safety, tolerability, and efficacy data to inform decision-making about initiating and discontinuing belzutifan, such as through a patient registry, particularly as belzutifan would likely be prescribed to patients starting in early adulthood and continued as a chronic therapy. Similarly, patient group input suggested that patients receiving belzutifan should be enrolled in a monitoring program to collect continuous, real-world safety and efficacy data to balance providing patients with earlier access to belzutifan against the need to address evidentiary uncertainty. As detailed in the following section, clinical experts discussed the implications of this evidentiary uncertainty for the use of belzutifan, including those related to clinical decision-making and informed consent.
Clinical experts noted that, while the trial population was broadly representative of the patient population that they encountered in clinical practice, there were some differences. The incidence of VHL disease is similar across racial and ethnic groups,15 and clinical experts expected the Canadian population of patients with VHL disease would be more ethnically and racially diverse than in LITESPARK-004, in which 90% of trial participants were white. However, they did not expect this to limit the generalizability of the trial results to a more diverse patient population. Rather, they noted that the lack of diversity within the pivotal trial was likely emblematic of a broader equity issue facing clinical trials, in which some demographic groups face greater challenges in accessing clinical trials, which tend to be run through specialized, tertiary centres. More broadly, the underrepresentation of racial, ethnic, and other marginalized groups, as well as women, in clinical trials, has been identified as ethically concerning.19 Diverse clinical trial participation is required to contribute to building trust in medical research and institutions (which can affect patients’ willingness to pursue treatment), promoting fairness for potential participants and their communities, and producing higher-quality biomedical knowledge.19 Clinical experts also noted that, in practice, clinicians would likely prescribe belzutifan on a case-by-case basis after assessing a patient’s best interests, and that they would include patients with an Eastern Cooperative Oncology Group Performance Status of 2, which exceeds that of the trial eligibility criteria (a score of ≤ 1).
As discussed in greater detail in the Pharmacoeconomic Report in this Review, the lack of long-term efficacy and comparative effectiveness data limits the ability to accurately model and assess cost-effectiveness of belzutifan. This limitation, which may affect cost-effectiveness analyses for drugs that treat rare diseases (and oncology drugs more generally) presents challenges for assessing the opportunity costs — or forgone benefits — associated with reimbursing and resourcing a particular intervention over others.20 Understanding opportunity costs is important for informing resource allocation decisions at a health systems level.
Ethical Considerations in the Use of Belzutifan
There are several important ethical considerations pertaining to the use of belzutifan for VHL disease for an associated nonmetastatic RCC, CNS hemangioblastoma, or nonmetastatic pNET not requiring immediate surgery, including those related to the harms and benefits associated with the use of belzutifan, access, and informed consent.
Balancing Benefits and Harms
As discussed in the Clinical Review Report for this reimbursement review, belzutifan demonstrated a promising durable response in the LITESPARK-004 trial. However, no definitive conclusions could be drawn about the safety and efficacy of belzutifan for adult patients with a VHL-associated nonmetastatic RCC, CNS hemangioblastoma, or nonmetastatic pNET not requiring immediate surgery based on currently available evidence. The clinical experts consulted for this review noted that such evidentiary uncertainty was not outside the norm when treating patients with VHL due to the rarity of the disease, but required consideration when weighing the potential benefits and harms associated with the use of belzutifan in clinical practice.
Clinical experts and clinician and patient group input noted that belzutifan may be beneficial for patients by offering the first systemic treatment for VHL-associated tumours. By targeting the underlying pathophysiology of the disease, belzutifan may alter the current treatment paradigm for VHL, delaying disease progression and potentially preserving patient function and avoiding the need for local treatments (e.g., surgery or radiation) and associated appointments, hospitalizations, and rehabilitation, all of which are physically, psychosocially, and financially burdensome for patients. The use of belzutifan also presents several potential risks for patients with VHL disease. Clinical experts noted that, in most cases, belzutifan presented a risk of anemia (reported in 90.2% of participants in the LITESPARK-004 trial), which could require blood transfusions (in 1.8% of participants in the LITESPARK-004 trial) or render patients transfusion-dependent. They also noted that belzutifan presented a risk of fatigue, hypoxia, and embryo-fetal toxicity. As a result, patients of childbearing age must use 2 contraceptives when taking belzutifan as oral contraceptives could be rendered less effective through interactions with belzutifan.
Clinical experts also acknowledged that there was insufficient clinical evidence to understand the long-term safety and efficacy of belzutifan, the impact of discontinuing treatment on disease progression, and the impact of chronic use for patients. They noted that it was particularly important to consider long-term safety (e.g., long-term impact on fertility and neurocognitive status), as patients can initiate belzutifan in early adulthood and continue treatment over the course of decades even while they are relatively healthy and not at immediate risk of harm due to VHL-associated tumours. They added that there was insufficient evidence regarding belzutifan’s impact on fertility. The product monograph cautions that there are no data concerning belzutifan’s effects on fertility in humans, but animal studies suggest that it may affect fertility in both males and females, and that the reversibility of this effect is unknown. Clinical experts noted the importance of considering belzutifan’s long-term tolerability, as patients without metastatic disease or serious manifestations of VHL-associated tumours may be less likely to continue with treatment if they do not tolerate belzutifan well.
On balance, clinical experts and clinician group input noted that they would prescribe belzutifan for patients with VHL based on available evidence concerning its potential systemic effects and in the absence of available alternative systemic therapies. They recognized that they were trying to balance patients’ currently unmet need for an effective systemic treatment for VHL-associated tumours (including treatment that could delay or reduce the need for invasive, local treatments) with a consideration of the risks of adverse events and the evidentiary uncertainty around the long-term safety, efficacy, and tolerability of belzutifan. Patient group input also reported that patients would be willing to tolerate moderate to severe side effects from a treatment that would help them avoid the need for surgery to remove VHL-associated cysts and tumours. Moreover, patient group input emphasized that patients could not afford to wait for greater evidentiary certainty before accessing a systemic therapy for VHL, given that they needed “to have the opportunity to benefit from extended periods of tumour-free remission.
As a result, and in recognition of the heterogenous presentation of VHL disease, patient group input and clinical experts noted the importance of physicians and patients (and families) engaging in an ongoing process of sharing and guiding clinical decision-making based on patients’ individual circumstances. Moreover, patients with VHL disease should be recognized as experts in their own condition, particularly due to the rarity and heterogeneity of phenotypic manifestations of the disease, and therefore need to be included in all aspects of decision-making about their treatment and care.8 Similarly, while the LITESPARK-004 trial required participants to have tumours measuring 3 cm or larger, as these are generally considered to require intervention in VHL disease, clinical experts noted that prescribing decisions for belzutifan should be based on individual patients’ circumstances as the location and nature of a particular tumour could have distinct implications for function and other important indicators.
Clinical experts also recommended that germline genetic testing should be required to confirm a VHL diagnosis (if it had not already been performed as a part of initial VHL diagnosis) before the initiation of belzutifan, as the biology of VHL-associated tumours, such as CNS hemangioblastomas, is distinct in the context of VHL disease. They also suggested that confirmatory genetic testing could help prevent “indication-creep,” or the use of belzutifan in cases in which patients presented with VHL-like, but nonetheless distinct, tumour manifestations for which there was no evidence of efficacy. Preventing off-label use was cited as important as it could potentially expose patients to unnecessary risks without accompanying benefits at a greater cost to the health care system.
Given the complexity of VHL disease, uncertainty about the safety and efficacy of belzutifan, and risk of potential adverse events, clinical experts and clinician group input recommended that belzutifan be prescribed by a medical specialist (e.g., a medical oncologist or equivalent) with the requisite knowledge about VHL disease and belzutifan who could oversee and coordinate a patient’s treatment and care. This was particularly important given the need for ongoing monitoring of treatment response and risks of adverse events that would require timely management. As a result, and as discussed in the following section, clinical experts and clinician and patient group input emphasized that the safe and effective use of belzutifan requires patients to have adequate access to ongoing specialist monitoring and care, as well as better coordination of care.
Considerations Related to Access
Several considerations also arise related to the equitable provision of, and access to, belzutifan and associated care, including geographic or diagnostic-related barriers to access. As a daily, orally administered pill, patients can self-administer belzutifan at home, which makes treatment with belzutifan relatively accessible. However, clinical experts and clinician group input noted that patients would still require ongoing access to specialist care, testing, and medical imaging to monitor treatment response (including via MRI or CT every 2 to 6 months depending on tumour type), tolerability, and adverse events. Due to the chronic nature of the therapy, clinical experts acknowledged that treatment with belzutifan could increase the frequency of specialist follow-up appointments and visits to tertiary centres compared to the appointments patients already required for active surveillance or for local treatments. Clinical experts noted that the ongoing need for monitoring and care associated with belzutifan could present geographic and financial barriers to, or disproportionately burden, patients residing far from tertiary centres who would need to travel to access testing and care. However, they noted that this was already the case for active surveillance and treatment for VHL disease. They recommended the use of telehealth and remote monitoring services, as well as coordination with local or community care (e.g., for testing or imaging), where possible, to make monitoring and follow-up treatments with belzutifan more accessible. At the same time, they emphasized the importance of coordinating patient treatment centrally through a specialized, tertiary centre.
Given the rarity and heterogenous presentation of VHL, clinical experts acknowledged that delays in diagnosis due to physicians’ unfamiliarity with the condition — particularly in de novo cases without a family history of VHL — could delay intervention and treatment with belzutifan. This could be further exacerbated by geographic considerations as specialists familiar with VHL and/or treatment with belzutifan tend to practise in large urban centres. Similarly, if confirmatory germline genetic testing were required, access to germline testing and associated genetic counselling could be a barrier for patients residing far from specialized centres.
Considerations Related to Informed Consent
There are at least 2 key considerations related to informed consent for the use of belzutifan, including 1 related to the limited available evidence to support clinical decision-making and the implications of chronic medication use for patients’ health and understandings of VHL. Clinical experts emphasized the importance of robust and informed consent to gauge patients’ knowledge of VHL disease, assess individual patients’ circumstances and needs, and transparently discuss potential adverse events (e.g., embryo-fetal toxicity, risk of anemia, and hypoxia). For example, clinical experts cited discussing the possible need for blood transfusions, including what transfusion entails as well as its risks and benefits, before initiating treatment with belzutifan due to the risk of anemia. They also noted that discussions of informed consent should transparently acknowledge the current state of evidence, including the evidentiary uncertainty about belzutifan’s long-term safety and efficacy, including its long-term impact on fertility, as well as uncertainty about the effects of discontinuing treatment.
Clinical experts also noted the need to disclose that belzutifan was a chronic or potentially life-long medication, and to recognize that this could also affect how patients understand their disease.18 As reported in published literature, patients’ understandings of the chronic and hereditary nature of VHL disease, including the requirement for life-long monitoring or treatment, could present psychosocial burdens for patients and families and may require access to appropriate psychosocial support and genetic counselling.8,10,14,16,17 As a chronic medication that may be initiated in early adulthood, it is also important that conversations about the potential harms and benefits, and evidentiary uncertainty, be revisited in a process of ongoing, shared decision-making as patients continue on treatment and transition through different life stages or care settings.
Health Systems Considerations
The reimbursement of belzutifan for VHL raises several ethical considerations relating to health systems and resource considerations, including opportunity costs, the sustainability of Canadian health care budgets, the ongoing need for specialist care and centrally coordinated care, and health information infrastructure. Expensive drugs for rare diseases, including belzutifan, raise ethical considerations related to distributive justice and equitable access, the sustainability of health care budgets, and fair pricing of pharmaceuticals.20,21 Although there is a significant unmet need for an effective disease-modifying treatment for VHL disease, assessing the opportunity costs of reimbursing belzutifan is complicated by the evidentiary uncertainty about the magnitude and durability of its therapeutic effect.
Clinical experts noted that the use of belzutifan may increase the frequency of visits required, as a specialist physician and blood draws or other testing are required to monitor treatment-related toxicity and treat adverse events. However, they also noted that the use of belzutifan was unlikely to notably increase the utilization of other health care resources such as germline genetic testing or resources (e.g., MRI) required to monitor disease progression. This is because patients — particularly those who had received treatment or care at a tertiary centre — would most likely have already undergone genetic testing due to a family history or presentation with VHL-associated morbidities, and would therefore already be under active surveillance even in the absence of belzutifan. Clinical experts and clinician group input also noted that, although no confirmatory evidence is available presently, they expected health care resource utilization associated with local treatments for VHL-associated tumours (e.g., surgeries, radiation therapy, neurologic assessment and treatment, and hospitalization) could decrease, or be delayed, were belzutifan used. However, they also acknowledged that safe and effective treatment of patients with VHL disease with belzutifan would benefit from ensuring that patients’ treatment is overseen and coordinated centrally by a specialist at a tertiary centre. In contrast, they cautioned that care for patients with VHL disease in Canada is not well coordinated and that specialists are often unaware of patients’ care and status once in the community.7,9 As a result, offering belzutifan in an equitable manner may require balancing more accessible monitoring and care close to home for patients (e.g., through virtual care and coordinating with local, community-based centres for testing and imaging) against ensuring that treatment with belzutifan is overseen by a specialist and that patients’ overall care is centrally coordinated given the complex, multidisciplinary nature of VHL disease care.5,7
Relatedly, there is presently no standardized or centralized health information database for patients with VHL disease in Canada.7,9 A clinical VHL database piloted with a cohort of patients in Toronto, Ontario, provides an example of a database that has the potential to benefit VHL patient treatment, management, screening, and follow-up, as well as to better understand genotypic and phenotypic heterogeneity in the VHL patient population.9 Recognizing the outstanding uncertainty in the clinical and pharmacoeconomic evidence used to evaluate belzutifan, health systems may also need to consider the potential resource implications and health systems infrastructure required to generate additional evidence about the use of belzutifan for the treatment of VHL-associated tumours, such as through patient registries, databases, or monitoring programs.9
Limitations
Little published literature discusses the ethical considerations related to the use of belzutifan for the treatment of VHL disease given both the rarity of the disease and the novelty of the drug under review. This does not imply that ethical considerations in the context of belzutifan for VHL disease are absent, and this review of ethical considerations was augmented by drawing from additional resources collected in the course of this reimbursement review, including patient group, clinician group, and drug program input, and discussion with clinical experts, as well as engagement with CADTH clinical and pharmacoeconomic review teams, to provide a comprehensive understanding of the ethical considerations related to the use of belzutifan to treat VHL disease.
Although this ethics report drew on and considered patient group, clinician group, drug program, and clinical expert input, it is possible that more direct engagement with key stakeholders (patients, caregivers, family members, and other decision-makers) regarding their specific experiences with VHL disease and/or belzutifan could have offered additional relevant ethical considerations or domains of analysis.
Conclusion
Input from patient groups, clinician groups, and provincial drug programs, as well as direct engagement with clinical experts and published literature were reviewed for ethical considerations relevant to the use of belzutifan for the treatment of adult patients with VHL disease who require therapy for an associated nonmetastatic RCC, CNS hemangioblastoma, or nonmetastatic pNET not requiring immediate surgery. Ethical considerations in the context of VHL disease highlighted the significant physical and psychosocial burden of the disease on patients, families, and caregivers, as well as the challenges associated with the hereditary nature of the disease for patients and entire families. There is a significant unmet need for a systemic treatment for VHL-associated tumours due to the morbidity of local treatment, including surgery and radiation, and the absence of alternative disease-modifying therapies. Clinical trial evidence indicated that there is presently evidentiary uncertainty concerning the safety and efficacy of belzutifan, particularly in the long term; this uncertainty limits assessment of clinical benefits and harms associated with treatment as well as pharmacoeconomic assessment of cost-effectiveness.
Belzutifan presents potential risks for patients, including common risks of anemia and embryo-fetal toxicity. Despite potential risks of adverse events and evidentiary uncertainty about belzutifan’s long-term safety and efficacy, patients and clinicians expressed a willingness to undertake some risks for the potential benefit of a therapy that could delay disease progression given the burden associated both with VHL-associated tumours and the invasive, local treatments require to remove them as well as the absence of alternative disease-modifying therapies. Robust informed consent processes are required to disclose risks of adverse events and evidentiary uncertainty about the safety, efficacy, and tolerability associated with the long-term use of belzutifan as patients continue on treatment and transition through different life stages or care settings. Equitable access to belzutifan requires attending to potential geographic and diagnostic barriers to access, including those associated with the specialist care and monitoring required for safe and effective use. Ethical considerations for health systems related to the implementation of belzutifan highlight the challenges of funding decisions and assessments of opportunity costs for expensive drugs for rare diseases, the need for better coordination of multidisciplinary and ongoing treatment, monitoring, and care for VHL, and improved health information systems infrastructure.
References
1.EUnetHTA Joint Action 2 Work Package 8, HTA Core Model version 3.0 2016; http://www.htacoremodel.info/BrowseModel.aspx.
2.Benkhalti M, Espinoza M, Cookson R, Welch V, Tugwell P, Dagenais P. Development of a checklist to guide equity considerations in health technology assessment. Int J Technol Assess Health Care. 2021;37(1). PubMed
3.Grey matters: a practical tool for searching health-related grey literature. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/grey-matters. Accessed 2023 Feb 16.
4.Sandelowski M. Whatever happened to qualitative description? Res Nurs Health. 2000;23(4):334-340. PubMed
5.Crespigio J, Berbel LCL, Dias MA, et al. Von Hippel-Lindau disease: a single gene, several hereditary tumors. J Endocrinol Invest. 2018;41(1):21-31. PubMed
6.Clinical Study Report: study number. Title of report [internal sponsor's report]. City (PROV): Sponsor name; 1800.
7.Bradley S, Dumas N, Ludman M, Wood L. Hereditary renal cell carcinoma associated with von Hippel-Lindau disease: a description of a Nova Scotia cohort. Canadian Urological Association Journal. 2009;3(1):32-36. PubMed
8.Methley A, Dawson B, Teager A, Morris C, Morris H. Von Hippel-Lindau syndrome: a literature review and clinical considerations. European Journal of Palliative Care. 2017;24(4):161-165.
9.Salama Y, Albanyan S, Szybowska M, et al. Comprehensive characterization of a Canadian cohort of von Hippel-Lindau disease patients. Clin Genet. 2019;96(5):461-467. PubMed
10.Nielsen SM, Rhodes L, Blanco I, et al. 2016.
11.Li FP. Identification and management of inherited cancer susceptibility. Environ Health Perspect. 1995;103 Suppl 8:297-300. PubMed
12.Tischkowitz M, Rosser E. Inherited cancer in children: practical/ethical problems and challenges. Eur J Cancer. 2004;40(16):2459-2470. PubMed
13.Levy M, Richard S. Attitudes of von Hippel-Lindau disease patients towards presymptomatic genetic diagnosis in children and prenatal diagnosis. J Med Genet. 2000;37(6):476-478. PubMed
14.Lips CJ, Höppener JW, Van Nesselrooij BP, Van der Luijt RB. Counselling in multiple endocrine neoplasia syndromes: from individual experience to general guidelines. J Intern Med. 2005;257(1):69-77. PubMed
15.Bond E, Yashar B, Else T, Osborne J, Marvin M. Disclosure of genetic risk to dating partners among young adults with von Hippel-Lindau disease. Fam Cancer. 2022;19:19. PubMed
16.Lammens CR, Bleiker EM, Verhoef S, et al. Psychosocial impact of Von Hippel-Lindau disease: levels and sources of distress. Clin Genet. 2010;77(5):483-491. PubMed
17.Lammens CR, Bleiker EM, Verhoef S, et al. Distress in partners of individuals diagnosed with or at high risk of developing tumors due to rare hereditary cancer syndromes. Psycho-Oncology. 2011;20(6):631-638. PubMed
18.Kasparian NA, Rutstein A, Sansom-Daly UM, et al. Through the looking glass: an exploratory study of the lived experiences and unmet needs of families affected by Von Hippel-Lindau disease. Eur J Hum Genet. 2015;23(1):34-40. PubMed
19.Schwartz AL, Alsan M, Morris AA, Halpern SD. Why Diverse Clinical Trial Participation Matters. New England Journal of Medicine. 2023. PubMed
20.Kacetl J, Marešová P, Maskuriy R, Selamat A. Ethical questions linked to rare diseases and orphan drugs - a systematic review. Risk Manag Healthc Policy. 2020;13:2125-2148. PubMed
21.Wagner M, Goetghebeur MM, Ganache I, et al. HTA challenges for appraising rare disease interventions viewed through the lens of an institutional multidimensional value framework. Expert Rev Pharmacoecon Outcomes Res. 2022:1-10. PubMed
Appendix 1: Details of Included Publications
Table 1: Details of Included Publications
First author, year | Publication type | Objective | Key ethical considerations | Funding source |
|---|---|---|---|---|
Bond (2022)15 | Qualitative interview study | To describe the young adults’ attitudes toward dating and decisions related to disclosing a VHL diagnosis to a dating partner |
| University of Michigan Rackham Graduate School Student Research Grant, National Society of Genetic Counselors Jane Engelberg Memorial Fellowship Student Research Award, National Society of Genetic Counselors Jane Engleberg Memorial Fellowship Student Research Award |
Bradley (2009)7 | Database study | To determine how many patients in Nova Scotia, Canada had VHL disease and how they were cared for, and to compare practice with published protocols |
| None declared |
Crespigio (2018)5 | Review | To describe the epidemiology, clinical presentation, diagnosis, and treatment of VHL |
| Portuguese Foundation for Science and Technology (FCT) PhD Grant |
Kacetl (2020)20 | Systematic review | To identify ethical questions related to rare diseases and orphan drugs and ethical principles or approaches applied to address them |
| University of Hradec Kralove Long-Term Development Plan |
Kasparian (2015) | Mixed-methods study (qualitative interviews and self-administered survey) | To describe the lived experiences and unmet needs of families affected by VHL in Australia |
| Career Development Fellowship from the National Health and Medical Research Council of Australia (NHMRC ID 1049238), Leukaemia Foundation of Australia PhD Scholarship, Early Career Researcher Award from UNSW Medicine from the University of New South Wales |
Lammens, (2010)16 | Survey study | To describe the psychosocial impact of VHL, including levels and sources of distress, for patients with VHL and their family members |
| Dutch Cancer Society (grant number 2005 to 3209) |
Lammens, (2011)17 | Survey study | To describe the prevalence of, and factors associated with, psychological distress among partners of individuals with or at high risk of Li Fraumeni syndrome or VHL |
| Dutch Cancer Society (grant number NKI 2005 to 3209) |
Levy (2000)13 | Qualitative interview study | To describe the attitudes of patients with VHL toward presymptomatic genetic diagnosis in children and prenatal diagnosis in France |
| Ligue Nationale contre le Cancer |
Li (1995)11 | Review | To describe the potential benefits and harms associated with the identification and management of inherited cancer susceptibility |
| None declared |
Lips (2005)14 | Review | To describe guidance for genetic and medical counselling for endocrine neoplasia syndromes, including VHL |
| None declared |
Methley (2017)8 | Review | To describe the diagnosis and treatment of VHL, including with respect to psychological and palliative care |
| None declared |
Nielsen (2016)10 | Review | To describe the genetics of VHL and the role and impact of genetic testing and counselling for patients with VHL |
| Authors reported relationships with GeneDx, Bioreference Laboratories, AstraZeneca, and N-of-One |
Salama (2019)9 | Database study | To describe the development of a VHL database capturing genetic and clinical information and report the findings from a patient cohort from Toronto, Ontario |
| Von Hippel-Lindau Association Research Grant, Garron Family Cancer Centre Studentship Award, Starbucks Clinical Genetics/Genomics Research Studentship Award |
Schwartz (2023)19 | Perspective | To identify the ethical considerations related to diverse clinical trial participation |
| Authors received support from Abbot Laboratories, Acorai, Boehringer Ingelheim, Cytokinetics, Edwards Lifesciences Corporation, Ionis Pharmaceuticals, Merck, Myokardia, Novartis, Aetna, Lown Institute, Tufts Medical Center, VBID Health |
Tischkowitz, (2004)12 | Review | To identify the ethical challenges for patients and families with inherited cancer in children, including for VHL |
| None reported |
Wagner (2022)21 | Review and expert opinion | To identify ethical challenges for appraising interventions for rare diseases, including key ethical tensions as well as approaches and principles for addressing these challenges |
| Institut national d'excellence en santé et en services sociaux (INESSS) |
Note that this appendix has not been copy-edited.
Stakeholder Input
Patient Input
The Canadian VHL Alliance
(with The Canadian Organization for Rare Disorders, Kidney Cancer Canada, Pancreatic Cancer Canada, and the Canadian Neuroendocrine Tumour Society)
About The Canadian VHL Alliance
The Canadian VHL Alliance (CVHLA) https://cvhla.ca raises money for research, provides education and support to Canadian VHL patients and their families, and advocates for improved treatment for patients with VHL disease.
The Canadian Organization for Rare Disorders (CORD) https://raredisorders.ca is Canada’s national network for organizations representing all those with rare disorders. CORD provides a strong common voice to advocate for health policy and a healthcare system that works for those with rare disorders. CORD works with governments, researchers, clinicians and industry to promote research, diagnosis, treatment and services for all rare disorders in Canada.
Kidney Cancer Canada https://kidneycancercanada.ca is a national community of patients, caregivers and health professionals who work to provide every Canadian touched by kidney cancer with support, education and advocacy for their care pathways and treatment options.
Pancreatic Cancer Canada https://pancreaticcancercanada.ca raises funds to ensure ground-breaking research, provides patient support services, education and raises awareness, with the goal to improve the rate of pancreatic cancer survival.
The Canadian Neuroendocrine Tumour Society (CNETS) https://cnets.ca was formed in 2007 to assist the Canadian neuroendocrine cancer community. CNETS supports patients through education, peer support programs both in person and virtually, and helps patients navigate the Canadian healthcare system. CNETS increases awareness about neuroendocrine cancers among the general population and the medical field, fundraise for research, manage their own annual research grant competition and advocate on behalf of patients for access to cutting edge treatments and diagnostics Canada-wide.
Information Gathering
In December 2022, CVHLA and Kidney Cancer Canada, conducted an online survey of patients and caregivers to assess the challenges VHL patients and caregivers face because of the disease. 123 patients and caregivers participated in the survey as follows:
Patients living with VHL: n=72 (59%)
Someone providing care to a person with VHL disease (either currently or previously): n=51 (41%)
Through this survey CVHLA identified 19 patients who had experience with belzutifan for the treatment of VHL disease.
Additionally, semi-structured telephone interviews were conducted with three patients and caregivers who have experience with the treatment under review.
Disease Experience
Summary
Overall, patients described living with VHL as an on-going series of physical and psychological struggles. Because VHL tumours can grow in different parts of the body (spine, organs, and brain), the symptoms are varied. Numerous participants reported not getting a diagnosis until the tumours had advanced causing serious problems affecting vision, hearing, and walking. They experience considerable discomfort, pain and interference with carrying out everyday activities.
Psychologically, knowing you or a family member has VHL is a source of constant worry and stress, in part, because it is a “hidden condition.” Some VHL patients reported their initial symptoms were dismissed or misdiagnosed by their local physicians; others said they were the ones who educated their healthcare providers in order to get access to appropriate care and services. Participants also talked about the huge burden of adhering to tumour screening guidelines, scheduling numerous different kinds of tests, sometimes traveling to major centres for tumour screenings, and paying for all of the expenses not covered by public healthcare or even private insurance. In fact, they often had to “fight” with the insurance companies to cover essential medicines.
Moreover, because tumours have to be monitored regularly, many VHL patients reported worrying about the potential adverse effects of frequent screenings (contrast, electromagnet images) as well as the stress caused by the “uncertainty” of tumour activity between scans. Overall, participants expressed the view that receiving a scan result rarely provides a feeling of “relief”; there is no such thing as a “good news” scan result since the best-case scenario is a report of “no change” in the tumour (it doesn’t go away on its own and can continue to grow).
What we heard was that unlike most single-site cancers where a “five-year cancer free” test result means no further screenings or worry, VHL is, at best, a lifetime of uncertainty.
Patients experience VHL as excruciatingly painful and debilitating, with cysts and tumours that can attack throughout the body, including the spine, brain, kidney, pancreas kidney, eyes/retina, epididymis, adrenal glands, endolymphatic sac, spine, brain/brainstem/cerebellum, neck, breast, inner ear, choroid arteries, jugular vein, lungs, duodenum, and groin. They also experience serious disruption to daily life and quality of life, including diminished ability to care for themselves, to engage in family and social activities, to plan for a family, and to participate in work. The last also affects their finances, feelings of self-worth, and engagement in meaningful activities. Given that the only treatment is surgery, it is not surprising that the overwhelming majority of patients have endured multiple surgeries on multiple sites, some with tremendous life-threatening risks. And, of course, it is not feasible to surgical remove tumours at some sites, such as the spine and the brain.
Detail
In our survey, overall, about 45% of participants reported a negative impact “4” or “5” on each of these activities, your ability to:
Work
Travel
Exercise
Conduct household chores
To spend time with family and friends, and
To fulfill family obligations.
We asked: Please let us know how surgeries have impacted your ability to work or your quality of life, including spending time with loved ones. 92 patients and caregivers provided commentary, some taking belzutifan.
One mother’s experience:
“I have had to watch one daughter go through losing their adrenal glands at age 18 & go on replacement steroids & enzymes daily & Lanreotide injections monthly & almost died due to HIB flu & strep & sepsis & lost lung, kidney, heart function & had to be put into a coma to survive due to lowered immune system. She had to decide to not have children due to VHL & damage done during surgeries & scar tissue from her pancreas surgeries betting attached to her reproductive organs & needing a hysterectomy. She is now in her late 40s & because of the replacement steroids she has a shrinking brain of a 70-year-old & bone loss due to osteoporosis brought on by the steroids. She also has eye & brain tumors that are being watched. She is also getting many other disabilities due to being immuno-compromised.”
“My other daughter has had one adrenal gland removed & part of the other & her spleen removed, etc. so she is immuno-compromised. She also has brain & eye tumors that are being watched. Now she has managed to have 2 children & one of the 2 has VHL & has had abdominal VHL surgery at age 12. I know how that horrible feel due to my children being 11 & 18 during their 1st surgeries & me being 6. Most of our tumors are found with MRIs but the kidney tumors need CT scans to define them before surgery & now every 3 months due to being on belzutifan trial. So, even more radiation, which has been shown to cause kidney cancer, etc.”
Others stated:
“Please approve belzutifan, so we can stop having so many invasive surgeries & procedures like RFA (radio frequency ablation) & radiation causing scans in our future. We are running out of organs to remove or partially remove & getting too much radiation.”
“Surgeries are very tough on the body and often very tough side effects.”
“I was born with VHL, passed on from my father who passed away when I was 2 due to VHL. I hope to find a cure for me and my child that inherited it.”
“My daughters & I all are immunocompromised due to our spleens being removed, etc. & needing to get the Splenectomy vaccines on top of flu, pneumonia, covid, Shingrix, Prevnar 13, etc.”
“Belzutifan is our kind of our last-ditch effort to slow down the bus.”
For more patient experiences, please refer to Appendix 1.
Experiences With Currently Available Treatments
Summary
Belzutifan is the only approved treatment for patients with VHL disease and associated RCC, central nervous system (CNS) hemangioblastoma, or pNET that does not require immediate surgery.
When asked about the number of surgeries experienced, prior to the introduction of belzutifan, numerous patients reported that they had had so many surgeries they were only able to say, “don’t know”, “multiple”, “too many to remember”, or “lost count”. Based on the 98 individuals who provided quantifiable responses, a total of 520 surgeries had been experienced, with 18 individuals (18.4%) reporting 10 or more surgeries.
The average number of surgeries was 5.3. Sadly, many patients qualified their count as the number “so far”, signaling more surgeries could be expected.
Among the most terrifying and high-risk surgeries that participants talked about are laser eye surgeries. Worse, many patients reported that their eye tumours could recur, necessitating repeated surgeries, with one patient reporting 24 laser eye surgeries to date.
Detail
Surgery remains the primary treatment for symptomatic lesions in VHL-disease. Of the 112 individuals who answered the question, 85% (n=95) reported having had surgery to remove VHL cysts and tumors, with 6% (n=7) reported having had no surgery, and 9% (n=10) reported that they have “NOT YET” had surgery.
87 individuals reported multiple tumor sites ranging from 2 to 8 sites. Based on the data collected, the average patient had tumors in 2.8 “sites”. However, many patients reported more than one tumor in one location/site. The sites reported included: kidney, pancreas, eyes/retina, epididymis, adrenal glands, endolymphatic sac, spine, brain/brainstem/cerebellum, neck, breast, inner ear, choroid arteries, jugular vein, lungs, duodenum, and groin. Patients reported not only having tumors resected, but in various cases having a whole kidney or lung removed.
We asked: How many surgeries have you (or the patient you care for) had with respect to the removal of VHL cysts and tumors?
98 individuals provide data that we were able to use. Unfortunately, numerous patients had so many surgeries that they reported comments like: “don’t know”, “multiple”, “too many to remember”, or “lost count.
Of the 98 individuals that provided usable numeric responses, there were a total of 520 surgeries reported, with 18 individuals (18.4%) reporting 10 or more surgeries.
The average number of surgeries reported = 5.3.
Some patients emphasized that the reported number was “so far” indicating that more surgeries were anticipated.
Many patients reported multiple laser eye surgeries in addition to surgeries in other locations on their body, including one patient who had 24 laser eye surgeries.
Many respondents spoke of the impact of surgeries on “your ability to work or your quality of life, including spending time with loved ones.”
Specifically, they said:
"Surgeries and threat of surgeries has made every day a struggle. Some physically as the surgeries have limited my ability to do the things, I once enjoyed like running and sports. Some mentally as the fear of surgery or possible surgery has affected every life decision I have ever made.”
“Confined to wheelchair following brain surgery. Needs fulltime personal care. Low quality of life.”
“The surgeries have impacted my work, quality of life and including spending time with loved ones quite a bit. I have struggled with pain on a daily basis, and it is hard to be active.”
“Because the surgery location is a cerebellar tumour, there were many concerns about the side effects and whether I would be able to live again after the surgery… I had to quit the company repeatedly due to symptoms and treatment. This results in hardship financially and mentally.”
“I have had spinal cord surgery three times, all in the lumbar spine. With each surgery the scar tissue becomes more extensive… causes pain and issues with sensation and strength. The doctors say the tumours are like salt and pepper all over the cord, from top to bottom. I’m terrified they will grow and require more surgery. I can’t keep doing this…”
“It has forced me to take a lot of time off work over the years to have surgery and recover, which in turn has deterred me from going further in school or taken a more serious role at my current jobs.”
Caregivers reported:
“Surgery on the brain stem tumours… It took away their ability to swallow, walk, breathe without oxygen, speak clearly.”
“The surgeries always impact the time we get to spend together because he’s away for surgery and then trying to recover at home. It has impacted the time we spend with him because he is so sick. He is away so much for medical reasons he’s missing out on so much family time. And as for work, he is not at all able to work. He has been sitting at home for the last year too sick for work.”
“The results of surgery impacted the patient and made him bedridden, and took away his ability to swallow, walk. Needed to used oxygen. Inability to speak clearly. Fighting pneumonia frequently. Needed all around care.”
Improved Outcomes
Summary
Patients with VHL disease overwhelmingly expressed the need for a treatment that can improve their physical condition by decreasing the size of (or stabilizing) tumours, reducing pain, improving breathing, offering long(er)-term stability or reduction of disease., and, most importantly, offering the opportunity to avoid surgery. Overall, patients indicated they were willing to tolerate moderate to severe side effects of a treatment that would allow avoidance of surgery to remove VHL related cysts and tumours.
Detail
Participants were asked to rate the importance of different types of outcomes in relation to a new therapy, from "not important" to "extremely important."
Moreover, respondents were also asked to rate the “severity of side effects” they would be willing to tolerate in order receive a surgery that would provide the “opportunity to avoid surgery.”
Table 1: Ratings of the Importance of Different Types of Outcomes in Relation to a New Therapy
Ratings of the Importance of Different Types of Outcomes in Relation to a New Therapy | ||||||
|---|---|---|---|---|---|---|
Improvement to your physical condition such as decreasing the size of (or stabilizing) the tumour(s), reducing pain, improving your breathing (N=89) | ||||||
1 (Not important) | 2 | 3 | 4 | 5 (Extremely important) | N/A | Weighted Average (WA) |
0pts (0%) | 0pts (0%) | 4pts (4.5%) | 9pts (10.11%) | 73pts (82%) | 3pts (3.37%) | 4.80 |
Overall Improvement to your quality of life (N=89) | ||||||
1pt (1.12%) | 3pts (3.37%) | 6pts (6.74%) | 7pts (7.87%) | 69pts (77.53%) | 3pts (3.37%) | 4.63 |
Chance for long-term stability or reduction of disease (N=112) | ||||||
0pts (0%) | 0pts (0%) | 1pt (1.12%) | 10pts (11.24%) | 76pts (85.39%) | 2pts (2.25%) | 4.86 |
Opportunity to avoid surgery(s) for the removal of VHL related cysts/tumours (N=88) | ||||||
0pts (0%) | 0pts (0%) | 2pts (2.27%) | 5pts (5.68%) | 79pts (89.77%) | 2pts (2.27%) | 4.9 |
Rate the severity of side effects that would provide the opportunity to avoid surgery (N=88) | ||||||
2pts (2.22%) | 14pts (15.56%) | 33pts (36.67%) | 23pts (25.56%) | 14pts (15.56%) | 4pts (4.44%) | 3.38 |
Experience With Drug Under Review
Summary
Given the known risks of surgery and the traumatic psychological and physical impact of tumour recurrence, the patient groups represented in this submission are unanimous in their recommendation that all patients with VHL should be given the opportunity to access belzutifan based on individual informed decision between the treating physician and the patient/family. Given the lack of clear biological and other criteria for belzutifan, we endorse individually approved access based on the clinician-patient assessment of the balance of risks and benefits of belzutifan versus other options (no treatment, surgery, and watchful waiting).
Obviously, patients with tumours in locations where surgery is not feasible or highly risky (spine, brain, eyes, nerves), patients who have had multiple surgeries, and surgeries with other underlying conditions or frailties, the drug should not limited to these patients. Rather, the decision should take into consideration the clinical status of the patient, the location, severity and prognosis of the tumours, history of surgery and outcomes, psychological and mental health status of the patient, and other relevant factors.
The patient groups represented in this submission recognize that the evidence to date does not indicate that belzutifan can shrink or eliminate all tumours; nor does it prevent all tumours from recurring for all patients living with VHL. However, we also recognize that belzutifan does work to shrink tumours to the point of being no longer problematic and many patients have not had the tumours recur post-treatment. To gain more knowledge, we recommend that all patients receiving belzutifan should be enrolled in a patient monitoring program to collect on-going real-world data on beneficial and adverse outcomes, which will be analyzed to further develop the treatment guidelines and protocol. This “managed access” approach has a high probability of success if monitored by designated specialists with appropriate clinical support. It is not desirable to have patients wait for more clinical trials to be conducted or for more evidence to be collected through other “controlled” settings.
Patients living with VHL cannot afford to wait for access until there is greater “certainty” in terms of outcomes based on additional or expanded clinical trials. Patients living with VHL need to have the opportunity to benefit from extended periods of tumour-free “remission.”
Detail
In Appendix 1, we supply patient stories from interviews conducted in January 2023. These stories detail a few individual cases to illustrate how the disease and the resulting surgeries can affect all aspects of the whole family.
From the discovery of the disease, across the whole family, to losing loved ones, at a very young age, VHL is a devastating disease. Those that survive the death of a family member, must themselves endure surgeries that leave them in constant pain and often render them bed-ridden. The surgeries can introduce fear of anesthetic dementia, continuous pain and digestive complications.
The psychological impact from the surgeries, their resulting effects on physical and emotion resilience caused mental breakdowns. Living with these ailments can make working impossible, changing contributing citizens and families into those reliant on the provincial and federal subsistence programs, for the rest of their lives.
In one case, it was noted that 30 members of one extended family have VHL. Stories of nephews becoming paralyzed following brain surgery spread quickly. It is very tough psychologically to hear about that and know that you could be next. Now family members can talk about the 6-8 members of his family that previously would be going “under the knife” for tumours that threaten some significant aspect of their physiology, to those people starting the new drug belzutifan. We talked to a family where this good news and that some are already reporting very positive results can be mentioned as hopeful news.
Overall, 19 of the survey participants reported having had experience with belzutifan to treat VHL disease.
When asked about the experience [of] side effects that were particularly difficult to tolerate, the following responses were received.
Seizures
Low hemoglobin levels
Anemia- very tired
Nothing has been intolerable so far
Headaches some dizziness and heart thumping
Fatigue, but F has no adrenals
Participants were asked to rate on a five-point scale quality of life while taking belzutifan, form "low/seriously impacted" to "high/normal living."
Table 2: Personal Experience With Belzutifan
Personal Experience With Belzutifan | |||||||
|---|---|---|---|---|---|---|---|
How would you rate belzutifan’ s effectiveness in controlling your VHL disease? (N=18) | |||||||
1 (Not effective) | 2 | 3 | 4 | 5 (Extremely effective) | N/A | Weighted Average (WA) | |
0pts (0%) | 0pts (0%) | 7pts (38.9%) | 4pts (22.22%) | 2pts (15.56%) | 5pts (27.78%) | 3.62 | |
How would you rate belzutifan’s side effects? (N=18) | |||||||
0pts (0%) | 0pts (0%) | 6pts (33.33%) | 5pts (27.78%) | 5pts (27.78%) | 2pts (11.11%) | 3.94 | |
How would you rate your quality of life while taking belzutifan? (N=18) | |||||||
0pts (0%) | 0pts (0%) | 5pts (27.78%) | 9pts (50%) | 1pts (5.56%) | 3pts (16.67%) | 3.73 | |
Participants were also asked to rate on a five-point scale the “tolerability” of eight specific side effects associated with belzutifan. The responses are as follows.
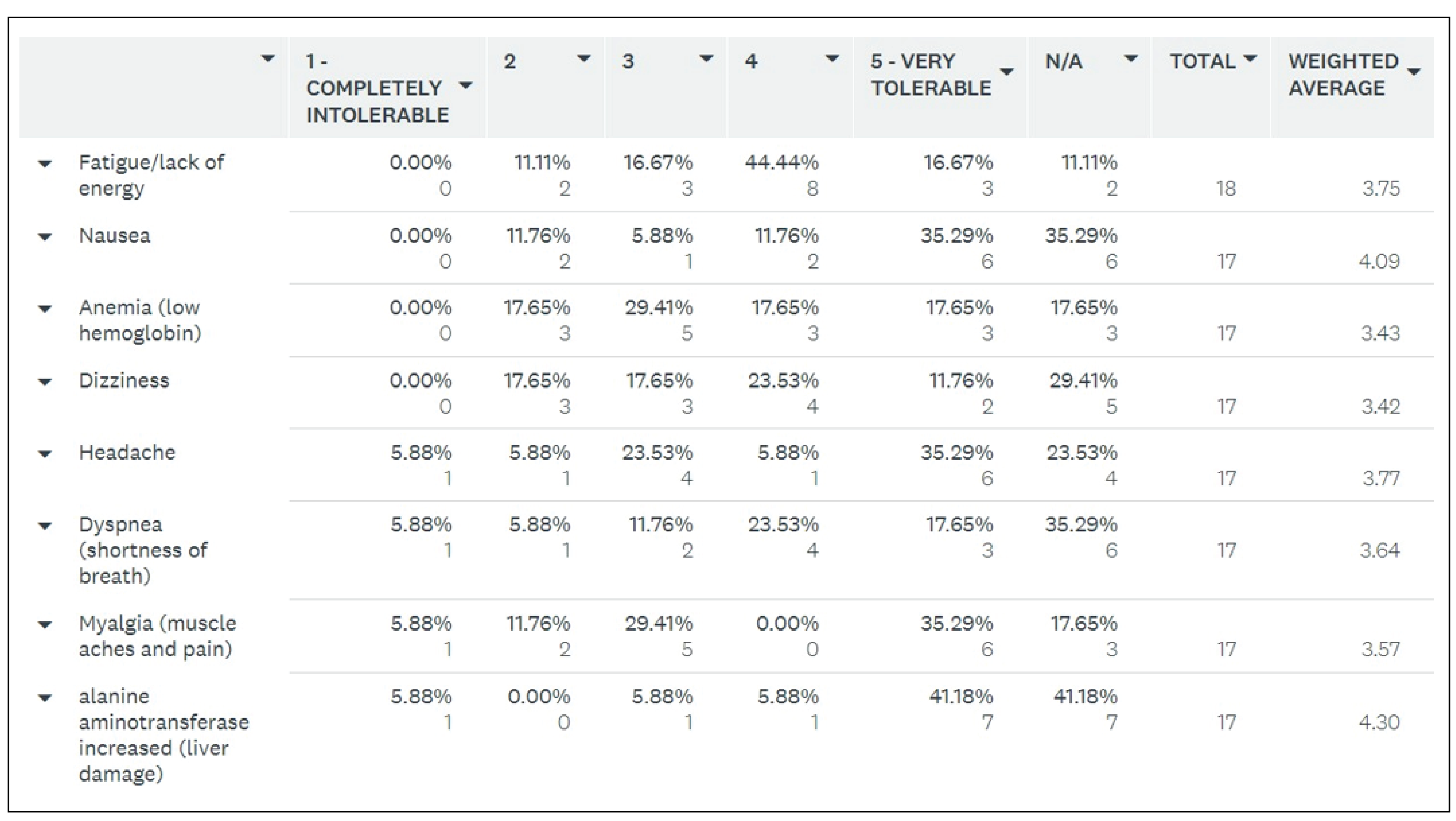
Finally, they were asked to provide open-ended comments about their experience. These are some of the comments received.
“Very hopeful this drug will help all VHL patients.”
“Hoping for great results for VHL patients.”
“We have never had a normal scan until now.”
“This medication is lifesaving in more ways than one, access is vital, and should be granted to those with vascular tumours beyond just RCCs, as it has been proven to be incredibly effective at controlling and reducing the size of CNS tumours of the brain, spine and eyes, and endocrine tumours like pheochromocytomas, and pNETs as well.”
In response to the request for changes in long-term health and well-being due to belzutifan, experienced and expected, the following comments were received.
“I am hoping for less surgeries and a longer life then my predecessors.”
“We hope that it helps to give him more quality of life with less surgeries and hopefully less tumours.”
“Peace.”
“If it can prevent more surgeries, this is a major improvement to wellbeing as neurosurgeon has said no more surgeries as possible. Progression of tumours will result in full loss of bodily functions.”
“Slow or stop the growth of VHL Kidney tumors specifically & hopefully the neuro- endocrine tumors associated with VH in my pancreas, adrenal gland & brain & paragangliomas.”
“Lifesaving.”
We further asked: Can you tell us about your story and why access to belzutifan and future therapies are so important to you?
“My dad has had VHL for all of his life…he has had about 15 different surgeries either on his kidney, his brain or his spine. He has been sick for most of his life because of this. We pray that the belzutifan will help him to have more healthy days than not. It is so important to us for him to continue to get those belzutifan. His tumours have been growing so much before this, that they have turned to cancer, and given him more sickness, we hope that this will work for him.”
“To keep my health the way it is currently and for my children and family members in the future. We have lost so many family members to VHL it’s hard to keep going in life when you see your own people falling over one by one with the same disease I am fighting.”
“I have seen many loved ones suffer from the symptoms that the tumours make and how it effects their quality of life and would love for you to help them as well as future generations fight this decease. There are too many children suffering from it as well and I hope you can find answers for them, thank you!”
“VHL patients deserve the right to live their lives as far and as healthily as they can, and if there are treatments available that can prolong and improve their lives and reduce their pain and tumours, they should have a right to access those treatments. To deny them is inhumane and cruel. Access should be easily managed through an oncology team and factors like a patient's location, gender, race, social status, insurance, or income should have no impact on their ability to access lifesaving treatments like belzutifan.”
Companion Diagnostic Test
Summary
The use of belzutifan does not require companion testing.
Anything Else?
Summary
Many belzutifan patients noted significant improvements with eye tumours. We realize this is not an indication within this submission, but it cannot be understated how large a side benefit this is for patients.
We believe this multi-site, in many cases proactive therapy, which addresses the root cause of the disease, is transformative, and has the potential to dramatically alleviate the burden of surgery, improve patients’ quality of life, and significantly reduce the massive health care costs associated with surgeries and hospitalizations.
The physical and emotional pain caused by the disease, then surgeries, then the aftermath of the surgeries is tremendous. Losing Canadians productivity and enjoyment of life to this disease can stop now.
We hope that you can find a way to make this a reality.
In recognition that VHL is a rare genetic disease with significant unmet need, we urge CADTH to apply the recommendations framework that includes “Considerations for Significant Unmet Need” as described in the Procedures for CADTH Reimbursement Reviews (March 2022), section 9.3.1.
We also request that CADTH report (in the draft recommendation) how the considerations for significant unmet need were applied in the review process.
Conflict of Interest Declaration — The Canadian VHL Alliance
To maintain the objectivity and credibility of the CADTH reimbursement review process, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission?
No, we did not get any outside help to prepare this submission.
Did you receive help from outside your patient group to collect or analyze data used in this submission?
No, we did not get any outside help to collect or analyze the data.
List any companies or organizations that have provided your group with financial payment over the past 2 years AND who may have direct or indirect interest in the drug under review.
Table 3: Financial Disclosures for the Canadian VHL Alliance
Organization | Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|---|
CVHLA - Sponsorship of 2022 International VHL Medical Symposium | Merck | — | — | X | — |
CORD | Merck | — | — | X | — |
KCC | Merck | — | — | — | X |
PCC | N/A | — | — | — | — |
CNET | N/A | — | — | — | — |
Appendix 1
Patient Stories
KS (Patient, interview date Jan 30, 2023)
KS is a 70-year-old woman living in Surrey BC. She was 6 years old when it was apparent that she had VHL as tumors were discovered on her adrenal gland. In her family, her father had VHL, with she and her two brothers also inheriting the syndrome. One brother died at the age of 18 as a result of VHL related surgery. Her two daughters and one grandchild also have VHL.
KS reports having used drug therapy and having undergone seven surgeries for the removal of cysts and tumors throughout her body, including in the: kidney, pancreas, adrenal glands, and brain, and an additional 10+ eye surgeries, having eventually lost one eye. One surgery resulted in damaged to her spine resulting in enduring pain and the need for intensive physiotherapy.
More recently, growing tumors were causing severe sciatica resulting in her being bed-ridden for 6 or 7 years. Finally, she had yet more abdominal surgery where they removed the body and tail of her pancreas, spleen, gall bladder and a paraganglioma from between her vena cava and aorta and removed a tumor from her left kidney.
Unfortunately, there is still tumor growth and now KS has pancreas NETs and (clear cell) renal cell carcinoma.
KS reports that VHL has had significant impact on her ability to work, travel, exercise, conduct household chores and spend time with family and friends.
“Each time I go under anesthesia it is one more step towards anesthetic dementia. Each CT scan I receive more radiation and more chance of my kidney tumors going cancerous. I had to retire early due to VHL adrenal and brain tumors causing me to have a mental breakdown at work due to stress and vertigo. I had to go for lots of therapy and I still see a psychiatrist monthly and take psychiatric medications to function well in society and at home.”
KS also reports that VHL has had tremendous impact on her financial well-being. When she was younger, as a single mother, she had to pay for childcare and/or seek accommodations for her children during her many surgeries and recovery times. She also reports having had to use holiday and sick days and having to go on Employment Insurance or disability insurance or welfare to accommodate scheduled surgeries and recovery. Eventually she went on CPP Disability which was only was good until she reached the age of 65. At that age she was switched to CPP, and her income has dropped drastically even though her actual level of disability has increased. She also reports having had to pay out-of-pocket for three new replacement eye orthotics (made by an Ocularist) as BC medical Insurance does not reimburse for eye orthotics.
Experience With Belzutifan
KS strongly advocated for access to belzutifan and is now taking 120 mg a day. belzutifan has had tremendous impact on her two brain tumors, with one disappearing completely, and the other having shrunk by half. She also reports that her vertigo has disappeared since commencing treatment with belzutifan. She has much hope that belzutifan will shrink (or halt the growth of) the remaining tumors in her kidney, pancreas, adrenal glands and brain. She also is holding out hope that this drug will be made available to her children and grandchild and future generations. KS says:
“We VHL Warriors need something other than surgeries and invasive procedures throughout our lives to slow or stop the growth of these tumors.”
JT (Caregiver, interview date Jan 30, 2023) Patient is her husband: FT
JT is the caregiver to her husband “FT”. They are both in their 50s.
FT’s mother discovered she had VHL in 1970 after a series of surgeries and ultimately losing vision in her right eye. She had already had three children at that point (including FT). As a result, it was assumed that the three children had VHL, which was later confirmed through genetic testing. One of FT’s brothers developed a brain tumor and subsequently passed away. FT’s sister developed a pancreatic tumor. FT and JT have two of their own children. JT reports that they were screened for VHL and are “thankfully negative”.
FT has had many surgeries for the removal of VHL-related cysts and tumors. One surgery was particularly consequential. In preparation for brain surgery FT was given an angiogram, which caused bleeding, which then caused a stroke. This stroke has left him permanently disabled and unable to work. FT now has trouble speaking, has permanent double-vision and needs to wear an eye patch. He has lost hearing in one ear and his jaw also doesn’t open properly and he cannot ingest food easily. JT told us that VHL has had a huge impact on FT’s ability to conduct day-to-day activities including work, exercise, and chores. Because of the disability incurred as a result of stroke, FT is no longer comfortable spending time with family and friends.
JT says that this disability is heartbreaking as FT was highly skilled, was entrepreneurial and ran his own business. Now he is unable to work with massive impacts on his mental health and happiness. JT reports that they now rely on financial support from FT’s elderly parents.
Experience With Belzutifan
FT started using belzutifan in February 2022. JT reports that FT’s scans in November 2022 revealed a significant reduction in size of his kidney tumors and pancreatic cysts. Further, a cyst that was growing (rapidly) on his neck, behind his right ear has now stabilized, and appears to be reducing in size. And JT reports that an endolymphatic sac tumor (ELST) in JT’s brain has stopped growing.
JT says that FT is finding belzutifan to be tolerable, with minimal side effects. However, there is treatment- related fatigue and shortness of breath.
JT told us that belzutifan is a very effective treatment, with manageable side effects and that FT will continue to use belzutifan as long as it works.
JT did significant work to access belzutifan and went to her Member of Parliament in December 2021 to get help with FT’s Special Access Program application to Health Canada. The treatment is currently being reimbursed by the manufacturer’s patient support program.
RW (caregiver, date of Interview January 31, 2023.) Patient is her husband: WW
RW is a caregiver to her 51-year-old husband “WW”. RW has been with WW for 31 years living in northern BC and has seen his whole journey with VHL.
WW knew he had VHL in approximately 1997 as his older sisters and father had VHL, and when he went for an eye exam, the specialist observed that he “had a twisted nerve in the eye” which was suspected to be VHL-related. He has since confirmed the VHL diagnosis with genetic testing.
WW has had numerous kidney surgeries and brain surgeries. Some of these surgeries were done in Edmonton and some at National Institutes of Health (NIH) in Washington as part of a VHL study. Also noted were an additional fifteen (15) surgeries of which many were eye surgeries/cryotherapy for retinal hemangioblastomas.
RW reports that VHL has significantly impacted WW’s ability to work, travel, exercise and do household chores. RW reports that VHL has had moderate to high impact on WW’s ability to spend time with family and friends and fulfill family obligations. RW and WW believe that access to new treatments for VHL is very important. WW was a logger (machine operator) and worked for 26 years with one blind eye. But, as a result of additional tumors and burden of disease, he is now permanently out of the workforce.
RW and WW have seen significant financial impact as a result of VHL. They have seen reduced income now that WW Is on long-term disability, but that ends in March 2023. RW reports that WW participating in the study at NIH had significant financial impact as their hotels were compensated at 50% when staying in Washington. When they go to Vancouver to see a VHL specialist, there are hotel costs, travel costs etc. related to staying in Vancouver. (They a 16-hour drive away).
30 members of WW’s extended family have VHL. Some are now blind. One nephew is paralyzed following brain surgery. About 6-8 members of his family are currently on belzutifan. Some are already reporting very positive results.
Experience With Belzutifan
WW accessed belzutifan through a patient support program sponsored by the manufacturer and started treatment in August 2022. The belzutifan tablets are delivered to his home.
By November many of WW’s brain and kidney tumors have shrunk significantly. RW believes that belzutifan will result in fewer surgeries for WW with a tremendous positive impact on his quality of life.
RW reports that WW finds the treatment to be quite tolerable, although his hemoglobin is now lower than optimal, he has some fatigue, and his oxygen is low.
RW reports that WW is hoping that belzutifan continues to shrink and/or stabilize his tumors so that he requires fewer surgeries and has a longer life expectancy. He is also hoping his offspring and extended family will benefit from this new treatment for VHL.
Other Patient and Caregiver Quotes
“I started having VHL surgeries at the age of 6 in 1965 & had my last open surgery at the age of 69 in 2021. Unfortunately, the St Pauls Hospital in Vancouver, BC Tumor Board refused to do any more surgery due to my age & that they called me frail. This caused me to be bed ridden for the last 5 to 8 years due to disabling sciatica-like symptoms & stop driving my car due to pain pill consumption. I also had nausea & lost 50 pounds without trying. My Urologist, Dr. Michael Eng, found a Pancreas/Liver surgeon at Vancouver General Hospital, Dr. Peter Kim, who was willing to do surgery on my pancreas & let my Urologist also do an extra surgical procedure to scrape off one kidney tumor that he cannot reach with an RFA procedure. I no longer have disabling Sciatica pain. But unfortunately, because they waited too long, my kidney & pancreas tumors grew & became cancerous. I am now up & about & just have weakened core muscles & stiffness & tire easily due to 5 to 8 years of being bed ridden.”
“I have had 7 VHL open abdominal organ sparing surgeries to remove tumors on my pancreas, kidneys, adrenal glands & paraganglioma from between my vena cava & aorta. They also removed my spleen & gall bladder this last time. Each surgery I have to go under general anesthetic which increases my risk of anesthetic dementia as I age & the cutting of my core muscles, etc. repeatedly & affects my stamina & physical strength. I have slow growing Hemangioblastoma brain tumors which they are watching. I also hope the belzutifan will shrink or stop the growth of my brain tumors. I had to have 2 C-Sections as I was told I would "most likely expire if I went into labour", due to my adrenal & brain tumors in the 1970s. I hope belzutifan proves to shrink or stop the growth of these tumors also.”
“I have had so many CT scans to keep watch on my abdominal tumors over the years which gives me so much radiation exposure in my lifetime which is not healthy. (Every year for approximately 50 years) I have also had MIBG & PET Cat scan, and RFA (radio frequency ablation) procedures which adds to my radiation exposure.”
When we asked: Please let us know how surgeries have impacted your ability to work or your quality of life, including spending time with loved ones. 92 patients and caregivers provided commentary.
Clinician Group Input
Ontario Health (Cancer Care Ontario) Genitourinary Cancer Drug Advisory Committee
About Ontario Health (Cancer Care Ontario) Genitourinary Cancer Drug Advisory Committee
OH-CCO’s Drug Advisory Committees provide timely evidence-based clinical and health system guidance on drug-related issues in support of CCO’s mandate, including the Provincial Drug Reimbursement Programs (PDRP) and the Systemic Treatment Program.
Information Gathering
Discussed jointly via emails and teleconference meeting.
Current Treatments and Treatment Goals
Currently, there are no standard systemic treatment options available for these patients – non-metastatic RCC with VHL syndrome, not planning for surgical management. Belzutifan will provide the first systemic option for these patients. The drug targets the biologic underpinning of the disease.
Important treatment goals include delaying further disease progression, nephron preservation as the disease recurs over and over (delay time to surgery and the need for partial nephrectomy), reduces the number of surgeries required in the patient’s lifetime.
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
Big unmet need. No current approved systemic therapy for this patient population. Additionally, surgical options would not be preferred in patients with renal lesions 1-3 cm.
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
Belzutifan will address the underlying disease process and is the first systemic treatment option available for these patients.
Belzutifan will cause a shift in the current treatment paradigm.
These patients currently have limited other treatment options as surgical option would not be preferred for renal lesions 1-3 cm.
Which patients would be best suited for treatment with the drug under review? Which patients would be least suitable for treatment with the drug under review?
Per the criteria in the clinical trial. Patients who are suitable for belzutifan should be prescribed by specialist physicians. For localized disease (i.e., non-metastatic disease).
What outcomes are used to determine whether a patient is responding to treatment in clinical practice? How often should treatment response be assessed?
Clinical and radiographic assessment by treating physician per standard of care.
What factors should be considered when deciding to discontinue treatment with the drug under review?
Safety, tolerability and efficacy.
What settings are appropriate for treatment with [drug under review]? Is a specialist required to diagnose, treat, and monitor patients who might receive [drug under review]?
Oral medication for take home administration, prescribed by specialists familiar with VHL and this patient population.
Additional Information
Although a phase 2 single arm study, the data is suitable as this is a younger, rare disease patient population. This drug impacts on the patient’s quality of life and loss of function. Maintenance of function is important in this patient population.
Belzutifan has multisystem benefits to patients with VHL associated tumours, including associated CNS tumours.
Conflict of Interest Declarations — Ontario Health (Cancer Care Ontario) Genitourinary Cancer Drug Advisory Committee
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please refer to the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission?
OH-CCO provided secretariat support to the group in completing this submission.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission?
No.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review.
Declaration for Clinician 1
Name: Dr. Girish Kulkarni
Position: Lead, OH-CCO GU DAC
Date: 08-02-2023
Table 4: COI Declaration for OH-CCO Genitourinary Cancer Drug Advisory Committee — Clinician 1
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In Excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Declaration for Clinician 2
Name: Dr. Aly-Khan Lalani
Position: Member, OH-CCO GU DAC
Date: 08-02-2023
Table 5: COI Declaration for OH-CCO Genitourinary Cancer Drug Advisory Committee — Clinician 2
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Merck | X | — | — | — |
Declaration for Clinician 3
Name: Dr. Sebastien Hotte
Position: Member, OH-CCO GU DAC
Date: 08-02-2023
Table 6: COI Declaration for OH-CCO Genitourinary Cancer Drug Advisory Committee — Clinician 3
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Merck | X | — | — | — |
Declaration for Clinician 4
Name: Dr. Chris Morash
Position: Member, OH-CCO GU DAC
Date: 08-02-2023
Table 7: COI Declaration for OH-CCO Genitourinary Cancer Drug Advisory Committee — Clinician 4
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Merck | X | — | — | — |
Declaration for Clinician 5
Name: Dr. Christina Canil
Position: Member, OH-CCO GU DAC
Date: 08-02-2023
Table 8: COI Declaration for OH-CCO Genitourinary Cancer Drug Advisory Committee — Clinician 5
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Merck | X | — | — | — |
Declaration for Clinician 6
Name: Dr. Reeta Barua
Position: Member, OH-CCO GU DAC
Date: 14-02-2023
Table 9: COI Declaration for OH-CCO Genitourinary Cancer Drug Advisory Committee — Clinician 6
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Merck | X | — | — | — |
Declaration for Clinician 7
Name: Dr. Akmal Ghafoor
Position: Member, OH-CCO GU DAC
Date: 17-02-2023
Table 10: COI Declaration for OH-CCO Genitourinary Cancer Drug Advisory Committee — Clinician 7
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In Excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Canadian Subspecialists Involved in VHL Care
About Canadian Subspecialists Involved in VHL Care
The clinician group involved in this submission consists of subspecialists across Canada who are involved in the care of patients with VHL disease, across the patients’ spectrum of needs. This group includes neurosurgeons, ophthalmologists, urologists, endocrinologists, hepatobiliary pancreatic surgeons, radiation oncologists, and medical oncologists.
Information Gathering
The literature has been reviewed to collect evidence and data to date on the care of patients with VHL.
Current Treatments and Treatment Goals
Von-Hippel Lindau (VHL) disease is an autosomal dominant inherited oncologic condition, affecting approximately 1 in 36,000 people [1]. This condition is a result of mutations in the VHL tumour suppressor gene, which subsequently activates cellular pathways that result in the development of multiorgan neoplasms. These include but are not limited to retinal hemangioblastomas, endolymphatic sac tumours affecting the middle ear, central nervous system (CNS) hemangioblastomas, pancreatic neuroendocrine tumours (pNETs), clear cell renal cell carcinomas (RCC), pheochromocytomas, and epididymal cystadenomas. Diagnosis is typically made based on clinical symptoms, radiographic presence of typified tumours, and/or family history. It may be confirmed by germline testing. VHL is typically diagnosed at a young age, often initially on retinal screening of individuals with a known family history. By the time many patients are diagnosed, they have often developed life altering end organ damage, such as visual impairment, renal impairment, or neurological symptoms.
Management of VHL disease involves close clinical and radiographic monitoring and appropriate timing of local strategies such as surgical resection, ophthalmologic interventions (such as laser photocoagulation) or radiation therapy. Patients with VHL will undergo multiple such interventions throughout their lives, with cumulative morbidity and risk for mortality. These invasive management strategies do not alter the natural history of the disease and are done with the goal of reducing the risk of further spread of disease and delaying symptomatic progression.
Ideal treatment goals for this patient population are to achieve cytoreduction of existing tumours, halt the development of new lesions, and prevent disease progression, thus reducing the need for multiple extensive surgical interventions. Additionally, treatment should reduce the risk for long-term sequelae of disease such as vision loss, renal impairment, and neurological deficits. As VHL-related RCCs occur recurrently and bilaterally, the necessary repeated resection and ablation of these ultimately compromises renal function, leading to chronic kidney disease and a need for dialysis.
Finally, effective treatment should prevent the development of metastatic RCC (mRCC) and reduce disease-related mortality. The leading causes of death in patients with VHL are complications from CNS hemangioblastomas and RCC [2]. In cases where metastatic RCC has developed, vascular endothelial growth factor receptor tyrosine kinase inhibitors (VEGFR TKIs) and/or immune checkpoint inhibitor-based systemic therapies are initiated with palliative intent.
Given that patients with VHL are typically quite young, effective systemic therapies which can defer the need for frequent surgical intervention can permit them to maintain better health-related quality of life, care for their young families, remain employed, maintain independence, and reduce psychosocial distress.
Previous clinical trials evaluated the use of the oral VEGFR TKIs, sunitinib and pazopanib, in management of VHL disease. Evidence from those clinical trials is outlined below. Neither of these drugs are approved by Health Canada for this indication.
Pazopanib
The role of pazopanib in VHL disease was studied in a non-randomized phase II clinical trial in which 31 patients with VHL received pazopanib 800mg orally daily for 24 weeks [3]. The primary endpoint was objective response rate and safety. Objective response rate in RCC tumours of 42% was reported, however organ specific response rates varied, and in CNS tumours was 4%. Treatment was generally tolerable but associated with grade 3/4 toxicities. Treatment-related toxicity led to discontinuation of pazopanib in 22.6% of patients.
Sunitinib
Sunitinib was studied in a phase II open-label clinical trial, in which 15 patients with VHL were treated with sunitinib 50mg oral daily for 28 days on, followed by 14 days off [4]. Evaluation of the primary endpoint of toxicity revealed that 67% of patients required a dose reduction, and grade 3 toxicity was reported in 33% of patients. Response rate of 0% in CNS hemangioblastomas, pNETs, renal cysts, retinal hemangiomas and pancreatic tumours was reported. In RCC lesions, response rate of 33% was reported.
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
There are currently no definitive curative treatment options for VHL, nor any which reverse the course of the disease. This is because the current management strategy does not target the underlying pathophysiology of disease and prevent the recurrent nature of tumour development. Serial surgical interventions are challenging to tolerate and may be associated with permanent side effects. For example, patients may experience permanent neurological deficits or chronic renal impairment post-operatively. In growing CNS lesions radiation and re-irradiation may also come with unwanted side effects, including permanent debilitating neurologic deficits. In some cases, local intervention may not be safe or feasible, and symptoms continue to progress as tumours grow, and focus is then on palliation. VHL patients need access to effective treatments which do in fact target the underlying pathophysiology of the disease; reducing the size and number of tumours, and thus deferring the need for frequent surgical interventions, and permitting them to maintain better health outcomes, health-related quality of life and reduce psychosocial distress.
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
Belzutifan is the first Health Canada approved systemic therapy option for patients with VHL disease and represents an important paradigm shift in management. This drug is an oral hypoxia-inducible factor-2α (HIF-2α) inhibitor. Mutations in the VHL gene result in dysfunctional VHL protein (pVHL). This protein normally functions to degrade HIF subunits.
When HIF subunits cannot be degraded due to dysfunctional pVHL, they result in stimulation of pathways associated with tumorigenesis, angiogenesis and ultimately, the multiorgan neoplasms seen in VHL. Therefore, targeting of HIF-2α addresses the underlying pathophysiology of VHL disease, and results regression of neoplasms.
As clinicians involved in the care of these patients, we support the use of belzutifan for the treatment of patients with VHL disease associated non-metastatic RCC, CNS hemangioblastomas or non-metastatic pNET. This will allow patients to benefit from systemic therapy to address multiorgan disease. While belzutifan will not eliminate the need for surgical intervention, it will reduce or indeed eliminate the need for surgery in many cases. This outcome was evaluated in the LITESPARK-004 clinical trial with compelling results, as shown below.
Results from the LITESPARK-004 clinical trial were published in November 2021 and led to Heath Canada approval for the use of belzutifan in patients with confirmed VHL [5]. This represents an important paradigm shift in the management of these patients. Belzutifan is currently available through a Patient Access Program.
LITESPARK-004 Study
The LITESPARK-004 study was a phase 2, open-label, single arm clinical trial which evaluated the efficacy of belzutifan in patients with VHL disease (N=61). The primary endpoint was objective response rate (ORR) in VHL associated RCC tumours (defined as partial or complete response on imaging). Secondary endpoints included duration of response, time to response, progression-free survival, and efficacy of belzutifan in non–RCC tumours. Patients in this trial received belzutifan 120mg oral daily until disease progression or unacceptable toxicity. Results and figures from the 36-month clinical trial follow-up are outlined below [6].
Response in VHL associated RCC: The ORR in VHL associated RCC was 64% (95% confidence interval [CI] 50.6-75.8), with a median time to response of 11.1 months (range 2.7-30.5 months) (Figure 2). Complete response was seen in 7% of cases. No patients experienced progression of RCC tumours while taking belzutifan. Amongst these patients, 92% had a reduction in the diameter of their target lesions (Figure 3). Median duration of response was not reached and 87% of patients continued to have ongoing response to treatment (Figure 4).
Response in VHL associated pNETs: In pNETs, response rate of 91% was seen, with 31.8% of patients achieving complete response. Median time to response was 8.4 months (range 2.5-19.1), and median duration of response was not reached.
Response in VHL associated CNS hemangioblastomas: In evaluation of CNS hemangioblastomas, ORR of 44%, and complete response rate 8% were reported. Median time to response in CNS hemangioblastomas was 3.2 months (range 2.3-16.6 months). A median 30% reduction in the size of cerebellar hemangioblastomas was reported, and in spinal hemangioblastomas, a 51% reduction was seen.
Response in VHL associated retinal hemangioblastomas: Response rate of 100% was seen in retinal hemangioblastomas. Median duration of response was not reached.
Figure 2: Best Objective Response Rates in RCC Tumours in the LITESPARK-004 Clinical Trial at 36-month Follow-Up
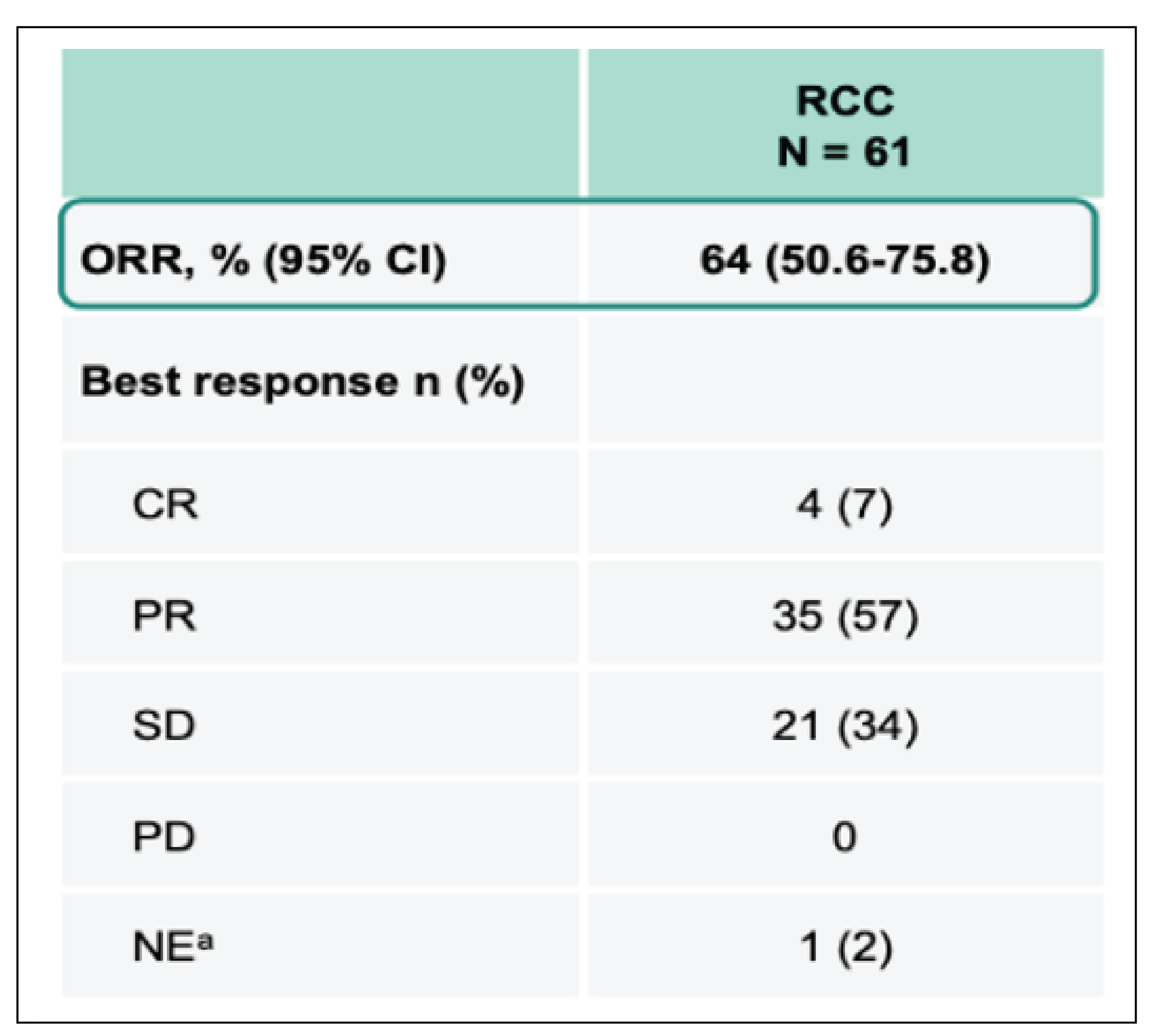
Figure 3: Waterfall Plot Demonstrating Best Change in Target RCC Tumour Size After Initiation of Belzutifan
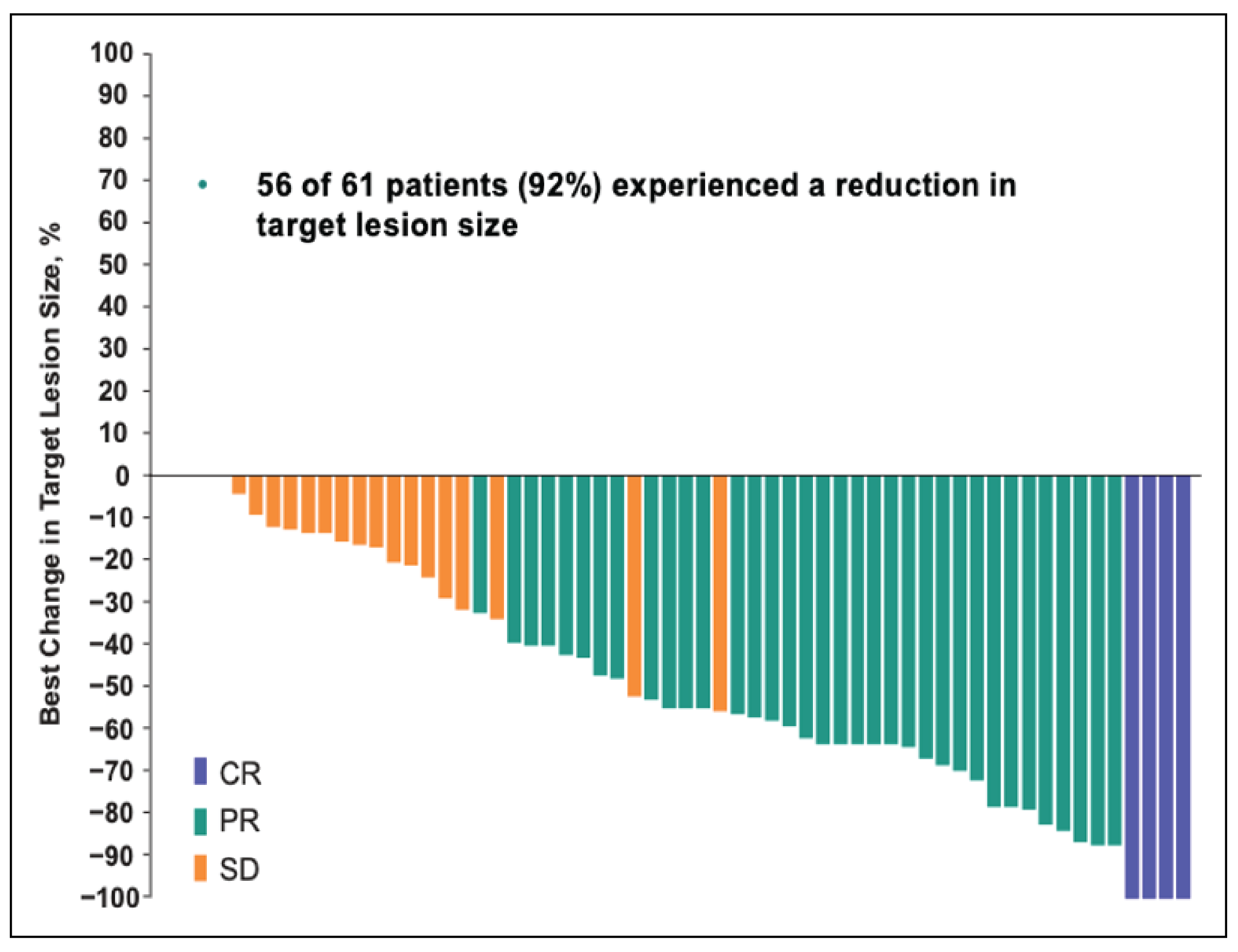
This data is from 36-month follow-up of the LITESPARK-004 clinical trial.
Figure 4: Duration of Treatment and Time to Response in RCC Tumours
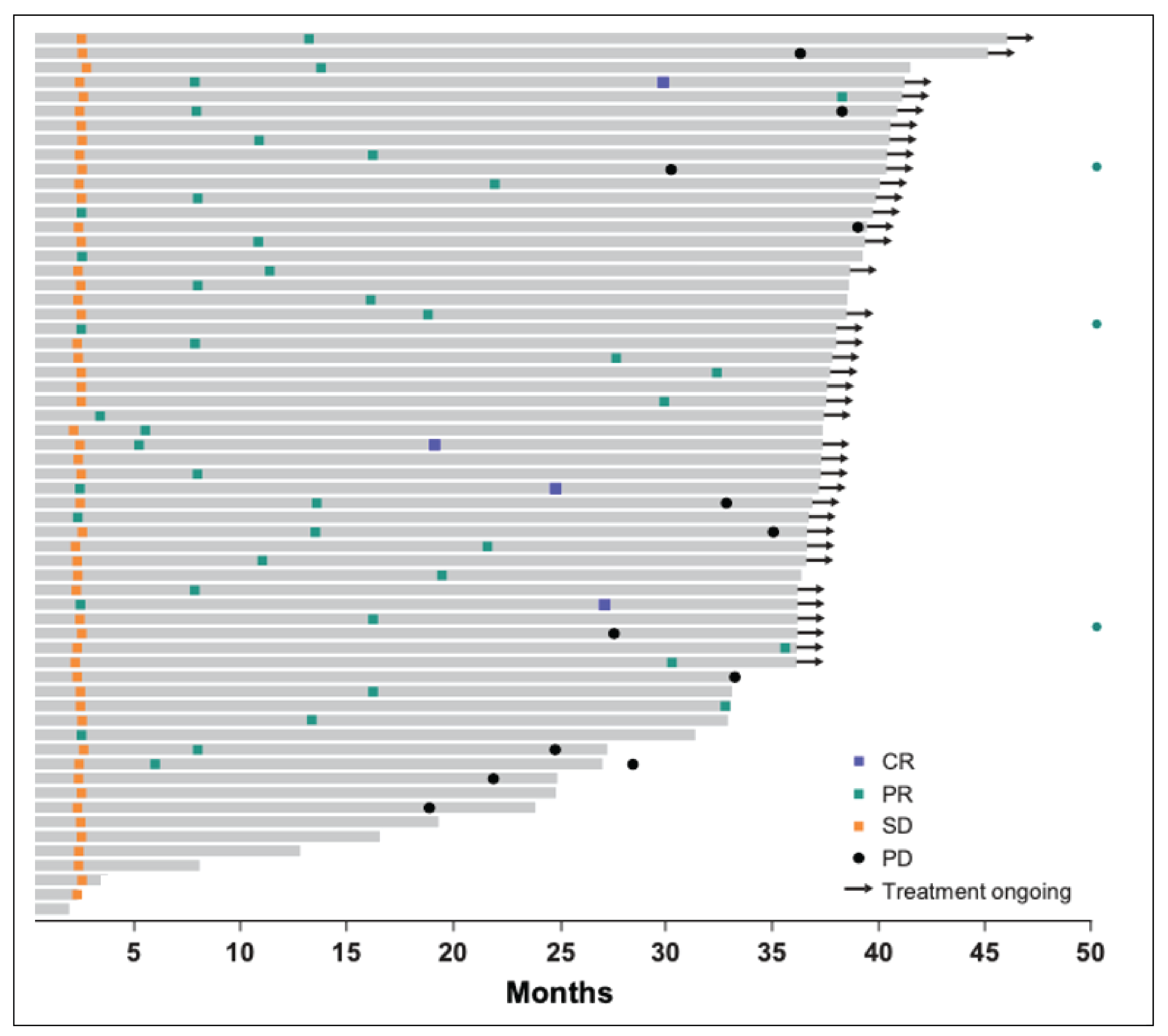
This data is from 36-month follow-up of the LITESPARK-004 clinical trial.
Safety: Safety and tolerability were well-maintained, with 18% of patients experiencing grade 3 treatment-related adverse events, and no grade 4-5 toxicities were treatment-related (Figure 5). The most common side effects were anemia, fatigue, headaches, and dizziness (Figure 6). 90% of patients experienced anemia, but only 8% experienced grade 3-5 anemia. Hypoxia, a known side effect of this medication, was observed in 1 patient, and this was managed with dose reduction. There were no treatment-related deaths.
Figure 5: Adverse Events of All Cause Reported in the Total Patient Population in the LITESPARK-004 Clinical Trial at 36-Month Follow-Up
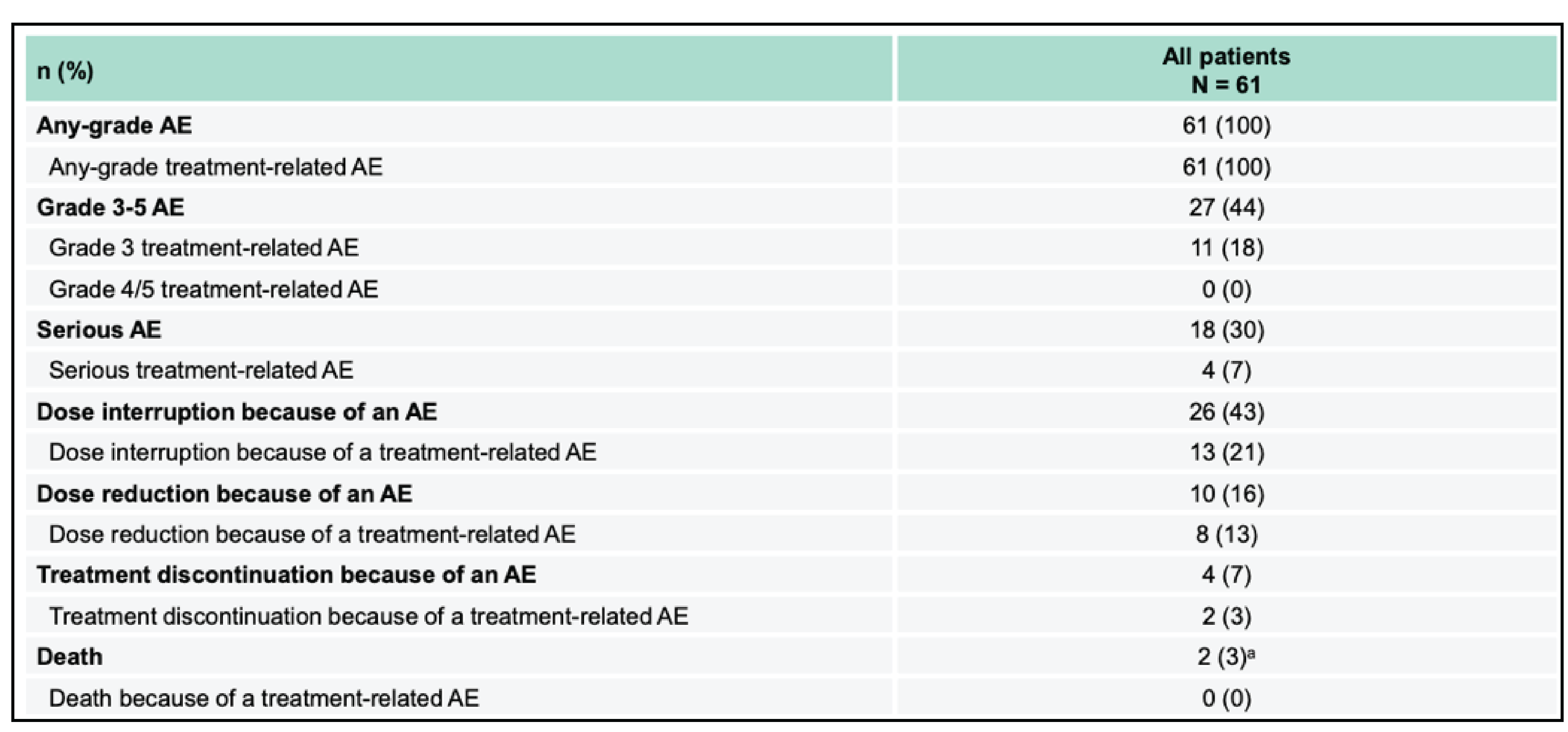
Figure 6: Adverse Events With Incidence of 20% or Greater While on Treatment With Belzutifan
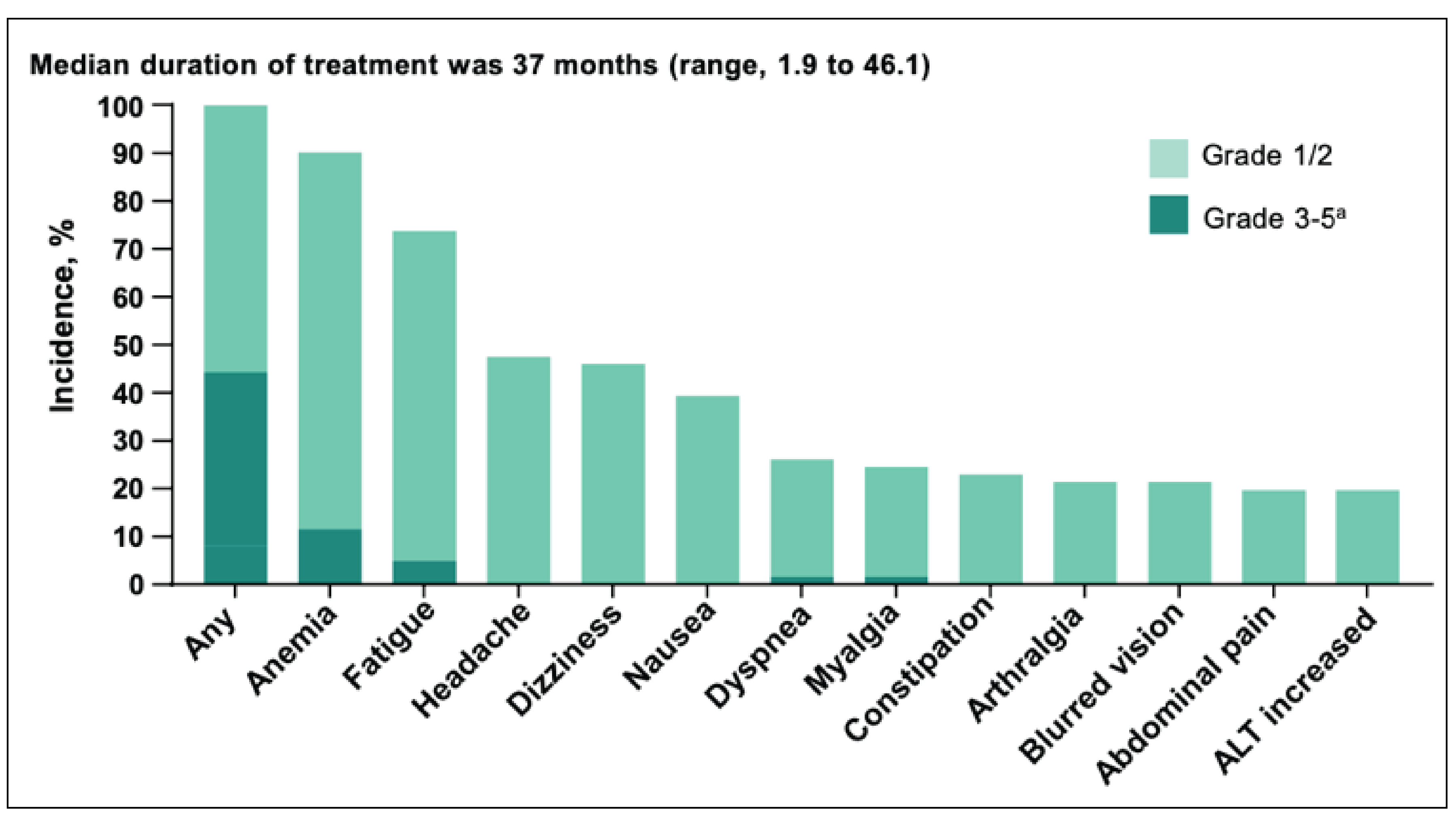
This data is from 36-month follow-up of the LITESPARK-004 clinical trial.
Tumour-Related Procedures on Belzutifan: Importantly, the LITESPARK-004 clinical trial reported on the frequency of surgical and other interventions for tumour control (adrenalectomy, craniotomy, cryoablation, cryotherapy, eye removal, intradural resection, laser ablation, laser surgery, laminectomy, laser photocoagulation, pancreatectomy, partial nephrectomy, radiation therapy, radiofrequency ablation, retinal surgery, total nephrectomy, tumor enucleation, and ventriculoperitoneal shunt placement) before and after initiation of belzutifan. Prior to starting belzutifan, 142 interventions were performed (in 61 patients), and after starting belzutifan, 4 interventions were performed. At the 36-month data update, 87 procedures (in 46 patients) were reported in the four years prior to initiation of belzutifan, and thereafter, 11 procedures (in 9 patients) were reported (Figure 7).
Figure 7: Distribution of Tumour Reduction Procedures Prior to and After Start of Belzutifan
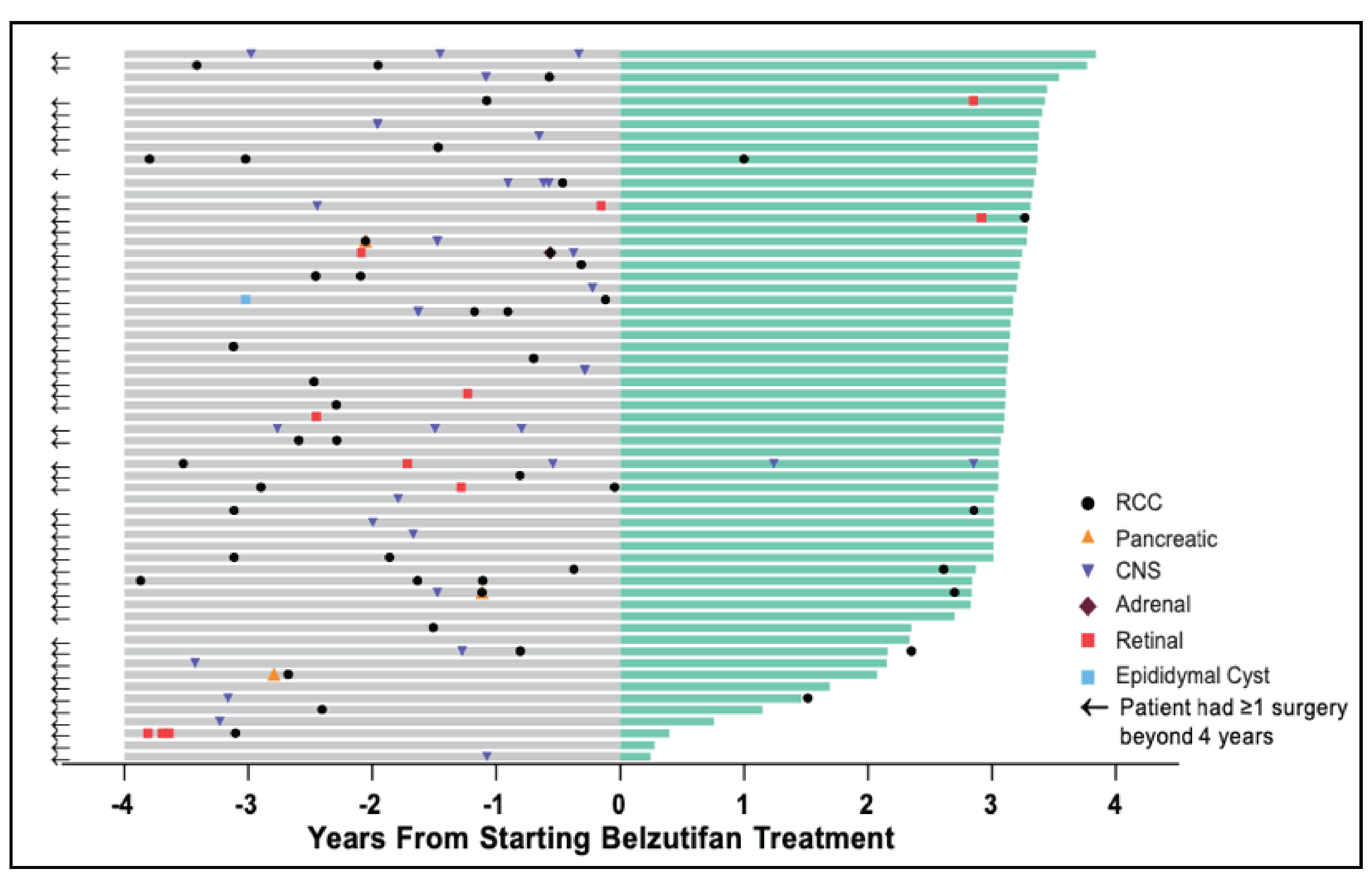
Time 0 years indicates when belzutifan was initiated. Type of tumours requiring intervention are indicated in the legend.
This data is from 36-month follow-up of the LITESPARK-004 clinical trial.
Which patients would be best suited for treatment with the drug under review? Which patients would be least suitable for treatment with the drug under review?
All adult patients (18 years of age or older) with VHL disease who require treatment for VHL associated neoplasms such as RCC, CNS hemangioblastomas and pNET without immediate need for surgery, should be considered for belzutifan. Patients who require immediate surgical management should defer treatment with belzutifan until surgery has been completed.
Patients should have ECOG performance status 0-2, adequate hemoglobin level (>100g/L) and liver function (AST and ALT < 2.5 × ULN, total bilirubin < 1.5 × ULN, and alkaline phosphatase ≤ 2.5 × ULN), and not require supplemental oxygen.
Pregnant women and women who are breastfeeding should not use belzutifan. Women of childbearing potential (WOCBP) must ensure that they are using a method of contraception while taking belzutifan, as the drug is associated with embryo-fetal toxicity. Oral contraceptives may interact with belzutifan such that they are rendered less effective, and thus clinicians must discuss this with WOCBP prior to initiating belzutifan.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice? How often should treatment response be assessed?
The outcomes used in clinical practice are aligned with those used in the clinical trial. In the LITESPARK-004 study, ORR was evaluated by radiographic assessments and ophthalmologic assessments while taking belzutifan. We agree that this is an appropriate strategy for assessing response. Response should be assessed by interval MRI abdomen and MRI spinal cord/brain every 12 weeks, and routine ophthalmologic assessment every 6 months (or sooner if deemed necessary by ophthalmologist). Clinical symptoms, laboratory evaluation (complete blood count and differential, serum chemistry) and tolerance should be assessed by clinicians every 4 weeks.
What factors should be considered when deciding to discontinue treatment with the drug under review?
Patients on belzutifan should be monitored for response and tolerance as outlined above. Should patients have evidence of disease progression radiographically, belzutifan should be stopped. Furthermore, tolerance must be evaluated based on clinical assessment of performance status, oxygen saturation, blood pressure measurement, weight stability, and evaluation of biochemical parameters, including complete blood count, creatinine, and liver enzymes. Should toxicity/tolerance be unacceptable based on shared discussion between patient and clinician, dose modification should be implemented, or the drug may need to be discontinued. Additionally, should pregnancy occur in a female patient while on belzutifan, the medication must be stopped immediately.
What settings are appropriate for treatment with belzutifan? Is a specialist required to diagnose, treat, and monitor patients who might receive belzutifan?
Treatment with belzutifan should be done under the guidance of a medical oncologist (or other specialist physician with equivalent expertise in the use of systemic therapies) in a cancer care centre, and where available at a specialized multidisciplinary VHL Clinic. Given the complexities of care for these patients, access to a large group of subspecialists, and specialized imaging is critical to inform decision-making in a timely manner.
Additional Information
Patients with VHL disease have a challenging and prolonged health trajectory that results in complex care needs. For decades, their care has been dictated by active surveillance and surgical intervention when tumours progress and/or when symptoms develop. This management strategy, and the inability to target the underlying pathophysiology of a disease state which has multisystem involvement, leads to significant psychosocial distress for these patients and their family members. The ability to improve outcomes and allow patients to live well with VHL is of paramount importance for this patient population. Belzutifan represents the first systemic therapy option to achieve this, and providing access to Canadian patients is of utmost priority. While at present there is no data to confirm this, we expect that in the long- term, belzutifan will also be cost-effective for the healthcare system as it will reduce the number of surgical interventions and hospitalizations.
VHL disease is a rare oncologic disorder with significant unmet need. As such, we urge CADTH to apply the recommendations framework that includes “Considerations for Significant Unmet Need” as described in the Procedures for CADTH Reimbursement Reviews (March 2022), section 9.3.1. We also urge CADTH to transparently report (in the draft recommendation) how the considerations for significant unmet need contributed to the draft recommendation.
Conflict of Interest Declarations — Canadian Subspecialists Involved in VHL Care
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please refer to the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission?
None.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission?
None.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review.
References
Maher ER, Neumann HP, Richard S. von Hippel-Lindau disease: a clinical and scientific review. Eur J Hum Genet. 2011 Jun;19(6):617-23.
Binderup ML, Jensen AM, Budtz-Jørgensen E, Bisgaard ML. Survival and causes of death in patients with von Hippel-Lindau disease. J Med Genet. 2017 Jan;54(1):11-18.
Jonasch E, McCutcheon IE, Gombos DS, Ahrar K, Perrier ND, Liu D, Robichaux CC, Villarreal MF, Weldon JA, Woodson AH, Pilie PG, Fuller GN, Waguespack SG, Matin SF. Pazopanib in patients with von Hippel-Lindau disease: a single-arm, single-centre, phase 2 trial. Lancet Oncol. 2018 Oct;19(10):1351-1359.
Jonasch E, McCutcheon IE, Waguespack SG, Wen S, Davis DW, Smith LA, Tannir NM, Gombos DS, Fuller GN, Matin SF. Pilot trial of sunitinib therapy in patients with von Hippel-Lindau disease. Ann Oncol. 2011 Dec;22(12):2661-2666.
Jonasch E, Donskov F, Iliopoulos O, Rathmell WK, Narayan VK, Maughan BL, Oudard S, Else T, Maranchie JK, Welsh SJ, Thamake S, Park EK, Perini RF, Linehan WM, Srinivasan R; MK-6482-004 Investigators. Belzutifan for Renal Cell Carcinoma in von Hippel-Lindau Disease. N Engl J Med. 2021 Nov 25;385(22):2036- 2046.
R. Srinivasan, O. Iliopoulos, W.K. Rathmell, V. Narayan, B.L. Maughan, S. Oudard, T. Else, J.K. Maranchie, S.J. Welsh, A.B. Bøndergaard Iversen, K. Chen, R.F. Perini, Y. Liu, W.M. Linehan, E. Jonasch. LBA69- Belzutifan, a HIF-2α Inhibitor, for von Hippel-Lindau (VHL) disease associated neoplasms: 36 months of follow-up of the phase II LITESPARK-004 study. Annals of Oncology (2022) 33 (suppl_7): S808-S869. 10.1016/annonc/annonc1089
Declaration for Clinician 1
Name: Rebecca Harrison
Position: Clinical Associate Professor, Neurology and Medical Oncology
Date: 30-01-2023
Table 11: COI Declaration for Canadian Subspecialists Involved in VHL Care — Clinician 1
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In Excess of $50,000 |
|---|---|---|---|---|
EMD Serono/Pfizer (honorarium) | X | — | — | — |
Declaration for Clinician 2
Name: Nicolas Dea
Position: Spine Surgeon, Clinical Associate Professor of Neurosurgery
Date: 30-01-2023
Table 12: COI Declaration for Canadian Subspecialists Involved in VHL Care — Clinician 2
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Baxter | X | — | — | — |
Stryker | — | X | — | — |
Medtronic | X | — | — | — |
Cerapedics | — | — | X | — |
Declaration for Clinician 3
Name: Susan Ellard
Position: Medical Oncologist, Department leader Medical Oncology BC Cancer Kelowna
Date: 31-01-2023
Table 13: COI Declaration for Canadian Subspecialists Involved in VHL Care — Clinician 3
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Merck (stock ownership) | — | X | — | — |
Declaration for Clinician 4
Name: Jean-Michel Lavoie
Position: Medical oncologist
Date: 31-01-2023
Table 14: COI Declaration for Canadian Subspecialists Involved in VHL Care — Clinician 4
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Bayer | X | — | — | — |
Pfizer | X | — | — | — |
TerSera | X | — | — | — |
Declaration for Clinician 5
Name: Lucia Nappi
Position: Medical oncologist – BC Cancer Vancouver Centre
Date: 31-01-2023
Table 15: COI Declaration for Canadian Subspecialists Involved in VHL Care — Clinician 5
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Bayer | X | — | — | — |
Astra Zeneca | X | — | — | — |
Ipsen | X | — | — | — |
Merck | X | — | — | — |
Pfizer | X | — | — | — |
Declaration for Clinician 6
Name: Corinne Maurice-Dror
Position: Medical Oncologist, BC Cancer-Vancouver
Date: 02-02-2023
Table 16: COI Declaration for Canadian Subspecialists Involved in VHL Care — Clinician 6
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Merck (MSD) | X | — | — | — |
BMS | X | — | — | — |
Novartis | X | — | — | — |
Medison | X | — | — | — |
Pfizer | X | — | — | — |
Biomica ltd. | — | X | — | — |
Declaration for Clinician 7
Name: Daniel Khalaf
Position: Medical Oncologist
Date: 02-02-2023
Table 17: COI Declaration for Canadian Subspecialists Involved in VHL Care — Clinician 7
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In Excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Declaration for Clinician 8
Name: Jeffrey Graham
Position: Medical Oncologist, CancerCare Manitoba
Date: 3-02-2023
Table 18: COI Declaration for Canadian Subspecialists Involved in VHL Care — Clinician 8
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Ipsen | X | — | — | — |
Pfizer | X | — | — | — |
Janssen | X | — | — | — |
BMS | X | — | — | — |
Merck | X | — | — | — |
Declaration for Clinician 9
Name: Eric Winquist
Position: Medical oncologist/Professor, Western University, London, Ontario
Date: 03-02-2023
Table 19: COI Declaration for Canadian Subspecialists Involved in VHL Care — Clinician 9
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Amgen | — | X | — | — |
Bayer | X | — | — | — |
Eisai | — | X | — | — |
Ipsen | — | X | — | — |
Medunik | X | — | — | — |
Merck | X | — | — | — |
Roche | X | — | — | — |
Declaration for Clinician 10
Name: Dr. Georg A. Bjarnason
Position: Medical Oncologist, Sunnybrook Odette Cancer Centre, Toronto, Ontario.
Date: 5-Feb-2023
Table 20: COI Declaration for Canadian Subspecialists Involved in VHL Care — Clinician 10
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Pfizer | — | X | — | — |
Merck | — | X | — | — |
BMS | — | X | — | — |
Ipsen | — | X | — | — |
Declaration for Clinician 11
Name: Naveen S. Basappa
Position: Assistant Professor, Dept of Medical Oncology, University of Alberta, Cross Cancer Institute, Edmonton, AB Canada
Date: 06-02-2023
Table 21: COI Declaration for Canadian Subspecialists Involved in VHL Care — Clinician 11
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Merck | X | — | — | — |
Ipsen | — | X | — | — |
AstraZeneca | X | — | — | — |
Bayer | X | — | — | — |
BMS | X | — | — | — |
Pfizer | X | — | — | — |
Janssen | — | X | — | — |
Seagen | X | — | — | — |
Eisai | X | — | — | — |
EMD Serono | X | — | — | — |
Declaration for Clinician 12
Name: Manik Chahal
Position: Medical Oncologist
Date: 06-02-2023
Table 22: COI Declaration for Canadian Subspecialists Involved in VHL Care — Clinician 12
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In Excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Declaration for Clinician 13
Name: Sunil Parimi
Position: Medical Oncologist, BC Cancer Victoria Cancer Centre, Victoria, British Columbia
Date: 06-02-2023
Table 23: COI Declaration for Canadian Subspecialists Involved in VHL Care — Clinician 13
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Pfizer | X | — | — | — |
BMS | X | — | — | — |
Merck | X | — | — | — |
Novartis | X | — | — | — |
Declaration for Clinician 14
Name: Seth Climans
Position: Neuro-Oncologist, London Health Sciences Centre
Date: 01-02-2023
Table 24: COI Declaration for Canadian Subspecialists Involved in VHL Care — Clinician 14
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In Excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Declaration for Clinician 15
Name: Daniel Heng
Position: Head, Medical Oncology, Tom Baker Cancer Centre
Date: 06-02-2023
Table 25: COI Declaration for Canadian Subspecialists Involved in VHL Care — Clinician 15
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Merck | X | — | — | — |
Declaration for Clinician 16
Name: Richard Gagnon
Position: Medical Oncologist – BC Cancer Victoria Centre, Victoria, British Columbia
Date: 06-02-2023
Table 26: COI Declaration for Canadian Subspecialists Involved in VHL Care — Clinician 16
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In Excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Declaration for Clinician 17
Name: Mary Jane Lim-Fat, MD
Position: Neuro-Oncologist, Odette Cancer Centre
Date: 07-02-2023
Table 27: COI Declaration for Canadian Subspecialists Involved in VHL Care — Clinician 17
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In Excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Declaration for Clinician 18
Name: Lyly Hanh Lê
Position: Medical Oncologist, BC Cancer - Surrey
Date: 07-02-2023
Table 28: COI Declaration for Canadian Subspecialists Involved in VHL Care — Clinician 18
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In Excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Declaration for Clinician 19
Name: Krista Noonan
Position: Medical Oncologist, BC Cancer - Surrey
Date: 07-02-2023
Table 29: COI Declaration for Canadian Subspecialists Involved in VHL Care — Clinician 19
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Astra Zeneca | X | — | — | — |
Pfizer | X | — | — | — |
Merck | X | — | — | — |
BMS | X | — | — | — |
Ipsen | X | — | — | — |
Essai | X | — | — | — |
Declaration for Clinician 20
Name: Michelle Johnson
Position: Clinical Associate Professor, University of British Columbia Division of Endocrinology
Date: 08-02-2023
Table 30: COI Declaration for Canadian Subspecialists Involved in VHL Care — Clinician 20
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In Excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Declaration for Clinician 21
Name: Charles Haw
Position: Neurosurgeon, Clinical Assistant Professor, University of British Columbia Division of Neurosurgery
Date: 08-02-2023
Table 31: COI Declaration for Canadian Subspecialists Involved in VHL Care — Clinician 21
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In Excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Declaration for Clinician 22
Name: Maryam Soleimani
Position: Medical Oncologist, BC Cancer Vancouver Centre; Clinical Assistant Professor, University of British Columbia
Date: 09-02-2023
Table 32: COI Declaration for Canadian Subspecialists Involved in VHL Care — Clinician 22
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Pfizer | X | — | — | — |
Bayer | X | — | — | — |
Ipsen | X | — | — | — |
Declaration for Clinician 23
Name: Adam Fundytus
Position: Medical Oncologist
Date: 09-02-2023
Table 33: COI Declaration for Canadian Subspecialists Involved in VHL Care — Clinician 23
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Bayer | X | — | — | — |
Seagen | X | — | — | — |
Astra Zeneca | X | — | — | — |
Declaration for Clinician 24
Name: Dr. Patrick E. Ma
Position: Clinical Profressor, UBC Ophthalmalogy
Date: 09-02-2023
Table 34: COI Declaration for Canadian Subspecialists Involved in VHL Care — Clinician 24
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Allergan | X | — | — | — |
Alcon | X | — | — | — |
Novartis | X | — | — | — |
Bayer | X | — | — | — |
Bausch and Lomb | X | — | — | — |
Declaration for Clinician 25
Name: Miles P. Mannas
Position: Urologic Oncologist
Date: 09/02/2023
Table 35: COI Declaration for Canadian Subspecialists Involved in VHL Care — Clinician 25
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Jaansen | X | — | — | — |
TerSera | X | — | — | — |
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
Redactions: Confidential information in this document may be redacted at the request of the sponsor in accordance with the CADTH Drug Reimbursement Review Confidentiality Guidelines
Stakeholder Input: The views expressed in each submission are those of the submitting organization or individual; not necessarily the views of CADTH or of other organizations. As such, they are independent of CADTH and do not necessarily represent or reflect the view of CADTH. No endorsement by CADTH is intended or should be inferred. By filing with CADTH, the submitting organization or individual agrees to the full disclosure of the information. CADTH does not edit the content of the submissions.
CADTH does use reasonable care to prevent disclosure of personal information in posted material; however, it is ultimately the submitter’s responsibility to ensure no identifying personal information or personal health information is included in the submission. The name of the submitting organization or individual and all conflict of interest information are included in the submission; however, the name of the author, including the name of an individual patient or caregiver submitting the patient input, are not posted.
Accessibility: CADTH is committed to treating people with disabilities in a way that respects their dignity and independence, supports them in accessing material in a timely manner, and provides a robust feedback process to support continuous improvement. All materials prepared by CADTH are available in an accessible format. Where materials provided to CADTH by a submitting organization or individual are not available in an accessible format, CADTH will provide a summary document upon request. More details on CADTH’s accessibility policies can be found here.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.