Drugs, Health Technologies, Health Systems
Reimbursement Review
Elranatamab (Elrexfio)
Sponsor: Pfizer Canada ULC
Therapeutic area: Relapsed or refractory multiple myeloma
This multi-part report includes:
Clinical_Review
Pharmacoeconomic_Review
Clinical_Review
Abbreviations
AE
adverse event
B2M
beta2-microglobulin
BCMA
B-cell maturation antigen
BICR
blinded independent central review
CAR
chimeric antigen receptor
CI
confidence interval
cilta-cel
ciltacabtagene autoleucel
CMRG
Canadian Myeloma Research Group
CRR
complete response rate
CRS
cytokine release syndrome
DOR
duration of response
ECOG PS
Eastern Cooperative Oncology Group Performance Status
EM
effect modifier
EORTC QLQ-MY20
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Multiple Myeloma 20
ESS
effective sample size
FISH
fluorescence in situ hybridization
GRADE
Grading of Recommendations Assessment, Development and Evaluation
HR
hazard ratio
HRQoL
health-related quality of life
ICANS
immune effector cell-associated neurotoxicity syndrome
IMiD
immunomodulatory drug
IMWG
International Myeloma Working Group
IPD
individual-level patient data
IPT
inverse probability of treatment
IPTW
inverse probability of treatment weighting
ISS
International Staging System
LDH
lactate dehydrogenase
mAb
monoclonal antibody
MAIC
matching-adjusted indirect comparison
MM
multiple myeloma
OH-CCO
Ontario Health (Cancer Care Ontario)
OR
objective response
ORR
objective response rate
OS
overall survival
PFS
progression-free survival
PI
proteasome inhibitor
PRO
patient-reported outcome
PS
propensity score
PV
prognostic variable
R-ISS
Revised International Staging System
RCT
randomized controlled trial
RR
risk ratio
RRMM
relapsed or refractory multiple myeloma
RW
real-world
RWD
real-world database
RWE
real-world evidence
SMD
standardized mean difference
SOC
standard of care
TCE
triple-class exposed
TCR
triple-class refractory
TEAE
treatment-emergent adverse event
ULN
upper limit of normal
URTI
upper respiratory tract infection
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Table 1: Background Information on Application Submitted for Review
Item | Description |
|---|---|
Drug product | Elranatamab (Elrexfio), 40 mg/mL, solution for subcutaneous injection supplied as:
|
Sponsor | Pfizer Canada ULC |
Indication | For the treatment of adult patients with relapsed or refractory multiple myeloma who have received at least 3 prior lines of therapy, including a proteasome inhibitor, an immunomodulatory agent, and an anti-CD38 monoclonal antibody, and who have demonstrated disease progression on the last therapy |
Reimbursement request | As per the indication |
Health Canada approval status | NOC/c |
Health Canada review pathway | NOC/c and Project Orbis |
NOC date | December 6, 2023 |
Recommended dosage | Step-up doses of 12 mg on day 1 and 32 mg on day 4 of week 1, followed by the first treatment dose of 76 mg on day 8, and then 76 mg weekly thereafter through week 24. Treatment with Elrexfio should continue until disease progression or unacceptable toxicity. |
NOC = Notice of Compliance; NOC/c = Notice of Compliance with Conditions.
Introduction
Multiple myeloma (MM) is a plasma cell cancer characterized by the clonal proliferation of malignant plasma cells (B-cells) and the overproduction of the abnormal immunoglobulin M protein. In 2022, it was estimated that 4,000 individuals living in Canada were diagnosed with MM and that 1,650 patients living in Canada died from MM. The 5-year survival rate for patients with MM is estimated to be approximately 50%, and although survival rates have improved in recent years due to advances in therapeutic options, MM remains incurable. The majority of patients with MM will relapse and many patients will become refractory to commonly used therapies. Patients with relapsed or refractory multiple myeloma (RRMM) often undergo multiple rounds of treatment, with the duration of remission, depth of response, progression-free survival (PFS), and overall survival (OS) decreasing with each subsequent line of therapy. According to the clinical experts consulted by CADTH, the main treatment goals for patients with RRMM are to prolong survival, improve symptoms, minimize toxicities, and maintain or improve health-related quality of life (HRQoL). Therapies for the treatment of patients with RRMM, and the sequencing of these treatments, depend on eligibility for autologous stem cell transplant at diagnosis, age, comorbidities, previous treatments, beforexicities, and line of therapy. According to the joint clinical practice guideline of Ontario Health (Cancer Care Ontario) (OH-CCO) and the American Society of Clinical Oncology, treatment for RRMM includes triplet therapy consisting of proteasome inhibitors (PIs), immunomodulatory drugs (IMiDs), and monoclonal antibodies (mAbs). There is no preferred therapy for RRMM in the fourth-line and beyond settings, and at this stage of the disease, patients may be treated with PIs, IMiDs, and anti-CD38 mAbs, and in some cases, receive more than 1 PI or IMiD, further limiting treatment options in later lines of therapy.
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of elranatamab 76 mg, subcutaneous injection, for the treatment of adults with RRMM who have received at least 3 prior lines of therapy.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient and clinician groups that responded to CADTH’s call for input and from clinical experts consulted by CADTH for the purpose of this review.
Patient Input
CADTH received 1 patient group submission from Myeloma Canada. Myeloma Canada conducted both patient and caregiver surveys from September 26 to October 23, 2023, across Canada and internationally via email and social media. A total of 67 complete responses to the patient survey were received, of which 38 responses were recorded based on the respondent’s eligibility criteria (receiving treatment with an IMiD, PI, and anti-CD38 antibody). Among these 38 patients, 24 patients were eligible for the drug under review and 14 patients had experience with it. A total of 32 caregivers responded to the caregiver survey, 11 of whose responses were recorded (8 based on eligibility and 3 based on experience with elranatamab).
Patient respondents indicated that among their daily activities and quality of life, their ability to work was the factor the most significantly impacted by symptoms associated with myeloma, followed by the ability to travel and to exercise. Regarding the most significant financial implication of myeloma treatment on patients and their household, 24 of 49 respondents (both patients and caregivers) identified loss of income or pension funds due to absence from work, disability, or early retirement as the most significant financial implication, and 20 of 49 respondents chose travel parking costs. Patient respondents felt that interruption of life goals or accomplishments had the greatest impact on their quality of life, followed by the loss of sexual desire and anxiety or worry. Patient and caregiver respondents identified the following factors as the most important to myeloma treatment: quality of life, manageable side effects, effectiveness of the treatment (especially in achieving remission and having a durable response), and treatment accessibility or portability (including fewer or minimal visits to the hospital or cancer centre). Infections were identified as the most important aspect to control identified by patients, followed by mobility and kidney problems.
In terms of treatment outcomes, 12 of the 23 respondents who would currently be eligible for treatment with elranatamab rated improved quality of life as extremely important, 6 of the respondents rated it as very important, and 5 of the respondents rated it as somewhat important. In addition, 17 of the 23 patients rated the aspect of life extension while considering a myeloma treatment as extremely important, and 4 patients rated it as very important. When asked about their tolerance of the most common side effects in patients who receive elranatamab, these patients perceived pneumonia, immune effector cell-associated neurotoxicity syndrome (ICANS), upper respiratory tract infections (URTIs), cytokine release syndrome (CRS), and infections to be the least tolerable side effects, followed by peripheral neuropathy, other infections, and COVID-19. Regarding the impact of the dosing schedule of elranatamab on the quality of life (weekly injections for at least 24 weeks, with the possibility of then switching to every 2 weeks), 11 of 24 patients chose the response of negative impact, indicating it would limit patients’ ability to travel or require a relocation (near their cancer centre) for the duration of treatment.
A total of 17 respondents (14 patients and 3 caregivers) indicated having experience with elranatamab. All 14 patients who had received or are currently receiving treatment with elranatamab mentioned they were admitted to the hospital at some point in the initial step-up dosing period. Regarding the most frequently experienced elranatamab side effects, all 14 patients rated cough as the least bearable side effect, followed by CRS, neutropenia, and URTI. Most of these patients mentioned the overall side effects while receiving elranatamab were manageable and found elranatamab effective in controlling their myeloma.
Clinician Input
Input From Clinical Experts Consulted by CADTH
Unmet Needs
The clinical experts indicated that since almost all patients with RRMM will become refractory to their therapy and continue on to the next line of therapy, the unmet needs of patients would be new effective treatments, with curative potential, which are tolerable by targeting a different mechanistic pathway. Both clinical experts highlighted that the balance between treatment efficacy, minimizing toxicities, and quality of life would be important.
Place in Therapy
The clinical experts agreed that because of elranatamab’s novel mechanism of action, it would provide an additional treatment option for patients who are refractory to other standard of care (SOC) treatments. They noted that elranatamab is a new class of treatment for which there should be no existing drug resistance, and given its unique mechanism of action and toxicity profile, it should create a treatment synergy with other current families of myeloma treatments. However, they noted that given the lack of direct evidence, it is not known yet if elranatamab is more effective than other therapies.
Patient Population
The clinical experts agreed that the patients best suited for elranatamab would be those who are triple-class refractory (TCR). One of the clinical experts noted that patients most likely to respond to this therapy would be those with a stronger and more intact immune system, and patients with significant pre-existing cytopenias may not be ideal candidates as the cytopenias may worsen during treatment and predispose patients to infection. The experts did not note any issues or challenges related to the diagnosis or misdiagnosis of RRMM, and the identification of patients likely to respond. Patients would be identified during routine cancer follow-up based on biochemical assessment (serum protein electrophoresis, serum free light chain) or other evidence of relapse.
Assessing the Response Treatment
The clinical experts agreed that in clinical practice, standard clinical response criteria can be used to determine whether a patient with RRMM is responding or progressing on treatment. The clinical experts noted that achieving a durable objective response (OR) lasting 6 months to 12 months would be a sign of successful treatment, and such a response would be associated with a reduction in disease-related symptoms, bone pain, fatigue, and transfusion requirements. They noted that toxicities, especially cytopenias such as neutropenia, infections, CRS, and hypogammaglobulinemia, would need to be monitored.
Discontinuing Treatment
The clinical experts indicated that treatment with elranatamab should be discontinued if the patient experiences disease progression (as defined radiologically or biochemically), loss of response, unacceptable toxicity such as grade 3 or grade 4 infection or CRS, light chain or renal dysfunction, or increasing transfusion requirement.
Prescribing Considerations
The clinical experts noted that patients receiving elranatamab should be under the care of a specialist (e.g., hematologist, oncologist) familiar with myeloma and the use of bispecific antibodies, and who can manage toxicity associated with the therapy. They noted that elranatamab can be given in most centres experienced with myeloma therapy, and that the first few doses usually require hospitalization.
Clinician Group Input
Clinician group input on the review of elranatamab was received from 2 clinician groups: the Canadian Myeloma Research Group (CMRG) and Ontario Health -Cancer Care Ontario Hematology Cancer Drug Advisory Committee (OH-CCO’s Drug Advisory Committees). A total of 33 clinicians provided input for this submission (26 clinicians from CMRG and 7 clinicians from OH-CCO’s Drug Advisory Committees).
Both CMRG and OH-CCO’s Drug Advisory Committees emphasized that the overall treatment goals are to delay progression, improve OS, minimize adverse effects, control the disease and associated symptoms, and improve quality of life. While discussing the unmet needs of patients, CMRG highlighted that myeloma remains incurable and patients eventually become refractory to all available funded drugs, similar to the statements of the clinical experts consulted by CADTH. CMRG emphasized that the highest unmet need consists of patients with advanced disease who have received multiple lines of treatment and have already received the 3 major classes of drugs (triple-class exposed [TCE] or refractory), including an IMiD, PI, and anti-CD38 mAb.
As with the clinical experts consulted by CADTH, both clinician groups agreed that elranatamab could be another option for TCE patients. CMRG indicated that patients with a good performance status, minimal or no comorbidities, relatively low tumour burden, adequate organ function, and satisfactory blood counts are those most likely to have the best outcomes with elranatamab. CMRG noted that overall, patients with poor disease-related prognostic factors, such as extramedullary myeloma and high-risk cytogenetics, should be eligible for the treatment under review.
CMRG added that clinically meaningful responses usually correlate with at least a partial remission as defined by International Myeloma Working Group (IMWG) consensus criteria. Both CMRG and OH-CCO’s Drug Advisory Committees agreed that treatment discontinuation is based on ongoing efficacy or response, disease progression, and long-term tolerability or significant toxicities. Given that prior anti–B-cell maturation antigen, or BCMA, exposure does not preclude responsiveness to subsequent anti-BCMA therapy, CMRG would suggest that patients with prior anti-BCMA therapy who did not progress during it (i.e., nonrefractory to anti-BCMA therapy) be allowed access to elranatamab.
Drug Program Input
Input was obtained from the drug programs that participate in the CADTH reimbursement review process. The following were identified as key factors that could potentially impact the implementation of a CADTH recommendation for elranatamab:
relevant comparators
considerations for the initiation of therapy
considerations for the discontinuation of therapy
considerations for the prescribing of therapy
generalizability
funding algorithm
care provision issues
system and economic issues.
The clinical experts consulted by CADTH provided advice on the potential implementation issues raised by the drug programs. Refer to Table 4.
Clinical Evidence
Systematic Review
Description of Studies
One ongoing trial, the MagnetisMM-3 study (N = 187), met the inclusion criteria for the systematic review conducted by the sponsor. The objective of the MagnetisMM-3 trial was to assess the efficacy and safety of elranatamab 76 mg, subcutaneous injection, in adults with RRMM. The trial enrolled adults who either had previous experience with BCMA-directed treatment (cohort B) or did not (cohort A), were disease-refractory to at least 1 PI, 1 IMiD, and 1 anti-CD38 antibody, and were disease-relapsed or disease-refractory to their last antimyeloma regimen. Patients had an Eastern Cooperative Oncology Group Performance Status (ECOG PS) score of less than or equal to 2, and adequate bone marrow, hepatic, and renal functions. The 2 noncomparative cohorts were analyzed separately. Patients received elranatamab 76 mg, subcutaneous injection, once a week on a 28-day cycle with a 2 step-up priming dose regimen of 12 mg on day 1 and 32 mg on day 4 during the first week. Patients who received dosing once a week for at least 6 cycles and attained a partial response or better persisting for at least 2 months had their dosing interval changed to once every 2 weeks. The outcomes relevant to the CADTH review included the primary outcome of the objective response rate (ORR) by blinded independent central review (BICR) per IMWG criteria, and secondary outcomes of PFS, OS, complete response rate (CRR), duration of response (DOR), and safety. HRQoL via the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Multiple Myeloma 20 (EORTC QLQ-MY20) tool was included as an exploratory outcome. The trial population was predominately white (███), with a similar proportion of male and female patients who had a mean age of ██ years. Most patients had an ECOG PS score of 1 (███) and 0 (███), indicating good overall performance, a Revised International Staging System (R-ISS) disease stage of II (███), standard cytogenetic risk (███), and a prior stem cell transplant (███). Patients had received an average of | prior lines of therapy, and ███ had penta-drug refractory disease (refractory to at least 2 PIs, 2 IMiDs, and 1 anti-CD38 antibody). Key characteristics were generally consistent between cohorts, although patients in cohort B had a longer mean time since first diagnosis ████████████████████████ and received on average more prior anticancer therapies ███████████████████████ than patients in cohort A.
Efficacy Results
Only those efficacy outcomes and analyses of subgroups identified as important to this review are reported. Efficacy and safety data were evaluated at a planned analysis data cut-off date of October 14, 2022, and additional follow-up data at a cut-off date of March 14, 2023.
Objective Response Rate
At the March 14, 2023, data cut-off, with a median follow-up of 14.7 months, the ORR in cohort A was 61.1% (95% confidence interval [CI], 51.8% to 69.6%; P < 0.0001) and ██████████████████████████████ in cohort B. In cohort A and cohort B, the ORR was greater than or equal to the prespecified alternative hypotheses of 48% and 34%, respectively. These findings were consistent with the results at the 9-month analysis (with a data cut-off date of October 14, 2022). In cohort A, the ORR results were consistent across subgroups by age, baseline cytogenetics risk, prior stem cell transplant, and number of prior lines of therapy. However, lower ORRs were observed in patients with R-ISS stage III. ███████████████████████████████████.
PFS by BICR
In total, ██ events had occurred in both cohorts by the March 14, 2023, data cut-off. The median follow-up for PFS was 14.7 months for cohort A and █████████ for cohort B. The median PFS was not reached (95% CI, 9.9 months to not estimable) in cohort A and █████████████████████████ in cohort B. The probability of being event-free at 12 months in cohort A was 56.6% (95% CI, 46.7% to 65.3%) ██████████████████████████ in cohort B.
Overall Survival
As of the March 14, 2023, data cut-off, the OS data were immature. A total of 55 (44.7%) patients in cohort A and █████████ patients in cohort B had died. Median OS had not yet been reached in cohort A and was █████████████████████████ ██████████ in cohort B. The probability of being alive at 12 months in cohort A ██████████████████████████████████████████████ in cohort B.
DOR and CRR
As of the March 14, 2023, data cut-off, the median DOR had not been reached among responders in both cohorts, with ███ of all patients censored at the time of the analysis. The probability of patients remaining in response at 12 months was 75.5% (95% CI, 58.8% to 80.9%) in cohort A ███ █████ ████ ███ ████ ██ █████ in cohort B. A complete response or better was attained in 43 patients (complete response = 35.0% [95% CI, 26.6% to 44.1%]) in cohort A ███ █ ██████ ███ ███ ███ ██ █████ patients in cohort B.
Harms Results
All patients in the trial reported at least 1 TEAE. The most frequently reported TEAEs in both cohorts were CRS █████, anemia █████, neutropenia █████ and diarrhea ██████ In both cohorts, ███ of patients experienced 1 or more serious TEAE. The type and number of events were similar in both cohorts, with the most frequently reported events being COVID-19 pneumonia ██████ and CRS ██████ Study treatment discontinuation due to TEAEs occurred in ███ of patients, and was similar in both cohorts. In cohort A and cohort B, 45% and ███ of patients died, respectively. Most deaths in both cohorts were attributed to disease progression. In the total population, the most frequently reported notable adverse events (AEs) were infections █████ and CRS ██████ followed by peripheral neuropathy ██████ hypogammaglobulinemia ██████ and ICANS (████ All CRS events were grade 1 or grade 2 in severity. The median time from the most recent elranatamab dose to CRS onset was | days and the median time to resolution was also | days. In general, the harms results of the MagnetisMM-9 trial were similar to those of the MagnetisMM-3 trial. According to the clinical experts, infection-related hospitalizations, hypogammaglobulinemia as measured by need for IV or subcutaneous immunoglobulin, and neurotoxicities were considered important outcomes, although they were not reported in the trials. As such, this represents a gap in the available evidence.
Critical Appraisal
The primary limitation of the MagnetisMM-3 trial was the absence of a comparator group to assess the efficacy and harms of elranatamab, and therefore the interpretation of the results is limited to its single-arm design. As such, it is difficult to make causal conclusions — in particular, to what extent the observed effects were attributable to elranatamab. The open-label design introduces a potential bias in the assessment of ORR, PFS, DOR, and CRR, and a potential reporting bias of the subjective outcomes HRQoL and safety. However, this bias was mitigated by the use of BICR for ORR, PFS, DOR, and CRR. To minimize the risk of differential measurement error, the trial performed tumour assessments using IMWG criteria and radiographic scans were assessed by BICR. Sample size and power calculations were based on ORR, which had a prespecified hypothesis that was tested; however, all other analyses were descriptive. These included PFS, OS, DOR, and CRR, and the exploratory HRQoL outcome (via the EORTC QLQ-MY20 tool), which are deemed clinically important outcomes for the disease. The sample sizes for the subgroup analyses were small, and not adjusted for multiplicity, which also made it difficult in interpreting the results. While the trial met its primary objective of assessing ORR, there was limited supporting evidence from important secondary outcomes — notably, the immature data for PFS and OS. Given the importance of these outcomes to patients and clinicians, longer follow-up for the PFS and OS analyses would have been preferred to determine the clinical value of treatment with elranatamab. In addition, patients were permitted to receive post-treatment anticancer medications after study treatment had been discontinued (33% of all patients), which may have influenced the assessment of OS. The results of the EORTC QLQ-MY20 questionnaire were subjected to bias potentially due to incomplete reporting or missing data, which could have influenced the results toward the null. Therefore, the potential differences regarding a patient’s quality of life remain uncertain.
In general, the population requested for reimbursement aligns with that of the Health Canada indication, and the dosing and administration of elranatamab were consistent with the Health Canada–approved product monograph. According to the clinical experts consulted by CADTH, the inclusion and exclusion criteria and baseline characteristics of the MagnetisMM-3 trial were generalizable to adults with RRMM in the Canadian setting. However, the clinical experts noted that the trial did not include patients with a poor ECOG PS score, which is not entirely representative of patients with RRMM in clinical practice. The trial included outcomes that were important to patients and clinicians. The patient group indicated that stopping disease progression, prolonging life, improving HRQoL, and reducing treatment side effects are important to them. However, assessing HRQoL as an exploratory outcome is a limitation to the evidence since no definitive conclusions can be drawn.
GRADE Summary of Findings and Certainty of the Evidence
Methods for Assessing the Certainty of the Evidence
For pivotal studies and randomized controlled trials (RCTs) identified in the sponsor’s systematic review, the Grading of Recommendations Assessment, Development and Evaluation (GRADE) tool was used to assess the certainty of the evidence for outcomes considered most relevant to inform CADTH’s expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group.1,2
Although GRADE guidance is not available for noncomparative studies, the CADTH review team assessed pivotal single-arm trials for study limitations (which refers to internal validity or risk of bias), inconsistency across studies, indirectness, and publication bias to present these important considerations. Because the lack of a comparator group does not allow for a conclusion to be drawn on the effect of the intervention versus any comparator, the certainty of evidence for single-arm trials started at very low certainty with no opportunity for rating up.
The selection of outcomes for GRADE assessment was based on the sponsor’s Summary of Clinical Evidence, consultation with clinical experts, and input received from patient and clinician groups and public drug plans. The following list of outcomes was finalized in consultation with expert committee members:
response outcomes (ORR, DOR, CRR)
survival outcomes (PFS, OS)
HRQoL outcomes (EORTC QLQ-MY20 functional and symptom scale scores).
Results of GRADE Assessments
Table 2 presents the GRADE summary of findings for elranatamab.
Table 2: Summary of Findings for Elranatamab for Patients with RRMM
Outcome and follow-up | Patients (MagnetisMM-3 study), N | Effect (95% CI) | Certainty | What happens |
|---|---|---|---|---|
OR | ||||
Proportion of patients who attained OR (PR or better) Median follow-up: 14.7 months | 123 (1 noncomparative trial: Cohort A) | 611 per 1,000 (518 to 696) | Very lowa | The evidence is very uncertain about the effect of elranatamab on OR when compared with any comparator. |
Proportion of patients who attained OR (PR or better) Median follow-up: ███ ██████ | ██ (1 noncomparative trial: Cohort B) | ███ ███ █████ ████ ██ ████ | Very lowa | The evidence is very uncertain about the effect of elranatamab on OR when compared with any comparator. |
PFS | ||||
Patients with probability of PFS at 12 months; median PFS, months Median follow-up: 14.7 months | 123 (1 noncomparative trial: Cohort A) | 566 per 1,000 (467 to 653); median PFS not reached (9.9 to NE) | Very lowa | The evidence is very uncertain about the effect of elranatamab on PFS when compared with any comparator. |
Patients with probability of PFS at 12 months; median PFS, months Median follow-up: ███ ██████ | ██ (1 noncomparative trial: Cohort B) | ███ ███ █████ ████ ██ █████ ██████ ███ ███ ███ ██████ ████ ██ ████ | Very lowa | The evidence is very uncertain about the effect of elranatamab on PFS when compared with any comparator. |
OS | ||||
Patients with probability of OS at 12 months; median OS, months Median follow-up: 14.7 months | 123 (1 noncomparative trial: Cohort A) | 630 per 1,000 (537 to 709); median OS not reached (13.9 to NE) | Very lowa | The evidence is very uncertain about the effect of elranatamab on OS when compared with any comparator. |
Patients with probability of OS at 12 months; median OS, months Median follow-up: ███ ██████ | ██ (1 noncomparative trial: Cohort B) | ███ ███ █████ ████ ██ █████ ██████ ██ ███ ████ ██████ ████ ██ ███ | Very lowa | The evidence is very uncertain about the effect of elranatamab on OS when compared with any comparator. |
DOR | ||||
Patients with probability of remaining in response (PR or better) at 12 months; median DOR, months Median follow-up: 14.7 months | 75 (1 noncomparative trial: Cohort A) | 753 per 1,000 (631 to 839); median DOR not reached (NE to NE) | Very lowa | The evidence is very uncertain about the effect of elranatamab on DOR when compared with any comparator. |
Patients with probability of remaining in response (PR or better) at 12 months; median DOR, months Median follow-up: ███ ██████ | ██ (1 noncomparative trial: Cohort B) | ███ ███ █████ ████ ██ █████ ██████ ███ ███ ███████ █████ ██ ███ | Very lowa | The evidence is very uncertain about the effect of elranatamab on DOR when compared with any comparator. |
CR | ||||
Proportion of patients who attained CR or better Median follow-up: 14.7 months | 123 (1 noncomparative trial: Cohort A) | 350 per 1,000 (266 to 441) | Very lowa | The evidence is very uncertain about the effect of elranatamab on CR or better when compared with any comparator. |
Proportion of patients who attained CR or better Median follow-up: ███ ██████ | ██ (1 noncomparative trial: Cohort B) | ██ ███ █████ ███ ██ ████ | Very lowa | The evidence is very uncertain about the effect of elranatamab on CR or better when compared with any comparator. |
EORTC QLQ-MY20 scale scores | ||||
████ ███████████ ██ ████ █████ ██████ ██████ █████ ████ █ | ██ ██ ███ | ████ ████ | Very lowa, b | The evidence is very uncertain about the effect of elranatamab on body image when compared with any comparator. |
████ ███████████ ██ ████ █████ ██████ ██████ █████ ████ █ | ██████████ | ████ ████ | Very lowa, b | The evidence is very uncertain about the effect of elranatamab on body image when compared with any comparator. |
████ ███████████ ██ ████ █████ ██████ ██████ █████ ████ █ | ██ ██ ███ | ████ ████ | Very lowa, b | The evidence is very uncertain about the effect of elranatamab on future perspective when compared with any comparator. |
████ ███████████ ██ ████ █████ ██████ ██████ █████ ████ █ | ██ ██ ███ | ████ ████ | Very lowa, b | The evidence is very uncertain about the effect of elranatamab on future perspective when compared with any comparator. |
████ ███████████ ██ ████ █████ ██████ ██████ █████ ████ █ | ██ ██ ███ | █████ ████ | Very lowa, b | The evidence is very uncertain about the effect of elranatamab on disease symptoms when compared with any comparator. |
████ ███████████ ██ ████ █████ ██████ ██████ █████ ████ █ | ██ ██ ███ | █████ ████ | Very lowa, b | The evidence is very uncertain about the effect of elranatamab on disease symptoms when compared with any comparator. |
████ ███████████ ██ ████ █████ ██████ ██████ █████ ████ █ | ██ ██ ███ | █████ ████ | Very lowa, b | The evidence is very uncertain about the effect of elranatamab on side effects of treatment when compared with any comparator. |
████ ███████████ ██ ████ █████ ██████ ██████ █████ ████ █ | ██ ██ ███ | █████ ████ | Very lowa, b | The evidence is very uncertain about the effect of elranatamab on side effects of treatment when compared with any comparator. |
+= censored observation; CI = confidence interval; CR = complete response; DOR = duration of response; EORTC QLQ-MY20 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Multiple Myeloma 20; NE = not estimable; NR = not reported; OR = objective response; OS = overall survival; PFS = progression-free survival; PR = partial response; RRMM = relapsed or refractory multiple myeloma.
Notes: Data, including effect estimates are based on the MagnetisMM-3 trial data cut-off date of March 14, 2023.
aIn the absence of a comparator arm, conclusions about efficacy relative to any comparator cannot be drawn and certainty of evidence started at the level of very low.
bRated down 1 level for risk of bias due to a large amount of missing outcome data.
Source: MagnetisMM-3 Clinical Study Report.3[Details included in the table are from the sponsor’s Summary of Clinical Evidence].
Long-Term Extension Studies
No long-term extension studies were submitted by the sponsor.
Indirect Comparisons
Description of Studies
In the absence of direct comparative evidence of elranatamab versus relevant comparators, 2 unanchored matching-adjusted indirect comparisons (MAICs) were conducted by the sponsor. The objective of MAIC 1 was to assess the relative treatment effect of elranatamab, using data from cohort A of the MagnetisMM-3 trial, compared to physician’s choice of treatment based on aggregated data from the CMRG database in patients with TCE or RRMM. The outcomes assessed included PFS and OS.
The objective of MAIC 2 was to assess the relative treatment effect of elranatamab compared to teclistamab from the MajesTEC-1 trial, physician’s choice of treatment from prospective real-world evidence (RWE) studies (the LocoMMotion and MAMMOTH trials), idecabtagene vicleucel from the KarMMa trial, and ciltacabtagene autoleucel (cilta-cel) from the CARTITUDE-1 trial in patients with TCE or RRMM. Since idecabtagene vicleucel is not used in Canada, as per the participating drug plans and clinical experts consulted by CADTH, comparisons to this treatment were not included in this report. The outcomes assessed included ORR, PFS, OS, and CRR. Both MAICs used the same methods to match study populations and quantify the relative effect of treatments using HRs with 95% CIs. Prognostic variables (PVs) and effect modifiers (EMs) were identified through a systematic literature review and validated with clinical expert opinion.
Efficacy Results
The results of both MAICs were generally in favour of elranatamab compared to relevant comparators, except for cilta-cel. In MAIC 1, the PFS and OS favoured elranatamab versus physician’s choice of treatment, although the proportional hazards assumption was violated for both outcomes, which could have biased the estimates. In MAIC 2, the ORR favoured elranatamab versus teclistamab and physician’s choice of treatment. For PFS, the hazard ratio (HR) favoured elranatamab versus teclistamab and physician’s choice of treatment and crossed the null for elranatamab versus cilta-cel. For OS, the HR crossed the null for elranatamab versus teclistamab, favoured cilta-cel versus elranatamab, and favoured elranatamab versus physician’s choice of treatment. The proportional hazards assumption was violated in most comparisons for both OS and PFS, except for the comparison to teclistamab. For CRR, the effect crossed the null for elranatamab versus teclistamab, and favoured elranatamab versus physician’s choice of treatment.
Harms Results
The MAICs did not include harms, and therefore no conclusions could be drawn on the relative safety of elranatamab versus relevant comparators from this evidence.
Critical Appraisal
Both MAIC 1 and MAIC 2 used the same methods to indirectly compare treatments, and their rationale and objectives were reported. In the case of both MAICs, the authors did not report a systematic literature search, describe their methods for data extraction, or conduct quality assessment of the included studies. The MAICs included relevant outcomes identified by the CADTH team (ORR, PFS, OS, CRR); however, important outcomes such as DOR, HRQoL, and safety were not included in the comparisons. The CMRG database did not capture DOR, HRQoL and safety outcomes, and therefore these outcomes were not included in MAIC 1. As such, their indirect comparative assessment remains unknown.
Across the included studies, there were similarities and notable differences in study design, inclusion and exclusion criteria, outcome definitions, and patient characteristics. For MAIC 2, a key difference of comparing elranatamab to teclistamab, cilta-cel, and physician’s choice of treatment based on the LocoMMotion study was that these studies included patients who were TCE, while the MagnetisMM-3 trial enrolled patients who were TCR. As TCE patients are potentially in better health than TCR patients, the treatment comparisons against these drugs would have been subjected to a certain degree of uncertainty in favour of the comparators. To account for between-study differences in patient baseline characteristics, several relevant PVs and EMs were matched in the weighting process, with separate sets of variables used across treatment comparisons and outcomes. These variables were selected based on a systematic literature search and clinical expert input; however, the authors did not differentiate PVs from EMs, and used them collectively in the weighting process. For MAIC 1 (elranatamab versus physician’s choice), ISS disease stage and cytogenetic risk could not be adjusted in the analyses for PFS and OS, as the definitions did not align across the MagnetisMM-3 trial and the CMRG study, a multicentre, retrospective, real-world (RW) study. The authors noted that, at the feasibility stage, because the definitions of ISS disease stage and cytogenetic risk were not comparable between the 2 studies, they were not included in the indirect treatment comparison. In the CMRG study, patient-level data regarding these 2 variables were captured at diagnosis rather than at the start of the trial period, as it was defined in the MagnetisMM-3 trial. Additionally, extramedullary disease was not adjusted for in the analysis as it was not reported in the CMRG study. For MAIC 2, these 2 important variables were missing for 2 comparisons: in the comparison of physician’s choice of treatment from the MAMMOTH study, extramedullary disease was not adjusted for, and in the comparison of physician’s choice of treatment from the LocoMMotion study, cytogenetic risk was not adjusted for. Not adjusting for these differences could introduce residual confounding due to unreported or unobserved cross-study differences, although the direction or extent of bias is unclear. For MAIC 1, following the weighting process, the effective sample size (ESS) for OS declined by approximately 34% of the original sample size in the comparison with physician’s choice of treatment. For the PFS comparison with physician’s choice of treatment, the ESS declined by approximately 33% of the original sample size. For MAIC 2, following adjustment, the ESS for OS declined by 37% of the original sample size in the comparison with teclistamab, by 73% of the original sample size in the comparison with cilta-cel, by 45% of the original sample size in the comparison with physician’s choice of treatment (the LocoMMotion study), and by 20% of the original sample size in the comparison with physician’s choice of treatment (the MAMMOTH study). These reductions in the ESS meant that the final matched patient population was more selective than the original patient population, and may lead to large uncertainty in estimated treatment effects, although the magnitude and direction of potential bias is unclear. For MAIC 1, the proportional hazards assumption was violated for both the PFS and OS outcomes, and for MAIC 2, the assumption was violated in most comparisons for the PFS and OS outcomes. These violations could have led to biased treatment effect estimates. In addition, since both MAICs only included cohort A from the MagnetisMM-3 trial and the Health Canada indication is for patients with and without prior exposure to BCMA-directed therapies, there is no indirect comparative evidence for the use of elranatamab in patients who have received prior BCMA-directed therapy. Due to these limitations in the MAICs and uncertainty in their estimates, no definitive conclusions could be drawn on the relative treatment effects of elranatamab versus relevant comparators.
Studies Addressing Gaps in the Evidence From the Systematic Review
This section summarizes 2 retrospective cohort studies with external control arms (Study C1071024 and Study C1071031) and 1 phase I and phase II dosing study (the MagnetisMM-9 trial) that were submitted to provide comparative evidence of elranatamab versus other active treatments.
RWE External Cohort Studies (Study C1071024 and Study C1071031)
Description of Studies
A retrospective cohort study, Study C1071024, was conducted to compare the efficacy outcomes ORR, time to response, and DOR observed in the participants of the MagnetisMM-3 trial (with at least 9 months of follow-up) and RW patients selected from 2 US-based oncology electronic health record databases, the Flatiron Health and COTA databases. Study C1071031 is the continuation of Study C1071024 with an available follow-up of the MagnetisMM-3 study participants of approximately 15 months. Study C1071031 aimed to compare the PFS and OS in participants of the MagnetisMM-3 study treated with elranatamab versus RW patients with TCR MM treated with RW physician’s choice of therapy. Study C1071031 also assessed patient-reported outcomes (PROs) (via the EORTC QLQ-MY20 tool) using other studies, Study C1071013 and Study C1071014, as the data sources for the external cohort. Patients were considered eligible for selection in the external control arm if they had MM that was refractory to at least 1 PI, 1 IMiD, and 1 anti-CD38, and had started at least 1 new treatment since the documentation of TCR status. The date of initiation of the first regimen after TCR MM eligibility was defined as the index date in establishing the external control arms from the Flatiron Health and COTA databases. Patients were only eligible if they had an index date occurring between November 16, 2015, and June 30, 2022.
For the main analysis in Study C1071024 and Study C1071031, differences in baseline and key covariate characteristics between participants in the MagnetisMM-3 study and each external control arm were balanced using inverse probability of treatment weighting (IPTW).
Between February 2021 and January 2022, the MagnetisMM-3 trial, cohort A, enrolled 123 patients with TCR MM, who were included in the main analysis for Study C1071031. For the external control arms for Study C1071024 and Study C1071031, 239 patients with TCR MM were selected from the COTA database and 152 patients from the Flatiron Health database. Median follow-up times for included patients were 14.7 months in the MagnetisMM-3 trial, cohort A; 8.8 months for patients with TCR MM from the COTA database; and 7.7 months for patients with TCR MM from the Flatiron Health database.
A systematic literature review was conducted to identify variables most strongly and consistently correlated with outcomes in real-world database (RWD) studies conducted among patients with RRMM and some additional variables were included in the analysis as confounders. To control baseline confounding, propensity scores (PSs) were estimated using logistic regression models.
For the PROs analysis (EORTC QLQ-MY20), a total of 67 patients from prospective cohort studies C1071013 and C1071014 were included. Baseline characteristics were compared between participants of the MagnetisMM-3 study and Study C1071013 and Study C1071014. Most baseline characteristics between Study C1071013 and Study C1071014 were generally similar, although compared to the MagnetisMM-3 study’s population, the population from the observational studies, Study C1071013 and Study C1071014, had higher proportions of ISS stage III (18.3% and 37.8%, respectively), an ECOG PS score of 2 (5.6% and 20.0%, respectively), and high-risk cytogenetics (24.4% and 42.2%, respectively). A higher proportion of participants in the MagnetisMM-3 study had extramedullary disease compared to patients from the observational studies (38.9% and 13.3%, respectively).
Efficacy Results
PFS (Study C1071031): During the study periods, PFS events (disease progression or death) were identified for 53 (43%) patients in the MagnetisMM-3 trial’s population, 136 (57%) patients in the COTA database population, and 88 (58%) patients in the Flatiron Health database population. Median PFS was longer with elranatamab versus RW SOC in the COTA database population, both before weighting (HR = 0.51 [95% CI, 0.37 to 0.71; P < 0.0001]) and after IPTW (HR = 0.37 [95% CI, 0.22 to 0.64; P = 0.0003]). In the restricted mean survival time analyses, the average PFS was longer with elranatamab versus RW SOC in the COTA database population at 9 months, 12 months, 15 months, 18 months, and 24 months using both weighted and unweighted analyses. Similarly, the average PFS time was longer with elranatamab versus RW SOC in the Flatiron Health database population.
OS (Study C1071031): During the study periods, deaths were identified for 55 (45%) patients in the MagnetisMM-3 trial’s population, 171 (72%) patients from the COTA database population, and 90 (59%) patients from the Flatiron Health database population. Median OS was longer with elranatamab versus RW SOC in the COTA database population, both before weighting (HR = 0.65 [95% CI, 0.47 to 0.88; P = 0.0062]) and after IPTW (HR = 0.46 [95% CI, 0.27 to 0.77; P = 0.0032]). In the restricted mean survival time analyses, the average OS time was longer with elranatamab versus RW SOC in the COTA database population at 12 months, 15 months, 18 months, and 24 months using the unweighted analyses, and was also longer at 9 months, 12 months, 15 months, 18 months, and 24 months using the inverse probability of treatment (IPT)-weighted analyses. Similarly, the average OS time was longer with elranatamab versus RW SOC in the Flatiron Health database population at 9 months, 12 months, 15 months, 18 months, and 24 months using the unweighted analyses.
ORR (Study C1071024): The ORR was higher for elranatamab compared to RW SOC in both unweighted and IPT-weighted analyses. In the unweighted analyses, the ORR was 61% (95% CI, 51.8% to 69.6%) in the MagnetisMM-3 trial’s population, 31.3% (95% CI, 25.4% to 37.7%) in the COTA database population, and 30.3% (95% CI, 23.1% to 38.2%) in the Flatiron Health database population, with higher values observed in the MagnetisMM-3 trial versus the COTA database population (risk ratio [RR] = 1.95 [95% CI, 1.54 to 2.47; P < 0.0001]) and versus the Flatiron Health database population (RR = 2.01 [95% CI, 1.52 to 2.67; P < 0.0001]). Similarly, after adjusting for baseline confounding using IPTW, higher ORR was observed in the MagnetisMM-3 trial versus the COTA database population (RR = 2.22 [95% CI, 1.69 to 2.90; P < 0.0001]) and versus the Flatiron Health database population (RR = 1.79 [95% CI, 1.01 to 3.15; P = 0.0447]).
DOR (Study C1071024): Among patients who attained an OR, the median DOR was longer with elranatamab compared to RW SOC from both databases. In the unweighted analysis, improved DOR was observed with elranatamab in the MagnetisMM-3 trial compared with RW SOC in the COTA database population (HR = 0.17 [95% CI, 0.09 to 0.31; P < 0.0001]) and in the Flatiron Health database population (HR = 0.22 [95% CI, 0.11 to 0.43; P < 0.0001]). After accounting for the baseline confounding in the IPT-weighted analysis, improved DOR was still observed with elranatamab in the MagnetisMM-3 trial compared with RW SOC in the COTA database population (HR = 0.11 [95% CI, 0.06 to 0.22; P < 0.0001]) and in the Flatiron Health database population (HR = 0.21 [95% CI, 0.10 to 0.45; P < 0.0001]).
PROs (MagnetisMM-3 Trial Versus Study C1071013 and Study C1071014)
The least squares mean difference values for the disease symptoms and side effects of treatment modules were inconclusive.
Harms Results
Safety data were not evaluated.
Critical Appraisal
Patients were compared using IPTW and doubly robust methods in an attempt to minimize the impact of confounding on the results. It should be noted that this method cannot control for substantial differences resulting from different study designs between the 2 cohorts (RCT versus retrospective registry review). The MagnetisMM-3 trial is a phase II, open-label, single-arm trial whereas the external control arms were derived from longitudinal RW cohorts from electronic health records in the US. For the retrospective cohorts, there was concern of potential time-related bias (e.g., treatment changes, informative censoring) due to the likely possibility of unequal number of dropouts for outcome assessment. The definition of censoring in the PFS analysis was not equivalent between participants of the MagnetisMM-3 trial and patients identified from RW sources, which is a potential source of measurement error in PFS measurements that may have biased the comparative effectiveness estimates in favour of the SOC treatment group. There might be important unknown or unmeasured residual confounding in the external control arms that were either not documented or could not be accounted for. Although the sponsor conducted IPTW, a few characteristics were not well balanced in the comparison of the MagnetisMM-3 trial and the Flatiron Health database populations (i.e., ECOG PS score, time since the initial MM diagnosis, Charlson Comorbidity Index score, the number of lines of therapy before the index date, and history of stem cell transplant). Therefore, there remains also a potential risk of residual confounding. The sponsor recognized that unlike clinical trial settings, which use specifically defined outcomes and scheduled assessments, RW data are subject to inconsistent assessments and evaluations of treatment response. The sponsor noted that further limitations on the data quality of RWDs such as key variables were either unavailable or not similarly reported, that missing data and the accuracy of recorded data may introduce an information bias and residual confounding, and that applying eligibility criteria from a clinical trial to an RWD requires adjustments, which could impact the comparability of the populations. Well-defined, reliable, and clinically meaningful outcomes that are typically used in randomized trials may be particularly difficult to ascertain and evaluate in a RWD source that is being considered for an externally controlled trial. As a general consideration, outcomes of interest are more likely to be recorded in clinical records when events are objective and/or require immediate medical attention. This might have led to the omission of some important outcomes in the RWE cohort, which may bias the results. In addition, the sponsor did not evaluate the consistency of the timing of outcome assessments in the treatment arm compared to the external control arms. For the analysis of PROs (EORTC QLQ-MY20), participation in Study C1071013 and Study C1071014 was dependent on physicians’ and patients’ ability and willingness to participate, which may have impacted patient representativeness and be a source of self-selection bias.
The patients chosen from these RWDs to generate the external cohorts were highly selective in nature and may not reflect the general population. It is not possible to know whether the results may have differed if data from different RRMM studies or databases had been used. Numerous therapies were used in the RW clinical practice groups from the MagnetisMM-3 trial cohort and the external cohorts, many of which may not be relevant to Canadian clinical practice. Additionally, treatment regimens reported from these sources were included from November 16, 2015, until June 30, 2022 (the index date), and may not be reflective of current treatment standards. The clinical experts consulted by CADTH indicated that the patient population included in the external control arms based on the US-based COTA and Flatiron Health databases may differ from the Canadian general population. The sponsor conducted a subgroup analysis according to treatments, providing the rationale that treatments included in the analysis aligned with the “relevant comparators” for this submission. However, according to the clinical experts consulted by CADTH, some important comparators (e.g., pomalidomide, bortezomib, dexamethasone, belantamab) used in Canada are missing from the RW treatment list used for the subgroup analysis. Furthermore, the clinical experts also noted that some of treatments included are not commonly used in Canada.
MagnetisMM-9 Trial
Description of Studies
The phase I and phase II MagnetisMM-9 trial was conducted to evaluate a dosing regimen with 2 step-up priming doses and longer dosing intervals of elranatamab. The primary objective was to assess the safety of a priming dose regimen that involves premedication and 2 step-up priming doses administered within the first week of elranatamab treatment in RRMM participants who are refractory to at least 1 PI, 1 IMiD, and 1 anti-CD38 mAb. At the time of submission, data were only available for an interim analysis up to July 29, 2022, at which point patients had only been enrolled in part 1(76 mg elranatamab) and part 2A, dose level 1(> 76 mg with more than 1 week dosing interval); efficacy data were only available for patients from part 1 and safety data were only available for patients from part 1 and part 2A, dose level 1. Both sets of patients received the same first cycle (premedication, 2 step-up priming doses of elranatamab [4 mg and 20 mg], and 76 mg doses of elranatamab); patients in part 1 continued elranatamab 76 mg every week for 6 cycles while patients in part 2A, dose level 1, received elranatamab 116 mg every 2 weeks for cycle 2 to cycle 6. Additional doses were considered in the MagnetisMM-9 trial design but were not summarized because data for those groups were not yet available. The primary outcome of the MagnetisMM-9 trial was the rate of grade 2 or higher CRS during cycle 1 in adult patients with TCR MM, which was evaluated against an a priori assumption that the mean grade 2 or higher CRS rate would be 35%. Outcomes in the MagnetisMM-9 study were analyzed descriptively and without a hierarchical testing strategy; several efficacy outcomes (the duration of complete response, PFS, OS, and minimal residual disease) were immature at the time of submission and are not summarized because data were not available at the time of the interim data cut-off date. The main inclusion and exclusion criteria for the MagnetisMM-9 study were similar to the eligibility criteria of the pivotal MagnetisMM-3 trial. The baseline demographic characteristics and clinical characteristics of patients who enrolled in the MagnetisMM-3 and MagnetisMM-9 trials were generally consistent with the characteristics of patients who have heavily pretreated RRMM.
Efficacy Results
At the latest data cut-off date (July 29, 2022), efficacy data were not available for the MagnetisMM-9 study. At this time, the trial included ██ patients, █████ of patients were receiving treatment, and █████ were under follow-up. In the overall population, the median treatment duration was ████ months in the MagnetisMM-9 study; the median treatment duration in part 1 of the MagnetisMM-9 study (████ months) was comparable to that in the overall MagnetisMM-3 study population. The median cumulative dose was higher in the MagnetisMM-3 study than in the MagnetisMM-9 study (█████ ██ ███ ███ ███ ████████████), which reflects the shorter time on treatment in the MagnetisMM-9 study at the data cut-off dates. However, relative dose intensities were similar between the MagnetisMM-3 study (███████ and the MagnetisMM-9 study (████████ No major differences were observed in the proportions of patients with dose reductions or interruptions in the MagnetisMM-3 study (██████ and the MagnetisMM-9 study (███████ which were predominantly due to AEs. A smaller proportion of patients re-escalated to the 76 mg or 116 mg doses of elranatamab in the MagnetisMM-9 trial. Patients in the overall populations of the MagnetisMM-9 study had heavily pretreated MM (median = | previous lines) that was refractory to the last line of therapy. Most patients (█████) were classified as being TCR. Similar to the MagnetisMM-3 trial, infection prophylaxis was common in the MagnetisMM-9 trial, most frequently involving antiviral medication (██████ and medication to prevent Pneumocystis jiroveci pneumonia (███████
Harms Results
All harms data reported in this section are from the data cut-off date of July 29, 2022. All patients in the trial reported at least 1 TEAE. The most frequently reported TEAEs in part 1 were CRS (███), anemia (███), neutropenia (███), diarrhea (███), decreased appetite (███), pyrexia (███) and fatigue (███). The most frequently reported TEAEs in part 2A, dose level 1, were CRS (███), anemia (███), neutropenia (███), diarrhea (███), fatigue (███), decreased appetite (███), injection site reaction (███), thrombocytopenia (███) and pain in extremity (███). In the total population, ███ of patients experienced at least 1 serious TEAE. The most frequently reported serious AEs in both part 1 and part 2A, dose level 1, were CRS ████ ███ ████ ██████████████ Study treatment discontinuation due to TEAEs in part 1 were ███ and ███ in part 2A, dose level 1. The most common TEAEs leading to the discontinuation of elranatamab included septic shock (██) and peripheral sensory neuropathy (██) for part 2A, dose level 1, and neutropenia (██) for part 1. In part 1 and part 2A, dose level 1, ███ ███ ███ of patients died, respectively. Most deaths in both cohorts were attributed to other reasons ███ ██ ████ █ ███ ███ ██ ████ ██ ████ █████ ███ The primary end point of the MagnetisMM-9 trial was the rate of grade 2 or higher CRS during cycle 1 (combining patients from part 1 and part 2A), which was ███████
Critical Appraisal
The MagnetisMM-9 study was an open-label, single-arm, phase I and phase II trial. The primary limitation of the MagnetisMM-9 study was the absence of a comparator group against which the benefits and harms of elranatamab could be compared. Single-arm trials are subject to several limitations that complicate their interpretation. Efficacy outcomes in the MagnetisMM-9 study were analyzed descriptively. As the primary outcome for the MagnetisMM-9 study, the rate of grade 2 or higher CRS during cycle 1 was evaluated against an a priori assumption. Efficacy data were immature. The trial was open label, which can result in a risk of bias in the measurement of the outcomes, particularly for subjective harms.
The baseline demographic characteristics and clinical characteristics of patients who enrolled in the MagnetisMM-3 and MagnetisMM-9 trials were generally consistent with the characteristics of patients who have heavily pretreated RRMM. Dose adjustments were allowed in the trial and the methods were outlined in the protocol. Dose adjustments or modifications are anticipated in a clinical practice setting to manage AEs while maintaining drug benefit.
Conclusions
Evidence of efficacy and safety from 1 ongoing, phase II, noncomparative, open-label trial (the MagnetisMM-3 trial) in adults with RRMM who had received at least 3 prior lines of therapy was included in the review for elranatamab. The clinical experts consulted by CADTH indicated that based on their experience treating patients with RRMM and the natural history of the disease, the ORR observed in patients without prior exposure to BCMA-directed therapy (cohort A) is clinically meaningful. However, it remains unknown whether elranatamab could improve PFS, OS, and DOR in patients with prior exposure to BCMA-directed therapy (cohort B) and without prior exposure to BCMA-directed therapy (cohort A) because of the lack of a comparator group, because data were immature, and because no definitive conclusions can be drawn on HRQoL due to the open-label design and large amount of missing outcome data. Overall, the results for patients in cohort B were not as favourable as those for patients in cohort A. There were no new safety signals identified and the safety of elranatamab was consistent with the known safety profile of the drug. Results from the indirect treatment comparisons and RWE studies consistently favoured elranatamab over comparators, except for cilta-cel. However, due to limitations of these studies, no conclusions can be drawn regarding the relative efficacy and safety of elranatamab compared to relevant comparators, including physician’s choice of treatment, teclistamab, and cilta-cel. The evidence submitted to CADTH did not include indirect comparative evidence between elranatamab and any comparator for patients with prior exposure to BCMA-directed therapy; this represents a gap in the available indirect evidence.
Introduction
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of elranatamab 40 mg/mL, subcutaneous injection, for the treatment of adults with RRMM who have received at least 3 prior lines of therapy.
Disease Background
Content in this section has been informed by materials submitted by the sponsor and clinical expert input. The following has been summarized and validated by the CADTH review team.
MM is a plasma cell cancer characterized by the clonal proliferation of malignant plasma cells (B-cells) and the overproduction of the abnormal immunoglobulin M protein.4 Older individuals and men (as opposed to women) are more likely to develop MM and it is twice as common in African-American individuals compared to Caucasian or Asian individuals.5,6 In 2022, it was estimated that 4,000 individuals living in Canada were diagnosed with MM and 1,650 patients living in Canada died from MM.7 The 5-year survival rate for patients with MM is estimated to be approximately 50%,8 and although survival rates have improved in recent years due to advances in therapeutic options, MM remains incurable.9,10 The majority of patients with MM will relapse and many patients will become refractory to commonly used therapies.11 Patients with RRMM often undergo multiple rounds of treatment, with the duration of remission, depth of response, PFS, and OS decreasing with each subsequent line of therapy.6
The most common symptoms of MM are fatigue and bone pain,6 with other symptoms including kidney problems, recurrent infections, fever, and nervous system problems.12 Disease stage, along with other factors, can impact MM prognosis. Commonly recognized factors that impact the prognosis of MM include beta2-microglobulin (B2M) (high levels are associated with poor prognosis), serum albumin (low levels are associated with poor prognosis), lactate dehydrogenase (LDH) (high activity is predictive of poor prognosis), and chromosomal changes (shorter remission duration is associated with chromosome deletions or translocations).13 In addition to these factors, prognosis may be influenced by age, creatinine levels, and performance status. In general, older patients, those with high creatinine levels, and those with poor overall function tend to have worse outcomes compared to younger individuals, those with lower creatinine levels, and those with better overall function.14
The diagnosis of MM typically occurs during a visit to a primary care physician, occurring either incidentally when laboratory tests for other conditions are ordered, or if MM is suspected based on signs and symptoms.15 The diagnosis of MM is based on the presence of 1 or more myeloma-defining events, along with either 10% or more clonal bone marrow plasma cells or biopsy-proven plasmacytoma.6 Myeloma-defining events include the presence of end-organ damage known as the CRAB criteria (hypercalcemia, renal insufficiency, anemia, and bone lesions) along with 3 specific biomarkers: a clonal bone marrow plasma cell percentage of 60% or more, a free light chain ratio of 100 or more, and more than 1 focal lesion on MRI scans.6
Several systems are used for staging MM: the International Staging System (ISS), R-ISS, and the Durie-Salmon staging system.4,16,17 The ISS is commonly used in Canada and uses blood tests that assess albumin levels and B2M levels to stage MM (advanced-stage MM is associated with lower albumin and higher B2M levels):16
stage I — B2M of less than 3.5 mg/L; serum albumin of 3.5 g/dL or more
stage II — B2M of less than 3.5 mg/L; serum albumin of less than 3.5 g/dL; or B2M of 3.5 mg/L to 5.5 mg/L, irrespective of serum albumin
stage III — B2M of more than 5.5 mg/L.
The preferred staging system for MM is the R-ISS,17 which combines elements of tumour burden (ISS) and disease biology (the presence of high-risk cytogenetic abnormalities or elevated LDH levels), to create a unified prognostic index that helps in clinical care as well as in the comparison of clinical trial data. R-ISS uses serum B2M, serum albumin, serum LDH, and bone marrow fluorescence in situ hybridization (FISH) results to stratify patients into 3 risk groups:16,17
stage I — B2M of less than 3.5 mg/L, serum albumin of 3.5 g/dL or more, normal LDH, and with no del(17p), t(4;14), t(14;16) by FISH
stage II — neither stage I nor stage III (There are 2 categories for stage II: serum 2-microglobulin 3.5 mg/L but serum albumin 3.5 g/dL; or serum 2-microglobulin 3.5 to 5.5 mg/L irrespective of the serum albumin level.
stage III — B2M of 5.5 mg/L or more, elevated LDH, and/or del(17p), t(4;14), t(14;16) by FISH.
According to the IMWG criteria, a patient is considered to have refractory MM when they are nonresponsive to therapy or experience disease progression within 60 days of their last line of therapy.18,19 A patient is considered to have relapsed MM if they experience disease progression after being previously treated and require a salvage therapy but do not meet the criteria for primary refractory MM or RRMM.18,19 Finally, a patient is considered to have relapsed and refractory MM if they have attained a minimal response or better at some point during previous treatments but the disease is currently nonresponsive on salvage therapy, or they experience disease progression within 60 days of their last therapy.18,19
Standards of Therapy
Content in this section has been informed by materials submitted by the sponsor and clinical expert input. The following has been summarized and validated by the CADTH review team.
According to the clinical experts consulted by CADTH, the main treatment goals for patients with RRMM are to prolong survival, improve symptoms, minimize toxicities, and maintain or improve HRQoL. Therapies for the treatment of patients with RRMM, and the sequencing of these treatments, depend on eligibility for autologous stem cell transplant at diagnosis, age, comorbidities, previous treatments, beforexicities, and line of therapy. According to the joint clinical practice guideline of OH-CCO and the American Society of Clinical Oncology, treatment for RRMM includes triplet therapy consisting of PIs, IMiDs, and mAbs.20 There is no preferred therapy for RRMM in the fourth-line and beyond settings, and at this stage of the disease, patients may be treated with PIs, IMiDs, and anti-CD38 mAbs,20,21 and in some cases receive more than 1 PI or IMiD, further limiting treatment options in later lines of therapy. According to the 2022 Provisional Funding Algorithm for MM developed by CADTH,21 patients with drug resistance cannot be treated again with the same drug, except for dexamethasone, which is found in all regimens. Depending on drug sensitivity, patients can be treated with carfilzomib and dexamethasone or pomalidomide and dexamethasone in combination with isatuximab; carfilzomib, lenalidomide, and dexamethasone; lenalidomide and dexamethasone; daratumumab, lenalidomide, and dexamethasone; or daratumumab, bortezomib, and dexamethasone. Alternative regimens with a different PI or immunomodulator backbone can be offered in the third and fourth lines, depending on drug sensitivity. Cyclophosphamide may be added to some regimens, such as pomalidomide and dexamethasone; carfilzomib and dexamethasone; and lenalidomide and dexamethasone.
Recent recommendations to reimburse drugs to treat triple RRMM with conditions by the pan-Canadian Oncology Drug Review Expert Review Committee include carfilzomib and dexamethasone; pomalidomide and dexamethasone; selinexor, bortezomib, and dexamethasone; and cilta-cel. According to the CADTH Provisional Funding Algorithm for MM, selinexor, bortezomib, and dexamethasone is recommended for third-line therapy and beyond in patients who are sensitive to bortezomib but not to anti-CD38 mAbs and lenalidomide. In Canada, coverage for pomalidomide and dexamethasone with or without cyclophosphamide, and carfilzomib and dexamethasone with or without cyclophosphamide, is determined on a case-by-case basis while cilta-cel is under consideration for negotiation at the pan-Canadian Pharmaceutical Alliance. Coverage for selinexor varies across provinces and territories in Canada.
Drug Under Review
Elranatamab injection is indicated for the treatment of adults with RRMM who have received at least 3 prior lines of therapy, including a PI, an IMiD, and an anti-CD38 mAb, and who have demonstrated disease progression on the last therapy. The reimbursement request aligns with the Health Canada indication for elranatamab.22
Elranatamab is a bispecific antibody consisting of humanized anti-BCMA and anti–CD3-epsilon targeting arms paired on a immunoglobulin G2a backbone with nullified Fc binding function, which leads to a longer half-life.23,24 Elranatamab binds to both BCMA-expressing MM cells and T-cells, effectively creating a bridge between them.24,25 Activated T-cells release perforin and granzyme B, leading to cytolysis of MM cells.23,25-27
The recommended dosing schedule for elranatamab, via subcutaneous injection, is 12 mg on day 1 and 32 mg on day 4 of week 1, followed by a full treatment dose of 76 mg administered weekly from week 2 to week 24.22 For patients who have received at least 24 weeks of treatment and have attained a response (i.e., an IMWG response category of partial response or better with responses persisting for at least 2 months), the dose interval should transition to a schedule of every 2 weeks.22
Key characteristics of elranatamab and other therapies for the treatment of adult patients with RRMM in fourth-line therapy and beyond, as indicated in CADTH's Provisional Funding Algorithm for MM,21 are presented in Table 3.
Table 3: Key Characteristics of Pharmacotherapies for Multiple Myeloma
Characteristics | Elranatamab | Ciltacabtagene autoleucel | Selinexor | PIs (carfilzomib) | IMiDs (pomalidomide) |
|---|---|---|---|---|---|
Mechanism of action | A bispecific BCMA-directed T-cell–engaging antibody binds BCMA on plasma cells, plasmablasts, MM cells, and CD3-epsilon on T-cells leading to selective cytolysis of the BCMA-expressing cells | BCMA-directed genetically modified autologous CAR T-cell immunotherapy | Selinexor is a compound that specifically blocks XPO1, a nuclear export protein that transports cargo proteins within the cell. XPO1 inhibition by selinexor leads to the reduction of cancer cells. | Proteasome inhibition leads to the accumulation of misfolded protein in endoplasmic reticulum, resulting in apoptosis and the inhibition of cell proliferation. | Immunomodulatory and antineoplastic activity; inhibits proliferation and induces apoptosis of hematopoietic tumour cells |
Indicationa | Treatment of adult patients with RRMM who have received at least 3 prior lines of therapy, including a PI, an IMiD, and an anti-CD38 mAb | For the treatment of adult patients with MM who have received at least 3 prior lines of therapy, including a PI, an IMiD, and an anti-CD38 antibody, and who are refractory to their last treatment | In combination with bortezomib and dexamethasone for the treatment of adult patients with MM who have received at least 1 prior therapy | In combination with dexamethasone alone, for patients with relapsed MM who have received 3 prior lines of therapy | In combination with dexamethasone for patients with MM for whom both bortezomib and lenalidomide have failed and who have received at least 2 prior regimens and demonstrated disease progression on the last regimen |
Route of administration | SC injection | IV infusion | Orally | IV infusion | Orally |
Recommended dosage | 12 mg on day 1 and 32 mg on day 4 of week 1, followed by a full treatment dose of 76 mg administered weekly from week 2 to week 24 | Single infusion of 0.5 × 106 to 1.0 × 106 CAR-positive viable T-cells per kg body weight |
|
|
|
Serious adverse effects or safety issues | Cytokine release syndrome, neurologic toxicity (including ICANS), infections, hypogamma-globulinemia, hepatotoxicity, neutropenia, and febrile neutropenia | Cytokine release syndrome, neurologic toxicities (including ICANS), hemophagocytic lymphohistio-cytosis, or macrophage activation syndrome | Fatigue, severe or life-threatening hyponatremia, nausea, vomiting, diarrhea, anorexia or weight loss, thrombocytopenia, neutropenia, infections, dizziness, cataracts | Infusion reactions, tumour lysis syndrome Infections, cardiac disorders, venous thrombosis, hypertension, hemorrhage, thrombocytopenia, hepatotoxicity, hepatitis B reactivation, posterior reversible encephalopathy syndrome, PML, acute renal failure, pulmonary toxicity | Neutropenia, thrombocytopenia, infections, DVT and pulmonary embolism, hepatotoxicity, anaphylaxis, hepatitis B reactivation, severe rash (SJS, TEN, DRESS), tumour lysis syndrome |
Other | None | None | Currently under negotiations | Premedication for carfilzomib is recommended with dexamethasone (at least 30 minutes prior) to reduce the incidence and severity of infusion reactions. | Antithrombotic prophylaxis is recommended. |
BCMA = B-cell maturation antigen; CAR = chimeric antigen receptor; DRESS = Drug Rash with Eosinophilia and Systemic Symptoms; DVT = deep venous thrombosis; ICANS = immune effector cell-associated neurotoxicity syndrome; IMiD = immunomodulatory drug; mAb = monoclonal antibody; MM = multiple myeloma; PI = proteasome inhibitor; PML = progressive multifocal leukoencephalopathy; RRMM = relapsed or refractory multiple myeloma; SC = subcutaneous; SJS = Stevens-Johnson syndrome; TEN = toxic epidermal necrolysis.
aHealth Canada–approved indication.
Sources: Product monographs for Elrexfio,22 Carvykti,28 Xpovio,29 Pomalyst,32 and Kyprolis,30 and Canadian Pharmacists Association.31
Stakeholder Perspectives
Patient Group Input
This section was prepared by the CADTH review team based on the input provided by a patient group. The full original patient input received by CADTH has been included in the Stakeholder section of this report.
CADTH received 1 patient group submission from Myeloma Canada. Myeloma Canada conducted both patient and caregiver surveys from September 26 to October 23, 2023, across Canada and internationally via email and social media. A total of 67 complete responses to the patient survey were received, of which 38 responses were recorded based on the respondent’s eligibility criteria (receiving treatment with an IMiD, PI, and anti-CD38 antibody). Among these 38 patients, 24 were eligible for the drug under review and 14 had experience with it. A total of 32 caregivers responded to the caregiver survey, 11 of whose responses were recorded (8 based on eligibility and 3 based on experience with elranatamab). Upon verifying their eligibility for or experience with elranatamab, respondents were divided into 4 subsets. These included patients (n = 24) who would currently be eligible for treatment with elranatamab; patients (n = 14) who have received or are currently receiving treatment with elranatamab; caregivers (n = 8) of patients who would currently be eligible for treatment with elranatamab; and caregivers (n = 3) of patients who have received or are currently receiving treatment with elranatamab. Regarding receiving prior lines of therapy, 13 patients and 3 caregivers indicated receiving 3 lines of therapy, 6 patients and 5 caregivers indicated receiving 4 lines of therapy, 6 patients and 1 caregiver indicated receiving 1 line of therapy, and 5 patients and 2 caregiver respondents indicated receiving 5 lines of therapy or more.
Patient respondents indicated that among their daily activities and quality of life, their ability to work was the factor the most significantly impacted by symptoms associated with myeloma, followed by the ability to travel and to exercise. Regarding the most significant financial implication of myeloma treatment on patients and their household, 24 of 49 respondents (both patients and caregivers) identified loss of income or pension funds due to absence from work, disability, or early retirement as the most significant financial implication, and 20 of 49 respondents chose travel parking costs. Patient respondents felt that interruption of life goals or accomplishments had the greatest impact on their quality of life, followed by loss of sexual desire and anxiety or worry. Patient and caregiver respondents identified the following factors as the most important to myeloma treatment: quality of life, manageable side effects, effectiveness of the treatment (especially in achieving remission and having a durable response), and treatment accessibility or portability (including fewer or minimal visits to the hospital or cancer centre). Infections were identified by patients as the most important aspect to control, followed by mobility and kidney problems.
In terms of treatment outcomes, 12 of the 23 respondents who would currently be eligible for treatment with elranatamab rated improved quality of life as extremely important, 6 respondents rated it as very important, and 5 respondents rated it as somewhat important. In addition, 17 of the 23 patients rated the aspect of life extension while considering a myeloma treatment as extremely important, and 4 patients rated it as very important. When asked about their tolerance of the most common side effects in patients who receive elranatamab, these patients perceived pneumonia, ICANS, URTI, CRS, and infections as the least tolerable side effects, followed by peripheral neuropathy, other infections, and COVID-19. Regarding the impact of the dosing schedule of elranatamab on quality of life (weekly injections for at least 24 weeks, with the possibility of then switching to every 2 weeks), 11 of 24 patients chose the response of negative impact, indicating that it would limit patients’ ability to travel or require a relocation (near their cancer centre) for the duration of treatment.
A total of 17 respondents (14 patients and 3 caregivers) indicated having experience with elranatamab. Among these, 12 respondents (10 patients and 2 caregivers) received elranatamab as monotherapy, 4 patients received elranatamab in combination with another drug, and 1 caregiver was unsure. All 14 patients who had received or were currently receiving treatment with elranatamab mentioned that they were admitted to the hospital at some point in the initial step-up dosing period. Regarding the most frequently experienced elranatamab side effects, all 14 patients rated cough as the least bearable side effect, followed by CRS, neutropenia, and URTI. Most of these patients mentioned that the overall side effects while receiving elranatamab were manageable and found elranatamab effective in controlling their myeloma.
Clinician Input
Input From Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of RRMM.
Unmet Needs
The clinical experts indicated that since almost all patients with RRMM will become refractory to their therapy and continue on to the next line of therapy, the unmet needs of patients would be new effective treatments, with curative potential, which are tolerable by targeting a different mechanistic pathway. Both clinical experts highlighted that the balance between treatment efficacy, minimizing toxicities, and quality of life would be important.
Place in Therapy
The clinical experts agreed that due to elranatamab’s novel mechanism of action, it would provide an additional treatment option for patients who are refractory to other SOC treatments. The clinical experts noted that elranatamab is a new class of treatment for which there should be no existing drug resistance, and given its unique mechanism of action and toxicity profile, it should create a treatment synergy with other current families of myeloma treatments. However, they noted that given the lack of direct evidence, it is not known yet if elranatamab is more effective than other therapies.
Patient Population
The clinical experts agreed that the patients best suited for elranatamab would be those who are TCR. One of the clinical experts noted that patients most likely to respond to this therapy would be those with a stronger and more intact immune system, and that patients with significant pre-existing cytopenias may not be ideal candidates as the cytopenias may worsen during treatment and predispose patients to infection. The experts did not note any issues or challenges related to the diagnosis or misdiagnosis of RRMM, and the identification of patients likely to respond. Patients would be identified during routine cancer follow-up based on biochemical assessment (serum protein electrophoresis, serum free light chain) or other evidence of relapse.
Assessing the Response Treatment
The clinical experts agreed that in clinical practice, standard clinical response criteria can be used to determine whether a patient with RRMM is responding or progressing on treatment. The clinical experts noted that achieving a durable OR lasting 6 months to 12 months would be a sign of successful treatment, and such a response would be associated with a reduction in disease-related symptoms, bone pain, fatigue, and transfusion requirements. They noted that toxicities, especially cytopenias such as neutropenia, infections, CRS, and hypogammaglobulinemia, would need to be monitored.
Discontinuing Treatment
The clinical experts indicated that treatment with elranatamab should be discontinued if the patient experiences disease progression (as defined radiologically or biochemically), loss of response, unacceptable toxicity such as grade 3 or grade 4 infection or CRS, light chain or renal dysfunction, or increasing transfusion requirement.
Prescribing Considerations
The clinical experts noted that patients receiving elranatamab should be under the care of a specialist (e.g., hematologist, oncologist) familiar with myeloma and the use of bispecific antibodies, and who can manage toxicity associated with the therapy. They noted that elranatamab can be given in most centres experienced with myeloma therapy, and that the first few doses usually require hospitalization.
Clinician Group Input
This section was prepared by the CADTH review team based on the input provided by clinician groups. The full original clinician group input received by CADTH has been included in the Stakeholder section of this report.
Clinician group input on the review of elranatamab was received from 2 clinician groups: the CMRG and OH-CCO’s Hematology Cancer Drug Advisory Committee (OH-CCO’s Drug Advisory Committees). A total of 33 clinicians (26 from CMRG and 7 from OH-CCO’s Drug Advisory Committees) provided input for this submission.
Both CMRG and OH-CCO’s Drug Advisory Committees emphasized that the overall treatment goals are to delay progression, improve OS, minimize adverse effects, control the disease and associated symptoms, and improve quality of life. While discussing the unmet needs of patients, CMRG highlighted that myeloma remains incurable and patients eventually become refractory to all available funded drugs, similar to the statements of the clinical experts consulted by CADTH. CMRG emphasized that the highest unmet need consists of patients with advanced disease who have received multiple lines of treatment and have already received the 3 major classes of drugs (TCE or refractory) including an IMiD, PI, and anti-CD38 mAb. Another unmet need noted by OH-CCO Drug Advisory Committees is to achieve ease of administration with elranatamab (i.e., subcutaneous injection and no need for apheresis).
Similar to the clinical experts consulted by CADTH, both clinician groups agreed that elranatamab could be another option for TCE patients. CMRG further stated that presently, this treatment would be used late in the current lines of myeloma treatment (i.e., after the failure of multiple drugs). Moreover, CMRG added that elranatamab is not expected to impact the sequencing of drugs earlier in the disease course or lead to a major change in treatment algorithms before patients becoming TCE or refractory.
CMRG indicated that patients with a good performance status, minimal or no comorbidities, relatively low tumour burden, adequate organ function, and satisfactory blood counts are the patients most likely to have the best outcomes with elranatamab. CMRG noted that overall, patients with poor disease-related prognostic factors, such as extramedullary myeloma and high-risk cytogenetics, should be eligible for the treatment under review.
OH-CCO Drug Advisory Committees noted that treatment responses with elranatamab are based on standard myeloma response measures, CRS, and ICANS toxicity grading scales. CMRG elaborated that responses are based on monoclonal protein markers in the serum and/or urine, a bone marrow biopsy, and in some instances, imaging studies. CMRG added that clinically meaningful responses usually correlate with at least a partial remission as defined by IMWG consensus criteria, including an improvement in symptoms (the cessation of bone destruction with less pain, fewer fractures, and less need for radiotherapy), an improvement in energy, and better ability to perform activities of daily living. Both CMRG and OH-CCO’s Drug Advisory Committees agreed that treatment discontinuation is based on ongoing efficacy or response, disease progression, and long-term tolerability or significant toxicities.
Given that prior anti-BCMA exposure does not preclude responsiveness to subsequent anti-BCMA therapy, CMRG suggests that patients with prior anti-BCMA therapy who did not progress during it (i.e., nonrefractory to anti-BCMA therapy) be allowed access to elranatamab.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 4.
Table 4: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Relevant comparators | |
The MagnetisMM-3 study is an open-label, single-arm, phase II trial. The CADTH submission is based on data from cohort A, which did not allow prior BCMA-directed therapies. Relevant comparators that are funded in some or most jurisdictions include Pd or PCd, Kd or KCd, and SVd. How does elranatamab compare to Pd or PCd, Kd or KCd, or SVd? | The CADTH team noted that the comparison between elranatamab and relevant comparators was to be addressed in the Clinical Review Report. The clinical experts noted that, to their knowledge, the direct comparative efficacy and safety between elranatamab and relevant comparators is unknown. |
Cilta-cel is also used in this setting; however, it is under active negotiation at the time of this input. The CADTH reimbursement conditions for cilta-cel specified that it should not be reimbursed in patients who have received prior treatment with therapy targeting BCMA. | This is a comment from the drug plans to inform pERC deliberations. |
Considerations for initiation of therapy | |
The elranatamab submission was based on the MagnetisMM-3 trial’s cohort A, which did not allow prior BCMA-directed therapy. Should patients previously treated with BCMA-directed therapy (e.g., belantamab mafodotin, cilta-cel) be eligible for elranatamab? Should patients treated with elranatamab be eligible for CAR T-cell therapy (e.g., cilta-cel)? What evidence is there to support the aforementioned sequences? | The clinical experts noted that although the results for cohort B (patients with prior BCMA-directed treatments) were not as promising as those for cohort A (patients with no prior BCMA-directed treatments), patients with previous BCMA-directed therapy should be eligible for elranatamab. The clinical experts indicated that there are no data to support whether patients treated with elranatamab would benefit from subsequent CAR T-cell therapy. They noted that the target of the treatments is the same; however, the T-cells are being activated through a different mechanism with CAR T-cell therapy and therefore may be active when elranatamab-activated T-cells fail. The clinical experts noted that, to their knowledge, there is no evidence to support the aforementioned sequences. |
Are 3 prior lines of therapy required if a patient is refractory to a proteosome inhibitor, an immunomodulatory drug, and an anti-CD38 monoclonal antibody as part of an earlier line of therapy (e.g., by second-line therapy)? | The clinical experts noted that 3 prior lines of therapy should not be required, and it would be more reasonable for patients to have been treated with a proteosome inhibitor, an immunomodulatory drug, and an anti-CD38 monoclonal antibody, or have been refractory to these therapies. The clinical experts indicated that with current therapies, they are combining multiple classes of antimyeloma drugs to treat patients. Upon progression, patients have fewer options with current standard of care drugs and, therefore, access to anti-BCMA therapy in these situations makes sense (and should be even more effective with less exhausted and/or damaged T-cells), although these patients were not included in the MagnetisMM-3 trial. |
Considerations for discontinuation of therapy | |
The product monograph has specific recommendations for restarting after dose delays, some of which require a re-administration of step-up dosing. | This is a comment from the drug plans to inform pERC deliberations. |
Considerations for prescribing of therapy | |
Elranatamab must be administered according to a step-up dosing schedule to minimize the risk and severity of CRS and ICANS: 12 mg SC on day 1 and 32 mg SC on day 4 of week 1, cycle 1, followed by 76 mg SC once weekly in 28-day cycles. After 6 cycles, patients who have attained and maintained a partial response or better for at least 2 months can be transitioned to dosing of once every 2 weeks (starting cycle 7, day 1). The MagnetisMM-3 trial allowed patients to go back to weekly dosing if the patient subsequently began to have a disease burden that did not yet qualify as progressive disease according to IMWG criteria. Can pERC confirm what the dosing schedule should be? | The clinical experts noted that it would be reasonable for patients to switch back to weekly dosing if patients begin to have disease burden that does not qualify as progressive disease. |
Teclistamab is under review for a similar indication. Should the reimbursement criteria for elranatamab be aligned with that of teclistamab? | The clinical experts indicated that it would be reasonable for the 2 drugs to have similar reimbursement criteria if they are recommended for reimbursement by pERC. |
Generalizability | |
The MagnetisMM-3 trial included patients with ECOG PS ≤ 2. Should elranatamab be used in the following patients:
| The clinical experts noted that although there are no data from the MagnetisMM-3 trial to answer this question, it would be reasonable to use elranatamab in patients with CNS disease that is under treatment or controlled, and plasma cell leukemia or amyloidosis. They noted that CNS myeloma is not common, and both plasma cell leukemia and amyloidosis are diseases mediated by plasma cell clones that express BCMA and, therefore, elranatamab would likely have activity. |
At the time of funding, should patients receiving alternative therapies (e.g., Pd or PCd, Kd or KCd, SVd) be eligible to switch to elranatamab? | The clinical experts noted that the option could be provided, especially for patients not responding or not responding well or experiencing toxicities associated with the alternative treatments. They noted that if a patient is responding to 1 of these drug combinations, they would likely maximize and maintain the response as long as possible. |
Funding algorithm (oncology only) | |
Complex therapeutic space with multiple lines of therapy, subpopulations, or competing products | This is a comment from the drug plans to inform pERC deliberations. |
Under what clinical circumstances would elranatamab be preferred over teclistamab or over cilta-cel, and vice versa? There may be interest in sequencing elranatamab with other BCMA-directed drugs. | One of the clinical experts noted that they would likely prioritize cilta-cell before a bispecific, if there are no clinical or logistical issues. The clinical experts noted that the toxicity profile and likelihood of CRS could be a consideration. They indicated that elranatamab is given subcutaneously, which could be an advantage over the other therapies where infusion access is limited, although elranatamab still needs to be given in a trained infusion or chemotherapy unit. They also noted that using a bispecific over CAR T-cell therapy may be necessary when geographic access or capacity is an issue and where immediate treatment is required. |
Care provision issues | |
Elranatamab is supplied as single use vials of 44 mg and 76 mg (both with a similar concentration of 40 mg/mL). A step-up dosing regimen of 12 mg and 32 mg is required during initiation and also during restarts, which would result in drug wastage. The drug may need to be initiated in the inpatient setting, in which case, the drug cost would be outside the drug program budget in some provinces and territories. | This is a comment from the drug plans to inform pERC deliberations. |
CRS and ICANS can occur with elranatamab, although the severity and incidence appeared to be low in the trial. The funding of tocilizumab needs to be incorporated as part of any implementation to ensure that sites have tocilizumab available to manage CRS and ICANS. Other therapies (i.e., anakinra) may be required to treat ICANS. | This is a comment from the drug plans to inform pERC deliberations. |
The monograph states that elranatamab should be administered by a health care professional with access to appropriate medical support to manage severe reactions, including CRS and neurologic toxicity. Is it safe to administer elranatamab in the outpatient setting? | The clinical experts noted that based on the very low frequency of grade 3 or greater CRS reported in the MagnetisMM-3 trial, it seems that CRS can be managed as an outpatient procedure, as long as the treating clinicians are experienced in diagnosing and managing CRS. They indicated that patients who are high risk for CRS (i.e., those with large disease burden, elevated creatinine) could be monitored more closely, perhaps as an inpatient. |
System and economic issues | |
There is concern about the feasibility of adoption (budget impact and capacity) but there is uncertainty on what the uptake for elranatamab will be. | This is a comment from the drug plans to inform pERC deliberations. |
There are additional costs associated with the requirement of tocilizumab for CRS, which impact drug program budgets (acute care). Additional resources would also be required for the management of infections, which can be quite severe. | This is a comment from the drug plans to inform pERC deliberations. |
Generic pomalidomide is available, and confidential pricing exists for carfilzomib and selinexor. | This is a comment from the drug plans to inform pERC deliberations. |
BCMA = B-cell maturation antigen; CAR = chimeric antigen receptor; cilta-cel = ciltacabtagene autoleucel; CNS = central nervous system; CRS = cytokine release syndrome; ECOG PS = Eastern Cooperative Oncology Group Performance Status; ICANS = immune effector cell-associated neurotoxicity syndrome; IMWG = International Myeloma Working Group; KCd = carfilzomib plus dexamethasone in combination with cyclophosphamide; Kd = carfilzomib plus dexamethasone; PCd = pomalidomide plus dexamethasone in combination with cyclophosphamide; Pd = pomalidomide plus dexamethasone; pERC = pan-Canadian Oncology Drug Review Expert Review Committee; SC = subcutaneous; SVd = selinexor plus bortezomib and dexamethasone.
Clinical Evidence
The objective of CADTH’s Clinical Review Report is to review and critically appraise the clinical evidence submitted by the sponsor on the beneficial and harmful effects of elranatamab 40 mg/mL, subcutaneous injection, for the treatment of adults with RRMM who have received at least 3 prior lines of therapy, including a PI, an IMiD, and an anti-CD38 mAb, and who have demonstrated disease progression on the last therapy. The focus will be placed on comparing elranatamab to relevant comparators and identifying gaps in the current evidence.
A summary of the clinical evidence included by the sponsor in the review of elranatamab is presented in 3 sections, with CADTH’s critical appraisal of the evidence included at the end of each section. The first section, the systematic review, includes pivotal studies and RCTs that were selected according to the sponsor’s systematic review protocol. CADTH’s assessment of the certainty of the evidence in this first section using the GRADE approach follows the critical appraisal of the evidence. The second section includes indirect evidence from the sponsor. The third section includes additional studies that were considered by the sponsor to address important gaps in the systematic review evidence.
Included Studies
Clinical evidence from the following is included in the CADTH review and appraised in this document:
One pivotal trial
Two indirect treatment comparisons
Three additional studies addressing gaps in the pivotal and/or RCT evidence.
In addition, a multicentre retrospective cohort study that used the CMRG database to describe RW outcomes in patients with anti-CD38 mAb refractory MM subsequently treated with SOC regimens is summarized in Appendix 1.
Systematic Review
Content in this section has been informed by materials submitted by the sponsor. The following has been summarized and validated by the CADTH review team.
Description of Studies
Characteristics of the included studies are summarized in Table 5.
The MagnetisMM-3 study is an ongoing, phase II, nonrandomized, noncomparative, open-label, multicentre trial that aims to assess the efficacy and safety of elranatamab 76 mg, subcutaneous injection, once weekly after 2 step-up priming doses followed by dosing every 2 weeks in adults with RRMM (Figure 1).3 The trial enrolled adults with a prior diagnosis of MM and measurable disease who either had previous experience with BCMA-directed treatment (cohort B) or did not (cohort A). Patients had to have been disease-refractory to at least 1 PI, 1 IMiD, and 1 anti-CD38 antibody, and disease-relapsed or disease-refractory to their last antimyeloma regimen. The 2 cohorts were analyzed separately.
The trial enrolled 187 patients (cohort A, n = 123; cohort B, n = 64) across 10 countries, including 13 patients from 5 Canadian centres. The trial included a screening phase up to 28 days, and a treatment phase that included 28-day cycles until discontinuation criteria were met, which included confirmed disease progression, unacceptable toxicity, withdrawal of consent, death, or study termination. All patients were followed up at 28 days to 35 days after treatment discontinuation, with long-term follow-up of 2 years or longer after enrolment.
The outcomes relevant to the CADTH review included the primary outcome of ORR by BICR per IMWG criteria, and secondary outcomes of PFS, OS, CRR, DOR, and safety. HRQoL measured via the EORTC QLQ-MY20 tool was included as an exploratory outcome.
Efficacy and safety data were evaluated at a planned analysis data cut-off date of October 14, 2022, and additional follow-up data to a cut-off date of March 14, 2023.
Table 5: Details of Studies Included in the Systematic Review
Detail | MagnetisMM-3 trial |
|---|---|
Designs and populations | |
Study design | Phase II, open-label, multicentre, noncomparative, nonrandomized trial
|
Locations | 53 centres across 10 countries: Australia, Belgium, Canada, Germany, Spain, France, Great Britain, Japan, Poland, and the US
|
Patient enrolment dates | Study initiation date: February 2, 2021 Planned analysis for primary end point for cohort A and cohort B: October 14, 2022 Data cut-off date for this submission: March 14, 2023 |
Randomization (N) | Patients were not randomized. A total of 187 eligible patients were assigned to treatment (cohort A, n = 123 patients; cohort B, n = 64 patients) |
Key inclusion criteria |
|
Key exclusion criteria |
|
Drugs | |
Intervention | Elranatamab 76 mg, injected subcutaneously:
|
Comparator(s) | None |
Study duration | |
Screening phase | Up to 28 days before starting study treatment |
Treatment phase | Treatment in 28-day cycles until treatment discontinuation or study withdrawal (i.e., because of confirmed disease progression, unacceptable toxicity, withdrawal of consent, or study termination) |
Follow-up phase | A follow-up visit was conducted at 28 days to 35 days after treatment discontinuation, with long-term follow-up for ≥ 2 years after enrolment |
Outcomes | |
Primary end point | ORR by BICR per IMWG criteria |
Secondary and exploratory end points | Key secondary (statistically tested):
Secondary (descriptive):
Exploratory (descriptive):
|
Publication status | |
Publications | Lesokhin et al. (2023)32 |
ADC = antibody-drug conjugate; ASTCT = American Society for Transplantation and Cellular Therapy; BCMA = B-cell maturation antigen; BICR = blinded independent central review; CAR = chimeric antigen receptor; CRR = complete response rate; CRS = cytokine release syndrome; DOCR = duration of complete response; DOR = duration of response; ECOG PS = Eastern Cooperative Oncology Group Performance Status; EMD = extramedullary disease; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EORTC QLQ-MY20 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Multiple Myeloma 20; GBS = Guillain-Barré syndrome; GVHD = graft-vs.-host disease; HBV = hepatitis B virus; HCV = hepatitis C virus; ICANS = immune effector cell-associated neurotoxicity syndrome; ICU = intensive care unit; IMiD = immunomodulatory drug; IMWG = International Myeloma Working Group; MM = multiple myeloma; MRD = minimal residual disease; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; PI = proteasome inhibitor; POEMS = polyneuropathy, organomegaly, endocrinopathy, myeloma protein, and skin changes; SARS-CoV-2 = severe acute respiratory syndrome coronavirus 2; TTR = time to response; ULN = upper limit of normal.
Note: Details included in Table 5 are from the sponsor’s Summary of Clinical Evidence.
Source: MagnetisMM-3 Clinical Study Report.3[Details included in the table are from the sponsor’s Summary of Clinical Evidence].
Populations
Inclusion and Exclusion Criteria
A detailed description of the inclusion and exclusion criteria for the MagnetisMM-3 trial is provided in Table 5. Eligible patients were adults with MM with measurable disease as defined by IMWG criteria. Patients had to have disease that was refractory (defined as having disease progression while on therapy, or within 60 days of the last dose in any line, regardless of response) to at least 1 or more PI, IMiD, and anti-CD38 antibody, and disease-relapsed or disease-refractory to their last regimen. Patients eligible for cohort A must not have received prior BCMA-directed therapy, while patients eligible for cohort B must have received prior BCMA-directed antibody-drug conjugate or BCMA-directed chimeric antigen receptor (CAR) T-cell therapy. Patients were required to have an ECOG PS of less than or equal to 2, a left ventricular ejection fraction greater than or equal to 40%, and adequate bone marrow, hepatic, and renal functions. Patients were excluded if they had smouldering MM; active plasma cell leukemia; amyloidosis or polyneuropathy, organomegaly, endocrinopathy, myeloma protein, skin changes syndrome; a stem cell transplant 12 weeks or less before enrolment or active graft-versus-host disease; or any active, uncontrolled bacterial, fungal, or viral infection. Patients were also excluded if they had impaired cardiovascular function or clinically meaningful cardiovascular disease for 6 months or less.
Figure 1: Study Design of MagnetisMM-3 Trial
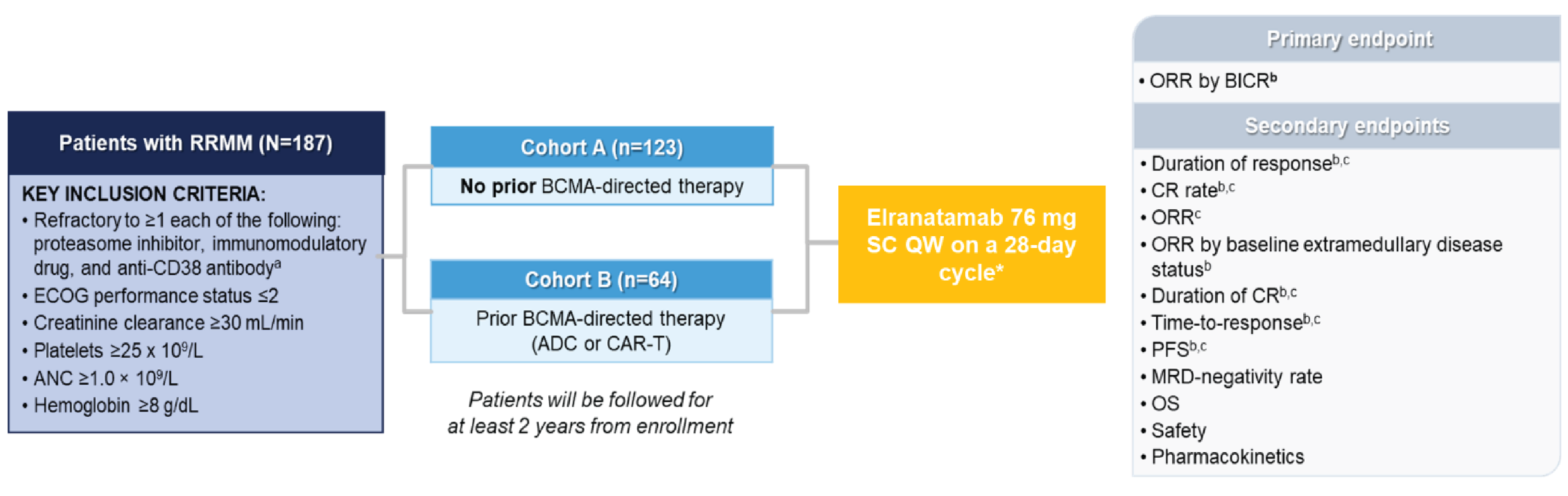
ADC = antibody-drug conjugate; ANC = absolute neutrophil count; BCMA = B-cell maturation antigen; BICR = blinded independent central review; BsAb = bispecific antibody; CAR t = chimeric antigen receptor T-cell therapy; CR = complete response; ECOG = Eastern Cooperative Oncology Group; IMWG = International Myeloma Working Group; min = minute; MM = multiple myeloma; MRD = minimal residual disease; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; POEMS = polyneuropathy, organomegaly, endocrinopathy, myeloma protein, and skin changes; Q2W = every 2 weeks; QW = every week; RRMM = relapsed or refractory multiple myeloma; SC = subcutaneous.
Note: Details included in Figure 1 are from the sponsor’s Summary of Clinical Evidence.
Prior BCMA-directed treatments included ADC or CAR-Ts (no prior BCMA-directed BsAb).
* If a patient attained an IMWG response category of partial response or better persisting for at least 2 months, the dosage interval could be changed from QW to Q2W.
a Refractory is defined as having disease progression while on therapy or within 60 days of the last dose in any line, regardless of response. MM with measurable disease is as defined by IMWG criteria. Patients with an active or clinically significant bacterial, fungal, or viral infection, POEMS syndrome, and those who received a stem cell transplant within 12 weeks before enrolment were excluded.
b BICR assessment per IMWG response criteria.
c Investigator assessment per IMWG response criteria.
Source: Bahlis et al. (2022).33
Interventions
Patients received elranatamab 76 mg by subcutaneous injection once a week on a 28-day cycle with a 2 step-up priming dose regimen of 12 mg on day 1 and 32 mg on day 4 during the first week (4 patients received a single 44 mg priming dose). Hospitalization was required for 48 hours following the first step-up dose and for 24 hours after the second step-up dose. Premedication with acetaminophen (650 mg), diphenhydramine (25 mg), and dexamethasone (20 mg) were required before each step-up dose and before the first full dose of elranatamab. Patients who received once a week dosing for at least 6 cycles and attained a partial response or better persisting for at least 2 months had their dosing interval changed to once every 2 weeks. Dose reductions and interruptions were permitted for toxicity. Elranatamab treatment was to be continued until patient refusal, loss to follow-up, death, disease progression, or unacceptable toxicity.
Outcomes
A list of efficacy end points assessed in this Clinical Review Report is provided in Table 6, followed by descriptions of the outcome measures. Summarized end points are based on outcomes included in the sponsor’s Summary of Clinical Evidence as well as any outcomes identified as important to this review according to the clinical experts consulted by CADTH and stakeholder input from patient and clinician groups and public drug plans. Using the same considerations, the CADTH review team selected end points that were considered to be the most relevant to inform CADTH’s expert committee deliberations and finalized this list of end points in consultation with members of the expert committee. All summarized efficacy end points were assessed using GRADE.
Table 6: Outcomes Summarized From the Studies Included in the Systematic Review
Outcome measure | Time point | MagnetisMM-3 trial |
|---|---|---|
ORR by BICR | At any time from the first dose of elranatamab until the first instance of confirmed progressive disease or the start of new anticancer therapy | Primarya |
PFS by BICR | At 6 months, 9 months, 12 months, and 15 months | Secondary |
Overall survival | At 6 months, 9 months, 12 months, and 15 months | Secondary |
CRR by BICR | At any time from the first dose of elranatamab until the first instance of confirmed progressive disease or the start of new anticancer therapy | Secondary |
Duration of response | At 6 months, 9 months, 12 months, and 15 months | Secondary |
CRR | At any time from the first dose of elranatamab until the first instance of confirmed progressive disease or the start of new anticancer therapy | Secondary |
EORTC QLQ-MY20 | At cycle 15 | Exploratory |
BICR = blinded independent central review; CRR = complete response rate; EORTC QLQ-MY20 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Multiple Myeloma 20; ORR = objective response rate; PFS = progression-free survival.
Note: Details included in Table 6 are from the sponsor’s Summary of Clinical Evidence.
aStatistical testing for this outcome was adjusted for multiple comparisons (e.g., hierarchical testing).
Source: MagnetisMM-3 Clinical Study Report.3
Objective Response Rate
The primary outcome for the MagnetisMM-3 trial was ORR assessed by BICR, defined as confirmed partial response or better according to IMWG criteria from the date of first dose until confirmed progressive disease, death, or the start of new anticancer therapy, whichever occurred first. Patients who did not have a postbaseline disease assessment due to early confirmed progressive disease, who received anticancer therapy other than the study intervention before achieving an OR, or who died, experienced confirmed progressive disease, or stopped disease assessments for any reason before achieving an OR were counted as nonresponders.
Progression-Free Survival
The secondary outcome of PFS was defined as the time from the date of first dose until confirmed progressive disease per IMWG criteria or death due to any cause, whichever occurred first, or censoring. PFS was censored on the date of the last adequate disease assessment for patients who did not have an event (i.e., confirmed progressive disease per IMWG criteria or death due to any cause), before the start of a new anticancer therapy, or when there were 2 consecutive missed disease assessments. Participants who did not have an adequate postbaseline disease assessment were censored on the date of the first dose unless death occurred on or before the time of the second planned disease assessment (i.e., ≤ 70 days after the date of the first dose), in which case the death was considered an event. Tumour assessments were done with CT or MRI at screening and at suspected complete response (if not performed within the prior 6 weeks), at the sign of progressive disease from extramedullary disease, and annually if not done within the past 12 months.
Overall Survival
The secondary outcome of OS was defined as the time from the first dose to death due to any cause or censoring. Patients not known to have died were censored at the last contact date.
Complete Response Rate
The secondary outcome of CRR assessed by BICR was defined as confirmed complete response or better according to IMWG criteria at any time from the first treatment dose until confirmed progressive disease or the start of new anticancer therapy.
Duration of Response
The secondary outcome of DOR was defined as the time from the first confirmed response to confirmed progressive disease or death due to any cause, whichever was earlier, or censoring. Patients were censored at the last valid assessment before the initiation of new anticancer therapy or when there were 2 consecutive missed efficacy assessments before an event.
Health-Related Quality of Life
The exploratory outcome HRQoL was measured by change in baseline in the EORTC QLQ-MY20 tool. A summary of its measurement properties is in Table 7. The EORTC QLQ-MY20 is an MM-specific module of the European Organisation for Research and Treatment of Cancer questionnaire that contains 20 items that use 4-point Likert scales, and are grouped into 2 functional scales (future perspective, body image) and 2 symptom scales (disease symptoms, side effects of treatment). Patients self-rate their current state for each item and scores are linearly transformed onto a scale of 0 to 100. Higher scores indicate worse symptoms (disease symptoms and side effects of treatment) or better support or functioning (future perspectives and body image). One study of patients with MM has estimated minimal important differences of 10 points for disease symptoms, 10 points for side effects of treatment, 13 points for body image, and 9 points for future perspective.34 Assessments were performed at baseline (day 1 and day 15), end of treatment (28 days to 35 days post–final dose), and once every 3 cycles after year 1.
Safety Outcomes
The assessment of safety was based on the incidence of treatment-emergent adverse events (TEAEs), serious TEAEs, notable TEAEs, TEAEs leading to discontinuation, TEAEs leading to dose modification, and deaths. AEs were reported throughout the study period and coded to preferred term and system organ class using the Medical Dictionary for Regulatory Activities and classified by severity using the National Cancer Institute’s Common Terminology Criteria for Adverse Events, version 5.0, except for CRS and ICANS, which were graded according to the criteria of the American Society for Transplantation and Cellular Therapy. TEAEs were defined as any event occurring from the first dose of elranatamab through the minimum of 90 days after the last elranatamab dose or the start of new anticancer therapy.
Table 7: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
EORTC QLQ-MY20 | A 20-item myeloma module intended for use only in conjunction with the EORTC QLQ-C30. The module consists of 3 multi-item subscales — disease symptoms, side effects of treatment, and future perspective — and 1 single item subscale, body image.35 | Validity: After removing the social support scale (4 items) in the EORTC QLQ-MY24 due to the ceiling effects, the psychometric properties of the resultant EORTC QLQ-MY20 were evaluated by Cocks et al.36 Patients had to be in a clinical trial at the time of this field study and have had either newly diagnosed MM (N = 225) or relapsed or refractory MM (N = 15).36 For known-groups comparison, the EORTC QLQ-MY20 scale scores for patients with a WHO performance status of 0, 1, or 2 (N = 200) were compared to patients with a WHO performance status of 3 or 4 (N = 25) at baseline. Only the disease symptoms, side effects of treatment, and body image scales demonstrated differences between patient groups according to their performance status (0,1, or 2 vs. 3 or 4).36 Reliability: Not assessed in patients with MM Responsiveness: In addition to validity, Cocks et al.36 evaluated the responsiveness of EORTC QLQ-MY20. For responsiveness to change, the scale scores at baseline were compared to follow-up (during or on completion of the respective trial treatment) for 137 (57%) patients who attained at least partial response. The scale scores for disease symptoms and body image decreased over time with treatment while the scale scores for treatment side effects increased.36 | The following estimated MIDs were derived for patients with MM (both newly diagnosed and relapsed or refractory):34
|
EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EORTC QLQ-MY20 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Multiple Myeloma 20; EORTC QLQ-MY24 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Multiple Myeloma 24; MID = minimal important difference; MM = multiple myeloma.
Statistical Analysis
A summary of the statistical analysis of efficacy outcomes is provided in Table 8.
Sample Size and Power Calculation
Sample sizes were calculated separately for cohort A and cohort B. In cohort A, 120 treated patients would provide approximately 98% power at a 1-sided significance level of 0.025 to reject the null hypothesis (ORR by BICR ≤ 30%) if the observed ORR was greater than or equal to 48%. In cohort B, 60 treated patients would provide approximately 95% power at a 1-sided significance level of 0.025 to reject the null hypothesis (ORR by BICR ≤ 15%) if the observed ORR was greater than or equal to 34%. The rationale for these thresholds was not reported in the sponsor’s submission.
Statistical Testing
Point estimates of ORR by BICR in cohort A and cohort B were calculated along with the 2-sided exact 95% CIs using the Clopper-Pearson method. The null hypotheses were tested at a 1-sided alpha of 0.025 independently in the 2 cohorts. PFS and OS were analyzed using the Kaplan-Meier method and displayed graphically, and median PFS and OS times with 2-sided 95% CIs were calculated using the Brookmeyer-Crowley method. The CIs for the survival function estimates at different time points were derived using the log-log method according to the Kalbfleisch-Prentice method. Point estimates for CRR were calculated using the same method as for ORR. If at least 3 participants attained an OR and subsequently had an event, DOR was estimated using the same method as described for PFS and OS. The analysis of the EORTC QLQ-MY20 scales were summarized using descriptive statistics. Efficacy outcomes were not adjusted for covariates or baseline variables, and sensitivity analyses or analyses used to handle missing data were not performed. No adjustments for multiple comparisons were made for the included outcomes.
Cohort A crossed the efficacy boundary at the first planned interim analysis (data cut-off date of March 23, 2022) based on the first 94 patients while cohort B crossed the efficacy boundary at the final analysis (data cut-off date of June 17, 2022). Additional data were provided at the March 14, 2023, data cut-off date.
Subgroup Analysis
The following prespecified subgroups of interest were assessed for the primary outcome of ORR: age (< 65 years versus ≥ 65 years; < 75 years versus ≥ 75 years), baseline cytogenetics risk groups (high risk versus standard risk), prior stem cell transplant (yes versus no), disease stage (I to II versus III) according to the R-ISS, and the number of prior lines of therapy (≤ 5 versus > 5). The subgroup analyses were not adjusted for multiplicity.
Sensitivity Analyses and Data Imputation Methods
Sensitivity analyses and data imputation were not performed.
Analysis Populations
The efficacy and safety outcomes were analyzed based on the safety analysis set, defined as patients who received at least 1 dose of elranatamab. The HRQoL outcome was analyzed based on all patients from the safety analysis set who completed a baseline assessment and at least 1 postbaseline assessment.
Table 8: Statistical Analysis of Efficacy End Points — MagnetisMM-3 Trial
End point | Statistical model | Adjustment factors | Handling of missing data | Sensitivity analyses |
|---|---|---|---|---|
ORR by BICR | Point estimates with 2-sided 95% CI were calculated using the Clopper-Pearson method. | None | None | Patients were treated as nonresponders, if untreated. |
PFS by BICR | Kaplan-Meier method and median values with 2-sided 95% CIs were calculated using the Brookmeyer-Crowley method. Survival rates at specific times estimated with 2-sided 95% CIs were calculated using the Kalbfleisch-Prentice method. | None | None | None |
Overall survival | ||||
DOR by BICR | ||||
CRR by BICR | Point estimates with 2-sided 95% CI were calculated using the Clopper-Pearson method. | None | None | None |
EORTC QLQ-MY20 | Summarized descriptively | None | None | None |
BICR = blinded independent central review; CI = confidence interval; CRR = complete response rate; DOR = duration of response; EORTC QLQ-MY20 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Multiple Myeloma 20; ORR = objective response rate; PFS = progression-free survival.
Note: Details included in Table 8 are from the sponsor’s Summary of Clinical Evidence.
Source: MagnetisMM-3 Clinical Study Report.3
Results
Patient Disposition
A summary of patient disposition is in Table 9. In total, 237 patients were screened, and 187 patients were assigned to elranatamab treatment (cohort A = 123; cohort B = 64). Reasons were not reported for the 45 patients who were screened out and 5 patients not enrolled. At the March 14, 2023, data cut-off, 82 (66.7%) patients in cohort A and 51 (79.7%) patients in cohort B discontinued treatment. The most common reason for discontinuation in both groups was disease progression (cohort A = 48; cohort B = 29), followed by AEs (cohort A = 17; cohort B = 7), and death (cohort A = 9; cohort B = 9).
Baseline Characteristics
A summary of baseline patient demographics and disease characteristics of the safety population are in Table 10. The characteristics outlined in the table are limited to those that are most relevant to this review or were felt to affect the outcomes or interpretation of the study results. The trial population was predominately white (███), with a similar proportion of male and female patients who had a mean age of ██ years ████ ████ ███████ ██ ███ ██ █████). Most patients had an ECOG PS score of 1 (███) and 0 (███), indicating good overall performance, an R-ISS disease stage of II (███), standard cytogenetic risk (███), and a prior stem cell transplant (███). Patients had received an average of | prior lines of therapy, ███ had TCR disease, and ███ had penta-drug refractory disease (refractory to at least 2 PIs, 2 IMiDs, and 1 anti-CD38 antibody). ████████ ███ ███████████████ ████ █████████ ██████████ ███████ ████████ ████████ ██████ █ ███ █ ██████ ████ ████ █████ █████ █████████ ██████ ██████ ████ ████████ ███ ████████ ██ ███████ ████ █████ ██████████ █████████ ██████████ ███ ██████████ ████ ██████ ██
Table 9: Summary of Patient Disposition — MagnetisMM-3 Trial
Patient disposition | MagnetisMM-3 trial | |
|---|---|---|
Cohort A | Cohort B | |
Screened, N (%) | 237 (100) | |
Did not meet screening criteria, N (%) | 45 (NR) | |
Met screening criteria but did not enrol, N (%) | 5 (NR) | |
Reason for not meeting screening criteria, n (%) | ||
Not reported | 5 (NR) | |
Treated, N (%) | 123 (100) | 64 (100) |
Discontinued from study, n (%) | 82 (66.7) | ██ ██████ |
Reason for discontinuation, n (%) | ||
Progressive disease | 48 (39.0) | ██ █████ |
Adverse event | 17 (13.8) | ██████ |
Death | 9 (7.3) | ██████ |
Withdrawal by patient | 4 (3.3) | █████ |
Lack of efficacy | 3 (2.4) | █████ |
Global deterioration of health status | 1 (0.8) | █████ |
Refused further study procedures | 0 | █████ |
Ongoing in study as of March 14, 2023, data cut-off, N (%) | 41 (33.3) | ██ ██████ |
Safety analysis set, N | 123 | ██ |
PRO analysis set, N (%) | ███ ██████ | ██ ██████ |
NR = not reported; PRO = patient-reported outcome.
Note: Details included in Table 9 are from the sponsor’s Summary of Clinical Evidence.
Source: MagnetisMM-3 Clinical Study Report.3
Table 10: Summary of Baseline Characteristics — MagnetisMM-3 Trial
Characteristic | MagnetisMM-3 trial | ||
|---|---|---|---|
Cohort A (N = 123) | Cohort B (N = 64) | Total (N = 187) | |
Age, years, mean (SD) | 67.1 (9.45) | ████ ██████ | ████ ██████ |
≥ 65 years, n (%) | 80 (65.0) | ██ ██████ | ███ ██████ |
≥ 75 years, n (%) | 24 (19.5) | ██ ██████ | ██ ██████ |
Sex, n (%) | |||
Female | 68 (55.3) | ██ ██████ | ██ ██████ |
Male | 55 (44.7) | ██ ██████ | ██ ██████ |
Race, n (%) | |||
White | 72 (58.5) | ██ ██████ | ███ ██████ |
Black or African American | 9 (7.3) | █████ | ██ █████ |
Asian | 16 (13.0) | █████ | ██ █████ |
Unknown | 2 (1.6) | █████ | ████ |
Not reported | 24 (19.5) | ██ ██████ | ██ ██████ |
ECOG PS, n (%) | |||
0 | 45 (36.6) | ██ ██████ | ██ ██████ |
1 | 71 (57.7) | ██ ██████ | ███ ██████ |
2 | 7 (5.7) | █████ | ██ █████ |
Disease stage (R-ISS), n (%) | |||
I | 28 (22.8) | ██ ██████ | ██ ██████ |
II | 68 (55.3) | ██ ██████ | ███ ██████ |
III | 19 (15.4) | ██ ██████ | ██ ██████ |
Unknown | 8 (6.5) | █████ | ██ █████ |
Cytogenetic risk, n (%) | |||
Standard | 83 (67.5) | ██ ██████ | ███ ██████ |
High | 31 (25.2) | ██ ██████ | ██ ██████ |
Missing | 9 (7.3) | ██████ | ██ █████ |
Extramedullary disease by BICR, n (%) | |||
Yes | 39 (31.7) | ██ ██████ | ██ ██████ |
No | 84 (68.3) | ██ ██████ | ███ ██████ |
Type of myeloma, n (%) | |||
IgG | 65 (52.8) | ██ ██████ | ███ ██████ |
IgA | 20 (16.3) | ██████ | ██ ██████ |
IgD | 1 (0.8) | █████ | █████ |
Light chain only | 24 (19.5) | ██ ██████ | ██ ██████ |
Unknown | 13 (10.6) | █████ | ██ █████ |
Baseline bone marrow plasma cells, n (%) | |||
< 50% | 89 (72.4) | ██ ██████ | ███ ██████ |
≥ 50% | 26 (21.1) | ██ ██████ | ██ ██████ |
Missing | 8 (6.5) | ██████ | ██ █████ |
Renal function, n (%) | |||
CrCl ≤ 60 mL per minute | ██ ██████ | ██ ██████ | ██ ██████ |
CrCl > 60 mL per minute | ██ ██████ | ██ ██████ | ███ ██████ |
Liver function, n (%) | |||
Normal | ███ ██████ | ██ ██████ | ███ ██████ |
Impaired | ██ ██████ | ██ ██████ | ██ ██████ |
Patients with ≥ 1 poor prognosis feature,a n (%) | 81 (65.9) | ██ ██████ | ███ ██████ |
Time since first diagnosis of plasma cell myeloma, months | |||
Mean (SD) | 78.7 (45.87) | █████ ███████ | ████ ███████ |
Prior anticancer therapies | |||
Mean (SD) | 5.2 (2.58) | ███ ██████ | ███ ██████ |
1 to 3 lines, n (%) | ██ ██████ | █████ | ██ ██████ |
4 to 5 lines, n (%) | ██ ██████ | ██ ██████ | ██ ██████ |
> 5 lines, n (%) | ██ ██████ | ██ ██████ | ██ ██████ |
Triple-class refractory, n (%) | 119 (96.7) | ██ ██████ | ███ ██████ |
Penta-drug refractory, n (%)b | 52 (42.3) | ██ ██████ | ██ ██████ |
Prior stem cell transplant, n (%) | 87 (70.7) | ██ ██████ | ███ ██████ |
Autologous | ██ ██████ | ██ ██████ | ███ ██████ |
Allogeneic | █████ | █████ | █████ |
Syngeneic | █████ | █████ | █████ |
Unknown | █████ | █████ | █████ |
Prior BCMA-targeted therapy, n (%) | 0 | ██ ███████ | ██ ██████ |
ADC | 0 | ██ ██████ | ██ ██████ |
CAR T-cell | 0 | ██ ██████ | ██ ██████ |
ADC and CAR T-cell | 0 | █████ | █████ |
Anti-BCMA bispecific | 0 | █████ | █████ |
Refractory to BCMA-targeted therapy, n (%) | 0 | ██ ██████ | ██ ██████ |
ADC = antibody-drug conjugate; BCMA = B-cell maturation antigen; BICR = blinded independent central review; CAR = chimeric antigen receptor; CrCl = creatinine clearance; ECOG PS = Eastern Cooperative Oncology Group Performance Status; IgA = immunoglobulin A; IgD = immunoglobulin D; IgG = immunoglobulin G; R-ISS = Revised International Staging System; SD = standard deviation.
Note: Details included in Table 10 are from the sponsor’s Summary of Clinical Evidence.
aThis included participants who had at least 1 of the following: an ECOG PS score of 2, an R-ISS score of 3, extramedullary disease at baseline by BICR, high cytogenetic risk, or bone marrow plasma cell involvement greater than or equal to 50%.
bPenta-drug refractory disease is defined as being refractory to at least 2 proteasome inhibitors, 2 immunomodulatory drugs, and 1 anti-CD38 antibody.
Source: MagnetisMM-3 Clinical Study Report.3[Details included in the table are from the sponsor’s Summary of Clinical Evidence].
Exposure to Study Treatments
By the March 14, 2023, data cut-off, the median duration of treatment observed in the total population was ████ months ██████ █ ████ ██ ████ ████████ The median durations of treatment for cohort A and cohort B were 5.6 months (range, 0.03 months to 24.4 months) and ███ ██████ ██████ █ ████ ██ ████ ███████, respectively. The average dose intensity per week was █████ ██████████ █████ with █████ of patients experiencing 1 or more dose reduction or interruption, mostly (██████ due to AEs. The most common AEs leading to dose reduction or interruption were not reported. Most patients re-escalated to the 76 mg dose of elranatamab after requiring a dose reduction (██████ or dose interruption (███████ All patients received at least 1 or more concomitant medication, and almost all (██ ██ █████ received the first, second, and third doses of all 3 premedication drugs (antipyretics, antihistamines, and corticosteroids) as CRS prophylaxis. Infection prophylaxis was also commonly provided, most frequently involving antiviral medication (██████ and medication to prevent Pneumocystis jiroveci pneumonia ████████ Exposure to concomitant medications was generally consistent between cohorts.
Subsequent Treatment
A summary of subsequent anticancer therapy is in Table 11. Overall, ███ of patients received subsequent anticancer therapy after receiving elranatamab. The most common therapies included dexamethasone █████, cyclophosphamide ███ ██, or carfilzomib ██████ Two patients ██████ underwent subsequent transplants and no patients received follow-up radiation therapy. In general, subsequent treatments for patients in cohort A and cohort B were similar.
Table 11: Summary of Subsequent Treatment — MagnetisMM-3 Trial
Exposure | MagnetisMM-3 trial | ||
|---|---|---|---|
Cohort A (N = 123) | Cohort B (N = 64) | Total (N = 187) | |
Received subsequent anticancer therapy, n (%) | 38 (30.9) | ██ ██████ | ██ ██████ |
Medication | 38 (30.9) | ██ ██████ | ██ ██████ |
Radiation therapy | 0 | █████ | █████ |
Transplant | 1 (0.8) | █████ | █████ |
Most frequent anticancer medications (≥ 5%), n (%) | |||
Dexamethasone | 29 (23.6) | ██ ██████ | ██ ██████ |
Cyclophosphamide | 17 (13.8) | █████ | ██ ██████ |
Carfilzomib | 13 (10.6) | █████ | ██ ██████ |
Bortezomib | 11 (8.9) | █████ | ██ █████ |
Pomalidomide | 10 (8.1) | █████ | ██ █████ |
Selinexor | 5 (4.1) | █████ | ██ █████ |
Note: Details included in Table 11 are from the sponsor’s Summary of Clinical Evidence.
Source: MagnetisMM-3 Clinical Study Report.3
Efficacy
Only those efficacy outcomes and analyses of subgroups identified as important to this review were reported. The findings presented are from the 15-month analysis (March 14, 2023, data cut-off).
ORR by BICR
At the March 14, 2023, data cut-off, with a median follow-up of 14.7 months, the ORR in cohort A was 61.1% (95% CI, 51.8% to 69.6%; P < 0.0001) and █████ ████ ███ ████ ██ █████████████ in cohort B. These findings were consistent with the results at the 9-month analysis (data cut-off date of October 14, 2022).
ORR Subgroup Analyses
Forest plots of ORRs by BICR for cohort A and cohort B are in Figure 2 and Figure 3, respectively. In cohort A, the ORR results were consistent across subgroups by age, baseline cytogenetics risk, prior stem cell transplant, and number of prior lines of therapy. However, lower ORRs were observed in patients with R-ISS stage III. ██ ██████ ██ ███ ███ ███████ █████████████ ██████ ███ ██████████
PFS by BICR
Table 12 provides a summary of results for PFS by BICR. In total, 95 events had occurred in both cohorts by the March 14, 2023, data cut-off. The median follow-up for PFS was 14.7 months for cohort A and ███ months for cohort B. The median PFS was not reached (95% CI, 9.9 months to not estimable) in cohort A and ███ ██████ ████ ███ ███ ██ ████ in cohort B. The probability of being event-free at 12 months in cohort A was 56.6% (95% CI, 46.7% to 65.3%) and █████ ████ ███ ████ ████ in cohort B.
Table 12: Progression-Free Survival — MagnetisMM-3 Trial, Safety Analysis Set
MagnetisMM-3 trial | |||
|---|---|---|---|
Progression-free survival by BICR | Cohort A (N = 123) | Cohort B (N = 64) | Total (N = 187) |
March 14, 2023, data cut-off | |||
Patients with events, n (%) | |||
Total | 53 (43.1) | ██ ██████ | ██ ██ |
Progressive disease | 36 (29.3) | ██ ██████ | ██ ██ |
Death | 17 (13.8) | ██ ██████ | ██ ██ |
Patients censored | 70 (56.9) | ██ ██████ | ██ ██ |
Reason for censoring, n (%) | |||
Start of new anticancer therapy | ██ ██████ | █████ | ██ ██ |
Event after missing or inadequate postbaseline assessments | █████ | █████ | ██ ██ |
Withdrawal of consent | █████ | █████ | █████ |
Ongoing without an event | ██ ██████ | ██ ██████ | ██ ██ |
Radiographic progression-free survival, months | |||
Median (95% CI)a | NE (9.9 to NE) | █████ | █████ |
Probability of being event-free, % (95% CI) | |||
At 12 monthsa | 56.6 (46.7 to 65.3) | █████ | █████ |
BICR = blinded independent central review; CI = confidence interval; NE = not estimable.
Note: Details included in Table 12 are from the sponsor’s Summary of Clinical Evidence.
aBased on Kaplan-Meier estimates.
Source: MagnetisMM-3 Clinical Study Report.3
Overall Survival
Table 13 provides a summary of OS findings. As of the March 14, 2023, data cut-off, the OS data were immature. A total of 55 (44.7%) patients in cohort A and ██ ███████ patients in cohort B had died. Median OS had not yet been reached in cohort A and was ████ ██████ ████ ██ ███ ██ ███ ██████████ in cohort B. The probability of being alive at 12 months in cohort A was 63.0% (95% CI, 53.7% to 70.9%) and █████ ████ ███ ████ ██ █████ in cohort B.
Table 13: Overall Survival — MagnetisMM-3 Trial, Safety Analysis Set
MagnetisMM-3 trial | |||
|---|---|---|---|
Overall survival | Cohort A (N = 123) | Cohort B (N = 64) | Total (N = 187) |
March 14, 2023, data cut-off | |||
Patients with events, n (%) | 55 (44.7) | ██ ██████ | ██ ██████ |
Patients censored n (%) | 68 (55.3) | ██ ██████ | ██ ██████ |
Reason for censoring, n (%) | |||
Withdrawal of consent | █████ | █████ | █████ |
Loss to follow-up | █████ | █████ | █████ |
Ongoing without an event | ██ ██████ | ██ ██████ | ██ ██████ |
Overall survival, months | |||
Median (95% CI)a | NE (13.9 to NE) | ████ ████ | ████ ███ |
Probability of being event-free, % (95% CI) | |||
At 12 monthsa | 63.0 (53.7 to 70.9) | ████ ██ | ████ ███ |
CI = confidence interval; NE = not estimable.
Note: Details included in Table 13 are from the sponsor’s Summary of Clinical Evidence.
aBased on Kaplan-Meier estimates.
Source: MagnetisMM-3 Clinical Study Report.3
DOR and CRR by BICR
Table 14 provides a summary of DOR findings. By the March 14, 2023 data cut-off, the ██████ ███ ███ ███ ███████ █████ ██████████ ██ ████ ████████ ████ ███ ██ ███ ████████ ████████ ██ ███ ████ ██ ███ ████████. The probability of patients remaining in response at 12 months was 75.5% (95% CI, 58.8% to 80.9%) in cohort A and █████ ████ ███ ████ ██ █████ in cohort B. A complete response or better was attained in 43 patients (complete response or better = 35.0% [95% CI, 26.6% to 44.1%]) in cohort A and █████ ███ ███ ███ ██ █████ in cohort B.
Table 14: Duration of Response Among Confirmed Responders — MagnetisMM-3 Trial, Safety Analysis Set
MagnetisMM-3 trial | |||
|---|---|---|---|
Duration of response | Cohort A (N = 123) | Cohort B (N = 64) | Total (N = 187) |
March 14, 2023, data cut-off | |||
Patients who attained PR or better, n | 75 | ██ | 97 |
Patients with events, n (%) | ██ ██████ | ██████ | 25 (25.8) |
Progressive disease | ██████ | ██████ | 12 (12.4) |
Death | ██ ██████ | ██████ | 13 (13.4) |
Patients censored n (%) | 56 (74.7) | ██ ██████ | 72 (74.2) |
Reason for censoring, n (%) | |||
Start of new anticancer therapy | ██████ | ██████ | 6 (6.2) |
Withdrawal of consent | ██████ | ██████ | 3 (3.1) |
Ongoing without an event | ██ ██████ | ██ ██████ | 63 (64.9) |
Duration of response, months | |||
Median (95% CI)a | NE (NE to NE) | ██ █████ | NE (NE to NE) |
Probability of being event-free, % (95% CI) | |||
At 12 monthsa | 75.3 (63.1 to 83.9) | ████ ██ | 73.3 (62.4 to 81.5) |
CI = confidence interval; NE = not estimable; PR = partial response.
Note: Details included in Table 14 are from the sponsor’s Summary of Clinical Evidence.
aBased on Kaplan-Meier estimates.
Source: MagnetisMM-3 Clinical Study Report.3
HRQoL by EORTC QLQ-MY20
███ ███████████ ███████ █████ ████████ █████ ██████ ███ ████████ ██ Table 15 ██ ███ █████ ███ ████ ████ ███ ████ ███ ████ █████ ██████ ████ ████████ ██ █████ ██ ██ ██████ █ ████ █████████ ███████████ █████ ██████ █████████ ██ ██████ █ ███ ████ ██ ██████ ██ ███ ███████ █████████ ██████████ █████ ██ ██ ███████ ██████ ███████████ ██████ █████████ ██ ████ ███████ ███ ███ ██████ ████ ████████ ████████ ███ ████████ ███ ██ █ ██████ ██ █████ ███ ███████ ███████ ██████ █████████ ██ ████ ███████ ███ ███ ███ ██████ ███ ████████ ███ ██ ██ ███████ ████ ███████ ██ █████████ ██████ █████████ ██ ████ ███████ ███ ███ ███ ██████ ███ ████████ ███ ██ ██ ██████.
Table 15: Mean Changes in EORTC QLQ-MY20 From Baseline to Cycle 15 — MagnetisMM-3 Trial, PRO Analysis Set [Redacted]
██████ | ████████████ | |||||
|---|---|---|---|---|---|---|
██████ █ ███ █ ████ | ██████ █ ███ █ ███ | |||||
███ | ███ | ███ | ███ | ███ | ███ | |
█████ ███ ████ ████ ███████ | ||||||
████ █████ ███████ ██████ ████████ ████████ ████ ██████ | ||||||
████████ | ███ | ███ | ███ | ███ | ███ | ███ |
█████ ██ | ███ | ███ | ███ | ███ | ███ | ███ |
██████ ███████████ ███████ ██████ ████████ ██████ | ||||||
████████ | ███ | ███ | ███ | ███ | ███ | ███ |
█████ ██ | ███ | ███ | ███ | ███ | ███ | ███ |
███████ ████████ ██████ ██████ ████████ █████████ | ||||||
████████ | ███ | ███ | ███ | ███ | ███ | ███ |
█████ ██ | ███ | ███ | ███ | ███ | ███ | ███ |
████ ███████ ██ █████████ ██████ ██████ █████ | ||||||
████████ | ███ | ███ | ███ | ███ | ███ | ███ |
█████ ██ | ███ | ███ | ███ | ███ | ███ | ███ |
CFB = change from baseline; EORTC QLQ-MY20 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Multiple Myeloma 20; PRO = patient-reported outcome; SD = standard deviation.
Note: Details included in Table 15 are from the sponsor’s Summary of Clinical Evidence.
Source: MagnetisMM-3 Clinical Study Report.3
Harms
Harms data reported in this section are from the data cut-off date of March 14, 2023. The key harms results for the safety (i.e., as-treated) population are summarized in Table 16.
Adverse Events
All patients in the trial reported at least 1 TEAE. The most frequently reported TEAEs in cohort A were CRS (58%), anemia (49%), neutropenia (49%), diarrhea (42%), and fatigue (37%). ███ ████ ██████████ ████████ █████ ██ ██████ █ ████ ████████ ███████ ████████ ██████ ██████ ██████ ████████████████ ██████ ███████████████ ███ ███████████ ██████
Serious Adverse Events
In the total population, ███ of patients experienced 1 or more serious TEAE. The type and number of events were similar in both cohorts, with the most frequently reported events being COVID-19 pneumonia █████, CRS █████, pneumonia ██ ██, and disease progression ████.
Withdrawals Due to Adverse Events
Study treatment discontinuation due to TEAEs in cohort A was 20% and ███ in cohort B. The most common TEAEs leading to the discontinuation of elranatamab across both cohorts were similar, and included septic shock ████, neutropenia ████ COVID-19 pneumonia ████, and peripheral sensory neuropathy ████.
Mortality
In cohort A and cohort B, 45% and ███ of patients died, respectively. Most deaths in both cohorts were attributed to disease progression (30% in cohort A and ████ in cohort B).
Notable Harms
The incidence of notable harms in the total population was ███, and was similar in both cohorts. In the total population, the most frequently reported notable AEs were infections █████ and CRS█████, followed by peripheral neuropathy █████, hypogammaglobulinemia █████, and ICANS ████. All CRS events were grade 1 or grade 2 in severity. The median time from the most recent elranatamab dose to CRS onset was | ████ ███████ █ ██ █ █████ and the median time to resolution was | ████ ███████ █ ██ ██ ██████
Table 16: Summary of Harms Results — MagnetisMM-3 Trial, Safety Analysis Set
Harm | Cohort A (N = 123) | Cohort B (N = 64) | Total (N = 187) |
|---|---|---|---|
March 14, 2023, data cut-off | |||
Most common TEAEs,a n (%) | |||
≥ 1 TEAE | 123 (100) | ██ █████ | ███ █████ |
Cytokine release syndrome | 71 (57.7) | ██ ██████ | ███ ██████ |
Anemia | 60 (48.8) | ██ ██████ | ███ ██████ |
Neutropenia | 60 (48.8) | ██ ██████ | ██ ██████ |
Diarrhea | 52 (42.3) | ██ ██████ | ██ ██████ |
Thrombocytopenia | 38 (30.9) | ██ ██████ | ██ ██████ |
Lymphopenia | 33 (26.8) | ██ ██████ | ██ ██████ |
Fatigue | 45 (36.6) | ██████ | ██ ██████ |
Decreased appetite | 41 (33.3) | ██ ██████ | ██ ██████ |
Pyrexia | 37 (30.1) | ██ ██████ | ██ ██████ |
Hypokalemia | 32 (26.0) | ██ ██████ | ██ ██████ |
Cough | 31 (25.2) | ██ ██████ | ██ ██████ |
Nausea | 33 (26.8) | ██████ | ██ ██████ |
Injection site reaction | 33 (26.8) | ██████ | ██ ██████ |
SARS-CoV-2 test positive | 28 (22.8) | ██ ██████ | ██ ██████ |
Headache | 29 (23.6) | ██████ | ██ ██████ |
Asthenia | 24 (19.5) | ██ ██████ | ██ ██████ |
Arthralgia | 24 (19.5) | ██████ | ██ ██████ |
Leukopenia | 19 (15.4) | ██ ██████ | ██ ██████ |
Constipation | 18 (14.6) | ██ ██████ | ██ ██████ |
Pneumonia | 20 (16.3) | ██████ | ██ ██████ |
Vomiting | 20 (16.3) | ██████ | ██ ██████ |
Upper respiratory tract infection | 20 (16.3) | ██████ | ██ ██████ |
Pain in extremity | 11 (8.9) | ██ ██████ | ██ ██████ |
Serious TEAEs,b n (%) | |||
Patients with ≥ 1 serious TEAE | 92 (74.8) | ██ ██████ | ███ ██████ |
COVID-19 pneumonia | 17 (13.8) | ██████ | ██ ██████ |
Cytokine release syndrome | 16 (13.0) | ██████ | ██ ██████ |
Pneumonia | 12 (9.8) | █████ | ██ █████ |
Disease progression | 6 (4.9) | █████ | ██ █████ |
Sepsis | 7 (5.7) | █████ | █████ |
Patients who stopped treatment due to TEAEs,c n (%) | |||
Patients who permanently discontinued elranatamab | 24 (19.5) | ██ ██████ | ██ ██████ |
Septic shock | 2 (1.6) | █████ | █████ |
Neutropenia | 3 (2.4) | █████ | █████ |
COVID-19 pneumonia | 1 (0.8) | █████ | █████ |
Peripheral sensory neuropathy | 1 (0.8) | █████ | █████ |
Deaths, n (%) | |||
Patients who died | 55 (44.7) | ██ ██████ | ██ ██████ |
Cause of death | |||
Disease progression | 37 (30.1) | ██ ██████ | ██ ██████ |
Other | 10 (8.1) | █████ | █████ |
Unknown | 4 (3.3) | █████ | █████ |
Study treatment toxicity | 4 (3.3) | █████ | █████ |
Notable harms, n (%) | |||
Infections | 87 (69.9) | ██ ██████ | ███ ██████ |
Cytokine release syndrome, n (%) | 71 (57.7) | ██ ██████ | ███ ██████ |
Peripheral neuropathy, n (%) | 25 (20.3) | ██ ██████ | ██ ██████ |
Hypogammaglobulinemia | 13 (10.6) | █████ | █████ |
ICANS, n (%) | 6 (4.9) | █████ | █████ |
ICANS = immune effector cell-associated neurotoxicity syndrome; SARS-CoV-2 = severe acute respiratory syndrome coronavirus 2; TEAE = treatment-emergent adverse event.
Note: Details included in Table 16 are from the sponsor’s Summary of Clinical Evidence.
aFrequency of 10% or more in at least 1 group.
bFrequency of 5% or more in at least 1 group.
cFrequency of 3 or more total patients.
Source: MagnetisMM-3 Clinical Study Report.3
Critical Appraisal
Internal Validity
The primary limitation of the MagnetisMM-3 trial was the absence of a comparator group to assess the efficacy and harms of elranatamab, and therefore the interpretation of the results is limited to its single-arm design. As such, it is difficult to make causal conclusions — in particular, to what extent the observed effects were attributable to elranatamab. The open-label design introduces a potential bias in the assessment of ORR, PFS, DOR, and CRR, and a potential reporting bias of the subjective outcomes HRQoL and safety. However, this bias was mitigated by the use of BICR for ORR, PFS, DOR, and CRR. To minimize the risk of differential measurement error, the trial performed tumour assessments using IMWG criteria and radiographic scans were assessed by BICR. Sample size and power calculations were based on ORR, which had a prespecified hypothesis that was tested; however, all other analyses were descriptive. These included PFS, OS, DOR, and CRR, and the exploratory HRQoL outcome (via the EORTC QLQ-MY20 tool), which are deemed clinically important outcomes for the disease. The sample sizes for the subgroup analyses were small and not adjusted for multiplicity, which also made it difficult in interpreting the results.
The median durations for PFS and OS were immature; therefore, the treatment benefit of PFS and OS based on the latest interim analysis would have been subjected to a certain degree of uncertainty. While the trial met its primary objective of assessing ORR, there was limited supporting evidence from important secondary outcomes — notably, the immature data for PFS and OS. Given the importance of these outcomes to patients and clinicians, longer follow-up for the PFS and OS analyses would have been preferred to determine the clinical value of treatment with elranatamab. In addition, patients were permitted to receive post-treatment anticancer medications after study treatment had been discontinued (33% of all patients), which may influence the assessment of OS. The EORTC QLQ-MY20 questionnaire has been validated in patients with RRMM with evidence of reliability, responsiveness, and minimal important difference. However, the results for this outcome were subjected to bias potentially due to incomplete reporting or missing data, which could have biased the results toward the null. Therefore, the potential differences regarding a patient’s quality of life remain uncertain.
External Validity
In general, the population requested for reimbursement aligns with that of the Health Canada indication, and the dosing and administration of elranatamab were consistent with the Health Canada–approved product monograph. According to the clinical experts consulted by CADTH, the eligibility criteria and baseline characteristics of the MagnetisMM-3 trial were generalizable to adults with RRMM in the Canadian setting, although the trial did not include patients with a poor ECOG PS. The clinical experts noted that enrolling patients with only an ECOG PS score of 0 and 1 is not entirely representative of patients with RRMM as they expect to encounter patients with higher ECOG PS scores in their practice.
Dose adjustments were allowed in the trial and the methods were outlined in the protocol. The clinical experts noted that dose adjustments or modifications are anticipated in a clinical practice setting to manage AEs while maintaining drug benefit.
The trial included outcomes that were important to patients and clinicians. The patient group indicated that stopping disease progression, prolonging life, improving HRQoL, and reducing treatment side effects are important to them. However, assessing HRQoL as an exploratory outcome is a limitation to the evidence since no definitive conclusions can be drawn. The clinical experts noted that the following safety outcomes were not reported in the trial: infection-related hospitalizations, hypogammaglobulinemia as measured by the need for IV or subcutaneous immunoglobulin, and neurotoxicities.
GRADE Summary of Findings and Certainty of the Evidence
Methods for Assessing the Certainty of the Evidence
For pivotal studies and RCTs identified in the sponsor’s systematic review, GRADE was used to assess the certainty of the evidence for outcomes considered most relevant to inform CADTH’s expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group:1,2
“High certainty: We are very confident that the true effect lies close to that of the estimate of the effect.
Moderate certainty: We are moderately confident in the effect estimate — The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. We use the word ‘likely’ for evidence of moderate certainty (e.g., X intervention likely results in Y outcome).
Low certainty: Our confidence in the effect estimate is limited — The true effect may be substantially different from the estimate of the effect. We use the word may for evidence of low certainty (e.g., X intervention may result in Y outcome).
Very low certainty: We have very little confidence in the effect estimate — The true effect is likely to be substantially different from the estimate of effect. We describe evidence of very low certainty as very uncertain.
Although GRADE guidance is not available for noncomparative studies, the CADTH review team assessed pivotal single-arm trials for study limitations (which refers to the internal validity or risk of bias), inconsistency across studies, indirectness, and publication bias to present these important considerations. Because the lack of a comparator arm does not allow for a conclusion to be drawn on the effect of the intervention versus any comparator, the certainty of evidence for single-arm trials started at the level of very low certainty with no opportunity for rating up.
Results of GRADE Assessments
Table 2 presents the GRADE summary of findings for elranatamab.
Long-Term Extension Studies
No long-term extension studies were submitted by the sponsor.
Indirect Evidence
Content in this section has been informed by materials submitted by the sponsor. The following has been summarized and validated by the CADTH review team.
Objectives for the Summary of Indirect Evidence
The aim of this section is to summarize and critically appraise 2 sponsor-submitted unanchored MAICs used to inform the pharmacoeconomic model and to fill gaps in the comparative evidence versus other relevant treatments for adults with RRMM who have received at least 3 prior lines of therapy.
Description of MAICs
For both MAICs, the sponsor did not report a systematic literature search or describe the methods for study selection, data extraction, and quality assessment.
MAIC Design
Objectives
MAIC 1: Elranatamab Versus Physician’s Choice
The objective of MAIC 137 was to assess the relative treatment effect of elranatamab, using data from cohort A of the MagnetisMM-3 trial, compared to physician’s choice of treatment based on RWE from the CMRG database38 and selinexor plus bortezomib in combination with dexamethasone treatment data from the BOSTON trial39 in patients with TCE or RRMM. The outcomes assessed included PFS and OS.
MAIC 2: Elranatamab Versus Teclistamab, Cilta-Cel, and Physician’s Choice
The objective of MAIC 240 was to assess the relative treatment effect of elranatamab, using data from cohort A of the MagnetisMM-3 trial, compared to teclistamab from the MajesTEC-1 trial,41 physician’s choice of treatment from prospective RWE studies (the LocoMMotion42 and MAMMOTH43,44 trials), idecabtagene vicleucel from the KarMMa trial,45 and cilta-cel from the CARTITUDE-1 trial46,47 in patients with TCE or RRMM.40 Since idecabtagene vicleucel is not used in Canada, as per the participating drug plans and clinical experts consulted by CADTH, it was not included in this report. The outcomes assessed included ORR, PFS, OS, and CRR.
MAIC Analysis Methods
MAIC 1: Elranatamab Versus Physician’s Choice
A feasibility assessment was carried out to compare the study design, patient population, and outcome definitions between the MagnetisMM-3 trial, the CMRG study, and the BOSTON trial. Compatibility considerations focused on similarities and differences between the studies, and whether these could be adequately adjusted in an MAIC. Based on the feasibility assessment, an MAIC comparing elranatamab to physician’s choice of treatment from the CMRG study was feasible. Due to key differences in trial design, inclusion and exclusion criteria, patient population, and the definitions of outcome measures between the MagnetisMM-3 and BOSTON trials, an MAIC between elranatamab and selinexor plus bortezomib in combination with dexamethasone was deemed unfeasible, and therefore not reported.
The authors performed an unanchored MAIC by combining individual-level patient data (IPD) from the MagnetisMM-3 trial and aggregate data from a subgroup analysis of patients with TCE or RRMM from the CMRG RWE study to compare elranatamab to physician’s choice of treatment. The main indirect comparative analysis was conducted on cohort A (no prior BCMA-directed therapy) of the MagnetisMM-3 trial, with a median follow-up duration of 14.7 months (with a data cut-off date of March 14, 2023).
To identify potential PVs to adjust for in the comparative analyses, univariate Cox proportional hazards models were performed to identify any potential PVs based on the MagnetisMM-3 trial data. Any variable that exhibited a P value greater than 0.05 was removed as a PV. EMs and additional PVs were identified through a systematic literature review and validated with clinical expert opinion. The list of PVs and EMs for PFS and OS are in Table 17.
To conduct the MAIC, weights were assigned such that the average baseline characteristics after reweighting matched the published aggregate characteristics of the CMRG population. For variables where the means and the distributions were reported in the aggregated data, weights were generated so that the weighted means and the standard deviations in the IPD from the MagnetisMM-3 study matched those as reported in the aggregated data. For continuous variables where only the medians were reported, binary variables were generated using the IPD based on the reported medians from the aggregated data and the weights were generated so that the weighted means of the binary variables were 0.5 (i.e., to match the median reported in the aggregated data).
A PS-type logistic regression equation was used to estimate the balancing weights; this equation predicted whether a given type of patient originated from the index trial or the comparator trial as a function of baseline characteristics. More specifically, weights were estimated by the odds calculated as  where
where  is the vector of baseline variables included for matching. The beta coefficients were determined by the method of moments. Once the coefficients were estimated, the equation was applied to the patients from the MagnetisMM-3 trial to calculate the individual patient weights. These weights were then used to calculate the ESS, attained after weighting patients. The ESS was calculated by (∑wi)2 ÷ (∑wi2). If the populations were perfectly balanced before adjustment, the ESS would equal the original size of the MagnetisMM-3 trial’s population. Adjustments for population differences assigned patients uneven weights, which led to the inevitable loss of ESS. A low ESS indicated an irregular distribution of weights across patients, meaning that only a small fraction of patients shared common characteristics. The relative effect of elranatamab versus physician’s choice of treatments was quantified as HRs with 95% CIs, as well as Kaplan-Meier curves. Differences were considered statistically significant at P values of less than 0.05. Sensitivity analyses were not performed.
is the vector of baseline variables included for matching. The beta coefficients were determined by the method of moments. Once the coefficients were estimated, the equation was applied to the patients from the MagnetisMM-3 trial to calculate the individual patient weights. These weights were then used to calculate the ESS, attained after weighting patients. The ESS was calculated by (∑wi)2 ÷ (∑wi2). If the populations were perfectly balanced before adjustment, the ESS would equal the original size of the MagnetisMM-3 trial’s population. Adjustments for population differences assigned patients uneven weights, which led to the inevitable loss of ESS. A low ESS indicated an irregular distribution of weights across patients, meaning that only a small fraction of patients shared common characteristics. The relative effect of elranatamab versus physician’s choice of treatments was quantified as HRs with 95% CIs, as well as Kaplan-Meier curves. Differences were considered statistically significant at P values of less than 0.05. Sensitivity analyses were not performed.
The assessed outcomes PFS and OS were defined based on the MagnetisMM-3 trial as the time from the date of first dose until confirmed progression per IMWG criteria or death due to any cause, and as the time from the date of first dose until death due to any cause, respectively. The proportional hazards assumption for PFS and OS was assessed using the threshold of the Schoenfeld test set at a P value of 0.05, and through visual inspection of the log cumulative hazard plots and the Schoenfeld residual plots.
MAIC 2: Elranatamab Versus Teclistamab, Cilta-Cel, and Physician’s Choice
MAIC 2 used the same methods as MAIC 1, and is briefly described here. A compatibility assessment was performed and the results suggested notable heterogeneity between the included studies, particularly differences in patient populations. For elranatamab, IPD from the MagnetisMM-3 trial were used with the same data cut-off date of March 14, 2023, and for comparators, aggregated data were derived from their respective pivotal trial or study publications. The main indirect comparative analysis was conducted on cohort A (no prior BCMA-directed therapy) of the MagnetisMM-3 trial. The same PVs and EMs were used in MAIC 1 (Table 17) for both time-to-event and response-related outcomes. The methods to applying weights and quantifying the relative effects of treatment were the same as the methods used in MAIC 1, although it also included a naive comparison without any adjustment to treatment effects. The assessed outcomes of ORR, PFS, OS, and CRR were defined based on the MagnetisMM-3 trial. For ORR and CRR, results were reported as between-group rate differences (i.e., elranatamab and the comparator) and odds ratios with respective 95% CIs. A sensitivity analysis was performed using imputed data for variables in the MagnetisMM-3 trial where there were missing data (imputed based on a random sample of the observed data).
Results of MAIC 1 and MAIC 2
Summary of Included Studies
MAIC 1: Elranatamab Versus Physician’s Choice
A summary of study characteristics for the MagnetisMM-3 trial and CMRG study is in Table 18.
The CMRG database captures both legacy data and prospectively collected data from 2007 up to a data cut-off date of June 30, 2022, and reflects the outcomes seen with the basket of treatments used in RW clinical practice in Canada. The most prevalent regimens used in the CMRG basket were IMiDs and PIs. In the CMRG study, ISS disease stage and cytogenetic risk were reported for patients with MM at diagnosis. These baseline characteristics did not match the definition in the MagnetisMM-3 trial (where it was captured at the initiation of the trial period). As a result of this discrepancy, ISS disease stage and cytogenetic risk were not adjusted in the analysis. Other baseline characteristics that were reported in the CMRG study, such as exposure to prior therapies and being refractory to prior therapies, were not included in the analysis as these variables were not identified as key PVs and EMs.
To perform matching with the MagnetisMM-3 trial’s population, patients were selected from the CMRG database if they were adults (≥ 18 years), had MM that was refractory to an anti-CD38 mAb (progressed on therapy or within 60 days of the last dose of the anti-CD38 mAb), and had TCR disease (refractory to at least 1 IMiD, at least 1 PI, and 1 anti-CD38 mAb).
Table 17: Prognostic Variables and Effect Modifiers Identified for PFS and OS for MAIC 1 and MAIC 2
Characteristic | PFS | OS |
|---|---|---|
Prognostic variables and effect modifiers |
|
|
ECOG PS = Eastern Cooperative Oncology Group Performance Status; IgA = immunoglobulin A; IgD = immunoglobulin D; IgG = immunoglobulin G; ISS = International Staging System; MAIC = matching-adjusted indirect comparison; MM = multiple myeloma; OS = overall survival; PFS = progression-free survival; R-ISS = Revised International Staging System.
Note: Details included in Table 17 are from the sponsor’s Summary of Clinical Evidence.
Source: MAIC 1 technical report.37
Table 18: Summary of Study Characteristics Included in MAIC 1 — Elranatamab Versus Physician’s Choice
Study characteristic | MagnetisMM-3 trial (cohort A) | CMRG study |
|---|---|---|
Key inclusion criteria |
|
|
Key exclusion criteria |
|
|
Study design | Single-arm, phase II, open-label trial | Multicentre, retrospective, real-world study |
Patient population | Patients with TCR MM (cohort A had not previously received BCMA-directed therapy) | Patients with TCR MM |
Age, median (years) | 68.0 | 67.4 |
Sex, male, n (%) | 68 (55%) | 108 (54%) |
Median time since initial diagnosis, years | 6.1 | 4.2 |
Prior lines of therapy, n | 5 | 3 |
Sample size | n = 123 (cohort A) | Total n = 466, TCR MM n = 199 |
Treatment arm | Elranatamab monotherapy | Physician’s choice |
Dosing and administration | Subcutaneously: 12 mg on cycle 1, day 1; 32 mg on cycle 1, day 4; 76 mg on cycle 1, day 8; and weekly thereafter | Real-world administration (not prespecified) |
Definition of outcomes | PFS: Time from the date of first dose until confirmed PD per IMWG criteria, or death due to any cause OS: Time from the date of first dose until death due to any cause | PFS: Time between initiation of subsequent therapy after progression on the index regimen to progression (as defined by the IMWG criteria) or death OS: Time between initiation of subsequent therapy and death or last known follow-up |
BCMA = B-cell maturation antigen; CMRG = Canadian Myeloma Research Group; ECOG PS = Eastern Cooperative Oncology Group Performance Status; IMiD = immunomodulatory drug; IMWG = International Myeloma Working Group; mAb = monoclonal antibody; MAIC = matching-adjusted indirect comparison; MM = multiple myeloma; OS = overall survival; PD = progressive disease; PFS = progression-free survival; PI = proteasome inhibitor; TCR = triple-class refractory.
Note: Details included in Table 18 are from the sponsor’s Summary of Clinical Evidence.
Source: MAIC 1 technical report.37
MAIC 2: Elranatamab Versus Teclistamab, Cilta-Cel, and Physician’s Choice
A summary of study characteristics is in Table 19.
Elranatamab Versus Teclistamab
Overall, the design of the pivotal trials of elranatamab (the MagnetisMM-3 study) and teclistamab (the MajesTEC-1 study) was similar except that in the MagnetisMM-3 study, enrolled patients were TCR whereas patients in the MajesTEC-1 study were TCE. Additionally, the MajesTEC-1 trial enrolled patients with an ECOG PS score of less than or equal to 1, which differs from the MagnetisMM-3 trial where patients with a performance score less than or equal to 2 were eligible for enrolment. To account for this difference, patients from the MagnetisMM-3 trial with an ECOG PS score greater than 1 were excluded from MAIC analyses. In the MajesTEC-1 trial, extramedullary disease was defined as the presence of 1 or more extramedullary soft-tissue lesions. This definition did not match the definition in the MagnetisMM-3 trial (defined as the presence of any plasmacytoma [extramedullary and/or paramedullary] with a soft-tissue component). To account for this, an additional baseline variable in the MagnetisMM-3 study’s IPD was created for the comparison versus teclistamab, which matched the definition of extramedullary disease in the MajesTEC-1 study. The definitions of PFS and OS were similar between the 2 trials.
Elranatamab Versus Cilta-Cel
A key difference between the designs of the MagnetisMM-3 and CARTITUDE-1 trials was patients in the MagnetisMM-3 trial were TCE, whereas patients in CARTITUDE-1 were TCR. There were notable differences between the number of patients with different disease stages, extramedullary disease, and creatine clearance. Other characteristics, including the definitions of PFS and OS, were similar between the 2 trials.
Elranatamab Versus Physician’s Choice
LocoMMotion Study
A key difference between the designs of the MagnetisMM-3 trial and the LocoMMotion study is that the latter is an observational, noninterventional study of patients who are TCE whereas the MagnetisMM-3 study is a single-arm, interventional clinical trial of patients who are TCR. In addition, the LocoMMotion study enrolled patients with an ECOG PS score of less than or equal to 1 (the MagnetisMM-3 trial enrolled patients with an ECOG PS score of 2 or less). However, when the baseline characteristics were captured, ECOG PS scores higher than 1 were recorded. As a result, ECOG PS score was not considered to be a discrepancy between the MagnetisMM-3 and LocoMMotion studies. Due to the large amount of missing data, cytogenetic risk was not included in the MAIC. This potentially led to bias as cytogenetic risk was identified as a PV and EM. Other characteristics, including the definitions of PFS and OS, were similar between the 2 studies.
Table 19: Summary of Study Characteristics Included in MAIC 2 — Elranatamab Versus Teclistamab, Cilta-Cel, and Physician’s Choice
Characteristic | MagnetisMM-3 trial (cohort A) | MajesTEC-1 trial | CARTITUDE-1 trial | LocoMMotion trial | MAMMOTH trial |
|---|---|---|---|---|---|
Drug | Elranatamab | Teclistamab | Cilta-cel | Physician’s choice | Physician’s choice |
Key inclusion criteria |
|
|
|
|
|
Key exclusion criteria |
|
|
| NR |
|
Study design | Single-arm, phase II, open-label trial | Single-arm, phase II, open-label trial | Single-arm, phase Ib and phase II, open-label trial | Ongoing, prospective, noninterventional study | Retrospective study |
Patient population | TCR MM (patients in cohort A had not previously received BCMA-directed therapy) | Patients with TCE or TCR MM | Patients with TCE or TCR MM | Patients with TCE or TCR MM | Patients with TCR MM |
Age, median, years | 68 | 64 | NR | 68 | 65 |
Sex, male, n (%) | 68 (55%) | 96 (58%) | 57 (59%) | 68 (55%) | 94 (53%) |
Time from initial diagnosis, median, years | 6.2 | 6.0 | 5.9 | 6.1 | 4.8 |
Sample size | n = 123 (cohort A) | n = 165 | n = 97 | n = 248a | n = 177 |
BCMA = B-cell maturation antigen; CAR = chimeric antigen receptor; cilta-cel = ciltacabtagene autoleucel; ECOG PS = Eastern Cooperative Oncology Group Performance Status; GVHD = graft-vs.-host disease; IMiD = immunomodulatory drug; IMWG = International Myeloma Working Group; mAb = monoclonal antibody; MAIC = matching-adjusted indirect comparison; MM = multiple myeloma; NR = not reported; PI = proteasome inhibitor; SCT = stem cell transplant; TCE = triple-class exposed; TCR = triple-class refractory.
Note: Details included in Table 19 are from the sponsor’s Summary of Clinical Evidence.
aThe LocoMMotion study is ongoing. Time-to-event data for this study were based on a data cut-off date of October 2022, after a median follow-up of 26.4 months.
Source: MAIC 2 technical report.40
MAMMOTH Study
Similar to the LocoMMotion study, the MAMMOTH study reflects the outcomes seen with the basket of treatments used in RW clinical practice. A key difference between the designs of the 2 studies is that the MAMMOTH study was an observational, noninterventional study whereas the MagnetisMM-3 study is a single-arm, interventional clinical trial. Only data from the TCR subgroup were used for comparison in analyses. Differences between the studies included patients who were penta-exposed and penta-refractory. Other characteristics, including the definitions of ORR, PFS, OS, and CRR, were similar between the 2 studies.
Results
MAIC 1: Elranatamab Versus Physician’s Choice
In the comparison of PFS with elranatamab versus physician’s choice of treatment (the CMRG study), weights were generated based on adjustment for median age, median time since initial diagnosis in years, and median prior lines of therapy. The same adjustments were made for the OS comparison, with the addition of sex. The authors noted that the proportional hazards assumption was violated for both OS and PFS.
Progression-Free Survival
Following MAIC adjustment and an ESS of 82, the PFS HR was 0.36 (95% CI, 0.23 to 0.54; P = 0.000) in favour of elranatamab versus physician’s choice of treatment.
Overall Survival
Following MAIC adjustment and an ESS of 81, the OS HR was 0.48 (95% CI, 0.32 to 0.73; P = 0.000) in favour of elranatamab versus physician’s choice of treatment.
MAIC 2: Elranatamab Versus Teclistamab, Cilta-Cel, and Physician’s Choice
A summary of PVs and EMs adjusted in the MAICs is in Table 20, and results for ORR, PFS, OS, and CRR are in Table 21. The authors noted that the proportional hazards assumption was violated in most comparisons for both OS and PFS, except for the comparison to teclistamab (PFS and OS) and the LocoMMotion study (OS only).
Objective Response Rate
Following MAIC adjustment, the ORR difference favoured elranatamab versus teclistamab and physician’s choice of treatment (for both the LocoMMotion and MAMMOTH studies). The results of the sensitivity analyses were consistent with the primary base-case analyses.
Progression-Free Survival
Following MAIC adjustment, the PFS HR favoured elranatamab versus teclistamab and physician’s choice of treatment (for both the LocoMMotion and MAMMOTH studies), and crossed the null for elranatamab versus cilta-cel. The results of the sensitivity analyses were consistent with the primary base-case analyses.
Overall Survival
Following MAIC adjustment, the OS HR crossed the null for elranatamab versus teclistamab, favoured cilta-cel versus elranatamab, and favoured elranatamab versus physician’s choice of treatment (for both the LocoMMotion and MAMMOTH studies). The results of the sensitivity analyses were consistent with the primary base-case analyses.
Complete Response Rate
Following MAIC adjustment, the CRR difference between elranatamab and teclistamab crossed the null, and favoured elranatamab versus physician’s choice of treatment (for both the LocoMMotion and MAMMOTH studies). The results of the sensitivity analyses were consistent with the primary base-case analyses.
Table 20: Summary of Variables Adjusted in MAIC 2, per Outcome
Comparator | ORR (ESS) | PFS (ESS) | OS (ESS) | CRR (ESS) |
|---|---|---|---|---|
Elranatamab vs. comparator | ||||
Teclistamab | Same as OS outcome, with the removal of sex | Same as OS outcome, with the removal of sex |
| Same as OS outcome, with the removal of sex |
Cilta-cel | NA | Same as OS outcome |
| NA |
Physician’s choice: LocoMMotion study | Same as OS outcome, with the removal of sex | Same as OS outcome, with the removal of sex |
| Same as OS outcome, with the removal of sex |
Physician’s choice: MAMMOTH study | Same as OS outcome, with the removal of sex | Same as OS outcome, with the removal of sex |
| Same as OS outcome, with the removal of sex |
Cilta-cel = ciltacabtagene autoleucel; CRR = complete response rate; ECOG PS = Eastern Cooperative Oncology Group Performance Status; ESS = effective sample size; ISS = International Staging System; MAIC = matching-adjusted indirect comparison; NA = not applicable; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; vs. = versus.
Note: Details included in Table 20 are from the sponsor’s Summary of Clinical Evidence.
Source: MAIC 2 technical report.40
Table 21: Summary of Adjusted MAIC 2 Results, per Outcome
Comparator | ORR (ESS) | PFS (ESS) | OS (ESS) | CRR (ESS) |
|---|---|---|---|---|
Elranatamab vs. comparator | ||||
Teclistamab | Rate difference = 12.3% (95% CI, 0.70% to 23.9%) OR = 1.791 (95% CI, 1.01 to 3.19) ESS = 75 | HR = 0.59 (95% CI, 0.39 to 0.89; P = 0.012) ESS = 75 | HR = 0.66 (95% CI, 0.42 to 1.03; P = 0.067) ESS = 73 | Rate difference = 3.63% (95% CI, –9.08% to 16.3%) OR = 1.16 (95% CI, 0.69 to 1.96) ESS = 75 |
█████████ | ██ | ██ ████ ███ █ ████ █████ ████ █ ██ | ██ ████ ███ █ ████ █████ ██ ███████ █ ██ | ██ |
Physician’s choice: LocoMMotion study | Rate difference = 37.5% (95% CI, 26.2% to 48.8%) OR = 4.85 (95% CI, 2.853 to 8.228) ESS = 68 | HR = 0.316 (95% CI, 0.20 to 0.49; P = 0.000) ESS = 68 | HR = 0.62 (95% CI, 0.40 to 0.94; P = 0.026) ESS = 68 | Rate difference = 42.3% (95% CI, 31.8% to 52.7%) OR = 184.0 (95% CI, 24.7 to 1,372.9) ESS = 68 |
Physician’s choice: MAMMOTH study | Rate difference = 28.1% (95% CI, 16.8% to 39.5%) OR = 3.24 (95% CI, 1.98 to 5.32) ESS = 100 | HR = 0.251 (95% CI, 0.17 to 0.37; P = 0.000) ESS = 100 | HR = 0.49 (95% CI, 0.33 to 0.71; P = 0.000) ESS = 100 | Rate difference = 26.2% (95% CI, 16.4% to 36.0%) OR = 5.48 (95% CI, 2.88 to 10.4) ESS = 100 |
CI = confidence interval; CRR = complete response rate; ESS = effective sample size; HR = hazard ratio; MAIC = matching-adjusted indirect comparison; NA = not applicable; OR = odds ratio; OS = overall survival; PFS = progression-free survival; RE = random effect; vs. = versus.
Note: Details included in Table 21 are from the sponsor’s Summary of Clinical Evidence.
Source: MAIC 2 technical report.40
Critical Appraisal of MAIC 1 and MAIC 2
Both MAIC 1 and MAIC 2 used the same methods to indirectly compare treatments, and their rationale and objectives were reported. In the case of both MAICs, the authors did not report a systematic literature search, describe their methods for data extraction, or conduct quality assessment of the included studies. In addition, only cohort A from the MagnetisMM-3 trial was included in the primary analyses. As such, the indirect comparative assessment remains unknown for patients with prior BCMA-directed therapy (cohort B).
The MAICs included relevant outcomes identified by the CADTH team (ORR, PFS, OS, CRR); however, important outcomes such DOR, HRQoL, and safety were not included in the comparisons. Across the included studies, there were notable differences in study designs (single-arm, open-label, phase II trial versus multicentre retrospective or prospective cohort studies), inclusion and exclusion criteria, and patient characteristics (refractory or relapse status, prior history of treatments, ECOG PS). For MAIC 2, a key difference of comparing elranatamab to teclistamab, cilta-cel, and physician’s choice of treatment based on the LocoMMotion study was that these studies included patients who were TCE, while the MagnetisMM-3 trial enrolled patients who were TCR. Therefore, there is significant concern that the MAIC results would have been subjected to biases due to the large amount of heterogeneity across the included studies.
To account for between-study differences in patient baseline characteristics, several relevant PVs and EMs were matched in the weighting process, with separate sets of variables used across treatment comparisons and outcomes. These variables were selected based on a systematic literature search and clinical expert input.
For MAIC 1 (elranatamab versus physician’s choice), ISS disease stage and cytogenetic risk could not be adjusted in the analyses for PFS and OS, as the definitions did not align across the MagnetisMM-3 trial and CMRG study. In the CMRG study, patient-level data regarding these 2 variables were captured at diagnosis rather than at the start of the trial period, as it was defined in the MagnetisMM-3 trial. Additionally, extramedullary disease was not adjusted for in the analysis as it was not reported in the CMRG study.
For MAIC 2, the following variables were missing for 2 comparisons: in the comparison of physician’s choice of treatment from the MAMMOTH study, extramedullary disease was not adjusted for, and in the comparison with physician’s choice of treatment from the LocoMMotion study, cytogenetic risk was not adjusted for. The authors noted that both cytogenetic risk and extramedullary disease were found to be important PVs based on the IPD of the MagnetisMM-3 study. These limitations, and differences in study design that could not be adjusted for in the analysis, could introduce residual confounding due to unreported or unobserved cross-study differences, although the direction or extent of bias is unclear.
For MAIC 1, following the weighting process, the ESS for OS declined by approximately 34% of the original sample size in the comparison with physician’s choice of treatment. For the PFS comparison with physician’s choice of treatment, the ESS declined by approximately 33% of the original sample size. For MAIC 2, following adjustment, the ESS for OS declined by 37% of the original sample size in the comparison with teclistamab, by 73% of the original sample size in the comparison with cilta-cel, by 45% of the original sample size in the comparison with physician’s choice of treatment (the LocoMMotion study), and by 20% of the original sample size in the comparison with physician’s choice of treatment (the MAMMOTH study). These reductions in the ESS meant the final matched patient population was more highly selective than the original patient population, and may lead to large uncertainty in estimated treatment effects, although the magnitude and direction of potential bias is unclear.
For MAIC 1, the proportional hazards assumption was violated for both PFS and OS outcomes, and for MAIC 2, the assumption was violated in most comparisons for PFS and OS outcomes. The assumptions were based on the Schoenfeld test, and through visual inspection of the log cumulative hazard plots and the Schoenfeld residual plots. These violations could have led to biased treatment effect estimates.
Studies Addressing Gaps in the Systematic Review Evidence
Content in this section has been informed by materials submitted by the sponsor. The following has been summarized and validated by the CADTH review team.
This section summarizes 2 retrospective cohort studies with external control arms (Study C107102448 and Study C107103149) and 1 phase I and phase II dosing study (the MagnetisMM-9 trial).50 The sponsor provided an article on a multicentre retrospective cohort study using the CMRG database,51 which has been included in Appendix 1. The following section summarizes the details of both Study C1071024 and Study C1071031.
Description of RWE External Cohort Studies (Study C1071024 and Study C1071031)
To help contextualize the results from the MagnetisMM-3 study, the sponsor provided 2 studies (Study C107102448 and Study C107103149) to retrospectively compare efficacy outcomes between elranatamab and 2 external control arms using a basket of RW treatments (refer to Table 22 for details) from the Flatiron Health and COTA databases.
A retrospective cohort study, Study C1071024, was conducted to compare the efficacy outcomes ORR and DOR observed in the participants of the MagnetisMM-3 study (with at least 9 months of follow-up) and RW patients selected from 2 US-based oncology electronic health record databases, the Flatiron Health and COTA databases. The Flatiron Health database is a longitudinally, demographically, and geographically diverse database covering more than 280 community cancer centres and academic institutions (approximately 800 sites of care) that represent more than 2.4 million active US cancer patients. The source population includes patients managed in at least 1 of the US oncology centres taking part in the Flatiron Health database network from January 1, 2011, onward. The COTA database is a longitudinal database derived from the electronic health records of more than 200 health care provider sites in the US (including academic institutions, community centres, and hospital systems) that represent 500,000 patients. Data elements were standardized across sources and ontologies to create a single, structured dataset to cover the full longitudinal history of a patient’s clinical care.
Study C1071031 is the continuation of Study C1071024 with an available follow-up of the MagnetisMM-3 study participants of approximately 15 months. Study C1071031 aimed to compare the PFS and OS in participants of the MagnetisMM-3 study treated with elranatamab versus RW patients with TCR MM treated with RW physician’s choice of therapy. Study C1071031 also assessed PROs (via the EORTC QLQ-MY20 tool) using other studies, Study C1071013 and Study C1071014, as the data sources for the external cohort. In Study C1071024 and Study C1071031, 2 external arms were constructed from these 2 cohorts of RW patients with TCR MM to maximize comparability to participants from the pivotal MagnetisMM-3 trial. The eligibility criteria for patients in the 2 external control arms were based on the eligibility criteria from the pivotal MagnetisMM-3 trial. Patients were considered eligible for selection in the external control arm if they had MM that was refractory to at least 1 PI, 1 IMiD, and 1 anti-CD38, and had started at least 1 new treatment since the documentation of TCR status. Refractory disease was defined as experiencing progression, according to IMWG criteria or clinical assessment, while on therapy or within 60 days of the last dose in any line of therapy, regardless of response.
The date of the initiation of the first regimen after TCR MM eligibility was defined as the index date in establishing the external control arms from the Flatiron Health and COTA databases for both Study C1071024 and Study C1071031. Patients were only eligible if they had an index date occurring between November 16, 2015 (the date that the US FDA approved the first anti-CD38 therapy), and March 31, 2022 (Study C1071024), or June 30, 2022 (Study C1071031). The study period comprised the baseline period (time preceding the index date) and the observational period (time following the index date). The observational period spanned from the index date to the date of death or the latest available patient record, whichever occurred first. The sequences of relevant study events are shown for the MagnetisMM-3 trial in Figure 2 and the external control arms in Figure 3.
Study C1071024 used the Flatiron Health and COTA databases as data sources for the external cohorts that were compared to the MagnetisMM-3 study for the outcomes ORR and DOR. Study C10710131 also used the Flatiron Health and COTA databases for the cohorts compared to the MagnetisMM-3 study for the outcomes of OS and PFS. In addition, study C1071031 assessed PROs (via the EORTC QLQ-MY20 tool) using other studies, Study C1071013 and Study C1071014, as the data sources for the external cohort. Data were extracted between November 16, 2015, and June 30, 2022. Similar inclusion and exclusion criteria from the MagnetisMM-3 trial were applied to the external control arms from Study C1071013 and Study C1071014 to maximize comparability to participants from the pivotal MagnetisMM-3 trial.
Figure 2: Baseline and Observation Periods in MagnetisMM-3 Trial
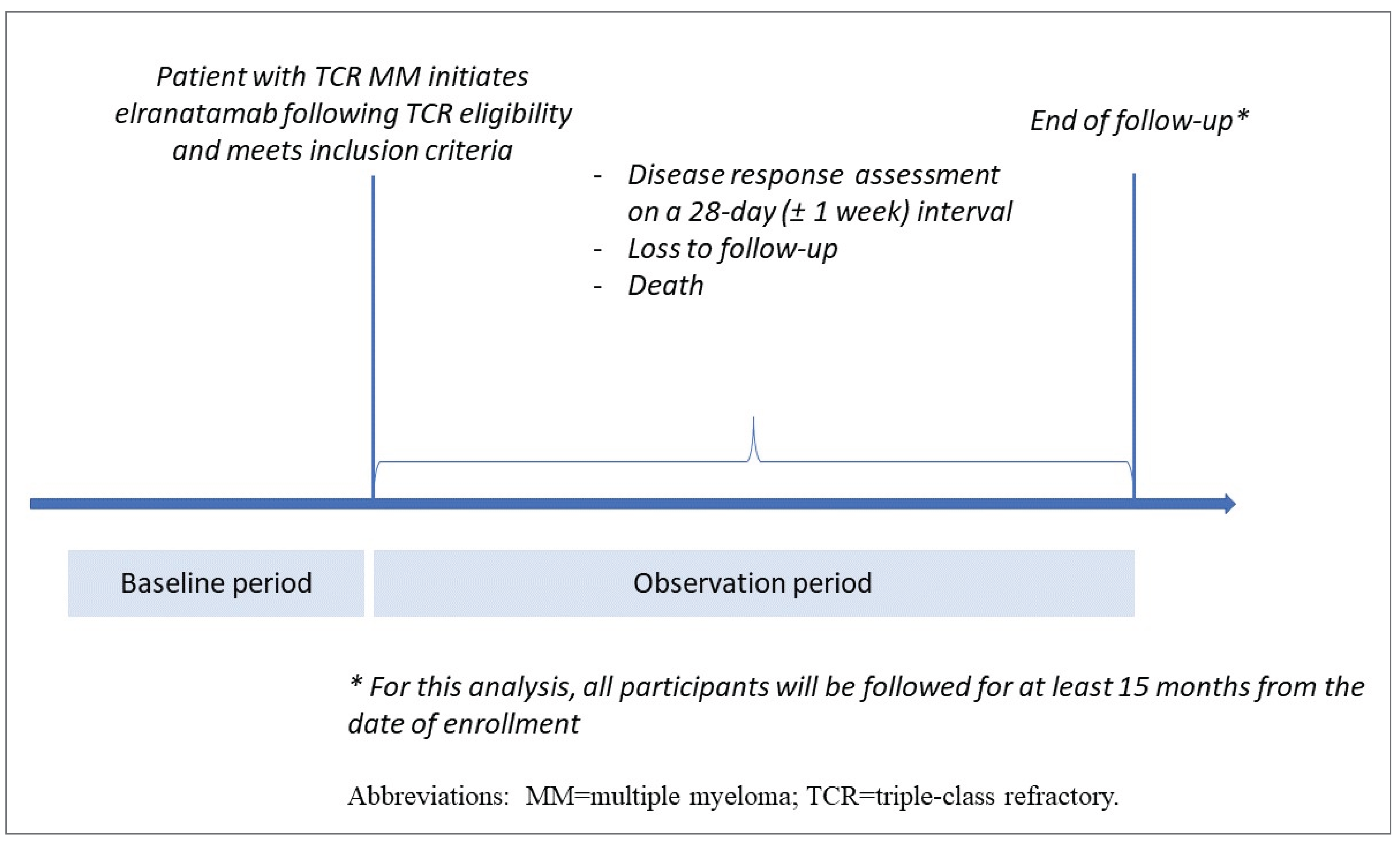
Sources: Study C1071024 and Study C1071031 technical reports.48,49
Study C1071013 is a noninterventional, observational, prospective, multinational (the US, Canada, France, Germany) study collecting IPD from RW patients with TCR MM who started a new line of systemic therapy at any point after they were TCR eligible. PRO measures (via the EORTC QLQ-MY20 tool) were collected at the start of this new line of systemic therapy and then monthly for 12 months. Study C1071013 is ongoing and a data cut-off from March 31, 2023, was used for this analysis.
Study C1071014 is a noninterventional, observational, prospective study in the US collecting IPD from RW patients with TCR MM who started a new line of systemic therapy at any point after they were classified as eligible based on having TCR disease. PRO measures (via the EORTC QLQ-MY20 tool) were collected at the start of this new line of systemic therapy and then monthly for 6 months. Study C1071014 is ongoing and a data cut-off date from April 2023 was used for this analysis. Only patients using regimens that included treatment options available in RW clinical practice such as alkylating drugs, IMiDs, PIs, anti-CD38 therapies, anti–signalling lymphocytic activation molecule family member 7 therapies, BCMAs (except BCMA bispecifics), and other select anti-MM systemic therapies such as panobinostat and selinexor were included in the external control arms from both Study C1071013 and Study C1071014 for the PRO analysis.
Figure 3: Baseline and Observation Periods in the Flatiron Health and COTA Database External Control Arms
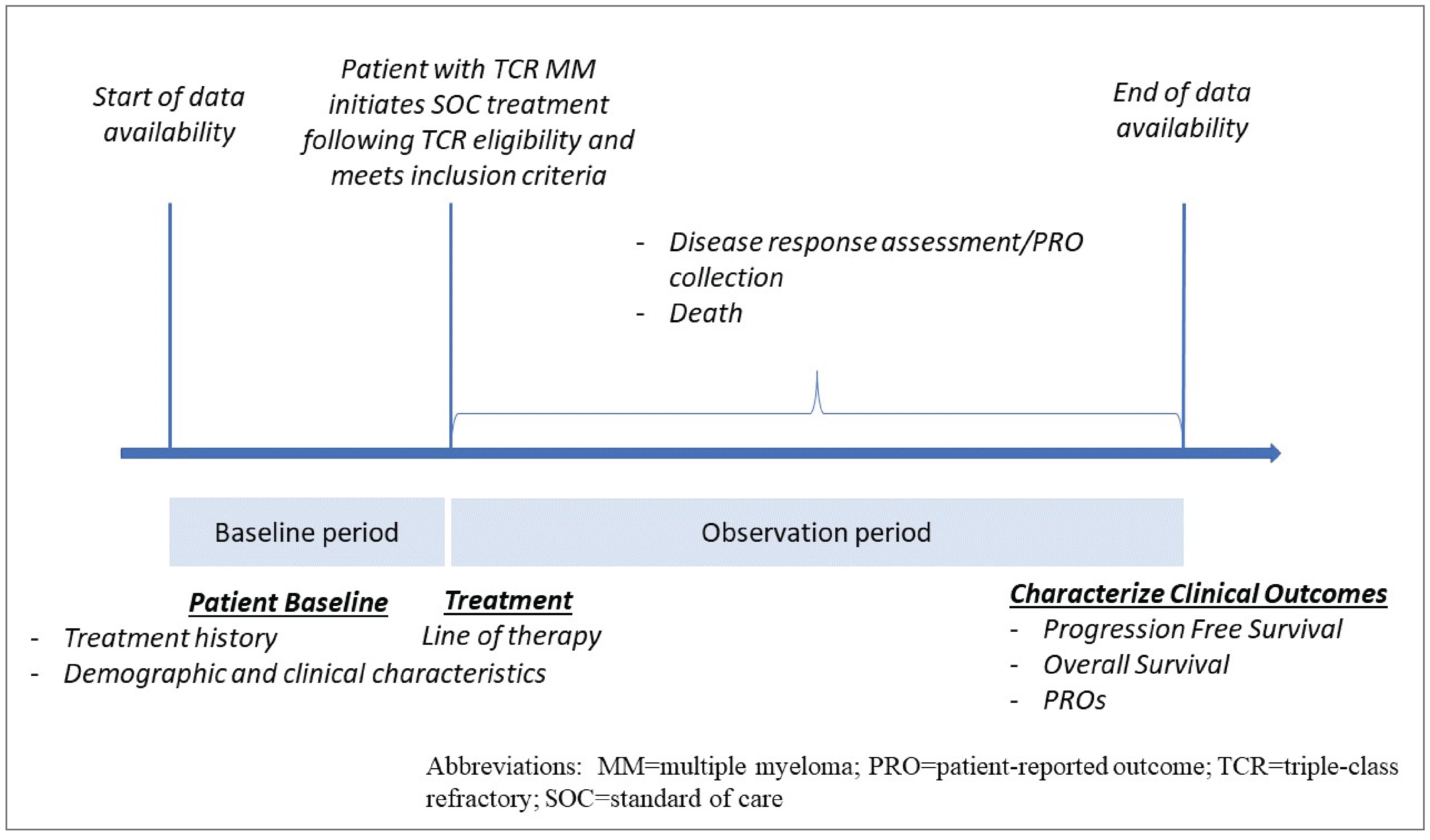
Source: Study C1071024 and Study C1071031 technical reports.48,49
Patients with TCR MM were defined as patients with MM with disease-refractory to 1 or more IMiD, 1 or more PI, and 1 or more anti-CD38 antibody treatment based on the refractory status recorded in the COTA and Flatiron Health databases. Refractory status was defined using IMWG-derived progression events or health care provider -reported progression. To minimize potential misclassification and to enhance the comparability of patients identified from the COTA and Flatiron Health databases, IMWG-derived progressions were reallocated to a specific line of therapy using a sponsor-developed algorithm. Various time windows were tested while developing this algorithm.
For the comparative analysis of PFS and OS, units used in reported laboratory values in the populations identified from RWD sources were standardized to those used in the MagnetisMM-3 study to permit proper comparisons between treatment groups.
Populations
Two types of eligibility criteria (critical and expanded) were used for the efficacy analysis in Study C1071024 and Study C1071031. The critical eligibility criteria were applied for the main analysis and additional analysis, and expanded eligibility criteria were additional criteria added for sensitivity analyses to assess the potential influence of the selection process based on the eligibility criteria.
The critical inclusion criteria, based on the MagnetisMM-3 study, that were applied to the COTA and Flatiron Health databases were as follows:
male or female patients aged 18 years or older
a prior diagnosis of MM as defined according to IMWG criteria
measurable disease, based on IMWG criteria
TCR MM, defined as refractory to at least 1 IMiD, at least 1 PI, and at least 1 anti-CD38 antibody
patient had started at least 1 anti-MM systemic therapy in the TCR MM setting
an ECOG PS score of 2 or less.
The critical exclusion criteria, based on the MagnetisMM-3 study, that were applied to the COTA and Flatiron Health databases were as follows:
active plasma cell leukemia
amyloidosis
previous treatment with an investigational drug within 30 days
smouldering MM
stem cell transplant within 12 weeks before enrolment or active graft-versus-host disease
active malignancy within 3 years before enrolment (except for adequately treated basal cell or squamous cell skin cancer, or carcinoma in situ)
active infections.
The same critical eligibility criteria were applied to Study C1071013 and Study C1071014 for the analysis of PROs (via the EORTC QLQ-MY20 tool).
In addition to the critical criteria, there was also expanded eligibility criteria.
The expanded inclusion criteria were as follows:
adequate hepatic function characterized by all of the following —
total bilirubin of 2 or less multiplied by the upper limit of normal (ULN) (≤ 3 × ULN if documented Gilbert syndrome)
aspartate aminotransferase of 2.5 or less multiplied by the ULN
alanine aminotransferase of 2.5 or less multiplied by the ULN
adequate renal function, defined by an estimated creatinine clearance of 30 mL per minute or more
adequate bone marrow function characterized by all of the following —
absolute neutrophil count of 1.0 or more multiplied by 109/L
platelets of 25 or more multiplied by 109/L
hemoglobin of 8 g/dL or more.
The expanded exclusion criteria were as follows:
impaired cardiovascular function or clinically significant cardiovascular diseases, defined based on the history of any of the following conditions within 6 months before enrolment —
acute myocardial infarction or acute coronary syndromes
clinically significant cardiac arrhythmias
thromboembolic or cerebrovascular events
prolonged QT syndrome (or triplicate average QT interval corrected for heart rate using the Fridericia formula greater than 470 milliseconds)
ongoing grade 2 or higher peripheral sensory or motor neuropathy
a history of any grade of peripheral sensory or motor neuropathy with prior BCMA-directed therapy (cohort B)
a history of Guillain-Barré syndrome or Guillain-Barré syndrome variants, or a history of any grade 3 or higher peripheral motor neuropathy.
Interventions
Patients were classified as having received elranatamab (in the MagnetisMM-3 trial) or any of the RW treatment options (in the COTA or Flatiron Health databases) in Study C1071024 and Study C1071031 that are described in Table 22. Only the first RW treatment option in the TCR setting during the index period was considered in the analyses; subsequent treatments were not considered.
Table 22: List of Treatments Available for MM Received by Patients in the COTA or Flatiron Health Databases
Class | Drug |
|---|---|
Alkylating drugs | Bendamustine, cisplatin, cyclophosphamide, melphalan, melphalan flufenamide, carmustine, bendamustine |
Anthracycline | Adriamycin, idarubicin, liposomal doxorubicin |
Anti-BCMA (ADC) | Belantamab mafodotin |
Anti-BCMA (CAR T-cell therapy) | Idecabtagene vicleucel, ciltacabtagene autoleucel |
BCL2 inhibitor | Venetoclax |
Anti-CD38–directed mAb | Daratumumab, daratumumab and hyaluronidase, isatuximab |
Corticosteroid | Dexamethasone, prednisone, methylprednisolone |
HDAC | Panobinostat |
IMiD | Lenalidomide, pomalidomide, thalidomide |
Nuclear export inhibitor | Selinexor |
PI | Bortezomib, carfilzomib, ixazomib |
Podophyllotoxin derivative | Etoposide |
Anti-SLAMF7 mAb | Elotuzumab |
Vinca alkaloid | Vincristine (also known as leurocristine) |
ADC = antibody-drug conjugate; anti-BCMA = anti–B-cell maturation antigen; CAR = chimeric antigen receptor; BCL2 = B-cell lymphoma 2; HDAC = histone deacetylase IMiD = immunomodulatory drug; mAb = monoclonal antibody; MM = multiple myeloma; PI = proteasome inhibitor ; Anti-SLAMF7 = anti-signalling lymphocytic activation molecule family member 7
Note: Details included in Table 22 are from the sponsor’s Summary of Clinical Evidence.
Sources: Study C1071024 and Study C1071031 technical reports.48,49[Details included in the table are from the sponsor’s Summary of Clinical Evidence].
Outcomes
Mortality data in the COTA database are collected via a third-party obituary source while mortality data in the Flatiron Health database are collected through an amalgamation of structured data elements and unstructured documents, and by linking to external mortality sources and the Social Security Death Index. Table 23 compares the definitions of PFS, OS, ORR, and DOR used in the MagnetisMM-3 study, the COTA database, and Flatiron Health database populations.
Table 23: Definitions of Primary Outcomes in MagnetisMM-3 Trial, and COTA and Flatiron Health Databases
Outcome | MagnetisMM-3 trial | COTA database | Flatiron Health database | |
|---|---|---|---|---|
Study C1071031 | ||||
PFS | Time from the date of the first dose until confirmed PD per IMWG criteria or death due to any cause, whichever occurs first | Time from initiation of the first-line therapy after patient identified as having TCR MM to either the date of progression or death due to any cause, whichever occurs first | Time from initiation of the first-line therapy after patient identified as having TCR MM to either the date of progression or death due to any cause, whichever occurs first | |
Implementation censoring rules for PFS | Participants who do not have an event (confirmed PD per IMWG criteria or death due to any cause) | Patients without an event were censored on the earliest date between the latest available record for the patient or the data cut-off date. | Patients without an event were censored on the earliest date between the latest available record for the patient or the data cut-off date. | |
Participants who started a new anticancer therapy before an event were censored on the date of the last adequate disease assessment before the new anticancer therapy. | Patients who started a new line of therapy before an event were censored on the day before the start date of the next line of therapy. | Patients who started a new line of therapy before an event were censored on the day before the start date of the next line of therapy. | ||
Participants with an event after a gap of 2 or more missing disease assessments were censored on the date of the last adequate disease assessment before the gap. | Cannot be implemented | Cannot be implemented | ||
Participants who did not have an adequate postbaseline disease assessment were censored on the date of the first dose of study intervention unless death occurred on or before the time of the second planned disease assessment (i.e., ≤ 70 days after the date of first dose), in which case the death was considered an event. | Cannot be implemented | Cannot be implemented | ||
OS | Time from the date of the first dose until death due to any cause | Time from initiation of the first-line therapy after patient identified as having TCR MM until the date of death due to any cause | Time from initiation of the first-line therapy after patient identified as having TCR MM until the date of death due to any cause | |
Study C1071024 | ||||
ORR | This was the proportion of participants with an OR based on blinded independent central review per IMWG criteria. OR is defined as having the best overall response of confirmed sCR, CR, VGPR, and PR per IMWG criteria, from the date of the first dose until confirmed PD, death, or the start of new anticancer therapy, whichever occurs first. | This was the proportion of patients who attained at least VGPR or PR based on IMWG criteria. | This was the proportion of patients who attained sCR, CR, VGPR, or PR based on IMWG criteria. | |
DOR | For participants with an OR per IMWG criteria, this was the time from the first documentation of OR that was subsequently confirmed, until confirmed PD per IMWG criteria, or death due to any cause, whichever occurred first. | Among patients who attained an OR (based on PR or VGPR), this was the time from the first documentation of OR until progression or death due to any cause, whichever occurred first. | Among patients who attained an OR, this was the time from the first documentation of OR until progression or death due to any cause, whichever occurred first. | |
CR = complete response; DOR = duration of response; FLC = free light chain; IMWG = International Myeloma Working Group; MM = multiple myeloma; OR = objective response; ORR = objective response rate; OS = overall survival; PD = progressive disease; PFS = progression-free survival; PR = partial response; sCR = stringent complete response; TCR = triple-class refractory; VGPR = very good partial response.
Note: Details included in Table 23 are from the sponsor’s Summary of Clinical Evidence.
The COTA database uses a third-party obituary data source to capture mortality data. COTA defines progression based on IMWG criteria. COTA defines a progression as an increase of 25% or more from the lowest response value in any 1 or more of the following criteria: Serum Protein Electrophoresis(SPEP) with an absolute increase of more than 0.5 g/dL; 24-hour Urine protein electrophoresis (UPEP) with an absolute increase of more than 200 mg per 24 hours; in patients without measurable serum and urine M protein, the absolute increase of more than 10 mg/dL in the difference between involved and uninvolved FLC levels; or an absolute bone marrow plasma cell percentage of more than 10%. The Flatiron Health database’s mortality variable is created through an amalgamation of structured data elements and unstructured documents, and by linking to external mortality sources and the Social Security Death Index. Flatiron Health defines progression based on IMWG criteria. Flatiron Health defines a progression as an increase of 25% or more from baseline or nadir value in any 1 or more of the following: an absolute increase in serum M protein by SPEP by 0.5 g/dL or more; serum M protein of 1 g/dL or more if the lowest M component was 5 g/dL or more; an absolute increase in urine M protein by UPEP by 200 mg or more per 24 hours; or in patients without measurable serum and urine M protein levels, an absolute increase in the difference between involved and uninvolved FLC levels of more than 10 mg/dL.
Sources: Study C1071024 and Study C1071031 technical reports.48,49
Statistical Analysis for Study C1071024 and Study C1071031
Methods
No formal sample size estimates were calculated for these study. The study sample was identified from the analysis of secondary data that had already been collected. Accordingly, the sample size was limited by the duration of the observation window.
A total of 6 datasets and 7 datasets were created using the various sources based on critical eligibility criteria and expanded eligibility criteria (additional criteria were added for sensitivity analyses to assess the potential influence of the selection process based on the eligibility criteria) in Study C1071024 and Study C1071031, respectively. Each dataset used the same patients from the MagnetisMM-3 trial along with varying RW patients.
For the main analysis and sensitivity analyses to address the primary and secondary objectives:
the MagnetisMM-3 trial, cohort A arm, plus the external control arm selected chose to use critical eligibility criteria from the COTA database
the MagnetisMM-3 trial, cohort A arm, plus the external control arm selected using critical eligibility criteria from the Flatiron Health database.
For a sensitivity analysis based on alternative inclusion and exclusion criteria:
the MagnetisMM-3 trial, cohort A arm, plus the external control arm selected using expanded eligibility criteria from the COTA database
the MagnetisMM-3 trial, cohort A arm, plus the external control arm selected using expanded eligibility criteria from Flatiron Health database.
For the additional analyses based on the MagnetisMM-3 trial, cohort A and cohort B:
the MagnetisMM-3 trial, cohort A and cohort B arms, plus the external control arm selected using critical eligibility criteria from the COTA database
the MagnetisMM-3 trial, cohort A and cohort B arms, plus the external control arm selected using critical eligibility criteria from the Flatiron Health database.
For the analysis of PROs (via the EORTC QLQ-MY20 tool):
the MagnetisMM-3 trial, cohort A and cohort B arms, plus the external control arm selected using critical eligibility criteria from the prospective observational Study C1071013 and Study C1071014.
For the main analysis in Study C1071024 and Study C1071031, differences in baseline and key covariate characteristics between participants in the MagnetisMM-3 trial and each external control arm, including treatment history and disease-related characteristics at the index date, were balanced using IPTW. In a sensitivity analysis, the robustness of the estimates from the primary analysis was assessed via doubly robust estimation using a semiparametric approach described by Yadlowsky et al.52 Furthermore, sensitivity analyses were conducted to evaluate the effect of alternative inclusion and exclusion criteria, and to evaluate any differences in the magnitude of treatment effect when also accounting for prior exposure to BCMA-directed therapy. Finally, a quantitative bias analysis (nullification analysis) was performed to evaluate the robustness of results in the presence of potential threats to internal validity.
A systematic literature review was conducted to identify variables most strongly and consistently correlated with outcomes in RWD studies conducted among patients with RRMM. Results from 57 identified studies supported adjustment for the following covariates that were strongly associated with outcomes in patients with RRMM:
age
sex
cytogenic risk
number of prior lines of therapy
ECOG PS score
time since initial MM diagnosis
penta-refractory status
ISS stage.
Additional confounders were identified and included in the analysis to optimize the balance between participants from the MagnetisMM-3 trial and each RW data source. The confounders identified were based on their clinical importance and relevance to disease prognosis and disease complications:
disease prognosis, severity, and complications — the level of serum albumin, calcium, hemoglobin, and serum creatinine; the presence of bone lesions; and extramedullary disease
liver dysfunction — the level of serum bilirubin, aspartate aminotransferase, and alanine aminotransferase
burden of comorbid conditions — the Charlson Comorbidity Index score.
The value of each confounding variable was measured on or before the index date; if before, the most recent measurement was used. Of note, the presence of extramedullary disease was only available for the analyses using the combined datasets of the MagnetisMM-3 trial and COTA database patients, because this variable was unavailable in the Flatiron Health database. Next, due to the high percentage of missing values in the COTA database, bilirubin, calcium in serum or plasma, and serum albumin were included only in the analyses using the combined datasets of the MagnetisMM-3 study and Flatiron Health database patients. Information used to construct the Charlson Comorbidity Index was assessed up to 12 months before the index date, inclusive. For RW patients, the Charlson Comorbidity Index was obtained directly from the data source; for MagnetisMM-3 study participants, it was derived from the Medical Dictionary for Regulatory Activities classification of available patient comorbidity information. Values for other clinical covariates identified as potential confounders were measured on or up to 90 days before the index date; if before, the most recent measurement was used.
PSs and IPTW
To control baseline confounding, PSs were estimated using logistic regression models as the probability of initiating elranatamab versus SOC conditional on patient characteristics described earlier for both Study C1071024 and Study C1071031. Standardized mean differences (SMDs) were used to assess the balance in baseline prognostic characteristics between elranatamab and SOC-treated patients before and after applying IPTW. The SMDs were estimated for means (continuous variables) and prevalence (dichotomous variables), which were considered balanced across exposure groups if the corresponding SMD was 20% or less. To ensure that the estimated IPTW would allow for obtaining unbiased estimates of the treatment effect, several assumptions were verified.
Weighted Analyses Of PFS, OS, and Resposnse Rates
The proportional hazards assumption was tested based on the visual assessment of the Kaplan-Meier curves and using the Schoenfeld residuals test. Because the proportional hazards assumption was not adjusted for when comparing survival curves (PFS and OS) in participants of the MagnetisMM-3 study and patients from the Flatiron Health database, unadjusted and IPT-weighted restricted mean survival time models were applied instead of the Cox proportional hazards regression model.
ORR was compared between treatment groups using unadjusted and IPT-weighted log-binomial models. Robust standard errors were used for IPT-weighted analysis. DOR was compared between treatment groups using HRs estimated from unadjusted and IPT-weighted Cox proportional hazards models. Differences were considered statistically significant at P values of less than 0.05.
Subgroup Analysis for PFS and OS
The sponsor provided a rationale for the subgroup analysis, stating that the treatment patterns described in the COTA and Flatiron Health databases may not be generalizable to all non-US countries. Subgroup analyses were performed to only include treatments frequently available for this patient population in non-US countries. For subgroups with a sufficient sample size, PFS and OS were compared between participants of the MagnetisMM-3 trial and patients from the Flatiron Health and COTA databases using IPTW analysis.
Missing Values
For both Study C1071024 and Study C1071031, incomplete dates of death (i.e., missing day) were imputed in the RW data to match the rules of the MagnetisMM-3 study. The Flatiron Health database provides only the month and year of death. Therefore, the date of death was imputed as the middle of the month (i.e., the 15th), unless the patient’s last record date was within the month of death, in which case the date of death was imputed as the date of the last record. The COTA database provides the precise date of death for most patients. When the date of death is missing, the COTA database by default imputes the date of the death as the middle of the month when the month is known, and as the middle of the year when only the year is known. For patients whose month of death is known, the date of death was imputed as the last record date if it was within 15 days of the date of death provided by the COTA database (otherwise, the default date of death was kept). For patients whose year of death only was known, the date of death was imputed as the last record date if it fell within 182 days of the date of death provided by the COTA database (otherwise, the default date of death was kept).
For the baseline characteristics, a missing day component was imputed as the last day of the corresponding month to decide whether the measurement lay within the baseline period for qualifying as the baseline value. A missing month component was not imputed, but if it was clear from the year component that the covariate fell within the baseline period, the measurement was taken into consideration. A missing year component was not imputed.
For each baseline covariate, the proportion of missing values was assessed. For covariates with a proportion of missing values of 30% or less, multiple imputation was performed under the assumption of missingness at random. Multiple imputation by chained equations was performed to address missing values, using the fully conditional specification method. Variables included in the imputation model were baseline characteristics used to estimate the PS, measured covariates related to missingness and those correlated with the covariate of interest, as well as the cumulative baseline hazard for time-to-event models.
The convergence of imputation models obtained via multiple imputation by chained equations was assessed. The distributions of covariates in the observed and imputed data were visually assessed using plots. Convergence was evaluated by plotting the mean and variance of each imputation run across iterations, to confirm that there were no apparent trends.
Sensitivity Analyses
A conditional average treatment effect and its associated HR were estimated using a semiparametric approach. This estimator provided a doubly robust comparison for PFS and OS between treatment arms. Standard errors and 95% CIs were obtained for this estimator using the nonparametric bootstrap.
To evaluate the robustness of primary analysis results, a sensitivity analysis was conducted using the set of all participants within cohort A of the MagnetisMM-3 study who received at least 1 dose of elranatamab and RW patients selected using expanded eligibility criteria. The analyses were conducted to compare the PFS and OS using IPT-weighted analyses. A nullification analysis was applied to assess the potential influence of unmeasured confounding on the observed associations. A sensitivity analysis was conducted to assess the potential influence of unmeasured confounders on the estimates described in the main analyses.
Analysis of PROs (EORTC QLQ-MY20)
For each treatment group (elranatamab or SOC), the number and percentage of participants who completed the EORTC QLQ-MY20at each visit and the timing of PRO completion by treatment group were described. An instrument was considered completed if at least half of the item was answered by the participant. In this study, 2 symptom scales (disease symptoms and side effects of treatment) for the EORTC QLQ-MY20 module were assessed. For this analysis, the PROs (via the EORTC QLQ-MY20 tool) collected at baseline and at monthly follow-up visits up to month 6 were analyzed. The time points for the follow-up measurements were determined after the assessment of the data completion status.
PROs (EORTC QLQ-MY20) were compared among MagnetisMM-3 study participants and patients from the Study C1071013 and Study C1071014 prospective observational studies in unadjusted analyses and analyses adjusted for age, sex, baseline values of ECOG PS scores, extramedullary disease, and high cytogenetic risk, and time of PROs completion (EORTC QLQ-MY20). A higher score for the EORTC QLQ-MY20 disease symptoms and side effects of treatment scales represented a higher perceived level of symptoms or problems.
A mixed model of repeated measures was fitted to the data to examine the effects of time (visit) among patients treated with elranatamab versus SOC. Mixed models of repeated measures were also used for the domains of EORTC QLQ-MY20 to examine the effects of time (visit) by cohort and overall. In the model, outcomes were postbaseline scores (and change scores separately), the predictor was the treatment group (elranatamab versus SOC), and the controlling covariates were the corresponding baseline PROs score (EORTC QLQ-MY20), age (< 65 years versus ≥ 65 years), sex, ECOG PS score (0 versus 1+), extramedullary disease (yes versus no), high cytogenetic risk (yes versus no), and time (visit).
Results
Patient Disposition (Study C1071031)
Between February 2021 and January 2022, the MagnetisMM-3 trial, cohort A, enrolled 123 patients with TCR MM who were included in the main analysis for Study C1071031. Applying the critical eligibility criteria to the databases identified 239 patients with TCR MM in the COTA database who had initiated a new line of therapy between November 2015 and June 2022 (Figure 4), as well as 152 patients with TCR MM in the Flatiron Health database who had initiated a new line of therapy between November 2015 and August 2021 (Figure 5) to create external control arms for Study C1071024 and Study C1071031. The median follow-up times for included patients were 14.7 months in the MagnetisMM-3 trial, cohort A; 8.8 months for patients with TCR MM from the COTA database; and 7.7 months for patients with TCR MM from the Flatiron Health database. Study C1071024 had similar patient disposition, with slight differences in the cohort from the COTA database.
Baseline Characteristics
Table 24 shows the baseline demographic and clinical characteristics of included patients from the MagnetisMM-3 study, cohort A, and the COTA and Flatiron Health databases included in Study C1071031. The characteristics for participants included in Study C1071024 are not described here, as the numbers are the same for both the MagnetisMM-3 study, cohort A, and the Flatiron Health database, with a slight difference in the COTA database (N = 239 in Study C1071031 and N = 233 in Study C1071024). Some differences were noted in the baseline characteristics among patients. The MagnetisMM-3 study population was slightly more pretreated than the COTA or Flatiron Health database populations (the number of mean treatment lines were 5.2 versus 4.9 versus 4.0, respectively) and more likely to have previously received stem cell transplant (70.7% versus 57.3% versus 36.2%, respectively). The MagnetisMM-3 study population was more likely to have extramedullary disease compared to the COTA database population (30.9% versus 13.4%, respectively), while the COTA database population was more likely to have bone lesions than the MagnetisMM-3 study population or the Flatiron Health database population (50.6% versus 27.6% versus 11.8%, respectively). No major differences in cytogenetic risk were noted between the 3 different databases.
Figure 4: Flow Chart for Selection of Cohort From COTA DATABASE Using the Critical Eligibility Criteria (Study C1071031)
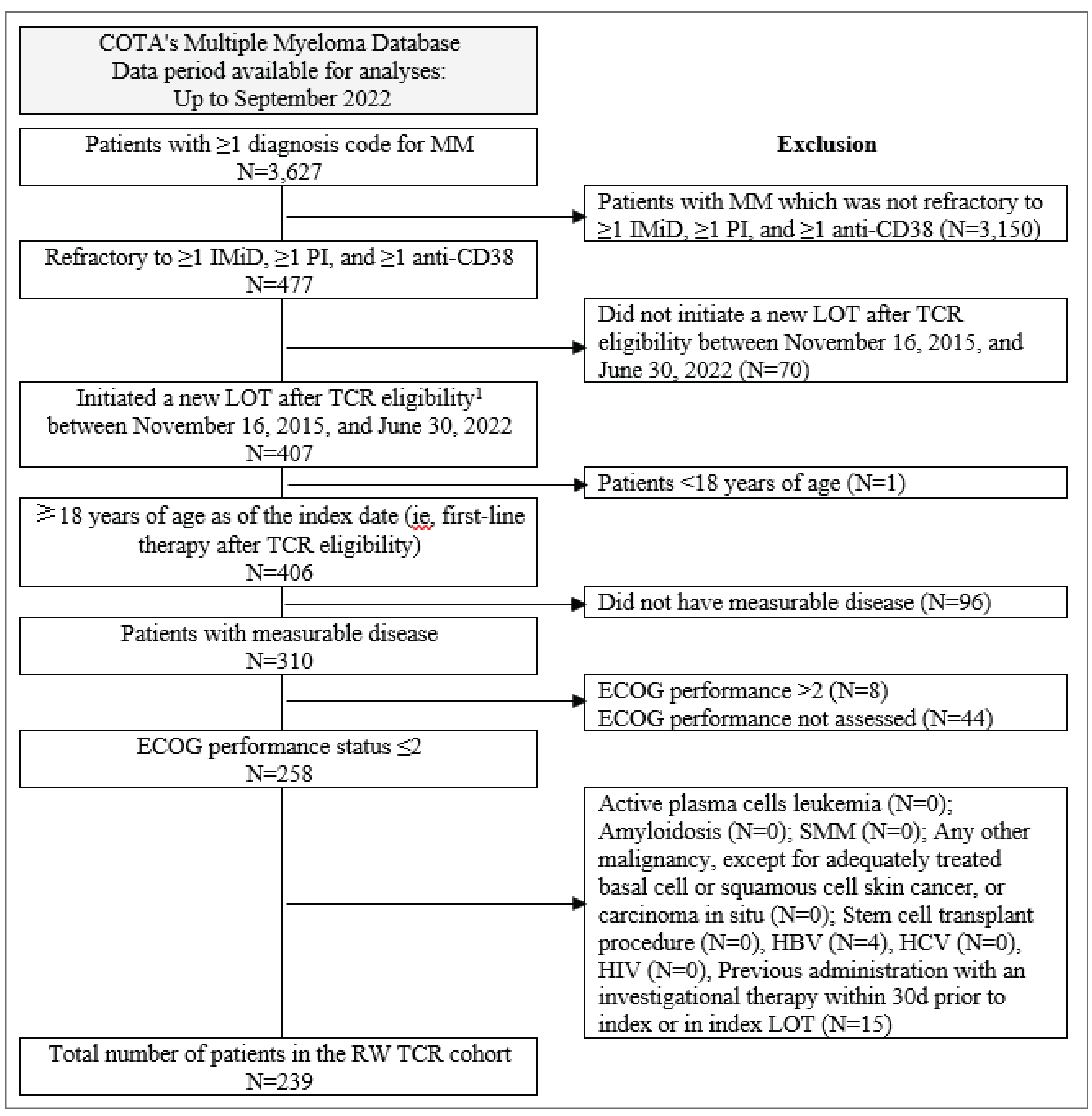
D = day; ECOG = Eastern Cooperative Oncology Group; HBV = hepatitis B virus; HCV = hepatitis C virus; IMiD = immunomodulatory drug; LOT = line of therapy; MM = multiple myeloma; PI = proteasome inhibitor; RW = real world; SMM = smouldering multiple myeloma; TCR = triple-class refractory.
1 TCR eligibility is defined as the earliest date on which patients were identified as having MM refractory to 1 or more IMiD, 1 or more PI, and 1 or more anti-CD38.
Source: Study C1071031 technical report.49
Figure 5: Flow Chart for Selection of Cohort from Flatiron Health Database Using the Critical Eligibility Criteria (Study C1071031)
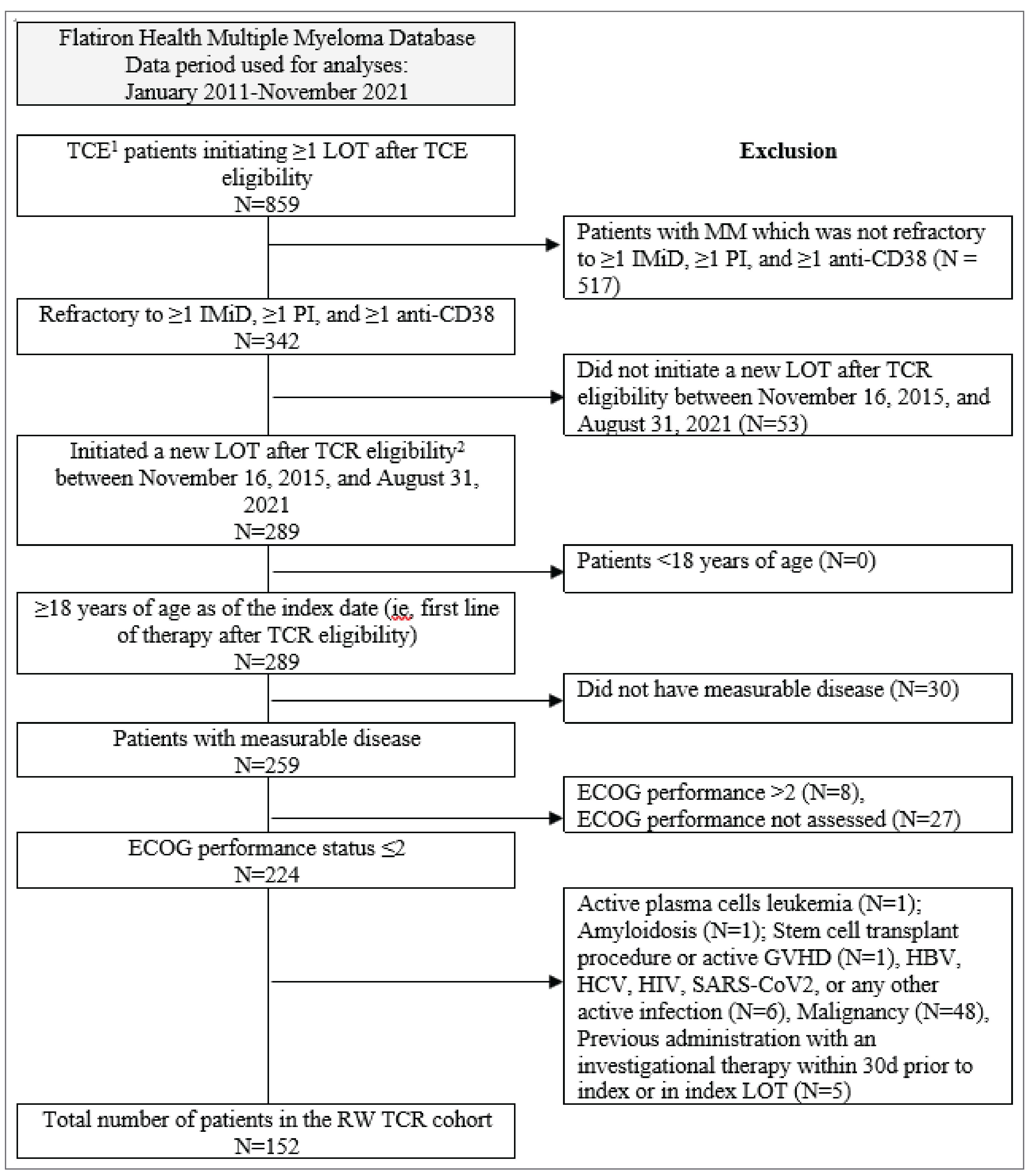
ECOG = Eastern Cooperative Oncology Group; GVHD = graft-versus-host disease; HBV = hepatitis B virus; HCV = hepatitis C virus; IMiD = immunomodulatory drug; LOT = line of therapy; MM = multiple myeloma; PI = proteasome inhibitor; RW = real world; SARS-CoV-2 = severe acute respiratory syndrome coronavirus 2; TCE = triple-class exposed; TCR = triple-class refractory.
1 The identification of patients in the Flatiron Health and COTA databases followed a different stepwise approach. TCE was defined as patients exposed to at least 1 PI, 1 IMiD, and 1 anti-CD38 monoclonal antibody.
2 TCR eligibility was defined as the earliest date on which patients were identified as having MM refractory to 1 or more IMiD, 1 or more PI, and 1 or more anti-CD38.
Source: Study C1071031 technical report.49
Multiple imputation by chained equations (for missing data) and IPTW were applied in an attempt to improve the balance of the 3 populations’ baseline demographic and disease characteristics. After applying these techniques, the SMDs were less than the prespecified threshold of 0.2 for all important prognostic factors in the comparison of the MagnetisMM-3 study and the COTA database populations, while a few characteristics were not balanced in the comparison of the MagnetisMM-3 study and the Flatiron Health database populations (ECOG PS score, time since initial MM diagnosis, Charlson Comorbidity Index score, the number of lines of therapy before the index date, and history of stem cell transplant). The details are in Table 25.
For the analysis of the PROs (EORTC QLQ-MY20), a total of 67 patients from prospective cohort studies Study C1071013 and Study C1071014 were included. Baseline characteristics were compared between participants of the MagnetisMM-3 trial and Study C1071013 and Study C1071014. Most baseline characteristics between Study C1071013 and Study C1071014 were generally similar, although compared to the MagnetisMM-3 trial’s population, the population from the observational studies had higher proportions of ISS stage III (18.3% for the MagnetisMM-3 trial participants and 37.8% for the Study C1071013 and Study C1071014 patients), an ECOG PS score of 2 (5.6% for the MagnetisMM-3 trial participants and 20.0% for the Study C1071013 and Study C1071014 patients), and high-risk cytogenetics (24.4% for the MagnetisMM-3 trial participants and 42.2% for the Study C1071013 and Study C1071014 patients). A higher proportion of participants in the MagnetisMM-3 trial had extramedullary disease compared to patients from the observational studies (38.9% for the MagnetisMM-3 trial participants and 13.3% for the Study C1071013 and Study C1071014 patients). Baseline demographic and clinical characteristics of the participants of the MagnetisMM-3 trial and patients in the prospective observational trials Study C1071013 and Study C1071014 are presented in Table 26.
Table 24: Baseline Demographics and Disease Characteristics of Participants of MagnetisMM-3 Trial, Cohort A, and RW Patients Identified From COTA and Flatiron Health Databases Before Matching (Study C1071031)
Characteristic | MagnetisMM-3 trial, cohort A (N = 123) | COTA database (N = 239) | Flatiron Health database (N = 152) |
|---|---|---|---|
Demographics | |||
Age at the index date in years, mean (SD) | 67.1 (9.4) | 68.0 (9.4) | 69.5 (10.0) |
Sex, n (%) | |||
Male | 68 (55.3) | 130 (54.4) | 80 (52.6) |
Female | 55 (44.7) | 109 (45.6) | 72 (47.4) |
Body mass index (kg/m2), mean (SD) | 26.6 (5.4) | 29.0 (6.2) | 27.4 (5.6) |
Race, n (%) | |||
White | 72 (58.5) | 175 (73.2) | 102 (67.1) |
Non-white | 51 (41.5) | 64 (26.8) | 50 (32.9) |
Disease characteristics | |||
ISS stage, within 90 days before or on the index date, n (%) | |||
I | 35 (28.5) | 31 (13.0) | 11 (7.2) |
II | 45 (36.6) | 26 (10.9) | 19 (12.5) |
III | 25 (20.3) | 22 (9.2) | 19 (12.5) |
ECOG PS, within 90 days before or on the index date, n (%) | |||
0 | 45 (36.6) | 71 (29.7) | 47 (30.9) |
1 | 71 (57.7) | 129 (54.0) | 81 (53.3) |
2 | 7 (5.7) | 39 (16.3) | 24 (15.8) |
Time from initial MM diagnosis to the index date (years), mean (SD) | 6.6 (3.8) | 5.4 (4.4) | 4.1 (2.2) |
Penta-refractory status at TCR eligibility date, n (%) | 52 (42.3) | 45 (18.8) | 23 (15.1) |
High cytogenetic risk, on or before the index date, n (%) | 31 (25.2) | 49 (20.5) | 38 (25.0) |
Presence of bone lesion on or before the index date, n (%) | 34 (27.6) | 121 (50.6) | 18 (11.8) |
Extramedullary disease on or before the index date, n (%) | 38 (30.9) | 32 (13.4) | Not reported |
MM treatment history | |||
Number of preindex treatment lines, mean (SD) | 5.2 (2.6) | 4.9 (2.4) | 4.0 (1.7) |
Stem cell transplant on or before the index date, n (%) | 87 (70.7) | 137 (57.3) | 55 (36.2) |
Comorbidity profile | |||
Charlson Comorbidity Index score before or on the index date, n (%) | |||
2 | 83 (67.5) | 200 (83.7) | 121 (79.6) |
3 | 21 (17.1) | 22 (9.2) | 14 (9.2) |
4 | 11 (8.9) | 11 (4.6) | 10 (6.6) |
5 | 6 (4.9) | 4 (1.7) | 4 (2.6) |
6 | 2 (1.6) | 2 (0.8) | 3 (2.0) |
ECOG PS = Eastern Cooperative Oncology Group Performance Status; ISS = International Staging System; MM = multiple myeloma; RW = real world; SD = standard deviation; TCR = triple-class refractory.
Note: Details included in Table 24 are from the sponsor’s Summary of Clinical Evidence.
Source: Study C1071031 technical report.49
Table 25: Baseline Demographics and Disease Characteristics of Participants of MagnetisMM-3 Trial, Cohort A, and RW Patients Identified From COTA and Flatiron Health Databases After Applying MICE and IPTW (Study C1071031)
Detail | After MICEa unweighted | After MICEa and IPT-weightingb | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
Characteristics | MagnetisMM-3 trial, cohort A (N = 123) | COTA database (N = 239) | SMDc | Flatiron Health database (N = 152) | SMDc | MagnetisMM-3 trial, cohort A (N = 113) | COTA database (N = 235.2) | SMDc | Flatiron Health database (N = 150.6) | SMDc |
Demographics | ||||||||||
Age at the index date in years, mean | 67.1 | 68.0 | 0.102 | 69.5 | 0.246 | 68.5 | 67.3 | 0.125 | 69.2 | 0.062 |
Sex, % | ||||||||||
Male | 55.3 | 54.4 | 0.018 | 52.6 | 0.053 | 49.9 | 53.7 | 0.076 | 55.6 | 0.041 |
Female | 44.7 | 45.6 | 47.4 | 50.1 | 46.3 | 44.4 | ||||
Body mass index (kg/m2), mean | 26.6 | 28.9 | 0.391 | 27.4 | 0.141 | 26.5 | 29.2 | 0.502 | 27.9 | 0.304 |
Race, % | ||||||||||
White | 58.5 | 73.2 | 0.314 | 67.1 | 0.178 | 67.0 | 69.7 | 0.059 | 63.2 | 0.122 |
Non-white | 41.5 | 26.8 | — | 32.9 | — | 33.0 | 30.3 | — | 36.8 | — |
Disease characteristics | ||||||||||
ISS stage, within 90 days before or on the index date, % | ||||||||||
I | 28.5 | 13.0 | 1.258 | 7.2 | 1.309 | 20.7 | 20.4 | 0.085 | 16.6 | 0.135 |
II | 36.6 | 10.9 | — | 12.5 | — | 20.8 | 17.9 | — | 29.1 | — |
III | 20.3 | 9.2 | — | 12.5 | — | 12.0 | 11.9 | — | 10.5 | — |
Unknown or not assessed | 14.6 | 66.9 | — | 67.8 | — | 46.5 | 49.8 | — | 43.9 | — |
ECOG PS score, within 90 days before or on the index date, % | ||||||||||
0 | 36.6 | 29.7 | 0.371 | 30.9 | 0.367 | 34.0 | 31.2 | 0.066 | 30.8 | 0.261 |
1 | 57.7 | 54.0 | — | 53.3 | — | 53.1 | 55.6 | — | 46.9 | — |
2 | 5.7 | 16.3 | — | 15.8 | — | 12.9 | 13.2 | — | 22.3 | — |
Time from initial MM diagnosis to the index date (years), mean | 6.6 | 5.4 | 0.280 | 4.1 | 0.798 | 6.2 | 5.7 | 0.135 | 4.8 | 0.349 |
High cytogenetic risk, % | 25.2 | 20.5 | 0.112 | 25.0 | 0.005 | 15.3 | 22.2 | 0.177 | 22.8 | 0.037 |
Presence of bone lesion during the baseline period or on the index date, % | 27.6 | 50.6 | 0.485 | 11.8 | 0.405 | 43.8 | 44.9 | 0.022 | 23.7 | 0.078 |
Extramedullary disease % | 30.9 | 13.4 | 0.431 | — | — | 31.0 | 22.6 | 0.192 | — | — |
MM treatment history | ||||||||||
Number of LOTs used before index date (T1), mean | 5.2 | 4.9 | 0.124 | 4.0 | 0.555 | 5.3 | 4.9 | 0.130 | 4.4 | 0.528 |
Refractory status at the time of TCR eligibility (T0), % | ||||||||||
Penta-refractory MM | 42.3 | 18.8 | 0.526 | 15.1 | 0.629 | 32.3 | 24.6 | 0.170 | 23.4 | 0.270 |
SCT during the baseline period, % | 70.7 | 57.3 | 0.282 | 36.2 | 0.738 | 65.4 | 62.5 | 0.060 | 44.9 | 0.416 |
Laboratory values, mean | ||||||||||
Aspartate aminotransferase (microkat/L) | 0.4 | 0.4 | 0.013 | 0.4 | 0.019 | 0.4 | 0.4 | 0.093 | 0.4 | 0.061 |
Alanine aminotransferase (microkat/L) | 0.3 | 0.4 | 0.237 | 0.3 | 0.036 | 0.3 | 0.4 | 0.198 | 0.3 | 0.030 |
Bilirubin | 9.0 | 8.5 | 0.074 | 8.3 | 0.112 | 9.6 | 9.1 | 0.072 | 9.4 | 0.004 |
Hemoglobin (g/L) | 104.0 | 105.2 | 0.066 | 103.5 | 0.025 | 103.7 | 104.4 | 0.038 | 104.0 | 0.025 |
Creatinine clearance (mL per minute) | 74.1 | 70.2 | 0.108 | 62.5 | 0.359 | 72.9 | 76.2 | 0.086 | 71.4 | 0.014 |
Calcium in serum or plasma (mmol/L) | 2.3 | 2.3 | 0.169 | 2.3 | 0.046 | 2.3 | 2.3 | 0.008 | 2.3 | 0.110 |
Serum albumin (g/dL) | 36.1 | 34.6 | 0.273 | 34.1 | 0.368 | 35.4 | 34.9 | 0.088 | 34.0 | 0.114 |
Comorbidity profile | ||||||||||
Charlson Comorbidity Index score during the year before or on the index date, % | ||||||||||
2 | 67.5 | 83.7 | 0.429 | 79.6 | 0.262 | 81.6 | 80.7 | 0.078 | 70.6 | 0.250 |
3 | 17.1 | 9.2 | — | 9.2 | — | 10.1 | 11.4 | — | 14.4 | — |
4 | 8.9 | 4.6 | — | 6.6 | — | 4.9 | 4.7 | — | 6.7 | — |
5 | 4.9 | 1.7 | — | 2.6 | — | 2.8 | 2.6 | — | 7.0 | — |
6+ | 1.6 | 0.8 | — | 2.0 | — | 0.7 | 0.7 | — | 1.2 | — |
ECOG PS = Eastern Cooperative Oncology Group Performance Status; IPT = inverse probability of treatment; IPTW = inverse probability of treatment weighting; ISS = International Staging System; LOT = line of therapy; MICE = multiple imputation by chained equation; MM = multiple myeloma; PS = propensity score; RW = real world; SCT = stem cell transplant; SMD = standardized mean difference; TCR = triple-class refractory.
Note: Details included in Table 25 are from the sponsor’s Summary of Clinical Evidence.
aMICE using the fully conditional specification method was performed to address missing values in baseline covariates included in the PS model. Summary statistics and standardized difference values reported in this table were first calculated individually within each of the imputed datasets, and then were averaged across the datasets. Due to rounding of descriptive statistics, some standardized differences are greater than 0 when there appears to be no difference in the balance of covariates.
bWeights used to produce these preliminary results were stabilized and truncated at the 99.5th percentile.
cUnlike t tests and other statistical tests of hypothesis, the standardized difference is not influenced by sample size and can therefore be used to compare balance in observed covariates between large study cohorts. It also allows for the comparison of the relative balance of continuous variables measured in different units (e.g., age vs. number of immunosuppressant medications) by calculating each in standard deviation units. For the purposes of the current study, a standardized difference threshold of more than |0.2| was used to identify imbalanced covariates. The proposed threshold aligns with the literature, where authors generally proposed thresholds ranging from more than |0.10| to more than |0.20| to define covariate imbalance.
Source: Study C1071031 technical report.49
Table 26: Baseline Demographics and Disease Characteristics of Participants of MagnetisMM-3 Trial, Cohort A and Cohort B, and Patients in Prospective Observational Studies C1071013 and C1071014 [Redacted]
Characteristic | MagnetisMM-3 trial, cohort A and cohort B (N = 180) | SOC, Study C1071013, no CAR T-cell therapy (N = 18) | SOC, Study C1071014, no CAR T-cell therapy (N = 27) | (Study C1071013 and Study C1071014) (N = 45)a |
|---|---|---|---|---|
████████████ | ||||
███ ██ ███ █████ ████ ██ ██████ █ | ████ █████ | ████ █████ | ████ █████ | ████ █████ |
████ █ ███ | ||||
████ | ██ ██████ | ██████ | ██ ██████ | ██ ██████ |
██████ | ██ ██████ | ██ ██████ | ██ ██████ | ██ ██████ |
█████████████ ███████████ | ████ █████ | ████ █████ | ████ █████ | ████ █████ |
█████ █ ███ | ||||
█████ | ███ ██████ | ███ ████████ | ██ ███████ | ███ ████████ |
█████████ | ██ ██████ | ███ ████████ | ███ | ███ ████████ |
█████████████ | ||||
███ ██████ ██ ██ ████ ██████ ██ ██ ███ █████ █████ | ||||
██ | ██ ██████ | ██████ | ██ ██████ | ██ ██████ |
██ | ███ ██████ | ██████ | ██████ | ██████ |
███ | ██ ██████ | ██ ██████ | ██████ | ██ ██████ |
███████ ██ ███ ████████ | ██ █████ | ██████ | ██████ | █████ |
████ ██████████ █████ █████ | ||||
██████ | ██████ | ██████ | ██████ | ██████ |
██████ | ██████ | ██████ | ██████ | ██████ |
██████ | ██████ | ██████ | ██████ | ██████ |
████ ████ ███████ ██ █████████ ██ ███ ███████████ | ██████ | ██████ | ██████ | ██████ |
████████ █ ███ | ██████ | ██████ | ██████ | ██████ |
████ ███████████ █████ ██ ██ ██████ | ██████ | ██████ | ██████ | ██████ |
████████ ██ █████ ██ ██ ██████ ███ | ██ ██████ | ███████ | ██████ | ███ ████████ |
█████████ | ██ ██████ | ██████ | ██████ | ██████ |
█████████ | ||||
█████████ | ███ █████ | ███ █████ | ██████ | ███ █████ |
█████████ | ███ ██████ | ██████ | ██████ | ███ ████████ |
████████████ | ||||
█████████████ | ||||
████ ████ | ███ █████ | ███ █████ | ███ █████ | ███ █████ |
██████ █████ | ███ ████ █ | ███ ████ █ | ███ ████ █ | ███ ████ █ |
BCMA = B-cell maturation antigen; CAR = chimeric antigen receptor; ECOG PS = Eastern Cooperative Oncology Group Performance Status; FLC = free light chain; ISS = International Staging System; LOT = line of therapy; MM = multiple myeloma; SD = standard deviation; SOC = standard of care.
Note: Details included in Table 26 are from the sponsor’s Summary of Clinical Evidence.
aThe SOC combined cohort included patients with no CAR T-cell therapy and no history of BCMA from either SOC Study C1071013 or SOC Study C1071014. When information on a given patient characteristic was unavailable for 1 of the 2 SOC studies, a missing value was reported for the combined cohort.
Source: Study C1071031 technical report.49
Efficacy
PFS (Study C1071031)
During the study periods, PFS events (disease progression or death) were identified for 53 (43%) patients in the MagnetisMM-3 trial’s population, 136 (57%) patients in the COTA database population, and 88 (58%) patients in the Flatiron Health database population. In the unweighted analyses, the rate of PFS events per 1,000 patient-months were 49.4 events (95% CI, 37.8 events to 64.7 events) in the MagnetisMM-3 trial’s population, 110.9 events (95% CI, 93.7 events to 131.2 events) in the COTA database population, and 137.8 events (95% CI, 111.8 events to 169.9 events) in the Flatiron Health database population. The median PFS was not reached in the MagnetisMM-3 trial’s population, was 4.7 months in the COTA database population, and was 3.7 months in the Flatiron Health database population. The median PFS was longer with elranatamab versus RW SOC in the COTA database population, both before weighting (HR = 0.51 [95% CI, 0.37 to 0.71; P < 0.0001]) and after IPTW (HR = 0.37 [95% CI, 0.22 to 0.64; P = 0.0003]) (Table 27 and Figure 6). However, due to violations of the proportional hazards assumption, the unweighted and IPT-weighted comparisons between elranatamab and SOC in the Flatiron Health database population were conducted using restricted mean survival time analyses, as prespecified in the statistical analysis plan.
The results of the restricted mean survival time analyses for COTA and Flatiron Health databases are presented in Figure 7 and Figure 8, respectively. In the restricted mean survival time analyses, the average PFS was longer with elranatamab versus RW SOC in the COTA database population at 9 months, 12 months, 15 months, 18 months, and 24 months using both weighted and unweighted analyses. Similarly, the average PFS time was longer with elranatamab versus RW SOC in the Flatiron Health database population.
Table 27: PFS Comparison Between Elranatamab in MagnetisMM-3 Trial, Cohort A, and RW External Control Arms
Detail | MagnetisMM-3 trial, | COTA database | P value | MagnetisMM-3 trial, | Flatiron Health database | P value |
|---|---|---|---|---|---|---|
Participants | (N = 123) | (N = 239) | — | (N = 123) | (N = 152) | — |
Unweighted analysis | ||||||
HR (95% CI)a | 0.51 (0.37 to 0.71) | Reference | < 0.0001b | —c | Reference | — |
IPTW analysis | ||||||
HR (95% CI)d | 0.37 (0.22 to 0.64) | Reference | 0.0003b | —c | Reference | — |
CI = confidence interval; HR = hazard ratio; IPT = inverse probability of treatment; IPTW = inverse probability of treatment weighting; PFS = progression-free survival; RW = real world.
Note: Details included in Table 27 are from the sponsor’s Summary of Clinical Evidence.
aHRs were estimated using unadjusted Cox proportional hazards models.
bSignificant at the 5% level.
cFor the MagnetisMM-3 trial vs. Flatiron study comparison, the proportional hazards assumption was violated, and the HR could not be estimated.
dFor the IPTW analysis, IPTW HRs were estimated using weighted Cox proportional hazards models and CIs were estimated using robust error variances. Stabilized IPT weights truncated at the 99.5th percentile were used.
Source: Study C1071031 technical report.49
Figure 6: Forest Plot Summarizing Hazard Ratios for PFS Analysis
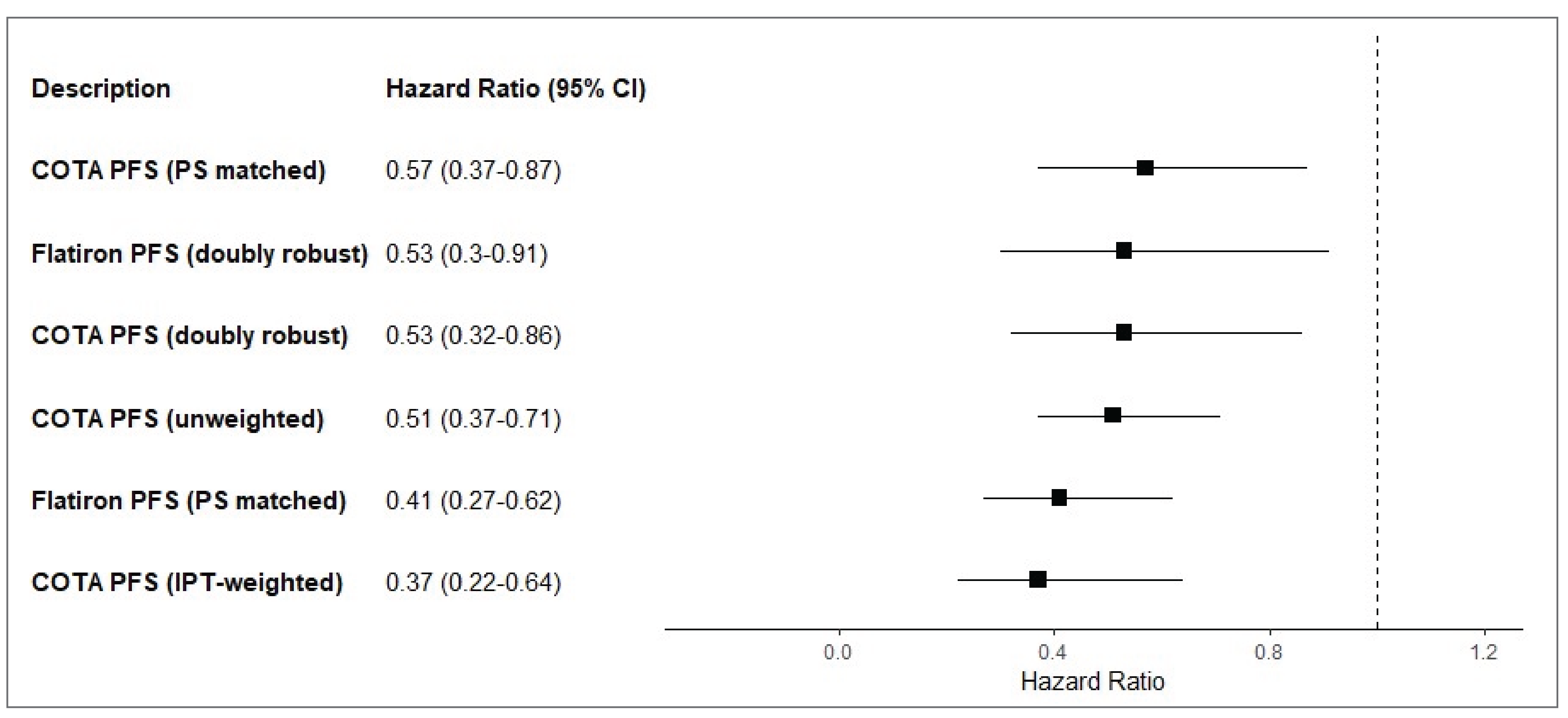
CI = confidence interval; IPT = inverse probability of treatment; PFS = progression-free survival; PS = propensity score.
Source: Study C1071031 technical report.49
OS (Study C1071031)
During the study periods, deaths were identified for 55 (45%) patients in the MagnetisMM-3 trial’s population, 171 (72%) patients from the COTA database population, and 90 (59%) patients from the Flatiron Health database population. In the unweighted analyses, the all-cause mortality rate (per 1,000 patient-months) was 37.7 (95% CI, 28.9 to 49.1) in the MagnetisMM-3 trial’s population, 52.9 (95% CI, 45.5 to 61.5) in the COTA database population, and 54.6 (95% CI, 44.4 to 67.1) in the Flatiron Health database population. The median OS was not reached in the MagnetisMM-3 trial and was 11.24 months in both the COTA and Flatiron Health database populations. The median OS was longer with elranatamab versus RW SOC in the COTA database population both before weighting (HR = 0.65 [95% CI, 0.47 to 0.88; P = 0.0062]) and after IPTW (HR = 0.46 [95% CI, 0.27 to 0.77; P = 0.0032]) (Table 28 and Figure 9). However, due to violations of the proportional hazards assumption, restricted mean survival time analyses were conducted for the COTA and Flatiron Health database populations (Figure 10 and Figure 11, respectively). In the restricted mean survival time analyses, the average OS time was longer with elranatamab versus RW SOC in the COTA database population at 12 months, 15 months, 18 months, and 24 months using the unweighted analyses, and was also longer at 9 months, 12 months, 15 months, 18 months, and 24 months using the IPT-weighted analyses. Similarly, the average OS time was longer with elranatamab versus RW SOC in the Flatiron Health database population at 9 months, 12 months, 15 months, 18 months, and 24 months using the unweighted analyses. A trend toward improved survival with elranatamab versus RW SOC in the Flatiron Health database population was observed using the IPT-weighted analyses, although the results did not reach statistical significance.
Figure 7: Kaplan-Meier Curves of PFS and RMST Estimates in MagnetisMM-3 Trial, Cohort A, and COTA Database External Control Arm Before IPTW (A) and After IPTW (B)
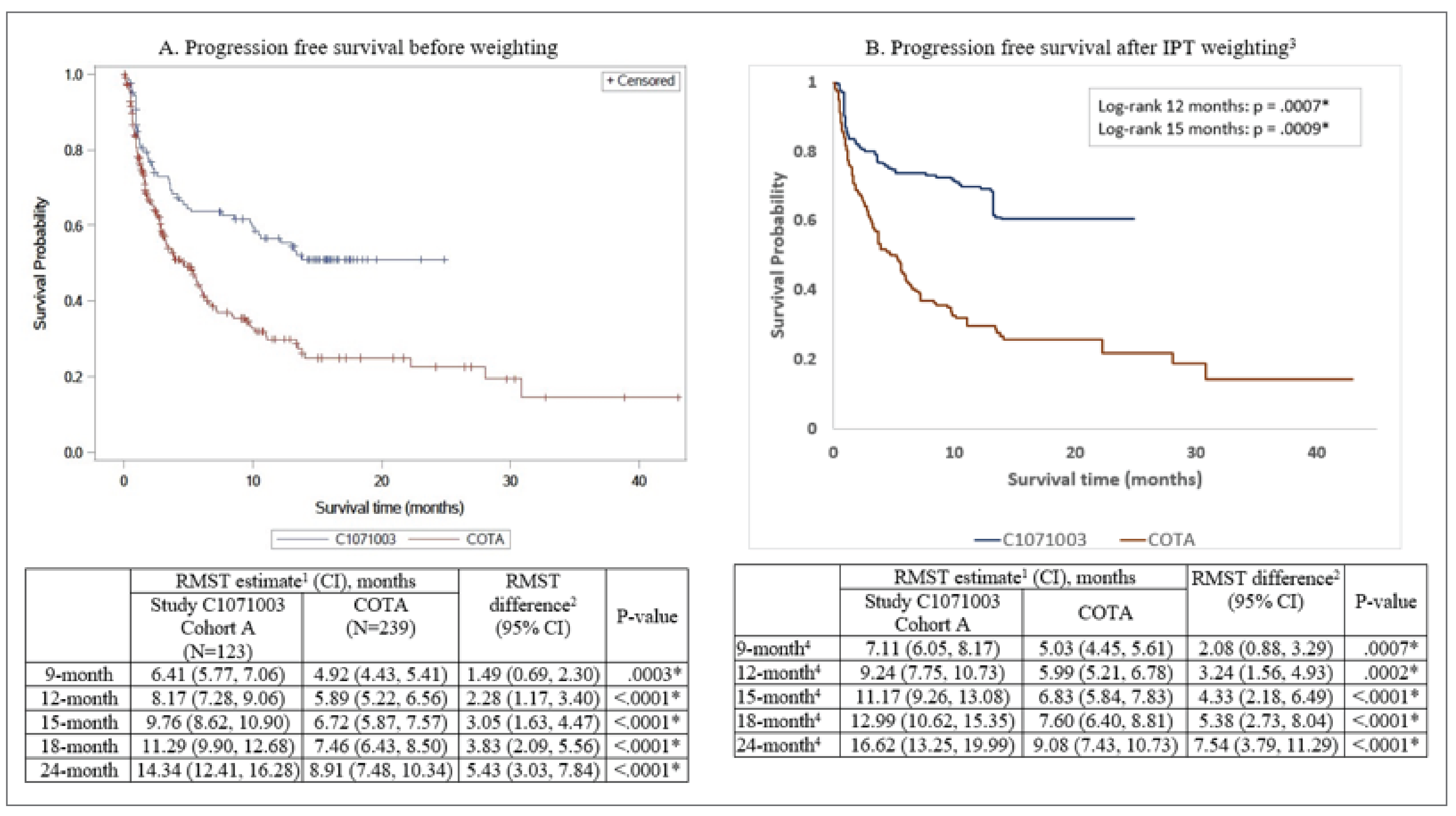
CI = confidence interval; IPT = inverse probability of treatment; IPTW = inverse probability of treatment weighting; PFS = progression-free survival; RMST = restricted mean survival time; RW = real world; TCR = triple-class refractory.
* Significant at the 5% level.
1 The RMST estimates correspond to the number of months patients in each cohort remain progression-free on average over a specified period following the date of the first dose for Study C1071003 patients and following the initiation of the first-line therapy after TCR for RW patients.
2 Unweighted RMST differences and P values were obtained using nonparametric Kaplan-Meier estimators, and IPT-weighted RMST differences and P values were obtained using adjusted RMST proposed by Conner et al. (Conner SC, Sullivan LM, Benjamin EJ, LaValley MP, Galea S, Trinquart L. Adjusted restricted mean survival times in observational studies. Stat Med. 2019 Sep 10;38(20):3832 to 3860.)
3 Kaplan-Meier estimates obtained from each of 5 imputed datasets were normalized using a complementary log-log transformation to satisfy the assumptions of Rubin’s pooling rules. The same transformation was applied to the standard errors for each Kaplan-Meier curve, which were obtained using the delta method. The transformed estimates and their standard errors were then analyzed as usual using the MIANALYZE procedure, and back-transformed to the original scale to produce a summary Kaplan-Meier plot.
4 Stabilized IPT weights truncated at the 99.5th percentile were used.
Source: Study C1071031 technical report.49
Figure 8: Kaplan-Meier Curves of PFS and RMST Estimates in MagnetisMM-3 Trial, Cohort A, and Flatiron Health Database External Control Arm Before IPTW (A) and After IPTW (B)
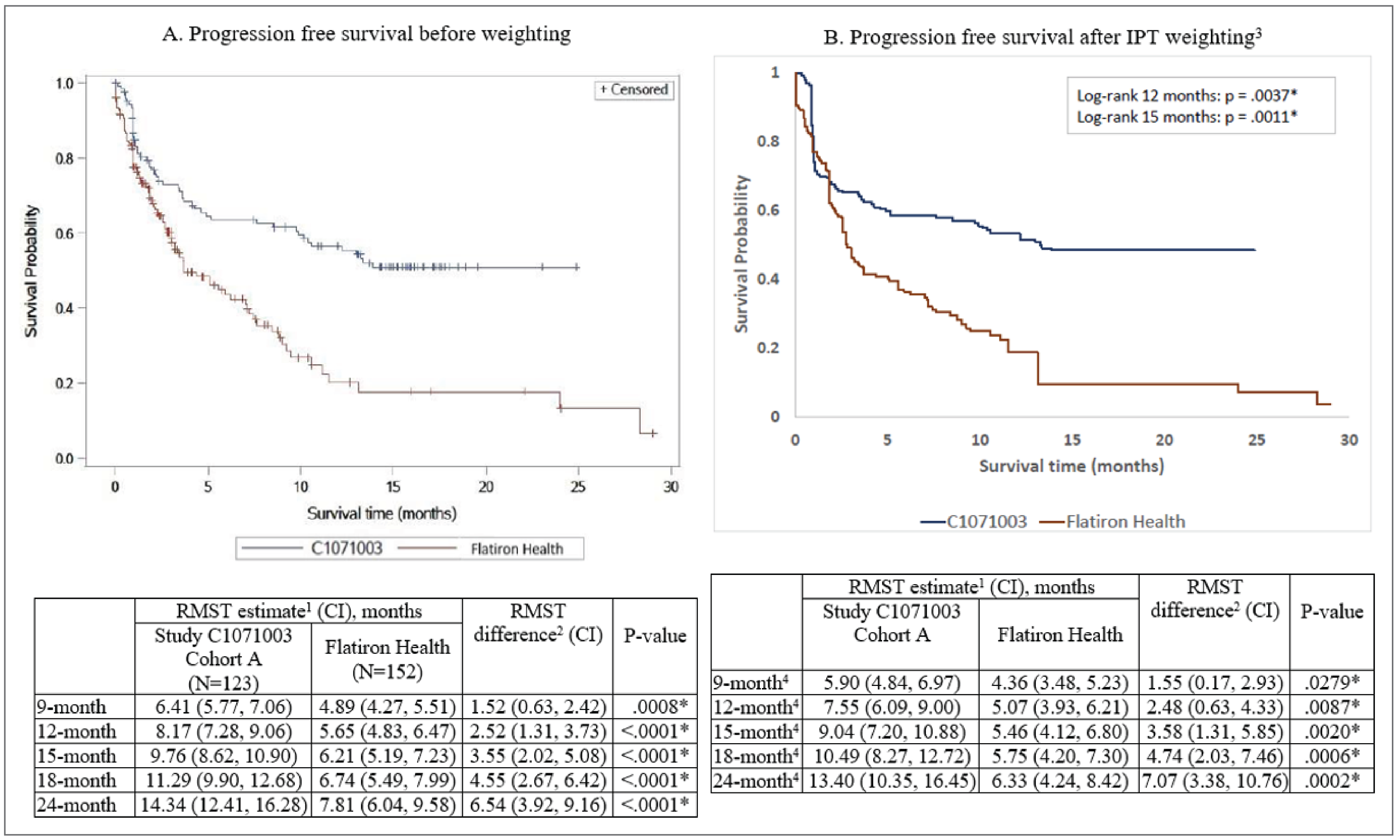
CI = confidence interval; IPT = inverse probability of treatment; IPTW = inverse probability of treatment weighting; PFS = progression-free survival; RMST = restricted mean survival time; RW = real world; TCR = triple-class refractory.
* Significant at the 5% level.
1 The RMST estimates correspond to the number of months patients in each cohort remain progression-free on average over a specified period following the date of the first dose for Study C1071003 patients and following the initiation of the first-line therapy after TCR for RW patients.
2 Unweighted RMST differences and P values were obtained using nonparametric Kaplan-Meier estimators, and IPT-weighted RMST differences and P values were obtained using adjusted RMST proposed by Conner et al. (Conner SC, Sullivan LM, Benjamin EJ, LaValley MP, Galea S, Trinquart L. Adjusted restricted mean survival times in observational studies. Stat Med. 2019 Sep 10;38(20):3832 to 3860.)
3 Kaplan-Meier estimates obtained from each of 5 imputed datasets were normalized using a complementary log-log transformation to satisfy the assumptions of Rubin’s pooling rules. The same transformation was applied to the standard errors for each Kaplan-Meier curve, which were obtained using the delta method (Oehlert 1992). The transformed estimates and their standard errors were then analyzed as usual using the MIANALYZE procedure, and back-transformed to the original scale to produce a summary Kaplan-Meier plot.
4 Stabilized IPT weights truncated at the 99.5th percentile were used.
Source: Study C1071031 technical report.49
Table 28: OS Comparison Between Elranatamab in MagnetisMM-3 Trial, Cohort A, and RW External Control Arms
Detail | MagnetisMM-3 trial, | COTA database | P value | MagnetisMM-3 trial, | Flatiron Health database | P value |
|---|---|---|---|---|---|---|
Participants | (N = 123) | (N = 239) | — | (N = 123) | (N = 152) | — |
Unweighted analysis | ||||||
HR (95% CI)a | 0.65 (0.47 to 0.88) | Reference | 0.0062b | —c | Reference | — |
IPTW analysis | ||||||
HR (95% CI)d | 0.46 (0.27 to 0.77) | Reference | 0.0032b | —c | Reference | — |
CI = confidence interval; HR = hazard ratio; IPT = inverse probability of treatment; IPTW = inverse probability of treatment weighting; OS = overall survival; RW = real world.
Note: Details included in Table 28 are from the sponsor’s Summary of Clinical Evidence.
aHRs were estimated using unadjusted Cox proportional hazards models.
bSignificant at the 5% level.
cFor the Study C1071003 vs. Flatiron study comparison, the proportional hazards assumption was violated, and the HR could not be estimated.
dFor the IPT-weighted analysis, IPT-weighted HRs were estimated using weighted Cox proportional hazards models and CIs were estimated using robust error variances. Stabilized IPT weights truncated at the 99.5th percentile were used.
Source: Study C1071031 technical report.49
Figure 9: Forest Plot Summarizing Hazard Ratios for OS Analysis
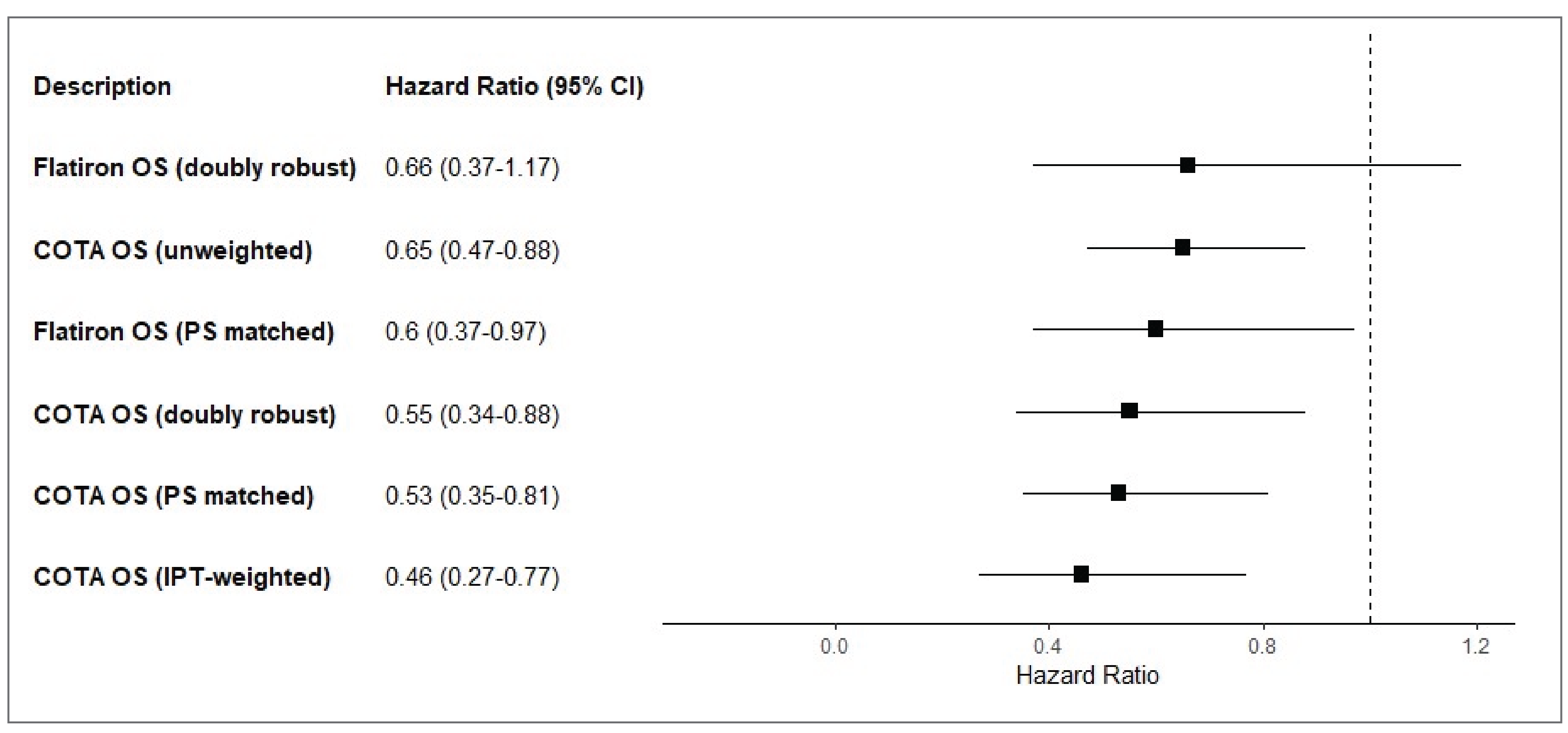
CI = confidence interval; IPT = inverse probability of treatment; OS = overall survival; PS = propensity score.
Source: Study C1071031 technical report.49
Sensitivity Analyses of OS and PFS (Study C1071031)
Doubly Robust Comparisons
Analyses with doubly robust adjustment for baseline confounding using a semiparametric approach revealed results that were consistent with the primary analyses.
Nullification Analysis
For the PFS analyses of the MagnetisMM-3 trial and COTA database populations, the estimated e-values were 2.54 for the unweighted analysis and 3.34 for the IPTW analysis. For the OS analyses of the MagnetisMM-3 trial and COTA database populations, the estimated e-values were 2.04 for the unweighted analysis and 2.82 for the IPTW analysis.
Additional Analyses of OS and PFS (Study C1071031)
Comparisons of PFS and OS in PS-Matched Populations
Matching based on PSs (1:1 on the 0.2 standard deviations of the logit of the PS) produced 89 matched pairs of patients from the MagnetisMM-3 trial and COTA database populations, as well as 69 matched pairs of patients from the MagnetisMM-3 trial and Flatiron Health database populations. After PS matching, the SMDs were about 0.2 for most of the important baseline prognostic characteristics, with the exception of ISS stage and Charlson Comorbidity Index score in matched patients from the MagnetisMM-3 trial, cohort A, and the Flatiron Health database. After matching, the Flatiron Health database population had a higher proportion of missing ISS stage values (Flatiron Health database = 40.5%; MagnetisMM-3 trial = 23.1%) and a lower proportion of Charlson Comorbidity Index scores of 4 or higher (Flatiron Health database = 9.4%; MagnetisMM-3 trial = 14.2%).
The results from the PS-matched populations were consistent with the findings from the main analyses, with elranatamab providing significantly longer PFS and OS versus RW SOC in both the COTA and Flatiron Health database populations (Table 29).
Table 29: PFS and OS Comparison Between Elranatamab in PS-Matched Participants of MagnetisMM-3 Trial, Cohort A, and RW External Control Arms
Characteristic | MagnetisMM-3 trial, cohort A | COTAadatabase | P value | MagnetisMM-3 trial, cohort A | Flatiron Health database | P value |
|---|---|---|---|---|---|---|
(N = 89)a | (N = 89)a | (N = 68.6)a | (N = 68.6)a | |||
PFS | ||||||
HR (95% CI)b | 0.57 (0.37 to 0.87) | Reference | 0.0101c | 0.41 (0.27 to 0.62) | Reference | < 0.0001c |
OS | ||||||
HR (95% CI)b | 0.53 (0.35 to 0.81) | Reference | 0.0032c | 0.60 (0.37 to 0.97) | Reference | 0.0380c |
CI = confidence interval; HR = hazard ratio; OS = overall survival; PFS = progression-free survival; PS = propensity score; RW = real world.
Note: Details included in Table 29 are from the sponsor’s Summary of Clinical Evidence.
aPatients from the Study C1071003 cohort were matched 1:1 without replacement to a patient from the RW cohort on PSs using a caliper of 0.2 standard deviations of the logit of the PS. The number of patients reported in this table were first calculated individually within each of the imputed datasets, and then were averaged across the datasets.
bHRs were estimated using unadjusted Cox proportional hazards models, with a robust variance estimator to account for the clustering within matched pairs.
cSignificant at the 5% level.
Source: Study C1071031 technical report.49
Figure 10: Kaplan-Meier Curves of OS and RMST Estimates in MagnetisMM-3 Trial, Cohort A, and COTA Database External Control Arm Before IPTW (A) and After IPTW (B)
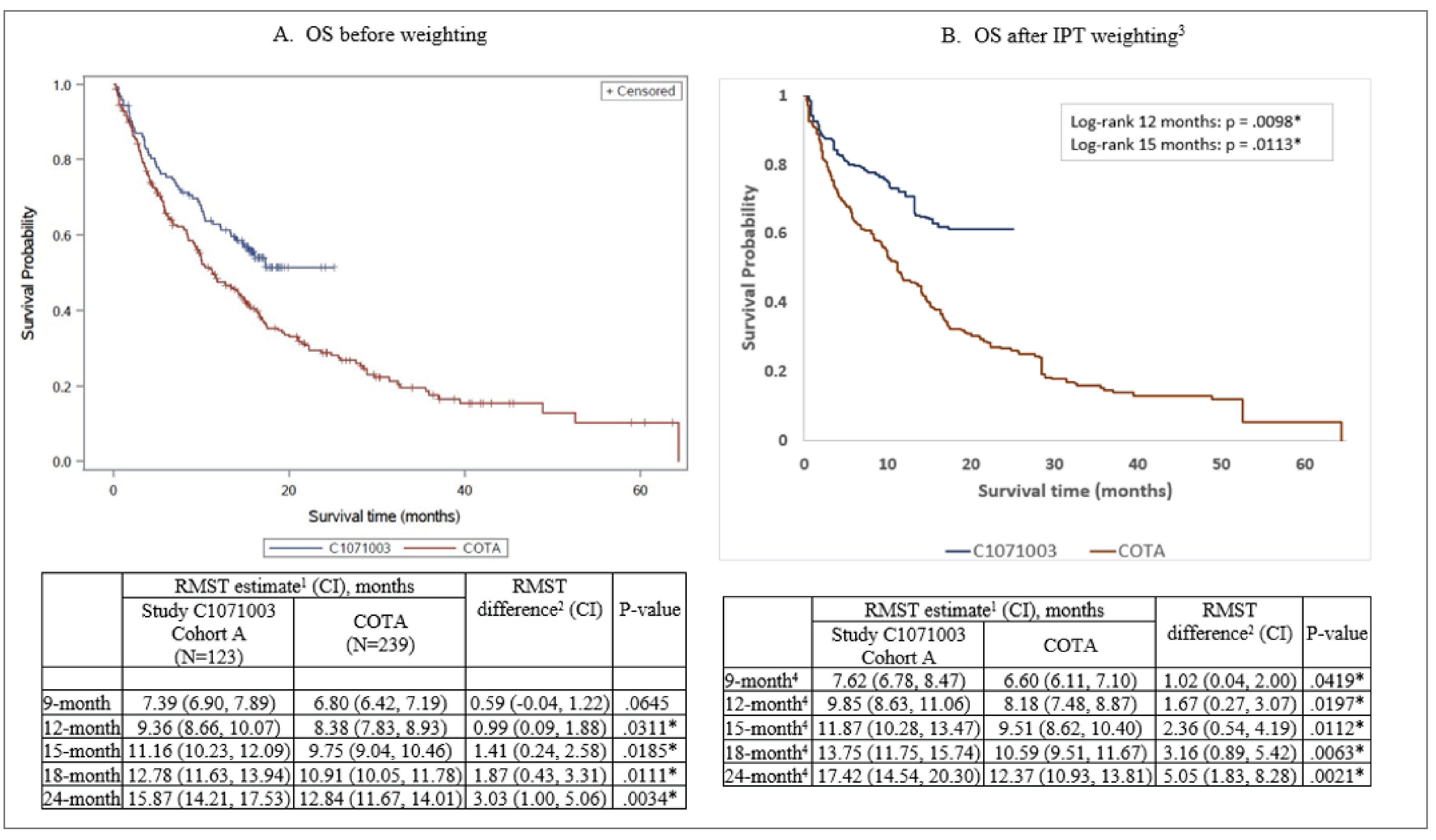
CI = confidence interval; IPT = inverse probability of treatment; IPTW = inverse probability of treatment weighting; OS = overall survival; RMST = restricted mean survival time; RW = real world; TCR = triple-class refractory.
* Significant at the 5% level.
1 The RMST estimates correspond to the number of months patients in each cohort remain progression-free on average over a specified period following the date of the first dose for Study C1071003 patients and following the initiation of the first-line therapy after TCR for RW patients.
2 Unweighted RMST differences and P values were obtained using nonparametric Kaplan-Meier estimators, and IPT-weighted RMST differences and P values were obtained using adjusted RMST proposed by Conner et al. (Conner SC, Sullivan LM, Benjamin EJ, LaValley MP, Galea S, Trinquart L. Adjusted restricted mean survival times in observational studies. Stat Med. 2019 Sep 10;38(20):3832 to 3860.)
3 Kaplan-Meier estimates obtained from each of 5 imputed datasets were normalized using a complementary log-log transformation to satisfy the assumptions of Rubin’s pooling rules. The same transformation was applied to the standard errors for each Kaplan-Meier curve, which were obtained using the delta method (Oehlert 1992). The transformed estimates and their standard errors were then analyzed as usual using the MIANALYZE procedure, and back-transformed to the original scale to produce a summary Kaplan-Meier plot.
4 Stabilized IPT weights truncated at the 99.5th percentile were used.
Source: Study C1071031 technical report.49
Figure 11: Kaplan-Meier Curves and RMST Estimates of OS in MagnetisMM-3 Trial, Cohort A, and Flatiron Health Database External Control Arm Before IPTW (A) and After IPTW (B)

CI = confidence interval; IPT = inverse probability of treatment; IPTW = inverse probability of treatment weighting; OS = overall survival; RMST = restricted mean survival time; RW = real world; TCR = triple-class refractory.
* Significant at the 5% level.
1 The RMST estimates correspond to the number of months patients in each cohort remain progression-free on average over a specified period following the date of the first dose for Study C1071003 patients and following the initiation of the first-line therapy after TCR for RW patients.
2 Unweighted RMST differences and P values were obtained using nonparametric Kaplan-Meier estimators, and IPT-weighted RMST differences and P values were obtained using adjusted RMST proposed by Conner et al. (Conner SC, Sullivan LM, Benjamin EJ, LaValley MP, Galea S, Trinquart L. Adjusted restricted mean survival times in observational studies. Stat Med. 2019 Sep 10;38(20):3832 to 3860.)
3 Kaplan-Meier estimates obtained from each of 5 imputed datasets were normalized using a complementary log-log transformation to satisfy the assumptions of Rubin’s pooling rules. The same transformation was applied to the standard errors for each Kaplan-Meier curve, which were obtained using the delta method (Oehlert 1992). The transformed estimates and their standard errors were then analyzed as usual using the MIANALYZE procedure, and back-transformed to the original scale to produce a summary Kaplan-Meier plot.
4 Stabilized IPT weights truncated at the 99.5th percentile were used.
Source: Study C1071031 technical report.49
ORR (Study C1071024)
Table 30 represents the ORR for elranatamab compared to RW SOC in both unweighted and IPT-weighted analyses. In the unweighted analyses, the ORR was 61% (95% CI, 51.8% to 69.6%) in the MagnetisMM-3 trial’s population, 31.3% (95% CI, 25.4% to 37.7%) in the COTA database population, and 30.3% (95% CI, 23.1% to 38.2%) in the Flatiron Health database population, with higher values observed in the MagnetisMM-3 trial population versus the COTA database population (RR = 1.95 [95% CI, 1.54 to 2.47; P < 0.0001]) and versus the Flatiron Health database population (RR = 2.01 [95% CI, 1.52 to 2.67; P < 0.0001]). Similarly, after adjusting for baseline confounding using IPTW, a higher ORR was observed in the MagnetisMM-3 trial population versus the COTA database population (RR = 2.22 [95% CI, 1.69 to 2.90; P < 0.0001]) and versus the Flatiron Health database population (RR = 1.79 [95% CI, 1.01 to 3.15; P = 0.0447]).
Table 30: ORR Comparison Between Elranatamab in MagnetisMM-3 Trial and RW External Control Arms
Characteristic | MagnetisMM-3 trial, cohort A | COTA database | P value | MagnetisMM-3 trial, cohort A | Flatiron Health database | P value |
|---|---|---|---|---|---|---|
Unweighted analysis | ||||||
N | 123 | 233 | — | 123 | 152 | — |
ORR (95% CI), % | 61.0 (51.8 to 69.6) | 31.3 (25.4 to 37.7) | — | 61.0 (51.8 to 69.6) | 30.3 (23.1 to 38.2) | — |
RR (95% CI) | 1.95 (1.54 to 2.47) | Reference | < 0.0001 | 2.01 (1.52 to 2.67) | Reference | < 0.0001 |
IPT-weighted analysis | ||||||
N | 123 | 213 | — | 122 | 149 | — |
ORR (95% CI), % | 75.7 (65.6 to 87.4) | 34.2 (27.2 to 43.0) | — | 56.0 (41.1 to 76.2) | 31.3 (19.4 to 50.4) | — |
RR (95% CI) | 2.22 (1.69 to 2.90) | Reference | < 0.0001 | 1.79 (1.01 to 3.15) | Reference | 0.0447 |
CI = confidence interval; IPT = inverse probability of treatment; ORR = objective response rate; RR = risk ratio; RW = real world.
Note: Details included in Table 30 are from the sponsor’s Summary of Clinical Evidence.
Source: Study C1071024 technical report.48
DOR (Study C1071024)
Among patients who attained an OR, the median DOR was longer with elranatamab compared to RW SOC from both databases (Table 31). In the unweighted analysis, improved DOR was observed with elranatamab in the MagnetisMM-3 trial compared with RW SOC in the COTA database (HR = 0.17 [95% CI, 0.09 to 0.31; P < 0.0001]) and in the Flatiron Health database (HR = 0.22 [95% CI, 0.11 to 0.43; P < 0.0001]). After accounting for the baseline confounding in the IPT-weighted analysis, improved DOR was still observed with elranatamab in the MagnetisMM-3 study compared with RW SOC in the COTA database (HR = 0.11 [95% CI, 0.06 to 0.22; P < 0.0001]) and in the Flatiron Health database (HR = 0.21 [95% CI, 0.10 to 0.45; P < 0.0001]).
Table 31: DOR Comparison Between Participants in MagnetisMM-3 Trial, Cohort A, and RW External Control Arms
Characteristic | MagnetisMM-3 trial, cohort A | COTA database | P value | MagnetisMM-3 trial, cohort A | Flatiron Health database | P value |
|---|---|---|---|---|---|---|
Unweighted analysis | ||||||
N | 75 | 73 | — | 75 | 46 | — |
HR (95% CI) | 0.17 (0.09 to 0.31) | Reference | < 0.0001 | 0.22 (0.11 to 0.43) | Reference | < 0.0001 |
IPT-weighted analysis | ||||||
N | 75 | 68 | — | 74 | 43 | — |
HR (95% CI) | 0.11 (0.06 to 0.22) | Reference | < 0.0001 | 0.21 (0.10 to 0.45) | Reference | < 0.0001 |
CI = confidence interval; DOR = duration of response; HR = hazard ratio; IPT = inverse probability of treatment; RW = real world.
Note: Details included in Table 31 are from the sponsor’s Summary of Clinical Evidence.
Source: Study C1071024 technical report.48
Expanded Eligibility Criteria Sample
The use of expanded eligibility criteria, compared to the critical eligibility criteria from the primary analyses, resulted in smaller samples of eligible patients: 72 patients with TCR MM initiated a new line of therapy between November 2015 and June 2022 in the COTA database population and 54 patients with TCR MM initiated a new line of therapy between November 2015 and August 2021 in the Flatiron Health database population. These populations of patients had similar demographic characteristics to those of patients from the MagnetisMM-3 trial. In this sample of patients, the median follow-up times were 14.7 months in the MagnetisMM-3 trial, 14.0 months in the COTA database, and 8.3 months in the Flatiron Health database.
Consistent with the results of the primary analyses, elranatamab provided improved PFS compared to RW SOC from the COTA database both before weighting (HR = 0.51 [95% CI, 0.34 to 0.77; P = 0.0012]) and after IPTW (HR = 0.34 [95% CI, 0.20 to 0.58; P < 0.0001]). Similarly, elranatamab provided improved OS compared to RW SOC from the COTA database in the IPTW analysis (HR = 0.38 [95% CI, 0.23 to 0.63; P = 0.0002]).
Restricted mean survival time analyses were conducted for the Flatiron Health database population due to violation of the proportional hazards assumption in that cohort. These analyses demonstrated significantly longer average PFS with elranatamab versus RW SOC in the Flatiron Health database population at 9 months, 12 months, 15 months, 18 months, and 24 months in both the unweighted and IPTW analyses (all P < 0.05). A similar benefit with elranatamab in terms of OS was observed in the IPTW analyses at all time points (all P < 0.05), although the benefit did not reach statistical significance in the unweighted analyses.
Subgroup Analyses According to Treatment Subgroups
Results from subgroup 2, as most closely aligned with the relevant comparators for this submission, are presented as follows. Subgroup 2 was created by selecting eligible patients with TCR MM from the COTA and Flatiron Health database populations who received RW treatment using only:
carfilzomib plus dexamethasone
panobinostat plus bortezomib plus dexamethasone
carfilzomib plus lenalidomide plus dexamethasone
carfilzomib plus cyclophosphamide plus dexamethasone
pomalidomide plus dexamethasone
pomalidomide plus cyclophosphamide plus dexamethasone.
As a result, despite the US-based data sources, this permits comparisons of elranatamab with a basket of RW treatments that is more closely aligned with the Canadian context. Results from the unweighted Kaplan-Meier curves demonstrate that elranatamab provided better PFS and OS compared to subgroup 2 from the COTA and Flatiron Health databases (Figure 12).
Figure 12: Unweighted Kaplan-Meier Curve of PFS and OS Based on Subgroup 2 From COTA and Flatiron Health Databases [Redacted]

OS = overall survival; PFS = progression-free survival.
Note: The blue curve reflects MagnetisMM-3 trial results.
Source: Study C1071031 technical report.49
PROs (MagnetisMM-3 Trial Versus Study C1071013 and Study C1071014)
A total of ███ patients from the MagnetisMM-3 trial completed at least 1 PRO questionnaire (EORTC QLQ-C30, EORTC QLQ-MY20, or EQ-5D-5L) at baseline, including ███ participants from cohort A and ██ participants from cohort B. A total of ██ patients (██ patients with no index CAR T-cell therapy and ██ patients with index CAR T-cell therapy) in prospective observational studies Study C1071013 and Study C1071014 completed at least 1 PRO questionnaire at baseline. The main group for this analysis was participants from the MagnetisMM-3 trial, cohort A and cohort B, and a combined group of patients from the observational studies (Study C1071013 and Study C1071014 with no index CAR T-cell therapy).
Results were compared over the first 6 monthly visits in each dataset. Completion rates for the PRO tools were similar between the MagnetisMM-3 trial and the observational studies at visit 1 to visit 4, although the completion rate was higher in the MagnetisMM-3 study at visit 5 and visit 6. Table 32 presents the mean difference for the EORTC QLQ-MY20 disease symptoms and side effects of treatment scales.
Table 32: Estimates of LSM Difference for EORTC QLQ-MY20 Obtained From Mixed Model for Study C1071003, Cohort A and Cohort B, and Observational Studies C1071013 and C1071014 With No Index CAR T-Cell Therapy [Redacted]
█████████ | ████ | ██ ████ ██████████ ███████ ██████ | ||
|---|---|---|---|---|
█████ ████████ | █████ | ██ ████ ████ | ██████████ ███ | ███████ |
███████ ██████████ | █████ | ██████ | ███████ █████ | █████ |
█████ | ██████ | ████████ █████ | █████ | |
█████ | █████ | ███████ █████ | █████ | |
█████ | ██████ | ███████ █████ | █████ | |
█████ | ██████ | ████████ █████ | █████ | |
█████ | █████ | ████████ █████ | █████ | |
████ ███████ | █████ | █████ | ███████ █████ | █████ |
█████ | █████ | ███████ █████ | █████ | |
█████ | █████ | ███████ █████ | █████ | |
█████ | ██████ | ███████ █████ | █████ | |
█████ | █████ | ███████ █████ | █████ | |
█████ | ██████ | ████████ █████ | █████ | |
CAR = chimeric antigen receptor; EORTC QLQ-MY20 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Multiple Myeloma 20; LSM = least squares mean.
Note: Details included in Table 32 are from the sponsor’s Summary of Clinical Evidence.
Source: Study C1071031 technical report.49
Harms
Safety data were not evaluated in any of the comparative studies described in this section. Analyses performed as part of this retrospective cohort study were based on information collected from electronic health records.
Critical Appraisal
Internal Validity
Given the lack of a comparator arm in the MagnetisMM-3 trial, the use of external RW data could be justified. Patients were compared using IPTW and doubly robust methods in an attempt to minimize the impact of confounding on the results. It should be noted that this method cannot control for substantial differences resulting from different study designs between the 2 cohorts (RCT versus retrospective registry review).
The longitudinal, RW Flatiron Health and COTA databases were selected and standardized as external control arms based on their inclusion and exclusion criteria and enrolled population, which aimed to reduce the potential for selection bias and heterogeneity. However, since there were differences among the definitions used across the COTA and Flatiron Health databases and the MagnetisMM-3 trial, the potential for bias and heterogeneity could be there. The RW cohorts were selected by applying patient characteristics of the MagnetisMM-3 trial to create 2 external cohorts of RW patients, though no other rationale was provided. Participants were not randomized to treatment, and the choice of treatment in the external control arms was determined by their physicians . . To reduce the impact of potential bias and improve exchangeability between the participants of the MagnetisMM-3 trial and patients from the external control arms, the sponsor reported measures taken to align these populations by applying similar inclusion and exclusion criteria, and by using advanced statistical methods. Since applying inclusion and exclusion criteria from a clinical trial to an RWD requires some adjustments due to data availability and differences in assessment in a clinical trial versus in an RW setting, these adjustments may impact the comparability between the RW cohorts and the MagnetisMM-3 trial population. Additionally, due to the lack of availability of certain tests for assessing organ function for RW patients, only a critical set of inclusion and exclusion criteria were applied to create the primary RW cohort of patients with TCR MM to balance the need for sample size and the comparability of patients.
Study Design
The MagnetisMM-3 trial is a phase II, open-label, single-arm trial, whereas the external control arms were derived from longitudinal RW cohorts from electronic health records in the US. For the retrospective cohorts, it is unclear how the index date (time 0) was defined for each and every patient on treatment as listed in the summary Table 22 for various periods on treatment and follow-up for outcomes over a long period from November 2015 to March 2022. Therefore, there was significant concern of potential time-related bias (e.g., treatment changes, informative censoring) due to the likely unequal possibility of dropouts for outcome assessment. This bias could bias the results in favour of the study treatment, despite the use of IPTW to adjust for known confounding bias.
Differences in Outcome Definitions and Analysis
The definition of censoring in the PFS analysis was not equivalent between participants of the MagnetisMM-3 trial and patients identified from RW sources; this is a potential source of measurement error in PFS measurements. For example, participants of the MagnetisMM-3 trial had scheduled visits for disease assessment, and in cases where a participant was switched to a new line of therapy before a progression event, or when a participant did not have a progression event during the observation period, the follow-up of such participants was censored on the date of the last disease assessment. On the other hand, patients in the RW setting did not have scheduled visits for disease assessments, and for those without a progression event, their follow-up was censored on the date of a new line of therapy initiation or the end of the period of observation. In all, these may result in longer PFS times for RW patients and bias the comparative effectiveness estimates in favour of the SOC treatment group.
Control of Confounding
There might be important unknown or unmeasured residual confounding in the external control arms that were either not documented or could not be accounted for. In databases not collected for research but for administration purposes, the misclassification of exposure or incomplete reporting may be a concern (e.g., adherence, dose, timing of initiation, duration of treatment) and the receipt of additional treatments. Although the sponsor IPTW, a few characteristics were not well balanced in the comparison of the MagnetisMM-3 trial and Flatiron Health database populations (ECOG PS score, time since initial MM diagnosis, Charlson Comorbidity Index score, the number of lines of therapy before the index date, and history of stem cell transplant). Therefore, there remains also a potential risk of residual confounding.
The sponsor recognized that unlike clinical trial settings, which use specifically defined outcomes and scheduled assessments, RW data are subject to inconsistent assessments and evaluations of treatment response. Furthermore, there is evidence that disease progression may be diagnosed later in the RW setting compared to a clinical study setting.53,54 Moreover, censoring for PFS events was not equivalent between the different datasets used in the present analyses, which could have led to prolonged PFS times in the RW patients due to the censoring rules. Both factors could have biased the comparison of elranatamab versus RW SOC favouring the SOC.
Data Quality Assessment
The sponsor noted further limitations on the data quality of RWDs. First, key variables to assess disease severity were either unavailable or not similarly reported in the different datasets (e.g., extramedullary disease was not recorded in the Flatiron Health database, despite being an important predictor of disease severity and prognosis). Second, missing data and the accuracy of recorded data on disease characteristics, lab results, and comorbidities in RWDs may introduce an information bias and residual confounding. Third, applying inclusion and exclusion criteria from a clinical trial to an RWD requires adjustments due to data availability and differences in assessment in a clinical trial versus an RW setting, which could impact the comparability of the MagnetisMM-3 trial, COTA database, and Flatiron Health database populations. Well-defined, reliable, and clinically meaningful outcomes that are typically used in randomized trials may be particularly difficult to ascertain and evaluate in an RWD source that is being considered for an externally controlled trial. For example, radiologic end points in controlled oncology trials (e.g., ORR, PFS) are based on prespecified imaging assessment frequency and standardized measurement criteria for Response Evaluation Criteria in Solid Tumours. In routine clinical care, however, radiologic assessment frequency is variable, and formal tumour measurement may not routinely be performed or documented, making a valid assessment of PFS or ORR using external control data, such as data from electronic health records, challenging. In some cases, and depending on the outcome, the occurrence of an event may not have been evaluated in clinical care or, if evaluated, may not have been recorded. As a general consideration, outcomes of interest are more likely to be recorded in clinical records when events are objective and/or require immediate medical attention. This might have led to the omission of some important outcomes, which may bias the results.
Timing of Outcome Assessment
When considering outcomes in the externally controlled trials, the sponsor did not evaluate the consistency of the timing of outcome assessments in the treatment arm compared to the external control arms. Since the timing and frequency of outcome assessments in RWDs will have been determined during clinical care and may have been influenced by the patient’s clinical status, whereas outcome assessments in the treatment arm are protocol-specified, this may lead to bias. The difference in the time frame between the external control arms (2015 to 2022) and the pivotal trial (2021 to 2023) may lead to inconsistency related to the outcome assessment.
For the analysis of PROs (via the EORTC QLQ-MY20 tool), participation in Study C1071013 and Study C1071014 was dependent on physicians’ and patients’ ability and willingness to participate, which may impact patient representativeness and be a source of self-selection bias. Similarly, results may not be translatable to geographic regions not captured by the COTA and Flatiron Health databases, with different health care systems and treatment approaches.
External Validity
The patients selected from these RWDs to generate the external cohorts were highly selective in nature and may not reflect the general population. It is not possible to know whether the results may have differed if data from different RRMM studies or databases had been used. Numerous therapies were used in the RW clinical practice groups from the MagnetisMM-3 trial cohort and the external cohorts, many of which may not be relevant to Canadian clinical practice. Additionally, treatment regimens reported from these sources were included from November 16, 2015, until June 30, 2022 (index date), and clinical practice might have changed since the enrolment of patients from these sources and may not be reflective of current treatment standards. Patients undergoing third-line treatment today may be worse off than patients who underwent third-line treatment at the time of the data collection for this study. The index date for the external control arms was spread over more than 6.5 years from 2015 until 2022, whereas the pivotal MagnetisMM-3 trial began in early 2021 and the data cut-off date was early 2023, which indicates some temporal differences in this date relative to treatment initiation or other important landmark times by treatment arm; this may bias any observed treatment effects. While the pivotal trial consists of a more recent treatment regimen, the external control arms include a wide range of treatments, some of which may not be suitable at this time. The wide range of the index date might include patients not receiving effective treatments to control their disease, thus favouring the benefits of the study drug.
The clinical experts consulted by CADTH indicated that the patient population included in the external control arms based on the COTA and Flatiron Health databases may differ from the general Canadian population. Since the external control arms population is based in the US, the patients receiving the treatments for this particular indication would have different health accessibility compared to the general Canadian population due to differences in the health care systems in the 2 countries. For this reason, the results from this RWE study may not be generalizable to the Canadian population.
The sponsors conducted a subgroup analysis according to treatments, providing the rationale that treatments included in the analysis aligned with the relevant comparators for this submission. However, according to the clinical experts consulted by CADTH, some important comparators used in Canada (e.g., pomalidomide, bortezomib, dexamethasone, belantamab belantamab) are missing from the RW treatment list used for the subgroup analysis. The experts also noted that panobinostat plus bortezomib plus dexamethasone are not available in Canada, that the carfilzomib plus lenalidomide plus dexamethasone combination is not likely funded as patients will be refractory to lenalidomide, and that for the carfilzomib plus cyclophosphamide plus dexamethasone combination, it may be possible to add cyclophosphamide to carfilzomib in some geographical locations in Canada, but not all.
MagnetisMM-9 Trial
Description of Studies: This section includes a dose-finding phase I and phase II study, the MagnetisMM-9 trial,50 to evaluate a dosing regimen with 2 step-up priming doses and longer dosing intervals of elranatamab. The primary objective of this study was to assess the safety (in particular, the rate of ≥ grade 2 CRS) of a priming dose regimen that involves premedication and 2 step-up priming doses administered within the first week of elranatamab treatment in RRMM participants who are refractory to at least 1 PI, 1 IMiD, and 1 anti-CD38 mAb. Characteristics of the MagnetisMM-9 trial are summarized in Table 33.
Table 33: Details of MagnetisMM-9 Trial
Detail | MagnetisMM-9 trial |
|---|---|
Designs and populations | |
Study design | Phase I and phase II, open-label, multicentre, noncomparative, nonrandomized trial in adult patients with MM who are refractory to at least 1 PI, 1 IMiD, and 1 anti-CD38 antibody |
Locations | 24 centres in Great Britain, Japan, Taiwan, and the US |
Patient enrolment dates | Study initiation date: October 7, 2021 Interim analysis date: July 29, 2022 |
Randomization (N) | Patients were not randomized. In total,46 patients were enrolled and 45 patients were treated. |
Key inclusion criteria |
|
Key exclusion criteria |
|
Drugs | |
Intervention | Elranatamab 76 mg, injected subcutaneously:
Twelve patients received elranatamab 116 mg q.2.w. for cycle 2 to cycle 6. The overall safety, tolerability, PK, PD, and preliminary antimyeloma activity of alternative regimens of elranatamab at dose levels > 76 mg (116 mg or 152 mg) starting from cycle 2 with different dosing intervals (q.w., q.2.w., q.4.w.) (part 2), and a regimen of elranatamab full dose of 76 mg q.w. for 6 cycles followed by 76 mg q.2.w. or RP2D q.4.w. (part 1) was also evaluated, but these dosages differ from the Health Canada recommended dosage. |
Comparator(s) | None |
Study duration | |
Screening phase | Up to 28 days before starting study treatment |
Treatment phase | Treatment in 28-day cycles until treatment discontinuation or study withdrawal (i.e., because of confirmed disease progression, unacceptable toxicity, withdrawal of consent, or study termination) |
Follow-up phase | A follow-up visit was conducted at 28 days to 35 days after treatment discontinuation, with long-term follow-up for ≥ 2 years after enrolment. |
Outcomes | |
Primary end point | ≥ grade 2 CRS during cycle 1 |
Secondary and exploratory end points | Secondary (descriptive):
Note: Additional outcomes were planned as part of this ongoing study but are not presented due to the lack of data at the data cut-off date. |
BCMA = B-cell maturation antigen; CRR = complete response rate; CRS = cytokine release syndrome; DOR = duration of response; ECOG PS = Eastern Cooperative Oncology Group Performance Status; GBS = Guillain-Barré syndrome; GVHD = graft-vs.-host disease; HBV = hepatitis B virus; HCV = hepatitis C virus; IMiD = immunomodulatory drug; IMWG = International Myeloma Working Group; MM = multiple myeloma; ORR = objective response rate; PD = pharmacodynamic; PI = proteasome inhibitor; PK = pharmacokinetic; POEMS = polyneuropathy, organomegaly, endocrinopathy, myeloma protein, and skin changes; q.2.w. = every 2 weeks; q.4.w. = every 4 weeks; q.w. = every week; RP2D = recommended phase II dose; SARS-CoV-2 = severe acute respiratory syndrome coronavirus 2; TTR = time to response.
Note: Details included in Table 33 are from the sponsor’s Summary of Clinical Evidence.
Source: MagnetisMM-9 Clinical Study Report.50
The primary objective of the MagnetisMM-9 trial was to determine the rate of grade 2 or higher CRS during cycle 1 (when all patients received the same dosing regimen) in adult patients with TCR MM (refractory to ≥ 1 IMiD, ≥ 1 PI, and ≥ 1 anti-CD38 antibody). Overall safety, tolerability, and efficacy outcomes were also assessed, as well as a recommended phase II dose and different dosing intervals. A study schematic is represented in Figure 13.
At the time of submission, data were only available for an interim analysis up to July 29, 2022, at which point patients had only been enrolled in part 1 and part 2A, dose level 1; efficacy data were only available for patients from part 1 and safety data were only available for patients from part 1 and part 2A, dose level 1. Both sets of patients received the same first cycle (premedication, 2 step-up priming doses of elranatamab [4 mg and 20 mg], and 76 mg doses of elranatamab); patients in part 1 continued on elranatamab 76 mg every week for 6 cycles while patients in part 2A, dose level 1, received elranatamab 116 mg every 2 weeks for cycle 2 to cycle 6. Note that the focus of the report is on the doses that align with the Health Canada recommended dosage (i.e., step-up doses of 12 mg on day 1 and 32 mg on day 4 of week 1, followed by the first treatment dose of 76 mg on day 8, and then 76 mg weekly thereafter through week 24). For patients who have received at least 24 weeks of treatment and have attained a response (i.e., a partial response or better that has been maintained for at least 2 months), the dosage interval should transition to a schedule of every 2 weeks.22
Figure 13: Study Design of MagnetisMM-9 Trial

C# = cycle and its number; D# = day and its number; PR = partial response; QW = every week.
Source: MagnetisMM-9 Clinical Study Report.50
Populations
Inclusion and Exclusion Criteria
The main inclusion and exclusion criteria for the MagnetisMM-9 trial were similar to the eligibility criteria of the pivotal MagnetisMM-3 trial that was previously described in the report.
Interventions
Slightly different elranatamab priming and dosing regimens were used for the MagnetisMM-9 trial compared to the ones described in the pivotal trial. For the part 1 and part 2A patient groups, the 2 step-up priming doses of elranatamab were 4 mg on cycle 1, day 1, and 20 mg on cycle 1, day 4, which were followed by a 76 mg dose in cycle 1 on day 8, day 15, and day 22. Patients in part 1 continued elranatamab 76 mg every week for 6 cycles while patients in part 2A, dose level 1, received elranatamab 116 mg every 2 weeks for cycle 2 to cycle 6. At cycle 7 and onward, patients who had attained partial response or better could be changed to a dosing interval of 76 mg every 2 weeks (part 1 patients) or 116 mg every 4 weeks (part 2A patients).
Additional doses were considered in the MagnetisMM-9 trial design but are not summarized here because data for those groups were not yet available.
Outcomes
The primary outcome of the MagnetisMM-9 study was to determine the rate of grade 2 or higher CRS during cycle 1 in adult patients with TCR MM. Outcomes in the MagnetisMM-9 study were analyzed descriptively and without a hierarchical testing strategy; several efficacy outcomes (the duration of complete response, PFS, OS, and minimal residual disease) were immature at the time of submission and are not summarized because data were not available at the time of the interim data cut-off date. PROs were not available for the MagnetisMM-9 study.
Statistical Analysis
Efficacy outcomes in the MagnetisMM-9 trial were analyzed descriptively and using the same methods as for the corresponding outcomes in the MagnetisMM-3 study. As the primary outcome for the MagnetisMM-9 trial, the rate of grade 2 or higher CRS during cycle 1 was evaluated against an a priori assumption that the mean grade 2 or higher CRS rate would be 35%.
Sample Size and Power Calculation
In the MagnetisMM-9 trial, a sample size of approximately 76 patients was selected to meet 2 criteria:
Bayesian statistical significance would be achieved if the posterior probability is 10% for the true grade 2 or higher CRS rate exceeding the a priori assumption of 35%
clinical relevance (i.e., justifying further clinical development) would be met if the median of the posterior distribution of the grade 2 or higher CRS rate is 27% or less.
Subgroup Analysis
In the MagnetisMM-9 trial, the following subgroup analyses were conducted for a smaller list of variables and were also not adjusted for multiplicity: BCMA status (exposed versus naive) and extramedullary disease status (yes versus no).
Analysis Populations
All efficacy and safety analyses were based on the corresponding safety analysis set, which included 45 patients in the MagnetisMM-9 trial (efficacy data were only available for 33 patients from part 1).
Results
Patient Disposition
A summary of patient disposition is in Table 34. At the latest data cut-off dates, the MagnetisMM-9 trial included ██ patients (July 29, 2022). At the July 29t, 2022 data cut-off date, a larger proportion of patients were still receiving treatment in MagnetisMM-9 ███████ than in the MagnetisMM-3 study (28.9%). The most common reasons for discontinuing treatment were progression of disease ███████ and AEs ███████. The proportion of patients still under follow-up was higher in the MagnetisMM-9 trial ███████ than in the MagnetisMM-3 study (47.6%) and death was the most common reason for study discontinuation ███████.
Table 34: Summary of Patient Disposition — MagnetisMM-9 Trial [Redacted]
███████ ████████████ | █████████████ | |
|---|---|---|
████ █ ███ █ ████ | ████ ██ ███ ██ █ ██████ | |
████████ █ ██ | ██ ██████ | ██ ██████ |
████████████ ██████████ █ ██ | ██ ██████ | ██████ |
██████ ███ ████████████████ █ ██ | ||
███████████ ████████ | ██████ | █████ |
███████ ██████ | █████ | ██████ |
██████ | █████ | █████ |
███████████ ████████ | █████ | ██ |
███████ ██ █████ ██ ██ ████ ███ ████ ████ ████████ █ █ | ██ ██████ | ██████ |
DL1 = dose level 1 (elranatamab 116 mg every 2 weeks for cycle 2 to cycle 6).
Note: Details included in Table 34 are from the sponsor’s Summary of Clinical Evidence.
Source: MagnetisMM-9 Clinical Study Report.50
Baseline Characteristics
The baseline demographic characteristics and clinical characteristics of patients who enrolled in the MagnetisMM-3 and MagnetisMM-9 studies were generally consistent with the characteristics of patients who had heavily pretreated RRMM (Table 35).
Table 35: Summary of Baseline Characteristics — MagnetisMM-9 Trial [Redacted]
█████████ | █████████████ | ||
|---|---|---|---|
████ █ ███ █ ███ | ████ ██ █ | ███████ | |
████ █████ | ████ ███████ | ████ ██████ | ████ ██████ |
██ █ ██ ██████ | ██ ██████ | ██████ | ██ ██████ |
██ █ ██ ██████ | █████ | █████ | █████ |
████ █ ██ | |||
██ ███████ | ██ ██████ | ██████ | ██ ██████ |
██ ████████ | ██ ██████ | ██████ | ██ ██████ |
█████ █ █████ | |||
██ ███████ | ██ ██████ | ██████ | ██ ██████ |
██ █████ ███ | ██ ███████ | ██ ███████ | ██ ███████ |
██ ███████ | ██ ██████ | ██████ | ██ ██████ |
██ █████████ | ██ ███████ | ██ ███████ | ██ ███████ |
██ ███ ██████ | ██ ███████ | ██ ███████ | ██ ███████ |
████ ███████████ ███████ █ ███ | |||
██ ██ | ██ ██████ | ██████ | ██ ██████ |
██ ██ | ██ ██████ | ██████ | ██ ██████ |
██ ██ | ██ ███████ | ██ ███████ | ██ ███████ |
███████ █████ ████████ █ ███ | |||
██ ██ | ██ ███████ | ██ ███████ | ██ ███████ |
██ ███ | ██ ██████ | ██████ | ██ ██████ |
██ ████ | ██████ | ██████ | ██████ |
██ ████████ | █████ | █████ | █████ |
███████████ █████ █ ███ | |||
██ ██████████ | ██ ███████ | ██ ███████ | ██ ███████ |
██ ██████ | ██ ███████ | ██ ███████ | ██ ███████ |
██ ████████ | ██ ███████ | ██ ███████ | ██ ███████ |
██████████████ ███████ ██ █████ █ ███ | |||
██ ████ | ██ ██████ | ██████ | ██ ██████ |
██ ███ | ██ ██████ | ██████ | ██ ██████ |
████ ██ ████████ █ ███ | |||
██ ████ | ██ ██████ | ██████ | ██ ██████ |
██ ████ | ██████ | ██████ | ██████ |
██ ████ | ██ ███████ | ██ ███████ | ██ ███████ |
██ ███████ | ██ ███████ | ██ ███████ | ██ ███████ |
██ ███████ | ██ ███████ | ██ ███████ | ██ ███████ |
████████ ████ ██████ ██████ ██████ █ ███| | |||
██ █ ████ | ██ ██████ | ██████ | ██ ██████ |
██ █ ████ | ██████ | █████ | ██████ |
██ ████████ | ██ ███████ | ██ ███████ | ██ ███████ |
█████ █████████ █ ███ | |||
██ ███████ | ██████ | ██████ | ██ ██████ |
██ ███████ | ██ ██████ | ██ ██████ | ██ ██████ |
█████ █████████ █ ██ | |||
██ ███████ | ██ ██████ | ██ ███████ | ██ ██████ |
██ ███████ | ██ ███████ | ██ ███████ | ██ ███████ |
██ ███████ | ██ ███████ | ██ ███████ | ██ ███████ |
████ █████ █████ █████████ ██ ██████ ████ ████████ ██████ | |||
████ █████ | ████ ███████ | ████ ███████ | ████ ███████ |
█████ ██████████ █████████ | |||
██ ████ █████ | ███████ | ███ ███████ | ███ ███████ |
██ ███ ██████ | ██████ | ██████ | ██ ██████ |
██ ███ ██████ | ██ ██████ | ██████ | ██ ██████ |
███████ █ ████ | ██ ██████ | ██████ | ██ ██████ |
██████████ | ██ ██████ | ██ ██████ | ██ ██████ |
██████████ | ██ ██████ | ██████ | ██ ██████ |
█████ █████ ██ | ██ ██████ | ██ ██████ | ██ ██████ |
██ ███████ | ██ ██████ | ██ ██████ | ██ ██████ |
██ ███████ | ██ ███████ | ██ ███████ | ██ ███████ |
██ ██████████ | ██ ███████ | ██ ███████ | ██ ███████ |
██ ████████ | ██ ███████ | ██ ███████ | ██ ███████ |
████████████ | ██ ███████ | ██ ███████ | ██ ███████ |
██ ████ | ██ ███████ | ██ ███████ | ██ ███████ |
██ ██████ | ██ ███████ | ██ ███████ | ██ ███████ |
██ ███ ███ ██████ | ██ ███████ | ██ ███████ | ██ ███████ |
██████████ █ | ██ ███████ | ██ ███████ | ██ ███████ |
ADC = antibody-drug conjugate; BCMA = B-cell maturation antigen; BICR = blinded independent central review; CAR = chimeric antigen receptor; CrCl = creatinine clearance; ECOG PS = Eastern Cooperative Oncology Group Performance Status; NR = not reported; R-ISS = Revised International Staging System; SD = standard deviation.
Note: Details included in Table 35 are from the sponsor’s Summary of Clinical Evidence.
aIncluded participants who had at least 1 of the following: an ECOG PS score of 2, an R-ISS score of 3, extramedullary disease at baseline by BICR, high cytogenetic risk, or bone marrow plasma cell involvement greater than or equal to 50%.
bPenta-drug refractory disease is defined as being refractory to at least 2 proteasome inhibitors, 2 immunomodulatory drugs, and 1 anti-CD38 antibody.
Source: MagnetisMM-9 Clinical Study Report.50
Exposure to Study Treatments
In the overall population, median treatment duration was ████ months in the MagnetisMM-9 trial; the median treatment duration in part 1 of the MagnetisMM-9 trial █████ ███████ was comparable to that in the overall MagnetisMM-3 trial’s population. The median cumulative dose was higher in the MagnetisMM-3 trial than in the MagnetisMM-9 trial ██████ ██ ███ ███ ███ █████████████, which reflects the shorter time on treatment in the MagnetisMM-9 study at the data cut-off dates. However, relative dose intensities were similar between the MagnetisMM-3 study (79.87%) and the MagnetisMM-9 study █████████ No major differences were observed in the proportions of patients with dose reductions or interruptions in the MagnetisMM-3 study (79.1%) and the MagnetisMM-9 study ███████, which were predominantly due to AEs. A smaller proportion of patients re-escalated to the 76 mg or 116 mg doses of elranatamab in the MagnetisMM-9 study. Patients in the overall populations of the MagnetisMM-9 study had heavily pretreated MM (median = | previous lines) that was refractory to the last line of therapy. Most patients ███████ were classified as being TCR. Similar to the MagnetisMM-3 trial, infection prophylaxis was common in the MagnetisMM-9 study, most frequently involving antiviral medication ███████ and medication to prevent Pneumocystis jiroveci pneumonia ████████
Subsequent Treatment
While patients were monitored for subsequent anticancer therapies in the MagnetisMM-9 study, there was limited information regarding these treatments; this may be related to the short follow-up intervals at the interim analysis.
Efficacy
As of the data cut-off date, incomplete efficacy data were available from the study.
Harms
Harms data reported in this section are from the data cut-off date of July 29, 2022. The key harms results for the safety (i.e., as-treated) population are summarized in Table 36.
Table 36: Summary of Harms Results — MagnetisMM-9 Trial, Safety Analysis Set [Redacted]
█████ | ██████ █ ███ | ████ ██ ███ | ████ |
|---|---|---|---|
████ ███ ████ ████ ███████ | |||
████ ██████ ███████ | |||
████ | ██ ███████ | ██ ███████ | ██ ███████ |
████████ ███████ ████████ | ██ ██████ | ██████ | ██ ██████ |
██████ | ██ ██████ | ██████ | ██ ██████ |
███████████ | ██ ██████ | ██████ | ██ ██████ |
████████ | ██ ██████ | ██████ | ██ ██████ |
████████████████ | ██████ | ██████ | ██████ |
███████████ | █████ | ██████ | ██████ |
███████ | ██ ██████ | ██████ | ██████ |
█████████ ████████ | ██ ██████ | ██████ | ██████ |
███████ | ██ ██████ | ██████ | ██████ |
███████████ | ██████ | ██████ | ██████ |
█████ | ██████ | ██████ | ██████ |
██████ | ██████ | ██████ | ██████ |
█████████ ████████ | ██████ | ██████ | ██████ |
█████████ ████████ | ██████ | ██████ | ██████ |
████████ | ██████ | ██████ | ██ ██████ |
████████ | ██████ | ██████ | ██ ██████ |
██████████ | ██████ | ██████ | ██ ██████ |
██████████ | ██████ | ██████ | ██ ██████ |
████████████ | ██████ | ██████ | ██ ██████ |
█████████ | ██████ | ██████ | ██ ██████ |
████████ | ██████ | ██████ | ██ ██████ |
█████████ ████████ | ██████ | ██████ | ██ ██████ |
█████████ ████████ | ██████ | ██████ | ██ ██████ |
█████████ ████████ | ██████ | ██████ | ██ ██████ |
████████ | ██████ | ██████ | ██ ██████ |
███████ ██████ | ██████ | ██████ | ██ ██████ |
████████ ██████████ ████ | ██████ | ██████ | ██ ██████ |
████████ █████████ | ██████ | ██████ | ██ ██████ |
████████ ███████ ████████ | ██████ | ██████ | ██ ██████ |
█████████ | ██████ | ██████ | ██ ██████ |
███████ ███████████ | ██████ | ██████ | ██ ██████ |
██████ | ██████ | ██████ | ██ ██████ |
███████ ███ ███████ █████████ ███ ██ ███████ | ██████ | ██████ | ██ ██████ |
████████ ███ ███████████ ████████████ ███████████ | ██████ | ██████ | ██ ██████ |
██████ █████ | ██████ | ██████ | ██ ██████ |
███████████ | ██████ | ██████ | ██ ██████ |
████████ █████████ | ██████ | ██████ | ██ ██████ |
██████████ ███████ ██████████ | ██████ | ██████ | ██ ██████ |
███████ █ ███ | ██████ | ██████ | ██ ██████ |
████████ ███ ████ | ██████ | ██████ | ██ ██████ |
█████ ██ █████ | ██████ | ██████ | ██ ██████ |
███████ ███████████ | ██████ | ██████ | ██ ██████ |
█████ | ██████ | ██████ | ██ ██████ |
███████ | ██████ | ██████ | ██ ██████ |
█████ █████████ ████████ | ██████ | ██████ | ██ ██████ |
███████ █████ █ ███ | ██████ | ██████ | ██ ██████ |
██████████ | ██████ | ██████ | ██ ██████ |
████████ ███████ ██████ | ██████ | ██████ | ██ ██████ |
██████████ ███████████ | ██████ | ██████ | ██ ██████ |
██████████████ | ██████ | ██████ | ██ ██████ |
██████ █ ███ | ██████ | ██████ | ██ ██████ |
CRS = cytokine release syndrome; ICANS = immune effector cell-associated neurotoxicity syndrome; SARS-CoV-2 = severe acute respiratory syndrome coronavirus 2; TEAE = treatment-emergent adverse event.
Note: Details included in Table 36 are from the sponsor’s Summary of Clinical Evidence.
aFrequency of 10% or more in at least 1 group.
bFrequency of 5% or more in at least 1 group.
cFrequency of 1 or more total patients.
Source: MagnetisMM-9 Clinical Study Report.50
Adverse Events
███ ████████ ██ ███ █████ ████████ ██ █████ █ █████ ███ ████ ██████████ ████████ █████ ██ ████ █ ████ ████████ ███████ ████████ ██████ ██████ ██████ ███████████ ██████ ████████ ██████ █████████ ████████ ██████ ███████ █████ ███ ███████ ██████ ███ ████ ██████████ ████████ █████ ██ ████ ██ ████ █████ █ ████ ████████ ███████ ████████ ██████ ██████ ██████ ███████████ ██████ ████████ ██████ ███████ ██████ █████████ ████████ ██████ █████████ ████ ████████ ██████ ████████████████ █████ ███ ████ ██ █████████ ██████
Serious Adverse Events
In the total population, ███ of patients experienced at least 1 serious TEAE. The most frequently reported serious AEs in both part 1 and part 2A, dose level 1, were CRS ████ ███ ████ ██████████████
Withdrawal Due to Adverse Events
Study treatment discontinuation due to TEAEs in part 1 were ███ ███ ███ in part 2A, dose level 1. The most common TEAEs leading to discontinuation of elranatamab included ██████ █████ ████ ███ ██████████ ███████ ██████████ ████ for part 2A, dose level 1, and ███████████ ████ for part 1.
Mortality
In part 1 and part 2A, dose level 1, ███ ███ ███ of patients died, respectively. Most deaths in both cohorts were attributed to other reasons (██ ██ ████ █ ███ ███ ██ ████ ██ ████ █████).
Notable Harms
The primary end point of the MagnetisMM-9 study was the rate of grade 2 or higher CRS during cycle 1 (combining patients from part 1 and part 2A), which was ███████
Critical Appraisal
Internal Validity
The MagnetisMM-9 study was an open-label, single-arm, phase I and phase II trial. The primary limitation of the MagnetisMM-9 study was the absence of a comparator group against which the benefits and harms of elranatamab could be compared. Single-arm phase I and phase II trials are generally not considered as confirmatory for efficacy and are subject to several limitations in their interpretation. As the primary outcome for the MagnetisMM-9 study, the rate of grade 2 or higher CRS during cycle 1 was evaluated against an a priori assumption that the mean grade 2 or higher CRS rate would be 35%. Efficacy data were only available for 33 patients from part 1 and were therefore incomplete. The trial was open label, which can result in a risk of bias in the measurement of the outcomes, particularly for subjective outcomes.
External Validity
The baseline demographic characteristics and clinical characteristics of patients who enrolled in the MagnetisMM-3 and MagnetisMM-9 studies were generally consistent with the characteristics of patients who have heavily pretreated RRMM.
Dose adjustments were allowed in the trial and the methods were outlined in the protocol. Dose adjustments or modifications are anticipated in a clinical practice setting to manage AEs while maintaining drug benefit.
Discussion
Summary of Available Evidence
One pivotal phase II, noncomparative, open-label trial, 2 MAICs, and 3 studies addressing gaps in the pivotal and RCT evidence submitted by the sponsor were summarized in this report.
One ongoing trial, the MagnetisMM-3 study (N = 187), met the inclusion criteria for the systematic review conducted by the sponsor. The objective of the MagnetisMM-3 trial was to assess the efficacy and safety of elranatamab 76 mg, subcutaneous injection, in adults with RRMM. The trial enrolled adults who either did (cohort B) or did not (cohort A) have previous experience with BCMA-directed treatment, were disease-refractory to at least 1 PI, 1 IMiD, and 1 anti-CD38 antibody, and were disease-relapsed or disease-refractory to their last antimyeloma regimen. The 2 cohorts were noncomparative and analyzed separately. The outcomes relevant to the CADTH review included the primary outcome of ORR by BICR per IMWG criteria, and the secondary outcomes of PFS, OS, DOR, CRR, and safety. HRQoL measured by EORTC QLQ-MY20 was an exploratory outcome. The trial population was predominately white █████, with a similar proportion of male and female patients who had a mean age of ██ years. Most patients had an ECOG PS score of 1 █████ and 0 █████, indicating good overall performance, an R-ISS disease stage of II █████, standard cytogenetic risk █████, and a prior stem cell transplant █████. Patients had received an average of | prior lines of therapy, and ███ had penta-drug refractory disease (refractory to at least 2 PIs, 2 IMiDs, and 1 anti-CD38 antibody). Key characteristics were generally consistent between cohorts, although patients in cohort B had a longer mean time since first diagnosis (█████ ██████ ████ ██████), and received on average more prior anticancer therapies ██████████ ███ ██████████ than patients in cohort A.
In the absence of direct comparative evidence of elranatamab versus relevant comparators, 2 unanchored MAICs were conducted by the sponsor. The objective of MAIC 1 was to assess the relative treatment effect of elranatamab, using IPD from cohort A of the MagnetisMM-3 trial, compared to physician’s choice of treatment based on aggregated data from the CMRG database in patients with TCE or RRMM. The outcomes assessed included PFS and OS. Similar to MAIC 1, the objective of MAIC 2 was to assess the relative treatment effect of elranatamab compared to teclistamab from the MajesTEC-1 trial, physician’s choice of treatment from prospective RWE studies (the LocoMMotion and MAMMOTH trials), and cilta-cel from the CARTITUDE-1 trial in patients with TCE or RRMM. The outcomes assessed included ORR, PFS, OS, and CRR.
The section on studies addressing gaps summarizes 2 retrospective cohort studies with external control arms (Study C1071024 and Study C1071031) and 1 phase I and phase II dosing study (the MagnetisMM-9 trial). Study C1071024 and Study C1071031 were conducted to retrospectively compare efficacy outcomes between elranatamab and 2 external control arms using a basket of RW treatments from the Flatiron Health and COTA databases. Study C1071024 assessed ORR and DOR. Study C1071031 is the continuation of Study C1071024, using data from the MagnetisMM-3 trial with a longer follow-up of approximately 15 months to assess PFS and OS. Study C1071031 also assessed PROs (via the EORTC QLQ-MY20 tool), using other studies as the data sources for the external cohort.
The primary objective of the dose-finding phase I and phase II MagnetisMM-9 trial was to assess the safety of a priming dose regimen that involves premedication and 2 step-up priming doses administered within the first week of elranatamab treatment in RRMM participants who are refractory to at least 1 PI, 1 IMiD, and 1 anti-CD38 mAb. The primary outcome of the MagnetisMM-9 trial was to determine the rate of grade 2 or higher CRS during cycle 1 in adult patients with TCR MM.
Interpretation of Results
The evidence from the pivotal trial, the MagnetisMM-3 study, addressed treatment outcomes noted to be important by both patients and clinicians. The patient group indicated that stopping disease progression, prolonging life, improving HRQoL, and reducing treatment side effects are important to them. Based on the GRADE assessment, the pivotal trial evidence is very uncertain about the effect of elranatamab when compared with any comparator. The lack of a control group limits the interpretation of the efficacy and safety results of the trial, as these findings could have been confounded by a potential placebo effect, the use of concomitant treatments, and the natural history of the disease. The 2 RWE studies attempted to provide the relative treatment effect of elranatamab, using primarily cohort A from the MagnetisMM-3 trial versus external cohorts identified from existing US databases, with relevant comparators including a basket of physician’s choices of treatments for the assessment of OS, ORR, and HRQoL outcomes. Safety data were not evaluated in any of the studies. Despite different data sources, these studies consistently appeared to favour elranatamab versus physician’s choices of treatments in particular; however, the studies would have potentially had several important methodological limitations, including a high risk of residual confounding and time-related biases (i.e., uneven dropouts due to informative censoring over different duration of follow-up). For these reasons, the RWE studies were deemed insufficient to draw definitive conclusions and are not further discussed in this section. In this report, the clinical relevance of the findings from the pivotal trial were contextualized based on clinical expert feedback on how they might compare to the usual clinical course of RRMM. The results of the MAICs were also summarized as they informed the pharmacoeconomic model.
Efficacy
The MagnetisMM-3 trial reached its primary outcome at the 9-month final planned analysis and 15-month interim analysis in cohort A and cohort B, demonstrating an ORR of 61% and 34%, respectively. The clinical experts consulted by CADTH considered the results for cohort A clinically meaningful but not for cohort B, based on their suggested clinically important threshold of 40%. In both cohorts, descriptive subgroup analysis results for ORR appeared generally consistent with the primary analysis, though they included a small number of patients. Among responders, the median DOR was not reached in both cohorts at the most recent data cut-off date of March 14, 2023, with ███ of all patients censored at the time of the analysis. The probability of patients remaining in response at 12 months was 76% in cohort A and █████ in cohort B. The clinical experts considered these DOR results to be clinically meaningful, based on their suggested threshold of 40%. A complete response or better was attained in 35% of patients in cohort A and ██ of patients in cohort B; the clinical experts considered the results for cohort A clinically meaningful, based on their suggested threshold of 20%.
At the first and second interim analyses, the PFS and OS data were immature, with medians and CIs not being reached for both cohorts, except for PFS in cohort B, which reached ███ months. Longer follow-up is needed to better understand whether elranatamab addresses patients’ needs for a treatment that improves survival outcomes. Due to the limitation of the lack of a control group, a causal conclusion of the clinically meaningful benefit is compromised. Moreover, due to insufficient data, whether these observed ORRs would be transferable to an improvement in OS remains unknown.
HRQoL is an important outcome to patients and clinicians, and was assessed as an exploratory outcome by measuring EORTC QLQ-MY20 scale scores. ██ █████ ███ ████ █████ ██████ ████ ████████ ██ █████ ██ ██ ██████ █ ████ █████████ ███████████ █████ ██ ████████ ██ ██████ █ ███ ████ ██ ██████ ██ ███ ███ ██ ██ ███████ ██████ ███████████ ██████ █████████ ██ ████ ███████ ███ ███ ██████ ████ ████████ ████████ ███ ████████ ███ ██ █ ███████ ███████ ███████ ████████ ██ ████ ███████ ███ ███ ███ ██████ ███ ████████ ███ ██ ██ ███████ ████ ███████ ██ █████████ ██████ ████████ ██ ████ ███████ ███ ███ ███ ██████ ███ ████████ ███ ██ ██ ███████ Interpretation of these results is limited and no conclusion could be drawn due to the lack of a control group, potential bias due to assessor knowledge of treatment assignment, and a large amount of missing outcome data over time. Of note, the clinical experts consulted for this review indicated that HRQoL measures such as the EORTC QLQ-MY20 tool are not used in routine clinical practice.
Based on the sponsor-submitted unanchored MAICs, the results were generally in favour of elranatamab compared to relevant comparators, except for cilta-cel. In MAIC 1, the PFS and OS results favoured elranatamab versus physician’s choice of treatment, although the proportional hazards assumption was violated for both outcomes, which could have biased the estimates. In MAIC 2, the ORR favoured elranatamab versus teclistamab and physician’s choice of treatment. For PFS, the HR favoured elranatamab versus teclistamab and physician’s choice of treatment, and crossed the null for elranatamab versus cilta-cel. For OS, the HR crossed the null for elranatamab versus teclistamab, favoured cilta-cel versus elranatamab, and favoured elranatamab versus physician’s choice of treatment. The proportional hazards assumption was violated in most comparisons for both OS and PFS, except for the comparison to teclistamab. For CRR, the effect crossed the null for elranatamab versus teclistamab, and favoured elranatamab versus physician’s choice of treatment. To account for between-study differences in patient baseline characteristics, several relevant PVs and EMs were matched in the weighting process, with separate sets of variables used across treatment comparisons. These variables were selected based on a systematic literature search and clinical expert input. However, whether the overall exchangeability assumption was held in both MAICs was a significant concern as there were several notable sources of heterogeneity and missing data for potential EMs, which limited the ability to adjust for differences between studies. Identified methodological issues of concern included study design characteristics, patient eligibility criteria, and baseline patient characteristics such as ISS disease stage, cytogenetic risk, and extramedullary disease. Of note, since the MAICs only included cohort A from the MagnetisMM-3 trial and the Health Canada indication is for patients both with and without prior exposure to BCMA-directed therapies, there is no indirect comparative evidence for the use of elranatamab in patients who have received prior BCMA-directed therapy. Due to these limitations in the MAICs and uncertainty in their estimates, no definitive conclusions could be drawn on the relative treatment effects of elranatamab versus relevant comparators.
Harms
All patients in the pivotal trial reported at least 1 TEAE. The most frequently reported TEAEs in both cohorts were CRS █████, anemia █████, neutropenia █████ and diarrhea █████. In both cohorts, ███ of patients experienced 1 or more serious TEAE. The type and number of events were similar in both cohorts, with the most frequently reported events being COVID-19 pneumonia █████ and CRS █████. Study treatment discontinuation due to TEAEs occurred in ███ of patients, and was similar in both cohorts. In cohort A and cohort B, 45% and ███ of patients died, respectively. Most deaths in both cohorts were attributed to disease progression. In the total population, the most frequently reported notable AEs were infections █████ and CRS █████, followed by peripheral neuropathy █████, hypogammaglobulinemia ██████ and ICANS █████ All CRS events were grade 1 or grade 2 in severity. The median time from the most recent elranatamab dose to CRS onset was | days and the median time to resolution was also | days. In general, the harms results of the phase I and phase II MagnetisMM-9 trial were similar to those of the MagnetisMM-3 trial. According to the clinical experts, infection-related hospitalizations, hypogammaglobulinemia as measured by the need for IV or subcutaneous immunoglobulin, and neurotoxicities were considered important outcomes, although they were not reported in the trials. As such, this represents a gap in the available evidence on harms.
The patient group that provided input for this review highlighted that there is a need for alternative tolerable treatments. However, since the trials did not include a relevant control or active comparator, no causal association can be drawn on elranatamab regarding the risk of any particular harm, and whether elranatamab is a more tolerable treatment compared to other treatment options. The clinical experts noted that the trials did not include patients with a poor ECOG PS score, which is not entirely representative of all patients with RRMM in clinical practice. Therefore, patients in the 2 trials may have been healthier than the broader population who could receive elranatamab in practice. It is also more likely that a healthier patient is better able to tolerate an AE and be willing to remain on the study drug, thereby lowering the number of patients who withdraw from treatment compared to clinical practice. The clinical experts indicated that the reported AEs were reasonable for what is known about RRMM and the study treatments (elranatamab and concomitant drugs) and that with appropriate care, the AEs would be manageable for many patients.
The sponsor-submitted MAICs did not include harms, and therefore no conclusions could be drawn on the relative safety of elranatamab versus relevant comparators.
Conclusion
Evidence of efficacy and safety from 1 ongoing, phase II, noncomparative, open-label trial (the MagnetisMM-3 study) in adults with RRMM who had received at least 3 prior lines of therapy was included in the review for elranatamab. The clinical experts consulted by CADTH indicated that based on their experience treating patients with RRMM and the natural history of the disease, the ORR observed in patients without prior exposure to BCMA-directed therapy (cohort A) is clinically meaningful. However, it remains unknown whether elranatamab could improve PFS, OS, and DOR in patients with (cohort B) and without (cohort A) prior exposure to BCMA-directed therapy because of the lack of a comparator group, because the data were immature, and because no definitive conclusions can be drawn on HRQoL due to the open-label design and large amount of missing outcome data. Overall, the results for patients in cohort B were not as favourable as for those in cohort A. There were no new safety signals identified and the safety of elranatamab was consistent with the known safety profile of the drug. Results from the indirect treatment comparisons and RWE studies consistently favoured elranatamab over comparators, except cilta-cel. However, due to limitations of these studies, no conclusions can be drawn regarding the relative efficacy and safety of elranatamab compared to relevant comparators, including physician’s choice of treatment, teclistamab, and cilta-cel. The evidence submitted to CADTH did not include indirect comparative evidence between elranatamab and any comparator for patients with prior exposure to BCMA-directed therapy; this represents a gap in the available indirect evidence.
References
1.Balshem H, Helfand M, Schünemann HJ, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011;64(4):401-406. PubMed
2.Santesso N, Glenton C, Dahm P, et al. GRADE guidelines 26: informative statements to communicate the findings of systematic reviews of interventions. J Clin Epidemiol. 2020;119:126-135. PubMed
3.Clinical Study Report: C1071003. An open-label, multicenter, non-randomized phase 2 study of elranatamab (pf-6863135) monotherapy in participants with multiple myeloma who are refractory to at least one proteasome inhibitor, one immunomodulatory drug and one anti-cd38 antibody [internal sponsor’s report]. New York (NY): Pfizer Inc; 2022 Dec 14.
4.Kyle RA, Rajkumar SV. Criteria for diagnosis, staging, risk stratification and response assessment of multiple myeloma. Leukemia. 2009;23(1):3-9. PubMed
5.Bird SA, Boyd K. Multiple myeloma: an overview of management. Palliat Care Soc Pract. 2019;13:1178224219868235. PubMed
6.Rajkumar SV. Multiple myeloma: 2022 update on diagnosis, risk stratification, and management. Am J Hematol. 2022;97(8):1086-1107. PubMed
7.Canadian Cancer Society. Multiple myeloma statistics [sponsor-submitted reference]. 2022; https://cancer.ca/en/cancer-information/cancer-types/multiple-myeloma/statistics. Accessed 2023 May.
8.Canadian Cancer Society. Survival statistics for multiple myeloma [sponsor-submitted reference]. https://cancer.ca/en/cancer-information/cancer-types/multiple-myeloma/prognosis-and-survival/survival-statistics. Accessed 2023 May.
9.Podar K, Leleu X. Relapsed/Refractory Multiple Myeloma in 2020/2021 and Beyond. Cancers (Basel). 2021;13(20):5154. PubMed
10.Mikhael J, Ismaila N, Cheung MC, et al. Treatment of Multiple Myeloma: ASCO and CCO Joint Clinical Practice Guideline. J Clin Oncol. 2019;37(14):1228-1263. PubMed
11.Kurtin SE. Relapsed or Relapsed/Refractory Multiple Myeloma. J Adv Pract Oncol. 2013;4(Suppl 1):5-14.
12.Canadian Cancer Society. Symptoms of multiple myeloma [sponsor-submitted reference]. https://cancer.ca/en/cancer-information/cancer-types/multiple-myeloma/signs-and-symptoms. Accessed 2023 May.
13.Myeloma Canada. Multiple Myeloma Patient Handbook [sponsor-submitted reference]. 2014; https://myeloma.ca/pixms/uploads/serve/ckeditor/mmph_en-2.pdf. Accessed 2023 May.
14.Canadian Cancer Society. Prognosis and survival for multiple myeloma [sponsor-submitted reference]. https://cancer.ca/en/cancer-information/cancer-types/multiple-myeloma/prognosis-and-survival. Accessed 2023 May.
15.Mayo Clinic. Multiple myeloma [sponsor-submitted reference]. https://www.mayoclinic.org/diseases-conditions/multiple-myeloma/diagnosis-treatment/drc-20353383. Accessed 2023 May.
16.Canadian Cancer Society. Stages of multiple myeloma [sponsor-submitted reference]. https://cancer.ca/en/cancer-information/cancer-types/multiple-myeloma/staging. Accessed 2023 May.
17.Greipp PR, San Miguel J, Durie BG, et al. International staging system for multiple myeloma. J Clin Oncol. 2005;23(15):3412-3420. PubMed
18.Bhatt P, Kloock C, Comenzo R. Relapsed/Refractory Multiple Myeloma: A Review of Available Therapies and Clinical Scenarios Encountered in Myeloma Relapse. Curr Oncol. 2023;30(2):2322-2347. PubMed
19.Rajkumar SV, Harousseau JL, Durie B, et al. Consensus recommendations for the uniform reporting of clinical trials: report of the International Myeloma Workshop Consensus Panel 1. Blood. 2011;117(18):4691-4695. PubMed
20.Mikhael J. Treatment Options for Triple-class Refractory Multiple Myeloma. Clin Lymphoma Myeloma Leuk. 2020;20(1):1-7. PubMed
21.Provisional Funding Algorithm: Multiple myeloma. (CADTH Reimbursement Review). Ottawa (ON): CADTH; 2023: https://www.cadth.ca/sites/default/files/DRR/2023/PH0031%20Multiple%20Myeloma_Algorithm-Secured.pdf. Accessed 2023 Aug.
22.Pfizer Canada ULC. Draft Product Monograph: ELREXFIO (elranatamab solution for injection) [sponsor-submitted reference]. 2023.
23.Karwacz K, Hooper AT, Chang CPB. Abstract 4557: BCMA-CD3 bispecific antibody PF-06863135: Preclinical rationale for therapeutic combinations. Cancer Res. 2020;80(16_Supplement):4557.
24.Lesokhin AM, Levy MY, Dalovisio AP. Preliminary Safety, Efficacy, Pharmacokinetics, and Pharmacodynamics of Subcutaneously (SC) Administered PF-06863135, a B-Cell Maturation Antigen (BCMA)-CD3 Bispecific Antibody, in Patients with Relapsed/Refractory Multiple Myeloma (RRMM). Blood. 2020;136(8-9).
25.Abramson HN. B-Cell Maturation Antigen (BCMA) as a Target for New Drug Development in Relapsed and/or Refractory Multiple Myeloma. Int J Mol Sci. 2020;21(15). PubMed
26.Panowski SH, Kuo TC, Zhang Y, et al. Preclinical Efficacy and Safety Comparison of CD3 Bispecific and ADC Modalities Targeting BCMA for the Treatment of Multiple Myeloma. Mol Cancer Ther. 2019;18(11):2008-2020. PubMed
27.Udata C, Wei D, Jiang S, et al. Abstract 5508: BCMA-CD3 bispecific antibodies: A modeling framework to characterize kinetics of bispecific antibody, T cell, cytokines, and serum M-protein. Cancer Res. 2020;80(16_Supplement):5508-5508.
28.Ciltacabtagene autoleucel (CARVYKTI) [product monograph; sponsor-submitted reference]. Toronto (ON): Janssen Inc.; 2023. Accessed 2023 Feb 9.
29.Xpovio (selinexor): tablets, 20 mg, oral [product monograph]. Oakville (ON): FORUS Therapeutics Inc; 2021.
30.Kyprolis® (carfilzomib): vial, 10, 30, 60 mg, injection [product monograph]. Mississauga (ON): Amgen Canada Inc.; 2019: https://pdf.hres.ca/dpd_pm/00051989.PDF. Accessed 2022 Dec 14.
31.e-CPS. Ottawa (ON): Canadian Pharmacists Association; 2022: https://www.e-therapeutics.ca. Accessed 2023 Nov 5.
32.Lesokhin AM, Tomasson MH, Arnulf B, et al. Elranatamab in relapsed or refractory multiple myeloma: phase 2 MagnetisMM-3 trial results. Nat Med. 2023;29(9):2259-2267. PubMed
33.Bahlis NJ, Tomasson MH, Mohty M, et al. Efficacy and Safety of Elranatamab in Patients with Relapsed/Refractory Multiple Myeloma Naïve to B-Cell Maturation Antigen (BCMA)-Directed Therapies: Results from Cohort a of the Magnetismm-3 Study. Blood. 2022;140(Supplement 1):391-393.
34.Sully K, Trigg A, Bonner N, et al. Estimation of minimally important differences and responder definitions for EORTC QLQ-MY20 scores in multiple myeloma patients. Eur J Haematol. 2019;103(5):500-509. PubMed
35.Osborne TR, Ramsenthaler C, Siegert RJ, Edmonds PM, Schey SA, Higginson IJ. What issues matter most to people with multiple myeloma and how well are we measuring them? A systematic review of quality of life tools. Eur J Haematol. 2012;89(6):437-457. PubMed
36.Cocks K, Cohen D, Wisloff F, et al. An international field study of the reliability and validity of a disease-specific questionnaire module (the QLQ-MY20) in assessing the quality of life of patients with multiple myeloma. Eur J Cancer. 2007;43(11):1670-1678. PubMed
37.Matching-adjusted indirect treatment comparison (MAIC) of elranatamab versus physicians’ choice of treatment in Canada for the treatment of adult patients with multiple myeloma who have received at least three prior lines of therapy, including one proteasome inhibitor, one immunomodulatory drug, and one anti-CD38 monoclonal antibody, and who have demonstrated disease progression on the last therapy [internal sponsor’s report]. In: Drug Reimbursement Review sponsor submission: Elrexfio (elranatamab), 76 mg subcutaneous injection. New York (NY): Pfizer Inc; 2023 Oct 4.
38.Pfizer Canada ULC. Real World Data on Outcomes of Anti-CD38 Antibody Treated, Including Triple Class Refractory, Patients with Multiple Myeloma: A Multi-Institutional Report from the Canadian Myeloma Research Group (CMRG) Database [sponsor-submitted reference]. 2023.
39.Grosicki S, Simonova M, Spicka I, et al. Once-per-week selinexor, bortezomib, and dexamethasone versus twice-per-week bortezomib and dexamethasone in patients with multiple myeloma (BOSTON): a randomised, open-label, phase 3 trial. Lancet. 2020;396(10262):1563-1573. PubMed
40.Matching-adjusted indirect treatment comparison (MAIC) of elranatamab versus relevant comparators in Canada for the treatment of adult patients with relapsed or refractory multiple myeloma who have received at least 3 prior lines of therapy, including a proteasome inhibitor, an immunomodulatory agent, and an anti-CD38 monoclonal antibody, and who have demonstrated disease progression on the last therapy [internal sponsor’s report]. In: Drug Reimbursement Review sponsor submission: Elrexfio (elranatamab), 76 mg subcutaneous injection. New York (NY): Pfizer Inc; 2023 Sept 1.
41.Moreau P, Garfall AL, van de Donk N, et al. Teclistamab in Relapsed or Refractory Multiple Myeloma. N Engl J Med. 2022;387(6):495-505. PubMed
42.Einsele H, Moreau P, Stefano VD. Subgroup analyses in patients with relapsed/refractory multiple myeloma (RRMM) receiving real-life current standard of care (SOC) in the LocoMMotion study. J Clin Oncol. 2022;40(16_suppl):8031-8031.
43.Gandhi UH, Cornell RF, Lakshman A, et al. Outcomes of patients with multiple myeloma refractory to CD38-targeted monoclonal antibody therapy. Leukemia. 2019;33(9):2266-2275. PubMed
44.Bal S, Malek E, Kansagra A, et al. Treatment outcomes of triple class refractory multiple myeloma: a benchmark for new therapies. Leukemia. 2022;36(3):877-880. PubMed
45.Munshi NC, Anderson LD, Jr., Shah N, et al. Idecabtagene Vicleucel in Relapsed and Refractory Multiple Myeloma. N Engl J Med. 2021;384(8):705-716. PubMed
46.Berdeja JG, Madduri D, Usmani SZ, et al. Ciltacabtagene autoleucel, a B-cell maturation antigen-directed chimeric antigen receptor T-cell therapy in patients with relapsed or refractory multiple myeloma (CARTITUDE-1): a phase 1b/2 open-label study. Lancet. 2021;398(10297):314-324. PubMed
47.Martin T, Usmani SZ, Berdeja JG, et al. Ciltacabtagene Autoleucel, an Anti-B-cell Maturation Antigen Chimeric Antigen Receptor T-Cell Therapy, for Relapsed/Refractory Multiple Myeloma: CARTITUDE-1 2-Year Follow-Up. J Clin Oncol. 2023;41(6):1265-1274. PubMed
48.Comparative Effectiveness of Elranatamab (PF-06863135) in Clinical Study C1071003 Versus Standard of Care (SOC) in Real-World (RW) External Control Arms in Patients with Triple-Class Refractory (TCR) Multiple Myeloma (MM) [sponsor-submitted reference]. 2022. Accessed 2022 Dec 7.
49.Comparative Effectiveness of Elranatamab (PF 06863135) in Clinical Study C1071003 Versus Standard of Care (SOC) in Real-World (RW) External Control Arms in Patients with Triple-Class Refractory (TCR) Multiple Myeloma (MM) [sponsor-submitted reference]. 2023. Accessed 2023 Aug 8.
50.Pfizer. Clinical Study Report: A Phase 1/2, Open-Label, Multicenter Study to Evaluate a Dosing Regimen With Two Step-Up Priming Doses and Longer Dosing Intervals of Elranatamab (PF-06863135) Monotherapy in Participants With Relapsed/Refractory Multiple Myeloma (MagnetisMM-9, data cut-off: 29 Jul 2022) [sponsor-submitted reference]. 2022.
51.Visram A, et al. Real World Data on Outcomes of Anti-CD38 Antibody Treated, Including Triple Class Refractory, Patients with Multiple Myeloma: A Multi-Institutional Report from the Canadian Myeloma Research Group (CMRG) Database [sponsor-submitted reference]. 2023.
52.Yadlowsky S, Pellegrini F, Lionetto F, Braune S, Tian L. Estimation and Validation of Ratio-based Conditional Average Treatment Effects Using Observational Data. J Am Stat Assoc. 2021;116(533):335-352. PubMed
53.Chakraborty R, Liu HD, Rybicki L, et al. Progression with clinical features is associated with worse subsequent survival in multiple myeloma. Am J Hematol. 2019;94(4):439-445. PubMed
54.Goldman-Mazur S, Visram A, Kapoor P, et al. Outcomes after biochemical or clinical progression in patients with multiple myeloma. Blood Adv. 2023;7(6):909-917. PubMed
55.Kumar S, Paiva B, Anderson KC, et al. International Myeloma Working Group consensus criteria for response and minimal residual disease assessment in multiple myeloma. Lancet Oncol. 2016;17(8):e328-e346. PubMed
Appendix 1: Description of Study
Please note that this appendix has not been copy-edited.
Visram et al. (2023)51
Visram et al. (2023)51 conducted a multicentre retrospective cohort study which used the CMRG database to describe RW outcomes (e.g., clinical characteristics, PFS, OS) in patients with anti-CD38 mAb refractory MM subsequently treated with SOC regimens. Outcomes of patients with TCR MM were evaluated as a distinct cohort in this study. The authors also compared PFS and OS outcomes among patients with TCE versus TCR MM, since both the US FDA and European Medicines Agency had approved the use of some immune therapies for MM in patients who were TCE and not necessarily TCR.
The CMRG database is a prospectively maintained national database including at least 8,700 patients diagnosed with MM since 2007 across 17 academic centres. The inclusion criteria for this study were patients with MM who were refractory to an anti-CD38 mAb-based index regimen after 4 weeks or more of treatment and were subsequently treated with available SOC regimens. Since anti-CD38 mAb-based regimens were not reimbursed in Canada in the front-line setting at the time of data cut-off (June 30, 2022), most patients received anti-CD38 mAb regimens at the time of relapse. Patients having a progression of MM on therapy or within 60 days of the last dose of the anti-CD38 mAb-containing regimen were considered refractory in this study, as defined by the IMWG response criteria.19 The exclusion criteria for this study were patients who discontinued anti-CD38 mAb therapy for any reasons other than having progressive disease, patients who were treated with an anti-CD38 mAb for a plasma cell disorder other than MM, patients who were lost to follow-up or relieved after anti-CD38 mAb progression, or patients who were treated on a clinical trial after anti-CD38 mAb progression with an investigational drug in the subsequent line of therapy.
The index regimen for this study was defined as the anti-CD38 mAb-containing regimen. SOC treatments applied at a subsequent time after progression on the index regimen in this study included IMiDs, PIs, anti-CD38 mAbs, alkylating drugs, anthracyclines, and steroids. Patients with TCR MM were defined as patients who were refractory to an IMiD, PI, and an anti-CD38 mAb. Penta-refractory disease was defined as having progression while on treatment or within 60 days of the last dose of 2 IMiDs, 2 PI’s, and1 CD38 mAb. Daratumumab, bortezomib, and dexamethasone was a common treatment regimen in this study. Patients with MM who did not fulfill TCR criteria were defined as being TCE if they had been previously treated with an IMiD, PI, and an anti-CD38 mAb.
Response rates for this study were selected as per modified IMWG guidelines. Complete response was described as the absence of a monoclonal protein on serum protein electrophoresis, serum immunofixation, and urine immunofixation even in cases where a bone marrow was not performed to confirm a response.55 The ORR was defined as a partial response or better according to IMWG criteria.55 PFS was defined as the time between initiation of subsequent therapy after progression on the index regimen until next confirmed progressive disease per IMWG criteria or death due to any cause.55 OS was defined as the time between starting a subsequent therapy and death or date of the last follow-up.
Statistical Analysis
Time-to-event analyses were used to evaluate the PFS and OS for this study. Multivariable analysis was applied to determine the impact of various risk factors on PFS and OS. Variables considered for the analyses of PFS and OS included age at time of progression on index regimen (≥ 75 years versus < 75 years), high-risk status at diagnosis (yes versus no versus unknown), sex (male versus female), number of prior treatment lines (≥ 3 prior lines including the index regimen versus < 3 prior lines), depth of response on index regimen (< very good partial response versus ≥ very good partial response), and time from diagnosis to progression on the index regimen (≥ 4 years versus < 4 years). Confounding was evaluated by monitoring the changes in the model parameters while adding new variables. Changes of more than 20% in the regression coefficients was considered an indication of confounding. Sensitivity analyses were conducted among patients with TCR MM to identify a subgroup with inferior outcomes.
Results
In this study, a total of 663 patients with MM who were refractory to anti-CD38 mAb therapy were identified from the CMRG database. Among these patients, 466 (70%) initiated a subsequent line of therapy, 145 (22%) had palliative care, and 52 (8%) patients were lost to follow-up. Of the 197 patients not initiating any subsequent regimen at the time of progression or lost to follow-up, the median age was 72 years, and the median OS from the time of index regimen progression was 1.3 months (95% CI, 0.4 months to 1.7 months). Of these untreated patients, 137 (70%) were patients with TCR MM, with a median age at progression on the index regimen of 71 years (range 42 to 91), as well as with a median of 4 (range, 2 to 9) lines of treatment including the index regimen. Among these 663 patients, 42 (6.3%) had penta-refractory MM status at progression on the index regimen; 22 patients did not initiate further treatment; and 20 patients got subsequent treatment on a clinical trial (n = 11) or with SOC regimens (n = 9).
Treatments and Efficacy Outcomes Post CD38-mAb Progression
Of the 466 patients getting subsequent treatment, 120 patients were on clinical trial and got excluded, ending with 346 patients treated with SOC regimens included in this study. Among these, 338 (98%) patients had MM refractory to daratumumab, with only 8 (2%) patients receiving isatuximab as part of the index regimen. Among the included patients, 218 (36%) previously received an autologous stem cell transplant, and most patients had MM refractory to lenalidomide (88%) or bortezomib (53%). Of the 109 patients with disease progression on daratumumab, bortezomib, and dexamethasone, 87 had bortezomib (and TCR) refractory disease and 22 had non-TCR MM at progression. The median age at initiation of subsequent regimen was 68 (range 40 to 90) years. The median time from diagnosis to the start of subsequent SOC regimen after progression on the index therapy was 57 (range 6 to 283) months, and the median number of prior treatment lines was 3 (range 1 to 9).
The most common SOC regimen in this study after progression on the index treatment was a PI or steroid doublet, followed by either a combination of PI or IMiDs with an alkylator (most commonly cyclophosphamide for this study). Among the included patients, 27 (8%) were re-treated with a CD38-mAb at the time of progression on the index regimen (25 of these patients moved to a different anti-CD38 mAb), with a median washout period of 1.1 (range 0 to 7.0) months. The median follow-up time from the date of initiation of subsequent SOC regimen was 8 months. Among the total cohort of patients with MM who were refractory to an anti-CD38 mAb and treated with subsequent SOC therapy (n = 346), the median PFS from the initiation of subsequent therapy was 4.6 months (95% CI, 4.1 months to 5.6 months), and the median OS was 13.3 months (95% CI, 10.6 months to 16.6 months). The median PFS and OS value was similar after excluding 7 patients who experienced disease relapse on front-line daratumumab (median PFS of 4.6 months [95% CI, 4.0 months to 5.5 months], median OS of 13.2 months [95% CI, 10.4 months to 15.3 months]). The ORR to first subsequent SOC regimen was 48% (131 of 273), and 7% (18 of 273) patients attained at least a CR.
Outcomes Among Patients With TCR Versus Non-TCR MM
Of the included study cohort, 199 (58%) patients had TCR MM and were treated with SOC treatments after their progression on anti-CD38 mAb. The next most common line of therapy among patients with TCR MM was a combination of PI or steroid (27%), IMiD or alkylator (23%), PI or alkylator (15%), or PI or IMiD (12%). Since anti-BCMA therapy, an XPO1 inhibitor, or venetoclax were not available as SOC in Canada, no patients received these treatments directly after progression on the index regimen. The ORR among patients was 40% (65 of 161) to the first subsequent line of therapy, with 5% (8 of 161) of patients gaining a complete response or better. Among patients with TCR MM, 14 (7%) were re-treated with an anti-CD38 mAb in combination with either an IMiD or PI in the next line of treatment after their progression on the index regimen. A total of 8 patients of these 14 (ORR 57%) attained at least a partial response. Of the 147 patients who had non-TCR MM at the time of progression on the index anti-CD38 mAb-containing regimen, 123 (84%) had TCE MM.
Among patients with TCR MM, the median follow-up time from the date of initiation of subsequent SOC treatment was 7.2 months. The median PFS value from the start of subsequent regimen was 4.4 months (95% CI, 3.6 months to 5.3 months), and the median OS value was 10.5 months (95% CI, 8.5 months to 13.8 months). Among the 48 of 199 (24%) patients with TCR MM and high-risk cytogenetic markers at diagnosis, the median PFS and OS values from the time of initiation of subsequent therapy after progression on the index therapy were 2.8 months (95% CI, 2.3 months to 6.1 months) and 8.5 months (95% CI, 4.7 months to 12.4 months), respectively. Similarly, 161 of 199 (81%) patients with TCR MM and a DOR on the index anti-CD38 mAb-containing regimen of less than 1 year had a median PFS of 3.9 months (95% CI, 3.0 months to 5.1 months), compared to 38 (19%) patients with a response of 1 year or more who had a median PFS of 6.1 months (95% CI, 3.9 months to 7.3 months).
While comparing the median PFS and OS for patients with non-TCR versus TCR MM when progressing on the index regimen from the start of the subsequent treatment, the median PFS values were 6.0 versus 4.4 months, respectively, P = 0.009; and median OS values were 17.5 versus 10.5 months, respectively, P = 0.003, among patients with non-TCR versus TCR MM. The median PFS of patients with TCR versus TCE MM was 4.4 months (95% CI, 3.6 months to 5.3 months) versus 4.5 months (95% CI, 3.9 months to 7.9 months), respectively, P = 0.06. The median OS values among patients with TCR versus TCE MM were 10.5 months (95% CI, 8.3 months to 13.4 months) versus 17.4 months (95% CI, 12.3 months to 26.6 months), respectively, P = 0.01.
Critical Appraisal
This was a RW retrospective cohort study which used a Canadian database (the CMRG database) to describe RW outcomes in patients with anti-CD38 mAb refractory MM subsequently treated with SOC regimens. This study also evaluated outcomes of patients with TCR MM as a distinct cohort. However, this study did not evaluate the effect of elranatamab and did not provide evidence about the efficacy and safety of this specific treatment.
Pharmacoeconomic_Review
Abbreviations
AE
adverse event
BCMA
B-cell maturation antigen
BIA
budget impact analysis
CAR
chimeric antigen receptor
cilta-cel
ciltacabtagene autoleucel
CMRG
Canadian Myeloma Research Group
CRS
cytokine release syndrome
CUA
cost-utility analysis
GRADE
Grading of Recommendations Assessment, Development and Evaluation
ICER
incremental cost-effectiveness ratio
IMiD
immunomodulatory drug
KCd
carfilzomib plus cyclophosphamide plus dexamethasone
Kd
carfilzomib plus dexamethasone
mAb
monoclonal antibody
MAIC
matching-adjusted indirect comparison
MM
multiple myeloma
NDMM
newly diagnosed multiple myeloma
OS
overall survival
PCd
pomalidomide plus cyclophosphamide plus dexamethasone
Pd
pomalidomide plus dexamethasone
PFS
progression-free survival
PI
proteasome inhibitor
QALY
quality-adjusted life-year
RDI
relative dose intensity
RRMM
relapsed or refractory multiple myeloma
SVd
selinexor plus bortezomib plus dexamethasone
TTD
time to treatment discontinuation
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Elranatamab (Elrexfio), solution for subcutaneous injection |
Indication | For the treatment of adult patients with relapsed or refractory multiple myeloma who have received at least 3 prior lines of therapy, including a proteasome inhibitor, an immunomodulatory agent, and an anti-CD38 monoclonal antibody, and who have demonstrated disease progression on the last therapy |
Health Canada approval status | NOC/c |
Health Canada review pathway | Advance consideration under NOC/c, Project Orbis |
NOC date | December 6, 2023 |
Reimbursement request | As per indication |
Sponsor | Pfizer Canada ULC |
Submission history | Previously reviewed: No |
NOC/c = Notice of Compliance with Conditions.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis PSM |
Target population | Adult patients with RRMM who have received at least 3 prior lines of therapy including a PI, an IMiD, and an anti-CD38 mAb, and who have demonstrated disease progression on the last therapy |
Treatment | Elranatamab |
Dosage regimen | Step-up dosing of 12 mg on day 1, followed by 32 mg on day 4; 76 mg is given once weekly thereafter. For patients who have received 24 weeks of treatment and have attained a response (i.e., a partial response or better that has been maintained for at least 2 months), the dose interval should transition to a schedule of every 2 weeks. |
Submitted price | Elranatamab, 40 mg/mL solution for subcutaneous injection, single-use vials:
|
Submitted treatment cost | The first 28-day costs of elranatamab are $25,053. Every 28 days after this, the costs are $28,000. If patients switch to a dosing schedule of every 2 weeks after 24 weeks of treatment, the 28-day treatment costs per patient are $14,000. |
Comparators |
|
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, life-years |
Time horizon | Lifetime (20 years) |
Key data sources |
|
Submitted results |
|
Key limitations |
|
CADTH reanalysis results |
|
Cilta-cel = ciltacabtagene autoleucel; CMRG = Canadian Myeloma Research Group; ICER = incremental cost-effectiveness ratio; IMiD = immunomodulatory drug; KCd = carfilzomib plus cyclophosphamide plus dexamethasone; Kd = carfilzomib plus dexamethasone; mAb = monoclonal antibody; PCd = pomalidomide plus cyclophosphamide plus dexamethasone; pCPA = pan-Canadian Pharmaceutical Alliance; Pd = pomalidomide plus dexamethasone; PFS = progression-free survival; PI = proteasome inhibitor; PSM = partitioned survival model; q.2.w. = every 2 weeks; QALY = quality-adjusted life-year; RDI = relative dose intensity; RRMM = relapsed or refractory multiple myeloma; SVd = selinexor plus bortezomib plus dexamethasone; TTD = time to treatment discontinuation; vs. = versus.
Conclusions
According to clinical experts consulted by CADTH, evidence from the single-arm, open-label, MagnetisMM-3 trial suggests that treatment with elranatamab may be associated with clinically meaningful benefit for objective response rate in those without prior exposure to B-cell maturation antigen (BCMA)-directed therapy. Based on the Grading of Recommendations Assessment, Development and Evaluation (GRADE) assessment of the MagnetisMM-3 study, CADTH categorized this evidence as having very low certainty, due to limitations associated with the lack of a comparator arm, which does not allow for any conclusions to be drawn on the relative effects of elranatamab versus any comparator. The CADTH clinical review identified limitations with the sponsor’s comparison of the MagnetisMM-3 trial to data from the Canadian Myeloma Research Group (CMRG), as well as the comparison of the MagnetisMM-3 trial to the CARTITUDE trial, which restricted the ability to interpret the relative treatment effects observed between elranatamab, physician’s choice (a basket of combination therapies), and ciltacabtagene autoleucel (cilta-cel). The evidence submitted to CADTH did not include indirect comparative evidence between elranatamab and any comparator for patients with prior exposure to BCMA-directed therapy; this represents a gap in the available indirect evidence. This clinical uncertainty is reflected in the submitted economic analysis.
A sequential analysis was not performed on the CADTH base case as different populations were used to inform each comparator. Pairwise comparisons are presented instead. In the CADTH base case, elranatamab was more effective (incremental quality-adjusted life-years [QALYs] = 1.03) and more costly (incremental costs = $215,242) compared to physician’s choice. This resulted in an incremental cost-effectiveness ratio (ICER) of $208,582 per QALY gained. Incremental QALYs were driven by a survival benefit associated with elranatamab relative to physician’s choice (incremental life-years = 1.38). Incremental costs were driven by higher drug costs ($182,040), as well as higher administration costs (e.g., inpatient hospitalizations) and adverse event (AE) management with elranatamab ($34,125). The main difference between the CADTH base case and the sponsor’s base case was the difference in incremental costs. The CADTH base-case changes increased the costs associated with elranatamab and decreased the costs of physician’s choice; estimates of clinical benefit (QALYs) were not substantially different. Relative to physician’s choice, the cost of elranatamab would need to decrease to approximately $1,960 per 76 mg/1.9 mL to be considered cost-effective at a $50,000 per QALY threshold. This translates to a 28-day cost of $3,920 for dosing every 2 weeks and $7,840 for dosing weekly. Relative to cilta-cel, elranatamab was found to be less costly and less effective (incremental costs = –$359,929; incremental QALYs = –1.34).
CADTH notes that the submitted analysis was based on a large, sustained impact on survival favouring elranatamab relative to physician’s choice, which predicts a survival benefit of 1.38 years. In the absence of robust, head-to-head, long-term clinical evidence, the extent of survival benefit for elranatamab, compared to physician’s choice, is highly uncertain. Consequently, the CADTH base case may overestimate the clinical benefits associated with elranatamab and therefore represent optimistic (upper bound) clinical benefits based on current clinical evidence. Higher price reductions may therefore be required for elranatamab to be cost-effective.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, clinician groups, and drug plans that participated in the CADTH review process.
Patient input was provided by Myeloma Canada. A survey of patients and caregivers living in Canada as well as international patients and caregivers indicated that multiple myeloma (MM) symptoms negatively impact daily life by decreasing quality of life, impacting the ability to work and travel, and resulting in the inability to exercise. Patients most frequently indicated requiring 3 lines of therapy for management of the disease. Patients indicated that control of infections, mobility, and kidney problems were treatment goals of high importance. They also reported experiencing nausea, gastrointestinal issues, and graft-versus-host disease with currently available treatments. Survey respondents indicated that pneumonia, immune effector cell-associated neurotoxicity syndrome, upper respiratory tract infections, cytokine release syndrome (CRS), and infections would be the least tolerable side effects associated with elranatamab. Patients expressed moderate concern with the potential side effects of elranatamab; however, approximately half of survey respondents who were eligible for treatment indicated that they would consider elranatamab as an option for their next treatment. Of the survey respondents who had been treated with elranatamab, most indicated currently undergoing treatment without relapse. All patients receiving elranatamab reported admission to the hospital in the initial step-up dosing period that ranged from 4 nights to 2 weeks. Patients receiving elranatamab indicated that cough, CRS, neutropenia, and upper respiratory tract infections were the least tolerable side effects experienced with treatment. Overall, approximately half of the patients being treated with elranatamab indicated that elranatamab completed or mostly improved overall quality of life, with the other half indicating no improvement or that it was too soon to tell. General feedback on the effectiveness of elranatamab controlling myeloma and meeting treatment expectations indicated positive experiences.
Registered clinician input was received from 2 groups: the CMRG and the Ontario Health (Cancer Care Ontario) Hematology Cancer Drug Advisory Committee (Drug Advisory Committees of Ontario Health [Cancer Care Ontario]). CMRG stated that newly diagnosed patients with myeloma in Canada are divided into 2 categories: those who are transplant-eligible and those who are transplant-ineligible, based on age and fitness. Transplant-eligible patients receive bortezomib-based induction with bortezomib plus lenalidomide plus dexamethasone or cyclophosphamide plus bortezomib plus dexamethasone followed by high-dose melphalan plus autologous stem cell transplant and lenalidomide maintenance until disease progression. Transplant-ineligible patients would have previously received lenalidomide plus dexamethasone or bortezomib plus lenalidomide plus dexamethasone followed by single-drug lenalidomide until disease progression. Recently, daratumumab-based combinations such as daratumumab plus lenalidomide plus dexamethasone, daratumumab plus cyclophosphamide plus bortezomib plus dexamethasone, and bortezomib plus melphalan plus prednisolone are preferred and include provisions for the long-term continuous administration of selected drugs. Second-line therapy depends on whether patients have progressed on lenalidomide. The inclusion of an anti-CD38 antibody (e.g., daratumumab and isatuximab) is key in second-line therapy, representing a high priority for patients. Other relevant anti-CD38 monoclonal antibody (mAb)-containing regimens have been approved by Health Canada and could be used in second-line therapy and beyond. Clinician groups also indicated that, since elranatamab is expected to be used after the failure of multiple drugs, it is not expected to impact the sequencing of drugs earlier in the disease course or lead to a major change in treatment algorithms before patients becoming triple-class exposed or triple-class refractory. However, elranatamab is expected to shift the current treatment paradigm for patients with advanced disease given that it will provide an additional, more readily accessible T-cell redirecting therapy for patients refractory to the most commonly used drugs.
Participating drug plans were interested in understanding how elranatamab compared with currently funded options, such as pomalidomide plus dexamethasone (Pd) or pomalidomide plus cyclophosphamide plus dexamethasone (PCd), carfilzomib plus dexamethasone (Kd) or carfilzomib plus cyclophosphamide plus dexamethasone (KCd), and selinexor plus bortezomib plus dexamethasone (SVd). Drug plans questioned whether patients previously treated with BCMA-targeted therapy (e.g., cilta-cel) should be eligible for elranatamab, and vice versa. Drug plans also questioned whether the reimbursement criteria for elranatamab should be aligned with that of teclistamab given their similar indication. Drug plans were further interested in clarifying whether patients are anticipated to switch from dosing weekly to dosing every 2 weeks. Finally, drug plans indicated that CRS and immune effector cell-associated neurotoxicity syndrome can occur with elranatamab, and that the administration of treatment should be administered by a health care professional to manage severe AEs. Drug plans noted that additional costs related to tocilizumab for CRS and the management of infections would impact drug program budgets.
Several of these concerns were addressed in the sponsor’s model.
The impact of disease and treatment on a patient’s quality of life was captured with utility values. AEs were incorporated as disutilities within the analysis.
To account for suggested risk monitoring for CRS and neurotoxicity during the step-up dosing period, the model assumed a 5-day hospitalization during treatment initiation based on clinical expert feedback.
In addition, CADTH addressed some of these concerns as follows.
In a scenario analysis, CADTH explored the impact of assuming that patients would not switch to dosing every 2 weeks after 24 weeks of treatment.
CADTH was unable to address the following concerns raised from stakeholder input.
Costs related to tocilizumab were not disaggregated by the sponsor but were assumed to be included in overall cost per inpatient stay.
Economic Review
The current review is for elranatamab (Elrexfio) for adult patients with relapsed or refractory multiple myeloma (RRMM) who have received at least 3 prior lines of therapy, including a proteasome inhibitor (PI), an immunomodulatory drug (IMiD), and an anti-CD38 mAb, and who have demonstrated disease progression on the last therapy.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis (CUA) of elranatamab compared with a basket of combination therapies (physician’s choice) and cilta-cel.1 Aligned with Health Canada’s indicated population, the modelled population comprised adult patients with RRMM who had received at least 3 prior lines of therapy, including a PI, an IMiD, and an anti-CD38 mAb, and who had demonstrated disease progression on the last therapy.1
Elranatamab is available as a solution for subcutaneous injection in 44 mg/1.1 mL and 76 mg/1.9 mL vials.2 The recommended starting dose is 12 mg on day 1, followed by 32 mg on day 4; 76 mg is then given once weekly thereafter.2 For patients who have received at least 24 weeks of treatment and have attained a response (i.e., a partial response or better that has been maintained for at least 2 months), the dosing interval should transition to a schedule of every 2 weeks.2 Patients are treated with elranatamab until disease progression or unacceptable toxicity. The submitted price of elranatamab is $4,053 for a 44 mg/1.1 mL vial and $7,000 for a 76 mg/1.9 mL vial, which at the recommended dosage corresponds to a 28-day cost of $25,053 (first month on treatment) and $28,000 (month 2 onward) per patient.1 If patients switch to an every 2-week dosing schedule after 24 weeks of treatment, monthly costs per patient are estimated to be $14,000.
Physician’s choice encompassed a mix of therapies commonly used in Canadian clinical practice based on the real-world CMRG study.3 Physician’s choice included 33% Kd, 10% KCd, 7% Pd, and 21% PCd. For the remaining 29%, less frequently used combinations of PI, IMiD, and mAb were estimated to be used at approximately 4% or less per treatment (Table 10 in Appendix 3).1 The sponsor estimated the weighted 28-day per-patient drug acquisition cost associated with physician’s choice to be approximately $11,351.1 Additionally, the sponsor applied a single cost at the time of cilta-cel infusion ($633,716) to the percentage of patients who ultimately received treatment in the weighted population of the CARTITUDE-1 trial (85%).1
The clinical outcomes modelled were overall survival (OS), progression-free survival (PFS), and time to treatment discontinuation (TTD). The economic outcomes of interest were QALYs and life-years. The economic evaluation was conducted over a lifetime time horizon (20 years) from the perspective of the Canadian public health care payer. Costs and outcomes were discounted at 1.5% per annum.
Model Structure
The sponsor submitted a partitioned survival model to capture costs and outcomes associated with elranatamab and comparators. The model included 3 health states: progression-free, progressed disease, and death, whereby transitions between health states occurred on a weekly cycle length (Figure 1).1 The proportion of patients in the progression-free, progressed disease, and death health states was estimated over time based on OS and PFS curves that were informed by the MagnetisMM-3 trial and matching-adjusted indirect comparisons (MAICs) comparing the efficacy of elranatamab to physician’s choice and cilta-cel.1 The proportion of patients with progressed disease was estimated as the difference between the proportion of living patients (estimated from the OS curve) and the proportion of progression-free patients (estimated from the PFS curve). PFS was defined as the time from the date of the first dose until confirmed progressed disease per International Myeloma Working Group criteria. Patients began in the progression-free health state, where they were assumed to initiate third-line treatment for RRMM, and over time could progress to either the progressed disease health state or transition to the death state. Patients transitioning to the death state remained there until the end of the model time horizon.
Model Inputs
Baseline patient characteristics were derived from the MagnetisMM-3 trial, a phase II, nonrandomized, open-label study of elranatamab monotherapy in patients with MM who are refractory to at least 1 PI, 1 IMiD, and 1 anti-CD38 antibody.1 Patients were assigned to 1 of the parallel cohorts: those naive to BCMA-directed therapies (cohort A) and those with previous exposure to BCMA-directed antibody-drug conjugates or chimeric antigen receptor (CAR) T-cells (cohort B). The mean patient age was 67 years, the mean patient weight was 74 kg, and 55% of patients were male.1 These characteristics were derived from the enrolled patient population of cohort A of the MagnetisMM-3 trial and were used to inform the drug dosage regimens and the age- and gender-specific distribution of the general population mortality risk in the model.
Clinical efficacy parameters used to characterize elranatamab, physician’s choice, and cilta-cel, including OS, PFS, and TTD, were derived from various data sources. Inputs for elranatamab were based on the MagnetisMM-3 trial and unanchored MAICs were conducted between elranatamab and comparators.1,4 Data from the retrospective CMRG study were used to derive inputs for physician’s choice and inputs for cilta-cel were informed from the CARTITUDE-1 trial.3,5 Data from the BOSTON trial were used to inform inputs for the scenario analysis including SVd as a comparator treatment.6 Parametric survival modelling was used to extrapolate OS, PFS, and TTD beyond time points available in the studies. Distributions were selected based on the clinical plausibility of long-term survival projections and visual inspection of model fit, as well as the Akaike information criterion and the Bayesian information criterion. OS for elranatamab was derived based on cohort A of the MagnetisMM-3 study and the sponsor selected a Weibull distribution based on visual inspection and long-term survival projection. PFS for elranatamab was also derived based on cohort A of the MagnetisMM-3 study and a Weibull distribution was selected based on best statistical fit. For physician’s choice and cilta-cel, the proportional hazards assumption did not hold, and hazard ratios derived from the MAICs could not be directly applied to the elranatamab survival curves. Instead, the sponsor derived adjusted parameters using data from the sponsor-conducted MAICs to extrapolate PFS and OS curves for each comparator. For treatments with median treatment duration available (e.g., elranatamab, SVd), TTD curves were derived based on median treatment duration assuming an exponential distribution for all treatments. It was assumed that patients receiving physician’s choice were treated until disease progression.
Health state–specific utility values were derived from an analysis of EQ-5D-5L index data collected from patients in the MagnetisMM-3 trial, with Canadian-specific utility weights. Utility values for the progression-free health state and the disease progression health state were 0.7860 and 0.7244, respectively. Disutilities related to blood and lymphatic system disorders, gastrointestinal disorders, general disorders, infections and infestations, investigations, psychiatric disorders, renal and urinary disorders, vascular disorders, and metabolism and nutrition disorders and their respective durations were sourced from published literature and included in the model.1 Disutility due to CRS and neurotoxicity were included and were assumed to occur for the same duration as observed for teclistamab from the MajesTEC-1 trial.
Costs captured in the model included primary and subsequent treatment costs (i.e., drug acquisition and drug administration), disease management costs, AE management costs, and terminal care costs. Drug acquisition costs for elranatamab were based on the sponsor’s submitted price. The dosing modelled for elranatamab is consistent with that described in the Overview section; however, dosage-switching to every 2 weeks was assumed to occur for 100% of patients after 24 weeks. Drug acquisition costs for physician’s choice therapies were sourced from the Ontario Drug Benefit Formulary, CADTH published reviews, and the Association québécoise des pharmaciens propriétaires with dosing schedules based on their corresponding clinical trials.7-10 Costs of cilta-cel included a 1-time per-patient cost associated with CAR T-cell procedure, in addition to costs associated with re-treatment, premedication, bridging therapy, administration, and monitoring.11 The sponsor applied a median relative dose intensity (RDI) value for each treatment based on their respective clinical trial or based on an assumption to derive drug acquisition costs.1
Health care resource use included monitoring costs and medical resource use costs. Monitoring costs were assumed by the sponsor to vary by health state and treatment received, and included complete blood count tests, liver function tests, and biochemistry tests. Medical resource use included physician office visits across all comparators, hospitalization associated with step-up dosing of elranatamab, and leukapheresis needed before CAR T-cell therapy. All health care resource use estimates were sourced from the Ontario Schedule of Benefits, the Ontario Case Costing Initiative, the Ontario Schedule of Benefits for Laboratory Services, or published literature.12,13 Costs associated with AEs such as blood and lymphatic system disorders, gastrointestinal disorders, general disorders, infections and infestations, investigations, psychiatric disorders, renal and urinary disorders, vascular disorders, and metabolism and nutrition disorders were estimated based on data from the Ontario Case Costing Initiative and included inpatient and outpatient unit costs per event.13
Costs related to AEs of special interest such as CRS and neurotoxicity were included based on inpatient unit costs and length of stay based on the MagnetisMM-3 study and published literature.1 The costs of subsequent treatment were applied as a 1-off cost based on dosage and median treatment of therapies in the CMRG physician’s choice basket, applied to 63.9% of all patients after progression aligned with the MagnetisMM-3 trial.1 All patients who transitioned to death were assumed to have incurred terminal care costs in the last cycle before death.14
Summary of Sponsor’s Economic Evaluation Results
All analyses were run probabilistically (1,000 iterations for the base case and 500 iterations for scenario analyses). The deterministic and probabilistic results were similar. The probabilistic findings are presented as follows.
Base-Case Results
In the sponsor’s base case, elranatamab was associated with an incremental cost of $79,250 and an incremental QALY gain of 1.07 compared with physician’s choice, resulting in an ICER of $73,938 per QALY gained. Compared with cilta-cel, elranatamab was less costly and less effective (incremental costs = –$468,938; incremental QALYs = –0.88). The sponsor’s analysis predicted that elranatamab was associated with a longer duration of life than physician’s choice, as well as a shorter duration of life than cilta-cel (i.e., incremental life-years are 1.39 and –1.27, respectively). Given the duration of the MagnetisMM-3 trial (i.e., a follow-up duration of 15 months) in contrast to the model’s time horizon (i.e., 20 years), the majority of the incremental QALYs realized by patients receiving elranatamab relative to physician’s choice (approximately 65%) was derived from the period beyond which there is observed trial data (i.e., an extrapolated period). The probability that elranatamab was cost-effective at a $50,000 per QALY gained threshold was 24%. The sponsor’s submitted analysis is based on the publicly available prices for all drug treatments. Additional results from the sponsor’s submitted economic evaluation base case are presented in Appendix 3.
Table 3: Summary of the Sponsor’s Economic Evaluation Results, Pairwise
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER ($/QALY) |
|---|---|---|---|---|---|
Elranatamab vs. physician’s choice | |||||
Physician’s choice | 150,442 | Reference | 0.76 | Reference | Reference |
Elranatamab | 229,692 | 79,250 | 1.84 | 1.07 | 73,938 |
Elranatamab vs. cilta-cel | |||||
Cilta-cel | 698,630 | Reference | 2.71 | Reference | Reference |
Elranatamab | 229,692 | –468,938 | 1.84 | –0.88 | Less costly and less effectivea |
Cilta-cel = ciltacabtagene autoleucel; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
aThis represents the ICER if cilta-cel were funded in replacement of elranatamab. Cilta-cel costs an additional $468,938 but generate an additional 0.88 QALYs.
Source: Sponsor’s pharmacoeconomic submission.1
Sensitivity and Scenario Analysis Results
In a key scenario analysis, SVd was included as a comparator using efficacy estimates obtained from the BOSTON trial. Results are presented in Appendix 3. CADTH notes that this scenario analysis relied on naive comparisons between elranatamab and SVd, indicating that results should be interpreted with caution due to the nature of the analysis as well as differences in patient populations between trials.
The sponsor assessed several model parameters and assumptions in additional scenario analyses. These included LocoMMotion trial data to parameterize physician’s choice, the removal of subsequent treatment, mean treatment duration for elranatamab (7.928 months) instead of median treatment duration (5.552 months), an RDI of 78% for physician’s choice, alternate durations of hospitalization for treatment initiation and CRS, 90% of patients switching from dosing weekly to dosing every 2 weeks, carfilzomib dosing of once a week, and various alternate assumptions regarding the extrapolation of OS and PFS. The ICER was most sensitive to changes in treatment duration and the use of LocoMMotion trial data instead of CMRG study data for physician’s choice, resulting in ICERs of $115,598 and $116,437, respectively, when comparing elranatamab to physician’s choice. ICERs ranged from $48,265 to $116,437 relative to physician’s choice across all scenarios.
The sponsor also conducted a scenario analysis from a societal perspective; this analysis included additional costs associated with lost productivity due to treatment administration. In this analysis, relative to physician’s choice, the ICER was $74,487 per QALY gained. This was similar to the sponsor’s base-case analysis using a health care payer perspective.
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations to the sponsor’s analysis that have notable implications for the economic analysis.
Comparative efficacy of elranatamab is highly uncertain: In the sponsor’s submitted pharmacoeconomic submission, the clinical efficacy of elranatamab, physician’s choice, and cilta-cel is characterized by PFS and OS. However, there is an absence of head-to-head clinical trial evidence comparing elranatamab to comparator treatments. To estimate comparative efficacy data, the sponsor instead applied an “MAIC-adjusted curve” to each comparator to estimate OS and PFS based on weighted data from the sponsor-conducted MAICs. The CADTH clinical review concluded that based on the noncomparative, open-label MagnetisMM-3 trial, it remains unknown whether elranatamab improves PFS, OS, and duration of response as data were immature. Results from the indirect treatment comparisons and real-world evidence studies consistently favoured elranatamab over comparators, except for cilta-cel. However, the CADTH clinical review states that no conclusions could be drawn on the relative efficacy and safety of elranatamab compared to physician’s choice and cilta-cel due to limitations with the indirect treatment comparisons and available real-world evidence data. The CADTH reanalysis is subject to a high degree of uncertainty due to uncertainty regarding the effects of treatment on PFS and OS. This uncertainty is compounded by the extent of clinical benefit predicted by the model beyond the trial period of 15 months (approximately 65% of total benefit).
CADTH could not address this limitation in reanalysis.
Modelling approach may overestimate comparative efficacy of elranatamab: In the absence of long-term clinical efficacy data, the sponsor extrapolated PFS and OS beyond the 15-month data available from the MagnetisMM-3 trial using parametric survival modelling. A Weibull distribution was selected for both PFS and OS curves. However, this led to results suggesting that after 30 months there would be no further progression for the 35% of patients who survive to that time point. This would indicate a potential cure. No clinical evidence was provided to support this. Clinical experts consulted by CADTH also stated that the sponsor’s extrapolation of PFS likely overestimated PFS for elranatamab and did not meet face validity when looking at 5-year, 10-year, and 15-year predictions. Due to the lack of robust data, PFS and OS beyond the trial data for elranatamab is uncertain.
The PFS Kaplan-Meier curve shows that in the first 4 months of treatment, approximately 30% of patients experience a progression or mortality event. From month 4 to month 8, only 7% of patients experience an event. This would indicate that over time, the risk of a progression event decreases. Therefore, when survival analysis is conducted on this data, there is a large continuing reduction in the likelihood of progression events over time. When examining the potential extrapolations of PFS, all the survival curves intersect OS (except for the exponential curve), which is clinically implausible. Although the sponsor caps PFS at OS, this would still indicate that a large proportion of patients who receive elranatamab will never progress even after discontinuing therapy. This would indicate that remaining progression-free has 0 impact on OS, which was considered unlikely.
One limitation with the survival analysis is the assumption that the population is homogeneous. This means all individuals in the cohort who are at risk at a specific point in time have the same probability of progression. However, for elranatamab, 40 of 125 patients did not attain a response. These patients made up most progression events. Given this heterogeneity in progression among the cohort, it would be more appropriate to conduct a survival analysis on responders and nonresponders separately. A survival analysis in heterogenous populations can lead to inaccurate extrapolations. The limitations of conducting a survival analysis in a heterogenous population have been discussed in the literature.15,16
Finally, the modelling approach for treatment discontinuation of elranatamab led to results that did not meet face validity. In the analysis, discontinuation is only used to estimate treatment costs. The sponsor derived TTD curves for elranatamab based on the median duration of treatment of 5.55 months and assuming a constant rate of discontinuation over time. Using the median ignores any skewness in the data and there is no clinical or methodological justification to extrapolate TTD any differently than OS and PFS. Second, this approach generated a survival curve for TTD that did not represent the data in the trial. Third, the sponsor’s approach assumes no correlation between treatment discontinuation and progression. A patient will discontinue therapy due to unacceptable toxicity or progression, meaning PFS and TTD are intrinsically linked. However, the sponsor assumed that despite remaining progression-free, many patients will come off treatment altogether, indicating that toxicity is responsible for nearly all treatment discontinuations. This goes against the clinical data, which shows progression is the most cited reason for discontinuation. Therefore, the sponsor’s approach underestimates the costs associated with elranatamab.
A more appropriate analysis may have been to conduct a survival analysis for OS, PFS, and TTD on responders and nonresponders separately. However, the appropriateness of this could not be determined as the sponsor declined to send CADTH survival data based on response when requested. Alternatively, a more sophisticated survival analysis may be warranted to accurately fit the data.
For the base-case analysis, CADTH assumed a gamma distribution when extrapolating TTD. For PFS, none of the options provided by the sponsor met face validity in that they either intersected OS or did not fit the trial data well. Therefore, a survival curve was created by applying a hazard ratio of 0.7 to the TTD survival rate. This assumes a strong correlation between PFS and TTD, which is confirmed by trial data as progression is responsible for most discontinuation events. A hazard ratio of 0.7 was chosen based on visual inspection of the data and assuming PFS would not intersect OS. For the scenario analyses, 2 alternative survival curves were extrapolated for PFS by applying a hazard ratio of 0.6 and 0.8 to the TTD event rate. This was considered the most plausible range for PFS. Applying a hazard ratio of 0.6 fits the first 6 months of data well but may underestimate long-term PFS with elranatamab. Applying a hazard ratio of 0.8 overestimates PFS in the first 6 months. After 12 months, patient numbers are small (< 50) and there is a high amount of censoring, increasing the uncertainty of extrapolation beyond this point. Figure 4 outlines the PFS survival curves considered by CADTH.
Generalizability of modelled population to Canadian clinical practice is unclear: CADTH notes that there is uncertainty regarding the expected survival benefit in a Canadian setting following the implementation of elranatamab to a broader population that expands beyond the selective patient population recruited within the clinical trial. The clinical data used to populate the submitted economic model was restricted to cohort A patients from the MagnetisMM-3 trial, which only included patients who did not have previous experience with BCMA-directed treatment and an Eastern Cooperative Oncology Group Performance Status score of 2 or less. The majority of patients (94%) enrolled in the MagnetisMM-3 trial had an Eastern Cooperative Oncology Group Performance Status score of 1 or less (59% of patients with a score of 1 and 35% of patients with a score of 0). According to the CADTH clinical review, the evidence submitted to CADTH did not include indirect comparative evidence between elranatamab and any comparator for patients with prior exposure to BCMA-directed therapy; this represents a gap in the available indirect evidence. If elranatamab were to become available in clinical practice, where patients are likely to have more diverse clinical and demographic profiles, the magnitude of clinical benefit is uncertain.
CADTH was unable to address this limitation owing to the lack of clinical data.
Dosing schedule for elranatamab is not aligned with the trial: As per the product monograph, the adoption of doses every 2 weeks is as follows: “for patients who have received at least 24 weeks of treatment and have attained a response (i.e., a partial response or better that has been maintained for at least 2 months), the dose interval should transition to an every two-week schedule.”2 However, the sponsor’s base case assumes that 100% of patients will transition to a dosing schedule of every 2 weeks as per “MagnetisMM-3 trial protocol.” As per the data from the latest September 11, 2023, MagnetisMM-3 trial data cut-off submitted by the sponsor, 61 patients remain on treatment after 24 weeks of treatment and 58 patients were recorded to have switched from dosing weekly to dosing every 2 weeks. The submitted data also indicates that 3 patients among those switching from dosing weekly to every 2 weeks ended up switching back to dosing every week, meaning that 55 patients switched and remained on a dosing schedule of every 2 weeks out of 61 total patients remaining on treatment. As such, CADTH readjusted the percentage of patients dosage-switching after 24 weeks in reanalysis to reflect the clinical trial data.
CADTH adjusted the percentage of patients (55 of 61 patients = 90.16%) who would switch to dosing every 2 weeks after 24 weeks, based on data from the MagnetisMM-3 trial provided by the sponsor.
Treatment schedule for carfilzomib and dexamethasone is not reflective of Canadian practice: The sponsor assumes patients receiving carfilzomib and dexamethasone will receive the treatment on a twice weekly schedule in the economic model. It was noted that most centres in Canada use the once weekly schedule in practice. The once weekly schedule was found to have a potentially improved efficacy profile compared to the twice weekly schedule, in addition to having a more convenient dosing schedule for patients since it requires less frequent administrations.17
CADTH updated the dosing schedule for carfilzomib and dexamethasone to align with the following once weekly dosing: 28-day cycle, cycle 1 — 20 mg/m2 on day 1, then 70 mg/m2 on day 8 and day 15; 28-day cycle, cycle 2 — 70 mg/m2 on day 1, day 8, and day 15.
Cost of pomalidomide is overestimated: In the analysis, the sponsor estimated the cost of pomalidomide to be $425 per 4 mg capsule. Using IQVIA DeltaPA, $125 per 4 mg capsule was cited in some Canadian jurisdictions and likewise matches the cost cited in the July 2023 pan-Canadian Pharmaceutical Alliance generics categories report.18
CADTH updated the cost of pomalidomide to $125 per capsule.
Application of RDI may underestimate drug costs: In the sponsor’s model, the median RDI was calculated for elranatamab to be 78.35% based on MagnetisMM-3 trial data using overall dose intensity (based on dose received) and planned dose intensity. For all other comparators, RDI was taken from published literature. Given elranatamab is administered using a single-dose vial, any dose reductions would not impact drug cost as 1 vial would still be required regardless of the dose. Dose interruptions or skipping would, however, reduce drug costs. As part of an additional information request, an analysis of RDI was provided by the sponsor assuming any dose administered greater than 0 mg was counted as a 76 mg dose (the full recommended dose). This means only dose skipping and interruption were included in the calculation. Based on this, the mean RDI was calculated to be 80.61% in cohort A, meaning that 80.61% of planned administrations were administered. However, RDI was calculated over the trial, which covered the period individuals switched to a dosing schedule of every 2 weeks. It is likely that once a stable dose has been attained and movement to a dosing schedule of every 2 weeks has occurred, there will be a reduction in skipped doses and RDI may trend closer to 100%.
In reanalysis, CADTH assumed an RDI of 80.61%, while assessing the impact of an RDI of 100% in a scenario analysis.
Proportion of patients who require subsequent therapy is uncertain: Based on the MagnetisMM-3 trial, the sponsor assumes that 63.9% of patients will require subsequent treatment after progression, which is applicable to elranatamab as well as all comparators. It is uncertain whether patients who receive elranatamab versus comparators would be similarly likely to receive a subsequent line of therapy. In the absence of robust head-to-head Canadian data, the impact that elranatamab has on subsequent therapy usage is uncertain. In the sponsor’s base case, costs related to subsequent therapy were less for patients receiving elranatamab because patients receiving elranatamab remained progression-free for a longer period and therefore more patients died before progression.
CADTH could not address this limitation in reanalysis due to the lack of comparative clinical data. Any cost savings due to delay or the avoidance of subsequent therapy is highly uncertain.
Cost-effectiveness relative to SVd is uncertain: To evaluate the cost-effectiveness of elranatamab to SVd, the sponsor conducted a naive comparison of the MagnetisMM-3 trial to the BOSTON trial.19 No analysis was conducted to account for the differing patient populations between the 2 cohorts. As the BOSTON trial included patients who had only 1 prior exposure to a therapy for MM, it likely represents a healthier cohort of patients than those evaluated in the MagnetisMM-3 trial. Results from this analysis are therefore highly uncertain.
CADTH could not address this limitation in reanalysis due to the lack of robust clinical data. The cost-effectiveness of elranatamab versus SVd is therefore unknown.
Uncertainty in the inclusion of tocilizumab costs: AEs such as CRS and neurotoxicity associated with treatment require patients to be treated with tocilizumab. In the sponsor’s submitted model, costs related to tocilizumab were not explicitly included. However, patients who experience CRS and neurotoxicity incur costs based on the average cost per inpatient day for cancer patients in Canada, and it is assumed that this includes drug costs for tocilizumab (as rescue medication). Notably, drug costs for tocilizumab as rescue medication were not disaggregated and CADTH could not validate if they were adequately captured in the submitted model. Based on data from the MagnetisMM-3 trial, the incidence of grade 1 and grade 2 CRS was 57.72% and as such, approximately half of patients in the model would therefore incur costs related to tocilizumab rescue medication. At the recommended dosage of 8 mg/kg on day 1, day 4, and day 8, tocilizumab is expected to cost approximately $1,371 per patient (this assumes wastage, 1 treatment cycle as observed in the MagnetisMM-3 trial, and the use of a body surface area of 1.82 m2 and weight of 71.8 kg as per trial data). CADTH notes that costs associated with elranatamab may therefore be underestimated.
CADTH notes that tocilizumab costs may not be adequately captured by the sponsor. This is unlikely to have a large impact on the results due to the cost of tocilizumab being substantially lower than all other costs considered in the analysis.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CADTH (refer to Table 4).
Table 4: Key Assumptions of the Submitted Economic Evaluation (Not Noted as Limitations to the Submission)
Sponsor’s key assumption | CADTH comment |
|---|---|
Hospitalization for elranatamab step-up administration was assumed to be 5 days at treatment initiation. | Acceptable. Based on clinical expert opinion obtained by the sponsor, it was assumed that a 5-day inpatient stay would be adequate to monitor AEs following treatment initialization of elranatamab. |
The sponsor assumed that subsequent treatment would be characterized by CMRG. | Acceptable. Physician’s choice was characterized by CMRG in the base case and would reflect treatment for patients living in Canada. |
AE = adverse event; CMRG = Canadian Myeloma Research Group.
CADTH Reanalyses of the Economic Evaluation
Base-Case Results
Several limitations with the sponsor’s submission could not be adequately addressed (i.e., a lack of head-to-head comparative clinical efficacy data and uncertainty regarding long-term clinical effectiveness). The CADTH base case was derived by making changes in model parameter values and assumptions, in consultation with clinical experts. CADTH undertook a stepped reanalysis that modelled elranatamab PFS as a function of TTD, applied a parametric curve (gamma distribution) to extrapolate elranatamab TTD, adjusted the proportion of patients switching to dosing every 2 weeks based on trial data, updated the cost of pomalidomide, assumed carfilzomib was administered weekly rather than twice weekly, and adjusted the RDI to reflect dose interruptions only.
Details for each stepwise change to derive the CADTH reanalysis are presented in Table 5. The summary results of the CADTH reanalyses are presented in Table 6 (disaggregated results are presented in Appendix 4).
In the CADTH base case, elranatamab was associated with an ICER of $208,582 per QALY gained compared to physician’s choice (incremental costs = $215,242; incremental QALYs = 1.03) (refer to Table 6). Compared with cilta-cel, elranatamab was less costly and less effective (incremental costs = –$359,929; incremental QALYs = –1.34). Hence, the ICER of cilta-cel versus elranatamab was $268,604 per QALY gained. Results were primarily driven by the effect of each treatment on OS and PFS as well as the duration of treatment.
Table 5: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Changes to derive the CADTH base case | ||
1. Extrapolating TTD and PFS | Assumed exponential distribution for TTD based on median treatment duration of elranatamab (5.5 months) from cohort A of the MagnetisMM-3 trial Weibull distribution to extrapolate PFS for elranatamab | Gamma distribution was used to extrapolate TTD for elranatamab. A survival curve for PFS was generated by applying a hazard ratio of 0.7 to the rate of treatment discontinuation. |
2. Proportion of patients switching to q.2.w. dosing after 24 weeks | 100.00% | 90.16% based on the proportion of patients switching to q.2.w. dosing relative to the total number patients remaining on treatment after 24 weeks (n = 55 of 61) |
3. Cost of pomalidomide | $425 per 4 mg capsule | $125 per 4 mg capsule |
4. Dosing schedule for carfilzomib + dexamethasone | 28-day cycles:
| 28-day cycles:
|
5. Application of elranatamab RDI | Median RDI of 78.35% applied to calculate drug acquisition costs for elranatamab | Mean RDI of 80.61% applied, adjusting for dose interruptions only and reflecting the proportion of doses administered in the MagnetisMM-3 trial |
CADTH base case | ― | Reanalysis 1 + 2 + 3 + 4 + 5 |
PFS = progression-free survival; q.2.w. = every 2 weeks; RDI = relative dose intensity; TTD = time to treatment discontinuation.
Table 6: Summary of the Stepped Analysis of the CADTH Reanalysis Results
Stepped analysis | Drug | Total costs ($) | Total QALYs | Pairwise ICER vs. elranatamab ($/QALY)a |
|---|---|---|---|---|
Sponsor’s base case (deterministic) | Physician’s choice | 152,087 | 0.73 | 65,233 |
Elranatamab | 223,416 | 1.82 | NA | |
Cilta-cel | 706,323 | 2.54 | Elranatamab is less costly and less effective. | |
CADTH reanalysis 1: TTD and PFS extrapolation | Physician’s choice | 152,087 | 0.73 | 165,592 |
Elranatamab | 327,639 | 1.79 | NA | |
Cilta-cel | 706,323 | 2.54 | Elranatamab is less costly and less effective. | |
CADTH reanalysis 2: Q.2.w. dosing switch after 24 weeks | Physician’s choice | 152,087 | 0.73 | 69,508 |
Elranatamab | 228,091 | 1.82 | NA | |
Cilta-cel | 706,323 | 2.54 | Elranatamab is less costly and less effective. | |
CADTH reanalysis 3: Cost of pomalidomide | Physician’s choice | 124,189 | 0.73 | 88,384 |
Elranatamab | 220,834 | 1.82 | NA | |
Cilta-cel | 691,317 | 2.54 | Elranatamab is less costly and less effective. | |
CADTH reanalysis 4: Dosing schedule for carfilzomib + dexamethasone | Physician’s choice | 142,135 | 0.73 | 74,980 |
Elranatamab | 224,123 | 1.82 | NA | |
Cilta-cel | 708,776 | 2.54 | Elranatamab is less costly and less effective. | |
CADTH reanalysis 5: Application of elranatamab RDI | Physician’s choice | 152,087 | 0.73 | 69,026 |
Elranatamab | 227,565 | 1.82 | NA | |
Cilta-cel | 706,323 | 2.54 | Elranatamab is less costly and less effective. | |
CADTH base case (1 + 2 + 3 + 4 + 5): (deterministic) | Physician’s choice | 114,237 | 0.73 | 210,405 |
Elranatamab | 337,298 | 1.79 | NA | |
Cilta-cel | 693,771 | 2.54 | Elranatamab is less costly and less effective. | |
CADTH base case (1 + 2 + 3 + 4 + 5): (probabilistic) | Physician’s choice | 112,396 | 0.78 | 208,582 |
Elranatamab | 327,637 | 1.82 | NA | |
Cilta-cel | 687,567 | 2.77 | Elranatamab is less costly and less effective.b |
Cilta-cel = ciltacabtagene autoleucel; ICER = incremental cost-effectiveness ratio; NA = not applicable; q.2.w. = every 2 weeks; QALY = quality-adjusted life-year; PFS = progression-free survival; RDI = relative dose intensity; TTD = time to treatment discontinuation; vs. = versus.
Note: The CADTH reanalysis is based on publicly available prices of the comparator treatments. The results of all steps are presented deterministically unless otherwise indicated, while the cumulative CADTH base case is always presented both deterministically and probabilistically.
aThis is not a sequential analysis given that the populations enrolled in the relevant studies examining the efficacy of cilta-cel and physician’s choice were different.
bCilta-cel costs an additional $359,929 but generates an additional 1.34 QALYs, leading to an ICER of $268,604 per QALY gained. This represents the ICER if cilta-cel were funded in replacement of elranatamab.
Scenario Analysis Results
CADTH undertook price reduction analyses based on the sponsor’s submitted results and the CADTH base-case reanalysis. The CADTH base case suggests that a 72% price reduction is required for elranatamab to be considered cost-effective at a willingness-to-pay threshold of $50,000 per QALY gained compared to physician’s choice. The 28-day cost of elranatamab would be approximately $7,840 at a 72% price reduction. This decreases to $3,920 if a dosing schedule of every 2 weeks is used. In the CADTH base case, cilta-cel costs more than elranatamab ($359,929) but also generates additional QALYs (1.34), leading to an ICER of $268,604 per QALY gained. Therefore, if the price of elranatamab decreased, the ICER would increase (cilta-cel becomes less cost-effective).
Table 7: CADTH Price Reduction Analyses
Analysis | Unit drug cost ($) | ICERs for elranatamab vs. physician’s choice ($/QALY) | |
|---|---|---|---|
Price reduction | $ | Sponsor’s base case | CADTH reanalysis |
No price reduction | 7,000 | 73,938 | 208,582 |
10% | 6,300 | 60,627 | 186,650 |
20% | 5,600 | 47,316 | 164,718 |
30% | 4,900 | 34,005 | 142,786 |
40% | 4,200 | 20,694 | 120,855 |
50% | 3,500 | 7,383 | 98,923 |
60% | 2,800 | Elranatamab is dominant | 76,991 |
70% | 2,100 | Elranatamab is dominant | 55,059 |
80% | 1,400 | Elranatamab is dominant | 33,127 |
90% | 700 | Elranatamab is dominant | 11,195 |
100% | 0 | Elranatamab is dominant | Elranatamab is dominant |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus.
CADTH conducted the following additional scenario analyses to determine the impact of alternate assumptions on the cost-effectiveness of elranatamab relative to physician’s choice and cilta-cel.
CADTH applied an RDI value of 100% to elranatamab.
CADTH implemented an alternative extrapolation of PFS by applying a hazard ratio of 0.6 to TTD.
CADTH implemented an alternative extrapolation of PFS by applying a hazard ratio of 0.8 to TTD.
When an RDI value of 100% was applied to elranatamab, the ICER of elranatamab relative to physician’s choice increased to $262,162 per QALY gained. Elranatamab remained less costly and less effective than cilta-cel. Alternative extrapolations of PFS did not have a substantial impact on the ICER. Assuming a more pessimistic extrapolation of PFS increased the ICER to $214,009 per QALY gained. A more optimistic extrapolation decreased the ICER to $188,658 per QALY gained. The results of these analysis are presented in Table 14.
Issues for Consideration
Teclistamab is currently under review for adult patients with RRMM who have received at least 3 prior lines of therapy, including a PI, an IMiD, and an anti-CD38 mAb, and who have demonstrated disease progression on the last therapy. The cost-effectiveness of teclistamab versus elranatamab is unknown.
Overall Conclusions
According to clinical experts consulted by CADTH, evidence from the single-arm, open-label, MagnetisMM-3 trial suggests that treatment with elranatamab may be associated with clinically meaningful benefit for objective response rate in those without prior exposure to BCMA-directed therapy. Based on the GRADE assessment of the MagnetisMM-3 study, CADTH categorized this evidence as having very low certainty due to limitations associated with the lack of a comparator arm; this does not allow for any conclusions to be drawn on the relative effects of elranatamab versus any comparator. The CADTH clinical review identified limitations with the sponsor’s comparison of the MagnetisMM-3 study to data from CMRG, as well as the comparison of the MagnetisMM-3 study to the CARTITUDE study, which restricted the ability to interpret the relative treatment effects observed between elranatamab, physician’s choice, and cilta-cel. The evidence submitted to CADTH did not include indirect comparative evidence between elranatamab and any comparator for patients with prior exposure to BCMA-directed therapy; this represents a gap in the available indirect evidence. This clinical uncertainty is reflected in the submitted economic analysis.
A sequential analysis was not performed on the CADTH base case as different populations were used to inform each comparator. Pairwise comparisons are presented instead. In the CADTH base case, elranatamab was more effective (incremental QALYs = 1.03) and more costly (incremental costs = $215,242) compared to physician’s choice. This resulted in an ICER of $208,582 per QALY gained. Incremental QALYs were driven by a survival benefit associated with elranatamab relative to physician’s choice (incremental life-years = 1.38). Incremental costs were driven by higher drug costs ($182,040), as well as higher administration costs (e.g., for inpatient hospitalizations) and AE management with elranatamab ($34,125). The main difference between the CADTH base case and the sponsor’s base case is the difference in incremental costs. The CADTH base-case changes increased the costs associated with elranatamab and decreased the costs of physician’s choice; estimates of clinical benefit (QALYs) were not substantially different. Relative to physician’s choice, the cost of elranatamab would need to decrease to approximately $1,960 per 76 mg/1.9 mL to be considered cost-effective at a $50,000 per QALY threshold. This translates to a 28-day cost of $3,920 for dosing every 2 weeks and $7,840 for weekly dosing. Relative to cilta-cel, elranatamab was found to be less costly and less effective (incremental costs = –$359,929; incremental QALYs = –1.34).
CADTH notes that the submitted analysis was based on a large, sustained impact on survival favouring elranatamab relative to physician’s choice, which predicts a survival benefit of 1.38 years. In the absence of robust, head-to-head, long-term clinical evidence, the extent of survival benefit for elranatamab, compared to physician’s choice, is highly uncertain. Consequently, the CADTH base case may overestimate the clinical benefits associated with elranatamab and therefore represent optimistic (upper bound) clinical benefits based on current clinical evidence. Higher price reductions may therefore be required for elranatamab to be cost-effective.
References
1.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Elrexfio (elranatamab), 44 mg/1.1 mL (40 mg/mL) solution for subcutaneous injection, 76 mg/1.9 mL (40 mg/mL) solution for subcutaneous injection. Kirkland (QC): Pfizer Canada; 2023 Nov 9.
2.Elrexfio (elranatamab): 44 mg/1.1 mL (40 mg/mL) solution for subcutaneous injection, 76 mg/1.9 mL (40 mg/mL) solution for subcutaneous injection [product monograph]. Kirkland (QC): Pfizer Canada ULC; 2023 Oct 20.
3.Visram A, De La Torre A, White D, et al. Real World Data on Outcomes of Anti-CD38 Antibody Treated, Including Triple Class Refractory, Patients with Multiple Myeloma: A Multi-Institutional Report from the Canadian Myeloma Research Group (CMRG) Database [sponsor-supplied reference]. 2023.
4.Matching-adjusted indirect treatment comparison (MAIC) of elranatamab versus physicians’ choice of treatment in Canada for the treatment of adult patients with multiple myeloma who have received at least three prior lines of therapy, including one proteasome inhibitor, one immunomodulatory drug, and one anti-CD38 monoclonal antibody, and who have demonstrated disease progression on the last therapy [internal sponsor's report]. In: Elrexfio (elranatamab), 44 mg/1.1 mL (40 mg/mL) solution for subcutaneous injection, 76 mg/1.9 mL (40 mg/mL) solution for subcutaneous injection. Kirkland (QC): Pfizer Canada; 2023 Oct 4.
5.Berdeja JG, Madduri D, Usmani SZ, et al. Ciltacabtagene autoleucel, a B-cell maturation antigen-directed chimeric antigen receptor T-cell therapy in patients with relapsed or refractory multiple myeloma (CARTITUDE-1): a phase 1b/2 open-label study. Lancet. 2021;398(10297):314-324. PubMed
6.Grosicki S, Simonova M, Spicka I, et al. Once-per-week selinexor, bortezomib, and dexamethasone versus twice-per-week bortezomib and dexamethasone in patients with multiple myeloma (BOSTON): a randomised, open-label, phase 3 trial. Lancet. 2020;396(10262):1563-1573. PubMed
7.Ontario Ministry of Health, Ontario Ministry of Long-Term Care. Ontario drug benefit formulary/comparative drug index [sponsor-supplied reference]. 2022; https://www.formulary.health.gov.on.ca/formulary/. Accessed 2023 Aug 10.
8.Carfilzomib (Kyprolis) for Multiple Myeloma (relasped) [sponsor-supplied reference]. Ottawa (ON): CADTH; 2017.
9.CADTH reimbursement review: Selinexor (Xpovio) [sponsor-supplied reference]. Can J Health Technol. 2022;2(10). https://www.cadth.ca/sites/default/files/DRR/2022/PC0276-Xpovio.pdf.
10.pCODR expert review committee (pERC) initial recommendation: Isatuximab (Sarclisa) [sponsor-supplied reference]. Ottawa (ON): CADTH; 2020: https://www.cadth.ca/sites/default/files/pcodr/Reviews2021/10220IsatuximabMM_inRec_pERC%20Chair%20Approved_Post4Feb2021_final.pdf.
11.CADTH reimbursement review: Ciltacabtagene Autoleucel (Carvykti) [sponsor-supplied reference]. Ottawa (ON): CADTH; 2023.
12.Schedule of Benefits for Laboratory Services [sponsor-supplied reference]. Toronto (ON): Ontario Ministry of Health: https://www.health.gov.on.ca/en/pro/programs/ohip/sob/lab/sob_lab_2023.pdf. Accessed 2023 Sep 4.
13.Ontario Case Costing Initiative (OCCI) [sponsor-supplied reference]. Toronto (ON): Ontario Health and Long-Term Care; 2017: https://data.ontario.ca/en/dataset/ontario-case-costing-initiative-occi. Accessed 2022 Oct 22.
14.Walker H, Anderson M, Farahati F, et al. Resource use and costs of end-of-life/palliative care: Ontario adult cancer patients dying during 2002 and 2003. J Palliat Care. 2011;27(2):79-88. PubMed
15.Tarride J-E, Cheung M, Hanna TP, et al. Platform, Basket, and Umbrella Trial Designs: Issues Around Health Technology Assessment of Novel Therapeutics. Can J Health Technol. 2022;2(7). PubMed
16.Zaric GS. The impact of ignoring population heterogeneity when Markov models are used in cost-effectiveness analysis. Med Decis Making. 2003;23(5):379-396. PubMed
17.Moreau P, Mateos MV, Berenson JR, et al. Once weekly versus twice weekly carfilzomib dosing in patients with relapsed and refractory multiple myeloma (A.R.R.O.W.): interim analysis results of a randomised, phase 3 study. Lancet Oncol. 2018;19(7):953-964. PubMed
18.Pan-Canadian Pharmaceutical Alliance. Generics Categories Report July 2023. 2023; https://www.pcpacanada.ca/generic-drug-framework. Accessed 2024 Mar 13.
19.Grosicki S, Simonova M, Spicka I, et al. Once-per-week selinexor, bortezomib, and dexamethasone versus twice-per-week bortezomib and dexamethasone in patients with multiple myeloma (BOSTON): a randomised, open-label, phase 3 trial. The Lancet. 2020;396(10262):1563-1573. PubMed
20.BC Cancer. BC Cancer Protocol Summary for Therapy of Multiple Myeloma Using Carfilzomib and Dexamethasone With or Without Cyclophosphamide. 2022; http://www.bccancer.bc.ca/chemotherapy-protocols-site/Documents/Lymphoma-Myeloma/MYCARDEX_Protocol.pdf. Accessed 2024 May.
21.Cancer Care Ontario. DEXAPOMA Regimen [sponsor-supplied reference]. 2023: https://www.cancercareontario.ca/en/drugformulary/regimens/46761.
22.Cancer Care Ontario. CYCLDEXAPOMA Regimen [sponsor-supplied reference]. 2023: https://www.cancercareontario.ca/en/drugformulary/regimens/47786.
23.Ontario Ministry of Health, Ontario Ministry of Long-Term Care. Ontario drug benefit formulary/comparative drug index. 2022; https://www.formulary.health.gov.on.ca/formulary/. Accessed 2023 Dec 15.
24.DeltaPA. [Ottawa (ON)]: IQVIA; 2022: https://www.iqvia.com/. Accessed 2023 Dec.
25.Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Elrexfio (elranatamab), 44 mg/1.1 mL (40 mg/mL) solution for subcutaneous injection, 76 mg/1.9 mL (40 mg/mL) solution for subcutaneous injection. Kirkland (QC): Pfizer Canada; 2023 Nov 9.
26.Myeloma Canada. Incidence & Prevalence in Canada [sponsor-supplied reference]. Accessed 2023 Jul 7.
27.Fonseca R, Usmani SZ, Mehra M, et al. Frontline treatment patterns and attrition rates by subsequent lines of therapy in patients with newly diagnosed multiple myeloma. BMC Cancer. 2020;20(1):1087. PubMed
28.Canadian Cancer Statistics - A 2022 Special Report on Cancer Prevalence. Toronto (ON): Canadian Cancer Society; 2022: https://cdn.cancer.ca/-/media/files/research/cancer-statistics/2022-statistics/2022-special-report/2022_prevalence_report_final_en.pdf. Accessed 2022 Dec 1.
29.McCurdy A, Mian H, LeBlanc R, et al. Redefining attrition in multiple myeloma (MM): a Canadian Myeloma Research Group (CMRG) analysis. Blood Cancer J. 2023;13(1):111. PubMed
30.Dhanasiri S, Hollier-Hann G, Stothard C, Dhanda DS, Davies FE, Rodriguez-Otero P. Treatment Patterns and Outcomes in Triple-Class Exposed Patients With Relapsed and Refractory Multiple Myeloma: Findings From the Multinational ITEMISE Study. Clin Ther. 2021;43(11):1983-1996.e1983.
31.Minakata D, Fujiwara SI, Yokoyama D, et al. Relapsed and refractory multiple myeloma: A systematic review and network meta-analysis of the efficacy of novel therapies. Br J Haematol. 2023;200(6):694-703. PubMed
Appendix 1: Cost Comparison Table
Table 8: CADTH Cost Comparison Table for Patients With Relapsed or Refractory Multiple Myeloma Who Have Received at Least 3 Prior Therapies
Treatment | Strength / concentration | Form | Price ($) | Recommended dosage | Daily cost ($) | 28-day cycle cost ($) |
|---|---|---|---|---|---|---|
Elranatamab (Elrexfio) | 44 mg 76 mg | Solution for subcutaneous injection | 4,053.0000 7,000.0000 | Step-up dosing schedule: 12 mg on day 1; 32 mg on day 4 Dosing schedule from week 2 onward: 76 mg on day 8 and 76 mg weekly thereafter. For patients who have received at least 24 weeks of treatment and have attained a response (i.e., a partial response or better that has been maintained for at least 2 months), dose interval should transition to q.2.w. | During first 28 days on treatment: 894.75 Subsequent 28 days: 1,000.00 Subsequent 28-day q.2.w. dosing schedule: 500.00 | During first 28 days on treatment: 25,053 Subsequent 28 days: 28,000 Subsequent 28-day q.2.w. dosing schedule: 14,000 |
Carfilzomib + dexamethasone20 | ||||||
Carfilzomib | 10 mg 30 mg 60 mg | Powder in vial | 255.5500a 766.6590 1,533.3300 | 28-day cycles: Cycle 1: 20 mg/m2 on day 1; 70 mg/m2 on day 8 and day 15 Cycle 2+: 70 mg/m2 on day 1, day 8, and day 15 | Cycle 1: 273.81 Cycles 2+: 355.95 | Cycle 1: 7,667 Cycles 2+: 9,967 |
Dexamethasone | 0.5 mg 4 mg | Tablet | 0.1564 0.6112 | 28-day cycles: 20 mg on day 1, day 2, day 8, day 9, day 15, day 16, day 22, and day 23 | 0.87 | 24 |
Carfilzomib + dexamethasone regimen | Cycle 1: 274.68 Cycle 2+: 356.82 | Cycle 1: 7,691 Cycle 2+: 9,991 | ||||
Carfilzomib + cyclophosphamide + dexamethasone20 | ||||||
Carfilzomib | 10 mg 30 mg 60 mg | Powder in vial | 255.5500a 766.6590 1,533.3300 | 28-day cycles: Cycle 1: 20 mg/m2 on day 1; 70 mg/m2 on day 8 and day 15 Cycle 2+: 70 mg/m2 on day 1, day 8, and day 15 | Cycle 1: 273.81 Cycles 2+: 355.95 | Cycle 1: 7,667 Cycles 2+: 9,967 |
Cyclophosphamide | 25 mg 50 mg | Tablet | 0.3545 0.4773 | 28-day cycles: 300 mg/m2 on day 1, day 8, and day 15 | 0.61 | 17 |
Dexamethasone | 0.5 mg 4 mg | Tablet | 0.1564 0.6112 | 28-day cycles: 40 mg on day 1, day 8, day 15, and day 22 | 0.87 | 24 |
Carfilzomib + cyclophosphamide + dexamethasone regimen | Cycle 1: 275.29 Cycles 2+: 357.44 | Cycle 1: 7,708 Cycles 2+: 10,008 | ||||
Dexamethasone + pomalidomide21 | ||||||
Dexamethasone | 0.5 mg 4 mg | Tablet | 0.1564 0.6112 | 28-day cycles: 20 to 40 mg on day 1, day 8, day 15, and day 22 | 0.44 to 0.87 | 12 to 24 |
Pomalidomide | 1 mg 2 mg 3 mg 4 mg | Capsule | 125.0000 | 28-day cycles: 4 mg on day 1 to day 21 | 93.75 | 2,625 |
Dexamethasone + pomalidomide regimen | 94.19 to 94.62 | 2,637 to 2,649 | ||||
Cyclophosphamide + dexamethasone + pomalidomide22 | ||||||
Cyclophosphamide | 25 mg 50 mg | Tablet | 0.3545 0.4773 | 28-day cycles: 400 mg on day 1, day 8, and day 15 | 0.41 | 11 |
Dexamethasone | 0.5 mg 4 mg | Tablet | 0.1564 0.6112 | 28-day cycles: 20 to 40 mg on day 1, day 8, day 15, and day 22 | 0.44 to 0.87 | 12 to 24 |
Pomalidomide | 1 mg 2 mg 3 mg 4 mg | Capsule | 125.0000 | 28-day cycles: 4 mg on day 1 to day 21 | 93.75 | 2,625 |
Cyclophosphamide + dexamethasone + pomalidomide regimen | 94.60 to 95.03 | 2,649 to 2,661 | ||||
Bortezomib + dexamethasone + selinexor | ||||||
Bortezomib | 1 mg 2.5 mg 3.5 mg | Powder in vial | 400.6900a 1,001.7300 1,402.4200 | 35-day cycles: 1.3 mg/m2 on day 1, day 8, day 15, and day 22 | 114.48 | 4,007 |
Dexamethasone | 0.5 mg 4 mg | Tablet | 0.1564 0.6112 | 35-day cycles: 40 mg on day 1, day 8, day 15, day 22, and day 29 | 0.87 | 31 |
Selinexor | 20 mg | Tablet | 550.0000a | 35-day cycles: 100 mg on day 1, day 8, day 15, day 22, and day 29 | 392.86 | 13,750 |
Bortezomib + dexamethasone + selinexor regimen | 508.21 | 17,787 | ||||
CAR T-cell therapy | ||||||
Ciltacabtagene autoleucel | 0.5 to 1.0 × 106 CAR-positive viable T-cells per kg, with a maximum of 1 × 108 T-cells | Cell suspension in patient-specific single infusion bag | 632,455.0000b | One-time dosec | NA | NA |
CAR = chimeric antigen receptor; q.2.w. = every 2 weeks.
The comparators presented in the above table have been deemed to be appropriate based on feedback from clinical experts. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Note: All prices are from the Ontario Drug Benefit Formulary (accessed December 2023),23 unless otherwise indicated, and do not include dispensing fees. Calculations assume a patient body weight of 74 kg and a body surface area of 1.85 m2, based on the MagnetisMM-3 trial.1
aIQVIA DeltaPA database, accessed October 2023.24
bSponsor submitted price reported in the CADTH pharmacoeconomic review of ciltacabtagene autoleucel.11
cCiltacabtagene autoleucel is delivered as a 1-time dose. Daily and annual costs were not calculated.
Note: This table has not been copy-edited.
Appendix 2: Submission Quality
Please note that this appendix has not been copy-edited.
Description | Yes or no | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | Yes | No comment. |
Model has been adequately programmed and has sufficient face validity | No | The sponsor’s use of a PSM introduces structural assumptions about the relationship between PFS and OS that likely do not accurately reflect causal relationships within the disease pathway. These assumptions may produce a survival bias that favours elranatamab. Due to the assumed independence between OS and PFS end points in a PSM, extrapolations for each end point may reflect within-trial trends in the rates of relapse and death. |
Model structure is adequate for decision problem | Yes | No comment. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | Yes | No comment. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | Yes | No comment. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | Yes | No comment. |
OS = overall survival; PFS = progression-free survival; PSM = partitioned survival model.
Appendix 3: Additional Information on the Submitted Economic Evaluation
Please note that this appendix has not been copy-edited.
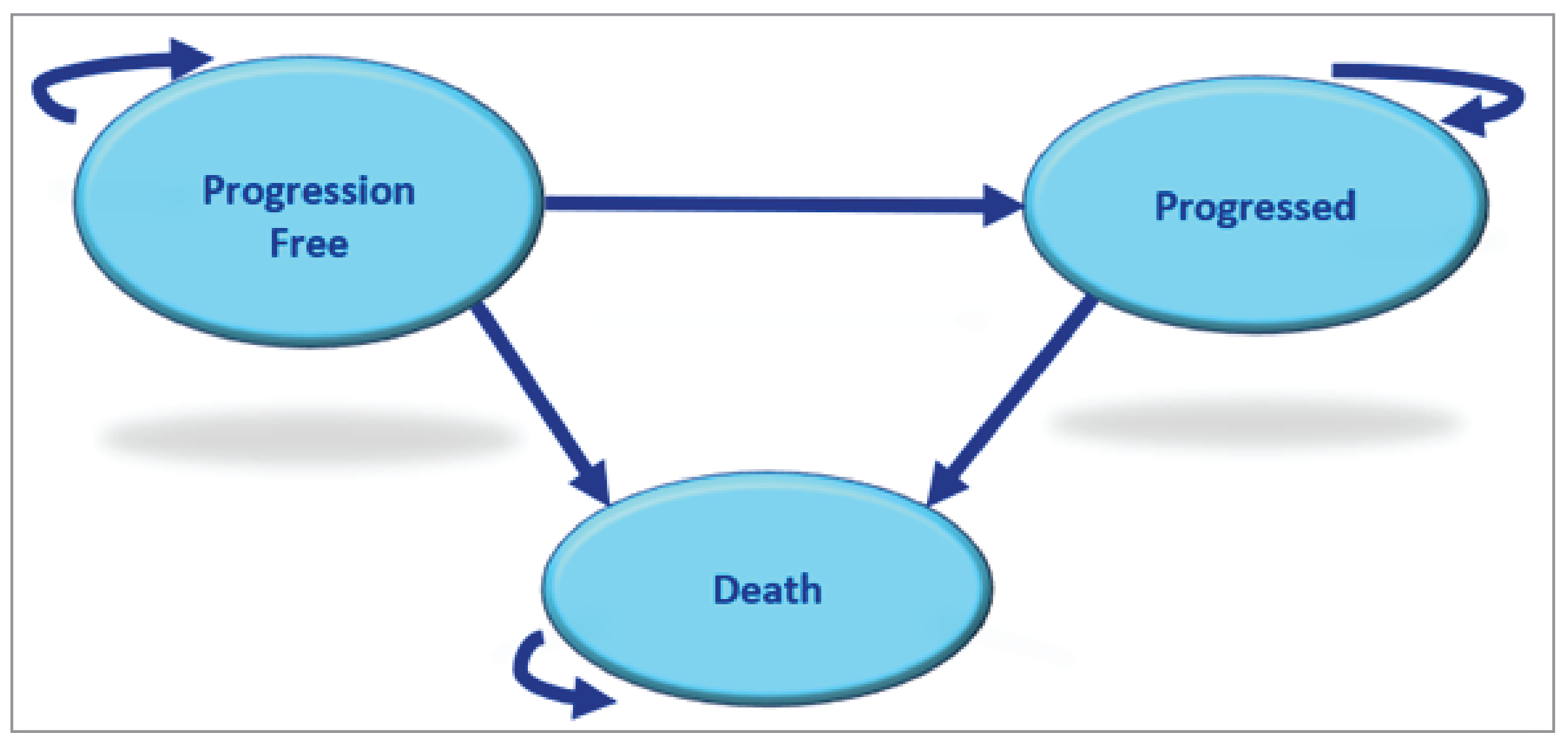
Detailed Results of the Sponsor’s Base Case
Table 10: Physician’s Choice (CMRG Basket) Regimens for TCE RRMM
Regimen | Distribution |
|---|---|
PI only | |
Carfilzomib, dexamethasone | 33.10% |
Bortezomib, dexamethasone | 1.26% |
IMID only | |
Pomalidomide, dexamethasone | 7.06% |
Lenalidomide, dexamethasone | 2.15% |
IMID + PI | |
Pomalidomide, carfilzomib, dexamethasone | 3.52% |
Pomalidomide, ixazomib, dexamethasone | 3.17% |
Pomalidomide, bortezomib, dexamethasone | 2.82% |
IMID + alkylator | |
Pomalidomide, cyclophosphamide, dexamethasone | 20.55% |
PI + alkylator | |
Carfilzomib, cyclophosphamide dexamethasone | 10.12% |
Bortezomib, cyclophosphamide, dexamethasone | 4.60% |
Ixazomib, cyclophosphamide, dexamethasone | 3.37% |
CD38 mAb + other | |
Daratumumab, pomalidomide, dexamethasone | 5.52% |
Isatuximab, pomalidomide, dexamethasone | 2.76% |
Bortezomib, cyclophosphamide, dexamethasone | 4.60% |
Ixazomib, cyclophosphamide, dexamethasone | 3.37% |
IMiD = immunomodulatory drugs; mAb = monoclonal antibody; PI = protease inhibitor; RRMM = relapsed or refractory multiple myeloma; TCE = triple-class exposed.
Source: Sponsor’s pharmacoeconomic submission.1
Figure 2: Sponsor’s Modelled PFS, OS, and TTD Curves for Elranatamab
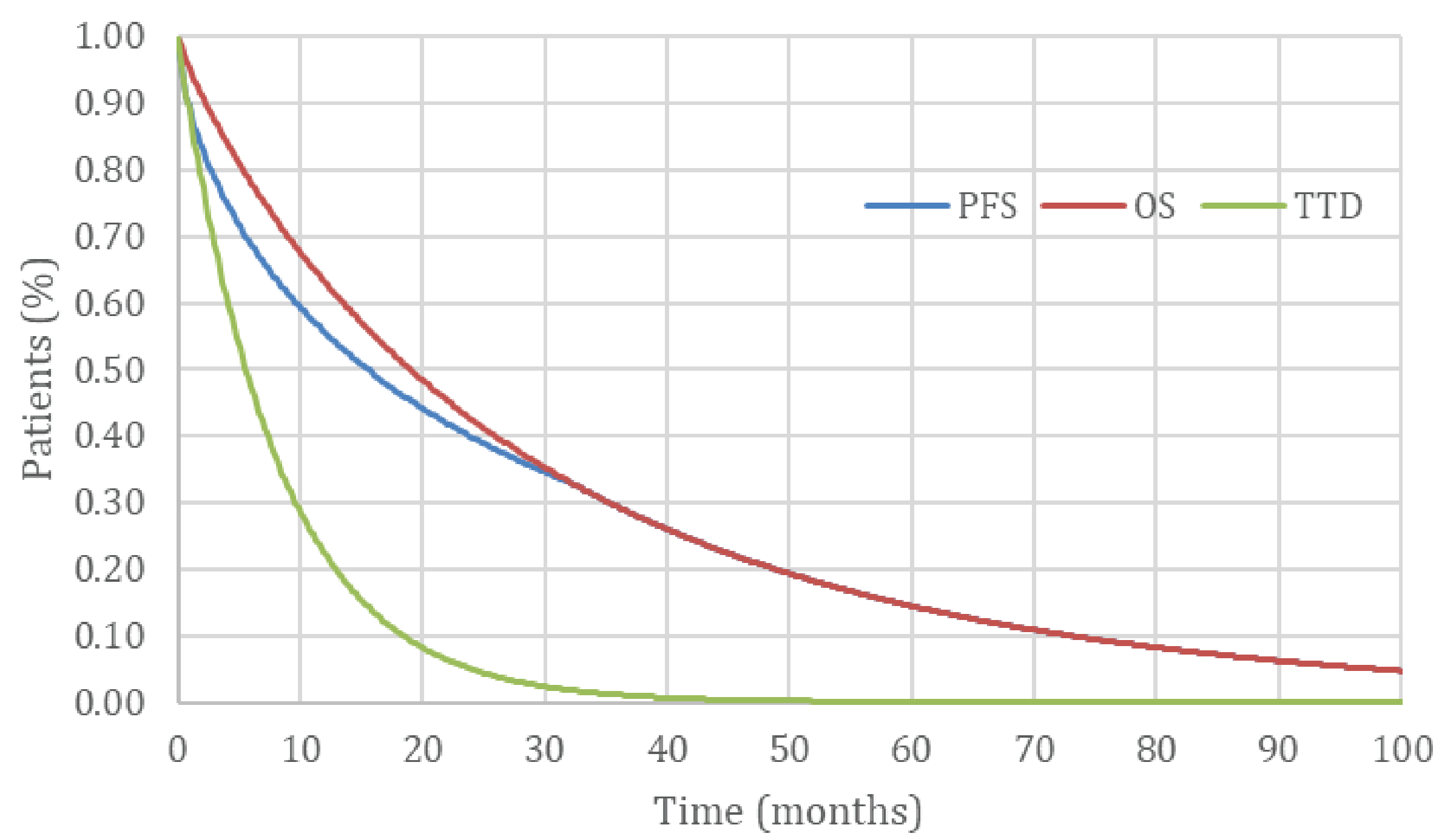
PFS = progression-free survival; OS = overall survival; TTD = time to treatment discontinuation
Source: Sponsor’s pharmacoeconomic submission.1
Table 11: Disaggregated Summary of the Sponsor’s Economic Evaluation Results
Parameter | Elranatamab | Cilta-cel | Physician’s choice |
|---|---|---|---|
Discounted LYs | |||
Total | 2.45 | 3.71 | 1.06 |
Preprogression | 2.18 | 2.19 | 0.52 |
Postprogression | 0.26 | 1.53 | 0.54 |
Discounted QALYs | |||
Total | 1.84 | 2.71 | 0.76 |
Preprogression | 1.72 | 1.72 | 0.41 |
Postprogression | 0.19 | 1.11 | 0.39 |
AE disutility | –0.07 | –0.12 | –0.03 |
Discounted costs ($) | |||
Total | 229,692 | 698,630 | 150,442 |
Preprogression (total) | 181,743 | 624,075 | 82,404 |
Drug acquisition cost of primary treatment | 142,114 | 558,908 | 77,316 |
Drug administration cost | 1,191 | 827 | 2,115 |
Medical resource use cost | 18,909 | 42,201 | 658 |
Monitoring test cost | 559 | 1,209 | 133 |
AE management | 18,971 | 20,931 | 2,182 |
Postprogression (total) | 16,330 | 43,831 | 35,652 |
Drug acquisition cost of subsequent treatment | 15,532 | 40,095 | 32,773 |
Drug administration cost | 401 | 1,105 | 2,064 |
Medical resource use cost | 330 | 2,239 | 677 |
Monitoring test cost | 67 | 392 | 137 |
Death cost | 31,619 | 30,724 | 32,386 |
AE = adverse event; ICER = incremental cost-effectiveness ratio; NA = not applicable; QALY = quality-adjusted life-year.
Source: Sponsor’s pharmacoeconomic submission.1
Scenario Analyses
Table 12: Scenario Analyses of the Sponsor’s Economic Evaluation Results
Scenario analysis | Drug | Total costs ($) | Total QALYs | ICER vs. elranatamab ($/QALY) |
|---|---|---|---|---|
Scenario 1: SVd included as comparator | SVd | 206,949 | 2.85 | Reference |
Elranatamab | 229,910 | 1.85 | Elranatamab is dominated by SVd |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Please note that this appendix has not been copy-edited.
Detailed Results of CADTH Base Case
Figure 3: CADTH’s Modelled PFS, OS, and TTD Curves for Elranatamab
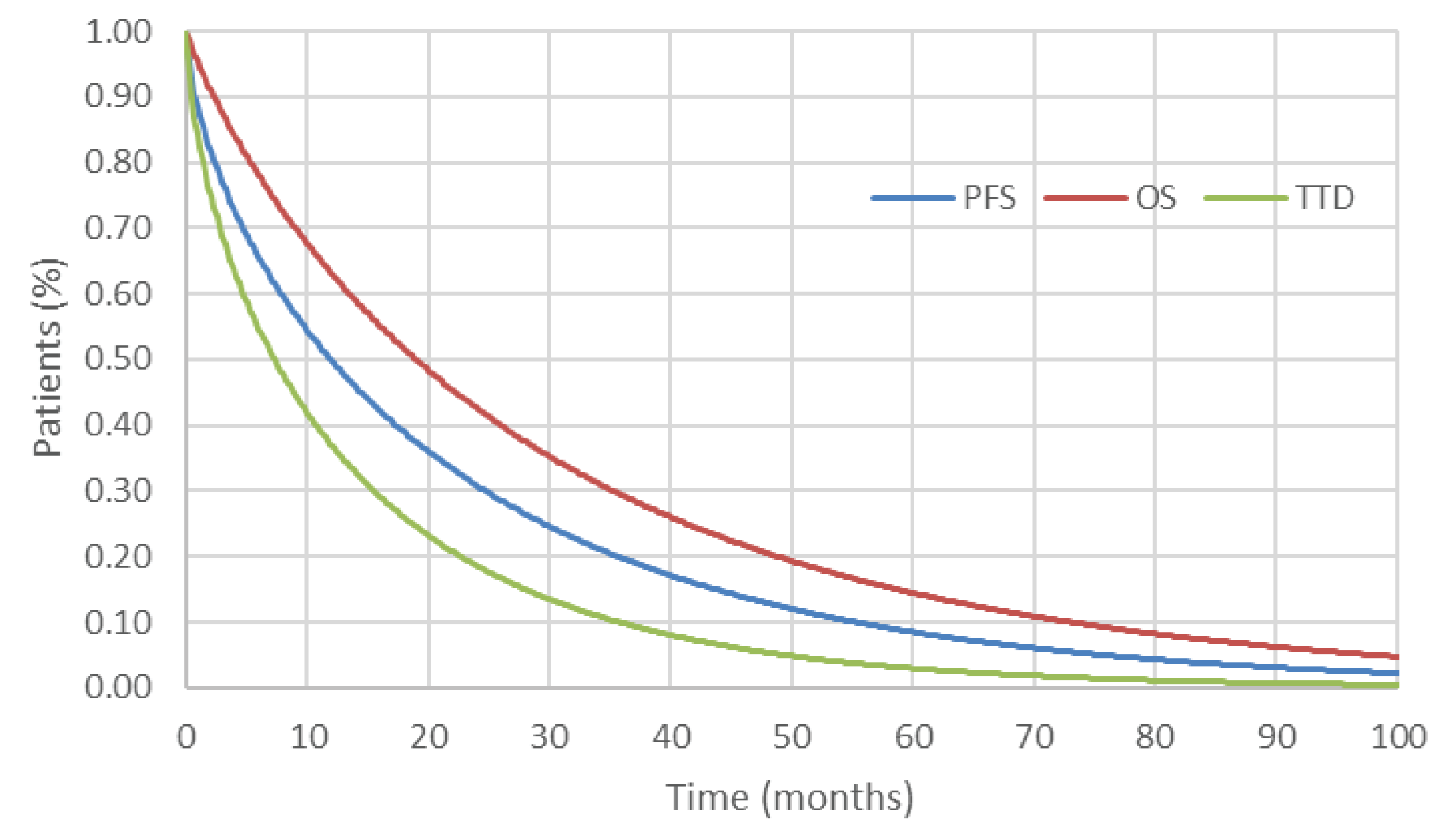
PFS = progression-free survival; OS = overall survival; TTD = time to treatment discontinuation.
Source: Sponsor’s pharmacoeconomic submission.1
Table 13: Disaggregated Summary of CADTH’s Economic Evaluation Results
Parameter | Elranatamab | Cilta-cel | Physician’s choice |
|---|---|---|---|
Discounted LYs | |||
Total | 2.46 | 3.80 | 1.09 |
Preprogression | 1.76 | 2.21 | 0.52 |
Postprogression | 0.70 | 1.59 | 0.56 |
Discounted QALYs | |||
Total | 1.82 | 2.77 | 0.78 |
Preprogression | 1.38 | 1.73 | 0.41 |
Postprogression | 0.51 | 1.15 | 0.41 |
AE disutility | –0.07 | –0.12 | –0.03 |
Discounted costs ($) | |||
Total | 327,637 | 687,567 | 112,396 |
Preprogression (total) | 267,209 | 619,685 | 49,955 |
Drug acquisition cost of primary treatment | 227,594 | 554,337 | 45,554 |
Drug administration cost | 1,846 | 727 | 1,416 |
Medical resource use cost | 18,470 | 42,519 | 660 |
Monitoring test cost | 451 | 1,214 | 134 |
AE management | 18,849 | 20,888 | 2,190 |
Postprogression (total) | 28,848 | 37,274 | 30,094 |
Drug acquisition cost of subsequent treatment | 26,983 | 33,466 | 27,157 |
Drug administration cost | 793 | 1,089 | 2,083 |
Medical resource use cost | 890 | 2,307 | 709 |
Monitoring test cost | 182 | 412 | 145 |
Death cost | 31,581 | 30,608 | 32,347 |
AE = adverse event; ICER = incremental cost-effectiveness ratio; NA = not applicable; QALY = quality-adjusted life-year.
Scenario Analyses
Table 14: Scenario Analyses of CADTH’s Economic Evaluation Results
Scenario analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|---|
CADTH base case | Physician’s choice | 114,237 | 0.73 | Reference |
Elranatamab | 337,298 | 1.79 | 210,405 | |
Scenario 1: Elranatamab RDI (100%) | Physician’s choice | 114,237 | 1.01 | Reference |
Elranatamab | 392,168 | 1.79 | 262,162 | |
Scenario 2: Pessimistic PFS extrapolation | Physician’s choice | 114,237 | 0.73 | Reference |
Elranatamab | 337,708 | 1.77 | 214,009 | |
Scenario 3: Optimistic PFS extrapolation | Physician’s choice | 114,237 | 0.73 | Reference |
Elranatamab | 318,288 | 1.81 | 188,658 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; RDI = relative dose intensity.
Note: All results presented deterministically.
Figure 4: Extrapolation of PFS for Elranatamab
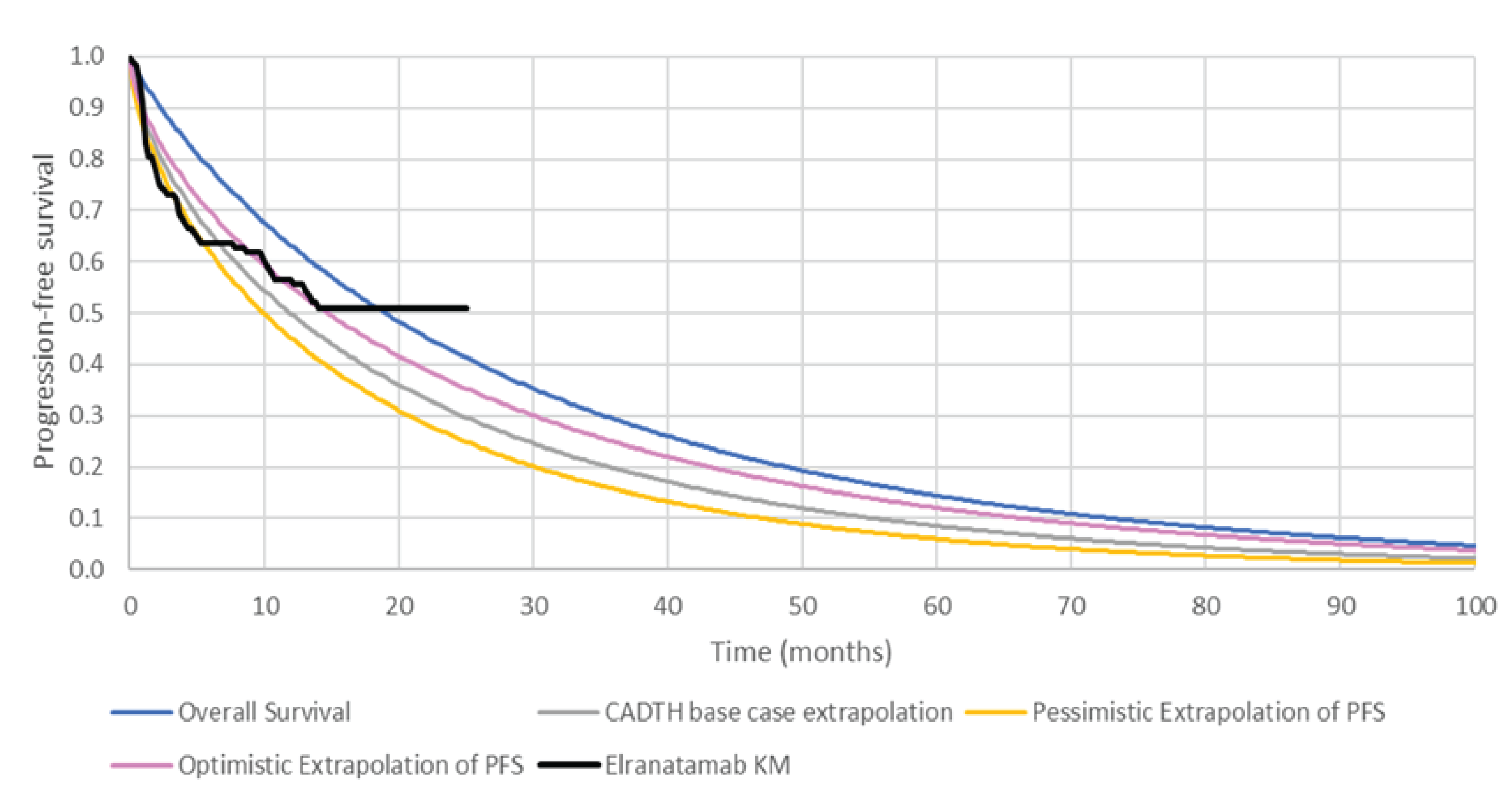
KM = Kaplan-Meier; PFS = progression-free survival.
Source: Sponsor’s pharmacoeconomic submission.1
Appendix 5: Submitted Budget Impact Analysis and CADTH Appraisal
Please note that this appendix has not been copy-edited.
Table 15: Summary of Key Takeaways
Key takeaways of the budget impact analysis (BIA) |
|---|
|
Summary of Sponsor’s BIA
The sponsor submitted a BIA to estimate the incremental 3-year budget impact of reimbursing elranatamab for the treatment of adult patients with RRMM who have received at least 3 prior lines of therapy, including a PI, an IMiD, and an anti-CD38 mAb, as per the submitted reimbursement request.25 The BIA was undertaken from the perspective of a Canadian public payer over a 3-year time horizon (2024 through 2027) using a prevalence-based epidemiologic approach. Data to inform the model were obtained from various sources, including the published literature, the sponsor’s internal data, and input from clinical experts consulted by the sponsor, and key inputs to the BIA are documented in Table 17.
The sponsor compared a reference scenario in which patients received current standard of care (i.e., physician’s choice defined as a weighted basket of Kd, KCd, Pd, PCd, and other CMRG treatments; SVd; cilta-cel; and a proportion of patients enrolled in clinical trials) to a new drug scenario in which elranatamab was reimbursed. The sponsor’s analysis included drug acquisition costs and dosing modelled for elranatamab reflected the product monograph.
Table 16: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1/year 2/year 3 if appropriate) |
|---|---|
Target population | |
Prevalence of multiple myeloma | 0.0004026 |
Incidence of multiple myeloma | 0.0001026 |
Proportion of adult patients who have received at least 3 prior lines of therapy, including a PI, IMiD and anti-CD38, and who have demonstrated disease progression on the last therapy | 18%27 |
Proportion of patients with public coverage | Jurisdiction-specific |
Number of patients eligible for drug under review | 1,570 / 1,588 / 1,607 |
Market uptake (3 years) | |
Uptake (reference scenario) Physician’s choice (CMRG basket)a SVd Cilta-cel Clinical trials | 69% / 59% / 49% 9% / 9% / 9% 10% / 20% / 30% 12% / 12% / 12% |
Uptake (new drug scenario) Elranatamab Physician’s choice (CMRG basket)a SVd Cilta-cel Clinical trials | 10%% / 14% / 15% 61% / 48% / 38% 7% / 6% / 5% 10% / 20% / 30% 12% / 12% / 12% |
Cost of treatment (per patient)b | |
Cost of treatment based on comparator duration of therapy Elranatamab Physician’s choice (CMRG basket) SVd Cilta-cel Clinical trials | $154,000 $123,741 $164,073 $640,072 $0 |
IMiD = immunomodulatory drug; PI = proteasome inhibitor; SVd = selinexor plus bortezomib plus dexamethasone.
aPhysician’s choice assumed to comprise 10% KCd (carfilzomib + cyclophosphamide + dexamethasone), 33% Kd (carfilzomib + dexamethasone), 21% PCd (pomalidomide + cyclophosphamide + dexamethasone), 7% Pd (pomalidomide + dexamethasone), and 29% other CMRG treatments (Vd: bortezomib, dexamethasone; Rd: lenalidomide, dexamethasone; KPd: pomalidomide, carfilzomib, dexamethasone; IxaPd: pomalidomide, ixazomib, dexamethasone; PVd: pomalidomide, bortezomib, dexamethasone; VCd/CyBorD: bortezomib, cyclophosphamide, dexamethasone; IxaCd: ixazomib, cyclophosphamide, dexamethasone; DPd: daratumumab, pomalidomide, dexamethasone; and IsaPd: isatuximab, pomalidomide, dexamethasone).
bCosts of treatment were calculated based on body surface area of 1.82 m2 and body weight of 72 kg based on the MagnetisMM-3 trial.25 Costs used dosing schedules as per each comparator’s respective product monograph and used duration of therapy from each treatment’s respective pivotal clinical trial to determine number of cycles on treatment. RDI was applied in the calculation of drug costs and all calculations included drug wastage in the base case.
Summary of the Sponsor’s BIA Results
The sponsor estimated that the 3-year budget impact of reimbursing elranatamab for the treatment of adult patients with RRMM who have received at least 3 prior lines of therapy, including a PI, an IMiD, and an anti-CD38 mAb would be $6,071,316 in year 1, $8,471,472 in year 2, and $8,672,744 in year 3, for a 3-year cumulative total of $23,215,531.
In a scenario analysis where the inpatient costs of elranatamab (e.g., first 3 doses in hospital) were excluded, the 3-year cumulative total budget impact of reimbursing elranatamab was estimated to be $12,989,438.
CADTH Appraisal of the Sponsor’s BIA
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
Uncertainty in the sponsor’s approach to calculating the BIA: To calculate target population, the sponsor uses published estimates of prevalence from 1993 to 2018 and incidence data based on the number of cases estimated in 2022.26 The sponsor then subtracts the number of incident patients from the number of prevalent patients. The remaining prevalent patients were multiplied by the proportion of patients who received 3 prior lines of therapy and who are triple-class exposed to determine the patients who are then eligible for fourth-line therapy.27 This approach is known as a prevalence-based approach to calculating a budget impact.
CADTH notes that there are notable cost implications associated with a prevalence-based versus an incidence-based approach. Using a prevalence-based approach, it is conventional to assign an annual cost of therapy to the size of the cohort every year. This is under the assumption of a static population (i.e., if a patient comes off therapy [for example due to death], they are replaced with a new patient [new diagnosis]). When using an incidence-based approach, the full costs of therapy incurred over the time horizon of the BIA should be applied to each incident case.
A prevalence-based approach is conventional when there is an expectation that the entry of a new drug will lead to patients switching to the new treatment from existing therapies. This means prevalent cases are relevant to the decision problem, not just new incident cases. However, there is no expectation that patients with RRMM would switch from current to new therapies unless they experienced unacceptable toxicity or progression at which point, they become an incident patient. Hence, only patients who do not experience improvement with a third line of therapy or beyond (i.e., incident cases) are relevant to the decision problem. Prevalence-based approaches are used in cases where there is no active therapy available, or patients are on therapy for a long time (e.g., asthma). It is unconventional to use a prevalence-based approach in oncology where usually only incident cases are relevant to the decision problem. Second, a prevalence-based model assumes a static population under the assumption that incident cases replace deaths. However, if a new therapy extends life, then the size of the prevalent cohort will increase until a new steady state is reached. Overall, a prevalence-based model imposes many strict assumptions that are problematic when most of the population relevant to the decision problem is made up of incident patients.
Given these reasons CADTH re-estimated the BIA using a corrected incidence-based approach. CADTH extracted costs from the sponsor’s CUA model to estimate the elranatamab drug costs incurred for each incident case in the BIA. The CUA model was run with a 1, 2, and 3-year time horizon at a 0% discount rate. When considering a 3-year time horizon, the CUA model indicates an average drug acquisition cost of $204,214 for patients treated with elranatamab. Over the 3-year time horizon of the BIA, the average cost per patient for each incident case that receives elranatamab in year 1 is expected to be $204,214 over 3 years. When considering a 2-year time horizon, the CUA model indicates an average drug acquisition cost of $182,123 for patients treated with elranatamab. Over the time horizon of the BIA, the average cost per patient for each incident case that receives elranatamab in year 2 is expected to be $182,123 over 2 years. Finally, when considering a 1-year time horizon, the CUA model indicates an average drug acquisition cost of $138,400 for patients treated with elranatamab. Over the time horizon of the BIA, the average cost per patient for each incident case that receives elranatamab in year 3 is expected to be $138,400 over 1 year.
CADTH updated the costs associated with elranatamab: incident cases in year 1 are assumed to experience 3 years of costs equating to $204,214 over 3 years; incident cases in year 2 are assumed to experience 2 years of costs equating to $182,123 over 2 years; and incident cases in year 3 are assumed to experience 1 year of costs equating to $138,400 over 1 year.
CADTH updated the costs associated with physician’s choice: based on the CUA nearly all costs are incurred in the first-year post-treatment. For every incident case $44,000 of costs were assumed for patients receiving physician’s choice.
The aforementioned costs reflect the base-case changes made in the CADTH base case for the CUA. This includes changes to treatment discontinuation, RDI, movement to dosing every 2 weeks, price of pomalidomide, administration schedule of carfilzomib.
Proportion of patients with newly diagnosed multiple myeloma (NDMM) receiving therapy in 4L is uncertain: The sponsor estimated the proportion of patients with NDMM who would become triple-refractory based on attrition rates from Fonseca et al. (2020).27 This publication leveraged data from US-based databases to examine treatment patterns and attrition rates by line of therapy in patients with NDMM.27 CADTH notes that Fonseca et al. likely overestimates attrition as it is challenging to capture reasons other than death for failing to receive a subsequent line of treatment. Fonseca et al. define attrition as the proportion of patients in a given line of therapy who receive only that line of therapy.27 However, it cannot be assumed that all patients who do not go on to receive subsequent therapy have either died or progressed without subsequent treatment. This is because there is a non-negligible proportion of patients treated with planned fixed-duration initial therapy who remain in remission, as well as a proportion of patients undergoing continuous first-line therapy who have maintained their response. These patients are incorrectly captured within the attrition rate estimated by Fonseca et al., thereby contributing to an overestimation of attrition. These patients may progress later, beyond the period of follow-up.
Given the aforementioned, CADTH attempted to re-estimate the eligible patient incident population using a different approach due to issues with the sponsor’s attrition rates. CADTH uses similar prevalence data from the Canadian Cancer Society showing that the 25-year prevalence of MM in Canada is 1 in 2,505 (or 0.04%).28 Applying this estimate to jurisdictions included in the CADTH base case resulted in a total of 11,780 patients. This means there are 11,780 patients estimated to be alive with a MM diagnosis in 2023. To estimate how many patients will be eligible for elranatamab each year an assumption must be made as to what percentage of these patients will not experience improvement with a third-line or later therapy each year. A Canadian-based study by McCurdy et al. (2023) analyzed retrospective cohort data from patients with NDMM who received at least 1 line of therapy from January 1, 2010, to December 31, 2020.29 McCurdy et al. categorized patients by transplant eligibility status and line of therapy. They further categorized patients receiving each therapy line based on whether they (1) were actively receiving treatment or were on remission off-treatment; (2) relapsed and went on to receive subsequent therapy; (3) progressed and opted to forego subsequent therapy; (4) died; or (5) were lost to follow-up.29 A summary of how this data were analyzed by CADTH is provided in Table 19. A total of 5,548 patients were identified. Of those, 1,409 patients died before reaching the fourth-line setting. Of the remaining 4,139 patients, 251 patients are alive and actively receiving third-line therapy, while 735 patients relapsed and went on to receive subsequent therapy in fourth-line setting and beyond. The study does not offer data regarding the distribution of patients in the fourth-line setting that are actively receiving therapy or have died. In the absence of data, CADTH assumed that 50% of patients who received therapy in the fourth line remained on active therapy. This assumption is based on the downward trend presented in the same study, which suggests that 10%, 17%, and 27% of patients treated in the first, second, and third-line settings, respectively, die before reaching the subsequent line.29 Assuming a 50% mortality risk in the fourth-line setting, the total number of patients who are alive in the cohort decreases to 3,771 (4,139 – (0.5 * 735)). Of those, 6.6% (251 of 3,771) are actively receiving third-line therapy, and 9.7% ((0.5 * 735) / 3,771) are actively receiving treatment in the fourth-line setting and beyond. From this it is estimated that 1,885 patients (11,780 * (0.16)) are actively receiving a third-line or later therapy for MM in jurisdictions included in the CADTH base case.
The final assumption is what proportion of these patients move on to the next line of therapy each year. Of those actively receiving therapy in the third-line and beyond, some will die before not experiencing improvement or do not receive further treatment after not experiencing improvement. In the McCurdy study, in the third-line setting, at the end of follow-up 40% of patients had gone on to receive a subsequent line and 40% did not.29 If we assume this same ratio applies to patients on active therapy this would mean 50% of patients who receive a third-line therapy will go on to receive a fourth-line therapy and 50% will not. As the average time on third-line therapy and beyond is close to a year on average it is likely that most people who progress will do so within a year. Based on this CADTH assumed that 50% of patients actively receiving a third-line or later therapy will not experience improvement and receive a subsequent line every year. This equates to 966 incident patients each year requiring a fourth-line or later therapy (50% of 1,885 is 966).
This approach is uncertain for several reasons. First, the data in McCurdy et al. is not broken down in the 4L or later setting so assumptions had to be made regarding the size of the surviving cohort. Second, this data are based on a time period (2010 to 2020) whereby some patients likely did not receive daratumumab. Daratumumab in the first-line setting in Canada has become more prominent in recent years and survival time on this regimen is much higher than alternative regimens. CADTH would therefore expect more patients being diagnosed in recent years remain on active therapy in the first-line setting longer and therefore die on first-line treatment, meaning less patients in the fourth-line and latter settings. Finally, the prevalence estimate looks at MM cases over the past 25 years whereas the data from McCurdy looks at 10 years’ worth of diagnoses. Although the expected surviving cohort from 10 to 25 years plus is likely to be small in a MM population these patients may be more likely to be on later lines of therapy.
CADTH conducted a reanalysis that revised the eligible patient population assuming 966 patients will require a fourth-line or later therapy in the starting year of the BIA. Based on population growth rates, the eligible target population was estimated to be 975 in year 1, 985 in year 2, and 994 in year 3.
Noting considerable uncertainty owing to the lack of data informing relevant parameters in the fourth-line setting, it is plausible that the CADTH estimate may represent the upper bound of the eligible population given the changing treatment landscape with daratumumab becoming more prevalent in the first-line setting. CADTH conducted a scenario analysis that assumed a 50% reduction in the eligible patient population to offer a potential estimate of the lower bound.
Market shares of elranatamab were likely underestimated: The sponsor assumed that elranatamab would have a market share of 10%, 14%, and 15% in Years 1, 2, and 3, respectively. However, clinical expert feedback noted that the sponsor’s market share projects were potentially lower than expected in practice if a treatment such as elranatamab were to be funded as fourth-line treatment. This aligned with the feedback received from registered clinician groups in Canada who noted that elranatamab was expected to shift the current treatment paradigm given that it will provide a more readily accessible T-cell redirecting therapy for patients with advanced diseases who are refractory to the most used drugs. Clinical experts indicated that if elranatamab were reimbursed, it would be reasonable to expect that approximately 30% of patients would likely be treated with elranatamab in the fourth-line setting. CADTH notes that these market share estimates apply to incident cases (patients who have recently not experienced improvement with either 3L or later therapy).
CADTH adjusted the projected market shares of elranatamab to reach 30% in year 3, based on feedback obtained from clinical experts.
Costs associated with SVd are overestimated: In the sponsor’s estimation of costs associated with SVd, treatment duration for SVd was assumed to be 48 weeks to reflect median duration of treatment from the BOSTON trial.19 The BOSTON trial included patients who had only 1 prior exposure to a therapy for MM and likely represents a healthier cohort than those evaluated in the MagnetisMM-3 trial. Compared to those with only 1 prior exposure to therapy, it is expected that progression would occur earlier in those who have been triple-class exposed due to their poor clinical prognosis.30 Similarly, duration of treatment is also expected to be shorter for those who have been triple-class exposed. A published network meta-analysis found that the relative efficacy of selinexor may not be better than other treatments included as physician’s choice in patients with RRMM.31 However this assumes relative efficacy is not influenced by line of therapy or prior exposure to certain therapies.
CADTH adjusted the duration of therapy for SVd to 24 weeks. This assumes time spent of SVd is similar to treatments included in physician’s choice.
Allocating market share to clinical trials is not appropriate: The sponsor assumed that 12% of patients were enrolled in clinical trials and as a result, received medications through the clinical trial – not incurring any treatment or drug costs. This artificially decreases the estimated market size. Patients currently enrolled in clinical trials could become eligible for elranatamab if reimbursed. This assumption underestimates the budget impact. Furthermore, patient enrolment in clinical trials in the new drug scenario is less likely if a new effective therapy is reimbursed. Since costs for clinical trials are assumed to be $0, this assumption omits potential treatment-related costs that may be incurred by drug plans from patients participating in clinical trials.
In the CADTH reanalysis, no market share was allocated to clinical trials in the new and reference drug scenario. Clinical trial market shares were evenly distributed among physician’s choice and SVd in year 0 and subsequently carried over for the duration of the analysis.
Face validity of total budget estimation: In the sponsor’s prevalence-based approach to estimating target population, adjustment was made for patients receiving CAR T-cell therapy such that patients who received treatment were excluded in subsequent years due to CAR T-cell therapy being administered as a single-dose infusion. CADTH notes that the estimated total budget appears to then decrease over time in both the reference and new drug scenario, which does not meet face validity when looking at incident cases. This has no impact on the estimated budget impact, however, because the estimated number of patients treated with CAR T-cell therapy does not differ in the reference versus new drug scenario.
CADTH noted that this did not impact the estimated budget impact and did not address this minor limitation in reanalysis.
Uncertainty in inclusion of tocilizumab costs: The sponsor states that the product monograph stipulates that tocilizumab should be administered to patients as premedication before administration of elranatamab, which was included by the sponsor in their submitted BIA model. CADTH notes that the product monograph does not include this stipulation. However, CADTH extracted costs from the sponsor’s CUA model to estimate the elranatamab drug costs incurred for each incident case in the BIA. The sponsor’s CUA model did not adequately capture the costs of tocilizumab premedication. At the recommended dose of 8 mg/kg on days 1, 4, and 8, tocilizumab is expected to cost approximately $1,371 per patient (assuming wastage, 1 treatment cycle as observed in the MagnetisMM-3 trial and using a body surface area of 1.82 m2 and weight of 71.8 kg as per trial data).
As a scenario analysis CADTH included the cost of tocilizumab ($1,371) for each patient who receive elranatamab.
CADTH Reanalyses of the BIA
The results of the CADTH stepwise reanalysis are presented in summary format in Table 18 and a more detailed breakdown is presented in Table 20. The CADTH reanalysis of the BIA estimated that the 3-year budget impact of reimbursing elranatamab for the treatment of adult patients with RRMM who have received at least 3 prior lines of therapy, including a PI, an IMiD, and an anti-CD38 mAb would be $15,819,100 in year 1, $30,815,799 in year 2, and $40,176,258 in year 3, for a 3-year cumulative total of $86,811,158.
Table 17: CADTH Revisions to the Submitted Budget Impact Analysis
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Changes to derive the CADTH base case | ||
1. Calculation of the budget impact |
|
|
2. Eligible patient population | Prevalent population Year 1: 1,570 Year 2: 1,588 Year 3: 1,607 | Incident population Year 1: 975 Year 2: 985 Year 3: 994 |
3. Market shares of elranatamab | Year 1: 10% Year 2: 14% Year 3: 15% | Year 1: 20% Year 2: 28% Year 3: 30% |
4. Clinical trials market share | 12% | 0% |
CADTH base case | Reanalysis 1 + 2 + 3 + 4 | |
Table 18: Summary of the CADTH Reanalyses of the BIA
Stepped analysis | 3-year total ($) |
|---|---|
Submitted base case | 23,215,531 |
CADTH reanalysis 1 – calculation of budget impact | 73,156,251 |
CADTH reanalysis 2 – revised eligible population | 14,394,100 |
CADTH reanalysis 3 – market shares of elranatamab | 121,976,812 |
CADTH reanalysis 4 – removal of clinical trial market shares | 23,215,531 |
CADTH base case | 86,811,158 |
BIA = budget impact analysis.
Table 19: Summary of Data Used From McCurdy et al.
Line of therapy | Transplant eligibility status | Total number of patientsa | Actively receiving treatment in the given lineb | Died on that line of therapy b |
|---|---|---|---|---|
1 | Transplant-eligible | 3,111 | 1,151 (37%) | 156 (5%) |
Transplant-ineligible | 2,437 | 463 (19%) | 414 (17%) | |
2 | Transplant-eligible | 1,455 | 437 (30%) | 146 (10%) |
Transplant-ineligible | 1,332 | 320 (24%) | 306 (23%) | |
3 | Transplant-eligible | 787 | 126 (16%) | 157 (20%) |
Transplant-ineligible | 657 | 125 (19%) | 230 (35%) | |
4 | Transplant-eligible | 472 | NR | NR |
Transplant-ineligible | 263 | NR | NR |
NR = not reported.
aValues in this column have been taken directly from McCurdy et al. (2023).29
bValues in these columns have been calculated by applying the percentage from McCurdy et al. (2023) to the total number of patients for each line.29
Source: McCurdy et al.29
CADTH conducted the following scenario analyses to address remaining uncertainty, using the CADTH base case (results are provided in Table 20:
Assuming a 50% reduction in the eligible patient population to offer a probable estimate of the lower bound.
Assuming the project market share of elranatamab is 30%, 40%, and 50% in Years 1, 2, and 3, respectively.
Assume all patients who receive elranatamab incur $1,371 in costs associated with tocilizumab.
Table 20: Detailed Breakdown of the CADTH Reanalyses of the BIA
Stepped analysis | Scenario | Year 0 (current situation) ($) | Year 1 ($) | Year 2 ($) | Year 3 ($) | 3-year total ($) |
|---|---|---|---|---|---|---|
Submitted base case | Reference | 174,553,508 | 257,674,108 | 242,224,807 | 226,319,697 | 726,218,613 |
New drug | 174,553,508 | 263,745,424 | 250,696,279 | 234,992,440 | 749,434,144 | |
Budget impact | 0 | 6,071,316 | 8,471,472 | 8,672,744 | 23,215,531 | |
CADTH base case | Reference | 48,015,502 | 106,563,275 | 103,863,638 | 101,079,741 | 311,506,654 |
New drug | 48,015,502 | 122,382,375 | 134,679,437 | 141,255,999 | 398,317,811 | |
Budget impact | 0 | 15,819,100 | 30,815,799 | 40,176,258 | 86,811,158 | |
CADTH scenario analysis 1: 50% reduction in eligible patient population | Reference | 24,007,751 | 53,281,637 | 51,931,819 | 50,539,870 | 155,753,327 |
New drug | 24,007,751 | 61,191,187 | 67,339,719 | 71,120,449 | 199,651,355 | |
Budget impact | 0 | 7,909,550 | 15,407,900 | 20,580,578 | 43,898,028 | |
CADTH scenario analysis 2: Elranatamab market shares reach 50% | Reference | 48,015,502 | 106,563,275 | 103,863,638 | 101,079,741 | 311,506,654 |
New drug | 48,015,502 | 130,477,437 | 149,351,736 | 166,405,140 | 446,234,312 | |
Budget impact | 0 | 23,914,162 | 45,488,098 | 65,325,399 | 134,727,659 | |
CADTH scenario analysis 3: Tocilizumab costs | Reference | 48,015,502 | 106,563,275 | 103,863,638 | 101,079,741 | 311,506,654 |
New drug | 48,015,502 | 122,649,840 | 134,679,437 | 141,255,999 | 398,585,277 | |
Budget impact | 0 | 16,086,565 | 30,815,799 | 40,176,258 | 87,078,623 |
BIA = budget impact analysis.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.