Drugs, Health Technologies, Health Systems
Reimbursement Review
Dostarlimab (Jemperli)
Sponsor: GlaxoSmithKline Inc.
Therapeutic area: Endometrial cancer
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Clinical Review
Abbreviations
AE
adverse event
BICR
blinded independent central review
CDA-AMC
Canada’s Drug Agency
CI
confidence interval
dMMR
mismatch repair deficient
ECOG
Eastern Cooperative Oncology Group
EORTC QLQ-C30
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30
FIGO
International Federation of Gynaecology and Obstetrics
GOC
Society of Gynecologic Oncology of Canada
GRADE
Grading of Recommendations Assessment, Development and Evaluation
HR
hazard ratio
HRQoL
health-related quality of life
ITT
intention to treat
KM
Kaplan-Meier
MID
minimal important difference
MMR
mismatch repair
MMRM
mixed-effects model for repeated measures
MSI
microsatellite instability
MSI-H
microsatellite instability–high
MSS
microsatellite stable
NE
not estimable
OH (CCO)
Ontario Health (Cancer Care Ontario)
OS
overall survival
PFS
progression-free survival
pMMR
mismatch repair proficient
RCT
randomized controlled trial
TEAE
treatment-emergent adverse event
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Table 1: Background Information on the Application Submitted for Review
Item | Description |
|---|---|
Drug product | Dostarlimab (Jemperli) 50 mg/mL solution for IV infusion in 500 mg/10 mL vial, 500 mg q.3.w. for 6 cycles followed by 1,000 mg q.6.w. |
Sponsor | GlaxoSmithKline Inc. |
Indication | Jemperli is indicated in combination with carboplatin and paclitaxel for the treatment of adult patients with primary advanced or first recurrent endometrial cancer who are candidates for systemic therapy |
Reimbursement request | As per indication |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | April 16, 2025 |
Recommended dose | The recommended dose as combination therapy is 500 mg Jemperli administered through IV infusion over 30 minutes q.3.w. for 6 doses followed by 1,000 mg q.6.w. for all cycles thereafter until progression of disease or unacceptable toxicity, or for up to 3 years |
NOC = Notice of Compliance; q.3.w. = every 3 weeks; q.6.w. = every 6 weeks.
Introduction
Endometrial cancer is the most common gynecologic cancer in high-income countries, with approximately 8,600 new cases estimated in Canada in 2024. Recurrence occurs in 10% to 15% of patients, with poor outcomes for advanced or recurrent cases. For patients with primary advanced or recurrent endometrial cancer, the current standard of care is platinum-based combination regimens, with response rates ranging from 40% to 62% in the first-line setting. However, for patients whose disease progresses after platinum-based chemotherapy, there is no standard second-line treatment. Current options, such as single-drug chemotherapies or hormonal therapies, have low response rates and limited survival benefits.
Dostarlimab (Jemperli), a PD-1 monoclonal antibody, is indicated for treating adults with primary advanced or recurrent endometrial cancer, particularly those with mismatch repair deficient (dMMR) or microsatellite instability–high (MSI-H) tumour status, which is found in approximately 13% to 30% of recurrent endometrial cancer cases. For this review, the approved Health Canada indication involves using dostarlimab in combination with carboplatin-paclitaxel for adult patients with primary advanced or first recurrent endometrial cancer who are candidates for systemic therapy. The recommended dose is 500 mg administered through IV every 3 weeks for 6 cycles in combination with carboplatin-paclitaxel followed by 1,000 mg monotherapy every 6 weeks for up to 3 years. Dostarlimab has also already been approved by Health Canada for patients with dMMR or MSI-H recurrent or primary advanced endometrial cancer in combination with carboplatin-paclitaxel. In 2024, the pan-Canadian Oncology Drug Review Expert Review Committee (pERC) recommended reimbursement for its use in combination therapy in this setting.
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of dostarlimab 500 mg administered through IV infusion every 3 weeks for 6 cycles in combination with carboplatin-paclitaxel followed by 1,000 mg monotherapy every 6 weeks starting at cycle 7 for up to 3 years for the treatment of adults with primary advanced or first recurrent endometrial cancer who are candidates for systemic therapy.
Perspectives of Patients, Clinicians, and Drug Programs
The information in this section is a summary of input provided by the patient and clinician groups who responded to CDA-AMC’s call for input and from clinical experts consulted by Canada’s Drug Agency (CDA-AMC) for the purpose of this review.
Patient Input
CDA-AMC received input from 1 patient group, the Colorectal Cancer Resource & Action Network (CCRAN), regarding the use of dostarlimab for advanced or recurrent endometrial cancer. CCRAN collaborated with the Canadian Cancer Survivor Network to collect perspectives from patients with endometrial cancer. The input was gathered through interviews with 4 patients (all of whom were females residing in Canada), and 2 clinicians. The patients had undergone a variety of treatments, including surgery, chemotherapy, immunotherapy, hormonal therapy, and targeted therapies.
Endometrial cancer had a significant impact on the daily lives of these patients and their families. Patients reported struggling with debilitating side effects, such as neuropathy, fatigue, sexual dysfunction, and digestive issues, all of which diminished their quality of life. In addition to the physical burdens, the patients highlighted the emotional strain of managing the disease, including inadequate mental health support and challenges accessing treatment, particularly for those in rural areas.
Key outcomes that were important to patients included better symptom control, improved survival, and reduced treatment-related side effects. There was a strong preference for therapies that would allow patients to maintain their quality of life and engage in day-to-day activities, such as work, hobbies, and family care.
The input from CCRAN highlighted several unmet needs in the current treatment landscape, particularly for patients with recurrent or metastatic disease. Patients expressed a need for new treatments that could strike a balance between effectiveness and tolerable side effects, which is critical for their ability to maintain a normal life while managing the disease. This perspective is essential for interpreting the clinical trial results for dostarlimab and assessing how the treatment may improve patient outcomes in the Canadian health care context.
Clinician Input
Input From Clinical Experts Consulted by CDA-AMC
The clinical experts indicated that the treatment goals for patients with primary advanced or recurrent endometrial cancer are to prolong survival, delay disease progression, and improve quality of life. The experts noted that the standard of care for the majority of patients is usually chemotherapy (often with carboplatin-paclitaxel) or immunotherapy, and to a lesser extent, hormonal therapy, surgery, or radiation, depending on extent of disease and sites of recurrence. The experts noted that most patients become refractory to current treatment options, and that subsequent therapies are limited to chemotherapies (e.g., doxorubicin, topotecan, paclitaxel, oxaliplatin, docetaxel, and bevacizumab), which offer poor response rates and have high toxicity. The experts also indicated that there is an important unmet need for an effective first-line treatment for patients with metastatic mismatch repair proficient (pMMR) endometrial cancer. The clinical experts considered dostarlimab’s mechanism of action as distinct from that of chemotherapy; consequently, its use would cause a significant shift in the current treatment paradigm. The clinical experts noted that dostarlimab would be used in the first-line setting in combination with carboplatin-paclitaxel for all patients with primary advanced, recurrent endometrial cancer, including those with dMMR mutations. The clinical experts agreed that the patients best suited for dostarlimab plus carboplatin-paclitaxel would be those with advanced or recurrent endometrial cancer. In their opinion, the patients who would benefit most would be those with dMMR status or, to a lesser extent, pMMR status. The experts highlighted that patients would be identified based on clinical examination and judgment; a companion diagnostic would not be needed. The clinical experts indicated that in clinical practice, a combination of radiographic and clinical parameters is used to determine whether a patient is responding or progressing on treatment. The experts indicated that treatment with dostarlimab plus carboplatin-paclitaxel should be discontinued if patients experience disease progression (defined radiologically or clinically) or if treatment is intolerable. They noted that discontinuation should be based on several cycles of treatment, given that tumour swelling or enlargement could occur with immunochemotherapy. They indicated that patients receiving dostarlimab plus carboplatin-paclitaxel should be under the care of a gynecologic oncologist or medical oncologist who can manage toxicity associated with the therapy. They noted that it would be reasonable for patients to receive the therapy in a community setting in which day-to-day follow-up is with a general practitioner in oncology.
Clinician Group Input
Two clinician groups, the Ontario Health (Cancer Care Ontario) (OH [CCO]) Gynecologic Cancer Drug Advisory Committee and the Society of Gynecologic Oncology of Canada (GOC), provided input for this review.
There were no significant contrary views between the input from the clinical experts consulted by CDA-AMC and the OH (CCO).
The clinician groups and CDA-AMC clinical experts agreed on key areas, such as the unmet need for durable responses to current treatments, the treatment goals of prolonging life and improving health-related quality of life (HRQoL), and the most appropriate patient population being those with dMMR tumours.
The clinician group highlighted that dostarlimab, in combination with chemotherapy, offers a valuable new option as a first-line treatment in clinical practice, particularly for patients with primary stage III or IV or recurrent pMMR endometrial cancer who have limited treatment options and poor outcomes with chemotherapy alone.
Drug Program Input
Input was obtained from the drug programs that participate in the CDA-AMC reimbursement review process. The following were identified as key factors that could potentially affect the implementation of a CDA-AMC recommendation for dostarlimab plus carboplatin-paclitaxel:
considerations for the initiation of therapy
generalizability
funding algorithm
care provision issues.
The clinical experts consulted by CDA-AMC provided advice on the potential implementation issues raised by the drug programs. Refer to Table 4.
Clinical Evidence
Systematic Review
Description of Studies
One trial, the RUBY trial, Part 1 (N = 494), met the inclusion criteria for the systematic review conducted by the sponsor. The objective was to assess the efficacy and safety of dostarlimab IV infusion plus carboplatin-paclitaxel, followed by dostarlimab monotherapy, compared with placebo plus carboplatin-paclitaxel, followed by placebo, in adults with primary advanced or recurrent endometrial cancer. The trial enrolled patients who were at least 18 years of age and had histologically or cytologically confirmed, primary advanced or first recurrent endometrial cancer that was not amenable to curative therapy; an Eastern Cooperative Oncology Group (ECOG) Performance Status score of 0 or 1; and adequate organ function. Patients were excluded if they had received neoadjuvant or adjuvant chemotherapy, with or without recurrence, in the 6 months before entering the trial or if they had received prior treatment with an anti–PD-L1 or anti–PD-1 antibody. The approved Health Canada indication and reimbursement request aligned with the trial population. The outcomes most relevant to the CDA-AMC review included the dual primary outcomes of overall survival (OS) and progression-free survival (PFS) per investigator assessment and the secondary outcomes of HRQoL (measured using the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 [EORTC QLQ-C30] Global Health Status) and safety. Efficacy and safety data were evaluated at the data cut-off dates of September 28, 2022 (interim analysis 1) and September 22, 2023 (interim analysis 2). Overall, key baseline characteristics were generally balanced between treatment groups. The trial population was predominantly white (approximately 77%), with a mean age of 64 years; half of patients were aged 19 years to 64 years. Most patients (approximately 63%) had an ECOG Performance Status score of 0, indicating good overall performance; endometrioid histology (adenocarcinoma type or adenocarcinoma variant) at diagnosis (approximately 55%); recurrent (48%) or primary stage IV (33%) disease status; International Federation of Gynaecology and Obstetrics (FIGO) stage III or IV at diagnosis (approximately 60%); mismatch repair (MMR) microsatellite instability (MSI) status of pMMR and microsatellite stable (MSS) (approximately 76%); had received prior surgery for endometrial cancer (approximately 90%); and had not received prior external pelvic radiotherapy (approximately 83%).
Efficacy Results
Only those efficacy outcomes and analyses of subgroups identified as important to this review are reported. The main findings for the efficacy outcomes for Part 1 of the RUBY trial are from the data cut-off dates of September 28, 2022 (interim analysis 1) and September 22, 2023 (interim analysis 2). The boundaries for statistical significance for the dual primary outcomes of PFS and OS were met in interim analysis 1 and interim analysis 2, respectively. PFS was not re-evaluated during interim analysis 2. HRQoL results are from interim analysis 1, while safety results are from interim analysis 2.
Overall Survival
By the interim analysis 2, the median duration of follow-up for all patients was 37.2 months (range, 31.0 months to 49.5 months). There were 109 deaths (44.5%) in the group receiving dostarlimab plus carboplatin-paclitaxel and 144 deaths (57.8%) in the group receiving placebo plus carboplatin-paclitaxel. The median OS was 44.6 months (95% confidence interval [CI], 32.6 months to not estimable [NE]) in the group receiving dostarlimab plus carboplatin-paclitaxel versus 28.2 months (95% CI, 22.1 months to 35.6 months) in the group receiving placebo plus carboplatin-paclitaxel (1-sided P value = 0.0020), with a between-group hazard ratio (HR) of 0.69 (95% CI, 0.54 to 0.89). The results of the sensitivity analysis were consistent with those of the primary analysis. The Kaplan-Meier (KM)-estimated probabilities of being alive at 24 months and 36 months were 70.1% (95% CI, ████ to ████) versus 54.3% (95% CI, ████ to ████; between-group difference: ████% [95% CI, ███ to ████]), and 54.9% (95% CI, ████ to ████) versus 42.9% (95% CI, ████ to ████; between-group difference: ████% [95% CI, ████ to ████]) in the groups receiving dostarlimab plus carboplatin-paclitaxel and placebo plus carboplatin-paclitaxel, respectively.
The efficacy results for OS were generally consistent across the subgroup analyses of interest (age and histology) in favour of dostarlimab plus carboplatin-paclitaxel; however, there was inconsistency in the effects across the disease status subgroup. The subgroup analyses did not include MMR or MSI status.
PFS by Investigator Assessment
At the time of the first interim analysis, the median duration of follow-up for all patients was 25.4 months (range, 19.2 months to 37.8 months), and PFS events had been reported for 135 patients (55.1%) in the group receiving dostarlimab plus carboplatin-paclitaxel and 177 patients (71.1%) in the group receiving placebo plus carboplatin-paclitaxel. The median PFS was 11.8 months (95% CI, 9.6 months to 17.1 months) in the group receiving dostarlimab plus carboplatin-paclitaxel versus 7.9 months (95% CI, 7.6 months to 9.5 months) in the group receiving placebo plus carboplatin-paclitaxel (1-sided P value < 0.0001), with a between-group HR of 0.64 (95% CI, 0.51 to 0.80). The results of the sensitivity analyses were consistent with those of the primary analysis. The KM-estimated probabilities of PFS at 12 months and 24 months were 48.2% (95% CI, ████ to ████) versus 29.0% (95% CI, ████ to ████; between-group difference: ████% [95% CI, ████ to ████]), and 36.1% (95% CI, ████ to ████) versus 18.1% (95% CI, ████ to ████; between-group difference: ████% [95% CI, ████ to ████) in the groups receiving dostarlimab plus carboplatin-paclitaxel and placebo plus carboplatin-paclitaxel, respectively. The results of the secondary outcome of PFS by blinded independent central review (BICR) assessment were consistent with those of the investigator assessment (data not shown).
The efficacy results for PFS were generally consistent across the exploratory subgroup analyses by MMR and MSI status at baseline, disease status at baseline, age, and histology, in favour of dostarlimab plus carboplatin-paclitaxel. The HRs for the subgroups of patients with dMMR or MSI-H and pMMR or MSS were 0.33 (95% CI, 0.19 to 0.57) and 0.76 (95% CI, 0.60 to 0.98), respectively. There were some inconsistent effects across the disease status subgroup, particularly for patients with primary stage III cancer.
HRQoL by EORTC QLQ-C30
At baseline and at cycles 7 and 13, the EORTC QLQ-C30 Global Health Status mean scores for the intention-to-treat (ITT) population were similar between treatment groups, and there were no clinically meaningful changes observed (defined by the sponsor as a change in score from baseline of ≥ 10 points) in either group at cycle 7 or 13. The between-group least squares mean differences in change from baseline at cycles 7 and 13 were ████ (95% CI, ████ to ███) and ████ (95% CI, ████ to ███), respectively.
Harms Results
Harms data reported in this section are from interim analysis 2 (data cut-off date of September 22, 2023). There were no significant changes in the incidence of treatment-emergent adverse events (TEAEs) from the time of interim analysis 1 to the time of interim analysis 2. All patients in both treatment groups reported at least 1 TEAE. The most frequently reported TEAEs in the groups receiving dostarlimab plus carboplatin-paclitaxel and placebo plus carboplatin-paclitaxel, respectively, were fatigue (52.3% versus 54.9%), alopecia (53.9% versus 50.0%), nausea (54.4% versus 46.3%), peripheral neuropathy (44.0% versus 41.9%), and anemia (37.8% versus 42.7%). Of these TEAEs, a higher proportion of patients taking dostarlimab plus carboplatin-paclitaxel reported nausea. A higher proportion of patients receiving dostarlimab plus carboplatin-paclitaxel experienced at least 1 grade 3 or higher TEAE (72.2%) versus those receiving placebo plus carboplatin-paclitaxel (60.2%). The most common grade 3 or higher TEAEs in both groups were anemia (14.9% versus 16.7%), neutropenia (9.5% versus 9.3%), and neutrophil count decrease (8.3% versus 13.8%). The incidence of serious TEAEs was higher in the group receiving dostarlimab plus carboplatin-paclitaxel (39.8%) versus the group receiving placebo plus carboplatin-paclitaxel (28.0%). The most frequently reported serious TEAEs in the group receiving dostarlimab plus carboplatin-paclitaxel were pulmonary embolism (3.3% versus 2.0%) and sepsis (3.3% versus 0.4%); the most common serious TEAEs in the group receiving placebo plus carboplatin-paclitaxel were anemia (2.4% versus 1.2%) and pulmonary embolism. A higher proportion of TEAEs that led to study treatment discontinuation was reported in patients treated with dostarlimab plus carboplatin-paclitaxel (24.9%) versus placebo plus carboplatin-paclitaxel (16.3%). The most common TEAEs leading to discontinuation in both groups were peripheral neuropathy (2.1% versus 2.8%), peripheral sensory neuropathy (2.9% versus 0.4%), and infusion-related reaction (2.1% versus 3.3%). A lower proportion of deaths was reported in the group receiving dostarlimab plus carboplatin-paclitaxel (39.4%) versus the group receiving placebo plus carboplatin-paclitaxel (54.1%), with the primary reason for death in both groups being disease progression (████% versus ████%). For notable harms, a higher proportion of any immune-related TEAE was reported in patients taking dostarlimab plus carboplatin-paclitaxel (58.5%) versus placebo plus carboplatin-paclitaxel (37.0%). The incidence of infusion-related reactions was similar between the groups (████% versus ████%).
Critical Appraisal
Part 1 of the RUBY trial was a randomized, double-blind, placebo-controlled, phase III trial. Randomization procedures, including stratification by MMR and MSI status, previous external pelvic radiotherapy, and disease status, were appropriate and conducted using an interactive response system. In general, the key baseline characteristics of patients appeared balanced between groups. Sample sizes and power calculations were based on the dual primary outcome of PFS. The trial was powered to detect significant differences for PFS and OS. The interim analyses were preplanned with adequately justified stopping boundaries, which provides confidence that the statistical significance of PFS and OS is not a result of type I error. The prespecified analyses of PFS and OS were appropriately controlled for multiple comparisons. All other analyses were descriptive, including the HRQoL outcome of EORTC QLQ-C30 Global Health Status, which was deemed a clinically important outcome for the disease. The sample sizes for the exploratory subgroup analyses of PFS and OS, including by MMR status, were small. Aside from PFS in the population of patients with dMMR, the trial was not powered to detect subgroup differences. To minimize the risk of bias in the measurement of PFS, the trial performed tumour assessments using Response Evaluation Criteria in Solid Tumours Version 1.1 per investigator assessment; radiographic scans were assessed by BICR as a secondary outcome. The PFS per BICR assessment results were similar to the investigator-assessed results. In addition, the findings of the sensitivity analyses for the dual primary outcomes of PFS and OS were consistent with those of the primary analysis. Patients were permitted to receive posttreatment anticancer medications after study treatment had been discontinued, which may have influenced the assessment of OS. Given that no sensitivity analyses were performed to test the treatment policy strategy for OS (e.g., to exclude the effect of subsequent therapies), the estimated effect would be a combination of treatment with dostarlimab plus carboplatin-paclitaxel versus placebo plus carboplatin-paclitaxel, plus subsequent treatments. Therefore, survival results might be partially attributable to treatments administered after disease progression rather than to the study treatment itself. However, this is a relevant comparison because it is reflective of how the intervention and comparator would be used in practice. The trial authors stated that the proportional hazards assumption was assessed through visual inspection of a survival curve fit to KM data, inspection of log-cumulative hazard plots over time, and statistical goodness of fit based on relative Akaike and Bayesian information criterion values; however, the assessment results were not reported. Despite the absence of these results, visual inspection of the KM curves for PFS and OS appear to indicate a clear separation (at approximately 5 months and 7 months, respectively), after which sustained proportionality appears present throughout the study treatment. The EORTC QLQ-C30 has been validated in patients with cancer, with evidence of reliability and minimal important difference (MID) ranges. Based on the MID ranges identified in the literature, the sponsor suggested a 10-point change from baseline score as a clinically meaningful change; this was considered reasonable by the review team. Additionally, the result of the EORTC QLQ-C30 Global Health Status outcome was subject to potential bias due to missing data (however, the direction and extent of bias are unclear).
The population requested for reimbursement aligns with the approved Health Canada indication and overall trial population. The dosing and administration of dostarlimab were consistent with the approved product monograph. According to the clinical experts consulted by CDA-AMC, the eligibility criteria and baseline characteristics of Part 1 of the RUBY trial were generalizable to adults with primary advanced or recurrent endometrial cancer in the Canadian setting. However, the trial did not include patients with an ECOG Performance Status score of greater than 1. The clinical experts indicated that patients with good ECOG Performance Status (i.e., a score of 0 to 2) should be eligible for dostarlimab plus carboplatin-paclitaxel, followed by dostarlimab maintenance, if they are able to tolerate the therapy. The timing of administering dostarlimab or placebo in combination with carboplatin-paclitaxel appears align with chemotherapy regimens in the current standard of care, according to the clinical experts consulted by CDA-AMC. In Part 1 of the RUBY trial, treatment duration was up to 3 years if patients did not experience disease progression, unacceptable toxicity, or death. The trial included outcomes that were important to patients and clinicians. The patient group indicated that stopping disease progression, prolonging life, improving HRQoL, and reducing treatment side effects are important.
GRADE Summary of Findings and Certainty of the Evidence
For the pivotal studies and randomized controlled trials (RCTs) identified in the sponsor’s systematic review, Grading of Recommendations Assessment, Development and Evaluation (GRADE) was used to assess the certainty of the evidence for the outcomes considered most relevant to inform the CDA-AMC’s expert committee deliberations, and a final certainty rating was determined, as outlined by the GRADE Working Group.
Following the GRADE approach, evidence from the RCTs started as high-certainty evidence and could be rated down for concerns related to study limitations (which refer to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, or publication bias.
When possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect; if this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., the clinical importance is unclear). In all cases, the target of the certainty of evidence assessment was based on the point estimate and its location relative to the threshold for a clinically important effect (when a threshold was available) or to the null.
The reference points for the certainty of evidence assessment for OS, PFS, any immune-related TEAEs, and any infusion-related reactions were set according to the presence or absence of an important effect based on thresholds informed by the clinical experts consulted for this review. The reference point for the certainty of the evidence assessment for EORTC QLQ-C30 Global Health Status score was set according to the presence or absence of an important effect based on a threshold suggested by the sponsor that was informed by the literature.
The selection of outcomes for GRADE assessment was based on the sponsor’s Summary of Clinical Evidence, consultation with clinical experts, and input received from patient and clinician groups and public drug plans. The following list of outcomes was finalized in consultation with expert committee members:
survival outcomes (OS and PFS)
HRQoL outcome (EORTC QLQ-C30 Global Health Status)
notable harms (any immune-related TEAEs or any infusion-related reactions).
Results of GRADE Assessments
Table 2 presents the GRADE summary of findings for dostarlimab plus carboplatin-paclitaxel versus placebo plus carboplatin-paclitaxel.
Long-Term Extension Studies
No long-term extension studies were submitted by the sponsor.
Indirect Comparisons
No indirect treatment comparisons were submitted by the sponsor.
Studies Addressing Gaps in the Evidence From the Systematic Review
No studies addressing gaps were submitted by the sponsor.
Conclusions
Evidence from 1 phase III, randomized, double-blind trial (the RUBY trial, Part 1) reported on outcomes that were important to both patients and clinicians. The trial showed high certainty of evidence that treatment with dostarlimab plus carboplatin-paclitaxel results in a clinically important increase in OS at 24 months and 36 months and in PFS at 12 months and 24 months compared to placebo plus carboplatin-paclitaxel in adults with primary advanced or first recurrent endometrial cancer. At cycle 7 of treatment, there was low certainty of evidence for little to no clinically important between-group difference in HRQoL; no definitive conclusions can be drawn about HRQoL at cycle 13 due to concerns about imprecision and missing outcome data. There were no new safety signals identified; the safety of dostarlimab plus carboplatin-paclitaxel was consistent with the known safety profiles of the individual drugs. However, the trial showed high certainty of evidence for a clinically important increase in the proportion of patients who experience any immune-related TEAE when compared with placebo plus carboplatin-paclitaxel.
Table 2: Summary of Findings for Dostarlimab Plus Carboplatin-Paclitaxel vs. Placebo Plus Carboplatin-Paclitaxel for Patients With Primary Advanced or First Recurrent Endometrial Cancer — RUBY Trial, Part 1
Outcome and follow-up | Patients (studies), N | Relative effect (95% CI) | Absolute effects (95% CI) | Certainty | What happens | ||
|---|---|---|---|---|---|---|---|
Placebo plus carboplatin-paclitaxel | Dostarlimab plus carboplatin-paclitaxel | Difference | |||||
OS – ITT population, interim analysis 2 (data cut-off date of September 22, 2023) | |||||||
Probability of survival at 24 months Median follow-up for all patients: 37.2 months | 494 (1 RCT) | NA | 543 per 1,000 | 701 per 1,000 (███ to ███) | ███ fewer per 1,000 (██ fewer to ███ fewer) | Higha | Dostarlimab plus carboplatin-paclitaxel results in a clinically important increase in the probability of survival at 24 months when compared with placebo plus carboplatin-paclitaxel. |
Probability of survival at 36 months Median follow-up for all patients: 37.2 months | 494 (1 RCT) | NA | 429 per 1,000 | 549 per 1,000 (███ to ███) | ███ fewer per 1,000 (███ fewer to ███ fewer) | Higha | Dostarlimab plus carboplatin-paclitaxel results in a clinically important increase in the probability of survival at 36 months when compared with placebo plus carboplatin -paclitaxel. |
PFS – ITT population, interim analysis 1 (data cut-off date of September 28, 2022) | |||||||
Probability of PFS at 12 months Median follow-up for all patients: 25.4 months | 494 (1 RCT) | NA | 290 per 1,000 | 482 per 1,000 (███ to ███) | ███ more per 1,000 (███ more to ███ more) | Highb | Dostarlimab plus carboplatin-paclitaxel results in a clinically important increase in the probability of PFS at 12 months when compared with placebo plus carboplatin-paclitaxel. |
Probability of PFS at 24 months Median follow-up for all patients: 25.4 months | 494 (1 RCT) | NA | 181 per 1,000 | 361 per 1,000 (███ to ███) | ███ more per 1,000 (███ more to ███ more) | Highb | Dostarlimab plus carboplatin-paclitaxel results in a clinically important increase in the probability of PFS at 24 months when compared with placebo plus carboplatin-paclitaxel. |
EORTC QLQ-C30 Global Health Status – ITT population, interim analysis 1 (data cut-off date of September 28, 2022) | |||||||
LS mean change from baseline in Global Health Status; scores range from 0 to 100, with higher scores indicating better health status Time point: cycle 7 | ███ (1 RCT) | NA | −2.3 | −1.8 (SD = 22.79) | ████ (████ to ███) | Lowc | Dostarlimab plus carboplatin-paclitaxel may result in little to no clinically important difference in Global Health Status at cycle 7 when compared with placebo plus carboplatin-paclitaxel. |
LS mean change from baseline in Global Health Status; scores range from 0 to 100, with higher scores indicating better health status Time point: cycle 13 | ███ (1 RCT) | NA | −0.9 | 3.3 (SD = 23.5) | ████ (████ to ███) | Very lowd | The evidence is very uncertain about the effect of dostarlimab plus carboplatin-paclitaxel on Global Health Status at cycle 13 when compared with placebo plus carboplatin-paclitaxel. |
Harms – safety population, interim analysis 2 (data cut-off date of September 22, 2023) | |||||||
Any immune-related TEAEs Median follow-up for all patients: 37.2 months | 487 (1 RCT) | NA | 370 per 1,000 | 585 per 1,000 (NA) | ███ more per 1,000 (███ more to ███ more) | Highe | Dostarlimab plus carboplatin-paclitaxel results in a clinically important increase in any immune-related TEAEs when compared to placebo plus carboplatin-paclitaxel. |
Any infusion-related reactions Median follow-up for all patients: 37.2 months | 487 (1 RCT) | NA | ███ per 1,000 | ███ per 1,000 (NA) | ██ fewer per 1,000 (██ fewer to ██ more) | Lowf | Dostarlimab plus carboplatin-paclitaxel may result in little to no difference in any infusion-related reactions when compared to placebo plus carboplatin-paclitaxel. |
CI = confidence interval; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; ITT = intention to treat; LS = least squares; NA = not applicable; OS = overall survival; PFS = progression-free survival; RCT = randomized controlled trial; SD = standard deviation; TEAE = treatment-emergent adverse event; vs. = versus.
Note: Study limitations (which refer to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias were considered when assessing the certainty of the evidence. All serious concerns in these domains that led to the rating down of the level of certainty are documented in the table footnotes.
aA between-group absolute risk difference of 5% (50 fewer or more events per 1,000 patients) at 24 months and 36 months was clinically important, according to the clinical experts. The point estimate and entire CI exceeded the threshold.
bA between-group absolute risk difference of 10% (100 fewer or more events per 1,000 patients) at 12 months and 24 months was clinically important, according to the clinical experts. The point estimate and entire CI exceeded the threshold.
cRated down 2 levels for risk of bias due to missing outcome data. There is no imprecision in the estimate (i.e., the point estimate and entire 95% CI for the between-group difference show little to no difference). Based on the ranges identified in the literature and suggested by the sponsor, a 10-point change from baseline in EORTC QLQ-C30 scale score was considered clinically important.
dRated down 1 level for serious imprecision because the 95% CI for the between-group difference included the possibility of both harm and little to no difference when compared with placebo plus carboplatin-paclitaxel; based on the ranges identified in the literature and suggested by the sponsor, a 10-point change from baseline in EORTC QLQ-C30 scale score was considered clinically important. Rated down 2 levels for risk of bias due to missing outcome data.
eA between-group absolute risk difference of 5% (50 fewer or more events per 1,000 patients) was clinically important, according to the clinical experts. The point estimate and entire CI exceeded the threshold (i.e., more TEAEs).
fRated down 2 levels for very serious imprecision because the 95% CI for the between-group absolute risk difference included the possibility of both important benefit and important harm; a between-group absolute risk difference of 5% (50 fewer or more events per 1,000 patients) was clinically important, according to the clinical experts.
Source: Clinical Study Report for Part 1 of the RUBY trial.1 Details included in the table are from the sponsor’s Summary of Clinical Evidence and additional information provided in the submission.
Introduction
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of dostarlimab (Jemperli) 500 mg administered through IV infusion every 3 weeks for 6 cycles in combination with carboplatin-paclitaxel followed by 1,000 mg monotherapy every 6 weeks starting at cycle 7 for up to 3 years for the treatment of adults with primary advanced or first recurrent endometrial cancer who are candidates for systemic therapy.
Disease Background
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following has been summarized and validated by the CDA-AMC review team.
Uterine cancer is caused by a malignant tumour that starts in the cells of the uterus and can spread to other parts of the body.2 More than 95% of all uterine cancers are endometrial.3 Endometrial cancer is the most common gynecologic cancer in high-income countries and the second most common gynecologic cancer worldwide.4,5
Patients with endometrial cancer may present with abnormal vaginal bleeding, pelvic pain, back pain, feeling of a mass, or unintentional weight loss.6 Signs and symptoms of metastatic disease may include vaginal, bladder, or rectal bleeding, abdominal pain, pelvic pain, lower abdominal or extremity swelling, anorexia, weight loss, shortness of breath, cough, chest pain, or bone pain.7
Diagnosis of endometrial cancer is based on histological evaluation of an endometrial biopsy, endometrial curettage, or hysterectomy specimen.8 Up to 18% of females with endometrial cancer experience recurrence, with risk increasing by stage at diagnosis.9-13
An estimated 8,600 females in Canada will be diagnosed with uterine cancer in 2024.2 An estimated 1,600 will die from it.2 According to the American Cancer Society, endometrial cancer affects mainly females who are in the postmenopausal stage. The average age of females diagnosed with endometrial cancer is 60 years.14 Endometrial cancer is uncommon in females younger than 45 years.14 Most patients with endometrial cancer are diagnosed with early-stage disease.15 Around 10% to 15% of females diagnosed with endometrial cancer will experience a recurrence.16 Less than 20% of patients with recurrent endometrial cancer survive 5 years.17-22 The median OS for patients with recurrent endometrial cancer is less than 3 years.18,20,23,24,
Standards of Therapy
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following has been summarized and validated by the CDA-AMC review team.
Treatment priorities for patients with primary advanced or recurrent endometrial cancer who are candidates for systemic therapy are prolonging survival, improving HRQoL, and minimizing TEAEs. According to the clinical experts consulted by the review team, the goals of treatment are dependent on the stage and extent of disease and previous treatments received. For patients with advanced disease, surgery is considered when macroscopic resection is feasible with acceptable morbidity following preoperative staging. If surgery is not feasible, patients may require systemic treatment as a frontline option or radiation before surgery. The current standard of care for first-line treatment is carboplatin-paclitaxel for advanced (i.e., stage III or IV) or recurrent endometrial cancer.25-27 Although single-drug chemotherapy may be considered in patients as first-line therapy, combination chemotherapy is favoured over monotherapy. Triplet combinations (e.g., cisplatin, doxorubicin, and paclitaxel) and hormonal therapies may also be considered in some frontline settings. Triplet combinations have demonstrated similar efficacy, but have a less favourable toxicity profile. Hormone therapies, such as megestrol, medroxyprogesterone, letrozole, or tamoxifen may be used for a small subset of patients with estrogen receptor–positive and/or progesterone receptor–positive status, low-grade histology, non–life-threatening disease, or for patients with significant comorbidities that preclude the use of chemotherapy.25-27 Second-line or later treatments are considered for patients who do not respond or have subsequently progressed despite receiving frontline treatment. There is currently no standard of care for this population.
Drug Under Review
The key characteristics of dostarlimab and other treatments available for patients with endometrial cancer are summarized in Table 3.
Dostarlimab (Jemperli) is an anti–PD-1 monoclonal antibody that binds with high affinity to the receptor, blocking its interaction with PD-L1 and PD-L2.28 This action restores cytotoxic T-cell activity, enabling T cells to target and kill tumour cells.
Dostarlimab in combination with carboplatin-paclitaxel has been approved by Health Canada for the treatment of adult patients with primary advanced or first recurrent endometrial cancer who are candidates for systemic therapy. The reimbursement request aligns with this indication. The recommended dosage for dostarlimab in combination with carboplatin-paclitaxel is 500 mg every 3 weeks for 6 cycles followed by 1,000 mg monotherapy every 6 weeks. This treatment continues until disease progression or unacceptable toxicity, or for up to 3 years. Dostarlimab is administered through IV infusion.
Dostarlimab was previously approved by Health Canada as monotherapy for adult patients with dMMR or MSI-H recurrent or advanced endometrial cancer that has progressed following prior platinum-based therapy. However, pERC recommended against reimbursing it for that indication in September 2022.29 In May 2024, pERC recommended reimbursement with conditions when used in combination with carboplatin-paclitaxel as first-line treatment for adult patients with primary advanced or recurrent dMMR or MSI-H endometrial cancer who are candidates for systemic therapy.30
Table 3: Key Characteristics of Dostarlimab, Carboplatin, and Paclitaxel
Characteristic | Dostarlimab | Carboplatin | Paclitaxel |
|---|---|---|---|
Mechanism of action | Monoclonal antibody; blocks the PD-1 receptor, allowing cytotoxic T cells to kill tumour cells. | Synthetic analogue of cisplatin; causes DNA crosslinks, leading to cell death. | Antimicrotubule drug; stabilizes microtubules, preventing depolymerization. |
Indicationa | Approved indications:
| Indication for endometrial cancer was not identified in the product monograph. | Indication for endometrial cancer was not identified in the product monograph. |
Route of administration | IV infusion | IV infusion | IV infusion |
Recommended dose | 500 mg every 3 weeks for 6 doses followed by 1,000 mg every 6 weeks as monotherapy (administered before chemotherapy, when combined) | 400 mg/m2 IV infusion over 15 minutes to 60 minutes | 175 mg/m2 IV infusion over 3 hours (varies by condition) |
Serious adverse effects or safety issues | Immune-mediated reactions (e.g., pneumonitis, colitis, endocrinopathies), infusion-related reactions | Hypersensitivity reactions, bone marrow suppression, renal and hepatic toxicity | Bone marrow suppression, cardiac abnormalities, hepatotoxicity |
dMMR = mismatch repair deficient; MSI-H = microsatellite instability–high.
aHealth Canada–approved indication.
Source: Product monographs for dostarlimab,28 carboplatin,31 and paclitaxel.32
Perspectives of Patients, Clinicians, and Drug Programs
Patient Group Input
This section was prepared by the CDA-AMC review team based on the input provided by patient groups. The full patient and clinician group submissions received are available in the consolidated patient and clinician group input document for this review on the project website.
Patient group input was received from 1 group, CCRAN, regarding the use of dostarlimab for advanced or recurrent endometrial cancer. CCRAN is a patient-driven organization that advocates for improved care, education, and support for patients with cancer, particularly those with colorectal cancer. In this submission, CCRAN collaborated with the Canadian Cancer Survivor Network to gather perspectives from patients with endometrial cancer. Information was collected through interviews conducted with 4 patients and 2 clinicians, who shared their perspectives on managing or experiencing advanced or recurrent endometrial cancer. All patients were females residing in Canada.
The 4 patients had undergone a variety of treatments, including surgery, chemotherapy, immunotherapy, hormonal therapy, and targeted therapies. Specific treatments included medications, such as pembrolizumab, carboplatin, paclitaxel, and letrozole. The patients reported significant side effects associated with these treatments, including neuropathy, fatigue, sexual dysfunction, vaginal discomfort (dryness, itching, tightening, and burning), constipation, bowel pain, nausea, loss of stamina, and fluid retention. Two of the patients had received chemotherapy, while the other 2 patients had undergone a combination of hormonal and immunotherapy treatments. Regardless of treatment regimen, all patients expressed difficulty tolerating the therapies, which left lasting impacts on their quality of life.
In addition to the physical challenges, patients also highlighted broader issues affecting their ability to manage their disease. These included a lack of early screening and diagnosis, insufficient after-care and mental health support, and logistical barriers to accessing treatment, particularly for those living in rural or remote areas. Winter travel to treatment centres was noted as a significant burden for some patients, further complicating their access to care.
The patients emphasized that current treatment options for advanced endometrial cancer are limited, particularly for those with recurrent or metastatic disease. They expressed the need for new therapies that could better control symptoms, improve survival outcomes, and minimize the severe side effects they experienced with existing treatments. There was a clear preference for treatments that strike a balance between effectiveness and manageable side effects, given that their previous therapies had often led to debilitating outcomes.
CCRAN highlighted that patients with advanced endometrial cancer are seeking new treatment options that would help them live longer while maintaining their quality of life. The organization stressed that current therapies often result in substantial side effects that significantly affect patients' day-to-day activities and overall well-being. Patients consistently called for increased access to treatments associated with more tolerable side effects, noting that this would allow them to continue participating in everyday tasks, such as working and caring for family members. These concerns formed a central theme in the feedback gathered by CCRAN.
Clinician Input
Input From Clinical Experts Consulted by CDA-AMC
All CDA-AMC review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of primary advanced endometrial cancer.
Unmet Needs
The clinical experts indicated that the treatment goals for patients with primary advanced or recurrent endometrial cancer are to prolong survival, delay disease progression, and improve quality of life. The experts noted that the standard of care for the majority of patients is chemotherapy (usually with carboplatin-paclitaxel) or immunotherapy, and to a lesser extent, hormonal therapy, surgery, or radiation, depending on the extent of disease and sites of recurrence. They noted that most patients become refractory to current treatment options and that subsequent therapies are limited to chemotherapies (e.g., doxorubicin, topotecan, paclitaxel, oxaliplatin, docetaxel and bevacizumab), which are associated with poor response rates and high toxicity. The experts also indicated that there is an important unmet need for effective first-line treatment for patients with metastatic, pMMR-mutated endometrial cancer, and that patients would appreciate receiving treatment closer to their homes in order to decrease the amount of time and travel needed to reach chemotherapy centres.
Place in Therapy
The clinical experts considered dostarlimab’s mechanism of action as distinct from that of chemotherapy and anticipated it would address the underlying disease process, thereby causing a shift in the current treatment paradigm. The clinical experts noted that dostarlimab would be used in the first-line setting in combination with carboplatin-paclitaxel for all patients with primary advanced recurrent endometrial cancer, including those with dMMR and pMMR mutations; however, in their opinion, the greatest effect would be observed in patients with dMMR mutations.
Patient Population
The clinical experts agreed that the patients best suited for dostarlimab plus carboplatin-paclitaxel would be those with advanced or recurrent endometrial cancer. In their opinion, the patients who would gain the most benefit are those with dMMR status and, to a lesser extent, pMMR status. The experts highlighted that patients would be identified based on clinical examination and judgment; a companion diagnostic would not be needed.
Assessing Response to Treatment
The clinical experts indicated that in clinical practice, a combination of radiographic and clinical parameters is used to determine whether a patient is responding or progressing on treatment. They noted that treatment response should be assessed every 3 cycles with combination therapy (less frequently with monotherapy). The experts agreed that a clinically meaningful response includes prolonged survival, radiological response or stabilization, improvement in patient symptoms, and maintenance of HRQoL.
Discontinuing Treatment
The clinical experts indicated that treatment with dostarlimab plus carboplatin-paclitaxel should be discontinued if patients experience disease progression (defined radiologically or clinically) or if treatment is intolerable. They noted that discontinuation should be based on several cycles of treatment because tumour swelling or enlargement could occur with immunochemotherapy.
Prescribing Considerations
The clinical experts indicated that patients receiving dostarlimab plus carboplatin-paclitaxel should be under the care of a gynecologic oncologist or medical oncologist who can manage toxicity associated with the therapy. They noted that it would be reasonable for patients to receive the therapy in a community setting where day-to-day follow-up is with a general practitioner in oncology.
Clinician Group Input
This section was prepared by the CDA-AMC review team based on the input provided by clinician groups. The full original clinician group inputs received by CDA-AMC have been included in this section of the report.
Two clinician groups, the OH (CCO) Gynecologic Cancer Drug Advisory Committee and GOC, provided input for this review.
According to OH (CCO), the current standard treatment for patients with primary advanced or recurrent endometrial cancer includes platinum-based chemotherapy, typically carboplatin-paclitaxel, and sometimes radiation therapy. Treatment goals include prolonging life, delaying disease progression, reducing symptoms, improving HRQoL, and potentially curing the disease.
The clinician group noted that many patients do not produce a durable response to the current carboplatin-paclitaxel regimen. They emphasized that there is an unmet need for new therapies to improve oncologic outcomes and extend survival.
GOC highlighted that the current treatment for pMMR endometrial cancer involves surgery (with or without adjuvant radiation) for early-stage disease and chemotherapy for advanced or recurrent cases. They noted that immunotherapy options are limited to later lines of therapy for recurrent disease, in combination with lenvatinib. Importantly, they stated that patients with primary stage III or IV or recurrent pMMR endometrial cancer would be best suited for dostarlimab plus chemotherapy, particularly those with limited treatment options and poor outcomes on chemotherapy alone.
Regarding place in therapy, OH (CCO) noted that dostarlimab combined with chemotherapy would be used as first-line therapy, followed by maintenance treatment, particularly for patients with dMMR tumours, who would likely experience the greatest benefit. GOC added that dostarlimab would represent the immunotherapy option as a first-line treatment for advanced or recurrent pMMR cases, addressing a significant unmet need.
According to the clinician groups, the patients best suited for treatment with dostarlimab are those with dMMR tumours and adequate ECOG Performance Status (i.e., score of 0 to 1). The least suitable patients would include those with contraindications to immunotherapy, poor ECOG Performance Status, or severe autoimmune conditions.
The key outcomes to determine response to therapy, as identified by both groups, include PFS, OS, and quality of life. Imaging and clinical exams are the primary tools for assessment, with evaluation intervals at the physician’s discretion. Treatment discontinuation would be based on disease progression, intolerable adverse effects, or significant patient deterioration.
The clinician groups also noted that the appropriate treatment setting for dostarlimab is an outpatient clinic or hospital where the patient is under the care of gynecologic oncology specialists who can monitor treatment and manage potential side effects.
No additional information was provided. Conflict of interest declarations were included for all contributors, with no external assistance noted for completing or analyzing the submission.
Drug Program Input
The drug programs provide input on each drug being reviewed through CDA-AMC’s reimbursement review processes by identifying issues that may affect their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CDA-AMC are summarized in Table 4.
Table 4: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Relevant comparators | |
The comparator in Part 1 of the RUBY trial was carboplatin in combination with paclitaxel, which is an appropriate comparator. Other comparators are hormonal therapies for hormone receptor–positive endometrial cancer. | Comment from the drug plans to inform pERC deliberations. |
Considerations for initiation of therapy | |
Testing for dMMR and pMMR status needs to be completed before initiation of therapy. | Comment from the drug plans to inform pERC deliberations. The CDA-AMC review team noted that, as per the approved Health Canada indication and reimbursement request, MMR and/or MSI testing may not be required to initiate therapy, given that patients with either pMMR or dMMR would be eligible. |
Is the recommendation for pMMR the same as dMMR (i.e., patients who progress while on or within 6 months of adjuvant therapy would not be eligible for dostarlimab plus carboplatin-paclitaxel)? | The clinical experts indicated that patients with pMMR and dMMR status should be eligible for dostarlimab plus carboplatin-paclitaxel. |
For the dMMR indication, pERC thought it would be reasonable to allow an additional 1 year of dostarlimab upon disease progression for those who had completed 3 years of dostarlimab. Can the same be said for the pMMR endometrial cancer indication? | The clinical experts noted that an additional 1 year of treatment with dostarlimab would be reasonable in patients with dMMR or pMMR status who experience disease progression after competing 3 years of dostarlimab treatment. |
Considerations for prescribing of therapy | |
Dostarlimab is administered as a 500 mg dose with carboplatin-paclitaxel on day 1 every 21 days for 6 cycles, followed by dostarlimab 1,000 mg IV monotherapy every 6 weeks up to a total of 3 years of therapy. | Comment from the drug plans to inform pERC deliberations. |
Dostarlimab is administered as a 30-minute IV infusion. | Comment from the drug plans to inform pERC deliberations. |
Generalizability | |
Patients with ECOG Performance Status > 1 were excluded from the trial. Can they be considered eligible for dostarlimab in combination with carboplatin-paclitaxel followed by dostarlimab maintenance? | The clinical experts indicated that patients with good ECOG Performance Status (or a score of 0 to 2) should be eligible for dostarlimab plus carboplatin-paclitaxel followed by dostarlimab maintenance, if they are able to tolerate the therapy. They noted that patients with an ECOG Performance Status greater than 2 would likely be unable to tolerate the combination of 2 chemotherapy drugs and immunotherapy. |
For patients who are currently receiving carboplatin-paclitaxel for first-line pMMR endometrial cancer, is it recommended to add dostarlimab to carboplatin-paclitaxel? If yes, what would be the maximum number of cycles recommended that a patient would receive of carboplatin-paclitaxel (e.g., patient should have no more than 3 cycles of carboplatin-paclitaxel if dostarlimab is to be added)? | The clinical experts noted that patients who are already on chemotherapy should be able to add dostarlimab within 3 cycles to 6 cycles of their last chemotherapy treatment. |
Funding algorithm (oncology only) | |
Durvalumab with carboplatin-paclitaxel followed by durvalumab and olaparib maintenance is currently under review for the first-line treatment of pMMR endometrial cancer. Is there a reason why a prescriber would choose dostarlimab plus chemotherapy instead of durvalumab plus chemotherapy followed by durvalumab plus olaparib maintenance, or vice versa? | The clinical experts noted that it is unclear who would benefit from the addition of a PARP inhibitor, and that the added toxicity of a fourth drug could be burdensome to patients. |
Care provision issues | |
More pharmacy preparation time is needed to prepare dostarlimab. | Comment from the drug plans to inform pERC deliberations. |
Dostarlimab is an immune checkpoint inhibitor and monitoring for immune-mediated toxicities will be required. | Comment from the drug plans to inform pERC deliberations. |
dMMR and pMMR testing is required. When is the best time to test for dMMR and pMMR status? | The clinical experts indicated that, while there is variability across cancer centres regarding the time frame for MMR and/or MSI testing (e.g., shortly upon diagnosis, after biopsy, or after surgery), the ideal time to test for dMMR and pMMR status is during diagnosis. As noted in the section of this table focusing on considerations for the initiation of therapy, the clinical experts indicated that patients with pMMR and dMMR status should be eligible for dostarlimab plus carboplatin-paclitaxel. |
System and economic issues | |
A large budget impact is anticipated if dostarlimab plus chemotherapy is recommended for pMMR endometrial cancer. | Comment from the drug plans to inform pERC deliberations. |
Generic carboplatin-paclitaxel are available with confidential prices. | Comment from the drug plans to inform pERC deliberations. |
It will be important to provide the economics for the population of patients with pMMR status, not the ITT population, as CDA-AMC has already issued its economic report and a recommendation for dMMR. It is anticipated, based on the results, that reimbursement for patients with pMMR will not be as cost-effective as for the dMMR indication (and that treatment of patients with pMMR will have a large budget impact) because approximately 75% of patients have pMMR tumours. | Comment from the drug plans to inform pERC deliberations. |
CDA-AMC = Canada’s Drug Agency; dMMR = mismatch repair deficient; ECOG = Eastern Cooperative Oncology Group; ITT = intention to treat; MMR = mismatch repair; MSI = microsatellite instability; pERC = pan-Canadian Oncology Drug Review Expert Review Committee; pMMR = mismatch repair proficient.
Clinical Evidence
The objective of this clinical review report is to review and critically appraise the clinical evidence submitted by the sponsor on the beneficial and harmful effects of dostarlimab 500 mg administered through IV infusion every 3 weeks for 6 cycles in combination with carboplatin-paclitaxel, followed by dostarlimab 1,000 mg monotherapy every 6 weeks starting at cycle 7 for up to 3 years for the treatment of adults with primary advanced or first recurrent endometrial cancer who are candidates for systemic therapy. The focus will be on comparing dostarlimab to relevant comparators and identifying gaps in the current evidence.
A summary of the clinical evidence included by the sponsor in the review of dostarlimab is presented in 4 sections, with CDA-AMC’s critical appraisal of the evidence included at the end of each. The first section, the systematic review, includes pivotal studies and RCTs that were selected according to the sponsor’s systematic review protocol. CDA-AMC’s assessment of the certainty of the evidence in this first section using the GRADE approach follows the critical appraisal of the evidence. The second, third, and fourth sections would typically include long-term extension studies, indirect evidence, and additional studies to address important gaps in the systematic review evidence, respectively; however, none were submitted by the sponsor.
Included Studies
Clinical evidence from the following is included in the CDA-AMC review and appraised in this document:
1 pivotal trial identified in the systematic review.1
Systematic Review
Contents within this section have been informed by materials submitted by the sponsor. The following has been summarized and validated by the CDA-AMC review team.
Description of Study
Characteristics of the included study are summarized in Table 5.
The RUBY trial, Part 1,1 is an ongoing, phase III, randomized, double-blind, multicentre trial that aims to assess the efficacy and safety of dostarlimab IV infusion plus carboplatin-paclitaxel followed by dostarlimab monotherapy versus placebo plus carboplatin-paclitaxel followed by placebo in adults with primary advanced or recurrent endometrial cancer. The trial enrolled patients who were at least 18 years of age and had histologically or cytologically confirmed, primary advanced or first recurrent endometrial cancer that was not amenable to curative therapy. The focus of the approved Health Canada indication and reimbursement request is aligned with the overall trial population. The RUBY trial, Part 2 evaluates the efficacy and safety of treatment with dostarlimab plus carboplatin-paclitaxel followed by dostarlimab plus niraparib versus placebo plus carboplatin-paclitaxel followed by placebo in patients with recurrent or primary advanced endometrial cancer. Because Part 2 has no available data yet, the focus of this review is on the results of Part 1.
The study design of the RUBY trial, Part 1 is depicted in Figure 1. Patients enrolled (N = 494) across 164 sites were randomly assigned through an interactive response system in a 1-to-1 ratio to receive dostarlimab plus carboplatin-paclitaxel (N = 245) or placebo plus carboplatin-paclitaxel (N = 249). Eight patients across 8 sites in Canada were included in the trial. Randomization was stratified by MMR and MSI status (i.e., dMMR and/or MSI-H or pMMR and/or MSS), prior external pelvic radiotherapy (yes or no), and disease status (recurrent, primary stage III, or primary stage IV). MMR and MSI status were identified through immunohistochemistry, polymerase chain reaction, and next-generation sequencing tests.
The trial included a screening phase (performed in the 28 days before starting treatment), a treatment phase lasting up to 3 years, and a follow-up phase. During the follow-up phase, patients were followed for safety assessments (90 days ± 7 days after the last dose of treatment) and for survival assessments (every 90 days ± 4 days until death or the end of study data collection).
Table 5: Details of Study Included in the Systematic Review
Detail | RUBY trial, Part 1 |
|---|---|
Design and population | |
Study design | Phase III, randomized, multicentre, double-blind study |
Locations | Patients enrolled across 164 sites in 20 countries (e.g., Canada, European countries, UK, US) |
Patient enrolment dates | Start: August 2019 End: January 2021 |
Data cut-off date | September 28, 2022 (interim analysis 1) September 22, 2023 (interim analysis 2) |
Randomized (N) | ITT (N = 494)
|
Key inclusion criteria |
|
Key exclusion criteria |
|
Drugs | |
Intervention | Dostarlimab 500 mg IV infusion over 30 minutes in combination with chemotherapy for the first 6 doses (carboplatin: area under the concentration time-curve, 5 mg per mL per minute; paclitaxel: 175 mg per square metre of body surface area), followed by dostarlimab 1,000 mg IV infusion once every 6 weeks for up to 3 years |
Comparator | Matching placebo IV infusion in combination with carboplatin-paclitaxel for the first 6 doses, followed by placebo IV infusion once every 6 weeks for up to 3 years |
Study duration | |
Screening phase | 28 days before starting treatment |
Treatment phase | Up to 3 years |
Follow-up phase |
|
Outcomes | |
Primary outcome | Dual primary outcomes:
|
Secondary and exploratory outcomes | Secondary:
Exploratory:
|
Publication status | |
Publications | ClinicalTrials.gov number, NCT03981796 Mirza et al. (2023)33 Powel et al. (2024)34 |
AE = adverse event; BICR = blinded independent central review; DCR = disease control rate; DoR = duration of response; EC = endometrial cancer; ECOG = Eastern Cooperative Oncology Group; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EORTC QLQ-EN24 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Endometrial Cancer Module (24 items); HRQoL = health-related quality of life; MMR = mismatch repair; MSI = microsatellite instability; ORR = objective response rate; OS = overall survival; PD = progressive disease; PFS = progression-free survival; PFS2 = progression-free survival from treatment randomization to the date of assessment of progression on the first subsequent anticancer therapy; RECIST 1.1 = Response Evaluation Criteria in Solid Tumours Version 1.1.
Source: RUBY trial, Part 1 Clinical Study Report.1 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Figure 1: Study Design of RUBY Trial, Part 1
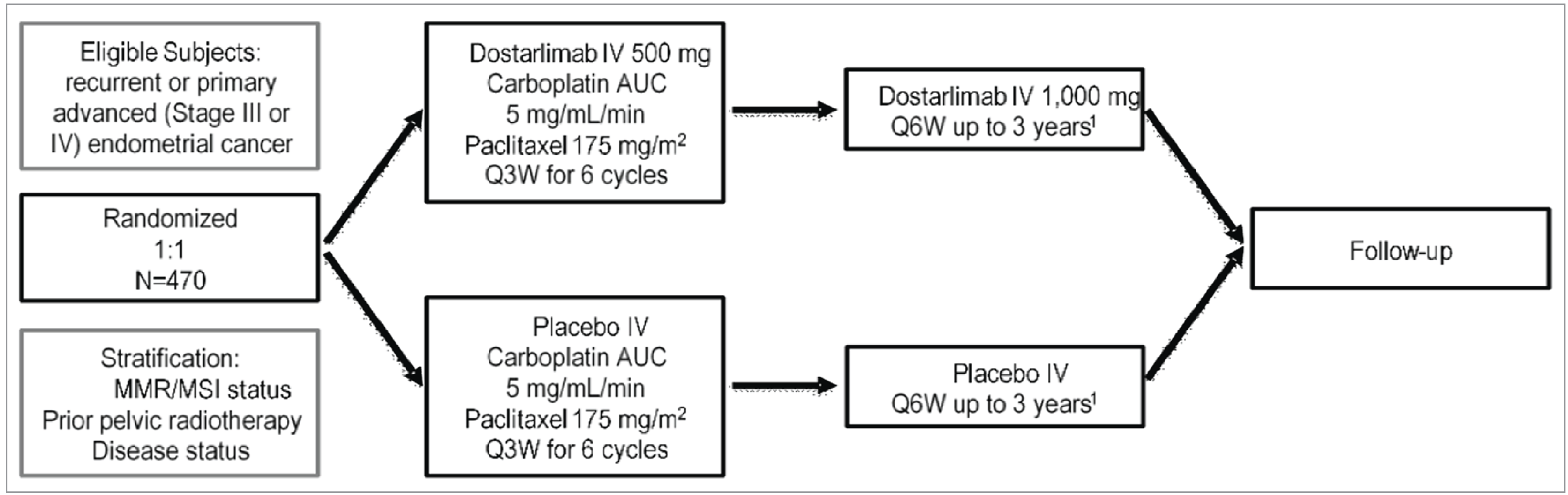
AUC = area under the plasma or serum concentration time-curve; MMR = mismatch repair; MSI = microsatellite instability; Q3W = every 3 weeks; Q6W = every 6 weeks.
Source: RUBY trial, Part 1 Clinical Study Report.1 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Populations
Inclusion and Exclusion Criteria
A detailed description of the key inclusion and exclusion criteria for the RUBY trial, Part 1, is in Table 5. Eligible patients were adults aged 18 years or older with histologically or cytologically diagnosed endometrial cancer with primary advanced (stage III or IV) or first recurrent disease and a low potential for cure through radiation therapy or surgery, alone or in combination. Patients also had to have an ECOG Performance Status score of 0 or 1 and adequate organ function. Patients were excluded if they had received neoadjuvant or adjuvant chemotherapy, with or without recurrence, in the 6 months before entering the trial, had experienced more than 1 previous disease recurrence, or had received prior treatment with an anti–PD-1, anti–PD-L1, or anti–PD-L2 antibody.
Interventions
Patients were randomized to receive dostarlimab 500 mg or placebo as a 30-minute IV infusion plus carboplatin (area under the concentration time-curve of 5 mg/mL/minute) and paclitaxel (175 mg/m2 every 3 weeks for 6 cycles starting at cycle 1 day 1) for the first 6 cycles, followed by dostarlimab 1,000 mg monotherapy or placebo through IV every 6 weeks starting at cycle 7. Dostarlimab monotherapy or placebo was continued for up to 3 years or until progressive disease, unacceptable toxicity, withdrawal of consent, investigator’s decision, or death; continuation of treatment for longer than 3 years was considered following discussion with the sponsor and investigator. All patients were to be pretreated with corticosteroids, diphenhydramine, and H2 antagonists, as indicated in the local product information, following the administration of dostarlimab or placebo and before the administration of carboplatin-paclitaxel.
Dosing modifications for the management of specific immune-related adverse events (AEs) (for dostarlimab or placebo) and hematologic AEs (for carboplatin-paclitaxel) were prespecified. Notably, treatments were to be withheld for study drug–related grade 3 or greater toxicities and for specific immune-related AEs. Dose reductions of carboplatin, paclitaxel, or both were permitted. Dose reductions of dostarlimab or placebo were not permitted. Doses of all 3 drugs were to be interrupted or discontinued for toxicity related to the combination therapy. Patients whose treatments were interrupted were to resume study treatment within 3 weeks of a scheduled interruption, for a maximum of 6 weeks. Patients were permitted to discontinue either the dostarlimab or placebo and continue on chemotherapy alone, or vice versa (i.e., to discontinue chemotherapy and continue on dostarlimab or placebo monotherapy). Paclitaxel was not to be replaced by other taxanes (e.g., docetaxel, nab-paclitaxel) because safety data for combining these with dostarlimab were not available. Patients who discontinued treatment after a treatment interruption of more than 4 weeks should have had their end-of-treatment visit within 2 weeks of the decision to discontinue treatment or before initiating alternate anticancer therapy, whichever occurred first.
Patients received rescue medications and/or supportive care for AEs experienced during treatment, including infusion-related reactions. Prophylactic cytokines (e.g., G-CSF) were permitted in cycles after cycle 1. Concomitant medications that were prohibited during the screening and treatment phase of the study included treatments other than the randomized study treatment (including systemic anticancer therapy, immunotherapy, chemotherapy, and investigational drugs); surgery to treat the underlying disease; blood products or colony-stimulating factors (e.g., G-CSF, GM-CSF, or recombinant erythropoietin) within 21 days before the first dose of study drug; systemic glucocorticoids, other than to manage symptoms of suspected immune-related AEs, unless deemed necessary (e.g., to treat acute asthma or chronic obstructive pulmonary disease), based on investigator judgment; and live virus and bacterial vaccines. Patients could start subsequent treatments (e.g., follow-up anticancer therapy) after stopping dostarlimab treatment (e.g., for disease progression or other reasons, as described).
Outcomes
A list of efficacy end points assessed in this Clinical Review Report is provided in Table 6, followed by descriptions of the outcome measures. Summarized end points are based on outcomes included in the sponsor’s Summary of Clinical Evidence as well as on any outcomes identified as important to this review according to the clinical experts consulted by CDA-AMC and the input from patient and clinician groups and public drug plans. Using the same considerations, the CDA-AMC review team selected end points that were considered most relevant to inform its expert committee deliberations and finalized this list of end points in consultation with members of the committee. All summarized efficacy end points were assessed using GRADE. Select notable harms outcomes considered important for informing CDA-AMC’s expert committee deliberations were also assessed using GRADE. The outcomes relevant to the CDA-AMC review included the dual primary outcomes of OS and PFS per investigator assessment and the secondary outcomes of HRQoL (measured using the EORTC QLQ-C30 Global Health Status) and safety. Efficacy and safety data were evaluated at the data cut-off dates of September 28, 2022 (interim analysis 1), and September 22, 2023 (interim analysis 2).
Table 6: Efficacy Outcomes Summarized From the Study Included in the Systematic Review
Outcome measure | Time point | RUBY trial, Part 1 |
|---|---|---|
Overall survival | At 24 and 36 months | Primarya |
Progression-free survival | At 12 and 24 months | Primarya |
EORTC QLQ-C30 Global Health Status | At cycle 7 and 13 | Secondary |
EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30.
aStatistical testing was performed hierarchically.
Source: RUBY trial, Part 1 Clinical Study Report.1 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Overall Survival
The dual primary outcome of OS was defined as the time from randomization to the date of death by any cause. OS was assessed at end of treatment and following this visit using acceptable means, such as telephone contact. Patients without documented death at the time of the analysis were censored at the last date on which they were known to be alive.
Progression-Free Survival
The dual primary outcome of PFS per investigator assessment was defined as the time from randomization to the earliest date of radiographic assessment of progressive disease per Response Evaluation Criteria in Solid Tumours Version 1.1 or death due to any cause in the absence of progressive disease, whichever occurred first. Tumour imaging of the chest, abdomen, pelvis, and other affected sites, as clinically indicated, was performed by CT or MRI, if clinically appropriate. Radiographic evaluations were to be conducted every 6 weeks until week 25 and then every 9 weeks until week 52. After 52 weeks, imaging was to be performed every 12 weeks until disease progression. If a patient discontinued treatment for a reason other than disease progression, death, withdrawal of consent, or loss of follow-up, radiographic scans were to be continued at specified time intervals. PFS was censored based on the following 3 criteria: no baseline tumour assessment and no death within 12 weeks; no disease progression, no death, and no initiation of new anticancer therapy; and no disease progression, no death, and initiation of new anticancer therapy.
Health-Related Quality of Life
The secondary outcome of HRQoL was measured by change in baseline in patient-reported Global Health Status using the EORTC QLQ-C30 Version 3.0. The questionnaire incorporates 5 functional scales (physical, role, cognitive, emotional, and social), 3 symptom scales (fatigue, pain, and nausea and vomiting), a Global Health Status and quality of life scale, and 6 single items assessing additional symptoms commonly reported by patients with cancer (dyspnea, appetite loss, insomnia, constipation, diarrhea, and financial difficulty). A score of 0 to 100 was derived for the Global Health Status scale, with higher scores indicating better health status. The validity, reliability, responsiveness, and MID of the EORTC QLQ-C30 instrument are summarized in Table 7. The sponsor suggested an absolute change greater than or equal to 10 points from baseline, which was informed by the literature and used in other trials, to define a clinically meaningful change. No MID was identified in the literature specifically for patients with endometrial cancer.
Harms Outcomes
The assessment of safety was based on the proportion of patients experiencing 1 or more TEAEs, serious TEAEs, and TEAEs leading to discontinuation, dose modification, or death. TEAEs were defined as any AE or serious AE that occurred on or after the start of treatment through 90 days after the last dose of study treatment or until the start of alternate anticancer therapy, whichever occurred earlier. No notable AEs were identified by the sponsor; however, based on feedback from the clinical experts consulted by CDA-AMC and the important potential harms identified in the product monograph for dostarlimab, immune-related AEs and infusion-related reactions were included in this report.
Table 7: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
EORTC QLQ-C30 | The EORTC QLQ-C30 is a 30-item, patient-reported, cancer-specific, HRQoL questionnaire using 4-point and 7-point Likert scales.35 There are 15 domains for the EORTC QLQ-C30. Functional scales, ranging from 0 to 100 (with higher scores indicating higher functioning) include Global Health Status and QoL, physical functioning, role functioning, emotional functioning, cognitive functioning, and social functioning. Symptom scales, ranging from 0 to 100 (with higher scores indicating a greater degree of symptoms or worse condition) include fatigue, pain, nausea and vomiting, dyspnea, insomnia, appetite loss, constipation, diarrhea, and financial difficulties.35 | Content validity: When mapping to WHO’s ICF framework, 25 of the 30 items in the EORTC QLQ-C30 were endorsed by 21 health care professionals, using the Delphi technique (≥ 70% agreement).36 Discriminant validity: Spearman’s rank correlations with external parameters, such as ECOG Performance Status, ranged from 0.02 to 0.56 among 150 patients in Canada with metastatic breast cancer.37 Convergent validity: Spearman’s rank correlations with scores on the Profile of Mood States and Psychosocial Adjustment to Illness Scale ranged from 0.02 to 0.76 among 150 patients in Canada with metastatic breast cancer.37 Inter-rater reliability: The median kappa coefficient for patient-observer agreement across the 30 items in the EORTC QLQ-C30 was 0.86, with a range of 0.48 to 1.00, in patients with metastatic breast cancer, representing substantial to near-perfect agreement for most items.38,39 Responsiveness: No literature was identified that assessed responsiveness in patients with breast cancer. | In a paper synthesizing data from 21 published EORTC QLQ-C30 phase III trials enrolling 13,015 patients across 9 cancer types, the anchor-based MID for the Global Health Status scale for between-group change over time in patients with breast cancer ranged from −13 to −6 for deterioration and from 8 to 11 for improvement.40 The sponsor suggested an absolute change ≥10 points from baseline, which was informed by the literature.41,42 |
ECOG = Eastern Cooperative Oncology Group; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; ICF = International Classification of Functioning, Disability and Health; MID = minimal important difference; QoL = quality of life.
Statistical Analysis
Sample Size and Power Calculation
The sample size was driven by the analysis of the dual primary outcome of PFS, as determined by investigator assessment. The sample size and power calculation were based on the following assumptions:
for patients with primary or advanced recurrent endometrial cancer, an HR of 0.67, corresponding to an increase in median PFS to 15 months in the group receiving dostarlimab plus carboplatin-paclitaxel from 10 months in the group receiving placebo plus carboplatin-paclitaxel
for the subpopulation of patients with dMMR or MSI-H, an HR of 0.50, corresponding to an increase in median PFS to 20 months in the group receiving dostarlimab plus carboplatin-paclitaxel from 10 months in the group receiving placebo plus carboplatin-paclitaxel
dMMR or MSI-H (expected in 25% of patients) and pMMR or MSS (expected in 75% of patients)
1-to-1 randomization
alpha equal to 0.02 (1-sided)
power of approximately 89% to detect a significant difference in PFS between the treatment groups among patients with dMMR or MSI-H tumours
accrual over a period of 22 months
an annual dropout rate of 5%
exponential distribution of PFS.
Based on these assumptions and a group sequential log-rank test design with 2 analyses planned (i.e., interim analysis 1, at approximately 84.6% information, and 1 final analysis based on a Lan-DeMets [O’Brien-Fleming] alpha spending function), a total sample size of 470 patients was planned, and approximately 118 patients were expected to have dMMR or MSI-H status. To maintain the natural distribution of patients in the overall population with dMMR or MSI-H status (25%) and pMMR or MSS status (75%), the numbers of patients enrolled were capped at approximately 120 patients and 350 patients, respectively. In addition, the total number of patients with carcinosarcoma was capped at 50 patients (approximately 10%) to prevent overrepresentation of this patient population. Subsequent to interim analysis 1, a second interim analysis (with a data cut-off date of September 22, 2023) was targeted to evaluate ongoing efficacy and monitor any emerging safety concerns.
Statistical Testing
A summary of the statistical analysis of efficacy outcomes is in Table 8. The dual primary outcomes of PFS and OS were analyzed using HRs and associated 2-sided CIs based on the stratified Cox proportional hazards model. The distributions of PFS and OS were estimated using the KM method and compared using a stratified log-rank test. Median PFS and OS for each treatment group were reported, with 95% CIs based on the Brookmeyer-Crowley method. Underlying assumptions of proportional hazards were checked based on a visual inspection of a survival curve fit to KM data, inspection of log-cumulative hazard plots over time, and statistical goodness of fit based on relative Akaike and Bayesian information criterion values.
The statistical analyses of PFS and OS were controlled for type I error for multiple hypotheses and interim analyses using a graphical method (Figure 2). The family-wise type I error was controlled at 2.5% (1-sided alpha allocation) for PFS and OS, including across interim analyses. The alpha level assigned to a subfamily was rolled over only if all the hypotheses within the subfamily were significant based on the weight for reallocation presented on the dashed lines connecting subfamilies (refer to Figure 2). Within each subfamily, weights for reallocation from each hypothesis to the other were represented on the solid lines connecting hypotheses. Hypothesis testing for PFS in the overall population was performed only if the null hypothesis of PFS was rejected in the subpopulation of patients with dMMR or MSI-H status. Hypothesis testing for OS in the overall population started at the time when the hypothesis testing for PFS was completed or at a reallocated alpha level (2.5%) if both null hypotheses were rejected for hypothesis 1 and hypothesis 2; otherwise, OS was tested at the initial alpha level (0.5%). To test hypothesis 1 (i.e., PFS in dMMR or MSI-H), interim analysis 1 and a final analysis were planned. Interim analysis 1 was planned to take place after approximately 77 PFS events had occurred, with the final analysis planned to take place after 91 PFS events had occurred. The boundary for declaring superiority of dostarlimab plus carboplatin-paclitaxel over placebo plus carboplatin-paclitaxel was based on a Lan-DeMets (O’Brien-Fleming) alpha spending function (1-sided alpha = 0.02, as previously noted). At the data cut-off date of September 28, 2022 (interim analysis 1), 66 PFS events were observed in the subpopulation of patients with dMMR or MSI-H status; therefore, the boundary for declaring superiority was adjusted to P equals 0.00630. To test for hypothesis 3 (i.e., OS in all patients), 3 interim analyses and 1 final analysis were planned at 321 OS events. The first interim analysis of OS was conducted at the same time as PFS in the population of patients with dMMR or MSI-H status, when 165 deaths were observed. The stopping boundary for this first interim analysis of OS was adjusted based on the actual observed number of deaths, with a P value stopping boundary of 0.00177.
For the HRQoL outcome of EORTC QLQ-C30 Global Health Status, descriptive statistics were used to summarize the observed values and changes from baseline data at each scheduled assessment time point. A mixed-effects model for repeated measures (MMRM) was performed to compare the between-treatment difference, adjusting for correlations across multiple time points within a patient and controlling for the baseline value. The adjustment factors for MMRM included fixed effects (treatment, analysis visit, and treatment-by-visit interaction) and a random effect (patient), with baseline value as a continuous covariate along with baseline-by-visit interaction. Adjusted mean differences and 95% CIs were presented to illustrate the effect of treatment. The analysis was not controlled for multiplicity. Safety data were summarized descriptively.
Subgroup Analysis
For the prespecified subgroups of interest, the unstratified HR and associated 95% CIs of OS and PFS were performed by MMR and MSI status at baseline (dMMR and/or MSI-H, pMMR and/or MSS, or dMMR [derived]), age (< 65 years or ≥ 65 years), disease status at baseline (recurrent, primary stage III, primary stage IV, or no disease), and histology (endometrioid carcinoma or other). Survival estimates were provided using KM curves and reported as medians with 95% CIs and presented as forest plots. The subgroup analyses were exploratory, and no inferential statistics (i.e., P values) were produced.
Sensitivity Analyses
The sensitivity analyses performed for PFS are summarized in Table 8.
Table 8: Statistical Analysis of Efficacy Outcomes
End point | Statistical model | Adjustment factors | Handling of missing data | Sensitivity analyses |
|---|---|---|---|---|
OS | Stratified log-rank test and stratified Cox model KM estimates | Unadjusted | Missing observations were generally treated as missing at random and were not imputed. | The same as the primary analysis, except MMR and MSI subsets are based on the MMR and MSI classifications entered for randomization instead of the source-verified MMR and MSI classifications collected in the eCRF. |
PFS | Stratified log-rank test and stratified Cox model | Unadjusted | Missing observations were generally treated as missing at random and were not imputed. |
|
EORTC QLQ-C30 Global Health Status | MMRM | Adjusted means, 95% CI, and P values from an MMRM with treatment, visit, and treatment-by-visit interaction as fixed effects; baseline as a continuous covariate along with baseline-by-visit interaction (fixed effects); and patient as a random effect | Single-item measures: If the item was missing, the score S was set to missing (i.e., applying linear transformation to 0 to 100 to obtain the score S) | NA |
BICR = blinded independent central review; CI = confidence interval; eCRF = electronic case report form; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; KM = Kaplan-Meier; MMR = mismatch repair; MMRM = mixed-effects model for repeated measures; MSI = microsatellite instability; NA = not applicable; OS = overall survival; PD = progressive disease; PFS = progression-free survival; RECIST 1.1 = Response Evaluation Criteria in Solid Tumours Version 1.1.
Source: RUBY trial, Part 1 Clinical Study Report.1 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Figure 2: Multiplicity Control Strategy for Comparisons Between Treatment Groups in Part 1 of the RUBY Trial
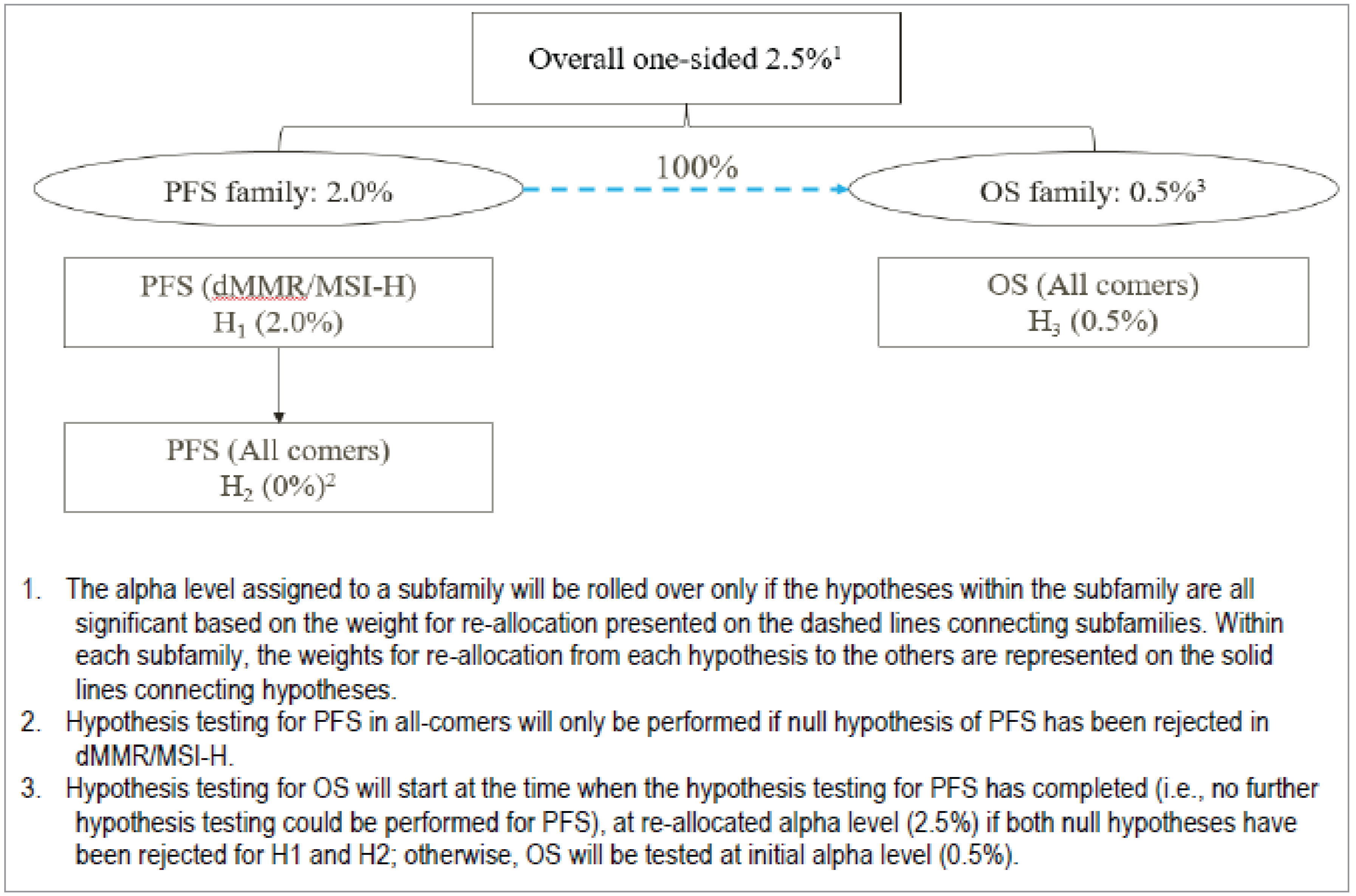
dMMR = mismatch repair deficient; H1 = hypothesis 1; H2 = hypothesis 2; H3 = hypothesis 3; MSI-H = microsatellite instability–high; OS = overall survival; PFS = progression-free survival.
Source: RUBY trial, Part 1 Clinical Study Report.1 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Analysis Populations
The efficacy outcomes, including HRQoL, were analyzed based on the ITT population. The safety outcomes were analyzed using the safety population, defined as patients who received any amount of the study drug.
Results
Patient Disposition
A summary of patient disposition for the data cut-off date of September 22, 2023 (interim analysis 2), is in Table 9. In total, 607 patients were screened, of whom 494 were randomized to receive dostarlimab plus carboplatin-paclitaxel (n = 245) or placebo plus carboplatin-paclitaxel (n = 249). For the 113 patients who were screened out, the most common reason was not meeting 1 or more of the eligibility criteria (n = 88), followed by meeting eligibility criteria but not enrolling (n = 25). In the groups receiving dostarlimab plus carboplatin-paclitaxel and placebo plus carboplatin-paclitaxel, 130 (53.1%) and 160 (64.3%) patients, respectively, discontinued from the trial. The main reason for study discontinuation for both treatment groups was death from any cause (39.2% versus 53.4%), with disease progression (████% versus ████) as the main cause of death. In both treatment groups, the most common reason for dostarlimab or placebo discontinuation was progressive disease according to Response Evaluation Criteria in Solid Tumours Version 1.1, per investigator assessment. The most common reason for carboplatin or paclitaxel discontinuation was completion of the planned treatment course.
Table 9: Summary of Patient Disposition — RUBY Trial, Part 1, Interim Analysis 2
Characteristics | Dostarlimab plus carboplatin-paclitaxel | Placebo plus carboplatin-paclitaxel |
|---|---|---|
Screened, N | 607 | |
Screened out | 113 | |
Reason for being screened out, n (%) | ||
Did not meet eligibility criteria | 88 (NR) | |
Met eligibility criteria, but did not enrol | 25 (NR) | |
Randomized, N (%) | 245 (NR) | 249 (NR) |
Treated, N (%) | 241 (NR) | 246 (NR) |
Discontinued from study, n (%) | 130 (53.1) | 160 (64.3) |
Reason for discontinuation, n (%) | ||
Withdrawal of consent | 26 (10.6) | 20 (8.0) |
Lost to follow-up | 5 (2.0) | 5 (2.0) |
Other | 3 (1.2) | 2 (0.8) |
Death from any cause | 96 (39.2) | 133 (53.4) |
Main cause of death, N (%) | ||
Disease progression | ██ ██████ | ███ ██████ |
Adverse event | █████ | █████ |
Unknown | █████ | ██ █████ |
Other | █████ | ██████ |
Ongoing in trial, n (%) | ███ ███████ | ██ ███████ |
On study treatment | 27 (11.0%) | 22 (8.8%) |
In follow-up | 88 (35.9%) | 67 (26.9%) |
ITT, N | 245 | 249 |
Safety, N | 241 | 246 |
ITT = intention to treat; NR = not reported.
Source: RUBY trial, Part 1 Clinical Study Report.1 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Baseline Characteristics
The baseline characteristics for the ITT population are outlined in Table 10 and are limited to those that are most relevant to this review or were thought to affect the outcomes or interpretation of the trial results. Overall, the key baseline characteristics were generally balanced between treatment groups. The trial population was predominantly white (approximately 77%), with a mean age of 64 years, with half of patients aged 19 years to 64 years. Most patients had an ECOG Performance Status of 0 (approximately 63%), indicating good overall performance; endometrioid histology (adenocarcinoma type or adenocarcinoma variant) at diagnosis (approximately 55%); recurrent (48%) or primary stage IV (33%) disease status; FIGO stage III or IV at diagnosis (approximately 60%); an MMR or MSI status of pMMR or MSS (approximately 76%); and had received prior surgery for endometrial cancer (approximately 90%). Most patients (approximately 83%) had not received prior external pelvic radiotherapy.
Table 10: Summary of Baseline Characteristics — ITT Population, RUBY Trial, Part 1
Characteristic | Dostarlimab plus carboplatin-paclitaxel (N = 245) | Placebo plus carboplatin-paclitaxel (N = 249) |
|---|---|---|
Age (years) | ||
Mean (SD) | 64.0 (9.20) | 63.9 (10.1) |
Range | 41 to 81 | 28 to 85 |
Age group (years), n (%) | ||
19 years to 64 years | 127 (51.8) | 114 (45.8) |
≥ 65 years | 118 (48.2) | 135 (54.2) |
Race, N (%) | ||
American Indian or Alaska Native [wording from original source] | 1 (0.4) | 1 (0.4) |
Asian | 7 (2.9) | 8 (3.2) |
Black or African American | 28 (11.4) | 31 (12.4) |
Native Hawaiian or other Pacific Islander | 1 (0.4) | 0 (0) |
White | 189 (77.1) | 191 (76.7) |
Not reported | 6 (2.4) | 10 (4.0) |
Unknown | 13 (5.3) | 8 (3.2) |
ECOG PS score, n (%) | ||
0 | 145 (60.2) | 160 (65.0) |
1 | 96 (39.8) | 86 (35.0) |
FIGO stage at diagnosis, n (%) | ||
I | 65 (26.5) | 71 (28.5) |
II | 13 (5.3) | 13 (5.2) |
III | 75 (30.6) | 65 (26.1) |
IV | 72 (29.4) | 84 (33.7) |
Unknown | 20 (8.2) | 16 (6.4) |
Disease status, n (%) | ||
Primary stage III | 45 (18.4) | 47 (18.9) |
Primary stage IV | 83 (33.9) | 83 (33.3) |
Recurrent | 117 (47.8) | 119 (47.8) |
Histology at diagnosis, n (%) | ||
Carcinosarcoma | 25 (10.2) | 19 (7.6) |
Clear cell adenocarcinoma | 8 (3.3) | 9 (3.6) |
Endometrioid (adenocarcinoma type or adenocarcinoma variant) | 134 (54.7) | 136 (54.6) |
Mixed carcinoma with ≥ 10% carcinosarcoma, clear cell, or serous histology | 10 (4.1) | 9 (3.6) |
Mucinous adenocarcinoma | 0 (0) | 1 (0.4) |
Serous adenocarcinoma | 50 (20.4) | 52 (20.9) |
Undifferentiated carcinoma | 1 (0.4) | 2 (0.8) |
Other | 17 (6.9) | 21 (8.4) |
MMR and/or MSI status, n (%) | ||
dMMR or MSI-H | 53 (21.6) | 65 (26.1) |
pMMR or MSS | 192 (78.4) | 184 (73.9) |
Prior intervention for study indication, n (%) | ||
Pharmacological treatment | 48 (19.6) | 52 (20.9) |
Surgery | 224 (91.4) | 224 (90.0) |
Radiotherapy | ██ ██████ | ██ ██████ |
Prior external pelvic radiotherapy, n (%) | ||
Yes | 41 (16.7) | 45 (18.1) |
No | 204 (83.3) | 204 (81.9) |
dMMR = mismatch repair deficient; ECOG PS = Eastern Cooperative Oncology Group Performance Status; FIGO = International Federation of Gynecology and Obstetrics; ITT = intention to treat; MMR = mismatch repair; MSI-H = microsatellite instability–high; MSS = microsatellite stable; pMMR = mismatch repair proficient; SD = standard deviation.
Source: RUBY trial, Part 1 Clinical Study Report.1 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Exposure to Study Treatments
By the data cut-off date of September 22, 2023 (interim analysis 2), the median durations of treatment with dostarlimab and placebo were 43 weeks (range, 3.0 weeks to 192.6 weeks) and 36 weeks (range, 2.1 weeks to 193.1 weeks), respectively. The median numbers of dosing cycles with dostarlimab were ████ (range, ██ to ██) and ███ (range, ██ to ██) with placebo. In the first 6 cycles of study treatment, the median relative dose intensity of carboplatin in the group receiving dostarlimab plus carboplatin-paclitaxel was ████% (range, ████% to █████%); it was ████% (range, ████% to █████%) in the group receiving placebo plus carboplatin-paclitaxel. The median relative dose intensity of paclitaxel in the group receiving dostarlimab plus carboplatin-paclitaxel was ████% (range, ███% to █████%); it was ████% (range, ███% to █████%) in the group receiving placebo plus carboplatin-paclitaxel.
In general, infusion interruptions were infrequent and similar between the treatment groups; ███% and ███% of patients had any infusion interruption in the groups receiving dostarlimab plus carboplatin-paclitaxel and placebo plus carboplatin-paclitaxel, respectively. The most common reasons for any infusion interruption in both groups were AEs (██%) and other (██%). The most common AE leading to any infusion interruption was infusion-related reaction, which occurred at similar rates in both groups (approximately ██%). Any missed infusions occurred in ███% of patients in the group receiving dostarlimab plus carboplatin-paclitaxel group and ███% in the group receiving placebo plus carboplatin-paclitaxel.
The most common concomitant medications taken by patients in the group receiving dostarlimab plus carboplatin-paclitaxel compared to the group receiving placebo plus carboplatin-paclitaxel, respectively, were dexamethasone (████% versus ████), paracetamol (████% versus ████%), ondansetron (████% versus ████%), famotidine (████% versus ████%), and diphenhydramine (████% versus ████%).
Subsequent Treatment
At the data cut-off date of September 22, 2023 (interim analysis 2), 59.3% of the ITT population had received subsequent anticancer therapy after discontinuing study treatment (Table 11). The proportion of patients receiving subsequent anticancer treatments was lower in the group receiving dostarlimab plus carboplatin-paclitaxel (49.0%) than in the group receiving placebo plus carboplatin-paclitaxel (69.5%). The most common therapies in both groups were chemotherapy (approximately ████% in both groups) and immunotherapy (17.1% in the dostarlimab plus carboplatin-paclitaxel group versus 38.2% in the placebo plus carboplatin-paclitaxel group).
Efficacy
Only those efficacy outcomes and analyses of subgroups identified as important to this review are reported. The main findings for the efficacy outcomes for the RUBY trial, Part 1 are from the data cut-off dates of September 28, 2022 (interim analysis 1), and September 22, 2023 (interim analysis 2). The boundary for statistical significance for the dual primary outcomes of PFS and OS were met in interim analysis 1 and interim analysis 2, respectively. PFS was not re-evaluated at interim analysis 2. HRQoL results are from interim analysis 1. Safety results are from interim analysis 2.
Table 11: Summary of Subsequent Treatment — ITT Population, RUBY Trial, Part 1
Received subsequent therapy, n (%) | Dostarlimab plus carboplatin-paclitaxel (N = 245) | Placebo plus carboplatin-paclitaxel (N = 249) |
|---|---|---|
Any | 120 (49.0) | 173 (69.5) |
Chemotherapy | ██ ██████ | ██ ██████ |
Immunotherapy | 42 (17.1) | 95 (38.2) |
Radiation therapy | ██ ██████ | ██ ██████ |
Hormonal therapy | ██ █████ | ██ ██████ |
Other | █████ | ██ █████ |
Unknown | █████ | █████ |
ITT = intention to treat.
Source: RUBY trial, Part 1 Clinical Study Report.1 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Overall Survival
A summary of OS findings is in Table 12. By the second interim analysis, the median duration of follow-up for all patients was 37.2 months (range, 31.0 months to 49.5 months), and there were 109 deaths (44.5%) in the group receiving dostarlimab plus carboplatin-paclitaxel versus 144 deaths (57.8%) in the group receiving placebo plus carboplatin-paclitaxel. The median OS was 44.6 months (95% CI, 32.6 months to NE) in the group receiving dostarlimab plus carboplatin-paclitaxel versus 28.2 months (95% CI, 22.1 months to 35.6 months) in the group receiving placebo plus carboplatin-paclitaxel (1-sided P value = 0.0020), with a between-group HR of 0.69 (95% CI, 0.54 to 0.89). The result of the sensitivity analysis was consistent with that of the primary analysis.
The KM-estimated probabilities of being alive at 24 months and 36 months (Figure 3) were 70.1% (95% CI, ████ to ████) versus 54.3% (95% CI, ████ to ████; between-group difference: ████% [95% CI, ███ to ████]) and 54.9% (95% CI, ████ to █████ versus 42.9% (95% CI, ████ to ████; between-group difference: ████% [95% CI, ████ to ████]) in the groups receiving dostarlimab plus carboplatin-paclitaxel and placebo plus carboplatin-paclitaxel, respectively.
OS Subgroup Analyses
The efficacy results for OS were generally consistent across the subgroup analyses of interest (age and histology) in favour of dostarlimab plus carboplatin-paclitaxel; however, there was inconsistency in effects across disease status subgroups (Figure 4). The subgroup analyses did not include MMR or MSI status.
Table 12: Overall Survival — ITT Population, RUBY Trial, Part 1
Overall survival | Dostarlimab plus carboplatin-paclitaxel (N = 245) | Placebo plus carboplatin-paclitaxel (N = 249) |
|---|---|---|
Interim analysis 2, data cut-off date of September 22, 2023 | ||
Deaths, N (%) | 109 (44.5) | 144 (57.8) |
Patients censored | 136 (55.5) | 105 (42.2) |
Median OS, months (95% CI) | 44.6 (32.6 to NE) | 28.2 (22.1 to 35.6) |
Stratified HR (95% CI)a | 0.69 (0.54 to 0.89) | |
1-sided P valueb | 0.0020 | |
KM probability of being event-free at 24 months, % (95% CI) | 70.1 (████ to ████) | 54.3 (████ to ████) |
Between-group difference, % (95% CI) | ████ (███ to █████ | |
KM probability of being event-free at 36 months, % (95% CI) | 54.9 (████ to ████) | 42.9 (████ to ████) |
Between-group difference, % (95% CI) | ████ (████ to ████) | |
CI = confidence interval; HR = hazard ratio; ITT = intention to treat; KM = Kaplan-Meier; NE = not estimable; OS = overall survival.
aBased on a stratified Cox proportional hazards model.
bBased on stratified log-rank test.
Source: RUBY trial, Part 1 Clinical Study Report.1 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
PFS by Investigator Assessment
A summary of results for PFS by investigator assessment is in Table 12. At the time of the first interim analysis, the median duration of follow-up for all patients was 25.4 months (range, 19.2 months to 37.8 months); PFS events had been reported for 135 patients (55.1%) receiving dostarlimab plus carboplatin-paclitaxel and for 177 patients (71.1%) receiving placebo plus carboplatin-paclitaxel. The median PFS durations were 11.8 months (95% CI, 9.6 months to 17.1 months) in the group receiving dostarlimab plus carboplatin-paclitaxel versus 7.9 months (95% CI, 7.6 months to 9.5 months) in the group receiving placebo plus carboplatin-paclitaxel (1-sided P value < 0.0001), with a between-group HR of 0.64 (95% CI, 0.51 to 0.80). The results of the sensitivity analyses were consistent with those of the primary analysis.
The KM-estimated probabilities of PFS at 12 months and 24 months (Figure 5) were 48.2% (95% CI, ████ to █████ versus 29.0% (95% CI, ████ to ████; between-group difference: ████% [95% CI, ████ to ████]), and 36.1% (95% CI, ████ to ████) versus 18.1% (95% CI, ████ to ████; between-group difference: ████% [95% CI, ████ to ████) in the groups receiving dostarlimab plus carboplatin-paclitaxel and placebo plus carboplatin-paclitaxel, respectively. The results of the secondary outcome of PFS by BICR assessment were consistent with those of the investigator assessment (data not shown).
PFS Subgroup Analyses
The efficacy results for PFS were generally consistent across the exploratory subgroup analyses by MMR and/or MSI status at baseline, age, disease status at baseline, and histology, in favour of dostarlimab plus carboplatin-paclitaxel. The HRs for the 2 subgroups (i.e., dMMR and/or MSI-H and pMMR and/or MSS) were 0.33 (95% CI, 0.19 to 0.57) and 0.76 (95% CI, 0.60 to 0.98), respectively. There were some inconsistent effects across the disease status subgroup, particularly for patients with primary stage III caner (Figure 4).
Figure 3: KM Plot of OS — ITT Population, RUBY Trial, Part 1
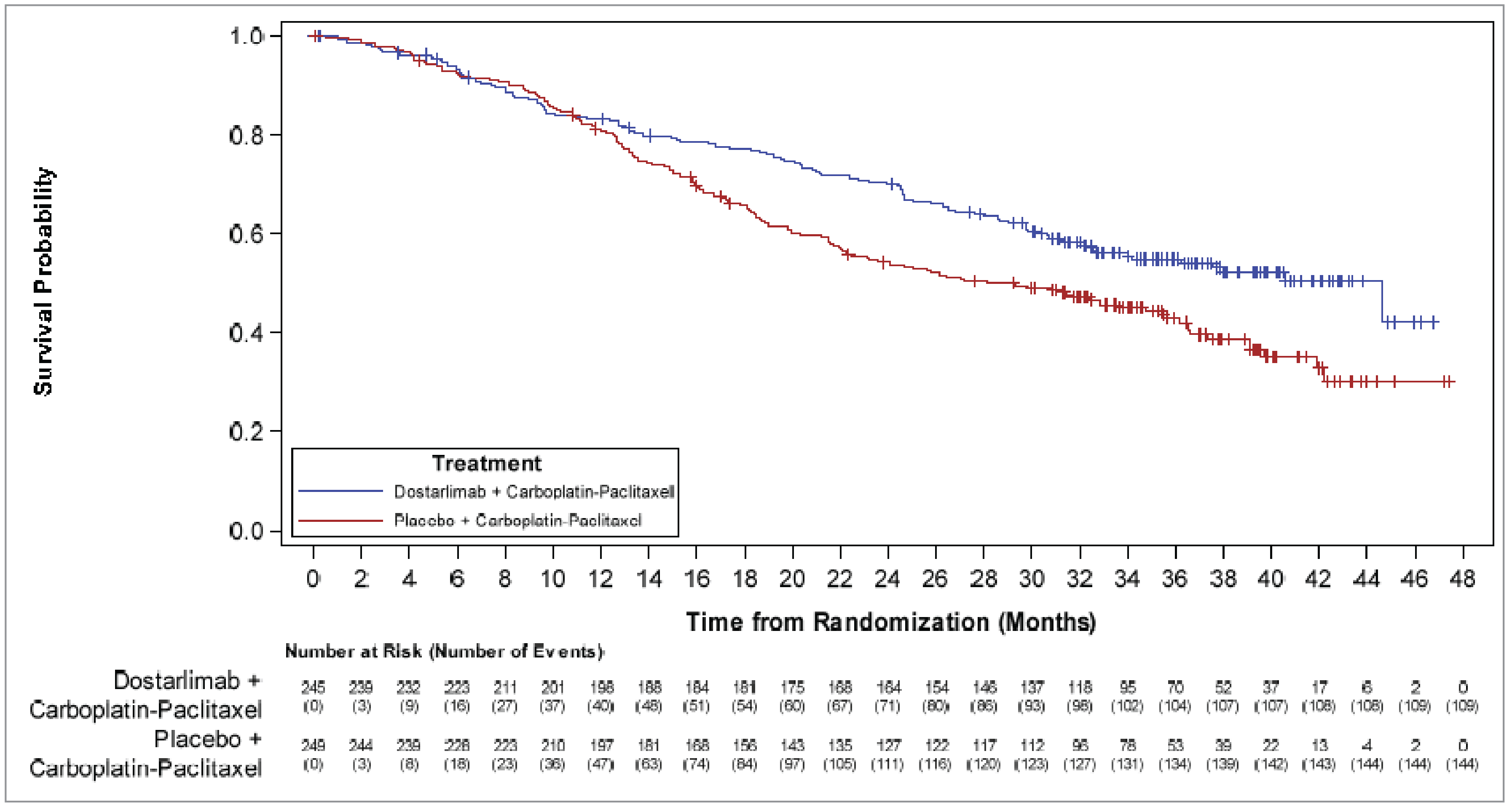
ITT = intention to treat; KM = Kaplan-Meier; OS = overall survival.
Source: RUBY trial, Part 1 Clinical Study Report. Details included in the table are from the sponsor’s Summary of Clinical Evidence.
HRQoL by EORTC QLQ-C30
The EORTC QLQ-C30 Global Health Status results for the ITT population are summarized in Table 14. At baseline, cycle 7, and cycle 13, Global Health Status mean scores were similar between treatment groups; there were no clinically meaningful changes observed (defined by the sponsor as change in score from baseline of ≥ 10 points) in either group at cycle 7 or cycle 13. The between-group least squares mean differences in change from baseline at cycles 7 and 13 were ████ (95% CI, ████ to ███) and ████ (95% CI, ████ to ███), respectively.
Table 13: Progression-Free Survival — ITT Population, RUBY Trial, Part 1
PFS by investigator assessment | Dostarlimab plus carboplatin-paclitaxel (N = 245) | Placebo plus carboplatin-paclitaxel (N = 249) |
|---|---|---|
Interim analysis 1, data cut-off date of September 28, 2022 | ||
Patients with events, N (%) | ||
Total | 135 (55.1) | 177 (71.1) |
Disease progression | ███ ██████ | ███ ██████ |
Death | ██ █████ | █████ |
Patients censored | 110 (44.9) | 72 (28.9) |
Median PFS, months (95% CI) | 11.8 (9.6 to 17.1) | 7.9 (7.6 to 9.5) |
Stratified HR (95% CI)a | 0.64 (0.51 to 0.80) | |
1-sided P valueb | < 0.0001 | |
KM probability of being event-free at 12 months, % (95% CI) | 48.2 (████ to ████) | 29.0 (████ to ████) |
Between-group difference, % (95% CI) | ████ (████ to ████) | |
KM probability of being event-free at 24 months, % (95% CI) | 36.1 (████ to ████) | 18.1 (████ to ████) |
Between-group difference, % (95% CI) | ████ (████ to ████) | |
CI = confidence interval; HR = hazard ratio; ITT = intention to treat; KM = Kaplan-Meier; PFS = progression-free survival.
aBased on a stratified Cox proportional hazards model.
bBased on stratified log-rank test.
Source: RUBY trial, Part 1 Clinical Study Report.1 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Table 14: Summary of EORTC QLQ-C30 Global Health Status Results — ITT Population, RUBY Trial, Part 1, Interim Analysis 1
Global Health Status (higher scores indicate better health status) | Dostarlimab plus carboplatin-paclitaxel (N = 245) | Placebo plus carboplatin-paclitaxel (N = 249) |
|---|---|---|
Baseline | ||
Number of patients contributing to the analysisa | ███ | ███ |
Mean (SD) | ████ ██████ | ████ ██████ |
Cycle 7 | ||
Number of patients contributing to the analysisa | ███ | ███ |
Mean (SD) | ████ ██████ | ████ ██████ |
Mean CFB (SD) | −1.8 (22.8) | −2.3 (23.1) |
Number of patients contributing to the MMRM between-group analysisb | ███ | ███ |
Between-group difference, LS mean (95% CI) | ████ (████ to ███) | |
Cycle 13 | ||
Number of patients contributing to the analysisa | ██ | ██ |
Mean (SD) | ████ ██████ | ████ ██████ |
Mean CFB (SD) | 3.3 (23.5) | −0.9 (19.3) |
Number of patients contributing to the MMRM between-group analysisb | ██ | ██ |
Between-group difference, LS mean (95% CI) | ████ (████ to ███) | |
CFB = change from baseline; CI = confidence interval; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; ITT = intention to treat; LS = least squares; MMRM = mixed-effects model for repeated measures; SD = standard deviation.
aNumber of participants with nonmissing value at both baseline and the corresponding postbaseline visit.
bBased on MMRM.
Source: RUBY trial, Part 1 Clinical Study Report.1 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Figure 4: Forest Plot of OS by Subgroups — ITT Population, RUBY Trial, Part 1
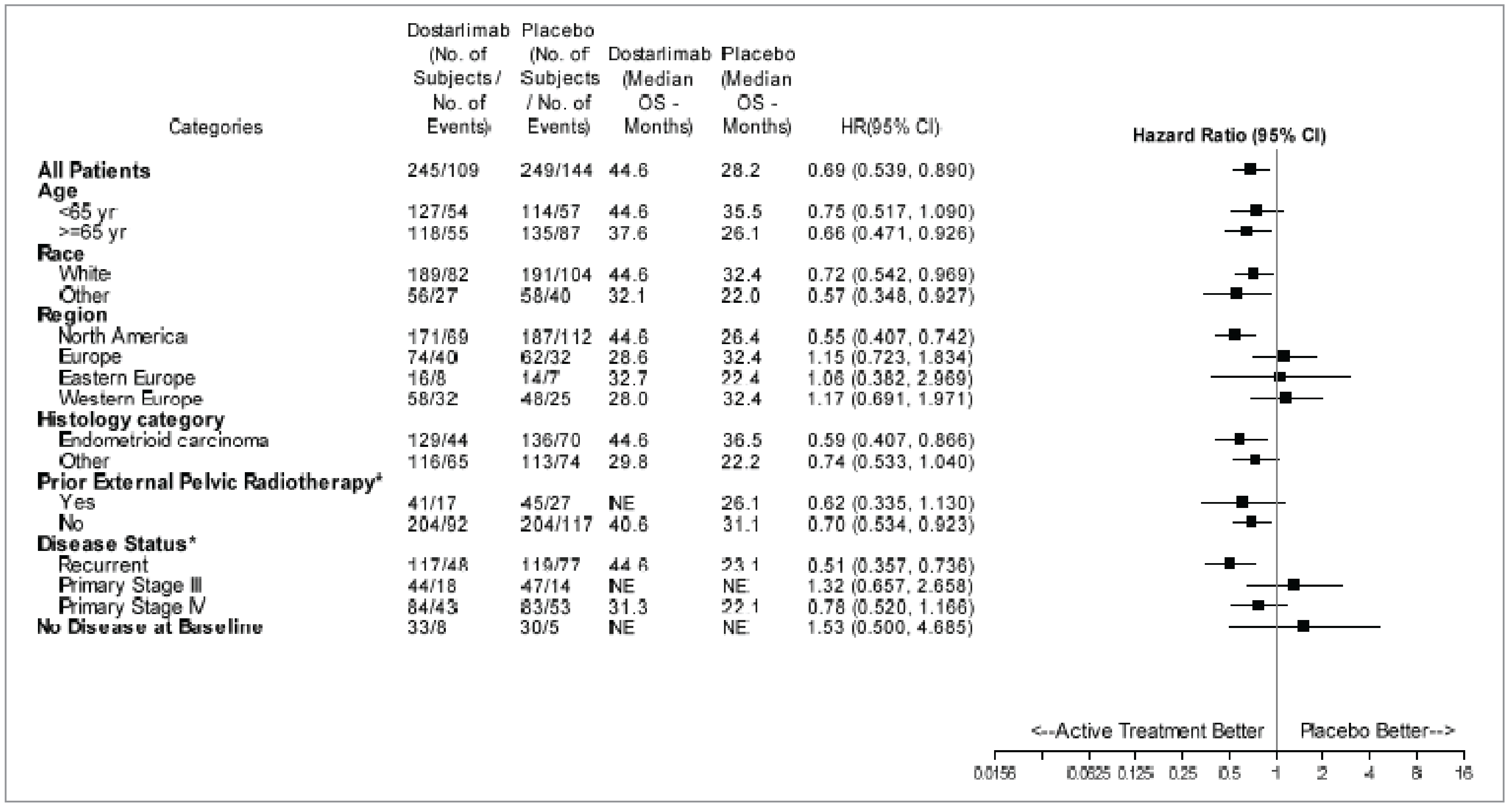
CI = confidence interval; HR = hazard ratio; ITT = intent to treat; NE = not estimable; OS = overall survival.
*Patients whose initial diagnosis differed from endometrioid carcinoma (e.g., disease with carcinosarcoma, clear cell, serous, or mixed histology [containing ≥ 10% carcinosarcoma, clear cell, or serous histology]).
Source: RUBY trial, Part 1 Clinical Study Report.1 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Figure 5: KM Plot of PFS — ITT Population, RUBY Trial, Part 1
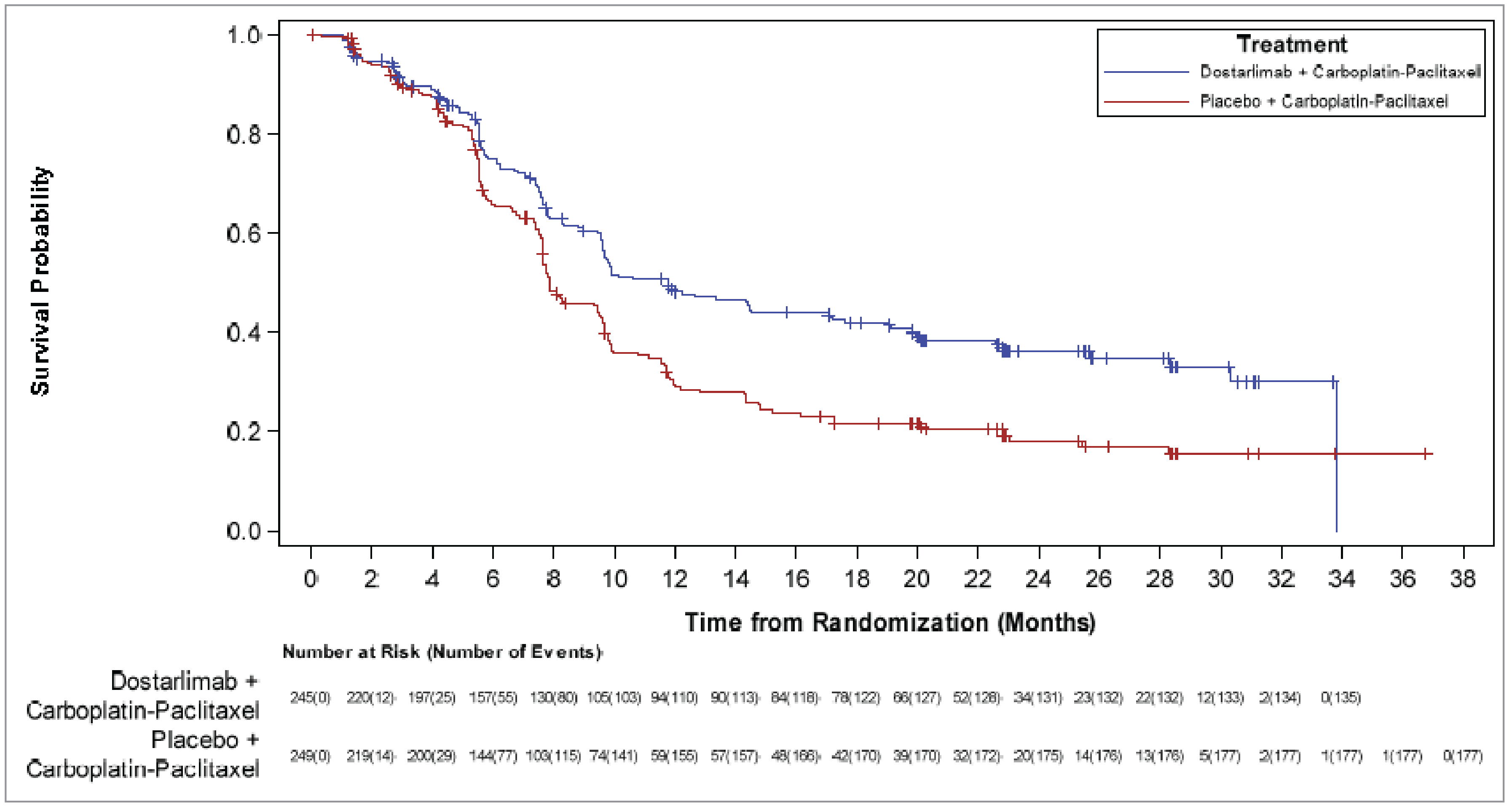
ITT = intention to treat; KM = Kaplan-Meier; PFS = progression-free survival.
Source: RUBY trial, Part 1 Clinical Study Report.1 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Harms
Harms data reported in this section are from the second interim analysis (data cut-off date of September 22, 2023). There were no significant changes in the incidences of TEAEs from the time of the first interim analysis to the time of the second interim analysis. The key harms results for the safety population are summarized in Table 15.
Adverse Events
All patients in both treatment groups reported at least 1 TEAE. The most frequently reported TEAEs in the groups receiving dostarlimab plus carboplatin-paclitaxel and placebo plus carboplatin-paclitaxel, respectively, were fatigue (52.3% versus 54.9%), alopecia (53.9% versus 50.0%), nausea (54.4% versus 46.3%), peripheral neuropathy (44.0% versus 41.9%), and anemia (37.8% versus 42.7%). Of these TEAEs, a higher proportion of patients taking dostarlimab plus carboplatin-paclitaxel reported nausea. A higher proportion of patients in the group receiving dostarlimab plus carboplatin-paclitaxel experienced at least 1 grade 3 or higher TEAE (72.2%) versus the group receiving placebo plus carboplatin-paclitaxel (60.2%). The most common grade 3 or higher TEAEs in both groups were anemia (14.9% versus 16.7%), neutropenia (9.5% versus 9.3%), and neutrophil count decrease (8.3% versus 13.8%).
Figure 6: Forest Plot of PFS by Subgroups — ITT Population, RUBY Trial, Part 1
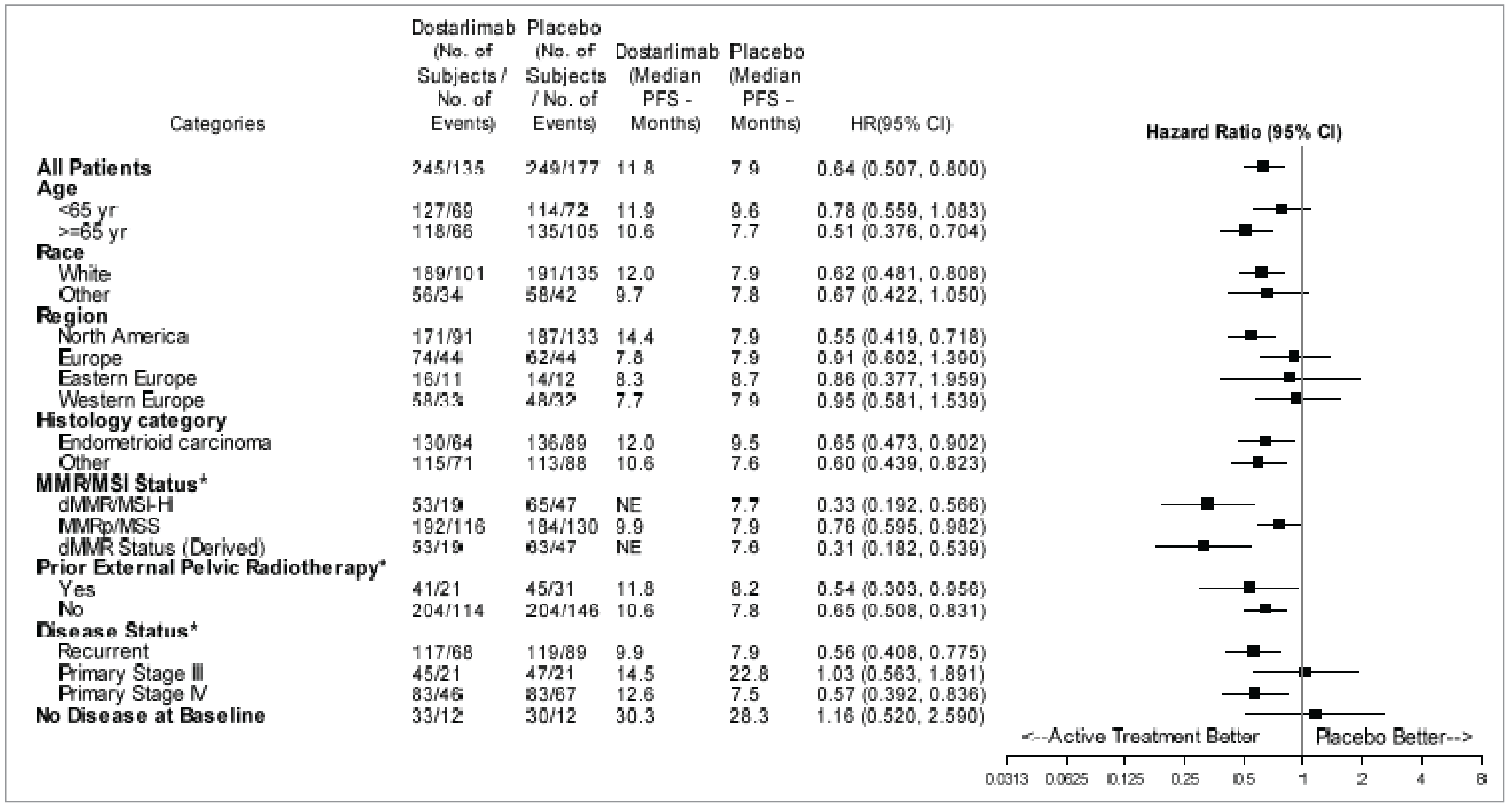
CI = confidence interval; dMMR = mismatch repair deficient; eCRF = electronic case report form; HR = hazard ratio; ITT = intent to treat; MMR = mismatch repair; MMRp = mismatch repair proficient; MSI = microsatellite instability; MSI-H = microsatellite instability–high; MSS = microsatellite stable; NE = not estimable; PFS = progression-free survival.
*Patients whose initial diagnosis differed from endometrioid carcinoma (e.g., disease with carcinosarcoma, clear cell, serous, or mixed histology [containing ≥ 10% carcinosarcoma, clear cell, or serous histology]).
Source: RUBY trial, Part 1 Clinical Study Report.1 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Serious AEs
The incidence of serious TEAEs was higher in the group receiving dostarlimab plus carboplatin-paclitaxel (39.8%) than in the group receiving placebo plus carboplatin-paclitaxel (28.0%). The most frequently reported serious TEAEs in the former group were pulmonary embolism (3.3% versus 2.0%) and sepsis (3.3% versus 0.4%); the most common in the latter were anemia (2.4% versus 1.2%) and pulmonary embolism.
Withdrawals Due to AEs
A higher proportion of TEAEs leading to study treatment discontinuation were reported in patients treated with dostarlimab plus carboplatin-paclitaxel (24.9%) versus placebo plus carboplatin-paclitaxel (16.3%). The most common TEAEs leading to discontinuation in both groups were peripheral neuropathy (2.1% versus 2.8%), peripheral sensory neuropathy (2.9% versus 0.4%), and infusion-related reaction (2.1% versus 3.3%).
Mortality
A lower proportion of deaths were reported in the group receiving dostarlimab plus carboplatin-paclitaxel (39.4%) versus the group receiving placebo plus carboplatin-paclitaxel (54.1%), with the primary reason for death in both groups being disease progression (████% versus ████%).
Notable Harms
A higher proportion of any immune-related TEAEs were reported in patients taking dostarlimab plus carboplatin-paclitaxel (58.5%) versus placebo plus carboplatin-paclitaxel (37.0%). The incidence of infusion-related reactions was similar between groups (████% versus ████%).
Table 15: Summary of Harms — Safety Population, RUBY Trial, Part 1, Interim Analysis 2
Harms | Dostarlimab plus carboplatin-paclitaxel (N = 241) | Placebo plus carboplatin-paclitaxel (N = 246) |
|---|---|---|
TEAEs experienced by > ██% of patients in either group, n (%) | ||
Any TEAEs | 241 (100) | 246 (100) |
Fatigue | 126 (52.3) | 135 (54.9) |
Alopecia | 130 (53.9) | 123 (50.0) |
Nausea | 131 (54.4) | 114 (46.3) |
Peripheral neuropathy | 106 (44.0) | 103 (41.9) |
Anemia | 91 (37.8) | 105 (42.7) |
Arthralgia | 90 (37.3) | 87 (35.4) |
Constipation | 84 (34.9) | 89 (36.2) |
Diarrhea | 76 (31.5) | 72 (29.3) |
Hypomagnesemia | ██ ██████ | ██ ██████ |
Myalgia | ██ ██████ | ██ ██████ |
Rash | ██ ██████ | ██ ██████ |
Dyspnea | ██ ██████ | ██ ██████ |
Decreased appetite | ██ ██████ | ██ ██████ |
Peripheral sensory neuropathy | ██ ██████ | ██ ██████ |
Vomiting | ██ ██████ | ██ ██████ |
Most common grade ≥ 3 TEAEs, n (%)b | ||
Any grade ≥ 3 TEAE | 174 (72.2) | 148 (60.2) |
Most common events | ||
Anemia | 36 (14.9) | 41 (16.7) |
Neutropenia | 23 (9.5) | 23 (9.3) |
Neutrophil count decrease | 20 (8.3) | 34 (13.8) |
Hypertension | 17 (7.1) | 8 (3.3) |
White blood cell count decrease | 16 (6.6) | 13 (5.3) |
Pulmonary embolism | 14 (5.8) | 12 (4.9) |
Lymphocyte count decrease | ██ █████ | ██ █████ |
Hypokalemia | ██ █████ | ██ █████ |
Rash | ██ █████ | ██ █████ |
Hyponatremia | ██ █████ | ██ █████ |
Lipase increase | ██ █████ | ██ █████ |
Thrombocytopenia | ██ █████ | ██ █████ |
Platelet count decrease | ██ █████ | ██ █████ |
Amylase increase | ██ █████ | ██ █████ |
Hyperglycemia | ██ █████ | ██ █████ |
Asthenia | ██ █████ | ██ █████ |
Most common serious TEAEs, n (%)a | ||
Any serious TEAE | 96 (39.8) | 69 (28.0) |
Pulmonary embolism | 8 (3.3) | 5 (2.0) |
Sepsis | 8 (3.3) | 1 (0.4) |
Pyrexia | 7 (2.9) | 2 (0.8) |
Anemia | 3 (1.2) | 6 (2.4) |
Asthenia | 2 (0.8) | 6 (2.4) |
Vomiting | 5 (2.1) | 3 (1.2) |
Dyspnea | 5 (2.1) | 1 (0.4) |
Muscular weakness | 5 (2.1) | 1 (0.4) |
Urinary tract infection | ██ █████ | ██ █████ |
Febrile neutropenia | ██ █████ | ██ █████ |
Most common TEAEs leading to any study treatment discontinuation, n (%)a | ||
Any TEAE leading to discontinuation of any study treatment | ██ ██████ | ██ ██████ |
Peripheral sensory neuropathy | ██ █████ | ██ █████ |
Peripheral neuropathy | ██ █████ | ██ █████ |
Infusion-related reaction | ██ █████ | ██ █████ |
Deaths, n (%) | ||
Death during study | 95 (39.4) | 133 (54.1) |
Primary reason for death | ||
Disease progression | ██ ██████ | ███ ██████ |
AE | ██ █████ | ██ █████ |
Unknown | ██ █████ | ██ █████ |
Other | ██ █████ | ██ █████ |
Notable harms, n (%) | ||
Any immune-related TEAEs | 141 (58.5%) | 91 (37.0%) |
Between-group difference, % (95% CI) | ████ (████ to ████) | |
Any infusion-related reactions | ██ (████%) | ██ (████%) |
Between-group difference, % (95% CI) | ████ (████ to ███) | |
AE = adverse event; CI = confidence interval; TEAE = treatment-emergent adverse event.
aThe most common AEs were those that were experienced by greater than or equal to 2% of patients in at least 1 of the treatment groups.
bThe most common AEs were those that were experienced by greater than or equal to 3% of patients in at least 1 of the treatment groups.
Source: RUBY trial, Part 1 Clinical Study Report.1 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Critical Appraisal
Internal Validity
Part 1 of the RUBY trial was a randomized, double-blind, placebo-controlled, phase III trial. Randomization procedures, including stratification by MMR and/or MSI status, previous external pelvic radiotherapy, and disease status, were appropriate and conducted through an interactive response system. In general, the key baseline characteristics of patients appeared balanced between groups, indicating that randomization was successful.
Important protocol deviations were slightly higher in the group receiving dostarlimab plus carboplatin-paclitaxel (████%) versus the group receiving placebo plus carboplatin-paclitaxel (████%); these were primarily due to assessment of time point completion (████% versus ████%). It is unclear if these deviations favoured 1 group or the other; therefore, the presence, magnitude, and direction of potential bias are unknown.
Sample sizes and power calculations were based on the dual primary outcome of PFS, and the trial was powered to detect significant differences for PFS and OS. The interim analyses were preplanned, with adequately justified stopping boundaries, which provides confidence that the statistical significance of PFS and OS are not a result of type I error. The prespecified analyses of PFS and OS were appropriately controlled for multiple comparisons. All other analyses were descriptive, including the HRQoL outcome of EORTC QLQ-C30 Global Health Status, deemed a clinically important outcome for the disease. The sample sizes for the exploratory subgroup analyses of PFS and OS, including by MMR status, were small. The trial may not have been powered to detect subgroup differences.
Although patients and investigators were blinded to treatment assignment, there was a potential for unblinding due to imbalances in TEAEs, particularly any immune-related TEAEs across treatment groups (i.e., numbers were higher in the group receiving dostarlimab plus carboplatin-paclitaxel). Knowledge of treatment assignment could increase the risk of bias in the measurement of subjective outcomes, including HRQoL and subjective harms; however, the extent and direction of bias cannot be predicted. Objective outcomes (like OS) are unlikely to be affected by bias due to unblinding. To minimize the risk of bias in the measurement of PFS, the trial performed tumour assessments using Response Evaluation Criteria in Solid Tumours Version 1.1 per investigator assessment, and radiographic scans were assessed by BICR as a secondary outcome. The PFS per BICR assessment results were similar to those of the investigator-assessed results. In addition, the findings of the sensitivity analyses for the dual primary outcomes of PFS and OS were consistent with those of the primary analysis.
Patients were permitted to receive posttreatment anticancer medications after study treatment had been discontinued (49% in the dostarlimab group versus 69.5% in the placebo group). This can influence the assessment of OS. Given that no sensitivity analyses were performed to test treatment policy strategy for OS (e.g., to exclude the effect of subsequent therapies), the estimated effect would be a combination of treatment with dostarlimab plus carboplatin-paclitaxel versus placebo plus carboplatin-paclitaxel, plus subsequent treatments. Therefore, survival results might be partially attributable to treatments administered after disease progression rather than to the study treatment itself; however, without the necessary analysis, the direction and magnitude of bias are unclear. Nonetheless, this is a relevant comparison because it is reflective of how the intervention and comparator would be used in practice.
The trial authors stated that the proportional hazards assumption was assessed by visual inspection of a survival curve fit to KM data, inspection of log-cumulative hazard plots over time, and statistical goodness of fit based on relative Akaike and Bayesian information criterion values. However, the assessment results were not reported. Despite the absence of these results, visual inspection of the KM curves for PFS and OS indicated a clear separation (at approximately 5 months and 7 months, respectively), after which there appeared to be sustained proportionality throughout the study treatment.
The EORTC QLQ-C30 has been validated in patients with cancer, with evidence of reliability and MID ranges. Based on the MID ranges identified in the literature, the sponsor suggested a 10-point change from baseline score as clinically meaningful, and this was considered reasonable by the review team. No evidence was identified in the literature for responsiveness. Additionally, the results of the Global Health Status outcome may be biased due to missing data; however, the direction and extent of bias are unclear because no models beyond MMRM were tested using alternative imputation methods or sensitivity analyses to assess the impact of missing data.
External Validity
The population requested for reimbursement aligns with the approved Health Canada indication and overall trial population. The dosing and administration of dostarlimab were consistent with the approved product monograph. The timing of administering dostarlimab or placebo in combination with carboplatin-paclitaxel appears to be aligned with the chemotherapy regimens in the current standard of care, according to the clinical experts consulted by CDA-AMC. The clinical experts noted that the carboplatin dose used in both treatment groups — an area under the concentration time-curve of 5 mg/mL/minute — was 1 mg/mL/minute lower than what is typically prescribed in Canada; however, they did not consider this lower dose to be unreasonable. In Part 1 of the RUBY trial, treatment duration was up to 3 years if patients did not experience disease progression, unacceptable toxicity, or death.
According to the clinical experts consulted by CDA-AMC, the eligibility criteria and baseline characteristics of Part 1 of the RUBY trial were generalizable to adults with primary advanced or first recurrent endometrial cancer in the Canadian setting. However, the trial did not include patients with an ECOG Performance Status of greater than 1. The clinical experts indicated that patients with a good ECOG Performance Status (or a score of 0 to 2) should be eligible for dostarlimab plus carboplatin-paclitaxel followed by dostarlimab maintenance if they are able to tolerate the therapy.
The trial included outcomes that were important to patients and clinicians. The patient group indicated that stopping disease progression, prolonging life, improving HRQoL, and reducing treatment side effects are important to them.
GRADE Summary of Findings and Certainty of the Evidence
Methods for Assessing the Certainty of the Evidence
For the pivotal studies and RCTs identified in the sponsor’s systematic review, GRADE was used to assess the certainty of the evidence for the outcomes considered most relevant to inform the CDA-AMC expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group:43,44
High certainty: We are very confident that the true effect lies close to that of the estimate of the effect.
Moderate certainty: We are moderately confident in the effect estimate. The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. We use the word “likely” for evidence of moderate certainty (e.g., “X intervention likely results in Y outcome”).
Low certainty: Our confidence in the effect estimate is limited. The true effect may be substantially different from the estimate of the effect. We use the word “may” for evidence of low certainty (e.g., “X intervention may result in Y outcome”).
Very low certainty: We have very little confidence in the effect estimate. The true effect is likely to be substantially different from the estimate of the effect. We describe evidence of very low certainty as “very uncertain.”
Following the GRADE approach, evidence from RCTs started as high-certainty evidence and could be rated down for concerns related to study limitations (which refer to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, or publication bias.
When possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect; if this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., the clinical importance is unclear). In all cases, the target of the certainty of evidence assessment was based on the point estimate and its location relative to the threshold for a clinically important effect (when a threshold was available) or to the null.
The reference points for the certainty of evidence assessment for OS, PFS, any immune-related TEAEs, and any infusion-related reactions were set according to the presence or absence of an important effect based on thresholds informed by the clinical experts consulted for this review. The reference points for the certainty of the evidence assessment for the EORTC QLQ-C30 Global Health Status score were set according to the presence or absence of an important effect based on a threshold suggested by the sponsor that was informed by the literature.
Results of GRADE Assessments
Table 2 presents the GRADE summary of findings for dostarlimab plus carboplatin-paclitaxel versus placebo plus carboplatin-paclitaxel.
Long-Term Extension Studies
No long-term extension studies were submitted by the sponsor.
Indirect Evidence
No indirect treatment comparisons were submitted by the sponsor.
Studies Addressing Gaps in the Systematic Review Evidence
No additional studies were submitted by the sponsor.
Discussion
Summary of Available Evidence
One ongoing, pivotal, phase III, randomized, double-blind trial submitted by the sponsor was summarized in this report.
The RUBY trial, Part 1 (N = 494) met the inclusion criteria for the systematic review conducted by the sponsor. The objective of the trial was to assess the efficacy and safety of dostarlimab IV infusion plus carboplatin-paclitaxel followed by dostarlimab monotherapy versus placebo plus carboplatin-paclitaxel followed by placebo in adults with primary advanced or recurrent endometrial cancer. The trial enrolled patients who were aged at least 18 years and had histologically or cytologically confirmed, primary advanced or first recurrent endometrial cancer that was not amenable to curative therapy, an ECOG Performance Status score of 0 or 1, and adequate organ function. Patients were excluded if they had received neoadjuvant or adjuvant chemotherapy, with or without recurrence, in the 6 months before entering the trial, or if they had received prior treatment with an anti–PD-L1, anti–PD-L2, or anti–PD-1 antibody. The approved Health Canada indication and reimbursement request aligned with the trial population. The outcomes most relevant to the CDA-AMC review included the dual primary outcomes of OS and PFS per investigator assessment and the secondary outcomes of HRQoL (measured using the EORTC QLQ-C30 Global Health Status) and safety. Efficacy and safety data were evaluated at the data cut-off dates of September 28, 2022 (interim analysis 1) and September 22, 2023 (interim analysis 2). Overall, the key baseline characteristics were generally balanced between the treatment groups. The trial population was predominantly white (approximately 77%), with a mean age of 64 years, with half of patients aged 19 years to 64 years. Most patients (approximately 63%) had an ECOG Performance Status of 0, indicating good overall performance; endometrioid histology (adenocarcinoma type or adenocarcinoma variant) at diagnosis (approximately 55%); recurrent (48%) or primary stage IV (33%) disease status; FIGO stage III or IV at diagnosis (approximately 60%); MMR and/or MSI status of pMMR and/or MSS (approximately 76%); had received prior surgery for endometrial cancer (approximately 90%); and had not received prior external pelvic radiotherapy (approximately 83%).
Interpretation of Results
The evidence from Part 1 of the pivotal RUBY trial addressed treatment outcomes that were noted to be important by both patients and clinicians. The patient group input indicated that stopping disease progression, prolonging life, improving HRQoL, and reducing treatment side effects are important to them. Similarly, the clinical experts consulted by the review team indicated that, because the treatment goal for patients is long-term disease control, patients’ unmet needs were for new treatments that would delay progression, prolong OS, and improve quality of life with minimal toxicity.
Efficacy
The RUBY trial, Part 1 supported a clinically meaningful improvement with dostarlimab plus carboplatin-paclitaxel over placebo plus carboplatin-paclitaxel for OS and PFS at the second interim analysis (data cut-off date of September 22, 2023) and first interim analysis (data cut-off date of September 28, 2022), respectively, in adults with primary advanced or first recurrent endometrial cancer who were candidates for systemic therapy. The median duration of follow-up for all patients was 37.2 months, with median OS durations of 44.6 months (95% CI, 32.6 to NE) in the group receiving dostarlimab plus carboplatin-paclitaxel versus 28.2 months (95% CI, 22.1 to 35.6) in the group receiving placebo plus carboplatin-paclitaxel. The between-group differences in probabilities of being alive at 24 months and 36 months were ████% (95% CI, ███ to ████) and ████% (95% CI, ████ to ████), respectively. For the GRADE assessment, the clinical experts consulted by CDA-AMC suggested a clinically important threshold of 2% to 5% between-group absolute risk difference for both time points. To align with the previous CDA-AMC review of dostarlimab informed by the same trial (i.e., the RUBY trial, Part 1), a 5% threshold was used for the GRADE assessment. Based on this threshold, there was high certainty of evidence for a clinically important increase in the probability of OS at 24 months and 36 months. The OS findings were generally consistent across the subgroup analyses by age and histology in favour of dostarlimab plus carboplatin-paclitaxel; however, there was inconsistency in the effects across the disease status subgroup. The subgroup analyses were exploratory and not powered to detect differences between groups. Because patients were permitted to receive posttreatment anticancer therapy (dostarlimab plus carboplatin-paclitaxel = 49.0%; placebo plus carboplatin-paclitaxel = 69.5%), the potential treatment benefit on OS would have been subject to a degree of uncertainty.
The between-group differences in probabilities of PFS at 12 months and 24 months were ████% (95% CI, ████ to ████) and ████% (95% CI, ████ to ████), respectively. For the GRADE assessment, the clinical experts suggested a clinically important threshold of a 10% between-group absolute risk difference for both time points. Based on this threshold, there was high certainty of evidence for a clinically important increase in the probability of PFS at 12 months and 24 months. The PFS findings were generally consistent across the exploratory subgroup analyses by MMR and MSI status at baseline, age, disease status at baseline, and histology, in favour of dostarlimab plus carboplatin-paclitaxel; however, there were some inconsistent effects across the disease status subgroup. The HRs for the subgroup of patients with dMMR or MSI-H were larger than for the subgroup of patients with pMMR or MSS, favouring dostarlimab plus carboplatin-paclitaxel.
For EORTC QLQ-C30 Global Health Status, the certainty of evidence at cycle 7 was low, resulting in little to no clinically important difference for dostarlimab plus carboplatin-paclitaxel compared to placebo plus carboplatin-paclitaxel, based on the sponsor’s suggested threshold of a 10-point change from baseline score. This low certainty of evidence was attributed to risk of bias due to missing outcome data. At cycle 13, the certainty of evidence was very low. This was attributed to serious imprecision (because the 95% CI for the between-group difference included the possibility of both harm and little to no difference) as well as to risk of bias due to missing outcome data.
Harms
All patients in both treatment groups reported at least 1 TEAE. The most frequently reported TEAEs in both groups were fatigue, alopecia, nausea, peripheral neuropathy, and anemia. More patients reported nausea in the group receiving dostarlimab plus carboplatin-paclitaxel. A higher proportion of patients in the group receiving dostarlimab plus carboplatin-paclitaxel experienced at least 1 grade 3 or higher TEAE versus the group receiving placebo plus carboplatin-paclitaxel, with anemia, neutropenia, and decreased neutrophil count being the most common in both groups. A higher proportion of patients receiving dostarlimab plus carboplatin-paclitaxel experienced serious TEAEs, with pulmonary embolism and sepsis being the most common. The clinical experts indicated that the incidence of these TEAEs is expected with dostarlimab plus carboplatin-paclitaxel, and that with appropriate care, TEAEs would be manageable for many patients. A higher proportion of TEAEs leading to study treatment discontinuation were reported in patients treated with dostarlimab plus carboplatin-paclitaxel, with peripheral neuropathy, peripheral sensory neuropathy, and infusion-related reaction being the most common in both groups. The incidence of death was lower among patients receiving dostarlimab plus carboplatin-paclitaxel; disease progression was the primary reason for death in both groups. For notable harms, a higher proportion of patients in the group receiving dostarlimab plus carboplatin-paclitaxel experienced any immune-related TEAEs, with a between-group absolute risk difference of ████%. For the GRADE assessment, the clinical experts consulted by CDA-AMC suggested a clinically important threshold of 5% for the between-group absolute risk difference. Based on this threshold, there was high certainty of evidence for a clinically important increase in the proportion of patients experiencing any immune-related TEAEs when compared to placebo plus carboplatin-paclitaxel. The incidence of infusion-related reactions was similar between groups, with a between-group absolute risk difference of ████%. Based on the 5% threshold, CDA-AMC judged that there was low certainty of evidence that dostarlimab plus carboplatin-paclitaxel may result in little to no difference in any infusion-related reactions compared to placebo plus carboplatin-paclitaxel. This low certainty of evidence was attributed to imprecision because the 95% CI for the between-group absolute risk difference included the possibility of both important benefit and important harm.
Conclusion
Evidence from 1 phase III, randomized, double-blind trial (the RUBY trial, Part 1) reported on outcomes that were important to patients and clinicians. The trial showed high certainty of evidence that treatment with dostarlimab plus carboplatin-paclitaxel results in a clinically important increase in OS at 24 months and 36 months and PFS at 12 months and 24 months compared to placebo plus carboplatin-paclitaxel in adults with primary advanced or first recurrent endometrial cancer. At cycle 7 of treatment, there was low certainty of evidence for little to no clinically important between-group difference in HRQoL; no definitive conclusions can be drawn about HRQoL at cycle 13 due to concerns relating to imprecision and missing outcome data. There were no new safety signals identified; the safety of dostarlimab plus carboplatin-paclitaxel was consistent with the known safety profiles of the individual drugs. However, the trial showed high certainty of evidence for a clinically important increase in the proportion of patients who experience any immune-related TEAEs compared with placebo plus carboplatin-paclitaxel.
References
1.GlaxoSmithKline Inc. Clinical Study Report: TMF-15689673. A phase 3, randomized, double-blind, multicenter study of dostarlimab (TSR-042) plus carboplatin-paclitaxel versus placebo plus carboplatin-paclitaxel in patients with recurrent or primary advanced endometrial cancer (RUBY Part 1) [internal sponsor’s report]. March 7, 2023.
2.Canadian Cancer Society. What is uterine cancer? Accessed September 13, 2024. https://cancer.ca/en/cancer-information/cancer-types/uterine/what-is-uterine-cancer
3.Canadian Cancer Society. Stages of uterine cancer. Accessed January 2, 2024. https://cancer.ca/en/cancer-information/cancer-types/uterine/staging
4.Global Cancer Observatory: Cancer Today. Cancer factsheet: Corpus uteri. 2020. Accessed June 1, 2021. https://gco.iarc.who.int/media/globocan/factsheets/cancers/24-corpus-uteri-fact-sheet.pdf
5.Global Cancer Observatory: Cancer Today. Cancer today online analysis (GLOBOCAN 2020): Estimated age-standardized incidence rates (World) in 2020, World, High income, females, all ages. 2020. Accessed May 23, 2022. https://gco.iarc.fr/today/online-analysis-multi-bars?v=2020&mode=cancer&mode_population=countries&population=900&populations=900_986&key=asr&sex=2&cancer=39&type=0&statistic=5&prevalence=0&population_group=0&ages_group%5B%5D=0&ages_group%5B%5D=17&nb_items=10&group_cancer=1&include_nmsc=0&include_nmsc_other=1&type_multiple=%257B%2522inc%2522%253Atrue%252C%2522mort%2522%253Afalse%252C%2522prev%2522%253Afalse%257D&orientation=horizontal&type_sort=0&type_nb_items=%257B%2522top%2522%253Atrue%252C%2522bottom%2522%253Afalse%257D#collapse-group-1-0-4 [sponsor supplied reference]
6.American Cancer Society. Endometrial cancer stages. Accessed January 2, 2024. https://www.cancer.org/cancer/types/endometrial-cancer/detection-diagnosis-staging/staging.html
7.Campos S, Cohn D. Post TW, ed. Initial treatment of metastatic endometrial cancer. UpToDate; 2023. Accessed January 2, 2024. http://www.uptodate.com
8.Plaxe S, Mundt A. Post TW, ed. Overview of resectable endometrial carcinoma. UpToDate; 2023. Accessed September 13, 2024. http://www.uptodate.com
9.Bricou A, Bendifallah S, Daix-Moreux M, et al. A proposal for a classification for recurrent endometrial cancer: Analysis of a French multicenter database from the FRANCOGYN Study Group. Int J Gynecol Cancer. 2018;28(7):1278-1284. doi: 10.1097/igc.0000000000001296 PubMed
10.Cosgrove CM, Backes FJ, O'Malley D, et al. Endometrial cancer: who lives, who dies, can we improve their story? Oncologist. 2021;26(12):1044-1051. doi: 10.1002/onco.13934 PubMed
11.Donkers H, Bekkers R, Massuger L, Galaal K. Socioeconomic deprivation and survival in endometrial cancer: The effect of BMI. Gynecol Oncol. 2020;156(1):178-184. doi: 10.1016/j.ygyno.2019.10.030 PubMed
12.Lubrano A, Benito V, Pinar B, Molano F, Leon L. Efficacy of endometrial cancer follow-up protocols: time to change? Rev Bras Ginecol Obstet. 2021;43(1):41-45. doi: 10.1055/s-0040-1721352 PubMed
13.Oaknin A, Gilbert L, Tinker AV, et al. Safety and antitumor activity of dostarlimab in patients with advanced or recurrent DNA mismatch repair deficient/microsatellite instability-high (dMMR/MSI-H) or proficient/stable (MMRp/MSS) endometrial cancer: interim results from GARNET-a phase I, single-arm study. J Immunother Cancer. 2022;10(1):e003777. doi: 10.1136/jitc-2021-003777 PubMed
14.American Cancer Society. Key statistics for endometrial cancer. Accessed October 11, 2022 https://www.cancer.org/cancer/endometrial-cancer/about/key-statistics.html
15.Brooks RA, Fleming GF, Lastra RR, et al. Current recommendations and recent progress in endometrial cancer. CA Cancer J Clin. 2019;69(4):258-279. doi: 10.3322/caac.21561 PubMed
16.Huijgens AN, Mertens HJ. Factors predicting recurrent endometrial cancer. Facts Views Vis Obgyn. 2013;5(3):179-86. Accessed May 28, 2025. https://pmc.ncbi.nlm.nih.gov/articles/PMC3987371/ PubMed
17.Makker V, Green AK, Wenham RM, Mutch D, Davidson B, Miller DS. New therapies for advanced, recurrent, and metastatic endometrial cancers. Gynecol Oncol Res Pract. 2017;4:19. doi: 10.1186/s40661-017-0056-7 PubMed
18.National Cancer Institute (NCI). Cancer Stat Facts: Uterine Cancer. 2022. Accessed February 2023. https://seer.cancer.gov/statfacts/html/corp.html
19.NCCN Guidelines. Uterine neoplasms, v2.2023. National Comprehensive Cancer Network; 2023. Accessed May 2023. https://www.nccn.org/
20.Nomura H, Aoki D, Takahashi F, et al. Randomized phase II study comparing docetaxel plus cisplatin, docetaxel plus carboplatin, and paclitaxel plus carboplatin in patients with advanced or recurrent endometrial carcinoma: a Japanese Gynecologic Oncology Group study (JGOG2041). Ann Oncol. 2011;22(3):636-642. doi: 10.1093/annonc/mdq401 PubMed
21.Oaknin A, Bosse TJ, Creutzberg CL, et al. Endometrial cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann Oncol. 2022;33(9):860-877. doi: 10.1016/j.annonc.2022.05.009 PubMed
22.Sorbe B, Andersson H, Boman K, Rosenberg P, Kalling M. Treatment of primary advanced and recurrent endometrial carcinoma with a combination of carboplatin and paclitaxel-long-term follow-up. Int J Gynecol Cancer. 2008;18(4):803-8. doi: 10.1111/j.1525-1438.2007.01094.x PubMed
23.Miller DS, Filiaci VL, Mannel RS, et al. Carboplatin and paclitaxel for advanced endometrial cancer: final overall survival and adverse event analysis of a phase III trial (NRG Oncology/GOG0209). J Clin Oncol. 2020;38(33):3841-3850. doi: 10.1200/jco.20.01076 PubMed
24.Coleman. Treatment Patterns and Outcomes Among Patients with Advanced or Recurrent Endometrial Cancer Initiating First-Line Therapy in the United States. J Health Econ Outcomes Res. 2023;10(2):82-90. PubMed
25.Guideline Resource Unit, Alberta Health Services. Cancer of the uterine cervix, version 5. 2015. Accessed July 17, 2023. https://www.albertahealthservices.ca/assets/info/hp/cancer/if-hp-cancer-guide-gyne002-endometrial.pdf [sponsor supplied reference]
26.BC Cancer. Endometrium: cancer management manual. 2023. Accessed July 17, 2023. http://www.bccancer.bc.ca/health-professionals/clinical-resources/cancer-management-manual/gynecology/endometrium
27.Gawlik C, Carey M, Faught W, Fung Kee Fung M, Chambers A, Members of the Gynecology Cancer Disease Site Group. Systemic therapy for advanced or recurrent endometrial cancer, and advanced or recurrent uterine papillary serous carcinoma, version 4. Cancer Care Ontario (CCO); 2019. Accessed July 17, 2023. https://www.cancercareontario.ca/en/guidelines-advice/types-of-cancer/501
28.GlaxoSmithKline Inc. Jemperli (dostarlimabfor injection): 500 mg/10 mL vial, solution for infusion [product monograph]. December 23, 2021. Updated January 31, 2023. Accessed September 16, 2024. https://pdf.hres.ca/dpd_pm/00069388.PDF
29.CADTH. Reimbursement Recommendation: dostarlimab (Jemperli). Can J Health Technol. 2022;2(9). doi: 10.51731/cjht.2022.441
30.CADTH. Reimbursement Recommendation: dostarlimab (Jemperli). Can J Health Technol. 2024;4(5). doi: 10.51731/cjht.2024.898
31.Accord Healthcare Inc. Carboplatin Injection BP: 10 mg/mL solution for intravenous injection [product monograph]. December 23, 2008. Updated December 19, 2022. Accessed May 27, 2025. https://pdf.hres.ca/dpd_pm/00068833.PDF
32.Bristol-Myers Squibb Canada. Taxol (paclitaxel): 6mg/mL injection [product monograph]. Updated February 10, 2010. Accessed May 27, 2025. https://pdf.hres.ca/dpd_pm/00009873.PDF
33.Mirza MR, Chase DM, Slomovitz BM, et al. Dostarlimab for Primary Advanced or Recurrent Endometrial Cancer. N Engl J Med. 2023;388(23):2145-2158. doi: 10.1056/NEJMoa2216334 PubMed
34.Powell MA, Bjorge L, Willmott L, et al. Overall survival in patients with endometrial cancer treated with dostarlimab plus carboplatin-paclitaxel in the randomized ENGOT-EN6/GOG-3031/RUBY trial. Ann Oncol. 2024;35(8):728-738. doi: 10.1016/j.annonc.2024.05.546 PubMed
35.Aaronson NK, Ahmedzai S, Bergman B, et al. The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst. 1993;85(5):365-76. doi: 10.1093/jnci/85.5.365 PubMed
36.Letellier ME, Dawes D, Mayo N. Content verification of the EORTC QLQ-C30/EORTC QLQ-BR23 with the International Classification of Functioning, Disability and Health. Qual Life Res. 2015;24(3):757-68. doi: 10.1007/s11136-014-0791-8 PubMed
37.McLachlan SA, Devins GM, Goodwin PJ. Validation of the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire (QLQ-C30) as a measure of psychosocial function in breast cancer patients. Eur J Cancer. 1998;34(4):510-517. doi: 10.1016/s0959-8049(97)10076-4 PubMed
38.Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977;33(1):159-74. PubMed
39.Groenvold M, Klee MC, Sprangers MA, Aaronson NK. Validation of the EORTC QLQ-C30 quality of life questionnaire through combined qualitative and quantitative assessment of patient-observer agreement. J Clin Epidemiol. 1997;50(4):441-50. doi: 10.1016/s0895-4356(96)00428-3 PubMed
40.Musoro JZ, Coens C, Sprangers MAG, et al. Minimally important differences for interpreting EORTC QLQ-C30 change scores over time: A synthesis across 21 clinical trials involving nine different cancer types. Eur J Cancer. 2023;188:171-182. doi: 10.1016/j.ejca.2023.04.027 PubMed
41.Osoba D, Rodrigues G, Myles J, Zee B, Pater J. Interpreting the significance of changes in health-related quality-of-life scores. J Clin Oncol. 1998;16(1):139-44. doi: 10.1200/JCO.1998.16.1.139 PubMed
42.de Vet HC, Terwee CB, Ostelo RW, Beckerman H, Knol DL, Bouter LM. Minimal changes in health status questionnaires: distinction between minimally detectable change and minimally important change. Health Qual Life Outcomes. 2006;4:54. doi: 10.1186/1477-7525-4-54 PubMed
43.Balshem H, Helfand M, Schünemann HJ, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011;64(4):401-6. doi: 10.1016/j.jclinepi.2010.07.015 PubMed
44.Santesso N, Glenton C, Dahm P, et al. GRADE guidelines 26: informative statements to communicate the findings of systematic reviews of interventions. J Clin Epidemiol. 2020;119:126-135. doi: 10.1016/j.jclinepi.2019.10.014 PubMed
Pharmacoeconomic Review
Abbreviations
AE
adverse event
AUC
area under the concentration time-curve
BIA
budget impact analysis
BSA
body surface area
CDA-AMC
Canada’s Drug Agency
CUA
cost-utility analysis
dMMR
mismatch repair deficient
IA2
interim analysis 2
ICER
incremental cost-effectiveness ratio
KM
Kaplan-Meier
MMR
mismatch repair
MSI
microsatellite instability
MSI-H
microsatellite instability–high
MSS
microsatellite stable
OS
overall survival
PFD
progression-free disease
PFS
progression-free survival
pMMR
mismatch repair proficient
PSM
partitioned survival model
QALY
quality-adjusted life-year
TTD
time to treatment discontinuation
WTP
willingness to pay
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Dostarlimab (Jemperli), solution for infusion, 500 mg/10 mL vial (50 mg/mL) |
Proposed indication | In combination with carboplatin and paclitaxel for the treatment of adult patients with primary advanced or recurrent endometrial cancer who are candidates for systemic therapy |
Health Canada approval status | NOC |
Health Canada review pathway | Standard review |
NOC date | April 16, 2025 |
Reimbursement request | As per indication |
Sponsor | GlaxoSmithKline Inc. |
Submission history | Previously reviewed: Yes Indication: In combination with carboplatin and paclitaxel for the treatment of adult patients with primary advanced or recurrent dMMR or MSI-H endometrial cancer who are candidates for systemic therapy Recommendation date: May 3, 2024 Recommendation: Reimburse with conditions Indication: Monotherapy for the treatment of adult patients with dMMR or MSI-H recurrent or advanced endometrial cancer who have progressed on or following prior treatment with a platinum-containing regimen Recommendation date: August 24, 2022 Recommendation: Do not reimburse |
dMMR = mismatch repair deficient; MSI-H = microsatellite instability–high; NOC = Notice of Compliance.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis PSM |
Target population | Adult patients with primary advanced or recurrent endometrial cancer who are candidates for systemic therapy |
Treatments | Dostarlimab plus carboplatin-paclitaxel |
Dose regimen | 500 mg administered as an IV infusion over 30 minutes every 3 weeks for 6 doses (in combination with carboplatin dosed at AUC 5 mg/mL and paclitaxel 175 mg/m2), followed by 1,000 mg every 6 weeks until progression of disease, unacceptable toxicity, or the maximum treatment duration of 3 years |
Submitted price | Dostarlimab, 50 mg/mL, solution for infusion, $10,031.08 per 500 mg vial |
Submitted treatment cost | Cycles 1 to 6: $14,515 per 3-week cycle (dostarlimab plus carboplatin-paclitaxel) Cycles 7 and onward: $20,062 per 6-week cycle (dostarlimab alone) |
Comparator | Carboplatin-paclitaxel |
Perspective | Publicly funded health care payers in Canada |
Outcomes | QALYs, LYs |
Time horizon | Lifetime (36.10 years) |
Key data sources | RUBY trial, Part 1, IA1 and IA2 |
Submitted results | Full population: ICER = $78,806 per QALY gained (incremental cost = $147,238; incremental QALYs = 1.87) |
Key limitations |
|
CDA-AMC reanalysis results |
|
AUC = area under the concentration curve; CDA-AMC = Canada’s Drug Agency; IA1 = interim analysis 1; IA2 = interim analysis 2; ICER = incremental cost-effectiveness ratio; LY = life-year; OS = overall survival; PSM = partitioned survival model; QALY = quality-adjusted life-year; WTP = willingness to pay.
Conclusions
The clinical review by Canada’s Drug Agency (CDA-AMC) highlighted the results from Part 1 of the RUBY trial, which indicated with high certainty of evidence that treatment with dostarlimab plus carboplatin-paclitaxel significantly improves overall survival (OS) at 24 months and 36 months and progression-free survival (PFS) at 12 months and 24 months compared to placebo plus carboplatin-paclitaxel in adults with primary advanced or first recurrent endometrial cancer. The benefits in OS and PFS were generally consistent across subgroup analyses by mismatch repair (MMR) and microsatellite instability (MSI) status at baseline. However, aside from PFS in the population of patients with mismatch repair deficient (dMMR) disease, these subgroup analyses were exploratory and not designed to detect differences between groups.
CDA-AMC undertook reanalysis to address some of the limitations identified in the model. The results of the CDA-AMC reanalysis were broadly aligned with the sponsor’s, suggesting that dostarlimab plus carboplatin-paclitaxel was more costly and more effective than carboplatin-paclitaxel alone for the treatment of patients with primary advanced or recurrent endometrial cancer who are candidates for systemic therapy. The CDA-AMC reanalysis resulted in an incremental cost-effectiveness ratio (ICER) for dostarlimab plus carboplatin-paclitaxel of $159,924 per quality-adjusted life-year (QALY) gained compared to placebo plus carboplatin-paclitaxel, with a 0% probability of being cost-effective at a threshold of $50,000 per QALY gained. A 56% price reduction for dostarlimab would be necessary to consider it cost-effective at this threshold. CDA-AMC conducted scenario analyses and found that the results are sensitive to assumptions regarding the extrapolation of OS for dostarlimab plus carboplatin-paclitaxel and carboplatin-paclitaxel alone, as well as to variations in subsequent treatment distribution, treatment duration, and health state utility values. Due to uncertainties around long-term OS and the costs and efficacy of subsequent therapies, a greater price reduction may be needed to ensure cost-effectiveness.
Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, clinician groups, and drug plans that participated in the CDA-AMC review process.
The patient input was submitted by the Colorectal Cancer Resource & Action Network in collaboration with the Canadian Cancer Survivor Network. The network gathered perspectives from 4 patients in Canada with advanced or metastatic endometrial cancer, 3 of whom had direct experience with dostarlimab in combination with carboplatin and paclitaxel. The feedback highlighted significant gaps in current treatments, especially for patients with mismatch repair proficient (pMMR) disease, who constitute the majority of endometrial cancer cases and have limited effective options. Patients experienced significant delays in diagnosis and limited quality of life under standard treatments, which often induce severe side effects. Those who accessed dostarlimab reported prolonged life, minimal side effects, and improved quality of life, and were able to re-engage in daily activities and family life.
The clinician input was provided by 2 gynecological clinician groups familiar with the population of patients with advanced endometrial cancer. Clinicians noted that while chemotherapy with carboplatin and paclitaxel is a current standard for endometrial cancer, it is often associated with important toxicities, like neuropathy, and limited efficacy in preventing recurrence. The unmet need is particularly acute for patients with pMMR tumours, who represent approximately 70% of endometrial cancer cases and have limited effective treatment options. Clinicians emphasized that adding dostarlimab could reduce toxicities, improve patient quality of life, and potentially extend survival, especially when combined with chemotherapy for patients with pMMR tumours. They highlighted that dostarlimab’s shorter infusion times and manageable side effects would benefit both the health care system and patient adherence.
The drug plans highlighted several key considerations for implementing dostarlimab. First, the plans emphasized that testing for dMMR and pMMR status should be completed before therapy to confirm patient eligibility. Additionally, there was a question of whether patients who complete an initial 3-year course of dostarlimab, but later experience disease progression, should be eligible for an additional year of treatment, similar to the protocol for patients with dMMR. Because dostarlimab is an immune checkpoint inhibitor, close monitoring for immune-mediated adverse events (AEs) is essential. The drug plans also raised questions about dostarlimab's positioning within the treatment pathway, especially regarding its potential use relative to other therapies, such as durvalumab, which is currently under review as an alternative. Finally, the plans noted potential delays in therapy administration due to the additional time required for drug preparation in pharmacies.
Several of these concerns were addressed in the sponsor’s model:
The treatment goals of prolonging survival and ability to maintain quality of life were considered.
Generic prices for carboplatin and paclitaxel were considered.
As requested by CDA-AMC, the sponsor provided a cost-effectiveness analysis of dostarlimab plus carboplatin-paclitaxel by MMR and MSI status.
In addition, CDA-AMC addressed some of the following concerns:
The cost of MMR and MSI status testing was included in a scenario analysis.
CDA-AMC conducted a scenario analysis adding 1 year of treatment with dostarlimab after completing 3 years of dostarlimab.
However, CDA-AMC was unable to address the following concerns raised in the input received from patients, clinicians, and drug plans:
The cost-effectiveness of dostarlimab plus carboplatin-paclitaxel relative to other therapies currently under review, such as durvalumab, could not be estimated.
Economic Review
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted an economic evaluation of dostarlimab plus carboplatin-paclitaxel compared to carboplatin-paclitaxel for the treatment of adult patients with primary advanced or recurrent endometrial cancer who are candidates for systemic therapy. This target population was aligned with the proposed Health Canada indication and the reimbursement request.
Dostarlimab is available as a solution for infusion at a concentration of 50 mg/mL and cost of $10,031.08 per 10 mL vial. The recommended dosage of dostarlimab is 500 mg every 3 weeks in combination with carboplatin-paclitaxel for 6 cycles, followed by 1,000 mg of dostarlimab monotherapy every 6 weeks until disease progression or unacceptable toxicity, or up to 3 years. At the submitted price, dostarlimab will cost $10,031 for every 21 days. Discontinuation criteria include disease progression, unacceptable toxicity, or the maximum treatment duration of 3 years. The carboplatin-paclitaxel regimen is composed of 2 separate treatments. Carboplatin is available as a solution for infusion at a concentration of 10 mg/mL in vial sizes of 5 mL ($70), 15 mL ($210), 45 mL ($600), and 60 mL ($778). As per the Cancer Care Ontario regimen monograph, carboplatin should be administrated at an area under the concentration time curve (AUC) of 5 mg per mL per minute. The calculation of the recommended dose should incorporate the direct relationship between glomerular filtration rate and carboplatin clearance.
A patient aged ████ years with a body surface area (BSA) of ████ m2 would receive a calculated dose of ██████ mg when administered with an AUC of 5 mg per mL per minute. Paclitaxel is available as a solution for infusion at a 6 mg/mL concentration in vial sizes of 5 mL ($300) and 50 mL ($3,740). At a recommended dose of 175 mg/m2 for paclitaxel, a patient with a BSA of ████ m2 would receive a calculated dose of ██████ mg. The 21-day cycle costs of the carboplatin-paclitaxel regimen with and without concomitant dostarlimab would be $14,515 for dostarlimab plus carboplatin-paclitaxel and $4,484 for carboplatin-paclitaxel alone. Carboplatin-paclitaxel was the only comparator included in the analysis, based on a deviation request submitted by the sponsor and accepted by CDA-AMC.
Modelled outcomes included life-years and QALYs. Costs were estimated from the perspective of the public health care payer in Canada. Model outputs were generated over a lifetime horizon of approximately 36 years, with a cycle length of 1 week. Costs and outcomes were discounted at 1.5%.
Model Structure
The costs and effects of each alternative were estimated using a partitioned survival model (PSM). This model structure tracked patients across 3 mutually exclusive health states: progression-free disease (PFD), progressed disease, and death. State membership was estimated using an AUC approach from 2 independent survival curves (PFS and OS). A third survival curve, time to treatment discontinuation (TTD), was used to determine the proportion of patients in the PFD state no longer on treatment. This allowed the model to incorporate the possibility of treatment withdrawal before progression.
Model Inputs
The modelled patient cohort comprised adults with primary advanced or recurrent endometrial cancer whose baseline characteristics reflected those of patients in Part 1 of the RUBY trial.1 This was a randomized, phase III trial that involved the direct comparison of dostarlimab added to carboplatin-paclitaxel versus placebo plus carboplatin-paclitaxel. Baseline characteristics of interest included age (mean = ████ years), sex (100% female), BSA (mean = ████ m2), and weight (mean = █████ kg).
The key clinical efficacy inputs (i.e., OS and PFS) and TTD for each treatment regimen were derived from the RUBY trial, Part 1. (The PFS, TTD, and health utility data cut-off date was September 28, 2022, while the OS data cut-off date was September 22, 2023.) PFS, OS, and TTD outcomes were extrapolated beyond the trial duration by fitting parametric survival models to the trial data (maximum duration of follow-up = approximately 3.9 years). Model selection was based on statistical fit (i.e., Akaike information criterion, Bayesian information criterion, visual inspection of goodness of fit to observed data, clinical plausibility, and external validation against real-world data). The sponsor selected a log-normal distribution to extrapolate the OS of patients on dostarlimab plus carboplatin-paclitaxel and on carboplatin-paclitaxel alone. For the long-term extrapolations of PFS, log-logistic distribution was selected for both dostarlimab plus carboplatin-paclitaxel and carboplatin-paclitaxel alone. The sponsor assumed that the efficacy of dostarlimab persisted for the entire time horizon. The sponsor fitted a Weibull distribution to extrapolate TTD curves for dostarlimab plus carboplatin-paclitaxel and carboplatin-paclitaxel alone based on treatment discontinuation data from the RUBY trial, Part 1. The submitted model assumed that all patients treated with dostarlimab plus carboplatin-paclitaxel would discontinue treatment after 3 years (156 weeks), while those receiving carboplatin-paclitaxel alone would stop at 18 weeks.
In addition to tracking the proportion of the cohort in each health state, the model also tracked the occurrence of AEs. The specific AEs included in the model were anemia, neutropenia, hypertension, hypokalemia, pulmonary embolism, and a decrease in lymphocyte count, neutrophil count, or white blood cell count. The treatment-specific risk of each AE was obtained from the RUBY trial, Part 1. It was assumed that patients were only at risk of an AE in the first cycle on treatment.
Health-related quality of life was reflected by the combination of health state utilities and AE-specific disutilities. The health state utility values were obtained from the indirect measurement of patient preferences in the RUBY trial, Part 1, using the EQ-5D-5L. Mean health state utilities of █████ (PFD state; 95% CI, ███████████) and █████ (PD state; 95% CI, ███████████) were obtained by applying tariffs that corresponded to the preferences of the patient population in Canada.2 In the base case, the sponsor adjusted the EQ-5D health state utilities by age and sex. This involved multiplying the EQ-5D health state utilities by age- and sex-specific decrements estimated from general population utilities obtained from the Health Utilities Index Mark 3.3 Values for AE-specific disutilities were sourced from prior technology appraisals and published literature.4-7
The sponsor considered the costs associated with drug acquisition and administration, state-specific follow-up and monitoring, subsequent therapy, and end-of-life care. Treatment acquisition costs were calculated from the price per units consumed based on the recommended dosage for each alternative considered in the model. The price of dostarlimab represented the sponsor’s submitted price, while all other drug prices were obtained from the IQVIA DeltaPA database.8 The sponsor’s model included the costs associated with AEs of grade 3 or greater with an incidence rate of 5% or more in the RUBY trial, Part 1.
Eligible second-line treatments included carboplatin-paclitaxel, paclitaxel, pembrolizumab, pembrolizumab-lenvatinib, letrozole, doxorubicin, and radiotherapy. Acquisition costs for these treatments were weighted by the percentage of patients who initiated each therapy following first-line discontinuation in the RUBY trial, Part 1. Treatment administration costs were applied for any treatment that required IV administration; these included infusion, chair time, the per-visit physician billing fee, and pharmacy and nursing workloads. Treatment monitoring costs reflected resource utilization associated with indication-specific disease pathway management procedures published by Cancer Care Ontario.9 Costs associated with outpatient consultation, imaging, laboratory testing, and physician or nurse visits were obtained from the Ontario Schedule of Benefits.10 Terminal care costs were applied to patients who transitioned to the death state; the estimate of costs was obtained from a study by de Oliveira et al. (2016) that reported the 5-year and lifetime net costs of the 21 most prevalent cancer sites in Ontario.11
Summary of Sponsor’s Economic Evaluation Results
All analyses were run probabilistically (i.e., 1,000 iterations for the base-case and scenario analyses). The deterministic and probabilistic results were similar. The probabilistic findings are presented here. Additional results from the sponsor’s submitted economic evaluation base case are presented in Appendix 3.
Base-Case Results
The submitted economic evaluation was based on the publicly available prices of the comparator treatments. The incremental costs and QALYs for dostarlimab plus carboplatin-paclitaxel relative to carboplatin-paclitaxel monotherapy were $147,238 and 1.87 QALYs, respectively, resulting in an ICER of $78,806 per QALY (Table 3). Eighty-four percent of the incremental QALYs were generated through extrapolation beyond the observed RUBY trial, Part 1 period (i.e., 3.9 years). At a willingness-to-pay (WTP) threshold of $50,000 per QALY gained, dostarlimab plus carboplatin-paclitaxel had a 3% probability of cost-effectiveness.
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER vs. reference ($/QALY) |
|---|---|---|---|---|---|
CP | $135,687 | Reference | 3.09 | Reference | Reference |
Dostarlimab plus CP | $282,925 | $147,238 | 4.96 | 1.87 | $78,806 |
CP = carboplatin-paclitaxel; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus.
Source: Sponsor’s pharmacoeconomic submission.
Sensitivity and Scenario Analysis Results
The sponsor provided scenario analyses exploring the impact of adopting alternative PFS, OS, and TTD exploration methods, using alternate data sources for subsequent treatments, and considering indirect costs. Dostarlimab plus carboplatin-paclitaxel was not cost-effective in any of these scenario analyses; the conclusions remained robust to alternative inputs and assumptions. The cost-effectiveness results were most sensitive to assumptions about the long-term OS modelling approach and subsequent treatment distributions. As requested by CDA-AMC, the sponsor submitted an exploratory cost-effectiveness analysis of dostarlimab plus carboplatin-paclitaxel stratified by MSI and MMR status. The analysis suggested an ICER of $32,383 per QALY gained for dMMR or microsatellite stability high (MSI-H) tumours and of $127,138 per QALY gained for pMMR or microsatellite stable (MSS) tumours. Additional information is available in Appendix 3.
CDA-AMC Appraisal of the Sponsor’s Economic Evaluation
CDA-AMC identified several key limitations to the sponsor’s analysis that have notable implications on the economic analysis.
The long-term extrapolation of OS may be overestimated. The sponsor applied parametric survival curves to extend the PFS and OS data for patients receiving dostarlimab plus carboplatin-paclitaxel and carboplatin-paclitaxel alone. This was based on Kaplan-Meier (KM) OS data available at the end of the trial follow-up (i.e., 3.9 years), assuming a sustained response following treatment discontinuation over a 36-year model horizon. Although the log-normal distribution was chosen for OS data based on statistical fit, visual inspection, and clinical plausibility, these extrapolations resulted in survival outcomes that clinical experts consulted by CDA-AMC considered overly optimistic. Consequently, due to these prolonged OS projections, the incremental QALYs calculated for both treatment regimens are likely overestimated. CDA-AMC subsequently selected less optimistic parametric distributions for the OS of these treatments.
Furthermore, given the limited availability of long-term PFS and OS data, the assumption by the sponsor of no treatment waning is uncertain and may lead to an underestimation of the ICER.
For the revised base-case analysis, CDA-AMC opted for Weibull distributions for the OS data of both treatments. Additionally, CDA-AMC conducted a scenario analysis using log-logistic distribution for OS for both treatments. Given the arbitrary nature of the cut-off time point for treatment waning, CDA-AMC applied immediate waning and gradual delays starting at 3 years and 5 years in the scenario analyses to explore the impact of different waning assumptions on the outcomes.
A postprogression survival benefit associated with dostarlimab plus carboplatin-paclitaxel is uncertain. The sponsor’s base-case results indicate that patients treated with dostarlimab plus carboplatin-paclitaxel experience longer survival after disease progression compared to those treated with carboplatin-paclitaxel alone. Specifically, about 85% of the reported incremental survival (i.e., 1.94 life-years) occurs after patients have progressed and discontinued combination therapy with dostarlimab. However, the use of a PSM raises concerns about the accuracy of these findings. This model imposes structural assumptions linking PFS and OS that may not accurately represent the true causal relationships within the disease pathway. These assumptions could introduce a bias in postprogression survival that favours the dostarlimab combination. In a PSM, the structural independence assumed between the OS and PFS end points means that extrapolations for each end point could merely reflect observed within-trial trends in progression and mortality rates rather than the actual effects of the treatment.
Moreover, the potential mechanisms through which dostarlimab plus carboplatin-paclitaxel could confer postprogression survival benefits remain unclear. This concern is compounded by the fact that a higher percentage of patients in the carboplatin-paclitaxel group of the RUBY trial, Part 1 received subsequent therapies compared to the patients in the dostarlimab group (69% versus 49%), including advanced treatments like pembrolizumab and pembrolizumab plus lenvatinib. Despite this, the PSM fails to consider how these subsequent therapies might affect survival, which complicates the interpretation of the OS data.
CDA-AMC was unable to address this limitation because it was unclear whether the implied postprogression benefit was due to the effect of treatment with dostarlimab or if the benefits stemmed from limitations inherent to the PSM.
The sponsor’s selection of subsequent treatments in the pharmacoeconomic model does not match clinical expectations. According to the submitted model, the distribution of subsequent treatments was based on RUBY trial, Part 1 interim analysis 2 (IA2) data and considered reimbursement conditions in Canada. The treatments included dostarlimab, carboplatin-paclitaxel, pembrolizumab, doxorubicin, pembrolizumab plus lenvatinib, letrozole, paclitaxel, and radiotherapy. Although the sponsor indicated that the assumptions were driven by Canadian reimbursement criteria, the model did not include several commonly reimbursed treatments, such as docetaxel monotherapy and pegylated liposomal doxorubicin monotherapy. Furthermore, there were discrepancies in the distribution of some treatments between the submitted model and the Clinical Study Report. For example, the submitted base case assumed that ████% of patients receiving dostarlimab plus carboplatin-paclitaxel and ███% of those receiving carboplatin-paclitaxel alone would receive re-treatment with carboplatin-paclitaxel as a subsequent therapy. In contrast, the Clinical Study Report suggests that only █████% of patients receiving dostarlimab plus carboplatin-paclitaxel and ███% of those receiving carboplatin-paclitaxel alone would be re-treated with carboplatin-paclitaxel.
More importantly, the sponsor assumed that all patients received some form of treatment after first-line therapies, which contradicts the data reported in IA2 of the RUBY trial, Part 1, previous CDA-AMC reports, and Canadian clinical practice. According to IA2, █████% of patients on dostarlimab plus carboplatin-paclitaxel and █████% of patients on carboplatin-paclitaxel alone received no subsequent treatment. Clinical experts consulted by CDA-AMC also indicated that 20% to 25% of patients would typically receive no treatment following first-line therapies. Neglecting the proportion of patients who receive no treatment likely leads to overestimating the total costs for both treatment regimens. However, the impact of this omission on the ICER remains unclear, given that the benefits of subsequent therapies were not explicitly captured in the PSM due to the previously described limitations of the model.
CDA-AMC addressed this limitation by setting the proportion of patients who received no treatment in both groups to 25% while retaining the sponsor's assumptions about the types of subsequent treatments considered. The proportions of subsequent treatments used in the model were based on data from IA2 in Part 1 of the RUBY trial.
CDA-AMC notes that adjusting the distribution of subsequent therapies in the model affects costs only. Because of the sponsor’s choice to use a PSM, variations in the efficacy and time on treatment for different comparators cannot be reflected in the model. Changes in the costs and QALYs associated with the lack of alignment between the values used in the trial and values reflecting current practice in Canada could not be estimated; these add uncertainty to the ICER.
Health state utility values lacked transparency. The sponsor assigned a health utility value of █████ to the progression-free health state and █████ to the progressed disease health state. However, CDA-AMC was unable to verify these estimates because the supplementary utility data analysis provided by the sponsor was based on the UK value set and included treatment groups in the regression model. Notably, the analysis reported significantly lower health utility values for the progression-free (█████) and progressed health states (█████). Using the lower utility values would result in a higher ICER for dostarlimab plus carboplatin-paclitaxel. Additionally, the sponsor's economic report stated that the model adjusted for age-related decrements using Health Utilities Index Mark 3 utility estimates derived from the general population in Canada by age and sex, as reported by Guertin et al. (2018).3 However, the sponsor’s model cited population norms derived using the EQ-5D-5L by Yan et al. (2024).12
To address this limitation, CDA-AMC conducted a scenario analysis using alternative health utility values to assess the uncertainty surrounding these health utility values.
Additional limitations were identified, but were not considered to be key limitations. These limitations are outlined subsequently.
Drug pricing for paclitaxel and carboplatin in the economic model did not reflect the current publicly available list prices, and extrapolated TTD was used to represent treatment duration. Specifically, the model applied unit costs of $971 for paclitaxel 100 mg and $775 for carboplatin 600 mg, which are slightly lower than the current list prices of $1,197 for paclitaxel and $778 for carboplatin. Furthermore, as per CDA-AMC’s recommended procedure for modelling time-to-event end points, the sponsor used extrapolated TTD data from the Weibull model for both treatments.
To address this limitation, CDA-AMC used the current list prices for paclitaxel and carboplatin in the corrected base case and applied KM TTD curves for both treatments in the revised base case due to insufficient follow-up data available for all patients.
Additionally, the following key assumptions were made by the sponsor and appraised by CDA-AMC (refer to Table 4).
CDA-AMC Reanalyses of the Economic Evaluation
Base-Case Results
The CDA-AMC base case was derived by changing model parameter values and assumptions in consultation with clinical experts. A summary of each of the changes applied to the economic evaluation is presented in Table 5. Each independent change was applied in the sequence detailed in the table to arrive at the CDA-AMC base case. Consistent with the sponsor’s base case, the costs and effects for each alternative treatment strategy were generated from a Monte Carlo simulation of 1,000 iterations.
Table 4: Key Assumptions of the Submitted Economic Evaluation (Not Noted as Limitations to the Submission)
Sponsor’s key assumption | CDA-AMC comment |
|---|---|
The baseline characteristics of participants in Part 1 of the RUBY trial were representative of the patient population in Canada. | Acceptable. The clinical experts consulted by CDA-AMC indicated that the baseline patient characteristics in the RUBY trial, Part 1 generally reflect those of patients with advanced and recurrent endometrial cancer in Canadian clinical practice. They expressed no concerns regarding the generalizability of the study findings. |
The sponsor assumed a lifetime time horizon of 36 years. | Acceptable. The clinical expert consulted by CDA-AMC noted that the time horizon was long, but acceptable, given that the same time horizon was used in a previous CDA-AMC submission.13 |
Dosage regimens for dostarlimab, carboplatin, and paclitaxel were based on Part 1 of the RUBY trial. | Acceptable. The clinical expert consulted by CDA-AMC deemed this assumption acceptable, but noted that a higher dose of carboplatin (6 AUC mg/mL) is more commonly used in Canadian clinical practice. The effects of this higher dose on clinical benefits and the ICER remain unknown. |
The sponsor assumed that all patients receiving dostarlimab would discontinue treatment at the 3-year mark, following a 3-year stopping rule, while all patients receiving carboplatin-paclitaxel would discontinue treatment at 18 weeks. | Appropriate. |
The sponsor excluded MMR and MSI-H testing costs. | Acceptable. The clinical experts consulted by CDA-AMC noted that MMR and/or MSI-H testing is expected to become part of clinical practice. They did not anticipate the need for test results for the requested indication. |
AUC = area under the curve; CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; MMR = mismatch repair; MSI-H = microsatellite instability–high.
Table 5: CDA-AMC Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
1. Carboplatin and paclitaxel pricing | Carboplatin 450 mg: $599.85 Carboplatin 600 mg: $775.00 Paclitaxel 100 mg: $971.00 | Carboplatin 450 mg: $600.00 Carboplatin 600 mg: $778.00 Paclitaxel 100 mg: $1,196.80 |
Changes to derive the CDA-AMC base case | ||
1. Extrapolation for OS curves for both treatments | Log-normal | Weibull |
2. Treatment durations for dostarlimab, carboplatin, and paclitaxel | Extrapolated using the Weibull model | Used observed Kaplan-Meier TTD data |
3. Proportion of patients not receiving subsequent treatmentsa | 0% | 25% |
CDA-AMC base case | ― | 1 + 2 + 3 |
CDA-AMC = Canada’s Drug Agency; OS = overall survival; TTD = time to treatment discontinuation.
aThe distribution of subsequent treatments was corrected to match what was reported for the intention-to-treat population in interim analysis 2 of the RUBY trial, Part 1.
Table 6: Summary of the Stepped Analysis of the CDA-AMC Reanalysis Results
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICERs ($/QALY) |
|---|---|---|---|---|
Sponsor’s base case | CP | 135,687 | 3.09 | Reference |
Dostarlimab plus CP | 282,925 | 4.96 | 78,806 | |
Sponsor’s corrected base case | CP | 141,818 | 3.08 | Reference |
Dostarlimab plus CP | 292,853 | 4.94 | 81,357 | |
CDA-AMC reanalysis 1 | CP | 131,761 | 2.31 | Reference |
Dostarlimab plus CP | 281,294 | 3.33 | 146,472 | |
CDA-AMC reanalysis 2 | CP | 141,818 | 3.08 | Reference |
Dostarlimab plus CP | 292,362 | 4.94 | 81,093 | |
CDA-AMC reanalysis 3 | CP | 121,094 | 3.08 | Reference |
Dostarlimab plus CP | 288,370 | 4.94 | 90,095 | |
CDA-AMC base case (1 + 2 + 3) | CP | 112,588 | 2.31 | Reference |
Dostarlimab plus CP | 277,127 | 3.34 | 161,142 | |
CDA-AMC base case (1 + 2 + 3) (probabilistic) | CP | 108,464 | 2.32 | Reference |
Dostarlimab plus CP | 272,426 | 3.34 | 159,924 |
CDA-AMC = Canada’s Drug Agency; CP = carboplatin-paclitaxel; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Note: The CDA-AMC reanalysis is based on publicly available prices of the comparator treatments. The results of all steps are presented deterministically unless otherwise indicated, while the cumulative CDA-AMC base case is always presented both deterministically and probabilistically.
In the CDA-AMC base-case analysis, the combination of dostarlimab plus carboplatin-paclitaxel was associated with an estimated total cost of $272,426 and total QALYs of 3.34. In comparison, patients receiving only carboplatin-paclitaxel incurred total costs of $108,464 and achieved total QALYs of 2.32. This results in an ICER of $159,924 per QALY gained for adult patients with primary advanced or recurrent endometrial cancer who are candidates for systemic therapy. The probability of this treatment combination being cost-effective at a WTP threshold of $50,000 per QALY gained was 0%. Notably, more than half (71%) of the incremental QALYs attributed to dostarlimab plus carboplatin-paclitaxel, compared to carboplatin-paclitaxel alone, were accrued beyond the trial follow-up period and based on the sponsor’s extrapolation of the trial data. Results of the stepped reanalysis are available in Table 6, with full disaggregated results available in Appendix 4, Table 10.
Scenario Analysis Results
A series of scenario analyses were conducted on CDA-AMC’s base case. These analyses explored the impact of altering the following model parameters and assumptions: assuming no treatment effect after treatment discontinuation (i.e., an immediate and a gradual delay in treatment waning effect); extending a stopping rule for dostarlimab to 4 years from 3 years; adopting an alternate source for subsequent treatment distribution (i.e., a sponsor’s commissioned clinician survey); using alternate health state utility values; using log-logistic distribution to extrapolate OS for both treatments; using log-normal distribution to extrapolate PFS for both treatments; and applying MSI and MMR testing costs to patients receiving dostarlimab plus carboplatin-paclitaxel.
Results from the scenario analyses (Appendix 4, Table 11) demonstrated that the cost-effectiveness findings were most sensitive to the survival models used to extrapolate OS data. If the log-logistic model was used to predict OS data for both treatments, the ICER would be reduced to $103,167 per QALY, but would still not be cost-effective. The assumptions about subsequent treatment distribution, treatment duration, and health utility values also influenced the ICER. When adopting subsequent treatment distribution obtained from a clinician survey commissioned by the sponsor, the ICER increased to $182,579 per QALY. When the treatment duration of dostarlimab was extended to 4 years, the ICER rose to $172,086 per QALY. Similarly, when the lower health state utility values were used, the ICER increased to $172,762 per QALY.
In addition, as requested by drug plans, a separate set of scenario analyses was performed to estimate the incremental cost-effectiveness of dostarlimab plus carboplatin-paclitaxel in patients with dMMR and pMMR separately. In patients with dMMR or MSI-H, dostarlimab plus carboplatin-paclitaxel was associated with $234,943 in incremental costs and 6.72 incremental QALYs compared to carboplatin-paclitaxel alone, resulting in an ICER of $34,971 per QALY gained. In patients with pMMR or MSS, dostarlimab plus carboplatin-paclitaxel was associated with $146,362 in incremental costs and 0.54 incremental QALYs compared to carboplatin-paclitaxel alone, resulting in an ICER of $273,097 per QALY gained. These scenarios are associated with a greater degree of uncertainty, given that the RUBY trial, Part 1 was not powered to detect differences in OS and PFS for these subgroups.
CDA-AMC undertook a price-reduction analysis based on the sponsor’s base case and CDA-AMC base case (Table 7). The results show that a price reduction of 56% is required for dostarlimab plus carboplatin-paclitaxel to be considered cost-effective at a WTP threshold of $50,000 per QALY when considering the CDA-AMC base case.
Table 7: CDA-AMC Price-Reduction Analyses
Analysis | Unit drug cost | ICERs for dostarlimab plus CP vs. CP ($/QALY) | |
|---|---|---|---|
Price reduction | ($) | Sponsor base case | CDA-AMC reanalysis |
No price reduction | 10,031 | 78,806 | 159,924 |
10% | 9,028 | 68,038 | 140,349 |
20% | 8,025 | 57,271 | 120,774 |
26.8% | 7,343 | 50,000 | 108,468 |
30% | 7,022 | 46,503 | 101,199 |
40% | 6,019 | 35,735 | 81,624 |
50% | 5,016 | 24,968 | 62,049 |
56.2% | 4,394 | 20,032 | 50,000 |
60% | 4,012 | 14,200 | 42,474 |
70% | 3,009 | 3,432 | 22,900 |
80% | 2,006 | Dostarlimab plus CP is dominant | 3,325 |
90% | 1,003 | Dostarlimab plus CP is dominant | Dostarlimab plus CP is dominant |
CDA-AMC = Canada’s Drug Agency; CP = carboplatin-paclitaxel; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus.
Issues for Consideration
CDA-AMC is currently reviewing 2 other therapeutic strategies for endometrial cancer: durvalumab combined with carboplatin-paclitaxel followed by durvalumab monotherapy for patients with dMMR; and durvalumab combined with carboplatin-paclitaxel, followed by durvalumab combined with olaparib, for patients with pMMR. The cost-effectiveness of dostarlimab in comparison to these therapies requires further investigation.
Based on drug plan feedback, in order to identify the patients eligible for treatment, companion MSI and/or MMR testing needs to be operationalized and funded for endometrial cancer. Testing costs were included in the CDA-AMC scenario analysis and had minimal impact on the cost-effectiveness results.
Overall Conclusions
The CDA-AMC clinical review highlighted a high certainty of evidence from the RUBY trial, Part 1, and indicated that treatment with dostarlimab plus carboplatin-paclitaxel significantly improves OS at 24 months and 36 months, and PFS at 12 months and 24 months, compared to placebo plus carboplatin-paclitaxel in adults with primary advanced or first recurrent endometrial cancer. The benefits in OS and PFS were generally consistent across subgroup analyses by MMR and/or MSI status at baseline. These subgroup analyses were exploratory and not designed to detect differences between groups.
However, CDA-AMC identified several limitations in the sponsor’s pharmacoeconomic evaluation that significantly affect the cost-effectiveness results. The survival models chosen by the sponsor may overestimate patient survival compared to clinical expectations. The PSM used also indicated a postprogression survival benefit, potentially due to a structural bias favouring dostarlimab plus carboplatin-paclitaxel. The extrapolation of these data beyond the period covered by KM data is uncertain, with about 84% of the incremental benefit coming from the extrapolated period versus 71% in the CDA-AMC base case.
Additionally, the distribution of subsequent treatments in the submitted model does not accurately reflect Canadian clinical practice, and the proportions used did not align with those reported in the Clinical Study Report. Clinical experts consulted by CDA-AMC advised that 20% to 25% of patients would typically receive no subsequent therapies. This view contradicts the model’s assumption that all patients received subsequent therapies.
To address the submitted model’s limitations, CDA-AMC made various adjustments to the base case, adopting less optimistic predictions for long-term OS. CDA-AMC corrected unit prices for carboplatin and paclitaxel and used observed treatment durations from the trial instead of extrapolated data. In the revised base case, CDA-AMC applied the Weibull distribution to predict OS for both treatments and aligned the distribution of patients receiving no treatment with Canadian clinical practice. The CDA-AMC reanalysis yielded an ICER for dostarlimab plus carboplatin-paclitaxel of $159,924 per QALY compared to placebo plus carboplatin-paclitaxel, with a 0% probability of being cost-effective at a $50,000 per QALY threshold. A 56% price reduction for dostarlimab plus carboplatin-paclitaxel would be necessary to consider it cost-effective at this threshold. CDA-AMC conducted scenario analyses and found that the results are sensitive to assumptions regarding the long-term OS benefit of dostarlimab plus carboplatin-paclitaxel compared to carboplatin-paclitaxel alone as well as to variations in subsequent treatment distribution, treatment duration, and health utility values. Due to uncertainties around long-term OS, a more significant price reduction might be justified.
References
1.Mirza MR, Chase DM, Slomovitz BM, et al. Dostarlimab for Primary Advanced or Recurrent Endometrial Cancer. N Engl J Med. 2023;388(23):2145-2158. PubMed
2.Xie F, Pullenayegum E, Gaebel K, et al. A Time Trade-off-derived Value Set of the EQ-5D-5L for Canada. Med Care. 2016;54(1):98-105. PubMed
3.Guertin JR, Feeny D, Tarride JE. Age- and sex-specific Canadian utility norms, based on the 2013-2014 Canadian Community Health Survey. CMAJ. 2018;190(6):E155-E161. PubMed
4.Swinburn P, Lloyd A, Nathan P, Choueiri TK, Cella D, Neary MP. Elicitation of health state utilities in metastatic renal cell carcinoma. Curr Med Res Opin. 2010;26(5):1091-1096. PubMed
5.Nafees B, Stafford M, Gavriel S, Bhalla S, Watkins J. Health state utilities for non small cell lung cancer. Health Qual Life Outcomes. 2008;6:84. PubMed
6.Hannouf MB, Sehgal C, Cao JQ, Mocanu JD, Winquist E, Zaric GS. Cost-effectiveness of adding cetuximab to platinum-based chemotherapy for first-line treatment of recurrent or metastatic head and neck cancer. PLoS One. 2012;7(6):e38557. PubMed
7.Christensen HN, Olsson U, From J, Breivik H. Opioid-induced constipation, use of laxatives, and health-related quality of life. Scandinavian journal of pain. 2016;11(1):104-110. PubMed
8.DeltaPA. Ottawa (ON): IQVIA; 2023: https://www.iqvia.com/. Accessed 1800 Jan 1.
9.Cancer Care Ontario: funded evidence-informed regimens. 2024; https://www.cancercareontario.ca/en/drugformulary/regimens. Accessed 1800 Jan 1.
10.Schedule of benefits for physician services under the Health Insurance Act: (June 29, 2023 (effective July 24, 2023)). Toronto (ON): Ontario Ministry of Health; 2023: https://www.health.gov.on.ca/en/pro/programs/ohip/sob/physserv/sob_master.pdf. Accessed 1800 Jan 1.
11.de Oliveira C, Pataky R, Bremner KE, et al. Phase-specific and lifetime costs of cancer care in Ontario, Canada. BMC Cancer. 2016;16(1):809. PubMed
12.Yan J, Xie S, Johnson JA, et al. Canada population norms for the EQ-5D-5L. Eur J Health Econ. 2024;25(1):147-155. PubMed
13.Drug Reimbursement Review pharmacoeconomic report: GENERIC NAME (BRAND NAME) for INDICATION. Ottawa (ON): CADTH; 1800: URL. Accessed 1800 Jan 1.
14.Statistics C. Population estimates on July 1st, by age and sex. Table: 17-10-0005-01 (formerly CANSIM 051-0001)2024.
15.Brenner DR, Gillis J, Demers AA, et al. Projected estimates of cancer in Canada in 2024. CMAJ. 2024;196(18):E615-e623. PubMed
16.Canadian Cancer S. Canadian Cancer Statistics. 2023.
17.Canadian Cancer S. Cancerous tumours of the uterus. 2024; https://cancer.ca/en/cancer-information/cancer-types/uterine/what-is-uterine-cancer/cancerous-tumours, 2024.
18.Canadian Cancer S. Canadian Cancer Statistics: A 2018 special report on cancer incidence by stage. 2018.
19.Huijgens AN, Mertens HJ. Factors predicting recurrent endometrial cancer. Facts Views Vis Obgyn. 2013;5(3):179-186. PubMed
20.Martins D, O'Sullivan DE, Boyne DJ, et al. Understanding Characteristics, Treatment Patterns, and Clinical Outcomes for Individuals with Advanced or Recurrent Endometrial Cancer in Alberta, Canada: A Retrospective, Population-Based Cohort Study. Curr Oncol. 2023;30(2):2277-2289. PubMed
21.Gsk. Data on file. RUBY IA1 (28Sep2022): Table 1.0101 and 1.1701 Summary of Demographic Characteristics (ITT Analysis Set), January 2023. 2023.
22.Gsk. Data on file. RUBY IA1 (28Sep2023): Utility analyses. 2023.
Appendix 1: Cost Comparison Table
Please note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical expert(s) and drug plans. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 8: CDA-AMC Cost Comparison Table for Primary Advanced or Recurrent Endometrial Cancer
Treatment | Strength / concentration | Form | Price | Recommended dosage | Daily cost ($) | 21-day cost ($)a |
|---|---|---|---|---|---|---|
Dostarlimab (Jemperli) | 50 mg/mL | 10 mL vial for IV infusion | 10,031.08 | Loading: 500 mg every 3 weeks for 6, 21-day cycles. Maintenance: 1,000 mg once every 6 weeks thereafter. | 477.67 | 10,031 |
Carboplatin (Generic) | 10 mg/mL | 5 mL Vial 15 mL Vial 45 mL Vial 60 mL Vial | 70.0000a 210.0000a 600.0000a 778.0000a | AUC 5b on day 1 for 6 21-day cycles | 46.90 | 985 |
Paclitaxel (Generic) | 6 mg/mL | 5 mL Vial 16 mL Vial 25 mL Vial 50 mL Vial | 300.0000a 1,196.8000a 1,870.0000a 3,740.0000a | 175 mg/m2 on day 1 for 6 21-day cycles | 206.67 | 4,340 |
Dostarlimab plus carboplatin-paclitaxel: Loading period | 731.24 | 15,356 | ||||
Dostarlimab: Maintenance period | 477.67 | 10,031 | ||||
Carboplatin-paclitaxel | ||||||
Carboplatin (Generic) | 10 mg/mL | 5 mL Vial 15 mL Vial 45 mL Vial 60 mL Vial | 70.0000a 210.0000a 600.0000a 778.0000a | AUC 4 to 6b on day 1 for 6, 21-day cycles | 36.90 | 775 |
Paclitaxel (Generic) | 6 mg/mL | 5 mL Vial 16 mL Vial 25 mL Vial 50 mL Vial | 300.0000a 1,196.8000a 1,870.0000a 3,740.0000a | 175 mg/m2 on day 1 for 6, 21-day cycles | 206.67 | 4,340 |
Carboplatin-paclitaxel | 243.57 | 5,115 | ||||
AUC = area under concentration time curve.
Note: All prices are from the Ontario Drug Benefit Formulary (accessed September 2024), unless otherwise indicated, and do not include dispensing fees.
aPrices reflect IQVIA DeltaPA wholesale list prices (accessed September 2024).
bText missing.
Appendix 2: Submission Quality
Please note that this appendix has not been copy-edited.
Description | Yes or no | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | Yes | No comment. |
Model has been adequately programmed and has sufficient face validity | No | The model appears to be overly complex. It incorporates unnecessary and lengthy functions, and the same variables are referenced across multiple sheets under different names. This approach could lead to errors and make the process of validating the model more challenging. |
Model structure is adequate for decision problem | Yes | No comment |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | No | Refer to the CDA-AMC appraisal section regarding uncertainty with subsequent treatment costs and health utilities |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | Yes | No comment |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | No | Refer to the CDA-AMC appraisal section. There is a discrepancy between the descriptions in the submitted economic report and the model itself. Additionally, the model lacks justification for the differing proportions of subsequent treatment distributions compared to those reported in the RUBY Part 1 IA2 report. |
CDA-AMC = Canada’s Drug Agency; IA = interim assessment.
Appendix 3: Additional Information on the Submitted Economic Evaluation
Please note that this appendix has not been copy-edited.
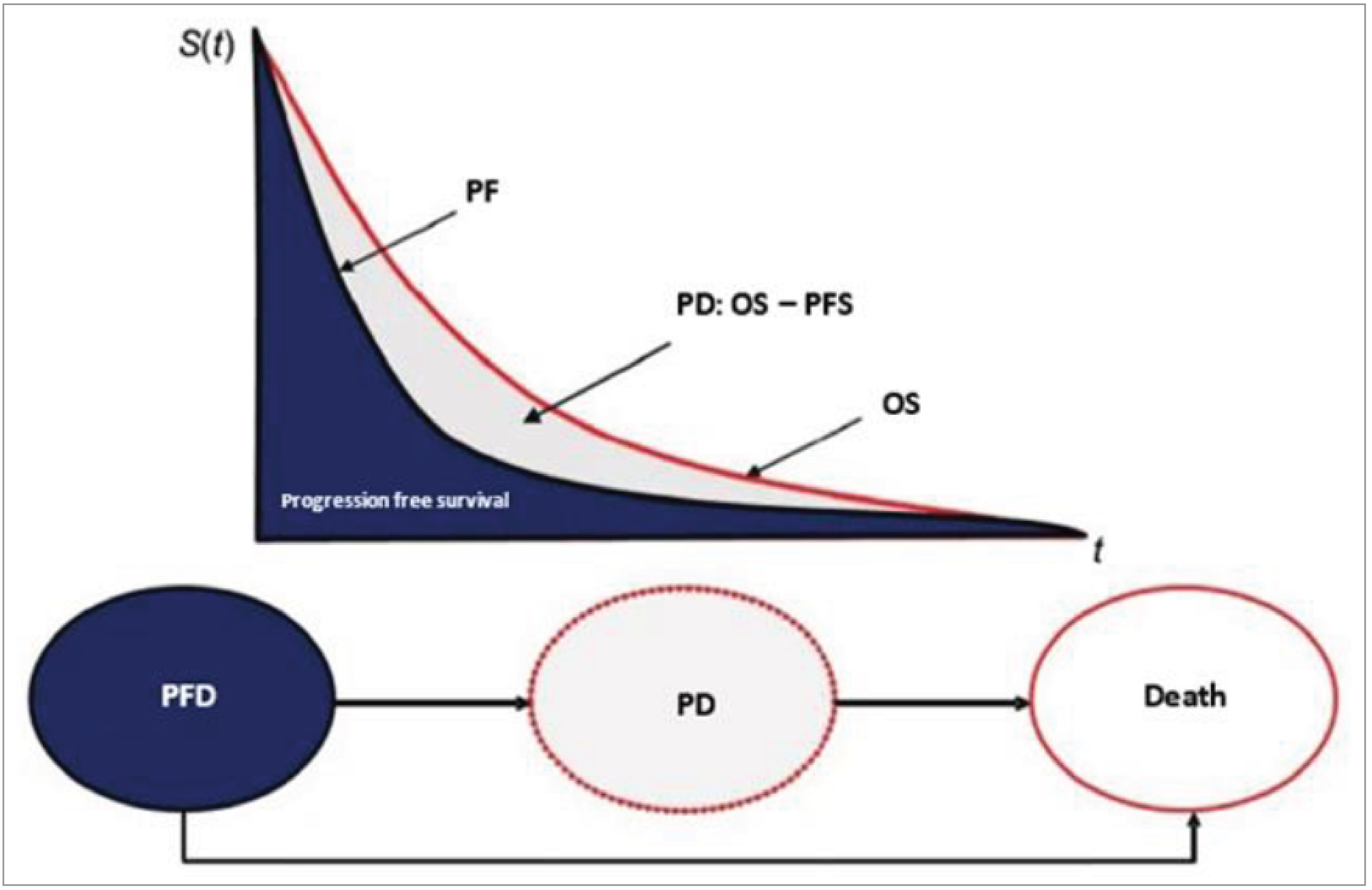
PD = progressed disease; PFD = progression-free disease; PFS = progression-free survival; OS = overall survival.
Source: Sponsor’s pharmacoeconomic submission.
Detailed Results of the Sponsor’s Base Case
Table 10: Disaggregated Summary of the Sponsor’s Economic Evaluation Results
Parameter | Dostarlimab + CP | CP |
|---|---|---|
Discounted LYs | ||
Total | 6.14 | 3.85 |
By health state | ||
Progression-free | 2.35 | 1.18 |
Progressed disease | 3.78 | 2.67 |
Discounted QALYs | ||
Total | 4.96 | 3.09 |
By health state | ||
Progression-free | 1.96 | 0.97 |
Progressed disease | 3.00 | 2.11 |
Discounted costs ($) | ||
Total | 282,925 | 135,687 |
Acquisition | 221,759 | 23,614 |
Administration | 4,720 | 2,579 |
Health state cost | 44,856 | 37,897 |
Adverse event cost | 268 | 265 |
Subsequent treatment cost | 11,322 | 71,332 |
CP = carboplatin-paclitaxel; LY = life-year; QALY = quality-adjusted life-year.
Source: Sponsor’s pharmacoeconomic submission.
Table 11: Sponsor’s Economic Evaluation Results by MMR Status
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER vs. reference ($/QALY) |
|---|---|---|---|---|---|
Full indicated population | |||||
CP | 135,687 | Reference | 3.85 | Reference | Reference |
Dostarlimab plus CP | 282,925 | 147,238 | 6.14 | 1.87 | 78,806 |
dMMR/MSI-H population | |||||
CP | 156,309 | Reference | 3.62 | Reference | Reference |
Dostarlimab plus CP | 378,408 | 222,100 | 10.48 | 6.86 | 32,383 |
pMMR/MSS population | |||||
CP | 121,052 | Reference | 2.92 | Reference | Reference |
Dostarlimab plus CP | 256,789 | 135,737 | 3.99 | 1.07 | 127,138 |
CP = carboplatin-paclitaxel; LY = life-year; QALY = quality-adjusted life-year; dMMR = mismatch repair deficient; pMMR = mismatch repair proficient; vs. = versus.
Appendix 4: Additional Details on the CDA-AMC Reanalyses and Sensitivity Analyses of the Economic Evaluation
Please note that this appendix has not been copy-edited.
Detailed Results of the CDA-AMC Base Case
Table 12: Disaggregated Summary of CDA-AMC’s Economic Evaluation Results
Parameter | Dostarlimab + CP | CP |
|---|---|---|
Discounted LYs | ||
Total | 4.10 | 2.87 |
By health state | ||
Progression-free | 2.18 | 1.15 |
Progressed disease | 1.92 | 1.72 |
Discounted QALYs | ||
Total | 3.34 | 2.31 |
By health state | ||
Progression-free | 1.82 | 0.95 |
Progressed disease | 1.52 | 1.36 |
Discounted costs ($) | ||
Total | 277,127 | 112,588 |
Acquisition | 229,395 | 28,704 |
Administration | 4,803 | 2,609 |
Health state cost | 35,857 | 33,386 |
Adverse event cost | 267 | 264 |
Subsequent treatment cost | 6,805 | 47,626 |
CP = carboplatin-paclitaxel; LY = life-year; QALY = quality-adjusted life-year.
Source: Sponsor’s pharmacoeconomic submission.
Table 13: CDA-AMC’s Economic Evaluation Results by MMR Status
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER vs. reference ($/QALY) |
|---|---|---|---|---|---|
Full indicated population | |||||
CP | 108,464 | Reference | 2.32 | Reference | Reference |
Dostarlimab plus CP | 272,426 | 163,962 | 3.34 | 1.03 | 159,924 |
dMMR/MSI-H population | |||||
CP | 129,434 | Reference | 2.58 | Reference | Reference |
Dostarlimab plus CP | 364,377 | 234,943 | 9.30 | 6.72 | 34,971 |
pMMR/MSS population | |||||
CP | 103,778 | Reference | 2.25 | Reference | Reference |
Dostarlimab plus CP | 250,141 | 146,362 | 2.79 | 0.54 | 273,097 |
CP = carboplatin- paclitaxel; dMMR = mismatch repair deficient; LY = life-year; MMR = mismatch repair; MSS = microsatellite stable; pMMR = mismatch repair proficient; QALY = quality-adjusted life-year; vs. = versus.
At the sponsor’s submitted price for dostarlimab and publicly available list prices for all other drugs, dostarlimab plus carboplatin-paclitaxel did not require a reduction in price to be cost-effective at a WTP threshold of $50,000 per QALY gained for patients with dMMR/MSI-H disease. A 67% price reduction was needed to achieve cost-effectiveness at this threshold for patients with pMMR/MSS disease. This price reduction is associated with a higher degree of uncertainty than the CDA-AMC base case.
Scenario Analyses
Table 14: Scenario Analyses Conducted on the CDA-AMC Base Case
Scenario analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|---|
CDA-AMC base case | CP | 108,464 | 2.32 | Reference |
Dostarlimab plus CP | 272,426 | 3.34 | 159,924 | |
Scenario 1a: Immediate treatment waning (at treatment discontinuation) | CP | 112,588 | 2.31 | Reference |
Dostarlimab plus CP | 279,225 | 3.32 | 165,024 | |
Scenario 1b: Apply delayed treatment waning (gradual decrease in treatment effect from treatment discontinuation [156 weeks] to 3 years) | CP | 108,727 | 2.32 | Reference |
Dostarlimab plus CP | 272,988 | 3.34 | 161,233 | |
Scenario 1c: Apply delayed treatment waning (gradual decrease in treatment effect from treatment discontinuation [156 weeks] to 5 years) | CP | 108,788 | 2.32 | Reference |
Dostarlimab plus CP | 272,483 | 3.34 | 159,929 | |
Scenario 2: Extend a stopping rule for dostarlimab to 4 years | CP | 109,041 | 2.32 | Reference |
Dostarlimab plus CP | 285,915 | 3.34 | 172,086 | |
Scenario 3: Use an alternate source of subsequent treatment distribution (sponsor’s commissioned clinician survey) | CP | 92,844 | 2.32 | Reference |
Dostarlimab plus CP | 280,694 | 3.35 | 182,579 | |
Scenario 4: Use alternate (lower) health state utility values | CP | 109,080 | 2.11 | Reference |
Dostarlimab plus CP | 272,529 | 3.06 | 172,762 | |
Scenario 5: Use log-logistic distribution to predict OS for both treatments | CP | 116,284 | 3.04 | Reference |
Dostarlimab plus CP | 281,415 | 4.64 | 103,167 | |
Scenario 6: Use log-normal distribution to predict PFS for both treatments | CP | 110,340 | 2.32 | Reference |
Dostarlimab plus CP | 272,804 | 3.34 | 158,342 | |
Scenario 7: Inclusion of MSI/MMR testing cost | CP | 109,191 | 2.32 | Reference |
Dostarlimab plus CP | 272,763 | 3.34 | 159,380 |
CDA-AMC = Canada’s Drug Agency; CP = carboplatin-paclitaxel; ICER = incremental cost-effectiveness ratio; MMR = mismatch repair; MSI = microsatellite instability; QALY = quality-adjusted life-year.
Appendix 5: Submitted Budget Impact Analysis and CDA-AMC Appraisal
Please note that this appendix has not been copy-edited.
Table 15: Summary of Key Take-Aways
Key take-aways of the budget impact analysis |
|---|
|
Summary of Sponsor’s Budget Impact Analysis
The sponsor submitted a budget impact analysis (BIA) estimating the incremental budget impact of reimbursing dostarlimab (Jemperli) plus carboplatin-paclitaxel for the treatment of patients with primary advanced or recurrent endometrial cancer that are candidates for systemic therapy. Their BIA was conducted from the perspective of the public drug plans in Canada (except Quebec) over a 3-year time horizon (2025 to 2027) plus the baseline year before the introduction of the regimen. Key inputs to the BIA are documented in Table 16.
The sponsor used an epidemiological approach to estimate the eligible population, drawing data from multiple sources. An annual female growth rate of 1.71% was applied and extrapolated over the 3-year time horizon.14 For uterine cancer, the sponsor used an incidence rate of 43.14 per 100,000 and applied a projected annual growth rate of 1.90%.15,16 They estimated that 95% of uterine cancers are endometrial and, among these: 75.5% are in stage I, with 6.5% expected to experience lifetime recurrence; 6.4% are in stage II, with a 20% recurrence rate; 11.3% are primary advanced stage III; and 6.7% are primary advanced stage IV.17-19 Among patients with recurrent stage I and II, as well as primary advanced endometrial cancer, the sponsor assumed that ████% would receive platinum-based chemotherapy (PBCT).20 They further assumed that all patients on PBCT would be eligible for dostarlimab plus carboplatin-paclitaxel or carboplatin-paclitaxel alone, treating both dMMR and pMMR endometrial cancer as a single population.
The sponsor’s estimates for time on treatment were based on PFS data extrapolated from their trial. The model differentiated between treatment arms (dostarlimab plus carboplatin-paclitaxel and carboplatin-paclitaxel), using PFS data to determine the proportion of patients alive in each arm and to calculate both treatment and subsequent treatment costs based on disease progression observed in the RUBY trial.21 In the base case, the market shares were based on internal GlaxoSmithKline Inc. market analysis.22
Key assumptions:
For patients that progressed following treatment with carboplatin-paclitaxel, the sponsor assumed that ████% will receive pembrolizumab monotherapy and another ████% will receive pembrolizumab and lenvatinib as subsequent therapy compared to █████% receiving either treatment following treatment with dostarlimab.
The sponsor assumed that the risk of recurrence in real-world Canadian practice was aligned with the recurrence rates observed in 2013 Dutch Study.19
Table 16: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1 / year 2 / year 3) | |
|---|---|---|
Target population | ||
Adult female population in Canada | 16,137,795 / 16,414,676 / 16,696,41714 | |
Annual % growth in the female population | 1.7%14 | |
Annual incidence of uterine cancer | 43.14 / 100,00015 | |
Annual % change in incidence of uterine cancer | 1.9%16 | |
Proportion with endometrial cancer | 95%17 | |
Proportion with stage I - EC | 75.5%18 | |
Proportion with stage II - EC | 6.4%18 | |
Proportion with stage III - EC | 11.3%18 | |
Proportion with stage IV - EC | 6.7%18 | |
Lifetime incidence of recurrent stage I | 6.5%19 | |
Lifetime incidence of recurrent stage II | 20.0%19 | |
Proportion receiving 1L - therapy | ████%20 | |
Proportion receiving PBCT | ████%20 | |
Number of patients eligible for drug under review | 868 / 900 / 932 | |
Market uptake (3 years) | ||
Uptake (reference scenario) Dostarlimab plus CP CP | 0% / 0% / 0%21 100% / 100% / 100%21 | |
Uptake (new drug scenario) Dostarlimab plus CP CP | ██% ██% / ██%21 ██% ██% / ██%21 | |
Cost of treatment (per patient, per month) | ||
Dostarlimab plus CP CP | $14,514.93 $4,483.85 | |
Proportion of subsequent treatment | Dostarlimab arm / CP arm21 | |
Dostarlimab Carboplatin and paclitaxel Pembrolizumab Doxorubicin Gemcitabine Pembrolizumab and lenvatinib Letrozole Paclitaxel Radiotherapy Docetaxel No treatment Carboplatin and liposomal doxorubicin Cisplatin and doxorubicin Liposomal doxorubicin Carboplatin Cisplatin | █████% █████% █████% █████% █████% █████% █████% █████% █████% █████% █████% █████% █████% █████% █████% █████% | █████% █████% █████% █████% █████% █████% █████% █████% █████% █████% █████% █████% █████% █████% █████% █████% |
1L = first line; CP = carboplatin-paclitaxel; EC = endometrial cancer; PBCT = platinum-based chemotherapy.
Summary of the Sponsor’s BIA Results
The cumulative net budget impact of funding dostarlimab plus carboplatin-paclitaxel for patients with advanced or recurrent endometrial cancer, accounting for subsequent therapy costs, was $23,451,262 in year 1, $54,745,529 in year 2, and $79,298,682 in year 3, resulting in a total budget impact of $157,495,473 over 3 years. Including subsequent therapy increases total costs in the carboplatin-paclitaxel arm, thereby reducing the overall net budget impact. The inclusion of subsequent therapy reflects current drug funding criteria in clinical practice.
Over 3 years, the net budget impact, excluding subsequent therapy costs, totalled $235,492,565, with $39,607,041 in year 1, $83,962,490 in year 2, and $111,923,034 in year 3.
CDA-AMC Appraisal of the Sponsor’s BIA
CDA-AMC identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
Subsequent treatment distributions may not reflect clinical practice in Canada: The sponsor’s model assumed that the distribution of subsequent therapies would follow the values from the RUBY 1 trial. These values are subject to the same set of limitations as described in the economic analysis.
In reanalysis, CDA-AMC used the same subsequent treatment distribution assumptions as the cost-utility analysis (CUA) reanalysis base case.
The uptake of dostarlimab is underestimated: The sponsor’s submitted BIA indicated that dostarlimab would result in a market uptake of ████% in year 1, ████% in year 2, and ████% in year 3 based on the sponsor’s internal market share analysis. However, CDA-AMC obtained clinical expert feedback indicating that the market uptake of 66% in year 3 does not align with clinical expectations and indicated the sponsor likely underestimated dostarlimab uptake. Unless dostarlimab posed to have a contraindication, clinical experts consulted by CDA-AMC expected higher than 66% market share in year 3.
CDA-AMC conducted a scenario analysis in which the market share for dostarlimab in the new drug scenario was increased by an arbitrary value of 10% (from ████% to ████%) in year 3.
CDA-AMC Reanalyses of the BIA
Table 17: CDA-AMC Revisions to the Submitted BIA
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
Correctionsa to sponsor’s base case | ||
1. Subsequent treatment cost | Sponsor’s estimate of subsequent therapy costs | Aligned with CUA model acquisition costs of subsequent therapies |
Changes to derive the CDA-AMC base case | ||
1. Distributions of subsequent therapy Dostarlimab Carboplatin and paclitaxel Pembrolizumab Doxorubicin Gemcitabine Pembrolizumab and lenvatinib Letrozole Paclitaxel Radiotherapy Docetaxel No treatment Carboplatin and liposomal doxorubicin Cisplatin and doxorubicin Liposomal doxorubicin Carboplatin Cisplatin | Dostarlimab plus CP arm / CP arm █████% █████% █████% █████% █████% █████% █████% █████% █████% █████% █████% █████% █████% █████% █████% █████% █████% █████% █████% █████% █████% █████% █████% █████% █████% █████% █████% █████% █████% █████% █████% █████% | Dostarlimab plus CP arm / CP arm █████% █████% █████% █████% █████% █████% █████% █████% █████% █████% █████% █████% █████% █████% █████% █████% █████% █████% █████% █████% █████% █████% █████% █████% █████% █████% █████% █████% █████% █████% █████% █████% |
CDA-AMC base-case | Reanalysis 1 | |
CDA-AMC = Canada’s Drug Agency; CP = carboplatin-paclitaxel; CUA = cost-utility analysis.
aCorrections are minor errors (e.g., transcription errors between report and model, misapplication of distributions or SEs in probabilistic analyses) that are not identified as limitations.
The results of the CDA-AMC step-wise reanalysis are presented in summary format in Table 18 and a more detailed breakdown is presented in Table 19.
Based on the CDA-AMC reanalysis, the budget impact of the reimbursement of dostarlimab with carboplatin-paclitaxel for the treatment of endometrial cancer is expected to be $29,283,835 in year 1, $65,325,514 in year 2, $91,420,845 in year 3, with a 3-year total of $186,030,194.
Aligning the relative proportion of subsequent treatments to the values used in the CDA-AMC CUA base case led to a 18% increase in the net budget impact.
Table 18: Summary of the CDA-AMC Reanalyses of the BIA
Stepped analysis | Three-year total ($) |
|---|---|
Submitted base case | $157,495,473 |
CDA-AMC reanalysis 1 (CDA-AMC base case) | $186,030,194 |
BIA = budget impact analysis; CDA-AMC = Canada’s Drug Agency.
CDA-AMC conducted the following scenario analysis to address remaining uncertainty, using the CDA-AMC base case. The results are provided in Table 19:
Assuming that the price of dostarlimab is reduced by 56.5% (CDA-AMC’s estimated price reduction from the CUA).
Dostarlimab plus carboplatin-paclitaxel market share was increased by 10% (from ████% to ████%) in year 3, with the balance of market shares redistributed to the carboplatin-paclitaxel arm.
Table 19: Detailed Breakdown of the CDA-AMC Reanalyses of the BIA
Stepped analysis | Scenario | Year 0 (current situation) | Year 1 | Year 2 | Year 3 | Three-year total |
|---|---|---|---|---|---|---|
Submitted base case | Reference | $59,768,253 | $61,939,789 | $71,823,589 | $76,066,381 | $209,829,759 |
New drug | $59,768,253 | $85,391,051 | $126,569,119 | $155,365,063 | $367,325,232 | |
Budget impact | $0 | $23,451,262 | $54,745,529 | $79,298,682 | $157,495,473 | |
CDA-AMC base case | Reference | $44,376,679 | $45,988,998 | $52,719,400 | $55,717,444 | $154,425,843 |
New drug | $44,376,679 | $75,272,833 | $118,044,914 | $147,138,290 | $340,456,037 | |
Budget impact | $0 | $29,283,835 | $65,325,514 | $91,420,845 | $186,030,194 | |
CDA-AMC scenario analysis: 56.5% price reduction | Reference | $44,376,679 | $45,988,998 | $52,719,400 | $55,717,444 | $154,425,843 |
New drug | $44,376,679 | $53,090,821 | $70,930,909 | $84,260,088 | $208,281,818 | |
Budget impact | $0 | $7,101,822 | $18,211,509 | $28,542,643 | $53,855,975 | |
CDA-AMC scenario analysis: 10% increase in dostarlimab market share year 3 | Reference | $44,376,679 | $45,988,998 | $52,719,400 | $55,717,444 | $154,425,843 |
New drug | $44,376,679 | $75,272,833 | $118,044,914 | $155,203,399 | $348,521,146 | |
Budget Impact | $0 | $29,283,835 | $65,325,514 | $99,485,955 | $194,095,303 |
BIA = budget impact analysis; CDA-AMC = Canada’s Drug Agency.
Based on publicly available prices of the comparator treatments.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.