Drugs, Health Technologies, Health Systems
Reimbursement Review
Isatuximab (Sarclisa)
Sponsor: Sanofi-Aventis Canada Inc.
Therapeutic area: Multiple myeloma
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Clinical Review
Abbreviations
AE
adverse event
AESI
adverse event of special interest
ASCT
autologous stem cell transplant
CDA-AMC
Canada’s Drug Agency
CI
confidence interval
CMRG
Canadian Myeloma Research Group
CR
complete response
CyBorD
cyclophosphamide-bortezomib-dexamethasone
DCyBorD
daratumumab-cyclophosphamide-bortezomib-dexamethasone
DRd
daratumumab-lenalidomide-dexamethasone
DVMP
daratumumab-bortezomib-melphalan-prednisone
ECOG PS
Eastern Cooperative Oncology Group Performance Status
EORTC QLQ-C30
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30
ESS
effective sample size
FISH
fluorescence in situ hybridization
GRADE
Grading of Recommendations Assessment, Development and Evaluations
HR
hazard ratio
HRQoL
health-related quality of life
Ig
immunoglobulin
IgG
immunoglobulin G
IMWG
International Myeloma Working Group
IPCW
inverse probability of censoring weighting
IPW
inverse probability weighting
IR
infusion-related
IRC
independent review committee
IRT
interaction response technology
IsaVRd
isatuximab-bortezomib-lenalidomide-dexamethasone
ISS
International Staging System
ITC
indirect treatment comparison
ITT
intention to treat
KM
Kaplan-Meier
LCH
log-cumulative hazard
LDH
lactate dehydrogenase
MAIC
matching-adjusted indirect comparison
MM
multiple myeloma
MRD
minimal residual disease
NC
not calculated
NICE
National Institute for Health and Care Excellence
NMA
network meta-analysis
OH CCO
Ontario Health (Cancer Care Ontario)
OR
odds ratio
ORR
overall response rate
OS
overall survival
PD
progressive disease
PFS
progression-free survival
PLD
patient-level data
QoL
quality of life
R-ISS
Revised International Staging System
RCT
randomized controlled trial
Rd
lenalidomide-dexamethasone
RMST
restricted mean survival time
RWE
real-world evidence
SAE
serious adverse event
SD
standard deviation
SLR
systematic literature review
TEAE
treatment-emergent adverse event
TT1R
time to first response
VGPR
very good partial response
VRd
bortezomib-lenalidomide-dexamethasone
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Table 1: Background Information on Application Submitted for Review
Item | Description |
|---|---|
Drug product | Isatuximab (Sarclisa), 20 mg/mL concentrate for solution for IV infusion |
Sponsor | Sanofi-Aventis Canada Inc. |
Indication | In combination with bortezomib, lenalidomide, and dexamethasone, for the treatment of patients with newly diagnosed multiple myeloma who are not eligible for ASCT |
Reimbursement request | As per indication |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | April 17, 2025 |
Recommended dosage | 10 mg/kg body weight administered as an IV infusion in combination with bortezomib-lenalidomide-dexamethasone |
ASCT = autologous stem cell transplant; NOC = Notice of Compliance.
Introduction
Multiple myeloma (MM) is an incurable, malignant plasma cell disease that originates from multipotent hematopoietic cells in the bone marrow. It is characterized by clonal proliferation of plasma cells in the bone marrow and excess production of monoclonal immunoglobulin (Ig). As the malignant plasma or myeloma cells accumulate in the bone marrow, they may form localized tumours or plasmacytomas. They also may interfere with normal blood cell production. When multiple plasmacytomas form either inside or outside bone, the condition is called MM. MM is the second most common hematologic cancer worldwide and the 15th most diagnosed cancer in Canada. There is limited information on the prevalence of MM in Canada; however, in 2024, it was estimated that 4,100 individuals living in Canada were diagnosed with MM and 1,750 of them would die from it.1 According to GLOBOCAN 2022 data, the 5-year prevalence for both sexes in North America was 117,011 cases or 21.7% of all prevalent cases worldwide. In Canada, the 1-year prevalence (2022 data for both sexes) was reported to be 4,044 cases or 10.5 cases per 100,000 population, whereas the 5-year prevalence was 14,553 cases or 37.9 cases per 100,000 population.
In eligible patients who were previously untreated, newly diagnosed MM is usually treated with an autologous stem cell transplant (ASCT) following induction therapy (i.e., typically with high-dose chemotherapy). However, the number of patients who may not be eligible for an ASCT is estimated to be as high as 81%. Further, not all patients who are eligible for an ASCT are willing to undergo therapy. Despite treatment advances over the past 2 decades, MM remains an incurable disease with the treatment options currently available.
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of isatuximab (10 mg/kg infusion) combined with bortezomib-lenalidomide-dexamethasone (IsaVRd), for the treatment of adult patients with transplant-ineligible, newly diagnosed MM. In April 2021, isatuximab (10 mg/kg IV infusion) combined with pomalidomide-dexamethasone received a recommendation from Canada’s Drug Agency (CDA-AMC) to reimburse with clinical criteria and/or conditions for the treatment of patients with relapsed or refractory MM who have received at least 2 prior therapies, including lenalidomide and a proteasome inhibitor. In February 2022, isatuximab (10 mg/kg IV infusion) combined with carfilzomib-dexamethasone also received a CDA-AMC recommendation to reimburse with clinical criteria and/or conditions for the treatment of adult patients with relapsed or refractory MM who have received at least 1 prior therapy.
Perspectives of Patients, Clinicians, and Drug Programs
The information in this section is a summary of input provided by the patient and clinician groups that responded to the call from CDA-AMC for input and from clinical experts consulted by CDA-AMC for the purpose of this review.
Patient Input
Myeloma Canada, an advocacy group supporting individuals with MM, provided input for the CDA-AMC review of isatuximab. Information for this submission was gathered through an online survey of patients and caregivers conducted by Myeloma Canada from October 11 to November 10, 2024. The survey was distributed via email and social media by Myeloma Canada and the Leukemia & Lymphoma Society of Canada.
Of the 43 survey responses, 24 were complete and eligible and divided into 2 subsets; 1 subset (named subset C) had 22 respondents ineligible for or not receiving an ASCT as first-line therapy and the second subset (named subset T) had 2 patients who received IsaVRd as first-line therapy.
Respondents rated the most important myeloma symptoms to control as bone issues such as fractures or pain (extremely important), followed by infections, mobility, and neuropathy. Myeloma symptoms were reported to have a significant impact on daily activities and quality of life (QoL), with respondents indicating an extreme effect on their ability to travel, work, and carry out household chores. The factors that patients considered most important to myeloma treatment consisted of effectiveness and remission, overall QoL, manageable side effects, the minimization of hospital visits, and ease of access.
The 2 respondents with IsaVRd experience reported having received the treatment for 1 year to 2 years. They found supportive care very effective, with treatment side effects and hospital visits having a slight to moderate negative impact on QoL. Both respondents rated IsaVRd as effective in controlling myeloma and manageable in terms of side effects. Despite side effects like diarrhea, infections, and neuropathy, they reported overall improved QoL, with 1 respondent noting significant health improvements.
Clinician Input
Input From Clinical Experts Consulted by CDA-AMC
According to the clinical experts consulted by CDA-AMC, newer and more cost-effective treatments are welcomed as the currently available options are limited.
Unmet Needs
In the absence of a cure for MM, the goal is to prevent disease progression and prolong QoL. Even so, a significant number of patients on the current standard of care in Canada (daratumumab-lenalidomide-dexamethasone [DRd]) progress after 8 months of treatment, therefore never reaching the landmark 5-year progression-free survival (PFS) average. The prognosis is even worse for patients with early relapses because no other therapy offers this duration of response. With the average age of individuals with MM being in the transplant-ineligible category, there is an unmet need for treatments that effectively delay first relapse, lessen frailty from progressive disease (PD), and minimize health care usage from the symptoms of PD.
Place in Therapy
According to the clinical experts, IsaVRd would be an alternative to the currently funded first-line therapy for patients with myeloma who are transplant-ineligible (e.g., DRd). It is expected that combinations using isatuximab would be equally considered for first-line treatment in this patient population. Subsequently, bortezomib-lenalidomide-dexamethasone (VRd) may be used more frequently due to starting patients on IsaVRd, given that some patients may not tolerate the side effects of isatuximab and remain on VRd only.
Patient Population
All patients requiring first-line therapy for transplant-ineligible MM would be eligible for treatment with IsaVRd.
Assessing the Response Treatment
Together with traditional measures of response as per International Myeloma Working Group (IMWG) response criteria, a reduction in the frequency and/or severity of symptoms such as bone pain and renal failure would be documented monthly with lab investigations. Improvement in QoL and function would be expected with better and faster response to therapy.
Discontinuing Treatment
The clinical experts consulted by CDA-AMC noted that treatment discontinuation is guided by IMWG response criteria or is clinically determined, and is also guided by PD and intolerable side effects (e.g., infusion reactions and infection).
Prescribing Considerations
IsaVRd would be considered as a first-line treatment option for individuals with transplant-ineligible MM. The clinical experts noted that a myeloma therapy expert would be needed to facilitate therapy.
Clinician Group Input
Two clinician groups comprising 19 clinicians provided input for this review: the Canadian Myeloma Research Group (CMRG) (13 clinicians contributed to the input) and the Ontario Health (Cancer Care Ontario) (OH [CCO]) Hematology Cancer Drug Advisory Committee (6 clinicians contributed to the input). Overall, the input was aligned with the input from the clinical experts consulted by CDA-AMC.
The OH (CCO) Hematology Cancer Drug Advisory Committee highlighted the lack of comparative data with DRd and noted that isatuximab’s IV administration may be less appealing than daratumumab’s subcutaneous option. The clinical experts consulted by CDA-AMC noted that this may be a less relevant issue once isatuximab evolves in the future to permit subcutaneous administration and this form of delivery is approved.
The CMRG pointed out that the key shift in treatment would involve adding bortezomib to the anti-CD38 monoclonal antibody, lenalidomide, and a steroid backbone, supporting IsaVRd as the new first-line standard of care for patients with newly diagnosed, transplant-ineligible MM due to its potential for greater efficacy than VRd alone. The CMRG also remarked that while isatuximab requires longer infusion times, shorter durations are feasible. Furthermore, patients who were refractory to bortezomib in the front-line setting could still benefit from carfilzomib-based regimens, making IsaVRd unlikely to alter the relapsed treatment landscape significantly.
Drug Program Input
The Provincial Advisory Group identified jurisdictional implementation issues related to relevant comparators, considerations for the initiation of therapy, considerations for the prescribing of therapy, generalizability, considerations for a funding algorithm, care provision issues, and system and economic issues. The clinical experts consulted by CDA-AMC weighed evidence from the pivotal IMROZ trial and other clinical considerations to provide responses to the Provincial Advisory Group’s implementation questions.
Clinical Evidence
Systematic Review
Description of Studies
The systematic review included 3 reports of 1 pivotal trial (the IMROZ study). The IMROZ study is an ongoing, prospective, international (no sites in Canada), multicentre, open-label, parallel-group, phase III randomized controlled trial (RCT) to assess the clinical benefit of IsaVRd compared to VRd alone in patients with newly diagnosed MM who are not eligible for an ASCT. A total of 446 patients were randomized in a 3:2 ratio to IsaVRd (N = 265) or VRd (N = 181). Randomization was stratified by country (China versus other countries), age (younger than 70 years versus 70 years or older), and Revised International Staging System (R-ISS) stage I to stage II versus stage III versus not classified (i.e., inconclusive fluorescence in situ hybridization [FISH] unless the randomization stratum could be determined based on lactate dehydrogenase [LDH], albumin, and beta2-microglobulin only). Patients in the IsaVRd group received isatuximab 10 mg/kg IV in 42-day cycles (cycle 1 to cycle 4) or 28-day cycles (after 4 cycles) in combination with VRd. Patients were treated until they died, experienced disease progression, experienced unacceptable toxicity, or decided to discontinue study treatment. The primary outcome was PFS, and the key secondary outcomes included minimal residual disease (MRD) and overall survival (OS). During the continuous treatment period, patients randomized to the VRd group who had confirmed PD during the VRd portion of the continuous treatment period (as assessed by the investigator) could cross over to the IsaVRd group. Harms including treatment-emergent adverse events (TEAEs), serious adverse events (SAEs), and adverse events (AEs) of special interest (AESI) were also measured and reported. Patient-reported outcomes (e.g., health-related quality of life [HRQoL]) were measured as well.
Patients were aged an average of 71.5 years (SD = 4.8 years), and 53.1% of patients were male while 46.9% were female. Most patients (89.0%) had an Eastern Cooperative Oncology Group Performance Status (ECOG PS) score of 0 or 1. The most common International Staging System (ISS) stage at study entry was stage I (53.0% of patients), followed by stage II (31.1% of patients), and stage III (15.2% of patients). The MM subtype at baseline was most frequently IgG (64.1% of patients) and the R-ISS stage at study entry was most frequently stage II (n = 286; 64.1% of patients). The median time from initial diagnosis to randomization was 1.18 months. The main reason for transplant ineligibility was being aged 65 years or older (95.7% of patients).
Unless otherwise specified, all data reported are from the second interim analysis for the IMROZ trial, corresponding with a data cut-off of September 26, 2023, and reported for the intention-to-treat (ITT) population. This data cut-off date corresponds with the planned second PFS interim analysis cut-off date (i.e., the date when 167 PFS events [with a 75% information fraction] from the global population were expected to be observed). By the September 26, 2023, data cut-off, a total of 162 PFS events had been observed, as determined by an independent review committee (IRC). The median follow-up at this data cut-off date was 59.73 months (range, 0.17 months to 68.99 months).
Efficacy Results
At the time of the September 26, 2023, data cut-off, 78 patients (43.1%) in the VRd group and 84 patients (31.7%) in the IsaVRd group experienced PFS events. The median PFS was 54.34 months (95% confidence interval [CI], 45.207 months to not calculated [NC]) in the VRd group and not reached in the IsaVRd group. The hazard ratio (HR) was 0.596 (98.5% CI, 0.406 to 0.876) in favour of the IsaVRd group compared to the VRd group. At 60 months, the PFS probability was 45.2% in the VRd group and 63.2% in the IsaVRd group. The risk difference at 60 months was 18.0% (95% CI, 6.5% to 29.5%). The results for sensitivity analyses (e.g., without censoring for further antimyeloma treatment, using investigator assessment of response, without censoring for progression or death occurring at least 13 weeks after the last valid disease assessment) and planned subgroup analyses (e.g., by age, sex, race, or geographic location) were consistent with those of the primary analysis.
At the time of the interim analysis, 128 deaths had occurred (VRd group = 59 deaths; IsaVRd group = 69 deaths), representing an OS information fraction of 63%. The median OS was not calculable at the data cut-off date for the IsaVRd or VRd group (HR = 0.776; 99.97% CI, 0.407 to 1.48). OS was not formally analyzed due to an earlier failure of the statistical hierarchy (the final OS analysis will be conducted once there have been 202 deaths). The OS event-free probability at 60 months was 66.3% in the VRd group and 72.3% in the IsaVRd group, representing an absolute risk difference of 5.9% (95% CI, –3.3% to 15.2%).
The overall response rate (ORR) was similar in the VRd group and the IsaVRd group at 92.3% versus 91.3%, respectively (odds ratio [OR] = 0.888; 95% CI, 0.439 to 1.794). The complete response (CR) rate (consisting of patients with stringent CR and CR) was statistically significant in favour of IsaVRd (OR = 1.656; 95% CI, 1.097 to 2.500) with a CR or better in 74.7% of patients in the IsaVRd group compared with 64.1% of patients in the VRd group. The MRD negativity rate for patients with a CR was statistically lower in the VRd group (40.9%) compared with the IsaVRd group (55.5%) (OR = 1.803; 95% CI, 1.229 to 2.646). The rate of very good partial response (VGPR) or better based on IRC assessment was 82.9% in the VRd group and 89.1% in the IsaVRd group (OR = 1.729; 95% CI, 0.994 to 3.008). The P value did not cross the multiplicity-adjusted efficacy boundary of 0.025. Most patients (> 90%) in both treatment groups achieved a tumour response.
HRQoL was assessed using the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC QLQ-C30). Completion rates were more than 90% of patients to cycle 14, and more than 80% of patients at each cycle among patients remaining in follow-up; however, the total number of patients declined over time. Global health status remained stable throughout the treatment period, with no apparent differences between groups with regard to change from baseline.
Harms Results
Most patients had a TEAE (IsaVRd group = 99.6%; VRd group = 98.3%), with the most frequently reported TEAEs (≥ 10% of patients) in the IsaVRd and the VRd treatment groups being peripheral sensory neuropathy (54.4% versus 60.8%, respectively), diarrhea (54.8% versus 48.6%, respectively), constipation (35.7% versus 40.9%, respectively), upper respiratory tract infection (34.2% versus 33.7%, respectively), peripheral edema (32.7% versus 32.6%, respectively), fatigue (34.6% versus 26.5%, respectively), and cataracts (38.0% versus 25.4%, respectively).
More individuals in the IsaVRd group had a grade 3 or higher TEAE compared to those in the VRd group (91.6% versus 84.0%, respectively). Similarly, more patients in the IsaVRd group had treatment-emergent SAEs than those in the VRd group (70.7% versus 67.4%, respectively). The most frequently reported SAE (≥ 10% of patients in either treatment group) was pneumonia (29.7% in the IsaVRd group versus 21.0% in the VRd group).
TEAEs leading to definitive treatment discontinuation were reported in 22.8% of patients receiving IsaVRd and 26.0% of patients receiving VRd. The most frequent reason for definitive treatment discontinuation was due to COVID-19 pneumonia (3.0% in the IsaVRd group versus 0.6% in the VRd group).
There were 128 deaths reported (IsaVRd group = 26.2%; VRd group = 32.6%). AEs accounted for 11.0% in the IsaVRd group and 6.1% in the VRd group.
Infusion reactions and infections were notable harms of interest to this review. Infusion reactions were more frequent with IsaVRd compared to VRd (23.6% versus 1.1%, respectively). The rate of infections was similar across groups, occurring in 91.3% of patients in the IsaVRd group and 86.7% of patients in the VRd group; they consisted primarily of pneumonia, upper respiratory tract infections, and COVID-19 infections.
Critical Appraisal
The randomization method and allocation concealment of the IMROZ trial were considered adequate. However, the IMROZ study was an open-label trial, and a lack of blinding may have biased results, particularly for subjective, patient-reported outcomes (e.g., HRQoL), harms reporting, or willingness to remain in the trial. Objective outcomes like death and assessment of outcomes like PFS were conducted by a blinded IRC and therefore were unlikely to have been influenced by a lack of blinding. Even so, there was an exploratory component to this trial in which patients in the VRd control group were allowed to cross over to the IsaVRd group after disease progression was confirmed. Multiplicity was controlled in the key secondary outcomes with the use of a hierarchical testing procedure; however, an early failure of the hierarchy meant that statistical testing was not conducted for OS, 1 of the key secondary outcomes, and no inferences could be drawn about differences between groups for this outcome. HRQoL was not included in the hierarchy, and differences between groups were not tested statistically; therefore, no conclusions could be drawn about this outcome. While the IMROZ trial is still ongoing, the available results were based on a planned interim analysis, with an information fraction of 75% for PFS; therefore, there is a risk of overestimation of the primary effect for PFS. However, given the statistically significant difference observed between the groups and the calculation of the 98.5% CIs, the potential for overestimation is unlikely to alter the conclusions. In the analysis of PFS, 18.8% of patients in the VRd group and 23.8% of patients in the IsaVRd group were censored due to not having a valid disease assessment in the 13 weeks before the data cut-off date (i.e., missed 2 or more scheduled disease assessments). Because the reason for missed assessments is not known, there is potential for a risk of bias due to informative censoring. There was no sensitivity analysis addressing this issue and the direction of potential bias cannot be ascertained. At the data cut-off date, the OS information fraction was 63%. This is important because while PFS can be viewed as a surrogate for OS, death is not an immediate consequence of treatment failure as further lines of treatment can prolong life. Furthermore, the OS analysis is confounded by crossovers (the risk of bias may be toward the null). As the trial progressed, more patients discontinued treatment or died. This may have led to attrition bias for outcomes analyzed based on change scores like HRQoL or the incidence of AEs, which were only documented for patients still being followed. For the latter, results were additionally reported after adjustment for the duration of exposure.
The IMROZ trial excluded patients aged older than 80 years and those with an ECOG PS score greater than 2; however, some patients with an ECOG PS score of 2 or more were enrolled. The clinical experts noted that the efficacy of VRd in the trial was higher than would normally be expected, which could be the result of a learning curve in jurisdictions that use VRd regularly. Further, in the IMROZ trial, bortezomib was not dosed at the Canadian and international standard of once weekly. Finally, while the study was conducted in 96 sites (in 21 countries or regions), none of the sites were in Canada.
GRADE Summary of Findings and Certainty of the Evidence
The selection of outcomes for the Grading of Recommendations Assessment, Development and Evaluations (GRADE) assessment was based on the sponsor’s Summary of Clinical Evidence, consultation with clinical experts, and input received from patient and clinician groups and public drug plans. The following list of outcomes was finalized in consultation with expert committee members:
PFS — median, 18 months, 36 months, and 60 months
OS — median and 60 months
HRQoL using the EORTC QLQ-C30 — change from baseline
individuals with SAEs — up to the data cut-off date.
Table 2: Summary of Findings for IsaVRd Versus VRd for Patients With Multiple Myeloma
Outcome and follow-up | Patients (studies), N | Relative effect (95% CI) | Absolute effects (95% CI) | Certainty | Interpretation | ||
|---|---|---|---|---|---|---|---|
IsaVRd | VRd | Difference | |||||
Survival outcomes (median follow-up = 59.7 months; range, 0.17 months to 68.99 months) | |||||||
Probability of PFS by IRC at 18 months | 446 (1 RCT) | ██ █████ █████ ██ █████ ██ ██████ | 882 per 1,000 (835 to 916 per 1,000) | 796 per 1,000 (726 to 850 per 1,000) | 86 more per 1,000 (13 to 159 more per 1,000) | Moderatea | IsaVRd likely results in an improvement in PFS compared to VRd. |
Probability of PFS by IRC at 36 months | 446 (1 RCT) | ██ █████ █████ ██ █████ ██ ██████ | 761 per 1,000 (702 to 809 per 1,000) | 664 per 1,000 (583 to 732 per 1,000) | 97 more per 1,000 (5 to 189 more per 1,000) | Moderatea | IsaVRd likely results in an improvement in PFS compared to VRd. |
Probability of PFS by IRC at 60 months | 446 (1 RCT) | ██ █████ █████ ██ █████ ██ ██████ | 632 per 1,000 (562 to 694 per 1,000) | 452 per 1,000 (356 to 542 per 1,000) | 180 more per 1,000 (65 to 295 more per 1,000) | Moderatea | IsaVRd likely results in an improvement in PFS compared to VRd. |
Probability of OS by IRC at 60 months | 446 (1 RCT) | ██ █████ █████ ██ █████ ██ ██████ | 723 per 1,000 (661 to 775 per 1,000) | 663 per 1,000 (585 to 731 per 1,000) | 59 more per 1,000 (33 fewer to 152 more per 1,000) | Lowb | IsaVRd may result in an improvement in OS compared to VRd. |
Patient-reported outcomes (HRQoL) | |||||||
EORTC QLQ-C30 global health status Follow-up: Up to 90 days after the last study treatment | 446 (1 RCT) | NA | NA | The mean difference between groups in change from baseline in assessments using the EORTC QLQ-C30 was not tested statistically. The mean global health status appeared relatively stable over time in both groups with wide overlapping CIs. | Lowc | IsaVRd may result in little to no difference in global health status compared to VRd. | |
Safety outcomes (treatment-emergent SAEs) | |||||||
SAEs Follow-up: Up to 20 days after the last dose of study treatmentd | 444 (1 RCT) | RR = 1.05 (0.92 to 1.19) | 707 per 1,000 (648 to 762 per 1,000) | 674 per 1,000 (601 to 742 per 1,000) | 33 more per 1,000 (54 fewer to 121 more per 1,000) | Moderatee | IsaVRd likely results in an increase in SAEs compared to VRd. |
CI = confidence interval; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; HRQoL = health-related quality of life; IRC = independent review committee; IsaVRd = isatuximab-bortezomib-lenalidomide-dexamethasone; NA = not applicable; OS = overall survival; PFS = progression-free survival; RCT = randomized controlled trial; RR = risk ratio; SAE = serious adverse event; VRd = bortezomib-lenalidomide-dexamethasone.
Note: Study limitations (which refer to internal validity or the risk of bias), inconsistency across studies, indirectness, the imprecision of effects, and publication bias were considered when assessing the certainty of the evidence. All serious concerns in these domains that led to the rating down of the level of certainty are documented in the table footnotes.
aNo threshold of clinical importance could be established. Effects were appraised using the null. Rated down 1 level for study limitations; 18.8% of patients in the VRd group and 23.8% in the IsaVRd group were censored due to not having a valid disease assessment in the 13 weeks before the data cut-off (i.e., missed 2 or more scheduled disease assessments). Because the reason for missed assessments was not known, there is a potential for a risk of bias due to informative censoring.
bRated down 1 level for study limitations. Results are from an interim analysis where OS was not formally tested, there is a risk of bias due to confounding as a result of crossover of patients from the VRd group to the IsaVRd group postprogression, and there is a potential for a risk of bias due to informative censoring. No threshold of clinical importance could be established; effects were appraised using the null. Rated down 1 level for imprecision. The point estimate suggests benefit and the CI includes no difference and potential harm.
cRated down 2 levels for study limitations. There is a risk of bias due to a lack of blinding and a subjective outcome, as well as due to substantial missing outcome data.
dFor patients in the VRd group who crossed over, the follow-up was to the crossover date minus 1 day.
eNo threshold of clinical importance could be established; effects were appraised using the null. Rated down 1 level for imprecision. The point estimate suggests harm and the CI includes no difference and potential benefit (i.e., lesser harm than VRd).
Source: IMROZ Clinical Study Report.32
Long-Term Extension Studies
There is no long-term extension phase planned for the IMROZ trial. The IMROZ trial remains ongoing with an anticipated completion date of June 30, 2027. No other long-term extension studies were included in the submission.
Indirect Comparisons
Description of Studies
Unanchored matching-adjusted indirect comparisons (MAICs) were used as the source of indirect treatment comparison (ITC) to compare individual patient-level data (PLD) for IsaVRd from the IMROZ trial to aggregate data from studies of DRd, lenalidomide-dexamethasone (Rd), daratumumab-bortezomib-melphalan-prednisone (DVMP), and daratumumab-cyclophosphamide-bortezomib-dexamethasone (DCyBorD). For the comparison to cyclophosphamide-bortezomib-dexamethasone (CyBorD) (Flatiron Health data source), a nonrandomized comparison using inverse probability weighting (IPW) methods was used because individual PLD were available for each group.
Efficacy Results
Progression-Free Survival
The MAIC of IsaVRd versus DRd resulted in HRs of ████ ████ ███ ████ ██ █████ at 1 year and ████ ████ ███ ████ ██ █████ at 5 years.
The MAIC of IsaVRd versus DVMP resulted in HRs of ████ ████ ███ ████ ██ ████ at 1 year and ████ ████ ███ ████ ██ █████ at 5 years.
The MAIC of IsaVRd versus DCyBorD resulted in HRs of ████ ████ ███ ████ ██ █████ at 1 year and ████ ████ ███ ████ ██ █████ at 5 years.
The MAIC of IsaVRd versus Rd using data from the MAIA study resulted in HRs of ████ ████ ███ ████ ██ █████ at 1 year and ████ ████ ███ ████ ██ █████ at 5 years. Using data from the FIRST study, the HR was ████ ████ ███ ████ ██ █████ at 1 year and ████ ████ ███ ████ ██ █████ at 5 years.
The observational comparison of IsaVRd versus CyBorD resulted in HRs of ████ ████ ███ ████ ██ █████ at 1 year and ████ ████ ███ ████ ██ █████ at 5 years.
Overall Survival
The MAIC of IsaVRd versus DRd resulted in HRs of ████ ████ ███ ████ ██ █████ at 1 year and ████ ████ ███ ████ ██ █████ at 5 years.
The MAIC of IsaVRd versus DVMP resulted in HRs of ████ ████ ███ ████ ██ █████ at 1 year and ████ ████ ███ ████ ██ █████ at 5 years.
There were no data available to compare OS for IsaVRd versus DCyBorD.
The MAIC of IsaVRd versus Rd using data from the MAIA study resulted in HRs of ████ ████ ███ ████ ██ █████ at 1 year and ████ ████ ███ ████ ██ █████ at 5 years. Using data from the FIRST study, the HR was ████ ████ ███ █████ █████ at 1 year and ████ ████ ███ █████ █████ at 5 years.
The observational comparison of IsaVRd versus CyBorD resulted in HRs of ████ ████ ███ ████ ██ █████ at 1 year and ████ ████ ███ ████ ██ █████ at 5 years.
Harms Results
Harms were not evaluated in the submitted ITCs.
Critical Appraisal
The ITC analyses were preceded by a feasibility appraisal, and the decision to use MAICs and IPW as the ITC method of choice (instead of network meta-analysis [NMA]) was adequately justified. However, the unanchored nature of the comparisons imposes an unrealistic assumption that all prognostic factors and effect modifiers are adequately adjusted for. The choice of the adjustment factors was based on internal expert opinion and availability and completeness of data in the trials. An assessment of the potential magnitude of residual confounding was not presented for any comparison; therefore, the extent of potential bias is unknown. The adjustment methods used cannot overcome methodological or design differences across the comparators, which can introduce bias (e.g., region or setting, length of follow-up, outcome definitions [event and censoring rules, schedule and method of assessments], cointerventions, or subsequent treatments). Important outcomes for decision-making like HRQoL and AEs were not included in the analyses, even though the MAIC included real-world evidence (RWE) that could have provided important insights and the generation of hypotheses for future confirmation. The OS data from the IMROZ trial is still immature and final data will not be available until 2027, so any MAIC based on this is premature. Generalizability may be an issue due to the small sample size remaining after the exclusions and matching in some of the analyses.
Studies Addressing Gaps in the Evidence From the Systematic Review
No studies addressing gaps were submitted.
Conclusions
One multinational, ongoing, open-label, phase III RCT (the IMROZ study) was included in the CDA-AMC review. In a population of 446 patients with newly diagnosed MM who were ineligible for an ASCT, IsaVRd resulted in a statistically significant improvement in PFS compared to VRd. Though the median PFS was not reached in the IsaVRd group, the clinical experts consulted by the review team considered the findings clinically meaningful. There was some concern for the potential risk of bias in the analysis of PFS due to missed disease assessments. The IMROZ trial is an ongoing study and though the results suggest that IsaVRd may improve OS compared to VRd, conclusions are limited because the data for OS were based on an interim analysis and were not formally tested. Additionally, the median results for OS had not been reached and results were considered immature. Because the final analysis of OS is not yet available, the results are only considered supportive of the overall findings. The findings for OS are also limited by potential confounding by crossovers, and imprecision in the estimates (i.e., CIs crossed the null). The addition of isatuximab to VRd increased the incidence of patients with grade 3 or higher TEAEs but the clinical experts consulted by the review team noted that the side effects were considered manageable. HRQoL seemed to be similar between groups, suggesting no detriment to QoL, but there was no statistical testing and there was increased attrition as the trial progressed.
Time-varying MAICs and IPW were used to derive comparative effect estimates for IsaVRd versus relevant comparators that were not included in the IMROZ trial. Despite the fact that these analyses suggested improved PFS with IsaVRd compared to DVMP and Rd (there was no difference detected compared to DRd, DCyBorD, and CyBorD), multiple methodological limitations rendered the evidence insufficient to draw definitive conclusions. These limitations included a high risk of bias resulting from unaddressed prognostic and effect-modifying variables, differences in study design and/or conduct that could not be adjusted for in the analyses, important reductions in ESS, and in some cases, imprecision (i.e., CIs crossing the null). Findings for OS are subject to additional uncertainty as the data for OS from the IMROZ trial remain immature. The lack of consideration of HRQoL and harms in the indirect comparisons limits the ability to comprehensively assess the balance of comparative benefits and harms.
Introduction
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of isatuximab, 10 mg/kg infusion in combination with VRd, for the treatment of adult patients with transplant-ineligible, newly diagnosed MM.
Disease Background
Content in this section has been informed by materials submitted by the sponsor and clinical expert input. The following has been summarized and validated by the CDA-AMC review team.
MM is an incurable, malignant plasma cell disease that originates from multipotent hematopoietic cells in bone marrow.2 It is characterized by clonal proliferation of plasma cells in the bone marrow and excess production of monoclonal Ig, usually of the IgG or IgA type, or free light chains (e.g., paraprotein, M protein, M component).2 As the malignant plasma or myeloma cells accumulate in the bone marrow, they may form localized tumours or plasmacytomas, which, in turn, grow inside (intramedullary) or outside (extramedullary or soft-tissue) bone.3 They also may interfere with normal blood cell production. When multiple plasmacytomas form either inside or outside bone, the condition is called MM.3 The natural history of MM depicts a heterogenous course characterized by 3 clinical stages: monoclonal gammopathy of undetermined significance, smouldering MM, and active MM.3 The timeline for movement through these stages is not linear.4,5 As myeloma cells proliferate and the disease progresses, patients face a heavy disease burden due to disease-related symptoms and complications such as hypercalcemia, anemia, weakness, fatigue, renal failure, exertional dyspnea, immunodeficiency, infection, bone destruction leading to pain and fractures, and treatment-related toxicities.6
MM is the second most common hematologic cancer worldwide and the 15th most diagnosed cancer in Canada.7 While there is limited information on its prevalence in Canada, in 2024, it was estimated that 4,100 individuals living in Canada would be diagnosed with MM and 1,750 would die from it.8 According to GLOBOCAN 2022 data, the 5-year prevalence of MM for both sexes in North America was 117,011 cases, or 21.7% of all prevalent cases of MM worldwide.9 In Canada, the 1-year prevalence (2022 data for both sexes) was reported to be 4,044 cases or 10.5 cases per 100,000 population, whereas the 5-year prevalence was 14,553 cases or 37.9 cases per 100,000 population.10
Timely diagnosis is key to prevent or limit irreversible injury to organs and to prolong survival.11 For patients with suspected MM, the initial diagnostic work-up usually includes baseline blood studies (e.g., complete blood count), and biological assessments to differentiate symptomatic and asymptomatic MM.11,12 Various serum and urine analyses are also conducted to evaluate the M protein components in serum (e.g., quantitative Ig tests for IgA, IgD, IgE, IgG, and IgM, serum protein electrophoresis and serum immunofixation electrophoresis) and in urine (e.g., 24-hour urine protein electrophoresis or urine immunofixation electrophoresis).12 A serum free light chain assay along with serum protein electrophoresis and serum immunofixation electrophoresis provide high sensitivity and prognostic value.12 Other evaluations include bone marrow aspiration and biopsy to detect quantitative and/or qualitative abnormalities of bone marrow plasma cells or whole body low-dose CT to identify lytic bone lesions.12 Cytogenetic testing such as karyotyping or chromosome analysis by FISH is used to identify specific chromosomal abnormalities associated with MM such as translocations, deletions, or amplifications, and to assist with risk stratification.11,12 Gene expression profiling also assists with prognosis and therapeutic decisions.13-15 Additional diagnostic tests include bone marrow immunohistochemistry, flow cytometry, whole body MRI, or PET or PET-CT scans.12
The diagnosis of symptomatic MM is made on the basis of the IMWG criteria: clonal bone marrow cells of more than 10% (or biopsy-proven bony or extramedullary plasmacytoma), end organ damage (hypercalcemia, renal insufficiency, anemia, or bone lesions), or myeloma defining events (clonal bone marrow plasma cells of 60% or more, a serum involved or uninvolved free light chain ratio of 100 or more, or more than 1 focal lesion on an MRI).16,17 Staging is then conducted using the Second Revision of the ISS.18 The ISS is based on serum beta2-microglobulin and serum albumin measurements.19 The ISS was revised in 2015 (R-ISS) and integrates high-risk chromosomal abnormalities detected by FISH and serum LDH as prognostic factors to better stratify patients who were newly diagnosed into homogeneous survival groups.20 In Canada, MM is most often staged using the Second Revision of the ISS and genetic information.21 There are no confirmed or anticipated statements in the Canadian product monograph regarding specific diagnostic technology that is recommended for isatuximab.
Standards of Therapy
Content in this section has been informed by materials submitted by the sponsor and clinical expert input. The following has been summarized and validated by the CDA-AMC review team.
Pharmacotherapy regimens for MM are complex and evolving rapidly as novel drugs and multidrug combination regimens of various drug classes are increasingly being incorporated into clinical practice. In eligible patients who were previously untreated, newly diagnosed MM is usually treated with an ASCT following induction therapy (i.e., typically with high-dose chemotherapy). It should be noted that more than 50% of patients may not be eligible for an ASCT because of health risks or other issues.22,23 Further, not all patients who are eligible for an ASCT are willing to undergo a transplant.
There are currently 3 main drug classes available for the treatment of MM: immunomodulatory drugs (e.g., thalidomide, lenalidomide, and pomalidomide), proteasome inhibitors (e.g., bortezomib, carfilzomib, and ixazomib), and monoclonal antibodies (e.g., anti-CD38 antibodies such as daratumumab and isatuximab). In 2019, the joint guideline from OH (CCO) and the American Society of Clinical Oncology recommended initial treatment of triplet therapy including a novel drug (e.g., immunomodulatory drugs) and steroids.24 In 2024, CDA-AMC recommended the prioritization of first-line daratumumab (e.g., DCyBorD or DRd) in patients with MM who were ineligible for a transplant.25 Despite treatment advances over the past 2 decades, MM remains an incurable disease, with the treatment options currently available reflecting the need for further innovative treatment options.
Drug Under Review
Isatuximab is a monoclonal antibody that binds to a specific extracellular epitope of CD38, triggering mechanisms that result in the death of CD38-expressing tumour cells.26 CD38 is a transmembrane glycoprotein with ectoenzymatic activity that is expressed in hematologic malignancies as well as other cell types and tissues. Isatuximab acts through IgG fragment crystallizable-dependent mechanisms, including antibody-dependent cell-mediated cytotoxicity, antibody-dependent cellular phagocytosis, and complement-dependent cytotoxicity, and may also trigger the death of tumour cells by inducing apoptosis through a fragment crystallizable-independent mechanism.26
Isatuximab is administered as an IV infusion, at a dose of 10 mg/kg, in combination with bortezomib-lenalidomide-dexamethasone for the treatment of patients with newly diagnosed MM who are not eligible for an ASCT. It has a Health Canada indication for the treatment of adult patients with relapsed or refractory MM who have received 1 to 3 prior lines of therapy. Each treatment cycle is 28 days; in cycle 1, isatuximab is administered on day 1, day 8, day 15, and day 22 (weekly), and, in cycle 2 and beyond, it is administered every 2 weeks. Treatment continues until disease progression or unacceptable toxicity. The sponsor’s reimbursement request is consistent with past Health Canada schedules for isatuximab. In April 2021, isatuximab (10 mg/kg) IV infusion combined with pomalidomide and dexamethasone received a CDA-AMC recommendation to reimburse with clinical criteria and/or conditions for the treatment of patients with relapsed or refractory MM who have received at least 2 prior therapies including lenalidomide and a proteasome inhibitor. In February 2022, isatuximab (10 mg/kg) IV infusion combined with carfilzomib and dexamethasone received a CDA-AMC recommendation to reimburse with clinical criteria and/or conditions for the treatment of adult patients with relapsed or refractory MM who have received 1 to 3 prior lines of therapy.
Key characteristics of isatuximab are summarized in Table 3 with other treatments available for the first-line treatment of transplant-ineligible MM.
Table 3: Key Characteristics of Isatuximab, Proteasome Inhibitors, Immunomodulatory Drugs, and Daratumumab
Characteristic | Isatuximab | Proteasome inhibitors | IMiDs | Daratumumab |
|---|---|---|---|---|
Mechanism of action | Binds to a specific extracellular epitope of CD38, triggering mechanisms that result in the death of CD38-expressing tumour cells | Proteasome inhibition leads to accumulation of misfolded protein in ER, resulting in apoptosis; inhibits cell proliferation | Immunomodulatory and antineoplastic activity; inhibits proliferation and induces apoptosis of hematopoietic tumour cells | mAb targeting CD38 is overexpressed on tumour cells in hematologic malignancies; induces cell lysis via a variety of mechanisms, including ADCC, CDC, and ADCP |
Indicationa | In combination with bortezomib, lenalidomide, and dexamethasone for the treatment of patients with newly diagnosed MM who are not eligible for an ASCT | Carfilzomib: In combination with dexamethasone and daratumumab, or lenalidomide and dexamethasone, or dexamethasone alone for patients with relapsed MM who have received 1 to 3 prior lines of therapy Bortezomib: Part of combination therapy for patients with previously untreated MM who are unsuitable for SCT Part of combination therapy for induction treatment of patients with previously untreated MM who are suitable for SCT Treatment of progressive MM in patients who have received at least 1 prior therapy and who have already undergone or are unsuitable for SCT Part of combination therapy for the treatment of patients with previously untreated mantle cell lymphoma who are unsuitable for SCT Treatment of patients with mantle cell lymphoma who have relapsed or were refractory to at least 1 prior therapy | Lenalidomide: In combination with dexamethasone for the treatment of patients with MM who are not eligible for SCT Pomalidomide: In combination with dexamethasone and bortezomib for patients with MM who have received at least 1 prior treatment regimen that included lenalidomide in combination with dexamethasone for patients with MM for whom both bortezomib and lenalidomide have failed and who have received at least 2 prior regimens and demonstrated disease progression on the last regimen | In combination with lenalidomide plus dexamethasone or bortezomib plus melphalan plus prednisone for patients with newly diagnosed MM who are ineligible for an ASCT In combination with lenalidomide plus dexamethasone or bortezomib plus dexamethasone for patients with MM who have received at least 1 prior therapy For the treatment of patients with MM who have received at least 3 prior lines of therapy, including a PI and an IMiD or who are refractory to both |
Route of administration | IV infusion | IV infusion | Oral | IV infusion |
Recommended dosage | 10 mg/kg weekly (day 1, day 8, day 15, and day 22 of the 28-day cycle) for cycle 1 and every 2 weeks (day 1 and day 15) for cycle 2 and beyond Treatment is repeated until disease progression or unacceptable toxicity. | Carfilzomib:
Treatment is continued until disease progression or unacceptable toxicity. Bortezomib: For MM, patients suitable for SCT:
For patients not suitable for SCT:
| Pomalidomide:
Lenalidomide:
Treatment is repeated until disease progression. | DRd (4-week cycle):
DVMP (6-week cycle):
DVd (3-week cycle):
Treatment is continued until disease progression |
Serious adverse effects or safety issues |
| Carfilzomib:
Bortezomib:
| Both:
|
|
Other | Premedication with dexamethasone, acetaminophen, H2 receptor antagonist or proton pump inhibitor, and diphenhydramine is recommended to reduce risk and severity of infusion-related reactions | Premedication for carfilzomib recommended with dexamethasone (at least 30 minutes prior) to reduce incidence and severity of infusion reactions Antiviral prophylaxis should be considered before initiating bortezomib to prevent reactivation of herpes zoster | Antithrombotic prophylaxis recommended Antibiotic prophylaxis recommended Only available under a controlled distribution program | Premedication with dexamethasone, antipyretics, and antihistamines is recommended; postinfusion (to prevent delayed infusion reactions), oral corticosteroid. Antibiotic and antiviral prophylaxis should also be considered to prevent reactivation of herpes zoster. |
ADCC = antibody-dependent cell-mediated cytotoxicity; ADCP = antibody-dependent cellular phagocytosis; ASCT = autologous stem cell transplant; CDC = complement-dependent toxicity; CHF = congestive heart failure; DKd = daratumumab-carfilzomib-dexamethasone; DRd = daratumumab-lenalidomide-dexamethasone; DRESS = drug reaction with eosinophilia and systemic symptoms; DVd = daratumumab-bortezomib-dexamethasone; DVMP = daratumumab-bortezomib-melphalan-prednisone; DVT = deep vein thrombosis; ER = endoplasmic reticulum; H2 = histamine subtype 2; IMiD = immunomodulatory drug; Kd = isatuximab-dexamethasone; KRd = isatuximab-lenalidomide-dexamethasone; mAb = monoclonal antibody; MM = multiple myeloma; NOC = Notice of Compliance; PE = pulmonary embolism; PI = proteasome inhibitor; PML = progressive multifocal leukoencephalopathy; Rd = lenalidomide-dexamethasone; SCT = stem cell transplant; SJS = Stevens-Johnson syndrome; TEN = toxic epidermal necrolysis; TLS = tumour lysis syndrome; VPd = bortezomib-pomalidomide-dexamethasone.
aHealth Canada–approved indication.
Source: CADTH Reimbursement Review: Isatuximab (Sarclisa).27
Perspectives of Patients, Clinicians, and Drug Programs
The full patient and clinician group submissions received by CDA-AMC are available in the consolidated patient and clinician group input document for this review on the project website.
Patient Group Input
This section was prepared by the CDA-AMC review team based on the input provided by patient groups.
Myeloma Canada, an advocacy group supporting individuals with MM, provided input for the CDA-AMC review of isatuximab. Information for this submission was gathered through an online survey of patients and caregivers conducted by Myeloma Canada from October 11 to November 10, 2024. The survey was distributed via email and social media by Myeloma Canada and the Leukemia & Lymphoma Society of Canada.
Among the 43 survey responses, 24 were complete and eligible and divided into 2 subsets; 1 subset (named subset C) had 22 respondents ineligible for or not receiving an ASCT as first-line therapy and the second subset (named subset T) had 2 patients who received IsaVRd as first-line therapy. Subset C included respondents primarily from British Columbia (n = 11), with others from across Canada and 2 international participants. Most were male (n = 15; female, n = 7), aged 70 years to 79 years (n = 15), and lived in urban areas (n = 19). Subset T included 2 patients from Ontario aged 70 years to 79 years, 1 male and 1 female. None of the respondents were currently eligible for the treatment under review.
Eligible respondents (n = 24) rated the importance of controlling myeloma symptoms on a scale of 1 (not important) to 5 (extremely important), with bone issues (e.g., fractures, pain) (n = 12) rated as extremely important, followed by infections (n = 10), mobility (n = 9), and neuropathy (n = 8). Myeloma symptoms were reported to have a significant impact on daily activities and QoL, with respondents indicating an extreme effect on their ability to travel (n = 5), work (n = 4), and carry out household chores (n = 3). Most respondents (n = 19) reported visiting the hospital or cancer centre monthly, with travel times of less than 30 minutes (n = 11) or 30 minutes to 1 hour (n = 9).
According to the survey, treatment costs were primarily linked to parking fees (n = 8), drug expenses (n = 5), and administration fees (n = 3). Furthermore, the psychological and social challenges associated with the disease that were reported to have an extreme impact on QoL included the loss of sexual desire (n = 4), followed by difficulty sleeping (n = 3) and anxiety or worry (n = 2). Of the 21 patient respondents, 11 reported needing caregiver support while 8 indicated they did not. When asked about the factors they consider most important to myeloma treatment, 22 respondents emphasized effectiveness and remission, overall QoL, manageable side effects, the minimization of hospital visits, and ease of access.
In subset C, 18 respondents were ineligible for an ASCT at diagnosis, and 4 were eligible but did not receive a transplant. The most used first-line treatments were dexamethasone (n = 21), lenalidomide (n = 18), and daratumumab (n = 13), with DRd being the most frequent treatment combination (n = 11), followed by Rd (n = 3). Respondents rated their treatment experience positively, with many reporting improved QoL, manageable side effects, and effective myeloma control, and stating that the experience completely or mostly met their expectations. When considering treatment, respondents from subset C rated infections and cataracts as the least bearable side effects, followed by neutropenia and fever.
The 2 respondents with IsaVRd experience reported having received the treatment for 1 to 2 years. They found supportive care very effective, with treatment side effects and hospital visits having a slight to moderate negative impact on QoL. Both respondents rated IsaVRd as effective in controlling myeloma and manageable in terms of side effects. Despite side effects like diarrhea, infections, and neuropathy, they reported overall improved QoL, with 1 respondent noting significant health improvements.
Clinician Input
Input From Clinical Experts Consulted by CDA-AMC
All CDA-AMC review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, or providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of MM.
Unmet Needs
The clinical experts noted that MM is an incurable disease despite the treatments available today. In the absence of a cure, the goal is to prevent disease progression and prolong QoL. It should be noted that QoL in clinical practice may be determined by a combination of validated QoL scales, patient reports, and clinical determination. A significant number of patients receiving the current standard of care in Canada (DRd) progress after 8 months of treatment, therefore never reaching the landmark 5-year PFS average. Prognosis is even worse for patients with early relapses because no other therapy offers this duration of response. With active myeloma, it takes typically 6 months for the symptoms (e.g., renal failure and extreme bone pain) to settle and to begin to experience alleviation. With relapsed disease, the symptoms of myeloma persist, and death can occur, so having more effective therapy in first-line treatment that would delay progression for as long as possible and prevent these issues and attrition is essential. With the average age of individuals with MM being in the transplant-ineligible category, there is an unmet need for treatments that effectively delay first relapse, lessen frailty from PD, and minimize health care usage from the symptoms of PD.
Place in Therapy
According to the clinical experts, IsaVRd would be an alternative to the currently funded first-line therapy for patients with myeloma who are ineligible for transplant (e.g., DRd). It is expected that combinations using isatuximab would be equally considered for first-line treatment in this patient population. The clinical experts also noted that isatuximab may also provide an alternative for drug shortages to meet patient preferences and frailty status. The clinical experts noted that, in the future, the evolution of isatuximab delivery with subcutaneous administration at home may help to decrease chair time and minimize health disparities for patients in rural settings who do not live in an urban environment and would otherwise refuse daratumumab. Further, combined with a bortezomib home injection, this would allow for a 4-drug combination to be delivered in the home, decreasing the burden on the health care system and further reducing health disparities. Also, the addition of proteosome inhibitors has consistently added 8 months of OS compared to the control group in other phase III myeloma clinical trials.
Patient Population
All patients requiring first-line therapy for transplant-ineligible MM would be eligible for treatment with IsaVRd.
Assessing the Response Treatment
Together with traditional measures of response as per IMWG response criteria, a reduction in the frequency and/or severity of symptoms such as bone pain and renal failure would be documented monthly with lab investigations. Improvement in QoL and function would be expected with better and faster response to therapy.
Discontinuing Treatment
The clinical experts noted that treatment discontinuation is guided by IMWG response criteria or is clinically determined, and is also guided by PD and intolerable side effects (e.g., infusion reactions and infection). The clinical experts also noted that consideration for the discontinuation of therapy based on sustained negative MRD response may allow for treatment-free intervals, but research on drug stoppage trials is ongoing. It should also be noted that deep and durable responses are needed first before entertaining the idea of the discontinuation of drug therapy.
Prescribing Considerations
IsaVRd would be considered as a first-line treatment option for individuals with transplant-ineligible MM. The clinical experts noted that a myeloma therapy expert would be needed to facilitate therapy.
Clinician Group Input
This section was prepared by the CDA-AMC review team based on the input provided by clinician groups.
Two clinician groups comprising 19 clinicians provided input for this review: CMRG (13 clinicians contributed to the input) and the OH (CCO) Hematology Cancer Drug Advisory Committee (6 clinicians contributed to the input). Overall, the input was aligned with the input from the clinical experts consulted by CDA-AMC.
According to clinician groups, patients who are newly diagnosed in Canada with myeloma and who are transplant-ineligible typically receive daratumumab-based regimens, such as DRd, until disease progression. A small proportion of patients with renal impairment or poor bone marrow reserve may start treatment with DCyBorD. Less often, patients with transplant ineligibility due to frailty may receive Rd or VRd (typically “lite”), with single drug lenalidomide also used until disease progression.
Both groups underscored the primary treatment goals: prolonging PFS and OS and controlling disease symptoms and complications (e.g., bone damage, kidney failure, hypercalcemia, or low blood counts). Additionally, CMRG stressed minimizing treatment-related AEs and improving QoL by tailoring care to individual patient needs.
While acknowledging multiple therapy lines for myeloma, both groups reiterated its incurable nature. The CMRG stressed that long-term survival depends on maximizing disease control during first-line treatment, emphasizing deep and durable response — including MRD negativity — to achieve prolonged remission. They noted that 19% of patients who are transplant-ineligible in Canada do not receive second-line therapy due to disease progression or death.
The OH (CCO) Hematology Cancer Drug Advisory Committee highlighted the lack of comparative data for IsaVRd with DRd and noted that the IV administration of isatuximab may be less appealing than subcutaneous daratumumab. The CMRG pointed out that the key shift in treatment would involve adding bortezomib to the anti-CD38 monoclonal antibody, lenalidomide, and a steroid backbone, supporting IsaVRd as the new first-line standard of care for patients who are transplant-ineligible with newly diagnosed MM due to its potential for greater efficacy than VRd alone. They also remarked that while isatuximab requires longer infusion times, shorter durations are feasible. Furthermore, patients who were refractory to bortezomib in the front-line setting could still benefit from carfilzomib-based regimens, making IsaVRd unlikely to alter the relapsed treatment landscape significantly.
The OH (CCO) Hematology Cancer Drug Advisory Committee highlighted the use of standard myeloma response criteria and noted that PFS is a key outcome. The CMRG elaborated on using monoclonal protein markers, bone marrow biopsy, and imaging studies per IMWG criteria while clinical trials also assess marrow MRD. Clinically meaningful responses (defined as at least partial remission) were linked to improvements in symptoms such as reduced bone pain, fewer fractures, a decreased need for radiotherapy, increased energy, and enhanced daily functioning. Response evaluations are typically conducted every 1 month to 3 months based on clinical stability and treatment regimen.
Both groups agreed that treatment discontinuation should be considered for significant intolerance. The OH (CCO) Hematology Cancer Drug Advisory Committee added that disease progression could also warrant discontinuation, while CMRG emphasized that bortezomib-related toxicity might necessitate stopping treatment.
The clinician groups concurred that isatuximab should be administered in systemic therapy centres. The CMRG specified that IsaVRd is suitable for centres experienced in managing isatuximab and bortezomib and should be overseen by hematologists or oncologists proficient in managing potential AEs, including in community and tertiary facilities.
Drug Program Input
The drug programs provide input on each drug being reviewed through the CDA-AMC reimbursement review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CDA-AMC are summarized in Table 4.
Table 4: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation question | Clinical expert response |
|---|---|
Relevant comparators | |
Funded treatment options for patients newly diagnosed with myeloma who are transplant-ineligible include VRd, DRd, DCyBorD, and DVMP. The IMROZ trial compared IsaVRd against VRd, with 4 induction cycles of VRd ± isatuximab followed by continuous Rd ± isatuximab until disease progression or unacceptable toxicity. How does IsaVRd compare to DRd, DCyBorD, or DVMP? | The clinicians theorized that IsaVRd would have better, if not similar, efficacy to DRd but that head-to-head trials would be needed to confirm this. They also noted that DCyBorD and DVMP are not commonly used due to their safety profiles and clinical inferiority compared with DRd. Additionally, the MRD response rates are higher with the drug combinations containing bortezomib. |
Considerations for initiation of therapy | |
Should the following patients be considered for IsaVRd? Patients with:
| The clinicians confirmed that these patient populations should be considered for IsaVRd on a case-by-case basis, and delivery of treatment would vary depending on the situation (e.g., may start oral treatments only in patients aged > 80 years, and add on other treatments if tolerated). It should also be noted that a frailty assessment would be better than age alone. Age does contribute to frailty, but it is not unto itself the only definition of frailty. The experts also noted that amyloidosis is a different disease from myeloma, and no treatments are given in patients with monoclonal gammopathy of undetermined significance or smouldering myeloma. Thus, treatment with IsaVRd is not warranted in these populations. |
Considerations for discontinuation of therapy | |
Should cyclophosphamide be added to IsaVRd upon biochemical progression, given the clinical practice of adding cyclophosphamide to other myeloma regimens to prolong the response? | The clinical experts noted that it is not recommended because cyclophosphamide is generally used as a bridging therapy and only adds more toxicity without an expectation of real benefit. |
Should treatments be resumed if prolonged treatment breaks occur? | The clinicians confirmed that treatment should be resumed if progression has not occurred before the prolonged treatment break. |
If 1 of the drugs is discontinued, can the other drugs in the regimen be continued until disease progression or unacceptable toxicity? | The clinicians confirmed that if 1 of the drugs in the regimen is discontinued, then the treatment can continue with the other drugs in the regimen until disease progression or unacceptable toxicity. |
Considerations for prescribing of therapy | |
The dosing schedule for VRd in the IMROZ trial appears different from that used in jurisdictions in Canada (weekly at a dose of 1.3 mg/m2 to 1.5 mg/m2). Are there alternative dosing schedules for bortezomib or VRd that can be used? | The clinical experts noted that bortezomib should be dosed at the Canadian and international standard of once weekly. |
Rapid infusion of isatuximab has been adopted by some jurisdictions to save on chair time. | This is a comment from the drug plans to inform pERC deliberations, though the clinical experts highlighted that this should be conducted when possible. |
Generalizability | |
On a time-limited basis, should isatuximab be added to treatment for patients receiving VRd? | The clinicians confirmed that it should be considered for this patient population. |
Funding algorithm | |
Under what clinical circumstances would IsaVRd be preferred over daratumumab-based regimens and vice versa? Note: If the patient’s disease progresses on an anti-CD38 biologic, then the patient would not be eligible for any downstream anti-CD38 biologic. | The clinicians noted that IsaVRd would be a substitute for daratumumab-based regimens, and the choice would come down to patient and clinician preference on a case-by-case basis. |
Care provision issues | |
Isatuximab interferes with blood compatibility testing; hence, the product monograph recommends that patients undergo phenotyping before the first isatuximab infusion. | This is a comment from the drug plans to inform pERC deliberations. |
System and economic issues | |
In the trial, prophylactic administration of G-CSF was given at the investigator’s discretion if there was recurrent neutropenia or if there were serious neutropenic complications. | This is a comment from the drug plans to inform pERC deliberations. |
Confidential prices exist for daratumumab. | This is a comment from the drug plans to inform pERC deliberations. |
DCyBorD = daratumumab-cyclophosphamide-bortezomib-dexamethasone; DRd = daratumumab-lenalidomide-dexamethasone; DVMP = daratumumab-bortezomib-melphalan-prednisone; ECOG PS = Eastern Cooperative Oncology Group Performance Status; G-CSF = granulocyte colony-stimulating factor; IsaVRd = isatuximab-bortezomib-lenalidomide-dexamethasone; MRD = minimal residual disease; pERC = pan-Canadian Oncology Drug Review Expert Review Committee; Rd = lenalidomide-dexamethasone; VRd = bortezomib-lenalidomide-dexamethasone.
Clinical Evidence
The objective of the CDA-AMC Clinical Review report is to review and critically appraise the clinical evidence submitted by the sponsor on the beneficial and harmful effects of isatuximab 20 mg/mL concentrate solution for IV infusion in the treatment of patients with newly diagnosed MM who are not eligible for an ASCT. The focus will be placed on comparing isatuximab to relevant comparators and identifying gaps in the current evidence.
A summary of the clinical evidence included by the sponsor in the review of isatuximab is presented in 2 sections with the CDA-AMC critical appraisal of the evidence included at the end of each section. The first section, the systematic review, includes the pivotal RCT that was selected according to the sponsor’s systematic review protocol. The CDA-AMC assessment of the certainty of the evidence in this first section using the GRADE approach follows the critical appraisal of the evidence. The second section includes indirect evidence from the sponsor and indirect evidence selected from the literature that met the selection criteria specified in the review. The third and fourth sections would normally include sponsor-submitted long-term extension studies and additional relevant studies that were considered to address important gaps in the evidence included in the systematic review. However, none were submitted by the sponsor.
Included Studies
Clinical evidence from the following is included in the CDA-AMC review and appraised in this document:
1 pivotal RCT identified in the systematic review (the IMROZ study)
an ITC analysis.
Systematic Review
Content in this section has been informed by materials submitted by the sponsor. The following has been summarized and validated by the CDA-AMC review team.
Description of Studies
One study (the IMROZ trial) was identified from the literature for inclusion in the systematic review. Characteristics of the included study are summarized in Table 5.
The IMROZ trial (ClinicalTrials.gov ID code NCT03319667) is an ongoing, prospective, international, multicentre, randomized, open-label, parallel-group, phase III trial to assess the clinical benefit of IsaVRd compared to VRd alone in patients with newly diagnosed MM who are not eligible for an ASCT. The IMROZ trial is being conducted at 96 sites in 21 countries or regions but there are no participating sites in Canada. A total of 446 patients who were enrolled were randomized using an interactive response technology (IRT) in a 3:2 ratio to IsaVRd (N = 265) and VRd (N = 181). Randomization was stratified by country (China versus other countries), age (younger than 70 years versus 70 years or older), and R-ISS stage I to stage II versus stage III versus not classified (i.e., inconclusive FISH unless the randomization stratum could be determined based on LDH, albumin, and beta2-microglobulin only). The primary objective of the IMROZ study was to demonstrate the benefit of IsaVRd in the prolongation of PFS using IMWG criteria. During the continuous treatment period, patients randomized to the VRd group who had confirmed PD during the VRd portion of the continuous treatment period (as assessed by the investigator) could cross over to the IsaVRd group. Unless otherwise specified, all data reported in this document are from the September 26, 2023, data cut-off. This corresponds with the second planned PFS interim analysis cut-off date (i.e., the date when 167 IRC-determined PFS events [information fraction of 75%] from the global population were expected to be observed). At the September 26, 2023, data cut-off (median follow-up = 59.73 months; range, 0.17 months to 68.99 months), a total of 162 PFS events had been observed.
Table 5: Details of Study Included in the Systematic Review
Detail | IMROZ study |
|---|---|
Designs and populations | |
Study design | Phase III, randomized, open-label, multicentre, parallel-group study |
Locations | 96 sites in 21 countries or regions, including France, the Czech Republic, Türkiye, Australia, Greece, and China |
Patient enrolment dates | Start date: December 27, 2017 End date: Ongoing (estimated completion date is June 30, 2027) |
Randomized (N) | N = 446
|
Inclusion criteria | Main study:
Crossover study:
|
Exclusion criteria |
|
Drugs | |
Intervention |
|
Comparator(s) |
|
Study duration | |
Screening phase | 4 weeks |
Run-in phase | Not reported |
Treatment phase | Induction period: 24 weeks (4 cycles of 42 days’ duration [6 weeks’ duration]) Continuous treatment period: Continuous cycles of 4 weeks’ duration (28 days’ duration) until PD, unacceptable AEs, or patient’s decision to discontinue |
Follow-up phase | Every 3 months (± 5 days) after last study treatment administration or every 4 weeks (± 3 days) after EOT |
Outcomes | |
Primary end point | PFS by IRC according to IMWG criteria |
Secondary and exploratory end points | Key secondary end points
Other secondary end points
Exploratory end points
|
Publication status | |
Publications | Facon et al. (2018),28 Orlowski et al. (2018),29 Facon et al. (2024),30 and Facon et al. (2024)31 ClinicalTrials.gov ID: NCT03319667 |
AE = adverse event; CR = complete response; CrCl = creatinine clearance; DOR = duration of response; ECOG PS = Eastern Cooperative Oncology Group Performance Status; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EORTC QLQ-MY20 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Multiple Myeloma 20; EOT = end of treatment; Fc = fragment crystallizable; Ig = immunoglobulin; IgM = immunoglobulin M; IMWG = International Myeloma Working Group; IRC = independent review committee; IsaRd = isatuximab-lenalidomide-dexamethasone; IsaVRd = isatuximab-bortezomib-lenalidomide-dexamethasone; MM = multiple myeloma; MRD = minimal residual disease; ORR = overall response rate; OS = overall survival; PD = progressive disease; PFS = progression-free survival; PFS2 = progression-free survival on next line of therapy; PK = pharmacokinetic; PRO = patient-reported outcome; q.4.w. = every 4 weeks; q.d. = every day; q.w. = every week; SAE = serious adverse event; SC = subcutaneous; SCT = stem cell transplant; TEAE = treatment-emergent adverse event; TT1R = time to first response; TTBR = time to best response; TTP = time to progression; VGPR = very good partial response; VRd = bortezomib-lenalidomide-dexamethasone.
Note: Outcomes were reported for a preplanned second interim PFS analysis (and interim analysis of OS) corresponding with a data cut-off date of September 26, 2023, with a median follow-up of 59.73 months.
Sources: IMROZ Clinical Study Report32
Populations
Inclusion and Exclusion Criteria
Patients who were enrolled were newly diagnosed with MM as defined by the IMWG criteria and evidence of measurable disease.16 Patients were not considered for high-dose chemotherapy due to their age (i.e., 65 years or older, or younger than 65 years with important comorbidities likely to have a negative impact on the tolerability of high-dose chemotherapy with stem cell transplant), or where high-dose chemotherapy was not indicated. To be eligible for crossover, patients must have confirmed PD in the VRd group before crossover and have not received any systemic anticancer therapy other than VRd in the IMROZ study. Key exclusion criteria were those younger than 18 years or those older than 80 years, a diagnosis of peripheral neuropathy greater than grade 1 or grade 1 with pain, amyloidosis, monoclonal gammopathy of undetermined significance, smouldering MM, Waldenström disease, or other conditions in which Ig M protein is present in the absence of a clonal plasma cell infiltration with lytic bone lesions. Patients were also excluded if they had prior or current systemic therapy or a stem cell transplant for MM (except for emergency use of a short course of corticosteroids if completed 14 days before randomization), concomitant plasma cell leukemia, a major procedure within 14 days of study initiation, an ECOG PS score greater than 2, or clinical laboratory parameters outside predefined limits.
Interventions
Isatuximab was supplied as a 20 mg/mL concentrate for solution for parenteral infusion. The appropriate volume of isatuximab based on patient weight was diluted in 250 mL of a 0.9% sodium chloride solution or a 5% dextrose solution to achieve the appropriate drug concentration for IV infusion. Infusion via a central line was preferred, if available; however, if patients experienced local intolerance after peripheral IV infusion, the decision to use a central line was at the discretion of the investigator. The length of infusion corresponded with the amount of time for the total dose to be administered and the presence or absence of infusion-related (IR) reactions. The dose of isatuximab administered was 10 mg/kg according to the following schedule. For cycle 1 (a 42-day cycle), the dose was administered once weekly on day 1, day 8, day 15, day 22, and day 29; for cycle 2 to cycle 4 (42-day cycles), the dose was administered every 2 weeks on day 1, day 15, and day 29; for cycle 5 to cycle 17 (28-day cycles), the dose was administered every 2 weeks on day 1 and day 15; and for cycles 18 and beyond (28-day cycles), the dose was administered every 4 weeks on day 1 in combination with the following:
bortezomib 1.3 mg/m2: Day 1, day 4, day 8, day 11, day 22, day 25, day 29, and day 32 of the first 42-day cycles only by subcutaneous injection; patients with a body surface area greater than 2.2 m2 were to use 2.2 m2 for the determination of the bortezomib dose
lenalidomide 25 mg: Once daily on day 1 to day 14 and day 22 to day 35 in a 42-day cycle (10 mg once daily if creatinine clearance was 30 mL or more per minute to less than 60 mL per minute) in induction period and 25 mg once daily on day 1 to day 21 of a 28-day cycle in the continuous treatment period and crossover by oral capsule
dexamethasone 20 mg: Once daily on day 1, day 2, day 4, day 5, day 8, day 9, day 11, day 12, day 15, day 22, day 23, day 25, day 26, day 29, day 30, day 32, and day 33 if aged younger than 75 years, or otherwise day 1, day 4, day 8, day 11, day 15, day 22, day 25, day 29, and day 32 for cycle 1 to cycle 4 and 20 mg once daily on day 1, day 8, day 15, and day 22 during the continuous treatment period by IV infusion on isatuximab infusion days or otherwise by oral tablet; dexamethasone was to be administered 15 minutes to 30 minutes (but no longer than 60 minutes) before isatuximab.
The dosing of VRd in the control group followed the same regimen as for the IsaVRd group. For both groups, there was no limitation on the number of treatment cycles to be administered in the absence of major toxicity, PD, or any other discontinuation criteria. Dose adjustments (i.e., dose delay, dose omission, or — specifically for VRd — dose reduction) were permitted for subsequent treatment cycles based on individual patient tolerance. No dose reductions were permitted for isatuximab.
Patients allocated to the IsaVRd group received premedications before the isatuximab infusion to reduce the risk and severity of IR reactions commonly observed with monoclonal antibodies. Recommended premedication included diphenhydramine 25 mg to 50 mg IV (or equivalent), dexamethasone IV or oral (as per previous dosing), ranitidine 50 mg IV (or equivalent), and acetaminophen 650 mg to 1,000 mg orally before isatuximab. The isatuximab infusion was to start immediately after completion of the premedication regimen. Patients who did not experience an IR reaction upon 4 consecutive administrations of isatuximab could have their subsequent premedication reconsidered at the investigator’s discretion. Thromboprophylaxis was applied continuously throughout the study period as per local practice.
Patients in the VRd group eligible for crossover treatment were dosed as follows:
dexamethasone 20 mg by IV infusion on the days of isatuximab administration and orally otherwise on day 1, day 8, day 15, and day 22 of each cycle between 15 minutes and 30 minutes (but not longer than 60 minutes) before isatuximab
isatuximab 10 mg/kg by IV infusion on day 1, day 8, day 15, and day 22 of the first crossover cycle, and then 10 mg/kg on day 1 and day 15 for subsequent cycles.
Outcomes
Disease assessments (e.g., M protein measurements) were performed by a central laboratory. An IRC, blinded to study treatment groups, determined disease response and progression according to efficacy MM laboratory data (central laboratory results), bone marrow assessment for plasma cell infiltration (based on local laboratory results), and centrally reviewed imaging as per IMWG criteria and in line with the IRC charter up to the final PFS analysis.33
A list of efficacy end points assessed in this Clinical Review report is provided in Table 6, followed by descriptions of the outcome measures. Summarized end points are based on outcomes included in the sponsor’s Summary of Clinical Evidence as well as any outcomes identified as important to this review according to the clinical experts consulted by CDA-AMC and input from patient and clinician groups and public drug plans. Using the same considerations, the CDA-AMC review team selected end points that were most relevant to informing the CDA-AMC expert committee deliberations and finalized this list of end points in consultation with members of the expert committee. All summarized efficacy end points were assessed using the GRADE tool. Select notable harms outcomes considered important for informing the CDA-AMC expert committee deliberations were also assessed using GRADE. The outcomes selected for GRADE appraisal were PFS, OS, HRQoL, and SAEs. Infusion reactions and infections were also noted as important by the clinical experts consulted for this review. The following outcomes were included in the text of the report as supportive information: ORR (and its components, including CR and VGPR), the MRD negativity rate, and time to first response (TT1R).
Table 6: Outcomes Summarized From the IMROZ Trial
Outcome measure | Time point | IMROZ study |
|---|---|---|
Progression-free survivala | 18 months, 36 months, and 60 months | Primary |
Overall survivala | 60 months | Secondary |
Clinical response outcomes (ORR, CR, VGPR) | 60 months | Secondary |
Minimal residual disease negativity | 60 months | Secondary |
Time to first response | 60 months | Secondary |
Health-related quality of life | Up to 90 days after the last study treatment | Secondary |
CR = complete response; ORR = overall response rate; OS = overall survival; PFS = progression-free survival; VGPR = very good partial response.
aStatistical testing for these end points was adjusted for multiple comparisons (e.g., hierarchical testing). The hierarchy failed after VGPR or better rate. An interim analysis of OS for futility and overwhelming efficacy was planned at the time of the interim analysis of PFS. The final analysis will be performed when there have been approximately 202 deaths.
Source: IMROZ Clinical Study Report.32
Progression-Free Survival
The primary outcome was PFS, defined as the time from the date of randomization to the date of first documented PD (determined by the IRC per IMWG criteria) or death from any cause, whichever came first. If PD and death were not observed before the data cut-off date or the date of initiation of further antimyeloma treatment, PFS was censored at the date of the last valid disease assessment not showing PD or the analysis cut-off date, whichever came first. Progressions or deaths occurring more than 13 weeks after the last valid disease assessment (i.e., after > 2 consecutive missed scheduled disease assessments) were to be censored at the date of the last valid disease assessment without evidence of progression before initiation of new antimyeloma treatment (if any) or the PFS analysis cut-off date, whichever came first. Patients without an event and without any valid postbaseline assessment were censored at the date of randomization. Responses (including progression) were evaluated by a blinded IRC according to IMWG criteria using central laboratory results and central radiological review. Response and progression based on serum and/or urine M protein were confirmed by 2 consecutive assessments.
Overall Survival
OS, a key secondary outcome, was defined as the time from the date of randomization to death from any cause. Patients without an event at the data cut-off date were to be censored at the last date that the patient was known to be alive or at the analysis cut-off date, whichever came first.
Clinical Response
ORR was defined as the proportion of patients with best overall response of stringent CR, CR, VGPR, and partial response, as assessed by the IRC using IMWG response criteria. The following assessments were considered for derivation of the best overall response:
Randomized groups: From the randomization date until the first documentation of PD, death, initiation of antimyeloma treatment, or crossover, whichever came first.
Crossover group: The best sequential response, from the first isatuximab drug intake until the first documentation of PD, death, or initiation of antimyeloma treatment, whichever came first.
Minimal Residual Disease
The MRD negativity rate, a key secondary outcome, was defined as the negativity rate for patients with a CR or better response, deemed as the proportion of patients for whom MRD is negative. Bone aspirates were collected at screening and for patients with a CR or VGPR at the end of the induction period, then every 6 months during the first 2 years (i.e., at 12 months, 18 months, and 24 months after randomization), and then once a year until PD or until the final PFS analysis cut-off date, whichever occurred first. The threshold for negativity by means of next-generation sequencing was assessed at 10-5 sensitivity.
Time to First Response
TT1R was defined as the time from randomization to the first IRC-determined response (partial response or better) that is subsequently confirmed.
Health-Related Quality of Life
HRQoL was assessed using EORTC QLQ-C30 (Table 7), a 30-item instrument with 15 items related to function (physical, role, cognitive, emotional, social), 7 questions related to symptoms (7 questions), single-item symptom scales (dyspnea, insomnia, appetite loss, constipation, diarrhea, and financial impact), and 2 items related to global QoL. All except global QoL are scored from 1 (“not at all”) to 4 (“very much”).34,35 The EORTC QLQ-C30 score range is 0 to 100, with higher scores indicating better functioning or global health status or QoL, and lower scores indicating a higher symptom burden. It was administered before treatment on day 1 of every cycle, at the end of treatment visit, and at 90 (± 5) days after the last study treatment administration.
Responses were not expected at a given visit for any of the following reasons: death, progression, dropout due to an AE, poor protocol compliance, or withdrawal by a patient. A questionnaire could be expected but not received for other reasons as well (e.g., failure to distribute the questionnaire, patient did not have the time to complete questionnaire).
Safety Outcomes
Safety outcomes included AEs, SAEs, and AESIs, including IR reactions.
Table 7: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusion about measurement properties | Within-group MID |
|---|---|---|---|
EORTC QLQ-C30 | The EORTC QLQ-C30 is a standardized, patient self-administered questionnaire for evaluating the HRQoL of patients with cancer. It consists of functional scales, 3 symptom scales, and 6 single-item scales. | Validity: All subscales shown to be impaired in patients with MM compared to population norms.36 No correlation of any subscale with the SEIQoL index suggesting independence (the SEIQoL index is an instrument that allows patients to select the 5 most important domains for their present QoL and measures their satisfaction in these domains).37 Reliability: Internal consistency measured using the Cronbach alpha in a study of patients with MM; all 5 of the functional scales reported an alpha > 0.7 except for cognitive function (alpha = 0.57).38 Responsiveness: Patients who reported significant improvements on the Global HRQoL scale had SRM values of 0.32. Patients who reported significantly deteriorated HRQoL had SRM values of 0.57.39 | Threshold estimates for small, moderate, and large effect sizes in the GHS or QoL in patients with MM:
The mean MIDs in patients whose disease improved was 7.6 points (95% CI, 2 points to 13 points) and –12.1 points (95% CI, –18 points to –6 points) in patients whose disease deteriorated.39 |
CI = confidence interval; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; GHS = global health status; HRQoL = health-related quality of life; MID = minimal important difference; MM = multiple myeloma; QoL = quality of life; SEIQoL = Schedule for the Evaluation of Individual Quality of Life; SRM = standardized response mean.
Statistical Analysis
Sample Size and Power Calculation
In determining sample size, the sponsor assumed that there would be a median PFS of 40 months in the VRd group, that the IsaVRd group would have an HR of 0.64 compared to the VRd group, and that, assuming proportional hazards, this was expected to correspond to an improvement in median PFS from 40 months to 62.5 months. The sponsor planned to perform a stratified log-rank test at a 1-sided significance level of 2.5% power and planned for a 3:2 randomization ratio, IsaVRd to VRd, as well as an interim analysis for PFS when 60% of the PFS events had been observed. Based on these assumptions, a total of 222 events were needed to achieve 90% power, and 440 patients (264 patients in the IsaVRd group and 176 patients in the VRd group) were needed to achieve the targeted number of PFS events. Assuming a uniform accrual of 30 patients per month, the final PFS cut-off date was expected to be approximately 60 months after the first patient had been enrolled. With the addition of 1 interim analysis when 75% of PFS events were observed, the power was to be decreased from 90.1% to 89.7 %. With the addition of a third interim analysis once 85% of PFS events had been observed, the power was to be decreased to 89.4%.
Statistical and Analytical Plans
Continuous data were summarized using the number of available data, the mean, standard deviation (SD), the median, quartile 1 and quartile 3, and minimum and maximum values for each treatment group, as applicable. Categorical and ordinal data were summarized using the number and percentage of patients in each treatment group.
All efficacy analyses were performed in the ITT population. All analyses using the stratification factors employed the stratification factors as per IRT; however, due to the low number of patients randomized in the stratum R-ISS not classified (N = 5), stratification factors R-ISS stage III and R-ISS not classified were pooled together. Statistical testing was only conducted for the induction and continuous portions of the IMROZ trial. Of note, the purpose of the crossover group was exploratory and no formal statistical testing was performed. The results of the crossover phase are not reported here.
The analyses presented in this document correspond with the preplanned second PFS interim analysis (Table 8).
Primary Outcome
Testing of the primary end point (PFS) was via a log-rank test stratified by age and R-ISS. The estimates for HR and corresponding 95% CI were provided using a Cox proportional hazards model stratified by the same stratification factors. The Kaplan-Meier (KM) method was used to estimate median PFS and probabilities of being progression-free at different time points, as well as corresponding CIs.
Testing of all relevant end points as well as adjustment factors, methods of handling missing data, and sensitivity analyses are described in Table 8.
Data Imputation Methods
If a postbaseline disease assessment of response was determined to be “not evaluable” based on IMWG criteria or the date of assessment was missing, the disease assessment was considered invalid. For PFS and OS, the trial reported nonmissing observations in the considered population.
Subgroup Analyses
The consistency of the results of the primary analysis was evaluated across the following predefined subgroups (if there were 10 patients in each treatment group within each subgroup):
age by IRT (aged younger than 70 years versus 70 years)
age (aged younger than 70 years versus 70 years; aged younger than 75 years versus 75 years)
sex (male versus female)
race (white versus other)
geographical region of the world (Europe versus North America versus Asia versus other countries or regions)
ECOG PS score at baseline (0 or 1 versus greater than 1)
ISS staging at study entry (stage I versus stage II versus stage III)
R-ISS staging at study entry by IRT (stage I or stage II versus stage III or not classified)
chromosomal abnormality (17p deletion, t[4;14], t[14;16]) (at least 1 versus none)
chromosomal abnormality 1q21+ (yes versus no)
MM type at study entry (IgG versus non-IgG)
extramedullary or paramedullary plasmacytoma at baseline by IRC (yes versus no)
plasmacytoma disease by IRC (both extramedullary and paramedullary disease versus only extramedullary disease versus only paramedullary disease versus no plasmacytoma disease)
baseline estimated glomerular filtration rate (modification of diet in renal disease formula) (less than 60 mL per minute per 1.73 m2 versus 60 mL per minute per 1.73 m2)
hemoglobin at baseline (less than 10 g/dL versus 10 g/dL).
For each predefined subgroup, the treatment effect HR and associated 2-sided 95% CI was estimated and a forest plot summarizing the results for the predefined subgroups was constructed. For each subgroup, PFS was analyzed using a nonstratified Cox proportional hazards model with terms for the factor, treatment, and their interaction. A test of the interaction was performed at the 10% alpha level. The prespecified subgroups were not included in the statistical hierarchical testing strategy nor adjusted for multiplicity.
Multiplicity Adjustment
Hypothesis testing of the key secondary outcomes was carried out using a closed test procedure to control the type I error rate. Testing on key secondary outcomes was performed only if the significance level had been reached on PFS and testing on subsequent outcomes continued only if the null hypothesis for the previously tested outcome was rejected. The hierarchical procedure was performed according to the following order:
CR rate at the time of the primary PFS analysis and/or the final PFS analysis
MRD negativity rate at the time of the primary PFS analysis and/or the final PFS analysis
VGPR or better rate at the time of the primary PFS analysis and/or the final PFS analysis
OS.
Three interim analyses for PFS were planned to be conducted after 60%, 75%, and 85% of events had been observed. The primary analysis of PFS corresponded to the positive interim analysis or the final PFS analysis. At the time of the positive PFS interim analysis, key secondary end points were tested sequentially up to the null hypothesis that failed to be rejected for a key secondary end point. At the final PFS analysis, the testing procedure will resume where it stopped at interim analysis. Except for OS and PFS on next line of therapy, other secondary end points were analyzed at the time of the primary analysis and/or the final analysis of PFS. The OS analysis will be conducted with up to 5 looks, including at the time of the interim and final analysis of PFS, and at the final OS analysis when approximately 202 deaths have occurred. In addition, up to 3 nonbinding futility analyses of OS will be performed; the data monitoring committee may have considered stopping the trial at the time of interim analysis 2 if the HR for OS was higher than 1.1. Control for multiplicity across the interim analyses of PFS was achieved using an O’Brien-Fleming alpha spending function. The efficacy boundaries were determined based on the actual number of events at each analysis. At the time of interim analysis 2, the P value boundary for PFS was 0.007423. Similarly, for key secondary end points, significance levels were determined based on alpha spending functions specific to each end point (O’Brien-Fleming alpha spending functions for CR and the MRD negativity rate and a user-defined alpha spending function for OS). Other end points were unadjusted for multiplicity.
Sensitivity Analyses
Ten different sensitivity analyses of the primary outcome were conducted and included: a PFS analysis without censoring for further antimyeloma treatment; a PFS analysis using investigator assessment of response and considering symptomatic deterioration; a PFS analysis using investigator assessment of response and ignoring symptomatic deterioration; initiation of further antimyeloma treatment considered as a PFS event; a PFS analysis without censoring of progression or death occurring greater than 13 weeks after the last valid disease assessment; analysis based on scheduled assessment dates instead of actual assessment dates; a final PFS analysis using the date of the last observed event as the cut-off date; an unstratified PFS analysis; a PFS analysis using stratification factors as per an electronic case report form (if relevant); and a PFS analysis censoring death events due to COVID-19 infections. Sensitivity analyses for other end points are described in Table 8.
Table 8: Statistical Analysis of Efficacy End Points of IMROZ Study
Statistical model | Adjustment factor | Handling of missing dataa | Sensitivity analysis |
|---|---|---|---|
PFS | |||
| Stratification factors (i.e., age and R-ISS) | Censored |
|
OS | |||
| Stratification factors (i.e., age and R-ISS) | Censored |
|
ORR | |||
| Stratification factors (i.e., age and R-ISS) | None | None |
MRD negativity rateb | |||
| Stratification factors (i.e., age and R-ISS) | Tipping point analysis Multiple imputation | Impact of missing data (e.g., multiple imputations, tipping point analysis) |
HRQoL (EORTC QLQ-C30) | |||
| None | Complete case analysis (no imputation of missing data) | None |
TT1R | |||
| None | None | None |
CMH = Cochran-Mantel-Haenszel; eCRF = electronic case report form; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; HRQoL = health-related quality of life; ITT = intention to treat; KM = Kaplan-Meier; MRD = minimal residual disease; ORR = overall response rate; OS = overall survival; PD = progressive disease; PFS = progression-free survival; R-ISS = Revised International Staging System; TT1R = time to first response.
aAnalyses and summaries of continuous and categorical variables were based on observed data only. Percentages were calculated using as denominator the number of patients with nonmissing observations in the considered population.
bPatients in the ITT population without MRD assessment were to be considered as having positive MRD.
Source: IMROZ Clinical Study Report and Statistical Analysis Plan.32
Analysis Populations
Analysis populations of the IMROZ trial are summarized in Table 9.
Table 9: Analysis Populations of IMROZ Trial
Population | Definition | Application |
|---|---|---|
ITT population | The ITT population is the randomized population. | Primary population for all efficacy analyses |
Population without trial impact (disruption) due to COVID-19 | All randomized populations meeting these requirements:
| Population used for additional analyses to address the impact of COVID-19 on the study |
Safety population | Patients from the ITT population who received at least 1 dose or part of a dose of study treatments | Primary population for analysis of safety, exposure, and safety data before crossover for patients receiving VRd who crossed over |
Pharmacokinetic population | Includes patients from the safety population who received at least 1 dose of isatuximab in the IsaVRd treatment group, even if incomplete, with data for at least 1 isatuximab concentration available postbaseline | Population used for pharmacokinetic analyses of isatuximab |
Immunogenicity population (ADA population) | Includes patients from the safety population from the IsaVRd group with at least 1 sample taken postbaseline after drug administration during the treatment or follow-up period that is appropriate for ADA testing with a reportable result (negative, positive, or inconclusive) | Population used for ADA analyses |
Biomarker population | Patients from the ITT population evaluable for at least 1 of the genetic biomarkers | Population for analysis of immune genetic biomarkers |
ADA = antidrug antibody; IsaVRd = isatuximab-bortezomib-lenalidomide-dexamethasone; ITT = intention to treat; VRd = bortezomib-lenalidomide-dexamethasone.
Source: IMROZ Clinical Study Report and Statistical Analysis Plan.32
Results
Patient Disposition
In the IMROZ trial, a total of 512 patients were screened and 446 patients (87.1%) were randomized (Table 10). Among patients who were randomized, the reason for transplant ineligibility was being aged 65 years or older (427 patients [95.7%]) and comorbidities (19 patients [4.3%]); these were not substantially different between the groups. The IMROZ study is an ongoing trial and at the time of the second PFS interim analysis data cut-off (September 26, 2023), 275 patients had discontinued treatment (137 patients [75.7%] in the VRd group and 138 patients [52.1%] in the IsaVRd group), mainly due to AEs (50 patients [27.6%] in the VRd group and 60 patients [22.6%] in the IsaVRd group). More patients in the VRd group (67 patients [37.0%]) than the IsaVRd group (38 patients [14.3%]) had discontinued treatment due to PD. As of the data cut-off date, 25 patients in the VRd group had crossed over to receive IsaVRd.
Table 10: Summary of Patient Disposition From the IMROZ Trial
Patient disposition | IMROZ study | |
|---|---|---|
VRd (N = 181) | IsaVRd (N = 265) | |
Screened, N | 512 | |
Reason for not advancing past screening, n (%) | ||
Did not meet inclusion criteria | 29 (5.7) | |
Met exclusion criteria | 37 (7.2) | |
Randomized, N | 181 | 265 |
Randomized and treated, n (%) | 181 (100) | 263 (99.2) |
Discontinued treatment, n (%) | 137 (75.7) | 138 (52.1) |
Reason for treatment discontinuation, n (%)a | ||
Adverse events | 50 (27.6) | 60 (22.6) |
Related to COVID-19 | 4 (2.2) | 8 (3.0) |
Progressive disease | 67 (37.0) | 38 (14.3) |
Poor adherence to protocol | 0 (0) | 6 (2.3) |
Withdrawal by patient | 16 (8.8) | 23 (8.7) |
Other | 4 (2.2) | 11 (4.2) |
Related to COVID-19 | 0 (0) | 1 (0.4) |
Discontinued from study, n (%) | 72 (39.8) | 87 (32.8) |
Reason for study discontinuation, n (%) | ||
Completed | 0 (0) | 0 (0) |
Death | 59 (32.6) | 69 (26.0) |
Poor adherence to protocol | 0 (0) | 0 (0) |
Withdrawal by patient | 12 (6.6) | 14 (5.3) |
Other | 1 (0.6) | 4 (1.5) |
ITT population, N | 181 | 265 |
Safety population, N | 181 | 263 |
Crossover population, N | 25 | NA |
Population without trial impact (disruption) due to COVID-19 | 171 | 247 |
IsaVRd = isatuximab-bortezomib-lenalidomide-dexamethasone; ITT = intention to treat; NA = not applicable; VRd = bortezomib-lenalidomide-dexamethasone.
aTreatment discontinuation reported in Table 10 refers to definitive treatment discontinuation, which was defined as the discontinuation of all study interventions. Per protocol, patients could discontinue only 1 component of combination therapy and continue the other(s).
Source: IMROZ Clinical Study Report.32
Baseline Characteristics
The baseline characteristics outlined in Table 11 are limited to those that are most relevant to this review or were felt to affect the outcomes or interpretation of the study results. At baseline, the 2 groups were balanced with regard to patient demographic and disease characteristics in the ITT population. Patients were aged an average of 71.5 years (SD = 4.8 years). Most patients (89.0%) had an ECOG PS score of 0 or 1. The most common ISS stage at study entry was stage I (53.0%), followed by stage II (31.1%) and stage III (15.2%). The MM subtype at baseline was most frequently IgG (64.1%) and the R-ISS stage at study entry was most frequently stage II (n = 286; 64.1%). The median time from initial diagnosis to randomization was 1.18 months. The main reason for transplant ineligibility was being aged 65 years or older (95.7%). It should be noted that there were fewer patients with kidney dysfunction (estimated glomerular filtration rate < 60 mL per minute per 1.73 m2) in the IsaVRd group at baseline compared to the VRd group (24.9% versus 34.3%, respectively).
Table 11: Summary of Baseline Characteristics From IMROZ Study
Characteristic | IMROZ study | |
|---|---|---|
VRd (N = 181) | IsaVRd (N = 265) | |
Age (years) | ||
Mean (SD) | 71.5 (4.8) | 71.7 (4.0) |
Median (range) | 72.0 (55 to 80) | 72.0 (60 to 80) |
Age group (years), n (%) | ||
< 65 | 9 (5.0) | 8 (3.0) |
65 to 75 | 115 (63.5) | 188 (70.9) |
≥ 75 | 57 (31.5) | 69 (26.0) |
Age group (years), n (%) | ||
< 70 | 56 (30.9) | 81 (30.6) |
≥ 70 | 125 (69.1) | 184 (69.4) |
Sex, n (%) | ||
Female | 87 (48.1) | 122 (46.0) |
Male | 94 (51.9) | 143 (54.0) |
Race, n (%) | ||
American Indian or Alaska Native | 1 (0.6) | 4 (1.5) |
Asian | 17 (9.4) | 31 (11.7) |
Black or African American | 2 (1.1) | 2 (0.8) |
Native Hawaiian or another Pacific Island | 1 (0.6) | 1 (0.4) |
White | 131 (72.4) | 192 (72.5) |
Not reported or missing | 29 (16.0) | 35 (13.2) |
Unknown | 0 (0) | 0 (0) |
Geographic region, n (%) | ||
Europe | 106 (58.6) | 169 (63.8) |
North America | 5 (2.8) | 3 (1.1) |
Asia | 15 (8.3) | 31 (11.7) |
Other countries | 55 (30.4) | 62 (23.4) |
Time from initial diagnosis of MM to randomization (months) | ||
Mean (SD) | 1.82 (3.27) | 2.03 (3.74) |
Median (range) | 1.18 (0.3 to 37.7) | 1.22 (0.3 to 48.9) |
MM subtype at study entry, n (%) | ||
IgG | 115 (63.5) | 171 (64.5) |
IgA | 41 (22.7) | 57 (21.5) |
IgM | 1 (0.6) | 1 (0.4) |
IgD | 2 (1.1) | 3 (1.1) |
IgE | 0 (0) | 0 (0) |
Kappa light chain only | 11 (6.1) | 21 (7.9) |
Lambda light chain only | 10 (5.5) | 11 (4.2) |
Unknown or undetected | 1 (0.6) | 1 (0.4) |
Biclonal status at study entry, n (%) | ||
Yes | 3 (1.7) | 3 (1.1) |
No | 178 (98.3) | 262 (98.9) |
ECOG PS score, n (%) | ||
0 or 1 | 162 (89.5) | 235 (88.7) |
≥ 2 | 19 (10.5) | 30 (11.3) |
Patients with plasmacytoma as per IRC, n (%) | ||
Both extramedullary and paramedullary disease | 1 (0.6) | 1 (0.4) |
Only extramedullary disease | 6 (3.3) | 18 (6.8) |
Only paramedullary disease | 49 (27.1) | 67 (25.3) |
No plasmacytoma disease | 125 (69.1) | 179 (67.5) |
Estimated GFR < 60 mL per minute per 1.73 m2, n (%) | 62 (34.3) | 66 (24.9) |
ISS stage at study entry, n (%) | ||
Stage I | 47 (26.0) | 90 (34.0) |
Stage II | 80 (44.2) | 107 (40.4) |
Stage III | 53 (29.3) | 67 (25.3) |
Unknown | 1 (0.6) | 1 (0.4) |
R-ISS stage at study entry, n (%) | ||
Stage I | 35 (19.3) | 66 (24.9) |
Stage II | 123 (68.0) | 163 (61.5) |
Stage III | 17 (9.4) | 27 (10.2) |
Not classified | 6 (3.3) | 9 (3.4) |
Measurable paraprotein at baseline, n (%) | ||
Only serum M protein | 109 (60.2) | 166 (62.6) |
Only urine M protein | 15 (8.3) | 25 (9.4) |
Both serum and urine M protein | 38 (21.0) | 46 (17.4) |
Only serum free light chain with serum M protein between 0.5 g/dL and 1 g/dL and no urine M protein measurable | 2 (1.1) | 9 (3.4) |
Only serum free light chain with serum M protein < 0.5 g/dL and no urine M protein measurable | 15 (8.3) | 15 (5.7) |
Nonmeasurable | 2 (1.1) | 4 (1.5) |
Cytogenetic risk at study entry, n (%) | ||
Standard | 140 (77.3) | 207 (78.1) |
Higha | 34 (18.8) | 40 (15.1) |
Not classified | 7 (3.9) | 18 (6.8) |
High-risk chromosomal abnormalities and 1q21+, n (%)b | 15 (8.3) | 19 (7.2) |
Chromosomal abnormality, n (%)c | ||
1q21+ | 70 (38.7) | 95 (35.8) |
Amplification 1q21 | 23 (12.7) | 32 (12.1) |
Del(17p) with a 50% cut-off | 9 (5.0) | 15 (5.7) |
1q21+ = chromosome arm 1q21; Del(17p) = 17p deletion; ECOG PS = Eastern Cooperative Oncology Group Performance Status; GFR = glomerular filtration rate; IgA = immunoglobulin A; IgD = immunoglobulin D; IgE = immunoglobulin E; IgG = immunoglobulin G; IgM = immunoglobulin M; IRC = independent review committee; IsaVRd = isatuximab-bortezomib-lenalidomide-dexamethasone; ISS = International Staging System; MM = multiple myeloma; R-ISS = Revised International Staging System; SD = standard deviation; VRd = bortezomib-lenalidomide-dexamethasone.
aHigh cytogenetic risk was defined as the presence of del(17p), t(4;14), t(14;16), or a combination of these.
bAbnormality was defined as present in at least 30% of abnormal bone marrow plasma cells for t(4;14), t(14;16), and 1q21+ (at least 3 copies) and at least 50% of abnormal plasma cells for del(17p). One patient in the IsaVRd group had 2 high-risk chromosomal abnormalities (del[17p] and t[4;14]).
cThe 1q21+ abnormality was defined as at least 3 copies of 1q21. The amplification 1q21 abnormality was defined as at least 4 copies of 1q21.
Sources: IMROZ Clinical Study Report32 and Facon et al. (2024).30
Exposure to Study Treatments
The median duration of overall exposure to study treatments was 31.28 months (range, 0.6 months to 67.2 months) in the VRd group and 53.16 months (range, 0.5 months to 68.8 months) in the IsaVRd group, as detailed in Table 12. The median number of cycles started was 29.00 cycles (range, 1 cycle to 69 cycles) in the VRd group and 52.00 cycles (range, 1 cycle to 69 cycles) in the IsaVRd group. The median duration of exposure to the IsaVRd regimen after exposure in the crossover population was 8.02 months (range, 2.0 months to 49.2 months) and the median number of cycles started was 9.00 cycles (range, 2 cycles to 53 cycles). At the time of data cut-off, 4 patients (16.0%) were still on crossover treatment, with the most common reason for treatment discontinuation being disease progression in 16 patients (64.0%).
Table 12: Summary of Patient Exposure From Studies Included in the Systematic Review
Exposure | IMROZ study | |
|---|---|---|
VRd (N = 181) | IsaVRd (N = 263) | |
Total number of cycles started | 5,718 | 10,795 |
Cumulative exposure to treatment (patient-years) | 490.75 | 909.60 |
Number of cycles started by patients | ||
Mean (SD) | 31.59 (21.76) | 41.05 (21.98) |
Median (range) | 29.00 (1.0 to 69.0) | 52.00 (1.0 to 69.0) |
Duration of exposure (weeks) | ||
Mean (SD) | 141.47 (94.38) | 180.46 (92.99) |
Median (range) | 136.00 (2.6 to 292.0) | 231.14 (2.0 to 299.0) |
Duration of exposure (months) | ||
Mean (SD) | 32.54 (21.71) | 41.50 (21.39) |
Median (range) | 31.28 (0.6 to 67.2) | 53.16 (0.5 to 68.8) |
IsaVRd = isatuximab-bortezomib-lenalidomide-dexamethasone; SD = standard deviation; VRd = bortezomib-lenalidomide-dexamethasone.
Source: IMROZ Clinical Study Report.32
Concomitant Medications and Cointerventions
Concomitant medications are those the patient used at any time during the treatment period (from the first dose of study treatment to the last dose + 30 days). Most patients in both treatment groups received at least 1 concomitant medication (IsaVRd group = 99.2%; VRd group = 100%). The most common medications were anti-infectives for systemic use (IsaVRd group = 99.2%; VRd group = 100%) and blood and blood-forming organs (IsaVRd group = 99.2%; VRd group = 100%).
Subsequent Treatment
In the ITT population, the time to the next treatment in the IsaVRd group was delayed compared with the VRd group (stratified HR = 0.376; 95% CI, 0.265 to 0.534). The median time to the next treatment was 63.57 months (range, 48.624 months to NC) for the VRd group and was not reached in the IsaVRd group.
Among patients who received further antimyeloma treatment (80 patients [44.2%] and 52 patients [19.6%] in the VRd and IsaVRd groups, respectively), the most frequent subsequent therapy given was corticosteroids (90.0% and 100% in the VRd group and the IsaVRd group, respectively) and immunomodulators (72.5% and 76.9% in the VRd group and the IsaVRd group, respectively). This included not only the second line of therapy, but all further lines of therapy received by the patients. Further antimyeloma treatment also included anti-CD38 drugs (monoclonal antibodies) in twice as many participants in the VRd group (68.8%) than in the IsaVRd group (34.6%) — primarily, daratumumab (37.5% and 28.8%, respectively). Patients treated with subsequent isatuximab (36.3% and 5.8% in the VRd and IsaVRd groups, respectively) included 25 patients (13.8%) in the VRd group opting to cross over to the IsaVRd group.
Efficacy
Only those efficacy outcomes and analyses of subgroups identified in the CDA-AMC review protocol are reported in this section. The median follow-up at the September 26, 2023, data cut-off was 59.73 months (range, 0.17 months to 68.99 months). A summary of the key efficacy results for the IMROZ trial is presented in Table 13.
Table 13: Summary of Key Efficacy Results From Studies Included in the Systematic Review
Variable | IMROZ study | |
|---|---|---|
VRd (N = 181) | IsaVRd (N = 263) | |
PFS by IRCa | ||
Number of patients with events, n (%) | 78 (43.1) | 84 (31.7) |
Disease progression | 66 (84.6) | 50 (59.5) |
Death without disease progression | 12 (15.4) | 34 (40.5) |
Number of patients censored, n (%) | 103 (56.9) | 181 (68.3) |
Censored, follow-up ongoing | 39 (21.5) | 89 (33.6) |
Censored, follow-up ended | 64 (35.4) | 92 (34.7) |
No postbaseline assessment | 0 | 2 (0.8) |
Lost to follow-upb | 34 (18.8) | 63 (23.8) |
Events more than 13 weeks from last valid disease assessment | 4 (2.2) | 11 (4.2) |
Further antimyeloma treatment | 26 (4.4) | 16 (6.0) |
PFS (months), median (95% CI) | 54.34 (45.207 to NC) | NC (NC to NC) |
Stratified HR (98.5% CI)c,d | 0.596 (0.406 to 0.876) | |
Stratified P valuec,d | 0.0005 | |
PFS probability (%) (95% CI)e | ||
6 months | 91.9 (86.7 to 95.1) | 95.3 (92.0 to 97.3) |
12 months | 86.4 (80.3 to 90.8) | 92.6 (88.6 to 95.2) |
18 months | 79.6 (72.6 to 85.0) | 88.2 (83.5 to 91.6) |
24 months | 72.2 (64.6 to 78.5) | 83.7 (78.5 to 87.7) |
30 months | 70.1 (62.2 to 76.6) | 80.3 (74.8 to 84.7) |
36 months | 66.4 (58.3 to 73.2) | 76.1 (70.2 to 80.9) |
42 months | 61.1 (52.8 to 68.4) | 72.2 (66.1 to 77.4) |
48 months | 53.5 (45.1 to 61.3) | 69.9 (63.7 to 75.3) |
54 months | 50.3 (41.7 to 58.2) | 66.6 (60.2 to 72.3) |
60 months | 45.2 (35.6 to 54.2) | 63.2 (56.2 to 69.4) |
66 months | 39.5 (26.4 to 52.3) | 63.2 (56.2 to 69.4) |
PFS risk difference (%) (95% CI) | ||
18 months | 8.6 (1.3 to 15.9) | |
36 months | 9.7 (0.5 to 18.9) | |
60 months | 18 (6.5 to 29.5) | |
OSa | ||
Number of deaths, n (%) | 59 (32.6) | 69 (26.0) |
Number of patients censored, n (%) | 122 (67.4) | 196 (74.0) |
OS (months), median (95% CI) | NC (NC to NC) | NC (NC to NC) |
Stratified HR (99.9725% CI)c | 0.776 (0.407 to 1.48) | |
Stratified P valuec,f | 0.0760 | |
Survival probability (%) (95% CI)c | ||
6 months | 95.6 (91.3 to 97.8) | 96.2 (93.0 to 97.9) |
12 months | 93.3 (88.5 to 96.1) | 94.6 (91.1 to 96.8) |
18 months | 91.0 (85.7 to 94.4) | 93.5 (89.7 to 95.9) |
24 months | 88.1 (82.4 to 92.1) | 91.1 (87.0 to 94.0) |
30 months | 85.3 (79.1 to 89.7) | 87.2 (82.5 to 90.8) |
36 months | 83.5 (77.2 to 88.2) | 81.0 (75.6 to 85.3) |
42 months | 77.7 (70.7 to 83.2) | 78.2 (72.7 to 82.8) |
48 months | 75.3 (68.1 to 81.0) | 76.6 (71.0 to 81.3) |
54 months | 72.2 (64.9 to 78.3) | 75.0 (69.2 to 79.9) |
60 months | 66.3 (58.5 to 73.1) | 72.3 (66.1 to 77.5) |
66 months | 61.3 (51.8 to 69.5) | 72.3 (66.1 to 77.5) |
OS risk difference (%) (95% CI) | ||
60 months | 5.9 (–3.3 to 15.2) | |
Clinical response | ||
ORR, n (%) | 167 (92.3) | 242 (91.3) |
95% CIb | 0.8736 to 0.9571 | 0.8726 to 0.9442 |
Stratified OR (95% CI)b | 0.888 (0.439 to 1.794) | |
Stratified CMH test P valuec,f | 0.6295 | |
sCR, n (%) | 10 (5.5) | 29 (10.9) |
CR, n (%) | 106 (58.6) | 169 (63.8) |
VGPR, n (%) | 34 (18.8) | 38 (14.3) |
VGPR risk difference (%) (95% CI) | –4.3 (–11.4 to 2.8) | |
PR, n (%) | 17 (9.4) | 6 (2.3) |
MRD negativity rate for patient with a CRa | ||
MRD negativity rate, n (%)g | 74 (40.9) | 147 (55.5) |
95% CIf | 0.3365 to 0.4842 | 0.4927 to 0.6155 |
Stratified OR (95% CI)b | 1.803 (1.229 to 2.646) | |
Stratified CMH test P valueb | 0.0013 | |
MRD-negative CR risk difference (%) (95% CI) | 14.6 (5.2 to 23.9) | |
TT1R | ||
TT1R (months), median (95% CI) | 1.48 (1.478 to 1.511) | 1.51 (NC to NC) |
CI = confidence interval; CMH = Cochran-Mantel-Haenszel; CR = complete response; HR = hazard ratio; IRC = independent review committee; IsaVRd = isatuximab-bortezomib-lenalidomide-dexamethasone; ITT = intention to treat; KM = Kaplan-Meier; MRD = minimal residual disease; NC = not calculated; OR = odds ratio; ORR = overall response rate; OS = overall survival; PFS = progression-free survival; PR = partial response; R-ISS = Revised International Staging System; sCR = stringent complete response; TT1R = time to first response; VGPR = very good partial response; VRd = bortezomib-lenalidomide-dexamethasone.
Note: Median follow-up time is 59.73 months. An HR of less than 1 or an OR of more than 1 favours the IsaVRd treatment group.
aTested according to a prespecified statistical hierarchy and P value has been adjusted for multiple testing.
bPatient is considered as lost to follow-up if the reason for censoring is last valid disease assessment before the cut-off date and if the time from the last disease assessment to the cut-off date is longer than 13 weeks.
cStratified by age (< 70 years versus ≥ 70 years) and R-ISS stage (stage I or stage II versus stage III or not classified) according to interactive response technology.
dThe 1-sided significance level was 0.007423 using the O’Brien-Fleming alpha spending function to control overall 1-sided type I error at 2.5%.
eEstimated using the KM method.
fNoninferential (nominal P value) due to break in statistical hierarchical testing procedure at VGPR rate or better.
gFor analysis purposes, patients in the ITT population but without MRD assessment by next-generation sequencing were considered as having positive MRD. Sensitivity of 1 in 10-5 nucleated cells.
Sources: IMROZ Clinical Study Report32 and Facon et al. (2024).30
Progression-Free Survival
There were 78 patients (43.1%) in the VRd group and 84 patients (31.7%) in the IsaVRd group in the ITT population who experienced PFS events after a median follow-up of 59.73 months as per Table 13. The HR was 0.596 (98.5% CI, 0.406 to 0.876; P = 0.0005), corresponding with a 40.4% reduction in the hazard of disease progression or death in the IsaVRd group compared to the VRd group. An early separation between the VRd and IsaVRd groups was observed in the KM PFS curves as depicted in Figure 1. The median PFS was 54.34 months (95% CI, 45.207 months to NC) in the VRd group and not reached in the IsaVRd group. At 60 months, the PFS probability was 45.2% in the VRd group and 63.2% in the IsaVRd group. The risk difference at 60 months was 18.0% (95% CI, 6.5% to 29.5%).
A number of sensitivity analyses of the primary outcome were performed (refer to Table 8). All results were consistent with those of the primary analysis. There were also several subgroup analyses, with most also demonstrating no significant interaction at the 10% level between treatment groups and subgroups of stratification factors, demographic characteristics, or baseline disease characteristics supporting an overall consistent treatment effect (Figure 2). Most subgroup analyses, including those of poor prognosis subgroups, showed a treatment effect that favoured IsaVRd over VRd, consistent with the primary PFS analysis. However, in the subgroup of MM type at study entry (IgG versus non-IgG), the subgroup of plasmacytoma disease per IRC (extramedullary disease versus only paramedullary disease versus no plasmacytoma disease), and the subgroup of chromosomal 1q21+ abnormality, the P value for interaction was less than 10%, suggesting there is some difference in the treatment effect across those subgroups. The effect of IsaVRd over VRd seems to be stronger, respectively, in the IgG subgroup and extramedullary disease subgroup, and in participants with chromosomal 1q21+ abnormality.
Figure 1: IMROZ Trial KM Curves for PFS by IRC (ITT Population)
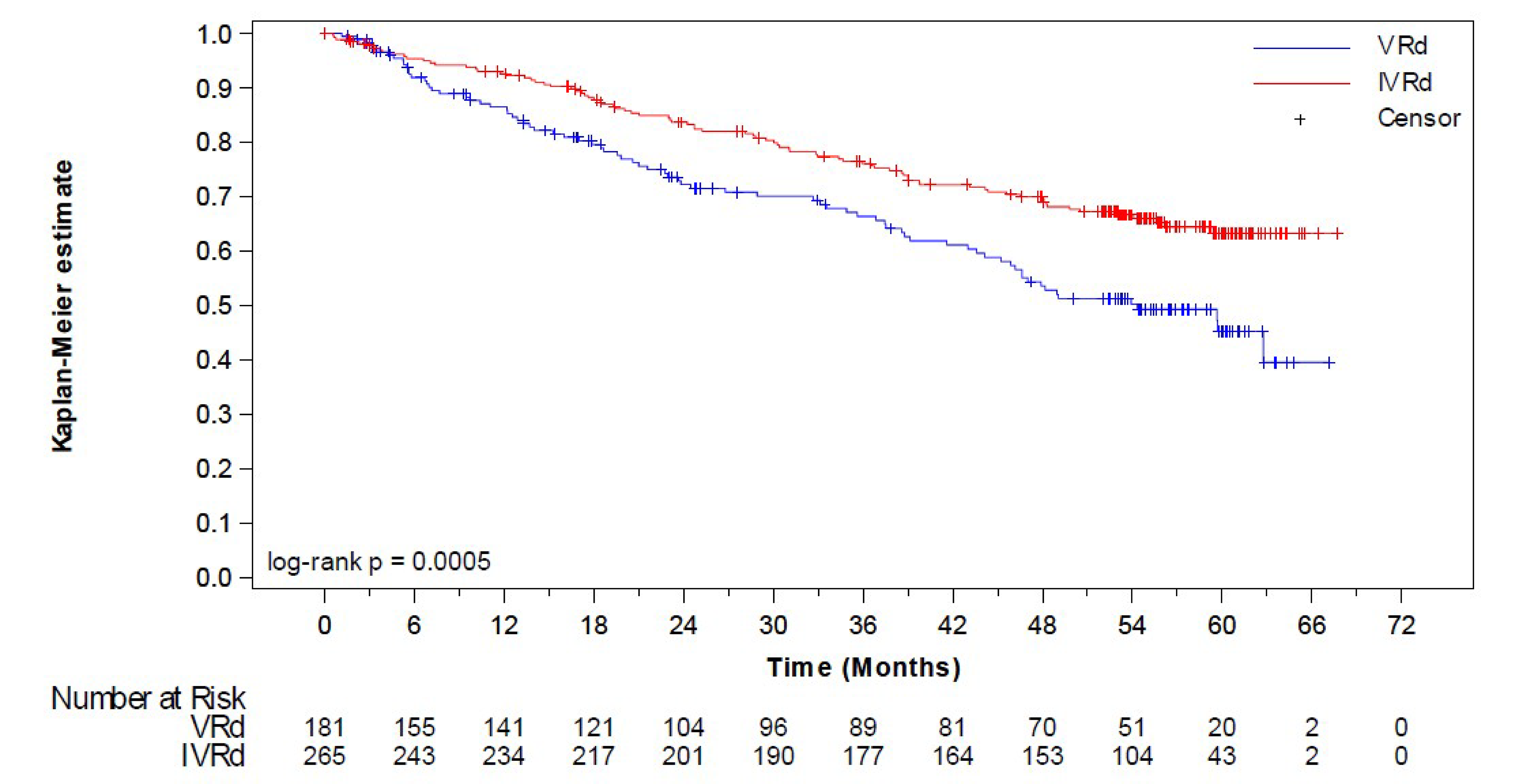
IRC = independent review committee; ITT = intention to treat; IVRd [IsaVRd] = isatuximab-bortezomib-lenalidomide-dexamethasone; KM = Kaplan-Meier; PFS = progression-free survival; R-ISS = Revised International Staging System; VRd = bortezomib-lenalidomide-dexamethasone.
Note: Log-rank test procedure stratified by age (< 70 years versus ≥ 70 years) and R-ISS stage (stage I or stage II versus stage III or not classified) according to interactive response technology. The 1-sided significance level was 0.007423.
Source: IMROZ Clinical Study Report.32
Figure 2: IMROZ Trial Forest Plot of Subgroup Analyses of PFS by IRC by Baseline Demographic Characteristics (ITT Population)
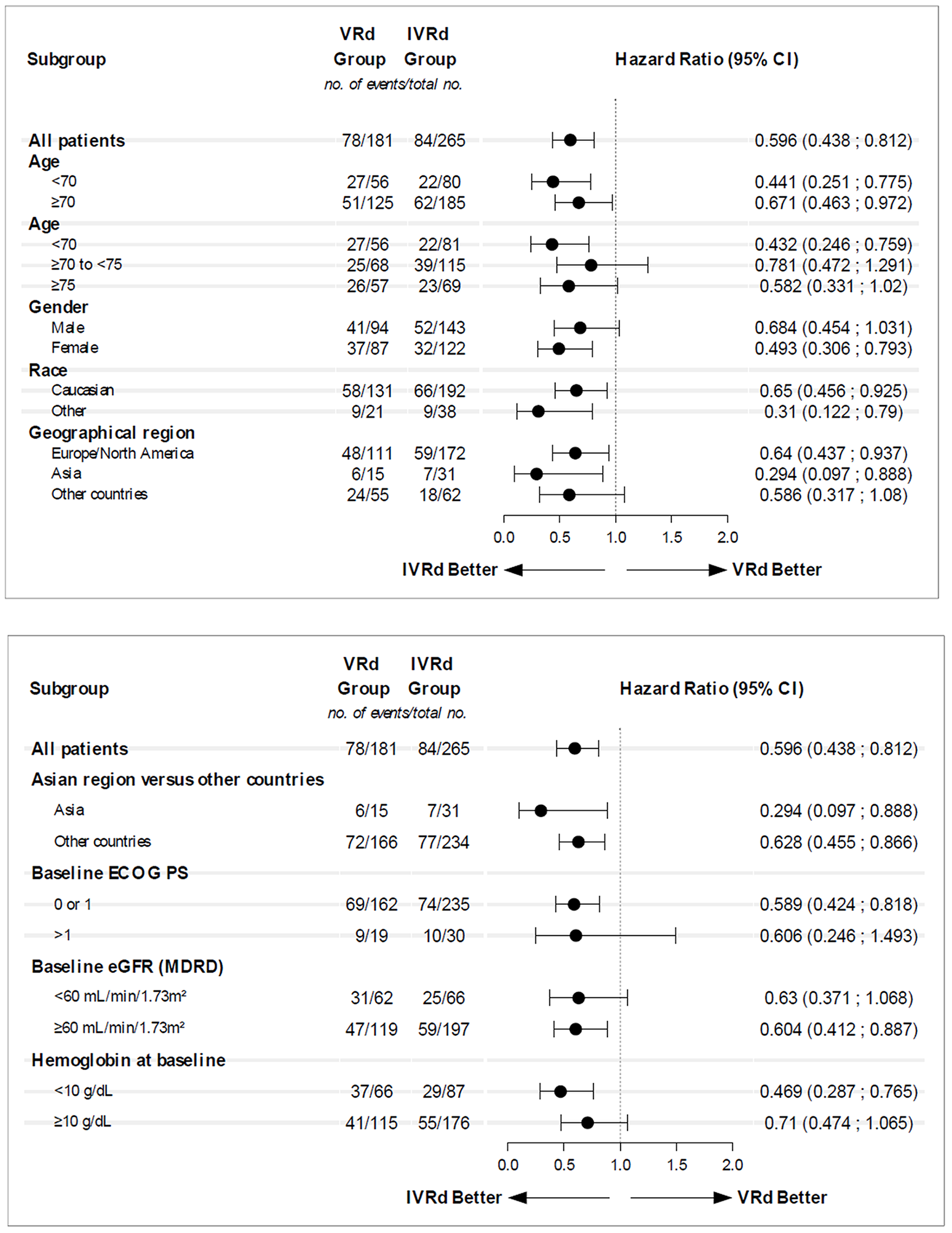
CI = confidence interval; ECOG PS = Eastern Cooperative Oncology Group Performance Status; eGFR = estimated glomerular filtration rate; IRC = independent review committee; ITT = intention to treat; IVRd [IsaVRd] = isatuximab-bortezomib-lenalidomide-dexamethasone; MDRD = Modification of Diet in Renal Disease; PFS = progression-free survival; VRd = bortezomib-lenalidomide-dexamethasone.
Source: IMROZ Clinical Study Report.32
Overall Survival
The interim analysis of OS for futility and overwhelming efficacy was planned at the time of the interim analysis of PFS. After a median follow-up of 59.73 months, there were 59 deaths (32.6%) in the VRd group and 69 deaths (26.0%) in the IsaVRd group as per Table 13. This represents an OS information fraction of 63% because the final OS analysis is to be conducted once there have been 202 deaths. The HR was 0.776 (99.97% CI, 0.407 to 1.48), which passed the prespecified futility threshold that was set to an HR of more than 1.1. The 1-sided nominal P value was 0.076. The KM curves follow a similar trajectory (and consequently crossed at times) and do not begin to separate until after 54 months. Median OS was not reached in either treatment group. The risk difference at 60 months was 0.059 (95% CI, –0.033 to 0.152). The KM curves for OS are provided in Figure 3.
Figure 3: IMROZ Trial KM Curves for OS (ITT Population)
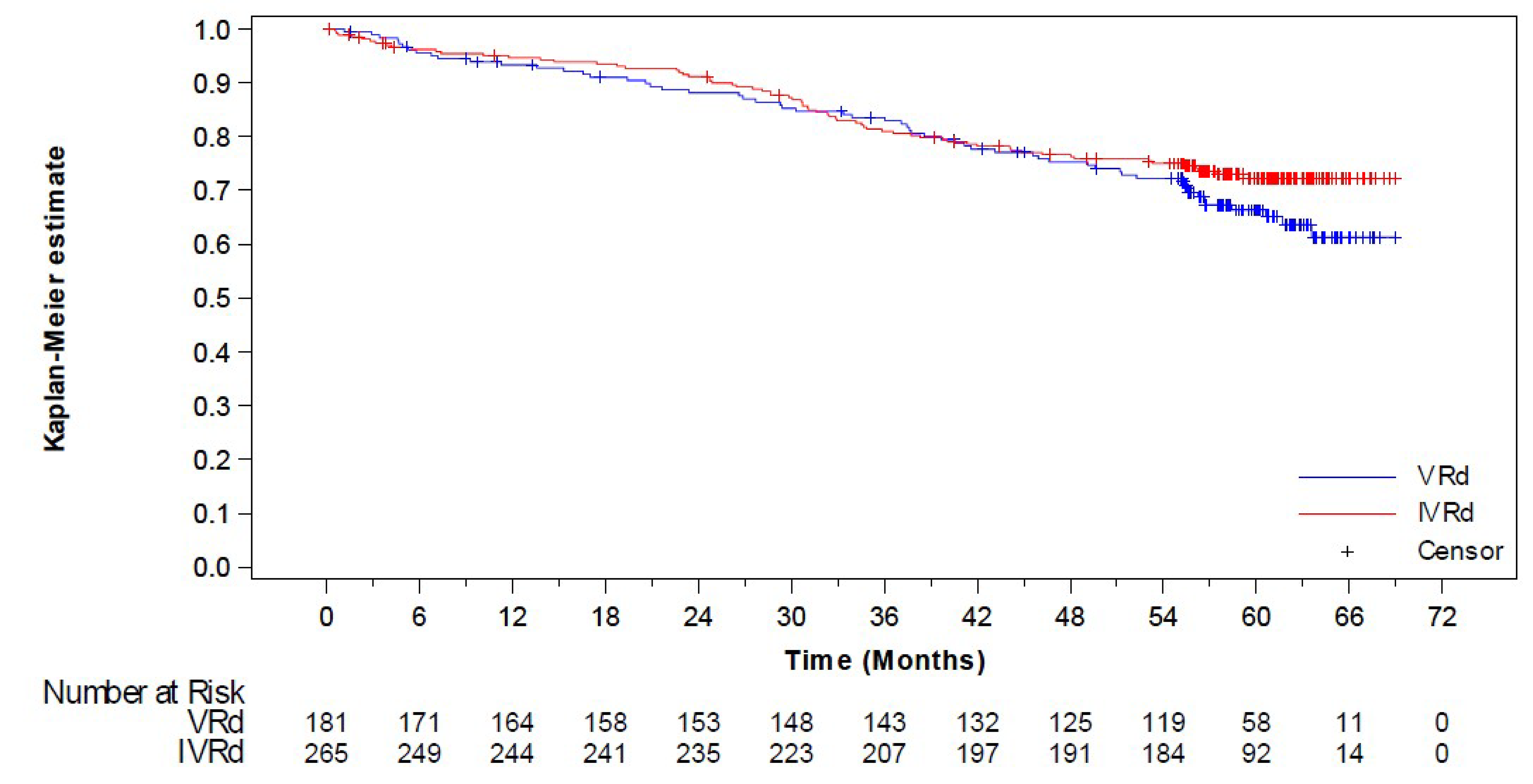
ITT = intention to treat; IVRd = isatuximab-bortezomib-lenalidomide-dexamethasone; KM = Kaplan-Meier; OS = overall survival; VRd = bortezomib-lenalidomide-dexamethasone.
Source: IMROZ Clinical Study Report.32
The effect of death due to COVID and crossover from the VRd group to the IsaVRd group were tested in sensitivity analyses for OS. In addition, a sensitivity analysis of OS adjusted by the switch to anti-CD38 therapies showed that the stratified HR was 0.837 (95% CI, 0.585 to 1.198) using the rank-preserving structural failure time model and 0.803 (95% CI, 0.557 to 1.158) using the inverse probability of censoring weighting (IPCW) method. These results were consistent with those of the primary analysis.
Clinical Response
Overall Response Rate
Most patients (> 90%) in both treatment groups obtained a tumour response. An ORR (i.e., total patients with stringent CR, CR, VGPR, or PR) were experienced by 167 patients (92.3%) in the VRd group and 242 patients (91.3%) in the IsaVRd group (OR = 0.888; 95% CI, 0.439 to 1.794). Subgroup analyses (e.g., poor prognosis subgroups) were consistent with the primary findings.
Complete Response
The CR rate was statistically significant in favour of IsaVRd (OR = 1.656; 95% CI, 1.097 to 2.500; P = 0.0080) with a CR or better in 74.7% of patients in the IsaVRd group compared with 64.1% of patients in the VRd group.
Very Good Partial Response
The rate of VGPR or better based on IRC assessment was 82.9% in the VRd group and 89.1% in the IsaVRd group (OR = 1.729; 95% CI, 0.994 to 3.008; P = 0.0259). The P value did not cross the multiplicity-adjusted efficacy boundary of 0.025.
MRD Negativity Rate
The MRD negativity rate for patients with a CR was statistically lower in the VRd group (40.9%) compared with the IsaVRd group (55.5%) (OR = 1.803; 95% CI, 1.229 to 2.646; P = 0.0013).
MRD Negativity Rate for Patients With a CR
The percentage of patients with at least 1 evaluable on-treatment sample was lower in the VRd group than in the IsaVRd group (75.7% and 84.2%, respectively) (Table 13). Sensitivity analyses of tipping point analysis and multiple imputations were conducted to assess the impact of missing data in the analysis of MRD negativity rate in patients with a CR or better. These results were consistent with those of the primary analysis.
Time to First Response
In the ITT population, the median TT1R was short in both treatment groups. In the VRd group, the median TT1R by IRC assessment was 1.48 months (95% CI, 1.478 months to 1.511 months) and 1.51 months (95% CI, NC to NC) in the IsaVRd group.
Health-Related Quality of Life
HRQoL was assessed using the EORTC QLQ-C30 tool. More than 90% of patients completed the questionnaire for at least the first 14 cycles and more than 80% of patients did so at each cycle. Results were reported for change from baseline in each treatment group, but no statistical analyses were planned. Figure 4 shows that at most time points, the results of the EORTC QLQ-C30 tool were similar between groups with overlapping CIs.
Figure 4: IMROZ Trial EORTC QLQ-C30 Mean (SD) Scores for GHS QoL Over Time (ITT Population Evaluable)
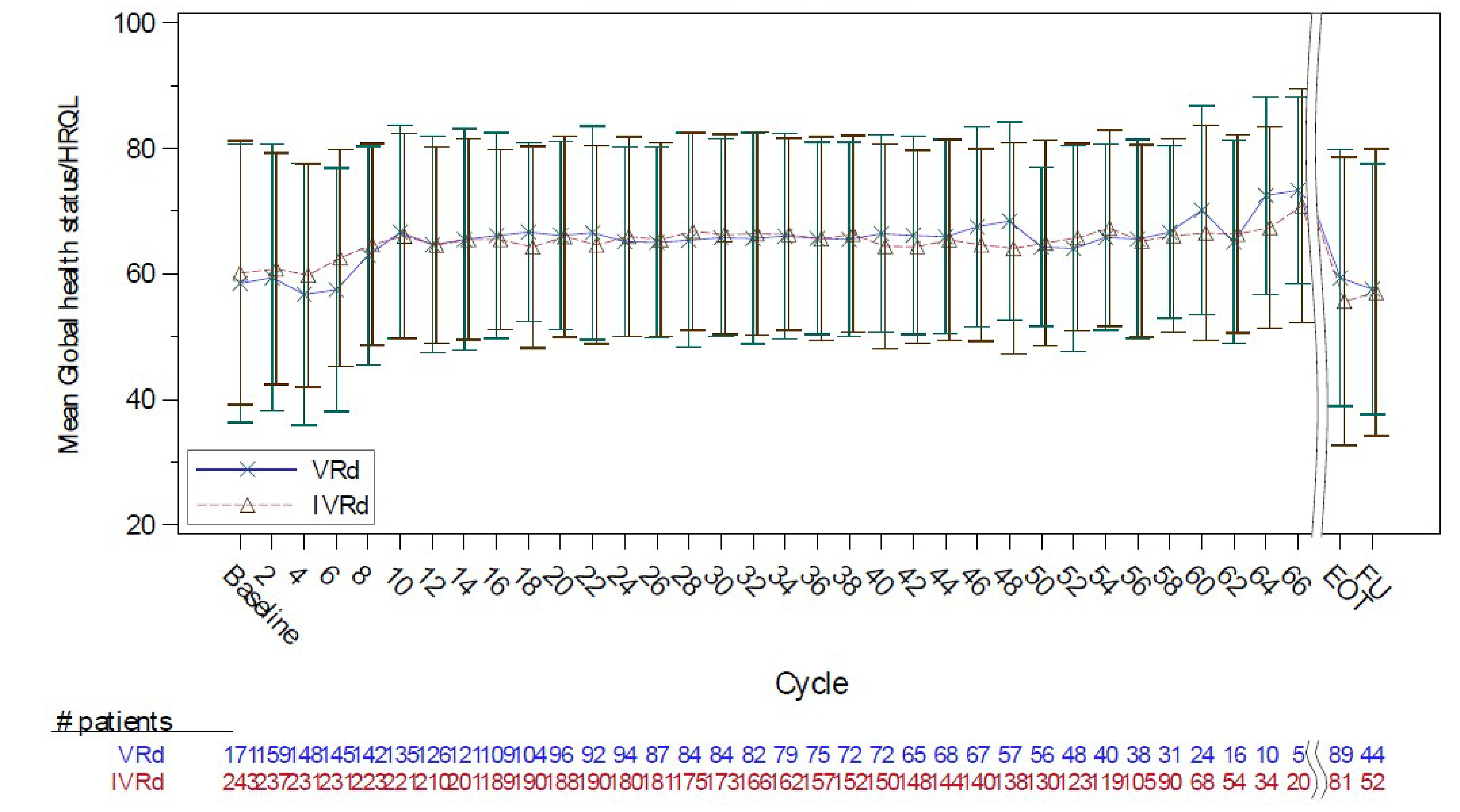
CI = confidence interval; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EOT = end of treatment; FU = follow-up; GHS = global health status; HRQoL = health-related quality of life; IVRd = isatuximab-bortezomib-lenalidomide-dexamethasone; ITT = intention to treat; QoL = quality of life; SD = standard deviation; VRd = bortezomib-lenalidomide-dexamethasone.
Note: A higher score represents better QoL. Cycles with fewer than 20 patients were not presented. EOT was 30 days after the last study treatment administration. FU was 90 days after the last study treatment administration.
Source: IMROZ Clinical Study Report.32
Harms
Safety outcomes for the IMROZ trial were reported for the safety population (i.e., all patients who received at least 1 dose of study treatment). A summary of the overall TEAEs experienced by patients in the IMROZ trial is provided in Table 14.
Adverse Events
In the study, 99.6% of patients in the IsaVRd group and 98.3% of patients in the VRd group had at least 1 TEAE; the percentage of patients who had at least a grade 3 AE was 70.7% versus 67.4%, respectively (Table 14). The most common AE in the IsaVRd group was diarrhea; it occurred in 54.8% of patients in the IsaVRd group and 48.6% of patients in the VRd group. Other common AEs in the IsaVRd group versus the VRd group, included peripheral sensory neuropathy (54.4% versus 60.8%), cataracts (38.0% versus 25.4%), constipation (35.7% versus 40.9%), fatigue (34.6% versus 26.5%), and upper respiratory tract infection (34.2% versus 33.7%).
Serious Adverse Events
SAEs occurred in 70.7% of patients in the IsaVRd group and 67.4% of patients in the VRd group (Table 14). The most common SAE was pneumonia (29.7% in the IsaVRd group versus 21.0% in the VRd group).
Withdrawal Due to Adverse Events
Overall, 26.0% of patients in the IsaVRd group and 22.8% of patients in the VRd group had an AE leading to definitive treatment discontinuation, which was defined as discontinuing all treatments (Table 14). The most frequent reason for definitive treatment discontinuation was due to COVID-19 pneumonia (3.0% in the IsaVRd group versus 0.6% in the VRd group).
Deaths
There were 128 deaths recorded in the IMROZ trial; death occurred in 26.2% of patients in the IsaVRd group and 32.6% of patients in the VRd group (Table 14). Death due to disease progression occurred more frequently in the VRd group (12.2%) while death due to an AE occurred more frequently in the IsaVRd group (11.0%).
Notable Harms
Infusion reactions and infections were notable harms of interest to this review. Infusion reactions were more frequent with IsaVRd compared to VRd (23.6% versus 1.1%, respectively). The rate of infections was similar across groups, occurring in 91.3% of patients in the IsaVRd group and 86.7% of patients in the VRd group; they consisted of pneumonia, upper respiratory tract infections, and COVID-19 infections. Among other AESIs in the trial, other than deaths, were primary malignancies, which occurred in 16.0% of patients in the IsaVRd group and 8.8% of patients in the VRd group, with squamous cell carcinoma of the skin being the most common (4.9% in the IsaVRd group versus 2.2% in the VRd group). There were no hematologic malignancies reported in either treatment group. Events of decreased neutrophil count occurred in 30.0% of patients in the IsaVRd group versus 21.5% of patients in the VRd group.
Table 14: Summary of Harms Results From the IMROZ Trial
AE | VRd (N = 181) | IsaVRd (N = 263) |
|---|---|---|
TEAEs, n (%) | ||
Patients with ≥ 1 TEAE | 178 (98.3) | 262 (99.6) |
Patients with any ≥ grade 3 TEAE | 152 (84.0) | 241 (91.6) |
Most common AEs, n (%)a | ||
Diarrhea | 88 (48.6) | 144 (54.8) |
Peripheral sensory neuropathy | 110 (60.8) | 143 (54.4) |
Cataract | 46 (25.4) | 100 (38.0) |
Constipation | 74 (40.9) | 94 (35.7) |
Fatigue | 48 (26.5) | 91 (34.6) |
Upper respiratory tract infection | 61 (33.7) | 90 (34.2) |
Peripheral edema | 59 (32.6) | 86 (32.7) |
Neutropenia | 39 (21.5) | 79 (30.0) |
Infusion-related reaction | 2 (1.1) | 62 (23.6) |
COVID-19 | 30 (16.6) | 59 (22.4) |
Insomnia | 44 (24.3) | 59 (22.4) |
Back pain | 31 (17.1) | 58 (22.1) |
Bronchitis | 32 (17.7) | 58 (22.1) |
Asthenia | 44 (24.3) | 57 (21.7) |
SAEs, n (%) | ||
Patients with ≥ 1 SAEb | 122 (67.4) | 186 (70.7) |
Pneumonia | 38 (21.0) | 78 (29.7) |
Upper respiratory tract infection | 7 (3.9) | 5 (1.9) |
Sepsis | 6 (3.3) | 6 (2.3) |
Bronchitis | 3 (1.7) | 7 (2.7) |
Syncope | 6 (3.3) | 6 (2.3) |
Transient ischemic attack | 5 (2.8) | 3 (1.1) |
Cataract | 2 (1.1) | 6 (2.3) |
Atrial fibrillation | 8 (4.4) | 8 (3.0) |
Cardiac failure | 6 (3.3) | 1 (0.4) |
Pulmonary embolism | 6 (3.3) | 11 (4.2) |
Diarrhea | 9 (5.0) | 5 (1.9) |
Pathological fracture | 7 (3.9) | 3 (1.1) |
Acute kidney injury | 4 (2.2) | 4 (1.5) |
General physical health deterioration | 4 (2.2) | 1 (0.4) |
Pyrexia | 3 (1.7) | 6 (2.3) |
Femur fracture | 1 (0.6) | 6 (2.3) |
Withdrawals due to AEs, n (%) | ||
Patients with any TEAE leading to definitive treatment discontinuationc | 47 (26.0) | 60 (22.8) |
COVID-19 pneumonia | 1 (0.6) | 8 (3.0) |
Pneumonia | 4 (2.2) | 6 (2.3) |
Diarrhea | 5 (2.8) | 0 (0) |
Deaths, n (%) | ||
Patients who diedd | 59 (32.6) | 69 (26.2) |
Disease progression | 22 (12.2) | 13 (4.9) |
AE | 11 (6.1) | 29 (11.0) |
Othere | 26 (14.4) | 27 (10.3) |
AE = adverse event; IsaRd = isatuximab-lenalidomide-dexamethasone; IsaVRd = isatuximab-bortezomib-lenalidomide-dexamethasone; SAE = serious adverse event; TEAE = treatment-emergent adverse event; VRd = bortezomib-lenalidomide-dexamethasone.
aTEAEs reported are all-grade TEAEs in at least 20% of patients in either treatment group.
bSAEs reported are all-grade SAEs in at least 2% of patients in either treatment group.
cDefinitive treatment discontinuations are all-grade TEAEs leading to definitive treatment discontinuation in 2% or more of patients in either treatment group. Definitive treatment discontinuation is defined as the discontinuation of all study interventions or the last ongoing study drug.
dTotal deaths during the treatment and posttreatment periods (including the crossover period for patients in the VRd group who switched to IsaRd).
eOther deaths mainly comprised the primary System Organ Class of infections and infestations (7.2% [n = 13] in the VRd group and 13.7% [n = 36] in the IsaVRd group).
Source: IMROZ Clinical Study Report.32
Critical Appraisal
Internal Validity
The IMROZ trial was planned with adequate power to meet the goals of the study’s primary outcome (PFS), randomizing 446 patients in a 3:2 ratio to the addition of isatuximab to VRd or VRd only. The assumptions made when performing power calculations were considered reasonable. The randomization method, and allocation concealment, appeared adequate. Further, the randomization was stratified based on important prognostic factors to minimize important differences in baseline characteristics between groups and to allow for the maintenance of randomization for exploratory subgroup analyses based on these baseline characteristics. The use of IRC assessments for the important outcomes provides objectivity to the outcome assessments. There were, however, some limitations and potential sources of bias, which are outlined in this section.
The reported results to date were based on a preplanned second PFS interim analysis (i.e., the date when 167 PFS events [with a 75% information fraction] were expected to be observed in the global population). The interim data cut-off date for these analyses occurred when 162 PFS events had been observed. Interim analyses are typically at risk of overestimating the true magnitude of benefit. However, given the statistical and clinical significance of the difference observed between the IsaVRd and VRd groups, and the relatively large information fraction, this is likely not a major concern. In the analysis of PFS, 18.8% of patients in the VRd group and 23.8% of patients in the IsaVRd group were censored due to not having a valid disease assessment in the 13 weeks before the data cut-off date (i.e., missed 2 or more scheduled disease assessments). Because the reason for missed assessments is not known, there is a potential for the risk of bias due to informative censoring. There was no sensitivity analysis addressing this issue and the direction of potential bias cannot be ascertained. Other sensitivity analyses of the primary end point were supportive of the primary analysis. At the data cut-off date, the OS information fraction was 63%. This is important because while PFS can be viewed as a surrogate for OS, death is not an immediate consequence of treatment failure as further lines of treatment can prolong life. Furthermore, the OS analysis is confounded by crossovers (the risk of bias may be toward the null). To account for this potential bias, the sponsor performed several sensitivity analyses of OS results, including IPCW and rank-preserving structural failure time models. However, these analyses are limited by unverifiable underlying assumptions (i.e., a key assumption of no unmeasured confounding for IPCW and a common treatment effect for IPCW). As the follow-up continues, the potential bias from treatment crossovers may increase, including the use of newer, highly effective therapies that delay death (e.g., chimeric antigen receptor T-cell therapy).
The IMROZ study is open-label, and a lack of blinding may bias results, particularly for subjective, patient-reported outcomes. HRQoL self-reporting and the reporting of more subjective AEs (e.g., injection-related AEs) may also be influenced by a lack of blinding because patients may anticipate known adverse effects of IsaVRd and thus may be more likely to report them when they do occur. Physician knowledge of their patient’s assigned treatment may also affect the way they manage their patient, and patient knowledge of their assigned treatment may make them more or less likely to remain in the study. Objective clinical outcomes such as PFS and OS are less likely to be influenced by a lack of blinding, especially when they are evaluated by a blinded IRC. Assessment of radiological and laboratory-related outcomes (such as ORR) were also conducted by a blinded IRC and therefore would not be less likely to be directly biased from a lack of blinding.
Multiplicity was controlled in the study by using a hierarchical testing procedure. The hierarchy was planned for 4 consecutive analyses following the testing of PFS (CR rate, MRD negativity rate, VGPR or better rate, then OS) and failed at the third analysis. Therefore, as described in the protocol, OS was not formally analyzed and is only expected in the final analysis in 2027. Additionally, the trial was not stratified for most subgroup analyses, and the subgroup analyses were not adjusted for multiplicity or powered to detect effect modification. As such, the conclusions of the subgroup analyses should only be used for hypothesis generation. Even so, the results of most sensitivity and subgroup analyses for the primary outcome, PFS, were generally consistent with the primary analysis supporting the consistency of the effect across subgroups.
By the time of the second interim analysis, most patients had discontinued treatment, mainly due to AEs or PD. This large level of treatment discontinuation may influence any potential comparative evaluation and interpretation of HRQoL and harms outcomes, which were not done in this study. Relatively few patients discontinued the study due to reasons other than death (7.2% in the VRd group and 6.8% in the IsaVRd group). However, the number of patients remaining to complete HRQoL assessments declined over time, resulting in a risk of bias due to missing outcome data given that only complete cases were reported.
External Validity
The IMROZ trial excluded patients older than 80 years and those with an ECOG PS score of greater than 2; however, some patients with an ECOG PS score of 2 or more were enrolled. In a real-world setting, these individuals may be eligible for treatment. The clinical experts noted that the efficacy of VRd in the trial was higher than would normally be expected, which could be the result of a learning curve in jurisdictions that use VRd regularly. For example, in the phase III SWOG S0777 trial, the median PFS for VRd was only 43 months40 compared to 54 months in the IMROZ trial. Further, in the IMROZ trial, bortezomib was not dosed at the Canadian and international standard of once weekly. In addition, the most commonly used drug in Canada for this population is based on daratumumab, which was not evaluated in this trial. This brings uncertainty with regard to the anticipated true effect relative to relevant comparators in a Canadian population, but it is expected to be more effective than the historic use of VRd and with a better side-effect profile due to once weekly dosing of bortezomib. Finally, while the IMROZ study was conducted in 96 sites (21 countries), none of the sites were in Canada. As such, data from patients in Canada cannot be directly compared to those of individuals from other countries to determine if the results were homogeneous or if there were uncontrolled factors related to geography or the health care system that could have affected the results, although the clinical experts considered that this may be a minor factor that could affect external validity in the context in Canada.
GRADE Summary of Findings and Certainty of the Evidence
Methods for Assessing the Certainty of the Evidence
For pivotal studies and RCTs identified in the sponsor’s systematic review, GRADE was used to assess the certainty of the evidence for outcomes considered most relevant to inform the CDA-AMC expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group41,42:
“High certainty: We are very confident that the true effect lies close to that of the estimate of the effect.
Moderate certainty: We are moderately confident in the effect estimate — The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. We use the word ‘likely’ for evidence of moderate certainty (e.g., ‘X intervention likely results in Y outcome’).
Low certainty: Our confidence in the effect estimate is limited — The true effect may be substantially different from the estimate of the effect. We use the word ‘may’ for evidence of low certainty (e.g., ‘X intervention may result in Y outcome’).
Very low certainty: We have very little confidence in the effect estimate — The true effect is likely to be substantially different from the estimate of effect. We describe evidence of very low certainty as ‘very uncertain.’”
Following the GRADE approach, evidence from the RCT started as high-certainty evidence and could be rated down for concerns related to study limitations (which refers to internal validity or a risk of bias), indirectness, the imprecision of effects, and publication bias.
When possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect; if this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., the clinical importance is unclear). In all cases, the target of the certainty of evidence assessment was based on the point estimate and where it was located relative to the threshold for a clinically important effect (when a threshold was available) or to the null. Certainty in the effects for OS, PFS, and SAEs was based on the presence or absence of any effect because a threshold of clinical importance could not be established. A literature-based minimal important difference was available for HRQoL; however, the difference between groups was not tested statistically. Therefore, a narrative description of the findings was used.
The selection of outcomes for GRADE assessment was based on the sponsor’s Summary of Clinical Evidence, consultation with clinical experts, and input received from patient and clinician groups and public drug plans. The following list of outcomes was finalized in consultation with expert committee members:
PFS — median, 18 months, 36 months, and 60 months
OS — median and 60 months
HRQoL using the EORTC QLQ-C30 — change from baseline
individuals with SAEs — up to the data cut-off date.
Results of GRADE Assessments
Table 2 presents the GRADE summary of findings for IsaVRd versus VRd in patients with newly diagnosed MM.
Long-Term Extension Studies
There is no long-term extension phase planned for the IMROZ trial. The IMROZ trial remains ongoing with an anticipated completion date of June 30, 2027. No other long-term extension studies were included in the submission.
Indirect Evidence
Content in this section has been informed by materials submitted by the sponsor. The following has been summarized and validated by the CDA-AMC review team.
Objectives for the Summary of Indirect and Nonrandomized Evidence
Currently, the only head-to-head randomized comparison of IsaVRd is the IMROZ trial. Given that there are several other treatment options in the setting in Canada, and given a recent recommendation by the Formulary Management Expert Committee to prioritize daratumumab, the sponsor submitted an ITC report in which an NMA and unanchored MAICs were conducted for most comparators for the outcomes PFS and OS. The MAICs used individual PLD from the IMROZ study and aggregate data for the comparator studies. Individual PLD were used in both groups in the comparison of IsaVRd (the IMROZ study) and CyBorD (the Flatiron Health database), which were considered as a nonrandomized study and compared using IPW methods.
Description of the ITCs and Nonrandomized Comparison
The sponsor-provided ITC report describes the proposed NMA, MAICs, and nonrandomized comparisons that were performed. A systematic review and feasibility assessment were done to identify studies to include in the ITC, the eligibility criteria for which are summarized in Table 15.
Table 15: Study Selection Criteria and Methods for ITCs Submitted by the Sponsor
Characteristic | Indirect comparison |
|---|---|
Population | Adult patients (aged ≥ 18 years) with newly diagnosed or previously untreated MM (patient populations who were both transplant-eligible and transplant-ineligible).a Only the studies that reported results in patients who were transplant-ineligible were included for the NMA. |
Intervention (transplant-ineligible) |
|
Comparator | Any, including but not limited to:
Any other pharmacological or nonpharmacological intervention (such as HSCT) |
Outcome | Overall survival, progression-free survival |
Study designs | Phase IIb, phase III, phase IV, and unclear RCTs |
Publication characteristics | Published studies, with results presented in articles, conference proceedings, or abstracts, or posted on clinical trial registries |
Language | English |
Time frame | Original SLR: Up to March 2021 First update: February 2021 to July 2022 onward Second update: June 2022 to August 2023 Third update: July 2023 to April 2024 |
Databases searched | Electronic bibliographical databases:
Conference proceedings:
Bibliographies of key systematic reviews and meta-analysis articles were also screened to ensure that initial searches captured all the relevant clinical studies. |
Selection process | Screening was performed by 2 independent reviewers who reviewed each reference identified in the literature search. Any uncertainty regarding the inclusion or exclusion decision of studies was checked by a third reviewer. |
Data extraction process | Data were extracted by a single reviewer. All extracted data were quality-checked against the original source article by a second senior reviewer. |
Quality assessment | All included studies were subject to a quality appraisal using the standard NICE checklist.43 |
ASCO = American Society of Clinical Oncology; ASH = American Society of Hematology; BSH = British Society for Haematology; CDSR = Cochrane Database of Systematic Reviews; CENTRAL = Cochrane Central Register of Controlled Trials; CTd = cyclophosphamide-thalidomide-dexamethasone; CyBorD = cyclophosphamide-bortezomib (Velcade)-dexamethasone; DCyBorD = daratumumab (Darzalex)-cyclophosphamide-bortezomib (Velcade)-dexamethasone; DRd = daratumumab-lenalidomide (Revlimid)-dexamethasone; DVMP = daratumumab-bortezomib (Velcade)-melphalan-prednisone; DVRd = daratumumab (Darzalex)-bortezomib (Velcade)-lenalidomide (Revlimid)-dexamethasone; EHA = European Hematology Association; EKRd = elotuzumab-carfilzomib (Kyprolis)-lenalidomide (Revlimid)-dexamethasone; ERd = elotuzumab-lenalidomide (Revlimid)-dexamethasone; ESMO = European Society for Medical Oncology; HSCT = hematopoietic stem cell transplant; ITC = indirect treatment comparison; IsaVRd = isatuximab (Sarclisa)-bortezomib (Velcade)-lenalidomide (Revlimid)-dexamethasone; MM = multiple myeloma; MPR = melphalan-prednisone-lenalidomide (Revlimid); MPT = melphalan-prednisone-thalidomide; NICE = National Institute for Health and Care Excellence; NMA = network meta-analysis; RCT = randomized controlled trial; Rd = lenalidomide (Revlimid)-dexamethasone; SLR = systematic literature review; Vd = bortezomib (Velcade)-dexamethasone; VMP = bortezomib (Velcade)-melphalan-prednisone; VRd = bortezomib (Velcade)-lenalidomide (Revlimid)-dexamethasone; VTd = bortezomib (Velcade)-thalidomid-dexamethasone.
aStudies assessing mixed populations with more than 80% of the population of interest or reporting separate subgroup data for the population of interest were included and extracted.
bMPR and MPT were newly added to the list of included interventions for the SLR update.
Source: Clinical Systematic Literature Review Update for Treatments in Newly Diagnosed Multiple Myeloma.44
ITC and Nonrandomized Study Design
Objectives
In the absence of direct comparison between IsaVRd and other available treatments in Canada, the overall aim of the ITC was to estimate the relative efficacy of IsaVRd compared with currently funded alternative treatments (DVMP, DRd, Rd, DCyBorD, and CyBorD) in patients with transplant-ineligible newly diagnosed MM.
Study Selection Methods
Three sources of data informed the ITC analyses. The first source was a systematic literature review (SLR) of RCTs that were used to compare IsaVRd with DVMP, DRd, and Rd in patients with untreated MM. DCyBorD and CyBorD were identified as being used in clinical practice but no RCTs were identified from the clinical SLR to support ITCs. Thus, 2 alternative sources were considered, including PLD from the real-world Flatiron Health Electronic Medical Record database, and a clinical SLR of non-RCTs and observational studies.
The RCT SLR was last updated in April 2024. Bibliographies of key systematic reviews and meta-analysis articles (identified in the update from 2023) were also screened to ensure that the initial searches done by CDA-AMC captured all the relevant clinical studies. Bibliographic searching was also conducted as per the original SLR (from 2023 onward) for the National Institute for Health and Care Excellence (NICE) (including the National Health Services Cancer Drugs Fund), the Scottish Medicines Consortium, the All Wales Medicines Strategy Group, CDA-AMC (including the pan-Canadian Oncology Drug Review), and the Pharmaceutical Benefits Advisory Committee to identify primary publications (i.e., completed trials whose results were available and published as full-text articles reporting primary end points).
To determine the final set of studies eligible for the clinical SLR of non-RCT and observational studies, explicit inclusion and exclusion criteria were applied to the literature search results. The criteria used for the inclusion and exclusion of studies in the systematic review are described in Table 16. These criteria were applied to the literature search results to identify the final set of studies that form the main body of the clinical evidence included in the review update.
Table 16: Inclusion and Exclusion Criteria for the Non-RCT and Observational SLR for the ITCs Submitted by the Sponsor
Category | Inclusion criteria | Exclusion criteria |
|---|---|---|
Population | Adult patients (aged 18 years or older) with newly diagnosed or previously untreated MM (both Te and Ti patient populations)a |
|
Interventions (transplant-eligible and transplant-ineligible) |
|
|
Comparators | Any, including but not limited to:
| No limit on comparators |
Outcomes |
| Trials assessing outcomes irrelevant to the review |
Treatment setting | Front-line Induction (for Te studies):
Consolidation (for Te studies):
Type of treatment not reported |
|
Trial design |
|
|
Databases searched | Electronic bibliographical databases:
Conference proceedings:
Bibliographies of key systematic reviews and meta-analysis articles were also screened to ensure that initial searches conducted by CDA-AMC captured all the relevant studies. | NA |
Language | Englishb | Non-English |
Countries | No restrictions | None |
Time frame | No limit on full-text articles 2023 onward for conference abstracts | NA |
ASCO = American Society of Clinical Oncology; ASCT = autologous stem cell transplant; BSH = British Society for Haematology; CDA-AMC = Canada’s Drug Agency; CDSR = Cochrane Database of Systematic Reviews; CENTRAL = Cochrane Central Register of Controlled Trials; CyBorD = cyclophosphamide-bortezomib-dexamethasone; DCyBorD = daratumumab-cyclophosphamide-bortezomib-dexamethasone; HSCT = hematopoietic stem cell transplant; ITC = indirect treatment comparison; MM = multiple myeloma; NA = not applicable; OS = overall survival; PFS = progression-free survival; PFS2 = progression-free survival on next line of therapy; RCT = randomized controlled trial; RRMM = relapsed or refractory multiple myeloma; SLR = systematic literature review; SOC = standard of care; Te = transplant-eligible; Ti = transplant-ineligible.
aStudies assessing mixed populations with more than 80% of the population of interest or reporting separate subgroup data for the population of interest were included and extracted. The studies were retained for information purposes only and the focus of the review in terms of data extraction and reporting of results was studies in the Ti population.
bNon-English citations that were potentially relevant to the SLR were to be flagged.
Source: Clinical Systematic Literature Review Update for Treatments in Newly Diagnosed Multiple Myeloma.44
All retrieved studies were assessed against the eligibility criteria. Primary screening (level 1, title and abstract) and secondary screening (level 2, full text) was conducted by 2 independent reviewers against the eligibility criteria. Any uncertainty regarding the inclusion of a study was checked by a third reviewer. Included studies were categorized according to the transplant status of the study participants (who were newly diagnosed with MM and were transplant-eligible or transplant-ineligible). Studies that included both populations were categorized as “both” and consideration was given as to whether the results of each population were reported separately. Studies were categorized as “unclear” where the transplant eligibility status of participants was not reported. Data were extracted by a single reviewer. All extracted data were quality-checked against the original source article by a second senior reviewer. All included studies were subject to a quality appraisal using the standard NICE checklist as per the original SLR.43 Quality assessment was done by a single independent reviewer and checked by a second senior reviewer.
Feasibility Assessment
A total of 76 RCTs were identified in the SLR; 30 studies included patients who were transplant-eligible, 33 studies included patients who were transplant-ineligible, 6 studies included patients who were both transplant-eligible and transplant-ineligible, and in 7 studies the transplant status was unclear. The 30 studies that included only patients who were transplant-eligible were not further considered (not relevant to the comparison of interest). The feasibility assessment considered the remaining 46 RCTs plus the IMROZ trial (47 studies).
The feasibility of conducting ITCs was based on the connectivity of the evidence base and the evaluation of the plausibility of key assumptions (similarity, homogeneity, and consistency). This was accomplished via qualitative evaluation of the comparability of study design, inclusion and exclusion criteria, treatment regimens, patient demographics, and outcome data. Following review, 31 studies were deemed not suitable for inclusion in ITCs and were excluded based on transplant status (n = 8), a lack of network connectivity (n = 17), study design (n = 4), differences in patient characteristics (n = 1), and a lack of relevant outcome data (n = 1). In total, 16 studies (including the IMROZ study) were deemed suitable for ITCs.
The potential to conduct an NMA was explored. The IMROZ study was connected to the network via the SWOG S0777 study, which compared VRd to Rd. There were potential imbalances in patient characteristics and differences in the administration of bortezomib between the SWOG S0777 study and the IMROZ study. Therefore, it was determined that the inclusion of the SWOG S0777 study to anchor the IMROZ study to the network would likely lead to substantial bias and unreliable relative efficacy estimates for IsaVRd compared to other treatments. As a suitable network of evidence could not be formed for comparisons, an unanchored MAIC (and IPW for the comparison to CyBorD) was deemed the most appropriate approach to assess comparative efficacy for IsaVRd versus relevant comparators.
Summary of Included Studies
SLR of RCTs in patients with untreated MM: Three comparator trials were identified that were deemed relevant suitable for unanchored MAICs — the MAIA study (DRd and Rd), the ALCYONE study (DVMP), and the FIRST study (Rd).
SLR of non-RCTs and observational studies: The SLR identified 1 single-arm study that assessed DCyBorD, in which only PFS data were available. Further, for the comparison with CyBorD, the SLR did not identify any study that was deemed suitable for ITCs. Therefore, RWE was required to fill this gap.
RWE using Flatiron Health data: RWE data from the Flatiron Health database was identified as the most appropriate source for the comparison with CyBorD. The Flatiron Health Electronic Medical Record database is a retrospective, observational cohort study that uses real-world PLD for patients with MM who received VRd and did not receive an ASCT in first-line therapy. The study period was from April 30, 2011, to January 31, 2022. A cohort of patients who underwent VRd followed by lenalidomide maintenance was used to extrapolate survival outcomes.
ITC and Nonrandomized Study Analysis Methods
MAIC Methods
Given that a common comparator was not available between the IMROZ trial and the comparator studies, an unanchored MAIC was required for comparisons between IsaVRd and other treatments. In the analysis, individual patients treated with IsaVRd from the IMROZ trial were assigned statistical weights that adjusted for their over-representation or under-representation relative to the average prognostic factors and treatment effect modifiers observed in each comparative evidence source. These weights were then incorporated into the analyses of PFS and OS outcomes.
IPW Methods
IPW was used to adjust for observed differences in patient characteristics between the IMROZ study population and the patients treated with CyBorD at first-line therapy from the Flatiron Health data source. Propensity scores for patients receiving IsaVRd in the IMROZ study and patients receiving CyBorD from the Flatiron Health data source were derived using logistic regression (known as the propensity score model). Statistical weights were derived for the average treatment effect on the treated estimand, with the target population being patients in the IMROZ study. The final propensity score model adjusted for the following covariates: age (continuous), ECOG PS score (0, 1, 2, or 3), ISS stage (stage I, stage II, stage III, or stage IV), time from MM diagnosis to treatment (continuous), cytogenetic risk (standard or high), and chromosomal abnormality 1q21+ (present or absent). Multiple imputation was used to impute missing baseline characteristics in the Flatiron Health data source, assuming that the data were missing at random.
Comparisons with DCyBorD were informed by aggregate data from a single-arm trial (the Yimer et al. study50); the single-arm nature of the Yimer et al. study meant an unanchored MAIC was required. This was the only source of evidence available for DCyBorD. Additionally, only PFS could be analyzed because OS data were not reported.
Identification of Prognostic Factors and Treatment Effect Modifiers
Unanchored MAICs require that all prognostic factors and treatment effect modifiers be adjusted for. The following sources were used to identify prognostic factors and treatment effect modifiers.
Clinical expertise: Consultations with clinicians indicated that the following characteristics were prognostic and/or effect-modifying for OS and PFS (ranked in descending order of importance) — age, frailty, ISS stage, cytogenetic risk, ECOG PS score, LDH levels, and renal impairment.
PLD analyses of the IMROZ clinical trial data:
PFS subgroup analyses32 conducted in the IMROZ trial indicated that there was some evidence (P value < 0.1) of a difference in the treatment effect across 2 subgroups — MM type IgG and chromosomal abnormality 1q21+
Cox proportional hazards models fitted to the IMROZ trial PLD indicated that ISS stage, chromosomal abnormality 1q21+, LDH levels, and creatinine clearance have a statistically significant effect on PFS outcomes.
PLD analyses of Flatiron Health data: Cox proportional hazards models fitted to the Flatiron Health data identified age, ECOG PS score, ISS stage, cytogenetic risk, and chromosomal abnormality 1q21+ as potential prognostic factors for OS and ISS stage, cytogenetic risk, and chromosomal abnormality 1q21+ as potential prognostic factors for PFS.45
Based on the aforementioned details, 9 patient characteristics were considered for adjustment in the MAICs: age, frailty, ISS stage, cytogenetic risk, chromosomal abnormality 1q21+, ECOG PS score, LDH levels, creatinine clearance (a proxy for renal impairment), and MM type IgG. Inclusion of these characteristics in the matching depended on data availability as reported in the clinical trials. Note that frailty was not reported in any comparator study so could not be adjusted for in analyses. Table 17 presents the characteristics included in the matching for each comparator study.
Statistical Analysis Methods
Following the estimation of statistical weights for the MAICs and IPW, adjusted and unadjusted KM curves as well as the mean difference in restricted mean survival time (RMST) were reviewed. Adjusted log-cumulative hazard (LCH) curves, Schoenfeld residual plots, and the Schoenfeld residual test were used to assess the proportional hazards assumption. In all cases, potential violations to the proportional hazards assumption resulted in time-varying models being preferred over constant HR models. Weighted parametric survival models were fit for each of the 7 standard distributions (exponential, gamma, generalized gamma, log-normal, log-logistic, Gompertz, and Weibull) with a multivariate treatment effect parameter. Relative effects were applied to 1 parameter (exponential) or 2 parameters (remaining distributions). A bootstrapping approach was used to estimate time-varying HRs and 95% CIs over time.
In the absence of justification for fitting different parametric models for each group, the same distribution was used for both groups for all comparisons. In the IMROZ trial ITT analysis, the gamma distribution was preferred for modelling PFS and the Gompertz distribution was preferred for modelling OS. For consistency, the same distributions were preferred in this ITC analysis, although all distributions were analyzed.
Table 17: Matching Variables Used in the MAICs
Characteristic | Evidence for consideration in matching | MAIA study (DRd, Rd) | ALCYONE study (DVMP) | FIRST study (Rd) | Yimer et al. study50 (DCyBorD) |
|---|---|---|---|---|---|
Age | Identified by clinicians | Mean | Mean | Mean | Mean |
Frailty | Identified by clinicians | Not reported | Not reported | Not reported | Not reported |
ISS stage | Identified by clinicians and exploratory analyses of Flatiron Health data and IMROZ study data | Stage I, stage II, stage III | Stage I, stage II, stage III | Stage I, stage II, stage III | Stage I, stage II, stage III |
Cytogenic risk | Identified by clinicians and exploratory analyses of Flatiron Health data | High, standard, missing | High, standard, missing | High, standard, missing | High, standard, missing |
Chromosomal abnormality 1q21+ | Identified as prognostic in exploratory analyses of Flatiron Health data and IMROZ study data | Not reported | Not reported | Not reported | Not reported |
ECOG PS score | Identified by clinicians and exploratory analyses of Flatiron Health data and IMROZ study data | 0 to 1, ≥ 2 | 0 to 1, ≥ 2 | 0 to 1, ≥ 2 | 0 to 1, ≥ 2 |
Multiple myeloma type | Potential treatment effect modifier based on the IMROZ study CSR32 | IgG, non-IgG | IgG, non-IgG | IgG, non-IgG | IgG, non-IgG |
LDH levels | Identified by clinicians and exploratory analyses of IMROZ study data | Not reported | Not reported | < 200 IU/L, ≥ 200 IU/L | Not reported |
Creatinine clearance, proxy for renal impairment | Identified by clinicians and exploratory analyses of IMROZ study data | ≤ 60 mL per minute, > 60 mL per minute | < 60 mL per minute, ≥ 60 mL per minute | < 60 mL per minute, ≥ 60 mL per minute | Not reported |
1q21+ = chromosome arm 1q21; CSR = Clinical Study Report; DCyBorD = daratumumab-cyclophosphamide-bortezomib-dexamethasone; DRd = daratumumab-lenalidomide-dexamethasone; DVMP = daratumumab-bortezomib-melphalan-prednisone; ECOG PS = Eastern Cooperative Oncology Group Performance Status; IgG = immunoglobulin G; ISS = International Staging System; LDH = lactate dehydrogenase; MAIC = matching-adjusted indirect comparison; Rd = lenalidomide-dexamethasone.
Source: Indirect Treatment Comparisons for Isatuximab Combined with Bortezomib, Lenalidomide and Dexamethasone in Transplant-Ineligible Newly Diagnosed Multiple Myeloma.46
Results of ITC and Nonrandomized Study
Results
Overview of Included Studies and Data Sources to Support the ITC and Nonrandomized Study
An overview of the set of studies used to support ITCs between IsaVRd and each of DRd, DVMP, DCyBorD, Rd, and CyBorD is provided in Table 18. An unanchored MAIC was required for comparisons with all treatments except CyBorD, in which IPW was conducted. A summary of the sources of heterogeneity between each trial and the IMROZ study is available in Table 19.
Evidence Networks
Given multiple MAICs were performed to compare IsaVRd and relevant comparators, there are no networks available. Networks were created for NMAs performed as exploratory analyses and are not presented herein.
Table 18: Summary of Data Sources Used for MAIC and IPW
Treatment | Study or data source | Sample size | Study design | Country | OS data source | PFS data source |
|---|---|---|---|---|---|---|
IsaVRd | IMROZ study | 265 | RCT, open-label, phase III | Multicentre international | Individual patient data | Individual patient data |
MAIC (unanchored) | ||||||
DRd | MAIA study | 368 | RCT, open-label, phase III | Multicentre international | Technical Appraisal guidance document TA91747 | Kumar et al. (2022)48 |
DVMP | ALCYONE study | 350 | RCT, open-label, phase III | Multicentre international | Mateos et al. (2022)49 | Mateos et al. (2022)49 |
DCyBorD | Yimer et al. study50 | 48 | Single-arm, open-label, phase II | US | Yimer et al. study50 | Not available |
Rd | MAIA study | 369 | RCT, open-label, phase III | Multicentre international | Technical Appraisal guidance document TA91747 | Kumar et al. (2022)48 |
FIRST study | 535 | RCT, open-label, phase III | Multicentre international | Facon et al. (2018)51 | Facon et al. (2018)51 | |
IPW | ||||||
CyBorD | Flatiron Health data source | 249 | Retrospective cohort study | US | Individual patient data45 | Individual patient data45 |
CyBorD = cyclophosphamide-bortezomib-dexamethasone; DCyBorD = daratumumab-cyclophosphamide-bortezomib-dexamethasone; DRd = daratumumab-lenalidomide-dexamethasone; DVMP = daratumumab-bortezomib-melphalan-prednisone; IPW = inverse probability weighting; IsaVRd = isatuximab-bortezomib-lenalidomide-dexamethasone; MAIC = matching-adjusted indirect comparison; OS = overall survival; PFS = progression-free survival; RCT = randomized controlled trial; Rd = lenalidomide-dexamethasone.
Source: Indirect Treatment Comparisons for Isatuximab Combined with Bortezomib, Lenalidomide and Dexamethasone in Transplant-Ineligible Newly Diagnosed Multiple Myeloma.46
Table 19: Summary of Heterogeneity Between IMROZ Study and Data Sources Used for MAIC and IPW
Study or data source | Comparison supported | Heterogeneity between comparator evidence and IMROZ study |
|---|---|---|
MAIA study | DRd, Rd |
|
ALCYONE study | DVMP |
|
Yimer et al. study50 | DCyBorD |
|
FIRST study | Rd |
|
Flatiron Health data | CyBorD |
|
ASCT = allogeneic stem cell transplant; CyBorD = cyclophosphamide-bortezomib-dexamethasone; DCyBorD = daratumumab-cyclophosphamide-bortezomib-dexamethasone; DRd = daratumumab-lenalidomide-dexamethasone; DVMP = daratumumab-bortezomib-melphalan-prednisone; IPW = inverse probability weighting; ISS = International Staging System; MAIC = matching-adjusted indirect comparison; OS = overall survival; Rd = lenalidomide-dexamethasone; SCT = stem cell transplant; vs. = versus.
Source: Indirect Treatment Comparisons for Isatuximab Combined with Bortezomib, Lenalidomide and Dexamethasone in Transplant-Ineligible Newly Diagnosed Multiple Myeloma.46
Efficacy
IsaVRd Versus DRd (MAIA Study)
Baseline Characteristics
The unanchored MAIC of IsaVRd compared to DRd using the MAIA study was conducted employing the following matching characteristics: age, ISS stage, ECOG PS score, cytogenetic risk, creatinine clearance, and MM type. Chromosomal abnormality 1q21+, LDH levels, and frailty were not reported in the MAIA study so were not included in the weighting. The effective sample size (ESS) of the weighted IsaVRd population was ███ patients after matching, which is ███ of the original sample size (N = 265).
Table 20 shows the patient baseline characteristics for IsaVRd and DRd before and after matching. Characteristics reported for the MAIC that were not included in the matching included sex, race, and time since diagnosis.
Table 20: Baseline Characteristics Before and After Matching — IsaVRd (IMROZ Study) Versus DRd (MAIA Study)
Characteristic | IMROZ study (IsaVRd) | MAIA study (DRd) N = 368 | |
|---|---|---|---|
Before matching (N = 265) | After matching (ESS = ███ ██████ | ||
Age, years, mean | 71.7 | ████ | ██ |
Male, % | 54 | ██ | ██ |
Race, % | |||
White | 73 | ██ | ██ |
Other | 14 | ██ | ██ |
Missing or not reported | 13 | ██ | ██ |
ISS stage, % | |||
I | 34 | ██ | ██ |
II | 41b | ██ | ██ |
III | 25 | ██ | ██ |
ECOG PS score, % | |||
0 to 1 | 89 | ██ | ██ |
≥ 2 | 11 | ██ | ██ |
Cytogenic risk, % | |||
High | 15 | ██ | ██ |
Standard | 78 | ██ | ██ |
Missing | 7 | ██ | ██ |
Time since diagnosis, months, mean | 2.03 | ████ | ████ |
Multiple myeloma type, % | |||
IgG | 65 | ██ | ██ |
Non-IgG | 35 | ██ | ██ |
Creatinine clearance, % | |||
< 60 mL per minute | 25 | ██ | ██ |
≥ 60 mL per minute | 75 | ██ | ██ |
LDH levels, IU/L, mean | 178 | █████ | ██ |
DRd = daratumumab-lenalidomide-dexamethasone; ECOG PS = Eastern Cooperative Oncology Group Performance Status; ESS = effective sample size; IgG = immunoglobulin G; IsaVRd = isatuximab-bortezomib-lenalidomide-dexamethasone; ISS = International Staging System; LDH = lactate dehydrogenase; NR = not reported.
Note: Matching characteristics included age, ISS stage, ECOG PS score, cytogenetic risk, and multiple myeloma type.
aAssumed based on the median.
bMissing ISS stage was grouped into ISS stage II because this was the largest group.
Source: Indirect Treatment Comparisons for Isatuximab Combined with Bortezomib, Lenalidomide and Dexamethasone in Transplant-Ineligible Newly Diagnosed Multiple Myeloma.46
Progression-Free Survival
The MAIC of IsaVRd versus DRd suggests that the relative treatment effect between IsaVRd and DRd is slightly less when adjusting for differences in patient characteristics. This is shown by the smaller difference in the KM curves and the corresponding change in the difference in restricted mean survival from ████ months (95% CI, ████ ██ ████ months) before weighting to ████ months (95% CI, █████ ██ ████ months) after weighting.
Proportional hazards between the adjusted IsaVRd and DRd PFS data were tested using LCH plots and Schoenfeld residual plots. The LCH curves overlapped initially and were not approximately parallel, indicating hazards are nonproportional. This is also reflected in the Schoenfeld plot, which showed a slight arc in the log HR. However, the Schoenfeld test was not statistically significant (P = 0.721). Findings suggest that the proportional hazards assumption may not be valid, meaning a constant HR may provide a biased estimate of the relative treatment effect. As such, time-varying HRs estimated from weighted parametric survival models are preferred.
Associated landmark HRs show an HR of ████ (95% CI, ████ ██ ████) at 1 year and ████ (95% CI, ████ ██ ████) at 5 years (Table 21). Following the end of the IMROZ trial follow-up (5.67 years), the HR was ████ (95% CI, ████ ██ ████). However, the 95% CIs overlap 1 throughout the time period, suggesting no statistically significant treatment effect.
Overall Survival
Similar to PFS, the relative treatment effect between IsaVRd and DRd was reduced following adjustment, shown by the smaller difference in the KM curves and by the smaller difference in restricted mean survival, which reduced from ████ months (95% CI, ████ ██ ████) before matching to ████ months (95% CI, █████ ██ ████) following adjustment.
Similar to PFS, the assessment of LCH and Schoenfeld residual plots showed that the proportional hazards assumption may not be appropriate for OS. As such, constant HRs may be subject to bias and not provide reliable relative effect estimates. Because of this, time-varying HRs estimated from weighted parametric survival models are preferred.
Results for all distributions suggest that IsaVRd provides a lower hazard of death (HR < 1) throughout the entire time period; however, results are not statistically significant. For the Gompertz distribution, the HR decreases linearly over time with an estimated HR of ████ (95% CI, ████ ██ ████) at 1 year and ████ (95% CI, ████ ██ ████) at 5 years (Table 22).
Table 21: Landmark HRs for PFS — IsaVRd (IMROZ Study) Vs. DRd (MAIA Study)
Time (years) | HR (95% CI) for IsaVRd vs. DRd | ||||||
|---|---|---|---|---|---|---|---|
Exponential | Gamma | Generalized gamma | Gompertz | Log-logistic | Log-normal | Weibull | |
1 | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
2 | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
5 | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
5.67a | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
10 | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
28 | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ ██████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
CI = confidence interval; DRd = daratumumab-lenalidomide-dexamethasone; HR = hazard ratio; IsaVRd = isatuximab-bortezomib-lenalidomide-dexamethasone; PFS = progression-free survival; vs. = versus.
Notes: An HR of less than 1 indicates a reduced hazard of progression or death for IsaVRd. Bolded values indicate the preferred model.
aMaximum IMROZ study follow-up.
Source: Indirect Treatment Comparisons for Isatuximab Combined with Bortezomib, Lenalidomide and Dexamethasone in Transplant-Ineligible Newly Diagnosed Multiple Myeloma.46
Table 22: Landmark HRs for OS — IsaVRd (IMROZ Study) Vs. DRd (MAIA Study)
Time (years) | HR (95% CI) for IsaVRd vs. DRd | ||||||
|---|---|---|---|---|---|---|---|
Exponential | Gamma | Generalized gamma | Gompertz | Log-logistic | Log-normal | Weibull | |
1 | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
2 | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
5 | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
5.67a | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
10 | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
28 | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ ██████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
CI = confidence interval; DRd = daratumumab-lenalidomide-dexamethasone; HR = hazard ratio; IsaVRd = isatuximab-bortezomib-lenalidomide-dexamethasone; OS = overall survival; vs. = versus.
Notes: An HR of less than 1 indicates reduced a hazard of death for IsaVRd. Bolded values indicate the preferred distribution.
aMaximum IMROZ study follow-up.
Source: Indirect Treatment Comparisons for Isatuximab Combined with Bortezomib, Lenalidomide and Dexamethasone in Transplant-Ineligible Newly Diagnosed Multiple Myeloma.46
IsaVRd Versus DVMP (ALCYONE Study)
Baseline Characteristics
The MAIC for IsaVRd versus DVMP was initially conducted using the following matching characteristics: age, ISS stage, ECOG PS score, cytogenetic risk, MM type, and creatinine clearance. However, the ESS of the weighted population was very low (██ █████████ ████ of the original sample size). Additionally, extreme weights were estimated for some patients (e.g., | ███████ ███ █ ██████ ██ ████). To preserve the ESS, creatinine clearance was excluded from the weighting as it was the variable ranked lowest (of those adjusted for) by clinicians. Additionally, chromosomal abnormality 1q21+, LDH levels, and frailty were not reported in the ALCYONE study, so they were not included in the weighting. The ESS of the weighted IsaVRd population following the exclusion of creatinine clearance was ███ █████████ █████ ██ ███ of the original sample size.
Table 23 shows the patient baseline characteristics before and after matching. Patient populations with respect to the matching variables were well balanced following adjustment. Characteristics reported for the ALCYONE study that were not part of the weighing included sex, race, time since diagnosis, and creatinine clearance. The matched IsaVRd population has a greater proportion of patients who were male, a lower proportion of patients who were white, and a marginally longer time since diagnosis compared with the DVMP population. Creatinine clearance was removed from the analyses to preserve ESS, so there is an imbalance between treatments for this characteristic. The matched IsaVRd population has a greater proportion of patients with creatinine clearance of more than 60 mL per minute compared with the DVMP population.
Progression-Free Survival
The MAIC of IsaVRd versus DVMP suggests that the relative treatment effect between IsaVRd and DVMP is less when adjusting for differences in patient characteristics. This is shown by the smaller difference in the KM curves and the corresponding change in the difference in restricted mean survival from █████ months (95% CI, ████ ██ █████ months) before matching to █████ months (95% CI, ████ ██ █████ months) after matching.
Proportional hazards between the adjusted IsaVRd and DVMP PFS data were tested using LCH plots and Schoenfeld residual plots. The LCH curves overlapped during the █████ ██ ██████ before separating, indicating hazards were nonproportional. This is also reflected in the Schoenfeld plot, which showed the log HR did not form an approximate straight line. However, the Schoenfeld test was not statistically significant (P = 0.687). Overall, findings suggest the proportional hazards assumption may not be valid, meaning a constant HR may provide a biased estimate of the relative treatment effect. As such, time-varying HRs estimated from weighted parametric survival models are preferred.
Results for the gamma distribution suggest IsaVRd provides a lower hazard of progression or death (HR < 1). The HR is estimated to be ████ (95% CI, ████ ██ ████) at 1 year and ████ (95% CI, ████ ██ ████) at 5 years (Table 24).
Overall Survival
The MAIC of IsaVRd versus DVMP suggests that the relative treatment effect between IsaVRd and DVMP is less when adjusting for differences in patient characteristics. This is shown by the smaller difference in the KM curves and the corresponding change in the difference in restricted mean survival from ████ months (95% CI, ████ ██ ████ months) before matching to ████ months (95% CI, █████ ██ ████ months) after matching.
Similar to PFS, the assessment of LCH and Schoenfeld residual plots showed the proportional hazards assumption may also not be appropriate for OS. The LCH curves were not approximately parallel, crossing at approximately ██ ██████ and overlapping from approximately ██ ██████. Furthermore, the Schoenfeld plot showed an arc in the log HR over time, suggesting nonproportional hazards, although the Schoenfeld test was not statistically significant (P = 0.191). As the proportional hazards assumption is questionable, constant HRs may be subject to bias and not provide reliable relative effect estimates. Because of this, time-varying HRs estimated from weighted parametric survival models are preferred.
For the Gompertz distribution, the time-varying HR was monotonically decreasing and tended toward 0 over time. The estimated HR was ████ (95% CI, ████ ██ █████ at 1 year and ████ (95% CI, ████ ██ █████ at 5 years. The extrapolated HR estimates toward the end of the time period are implausible, with an estimate of ████ (95% CI, ████ ██ █████ at 28 years (Table 25).
Table 23: Baseline Characteristics Before and After Matching — IsaVRd (IMROZ Study) Versus DVMP (ALCYONE Study)
Characteristic | IMROZ study (IsaVRd) | ALCYONE study (DVMP) N = 350 | |
|---|---|---|---|
Before matching (N = 265) | After matching (ESS = ███ ██████ | ||
Age, years, mean | 72 | ██ | ██ |
Male, % | 54 | ██ | ██ |
Race, % | |||
White | 73 | ██ | ██ |
Other | 14 | ██ | ██ |
Missing or not reported | 13 | ██ | ██ |
ISS stage, % | |||
I | 34 | ██ | ██ |
II | 41a | ██ | ██ |
III | 25 | ██ | ██ |
ECOG PS score, % | |||
0 to 1 | 89 | ██ | ██ |
≥ 2 | 11 | ██ | ██ |
Cytogenic risk, % | |||
High | 15 | ██ | ██ |
Standard | 78 | ██ | ██ |
Missing | 7 | ██ | ██ |
Time since diagnosis, months, mean | 2.03 | ███ | ████ |
Multiple myeloma type, % | |||
IgG | 65 | ██ | ██ |
Non-IgG | 35 | ██ | ██ |
Creatinine clearance, % | |||
< 60 mL per minute | 25 | ██ | ██ |
≥ 60 mL per minute | 75b | ██ | ██ |
LDH levels, IU/L, mean | 178 | █████ | ██ |
DVMP = daratumumab-bortezomib-melphalan-prednisone; ECOG PS = Eastern Cooperative Oncology Group Performance Status; ESS = effective sample size, IgG = immunoglobulin G; IsaVRd = isatuximab-bortezomib-lenalidomide-dexamethasone; ISS = International Staging System; LDH = lactate dehydrogenase; NR = not reported.
Note: Matching characteristics included age, ISS stage, ECOG PS score, cytogenetic risk, and multiple myeloma type.
aMissing ISS stage was grouped into ISS stage II because this was the largest group.
bAssumed based on the median.
Source: Indirect Treatment Comparisons for Isatuximab Combined with Bortezomib, Lenalidomide and Dexamethasone in Transplant-Ineligible Newly Diagnosed Multiple Myeloma.46
Table 24: Landmark HRs for PFS — IsaVRd (IMROZ Study) Vs. DVMP (ALCYONE Study)
Time (years) | HR (95% CI) for IsaVRd vs. DVMP | ||||||
|---|---|---|---|---|---|---|---|
Exponential | Gamma | Generalized gamma | Gompertz | Log-logistic | Log-normal | Weibull | |
1 | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
2 | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
5 | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
5.67a | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
10 | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
28 | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ ██████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
CI = confidence interval; DVMP = daratumumab-bortezomib-melphalan-prednisone; HR = hazard ratio; IsaVRd = isatuximab-bortezomib-lenalidomide-dexamethasone; PFS = progression-free survival; vs. = versus.
Notes: An HR of less than 1 indicates a reduced hazard of death for IsaVRd. Bolded values indicate the preferred distribution.
aMaximum IMROZ study follow-up.
Source: Indirect Treatment Comparisons for Isatuximab Combined with Bortezomib, Lenalidomide and Dexamethasone in Transplant-Ineligible Newly Diagnosed Multiple Myeloma.46
Table 25: Landmark HRs for OS — IsaVRd (IMROZ Study) Vs. DVMP (ALCYONE Study)
Time (years) | HR (95% CI) for IsaVRd vs. DVMP | ||||||
|---|---|---|---|---|---|---|---|
Exponential | Gamma | Generalized gamma | Gompertz | Log-logistic | Log-normal | Weibull | |
1 | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
2 | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
5 | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
5.67a | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
10 | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
28 | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
CI = confidence interval; DVMP = daratumumab-bortezomib-melphalan-prednisone; HR = hazard ratio; IsaVRd = isatuximab-bortezomib-lenalidomide-dexamethasone; OS = overall survival; vs. = versus.
Notes: An HR of less than 1 indicates a reduced hazard of death for IsaVRd. Bolded values indicate the preferred distribution.
aMaximum IMROZ study follow-up.
Source: Indirect Treatment Comparisons for Isatuximab Combined with Bortezomib, Lenalidomide and Dexamethasone in Transplant-Ineligible Newly Diagnosed Multiple Myeloma.46
IsaVRd Versus DCyBorD
Baseline Characteristics
The MAIC for IsaVRd versus DCyBorD could only be conducted for PFS as OS data were not reported for the Yimer et al. study.50 Analyses were conducted using the following matching characteristics: age, ECOG PS score, ISS stage, cytogenetic risk, and MM type. Chromosomal abnormality 1q21+, LDH levels, creatinine clearance levels, and frailty were not reported in the Yimer et al. study, so were not included in the weighting. The ESS of the weighted IsaVRd population was ██ █████████ █████ ██ ███ of the original sample size. In addition, there was evidence of extreme (very high or very low) weights. This low ESS is likely due to the small overlap in cytogenetic risk distributions, where ███ of the IsaVRd population were high-risk compared with ███ in the Yimer et al. study.
Table 26 shows the patient baseline characteristics for IsaVRd and DCyBorD before and after weighting. Patient populations with respect to the matching variables were well balanced following adjustment. Characteristics reported for the Yimer et al. study that were not part of the matching included sex and time since diagnosis. The weighted IsaVRd population had a lower proportion of patients who were male and shorter mean time since diagnosis.
Table 26: Baseline Characteristics Before and After Matching — IsaVRd (IMROZ Study) Versus DCyBorD (Yimer et al. Study50)
Characteristic | IMROZ study (IsaVRd) | Yimer et al. study (DCyBorD) N = 48 | |
|---|---|---|---|
Before matching (N = 265) | After matching (N = ██ ██████ | ||
Age, years, mean | 72 | ██ | ██| |
Male, % | 54 | ██ | ██ |
Race, % | |||
White | 73 | ██ | ██ |
Other | 14 | ██ | ██ |
Missing or not reported | 13 | ██ | ██ |
ISS stage, % | |||
I | 34 | ██ | ██ |
II | 41b | ██ | ██ |
III | 25 | ██ | ██ |
ECOG PS score, % | |||
0 to 1 | 89 | ██ | ██ |
≥ 2 | 11 | ██ | ██ |
Cytogenic risk, % | |||
High | 15 | ██ | ██ |
Standard | 78 | ██ | ██ |
Missing | 7 | ██ | ██ |
Time since diagnosis, months, mean | 2.03 | ███ | ████ |
Multiple myeloma type, % | |||
IgG | 65 | ██ | ██ |
Non-IgG | 35 | ██ | ██ |
Creatinine clearance, % | |||
< 60 mL per minute | 25 | ██ | ██ |
≥ 60 mL per minute | 74 | ██ | ██ |
LDH levels, IU/L, mean | 178 | █████ | ██ |
DCyBorD = daratumumab-cyclophosphamide-bortezomib-dexamethasone; ECOG PS = Eastern Cooperative Oncology Group Performance Status; IgG = immunoglobulin G; IsaVRd = isatuximab-bortezomib-lenalidomide-dexamethasone; ISS = International Staging System; LDH = lactate dehydrogenase; NR = not reported.
Notes: Matching characteristics included age, ISS stage, ECOG PS score, cytogenetic risk, and multiple myeloma type.
aAssumed based on the median.
bMissing ISS stage was grouped into ISS stage II because this was the largest group.
Source: Indirect Treatment Comparisons for Isatuximab Combined with Bortezomib, Lenalidomide and Dexamethasone in Transplant-Ineligible Newly Diagnosed Multiple Myeloma.46
Progression-Free Survival
The MAIC of IsaVRd versus DCyBorD suggests that the relative treatment effect between IsaVRd and DCyBorD is greater when adjusting for differences in patient characteristics. This is shown by the larger difference in the KM curves and the corresponding change in the difference in restricted mean survival from ████ months (95% CI, █████ ██ ████ months) before matching to ████ months (95% CI, █████ ██ ████ months) after matching.
Proportional hazards between the adjusted IsaVRd and DCyBorD PFS data were tested using LCH plots and Schoenfeld residual plots. The LCH curves crossed once initially but appeared approximately proportional thereafter. The Schoenfeld plot showed a decreasing log HR over time, suggesting nonproportionality. However, the Schoenfeld test was not statistically significant (P = 0.241). There is some doubt that the proportional hazards assumption may not be valid given the shape of the Schoenfeld plot; however, the LCH curves did not show obvious signs of nonproportional hazards.
Results for the gamma distribution suggest IsaVRd provides a lower hazard of progression or death (HR < 1) over time; however, results are not statistically significant because the 95% CI overlaps 1 throughout time. The HR is estimated to be ████ (95% CI, ██████ ████) at 1 year and ████ (95% CI, ████ ██ █████ at 5 years (Table 27).
Table 27: Landmark HRs for PFS — IsaVRd (IMROZ Study) Vs. DCyBorD (Yimer et al. study50)
Time (years) | HR (95% CI) for IsaVRd vs. DCyBorD | |||||
|---|---|---|---|---|---|---|
Exponential | Gamma | Generalized gamma | Log-logistic | Log-normal | Weibull | |
1 | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
2 | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
5 | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
5.67a | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
10 | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
28 | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ ██████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ ██████ |
CI = confidence interval; DCyBorD = daratumumab-cyclophosphamide-bortezomib-dexamethasone; HR = hazard ratio; IsaVRd = isatuximab-bortezomib-lenalidomide-dexamethasone; PFS = progression-free survival; vs. = versus.
Notes: An HR of less than 1 indicates a reduced hazard of progression or death for IsaVRd. Bolded values indicate the preferred distribution. Gompertz has been removed due to implausible estimates of survival.
aMaximum IMROZ study follow-up.
Source: Indirect Treatment Comparisons for Isatuximab Combined with Bortezomib, Lenalidomide and Dexamethasone in Transplant-Ineligible Newly Diagnosed Multiple Myeloma.46
IsaVRd Versus Rd (MAIA Study)
Baseline Characteristics
For analyses versus Rd using the MAIA study, the following characteristics were adjusted for in analyses: age, ISS stage, ECOG PS score, cytogenetic risk, creatinine clearance, and MM type. Chromosomal abnormality 1q21+, LDH levels, and frailty were not reported in the MAIA study, so were not included in the weighting. The ESS of the weighted IsaVRd population was ███ ████████ after weighting, which is ███ of the original sample size (N = 265). Table 28 shows the patient baseline characteristics for IsaVRd and Rd before and after weighting. Patient populations with respect to the matching variables were well balanced following adjustment. Characteristics reported for the MAIA study that were not included in the weighting included sex, race, and time since diagnosis. Patients receiving IsaVRd and Rd had similar proportions of patients who were male and mean time since diagnosis before and after weighting. Patients receiving Rd had a greater proportion of patients who were white than patients receiving IsaVRd.
Table 28: Baseline Characteristics of IsaVRd and Rd Before and After Matching
Characteristic | IsaVRd (IMROZ study) | Rd (MAIA study) N = 369 | |
|---|---|---|---|
Before matching N = 265 | After matching ESS = ███ █████ | ||
Age, years, mean | 72 | ██ | ██ |
Male, % | 54 | ██ | ██ |
Race, % | |||
White | 73 | ██ | ██ |
Other | 14 | ██ | ██ |
Missing or not reported | 13 | ██ | ██ |
ISS stage, % | |||
I | 34 | ██ | ██ |
II | 41a | ██ | ██ |
III | 25 | ██ | ██ |
ECOG PS score, % | |||
0 to 1 | 89 | ██ | ██ |
≥ 2 | 11 | ██ | ██ |
Cytogenetic risk, % | |||
High | 15 | ██ | ██ |
Standard | 78 | ██ | ██ |
Missing | 7 | ██ | ██ |
Multiple myeloma type, % | |||
IgG | 65 | ██ | ██ |
Non-IgG | 35 | ██ | ██ |
Creatinine clearance, % | |||
≤ 60 mL per minute | 25 | ██ | ██ |
> 60 mL per minute | 75b | ██ | ██ |
LDH levels, IU/L, mean | 178 | █████ | ██ |
Time since diagnosis, months, mean | 2.03 | ███ | ████ |
ECOG PS = Eastern Cooperative Oncology Group Performance Status; ESS = effective sample size, IgG = immunoglobulin G; IsaVRd = isatuximab-bortezomib-lenalidomide-dexamethasone; ISS = International Staging System; LDH = lactate dehydrogenase; NA = not applicable; NR = not reported; Rd = lenalidomide-dexamethasone.
Note: Matching characteristics included age, ISS stage, ECOG PS score, cytogenetic risk, creatinine clearance, and multiple myeloma type.
aMissing patients were grouped into the largest category.
bAssumed based on the median.
Source: Indirect Treatment Comparisons for Isatuximab Combined with Bortezomib, Lenalidomide and Dexamethasone in Transplant-Ineligible Newly Diagnosed Multiple Myeloma.46
Progression-Free Survival
The MAIC of IsaVRd versus Rd suggests that the relative treatment effect between IsaVRd and Rd is slightly less when adjusting for differences in patient characteristics. This is shown by the smaller difference in the KM curves and the difference in restricted mean survival. Following adjustment, the difference in restricted mean survival reduces from █████ months (95% CI, █████ ██ █████ months) before matching to █████ months (95% CI, ████ ██ █████ months) after matching. Proportional hazards between the adjusted IsaVRd and Rd PFS data were tested using LCH plots and Schoenfeld residual plots. The Schoenfeld plot suggests a mostly horizontal log HR with no statistical significance on the Schoenfeld test (P > 0.05); however, the LCH curves cross at approximately | ██████ indicating nonproportional hazards. Therefore, constant HRs may provide a biased estimate of the relative treatment effect. As such, time-varying HRs estimated from weighted parametric survival models are preferred.
Results suggest IsaVRd provides a significantly lower hazard of progression or death (HR < 1). Associated landmark HR estimates show an HR of ████ (95% CI, ████ ██ ████) at 1 year and ████ (95% CI, ████ ██ ████) at 5 years for the gamma distribution (Table 29).
Table 29: Landmark HRs for PFS — IsaVRd (IMROZ Study) Vs. Rd (MAIA Study)
Time (years) | HR (95% CI) for IsaVRd vs. Rd | ||||||
|---|---|---|---|---|---|---|---|
Exponential | Gamma | Generalized gamma | Gompertz | Log-logistic | Log-normal | Weibull | |
1 | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
2 | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
5 | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
5.67a | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
10 | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
28 | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ ██████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
CI = confidence interval; HR = hazard ratio; IsaVRd = isatuximab-bortezomib-lenalidomide-dexamethasone; PFS = progression-free survival; Rd = lenalidomide-dexamethasone; vs. = versus.
Notes: An HR of less than 1 indicates a reduced hazard of progression or death for IsaVRd. Bolded values indicate the preferred model.
aMaximum IMROZ study follow-up.
Source: Indirect Treatment Comparisons for Isatuximab Combined with Bortezomib, Lenalidomide and Dexamethasone in Transplant-Ineligible Newly Diagnosed Multiple Myeloma.46
Overall Survival
Similar to PFS, the relative treatment effect between IsaVRd and Rd is reduced following adjustment as shown by the smaller difference in KM curves and restricted mean survival. Following adjustment, the difference in restricted mean survival reduced from ████ months (95% CI, ████ ██ █████ months) to ████ months (95% CI, ████ ██ ████ months).
Similar to PFS, the assessment of LCH and Schoenfeld residual plots showed the proportional hazards assumption may not be appropriate for OS. Results suggest a potential violation of the proportional hazards assumption. The Schoenfeld plot suggests a mostly horizontal log HR with no statistical significance on the Schoenfeld test (P > 0.05); however, the LCH curves cross at approximately ██ ██████. As such, constant HRs may provide a biased estimate of the relative treatment effect; time-varying HRs estimated from weighted parametric survival models are preferred.
Landmark HR estimates show an HR of ████ (95% CI, ████ ██ ████) at 1 year and ████ (95% CI, ████ ██ ████) at 5 years (Table 30). The HR for the Gompertz distribution is monotonically decreasing and tends toward 0 at 28 years, meaning results at later time points may be implausible.
Table 30: Landmark HRs for OS — IsaVRd (IMROZ Study) Vs. Rd (MAIA Study)
Time (years) | HR (95% CI) for IsaVRd vs. Rd | ||||||
|---|---|---|---|---|---|---|---|
Exponential | Gamma | Generalized gamma | Gompertz | Log-logistic | Log-normal | Weibull | |
1 | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
2 | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
5 | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
5.67a | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
10 | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
28 | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ ██████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
CI = confidence interval; HR = hazard ratio; IsaVRd = isatuximab-bortezomib-lenalidomide-dexamethasone; OS = overall survival; Rd = lenalidomide-dexamethasone; vs. = versus.
Notes: An HR of less than 1 indicates a reduced hazard of death for IsaVRd. Bolded values indicate the preferred distribution.
aMaximum IMROZ study follow-up.
Source: Indirect Treatment Comparisons for Isatuximab Combined with Bortezomib, Lenalidomide and Dexamethasone in Transplant-Ineligible Newly Diagnosed Multiple Myeloma.46
IsaVRd Versus Rd (FIRST Study)
Baseline Characteristics
For analyses versus Rd using the FIRST study, the following characteristics were adjusted for in analyses: age, ISS stage, ECOG PS score, cytogenetic risk, creatinine clearance, MM type, and LDH level. Chromosomal abnormality 1q21+ and frailty were not reported in the FIRST study, so they were not included in the weighting. The ESS of the weighted IsaVRd population was ███ █████████ ███ of the original sample size (N = 265). Table 31 shows the patient baseline characteristics for IsaVRd and Rd before and after weighting. Patient populations with respect to the matching variables were well balanced following adjustment. Characteristics reported for the FIRST study that were not used in the weighting included sex. The IsaVRd and Rd patients had similar proportions of male patients before and after weighting.
Table 31: Baseline Characteristics of IsaVRd and Rd Before and After Matching
Characteristic | IsaVRd (IMROZ study) | Rd (FIRST study) N = 535 | |
|---|---|---|---|
Before matching N = 265 | After matching ESS = ███ █████ | ||
Age, years, mean | 72 | ██ | ██ |
Male, % | 54 | ██ | ██ |
Race, % | |||
White | 73 | ██ | ██ |
Other | 14 | ██ | ██ |
Missing or not reported | 13 | ██ | ██ |
ISS stage, % | |||
I | 34 | ██ | ██ |
II | 41a | ██ | ██ |
III | 25 | ██ | ██ |
ECOG PS score, % | |||
0 to 1 | 89 | ██ | ██ |
≥ 2 | 11 | ██ | ██ |
Cytogenetic risk, % | |||
High | 15 | ██ | ██ |
Standard | 78 | ██ | ██ |
Missing | 7 | || | || |
Multiple myeloma type, % | |||
IgG | 65 | ██ | ██ |
Non-IgG | 35 | ██ | ██ |
Creatinine clearance, % | |||
≤ 60 mL per minute | 25 | ██ | ██ |
> 60 mL per minute | 75b | ██ | ██ |
LDH levels, % | |||
< 200 IU/L | 66 | ██ | ██ |
≥ 200 IU/L | 34 | ██ | ██ |
Time since diagnosis, months, mean | 2.03 | ███ | ██ |
ECOG PS = Eastern Cooperative Oncology Group Performance Status; ESS = effective sample size, IgG = immunoglobulin G; IsaVRd = isatuximab-bortezomib-lenalidomide-dexamethasone; ISS = International Staging System; LDH = lactate dehydrogenase; NR = not reported; Rd = lenalidomide-dexamethasone.
Note: Matching characteristics included age, ISS stage, ECOG PS score, cytogenetic risk, creatinine clearance, and multiple myeloma type.
aMissing patients were grouped into the largest category.
bAssumed based on the median.
Source: Indirect Treatment Comparisons for Isatuximab Combined with Bortezomib, Lenalidomide and Dexamethasone in Transplant-Ineligible Newly Diagnosed Multiple Myeloma.46
Progression-Free Survival
The relative treatment effect between IsaVRd and Rd reduces when adjusting for differences in patient characteristics, shown by the smaller difference in the KM curves. The difference in RMST following adjustment decreases from ██ months (95% CI, █████ ██ █████ months) to █████ months (95% CI, █████ ██ █████ months).
Proportional hazards between the adjusted IsaVRd and Rd PFS data were tested using LCH plots and Schoenfeld residual plots. Results suggest a potential violation of the proportional hazards assumption. The Schoenfeld plot suggests a mostly horizontal log HR with no statistical significance on the Schoenfeld test (P > 0.05); however, the LCH curves cross up to approximately | ██████. Therefore, constant HRs may provide a biased estimate of the relative treatment effect. As such, time-varying HRs estimated from weighted parametric survival models are preferred.
Results suggest IsaVRd provides a significantly lower hazard of progression or death (HR < 1). Associated landmark HR estimates (Table 32) show an HR of ████ (95% CI, ████ ██ ████) at 1 year and ████ (95% CI, ████ ██ ████) at 5 years for the gamma distribution.
Overall Survival
Similar to PFS, the relative treatment effect between IsaVRd and Rd is reduced following adjustment, as shown by the KM curve and the difference in RMST. Following adjustment, the difference in RMST reduced from ████ months (95% CI, ████ ██ █████ months) to ████ months (95% CI, ████ ██ █████ months).
Proportional hazards between the adjusted IsaVRd and Rd PFS data were tested using LCH plots and Schoenfeld residual plots. Results suggest a potential violation of the proportional hazards assumption. The Schoenfeld plot suggests a mostly horizontal log HR with no statistical significance on the Schoenfeld test (P > 0.05); however, the LCH curves are not parallel throughout the time period. Therefore, constant HRs may provide a biased estimate of the relative treatment effect. As such, time-varying HRs estimated from weighted parametric survival models are preferred.
Landmark HR estimates (Table 33) show an HR of ████ (95% CI, █████ ████) at 1 year and ████ (95% CI, █████ ████) at 5 years for the Gompertz distribution. The HR for the Gompertz distribution is monotonically decreasing, meaning results at later time points may be implausible.
Table 32: Landmark HRs for PFS — IsaVRd (IMROZ Study) Vs. Rd (FIRST Study)
Time (years) | HR (95% CI) for IsaVRd vs. Rd | ||||||
|---|---|---|---|---|---|---|---|
Exponential | Gamma | Generalized gamma | Gompertz | Log-logistic | Log-normal | Weibull | |
1 | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
2 | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
5 | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
5.67a | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
10 | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
28 | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | █████ ██████ ███████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
CI = confidence interval; HR = hazard ratio; IsaVRd = isatuximab-bortezomib-lenalidomide-dexamethasone; PFS = progression-free survival; Rd = lenalidomide-dexamethasone; vs. = versus.
Notes: An HR of less than 1 indicates a reduced hazard of progression or death for IsaVRd. Bolded values indicate the preferred distribution.
aMaximum IMROZ study follow-up.
Source: Indirect Treatment Comparisons for Isatuximab Combined with Bortezomib, Lenalidomide and Dexamethasone in Transplant-Ineligible Newly Diagnosed Multiple Myeloma.46
Table 33: Landmark HRs for OS — IsaVRd (IMROZ Study) Vs. Rd (FIRST Study)
Time (years) | HR (95% CI) for IsaVRd vs. Rd | ||||||
|---|---|---|---|---|---|---|---|
Exponential | Gamma | Generalized gamma | Gompertz | Log-logistic | Log-normal | Weibull | |
1 | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
2 | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
5 | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
5.67a | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
10 | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
28 | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ ██████ | ████ ██████ ██████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
CI = confidence interval; HR = hazard ratio; IsaVRd = isatuximab-bortezomib-lenalidomide-dexamethasone; OS = overall survival; Rd = lenalidomide-dexamethasone; vs. = versus.
Notes: An HR of less than 1 indicates a reduced hazard of death for IsaVRd. Bolded values indicate the preferred distribution.
aMaximum IMROZ study follow-up.
Source: Indirect Treatment Comparisons for Isatuximab Combined with Bortezomib, Lenalidomide and Dexamethasone in Transplant-Ineligible Newly Diagnosed Multiple Myeloma.46
IsaVRd Versus CyBorD (Flatiron Health Data Source)
Baseline Characteristics
This section presents the results of the population-adjusted comparisons for IsaVRd versus CyBorD using the IMROZ trial and data from the Flatiron Health dataset, respectively. Unlike the MAICs presented in the preceding sections, these analyses used IPW to balance populations due to the availability of PLD for each treatment. It was also possible to weight the CyBorD population to be similar to the IsaVRd population, unlike the MAICs, which weighed the IsaVRd population to be more similar to the comparator population due to the lack of PLD in the comparator study. The ESS of the weighted CyBorD population was ███ ████████ following adjustment, which is ███ of the original sample size. Note that a 99th percentile trimming approach was applied due to the estimation of extreme weights. As such, the | ████████ with the largest weights ████ ███ ██████ ████ █████ ██ ████
Table 34 shows the patient baseline characteristics for IsaVRd and CyBorD before and after matching. Six characteristics were adjusted for in the analyses: age, ECOG PS score, ISS stage, time since diagnosis, cytogenetic risk, and chromosomal abnormality 1q21+. Patient populations with respect to these variables were well balanced following adjustment. Two characteristics available in the Flatiron Health dataset were not adjusted for in analyses (sex and race) as neither characteristic was identified as a prognostic factor or treatment effect modifier.
Table 34: Baseline Characteristics Before and After Weighting — IsaVRd (IMROZ Study) Versus CyBorD (Flatiron Health Data Source)
Characteristic | IMROZ study (IsaVRd) N = 265 | Flatiron Health data source (CyBorD) | |
|---|---|---|---|
Before weighting (N = ████ | After weighting (N = ███ ██████ | ||
Age, years, mean | 72 | ██ | ██ |
Male, % | 54 | ██ | ██ |
Race, % | |||
White | 73 | ██ | ██ |
Other | 14 | ██ | ██ |
Missing or not reported | 13 | ██ | ██ |
ISS stage, % | |||
I | 35 | ██ | ██ |
II | 41 | ██ | ██ |
III | 24 | ██ | ██ |
ECOG PS score, % | |||
0 | 46 | ██ | ██ |
1 | 42 | ██ | ██ |
≥ 2 | 11 | ██ | ██ |
Cytogenic risk, % | |||
High | 15 | ██ | ██ |
Standard | 78 | ██ | ██ |
Missing | 7 | ██ | ██ |
Chromosomal abnormality 1q21+, % | |||
Present | 36 | ██ | ██ |
Absent | 57 | ██ | ██ |
Missing | 7 | ██ | ██ |
Time since diagnosis, months, mean | 2.05 | ████ | ███ |
1q21+ = chromosome arm 1q21; CyBorD = cyclophosphamide-bortezomib-dexamethasone; ECOG PS = Eastern Cooperative Oncology Group Performance Status; IsaVRd = isatuximab-bortezomib-lenalidomide-dexamethasone; ISS = International Staging System.
Notes: Characteristics adjusted for in the analysis included age, ECOG PS score, ISS stage, time since diagnosis, cytogenic risk, and chromosomal abnormality 1q21+.
Source: Indirect Treatment Comparisons for Isatuximab Combined with Bortezomib, Lenalidomide and Dexamethasone in Transplant-Ineligible Newly Diagnosed Multiple Myeloma.46
Progression-Free Survival
The adjustment for differences in patient characteristics had little impact on the PFS of patients receiving CyBorD. The difference in RMST is slightly reduced from █████ months (95% CI, █████ ██ █████ months) to █████ months (95% CI, █████ ██ █████ months). Following adjustment, results suggest that IsaVRd provides a statistically significant reduced hazard of progression or death compared with CyBorD (HR = ████ ████ ███ ████ ██ ████).
Proportional hazards between the adjusted IsaVRd and CyBorD PFS data were tested using LCH plots and Schoenfeld residual plots. Results suggest no violation of the proportional hazards assumption. The LCH plot presents approximately parallel curves and the Schoenfeld plot suggests a mostly horizontal log HR. For consistency, time-varying HRs estimated from weighted parametric survival models are preferred.
Results suggest IsaVRd provides a statistically significant lower hazard of progression or death (HR < 1) from approximately ██ months. Associated landmark HR estimates (Table 35) are reasonably constant and show an HR of ████ (95% CI, ████ ██ ████) at 1 year and ████ (95% CI, ████ ██ ████) at 5 years. This estimate aligns with the HR estimated from the Cox proportional hazards model █████ [95% CI, ████ ██ ████]), suggesting that a constant HR may be a reasonable estimate for this comparison.
Table 35: Landmark HRs for PFS — IsaVRd (IMROZ Study) Vs. CyBorD (Flatiron Health Data Source)
Time (years) | HR (95% CI) for IsaVRd vs. CyBorD | ||||||
|---|---|---|---|---|---|---|---|
Exponential | Gamma | Generalized gamma | Gompertz | Log-logistic | Log-normal | Weibull | |
1 | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
2 | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
5 | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
5.67a | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
10 | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
28 | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ ██████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
CI = confidence interval; CyBorD = cyclophosphamide-bortezomib-dexamethasone; HR = hazard ratio; IsaVRd = isatuximab-bortezomib-lenalidomide-dexamethasone; PFS = progression-free survival; vs. = versus.
Notes: An HR of less than 1 indicates a reduced hazard of progression or death for IsaVRd. Bolded values indicate the preferred model.
aMaximum IMROZ study follow-up.
Source: Indirect Treatment Comparisons for Isatuximab Combined with Bortezomib, Lenalidomide and Dexamethasone in Transplant-Ineligible Newly Diagnosed Multiple Myeloma.46
Overall Survival
The adjustment for differences in patient characteristics had little impact on the OS of CyBorD patients. Following adjustment, results suggest that IsaVRd provides a statistically significant reduced hazard of death compared with CyBorD (HR = ████ 95% CI, ████ ██ ████). The difference in RMST is slightly larger following adjustment, increasing from ████ months (95% CI, ████ ██ █████ months) to █████ months (95% CI, ████ ██ █████ months).
Similar to PFS, the assessment of LCH and Schoenfeld residual plots showed no clear violation of the proportional hazards assumption for OS. The LCH plot presents approximately parallel curves and the Schoenfeld plot suggests a mostly horizontal log HR. For consistency, time-varying HR methods are preferred for analyses.
Results for the Gompertz distribution suggest IsaVRd provides a statistically significant lower hazard of death (HR < 1) up to approximately ██ █████. Associated landmark HR estimates (Table 36) show an HR of ████ (95% CI, ████ ██ ████) at 1 year and ████ (95% CI, ████ ██ ████) at 5 years. This suggests that there is an increasing treatment effect for IsaVRd over time and that the assumption of proportional hazards may not be appropriate. This also indicates that the HR estimated based on the Cox proportional hazards model (████ 95% CI, ████ ██ ████) may be subject to bias.
Table 36: Landmark HRs for OS — IsaVRd (IMROZ Study) Vs. CyBorD (Flatiron Health Data Source)
Time (years) | HR (95% CI) for IsaVRd vs. CyBorD | ||||||
|---|---|---|---|---|---|---|---|
Exponential | Gamma | Generalized gamma | Gompertz | Log-logistic | Log-normal | Weibull | |
1 | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
2 | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
5 | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
5.67a | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
7.17 | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
10 | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
28 | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
CI = confidence interval; CyBorD = cyclophosphamide-bortezomib-dexamethasone; HR = hazard ratio; IsaVRd = isatuximab-bortezomib-lenalidomide-dexamethasone; OS = overall survival; vs. = versus.
Notes: An HR of less than 1 indicates a reduced hazard of death for IsaVRd. Bolded values indicate the preferred model.
aMaximum IMROZ study follow-up.
Source: Clinical Systematic Literature Review Update for Treatments in Newly Diagnosed Multiple Myeloma.44
Harms
Safety outcomes were not evaluated in the ITCs performed for this submission.
Critical Appraisal of MAIC and Nonrandomized Study
No major issues were identified with regard to the systematic search for identifying relevant studies for the MAIC. However, it should be noted that the search parameters (e.g., databases searched, keywords, and free text) differed from those used in identifying clinical trials for the main analysis. Furthermore, it is uncertain if there was a systematic evaluation of options that led to choosing the Flatiron Health database for the IPW analyses, and if there are other potential databases that could have been used instead. It is possible that the use of another data source could have resulted in different conclusions. The ITC analyses were preceded by a feasibility appraisal and the decision to use MAICs and IPW as the ITC method of choice (instead of an NMA) was adequately justified.
In the MAICs, the unanchored nature of the comparison imposes the assumption that all prognostic factors and effect modifiers are adequately adjusted for, which is unlikely to be the case. As for the choice of the matching factors, it was based on internal expert opinion (rather than a survey of clinical experts) and the availability and completeness of data in the trials (which is inconsistent with the NICE Decision Support Unit guidelines, which recommend that all necessary factors be identified, regardless of availability in the data). While the availability of individual PLD for both groups in the IPW comparison allowed for the weighing of patients receiving CyBorD to resemble the IsaVRd population, it similarly required that all confounding and effect-modifying variables be adequately adjusted for to produce a valid comparison. Notably, each of the MAICs and the IPW excluded known effect-modifying or prognostic variables due to these not being reported either in the IMROZ study or the comparator studies. Chromosomal abnormality 1q21+, LDH level, and frailty were commonly missing. Many of the adjustment factors were categorized or dichotomized, which discards information and may result in residual confounding and inadequate adjustment. An assessment of the potential magnitude of residual confounding was not presented for any comparison; therefore, the extent of potential bias is unknown. The adjustment methods used cannot overcome methodological (e.g., RCT, single-arm trial, retrospective observational study design) or design differences across the comparators, which can introduce bias (e.g., region or setting, length of follow-up, outcome definitions [event and censoring rules, schedule and method of assessments], cointerventions, subsequent treatments). This is likely to be of particular concern for comparison to the RWE source, where outcome assessments and patient follow-up may differ substantially from a trial setting. Multiple imputation was used to impute missing data in the RWE data source, assuming that the data were missing at random. However, it is not clear whether this assumption is reasonable given that the extent and reasons for missing data were not described. Important outcomes for decision-making like HRQoL and AEs were not included in the analyses, even though the nonrandomized comparison included RWE, which could have provided important insights and the generation of hypotheses for future confirmation. This limits the ability to evaluate the balance of comparative benefits and harms. The MAICs and IPW for OS are subject to increased uncertainty as the data from the IMROZ trial is still immature and final data will not be available until 2027. In several cases, the CIs were wide and crossing the null, introducing further imprecision and uncertainty into the comparative effects. Generalizability may be an issue due to the small sample size remaining after the exclusions and weighting in some of the analyses. This suggests that the results are being driven by a subset of patients in the IMROZ trial (for the MAICs) or the RWE source (for the IPW). In some cases, the small ESSs after matching could also render the results unstable, with reductions ranging from ███ ██ ███ across analyses. Weighting in the MAICs makes the population for comparison more similar to the comparator studies, which might also adversely affect generalizability. Results extending beyond the follow-up period of the included studies are considered uncertain because they are based on extrapolations. In some cases, these extrapolations were clinically implausible.
Studies Addressing Gaps in the Systematic Review Evidence
No additional studies were submitted by the sponsor.
Discussion
Summary of Available Evidence
One ongoing, randomized, open-label, parallel-group, phase III trial (the IMROZ study) assessing the clinical benefit of IsaVRd compared to VRd alone in patients with newly diagnosed MM who are not eligible for an ASCT was included in the CDA-AMC review. In total, 446 patients were randomized in a 3:2 ratio to IsaVRd or VRd. Randomization was stratified by country (China versus other countries), age (younger than 70 years versus 70 years or older), and R-ISS stage (stage I to stage II versus stage III versus not classified). The primary outcome was PFS, and key secondary outcomes included OS, MRD negativity in patients with VGPR or better, and ORR. All results presented were from a second planned interim analysis, with final results for OS not expected until 2027.
In the absence of direct comparison between IsaVRd and other available treatments in Canada, the sponsor-submitted MAICs were based on individual-level data from the IMROZ study and summary data from nonrandomized studies for DVMP, DRd, Rd, and DCyBorD, and a nonrandomized comparison employing IPW methods to compare IsaVRd to CyBorD using individual PLD from an RWE source. In total, IsaVRd was compared to 4 other treatments for PFS and 5 other treatments for OS. The main comparator for the context in Canada compared isatuximab with daratumumab-based regimens (e.g., DRd, DVMP, DCyBorD). There were limited data available for assessing HRQoL or safety. No other evidence was submitted by the sponsor because no extension studies had been conducted to date.
In the IMROZ study, patients were aged an average of 71.5 years (SD = 4.8 years), and 53.1% of patients were male while 46.9% were female. Most patients had MM of the IgG subtype (64.1%) at diagnosis. The most common ISS stage at study entry was stage I (53.0%), followed by stage II (31.1%) and stage III (15.2%). Most patients (89.0%) had an ECOG PS score of 0 or 1, and some patients with an ECOG PS score of 2 or more were enrolled despite this being an exclusion criterion. The median time from initial diagnosis to randomization was 1.18 months. The main reason for transplant ineligibility was being aged 65 years or older (95.7%).
Interpretation of Results
Efficacy
Patient and clinician input received by CDA-AMC for this review indicated that outcomes such as PFS, OS, HRQoL, and safety are highly valued. The clinical experts consulted for this review confirmed that MM is not yet curable with currently available treatments, reflecting an unmet clinical need for new treatment options. Though there remains uncertainty about whether PFS can act as a valid surrogate for OS in this setting, clinical experts highlighted PFS as a key outcome of interest in trials of treatments for patients with newly diagnosed MM. Data for OS will take an extended time to accrue and are likely to be confounded by subsequent treatments.
In the IMROZ trial, IsaVRd improved PFS in comparison with VRd in patients with newly diagnosed MM who were not eligible for an ASCT or with no intent for an ASCT as initial therapy. The greatest benefit was seen on longer follow-up (e.g., 60 months). There was some risk of bias concern due to an important degree of missed disease assessments. In the VRd control group, the median PFS was 54.34 months. The addition of isatuximab to VRd improved PFS, making it “not reached” in the IsaVRd group. Therefore, more than half of the patients in the IsaVRd group had not yet experienced disease progression or death during the observation period. This would indicate that the addition of isatuximab is particularly effective, leading to longer periods without progression for many patients. The clinical experts consulted by the review team confirmed that this is clinically meaningful.
The findings related to OS are subject to several limitations, including a lack of formal testing (because the hierarchy had failed), the need for longer follow-up for the data to mature, the CIs crossing the null, and confounding due to crossover that is likely to worsen over time. PFS is not always a good surrogate for OS due to methodological challenges and sometimes weak correlations between the 2 outcome measures.52-54 Similarly, between-group comparisons of HRQoL were not formally assessed in the IMROZ study but visual inspection of the results presented in a graphical format seem to suggest that the results were similar between the groups and there was no detriment to HRQoL. The lack of statistically analyzed HRQoL data are an important limitation, given the significant impact of MM on HRQoL and the importance of this outcome to patients. It should also be noted that the clinicians commented that the currently available QoL scales need to be improved to be more user-friendly to be more incorporated into clinical practice.
While the IMROZ trial only compared the addition of isatuximab to VRd compared with VRd alone, numerous other relevant comparators were identified in the systematic review protocol, for which data were lacking head-to-head comparisons from RCTs. Of important note is daratumumab (e.g., DVMP, DRd, Rd, DCyBorD, CyBorD), which the CADTH Reimbursement Review Provisional Funding Algorithm for MM and the Formulary Management Expert Committee recommendation noted should be prioritized in this patient population.25,55 As such, alternative sources of evidence were used (e.g., PLD from the real-world Flatiron Health Electronic Medical Record database and data from non-RCTs and observational studies) to allow 2 unanchored MAIC analyses of isatuximab-containing regimens versus daratumumab-containing regimens (i.e., DRd and DVMP) to be performed. The results showed no consistent benefit with regard to PFS for isatuximab-containing regimens in the MAICs. It should also be noted that while MAICs for OS were performed, given that the final analysis for OS from the IMROZ trial will not be complete until 2027, the results are subject to important uncertainty at this time. The major limitations of the MAICs include the fact that they involved unanchored comparisons that impose the assumption that all prognostic factors and effect modifiers are adequately adjusted for, which is unlikely to be the case (and several were left out due to being unavailable), and that the final data for OS may not be available for years. Consequently, there is great uncertainty in the results obtained from the MAICs due to bias resulting from unaddressed prognostic and effect-modifying variables, differences in study design and/or conduct that cannot be adjusted for in the analyses, important reductions in ESS, and in some cases, imprecision. Finally, there was no attempt to compare HRQoL in any of the ITC analyses; however, this was expected, given that this outcome was not formally assessed in the IMROZ study.
Harms
Almost all patients in the IMROZ trial had at least 1 TEAE. There were some numerical differences in some notable harms. Diarrhea (higher in the IsaVRd group), constipation (higher in the VRd group), cataracts (higher in the VRd group), and second primary malignancies (higher in the IsaVRd group) were different between the groups. Grade 3 or higher AEs were also higher in the IsaVRd group but the risk of developing treatment-emergent SAEs was not significantly different between the groups. Further, it should be noted that these harms may be associated with the disease itself and not caused by the interventions. Infusion reactions were more common in the IsaVRd group, and though numerically more instances of infections occurred in the IsaVRd group, the overall proportions were similar between groups. Other notable harms mentioned in the product monograph for isatuximab include cardiotoxicity, second primary malignancies, neutropenia, and thrombocytopenia. Cardiotoxicity is particularly concerning in this population given that patients are often older (aged 65 years or older) and at higher baseline risk of cardiovascular disease. There was no clear and consistent indication in the IMROZ trial that the addition of isatuximab to VRd caused additional cardiotoxicity. Overall discontinuations of all study treatment were less common with IsaVRd than with VRd (52.1% versus 75.7%, respectively), with more patients in the VRd group than in the IsaVRd group discontinuing treatment due to PD (37.0% versus 14.3%, respectively). There were numerically more cases of neutropenia with IsaVRd than with VRd (30.0% versus 21.5%, respectively). Harms were not outcomes in the proposed NMAs or the MAICs submitted to CDA-AMC, and this should be considered a limitation of the indirect evidence. Therefore, the safety and tolerability of IsaVRd relative to other regimens used in MM are unknown.
Conclusion
One multinational, ongoing, open-label, phase III RCT (the IMROZ study) was included in the CDA-AMC review. In a population of 446 patients with newly diagnosed MM who were ineligible for an ASCT, IsaVRd resulted in a statistically significant improvement in PFS compared to VRd. Though the median PFS was not reached in the IsaVRd group, the clinical experts consulted by the review team considered the findings clinically meaningful. There was some concern for the potential risk of bias in the analysis of PFS due to missed disease assessments. The IMROZ trial is an ongoing study and though the results suggest that IsaVRd may improve OS compared to VRd, conclusions are limited because the data for OS were based on an interim analysis and were not formally tested. Additionally, the median results for OS had not been reached and results were considered immature. As the final analysis of OS is not yet available, the results are only considered supportive of the overall findings. The findings for OS are also limited by potential confounding by crossovers, and imprecision in the estimates (i.e., CIs crossed the null). The addition of isatuximab to VRd increased the incidence of patients with grade 3 or higher TEAEs, but the clinical experts consulted by the review team noted that the side effects were considered manageable. HRQoL seemed to be similar between groups, suggesting no detriment to QoL, but there was no statistical testing and there was increased attrition as the trial progressed.
Time-varying MAICs and IPW were used to derive comparative effect estimates for IsaVRd versus relevant comparators that were not included in the IMROZ trial. Despite the fact that these analyses suggested improved PFS with IsaVRd compared to DVMP and Rd (there was no difference detected compared to DRd, DCyBorD, and CyBorD), multiple methodological limitations rendered the evidence insufficient to draw definitive conclusions. These included a high risk of bias resulting from unaddressed prognostic and effect-modifying variables, differences in study design and/or conduct that could not be adjusted for in the analyses, important reductions in ESS, and in some cases, imprecision (i.e., CIs crossing the null). Findings for OS are subject to additional uncertainty as the data for OS from the IMROZ trial remain immature. The lack of consideration of HRQoL and harms in the indirect comparisons limits the ability to comprehensively assess the balance of comparative benefits and harms.
References
1.Brenner DR, Gillis J, Demers AA, et al. Projected estimates of cancer in Canada in 2024. CMAJ. 2024;196(18):E615-E623. doi: 10.1503/cmaj.240095 PubMed
2.Kuehl WM, Bergsagel PL. Molecular pathogenesis of multiple myeloma and its premalignant precursor. J Clin Invest. 2012;122(10):3456-63. doi: 10.1172/JCI61188 PubMed
3.International Myeloma Foundation. What is multiple myeloma? Accessed July 8, 2024. https://www.myeloma.org/what-is-multiple-myeloma
4.Yong K, Delforge M, Driessen C, et al. Multiple myeloma: patient outcomes in real-world practice. Br J Haematol. 2016;175(2):252-264. doi: 10.1111/bjh.14213 PubMed
5.Kurtin S. Relapsed or relapsed/refractory multiple myeloma. J Adv Pract Oncol. 2013;4:5-14. Accessed May 22, 2025. https://jadpro.com/media/gy1p210r/relapsed-or-relapsed-refractory-mm_kurtin.pdf
6.Usmani S, Ahmadi T, Ng Y, et al. Analysis of real-world data on overall survival in multiple myeloma patients with ≥3 prior lines of therapy including a proteasome inhibitor (PI) and an immunomodulatory drug (IMiD), or double refractory to a PI and an IMiD. Oncologist. 2016;21(11):1355-1361. doi: 10.1634/theoncologist.2016-0104 PubMed
7.Kazandjian D. Multiple myeloma epidemiology and survival: A unique malignancy. Semin Oncol. 2016;43(6):676-681. doi: 10.1053/j.seminoncol.2016.11.004 PubMed
8.Canadian Cancer Society. Multiple myeloma statistics. 2024. Accessed July 8, 2024. https://cancer.ca/en/cancer-information/cancer-types/multiple-myeloma/statistics
9.Global Cancer Observatory: Cancer Today. Multiple myeloma. International Agency for Research on Cancer; 2022. Accessed July 8, 2024. https://gco.iarc.who.int/media/globocan/factsheets/cancers/35-multiple-myeloma-fact-sheet.pdf
10.Global Cancer Observatory: Cancer Today. Country Fact Sheet: Canada. International Agency for Research on Cancer; 2022. Accessed July 8, 2024. https://gco.iarc.who.int/media/globocan/factsheets/populations/124-canada-fact-sheet.pdf
11.Bergstrom DJ, Kotb R, Louzada ML, Sutherland HJ, Tavoularis S, Venner CP. Consensus Guidelines on the Diagnosis of Multiple Myeloma and Related Disorders: Recommendations of the Myeloma Canada Research Network Consensus Guideline Consortium. Clin Lymphoma Myeloma Leuk. 2020;20(7):e352-e367. doi: 10.1016/j.clml.2020.01.017 PubMed
12.Canadian Cancer Society. Diagnosis of multiple myeloma. Accessed July 8, 2024. https://cancer.ca/en/cancer-information/cancer-types/multiple-myeloma/diagnosis
13.NCCN Guidelines. Multiple Myeloma, version 1.2025. National Comprehensive Cancer Network (NCCN); 2024. Accessed November 18, 2024. https://www.nccn.org/
14.Chng WJ, Dispenzieri A, Chim CS, et al. IMWG consensus on risk stratification in multiple myeloma. Leukemia. 2014;28(2):269-77. doi: 10.1038/leu.2013.247 PubMed
15.Sonneveld P, Avet-Loiseau H, Lonial S, et al. Treatment of multiple myeloma with high-risk cytogenetics: a consensus of the International Myeloma Working Group. Blood. 2016;127(24):2955-62. doi: 10.1182/blood-2016-01-631200 PubMed
16.Rajkumar SV. Updated Diagnostic Criteria and Staging System for Multiple Myeloma. Am Soc Clin Oncol Educ Book. 2016;35:e418-23. doi: 10.1200/EDBK_159009 PubMed
17.International Myeloma Foundation. International Myeloma Working Group (IMWG) criteria for the diagnosis of multiple myeloma. Accessed July 8, 2024. https://www.myeloma.org/international-myeloma-working-group-imwg-criteria-diagnosis-multiple-myeloma
18.D'Agostino M, Cairns DA, Lahuerta JJ, et al. Second Revision of the International Staging System (R2-ISS) for Overall Survival in Multiple Myeloma: A European Myeloma Network (EMN) Report Within the HARMONY Project. J Clin Oncol. 2022;40(29):3406-3418. doi: 10.1200/JCO.21.02614 PubMed
19.Greipp PR, San Miguel J, Durie BG, et al. International staging system for multiple myeloma. J Clin Oncol. 2005;23(15):3412-20. doi: 10.1200/JCO.2005.04.242 PubMed
20.Palumbo A, Avet-Loiseau H, Oliva S, et al. Revised International Staging System for Multiple Myeloma: A Report From International Myeloma Working Group. J Clin Oncol. 2015;33(26):2863-9. doi: 10.1200/JCO.2015.61.2267 PubMed
21.Canadian Cancer Society. Stages of multiple myeloma. 2024. Accessed July 8, 2024. https://cancer.ca/en/cancer-information/cancer-types/multiple-myeloma/staging
22.Atrash S, Bhutani M, Paul B, Voorhees PM, Usmani SZ. Management of newly diagnosed transplant ineligible multiple myeloma. Leuk Lymphoma. 2020;61(11):2549-2560. doi: 10.1080/10428194.2020.1786558 PubMed
23.Kumar SK, Callander NS, Alsina M, et al. Multiple Myeloma, Version 3.2017, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2017;15(2):230-269. doi: 10.6004/jnccn.2017.0023 PubMed
24.Mikhael J, Ismaila N, Cheung MC, et al. Treatment of Multiple Myeloma: ASCO and CCO Joint Clinical Practice Guideline. J Clin Oncol. 2019;37(14):1228-1263. doi: 10.1200/JCO.18.02096 PubMed
25.CADTH. Reimbursement Recommendation: optimal pharmacotherapy for transplant-ineligible multiple myeloma. (Therapeutic Review). 2024. Accessed May 22, 2025. https://www.cadth.ca/sites/default/files/DRR/2024/TR0014%20Final%20Recommendation%20and%20Reasons.pdf
26.sanofi-aventis Canada Inc. Sarclisa (Isatuximab for injection): 100 mg/5 mL or 500 mg/25 mL, concentrate for solution for infusion [product monograph]. Updated April 17, 2025.
27.CADTH. Reimbursement Review: isatuximab (Sarclisa). Can J Health Technol. 2022;2(4). doi: 10.51731/cjht.2022.305
28.Facon T, Goldschmidt H, Cavo M, et al. PB2185: Phase III (IMROZ) study design: Isatuximab plus bortezomib, lenalidomide, and dexamethasone (VRD) versus VRD in transplant-ineligible patients with newly diagnosed multiple myeloma. Hemasphere. 2018;2(S1):976. doi: 10.1097/HS9.0000000000000060
29.Orlowski RZ, Goldschmidt H, Cavo M, et al. Phase III (IMROZ) study design: Isatuximab plus bortezomib (V), lenalidomide (R), and dexamethasone (d) vs VRd in transplant-ineligible patients (pts) with newly diagnosed multiple myeloma (NDMM). J Clin Oncol. 2018;36(15 suppl):TPS8055. doi: 10.1200/jco.2018.36.15_suppl.tps8055
30.Facon T, Dimopoulos MA, Leleu XP, et al. Isatuximab, Bortezomib, Lenalidomide, and Dexamethasone for Multiple Myeloma. N Engl J Med. 2024;391(17):1597-1609. doi: 10.1056/NEJMoa2400712 PubMed
31.Facon T, Dimopoulos M-A, Leleu XP, et al. Phase 3 study results of isatuximab, bortezomib, lenalidomide, and dexamethasone (Isa-VRd) versus VRd for transplant-ineligible patients with newly diagnosed multiple myeloma (IMROZ). J Clin Oncol. 2024;42(16 suppl):7500. doi: 10.1200/JCO.2024.42.16_suppl.7500
32.Sanofi-Aventis Recherche & Developpement. Clinical Study Report: EFC12522, Interim 1. A Phase 3 randomized, open-label, multicenter study assessing the clinical benefit of isatuximab (SAR650984) in combination with bortezomib (Velcade®), lenalidomide and dexamethasone versus bortezomib, lenalidomide and dexamethasone in patients with newly diagnosed multiple myeloma not eligible for transplant [internal sponsor's report]. February 29, 2024.
33.Kumar S, Paiva B, Anderson KC, et al. International Myeloma Working Group consensus criteria for response and minimal residual disease assessment in multiple myeloma. Lancet Oncol. 2016;17(8):e328-e346. doi: 10.1016/S1470-2045(16)30206-6 PubMed
34.Aaronson NK, Ahmedzai S, Bullinger M, et al. The EORTC Core Quality of Life Questionnaire: Interim Results of an International Field Study. In: Osoba D, ed. Effect of Cancer on Quality of Life. CRC Press; 1991:185-202.
35.Aaronson NK, Ahmedzai S, Bergman B, et al. The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst. 1993;85(5):365-76. doi: 10.1093/jnci/85.5.365 PubMed
36.Osborne TR, Ramsenthaler C, Siegert RJ, Edmonds PM, Schey SA, Higginson IJ. What issues matter most to people with multiple myeloma and how well are we measuring them? A systematic review of quality of life tools. Eur J Haematol. 2012;89(6):437-57. doi: 10.1111/ejh.12012 PubMed
37.Frick E, Borasio GD, Zehentner H, Fischer N, Bumeder I. Individual quality of life of patients undergoing autologous peripheral blood stem cell transplantation. Psychooncology. 2004;13(2):116-24. doi: 10.1002/pon.730 PubMed
38.Kontodimopoulos N, Samartzis A, Papadopoulos AA, Niakas D. Reliability and validity of the Greek QLQ-C30 and QLQ-MY20 for measuring quality of life in patients with multiple myeloma. ScientificWorldJournal. 2012;2012:842867. doi: 10.1100/2012/842867 PubMed
39.Kvam AK, Fayers PM, Wisloff F. Responsiveness and minimal important score differences in quality-of-life questionnaires: a comparison of the EORTC QLQ-C30 cancer-specific questionnaire to the generic utility questionnaires EQ-5D and 15D in patients with multiple myeloma. Eur J Haematol. 2011;87(4):330-7. doi: 10.1111/j.1600-0609.2011.01665.x PubMed
40.Durie BGM, Hoering A, Abidi MH, et al. Bortezomib with lenalidomide and dexamethasone versus lenalidomide and dexamethasone alone in patients with newly diagnosed myeloma without intent for immediate autologous stem-cell transplant (SWOG S0777): a randomised, open-label, phase 3 trial. Lancet. 2017;389(10068):519-527. doi: 10.1016/S0140-6736(16)31594-X PubMed
41.Santesso N, Glenton C, Dahm P, et al. GRADE guidelines 26: informative statements to communicate the findings of systematic reviews of interventions. J Clin Epidemiol. 2020;119:126-135. doi: 10.1016/j.jclinepi.2019.10.014 PubMed
42.Balshem H, Helfand M, Schünemann HJ, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011;64(4):401-406. doi: 10.1016/j.jclinepi.2010.07.015 PubMed
43.National Institute for Health and Care Excellence. Single technology appraisal: User guide for company evidence submission template. 2015. Accessed November 24, 2020. https://www.nice.org.uk/process/pmg24
44.sanofi-aventis Canada Inc. EVG-35528-01: clinical systematic literature review update for treatments in newly diagnosed multiple myeloma, version 5.1 [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Sarclisa (isatuximab for injection), 20 mg/mL concentrate for solution for infusion. June 14, 2024.
45.sanofi-aventis Canada Inc. 3842 Report: Weighting Flatiron Electronic Medical Records Data to IMROZ Trial Data in Transplant-ineligible Newly Diagnosed Multiple Myeloma, draft 3 (final) [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Sarclisa (isatuximab for injection), 20 mg/mL concentrate for solution for infusion. August 16, 2024.
46.sanofi-aventis Canada Inc. PRJ000005: Indirect Treatment Comparisons for Isatuximab Combined with Bortezomib, Lenalidomide and Dexamethasone in Transplant-Ineligible Newly Diagnosed Multiple Myeloma – Technical Report, final [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Sarclisa (isatuximab for injection), 20 mg/mL concentrate for solution for infusion. October 18, 2024.
47.National Institute for Health and Care Excellence. Single Technology Appraisal: Daratumumab in combination for untreated multiple myeloma when stem cell transplant is suitable [ID1510]. Supporting evidence: committee papers. 2021. Accessed by sponsor, no date provided. https://www.nice.org.uk/guidance/ta763/documents/committee-papers-3
48.Kumar SK, Moreau P, Bahlis NJ, et al. Daratumumab plus lenalidomide and dexamethasone (D-Rd) versus lenalidomide and dexamethasone (Rd) alone in transplant-ineligible patients with newly diagnosed multiple myeloma (NDMM): updated analysis of the phase 3 Maia study. Blood. 2022;140(Supplement 1):10150-10153. doi: 10.1182/blood-2022-163335
49.Mateos M-V, San-Miguel J, Cavo M, et al. Daratumumab plus bortezomib, melphalan, and prednisone (D-VMP) versus bortezomib, melphalan, and prednisone (VMP) alone in transplant-ineligible patients with newly diagnosed multiple myeloma (NDMM): updated analysis of the phase 3 Alcyone study. Blood. 2022;140(Supplement 1):10157-10159. doi: 10.1182/blood-2022-163347
50.Yimer H, Melear J, Faber E, et al. Daratumumab, bortezomib, cyclophosphamide and dexamethasone in newly diagnosed and relapsed multiple myeloma: LYRA study. Br J Haematol. 2019;185(3):492-502. doi: 10.1111/bjh.15806 PubMed
51.Facon T, Dimopoulos MA, Dispenzieri A, et al. Final analysis of survival outcomes in the phase 3 FIRST trial of up-front treatment for multiple myeloma. Blood. 2018;131(3):301-310. doi: 10.1182/blood-2017-07-795047 PubMed
52.Adunlin G, Cyrus JW, Dranitsaris G. Correlation between progression-free survival and overall survival in metastatic breast cancer patients receiving anthracyclines, taxanes, or targeted therapies: a trial-level meta-analysis. Breast Cancer Res Treat. 2015;154(3):591-608. doi: 10.1007/s10549-015-3643-5 PubMed
53.Paoletti X, Oba K, Bang YJ, et al. Progression-free survival as a surrogate for overall survival in advanced/recurrent gastric cancer trials: a meta-analysis. J Natl Cancer Inst. 2013;105(21):1667-70. doi: 10.1093/jnci/djt269 PubMed
54.Belin L, Tan A, De Rycke Y, Dechartres A. Progression-free survival as a surrogate for overall survival in oncology trials: a methodological systematic review. Br J Cancer. 2020;122(11):1707-1714. doi: 10.1038/s41416-020-0805-y PubMed
55.CADTH. Reimbursement Review Provisional Funding Algorithm: multiple myeloma. 2024. Accessed May 22, 2025. https://www.cda-amc.ca/sites/default/files/DRR/2024/PH0047_Multiple_Myeloma.pdf
Pharmacoeconomic Review
Abbreviations
AE
adverse event
ASCT
autologous stem cell transplant
BIA
budget impact analysis
CDA-AMC
Canada’s Drug Agency
CUA
cost-utility analysis
CyBorD
cyclophosphamide-bortezomib-dexamethasone
DCyBorD
daratumumab-cyclophosphamide-bortezomib-dexamethasone
DoT
duration of treatment
DRd
daratumumab-lenalidomide-dexamethasone
DVMP
daratumumab-bortezomib-melphalan-prednisone
HR
hazard ratio
ICER
incremental cost-effectiveness ratio
IPW
inverse probability weighting
IsaVRd
isatuximab-bortezomib-lenalidomide-dexamethasone
ITC
indirect treatment comparison
ITT
intention to treat
MAIC
matching-adjusted indirect comparison
MM
multiple myeloma
NDMM
newly diagnosed multiple myeloma
OS
overall survival
PFS
progression-free survival
PSM
partitioned survival model
QALY
quality-adjusted life-year
Rd
lenalidomide-dexamethasone
RDI
relative dose intensity
TTD
time to treatment discontinuation
VRd
bortezomib-lenalidomide-dexamethasone
WTP
willingness to pay
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Isatuximab (Sarclisa), 20 mg/mL, concentrate for solution for IV infusion |
Indication | In combination with bortezomib, lenalidomide, and dexamethasone, for the treatment of patients with newly diagnosed multiple myeloma who are not eligible for ASCT |
Health Canada approval status | NOC |
Health Canada review pathway | Standard review |
NOC date | April 17, 2025 |
Reimbursement request | As per indication |
Sponsor | Sanofi-Aventis Canada Inc. |
Submission history | Previously reviewed: Yes Indication: In combination with carfilzomib and dexamethasone, for the treatment of adult patients with relapsed or refractory MM who have received 1 to 3 prior lines of therapy Recommendation date: January 28, 2022 Recommendation: Reimburse with clinical criteria and/or conditions Indication: In combination with pomalidomide and dexamethasone, for the treatment of patients with relapsed and refractory MM who have received at least 2 prior therapies including lenalidomide and a proteasome inhibitor Recommendation date: February 4, 2021 Recommendation: Reimburse with clinical criteria and/or conditions |
ASCT = autologous stem cell transplant; MM = multiple myeloma; NOC = Notice of Compliance.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis PSM |
Target population | Adult patients with NDMM who are not eligible for ASCT |
Treatment | IsaVRd |
Dosage regimen | Cycle 1 (42-day cycle), isatuximab (10 mg/kg) is dosed weekly on day 1, day 8, day 15, day 22, and day 29 Cycle 2 to cycle 4 (42-day cycles), isatuximab (10 mg/kg) is dosed every 2 weeks on day 1, day 15, and day 29 Cycle 5 to cycle 17 (28-day cycles), isatuximab (10 mg/kg) is dosed every 2 weeks on day 1 and day 15 Cycles 18 and beyond (28-day cycles), isatuximab (10 mg/kg) is dosed every 4 weeks on day 1 |
Submitted price | Isatuximab: $757.90 per 100 mg/5 mL Isatuximab: $3,789.49 per 500 mg/25 mL |
Submitted treatment cost | $33,695 in cycle 1, $20,217 in cycle 2 to cycle 4, $11,669 in cycle 5 to cycle 17, and $5,835 in cycles 18 and beyond |
Comparators |
|
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | Lifetime (29 years) |
Key data sources |
|
Submitted results |
|
Key limitations |
|
CDA-AMC reanalysis results |
|
ASCT = autologous stem cell transplant; CDA-AMC = Canada’s Drug Agency; CyBorD = cyclophosphamide-bortezomib-dexamethasone; DCyBord = daratumumab-cyclophosphamide-bortezomib-dexamethasone; DoT = duration of treatment; DRd = daratumumab-lenalidomide-dexamethasone; DVMP = daratumumab-bortezomib-melphalan-prednisone; HR = hazard ratio; ICER = incremental cost-effectiveness ratio; IsaVRd = isatuximab-bortezomib-lenalidomide-dexamethasone; ITC = indirect treatment comparison; LY = life-year; NDMM = newly diagnosed multiple myeloma; OS = overall survival; PFS = progression-free survival; PSM = partitioned survival model; QALY = quality-adjusted life-year; Rd = lenalidomide-dexamethasone; TTD = time to treatment discontinuation; VRd = bortezomib-lenalidomide-dexamethasone; vs. = versus; WTP = willingness to pay.
Conclusions
Evidence from the ongoing, open-label, phase III IMROZ trial comparing the efficacy and safety of isatuximab-bortezomib-lenalidomide-dexamethasone (IsaVRd) and bortezomib-lenalidomide-dexamethasone (VRd) shows that IsaVRd resulted in a statistically significant improvement in progression-free survival (PFS) compared to VRd among adult patients with newly diagnosed multiple myeloma (NDMM) who were ineligible for an autologous stem cell transplant (ASCT) or with no intent for an ASCT as initial therapy. Specifically, the Clinical Review conducted by Canada’s Drug Agency (CDA-AMC) noted that IsaVRd likely results in an increase in the probability of being progression-free at 18 months, 36 months, and 60 months compared to VRd, with moderate certainty of evidence. The Clinical Review further noted that while results suggest IsaVRd may improve overall survival (OS) compared to VRd at 60 months of follow-up, conclusions are limited as the OS data were based on an interim analysis (data cut-off date = September 26, 2023; median follow-up = 59.73 months). Additionally, the median OS was not reached, the results were considered immature, and the between-group difference in OS was not statistically significant, representing low-certainty evidence.
The comparative clinical efficacy against other comparators was not evaluated in the IMROZ trial; consequently, uncertainty persists due to the absence of head-to-head clinical evidence and several methodological limitations in the sponsor's indirect treatment comparisons (ITCs). The CDA-AMC Clinical Review noted uncertainty associated with the results of the matching-adjusted indirect comparison (MAIC) and inverse probability weighting (IPW) analyses owing to unaddressed prognostic and effect-modifying variables, study design differences, reductions in effective sample size, and imprecision in some estimates. These issues undermine the ability to draw definitive conclusions. Furthermore, the Clinical Review noted that indirect comparisons regarding OS are particularly uncertain due to the immaturity of the data from the IMROZ trial.
The CDA-AMC base case focused on comparing IsaVRd and daratumumab-lenalidomide-dexamethasone (DRd) because clinical experts identified DRd as the most relevant comparator and ITC limitations restricted other comparisons. As part of the pairwise base-case reanalysis, CDA-AMC assumed equal OS, excluded subsequent therapy costs, and aligned time to treatment discontinuation (TTD) with PFS. In the CDA-AMC base case, IsaVRd is associated with an incremental cost-effectiveness ratio (ICER) of $311,681 per quality-adjusted life-year (QALY) gained relative to DRd (incremental costs = $22,340; incremental QALYs = 0.07). The estimated ICER was driven by assumptions regarding TTD. Based on the CDA-AMC base-case reanalysis, a 2.5% price reduction for isatuximab is required for IsaVRd to be considered cost-effective relative to DRd at a willingness-to-pay (WTP) threshold of $50,000 per QALY gained. This would reduce the price of isatuximab from $757.90 to $738.95 (per 100 mg/5 mL vial), and from $3,789.49 to $3,694.75 (per 500 mg/25 mL vial).
The CDA-AMC base case relies on a sustained PFS benefit for IsaVRd, where patients receiving IsaVRd gain 0.07 additional QALYs compared to those treated with DRd because they spend comparatively more time in the progression-free health state. In the absence of long-term head-to-head clinical evidence, the extent of this benefit is highly uncertain. Should the PFS benefit for IsaVRd be lower than predicted, the resulting ICER would exceed the CDA-AMC base case, necessitating larger price reductions to achieve cost-effectiveness. Moreover, when comparing the duration of follow-up in the IMROZ trial to the time horizon of the model (69 months [approximately 5.8 years] versus 29 years), it is important to note that most of the QALY benefit (82%) predicted by the model for patients treated with IsaVRd is accrued in the post-trial period of the model on the basis of extrapolation.
Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, clinician groups, and drug plans that participated in the CDA-AMC review process.
Patient group input was gathered from Myeloma Canada, using data from a survey conducted from October to November 2024. Survey eligibility was based on patient and caregiver self-reported experiences with multiple myeloma (MM). Participants qualified if they or the person they cared for was deemed ineligible for an ASCT at diagnosis and/or did not undergo an ASCT as first-line therapy. Of 43 responses, 24 were eligible and were divided into 2 groups; 1 group (named subset C) had 22 respondents who were ineligible for or did not receive an ASCT as first-line therapy and a second group (named subset T) had 2 respondents who received IsaVRd. Respondents highlighted the profound impact of MM symptoms, such as bone issues and neuropathy, on their quality of life, daily activities, and finances. Most required monthly hospital visits. Effective treatment, remission, improved quality of life, and manageable side effects were top priorities for respondents. In subset C, current MM regimens received positive feedback for improving quality of life and meeting expectations. However, opinions on IsaVRd were mixed, with respondents acknowledging potential benefits but raising concerns about side effects and frequent hospital visits. Among those with IsaVRd experience, both respondents reported effective disease control, manageable side effects, and improved quality of life despite challenges such as infections and neuropathy. Overall, the survey underscored the need to balance treatment efficacy with the burden on patients’ daily lives and mental well-being.
Two clinician groups, the Canadian Myeloma Research Group and the Ontario Health (Cancer Care Ontario) (OH-CCO) Hematology Cancer Drug Advisory Committee, provided input for this review. Both emphasized that the primary treatment goals are prolonging PFS and OS, controlling disease symptoms, and minimizing adverse events (AEs) to improve quality of life. The Canadian Myeloma Research Group highlighted the importance of maximizing disease control during first-line therapy, aiming for deep and durable responses, including minimal residual disease negativity, to achieve prolonged remission. The groups endorsed IsaVRd as a first-line quadruplet regimen for patients with NDMM who are transplant-ineligible, citing its superior efficacy compared with VRd, despite the longer infusion times. The OH-CCO Hematology Cancer Drug Advisory Committee group highlighted the absence of comparative data with DRd and noted the less convenient IV administration of isatuximab compared with daratumumab’s subcutaneous option. Both groups emphasized that isatuximab treatment requires specialized centres with expertise in managing AEs. Clinically meaningful responses, such as partial remission, were associated with symptom improvement. Treatment discontinuation was recommended in cases of substantial intolerance, disease progression, or bortezomib toxicity.
Those drug plans participating in the CDA-AMC review process questioned the clinical circumstances under which IsaVRd would be preferred over daratumumab-based regimens. The plans noted that if a patient’s disease progresses on an anti-CD38 biologic, they would no longer be eligible for additional anti-CD38 biologics. Concerns were raised about the anticipated budget impact because the sponsor assumed that most of the market share would be captured from DRd. The drug plans raised concerns about potential costs associated with AEs, such as neutropenia. They also questioned whether isatuximab should be added to the regimen for patients currently receiving VRd.
Several of these concerns were addressed in the sponsor’s model:
PFS and OS were included in the model.
The impact of disease and treatment on a patient’s quality of life was captured with utility values.
AEs, including neutropenia, were incorporated as disutilities and applied as a 1-time decrement in the analysis.
In addition, CDA-AMC addressed some of these concerns as follows:
CDA-AMC performed a scenario analysis to assess the budgetary impact of reducing the market uptake of IsaVRd.
CDA-AMC was unable to address the following concerns raised by patients, clinicians, and drug programs who provided input:
Due to uncertainties associated with the distribution of subsequent therapy in the sponsor’s submitted model, CDA-AMC excluded subsequent therapy costs from the base-case reanalysis.
Economic Review
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis (CUA) of IsaVRd compared with cyclophosphamide-bortezomib-dexamethasone (CyBorD), daratumumab-cyclophosphamide-bortezomib-dexamethasone (DCyBorD), DRd, daratumumab-bortezomib-melphalan-prednisone (DVMP), lenalidomide-dexamethasone (Rd), and VRd for the treatment of adult patients with NDMM who are not eligible to undergo a transplant or with no intent for an ASCT as initial therapy.1 The modelled population is aligned with the Health Canada indication and with patients enrolled in the IMROZ trial.2
Isatuximab is supplied in single-use vials containing 100 mg/5 mL or 500 mg/25 mL of concentrate for solution for infusion. The submitted price for isatuximab is $757.90 for the 100 mg/5 mL vial and $3,789.49 for the 500 mg/25 mL vial. The recommended dose of isatuximab is 10 mg/kg administered as an IV infusion in combination with bortezomib-lenalidomide-dexamethasone. Dosing cycles range between 28- and 42-day cycles.3 In cycle 1 (42 days), isatuximab is administered weekly on day 1, day 8, day 15, day 22, and day 29. In cycle 2 to cycle 4 (42 days), isatuximab is administered every 2 weeks on day 1, day 15, and day 29. In cycle 5 to cycle 17 (28 days), isatuximab is administered every 2 weeks on day 1 and day 15. In cycles 18 and beyond (28 days), isatuximab is administered every 4 weeks on day 1. Using the submitted price for isatuximab, the sponsor estimated the per-patient, 28-day cycle cost of IsaVRd to range from $5,835 (cycle 18 and beyond) to $33,695 (cycle 1). The sponsor estimated drug acquisition costs by factoring in wastage and relative dose intensity (RDI).
The clinical outcomes modelled were OS, PFS, and TTD. The model simulated life-years, QALYs, and costs for each treatment over a lifetime time horizon (29 years), discounted at a rate of 1.5% per year. The analysis was undertaken from the perspective of Canada’s publicly funded health care system.
Model Structure
The sponsor submitted a partitioned survival model (PSM) with 3 health states: progression-free, postprogression, and death, whereby transitions between health states occurred on a 2-week cycle length (Figure 1). The proportion of patients in each health state was estimated over time based on the OS and PFS curves for each intervention. All patients entered the model in the progression-free health state, where they received either IsaVRd, CyBorD, DCyBorD, DRd, DVMP, Rd, or VRd, with state occupancy defined by PFS. During each cycle, patients either remained progression-free, transitioned to the postprogression state, or died. Death was modelled as an absorbing state. The proportion of patients in the postprogression state was calculated by subtracting the proportion of patients alive and progression-free (based on the PFS curve) from the proportion of patients alive (based on the OS curve). Patients in the postprogression state either remained in this state or died (i.e., patients could not return to the progression-free state).
Model Inputs
Baseline patient characteristics in the model were reflective of the intention-to-treat (ITT) population in the IMROZ trial.4 The average patient in the modelled cohort, which the sponsor assumed reflected the patient population in Canada, was aged 72 years, weighed 74 kg, had a mean body surface area of 1.8 m2, and was predominantly male (53% male, 47% female). These characteristics were used to inform the drug dosage regimens, as well as the age-specific and sex-specific distribution of the general population mortality risk, which the sponsor used to cap the lower bound for all-cause mortality in the model.
Key clinical efficacy inputs, including OS, PFS, and TTD, for patients receiving IsaVRd and VRd were derived from the ITT population of the IMROZ trial (data cut-off date = September 26, 2023). Kaplan-Meier estimates of OS, PFS, and TTD from the IMROZ trial were used to fit parametric survival curves to extrapolate the treatment effect beyond the observed trial period (median follow-up = 59.73 months; maximum follow-up = 69 months) over the entire model time horizon (29 years). Several parametric functions were fitted to the OS, PFS, and TTD data to select candidate distributions based on goodness-of-fit statistics, visual inspection, and clinical plausibility of long-term projections as determined by clinical experts in Canada. The sponsor selected the Gompertz distribution for OS for both IsaVRd and VRd. For PFS and TTD, the sponsor selected the gamma and exponential distributions, respectively, to extrapolate outcomes for both IsaVRd and VRd. OS and PFS for all other comparators (CyBorD, DCyBorD, DRd, DVMP, and Rd) were derived from ITCs conducted by the sponsor. Due to a lack of a common anchor and the absence of a valid network connection with the IMROZ study, the sponsor conducted an MAIC and inverse probability of treatment weighting, specifically for CyBorD. Nonproportional hazards were applied to the base curves to determine OS and PFS for comparators that were not captured in the IMROZ trial. TTD curves for comparators not included in the IMROZ trial were derived by applying a hazard ratio (HR) to the PFS curves for CyBorD, DCyBorD, DVMP, and Rd, and using an HR from the MAIA trial for DRd.
The health state utility values for the progression-free (0.62) and postprogression (0.59) health states were derived from Hatswell et al.,5 who conducted a metaregression and presented health state utilities in MM. It was assumed that the progression-free health state was informed by the utility reported for first-line MM, and progressed disease was informed by the utility reported for second-line MM. The model incorporated the decremental effect of aging on patients’ quality of life, as well as sex differences, derived from the Guertin et al. study.6
AEs were modelled as a 1-time cost in the first cycle of the model because the sponsor assumed that the AEs mostly occurred shortly after treatment initiation. AEs for VRd and IsaVRd were derived from the IMROZ trial.4 AEs for all remaining comparators were sourced from trial data included in the sponsor-submitted ITC.7,8 Grade 3 or higher AEs occurring in 5% or more of patients across the relevant trials, except for grade 3 or grade 4 AEs occurring in 10% or more of patients in the ALCYONE trial,7 were considered. AE-related utility decrements were calculated for a specified duration and applied in the first cycle of the model. Duration in days and disutility values were informed by National Institute for Health and Care Excellence technical appraisal guidance documents TA917,9 TA870,10 or TA970.11
The analysis included the following costs: drug acquisition, drug administration, subsequent treatment, follow-up, monitoring, management of AEs, and terminal care costs. Costs were obtained from IQVIA DeltaPA,12 Ontario Drug Benefit Formulary,13 previous CDA-AMC reimbursement reviews,14 Ontario Drug Benefit physician services,15 and published literature.16 Dosing regimens were informed by OH-CCO. Inpatient AE management costs were derived from the Canadian Institute for Health Information’s Patient Cost Estimator. Subsequent treatment costs for second-line, third-line, and fourth-line settings were included in the model. The distribution of subsequent treatments was obtained from a survey of clinical experts obtained by the sponsor. The type of subsequent therapy received and the length of time the patient would remain on subsequent therapy differed based on the initial therapy. Unit costs for routine monitoring were derived from published literature, with the frequency based on clinical expert feedback. Terminal care costs included in the model were informed by published literature.16,17
Summary of Sponsor’s Economic Evaluation Results
All analyses were run probabilistically (1,000 iterations). The deterministic and probabilistic results were similar. The probabilistic findings are presented as follows. The submitted analysis was based on the submitted price for isatuximab and public list prices for comparators. Additional results from the sponsor’s submitted economic evaluation base case are presented in Appendix 3.
Base-Case Results
In the sponsor’s submitted base case, the expected total costs and QALYs over a lifetime horizon for IsaVRd were $1,227,580 and 5.62, respectively (Table 3). In the sequential analysis, IsaVRd was associated with an ICER of $395,725 (incremental cost = $400,275; incremental QALYs = 1.011). Approximately 78% of incremental QALYs for IsaVRd, relative to DVMP, was gained in the extrapolated period of the model (i.e., beyond the 5.67 years observed in the IMROZ trial).
At a WTP threshold of $50,000 per QALY gained, IsaVRd has a 0% probability of being considered the optimal treatment. Submitted analyses are based on the publicly available prices of the comparator treatments.
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Total QALYs | Sequential ICER ($ per QALY) |
|---|---|---|---|
DVMP | 827,304 | 4.61 | Reference |
IsaVRd | 1,227,580 | 5.62 | 395,725 |
Dominated treatments | |||
DCyBorD | 904,704 | 4.59 | Dominated by DVMP |
Rd | 985,146 | 4.29 | Dominated by DVMP |
CyBorD | 1,023,626 | 3.34 | Dominated by DVMP |
VRd | 1,238,658 | 3.96 | Dominated by DVMP |
DRd | 1,307,996 | 5.22 | Dominated by IsaVRd |
CyBorD = cyclophosphamide-bortezomib-dexamethasone; DCyBorD = daratumumab-cyclophosphamide-bortezomib-dexamethasone; DRd = daratumumab-lenalidomide-dexamethasone; DVMP = daratumumab-bortezomib-melphalan-prednisone; ICER = incremental cost-effectiveness ratio; IsaVRd = isatuximab-bortezomib-lenalidomide-dexamethasone; QALY = quality-adjusted life-year; Rd = lenalidomide-dexamethasone; VRd = bortezomib-lenalidomide-dexamethasone.
Source: Sponsor’s pharmacoeconomic submission.1
Sensitivity and Scenario Analysis Results
The sponsor conducted several pairwise deterministic scenario analyses using alternative discount rates and time horizons, excluding wastage, using alternative survival extrapolations for IsaVRd, using HR-based extrapolations for comparators, adopting utilities from the IMROZ trial, excluding disutilities due to AEs, incorporating a lump-sum cost for subsequent therapies, and excluding RDI.
Assuming proportional and constant hazards resulted in higher ICERs for IsaVRd compared to CyBorD, DCyBorD, DRd, DVMP, and Rd. Excluding RDI resulted in higher ICERs for IsaVRd versus all comparators. Finally, reducing the time horizon to 15 years increased the ICER for IsaVRd versus all comparisons.
The sponsor conducted a scenario analysis from a societal perspective; this analysis included additional costs associated with patient and caregiver productivity impairment, as well as out-of-pocket costs. In this analysis, relative to VRd, the ICER for IsaVRd was $16,335 per QALY gained.
CDA-AMC Appraisal of the Sponsor’s Economic Evaluation
CDA-AMC identified several key limitations to the sponsor’s analysis that have notable implications for the economic analysis.
Comparative clinical evidence of IsaVRd and relevant comparators is highly uncertain. In the absence of direct head-to-head evidence comparing IsaVRd with treatments commonly used in clinical practice in Canada, the sponsor relied on an ITC approach to derive relative effectiveness in terms of PFS and OS. This included unanchored MAIC and IPW analyses. Individual patient data were used specifically for comparisons between IsaVRd and CyBorD. According to the clinical review team, the sponsor’s indirect evidence suggests that IsaVRd may offer improved outcomes for PFS and OS compared to DVMP and Rd. However, comparisons with CyBorD, DRd, and DCyBorD did not yield significant differences. There remain several critical limitations to these analyses, including unaddressed prognostic and effect-modifying variables, differences in study design and conduct that could not be adequately adjusted for, important reductions in effective sample size, and imprecision in some estimates. Furthermore, findings related to OS are particularly uncertain due to immature data from the IMROZ trial. Extrapolated results beyond the follow-up period of the included studies further contribute to uncertainty regarding long-term outcomes.
Given the absence of direct evidence comparing IsaVRd to relevant comparators and the limitations of the sponsor’s ITC, the extent to which IsaVRd offers a net benefit over any funded regimen beyond VRd remains uncertain.
Due to the uncertainties associated with the results of the MAIC and IPW analyses, all comparators except DRd were excluded from the CDA-AMC reanalysis.
The impact of IsaVRd on long-term OS is highly uncertain. The sponsor submitted a PSM based on the ITT population enrolled in the IsaVRd treatment group of the IMROZ trial. OS for IsaVRd was extrapolated from the Kaplan-Meier curve observed in the IMROZ trial, which had a median follow-up of 59.73 months. The sponsor estimated that 73% of patients receiving IsaVRd would be alive at 5 years. At 10 years and 15 years, the projected survival rates were 52% and 36%, respectively. Notably, at 20 years — when the cohort’s average age exceeds 90 years — more than 20% of patients were still predicted to be alive. This suggests a substantial reduction in mortality risk over time. The only plausible rationale for such a reduction would be if IsaVRd had a curative effect, eliminating the mortality risk associated with MM, even in patients who were relapsed and refractory to multiple lines of therapy. However, there is no evidence from the IMROZ trial to support a curative effect for IsaVRd. Therefore, the predicted reduction in mortality appears to be based on assumption rather than trial-based evidence.
According to the clinical review team, as of the data cut-off on September 26, 2023, median OS had not been reached in either intervention group of the IMROZ trial, highlighting the immaturity of the OS data. Additionally, the clinical review team noted that OS estimates derived from the sponsor's ITCs are subject to further uncertainty. Given the lack of robust long-term data, the projected OS benefit for patients receiving IsaVRd in the post-trial period of the model is highly uncertain.
Moreover, clinical expert feedback highlighted that VRd is rarely prescribed in current clinical practice in Canada. This was corroborated by the sponsor’s budget impact analysis (BIA), which projected VRd to capture less than 5% of the market in Canada. Clinical experts emphasized that DRd is the most relevant comparator for this indication.
Due to this limitation, reanalysis by CDA-AMC equated the OS curves for IsaVRd and DRd, the latter of which was identified as the most relevant comparator in clinical practice in Canada.
Subsequent therapy costs are associated with significant uncertainty. In the sponsor’s base-case analysis, subsequent therapy costs were applied as a 1-time cost when a patient transitioned to the postprogression health state. The cost of subsequent treatment was calculated as a weighted distribution of treatment regimens, with proportions informed by clinical expert input. The sponsor assumed that all patients in subsequent lines of therapy would be treated until progression, but this approach was deemed inappropriate for several reasons. Applying a single 1-off cost likely overestimates subsequent therapy expenses because it fails to account for the relationship between time in the progressed health state and time on treatment. Additionally, clinical experts consulted by CDA-AMC noted that assuming the same subsequent therapies regardless of prior treatment history is unrealistic, as treatment selection is often influenced by previous therapy exposure; for instance, patients treated with an anti-CD38 regimen like daratumumab or isatuximab would typically not receive another anti-CD38 therapy. While CDA-AMC acknowledges that subsequent treatment efficacy and costs may differ between IsaVRd and its comparators, the lack of a more granular, line-specific model introduces substantial uncertainty.
Due to limitations in the PSM structure and uncertainties surrounding the distribution of subsequent therapies, CDA-AMC excluded subsequent therapy costs from the base-case analysis. The impact of these costs on the cost-effectiveness of IsaVRd remains unknown. Any estimates derived from the current model would be misleading, as the model fails to account for the complexities inherent to MM treatment pathways.
TTD was inappropriately modelled for comparators. For comparators not included in the IMROZ trial, such as CyBorD, DCyBorD, DVMP, and Rd, TTD was not reported as an outcome. In the sponsor’s model, median duration of treatment (DoT) was used as a proxy for median TTD. For most comparators, the ratio between median PFS and median DoT was applied as an HR to each of the comparator PFS curves to calculate an exponential distribution. This approach assumes that the relationship between median PFS and median DoT follows an exponential distribution, which may not accurately reflect the true distribution of TTD. Additionally, median DoT does not account for censoring, which may bias the estimates of TTD, especially if there is a high rate of patient dropout or early discontinuation. This lack of censoring consideration may lead to an overestimation of treatment persistence, introducing substantial uncertainty into the model.
For DRd, however, the sponsor derived TTD by applying the HR of TTD versus PFS from the MAIA trial to the ITC-derived DRd PFS curve. This approach assumes that the relationship between TTD and PFS is consistent across the MAIA trial and IMROZ study populations, which may not hold true. Additionally, the use of a parametric curve fit — specifically, a Gompertz distribution — to model DRd TTD based on the MAIA study’s DRd TTD Kaplan-Meier data may not accurately reflect the true distribution of TTD in the IMROZ study population. This approach also leads to a naive comparison because it assumes that DRd TTD from the MAIA trial can be directly applied to the IMROZ study population without accounting for important differences between these trial populations. Furthermore, the approach is susceptible to biases due to differences in trial methodologies, patient populations, and treatment regimens, which could impact the accuracy and applicability of the TTD estimates.
To address this limitation, CDA-AMC performed a reanalysis equating TTD to PFS for both IsaVRd and its comparators. This approach simplifies the analysis by eliminating the need for complex assumptions about distributions or censoring, and enhancing transparency and ease of implementation. Equating TTD to PFS across the intervention and its comparators ensures consistency and avoids bias because the incremental benefit is the primary focus of the cost-effectiveness analysis.
CDA-AMC conducted a scenario analysis to assess the impact of using an HR of median TTD versus median PFS to extrapolate long-term TTD for IsaVRd and DRd.
The model lacked transparency due to poor modelling practices. The sponsor’s submitted model included numerous IFERROR and ISERROR statements, which lead to situations in which the parameter value is overwritten with an alternative value without alerting the user to the automatized overwriting. The systematic use of IFERROR statements makes thorough auditing of the sponsor’s model impractical and it remains unclear whether the model is running inappropriately by overriding errors.
CDA-AMC was unable to address this limitation and notes that a thorough validation of the sponsor’s model was not possible.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CDA-AMC (refer to Table 4).
Table 4: Key Assumptions of the Submitted Economic Evaluation
Sponsor’s key assumption | CDA-AMC comment |
|---|---|
Wastage was not included for subsequent therapies. | Inappropriate. Due to uncertainties associated with the inclusion of subsequent therapies, the CDA-AMC base case did not include subsequent therapy costs. |
CDA-AMC = Canada’s Drug Agency.
CDA-AMC Reanalyses of the Economic Evaluation
Base-Case Results
CDA-AMC undertook the reanalyses outlined in Table 5 to address, where possible, the limitations within the sponsor’s submitted economic model. The CDA-AMC base case was derived by making changes in model parameter values and assumptions, in consultation with clinical experts.
Table 5: CDA-AMC Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
Changes to derive the CDA-AMC base case | ||
1. Comparators |
|
|
2. Subsequent therapy cost | One-off cost at the time of progression | Excluded |
3. OS |
|
|
4. TTD |
|
|
CDA-AMC base case | Reanalyses 1 + 2 + 3 + 4 | |
CDA-AMC = Canada’s Drug Agency; CyBorD = cyclophosphamide-bortezomib-dexamethasone; DCyBorD = daratumumab-cyclophosphamide-bortezomib-dexamethasone; DRd = daratumumab-lenalidomide-dexamethasone; DVMP = daratumumab-bortezomib-melphalan-prednisone; HR = hazard ratio; IsaVRd = isatuximab-bortezomib-lenalidomide-dexamethasone; ITC = indirect treatment comparison; MAIC = matching-adjusted indirect comparison; OS = overall survival; PFS = progression-free survival; Rd = lenalidomide-dexamethasone; TTD = time to treatment discontinuation; VRd = bortezomib-lenalidomide-dexamethasone; vs. = versus.
The CDA-AMC base case was based on publicly available prices of the comparator treatments. Results from the CDA-AMC base case are presented in Table 6. Additional results from the CDA-AMC base case, including the results of the stepwise analyses, are presented in Appendix 4.
In the CDA-AMC base case, the expected total costs and QALYs over a lifetime horizon for IsaVRd were $1,023,257 and 5.62, respectively. IsaVRd was associated with an ICER of $311,681 per QALY gained relative to DRd (incremental costs = $22,340; incremental QALYs = 0.07). Approximately 82% of incremental QALYs for IsaVRd, relative to DRd, were gained in the extrapolated period of the model (i.e., beyond the 5.67 years observed in the IMROZ trial).
Table 6: Summary of the CDA-AMC Reanalysis Results
Drug | Total costs ($) | Total QALYs | ICER ($ per QALY) |
|---|---|---|---|
CDA-AMC base case (probabilistic) | |||
DRd | 1,000,917 | 5.55 | Reference |
IsaVRd | 1,023,257 | 5.62 | 311,681 |
CDA-AMC = Canada’s Drug Agency; DRd = daratumumab-lenalidomide-dexamethasone; ICER = incremental cost-effectiveness ratio; IsaVRd = isatuximab-bortezomib-lenalidomide-dexamethasone; QALY = quality-adjusted life-year.
Source: Sponsor’s pharmacoeconomic submission.1
Scenario Analysis Results
CDA-AMC undertook price reduction analyses based on the sponsor’s results and the CDA-AMC base case. The CDA-AMC base case suggested that a 2.5% price reduction for isatuximab would be required for IsaVRd to achieve cost-effectiveness relative to DRd at a WTP threshold of $50,000 per QALY gained (Table 7).
Table 7: CDA-AMC Price Reduction Analyses
Analysis | Unit drug cost ($) | ICERs for IsaVRd vs. comparator (as indicated) ($ per QALY) | ||
|---|---|---|---|---|
Price reduction | 100 mg/5 mL | 500 mg/25 mL | Sponsor base case | CDA-AMC reanalysis |
No price reduction | 757.90 | 3,789.49 | 395,725 (vs. DVMP) | 311,681 (vs. DRd) |
10% | 682.11 | 3,410.54 | 341,442 (vs. DVMP) | IsaVRd is dominant |
20% | 606.32 | 3,031.59 | 287,158 (vs. DVMP) | IsaVRd is dominant |
30% | 530.53 | 2,652.64 | 232,875 (vs. DVMP) | IsaVRd is dominant |
40% | 454.74 | 2,273.69 | 178,591 (vs. DVMP) | IsaVRd is dominant |
50% | 378.95 | 1,894.75 | 124,307 (vs. DVMP) | IsaVRd is dominant |
60% | 303.16 | 1,515.80 | 70,024 (vs. DVMP) | IsaVRd is dominant |
70% | 227.37 | 1,136.85 | 15,740 (vs. DVMP) | IsaVRd is dominant |
80% | 151.58 | 757.90 | IsaVRd is dominant | IsaVRd is dominant |
90% | 75.79 | 378.95 | IsaVRd is dominant | IsaVRd is dominant |
CDA-AMC = Canada’s Drug Agency; DRd = daratumumab-lenalidomide-dexamethasone; DVMP = daratumumab-bortezomib-melphalan-prednisone; ICER = incremental cost-effectiveness ratio; IsaVRd = isatuximab-bortezomib-lenalidomide-dexamethasone; QALY = quality-adjusted life-year; vs. = versus.
CDA-AMC conducted a scenario analysis to explore the impact of using an HR of median TTD versus median PFS to extrapolate long-term TTD for IsaVRd and DRd. In this scenario, IsaVRd dominated DRd, providing more QALYs at a lower cost. However, this scenario is subject to greater uncertainty due to potential biases arising from differences in trial methodologies, patient populations, and treatment regimens that may affect the accuracy of the TTD estimates. Results of the scenario analysis are presented in Appendix 4, Table 13.
Issues for Consideration
CDA-AMC reanalyses are based on the public list prices of IsaVRd and other comparator treatments, which may differ from any confidential prices paid by those drug plans participating in the CDA-AMC review process and may influence the results of the cost-effectiveness and BIA.
Overall Conclusions
Evidence from the ongoing, open-label, phase III IMROZ trial comparing the efficacy and safety of IsaVRd and VRd shows that IsaVRd resulted in a statistically significant improvement in PFS compared to VRd among adult patients with NDMM who were ineligible for an ASCT or with no intent for an ASCT as initial therapy. Specifically, the CDA-AMC Clinical Review noted that IsaVRd likely results in an increase in the probability of being progression-free at 18 months, 36 months, and 60 months compared to VRd, with moderate certainty of evidence. The Clinical Review further noted that while results suggest IsaVRd may improve OS compared to VRd at 60 months of follow-up, conclusions are limited as the OS data were based on an interim analysis (data cut-off date = September 26, 2023; median follow-up = 59.73 months). Additionally, the median OS was not reached, and the results were considered immature.
The comparative clinical efficacy against other comparators was not evaluated in the IMROZ trial; consequently, uncertainty persists due to the absence of head-to-head clinical evidence and several methodological limitations in the sponsor's ITCs. The CDA-AMC Clinical Review noted uncertainty associated with the results of the MAIC and IPW analyses owing to unaddressed prognostic and effect-modifying variables, study design differences, reductions in effective sample size, and imprecision in some estimates. These issues undermine the ability to draw definitive conclusions. Furthermore, the Clinical Review noted that indirect comparisons regarding OS are particularly uncertain due to the immaturity of the data from the IMROZ trial.
The CDA-AMC base case focused on comparing IsaVRd and DRd because clinical experts identified DRd as the most relevant comparator and ITC limitations restricted other comparisons. As part of the pairwise base-case reanalysis, CDA-AMC assumed equal OS, excluded subsequent therapy costs, and aligned TTD with PFS. In the CDA-AMC base case, IsaVRd is associated with an ICER of $311,681 per QALY gained relative to DRd (incremental costs = $22,340; incremental QALYs = 0.07). The estimated ICER was driven by assumptions regarding TTD. Based on the CDA-AMC base-case reanalysis, a 2.5% price reduction for isatuximab is required for IsaVRd to be considered cost-effective relative to DRd at a WTP threshold of $50,000 per QALY gained. This would reduce the price of isatuximab from $757.90 to $738.95 (per 100 mg/5 mL vial), and $3,789.49 to $3,694.75 (per 500 mg/25 mL vial).
The CDA-AMC base case relies on a sustained PFS benefit for IsaVRd, where patients receiving IsaVRd gain 0.07 additional QALYs compared to those treated with DRd because they spend comparatively more time in the progression-free health state. In the absence of long-term head-to-head clinical evidence, the extent of this benefit is highly uncertain. Should the PFS benefit for IsaVRd be lower than predicted, the resulting ICER would exceed the CDA-AMC base case, necessitating larger price reductions to achieve cost-effectiveness. Moreover, when comparing the duration of follow-up in the IMROZ trial to the time horizon of the model (69 months [approximately 5.8 years] versus 29 years), it is important to note that most of the QALY benefit (82%) predicted by the model for patients treated with IsaVRd is accrued in the post-trial period of the model on the basis of extrapolation.
References
1.sanofi-aventis Canada Inc. Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Sarclisa (isatuximab for injection), 20 mg/mL concentrate for solution for infusion. October 30, 2024.
2.sanofi-aventis Canada Inc. 3842 Report: Weighting Flatiron Electronic Medical Records Data to IMROZ Trial Data in Transplant-ineligible Newly Diagnosed Multiple Myeloma, draft 3 (final) [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Sarclisa (isatuximab for injection), 20 mg/mL concentrate for solution for infusion. August 16, 2024.
3.sanofi-aventis Canada Inc. Sarclisa (Isatuximab for injection): 100 mg/5 mL or 500 mg/25 mL, concentrate for solution for infusion [product monograph]. Updated April 17, 2025.
4.Sanofi Group. Clinical Trial Protocol: EFC12522, amended 6. A phase 3 randomized, open-label, multicenter study assessing the clinical benefit of isatuximab (SAR650984) in combination with bortezomib (Velcade®), lenalidomide and dexamethasone versus bortezomib, lenalidomide and dexamethasone in patients with newly diagnosed multiple myeloma not eligible for transplant [internal sponsor's report]. June 9, 2022.
5.Hatswell AJ, Burns D, Baio G, Wadelin F. Frequentist and Bayesian meta-regression of health state utilities for multiple myeloma incorporating systematic review and analysis of individual patient data. Health Econ. 2019;28(5):653-665. doi: 10.1002/hec.3871 PubMed
6.Guertin JR, Feeny D, Tarride JE. Age- and sex-specific Canadian utility norms, based on the 2013-2014 Canadian Community Health Survey. CMAJ. 2018;190(6):E155-E161. doi: 10.1503/cmaj.170317 PubMed
7.Mateos MV, Dimopoulos MA, Cavo M, et al. Daratumumab plus Bortezomib, Melphalan, and Prednisone for Untreated Myeloma. N Engl J Med. 2018;378(6):518-528. doi: 10.1056/NEJMoa1714678 PubMed
8.Orlowski RZ, Moreau P, Niesvizky R, et al. Carfilzomib-Dexamethasone Versus Bortezomib-Dexamethasone in Relapsed or Refractory Multiple Myeloma: Updated Overall Survival, Safety, and Subgroups. Clin Lymphoma Myeloma Leuk. 2019;19(8):522-530 e1. doi: 10.1016/j.clml.2019.04.018 PubMed
9.National Institute for Health and Care Excellence. Daratumumab with lenalidomide and dexamethasone for untreated multiple myeloma when a stem cell transplant is unsuitable. (Technology appraisal guidance TA917). October 25, 2023. Accessed June 2024. https://www.nice.org.uk/guidance/ta917
10.National Institute for Health and Care Excellence. Ixazomib with lenalidomide and dexamethasone for treating relapsed or refractory multiple myeloma. (Technology appraisal guidance TA870). February 22, 2023. Accessed July 2, 2024. https://www.nice.org.uk/guidance/ta870
11.National Institute for Health and Care Excellence. Selinexor with dexamethasone for treating relapsed or refractory multiple myeloma after 4 or more treatments. (Technology appraisal guidance TA970). May 8, 2024. https://www.nice.org.uk/guidance/ta970
12.IQVIA. DeltaPA. 2023. Accessed December 2024. https://www.iqvia.com/
13.Ontario Ministry of Health. Ontario drug benefit formulary/comparative drug index. Accessed August 2024. https://www.formulary.health.gov.on.ca/formulary/
14.CADTH. Reimbursement Review provisional funding algorithm: multiple myeloma. August 2024. Accessed by sponsor, no date provided. https://www.cadth.ca/sites/default/files/DRR/2024/PH0047_Multiple_Myeloma.pdf
15.Ontario Ministry of Health. Schedule of benefits for physician services under the Health Insurance Act: (February 20, 2024 (effective April 1, 2024)). Accessed by sponsor, no date provided. https://www.ontario.ca/files/2024-08/moh-schedule-benefit-2024-08-30.pdf
16.de Oliveira C, Pataky R, Bremner KE, et al. Phase-specific and lifetime costs of cancer care in Ontario, Canada. BMC Cancer. 2016;16(1):809. doi: 10.1186/s12885-016-2835-7 PubMed
17.Garaszczuk R, Yong JHE, Sun Z, de Oliveira C. The Economic Burden of Cancer in Canada from a Societal Perspective. Curr Oncol. 2022;29(4):2735-2748. doi: 10.3390/curroncol29040223 PubMed
18.Brenner DR, Gillis J, Demers AA, et al. Projected estimates of cancer in Canada in 2024. CMAJ. 2024;196(18):E615-E623. doi: 10.1503/cmaj.240095 PubMed
19.Statistics C. Projected population, by projection scenario, age and sex, as of July 1 (Table: 17-10-0057-01). 2024. Accessed February. https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1710005701
20.sanofi-aventis Canada Inc. Sarclisa (isatuximab): clinician survey for the treatment of adult patients with newly diagnosed multiple myeloma ineligible for transplant [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Sarclisa (isatuximab for injection), 20 mg/mL concentrate for solution for infusion. July 2024.
21.Facon T, Dimopoulos MA, Leleu XP, et al. Isatuximab, Bortezomib, Lenalidomide, and Dexamethasone for Multiple Myeloma. N Engl J Med. 2024. doi: 10.1056/NEJMoa2400712 PubMed
22.Molle P, Reynolds J, Janowski W, al e. A Randomized Study of Bortezomib, Cyclophosphamide and Dexamethasone Induction (VCD) Versus VCD and Daratumumab Induction Followed By Daratumumab Maintenance (VCDD) for the Initial Treatment of Transplant-Ineligible Patients with Multiple Myeloma (AMaRC 03-16). Blood. 2021;138(S1):2728-2729.
23.Facon T, Kumar SK, Plesner T, et al. Daratumumab, lenalidomide, and dexamethasone versus lenalidomide and dexamethasone alone in newly diagnosed multiple myeloma (MAIA): overall survival results from a randomised, open-label, phase 3 trial. Lancet Oncol. 2021;22(11):1582-1596. doi: 10.1016/S1470-2045(21)00466-6 PubMed
24.Mateos MV, Sonneveld P, Hungria V, et al. Daratumumab, Bortezomib, and Dexamethasone Versus Bortezomib and Dexamethasone in Patients With Previously Treated Multiple Myeloma: Three-year Follow-up of CASTOR. Clin Lymphoma Myeloma Leuk. 2020;20(8):509-518. doi: 10.1016/j.clml.2019.09.623 PubMed
Appendix 1: Cost Comparison Table
Please note that this appendix has not been copy-edited.
The comparators presented in Table 8 have been deemed to be appropriate based on feedback from clinical experts and drug plan. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in Table 8 and as such, the table may not represent the actual costs to public drug plans.
Table 8: CDA-AMC Cost Comparison Table for Multiple Myeloma Not Eligible for ASCT
Treatment | Strength / concentration | Form | Price ($) | Recommended dosage | Daily cost ($) | 28-day cost ($) |
|---|---|---|---|---|---|---|
IsaVRd (28- and 42-day cycle) | ||||||
Isatuximab | 100 mg/5 mL 500 mg/25 mL | Solution for injection | 757.9000a 3,789.4900a | Cycle 1 (42-day cycle): 10 mg/kg on days 1, 8, 15, 22, and 29 Cycle 2 to 4 (42-day cycles): 10 mg/kg days 1, 15, and 29 Cycles 5 to 17 (28-day cycle): 10 mg/kg days 1 and 15 Cycles 18+ (28-day cycles): 10 mg/kg on day 1 | Cycle 1: 722 Cycles 2 to 4: 433 Cycles 5 to 17: 433 Cycles 18+: 217 | Cycle 1: 20,211 Cycles 2 to 4: 12,126 Cycles 5 to 17: 12,126 Cycles 18+: 6,063 |
Bortezomibb | 2.5 mg 3.5 mg | Injection | 1,001.7300a 654.3100a | Cycle 1 to 4: 1.3 mg/m2 on days: 1, 4, 8, 11, 22, 25, 29 and 32 | Cycle 1 to 4: 70 | Cycle 1 to 4: 1,963 |
Lenalidomide | 10 mg 25 mg | Tablet | 90.2500 106.0000 | Cycle 1 to 4: 25 mg (10 mg for patients with creatinine clearance CrCl ≥ 30 to < 60 mL/min) on days 1 to 14 and days 22 to 35 Cycle 5+: 25 mg (10 mg for patients with creatinine clearance CrCl ≥ 30 to < 60 mL/min) on days 1 to 21 | Cycle 1 to 4: 58 to 68 Cycles 5+: 45 to 53 | Cycle 1 to 4: 1,625 to 1,908 Cycles 5+: 1,264 to 1,484 |
Dexamethasonec | 0.5 mg 4 mg | Tablet | 0.1564 0.6112 | Cycle 1 to 4: 20 mg on days 1, 2, 4, 5, 8, 9, 11, 12, 15, 22, 23, 25, 26, 29, 30, 32, and 33 Cycles 5+: 20 mg on days 1, 8, 15, and 22 | Cycle 1 to 4: 1.24 Cycles 5+: 0.29 | Cycle 1 to 4: 35 Cycles 5+: 8 |
IsaVRd regimen | Cycle 1: 906 to 916 Cycles 2 to 4: 617 to 627 Cycles 5 to 17: 479 to 486 Cycles 18+: 262 to 270 | Cycle 1: 25,359 to 25,643 Cycles 2 to 4: 17,275 to 17,559 Cycles 5 to 17: 13,398 to 13,619 Cycles 18+: 7,335 to 7,555 | ||||
CyBorD (28-day cycle) | ||||||
Bortezomibb | 2.5 mg 3.5 mg | Injection | 1,001.7300a 654.3100a | 1.3 mg/m2 on days 1, 8, 15, and 22 | 93 | 2,617 |
Cyclophosphamide | 25 mg 50 mg | Tablet | 0.3545 0.4773 | 300 mg/m2 on days 1, 8, 15, and 22 | 0.75 | 21 |
Dexamethasonec | 0.5 mg 4 mg | Tablet | 0.1564 0.6112 | Cycle 1 to 2: 40 mg on days: 1 to 4, 9 to 12, and 17 to 20 Cycles 3+: 40 mg on days 1, 8, 15, and 22 | Cycle 1 to 2: 2.62 Cycles 3+: 0.87 | Cycle 1 to 2: 73 Cycle 3+: 24 |
CyBorD regimen | Cycle 1 to 2: 97 Cycles 3+: 95 | Cycle 1 to 2: 2,712 Cycles 3+: 2,663 | ||||
DCyBorD (28-day cycle) | ||||||
Bortezomibb | 2.5 mg 3.5 mg | Injection | 1,001.7300a 654.3100a | Cycle 1 to 8: 1.3 mg/m2 on days 1, 8, 15, and 22 | Cycle 1 to 8: 93 | Cycle 1 to 8: 2,617 |
Cyclophosphamide | 25 mg 50 mg | Tablet | 0.3545 0.4773 | Cycle 1 to 8: 300 mg/m2 on days: 1, 8, 15, and 22 | Cycle 1 to 8: 0.75 | Cycle 1 to 8: 21 |
Daratumumab | 1,800 | Injection | 7,712.0500a | Cycle 1 to 2: 1,800 mg on days 1, 8, 15, and 22 Cycle 3 to 6: 1,800 mg on days 1 and 15 Cycle 7+: 1,800 mg on day 1 | Cycle 1 to 2: 1,102 Cycle 3 to 6: 551 Cycle 7+: 275 | Cycle 1 to 2: 30,848 Cycle 3 to 6: 15,424 Cycle 7+: 7,712 |
Dexamethasonec | 4 mg | Tablet | 0.6112 | 40 mg on days 1, 8, 15, and 22 | 0.87 | 24 |
DCyBorD regimen | Cycles 1, 2: 1,197 Cycles 3 to 6: 646 Cycles 7 to 8: 371 Cycle 9+: 276 | Cycles 1, 2: 33,511 Cycles 3 to 6: 18,087 Cycles 7 to 8: 10,375 Cycle 9+: 7,712 | ||||
DRd (28-day cycle) | ||||||
Daratumumab | 1,800 | Injection | 7,712.0500a | Cycle 1 to 2: 1,800 mg on days 1, 8, 15, and 22 Cycle 3 to 4: 1,800 mg on days 1 and 15 Cycle 5+: 1,800 mg on day 1 | Cycle 1 to 2: 1,102 Cycle 3 to 6: 551 Cycle 7+: 275 | Cycle 1 to 2: 30,848 Cycle 3 to 6: 15,424 Cycle 7+: 7,712 |
Dexamethasonec | 0.5 mg 4 mg | Tablet | 0.1564 0.6112 | 40 mg on days 1, 8, 15, and 22 | 0.87 | 24 |
Lenalidomide | 10 mg 25 mg | Tablet | 90.2500 106.0000 | 25 mg (10 mg for patients with creatinine clearance CrCl ≥ 30 to < 60 mL/min) on days 1 to 21 | 79.50 | 2,226 |
DRd regimen | Cycle 1 to 2: 1,182 Cycle 3 to 4: 631 Cycle 5+: 356 | Cycle 1 to 2: 33,099 Cycle 3 to 4: 17,675 Cycle 5+: 9,963 | ||||
DVMPd (42-day cycle for melphalan-prednisone-bortezomib) | ||||||
Bortezomibb | 2.5 mg 3.5 mg | Injection | 1,001.7300a 654.3100a | Cycle 1: 1.3 mg/m2 on days 1, 4, 8, 11, 22, 25, 29, and 32 Cycle 2 to 9: 1.3 mg/m2 on days 1, 8, 22, and 29 | Cycle 1: 125 Cycle 2 to 9: 62 | Cycle 1: 3,490 Cycle 2 to 9: 1,745 |
Daratumumab | 1,800 | Injection | 7,712.0500a | Cycle 1: 1,800 mg o days 1, 8, 15, 22, 29, and 36 Cycle 2 to 9: 1,800 mg on days 1 and 22 | Cycle 1 to 2: 1,102 Cycle 2 to 9: 367 | Cycle 1 to 2: 30,848 Cycle 2 to 9: 10,283 |
Melphalan | 2 mg | Tablet | 2.3297a | Cycle 1 to 9: 9 mg/m2 on days 1, 2, 3, and 4 | Cycle 1 to 9: 1.78 | Cycle 1 to 9: 50 |
Prednisone | 5 mg 50 mg | Tablet | 0.0220 0.1735 | Cycle 1 to 9: 60 mg/m2 on days 1, 2, 3, and 4 | Cycle 1 to 9: 0.03 | Cycle 1 to 9: 0.93 |
DVMP regimen | Cycle 1 to 2: 1,228 Cycle 2 to 9: 494 | Cycle 1 to 2: 34,388 Cycle 2 to 9: 13,823 | ||||
VRd (21-day cycle) | ||||||
Bortezomibb | 2.5 mg 3.5 mg | Injection | 1,001.7300a 654.3100a | Cycle 1 to 8: 1.3 mg/m2 on days 1, 8, and 15 | Cycle 1 to 8: 93 | Cycle 1 to 8: 2,617 |
Lenalidomide | 10 mg 25 mg | Tablet | 90.2500 106.0000 | 25 mg (10 mg for patients with creatinine clearance CrCl ≥ 30 to < 60 mL/min) on days 1 to 14 | 60 to 71 | 1,685 to 1,977 |
Dexamethasonec | 0.5 mg 4 mg | Tablet | 0.1564 0.6112 | 40 mg on days 1, 8, and 15 | 0.87 | 24 |
VRd regimen | Cycle 1 to 8: 155 to 165 Cycle 9+: 61 to 72 | Cycle 1 to 8: 4,326 to 4,620 Cycle 9+: 1,709 to 2,003 | ||||
Rd (28-day cycle) | ||||||
Lenalidomide | 10 mg 25 mg | Tablet | 90.2500 106.0000 | 25 mg on days 1 to 21 | 80 | 2,226 |
Dexamethasonec | 0.5 mg 4 mg | Tablet | 0.1564 0.6112 | 40 mg on days 1, 8, 15, and 22 | 0.87 | 24 |
Rd regimen | 80 | 2,250 | ||||
CDA-AMC = Canada’s Drug Agency; CrCl = creatine clearance; CyBorD = cyclophosphamide-bortezomib-dexamethasone; DCyBorDd = daratumumab-cyclophosphamide-bortezomib-dexamethasone; DRd = daratumumab-lenalidomide-dexamethasone; DVMP = daratumumab-bortezomib-melphalan-prednisone- bortezomib; IsaVRd = isatuximab-bortezomib-lenalidomide-dexamethasone; mm = multiple myeloma; Rd = lenalidomide-dexamethasone; VRd = bortezomib-lenalidomide-dexamethasone.
Note: All prices are from the Ontario Drug Benefit Formulary (accessed December 2024),13 unless otherwise indicated, and do not include dispensing fees. Wastage was included for all regimens and RDI was assumed to be 100%.
aDrug price from IQVIA DeltaPA (accessed December 2024).12
bIt was noted a higher dose of 1.5 mg/m2 is sometimes adopted for bortezomib.
cDexamethasone is also available as an IV formulation for infusion. The price of dexamethasone IV is $1.69 per 4mg/mL vial.
dDVMP regimen is rarely used in clinical practice in Canada and the monograph is for an IV form of daratumumab which is also rarely used. Here the subcutaneous version of daratumumab is assumed, aligning with all other regimens. As the cycle length is not 28 days in the 28-day cost column this represents the cost per 28-day cycle.
Appendix 2: Submission Quality
Please note that this appendix has not been copy-edited.
Description | Yes or no | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | Yes | No comment. |
Model has been adequately programmed and has sufficient face validity | No | Refer to key limitation “Model lacked transparency due to poor modelling practices.” |
Model structure is adequate for decision problem | Yes | No comment. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | Yes | No comment. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | Yes | No comment. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | Yes | No comment. |
Appendix 3: Additional Information on the Submitted Economic Evaluation
Please note that this appendix has not been copy-edited.
Figure 1: Partitioned Survival Model
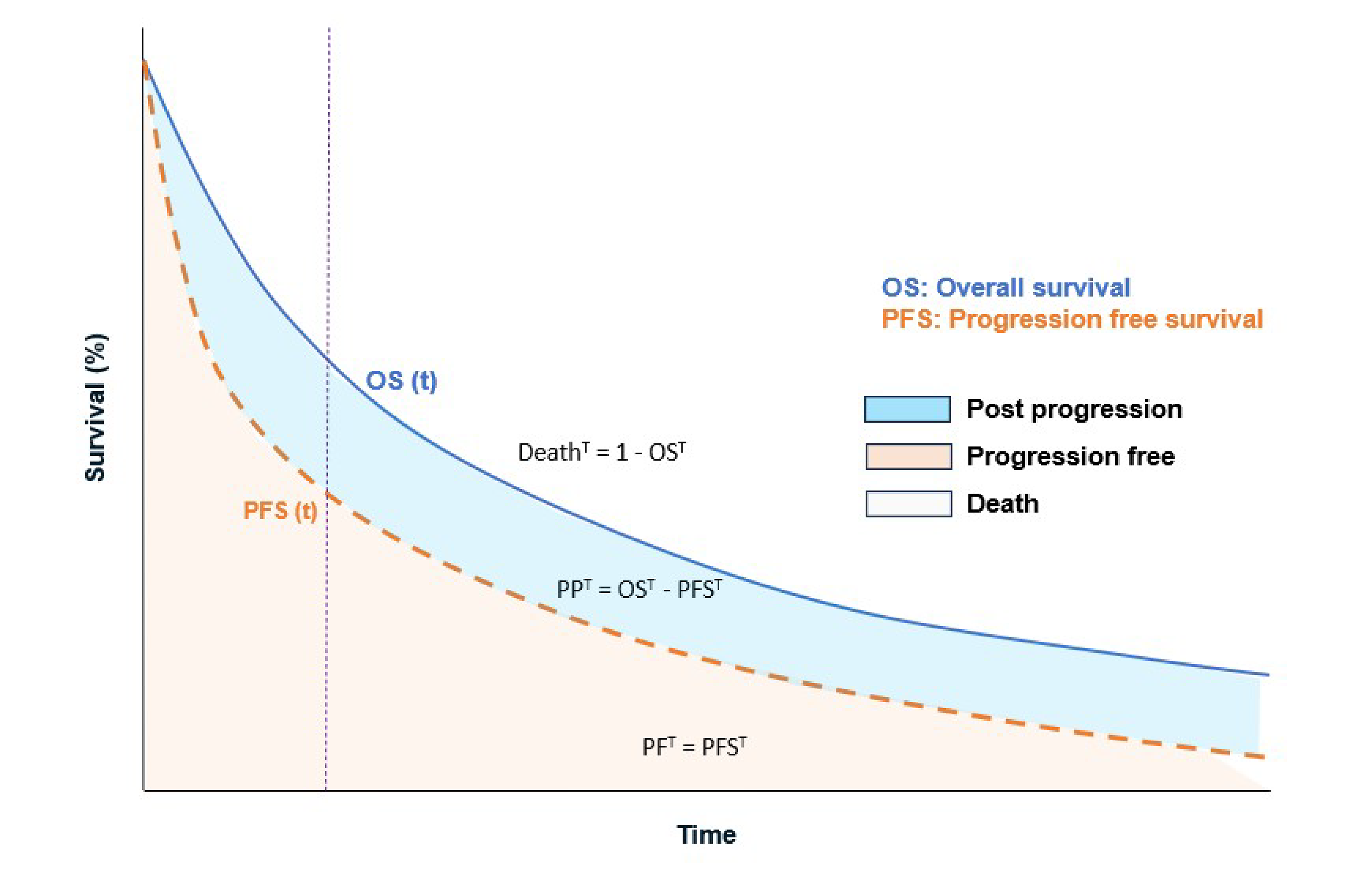
OS = overall survival; PF = progression-free; PFS = progression-free survival; PP = postprogression; t = time.
Source: Sponsor’s pharmacoeconomic submission.1
Detailed Results of the Sponsor’s Base Case
Table 10: Disaggregated Summary of the Sponsor’s Economic Evaluation Results
Parameter | IsaVRd | VRd | DRd | DCyBorD | DVMP | CyBorD | Rd |
|---|---|---|---|---|---|---|---|
Discounted LYs | |||||||
Total | 11.18 | 7.29 | 10.41 | 9.03 | 9.02 | 6.34 | 8.42 |
PF | 9.09 | 5.31 | 7.12 | 4.59 | 5.14 | 3.61 | 4.39 |
PD | 2.09 | 1.98 | 3.30 | 4.44 | 3.88 | 2.74 | 4.03 |
Discounted QALYs | |||||||
Total | 5.62 | 3.96 | 5.22 | 4.59 | 4.61 | 3.34 | 4.29 |
PF | 4.71 | 2.98 | 3.77 | 2.47 | 2.83 | 2.04 | 2.45 |
PD | 0.91 | 0.98 | 1.44 | 2.12 | 1.77 | 1.30 | 1.84 |
Discounted costs ($) | |||||||
Total | 1,227,580 | 1,238,658 | 1,307,996 | 904,704 | 827,304 | 1,023,626 | 985,146 |
Drug acquisition | 691,215 | 106,610 | 768,966 | 487,710 | 546,522 | 90,798 | 5,065 |
Administration | 20,075 | 1,881 | 12,285 | 7,465 | 10,690 | 2,757 | 0 |
Subsequent treatment | 410,584 | 997,559 | 410,509 | 308,091 | 178,160 | 812,868 | 777,059 |
Subsequent administration | 17,885 | 51,109 | 17,862 | 14,110 | 4,364 | 25,356 | 36,838 |
AE management | 11,633 | 8,370 | 21,235 | 12,115 | 12,079 | 20,946 | 13,919 |
Resource use | 22,212 | 16,170 | 22,560 | 19,566 | 19,835 | 13,071 | 16,109 |
End-of-life care | 53,976 | 56,959 | 54,579 | 55,647 | 55,653 | 57,830 | 56,156 |
AE = adverse event; CyBorD = cyclophosphamide-bortezomib-dexamethasone; DCyBorD = daratumumab-cyclophosphamide-bortezomib-dexamethasone; DRd = daratumumab-lenalidomide-dexamethasone; DVMP = daratumumab-bortezomib-melphalan-prednisone; IsaVRd = isatuximab-bortezomib-lenalidomide-dexamethasone; LY = life-year; PD = progressed disease; PF = progression-free; QALY = quality-adjusted life-year; Rd = lenalidomide-dexamethasone; VRd = bortezomib-lenalidomide-dexamethasone.
Source: Sponsor’s pharmacoeconomic submission.1
Appendix 4: Additional Details on the CDA-AMC Reanalyses and Sensitivity Analyses of the Economic Evaluation
Please note that this appendix has not been copy-edited.
Table 11: Summary of the Stepped Analysis of the CDA-AMC Base-Case Results
Stepped analysis | Drug | Total costs ($) | Total QALYs | Sequential ICER ($/QALY) |
|---|---|---|---|---|
Sponsor’s base case | DVMP | 827,304 | 4.61 | Reference |
IsaVRd | 1,227,580 | 5.62 | 395,725 | |
Dominated treatments | ||||
DCyBorD | 904,704 | 4.59 | Strictly dominated | |
Rd | 985,146 | 4.29 | Strictly dominated | |
CyBorD | 1,023,626 | 3.34 | Strictly dominated | |
VRd | 1,238,658 | 3.96 | Strictly dominated | |
DRd | 1,307,996 | 5.22 | Strictly dominated | |
CDA-AMC reanalysis 1: Comparators | DRd | 1,298,006 | 5.43 | Reference |
IsaVRd | 1,233,489 | 5.87 | Dominant | |
CDA-AMC reanalysis 2: Subsequent therapy | DRd | 878,612 | 5.43 | Reference |
IsaVRd | 814,729 | 5.87 | Dominant | |
CDA-AMC reanalysis 3: OS | DRd | 1,297,368 | 5.79 | Reference |
IsaVRd | 1,233,489 | 5.87 | Dominant | |
CDA-AMC reanalysis 4: TTD | DRd | 1,448,411 | 5.43 | Reference |
IsaVRd | 1,507,899 | 5.87 | 134,045 | |
CDA-AMC base case (deterministic) (reanalyses 1 + 2 + 3 + 4) | DRd | 1,029,956 | 5.79 | Reference |
IsaVRd | 1,089,140 | 5.87 | 731,361 | |
CDA-AMC base case (probabilistic) (reanalyses 1 + 2 + 3 + 4) | DRd | 1,000,917 | 5.55 | Reference |
IsaVRd | 1,023,257 | 5.62 | 311,681 | |
CDA-AMC = Canada’s Drug Agency; CyBorD = cyclophosphamide-bortezomib-dexamethasone; DCyBorD = daratumumab-cyclophosphamide-bortezomib-dexamethasone; DRd = daratumumab-lenalidomide-dexamethasone; DVMP = daratumumab-bortezomib-melphalan-prednisone; ICER = incremental cost-effectiveness ratio; IsaVRd = isatuximab-bortezomib-lenalidomide-dexamethasone; OS = overall survival; QALY = quality-adjusted life-year; Rd = lenalidomide-dexamethasone; TTD = time to treatment discontinuation; VRd = bortezomib-lenalidomide-dexamethasone.
Note: The CDA-AMC reanalysis is based on publicly available prices of the comparator treatments. The results of all steps are presented deterministically unless otherwise indicated, while the cumulative CDA-AMC base case is always presented both deterministically and probabilistically. Notably, the results of the CDA-AMC reanalyses 2, 3, and 4 are presented as pairwise comparisons between IsaVRd and DRd.
Table 12: Disaggregated Summary of CDA-AMC Economic Evaluation Results
Parameter | IsaVRd | DRd |
|---|---|---|
Discounted LYs | ||
Total | 11.19 | 11.19 |
PF | 9.03 | 7.16 |
PD | 2.16 | 4.02 |
Discounted QALYs | ||
Total | 5.62 | 5.55 |
PF | 4.68 | 3.79 |
PD | 0.93 | 1.75 |
Discounted costs ($) | ||
Total | 1,023,257 | 1,000,917 |
Drug acquisition | 909,297 | 886,971 |
Administration | 25,886 | 14,174 |
Subsequent treatment | 0 | 0 |
Subsequent administration | 0 | 0 |
AE management | 11,673 | 21,250 |
Resource use | 22,169 | 24,290 |
End-of-life care | 54,232 | 54,232 |
AE = adverse event; CDA-AMC = Canada’s Drug Agency; DRd = daratumumab-lenalidomide-dexamethasone; ICER = incremental cost-effectiveness ratio; IsaVRd = isatuximab-bortezomib-lenalidomide-dexamethasone; LY = life-year; PD = progressed disease; PF = progression-free; QALY = quality-adjusted life-year; vs. = versus.
Scenario Analyses
Table 13: Scenario Analysis Conducted on the CDA-AMC Base Case
Stepped analysis | Drug | Total costs ($) | Total QALYs | Sequential ICER ($/QALY) |
|---|---|---|---|---|
CDA-AMC base case (probabilistic) | DRd | 1,000,917 | 5.55 | Reference |
IsaVRd | 1,023,257 | 5.62 | 311,681 | |
CDA-AMC scenario 1: HR of median TTD vs. median PFS | DRd | 860,395 | 5.63 | Reference |
IsaVRd | 776,232 | 5.70 | Dominant |
CDA-AMC = Canada’s Drug Agency; DRd = daratumumab-lenalidomide-dexamethasone; HR = hazard ratio; ICER = incremental cost-effectiveness ratio; IsaVRd = isatuximab-bortezomib-lenalidomide-dexamethasone; PFS = progression-free survival; QALY = quality-adjusted life-year; TTD = time to treatment discontinuation.
Appendix 5: Submitted BIA and CDA-AMC Appraisal
Please note that this appendix has not been copy-edited.
Table 14: Summary of Key Take-Aways
Key take-aways of the BIA |
|---|
|
ASCT = autologous stem cell transplant; BIA = budget impact analysis; CDA-AMC = Canada’s Drug Agency; IsaVRd = isatuximab-bortezomib-lenalidomide-dexamethasone; NDMM = newly diagnosed multiple myeloma; RDI = relative dose intensity.
Summary of Sponsor’s BIA
The sponsor submitted a BIA to estimate the budget impact of reimbursing IsaVRd for the treatment of patients with NDMM who are not eligible for an ASCT or with no intent for an ASCT as initial therapy. The analysis was undertaken from a pan-Canadian public drug program perspective over a 3-year time horizon (2025 to 2027). The target population size was derived with an epidemiological approach, considering incident cases of MM in Canada. Key inputs to the BIA are documented in Table 15.
The following key assumptions were made by the sponsor:
RDI was not assumed to be 100%.
Proportion of patients either eligible for an ASCT but not intending to undergo it as initial therapy (███), or those ineligible for an ASCT (███), was based on clinical expert opinion.
DVMP is ███ ████████ ██ ███████ ███ share of the market.
██ of patients were expected to receive no active treatment.
IsaVRd is ███ ████████ ██ ███████ ███ market from CyBorD.
Table 15: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1 / year 2 / year 3 if appropriate) |
|---|---|
Target population | |
MM incidence (NDMM)
| 0.0084%18,19 (2,186 / 2,220 / 2,253) █████ ██████ █ █████ █ ████████████ ██████ █ █████ █ ████████████ ████ █ ███ █ ████ |
Number of patients eligible for drug under review | █████ █ █████ █ █████ |
Market uptake (3 years) | |
Uptake (reference scenario) | |
VRd | ██ █ ██ █ █████ █ ██ █ ██████ █ ███ █ ██████ █ ██ █ █████ █ ██ █ █████ █ ██ █ █████ █ ██ █ ██ |
Rd | |
DRd | |
DVMP | |
CyBorD | |
DCyBorD | |
No active treatment | |
Uptake (new drug scenario) | |
IsaVRd | ███ █ ███ █ ██████ █ ██ █ █████ █ ██ █ ██████ █ ███ █ ██████ █ ██ █ █████ █ ██ █ █████ █ ██ █ █████ █ ██ █ ██ |
VRd | |
Rd | |
DRd | |
DVMP | |
CyBorD | |
DCyBorD | |
No active treatment | |
Cost of treatment (per-patient, per 28-day cycle) | |
IsaVRda VRd Rd DRd DVMP CyBorD DCyBorD | $8,206 to $41,230 $2,136 to $10,873 $2,142 $10,164 to 34,230 $8,022 to $56,232 $4,040 to $4,064 $8,022 to $36,128 |
ASCT = autologous stem cell transplant; CyBorD = cyclophosphamide-bortezomib-dexamethasone; DCyBorD = daratumumab-cyclophosphamide-bortezomib-dexamethasone; DRd = daratumumab-lenalidomide-dexamethasone; DVMP = daratumumab-bortezomib-melphalan-prednisone; IsaVRd = isatuximab-bortezomib-lenalidomide-dexamethasone; MM = multiple myeloma; NDMM = newly diagnosed multiple myeloma; Rd = lenalidomide-dexamethasone; VRd = bortezomib-lenalidomide-dexamethasone.
aIsaVRd costs vary by cycle: $41,230 (cycle 1; 42 days/cycle), $29,090 (cycles 2 to 4; 42 days/cycle), $14,276 (cycles 5 to 17; 28 days/cycle), $8,206 (cycles 18+; 28 days/cycle)
Summary of the Sponsor’s BIA Results
In the sponsor’s base-case analysis, the estimated incremental budget impact of funding IsaVRd for the treatment of adult patients with NDMM who are not eligible for an ASCT or with no intent for an ASCT as initial therapy resulted in cost savings of $9,105,499 in year 1, $10,488,860 in year 2, and $27,756,430 in year 3, for a cumulative total cost savings of $47,350,789 over the 3-year projection period.
CDA-AMC Appraisal of the Sponsor’s BIA
CDA-AMC identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
Use of RDI to estimate actual drug costs is not appropriate. In the sponsor’s submitted BIA model, the cost of treatment regimens was calculated based on the RDI reported in the IMROZ trial21 for IsaVRd and VRd, and respective clinical trials7,22-24 for the remaining comparators. This consideration of RDI is problematic as this parameter can be influenced by several factors. The dose received by a patient may differ from the full planned dose of the drug due to dose delays, missed doses, dose reductions to manage toxicity, or subsequent dose re-escalation; each of these have differing impacts on drug costs. Furthermore, it is unclear how these assumptions interact with considerations about vial size and wastage. Additionally, for the oral comparators, prescriptions may be filled and reimbursed regardless of treatment adherence.
In the CDA-AMC reanalysis, RDI for the IsaVRd and comparators was set to 100%.
Market uptake of IsaVRd may be overestimated. The sponsor’s submitted BIA indicated that IsaVRd would result in a market uptake of ██% in year 1, ██% in year 2, and ██% in year 3, mostly capturing market from DRd. Market share assumptions were based on a survey of clinicians conducted by the sponsor.20 Clinical expert feedback obtained by CDA-AMC noted that while it is reasonable to assume that IsaVRd would capture market mostly from DRd, its ability to capture a substantial portion from other relevant comparators remains uncertain. Additionally, considering the significant uncertainty surrounding the comparative efficacy of IsaVRd versus DRd, as indicated by the appraisal of the sponsor-submitted CUA, it is reasonable to assume that IsaVRd may capture a smaller share of the current DRd market.
To mitigate this uncertainty, CDA-AMC performed a scenario analysis assuming a 25% decrease in IsaVRd’s market capture from DRd.
Subsequent therapy costs were not included in the BIA. In the sponsor’s submitted BIA model, subsequent therapy costs were not included in the base case or as a scenario analysis. As these costs were not included, it was not possible to estimate the budgetary impact of subsequent therapies. This does not align with the sponsor’s submitted CUA, which included subsequent therapy costs, informed by the relevant trials.
CDA-AMC was unable to address this limitation.
CDA-AMC Reanalyses of the BIA
Table 16: CDA-AMC Revisions to the Submitted BIA
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
Changes to derive the CDA-AMC base case | ||
1. RDIa | IsaVRd
VRd
Rd
DRd
| IsaVRd
VRd
Rd
DRd
|
CDA-AMC base case | Reanalysis 1 | |
BIA = budget impact analysis; CDA-AMC = Canada’s Drug Agency; CyBorD = cyclophosphamide-bortezomib-dexamethasone; DCyBorD = daratumumab-cyclophosphamide-bortezomib-dexamethasone; DRd = daratumumab-lenalidomide-dexamethasone; DVMP = daratumumab-bortezomib-melphalan-prednisone; IsaVRd = isatuximab-bortezomib-lenalidomide-dexamethasone; Rd = lenalidomide-dexamethasone; RDI = relative dose intensity; VRd = bortezomib-lenalidomide-dexamethasone.
aThe sponsor assumed 100% RDI for all other comparators, including CyBorD, DCyBorD, and DVMP.
The results of the CDA-AMC stepwise reanalysis are summarized in Table 17, with a more detailed breakdown provided in Table 18. The analysis indicates that funding IsaVRd for the treatment of adult patients with NDMM who are not eligible for an ASCT or with no intent for an ASCT as initial therapy resulted in cost savings of $3,304,157 in year 1, $2,016,456 in year 2, and $17,863,532 in year 3. This results in cumulative cost savings of $23,184,144 over 3 years.
Table 17: Summary of the CDA-AMC Reanalyses of the BIA
Stepped analysis | Three-year total ($) |
|---|---|
Submitted base case | –47,350,789 |
CDA-AMC base case | –23,184,144 |
BIA = budget impact analysis; CDA-AMC = Canada’s Drug Agency.
CDA-AMC conducted the following scenario analyses to address remaining uncertainty, using the CDA-AMC base case (results are provided in Table 18:
assuming a 25% reduction in market uptake of IsaVRd
assuming that the price of isatuximab is reduced by 2.5%.
Table 18: Detailed Breakdown of the CDA-AMC Reanalyses of the BIA
Stepped analysis | Scenario | Year 0 (current situation) ($) | Year 1 ($) | Year 2 ($) | Year 3 ($) | Three-year total ($) |
|---|---|---|---|---|---|---|
Submitted base case | Reference | 232,665,528 | 375,210,953 | 514,498,005 | 648,008,657 | 1,537,717,614 |
New drug | 232,665,528 | 366,105,454 | 504,009,144 | 620,252,227 | 1,490,366,825 | |
Budget impact | 0 | –9,105,499 | –10,488,860 | –27,756,430 | –47,350,789 | |
CDA-AMC base case | Reference | 243,433,925 | 396,730,921 | 546,879,631 | 690,773,045 | 1,634,383,596 |
New drug | 243,433,925 | 393,426,764 | 544,863,175 | 672,909,513 | 1,611,199,451 | |
Budget impact | 0 | –3,304,157 | –2,016,456 | –17,863,532 | –23,184,144 | |
CDA-AMC scenario analysis 1: 25% reduction in market capture for isatuximab | Reference | 243,433,925 | 396,730,921 | 546,879,631 | 690,773,045 | 1,634,383,596 |
New drug | 243,433,925 | 391,177,351 | 540,889,258 | 672,123,946 | 1,604,190,555 | |
Budget impact | 0 | –5,553,569 | –5,990,373 | –18,649,099 | –30,193,041 | |
CDA-AMC scenario analysis 2: 2.5% price reduction for isatuximab | Reference | 243,433,925 | 396,730,921 | 546,879,631 | 690,773,045 | 1,634,383,596 |
New drug | 243,433,925 | 391,064,361 | 540,647,368 | 667,219,813 | 1,598,931,542 | |
Budget impact | 0 | –5,666,559 | –6,232,263 | –23,553,232 | –35,452,054 |
BIA = budget impact analysis; CDA-AMC = Canada’s Drug Agency.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.