Drugs, Health Technologies, Health Systems
Reimbursement Review
Pembrolizumab (Keytruda)
Sponsor: Merck Canada Inc.
Therapeutic area: Advanced or recurrent endometrial carcinoma
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Clinical Review
Abbreviations
AE
adverse event
AEOSI
adverse event of special interest
CCRAN
Colorectal Cancer Resource & Action Network
CDA-AMC
Canada’s Drug Agency
CI
confidence interval
dMMR
deficient mismatch repair
EC
endometrial cancer
ECOG PS
Eastern Cooperative Oncology Group Performance Status
EUR
efficacy updated report
FACT-En TOI
Trial Outcome Index of the Functional Assessment of Cancer Therapy-Endometrial
FIGO
International Federation of Gynecology and Obstetrics
GRADE
Grading of Recommendations Assessment, Development and Evaluation
HR
hazard ratio
HRQoL
health-related quality of life
IA1
first Interim analysis
IHC
immunohistochemistry
ITC
indirect treatment comparison
ITT
intention to treat
KM
Kaplan-Meier
LS
least squares
MAIC
matching-adjusted indirect comparison
MID
minimal important difference
MMR
mismatch repair
MSI
microsatellite instability
MSI-H
microsatellite instability-high
OS
overall survival
PFS
progression-free survival
pMMR
proficient mismatch repair
QoL
quality of life
RCT
randomized controlled trial
RD
risk difference
RECIST 1.1
Response Evaluation Criteria in Solid Tumours Version 1.1
SAE
serious adverse event
SLR
systematic literature review
SUR
safety update report
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Table 1: Background Information of Application Submitted for Review
Item | Description |
|---|---|
Drug product | Pembrolizumab (Keytruda), 100 mg/4 mL vial, IV injection |
Sponsor | Merck Canada Inc. |
Indication | Pembrolizumab is indicated for the treatment of adult patients with primary advanced or recurrent endometrial carcinoma, in combination with carboplatin and paclitaxel, and then continued as monotherapy |
Reimbursement request | As per indication |
Health Canada approval status | post-NOC |
Health Canada review pathway | Standard |
NOC date | March 5, 2025 |
Recommended dose | 200 mg of pembrolizumab administered intravenously in a 30-minute infusion every 3 weeks in combination with carboplatin-paclitaxel for 6 cycles, followed by 400 mg of pembrolizumab maintenance therapy administered intravenously in a 30-minute infusion every 6 weeks for up to 14 cycles |
NOC = Notice of Compliance.
Introduction
Endometrial cancer (EC) is a type of uterine cancer that originates in the lining of the uterus and is the most common gynecological malignancy,1 accounting for approximately 95% of uterine cancers.2 In 2024, the Canadian Cancer Society estimated that 8,600 women in Canada would be diagnosed with EC, and that 1,600 would die from it.3 EC primarily affects postmenopausal women, with an average age at diagnosis of 60 years.4 EC is staged using the International Federation of Gynecology and Obstetrics (FIGO) system: stage I indicates a tumour confined to the uterus; stage II indicates cervical stroma invasion; stage III indicates regional spread; and stage IV indicates spread to bladder, bowel, or distant organs.5 In Canada, the overall 5-year net survival rate for patients with uterine cancer is 82%. According to the American Cancer Society, the 5-year relative survival rate by stage at diagnosis for the 2014 to 2020 time period was 81% for all stages, 19% for patients with distant metastasis, 95% for patients with localized metastasis, and 70% for patients with regional metastasis.6
Advanced-stage disease is defined as stage III or IV EC, in which the cancer extends beyond the uterus, whereas recurrent EC refers to a return of the disease after primary treatment.7 Recurrence can occur in various locations, which commonly include the abdominal cavity, lymph nodes, lungs, and vagina.8 Both primary advanced and recurrent EC are associated with numerous debilitating symptoms that significantly impair physical functioning and health-related quality of life (HRQoL). Key symptoms include abnormal vaginal bleeding, which may be periodic or continuous.9,10 Additional manifestations encompass pelvic or lower back pain, the presence of a palpable mass in the lower abdomen, and unintentional weight loss.9 Patients often experience abdominal distension, early satiety, alterations in bowel or bladder habits, bowel obstruction, and dyspareunia.11 The debilitating nature of the disease can have a profound impact on a patient’s daily activities, confidence, and self-esteem. Symptoms such as menopausal-like effects, sexual dysfunction, anxiety, depression, and long-term side effects of chemotherapy and radiotherapy can further diminish HRQoL.1,11,12 According to the clinical experts consulted by the review team, mismatch repair (MMR) testing, assessed by immunohistochemistry (IHC), is currently performed as the standard of care for patients with EC in Canada.6
Perspectives of Patient, Clinicians, and Drug Programs
The information in this section is a summary of input provided by the patient and clinician groups that responded to our call for input and from the clinical experts consulted for the purpose of this review.
Patient Input
One patient group, the Colorectal Cancer Resource & Action Network (CCRAN), submitted input on pembrolizumab (Keytruda) for the treatment of adult patients with primary advanced or recurrent EC in collaboration with the Canadian Cancer Survivor Network and HPV Global Action.
The patients interviewed for the input reported that the diagnosis of EC is very distressing and triggers intense emotions, such as extreme fear, stress, anxiety, and shock. The caregivers expressed similar issues they encountered as caregivers to patients with EC, such as emotional drain, anxiety and/or worry, inability to plan ahead, feeling isolated, and feelings of helplessness. Respondents in this input further noted that pain management was the immediate concern to be controlled for patients experiencing pain. On the other hand, longevity and robust treatment options were prioritized by patients not experiencing acute pain. Respondents to the EC survey reported receiving various treatment options, including radiation therapy, surgical resection, targeted therapy, hormonal therapy, immunotherapy, chemotherapy, and complementary medicines. Common side effects of these treatments experienced by the patients who contributed to the input included neuropathy, fatigue, dryness, itching, tightening and/or burning in the vagina, changes in sexual functioning, fluid retention, nausea, constipation, and “chemo brain.” The input from patients indicated that the effects of treatment often impact sexual health and functioning, which is frequently overlooked in clinical care and research.
In terms of improved outcomes, patients who contributed to this input expressed a desire to see a decrease in the time from drug development to access, along with an increase in the availability of additional lines of therapy, the development of treatments given by oral administration, improved access to targeted therapeutics rather than cytotoxic chemotherapeutics, increased funding for EC drug research, and the availability of tumour-agnostic access to biomarker-informed therapeutics. Last, the patient input highlighted the significant and urgent unmet need for additional precision therapeutics for the management of advanced or recurrent EC in Canada, particularly for the patient population with microsatellite stable (MSS) or proficient mismatch repair (pMMR) EC.
For the 6 patients who had experience with pembrolizumab, all noted a robust response, evidenced radiographically, biochemically, and/or clinically. Side effects reported by patients receiving pembrolizumab monotherapy included hyperthyroidism, hypothyroidism, joint pain, fatigue, diarrhea, skin changes, and worsening allergies and/or asthma. Patients who contributed to the input reported that these side effects were quite tolerable and manageable, and perceived a notable difference when they transitioned from the combination therapy to the monotherapy.
Clinician Input
Input From Clinical Experts Consulted for This Review
All Canada's Drug Agency (CDA-AMC) review teams include at least 1 clinical specialist with expertise in the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of primary advanced or recurrent EC.
The clinical experts indicated that the treatment goals for patients with primary advanced or recurrent EC are to control metastatic or recurrent disease, prolong progression-free survival (PFS), prolong overall survival (OS), and improve symptoms and quality of life (QoL). The experts noted that initial therapy after diagnosis can often involve a combination of surgery, systemic therapies (carboplatin with paclitaxel chemotherapy with or without immunotherapy or targeted therapy), hormonal therapy, and radiation therapy. They noted that, recently, dostarlimab has been approved in combination with chemotherapy for patients who have deficient mismatch repair (dMMR) disease. The CDA-AMC clinical experts indicated that dMMR cancers make up only 20% of ECs; the other 80% are pMMR ECs. For patients with dMMR EC, there is an unmet need for better therapies. Currently available combination treatments are associated with toxicity. As a result, many patients are not well enough to move to a second-line chemotherapy. Currently, there are not any treatments with limited toxicity, according to the clinical experts. The clinical experts noted that pembrolizumab in addition to platinum-based chemotherapy would be used in the first-line setting in combination with carboplatin and paclitaxel (carboplatin-paclitaxel) for all patients with primary advanced recurrent EC, including those with dMMR and pMMR mutations. Currently, it is the opinion of the clinical experts that, based on available evidence, pembrolizumab is a suitable choice for the dMMR population but its efficacy in the pMMR population may be more modest.
The clinical experts agreed that the patients best suited for pembrolizumab plus carboplatin-paclitaxel would be those with advanced or recurrent EC. In their opinion, because carcinosarcomas were excluded from the pivotal study, the response of such patients to pembrolizumab is uncertain. The experts emphasized that patients suitable for this treatment can be identified by physical examination, diagnostic tools (such as CT scans), and whether they have undergone previous surgery for EC. Clinicians consulted for this report noted that MMR status testing is routine for patients with EC. Having these results can guide the selection of the most appropriate treatment, based on available options. The clinical experts indicated that in clinical practice, physical examination and diagnostic imaging (CT scan mostly) are used to determine progression during treatment. They noted that treatment response should be assessed every 3 to 4 cycles in patients receiving combination therapy and less frequently in patients receiving monotherapy.
The experts agreed that a clinically meaningful response includes a reduction in tumour size observed on physical examination and CT scan. The clinical experts indicated that treatment with pembrolizumab plus carboplatin-paclitaxel should be discontinued if a patient develops progressive disease, suggested by the presence of symptoms and findings from physical examination or imaging. In addition, treatment should be discontinued if the patient cannot tolerate the toxicities (e.g., hematologic, neuropathic, renal, and organ-specific grade 4 immune-related toxicities). The clinical experts indicated that patients should be assessed for the appropriateness of pembrolizumab in a specialty clinic, and either a gynecologic oncologist or a medical oncologist should be involved in the initial decision-making. Once the patient has been assessed and a decision is made regarding treatment, it would be appropriate for patients to receive treatment in a community setting and be managed by clinicians with experience in the management of patients undergoing immunotherapy.
Clinician Group Input
Input from the Ontario Health Cancer Care Ontario Gynecologic Cancer Drug Advisory Committee was provided for this review. A total of 5 clinicians provided input. The clinician group noted that the treatment goals for patients include prolonging survival, delaying disease progression, reducing symptoms, improving HRQoL, and curing the disease whenever possible. Regarding the unmet needs, the group emphasized the need for new therapy to improve oncologic outcomes and prolong life in the pMMR population, and indicated that the only treatment available for this patient population is carboplatin-paclitaxel, which they said fails to produce a durable response.
The clinician group suggested that pembrolizumab be used as a first-line option for patients with EC undergoing chemotherapy, followed by maintenance monotherapy, or for patients with platinum-sensitive recurrent EC. The group specified that pembrolizumab may be used in settings similar to those in which dostarlimab and durvalumab are used. The group added that patients least suited for pembrolizumab are those with a contraindication to immunotherapy or a poor Eastern Cooperative Oncology Group Performance Status (ECOG PS). The clinician group noted that treatment response is assessed with a combination of imaging and clinical exam, per physician discretion. The clinician group indicated that treatment may be withheld because of disease progression and intolerable toxicity. The group stated that the treatment regimen should be administered in an outpatient setting by a physician who can give systemic therapy.
Drug Program Input
Input was obtained from the drug programs that participate in the CDA-AMC reimbursement review process. The following were identified as key factors that could potentially impact the implementation of a CDA-AMC recommendation for pembrolizumab plus carboplatin-paclitaxel:
consideration for initiation of therapy
generalizability
funding algorithms
care provision issues.
The clinical experts consulted by CDA-AMC provided advice on the potential implementation issues raised by the drug programs (refer to Table 5).
Clinical Evidence
Systematic Review
Description of Studies
One trial, NRG-GY018 (N = 819), was included in the systematic review conducted by the sponsor. NRG-GY018 is an ongoing phase III, randomized, multicentre, double-blind, placebo-controlled, parallel-group interventional study that included female adult patients with newly diagnosed, measurable, stage III or stage IVA EC, or stage IVB or recurrent EC. The study was designed essentially as 2 parallel trials to assess efficacy and safety among patients who had pMMR and dMMR tumours, separately. Enrolled patients had not received prior chemotherapy, unless it was adjuvant chemotherapy that had been completed at least 12 months before the study. The main objectives of the NRG-GY018 trial were to compare the efficacy and safety of pembrolizumab plus carboplatin-paclitaxel followed by continued pembrolizumab monotherapy with placebo plus carboplatin-paclitaxel followed by continued placebo in patients with advanced-stage (measurable stage III or IVA), stage IVB, and recurrent EC. The primary outcome was PFS. The additional (secondary) outcomes of interest to this review were OS and Trial Outcome Index of the Functional Assessment of Cancer Therapy-Endometrial (FACT-En TOI), and immune-mediated adverse reactions. PFS, OS, and immune-mediated adverse reactions outcomes were analyzed in pMMR and dMMR populations at the preplanned first interim analysis (IA1), with data cut-off dates of December 6, 2022, and December 16, 2022, respectively. After positive PFS results in both populations at IA1, the trial was unblinded. The sponsor provided a post hoc analysis (efficacy update report [EUR] and/or safety update report [SUR] analysis), which pooled the data from both MMR populations to provide findings for the all-comers population (as well as the dMMR and pMMR populations, separately), with approximately 9 months of additional follow-up (data cut-off date: August 18, 2023).
Approximately 74% of the included population in the study was white and 98% were recruited from North America. The median age of the participants was around 66 years (range 29 to 94 years), and more than half of the patients were 65 years or older. Most patients had an ECOG PS of 0 (approximately 66%), indicating good overall performance status, endometroid histology at diagnosis (approximately 59%), recurrent (57%) or primary stage IV (41%) disease status, FIGO stage III or IV disease at diagnosis (approximately 52%), central MMR status of pMMR (72%), and had received no prior radiotherapy (approximately 58%) or chemotherapy (approximately 80%).
This report will focus on outcomes based on results from the EUR and/or SUR analysis, which will serve as efficacy outcomes for the all-comers population and align with the reimbursement request. Results for the dMMR and pMMR populations are provided for additional context. Data for HRQoL end points, which are not reported in the EUR and/or SUR clinical study reports, are based on the IA1 analysis for the pMMR population (they have not yet been tested in the dMMR population).
Efficacy Results
The outcomes relevant to the CDA-AMC review included the primary outcome of PFS per investigator assessment and secondary outcomes of OS and HRQoL, measured with FACT-En TOI. At the IA1 data cut-off date, the median follow-up duration was 13.3 months in the pembrolizumab plus carboplatin-paclitaxel group and 13.7 months in the placebo plus carboplatin-paclitaxel group. At the data cut-off date of August 18, 2023 (EUR and/or SUR analysis), the median follow-up duration was 16.7 months in the pembrolizumab plus carboplatin-paclitaxel and 16.0 months in the placebo plus carboplatin-paclitaxel in the all-comers cohort.
Progression-Free Survival (All Comers)
IA1: The success criterion for the primary PFS hypothesis was met for both the pMMR (1-sided P < 0.001162) and dMMR (1-sided P < 0.002074) populations at IA1. The hazard ratio [HR] was 0.57 (95% confidence interval [CI], 0.44 to 0.74; 1-sided P < 0.001) in the pMMR population and 0.34 (95% CI, 0.22 to 0.53; 1-sided P < 0.001) in the dMMR population, both in favour of pembrolizumab plus carboplatin-paclitaxel. In a post hoc analysis for this submission, the HR in the all-comers population was 0.49 (95% CI, 0.39 to 0.62; 1-sided P < 0.0001) in favour of pembrolizumab plus carboplatin-paclitaxel.
EUR and/or SUR analysis: PFS events were reported for 199 (48.8%) patients in the pembrolizumab plus carboplatin-paclitaxel group and 257 (62.5%) patients in the placebo plus carboplatin-paclitaxel group. Median PFS was 16.8 months (95% CI, 13.1 to 19.8 months) in the pembrolizumab plus carboplatin-paclitaxel group versus 9.4 months (95% CI, 8.5 to 11.2 months) in the placebo plus carboplatin-paclitaxel group. The between-group HR was 0.62 (95% CI, 0.51 to 0.75), favouring pembrolizumab plus carboplatin-paclitaxel (1-sided P value < 0.0001). The Kaplan-Meier (KM)-estimated probability of being progression-free was 55.9% (95% CI, 50.7% to 60.8%) in the pembrolizumab plus carboplatin-paclitaxel group versus 38.5% (95% CI, 33.4% to 43.6%) in the placebo plus carboplatin-paclitaxel group at 12 months (risk difference [RD] = 17.4%; 95% CI, 10.2% to 24.6%), and 43.2% (95% CI, 37.4% to 48.8%) versus 24.9% (95% CI, 19.6% to 30.5%) at 24 months (RD = 18.3%; 95% CI, 10.4% to 26.2%), respectively. Results for the pMMR group and the dMMR group were consistent in direction with the overall population. The magnitude of effect was larger in the dMMR group than in the pMMR group. Sensitivity analyses in each MMR group showed results similar to those in the primary analysis.
Point estimates of most subgroup analyses were aligned in direction with the overall population. Tests of treatment-by-subgroup interaction were significant at a 0.05 alpha level for prior chemotherapy, prior radiation therapy, disease status, and MMR status at baseline. The magnitude of benefit was smaller for patients with prior chemotherapy (versus no prior chemotherapy), prior radiation therapy (versus no prior radiation therapy), recurrent and/or persistent disease (versus primary disease), and pMMR status (versus dMMR status).
Overall Survival (All Comers)
IA1: The information fraction was approximately 27% in the pMMR population and 18% in the dMMR population at IA1. The HR was 0.79 (95% CI, 0.53 to 1.17; 1-sided P = 0.1157) in the pMMR population and 0.55 (95% CI, 0.25 to 1.19; 1-sided P = 0.0617) in the dMMR population. Sensitivity analyses were generally consistent with the primary analyses. Results for the all-comers population were not reported.
EUR and/or SUR analysis: At the time of the EUR and/or SUR analysis, the information fraction was approximately 46% in the pMMR population and 29% in the dMMR population. The number of patients who died was 94 (23.0%) in the pembrolizumab plus carboplatin-paclitaxel group and 119 (29.0%) in the placebo plus carboplatin-paclitaxel group. Median OS was not reached in the pembrolizumab plus carboplatin-paclitaxel group and was 32.2 months (95% CI = 27.4 to 42.7 months) in the placebo plus carboplatin-paclitaxel group. The HR was 0.74 (95% CI, 0.57 to 0.97; 1-sided P = 0.0153), favouring pembrolizumab plus carboplatin-paclitaxel. The KM-estimated probability of OS at 18 months was 75.8 (CI, 70.3 to 80.4) versus 69.2 (CI, 63.4 to 74.2) (RD = 6.6%; 95% CI, −0.8% to 14.0%) in the pembrolizumab plus carboplatin-paclitaxel and placebo plus carboplatin-paclitaxel groups, respectively, and at 36 months was 59.8% (95% CI, 50.9% to 67.6%) versus 45.9% (95% CI, 34.6% to 56.5%) (RD = 13.9%; 95% CI, 0.1% to 27.7%), respectively. The sponsor did not provide a sensitivity analysis of the all-comers population for the EUR and/or SUR analysis. Results in the dMMR and pMMR populations were aligned in direction with the all-comers population, but statistical significance was not reached in either group. Point estimates suggested a somewhat larger magnitude of effect in the dMMR population, but CIs overlapped. Sensitivity analyses in each MMR group showed results similar to those in the primary analysis.
Point estimates of most subgroup analyses were aligned in direction with the overall population. Tests of treatment-by-subgroup interaction were significant at a 0.05 alpha level for prior chemotherapy, prior radiation therapy, and measurable disease at baseline. The magnitude of OS benefit was smaller for patients with prior chemotherapy (versus no prior chemotherapy), prior radiation therapy (versus no prior radiation therapy), and no measurable disease at baseline (versus measurable disease at baseline).
HRQoL by FACT-En TOI (pMMR Population)
The sponsor did not report patient-reported outcomes (PROs), including FACT-En TOI, in the updated (EUR and/or SUR) analysis. Therefore, data reported in this section are from the IA1 analysis. Baseline scores for FACT-En TOI in the pMMR population were similar in both treatment groups. At week 18, both treatment groups had slight decreases (worsening) in FACT-En TOI scores. The between-group difference in least squares (LS) mean change from baseline was −3.17 points (95% CI, −5.48 to −0.85 points; P = 0.0075), favouring placebo plus carboplatin-paclitaxel. No results were available for the all-comers population (or for the dMMR population).
Harms Results
The sponsor reported that 775 patients experienced at least 1 adverse event (AE), 99.2% in the pembrolizumab plus carboplatin-paclitaxel arm and 99.7% in the placebo plus carboplatin-paclitaxel arm. Overall, similar frequencies of AEs, grade 3 or grade 4 AEs, and serious adverse events (SAEs) were observed in the dMMR and pMMR cohorts. The most frequent AEs in the pembrolizumab plus carboplatin-paclitaxel and placebo plus carboplatin-paclitaxel arms were fatigue (70.3% versus 63.9%), anemia (59.8% versus 56.7%), alopecia (55% versus 57.5%), nausea (51.2% versus 45.9%), constipation (47.1% versus 41.8%), and diarrhea (42.2% versus 35.6%). Grade 3 or higher AEs were reported in 21.3% of patients in the pembrolizumab plus carboplatin-paclitaxel group and in 18.5% of patients in the placebo plus carboplatin-paclitaxel group. Exposure-adjusted event rates of frequently reported grade 3 to grade 5 AEs (incidence ≥ 5%) remained generally low and were similar in the 2 treatment groups (877 per 100 patient-months in the pembrolizumab plus carboplatin-paclitaxel group versus 511 per 100 patient-months in the placebo plus carboplatin-paclitaxel group). The most frequently reported grade 3 or higher AEs in the pembrolizumab plus carboplatin-paclitaxel and placebo plus carboplatin-paclitaxel arms were anemia (16.9% versus 11.6%) and decreased neutrophil count (14.1% versus 14.4%).
In addition, 237 patients experienced at least 1 SAE, 39.6% in the pembrolizumab plus carboplatin-paclitaxel group and 21.1% in the placebo plus carboplatin-paclitaxel group. The most frequently reported SAEs in the pembrolizumab plus carboplatin-paclitaxel group and placebo plus carboplatin-paclitaxel group were anemia (4.1% versus 4.1%), febrile neutropenia (2.8% versus 1.3%), urinary tract infection (2.6% versus 1.5%), dyspnea (2.3% versus 0.0%), hyperglycemia (2.3% versus 0.0%), pulmonary embolism (2.3% versus 2.1%), and sepsis (2.0% versus 1.3%). Anemia (56.7%) and pulmonary embolism (2.1%) were the most frequent SAEs reported in the placebo plus carboplatin-paclitaxel group. Adverse events of special interest (AEOSI) were reported as immune-mediated events and infusion-related events. The overall pattern of AEOSI associated with the combination treatment of pembrolizumab plus carboplatin-paclitaxel is similar to that for the AEOSI identified in IA1, with no meaningful changes in AEOSI. AEOSIs were reported in 39.6% of patients in the pembrolizumab plus carboplatin-paclitaxel group and 26.3% in the placebo plus carboplatin-paclitaxel group.
Critical Appraisal
Randomization and allocation concealment procedures were appropriate. The key baseline characteristics of patients, including disease severity, appeared to be balanced between groups (for the all-comers population and for both the pMMR and dMMR populations).
The planned NRG-GY018 analyses were conducted separately for the pMMR and dMMR populations. The success criterion for PFS was met in both groups at IA1. The post hoc EUR and/or SUR analysis had a longer follow-up and combined results from the pMMR and dMMR populations. The post hoc EUR and/or SUR analyses were not adjusted for multiplicity but produced PFS results similar to those from the protocol-defined IA1 analyses in the pMMR and dMMR populations. Sensitivity analyses supported the robustness of the PFS analyses.
Participants, study personnel, and the investigator were blinded until the database lock at IA1. Thereafter, the study became unblinded, and a substantial number of patients in the placebo plus carboplatin-paclitaxel group discontinued the protocol treatment to receive anti-PD-1 and/or PD-L1 therapies (primarily pembrolizumab with or without lenvatinib) before progression. As a result, there is a risk of bias in the PFS and OS results from the EUR and/or SUR analysis that is directed toward the null.
There was a small information fraction for OS. In the post hoc EUR and/or SUR analysis, a benefit in OS in the all-comers population was observed, although this analysis was unadjusted for multiplicity and at increased risk of type I error (false-positive results). The separate analyses of the pMMR and dMMR populations did not reach statistical significance.
Disease-related HRQoL was measured in the NRG-GY018 study using the FACT-En TOI, with results available only for the pMMR population at IA1. This tool is not routinely used in clinical practice. Results of the HRQoL outcome are at risk of bias, owing to missing data, but the direction and extent of the bias are unclear. It is not possible to generalize the results to the dMMR population.
Clinicians consulted by the CDA-AMC indicated that the population included in the NRG-GY018 trial reflects patients with advanced or recurrent EC commonly seen in clinical practice in Canada. However, the proportion of patients with an ECOG PS of 2 was lower in the NRG-GY018 trial than in their own clinical practice. Patients with carcinosarcomas were not eligible for inclusion in the study, so it is not possible to generalize the findings to that group.
The timing and dose of pembrolizumab administration in combination with carboplatin-paclitaxel align with clinical practice in Canada.
GRADE Summary of Findings and Certainty of the Evidence
The selection of outcomes for Grading of Recommendations Assessment, Development and Evaluation (GRADE) was based on the sponsor’s Summary of Clinical Evidence, consultation with clinical experts, and input received from patient and clinician groups and public drug plans. The following list of outcomes was finalized in consultation with expert committee members:
PFS
OS
FACT-En TOI
Immune-mediated and injection-related adverse reactions.
Table 2: Summary of Findings for Pembrolizumab Plus Carboplatin-Paclitaxel Versus Placebo Plus Carboplatin-Paclitaxel for Patients With Primary Advanced or Recurrent Endometrial Cancer (All Comers)
Outcome and follow-up | Patients (studies), N | Relative effect (95% CI) | Absolute effects (95% CI) | Certainty | What happens | ||
|---|---|---|---|---|---|---|---|
Placebo plus carboplatin-paclitaxel | Pembrolizumab plus carboplatin-paclitaxel | Difference | |||||
PFS (ITT population), EUR and/or SUR analysis data cut-off date of August 18, 2023 | |||||||
Probability of PFS at 12 months Median follow-up for all patients: 16.3 months | 819 (1 RCT) | NA | 385 per 1,000 | 559 per 1,000 (507 to 608) | 174 more per 1,000 (102 to 246 more per 1,000) | Higha | Pembrolizumab plus carboplatin-paclitaxel results in a clinically important increase in PFS at 12 months compared with placebo plus carboplatin-paclitaxel |
Probability of PFS at 24 months Median follow-up for all patients: 16.3 months | 819 (1 RCT) | NA | 249 per 1,000 | 432 per 1,000 (374 to 488) | 184 more per 1,000 (104 to 262 more per 1,000). | Highb | Pembrolizumab plus carboplatin-paclitaxel results in a clinically important increase in PFS at 24 months compared with placebo plus carboplatin-paclitaxel |
OS (ITT population), EUR and/or SUR analysis data cut-off date of August 18, 2023 | |||||||
Probability of survival at 18 months Median follow-up for all patients: 16.3 months | 819 (1 RCT) | NA | 692 per 1,000 | 758 per 1,000 (703 to 804) | 66 more per 1,000 (8 fewer to 140 more per 1,000) | Lowc | Pembrolizumab plus carboplatin-paclitaxel may result in a clinically important increase in survival at 18 months compared with placebo plus carboplatin-paclitaxel |
Probability of survival at 36 months Median follow-up for all patients: 16.3 months | 819 (1 RCT) | NA | 459 per 1,000 | 598 per 1,000 (509 to 676) | 139 more per 1,000 (1 to 277 more per 1,000) | Lowd | Pembrolizumab plus carboplatin-paclitaxel may result in a clinically important increase in survival at 36 months compared with placebo plus carboplatin-paclitaxel |
FACT-En TOI for pMMR population (ITT population), first interim analysis data cut-off date of December 6, 2022 | |||||||
LS mean change from baseline in global health status; scores range from 0 to 120, with higher scores indicating better health status Follow-up: 18 weeks | 534 (1 RCT) | NA | −0.84 | −4.01 (−5.65 to −2.36) | −3.17 (−5.48 to −0.85) | Moderatee | Pembrolizumab plus carboplatin-paclitaxel likely results in little-to-no clinically important difference in FACT-En TOI compared to placebo plus carboplatin-paclitaxel in the pMMR population; no evidence is available for the all-comer population (or for the dMMR population) |
Harms (safety population), second interim analysis data cut-off date of August 18, 2023 | |||||||
Any immune-related AEs and infusion-related reactions Median follow-up for all patients: 16.3 months | 779 (1 RCT) | RR, 1.51 (1.23 to 1.85) | 263 per 1,000 | 396 per 1,000 (NR) | 134 more per 1,000 (68 more to 198 more) | Highf | Pembrolizumab plus carboplatin-paclitaxel results in a clinically important increase in immune-related AEs and infusion-related reactions compared with placebo plus carboplatin-paclitaxel |
AE = adverse event; CI = confidence interval; EUR and/or SUR = efficacy update report and/or safety update report; FACT-En TOI = Trial Outcome Index of the Functional Assessment of Cancer Therapy-Endometrial; ITT = intention to treat; LS = least squares; NA = not applicable; NR = not reported; OS = overall survival; PFS = progression-free survival; pMMR = proficient mismatch repair; RCT = randomized controlled trial; RR = risk ratio.
Note: Study limitations (which refer to internal validity or risk of bias), indirectness, imprecision of effects, and publication bias were considered when assessing the certainty of the evidence. All serious concerns in these domains that led to the rating down of the level of certainty are documented in the table footnotes.
aA threshold of 10% (100 per 1,000 patients) for a clinically important between-group difference, informed by the clinical experts consulted, was used to inform the target of the certainty rating and the precision of the effect estimate.
bA between-group threshold of 10% (100 per 1,000 patients) for a clinically important between-group difference, informed by the clinical experts consulted, was used to inform the target of the certainty rating and the precision of the effect estimate.
cRated down 1 level for serious study limitations; the OS data have not yet matured, and the analysis was undertaken with a relatively small information fraction, which increases the uncertainty in the results. Not rated down for unblinding or for substantial use of anti-PD-1 and/or PD-L1 therapies in the placebo group after IA1, as the bias is directed toward the null. Rated down 1 level for serious imprecision; the 95% CI included the possibility of little-to-no difference based on the threshold of 5% (50 per 1,000 patients) suggested by the clinical experts.
dRated down 1 level for serious study limitations; the OS data have not yet matured, and the analysis was undertaken with a relatively small information fraction, which increases the uncertainty in the results. Not rated down for unblinding or for substantial use of anti-PD-1 and/or PD-L1 therapies in the placebo group after IA1, as the bias is directed toward the null. Rated down 1 level for serious imprecision; the 95% CI difference included the possibility of little-to-no difference based on the threshold of 5% (50 per 1,000 patients) suggested by the clinical experts.
eRated down 1 level for serious study limitations; there is a risk of bias because of missing outcome data.
fA between-group difference of 5% (50 per 1,000 patients) was clinically important, according to the clinical experts. The point estimate and entire CI exceeded the threshold. The relative risk and risk difference were supplied by the sponsor after an additional information request by the review team and was not part of the sponsor’s testing strategy.
Sources: NRG-GY018 Clinical Study Report,13 sponsor’s Summary of Clinical Evidence.
Long-Term Extension Studies
No long-term extension studies were submitted by the sponsor.
Indirect Comparisons
Description of Studies
Given the lack of direct comparative evidence between pembrolizumab and dostarlimab (each in combination with carboplatin-paclitaxel), the sponsor performed an anchored matching-adjusted indirect comparison (MAIC) to estimate the comparative PFS benefits in patients with advanced or recurrent dMMR EC. The analysis was informed by a systematic literature review (SLR) that identified the randomized, double-blinded, placebo-controlled, phase III RUBY-I trial as a comparator to the NRG-GY018 trial.
Efficacy Results
There was insufficient evidence to show a difference between pembrolizumab and dostarlimab (each in combination with carboplatin-paclitaxel) for PFS events based on the MAIC analysis (HR, 1.00; 95% CI 0.48 to 2.08) for advanced or recurrent dMMR EC.
Harms Results
No indirect evidence for harms was provided.
Critical Appraisal
Dostarlimab plus carboplatin-paclitaxel is a relevant comparator for advanced or recurrent dMMR EC. However, the results of the MAIC are highly uncertain, given numerous limitations. Namely, there was a risk of selection bias in the SLR in the absence of a priori selection criteria. There was heterogeneity in the patient populations and design of the trials (for example, time of chemotherapy interval for recurrent disease, inclusion of carcinosarcoma, and differences in censoring rules). There were wide 95% CIs for the treatment-effect estimates and there was a difference in the KM curves between the control arms, with more PFS events occurring in the control arm of the RUBY-I trial than in the control arm of the NRG-GY018 trial. These limitations suggest the possibility of heterogeneity between trials. Effect modifiers were justified, but unknown and/or unidentified effect modifiers could have potentially biased the MAIC results. Overall, the direction of bias cannot be determined. Beyond the methodological limitations of the approach, the CI around the point estimate was too wide to determine which treatment regimen might be favoured. Therefore, the results of the MAIC between pembrolizumab and dostarlimab (each in combination with carboplatin-paclitaxel) for advanced and recurrent dMMR EC should be considered highly uncertain. There is also an evidence gap, in that OS, HRQoL, and harms outcomes were not included in this analysis, which precludes a comprehensive understanding of the balance of comparative benefits and harms.
Studies Addressing Gaps in the Evidence From the Systematic Review
No studies addressing gaps in the evidence from the systematic review were submitted by the sponsor.
Conclusions
Evidence from 1 phase III, randomized, double-blind trial (NRG-GY018) informed on the efficacy and safety of pembrolizumab plus carboplatin-paclitaxel followed by pembrolizumab monotherapy, compared with placebo plus carboplatin-paclitaxel followed by placebo, in adults with pMMR and dMMR primary advanced or recurrent EC. Evidence from the trial showed that pembrolizumab plus carboplatin-paclitaxel results in clinically important increases in PFS at 12 months and 24 months. The magnitude of benefit in PFS was smaller for patients with prior chemotherapy (versus no prior chemotherapy), prior radiation therapy (versus no prior radiation therapy), recurrent and/or persistent disease (versus primary disease), and pMMR status (versus dMMR status), but the trial was not designed to confirm differences across populations. Evidence from the trial suggested that pembrolizumab plus carboplatin-paclitaxel may improve OS at 18 months and 36 months compared to placebo plus carboplatin-paclitaxel. Conclusions regarding OS were limited because the data are not yet mature, and results in the all-comers population were post hoc and unadjusted for multiplicity. There is some uncertainty in the generalizability of the OS findings to patients with prior chemotherapy, prior radiation therapy, and no measurable disease at baseline. At 18 weeks of treatment, there was likely to be little-to-no clinically important difference in HRQoL for pembrolizumab plus carboplatin-paclitaxel compared to placebo plus carboplatin-paclitaxel among patients with pMMR disease. There is no evidence available for the all-comers population, or for the dMMR population. Patients with carcinosarcoma were excluded, and there were few patients with an ECOG PS of 2,so generalizability to these groups is unknown. There were no new safety signals identified, and the safety of pembrolizumab plus carboplatin-paclitaxel was consistent with the known safety profiles of the individual drugs. As expected, there was an increase in the proportion of patients in the pembrolizumab plus carboplatin-paclitaxel group who experienced any immune-related AEs or infusion reactions compared with the placebo plus carboplatin-paclitaxel group.
According to the clinical experts consulted by the review team, MMR testing assessed by IHC is currently performed as the standard of care for patients with EC in Canada.
An indirect treatment comparison (ITC) of PFS between pembrolizumab and dostarlimab (each in combination with carboplatin-paclitaxel) for advanced and recurrent dMMR EC suggested uncertainty about which regimen may be favoured because of methodological limitations and important imprecision.
Introduction
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of pembrolizumab, 100 mg/4 mL vial, administered by IV injection, in the treatment of adult patients with primary advanced or recurrent EC.
Disease Background
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following information has been summarized and validated by the review team.
EC is a type of uterine cancer that originates in the lining of the uterus and is the most common gynecological malignancy,1 accounting for approximately 95% of uterine cancers.2 In 2024, the Canadian Cancer Society estimated that 8,600 women in Canada would be diagnosed with EC, and 1,600 would die from it.3 EC primarily affects postmenopausal women; the average age at diagnosis is 60 years.4
EC is staged using the FIGO system: stage I indicates a tumour confined to the uterus, stage II indicates cervical stroma invasion, stage III indicates regional spread, and stage IV indicates spread to bladder, bowel, or distant organs.5 In Canada, the overall 5-year net survival rate for uterine cancer is 82%. According to the American Cancer Society, the 5-year relative survival rate by stage at diagnosis for the 2014 to 2020 time period was 81% for all stages, 19% for distant metastasis, 95% for localized metastasis, and 70% for regional metastasis.6
Advanced-stage is defined as stage III or stage IV EC, in which the cancer extends beyond the uterus, whereas recurrent EC refers to its return after primary treatment.7 Recurrence can occur in various locations, commonly including the abdominal cavity, lymph nodes, lungs, and vagina.8
Both primary advanced and recurrent EC are associated with numerous debilitating symptoms that significantly impair physical functioning and HRQoL. Key symptoms include abnormal vaginal bleeding, which may be periodic or continuous.9,10 Additional manifestations encompass pelvic or lower back pain, the presence of a palpable mass in the lower abdomen, and unintentional weight loss.9 Patients often experience abdominal distension, early satiety, alterations in bowel or bladder habits, bowel obstruction, and dyspareunia.11 The debilitating nature of the disease has a profound impact on a patient’s daily activities, confidence, and self-esteem. Symptoms such as menopausal-like effects, sexual dysfunction, anxiety, and depression, and the long-term side effects of chemotherapy and radiotherapy can further diminish HRQoL.1,11,12
Standards of Therapy
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following information has been summarized and validated by the review team.
Treatment Goals
For patients with primary advanced or recurrent EC, treatment goals include disease control, prolonging life, symptom relief, improving or maintaining HRQoL, preventing disease recurrence, and minimizing toxicities.14-18 Treatment options currently used in the management of patients with advanced or recurrent EC can consist of surgery, chemotherapy, radiation therapy, hormonal therapy, or immune checkpoint inhibitors.17,19-25 Surgery or chemotherapy are generally the primary step for all patients with advanced (stage III and stage IV) or recurrent EC. The goals of surgery in these patients are to resect the tumour as much as possible and establish the extent of the cancer.17,19,20
Radiation therapy is indicated for patients in whom surgery would not be possible, to decrease the number of cancerous cells in the affected area after surgery, to manage EC symptoms (e.g., control heavy vaginal bleeding), or to shrink the tumour before surgical removal, and may be given in addition to chemotherapy.20,21,23,24,26 Hormonal therapy may be offered to patients who cannot undergo surgery, radiation therapy, or chemotherapy to relieve symptoms of distant metastases, or to control the growth of recurrent disease, and may also be used along with chemotherapy or radiation therapy in some patients.20,21,23,24,27 Response rates associated with radiation and hormonal therapy have been less favourable than those associated with chemotherapy.28-30 As such, radiation and hormonal therapy generally have a limited role and are not standard in the first-line treatment of patients with advanced or recurrent EC.20-24 Recent National Comprehensive Cancer Network guidelines for EC recommend checkpoint inhibitors and monoclonal antibodies, such as pembrolizumab and dostarlimab, as the first-line treatment for patients with primary advanced or recurrent EC.25
Patients in Canada with advanced or recurrent EC continue to need therapies that provide improved disease control, improved survival, and maintenance of HRQoL, with manageable safety profiles.31-34
Drug Under Review
Pembrolizumab administered in combination with carboplatin-paclitaxel chemotherapy and then continued as monotherapy is currently under review by Health Canada for the treatment of adult patients with primary advanced or recurrent EC. The recommended dose is 200 mg of pembrolizumab administered intravenously in a 30-minute infusion every 3 weeks in combination with chemotherapy for 6 cycles, followed by 400 mg of pembrolizumab maintenance therapy administered intravenously in a 30-minute infusion every 6 weeks for up to 14 cycles. The total treatment duration is until disease progression, unacceptable toxicity, or a maximum of 20 cycles (up to 24 months).35 The sponsor’s reimbursement request is the same as the proposed Health Canada indication.
Pembrolizumab is a high-affinity antibody against PD-1, which exerts dual ligand blockade of the PD-1 pathway, including PD-L1 and PD-L2, on antigen-presenting or tumour cells. By inhibiting the PD-1 receptor from binding to its ligands, pembrolizumab reactivates tumour-specific cytotoxic T lymphocytes in the tumour microenvironment.35
The key characteristics of pembrolizumab are summarized in Table 3, as are other treatments available for primary advanced or recurrent EC.
Table 3: Key Characteristics of Pembrolizumab, Dostarlimab, Carboplatin, and Paclitaxel
Characteristic | Pembrolizumab | Dostarlimab | Carboplatin | Paclitaxel |
|---|---|---|---|---|
Mechanism of action | Antibody against PD-1; inhibits the PD-1 receptor from binding to its ligands, reactivating tumour-specific cytotoxic T lymphocytes | Monoclonal antibody; blocks the PD-1 receptor, allowing cytotoxic T-cells to kill tumour cells | Synthetic analogue of cisplatin; causes DNA crosslinking of cancer cells, preventing proper DNA replication and transcription, triggering apoptosis (cell death) and inhibiting tumour growth | Antimicrotubule drug that promotes abnormal microtubule assembly, disrupting the cell's ability to divide by blocking the G2 and M phases of the cell cycle |
Indicationa | Proposed indication under review: Pembrolizumab in combination with chemotherapy, and then continued as pembrolizumab monotherapy, for the treatment of adult patients with primary advanced or recurrent endometrial cancer | In combination with carboplatin and paclitaxel for the treatment of adult patients with primary advanced or recurrent dMMR and/or MSI-H endometrial cancer who are candidates for systemic therapy | Although this regimen is considered appropriate as part of the first-line standard of care for patients,25 the indication for endometrial cancer is not specified in the product monograph | Although this regimen is considered appropriate as part of the standard of care for patients, the indication for endometrial cancer is not specified in the product monograph |
Route of administration | IV infusion | IV infusion | IV infusion | IV infusion |
Recommended dose | 200 mg of pembrolizumab administered intravenously every 3 weeks in combination with chemotherapy for 6 cycles, followed by 400 mg of pembrolizumab maintenance monotherapy administered intravenously every 6 weeks. The total treatment duration is until disease progression, unacceptable toxicity, or up to 24 months | 500 mg every 3 weeks for 6 doses, followed by 1,000 mg every 6 weeks for all cycles thereafter | 6 mg/mL per min administered every 3 weeks for a maximum of 6 cycles | 175 mg/m2 IV infusion over 3 hours administered every 3 weeks for a maximum of 6 cycles |
Serious adverse effects or safety issues | Immune-mediated adverse reactions, immune-mediated pneumonitis, colitis, hepatitis, nephritis, and severe skin reactions Severe endocrinopathies, including adrenal insufficiency (primary and secondary), hypophysitis, type 1 diabetes mellitus, diabetic ketoacidosis, hypothyroidism, hyperthyroidism, and thyroiditis Adrenal insufficiency (primary and secondary), hypophysitis, SJS and TEN; myocarditis, sclerosing cholangitis, and aplastic anemia; solid organ transplant rejection | Immune-mediated reactions (e.g., pneumonitis, colitis, endocrinopathies), infusion-related reactions | Hypersensitivity reactions, bone marrow suppression, renal and hepatic toxicity | Bone marrow suppression, cardiac abnormalities, hepatotoxicity |
dMMR = deficient mismatch repair; MSI-H = microsatellite instability-high; SJS = Stevens-Johnson syndrome; TEN = toxic epidermal necrolysis.
Note: At the time of this review, durvalumab in combination with carboplatin and paclitaxel and dostarlimab in combination with carboplatin and paclitaxel were being reviewed by CDA-AMC for the treatment of adult patients with primary advanced or recurrent endometrial cancer who are candidates for systemic therapy.
aHealth Canada–approved indication.
Sources: Product monographs for pembrolizumab,35 durvalumab,36 dostarlimab,37 carboplatin,38 and paclitaxel.39
Testing Procedure Considerations
For patients with EC, risk stratification models based on molecular subtypes can help in clinical decision-making by informing treatment algorithms.40-43 Molecular subtypes are grouped according to the presence or absence of certain alterations, such as a dMMR or microsatellite instability-high (MSI-H) status, p53 or TP53 aberrations, POLE mutations, or no specific molecular profile.40,42,43 Tumours that are dMMR occur when genetic or epigenetic changes affect the function of specific proteins involved in DNA repair pathways.44 Confirmation of MMR status (i.e., dMMR or pMMR) can inform the eligibility of patients for immune checkpoint inhibitor therapy and, further, for germline testing for inherited conditions such as Lynch syndrome.45 Current international guidelines recommend testing all EC tumours for MMR status, along with other molecular or genetic tests, such as those for p53 aberrations and, when indicated, POLE mutations.40,42,43
MMR testing is performed using IHC on the tumour tissue collected during diagnostic endometrial biopsy or after hysterectomy. IHC uses antibodies to target and stain specific MMR proteins, such as MLH1, MSH2, MSH6, and PMS2, which are the most clinically relevant in cancer.45,46 MMR is considered deficient (i.e., dMMR) if there is an absence of staining in any of the 4 MMR proteins.45 Each of the MMR proteins pairs with another to form heterodimer pairs (i.e., PMS2 with MLH1 and MSH6 with MSH2), and the use of a 2-antibody approach that targets PMS2 and MSH6 first before targeting all 4 proteins is a cost-effective and quick alternative already being implemented in some jurisdictions in Canada.21,47 The clinical experts consulted for this review agreed that all jurisdictions in Canada are routinely testing for the MMR status with IHC as the current standard of care for EC. They confirmed that IHC for MMR testing is widely available and funded in Canada and is relatively inexpensive.
Microsatellite instability (MSI) is a form of DNA alteration that can result from dysfunctional MMR mechanisms.44 MSI status can be detected with next-generation sequencing (NGS) or polymerase chain reaction (PCR).48 Although molecular genetic testing to assess MSI status in patients with EC is not as frequently used in Canada as IHC testing for MMR status, the clinical experts noted that its use may increase in the next 5 years, especially in larger cancer centres. They also stated that using NGS or PCR to determine MSI status is an acceptable alternative to using IHC testing to determine MMR status.49 When considering immune checkpoint inhibitor therapy, using IHC to determine MMR status is recommended over other methods, such as using NGS or PCR to determine MSI status, because of lower costs, shorter turnaround times, and being less resource-intensive.47,50,51
CDA-AMC considered the potential impacts of MMR testing in case it is used to ascertain eligibility for pembrolizumab in adult patients with primary advanced or recurrent EC, including impacts on health systems, patients (including families and caregivers), and costs. No new impacts are anticipated because MMR testing is currently performed as the standard of care for EC in Canada. Key considerations and relevant information available from materials submitted by the sponsor, input from the clinical experts consulted by the review team, and sources from the literature were validated by the review team when possible and are summarized in Table 4.
Table 4: Considerations for MMR Testing if Used to Establish Treatment Eligibility With Pembrolizumab in Primary Advanced or Recurrent EC
Consideration | Criterion | Available Information |
|---|---|---|
Health system–related | Number of individuals in Canada expected to require the test (e.g., per year) | The sponsor estimated that around 6,100 patients in Canada, excluding Quebec, would be diagnosed with incident EC in 2024.52 The clinical experts consulted for this review agreed with this estimate and mentioned that 90% to 95% of these individuals would receive MMR testing. Because MMR testing with IHC is already part of the standard of care for all patients with EC, the testing volume is not expected to increase if pembrolizumab becomes funded and MMR status is shown to inform eligibility. |
Availability and reimbursement status of the testing procedure in jurisdictions across Canada | According to the clinical experts, MMR testing with IHC is broadly available and funded across all jurisdictions in Canada. | |
Testing procedure as part of routine care | According to the clinical experts, MMR testing with IHC is currently performed as part of the diagnostic standard of care for all patients with EC. | |
Repeat testing requirements | According to the clinical experts, MMR testing usually only needs to be performed once and does not need to be repeated. A repeat test may be required if the biopsy sample is insufficient. The experts also confirmed that most individuals with recurrent EC would have been tested for MMR status at the time of their initial diagnosis. They did note, however, that that MMR status could change from the initial status in less than 10% of patients with recurrent EC cases.53 At present, individuals with recurrent EC are generally not retested for MMR status. | |
Impacts on human and other health care resources by provision of the testing procedure | Testing for MMR status with IHC is currently the standard of care for all patients with EC. Therefore, no additional impact on human health or other resources is anticipated from the testing if pembrolizumab becomes funded and MMR status is shown to inform eligibility. | |
Patient-related | Accessibility of the testing procedure in jurisdictions across Canada | Based on the input from the clinical experts, testing for MMR status with IHC is accessible to most, if not all, patients with EC across the country. |
Expected turnaround times for the testing procedure | According to the clinical experts, turnaround times for IHC testing of MMR status are short. The test is typically conducted using the diagnostic biopsy sample, and the results are usually available in 2 to 4 weeks, or by the time the patient sees the oncologist for the diagnosis. MMR testing on the surgically resected tissue can also be ordered by the treating oncologist, and results are usually ready before the 4-week follow-up visit. The clinical experts anticipate no or minimal additional impact on patients or caregivers related to turnaround times if pembrolizumab becomes funded and MMR status is shown to inform eligibility. | |
Burden associated with the testing procedure for patients, families, and/or caregivers | In patients with EC, IHC testing for MMR status is routinely conducted on biopsy samples collected as part of the diagnostic work-up. Individuals whose results show a dMMR status and their families would likely need genetic counselling and additional testing to determine the presence of a hereditary condition (e.g., Lynch syndrome).54 However, because MMR testing with IHC is already part of the standard of care for all patients with EC, there is no additional burden to patients, families, and/or caregivers anticipated from the testing if pembrolizumab becomes funded and MMR status is shown to inform eligibility. | |
Clinical | Clinical utility and validity of the testing procedure | There is evidence that demonstrates the diagnostic accuracy and clinical utility of IHC testing for MMR status.a,45,47 |
Risks of harm associated with the testing procedure | According to the clinical experts, because testing for MMR status with IHC is part of the standard of care at diagnosis for all patients with EC, there is no additional risk of harm anticipated from the testing if pembrolizumab becomes funded and MMR status is shown to inform eligibility. | |
Cost | Projected cost of the testing procedure | IHC testing for MMR status costs around $150 per test.55 Because this testing is currently part of the standard of care for the diagnosis of EC, there is no additional cost anticipated from the testing if pembrolizumab becomes funded and MMR status is shown to informs eligibility. |
dMMR = deficient mismatch repair; EC = endometrial cancer; IHC = immunohistochemistry; MMR = mismatch repair.
aCDA-AMC has not evaluated or critically appraised this evidence to determine its validity or reliability.
Perspectives of Patients, Clinicians, and Drug Programs
The full patient and clinician group submissions received are available in the consolidated patient and clinician group input document for this review on the project website.
Patient Group Input
This section was prepared by the review team based on the input provided by patient groups.
One patient group, the CCRAN, submitted input on pembrolizumab for the treatment of adult patients with primary advanced or recurrent EC in collaboration with the Canadian Cancer Survivor Network and HPV Global Action.
Information for this submission was gathered through outreach by the CCRAN to 14 Canadian gynecological oncology clinicians and/or clinical trial investigators in 2024. Additional information was gathered through outreach to a Canadian patient advocate, as well as 5 additional Canadian gynecological oncologists. CCRAN reached out to 16 US-based clinical trial investigators involved in the NRG-GY018 trial, and 2 patient organization in women’s cancer (SHARE Cancer Support based in the US and Peaches Womb Cancer Trust based in the UK), and the Society of Gynecologic Oncology. Additionally, a social media outreach campaign was shared within CCRAN, the Canadian Cancer Survivor Network, and HPV Global Action’s networks. Interviews were conducted with a Canadian patient and 5 international EC patients who had experience with the drug under review. Data from a 2023 survey were also used to inform this submission in respect of the disease experience and experience with previously available treatments.
Referring to a recent submission, the input indicated that gynecological cancers are plagued with inequities, including underfunding in research and treatments. The input also pointed to rising incidence and mortality rates for EC, despite advancements in oncology. As indicated in the input, EC symptoms primarily manifest as abnormal vaginal bleeding in premenopausal females and any vaginal bleeding in postmenopausal females. Abnormal vaginal bleeding is the most common symptom in both age groups and is experienced by more than 90% of patients with EC. Other symptoms may include abnormal vaginal discharge, difficulty or pain during urination, pain during intercourse, pelvic pain, and unexplained weight loss.
The patients who contributed to the input reported the diagnosis of EC as distressing and triggering intense emotions, such as extreme fear, stress, anxiety, and shock. The caregivers of patients with EC also expressed similar issues they encountered, such as emotional drain, anxiety and/or worry, inability to plan ahead, feelings of isolation, and feelings of helplessness. The input further emphasized that stigma, shame, and blame could be felt by individuals experiencing EC, considering the intimate nature of gynecological cancers. In additional to the psychological trauma of receiving a cancer diagnosis, many women reported experiencing pain related to their cancer symptoms. Respondents who contributed to this input further noted that pain management was an immediate concern for patients experiencing pain. For patients not experiencing acute pain, longevity and robust treatment options were prioritized.
Survey respondents reported receiving various treatment options, including radiation therapy, surgical resection, targeted therapy, hormonal therapy, immunotherapy, chemotherapy, and complementary medicines. Common side effects of these treatments experienced by the respondents included neuropathy, fatigue, dryness, itching, tightening and/or burning in the vagina, changes in sexual functioning, fluid retention, nausea, constipation, and chemo brain. The input highlighted the effects of treatment on the sexual health and functioning of the patient, which are frequently overlooked in clinical care and research.
In terms of improved outcomes, patients who contributed to this input expressed their desires to see a decrease in the time from drug development to access, along with an increase in the availability of additional lines of therapy, an increase in the development of treatments given by oral administration, improved access to targeted therapeutics (as opposed to cytotoxic chemotherapeutics), increased funding for EC drug research, and an increase in the availability of tumour-agnostic access to biomarker-informed therapeutics. In addition, 60% of patients with EC ranked “prolong life” as the most important issue they hope new treatments will address. Last, the patient input highlighted the significant and urgent unmet need for additional precision therapeutics in the management of advanced or recurrent EC in Canada, particularly for the MSS or pMMR EC patient population.
All 6 patients who had experience with pembrolizumab reported a robust response, evidenced radiographically, biochemically and/or clinically. Side effects reported by patients while on pembrolizumab monotherapy included hyperthyroidism, hypothyroidism, joint pain, fatigue, diarrhea, skin changes, and worsening allergies and/or asthma. Patients reported these side effects to be quite tolerable and manageable, and perceived a notable difference when moving from the combination therapy to the monotherapy.
Clinician Input
Input From Clinical Experts Consulted for This Review
All CDA-AMC review teams include at least 1 clinical specialist with expertise in the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of primary advanced or recurrent EC.
Unmet Needs
The clinical experts indicated that the treatment goals for patients with primary advanced or recurrent EC are to control metastatic or recurrent disease, prolong PFS, prolong OS, and improve patients' symptoms and QoL. The experts noted that initial therapy after diagnosis can often involve a combination of surgery, systemic therapies (carboplatin-paclitaxel chemotherapy with or without immunotherapy or targeted therapy), hormonal therapy, and radiation therapy. They noted that, recently, dostarlimab has been approved in combination with chemotherapy for patients with dMMR disease. The CDA-AMC clinical experts indicated that dMMR cancers make up only 20% of ECs; the other 80% are pMMR ECs. For patients with dMMR EC, there is an unmet need for better therapies. Currently, there are not any treatments with limited toxicity, according to the clinical experts.
Place in Therapy
The clinical experts noted that pembrolizumab plus carboplatin-paclitaxel would be used in the first-line setting for all patients with primary advanced recurrent EC, including those with dMMR and pMMR mutations.
The clinical experts noted that, currently, based on available evidence, pembrolizumab is a suitable choice for the dMMR population. Although efficacy in the pMMR population remains modest, the experts, nevertheless, noted that there is hope that recent evidence on pembrolizumab will support its use in combination with platinum-based chemotherapy in the pMMR population.
Patient Population
The clinical experts agreed that the patients best suited for pembrolizumab plus carboplatin-paclitaxel would be those with advanced or recurrent EC. Because patients with carcinosarcomas were excluded from the pivotal study, their response to pembrolizumab is uncertain. The experts noted that patients eligible for this treatment can be identified by physical examination, diagnostic tools (such as CT scans), and whether the patient has had previous surgery for EC. The clinicians consulted for this report noted that MMR status testing is routine for patients with EC and that the results can guide the selection of the most appropriate treatment based on available options.
Assessing the Response to Treatment
The clinical experts indicated that in clinical practice, physical examination and diagnostic imaging (CT scan mostly) are used to determine disease progression in a patient on treatment. They noted that treatment response should be assessed every 3 to 4 cycles during combination therapy and less frequently during monotherapy. The experts agreed that a clinically meaningful response includes a reduction in tumour size on physical examination, symptom improvement on clinical assessments, and improvements on CT scans.
Discontinuing Treatment
The clinical experts indicated that treatment with pembrolizumab plus carboplatin-paclitaxel should be discontinued if patients have progressive disease, suggested by the presence of symptoms and findings from physical examination or imaging. In addition, treatment should be discontinued in the case of intolerable, severe grade 4 toxicities (hematologic, neuropathic, renal, organ-specific grade 4 immune-related toxicities).
Prescribing Considerations
The clinical experts indicated that patients should be assessed for the appropriateness of pembrolizumab in a specialty clinic, and either a gynecologic oncologist or a medical oncologist should be involved in the initial decision-making. Once patients have been assessed and a decision has been made regarding treatment, it would be appropriate that they receive treatment in a community setting and that they be managed by clinicians with experience in the management of patients undergoing immunotherapy.
Clinician Group Input
This section was prepared by the review team based on the input provided by clinician groups.
One input submission from the Ontario Health (Cancer Care Ontario) Gynecologic Cancer Drug Advisory Committee was provided for this review. A total of 5 clinicians contributed input.
The clinician group noted that treatment goals for patients include prolonging survival, delaying disease progression, reducing symptoms, improving HRQoL, and curing the disease whenever possible. Regarding unmet needs, the group emphasized the need for new therapy for the pMMR population to improve oncologic outcomes and prolong life, and they indicated that the only treatment for this patient population is carboplatin-paclitaxel, which fails to produce a durable response.
The clinician group suggested that pembrolizumab be used as a first-line option for patients with chemotherapy, followed by maintenance therapy, or for patients with platinum-sensitive, recurrent disease. The group specified that pembrolizumab may be used in settings similar to those for dostarlimab and durvalumab. The group added that patients least suited for pembrolizumab would be those with a contraindication to immunotherapy or a poor ECOG PS.
The clinician group noted that treatment response is assessed through a combination of imaging and clinical exam, per physician discretion. The clinician group indicated that treatment may be withheld because of disease progression or intolerable toxicity. The group stated that the treatment regimen should be administered in outpatient settings under the care of a physician who can administer systemic therapy.
Drug Program Input
The drug programs provide input on each drug being reviewed through the reimbursement review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by for this review are summarized in Table 5.
Table 5: Summary of Drug Plan Input and Clinical Expert Responses
Drug program implementation questions | Clinical expert response |
|---|---|
Relevant comparators | |
Comparator in the NRG-GY018 clinical trial: placebo. At the time of this input, dostarlimab plus carboplatin-paclitaxel for patients with MSI-H and/or dMMR disease is under funding consideration by some jurisdictions; under CDA-AMC review are dostarlimab plus carboplatin-paclitaxel for the all-comers population and durvalumab plus chemotherapy with or without olaparib. How does pembrolizumab compare with dostarlimab-containing or durvalumab-containing regimens? Can patients with MSI-H and/or dMMR mutations who experience toxicity switch between dostarlimab plus chemotherapy and durvalumab plus chemotherapy? | The clinical experts indicated that, in their experience, both treatments are generally well tolerated and have similar toxicity profiles. They mentioned that, although they are not aware of any evidence currently available to address this question directly, switching between these treatments because of intolerable toxicity should be possible. |
Considerations for initiation of therapy | |
Clinical trial eligibility included patients who had received previous adjuvant chemotherapy if the chemotherapy-free interval was at least 12 months. Would it be appropriate to fund treatment for patients with a chemotherapy-free interval of less than 12 months? | The clinical experts noted that, currently, there is no evidence available on the use of pembrolizumab in patients with a chemotherapy-free interval of less than 12 months. However, dostarlimab was used in patients with a chemotherapy-free interval of at least 6 months in the RUBY-I trial. Therefore, our clinical experts agreed that it would be reasonable for pembrolizumab to be used in patients with a chemotherapy-free interval of less than 12 months, especially patients with dMMR mutations. |
If pembrolizumab is discontinued for reasons other than disease progression or intolerability after the initial 24 months of treatment, are patients eligible for an additional 12 months of treatment if disease recurs? | The clinical experts indicated that although they are not aware of any evidence to address this question, it would be reasonable to have a 12-month or 24-month treatment-free interval before a patient could be eligible for re-treatment if the disease were to recur. |
Consider alignment with dostarlimab for the dMMR patient population. | This is a comment from the drug plans to inform pERC deliberations. |
Considerations for prescribing of therapy | |
Jurisdictions will likely use weight-based dosing (2 mg/kg every 3 weeks to a maximum of 200 mg), as for to other indications. Dosing every 6 weeks was not used in the clinical trial. Would it be a reasonable option when funded? | The clinical experts indicated that, in their view, there is no difference between dosing every 3 weeks and every 6 weeks in terms of efficacy. They said they are not aware of any data regarding EC but mentioned that the efficacy of pembrolizumab plus chemotherapy administered every 6 weeks was similar to that of therapy administered every 3 weeks in the treatment of other cancers. |
Can alternate chemotherapy regimens be used in combination with pembrolizumab if there is a contraindication to platinum-containing chemotherapy? If the patient is not able to tolerate the platinum-containing chemotherapy, can treatment be continued with pembrolizumab monotherapy? | The clinical experts mentioned that the standard chemotherapy used in combination with pembrolizumab is platinum-based chemotherapy. Alternative chemotherapy in addition to pembrolizumab can be used. However, they said that they are not aware of any available data on alternative therapies that could be used in combination with pembrolizumab for this indication in patients with severe allergies to platinum regimens. The clinical experts agreed that if patients cannot tolerate pembrolizumab plus platinum-based therapy, it is reasonable to use pembrolizumab monotherapy, especially in patients with dMMR mutations. However, they said they are not aware of any available data to support this statement. |
Generalizability | |
Can patients currently on alternate treatment regimens (e.g., dostarlimab) who meet the eligibility criteria for pembrolizumab be eligible to switch to pembrolizumab plus chemotherapy? | The clinical experts agreed that it would be reasonable for patients to switch treatment regimens on a time-limited basis if pembrolizumab were to be reimbursed. However, the clinical experts indicated that they generally would not switch patients to pembrolizumab who are doing well on their current treatment regimen. The clinical experts noted that the duration of therapy and patient preference (i.e., shorter therapy and cost-related considerations) may be factors that could influence the decision to switch treatments. |
Funding algorithm (oncology only) | |
Under what clinical circumstances would pembrolizumab plus chemotherapy be preferred (or not preferred) over dostarlimab plus chemotherapy or durvalumab plus chemotherapy with or without olaparib? | The clinical experts indicated that, based on the available evidence and the absence of direct comparisons, they do not currently perceive any meaningful differences among these treatments. The clinical experts noted that there may be individual preferences based on the duration of therapy, which differs by treatment. |
dMMR = deficient mismatch repair; EC = endometrial cancer; pERC = pan-Canadian Oncology Review Expert Review Committee; MSI-H = microsatellite instability-high.
Clinical Evidence
The objective of this Clinical Review Report is to review and critically appraise the clinical evidence submitted by the sponsor on the beneficial and harmful effects of pembrolizumab plus carboplatin-paclitaxel for the treatment of adult patients with primary advanced or recurrent EC and then continued as monotherapy. The focus will be placed on comparing pembrolizumab to relevant comparators and identifying gaps in the current evidence.
A summary of the clinical evidence included by the sponsor in the review of pembrolizumab is presented in 4 sections, with a critical appraisal of the evidence included at the end of each section. The first section, the Systematic Review, includes pivotal studies and randomized controlled trials (RCTs) that were selected in accordance with the sponsor’s systematic review protocol. Our assessment of the certainty of the evidence in this first section, using the GRADE approach, follows the critical appraisal of the evidence. The second and fourth sections typically include long-term extension studies and studies considered by the sponsor to address important gaps in the systematic review evidence, respectively; however, such evidence was not submitted by the sponsor. The third section includes indirect evidence from the sponsor.
Included Studies
Clinical evidence from the following is included in the review and appraised in this document:
1 pivotal trial identified in the sponsor-conducted systematic review (NRG-GY018)56
1 ITC.
Systematic Review
Contents within this section have been informed by materials submitted by the sponsor. The following information has been summarized and validated by the review team.
Description of Study
Characteristics of the included study are summarized in Table 6.
NRG-GY018 is an ongoing phase III, randomized, multicentre, double-blind, placebo-controlled, parallel-group interventional study of female adult patients with newly diagnosed, measurable stage III or stage IVA EC, or stage IVB or recurrent EC. Patients were eligible if they had not received prior chemotherapy for the treatment of EC, or if they received adjuvant chemotherapy that had been completed at least 12 months before the study. The main objective of the NRG-GY018 trial was to compare the efficacy and safety of pembrolizumab in combination with carboplatin-paclitaxel followed by continued pembrolizumab monotherapy with placebo plus carboplatin-paclitaxel followed by continued placebo in patients with advanced-stage (measurable stage III or stage IVA), stage IVB, or recurrent EC.
Table 6: Details of the NRG-GY018 Study Included in the Systematic Review
Detail | NRG-GY018 |
|---|---|
Designs and populations | |
Study design | Ongoing, phase III, randomized, placebo-controlled, double-blind, parallel-group study |
Locations | 395 centres in 4 countries (Canada [14 sites], Japan, South Korea, US) |
Patient enrolment dates | Start date: August 12, 2019 (ongoing) Data cut-off dates:
|
Randomized (N) | Total n = 819 Pembrolizumab plus carboplatin-paclitaxel pMMR group n = 299 Placebo plus carboplatin-paclitaxel pMMR group n = 298 Pembrolizumab plus carboplatin-paclitaxel dMMR group n = 112 Placebo plus carboplatin-paclitaxel dMMR group n = 110 |
Key inclusion criteria |
|
Key exclusion criteria |
|
Drugs | |
Intervention |
|
Comparator(s) |
|
Study duration | |
Screening phase | 28 days |
Run-in phase | Not applicable |
Treatment phase | Maximum of 20 cycles of pembrolizumab or placebo (6 cycles with pembrolizumab or placebo plus carboplatin-paclitaxel; 14 cycles for pembrolizumab or placebo maintenance)b |
Follow-up phase | Up to 5 years |
Outcomes | |
Primary end point | PFS based on investigator assessment using RECIST 1.1 |
Secondary and exploratory end points | Secondary:
Exploratory: Quality of life and patient-reported outcomes: FACT-GOG-Ntx subscale (short), and a single-item GP5 of the FACT-G measuring bother from side effects of cancer therapy |
Safety end points | Adverse events as assessed by CTCAE. |
Publications | ClinicalTrials.gov Identifier: NCT03914612 |
ALT = alanine transaminase; AST = aspartate transaminase; AUC = area under the curve; BICR = blinded independent central review; CTCAE = Common Terminology Criteria for Adverse Events; dMMR = deficient mismatch repair; DoR = duration of response; EC = endometrial cancer; ECOG PS = Eastern Cooperative Oncology Group Performance Status; EUR and/or SUR = efficacy updated report and/or safety updated report; FACT-En TOI = Trial Outcome Index of the Functional Assessment of Cancer Therapy-Endometrial; FACT-G = Functional Assessment of Cancer Therapy-General; FACT-GOG-Ntx = Functional Assessment of Cancer Therapy Gynecologic Oncology Group-Neurotoxicity; IA1 = first interim analysis; MMR = mismatch repair; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; pMMR = proficient mismatch repair; PROMIS = Patient-Reported Outcomes Measurement Information System; RECIST 1.1 = Response Evaluation Criteria in Solid Tumours Version 1.1.
aPatients with treated brain metastases are eligible if follow-up brain imaging after central nervous system–directed therapy shows no evidence of progression and they have been off steroids for at least 4 weeks before Step 2 registration and remain clinically stable.
bAfter October 14, 2020, maintenance changed to every 6 weeks (from every 3 weeks), with a 400 mg pembrolizumab dose (from 200 mg). Treatment changed from 29 to 20 total cycles (combination and maintenance therapy).
Source: NRG-GY018 Clinical Study Report.13
The study design is presented in Figure 1. A total of 819 patients were randomized in a 1:1 ratio to each study group across 395 sites in 4 countries, including 14 sites in Canada. Randomization was generated with a computerized system, provided by Interactive Response Technology, and was stratified by MMR tumour status (dMMR or pMMR), ECOG PS, and prior adjuvant chemotherapy. MMR status for stratification was determined with centralized tissue testing (i.e., based on centralized MMR IHC) or, after amendment 9, with an institutional (local) MMR IHC test (although final central confirmation of the MMR IHC test was still required).
The trial included a 28-day screening phase. In the treatment phase, patients received either IV pembrolizumab or IV placebo plus carboplatin-paclitaxel for 6 cycles (combination phase), followed by IV pembrolizumab or IV placebo monotherapy for up to 14 additional cycles (maintenance phase). The maintenance phase initially consisted of treatment administered every 3 weeks for up to 29 maintenance cycles. However, after amendment 5, patients received treatment every 6 weeks for up to 14 maintenance cycles, as shown in Figure 1. The follow-up phase was planned to continue for up to 5 years.
NRG-GY018 is a study of 2 MMR populations, making it essentially 2 clinical trials with separate hypothesis testing in each group (pMMR and dMMR). The study is ongoing, and IA1, with data cut-off dates of December 6, 2022 (for the pMMR population), and December 16, 2022 (for the dMMR population), has been conducted. Since then, EUR60 and SUR61 analyses, with a data cut-off date of August 18, 2023, were completed, with additional follow-up data of approximately 9 months, and included for regulatory review by Health Canada. After positive efficacy results for the primary PFS hypothesis were achieved at IA1, the study was unblinded. This report will present outcomes based on the results from the EUR and/or SUR analyses, which will serve as the efficacy outcomes in the all-comers population, which is the focus of the reimbursement request. Results for the dMMR and pMMR populations are presented alongside the overall population for additional context. Data for HRQoL end points, which are not reported in EUR and/or SUR clinical study reports, will be presented based on the IA1 for the pMMR population (HRQoL has not yet been tested in the dMMR population, so results are not available for all comers).
Figure 1: Study Design of the NRG-GY018 Trial
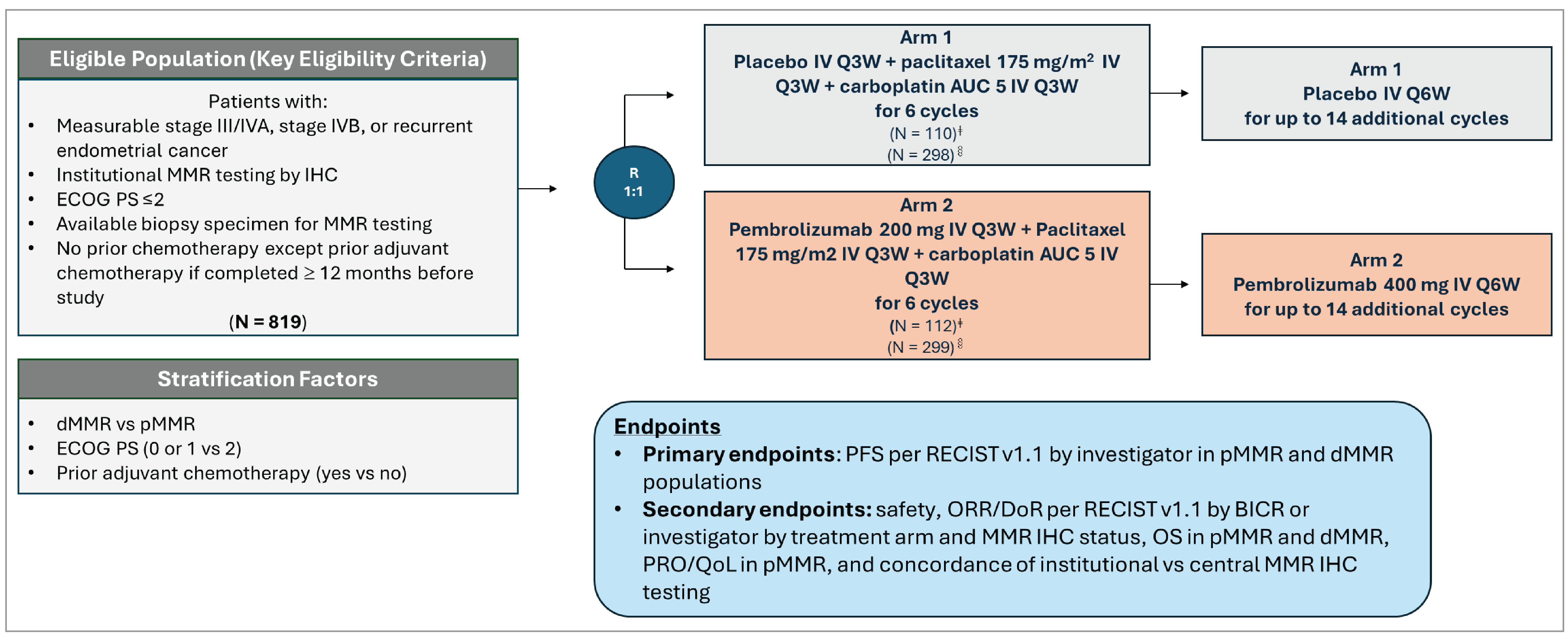
AUC = area under the curve; BICR = blinded independent central review; dMMR = deficient mismatch repair; ECOG PS = Eastern Cooperative Oncology Group Performance Status; MMR = mismatch repair proteins (MLH1, MSH2, MSH6, PMS2); ORR = objective response rate; OS = overall survival; PFS = progression-free survival; pMMR = proficient mismatch repair; PRO = patient-reported outcome; Q3W = every 3 weeks; Q6W = every 6 weeks; QoL = quality of life; R = ratio; RECIST v1.1 = Response Evaluation Criteria in Solid Tumours Version 1.1; vs = versus.
ǂNumber of patients included in the intention-to-treat population with dMMR.
§Number of patients included in the intention-to-treat population with pMMR.
Source: NRG-GY018 Clinical Study Report.62
Populations
Inclusion and Exclusion Criteria
A detailed description of the key inclusion and exclusion criteria for the NRG-GY018 trial is presented in Table 6. Eligible patients were adults 18 years and older with advanced-stage, metastatic, or recurrent EC, including stage III or stage IVA with measurable disease, per RECIST 1.1, or stage IVB or recurrent EC with or without measurable disease. All histologic subtypes were eligible except carcinosarcoma. Patients were required to have institutional results on immunohistochemical analysis of MMR status, have a biopsy specimen available for central immunohistochemical assessment (i.e., MMR and PD-L1 testing), demonstrate adequate organ function, and have an ECOG PS of 0, 1, or 2. Patients were excluded from the study if they had received prior chemotherapy for EC (except patients who had received prior adjuvant chemotherapy were eligible if the treatment was completed at least 12 months before the study), hormonal therapy in the previous 3 weeks, or radiation therapy in the previous 4 weeks, or if they had received prior treatment with anti-PD-1, anti-PD-L1, or anti-CTLA-4 therapies. Patients with treated brain metastases were eligible if follow-up brain imaging after central nervous system–directed therapy showed no evidence of progression and they had been off steroids for at least 4 weeks before Step 2 registration and remained clinically stable.
Interventions
Patients were randomized to receive either pembrolizumab 200 mg or placebo as a 30-minute IV infusion every 3 weeks in combination with carboplatin IV (area under the concentration-time curve of 5 mg/mL per minute) and paclitaxel IV (175 mg/m2 of body surface area) every 3 weeks, starting at cycle 1, day 1, for the first 6 cycles in the combination phase. In the maintenance phase, IV pembrolizumab 200 mg or IV placebo was given as monotherapy every 3 weeks, starting at cycle 7, day 1, in the maintenance phase. A total maximum of 35 cycles of combination and maintenance regimens was allowed. It is important to note that maintenance intervention changed after October 14, 2020, when maintenance changed to every 6 weeks (from every 3 weeks), pembrolizumab dose changed to 400 mg (from 200 mg), and total treatment cycles changed to 20 combination and maintenance cycles (from 35 cycles).
Dose modifications were allowed in the pembrolizumab and placebo components if the patient experienced immune-related AEs and for the chemotherapy component if the patient experienced hematologic AEs. Patients whose treatment was interrupted for drug-related reasons were to resume study treatment at the next planned treatment cycle or during the 9-week delay period. Patients were allowed to interrupt study treatment for situations other than treatment-related AEs, such as medical and surgical events or logistical reasons not related to study therapy. Patients were expected to resume study therapy within 3 weeks.
The study allowed the concomitant use of all prescription and over-the-counter medications, herbal supplements, and IV medications and fluids. During the screening period and throughout the study, patients could receive a preparative regimen to reduce the risk of hypersensitivity reactions associated with paclitaxel, as well as an antiemetic regimen to manage nausea and vomiting caused by carboplatin administration. Additionally, any treatments deemed necessary for the patient's welfare could be administered at the investigator’s discretion, in accordance with community standards of medical care.
Patients could initiate subsequent treatments, such as follow-up anticancer therapy, once pembrolizumab treatment was discontinued, whether because of disease progression or other reasons.
Outcomes
A list of efficacy end points assessed in this Clinical Review Report is provided in Table 7, followed by descriptions of the outcome measures. Summarized end points are based on outcomes included in the sponsor’s Summary of Clinical Evidence, as well as any outcomes identified as important to this review by the clinical experts consulted for this review and input from patient and clinician groups and public drug plans. Using the same considerations, the end points selected were considered most relevant to expert committee deliberations, and this list of end points was finalized in consultation with members of the expert committee. All summarized efficacy end points were assessed using GRADE. Select notable harms outcomes considered important to expert committee deliberations were also assessed using GRADE. The outcomes relevant to the CDA-AMC review included the primary outcome of PFS per investigator assessment and secondary outcomes of OS, HRQoL measured with FACT-En TOI, and immune-mediated AEs.
Table 7: Outcomes Summarized From the NRG-GY018 Study Included in the Systematic Review
Outcome measure | Time point | Hierarchy |
|---|---|---|
PFS (investigator assessed) | 12 months, 24 months | Primary |
OS | 18 months, 30 months | Secondary |
FACT-En TOI | 18 weeks | Secondary |
Immune-related AEs and infusion reactions | Up to 30 days after the last placebo plus carboplatin-paclitaxel dose or the last dose of pembrolizumab plus carboplatin-paclitaxel dose | Notable harm |
AE = adverse event; FACT-En TOI = Trial Outcome Index of the Functional Assessment of Cancer Therapy-Endometrial; OS = overall survival; PFS = progression-free survival.
Source: NRG-GY018 Clinical Study Report.63
Progression-Free Survival
The primary outcome, PFS per investigator assessment, was defined as the time from randomization to the earliest date of radiographic assessment of progressive disease, per RECIST 1.1, or death from any cause in the absence of progressive disease, whichever occurred first. Tumour imaging of the chest, abdomen, and pelvis, to determine the location and extent of disease, was performed using contrast-enhanced CT (the preferred method) or MRI if clinically appropriate (e.g., for body scans but not for the lungs). The imaging method used at baseline was maintained throughout the study. PET scans were not permitted for RECIST 1.1 response criteria. Radiographic evaluations were to be conducted every 9 weeks for the first 9 months. Afterward, imaging was done every 12 weeks until disease progression was documented by RECIST 1.1 or until the patient started a new cancer therapy. Imaging assessments could be discontinued if disease progression occurred. If study treatment was discontinued for reasons other than disease progression, imaging studies continued every 9 weeks until disease progression was documented.
The true date of disease progression was approximated by the date of the first assessment at which progressive disease is objectively documented, per RECIST 1.1, by investigator. Death was always considered a confirmed PFS event. The date of documented progressive disease or death was considered the event date, regardless of missed disease assessments. Participants who did not experience a PFS event were censored at the last contact date for the primary analysis, whether or not a subsequent anticancer therapy was initiated.
Overall Survival
OS was a secondary end point and was defined as the time from study entry to either the date of death or the day after the last known alive date if the date of death was completely missing. Patients who were not known to have died by the time of the analysis were censored on the day after the last date they were confirmed to be alive.
FACT-En TOI
The FACT-En TOI is a composite measure derived from the Functional Assessment of Cancer Therapy-General (FACT-G) scale, designed to assess overall QoL in patients with cancer. This measurement system has 3 clinically relevant subscales: 2 general subscales applicable to all cancers, and 1 subscale specifically targeted at EC. Specifically, the 3 subscales consist of, respectively, a 7-item physical well-being scale, a 7-item functional well-being scale, and a 16-item EC subscale. The total score ranges from 0 to 120, with a higher score indicating a better QoL or fewer symptoms or concerns.64
The validity, reliability, responsiveness, and estimates of the minimal important difference (MID) of the FACT-En TOI are summarized in Table 8.
Table 8: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
FACT-En TOI | The FACT-En TOI is a composite measure derived from the FACT-G scale, designed to assess overall quality of life in patients with cancer. This measurement system has 3 clinically relevant subscales: 2 general subscales applicable to all cancers, and 1 subscale specifically targeted at EC. Specifically, the 3 subscales consist of, respectively, a 7-item physical well-being scale, a 7-item functional well-being scale, and a 16-item EC subscale.65 Each item in the FACT-En TOI scale is scored on a 5-point scale (0 = not at all; 1 = a little bit; 2 = somewhat; 3 = quite a bit; 4 = very much). For negative statements, scores were reversed before calculation. The total FACT-En TOI score was the sum of the subscale scores if more than 80% of the FACT-En TOI items were valid and all component subscales had valid scores. Total scores range from 0 to 120 for FACT-En TOI, with higher scores indicating better quality of life or fewer symptoms and/or concerns.65 | Validity: The convergent and discriminant validity was acceptable; the EC subscales demonstrated generally acceptable levels of item correlation (≥ 0.40). The convergent and discriminant validity of the subscales had a moderate-to-high correlation with the EORTC QLQ-EN24 scale (r, −0.54 to −0.35), except for sexual interest, sexual activity, and hair loss (r = 0.05, −0.01, and −0.23, respectively), as well as the MENQOL questionnaire (r, −0.71 to −0.30). The subscales also demonstrated a moderate-to-high correlation with the K-PROMIS-29 v2.1 scale (r, −0.63 to 0.52).66 Reliability: Minimum reliability, with Cronbach alpha > 0.70, was met for the 5 scales of the EC subscales (range, 0.78 to 0.91) and the total score (0.93).66 In the test-retest reliability, the ICC of EC subscales was 0.76 (95% CI, 0.62 to 0.84), which was a satisfactory consistency.66 Responsiveness: There were no data available for responsiveness. | The sponsor proposed that the MID for the FACT-En TOI scale be estimated as 6 points, as used in other EC trials.67,68 This MID was based on a recommendation in the Yost and Eton (2005)69 study, using both anchor-based and distribution-based methods. |
CI = confidence interval; EC = endometrial cancer; EORTC QLQ-EN24 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire-Endometrial Cancer; FACT-En TOI = Trial Outcome Index of the Functional Assessment of Cancer Therapy-Endometrial; FACT-G = Functional Assessment of Cancer Therapy-General; ICC = intraclass correlation coefficient; MENQOL = Menopause-Specific Quality of Life; MID = minimal important difference.
Statistical Analysis
Based on the protocol, the sample size, power calculations, and statistical analyses were planned separately for the pMMR and dMMR populations. The all-comers population results reported by the sponsor in its clinical review are from a post hoc analysis that combined pMMR and dMMR data to align with the reimbursement request.
Sample Size and Power Calculations
A total sample size of 810 was initially planned for the study, with 590 patients and 220 patients in the pMMR and dMMR populations, respectively. The maximal accrual rate was expected to be about 25 patients per month (20 for the pMMR population and 5 for the dMMR population), leading to an expected period of active accrual of 29.5 months and 44.0 months in the pMMR and dMMR populations, respectively. When a population meets its accrual goals, further accrual to that population is to be avoided. For the pMMR population, based on Schoenfeld’s equation,70 394 PFS events were required, with an assumed HR of 0.70, and 590 patients were accrued. For the dMMR population, 168 PFS events were required, with an assumed HR of 0.60, and 220 patients were accrued. An HR of 0.70 for OS was assumed for both MMR populations. The type I error (alpha) was set at 0.0125 for each population, and the type II error (beta) was 10% for the pMMR population (providing 90% power) and 15% for the dMMR population (providing 85% power). At the interim efficacy analysis, power was expected to be 58% and 50% for pMMR and dMMR populations, respectively. The power for secondary end points was based on the sample size used for the primary end points. Because of the lack of sufficient statistical power in the dMMR group, the analysis for QoL (FACT-En TOI) was conducted only in the pMMR patient population at IA1. At least 80% of evaluable patients were expected for the QoL-PRO analysis.
Statistical Testing
A summary of the statistical analysis of efficacy outcomes is in Table 24 in Appendix 1. For the primary study end point of PFS, the null hypothesis (H0: HR ≥ 1 for the pembrolizumab plus carboplatin-paclitaxel arm versus the placebo plus carboplatin-paclitaxel arm) was tested separately in the pMMR and dMMR populations. Analyses of the all-comers population were post hoc and not part of the trial’s predefined testing strategy.
The KM method was used to estimate the survival curves for all time-to-event outcomes. For PFS and OS, KM estimates and HRs, along with their 95% CIs, were reported. A stratified Cox model with Efron’s method for handling ties, with treatment as a covariate, stratified by MMR status (pMMR versus dMMR) for the pooled population and by prior chemotherapy (yes versus no), was used to assess the magnitude of the treatment difference between the treatment arms. The distributions of PFS, assessed by RECIST 1.1, and OS were compared between the 2 treatment groups using a stratified log-rank test at a significance level of 0.0125 (1-sided).
A linear mixed model for repeated measures was used to estimate and compare the mean differences (with 95% CIs) between the treatment groups in changes from baseline over time in PROs. Analyses were based on the pMMR population at the data cut-off date of December 6, 2022. Model covariates included the patients randomly assigned study treatment, age at enrolment in the study, pretreatment QoL-PRO score, assessment time, and treatment-by-time interaction. The stratification factors used were the same as those used in the primary analysis. The model implicitly handles missing data under the missing-at-random assumption. Hochberg’s step-up multiple testing procedure was used to adjust P values for each assessment time point estimated from the fitted model.71
Interim Analysis and Multiple Testing Procedure
An interim efficacy analysis occurred after the population (both pMMR and dMMR) completed accrual, and a sufficient number of PFS events (50% information fraction) were observed, whichever was later. Each population (the dMMR and the pMMR groups) was evaluated separately and independently. If a population was at least 50% information time when the study closed (both populations), then the efficacy interim analysis for that population was conducted at that time. In each group, at the time of the final PFS analysis (significant interim or final analysis), an interim OS futility analysis will be performed and the OS interim analysis results will be released along with the PFS results. The final OS analysis will be performed when about 364 OS events have been observed in pMMR population, or 150 OS events in the dMMR population. This corresponds to about 60 months and 86 months after trial activation in the pMMR and dMMR populations, respectively. It is anticipated that there will be about 250 deaths in the pMMR population and 115 deaths in the dMMR population at their respective interim OS analyses (at the time of final PFS analyses).
The family-wise type I error was controlled at 2.5% (1-sided alpha-allocation) for PFS across multiple hypotheses and interim analyses using the graphical method of Maurer and Bretz. An O’Brien-Fleming type of stopping boundary was used with a Lan-Demets alpha spending function. The total alpha for each population started at 0.0125. The initial 1-sided alpha level allocated to the dMMR group was rolled over only if the hypothesis of the pMMR group was significant, based on the weight for reallocation presented in the boxes on the lines connecting the 2 hypotheses in Figure 2. If the null hypothesis testing for PFS in the pMMR group was rejected before the dMMR group was tested, then all of the alpha (a total of 0.0125) would be forwarded to the dMMR group. The alpha that was spent on the other group by means of the O’Brien-Fleming function was adjusted in accordance with the rules outlined by Maurer and Bretz. Because the prespecified primary hypotheses testing for PFS in the dMMR and pMMR populations achieved statistical significance at IA1 (data cut-off dates of December 6, 2022, and December 16, 2022, respectively), no formal hypothesis testing for PFS was performed at the data cut-off date of August 18, 2023, and all P values were nominal.
The QoL-PRO end points were tested at a significance level of 5% (2-sided). To control the overall type I error for the multiple QoL-PRO end points (the FACT-En TOI), each of the QoL-PRO end points were tested at a significant level of 1.67% (2-sided).
During the interim OS analysis for futility, the null hypothesis (H0: HR = 1.0) was tested against the alternative (Ha: HR > 0) at the 10% level of significance. The null hypothesis rejection of H0 indicated that the risk of death would be lower in the pembrolizumab plus carboplatin-paclitaxel group than in the placebo plus carboplatin-paclitaxel group.
Post hoc analyses in the all-comers population were not adjusted for multiplicity.
Figure 2: Multiplicity Diagram for Type I Error Control
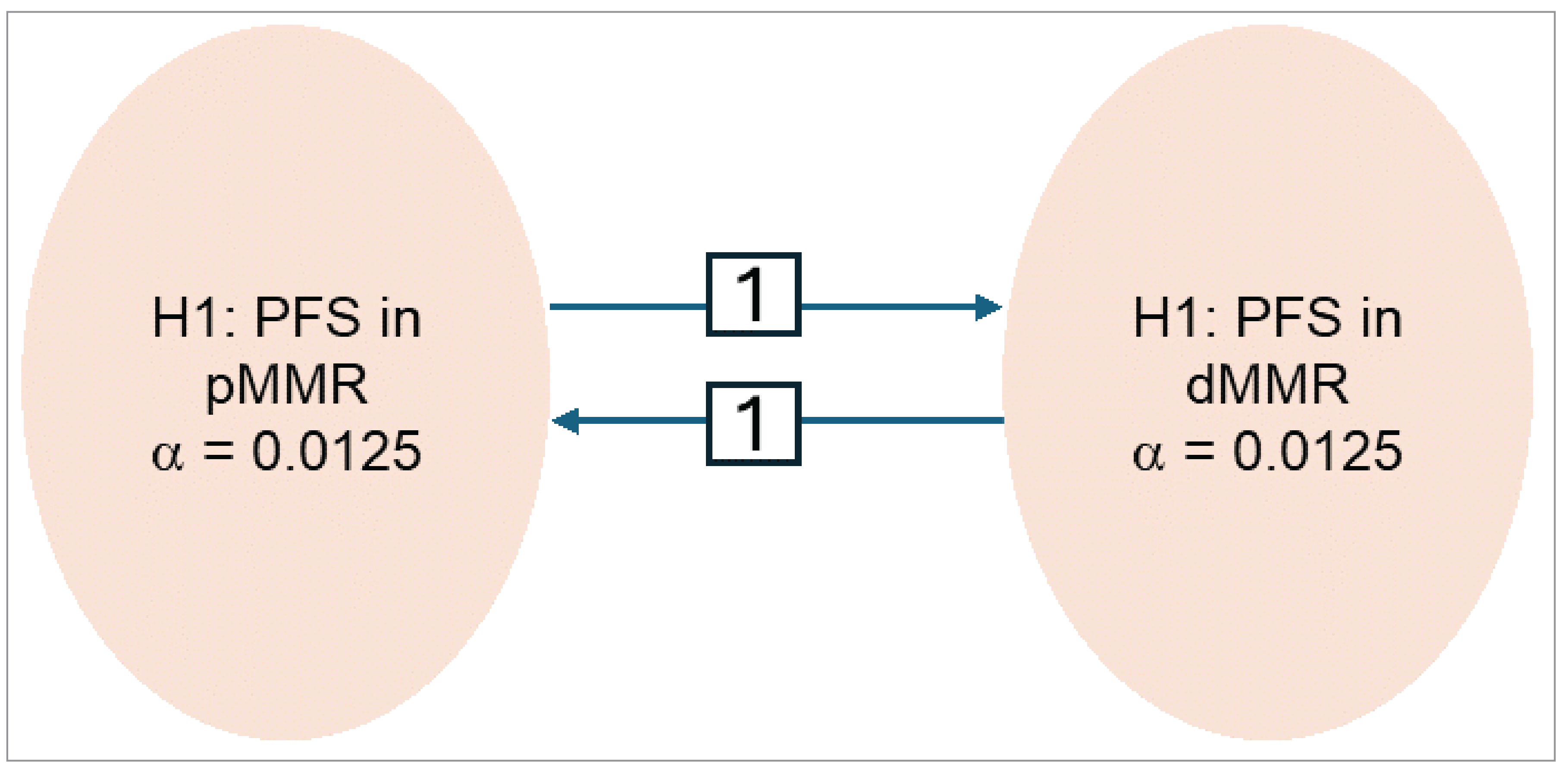
dMMR = deficient mismatch repair; PFS = progression-free survival; pMMR = proficient mismatch repair.
Source: NRG-GY018 Supplemental Statistical Analysis Plan.72
Subgroup Analyses
Subgroup analyses for PFS and OS were performed in the pMMR and dMMR populations using an unstratified Cox regression model with Efron’s method for handling ties, with treatment as a covariate. Results were reported as HRs with 95% CIs. Subgroup analyses were not performed if the number of patients in a subgroup category was less than 5% of the intention-to-treat (ITT) population, or if there were no events in a subgroup category. The subgroups included were age (younger than 65 years, 65 years to younger than 75 years, 75 years and older), race (white, all others), ECOG PS (0 versus 1 or 2), histology (endometrioid carcinoma or other), prior chemotherapy, prior radiotherapy, measurable disease at baseline, status of disease at baseline (primary or recurrent and/or persistent), and MMR status (pMMR versus dMMR).
In the post hoc all-comers analysis, the consistency of the treatment effects across subgroup categories for PFS was assessed using an unstratified Cox regression model, with treatment and subgroup as covariates and a treatment-by-subgroup interaction. The interaction P value from the treatment-by-subgroup interaction test (likelihood ratio test) was presented for each subgroup analysis.
Sensitivity Analyses
Details of sensitivity analyses and censoring rules for PFS are summarized in Table 9. Sensitivity analyses for PFS by investigator assessment and OS in the pMMR and dMMR subpopulations were used to test the robustness of the primary PFS and OS findings under various assumptions used in the analyses. The censoring rules were applied to the ITT MMR population, which included all patients who were randomized on or before the data cut-off dates for the 2 study populations. Patients were included in the treatment group to which they were randomized, based on institutional (local) or centralized MMR IHC test results. The stratification factor applied in the primary censoring and in sensitivity analyses 1, 2, 3, and 4 was prior adjuvant chemotherapy. The stratification factors applied in the primary censoring and in sensitivity analyses 5 and 6 were prior adjuvant chemotherapy and ECOG PS. There were no sensitivity analyses in the all-comers population either in IA1 or the EUR and/or SUR analysis.
Results
Patient Disposition
A summary of patient disposition for the data cut-off date of August 18, 2023 (EUR and/or SUR analysis), is presented in Table 11. In total, 1,064 patients were screened, 819 of whom were randomized to either pembrolizumab plus carboplatin-paclitaxel (n = 408) or placebo plus carboplatin-paclitaxel (n = 411). For the 248 patients who were screened out, the most common reason was that patient declined to participate (n = 68). In the pembrolizumab plus carboplatin-paclitaxel and the placebo plus carboplatin-paclitaxel groups, respectively, 121 (29.7%) and 147 (35.8%) patients discontinued the trial. The main reason for study discontinuation in both treatment groups was death from any cause (23.0% versus 28.9%). More patients in the placebo plus carboplatin-paclitaxel group discontinued the study drug (97.7%) than in the pembrolizumab plus carboplatin-paclitaxel group (69.3%). The most common reasons for discontinuation (pembrolizumab plus carboplatin-paclitaxel versus placebo plus carboplatin-paclitaxel) were progression during active treatment (37.6% versus 43.3%), AEs (18.2% versus 7.2%), and other (2.8% versus 38.7%). The sponsor noted that the imbalance in discontinuation for other reasons was primarily due to a substantial number of participants in the placebo plus carboplatin-paclitaxel group receiving subsequent anti-PD-1 and/or PD-L1 therapies with or without lenvatinib after unblinding of the study following the positive results at IA1. The imbalance in patients discontinuing for other reasons was much less apparent at IA1.
Table 9: Censoring Rules for Primary and Sensitivity Analyses of PFS and OS
NRG-GY018 | |||||||
|---|---|---|---|---|---|---|---|
Situation | Primary analysisa | Sensitivity analysis 1b | Sensitivity analysis 2c | Sensitivity analysis 3d | Sensitivity analysis 4e | Sensitivity analysis 5f | Sensitivity analysis 6g |
PFS | |||||||
PD or death documented after ≤ 1 missed disease assessment and before new anticancer therapy, if any | Progressed at date of documented PD or death | Progressed at date of documented PD or death | Progressed at date of documented PD or death | Progressed at date of documented PD or death | Same as the primary analysis, except only the central MMR data source was used. | Same as the primary analysis, except both stratification factors (prior adjuvant chemotherapy and ECOG PS) were used in the analysis instead of only prior adjuvant chemotherapy (Cox model and log-rank test). | Same as the primary analysis. The MMR population source is as follows: if a participant had central MMR results at the time of the DMC, those results were used; otherwise, institutional (local) MMR results were used. Three patients with indeterminate central MMR results were excluded. Data sources to determine PFS events were different from those used for the primary PFS analysis and reflect the analysis prepared for the DMC. Death and PD information were obtained from NRG Oncology’s follow-up CRF. |
PD or death documented immediately after ≥ 2 consecutive missed disease assessments or after new anticancer therapy, if any | Progressed at date of documented PD or death | Censored at last disease assessment before the earlier date of ≥ 2 consecutive missed disease assessments or new anticancer therapy, if any | Progressed at date of documented PD or death | Progressed at date of documented PD or death | |||
No PD and no death; new anticancer treatment is not initiated | Censored at last contact date | Censored at last disease assessment | Censored at last disease assessment | Progressed at treatment discontinuation; otherwise censored at last disease assessment | |||
No PD and no death; new anticancer treatment is initiated | Censored at last contact date | Censored at last disease assessment before new anticancer treatment | Censored at last disease assessment | Progressed at date of initiation of new anticancer treatment or discontinuation of treatment, whichever occurs later | |||
OS | |||||||
Completely missing death date | Event on the day after last known alive date (day A + 1) | Not applicable | Censored on the last known alive date (day A) | Event on the midpoint of last known alive date, and death confirmation date (day A + day B)/2 | Same as the primary analysis, except only the central MMR data source was used | Same as the primary analysis, except both stratification factors (prior adjuvant chemotherapy and ECOG PS) were used in the analysis instead of only prior adjuvant chemotherapy (Cox model and log-rank test) | Not applicable |
CRF = case report form; DMC = data monitoring committee; ECOG PS = Eastern Cooperative Oncology Group Performance Status; MMR = mismatch repair; OS = overall survival; PD = progressive disease; PFS = progression-free survival.
Note: A missed disease assessment includes any assessment that is not obtained or is considered inadequate for the evaluation of response.
aReferred to as protocol censoring rule in the clinical study reports.
bReferred to as primary (preferred) censoring rule in the clinical study reports.
cReferred to as sensitivity censoring rule 1 in the clinical study reports.
dReferred to as sensitivity censoring rule 2 in the clinical study reports.
eReferred to as protocol censoring rule by central MMR determination in the clinical study reports.
fReferred to as protocol censoring rule with both stratification factors by ITT MMR in the clinical study reports.
gReferred to as DMC censoring rule by DMC MMR in the clinical study reports.
Sources: NRG-GY018 Supplemental Statistical Analysis Plan,72 trial statistical report (efficacy update report).60
Table 10: Analysis Populations of the NRG-GY018 Trial
Population | Definition | Application |
|---|---|---|
ITT | All randomized patients in the treatment arm to which they are randomized | All efficacy analyses (all comers, pMMR, dMMR) |
APaT | All randomized patients who received at least 1 study intervention in the treatment arm corresponding to the treatment they received | Safety analyses (all comers, pMMR, dMMR) |
PRO FAS | Centrally determined patients who received at least 1 dose of study treatment and have at least 1 valid PRO end point assessment | PRO analyses (pMMR) |
APaT = all participants as treated; dMMR = deficient mismatch repair; FAS = full analysis set; ITT = intention to treat; pMMR = proficient mismatch repair; PRO = patient-reported outcome.
Sources: NRG-GY018 Clinical Study Report,62 Eskander et al. (2023).57
Table 11: Summary of Patient Disposition in the NRG-GY018 Trial
Patient disposition | Pembrolizumab plus carboplatin-paclitaxel (N = 408) | Placebo plus carboplatin-paclitaxel (N = 411) |
|---|---|---|
Screened, N | 1,064 | |
Randomized, N | 408 | 411 |
Discontinued study drug, n (%) | 271 (69.3) | 379 (97.7) |
Reason for discontinuation, n (%) | ||
Adverse event | 71 (18.2) | 28 (7.2) |
Drug not given | 0 | 1 (0.3) |
Alternative therapy in the absence of progression | 5 (1.3) | 5 (1.3) |
Death | 10 (2.6) | 4 (1.0) |
Progression during active treatment | 147 (37.6) | 168 (43.3) |
Other complicating disease | 6 (1.5) | 2 (0.5) |
Patient withdrawal or refusal | 19 (4.9) | 16 (4.1) |
Symptomatic deterioration | 2 (0.5) | 5 (1.3) |
Other | 11 (2.8) | 150 (38.7) |
Discontinued from study, n (%) | 121 (29.7) | 147 (35.8) |
Reason for discontinuation, n (%) | ||
Death | 94 (23.0) | 119 (29.0) |
Lost to follow-up | 1 (0.2) | 1 (0.2) |
Patient’s decision to withdraw | 23 (5.6) | 24 (5.8) |
Other | 3 (0.7) | 3 (0.7) |
Analysis sets | ||
ITT, N (%) | 408 (100.0) | 411 (100.0) |
APaT, N | 391 | 388 |
PRO FAS (pMMR only), N | 268 | 266 |
APaT = All participants as treated; FAS = full analysis set; ITT = intention to treat; pMMR = proficient mismatch repair; PRO = patient-reported outcome.
Source: Safety update report from the NRG-GY018 study.61
Baseline Characteristics
The baseline characteristics outlined in Table 12 are limited to those that are most relevant to this review or were felt to affect the outcomes or interpretation of the study results. Overall, the key baseline characteristics were generally balanced between treatment groups. The trial population had a mean age of 65 years, was predominately white (approximately 74%), and more than half of the patients were 65 years or older. The majority of patients (98%) were located in North America.
Most patients had an ECOG PS of 0 (approximately 66%), endometrioid (grade 1, grade 2, or grade 3) histology at diagnosis (approximately 60%), recurrent disease (57%), FIGO stage IA or stage IVB at diagnosis (approximately 24% and 33%, respectively), MMR status of pMMR (approximately 71%), and had not received prior radiation therapy (approximately 58%).
Table 12: Summary of Baseline Characteristics From the NRG-GY018 Trial
Characteristic | Pembrolizumab plus carboplatin-paclitaxel (N = 408) | Placebo plus carboplatin-paclitaxel (N = 411) |
|---|---|---|
Sex, female, n (%) | 408 (100.0) | 411 (100.0) |
Age, years | ||
Younger than 65, n (%) | 183 (44.9) | 191 (46.5) |
65 or older, n (%) | 225 (55.1) | 220 (53.5) |
Mean (SD) | 65.6 (9.2) | 65.3 (9.6) |
Median (range) | 66.3 (31.0 to 94.0) | 66.0 (29.0 to 91.0) |
Race, n (%) | ||
American Indian or Alaska native | 2 (0.5) | 4 (1.0) |
Asian | 20 (4.9) | 19 (4.6) |
Black or African American | 56 (13.7) | 60 (14.6) |
Multiple | 1 (0.2) | 1 (0.2) |
Native Hawaiian or other Pacific Islander | 1 (0.2) | 3 (0.7) |
White | 307 (75.2) | 300 (73.0) |
Missing | 21 (5.1) | 24 (5.8) |
Ethnicity, n (%) | ||
Hispanic or Latino | 27 (6.6) | 22 (5.4) |
Not Hispanic or Latino | 371 (90.9) | 375 (91.2) |
Not reported | 5 (1.2) | 7 (1.7) |
Unknown | 5 (1.2) | 7 (1.7) |
Region, n (%) | ||
North America | 401 (98.3) | 402 (97.8) |
Rest of the world | 7 (1.7) | 9 (2.2) |
Central MMR status, n (%) | ||
dMMR | 111 (27.2) | 112 (27.3) |
pMMR | 291 (71.3) | 295 (71.8) |
Intermediate | 2 (0.5) | 1 (0.2) |
Missing | 4 (1.0) | 3 (0.7) |
ECOG PS, n (%) | ||
0 | 270 (66.2) | 273 (66.4) |
1 | 128 (31.4) | 124 (30.2) |
2 | 10 (2.5) | 14 (3.4) |
Prior chemotherapy, n (%) | ||
Yes | 79 (19.4) | 85 (20.7) |
No | 329 (80.6) | 326 (79.3) |
Prior radiation therapy, n (%) | ||
Yes | 162 (39.7) | 180 (43.8) |
No | 246 (60.3) | 231 (56.2) |
Elapsed time from initial diagnosis years | ||
Mean (SD) | 1.8 (2.5) | 1.8 (2.3) |
Median (range) | 0.9 (0.0 to 18.3) | 1.0 (0.0 to 14.4) |
Histology, n (%) | ||
Endometrioid, grade 1 | 76 (18.6) | 80 (19.5) |
Endometrioid, grade 2 | 104 (25.5) | 102 (24.8) |
Endometrioid, grade 3 | 68 (16.7) | 61 (14.8) |
Serous | 85 (20.8) | 78 (19.0) |
Clear cell | 19 (4.7) | 20 (4.9) |
Dedifferentiated and/or undifferentiated | 11 (2.7) | 10 (2.4) |
Mixed epithelial | 9 (2.2) | 12 (2.9) |
Adenocarcinoma | 36 (8.8) | 47 (11.4) |
Missing | 0 (0.0) | 1 (0.2) |
FIGO stage at initial diagnosis, n (%) | ||
IA | 98 (24.0) | 102 (24.8) |
IB | 52 (12.7) | 59 (14.4) |
II | 38 (9.3) | 38 (9.2) |
IIIA | 16 (3.9) | 17 (4.1) |
IIIB | 9 (2.2) | 7 (1.7) |
IIIC1 | 28 (6.9) | 21 (5.1) |
IIIC2 | 22 (5.4) | 13 (3.2) |
IVA | 13 (3.2) | 9 (2.2) |
IVB | 131 (32.1) | 145 (35.3) |
Missing | 1 (0.2) | 0 (0.0) |
Status of disease, n (%) | ||
Recurrent | 239 (58.6) | 233 (56.7) |
Persistent | 4 (1.0) | 3 (0.7) |
Primary | 165 (40.4) | 175 (42.6) |
dMMR = deficient mismatch repair; ECOG PS = Eastern Cooperative Oncology Group Performance Status; FIGO = International Federation of Gynecology and Obstetrics; MMR = mismatch repair; pMMR = proficient mismatch repair; SD = standard deviation.
Source: Trial statistical report (efficacy update report).60
Exposure to Study Treatments
Exposure to randomized study treatments in the ITT population, which includes patients with dMMR and with pMMR, is summarized in Table 13.
The median duration of exposure to the study intervention was longer in the pembrolizumab plus carboplatin-paclitaxel group (███████) than in the placebo plus carboplatin-paclitaxel group (███████) up to the data cut-off date of August 18, 2023 (EUR and/or SUR analysis). Patients with a duration of exposure to the study intervention of more than 6 months and 12 months was higher in the pembrolizumab plus carboplatin-paclitaxel group than in the placebo plus carboplatin-paclitaxel group (███████████████████████████████████████).
Table 13: Summary of Patient Exposure From the NRG-GY018 Trial, All Comers (APaT Population)
Exposure | Pembrolizumab plus carboplatin-paclitaxel (N = 391) | Placebo plus carboplatin-paclitaxel (N = 388) |
|---|---|---|
Duration on therapya (days) | ||
Duration, mean (SD) | ████████████ | ████████████ |
Duration, median (range) | ███████████ | ███████████ |
Duration of exposureb | ||
More than 6 months, N (person-months) | ████████████ | ████████████ |
More than 12 months, N (person-months) | ████████████ | █████████ |
More than 18 months, N (person-months) | ███████████ | █████████ |
APaT = All participants as treated; SD = standard deviation.
aDuration of exposure is the time from the first dose date to the last dose date.
bDuration on therapy is calculated as the days between first dose date and last dose date of any study medication.
Source: Safety update report.61
Concomitant Medications
All concomitant medications were documented in clinical study reports. All patients in the dMMR cohort (100.0%) and most in the pMMR cohort (99.5%) reported taking concomitant medications. In the pMMR population, the use of antidiarrheals, intestinal anti-inflammatory and/or anti-infective drugs, homeopathic preparations, and thyroid therapy was more than 10% higher in the pembrolizumab plus carboplatin-paclitaxel group than in the placebo plus carboplatin-paclitaxel group. The use of other concomitant medications was balanced between the treatment groups. In the dMMR population, the use of several types of concomitant medications was more than 10% higher in the pembrolizumab plus carboplatin-paclitaxel group than in the placebo plus carboplatin-paclitaxel group. These included antidiarrheals, intestinal anti-inflammatory and/or anti-infective drugs, drugs used in diabetes, mineral supplements, other alimentary tract and metabolism products, stomatological preparations, antianemic preparations, antibacterials for systemic use, antithrombotic drugs, drugs that act on the renin-angiotensin system, lipid-modifying drugs, and other dermatological preparations. For other medication categories, use was generally balanced between the 2 treatment groups.
Subsequent Treatments
At the data cut-off date of August 18, 2023 (EUR and/or SUR analysis), 48.1% of patients received subsequent systemic anticancer treatment; the percentage was higher in placebo plus carboplatin-paclitaxel group (60.3%) than in the pembrolizumab plus carboplatin-paclitaxel group (35.8%) (Table 14). The main contributors to the difference between groups were anti-PD-1 and/or PD-L1 and antiangiogenic therapies. As previously noted and as the sponsor indicated, because enrolment was predominantly in the US, where there is access to poststudy immune-oncology therapy, when the study was unblinded after positive PFS results at IA1, it was expected that a substantial number of participants in the placebo plus carboplatin-paclitaxel group would receive subsequent anti-PD-1 and/or PD-L1 therapies with or without lenvatinib. As such, among those in the placebo plus carboplatin-paclitaxel group, 42.8% and 29.9% received subsequent anti-PD-1 and/or PD-L1 and antiangiogenic therapies, respectively, which is higher than the 15.0% and 14.7%, respectively, in the pembrolizumab plus carboplatin-paclitaxel group. The most common subsequent anti-PD-1 and/or PD-L1 therapy was pembrolizumab (14.2% in the pembrolizumab plus carboplatin-paclitaxel group versus 40.1% in the placebo plus carboplatin-paclitaxel group), and the most commonly used subsequent antiangiogenic therapy was lenvatinib (9.3% versus 21.4%). This difference was less pronounced at IA1, particularly in the pMMR group.
Table 14: Summary of Subsequent Treatment From the NRG-GY018 Trial, All Comers (ITT Population, EUR and/or SUR Analysis)
Exposure | Pembrolizumab plus carboplatin-paclitaxel (N = 408) | Placebo plus carboplatin-paclitaxel (N = 411) |
|---|---|---|
Subsequent therapy, n (%) | 146 (35.8) | 248 (60.3) |
Anti-PD-1 and/or PD-L1, n (%) | 61 (15.0) | 176 (42.8) |
Antiangiogenic, n (%) | 60 (14.7) | 123 (29.9) |
Chemotherapy, n (%) | 64 (15.7) | 67 (16.3) |
Hormonal drugs, n (%) | 25 (6.1) | 36 (8.8) |
Procedures, other nontherapeutic products or drugs, n (%) | 3 (0.7) | 10 (2.4) |
Radiotherapy, n (%) | 28 (6.9) | 33 (8.0) |
Other investigational or approved drugs, n (%) | 20 (4.9) | 34 (8.3) |
EUR and/or SUR = efficacy update report and/or safety update report; ITT = intention to treat.
Source: Trial statistical report (efficacy update report).60
Efficacy
Only efficacy outcomes and analyses of subgroups identified as important to this review are reported. At the IA1 data cut-off, the median follow-up duration was 9.9 months in the pembrolizumab plus carboplatin-paclitaxel group and 10.1 months in the placebo plus carboplatin-paclitaxel group in the all-comers cohort. At the data cut-off date of August 18, 2023 (EUR and/or SUR analysis), the median follow-up duration was 16.7 months in the pembrolizumab plus carboplatin-paclitaxel group and 16.0 months in the placebo plus carboplatin-paclitaxel in the all-comers cohort.
Progression-Free Survival
Interim Analysis 1
The success criterion for the primary PFS hypothesis was met for both the pMMR (1-sided P < 0.001162) and dMMR (1-sided P < 0.002074) populations at IA1. The HR was 0.57 (95% CI, 0.44 to 0.74; 1-sided P < 0.001) in the pMMR population and 0.34 (95% CI, 0.22 to 0.53; 1-sided P < 0.001) in the dMMR population, both in favour of pembrolizumab plus carboplatin-paclitaxel. Results of sensitivity analyses generally supported those of the primary analyses. The results of the Merck Sharp & Dohme censoring rule 2 in the pMMR population, where treatment discontinuation and new anticancer treatment initiation were considered to be events, were directionally aligned with the primary analysis, but the magnitude of effect was smaller and not statistically significant, with an HR of 0.81 (95% CI, 0.65 to 1.01). Results of subgroup analyses in both populations were directionally aligned with the primary analysis.
In a post hoc analysis for this submission, the HR in the all-comers population was 0.49 (95% CI, 0.39 to 0.62; 1-sided P < 0.0001) in favour of pembrolizumab plus carboplatin-paclitaxel.
EUR and/or SUR analysis (all comers): A summary of results for PFS by investigator assessment is in Table 15. PFS events were reported for 199 patients (48.8%) in the pembrolizumab plus carboplatin-paclitaxel group and 257 patients (62.5%) in the placebo plus carboplatin-paclitaxel group. Median PFS was 16.8 months (95% CI, 13.1 to 19.8 months) in the pembrolizumab plus carboplatin-paclitaxel group versus 9.4 months (95% CI, 8.5 to 11.2 months) in the placebo plus carboplatin-paclitaxel group. The HR was 0.62 (95% CI, 0.51 to 0.75; 1-sided P < 0.0001), favouring pembrolizumab plus carboplatin-paclitaxel. The KM-estimated probability of being progression-free was 55.9% (95% CI, 50.7% to 60.8%) versus 38.5% (95% CI, 33.4% to 43.6%) at 12 months (RD = 17.4%; 95% CI, 10.2% to 24.6%) and 43.2% (95% CI, 37.4% to 48.8%) versus 24.9% (95% CI, 19.6% to 30.5%) at 24 months (RD = 18.3%; 95% CI, 10.4% to 26.2%) in the pembrolizumab plus carboplatin-paclitaxel and placebo plus carboplatin-paclitaxel groups, respectively. The results of the EUR and/or SUR analysis for PFS in the all-comers population were generally consistent with the results of IA1.
Table 15: Summary of Key Efficacy Results From the NRG-GY018 Trial (ITT Population, EUR and/or SUR Analysis)
Variable | Pembrolizumab plus carboplatin-paclitaxel (N = 408) | Placebo plus carboplatin-paclitaxel (N = 411) |
|---|---|---|
PFS | ||
Number of events (%) | 199 (48.8) | 257 (62.5) |
Death, n (%) | 31 (7.6) | 30 (7.3) |
Progression, n (%) | 168 (41.2) | 227 (55.2) |
PFS, months, median (95% CI)a | 16.8 (13.1 to 19.8) | 9.4 (8.5 to 11.2) |
HR (95% CI)b | 0.62 (0.51 to 0.75) | |
P valuec | < 0.0001 | |
PFS rate at month 6, % (95% CI) | 86.9 (83.2 to 89.9) | 78.5 (74.1 to 82.2) |
Risk difference, % (95% CI)d | 8.4 (3.1 to 13.7) | |
PFS rate at month 12, % (95% CI) | 55.9 (50.7 to 60.8) | 38.5 (33.4 to 43.6) |
Risk difference, % (95% CI)d | 17.4 (10.2 to 24.6) | |
PFS rate at month 18, % (95% CI) | 47.0 (41.5 to 52.4) | 29.5 (24.2 to 34.9) |
Risk difference, % (95% CI)d | 17.5 (9.9 to 25.1) | |
PFS rate at month 24, % (95% CI) | 43.2 (37.4 to 48.8) | 24.9 (19.6 to 30.5) |
Risk difference, % (95% CI)d | 18.3 (10.4 to 26.2) | |
PFS rate at month 30, % (95% CI) | 40.4 (33.6 to 47.0) | 22.0 (16.1 to 28.5) |
Risk difference, % (95% CI)d | 18.4 (9.3 to 27.5) | |
PFS rate at month 36, % (95% CI) | 38.1 (30.5 to 45.7) | 18.4 (10.9 to 27.4) |
Risk difference, % (95% CI)d | 19.7 (8.5 to 30.9) | |
OS | ||
Number of events (%) | 94 (23.0) | 119 (29.0) |
OS, months, median (95% CI)a | NR (NR to NR) | 32.2 (27.4 to 42.7) |
HR (95% CI)b | 0.74 (0.57 to 0.97) | |
P valuec | 0.0153 | |
OS rate at month 6, % (95% CI) | 95.2 (92.6 to 96.9) | 93.7 (90.8 to 95.7) |
Risk difference, % (95% CI)d | 1.5 (−1.8 to 4.8) | |
OS rate at month 12, % (95% CI) | 86.1 (82.1 to 89.2) | 82.5 (78.2 to 86.0) |
Risk difference, % (95% CI)d | 3.6 (−1.7 to 8.9) | |
OS rate at month 18, % (95% CI) | 75.8 (70.3 to 80.4) | 69.2 (63.4 to 74.2) |
Risk difference, % (95% CI)d | 6.6 (−0.8 to 14.0) | |
OS rate at month 24, % (95% CI) | 68.9 (62.4 to 74.5) | 62.3 (55.8 to 68.1) |
Risk difference, % (95% CI)d | 6.6 (−2.0 to 15.2) | |
OS rate at month 30, % (95% CI) | 59.8 (50.9 to 67.6) | 51.7 (42.1 to 60.4) |
Risk difference, % (95% CI)d | 8.1 (−4.3 to 20.5) | |
OS rate at month 36, % (95% CI) | 59.8 (50.9 to 67.6) | 45.9 (34.6 to 56.5) |
Risk difference, % (95% CI)d | 13.9 (0.1 to 27.7) | |
OS rate at month 42, % (95% CI) | 59.8 (50.9 to 67.6) | 36.7 (19.2 to 54.5) |
Risk difference, % (95% CI)d | 23.1 (3.6 to 42.6) | |
OS rate at month 48, % (95% CI) | NR (NR to NR) | NR (NR to NR) |
CI = confidence interval; EUR and/or SUR = efficacy update report and/or safety update report; HR = hazard ratio; ITT = intention to treat; NR = not reached; OS = overall survival; PFS = progression-free survival.
aFrom the product-limit (Kaplan-Meier) method for censored data.
bBased on the Cox regression model with Efron’s method of tie handling, with treatment as a covariate stratified by prior chemotherapy.
cOne-sided P value is based on the log-rank test stratified by prior chemotherapy. The analysis is not adjusted for multiple comparisons.
d95% CI is based on the pooled standard error from both treatment arms.
Source: Trial statistical report (efficacy update report).60
Point estimates of most subgroup analyses were aligned in direction with the overall population. Tests of treatment-by-subgroup interaction were significant at a 0.05 alpha level for prior chemotherapy, prior radiation therapy, disease status, and MMR status at baseline. The magnitude of benefit was smaller for patients with prior chemotherapy (versus no prior chemotherapy), prior radiation therapy (versus no prior radiation therapy), recurrent and/or persistent disease (versus primary disease), and pMMR status (versus dMMR status).
Figure 3: KM Plot of PFS (ITT Population, All Comers, EUR and/or SUR Analysis)
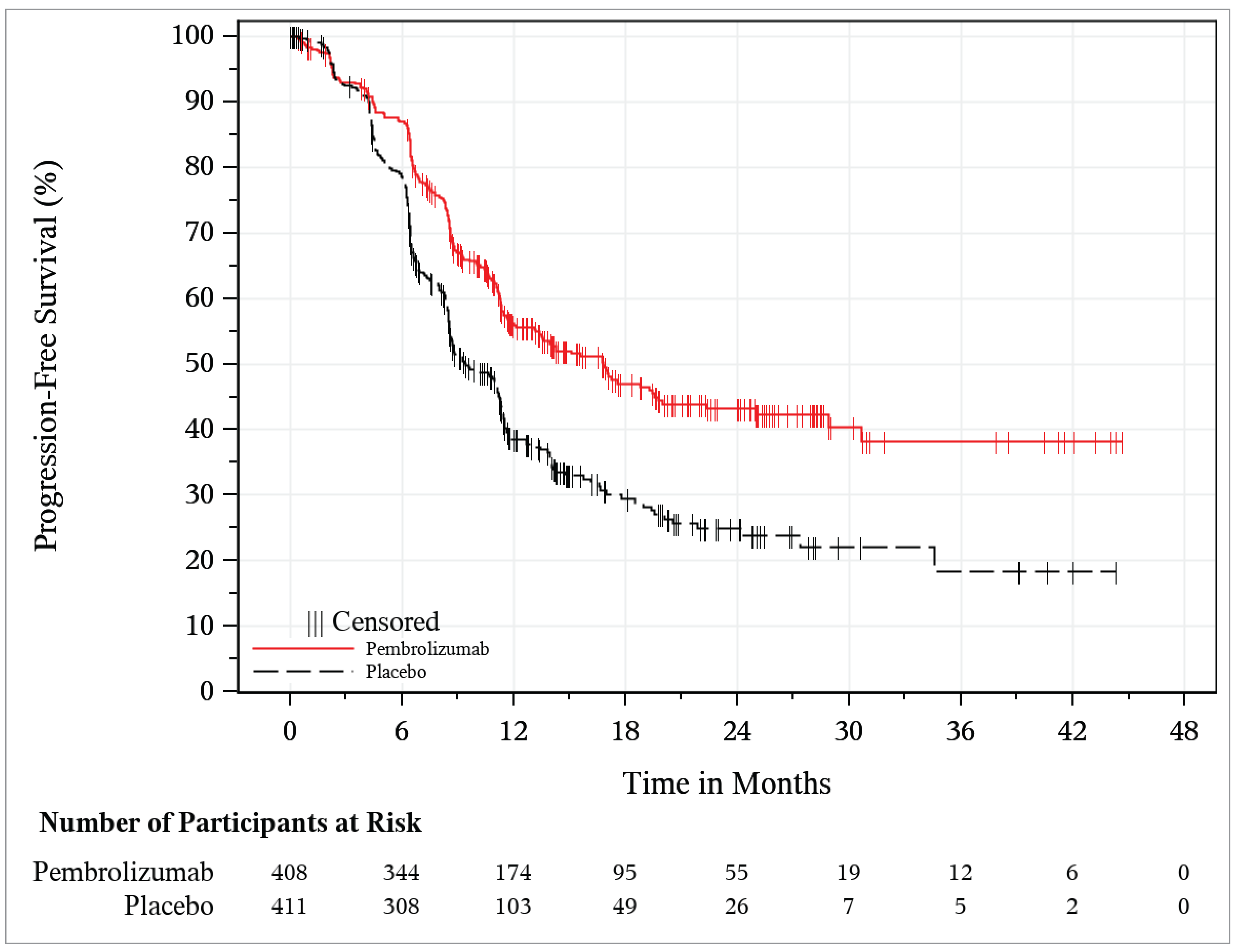
EUR and/or SUR = efficacy update report and/or safety update report; ITT = intention to treat; KM = Kaplan-Meier; PFS = progression-free survival.
Source: Trial statistical report (efficacy update report).60
EUR and/or SUR analysis (pMMR and dMMR cohorts): In the pMMR cohort, there were ███ PFS events observed (███ ██████ in the pembrolizumab plus carboplatin-paclitaxel group and ███ ███████ in the placebo plus carboplatin-paclitaxel group). Median PFS was ████ ████ ██ █ ████ ██ █████ months with pembrolizumab plus carboplatin-paclitaxel and ████ ████ ██ █ ███ ██ █████ months with placebo plus carboplatin-paclitaxel (Table 16). The HR was ████ ████ ██ █ ████ ██ █████ ████████████), favouring pembrolizumab plus carboplatin-paclitaxel. Results were directionally aligned with those at IA1, but the magnitude of benefit was smaller. The 12 month and 24 month investigator-assessed PFS probability (95% CI) was █████ ████ ██ █ ████ ██ █████ and █████ ████ ██ █ ████ ██ █████ (███ █████ ████ ███ ███ ██ █████), and ████ ████ ███ ████ ██ █████ and ████ ████ ██ █ ████ ██ █████ █████████ ████ ██ ███ ██ █████) in the pembrolizumab plus carboplatin-paclitaxel and placebo plus carboplatin-paclitaxel groups, respectively (Figure 3). Sensitivity analyses showed similar results to the primary analysis.
In the dMMR cohort, there were ███ PFS events observed (██ in the pembrolizumab plus carboplatin-paclitaxel group and ██ in the placebo plus carboplatin-paclitaxel group). Median PFS was ███ ███████ ████ ██ █ ████ ██████ ██ ███ ███████) with pembrolizumab plus carboplatin-paclitaxel and was ███ ████ ██ █ ███ ██ █████ months with placebo plus carboplatin-paclitaxel (Table 16). The HR was ████ ████ ██ █ ████ ██ █████ ████████████), favouring pembrolizumab plus carboplatin-paclitaxel. Results were aligned with those at IA1. The KM-estimated probability of being progression-free was █████ ████ ██ █ ████ ██ █████ versus ███ ████ ██ █ ████ ██ █████ █████████ ████ ███ ████ ██ ██████ at 12 months and ███ ████ ██ █ ████ ██ █████ versus █████ ████ ██ █ ████ ██ █████ ███ █ █████ ████ ███ ████ ██ ██████ at 24 months in the pembrolizumab plus carboplatin-paclitaxel and placebo plus carboplatin-paclitaxel groups, respectively (Figure 5). Sensitivity analyses showed similar results to the primary analysis.
Table 16: PFS Based on Investigator Assessment per RECIST 1.1 of the pMMR and dMMR Cohorts (ITT Population, EUR and/or SUR Analysis)
PFS groups | Pembrolizumab plus carboplatin-paclitaxel | Placebo plus carboplatin-paclitaxel |
|---|---|---|
pMMR population | ||
Sample size | ███ | ███ |
Number of events (%) | ███ ██████ | ███ ██████ |
Death, n (%) | ██ █████ | ██ ████ |
Progression, n (%) | ███ ██████ | ███ ██████ |
PFS, months, median (95% CI)a | ████ █████ ██ ██ | ████ ████ ██ ██ |
HR (95% CI)b | ████ █████ ██ █████ | |
P valuec | ██████ | |
PFS rate at month 6, % (95% CI) | ████ █████ ██ | ████ █████ ██ |
Risk difference, % (95% CI)d | ███ █████ ██ █████ | |
PFS rate at month 12, % (95% CI) | ████ █████ ██ ██ | ████ █████ ██ |
Risk difference, % (95% CI)d | ████ ████ ██ █████ | |
PFS rate at month 18, % (95% CI) | ████ █████ ██ | ████ █████ ██ |
Risk difference, % (95% CI)d | ████ ████ ██ █████ | |
PFS rate at month 24, % (95% CI) | ████ █████ ██ █ | ████ █████ ██ |
Risk difference, % (95% CI)d | ████ ████ ██ █████ | |
PFS rate at month 30, % (95% CI) | ████ █████ ██ █ | ████ █████ ██ |
Risk difference, % (95% CI)d | ████ █████ ██ █████ | |
PFS rate at month 36, % (95% CI) | ████ █████ ██ | ████ ████ ██ ██ |
Risk difference, % (95% CI)d | ████ ████ ██ █████ | |
dMMR population | ||
Sample size | ███ | ███ |
Number of events (%) | ██ ██████ | ██ ██████ |
Death, n (%) | █████ | █████ |
Progression, n (%) | ██ ██████ | ██ ██████ |
PFS, months, median (95% CI)a | ██ █████ ██ ███ | ███ ████ ██ ███ |
HR (95% CI)b | ████ █████ ██ █████ | |
P valuec | ███████ | |
PFS rate at month 6, % (95% CI) | ████ █████ ██ █ | ████ █████ ██ |
Risk difference, % (95% CI)d | ████ ████ ██ █████ | |
PFS rate at month 12, % (95% CI) | ████ █████ ██ | ████ █████ ██ |
Risk difference, % (95% CI)d | ████ █████ ██ █████ | |
PFS rate at month 18, % (95% CI) | ████ █████ ██ | ████ █████ ██ |
Risk difference, % (95% CI)d | ████ █████ ██ █████ | |
PFS rate at month 24, % (95% CI) | ████ █████ ██ | ████ █████ ██ |
Risk difference, % (95% CI)d | ████ █████ ██ █████ | |
PFS rate at month 30, % (95% CI) | ████ █████ ██ | ████ █████ █ |
Risk difference, % (95% CI)d | ████ █████ ██ █████ | |
PFS rate at month 36, % (95% CI) | ████ █████ ██ | ████ █████ ██ |
Risk difference, % (95% CI)d | ████ █████ ██ █████ | |
CI = confidence interval; dMMR = deficient mismatch repair; EUR and/or SUR = efficacy update report and/or safety update report; HR = hazard ratio; ITT = intention to treat; NR = not reached; PFS = progression-free survival; pMMR = proficient mismatch repair; RECIST 1.1 = Response Evaluation Criteria in Solid Tumours Version 1.1.
aFrom the product-limit (Kaplan-Meier) method for censored data.
bBased on the Cox regression model with Efron’s method of tie handling, with treatment as a covariate stratified by prior chemotherapy. Analyses are not adjusted for multiplicity, but statistical significance was previously reached in a multiplicity-adjusted analysis at IA1.
cOne-sided P value is based on the log-rank test stratified by prior chemotherapy.
d95% CI is based on the pooled standard error from both treatment arms.
Source: Trial statistical report (efficacy update report).60

Note: Figure 4 contained confidential information and was removed at the request of the sponsor.

Note: Figure 5 contained confidential information and was removed at the request of the sponsor.
Overall Survival
Interim Analysis 1
The information fraction was approximately 27% in the pMMR population and 18% in the dMMR population at IA1. The HR was 0.79 (95% CI, 0.53 to 1.17; 1-sided P = 0.1157) in the pMMR population and 0.55 (95% CI, 0.25 to 1.19; 1-sided P = 0.0617) in the dMMR population. Sensitivity analyses were generally consistent with the primary analyses. Results for the all-comers population were not reported. No data were provided by the sponsor for OS in the all-comers population at the IA1 analysis.
EUR and/or SUR Analysis: All Comers
A summary of OS findings is presented in Table 15. The number of patients who died was 94 (23.0%) in the pembrolizumab plus carboplatin-paclitaxel and 119 (29.0%) in the placebo plus carboplatin-paclitaxel group. Median OS was not reached in the pembrolizumab plus carboplatin-paclitaxel group and was 32.2 months (95% CI, 27.4 to 42.7 months) in the placebo plus carboplatin-paclitaxel group (Figure 6). The HR was 0.74 (95% CI, 0.57 to 0.97; 1-sided P = 0.0153), favouring pembrolizumab plus carboplatin-paclitaxel. The KM-estimated probability of OS was 75.8 (95% CI, 70.3 to 80.4) versus 69.2 (CI, 63.4 to 74.2) at 18 months (RD = 6.6%; 95% CI, −0.8% to 14.0%) and 59.8% (95% CI, 50.9% to 67.6%) versus 45.9% (95% CI, 34.6% to 56.5%) at 36 months (RD = 13.9%; 95% CI, 0.1% to 27.7%) in the pembrolizumab plus carboplatin-paclitaxel and placebo plus carboplatin-paclitaxel groups, respectively. The sponsor did not provide a sensitivity analysis for all comers in the EUR and/or SUR analysis.
Point estimates of most subgroup analyses were aligned in direction with the overall population. Tests of treatment-by-subgroup interaction were significant at a 0.05 alpha level for prior chemotherapy, prior radiation therapy, and measurable disease at baseline.
The magnitude of effect was smaller for patients who had received prior chemotherapy (versus no prior chemotherapy), prior radiation (versus no prior radiation therapy), and who had no measurable disease at baseline (versus measurable disease at baseline).
Figure 6: KM Plot of OS (ITT Population, All Comers, EUR and/or SUR Analysis)
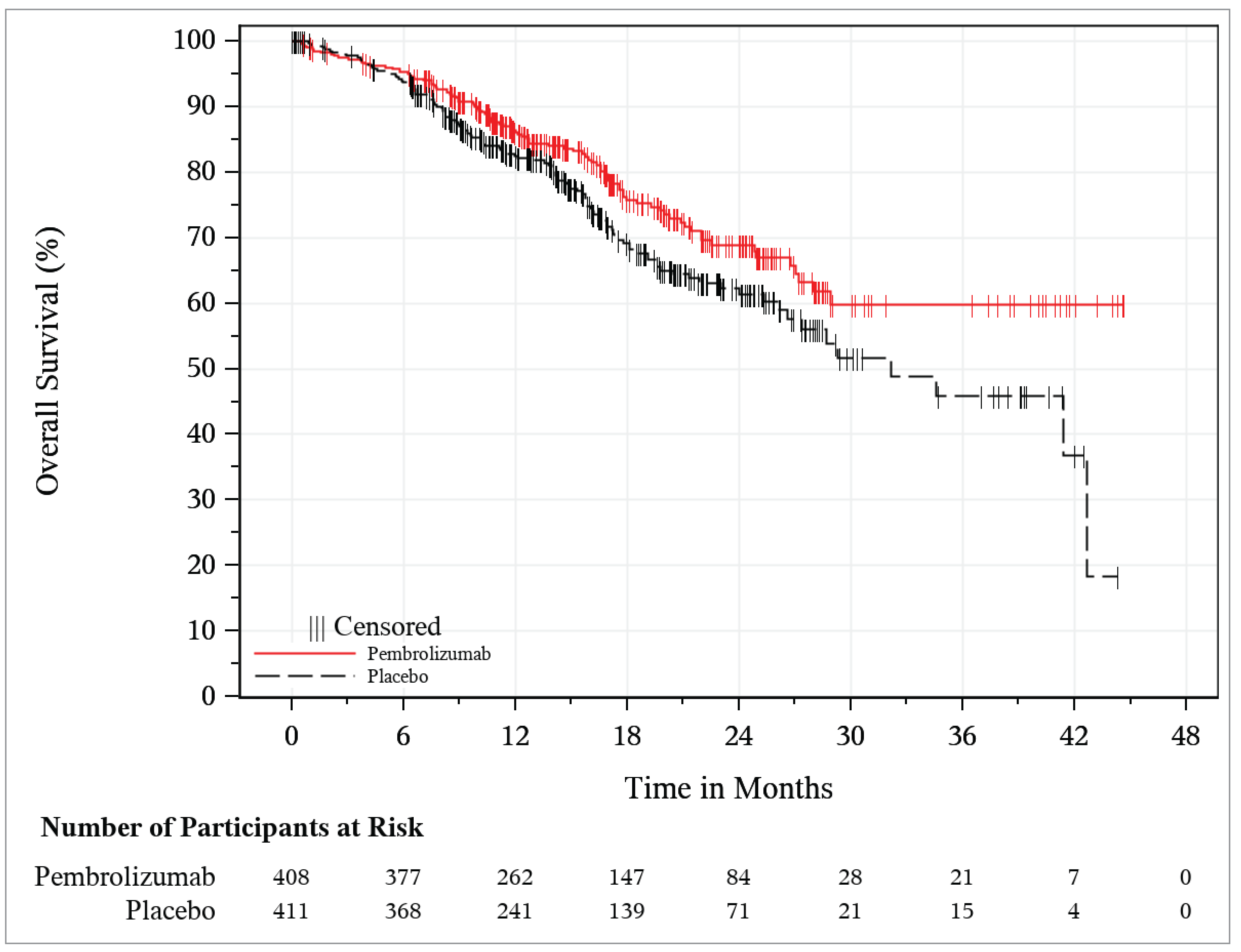
EUR and/or SUR = efficacy update report and/or safety update report; ITT = intention to treat; KM = Kaplan-Meier; OS = overall survival.
Source: Trial statistical report (efficacy update report).60
EUR and/or SUR Analysis: pMMR and dMMR Cohorts
At the time of the EUR and/or SUR analysis, the information fraction was approximately 46% in the pMMR population and 29% in the dMMR population. In the pMMR cohort, the number of patients who died was 77 (25.8%) in the pembrolizumab plus carboplatin-paclitaxel group and 92 (30.8%) in the placebo plus carboplatin-paclitaxel group. Median OS was 28.9 months (95% CI = 26.8 months to not reached) in the pembrolizumab plus carboplatin-paclitaxel group and 28.7 months (95% CI = 24.0 to 34.6 months) in the placebo plus carboplatin-paclitaxel group (Figure 7). The HR was 0.80 (95% CI = 0.59 to 1.08; 1-sided P = 0.0683). Results were consistent with those at IA1. The KM-estimated probability of OS was 72.9% (95% CI, 66.1% to 78.6%) versus 67.1% (95% CI, 59.9% to 73.2%) at 18 months (RD = 5.8%; 95% CI, −3.3 to 14.9) and 49.5% (95% CI, 37.9% to 60.1%) versus 35.3% (CI, 21.6% to 49.4%) at 36 months (RD = 14.2%; 95% CI, −3.6% to 32.0%) in the pembrolizumab plus carboplatin-paclitaxel and placebo plus carboplatin-paclitaxel groups, respectively. Sensitivity analyses showed similar results to the primary analysis.
In the dMMR cohort, the number of patients who died was 17 (15.5%) in the pembrolizumab plus carboplatin-paclitaxel group and 27 (24.1%) in the placebo plus carboplatin-paclitaxel group. Median OS was not reached in the pembrolizumab plus carboplatin-paclitaxel group and was 42.7 months (95% CI, 42.7 months to not reached) in the placebo plus carboplatin-paclitaxel group (Figure 8). The HR was 0.57 (95% CI, 0.31 to 1.04; 1-sided P = 0.0323). The KM-estimated probability of OS was 82.3% (95% CI, 72.4% to 88.9%) versus 73.9% (95% CI, 63.3% to 81.9%) at 18 months (RD = 8.4%; 95% CI, −4.0% to 20.8%) and 80.7% (95% CI, 70.3% to 87.7%) versus 70.9% (95% CI, 59.8% to 79.4%) at 36 months (RD = 9.8%; 95% CI, −3.3% to 22.9%) in the pembrolizumab plus carboplatin-paclitaxel and placebo plus carboplatin-paclitaxel groups, respectively. Sensitivity analyses showed similar results to the primary analysis.
Table 17: OS in the pMMR and dMMR Cohorts (ITT Population)
OS groups | Pembrolizumab plus carboplatin-paclitaxel (N = 298) | Placebo plus carboplatin-paclitaxel (N = 299) |
|---|---|---|
pMMR population | ||
Number of events (%) | 77 (25.8) | 92 (30.8) |
OS, months, median (95% CI)a | 28.9 (26.8 to NR) | 28.7 (24 to 34.6) |
HR (95% CI)b | 0.8 (0.59 to 1.08) | |
P valuec | 0.0683 | |
OS rate at month 6, % (95% CI) | 94.5 (91.2 to 96.6) | 93.4 (89.9 to 95.7) |
Risk difference, % (95% CI)d | 1.1 (−2.9 to 5.1) | |
OS rate at month 12, % (95% CI) | 83.8 (78.7 to 87.7) | 81.2 (75.9 to 85.4) |
Risk difference, % (95% CI)d | 2.6 (−3.9 to 9.1) | |
OS rate at month 18, % (95% CI) | 72.9 (66.1 to 78.6) | 67.1 (59.9 to 73.2) |
Risk difference, % (95% CI)d | 5.8 (−3.3 to 14.9) | |
OS rate at month 24, % (95% CI) | 63.0 (54.5 to 70.3) | 58.3 (50.1 to 65.6) |
Risk difference, % (95% CI)d | 4.7 (−6.4 to 15.8) | |
OS rate at month 30, % (95% CI) | 49.5 (37.9 to 60.1) | 44.2 (32.6 to 55.1) |
Risk difference, % (95% CI)d | 5.3 (−10.5 to 21.1) | |
OS rate at month 36, % (95% CI) | 49.5 (37.9 to 60.1) | 35.3 (21.6 to 49.4) |
Risk difference, % (95% CI)d | 14.2 (−3.6 to 32.0) | |
OS rate at month, 42% (95% CI) | 49.5 (37.9 to 60.1) | 17.7 (1.9 to 47.1) |
Risk difference, % (95% CI)d | 31.8 (6.6 to 57.0) | |
OS rate at month 48, % (95% CI) | NR (NR) | NR (NR) |
dMMR population | ||
Number of events (%) | 17 (15.5) | 27 (24.1) |
OS, months, median (95% CI)a | NR (NR) | 42.7 (42.7 to NR) |
HR (95% CI)b | 0.57 (0.31 to 1.04) | |
P valuec | 0.032 | |
OS rate at month 6, % (95% CI) | 97.3 (91.7 to 99.1) | 94.4 (88.0 to 97.4) |
Risk difference, % (95% CI)d | 2.9 (−3.1 to 8.9) | |
OS rate at month 12, % (95% CI) | 91.7 (84.6 to 95.6) | 85.7 (77.4 to 91.1) |
Risk difference, % (95% CI)d | 6.0 (−2.8 to 14.8) | |
OS rate at month 18, % (95% CI) | 82.3 (72.4 to 88.9) | 73.9 (63.3 to 81.9) |
Risk difference, % (95% CI)d | 8.4 (−4.0 to 20.8) | |
OS rate at month 24, % (95% CI) | 80.7 (70.3 to 87.7) | 70.9 (59.8 to 79.4) |
Risk difference, % (95% CI)d | 9.8 (−3.3 to 22.9) | |
OS rate at month 30, % (95% CI) | 80.7 (70.3 to 87.7) | 70.9 (59.8 to 79.4) |
Risk difference, % (95% CI)d | 9.8 (−3.3 to 22.9) | |
OS rate at month 36, % (95% CI) | 80.7 (70.3 to 87.7) | 70.9 (59.8 to 79.4) |
Risk difference, % (95% CI)d | 9.8 (−3.3 to 22.9) | |
OS rate at month 42, % (95% CI) | 80.7 (70.3 to 87.7) | 70.9 (59.8 to 79.4) |
Risk difference, % (95% CI)d | 9.8 (−3.3 to 22.9) | |
OS rate at month 48, % (95% CI) | NR (NR) | NR (NR) |
CI = confidence interval; dMMR = deficient mismatch repair; HR = hazard ratio; ITT = intention to treat; NR = not reached; OS = overall survival; pMMR = proficient mismatch repair.
aFrom the product-limit (Kaplan-Meier) method for censored data.
bBased on the Cox regression model with Efron’s method of tie handling, with treatment as a covariate stratified by prior chemotherapy.
cOne-sided P value is based on the log-rank test stratified by prior chemotherapy. Not adjusted for multiplicity.
dBased on the pooled standard error from both treatment arms.
Source: Trial statistical report (efficacy update report).60
HRQoL Assessed by FACT-En TOI (pMMR Population)
The sponsor did not report PROs from the FACT-En TOI in the updated (EUR and/or SUR) analysis. Therefore, this section is from IA1. The FACT-En TOI results for the pMMR population at IA1 are summarized in Table 18. Baseline scores for FACT-En TOI in the pMMR population were similar for both treatment groups. At week 18, both treatment groups had slight decreases (worsening) in FACT-En TOI scores. Directionally smaller decreases occurred in the placebo plus carboplatin-paclitaxel group than in the pembrolizumab plus carboplatin-paclitaxel group (LS mean change, −0.84 versus −4.01 points). The between-group difference in LS mean change from baseline was −3.17 points (95% CI, −5.48 to −0.85 points; P = 0.0075).
Figure 7: KM Plot of OS in the pMMR Cohort (ITT Population, EUR and/or SUR Analysis)

EUR and/or SUR = efficacy update report and/or safety update report; ITT = intention to treat; KM = Kaplan-Meier; OS = overall survival; pMMR = proficient mismatch repair.
Source: Trial statistical report (efficacy update report).60
Table 18: Summary of FACT-En TOI Results for the pMMR Population in the NRG-GY018 Trial (Interim Analysis 1)
FACT-En TOI results | Pembrolizumab plus carboplatin-paclitaxel (N = 268) | Placebo plus carboplatin-paclitaxel (N = 266) |
|---|---|---|
Baseline | ||
N with nonmissing assessmentsa | 252 | 253 |
Mean (SD) | 95.29 (16.51) | 94.34 (18.54) |
Week 18 | ||
N with nonmissing assessmentsa | 168 | 165 |
Mean (SD) | 89.98 (15.60) | 93.65 (16.22) |
Change from baseline to week 18b | ||
LS mean (95% CI)c | −4.01 (−5.65 to −2.36) | −0.84 (−2.47 to 0.78) |
Difference in LS mean (95% CI)c | −3.17 (−5.48 to −0.85) | |
P value | 0.0075 | |
CI = confidence interval; FACT-En TOI = Trial Outcome Index of the Functional Assessment of Cancer Therapy-Endometrial; LS = least squares; pMMR = proficient mismatch repair; SD = standard deviation.
Note: FACT-En TOI scores range from 0 to 100, with higher scores indicating better health status.
aFor baseline and week 18, N is the number of patients in each treatment group with nonmissing assessments at the specific time point;
bFor change from baseline, N is the number of patients in the analysis population in each treatment group.
cRepeated measures model based on the missing-at-random assumption. Model covariates included study treatment, age at enrolment in the study, pretreatment FACT-En TOI score, assessment time, and treatment-by-time interaction.
Source: NRG-GY018 Clinical Study Report.62
Figure 8: KM Plot of OS in the dMMR Cohort (ITT Population, EUR and/or SUR Analysis)
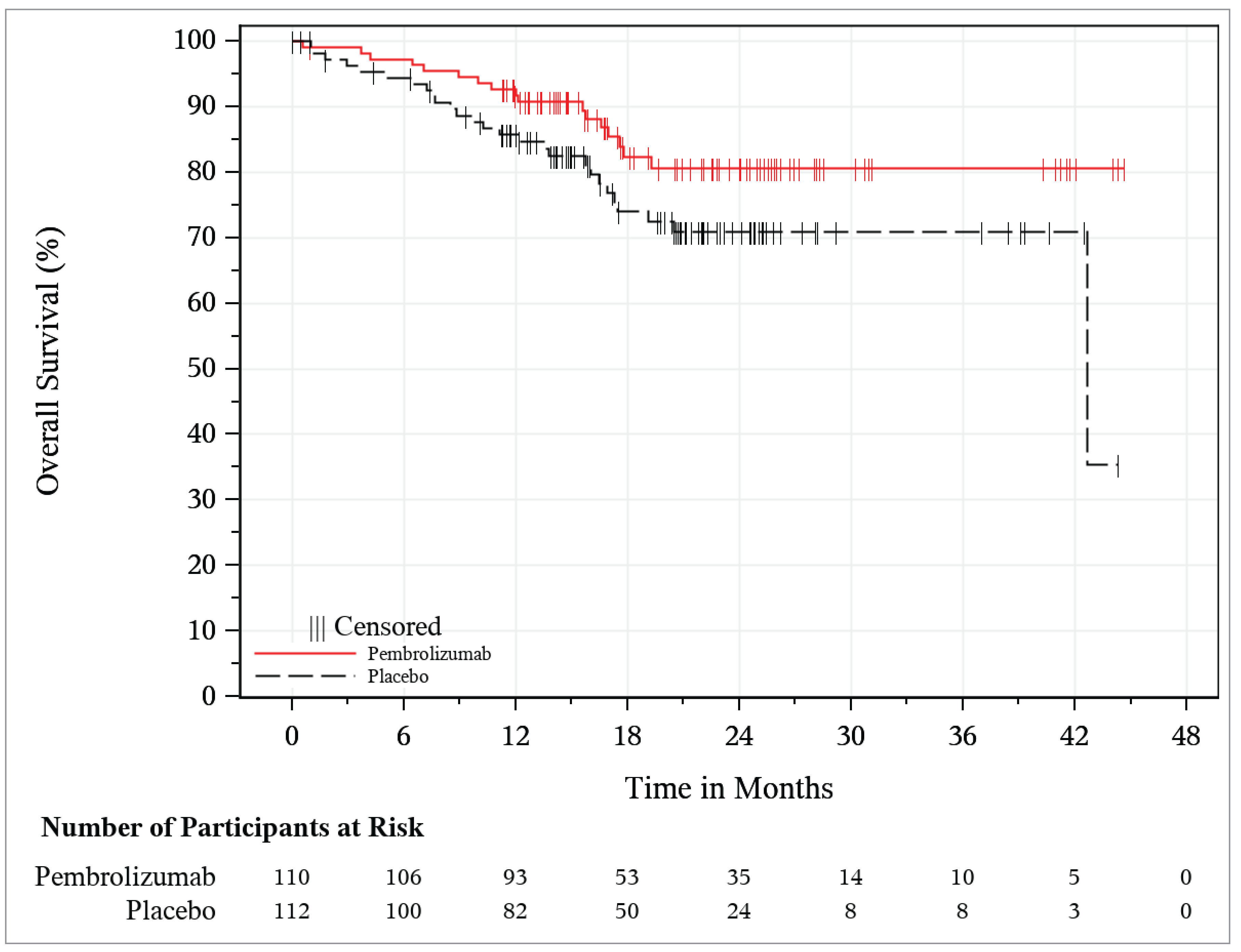
EUR and/or SUR = efficacy update report and/or safety update report; dMMR = deficient mismatch repair; ITT = intention to treat; KM = Kaplan-Meier; OS = overall survival.
Source: Trial statistical report (efficacy update report).60
Harms
Harms data reported in this section are from the SUR analysis for the all-comers population (data cut-off date: August 18, 2023).
The key harm results for the safety population are summarized in Table 19. Overall, frequencies of AEs, grade 3 or 4 AEs, and SAEs were similar in the dMMR and pMMR cohorts.
Adverse Events
Almost all patients experienced at least 1 AE (99.2% in the pembrolizumab plus carboplatin-paclitaxel arm and 99.7% in the placebo plus carboplatin-paclitaxel arm) (Table 19). The most frequent AEs in the pembrolizumab plus carboplatin-paclitaxel versus placebo plus carboplatin-paclitaxel groups were fatigue (70.3% versus 63.9%), anemia (59.8% versus 56.7%), alopecia (55% versus 57.5%), nausea (51.2% versus 45.9%), constipation (47.1% versus 41.8%), and diarrhea (42.2% versus 35.6%). Grade 3 or higher AEs were reported in 21.3% of patients in the pembrolizumab plus carboplatin-paclitaxel arm and in 18.5% of patients in the placebo plus carboplatin-paclitaxel arm. The most frequently reported grade 3 or higher AEs in the pembrolizumab plus carboplatin-paclitaxel and placebo plus carboplatin-paclitaxel arms were anemia (58.2%) and decreased neutrophil count (28.8%).
Serious Adverse Events
The sponsor reported that 237 patients experienced at least 1 SAE (39.6% in the pembrolizumab plus carboplatin-paclitaxel arm and 21.1% in the placebo plus carboplatin-paclitaxel arm) (Table 19). The most frequently reported SAEs in the pembrolizumab plus carboplatin-paclitaxel group and the placebo plus carboplatin-paclitaxel group were anemia (4.1% versus 4.1%), febrile neutropenia (2.8% versus 1.3%), urinary tract infection (2.6% versus 1.5%), dyspnea (2.3% versus 0.0%), hyperglycemia (2.3% versus 0.0%), pulmonary embolism (2.3% versus 2.1%), and sepsis (2.0% versus 1.3%).
The exposure-adjusted rate of SAEs remained similar between the 2 treatment groups (374 events per 100 patient-months in the pembrolizumab plus carboplatin-paclitaxel group versus 185 events per 100 patient-months in the placebo plus carboplatin-paclitaxel group). Individual SAEs reported with a higher incidence (more than a 2%-point difference) in the pembrolizumab plus carboplatin-paclitaxel group than in the placebo plus carboplatin-paclitaxel group were dyspnea and hyperglycemia (2.3% versus 0.0% for both).
Notable Harms
Notable harms were reported as immune-mediated events and infusion-related reactions. The infusion-related and immune-mediated reactions associated with the combination treatment of pembrolizumab plus carboplatin-paclitaxel are similar to the AEOSIs identified at IA1. AEOSIs were reported in 39.6% of patients in the pembrolizumab plus carboplatin-paclitaxel group and in 26.3% of patients in the placebo plus carboplatin-paclitaxel group.
Overall, grade 3 AEOSIs were reported in 9.7% of patients in the pembrolizumab plus carboplatin-paclitaxel group and in 4.1% of patients in the placebo plus carboplatin-paclitaxel group. The most frequently reported AEOSIs (with an incidence of more than 10%) in the pembrolizumab plus carboplatin-paclitaxel arm and the placebo plus carboplatin-paclitaxel arm were hypothyroidism (13.8% versus 3.9%) and infusion reactions (18.9% versus 18.6%). Most AEOSIs remained nonserious, of grade 1 or grade 2 in severity, and manageable with standard clinical practice, such as the administration of systemic corticosteroids and/or treatment interruption or discontinuation.
Withdrawals Due to AEs
AEs leading to discontinuation of the study treatment were reported in 71 of 391 patients (18.2%) in the pembrolizumab plus carboplatin-paclitaxel group and in 28 of 388 patients (7.2%) in the placebo plus carboplatin-paclitaxel group (Table 19).
Based on the NRG-GY018 trial protocol, the sponsor did not report which specific AEs led to treatment discontinuation.
Mortality
At the latest data cut-off date, death due to AEs was reported for 10 of 391 patients (2.6%) in the pembrolizumab plus carboplatin-paclitaxel group and 4 of 388 patients (1.0%) in the placebo plus carboplatin-paclitaxel group. Reasons for death due to AEs are detailed in Table 19.
Table 19: Summary of Harms Results From the NRG-GY018 Trial, All Comers (APaT Population, EUR and/or SUR Analysis)
Adverse events | Pembrolizumab plus carboplatin-paclitaxel (N = 391) | Placebo plus carboplatin-paclitaxel (N = 388) |
|---|---|---|
Any AE, n (%) | ||
Patients with ≥ 1 AE | 388 (99.2) | 387 (99.7) |
Most common AEs (≥ 10%) | ||
Blood and lymphatic system disorders | 258 (66.0) | 235 (60.6) |
Anemia | 234 (59.8) | 220 (56.7) |
Endocrine disorders | 79 (20.2) | 26 (6.7) |
Hypothyroidism | 54 (13.8) | 15 (3.9) |
Cardiac disorders | 60 (15.3) | 33 (8.5) |
Eye disorders | 76 (19.4) | 52 (13.4) |
Vision blurred | 45 (11.5) | 28 (7.2) |
Gastrointestinal disorders | 349 (89.3) | 325 (83.8) |
Abdominal pain | 68 (17.4) | 55 (14.2) |
Constipation | 184 (47.1) | 162 (41.8) |
Diarrhea | 165 (42.2) | 138 (35.6) |
Nausea | 200 (51.2) | 178 (45.9) |
Stomatitis | 42 (10.7) | 21 (5.4) |
Vomiting | 83 (21.2) | 50 (12.9) |
General disorders and administration-site conditions | 322 (82.4) | 287 (74.0) |
Fatigue | 275 (70.3) | 248 (63.9) |
Edema peripheral | 54 (13.8) | 44 (11.3) |
Infections and infestations | 188 (48.1) | 131 (33.8) |
COVID-19 | 41 (10.5) | 28 (7.2) |
Urinary tract infection | 60 (15.3) | 45 (11.6) |
Injury, poisoning, and procedural complications | 132 (33.8) | 89 (22.9) |
Fall | 44 (11.3) | 26 (6.7) |
Infusion-related reaction | 60 (15.3) | 56 (14.4) |
Investigations | 292 (74.7) | 265 (68.3) |
Increased alanine aminotransferase | 72 (18.4) | 39 (10.1) |
Increased aspartate aminotransferase | 61 (15.6) | 27 (7.0) |
Increased blood alkaline phosphatase | 60 (15.3) | 47 (12.1) |
Increased blood creatinine | 76 (19.4) | 36 (9.3) |
Decreased lymphocyte count | 94 (24.0) | 75 (19.3) |
Decreased neutrophil count | 111 (28.4) | 114 (29.4) |
Decreased platelet count | 131 (33.5) | 102 (26.3) |
Decreased weight | 41 (10.5) | 34 (8.8) |
Decreased white blood cell count | 137 (35.0) | 134 (34.5) |
Musculoskeletal and connective tissue disorders | 278 (71.1) | 259 (66.8) |
Arthralgia | 128 (32.7) | 140 (36.1) |
Back pain | 52 (13.3) | 49 (12.6) |
Muscular weakness | 40 (10.2) | 23 (5.9) |
Myalgia | 79 (20.2) | 70 (18.0) |
Pain in extremity | 64 (16.4) | 48 (12.4) |
Nervous system disorders | 344 (88.0) | 325 (83.8) |
Dizziness | 72 (18.4) | 62 (16.0) |
Peripheral neuropathy | 135 (34.5) | 116 (29.9) |
Peripheral sensory neuropathy | 146 (37.3) | 158 (40.7) |
Dysgeusia | 41 (10.5) | 43 (11.1) |
Headache | 73 (18.7) | 48 (12.4) |
Paresthesia | 40 (10.2) | 38 (9.8) |
Metabolism and nutrition disorders | 260 (66.5) | 240 (61.9) |
Decreased appetite | 88 (22.5) | 89 (22.9) |
Hyperglycemia | 93 (23.8) | 71 (18.3) |
Hypoalbuminemia | 56 (14.3) | 38 (9.8) |
Hypokalemia | 62 (15.9) | 76 (19.6) |
Hypomagnesemia | 82 (21.0) | 67 (17.3) |
Hyponatremia | 58 (14.8) | 36 (9.3) |
Psychiatric disorders | 101 (25.8) | 85 (21.9) |
Anxiety | 41 (10.5) | 31 (8.0) |
Insomnia | 53 (13.6) | 44 (11.3) |
Renal and urinary disorders | 107 (27.4) | 71 (18.3) |
Reproductive system and breast disorders | 67 (17.1) | 53 (13.7) |
Respiratory, thoracic, and mediastinal disorders | 188 (48.1) | 150 (38.7) |
Cough | 69 (17.6) | 55 (14.2) |
Dyspnea | 97 (24.8) | 72 (18.6) |
Skin and subcutaneous tissue disorders | 301 (77.0) | 260 (67.0) |
Alopecia | 215 (55.0) | 223 (57.5) |
Pruritus | 72 (18.4) | 46 (11.9) |
Rash | 63 (16.1) | 36 (9.3) |
Maculopapular rash | 56 (14.3) | 23 (5.9) |
Vascular disorders | 133 (34.0) | 119 (30.7) |
Hypertension | 62 (15.9) | 62 (16.0) |
SAEs, n (%) | ||
Patients with ≥ 1 SAEs | 155 (39.6) | 82 (21.1) |
Anemia | 16 (4.1) | 16 (4.1) |
Febrile neutropenia | 11 (2.8) | 5 (1.3) |
Urinary tract infection | 10 (2.6) | 6 (1.5) |
Dyspnea | 9 (2.3) | 0 (0.0) |
Hyperglycemia | 9 (2.3) | 0 (0.0) |
Pulmonary embolism | 9 (2.3) | 8 (2.1) |
Sepsis | 8 (2.0) | 5 (1.3) |
Decreased white blood cell count | 8 (2.0) | 4 (1.0) |
Patients who stopped treatment due to AEs, n (%) | ||
Patients who stopped treatment | 71 (18.2) | 28 (7.2) |
Deaths, n (%) | ||
Patients who died | 10 (2.6) | 4 (1.0) |
Cardiac arrest | 3 (0.8) | 0 (0.0) |
General disorders and administration-site conditions | 2 (0.5) | 0 (0.0) |
COVID-19 | 2 (0.5) | 0 (0.0) |
Sepsis | 1 (0.3) | 2 (0.5) |
Notable harms, n (%) | ||
With 1 or more AEs of special interest (immune-related AEs and infusion reactions) | 155 (39.6) | 102 (26.3) |
Hyperthyroidism | 32 (8.2) | 10 (2.6) |
Hypothyroidism | 54 (13.8) | 15 (3.9) |
Drug hypersensitivity | 9 (2.3) | 8 (2.1) |
Hypersensitivity | 9 (2.3) | 10 (2.6) |
Infusion reactions | 74 (18.9) | 72 (18.6) |
Drug hypersensitivity | 9 (2.3) | 8 (2.1) |
Hypersensitivity | 9 (2.3) | 10 (2.6) |
Infusion-related reaction | 60 (15.3) | 56 (14.4) |
AE = adverse event; APaT = all participants as treated; EUR and/or SUR = efficacy update report and/or safety update report; SAE = serious adverse event.
Source: Safety update report.61
Critical Appraisal
Internal Validity
NRG-GY018 is a randomized, double-blind, placebo-controlled, phase III trial. Randomization and allocation concealment procedures, including stratification by MMR tumour status, were appropriate and conducted by an interactive response system. In general, the key baseline characteristics of patients, including disease severity, appeared balanced between groups (for the all-comers population and both the pMMR and dMMR populations).
The NRG-GY018 trial was essentially 2 trials, with the sample size calculation and analysis conducted for the pMMR and dMMR populations separately. Sample size and power calculations were based on the primary outcome (PFS), and the trial was powered to detect significant differences for PFS in both the pMMR and dMMR groups. The primary success criterion for PFS was met in both the pMMR and dMMR groups at IA1. This analysis was preplanned with adequately justified stopping boundaries, which provides confidence that the statistical significance of PFS was not the result of type I error. The sponsor conducted a post hoc analysis (the EUR and/or SUR analysis) that combined the results of the pMMR and dMMR populations to align with the reimbursement request. The post hoc EUR and/or SUR analyses were not adjusted for multiplicity but produced PFS results similar to those in the protocol-defined IA1 analyses in the pMMR and dMMR populations. Sensitivity analyses supported the robustness of the PFS analyses.
The sponsor noted that participants, study personnel, and the investigator were blinded to the study treatment from the time of randomization until the database lock at IA1. There was a risk of unblinding among patients who experienced an AE that is likely to be related to the study drug (in the pembrolizumab plus carboplatin-paclitaxel group) during study treatment, particularly when monotherapy of pembrolizumab plus carboplatin-paclitaxel was not administered in either treatment group. However, there is no evidence of deviations from the intended interventions at IA1. Important protocol deviations at the EUR and/or SUR analysis were similar in the pembrolizumab plus carboplatin-paclitaxel group (2.4% in the pMMR cohort and 10.9% in the dMMR cohort) and the placebo plus carboplatin-paclitaxel group (3.4% in the pMMR cohort and 6.3% in the dMMR cohort). After positive PFS results at IA1, the study was unblinded and a substantial number of patients in the placebo plus carboplatin-paclitaxel group discontinued the protocol treatment so that they could receive anti-PD-1 and/or PD-L1 therapies (primarily pembrolizumab with or without lenvatinib) before progression. As a result, there is a risk of bias in the PFS results from the EUR and/or SUR analysis that is directed toward the null.
At the time of both the IA1 and EUR and/or SUR analyses, there was a small information fraction (i.e., proportion of expected events in the final analysis) for the analyses of OS. In the post hoc EUR and/or SUR analysis, a benefit in OS in the all-comers population was observed, although this analysis was unadjusted for multiplicity and at increased risk of type I error (false-positive results). The separate analyses of the pMMR and dMMR populations, per the trial design, did not reach statistical significance at IA1 or the post hoc EUR and/or SUR analysis. The aforementioned substantial use of anti-PD-1 and/or PD-L1 therapies (including before progression) in the placebo plus carboplatin-paclitaxel group following unblinding after IA1 introduces a bias that is directed toward the null. Although post hoc sensitivity analyses were undertaken in each population in an attempt to adjust for the effect of subsequent treatments, reliance on these results is compromised because their validity hinges on strong unverifiable assumptions.73
The double-blind nature of the trial up to IA1 mitigated any potential concern about bias in the measurement of the outcomes. Additionally, at that time point, a sensitivity analysis conducted by blinded independent central review (as opposed to investigator assessment) aligned with the primary analyses for PFS. Because the study became unblinded after IA1, the possibility for bias in the measurement of PFS after that time point may be increased, although consistency in the results across time points is reassuring. OS is an objective outcome, and HRQoL was measured only at IA1 (before unblinding), so would be unaffected. Safety results may have been affected by the unblinding and subsequent treatments.
Point estimates of subgroup analyses for PFS and OS in the all-comers population were generally aligned with results in the primary analysis of the overall population, but differences at the P < 0.05 level were identified for some subgroups. In PFS analyses, the magnitude of benefit was smaller for patients who had received prior chemotherapy (versus no prior chemotherapy), prior radiation therapy (versus no prior radiation therapy), recurrent and/or persistent disease (versus primary disease), and pMMR status (versus dMMR status). In OS analyses, the magnitude of effect was smaller for patients who had received prior chemotherapy (versus no prior chemotherapy), prior radiation (versus no prior radiation), and who had no measurable disease at baseline (versus measurable disease at baseline).
Tests for subgroup differences were not preplanned, and the trial was not designed to detect these differences. It is not clear how unblinding after IA1 affected the subgroup findings, and some subgroups (patients with prior chemotherapy, patients with no measurable disease) were relatively small. Therefore, it is not possible to draw a credible conclusion about effect modification.
Disease-related HRQoL was measured in the NRG-GY018 study using the FACT-En TOI questionnaire, which has been validated in patients with EC and has evidence of reliability and MID ranges.64,66 Based on the MID ranges identified in the literature, the sponsor suggested a 6-point change from baseline score as a clinically meaningful change, which was considered reasonable by the review team. The sponsor reported results of the FACT-En TOI for the pMMR population only based on the IA1 data. Additionally, results of the HRQoL outcome were subject to risk of bias due to missing data (33% in the pembrolizumab plus carboplatin-paclitaxel group and 34% in the placebo plus carboplatin-paclitaxel group). A missing-at-random mechanism was assumed, but there is no evidence to support the validity of this assumption. The direction and extent of bias is unclear because no sensitivity analyses that applied alternative imputation methods were used to assess the impact of missing data.
External Validity
The clinicians consulted by CDA-AMC indicated that the population included in the NRG-GY018 trial reflects patients with advanced or recurrent EC commonly seen in clinical practice in Canada. The proportion of patients with an ECOG PS of 2 was lower in the NRG-GY018 trial than in their own clinical practice, they noted.
The clinicians also noted that the timing of the administration of pembrolizumab or placebo plus carboplatin-paclitaxel aligns with the chemotherapy regimens currently used in practice in Canada. In the NRG-GY018 trial, the number of combination therapy cycles was adjusted from every 3 weeks to every 6 weeks, and the dose of pembrolizumab was increased from 200 mg to 400 mg, which reflects the current practice of the clinicians consulted by CDA-AMC. The clinicians noted that the changes in the number of cycles and the pembrolizumab dose are unlikely to affect the efficacy of the interventions before and after these adjustments, based on their experience and data from other trials of similar treatments for other cancers.
In the NRG-GY018 trial, the comparator to pembrolizumab plus carboplatin-paclitaxel was placebo plus carboplatin-paclitaxel, followed by pembrolizumab or placebo as monotherapy. According to the clinicians consulted by CDA-AMC, platinum-based chemotherapy (carboplatin and paclitaxel) aligns with current practice in Canada for patients with advanced-stage or recurrent EC.
Concomitant medications were permitted during NRG-GY018 trial, including systemic glucocorticoids and antibiotics for the management of AEs. Although the use of systemic glucocorticoids and antibiotics is aligned with clinical practice in Canada, the clinical experts indicated that using these 2 concomitant medications could be associated with poor outcomes in the pembrolizumab plus carboplatin-paclitaxel group.
Key outcomes for clinical decision-making included PFS and OS, as indicated by the clinicians consulted by CDA-AMC, and both were assessed in NRG-GY018 trial. The clinical experts consulted by CDA-AMC agreed on the value of PFS at 12 months to evaluate effects on disease progression that tend to occur early in treatment, and at 24 months to assess sustained treatment effects, with added value for the assessment of treatment response among trial participants lacking measurable disease. The clinical experts noted that FACT-En TOI is reasonable for evaluating HRQoL and assessing QoL, it is not routinely used in day-to-day practice. Given that results were provided only for the pMMR population, it is not possible to generalize the effects of the intervention on HRQoL to all comers or to the dMMR group.
The magnitude of benefit on PFS was smaller for patients who had received prior chemotherapy (versus no prior chemotherapy), prior radiation therapy (versus no prior radiation therapy), recurrent and/or persistent disease (versus primary disease), and pMMR status (versus dMMR status). Subgroup analyses raised uncertainty about the generalizability of beneficial effects on OS for patients who had received prior chemotherapy, prior radiation therapy, and who had no measurable disease at baseline. Given the small number of patients with an ECOG PS of 2, generalizability to these patients is uncertain. Patients with carcinosarcomas were not eligible for inclusion in the trial, so it is not possible to generalize the findings to that group.
GRADE Summary of Findings and Certainty of the Evidence
Methods for Assessing the Certainty of the Evidence
For the pivotal studies and RCTs identified in the sponsor’s systematic review, GRADE was used to assess the certainty of the evidence for outcomes considered most relevant to expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group.74,75
High certainty: We are very confident that the true effect lies close to that of the estimate of the effect.
Moderate certainty: We are moderately confident in the effect estimate. The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. We use the word likely for evidence of moderate certainty (e.g., X intervention likely results in Y outcome).
Low certainty: Our confidence in the effect estimate is limited. The true effect may be substantially different from the estimate of the effect. We use the word may for evidence of low certainty (e.g., X intervention may result in Y outcome).
Very low certainty: We have very little confidence in the effect estimate. The true effect is likely to be substantially different from the estimate of effect. We describe evidence of very low certainty as very uncertain.
When possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect; if this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., the clinical importance is unclear). In all cases, the target of the certainty of evidence assessment was based on the point estimate and where it was located relative to the threshold for a clinically important effect (when a threshold was available) or to the null.
The selection of outcomes for GRADE was based on the sponsor’s Summary of Clinical Evidence, consultation with clinical experts, and input received from patient and clinician groups and public drug plans. The following list of outcomes was finalized in consultation with expert committee members:
PFS
OS
FACT-En TOI
immune-mediated and injection-related adverse reactions.
In all cases, the target of the certainty of evidence assessment was based on the point estimate and where it was located relative to the threshold for a clinically important effect (when a threshold was available) or to the null. The target of the certainty of evidence assessment was the presence or absence of a clinically important effect for the probability of survival (OS and PFS) and harms (immune-related AEs, and infusion-related reactions), based on a threshold informed by the clinical experts consulted by CAD-AMC for this review. The target of the certainty of evidence assessment was the presence or absence of a clinically important effect for HRQoL (FACT-En TOI), based on an MID threshold identified in the literature.
Results of GRADE
Table 2 presents the GRADE summary of findings for pembrolizumab plus carboplatin-paclitaxel for the treatment of adult patients with primary advanced or recurrent EC and then continued as monotherapy.
Long-Term Extension Studies
Contents within this section have been informed by materials submitted by the sponsor. The following has been summarized and validated by the review team.
No long-term extension studies were submitted in the systematic review evidence.
Indirect Evidence
Contents within this section have been informed by materials submitted by the sponsor. The following has been summarized and validated by the review team.
Objectives for the Summary of Indirect Evidence
Because of a lack of studies directly comparing pembrolizumab with any other systemic treatments beyond paclitaxel in combination with carboplatin for patients with advanced or recurrent dMMR EC, indirect evidence was considered.
Description of Indirect Comparison
One sponsor-conducted anchored ITC is included in this review to compare pembrolizumab in combination with chemotherapy (paclitaxel and carboplatin) versus dostarlimab plus chemotherapy (paclitaxel and carboplatin) for the outcome of PFS in patients with advanced or recurrent dMMR EC. It should be noted that the results of the ITC only apply to dMMR EC.
Table 20: Study Selection Criteria and Methods for ITCs Submitted by the Sponsor
Characteristics | Indirect comparison |
|---|---|
Population | Stage III, stage IV, or recurrent dMMR EC |
Intervention | Pembrolizumab: IV 200 mg every 3 weeks for 6 cycles, followed by 400 mg of pembrolizumab maintenance therapy administered every 6 weeks, plus carboplatin and paclitaxel |
Comparator | Dostarlimab: 500 mg every 3 weeks for 6 cycles, followed by 1,000 mg of dostarlimab maintenance therapy and carboplatin plus paclitaxel |
Outcome | PFS |
Study designs | RCTs |
Publication characteristics | Journal articles Conference presentations Conference abstracts Trial statistical reports |
Exclusion criteria | No population of interest reported No outcome of interest reported Noninterventional studies |
Databases searched | Embase, MEDLINE, Cochrane |
Selection process | Articles were screened independently by 2 reviewers, with a third reviewer to resolve discrepancies |
Data extraction process | Data were extracted independently by 2 reviewers, with a third reviewer to resolve discrepancies |
Quality assessment | Study quality was assessed independently by 2 reviewers, with a third investigator included to reach consensus for any remaining discrepancies; the Cochrane risk-of-bias tool for randomized trials, version 2, was used for RCTs |
dMMR = deficient mismatch repair; EC = endometrial cancer; ITC = indirect treatment comparison; PFS = progression-free survival; RCT = randomized controlled trial.
Source: Sponsor-submitted ITC technical report.76
ITC Design
Objectives
The primary objective of the sponsor-submitted ITC was to compare PFS between pembrolizumab plus carboplatin-paclitaxel and dostarlimab plus carboplatin-paclitaxel in patients with advanced or recurrent dMMR EC.
Study Selection Methods
An SLR was conducted with a broader scope to identify relevant RCTs that evaluated the efficacy and safety of systemic treatments for patients with advanced or recurrent dMMR EC. The objective of the SLR was to search for studies that compared the treatment effect of pembrolizumab plus carboplatin-paclitaxel with alternative treatments used in Canada. The selection criteria for the SLR are described in Table 20. The search criteria did not include dates. It was not stated whether studies that included treatments other than dostarlimab or outcomes other than PFS were considered. All abstracts, proceedings, and full-text studies were screened independently by 2 reviewers; a third reviewer helped resolve disagreements. Reasons for exclusion were not documented. Data extraction and risk of bias appraisal (using the Cochrane risk-of-bias tool for RCTs, version 2) were performed by 2 independent reviewers; a third reviewer helped resolve disagreements.
ITC Analysis Methods
Two trials for the treatment of advanced or recurrent dMMR EC met the inclusion criteria for the SLR: the NRG-GY018 trial for pembrolizumab plus carboplatin-paclitaxel; and the RUBY-I trial for dostarlimab plus carboplatin-paclitaxel. The sponsor performed an MAIC. A summary of the analysis methods for the MAIC is shown in Table 21. An anchored MAIC approach was selected for the indirect comparison of advanced or recurrent dMMR EC between pembrolizumab plus carboplatin-paclitaxel and dostarlimab plus carboplatin-paclitaxel. The rationale for choosing an anchored MAIC over a network meta-analysis was not provided. Covariates used for matched adjustment chosen as potential effect modifiers were identified through targeted literature searches based on baseline characteristics from the RUBY-I trial, discussions with clinical experts, and reviews of the PFS forest plots reported for each trial. However, justification for the inclusion of these covariates or exclusion of others was not provided. Adaptations were applied to covariates to account for the limitations of the data (e.g., regrouping of race categories for 18 patients in the NRG-GY018 trial who had missing race information; these patients were grouped into the other category, excluding 7 patients with an ECOG PS of 2). Individual patient data from the NRG-GY018 trial were then weighted to match baseline characteristics in the comparator trial (RUBY-I) using weights estimated with the method of moments, described in Signorovitch et al.77 Weights were examined for extreme values, although a description of the weights was not provided. The effective sample size was calculated as the square of the summed weights divided by the sum of the squared weights. The covariate characteristics of patients before and after weighting in the NRG-GY018 trial were presented. A weighted Cox proportional hazards model with the MAIC weights applied was used to produce the results for the outcome of PFS. No sensitivity or subgroup analyses were performed.
Table 21: ITC Analysis Methods
Methods | Description |
|---|---|
ITC methods | Anchored matching-adjusted indirect comparison |
Covariates used for match adjustment |
|
Outcomes | Progression-free survival |
Sensitivity analyses | Not performed |
Subgroup analysis | Not performed |
ECOG PS = Eastern Cooperative Oncology Group Performance Status; ITC = indirect treatment comparison.
Source: Sponsor-submitted ITC technical report.76
Results of the MAIC
Summary of Included Studies
The number of citations that were screened by title and abstract, the number of citations reviewed by full-text screening, and the number of studies that met the selection criteria were not described. One published study (RUBY-I) was selected by the sponsor as the comparator study for the MAIC.78
The characteristics from the NRG-GY018 and RUBY-I trials are summarized in Table 22. The risk of bias (per the Cochrane risk-of-bias tool for randomized trials version 2) was described as low for all 6 domains.
Results
Patient characteristics from the ITT population of the NRG-GY018 trial (unadjusted and match-adjusted) and the RUBY-I trial are presented in Table 23. Both trials included an overall population with dMMR MSI-H and pMMR EC; however, the data included in the MAIC were limited to the dMMR MSI-H population. The sample size, power calculations, and statistical analyses were planned separately for the pMMR and dMMR groups for both trials. The NRG-GY018 trial was 2 trials within a trial: 1 for patients with dMMR EC and 1 for patients with pMMR EC. The primary analysis for the RUBY-I trial was conducted in the dMMR population.78 There were 222 patients (110 in the pembrolizumab plus carboplatin-paclitaxel arm and 112 in the placebo plus carboplatin-paclitaxel arm) with dMMR EC in the NRG-GY018 trial. However, because 7 patients with an ECOG PS of 2 were excluded from the MAIC analysis, 215 patients were analyzed (109 in the pembrolizumab plus chemotherapy arm and 106 in the placebo plus chemotherapy arm). There were 118 patients (53 in the dostarlimab plus carboplatin-paclitaxel arm and 106 in the placebo plus carboplatin-paclitaxel arm) with dMMR EC in the RUBY-I trial. The effective sample size for pembrolizumab plus carboplatin-paclitaxel after match adjustment was 156.14, which represented 72.6% of the original sample size from the NRG-GY018 trial.
Table 22: Summary of Included Studies in the MAIC
Study details | NRG-GY018 (index trial) | RUBY-I (comparator trial) |
|---|---|---|
Study design | Phase III, multicentre, double-blind, placebo-controlled RCT | Phase III, multicentre, double-blind, placebo-controlled RCT |
Sample size | 816 total 215 dMMR | 494 total 118 dMMR |
Population | Measurable stage III or stage IVA EC, or stage IVB or recurrent EC dMMR MSI-H
| Primary advanced-stage III or stage IV EC or first recurrent EC dMMR MSI-H
|
Intervention | Pembrolizumab 200 mg IV + paclitaxel 175 mg/m2 + carboplatin AUC 5 mg/mL per min every 3 weeks for 6 cycles (combination phase), followed by pembrolizumab 400 mg IV monotherapy (maintenance phase) every 6 weeks for up to 20 cycles | Dostarlimab 500 mg + paclitaxel 175 mg/m2 + + carboplatin AUC 5 mg/mL per min every 3 weeks for 6 cycles, followed by dostarlimab 1,000 mg IV every 6 weeks for up to 3 years |
Comparison | Placebo + paclitaxel 175 mg/m2 + carboplatin AUC 5 mg/mL per min every 3 weeks for 6 cycles (combination phase), followed by placebo monotherapy (maintenance phase) every 6 weeks | Placebo + paclitaxel 175 mg/m2 + carboplatin AUC 5 mg/mL per min every 3 weeks for 6 cycles, followed by placebo IV every 6 weeks for up to 3 years |
Outcome of interest (PFS) | Time from randomization to the first documented PD per RECIST 1.1 by investigator, or death from any cause, whichever occurs first | Time from randomization to the first documented PD per RECIST 1.1 by investigator, or death from any cause, whichever occurs first |
Median follow-up | 19.2 monthsa (actual follow-up) and 22.5 monthsb (theoretical follow-up); data cut-off date of August 18, 2023 | 24.8 months; data cut-off date |
AUC = area under the curve; dMMR = deficient mismatch repair; EC = endometrial cancer; ECOG PS = Eastern Cooperative Oncology Group Performance Status; MAIC = matching-adjusted indirect comparison; MSI-H = microsatellite instability-high; PD = progressive disease; PFS = progression-free survival; RCT = randomized controlled trial; RECIST 1.1 = Response Evaluation Criteria in Solid Tumours Version 1.1.
aCalculated from the date of randomization until the date of death or database cut-off date for patients without documented death at the time of database cut-off date.
bCalculated from the date of randomization until the database cut-off date for all patients. This represents the length of the trial.
Source Sponsor-submitted ITC technical report.76
Table 23: Summary of Model Covariates in the MAIC
Characteristic | Pembrolizumab | Dostarlimab | |
|---|---|---|---|
NRG-GY018 (unadjusted) | NRG-GY018 (match-adjusted) | RUBY-I | |
N (or ESS) | N = 215 | ESS = 156.14 | N = 118 |
Median age, years | 66.0 | 64.0 | 64.0 |
White (%) | 79.1 | 84.7 | 84.7 |
ECOG PS 0 (%)a | 65.1 | 57.3 | 57.0 |
Endometrioid histology (%) | 81.4 | 84.7 | 84.7 |
Recurrent disease (%) | 61.4 | 50.0 | 50.0 |
No prior radiotherapy (%) | 57.2 | 82.2 | 82.2 |
ECOG PS = Eastern Cooperative Oncology Group Performance Status; ESS = effective sample size; MAIC = matching-adjusted indirect comparison.
aPatients with an ECOG PS of 2 at baseline were excluded from the NRG-GY018 trial.
Source: Sponsor-submitted ITC technical report.76
The MAIC of PFS between pembrolizumab plus carboplatin-paclitaxel and dostarlimab plus carboplatin-paclitaxel for advanced or recurrent dMMR EC is summarized in Table 24. The KM curves for PFS from the MAIC analysis are shown in Figure 9.
There was insufficient evidence to show a difference between pembrolizumab plus carboplatin-paclitaxel and dostarlimab plus carboplatin-paclitaxel in PFS events based on the MAIC analysis (HR, 1.00; 95% CI, 0.48 to 2.08) for advanced or recurrent dMMR EC. The 95% CI included the possibility that either treatment regimen could be favoured.
Some of the statistical tests of proportional hazards suggest deviations from the proportional hazards assumptions used for the NRG-GY018 trial after matching, the RUBY-I trial data, and the NRG-GY018 trial data versus the RUBY-I trial data both before and after matching. In particular, the Grambsch and Therneau test (P value = 0.0275) and the time-dependent variable test (P value = 0.0023) for pembrolizumab plus carboplatin-paclitaxel versus dostarlimab plus carboplatin-paclitaxel after matching had P values less than 0.05.
Table 24: PFS Results in the MAIC for PFS for Advanced or Recurrent dMMR and/or MSI-H EC
Event | Pembrolizumab | Dostarlimab | |
|---|---|---|---|
NRG-GY018 (unadjusted) | NRG-GY018 (match-adjusted) | RUBY-I | |
Na (or ESS) | 109 | 93.8 | 53 |
PFS event, n (%) | 36 (33.0) | 29.1 (31.1) | 19 (35.8) |
PFS, months, median (95% CI) | NR (30.65 to NR) | NR (30.65 to NR) | NR (11.74 to NR) |
Hazard ratio (95% CI) versus dostarlimab | 1.05 (0.53 to 2.07) | 1.00 (0.48 to 2.08) | Reference |
CI = confidence interval; dMMR = deficient mismatch repair; EC = endometrial cancer; ESS = effective sample size; MAIC = matching-adjusted indirect comparison; MSI-H = microsatellite instability-high; NR = not reached; PFS = progression-free survival.
aIntention-to-treat population of patients who received active treatment in each trial.
bFrom the product-limit (Kaplan-Meier) method.
Source: Sponsor-submitted ITC technical report.76
Critical Appraisal of the Sponsor-Submitted MAIC
The MAIC was conducted based on studies identified by an SLR. However, there was no a priori protocol described for the SLR, so it is unclear if the sponsor adhered to predefined objectives, eligibility criteria, or methods. It appears that the selection process was refined to select studies that align with the MAIC study objectives; however, there is potential for selection bias because the criteria for selecting the comparator trial were not described a priori. The search did not include clinical trial registries or a supplementary manual search. The study selection and data extraction process were appropriate, as they involved at least 2 independent reviewers. The sponsor has not reported a list of excluded studies with justification for the exclusions.
Figure 9: KM Plot of PFS From the MAIC
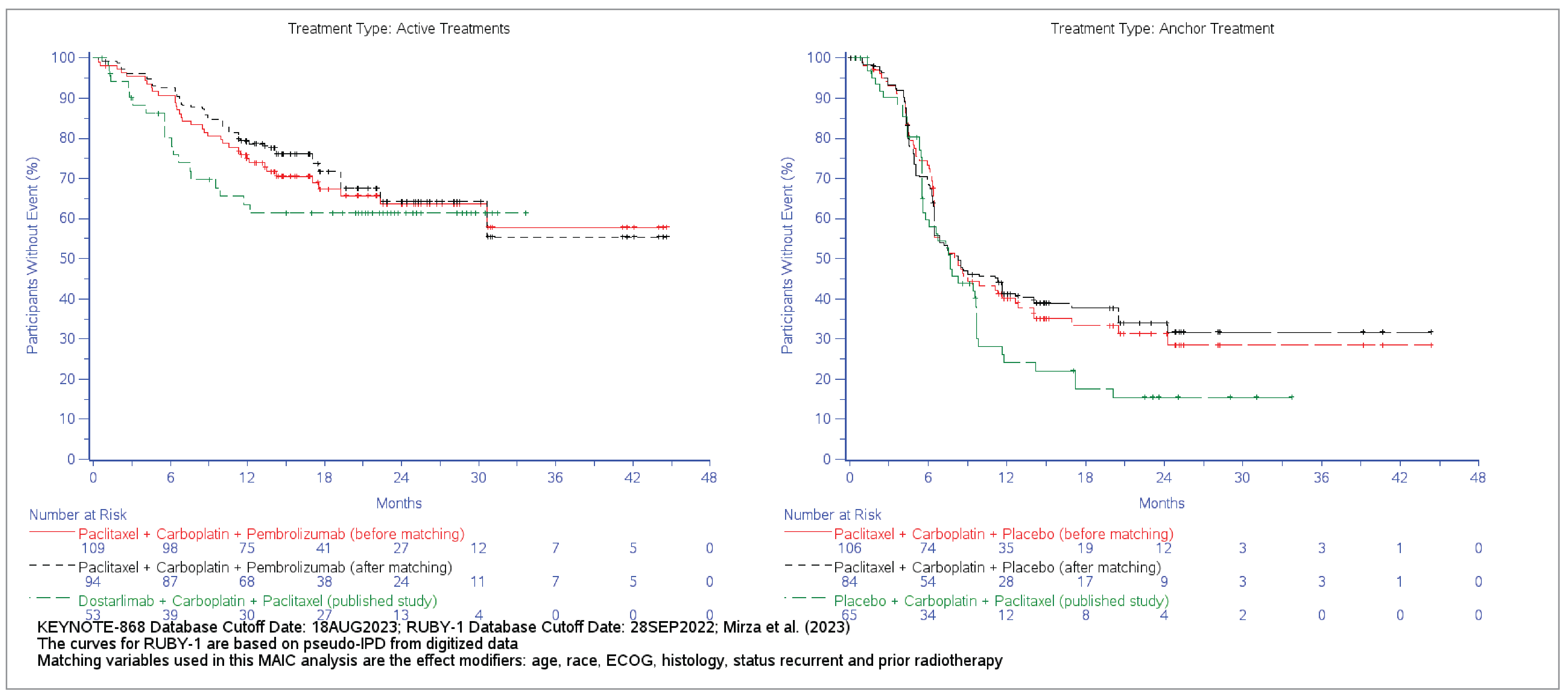
ECOG = Eastern Cooperative Oncology Group Performance Status; IPD = individual patient data; KM = Kaplan-Meier; MAIC = matching-adjusted indirect comparison; PFS = progression-free survival.
No justification was provided for the choice to conduct an MAIC instead of a network meta-analysis, given the common comparator with carboplatin-paclitaxel chemotherapy. A list of patient characteristics across the 2 trials, with rationale for the heterogeneity that would bias relative treatment-effect estimates in a network meta-analysis, if performed, was not provided. However, given this heterogeneity, the choice to perform an MAIC is reasonable. The covariates used for model adjustment (effect modifiers) were identified through discussions with clinical experts and reviews of the PFS forest plots reported in each trial. Rationale for the inclusion or exclusion of effect modifiers was not described, so there is uncertainty about the appropriateness of the identified factors and the direction of the potential bias.
Both trials included were phase III, double-blinded, placebo-controlled RCTs. Both the NRG-GY018 trial and the RUBY-I trial were conducted in an overall population that included patients with either dMMR EC or pMMR EC. For each trial, the sample size, power calculations, and statistical analyses were planned separately for the pMMR and dMMR populations; therefore, there was adequate power and control for type I error for a separate analysis of the pMMR and dMMR groups. The NRG-GY018 trial was 2 trials within a trial (for patients with dMMR EC and for patients with pMMR EC). The primary analysis of the RUBY-I trial was conducted in the dMMR population.78
Heterogeneity in patient populations between the trials beyond the match-adjusted baseline covariates likely contributes to uncertainty in the results of the MAIC. Namely, there were differences in the inclusion criteria of time since progression (the RUBY-I trial allowed prior neoadjuvant or adjuvant systemic therapy if disease had recurred or progressed at least 6 months after the completion of treatment; in the NRG-GY018 trial, prior adjuvant chemotherapy was permitted if the interval was at least 12 months). The index trial was somewhat narrower than the comparator trial with respect to the inclusion of patients with stage IVA and stage IVB EC, and patients with carcinosarcomas were excluded, whereas the RUBY-I trial included all patients with stage IV EC and patients with carcinosarcomas. In addition, patients with an ECOG PS of 2 were excluded from the match, as RUBY-I did not include such patients; however, this excluded relatively few patients. These differences in patient populations could not all be accounted for in the MAIC; however, the impact of these patients on the analysis was not described.
Unadjusted and match-adjusted baseline covariates were reported; however, the distribution of scaled weights was not reported. There was a notable reduction in the effective sample size, which was 72.6% of the original sample size after the weighting process. This suggests a discrepancy in population overlap and contributes to the imprecision and increased uncertainty of the findings.
Other sources of heterogeneity across the trials may be present that could contribute to the uncertainty of the findings from the MAIC. The follow-up duration was slightly longer for the RUBY-I trial (median, 24.8 months) than in the NRG-GY018 trial (median, 19.2 months of actual follow-up), although this follow-up period was reasonable, the clinical experts noted. There were some differences in the censoring rules used for the primary PFS analyses across the trials.78 The PFS KM curves in the control arms of the NRG-GY018 trial and the RUBY-I trial were different, with more PFS events in the comparator arm in the RUBY-I trial. Some tests of proportional hazards suggest deviations from the proportional hazards assumptions for model fit; therefore, the HR is at risk of being misleading, as it may be nonproportional over time. This suggests that differences in the patient population, study conditions, or outcome identification may contribute to heterogeneity in the trials and increase the uncertainty of the MAIC findings. Overall, the direction of bias due to this heterogeneity cannot be determined, which further contributes to the uncertainty of the findings from the MAIC.
It is possible that there are important effect modifiers that were not identified or included in the weighting, contributing to the uncertainty of the findings. For example, location and type of prior radiotherapy, tumour grade, or response to prior chemotherapy may be effect modifiers that were not included as covariates used for match adjustment. Unreported, unknown, or unmeasured effect modifiers between the study populations may contribute uncertainty to the findings from the MAIC. Notwithstanding other methodological concerns, the observed HR for PFS had wide 95% CIs that limited conclusions about which treatment regimen might be favoured.
Considering external validity, the results of the MAIC are only applicable to the population with advanced or recurrent dMMR EC, and only in the setting of patients with an ECOG PS 0 or 1. Some patient characteristics differ between the NRG-GY018 trial and the RUBY-I trial (more patients in the NRG-GY018 trial had received prior radiation, had recurrent disease, and had an ECOG PS of 0), which may impact the generalizability of the MAIC findings to the current clinical practice setting in Canada. The matching resulted in a population that was more similar to the RUBY-I population than to the original NRG-GY018 trial; however, the clinical experts noted that the baseline characteristics, both before and after matching, that were reported were reasonably generalizable to the clinical practice setting in Canada, so the effect of this is likely minimal. In addition, the MAIC assessed only PFS; OS and other efficacy outcomes of interest, such as HRQoL and harms, were not reported. Therefore, a comprehensive assessment of the balance of benefits and harms is not possible.
Studies Addressing Gaps in the Systematic Review Evidence
Contents within this section have been informed by materials submitted by the sponsor. The following has been summarized and validated by the review team.
No additional studies that address important gaps in the systematic review evidence were identified.
Discussion
Summary of Available Evidence
One ongoing pivotal phase III, randomized, double-blind trial (NRG-GY018) submitted by the sponsor met the inclusion criteria and is summarized in this report. The objective of the trial was to compare the efficacy and safety of pembrolizumab IV infusion plus carboplatin-paclitaxel followed by pembrolizumab monotherapy with placebo plus carboplatin-paclitaxel followed by placebo monotherapy in adults with primary advanced or recurrent EC in both pMMR and dMMR populations. The design was akin to 2 separate trials within a trial, in which hypothesis testing occurred separately for the pMMR and dMMR populations. After positive PFS results in both populations at IA1, the trial was unblinded. The sponsor conducted a post hoc analysis (the EUR and/or SUR analysis) that provided findings for the all-comers population (i.e., combined pMMR and dMMR populations) and included approximately 9 additional months of follow-up. This analysis is the focus of the submission, as it aligns with the proposed Health Canada indication and reimbursement request. Findings for HRQoL (measured by FACT-En TOI) were available only from the pMMR population at IA1.
The trial enrolled patients who were aged at least 18 years and had confirmed advanced-stage EC and metastatic or recurrent EC of any histologic subtype, except for carcinosarcoma. Patients with newly diagnosed stage III or stage IVA disease per RECIST 1.1 for measurable disease, or stage IVB or recurrent EC with or without measurable disease were also included in this study. Previous adjuvant chemotherapy was allowed if the chemotherapy-free interval was at least 12 months. Patients who received prior treatment with anti-PD-1, anti-PD-L1, or anti-CTLA-4 therapeutic antibodies were excluded from the NRG-GY018 trial. The outcomes most relevant to the CDA-AMC review included the primary outcome of PFS per investigator assessment and secondary outcomes of OS, HRQoL measured with the FACT-En TOI, and harms.
Overall, key baseline characteristics were generally balanced between treatment groups. Approximately 74% of the included population in the study was white and 98% of the participants were recruited from North America. The median age of the participants was around 66 years (range, 29 to 94 years), and more than half of the patients were 65 years or older. Most patients had an ECOG PS of 0 (approximately 66%), indicating good overall performance status, endometroid histology at diagnosis (approximately 59%), recurrent (57%) or primary stage IV (41%) disease, FIGO stage III or stage IV disease at diagnosis (approximately 52%), a central MMR status of pMMR (72%), and had not received prior radiotherapy (approximately 58%) or chemotherapy (approximately 80%).
Interpretation of Results
The evidence from the pivotal trial, NRG-GY018, included outcomes noted to be important by both patients and clinicians. The patient group input indicated that stopping disease progression, prolonging life, improving HRQoL and reducing treatment side effects are important to them. Similarly, the clinical experts consulted by CDA-AMC indicated that because the treatment goal for patients is long-term disease control, the unmet needs of patients would be new treatments that would delay progression, prolong OS, and improve QoL, while exposing patients to minimal toxicity.
Efficacy
The NRG-GY018 trial and the post hoc analysis for the all-comers population both suggested a clinically meaningful benefit of pembrolizumab plus carboplatin-paclitaxel over placebo plus carboplatin-paclitaxel for PFS in adults with primary advanced or recurrent EC. PFS was the primary end point of the NRG-GY018 trial, and the success criterion was met in both MMR groups at the planned IA1. The post hoc EUR and/or SUR analyses for the all-comer population produced similar results. This analysis of PFS was not preplanned or adjusted for multiplicity, and there were no sensitivity analyses. However, the robustness of the findings for the 2 MMR populations that contributed to the analysis of the all-comers population was supported by sensitivity analyses, and results in the pMMR and dMMR populations were similar to the findings at IA1. This mitigated concern regarding the post hoc all-comers PFS analysis. When interpreting the PFS results, the review team considered that the unblinding of the trial after IA1 resulted in a substantial proportion of patients in the placebo plus carboplatin-paclitaxel group discontinuing treatment and going on to receive anti-PD-1 and/or PD-L1 therapies (primarily pembrolizumab with or without lenvatinib) before progression. This may have introduced bias directed toward the null. The magnitude of benefit on PFS was more pronounced in the dMMR population than in the pMMR population (P < 0.05 in post hoc subgroup analyses); however, it was not the intent of the trial to detect differences between these groups.
Although patients and clinicians indicated that prolongation of OS is important, the clinical experts consulted by CDA-AMC noted that improvements in OS may be difficult to demonstrate. Results of the post hoc EUR and/or SUR all-comers analysis provided evidence that pembrolizumab plus carboplatin-paclitaxel may result in a clinically important improvement in survival compared to placebo plus carboplatin-paclitaxel. There was imprecision in the estimates, and CIs for absolute differences at 18 months and 36 months included effects that might not be clinically important or crossed the null. Aside from imprecision, there were some sources of uncertainty in the OS findings. Although the EUR and/or SUR all-comers analysis produced a statistically significant HR, this analysis is at increased risk of type I error because it was post hoc and not adjusted for multiplicity. Statistical significance was not reached in either of the protocol-defined MMR groups alone (IA1 or EUR and/or SUR). At the time of the IA1 and the EUR and/or SUR analyses, the OS data were not considered mature and the analyses were based on a relatively small information fraction. Although additional follow-up would be informative, the findings are confounded by the aforementioned use of anti-PD-1 and/or PD-L1 therapies in the placebo plus carboplatin-paclitaxel group, which is likely to be exacerbated over time. Post hoc sensitivity analyses were conducted on each MMR group in an attempt to address the issue; however, the validity of these analyses is reliant on assumptions that cannot be verified. Although PFS may be a surrogate for OS, there is some uncertainty in this setting. The sponsor provided a study showing that the within-arm change (i.e., level 2 suggestive evidence) in PFS was strongly correlated with OS among patients with primary advanced or recurrent EC.79 However, evidence of the ability of the treatment effect on PFS (i.e., level 1 trial-based evidence) to predict the treatment effect on OS is not available. The OS findings were consistent across the MMR groups, although the magnitude of effect was somewhat smaller in the pMMR group than in the dMMR group.
For FACT-En TOI, evidence in the pMMR population at 18 weeks of follow-up at IA1 indicated that pembrolizumab plus carboplatin-paclitaxel likely results in little-to-no clinically important difference compared to placebo plus carboplatin-paclitaxel, based on the sponsor’s suggested MID of 6 points, which was considered appropriate by the clinicians consulted by CDA-AMC for this review. The moderate certainty of the evidence was attributed to risk of bias related to missing outcome data. Findings for the all-comers population (and the dMMR group) were not available, and it is uncertain whether the findings can be generalized to that population in the absence of this evidence.
Clinicians consulted by CDA-AMC indicated that the patients included in the NRG-GY018 trial reflected the patients who they expected would receive pembrolizumab plus carboplatin-paclitaxel in clinical practice in Canada. However, patients with carcinosarcoma were excluded and there were few patients with an ECOG PS of 2, which reduces generalizability to those populations. Although credible effect modification cannot be confirmed, this introduces uncertainty about whether the benefits observed in the trial are generalizable to these patients.
Harms
All patients in the 2 treatment groups reported at least 1 AE. The most frequently reported SAEs in the pembrolizumab plus carboplatin-paclitaxel group and placebo plus carboplatin-paclitaxel group were anemia (4.1% versus 4.1%), febrile neutropenia (2.8% versus 1.3%), urinary tract infection (2.6% versus 1.5%), dyspnea (2.3% versus 0.0%), hyperglycemia (2.3% versus 0.0%), pulmonary embolism (2.3% versus 2.1%) and sepsis (2.0% versus 1.3%). Grade 3 or higher AEs were reported in more patients in the pembrolizumab plus carboplatin-paclitaxel arm than in the placebo plus carboplatin-paclitaxel arm. The most frequently reported grade 3 or higher AEs in the 2 treatment groups were anemia and decreased neutrophil count.
SAEs were experienced by about twice as many patients in the pembrolizumab plus carboplatin-paclitaxel group as in the placebo plus carboplatin-paclitaxel group, with anemia and febrile neutropenia being the most common. However, the difference between groups did not appear to be attributed to any particular SAE. A higher proportion of AEs that led to study treatment discontinuation was reported in the pembrolizumab plus carboplatin-paclitaxel group than in placebo plus carboplatin-paclitaxel group. However, the sponsor did not report which specific AEs led to treatment discontinuation. The incidence of death was higher in the pembrolizumab plus carboplatin-paclitaxel group, with cardiac arrest being the most common cause of death in this group. For notable harms, a higher proportion of patients in the pembrolizumab plus carboplatin-paclitaxel than in placebo plus carboplatin-paclitaxel group experienced immune-related AEs and infusion reactions. These AEs are manageable, according to the clinicians consulted by CDA-AMC. This trial did not report any new safety signals for pembrolizumab beyond the AEs identified in earlier studies.
Indirect Evidence
One sponsor-submitted MAIC was summarized and critically appraised. Given the lack of direct comparative evidence between pembrolizumab and dostarlimab (both in combination with carboplatin-paclitaxel), the sponsor performed an anchored MAIC to estimate the comparative PFS benefits of the 2 interventions in patients with advanced or recurrent dMMR EC. The analysis was informed by an SLR that identified the randomized, double-blinded, placebo-controlled, phase III RUBY-I trial as a comparator trial. Dostarlimab plus carboplatin-paclitaxel is a relevant comparator for patients with advanced or recurrent dMMR EC.
However, the results of the MAIC are highly uncertain, given numerous limitations. Namely, there was a risk of selection bias in the SLR in the absence of a priori selection criteria. There was heterogeneity in the patient populations and design of the trials (for example, time of chemotherapy interval for recurrent disease, the inclusion of carcinosarcoma, and differences in censoring). There were wide 95% CIs for the treatment-effect estimates and a difference in the KM curves between the control arms, with more PFS events occurring in the control arm of the RUBY-I trial than in the control arm of the NRG-GY018 trial. Identified effect modifiers were relevant, but it is likely that there are unknown or unidentified effect modifiers that could have potentially biased the MAIC results. Overall, the direction of bias cannot be determined. Beyond the methodological limitations of the approach, the CI around the point estimate was too wide to determine which treatment regimen might be favoured. Therefore, the results of the MAIC between pembrolizumab plus carboplatin-paclitaxel and dostarlimab plus carboplatin-paclitaxel for advanced and recurrent dMMR EC should be considered highly uncertain. It should be noted that the results of the MAIC only apply to advanced recurrent dMMR EC. There is also an evidence gap, in that OS, HRQoL, and harms outcomes were not included in this analysis, which precludes a comprehensive understanding of the balance of comparative benefits and harms.
Conclusion
Evidence from 1 phase III, randomized, double-blind trial (NRG-GY018) informed on the efficacy and safety of pembrolizumab plus carboplatin-paclitaxel followed by pembrolizumab monotherapy, compared with placebo plus carboplatin-paclitaxel followed by placebo, in adults with pMMR and dMMR primary advanced or recurrent EC. Evidence from the trial showed that pembrolizumab plus carboplatin-paclitaxel results in a clinically important increase in PFS at 12 months and 24 months. The magnitude of benefit on PFS was smaller for patients who had received prior chemotherapy (versus no prior chemotherapy), prior radiation therapy (versus no prior radiation therapy), recurrent and/or persistent disease (versus primary disease), and pMMR status (versus dMMR status), but the trial was not designed to confirm differences across populations. Evidence from the trial suggested that pembrolizumab plus carboplatin-paclitaxel may improve OS at 18 months and 36 months compared to placebo plus carboplatin-paclitaxel. Conclusions regarding OS were limited because the data are not yet mature and results in the all-comers population were post hoc and unadjusted for multiplicity. There is some uncertainty in the generalizability of the OS findings to patients who had received prior chemotherapy or prior radiotherapy or to patients who had no measurable disease at baseline. After 18 weeks of treatment, there was likely to be little-to-no clinically important difference in HRQoL for pembrolizumab plus carboplatin-paclitaxel compared to placebo plus carboplatin-paclitaxel among pMMR patients. There is no evidence available for all comers or for the dMMR group. Patients with carcinosarcoma were excluded, and there were few patients with an ECOG PS of 2, so generalizability to these groups is unknown. There were no new safety signals identified, and the safety of pembrolizumab plus carboplatin-paclitaxel was consistent with the known safety profiles of the individual drugs. As expected, there was an increase in the proportion of patients treated with pembrolizumab plus carboplatin-paclitaxel who experienced any immune-related AEs or infusion reactions.
According to the clinical experts consulted by the review team, MMR testing assessed with IHC is currently performed as the standard of care for patients with EC in Canada.
An ITC comparing PFS between pembrolizumab plus carboplatin-paclitaxel and dostarlimab plus carboplatin-paclitaxel for advanced and recurrent dMMR EC suggested uncertainty about which regimen may be favoured, owing to methodological limitations and important imprecision.
References
1.Makker V, MacKay H, Ray-Coquard I, et al. Endometrial cancer. Nat Rev Dis Primers. 2021;7(1):88. doi:10.1038/s41572-021-00324-8 PubMed
2.Canadian Cancer Society. Cancerous tumours of the uterus. 2024. Accessed May 28, 2024. https://cancer.ca/en/cancer-information/cancer-types/uterine/what-is-uterine-cancer/cancerous-tumours
3.Canadian Cancer Society. Uterine Cancer Statistics. 2024. Accessed 25 November, 2024. https://cancer.ca/en/cancer-information/cancer-types/uterine/statistics
4.National Cancer Institute. Endometrial Cancer Prevention (PDQ®)–Health Professional Version. National Institutes of Health (NIH); 2024. Accessed 25 November, 2024. https://www.cancer.gov/types/uterine/hp/endometrial-prevention-pdq
5.American Cancer Society. Endometrial cancer stages. 2019. Accessed 25 November, 2024. https://www.cancer.org/cancer/types/endometrial-cancer/detection-diagnosis-staging/staging.html
6.American Cancer Society. Cancer Statistics Center: Uterine corpus cancer stastistics. 2024. https://cancerstatisticscenter.cancer.org/types/uterine-corpus
7.Elshaikh MA, Yashar CM, Wolfson AH, et al. ACR appropriateness Criteria(R) advanced stage endometrial cancer. Am J Clin Oncol. 2014;37(4):391-6. doi:10.1097/COC.0000000000000098 PubMed
8.Kurra V, Krajewski KM, Jagannathan J, Giardino A, Berlin S, Ramaiya N. Typical and atypical metastatic sites of recurrent endometrial carcinoma. Cancer Imaging. 2013;13(1):113-22. doi:10.1102/1470-7330.2013.0011 PubMed
9.American Cancer Society. Signs and Symptoms of Endometrial Cancer. 2024. Accessed November 15, 2024. https://www.cancer.org/cancer/types/endometrial-cancer/detection-diagnosis-staging/signs-and-symptoms.html
10.Braun MM, Overbeek-Wager EA, Grumbo RJ. Diagnosis and management of endometrial cancer. Am Fam Physician. 2016;93(6):468-474. PubMed
11.Passarello K, Kurian S, Villanueva V. Endometrial Cancer: An Overview of Pathophysiology, Management, and Care. Semin Oncol Nurs. 2019;35(2):157-165. doi:10.1016/j.soncn.2019.02.002 PubMed
12.Ferrandina G, Petrillo M, Mantegna G, et al. Evaluation of quality of life and emotional distress in endometrial cancer patients: a 2-year prospective, longitudinal study. Gynecol Oncol. 2014;133(3):518-25. doi:10.1016/j.ygyno.2014.03.015 PubMed
13.Merck Canada Inc. Clinical Study Report: NRG-GY018. Pembrolizumab (MK-3475) in Combination with Paclitaxel and Carboplatin. Indication: Measurable Stage III or IVA, Stage IVB or Recurrent Endometrial Cancer [internal sponsor's report]. 2024.
14.BC Cancer. BC Cancer Protocol Summary for Treatment of Advanced or Recurrent Endometrial Cancer using CARBOplatin and PACLitaxel (GOENDAVCAT). Provincial Health Services Authority; 2023. Accessed December 1, 2023. http://www.bccancer.bc.ca/chemotherapy-protocols-site/Documents/Gynecology/GOENDAVCAT_Protocol.pdf
15.pan-Canadian Pharmaceutical Alliance. Jemperli (dostarlimab). Accessed June 19, 2024, https://www.pcpacanada.ca/negotiation/22696
16.Canadian Cancer Society. Chemotherapy for uterine cancer. Accessed April 16, 2024. https://cancer.ca/en/cancer-information/cancer-types/uterine/treatment/chemotherapy
17.Saskatchewan Cancer Agency. Provincial Endometrium Cancer Treatment Guidelines. 2013. Accessed April 16, 2024. http://www.saskcancer.ca/images/pdfs/health_professionals/clinical_resources/clinical_practice_guidelines/gyne-oncolog/Endometrium_Cancer_Treatment_Guidelines_-_01-2013.pdf
18.Canadian Cancer Society. Stages of uterine cancer. 2024. Accessed April 12, 2024. https://cancer.ca/en/cancer-information/cancer-types/uterine/staging
19.American Cancer Society. Treatment Choices for Endometrial Cancer, by Stage. 2024. Accessed April 12, 2024. https://www.cancer.org/cancer/types/endometrial-cancer/treating/by-stage.html
20.Canadian Cancer Society. Treatments for endometrial carcinoma. 2024. Accessed April 12, 2024. https://cancer.ca/en/cancer-information/cancer-types/uterine/treatment/endometrial-carcinoma
21.BC Cancer. Endometrium. Provincial Health Services Authority. Accessed April 12, 2024. http://www.bccancer.bc.ca/health-professionals/clinical-resources/cancer-management-manual/gynecology/endometrium
22.Cancer Care O. Systemic Therapy for Advanced or Recurrent Endometrial Cancer, and Advanced or Recurrent Uterine Papillary Serous Carcinoma. Updated July 2019. Accessed April 16, 2024. https://www.cancercareontario.ca/en/guidelines-advice/types-of-cancer/501
23.Cancer Care Ontario. Endometrial Cancer Treatment and Follow Up Pathway Map. Version 2021.11. Accessed April 12, 2024, https://www.cancercareontario.ca/sites/ccocancercare/files/assets/EndometrialCancerTreatmentPathwayMap.pdf
24.National Cancer Institute. Endometrial Cancer Treatment (PDQ®)–Health Professional Version. National Institutes of Health (NIH); 2024. Accessed February 8, 2024. https://www.cancer.gov/types/uterine/hp/endometrial-treatment-pdq
25.National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®): Uterine Neoplasms Version 2.2024. Accessed May 9, 2024, https://www.nccn.org/professionals/physician_gls/pdf/uterine.pdf
26.American Cancer Society. Radiation Therapy for Endometrial Cancer. 2024. Accessed June 7, 2024. https://www.cancer.org/cancer/types/endometrial-cancer/treating/radiation.html
27.American Cancer Society. Hormone Therapy for Endometrial Cancer. Accessed June 7, 2024. https://www.cancer.org/cancer/types/endometrial-cancer/treating/hormone-therapy.html
28.Pijnenborg JMA, van Weelden WJ, Reijnen C, Xanthoulea S, Romano A. Redefining the Position of Hormonal Therapy in Endometrial Cancer in the Era of Molecular Classification. J Clin Oncol. 2024;42(1):8-12. doi:10.1200/JCO.23.00470 PubMed
29.Matei D, Filiaci V, Randall ME, et al. Adjuvant Chemotherapy plus Radiation for Locally Advanced Endometrial Cancer. N Engl J Med. 2019;380(24):2317-2326. doi:10.1056/NEJMoa1813181 PubMed
30.Randall ME, Filiaci VL, Muss H, et al. Randomized phase III trial of whole-abdominal irradiation versus doxorubicin and cisplatin chemotherapy in advanced endometrial carcinoma: a Gynecologic Oncology Group Study. J Clin Oncol. 2006;24(1):36-44. doi:10.1200/JCO.2004.00.7617 PubMed
31.CADTH. Reimbursement Review: Jemperli (dostarlimab) for endometrial cancer. 2024. Accessed April 17, 2024. https://www.cadth.ca/dostarlimab-0
32.CADTH. Reimbursement Review: Jemperli (dostarlimab) for endometrial cancer. 2022. Accessed April 25, 2024. https://www.cadth.ca/dostarlimab
33.CADTH. Reimbursement Review: Keytruda (pembrolizumab) for advanced endometrial cancer. 2023. Accessed April 25, 2024. https://www.cadth.ca/pembrolizumab-8
34.CADTH. Reimbursement Review: Keytruda and Lenvima (Pembrolizumab and Lenvatinib) for advanced endrometrial cancer. 2022. Accessed April 25, 2024. https://www.cadth.ca/pembrolizumab-and-lenvatinib-0
35.Merck Canada Inc. PrKEYTRUDA® (pembrolizumab): solution for infusion 100 mg/4 mL vial [product monograph]. Accessed June 7, 2024, https://pdf.hres.ca/dpd_pm/00075758.PDF
36.AstraZeneca Canada Inc. PrIMFINZI® (durvalumab) for injection. Concentrate for solution for infusion, 50 mg / mL, Intravenous [product monograph]. 2022.
37.GlaxoSmithKline I. PrJEMPERLI (dostarlimab) for injection. Solution for infusion 500 mg/10 mL vial (50 mg/mL) [product monograph]. 2021;
38.Pfizer Canada ULC. PrCARBOPLATIN INJECTION BP (Carboplatin Injection). Sterile solution 10 mg / mL (50 mg, 150 mg, 450 mg, 600 mg of carboplatin per vial) [product monograph]. 2019.
39.Celgene Inc. PrABRAXANE® (paxlitaxel) for Injectable Suspension. Paclitaxel powder for injectable suspension nanoparticle, albumin-bound (nab®) paclitaxel [product monograph]. 2018.
40.National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®): Uterine Neoplasms Version 1.2025 2024. Accessed January 22, 2025. https://www.nccn.org/professionals/physician_gls/pdf/uterine.pdf
41.Berek JS, Matias-Guiu X, Creutzberg C, et al. FIGO staging of endometrial cancer: 2023. Int J Gynaecol Obstet. 2023;162(2):383-394. doi:10.1002/ijgo.14923 PubMed
42.Oaknin A, Bosse TJ, Creutzberg CL, et al. Endometrial cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann Oncol. 2022;33(9):860-877. doi:10.1016/j.annonc.2022.05.009 PubMed
43.Concin N, Matias-Guiu X, Vergote I, et al. ESGO/ESTRO/ESP guidelines for the management of patients with endometrial carcinoma. Int J Gynecol Cancer. 2021;31(1):12-39. doi:10.1136/ijgc-2020-002230 PubMed
44.Li GM. Mechanisms and functions of DNA mismatch repair. Cell Res. 2008;18(1):85-98. doi:10.1038/cr.2007.115 PubMed
45.Yoshida H, Takigawa W, Kobayashi-Kato M, Nishikawa T, Shiraishi K, Ishikawa M. Mismatch Repair Protein Expression in Endometrial Cancer: Assessing Concordance and Unveiling Pitfalls in Two Different Immunohistochemistry Assays. J Pers Med. 2023;13(8)doi:10.3390/jpm13081260 PubMed
46.Bateman AC. DNA mismatch repair proteins: scientific update and practical guide. J Clin Pathol. 2021;74(4):264-268. doi:10.1136/jclinpath-2020-207281 PubMed
47.Aiyer KTS, Doeleman T, Ryan NA, et al. Validity of a two-antibody testing algorithm for mismatch repair deficiency testing in cancer; a systematic literature review and meta-analysis. Mod Pathol. 2022;35(12):1775-1783. doi:10.1038/s41379-022-01149-w PubMed
48.Shimozaki K, Hayashi H, Tanishima S, et al. Concordance analysis of microsatellite instability status between polymerase chain reaction based testing and next generation sequencing for solid tumors. Sci Rep. 2021;11(1):20003. doi:10.1038/s41598-021-99364-z PubMed
49.Stelloo E, Jansen AML, Osse EM, et al. Practical guidance for mismatch repair-deficiency testing in endometrial cancer. Ann Oncol. 2017;28(1):96-102. doi:10.1093/annonc/mdw542 PubMed
50.Vikas P, Messersmith H, Compton C, et al. Mismatch Repair and Microsatellite Instability Testing for Immune Checkpoint Inhibitor Therapy: ASCO Endorsement of College of American Pathologists Guideline. J Clin Oncol. 2023;41(10):1943-1948. doi:10.1200/JCO.22.02462 PubMed
51.Bartley AN, Mills AM, Konnick E, et al. Mismatch Repair and Microsatellite Instability Testing for Immune Checkpoint Inhibitor Therapy: Guideline From the College of American Pathologists in Collaboration With the Association for Molecular Pathology and Fight Colorectal Cancer. Arch Pathol Lab Med. 2022;146(10):1194-1210. doi:10.5858/arpa.2021-0632-CP PubMed
52.Merck. Sponsor's Clinical Evidence Template: NRG-GY018 . Pembrolizumab (MK-3475) in Combination with Paclitaxel and Carboplatin Indication: Measurable Stage III or IVA, Stage IVB or Recurrent Endometrial Cancer [internal sponsor's report]. . 2024.
53.Ta RM, Hecht JL, Lin DI. Discordant loss of mismatch repair proteins in advanced endometrial endometrioid carcinoma compared to paired primary uterine tumors. Gynecol Oncol. 2018;151(3):401-406. doi:10.1016/j.ygyno.2018.10.012 PubMed
54.Lawrence J, Richer L, Arseneau J, et al. Mismatch Repair Universal Screening of Endometrial Cancers (MUSE) in a Canadian Cohort. Curr Oncol. 2021;28(1):509-522. doi:10.3390/curroncol28010052 PubMed
55.Peterse EFP, Naber SK, Daly C, et al. Cost-effectiveness of Active Identification and Subsequent Colonoscopy Surveillance of Lynch Syndrome Cases. Clin Gastroenterol Hepatol. 2020;18(12):2760-2767 e12. doi:10.1016/j.cgh.2019.10.021 PubMed
56.Eskander R, Sill M, Beffa L, et al. Pembrolizumab versus placebo in addition to carboplatin and paclitaxel for measurable stage 3 or 4a, stage 4b or recurrent endometrial cancer: The phase 3, NRG GY018 study (LBA 10). Gynecologic Oncology. 2023;176:S42-S43. doi:10.1016/j.ygyno.2023.06.523
57.Eskander RN, Sill MW, Beffa L, et al. Pembrolizumab plus Chemotherapy in Advanced Endometrial Cancer. N Engl J Med. 2023;388(23):2159-2170. doi:10.1056/NEJMoa2302312 PubMed
58.Eskander R, Sill M, Miller A, Beffa L, Moore R, Hope J. Overall survival, progression-free survival by PD-L1 status, and blinded independent central review results with pembrolizumab plus carboplatin/paclitaxel (CP) versus placebo plus CP in patients with endometrial cancer: results from the NRG GY018 trial. 2024:
59.Eskander R, Sill M, Miller A, et al. LBA43 Updated response data and analysis of progression free survival by mechanism of mismatch repair loss in endometrial cancer (EC) patients (pts) treated with pembrolizumab plus carboplatin/paclitaxel (CP) as compared to CP plus placebo (PBO) in the NRG GY018 trial. Ann Oncol. 2023;34:S1284.
60.Merck. Pembrolizumab – P868V01MK3475: Statistical Report. Efficacy Update Report of NRG-GY018/KEYNOTE-868. Primary advanced or recurrent endometrial cancer. Safety Update Report: Endometrial Cancer [internal sponsor's report].
61.Merck. Pembrolizumab – P868V01MK3475: 2.7.4 Summary of Clinical Safety. Safety Update Report: Endometrial Cancer [internal sponsor's report].
62.Merck Inc. Clinical Study Report (P868V01MK3475): A Phase III Randomized, Placebo-controlled Study of Pembrolizumab (MK-3475, NSC #776864) in Addition to Paclitaxel and Carboplatin for Measurable Stage III or IVA, Stage IVB or Recurrent Endometrial Cancer [internal sponsor's report]. 2023.
63.Clinical Study Report PVM. A Phase III Randomized, Placebo-controlled Study of Pembrolizumab (MK-3475, NSC #776864) in Addition to Paclitaxel and Carboplatin for Measurable Stage III or IVA, Stage IVB or Recurrent Endometrial Cancer. National Cancer Institute, Cancer Therapy Evaluation Program; 2024.
64.Functional Assessment of Chronic Illness Therapy Group. Functional Assessment of Cancer Therapy – Endometrial. FACIT. Accessed October 22, 2024, https://www.facit.org/measures/fact-en
65.Functional Assessment of Chronic Illness Therapy Group. Functional Assessment of Chronic Illness Therapy - Item GP5. FACIT. Accessed May 28, 2025, https://www.facit.org/measures/facit-item-gp5#:~:text=Item%20GP5%20from%20the%20FACIT%20Measurement%20System&text=The%20single%20FACT%2DG%20item,adverse%20events%20in%20clinical%20trials.
66.Kim S, Noh JJ, Kim Y, Cho J, Kang D, Lee YY. Psychometric validation of the Functional Assessment of Cancer Therapy-Endometrial among endometrial cancer patients. Cancer Med. 2024;13(5):e7096. doi:10.1002/cam4.7096 PubMed
67.Powell MA, Filiaci VL, Hensley ML, et al. Randomized Phase III Trial of Paclitaxel and Carboplatin Versus Paclitaxel and Ifosfamide in Patients With Carcinosarcoma of the Uterus or Ovary: An NRG Oncology Trial. J Clin Oncol. 2022;40(9):968-977. doi:10.1200/JCO.21.02050 PubMed
68.Matulonis UA, Huang HQ, Filiaci VL, et al. Patient reported outcomes for cisplatin and radiation followed by carboplatin/paclitaxel versus carboplatin/paclitaxel for locally advanced endometrial carcinoma: An NRG oncology study. Gynecol Oncol. 2022;164(2):428-436. doi:10.1016/j.ygyno.2021.11.021 PubMed
69.Yost KJ, Eton DT. Combining distribution- and anchor-based approaches to determine minimally important differences: the FACIT experience. Eval Health Prof. 2005;28(2):172-91. doi:10.1177/0163278705275340 PubMed
70.Schoenfeld DA. Sample-size formula for the proportional-hazards regression model. Biometrics. 1983:499-503. PubMed
71.Hochberg Y. A sharper Bonferroni procedure for multiple tests of significance. Biometrika. 1988;75(4):800-802.
72.Merck. MK-3475: Protocol No. 868-11. Supplemental Statistical Analysis Plan (sSAP) [internal sponsor's report]. 2023.
73.European Medicines Agency. Question and answer on adjustment for cross-over in estimating effects in oncology trials. 2018. Accessed May 28 2024. https://www.ema.europa.eu/en/adjustment-cross-over-estimating-effects-oncology-trials-scientific-guideline
74.Balshem H, Helfand M, Schunemann HJ, et al. GRADE guidelines: 3. Rating the quality of evidence. Journal of clinical epidemiology. 2011;64(4):401-6. doi:10.1016/j.jclinepi.2010.07.015 PubMed
75.Santesso N, Glenton C, Dahm P, et al. GRADE guidelines 26: informative statements to communicate the findings of systematic reviews of interventions. Journal of clinical epidemiology. 2020;119:126-135. doi:10.1016/j.jclinepi.2019.10.014 PubMed
76.Merck, Co I. Pembrolizumab (MK-3475) in Combination with Paclitaxel and Carboplatin for Participants with Measurable Stage III or IVA, Stage IVB or Recurrent Endometrial Cancer: Matching Adjusted Indirect Comparison (MAIC) [internal sponsor's report]. November 13 2024.
77.Signorovitch JE, Wu EQ, Yu AP, et al. Comparative effectiveness without head-to-head trials: a method for matching-adjusted indirect comparisons applied to psoriasis treatment with adalimumab or etanercept. Pharmacoeconomics. 2010;28(10):935-45. doi:10.2165/11538370-000000000-00000 PubMed
78.Mirza MR, Chase DM, Slomovitz BM, et al. Dostarlimab for Primary Advanced or Recurrent Endometrial Cancer. N Engl J Med. 2023;388(23):2145-2158. doi:10.1056/NEJMoa2216334 PubMed
79.Garside J, Shen Q, Westermayer B, et al. Association Between Intermediate End Points, Progression-free Survival, and Overall Survival in First-line Advanced or Recurrent Endometrial Cancer. Clinical Therapeutics. 2023;45(10):983-990. PubMed
Appendix 1: Detailed Outcome Data
Please note that this appendix has not been copy-edited.
Sensitivity analyses for PFS by investigator assessment and OS in the pMMR and dMMR subpopulations were reported in the Clinical Study Report. The censoring rules were reported for the ITT MMR population. The stratification factor applied in the primary censoring and sensitivity analyses 1, 2, 3, and 4 was prior adjuvant chemotherapy (yes or no). The stratification factors applied in the primary censoring and sensitivity analyses 5 and 6 were prior adjuvant chemotherapy (yes or no) and ECOG PS (0 and 1/2).
Table 25: Statistical Analysis of Efficacy End Points in the NRG-GY018 Trial
End point | Statistical model | Adjustment factors | Handling of missing data | Sensitivity analyses |
|---|---|---|---|---|
PFS (all-comersa, dMMR and pMMR) | Based on Cox regression model with Efron’s method of tie handling with treatment as a covariate | Stratified by prior chemotherapy | Censored |
|
OS (all comers, dMMR and pMMR) | Based on Cox regression model with Efron’s method of tie handling with treatment as a covariate | Stratified by prior chemotherapy OS adjusted for the treatment switchover to subsequent anti-PD-1/PD-L1 using IPCW and 2-stage model | Censored |
|
HRQoLb (FACT-En TOI) | Linear mixed model for repeated measures to estimate and compare the mean differences in change from baseline between the treatment groups | Treatment, age, pretreatment QOL/PRO score, assessment time and treatment-by-time interaction | Missing-at-random assumption | None |
AEOSI = adverse event of special interest; HRQoL = health-related quality of life; ITT = intention to treat; MMR = mismatch repair; OS = overall survival; ORR = objective response rate; PFS = progression-free survival; FACT-En TOI = Trial Outcome Index of the Functional Assessment of Cancer Therapy-Endometrial
aAll-comers analysis is an additional analysis post hoc from the sponsor.
bBased on information from the study protocol.57
Source: NRG-GY018 study protocol72
Table 26: PFS Sensitivity Analysis (ITT Population) for the pMMR and dMMR Populations
Sensitivity Analysis | HR (95% CI) |
|---|---|
pMMR | |
sensitivity analysis 1 | 0.70 (0.56 to 0.87) |
sensitivity analysis 2 | 0.72 (0.58 to 0.89) |
sensitivity analysis 3 | 0.58 (0.49 to 0.69) |
sensitivity analysis 4 | 0.73 (0.59 to 0.90) |
sensitivity analysis 5 | 0.74 (0.60 to 0.91) |
sensitivity analysis 6 | 0.67 (0.55 to 0.83) |
dMMR | |
sensitivity analysis 1 | 0.30 (0.19 to 0.46) |
sensitivity analysis 2 | 0.31 (0.20 to 0.47) |
sensitivity analysis 3 | 0.27 (0.19 to 0.38) |
sensitivity analysis 4 | 0.35 (0.24 to 0.53) |
sensitivity analysis 5 | 0.34 (0.23 to 0.51) |
sensitivity analysis 6 | 0.34 (0.23 to 0.51) |
HR = Hazard Ratio; ITT = intention to treat; PFS = progression-free survival; dMMR = deficient mismatch repair; pMMR = proficient mismatch repair
Source: NRG-GY018_Clinical Evidence Template.52
Table 27: OS Sensitivity Analysis (ITT Population) for the pMMR and dMMR Populations
Sensitivity Analysis | HR (95% CI) |
|---|---|
pMMR | |
sensitivity analysis 2 | 0.78 (95%CI = 0.58 to 1.06) |
sensitivity analysis 3 | 0.79 (95%CI = 0.59 to 1.07) |
sensitivity analysis 4 | 0.80 (95%CI = 0.59 to 1.08) |
sensitivity analysis 5 | 0.81 (95%CI = 0.60 to 1.10) |
dMMR | |
sensitivity analysis 4 | 0.56 (95%CI = 0.31 to 1.03) |
sensitivity analysis 5 | 0.58 (95%CI = 0.32 to 1.07) |
dMMR = deficient mismatch repair; HR = hazard ratio; ITT = intention to treat; OS = overall survival; pMMR = proficient mismatch repair.
Note: Sensitivity analyses 2, 3, 4, and 5 were conducted in the pMMR cohort, while sensitivity analyses 4 and 5 were performed in the dMMR cohort.
Source: NRG-GY018_Clinical Evidence Template.52
Table 28: Comparison of Summaries of Primary Efficacy Results Between Investigator Assessment and BICR in pMMR Participants in the NRG-GY018 Trial (ITT Population), Interim Analysis 1
Variable | By investigator assessment | By BICR | ||
|---|---|---|---|---|
Pembrolizumab plus carboplatin-paclitaxel (N = 294) | Placebo plus carboplatin-paclitaxel (N = 294) | Pembrolizumab plus carboplatin-paclitaxel (N = 294) | Placebo plus carboplatin-paclitaxel (N = 294) | |
PFS per RECIST 1.1 | ||||
Median PFSa, months (95% CI) | 13.1 (10.6, 19.5) | 8.7 (8.4, 11.0) | 19.5 (13.1, 28.0) | 11.0 (9.0, 11.5) |
HR (95% CI)b P valuec | 0.57 (0.44, 0.74) < 0.0001 | 0.64 (0.49, 0.85) 0.0008d | ||
PFS Rate per RECIST 1.1 | ||||
12 months % (95% CI) | 52.0 (43.8, 59.5) | 29.5 (22.4, 37.0) | 60.1 (52.1, 67.2) | 39.7 (31.8, 47.4) |
18 months % (95% CI) | 43.8 (35.0, 52.2) | 20.8 (14.1, 28.3) | 50.4 (41.1, 58.9) | 29.1 (21.3, 37.4) |
BICR = blinded independent central review; CI = confidence interval; HR = hazard ratio; ITT = intent-to-treat population; PFS = progression-free survival; pMMR = mismatch repair proficient; RECIST 1.1 = Response Evaluation Criteria in Solid Tumours version 1.1.
aFrom product-limit (Kaplan-Meier) method for censored data.
bBased on Cox regression model with Efron’s method of tie handling with treatment as a covariate stratified by prior chemotherapy
cOne-sided P value based on log-rank test stratified by prior chemotherapy.
dNominal P value.
Source: Statistical Report, Efficacy Results Based on BICR Assessment per RECISIT 1.1 in Interim Analysis of NRG-GY018/KEYNOTE-86860
Table 29: Comparison of Summaries of Primary Efficacy Results Between Investigator Assessment and BICR in dMMR Participants in the NRG-GY018 Trial (ITT Population), Interim Analysis 1
Variable | By investigator assessment | By BICR | ||
|---|---|---|---|---|
Pembrolizumab plus carboplatin-paclitaxel (N = 294) | Placebo plus carboplatin-paclitaxel (N = 294) | Pembrolizumab plus carboplatin-paclitaxel (N = 294) | Placebo plus carboplatin-paclitaxel (N = 294) | |
PFS per RECIST 1.1 | ||||
Median PFSa, months (95% CI) | NR (30.7, NR) | 8.3 (6.5, 12.3) | NR (NR, NR) | 14.1 (8.5, NR) |
HR (95% CI)b P valuec | 0.34 (0.22, 0.53) < 0.0001 | 0.45 (0.27, 0.73) 0.0005d | ||
PFS Rate per RECIST 1.1 | ||||
12 months % (95% CI) | 73.0 (62.0, 81.3) | 40.0 (29.3, 50.4) | 77.5 (66.9, 85.1) | 54.3 (42.9, 64.3) |
18 months % (95% CI) | 65.2 (52.7, 75.2) | 32.9 (22.5, 43.8) | 68.2 (55.8, 77.8) | 45.7 (32.3, 58.1) |
BICR = blinded independent central review; CI = confidence interval; HR = hazard ratio; ITT = intent-to-treat population; PFS = progression-free survival; pMMR = mismatch repair proficient; RECIST 1.1 = Response Evaluation Criteria in Solid Tumours version 1.1
aFrom product-limit (Kaplan-Meier) method for censored data.
bBased on Cox regression model with Efron’s method of tie handling with treatment as a covariate stratified by prior chemotherapy
cOne-sided P value based on log-rank test stratified by prior chemotherapy.
dNominal P value.
Source: Statistical Report, Efficacy Results Based on BICR Assessment per RECISIT 1.1 in Interim Analysis of NRG-GY018/KEYNOTE-86860
Table 30: Analysis of OS in pMMR Participants With PD-L1 CPS > = 1 (ITT Population), Interim Analysis 1
OS groups | Pembrolizumab plus carboplatin-paclitaxel ███████ | Placebo plus carboplatin-paclitaxel ███████ |
|---|---|---|
pMMR population | ||
Number of events (%) | ███████████ | ███████████ |
OS (months), median (95% CI) a | ███████████ | ███████████ |
HR (95% CI)b | ███████████ | |
P valuec | ███████████ | |
OS rate at month 6, % (95% CI) | ███████████ | ███████████ |
OS rate at month 12% (95% CI) | ███████████ | ███████████ |
OS rate at month 18 (%) (95% CI) | ███████████ | ███████████ |
OS rate at month 24 (%) (95% CI) | ███████████ | ███████████ |
OS rate at month 30 (%) (95% CI) | ███████████ | ███████████ |
OS rate at month 36 (%) (95% CI) | ███████████ | ███████████ |
dMMR population | ||
Number of events (%) | ████████ | ████████ |
OS (months), median (95% CI)a | ███████████ | ███████████ |
HR (95% CI)b | ███████████████ | |
P valuec | ██████ | |
OS rate at month 6 (%) (95% CI) | ███████████ | ███████████ |
OS rate at month 12 (%) (95% CI) | ███████████ | ███████████ |
OS rate at month 18 (%) (95% CI) | ███████████ | ███████████ |
OS rate at month 24 (%) (95% CI) | ███████████ | ███████████ |
OS rate at month 30 (%) (95% CI) | ███████████ | ███████████ |
OS rate at month 36 (%) (95% CI) | ███████████ | ███████████ |
CI = confidence interval; CP = carboplatin + paclitaxel; dMMR = deficient mismatch repair; HR = hazard ratio; ITT = intention to treat; NR = not reached; OS = overall survival; pMMR = proficient mismatch repair
aFrom product-limit (Kaplan-Meier) method for censored data.
bBased on Cox regression model with Efron’s method of tie handling with treatment as a covariate.
cOne-sided P value based on log-rank test stratified by prior chemotherapy. Not adjusted for multiplicity.
Source: Trial statistical report (efficacy update report).64
Pharmacoeconomic Review
Abbreviations
AE
adverse event
BIA
budget impact analysis
CDA-AMC
Canada’s Drug Agency
dMMR
deficient mismatch repair
EC
endometrial cancer
ICER
incremental cost-effectiveness ratio
LY
life-year
MAIC
matching-adjusted indirect comparison
MMR
mismatch repair
OS
overall survival
pCPA
pan-Canadian Pharmaceutical Alliance
PFS
progression-free survival
pMMR
proficient mismatch repair
PSM
partitioned survival model
QALY
quality-adjusted life-year
ToT
time on treatment
TTDC
time to treatment discontinuation or completion
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Pembrolizumab (Keytruda), 100 mg/4 mL vial |
Indication | Pembrolizumab in combination with carboplatin and paclitaxel and then continued as monotherapy for the treatment of primary advanced (stage III and stage IV) or recurrent endometrial carcinoma |
Health Canada approval status | NOC |
Health Canada review pathway | Standard review |
NOC date | March 5, 2025 |
Reimbursement request | As per indication |
Sponsor | Merck Canada Inc. |
Submission history | Previously reviewed: Yes Pembrolizumab has been reviewed for multiple indications at CDA-AMC. The following indications were reviewed for endometrial cancer. Indication: Unresectable or metastatic MSI-H or dMMR endometrial cancer in patients whose tumours have progressed following prior therapy and who have no satisfactory alternative treatment options, as monotherapy
In combination with lenvatinib Indication: Advanced endometrial carcinoma that is not MSI-H or dMMR in patients who have disease progression following prior platinum-based systemic therapy and are not candidates for curative surgery or radiation
|
CDA-AMC = Canada’s Drug Agency; dMMR = deficient mismatch repair; MSI-H = microsatellite instability–high; NOC = Notice of Compliance.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Partitioned survival model |
Target populations | Adults with primary advanced (stage III and stage IV) or recurrent endometrial cancer Subgroup analyses submitted by MMR status (i.e., dMMR and pMMR) |
Treatments | Pembrolizumab in combination with carboplatin-paclitaxel and then continued as monotherapy for the maintenance phase |
Dose regimen | Combination phase: Pembrolizumab 200 mg every 3 weeks for 6 cycles, in combination with carboplatin-paclitaxel, administered at doses of 750 mg and 175 mg/m2, respectively, every 3 weeks for up to 6 cycles Maintenance phase: 400 mg of pembrolizumab every 6 weeks until progression or for up to a maximum of 14 cycles |
Submitted price | $4,400.00 per 100 mg/4 mL vial |
Submitted treatment cost | Combination phase: Pembrolizumab: $8,800 every 3 weeks Maintenance phase: Pembrolizumab: $17,600 every 6 weeks |
Comparators |
|
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | Lifetime (35 years) |
Key data sources |
|
Submitted results |
|
Key limitations |
|
CDA-AMC reanalysis results |
|
CDA-AMC = Canada’s Drug Agency; dMMR = deficient mismatch repair; ICER = incremental cost-effectiveness ratio; LY = life-year; MMR = mismatch repair; OS = overall survival; PFS = progression-free survival; pMMR = proficient mismatch repair; PSM = partitioned survival model; QALY = quality-adjusted life-year.
Conclusions
The Canada’s Drug Agency (CDA-AMC) clinical review concluded that the results of the NRG-GY018 trial showed that pembrolizumab (Keytruda) plus carboplatin-paclitaxel compared to carboplatin-paclitaxel likely results in a clinically important improvement in progression-free survival (PFS) at 12 months and 24 months and may improve overall survival (OS) at 18 months and 36 months in adults with primary advanced or recurrent endometrial cancer (EC). However, conclusions regarding OS were limited because the data are not yet mature, and statistically significant results in the all-comers population were post hoc and unadjusted for multiplicity. Because of the lack of direct comparative evidence against dostarlimab (Jemperli) plus carboplatin-paclitaxel, an anchored matching-adjusted indirect comparison (MAIC) was conducted by the sponsor in the subgroup of patients with deficient mismatch repair (dMMR). The MAIC was limited, given the risk of selection bias and the heterogeneity in both the patient populations and trial designs. The results of the MAIC should therefore be viewed as highly uncertain, and insufficient evidence exists to suggest a PFS difference between the 2 immunotherapies combined with carboplatin-paclitaxel.
CDA-AMC was unable to address all identified limitations, given inherent assumptions imposed by the partitioned survival model (PSM) structure and the limited face validity of the available OS distributions. The CDA-AMC reanalysis used a stratified approach based on mismatch repair (MMR) status, in which weight-based dosing for pembrolizumab was applied and alternative health state utility values were sourced. The CDA-AMC reanalysis resulted in an incremental cost-effectiveness ratio (ICER) of $57,334 per quality-adjusted life-year (QALY) gained for pembrolizumab plus carboplatin-paclitaxel compared to carboplatin-paclitaxel in the overall population. Pembrolizumab was associated with a lower ICER in the dMMR population ($53,432 per QALY gained) than in the proficient mismatch repair (pMMR) population ($58,778 per QALY gained). Because OS could not be modified in the economic model to reflect more realistic long-term survival expectations, the results are dependent on patients receiving pembrolizumab plus carboplatin-paclitaxel gaining 2.02 additional LYs compared to carboplatin-paclitaxel.
The majority of the incremental clinical benefits for pembrolizumab (95%) were derived in the period beyond which there are observed trial data (i.e., the extrapolated period). The survival models chosen by the sponsor may overestimate patient survival compared to clinical expectations. The PSM used also indicated a postprogression survival benefit, likely owing to assumptions with the PSM model structure, favouring pembrolizumab plus carboplatin-paclitaxel. Additionally, the distribution of subsequent treatments in the submitted model does not accurately reflect Canadian clinical practice, and the proportions used did not align with those reported in the Clinical Study Report. As such, the cost-effectiveness of pembrolizumab and the price-reduction estimates are highly uncertain.
Clinical expert feedback suggested that pembrolizumab and dostarlimab may have a similar efficacy. There was no clinical evidence suggesting that the total treatment cost of pembrolizumab plus carboplatin-paclitaxel should be higher than the total treatment cost of dostarlimab plus carboplatin-paclitaxel in the dMMR subgroup.
Perspectives of Patients, Clinicians, and Drug Programs Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, clinician groups, and drug plans that participated in the CDA-AMC review process.
Patient input was provided by the Colorectal Cancer Resource & Action Network, in collaboration with the Canadian Cancer Survivor Network and HPV Global Action. This input was collected with a combination of virtual interviews, surveys, and literature reviews. The Colorectal Cancer Resource & Action Network conducted interviews with 6 patients (1 from Canada and 5 internationally) who had experience with pembrolizumab. More than 90% of the patients with EC reported abnormal vaginal bleeding, with some noting symptoms such as abnormal vaginal discharge, difficulty or pain during urination, pain during sexual intercourse, pelvic pain, and unexplained weight loss. The findings revealed dissatisfaction with current treatment options, including chemotherapy, radiation, and surgery, which are often associated with side effects such as fatigue, neuropathy, and sexual health issues. Patients expressed a need for treatments that prolong life. The patients interviewed who had experience with pembrolizumab, either as monotherapy or in combination with chemotherapy, reported robust responses (defined radiographically, biochemically, or chemically), improved quality of life, reduced symptoms (allergic reactions, hair loss, neutropenia), and manageable side effects. Pembrolizumab enabled these patients to regain independence, resume daily activities, and achieve prolonged remission or disease stability.
Clinician input was provided by the Ontario Health (Cancer Care Ontario) Gynecologic Cancer Drug Advisory Committee. The clinician group emphasized that the current treatment pathway for advanced or recurrent EC primarily relies on platinum-based chemotherapy, typically carboplatin-paclitaxel, often combined with radiation therapy. However, these treatment options fail to provide durable responses, particularly in patients with pMMR EC. Immunotherapies (e.g., dostarlimab and durvalumab) are under review for public reimbursement, and currently only accessible through compassionate-use programs. Treatment goals include prolonging survival, delaying disease progression, reducing symptoms, improving quality of life, and potentially curing the disease. Pembrolizumab is expected to have a place in therapy similar to the other immunotherapies and will likely be used in the first-line treatment setting and in patients with platinum-sensitive recurrent disease. The clinicians noted that some patients may not be suitable candidates for immunotherapy, particularly those with contraindications to such treatments or those who have a poor Eastern Cooperative Oncology Group Performance Status (ECOG PS).
The drug plans highlighted several key considerations regarding the reimbursement of pembrolizumab, particularly its dosing and overall budget impact. It was noted that pembrolizumab would likely be funded as weight-based dosing. Concerns were raised regarding the potential budget impact of reimbursing pembrolizumab in the first-line setting.
Several of these concerns were addressed in the sponsor’s model:
The model was structured based on the survival outcomes of PFS and OS. Furthermore, quality of life was captured through utility values that were measured with the EQ-5D system, which captures dimensions such as pain, usual activities, and self care.
CDA-AMC addressed some of these concerns, as follows:
Given that pan-Canadian Pharmaceutical Alliance (pCPA) negotiations of dostarlimab for the treatment of dMMR EC have concluded with a letter of intent, the CDA-AMC base case included dostarlimab as a relevant comparator in the dMMR subgroup.1
Weight-based dosing was assumed for pembrolizumab.
Economic Review
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis comparing the costs and outcomes of pembrolizumab plus carboplatin-paclitaxel to carboplatin-paclitaxel for the treatment of adults with primary advanced (stage III and stage IV) or recurrent EC. The modelled population reflects the Health Canada indication.2 The sponsor also submitted subgroup analyses by MMR status (i.e., dMMR and pMMR). In the dMMR population, dostarlimab plus carboplatin-paclitaxel was also considered a comparator.3
Pembrolizumab is available as a powder for solution for IV infusion (100 mg per 4 mL vial). In the combination phase, the recommended dosage of pembrolizumab is 200 mg every 3 weeks for 6 cycles in combination with carboplatin-paclitaxel.2,4 Carboplatin is dosed at 750 mg and paclitaxel is dosed at 175 mg/m2 every 3 weeks for up to 6 cycles.4 For the maintenance phase, pembrolizumab was assumed to be administrated at a dose of 400 mg every 6 weeks until disease progression, or for up to a maximum of 14 cycles.4 At the submitted price of $4,400 per 4 mL vial and assuming 100% relative dose intensity, the acquisition cost of pembrolizumab in the combination phase was estimated to be $8,800 for each 21-day cycle, and the total regimen cost of pembrolizumab plus carboplatin-paclitaxel was $13,185 per cycle. In the maintenance phase, in which pembrolizumab is recommended as monotherapy, the sponsor calculated the acquisition cost to be $17,600 per 6-week treatment cycle. The total regimen cost for chemotherapy alone was $4,384 per cycle, and the total regimen cost for dostarlimab plus carboplatin-paclitaxel was $14,416 per loading cycle (21 days) and $24,447 per maintenance cycle (6 weeks). No wastage was assumed, as the sponsor assumed vial sharing.4
Modelled outcomes included both life-years (LYs) and QALYs over a 35-year lifetime horizon with weekly cycles. The base-case analysis adopted the perspective of the Canadian public health care payer. Both costs and health outcomes were discounted at an annual rate of 1.5%.4
Model Structure
The sponsor submitted a PSM that comprised 3 health states: progression-free, progressed-disease, and death (Figure 1 in Appendix 3).4 The proportion of patients who were in the progression-free, progressed-disease, or death health states at any time point over the model’s time horizon was derived from nonmutually exclusive survival curves, based on the area under the survival curve. Patients with advanced or recurrent EC entered the model in the progression-free health state and were assumed to have stable or responding disease. The proportion of patients in the progression-free health state during each model cycle was estimated from the PFS curve.4 Progression was defined by the Response Evaluation Criteria in Solid Tumours Version 1.1 (RECIST 1.1), which was adopted in the NRG-GY018 trial.4 OS was partitioned to estimate the proportion of patients in the death state and in the postprogression state, reflecting live patients whose disease had progressed. Specifically, the proportion of patients in the progressed-disease health state was based on the difference between the OS and the PFS curves.4
Model Inputs
Patient baseline characteristics used to inform the model were derived from the NRG-GY018 trial, which assessed the efficacy and safety of pembrolizumab in adult patients with primary advanced (stage III and stage IV) or recurrent EC. For the overall population, the mean age was 65.4 years, the mean weight was 87.9 kg, and the mean body surface area was 1.95 m2. For the dMMR subgroup, the mean age was 65.7 years, the mean weight was 87.6 kg, and the mean body surface area was 1.96 m2. For the pMMR subgroup, the mean age was 65.4 years, the mean weight was 88.0 kg, and the mean body surface area was 1.95 m2.4,5
Key clinical efficacy inputs (OS and PFS) and time to treatment discontinuation or completion (TTDC) for pembrolizumab plus carboplatin-paclitaxel compared to chemotherapy alone were derived from the NRG-GY018 trial (data cut-off date: August 18, 2023).5 OS, PFS, and TTDC were extrapolated beyond the trial duration. The fitted models were assessed through visual inspection, goodness-of-fit statistics, external data, and clinical validation.4 The sponsor selected independent distributions for OS, PFS, and TTDC for the overall population and the 2 subgroups (Table 11). In the sponsor’s base case, the treatment effect of pembrolizumab was assumed to persist for a patient’s lifetime, even after discontinuation (i.e., no treatment-effect waning).4
For the scenario analysis that included dostarlimab plus carboplatin-paclitaxel as a comparator, the sponsor assumed identical efficacy (i.e., OS and PFS) with pembrolizumab plus carboplatin-paclitaxel, in the dMMR and/or microsatellite instability–high EC population. This was based on the PFS results of the conducted MAIC that compared pembrolizumab plus carboplatin-paclitaxel to dostarlimab plus paclitaxel-carboplatin.4 In the model, for dostarlimab treatment arm, PFS data were used as a proxy for TTDC.
Patients who discontinue their initial therapy would be eligible for subsequent treatment. Specifically, 23% of patients in the pembrolizumab plus carboplatin-paclitaxel arm and 54% in the chemotherapy arm would receive subsequent therapy. The distribution of subsequent treatments assumed in the sponsor’s model are reported in Table 12.
Adverse events (AEs) captured in the submitted model included any grade 3 or higher treatment-related AEs that occurred in at least 5% of patients in either arm of the NRG-GY018 trial, along with 3 AEs of special interest — diarrhea (grade 2+), neutropenia (any grade), and pneumonitis (grade 2+) — informed by the NRG-GY018 trial (data cut-off date: August 18, 2023).5 In addition, relevant AEs related to dostarlimab in the RUBY-I trial were included in the model.4
In the sponsor’s base case, 2 different health utility values were used: 0.82 for the progression-free health state; and 0.85 for the progressed-disease health state.4 Utility values were adjusted for age-related quality-of-life decline, using 3-Level EQ-5D data from published literature.4 AE utility decrements were sourced from literature, and total AE disutility was estimated based on AE incidence, duration, and its associated disutility values.
Costs in the model included drug acquisition, drug administration, subsequent treatment, disease management, AEs, and terminal care. Drug-acquisition costs were calculated by the sponsor as a function of the drug’s unit price, dosing schedule, and the proportion of patients on treatment, assuming 100% compliance and vial sharing for pembrolizumab.4 The price of pembrolizumab was based on the sponsor’s submitted price, whereas the prices of all other treatments were sourced from CDA-AMC Recommendation Reviews and the IQVIA database.6-8 Administration costs for therapies administered by IV infusion, including pembrolizumab, paclitaxel, and carboplatin, were based on the hourly wage of a nurse with more than 8 years of experience in Ontario.9 The model accounted for subsequent treatment costs after treatment discontinuation. The proportion of patients receiving subsequent treatments was based on clinical input sought by the sponsor, with costs calculated based on the duration of subsequent treatment reported in the NRG-GY018 trial,5 drug-acquisition costs, and associated administration costs.5 Drug-acquisition costs and administration costs were from the same sources, as noted previously. Disease-management costs for the progressed-disease and progression-free states were also included in the model and were derived from the Ontario Ministry of Health Schedule of Benefits for Laboratory Services and Schedule of Benefits for Physician Services.10,11 The costs of managing AEs were primarily sourced from the Canadian Institute for Health Information (2021–2022).12 Terminal-care costs were applied as a 1-time cost and were derived from published literature.13
Summary of Sponsor’s Economic Evaluation Results
All analyses were run probabilistically (5,000 iterations).4 The deterministic and probabilistic results were similar for the overall population and the pMMR subgroup but not for the dMMR subgroup; probabilistic results are therefore reported here, although the deterministic findings for the dMMR subgroup are also reported in Table 14 (Appendix 3). The submitted analyses were based on the submitted price for pembrolizumab and publicly available prices for other drugs. Additional results from the sponsor’s submitted economic evaluation base case are presented in Appendix 3.
Base-Case Results
In the sponsor’s base case, pembrolizumab plus carboplatin-paclitaxel resulted in an incremental cost of $101,912 and an incremental gain of 2.70 incremental QALYs over a lifetime horizon of 35 years. This produced an ICER of $37,682 per QALY gained compared to carboplatin-paclitaxel (Table 3). In addition, the sponsor’s model estimated that there would be an incremental LY gain of 3.46 associated with pembrolizumab plus carboplatin-paclitaxel. Pembrolizumab plus carboplatin-paclitaxel had a 78% probability of being cost-effective at a willingness-to-pay threshold of $50,000 per QALY compared to carboplatin-paclitaxel.4
The results were driven by the difference in OS. For the deterministic analysis, the sponsor’s model estimated that pembrolizumab plus carboplatin-paclitaxel would generate 2.78 incremental QALYs (Table 13) over a lifetime horizon; a majority (98%) of the incremental QALY benefits were derived from the extrapolation period (i.e., 2.72). The key cost driver was drug-acquisition costs, which represented 66% of the total costs of pembrolizumab. However, this was offset by the higher cost of subsequent treatment required in patients initially treated with carboplatin-paclitaxel compared to that of those who received pembrolizumab plus carboplatin-paclitaxel.
The sponsor further reported subgroup analyses for the dMMR and pMMR subgroups. Pembrolizumab plus carboplatin-paclitaxel, compared to carboplatin-paclitaxel, was associated with an ICER of $90,189 per QALY gained for the dMMR subpopulation and $65,041 per QALY gained for the pMMR subpopulation. Specific to the dMMR population, pembrolizumab plus paclitaxel-carboplatin dominated dostarlimab plus carboplatin-paclitaxel (i.e., less costly, equally effective).4
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER vs. paclitaxel-carboplatin ($/QALY) |
|---|---|---|---|---|---|
Overall population | |||||
Carboplatin-paclitaxel | 149,526 | Reference | 3.41 | Reference | Reference |
Pembrolizumab plus carboplatin-paclitaxel | 251,438 | 101,912 | 6.11 | 2.70 | 37,682 |
dMMR subgroup | |||||
Carboplatin-paclitaxel | 140,618 | Reference | 4.85 | Reference | Reference |
Pembrolizumab plus carboplatin-paclitaxel | 291,984 | 151,366 | 6.53 | 1.68 | 90,189 |
Dostarlimab plus carboplatin-paclitaxel | 504,734 | 212,750 | 6.53 | 0.00 | Dominated by pembrolizumab plus paclitaxel-carboplatin |
pMMR subgroup | |||||
Carboplatin-paclitaxel | 153,586 | Reference | 2.61 | Reference | Reference |
Pembrolizumab plus carboplatin-paclitaxel | 233,812 | 80,226 | 3.84 | 1.23 | 65,041 |
dMMR = deficient mismatch repair; ICER = incremental cost-effectiveness ratio; pMMR = proficient mismatch repair; QALY = quality-adjusted life-year; vs. = versus.
Note: For the dMMR subgroup, total QALYs are identical for pembrolizumab plus carboplatin-paclitaxel and dostarlimab plus carboplatin-paclitaxel, as the sponsor assumed OS and PFS with dostarlimab plus carboplatin-paclitaxel to be equivalent to OS and PFS with pembrolizumab plus carboplatin-paclitaxel.
Source: Sponsor’s pharmacoeconomic submission.4
Sensitivity and Scenario Analyses Results
The sponsor submitted several deterministic sensitivity analyses that explored the impact of changes in cohort baseline characteristics, alternative assumptions about costs, different methods of incorporating health state utilities, various model settings (such as discount rate), and the adoption of different assumptions (e.g., assuming that treatment waning occurs or that vial wastage is permitted).4 The results were largely aligned with the sponsor’s base-case analysis, although the results were most sensitive to changes in patient age and the exclusion of subsequent treatment costs. Of note, survival model parameters were not investigated as part of the sponsor’s sensitivity analysis.
No scenario analysis was conducted using a perspective other than the health care payer.4
CDA-AMC Appraisal of the Sponsor’s Economic Evaluation
CDA-AMC identified several key limitations to the sponsor’s analysis that have notable implications on the economic analysis:
Impact of MMR status and methods to derive the overall population estimates: In the submitted economic model, the sponsor separately estimated the cost-effectiveness of pembrolizumab plus carboplatin-paclitaxel versus carboplatin-paclitaxel in the overall population and in 2 relevant subgroups based on MMR status.4 It is reasonable to conduct the economic evaluation separately by subgroup, given that the NRG-GY018 trial explicitly stratified participants based on MMR status and reported greater clinical benefits in PFS, overall response rate, and duration of response with pembrolizumab plus carboplatin-paclitaxel in the dMMR cohort than in the pMMR subgroup.5 Clinical expert consultation further confirmed the appropriateness of these subgroups. However, to derive cost-effectiveness estimates for the overall population, CADTH health economics guidelines state that the appropriate estimate of the overall population results is determined by weighting the estimates for each subgroup by their respective prevalence.14 The sponsor’s approach to separately model the overall population and independently sample a new set of OS and PFS curves is therefore inappropriate. This resulted in nonsensical results, as the ICER for the overall population was lower than for the dMMR subpopulation and for the pMMR subpopulation in the sponsor’s analyses, which is not logically consistent.
In the CDA-AMC reanalysis, a stratified analysis based on MMR status was adopted. The estimate for cost and QALY for the overall population was determined by weighting the estimates for each subgroup by their respective prevalence reported in the NRG-GY018 trial.5
Uncertainty related to long-term extrapolation of OS: The median OS was not reached in the pembrolizumab plus carboplatin-paclitaxel arm and was reached at 32.2 months in the carboplatin-paclitaxel arm. As such, in the submitted model, OS was extrapolated beyond the trial duration. Clinical expert input received by CDA-AMC confirmed that the OS extrapolation in both the carboplatin-paclitaxel and pembrolizumab plus carboplatin-paclitaxel groups (in the pMMR and dMMR subgroups) did not align with clinical expectations or real-world survival outcomes, resulting in unrealistic long-term survival predictions. Indeed, in a multicentre, retrospective study, it was reported that the median OS from second-line platinum-based therapy in patients with advanced and/or recurrent EC was 12 months.15 The fact that a significant portion of the incremental QALYs was derived from data beyond the trial period underscores the substantial impact extrapolation assumptions can have on the model’s results. Together, this introduces a high level of uncertainty to the economic evaluation results.
CDA-AMC could not address this limitation as part of its base-case analyses. Clinical expert input obtained by CDA-AMC noted that all the available distributions produced overtly optimistic OS rates for the treatments being evaluated.
To explore the uncertainty around the OS benefit, CDA-AMC conducted scenario analyses using the most conservative OS curves for pembrolizumab plus carboplatin-paclitaxel and carboplatin-paclitaxel in the dMMR and pMMR subgroups. However, the results of this sensitivity analysis should be interpreted with caution, given that even these OS curves were noted to produce optimistic survival estimates, according to clinical expert input obtained by CDA-AMC.
Inherent assumptions of the PSM impact the ability to model subsequent treatments and result in unsubstantiated postprogression benefits associated with pembrolizumab: In the NRG-GY018 trial, approximately 30% of patients in the pembrolizumab plus carboplatin-paclitaxel arm and 58% of patients in the carboplatin-paclitaxel arm received subsequent therapy. In the submitted economic model, those proportions were lower than the values reported in the trial, with 23% and 54% of patients in the pembrolizumab plus carboplatin-paclitaxel and carboplatin-paclitaxel, respectively, receiving subsequent therapy. Furthermore, the distribution of subsequent therapies differed between the trial and the economic model, with the sponsor’s model distribution informed by clinical input and realignment to remove unlicensed treatments and regimens that are not available in Canada. The sponsor’s model assumed that patients who initially receive carboplatin-paclitaxel would be eligible for pembrolizumab with or without lenvatinib, and that nearly all patients (98%) would receive this immunotherapy as their next line of treatment. Clinical expert feedback received by CDA-AMC noted that such an assumption was appropriate; yet, in the NRG-GY018 trial, only about 65% of patients who initially received carboplatin-paclitaxel and then required subsequent treatment received a pembrolizumab-based regimen. Given that a higher proportion of patients receiving carboplatin-paclitaxel is modelled to receive pembrolizumab as subsequent therapy, which may be more effective than the subsequent treatment regimens studied in the NRG-GY08 trial, this is likely to impact OS. However, the PSM imposes the structural assumption that OS is independent of receipt of subsequent therapies. This lacks face validity and may overestimate the observed OS benefit in the pembrolizumab arm.
Furthermore, the sponsor’s base-case results indicated that patients treated with pembrolizumab plus carboplatin-paclitaxel experience longer survival after disease progression than those treated with carboplatin-paclitaxel. Specifically, about 8% of the reported incremental survival (0.29 LYs) occurred after a patient’s disease had progressed and pembrolizumab was discontinued. Although the NRG-GY018 trial showed an impact on PFS, there was no clear mechanism by which pembrolizumab plus carboplatin-paclitaxel would be expected to continue to provide clinical benefit after relapse. The sponsor’s use of a PSM raises concerns about the accuracy of these findings, as the structural independence assumed between the OS and PFS end points means that extrapolations for each end point could merely reflect observed within-trial trends in progression and mortality rates, rather than the actual effects of treatment. The PSM may not be able to accurately represent the true causal relationship within the disease pathway, and it introduces a bias in postprogression survival that favours pembrolizumab plus carboplatin-paclitaxel.
CDA-AMC was unable to address these limitations, given the inherent assumptions associated with PSM, in which changes in subsequent treatment do not impact OS. It remains unclear whether the implied postprogression benefit was related to the effect of treatment with pembrolizumab or stemmed from limitations inherent to the PSM. Clinical expert input received by CDA-AMC noted that a higher proportion of patients would, in fact, receive subsequent therapy in Canada than is assumed in the sponsor’s model. The effects of this could not be fully captured because differences in subsequent treatment would impact costs only and not the clinical effects modelled. As such, CDA-AMC conducted a scenario analysis testing alternative assumptions for the proportion and distribution of subsequent therapies in both the chemotherapy and pembrolizumab arms.
Health state utility values lacked face validity: The sponsor claimed that the time-to-death utility approach was applied to inform the utility weights employed in the sponsor’s base case. Yet, within the submitted Excel model, health state utility scores were applied (0.82 for the progressed-disease health state and 0.85 for the progression-free health state) that could not be validated, given that the source of these values were unclear. The selection of these utility weights would suggest that patients with progression-free, advanced or recurrent EC have a similar quality of life as people in the general population in Canada (0.864 for females aged 65 to 74 years).16 Furthermore, the utility values for patients in the progressed-disease health state (0.82) were similar to those in the progression-free health state (0.85). The clinical experts consulted by CDA-AMC confirmed that a patient’s quality of life typically worsens with disease progression.
In the CDA-AMC base case, CDA-AMC explored alternative utility values from other sources. According to clinical expert feedback received, it is reasonable to use ovarian cancer as a proxy for the quality of life experienced by patients with EC. As such, CDA-AMC applied alternate utility values for the progression-free and progressed-disease health states from National Institute for Health and Care Excellence (NICE) TA784 guidance (0.812 and 0.728, respectively), which was an economic evaluation conducted on patients with relapsed ovarian, fallopian tube, and peritoneal cancer.17
Uncertainty related to time on treatment for dostarlimab therapy: For dostarlimab only, time on treatment (ToT) was based on the PFS observed in the pembrolizumab plus carboplatin-paclitaxel arm of the NRG-GY018 trial. However, PFS and ToT are distinct concepts; PFS measures the time a patient remains free from disease progression, whereas ToT reflects the duration a patient stays on therapy, which can be impacted by many factors. Because patients may discontinue treatment while still experiencing prolonged disease control, aligning the duration of treatment with PFS could lead to an overestimation of dostarlimab’s costs in the model.
CDA-AMC was unable to address this limitation because of the constraint of the structure of the submitted model.
Uncertainty related to treatment-effect waning: In the sponsor’s base-case model, pembrolizumab’s treatment effect was assumed to persist for the patient’s lifetime, even after discontinuation (i.e., no treatment-effect waning). Although the evidence suggests that immunotherapeutic treatments like pembrolizumab may offer lasting benefits, even after discontinuation, the model does not fully account for the possibility that the treatment effect could diminish over time. The clinical experts consulted by CDA-AMC agreed that pembrolizumab was unlikely to continue influencing the probability of an event indefinitely and said that they expect a decline over time. Although the model provides an option to explore the effect of including treatment waning, the choice of the timing and distribution of waning effects (e.g., the start and end points) is dependent on many assumptions. For instance, the suggested start of treatment waning at 60 months and the end at 84 months, with 52.7% of patients experiencing waning, may not reflect the actual clinical experience of all patients or across indications.
CDA-AMC conducted 2 scenario analyses that similarly assumed treatment waning. In 1 scenario, immediate treatment waning was assumed to begin at 60 months but was applied to all patients. The other scenario assumed a gradual decline in treatment effect starting at year 5 and ending 3 years later.
Weight-based dosing for pembrolizumab reflects clinical practice: The sponsor assumed a fixed dosing regimen of pembrolizumab at a dose of 200 mg administered intravenously every 3 weeks, followed by 400 mg every 6 weeks, in the base-case model. However, CDA-AMC noted that, in line with other indications for pembrolizumab, jurisdictions would likely implement a weight-based dose of 2 mg/kg (up to a cap of 200 mg) every 3 weeks and then extended dosing intervals every 6 weeks (4 mg/kg, up to a 400 mg cap). Clinical expert input agreed that this approach to dosing would be reasonable.
In the reanalysis, CDA-AMC adopted a weight-based dosing regimen based on the average weight used by the sponsor.
Uncertainty has not been adequately specified in the probabilistic analysis: For the probabilistic analysis, a standard error of 10% from the mean was assumed for many model parameters. Given that the model parameters were informed by a variety of sources, including epidemiological studies and published clinical trials, the assumption of an arbitrary 10% of the mean is unnecessary and not reflective of the available information.
Furthermore, as noted previously, the deterministic and probabilistic results did not align in the dMMR population. Specifically, the absolute deterministic QALYs and LYs were consistently lower than the probabilistic QALYs and LYs for carboplatin-paclitaxel. Upon further investigation, CDA-AMC identified that the OS and PFS curves defined by a multivariate normal distribution had blank standard errors programmed.
Given that the standard error to define the parameters of the multivariate normal distribution for many of the OS and PFS curves were not reported, CDA-AMC set an undefined standard error for the multivariate normal distribution to zero. Although this resulted in the deterministic and probabilistic analyses aligning, the CDA-AMC reanalysis does not adequately account for the parameter uncertainties surrounding OS and PFS estimates.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CDA-AMC (refer to Table 4).
Table 4: Key Assumptions of the Submitted Economic Evaluation (Not Noted as Limitations to the Submission)
Sponsor’s key assumption | CDA-AMC comment |
|---|---|
A 35-year time horizon was chosen, assuming that no patients would survive beyond a mean age of 100 years. | Appropriate. This time horizon is sufficient to capture all lifetime costs and outcomes for the target population. |
Patients receiving pembrolizumab plus carboplatin-paclitaxel stopped treatment with pembrolizumab at 24 months. | Reasonable, as it aligns with the expected administration schedule, according to clinical expert feedback received by CDA-AMC. |
The efficacy (OS and PFS) of dostarlimab plus carboplatin-paclitaxel was equivalent to that of pembrolizumab plus carboplatin-paclitaxel. | Uncertain. This assumption was informed by the sponsor’s submitted MAIC. Although the CDA-AMC Clinical Review Report noted that there is insufficient evidence to demonstrate a difference in PFS between pembrolizumab plus carboplatin-paclitaxel and dostarlimab plus carboplatin-paclitaxel for advanced and recurrent dMMR EC, based on the submitted MAIC analysis, these results are highly uncertain because of concerns about the risk of selection bias and heterogeneity in both the patient populations and trial designs. The 95% confidence intervals for the treatment-effect estimates were wide and there was a noticeable difference in the KM curves between the control arms, with more PFS events occurring in the control arm of the RUBY-I trial than in the control arm of the NRG-GY018 trial. |
Grade ≥ 3 AEs in the ITT population of the NRG-GY018 trial for the subgroup of interest, in addition to AEs of special interest, have been included. | Uncertain, but unlikely to impact the economic results. The NRG-GY018 trial showed a clinically significant increase in immune-related AEs and infusion reactions with pembrolizumab plus carboplatin-paclitaxel compared to placebo plus carboplatin-paclitaxel, which was captured in the sponsor’s submitted model. |
Utility estimates are independent of MMR status. | Reasonable. |
No drug wastage. | Likely reasonable. Despite the pembrolizumab product monograph specifying that any unused portion left in the vial should be discarded, pembrolizumab is indicated for several other indications and vial sharing may be possible. CDA-AMC noted that assuming drug wastage is expected to have minimal impact on the results. |
No additional testing procedures will occur to determine MMR status. | Reasonable. Because MMR testing with IHC is already routinely available to all patients, it is acceptable to exclude its cost, as pembrolizumab is not expected to increase testing costs. |
AE = adverse event; CDA-AMC = Canada’s Drug Agency; dMMR = deficient mismatch repair; EC = endometrial cancer; IHC = immunohistochemistry; ITT = intention-to-treat; KM = Kaplan-Meier; MAIC = matching-adjusted indirect comparison; MMR = mismatch repair; OS = overall survival; PFS = progression-free survival.
CDA-AMC Reanalyses of the Economic Evaluation
Base-Case Results
The CDA-AMC base case was derived by making changes to model parameter values and assumptions, in consultation with clinical experts. The CDA-AMC base case adopted a stratified analysis based on MMR status. The estimate for costs and QALYs for the overall population was determined by weighting the estimates of the dMMR and pMMR subgroups by their respective prevalence reported in the NRG-GY018 trial (i.e., 27% for dMMR and 73% for pMMR). The CDA-AMC base case further adopted alternate health state utilities and applied weight-based dosing for pembrolizumab.
Table 5: CDA-AMC Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
1. Treatment compliance | — | Treatment compliance = 1 for all regimens |
Changes to derive the CDA-AMC base case | ||
1. Utility weights | Progression-free: 0.850 Progressed-disease: 0.820 | Progression-free: 0.812 Progressed-disease: 0.728 |
2. Dosing for pembrolizumab | Fixed dose | Weight-based dose |
CDA-AMC base case | ― | Reanalysis 1 + 2 |
CDA-AMC = Canada’s Drug Agency.
Results from the CDA-AMC base case suggest that pembrolizumab plus carboplatin-paclitaxel in the overall population was associated with higher costs ($90,334) than carboplatin-paclitaxel and improved QALYs (1.60 QALYs), resulting in an ICER of $57,334 per QALY gained (Table 7). The sponsor’s model estimated that there would be an incremental LY gain of 2.02 associated with pembrolizumab plus carboplatin-paclitaxel compared to carboplatin-paclitaxel.
For the dMMR subgroup, pembrolizumab plus carboplatin-paclitaxel was $139,066 more costly than carboplatin-paclitaxel and provided an additional 2.60 QALYs. This resulted in an ICER of $53,432 per QALY gained. Pembrolizumab plus carboplatin-paclitaxel dominated dostarlimab plus carboplatin-paclitaxel.
In the pMMR subgroup, pembrolizumab plus carboplatin-paclitaxel was associated with an incremental cost of $72,310 and an incremental QALY improvement of 1.23. This resulted in an ICER of $58,778 per QALY gained.
Although no changes were made to the OS and PFS curves in the CDA-AMC base case, the proportion of incremental QALY benefits derived from the extrapolated period differed from the sponsor’s base case, given that the analyses were stratified by MMR subgroup. Based on the deterministic results, in both subpopulations, approximately 95% of the incremental QALYs gained were from the period beyond the observed trial data. Consistent with the sponsor’s results, the majority (95%) of the incremental QALYs in the CDA-AMC analysis for the overall population were gained from the period beyond the observed trial data. Of note, the CDA-AMC reanalysis does not adequately account for the parameter uncertainties surrounding OS and PFS estimates, which are key drivers of the model results.
Table 6: Summary of the CDA-AMC Reanalysis Results (Probabilistic)
Analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|---|
dMMR population | ||||
Sponsor’s base case (corrected) | Carboplatin-paclitaxel | 141,213 | 3.93 | Reference |
Pembrolizumab plus carboplatin-paclitaxel | 303,916 | 6.53 | 62,571 | |
Dostarlimab plus carboplatin-paclitaxel | 504,670 | 6.53 | Dominated by pembrolizumab plus paclitaxel-carboplatin | |
CDA-AMC base case (reanalysis 1 + 2) | Carboplatin-paclitaxel | 141,213 | 3.58 | Reference |
Pembrolizumab plus carboplatin-paclitaxel | 280,279 | 6.18 | 53,432 | |
Dostarlimab plus carboplatin-paclitaxel | 504,670 | 6.18 | Dominated by pembrolizumab plus paclitaxel-carboplatin | |
pMMR population | ||||
Sponsor’s base case (corrected) | Carboplatin-paclitaxel | 153,998 | 2.55 | Reference |
Pembrolizumab plus carboplatin-paclitaxel | 242,448 | 3.80 | 70,261 | |
CDA-AMC base case (reanalysis 1 + 2) | Carboplatin-paclitaxel | 153,998 | 2.35 | Reference |
Pembrolizumab plus carboplatin-paclitaxel | 226,308 | 3.58 | 58,778 | |
CDA-AMC = Canada’s Drug Agency; dMMR = deficient mismatch repair; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Scenario Analysis Results
CDA-AMC conducted price analyses based on the sponsor’s base case and the CDA-AMC base-case reanalysis. Based on the CDA-AMC base case, a price reduction of approximately 10% would be required to achieve cost-effectiveness at a willingness-to-pay threshold of $50,000 per QALY gained (Table 7).
CDA-AMC conducted scenario analyses based on the CDA-AMC base-case analysis to assess the impact of alternative assumptions on the cost-effectiveness of adding pembrolizumab to carboplatin-paclitaxel. This included:
Adopting alternative extrapolated OS curves: In the dMMR subgroup, a gamma distribution was selected for the chemotherapy-alone arm, whereas a log-logistic distribution was used for the pembrolizumab arm. In the pMMR subgroup, a log-logistic distribution was selected for the chemotherapy-alone arm. Additionally, all selected distributions were 1-piece models, owing to the lack of clinically significant evidence to justify a breakpoint for a two-piece approach.
Applying different assumptions about the proportion and distribution of subsequent therapies: In the dMMR subgroup, 80% of patients in the chemotherapy-only arm received subsequent treatment, all of whom received pembrolizumab. In the pembrolizumab arm, the percentage of patients who received no subsequent treatment decreased from 87.5% to 60.0%. Of the 40% of patients who received subsequent treatment, 27.5% received chemotherapy and 12.5% received liposomal doxorubicin. In the pMMR subgroup, 55% of patients in the chemotherapy-only arm received subsequent treatment with pembrolizumab plus lenvatinib, whereas in the pembrolizumab arm, 60% of patients received no subsequent treatment; of the 40% who did, 13.5% received secondary chemotherapy and 26.5% received liposomal doxorubicin.
Applying the treatment-waning assumptions: One scenario assumed that treatment waning would begin at 60 months and apply to all patients immediately (scenario 3), whereas the other scenario assumed a gradual decrease in treatment effect that started at year 5 and lasted 3 years (scenario 4).
The results of these scenario analyses are present in Appendix 4. The results of the scenario analyses emphasize that the model is sensitive to OS assumptions in both the dMMR and pMMR subpopulations. The incorporation of a treatment-waning assumption, especially when applied to all patients, could also significantly impact the results of the model. The assumption that treatment would wane immediately at year 5 increased the ICER to $124,175 per QALY in the dMMR group and to $139,287 per QALY in the pMMR group, resulting in an ICER of $135,207 per QALY for the overall population. In the scenario that assumed gradual waning, the ICER increased to $112,183 per QALY for the overall population, to $114,612 per QALY for the pMMR subpopulation, and to $105,615 QALY for the dMMR subpopulation. The application of different assumptions about subsequent treatment resulted in a lower ICER for the dMMR subpopulation ($47,623 per QALY), whereas the change in ICER for the pMMR subgroup was less significant ($57,495 per QALY).
Table 7: CDA-AMC Price-Reduction Analyses
Analysis: price reduction | Unit drug cost | ICERs for pembrolizumab plus carboplatin-paclitaxel vs. comparators | CDA-AMC reanalysis, pMMR population | |
|---|---|---|---|---|
CDA-AMC reanalysis, overall population | CDA-AMC reanalysis, dMMR population | |||
No price reduction | $4,400 | If WTP is < $56,459, CP is optimal If WTP is < $56,459, pembrolizumab plus CP is optimal | If WTP is < $53,487, CP is optimal If WTP is < $53,487, pembrolizumab plus CP is optimal | If WTP is < $58,789, CP is optimal If WTP is < $58,789, pembrolizumab plus CP is optimal |
10% | $3,960 | If WTP is < $50,724, CP is optimal If WTP is < $50,724, pembrolizumab plus CP is optimal | If WTP is < $49,004, CP is optimal If WTP is < $49,004, pembrolizumab plus CP is optimal | If WTP is < $52,341, CP is optimal If WTP is < $52,341, pembrolizumab plus CP is optimal |
20% | $3,520 | If WTP is < $44,986, CP is optimal If WTP is < $44,986, pembrolizumab plus CP is optimal | If WTP is < $43,620 CP is optimal If WTP is < $43,620, pembrolizumab plus CP is optimal | If WTP is < $46,054 CP is optimal If WTP is < $46,054, pembrolizumab plus CP is optimal |
CDA-AMC = Canada’s Drug Agency; CP = carboplatin-paclitaxel; dMMR = deficient mismatch repair; ICER = incremental cost-effectiveness ratio; pMMR = proficient mismatch repair; vs. = versus; WTP = willingness to pay.
Issues for Consideration
The pCPA negotiation for dostarlimab plus carboplatin-paclitaxel was recently completed, with a letter of intent for the treatment of adult patients with primary advanced or recurrent dMMR and/or microsatellite instability–high EC who are candidates for systemic therapy. Clinical expert feedback received by CDA-AMC noted that the RUBY-I trial included adult patients with pMMR recurrent or advanced EC, although it does not have a Health Canada indication for this subgroup.
At the time of this review, durvalumab plus carboplatin-paclitaxel is under review by CDA-AMC for the first-line treatment of adults with primary advanced or recurrent pMMR EC who are candidates for systemic therapy, followed by durvalumab in combination with olaparib. The submitted model did not have an option to include this comparator.
Clinical expert input noted that there may be emerging drugs for the treatment of primary advanced or recurrent EC, such as CDK4/6 inhibitors like palbociclib, abemaciclib, and ribociclib, which are currently being investigated.
As in all CDA-AMC pharmacoeconomic reports, the economic evaluation presented here is based on publicly available list prices for all comparators, including pembrolizumab, dostarlimab, and chemotherapy. Negotiated prices are in place for all drugs in this evaluation. The finding of similar QALYs for pembrolizumab plus carboplatin-paclitaxel and dostarlimab plus carboplatin-paclitaxel is not affected by changes in drug prices; however, it is possible that the conclusion of similar costs would not hold if negotiated prices had been used in the analysis.
Overall Conclusions
The CDA-AMC clinical review concluded that the results of the NRG-GY018 trial showed that pembrolizumab plus carboplatin-paclitaxel compared to carboplatin-paclitaxel likely results in a clinically important improvement in PFS at 12 months and 24 months and may improve OS at 18 months and 36 months in adults with primary advanced or recurrent EC. However, conclusions regarding OS were limited because the data are not yet mature and statistically significant results in the all-comers population were post hoc and unadjusted for multiplicity. Because of the lack of direct comparative evidence against dostarlimab plus carboplatin-paclitaxel, an anchored MAIC was conducted by the sponsor in the subgroup of patients with dMMR. The MAIC was limited, given the risk of selection bias and the heterogeneity in both the patient populations and trial designs. The results of the MAIC should therefore be viewed as highly uncertain, and insufficient evidence exists to suggest a PFS difference between the 2 immunotherapies combined with carboplatin-paclitaxel.
CDA-AMC was unable to address all identified limitations, given inherent assumptions imposed by the PSM structure and the limited face validity of the available OS distributions. The CDA-AMC reanalysis used a stratified approach based on MMR status, in which weight-based dosing for pembrolizumab was applied and alternative health state utility values were sourced. The CDA-AMC reanalysis resulted in an ICER of $57,334 per QALY gained for pembrolizumab plus carboplatin-paclitaxel compared to carboplatin-paclitaxel in the overall population. Pembrolizumab was associated with a lower ICER in the dMMR population ($53,432 per QALY gained) than in the pMMR population ($58,778 per QALY gained). Because OS could not be modified in the economic model to reflect more realistic long-term survival expectations, the results are dependent on patients receiving pembrolizumab plus carboplatin-paclitaxel gaining 2.02 additional LYs compared to carboplatin-paclitaxel.
The majority of the incremental clinical benefits for pembrolizumab (95%) were derived in the period beyond which there are observed trial data (i.e., extrapolated period). The survival models chosen by the sponsor may overestimate patient survival compared to clinical expectations. The PSM used also indicated a postprogression survival benefit, likely owing to assumptions with the PSM model structure, favouring pembrolizumab plus carboplatin-paclitaxel. Additionally, the distribution of subsequent treatments in the submitted model does not accurately reflect Canadian clinical practice, and the proportions used did not align with those reported in the Clinical Study Report. As such, the cost-effectiveness of pembrolizumab and the price-reduction estimates are highly uncertain.
Clinical expert feedback suggested that pembrolizumab and dostarlimab may have a similar efficacy. There was no clinical evidence suggesting that the total treatment cost of pembrolizumab plus carboplatin-paclitaxel should be higher than the total treatment cost of dostarlimab plus carboplatin-paclitaxel in the dMMR subgroup.
References
1.Pan-Canadian Pharmaceutical Alliance. Jemperli (dostarlimab). 2024. Accessed February 10, 2025. https://www.pcpacanada.ca/negotiation/22696
2.KEYTRUDA®(pembrolizumab): solution for infusion 100 mg/4 mL vial [product monograph]. Merck Canada Inc.; 2024.
3.Francoeur A, Richardson M, Johnson C, Liang S-Y, Tewari K, Chan J. Cost-effectiveness analysis of immunotherapy regimens in advanced or recurrent endometrial cancer: An analysis of the NRG-GY018 and RUBY trials. Gynecologic Oncology. 2024;190:S54. doi:10.1016/j.ygyno.2024.07.082
4.Pharmacoeconomic evaluation [internal sponsor’s report]. In: Drug Reimbursement Review sponsor submission: pembrolizumab (Keytruda®), solution for infusion 100 mg/4 mL vial [internal sponsor’s package]. Kirkland (QC): Merck Canada Inc.; 2024 Nov 15.
5.Clinical Study Report: study number. A Phase III Randomized, Placebo-controlled Study of Pembrolizumab (MK-3475, NSC #776864) in Addition to Paclitaxel and Carboplatin for Measurable Stage III or IVA, Stage IVB or Recurrent Endometrial Cancer. [internal sponsor’s report]. National Cancer Institute, Cancer Therapy Evaluation Program; 2023.
6.DeltaPA [sponsor supplied reference]. IQVIA; 2023. https://www.iqvia.com/
7.CADTH. Drug Reimbursement Review: JEMPERLI (Dostarlimab) for primary advanced or recurrent mismatch repair deficient (dMMR)/microsatellite instability-high (MSI-H) endometrial cancer. 2024. Accessed February 10, 2025. https://www.cda-amc.ca/dostarlimab-0
8.CADTH Reimbursement Review: Pembrolizumab in Combination with Lenvatinib (Keytruda and Lenvima). Can J Health Technol. CADTH; 2022;2(12). Accessed February 10, 2025. https://www.cda-amc.ca/sites/default/files/DRR/2022/PC0288-Keytruda-Lenvima.pdf
9.Ontario Nurses Association. Highlights of Collective Agreement Changes as a Results of the Kaplan Decision and Items in agreement between ONA and Participating Hospitals [sponsor provided reference]. 2024. Accessed October 2024. https://www.ona.org/wp-content/uploads/2023-hospital-central-contract-highlights.pdf
10.Schedule of benefits for laboratory services [sponsor supplied reference]. Ontario Ministry of Health; 2023. https://www.health.gov.on.ca/en/pro/programs/ohip/sob/lab/sob_lab_2023.pdf
11.Schedule of benefits for physician services under the Health Insurance Act: (June 29, 2023 (effective July 24, 2023)) [sponsor provided reference]. Ontario Ministry of Health; 2023. https://www.health.gov.on.ca/en/pro/programs/ohip/sob/physserv/sob_master.pdf
12.Patient cost estimator. Canadian Institute for Health Information. Accessed October 2, 2024. https://www.cihi.ca/en/patient-cost-estimator
13.De Oliveira C, Pataky R, Bremner KE, et al. Estimating the Cost of Cancer Care in British Columbia and Ontario: A Canadian Inter-Provincial Comparison. Healthc Policy. 2017;12(3):95-108. PubMed
14.Guidelines for the economic evaluation of health technologies: Canada [sponsor provided reference]. 4th ed. CADTH; 2017. https://www.cadth.ca/guidelines-economic-evaluation-health-technologies-canada-4th-edition
15.Prabhu V, Kelkar S, Zhang J, et al. Real-world treatment patterns and clinical outcomes in patients with advanced or recurrent endometrial cancer re-challenged with platinum-based chemotherapy in Europe. Int J Gynecol Cancer. 2025;35(4):101658. doi:10.1016/j.ijgc.2025.101658 PubMed
16.Yan J, Xie S, Johnson JA, et al. Canada population norms for the EQ-5D-5L. Eur J Health Econ. 2024;25(1):147-155. doi:10.1007/s10198-023-01570-1 PubMed
17.Niraparib for maintenance treatment of relapsed, platinum-sensitive ovarian, fallopian tube and peritoneal cancer (CDF review TA528) [ID1644]. National Institute for Health and Care Excellence (NICE); 2021. Accessed February 14, 2025. https://www.nice.org.uk/guidance/TA784/documents/committee-papers-2
18.Keytruda® Budget Impact Analysis Report [internal sponsor’s report]. In: Drug Reimbursement Review sponsor submission: pembrolizumab (Keytruda®), solution for infusion 100 mg/4 mL vial [internal sponsor's package]. Kirkland (QC): Merck Canada Inc.; 2024 Nov 15.
19.Brenner DR, Gillis J, Demers AA, et al. Projected estimates of cancer in Canada in 2024. CMAJ. 2024;196(18):E615-E623. doi:10.1503/cmaj.240095 PubMed
20.American Cancer Society. Key Statistics for Endometrial Cancer [sponsor provided reference]. Accessed October 2, 2024. https://www.cancer.org/cancer/types/endometrial-cancer/about/key-statistics.html
21.Canadian Cancer Statistics Advisory Committee in collaboration with the Canadian Cancer Society, Statistics Canada and the Public Health Agency of Canada. Canadian Cancer Statistics 2018. Toronto, ON: Canadian Cancer Society; 2018 [sponsor provided reference]. 2018. Accessed October 2024.
22.Fung-Kee-Fung M, Dodge J, Elit L, et al. Follow-up after primary therapy for endometrial cancer: a systematic review. Gynecol Oncol. 2006;101(3):520-9. doi:10.1016/j.ygyno.2006.02.011 PubMed
Appendix 1: Cost Comparison Table
Please note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical experts and drug plans. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 8: CDA-AMC Cost Comparison for Primary Advanced or Recurrent Endometrial Cancer
Treatment | Strength/ concentration | Form | Price | Recommended dosage | Daily cost ($) | 21-Day cost ($)a |
|---|---|---|---|---|---|---|
Pembrolizumab | 25 mg/mL | 4 mL Vial | $4,400.0000 | 200 mg on day 1 of each 21-day cycle (6 cycles) Maintenance: 400 mg once every 6 weeks until progression | $419.05 | $8,800 |
Carboplatin | 10 mg/mL | 5 mL Vial 15 mL Vial 45 mL Vial 60 mL Vial | $70.0000 $210.0000 $600.0000 $775.0000 | AUC 4 to 6 on day 1 of each 21-day cycle | $36.90 to | $775 to |
Paclitaxel | 6 mg/mL | 5 mL Vial 16 mL Vial 25 mL Vial 50 mL Vial | $300.0000 $1,196.8000 $1,870.0000 $3,740.0000 | 175 mg/m2 on day 1 of each 21-day cycle | $206.67 | $4,340 |
Pembrolizumab plus carboplatin-paclitaxel: Combination period | $1,919.76 to | $13,915 to | ||||
Pembrolizumab plus carboplatin-paclitaxel: Maintenance period | $419.05 | $8,800 | ||||
Carboplatin-paclitaxel (CAR-PAC) | ||||||
Carboplatin | 10 mg/mL | 5 mL Vial 15 mL Vial 45 mL Vial 60 mL Vial | $70.0000 $210.0000 $600.0000 $775.0000 | AUC 4 to 6 on day 1 of each 21-day cycle | $36.90 to | $775 to |
Paclitaxel | 6 mg/mL | 5 mL Vial 16 mL Vial 25 mL Vial 50 mL Vial | $300.0000 $1,196.8000 $1,870.0000 $3,740.0000 | 175 mg/m2 on day 1 of each 21-day cycle | $206.67 | $4,340 |
Carboplatin-paclitaxel | $243.57 to | $5,115 to | ||||
Dostarlimab plus carboplatin-paclitaxel (DOST + CAR-PAC) | ||||||
Dostarlimab | 50 mg/mL | 10 mL vial | $10,031.0800 | 500 mg on day 1 of each 21-day cycle (6 cycles) Maintenance: 1,000 mg once every 6 weeks thereafter. | $477.67 | $10,031 |
Carboplatin | 10 mg/mL | 5 mL vial 15 mL vial 45 mL vial 60 mL vial | $70.0000 $210.0000 $600.0000 $775.0000 | AUC 5 on day 1 of each 21-day cycle | $46.90 | $985 |
Paclitaxel | 6 mg/mL | 5 mL vial 16 mL vial 25 mL vial 50 mL vial | $300.0000 $1,196.8000 $1,870.0000 $3,740.0000 | 175 mg/m2 on day 1 of each 21-day cycle | $206.67 | $4,340 |
Dostarlimab plus carboplatin-paclitaxel: Loading period | $731.24 | $15,356 | ||||
Dostarlimab: Maintenance period | $477.67 | $10,031 | ||||
Note: All prices are from the Ontario Drug Benefit Formulary (accessed September 2000), unless otherwise indicated, and do not include dispensing fees. For the purposes of dosage calculation, the average patient was assumed to weigh 88 kg, have a body surface area of 1.95 mg2 and included wastage of unused medication in vials.
aSponsor’s submitted price.
bIQVIA Delta Price Advisor wholesale price. Accessed February 2025.
Table 9: CDA-AMC Cost Comparison for Primary Advanced or Recurrent Endometrial Cancer — Off-Label Therapies
Treatment | Strength / concentration | Form | Price | Recommended dosage | Daily cost ($) | 21-Day cost ($) |
|---|---|---|---|---|---|---|
Bevacizumab plus carboplatin-paclitaxel (BEVA + CAR-PAC) | ||||||
Bevacizumab | 25 mg/mL | 4 mL vial 16 mL vial | $347.0000a $1,388.0000a | 15 mg/kg on day 1 of each 21-day cycle | $231.33 | $4,858 |
Carboplatin | 10 mg/mL | 5 mL Vial 15 mL Vial 45 mL Vial 60 mL Vial | $70.0000a $210.0000a $600.0000a $775.0000a | AUC 4 to 6 on day 1 of each 21-day cycle | $36.90 to | $775 to |
Paclitaxel | 6 mg/mL | 5 mL vial 16 mL vial 25 mL vial 50 mL vial | $300.0000a $1,196.8000a $1,870.0000a $3,740.0000a | 175 mg/m2 on day 1 of each 21-day cycle | $206.67 | $4,340 |
Regimen Cost | $474.90 to | $9,973 to $10,393 | ||||
Monotherapies | ||||||
Progesterone | 100 mg | Capsule | $1.4358b | 200 to 400 mg daily | $2.87 to $5.74 | $60 to $121 |
Letrozole | 2.5 mg | Tablet | $1.3780b | 2.5 mg daily | $1.38 | $29 |
Note: All prices are from the Ontario Drug Benefit Formulary (accessed September 2000), unless otherwise indicated, and do not include dispensing fees. For the purposes of dosage calculation, the average patient was assumed to weigh 88kg, have a body surface area of 1.95 mg2 and included wastage of unused medication in vials.
aIQVIA Delta Price Advisor wholesale price. Accessed February 2025.
bOntario Drug Benefit Formulary (Accessed February 2025).
Appendix 2: Submission Quality
Please note that this appendix has not been copy-edited.
Description | Yes or No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | Yes | — |
Model has been adequately programmed and has sufficient face validity | No | Refer to the key limitations. The OS extrapolations lacked face validity and issues were present regarding the transparency and flexibility within the submitted model. |
Model structure is adequate for decision problem | No | Refer to the key limitations regarding the partitioned survival modelling approach and its ability for changes in subsequent treatment to impact overall survival. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | No | The pharmacoeconomic report does not provide details about the value and sources of the parameters used in the probabilistic analysis. It is only noted that parameter distributions were estimated from the available data sources whenever possible. Furthermore, the probabilistic results for the dMMR subgroup misaligned with its deterministic results. OS and PFS curves defined by a multivariate normal distribution had blank standard errors programmed. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | Yes | No comments. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | Yes | No comments. |
Appendix 3: Additional Information on the Submitted Economic Evaluation
Please note that this appendix has not been copy-edited.
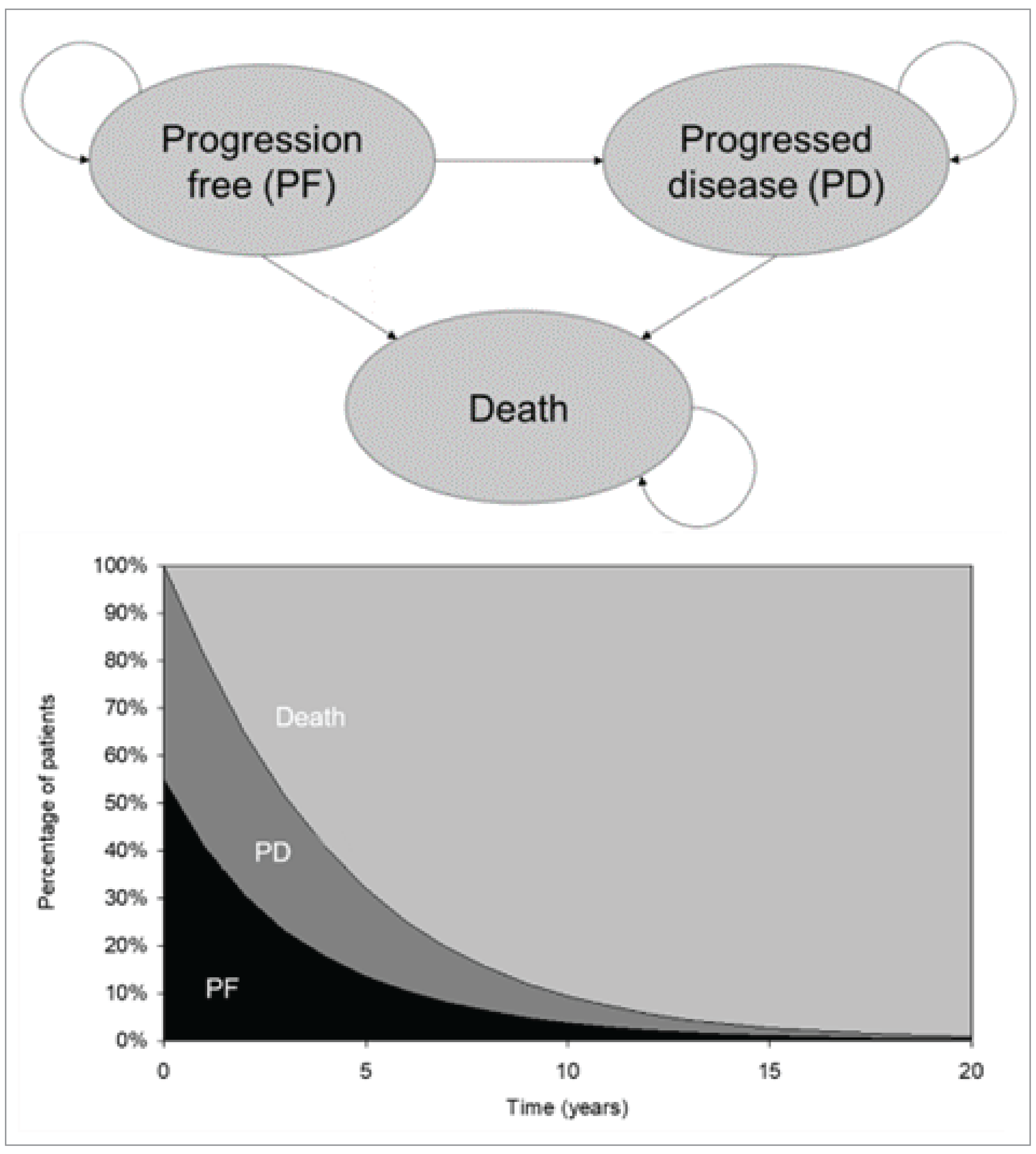
Table 11: Sponsor-Selected Statistical Distributions for OS, PFS, and TTDC
Curve | Pembrolizumab plus carboplatin + paclitaxel | Carboplatin + paclitaxel |
|---|---|---|
Overall population | ||
OS | Log normal distribution with two-piece extrapolation (breakpoint at Week 40) | Log-logistic distribution |
PFS | Log normal distribution with two-piece extrapolation (breakpoint at Week 38) | Log-logistic distribution with two-piece extrapolation (breakpoint at Week 38) |
TTDC | Kaplan-Meier | Kaplan-Meier |
dMMR subgroup | ||
OS | Gamma distribution | Gompertz distribution |
PFS | Log normal distribution with two-piece extrapolation (breakpoint at Week 27) | Log-logistic distribution |
TTDC | Kaplan-Meier | Kaplan-Meier |
pMMR subgroup | ||
OS | Log normal distribution with two-piece extrapolation (breakpoint at Week 60) | Weibull distribution with two-piece extrapolation (breakpoint at Week 60) |
PFS | Log-logistic distribution with two-piece extrapolation (breakpoint at Week 37) | Log-logistic distribution |
TTDC | Kaplan-Meier | Kaplan-Meier |
dMMR = deficient mismatch repair; OS = overall survival; pMMR = proficient mismatch repair; PFS = progression-free survival; TTDC = time to discontinuation or completion.
Table 12: Subsequent Treatment Distribution Reported in the NRG-GY018 Trial Versus the Sponsor’s Submitted Model
Subsequent treatment | dMMR | pMMR | ||||||
|---|---|---|---|---|---|---|---|---|
NRG-GY018 trial | Model | NRG-GY018 trial | Model | |||||
Pembrolizumab | Chemo | Pembrolizumab | Chemo | Pembrolizumab | Chemo | Pembrolizumab | Chemo | |
Bevacizumab | 0.00% | 1.10% | 0.00% | 0.00% | 0.59% | 1.67% | 0.00% | 0.00% |
Bevacizumab + liposomal doxorubicin | 0.00% | 1.10% | 0.00% | 0.00% | 3.53% | 0.84% | 0.00% | 0.00% |
Carboplatin | 1.56% | 0.00% | 0.00% | 0.00% | 0.00% | 1.26% | 0.00% | 0.00% |
Carboplatin + docetaxel | 4.69% | 1.10% | 0.00% | 0.00% | 4.12% | 6.69% | 0.00% | 0.00% |
Carboplatin + paclitaxel | 1.56% | 0.00% | 0.00% | 0.00% | 0.00% | 1.26% | 0.00% | 0.00% |
Dostarlimab | 0.00% | 0.00% | 0.00% | 0.00% | 0.00% | 0.00% | 0.00% | 0.00% |
Doxorubicin | 1.56% | 0.00% | 0.00% | 0.00% | 5.29% | 0.84% | 0.00% | 0.00% |
liposomal doxorubicin | 4.69% | 0.00% | 12.50% | 1.35% | 1.18% | 0.42% | 26.46% | 1.15% |
Everolimus + letrozole | 3.13% | 1.10% | 0.00% | 0.00% | 1.76% | 2.51% | 0.00% | 0.00% |
Lenvatinib + pembrolizumab | 1.56% | 1.10% | 0.00% | 0.00% | 2.94% | 0.42% | 0.00% | 0.00% |
Letrozole | 0.00% | 0.00% | 0.00% | 0.00% | 0.00% | 1.26% | 0.00% | 0.00% |
Megestrol (acetate) | 0.00% | 2.20% | 0.00% | 0.00% | 2.94% | 2.09% | 0.00% | 0.00% |
Megestrol (acetate) + tamoxifen | 0.00% | 0.00% | 0.00% | 0.00% | 2.35% | 0.00% | 0.00% | 0.00% |
Paclitaxel | 0.00% | 41.76% | 0.00% | 0.00% | 0.00% | 13.81% | 0.00% | 0.00% |
Pembrolizumab | 0.00% | 1.10% | 0.00% | 51.40% | 0.00% | 18.41% | 0.00% | 50.32% |
Radiotherapy | 1.56% | 4.40% | 0.00% | 0.00% | 9.41% | 5.44% | 0.00% | 0.00% |
No treatment | 79.69% | 45.05% | 87.50% | 47.24% | 65.88% | 43.10% | 73.54% | 48.53% |
Detailed Results of the Sponsor’s Base Case
Table 13: Disaggregated Summary of the Sponsor’s Economic Evaluation Results (Overall Population, Deterministic)
Parameter | Pembrolizumab plus carboplatin-paclitaxel | Carboplatin-paclitaxel |
|---|---|---|
Discounted LYs | ||
Total | 7.75 | 4.18 |
Progression-free | 5.47 | 2.18 |
Progressed | 2.28 | 2.00 |
Discounted QALYs | ||
Total | 6.16 | 3.38 |
Progression-free | 4.65 | 1.86 |
Progressed | 1.86 | 1.63 |
Adverse Event Disutility | −0.01 | 0.00 |
Age disutility | −0.35 | −0.11 |
Discounted costs | ||
Total | 251,992 | 149,616 |
Acquisition | 165,507 | 23,707 |
Administration | 1,087 | 770 |
Subsequent treatment cost | 2,428 | 47,042 |
Adverse event costs | 408 | 170 |
Terminal-care costs | 64,700 | 69,147 |
Disease-management costs in progressed state | 2,899 | 2,549 |
Disease-management costs in progression-free state | 14,572 | 5,816 |
LY = life-year; QALY = quality-adjusted life-year.
Source: Sponsor’s pharmacoeconomic submission.4
Table 14: Sponsor’s Economic Evaluation Results — dMMR Subgroup (Deterministic)
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER vs. paclitaxel-carboplatin ($/QALY) |
|---|---|---|---|---|---|
Carboplatin-paclitaxel | 140,789 | Reference | 3.93 | Reference | Reference |
Pembrolizumab plus carboplatin-paclitaxel | 292,231 | 151,442 | 6.55 | 2.62 | 57,925 |
Dostarlimab plus carboplatin-paclitaxel | 508,764 | 216,533 | 6.55 | 0 | Dominated by pembrolizumab plus paclitaxel and carboplatin |
dMMR = deficient mismatch repair; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus.
Appendix 4: Additional Details on the CDA-AMC Reanalyses and Sensitivity Analyses of the Economic Evaluation
Please note that this appendix has not been copy-edited.
Table 15: Summary of the Stepped Analysis of the CDA-AMC Reanalysis Results
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|---|
pMMR population | ||||
Sponsor’s base case (corrected) | Carboplatin-paclitaxel | 154,171 | 2.55 | Reference |
Pembrolizumab plus carboplatin-paclitaxel | 242,413 | 3.81 | 70,098 | |
CDA-AMC reanalysis 1: Utility weights | Carboplatin-paclitaxel | 154,171 | 2.35 | Reference |
Pembrolizumab plus carboplatin-paclitaxel | 242,413 | 3.58 | 71,725 | |
CDA-AMC reanalysis 2: Weight-based dosing for pembrolizumab | Carboplatin-paclitaxel | 154,171 | 2.55 | Reference |
Pembrolizumab plus carboplatin-paclitaxel | 226,251 | 3.81 | 57,259 | |
CDA-AMC base case (reanalysis 1 + 2, deterministic) | Carboplatin-paclitaxel | 154,171 | 2.35 | Reference |
Pembrolizumab plus carboplatin-paclitaxel | 226,251 | 3.58 | 58,588 | |
CDA-AMC base case (reanalysis 1 + 2, probabilistic) | Carboplatin-paclitaxel | 153,998 | 2.35 | Reference |
Pembrolizumab plus carboplatin-paclitaxel | 226,308 | 3.58 | 58,778 | |
dMMR population | ||||
Sponsor’s base case (corrected) | Carboplatin-paclitaxel | 141,203 | 3.93 | Reference |
Pembrolizumab plus carboplatin-paclitaxel | 303,950 | 6.55 | 62,249 | |
Dostarlimab plus carboplatin-paclitaxel | 508,764 | 6.55 | Dominated by pembrolizumab plus carboplatin-paclitaxel | |
CDA-AMC reanalysis 1: Utility weights | Carboplatin-paclitaxel | 141,203 | 3.59 | Reference |
Pembrolizumab plus carboplatin-paclitaxel | 303,950 | 6.20 | 60,842 | |
Dostarlimab plus carboplatin-paclitaxel | 508,764 | 6.19 | Dominated by pembrolizumab plus carboplatin-paclitaxel | |
CDA-AMC reanalysis 2: Weight-based dosing for pembrolizumab | Carboplatin-paclitaxel | 141,203 | 3.93 | Reference |
Pembrolizumab plus carboplatin-paclitaxel | 280,327 | 6.55 | 53,213 | |
Dostarlimab plus carboplatin-paclitaxel | 508,764 | 6.55 | Dominated by pembrolizumab plus carboplatin-paclitaxel | |
CDA-AMC base case (reanalysis 1 + 2, deterministic) | Carboplatin-paclitaxel | 141,203 | 3.57 | Reference |
Pembrolizumab plus carboplatin-paclitaxel | 280,327 | 6.20 | 53,057 | |
Dostarlimab plus carboplatin-paclitaxel | 508,764 | 6.19 | Dominated by pembrolizumab plus carboplatin-paclitaxel | |
CDA-AMC base case (reanalysis 1 + 2, probabilistic) | Carboplatin-paclitaxel | 141,213 | 3.58 | Reference |
Pembrolizumab plus carboplatin-paclitaxel | 280,279 | 6.18 | 53,432 | |
Dostarlimab plus carboplatin-paclitaxel | 507,670 | 6.18 | Dominated by pembrolizumab plus carboplatin-paclitaxel | |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Note: The CDA-AMC reanalysis is based on publicly available prices of the comparator treatments. The results of all steps are presented deterministically unless otherwise indicated. The ICERs displayed in the table are accurate according to the model files accounting from all decimals omitted from this table.
Table 16: Disaggregated Summary of the CDA-AMC Economic Evaluation Results — pMMR Subgroup
Parameter | Pembrolizumab plus carboplatin-paclitaxel | Carboplatin-paclitaxel |
|---|---|---|
Discounted LYs | ||
Total | 4.70 | 3.12 |
By health state or data source | ||
Progression-free | 3.23 | 1.33 |
Progressed | 1.47 | 1.79 |
Discounted QALYs | ||
Total | 3.58 | 2.35 |
By health state or data source | ||
Progression-free | 2.65 | 1.09 |
Progressed | 1.07 | 1.30 |
Discounted costs ($) | ||
Total | 226,308 | 153,998 |
Acquisition cost | 142,537 | 23,681 |
Administration cost | 1,059 | 769 |
Subsequent treatment cost | 2,808 | 52,502 |
Adverse event costs | 343 | 191 |
Terminal-care costs | 68,668 | 70,604 |
Disease-management costs in progressed state | 1,869 | 2,276 |
Disease-management costs in progression-free state | 8,611 | 3,550 |
CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; LY = life-year; NA = not applicable; PD = Progressed; PFS = Progression-free; QALY = quality-adjusted life-year; Ref. = reference.
Table 17: Disaggregated Summary of the CDA-AMC Economic Evaluation Results — dMMR Subgroup
Parameter | Pembrolizumab plus carboplatin-paclitaxel | Carboplatin-paclitaxel | Dostarlimab plus carboplatin-paclitaxel |
|---|---|---|---|
Discounted LYs | |||
Total | 8.08 | 4.88 | 8.08 |
By health state or data source | |||
Progression-free | 7.28 | 1.52 | 7.28 |
Progressed | 0.80 | 3.36 | 0.80 |
Discounted QALYs | |||
Total | 6.18 | 3.58 | 6.18 |
By health state or data source | |||
Progression-free | 5.91 | 1.24 | 5.91 |
Progressed | 0.58 | 2.44 | 0.58 |
Discounted costs ($) | |||
Total | 280,279 | 141,213 | 507,670 |
Acquisition cost | 191,151 | 23,769 | 416,036 |
Administration cost | 1,151 | 770 | 1,441 |
Subsequent treatment cost | 1,325 | 39,142 | 1,305 |
Adverse event costs | 1,124 | 112 | 3,360 |
Terminal-care costs | 64,735 | 68,667 | 64,734 |
Disease-management costs in progressed state | 1,020 | 4,276 | 1,021 |
Disease-management costs in progression-free state | 19,389 | 4,052 | 19,388 |
CDA-AMC = Canada’s Drug Agency; dMMR = deficient mismatch repair; LY = life-year; QALY = quality-adjusted life-year.
Scenario Analyses
Table 18: Scenario Analyses Conducted on the CDA-AMC Base Case (Probabilistic)
Scenarios | Population | Treatment | Total costs ($) | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|---|
Sponsor’s base case (corrected) | dMMR subgroup | CP | 141,213 | 3.93 | Reference |
Pembrolizumab plus CP | 303,916 | 6.53 | 62,571 | ||
Dostarlimab plus CP | 504,670 | 6.53 | Dominated by pembrolizumab plus paclitaxel and carboplatin | ||
pMMR subgroup | CP | 153,998 | 2.55 | Reference | |
Pembrolizumab plus CP | 242,448 | 3.80 | 70,261 | ||
CDA-AMC Scenario analysis 1: Alternative OS curve | dMMR subgroup | CP | 141,217 | 3.60 | Reference |
Pembrolizumab plus CP | 282,132 | 7.37 | 37,319 | ||
Dostarlimab plus CP | 509,576 | 7.37 | Dominated by Pembrolizumab plus CP | ||
pMMR subgroup | CP | 153,987 | 2.55 | Reference | |
Pembrolizumab plus CP | 226,308 | 3.58 | 70,710 | ||
CDA-AMC Scenario analysis 2: Alternative subsequent treatment assumptions | dMMR subgroup | CP | 162,755 | 3.58 | Ref. |
Pembrolizumab plus CP | 286,703 | 6.18 | 47,623 | ||
Dostarlimab plus CP | 507,670 | 6.18 | Dominated by Pembrolizumab plus CP | ||
pMMR subgroup | CP | 158,746 | 2.35 | Reference | |
Pembrolizumab plus CP | 229,428 | 3.58 | 57,495 | ||
CDA-AMC Scenario analysis 3: Including treatment-waning assumption, Immediate waning at year 5 | dMMR subgroup | CP | 141,213 | 3.58 | Ref. |
Pembrolizumab plus CP | 277,271 | 4.67 | 124,175 | ||
Dostarlimab plus CP | 504,663 | 4.67 | Dominated by pembrolizumab plus CP | ||
pMMR subgroup | CP | 153,998 | 2.35 | Reference | |
Pembrolizumab plus CP | 225,047 | 2.86 | 139,287 | ||
CDA-AMC Scenario analysis 4: Including treatment-waning assumption, gradual decrease in treatment effect | dMMR subgroup | CP | 141,213 | 3.58 | Reference |
Pembrolizumab plus CP | 277,852 | 4.87 | 105,615 | ||
Dostarlimab plus CP | 505,244 | 4.87 | Dominated by pembrolizumab plus CP | ||
pMMR subgroup | CP | 153,998 | 2.35 | Reference | |
Pembrolizumab plus CP | 225,283 | 2.97 | 114,612 |
CP = carboplatin-paclitaxel; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; Ref. = reference.
Note: The ICERs displayed in the table are accurate according to the model files accounting from all decimals omitted from this table.
Appendix 5: Submitted Budget Impact Analysis and CDA-AMC Appraisal
Please note that this appendix has not been copy-edited.
Table 19: Summary of Key Take-Aways
Key Take-aways of the budget impact analysis |
|---|
|
Summary of Sponsor’s Budget Impact Analysis
The sponsor submitted a budget impact analysis (BIA) to estimate the three-year budget impact of reimbursing pembrolizumab plus carboplatin-paclitaxel to treat adult patients with primary advanced or recurrent endometrial cancer (EC).18 The analysis was conducted from the perspective of pan-Canadian public drug plans over a 3-year time horizon from 2026 to 2028 with only drug-acquisition costs (including subsequent therapy costs) incorporated in the base-case analysis.18
The sponsor utilized an incidence-based approach to define the eligible population. The only treatment considered in the reference scenario was carboplatin-paclitaxel chemotherapy. A subgroup analysis was further provided only for the dMMR subgroup in which dostarlimab was included as another treatment in the reference scenario. To derive the eligible dMMR subpopulation size, the sponsor assumed that the proportion of dMMR patients comprised 27% of the total EC population.4 Specific to this subgroup analysis, the sponsor projected that dostarlimab would capture 14% of the market share by year 3 in the new drug scenario. The sponsor derived treatment duration estimates for pembrolizumab plus carboplatin-paclitaxel and carboplatin-paclitaxel from the NRG-GY018 trial based on the time to discontinuation curves. The duration on treatment for dostarlimab was based on the PFS of pembrolizumab from the same trial. The sponsor assumed a market share maximum of 50% for pembrolizumab, achieved at year 3, in both the overall analysis and subgroup analysis.18 Key inputs to the overall population’s BIA are documented in Table 20.
Key model assumptions included:
76.6% of patients receiving oral oncology therapies are publicly covered.
100% RDI and 5% drug wastage for all treatments.
Pembrolizumab costs were calculated by assuming it is prescribed as a fixed dose while the comparators were costed based on weight-based dosing.
Table 20: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1 / year 2 / year 3 if appropriate) | |
|---|---|---|
Target population | ||
Population growth rate | 2.48%19 | |
Incidence rate of uterine cancer | 36.7 per 100,00019 | |
Proportion of endometrial cancer | 90.0%20 | |
Proportion with advanced or metastatic disease | 17.7%21 | |
Proportion referred to medical specialist | 95.0%18 | |
Proportion with advanced stage disease | 87%22 | |
Proportion with recurrent disease | 13%22 | |
Proportion receiving 1L treatment who are candidates for systemic therapy | 90.0%18 | |
Number of patients eligible for drug under review | 1,571 / 1,610 / 1,650 | |
Market Uptake (3 years)18 | ||
Uptake (reference scenario) Carboplatin-paclitaxel | 100% / 100% / 100% | |
Uptake (new drug scenario) Pembrolizumab plus carboplatin-paclitaxel Carboplatin-paclitaxel | 17% / 46% / 50% 83% / 54% / 50% | |
Cost of treatment (per patient, per 21-day cycle)18 | ||
Pembrolizumab plus carboplatin-paclitaxel Carboplatin-paclitaxel | $13,184.78 $4,384.78 | |
2L Treatment rate18 | ||
Pembrolizumab plus carboplatin-paclitaxel Carboplatin-paclitaxel | 11% 48% | |
Type of subsequent treatment bases on 1L therapy | Pembrolizumab arm / CAR-PAC arm18 | |
Pembrolizumab plus lenvatinib Pembrolizumab Liposomal doxorubicin | — — 100% | 45% 53% 2% |
1L = first-line; 2L = second-line, CAR-PAC = carboplatin-paclitaxel.
Summary of the Sponsor’s BIA Results
The sponsor estimated the budget impact of reimbursing pembrolizumab for the treatment of adult patients with advanced or recurrent EC to be $12,239,648 in year 1, $58,715,219 in year 2 and $89,656,490 in year 3, for a three-year total budget impact of $160,611,357.
CDA-AMC Appraisal of the Sponsor’s BIA
CDA-AMC identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
The proportion starting second-line (2L) treatment and distributions of subsequent treatments are uncertain: The proportion of patients initiating subsequent therapy was based on assumptions made by the sponsor. Yet, these values did not align with the estimates for the same parameters within the submitted economic evaluation. Clinical expert feedback received by CDA-AMC indicated that the proportion of patients initiating second-line (2L) therapy in the Canadian context would likely be significantly higher than those reported in the trial or assumed in both models.
To explore the uncertainties surrounding these parameters, CDA-AMC conducted a scenario analysis. The proportion of patients initiating 2L therapy and the distribution of subsequent therapies were adjusted to estimates that were considered more closely aligned with Canadian clinical practice based on input from clinical expert consultations. The changes made in this scenario analysis is consistent with the input values used in the CDA-AMC scenario analysis of the economic evaluation.
The market uptake of pembrolizumab is likely underestimated: The sponsor assumed that pembrolizumab’s market uptake would increase linearly, reaching a maximum of 50% by year 3.18 However, clinical expert input obtained by CDA-AMC indicated that this assumption significantly underestimates pembrolizumab’s market share. As Canadian physicians are familiar with pembrolizumab because of its broad range of indications and extensive use in oncology, it is anticipated that pembrolizumab’s uptake would be higher than the sponsor’s projected estimate, especially in the first year.
CDA-AMC reanalyzed the market share assumptions based on feedback from clinical experts, incorporating considerations of physician familiarity with pembrolizumab because of its extensive use across multiple existing indications.
Dostarlimab’s market capture may be underestimated: The sponsor included dostarlimab as part of a scenario analysis, assuming that upon its reimbursement for the dMMR population, it would capture 19%, 15%, and 14% of the market share in years 1, 2, and 3, respectively.18 The sponsor further assumed that pembrolizumab would maintain a market share of 17%, 46%, and 50% over the same period, with the remaining shares held by carboplatin-paclitaxel.18 However, given the recent positive recommendation for the reimbursement of dostarlimab in the dMMR subgroup and the letter of intent finalized with pCPA, clinical expert feedback received by CDA-AMC indicated that dostarlimab is expected to impact pembrolizumab’s market share within the dMMR population.1,7 Expert input suggested that clinical evidence supports dostarlimab’s efficacy in patients with dMMR EC and given it is the first immunotherapy funded for this line of treatment, it could lead physicians to favour its use for this subgroup.
CDA-AMC conducted a scenario analysis to estimate the budget impact of reimbursing dostarlimab, incorporating clinical expert feedback which projected dostarlimab and pembrolizumab achieving equal market shares, with combined uptake reaching 60%, 70%, and 80% in years 1, 2, and 3, respectively.
Time on treatment assumptions for dostarlimab may be inappropriate: For dostarlimab only, ToT was modelled based on the PFS observed in the pembrolizumab plus carboplatin-paclitaxel arm of the NRG-GY018 trial and capped to the maximum number of treatment cycles specified in its product monograph.2 Yet, PFS and ToT are distinct concepts: PFS measures the time a patient remains free from disease progression while ToT reflects the duration a patient remains on therapy, which can be influenced by many factors. These parameters are not the same as patients may discontinue treatment yet continue to experience prolonged disease control. By setting duration of treatment to reflect PFS, the BIA model may overestimate the costs of dostarlimab particularly if the drug provides extended progression-free periods following treatment discontinuation.
CDA-AMC could not address this limitation through reanalyses given the paucity of data informing treatment duration in the dostarlimab arm.
The budget impact model does not fully capture costs of treatment: The sponsor assumed gradual weekly initiation of treatment, with a total of 17% of patients starting pembrolizumab over a 52-week period in year 1. This approach was further utilized to project market capture of pembrolizumab in years 2 and 3. In an incidence-based model, market shares represent the proportion of new patients on treatment at any point during the year, inherently accounting for changes in treatment over the course of the year. The sponsor’s assumption of a gradual treatment initiation may underestimate total treatment costs associated with the reimbursement of pembrolizumab.
CDA-AMC could not address this limitation given how initiation of treatment was coded in the sponsor’s submitted BIA.
The fixed dosing of pembrolizumab does not reflect clinical practice: The sponsor’s model assumed fixed dosing for pembrolizumab. However, as noted in the appraisal of the economic evaluation, current clinical practice and public drug plan policies prefer a weight-based dose for pembrolizumab. As a result, the average administered dose and associated treatment costs of pembrolizumab in the sponsor’s model are likely overestimated.
The CDA-AMC base case was revised to incorporate weight-based dosing, aligning with the approach used in the CUA.
CDA-AMC Reanalyses of the BIA
CDA-AMC revised the sponsor’s base case by modifying the market uptake to reflect Canadian clinical practice. The changes to the derived CDA-AMC base case are described in Table 21.
Table 21: CDA-AMC Revisions to the Submitted Budget Impact Analysis
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
Changes to derive the CDA-AMC base case | ||
1. Pembrolizumab’s market uptake assumption | 17% / 46% / 50% | 60% / 70% / 80% |
2. Dosing for pembrolizumab | Fixed dose | Weight-based dose |
CDA-AMC base case | Reanalysis 1 + 2 | |
The results of the CDA-AMC step-wise reanalysis are presented in summary format in Table 22 and a more detailed breakdown is presented in Table 23.
Based on the CDA-AMC reanalysis, the budget impact of the reimbursement of pembrolizumab for the treatment of EC is expected to be $49,400,994 in year 1, $97,116,184 in year 2 and $117,958,173 in year 3, with a three-year total of $264,475,351.
The estimated budget impact of reimbursing pembrolizumab is sensitive to change in market uptake assumptions. The modifications to the sponsor’s base case increased the estimated budget impact by 93%.
Table 22: Summary of the CDA-AMC Reanalyses of the Budget Impact Analysis
Stepped analysis | Three-year total ($) |
|---|---|
Submitted base case | 160,611,357 |
CDA-AMC reanalysis 1 | 309,637,022 |
CDA-AMC reanalysis 2 | 137,644,077 |
CDA-AMC base case | 264,475,351 |
Based on publicly available prices of the comparator treatments.
CDA-AMC presented the disaggregated results of the CDA-AMC base case for the dMMR subgroup which were derived by reducing the total eligible population by 27% (i.e., to reflect the proportion of dMMR patients relative to the total population). CDA-AMC further conducted the following scenario analyses (in the overall population) to address remaining uncertainty, using the CDA-AMC base case (results are provided in Table 23):
In scenario 1, the proportion of patients initiating 2L therapy was increased to 40% for those patients who initially received pembrolizumab plus carboplatin-paclitaxel and 61.75% for those who initially received carboplatin-paclitaxel. The distribution of subsequent therapies was recalculated to be consistent with the economic evaluation. Specifically, for those who initially received carboplatin-paclitaxel and proceed to initiate 2L therapy, all pMMR patients (73%) would receive pembrolizumab plus lenvatinib while all dMMR patients (27%) would receive pembrolizumab only.
In scenario 2, where dostarlimab is reimbursed for the dMMR population, the combined market share of immunotherapies was 60%, 70%, and 80% in years 1, 2, and 3, respectively. As dostarlimab is indicated for the dMMR subgroup only, it was assumed that the market shares of pembrolizumab and dostarlimab would be evenly split within this subgroup. For example, in year 1, 60% of patients would be on immunotherapy. Within the dMMR population (27%), this would mean 16.2% of patients would be on immunotherapy in which half would be on pembrolizumab while the other half would be on dostarlimab (8.1%). As 60% of pMMR population would also be pembrolizumab, the total market share for pembrolizumab in year 1 would therefore be 52% (i.e., 60%*(1 – 0.27) + 60%*(0.5*0.27)). Consequently, dostarlimab’s market share was calculated to be 8%, 9%, and 11% while the market share for pembrolizumab was 52%, 61% and 69% in years 1, 2, and 3, respectively.
Table 23: Detailed Breakdown of the CDA-AMC Reanalyses of the Budget Impact Analysis
Stepped analysis | Scenario | Year 0 (current situation) ($) | Year 1 ($) | Year 2 ($) | Year 3 ($) | Three-year total ($) |
|---|---|---|---|---|---|---|
Submitted base case | Reference | 38,806,288 | 73,377,039 | 91,467,930 | 99,707,888 | 264,552,857 |
New drug | 38,806,288 | 85,616,687 | 150,183,149 | 189,364,378 | 425,164,214 | |
Budget impact | 0 | 12,239,648 | 58,715,219 | 89,656,490 | 160,611,357 | |
CDA-AMC base case | Reference | 38,806,288 | 73,377,039 | 91,467,930 | 99,707,888 | 264,552,857 |
New drug | 38,806,288 | 122,778,033 | 188,584,114 | 217,666,061 | 529,028,208 | |
Budget impact | 0 | 49,400,994 | 97,116,184 | 117,958,173 | 264,475,351 | |
CDA-AMC base case for dMMR subgroup | Reference | 17,833,449 | 35,592,372 | 46,702,583 | 52,447,614 | 134,742,569 |
New drug | 17,833,449 | 45,789,873 | 65,649,526 | 73,199,570 | 184,638,969 | |
Budget impact | 0 | 10,197,501 | 18,946,943 | 20,751,955 | 49,896,399 | |
CDA-AMC scenario analysis 1: subsequent treatment assumptions | Reference | 40,808,850 | 82,765,485 | 104,421,208 | 114,164,394 | 301,351,088 |
New drug | 40,808,850 | 130,973,214 | 195,697,131 | 223,156,202 | 549,826,547 | |
Budget impact | 0 | 48,207,729 | 91,275,922 | 108,991,808 | 248,475,459 | |
CDA-AMC scenario analysis 2: market share of dostarlimab (dMMR subgroup only) | Reference | 66,049,810 | 131,823,600 | 172,972,530 | 194,250,424 | 499,046,554 |
New drug | 66,049,810 | 157,106,751 | 221,332,720 | 249,751,176 | 628,190,647 | |
Budget impact | 0 | 25,283,152 | 48,360,189 | 55,500,752 | 129,144,093 |
BIA = budget impact analysis; dMMR = deficient mismatch repair.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@cda-amc.ca.