CADTH Reimbursement Review
Olaparib (Lynparza)
Sponsor: AstraZeneca Canada Inc.
Therapeutic area: Metastatic castration-resistant prostate cancer (mCRPC)
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Stakeholder Input
Clinical Review
Abbreviations
ADT
androgen deprivation therapy
AE
adverse event
AML
acute myeloid leukemia
ARPI
androgen receptor pathway inhibitor
BICR
blinded independent central review
BPI-SF
Brief Pain Inventory-Short Form
BRCAm
breast cancer susceptibility gene–mutated
CCS
Canadian Cancer Society
CCSN
Canadian Cancer Survivor Network
CI
confidence interval
CRPC
castration-resistant prostate cancer
CSR
Clinical Study Report
CYP
cytochrome P450
DCO
data cut-off
DDR
DNA damage response
ECOG PS
Eastern Cooperative Oncology Group Performance Status
EFR
evaluable for response analysis set
FACT-P
Functional Assessment of Cancer Therapy – Prostate
FAS
full analysis set
GRADE
Grading of Recommendations Assessment, Development, and Evaluation
HR
hazard ratio
HRQoL
health-related quality of life
HRR
homologous recombination repair
HRRm
homologous recombination repair gene mutation
mCRPC
metastatic castration-resistant prostate cancer
mCSPC
metastatic castration-sensitive prostate cancer
MDS
myelodysplastic syndrome
mHSPC
metastatic hormone-sensitive prostate cancer
MID
minimal important difference
NHA
new hormonal agent
OH-CCO
Ontario Health (Cancer Care Ontario)
ORR
objective response rate
OS
overall survival
PARP
poly(adenosine diphosphate ribose) polymerase
PCWG3
Prostate Cancer Clinical Trials Working Group 3
PFS
progression-free survival
PSA
prostate-specific antigen
RCT
randomized controlled trial
RECIST 1.1
Response Evaluation Criteria in Solid Tumours version 1.1
rPFS
radiological progression-free survival
SAE
serious adverse event
SAF
safety analysis set
SD
standard deviation
SE
standard error
SSRE
symptomatic skeletal-related event
TFST
time to first subsequent anticancer therapy or death
WDAE
withdrawal due to adverse event
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Table 1: Background Information of Application Submitted for Review
Item | Description |
|---|---|
Drug product | Olaparib (Lynparza), 100 mg and 150 mg tablet, administered orally |
Sponsor | AstraZeneca Canada Inc. |
Indication | Olaparib is indicated in combination with abiraterone and prednisone or prednisolone for the treatment of adult patients with deleterious or suspected deleterious germline and/or somatic BRCA mutated metastatic castration resistant prostate cancer (mCRPC) in whom chemotherapy is not clinically indicated. BRCA mutation must be confirmed before olaparib treatment is initiated. |
Reimbursement request | Olaparib in combination with abiraterone and prednisone or prednisolone for the first-line treatment of adult patients with deleterious or suspected deleterious germline and/or somatic BRCA-mutated mCRPC in whom chemotherapy is not clinically indicated. |
Health Canada approval status | NOC/c |
Health Canada review pathway | Standard |
NOC date | July 11, 2023 |
Recommended dose | Olaparib, 600 mg (2 × 150 mg tablets, twice daily), orally Abiraterone, 1,000 mg (2 × 500 mg tablets or 4 × 250 mg tablets, daily), orally Prednisone or prednisolone, 10 mg (2 × 5 mg tablets, daily), orally |
mCRPC = metastatic castration-resistant prostate cancer; NOC = Notice of Compliance; NOC/c = Notice of Compliance with conditions.
Introduction
Prostate cancer is the most common cancers in Canada, affecting 1 in 8 males during their lifetime.1 It was estimated that in 2022, 24,600 males in Canada would be diagnosed with prostate cancer; this represents 20% of new cancer cases.1 Previous research demonstrated that 10% to 20% of patients with prostate cancer would develop castration-resistant prostate cancer (CRPC) within 5 years of follow-up, and of these patients, approximately 90% will have metastatic disease.2 When the disease progresses to the metastatic CRPC (mCRPC) stage, the 5-year survival rate decreases to approximately 26% to 28%.3,4 Metastatic disease is also debilitating and detrimental to patient’s health-related quality of life (HRQoL), with symptoms including pain, sexual dysfunction, discomfort, skeletal-related events, anxiety, depression, fatigue, cognitive impairment, urinary and bowel incontinence, nausea, and diarrhea.5-7 Certain gene mutations in patients with prostate cancer are associated with poor prognosis.8 They are associated with increased risk of prostate cancer and have more aggressive disease features, for example, early onset, metastatic involvement, and higher Gleason score.9-11 Patients with breast cancer susceptibility gene BRCA1 or BRCA2 mutations are considered to be more responsive to the effects of poly (adenosine diphosphate ribose) polymerase (PARP) inhibitors. Therefore, these patients may benefit from treatment with PARP inhibitors, and testing for genetic alterations can inform about prognosis and assist in the selection of optimal therapies.9,12,13
At the mCRPC stage, prostate cancer becomes uncurable, and the main treatment goals are to prolong patients’ survival, to delay disease progression, and to improve patients’ HRQoL. Currently, treatments available for patients with mCRPC usually include new hormonal agents (NHAs) (e.g., abiraterone or enzalutamide), taxane-based chemotherapies (e.g., docetaxel or cabazitaxel), and other therapies such as bone-targeted agents (e.g., radium-223), olaparib monotherapy, and lutetium vipivotide tetraxetan.14
Olaparib is a selective inhibitor of human PARP enzymes. Its primary mechanism of action is via inhibition of the growth of select tumour cell lines and induction of synthetic lethality in cells with deficiencies in BRCA and non-BRCA proteins involved in the homologous recombination repair (HRR) pathway.
Olaparib alone has been approved by Health Canada for the treatment of adult patients with deleterious germline and/or somatic BRCA- or ATM-mutated mCRPC who have progressed following prior treatment with an NHA. A combined antitumour effect with administration of PARP inhibitors (e.g., olaparib) and NHAs (e.g., abiraterone) has been reported in preclinical studies in prostate cancer models.15 On July 11, 2023, olaparib in combination with abiraterone and prednisone or prednisolone (referred to as olaparib plus abiraterone) was approved by Health Canada for the treatment of adult patients with deleterious or suspected deleterious germline and/or somatic BRCA-mutated mCRPC in whom chemotherapy is not clinically indicated. BRCA mutation must be confirmed before the combination regimen is initiated. The sponsor’s reimbursement request aligns with the Health Canada indication. Olaparib is administered orally. The recommended total daily dose of olaparib is 600 mg, taken as two 150 mg tablets twice daily. In the combination regimen, the dose of abiraterone is 1,000 mg orally once daily. Abiraterone should be given with prednisone or prednisolone 5 mg orally twice daily. It is recommended that treatment be continued until progression of the underlying disease or unacceptable toxicity.15
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient and clinician groups who responded to CADTH’s call for input and from clinical experts consulted by CADTH for the purpose of this review.
Patient Input
Two patient groups, the Canadian Cancer Society (CCS) and the Canadian Cancer Survivor Network (CCSN), provided input for the review of olaparib used in combination with abiraterone for mCRPC. The CCS, a national charitable organization, collected inputs from patients and caregivers through a survey that was open until April 27, 2023 (a start date for this survey was not provided). In total, 23 respondents provided input, none of whom had been treated with olaparib. The CCSN is a national network of patients, families and friends, community partners, funders and sponsors that aims to promote the best standard of care for cancer patients. The CCSN gathered patient input through an online survey from May 10 to 19, 2023. Of the 7 survey respondents, 1 had experience with olaparib monotherapy.
Based on the patient input, the majority of the patients had received multiple lines of treatment. None of the patient inputs specified whether these treatments were received at the mCRPC stage or since the patients’ initial diagnosis of prostate cancer. mCRPC disease and the currently available treatments have significant negative impact on patients’ physical and psychosocial well-being, affecting their everyday life, work, and family. Financial stress is 1 of the key barriers for patients who are receiving treatments for mCRPC.
Respondents from both patient groups indicated that there is a need for new treatments that can improve HRQoL, relieve symptoms, prolong survival, and have fewer side effects, as well as being affordable and easily accessed.
Clinician Input
Input From Clinical Experts Consulted by CADTH
The clinical experts indicated that for patients with mCRPC, the most important goals of treatment are to prolong survival, relieve symptoms, and improve quality of life. The experts identified the following unmet needs associated with the current treatments for mCRPC: therapies that are curative, therapies that improve survival outcomes better than the current treatments, and better-targeted therapies based on specific gene mutations.
The clinical experts indicated that of the current treatment options for adult patients with mCRPC, androgen receptor pathway inhibitors (ARPIs) (e.g., abiraterone or enzalutamide) or docetaxel can be used as first-line therapy, while ARPIs, docetaxel, or radium-223 may be considered as the second-line therapies, depending on what first-line therapy is used. Lutetium vipivotide tetraxetan, olaparib monotherapy (in patients with BRCA or ATM mutation), radium-223, or cabazitaxel can be used as later lines of treatment, thereafter. The experts also noted that, in certain patients, the combination of docetaxel and ARPI can be used as first-line treatment.
With the emergence of the combination regimen of olaparib plus abiraterone, and based on the study findings from the clinical trials (such as the PROpel trial16), the experts expected that there would be a shift in the current treatment paradigm. The experts anticipated that the combination regimen should be considered as a first-line therapy option in patients with mCRPC, in particular for those with BRCA mutation.
The clinical experts indicated that patients with BRCA mutations would be best suited for treatment with the combination of olaparib plus abiraterone and prednisone or prednisolone, based on the study findings from the clinical trials. The experts noted that the patients for whom chemotherapy is not clinically indicated include those who are deemed physically unfit (such as those with poor renal function or poor performance status) or those who have received prior docetaxel treatment in the metastatic castration-sensitive prostate cancer (mCSPC) phase. They also considered patients who refuse chemotherapy as patients who would potentially fall under this indication. The clinical experts noted that the proportion of patients in the first-line mCRPC who are likely to be clinically indicated to receive chemotherapy was no more than 10% to 15%. The experts also indicated that for patients who may be clinically indicated to receive a taxane-based chemotherapy but who are unwilling to receive docetaxel or cabazitaxel, the combination of olaparib plus abiraterone would only be considered as a treatment option if the patients have BRCA mutation. The experts noted that there is a lack of evidence to support the treatment with olaparib and ARPIs of patients with non–HRR-mutated cancers.
The clinical experts noted that in clinical practice, the criteria that are used to determine whether a patient with mCRPC is responding to treatment include prolonged survival, symptom (e.g., pain) relief, improved HRQoL, improved prostate-specific antigen (PSA) response, and improved results on an imaging scan. Typically, these assessments are reviewed once a month after initiation of a new therapy.
According to the clinical experts, treatment with the combination of olaparib plus abiraterone would be discontinued if disease progression is detected, based on the results of an imaging scan, PSA response, or worsening of symptoms, or if adverse effects of the treatment are intolerable.
The clinical experts noted that, in general, all centres that can prescribe ARPIs are appropriate for providing treatment with the combination of olaparib plus abiraterone. Germline testing and/or somatic testing must be available in these centres to assist in selecting the patients who are suitable for this treatment. In addition, due to the high rate of anemia and the possible need for blood transfusions in patients receiving combination therapy, the centres should be able to quickly and efficiently provide transfusions when required.
Clinician Group Input
Two clinician groups provided input for the review of olaparib plus abiraterone combination therapy: Ontario Health (Cancer Care Ontario) (OH-CCO) Genitourinary Cancer Drug Advisory Committee (GU DAC) and clinicians in Canada with expertise in managing advanced prostate cancer.
In general, the clinician group input was consistent with the input provided by the experts consulted by CADTH for this review. They indicated that mCRPC is an incurable disease. The quick progression of the disease at this stage precludes patients from being eligible for second-line therapies and beyond. Effective treatments that are available early in the metastatic stage are lacking, with no effective combination therapy approved to date. Therefore, a new early treatment option that could also prolong the duration of treatment with available therapies, delay disease progression, and improve long-term outcomes is warranted and critically needed. Both clinician groups stated that olaparib plus abiraterone fulfills this unmet need for an effective and tolerable first-line combination, and that all patients with mCRPC would benefit from this combination therapy. One clinician group added that this treatment also suits patients for whom docetaxel is not yet clinically indicated or who were previously treated with docetaxel in the mCSPC setting.
The clinician groups noted that assessing response to treatment should be based on outcomes such as radiological progression-free survival (rPFS), PSA response, symptom improvement, and HRQoL improvement.
Drug Program Input
Input was obtained from the drug programs that participate in the CADTH reimbursement review process. The following were identified as key factors that could potentially impact the implementation of a CADTH recommendation for the olaparib plus abiraterone combination therapy:
relevant comparators
considerations for initiation of therapy
considerations for discontinuation of therapy
considerations for prescribing of therapy
generalizability
funding algorithm
care provision issues
system and economic issues.
The clinical experts consulted by CADTH provided advice on the potential implementation issues raised by the drug programs.
Clinical Evidence
Systematic Review
Description of Studies
One phase III, randomized, double-blind, placebo-controlled, multicentre trial, PROpel (N = 796) met the inclusion criteria for the systematic review conducted by the sponsor, and a subgroup of patients who had a BRCA mutation (n = 85) was enrolled in the study. Even though the purpose of the PROpel trial was to evaluate the efficacy and safety of the combination of olaparib plus abiraterone versus abiraterone and placebo with prednisone or prednisolone (referred to as “abiraterone”) in all patients with mCRPC who had received no prior cytotoxic chemotherapy or NHAs at the mCRPC stage, to align with the Health Canada–approved indication the focus of this review was the evidence in the subgroup of patients with BRCA mutation.
In the PROpel trial, patients were randomized to either a combination of olaparib (300 mg twice daily) and abiraterone (1,000 mg once daily) and prednisolone or prednisone (5 mg twice daily) (n = 399; BRCA-mutated n = 47) or placebo (matched to olaparib; twice daily) and abiraterone (1,000 mg once daily) prednisolone or prednisone 5 mg twice daily (n = 397; BRCA-mutated n = 38). The primary efficacy end point in the PROpel trial was rPFS by investigator assessment. Other outcomes in this study included overall survival (OS), time to first subsequent anticancer therapy or death (TFST), HRQoL measured using the Functional Assessment of Cancer Therapy – Prostate (FACT-P) questionnaire, objective response rate (ORR), PSA50 response rate, and safety. In the subgroup population of patients with a BRCA mutation, all outcomes analyzed (rPFS, OS, TFST, ORR, PSA50 response rate, FACT-P total score, and safety) were exploratory.
Among the patients with a BRCA mutation in the olaparib plus abiraterone treatment group (n = 47), the median age at baseline was 67.0 years (range, 43 years to 83 years), 30 (63.8%) were aged more than 65 years, 34 (72.4%) had a Gleason score of 8 to 10, 8 (17.0%) had previously been treated with docetaxel at the mCSPC stage, 36 (76.6%) had an Eastern Cooperative Oncology Group Performance Status (ECOG PS) of 0, 31 (66.0%) had no or mild or no pain, and the median PSA level was 29.0 (range not reported). Among the patients with a BRCA mutation in the abiraterone treatment group (n = 38), the median age at baseline was 70.0 years (range, 46 years to 85 years), 27 (71.1%) were aged more than 65 years, 25 (65.8%) had a Gleason score of 8 to 10, 10 (26.3%) had previously been treated with docetaxel at the mCSPC stage, 20 (52.6%) had an ECOG PS of 0, 26 (68.4%) had no or mild or no pain, and the median PSA level was 22.5 (range not reported). Other important baseline characteristics, for example, TNM classification (a standard for cancer staging that includes the extent of the tumour [T], extent of spread to the lymph nodes [N], and presence of metastasis [M]) and prior treatments were not reported.
Efficacy Results
The investigator-assessed rPFS was the primary outcome in the PROpel trial. rPFS had a hazard ratio (HR) of 0.23 (95% confidence interval [CI], 0.12 to 0.43) for the patients with BRCA mutation. The median rPFS was not reached in the olaparib plus abiraterone group and was 8.4 months in the abiraterone group. According to the clinical expert consulted by CADTH, the survival benefit gained from treatment with olaparib plus abiraterone may be considered moderate and clinically important, despite that a median rPFS had yet to be reached at the time of the data cut-off (DCO) date. Results of the blinded independent central review (BICR)-assessed rPFS were consistent with those from the primary analysis.
Treatment with olaparib plus abiraterone may be associated with prolonged OS. Results from the OS analyses in the subgroup of patients with BRCA mutation (referred to as the BRCAm subgroup) showed that the HR of OS was 0.29 (95% CI, 0.14 to 0.56). Due to the immaturity of the data at the final OS analysis, the median OS was not reached in the olaparib plus abiraterone group and was 23.0 months in the abiraterone group. The clinical experts considered the improvement in OS to be clinically important. Overall, treatment with olaparib plus abiraterone was associated with prolonged OS, although the benefit gained in these patients was considered small compared to the abiraterone group, given the limitations of the available data. A longer follow-up time for the survival outcomes is desired.
The HR for TFST was 0.35 (95% CI, 0.21 to 0.61). The median TFST was 37.39 months in the olaparib plus abiraterone group and 14.75 months in the abiraterone group. The clinical experts considered the benefit from TFST clinically important and consistent with the primary outcome, rPFS. Given the available evidence, treatment with olaparib plus abiraterone was associated with longer time required for the first subsequent anticancer treatment compared to treatment with abiraterone.
HRQoL was assessed based on the least squares mean change from baseline in FACT-P total score. The change from baseline in the total score was 2.43 in the olaparib plus abiraterone group and –1.21 in the abiraterone group. The between-group difference in the mean change from baseline with 95% CI was not reported. Based on the data on FACT-P total score, the treatment effect of olaparib plus abiraterone on improving patients’ HRQoL, compared to that of abiraterone, remains uncertain.
Two exploratory outcomes, ORR and PSA50 response, were also measured in the PROpel trial to provide evidence on treatment response. The proportion of patients achieved complete response or partial response was 50.0% in the olaparib plus abiraterone group and 26.7% in the abiraterone group. The proportion of patients with a PSA50 response was 85.1% in the olaparib plus abiraterone group and 51.4% in the abiraterone group. Results of ORR and PSA50 response suggested that patients treated with olaparib plus abiraterone were associated with higher response rate and higher PSA50 response rate compared to those treated with abiraterone. However, definite conclusions on the response rate related to the treatment with the combination of olaparib plus abiraterone cannot be made because of concerns about the risk of bias related to baseline imbalances in patient characteristics and the high proportion of patients who were not evaluable, imprecision related to the small sample size of the subgroup, and lack of details in data reporting.
Harms Results
Limited results were reported for harms among patients in the BRCAm subgroup.
The overall frequency of adverse events (AEs) was similar between the olaparib plus abiraterone group and the abiraterone group in the PROpel trial, with 100% versus 89.5% of patients experiencing at least 1 AE in the 2 treatment groups, respectively. The most frequently reported AEs were anemia, fatigue, nausea, back pain, and arthralgia. The proportion of patients experiencing at least 1 serious adverse event (SAE) was similar between the olaparib plus abiraterone and abiraterone groups (29.8% versus 31.6%, respectively). The proportion of patients who withdrew from treatment due to AEs was 12.8% in the olaparib plus abiraterone group and 10.5% in the abiraterone group. The proportion of AEs leading to death was 2.1% in the olaparib plus abiraterone group and 5.3% in the abiraterone group. The causes of deaths were not given in the BRCAm subgroup. In this subgroup, 5 (10.6%) patients in the olaparib plus abiraterone group reported pulmonary embolism; no pulmonary embolisms were reported in the abiraterone group. Other notable harms were not reported in this subgroup. The small sample size and low number of events in the BRCAm subgroup resulted in an assessment of certainty rated low to very low. Nevertheless, the proportion of patients reported as having experienced SAEs, withdrawals due to adverse event (WDAEs), and notable harms (pulmonary embolisms) were aligned with the expectations of the clinical experts consulted by CADTH, based on their experience treating patients with mCRPC, and did not raise significant safety concerns.
Critical Appraisal
The current CADTH review focuses on the subgroup of patients with BRCA mutation in the PROpel trial (which aligned with Health Canada–approved indication) and not the overall population. One of the key limitations of this study was the small sample size. Although the sample size of the full population in the PROpel trial was approximately 800 patients, only 85 patients had a BRCA mutation, 47 in the olaparib plus abiraterone group and 38 in the abiraterone group.
Prognostic balance cannot be ensured across the treatment groups in this subgroup of patients as the randomization was not stratified by BRCA mutation status. There was an imbalance between the treatment groups based on several patient baseline characteristics (e.g., age, baseline pain scores, baseline Gleason score, and location of metastases), and several important patient characteristics (e.g., TNM classification, prior treatments for mCRPC) were not reported. Patients in the olaparib plus abiraterone treatment group tended to be younger and had more moderate or severe pain, slightly higher PSA levels at baseline, and better performance status. It is unclear how these factors, in combination, may have biased the study results. Small sample size resulted in imprecision in many of the effect estimates. Further, between-group differences (relative or absolute) were not provided for some outcomes (such as HRQoL and ORR), precluding the comprehensive appraisal of comparative efficacy.
In the PROpel trial, all subgroup analyses were considered exploratory and were not adjusted for multiple comparisons, so there is an increased risk of type I error (i.e., a false-positive result) for statistically significant findings.
In the subgroup of patients with BRCA mutation, efficacy and safety outcomes were not reported in sufficient detail. As a result, these outcomes were affected by concerns regarding imprecision, uncertainties, and study limitations (e.g., imbalanced baseline characteristics between the 2 treatment groups). This often precludes a robust critical appraisal, for example, reasons for censoring patients were not provided, information about the proportion of patients who completed HRQoL assessments in each group was not reported, and baseline values for HRQoL outcomes were not reported. As a result, it is difficult to fully explore the magnitude of treatment effect on these outcomes. The sponsor noted that, according to an FDA briefing document,17 adjustment by a known prognostic model in mCRPC did not produce overall divergent results from the unadjusted results. However, the CADTH review team did not have access to the adjusted model. Without any knowledge of the model and the variables within it, the team cannot fully interpret the results of the adjusted analysis. Furthermore, longer follow-ups are needed to examine the long-term clinical benefits or risks of this combination regimen, given the immature survival data at the third data cut-off (DCO3) date.
Updated analyses at DCO3 were not provided for all outcomes (e.g., rPFS, FACT-P total score, and PSA50 response). Missing data in the subgroup of patients with BRCA mutation raises concerns regarding the potential for bias in the study results.
External Validity
The clinical experts consulted by CADTH considered the eligibility criteria and baseline characteristics of the PROpel trial, and suggested that the study population is reflective of typical patient population that would receive combination therapy of olaparib plus abiraterone in Canada, except that patients in the PROpel trial were not allowed to have received prior abiraterone therapy before study entry and they were somewhat healthier (with, for example, better performance status and less pain). However, in clinical practice, patients at the mCRPC stage usually would have been treated with other active treatments including abiraterone. Therefore, the study findings may only be generalizable to patients who have not received abiraterone previously. The experts indicated that the outcome measures in the PROpel trial are appropriate and clinically relevant in clinical trials of metastatic prostate cancer. However, some important outcomes were not reported for the BRCAm subgroup (such as pain symptoms and symptomatic skeletal-related events [SSREs]). Results for certain AEs were not reported in this subgroup.
The combination therapy under review is indicated for the treatment of adult patients with deleterious or suspected deleterious germline and/or somatic BRCA-mutated mCRPC in whom chemotherapy is not clinically indicated. The drug is intended for use in the first-line setting at mCRPC. According to the clinical experts consulted by CADTH, there are no consistent criteria used in clinical practice to identify patients for whom chemotherapy are not clinically indicated. This patient group may include those who are deemed physically unfit (such as those with poor renal function or poor performance status), those who refuse chemotherapy, or those who have received prior docetaxel treatment. The clinical experts noted that the proportion of patients in the first-line mCRPC setting who are likely to be clinically indicated to receive chemotherapy was no greater than 10% to 15%, suggesting that 85% to 90% of these patients would be eligible for treatment with olaparib plus abiraterone. In the PROpel trial, the combination of olaparib plus abiraterone was compared to abiraterone, which was a relevant comparator. Evidence for the comparisons between olaparib plus abiraterone and other comparators is lacking.
GRADE Summary of Findings and Certainty of the Evidence
Methods for Assessing the Certainty of the Evidence
For pivotal studies and randomized controlled trials (RCTs) identified in the sponsor’s systematic review, Grading of Recommendations Assessment, Development, and Evaluation (GRADE) was used to assess the certainty of the evidence for outcomes considered most relevant to informing CADTH’s expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group.18,19
Following the GRADE approach, evidence from RCTs started as high certainty, and could be rated down for concerns related to: study limitations (which refers to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias.
Whenever possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect; if this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., the clinical importance is unclear). In all cases, the target of the certainty of evidence assessment was based on the point estimate and where it was located relative to the threshold for a clinically important effect (when a threshold was available) or to the null. The reference points for the certainty of evidence assessment for OS and rPFS was set to null, since there were no absolute effects for these outcomes. The reference point for the certainty of the evidence assessment for FACT-P total score was set according to the presence or absence of an important effect based on thresholds identified in the literature. The target of the certainty of evidence assessment was the presence or absence of any (non-null) effect for the TFST due to the lack of a formal minimal important difference (MID) estimate, and for harm events due to the unavailability of the absolute difference in effects, the certainty of evidence was summarized narratively.
The selection of outcomes for GRADE assessment was based on the sponsor’s Summary of Clinical Evidence, consultation with clinical experts, and input received from patient and clinician groups and public drug plans. The following list of outcomes was finalized in consultation with expert committee members:
survival outcomes (rPFS, OS, TSFT, SSRE)
response (ORR, PSA50 response)
HRQoL (FACT-P total score, Brief Pain Inventory-Short Form [BPI-SF] questionnaire)
harms (any AEs, SAEs, WDAEs, notable harms).
Results of GRADE Assessment
Table 2 presents the GRADE summary of findings for olaparib plus abiraterone versus abiraterone.
Table 2: Summary of Findings for Olaparib Plus Abiraterone Versus Abiraterone for Patients With BRCA-Mutated mCRPC
Outcome and follow-up | Patients (studies), N | Effect | Certainty | What happens |
|---|---|---|---|---|
rPFS | ||||
rPFS at DCO1 (July 30, 2021) Median follow-up:
| 1 RCT, 85 patients with BRCA mutation | Events at DCO1:
Median (95% CI) rPFS at DCO1, months:
Survival probability (95% CI): not reported at 1 or 2 years | Lowa | Olaparib plus abiraterone may result in a clinically important increase in rPFS when compared with abiraterone. |
OS | ||||
OS at DCO3 (October 12, 2022) Median follow-up:
| 1 RCT, 85 patients with BRCA mutation | Deaths at DCO3:
Median (95% CI) OS at DCO3, months:
Survival probability (95% CI): not reported at 1 or 2 years | Lowb | Olaparib plus abiraterone may result in a clinically important increase in OS when compared with abiraterone. |
TFST | ||||
Time to first subsequent anticancer therapy at DCO3 (October 12, 2022) Median follow-up:
| 1 RCT, 85 patients with BRCA mutation | Events at DCO3:
Median (95% CI) rPFS at DCO1, months:
Survival probability (95% CI): not reported at 1 or 2 years | Lowc | Olaparib plus abiraterone may result in a clinically important increase in the time to the first subsequent anticancer therapy when compared with abiraterone. |
SSRE | ||||
Not reported | — | NA | NA | There was no evidence on the effect of olaparib plus abiraterone on SSRE when compared with the effect of abiraterone. |
ORR | ||||
ORR at DCO1 (July 30, 2021) Median follow-up:
| 1 RCT, 35 patients with BRCA mutation | Response at DCO1:
| Very lowd | The evidence is very uncertain on the effect of olaparib plus abiraterone on ORR when compared to the effect of abiraterone. |
FACT-P | ||||
LSM change from baseline in FACT-P total score at DCO3 (October 12, 2022) (range of scores, from worst to best: 0 to 156) Median follow-up:
| 1 RCT, N not reported | Baseline, mean (SD):
At DCO3, mean change from baseline (95% CI):
| Very lowe | The evidence is very uncertain on the effect of olaparib plus abiraterone on HRQoL, measured with a disease-specific questionnaire, compared to the effect of abiraterone. |
BPI-SF | ||||
Not reported | — | NA | NA | There was no evidence on the effect of olaparib plus abiraterone on BPI-SF score when compared with the effect of abiraterone. |
PSA50 response | ||||
PSA50 response at DCO1 (July 30, 2021) Median follow-up:
| 1 RCT, 85 patients with BRCA mutation | Response at DCO1:
| Very lowf | The evidence is very uncertain about the effect of olaparib plus abiraterone on PSA50 response when compared to the effect of abiraterone. |
Harms | ||||
Any AEs at DCO3 (October 12, 2022) Median follow-up:
| 1 RCT, 85 patients with BRCA mutation | In the subgroup of patients with BRCA mutation, the proportion of AEs was 100% in the olaparib plus abiraterone group and 89.5% in the abiraterone group. | Lowg | Olaparib plus abiraterone may result in little to no difference in the number of patients experiencing ≥ 1 AEs when compared to abiraterone. |
Any SAEs at DCO3 (October 12, 2022) Median follow-up:
| 1 RCT, 85 patients with BRCA mutation | In the subgroup of patients with BRCA mutation, the proportion of SAEs was 29.8% in the olaparib plus abiraterone group and 31.6% in the abiraterone group. | Very lowh | The evidence is very uncertain about the effect of olaparib plus abiraterone on the number of patients experiencing ≥ 1 SAEs when compared to the effect of abiraterone. |
WDAEs at DCO3 (October 12, 2022) Median follow-up:
| 1 RCT, 85 patients with BRCA mutation | In the subgroup of patients with BRCA mutation, the proportion of WDAEs was 12.8% in the olaparib plus abiraterone group and 10.5% in the abiraterone group. | Very lowh | The evidence is very uncertain about the effect of olaparib plus abiraterone on the number of patients withdrawing from treatment due to AEs when compared to the effect of abiraterone. |
Pulmonary embolisms at DCO3 (October 12, 2022) Median follow-up:
| 1 RCT, 85 patients with BRCA mutation | In the subgroup of patients with BRCA mutation, 5 patients (10.6%) in the olaparib plus abiraterone group reported pulmonary embolism, compared to 0 patients in the abiraterone group. | Very lowh | The evidence is very uncertain about the effect of olaparib plus abiraterone on the number of patients who experience a pulmonary embolism when compared to the effect of abiraterone. |
AE = adverse event; BRCAm = breast cancer susceptibility gene–mutated; BPI-SF = Brief Pain Inventory-Short Form; CI = confidence interval; DCO = data cut-off; EFR = evaluable for response analysis set; FACT-P = Functional Assessment of Cancer Therapy – Prostate; HR = hazard ratio; HRQoL = health-related quality of life; LSM = least squares mean; mCRPC = metastatic castration-resistant prostate cancer; MID = minimal important difference; NA = not applicable; ORR = objective response rate; OS = overall survival; PSA = prostrate-specific antigen; PSA50 = prostrate-specific antigen response (proportion of patients achieving ≥ 50% decrease in PSA score from baseline to the lowest PSA result); RCT = randomized controlled trial; rPFS = radiological progression-free survival; SAE = serious adverse event; SD = standard deviation; SSRE = symptomatic skeletal-related event; TFST = time to first subsequent anticancer therapy or death; WDAE = withdrawal due to adverse event.
Note: Study limitations (which refer to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias were considered when assessing the certainty of the evidence. All serious concerns in these domains that led to the rating down of the level of certainty are documented in the table footnotes. All analyses for the BRCAm subgroup presented within this report were exploratory; as such, there were no adjustments for multiple comparisons, and statistically significant results are at increased risk of type I error.
aRated down 1 level for serious risk of bias. Randomization was not stratified by BRCA mutation status, and there were baseline imbalances in important patient characteristics. Rated down 1 level for serious imprecision. In the absence of available data for the between-group difference in event probabilities at clinically relevant time points, the judgment of precision was based on the 95% CI for the HR using the null as the threshold and the number of events at the DCO. The clinical importance of the between-group difference was judged based on the difference in median event rates and the input of the clinical experts consulted by CADTH for the review. Although the null was not crossed by the 95% CI, the small sample size (n = 85) and number of events (n = 42) raise concerns regarding potential overestimation of the true effect, and there is evidence of prognostic imbalance. The clinical experts indicated that the improvement in rPFS was clinically meaningful.
bRated down 1 level for serious risk of bias. Randomization was not stratified by BRCA mutation status, and there were baseline imbalances in important patient characteristics. Rated down 1 level for serious imprecision. In the absence of available data for the between-group difference in event probabilities at clinically relevant time points, the judgment of precision was based on the 95% CI for the HR using the null as the threshold and the number of events at the DCO. The clinical importance of the between-group difference was judged based on the difference in median event rates and the input of the clinical experts consulted by CADTH for the review. Although the null was not crossed by the 95% CI, the small sample size (n = 85) and number of events (n = 38) raise concerns regarding potential overestimation of the true effect, and there is evidence of prognostic imbalance. The clinical experts indicated that the improvement in OS was clinically meaningful.
cRated down 1 level for serious risk of bias. Randomization was not stratified by BRCA mutation status, and there were baseline imbalances in important patient characteristics. Rated down 1 level for serious imprecision. In the absence of available data for the between-group difference in event probabilities at clinically relevant time points, the judgment of precision is based on the 95% CI for the HR using the null as the threshold, and the number of events at the DCO. The clinical importance of the between-group difference was judged based on the difference in median event rates and the input of the clinical experts consulted by CADTH for the review. Although the null was not crossed by the 95% CI, the small sample size (n = 85) and number of events (n = 54) raise concerns regarding potential overestimation of the true effect, and there is evidence of prognostic imbalance. The clinical experts indicated that the improvement in TFST was clinically meaningful.
dRated down 2 levels for very serious risk of bias. Randomization was not stratified by BRCA mutation status, and there were baseline imbalances in important patient characteristics. A large proportion of patients were not included in the EFR (57.4% and 60.5% of patients were not evaluable in the olaparib plus abiraterone and abiraterone groups, respectively). Rated down 2 levels for serious imprecision. There was no point estimate (and 95% CI) for the assessment of between-group difference. The sample size (n = 35) was small, and there were few events (n = 14).
eRated down 2 levels for very serious risk of bias. Randomization was not stratified by BRCA mutation status, and there were baseline imbalances in important patient characteristics. It is unknown how many patients with mCRPC with BRCA mutation completed this assessment; however, in the overall population the completion rates for FACT-P were 67.6% in the olaparib plus abiraterone group and 66.3% in the abiraterone group. Rated down 1 level for serious imprecision. There was no point estimate (and 95% CI) for the assessment of between-group difference. MID of FACT-P total score ranged from 6 to 10; however, the between-group difference appeared smaller than the MID. The sample size was small (n = 85 or less [total analyzed not reported]), and there is evidence of prognostic imbalance.
fRated down 1 level for serious risk of bias. Randomization was not stratified by BRCA mutation status, and there were baseline imbalances in important patient characteristics. Rated down 1 level for serious imprecision. There was no point estimate (and 95% CI) for the assessment of between-group difference. The small sample size (n = 85) and number of events (n = 59) raise concerns regarding potential overestimation of the true effect, and there is evidence of prognostic imbalance. Rated down 1 level for serious indirectness. There is a lack of consistent evidence to inform whether this surrogate outcome correlates with OS.20
gRated down 1 level for serious risk of bias. Randomization was not stratified by BRCA mutation status, and there were baseline imbalances in important patient characteristics. Rated down 1 level for serious imprecision. The sample size (n = 85) and total number of events were small, and there is evidence of prognostic imbalance.
hRated down 1 level for serious risk of bias. Randomization was not stratified by BRCA mutation status, and there were baseline imbalances in important patient characteristics. Rated down 2 levels for very serious imprecision. The sample size was small (n = 85), and there were very few or no events in either group.
Sources: PROpel DCO1 Clinical Study Report,21 PROpel DCO3 Clinical Study Report,22 and Oncologic Drugs Advisory Committee Briefing Document.23 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Long-Term Extension Studies
No relevant long-term extension studies were submitted by the sponsor.
Indirect Comparisons
No relevant indirect treatment comparisons of patients with mCRPC and BRCA mutations were submitted by the sponsor.
Studies Addressing Gaps in the Evidence From the Systematic Review
No relevant studies addressing gaps in the evidence from the systematic review were submitted by the sponsor.
Conclusions
One phase III, double-blind, placebo-controlled RCT (PROpel) evaluated the efficacy and safety of first-line treatment with olaparib plus abiraterone with prednisone or prednisolone compared to abiraterone with prednisone or prednisolone in patients with mCRPC. Data from a subgroup of patients in this trial with a BRCA mutation is the most relevant evidence available at this time to inform the review of olaparib as per the indication approved by Health Canada. Compared with abiraterone, olaparib plus abiraterone may result in a clinically important increase in rPFS (median follow-up = 16.5 months at DCO1, July 30, 2021); OS (median follow-up = 18.5 months, at DCO3, October 12, 2022); and TFST (median follow-up = 18.5 months at DCO3, October 12, 2022), which were identified as important outcomes by patients and clinical experts. However, a longer duration of follow-up is needed to examine the long-term clinical benefits or risks of this combination regimen, particularly for OS, given the immature OS data at DCO3 in this trial. The results for HRQoL, ORR, and PSA response were very uncertain owing to reporting deficiencies and methodological limitations. As such, a definitive conclusion could not be drawn for these outcomes. There were no results reported for SSRE or pain among patients in the BRCAm subgroup, outcomes that were important to patients and clinical experts.
The proportion of patients who received treatment with olaparib plus abiraterone who experienced AEs was similar to the proportion of patients who received abiraterone. The proportion of patients who experienced SAEs, WDAEs, and notable harms was also similar in the treatment groups; however, the evidence was associated with very low certainty, due in part to the low sample size and event rate. The harms experienced by the patients were considered manageable and aligned with the clinical expectations.
Introduction
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of olaparib (tablets, 100 mg and 150 mg, oral use) in combination with abiraterone and prednisone or prednisolone for the treatment of adult patients with deleterious or suspected deleterious germline and/or somatic BRCA-mutated mCRPC, in whom chemotherapy is not clinically indicated.
Disease Background
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following have been summarized and validated by the CADTH review team.
Prostate cancer is the most common cancer among males in Canada, affecting 1 in 8 males during their lifetime.1 It was estimated that 24,600 males in Canada would be diagnosed with prostate cancer in 2022; this represents 20% of new cancer cases.1 The stages of prostate cancer are classified as localized, locally advanced, or metastatic disease, with further subcategorization according to hormonal therapy status, whether hormone-naive or sensitive, or whether the disease has progressed to mCRPC.24 A patient may progress to mCRPC from mCSPC, based on biochemical recurrence (characterized by rising PSA levels despite medical or surgical castration), or from nonmetastatic CRPC, based on presentation of metastases, which can be assessed radiographically.25,26 Based on the results of a systematic review that evaluated the epidemiology, progression, and outcomes of prostate cancer, 10% to 20% of patients with prostate cancer develop CRPC within 5 years of follow-up, and of these patients, approximately 90% will have metastatic disease.2
Prostate cancer accounts for 10% of cancer-related deaths in males in Canada.27 Even though the expected 5-year survival for males diagnosed with prostate cancer in Canada is high, at 91% for all stages combined,28 when the disease progresses to the mCRPC stage, the 5-year survival rate decreases to approximately 26% to 28%.3,4 Metastatic disease is debilitating and detrimental to patients’ HRQoL, with symptoms that include pain, sexual dysfunction, discomfort, skeletal-related events, anxiety, depression, fatigue, cognitive impairment, urinary and bowel incontinence, nausea, and diarrhea.5-7
Important factors that can influence the patient’s survival include site and extent of metastasis involvement, PSA kinetics, performance status, presence or absence of visceral metastases, use of opioids for pain relief, elevated serum lactate dehydrogenase, increasing serum PSA, increasing serum alkaline phosphatase, lower serum albumin and a lower hemoglobin level.29
In addition, certain gene mutations in patients with prostate cancer are associated with poor prognosis.8 CRPC is a molecularly heterogeneous disease. Previous research has found genomic defects in DNA damage repair (DDR), including HRR gene alterations, in approximately 20% to 30% of patients with CRPC.8,9 Mutations in the genes encoding components of DDR, such as BRCA1 and BRCA2, are common in prostate cancer. They are associated with an increased risk of prostate cancer and have more aggressive disease features, such as early onset, metastatic involvement, and higher Gleason grade.9-11 In a large prostate cancer sample (the PROfound study, a phase III study that examined the benefits of olaparib, a PARP inhibitor, in patients with mCRPC), of the 2,792 biopsies for aberrations in 15 DDR genes involved in the HRR pathway, the most common DDR genes were BRCA1, BRCA2, CDK12, ATM, and CHEK2.30 Furthermore, patients with BRCA1 or BRCA2 mutations were considered more responsive to the effects of PARP inhibitors. Therefore, these patients may benefit from treatment with PARP inhibitors, and testing for genetic alterations can inform about prognosis and assist in the selection of optimal therapies.9,12,13 The proportion of prostate tumours with germline and somatic DDR mutations are similar in patients with prostate cancer.30 Germline testing can be performed on peripheral blood or saliva. Somatic testing is typically performed using archived formalin-fixed paraffin-embedded tumour tissue from biopsies from the prostate or metastases, or radical prostatectomy specimens; it can also be performed on fresh frozen specimens. In addition, somatic testing can be obtained via liquid biopsy approaches using peripheral blood samples.12
Standards of Therapy
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following have been summarized and validated by the CADTH review team.
According to the clinical experts consulted by CADTH, at the mCRPC stage, prostate cancer becomes uncurable, and the main treatment goals are to prolong patients’ survival, delay disease progression, and improve patients’ HRQoL. This may include relieving mCRPC symptoms, reducing complications from metastases, and reducing the need for chemotherapy or other therapies with associated toxicities.
According to the practice guidelines in Canada, treatments available for patients with mCRPC usually include NHAs (i.e., abiraterone or enzalutamide), taxane-based chemotherapies (i.e., docetaxel or cabazitaxel), and other therapies such as bone-targeted agent (radium-223), olaparib monotherapy, and lutetium vipivotide tetraxetan.14 Abiraterone and enzalutamide are both potent, orally administered ARPIs. They have been shown to lead to improvements in rPFS, OS, and time to initiation of chemotherapy in the first-line chemotherapy-naive setting.31-34 The clinicians also suggested that abiraterone plus prednisone or enzalutamide is the preferred first-line treatment for mCRPC.35 Results of previous clinical trials have demonstrated that taxane-based chemotherapy in the first-line setting was associated with survival benefit and tumour regression in some patients, for example, those who progress with minimal change in PSA levels or who have significant visceral metastases.14,36-38 Radium-223 is recommended for patients with bone-only metastases who have progressed following taxane-based chemotherapy or are unfit for chemotherapy and do not have visceral metastases.14 Olaparib monotherapy is indicated for the treatment of adult patients with deleterious or suspected deleterious germline and/or somatic BRCA- or ATM-mutated mCRPC who have progressed following prior treatment with an NHA. BRCA or ATM mutations must be confirmed before olaparib treatment is initiated.15 Lutetium vipivotide tetraxetan for up to 6 cycles is recommended for patients with prostate-specific membrane antigen–positive mCRPC who have progressed on at least 1 previous taxane-based chemotherapy and an NHA. Compared to standard of care, lutetium vipivotide tetraxetan has shown benefit in median OS in this particular patient population.39
There is a lack of guidance regarding the optimal sequencing of NHAs and taxanes. For patients with mCRPC and no prior exposure to docetaxel or NHA, clinical practice guidelines recommend either treatment as the preferred frontline therapy. In practice, NHAs are the preferred frontline therapy, accounting for approximately two-thirds of the treatments received in the first-line setting.40 Abiraterone is among the most frequently used first-line treatments for mCRPC, and it is an established standard of care.41,42 Data from the US show that, of approximately 3,000 to 14,780 patients (from across large databases) with mCRPC, the most frequently used first-line monotherapies were abiraterone (35% to 36%), followed by enzalutamide (28% to 34%), and docetaxel (14% to 16%).41,42 The clinical experts consulted by CADTH noted that at present, most patients in the first-line setting for mCRPC are not treated with chemotherapy (or for whom chemotherapy is considered “not clinically indicated”).
There are safety and tolerability concerns related to the treatments currently available for patients with mCRPC. Docetaxel and cabazitaxel are associated with numerous SAEs including hypersensitivity and gastrointestinal and hematological AEs. Enzalutamide is associated with neuropsychiatric AEs. Use requires monitoring for signs and symptoms of ischemic heart disease as well as management optimization of cardiovascular risk factors, such as hypertension, diabetes, or dyslipidemia.43-45 A high unmet need exists for a treatment that can improve survival without compromising the quality of life for patients with mCRPC.
Drug Under Review
Olaparib is a selective inhibitor of human PARP enzymes, including PARP1, PARP2, and PARP3, that are required for the repair of DNA strand breaks. Its primary mechanism of action is via inhibition of the growth of certain tumour cell lines and induction of synthetic lethality into cells with deficiencies in BRCA and non-BRCA proteins involved in the HRR pathway.
Olaparib alone has been approved by Health Canada for the treatment of adult patients with deleterious germline and/or somatic BRCA- or ATM-mutated mCRPC who have progressed following prior treatment with an NHA.15 Olaparib monotherapy was previously reviewed in 2020 by CADTH for adult patients with mCRPC and deleterious or suspected deleterious germline and/or somatic mutations in the HRR genes BRCA or ATM who have progressed following prior treatment with an NHA. A recommendation to reimburse with conditions was issued by pERC in April 2021.
A combined antitumour effect with administration of PARP inhibitors (e.g., olaparib) and NHAs (e.g., abiraterone) has been reported in preclinical studies in prostate cancer models.15 This mechanism of action leads to increased accumulation of DNA damage that can enhance the antitumour effect of the combination compared to either agent alone in both non-HRR mutation and non–BRCA-mutated metastatic prostate cancer models. On July 11, 2023, olaparib in combination with abiraterone and prednisone or prednisolone was approved by Health Canada for the treatment of adult patients with deleterious or suspected deleterious germline and/or somatic BRCA-mutated mCRPC in whom chemotherapy is not clinically indicated. BRCA mutation must be confirmed before the combination regimen is initiated. The sponsor’s reimbursement request aligns with the Health Canada indication, which is for the first-line treatment of adult patients with deleterious or suspected deleterious germline and/or somatic BRCA-mutated mCRPC in whom chemotherapy is not clinically indicated.
Olaparib is administered orally. The recommended total daily dose of olaparib is 600 mg, taken as two 150 mg tablets twice daily. The 100 mg tablet is available for dose reduction.15 In the combination regimen, the dose of abiraterone is 1,000 mg orally once daily. Abiraterone should be given with prednisone or prednisolone 5 mg orally twice daily. It is recommended that treatment be continued until progression of the underlying disease or unacceptable toxicity.15
Key characteristics of olaparib and other treatments available for patients with mCRPC are summarized in Table 3.
Table 3: Key Characteristics of Current Treatments for Patients With mCRPC
Characteristic | Olaparib | Abiraterone | Enzalutamide | Docetaxel |
|---|---|---|---|---|
Mechanism of action | PARP inhibitor | Androgen biosynthesis inhibitor | Androgen receptor pathway inhibitor | Microtubular depolymerization inhibitor |
Indicationa | As monotherapy for the treatment of adult patients with deleterious or suspected deleterious germline and/or somatic BRCA- or ATM-mutated mCRPC who have progressed following prior treatment with an NHA. BRCA or ATM mutations must be confirmed before olaparib treatment is initiated. Combination regimen of olaparib plus abiraterone is indicated for the treatment of adult patients with deleterious or suspected deleterious germline and/or somatic BRCA-mutated mCRPC in whom chemotherapy is not clinically indicated. | In combination with prednisone for the treatment of mCRPC in patients who:
| In the setting of medical or surgical castration for the treatment of patients with mCRPC who:
| In combination with prednisone or prednisolone for the treatment of patients with androgen-independent (hormone-refractory) metastatic prostate cancer |
Route of administration | Oral | Oral | Oral | IV |
Recommended dose | Combination regimen: Olaparib: 600 mg per day (2 × 150 mg tablets twice daily) Abiraterone: 1,000 mg once daily Prednisone or prednisolone: 5 mg twice daily | 1 g (2 × 500 mg tablets or 4 × 250 mg tablets) as a single dose used with 10 mg prednisone daily | 160 mg (4 × 40 mg capsules) as a single oral daily dose | 75 mg/m2 administered as a 1-hour infusion every 3 weeks. Concomitant treatment with prednisone or prednisolone 5 mg orally twice daily is administered continuously |
Serious adverse effects or safety issues | Boxed warnings regarding the risk of myelodysplastic syndrome or acute myeloid leukemia and pneumonitis | Boxed warnings regarding the risk of hypertension, hypokalemia, fluid retention, and hepatotoxicity | Boxed warnings regarding the risk of seizures and posterior reversible encephalopathy syndrome | Boxed warnings regarding the risk of toxic deaths, enterocolitis, hepatotoxicity, neutropenia, hypersensitivity reactions, and fluid retention |
ADT = androgen deprivation therapy; mCRPC = metastatic castration-resistant prostate cancer; NHA = new hormonal agent; PARP = poly(adenosine diphosphate ribose) polymerase.
aHealth Canada–approved indication.
Sources: Product monographs on olaparib,15 abiraterone,46 enzalutamide,45 and docetaxel.44
Stakeholder Perspectives
Patient Group Input
This section was prepared by the CADTH review team based on the input provided by patient groups. The full original patient inputs received by CADTH have been included in the Stakeholder Perspectives section of this report.
Two patient groups, the CCS and the CCSN, provided input for the review of olaparib used in combination with abiraterone and prednisone or prednisolone for mCRPC.
The CCS is a national charitable organization dedicated to improving the lives of all those affected by cancer, through research, advocacy, and support. The CCSN works to increase advocacy and to train patients and survivors to engage in the development of policy for optimal cancer care for patients, survivors, their families, and communities.
Information from the CCS was based on a survey of patients and caregivers in Canada that was open until April 27, 2023 (a start date was not provided). In total, 23 respondents provided their input. The CCSN gathered data on olaparib through an online survey that was open in Canada from May 10, 2023, to May 19, 2023. Of the 7 patient respondents, 1 had experience with olaparib.
Patients surveyed by the CCS reported that their disease and the pain associated with it had a negative effect on their HRQoL and their ability to perform day-to-day activities. For example, of the 23 respondents to the CCS survey, 70% reported that the disease had a moderate-to-significant impact on their ability to engage in sexual activity, 48% indicated that it had a moderate-to-significant impact on their ability to work, and 43% stated that it had a moderate-to-significant impact on their ability to exercise and maintain positive mental health. Respondents from the CCSN survey reported a negative impact of the disease on the physical, mental, HRQoL and day-to-day living aspects of patients and caregivers.
None of the 23 respondents to the CCS survey had experience with olaparib. The majority of respondents (91%) had received hormonal therapy, 73% received radiotherapy, 41% received surgery, 27% received chemotherapy, and 27% received corticosteroids. Most (65%) indicated that they had undergone 3 or more lines of therapy. The respondents also reported AEs as a result of their treatments, including but not limited to reduction in libido and sexual function (65%), hot flashes (65%), fatigue (52%), and weight changes (48%). The AEs described by the CCSN survey respondents were similar. When asked about barriers to receiving treatment, 65% of CCS survey respondents reported experiencing at least 1 barrier, with cost of transportation to appointments being the most frequently reported barrier, followed by lack of familiarity with the health care system and the financial burden of the disease. None of the patient inputs specified whether the treatments were received in the mCRPC setting only or since the patients’ initial diagnosis of prostate cancer.
Respondents from both patient group inputs described some of outcomes they would expect from a new treatment, namely affordability and accessibility of efficacious treatments with fewer side effects that can improve HRQoL, delay the onset of symptoms, prolong life, and provide a cure.
Clinician Input
Input From Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise in the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of prostate cancer.
Unmet Needs
The clinical experts indicated that for patients with mCRPC, which is an incurable disease, the most important goals of treatment are to prolong survival, relieve symptoms, and improve the patient’s quality of life. The experts identified these unmet needs associated with the current treatments for mCRPC: therapies that are curative, therapies that improve survival outcomes to a greater extent than the current treatments, and better-targeted therapies based on specific gene mutations. The experts also indicated that with the multiple lines of therapy available, there is a need for approaches to predict patients’ response to a specific treatment, as well as to determine the optimal sequence of the treatments for patients with mCRPC.
Place in Therapy
The clinical experts indicated that the current treatment options for adult patients with mCRPC include ARPIs (e.g., abiraterone and enzalutamide), chemotherapies (e.g., docetaxel or cabazitaxel), bone-targeted therapies (e.g., radium-223), PARP inhibitors (e.g., olaparib, niraparib, or rucaparib), and prostate-specific membrane antigen–targeted radionuclide therapy (e.g., lutetium vipivotide tetraxetan). ARPIs or docetaxel can be used as first-line therapy, while ARPIs, docetaxel, or radium-223 may be considered as second-line therapies, depending on what first-line therapy is used. Lutetium vipivotide tetraxetan, olaparib monotherapy (in patients with BRCA or ATM mutation), radium-223, or cabazitaxel can be used as third-line therapy. The experts also noted that in some patients, a combination of docetaxel and ARPI can be used as first-line treatment.
With the emergence of the combination regimen of olaparib plus abiraterone, and based on the study findings from the clinical trials (such as the PROpel trial), the experts expected that there would be a shift in the current treatment paradigm. The experts anticipated that the combination regimen will be considered as a first-line therapy option in patients with mCRPC, in particular for those patients with BRCA mutation. The experts also noted that the combination regimen necessitates the germline and/or somatic genomic testing in all patients with incurable prostate cancer. Therefore, the volume of testing for HRR or BRCA mutations would increase accordingly.
Patient Population
The clinical experts indicated that patients with BRCA mutations would be best suited for treatment with the combination of olaparib plus abiraterone and prednisone or prednisolone. The experts also noted that the disease would progress more rapidly and have worse prognosis in patients with BRCA mutations compared to those without BRCA mutations. Moreover, even though several dozen proteins are involved in HRR functionality, only the patients with BRCA-mutated cancers appear to benefit from the addition of PARP inhibitor therapy.
The experts noted that patients for whom chemotherapy is not clinically indicated include those who are deemed physically unfit (because they have, for example, poor renal function or poor performance status), those who refuse chemotherapy, or those who have received prior docetaxel treatment in the mCSPC phase. The clinical experts noted that the proportion of patients in the first-line mCRPC who are likely to be clinically indicated to receive chemotherapy was no greater than 10% to 15%. The experts also indicated that, for patients who may be clinically indicated to receive a taxane-based chemotherapy but who are unwilling to receive docetaxel or cabazitaxel, the combination of olaparib plus abiraterone would only be considered as a treatment option if the patients have a BRCA mutation.
The experts indicated that there is a lack of evidence to support the use of olaparib and ARPIs in patients with non–HRR-mutated cancers.
Assessing the Response Treatment
The clinical experts noted that in clinical practice, the criteria that are used to determine whether a patient with mCRPC is responding to treatment include prolonged survival, symptom (e.g., pain) relief, improved HRQoL, improved PSA response, and improved results on an imaging scan. Typically, these assessments are reviewed once a month after initiation of a new therapy for patients with mCRPC.
Discontinuing Treatment
According to the clinical experts consulted by CADTH, treatment with the combination of olaparib plus abiraterone would be discontinued if disease progression were detected, based on results of an imaging scan, PSA response, or worsening of symptoms, or if adverse effects of the treatment become intolerable.
Prescribing Considerations
The clinical experts noted that in general, all centres that can prescribe ARPIs are appropriate for providing treatment with the combination of olaparib plus abiraterone. Germline testing and/or somatic testing must be accessible in these centres, to assist in selecting the patients who are suitable for this treatment. In addition, due to the high rate of anemia and possible need of blood transfusions in patients receiving combination therapy, the centres should be able to quickly and efficiently provide patients with transfusions whenever required.
Clinician Group Input
This section was prepared by the CADTH review team based on the input provided by clinician groups. The full original clinician group inputs received by CADTH have been included in the Stakeholder Perspectives section of this report.
Two groups of clinicians responded to CADTH’s call for input: the OH-CCO Genitourinary Cancer Drug Advisory Committee (GU DAC), which provides timely evidence-based guidance on drug-related issues, and clinicians in Canada with expertise in managing advanced prostate cancer. Information for this input was collected through videoconferencing and emails with the OH-COO and through the gathered clinicians’ collective input.
According to the clinicians’ input, prostate cancer is not only among the most common cancers diagnosed, but it is the third leading cause of death from cancer among males in Canada. Those who experience debilitating disease and die from prostate cancer are all patients with mCRPC. The quick progression of the disease precludes eligibility for second-line therapies and beyond.
Both clinician groups stated that treatment options for patients with mCRPC, including androgen receptor-axis-targeted therapies such as abiraterone and enzalutamide, are the preferred first-line therapies. The OH-COO group stated that chemotherapies such as docetaxel are only used in some patients with good performance status, and radium-223 is restricted to symptomatic bone-only metastases after chemotherapy failure.
According to both clinician groups, mCRPC is an incurable disease; as such, treatment goals are typically focused on maintaining HRQoL and slowing the progression of metastatic disease. The clinicians’ group added that mCRPC patients cannot access second-line therapy due to various clinical factors. While androgen receptor-axis-targeted therapies are the preferred option, no single standard of care exists, and current treatment options do not offer curative intent; in addition, there are many safety and tolerability limitations. Effective treatments that are available early in the metastatic stage are lacking, with no effective combination therapy approved to date. Therefore, a new early treatment option that could also prolong the treatment duration of available therapies, delay disease progression, and improve long-term outcomes is warranted and critically needed.
Both clinician groups stated that olaparib added to abiraterone fulfills this unmet need for an effective and tolerable first-line combination. The clinicians stated that olaparib combines 2 known mechanisms of action that were already approved as monotherapies for patients with mCRPC and, as such, would be a novel treatment option for physicians to consider in first-line to manage the progression of mCRPC.
According to both clinician groups, patients with mCRPC in the first-line setting would be best suited for this regimen, especially those with BRCA mutation. In addition, the clinicians’ group indicated that this treatment also suit patients where docetaxel is not yet clinically indicated or those previously treated with docetaxel in the mCSPC setting.
The 2 clinician groups indicated that the most meaningful outcome of interest is radiographically assessed disease progression. Biochemical response via PSA and symptom improvement would also inform decision-making, according to the OH-CCO. The clinicians’ group added that improving HRQoL, compared to the current standard of care, for this patient population is another outcome of interest.
The 2 clinician groups noted that discontinuation of therapy should be considered in patients with disease progression or for those who cannot tolerate treatment. The OH-COO group indicated that treating patients with this drug should be limited to outpatient specialty clinics with training in advanced genitourinary oncology. The clinicians’ group mentioned that there is no anticipated change in the treatment setting, specialist visits, or monitoring requirements for patients, given that the individual components of the regimen are already available and funded for patients with mCRPC.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s Reimbursement Review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 4.
Table 4: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Relevant comparators | |
In the pivotal trial PROpel, the treatment effect of the combination of olaparib plus abiraterone was compared to the treatment effect of abiraterone. How does olaparib plus abiraterone compare to olaparib monotherapy? Enzalutamide is another comparator for the combination of olaparib plus abiraterone in the first-line setting of patients with mCRPC. How does olaparib plus abiraterone compare to enzalutamide? | The clinical experts indicated that currently, olaparib monotherapy is not a standard of care for patients with mCRPC in the first-line setting. There is a lack of direct evidence to explore the relative efficacy of olaparib plus abiraterone vs. olaparib monotherapy in the first-line setting. Also, there is no evidence to compare treatment of olaparib plus abiraterone with enzalutamide treatment in the first-line setting of patients with mCRPC. |
Considerations for initiation of therapy | |
In the PROpel trial, eligible patients had an ECOG PS of 0 or 1. Should the use of olaparib plus abiraterone be extended to patients with ECOG PS > 1? | The clinical experts suggested that generalizing the study findings of patients with ECOG PS of 0 or 1 to those with performance status of 2 should be done very cautiously. |
Considerations for discontinuation of therapy | |
In the PROpel trial, the study drug could be continued even after objective disease progression if the investigator considered that there was continuous clinical benefit, no serious toxicity, and no better alternative treatment available. What objective parameters should be used to determine when the patient should no longer be eligible for further treatment with olaparib plus abiraterone? | The clinical experts noted that in clinical practice, there is no single objective parameter to consider for treatment discontinuation. This treatment may be discontinued if the disease or symptoms cannot be adequately controlled or intolerable toxicities. However, if the patient can tolerate it, the treatment may continue even if the patient’s PSA level is rising slightly. If the patient plans to switch to a different therapy, the combination treatment of olaparib plus abiraterone should be stopped. |
Considerations for prescribing of therapy | |
In the PROpel trial, patients were allowed to continue on olaparib if abiraterone was discontinued (and vice-versa). Is this consistent with practice in Canada? Is evidence available to support this treatment regimen? Should this approach be allowed in public listing? | The clinical experts indicated that the main reason for treatment discontinuation is likely related to disease progression or intolerable toxicity. In this case, usually both agents would be discontinued in practice, unless there is a clear signal that the intolerable toxicity is linked to 1 of the agents. If 1 agent needs to be stopped, usually the clinician would stop olaparib first and keep abiraterone (as this is a traditional drug for prostate cancer that has been used for long time and is well-tolerated). The experts assumed that the evidence to support this treatment regimen (continue on olaparib, but discontinue abiraterone) may be from the PROfound study (an open-label RCT that compared olaparib monotherapy to enzalutamide or abiraterone in patients with mCRPC who progressed while receiving enzalutamide or abiraterone).30 This study found that patients in the second-line setting may benefit from olaparib monotherapy if previous abiraterone treatment had failed, which is supportive of the scenario of continuing olaparib even if abiraterone has been stopped. Given that this approach was allowed in the research protocol of the PROpel trial, the experts assumed that it is probably consistent with practice in Canada, since most clinicians would treat patients according to the protocol. The decision should be made on a case-by-case basis. |
Generalizability | |
For patients with mCRPC who are currently receiving first-line abiraterone treatment, can olaparib be added? | The experts noted that there is no evidence to support adding olaparib for patients who are already on first-line abiraterone treatment. If olaparib needs to be added, the experts suggested that the patient should only be on abiraterone for a shorter period of time, i.e., the addition of olaparib occurs within 3 months. |
Funding algorithm | |
In the PROpel trial, patients might have prior docetaxel treatment in the localized or mCSPC setting. Under what circumstances would first-line olaparib plus abiraterone be preferred over other available systemic treatment options? Is there evidence to support the treatment sequencing? | The experts indicated that for patients with a known BRCA1 or BRCA2 mutation, first-line olaparib plus abiraterone would be preferred over other available systemic treatment options, unless there is a contraindication or the patients could not tolerate the incremental toxicities related to the combination therapy. In terms of sequencing, the experts suggested that for patients with mCRPC with a BRCA1 or BRCA2 mutation, olaparib plus abiraterone can be given first, followed by radium-223, docetaxel, or cabazitaxel, which are less effective as combination therapy in this subgroup of patients. |
Care provision issues | |
Companion diagnostics: Does BRCA mutation need to be confirmed before olaparib therapy is initiated to align with Health Canada NOC? Are there instances where dual therapy is preferred over triplet therapy? | The clinical experts agreed that BRCA testing will likely become mandatory for the treatment for mCRPC. The experts noted that the availability of testing for BRCA mutations varies widely across jurisdictions in Canada. They anticipated that germline testing would be widespread much sooner because of its ease of use, while somatic testing will probably not be widely implemented for another 5 years. The experts also indicated that it is unlikely that a triplet therapy would be given in the first-line setting to patients with mCRPC. |
System and economic issues | |
PAG has concerns about the budget impact of this combination regimen. | Comment from the drug programs to inform pERC deliberations. |
Generic abiraterone is available. | Comment from the drug programs to inform pERC deliberations. |
ECOG PS = Eastern Cooperative Oncology Group Performance Status; mCRPC = metastatic castration-resistant prostate cancer; mCSPC = metastatic castration-sensitive prostate cancer; NOC = notice of compliance; PAG = Provincial Advisory Group; pERC = CADTH pan-Canadian Oncology Review Expert Review Committee; PSA = prostate-specific antigen; RCT = randomized controlled trial; vs. = versus.
Clinical Evidence
The objective of CADTH’s Clinical Review Report is to review and critically appraise the clinical evidence submitted by the sponsor on the beneficial and harmful effects of olaparib (100 mg and 150 mg, tablets, oral use) in combination with abiraterone and prednisone or prednisolone for the treatment of adult patients with deleterious or suspected deleterious germline and/or somatic BRCA-mutated mCRPC in whom chemotherapy is not clinically indicated. The focus is on comparing olaparib plus abiraterone to relevant comparators and identifying gaps in the current evidence.
A summary of the clinical evidence included by the sponsor in the review of olaparib in combination with abiraterone and prednisone or prednisolone is presented in 4 sections with CADTH’s critical appraisal of the evidence included at the end of each section. The first section, the systematic review, includes pivotal studies and RCTs that were selected according to the sponsor’s systematic review protocol. The second, third, and fourth sections include sponsor-submitted long-term extension studies, indirect evidence provided by the sponsor, and additional studies that were considered by the sponsor to address important gaps in the systematic review evidence, respectively; however, no studies relevant to these sections were submitted.
Included Studies
Clinical evidence from the following is included in the CADTH review and appraised in this document:
1 pivotal study identified in the systematic review (PROpel).21
Systematic Review
Contents within this section have been informed by materials submitted by the sponsor. The following have been summarized and validated by the CADTH review team.
Description of Studies
The PROpel trial is a phase III, randomized, double-blind, placebo-controlled, multicentre, international trial. The purpose of this study is to evaluate the efficacy and safety of the combination of olaparib plus abiraterone versus abiraterone in patients with mCRPC who have received no prior cytotoxic chemotherapy or NHAs at the mCRPC stage. Patients were randomized 1:1 centrally via Interactive Response Technology to either a combination of olaparib (300 mg twice daily) and abiraterone (1,000 mg once daily) and prednisolone or prednisone (5 mg twice daily) (n = 399) or placebo (matched to olaparib, twice daily) and abiraterone (1,000 mg once daily) and prednisolone or prednisone (5 mg twice daily) (n = 397). Randomization was stratified by site of different metastases (bone only versus visceral versus other) and prior treatment with taxane at metastatic hormone-sensitive prostate cancer (mHSPC) (yes versus no), but not by HRR status. The patient, the investigator, and study centre staff were blinded to study drug allocation. The primary efficacy end point in the PROpel trial was rPFS by investigator assessment of all randomized patients.
Three DCOs were planned for this study:
DCO1 (July 30, 2021): interim analysis of the primary end point (rPFS) and first interim analysis of the key secondary end point (OS)
DCO2 (March 14, 2022): final analysis of rPFS and second interim analysis of OS
DCO3 (October 12, 2022): final analysis of OS (expected to occur approximately 48 months after the first patient was randomized, when a minimum follow-up of 32 months would be expected)
Patients were eligible regardless of HRR status. In the PROpel trial, 14 genes were included in the aggregated HRR panel: ATM, BARD1, BRCA1, BRCA2, BRIP1, CDK12, CHEK1, CHEK2, FANCL, PALB2, RAD51B, RAD51C, RAD51D, and RAD54L. HRR mutation status by both tumour tissue test and a circulating tumour (ctDNA-based) test were determined after randomization and before the primary analysis.
Given that the Health Canada indication for olaparib combination therapy targets patients with deleterious or suspected deleterious BRCA-mutated mCRPC and that patients must have confirmation of BRCA mutation before treatment is initiated, this review focuses on the subgroup of patients with BRCA-mutated mCRPC only.
Characteristics of the PROpel trial are summarized in Table 5.
Table 5: Details of Study Included in the Systematic Review
Detail | PROpel |
|---|---|
Design and population | |
Study design | Phase III, double-blind, placebo-controlled, randomized trial |
Locations | 126 sites in 17 countries in Asia, Europe, North America (including 10 in Canada), and South America |
Patient enrolment dates | Start date: October 2018 End date: October 2022 |
Randomized (N) | N = 796 (85 with BRCA mutation) Olaparib plus abiraterone: 399 (47 with BRCA mutation) Abiraterone: 397 (38 with BRCA mutation) |
Inclusion criteria |
|
Exclusion criteria |
|
Drugs | |
Intervention | Olaparib, 300 mg (2 × 150 mg tablets) taken orally twice daily, in combination with abiraterone 1,000 mg taken orally once daily and prednisone or prednisolone 5 mg taken orally twice daily |
Comparator(s) | Matching placebo, 2 tablets (matched to olaparib) taken orally twice daily, in combination with abiraterone 1,000 mg taken orally once daily and prednisone or prednisolone 5 mg taken orally twice daily |
Study duration | |
Screening phase | 28 days |
Treatment phase | Tumour assessment according to RECIST 1.1 criteria for soft tissues and PCWG3 criteria for bone metastasis every 8 weeks (± 7 days) for 24 weeks and then every 12 weeks (± 7 days) relative to randomization date |
Follow-up phase | 30 days (± 7 days) after last dose of study treatment |
Outcomes | |
Primary end point | Investigator-assessed rPFS |
Secondary and exploratory end points | Secondary end points:
Exploratory end points:
|
Safety | AEs, SAEs, physical examination findings, vital signs, ECG findings, and lab rest results |
Publication status | |
Publications | Clarke Noel W, Armstrong Andrew J, Thiery-Vuillemin A, et al. Abiraterone and olaparib for metastatic castration-resistant prostate cancer. NEJM Evidence. 2022;0(0):EVIDoa2200043. Doi:10.1056/EVIDoa2200043. Saad F, Armstrong AJ, Thiery-Vuillemin A, et al. PROpel: Phase III trial of olaparib (ola) and abiraterone (abi) versus placebo (pbo) and abi as first-line (1L) therapy for patients (pts) with metastatic castration-resistant prostate cancer (mCRPC). Journal of Clinical Oncology. 2022/02/20 2022;40(6_suppl):11-11. Doi:10.1200/JCO.2022.40.6 suppl.011 Clinical trial registration (ClinicalTrials.gov): NCT03732820 |
ADT = androgen deprivation therapy; AE = adverse event; AML = acute myeloid leukemia; BICR = blinded independent central review; BP = blood pressure; BPI-SF = Brief Pain Inventory-Short Form; CTC = circulating tumour cell; CTCAE = Common Terminology Criteria for Adverse Events; CYP = cytochrome P450; dUCBT = double umbilical cord blood transplant; ECG = electrocardiogram; ECOG PS = Eastern Cooperative Oncology Group Performance Status; EQ-5D-5L = 5-level EQ-5D; FACT-P = Functional Assessment of Cancer Therapy – Prostate; FFPE = formalin-fixed paraffin-embedded; mcg = microgram; mCRPC = metastatic castration-resistant prostate cancer; MDS = myelodysplastic syndrome; ORR = objective response rate; OS = overall survival; PARP = poly(adenosine diphosphate ribose) polymerase; PCWG3 = Prostate Cancer Clinical Trials Working Group 3; PFS2 = second progression-free survival; PSA = prostate-specific antigen; PSA50 = prostrate-specific antigen response (proportion of patients achieving ≥ 50% decrease in PSA score from baseline to the lowest PSA result); RECIST 1.1 = Response Evaluation Criteria in Solid Tumours version 1.1; rPFS = radiological progression-free survival; SAE = serious adverse event; SSRE = symptomatic skeletal-related event; TFST = time to first subsequent anticancer therapy or death.
Source: PROpel DCO1 Clinical Study Report.21 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Populations
Inclusion and Exclusion Criteria
A summary of inclusion and exclusion criteria for the PROpel trial is provided in Table 5. Briefly, patients eligible for inclusion in this study were required to be aged at least 18 years, or 19 years in the Republic of South Korea. Patients had to have an ECOG PS 0 or 1, histologically or cytologically confirmed prostate adenocarcinoma with at least 1 documented metastatic lesion on a bone scan, CT, or MRI. With the exception of androgen deprivation therapy (ADT) and first-generation antiandrogen agents with a 4-week washout period, prior systemic treatment in the mCRPC first-line setting was not allowed.
First-line mCRPC was defined as:
Patients had to be treatment-naive at the mCRPC stage, with no cytotoxic chemotherapy, NHA, or other systemic treatment in the mCRPC setting. ADT was the exception (gonadotropin-releasing hormone analogue or bilateral orchiectomy within 28 days before randomization; patients receiving ADT at study entry should continue to do so throughout the study).
Treatment with first-generation antiandrogen agents (e.g., bicalutamide) before randomization was allowed, but a washout period of 4 weeks was required.
Docetaxel treatment was allowed during neoadjuvant or adjuvant treatment of localized prostate cancer and at the mHSPC stage.
Prior to the mCRPC stage, treatment with the second-generation antiandrogen agents (except for abiraterone) without PSA progression, clinical progression, or objective radiological disease progression during treatment was allowed, provided the treatment was stopped at least 12 months before randomization.
Key exclusion criteria were associated with underlying medical conditions, active infection, previous exposure to PARP inhibitors including olaparib, concomitant use of known strong CYP3A inhibitors or inducers, and poor performance status.
Interventions
In the PROpel trial, patients received olaparib 300 mg (2 × 150 mg tablets) twice daily plus abiraterone 1,000 mg once daily and prednisone or prednisolone 5 mg twice daily, or 2 placebo tablets (matched to olaparib) twice daily and abiraterone 1,000 mg once daily and prednisone or prednisolone 5 mg twice daily. Patients started treatment as soon as possible after randomization (ideally, within 24 hours of randomization), and continued treatment until objective radiological disease progression according to the investigator (using Response Evaluation Criteria in Solid Tumours version 1.1 [RECIST 1.1] criteria for soft tissue lesions47 and Prostate Cancer Clinical Trials Working Group 3 [PCWG3] criteria for bone lesions),24 occurrence of unacceptable toxicity, severe noncompliance with the protocol, or patient withdrawal of consent. Crossover from abiraterone to olaparib plus abiraterone was not allowed in this study.
Toxicities observed during the study could be managed by dose interruptions or reductions of olaparib. The dose of olaparib could be reduced to 250 mg twice daily, then to 200 mg twice daily, if needed. If a dose reduction to less than 200 mg twice daily was required, then olaparib was to be discontinued. Once the olaparib dose was reduced, it could not be re-escalated (except following treatment with CYP3A4 inhibitors). Toxicities related to abiraterone were managed by the investigators following locally applicable prescribing information.
At the end of the study, the patients could continue to receive treatment as open-labelled drug if they were continuing to derive benefit from olaparib. Following objective disease progression, further treatment options were at the discretion of the investigator. Patients were allowed to continue the study drug if there was continuous clinical benefit, no serious toxicities, and no better alternative treatment available.
During the study, patients could not receive any other concurrent anticancer therapy including chemotherapy, immunotherapy, radiotherapy (except for palliatives), biological therapy, or other novel agents. Live virus vaccines were not allowed either. The use of moderate or strong CYP3A inhibitors was restricted; if no suitable alternative was available, the dose of olaparib could be reduced during the period of concomitant administration. Olaparib could be re-escalated following washout of the CYP3A inhibitor.
Outcomes
A list of efficacy end points assessed in this Clinical Review Report is provided in Table 6; descriptions of the outcome measures follow. Summarized end points are based on outcomes included in the sponsor’s Summary of Clinical Evidence as well as any outcomes identified as important to this review according to the clinical experts consulted by CADTH and stakeholder input from patient and clinician groups and public drug plans. Using the same considerations, the CADTH review team selected end points that were considered to be most relevant to inform CADTH’s expert committee deliberations and finalized this list of end points in consultation with members of the expert committee. All summarized efficacy end points were assessed using GRADE. Certain notable harms outcomes considered important for informing CADTH’s expert committee deliberations were also assessed using GRADE.
Table 6: Outcomes Summarized From the PROpel Trial
Outcome measure | Time point | PROpel, overall population | PROpel, BRCAm subgroup analysis |
|---|---|---|---|
rPFS | Tumour imaging assessments were performed at baseline, and then every 8 weeks until week 24, and every 12 weeks thereafter, until objective radiological disease progression was confirmed by the investigator | Primary outcome in the overall study populationa HR, median rPFS, and rPFS rates reported at DCO1 and DCO2 rPFS rates reported at 6, 12, 18, 24, and 30 months for the overall population | Exploratory Ad-hoc subgroup analysis of the primary outcome HR and median rPFS reported at DCO1 and DCO2 No rPFS rates available at various time points |
OS | From randomization to study completion | Key secondary outcome in the overall study populationa HR and median OS reported at DCO1, DCO2, and DCO3. OS rates reported at 6, 12, 18, 24, 30, 36 and 42 months | Exploratory HR and median OS from the final OS analysis reported at DCO3 No OS rates available at various time points |
TFST | From randomization to study completion | Secondarya HR and median TFST reported at DCO1, DCO2, and DCO3 | Exploratory HR and median TFST reported at DCO3 |
SSRE | From randomization to study completion | Secondary HR and median SSRE reported at DCO1, DCO2, and DCO3 | Exploratory SSRE results not available |
ORR | From randomization to study completion Results at 24 weeks are reported | Exploratory ORR reported at DCO1 and DCO2 | Proportion of patients with ORR at DCO1 |
FACT-P | Every 4 weeks from day 1 until week 52, at week 52, then every 8 weeks, and at treatment discontinuation visit | Secondary Mean change from baseline in FACT-P total score reported at DCO1, DCO2, and DCO3 | Exploratory Results of FACT-P total score reported at DCO3 |
BPI-SF | To be completed by patients each day for 7 consecutive days every 4 weeks (not required to be at site), with day 1 as the baseline visit date | Secondary Mean change from baseline in BPI-SF scores reported at DCO1, DCO2 and DCO3 | Results of BPI-SF scores were not available |
PSA50 or time to PSA50 progression | Measured at baseline, at 1, 2, and 3 months, every 4 weeks thereafter, and at treatment discontinuation visit date | Exploratory Proportion of patients with PSA50 response reported at DCO1, DCO2, and DCO3 | Exploratory Results of patients with PSA50 response reported at DCO3 |
Safety | Measured at baseline, at every visit (every 2 weeks before week 13, every 4 weeks starting at week 13) and at treatment discontinuation visit date | Safety Results reported at DCO1, DCO2, and DCO3 | Exploratory Results reported at DCO3 |
Any AE | From date of informed consent until 30 days after the last dose of study treatment | Safety Results reported at DCO1, DCO2, and DCO3 | Exploratory Results reported at DCO3 |
Any SAE | From date of informed consent until 30 days after the last dose of study treatment | Safety Results reported at DCO1, DCO2, and DCO3 | Exploratory Results reported at DCO3 |
Mortality | From date of informed consent until 30 days after the last dose of study treatment | Safety Results reported at DCO1, DCO2, and DCO3 | Exploratory Results reported at DCO3 |
WDAE | From date of informed consent until 30 days after the last dose of study treatment | Safety Results reported at DCO1, DCO2, and DCO3 | Exploratory Results reported at DCO3 |
Notable harms:
| From date of informed consent until 30 days after the last dose of study treatment | Safety Results reported at DCO1, DCO2, and DCO3 | Exploratory Results reported at DCO3 |
AE = adverse event; AML = acute myeloid leukemia; BPI-SF = Brief Pain Inventory-Short Form; BRCAm = breast cancer susceptibility gene–mutated; DCO = data cut-off; FACT-P = Functional Assessment of Cancer Therapy – Prostate; HR = hazard ratio; MDS = myelodysplastic syndrome; ORR = objective response rate; OS = overall survival; PSA = prostate-specific antigen; rPFS = radiological progression-free survival; SAE = serious adverse event; SSRE = symptomatic skeletal-related event; TFST = time to first subsequent anticancer therapy or death; WDAE = withdrawal due to adverse event.
aStatistical testing for these end points was adjusted for multiple comparisons (e.g., hierarchal testing) in the overall population, but not in the BRCAm subpopulation. In the PROpel trial, all the subgroup analyses were considered exploratory as supportive of the primary analysis of rPFS.
Source: PROpel DCO1 Clinical Study Report.21 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Radiological Progression-Free Survival
Investigator-assessed rPFS was the primary efficacy outcome in the PROpel trial. This was defined as time from randomization until the earliest date of radiological progression or death from any cause, whichever occurred first. rPFS was also assessed by BICR, but the BICR assessments were not communicated to investigators, and patient management was based only on the investigators’ assessments.
Soft tissue lesions were assessed via CT or MRI scans according to RECIST 1.1 criteria,47 while bone lesions were assessed via bone scintigraphy according to PCWG3 criteria.24 Baseline assessments were performed as close as possible to treatment assignment (and no more than 28 days before treatment assignment). Subsequent assessments were performed every 8 weeks (± 7 days) until week 24 and every 12 weeks (± 7 days) thereafter, until objective radiological disease progression according to the investigator. After the initial assessment of progression, 1 follow-up scan was collected (preferably at the next scheduled imaging visit), regardless of whether the patient received subsequent therapy.
Overall Survival
OS was the key secondary efficacy outcome in the PROpel trial. It was defined as time from randomization to death from any cause. Assessments for survival were conducted every 12 weeks following objective disease progression or treatment discontinuation.
Time to First Subsequent Therapy
TFST was defined as time from randomization to the start of the first subsequent anticancer therapy or, if earlier, to death from any cause.
Symptomatic Skeletal-Related Event
An SSRE was defined as the use of radiation therapy to bone to prevent or relieve skeletal complications; occurrence of new symptomatic pathological bone fractures (vertebral or nonvertebral, resulting from minimal or no trauma); occurrence of radiologically confirmed spinal cord compression; or a tumour-related orthopedic surgical intervention. In the PROpel trial, this outcome was measured as time from randomization to the first SSRE.
Objective Response Rate
ORR was defined as the proportion of patients with measurable soft tissue or bone disease at baseline who had a tumour response (complete response and partial response) determined as overall radiological response assessed based on RECIST 1.1 (for soft tissue)47 or PCWG3 criteria (for bone),24 according to the investigator and BICR assessment. ORR was an exploratory outcome in the PROpel trial.
FACT-P Questionnaire
FACT-P is a disease-specific, 39-item questionnaire specifically developed for patients with advanced prostate cancer that has been found to be reliable and valid in this population.48 FACT-P is used to assess patients’ HRQoL and prostate cancer–specific symptoms. It consists of 5 subscales: physical well-being (7 items), functional well-being (7 items), emotional well-being (6 items) social well-being (7 items), and additional concerns specific to prostate cancer or the prostate cancer subscale (12 items). The internal consistency of the prostate cancer subscale ranged from 0.65 to 0.69. Construct validity was confirmed by the ability to discriminate patients by disease stage, performance status, and baseline PSA level. All FACT-P questions are scored on a 5-point Likert scale from 0 to 4 (0 being not at all and 4 being very much). Negatively stated items are reversed by subtracting the response from 4. For all subscales, symptoms index and individual item scores, the higher the score, the better the HRQoL or symptom. The MID for the FACT-P total score was estimated to be from 6 to 10.49
FACT-P total score was a secondary end point in the PROpel trial.
Brief Pain Inventory-Short Form
The BPI-SF is a 15-item domain-specific instrument designed to assess the severity of pain and the impact or interference of pain on daily functions. All BPI-SF pain items, including “worst pain,” are scored on a 0 to 10 numeric rating scale where 0 equals “no pain” and 10 equals “worst pain imaginable.” This instrument consists of 2 domains: pain severity and pain interference. The pain severity domain consists of 4 items (items 3, 4, 5, and 6) that assess pain at its “worst,” “least,” “average,” and “now” (current pain), respectively, on the 11-point numeric rating scale. These 4 items may be averaged as a composite pain severity score or they may be interpreted individually. Strong correlations between worst pain and average pain items (r = 0.79) and between the worst pain item and the current pain (r = 0.52) were observed. Good internal consistency reliability (Cronbach alpha ≥ 0.89 and intraclass correlation coefficient values ≥ 0.73) were reported in studies with patients with mCRPC.50,51 In the PROpel trial, the “worst pain” (item 3) was used as a single item in assessing pain progression. An MID for BPI-SF in the study population is not available.
This was a secondary end point in the PROpel trial. However, no BPI-SF results were reported for the BRCAm subgroup.
PSA50 Response
PSA50 response was the proportion of patients achieving a 50% or greater decrease in PSA from baseline to the lowest post-baseline PSA result, confirmed by a consecutive PSA assessment at least 3 weeks later. Time to PSA progression was defined as the time from randomization to PSA progression per PCWG-3 criteria. This was an exploratory outcome in the PROpel trial.
Safety
AEs, including SAEs, were collected from time of signature of informed consent form, throughout the treatment period, including study treatment discontinuation ( + 7 days of last study drug dose), and the 30-day ( + 7 days) follow-up after last study drug dose. The notable harms identified by the clinical experts consulted by CADTH for this review included myelodysplastic syndrome (MDS) or acute myeloid leukemia (AML), new primary malignancy other than MDS or AML, and pneumonitis.
Table 7: Summary of Outcome Measures and Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
FACT-P | The FACT-P is a questionnaire used to assess HRQoL in males with prostate cancer. The instrument was tested in 3 independent samples: a subscale development sample (n = 43), validity sample 1 (n = 34), and validity sample 2 (n = 96).48 The FACT-P consists of a 27-item self-reported questionnaire measuring general HRQoL in cancer patients, the FACT-G, and a 12-item prostate cancer subscale, the PCS, designed to measure prostate cancer–specific quality of life. The FACT-P total score includes the FACT-G and the PCS. A higher overall score indicates better HRQoL. The FACT-P total score ranges from 0 to 156.49 | Validity: Concurrent validity of the FACT-P instrument was confirmed by the ability to differentiate between prostate cancer patients by disease stage, performance status, and baseline PSA level.48 Reliability: Internal consistency of the PCS ranged from 0.65 to 0.69, with coefficients for FACT-G subscales and aggregated scores ranging from 0.61 to 0.90. The coefficients for FACT-G total score ranged from 0.85 to 0.87, and the range for FACT-P was from 0.87 to 0.89.48 Responsiveness: Sensitivity to change in performance status and PSA score over a 2-month period suggested that some subscales of the FACT-P (including the PCS) are sensitive to meaningful clinical change.48 | Clinically meaningful changes were estimated as 6 to 10 for FACT-P total score using both anchor- and distribution-based methods.49 |
FACT-G = Functional Assessment of Cancer Therapy – General; FACT-P = Functional Assessment of Cancer Therapy – Prostate; HRQoL = health-related quality of life; MID = minimal important difference; PCS = prostate cancer subscale; PSA = prostate-specific antigen.
Statistical Analysis
Sample Size and Power Calculation
Approximately 720 patients were planned to be randomized across about 200 study sites in about 20 countries worldwide; in total, 796 patients were randomized. DCO1 was planned to occur when approximately 379 progression or death events had accrued in 796 patients (47.6% of patients had an event [maturity]; information fraction = 83.7%) to provide 94.1% power to show a statistically significant difference in rPFS. DCO1 was anticipated to occur approximately 31 months after the first patient was randomized. Since the BRCAm subgroup is the focus of this review, the power calculation for the overall population is not relevant.
Statistical Testing
In the PROpel trial, descriptive statistics were used for all variables, as appropriate. Continuous variables were summarized by number of observations, mean, standard deviation (SD), median, upper and lower quartiles, and minimum and maximum values. For log-transformed data, geometric mean, coefficient of variation, and median, minimum, and maximum values were presented. Categorical variables were summarized by frequency counts and percentages for each category. Results of statistical analyses were presented in tables using corresponding 95% CIs and P values from 2-sided tests, where appropriate. In general, for efficacy end points, the last non-missing measurement before randomization was considered the baseline measurement. If an evaluable assessment was only available after randomization but before the first dose of randomized treatment, then this assessment was used as baseline. For safety and patient-reported outcomes, the last observation before the first dose of study treatment was considered the baseline measurement unless otherwise specified. Change from baseline variables were calculated as the posttreatment value minus the value at baseline. Percentage change from baseline was calculated as (post-baseline value minus baseline value) / baseline value × 100.
The primary end point of rPFS (according to the investigator) was analyzed using a log-rank test stratified by metastases (bone only versus visceral versus other) and docetaxel treatment at the mHSPC stage (yes versus no) (Table 8). For both the overall population and the BRCAm subgroup, the HR and corresponding 95% CI were estimated using a Cox proportional hazards model (with ties handled using the Efron approach and the stratification variables as covariates) and the 2-sided CI calculated using a profile likelihood approach. A Kaplan-Meier (KM) plot of rPFS was presented by treatment group. For each treatment group, the rPFS rate and its 95% CI were not reported for the BRCAm subgroup. The assumption of proportionality was assessed. In the presence of nonproportionality, the HR was to be interpreted as an average HR over the observed extent of follow-up. Proportionality was tested first by producing plots of complementary log-log (event times) versus log (time), and if these raised concerns, a time-dependent covariate was fitted to assess the extent to which this represented random variation. In the PROpel trial, patients who did not progress (e.g., who had a complete response, partial response, or stable disease according to RECIST 1.1 criteria or nonprogressive disease according to PCWG3 criteria) and had not died at the time of analysis were censored at the earliest date of their last evaluable RECIST 1.1 or bone scan assessment that showed no disease progression.
Analyses of secondary end points (e.g., OS, TFST, and HRQoL) used the same method as used for the analysis of rPFS.
Safety and tolerability data were summarized using descriptive measures.
Multiplicity
In the overall population, the primary end point of rPFS was formally analyzed at DCO1 and DCO2 using an O’Brien and Fleming spending function to control the overall 1-sided type I error rate at 2.5%. A multiplicity testing procedure, based on the graphical approach in group sequential trials of Maurer and Bretz, was applied to TFST, time to pain progression, and OS, to control the overall 1-sided type I error rate at 2.5%. However, multiplicity adjustments were not applied to the subgroup analyses in the BRCAm subpopulation.
Subgroup Analyses
In the PROpel trial, prespecified subgroup analyses of the rPFS primary end point were performed to assess the consistency of the treatment effect across potential or expected prognostic factors. The following subgroups of the full analysis set (FAS) were analyzed for rPFS:
metastases (bone only, visceral, or other)
docetaxel treatment at the mHSPC stage (yes or no)
HRR gene mutation (HRRm) status subgroup (HRRm, non-HRRm, unknown) based on a circulating tumour (ctDNA)-based test (FoundationOne Liquid CDx)
HRRm status subgroup (HRRm, non-HRRm, unknown) based on a tissue test (FoundationOne CDx)
HRRm status subgroup (HRRm, non-HRRm, unknown) based on a germline blood test (Myriad myRisk)
ECOG PS at baseline (0 or 1)
age at randomization (< 65 years, ≥ 65 years)
region (Asia, Europe, North and South America)
racial and/or ethnic identity (white, Black or African American, Asian, other)
baseline PSA (above or below median baseline PSA of the patients across both treatment groups).
As previously noted, subgroup analyses in the BRCAm subpopulation were the focus of the review of the PROpel trial based on the indication for olaparib that was approved by Health Canada. The HRs for investigator-assessed radiological progression (olaparib plus abiraterone versus abiraterone) and associated 2-sided CIs were estimated using a Cox proportional hazards model with the Efron method used for handling ties that contained the treatment term, factor, and treatment-by-factor interaction term. The HRs and 95% CIs were presented on a forest plot. No adjustment to the significance level for testing of subgroups was made, and these subgroup analyses were considered exploratory as supportive of the primary analysis of rPFS in the overall population.
In the PROpel trial, the proportion of patients with a BRCA mutation was 11% of the overall population (n = 85). Per the Health Canada–approved indication for olaparib plus abiraterone and the sponsor’s reimbursement request, the review of efficacy outcomes was limited to the patients with a BRCA mutation, while safety outcomes were reported for both the overall population and the BRCAm subgroup.
Sensitivity Analyses
Preplanned sensitivity analyses for rPFS were performed for the overall population in the PROpel trial (Table 8). No sensitivity analyses were performed for the BRCAm subgroup.
Table 8: Statistical Analysis of Efficacy End Points in the PROpel Trial
End point | Statistical model | Adjustment factors, handling of missing data, and sensitivity analyses |
|---|---|---|
rPFS (primary end point) |
| For the BRCAm subgroup:
|
OS |
| For the BRCAm subgroup:
|
TFST |
| For the BRCAm subgroup:
|
FACT-P |
| N/A |
ORR | Methods not specified | N/A |
PSA50 response | Methods not specified | N/A |
BRCAm = breast cancer susceptibility gene–mutated; FACT-P = Functional Assessment of Cancer Therapy – Prostate; KM = Kaplan-Meier; mHSPC = metastatic hormone-sensitive prostate cancer; MMRM = mixed model for repeated measures; N/A = not available; ORR = objective response rate; OS = overall survival; PSA = prostate-specific antigen; rPFS = radiological progression-free survival; TFST = time to first subsequent anticancer therapy or death.
Source: PROpel DCO1 Clinical Study Report.21 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Analysis Populations
The FAS was used as the primary population for reporting efficacy data. The FAS comprised all randomized patients.
The evaluable for response analysis set (EFR) consisted of patients with measurable disease at baseline as determined by investigator assessment and BICR assessment. This dataset was used in the analysis for ORR. The EFR is a subset of the FAS.
The safety analysis set (SAF) consisted of all randomized patients who received any amount of olaparib, placebo, or abiraterone. Patients were analyzed according to the treatment received.
The analysis population is summarized in Table 9.
Table 9: Analysis Populations of the PROpel Trial
Population | Definition | Application |
|---|---|---|
FAS | The FAS was used as the primary population for reporting efficacy data and to summarize demographic and patient baseline characteristics. This comprised all patients randomized into the study, to be analyzed according to randomized treatment (ITT principle). | All efficacy analyses |
EFR | This subset of the FAS had measurable disease at baseline, as per RECIST 1.1. Measurable disease was defined using the investigator assessment for analyses of investigator data and using BICR assessment data for analyses of BICR assessment. | Used to measure tumour response, radiological ORR, best objective response, disease control rate, and DOR |
SAF | The SAF consisted of all randomized patients who received any amount of olaparib, placebo, or abiraterone. Patients were analyzed according to the treatment received. | Used to measure duration of exposure, deaths, cumulative exposure over time, AEs, new primary malignancies, SAEs, CTCAEs |
AE = adverse event; BICR = blinded independent central review; CTCAE = Common Terminology Criteria for Adverse Events; DoR = ; duration of response; EFR = evaluable for response analysis set; FAS = full analysis set; ITT = intention to treat; ORR = objective response rate; RECIST 1.1 = Response Evaluation Criteria in Solid Tumours version 1; SAE = serious adverse event; SAF = safety analysis set.
Source: PROpel DCO1 Clinical Study Report.21 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Results
Patient Disposition
A summary of patient disposition at DCO3 (October 12, 2022) for the overall population is presented in Table 10. Overall, 399 patients were randomized to the olaparib plus abiraterone group and 397 to the abiraterone group. Of these, 47 patients in the olaparib plus abiraterone group and 38 in the abiraterone group had the BRCA mutation. At DCO3, 72.4% of patients in the olaparib plus abiraterone group and 80.1% in the abiraterone group had discontinued olaparib or placebo. The most common reasons for discontinuation in both groups were objective disease progression, followed by “Other” (e.g., clinical progression, PSA progression, death) and AEs. The olaparib plus abiraterone group reported a higher proportion of AEs, while the abiraterone group were more likely to report disease progression as a reason for treatment discontinuation. Among patients in either group who discontinued abiraterone only, the main reasons were objective disease progression and “Other.” Fewer patients in the olaparib plus abiraterone group than in the abiraterone group discontinued abiraterone due to disease progression.
There is no patient disposition information specific to the patients included in the BRCAm subgroup.
Table 10: Summary of Patient Disposition of All Patients in the PROpel Trial at DCO3
Patient disposition | Olaparib + abiraterone (N = 399) | Abiraterone (N = 397) |
|---|---|---|
Randomized, N (%) | 399 (100) | 397 (100) |
Discontinued olaparib or placebo at DCO3, N (%) | 288 (72.4) | 317 (80.1) |
Patient decision | 29 (7.3) | 19 (4.8) |
Adverse event | 61 (15.3) | 29 (7.3) |
Severe noncompliance to protocol | 3 (0.8) | 3 (0.8) |
Objective disease progression | 125 (31.4) | 186 (47.0) |
Lost to follow-up | 0 | 1 (0.3) |
Othera | 70 (17.6) | 79 (19.9) |
Due to COVID-19 pandemic | 0 | 0 |
Discontinued abiraterone at DCO3, N (%) | ||
Patient decision | 30 (7.5) | 22 (5.6) |
Adverse event | 37 (9.3) | 30 (7.6) |
Severe noncompliance to protocol | 4 (1.0) | 3 (0.8) |
Objective disease progression | 137 (34.4) | 183 (46.2) |
Lost to follow-up | 0 | 1 (0.3) |
Other | 80 (20.1) | 78 (19.7) |
Due to COVID-19 pandemic | 0 | 0 |
Patients ongoing treatment at DCO3, N (%) | 110 (27.6) | 79 (19.9) |
Ongoing both olaparib + placebo and abiraterone | 103 (25.9) | 77 (19.4) |
Discontinued olaparib + placebo alone | 7 (1.8) | 2 (0.5) |
Patient decision | 1 (0.3) | 0 |
Adverse event | 6 (1.5) | 2 (0.5) |
Due to COVID-19 pandemic | 0 | 0 |
FAS, n (%) | 399 (100) | 397 (100) |
EFR, n (%) | 161 (40.4) | 160 (40.3) |
SAF, n (%) | 399 (100) | 397 (100) |
DCO = data cut-off; EFR = evaluable for response analysis set; FAS = full analysis set; SAF = safety analysis set.
Note: DCO3 occurred on October 12, 2022.
a“Other” reason for discontinuation of treatment, as provided by the investigator, included (but were not limited to) clinical progression, PSA progression, and death.
Source: PROpel DCO3 Clinical Study Report.22 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Baseline Characteristics
In the overall population, the baseline patient characteristics were generally balanced between treatment groups, with some differences observed for age (32.6% in the olaparib plus abiraterone group versus 24.4% in the abiraterone group were younger than 65 years) and previous hormonal therapy (75.9% in the olaparib plus abiraterone group versus 81.9% in the abiraterone group received prior hormonal therapy).
In the PROpel trial, the prevalence of BRCA mutation was 11% (n = 85). Limited baseline characteristic data were reported for patients with a BRCA mutation, but there were notable baseline imbalances in the reported characteristics. Patients in the olaparib plus abiraterone group were younger (36.2% were aged < 65 years, versus 28.9% in the abiraterone group) and had higher Gleason scores (72.4% had a score of 8 to 10, versus 65.8% in the abiraterone group). Compared to the abiraterone group, a lower proportion of patients in the olaparib plus abiraterone group received docetaxel during the mCSPC phase (17.0% versus 26.3%), while a higher proportion had better performance status (76.6% versus 52.6% had an ECOG PS of 0).
A summary of baseline patient demographics and disease characteristics of the overall and BRCAm subgroup are presented in Table 11.
Table 11: Summary of Baseline Characteristics in the FAS and FAS BRCAm Subgroup of the PROpel Trial at DCO1
Characteristic | All patients | BRCAm subgroup | ||
|---|---|---|---|---|
Olaparib + abiraterone (N = 399) | Abiraterone (N = 397) | Olaparib + abiraterone (N = 47) | Abiraterone (N = 38) | |
Median age (years), range | 69.0 (43 to 91) | 70.0 (46 to 86) | 67.0 (43 to 83) | 70.0 (46 to 85) |
Age group (years), n (%) | ||||
< 65 | 130 (32.6) | 97 (24.4) | 17 (36.2) | 11 (28.9) |
> 65 | 269 (67.4) | 300 (75.6) | 30 (63.8) | 27 (71.1) |
Race, n (%) | ||||
White | 282 (70.7) | 275 (69.3) | NR | |
Black or African American | 14 (3.5) | 11 (2.8) | NR | |
Asian | 66 (16.5) | 72 (18.1) | NR | |
Native Hawaiian or Other Pacific Islander | 2 (0.5) | 0 | NR | |
American Indian or Alaska Native | 1 (0.3) | 0 | NR | |
Other | 12 (3.0) | 9 (2.3) | NR | |
Missing | 22 (5.5) | 30 (7.6) | NR | |
Weight (kg), mean (SD) | 83.6 (16.44) | 81.9 (15.69) | NR | |
Patients with any previous treatment modalities, n (%) | 365 (91.5) | 380 (95.7) | NR | |
Immunotherapy | 4 (1.0) | 3 (0.8) | NR | |
Hormonal therapy | 303 (75.9) | 325 (81.9) | NR | |
Cytotoxic chemotherapy | 98 (24.6) | 100 (25.2) | NR | |
Targeted therapy | 0 | 1 (0.3) | NR | |
Radiotherapy | 206 (51.6) | 194 (48.9) | NR | |
Other | 6 (1.5) | 4 (1.0) | NR | |
Histology type, n (%) | ||||
Adenocarcinoma | 398 (99.7) | 397 (100) | NR | |
Other | | ||||| | ||| | NR | |
Total Gleason score, n (%) | ||||
≤ 7 | 121 (30.4) | 134 (33.8) | 10 (21.3) | 12 (31.6) |
8 to 10 | 265 (66.4) | 258 (64.9) | 34 (72.4) | 25 (65.8) |
Missing | 13 (3.3) | 5 (1.3) | 3 (6.3) | 1 (2.6) |
Distant metastases according to TNM classification at diagnosis, n (%) | ||||
M0 | ||| |||||| | ||| |||||| | NR | |
MX | || ||||| | || ||||| | NR | |
M1 | ||| |||||| | ||| |||||| | NR | |
M1a | || ||||| | || ||||| | NR | |
M1b | || |||||| | || |||||| | NR | |
M1c | || ||||| | || ||||| | NR | |
Missing | 1 (0.3) | 1 (0.3) | NR | |
Time from initial diagnosis (months), mean (SD) | |||| ||||||| | |||| ||||||| | NR | |
Time from mCRPC to randomization (months), mean (SD) | ||| |||||| | ||| ||||||| | NR | |
Prior treatment with second-generation antiandrogen agents before mCRPC stage, n (%) | ||||
Yes (enzalutamide) | 1 (0.3) | 0 | NR | |
No | ||| |||||| | ||| ||||| | NR | |
Prior docetaxel treatment at mHSPC stage, n (%) | ||||
Yes | 90 (22.6) | 89 (22.4) | 8 (17.0) | 10 (26.3) |
Type of prostate cancer progression, n (%) | ||||
PSA progression | 172 (43.1) | 173 (43.6) | NR | |
Radiological progression | 92 (23.1) | 73 (18.4) | NR | |
Both | 134 (33.6) | 150 (37.8) | NR | |
Missing | 1 (0.3) | 1 (0.3) | NR | |
ECOG PS, n (%) | ||||
0 | 286 (71.7) | 272 (68.5) | 36 (76.6) | 20 (52.6) |
1 | 112 (28.1) | 124 (31.2) | 11 (23.4) | 18 (47.4) |
Missing | 1 (0.3) | 1 (0.3) | | ||||| | | ||| |
Baseline pain score (BPI-SF item 3 “worst pain” score), n (%) | ||||
0 (no pain) | 133 (33.3) | 137 (34.5) | 31 (66.0) | 26 (68.4) |
> 0 to < 4 (mild pain) | 151 (37.8) | 173 (43.6) | ||
4 to < 6 (moderate pain) | 53 (13.3) | 36 (9.1) | 15 (31.9) | 10 (26.3) |
≥ 6 (severe pain) | 32 (8.0) | 28 (7.1) | ||
Missing | 30 (7.5) | 23 (5.8) | 1 (2.1) | 2 (5.3) |
Baseline serum PSA (mcg/L), median (range) | |||| ||||| ||||||| | |||| |||||| ||||||| | 29.0 (NR) | 22.5 (NR) |
Site of distant metastases, n (%) | ||||
Bone only | ||| |||||| | ||| |||||| | 25 (53.2) | 20 (52.6) |
Visceral | || |||||| | || |||||| | 5 (10.6) | 8 (21.1) |
Other | ||| |||||| | ||| |||||| | 17 (36.2) | 10 (26.3) |
BPI-SF = Brief Pain Inventory-Short Form; BRCAm = breast cancer susceptibility gene–mutated; DCO = data cut-off; ECOG PS = Eastern Cooperative Oncology Group Performance Status; FAS = full analysis set; mCRPC = metastatic castration-resistant prostate cancer; mHSPC = metastatic hormone-sensitive prostate cancer; M0 = no distant metastasis; M1 = distant metastasis; mcg = microgram; MX = metastasis cannot be evaluated; NR = not reported; PSA = prostate-specific antigen; SD = standard deviation; TNM = tumour, node, metastasis.
Sources: PROpel DCO1 Clinical Study Report,21 and Oncologic Drugs Advisory Committee Briefing Document.23 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Exposure to Study Treatments
In the overall population, the median duration of exposure was 564 days in the olaparib plus abiraterone group and 477 days in the abiraterone group. In the BRCAm subgroup, the median duration of treatment was 957 days and 300 days in the olaparib plus abiraterone and abiraterone groups, respectively.
Efficacy
Only those efficacy outcomes identified as important to this review are reported. The main findings presented for the BRCAm subgroup in the PROpel trial are from DCO1 (time of the primary rPFS analysis; July 30, 2021) and DCO3 (October 12, 2022).
Table 12: Summary of Patient Exposure in the SAF and SAF BRCAm Subgroup of the PROpel Trial at DCO3
Exposure | All patients | BRCAm subgroup | ||
|---|---|---|---|---|
Olaparib + abiraterone (N = 398) | Abiraterone (N = 398) | Olaparib + abiraterone (N = 47) | Abiraterone (N = 38) | |
Total treatment (days) | ||||||| | ||||||| | NR | NR |
Duration (days), median (range) | 564.0 (NR) | 476.5 (NR) | 957.0 (NR) | 300.0 (NR) |
BRCAm = breast cancer susceptibility gene–mutated; DCO = data cut-off; NR = not reported; SAF = safety analysis set.
Note: DCO3 occurred on October 12, 2022.
Sources: PROpel DCO3 Clinical Study Report22 and Oncologic Drugs Advisory Committee Briefing Document.23 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Radiographic Progression-Free Survival
The rPFS is the primary efficacy outcome in the PROpel trial. In the BRCAm subgroup at DCO1 (July 30, 2021), the median duration of follow-up in all patients was |||| months on the olaparib plus abiraterone group and |||| months on the abiraterone group. The median duration of follow-up for patients in the BRCAm subgroup was not reported.
At the time of the DCO1, 14 (29.8%) patients in the olaparib plus abiraterone group and 28 (73.7%) in the abiraterone group had experienced a rPFS event per the investigator’s assessment. The HR for investigator-assessed rPFS was 0.23 (95% CI, 0.12 to 0.43). The median rPFS was not reached (95% CI, not reported) in the olaparib plus abiraterone group and was 8.4 months (95% CI, not reported) in the abiraterone group. KM estimates of the probability of rPFS in each group at clinically relevant follow-up times were not reported.
The BICR-assessed rPFS was consistent with the investigator-assessed rPFS. The HR was 0.18 (95% CI, 0.09 to 0.34). The median rPFS was not reached (95% CI, not reported) in the olaparib plus abiraterone group and was 8.4 months (95% CI, not reported) in the abiraterone group.
The percentage of patients alive and without disease progression over time was not reported in this subgroup.
Note that rPFS analysis was formally performed at DCO1. At DCO2, formal rPFS analysis was not performed and analysis at this point was considered descriptive only. A final exploratory analysis of rPFS was performed at DCO3.
Table 13: Summary of rPFS Results in the FAS BRCAm Subgroup of the PROpel Trial at DCO1
Primary outcome: investigator-assessed rPFSa | Olaparib + abiraterone (n = 47) | Abiraterone (n = 38) |
|---|---|---|
Events,a n (%) | 14 (29.8) | 28 (73.7) |
Censored patients, n (%) | NR | |
No post-baseline assessment | NR | |
HR (95% CI)b | 0.23 (0.12 to 0.43) | |
Median rPFS, months (95% CI) | Not reached | 8.38 (NR to NR) |
Rate of rPFS at various time points, % (95% CI) | NR | |
BRCAm = breast cancer susceptibility gene–mutated; CI = confidence interval; DCO = data cut-off; FAS = full analysis set; HR = hazard ratio; mHSPC = metastatic hormone-sensitive prostate cancer; NR = not reported; rPFS = radiological progression-free survival.
Note: DCO1 occurred on July 30, 2021.
aFurther analyses on rPFS post DCO1 (primary end point) are considered exploratory only.
bHR and CI calculated using a Cox proportional hazards model adjusted for the variables selected in the primary pooling strategy: metastases (bone only, visceral, other) and docetaxel treatment at mHSPC stage. The Efron approach was used for handling ties. HR < 1 favours olaparib with abiraterone.
Source: Oncologic Drugs Advisory Committee Briefing Document.23
Figure 1: rPFS Change in the FAS BRCAm Subgroup of the PROpel Trial Based on Investigator Assessment and BICR
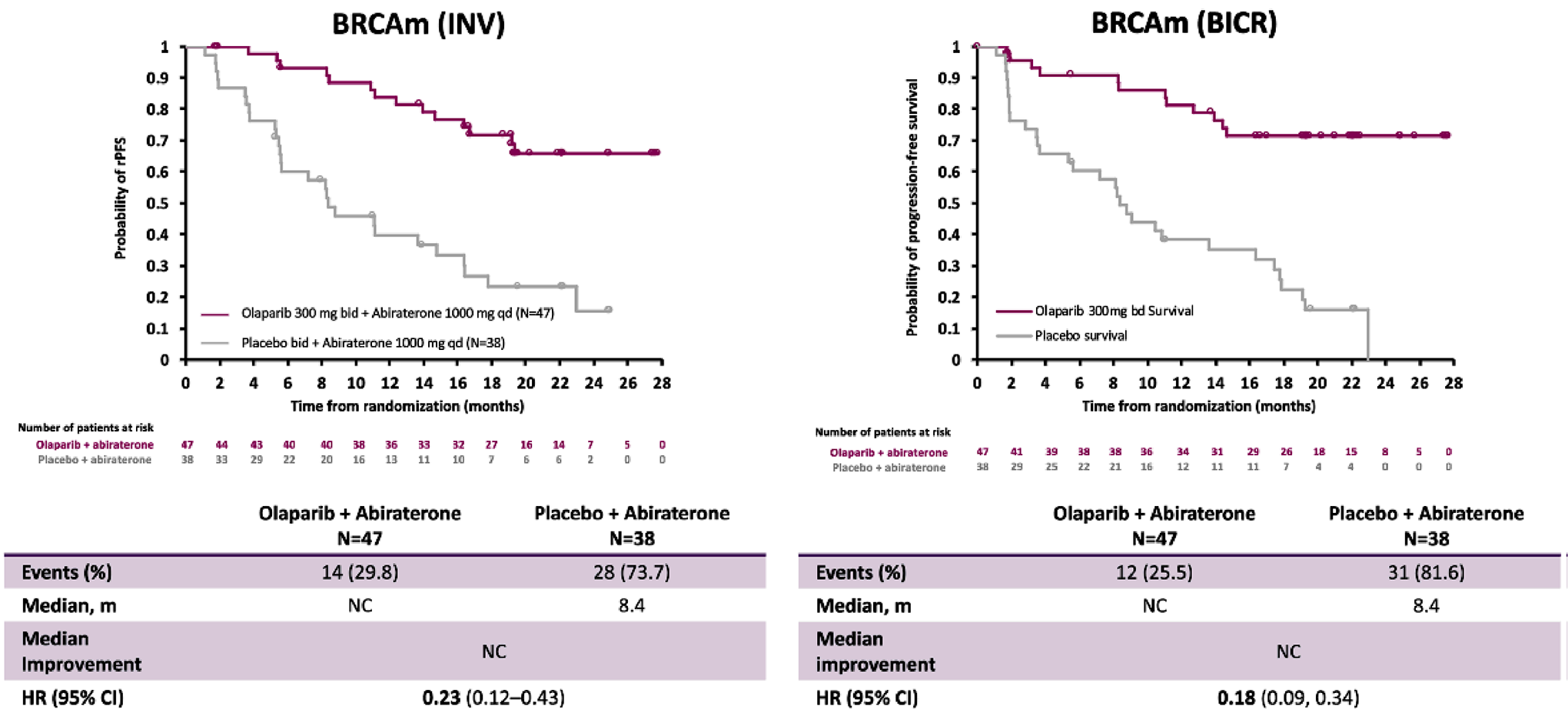
BICR = blinded independent central review; bid = twice daily; BRCAm = breast cancer susceptibility gene–mutated; CI = confidence interval; DCO = data cut-off; FAS = full analysis set; HR = hazard ratio; INV = investigator assessment; m = months; NC = not calculable/calculated; qd = once daily; rPFS = radiological progression-free survival.
Note: DCO1 occurred on July 30, 2021.
Source: Oncologic Drugs Advisory Committee Briefing Document.23
Overall Survival
At final analysis of OS at DCO3 (October 12, 2022), 13 (27.7%) patients in the olaparib plus abiraterone group and 25 (65.8%) in the abiraterone group had experienced an event. Results from the analyses in the BRCAm subgroup showed that the HR was 0.29 (95% CI, 0.14 to 0.56). The median OS was not reached (95% CI not reported) in the olaparib plus abiraterone group and was 23.0 (95% CI not reported) months in the abiraterone group. KM estimates of the probability of survival in each group at clinically relevant follow-up times were not reported.
The survival rate over time was not reported in this subgroup.
Table 14: Summary of OS Results in the FAS BRCAm Subgroup of the PROpel Trial at DCO3
Results | Olaparib with abiraterone (n = 47) | Placebo with abiraterone (n = 38) |
|---|---|---|
Deaths, n (%) | 13 (27.7) | 25 (65.8) |
Median OS, months a | Not reached | 22.97 |
HR (95% CI) b | 0.29 (0.14 to 0.56) | |
Rate of OS at various time points, % (95% CI) | NR | |
BRCAm = breast cancer susceptibility gene–mutated; CI = confidence interval; DCO = data cut-off; FAS = full analysis set; HR = hazard ratio; mHSPC = metastatic hormone-sensitive prostate cancer; NR = not reported; OS = overall survival.
Note: DCO3 occurred on October 12, 2022.
aCalculated using the Kaplan-Meier technique.
bHR and CI were calculated using a Cox proportional hazards model adjusted for the variables selected in the primary pooling strategy: metastases (bone only, visceral, other) and docetaxel treatment at mHSPC stage. The Efron approach was used for handling ties. HR < 1 favours olaparib with abiraterone.
Source: Oncologic Drugs Advisory Committee Briefing Document.23
Time to First Subsequent Anticancer Therapy or Death
At DCO3 (October 12, 2022), in the BRCAm subgroup, 24 (51.1%) patients in the olaparib plus abiraterone group and 30 (78.9%) in the abiraterone group had experienced a TFST event. The HR of TFST was 0.35 (95% CI, 0.21 to 0.61). The median TFST was 37.39 months (95% CI, not reported) in the olaparib plus abiraterone group and 14.75 months (95% CI, not reported) in the abiraterone group. KM estimates of the probability of a TFST event in each group at clinically relevant follow-up times were not reported.
Symptomatic Skeletal-Related Event
No data were available for the BRCAm subgroup.
Objective Response Rate
At DCO1 (July 30, 2021), there were 20 (42.6%) evaluable patients in the olaparib plus abiraterone group and 15 (39.5%) in the abiraterone groups. Of these patients, the proportion who achieved complete response or partial response was 50.0% (n = 10 out of 20) in the olaparib plus abiraterone group and 26.7% (n = 4 of 15) in the abiraterone group. Neither relative nor absolute between-group differences in tumour response rates were reported.
ORR results were available at DCO1 only.
Figure 2: OS Change in the FAS BRCAm Subgroup of the PROpel Trial
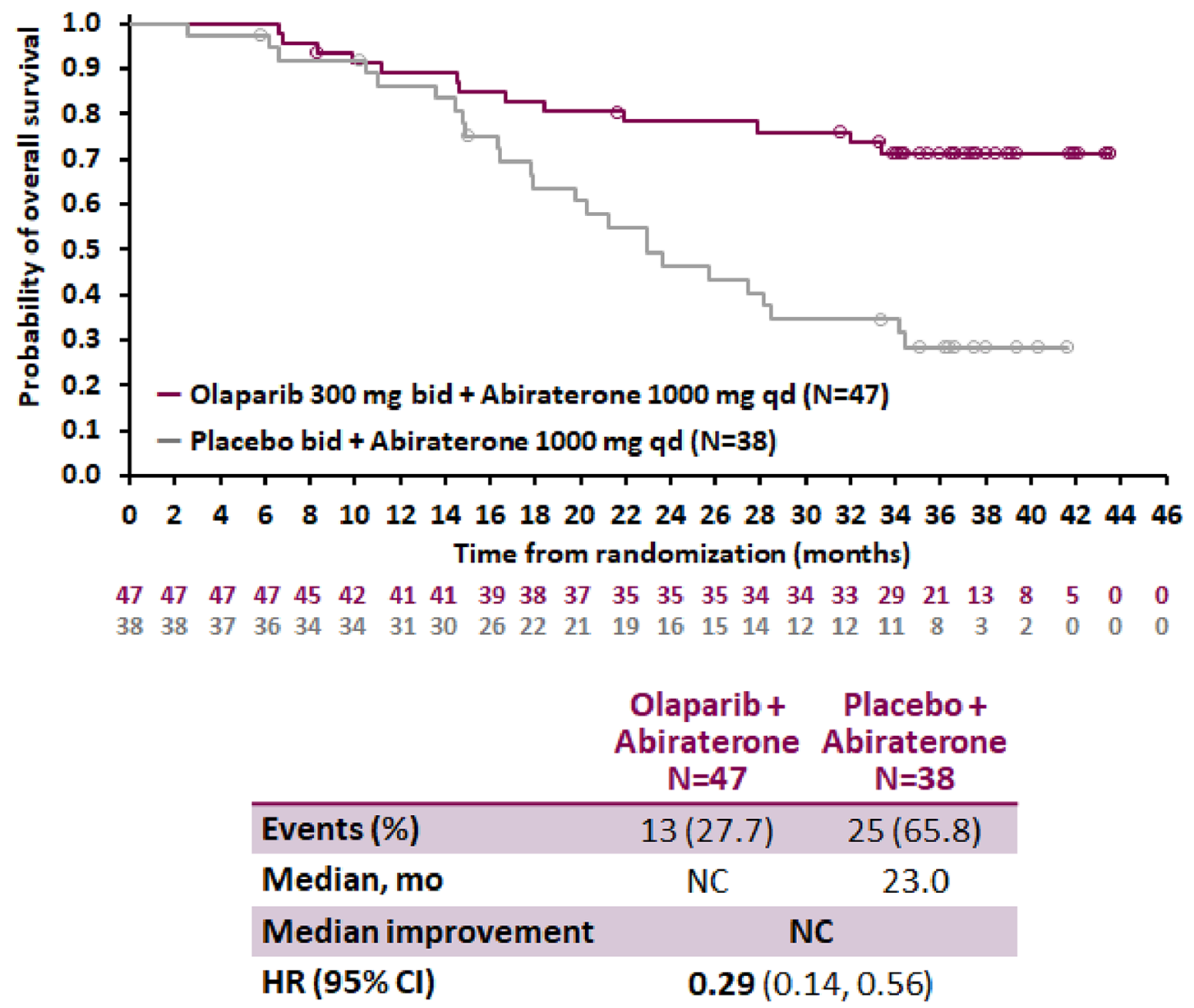
bid = twice daily; BRCAm = breast cancer susceptibility gene–mutated; CI = confidence interval; DCO = data cut-off; FAS = full analysis set; HR = hazard ratio; mo = months; NC = not calculable/calculated; OS = overall survival; qd = once daily.
Note: DCO3 occurred on October 12, 2022.
Source: Oncologic Drugs Advisory Committee Briefing Document.23
Table 15: Summary of TFST Results in the FAS BRCAm Subgroup in the PROpel Trial at DCO3
Results | Olaparib + abiraterone (n = 47) | Abiraterone (n = 38) |
|---|---|---|
Number of events, n (%) | 24 (51.1) | 30 (78.9) |
Median TFST (months)a | 37.39 | 14.75 |
HR (95% CI)b | 0.35 (0.21 to 0.61) | |
BRCAm = breast cancer susceptibility gene–mutated; CI = confidence interval; DCO = data cut-off; mHSPC = metastatic hormone-sensitive prostate cancer; TFST = time to first subsequent therapy or death; HR = hazard ratio.
Note: DCO3 occurred on October 12, 2022.
aCalculated using the Kaplan-Meier technique.
bHR and CI were calculated using a Cox proportional hazards model adjusted for the variables selected in the primary pooling strategy, i.e., metastases (bone only, visceral, other) and docetaxel treatment at mHSPC stage. The Efron approach was used for handling ties. HR < 1 favours olaparib with abiraterone.
Source: Oncologic Drugs Advisory Committee Briefing Document.23
Table 16: Summary of ORR Results in the EFR BRCAm Subgroup of the PROpel Trial at DCO1
Results | Olaparib + abiraterone (N = 47) | Abiraterone (N = 38) |
|---|---|---|
Patients in the EFR, n | 20 | 15 |
Proportion of patients with ORR, n (%) | 10 (50.0) | 4 (26.7) |
Odds ratio (95% CI) | NR | |
P value | NR | |
BRCAm = breast cancer susceptibility gene–mutated; CI = confidence interval; DCO = data cut-off; EFR = evaluable for response analysis set; ORR = objective response rate.
Notes: ORR was an exploratory outcome in the PROpel trial. Descriptive statistics were reported for this outcome.
DCO1 occurred on July 30, 2021.
Source: Oncologic Drugs Advisory Committee Briefing Document.23
Functional Assessment of Cancer Therapy – Prostate
At DCO3, in the BRCAm subgroup, the change from baseline in the FACT-P total score was 2.43 (standard error [SE] not reported) in the olaparib plus abiraterone group and –1.21 (SE not reported) in the abiraterone group. The between-group difference in the change from baseline was not reported.
There was no information available on the percentage of patients that completed the questionnaire at DCO3. In the overall population, the completion rate was 69.8% in the olaparib plus abiraterone group and 74.5% in the abiraterone group at DCO3.
Table 17: Summary of FACT-P Results at DCO3 in the FAS BRCAm Subgroup in the PROpel Trial
Results | Olaparib + abiraterone (N = 47) | Abiraterone (N = 38) |
|---|---|---|
Change from baseline, LSM (SE) | 2.43 (NR)a | –1.21 (NR) |
Difference in LSM (95% CI) | NR | |
2-sided P value | NR | |
BRCAm = breast cancer susceptibility gene–mutated; DCO = data cut-off; FACT-P = Functional Assessment of Cancer Therapy – Prostate; FAS = full analysis set; LSM = least squares mean; mHSPC = metastatic hormone-sensitive prostate cancer; SE = standard error.
Notes: FACT-P total score change from baseline values can range from a minimum of –156 to a maximum of 156. A clinically meaningful change value of 10 points was implemented in PROpel for the FACT-P total score–based end point.
DCO3 occurred on October 12, 2022.
aThe analysis was performed using a mixed model for repeated measures with treatment, visit, treatment-by-visit interaction, baseline FACT-P total score, and baseline-score-by-visit interaction, metastases and docetaxel treatment at mHSPC stage as fixed effects.
Source: Oncologic Drugs Advisory Committee Briefing Document.23
Brief Pain Inventory-Short Form
No data were available for the BRCAm subgroup.
PSA50 Response
Forty-seven (100%) patients in the olaparib plus abiraterone group and 37 (97.4%) in the abiraterone group had PSA results at baseline, and were included in the analysis of PSA50 response. At DCO1 (July 30, 2021), the proportion of patients with a PSA50 response was 85.1% in the olaparib plus abiraterone group and 51.4% in the abiraterone group. Neither relative nor absolute between-group differences in PSA50 response rates were reported.
PSA50 response results were available at DCO1 only.
Table 18: Summary of PSA50 Response Results at DCO1 in the FAS BRCAm Subgroup in the PROpel Trial
Results | Olaparib + abiraterone (N = 47) | Abiraterone (N = 38) |
|---|---|---|
Patients with a PSA result at baseline, n (%) | 47 (100) | 37 (97.4) |
Patients with confirmed response, n (%) | 40 (85.1) | 19 (51.4) |
BRCAm = breast cancer susceptibility gene–mutated; DCO = data cut-off; FAS = full analysis set; PSA = prostate-specific antigen.
Notes: PSA50 response was an exploratory outcome in the PROpel trial. Descriptive statistics were reported for this outcome.
DCO1 occurred on July 30, 2021.
Source: Oncologic Drugs Advisory Committee Briefing Document.23
Harms
Harms data reported for the SAF and the BRCAm subgroup of the SAF at DCO3 (October 12, 2022) are summarized in Table 19.
Adverse Events
In the overall population, the proportion of patients who experienced at least 1 AE was 97.7% in the olaparib plus abiraterone group and 96.0% in the abiraterone group. For the BRCAm subgroup, the proportion of patients who experienced at least 1 AE was 100% in the olaparib plus abiraterone group and 89.5% in the abiraterone group. Commonly reported AEs in the BRCAm subgroup included anemia (100%), fatigue (40.4%), nausea (40.4%), back pain (27.7%), and arthralgia (23.4%) (percentages shown are for the olaparib plus abiraterone group).
Serious Adverse Events
In the overall population at DCO3, 161 patients (40.5%) in the olaparib plus abiraterone group and 126 patients (31.8%) in the abiraterone group experienced 1 or more SAEs. Infections and infestations were the most common SAE in the olaparib plus abiraterone group, with ||||| versus ||||| in the abiraterone group. Other SAEs occurred infrequently in either group.
In the BRCAm subgroup, 29.8% of the patients in the olaparib plus abiraterone group and 31.6% of the patients in the abiraterone group reported at least 1 SAE. Data related to specific SAEs were not reported.
Withdrawals Due to Adverse Events
In the overall population at DCO3, 69 patients (17.3%) in the olaparib plus abiraterone group and 34 patients (8.6%) in the abiraterone group discontinued treatment with olaparib or placebo due to an AE. In the overall population, 45 patients (11.3%) in the olaparib plus abiraterone group and 37 patients (9.3%) in the abiraterone group discontinued abiraterone due to AEs.
In the BRCAm subgroup, the proportion of patients who discontinued olaparib or placebo due to AEs was 12.8% in the olaparib- abiraterone group and 10.5% in the abiraterone group. Three patients (6.4%) in the olaparib plus abiraterone group and 4 (10.5%) in the abiraterone group discontinued abiraterone due to AEs. The AEs that led to treatment discontinuations were not reported.
Mortality
In the overall population, AEs leading to death were reported for 6.5% of patients (n = 26 out of 398) in the olaparib plus abiraterone group and 5.1% (n = 20 out of 396) in the abiraterone group. Infections and infestations were a common reason for AEs leading to death, occurring for |||| patients in the olaparib plus abiraterone group and |||| in the abiraterone group.
In the BRCAm subgroup, AEs leading to death occurred for 1 (2.1%) patient in the olaparib plus abiraterone group and 2 (5.3%) patients in the abiraterone group. The AEs that resulted in death in either group were no reported.
Table 19: Summary of Harms Results in the SAF and the SAF BRCAm Subgroup of the PROpel Trial at DCO3
Adverse events | All patients | BRCAm subgroup | ||
|---|---|---|---|---|
Olaparib + abiraterone (n = 398) | Abiraterone (n = 396) | Olaparib + abiraterone (n = 47) | Abiraterone (n = 38) | |
AEs, n (%)a | ||||
≥ 1 AE | 389 (97.7) | 380 (96.0) | 47 (100) | 34 (89.5) |
Anemia | 197 (49.5) | 69 (17.4) | 47 (100.0) | 34 (89.5) |
Fatigue | 114 (28.6) | 81 (20.5) | 19 (40.4) | 5 (13.2) |
Nausea | 122 (30.7) | 57 (14.4) | 19 (40.4) | 7 (18.4) |
Back pain | 86 (21.6) | 79 (19.9) | 13 (27.7) | 8 (21.1) |
Arthralgia | 58 (14.6) | 77 (19.4) | 11 (23.4) | 7 (18.4) |
SAEs, n (%)b | ||||
Patients with ≥ 1 SAE | 161 (40.5) | 126 (31.8) | 14 (29.8) | 12 (31.6) |
Infections and infestations | || |||||| | || |||||| | NR | NR |
COVID-19 | 15 (3.8) | 10 (2.5) | NR | NR |
COVID-19 pneumonia | 7 (1.8) | 3 (0.8) | NR | NR |
Pneumocystis jirovecii pneumonia | 4 (1.0) | 0 | NR | NR |
Pneumonia | 11 (2.8) | 5 (1.3) | NR | NR |
Withdrawals due to adverse events, n (%) | ||||
Any AE leading to discontinuation of olaparib or placebo | 69 (17.3) | 34 (8.6) | 6 (12.8) | 4 (10.5) |
Any AE leading to discontinuation of abiraterone | 45 (11.3) | 37 (9.3) | 3 (6.4) | 4 (10.5) |
COVID-19 | | ||||| | ||| | NR | NR |
Pneumocystis jirovecii pneumonia | | ||||| | ||| | NR | NR |
Pneumonia | | ||||| | ||| | NR | NR |
Blood and lymphatic system disorders | || ||||| | | ||||| | NR | NR |
Anemia | || ||||| | | ||||| | NR | NR |
Deaths, n (%) | ||||
Total deaths | 176 (44.1) | 205 (51.6) | 13 (27.7) | 25 (65.8) |
AEs leading to death | 26 (6.5) | 20 (5.1) | 1 (2.1) | 2 (5.3) |
Infections and infestations | | ||||| | | ||||| | NR | NR |
Neoplasms benign, malignant and unspecified (including cysts and polyps) | ||| | | ||||| | NR | NR |
Nervous system disorders | ||| | | ||||| | NR | NR |
Cardiac disorders | | ||||| | | ||||| | NR | NR |
Respiratory, thoracic, and mediastinal disorders | | ||||| | | ||||| | NR | NR |
AE of special interest, n (%) | ||||
MDS or AML | 2 (0.5) | 0 | NR | NR |
New primary malignancies other than MDS or AML | 18 (4.5) | 14 (3.5) | NR | NR |
Pneumonitis | 5 (1.3) | 3 (0.8) | NR | NR |
Pulmonary embolism | 29 (7.3) | 9 (2.3) | 5 (10.6) | 0 |
AE = adverse event; AML = acute myeloid leukemia; BRCAm = breast cancer susceptibility gene–mutated; DCO = data cut-off; MDS = myelodysplastic syndrome; NR = not reported; SAE = serious adverse events; SAF = safety analysis set.
aSpecific AEs that occurred with a frequency of ≥ 15% in either group are presented in this table.
bSpecific SAEs that occurred with a frequency of ≥ 1% in either group are presented in this table.
Sources: PROpel DCO3 Clinical Study Report,22 and Oncologic Drugs Advisory Committee Briefing Document.23 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Notable Harms
The clinical experts consulted by CADTH identified the risks of MDS or AML, other new primary malignancies, pulmonary embolism, and pneumonitis as notable harms. Up to DCO3, there were 2 patients with MDS events in the olaparib plus abiraterone group and no patients with MDS or AML events in the abiraterone group; and 18 patients (4.5%) with AEs classified as “new primary malignancies other than MDS or AML” in the olaparib plus abiraterone group and 14 patients (3.5%) with these AEs in the abiraterone group. Pulmonary embolism was reported in 29 patients (7.3%) in the olaparib plus abiraterone group and 9 patients (2.3%) in the abiraterone group.
In the BRCAm subgroup, 5 (10.6%) patients in the olaparib plus abiraterone group reported pulmonary embolism. No patients in the abiraterone group experienced this notable harm. The frequency of occurrence of other notable harms were not reported for this subgroup of patients.
Critical Appraisal
Internal Validity
PROpel was a generally well conducted phase III, double-blind, multicentre RCT. The randomization was stratified on relevant prognostic factors, with the exception of BRCA mutation status. However, data from a subgroup of patients in the PROpel trial with a BRCA mutation are the most relevant evidence available at this time to inform the review of olaparib as per the indication approved by Health Canada. The small sample size of the BRCAm subgroup and imbalances in patient characteristics at baseline represent key limitations to the subgroup analysis of the PROpel trial.
Although the PROpel trial included approximately 800 patients, only 85 patients had a BRCA mutation, 47 in the olaparib plus abiraterone group and 38 in the abiraterone group. The trial was powered to detect a statistical difference in rPFS in the overall population; details about the trial’s power to detect differences in rPFS in the relevant subgroup were not reported.
Prognostic balance cannot be ensured across treatment groups in this subgroup of patients as the randomization was not stratified by BRCA mutation status. There was an imbalance between the treatment groups based on several patient baseline characteristics, such as age, baseline pain scores, baseline Gleason score, and location of metastases. Patients in the olaparib plus abiraterone treatment group tended to be younger and to have more higher levels of pain (moderate or severe), fewer visceral metastases but more “other” metastases, and better performance status. As such, there is a risk of bias arising from the randomization process; however, it is unclear how these factors in combination may have biased the study results. In addition, some important prognostic characteristics and/or treatment effect modifiers were not measured or reported in this particular subgroup; these include TNM classification at baseline and prior treatment for mCRPC. Due to the lack of information and the imbalances in baseline characteristics, the CADTH review team could not judge whether there was a risk of bias in the estimated treatment effects. Small sample sizes resulted in imprecision in many of the effect estimates. Further, between-group differences (relative or absolute) were not provided for some outcomes (e.g., HRQoL, ORR) precluding the comprehensive appraisal of comparative efficacy. To minimize the risk of bias in the measurement of the outcomes, tumours were assessed by investigators blinded to treatment assignment and by BICR, using RECIST 1.1 criteria and radiographic scans. Since the PROpel trial was a double-blind trial, it is also unlikely that there was risk of bias in measurement of other investigator-assessed (e.g., ORR) and self-reported (e.g., FACT-P questionnaire, subjective harms) outcomes. Risk of selective reporting bias was low, as the data were analyzed in accordance with the prespecified statistical plan.
A multiplicity testing procedure was applied to rPFS, TFST, time to pain progression, and OS to control the type I error rate in the overall population. However, other important efficacy outcomes were analyzed without multiplicity adjustment, for example, HRQoL was assessed using the FACT-P questionnaire. Further, the subgroup results presented herein were not adjusted for multiple comparisons, so statistically significant results are at an increased risk of being false positives. All subgroup analyses were intended to be exploratory.
In the subgroup of patients with BRCA mutation, efficacy and safety outcomes were not reported in sufficient detail. As a result, these outcomes were mostly affected by concerns regarding imprecision, uncertainties (e.g., it is unclear if the 95% CI for between-group difference included null), and study limitations (e.g., imbalanced baseline characteristics between the 2 treatment groups). This often precludes a robust critical appraisal, for example, reasons for censoring patients were not provided, information about the proportion of patients who completed HRQoL assessments in each group was not reported, and baseline values for HRQoL outcomes were not reported. As a result, it is difficult to explore the magnitude of treatment effect on these outcomes. Of note, the CADTH review team did not have access to the adjusted model. Without any knowledge of the model and the variables within it, the team cannot fully interpret the results of the adjusted analysis. Furthermore, longer follow-ups are needed to examine the long-term clinical benefits or risks of this combination regimen, given the immature survival data at DCO3. Results of confirmatory trial may be available next year.
According to the available data, results at DCO3 were missing for outcomes such as rPFS, FACT-P total score, and PSA50 response. Furthermore, missing data in the subgroup of patients with BRCA mutation raises concerns regarding the potential for bias in the study results. For example, for the ORR analysis, data were available for only 35 patients in the BRCAm subgroup (n = 85), and 50 patients did not have measurable disease at baseline and therefore were excluded from the EFR. In the FACT-P total score analysis, the number of patients who completed the questionnaire was not reported in the BRCAm subgroup, and in the overall population, approximately 70% of patients completed the questionnaire at DCO3. This large amount of missing data may affect the evaluation of rPFS.
In the PROpel trial, change in rPFS was consistent with OS in the subgroup of patients with BRCA mutation. In general, it is unclear if benefits in rPFS would translate into improvements in OS. For many new drugs that reported improvement in PFS, further analysis has demonstrated no improvement in OS.52 On the other hand, some studies have reported the correlation coefficient between rPFS and OS as being between 0.72 and 0.3 in patients with mCRPC,53,54 which demonstrates inconsistent evidence on the relationship between OS and rPFS. This may be due to different factors, including the varying definitions of rPFS used and relatively short follow-up periods. In addition, there is a lack of consistent evidence to inform whether PSA50 response, another surrogate outcome for survival, correlates well with OS.20
External Validity
Based on feedback from the clinical experts consulted by CADTH, the eligibility criteria and baseline characteristics of the PROpel trial study population generally aligned with the characteristics of patients in clinical practice in Canada who would receive olaparib plus abiraterone combination therapy, although the PROpel trial population was somewhat healthier, with better performance status and less pain reported at baseline, for example. An exception was that patients in the PROpel trial were not allowed to have received prior abiraterone therapy before entering the study; in clinical practice, patients at the mCRPC stage usually would have been treated with other active treatments including abiraterone. Therefore, the study findings may only be generalizable to patients who have not previously received abiraterone. The experts indicated that the outcome measures in the PROpel trials are appropriate and clinically relevant in clinical trials of metastatic prostate cancer. Even though a number of outcomes were judged to be clinically important by patient groups and clinicians, such as pain score or SSRE, data were not available for these outcomes in the subgroup of patients with a BRCA mutation. Results for certain AEs were not reported in this subgroup either.
In the PROpel trial, olaparib plus abiraterone combination therapy was compared with abiraterone. The clinical experts consulted for this review indicated that abiraterone is a relevant comparator for olaparib plus abiraterone in the study population. There is a lack of direct or indirect evidence to examine the relative efficacy and safety of the study drug to other currently active treatments, such as chemotherapy or other NHAs.
The combination therapy under review is indicated for the treatment of adult patients with deleterious or suspected deleterious germline and/or somatic BRCA-mutated mCRPC in whom chemotherapy is not clinically indicated. The combination therapy is intended for use in the first-line setting for patients with mCRPC. According to the clinical experts consulted by CADTH, there are no consistent criteria used in clinical practice to identify patients for whom chemotherapy is not clinically indicated. This patient group includes those who are deemed physically unfit (e.g., with poor renal function or poor performance status), those who refuse chemotherapy, or those who have received prior docetaxel treatment. The clinical experts noted that the proportion of patients in the first-line mCRPC setting who are likely to be clinically indicated to receive chemotherapy was no greater than 10% to 15%, suggesting that 85% to 90% of these patients are not clinically indicated to receive chemotherapy and therefore eligible for treatment with olaparib plus abiraterone.
GRADE Summary of Findings and Certainty of the Evidence
Methods for Assessing the Certainty of the Evidence
For pivotal studies and RCTs identified in the sponsor’s systematic review, GRADE was used to assess the certainty of the evidence for outcomes considered most relevant to inform CADTH’s expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group:18,19
“High certainty: We are very confident that the true effect lies close to that of the estimate of the effect.
Moderate certainty: We are moderately confident in the effect estimate — The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. We use the word ‘likely’ for evidence of moderate certainty (e.g., ‘X intervention likely results in Y outcome’).
Low certainty: Our confidence in the effect estimate is limited — The true effect may be substantially different from the estimate of the effect. We use the word ‘may’ for evidence of low certainty (e.g., ‘X intervention may result in Y outcome’).
Very low certainty: We have very little confidence in the effect estimate — The true effect is likely to be substantially different from the estimate of effect. We describe evidence of very low certainty as ‘very uncertain.’”
Following the GRADE approach, evidence from RCTs started as high certainty and could be rated down for concerns related to: study limitations (which refers to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias.
Whenever possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect; if this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., the clinical importance is unclear). In all cases, the target of the certainty of evidence assessment was based on the point estimate and where it was located relative to the threshold for a clinically important effect (when a threshold was available) or to the null. The reference points for the certainty of evidence assessment for OS and rPFS was set to null. The reference point for the certainty of the evidence assessment for FACT-P total score was set according to the presence or absence of an important effect based on thresholds identified in the literature. The target of the certainty of evidence assessment was the presence or absence of any (non-null) effect for the TFST due to the lack of a formal MID estimate, and for harm events due to the unavailability of the absolute difference in effects, the certainty of evidence was summarized narratively.
Results of GRADE Assessments
Drug Versus Placebo
Table 2 presents the GRADE summary of findings for olaparib plus abiraterone treatment versus abiraterone treatment.
Long-Term Extension Studies
There were no relevant long-term extension studies submitted for this review.
Indirect Evidence
There was no relevant indirect evidence submitted for this review.
Studies Addressing Gaps in the Systematic Review Evidence
There were no relevant studies addressing the gaps in the systematic review evidence submitted for this review.
Discussion
Summary of Available Evidence
The evidence included in this review consisted of 1 pivotal phase III, double-blind RCT. The PROpel (N = 796) trial met the inclusion criteria for the systematic review conducted by the sponsor. A subgroup of patients with BRCA mutation (n = 85) was enrolled in the study. The purpose of this study was to evaluate the efficacy and safety of olaparib plus abiraterone versus abiraterone in patients with mCRPC who have received no prior cytotoxic chemotherapy or NHAs at the mCRPC stage. Patients were randomized to either a combination of olaparib (300 mg twice daily) and abiraterone (1,000 mg once daily) (n = 399; BRCA-mutated n = 47) or abiraterone (1,000 mg once daily) (n = 397; BRCA-mutated n = 38). The primary efficacy end point in the PROpel trial was investigator-assessed rPFS. Other outcomes in this study included OS, TFST, HRQoL measured using the FACT-P questionnaire, ORR, PSA50 response, and safety. In the subgroup population of patients with BRCA mutation, all outcomes analyzed (rPFS, OS, TFST, ORR, PSA50 response rate, FACT-P total score, and safety) were exploratory. Despite randomization, there were some baseline patient characteristics that were imbalanced across treatment groups, including age, Gleason score at initial diagnosis, performance status at baseline, and PSA level at baseline in the subgroup of patients with BRCA mutation. In this population, 66% to 72% had a baseline Gleason score 8 to 10, and the approximate mean age of was 67 to 70 years. Seventeen percent to 26% had received prior docetaxel at the mHSPC stage, 53% to 77% had ECOG PS of 0, and baseline PSA level was 23 to 29 mcg/L.
Note that testing for BRCA mutation should be performed before olaparib treatment is initiated, according to the Health Canada–approved indication for olaparib.
Interpretation of Results
Efficacy
According to the patient groups and clinicians, mCRPC is an incurable disease. The important unmet needs that exist in the current treatments for mCRPC include: therapies that are curative, therapies that improve survival outcomes better than the current treatments, and, better-targeted therapies based on specific gene mutations. Patients with certain gene mutations have different disease characteristics and may respond differently compared to those without such mutations. Approximately 20% to 30% of the patients with mCRPC have gene mutations. Therefore, there may be a lack of quality evidence to justify the treatment selection in this subgroup of patients.
To align with the Health Canada–approved indication for the combination therapy of olaparib plus abiraterone (for adult patients with BRCA-mutated mCRPC in whom chemotherapy is not clinically indicated), the evidence examined in this current review was informed by evidence from a subgroup of patients with BRCA mutation in the PROpel trial. The PROpel trial provided comparative evidence to abiraterone with prednisone or prednisolone; however, no other comparative evidence was identified for this review. As such, a comparison to enzalutamide represents a gap in the evidence.
The reimbursement criteria requested by the sponsor for the combination therapy was for the first-line treatment of adult patients with BRCA-mutated mCRPC in whom chemotherapy is not clinically indicated. Based on the input from the clinical experts consulted by CADTH, patients “for whom chemotherapy is not clinically indicated” could include those who are deemed physically unfit (e.g., with poor renal function or poor performance status), those who refuse chemotherapy, or those who have received prior docetaxel treatment in the mCSPC phase. The experts estimated that the proportion of such patients in the first-line mCRPC setting would be 85% to 90%, and they would be eligible for the treatment with olaparib plus abiraterone. Despite the CADTH review team consulting with Health Canada, the clinical experts, and the drug programs to try to clarify the definition of “chemotherapy not clinically indicated,” it remains vague. As such, the interpretation depends on the clinical judgment of the treating physician. There is no standard definition of this particular patient group.
Preventing or delaying disease progression as well as prolonging life were identified as outcomes of importance to patients with mCRPC. OS and rPFS were assessed in the PROpel trial, reflecting patients’ needs. Managing symptoms that affect patients’ HRQoL and reducing skeletal pain are also important according to patient group input. In the PROpel trial, these outcomes were assessed by FACT-P, SSRE, and BPI-SF, although there were no results for SSRE or BPI-SF in the subgroup of patients with BRCA mutation.
The investigator-assessed rPFS was the primary outcome in the PROpel trial. rPFS had an HR of 0.23 (95% CI, 0.12 to 0.43) at DCO1 for the BRCAm subgroup, suggesting a reduction in rPFS associated with the treatment with olaparib plus abiraterone compared to treatment with abiraterone. The median rPFS had not been reached in the olaparib plus abiraterone group and was 8.4 months in the abiraterone group. According to the clinical experts consulted by CADTH, based on visual inspection of the KM curve and median rPFS in each group, the effect appeared clinically meaningful. The survival benefit gained from the treatment can be considered moderate and clinically important, despite that the median rPFS had yet to be reached at the data cut-off date. Results of the BICR-assessed rPFS are consistent with those from the primary analysis.
Results from the OS analyses in the BRCAm subgroup showed that the HR of OS was 0.29 (95% CI, 0.14 to 0.56), suggesting an increase in OS for patients treated with olaparib plus abiraterone, compared to those treated with abiraterone. Due to the immaturity of the data at the final OS analysis, the median OS was not reached in the olaparib plus abiraterone group and was 23.0 months in the abiraterone group. Given the trend shown in the KM curve, the clinical experts considered the improvement in OS clinically important. Results of the GRADE assessment noted that there was uncertainty in the results for rPFS and OS, owing to considerable imprecision in the effect estimates, due to the limited number of patients and the number of events, and risk of bias due to imbalanced baseline characteristics between treatment groups in this subgroup. Overall, treatment with olaparib plus abiraterone was associated with prolonged OS, although the benefit gained in these patients was considered small compared to the abiraterone group, given the limitations of the available data. According to an FDA briefing document,17 adjustment by a known prognostic model in mCRPC did not produce overall divergent results from the unadjusted results. However, the CADTH review team did not have access to the adjusted model. Without any knowledge of the model and the variables within it, the team cannot fully interpret the results of the adjusted analysis. A longer follow-up time for the survival outcomes is desired. Confirmatory trials are under way to provide further information regarding the long-term clinical benefit, such as OS, in the PROpel trial; the results may be available in 2025. In the PROpel trial, change in rPFS was consistent with OS. In general, it is unclear if benefits in rPFS would translate into improvements in OS. For many new drugs that reported improvement in PFS, further analysis demonstrated no improvement in OS.52 On the other hand, some studies have reported the correlation coefficient between rPFS and OS ranges from 0.7253 to 0.354 in patients with mCRPC, which demonstrates inconsistent evidence on the relationship between OS and rPFS. This may be due to different factors, including the varying definitions of rPFS used and relatively short follow-up periods.53,55
The HR for TFST was 0.35 (95% CI, 0.21 to 0.61). The median TFST was 37.39 months in the olaparib plus abiraterone group and 14.75 months in the abiraterone group. The GRADE assessment suggested that the benefit gained for TFST was with low certainty, due to the small sample size (resulting in imprecision) and imbalanced baseline characteristics (resulting in risk of bias). Based on the median TFST in each group, the clinical experts considered the benefit of olaparib plus abiraterone relative to abiraterone to be clinically important and consistent with the primary outcome (i.e., rPFS). Overall, given the available evidence, treatment with olaparib plus abiraterone was associated with longer time required for the first subsequent anticancer treatment compared to treatment with abiraterone.
HRQoL was assessed based on the least squares mean change from baseline in FACT-P total score. FACT-P is a disease-specific tool that is commonly used in clinical trials of prostate cancer. The mean change from baseline in the total score was 2.43 (SE not reported) in the olaparib plus abiraterone group and –1.21 (SE not reported) in the abiraterone group. The mean difference in the change from baseline between groups (and the 95% CI) were not reported. According to the GRADE assessment, the evidence on the effect of olapariband abiraterone on HRQoL, compared to that of abiraterone, is very uncertain. The MID for the FACT-P total score established in the literature is 10; therefore, the between-group difference in the mean change from baseline in FACT-P total score did not exceed the MID. Concerns also arose regarding risk of bias due to imbalanced baseline characteristics and the small number of patients who completed the FACT-P questionnaire (resulting in imprecision). These factors led to the GRADE certainty of evidence being downgraded to very low. Overall, based on the data on FACT-P total score, the treatment effect of olaparib plus abiraterone on improving patients’ HRQoL, compared to that of abiraterone, remains uncertain. A firm conclusion regarding the effect of the study drug on HRQoL cannot be drawn.
Two exploratory outcomes, ORR and PSA response, were also measured in the PROpel trial to provide evidence for the treatment effect of olaparib plus abiraterone. The ORR and PSA50 response results suggest that patients treated with olaparib plus abiraterone had a higher ORR (complete response and/or partial response) and higher PSA50 response rate than those treated with abiraterone. However, these outcomes were affected by serious concerns about risk of bias related to baseline imbalances in patient characteristics and the high proportion of patients who were not evaluable, imprecision related to the small sample size of the subgroup, and lack of details in data reporting. Definite conclusions on the response rates related to the treatment with the combination of olaparib plus abiraterone cannot be made.
Harms
Limited results are reported for harms in the subgroup of patients with BRCA mutation. The overall frequency of AEs was similar in the olaparib plus abiraterone and abiraterone groups in the PROpel trial; that is, 100% versus 89.5% experienced at least 1 AE, respectively, with the most frequently reported AEs being anemia, fatigue, nausea, back pain, and arthralgia. The proportion of patients with BRCA mutation experiencing at least 1 SAE was similar in the olaparib plus abiraterone and abiraterone groups (29.8% versus 31.6%, respectively). The proportion of patients who withdrew from treatment due to AEs was 12.8% in the olaparib plus abiraterone group and 10.5% in the abiraterone group. The proportion of AEs leading to death was 2.1% in the olaparib plus abiraterone group and 5.3% in the abiraterone group; causes for the deaths were not provided in this subgroup. In this subgroup, 5 patients in the olaparib plus abiraterone group reported pulmonary embolism. No other notable harms were reported in this subgroup. The certainty of the evidence for harm outcomes in the PROpel trial was assessed using GRADE. The small sample size and low number of events in the subgroup of patients with a BRCA mutation resulted in an assessment of certainty rated low to very low; however, the proportions of patients reported as having experienced SAEs, WDAEs, and notable harms (pulmonary embolisms) were aligned with the expectations of the clinical experts consulted by CADTH based on their experience treating patients with mCRPC, and did not raise significant safety concerns.
Because of the small sample size of the subgroup of interest, results of the harms outcomes in the overall population are also presented in Table 19. The clinical experts noted that there may be no biological basis to expect a difference in harms between the overall population and the BRCAm subgroup; however, this could not be confirmed based on the currently available evidence. The clinical experts also acknowledged that the patients with BRCA mutation in general are sicker than the overall population and have poorer prognosis. Adding more treatments may increase the risk of toxicity, and it would be difficult to identify which drug in the combination regimen is causing the AEs. Overall, the experts considered the harms related to treatment with olaparib plus abiraterone manageable, with no unexpected safety signal observed.
Conclusion
One phase III, double-blind, placebo-controlled RCT (PROpel) evaluated the efficacy and safety of first-line treatment with olaparib plus abiraterone with prednisone or prednisolone compared to abiraterone with prednisone or prednisolone in patients with mCRPC. Data from a subgroup of patients with a BRCA mutation is the most relevant evidence available at this time to inform the review of olaparib as per the indication approved by Health Canada. Compared with abiraterone, olaparib plus abiraterone may result in a clinically important increase in rPFS (median follow-up = 16.5 months; DCO1 date July 30, 2021), OS (median follow-up = 18.5 months; DCO3 date October 12, 2022), and TFST (median follow-up = 18.5 months; DCO3 date October 12, 2022), which were identified as important outcomes by patients and clinical experts. However, a longer duration of follow-up is needed to examine the long-term clinical benefits or risks of this combination regimen, particularly for OS, given the immature OS data at DCO3 in this trial. The results for HRQoL, ORR, and PSA response were very uncertain owing to reporting deficiencies and methodological limitations. As such, a definitive conclusion could not be drawn for these outcomes. There were no results reported for SSRE or pain among patients in the BRCAm subgroup, both of which were outcomes that were important to patients and clinical experts.
The proportion of patients who received treatment with olaparib plus abiraterone who experienced AEs was similar to those who received abiraterone treatment. The proportion of patients who experienced SAEs, WDAEs, and notable harms was also similar across treatment groups; however, the evidence was associated with very low certainty, due in part to the low sample size and event rate. The harms experienced by the patients were considered manageable and aligned with the clinical expectations.
References
1.What is prostate cancer? Toronto (ON): Canadian Cancer Society; 2021: https://cancer.ca/en/cancer-information/cancer-types/prostate/what-is-prostate-cancer. Accessed 2023 Jun 2.
2.Kirby M, Hirst C, Crawford ED. Characterising the castration-resistant prostate cancer population: a systematic review. Int J Clin Pract. 2011;65(11):1180-1192. PubMed
3.Survival statistics for prostate cancer. Toronto (ON): Canadian Cancer Society; 2023: https://www.cancer.ca/en/cancer-information/cancer-type/prostate/prognosis-and-survival/survival-statistics/?region=on. Accessed 2023 Oct 10.
4.Francini E, Gray KP, Shaw G, et al. Impact of new systemic therapies on overall survival (OS) of patients (pts) with metastatic castration resistant prostate cancer (mCRPC) in a hospital-based registry [abstract]. J Clin Oncol. 2018;36(6_suppl):203.
5.Hechmati G, Arellano J, Haynes I, Gunther O, Worsfold A, Rider A. Impact of bone metastases on quality of life in patients with castration-resistant prostate cancer (CRPC) at high risk for developing bone metastases [abstract]. Value Health. 2012;15(7):A431.
6.Sartor O, Flood E, Beusterien K, et al. Health-related quality of life in advanced prostate cancer and its treatments: biochemical failure and metastatic disease populations. Clin Genitourin Cancer. 2015;13(2):101–112. PubMed
7.Wolff JM, Donatz V, Klier J, Erhardt W, Dass RN, Geiges G. Quality of life among German patients with metastatic castration-resistant prostate cancer. Value Health. 2012;15(7):A431.
8.Mateo J, Boysen G, Barbieri CE, et al. DNA repair in prostate cancer: biology and clinical implications. Eur Urol. 2017;71(3):417-425. PubMed
9.Lozano R, Castro E, Aragón IM, et al. Genetic aberrations in DNA repair pathways: a cornerstone of precision oncology in prostate cancer. Br J Cancer. 2021;124(3):552-563. PubMed
10.Prostate cancer causes, risk factors, and prevention. Atlanta (GA): American Cancer Society; 2023: https://www.cancer.org/content/dam/CRC/PDF/Public/8794.00.pdf. Accessed 2023 Jul 27.
11.Cheng HH, Nelson PS. Genetic risk factors for prostate cancer. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2022: http://www.uptodate.com. Accessed 2023 Jul 26.
12.Selvarajah S, Schrader KA, Kolinsky MP, et al. Recommendations for the implementation of genetic testing for metastatic prostate cancer patients in Canada. Can Urol Assoc J. 2022;16(10):321-332. PubMed
13.Scott RJ, Mehta A, Macedo GS, Borisov PS, Kanesvaran R, El Metnawy W. Genetic testing for homologous recombination repair (HRR) in metastatic castration-resistant prostate cancer (mCRPC): challenges and solutions. Oncotarget. 2021;12(16):1600-1614. PubMed
14.Saad F, Aprikian A, Finelli A, et al. 2022 Canadian Urological Association (CUA)-Canadian Uro Oncology Group (CUOG) guideline: management of castration-resistant prostate cancer (CRPC). Can Urol Assoc J. 2022;16(11):E506-e515. PubMed
15.PrLynparza® (olaparib): 100 mg and 150 mg tablets [product monograph]. Mississauga (ON): AstraZeneca Canada; 2023 Jul 10.
16.Clarke Noel W, Armstrong Andrew J, Thiery-Vuillemin A, et al. Abiraterone and olaparib for metastatic castration-resistant prostate cancer. NEJM Evidence. 2022;0(0):EVIDoa2200043.
17.Oncologic Drugs Advisory Committee Meeting: olaparib (Lynparza). FDA Briefing Document. Silver Spring (MD): US Food and Drug Administration; 2023: https://www.fda.gov/media/167483/download. Accessed 2023 Nov 1.
18.Balshem H, Helfand M, Schünemann HJ, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011;64(4):401-406. PubMed
19.Santesso N, Glenton C, Dahm P, et al. GRADE guidelines 26: informative statements to communicate the findings of systematic reviews of interventions. J Clin Epidemiol. 2020;119:126-135. PubMed
20.Iwamoto H, Izumi K, Kadono Y, Mizokami A. Prognosis of patients with prostate cancer and middle range prostate - specific antigen levels of 20 - 100 ng / mL. Int Braz J Urol. 2019;45(1):61-67. PubMed
21.Clinical Study Report: D081SC00001 (PROpel). A randomised, double-blind, placebo-controlled, multicentre phase III study of olaparib plus abiraterone relative to placebo plus abiraterone as first-line therapy in men with metastatic castration-resistant prostate cancer [internal sponsor's report], first data cutoff (DCO1) on July 30, 2021. In: Drug Reimbursement Review sponsor submission: Lynparza (olaparib), 100 mg and 150 mg tablets. Mississauga (ON): AstraZeneca Canada; 2023 May 19.
22.Clinical Study Report. D081SC00001 (PROpel). A randomised, double-blind, placebo-controlled, multicentre phase iii study of olaparib plus abiraterone relative to placebo plus abiraterone as first-line therapy in men with metastatic castration-resistant prostate cancer [internal sponsor's report], third data cutoff (DCO3) on October 12, 2022. In: Drug Reimbursement Review sponsor submission: Lynparza (olaparib), 100 mg and 150 mg tablets. Mississauga (ON): AstraZeneca Canada; 2023 May 19.
23.Lynparza® (olaparib) in combination with abiraterone and prednisone or prednisolone for the treatment of adult patients with metastatic castration-resistant prostate cancer. Sponsor Briefing Document. Oncologic Drugs Advisory Committee Meeting of 28 April 2023. Silver Spring (MD): US Food and Drug Administration; 2023.
24.Scher HI, Morris MJ, Stadler WM, et al. Trial design and objectives for castration-resistant prostate cancer: updated recommendations from the Prostate Cancer Clinical Trials Working Group 3. J Clin Oncol. 2016;34(12):1402-1418. PubMed
25.Malone S, Shayegan B, Basappa NS, et al. Management algorithms for metastatic prostate cancer. Can Urol Assoc J. 2019;14(2):50-60. PubMed
26.So AI, Chi KN, Danielson B, et al. Update: Canadian Urological Association-Canadian Urologic Oncology Group guideline on metastatic castration-naive and castration-sensitive prostate cancer. Can Urol Assoc J. 2022 [epub ahead of print].
27.Brenner DR, Weir HK, Demers AA, et al. Projected estimates of cancer in Canada in 2020. Can Med Assoc J. 2020;192(9):E199. PubMed
28.Canadian Cancer Statistics Advisory Committee in collaboration with the Canaidan Cancer Society, Statistics Canada, and the Public Health Agency of Canada. Canadian cancer statistics 2022: a special report on cancer prevalence. Toronto (ON): Canadian Cancer Society; 2022: https://cancer.ca/en/cancer-information/resources/publications/canadian-cancer-statistics-a-2022-special-report-on-cancer-prevalence. Accessed 2023 Oct 10.
29.Dawson NA, Leger P. Overview of the treatment of castration-resistant prostate cancer (CRPC). In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2023: http://www.uptodate.com. Accessed 2023 Jul 26.
30.de Bono J, Mateo J, Fizazi K, et al. Olaparib for metastatic castration-resistant prostate cancer. N Eng J Med. 2020;382(22):2091-2102. PubMed
31.Beer TM, Armstrong AJ, Rathkopf D, et al. Enzalutamide in men with chemotherapy-naive metastatic castration-resistant prostate cancer: extended analysis of the phase 3 PREVAIL study. Eur Urol. 2017;71(2):151–154. PubMed
32.Beer TM, Armstrong AJ, Rathkopf DE, et al. Enzalutamide in metastatic prostate cancer before chemotherapy. N Engl J Med. 2014;371(5):424-433. PubMed
33.Ryan CJ, Smith MR, de Bono JS, et al. Abiraterone in metastatic prostate cancer without previous chemotherapy. N Engl J Med. 2013;368(2):138-148. PubMed
34.Ryan CJ, Smith MR, Fizazi K, et al. Abiraterone acetate plus prednisone versus placebo plus prednisone in chemotherapy-naive men with metastatic castration-resistant prostate cancer (COU-AA-302): final overall survival analysis of a randomised, double-blind, placebo-controlled phase 3 study. Lancet Oncol. 2015;16(2):152–160. PubMed
35.Saad F, Canil C, Finelli A, et al. Controversial issues in the management of patients with advanced prostate cancer: results from a Canadian consensus forum. Can Urol Assoc J. 2020;14(4):E137-e149. PubMed
36.Petrylak DP, Tangen CM, Hussain MH, et al. Docetaxel and estramustine compared with mitoxantrone and prednisone for advanced refractory prostate cancer. N Engl J Med. 2004;351(15):1513–1520. PubMed
37.Tannock IF, de Wit R, Berry WR, et al. Docetaxel plus prednisone or mitoxantrone plus prednisone for advanced prostate cancer. N Engl J Med. 2004;351(15):1502–1512. PubMed
38.Hussain A, Dawson NA. Chemotherapy in advanced castration-resistant prostate cancer. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2022: http://www.uptodate.com. Accessed 2023 Aug 2.
39.Sartor O, de Bono J, Chi KN, et al. Lutetium-177–PSMA-617 for metastatic castration-resistant prostate cancer. N Engl J Med. 2021;385(12):1091-1103. PubMed
40.Shore ND, Ionescu-Ittu R, Laliberté F, et al. Beyond frontline therapy with abiraterone and enzalutamide in metastatic castration-resistant prostate cancer: a real-world US study. Clin Genitourin Cancer. 2021;19(6):480-490. PubMed
41.Freedland SJ, Davis M, Epstein AJ, Arondekar B, Ivanova JI. Real-world treatment patterns among men with metastatic castration-resistant prostate cancer (mCRPC) in the U.S. Medicare population [abstract]. J Clin Oncol. 2022;40(28_suppl):406.
42.Malangone-Monaco E, Li W, Noxon B, et al. Real-world treatment patterns among patients with metastatic castration-resistant prostate cancer (mCRPC) in the US [abstract]. J Clin Oncol. 2022;40(6_suppl):49.
43.PrJevtana® (cabazitaxel): 40 mg/mL concentrated solution for injection. [product monograph]. Laval (QC): sanofi-aventis Canada; 2017 Sep 7.
44.PrTaxotere® (docetaxel): 80 mg/2.0 mL, 20 mg/0.5 mL concentrated solutionn for injection [product monograph]. Laval (QC): sanofi-aventis Canada; 2017 Nov 3.
45.PrXtandi® (enzalutamide): 40 mg capsules [product monograph]. Markham (ON): Astellas Pharma Canada; 2020 Jun 1.
46.Zytiga® (abiraterone acetate): 250 mg uncoated tablets, 500 mg film-coated tablets [product monograph]. Toronto (ON): Janssen; 2019 Oct 17.
47.Eisenhauer EA, Therasse P, Bogaerts J, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009;45(2):228-247. PubMed
48.Esper P, Mo F, Chodak G, Sinner M, Cella D, Pienta KJ. Measuring quality of life in men with prostate cancer using the functional assessment of cancer therapy-prostate instrument. Urology. 1997;50(6):920-928. PubMed
49.Cella D, Nichol MB, Eton D, Nelson JB, Mulani P. Estimating clinically meaningful changes for the Functional Assessment of Cancer Therapy--Prostate: results from a clinical trial of patients with metastatic hormone-refractory prostate cancer. Value Health. 2009;12(1):124-129. PubMed
50.Robinson DW, Jr., Zhao N, Dawkins F, Qi M, Revicki D. Pain questionnaire performance in advanced prostate cancer: comparative results from two international clinical trials. Qual Life Res. 2013;22(10):2777-2786. PubMed
51.Gater A, Abetz-Webb L, Battersby C, et al. Pain in castration-resistant prostate cancer with bone metastases: a qualitative study. Health Qual Life Outcomes. 2011;9:88. PubMed
52.Tannock IF, Pond GR, Booth CM. Biased evaluation in cancer drug trials-how use of progression-free survival as the primary end point can mislead. JAMA Oncol. 2022;8(5):679-680. PubMed
53.Morris MJ, Molina A, Small EJ, et al. Radiographic progression-free survival as a response biomarker in metastatic castration-resistant prostate cancer: COU-AA-302 results. J Clin Oncol. 2015;33(12):1356-1363. PubMed
54.Halabi S, Roy A, Yang Q, Xie W, Kelly WK, Sweeney C. Radiographic progression-free survival as a surrogate endpoint of overall survival in men with metastatic castrate-resistant prostate cancer [abstract]. J Clin Oncol. 2021;39(15_suppl):5057.
55.Halabi S, Vogelzang NJ, Ou SS, Owzar K, Archer L, Small EJ. Progression-free survival as a predictor of overall survival in men with castrate-resistant prostate cancer. J Clin Oncol. 2009;27(17):2766-2771. PubMed
Pharmacoeconomic Review
Abbreviations
AE
adverse event
AIC
Akaike information criterion
ARAT
androgen receptor-axis-targeted
BIC
Bayesian information criterion
BIA
budget impact analysis
ECOG PS
Eastern Cooperative Oncology Group Performance Status
HR
hazard ratio
HRQoL
health-related quality of life
ICER
incremental cost-effectiveness ratio
mCRPC
metastatic castration-resistant prostate cancer
mCSPC
metastatic castration-sensitive prostate cancer
NHA
new hormonal agent
OCCI
Ontario Case Costing Initiative
OS
overall survival
pCPA
pan-Canadian Pharmaceutical Alliance
PSM
partitioned survival model
QALY
quality-adjusted life-year
RDI
relative dose intensity
rPFS
radiological progression-free survival
RR
relative risk
RWE
real-world evidence
SRE
skeletal-related events
WTP
willingness to pay
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Olaparib (Lynparza), 100 mg and 150 mg tablets |
Submitted price | Olaparib, 100 mg or 150 mg: $69.95 per tablet |
Indication | Olaparib is indicated in combination with abiraterone and prednisone or prednisolone for the treatment of adult patients with deleterious or suspected deleterious germline and/or somatic BRCA mutated metastatic castration resistant prostate cancer (mCRPC) in whom chemotherapy is not clinically indicated. BRCA mutation must be confirmed before olaparib treatment is initiated. |
Health Canada approval status | NOC/c |
Health Canada review pathway | Standard |
NOC date | July 11, 2023 |
Reimbursement request | As per Health Canada indication |
Sponsor | AstraZeneca Canada Inc. |
Submission history | Previously reviewed: Yes Indication: Adjuvant treatment of adult patients with deleterious or suspected deleterious germline BRCA-mutated, HER2-negative high-risk early breast cancer who have been treated with neoadjuvant or adjuvant chemotherapy. Recommendation date: March 1, 2023 Recommendation: Reimburse with clinical criteria and/or conditions. Indication: As monotherapy for the treatment of adult patients with mCRPC and HRR gene mutations (germline and/or somatic) who have progressed following prior treatment with a new hormonal agent. Recommendation date: April 21, 2021 Recommendation: Reimburse with clinical criteria and/or conditions. Indication: As monotherapy for the maintenance treatment of adult patients with newly diagnosed advanced BRCA-mutated high-grade epithelial ovarian, fallopian tube, or primary peritoneal cancer who are in response (complete response or partial response) to first-line platinum-based chemotherapy, until disease progression or up to 2 years if no evidence of disease. Recommendation date: December 5, 2019 Recommendation: Reimburse with clinical criteria and/or conditions. |
HRR = homologous recombination repair; mCRPC = metastatic castration-resistant prostate cancer; NOC = Notice of Compliance; NOC/c = Notice of Compliance with conditions.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis PSM |
Target population | Adult patients with first-line BRCA1- or BRCA2-mutated mCRPC who are NHA-naive and are not clinically indicated for chemotherapy in Canada. Note: The target population is not aligned with the Health Canada–indicated population, which is line-agnostic and NHA-agnostic. It is also narrower than the reimbursement request population, which is NHA-agnostic. |
Treatment | Olaparib, in combination with abiraterone and prednisone or prednisolone (referred to as olaparib + abiraterone). |
Comparators |
|
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | 20 years |
Key data sources |
|
Submitted results |
|
Key limitations |
|
CADTH reanalysis results |
|
ICER = incremental cost-effectiveness ratio; LY = life-year; mCRPC = metastatic castration-resistant prostate cancer; NHA = new hormonal agent; PSM = partitioned survival model; OS = overall survival; QALY = quality-adjusted life-year; RDI = relative dose intensity; rPFS = radiological progression-free survival; TTD = time to treatment discontinuation of olaparib; TTDA = time to treatment discontinuation of abiraterone; vs. = versus.
Conclusions
Evidence from a subgroup of patients in the phase III double-blind PROpel randomized controlled trial who have a BRCA mutation suggests that treatment with olaparib in combination with abiraterone and prednisone or prednisolone (referred to as “olaparib plus abiraterone”) may result in a clinically important increase in overall survival (OS) and radiological progression-free survival (rPFS), compared to abiraterone, when used as first-line treatment for patients with metastatic castration-resistant prostate cancer (mCRPC) who are new hormonal agent (NHA)-naive and are not clinically indicated for chemotherapy. However, the CADTH Clinical Review Report described the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) of the available evidence as at low level of certainty, and concluded that longer duration of follow-up is needed to examine the long-term clinical benefits and risks of this combination regimen given the immaturity of the available data. The CADTH Clinical Review Report indicated that since randomization was not stratified by BRCA mutation status, the small sample size and number of events raised concerns regarding potential overestimation of the true effect. Moreover, there is evidence of prognostic imbalance across important baseline patient characteristics, which may bias the results in favour of olaparib plus abiraterone. Evidence for olaparib plus abiraterone versus other active treatments in the subgroup of patients with BRCA mutation in the first-line setting was not available at the time of this review.
In the CADTH base case, olaparib plus abiraterone was associated with an incremental cost-effectiveness ratio (ICER) of $160,535 per QALY gained, compared with abiraterone. The estimated ICER was higher than the sponsor’s estimate, driven primarily by the use of alternative parametric distributions to extrapolate the OS of olaparib plus abiraterone, as well as predictions for time to treatment discontinuation of olaparib and time to treatment discontinuation of abiraterone. The CADTH analysis conferred a sizable survival benefit to olaparib and abiraterone (3.73 life-years), which is more closely aligned with clinical expert expectations than the sponsor’s estimate. As a result of the longer time to discontinuation for both drugs within the olaparib plus abiraterone regimen in the CADTH reanalysis, patients are expected to incur an increase in treatment costs of more than $500,000 over the course of their lifetime, while other health care costs remain similar. Given the cost of olaparib ($102,000 per patient annually) and the Health Canada–indicated requirement that it be taken in combination with abiraterone, there are no price reductions for olaparib where a $50,000 per QALY gained threshold could be achieved. Were a decision-maker to consider other willingness-to-pay (WTP) thresholds, a price reduction for olaparib may be reached that could achieve cost-effectiveness for the olaparib and abiraterone regimen. CADTH also notes that olaparib, abiraterone, and enzalutamide went through the pan-Canadian Pharmaceutical Alliance (pCPA), and negotiations concluded with a letter of intent, suggesting there are already negotiated prices for the treatments considered in the analysis.
CADTH could not address the lack of clinical information for olaparib plus abiraterone in the NHA-experienced population or the uncertainty regarding the definition of clinical indication for chemotherapy in clinical practice. As a result, the cost-effectiveness results may not be generalizable to the patient population that is most likely to receive olaparib plus abiraterone in Canada.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, clinician groups, and drug plans that participated in the CADTH review process.
Two patient groups, the Canadian Cancer Society, and the Canadian Cancer Survivor Network, provided input through data collected via online surveys. The surveys, conducted in 2023, collected input from 30 patients with mCRPC living in Canada. The most important outcomes for patients included delaying disease progression, achieving long-term remission, improving survival, reducing skeletal pain, experiencing fewer side effects, and achieving better quality of life. The majority of patients surveyed had received 3 lines of therapy (65%), while 13% had received 2 and 9% had received 1. Luteinizing hormone-releasing hormone agonists and antagonists and antiandrogen therapies (91%) were the most commonly prescribed treatments, followed by radiotherapy (including teletherapy and brachytherapy) (73%), surgery (41%), chemotherapy (27%), and corticosteroids (27%). Important side effects included changes in sexual function and fertility, hot flashes, fatigue, and weight changes. Patients emphasized the need for more accessible therapies that minimize travel and out-of-pocket costs to patients. Patients who had experience with olaparib reported no difference in symptom management, management of side effects, ease of use, and disease progression. They reported side effects that included nausea, vomiting, tiredness, weakness, diarrhea, loss of appetite, headache, and dysgeusia.
Registered clinician input was received from the Ontario Health (Cancer Care Ontario) Genitourinary Cancer Drug Advisory Committee and a group of clinicians with expertise in management of advanced prostate cancer in Canada. According to clinician input, the current pathway of care for patients with mCRPC in the first-line setting includes androgen receptor-axis-targeted (ARAT) therapy (i.e., abiraterone, enzalutamide, and apalutamide) as well as chemotherapy (i.e., docetaxel and cabazitaxel). The clinicians noted that radiotherapy is available after chemotherapy failure, although it is restricted to symptomatic bone-only metastases. The clinician groups indicated that for patients entering first-line mCRPC, ARAT therapy is an effective option. However, since mCRPC is an incurable disease, the goal of treatment in the first-line setting is to slow the progression of metastatic disease. The clinician groups highlighted that olaparib plus abiraterone may fulfill the unmet need for an effective and tolerable first-line therapy and that it may be preferred by patients eligible to receive ARAT therapy. It was also noted that olaparib should be considered a treatment option for all patients with mCRPC in the first-line setting, although patients with adequate bone marrow function would be best suited given the risk of cytopenia. The clinicians also noted that there is no evidence to determine whether olaparib plus abiraterone should be used preferentially before or after docetaxel, so prior experience with chemotherapy should not be a requirement for reimbursement. Additionally, clinicians suggested mutation status should not be an exclusion criterion for reimbursement.
Participating drug plans were interested in obtaining clarification as to whether treatment with olaparib plus abiraterone may be considered for patients with greater disease severity than that observed in the PROpel trial (i.e., for patients with an Eastern Cooperative Oncology Group Performance Status [ECOG PS] > 1), and whether objective parameters could be used to determine treatment discontinuation beyond disease progression. The drug programs inquired about the clinical circumstances under which olaparib plus abiraterone would be preferred over other available systemic treatment options (i.e., optimal treatment sequencing). Finally, drug plans noted concerns regarding the anticipated budget impact and the potential requirement of diagnostic testing to determine gene mutation status.
Several of these concerns were addressed in the sponsor’s model:
The impact of disease and treatment on patients’ quality of life was captured with utility values. Adverse events (AEs) were incorporated as disutilities within the analyses.
Companion diagnostic test costs were incorporated.
In addition, CADTH addressed some of these concerns as follows:
In line with clinicians’ expectations that olaparib plus abiraterone use would likely shift the current treatment paradigm by replacing abiraterone and enzalutamide as the new preferred first-line treatment for patients with BRCA1- or BRCA2-mutated mCRPC who are NHA-naive, CADTH revised the sponsor’s projected market share in the budget impact analysis (BIA).
Economic Review
The current review is for olaparib (Lynparza), in combination with abiraterone and prednisone or prednisolone (henceforth, olaparib plus abiraterone), for the treatment of adult patients with first-line BRCA1- or BRCA2-mutated mCRPC who are NHA-naive and are not clinically indicated for chemotherapy in Canada.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis of olaparib plus abiraterone compared with abiraterone (with supportive prednisone or prednisolone) and enzalutamide. The target population was adult patients with first-line BRCA1- or BRCA2-mutated mCRPC who are NHA-naive and are not clinically indicated for chemotherapy in Canada.1 As such, although the patient cohort modelled in the sponsor’s base case is aligned with the available clinical evidence, it is narrower than the Health Canada–indicated population, which is line-agnostic and NHA-agnostic.
Olaparib is an oral inhibitor of poly(adenosine diphosphate)-ribose polymerase that exploits deficiencies in DNA repair pathways and selectively targets cancer cells with these deficiencies that are absent in normal cells.1 Olaparib is available as a 100 mg and 150 mg oral tablet.2 The recommended total daily dose of olaparib tablets is 600 mg, taken as two 150 mg tablets twice daily, in combination with abiraterone (1,000 mg once daily) and supportive prednisone or prednisolone (5 mg twice daily).2 The olaparib and abiraterone treatment captured in the economic model reflects the Health Canada–recommended dosing regimen.1 The submitted price of olaparib is $69.95 per 100 mg or 150 mg tablet, which at the recommended dose corresponds to an annual per-patient cost of $102,194. The sponsor-adjusted drug acquisition cost for all therapies used the relative dose intensities (RDIs) observed in the PROpel trial. For the combination treatment, the sponsor estimated an annual cost of $36,640 for abiraterone (with supportive prednisone or prednisolone) (RDI = |||||) and $93,712 for olaparib (RDI = |||||). This resulted in an annual per-patient cost of $130,352 for olaparib and abiraterone. The comparators for this analysis included abiraterone (RDI = ||||||) and enzalutamide (RDI = |||||), with corresponding annual per-patient costs of $36,982 and $38,816, respectively. Wastage was included in the base-case analysis and applied on a per administration basis for subsequent chemotherapy.1
The clinical outcomes modelled were rPFS and OS.1 The economic outcomes of interest were quality-adjusted life-years (QALYs) and life-years. The economic evaluation was conducted over a model horizon of 20 years, from the perspective of the public health care payer in Canada.1 Costs and outcomes were discounted at 1.5% per annum.
Model Structure
The sponsor submitted a partitioned survival model (PSM) to capture all costs and outcomes associated with olaparib plus abiraterone and comparators. The model included 3 health states: progression-free, progressed disease, and death, whereby transitions between health states occurred on a monthly cycle length (Figure 1).1 The proportion of patients in progression-free, progressed disease, and death states was estimated over time based on the OS and rPFS curves for each intervention; the OS and rPFS curves were informed by the PROpel trial, as well as the prospective registry study.1 The proportion of patients with progressed disease (i.e., postprogression state) was estimated as the difference between the proportion of living patients (estimated from the OS curve) and the proportion of progression-free patients (estimated from the rPFS curve). rPFS was defined as the time from randomization to either radiological progression or death due to any cause.1 Patients began in the progression-free health state, where they were assumed to initiate first-line treatment for mCRPC, and over time could progress to either the progressed disease health state or transition to the death state.1 Consistent with the natural history of progressive mCRPC, it was assumed that disease progression is irreversible, hence, patients in the progressed disease health state could either remain in this health state or transition to the death state (i.e., patients could not return to the progression-free health state).1
Model Inputs
Baseline patient characteristics were derived from PROpel, a phase III, placebo-controlled, multicentre, international trial designed to evaluate the efficacy and safety of olaparib plus abiraterone versus abiraterone with placebo in patients with mCRPC who have received no prior cytotoxic chemotherapy or NHAs in that stage of disease (N = 796). As the Health Canada indication was specific to patients testing positive for BRCA1 and/or BRCA2 gene alterations, information from that cohort was used to inform the economic analysis (n = 85).3,4 The average patient in the modelled cohort, which the sponsor assumed reflected the patient population in Canada, was aged 69 years, weighed 83 kg, and had a mean body surface area of 2.01 m2.1 The average weight and body surface area characteristics were derived from the patient population enrolled in the PROpel and TROPIC trials, respectively, and were used to inform the drug dosage regimens and the age- and sex-specific distribution of the general population mortality risk.3,5
Clinical efficacy parameters used to characterize olaparib plus abiraterone and abiraterone, including OS and rPFS, were derived from the final analysis of the PROpel trial (DCO3), using the October 12, 2022, data cut-off date (median follow-up for olaparib plus abiraterone group = 18.5 months; median follow-up for abiraterone group = 14.3 months).1 Parametric survival modelling was used to extrapolate OS and rPFS, as well as 2 end points representing the time to treatment discontinuation of olaparib and time to treatment discontinuation of abiraterone beyond time points available in the trial. Dependent parametric models were explored statistically through the assessment of the proportional hazard assumption (i.e., constant treatment effect on the hazards) and the accelerated failure time assumption (i.e., constant treatment effect on the time scales). Candidate distributions were selected based on clinical plausibility of long-term survival projections, visual inspection of model fit, as well as Akaike information criterion (AIC) and Bayesian information criterion (BIC). Moreover, the sponsor compared smoothed hazard functions from the observed PROpel trial data with the pattern of extrapolated hazards produced by different parametric distributions. The sponsor selected the log-normal distribution to model OS and rPFS beyond time points available in the trial for patients receiving olaparib plus abiraterone, and for those receiving abiraterone alone. The sponsor selected the gamma distribution to extrapolate time to treatment discontinuation of olaparib and time to treatment discontinuation of abiraterone in the olaparib plus abiraterone group and the log-logistic distribution to extrapolate time to treatment discontinuation of abiraterone in the abiraterone group.
Comparisons of olaparib plus abiraterone with enzalutamide required the use of an external real-world evidence (RWE) study. The estimation of transition probabilities for patients receiving enzalutamide were modelled via hazard-mapping using the hazard ratio (HR) of enzalutamide relative to abiraterone from a prospective registry study. Constant HRs were applied to the OS curve (HR for enzalutamide = 1.00) and the rPFS curve (HR for enzalutamide = 0.96) of abiraterone (the reference) to derive the long-term OS and rPFS for patients receiving enzalutamide.
Health state–specific utility values were derived from an analysis of 5-Level EQ-5D index data collected for all comers (i.e., irrespective of biomarker status) in the PROpel trial, with Canadian tariffs applied.6 The sponsor calculated utility values of ||||| and ||||| for the progression-free and progressed disease states, respectively. The sponsor stated that genetic mutations are not anticipated to be a predictor of health-related quality of life (HRQoL); hence, utilities captured in the model reflect all patients irrespective of the biomarker-selected subgroups.1 The sponsor incorporated disutilities associated with AEs greater than or equal to grade 3, with greater than or equal to 5% rate in any of the treatments considered.1 Treatment-related AE prevalence were informed by the PROpel trial (for olaparib plus abiraterone, and abiraterone)3,4 and the PREVAIL trial (for enzalutamide).7,8 AE-specific marginal disutilities were estimated from values reported in the literature, which derived UK-based preference values applied to EQ-5D descriptive questionnaire responses in the Medical Expenditure Panel Survey (n = 79,522).9 Disutilities were applied as a 1-time decrement during the first model cycle, assuming that serious AEs likely occurred at the time of treatment initiation.1 Treatment-related total mean utility decrements were calculated as the weighted sum of the treatment-specific prevalence of each AE and its associated disutility. In addition, given the high susceptibility of mCRPC to metastasize to bone tissue, skeletal-related events (SREs) were applied as a 1-time decrement during the first cycle following disease progression, irrespective of treatment. All patients had the same probability of experiencing an SRE upon progression; this probability was derived from the PROpel trial data.1
Costs captured in the model included those associated with drug acquisition, diagnostic testing, disease monitoring and medical follow-up, AE management, SRE management, subsequent treatment, and terminal care costs.1 Drug acquisition costs for olaparib were based on the sponsor’s submitted price.1 The dosing modelled for olaparib plus abiraterone was consistent with that described in the Overview section. In the model, each first-line treatment was adjusted to an RDI based on the PROpel clinical trial (for olaparib plus abiraterone, and for abiraterone)3,4 and RWE (for enzalutamide).10 Drug acquisition costs were sourced from the Ontario Drug Benefit Formulary11 and previous CADTH submissions,12,13 while dosing schedules were based on Ontario Health (Cancer Care Ontario) monographs.14
The sponsor assumed that, following the introduction of olaparib, diagnostic testing costs would apply to all patients with first-line mCRPC. Genetic testing costs are presented in Table 11. Proportion of patients pretested for mutation status (75%), mutation prevalence (11%),15 detection rate (58%),16 and unit cost per test ($1,304)17 were used to calculate the prevalence of mutation confirmed by testing (5%), the number of tests required to identify 1 patient who was BRCA mutation positive (22) and the total testing cost per patient treated ($28,317). After progressing on initial treatment, 65% of patients were assumed to receive subsequent therapy (Table 12). The total weighted costs of subsequent therapy differed by prior treatment (i.e., those who received olaparib plus abiraterone versus abiraterone or enzalutamide as first-line therapy) and were applied as a one-off cost in the first model cycle after progression. The weighted cost associated with subsequent therapy among patients receiving olaparib and abiraterone plus abiraterone or enzalutamide in the first-line setting was estimated to be $24,472 and $26,256, respectively. Treatment monitoring costs and health care resource use costs were sourced from the Ontario Ministry of Health Schedule of Benefits for Laboratory and Physician Services.18 Treatment-specific AE costs were estimated based on data from the Ontario Case Costing Initiative (OCCI),19 and applied as a 1-time cost in the first model cycle. Additionally, SRE costs were estimated based on data from the OCCI19 and the Canadian Institute for Health Information,20 and applied as a one-off cost upon progression. All patients who died were assumed to incur end-of-life costs ($8,518) in the last cycle before death based on the average cost for patients receiving palliative care according to the OCCI.19
Summary of Sponsor’s Economic Evaluation Results
The sponsor conducted the base case via a probabilistic sensitivity analysis with 1,000 simulations.1 The deterministic and probabilistic results were similar. The probabilistic findings are presented in the following.
Base-Case Results
In the sponsor’s base case, olaparib plus abiraterone was associated with an incremental cost of $431,466 and an incremental QALY gain of 4.27 compared with abiraterone, resulting in an ICER of $100,929 per QALY gained. Enzalutamide was associated with higher costs and more QALYs than abiraterone, but when compared with abiraterone, had a higher ICER than olaparib plus abiraterone, and thus was considered extendedly dominated through abiraterone plus olaparib and abiraterone.
The sponsor’s analysis predicted that olaparib plus abiraterone was associated with a longer duration of life than abiraterone and enzalutamide (i.e., incremental life-years: 5.06 and 5.04, respectively). Given the duration of the PROpel trial (i.e., median follow-up for the olaparib plus abiraterone group = 18.5 months; median follow-up for the abiraterone group = 14.3 months) in contrast to the model’s time horizon (i.e., 20 years), it is important to note that the majority of the incremental QALYs (83%) realized by patients receiving olaparib plus abiraterone relative to both abiraterone and enzalutamide was derived from the period beyond which there is observed trial data (i.e., extrapolated period). The key cost driver among patients receiving olaparib plus abiraterone was the drug acquisition cost, accounting for 79% of the total cost incurred. Likewise, the main cost driver among patients receiving abiraterone and enzalutamide was the cost of drug acquisition, which accounted for 52% and 55% of the total estimated cost, respectively. Diagnostic testing accounted for 5% of total costs among patients treated with olaparib plus abiraterone.
The probability that olaparib plus abiraterone was cost-effective at a $50,000 per QALY gained threshold was 0% when compared to both abiraterone and enzalutamide. The sponsor’s submitted analysis is based on the publicly available prices for all drug treatments. Additional results from the sponsor’s submitted economic evaluation base case are presented in Appendix 3.
Table 3: Summary of the Sponsor’s Economic Evaluation Results, Sequential
Drug | Total costs ($) | Total LYs | Total QALYs | Sequential ICER ($ per QALY) |
|---|---|---|---|---|
Sponsor’s base case | ||||
ABI | 92,125 | 2.75 | 2.30 | Reference |
OLA + ABI | 523,590 | 7.81 | 6.57 | 100,929 |
Dominated treatments | ||||
ENZA | 96,106 | 2.77 | 2.32 | Extendedly dominated through abiraterone and OLA-ABI |
ABI = abiraterone; ENZA = enzalutamide; ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year; OLA + ABI = olaparib plus abiraterone.
Source: Sponsor’s pharmacoeconomic submission.1
Sensitivity and Scenario Analysis Results
The sponsor assessed several model parameters and assumptions in probabilistic scenario analyses. These included applying different model time horizons; using alternative parametric distributions to extrapolate the OS and rPFS of olaparib plus abiraterone and abiraterone; assessing the impact of different treatment stopping rules; excluding specific cost components across interventions; and varying the source informing relevant utility values. The most influential parameters were alternative assumptions regarding efficacy, particularly as it regards the selection of OS extrapolations; time to treatment discontinuation; and varying model time horizons. When selecting the generalized gamma distribution to extrapolate time to treatment discontinuation of olaparib across interventions, the ICER increased to $149,748 per QALY gained (relative to abiraterone) and $150,129 per QALY gained (relative to enzalutamide). Moreover, when applying a 5-year treatment stopping rule, the ICER decreased to $85,852 per QALY gained (relative to abiraterone) and $85,786 per QALY gained (relative to enzalutamide). All other scenarios resulted in ICERs ranging between $89,457 and $128,046 per QALY gained.
In addition, the sponsor reported a subgroup analysis for treatment with olaparib plus abiraterone as first-line therapy for patients with mCRPC who have mutations of the HRR genes. For patients with HRR mutations, first-line treatment with olaparib plus abiraterone resulted in ICERs of $126,579 per QALY gained (relative to abiraterone) and $125,334 per QALY gained (relative to enzalutamide). No scenario analysis was conducted using a perspective other than the health care payer.
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the economic analysis:
Submitted model does not align with the indicated population: The approved indication for olaparib plus abiraterone is for the treatment of adult patients with deleterious or suspected deleterious germline and/or somatic BRCA-mutated mCRPC for whom chemotherapy is not clinically indicated, irrespective of prior NHA treatment. The PROpel trial was restricted to patients who were NHA-naive. As such, the sponsor’s modelled cohort focuses exclusively on patients with mCRPC who have not received prior treatment with an NHA. The sponsor indicated that there is no clinical evidence regarding the efficacy or effectiveness of olaparib plus abiraterone in this subpopulation. The clinical experts consulted by CADTH for this review indicated that results from the PROpel trial are not generalizable to the NHA-experienced population.
CADTH could not address this limitation given the lack of clinical data on the efficacy of olaparib plus abiraterone among NHA-experienced patients. As such, the cost-effectiveness of olaparib plus abiraterone in this population is unknown.
Generalizability of modelled population to Canadian clinical practice is unclear: The indication of olaparib plus abiraterone stipulates that it is for use in patients “in whom chemotherapy is not clinically indicated.” However, it is uncertain how the clinical indication for chemotherapy would be defined in clinical practice. According to the clinical experts consulted by CADTH, no consistent criteria are used in clinical practice to identify patients for whom chemotherapy is not clinically indicated. This group may include patients who are deemed physically unfit (e.g., patients with poor renal function or poor performance status), who refuse chemotherapy, or who received prior docetaxel treatment during the metastatic castration-sensitive prostate cancer (mCSPC) phase. The clinical experts consulted by CADTH for this review estimated that the proportion of patients in the first-line mCRPC setting who are likely to be clinically indicated to receive chemotherapy could be no more than 10% to 15%, thereby implying that 85% to 90% of patients would be eligible for treatment with olaparib plus abiraterone. The clinical experts also indicated that among patients who may be clinically indicated to receive taxane-based chemotherapy but who are unwilling to receive docetaxel or cabazitaxel, olaparib plus abiraterone would only be considered for those with a BRCA mutation. CADTH notes that although olaparib plus abiraterone was compared to abiraterone in the PROpel trial, evidence for the comparisons between olaparib plus abiraterone and other comparators is lacking.
CADTH also notes that PROpel consisted exclusively of patients with an ECOG PS less than or equal to 1 and a median age of 70 years. According to the clinical experts consulted by CADTH, the PROpel study population generally reflects patients in Canada with first-line BRCA-mutated mCRPC who would receive olaparib plus abiraterone. However, the clinical experts noted that clinical practice includes patients with lower (worse) ECOG PS. The clinical experts also noted that the proportion of patients in PROpel experiencing moderate to severe pain (29%) was lower than that observed for patients with mCRPC in clinical practice. The clinical experts further indicated that the lower prevalence of pain may be associated with the relatively high prevalence of patients with an ECOG PS of 0 (66%) in the PROpel trial. As such, if olaparib plus abiraterone were to become available in clinical practice, where patients are likely to have more diverse clinical and demographic profiles, there is uncertainty regarding the presence and magnitude of the OS benefit that could be expected. The clinical experts noted that the patients in the experimental arm of the PROpel trial were younger and had higher disease burden than the patients in the control arm, which may bias the results in favour of olaparib plus abiraterone.
CADTH notes that given this uncertainty, the cost-effectiveness results may not be generalizable to the patient population most likely to receive olaparib plus abiraterone in Canada.
Impact of olaparib plus abiraterone on long-term OS is uncertain. The sponsor predicted that olaparib plus abiraterone would be associated with approximately 5 additional years of life, compared with either abiraterone or enzalutamide, based on data from the final analysis (data cut-off date = October 12, 2022) of the PROpel study cohort with BRCA mutation (n = 85). Although olaparib plus abiraterone was associated with an HR of 0.29 (95% confidence interval, 0.14 to 0.56) compared with abiraterone in this population, CADTH noted that BRCA mutation status was not prespecified; the sample size of the BRCA-mutated subgroup was small and characterized by imbalances between treatment groups; and that the median OS for the full study population (N = 796) was not reached in the olaparib plus abiraterone group and was 23 months in the abiraterone group. Evidence suggests that the clinical benefit of cancer agents demonstrated in primary publications often differs from clinical evidence of updated mature data.21 Hence, CADTH contends that, in the absence of mature OS data, the extent to which the extrapolations of OS for olaparib plus abiraterone over- or underestimate the true incremental life-years is uncertain.
The sponsor selected parametric distributions based on goodness-of-fit criteria, visual inspection, and clinical plausibility, in accordance with Decision Support Unit guidance.22 While CADTH agrees that models should be compared based on their statistical fit, this pertains only to the observed trial period, not to the extrapolation period. The weight given to the comparative fit of alternative parametric models to the observed data depends on the extent to which extrapolation is required and the degree of censoring present. Given the length of time required for extrapolation and the size of the censored population in the PROpel trial, the clinical plausibility of the extrapolated portion of alternative models is of greater importance than the statistical fit to the observed data.23 According to the clinical experts consulted by CADTH for this review, although the PROpel trial findings appeared favourable and clinically important, the magnitude and durability of such a benefit was highly uncertain in the absence of longer-term evidence. An analysis of the sponsor’s submitted data for time to death was performed by CADTH and is presented in Figure 2 (Appendix 3). By characterizing the long-term OS of olaparib plus abiraterone with the log-normal distribution, the sponsor implicitly assumed that the survival benefit of olaparib plus abiraterone is stable during the extrapolated period. That is, the relative risk (RR) of death among patients treated with olaparib plus abiraterone (compared with patients treated with abiraterone) estimated at the end of year 2 from the sponsor’s analysis (RR = 0.27) is maintained until year 15 (RR = 0.33) (Figure 2). The clinical experts consulted by CADTH for this review disagreed with the use of a parametric distribution that would extrapolate a stable treatment effect on OS for 15 years, especially when considering data immaturity and the limited follow-up time of the PROpel trial. In accordance with clinical expert input, CADTH selected the gamma distribution to extrapolate the long-term OS of olaparib and abiraterone, which assumes that the survival benefit of olaparib and abiraterone decreases with time. That is, the RR of death for patients treated with olaparib plus abiraterone (compared to patients treated with abiraterone) estimated at the end of year 2 (RR = 0.26) from the CADTH reanalysis increases gradually throughout the lifetime horizon of the model (RR = 0.36, 0.53, 0.68, and 0.83 at years 5, 10, 15, and 20, respectively) (Figure 2). The clinical experts agreed that a progressive return to an RR of 1 throughout the 20-year model horizon was aligned with disease progression for mCRPC, and hence would better reflect progressive deterioration of patients with time.
CADTH conducted a reanalysis using the gamma distribution to extrapolate OS for olaparib plus abiraterone.
Modelling approach may overestimate comparative efficacy: Results from the sponsor's model suggested that olaparib and abiraterone was associated with longer survival after progression (1.2 years) relative to both abiraterone and enzalutamide, suggesting that treatment with olaparib plus abiraterone is associated with reductions in the rate of postprogression mortality. Specifically, the sponsor’s modelling approach predicts a 23% survival benefit in the postprogression period for olaparib plus abiraterone compared to abiraterone, which does not align with clinical expectations or available clinical evidence. CADTH notes that while the PROpel trial showed a clinically meaningful impact of olaparib plus abiraterone on rPFS and OS, there was no robust evidence that olaparib plus abiraterone would continue to provide clinical benefit after patients experience progression. The sponsor’s use of a PSM introduces structural assumptions about the relationship between rPFS and OS that likely do not accurately reflect causal relationships within the disease pathway. These assumptions may produce a postprogression survival bias that favours olaparib plus abiraterone. Due to the assumed independence between OS and rPFS end points in a PSM, extrapolations for each end point may reflect within-trial trends in the rates of relapse and death. However, as the postprogression mortality transition is not modelled directly on the PSM approach, it is not possible to establish from the model whether this effect was supported by the trial data or was generated entirely during extrapolation.
CADTH was unable to determine the extent to which the implied postprogression benefit was due to the effect of treatment or due to structural bias within the PSM, and could not address this in reanalysis.
Time to treatment discontinuation for patients receiving olaparib plus abiraterone is uncertain. In the sponsor’s base case, time on treatment for patients receiving olaparib plus abiraterone was informed by parametric distributions fitted to patient-level data on time to discontinuation of olaparib and time to discontinuation of abiraterone from the PROpel trial. Although the log-normal distribution had the best fit based on AIC and BIC for both treatments in patients receiving olaparib plus abiraterone, the sponsor selected the gamma distribution for the base-case analysis (which ranked sixth based on AIC and BIC), stating that it provided a more clinically plausible extrapolation with sufficient statistical fit. CADTH notes that the gamma distribution selected by the sponsor for time to treatment discontinuation of olaparib and time to treatment discontinuation of abiraterone estimated that 100% of patients would discontinue olaparib, and 99% of patients would discontinue abiraterone, 15 years after treatment initiation. In contrast, the sponsor’s extrapolation of rPFS (generated using the log-normal distribution) estimated that 12% of patients treated with olaparib plus abiraterone would be progression-free 15 years after treatment initiation. That is, 12% of patients receiving olaparib plus abiraterone would continue to experience rPFS benefit after treatment with olaparib is discontinued. Clinical expert feedback indicated that although assumptions regarding time on treatment are associated with uncertainty, time to treatment discontinuation of olaparib and time to treatment discontinuation of abiraterone should be better aligned with time to radiological progression among patients treated with olaparib plus abiraterone. The clinical experts indicated that the gamma distribution selected by the sponsor lacked face validity considering the discrepancy generated between time to treatment discontinuation of olaparib, time to treatment discontinuation of abiraterone, and rPFS extrapolations. Furthermore, the clinical experts remarked that if it is assumed that rPFS is durable over time, then it should also be reasonable to assume that time on treatment is maintained for a comparable period of time. Since the sponsor estimated that 7% of patients receiving olaparib plus abiraterone remain radiologically progression-free at the end of the model’s 20-year lifetime horizon, the log-normal distribution for time to treatment discontinuation of olaparib and time to treatment discontinuation of abiraterone that estimates that 3% and 4% of patients remain on treatment with olaparib plus abiraterone, respectively, by the 20-year landmark was deemed more clinically plausible. The clinical experts confirmed that the log-normal distribution generated extrapolations of time to treatment discontinuation of olaparib and time to treatment discontinuation of abiraterone that reflected the extrapolated rPFS for olaparib plus abiraterone.
CADTH conducted a reanalysis using the log-normal parametric distribution to extrapolate time to treatment discontinuation of olaparib and time to treatment discontinuation of abiraterone, which, together with meeting clinical face validity, were assessed as representing the best statistical fit among all the standard parametric curves considered.
Utility values associated with uncertainty: The sponsor derived utility estimates from an analysis of 5-Level EQ-5D index data collected in the PROpel trial with Canadian tariffs applied. However, in selecting this approach, patients receiving olaparib plus abiraterone, as well as those receiving abiraterone, would have better quality of life in preprogression (|||||) than the reported general age-adjusted male population in Canada (0.842).24 Clinical expert feedback sought by CADTH noted that patients receiving first-line treatment for mCRPC are expected to have a lower quality of life than the average male of the same age in Canada. CADTH acknowledges that the trial-based utility values may overestimate the progression-free utilities giving that the PROpel population was biologically fitter by design (refer to key limitation previously mentioned). In addition, the trial-based utility value calculated for patients with progressed metastatic disease (|||||) was marginally lower than the mean utility value reported for the average male aged 65 to 69 years in Canada. The clinical experts consulted by CADTH further indicated that the trial-based postprogression utility estimates lacked face validity considering the severity of the disease (i.e., the disease is biologically more aggressive) and the toxicity associated with treatments available beyond progression. Clinical expert input indicated that a utility decrement of 0.02 among patients with progressed mCRPC relative to the general population in Canada of the same age does not reflect the patient population, based on clinical practice, and would be inappropriate. In addition, the |||% decline in well-being experienced by patients with progressed metastatic disease in the submitted base case did not align with clinical expectation, owing to what was perceived to be a high postprogression utility value. CADTH also notes that the relatively short duration of follow-up in the PROpel trial suggests that trial-based utility inputs characterizing postprogression may result in a high degree of uncertainty.
CADTH conducted a reanalysis by sourcing utilities from alternative sources. The progression-free utility value assigned to patients irrespective of treatment (0.830) was sourced from the COU-AA-302 clinical trial that reported preference-based EQ-5D index scores for mCRPC in the pre-docetaxel treatment line with abiraterone as the main therapy of interest.25 In addition, CADTH considered 2 sources from the literature reporting utility estimates in postprogression. Diels et al. (2015) collected HRQoL data from patients with mCRPC who were enrolled in an observational study conducted in 47 centres across 6 European countries (N = 602).26 Sandblom et al. (2004) undertook an analysis of patients with prostate cancer in Sweden that explored changes in HRQoL toward the end of life (n = 1,243).27 Although the Diels et al. (2015) study included fewer patients, the rapidly evolving treatment landscape associated with prostate cancer in recent years suggests that the more recent publication would offer a more robust source as a base-case input. Hence, the base-case utility value assigned to patients in postprogression (0.600) was sourced from Diels et al. (2015).
CADTH explored an additional analysis that considered the impact of using the postprogression utility value derived from PROfound, a study of olaparib monotherapy in adult patients with BRCA-mutated mCRPC who progressed following prior treatment with an NHA.28 The study reported a postprogression utility value of |||||.
Use of RDI underestimated drug acquisition costs. In the sponsor’s base-case analysis, the mean RDI observed in the PROpel trial was used to derive the drug acquisition cost for all therapies (i.e., expected versus observed doses). The inclusion of RDI may underestimate the total cost of olaparib in real-world clinical practice as the dose received by patients may be different from the planned dose for several reasons (i.e., missed, delayed, or deescalated doses). CADTH notes that, when considering wastage, each reason determining a reduction in RDI may have a different impact on drug costs. Likewise, it is unclear how treatment discontinuation influences RDI. Furthermore, for oral therapies, pharmacies in Canada are likely to fill and dispense prescriptions in full. Without evidence to suggest that patients will delay filling prescriptions, it is not certain that unused tablets will result in lower drug costs. In addition, the sponsor did not provide justification as to why compliance in the real-world setting would be expected to be different across treatments included in the model. Consistent with previous reviews, given the inability to link distinct dose intensity levels with outcomes, the CADTH base case does not incorporate RDI.
CADTH conducted a reanalysis by assuming 100% RDI for all therapies considered.
Proportion of patients pretested for mutation status is uncertain. Olaparib plus abiraterone is indicated for the first-line treatment of adult patients with deleterious or suspected deleterious germline and/or somatic BRCA-mutated mCRPC, for whom chemotherapy is not clinically indicated. As such, BRCA1 or BRCA2 mutation must be confirmed before the treatment is initiated. The sponsor considered that, following the introduction of olaparib plus abiraterone, diagnostic testing costs would apply to all patients with first-line mCRPC. The model included a 1-time testing cost for genetic alterations, where tumour testing was assumed to be performed using archived formalin-fixed paraffin-embedded tumour tissue from biopsies from the prostate or metastases or from radical prostatectomy specimens. Based on the assumption that 75% of patients with mCRPC would be pretested for mutation status, the sponsor estimated that 22 tissue tests would be required to identify 1 patient with a BRCA mutation-positive diagnosis, resulting in the total testing cost of $28,317 per patient treated (Table 11). Clinical expert input sought by CADTH for this review indicated that the estimated proportion of patients assumed to be pretested for mutation status is highly uncertain and likely varies across jurisdictions and centres. The clinical experts further noted that the proportion assumed by the sponsor was likely an overestimate of the true proportion in current clinical practice in Canada.
CADTH notes that the cost-effectiveness results are generally robust to differing assumptions regarding the proportion of patients with mCRPC that would be pretested for mutation status.
Exclusion of a comparator relevant to the indicated population: Given that the submitted model focuses exclusively on patients with mCRPC who have not received prior treatment with an NHA, the sponsor excluded radium-223 as a relevant comparator from the economic analysis. The clinical experts consulted by CADTH for this review noted that radium-223 is indicated for patients for whom prior NHA treatment failed as well as for patients with symptomatic bone metastases and no known visceral metastatic disease. CADTH notes that radium-223 is currently reimbursed for the first-line treatment of mCRPC by 4 participating provincial drug programs, British Columbia, Manitoba, Ontario, and Saskatchewan. In accordance with the CADTH procedures and economic guidelines, radium-223 is considered to be a relevant comparator for the reimbursement request population, which includes NHA-experienced patients. However, CADTH notes that the use of radium-223 for the first-line treatment of mCRPC is infrequent. In a recent real-world study investigating use of systemic therapies in males with mCRPC in Canada, Shayegan et al. (2022) estimated that 3% received radium-223.29 As such, it is unlikely that the omission of radium-223 impacted the cost-effectiveness results.
CADTH was unable to address this limitation in the submitted model.
Poor modelling practices were employed. The sponsor’s submitted model included numerous IFERROR statements, resulting in situations where the parameter value was over-written with an alternative value without alerting the user to the automatized overwriting. The systematic use of IFERROR statements rendered thorough auditing of the sponsor’s model impractical, as it remains unclear whether the model ran inappropriately by overriding errors.
CADTH was unable to address this limitation, noting that a thorough validation of the submitted model was not possible.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CADTH (refer to Table 4).
Table 4: Key Assumptions of the Submitted Economic Evaluation
Sponsor’s key assumption | CADTH comment |
|---|---|
The sponsor assumed that 57.5% of tissue samples would result in a conclusive genetic test result. This detection rate was sourced from Hussain et al. (2022).16 | Reasonable. Clinical experts noted that the detection rate (i.e., tissue samples yielding a sequencing readout) obtained in the PROfound trial (n = 4,858 tissue samples) is generalizable to real-world clinical practice in Canada. CADTH noted that the PROfound trial required training in sample collection to improve generation of sequencing results due to the lower than anticipated detection rates observed in the early stages of the trial (52%). Using the detection rate from the PROfound trial obtained before within-trial training does not have a substantial impact on the cost-effectiveness of olaparib + abiraterone. |
CADTH Reanalyses of the Economic Evaluation
Base-Case Results
CADTH reanalyses were derived by making changes to model parameter values and assumptions, in consultation with clinical experts. The following changes were made to address several limitations within the economic model: using the gamma distribution to extrapolate OS for olaparib plus abiraterone; using the log-normal parametric distribution to extrapolate time to treatment discontinuation of olaparib and time to treatment discontinuation of abiraterone; sourcing utilities from alternative sources; and assuming 100% RDI for all therapies considered. These changes are summarized in Table 5.
Table 5: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
None | — | — |
Changes to derive the CADTH base case | ||
1. Impact of OLA + ABI on long-term OS is uncertain | OS for OLA + ABI was modelled using the log-normal distribution | OS for OLA + ABI was modelled using the gamma distribution |
2. TTD and TTDA for patients receiving OLA + ABI is uncertain. | TTD and TTDA in the OLA + ABI group were modelled using the gamma distribution. | TTD and TTDA in the OLA + ABI group were modelled using the log-normal distribution. |
3. Utility values |
|
|
4. Use of RDI underestimated drug acquisition costs | OLA + ABI:
ABI:
ENZA: ||||| | OLA + ABI:
ABI:
ENZA: 100% |
CADTH base case | Reanalyses 1 + 2 + 3 + 4 | |
ABI = abiraterone; ENZA = enzalutamide; OLA = olaparib; OLA + ABI = olaparib plus abiraterone; OS = overall survival; RDI = relative dose intensity; TTD = time to treatment discontinuation of olaparib; TTDA = time to treatment discontinuation of abiraterone.
In the CADTH base case, olaparib plus abiraterone was more costly and produced more QALYs than all comparators. The cost-effectiveness frontier constituted abiraterone and olaparib plus abiraterone (representing the optimal therapies). Enzalutamide was extendedly dominated. Compared with abiraterone, olaparib plus abiraterone was associated with an incremental QALY gain of 3.17 at an incremental cost of $508,237, resulting in an ICER of $160,535 per QALY gained. The probability that olaparib plus abiraterone was cost-effective at a WTP threshold of $50,000 per QALY was 2%.
The estimated ICER was higher than the sponsor’s base-case value, driven primarily by the use of alternative parametric distributions based on Kaplan-Meier data from the PROpel trial to extrapolate the OS of olaparib plus abiraterone, as well as time to treatment discontinuation of olaparib and time to treatment discontinuation of abiraterone. In line with clinical expert advice, the CADTH reanalysis achieved more plausible estimates in the absence of long-term evidence, while still conferring a survival benefit with olaparib and abiraterone. Most incremental QALYs were due to improvements in life-years. Furthermore, 73% of incremental QALYs gained by patients receiving olaparib and abiraterone were derived from the extrapolated period for which there are no observed trial data. The majority of the total cost of patients receiving olaparib and abiraterone was associated with drug acquisition costs (85%). The key cost driver among patients receiving abiraterone was also drug acquisition costs (52%). Diagnostic testing accounted for 5% of total costs among patients treated with olaparib and abiraterone.
The CADTH base case is based on publicly available prices of the comparator treatments. A detailed breakdown of the disaggregated results is available in Table 15.
Table 6: Summary of the Stepped Analysis of the CADTH Reanalysis Results, Deterministic
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|---|
Sponsor’s base case: Deterministic | ABI | 90,900 | 2.26 | Reference |
OLA + ABI | 522,681 | 6.71 | 96,957 | |
CADTH reanalysis 1: OS for OLA + ABI | ABI | 90,900 | 2.26 | Reference |
OLA + ABI | 509,814 | 5.54 | 127,919 | |
CADTH reanalysis 2: TTD and TTDA | ABI | 90,900 | 2.26 | Reference |
OLA + ABI | 619,785 | 6.71 | 118,762 | |
CADTH reanalysis 3: Utility values | ABI | 90,900 | 1.94 | Reference |
OLA + ABI | 522,681 | 6.03 | 105,583 | |
CADTH reanalysis 4: RDI | ABI | 92,267 | 2.26 | Reference |
OLA + ABI | 553,610 | 6.71 | 103,596 | |
CADTH base case: (1 + 2 + 3 + 4) | ABI | 92,267 | 1.94 | Reference |
OLA + ABI | 645,395 | 5.16 | 171,856 | |
CADTH base case: Probabilistic | ABI | 91,832 | 2.31 | Reference |
OLA + ABI | 600,069 | 5.47 | 160,535 |
ABI = abiraterone; ICER = incremental cost-effectiveness ratio; OLA + ABI = olaparib plus abiraterone; OS = overall survival; QALY = quality-adjusted life-year; RDI = relative dose intensity; TTD = time to treatment discontinuation of olaparib; TTDA = time to treatment discontinuation of abiraterone.
Table 7: Summary of the CADTH Reanalysis Results, Probabilistic
Drug | Total costs ($) | Total LYs | Total QALYs | Sequential ICER ($/QALY) |
|---|---|---|---|---|
CADTH base case | ||||
ABI | 91,832 | 2.76 | 2.31 | Reference |
OLA + ABI | 600,069 | 6.49 | 5.47 | 160,535 |
Dominated treatments | ||||
ENZA | 94,633 | 2.78 | 2.32 | Dominated |
ABI = abiraterone; ENZA = enzalutamide; ICER = incremental cost-effectiveness ratio; LY = life-year; OLA = olaparib; OLA + ABI = olaparib plus abiraterone; QALY = quality-adjusted life-year.
Scenario Analysis Results
CADTH undertook price reduction analyses based on the sponsor’s results and CADTH’s reanalyses. Results of the CADTH reanalysis suggest that there is no price reduction upon which olaparib plus abiraterone would be considered cost-effective relative to abiraterone at the WTP threshold of $50,000 per QALY gained (Table 8). This is because patients are assumed to receive abiraterone for longer when it is used in combination with olaparib than when it used as monotherapy. As such, when reducing the price of olaparib by 100%, the drug acquisition cost of the abiraterone component of the combination regimen is substantially higher than the drug acquisition cost of abiraterone alone. Given the longer time on treatment with the combination regimen in CADTH’s base case, a price reduction of approximately 60% is required to achieve an ICER of $100,000 per QALY gained.
Table 8: CADTH Price Reduction Analyses
Analysis (price reduction for OLA) | ICERs for OLA + ABI vs. ABI ($/QALY) | |
|---|---|---|
Sponsor’s base case | CADTH’s reanalysis | |
No price reduction | 96,958 | 171,856 |
10% | 90,472 | 159,700 |
20% | 83,986 | 147,544 |
30% | 77,500 | 135,388 |
40% | 71,014 | 123,231 |
50% | 64,528 | 111,075 |
60% | 58,042 | 98,919 |
70% | 51,557 | 86,763 |
80% | 45,071 | 74,607 |
90% | 38,585 | 62,451 |
100% | 32,099 | 50,295 |
ABI = abiraterone; ICER = incremental cost-effectiveness ratio; OLA = olaparib; OLA + ABI = olaparib and abiraterone; QALY = quality-adjusted life-year; vs. = versus.
Note: Based on deterministic analysis results.
Although there is no price reduction upon which olaparib plus abiraterone would be considered cost-effective at the WTP threshold of $50,000 per QALY gained, CADTH acknowledges that a 100% price reduction could not be expected to be practically implemented by decision-makers. CADTH explored revising the extrapolation of time to treatment discontinuation of olaparib and of abiraterone among patients treated with olaparib plus abiraterone back to the gamma distribution, in line with the sponsor’s submission. As noted in Table 17, which presents the proportion of patients receiving olaparib plus abiraterone as part of the combination therapy at different years in the model, when using the gamma distribution to extrapolate time to treatment discontinuation of olaparib and time to treatment discontinuation of abiraterone, a shorter average time on treatment for patients treated with olaparib plus abiraterone is assumed. However, this results in an assumed rPFS benefit beyond treatment duration that does not align with available evidence and clinical expert feedback. Based on this analysis, a 91% price reduction would be required for olaparib plus abiraterone to be cost-effective at a WTP threshold of $50,000 per QALY gained.
CADTH explored another analysis to determine the price reduction required for the full regimen of olaparib plus abiraterone to be cost-effective at a WTP threshold of $50,000 per QALY gained. In this scenario, a 79% price reduction for both olaparib and abiraterone were required. The price reductions for abiraterone were assumed to apply to both the regimen under review and the comparator treatment. CADTH presented this analysis to further highlight pricing considerations for olaparib in this setting, acknowledging that different manufacturers are responsible for the treatment, and as such, implementing this approach may not be feasible.
To address concerns regarding the uncertainty associated with the postprogression utility values, CADTH explored yet another analysis that considered the impact of using the postprogression utility value derived from the PROfound trial. In this scenario, the ICER of olaparib plus abiraterone decreased to $154,774 per QALY gained, relative to abiraterone. Based on this scenario, aligned with the CADTH reanalysis results, there is no price reduction upon which olaparib plus abiraterone would be considered cost-effective relative to abiraterone at a WTP threshold of $50,000 per QALY gained.
Issues for Consideration
Olaparib has previously been reviewed by CADTH for several conditions. The CADTH pan-Canadian Oncology Drug Review Expert Review Committee recommended olaparib be reimbursed in 4 of the 5 submissions to CADTH. In each recommendation to reimburse, there has been the condition of a price reduction. The pCPA concluded negotiations with a letter of intent for olaparib for multiple indications, including as monotherapy for the treatment of adult patients with mCRPC and deleterious or suspected deleterious BRCA or ATM with germline/somatic mutations in the HRR genes who have progressed following prior treatment with an NHA.30 As such, the negotiated price of olaparib is confidential, and it is currently funded by jurisdictional cancer formularies.
The clinical experts consulted by CADTH noted changes in the treatment landscape for patients with prostate cancer in recent years. In many treatment settings in Canada, patients with mCSPC receive treatment intensification such that they are treated with NHAs (including abiraterone and enzalutamide) in the metastatic setting. As a result, most of the patients who progress to mCRPC will have already received treatment with an NHA and would likely not to be retreated. For these patients, the most common approach to first-line mCRPC treatment is taxane-based chemotherapy (i.e., docetaxel). It is important to note that there is no direct comparative efficacy data for olaparib plus abiraterone compared to docetaxel and the relative cost-effectiveness is unknown. The use of olaparib plus abiraterone in place of docetaxel would have additional budget impact implications that not have been explored in this review.
At the time of writing this report, niraparib (Akeega) in combination with abiraterone and prednisone is under review for the treatment of adult patients with deleterious or suspected deleterious germline and/or somatic BRCA-mutated mCRPC, who are asymptomatic or mildly symptomatic, and for whom chemotherapy is not clinically indicated. Given that this indication overlaps with the population being assessed in the current review for olaparib plus abiraterone, niraparib may be a relevant comparator that could not be included in the present analysis. The cost-effectiveness of olaparib plus abiraterone compared to niraparib in combination with abiraterone is unknown. In addition, it is uncertain how the introduction of niraparib-abiraterone will affect market share expectations and, subsequently, the budgetary impact.
To receive treatment with olaparib and abiraterone, patients must have a germline or somatically confirmed BRCA mutation. As this will be the first first-line treatment for mCRPC that is dependent on genetic testing results, it is anticipated that there will be an increase in the overall number of genetic tests undertaken by patients with prostate cancer. Drug program input noted that while some provinces may already test for BRCA mutations before olaparib monotherapy as a later-line therapy, genetic testing at diagnosis (i.e., before first-line treatment) is not standard practice in all CADTH-participating jurisdictions. The increase in genetic testing of prostate cancer patients represents an added cost to the health care system. Further, the actual cost of companion diagnostic tests is uncertain due to the use of different platforms and testing methods (e.g., multipanel somatic gene testing or next-generation sequencing).
The pCPA concluded negotiations with a letter of intent for enzalutamide for multiple indications: mCSPC, nonmetastatic castrate-resistant prostate cancer, and first- and subsequent-line mCRPC.31-34 As such enzalutamide has a confidential negotiated price, and is currently funded by jurisdictional cancer formularies.35,36 The CADTH reanalyses are based on the publicly available price of enzalutamide, which may be different from the confidential price and may influence the results of the cost-effectiveness and BIAs.
The pCPA concluded negotiations with a letter of intent for abiraterone acetate for the treatment of mCRPC. As such, abiraterone acetate has a confidential negotiated price, and is currently funded by jurisdictional cancer formularies.35-37 The CADTH reanalyses are based on the publicly available price of abiraterone acetate, which may be different from the confidential price and may influence the results of the cost-effectiveness and BIAs.
Overall Conclusions
Evidence from a subgroup of patients with a BRCA mutation in the PROpel trial, a phase III, double-blind randomized controlled trial, suggests that treatment with olaparib plus abiraterone and prednisone or prednisolone may result in a clinically important increase in OS and rPFS when compared with abiraterone, when used as first-line treatment for patients with mCRPC who are NHA-naive and are not clinically indicated for chemotherapy. However, the CADTH Clinical Review Report described the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) of the available evidence as at a low level of certainty, and concluded that longer duration of follow-up is needed to examine the long-term clinical benefits and risks of this combination regimen given the immaturity of the available data. The CADTH Clinical Review Report indicated that since randomization was not stratified by BRCA mutation status, the small sample size and number of events raised concerns regarding potential overestimation of the true effect. Moreover, there is evidence of prognostic imbalance across important baseline patient characteristics, which may bias the results in favour of olaparib plus abiraterone. Evidence for olaparib plus abiraterone versus other active treatments in the subgroup of patients with BRCA mutation in the first-line setting was not available at the time of this review.
In addition to the previously mentioned limitations, CADTH identified several limitations with the sponsor’s economic submission that could be addressed through reanalyses. For the CADTH base-case analysis, CADTH revised the OS assumptions for olaparib plus abiraterone, which led to more plausible estimates of survival benefit; used alternative parametric distributions to extrapolate time to treatment discontinuation of olaparib and time to treatment discontinuation of abiraterone, which were aligned with the extrapolated rPFS for olaparib plus abiraterone; applied alternative health state utility values derived from published sources, which met clinical face validity; and removed RDI assumptions across treatments. In the CADTH base case, olaparib plus abiraterone was associated with an ICER of $160,535 per QALY gained, compared with abiraterone (incremental cost: $508,237; incremental QALYs: 3.17). Enzalutamide was similarly effective but more costly than abiraterone. The probability that olaparib plus abiraterone would be cost-effective at a WTP threshold of $50,000 per QALY was 2%. The estimated ICER was higher than the sponsor’s estimate, driven primarily by the use of alternative parametric distributions to extrapolate the OS of olaparib plus abiraterone, as well as predictions for time to treatment discontinuation of olaparib and time to treatment discontinuation of abiraterone. The CADTH base case conferred a sizable survival benefit to olaparib plus abiraterone (3.73 life-years), which is more closely aligned with clinical expert expectations, relative to the sponsor’s estimate.
As a result of the longer time to discontinuation for both drugs within the olaparib plus abiraterone regimen in the CADTH reanalysis, patients are expected to incur an increase in treatment costs of more than $500,000 over the course of their lifetime, while other health care costs remain similar. Given the cost of olaparib ($102,000 per patient annually) and the fact that it is taken in combination with abiraterone, there is no price reduction upon which olaparib plus abiraterone would be considered cost-effective relative to abiraterone at the WTP threshold of $50,000 per QALY gained. Were a decision-maker to consider other WTP thresholds, a price reduction for olaparib could be reached that achieves cost-effectiveness for the olaparib plus abiraterone regimen. For example, using the CADTH base case, a 60% price reduction could achieve an ICER of $100,000 per QALY gained. This is because patients are assumed to receive abiraterone longer when used in combination with olaparib than when used as monotherapy. Therefore, when reducing the price of olaparib by 100%, the drug acquisition cost of the abiraterone component of the combination regimen is substantially higher than the drug acquisition cost of abiraterone alone.
To highlight the impact of longer treatment duration, CADTH explored reducing the time to treatment discontinuation for olaparib plus abiraterone using the sponsor’s assumptions, despite that this analysis resulted in an assumed rPFS benefit beyond treatment duration. This analysis indicated that a price reduction of at least 91% would be required to achieve an ICER of $50,000 per QALY gained. An additional analysis explored the price reduction required for the olaparib plus abiraterone regimen to be considered cost-effective at a WTP threshold of $50,000 per QALY gained, although CADTH acknowledges the challenges with feasibly implementing such a pricing condition. CADTH acknowledges that olaparib, abiraterone, and enzalutamide each went through pCPA and that negotiations concluded with a letter of intent, suggesting there are already negotiated prices for the treatments considered in the analysis.
CADTH could not address some considerations, such as the lack of comparative evidence for olaparib plus abiraterone in the NHA-experienced population. Furthermore, the indication for olaparib plus abiraterone stipulates that it is for use in patients “in whom chemotherapy is not clinically indicated” and how the clinical indication for chemotherapy would be defined in clinical practice is uncertain. In light of this uncertainty, the cost-effectiveness results may not be generalizable to the patient population that is most likely to receive olaparib and abiraterone in Canada.
References
1.Cost-effectiveness model for olaparib plus abiraterone and prednisone/prednisolone for the first-line treatment of metastatic castration-resistant prostate cancer (mCRPC) [internal sponsor's report]. Mississauga (ON): AstraZeneca Canada; 2023 May 19.
2.PrLynparza® (olaparib): 100 mg and 150 mg tablets [product monograph]. Mississauga (ON): AstraZeneca Canada; 2023 Jul 10.
3.Saad F, Armstrong AJ, Thiery-Vuillemin A, et al. PROpel: phase III trial of olaparib (ola) and abiraterone (abi) versus placebo (pbo) and abi as first-line (1L) therapy for patients (pts) with metastatic castration-resistant prostate cancer (mCRPC) [abstract]. J Clin Oncol. 2022;40(6_suppl):11.
4.Clarke N, Armstrong A, Thiery-Vuillemin A, et al. Abiraterone and olaparib for metastatic castration-resistant prostate cancer. NEJM. 2022;1(9). PubMed
5.Kearns B, Pandor A, Stevenson M, et al. Cabazitaxel for hormone-relapsed metastatic prostate cancer previously treated with a docetaxel-containing regimen: an evidence review group perspective of a NICE single technology appraisal. Pharmacoeconomics. 2017;35(4):415-424. PubMed
6.Xie F, Pullenayegum E, Gaebel K, et al. A Time Trade-off-derived Value Set of the EQ-5D-5L for Canada. Med Care. 2016;54(1):98-105. PubMed
7.Armstrong AJ, Lin P, Tombal B, et al. Five-year survival prediction and safety outcomes with enzalutamide in men with chemotherapy-naïve metastatic castration-resistant prostate cancer from the PREVAIL trial. Eur Urol. 2020;78(3):347-357. PubMed
8.Evans CP, Higano CS, Keane T, et al. The PREVAIL study: primary outcomes by site and extent of baseline disease for enzalutamide-treated men with chemotherapy-naïve metastatic castration-resistant prostate cancer. Eur Urol. 2016;70(4):675-683. PubMed
9.Sullivan PW, Slejko JF, Sculpher MJ, Ghushchyan V. Catalogue of EQ-5D scores for the United Kingdom. Med Decis Making. 2011;31(6):800-804. PubMed
10.Rowe MP, Walter S, Hidayat A, et al. An analysis of survival in patients with castrate-resistant prostate cancer receiving enzalutamide with treatment breaks. J Clin Urolog. 2022;15(3):257-263.
11.Ontario Ministry of Health, Ontario Ministry of Long-Term Care. Ontario drug benefit formulary/comparative drug index. 2023; https://www.formulary.health.gov.on.ca/formulary/. Accessed 2023 Aug 10.
12.pan-Canadian Oncology Drug Review final economic guidance report: pembrolizumab (Keytruda) for metastatic urothelial carcinoma. Ottawa (ON): CADTH; 2018: https://www.cadth.ca/sites/default/files/pcodr/pcodr_pembrolizumab_keytruda_muc_fn_egr.pdf. Accessed 2023 Jun 9.
13.pCODR Expert Review Committee (pERC) final recommendation: avelumab (Bavenclo) for mMCC. Ottawa ON): CADTH; 2018: https://www.cadth.ca/sites/default/files/pcodr/pcodr_avelumab_bavencio_mcc_fn_rec.pdf. Accessed 2023 Jun 9.
14.Cancer Care Ontario. Drug Formulary. GDP - provider monograph. 2019; https://www.cancercareontario.ca/en/drugformulary/regimens/monograph/46166. Accessed 2022 Aug 15.
15.Pritchard CC, Mateo J, Walsh MF, et al. Inherited DNA-repair gene mutations in men with metastatic prostate cancer. NEJM. 2016;375(5):443-453. PubMed
16.Hussain M, Corcoran C, Sibilla C, et al. Tumor genomic testing for >4,000 men with metastatic castration-resistant prostate cancer in the phase III trial PROfound (olaparib). Clin Cancer Res. 2022;28(8):1518-1530. PubMed
17.Patel YP, Husereau D, Leighl NB, Melosky B, Nam J. Health and budget impact of liquid-biopsy-based Comprehensive Genomic Profile (CGP) testing in tissue-limited advanced non-small cell lung cancer (aNSCLC) patients. Curr Oncol. 2021;28(6):5278-5294. PubMed
18.Trapani D, Tay-Teo K, Tesch ME, et al. Implications of oncology trial design and uncertainties in efficacy-safety data on health technology assessments. Curr Oncol. 2022;29(8):5774-5791. PubMed
19.Ontario Case Costing Initiative (OCCI). Ambulatory care 2017/2018 by procedure Toronto (ON): Ontario Ministry of Health and Long-Term Care: https://data.ontario.ca/dataset/ontario-case-costing-initiative-occi. Accessed 2023 Dec 1.
20.Canadian Institute for Health Information (CIHI). https://www.cihi.ca/en. Accessed 2023 Mar 23.
21.Everest L, Blommaert S, Chu RW, Chan KKW, Parmar A. Parametric survival extrapolation of early survival data in economic analyses: a comparison of projected versus observed updated survival. Value Health. 2022;25(4):622-629. PubMed
22.Latimer N. NICE DSU Technical Support Document 14: survival analysis for economic evaluations alongside clinical trials - extrapolation with patient-level data. Sheffield (UK): University of Sheffield; 2011: https://www.ncbi.nlm.nih.gov/books/NBK395885/pdf/Bookshelf_NBK395885.pdf. Accessed 2023 Aug 15.
23.Latimer N. Survival analysis for economic evaluations alongside clinical trials—extrapolation with patient-level data: Inconsistencies, limitations, and a practical guide. Med Decis Making. 2013;33(6):743-754. PubMed
24.Guertin JR, Feeny D, Tarride JE. Age- and sex-specific Canadian utility norms, based on the 2013-2014 Canadian Community Health Survey. CMAJ. 2018;190(6):E155-E161. PubMed
25.Ryan CJ, Smith MR, Fizazi K, et al. Abiraterone acetate plus prednisone versus placebo plus prednisone in chemotherapy-naive men with metastatic castration-resistant prostate cancer (COU-AA-302): final overall survival analysis of a randomised, double-blind, placebo-controlled phase 3 study. Lancet Oncol. 2015;16(2):152-160. PubMed
26.Diels J, Hamberg P, Ford D, Price PW, Spencer M, Dass RN. Mapping FACT-P to EQ-5D in a large cross-sectional study of metastatic castration-resistant prostate cancer patients. Qual Life Res. 2015;24(3):591-598. PubMed
27.Sandblom G, Carlsson P, Sennfält K, Varenhorst E. A population-based study of pain and quality of life during the year before death in men with prostate cancer. Br J Cancer. 2004;90(6):1163-1168. PubMed
28.Hussain M, Mateo J, Fizazi K, et al. Survival with olaparib in metastatic castration-resistant prostate cancer. N Engl J Med. 2020;383(24):2345-2357. PubMed
29.Shayegan B, Wallis CJD, Malone S, et al. Real-world use of systemic therapies in men with metastatic castration resistant prostate cancer (mCRPC) in Canada. Urol Oncol. 2022;40(5):192.e191-192.e199. PubMed
30.pan-Canadian Pharmaceutical Alliance. Lynparza (olaparib). 2022; https://www.pcpacanada.ca/negotiation/21464. Accessed 2023 Aug 21.
31.pan-Canadian Pharmaceutical Alliance. Xtandi (enzalutamide). 2015; https://www.pcpacanada.ca/negotiation/20809. Accessed 2023 Aug 21.
32.pan-Canadian Pharmaceutical Alliance. Xtandi (enzalutamide). 2020; https://www.pcpacanada.ca/negotiation/21112. Accessed 2023 Aug 21.
33.pan-Canadian Pharmaceutical Alliance. Xtandi (enzalutamide). 2021; https://www.pcpacanada.ca/negotiation/21298. Accessed 2023 Aug 21.
34.pan-Canadian Pharmaceutical Alliance. Xtandi (enzalutamide). 2013; https://www.pcpacanada.ca/negotiation/20762. Accessed 2023 Aug 21.
35.Saskatchewan Cancer Agency. Drug Formulary. 2023; http://www.saskcancer.ca/health-professionals-article/drug-formulary. Accessed 2023 Aug 21.
36.Cancer Care Ontario: funded evidence-informed regimens. 2022; https://www.cancercareontario.ca/en/drugformulary/regimens. Accessed 2023 Aug 23.
37.pan-Canadian Pharmaceutical Alliance. Zytiga (abiraterone). 2014; https://www.pcpacanada.ca/negotiation/20774. Accessed 2023 Aug 21.
38.Woon DT, Chandrasekar T, Aaron L, et al. Disparity in public funding of therapies for metastatic castrate-resistant prostate cancer across Canadian provinces. Can Urolog Assoc J. 2018;12(10):328. PubMed
39.Budget-Impact Model for olaparib in combination with abiraterone and prednisone/prednisolone for the first-line treatment of BRCA1/2-mutated adult patients with metastatic castration-resistant prostate cancer (mCRPC) who are NHA-naïve and for whom chemotherapy is not clinically indicated: Canadian perspective [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Lynparza (olaparib), 100 mg and 150 mg tablets. Mississauga (ON): AstraZeneca Canada; 2023 May 19.
40.A real world observational study characterizing Canadian Advanced Prostate cancer patients treated with or without Androgen receptor-axis-targeted therapies (ARATs) [internal sponsor's report]. Mississauga (ON): AstraZeneca Canada Inc.; 2023 May 19.
41.Clinical Study Report D081SC00001 (PROpel): A randomised, double-blind, placebo- controlled, multicentre phase iii study of olaparib plus abiraterone relative to placebo plus abiraterone as first-line therapy in men with metastatic castration-resistant prostate cancer [internal sponsor's report]. Mississauga (ON): AstraZeneca Canada; 2023 May 19.
42.Chowdhury S, Bjartell A, Lumen N, et al. Real-world outcomes in first-line treatment of metastatic castration-resistant prostate cancer: the Prostate Cancer Registry. Target Oncol. 2020;15(3):301-315. PubMed
43.Table 17-10-0005-01. Population estimates on July 1st, by age and sex. Ottawa (ON): Statistics Canada; 2022: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1710000501. Accessed 2023 May 30.
44.Thurin NH, Rouyer M, Gross-Goupil M, et al. Epidemiology of metastatic castration-resistant prostate cancer: a first estimate of incidence and prevalence using the French nationwide healthcare database. Cancer Epidemiol. 2020;69:101833. PubMed
45.Shayegan B, Wallis CJD, Hamilton RJ, et al. Real-world utilization and outcomes of docetaxel among older men with metastatic prostate cancer: a retrospective population-based cohort study in Canada. Prostate Cancer Prostatic Dis. 2023;26(1):74-79. PubMed
Appendix 1: Cost Comparison Table
Note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical experts and drug plans. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 9: CADTH Cost Comparison Table for Metastatic Castration-Resistant Prostate Cancer
Treatment | Strength / concentration | Form | Price | Recommended dosage | Daily cost | Average 28-day cost |
|---|---|---|---|---|---|---|
Olaparib (Lynparza) | 100 mg 150 mg | Tablet | 69.9482a | 300 mg twice daily | 280 | 7,834 |
Abiraterone (generic) | 250 mg 500 mg | Tablet | 26.0313 52.0625 | 1,000 mg daily | 104 | 2,916 |
Prednisone (generic) | 5 mg | Tablet | 0.0220 | 10 mg daily | 0.04 | 1 |
Olaparib and abiraterone, with prednisone | — | — | — | — | — | 10,751 |
Androgen receptor-axis-targeted (ARAT) therapy | ||||||
Abiraterone (generic) | 250 mg 500 mg | Tablet | 26.0313 52.0625 | 1,000 mg daily | 104 | 2,916 |
Prednisone (generic) | 5 mg | Tablet | 0.0220 | 10 mg daily | 0.04 | 1 |
Abiraterone, taken with prednisone | — | — | — | — | 104 | 2,917 |
Enzalutamide (Xtandi) | 40 mg | Tablet | 29.1954 | 160 mg daily | 117 | 3,270 |
Radiopharmaceutical | ||||||
Radium-223 (Xofigo) | 1,100 kBq/mL | Vial | 5,640.0000b | 55 kBq per kg, given at 4-week intervals for a total of 6 injections | 201 | 5,640 |
Note: All prices are wholesale from IQVIA Delta PA (accessed June 2023), unless otherwise indicated, and do not include dispensing fees.
aSponsor’s submitted price.1
bPrice sourced from Woon et al. 2018.38
Appendix 2: Submission Quality
Note that this appendix has not been copy-edited.
Description | Yes/No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | No | Although the indicated population is NHA-agnostic, the population included in the PROpel trial was restricted to patients who are NHA-naive. As such, the modelled cohort excludes patients with mCRPC who have failed on prior treatment with an NHA. Clinical experts noted that radium-223 is indicated for patients who are NHA-experienced, therefore, the sponsor omitted a relevant comparator for the reimbursement request population. The model also has generalizability concerns given the degree of uncertainty around defining the clinical indication for chemotherapy. |
Model has been adequately programmed and has sufficient face validity | Yes | No comment |
Model structure is adequate for decision problem | No | The PSM further introduces structural assumptions about the relationship between rPFS and OS (i.e., non-mutually exclusive curves), which is potentially problematic since they are likely dependent outcomes. Clinical expert opinion suggested that survival is linked to the occurrence of progressive disease and thus the transition probability to death should vary for patients within the progression-free state compared to those in the progressed disease state. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | No | Poor modelling practices were employed. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | Yes | No comment |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | Yes | No comment |
NHA = next-generation hormonal agent; OS = overall survival; PSM = partitioned survival model; rPFS = radiological progression-free survival.
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note that this appendix has not been copy-edited.
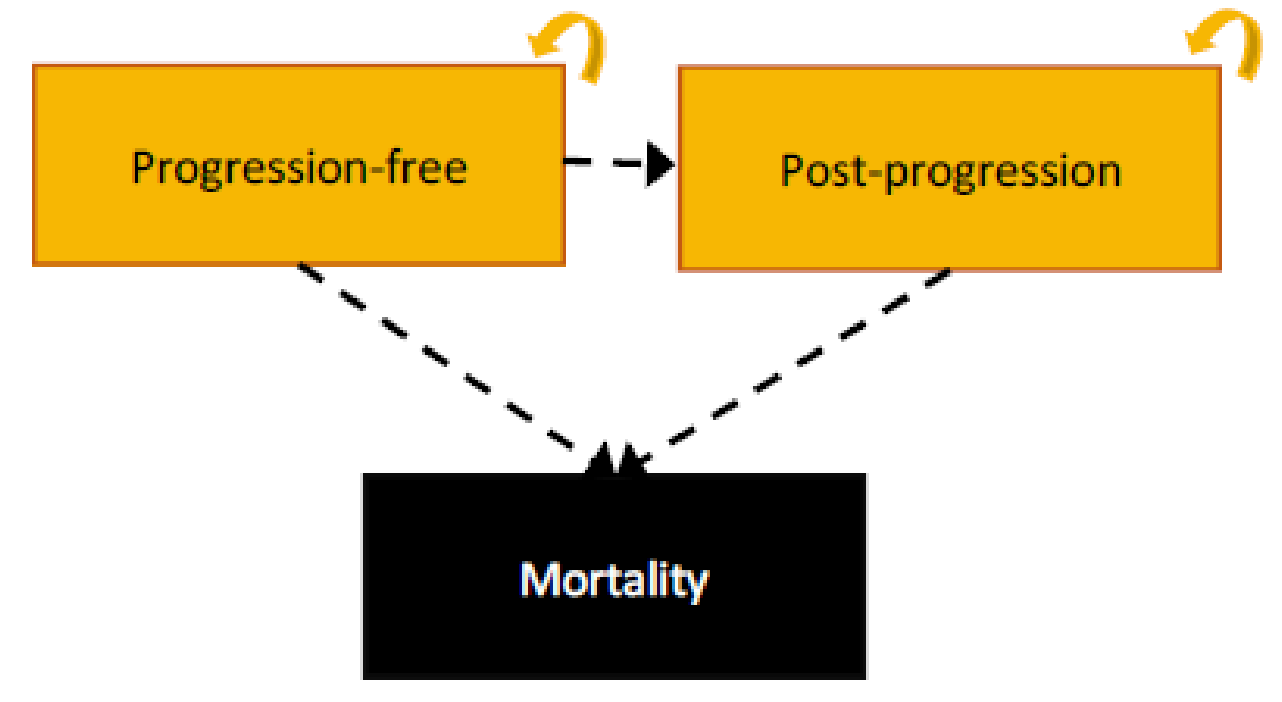
Figure 2: Relative Risk of Death for Olaparib Plus Abiraterone in Comparison With Abiraterone
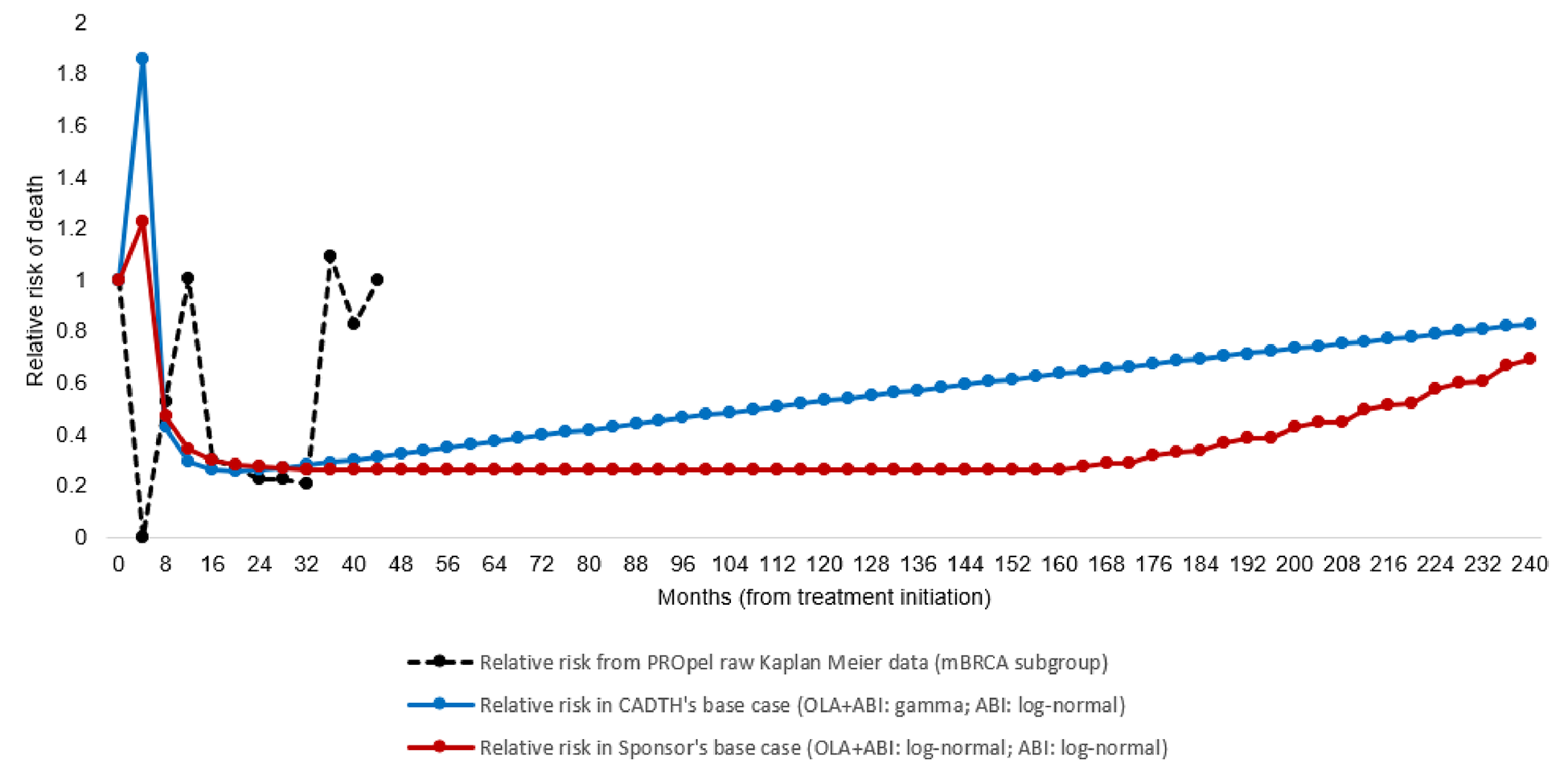
Source: CADTH calculation based on the PROpel trial Kaplan-Meier data and parametric extrapolations presented in the sponsor’s pharmacoeconomic model.
The dashed line represents the relative risk (RR) of death with olaparib plus abiraterone versus abiraterone over four-month periods, based on the raw data from the PROpel clinical trial. Data shown in the figure are simply “1 - survival at time t+1/survival at time t”. The data suggested that (1) up to month 20, the relative risk of death for patients treated with olaparib plus abiraterone compared with abiraterone fluctuates above and below 1 (matching the period when the KM curves cross); (2) from months 20 to 32, the risk of death is lower among patients treated with olaparib plus abiraterone compared with abiraterone (matching the period when the KM curves diverge); and (3) from month 32 onwards, there are limited relative effects, that is, the risk of death is similar and constant between the 2 treatment groups (i.e., RR marginally below 1). This suggests that while olaparib plus abiraterone prevented death between months 20 and 32, there is no evidence of a reduction in the relative risk of death beyond this period. The red line represents the RR of death in the sponsor’s submission, which assumed a stable risk for the majority of the extrapolated period. The blue line represents the RR of death in the CADTH base case, which assumes a gradual increase of risk throughout the model’s horizon.
Table 11: Parameters Used to Calculate Genetic Testing Costs
Component | Estimate | Source |
|---|---|---|
Proportion pre-tested for mutation status (a) | 75% | Assumptiona |
Prevalence of BRCA1 or BRCA2 mutation (b) | 10.7% | PROpel clinical trial4 |
Detection rate (c) | 57.5% | Hussain et al., 202216 |
Number of tests per patient treated (d) | 21.7 | Calculation [1/(a*b*c)] |
Unit cost of testing – Archival tumour tissue (e) | 1,304 | Patel et al., 202117 |
Proportion of tests using archival tissue (f) | 100% | Assumption |
Total testing cost per patient treated | 28,317 | Calculation (d*e*f) |
aDerived from sponsor’s internal forecasting and market research.
Source: Sponsor’s pharmacoeconomic submission.1
Table 12: Distribution of Subsequent Therapy
Subsequent therapy | First line therapy on which patients have progressed | ||
|---|---|---|---|
OLA + ABI | ABI | ENZA | |
OLA monotherapy | 0% | 10% | 10% |
ABI | 0% | 0% | 0% |
Docetaxel | 50% | 50% | 50% |
ENZA | 0% | 0% | 0% |
Cabazitaxel | 25% | 20% | 20% |
Carboplatin | 0% | 0% | 0% |
Carboplatin + cabazitaxel | 0% | 0% | 0% |
Radium-223 | 25% | 20% | 20% |
ABI = abiraterone; ENZA = enzalutamide; OLA = olaparib.
Source: Sponsor’s pharmacoeconomic submission.1
Table 13: Disaggregated Summary of the Sponsor’s Economic Evaluation Results
Parameter | OLA + ABI | ABI | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 7.81 | 2.75 | 5.06 |
Pre-progression | 5.32 | 1.41 | 3.91 |
Post-progression | 2.49 | 1.34 | 1.15 |
Discounted QALYs | |||
Total | 6.57 | 2.30 | 4.27 |
Pre-progression | 4.53 | 1.20 | 3.33 |
Post-progression | 2.05 | 1.10 | 0.95 |
Discounted costs ($) | |||
Total | 523,590 | 92,125 | 431,466 |
Diagnostic costs | 28,302 | 0 | 28,302 |
Primary therapy costs | |||
Primary therapy acquisition costs (Total) | 414,968 | 47,955 | 367,012 |
Primary therapy acquisition costs (Olaparib) | 289,248 | 289,248 | |
Primary therapy acquisition costs (Abiraterone) | 125,719 | 125,719 | |
Primary therapy routine monitoring costs | 11,207 | 4,991 | 6,216 |
Secondary therapy costs | |||
Secondary therapy acquisition and admin costs | 11,402 | 13,686 | −2,284 |
Secondary therapy routine monitoring costs | 46,935 | 14,734 | 32,201 |
Skeletal-related event costs | 1,379 | 1,543 | −164 |
Adverse event costs | 2,721 | 965 | 1,756 |
End of life costs | 6,677 | 8,250 | −1,573 |
ICER ($/QALY) | 100,929 | ||
Time to treatment discontinuation | |||
Median TTD (OLA + ABI) | 2.3 years | N/A | N/A |
Median TTDA (OLA + ABI) a | 2.6 years | N/A | N/A |
Median TTDA (ABI) | N/A | 0.8 years | N/A |
ABI = abiraterone; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; OLA = olaparib; TTD = time to treatment discontinuation of olaparib; TTDA = time to treatment discontinuation of abiraterone.
aTTDA (OLA + ABI) refers to the time to treatment discontinuation of abiraterone when used in combination with olaparib. The time to treatment discontinuation of abiraterone when used as monotherapy was not changed, in line with clinical expert opinion.
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Note that this appendix has not been copy-edited.
Detailed Results of CADTH Base Case
Table 14: Summary of CADTH’s Economic Evaluation Results, Pair-Wise
Drug | Total costs($) | Incremental costs($) | Total QALYs | Incremental QALYs | ICER($ per QALY) |
|---|---|---|---|---|---|
OLA + ABI vs. ABI | |||||
ABI | 91,832 | Reference | 2.31 | Reference | Reference |
OLA + ABI | 600,069 | 508,237 | 5.47 | 3.17 | 160,535 |
OLA + ABI vs. ENZA | |||||
ENZA | 94,633 | Reference | 2.32 | Reference | Reference |
OLA + ABI | 600,069 | 505,436 | 5.47 | 3.15 | 160,450 |
ABI = abiraterone; ENZA = enzalutamide; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; OLA = Olaparib.
Table 15: Disaggregated Summary of CADTH’s Economic Evaluation Results
Parameter | OLA + ABI | ABI | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 6.49 | 2.76 | 3.73 |
Pre-progression | 4.99 | 1.40 | 3.59 |
Post-progression | 1.50 | 1.36 | 0.14 |
Discounted QALYs | |||
Total | 5.47 | 2.31 | 3.17 |
Pre-progression | 4.24 | 1.19 | 3.05 |
Post-progression | 1.23 | 1.12 | 0.11 |
Discounted costs ($) | |||
Total | 600,069 | 91,832 | 508,237 |
Diagnostic costs | 28,322 | 0 | 28,322 |
Primary therapy costs | |||
Primary therapy acquisition costs (Total) | 508,040 | 47,785 | 460,255 |
Primary therapy acquisition costs (Olaparib) | 357,720 | 0 | 357,720 |
Primary therapy acquisition costs (Abiraterone) | 150,320 | 0 | 150,320 |
Primary therapy routine monitoring costs | 13,794 | 4,942 | 8,852 |
Secondary therapy costs | |||
Secondary therapy acquisition and admin costs | 11,548 | 13,356 | −1,808 |
Secondary therapy routine monitoring costs | 26,858 | 14,970 | 11,888 |
Skeletal-related event costs | 1,399 | 1,548 | −149 |
Adverse event costs | 2,716 | 964 | 1,752 |
End of life costs | 7,392 | 8,267 | −875 |
ICER ($/QALY) | 160,535 | ||
Time to treatment discontinuation | |||
Median TTD (OLA + ABI) | 2.3 years | N/A | N/A |
Median TTDA (OLA + ABI) a | 2.5 years | N/A | N/A |
Median TTDA (ABI) | N/A | 0.8 years | N/A |
ABI = abiraterone; ICER = incremental cost-effectiveness ratio; OLA = olaparib; QALY = quality-adjusted life-year; TTD = time to treatment discontinuation of olaparib; TTDA = time to treatment discontinuation of abiraterone.
aTTDA (OLA + ABI) refers to the time to treatment discontinuation of abiraterone when used in combination with olaparib. The time to treatment discontinuation of abiraterone when used as monotherapy was not changed, in line with clinical expert opinion.
Table 16: Exploratory Analysis of CADTH’s Economic Evaluation Results, Deterministic
Scenario analysis | Drug | Total costs ($) | Total QALYs | ICER ($ per QALYs) |
|---|---|---|---|---|
CADTH base case | ABI | 92,267 | 1.94 | Reference |
OLA + ABI | 645,395 | 5.16 | 171,856 | |
CADTH exploratory analysis 1: TTD and TTDA (gamma distribution) | ABI | 92,267 | 1.94 | Reference |
OLA + ABI | 540,743 | 5.16 | 139,341 | |
CADTH exploratory analysis 2: Reducing the price of OLA and ABI simultaneously by 79% | ABI | 51,128 | 1.94 | Reference |
OLA + ABI | 208,032 | 5.16 | 48,750 | |
CADTH exploratory analysis 3: Alternative utility value for the post-progression health state (0.757) | ABI | 91,772 | 2.30 | Reference |
OLA + ABI | 596,832 | 5.56 | 154,774 |
ABI = abiraterone; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; OLA = olaparib; TTD = time to treatment discontinuation of olaparib; TTDA = time to treatment discontinuation of abiraterone.
Note: all results reported above are deterministic analyses.
aTTDA refers to the time to treatment discontinuation of abiraterone when used in combination with olaparib. The time to treatment discontinuation of abiraterone when used as monotherapy was not changed, in line with clinical expert opinion.
Based on the results from exploratory analysis 1, CADTH notes that a 91% price reduction would be required for olaparib + abiraterone to be cost-effective at a willingness-to-pay threshold of $50,000 per QALY gained, and a 60% price reduction to achieve cost-effectiveness at a willingness-to-pay threshold of $100,000 per QALY gained.
Table 17: Time to Treatment Discontinuation of Olaparib and Time to Treatment Discontinuation of Abiraterone
Parameter | 1 year | 2 years | 3 years | 5 years | 10 years | 15 years | 20 years | Mediana |
|---|---|---|---|---|---|---|---|---|
TTD (OLA + ABI) | ||||||||
CADTH base case (log-normal) | 75% | 54% | 40% | 25% | 10% | 5% | 3% | 2.3 years |
CADTH scenario 1 (gamma)b | 78% | 56% | 40% | 20% | 3% | 0% | 0% | 2.3 years |
PROpel Kaplan-Meier data | 74% | 51% | 47% | — | — | — | — | — |
TTDA (OLA + ABI)c | ||||||||
CADTH base case (Log-normal) | 77% | 57% | 44% | 29% | 13% | 7% | 4% | 2.5 years |
CADTH scenario 1 (Gamma)b | 79% | 60% | 44% | 24% | 5% | 1% | 0% | 2.6 years |
PROpel Kaplan-Meier data | 74% | 53% | 49% | — | — | — | — | — |
ABI = abiraterone; OLA = olaparib; TTD = time to treatment discontinuation of olaparib; TTDA = time to treatment discontinuation of abiraterone.
aMean time to discontinuation could not be determined by CADTH based on the way it was presented in the submitted model.
bCADTH scenario 1 uses the same approach as the sponsor initially submitted.
cTTDA (OLA + ABI) refers to the time to treatment discontinuation of abiraterone when used in combination with olaparib. The time to treatment discontinuation of abiraterone when used as monotherapy was not changed, in line with clinical expert opinion.
Appendix 5: Submitted BIA and CADTH Appraisal
Note that this appendix has not been copy-edited.
Table 18: Summary of Key Take-Aways
Key Take-Aways of the BIA |
|---|
|
Summary of Sponsor’s BIA
The sponsor submitted a BIA to estimate the incremental 3-year budget impact of reimbursing olaparib plus abiraterone for the first-line treatment of adult patients with BRCA1- or BRCA2-mutated mCRPC who are NHA-naive, and for whom chemotherapy is not clinically indicated, as per its reimbursement request.39 The analysis was performed from the perspective of the Canadian public drug plan formulary. The sponsor estimated the budget impact by comparing 2 scenarios: a reference scenario that estimated the total costs associated with the current standard of care (i.e., abiraterone and enzalutamide monotherapy) for the first-line treatment of patients with BRCA1- or BRCA2-mutated mCRPC who are NHA-naive, and for whom chemotherapy is not clinically indicated; and a new drug scenario, where olaparib plus abiraterone is funded in the first line setting. The sponsor estimated the eligible population using an incidence-based approach, leveraging data from multiple sources in the scientific literature and assumptions based on clinical expert input. Under the drug plan perspective, the sponsor included drug acquisition costs, as well as costs associated with subsequent therapy. In addition, the model has the option to include costs associated with drug administration, AEs, skeletal events, routine care, and genetic testing to assess the broader budgetary impact of funding olaparib plus abiraterone on the health care system. The dosing modelled for olaparib plus abiraterone reflected the product monograph. Key inputs to the BIA are documented in Table 19.
Key assumptions made by the sponsor include:
44% of patients with mCRPC are NHA-naive.40
4% of patients with mCRPC who are NHA-naive receive docetaxel as first-line therapy.29
Patients survive for a maximum of 24 months and those surviving beyond 1 year receive continuous treatment with either primary or subsequent therapy throughout this period.
Uptake of olaparib plus abiraterone in the NHA-naive setting is assumed to decrease from 38% in year 1 to 37% in year 3.
Trial-41 and RWE-based42 TTD and OS data for olaparib plus abiraterone and comparators, which were used to estimate treatment durations for primary and subsequent therapies, were assumed reflective of clinical practice in Canada.
Each regimen was adjusted to a relative dose adjustment based on the PROpel trial and external RWE.10,41
Table 19: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as Year 1 / Year 2 / Year 3 if appropriate) |
|---|---|
Target population | |
At risk populationa43 | 12,289,699 |
Incidence rate of mCRPC44 | 21 per 100,000 |
4.61% | |
% NHA-naive40 | 43.8% |
% receiving docetaxel as 1L therapy45 | 3.9% |
Number of patients eligible for olaparib + abiraterone | 39 / 31 / 24 |
Market uptake (3 years) | |
Uptake NHA-naive (reference scenario) Abiraterone Enzalutamide | 56.2% / 56.2% / 56.2% 43.8% / 43.8% / 43.8% |
Uptake NHA-naive (new drug scenario) Olaparib + abiraterone Abiraterone Enzalutamide | 38.0% / 37.0% / 37.0% 34.8% / 35.4% / 35.4% 27.2% / 27.6% / 27.6% |
Cost of treatment (per patient) | |
Cost of treatment (per month) Olaparib + abiraterone Abiraterone Enzalutamide | $10,863 $3,082 $3,235 |
Genetic testing costs | |
Proportion pretested for mutation status | 75% |
Prevalence of BRCA1 or BRCA2 mutation4 | 10.7% |
Detection rate16 | 57.50% |
Number of tests per patient treated | 21.7 |
Unit cost of testing – Archival tumour tissue17 | 1,304 |
Proportion of tests using archival tissue | 100% |
Total testing cost per patient treated | 28,317 |
1L = first line; mCRPC = metastatic castration-resistant prostate cancer; NHA = next-generation hormonal agent.
aThe at-risk population represents the pan-Canadian population of adult men and excludes Quebec.
Summary of the Sponsor’s BIA Results
Results of the sponsor’s base case BIA suggest that the incremental expenditures associated with the reimbursement of olaparib plus abiraterone for the first-line treatment of patients with BRCA1- or BRCA2-mutated mCRPC who are NHA-naive, and for whom chemotherapy is not clinically indicated, as per its reimbursement request, would be $1,403,578 in year 1, $2,554,566 in year 2, and $1,968,173 in year 3, for a 3-year cumulative total of $5,926,318. When considering the broader health care system perspective, the estimated budgetary impact is $2,529,896 in year 1, $3,477,864 in year 2, and $2,689,710 in year 3, for a 3-year cumulative total of $8,697,471.
CADTH Appraisal of the Sponsor’s BIA
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
Model does not align with the indicated population. The approved indication for olaparib plus abiraterone is for the treatment of adult patients with deleterious or suspected deleterious germline and/or somatic BRCA mutated mCRPC in whom chemotherapy is not clinically indicated, irrespective of prior NHA treatment. The PROpel trial was restricted to patients who are NHA-naive. Hence, patients who have had prior treatment with an NHA were excluded from the BIAs.
CADTH conducted a scenario analysis that included patients who are NHA-experienced. The NHA-experienced population is estimated to account for 56% of patients with mCRPC.40 This approach is not without limitations, considering that radium-223, which was identified as a relevant comparator for the NHA-experienced population by clinical experts, is omitted from the analysis. Given this limitation, the estimated magnitude of the budgetary impact may be overestimated since it does not reflect the potential market uptake that may be attributed to radium-223 (a more costly treatment than the other included comparators).
Definition of clinical indication for chemotherapy in clinical practice is uncertain: The indication of olaparib plus abiraterone stipulates that it is for use in patients “in whom chemotherapy is not clinically indicated.” The sponsor assumed that 96% of patients with mCRPC who are NHA-naive would not be considered clinically indicated to receive chemotherapy in first-line.45 However, there is uncertainty regarding how the clinical indication for chemotherapy would be defined in clinical practice. According to the clinical experts consulted by CADTH, there are no consistent criteria used in clinical practice to identify patients for whom chemotherapy is not clinically indicated. This group may include patients who are deemed physically unfit (e.g., patients with poor renal function or poor performance status), patients who refuse chemotherapy, or patients who received prior docetaxel treatment in the mCSPC phase. Clinical experts consulted by CADTH for this review estimated that the proportion of patients in the first-line mCRPC setting who are likely to be clinically indicated to receive chemotherapy could be no more than 10% to 15%, thereby implying that 85% to 90% of patients would be eligible for treatment with olaparib plus abiraterone.
In light of the uncertainty regarding the proportion of the population that may not be considered clinically indicated to receive chemotherapy, CADTH conducted scenario analyses, which assumed that 20% (scenario 2) and 80% (scenario 3) of patients with mCRPC would be considered ineligible to receive chemotherapy.
Projected market share of olaparib and abiraterone is underestimated: The sponsor assumed that olaparib plus abiraterone would have a market share of 38%, 37%, and 37% in years 1, 2, and 3, respectively. Clinical expert feedback emphasized that the sponsor’s market share projections were substantially lower than they would anticipate in practice if the combination therapy were to be funded in first-line. Clinical experts consulted by CADTH noted that since the goal of treatment in the first-line setting is to slow the progression of metastatic disease, they would expect olaparib plus abiraterone to shift the current treatment paradigm by replacing abiraterone and enzalutamide as the new preferred first-line treatment for patients with BRCA1- or BRCA2-mutated mCRPC, who are NHA-naive, and for whom chemotherapy is not clinically indicated. This is aligned with the feedback received from registered clinician groups in Canada who noted that olaparib plus abiraterone is positioned to fulfill the unmet need for an effective and tolerable first-line therapy and may, thus, be preferred among patients eligible to receive NHA treatment. Clinical experts indicated that given the expectation of a potential paradigm shift, the future market uptake for olaparib plus abiraterone is likely to reach 100% by year 3.
CADTH conducted a reanalysis by adjusting the projected market share of olaparib plus abiraterone to 80%, 90% and 100% in Years 1, 2, and 3, respectively based on feedback sought from clinical experts.
Use of RDI underestimated drug acquisition costs. In the sponsor’s base-case analysis, the mean RDI observed in the PROpel trial was used to derive the drug acquisition cost for all therapies (i.e., expected vs observed doses). The inclusion of RDI may underestimate the total cost of olaparib in real-world clinical practice as the dose received by patients may be different from the planned dose for several reasons (i.e., missed, delayed, or deescalated doses). CADTH notes that, when considering wastage, each reason determining a reduction in RDI may have a different impact on drug costs. Likewise, it is unclear how treatment discontinuation influences RDI. Consistent with previous reviews, given the inability to link distinct dose intensity levels with outcomes, the CADTH base case does not incorporate RDI.
CADTH conducted a reanalysis by assuming 100% RDI for all therapies considered.
Prevalence of clinically confirmed BRCA1 or BRCA2 mutation is uncertain. The sponsor calculated that the prevalence of patients who are clinically confirmed to have a BRCA1 or BRCA2 mutation through genetic testing is 4.6%. This estimate is the product of (1) the proportion of patients assumed to be pretested for mutation (75%); (2) the prevalence of BRCA1 or BRCA2 mutation (11%); and (3) the detection rate (58%). Clinical expert input sought by CADTH for this review indicated that the estimated proportion of patients assumed to be pre-tested for mutation status is highly uncertain and likely variable across jurisdictions and centres. Clinical experts further noted that the proportion assumed by the sponsor was likely an overestimate of the true proportion in current clinical practice in Canada.
CADTH conducted a scenario analysis assuming that 50% of patients with mCRPC would be pretested for mutation status to assess the impact of the revised prevalence of confirmed BRCA1 or BRCA2 mutation (3.1%) on the budget.
Proportion of patients pretested for mutation status is uncertain. Olaparib and abiraterone is indicated for the first-line treatment of adult patients with deleterious or suspected deleterious germline and/or somatic BRCA-mutated mCRPC, for whom chemotherapy is not clinically indicated, whereby BRCA1 or BRCA2 mutation must be confirmed before the treatment is initiated. Hence, the sponsor considered that following the introduction of olaparib and abiraterone, diagnostic testing costs would apply to all patients with first-line mCRPC. Under the health care system perspective, the budget impact model included a 1-time testing cost for genetic alterations, where tumour testing was assumed to be performed using archived formalin-fixed paraffin-embedded tumour tissue from biopsies from the prostate or metastases, or from radical prostatectomy specimens. Based on the assumption that 75% of patients with mCRPC would be pre-tested for mutation status, the sponsor estimated that 22 tissue tests would be required to identify 1 patient with a BRCA mutation-positive diagnosis, which resulted in the total testing cost of $28,317 per patient treated (Table 11). Clinical expert input sought by CADTH for this review indicated that the estimated proportion of patients assumed to be pre-tested for mutation status is highly uncertain and likely variable across jurisdictions and centres. Clinical experts further noted that the proportion assumed by the sponsor was likely an overestimate of the true proportion in current clinical practice in Canada.
CADTH conducted a scenario analysis assuming that 50% of patients with mCRPC would be pre-tested for mutation status to assess the impact of this assumption on the broader health care system budget.
CADTH Reanalyses of the BIA
CADTH revised the sponsor’s submitted analysis by adjusting the projected market share of olaparib plus abiraterone in line with clinical expert input and assuming 100% RDI across all therapies considered. The changes applied to derive the CADTH base case are described in Table 20.
Table 20: CADTH Revisions to the Submitted BIA
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
None | — | — |
Changes to derive the CADTH base case | ||
1. Projected market share of olaparib + abiraterone is underestimated |
|
|
2. Use of RDI underestimated drug acquisition costs | OLA + ABI:
ABI:
ENZA: ||||| | OLA + ABI:
ABI:
ENZA: 100% |
CADTH base case | Re-analysis 1 + 2 | |
ABI = abiraterone; BIA = budget impact analysis; ENZA = enzalutamide; OLA = olaparib; RDI = relative dose intensity.
The results of the CADTH step-wise reanalysis are presented in summary format in Table 21 and a more detailed breakdown is presented in Table 22. The CADTH reanalysis suggests that reimbursing olaparib plus abiraterone for the first-line treatment of patients with BRCA1- or BRCA2-mutated mCRPC who are NHA-naive, and for whom chemotherapy is not clinically indicated, as per its reimbursement request, would be associated with an incremental cost of $3,191,277 in year 1, $6,208,353 in year 2, and $5,434,236 in year 3, for a 3-year budgetary impact of $14,833,866. The eligible patient population in the CADTH base case is 39, 31, and 24 in years 1, 2, and 3, respectively.
Table 21: Summary of the CADTH Reanalyses of the BIA
Stepped analysis | Three-year total |
|---|---|
Submitted base case | 5,926,318 |
CADTH reanalysis 1 | 13,696,343 |
CADTH reanalysis 2 | 6,419,036 |
CADTH base case | 14,833,866 |
BIA = budget impact analysis.
CADTH conducted additional scenario analyses to address remaining uncertainty, using the CADTH base case. Results are provided in Table 21.
Including the NHA-experienced population to reflect the Health Canada indicated population. This scenario increases the eligible patient population to 74, 70, and 67 in years 1, 2, and 3, respectively.
Assuming that 20% of patients are not clinically indicated to receive chemotherapy. This scenario decreases the eligible patient population to 8, 6, and 5 in years 1, 2, and 3, respectively.
Assuming that 80% of patients are not clinically indicated to receive chemotherapy. This scenario decreases the eligible patient population to 33, 25, and 20 in years 1, 2, and 3, respectively.
Assuming that 50% of patients with mCRPC would be pretested for mutation status, thus revising the prevalence of confirmed BRCA1 or BRCA2 mutation to 3.1%. This scenario decreases the eligible patient population to 26, 20, and 16 in years 1, 2, and 3, respectively.
Assuming that 50% of patients with mCRPC would be pre-tested for mutation status to assess the impact of this assumption on the broader health care system budget. This scenario decreases the eligible patient population to 26, 20, and 16 in years 1, 2, and 3, respectively.
Table 22: Detailed Breakdown of the CADTH Reanalyses of the BIA
Stepped analysis | Scenario | Year 0 | Year 1 | Year 2 | Year 3 | Three-year total |
|---|---|---|---|---|---|---|
Submitted base case | Reference | 1,800,214 | 2,216,673 | 1,734,379 | 1,357,020 | 5,308,072 |
New drug | 1,800,214 | 3,620,251 | 4,288,945 | 3,325,193 | 11,234,390 | |
Budget impact | 0 | 1,403,578 | 2,554,566 | 1,968,173 | 5,926,318 | |
CADTH base case | Reference | 1,917,330 | 2,313,426 | 1,810,081 | 1,416,251 | 5,539,758 |
New drug | 1,917,330 | 5,504,703 | 8,018,433 | 6,850,488 | 20,373,624 | |
Budget impact | 0 | 3,191,277 | 6,208,353 | 5,434,236 | 14,833,866 | |
CADTH scenario analysis 1: Inclusion of NHA-experienced patients | Reference | 3,036,987 | 4,122,043 | 3,892,339 | 3,723,335 | 11,737,717 |
New drug | 3,036,987 | 7,777,510 | 11,205,680 | 10,476,055 | 29,459,245 | |
Budget impact | 0 | 3,655,467 | 7,313,340 | 6,752,721 | 17,721,528 | |
CADTH scenario analysis 2: Assuming 20% of patients are not clinically indicated to receive chemotherapy | Reference | 399,028 | 481,462 | 376,708 | 294,745 | 1,152,915 |
New drug | 399,028 | 1,145,620 | 1,668,769 | 1,425,700 | 4,240,088 | |
Budget impact | 0 | 664,158 | 1,292,061 | 1,130,954 | 3,087,173 | |
CADTH scenario analysis 3: Assuming 80% of patients are not clinically indicated to receive chemotherapy | Reference | 1,596,112 | 1,925,849 | 1,506,831 | 1,178,981 | 4,611,661 |
New drug | 1,596,112 | 4,582,479 | 6,675,075 | 5,702,799 | 16,960,353 | |
Budget impact | 0 | 2,656,630 | 5,168,244 | 4,523,818 | 12,348,692 | |
CADTH scenario analysis 4: Assuming 3.1% prevalence of confirmed BRCA1 or BRCA2 mutation | Reference | 1,278,220 | 1,542,284 | 1,206,721 | 944,168 | 3,693,172 |
New drug | 1,278,220 | 3,669,802 | 5,345,622 | 4,566,992 | 13,582,416 | |
Budget impact | 0 | 2,127,518 | 4,138,902 | 3,622,824 | 9,889,244 | |
CADTH scenario analysis 5: Health care system perspectivea | Reference | 2,325,529 | 2,658,932 | 2,080,414 | 1,627,766 | 6,367,112 |
New drug | 2,325,529 | 6,996,384 | 9,278,542 | 7,848,054 | 24,122,979 | |
Budget impact | 0 | 4,337,451 | 7,198,128 | 6,220,287 | 17,755,867 | |
CADTH scenario analysis 6: Revision of pretested proportion (Health care system perspectivea) | Reference | 1,550,352 | 1,772,622 | 1,386,942 | 1,085,178 | 4,244,742 |
New drug | 1,550,352 | 5,033,707 | 6,474,762 | 5,458,209 | 16,966,678 | |
Budget impact | 0 | 3,261,085 | 5,087,820 | 4,373,032 | 12,721,936 | |
CADTH scenario analysis 7: 100% price reduction | Reference | 1,896,839 | 2,127,503 | 1,664,610 | 1,302,431 | 5,094,544 |
New drug | 1,896,839 | 2,131,588 | 2,325,833 | 1,884,419 | 6,341,840 | |
Budget impact | 0 | 4,085 | 661,224 | 581,988 | 1,247,297 |
BIA = budget impact analysis; NHA = next-generation hormonal agent.
aHealth care perspective includes costs associated with drug administration, adverse events, skeletal events, routine care, and genetic testing
Stakeholder Input
Patient Input
Canadian Cancer Survivor Network
About Canadian Cancer Survivor Network
The Canadian Cancer Survivor Network (CCSN) is a national network of patients, families, survivors, friends, community partners, funders, and sponsors who have come together to take action to promote the very best standard of care, whether it be it be early diagnosis, timely treatment and follow-up care, support for cancer patients, or issues related to survivorship or quality of end-of-life care. https://survivornet.ca/
Information Gathering
The Canadian Cancer Survivor Network utilized SurveyMonkey to create and collect all data for the survey on Olaparib. We then utilized our newsletter as well as our social media platforms to disseminate the survey to collect responses. The survey was open from May 10, 2023, to May 19, 2023, to obtain responses. All respondents to the survey are from Canada. All seven respondents to the survey are patients. Out of the seven respondents, six are male and one is female. When the survey data was analyzed, it was clear that one of the seven patients (1 of 7) had experience with Olaparib, and six of seven patients (6 of 7) do not have experience with Olaparib.
Disease Experience
When asked what stage of prostate cancer they had been diagnosed with, the following responses were received from six of the seven respondents:
Late Stage (4) or metastatic: 6
Current treatments that were identified include:
Radiation: 2
Surgery: 3
Targeted Therapy: 5
Immunotherapy: 1
Clinical Trials: 1
ADT: 3
Chemotherapy: 1
ADT+ Chemotherapy: 1
Other: 1 (Aberaterone and Dexamethazone)
When asked if there was an aspect of their disease that is most important to them to control, three respondents answered:
“Making sure that there is little pain as possible in my skeletal areas.”
“I want to be free of this Cancer.”
“Spreading to other organs.”
Respondents were asked if they have had any issues accessing any therapies. The following issues were highlighted by their responses:
Limited availability in my community: 3
Financial hardship due to cost: 2
Travel costs associated with accessing therapy/treatment: 2
Supplies or issues with administration: 2
When asked if there was anything that they would like to share about their cancer journey, six respondents shared these comments:
“No but I would like to know that there is one more effective drug in trial or development to prevent expansion of my metastatic prostate cancer. I’m currently on my last effective drug called cabazetaxil.”
“I was diagnosed 20 years ago and have been extremely fortunate that therapies following surgery were effective for so long.”
“The lies and over treatments in the medical community should be stopped. Unnecessary surgeries have ruined my life and I regret ever seeking out treatment that I was offered.”
“Physical change, mental stress, cause stress in marriage.”
“Keep as busy as possible and don’t give in.”
“I am a long-term cancer survivor and advocate for early diagnosis and surgical.”
There were no caregivers identified, however there were three respondents to our caregiver questions.
We asked what the issues are that they have encountered as a caregiver for someone with prostate cancer. Three respondents selected these issues:
Emotional drain: 2
Anxiety/Worrying: 3
Management of side effects: 1
Hours spent in medical appointments: 1
Lifestyle changes: 2
Inability to plan ahead: 2
Anger: 1
Feelings of "doom" due to challenging prognosis: 1
Feelings of helplessness: 2
Other: 1 (Loss of intimacy)
When asked how caring for someone with prostate cancer has affected their daily routine or lifestyle, two respondents had these thoughts to share:
“Difficulty in planning ahead. Last few years, limited ability to travel.”
“More sensitive to their needs.”
When asked if there was anything that they would like to share about their experiences in being a caregiver, two respondents shared these comments:
“Limited support for caregivers.”
“Mentally and emotionally challenging.”
Experiences With Currently Available Treatments
With the use of currently available treatments, patients reported that the following symptoms affected their quality of life and day-to-day living:
Frequency in urination: 2
Difficulty urinating: 1
Loss of appetite: 1
Bone/Skeletal Pain: 2
Indigestion: 1
Erectile Dysfunction (ED): 5
Nausea and vomiting: 1
Loss of quality of life: 3
Other: 4 (1 Fatigue and reduced concentration, 1 Have not been prescribed LYNPARZA as yet, weight gain, no energy, 1 Mental stress, 1 Fatigue)
When asked if any needs in their current therapy are not yet being met, six patients said no and one patient responded that they, “Require Support groups.”
Respondents were asked to select what adverse effects they are currently dealing with while on their treatments. Seven respondents selected the following:
Diarrhea: 1
Nausea/Vomiting: 1
Incontinence: 2
Erectile Dysfunction (ED): 4
Urinary issues: 1
Hot flashes: 5
Weight gain: 3
Loss of muscle: 4
Bruising:1
Anemia: 1
Infection: 1
Fatigue: 6
Osteoporosis: 2
Breast enlargement: 3
When asked if their adverse effects were tolerated, two said no, and five said yes with these responses on how they did:
“By regular exercises such as gym, swimming and biking.”
“Positive outlook. Live with them.”
“Supplements and Immunotherapy vaccinations.”
“Exercising.”
“Rest, attitude.”
We asked respondents to respond with how they are managing on their current treatment as if they were talking to a friend and what they would tell them. These are their responses:
“I am on my last type of chemo drug to control my metastatic prostate cancer called cabazitaxel.”
“Just finished steriotactic radiation therapy for 1 spot on each 6th rib and one spot on T8. The only side effect to date is some fatigue. Currently on Lupron and darolutamide. Side effects as mentioned above but managing to go on with life.”
“I am on Aberaterone and Dexamethazone and Eligard. The ADT treatments are tolerated as well as can be expected. low energy and weight gain are the worst symptoms.”
“Adt.”
“Seems to be working.”
“Collaboration of medication.”
Improved Outcomes
When asked about the following issues that they would hope to see a new drug address to manage their disease, seven respondents answered as follows:
Maintain quality of life: 6
Delay onset of symptoms: 3
Access to a new option for treatment: 4
Reduce side effects from current medications or treatments: 4
Ease of use: 1
Prolong life: 6
Provide a cure: 5
Patients were asked to describe how much of an improvement would be needed from the new drug to make it better than the current treatment:
“I would need about 40% better treatment.”
“A few extra years would be wonderful.”
“Provide a CURE to this nightmare disease.”
“Remove hot flashes, fatigue, weight gain, enlarged breast.”
“More energy is the big one for me.”
We then followed up with the question of how might their quality of life be different with those improvements:
“More energy and feeling better overall.”
“Spend more time with family.”
“Weight loss would help greatly.”
“Feel better physically and mentally.”
“That would help me live more fully.”
“Mobility, stable colon and bowel, less fatigue.”
We asked what considerations patients make when it comes to balancing the advantages and disadvantages of a treatment. Six respondents shared these thoughts:
“Making sure I do my physical workouts before treatment.”
“Will it delay progression.”
“I have no choices, if I refuse the treatments offered by my Oncologist, he will simply walk away from me and let nature take its course. In the past, I have had to fire my previous doctor.”
“Does benefit of treatment reduce cancer progression outweigh side effects.”
“I only know of the treatment I am taking now.”
“Quality of life and side effects.”
We asked the caregivers to rate (on a scale of excellent, good, poor, and very poor) how they feel current treatments address the needs of prostate cancer patients. Out of the three respondents, one selected ‘excellent’ and two selected ‘good’.
We asked caregivers to highlight the most challenging adverse effects related to their loved one’s current therapy or treatment. Two respondents shared these comments:
“ED and loss of libido.”
“Hot flashes, mood changes.”
When asked what they would most like to see out of a new treatment for patients with prostate cancer, two caregiver responses had this to say:
“A cure!”
“Cure and Reduce cancer progression.”
Experience With Drug Under Review
Patients reported nausea, vomiting, tiredness, weakness, diarrhea, loss of appetite, headache, and changes in the way food tastes as adverse effects caused by taking Olaparib.
Patients managed the adverse effects by exercise, massage, foods, and mindfulness.
The individual who has taken Olaparib gained access through a clinical trial.
We asked respondents to describe in their own words to advantages and disadvantages of Olaparib and how they made an impact on their life. One respondent shared that they had a bad reaction.
We asked respondents to rate on a scale of 1-5 how likely they would be to recommend that Olaparib be available to all patients who qualify for it. One respondent answered with a level one and three respondents answered with a level five.
When asked in comparison to other therapies how was their treatment experience with Olaparib in treating their prostate cancer, the respondents rated the following areas on a scale of much better, little or no difference, and much worse:
Symptom management: Little to no difference
Side effects: 1 Little to no difference, 1 Much worse
Ease of use: 1 Much better, 1 Much worse
Disease progression: 1 Much better, 1 Much worse
Companion Diagnostic Test
Not applicable.
Anything Else?
CCSN is aware of the limitations of this submission given the small number of respondents and with only one patient on Olaparib. However, the comments made and desires of the patients and caregivers in this submission are shared with many other individuals who have participated in past surveys for other submissions made regarding prostate cancer. From previous submissions it is clear that these individuals need more hope in continuing to live and control their disease over what can be many years. Besides the hope for a cure, many individuals in this submission, and past, are looking to have better quality of life so that they can contribute and have more time with the ones they love.
Conflict of Interest Declaration — Canadian Cancer Survivor Network
To maintain the objectivity and credibility of the CADTH reimbursement review process, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission?
No.
Did you receive help from outside your patient group to collect or analyze data used in this submission?
No.
List any companies or organizations that have provided your group with financial payment over the past 2 years AND who may have direct or indirect interest in the drug under review.
Table 1: Financial Disclosures for Canadian Cancer Survivor Network
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Astra Zeneca-2022 | — | — | — | X |
Astra Zeneca-2023 | — | — | — | X |
Canadian Cancer Society
About Canadian Cancer Society
Website Link: https://cancer.ca/en
Our purpose: To unite and inspire all Canadians to take control of cancer.
Our mission: In trusted partnership with donors and volunteers, we improve the lives of all those affected by cancer through world-class research, transformative advocacy and compassionate support.
We set ourselves apart from other cancer charities by taking a comprehensive approach against cancer. We are also the only national charity that supports all Canadians living with all cancers across the country. We shared our survey to through relevant CCS communication channels and support programs as well as through patient panels.
Information Gathering
The Canadian Cancer Society gathered perspectives through survey responses from patients and caregivers. The survey was open to people in Canada until April 27, 2023, for this submission.
Disease Experience
How much of an impact have symptoms associated with metastatic castration resistant prostate cancer had on your day-to-day activities and quality of life?
Please refer to Table 2 for more details. Out of a total of 23 respondents, the ability to engage in sexual activity was most affected with 16 (70%) respondents reporting moderate to significant impact. The second most affected ability was the ability to work, with 11 (48%) respondents reporting moderate to significant impact. The ability to exercise and the ability to maintain positive mental health were the next most affected with 10 (43%) respondents reporting moderate to significant impact in each.
Specify any other areas of your life that have been impacted and how significant the impact has been.
One patient felt that “once the cancer got to [the] bones, life became painful and quality of life declined significantly”. Another patient reported “headaches and joint pain have become debilitating”.
One patient elaborated on the impact their disease had on exercise, sharing that “cycling is painful”.
Two patients noted significant impact on sleep, with one saying “…I have bouts of sleepless nights and am being treated for constant daily crying.”, also touching on the impact in maintenance of positive mental health.
Experiences With Currently Available Treatments
Which of the following barriers have you faced when receiving treatment for your cancer?
Please refer to Figure 1 for more details. Out of 23 respondents, 15 (65%) reported facing at least one barrier when receiving treatment and identified 34 barriers. Of these barriers, transporation costs associated with appointments was the largest barrier to care (29%), followed by lack of familiarity with navigating the health care system (12%) and long wait times to receive tests or treatments (10%). Financial barriers in general (including costs associated with treatment and loss of income) encompassed 65% of the barriers identified by respondents.
How many lines of treatment have you undergone since your initial diagnosis of prostate cancer?
A description of what a line of treatment entails was provided. The majority of patients indicated they had undergone 3 or more lines of therapy (65%). Two patients underwent 1 line of therapy, 3 patients underwent 2 lines of therapy, and 3 patients were unsure.
Since your initial diagnosis of prostate cancer, which treatments have you tried?
Respondents were able to select from 14 options including a variety of treatments, watchful waiting and options to indicate they were unsure, or to provide additional information. The majority of respondents indicated that they used hormone therapy such as luteinizing hormone-releasing hormone (LHRH) agonists, LHRH antagonists and anti-androgen therapies (91%), followed by radiotherapy such as external beam radiation treatment or brachytherapy (73%), surgery (41%), and chemotherapy (27%). At one point during their treatments, 27% of respondents reported being treated with corticosteroids.
One respondent reported trying immunotherapy over the course of their treatment, and two respondents reported not being sure of some of the treatments they received. One respondent shared that they were treated with high intensity focused ultrasound.
How much of an impact do the following cancer treatment side effects have on your daily life?
Respondents were given a total of 31 different side-effects to rank as having no impact, small impact, moderate impact, severe impact or as N/A. Out of 23 respondents, there were a total of 182 side-effects causing moderate to severe impact on daily life. Please refer to Figure B for more details on side effects ranked as having moderate to severe impact on daily life. The most significant side effects in this regard were changes in libido, sexual function, and fertility (65%), and hot flashes (65%). This was followed by fatigue/low energy, and weight changes with 52% and 48% reporting moderate or severe impact on daily life respectively.
How willing would you be to tolerate new side effects from therapies if they could offer better control of disease progression?
Respondents were asked to rank willingness on a scale of 1 (will not tolerate side effects at all) to 5 (will tolerate significant side effects). Thirty-five percent ranked their willingness as a “5”, followed by 26% ranking “4”, 22% ranking “3”, 4% ranking “2” and 4% ranking “1”.
Improved Outcomes
What improvements would you like to see in new treatments that are not achieved in currently available treatments?
One patient commented on difficulty travelling to access treatment, saying they were “…not able to navigate larger cities (only have one working eye)” and that they were “…not able to contend with traffic…”. They also commented on the costs associated with travelling to appointments, saying “being retired I have to watch my budget.”
Table 2: Symptoms of Metastatic Castration Resistant Prostate Cancer and Impact on Quality of Life
Task | Small impact | Moderate impact | Significant impact | I’m not sure | N/A or no impact |
|---|---|---|---|---|---|
Ability to work | 4 (17.39%) | 4 (17.39%) | 7 (30.43%) | 0 (0%) | 8 (34.78%) |
Ability to travel | 2 (8.70%) | 4 (17.39%) | 5 (21.74%) | 1 (4.34%) | 11 (47.83%) |
Ability to exercise | 5 (21.74%) | 7 (30.43%) | 3 (13.04%) | 0 (0%) | 8 (34.78%) |
Ability to conduct household chores | 5 (21.74%) | 5 (21.74%) | 2 (8.70%) | 1 (4.34%) | 10 (43.48%) |
Ability to fulfill family obligations | 6 (26.09%) | 0 (0%) | 4 (17.39%) | 1 (4.34%) | 12 (52.17%) |
Ability to spend time with family and friends | 4 (17.39%) | 3 (13.04%) | 2 (8.70%) | 0 (0%) | 14 (60.87%) |
Ability to concentrate | 1 (4.34%) | 4 (17.39%) | 5 (21.74%) | 1 (4.34%) | 12 (52.17%) |
Ability to fulfill practical needs (dressing, bathing, preparing meals) | 2 (8.70%) | 2 (8.70%) | 2 (8.70%) | 0 (0%) | 17 (73.91%) |
Ability to maintain positive mental health | 3 (13.04%) | 4 (17.39%) | 6 (26.09%) | 1 (4.34%) | 9 (39.13%) |
Ability to engage in sexual activity | 1 (4.34%) | 1 (4.34%) | 15 (65.22%) | 1 (4.34%) | 5 (21.74%) |
Table provides a breakdown of respondents stated symptoms and impact on quality of life.
Another patient noted “affordability, availability” as an improvement they would like to see, saying that “none of the treatments [they] hear about in the US and Germany are available here. No PSMA scans or trials either.” The same patient noted significant side-effects with treatments that were available to them, saying “all of the treatments from chemo, all the drugs are literally almost as bad as the prostate cancer itself. Pain management is not readily accessible either.”
This sentiment was echoed by another patient who said they wanted to see “fewer or less severe side effects.”
The last patient expressed they wanted to see improved outcomes in terms of progression-free survival, saying “better and longer lasting effectiveness”.
Experience With Drug Under Review
No respondents had experience with the drug under review. As such, our submission focuses on experience with the disease and what respondents would like to see with new treatments.
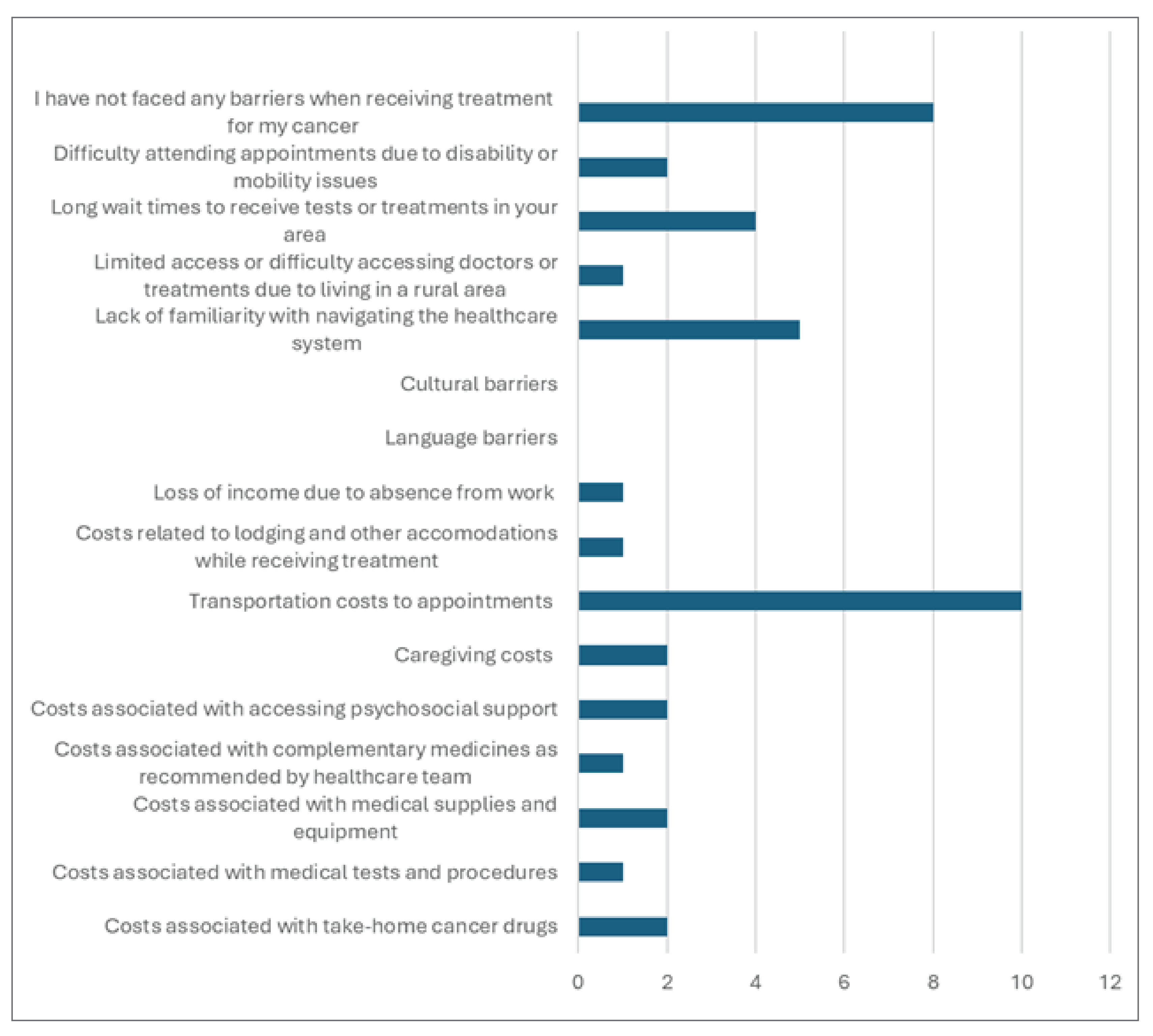
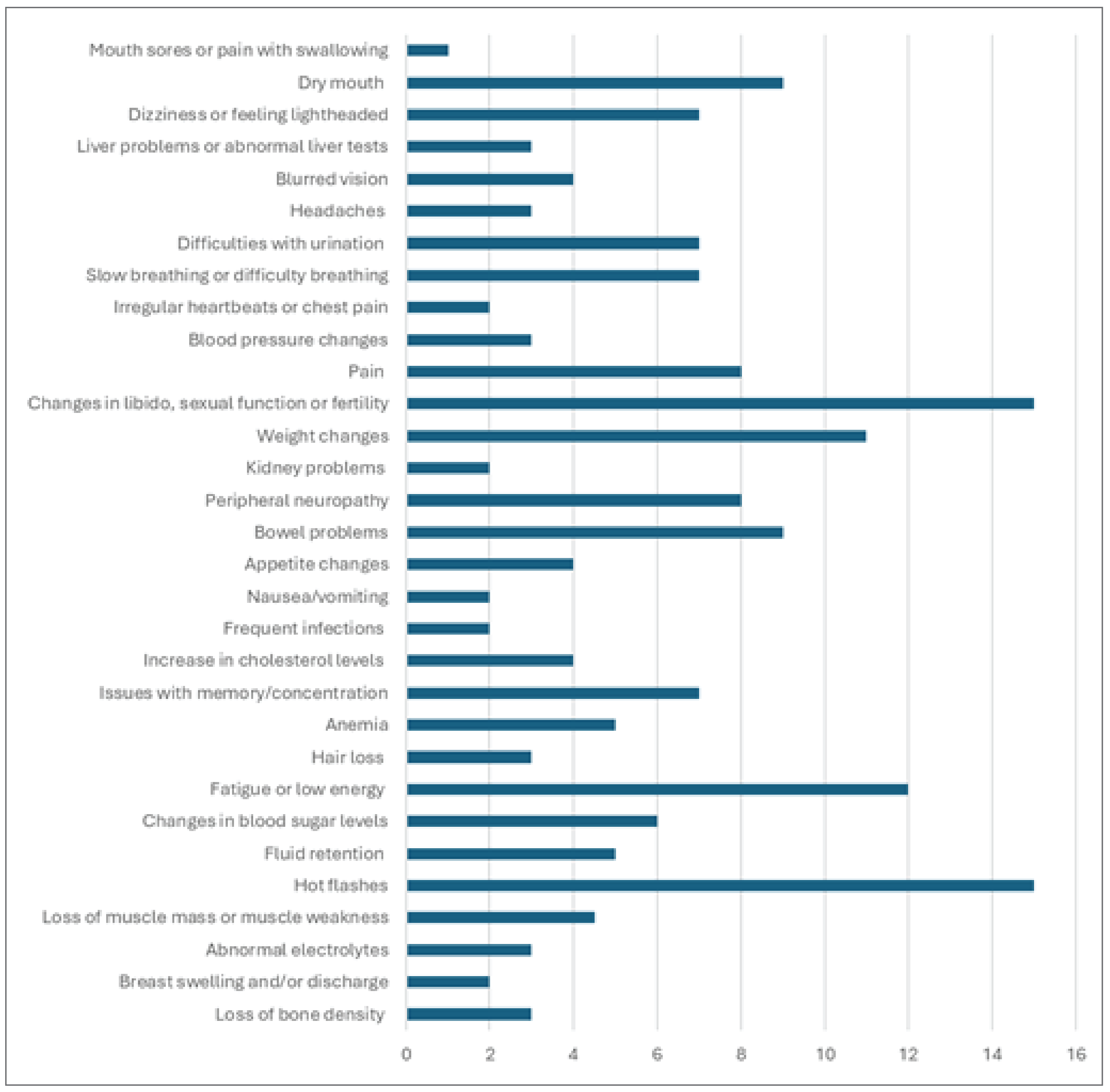
Conflict of Interest Declaration — Canadian Cancer Society
To maintain the objectivity and credibility of the CADTH reimbursement review process, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission?
No.
Did you receive help from outside your patient group to collect or analyze data used in this submission?
No.
List any companies or organizations that have provided your group with financial payment over the past 2 years AND who may have direct or indirect interest in the drug under review.
Table 3: Financial Disclosures for Canadian Cancer Society
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
AstraZeneca | — | — | — | X |
Merck | — | — | — | X |
Clinician Input
Canadian clinicians with expertise in managing advanced prostate cancer
Coordinated by the Canadian Cancer Society
About Canadian clinicians with expertise in managing advanced prostate cancer
We are responding to this call for clinician input as medical experts in support of olaparib in combination with abiraterone and prednisone or prednisolone for the treatment of patients with mCRPC, for whom chemotherapy is not clinically indicated. As lead of this group, I am the head of Urology at Le Centre hospitalier de l’Universite de Montreal (CHUM), the director of prostate cancer research at the Montreal Cancer Institute (CRCHUM), and full professor in the department of surgery at the Universite de Montreal. I also hold the Raymond Garneau Chair in prostate cancer at the Universite de Montreal. In my practice, I have been treating advanced prostate cancer for the past 30 years and have been a contributor and leader for many global clinical research studies in prostate cancer.
The group of clinicians being represented includes several leading experts specialized in the treatment of advanced prostate cancer from across Canada.
Information Gathering
Members of the group were asked to review a draft clinician input response developed by Dr. Saad. That collective input was then shared amongst the group members and a final document was developed based on the clinician group’s collective input. Any disagreements or regional specific issues were maintained in the document to provide CADTH with a full sense of how this regimen is anticipated to impact clinical practice across the provinces that are being represented by the clinician group.
Current Treatments and Treatment Goals
Prostate cancer is amongst the most common cancers diagnosed in Canadian men, with an estimated 1 out of 8 men being diagnosed with prostate cancer during his lifetime.1 Not only is prostate cancer highly prevalent, but it is also extremely deadly. Prostate cancer is the third leading cause of death from cancer; it is estimated that 1 out of 29 men will die from prostate cancer.2 To put this into perspective, this year, it is estimated that:
~ 25,000 Canadian men will be diagnosed with prostate cancer, representing 20% of all new cancer cases in men.1
> 4,000 Canadian men will die of prostate cancer, representing 10% of all cancer deaths in men.3
Patients who suffer and die of prostate cancer are all patients with mCRPC. Patients with mCRPC often progress quickly on current therapies with a significant number of patients not being eligible for second line therapies and beyond due to various clinical factors (refer to Figure 3).4 Data from Ontario has shown that most patients who receive mCRPC therapy only receive one line of proven life-prolonging therapy.5
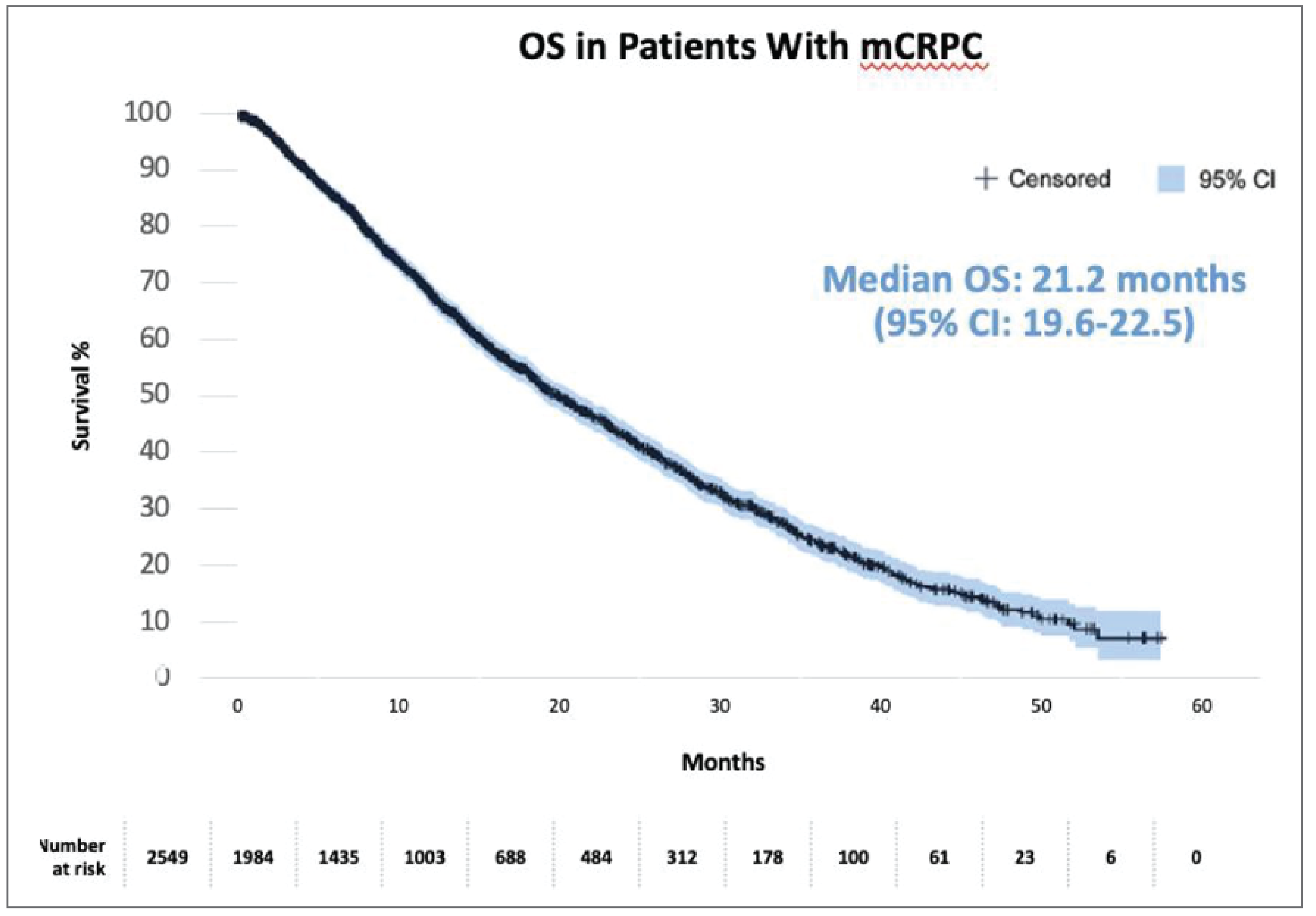
Treatment options for localized prostate cancer include prostatectomy and radiation therapy with the potential for watch and wait or active surveillance for patients with lower risk disease. For nearly three- quarters of a century, medical or surgical castration, i.e., androgen deprivation therapy (ADT), has been the first-line therapy for patients with biochemical recurrence or metastatic castration-sensitive prostate cancer (mCSPC). Although nearly all patients with mCSPC initially respond to ADT, almost all will eventually progress to mCRPC and eventually succumb to their disease.
For patients with mCRPC, androgen receptor-axis-targeted (ARAT) therapies such as enzalutamide6,7 and abiraterone8,9 are the preferred therapies with chemotherapies such as docetaxel10 being used in select patients with a good performance status and cabazitaxel11, with the latter only being funded after progression on docetaxel. Radium-22312 (Ra-223) is also available, but restricted to symptomatic bone-only metastases and often only after failing chemotherapy.
Olaparib monotherapy has recently been reviewed with funding limited to later in the treatment path, after ARAT, and only in patients with BRCA and ATM mutations [homologous recombination repair (HRR) genes].
Approximately ~20-25% of patients harbor mutations in HRR genes. For these patients, there is a need to find the best treatment options early on, including scenarios where HRR gene mutation status is unknown. There is an ongoing practical challenge in the clinic to secure genetic testing for HRR genes, and if secured, the results are not always available in time, and in many cases testing can fail (~20-30% failures).
Refer to Figure 4 for a depiction of the current prostate cancer landscape.
Figure 4: The Prostate Cancer Landscape
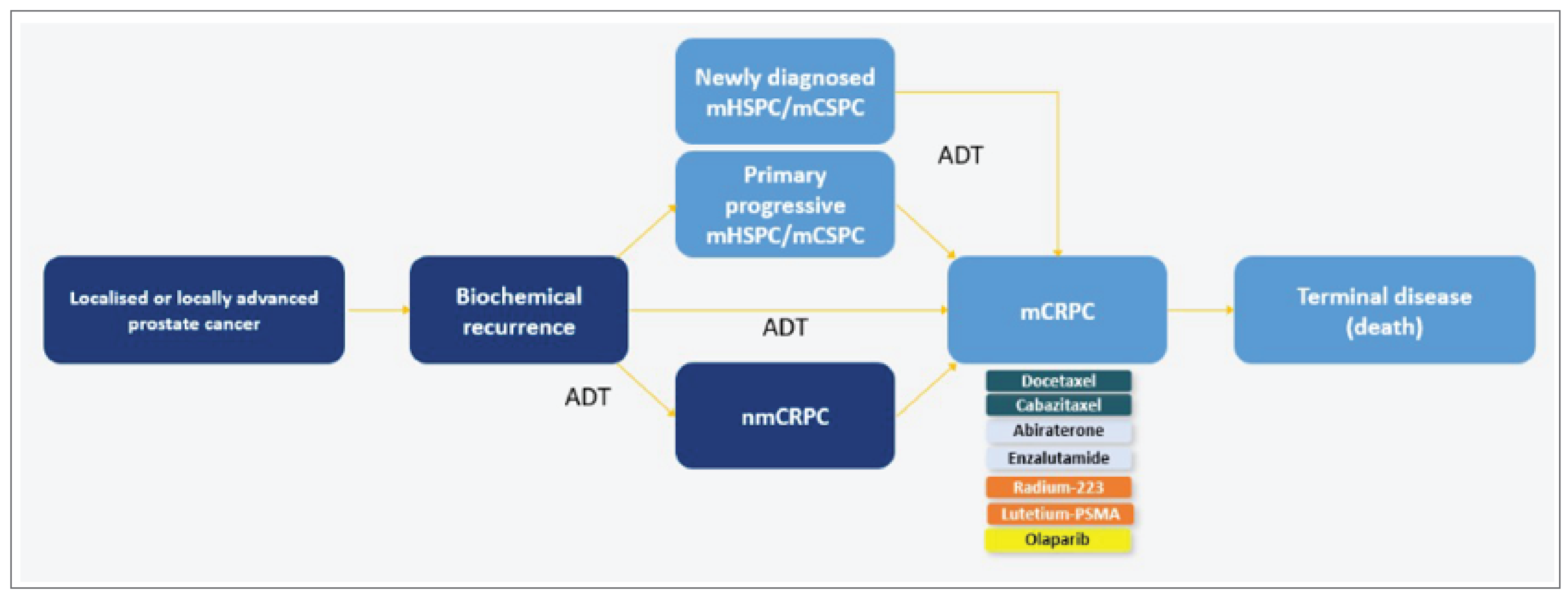
Sources: 1. Tannock IF et al. N Engl J Med 2004; 351:1502–12. 2. Ryan CJ et al. Lancet Oncol 2015;16:152–60. 3. Rathkopf DE et al. Eur Urol 2014;66:815–25. 4. Beer TM et al. Eur Urol 2017;71:151–4. 5. Armstrong AJ et al. Cancer 2017;123:2303–11. 6. de Bono JS et al. Lancet 2010;376:1147–54. 7. Hoskin P et al. Lancet Oncol 2014;15:1397-406.
Given mCRPC is an incurable disease, treatment is typically focused on delaying disease progression and maintaining quality of life. For patients entering first-line mCRPC, currently ARAT therapy is an effective option. However, the goal of treatment in the first line setting is to be as effective as possible to give patients the best chance possible. Thus, the most effective treatment in the first line setting is needed to slow the progression of metastatic disease. Building on effective first line options for mCRPC is critically needed.
Olaparib added to abiraterone fulfills this unmet need for an effective and tolerable first line combination.
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
In the mCRPC patient population, there is a continued need for new treatment options. The patient population in the funding request aligns with clinical practice and represents a significant unmet need as patients progress quickly, with a significant number not reaching second line therapy due to various clinical factors. Thus, the most effective treatment in the first line setting is needed to slow the progression of metastatic disease.
Treatment with an ARAT is currently the preferred option for mCRPC patients; however, no single standard of care exists. Currently available treatments do not offer patients curative intent. Rather, they provide some benefit in slowing the progression of metastatic disease or may provide patients with some limited palliation. However, there is room to improve on current therapies. As previously mentioned, efficacy is limited as most patients do not reach second line therapy. Moreover, current front-line mCRPC therapies have safety and tolerability limitations requiring patients and physician to consider the risk/benefit profile of each regimen. For example, docetaxel is associated with significant warnings and since it is administered by intravenous infusion, it is a more resource intensive therapy for patients. Consequently, the 2022 CUA-CUOG guidelines only recommend docetaxel for “select cases” when patients present with signs of rapid progression and symptomatic or visceral metastatic disease.
In current clinical practice, first-line treatment options fail within ~16 months of initiation and, since only a limited number of patients receive more than one line of treatment, there is a substantial unmet need for effective treatments that are available early in the metastatic setting. To date no effective combination therapy has been approved for mCRPC.
The rationale for combining olaparib and abiraterone was based on available pre-clinical and clinical data to combine two effective treatments in prostate cancer where improvement in clinical outcomes can be most impactful to patients. Interaction between PARP signaling and AR signaling pathways may explain the combined effect of agents observed in preclinical models.13 The proposed PARP-1 co-regulation of the androgen receptor pathway is supported by the observation that PARP inhibition may suppress transcription of several AR targets, in line with the observed improved efficacy.14 Furthermore, there is evidence that supports that inhibition of the AR signalling axis by ARATs induces an HRR deficient phenotype, which sensitizes cells to olaparib, despite resistance to an initial androgen deprivation therapy.15-16 Refer to Figure 5 for an illustrative summary.
Although there are several treatment options for mCRPC, the disease is incurable. Median progression-free survival (PFS) of approximately 16 months is obtained with early treatment initiation with ARATs, and they are the preferred treatment choice in the first line setting. There is also evidence of significantly diminishing efficacy with subsequent lines of ARAT therapy, with no additional efficacy benefit of taxane-based therapies. As such, a new treatment option that would allow for early intervention in the course of mCRPC and that could also prolong the treatment duration of available therapies, delay disease progression, and improve long-term outcomes in this setting is warranted. Olaparib (PARP inhibitor) added to abiraterone (ARAT) fulfills this unmet need for an effective and tolerable first line combination.
Figure 5: Rationale for Combining PARP Inhibitors and ARATs
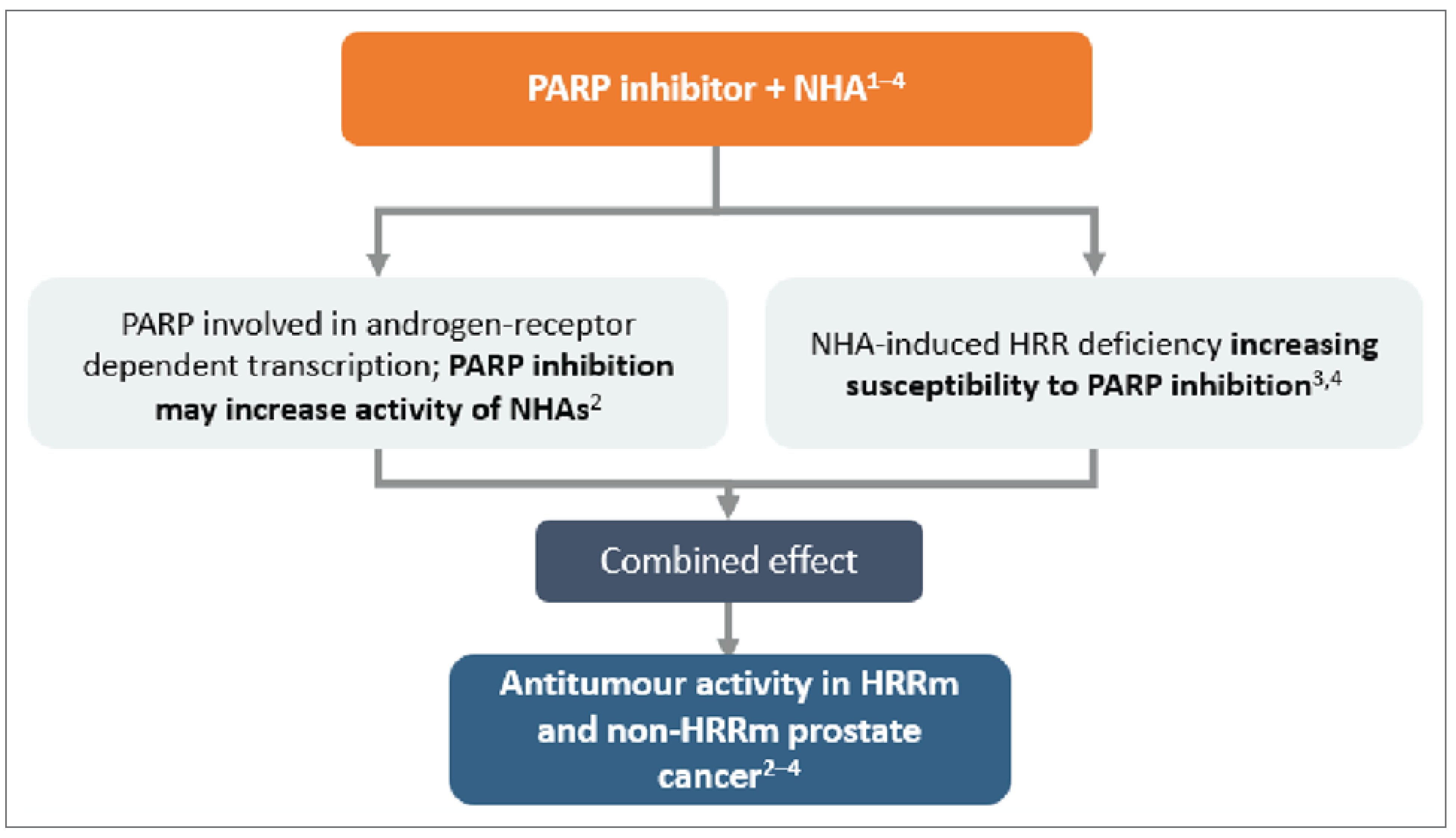
1 Mateo J, et al. N Engl J Med 2015;373:1697–1708
2 Schiewer MJ, et al Cancer Discov 2012;2:1134–1149
3 Polkinghorn WR, et al. Cancer Discov 2013;3:1245–1153
4 Asim M, et al. Nat Commun 2017;8:374
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
The drug under review combines two known mechanisms of action already approved as monotherapies for patients with mCRPC. The combination of these two established mechanisms of actions has been tested in both the pre-clinical and clinical setting and would be a novel option for physicians to consider in first line mCRPC. The combination of abiraterone + olaparib will be used as a first-line agent in mCRPC to manage the progression of the disease. As supported by the primary endpoint of the PROpel study, abiraterone + olaparib demonstrated radiographic PFS (rPFS) of over 24 months, which is a clinically meaningful addition of approximately 8 months over abiraterone. A consistent positive trend towards improved OS over current standard of care was also observed. Based on these results and the combination of the established mechanisms of action, the regimen under review would be considered as 1) first line mCRPC treatment for both ARAT experienced (any setting) and naïve patients, 2) for patients where docetaxel is not yet clinically indicated or previously treated with docetaxel in the mCSPC setting.
The regimen under review would not replace an available treatment but would be preferred to other therapies for patients that would be likely to receive an ARAT, due to the efficacy of the regimen. There is a dearth of sufficient evidence to determine whether olaparib with abiraterone should preferentially be used either before or after docetaxel. Further, the subgroup analysis from the PROpel trial suggested a benefit in patients irrespective of HRRm and BRCAm status; thus, mutation status should not be used as an exclusion for reimbursement of olaparib with abiraterone.
Survival of men with mCRPC in the real world remains a problem. Once prostate cancer progresses to mCRPC, the disease is not curable, and treatment focuses on delaying disease progression while maintaining quality of life. Available data suggests that the majority of patients will not go on to receive additional lines of therapy. The combination approach has a unique mechanism of action and potentially expands the clinical opportunity for olaparib to address a significant unmet need in a broader and earlier population. Given the poor prognosis of mCRPC, selecting the most appropriate treatment early is imperative.
Which patients would be best suited for treatment with the drug under review? Which patients would be least suitable for treatment with the drug under review?
The regimen under review would be considered as 1) first line mCRPC treatment for both ARAT experienced (any setting) and naïve patients, 2) for patients where docetaxel is not yet clinically indicated or previously treated with docetaxel in the mCSPC setting. There is no evidence to determine whether olaparib with abiraterone should preferentially be used either before or after docetaxel, thus prior use of docetaxel should not be a requirement for reimbursement. In addition, HRRm and BRCAm status should not be used as an exclusion for reimbursement of Olaparib with abiraterone.
As long as genetic testing is not required, there are no anticipated issues related to diagnosis. However, should a requirement for genetic testing be enforced, there are multiple issues related to the companion diagnostic test. There is a need to find the best treatment option early on, including scenarios where patient HRR mutation status is unknown. There is an ongoing practical challenge in the clinic to secure genetic testing for HRR genes, and if secured, the results are not always available in time, and in many cases testing can fail (~20-30% failures). Given about 20-40% of patients fail genetic testing for various reasons, HRRm and BRCAm status should not be used as an exclusion for reimbursement of olaparib with abiraterone, as it would exclude a large number of patients that would otherwise benefit from the combination regimen.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice? How often should treatment response be assessed?
The most meaningful clinical response to treatment at this stage of disease would be to 1) avoid progression [either radiographic progression (defined by PCWG3 criteria and/or RECIST) or clinical progression], and 2) maintain or improve quality of life (QoL) compared to the current standard of care for this patient population to ensure new regimens are either better tolerated or more convenient (e.g., less need for supportive medications, less frequent administration, etc.).
None of the existing treatments for mCRPC are curative; instead, they prolong survival and/or delay progression and maintain quality of life. mCRPC is associated with a range of symptoms but is predominantly characterized by bone pain, fatigue, and urinary dysfunction. These can further lead to significant morbidity, including pain and skeletal-related events such as spinal cord compression and pathological fractures, which require interventions such as bone surgery or radiation therapy. Living with prostate cancer affects everyday life, work, and relationships. Since curative therapy is not possible in the metastatic setting, reducing disease burden and symptoms are critical objectives of any therapeutic intervention.
What factors should be considered when deciding to discontinue treatment with the drug under review?
Patients should continue to receive treatment until objective radiological disease progression or clinical progression by investigator assessment or until they were unable to tolerate treatment.
What settings are appropriate for treatment with [drug under review]? Is a specialist required to diagnose, treat, and monitor patients who might receive [drug under review]?
Given the individual components of the regimen are already available and funded for patients with mCRPC, there is no anticipated change in treatment setting, specialist visits, or monitoring requirements for patients.
Additional Information
Should a requirement for genetic testing be enforced, there are multiple issue related to the companion diagnostic test. Approximately ~20-25% of patients harbor mutations in HRR genes. There is a need to find the best treatment options early on, including scenarios where patient HRR mutation status is unknown.
There is an ongoing practical challenge in the clinic to secure genetic testing for HRR genes, and if secured, the results are not always available in time, and in many cases testing can fail (~20-30% failures). Given about 20-40% of patients fail genetic testing for various reasons, HRRm and BRCAm status should not be used as an exclusion for reimbursement of Olaparib with abiraterone as it would exclude a large number of patients that would otherwise benefit from the combination regimen.
Conflict of Interest Declarations — Canadian clinicians with expertise in managing advanced prostate cancer
Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please refer to the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission?
No.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission?
No.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician who contributed to the input.
Declaration for Clinician 1
Name: Fred Saad
Position: Professor and Chief of Urology and Director of GU Oncology, CHUM
Date: 15-05-2023
Table 4: COI Declaration for Canadian Clinicians With Expertise in Managing Advanced Prostate Cancer — Clinician 1
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
AstraZeneca | — | — | X | — |
Astellas | — | — | X | — |
Pfizer | — | — | X | — |
Janssen | — | — | X | — |
Bayer | — | — | X | — |
Novartis | — | — | X | — |
Merck | — | X | — | — |
Bayer | — | — | X | — |
Tersera | — | X | — | — |
ABBVIE | — | X | — | — |
Tolmar | — | — | X | — |
Declaration for Clinician 2
Name: Christopher Wallis, MD PhD FRCSC
Position: Urologic Oncologist; Assistant Professor
Date: 08-05-2023
Table 5: COI Declaration for Canadian Clinicians With Expertise in Managing Advanced Prostate Cancer — Clinician 2
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Janssen Oncology | — | — | — | X |
SESEN Bio | — | — | X | — |
Precision Point Specialty LLC | — | X | — | — |
Bayer | — | — | X | — |
EMD Serono | X | — | — | — |
Haymarket Media | X | — | — | — |
Healing and Cancer Foundation | X | — | — | — |
Knight Therapeutics | X | — | — | — |
TerSera Canada | X | — | — | — |
Tolmar Pharmaceuticals | X | — | — | — |
Nanostics Inc | — | X | — | — |
AstraZeneca | X | — | — | — |
Merck | — | X | — | — |
Declaration for Clinician 3
Name: Geoffrey Gotto
Position: Clinical Associate Professor, University of Calgary
Date: 19-05-2023
Table 6: COI Declaration for Canadian Clinicians With Expertise in Managing Advanced Prostate Cancer — Clinician 3
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
BMS | X | — | — | — |
Ferring | — | X | — | — |
EMD Serono | — | X | — | — |
AstraZeneca | — | — | X | — |
Astellas | — | — | X | — |
Janssen | — | — | X | — |
Bayer | — | — | X | — |
Merck | — | — | X | — |
Tolmar | — | X | — | — |
Declaration for Clinician 4
Name: Ricardo Fernandes
[Declaration pending]
References
Canadian Cancer Statistics Advisory Committee., Canadian Cancer Statistics 2022. Canadian Cancer Society; 2022. Accessed at: https://cancer.ca/en/research/cancer-statistics.
Canadian Cancer Statistics Advisory Committee. Canadian Cancer Statistics 2021. Canadian Cancer Society; 2021.
Canadian Cancer Society. Survival statistics for prostate cancer. (https://www.cancer.ca/en/cancer- information/cancer-type/prostate/prognosis-and-survival/survival-statistics/?region=on).
George DJ et al. Clin Genitourin Cancer. 2020;18(4):284-294
Shayegan B et al. Urol Oncol 2022; 40 (5):192e1-192.e9
Beer TM et al. Eur Urol 2017;71:151–4.
Armstrong AJ et al. Cancer 2017;123:2303–11
Ryan CJ et al. Lancet Oncol 2015
Rathkopf DE et al. Eur Urol 2014;66:815–25
Tannock IF et al. N Engl J Med 2004
de Bono JS et al. Lancet 2010;376:1147–54.
Hoskin P et al. Lancet Oncol 2014;15:1397-406
Mateo J, et al. N Engl J Med 2015;373:1697–1708;
Schiewer MJ, et al Cancer Discov 2012;2:1134–1149
Polkinghorn WR, et al. Cancer Discov 2013;3:1245–1153
Asim M, et al. Nat Commun 2017;8:374
Ontario Health (Cancer Care Ontario) Genitourinary Cancer Drug Advisory Committee
About Your Clinician Group Ontario Health (Cancer Care Ontario) Genitourinary Cancer Drug Advisory Committee
OH-CCO’s Drug Advisory Committees provide timely evidence-based clinical and health system guidance on drug-related issues in support of CCO’s mandate, including the Provincial Drug Reimbursement Programs (PDRP) and the Systemic Treatment Program.
Information Gathering
Information was gathered via videoconferencing and email.
Current Treatments and Treatment Goals
The current treatment options in the first line setting of metastatic castrate resistant prostate cancer include docetaxel, abiraterone, apalutamide and enzalutamide.
The treatment goals are to prolong life, delay disease progression, delay time to initiate chemotherapy and improve health-related quality of life. An advantage to using this treatment over chemotherapy is the reduction in number of clinic visits, and it is an oral therapy as opposed to intravenous therapy.
Docetaxel is a cytotoxic chemotherapy that inhibits cell division, and the oral therapies all inhibit the androgen receptor pathways. Olaparib has a different mechanism of action in that inhibits the enzyme poly (ADP-ribose) polymerase, and thereby inhibits a cell’s ability to repair DNA.
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
As per the PROpel trial, the combination of olaparib with abiraterone demonstrates improvement in progression free survival. This is an incurable disease, so there is a need to prevent disease progression.
This effect appears to be more pronounced in those with germline or BRCA mutations.
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
As per the PROpel trial, Olaparib would be added to the current standard which is abiraterone. It would not be given as monotherapy.
Which patients would be best suited for treatment with the drug under review? Which patients would be least suitable for treatment with the drug under review?
All patients with metastatic castrate resistant prostate cancer in the first line setting would be best suited for this treatment.
This effect appears to be more pronounced in those with germline or somatic BRCA mutations. Patients with adequate bone marrow function would be best suited, given the risk of cytopenias with Olaparib.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice? How often should treatment response be assessed?
Radiographic progression free survival indicates patient response to treatment. Imaging would occur at least every 3 months. Biochemical response via PSA and symptom improvement would also inform decision making – this could occur every 4 to 12 weeks at the treating physician’s discretion.
What factors should be considered when deciding to discontinue treatment with the drug under review?
Disease progression and/or toxicity
What settings are appropriate for treatment with [drug under review]? Is a specialist required to diagnose, treat, and monitor patients who might receive [drug under review]?
Outpatient specialty clinic with training in advanced genitourinary oncology.
Additional Information
This treatment should be available agnostic to HRR status.
Conflict of Interest Declarations — Ontario Health (Cancer Care Ontario) Genitourinary Cancer Drug Advisory Committee
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please refer to the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission?
No.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission?
No.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician who contributed to the input.
Declaration for Clinician 1
Name: Dr. Girish Kulkarni
Position: Lead, Ontario Health CCO Genitourinary Cancer Drug Advisory Committee
Date: 14-04-2023
Table 7: COI Declaration for OH-CCO Genitourinary Cancer Drug Advisory Committee — Clinician 1
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Declaration for Clinician 2
Name: Dr. Reeta Barua
Position: Member, Ontario Health CCO Genitourinary Cancer Drug Advisory Committee
Date: 05-05-2023
Table 8: COI Declaration for OH-CCO Genitourinary Cancer Drug Advisory Committee — Clinician 2
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Janssen | X | — | — | — |
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
Redactions: Confidential information in this document may be redacted at the request of the sponsor in accordance with the CADTH Drug Reimbursement Review Confidentiality Guidelines.
Stakeholder Input: The views expressed in each submission are those of the submitting organization or individual; not necessarily the views of CADTH or of other organizations. As such, they are independent of CADTH and do not necessarily represent or reflect the view of CADTH. No endorsement by CADTH is intended or should be inferred. By filing with CADTH, the submitting organization or individual agrees to the full disclosure of the information. CADTH does not edit the content of the submissions.
CADTH does use reasonable care to prevent disclosure of personal information in posted material; however, it is ultimately the submitter’s responsibility to ensure no identifying personal information or personal health information is included in the submission. The name of the submitting organization or individual and all conflict of interest information are included in the submission; however, the name of the author, including the name of an individual patient or caregiver submitting the patient input, are not posted.
Accessibility: CADTH is committed to treating people with disabilities in a way that respects their dignity and independence, supports them in accessing material in a timely manner, and provides a robust feedback process to support continuous improvement. All materials prepared by CADTH are available in an accessible format. Where materials provided to CADTH by a submitting organization or individual are not available in an accessible format, CADTH will provide a summary document upon request. More details on CADTH’s accessibility policies can be found here.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec