Drugs, Health Technologies, Health Systems
Reimbursement Review
Pembrolizumab (Keytruda)
Sponsor: Merck Canada Inc.
Therapeutic area: Non–small cell lung cancer, neoadjuvant
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Clinical Review
Abbreviations
AE
adverse event
AESI
adverse event of special interest
AJCC
American Joint Committee on Cancer
BICR
blind independent central review
CDA-AMC
Canada’s Drug Agency
CI
confidence interval
CrI
credible interval
DFS
disease-free survival
DIC
deviance information criterion
ECOG PS
Eastern Cooperative Oncology Group Performance Status
EFS
event-free survival
EORTC QLQ-C30
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30
EORTC QLQ-LC13
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Lung Cancer 13
ePRO
electronically administered patient-reported outcome
FP
fractional polynomial
GRADE
Grading of Recommendations Assessment, Development and Evaluation
HR
hazard ratio
HRQoL
health-related quality of life
IA
interim analysis
IA1
first interim analysis
IA2
second interim analysis
ICI
immune checkpoint inhibitor
ITC
indirect treatment comparison
ITT
intention to treat
LSM
least squares mean
NGS
next-generation sequencing
NIF
nodal immune flare
NMA
network meta-analysis
NSCLC
non–small cell lung cancer
OH-CCO
Ontario Health (Cancer Care Ontario)
OS
overall survival
pCR
pathological complete response
PFS
progression-free survival
PRO
patient-reported outcome
QoL
quality of life
RCT
randomized controlled trial
RT
radiation therapy
SAE
serious adverse event
SLR
systematic literature review
TPS
tumour proportion score
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Table 1: Background Information on Application Submitted for Review
Item | Description |
|---|---|
Drug product | Pembrolizumab (Keytruda), 100 mg/4 mL vial, solution for infusion |
Sponsor | Merck Canada Inc. |
Indication | For the treatment of adult patients with resectable stage II, IIIA, or IIIB (T3 to 4N2) NSCLC in combination with platinum-containing chemotherapy as neoadjuvant treatment, and then continued as monotherapy as adjuvant treatment after surgery |
Reimbursement request | As per indication |
Health Canada approval status | NOC |
Health Canada review pathway | Standard review |
NOC date | February 6, 2025 |
Recommended dosage | For the neoadjuvant and adjuvant treatment of resectable NSCLC, patients should be treated with 4 doses of 200 mg q.3.w. or 2 doses of 400 mg q.6.w. of neoadjuvant pembrolizumab in combination with chemotherapy or until disease progression that precludes definitive surgery or unacceptable toxicity, followed by adjuvant treatment with pembrolizumab as monotherapy for up to 13 doses of 200 mg q.3.w. or 7 doses of 400 mg q.6.w. or until disease recurrence or unacceptable toxicity. Pembrolizumab should be administered before chemotherapy when given on the same day. |
NOC = Notice of Compliance; NSCLC = non–small cell lung cancer; q.3.w. = every 3 weeks; q.6.w. = every 6 weeks.
Introduction
Lung cancer is the most common malignancy and the leading cause of cancer-related death in Canada, with non–small cell lung cancer (NSCLC) accounting for approximately 88% of cases. In 2024, it was expected that an estimated 32,100 of people living in Canada would be diagnosed with lung cancer and 20,700 deaths would occur due to the disease. Most NSCLC cases are diagnosed at an advanced stage but about 30% to 35% are classified as early stage and potentially resectable. Despite surgery or definitive chemoradiotherapy being the only potentially curative options, high recurrence rates — ranging from 30% to 70% depending on the stage — remain a major challenge, and 5-year survival rates for stage II and stage III NSCLC are poor at 39% and 16%, respectively. Immunotherapy has been integrated into treatment regimens to improve outcomes, with drugs like nivolumab and atezolizumab demonstrating benefits in neoadjuvant or adjuvant settings. However, unmet needs persist, particularly in reducing recurrence and improving survival in resectable NSCLC.
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of pembrolizumab, 100 mg/4 mL vial, solution for infusion, in the treatment of adult patients with resectable stage II, stage IIIA, or stage IIIB (T3 to 4N2) NSCLC as neoadjuvant and adjuvant treatment.
Perspectives of Patient, Clinicians, and Drug Programs
The information in this section is a summary of input provided by the patient and clinician groups that responded to the call by Canada’s Drug Agency (CDA-AMC) for input and from clinical experts consulted for the purpose of this review.
Patient Input
One patient group input was received as a joint submission by the Canadian Cancer Survivor Network, Lung Cancer Canada, and the Lung Health Foundation regarding the use of pembrolizumab (Keytruda) for resectable stage II, stage IIIA, or stage IIIB NSCLC. Together, these organizations gathered patient perspectives through a survey conducted from August 1 to September 16, 2024. It included responses from 3 patients and 1 caregiver, all of whom were from Canada. All respondents reported having experience with pembrolizumab; however, it was unclear whether their use aligned specifically with the indication under review (resectable stage II, stage IIIA, or stage IIIB NSCLC) given that pembrolizumab is approved for multiple indications in lung cancer and may have been used in different phases of treatment.
The patients reported varying stages of NSCLC ranging from stage IB to stage IV. They had undergone various treatments, including surgery, radiation, chemotherapy, and immunotherapy, and in some cases had participated in clinical trials. Symptoms such as cough, shortness of breath, fatigue, and nausea were commonly reported, with significant impacts on their daily lives, including their ability to work, pursue hobbies, perform household tasks, and engage in physical activities. Emotional well-being, family relationships, and financial burdens were also identified as being negatively impacted by the disease.
When asked about their experiences with current treatments, patients highlighted both the benefits and challenges of their therapies. They reported that pembrolizumab, in combination with other treatments, helped reduce fatigue, manage cough, and improve appetite, energy, and pain levels. However, side effects such as fatigue, low energy, edema, and weight gain were noted. Most respondents found these side effects manageable with medications, allowing the respondents to continue participating in daily activities. While 1 respondent faced access challenges, such as travel costs and availability of targeted therapies, others reported no significant barriers to treatment.
Respondents emphasized that new treatments should focus on improving symptom control and quality of life (QoL) and maintaining stability even when a cure is not possible. Reduced cost was also a priority. Pembrolizumab was viewed positively, with 1 patient noting that it provided them with additional time to spend with loved ones and continue with their daily life. The extended event-free survival (EFS) reported in clinical trials was seen as particularly valuable, offering patients more time to enjoy meaningful activities.
Adverse effects such as colitis, hypothyroidism, and rheumatoid arthritis were reported, but most respondents found these side effects tolerable in exchange for the benefits of pembrolizumab. Overall, the treatment was rated favourably, with respondents appreciating its ability to control their disease and improve their QoL.
The patient groups acknowledged the small sample size of this submission but emphasized that the responses still highlight the positive impact of pembrolizumab for patients with lung cancer. The groups emphasized that the option to use pembrolizumab as part of a perioperative (i.e., both neoadjuvant and adjuvant) treatment plan offers patients a valuable new approach to managing their disease at multiple stages.
Clinician Input
Input From Clinical Experts Consulted for This Review
Clinical experts consulted for this review highlighted several unmet needs in the treatment of resectable NSCLC, particularly in stage II, stage IIIA, and stage IIIB, where optimizing cure rates and targeting micrometastatic disease are critical. Current therapies, such as neoadjuvant chemoimmunotherapy with nivolumab, have demonstrated efficacy but leave substantial room for improvement, according to the clinical experts. However, the clinical experts mentioned that the added value of adjuvant immunotherapy after neoadjuvant therapy remains unproven. Additional gaps were noted, such as uncertainties regarding the benefits of immunotherapy in PD-L1–negative tumours and specific subgroups within the early-stage NSCLC population.
Regarding pembrolizumab’s place in therapy, the experts indicated it would serve as an alternative to nivolumab in the neoadjuvant chemoimmunotherapy setting, particularly for stage II and stage IIIA, with potential applicability in stage IIIB. The experts emphasized the importance of assessing neoadjuvant response through imaging while recognizing challenges such as nodal immune flare (NIF), which could mimic progression. The clinical experts noted that discontinuation due to progression or severe toxicity may occur but also acknowledged that an immune phenomenon can sometimes be difficult to immediately distinguish from progression.
Clinician Group Input
Two clinician groups including a total of 25 clinicians — the Ontario Health (Cancer Care Ontario) (OH-CCO) Lung Cancer Drug Advisory Committee and the Lung Cancer Canada Medical Advisory Committee — provided input to this review.
According to both groups, the current standard treatment for patients with resectable stage II or stage III NSCLC includes neoadjuvant platinum-based chemotherapy, often combined with nivolumab. However, there is no access to adjuvant immunotherapy for patients who have undergone neoadjuvant chemoimmunotherapy. The treatment goals include curing the disease, improving overall survival (OS), and reducing the chance of recurrence, as measured by disease-free survival (DFS).
The clinician groups noted that a key unmet need is the lack of adjuvant immunotherapy for patients who have received neoadjuvant chemoimmunotherapy.
Regarding place in therapy, pembrolizumab combined with chemotherapy would represent an alternative to neoadjuvant chemoimmunotherapy with nivolumab. The clinician groups suggested that pembrolizumab could be a potential option for patients with resectable stage II or stage III disease who do not have EGFR or ALK mutations and who have no contraindications to immunotherapy. Patients least suited for treatment would include those with significant comorbidities, poor surgical candidacy, or contraindications to immunotherapy.
The clinician groups stated that treatment response would be assessed using imaging, including CT scans, both before surgery and during follow-up to monitor for disease recurrence. In the adjuvant phase, CT scans should be performed every 3 months to 6 months. Treatment discontinuation would occur due to disease progression, severe adverse events (AEs), or completion of the treatment course.
The clinician groups also noted that the appropriate treatment setting for pembrolizumab is in an outpatient clinic under the supervision of medical oncologists and thoracic surgeons experienced in managing thoracic malignancies. Surgery remains a key part of the treatment plan, and perioperative pembrolizumab is expected to improve surgical outcomes by increasing complete resection (R0) and improving lymph node downstaging.
Drug Program Input
Clinical experts reviewed and provided feedback on questions from public drug plans about pembrolizumab’s role in NSCLC treatment, specifically regarding eligibility, comparator treatments, and potential therapy adjustments.
Drug plans questioned how pembrolizumab in the perioperative setting compares with existing treatments. Experts noted that the KEYNOTE-671 trial (NCT03425643) — the pivotal study included in this submission — studied pembrolizumab with a cisplatin-doublet regimen followed by adjuvant pembrolizumab, which differs from real-world comparators like neoadjuvant nivolumab or adjuvant atezolizumab based on PD-L1 status; this allowed carboplatin to be the platinum partner of choice. Experts mentioned that if pembrolizumab is to be reimbursed for funding, it could be partnered with carboplatin or cisplatin as the platinum drug, even though only cisplatin was used in the trial.
Drug plans asked whether patients with EGFR mutations or ALK translocations should be eligible for perioperative pembrolizumab. Experts expressed caution here, explaining that due to the limited representation of these patients in the trials, pembrolizumab may not be well supported for these specific mutations. While some patients with EGFR or ALK alterations were included in the body of evidence, the small sample size makes conclusions difficult, leading experts to recommend against including these patients without further evidence.
On the question about the potential for drug plans to switch patients from neoadjuvant nivolumab to perioperative pembrolizumab, the experts agreed that this scenario would be rare but could be considered if clinicians observe potential benefits from the adjuvant pembrolizumab component. They stressed that any such switch would require careful clinical judgment and would apply only to a limited subset of patients.
In terms of the continuation or discontinuation of therapy, the drug plans sought guidance on circumstances for continuing or discontinuing pembrolizumab based on response. Experts indicated that disease progression, assessed through CT scans, is a primary reason to discontinue pembrolizumab. However, they noted that imaging results can sometimes show NIF, which is not true progression. Serious immune-related AEs, like pneumonitis or colitis, were also noted as valid reasons for discontinuation.
When assessing the generalizability of therapy to patients, the drug plans asked whether patients with an Eastern Cooperative Oncology Group Performance Status (ECOG PS) score of greater than 1 should be considered for pembrolizumab. Experts suggested that patients with an ECOG PS score of 2, especially those with stage III disease who are otherwise fit, may be eligible. However, they did not recommend pembrolizumab for patients with an ECOG PS score of 3, who would likely be unable to tolerate the treatment. Suitability for surgery was seen as the primary eligibility factor, with ECOG PS taking a secondary role in assessing operability.
Clinical Evidence
Systematic Review
Description of Studies
One pivotal study was included in this submission. The KEYNOTE-671 trial was a phase III, randomized, double-blind, placebo-controlled trial that evaluated pembrolizumab in combination with platinum-based chemotherapy as neoadjuvant treatment, followed by pembrolizumab monotherapy as adjuvant treatment, in patients with resectable stage II, stage IIIA, or selected stage IIIB (T3 to 4N2) NSCLC. In total, 797 patients were randomized 1:1 to receive either pembrolizumab or placebo, each in combination with chemotherapy for 4 cycles, followed by 13 cycles of pembrolizumab monotherapy or placebo after surgery. The coprimary end points were EFS and OS. Other outcomes included health-related quality of life (HRQoL) and safety measures. The study aimed to assess the efficacy of pembrolizumab in reducing the risk of recurrence, progression, or death and in improving long-term survival in this population.
The baseline characteristics of the study population were well balanced between treatment arms. The median age of participants was approximately 64 years, with the majority being male (74%) (female 26%). Most patients had stage IIIA disease (53%) and had an ECOG PS score of 0 or 1. Both squamous and nonsquamous histologies were well represented and around one-third of the participants had a PD-L1 tumour proportion score (TPS) of 50% or more.
Efficacy Results
In the KEYNOTE-671 trial, pembrolizumab demonstrated a statistically significant and clinically meaningful improvement in OS compared to placebo. At the second interim analysis (IA2), the hazard ratio (HR) was 0.72 (95% confidence interval [CI], 0.56 to 0.93; P = 0.00517). The median OS was not reached in the pembrolizumab arm whereas it was 52.4 months in the placebo arm. At 48 months, █████ of patients in the pembrolizumab arm were alive compared to 51.5% of patients in the placebo arm, an absolute difference of █████ ████ ███ ███ ██ ██████.
EFS, a coprimary end point in the KEYNOTE-671 study, also showed significant improvement with pembrolizumab. At IA2, the median EFS in the pembrolizumab arm was 47.2 months (95% CI, 32.9 months to not reached) compared to 18.3 months (95% CI, 14.8 months to 22.1 months) in the placebo arm, representing an approximate 29-month extension. At 48 months, the EFS rate was █████ for pembrolizumab versus 26.2% for placebo, a risk difference of █████ ████ ███ ████ ██ ██████. The HR for EFS was 0.59 (95% CI, 0.48 to 0.72; P < 0.00001). Kaplan-Meier curves showed separation beginning at approximately 5 months, with consistent benefits across prespecified subgroups, emphasizing pembrolizumab’s robust efficacy in reducing disease recurrence and progression.
The European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC QLQ-C30) ranges in score from 0 to 100, with higher scores indicating better health status. The difference in least squares mean (LSM) change from baseline in global health status for pembrolizumab versus placebo was 1.43 points (95% CI, –1.64 points to 4.49 points) at neoadjuvant week 11 and 2.22 points (95% CI, –0.58 points to 5.02 points) at adjuvant week 10. Physical and role functioning scores showed declines in the neoadjuvant phase in both arms but stabilized during the adjuvant phase. Overall, most patients reported stable or improved scores in the global health status scale and quality of life scale, with a slightly higher proportion favouring the pembrolizumab arm (58.7% versus 51.8%), and with a between-group difference of 7.0% (95% CI, 0.1% to 13.9%).
Harms Results
AEs were nearly universal in both treatment groups, with rates of 99.5% in the pembrolizumab arm and 98.7% in the placebo arm. Common AEs included nausea, decreased neutrophil counts, and anemia, with slightly higher incidences observed in the pembrolizumab group. Fatigue, decreased appetite, and rash were more frequent with pembrolizumab whereas asthenia was marginally more prevalent in the placebo arm. Serious adverse events (SAEs) occurred in 41.7% of patients in the pembrolizumab arm compared to 33.3% of patients in the placebo arm, with pneumonia and pulmonary embolism being the most common SAEs in both groups.
AEs led to higher treatment discontinuation rates in the pembrolizumab group, with 21.5% of patients discontinuing pembrolizumab or placebo and 25.8% of patients discontinuing any drug in the regimen, compared to 9.5% and 17.5% of patients in the placebo arm, respectively. Pneumonitis, anemia, and decreased neutrophil counts were among the most common reasons for discontinuation in the pembrolizumab arm. Mortality related to AEs was also higher in the pembrolizumab group (6.6%) compared to the placebo group (3.8%). Adverse events of special interest (AESIs), particularly immune-mediated events such as hypothyroidism (10.9%) and pneumonitis (6.1%), were notably more frequent in the pembrolizumab arm. The impact of AEs on surgical outcomes was also highlighted, as 6.3% of patients in the pembrolizumab arm were unable to undergo in-study surgery due to AEs compared to 4.3% of patients in the placebo arm.
Critical Appraisal
The KEYNOTE-671 trial had a rigorous double-blind, placebo-controlled design and a robust randomization process, which was stratified by disease stage, PD-L1 TPS, histologic features, and geographic region. These measures minimized bias and ensured methodological rigour. Baseline characteristics were well balanced between treatment arms, supporting valid comparisons. The study assessed OS and EFS using robust statistical methods, including stratified Cox regression and Kaplan-Meier survival analysis, with appropriate control for multiplicity. However, potential unblinding due to the distinct AE profiles of pembrolizumab may have introduced bias in subjective outcomes like HRQoL. The higher rates of treatment discontinuation and differences in subsequent antineoplastic therapy usage between the arms could also confound long-term outcome assessments, particularly OS. There was an increased risk of bias for HRQoL end points at longer follow-up (adjuvant week 10), where the amount of missing outcome data exceeded 30% in both groups. HRQoL analyses were unadjusted for multiplicity; therefore, statistically significant results for any subscale are at an increased risk of type I error (i.e., erroneously rejecting the null hypothesis).
For external validity, the KEYNOTE-671 trial enrolled a population reflective of patients with resectable stage II, stage IIIA, or stage IIIB NSCLC, aligning broadly with clinical practice in Canada, although an underrepresentation of patients who are Black may slightly limit its generalizability. Differences in the standard of care comparator used in the study versus current practices in Canada, such as the widespread use of neoadjuvant chemoimmunotherapy with nivolumab, may affect the applicability of the results. The clinical experts mentioned that the comparator arm of the KEYNOTE-671 study does not fully align with current practices in Canada, leaving unanswered questions about pembrolizumab’s potential advantages over existing standards of care. The design of the trial does not provide the ability to separate the effects of using pembrolizumab in the neoadjuvant and/or adjuvant phases. Additionally, the inclusion of patients with EGFR or ALK mutations, the reliance on cisplatin-based chemotherapy, and the ineligibility of some patients with comorbidities or contraindications to immunotherapy further constrain the trial’s relevance to certain patient subgroups. These factors highlight the need for careful interpretation when applying the trial findings to diverse real-world populations and evolving treatment landscapes.
GRADE Summary of Findings and Certainty of the Evidence
For pivotal studies and randomized controlled trials (RCTs) identified in the sponsor’s systematic review, the Grading of Recommendations Assessment, Development and Evaluation (GRADE) tool was used to assess the certainty of the evidence for outcomes considered most relevant to inform expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group.
The selection of outcomes for GRADE assessment was based on the sponsor’s Summary of Clinical Evidence, consultation with clinical experts, and input received from patient and clinician groups and public drug plans. The following list of outcomes was finalized in consultation with expert committee members:
OS at 24 months, 36 months, and 48 months
EFS at 24 months, 36 months, and 48 months
HRQoL
harms
AESI.
For the GRADE assessments, findings from the pivotal KEYNOTE-671 study were evaluated and summarized by outcome. Where deemed appropriate by the team at CDA-AMC, outcomes were presented narratively, reflecting the similarity across studies in terms of population, interventions, design, and outcome measures. In such cases, a single narrative statement was used to represent the overall body of evidence, providing a cohesive and streamlined interpretation.
Results of GRADE Assessments
Table 2 presents the GRADE summary of findings for neoadjuvant pembrolizumab versus placebo and chemotherapy for patients with NSCLC.
Table 2: Summary of Findings for Perioperative Pembrolizumab Versus Chemotherapy for Patients With NSCLC
Outcome and follow-up | Patients (studies), N | Relative effect (95% CI) | Absolute effect | Certainty | What happens | ||
|---|---|---|---|---|---|---|---|
Chemotherapy | Pembrolizumab | Difference (95% CI) | |||||
Survival (median follow-up = 29.8 months; range, 0.4 month to 62.0 months) | |||||||
Overall survival probability at 24 months | 797 (1 RCT) | NA | 747 per 1,000 | ███ ███ | ███ ███ | Moderatea | Pembrolizumab likely results in a clinically important increase in overall survival when compared with chemotherapy. |
Overall survival probability at 36 months | 797 (1 RCT) | NA | 640 per 1,000 | ███ ███ | ███ ███ | Moderatea | Pembrolizumab likely results in a clinically important increase in overall survival when compared with chemotherapy. |
Overall survival probability at 48 months | 797 (1 RCT) | NA | 515 per 1,000 | ███ ███ | ███ ███ | High | Pembrolizumab results in a clinically important increase in overall survival when compared with placebo and chemotherapy. |
EFS probability at 24 months | 797 (1 RCT) | NA | 414 per 1,000 | ███ ███ | ███ ███ | Highb | Pembrolizumab results in a clinically important increase in EFS when compared with chemotherapy. |
EFS probability at 36 months | 797 (1 RCT) | NA | 354 per 1,000 | ███ ███ | ███ ███ | Highb | Pembrolizumab results in a clinically important increase in EFS when compared with chemotherapy. |
EFS probability at 48 months | 797 (1 RCT) | NA | 262 per 1,000 | ███ ███ | ███ ███ | Highb | Pembrolizumab results in a clinically important increase in EFS when compared with chemotherapy. |
HRQoL | |||||||
HRQoL, EORTC QLQ-C30, and EORTC QLQ-LC13 | 785 (1 RCT) | Assessment of all EORTC QLQ-C30 global health status scale showed no evidence of difference of effects on HRQoL scores between treatment groups at 1.43 (95% CI, –1.64 to 4.49), with CIs including the null effect but not greater than or less than an MID of 5. | Moderatec | Pembrolizumab likely result in little to no difference in HRQoL when compared with chemotherapy. | |||
Harms | |||||||
AEs | 797 (1 RCT) | AEs were similar overall between groups. At least 1 AE was reported in 394 (99.5%) patients in the pembrolizumab arm and 394 (98.7%) patients in the placebo and chemotherapy arm. The most common AEs (> 15% of patients) were nausea (58% vs. 53%), decreased neutrophils (44% vs. 42%), constipation (39% vs. 37%), fatigue (32% vs. 25%), decreased appetite (29% vs. 25%), decreased white blood cells (28% vs. 25%), vomiting (21% vs. 17%), diarrhea (20% vs. 19%), and dyspnea (18% vs. 13%) in the pembrolizumab arm vs. the placebo and chemotherapy arm, respectively. | High | Pembrolizumab results in little to no difference in AEs when compared with chemotherapy. | |||
SAEs | 797 (1 RCT) | SAEs were more frequent in the pembrolizumab arm, with 165 (41.7%) patients having at least 1 SAE, compared to the placebo arm (133 [33.3%] patients). Pneumonia, pulmonary embolism, anemia, pyrexia, and elevated liver enzymes were most commonly reported. | Highd | Pembrolizumab results in an increase in SAEs when compared with chemotherapy. The clinical relevance of the difference is uncertain. | |||
AEs of special interest | 797 (1 RCT) | In the pembrolizumab arm as compared to the placebo and chemotherapy arm, respectively, the following AEs were more commonly reported: hypothyroidism (11% vs. 1.5%), pneumonitis (6.1% vs. 1.8%), hyperthyroidism (5.1% vs. 2%), severe skin reactions (2% vs. 0%), and colitis (1.3% vs. 0%). | Moderatee | Pembrolizumab likely results in more AEs of special interest when compared with chemotherapy. | |||
AE = adverse event; CI = confidence interval; EFS = event-free survival; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EORTC QLQ-LC13 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Lung Cancer 13; HRQoL = health-related quality of life; MID = minimal important difference; NA = not available: NSCLC = non–small cell lung cancer; RCT = randomized controlled trial; SAE = serious adverse event; vs. = versus.
Note: Study limitations (which refer to internal validity or risk of bias), inconsistency across studies, indirectness, the imprecision of effects, and publication bias were considered when assessing the certainty of the evidence. All serious concerns in these domains that led to the rating down of the level of certainty are documented in the table footnotes.
aA threshold of 50 more patients surviving per 1,000 patients treated with pembrolizumab (vs. placebo and chemotherapy) was considered clinically meaningful. The 95% CI crosses this threshold, denoting imprecision for establishing a meaningful effect at the time point of 24 months and 36 months but not at 48 months, when the estimate and its 95% CI included a clinically meaningful effect without imprecision.
bA threshold of 100 more patients surviving without events (EFS, as defined in the study) per 1,000 patients treated with pembrolizumab (vs. placebo and chemotherapy) was considered clinically meaningful. The 95% CI excludes this threshold, denoting no imprecision at this time point.
cAll estimates of effects from all assessments showed CIs that included the null effect but did not cross a conservative estimate of an MID of 5 points; hence, the effects were not rated down for imprecision but were rated down 1 level for risk of bias due to more than 30% missing data (non–randomly missing).
dThe total sample size was greater than a conservative estimate of a review information size of 400 patients per study. Furthermore, the total number of events was deemed appropriate for the outcome.
eAlthough the total sample size was greater than a conservative estimate of a review information size of 400 patients per study, certain events were small in number to draw strong conclusions, even though the total number of events was deemed appropriate for some outcomes. Hence, the overall effect was rated down 1 level for imprecision.
The OS and EFS end points were assessed at 24 months, 36 months, and 48 months as these time points were deemed important by experts consulted by CDA-AMC.
In OS, the 48-month end point assessment was considered high certainty and with an effect of clinical importance. The estimates at 24 months and 36 months were rated down 1 level for imprecision because the estimates showed wide CIs that included a threshold of benefit.
All EFS estimates were deemed of high certainty. HRQoL presented estimates with a 95% CI that included the null effect but did not cross any threshold of a minimally important difference of 10 points, denoting that there was likely to be little to no difference of effects between groups.
In AEs, the evidence showed that pembrolizumab results in little to no difference in the number of patients with at least 1 AE between pembrolizumab and placebo combined with chemotherapy (high certainty), and more SAEs in the pembrolizumab arm (high certainty). Also, pembrolizumab increased the number of AESIs such as hyperthyroidism, pneumonitis, or hypothyroidism (moderate certainty).
Long-Term Extension Studies
No long-term extension studies materials were submitted by the sponsor.
Indirect Comparison
Description of Studies
The indirect treatment comparison (ITC) employed a network meta-analysis (NMA) of 8 RCTs to evaluate the efficacy and safety of pembrolizumab in the perioperative treatment of resectable NSCLC. The included studies were identified through a systematic literature review (SLR) and selected based on predefined criteria, including patient population, interventions, comparators, and outcomes. The trials assessed therapies across various stages of early-stage resectable NSCLC, with a focus on EFS as the end point of interest.
Given that nonproportional hazards were identified for some comparisons, a fractional polynomial (FP) NMA allowing for time-varying hazards was also presented, including the same studies.
Efficacy Results
The constant hazards NMA demonstrated favourable EFS outcomes for perioperative pembrolizumab compared to surgery alone ████ █████ ███ ████ █████ ██████. However, when compared to chemotherapy ████ █████ ███ ████ ████ ██ ██████ chemoradiotherapy ███ █████ ███ ████ ████ ██ ██████ and neoadjuvant nivolumab ████ █████ ███ ████ ████ ██ ██████ no statistically significant differences were observed, with wide credible intervals (CrIs) that included the null effect.
Among the best-fitting FP models was the time-varying second-order FP (p1 = 0, p2 = 0) with treatment effects on scale and first shape. Results suggested that pembrolizumab was favoured over chemotherapy (time windows after 6 months), chemoradiotherapy (time windows after 12 months), and surgery alone. Earlier time windows for the chemotherapy and chemoradiotherapy comparisons had CrIs that were crossing the null. Comparisons to neoadjuvant nivolumab had wide CrIs on both sides of the null in all time windows.
Harms Results
No harms effects were assessed in the ITC and NMA submitted.
Critical Appraisal
The ITC was conducted using a rigorous SLR with prespecified criteria for population, intervention, comparison, and outcome, dual independent review, and quality assessment using the Cochrane Risk of Bias tool. Key limitations included the exclusion of adjuvant trials due to differences in end points (EFS versus DFS) and patient populations, which restricts comparisons with important treatment strategies (e.g., comparisons to adjuvant chemotherapy followed by pembrolizumab or atezolizumab). Differences in randomization timing (e.g., pretreatment in the KEYNOTE-671 study versus postsurgery in adjuvant trials) and the noninterchangeability of surrogate end points violate assumptions of similarity, homogeneity, and consistency, resulting in potentially biased estimates of relative treatment effects.
Imbalances in treatment effect modifiers, such as PD-L1 status, disease stage, and regional enrolment, further undermine the transitivity assumption and limit the robustness of the ITC findings. Additionally, full information on treatment effect modifiers was not always available to allow for a comprehensive assessment of the heterogeneity. Methodological choices, including assumptions regarding the pooled chemotherapy node and reliance on the constant HR model despite proportional hazards violations in some trials, exacerbate the uncertainty. The second-order FP NMA would overcome violations of the proportional hazards assumption but could not overcome the heterogeneity and other concerns previously noted. Additionally, interpretation is limited to discrete time windows and the sponsor noted that sample sizes were decreased at longer follow-up durations, introducing uncertainty into the comparative effect estimates. The exclusion of OS, HRQoL, and AE data reduces the analysis’s comprehensiveness while the omission of emerging therapies weakens its relevance in the evolving treatment landscape in Canada. The estimates relative to the most relevant comparator, neoadjuvant nivolumab, were particularly affected by wide CrIs that further increased the uncertainty. Although the ITC provides some insights into pembrolizumab’s perioperative efficacy, its use for clinical decision-making is constrained by methodological challenges, violations of key assumptions, and significant gaps in the evidence.
Conclusions
Evidence from the pivotal KEYNOTE-671 trial demonstrates that pembrolizumab (neoadjuvant in combination with chemotherapy, then as monotherapy in the adjuvant period) provides a clinically meaningful benefit in the treatment of resectable stage II, stage IIIA, and selected stage IIIB NSCLC, particularly in improving EFS and OS when compared to neoadjuvant chemotherapy alone. These benefits align with the priorities of patients and clinicians, especially in early-stage NSCLC, where the primary goals are curative intent and long-term survival. However, the evidence to determine an impact on HRQoL is still uncertain. Furthermore, pembrolizumab presents unique challenges, including increased rates of immune-mediated AEs, which may need careful patient monitoring and appropriate management strategies.
The evidence supports pembrolizumab as a potential alternative to existing standards, although indirect comparisons to highly relevant comparators, such as neoadjuvant nivolumab, suggest uncertainty about which regimen might be favoured. Uncertainties persist regarding the incremental value of the extended adjuvant regimen, particularly for certain subgroups that may derive limited additional benefit. The absence of direct head-to-head comparisons with nivolumab or other immune checkpoint inhibitors (ICIs) further complicates a definitive positioning of pembrolizumab within the current treatment paradigm. Notable gaps in the evidence include immature OS data and a lack of long-term safety data.
Overall, while the efficacy of pembrolizumab against chemotherapy in the neoadjuvant phase is established in the KEYNOTE-671 study, the necessity and added value of the extended adjuvant regimen, as well as its comparative effectiveness within current clinical practice, remain areas requiring further clarification. Long-term follow-up and real-world evidence may address these questions and refine pembrolizumab’s role in the evolving treatment landscape.
Introduction
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of pembrolizumab, 100 mg/4 mL vial, solution for infusion, in the treatment of adult patients with resectable stage II, stage IIIA, or stage IIIB (T3 to 4N2) NSCLC as neoadjuvant treatment.
Disease Background
Content in this section has been informed by materials submitted by the sponsor and clinical expert input. The following has been summarized and validated by the review team.
Lung cancer is the most common malignancy and the leading cause of cancer-related death in Canada. In 2024, it was expected that an estimated 32,100 patients in Canada (14,800 men and 17,300 women)1,2 would be diagnosed with lung cancer.3 Accounting for 1 in 4 cancer deaths, lung cancer would be responsible for about 20,700 deaths in Canada in 2024.1,2 NSCLC accounts for about 88% of all lung cancers. Most NSCLCs are diagnosed at a locally advanced or metastatic stage, precluding potentially curative surgery,4 but 30% to 35% of patients are diagnosed with an early-stage resectable disease.5-7
The stage of disease at diagnosis is the most important prognostic factor.3 The 5-year survival estimates by stage at diagnosis are 62% for patients with stage I disease, 39% for patients with stage II disease, 16% for patients with stage III disease, and 3% for patients with stage IV disease.8
Surgery or definitive chemoradiotherapy remain the only potentially curative treatments for early-stage NSCLC. However, 30% to 70% of patients with NSCLC develop recurrence after surgical resection, with distant metastases being 2 to 3 times more common than local recurrences.9-12 Most patients who develop locally recurrent or metastatic disease after resection are incurable with salvage therapy.13 Neoadjuvant and adjuvant systemic therapy strategies have been developed to prevent recurrence and improve prognosis in surgical resection candidates, but survival outcomes could still be improved.
NSCLC diagnosis requires imaging and a biopsy to confirm stage II, stage IIIA, or stage IIIB disease as per criteria for the American Joint Committee on Cancer (AJCC) cancer staging manual, eighth edition.14 Specific diagnostic tests for pembrolizumab are not detailed in the Canadian product monograph.
Standards of Therapy
Content in this section has been informed by materials submitted by the sponsor and clinical expert input. The following has been summarized and validated by the review team.
The main goal of systemic treatment for resectable stage II or stage III NSCLC is to prolong survival by reducing postsurgery recurrence, which affects up to 50% of patients in stage II15 and 70% of patients in stage III.12 Historically, platinum-based adjuvant chemotherapy was the standard of care, offering a 5% absolute 5-year OS improvement compared to surgery alone.16,17 However, recurrence rates and OS remain suboptimal with chemotherapy alone.
To address these gaps, immunotherapy has been integrated into neoadjuvant and adjuvant settings in Canada:
Neoadjuvant nivolumab with platinum-doublet chemotherapy — For resectable NSCLC (tumour ≥ 4 cm or node-positive); funded for 3 cycles in most jurisdictions.18-24
Atezolizumab postresection with adjuvant chemotherapy — For stage II and stage IIIA NSCLC with PD-L1 TPS of 50% or more and no EGFR or ALK mutations; reimbursed in most provinces and territories.20-22,24,25
Pembrolizumab postresection with adjuvant chemotherapy — Approved by Health Canada for stage IB and stage IIIA NSCLC and under review for tumours with PD-L1 TPS of less than 50%.26
These therapies improve outcomes such as EFS, pathological complete response (pCR), and DFS. Patients previously treated with immunotherapy are eligible for PD-1 and PD-L1 inhibitors in metastatic settings if at least 6 months have passed since the completion of therapy.18
For EGFR-mutated NSCLC, adjuvant osimertinib is recommended after the resection of stage IB and stage IIIA tumours to improve OS, either alone or after chemotherapy.27-30
Canadian guidelines recommend neoadjuvant chemotherapy with immunotherapy for stage II or stage IIIA NSCLC without EGFR or ALK alterations, and adjuvant chemotherapy and immunotherapy for patients who did not receive neoadjuvant therapy.15 Similar recommendations have been made by the National Institute for Health and Care Excellence and the National Comprehensive Cancer Network for adjuvant atezolizumab and neoadjuvant nivolumab.28,31,32
In Canada, the CDA-AMC provisional funding algorithm includes atezolizumab and nivolumab as standard of care for distinct patient populations based on tumour characteristics and treatment timing.18
Drug Under Review
Key characteristics of pembrolizumab are summarized in Table 3 with other treatments available for the treatment of adult patients with resectable stage II, stage IIIA, or stage IIIB (T3 to 4N2) NSCLC as neoadjuvant treatment.
Pembrolizumab (Keytruda) is a high-affinity monoclonal antibody targeting PD-1, which blocks its interaction with PD-L1 and PD-L2. This mechanism restores cytotoxic T-cell activity, enabling T-cells to target and eliminate tumour cells. Pembrolizumab has been approved by Health Canada for the treatment of adult patients with resectable stage II, stage IIIA, or stage IIIB (T3 to 4N2) NSCLC in combination with platinum-containing chemotherapy as neoadjuvant treatment, followed by monotherapy as adjuvant treatment after surgery. The Notice of Compliance was granted on February 6, 2025. The reimbursement request aligns with the Health Canada indication.26
The dosing regimen involves 200 mg every 3 weeks or 400 mg every 6 weeks of pembrolizumab in combination with chemotherapy for 4 doses as neoadjuvant treatment, followed by pembrolizumab monotherapy for up to 13 doses (200 mg every 3 weeks) or 7 doses (400 mg every 6 weeks) as adjuvant treatment, or until disease recurrence or unacceptable toxicity. Pembrolizumab should be administered before chemotherapy when given on the same day.26
There are no prescribing restrictions in the Canadian product monograph, and the drug may be prescribed and administered by qualified oncology professionals.
Table 3: Key Characteristics of Pembrolizumab, Platinum-Based Chemotherapy, and Nivolumab
Drug | Indication | Route and dosage | Serious adverse effect or safety issue |
|---|---|---|---|
Pembrolizumab26,33 + platinum-based chemotherapy22,33 and pembrolizumab33 | For the treatment of adult patients with resectable stage II, stage IIIA, or stage IIIB (T3 to 4N2) NSCLC in combination with platinum-containing chemotherapy as neoadjuvant treatment, and then continued as monotherapy as adjuvant treatment after surgerya | Pembrolizumab 200 mg IV q.3.w. plus 1 of the following:
For 4 cycles before surgery and then (after surgery):
| Pneumonitis, colitis, hepatitis, endocrinopathies, nephritis, and severe skin reactions |
Treatment of NSCLC | One of the following:
For 4 cycles before surgery | Several effects, including nephrotoxicity, neurotoxicity, myelosuppression, hypersensitivity reactions, cardiotoxicity, hepatotoxicity, and secondary malignancies | |
Neoadjuvant treatment of adult patients with resectable NSCLC (tumours ≥ 4 cm or node-positive) when used in combination with platinum-doublet chemotherapy | Nivolumab 360 mg IV q.3.w. plus 1 of the following:
For 3 cycles before surgery | Pneumonitis, colitis, hepatitis, endocrinopathies, skin and infusion-related reactions, and nephritis |
AUC = area under the curve; NSCLC = non–small cell lung cancer; q.3.w. = every 3 weeks.
aHealth Canada–approved indication.
Source: Product monographs from pembrolizumab,26,33 platinum-based chemotherapy,33-35 and nivolumab22,36 plus platinum-based chemotherapy.22
Perspectives of Patients, Clinicians, and Drug Programs
The full patient and clinician group submissions received by CDA-AMC are available in the consolidated patient and clinician group input document for this review on the project website.
Patient Group Input
This section was prepared by the review team based on the input provided by patient groups.
One patient group input was received as a joint submission by the Canadian Cancer Survivor Network, Lung Cancer Canada, and the Lung Health Foundation regarding the use of pembrolizumab (Keytruda) for resectable stage II, stage IIIA, or stage IIIB NSCLC. Together, these organizations gathered patient perspectives through a survey conducted from August 1 to September 16, 2024. This included responses from 3 patients and 1 caregiver, all of whom were from Canada. All respondents reported having experience with pembrolizumab; however, it was unclear whether the drug’s use aligned specifically with the indication under review (resectable stage II, stage IIIA, or stage IIIB NSCLC), as pembrolizumab is approved for multiple indications in lung cancer and may have been used in different phases of treatment.
The patients reported varying stages of NSCLC, ranging from stage IB to stage IV. They had undergone various treatments, including surgery, radiation, chemotherapy, and immunotherapy, and in some cases had participated in clinical trials. Symptoms such as cough, shortness of breath, fatigue, and nausea were commonly reported, with significant impacts on their daily lives, including their ability to work, pursue hobbies, perform household tasks, and engage in physical activities. Emotional well-being, family relationships, and financial burdens were also identified as being negatively impacted by the disease.
When asked about their experiences with current treatments, patients highlighted both the benefits and challenges of their therapies. They reported that pembrolizumab, in combination with other treatments, helped reduce fatigue, manage cough, and improve appetite, energy, and pain levels. However, side effects such as fatigue, low energy, edema, and weight gain were noted. Most respondents found these side effects manageable with medications, allowing the respondents to continue participating in daily activities. While 1 respondent faced access challenges, such as travel costs and availability of targeted therapies, others reported no significant barriers to treatment.
Respondents emphasized that new treatments should focus on improving symptom control and QoL and maintaining stability even when a cure is not possible. Reduced cost was also a priority. Pembrolizumab was viewed positively, with 1 patient noting that it provided them with additional time to spend with loved ones and continue with their daily life. The extended EFS reported in clinical trials was seen as particularly valuable, offering patients more time to enjoy meaningful activities.
Adverse effects such as colitis, hypothyroidism, and rheumatoid arthritis were reported but most respondents found these side effects tolerable in exchange for the benefits of pembrolizumab. Overall, the treatment was rated favourably, with respondents appreciating its ability to control their disease and improve their QoL.
The patient groups acknowledged the small sample size of this submission but emphasized that the responses still highlight the positive impact of pembrolizumab for patients with lung cancer. The groups emphasized that the option to use pembrolizumab as part of a perioperative treatment plan offers patients a valuable new approach to managing their disease at multiple stages.
Clinician Input
Input From Clinical Experts Consulted for This Review
All CDA-AMC review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of lung cancer.
Unmet Needs
The clinical experts acknowledged that the primary goal is to improve OS, offering a potential cure while preserving QoL, and acknowledging that some patients may have long-term survival potential. The unmet needs in treating resectable NSCLC at stage II, stage IIIA, and stage IIIB focus on optimizing cure rates and enhancing survival through systemic therapies that target micrometastatic disease.
The experts highlighted several unmet needs in early-stage NSCLC treatment, emphasizing the need for more effective therapies given current limitations. The clinicals experts indicated that currently available chemoimmunotherapy options have limitations and patient outcomes (e.g., EFS) could be improved, with specific subgroups such as those only having a partial response to the treatment having worse outcomes. Experts suggested that adding adjuvant pembrolizumab might benefit patients who do not reach pCR with neoadjuvant therapy alone, although this benefit remains unproven.
The experts also pointed out additional gaps in understanding which subgroups may not benefit from neoadjuvant immunotherapy, such as those within specific stages or with PD-L1–negative tumours. Moreover, the experts highlighted a significant gap in knowledge regarding the potential added value of adjuvant immunotherapy following neoadjuvant immunotherapy. Collectively, these insights underscore the critical need for further advancements to improve cure rates and outcomes in NSCLC.
Place in Therapy
The clinical experts mentioned that current standard treatment includes 3 cycles of neoadjuvant platinum-doublet chemotherapy with immunotherapy (nivolumab) for eligible patients. Although patients with stage IIIB disease were not included in the CheckMate 816 trial, the clinical experts were of the opinion that extrapolation of data supports the use of this regimen. However, limitations exist for patients with specific contraindications, such as autoimmune conditions or severe cardiorespiratory issues, and those with molecular aberrations (e.g., EGFR or ALK mutations) where targeted therapies like tyrosine kinase inhibitors are preferred.
The experts indicated that pembrolizumab would fit into the existing treatment paradigm for resectable NSCLC by offering an alternative in settings where neoadjuvant chemoimmunotherapy with nivolumab is currently used. Both experts noted the similarity between pembrolizumab and nivolumab in terms of toxicity, cost, and efficacy, suggesting that pembrolizumab would likely share the same patient population.
Patient Population
The clinical experts stated that the best candidates for pembrolizumab in the neoadjuvant chemoimmunotherapy setting are generally the same as those currently eligible for chemotherapy plus nivolumab, with a focus on patients with resectable NSCLC in stage II, stage IIIA, and stage IIIB. Patients in stage IIIB were included in the KEYNOTE-671 study, which provided important information about the rationale for their inclusion in the indication for pembrolizumab. However, the nivolumab plus chemotherapy regimen is already funded for stage IIIB patients, suggesting that pembrolizumab may be seen as an alternative rather than a replacement.
The experts emphasized that PD-L1 status remains a relevant factor, although uncertainties persist about the benefit of immunotherapy in patients with PD-L1–negative tumours. Additionally, EGFR and ALK status are important considerations, ideally assessed through next-generation sequencing (NGS). According to the clinical experts, this is already standard of care in most jurisdictions, but not all. However, patients eligible to receive neoadjuvant therapy are not required to undergo PDL1 or NGS testing as logistically this can sometimes be an issue in NSCLC where diagnostic tissue specimens are often scant and unfit for further testing. This limits the necessity for PD-L1 and NGS testing in all eligible patients. Both experts agreed that contraindications for pembrolizumab are similar to those for nivolumab, notably excluding patients with active autoimmune diseases.
Assessing the Response Treatment
The clinical experts mentioned that an appropriate assessment of the response to neoadjuvant chemoimmunotherapy in NSCLC would be through imaging (typically CT scans of the chest, abdomen, and pelvis) at the end of treatment (i.e., after 4 cycles) or sooner if clinically indicated. This assessment helps to ensure that there is no overt disease progression before surgical resection. However, the experts noted that imaging could be misleading due to NIF, where tumour and lymph nodes appear worse due to immune cell infiltration but are pathologically cancer-free. Therefore, PET scans are not recommended unless CT suggests new distant metastasis.
The experts mentioned that assessing adjuvant therapy is less practical, as there is no measurable disease postsurgery. Instead, the decision to continue adjuvant treatment relies on trial data supporting OS benefits.
Patients are monitored throughout treatment for toxicity through physical exams and blood tests every 1 to 2 cycles. For longer-term surveillance, CT scans are recommended every 3 months to 6 months during adjuvant therapy, every 6 months for the first 2 years post-therapy, and then annually as per OH-CCO guidelines. The clinical experts agree that a clinically meaningful response in neoadjuvant therapy involves no evidence of new lesions or metastasis, allowing patients to proceed with surgery. The frequency and timing of assessments are largely reflective of clinical practices in Canada, particularly regarding the use of CT imaging and periodic surveillance postsurgery.
Discontinuing Treatment
The experts considered that disease progression, as confirmed by periodic CT scans, is a primary reason to discontinue pembrolizumab treatment. However, progression observed on CT scans at the end of neoadjuvant therapy should be interpreted cautiously, as NIF can mimic progression but does not represent actual cancer growth. Only confirmed progression, verified after accounting for NIF, would warrant discontinuation.
Additionally, serious immune-related AEs, such as pneumonitis, colitis, or severe rash, are common reasons for stopping treatment. While patients with mild toxicities may be rechallenged with pembrolizumab, those experiencing severe or nonreversible toxicities typically discontinue therapy.
Prescribing Considerations
This treatment is ideally administered in cancer centres under the supervision of a medical oncologist to monitor these potential AEs and manage them promptly. While private infusion clinics may provide immunotherapy if the regimen is not publicly funded, medical oncologist oversight is still required to ensure safe and appropriate management.
Clinician Group Input
This section was prepared by the review team based on the input provided by clinician groups.
Two clinician groups including a total of 25 clinicians — the OH-CCO Lung Cancer Drug Advisory Committee and the Lung Cancer Canada Medical Advisory Committee — provided input to this review.
According to both groups, the current standard treatment for patients with resectable stage II or stage III NSCLC includes neoadjuvant platinum-based chemotherapy, often combined with nivolumab. However, there is no access to adjuvant immunotherapy for patients who have undergone neoadjuvant chemoimmunotherapy. The treatment goals include curing the disease, improving OS, and reducing the chance of recurrence, as measured by DFS.
The clinician groups noted that a key unmet need is the lack of adjuvant immunotherapy for patients who have received neoadjuvant chemoimmunotherapy.
Regarding the place in therapy of pembrolizumab, the clinician group considered that pembrolizumab combined with chemotherapy would represent an alternative to neoadjuvant chemoimmunotherapy with nivolumab. The clinician groups suggested that pembrolizumab could be a potential option for patients with resectable stage II or stage III disease who do not have EGFR or ALK mutations and who have no contraindications to immunotherapy. Patients least suited for treatment would include those with significant comorbidities, poor surgical candidacy, or contraindications to immunotherapy.
The clinician groups stated that treatment response would be assessed using imaging, including CT scans, both before surgery and during follow-up to monitor for disease recurrence. In the adjuvant phase, CT scans should be performed every 3 months to 6 months. Treatment discontinuation would occur due to disease progression, severe AEs, or completion of the treatment course.
The clinician groups also noted that the appropriate treatment setting for pembrolizumab is in an outpatient clinic under the supervision of medical oncologists and thoracic surgeons experienced in managing thoracic malignancies. Surgery remains a key part of the treatment plan, and perioperative pembrolizumab is expected to improve surgical outcomes by increasing R0 resections and improving lymph node downstaging.
Drug Program Input
The drug programs provide input on each drug being reviewed through the CDA-AMC reimbursement review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted for this review are summarized in Table 4.
Table 4: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation question | Clinical expert response |
|---|---|
Relevant comparators | |
The KEYNOTE-671 study compared neoadjuvant pembrolizumab plus cisplatin-doublet followed by surgery and adjuvant pembrolizumab to neoadjuvant cisplatin-doublet followed by surgery and placebo. At the time of this input, adjuvant platinum-based chemotherapy followed by pembrolizumab (if PD-L1 TPS < 50%) or perioperative durvalumab are under review. Funded comparators include:
| This is a comment to inform pERC deliberations. |
Considerations for initiation of therapy | |
Less than 5% of the pembrolizumab population was either EGFR-positive or had ALK translocation. Can pERC confirm whether patients with EGFR mutation or ALK translocation should be eligible for perioperative pembrolizumab? | The clinical experts consulted by CDA-AMC expressed a preference against using this treatment in this population due to the limited representation of patients with these specific characteristics in the trial. While acknowledging that some patients from this subgroup were included in the KEYNOTE-671 trial, the experts noted that the small sample size makes it challenging to draw definitive conclusions about the treatment’s efficacy for this subgroup. |
Under what clinical circumstances might perioperative pembrolizumab be preferred over perioperative durvalumab, neoadjuvant nivolumab, adjuvant atezolizumab, or adjuvant pembrolizumab? | The clinical experts indicated that while each of these immunotherapy options has shown some potential benefits in certain settings, the data are still evolving and direct comparisons between these treatments are limited. Consequently, they emphasized the need for more robust evidence to determine clear clinical advantages for 1 approach over another in the perioperative or adjuvant setting. |
Can pembrolizumab be administered with alternate chemotherapy if a patient cannot receive or tolerate platinum-based chemotherapy in the neoadjuvant phase? | If a patient is unable to receive or tolerate platinum-based chemotherapy in the neoadjuvant phase, the experts clarified that platinum-based chemotherapy is essential for achieving the intended efficacy of the treatment regimen. If an alternative to cisplatin is needed due to tolerance issues or specific contraindications, the experts would recommend carboplatin as a substitute when used in combination with pembrolizumab. They believe that carboplatin may provide a more tolerable option for some patients while maintaining the treatment’s effectiveness, as it still falls within the platinum-based category critical to the therapeutic protocol. |
Perioperative durvalumab is also under review. Where possible, the reimbursement criteria should align. | This is a comment to inform deliberations. |
Considerations for prescribing of therapy | |
PAG would like to inform pERC that most jurisdictions use weight-based dosing up to a cap for pembrolizumab (2 mg/kg up to 200 mg every 3 weeks or 4 mg/kg up to 400 mg every 6 weeks). | This is a comment to inform pERC deliberations. |
Would patients be eligible for pembrolizumab for downstream immunotherapy in the following situations? 1. The patient’s disease progresses during neoadjuvant pembrolizumab. 2. The patient receives neoadjuvant pembrolizumab but is not able to proceed to surgery. 3. The patient’s disease progresses during or recurs shortly after adjuvant pembrolizumab. 4. The patient has started but is not able to complete adjuvant pembrolizumab for reasons other than disease progression. | In these various scenarios, the experts outlined specific considerations. 1. For patients whose disease progresses during neoadjuvant pembrolizumab, the experts would not recommend continuing pembrolizumab if progression occurs during the neoadjuvant phase because this would indicate a lack of response to the therapy, and further immunotherapy would likely be ineffective. 2. For patients who receive neoadjuvant pembrolizumab but are unable to proceed to surgery, the experts noted that eligibility would depend on the reason for not proceeding with surgery. If surgery is cancelled due to disease progression or patient health issues, further immunotherapy may not be suitable. However, specific details of the case could affect this decision. 3. For patients whose disease progresses during or recurs shortly after adjuvant pembrolizumab, experts would consider re-treating with pembrolizumab if the recurrence occurs more than 6 months after completing the initial adjuvant therapy, because this suggests a delayed progression. If recurrence happens within 6 months, additional pembrolizumab would likely not be effective. 4. For patients unable to complete adjuvant pembrolizumab for reasons other than disease progression, re-treatment could be considered if a reasonable interval has passed since the last dose, allowing some recovery time. However, eligibility would again depend on the specific circumstances, with a preference for longer intervals before reinitiating therapy. Overall, the experts suggest a cautious approach, emphasizing the response to prior treatment, the interval duration since the last immunotherapy, and the specific clinical context in determining re-treatment eligibility. |
Generalizability | |
Should patients with ECOG PS > 1 be eligible? Should the ability to continue to surgery following neoadjuvant therapy be a consideration? | The experts suggested that patients with an ECOG PS score of 2 could potentially be eligible for neoadjuvant pembrolizumab, especially those with resectable stage III disease who are otherwise young and relatively fit. However, they clarified that patients with an ECOG PS score of 3 should not be considered eligible because the level of functional impairment would likely make them unsuitable candidates for such intensive therapy. The experts emphasized that the key criterion for neoadjuvant treatment is a patient’s suitability for surgery (i.e., if a surgeon has assessed a patient and determined they are fit for a thoracotomy, it implies a sufficient performance status for neoadjuvant therapy). Consequently, they would not place excessive emphasis on minor differences in ECOG PS if a patient is deemed surgically operable. For the experts, the primary consideration is ensuring that the patient’s overall condition allows them to complete the treatment pathway, which includes both neoadjuvant therapy and subsequent surgery. |
Should patients currently on or who were treated with neoadjuvant nivolumab plus chemotherapy be eligible for a switch to perioperative pembrolizumab? | The experts indicated that while this scenario may arise infrequently, it could be a viable option. They noted that patients could potentially benefit from the additional adjuvant immunotherapy provided in the perioperative pembrolizumab regimen. Given that most patients initially receive neoadjuvant nivolumab plus chemotherapy, the number of patients needing or opting for a switch is expected to be small. However, they agreed that if a clinician decided that a switch was appropriate for a particular patient, it could be considered within the same eligible population (i.e., personalized treatment adjustments based on the clinical judgment of the treating physician). |
System and economic issues | |
The sponsor estimated a 3-year incremental budget of $17.4 million ($930,000 in year 1, $6.3 million in year 2, and $10.1 million in year 3). This is significantly lower than the estimated 3-year incremental budget impact of $65.2 million for perioperative durvalumab (which was not considered in the sponsor’s BIA for perioperative pembrolizumab). PAG is concerned that if these estimates are low, there would be a resulting higher budget impact. | This is a comment to inform pERC deliberations. |
Durvalumab, atezolizumab, and nivolumab have confidential prices negotiated. | This is a comment to inform pERC deliberations. |
BIA = budget impact analysis; CDA-AMC = Canada’s Drug Agency; ECOG PS = Eastern Cooperative Oncology Group Performance Status; PAG = Provincial Advisory Group; pERC = pan-Canadian Oncology Drug Review Expert Review Committee; TPS = tumour proportion score.
Clinical Evidence
The objective of this Clinical Review Report is to review and critically appraise the clinical evidence submitted by the sponsor on the beneficial and harmful effects of pembrolizumab, 100 mg/4 mL vial, solution for IV infusion, in the treatment of adult patients with resectable stage II, stage IIIA, or stage IIIB NSCLC. The focus has been placed on comparing pembrolizumab to relevant comparators and identifying gaps in the current evidence.
A summary of the clinical evidence included by the sponsor in this submission review of pembrolizumab is presented in 2 sections with critical appraisal by CDA-AMC of the evidence included at the end of each section. The first section, the systematic review, includes pivotal studies and RCTs that were selected according to the sponsor’s systematic review protocol. The CDA-AMC assessment of the certainty of the evidence in this first section using the GRADE approach follows the critical appraisal of the evidence. The second section includes indirect evidence from the sponsor. Long-term extensions and studies addressing gaps were not submitted.
Included Studies
Clinical evidence from the following was included in the review and appraised in this document:
one pivotal study identified in the systematic review
one ITC.
Systematic Review
Content in this section has been informed by materials submitted by the sponsor. The following has been summarized and validated by the review team.
Description of Studies
Characteristics of the included study are summarized in Table 5.
Table 5: Details of the Pivotal Study Included in the Systematic Review
Detail | KEYNOTE-671 study |
|---|---|
Designs and populations | |
Study design | Phase III, multicentre, efficacy, safety, parallel assignment, double-blind, placebo-controlled intervention |
Locations | 227 sites in 25 countries (Argentina, Australia, Belgium, Brazil, Canada, China, Estonia, France, Germany, Ireland, Italy, Japan, Latvia, Lithuania, Malaysia, Poland, Romania, Russia, South Africa, South Korea, Spain, Taiwan, the UK, Ukraine, and the US) |
Patient enrolment dates | Start date: April 24, 2018 End date: December 15, 2021 |
Randomized (N) | Total N = 797 patients PEMBRO + chemotherapy and PEMBRO = 397 patients Placebo + chemotherapy and placebo = 400 patients |
Inclusion criteria |
|
Exclusion criteria |
|
Drugs | |
Intervention | Pembro: 200 mg IV on day 1 of each 21-day cycle for 4 cycles, followed by surgery and 13 cycles Cisplatin: 75 mg/m2 IV on day 1 of each 21-day cycle for 4 cycles Gemcitabine (squamous tumours): 1,000 mg/m2 IV on day 1 and day 8 of each 21-day cycle for 4 cycles Pemetrexed (nonsquamous tumours): 500 mg/m2 IV on day 1 of each 21-day cycle for 4 cycles Radiotherapy (selected circumstances): Up to 60 Gy (patients with microscopic positive margins or extracapsular nodal extensions) or up to 70 Gy (patients who do not have surgery or who have gross residual disease after surgery) to begin within 4 weeks to 8 weeks after surgery and within 2 weeks to 4 weeks of the start of adjuvant therapy |
Comparator | Placebo: IV, day 1 of each 21-day cycle for 4 cycles followed by surgery and 13 cycles Cisplatin: 75 mg/m2 IV on day 1 of each 21-day cycle for 4 cycles Gemcitabine (squamous tumours): 1,000 mg/m2 IV on day 1 and day 8 of each 21-day cycle for 4 cycles Pemetrexed (nonsquamous tumours): 500 mg/m2 IV on day 1 of each 21-day cycle for 4 cycles Radiotherapy (selected circumstances): Up to 60 Gy (patients with microscopic positive margins or extracapsular nodal extensions) or up to 70 Gy (patients who do not have surgery or who have gross residual disease after surgery) to begin within 4 weeks to 8 weeks after surgery and within 2 weeks to 4 weeks of the start of adjuvant therapy |
Study duration | |
Screening phase | Approximately 28 days before treatment randomization |
Treatment phase | Until the maximum number of administrations was reached (a total of 17 cycles of preoperative and postoperative pembrolizumab and placebo) or for any of the following reasons:
|
Follow-up phase | Efficacy and patient-reported outcome follow-up: Every 16 weeks (± 21 days) through to the end of year 3, and then every 6 months (± 28 days) for year 4 and year 5. Safety follow-up: AEs occurring up to 30 days (± 3 days) following end of study treatment. SAEs occurring up to 90 days following end of treatment or 30 days if the patient initiates new anticancer therapy. Treatment-related late toxicity may be collected for up to 5 years. |
Outcomes | |
Primary end points | Event-free survival and overall survival |
Secondary and exploratory end points | Secondary end points:
Exploratory and tertiary end points:
|
Publication status | |
Publications | Wakelee et al. (2023)37 Spicer et al. (2023)38 ClinicalTrials.gov identifier: NCT0342564339 EudraCT number: 2017 to 001832 to 2140 |
Unpublished reports | Clinical study report: P671V02MK347533 (data cut-off date of July 10, 2023) |
AE = adverse event; AJCC = American Joint Committee on Cancer: ECOG PS = Eastern Cooperative Oncology Group Performance Status; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EORTC QLQ-LC13 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Lung Cancer 13; FFPE = formalin-fixed paraffin embedded; IHC = immunohistochemistry; LCNEC = large cell neuroendocrine cancer; NSCLC = non–small cell lung cancer; PEMBRO = pembrolizumab; QoL = quality of life, RNA = ribonucleic acid; SAE = serious adverse event.
Sources: KEYNOTE-671 Clinical Study Report (second interim analysis),33 ClinicalTrials.gov.39
The KEYNOTE-671 trial is an ongoing phase III, multicentre, randomized, placebo-controlled, double-blind study designed to evaluate perioperative pembrolizumab in adult patients with early-stage NSCLC (Figure 1). The KEYNOTE-671 trial has been conducted at 227 medical centres in 25 countries, including 5 centres in Canada. Patients were randomized 1:1 to receive concomitant neoadjuvant platinum-doublet chemotherapy plus pembrolizumab (every 3 weeks for 4 cycles) followed by surgery and adjuvant pembrolizumab (every 3 weeks for 13 cycles) or concomitant neoadjuvant platinum-doublet chemotherapy plus placebo (every 3 weeks for 4 cycles) followed by surgery and adjuvant placebo (every 3 weeks for 13 cycles). Randomization was stratified according to disease stage (stage II versus stage III), PD-L1 TPS (< 50% versus ≥ 50%), histologic features (squamous versus nonsquamous), and geographic region (East Asia versus non–East Asia).
Populations
Inclusion and Exclusion Criteria
Eligible patients were aged 18 years or older with previously untreated, pathologically confirmed stage II, stage IIIA, or stage IIIB (T3 to 4N2) NSCLC according to the AJCC staging system manual, eighth edition, that was considered resectable based on surgical consultation and investigator assessment. Patients were able to undergo protocol therapy and surgery, had an ECOG PS score of 0 or 1 (on a 5-point scale, with higher scores indicating greater disability) within 10 days before randomization, and an ability to provide a tumour sample for PD-L1 assessment at a central laboratory. Patients should have had adequate organ function and been able to provide a tumour sample for PD-L1 testing. Full eligibility criteria are provided in Table 5.
Figure 1: KEYNOTE-671 Clinical Trial Design
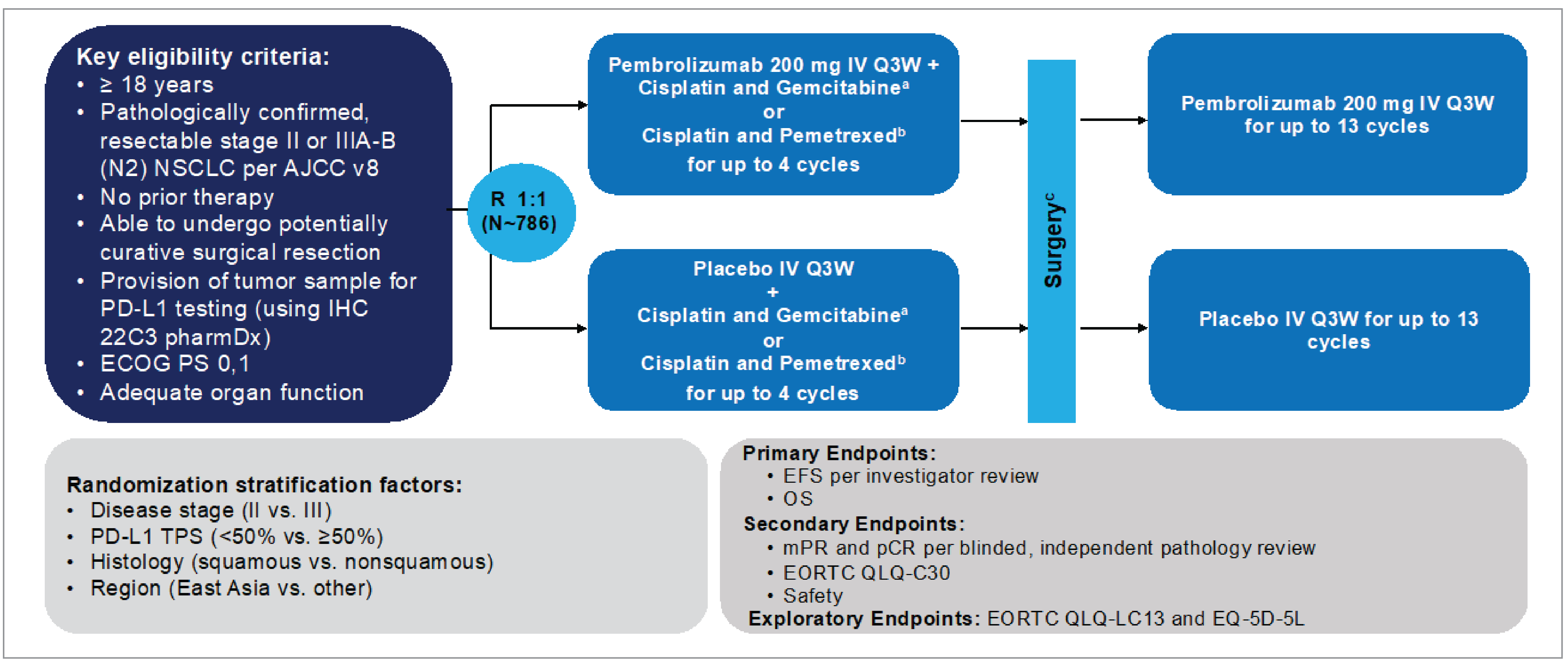
AJCC v8 = American Joint Committee on Cancer version 8; ECOG = Eastern Cooperative Oncology Group; EFS = event-free survival; EORTC QLQ-C30: European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EORTC QLQ-LC13: European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Lung Cancer 13; IHC = immunohistochemistry; mPR = major pathologic response; NSCLC = non–small cell lung cancer; OS = overall survival; pCR = pathologic complete response; PD-L1 = programmed cell death-ligand 1; PS = performance status; Q3W = every 3 weeks; QoL = quality of life; TPS = tumour proportion score; vs. = versus.
aCisplatin 75 mg/m2 IV Q3W + gemcitabine 1,000 mg/m2 IV on days 1 and 8 Q3W for squamous histology only.
bCisplatin 75 mg/m2 IV Q3W + pemetrexed 500 mg/m2 IV Q3W for nonsquamous histology only.
cRadiotherapy was indicated in participants with microscopic positive margins, gross residual disease, or extracapsular nodal extension following surgery and to participants who did not undergo planned surgery for any reason other than local progression or metastatic disease.
Source: KEYNOTE-671 study protocol (in Appendix 16.1.1.1 of the Clinical Study Report).33
Interventions
The neoadjuvant chemotherapy regimens were cisplatin plus gemcitabine for patients with squamous histology and cisplatin plus pemetrexed for patients with nonsquamous histology.
Pembrolizumab was administered at a dose of 200 mg in the neoadjuvant and adjuvant phases. All systemic treatments were given intravenously. Potentially curative surgical resection was to be performed no later than 20 weeks after the first dose of neoadjuvant pembrolizumab or placebo plus chemotherapy. The adjuvant phase was to be initiated at least 4 weeks and no later than 12 weeks after surgery. Patients in both treatment arms were to receive postoperative radiation therapy (RT) if microscopic residual disease or gross residual disease remained after surgery. Pembrolizumab, placebo, chemotherapy, and (in some patients) RT were continued until the maximum number of administrations was reached or until the occurrence of disease progression, recurrence, unacceptable toxicity, an investigator decision to discontinue, the withdrawal of consent, or other reasons, whichever occurred first.
For this document, the pembrolizumab arm and placebo arm refer to all treatment phases (neoadjuvant and surgery phase + adjuvant phase) and combine study treatments of all phases (Figure 2).
Figure 2: KEYNOTE-671 Study Phases
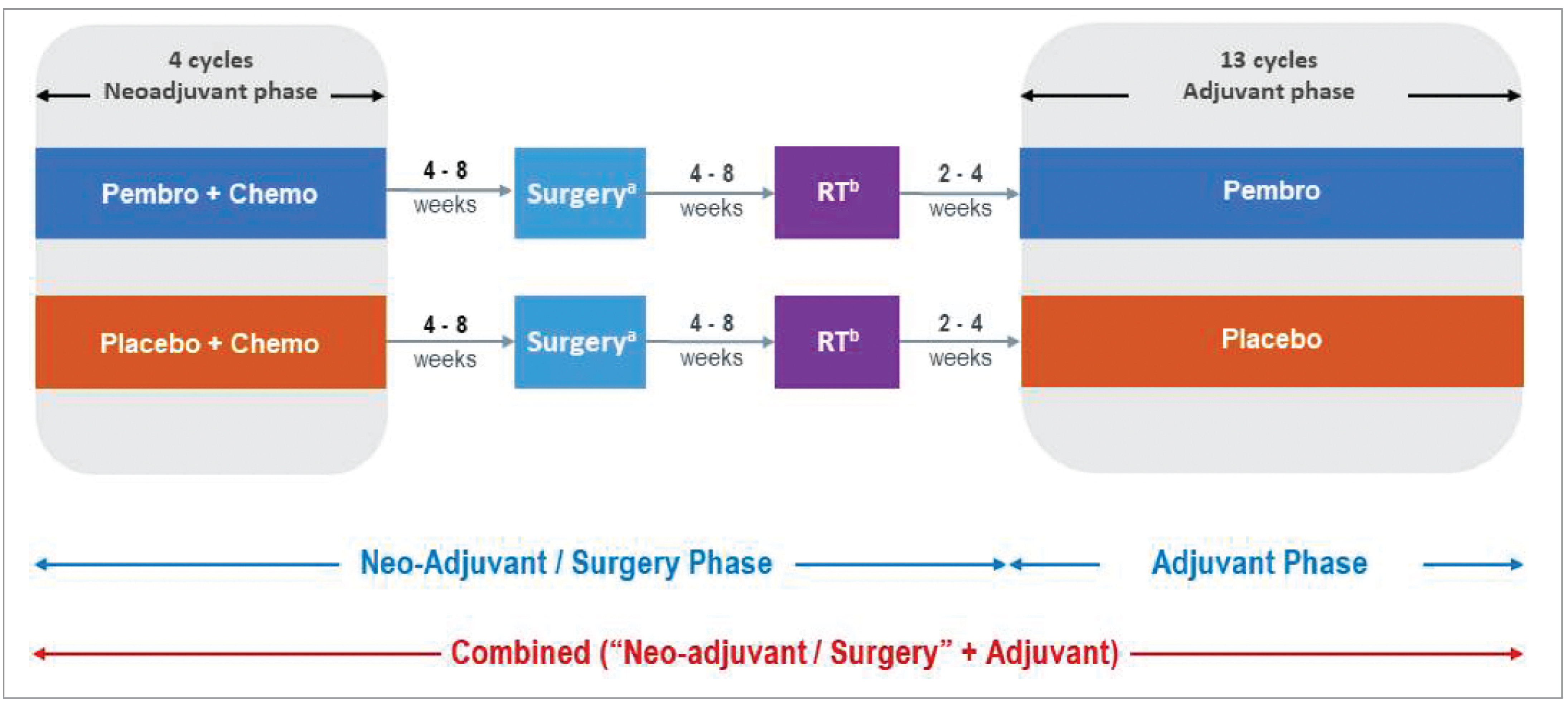
Chemo = chemotherapy; NAC = neoadjuvant chemotherapy; Pembro = pembrolizumab; RT = radiotherapy.
aIf a participant did not undergo surgery due to refusal, physician decision, medical illness, or any reason other than local progression or metastatic disease, they were to receive RT and continue to the adjuvant phase.
bOnly participants with microscopic residual disease or gross residual disease in the tumour bed after surgery were to undergo RT.
Source: KEYNOTE-671 Clinical Study Report (second interim analysis).33
Outcomes
The efficacy end points assessed in this Clinical Review Report, along with descriptions of the outcome measurement methods, are detailed in Table 6. These end points were selected based on the outcomes outlined in the sponsor’s Summary of Clinical Evidence33 and deemed important through consultations with clinical experts engaged by CDA-AMC, as well as feedback from patient and clinician groups and public drug plans. Using this collective input, the most relevant end points for informing expert committee deliberations were identified and finalized in collaboration with members of the expert committee. All efficacy end points were evaluated using the GRADE framework and are presented in order of importance, as determined through this process. Additionally, key harms outcomes identified as critical for expert committee deliberations were also assessed using the GRADE framework.
Table 6: Summary of Relevant Outcomes and Their Measures in the KEYNOTE-671 Study
Outcome measure | Time point | KEYNOTE-671 study end point |
|---|---|---|
Efficacy outcomes | ||
OS | 24 months, 36 months, and 48 months | Primarya |
EFS | 24 months, 36 months, and 48 months | Primarya |
Safety outcomes | ||
AEs | Any reported event from randomization until data cut-off (July 10, 2023) | Secondary |
SAEs | Any reported event from randomization until data cut-off (July 10, 2023) | Secondary |
Discontinuations due to AEs | Any reported event from randomization until data cut-off (July 10, 2023) | Secondary |
Deaths due to AEs | Any reported event from randomization until data cut-off (July 10, 2023) | Secondary |
Patient-reported outcomes | ||
EORTC QLQ-C30 | Randomization until data cut-off (July 10, 2023). Key time points of interest: Neoadjuvant week 11 and adjuvant week 10 | Secondary (item 29 and item 30), tertiary or exploratory (item 1 to item 8) |
EORTC QLQ-LC13 | Randomization until data cut-off (July 10, 2023). Key time points of interest: Neoadjuvant week 11 and adjuvant week 10 | Tertiary or exploratory |
AE = adverse event; EFS = event-free survival; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EORTC QLQ-LC13 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Lung Cancer 13; OS = overall survival; SAE = serious adverse event.
aStatistical testing for these end points was adjusted for multiple comparisons.
Source: KEYNOTE-671 Clinical Study Report (second interim analysis).33
In the KEYNOTE-671 trial, the dual primary end points were OS and EFS as assessed by biopsy by a local pathologist or by investigator-assessed imaging using Response Evaluation Criteria in Solid Tumours, version 1.1. Key secondary end points included change from baseline in the global health status scale and quality of life scale scores of the EORTC QLQ-C30 and safety. Other patient-reported outcomes (PROs) based on EORTC QLQ-C30, as well as PROs based on the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Lung Cancer (EORTC QLQ-LC13) module, were exploratory end points.
Outcomes studied in the KEYNOTE-671 trial and selected for this submission were defined as follows.
OS: This is the time from randomization to death due to any cause. The clinical experts consulted by the review team considered an absolute between-group difference of at least 5% (or 50 patients per 1,000 patients) to be clinically important.
EFS: This is the time from randomization to radiographic disease progression per Response Evaluation Criteria in Solid Tumours version 1.1 (for patients who have not had or will not have surgery, or patients who have gross residual disease after an incomplete resection), local progression (primary tumour or regional lymph nodes) precluding planned surgery, the inability to resect the tumour, local or distant recurrence (for patients who are disease-free after surgery or patients with microscopic positive margins), or death from any cause. Patients who reached the data cut-off date without an event (regardless of whether a new anticancer treatment was started) were censored at the last disease assessment. Patients with an EFS event after 2 or more missed disease assessments were considered to have progressed at the date of documented progressive disease, recurrence, surgery, or death. The clinical experts consulted by the review team considered an absolute between-group difference of at least 10% (or 100 patients per 1,000 patients) to be clinically important.
AEs: AEs, irrespective of causality, are reported from the time of treatment randomization through 30 days after the last dose of study treatment (severity is graded by the investigator according to the guidelines outlined in the National Cancer Institute Common Terminology Criteria for Adverse Events, version 4.0).
SAEs: SAEs are reported from the time of treatment randomization through 90 days after the last dose of study treatment or 30 days following the discontinuation of study treatment if the patient initiates a new anticancer treatment, whichever occurs first (intensity is assessed by the investigator according to the National Cancer Institute Common Terminology Criteria for Adverse Events, version 4.0). SAEs are AEs resulting in death or those that are life-threatening, require inpatient hospitalization or the prolongation of existing hospitalization, or result in persistent or significant disability and/or incapacity, congenital anomaly and/or birth death, or other important medical events.
Withdrawals due to AEs: These are withdrawals from study treatment (permanent discontinuation of study treatment) due to any study intervention–related toxicity specified as a reason for permanent discontinuation as defined in the guidelines for dose modification due to AEs.
AESIs: AESIs are immune-mediated events and infusion-related reactions associated with pembrolizumab. A predefined list of preferred terms was developed by the sponsor to consistently characterize the nature and frequency of each AESI regardless of causality as reported by investigators. These preferred terms are considered medically equivalent to the immune-mediated events and infusion-related reactions. AESIs are reported from the time of randomization through 90 days after the last dose of study treatment or 30 days following the discontinuation of study treatment if the patient initiates a new anticancer treatment, whichever occurs first.
EORTC QLQ-C30: EORTC QLQ-C30 is an HRQoL instrument that contains 30 items and measures 5 functional dimensions (physical, role, emotional, cognitive, and social), 3 symptom items (fatigue, nausea, and vomiting, and pain), 6 single items (dyspnea, sleep disturbance, appetite loss, constipation, diarrhea, and financial impact), and the global health status scale and quality of life scale (Table 7).
EORTC QLQ-LC13: EORTC QLQ-LC13 is a lung cancer module to the EORTC QLQ-C30 that measures HRQoL relevant to specific symptoms (chest pain, cough, and dyspnea) common in lung cancer. The lung cancer module is meant for use among a wide range of patients with lung cancer varying in disease stage and treatment modality. The module comprises 13 questions assessing lung cancer-associated symptoms (cough, hemoptysis, dyspnea, and site-specific pain), treatment-related side effects (sore mouth, dysphagia, peripheral neuropathy, and alopecia), and pain medication.
In the neoadjuvant phase, patients were to have an imaging assessment 3 weeks after cycle 2 and cycle 4 (if receiving all 4 cycles), 3 weeks after cycle 2 and 4 weeks after cycle 3 (if receiving 3 cycles), 3 weeks after cycle 2 (if receiving 2 cycles), and 3 weeks after cycle 1 (if receiving 1 cycle) (± 7 days). Following surgery, patients were to have new baseline imaging within 4 weeks before the start of adjuvant pembrolizumab or placebo treatment, then every 16 weeks (± 14 days) from the date of randomization during year 1, every 16 weeks (± 21 days) during year 2 and year 3, and every 6 months (± 28 days) during year 4 and year 5. Patients who did not undergo surgery and did not receive RT were not required to have new baseline imaging and were to have follow-up scans every 16 weeks (± 21 days) from the date of randomization. All imaging assessments were evaluated by the investigator and submitted for blind independent central review (BICR).
Table 7: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
EORTC QLQ-C30 | This is a 30-item, patient-reported, cancer-specific, HRQoL questionnaire using 4-point and 7-point Likert scales.41 There are 15 domains for EORTC QLQ-C30. Functional scales, ranging from 0 to 100 (with higher scores indicating higher functioning) include the global health status scale and quality of life scale, physical functioning, role functioning, emotional functioning, cognitive functioning, and social functioning. Symptom scales, ranging from 0 to 100 (with higher scores indicating a greater degree of symptoms or worse condition) include fatigue, pain, nausea and vomiting, dyspnea, insomnia, appetite loss, constipation, diarrhea, and financial difficulties.41 | Content validity: When mapping to WHO’s ICF framework, 25 of the 30 items in the EORTC QLQ-C30 were endorsed by 21 health care professionals, using the Delphi technique (≥ 70% agreement).42 Validity: Physical functioning correlations between items and the overall scale ranged from 0.60 to 0.80, indicating a strong internal structure. This was also indicated with clinical measures. An example is the correlation between EORTC QLQ-C30 global health status and ECOG PS: 0.50 to 0.60 (moderate validity).43 Cognitive functioning: Some lower correlations (below 0.40) were reported, suggesting a weaker construct validity for this scale.43 Reliability: Internal consistency has been reported with a Cronbach alpha greater than 0.7 and test reliability coefficients of 0.82 (SEM = 8.6).43 Responsiveness: No literature was identified that assessed responsiveness in patients with breast cancer. | In a paper synthesizing data from 21 published EORTC phase III trials enrolling 13,015 patients across 9 cancer types, the anchor-based MID for the global health status scale for between-group change over time in patients with lung cancer was 5 points for improvement and –5 points for deterioration or improvement. Estimated MIDs on other scales ranged from 6 points to 13 points for improvement and –5 points to –15 points for deterioration.44 The sponsor suggested an absolute within-group change greater than or equal to 10 points from baseline, which was informed by the literature.45,46 |
EORTC QLQ-LC13 | The EORTC QLQ-LC13 is a tumour-specific questionnaire used to supplement the EORTC QLQ-C30. It contains 13 items related to lung cancer symptoms and treatment side effects, including a 3-item scale assessing dyspnea and 9 single items: pain in chest, pain in arm or shoulder, pain in other parts, coughing, hemoptysis, sore mouth or tongue, dysphagia, peripheral neuropathy, and alopecia.41 Total raw scores can be transformed to a scale of 0 to 100. Higher scores on the symptom scales indicate worse symptoms.41 | Validity: Construct validity has been established between pain score and disease type (P < 0.001). Also, based on ECOG PS, construct validity was confirmed in dyspnea, coughing, and pain scores (P < 0.001).47 Correlation between spirometry result and dyspnea score was found to be weak (r = 0.24). BPI intensity score and EORTC QLQ-LC13 pain score were found to be modestly correlated (r > 0.4).48 Reliability: Good internal consistency reliability for the dyspnea multi-item scale (alpha = 0.81).47 However, internal consistency was found to be unacceptable for pain scores (alpha = 0.53 to 0.54) when EORTC QLQ-LC13 was used alone without EORTC QLQ-C30 questionnaire pain items.47 The reliability estimate for the dyspnea scale has been confirmed to be acceptable (i.e., alpha = 0.76 in another study).48 Responsiveness: Dyspnea, coughing, and pain scores improved significantly over time between the pretreatment and on-treatment period (P < 0.001 for all except for extra thoracic pain, which showed P < 0.05). Responsiveness of chest pain (P < 0.01), dyspnea (P < 0.001), and coughing (P < 0.001) to change in ECOG PS was also noted.47 | No relevant studies were identified in patients with NSCLC. A minimum clinically relevant change was defined by the sponsor as a change in the score from baseline of ≥ 10 for scales and items from the EORTC QLQ-LC13. |
BPI = Brief Pain Inventory; ECOG PS = Eastern Cooperative Oncology Group Performance Status; EORTC = European Organisation for Research and Treatment of Cancer; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EORTC QLQ-LC13 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Lung Cancer 13; HRQoL = health-related quality of life; ICF = International Classification of Functioning, Disability, and Health; MID = minimal important difference; NSCLC = non–small cell lung cancer; QoL = quality of life; SEM = standard error of the mean.
All PRO instruments operated as electronically administered patient-reported outcomes (ePROs) before all procedures and/or assessments at the hospital during scheduled visits. Year 1 included the neoadjuvant treatment phase, the surgery, and the adjuvant treatment phase. In the neoadjuvant phase, ePROs were administered at treatment cycle 1 (baseline) and cycle 4 (week 11); in the adjuvant phase, ePROs were administered at treatment cycle 1, cycle 2, cycle 3, cycle 4 (week 10), cycle 7, cycle 10, and cycle 13. In the posttreatment phase, ePROs were administered at the safety follow-up visit (30 days from the last dose), and then every 4 months in year 2, every 6 months in year 3, and yearly in year 4 and year 5.
Statistical Analysis
The hypotheses were evaluated by comparing pembrolizumab plus chemotherapy to placebo plus chemotherapy with respect to EFS and OS using a stratified log-rank test. For EFS and OS, HRs and corresponding 95% CIs were estimated using a stratified Cox regression model. Event rates were estimated within each treatment arm using the Kaplan-Meier method. The trial was considered positive if a statistically significant benefit of pembrolizumab was observed for either EFS or OS at an interim or final analysis. Details about the statistical model, adjustment factors, handling of missing data, and sensitivity analyses of efficacy end points are described in Table 8.
Table 8: Statistical Analysis of Efficacy End Points in the KEYNOTE-671 Study
End point | Statistical model | Adjustment factors | Handling of missing data | Sensitivity analyses |
|---|---|---|---|---|
OS | Test: Stratified log-rank test to assess the treatment difference Estimation: Stratified Cox model with Efron’s tie-handling method to assess the magnitude of treatment difference |
| Censored at last known alive date | Restricted mean survival time method was conducted for OS to account for the possible nonproportional hazards effect as a sensitivity analysis. |
EFS | Test: Stratified log-rank test to assess the treatment difference Estimation: Stratified Cox model with Efron’s tie-handling method to assess the magnitude of treatment difference |
| Censored at the last disease assessment | A sensitivity analysis by using the central review of imaging and biopsy Sensitivity analyses using different censoring rules |
Change from baseline in EORTC QLQ-C30 and EORTC QLQ-LC13 | Constrained longitudinal data analysis model for difference in LSM change from baseline | Treatment, time, treatment by visit interaction, and stratification variables of stage (stage II vs. stage III), TPS (≥ 50% vs. < 50%), histology (squamous vs. nonsquamous), and region (East Asia vs. non–East Asia) | Model-based | None |
EFS = event-free survival; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EORTC QLQ-LC13 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Lung Cancer 13; LSM = least squares mean; OS = overall survival; TPS = tumour proportion score; vs. = versus.
Source: KEYNOTE-671 Clinical Study Report (second interim analysis).33
Sample Size and Power Calculation
The study was designed to enrol approximately 786 patients to achieve a 90% power to detect an EFS HR of 0.7 at a 1-sided alpha of 0.01 (based on approximately 416 EFS events) and an OS HR of 0.7 at a 1-sided alpha of 0.0148 (based on approximately 386 deaths).
Statistical Testing
The KEYNOTE-671 study protocol planned 4 event-driven interim analyses and 1 final analysis with familywise type I error rate strongly controlled at a 1-sided alpha level of 0.025 across the EFS, OS, major pathological response, and pCR hypotheses using the graphical method of Maurer and Bretz. This method provides strong multiplicity control for multiple hypotheses as well as interim efficacy analyses by testing individual hypotheses in a group sequential fashion using an error spending approach. Figure 3 shows the initial 1-sided alpha allocation for each hypothesis in the ellipse representing the hypothesis. The initial weights for reallocation from each hypothesis to others are represented in the boxes on the lines connecting hypotheses.
Analyses of OS were planned in all analyses conducted for EFS. Additional OS analyses were also planned after the final EFS analysis. The final OS analysis will be conducted when approximately 386 deaths have been observed (approximately 96 months after the first patient was randomized).
At the time of writing this submission, the study is still ongoing, and the results reported here are based on the protocol prespecified for IA2 with a data cut-off date of July 10, 2023. The first patient was randomized on May 11, 2018, and the last patient was randomized on December 15, 2021. The IA2 data cut-off date is the primary completion date for the KEYNOTE-671 study. Data from the first interim analysis (IA1) (data cut-off date of July 29, 2022) were published in The New England Journal of Medicine on June 3, 2023.37
Figure 3: Multiplicity Graph for Type I Error Control in the KEYNOTE-671 Study
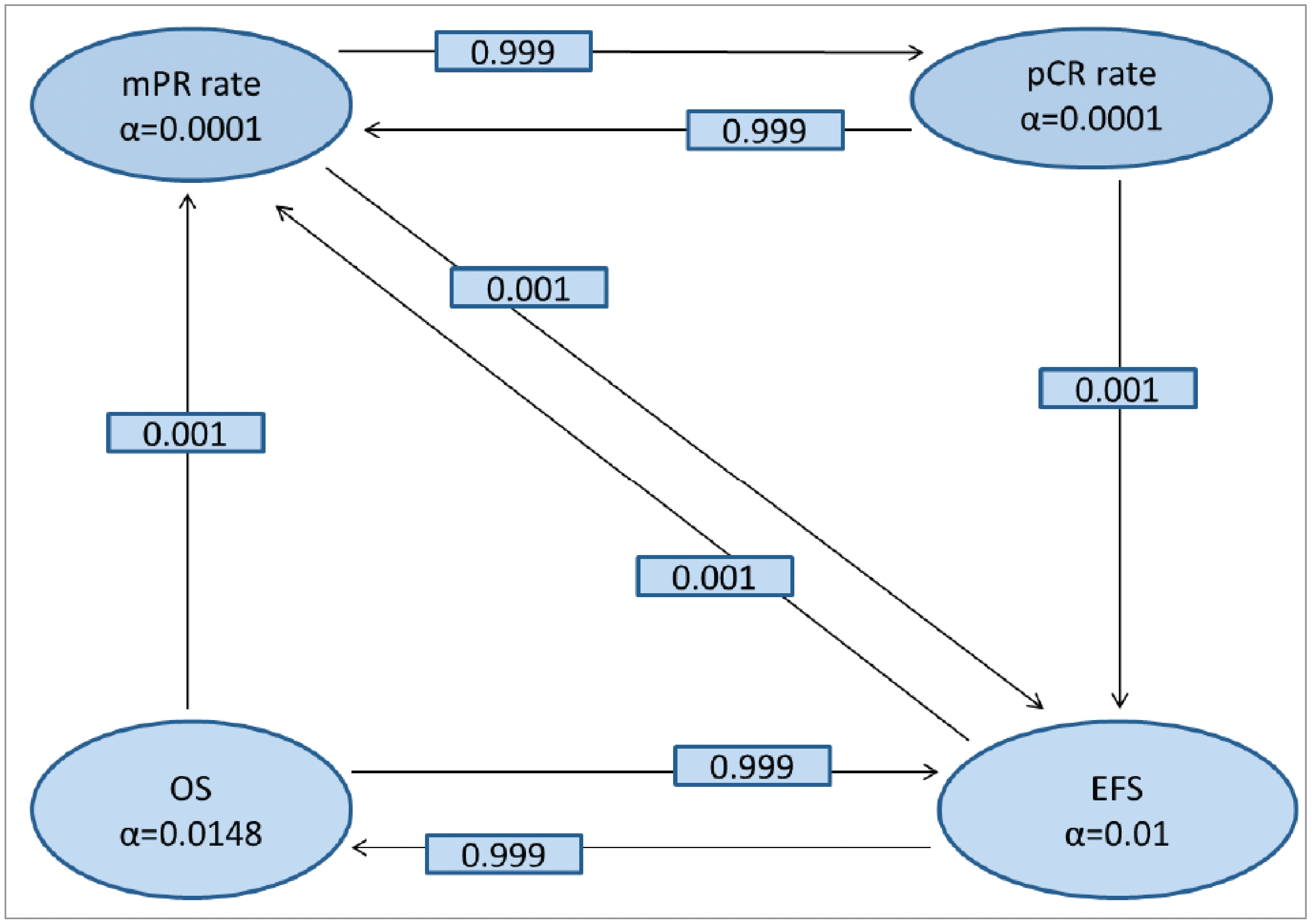
EFS = event-free survival; mPR = major pathological response; pCR = pathological complete response; OS = overall survival.
Source: KEYNOTE-671 Clinical Study Report (second interim analysis).33
Subgroup Analyses
To determine whether the treatment effect is consistent across various subgroups, the KEYNOTE-671 trial assessed the between-group treatment effect (with a nominal 95% CI) for the primary end points and plotted by treatment group within each category of the following classification variables:
tumour stage (stage II or stage III)
TPS (< 50% or ≥ 50%)
histology (squamous or nonsquamous)
geographic region (East Asia or non–East Asia)
age category (< 65 years or ≥ 65 years)
sex (female or male)
race (white or other [American Indian or Alaska Native, Asian, Black, or African American])
smoking status (never, former, or current)
known EGFR activating mutation status (yes or no)
ALK translocation status (yes or no).
The consistency of the treatment effect was assessed descriptively via summary statistics by category for the classification variables listed previously. Only the subgroup analyses for subgroups that had at least 30 patients in all groups were done. Subgroup analyses for efficacy end points were conducted using unstratified methods.
Analysis Populations
Analyses of primary and secondary efficacy end points were conducted on all randomized patients according to the intention-to-treat (ITT) principle. Safety analyses were based on all patients who received at least 1 dose of study treatment (all patients as treated population). PRO analyses were based on the PRO full analysis set population, which included all randomized patients who had at least 1 PRO assessment available and had received at least 1 dose of study treatment. Finally, perioperative complication (postoperative safety observation) analyses were performed on all randomized patients who received at least 1 dose of neoadjuvant study treatment and underwent in-study surgery (all patients receiving surgery population).
The analyses populations, as defined in the KEYNOTE-671 Clinical Study Report, are defined in Table 9.
Table 9: Analysis of Populations in KEYNOTE-671 Study
Population | Pembrolizumab arm | Placebo arm | Total | Definition | Application | |
|---|---|---|---|---|---|---|
ITT | 397 | 400 | 797 | All randomized patients. Patients were included in the treatment group to which they were randomized. | Efficacy outcomes | |
APaT | 396 | 399 | 795 | All randomized patients who received at least 1 dose of study treatment. Patients were included in the treatment group corresponding to the study treatment they actually received. | Safety outcomes | |
PRO FASa | EORTC QLQ-C30 | 388 | 391 | 779 | Patients who had at least 1 PRO assessment available and had received at least 1 dose of study medication. | PROs |
EORTC QLQ-LC13 | 386 | 388 | 774 | |||
APaT = all patients as treated; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EORTC QLQ-LC13 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Lung Cancer 13; FAS = full analysis set; ITT = intention to treat; PRO = patient-reported outcome.
aThe number of patients refers to the patients with a PRO assessment at baseline; the number of patients at follow-up varies by follow-up time point and PRO assessment.
Source: KEYNOTE-671 Clinical Study Report (second interim analysis).33
Results
Patient Disposition
Patient disposition is described in Table 10. Among the 1,364 patients screened, a total of 567 patients were not randomized — the majority of them (565 patients) for not meeting the selection criteria. The proportion of patients who discontinued from the study was similar in the 2 treatment arms (30.5% in the pembrolizumab arm and 38.3% in the placebo arm), with death as the most common cited reason (27.5% in the pembrolizumab arm and 35.3% in the placebo arm). Two patients (1 in each arm) were randomized but not treated.
In the pembrolizumab arm, 396 patients received at least 1 dose of neoadjuvant pembrolizumab plus chemotherapy for a median of 4 cycles, 325 patients (81.9%) underwent in-study surgery, 35 patients (8.8%) received in-study radiotherapy, and 290 patients (73.0%) received at least 1 dose of adjuvant pembrolizumab (Table 11). In the placebo arm, 399 patients received at least 1 dose of neoadjuvant plus chemotherapy for a median of 4 cycles, 317 patients (79.3%) underwent in-study surgery, 53 patients (13.3%) received in-study radiotherapy, and 267 (66.8%) patients received at least 1 dose of adjuvant placebo. In the adjuvant phase, the proportion of patients who discontinued study treatment was similar in both treatment arms (34.1% in the pembrolizumab arm versus 34.8% in the placebo arm). The most frequent reason for the discontinuation of pembrolizumab was AEs (14.1%) and the most frequent reason for the discontinuation of placebo was progressive disease (24.3%). A similar proportion of patients completed the 13 cycles of adjuvant study medication in both arms.
Among patients who underwent in-study surgery, 92.0% of those in the pembrolizumab arm and 84.2% of those in the placebo arm had complete resection.
For the ITT population at the data cut-off date for IA2, the median follow-up duration — defined as the time from randomization to the date of death or the data cut-off date if the patient was still alive — was 29.8 months (range, 0.4 months to 62.0 months); this was similar between the 2 treatment arms at 31.5 months (range, 0.4 months to 61.7 months) in the pembrolizumab arm and 28.9 months (range, 0.6 months to 62.0 months) in the placebo arm.
Table 10: Summary of Patient Disposition From the KEYNOTE-671 Study
Patient dispositiona | Pembrolizumab arm N (%) | Placebo arm N (%) |
|---|---|---|
Screened | 1,364 | |
Not randomized | 567 | |
Did not meet inclusion criteria or did meet exclusion criteria | 565 | |
Randomized (ITT) | 397 | 400 |
Status for study treatment (neoadjuvant in combination with surgery + adjuvant) | ||
Started | 396 | 399 |
Completed | 192 (48.2) | 174 (43.6) |
Discontinued | 205 (51.8) | 225 (56.4) |
Reasons for treatment discontinuation | ||
Adverse event | 86 (21.7) | 39 (9.8) |
Associated with COVID-19 | 3 (0.8) | 0 (0.0) |
Clinical progression | 2 (0.5) | 3 (0.8) |
Local progression preventing surgery | 1 (0.3) | 6 (1.5) |
Nonstudy anticancer therapy | 2 (0.5) | 6 (1.5) |
Associated with COVID-19 | 0 (0.0) | 1 (0.3) |
Physician decision | 22 (5.6) | 17 (4.3) |
Associated with COVID-19 | 1 (0.3) | 1 (0.3) |
Progressive disease | 62 (15.7) | 106 (26.6) |
Protocol violation | 1 (0.3) | 1 (0.3) |
Associated with COVID-19 | 0 (0.0) | 1 (0.3) |
Tumour found to be surgically unresectable | 5 (1.3) | 15 (3.8) |
Withdrawal by patient | 24 (6.1) | 32 (8.0) |
Associated with COVID-19 | 2 (0.5) | 0 (0.0) |
Status for trial | ||
Discontinued | 121 (30.5) | 153 (38.3) |
Reasons for study discontinuation | ||
Death | 109 (27.5) | 141 (35.3) |
Associated with COVID-19 | 5 (1.3) | 4 (1.0) |
Lost to follow-up | 2 (0.5) | 0 (0.0) |
Withdrawal by patient | 10 (2.5) | 12 (3.0) |
COVID-19 association unspecified, subsequently died | 1 (0.3) | 3 (0.8) |
Patients ongoing | 276 (69.5) | 247 (61.8) |
ITT = intention to treat; PRO = patient-reported outcome.
aThe number of patients refers to the patients with a PRO assessment at baseline; the number of patients at follow-up varies by follow-up time point and PRO assessment.
Source: KEYNOTE-671 Clinical Study Report (second interim analysis).33
Table 11: Detailed Patient Disposition From the KEYNOTE-671 Study, ITT Population
Patient disposition | Pembrolizumab arm N = 397 | Placebo arm N = 400 |
|---|---|---|
Status of study medication (neoadjuvant), n (%) | ||
Started study treatment | 396 | 399 |
Completed 4 cycles of pembrolizumab or placebo | 295 (74.5) | 297 (74.4) |
Discontinued before completing 4 cycles | 101 (25.5) | 102 (25.6) |
Started next study treatment | 70 (17.7) | 66 (16.5) |
Adverse event | 20 (5.1) | 22 (5.5) |
Physician decision | 49 (12.4) | 43 (10.8) |
Progressive disease | 1 (0.3) | 0 (0.0) |
Withdrawal by patient | 0 (0.5) | 1 (0.3) |
Discontinued without intent to receive any further study treatmenta | 31 (7.8) | 36 (9.0) |
Adverse event | 16 (4.0) | 13 (3.3) |
Clinical progression | 1 (0.3) | 1 (0.3) |
Local progression preventing surgery | 1 (0.3) | 1 (0.3) |
Nonstudy anticancer therapy | 0 (0.0) | 1 (0.3) |
Physician decision | 2 (0.5) | 4 (1.0) |
Progressive disease | 5 (1.3) | 14 (3.5) |
Withdrawal by patient | 6 (1.5) | 2 (0.5) |
Status of in-study surgery, n (%) | ||
Started | 325 | 317 |
Complete resection R0 | 299 (92.0) | 267 (84.2) |
Incomplete resection R1 | 17 (5.2) | 31 (9.8) |
Incomplete resection R2 | 4 (1.2) | 4 (1.3) |
Unresectable | 5 (1.5) | 15 (4.7) |
Discontinued without intent to receive any further study treatmenta | 45 (13.8) | 60 (18.9) |
Adverse event | 19 (5.8) | 10 (3.2) |
Clinical progression | 0 (0.0) | 1 (0.3) |
Nonstudy anticancer therapy | 2 (0.6) | 5 (1.6) |
Physician decision | 7 (2.2) | 6 (1.9) |
Progressive disease | 6 (1.8) | 10 (3.2) |
Protocol violation | 1 (0.3) | 1 (0.3) |
Tumour found to be unresectable | 5 (1.5) | 15 (4.7) |
Withdrawal by patient | 5 (1.5) | 12 (3.8) |
Status of in-study radiotherapy, n (%) | ||
Started | 35 | 53 |
Discontinued without intent to receive any further study treatmenta | 7 (20.0) | 8 (15.1) |
Adverse event | 2 (5.7) | 0 (0.0) |
Physician decision | 0 (0.0) | 1 (1.9) |
Progressive disease | 4 (11.4) | 5 (9.4) |
Withdrawal by patient | 1 (2.9) | 2 (3.8) |
Status of study medication (adjuvant), n (%) | ||
Started | 290 | 267 |
Completed 13 cycles of pembrolizumab or placebo | 191 (65.9) | 174 (65.2) |
Discontinued before completing 13 cycles | 99 (34.1) | 93 (34.8) |
Adverse event | 41 (14.1) | 15 (5.6) |
Clinical progression | 1 (0.3) | 1 (0.4) |
Physician decision | 12 (4.1) | 2 (0.7) |
Progressive disease | 37 (12.8) | 65 (24.3) |
Withdrawal by patient | 8 (2.8) | 10 (3.7) |
ITT = intention to treat.
aStudy treatment includes study medication, in-study surgery, and in-study radiotherapy.
Source: KEYNOTE-671 Clinical Study Report (second interim analysis).33
Baseline Characteristics
The baseline sociodemographic and disease characteristics of patients in the overall ITT population are summarized in Table 12, focusing on those most relevant to this review or likely to influence outcomes or the interpretation of study results. Baseline characteristics were well balanced between the treatment arms and broadly representative of patients newly diagnosed with early-stage resectable NSCLC. The majority of patients were white (61.4%), male (70.6%), aged younger than 65 years (54.6%), had stage III disease (70.0%), were former smokers (62.4%), and had an ECOG PS score of 0 (62.6%). PD-L1 TPSs of 50% or more were reported in 33.4% of patients.
Table 12: Summary of Baseline Characteristics in the KEYNOTE-671 Study, ITT Population
Characteristic | Pembrolizumab arm (N = 397) | Placebo arm (N = 400) |
|---|---|---|
Sex, n (%) | ||
Female | 118 (29.7) | 116 (29.0) |
Male | 279 (70.3) | 284 (71.0) |
Age (years), n (%) | ||
< 65 | 221 (55.7) | 214 (53.5) |
65 to 74 | 153 (38.5) | 152 (38.0) |
75 to 84 | 23 (5.8) | 34 (8.5) |
Age (continuous, years) | ||
Mean | 62.7 | 63.6 |
SD | 8.5 | 8.1 |
Median | 63 | 64 |
Range | 26 to 83 | 35 to 81 |
Race, n (%) | ||
American Indian or Alaska Native | 1 (0.3) | 0 (0.0) |
Asian | 124 (31.2) | 125 (31.3) |
Black or African American | 6 (1.5) | 10 (2.5) |
Multiple | 3 (0.8) | 10 (2.5) |
White | 250 (63.0) | 239 (59.8) |
Missing | 13 (3.3) | 16 (4.0) |
Ethnicity, n (%) | ||
Hispanic or Latino | 36 (9.1) | 34 (8.5) |
Not Hispanic or Latino | 329 (82.9) | 333 (83.3) |
Not reported | 18 (4.5) | 25 (6.3) |
Unknown | 14 (3.5) | 8 (2.0) |
Region (EU vs. formerly EU), n (%) | ||
EU | 136 (34.3) | 131 (32.8) |
Ex-EU | 261 (65.7) | 269 (67.3) |
Region (East Asia vs. non–East Asia), n (%) | ||
East Asia | 123 (31.0) | 121 (30.3) |
Non–East Asia | 274 (69.0) | 279 (69.8) |
Overall cancer staging at baseline, n (%) | ||
II | 118 (29.7) | 121 (30.3) |
III | 279 (70.3) | 279 (69.8) |
PD-L1 expression level, n (%) | ||
TPS ≥ 50% | 132 (33.2) | 134 (33.5) |
TPS = 1% to 49% | 127 (32.0) | 115 (28.8) |
TPS < 1% | 138 (34.8) | 151 (37.8) |
Smoking status, n (%) | ||
Never smoker | 54 (13.6) | 47 (11.8) |
Former smoker | 247 (62.2) | 250 (62.5) |
Current smoker | 96 (24.2) | 103 (25.8) |
Baseline ECOG PS, n (%) | ||
0 | 253 (63.7) | 246 (61.5) |
1 | 144 (36.3) | 154 (38.5) |
Histology, n (%) | ||
Squamous | 171 (43.1) | 173 (43.3) |
Nonsquamous | 226 (56.9) | 227 (56.8) |
EGFR activating mutation status, n (%) | ||
Yes | 14 (3.5) | 19 (4.8) |
No | 111 (28.0) | 124 (31.0) |
Unknown or missing | 272 (68.5) | 257 (64.3) |
ALK translocation status, n (%) | ||
Yes | 12 (3.0) | 9 (2.3) |
No | 104 (26.2) | 132 (33.0) |
Unknown or missing | 281 (70.8) | 259 (64.8) |
ECOG PS = Eastern Cooperative Oncology Group Performance Status; EU = European Union; ITT = intention to treat; SD = standard deviation; TPS = tumour proportion score; vs. = versus.
Source: KEYNOTE-671 Clinical Study Report (second interim analysis).33
Exposure to Study Treatments
Study Treatments
As of the data cut-off date for IA2 (July 10, 2023), the median duration of exposure to study treatments across the combined phases (neoadjuvant and surgery + adjuvant) was longer in the pembrolizumab arm at 375.5 days (range, 1.0 day to 728.0 days) compared with the placebo arm at 337.0 days (range, 1.0 day to 644.0 days) (Table 13). Among patients who received at least 1 dose of the assigned study treatment, 288 (72.7%) patients in the pembrolizumab arm and 263 (65.9%) patients in the placebo arm remained on study treatment for at least 6 months during the combined phases (Table 14).
Table 13: Patient Exposure, Combined Phases (Neoadjuvant in Combination With Surgery Plus Adjuvant) in the KEYNOTE-671 Study, APaT Population
Exposure | Pembrolizumab arm N = 396 | Placebo arm N = 399 |
|---|---|---|
Study days on treatment | ||
Patients, N | 396 | 399 |
Mean (SD) | 300.1 (158.7) | 281.1 (161.5) |
Median | 375.5 | 337.0 |
Range | 1.0 to 728.0 | 1.0 to 644.0 |
Study days on pembrolizumab or placebo | ||
Patients, N | 396 | 399 |
Mean (SD) | 292.2 (168.5) | 271.6 (172.0) |
Median | 375.5 | 337.0 |
Range | 1.0 to 728.0 | 1.0 to 644.0 |
Number of administrations of pembrolizumab or placebo | ||
Patients, N | 396 | 399 |
Mean (SD) | 11.3 (6.0) | 10.6 (6.1) |
Median | 15.0 | 12.0 |
Range | 1.0 to 17.0 | 1.0 to 17.0 |
APaT = all patients as treated; SD = standard deviation.
Note: Treatment includes study drugs, in-study surgery, and in-study radiotherapy.
Source: KEYNOTE-671 Clinical Study Report (second interim analysis).33
Table 14: Patient Exposure by Duration in the KEYNOTE-671 Study, APaT Population
Duration of exposure (months) | Pembrolizumab arm N = 396 | Placebo arm N = 399 | ||
|---|---|---|---|---|
n (%) | Person-months | n (%) | Person-months | |
Combined phases (neoadjuvant in combination with surgery + adjuvant) | ||||
> 0 | 396 (100.0) | 3,904.0 | 399 (100.0) | 3,684.6 |
≥ 1 | 380 (96.0) | 3,896.7 | 377 (94.5) | 3,674.5 |
≥ 3 | 330 (83.3) | 3,791.4 | 323 (81.0) | 3,560.4 |
≥ 6 | 288 (72.7) | 3,620.5 | 263 (65.9) | 3,321.5 |
≥ 12 | 202 (51.0) | 2,889.0 | 188 (47.1) | 2,652.7 |
≥ 15 | 51 (12.9) | 825.8 | 41 (10.3) | 660.6 |
Neoadjuvant and surgery phase | ||||
> 0 | 396 (100.0) | 1,377.2 | 399 (100.0) | 1,413.9 |
≥ 1 | 379 (95.7) | 1,368.9 | 377 (94.5) | 1,403.9 |
≥ 3 | 291 (73.5) | 1,173.9 | 293 (73.4) | 1,212.9 |
≥ 6 | 25 (6.3) | 166.3 | 26 (6.5) | 179.5 |
APaT = all patients as treated.
Note: Each patient is counted once on each applicable duration category row. The duration of exposure is the time from the first treatment date to the last treatment date. The duration of exposure in person-months is calculated as the total of all individual patient duration values in days divided by days per month (1 month = 30.4367 days). Treatment includes study drugs, in-study surgery, and in-study radiotherapy.
Source: KEYNOTE-671 Clinical Study Report (second interim analysis).33
Concomitant Medications and Cointerventions
The reported medical history conditions were generally as expected for patients with newly diagnosed stage II, stage IIIA, or stage IIIB NSCLC and were generally balanced between the treatment arms. Consistent with the selection criteria, no patients had received prior oncologic therapies. Reported concomitant interventions were generally balanced between the treatment arms.
Subsequent Treatment
Fewer patients initiated subsequent antineoplastic therapy in the pembrolizumab arm than in the placebo arm (24.7% versus 45.0%, respectively) (Table 15). Similarly, fewer subsequent uses of ICIs were reported in the pembrolizumab arm than in the placebo arm (7.6% versus 28.6%, respectively). The most prescribed (> 2%) subsequent systemic anticancer therapies in pembrolizumab-treated patients were carboplatin (11.3%), paclitaxel (6.3%), docetaxel (5.0%), gemcitabine (4.5%), pembrolizumab (3.3%), pemetrexed (3.3%), cisplatin (2.8%), and vinorelbine (2.3%). In placebo-treated patients, the most prescribed subsequent therapies were carboplatin (23.5%), paclitaxel (16.0%), pembrolizumab (13.0%), docetaxel (8.0%), pemetrexed (6.8%), nivolumab (5.3%), atezolizumab (4.8%), cisplatin (4.5%), durvalumab (4.3%), gemcitabine (3.8%), vinorelbine (3.8%), nab-paclitaxel (2.8%), etoposide (2.5%), ipilimumab (2.5%), bevacizumab (2.3%), and ramucirumab (2.3%).
Table 15: Subsequent Antineoplastic Therapies in the KEYNOTE-671 Study, ITT Population
Exposure | Pembrolizumab arm N (%) | Placebo arm N (%) |
|---|---|---|
Patients in population | 397 | 400 |
With 1 or more subsequent oncologic therapies | 98 (24.7) | 180 (45.0) |
Antineoplastic agents (> 3% of patients in 1 or more treatment groups) | 98 (24.7) | 180 (45.0) |
Atezolizumab | 4 (1.0) | 19 (4.8) |
Carboplatin | 45 (11.3) | 94 (23.5) |
Cisplatin | 11 (2.8) | 18 (4.5) |
Docetaxel | 20 (5.0) | 32 (8.0) |
Durvalumab | 5 (1.3) | 17 (4.3) |
Gemcitabine | 18 (4.5) | 15 (3.8) |
Nivolumab | 6 (1.5) | 21 (5.3) |
Paclitaxel | 25 (6.3) | 64 (16.0) |
Pembrolizumab | 13 (3.3) | 52 (13.0) |
Pemetrexed disodium | 12 (3.0) | 25 (6.3) |
Vinorelbine tartrate | 9 (2.3) | 15 (3.8) |
ITT = intention to treat.
Note: Every patient is counted a single time for each subsequent oncologic therapy. A patient with multiple subsequent therapies within a subsequent therapy category is counted a single time for that category. A medication class or specific medication appears only if its incidence meets the incidence criterion in the report title, after rounding.
Source: KEYNOTE-671 Clinical Study Report (second interim analysis).33
Efficacy
The outcomes in this section are presented in order of importance, as determined by the CDA-AMC team based on input from clinical experts, patient and clinician groups, and others with relevant interests in this issue. A summary of the primary and secondary efficacy end points for patients included in the KEYNOTE-671 trial is provided in Table 16.
Table 16: Key Survival Outcomes in the KEYNOTE-671 Study, ITT Population
Variables | Pembrolizumab arm (N = 397) | Placebo arm (N = 400) |
|---|---|---|
OS | ||
Number of events (%) | 110 (27.7) | 144 (36.0) |
Kaplan-Meier estimates (months)a | ||
Median (95% CI) | NR (NR to NR) | 52.4 (45.7 to NR) |
HR for pembrolizumab vs. placebo (95% CI)b | 0.72 (0.56 to 0.93) | |
P valuec | 0.00517 | |
OS rate at month 24, % (95% CI) | ████ █████ | 74.7 (70.1 to 78.7) |
Risk difference, % (95% CI) | ███ ██████ █████ | |
OS rate at month 36, % (95% CI) | ████ ██████ | 64.0 (58.5 to 68.9) |
Risk difference, % (95% CI) | ███ █████ █████ | |
OS rate at month 48, % (95% CI) | ████ ██████ | 51.5 (43.9 to 58.6) |
Risk difference, % (95% CI) | ████ █████ █████ | |
EFS (investigator assessment) | ||
Number of events (%) | 174 (43.8) | 248 (62.0) |
Progression or recurrence | 118 (29.7) | 187 (46.8) |
Local progression preventing surgery | 1 (0.3) | 6 (1.5) |
Inability to resect the tumour | 5 (1.3) | 15 (3.8) |
Death | 50 (12.6) | 40 (10.0) |
Kaplan-Meier estimates in months | ||
Median (95% CI) | 47.2 (32.9 to NR) | 18.3 (14.8 to 22.1) |
HR for pembrolizumab vs. placebo (95% CI)d | 0.59 (0.48 to 0.72) | |
P valuee | < 0.00001 | |
EFS rate at month 24, % (95% CI) | ████ ██████ | 41.4 (36.3 to 46.4) |
Risk difference, % (95% CI) | ████ ██████ █████ | |
EFS rate at month 36, % (95% CI) | ████ ██████ | 35.4 (30.3 to 40.6) |
Risk difference, % (95% CI) | ████ ██████ █████ | |
EFS rate at month 48, % (95% CI) | ████ ██████ | 26.2 (20.0 to 32.9) |
Risk difference, % (95% CI) | ████ ██████ █████ | |
CI = confidence interval; EFS = event-free survival; HR = hazard ratio; IA1 = first interim analysis; ITT = intention to treat; NR = not reached; OS = overall survival; Q = quartile; TPS = tumour proportion score; vs. = versus.
aFrom product-limit (Kaplan-Meier) method for censored data.
bBased on a Cox regression model with treatment as a covariate stratified by stage (stage II vs. stage III), TPS (≥ 50% vs. < 50%), histology (squamous vs. nonsquamous), and region (East Asia vs. non–East Asia), where region was collapsed for stage II TPS of 50% or more nonsquamous and stage II TPS of 50% or more squamous.
cOne-sided P value based on log-rank test stratified by stage (stage II vs. stage III), TPS (≥ 50% vs. < 50%), histology (squamous vs. nonsquamous), and region (East Asia vs. non–East Asia), where region was collapsed for stage II TPS of 50% or more nonsquamous and stage II TPS of 50% or more squamous. The multiplicity-adjusted 1-sided P value boundary for statistical significance was P equals 0.005426.
dBased on a Cox regression model with treatment as a covariate stratified by stage (stage II vs. stage III), TPS (≥ 50% vs. < 50%), histology (squamous vs. nonsquamous), and region (East Asia vs. non–East Asia), where region and histology were collapsed for stage II TPS of 50% or more (region was collapsed for stage III TPS ≥ 50% squamous and stage II TPS < 50% nonsquamous).
eOne-sided P value based on log-rank test stratified by stage (stage II vs. stage III), TPS (≥ 50% vs. < 50%), histology (squamous vs. nonsquamous), and region (East Asia vs. non–East Asia), where region and histology were collapsed for stage II TPS of 50% or more (region was collapsed for stage III TPS ≥ 50% squamous and stage II TPS < 50% nonsquamous). The P value was unadjusted for multiplicity because statistical significance was previously reached during the multiplicity-controlled testing procedure at IA1.
Source: KEYNOTE-671 Clinical Study Report (second interim analysis).33
Overall Survival
In the KEYNOTE-671 trial, OS was formally tested at IA2 using a multiplicity-adjusted 1-sided P value boundary of 0.005426. At IA2, a total of 254 patients had died: 110 patients (27.7%) in the pembrolizumab arm and 144 patients (36.0%) in the placebo arm. A statistically significant improvement in OS was observed in the pembrolizumab arm compared to the placebo arm, based on the Kaplan-Meier estimate (HR = 0.72; 95% CI, 0.56 to 0.93; P = 0.00517). The median OS was not reached in the pembrolizumab arm whereas it was 52.4 months (95% CI, 45.7 months to not reached) in the placebo arm. At 48 months, ████% of patients in the pembrolizumab arm were alive compared to 51.5% of patients in the placebo arm. This denotes a risk difference of █████ ████ ███ ███ ██ ██████.
The Kaplan-Meier plot showed that the pembrolizumab arm curve separated from the placebo arm curve at approximately month 16 and remained separated over time, with the separation widening after approximately month 42 (Figure 4). The estimated difference in restricted mean survival time in months was ████ ████ ███ █████ ██ █████ at month 36, ████ ████ ███ █████ ██ █████ at month 48, and ████ ████ ███ ████ ██ █████ at month 60, with point estimates favouring the pembrolizumab arm.
The OS benefit was generally consistent across the majority of prespecified subgroups (Figure 5). The point estimates suggested a smaller magnitude of effects for the following subgroups: those aged 65 years and older, races other than white (American Indian or Alaska Native, Asian, Black, or African American), those living in regions of East Asia, a TPS of less than 1%, and never smokers. However, CIs overlapped with the corresponding subgroup populations.
EFS by Investigator Assessment
In the KEYNOTE-671 trial, the success criterion for the primary EFS hypothesis was met at IA1 (data cut-off date of July 29, 2022), with a P value that exceeded the prespecified boundary for statistical significance. As shown in Table 16, at IA2, a total of 422 patients had an event (progression or recurrence, an inability to resect a tumour) or had died, including 174 patients (43.8%) in the pembrolizumab arm and 248 patients (62.0%) in the placebo arm. The majority of events were disease progression or recurrence (29.7% in the pembrolizumab arm and 46.8% in the placebo arm).
At 48 months, █████ of patients in the pembrolizumab arm were alive without an event compared to 26.2% of patients in the placebo arm, a risk difference of █████ ████ ███ ████ ██ ██████ The median EFS was approximately 29 months longer in the pembrolizumab arm at 47.2 months (95% CI, 32.9 months to not reached) compared to the placebo arm at 18.3 months (95% CI, 14.8 months to 22.1 months). The HR for EFS was 0.59 (95% CI, 0.48 to 0.72; P < 0.00001). These EFS results from IA2 are consistent with those from IA1.
A sensitivity analysis of EFS by BICR showed similar findings with an HR of 0.62 (95% CI, 0.51 to 0.76). A second sensitivity analysis used different censoring rules; events occurring immediately after 2 or more consecutive missed disease assessments or after new anticancer therapy were censored at the last disease assessment before the earlier date of the 2 or more consecutive missed disease assessments and new anticancer therapy. This sensitivity analysis also produced similar results to the primary analysis, with an HR of 0.59 (95% CI, 0.48 to 0.72).
Figure 4: Kaplan-Meier Plot of Overall Survival, ITT Population
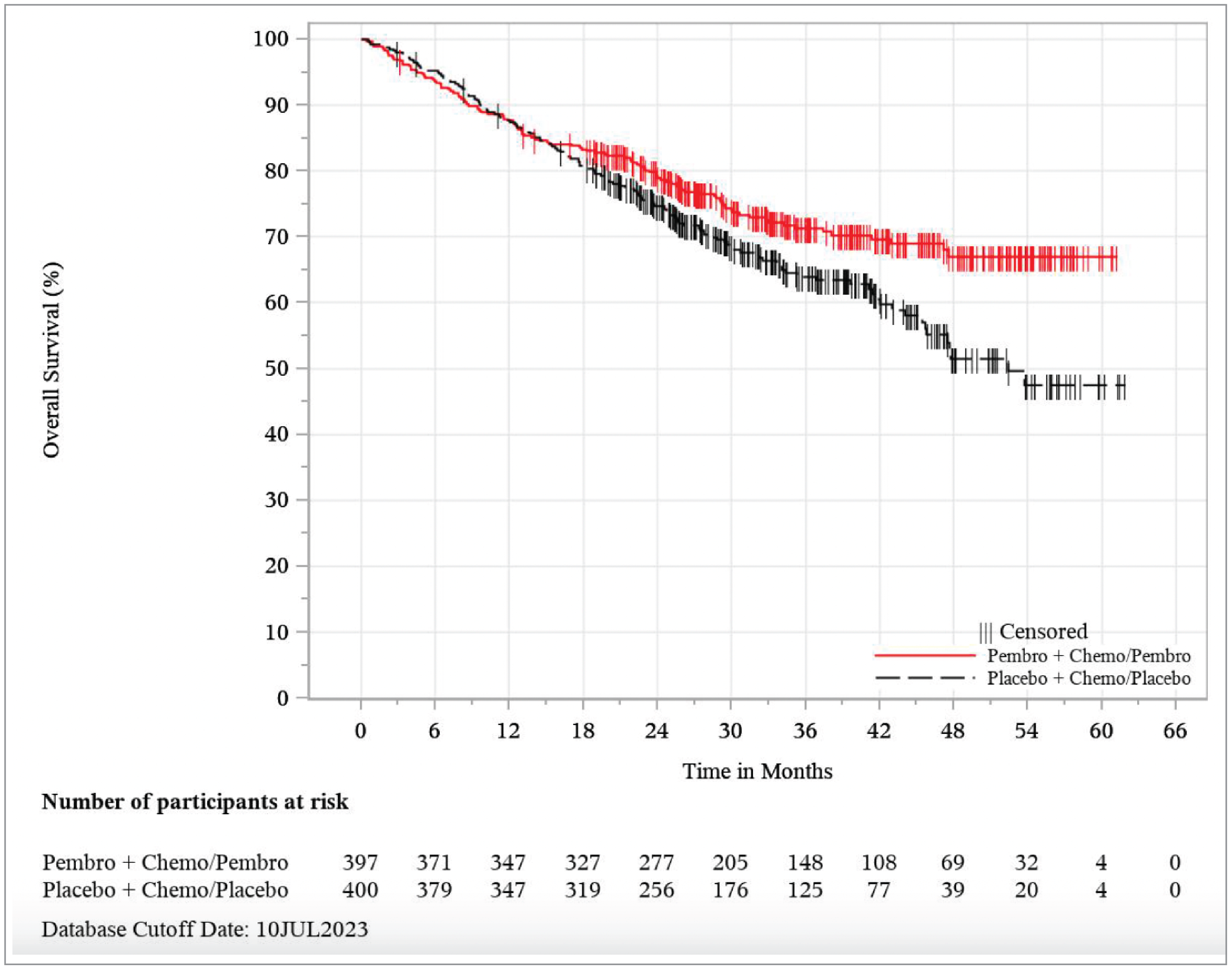
Chemo = chemotherapy; ITT = intention to treat; JUL = July; Pembro = pembrolizumab.
Source: KEYNOTE-671 Clinical Study Report (second interim analysis).33
The Kaplan-Meier plot showed that the pembrolizumab arm curve separated from the placebo arm curve at approximately month 5 and remained separated over time (Figure 6). The EFS benefit of pembrolizumab over placebo was consistent in direction across all prespecified subgroups (Figure 7).
Patient-Reported Outcomes
The completion rates for both the EORTC QLQ-C30 and EORTC QLQ-LC13 end points were greater than 90% at baseline and similar in both the pembrolizumab arm and the placebo arm. At week 11 in the neoadjuvant phase, the completion rate was 87.1% in the pembrolizumab group and 88.9% in the placebo group. At week 10 in the adjuvant phase, the completion rate was 68.6% in the pembrolizumab group and 62.1% in the placebo group. Compliance rates were the same at baseline for EORTC QLQ-C30 in both the pembrolizumab arm and the placebo arm (98.2% versus 98.2%, respectively) and remained similar at both week 11 in the neoadjuvant phase (89.1% versus 90.3%, respectively) and at week 10 in the adjuvant phase (92.2% versus 92.9%, respectively). Similar completion and compliance rates were observed at baseline, at week 11 for the neoadjuvant phase, and at week 10 for the adjuvant phase for EORTC QLQ-LC13.
Figure 5: Forest Plot of OS Hazard Ratio by Subgroup Factors Based on Investigator Assessment — ITT Population
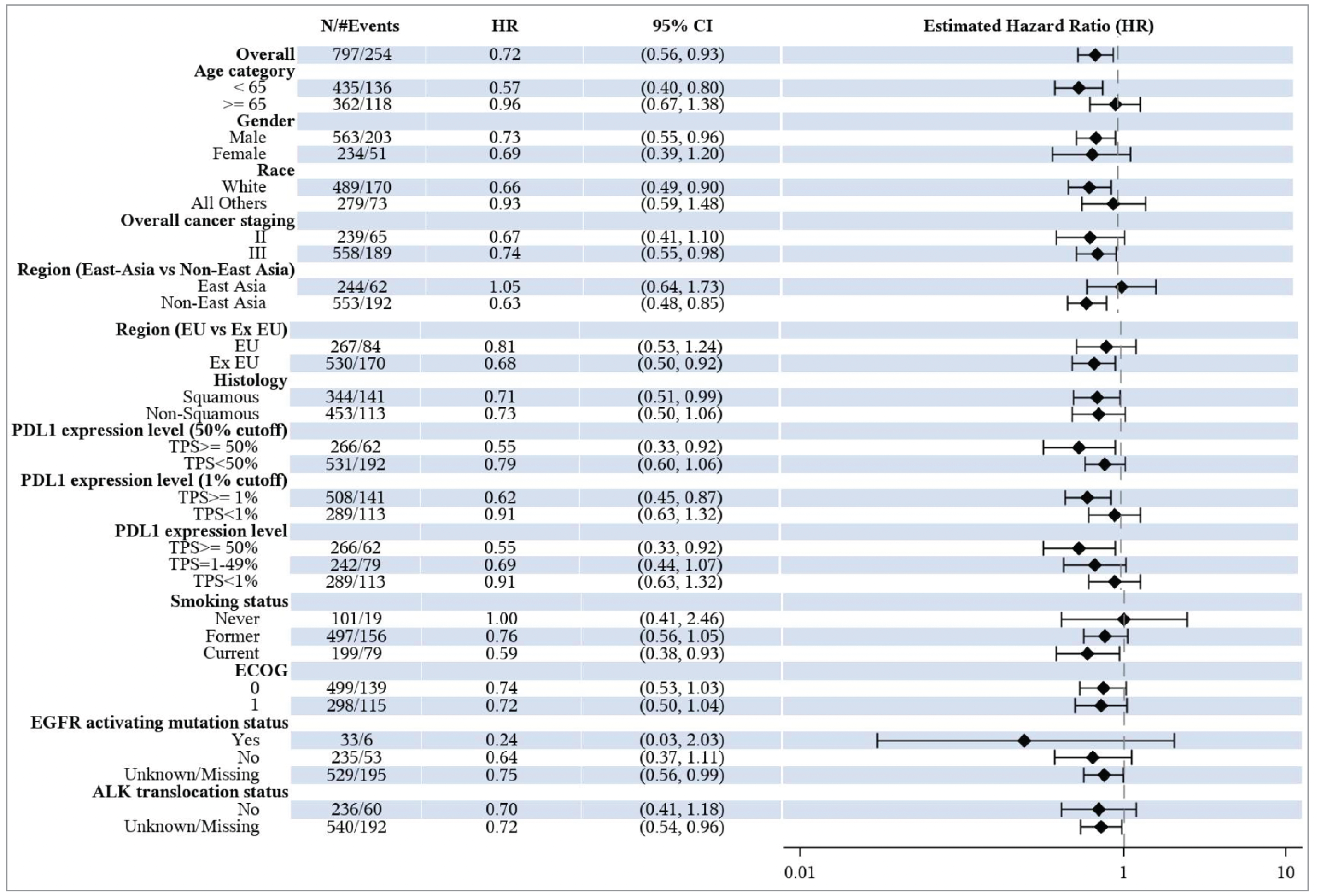
CI = confidence interval; ECOG = Eastern Cooperative Oncology Group; EU = European Union; HR = hazard ratio; ITT = intention to treat; OS = overall survival; TPS = tumour proportion score; vs = versus.
Source: KEYNOTE-671 Clinical Study Report (second interim analysis).33
Figure 6: Kaplan-Meier Plot of Event-Free Survival Based on Investigator Assessment — ITT Population
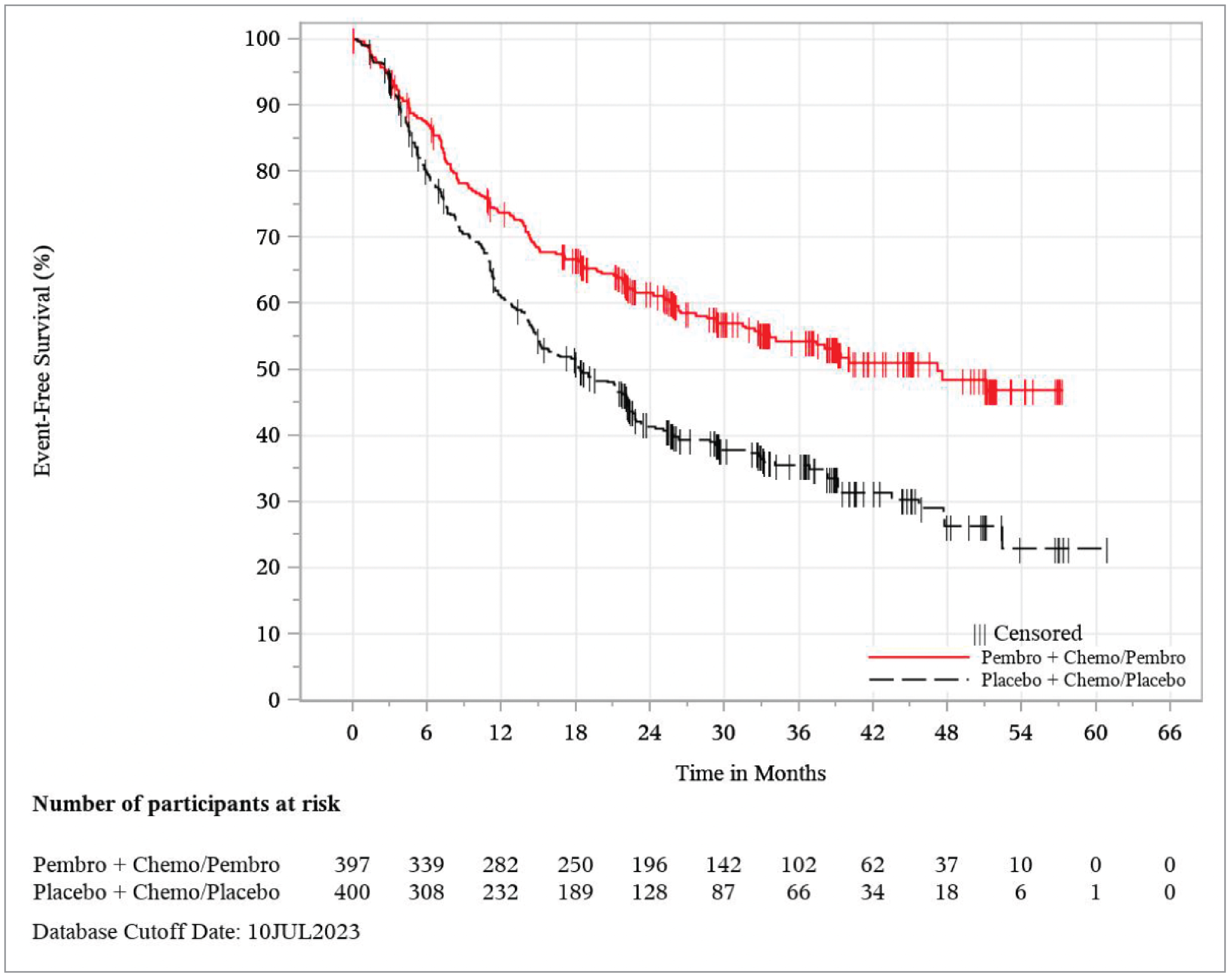
Chemo = chemotherapy; ITT = intention to treat; JUL = July; Pembro = pembrolizumab.
Source: KEYNOTE-671 Clinical Study Report (second interim analysis).33
The LSM change from baseline to neoadjuvant week 11 in the global health status scale and quality of life scale scores was –9.31 points (95% CI, –11.67 points to –6.94 points) in the pembrolizumab arm and –10.73 points (95% CI, –13.07 points to –8.40 points) in the placebo arm. The evidence was insufficient to show a difference in LSM change from baseline between the treatment arms at 1.43 points (95% CI, –1.64 points to 4.49 points).
The LSM change from baseline to adjuvant week 10 in the global health status scale and quality of life scale scores was –1.52 points (95% CI, –3.67 points to 0.63 points) in the pembrolizumab arm and –3.74 points (95% CI, –5.96 points to –1.52 points) in the placebo arm. The evidence was insufficient to show a difference in LSM change from baseline between the treatment arms at 2.22 points (95% CI, –0.58 points to 5.02 points).
Figure 7: Forest Plot of EFS Hazard Ratio by Subgroup Factors Based on Investigator Assessment — ITT Population
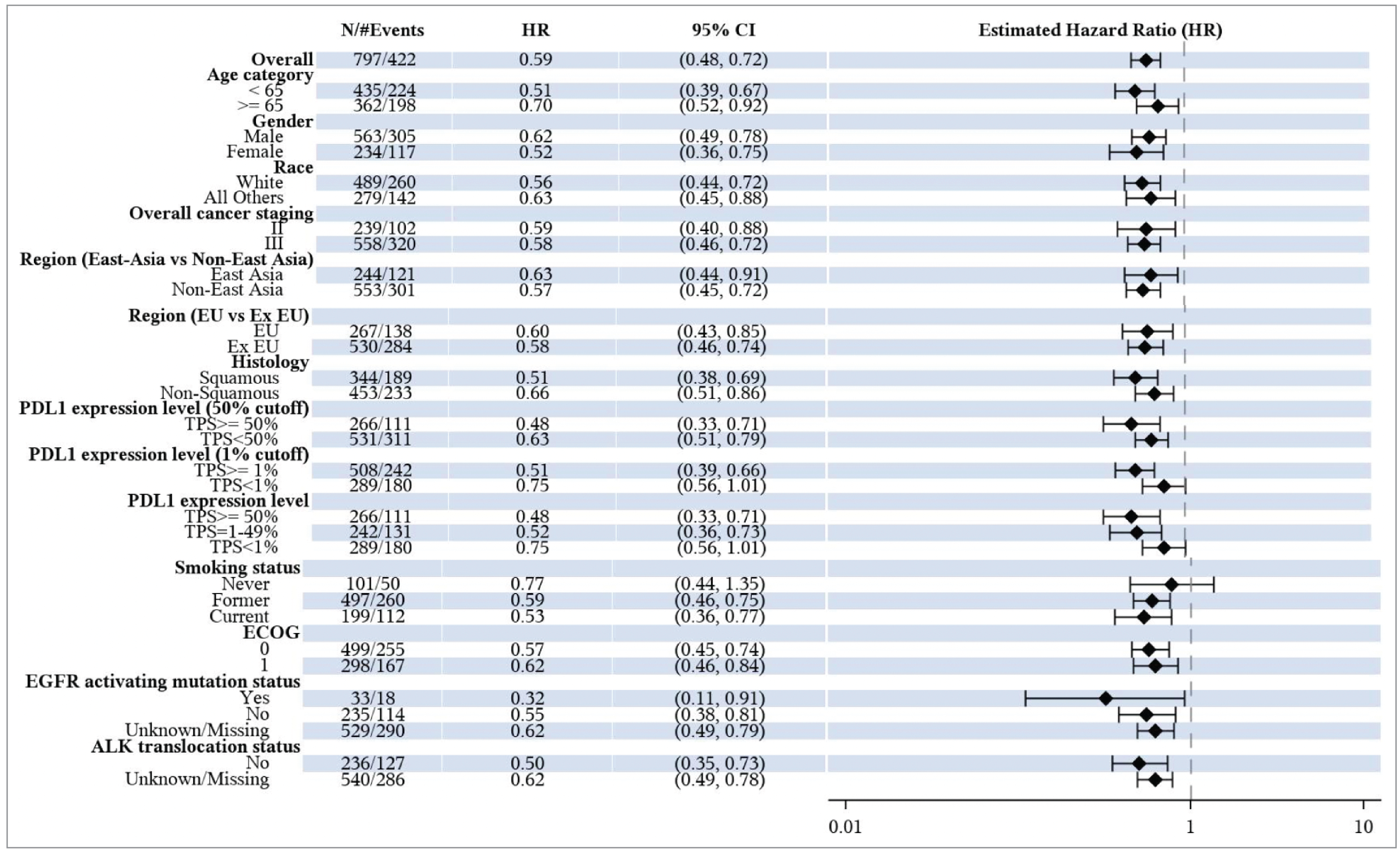
CI = confidence interval; ECOG = Eastern Cooperative Oncology Group; EFS = event-free survival; EU = European Union; HR = hazard ratio; ITT = intention to treat; TPS = tumour proportion score; vs = versus.
Source: KEYNOTE-671 Clinical Study Report (second interim analysis).33
Most patients reported stable plus improved in the global health status scale and quality of life scale scores over time in both the pembrolizumab arm at 58.7% (95% CI, 53.7% to 63.6%) and in the placebo arm at 51.8% (95% CI, 46.7% to 56.8%). The difference in the proportion that achieved stable plus improved in the global health status scale and quality of life scale scores over time across treatment arms was 7.0% (95% CI, 0.1% to 13.9%) in favour of the pembrolizumab arm.
Functioning domain scores declined, indicating worsening in the pembrolizumab arm and placebo arm in the neoadjuvant phase (Table 17) and in the adjuvant phase (Table 18). The scores were relatively stable in both arms, indicating no difference relative to baseline. Scores for other domains such as symptom, physical functioning, and role functioning are shown in the tables.
Physical and role functioning scores decreased relative to baseline in both the pembrolizumab arm and the placebo arm at neoadjuvant week 11. Deterioration was more pronounced in the placebo arm but the difference between the treatment arms was not significant. Similar findings were seen for physical and role functioning scores in the adjuvant phase at week 10.
Table 17: Key Patient-Reported Outcomes — Change From Baseline to Neoadjuvant Week 11
Treatment | N | Mean at neoadjuvant week 11 (SD) | N | LSM change from baseline (95% CI)a | Difference in LSM change from baselinea (95% CI) | P valueb |
|---|---|---|---|---|---|---|
EORTC QLQ-C30 global health status scale and quality of life scale | ||||||
Pembrolizumab arm | 344 | 64.10 (22.44) | 390 | –9.31 (–11.67 to –6.94) | 1.43 (–1.64 to 4.49) | 0.3611 |
Placebo arm | 354 | 62.12 (20.85) | 395 | –10.73 (–13.07 to –8.40) | ||
EORTC QLQ-C30 physical functioning | ||||||
Pembrolizumab arm | 344 | 81.74 (19.22) | 390 | –6.30 (–8.00 to –4.60) | 0.35 (–1.99 to 2.68) | 0.7714 |
Placebo arm | 354 | 81.07 (18.96) | 395 | –6.65 (–8.32 to –4.97) | ||
EORTC QLQ-C30 role functioning | ||||||
Pembrolizumab arm | 344 | 76.60 (27.01) | 390 | –9.43 (–12.00 to –6.87) | 1.04 (–2.41 to 4.49) | 0.5546 |
Placebo arm | 354 | 75.80 (26.43) | 395 | –10.47 (–13.00 to –7.94) | ||
EORTC QLQ-C30 symptom: dyspnea | ||||||
Pembrolizumab arm | 344 | 23.35 (25.59) | 390 | 2.16 (–0.35 to 4.67) | –1.77 (–5.10 to 1.55) | 0.2953 |
Placebo arm | 354 | 24.95 (25.63) | 395 | 3.94 (1.46 to 6.42) | ||
EORTC QLQ-LC13 symptom: cough | ||||||
Pembrolizumab arm | 343 | 20.70 (21.98) | 390 | –11.40 (–13.92 to –8.88) | –1.82 (–5.01 to 1.36) | 0.2607 |
Placebo arm | 352 | 23.48 (25.37) | 394 | –9.57 (–12.07 to –7.08) | ||
EORTC QLQ-LC13 symptom: chest pain | ||||||
Pembrolizumab arm | 343 | 12.44 (19.60) | 390 | 1.13 (–1.02 to 3.28) | 0.72 (–2.03 to 3.47) | 0.6065 |
Placebo arm | 352 | 11.74 (20.31) | 394 | 0.41 (–1.72 to 2.54) | ||
CI = confidence interval; cLDA = constrained longitudinal data analysis; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EORTC QLQ-LC13 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Lung Cancer 13; LSM = least squares mean; PRO = patient-reported outcome; SD = standard deviation; TPS = tumour proportion score.
Note: N is the number of patients in each treatment group with nonmissing assessments at the specific time point; for change from baseline, N is the number of patients in the analysis population in each treatment group.
aBased on a cLDA model with the PRO scores as the response variable with covariates for treatment, time, and treatment by visit interaction, and stratification factors (stage [stage II vs. stage III], TPS [≥ 50% vs. < 50%], histology [squamous vs. nonsquamous], and region [East Asia vs. non–East Asia]).
bThe P value was based on a 2-sided t test and was not adjusted for multiplicity.
Source: KEYNOTE-671 Clinical Study Report (second interim analysis).33
Cough-related disease symptom showed a reduction or improvement relative to baseline in both the pembrolizumab arm and the placebo arm at neoadjuvant week 11, with improvement more pronounced in the pembrolizumab arm. Dyspnea and chest pain–related symptom scores deteriorated relative to baseline in both the pembrolizumab arm and the placebo arm at neoadjuvant week 11, with no differences between the treatment groups observed. Similar findings were seen for cough, dyspnea, and chest pain disease–related symptom scores in the adjuvant phase at week 10.
Table 18: Key Patient-Reported Outcomes — Change From Baseline to Adjuvant Week 10
Treatment | N | Mean (SD) | N | LSM (95% CI)a | Difference in LSM (95% CI)a | P valueb |
|---|---|---|---|---|---|---|
EORTC QLQ-C30 global health status scale and quality of life scale | ||||||
Pembrolizumab arm | 271 | 72.88 (17.84) | 395 | –1.52 (–3.67 to 0.63) | 2.22 (–0.58 to 5.02) | 0.1197 |
Placebo arm | 247 | 70.28 (17.53) | 397 | –3.74 (–5.96 to –1.52) | ||
EORTC QLQ-C30 physical functioning | ||||||
Pembrolizumab arm | 271 | 84.21 (15.95) | 395 | –5.06 (–6.77 to –3.35) | 0.75 (–1.63 to 3.13) | 0.5356 |
Placebo arm | 247 | 83.24 (16.86) | 397 | –5.81 (–7.58 to –4.04) | ||
EORTC QLQ-C30 role functioning | ||||||
Pembrolizumab arm | 271 | 83.33 (22.73) | 395 | –4.86 (–7.39 to –2.34) | 2.14 (–1.33 to 5.61) | 0.2266 |
Placebo arm | 247 | 80.50 (23.92) | 397 | –7.00 (–9.62 to –4.39) | ||
EORTC QLQ-C30 symptom: dyspnea | ||||||
Pembrolizumab arm | 271 | 26.45 (23.69) | 395 | 5.78 (2.96 to 8.59) | –3.86 (–7.63 to –0.09) | 0.0449 |
Placebo arm | 247 | 29.96 (24.46) | 397 | 9.64 (6.73 to 12.55) | ||
EORTC QLQ-LC13 symptom: cough | ||||||
Pembrolizumab arm | 270 | 25.06 (23.03) | 395 | –6.78 (–9.73 to –3.84) | –2.15 (–5.95 to 1.65) | 0.2670 |
Placebo arm | 247 | 27.94 (24.19) | 397 | –4.63 (–7.67 to –1.59) | ||
EORTC QLQ-LC13 symptom: chest pain | ||||||
Pembrolizumab arm | 270 | 13.58 (19.41) | 395 | 2.99 (0.38 to 5.59) | –3.04 (–6.53 to 0.45) | 0.0876 |
Placebo arm | 247 | 16.60 (23.06) | 397 | 6.03 (3.33 to 8.73) | ||
CI = confidence interval; cLDA = constrained longitudinal data analysis; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EORTC QLQ-LC13 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Lung Cancer 13; LSM = least squares mean; PRO = patient-reported outcome; QoL = quality of life; SD = standard deviation; TPS = tumour proportion score.
Note: N is the number of patients in each treatment group with nonmissing assessments at the specific time point; for change from baseline, N is the number of patients in the analysis population in each treatment group.
aBased on a cLDA model with the PRO scores as the response variable with covariates for treatment by visit interaction and stratification factors (stage [stage II vs. stage III], TPS [≥ 50% vs. < 50%], histology [squamous vs. nonsquamous], and region [East Asia vs. non–East Asia]).
bThe P value was based on a 2-sided t test.
Source: KEYNOTE-671 Clinical Study Report (second interim analysis).33
Harms
Key harms data from the KEYNOTE-671 study are reported in Table 19. The safety data submitted and presented here align with those of the safety population that is used in the product monograph. However, the monograph reports data from IA1 and the submitted data reports from IA2. With approximately 1 year of additional follow-up from the IA1 data cut-off date, IA2 safety data are consistent with those reported at IA1. All patients had completed study treatment by the IA2 data cut-off date. No new safety concerns were identified.
Table 19: Key Harms Data — APaT Population
Adverse events | Pembrolizumab arm (N = 396) | Placebo arm (N = 399) |
|---|---|---|
Most common adverse events, n (%) (incidence ≥ 15% in 1 or more treatment groups), n (%)a,b,c,d | ||
Patients with 1 or more adverse events | 394 (99.5) | 394 (98.7) |
Nausea | 229 (57.8) | 213 (53.4) |
Neutrophil count, decreased | 174 (43.9) | 170 (42.6) |
Anemia | 169 (42.7) | 166 (41.6) |
Constipation | 155 (39.1) | 146 (36.6) |
Fatigue | 125 (31.6) | 101 (25.3) |
Decreased appetite | 115 (29.0) | 102 (25.6) |
White blood cell count, decreased | 112 (28.3) | 102 (25.6) |
Vomiting | 83 (21.0) | 69 (17.3) |
Diarrhea | 79 (19.9) | 75 (18.8) |
Platelet count, decreased | 76 (19.2) | 77 (19.3) |
Cough | 74 (18.7) | 60 (15.0) |
Dyspnea | 73 (18.4) | 52 (13.0) |
Blood creatinine, increased | 69 (17.4) | 60 (15.0) |
Rash | 69 (17.4) | 34 (8.5) |
Procedural pain | 61 (15.4) | 59 (14.8) |
Alanine aminotransferase, increased | 59 (14.9) | 41 (10.3) |
Asthenia | 58 (14.6) | 65 (16.3) |
Serious adverse events (sorted by decreasing incidence) (incidence ≥ 2% in 1 or more treatment groups), n (%)e,f,g | ||
With 1 or more adverse events | 165 (41.7) | 133 (33.3) |
Pneumonia | 21 (5.3) | 19 (4.8) |
Pulmonary embolism | 9 (2.3) | 9 (2.3) |
Anemia | 8 (2.0) | 3 (0.8) |
Pyrexia | 8 (2.0) | 1 (0.3) |
Aspartate aminotransferase, increased | 7 (1.8) | 1 (0.3) |
Patients who stopped treatment due to adverse events, n (%) | ||
Discontinued any chemotherapy | 44 (11.1) | 52 (13.0) |
Discontinued pembrolizumab or placebo | 85 (21.5) | 38 (9.5) |
Deaths, n (%) | ||
Patients who died | 26 (6.6) | 15 (3.8) |
Adverse events of special interest, n (%)a,b,e | ||
Hypothyroidism | 43 (10.9) | 6 (1.5) |
Pneumonitis | 24 (6.1) | 7 (1.8) |
Hyperthyroidism | 20 (5.1) | 8 (2.0) |
Severe skin reactions | 8 (2.0) | 0 (0.0) |
Colitis | 5 (1.3) | 0 (0.0) |
APaT = all patients as treated; MedDRA = Medical Dictionary for Regulatory Activities.
aTreatment includes study medications, in-study surgery, and in-study radiotherapy.
bNonserious adverse events up to 30 days of last treatment and serious adverse events up to 90 days of last treatment are included.
cThe MedDRA-preferred terms “neoplasm progression,” “malignant neoplasm progression,” and “disease progression” not related to the drug were excluded.
dDrug includes pembrolizumab or placebo, and chemotherapy.
eEvery patient is counted a single time for each applicable row and column.
fA specific adverse event appears only if its incidence in 1 or more of the columns met the incidence criterion in the report title, after rounding.
gSerious adverse events up to 90 days of the last treatment are included.
Source: KEYNOTE-671 Clinical Study Report (second interim analysis).33
Adverse Events
Overall, nearly all patients in both groups experienced at least 1 AE, with similar rates in the pembrolizumab group (99.5%) and the placebo group (98.7%). Common AEs included nausea, neutrophil count decrease, and anemia, with the pembrolizumab arm consistently showing marginally higher incidences. Notably, fatigue (31.6% versus 25.3%), decreased appetite (29.0% versus 25.6%), and rash (17.4% versus 8.5%) were more prevalent in the pembrolizumab group versus the placebo group, respectively. Conversely, asthenia was slightly higher in the placebo arm (16.3%) than in the pembrolizumab arm (14.6%).
Serious Adverse Events
As shown in Table 19, SAEs were more frequent in the pembrolizumab arm (165 patients [41.7%]) compared to the placebo arm (133 patients [33.3%]), with pneumonia (5.3% in the pembrolizumab arm versus 4.8% in the placebo arm) and pulmonary embolism (2.3% in the pembrolizumab arm versus 2.3% in the placebo arm) being the most common, but similar across both groups.
Withdrawals Due to AEs
Treatment discontinuation of pembrolizumab or placebo due to AEs was higher in the pembrolizumab arm than in the placebo arm (85 patients [21.5%] and 38 patients [9.5%], respectively). AEs leading to discontinuation of any drug in the assigned study regimen occurred in 102 patients (25.8%) in the pembrolizumab arm and 70 patients (17.5%) in the placebo arm. The most common AEs leading to discontinuation (≥ 1% of patients) were pneumonitis (1.8%), anemia (1.5%), decreased neutrophil count (1.5%), increased aspartate aminotransferase (1.3%), increased blood creatinine (1.0%), diarrhea (1.0%), and pneumonia (1.0%) in the pembrolizumab arm and nausea (2.0%), decreased neutrophil count (1.8%), increased blood creatinine (1.5%), pneumonia (1.3%), and acute kidney injury (1.0%) in the placebo arm.
Mortality
Overall, the number of deaths due to AEs was more frequent in the pembrolizumab group (26 patients [6.6%]) compared to the chemotherapy group (15 patients [3.8%]).
Notable Harms
AESIs, such as hypothyroidism and pneumonitis, were substantially more common in the pembrolizumab arm. The percentage of patients with an AESI was higher in the pembrolizumab group (103 patients [26.0%]) compared with the placebo group (36 patients [9.0%]). No new immune-mediated AEs were identified for pembrolizumab in the NSCLC perioperative setting. The most frequently reported notable harms (≥ 2% of patients) in the pembrolizumab group were hypothyroidism (10.9%), pneumonitis (6.1%), hyperthyroidism (5.1%), and severe skin reactions (2.0%). The majority of these events were effectively managed by standard clinical practice, including via corticosteroids and hormone replacement therapy.
Clinical experts consulted by the CDA-AMC team highlighted the importance of assessing the impact of AEs on in-study surgeries. In this context, 25 patients (6.3%) in the pembrolizumab arm were unable to undergo in-study surgery due to AEs, compared to 17 patients (4.3%) in the placebo arm.
Critical Appraisal
Internal Validity
The KEYNOTE-671 study employed a rigorous double-blind, placebo-controlled design, with randomization conducted centrally through an interactive response system. Allocation was stratified by critical factors such as disease stage, PD-L1 TPS, histologic features, and geographic region. Baseline demographic and clinical characteristics were well balanced between treatment groups, supporting the validity of the comparisons. These measures effectively minimized the risk of bias and enhanced the study's methodological robustness.
Blinding was appropriate, with both patients and investigators masked to treatment assignments. The use of a placebo control ensured the effectiveness of the blinding process. However, the potential for unblinding due to the distinct AE profiles, particularly immune-mediated events such as hypothyroidism and pneumonitis, was noted. This may introduce bias in the subjective assessment of outcomes, such as QoL measures, and subjective harms. However, the potential for bias was likely to be low for EFS because a sensitivity analysis using data adjudicated by BICR showed very similar results.
Adherence was adequate, with 74.5% of patients in the pembrolizumab group and 74.4% of patients in the placebo group completing the neoadjuvant phase. Exposure to the study treatments was higher in the pembrolizumab group, which might be expected given the longer time to disease progression in this group. Reasons for treatment discontinuation were more commonly due to AEs and less commonly due to progression in the pembrolizumab group compared to the placebo group. This seems likely to reflect expected reasons for discontinuation.
The dual primary end points — EFS and OS — were assessed in the ITT population. The analysis applied robust statistical methods, including stratified Cox regression and Kaplan-Meier survival analysis, with multiplicity adequately controlled using the Maurer and Bretz graphical method. The validity of the HRs from the Cox regression model (EFS and OS) relies on the proportional hazards assumption. Results of the assessment of this assumption were not readily available, although inspection of the Kaplan-Meier plots suggests that this assumption may be violated for OS. Nevertheless, the restricted mean survival time estimates were provided and assessment of the certainty of evidence relied on absolute between-group differences at clinically relevant time points, which would not be impacted by violation of the proportional hazards assumption. The OS findings are a result of an interim analysis; this increases the risk of overestimating the true magnitude of the treatment effect (OS was analyzed at a 65.8% information fraction).49 The analyses of HRQoL were uncontrolled for multiple comparisons; therefore, statistically significant results for any particular subscale can be considered to be at an increased risk of type I error (i.e., erroneously rejecting the null hypothesis).
AE reporting was comprehensive, with detailed grading and attribution. Higher rates of treatment stopping due to AEs were observed with pembrolizumab (21.5% versus 9.5% in the pembrolizumab and placebo groups, respectively), implying a transparent safety profile. However, the imbalance in subsequent therapies (24.7% versus 45.0% in the pembrolizumab and placebo groups, respectively) poses a potential confounder for OS outcomes. As such, end points such as OS may be considered as the combined effect of the study treatment and other subsequent treatments. Additionally, the impact of cointerventions such as radiotherapy on treatment effects was not extensively evaluated and was somewhat more common in the placebo group (received by 9% of patients in the pembrolizumab group and 13% of patients in the placebo group).
Few patients withdrew from the trial for reasons other than death (3% per group), suggesting a low risk of bias related to missing outcome data for EFS and OS. For HRQoL, the proportion of patients available for analysis declined over time. The analysis employed model-based imputation of missing data, but the presented reasons for the missing outcome data do not suggest that they are predominantly randomly missing. As such, there is an increased risk of bias, particularly for the adjuvant week 10 time point when the amount of missing outcome data exceeded 30% in both groups.
Subgroup analyses consistently demonstrated the efficacy of pembrolizumab on EFS across various strata, including PD-L1 expression levels, histologic features, and smoking status. For OS, the point estimates suggested a smaller magnitude of effects for the following subgroups: those aged 65 years and older, races other than white (American Indian or Alaska Native, Asian, Black or African American), those living in regions of East Asia, a TPS of less than 1%, and never smokers. Nonetheless, the intent of the subgroup analyses was to demonstrate consistency. As such, these were underpowered, resulting in wide CIs and limited credible conclusions regarding effect modification. There were no multiplicity adjustments for subgroup analyses.
In conclusion, the KEYNOTE-671 trial employed a robust study design, including adequate procedures for randomization and blinding. Potential unblinding due to AE profiles, imbalances in subsequent therapies, missing outcome data for HRQoL at later time points, and the need for further follow-up highlight areas at higher risk of bias when interpreting the results.
External Validity
The KEYNOTE-671 trial predominantly enrolled patients with resectable stage II, stage IIIA, or stage IIIB NSCLC representative of current practice in Canada, except for an underrepresentation of patients who are Black. Clinical experts consulted by CDA-AMC suggested that this demographic limitation may not significantly impact the generalizability of the findings to the population of patients in Canada.
In Canada, the standard of care for resectable NSCLC continues to evolve, according to the clinical experts. The current approach includes 3 cycles of neoadjuvant platinum-doublet chemotherapy with immunotherapy (e.g., nivolumab) for eligible patients, followed by surgical resection and potential adjuvant chemotherapy. Clinical experts highlight that the comparator arm in the KEYNOTE-671 trial may not fully reflect contemporary real-world practice. While the trial provides evidence for the efficacy and tolerability of perioperative pembrolizumab, a key question remains on whether its inclusion, particularly the adjuvant immunotherapy component, provides additional survival benefits compared to the current standard of care. Additionally, the design of the trial does not provide the ability to separate the effects of using pembrolizumab in the neoadjuvant and/or adjuvant phases.
Further concerns about applicability arise for specific subgroups of patients. Those with contraindications to immunotherapy, such as autoimmune conditions or severe cardiorespiratory impairments, may not benefit from this regimen. Similarly, patients with molecular anomalies (e.g., EGFR or ALK mutations) often derive greater benefit from targeted therapies like tyrosine kinase inhibitors. Also, experts pointed out ongoing speculation about certain subgroups — particularly those not achieving a pCR — that might benefit from adjuvant immunotherapy. The trial’s exclusive use of cisplatin-based chemotherapy also raises concerns, as cisplatin may be unsuitable for older patients or those with renal or auditory impairments, potentially limiting the regimen’s applicability.
GRADE Summary of Findings and Certainty of the Evidence
Methods for Assessing the Certainty of the Evidence
For pivotal studies and RCTs identified in the sponsor’s systematic review, GRADE was used to assess the certainty of the evidence for outcomes considered most relevant to inform expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group:
“High certainty: We are very confident that the true effect lies close to that of the estimate of the effect.
Moderate certainty: We are moderately confident in the effect estimate — The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. We use the word ‘likely’ for evidence of moderate certainty (e.g., ‘X intervention likely results in Y outcome’).
Low certainty: Our confidence in the effect estimate is limited — The true effect may be substantially different from the estimate of the effect. We use the word ‘may’ for evidence of low certainty (e.g., ‘X intervention may result in Y outcome’).
Very low certainty: We have very little confidence in the effect estimate — The true effect is likely to be substantially different from the estimate of effect. We describe evidence of very low certainty as ‘very uncertain.’”
Following the GRADE approach, evidence from RCTs started as high-certainty evidence and could be rated down for concerns related to study limitations (which refers to internal validity or risk of bias), inconsistency (heterogeneity) across studies when applicable, indirectness (applicability or generalizability issues), the imprecision of effects (wide CIs, small sample size, or low number of events), and publication bias.
When possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect; if this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., the clinical importance is unclear). In all cases, the target of the certainty of evidence assessment was based on the point estimate and where it was located relative to the threshold for a clinically important effect (when a threshold is available) or to the null.
For the GRADE assessments, findings from the pivotal KEYNOTE-671 study were considered and summarized per outcome.
Results of GRADE Assessments
Table 2 presents the GRADE summary of findings for neoadjuvant pembrolizumab versus placebo and chemotherapy for patients with NSCLC.
Long-Term Extension Studies
No long-term extension studies materials were submitted by the sponsor.
Indirect Evidence
Content in this section has been informed by materials submitted by the sponsor. The following has been summarized and validated by the review team.
Objectives for the Summary of Indirect Evidence
In the absence of head-to-head clinical trial evidence of perioperative pembrolizumab versus all alternative interventions of interest in the setting of early-stage resectable NSCLC, an ITC using an NMA of RCTs was conducted and submitted by the sponsor with the aim of providing a valid alternative.50-52
This section summarizes the NMA conducted to support the reimbursement submission of perioperative pembrolizumab in Canada by providing an indirect comparison between this treatment and neoadjuvant nivolumab for inclusion in the economic model.53
ITC Design
Objectives
The specific objectives of the ITC are as follows:
to identify and summarize RCT evidence regarding the efficacy and safety of perioperative pembrolizumab and other pharmacological treatments in the neoadjuvant, perioperative, or adjuvant setting for patients with early-stage resectable NSCLC by means of an SLR
to assess the feasibility of performing credible indirect or between-trial comparisons
if feasible, to estimate relative treatment effects for perioperative pembrolizumab and other pharmacological treatments in the neoadjuvant or perioperative setting for the population of interest by means of an NMA.
Study Selection Methods
An ITC between the KEYNOTE-671 study and adjuvant chemotherapy with or without immunotherapy was not possible to perform due to methodological challenges and limitations of the evidence. First, the timing of randomization was different, with patients in the KEYNOTE-671 study randomized after diagnosis but before any treatment whereas patients in the adjuvant chemotherapy with or without immunotherapy trials were randomized after undergoing complete resection of their tumour. This results in different study populations, with 1 population being untreated and only considered eligible for surgery that may result in R0, R1 (microscopic residual tumour), R2 (macroscopic residual tumour) resection while the other population underwent R0 resection. Thus, chemotherapy may have a different contribution to EFS and OS benefits when administered before versus after surgery as part of an immunotherapy-based approach, and these differences cannot be accounted for. Second, the surrogate end points (EFS in the KEYNOTE-671 study and DFS in the adjuvant chemotherapy with or without immunotherapy trials) are different (i.e., EFS includes progression that precludes potentially curative surgery) and were estimated at different time points after randomization. To account for differences in end point definition, there would be a need to recalculate EFS in patients in the KEYNOTE-671 trial who initiated adjuvant treatment after R0 resection; this would introduce a break in randomization and a potential for immortal time bias. Because OS was immature in the adjuvant chemotherapy with or without immunotherapy trials, it could not be used as a treatment outcome to avoid the use of EFS and DFS. Finally, there were differences in the patient populations, such as the inclusion of different stages using different versions of the AJCC cancer staging manual and the lack of substage information from older adjuvant chemotherapy trials. Because of these differences, the assumptions of similarity, homogeneity, and consistency were considered to be violated, which would lead to biased estimates of treatment effects and justify the infeasibility of ITCs.
The evidence base for the feasibility assessment and NMA was obtained from an SLR conducted on January 11, 2024, to identify and describe evidence from randomized trials on the efficacy and safety of neoadjuvant, perioperative (i.e., both neoadjuvant and adjuvant), or adjuvant treatments for early-stage resectable NSCLC. Interventions of interest for comparison to perioperative pembrolizumab included treatments recommended by the National Comprehensive Cancer Network,54 European Society for Medical Oncology,55 or National Institute for Health and Care Excellence;32 regulatory approved treatments; treatments currently in clinical trials; and placebo or watchful waiting. Studies were eligible only if the interventions of interest were delivered in patients who had not received any prior treatment (systemic and/or surgery) and thus, adjuvant trials were ultimately excluded. Because the goal of the SLR was to identify an evidence base to perform an NMA of relative treatment effects, only RCTs were of interest. Published systematic reviews and meta-analyses were not included in the SLR but, when identified, were flagged for handsearching of references lists. No time restriction was used for trial identification or selection.
Overall, 64 records pertaining to 32 unique clinical trials were identified. The criteria for population, intervention, comparison, outcomes, and study design and methods of the SLR are described in Table 20.
Table 20: Study Selection Criteria and Methods for the ITC Submitted by the Sponsor
Characteristics | Indirect comparison |
|---|---|
Population | Inclusion criteriaa Adult patients (18+ years) with newly diagnosed early-stage resectable NSCLC as defined by the study investigators:
Exclusion criteria Population exclusively consists of patients with:
|
Interventions or comparators | Any of the following systemic treatments, alone or in combination with other systemic treatments or radiotherapy, used in the neoadjuvant or perioperative setting:
Exclusion criterion: Any aforementioned listed treatment used in the adjuvant setting alone. |
Outcome | Efficacy outcomes:
Safety outcomes:
Patient-reported outcomes (e.g., EORTC QLQ-C30, EORTC QLQ-LC13, EQ-5D-5L). |
Study designs | RCT |
Publication characteristics | Inclusion of published and/or unpublished studies English language only |
Databases searched | Relevant studies were identified by searching the Embase, MEDLINE, and CENTRAL databases through the Ovid platform. The complete search strategy was peer reviewed by an information specialist who was not involved in the search strategy design, using the PRESS 2015 Guideline Evidence-Based Checklist.56 Reviews of the following proceedings of conferences from the past 3 years that took place before the search execution date were performed to identify any new RCTs that have not yet been published but are potentially eligible for inclusion:
|
Selection process | Two reviewers, working independently, reviewed all titles and abstracts identified in the literature search according to the study eligibility criteria, with the exception of outcome criteria, which were only applied during the screening of full-text publications. All studies identified as eligible during title and abstract screening were then screened at a full-text stage by the same 2 reviewers. Following reconciliation between the 2 investigators, a third reviewer was included to reach consensus on any remaining discrepancies in all stages of study selection. |
Data extraction process | Two reviewers, working independently, extracted data from the final list of included trials. Following reconciliation between the 2 reviewers, a third reviewer was included to reach consensus on any remaining discrepancies. |
Quality assessment | The risk of bias of individual RCTs was assessed using Cochrane Collaboration’s Risk of Bias tool version 2.0.57 This instrument was used to evaluate 5 key domains: bias arising from the randomization process, bias due to deviations from intended interventions, bias due to missing outcome data, bias in the measurement of the outcome, and bias in the selection of the reported result. These domains were assessed independently and in aggregate for an overall risk of bias judgment based on the following scale: a low risk of bias, some concerns, or a high risk of bias. Study quality was assessed by 2 independent reviewers. Where disagreements between reviewers occurred, a third reviewer provided arbitration. |
AACR = American Association for Cancer Research; AE = adverse event; ASCO = American Society of Clinical Oncology; DFS = disease-free survival; EFS = event-free survival; ELCC = European Lung Cancer Congress; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EORTC QLQ-LC13 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Lung Cancer 13; ESMO = European Society for Medical Oncology; IASLC = International Association for the Study of Lung Cancer; ITC = indirect treatment comparison; mPR = major pathological response; NSCLC = non–small cell lung cancer; OS = overall survival; pCR = pathological complete response; PFS = progression-free survival; RCT = randomized controlled trial; SAE = serious adverse event; WCLC = World Conference on Lung Cancer.
aStudies of adjuvant treatments were ineligible because they included a different population and had different end points.
bIn selected markets.
cAnalogues of EFS (i.e., DFS and PFS) were also considered.
Source: Sponsor’s Summary of Clinical Evidence.
ITC Analysis Methods
EFS, 1 of the primary end points of the KEYNOTE-671 study, was the main outcome evaluated in the analyses for the overall network of evidence. The sponsor indicated that an NMA for OS was done but did not contribute to the economic model. As a result, OS end points were not included in the ITC report from the sponsor.
All EFS analyses were performed in a Bayesian framework and involved a model with parameters, data, a likelihood distribution, and prior distributions. Under the assumption of consistency, the NMA model related the data from the individual studies to basic parameters reflecting the relative treatment effect of each intervention compared to the control (e.g., placebo). Based on these basic parameters, the relative treatment effects between each of the contrasts in the network were obtained.
Results using the investigator-assessed EFS were reported in this ITC. The following key assumptions were made in the analyses. First, to facilitate a network connection between the KEYNOTE-671 study and the other trials, the network assumes that cisplatin plus gemcitabine and cisplatin plus pemetrexed have similar efficacy when administered with perioperative pembrolizumab. The network also assumes that no adjuvant therapy is equivalent to receiving placebo in the adjuvant setting and that the effect of treatments pooled within each node are similar. The similarity of chemotherapy regimens was supported by a meta-analysis comparing chemotherapy to surgery, in which no difference in treatment effect was observed between chemotherapy regimens regardless of treatment drug, treatment regimen (including whether it was administered in the neoadjuvant or perioperative setting), trial design, or patient characteristics. Any delays between neoadjuvant therapy and surgery were assumed to not have an impact on treatment efficacy. The primary end point of interest was EFS as reported in the KEYNOTE-671 study; however, not all studies within the SLR reported EFS so CDA-AMC used progression-free survival (PFS) and DFS as a proxy for EFS. Finally, it was assumed that any differences in study characteristics, surgery characteristics, and patient baseline characteristics did not significantly alter the relative treatment effects.
Models, Likelihood, and Priors
For each subgroup of interest, both fixed-effects and random-effects models were considered. In general, the assumptions of random-effects models were preferred as they were expected to be more plausible than those of fixed-effects models. For the random-effects models, 1 parameter for the between-study heterogeneity was used, assuming that the between-study heterogeneity was the same for each intervention relative to the overall reference treatment of choice. If there was insufficient evidence to estimate between-study heterogeneity, fixed-effects models were used.
The NMA of reported HRs in terms of EFS assuming proportional hazards between treatments was performed using a regression model with a contrast-based normal likelihood for the log HR (and corresponding standard error) of each trial (or comparison) in the network, according to Dias et al.58 Normal noninformative prior distributions for the parameters were estimated with a mean of 0 and a variance of 10,000.
Traditional NMAs for survival outcomes are based on HR estimates and rely on the proportional hazards assumption, which the sponsor noted might not have been plausible for the presented comparisons. To address this limitation, Ouwens et al. have presented methods for an NMA of survival data using a multidimensional treatment effect as an alternative to the synthesis of the constant HRs.59,60 The hazard functions of the interventions in a trial are modelled using known parametric survival functions or FPs, and the difference in the parameters are considered the multidimensional treatment effect, which are synthesized (and indirectly compared) across studies. With this approach, the treatment effects are represented by multiple parameters rather than a single parameter. The model introduced by Jansen was used for the NMA of EFS.60,61
For EFS, the following competing survival distributions were considered using the multivariate NMA framework: Weibull, Gompertz, and second-order FPs including p1 = 0 or p1 = 1 and p2 = –1, p2 = –0.5, p2 = 0, p2 = 0.5, or p2 = 1. Powers of 2 or 3 were not explored as the resulting squared or cubed time transformations result in associated parameter estimates close to 0. For the relative treatment effects in the second-order FP framework, the sponsor assessed models that assume the following: treatment only has an impact on 2 of the 3 parameters describing the hazard function over time (i.e., 1 scale and 1 shape parameter); treatment has an impact on all 3 parameters describing the hazard function over time (i.e., 1 scale and 2 shape parameters). Fixed-effects analyses were conducted using each of the 22 models resulting from the combination of p1 and p2 values specified previously. Analyses using the first-order models and the 6 second-order FP models with the lowest fixed-effects deviance information criteria (DICs) were then conducted using random-effects models.
Model Selection
The DIC was used to compare the goodness-of-fit of competing survival models.62 For the analyses presented here, the model with the lowest DIC was selected as the base case unless there was a compelling reason to prefer 1 model (e.g., random effects being more plausible than fixed effects) and the models were reasonably close in DIC (using the 5-point cut-off).63 In the case of survival models, the plausibility of the HRs was also considered. Model diagnostics were checked using Gelmin-Rubin plots, trace plots, density plots, and autocorrelation plots. Overlays of the modelled survival data with the trial Kaplan-Meier curves were also used to validate the lowest DIC model.
Presentation of Results
The results of the NMA were presented in terms of cross-tables with relative treatment effect estimates between all interventions of interest along with 95% CrIs for all outcomes.
Software
The parameters of the different models were estimated within a Bayesian framework using a Markov Chain Monte Carlo method as implemented in the JAGS software package.64 A first series of 30,000 iterations (for constant HR NMAs) or 20,000 iterations (for time-varying HR NMAs) from the JAGS sampler was discarded as “burn-in” and the inferences were based on additional iterations using 2 chains of 20,000 iterations each. Convergence of the chains was confirmed by the Gelman-Rubin statistic.
Results of ITC
Summary of Included Studies
The 32 trials included in the SLR were evaluated for the feasibility of conducting an NMA.
The sponsor assumed that the between-trial differences noted in Table 22 would not have a significant impact on relative treatment effects; however, this could not always be evaluated due to limited reporting of baseline patient characteristics and subgroup data. In the stage and histology-based scenarios, most of the treatment comparisons in the networks were informed by only a single trial so there was also limited ability to account for between-trial heterogeneity and insufficient data to adjust for it by means of a meta-regression analysis. The paucity of data within these subgroups also means that perioperative pembrolizumab could not be compared to all treatments of interest. For all histology scenarios and the stage I to stage II time-varying HR scenario, the KEYNOTE-671 study (perioperative pembrolizumab) and the CheckMate 816 study (neoadjuvant nivolumab) were the only trials informing the analyses; however, there were imbalances in multiple trial baseline patient characteristics that showed evidence of treatment effect modification between the KEYNOTE-671 and CheckMate 816 trials.
With the inability to adjust for these variations as a main limitation of an NMA, and with the availability of individual patient-level data for the KEYNOTE-671 study, an anchored matching-adjusted indirect comparison was also conducted. However, the sponsor noted limitations, including the inability to adjust for key effect modifiers, so the results were not submitted for this report.
Evidence Networks
A network-of-evidence diagram was developed for the ITT populations of the 8 included trials and the end point of interest, EFS (Figure 8). Where available, subgroup data of patients from trials specifying investigator-assessed and BICR-assessed outcomes were used.
Treatment drugs (including PD-L1 and PD-1 inhibitors, tyrosine kinase inhibitors, and monoclonal antibodies) that are not currently approved or standard of care for the treatment of early-stage NSCLC were not of interest for the ITC analyses, which excluded 14 trials from the NMA evidence base: the AEGEAN study (durvalumab), the Altorki (2021) study (durvalumab), the CheckMate 77T study (perioperative nivolumab), the Elias 2022 study (radiotherapy alone), the EMERGING-CTONG1103 study (erlotinib), the NADIM II study (perioperative nivolumab), the NeoCOAST study (durvalumab, oleclumab, monalizumab, and danvatirsen), the NEOpredict-Lung study (nivolumab + relatlimab), the neoSCORE study (sintilimab), the NEOSTAR study (nivolumab + ipilimumab), the NeoTorch study (toripalimab), the PIT-1 study (bevacizumab), the RATIONALE-305 study (tislelizumab), and the TD-FOREKNOW study (camrelizumab). Perioperative durvalumab and perioperative nivolumab are not currently approved for the treatment of early-stage NSCLC and therefore were not eligible for inclusion in the NMA. In addition to perioperative pembrolizumab, treatments of interest for the NMA included neoadjuvant nivolumab, surgery alone, neoadjuvant or perioperative chemotherapy, and neoadjuvant or perioperative chemoradiotherapy. Six trials were excluded from the NMA evidence base because they only evaluated chemotherapy regimens (the Berghmans [2012] study, the Esteban [2007] study, and the IFCT 0002 study) or chemoradiotherapy regimens (the NRG Oncology RTOG 0839 study, the Roy [2016] study, and the Yokomise [2007] study) and would therefore collapse into a single treatment node in the network, which pooled all chemotherapy treatments and all chemoradiotherapy treatments. Of the 12 remaining trials, 3 were excluded because they did not report EFS or an analogue outcome (i.e., DFS or PFS) and 1 was excluded because the outcome of interest was assessed from diagnosis and not from randomization. The flow diagram of studies assessed in the NMA are depicted in Figure 9. The process of identifying trials suitable for inclusion in the analyses is detailed in the NMA report.53 The study design of the 8 trials included in the ITC analysis are described in Table 21.
Figure 8: Network of Evidence for EFS — ITT Population
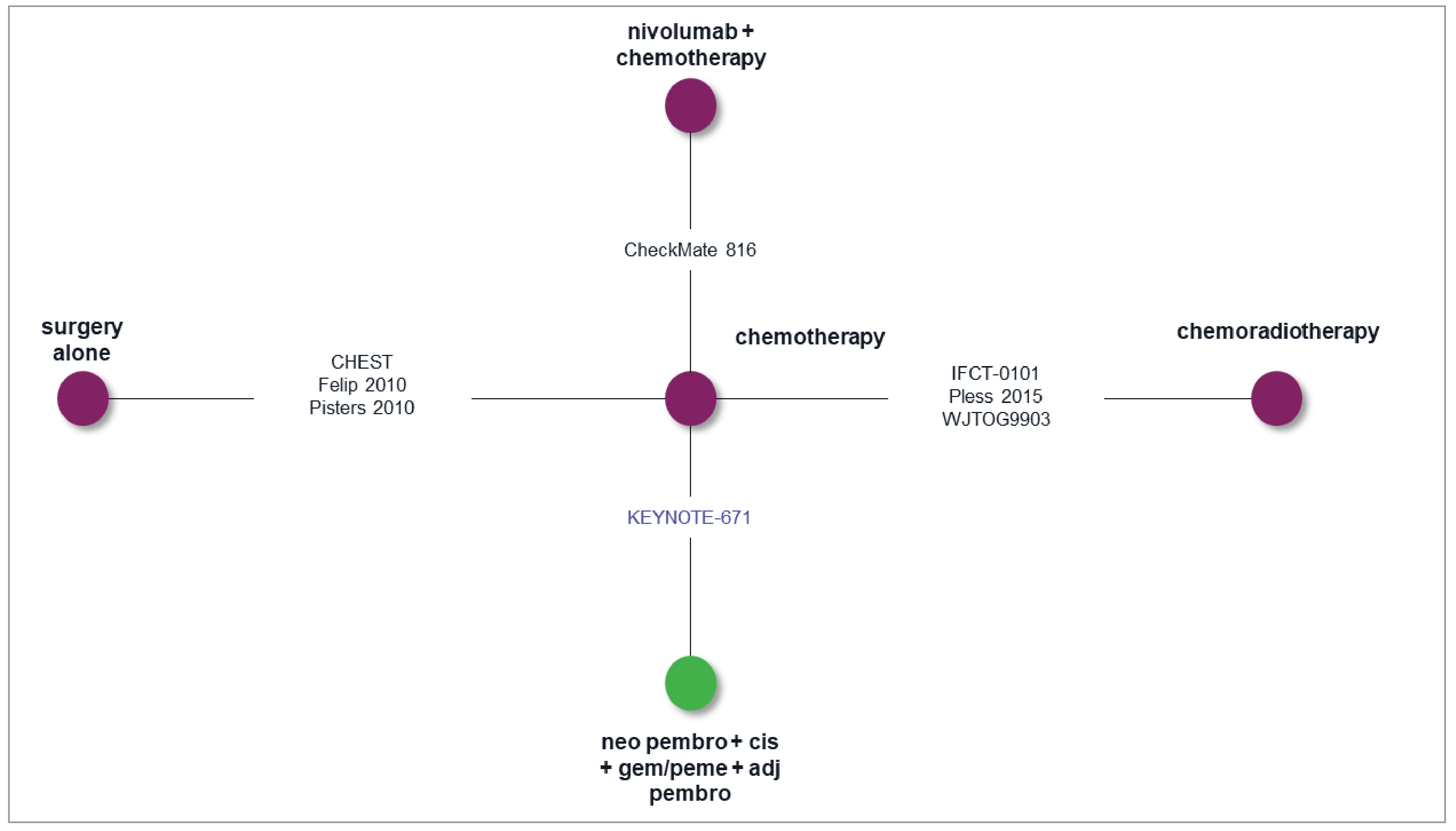
Adj = adjuvant; cis = cisplatin; EFS = event-free survival; gem = gemcitabine; ITT = intention to treat; neo = neoadjuvant; NMA = network meta-analysis; pembro = pembrolizumab; peme = pemetrexed.
Note: For illustration purposes only; the network diagram is not specific to a particular outcome or population of interest. Blue text (i.e., Keynote-671) indicates perioperative trials.
Source: Precision AQ network meta-analysis report (2024).53
The feasibility assessment demonstrated the appropriateness of proceeding with an NMA for the EFS outcomes but not for HRQoL and AEs. An analysis of pCR was only feasible between the KEYNOTE-671 and CheckMate 816 studies. However, because an NMA of pCR was not within the scope of addressing the data gaps in this submission for the purpose of economic modelling, results are not reported.
Table 22 highlights the key differences between the included trials that could be potential sources of heterogeneity and act as treatment effect modifiers in the NMA.
Figure 9: PRISMA Flow Diagram for the NMA
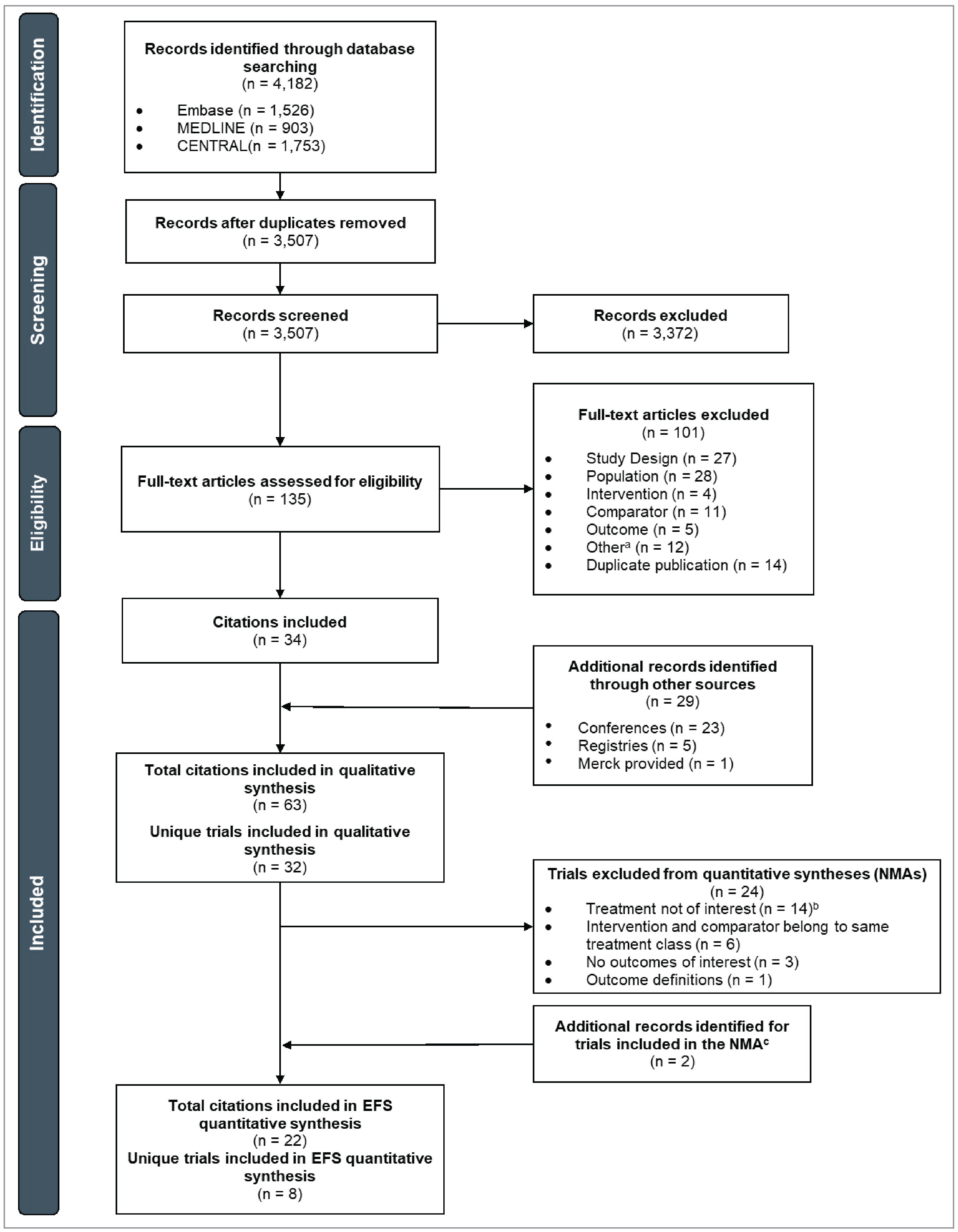
EFS = event-free survival; NMA = network meta-analysis; PRISMA = Preferred Reporting Items for Systematic Reviews and Meta-Analyses; SLR = systematic literature review.
aThe “Other” exclusion category includes conference abstracts, trial registries and protocols, and errata.
bAlthough the treatments evaluated in the AEGEAN and CheckMate 77T trials were not approved at the time of the analyses, additional indirect treatment comparisons comparing the KEYNOTE-671 study to these trials may be conducted separately in anticipation of upcoming treatment approvals.
cAfter finalizing the list of included trials identified in the SLR, hand searches were performed for the trials that had previously been included in indirect treatment comparisons to locate associated publications with additional trial data that had not been captured.
Source: Precision AQ network meta-analysis report (2024).53
Table 21: Study Design of Included Trials
Trial ID | Phase | Patient enrolment | Trial initiation | Trial completion | Masking | Region | Multicentre (Y/N) |
|---|---|---|---|---|---|---|---|
Perioperative pembrolizumab vs. chemotherapy | |||||||
KEYNOTE-671 trial | III | 797 | 2018 | 2026 | Double-blind | Multinational | Y |
Neoadjuvant nivolumab vs. chemotherapy | |||||||
CheckMate 816 trial | III | 358 | 2017 | 2028 | Open label | Multinational | Y |
Chemotherapy vs. surgery | |||||||
CHEST trial | III | 270 | 2000 | 2007 | Open label | Multinational | Y |
Felip (2010) trial | III | 413 | 2000a | NR | NR | Multinational (Europe) | Y |
Pisters (2010) trial | III | 337 | 1999 | NR | NR | NR | NR |
Chemoradiotherapy vs. chemotherapy | |||||||
IFCT-0101 trial | II | 46 | 2003 | 2012 | Open label | France | Y |
Pless (2015) trial | III | 232 | 2001 | 2037 | Open label | Multinational (Europe) | Y |
WJTOG9903 trial | III | 60 | 2000a | NR | NR | Japan | Y |
N = no; NR = not reported; vs. = versus; Y = yes.
aPatient enrolment dates; trial initiation dates were not reported.
Source: Precision AQ network meta-analysis report (2024).53
Table 22: Assessment of Homogeneity
Characteristic | Description and handling of potential effect modifier |
|---|---|
Trial eligibility criteria |
|
Patient characteristics |
|
Treatment characteristics | Lobectomy was the most common surgical procedure across the trials. Only 2 trials (the CheckMate 816 and CHEST studies) reported the time between receiving neoadjuvant therapy and surgery, so the NMAs assumed that any delays between neoadjuvant therapy and surgery did not impact treatment efficacy. The NMAs also assumed that differences in the proportion of patients who received surgery (which ranged from 75% in the chemotherapy arm of the CheckMate 816 study to 100% in the cisplatin + vinorelbine + radiotherapy arm and the carboplatin + paclitaxel + radiotherapy arm of the IFCT-0101 study) or in the proportion of patients who had complete resections (ranging from 67% in the cisplatin + gemcitabine or pemetrexed arm of the KEYNOTE-671 study to 93% in the paclitaxel + carboplatin arm of the Pisters [2010] study) did not significantly impact treatment efficacy or relative treatment effects. All trials except the CHEST, Pisters (2010), Pless (2015), and WJTOG9903 trials allowed select patients to undergo postoperative radiotherapy if they had unresectable lesions or incomplete resections, but only 2 trials (the KEYNOTE-671 and CheckMate 816 studies) reported the proportion of patients who received radiotherapy, ranging from 8% (the CheckMate 816 study, neoadjuvant nivolumab arm) to 13% (the KEYNOTE-671 study, cisplatin + gemcitabine or pemetrexed arm). The CheckMate 816 trial also administered adjuvant chemotherapy at the discretion of the investigator. However, a meta-analysis of neoadjuvant or perioperative chemotherapy vs. surgery alone noted that no difference in survival outcomes was observed when either chemotherapy or radiotherapy was administered postoperatively.65 |
Clinical trial setting | The earliest trial was initiated in 1999 (the Pisters [2010] study), and the latest trial is estimated to be completed in 2037 (the Pless [2015] study). Five trials were multinational (the CheckMate 816, CHEST, Felip [2010], KEYNOTE-671, and Pless [2015] studies), 1 trial was conducted in France (the IFCT-0101 study), and 1 trial was conducted in Japan (the WJTOG9903 study). The Pisters (2010) study did not report trial region. Seven trials were multicentre; the Pisters (2010) study did not report whether the trial was multicentre or single centre. |
Study design | All 8 included trials were phase III RCTs except for the IFCT-0101 study, which was a phase II RCT. Patient enrolment ranged from 46 patients (the IFCT-0101 study) to 797 patients (the KEYNOTE-671 study). Four trials were open label (the CheckMate 816, CHEST, IFCT-0101, and Pless [2015] studies), 1 trial was double-blind (the KEYNOTE-671 study), and the rest of the trials did not report masking. |
AJCC = American Joint Committee on Cancer; ECOG PS = Eastern Cooperative Oncology Group Performance Status; NMA = network meta-analysis; RCT = randomized controlled trial; TNM = tumour-nodes-metastasis; TPS = tumour proportion score.
Source: Precision AQ network meta-analysis report (2024).53
Results
Efficacy
NMAs were performed based on both HRs and Kaplan-Meier curves. NMAs for survival outcomes based on HRs rely on the proportional hazards assumption, which is implausible if the HRs of competing interventions are not constant over time.
Unless there were insufficient data to estimate between-study heterogeneity, the random-effects model was selected for the analyses based on the assumption that each trial contains unobserved heterogeneity uncorrelated with other trials. In analyses using the fixed-effects model, the variance in the analyses may be underestimated, so results should be interpreted with caution. Additionally, because the sample size decreases at longer follow-up durations, caution should be given to the interpretation of time-varying HRs at later time points due to increased uncertainty in the estimates. Results using the best-fitting random-effects or fixed-effects model are presented in this document.
EFS (Investigator-Assessed)
In both the constant and time-varying hazards NMA, EFS in ITT patients was reported in 8 trials across 5 unique treatments. Data sources for the clinical end points included in the EFS analyses by ITT population are available in Table 23.
In the random-effects constant HR model (Table 24), perioperative pembrolizumab demonstrated favourable EFS when compared to surgery ████ █████ ███ ████ █████ ██████ When comparing perioperative pembrolizumab to chemotherapy, chemoradiotherapy, and neoadjuvant nivolumab, no statistically significant result was observed (wide CrIs including the null effect).
The best-fitting survival model for the FP NMAs was the constant HR FP model (p1 = 0, p2 = 0) with treatment effects on scale (Table 25) and the best time-varying HR model was the second-order FP model (p1 = 0, p2 = 0) with treatment effects on scale and first shape (Table 26).
Table 23: Reported Within-Trial EFS (Investigator-Assessed) Outcomes — ITT Population
Trial | Data source (first author, year) | Reference treatment | Intervention | HR (95% CI) | ||
|---|---|---|---|---|---|---|
Regimen | N | Regimen | N | |||
Perioperative pembrolizumab vs. chemotherapy | ||||||
KEYNOTE-671 trial | Merck (2023) | CIS + GEM | 400 | Neoadjuvant PEMBRO + CIS + GEM or PEME + adjuvant PEMBRO | 397 | ████ █ |
███████████ █████████ ███ ████████████ | ||||||
CheckMate 816 trial | Spicer (2024) | Chemo | 179 | NIVO + chemo | 179 | ████ █ |
████████████ ███ ███████ | ||||||
CHEST trial | Scagliotti (2012) | Surgery | 141 | CIS + GEM | 129 | ████ █ |
Felip (2010) trial | Felip (2010) | Surgery | 210 | CAR + PAC | 199 | █████ |
Pisters (2010) trial | Pisters (2010) | Surgery | 168 | CAR + PAC | 169 | █████ |
█████████████████ ███ ████████████ | ||||||
IFCT-0101 trial | Girard (2010) | CIS + GEM | 14 | CAR + PAC + RT or CIS + VIN + RT | 32 | ██████ |
Pless (2015) trial | Pless (2015) | CIS + DOC | 115 | CIS + DOC + RT | 117 | ██████ |
WJTOG9903 trial | Katakami (2012) | CIS + DOC | 29 | CAR + DOC + RT | 31 | ██████ |
CAR = carboplatin; chemo = chemotherapy; CI = confidence interval; CIS = cisplatin; DOC = docetaxel; EFS = event-free survival; GEM = gemcitabine; HR = hazard ratio; ITT = intention to treat; NIVO = nivolumab; PAC = paclitaxel; PEMBRO = pembrolizumab; PEME = pemetrexed; RT = radiotherapy; VIN = vinorelbine; vs. = versus.
Source: Precision AQ network meta-analysis report (2024).53
Table 24: Random-Effects NMA [Redacted]
████ ██████ | ████ ██████ | ████ ██████ | ████ ██████ |
|---|---|---|---|
████ ██████ | ████ ██████ █ | ████ ██████ █ | ████ ██████ █ |
████ ██████ | ████ ██████ █ | ████ ██████ █ | ████ ██████ █ |
██████ ████████ ███████████ ██████████ ██████ █████████ █████ ███████████████ ███ █ █████████ ███ █ █████████████ ███ █ ██████████ ███ █ ████████ █████████ ███ █ ██████████ █████████ ███ █ ████████████ ███ █ ███████████████████ ███ █ ████████████ ████ █ ██████████ ███ █ ███████ ██████████████ ██████ █ ██████████████ ████ █ ███████████████████ █████████ ██ ███ ██████ █████56
Table 25: Estimated EFS [Redacted]
████ ██████ | ████ ██████ | ████ ██████ | ████ ██████ |
|---|---|---|---|
████ ██████ | ████ ██████ █ | ████ ██████ █ | ████ ██████ █ |
████ ██████ | ████ ██████ █ | ████ ██████ █ | ████ ██████ █ |
██████ ████ ████ ██████████ ███ ██████████ ███████ █████ ███ ███ ████ ██ ███ ███ █████████ ██████ ███ ██████ ██████████ ███ ██████ ██████ ███ █████████████ ███████████ ██ ███ ████ ████████████ ██████████████ ██████ █ ██████████████ ████ █ ███████████████████ █████████ ██ ███ ██████ █████56
Table 26: Estimated EFS [Redacted]
████ ██████ | ████ ██████ | ████ ██████ | ████ ██████ |
|---|---|---|---|
████ ██████ | ████ ██████ █ | ████ ██████ █ | ████ ██████ █ |
████ ██████ | ████ ██████ █ | ████ ██████ █ | ████ ██████ █ |
██████ ████ ████ ██████████ ███ ██████████ ███████ █████ ███ ███ ████ ██ ███ ███ █████████ ██████ ████████████ ███ █ ███████████████████ ███ █ ████████████ ████ █ ██████████ ███ █ ███████ ██████████████ ██████ █ ██████████████ ████ █ ███████████████████ █████████ ██ ███ ██████ █████56
Harms
Harms were not compared in the ITC analyses (not feasible).
Critical Appraisal of ITC
The ITC conducted an SLR using prespecified criteria for population, intervention, comparison, and outcome, and appropriate databases, including robust processes like dual independent review. Although authors report assessing the quality using the Cochrane Risk of Bias tool, the specific risk of bias of individual studies was not reported. The exclusion of adjuvant trials due to differences in patient populations and end points (e.g., EFS versus DFS) is a significant limitation because it precludes direct comparison with key treatment strategies including neoadjuvant chemotherapy, followed by pembrolizumab or atezolizumab.
Other critical methodological challenges from the included studies include the use of surrogate end points (EFS versus DFS versus PFS) that are not interchangeable due to different definitions (censoring rules were not provided), methods of measurement (most trials did not report whether this was investigator-assessed or assessed by BICR), and timing and length of follow-up. The ITC acknowledges potential differences in treatment effect modifiers, including stage, histology, PD-L1 status, and geographic region. Additionally, the information was not always available in the included studies to thoroughly assess for these potential differences. However, imbalances in key characteristics (e.g., PD-L1 TPS ≥ 50% being higher in the KEYNOTE-671 study, regional enrolment differences) likely influence outcomes. The small number did not allow these differences to be accounted for in the NMA (e.g., via network meta-regression). Additionally, a matching-adjusted indirect comparison was attempted for the KEYNOTE-671 study versus the CheckMate 816 study but was unsuccessful in resolving the heterogeneity in treatment effect modifiers across the trials, so results were not presented. The limited ability to adjust for these imbalances weakens the interpretation of the findings as it suggests that the assumptions of similarity, homogeneity, and consistency are violated, leading to biased estimates of relative treatment effects.
The ITC used robust methods such as Bayesian models (a proportional hazards NMA) and FP methods (a time-varying NMA). However, assumptions of proportional hazards were not met in some trials (e.g., the Pisters [2010] study), questioning the validity of the proportional hazards NMA model. The second-order FP model (with treatment effects on scale and shape) overcomes violation of the proportional hazards assumption but cannot overcome the heterogeneity and other concerns previously noted. Interpretation is limited to discrete time windows and the sponsor noted that sample sizes were decreased at longer follow-up durations, introducing uncertainty into the comparative effect estimates. The estimates relative to the most relevant comparator, neoadjuvant nivolumab, were particularly affected by wide CrIs that further increased the uncertainty. Small sample sizes in some trials and reliance solely on indirect evidence exacerbate this uncertainty. This may result in effect estimates that are sensitive to methodological choices, and lead to wide CrIs and reduced precision.
In terms of external validity, the ITC focused primarily on EFS. OS, a critical end point for those with relevant interests in this issue, was not reported. The ability of findings for EFS to predict a treatment effect on OS for all relevant comparisons is uncertain. Similarly, HRQoL was not assessed. Harms and AEs were also not assessed, limiting the safety profile analysis and ability to weigh the comparative benefits and harms. The exclusion of adjuvant trials and emerging therapies from the network diminishes the relevance of the findings in the context of the evolving treatment landscape in Canada. Even though the ITC was primarily developed for the economic model, this undermines the comprehensiveness and use of the ITC for clinical decision-making. These, together with differences in inclusion criteria (e.g., EGFR and ALK mutation status, PD-L1 expression) and geographic enrolment (e.g., higher representation in countries in Asia in the CheckMate 816 study) limit the generalizability to clinical practice in Canada.
Overall, acknowledging that NMAs are inherently limited by the extent to which the included studies meet the assumptions of the proposed methodology, the submitted ITC provides some insights into the comparative efficacy of perioperative pembrolizumab, but it is limited by methodological challenges, assumptions, and data gaps. Key issues include violations of transitivity, heterogeneity in study populations, and the omission of clinically important outcomes like OS, HRQoL, and safety.
Studies Addressing Gaps in the Systematic Review Evidence
No material with studies addressing gaps in the systematic review evidence were identified and submitted by the sponsor.
Discussion
Summary of Available Evidence
The body of evidence informing this submission consists of 1 pivotal study (the KENOTE-671 trial) and 1 ITC submitted by the sponsor.
The KEYNOTE-671 trial was a phase III, multicentre, randomized, double-blind study evaluating the efficacy and safety of pembrolizumab in combination with chemotherapy as neoadjuvant treatment, followed by pembrolizumab monotherapy as adjuvant treatment, in patients with resectable stage II, stage IIIA, or stage IIIB (T3 to 4N2) NSCLC. A total of 797 patients were enrolled, randomized 1:1 to receive either pembrolizumab plus platinum-based chemotherapy (cisplatin and gemcitabine or pemetrexed) or placebo plus chemotherapy in the neoadjuvant phase, followed by either pembrolizumab monotherapy or placebo for up to 13 adjuvant cycles. The main end points of relevance for this review, which were obtained from the study, were OS, EFS, HRQoL, and harms. Baseline characteristics of the study population were well balanced between treatment arms. The median age was approximately 64 years, with most patients being male (approximately 74%) and having an ECOG PS score of 0 or 1. The majority of patients had stage IIIA disease, and squamous and nonsquamous histologies were nearly equally represented. Around one-third of patients in both arms had a PD-L1 TPS of 50% or more.
The ITC submitted by the sponsor aimed to evaluate the relative efficacy of perioperative pembrolizumab compared to neoadjuvant nivolumab and other treatment options for early-stage resectable NSCLC. The ITC relied on an NMA of 8 RCTs identified through an SLR. EFS was the primary end point, but other clinically important outcomes such as OS, HRQoL, and AEs were not included.
Interpretation of Results
Efficacy
Outcomes such as OS, EFS, HRQoL, and safety (including harms and AEs) are highly valued by patients with resectable NSCLC, as well as by clinicians, drug programs, and committee members. These outcomes are pivotal in assessing the effectiveness and tolerability of new treatment regimens, particularly in early-stage NSCLC, where the primary goal is curative intent. For many with relevant interests in this issue, OS remains the gold standard for evaluating the long-term benefit of any new therapy.
OS was identified as the most critical outcome by patients and clinicians, as it directly reflects the intervention’s ultimate benefit in prolonging life. In the KEYNOTE-671 trial, pembrolizumab demonstrated a clinically meaningful improvement in OS compared to placebo; however, with immature data at the time of the interim analysis, the median OS was not reached in the pembrolizumab arm. At 48 months, the absolute difference in survival suggested an important and clinically meaningful effect. This finding reinforces pembrolizumab’s potential to improve long-term outcomes in resectable NSCLC, although further follow-up is needed to confirm the durability of this benefit. No credible subgroup effects were identified, although these were not a main aim of the study or powered enough to be detected.
EFS, a coprimary end point in the KEYNOTE-671 trial, serves as a surrogate end point for OS in early-stage NSCLC, facilitating earlier assessment of treatment efficacy. Pembrolizumab resulted in a clinically important improvement in EFS compared to placebo. The benefit was observed consistently across key subgroups, including those of patients with PD-L1 expression of 50% or more, stage IIIA disease, and both squamous and nonsquamous histologies. This underscores pembrolizumab’s robust efficacy across diverse patient populations, reinforcing its role in reducing the risk of recurrence or progression in resectable NSCLC.
HRQoL remains a critical consideration in curative treatment settings, where the focus is not only on survival but also on maintaining patients’ well-being during and after therapy. Evidence from the KEYNOTE-671 study suggests that pembrolizumab has a similar impact on HRQoL when compared to placebo and chemotherapy. However, the potential long-term effects of extended pembrolizumab dosing on QoL remain underexplored and warrant further study.
Some considerations are to be mentioned in terms of generalizability of the KEYNOTE-671 study results influenced by the study’s population and design. The higher proportion of patients of Asian ethnicity and stage IIIB cases may limit the applicability to clinical practice in Canada. Furthermore, the comparator arm of placebo plus chemotherapy does not fully align with current standards of care in Canada, which often involve nivolumab in combination with chemotherapy as neoadjuvant therapy. Clinical experts emphasize that pembrolizumab should be considered an alternative to nivolumab, noting their comparable efficacy and safety profiles. However, the extended treatment duration in the KEYNOTE-671 study, which includes additional adjuvant cycles, distinguishes pembrolizumab but highlights the uncertainty about whether this prolonged regimen provides a significant survival advantage. The KEYNOTE-671 trial was not designed such that the contribution of the individual components of the treatment regimen to overall efficacy could be distinguished.
Clinical experts acknowledged pembrolizumab’s potential to improve outcomes for patients with resectable NSCLC, particularly those at a high risk of recurrence. However, they highlighted the uncertainty regarding the necessity of additional adjuvant cycles, as the incremental benefit over established regimens, such as 3 cycles of neoadjuvant nivolumab with chemotherapy, remains unclear. According to the experts, both drugs share similar efficacy, toxicity, and cost profiles, but pembrolizumab’s extended regimen, including an additional neoadjuvant cycle and 13 adjuvant doses, raises questions about whether these additional doses provide a meaningful survival advantage.
In the ITC and constant hazards NMA submitted by the sponsor, the results suggested favourable EFS for perioperative pembrolizumab over surgery alone, but no statistically significant differences were observed compared to chemotherapy, chemoradiotherapy, or neoadjuvant nivolumab. To overcome non–proportional hazards in some comparisons, an FP NMA was used, which suggested favourable EFS for perioperative pembrolizumab over chemotherapy, chemoradiotherapy, and surgery alone. The CrIs for comparisons to neoadjuvant nivolumab were wide CrIs, suggesting that either regimen could be favoured. Key methodological challenges for both NMA approaches, such as differences in trial designs, populations, and surrogate end points (e.g., EFS in neoadjuvant trials versus DFS or PFS in adjuvant trials), violated the assumptions of homogeneity and transitivity, undermining the robustness of the findings. Additionally, critical gaps in the evidence, including the lack of head-to-head comparisons, limited confidence in the conclusions. Variability in trial populations and comparators contributed to inconsistencies in the ITC results. For instance, differences in PD-L1 expression, geographic enrolment, and disease stage were identified as potential effect modifiers. These imbalances may favour perioperative pembrolizumab in some scenarios and neoadjuvant nivolumab in others, further complicating the interpretation. The exclusion of adjuvant trials and emerging therapies from the network diminishes the relevance of the findings in the context of the treatment landscape in Canada (e.g., comparisons to adjuvant chemotherapy followed by pembrolizumab or atezolizumab are unavailable). The limited ability to account for between-study heterogeneity and the reliance on assumptions about pooled chemotherapy regimens also reduced the reliability of the results. Overall, while the ITC provides valuable indirect evidence, its internal validity limitations, combined with significant gaps in efficacy and safety outcomes, raise concerns about its external validity and applicability to real-world practice.
Harms
Safety and tolerability are crucial factors in treatment decision-making, particularly in potentially curative settings. Overall, pembrolizumab exhibited a safety profile consistent with chemotherapy regarding general AEs. However, it was associated with higher rates of immune-mediated AEs, such as hypothyroidism and pneumonitis, and an increased incidence of treatment discontinuations due to AEs compared to placebo. According to clinical experts consulted by CDA-AMC, these findings align with the established safety profile of other ICIs. Experts emphasized that while these AEs are expected, they are generally manageable and considered acceptable by many patients who prioritize improvements in OS and EFS.
The management of immune-mediated AEs requires specialized oncology care and careful monitoring, particularly in the context of the extended adjuvant treatment phase outlined in the KEYNOTE-671 study. Clinical experts noted that effective mitigation strategies, including timely intervention and patient education and heightened vigilance, are necessary for populations at an increased risk of immune-related complications, such as those with pre-existing autoimmune conditions or other vulnerabilities.
The ITCs submitted by the sponsor provided no information on comparative harms versus other relevant treatment regimens such as neoadjuvant nivolumab.
Conclusion
Evidence from the pivotal KEYNOTE-671 trial demonstrates that pembrolizumab (neoadjuvant in combination with chemotherapy, then as monotherapy in the adjuvant period) provides a clinically meaningful benefit in the treatment of resectable stage II, stage IIIA, and selected stage IIIB NSCLC, particularly in improving EFS and OS when compared to neoadjuvant chemotherapy alone. These benefits align with the priorities of patients and clinicians, especially in early-stage NSCLC, where the primary goals are curative intent and long-term survival. However, the evidence to determine an impact on HRQoL is still uncertain. Furthermore, pembrolizumab presents unique challenges, including increased rates of immune-mediated AEs, which may need careful patient monitoring and appropriate management strategies.
The evidence supports pembrolizumab as a potential alternative to existing standards, although indirect comparisons to highly relevant comparators, such as neoadjuvant nivolumab, suggest uncertainty about which regimen might be favoured. Uncertainties persist regarding the incremental value of the extended adjuvant regimen, particularly for certain subgroups that may derive limited additional benefit. The absence of direct head-to-head comparisons with nivolumab or other ICIs further complicates a definitive positioning of pembrolizumab within the current treatment paradigm. Notable gaps in the evidence include immature OS data and a lack of long-term safety data.
Overall, while the efficacy of pembrolizumab against chemotherapy in the neoadjuvant phase is established in the KEYNOTE-671 study, the necessity and added value of the extended adjuvant regimen, as well as its comparative effectiveness within current clinical practice, remain areas requiring further clarification. Long-term follow-up and real-world evidence may address these questions and refine pembrolizumab’s role in the evolving treatment landscape.
References
1.Canadian Cancer Statistics Advisory Committee in collaboration with the Canadian Cancer Society, Statistics Canada, and the Public Health Agency of Canada. Canadian Cancer Statistics 2024. Canadian Cancer Society; 2024. Accessed July 17, 2024. https://cdn.cancer.ca/-/media/files/research/cancer-statistics/2024-statistics/2024-cmaj/2024_cancer-specific-stats.pdf
2.Brenner DR, Gillis J, Demers AA, et al. Projected estimates of cancer in Canada in 2024. CMAJ. 2024;196(18):E615-E623. doi: 10.1503/cmaj.240095 PubMed
3.National Cancer Institute. SEER Program. Cancer Stat Facts: Lung and Bronchus Cancer. Accessed July 17, 2024. https://seer.cancer.gov/statfacts/html/lungb.html
4.Canadian Cancer Statistics Advisory Committee. Canadian Cancer Statistics: A 2020 special report on lung cancer. Canadian Cancer Society; 2020. Accessed June 12, 2024. https://cdn.cancer.ca/-/media/files/research/cancer-statistics/2020-statistics/canadian-cancer-statistics/2020-special-report/res-cancerstatistics-canadiancancerstatistics-2020_special-report_en.pdf
5.Ehrenstein V, Eriksen K, Taylor A, Servidio L, Jakobsen E. Characteristics and overall survival of patients with early-stage non-small cell lung cancer: A cohort study in Denmark. Cancer Med. 2023;12(1):30-37. doi: 10.1002/cam4.4946 PubMed
6.Molina JR, Yang P, Cassivi SD, Schild SE, Adjei AA. Non-small cell lung cancer: Epidemiology, risk factors, treatment, and survivorship. Mayo Clin Proc. 2008;83(5):584-94. doi: 10.4065/83.5.584 PubMed
7.Muthusamy B, Patil PD, Pennell NA. Perioperative systemic therapy for resectable non-small cell lung cancer. J Natl Compr Canc Netw. 2022;20(8):953-961. doi: 10.6004/jnccn.2022.7021 PubMed
8.Canadian Cancer Statistics Advisory Committee in collaboration with the Canadian Cancer Society, Statistics Canada, and the Public Health Agency of Canada. Canadian Cancer Statistics 2023. Canadian Cancer Society; 2023. Accessed July 17, 2024. https://cdn.cancer.ca/-/media/files/research/cancer-statistics/2023-statistics/2023_pdf_en
9.Uramoto H, Tanaka F. Recurrence after surgery in patients with NSCLC. Transl Lung Cancer Res. 2014;3(4):242-9. doi: 10.3978/j.issn.2218-6751.2013.12.05 PubMed
10.Taylor MD, Nagji AS, Bhamidipati CM, et al. Tumor recurrence after complete resection for non-small cell lung cancer. Ann Thorac Surg. 2012;93(6):1813-20; discussion 1820-1. doi: 10.1016/j.athoracsur.2012.03.031 PubMed
11.Besse B, Le Chevalier T. Adjuvant chemotherapy for non-small-cell lung cancer: A fading effect? J Clin Oncol. 2008;26(31):5014-7. doi: 10.1200/JCO.2008.18.1081 PubMed
12.West H, Hu X, Zhang S, et al. Treatment patterns and outcomes in resected early-stage non-small cell lung cancer: An analysis of the SEER-Medicare data. Clin Lung Cancer. 2023;24(3):260-268. doi: 10.1016/j.cllc.2022.12.005 PubMed
13.Shukla N, Hanna N. Neoadjuvant and adjuvant immunotherapy in early-stage non-small cell lung cancer. Lung Cancer (Auckl). 2021;12:51-60. doi: 10.2147/LCTT.S277717 PubMed
14.Amin MB, Greene FL, Edge SB, et al. The Eighth Edition AJCC Cancer Staging Manual: Continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA Cancer J Clin. 2017;67(2):93-99. doi: 10.3322/caac.21388
15.Tankel J, Spicer J, Chu Q, et al. Canadian consensus recommendations for the management of operable stage II/III non-small-cell lung cancer: Results of a modified Delphi process. Curr Oncol. 2023;30(12):10363-10384. doi:10.3390/curroncol30120755 PubMed
16.Saw SPL, Ong BH, Chua KLM, Takano A, Tan DSW. Revisiting neoadjuvant therapy in non-small-cell lung cancer. Lancet Oncol. 2021;22(11):e501-e516. doi: 10.1016/S1470-2045(21)00383-1 PubMed
17.Chaft JE, Dziadziuszko R, Haddock Lobo Goulart B. Moving immunotherapy into the treatment of resectable non-small cell lung cancer. Am Soc Clin Oncol Educ Book. 2024;44(3):e432500. doi: 10.1200/EDBK_432500 PubMed
18.CADTH Reimbursement Review Provisional Funding Algorithm. Non-small cell lung cancer without actionable oncogenic alterations. CDA-AMC; 2024. Accessed July 29, 2024. https://www.cadth.ca/sites/default/files/DRR/2024/PH0046_Final_Report_NSCLC.pdf
19.CADTH Reimbursement Recommendation: Nivolumab (Opdivo). Can J Health Technol. 2023;3(4). doi:10.51731/cjht.2023.621
20.Alberta Health Services. Outpatient Cancer Drug Benefit Program. Accessed September 5, 2024. https://www.albertahealthservices.ca/assets/programs/ps-1025651-drug-benefit-list.pdf
21.BC Cancer Agency. Benefit Drug List. Accessed September 5, 2024. http://www.bccancer.bc.ca/systemic-therapy-site/documents/policy%20and%20forms/benefit%20drug%20list.pdf
22.Cancer Care Ontario. Drug Formulary. Accessed August 5, 2024. https://www.cancercareontario.ca/en/drugformulary/search
23.Health PEI. Health PEI formulary drugs for oncology. Accessed September 7, 2024. https://www.princeedwardisland.ca/en/publication/health-pei-formulary-drugs-for-oncology
24.Saskatchewan Cancer Agency. Drug formulary. Accessed September 5, 2024. http://www.saskcancer.ca/health-professionals-article/drug-formulary
25.CADTH Reimbursement Recommendation: Atezolizumab (Tecentriq). Can J Health Technol. 2022;2(9). doi:10.51731/cjht.2022.449
26.Merck Canada Inc. Keytruda (pembrolizumab): solution for infusion, 100 mg/4 mL vial [draft product monograph]. March 8, 2024.
27.Remon J, Soria JC, Peters S, ESMO Guidelines Committee. Early and locally advanced non-small-cell lung cancer: An update of the ESMO Clinical Practice Guidelines focusing on diagnosis, staging, systemic and local therapy. Ann Oncol. 2021;32(12):1637-1642. doi: 10.1016/j.annonc.2021.08.1994 PubMed
28.NCCN Clinical Practice Guidelines in Oncology: Non-Small Cell Lung Cancer. v7.2024. National Comprehensive Cancer Network. Accessed July 18, 2024. https://www.nccn.org/
29.CADTH Reimbursement Recommendation: Osimertinib (Tagrisso). Can J Health Technol. 2022;2(1). doi:10.51731/cjht.2022.248 https://www.cadth.ca/osimertinib
30.Herbst RS, Tsuboi M, John T, et al. Overall survival analysis from the ADAURA trial of adjuvant osimertinib in patients with resected EGFR-mutated (EGFRm) stage IB–IIIA non-small cell lung cancer (NSCLC). J Clin Oncol. 2023;41(17_suppl):LBA3-LBA3. doi: 10.1200/JCO.2023.41.17_suppl.LBA3
31.National Institute for Health and Care Excellence. Atezolizumab for adjuvant treatment of resected non-small-cell lung cancer (NICE technology appraisal TA823). Accessed March 12, 2024. https://www.nice.org.uk/guidance/ta823
32.National Institute for Health and Care Excellence. Nivolumab with chemotherapy for neoadjuvant treatment of resectable non-small-cell lung cancer (NICE technology appraisal TA876). Accessed March 12, 2024. https://www.nice.org.uk/guidance/ta876
33.Merck Sharp & Dohme LLC. P671V02MK3475: A phase III, randomized, double-blind trial of platinum doublet chemotherapy +/− pembrolizumab (MK −3475) as neoadjuvant/adjuvant therapy for participants with resectable satge II, IIIA, and resectable IIIB (T3-4N2) non-small cell lung cancer (NSCLC) (KEYNOTE-671) [internal sponsor's report] In: Drug Reimbursement Review sponsor submission: Keytruda (pembrolizumab), solution for infusion, 100 mg/4 mL vial. November 27, 2023. P671V02MK3475.
34.Cancer Care Ontario. Drug Formulary: CISPPEME. Accessed June 10, 2024. https://www.cancercareontario.ca/en/drugformulary/regimens/48361
35.Cancer Care Ontario. Drug Formulary: CISPGEMC. Accessed August 1, 2024. https://www.cancercareontario.ca/en/drugformulary/regimens/monograph/48116
36.Bristol-Myers Squibb Canada. OPDIVO (nivolumab): Intravenous Infusion, 10 mg nivolumab /mL 40 mg and 100 mg single-use vials [product monograph]. September 25, 2015. Updated June 28, 2024. Accessed August 5, 2024. https://www.bms.com/assets/bms/ca/documents/productmonograph/OPDIVO_EN_PM.pdf
37.Wakelee H, Liberman M, Kato T, et al. Perioperative pembrolizumab for early-stage non-small-cell lung cancer. N Engl J Med. 2023;389(6):491-503. doi: 10.1056/NEJMoa2302983 PubMed
38.Spicer JD, Gao S, Liberman M, et al. LBA56 Overall survival in the KEYNOTE-671 study of perioperative pembrolizumab for early-stage non-small-cell lung cancer (NSCLC). Ann Oncol. 2023;34:S1297-S1298. doi: 10.1016/j.annonc.2023.10.052
39.Merck Sharp & Dohme LLC. NCT03425643: Efficacy and Safety of Pembrolizumab (MK-3475) With Platinum Doublet Chemotherapy as Neoadjuvant/Adjuvant Therapy for Participants With Resectable Stage II, IIIA, and Resectable IIIB (T3-4N2) Non-small Cell Lung Cancer (MK-3475-671/KEYNOTE-671) [accessed by sponsor]. ClinicalTrials.gov. Accessed June 2023. https://clinicaltrials.gov/study/NCT03425643
40.Merck Sharp & Dohme LLC. A Phase III, Randomized, Double-blind Trial of Platinum Doublet Chemotherapy +/− Pembrolizumab (MK-3475) as Neoadjuvant/Adjuvant Therapy for Participants with Resectable Stage II, IIIA, and Resectable IIIB (T3-4N2) Non-small Cell Lung Cancer (NSCLC) (KEYNOTE-671) [accessed by sponsor]. European Medicines Agency; 2022. Accessed June 2023. https://www.clinicaltrialsregister.eu/
41.Aaronson NK, Ahmedzai S, Bergman B, et al. The European Organization for Research and Treatment of Cancer QLQ-C30: A quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst. 1993;85(5):365-76. doi: 10.1093/jnci/85.5.365 PubMed
42.Letellier ME, Dawes D, Mayo N. Content verification of the EORTC QLQ-C30/EORTC QLQ-BR23 with the International Classification of Functioning, Disability and Health. Qual Life Res. 2015;24(3):757-68. doi: 10.1007/s11136-014-0791-8 PubMed
43.Nicklasson M, Bergman B. Validity, reliability and clinical relevance of EORTC QLQ-C30 and LC13 in patients with chest malignancies in a palliative setting. Qual Life Res. 2007;16(6):1019-28. doi: 10.1007/s11136-007-9210-8 PubMed
44.Musoro JZ, Coens C, Sprangers MAG, et al. Minimally important differences for interpreting EORTC QLQ-C30 change scores over time: A synthesis across 21 clinical trials involving nine different cancer types. Eur J Cancer. 2023;188:171-182. doi: 10.1016/j.ejca.2023.04.027 PubMed
45.Osoba D, Rodrigues G, Myles J, Zee B, Pater J. Interpreting the significance of changes in health-related quality-of-life scores. J Clin Oncol. 1998;16(1):139-44. doi: 10.1200/JCO.1998.16.1.139 PubMed
46.de Vet HC, Terwee CB, Ostelo RW, Beckerman H, Knol DL, Bouter LM. Minimal changes in health status questionnaires: Distinction between minimally detectable change and minimally important change. Health Qual Life Outcomes. 2006;4:54. doi: 10.1186/1477-7525-4-54 PubMed
47.Bergman B, Aaronson NK, Ahmedzai S, Kaasa S, Sullivan M. The EORTC QLQ-LC13: A modular supplement to the EORTC Core Quality of Life Questionnaire (QLQ-C30) for use in lung cancer clinical trials. EORTC Study Group on Quality of Life. Eur J Cancer. 1994;30A(5):635-42. doi: 10.1016/0959-8049(94)90535-5 PubMed
48.Nicklasson M, Bergman B. Validity, reliability and clinical relevance of EORTC QLQ-C30 and LC13 in patients with chest malignancies in a palliative setting. Qual Life Res. 2007;16(6):1019-28. PubMed
49.Bassler D, Briel M, Montori VM, et al. Stopping randomized trials early for benefit and estimation of treatment effects: Systematic review and meta-regression analysis. JAMA. 2010;303(12):1180-7. doi: 10.1001/jama.2010.310 PubMed
50.Ades AE. A chain of evidence with mixed comparisons: Models for multi-parameter synthesis and consistency of evidence. Stat Med. 2003;22(19):2995-3016. doi: 10.1002/sim.1566 PubMed
51.Caldwell DM, Ades AE, Higgins JP. Simultaneous comparison of multiple treatments: Combining direct and indirect evidence. BMJ. 2005;331(7521):897-900. doi: 10.1136/bmj.331.7521.897 PubMed
52.Lu G, Ades AE. Combination of direct and indirect evidence in mixed treatment comparisons. Stat Med. 2004;23(20):3105-24. doi: 10.1002/sim.1875 PubMed
53.Precision AQ. Systematic literature review and network meta-analysis of the efficacy and safety of neoadjuvant and perioperative treatments for patients with early-stage resectable non-small cell lung cancer. Canadian NMA report, Version 1 (EFS results) [accessed by sponsor]. August 28, 2024.
54.NCCN Clinical Practice Guidelines in Oncology: Non-Small Cell Lung Cancer. v3.2023 [accessed by sponsor]. National Comprehensive Cancer Network; 2023. https://www.nccn.org/
55.Postmus PE, Kerr KM, Oudkerk M, et al. Early and locally advanced non-small-cell lung cancer (NSCLC). ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. ESMO Slide Set [accessed by sponsor]. European Society for Medical Oncology; 2017. https://www.esmo.org/
56.McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 guideline statement. J Clin Epidemiol. 2016;75:40-6. doi: 10.1016/j.jclinepi.2016.01.021 PubMed
57.Higgins JP, Thomas J, Chandler J, et al. Cochrane handbook for systematic reviews of interventions. John Wiley & Sons; 2019.
58.Dias S, Welton NJ, Sutton AJ, Ades A. NICE DSU technical support document 2: A generalised linear modelling framework for pairwise and network meta-analysis of randomised controlled trials [accessed by spsonsor]. National Institute for Health and Care Excellence; 2011.
59.Ouwens MJ, Philips Z, Jansen JP. Network meta-analysis of parametric survival curves. Res Synth Methods. 2010;1(3-4):258-71. doi: 10.1002/jrsm.25 PubMed
60.Jansen JP. Network meta-analysis of survival data with fractional polynomials. BMC Med Res Methodol. 2011;11(1):61. doi: 10.1186/1471-2288-11-61 PubMed
61.Jansen JP, Cope S. Meta-regression models to address heterogeneity and inconsistency in network meta-analysis of survival outcomes. BMC Med Res Methodol. 2012;12(1):152. doi: 10.1186/1471-2288-12-152 PubMed
62.Dempster AP. The direct use of likelihood for significance testing. Statistics and Computing. 1997;7(4):247-252. doi: 10.1023/a:1018598421607
63.Medical Research Council Biostatistics Unit. DIC: Deviance Information Criteria. University of Cambridge; 2024. Accessed February 23, 2024. https://www.mrc-bsu.cam.ac.uk/software/bugs/the-bugs-project-dic/
64.Plummer M. JAGS Version 4.3.0 user manual [accessed by sponsor]. June 28, 2017. https://people.stat.sc.edu/hansont/stat740/jags_user_manual.pdf
65.NSCLC Meta-analysis Collaborative Group. Preoperative chemotherapy for non-small-cell lung cancer: A systematic review and meta-analysis of individual participant data. Lancet. 2014;383(9928):1561-71. doi: 10.1016/S0140-6736(13)62159-5 PubMed
Pharmacoeconomic_Review
Abbreviations
AE
adverse event
BIA
budget impact analysis
CDA-AMC
Canada’s Drug Agency
DM
distant metastasis
EFS
event-free survival
HR
hazard ratio
ICER
incremental cost-effectiveness ratio
ITC
indirect treatment comparison
LRR-P
local-regional recurrence or progression
NICE
National Institute for Health and Care Excellence
NMA
network meta-analysis
NSCLC
non–small cell lung cancer
OS
overall survival
QALY
quality-adjusted life-year
WTP
willingness to pay
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Pembrolizumab (Keytruda), 100 mg/4 mL solution for IV infusion |
Indication | For the treatment of adult patients with resectable stage II, IIIA, or IIIB (T3-4N2) NSCLC in combination with platinum-containing chemotherapy as neoadjuvant treatment, and then continued as monotherapy as adjuvant treatment |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | February 6, 2025 |
Reimbursement request | As per indication |
Sponsor | Merck Canada Inc. |
Submission history | Previously reviewed: Yes Indication: For the treatment of adult patients with stage IB (T2a ≥ 4 cm), II, or IIIA NSCLC who have undergone complete resection and platinum-based chemotherapy Recommendation date: January 30, 2025 Recommendation: Reimburse with clinical criteria and/or conditions Indication: For the treatment of patients with metastatic squamous NSCLC in combination with carboplatin and either paclitaxel or nab-paclitaxel in adults with no prior systemic chemotherapy treatment for metastatic NSCLC Recommendation date: January 3, 2020 Recommendation: Reimburse with clinical criteria and/or conditions. Indication: In combination with pemetrexed and platinum chemotherapy, for the treatment of metastatic nonsquamous NSCLC, in adults with no EGFR or ALK genomic tumor aberrations, and no prior systemic chemotherapy treatment for metastatic NSCLC. Recommendation date: May 31, 2019 Recommendation: Reimburse with clinical criteria and/or conditions. Indication: For previously untreated patients with metastatic NSCLC whose tumours express PD-L1 and who do not harbor a sensitizing EGFR mutation or ALK translocation Recommendation date: August 23, 2017 Recommendation: Reimburse with clinical criteria and/or conditions. Indication: For the treatment of patients with metastatic NSCLC whose tumours express PD-L1 (as determined by a validated test) and who have disease progression on or after platinum-containing chemotherapy Recommendation date: November 3, 2016 Recommendation: Reimburse with clinical criteria and/or conditions. |
NOC = Notice of Compliance; NSCLC = non–small cell lung cancer; T2a = tumour stage IIA.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Markov model |
Target population | Adult patients with resectable stage II, stage IIIA, or stage IIIB (T3-4N2) NSCLC |
Treatment | Neoadjuvant pembrolizumab plus chemotherapya followed by adjuvant pembrolizumab |
Dosage regimen |
|
Submitted price | Pembrolizumab: $4,400 per 100 mg/4 mL vial |
Submitted treatment cost |
|
Comparators |
|
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | Lifetime (36.9 years) |
Key data source | KEYNOTE-671 trial, sponsor-submitted NMA |
Submitted results |
|
Key limitations | The sponsor’s submitted model used a multistate model to estimate relative efficacy for neoadjuvant pembrolizumab and all comparators. While relative efficacy was informed by the sponsor’s NMA, the multistate modelling approach uses a distinct set of methods to estimate survival. While the approach is appropriate for the decision problem, the literature informing the use of these methods is still evolving. In addition to the methodological concerns, there were model transparency concerns that created barriers to validating some key assumptions. Due to resource and time constraints, CDA-AMC was unable to verify whether the calculations used to predict the transition probabilities from the event-free state were consistent with the selected methodology. |
CDA-AMC reanalysis results | The sponsor’s base case was maintained. The ICER was $119,365 per QALY gained (incremental costs = $59,658; incremental QALYs = 0.50). CDA-AMC did not identify any limitations that could be addressed through reanalysis. At least a 30% reduction in the price of pembrolizumab is needed for neoadjuvant pembrolizumab plus chemotherapy with adjuvant pembrolizumab to be considered cost-effective compared to neoadjuvant nivolumab at a WTP threshold of $50,000 per QALY gained. The identified internal validity concerns within the sponsor’s NMA and the lack of direct comparative evidence against neoadjuvant nivolumab means that a higher price reduction may be warranted. |
CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; LY = life-year; NMA = network meta-analysis; NSCLC = non–small cell lung cancer; QALY = quality-adjusted life-year; vs. = versus; WTP = willingness to pay.
aIncludes squamous (cisplatin + gemcitabine) or nonsquamous (cisplatin + pemetrexed) chemotherapy.
Conclusions
The Clinical Review by Canada’s Drug Agency (CDA-AMC) of the KEYNOTE-671 study concluded with high and moderate certainty that pembrolizumab demonstrated a statistically significant and clinically meaningful improvement in overall survival (OS) compared to chemotherapy alone in patients with resectable stage II, stage IIIA, and selected stage IIIB non–small cell lung cancer (NSCLC). Similar conclusions were reached for event-free survival (EFS) with the submitted evidence graded to be of high certainty. Results from the network meta-analysis (NMA) for EFS did not reveal statistically significant differences between perioperative pembrolizumab and surgery alone or neoadjuvant nivolumab. These findings were subject to uncertainty attributed to imprecision (wide credible intervals), methodological challenges, and gaps in the underlying evidence base.
The economic analysis relied on a multistate survival analysis to estimate survival and time in various health states. While the sponsor’s use of this approach was deemed appropriate for this decision problem, the literature on its implementation and appraisal is still evolving. A formal appraisal of the strength of this evidence could not be conducted, and its implications for the interpretation of the model output are unknown. Broadly, the results of the cost-effectiveness model were aligned with the findings from the KEYNOTE-671 trial and the sponsor’s NMA.
CDA-AMC was unable to address identified limitations in reanalysis. In the sponsor’s base case, neoadjuvant pembrolizumab plus chemotherapy followed by adjuvant pembrolizumab was more costly (incremental costs = $59,658) and more effective (incremental quality-adjusted life-years [QALYs] = 0.50) than neoadjuvant nivolumab plus chemotherapy. The incremental cost-effectiveness ratio (ICER) for perioperative pembrolizumab relative to neoadjuvant nivolumab was estimated to be $119,365 per QALY gained. In total, 74% of incremental QALYs were estimated during the extrapolated period of the KEYNOTE-671 trial. A price reduction of 30% is required for perioperative pembrolizumab to be considered cost-effective at a $50,000 per QALY gained threshold.
Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, clinician groups, and drug plans that participated in the CDA-AMC review process.
Patient input was received in a joint submission from the Canadian Cancer Survivor Network, Lung Cancer Canada, and the Lung Health Foundation. Information was collected using an online survey of patients in Canada conducted between August 1 and September 16, 2024. Respondents included 1 caregiver and 3 patients, all of whom had experience with the existing treatment options. All 3 patient respondents had experience with pembrolizumab and reported effective treatment with manageable side effects. One patient reported it was ineffective due to a low PD-L1 level.
Clinician input was received from 2 groups: Ontario Health (Cancer Care Ontario) Lung Cancer Drug Advisory Committee and Lung Cancer Canada’s Medical Advisory Committee. The consensus among both submissions was that the goal of therapy was curative and to improve OS. Current treatment options include neoadjuvant platinum-based chemotherapy alone or in combination with nivolumab. There is no approved regimen that includes adjuvant immunotherapy for patients who have undergone neoadjuvant chemoimmunotherapy. Neoadjuvant pembrolizumab in combination with chemotherapy followed by adjuvant pembrolizumab is expected to offer an alternative effective regimen to existing options.
Drug plan input identified concerns relating to the estimated budget impact and the presence of confidential negotiated prices for comparator treatments.
Several of these concerns were addressed in the sponsor’s model:
The comparators in the economic evaluation included current standards of care comprising surgery only.
Treatment prices were based on wholesale list prices compiled by a third-party organization.
CDA-AMC was unable to address the following concerns raised from input:
The estimated budget impact is subject to uncertainty.
Economic Review
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted an economic evaluation of neoadjuvant pembrolizumab in combination with platinum-based chemotherapy (cisplatin plus pemetrexed or gemcitabine) followed by adjuvant pembrolizumab for the treatment of adult patients with resectable stage II, stage IIIA, or stage IIIB (T3-4N2) NSCLC.1 This target population was aligned with the proposed Health Canada indication and the reimbursement request.
Pembrolizumab is available as a solution for IV infusion (100 mg/4 mL vial) at a submitted price of $4,400 per vial. For the stated indication, the prescribed regimen comprises neoadjuvant pembrolizumab in combination with cisplatin and pemetrexed or gemcitabine. The recommended dose for pembrolizumab is 200 mg every 3 weeks for a maximum of 4 cycles in the neoadjuvant setting and a maximum of 13 cycles in the adjuvant setting.2 At the submitted price, pembrolizumab alone will cost $8,800 in each 21-day cycle. Cisplatin and gemcitabine are available as solutions for IV infusions at concentrations of 10 mg/mL and 38 mg/mL with prices of $2.70 per mg and $0.27 per mg. Pemetrexed is available as a solution for IV infusion at a concentration of 10 mg/mL and a price of $2,145 per 50 mL vial. The recommended dose in the neoadjuvant setting is 75 mg/m2 of cisplatin in combination with 500 mg/m2 of pemetrexed or 1,000 mg/m2 of gemcitabine.2 A patient with a body surface area of 1.9 m2 would receive 143 mg of cisplatin, 950 mg of pemetrexed, and 1,900 mg of gemcitabine.1 The 21-day regimen cost for neoadjuvant therapy would be $13,495 and $9,745 for pembrolizumab in combination with cisplatin and pemetrexed or gemcitabine, respectively.
Three comparators were included in the economic evaluation. The first was a regimen of neoadjuvant chemotherapy equivalent to the control arm of the KEYNOTE-671 pivotal trial.1,3 This consisted of neoadjuvant cisplatin (75 mg/m2) in combination with pemetrexed (500 mg/m2) or gemcitabine (1,000 mg/m2). For a patient with a body surface area of 1.9 m2, the 21-day regimen cost would be $4,695 and $945 for cisplatin in combination with pemetrexed or gemcitabine, respectively. The second comparator was a regimen of neoadjuvant nivolumab in combination with chemotherapy. Nivolumab is available as a solution for IV infusion (10 mg/mL) in single-use vials of 4 mL (40 mg) and 10 mL (100 mg), which cost $782 and $1,956 per vial, respectively. It was assumed that neoadjuvant chemotherapy for this regimen would include pemetrexed or gemcitabine in combination with cisplatin or paclitaxel and carboplatin. Optional adjuvant chemotherapy using carboplatin, cisplatin, docetaxel, gemcitabine, paclitaxel, pemetrexed, or vinorelbine was also considered. The average 21-day cycle cost was $10,378 for neoadjuvant therapy and $1,469 for adjuvant therapy, leading to a total cycle cost (for all regimen combinations) of $11,846.1 The final comparator of the economic evaluation was surgery only, in which no neoadjuvant or adjuvant therapy was offered to patients.1
Modelled outcomes included life-years and QALYs. Costs were estimated from the perspective of the Canadian public health care payer. Model outputs were generated over a lifetime horizon of 36.9 years, with a cycle length of 1 week. Costs and outcomes were discounted at 1.5%.1
Model Structure
The sponsor submitted a Markov model that tracked a hypothetical cohort of patients across 4 health states. As depicted in Figure 1, these included the event free, local-regional recurrence or progression (LRR-P), distant metastasis (DM), and death states. Patients entered the model in the event-free state and initiated 1 of the mutually exclusive alternatives (neoadjuvant pembrolizumab plus adjuvant pembrolizumab, neoadjuvant chemotherapy, neoadjuvant nivolumab plus chemotherapy, and surgery). After each cycle, patients may remain in their existing state or transition to a different state representing a change in prognosis or death. It was assumed that patients could not transition to a previously occupied state (which represented a better prognosis). The transition probabilities were subject to time dependencies with respect to time in the model and time in each state.
Model Inputs
All data summarizing baseline characteristics were obtained from the KEYNOTE-671 trial.1,3,4 This was a randomized, phase III trial that involved the direct comparison of pembrolizumab in combination with platinum-doublet chemotherapy in the neoadjuvant phase, followed by adjuvant pembrolizumab with placebo in combination with platinum-doublet chemotherapy.3,4 Baseline characteristics of interest included age (mean = 63.1 years), sex (29.4% female; 71.6% male), histology (43.2% squamous; 56.8% nonsquamous), body surface area (mean = 1.9 m2; standard error = 0.01), and weight (mean = 73.7 kg; standard error = 0.6).1,3,4 The submission also considered a baseline glomerular filtration rate of 75 mL per minute per 1.73 m2 obtained from a published technology assessment of pemetrexed for the first-line treatment of NSCLC.1,5
Estimates of relative efficacy for the economic evaluation were obtained from the sponsor-submitted systematic review and NMA. This indirect treatment comparison (ITC) was necessary because the KEYNOTE-671 trial did not include a direct comparison with neoadjuvant nivolumab or surgery only. Eight identified trials formed a connected network that used chemotherapy as a common comparator.6 The outcome of interest from the NMA, as it related to the economic evaluation, was EFS. In the submitted base case, the economic evaluation relied on results from a random-effects model. The corresponding time-constant hazard ratios (HRs) for neoadjuvant nivolumab plus chemotherapy and surgery only, relative to perioperative pembrolizumab, were ████ ████ ████ ████ ██ █████ and ████ ████ ████ ████ ██ █████ respectively.
Transition probabilities from the event-free state were estimated using patient-level data from the KEYNOTE-671 trial.1 Consistent with the approach summarized by Williams et al. trial data were analyzed by performing a multistate survival analysis.7,8 Unlike traditional survival analysis, which considers a single event, a multistate survival analysis provides a mechanism to capture the effect of treatment on intermediate (LRR-P and DM) and final (death) outcomes.9 This type of model can be obtained by fitting individual parametric models for each possible transition (event free to LRR-P, event free to DM, and event free to death). However, any event that is not an event of interest is treated as a censoring event. For each transition, parametric models were fit using the exponential, Weibull, Gompertz, log-normal, log-logistic, gamma, and generalized gamma distributions. These models were fit under 3 different approaches considered by the sponsor. In the first approach, independent parametric models were fit to each treatment arm from the KEYNOTE-671 trial. In the second approach, joint parametric models (with a treatment arm covariate) were fit to the trial data. In the third approach, joint parametric models were fit with covariates specific to the treatment arm and period of follow-up (allowing for a time-varying HR before or after 1 year). This resulted in 343, 27, and 27 possible combinations of multistate model configurations to select from for each approach and 397 total possible combinations. From the 397 total possible combinations, the base configuration was selected following an assessment of statistical fit, proportional hazards, visual assessment of fit, and clinical plausibility of long-term extrapolations. This resulted in the selection of the independent parametric survival models, assuming a generalized gamma distribution for the event free to LRR-P and DM transitions and a log-normal distribution for the event free to death transition.1
For all comparators of the decision model, the selected configuration of the multistate survival analysis was used to predict the hazard at each point in the specified time horizon. Transition probabilities for the neoadjuvant pembrolizumab and neoadjuvant chemotherapy arms were obtained by converting these hazards to probabilities. This same procedure was applied to the neoadjuvant nivolumab plus chemotherapy and surgery only arms. However, the hazards for each arm were obtained by adjusting the estimated hazards for perioperative pembrolizumab using the HRs obtained from the sponsor’s NMA.1
Transition probabilities from the LRR-P state had to be estimated independently from the KEYNOTE-671 trial. This was attributable to the fact that follow-up imaging data were not routinely collected for patients who experienced LRR-P as their first event. In response, the sponsor matched observational data from the US SEER-Medicare database to patient characteristics from the KEYNOTE-671 trial. Using a dataset of 43 patients, the sponsor fitted a separate survival model (using an exponential distribution) to obtain the probability of transitioning from LRR-P to DM and death. In other words, the model assumed that an initial neoadjuvant treatment strategy (or surgery alone) would have no impact on the risk of DM or death for patients occupying the LRR-P state.
Transition probabilities between DM and death were dependent on the distribution of first-line treatments for metastatic NSCLC. Data informing the risk of death were obtained from parametric models estimated directly or indirectly based on the available evidence for each metastatic treatment strategy for each relevant subgroup. Parametric survival models, following an exponential distribution, were fit for 3 treatment strategies with direct evidence available: pembrolizumab plus pemetrexed plus platinum-based chemotherapy (nonsquamous NSCLC) or paclitaxel (squamous NSCLC), and osimertinib (EGFR–positive NSCLC).10-14 Time-constant HRs were used to adjust the directly estimated survival probabilities for label-indicated regimens that were identified from published evidence syntheses.15,16 For therapies that were not included in the evidence synthesis, the sponsor relied on directly estimated HRs or the median OS and progression-free survival reported from relevant clinical trials.17-25
Two additional adjustments were made to the estimated transition probabilities. First, all transitions to the death state were constrained by age-matched general population mortality risks weighted by sex. These estimates were obtained from Canadian life tables published by Statistics Canada.1,26 Second, the sponsor applied a cure assumption to patients who remained in the event-free state 7 years after model entry. This was implemented as a linear increase in the percentage reduction in the per cycle risk of transitioning from the event-free state to the LRR-P, DM, or death states from 0% to 95%.1
In addition to tracking the proportion of the cohort occupying each health state, the model also tracked the occurrence of adverse events (AEs). This was restricted to grade 3 and higher AEs occurring in the neoadjuvant or adjuvant setting such as anemia, neutropenia, or decreases in neutrophil count, platelet count, and white blood cell count.1 The risk of each AE for the perioperative pembrolizumab and chemotherapy regimens was obtained from the KEYNOTE-671 trial.1,3,4 Meanwhile, the AE event risks for the neoadjuvant nivolumab plus chemotherapy regimen were obtained from the CheckMate 816 trial.1,27 Patients in the surgery only arm of the model were assumed to face no risk of AEs.1
Health-related quality of life was incorporated into the model using utility values specific to each health state and AE. Values for the health state utilities were obtained from the indirect measurement of patient preferences using the EQ-5D-5L and EQ-5D-3L questionnaires.1 Canadian population tariffs were applied to data collected from the KEYNOTE-671 trial to obtain utility estimates for the event free (0.865), LRR-P (0.831), and DM (preprogression; 0.793) health states.1,28 Patients who entered the DM state postprogression were assigned utility estimates from the KEYNOTE-407 trial (squamous histology; 0.657) and the KEYNOTE-189 (nonsquamous histology; 0.679) trial.1 While it was assumed that these postprogression utility values were generalizable to the context in Canada, they represented the preferences of the general population from the UK.1 The base case also considered changes in use corresponding to the incidence of each AE. A decrement of –0.027 was applied as a 1-time event in the first model cycle. This was calculated as a function of treatment-specific AE risks, the mean duration per AE episode, the mean number of episodes per patient, and the estimated disutility associated with AE using data collected in the KEYNOTE-671 trial.1,3,4
In the submitted base case, costs were restricted to direct costs incurred by the public health care payer. This consisted of costs relating to treatment acquisition, treatment administration, surgery, and radiotherapy, AE management, non–drug disease management, and terminal care.1 Treatment acquisition costs were calculated from the price per unit consumed for the recommended dosage of treatments prescribed as neoadjuvant, adjuvant, and subsequent therapy. The price of pembrolizumab reflected the sponsor’s submitted price, while all other drug prices were obtained from IQVIA’s DeltaPA database and published formulary reviews.1,29-33 Treatment administration costs were restricted to therapies that were delivered intravenously. This was calculated as the product of the median hourly wage of registered nurses in Canada ($40.39) and the relevant infusion time from the KEYNOTE-671 and CheckMate-816 trial protocols.1,27,34,35
Surgery costs were applied for patients occupying the event-free state. The cost of initial surgery was assumed to be $14,645.24 while the cost for subsequent radiotherapy was assumed to be $16,211.61.1,36,37 Patients undergoing neoadjuvant treatment were eligible for initial surgery if they had completed the neoadjuvant regimen. This was assumed to occur at week 15 (perioperative pembrolizumab and neoadjuvant chemotherapy) and week 11 (neoadjuvant nivolumab). Patients occupying the LRR-P state were assumed to incur 1-time costs relating to chemotherapy, radiotherapy, and salvage surgery. The frequency of each intervention reflected estimates reported in a retrospective cohort study of patients in Canada.1,38 Unit costs for each type of salvage surgery (rib excision, partial lung resection, metastasectomy, lung lobectomy, and lung wedge resection) were obtained from a Canadian patient cost estimator and a prior formulary review report.1,31,36
Costs associated with the management of AEs were applied as a lump-sum at model entry. It was assumed costs would be incurred for the management of anemia and neutropenia. Unit costs reflected Ontario estimates from a Canadian patient cost estimator.1,36 While the model incorporated non–drug disease management costs, the specific components captured in this type of cost were not described. Terminal care costs were assumed to be incurred upon entry to the death state and represented a 1-time cost ($81,058) associated with palliative care in the last 30 days of life.1,39
Summary of Sponsor’s Economic Evaluation Results
In the submitted base case, the costs and QALYs for each alternative were generated in a Monte Carlo simulation of 5,000 iterations. Results were similar between the probabilistic and deterministic simulations. The probabilistic findings are presented as follows.
Base-Case Results
The submitted analysis was based on the publicly available prices of the comparator treatments. Results from the base case of the submitted economic evaluation are presented in Table 3. Neoadjuvant pembrolizumab plus chemotherapy followed by adjuvant pembrolizumab was more costly (incremental costs = $59,658) and more effective (incremental QALYs = 0.50) than neoadjuvant nivolumab plus chemotherapy.1 With a calculated ICER of $119,365, the pembrolizumab regimen was not cost-effective at a willingness-to-pay (WTP) threshold of $50,000 per QALY gained.1 There was a 38% probability of neoadjuvant pembrolizumab plus chemotherapy with adjuvant pembrolizumab being cost-effective compared to neoadjuvant nivolumab plus chemotherapy at this threshold.
While the methods used to estimate survival in the sponsor’s pharmacoeconomic model differed from those of the KEYNOTE-671 trial (i.e., the use of a multistate survival approach with relative efficacy from an NMA), the survival results from the model were broadly similar. At 48 months, █████ of KEYNOTE-671 study participants who had received neoadjuvant pembrolizumab plus chemotherapy with adjuvant pembrolizumab remained alive, while 63.9% were still alive at that time point in the corresponding arm of the pharmacoeconomic model. The estimated survival was 51.5% and 51.1% at 48 months for the KEYNOTE-671 trial and pharmacoeconomic model, respectively, among patients who received neoadjuvant chemotherapy. The incremental survival difference was smaller (█████ ████████) in the pharmacoeconomic model than in the trial, which suggests that any differences in observed versus modelled survival did not favour the cost-effectiveness of pembrolizumab.
While total costs were broadly similar for all comparators (range, $208,689 to $268,346), costs were higher in the event-free state for neoadjuvant pembrolizumab and neoadjuvant nivolumab than they were for both dominated treatments (neoadjuvant chemotherapy and surgery alone). Conversely, the modelled cohort generated lower costs in the DM state for neoadjuvant pembrolizumab and neoadjuvant nivolumab than for the other comparators. The sponsor’s model results suggest that higher upfront costs for neoadjuvant and perioperative therapies were offset by avoided downstream costs of metastatic treatment (which may comprise regimens that include pembrolizumab or nivolumab).
Approximately 74% of the incremental QALYs for neoadjuvant pembrolizumab plus chemotherapy with adjuvant pembrolizumab compared with neoadjuvant nivolumab plus chemotherapy was derived beyond the median follow-up period from the KEYNOTE-671 trial.1
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|
Neoadjuvant nivolumab plus chemotherapy | 208,689 | 7.62 | Reference |
Neoadjuvant pembrolizumab plus chemotherapy with adjuvant pembrolizumab | 268,346 | 8.12 | 119,365 |
Dominated treatments | |||
Surgery only | 227,767 | 4.69 | NAa |
Neoadjuvant chemotherapy | 254,323 | 5.25 | NAa |
ICER = incremental cost-effectiveness ratio; NA = not applicable; QALY = quality-adjusted life-year.
aDominated by neoadjuvant nivolumab plus chemotherapy.
Source: Sponsor’s pharmacoeconomic submission.1
Additional results from the sponsor’s submitted economic evaluation base case are presented in Appendix 3.
Sensitivity and Scenario Analysis Results
In addition to the submitted base case, the sponsor considered 26 scenario analyses that examined alternative inputs or assumptions relating to the time horizon, discount rates, parametric distributions, cure, treatment waning, mortality, time-varying HRs of EFS failure, adjustments to the risk of death from DM, the mix of first-line and second-line treatments following entry to the DM state, alternate market shares for treatment in the LRR-P state, the source of evidence informing the risk of surgery from the LRR-P state, vial sharing, and the source of health state utilities. While each scenario had a slight impact on the expected costs and benefits, none had a meaningful effect on the conclusion for the cost-effectiveness of neoadjuvant pembrolizumab plus chemotherapy followed by adjuvant pembrolizumab.
The sponsor conducted a scenario analysis from a societal perspective; this analysis included additional costs associated with a loss in patient productivity (due to absenteeism and death) and lost income for informal caregivers. In this analysis, relative to neoadjuvant nivolumab plus chemotherapy, the ICER was $97,377 per QALY gained.
CDA-AMC Appraisal of the Sponsor’s Economic Evaluation
CDA-AMC identified several key limitations to the sponsor’s analysis that have notable implications for the economic analysis.
Distinct methods were used to estimate comparative clinical efficacy: The Clinical Review concluded with moderate to high levels of certainty that neoadjuvant pembrolizumab plus chemotherapy with adjuvant pembrolizumab was associated with improvements in EFS and OS compared to placebo. The Clinical Review identified several concerns within the NMA comparing perioperative pembrolizumab to other comparators (neoadjuvant nivolumab plus chemotherapy, neoadjuvant chemotherapy, and surgery alone), and determined that the ability to draw conclusions about the comparative efficacy of perioperative pembrolizumab to these comparators was constrained by methodological and data constraints.
In the submitted pharmacoeconomic model, the sponsor used a multistate survival analysis approach to incorporate the risk of competing events. This methodology involved fitting parametric regressions for each transition, after censoring competing events (i.e., LRR-P, DM, and death). The sponsor considered a complex analysis strategy in which transition-specific models were fit to each arm of the KEYNOTE-671 trial independently, to the full trial dataset using a treatment covariate, and to the full trial dataset using covariates for treatment arm and the period of follow-up. The CDA-AMC Clinical Review’s appraisal of the strength of the comparative efficacy evidence from the NMA may not directly translate to the economic evaluation. The use of a multistate model was deemed appropriate for this submission, and the sponsor’s approach appeared to follow methodological guidance available in the literature.7,8 In addition, the sponsor’s submission to CDA-AMC proactively addressed the primary limitations identified in a recent independent technology appraisal for a similar model submitted to the National Institute for Health and Care Excellence (NICE) in the UK.40 However, CDA-AMC did not perform a formal appraisal of the quality of this evidence. The survival estimates produced by the pharmacoeconomic model were broadly aligned with the evidence presented in the Clinical Review, but the divergence in methods used to estimate comparative efficacy may introduce biases of unknown direction and magnitude in the estimated ICER.
CDA-AMC was unable to address the uncertainty around the methods used to estimate the relative efficacy of the various comparators within the model.
Model transparency was degraded by unnecessary complexity: The sponsor’s approach to survival analysis resulted in the specification of 343, 27, and 27 possible combinations of multistate model configurations to select from. Despite the specification of 397 possible scenarios for a single set of parameters, the sponsor only considered the impact of 8 alternatives in scenario analysis, none of which had a meaningful impact on the conclusions of the economic evaluation. This was confirmed in the appraisal of a similar version of this model by NICE.40 The independent evidence review group concluded that the results of the economic evaluation were not sensitive to alternate multistate model configurations. This was attributed to 2 factors. The first was that the patient-level data used for the multistate survival analysis had a maximum duration of follow-up of 62 months (5.2 years). The second was the cure assumption applied to patients who occupied the event-free state for more than 7 years.40 By year 10 in the model, it was assumed 95% of these patients had a 0% probability of progression and the risk of death was equal to that of the general population.1,40 In other words, after 7 years, the predicted probabilities from the selected configuration of the multistate survival analysis were substituted with values that reflected the requirements of the cure assumption. This meant that the values from the survival analysis only influenced the transition probabilities at points in time that overlapped with the trial period, rather than the extrapolated period where the predicted values would have been the most uncertain. Given the scope of the review, it was not possible to fully examine and verify that this important assumption was happening within the model as expected. The complex method for programming the model file may have introduced errors that could not be detected, which may have introduced bias into the analysis that could not be detected.
CDA-AMC was unable to address this limitation. The extent to which the sponsor’s results were affected by calculation or programming errors could not be determined.
CDA-AMC Reanalyses of the Economic Evaluation
Base-Case Results
CDA-AMC did not specify a base case or conduct a reanalysis of the submitted economic evaluation. This was attributable to an inability to identify any key limitations that could be addressed through modification. The sponsor’s use of a multistate survival analysis meant that evidence from the KEYNOTE-671 trial could be incorporated into the economic evaluation in a way that treated the transitions from the event-free state as competing risks. While this methodology is an emerging best practice in the development of economic evaluations that rely on time-to-event data, the literature reflecting its implementation and appraisal remains immature.7,8 Furthermore, it was noted that the submission to CDA-AMC was prepared in a manner that addressed the primary limitations identified in the recent independent technology appraisal for a similar model submitted to NICE in the UK. However, CDA-AMC remains concerned that the unnecessary programming complexity of the submitted economic evaluation may have resulted in errors that could not be identified in this review.
Scenario Analysis Results
A series of scenario analyses was conducted to explore the impact of reductions to the price of pembrolizumab on the results of the sponsor’s base case. In the CDA-AMC base case, a price reduction of 30% (i.e., the pembrolizumab price of $3,080 per vial; $6,160 per 21-day cycle) is required for pembrolizumab to be considered cost-effective at a WTP threshold of $50,000 per QALY gained. Additional details about price reduction are presented in Table 4.
Table 4: CDA-AMC Price Reduction Analyses
Analysis | Unit drug cost ($) | ICER ($/QALY) |
|---|---|---|
Price reduction | $ | Sponsor base casea |
No price reduction | 4,400 | 119,365 |
10% | 3,960 | 95,676 |
20% | 3,520 | 71,976 |
30% | 3,080 | 48,275 |
40% | 2,640 | 24,575 |
50% | 2,200 | 874 |
60% | 1,760 | Dominates |
70% | 1,320 | Dominates |
80% | 880 | Dominates |
90% | 440 | Dominates |
CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
aNeoadjuvant pembrolizumab plus chemotherapy with adjuvant pembrolizumab versus neoadjuvant nivolumab plus chemotherapy.
Issues for Consideration
Pembrolizumab has been previously reviewed by CDA-AMC for several conditions, including for the treatment of patients with NSCLC who have undergone complete resection and platinum-based chemotherapy;41 for the treatment of patients with metastatic NSCLC whose tumours express PD-L1 greater than or equal to 1% and who have disease progression on or after platinum-containing chemotherapy;42 for the treatment of patients with untreated metastatic, squamous NSCLC;43 for the treatment of patients with previously untreated metastatic NSCLC whose tumours express PD-L1 greater than or equal to 50% and who do not harbour a sensitizing EGFR mutation or ALK translocation;44 and for the treatment of patients with metastatic nonsquamous NSCLC with no EGFR or ALK genomic tumour aberrations and no prior systematic chemotherapy treatment for metastatic NSCLC.45 The cost-effectiveness results of these evaluations may not be directly comparable to those in the current review, owing to differences in target population, model structure, clinical effectiveness parameters, health state utility values, and cost inputs. CDA-AMC further notes that the pan-Canadian Pharmaceutical Alliance concluded negotiations with a letter of intent for pembrolizumab for the specified indications.46,47 Therefore, pembrolizumab has a confidential negotiated price that may differ from the submitted price used to calculate the acquisition costs of pembrolizumab. Differences in these prices may influence the conclusions of the economic evaluation and budget impact analysis (BIA).
Pembrolizumab was considered by the pan-Canadian Oncology Drug Review Expert Review Committee on December 4, 2024, for the treatment of adult patients with stage IB (tumour stage IIA ≥ 4 cm), stage II, or stage IIIA NSCLC who have undergone complete resection and platinum-based chemotherapy. The final recommendation was not available at the time of this report.
Overall Conclusions
The CDA-AMC Clinical Review of the KEYNOTE-671 trial concluded that perioperative pembrolizumab provides a clinically meaningful benefit in the treatment of resectable stage II, stage IIIA, and selected stage IIIB NSCLC. For OS, perioperative pembrolizumab demonstrated a statistically significant and clinically meaningful improvement compared to placebo. This evidence was determined to be at high certainty at 48 months and moderate certainty at 24 months and 36 months. Similar conclusions were reached for EFS at all 3 time points. However, the CDA-AMC Clinical Review noted that the conclusions for EFS may have been influenced by potential unblinding because of the distinct AE profiles for perioperative pembrolizumab that were not observed in the placebo arm of the trial. Indirect evidence submitted by the sponsor suggested that perioperative pembrolizumab was more effective, in terms of EFS, than surgery alone. However, statistically significant differences were not observed between perioperative pembrolizumab and any other comparator included in the ITC. The ITC results were subject to uncertainty attributed to imprecision (wide credible intervals), methodological challenges, the violation of key assumptions, and gaps in the underlying evidence base. While the OS and EFS results from the KEYNOTE-671 trial were not incorporated as input parameters into the economic evaluation, the HRs from the ITC were used to adjust the event-free transition probabilities for the indirect comparators. Because the economic model incorporates the NMA into its estimation of relative effectiveness, the results are subject to the limitations identified within the NMA. However, the use of a multistate survival analysis within the economic analysis adds additional complexity to the interpretation of findings, as it represents a distinct method for estimating survival in the patient cohort.
Interpretation of the results was further affected by the programming approach used in the economic model, which was highly complex and interfered with the ability of CDA-AMC to validate the formulas and outputs. An appraisal of an alternate version of this model by NICE concluded that the results of the economic evaluation were not sensitive to changes in the configuration of the multistate model due to assumptions related to how the model reflected the possibility of being cured of disease. Despite the model’s lack of sensitivity to changes in the survival analysis, the sponsor devoted multiple sheets within the model file to explorations of different survival assumptions. This made the file difficult to validate, despite having little discernible impact on cost-effectiveness. This complexity may have introduced errors that could not be detected within the review period.
The sponsor’s use of a multistate survival analysis is consistent with an emerging best practice in the development of economic evaluations that rely on time-to-event data.7,8 However, the literature regarding the implementation and appraisal of this methodology remains immature. CDA-AMC notes the proactive efforts taken by the sponsor to address the primary limitations identified in the recent independent technology appraisal for a similar model submitted to NICE in the UK. The survival outputs from the model were broadly aligned with the results of the KEYNOTE-671 trial (OS for patients treated with pembrolizumab at 48 months was 63.9% and █████ respectively) and the submitted NMA (OS for patients treated with chemotherapy at 48 months was 51.1% and 51.5%, respectively), but the methodological and programming complexity within the submission may have introduced biases of unknown magnitude and direction during the extrapolated period of the analysis.
CDA-AMC did not conduct a reanalysis. In the sponsor’s base case, neoadjuvant pembrolizumab plus chemotherapy followed by adjuvant pembrolizumab was more costly (incremental costs = $59,658) and more effective (incremental QALYs = 0.50) than neoadjuvant nivolumab plus chemotherapy. The ICER for perioperative pembrolizumab relative to neoadjuvant nivolumab was estimated to be $119,365 per QALY gained. A 30% reduction in the price of pembrolizumab is required for neoadjuvant pembrolizumab plus chemotherapy with adjuvant pembrolizumab to be considered cost-effective compared to neoadjuvant nivolumab plus chemotherapy at a WTP threshold of $50,000 per QALY gained. Given the absence of direct comparative evidence against neoadjuvant nivolumab and the identified internal validity concerns within the indirect evidence, additional price reduction may be warranted.
References
1.Merck Canada Inc. Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Keytruda (pembrolizumab), solution for infusion 100 mg/4 mL vial. September 7, 2024.
2.Merck Canada Inc. Keytruda (pembrolizumab): solution for infusion 100 mg/4 mL vial [product monograph]. March 8, 2024.
3.Merck Sharp & Dohme LLC. Clinical Study Report P671V02MK3475: A phase III, randomized, double-blind trial of platinum doublet chemotherapy +/− pembrolizumab (MK −3475) as neoadjuvant/adjuvant therapy for participants with resectable satge II, IIIA, and resectable IIIB (T3-4N2) non-small cell lung cancer (NSCLC) (KEYNOTE-671) [internal sponsor's report]. November 27, 2023.
4.Spicer JD, Gao S, Liberman M, et al. Overall survival in the KEYNOTE-671 study of perioperative pembrolizumab for early-stage NSCLC [accessed by sponsor]. ESMO Congress 2023, Madrid, Spain.
5.National Institute for Health and Care Excellence. Pemetrexed for the first-line treatment of non-small-cell lung cancer (NICE technology appraisal TA181) [accessed by sponsor]. 2009. https://www.nice.org.uk/guidance/ta181
6.Merck Canada Inc. Sponsor's NMA report title [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Keytruda (pembrolizumab), solution for infusion 100 mg/4 mL vial. September 7, 2024.
7.Williams C, Lewsey JD, Briggs AH, Mackay DF. Cost-effectiveness analysis in R using a multi-state modeling survival analysis framework: A tutorial. Med Decis Making. 2017;37(4):340-352. doi: 10.1177/0272989X16651869 PubMed
8.Williams C, Lewsey JD, Mackay DF, Briggs AH. Estimation of survival probabilities for use in cost-effectiveness analyses: A comparison of a multi-state modeling survival analysis approach with partitioned survival and markov decision-analytic modeling. Med Decis Making. 2017;37(4):427-439. doi: 10.1177/0272989X16670617 PubMed
9.Putter H, Fiocco M, Geskus RB. Tutorial in biostatistics: Competing risks and multi-state models. Stat Med. 2007;26(11):2389-430. doi: 10.1002/sim.2712 PubMed
10.Gadgeel S, Rodriguez-Abreu D, Speranza G, et al. Updated analysis from KEYNOTE-189: Pembrolizumab or placebo plus pemetrexed and platinum for previously untreated metastatic nonsquamous non-small-cell lung cancer. J Clin Oncol. 2020;38(14):1505-1517. doi: 10.1200/JCO.19.03136 PubMed
11.Gandhi L, Rodriguez-Abreu D, Gadgeel S, et al. Pembrolizumab plus chemotherapy in metastatic non-small-cell lung cancer. N Engl J Med. 2018;378(22):2078-2092. doi: 10.1056/NEJMoa1801005 PubMed
12.Paz-Ares L, Luft A, Vicente D, et al. Pembrolizumab plus chemotherapy for squamous non-small-cell lung cancer. N Engl J Med. 2018;379(21):2040-2051. doi: 10.1056/NEJMoa1810865 PubMed
13.Ramalingam SS, Vansteenkiste J, Planchard D, et al. Overall survival with osimertinib in untreated, EGFR-mutated advanced NSCLC. N Engl J Med. 2020;382(1):41-50. doi: 10.1056/NEJMoa1913662 PubMed
14.Soria JC, Ohe Y, Vansteenkiste J, et al. Osimertinib in untreated EGFR-mutated advanced non-small-cell lung cancer. N Engl J Med. 2018;378(2):113-125. doi: 10.1056/NEJMoa1713137 PubMed
15.Zhang H, Chen J, Liu T, Dang J, Li G. First-line treatments in EGFR-mutated advanced non-small cell lung cancer: A network meta-analysis. PLoS One. 2019;14(10):e0223530. doi: 10.1371/journal.pone.0223530 PubMed
16.Merck, Co. Network meta-analysis of interventions for the first-line treatment of metastatic NSCLC patients: technical report [Data on file]. September 1, 2023.
17.Roszkowski K, Pluzanska A, Krzakowski M, et al. A multicenter, randomized, phase III study of docetaxel plus best supportive care versus best supportive care in chemotherapy-naive patients with metastatic or non-resectable localized non-small cell lung cancer (NSCLC). Lung Cancer. 2000;27(3):145-57. doi: 10.1016/s0169-5002(00)00094-5 PubMed
18.Herbst RS, Giaccone G, de Marinis F, et al. Atezolizumab for first-line treatment of PD-L1-selected patients with NSCLC. N Engl J Med. 2020;383(14):1328-1339. doi: 10.1056/NEJMoa1917346 PubMed
19.Ozguroglu M, Kilickap S, Sezer A, et al. First-line cemiplimab monotherapy and continued cemiplimab beyond progression plus chemotherapy for advanced non-small-cell lung cancer with PD-L1 50% or more (EMPOWER-Lung 1): 35-month follow-up from a mutlicentre, open-label, randomised, phase 3 trial. Lancet Oncol. 2023;24(9):989-1001. doi: 10.1016/S1470-2045(23)00329-7 PubMed
20.Gogishvili M, Melkadze T, Makharadze T, et al. Cemiplimab plus chemotherapy versus chemotherapy alone in non-small cell lung cancer: A randomized, controlled, double-blind phase 3 trial. Nat Med. 2022;28(11):2374-2380. doi: 10.1038/s41591-022-01977-y PubMed
21.Wong ML, McMurry TL, Stukenborg GJ, et al. Impact of age and comorbidity on treatment of non-small cell lung cancer recurrence following complete resection: A nationally representative cohort study. Lung Cancer. 2016;102:108-117. doi: 10.1016/j.lungcan.2016.11.002 PubMed
22.Zhou C, Solomon B, Loong HH, et al. First-line selpercatinib or chemotherapy and pembrolizumab in RET fusion-positive NSCLC. N Engl J Med. 2023;389(20):1839-1850. doi: 10.1056/NEJMoa2309457 PubMed
23.Georgoulias V, Ardavanis A, Agelidou A, et al. Docetaxel versus docetaxel plus cisplatin as front-line treatment of patients with advanced non-small-cell lung cancer: A randomized, multicenter phase III trial. J Clin Oncol. 2004;22(13):2602-9. doi: 10.1200/JCO.2004.11.004 PubMed
24.Georgoulias V, Androulakis N, Kotsakis A, et al. Docetaxel versus docetaxel plus gemcitabine as front-line treatment of patients with advanced non-small cell lung cancer: A randomized, multicenter phase III trial. Lung Cancer. 2008;59(1):57-63. doi: 10.1016/j.lungcan.2007.07.021 PubMed
25.de Castro G, Jr., Kudaba I, Wu YL, et al. Five-year outcomes with pembrolizumab versus chemotherapy as first-line therapy in patients with non-small-cell lung cancer and Programmed Death Ligand-1 Tumor Proportion Score >/= 1% in the KEYNOTE-042 Study. J Clin Oncol. 2023;41(11):1986-1991. doi: 10.1200/JCO.21.02885 PubMed
26.Statistics Canada. Table: 13-10-0114-01. Life expectancy and other elements of the life table, Canada, all provinces except Prince Edward Island. 2023. Accessed November 4, 2024. https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310011401
27.Forde PM, Spicer J, Lu S, et al. Neoadjuvant nivolumab plus chemotherapy in resectable lung cancer. N Engl J Med. 2022;386(21):1973-1985. doi: 10.1056/NEJMoa2202170 PubMed
28.Xie F, Pullenayegum E, Gaebel K, et al. A Time Trade-off-derived Value Set of the EQ-5D-5L for Canada. Med Care. 2016;54(1):98-105. doi: 10.1097/MLR.0000000000000447 PubMed
29.IQVIA. DeltaPA. 2024. Accessed October 21, 2024. https://www.iqvia.com/
30.CADTH Reimbursement Review: Cemiplimab (Libtayo). Can J Health Technol. 2022;2(8). doi:10.51731/cjht.2022.433
31.CADTH Reimbursement Review: Nivolumab (Opdivo). Can J Health Technol. 2023;3(7). doi:10.51731/cjht.2023.684
32.CADTH Reimbursement Review: Nivolumab (Opdivo) in combination with Ipilimumab (Yervoy). Can J Health Technol. 2021;1(9). doi:10.51731/cjht.2021.168
33.CADTH Reimbursement Review: Osimertinib (Tagrisso). Can J Health Technol. 2022;2(3). doi:10.51731/cjht.2022.280
34.Government of Canada. Prevailing Wages. Registered Nurse (R.N.) in Canada. Labour market information [accessed by sponsor]. 2023. https://www.jobbank.gc.ca/marketreport/wages-occupation/993/ca
35.Wakelee H, Liberman M, Kato T, et al. Perioperative pembrolizumab for early-stage non-small-cell lung cancer. N Engl J Med. 2023;389(6):491-503. doi: 10.1056/NEJMoa2302983 PubMed
36.Canadian Institute for Health Information. Patient Cost Estimator [accessed by sponsor]. 2021. https://www.cihi.ca/en/patient-cost-estimator
37.Mittmann N, Liu N, Cheng SY, et al. Health system costs for cancer medications and radiation treatment in Ontario for the 4 most common cancers: A retrospective cohort study. CMAJ Open. 2020;8(1):E191-E198. doi: 10.9778/cmajo.20190114 PubMed
38.Agulnik J, Kasymjanova G, Pepe C, et al. Understanding clinical practice and survival outcomes in patients with unresectable stage III non-small-cell lung cancer in a single centre in Quebec. Curr Oncol. 2020;27(5):e459-e466. doi: 10.3747/co.27.6241 PubMed
39.De Oliveira C, Pataky R, Bremner K, et al. Estimating the cost of cancer care in British Columbia and Ontario: A Canadian inter-provincial comparison. Healthc Policy. 2017;12(3):95-108. doi: 10.12927/hcpol.2017.25024 PubMed
40.National Institute for Health and Care Excellence. Pembrolizumab as neoadjuvant (with chemotherapy) and adjuvant (as monotherapy) treatment for resectable non-small-cell lung cancer (Technology appraisal guidance ID5094. Supporting Evidence: committee papers). 2024. Accessed October 30, 2024. https://www.nice.org.uk/guidance/indevelopment/gid-ta11174
41.CADTH Reimbursement Review: Pembrolizumab. 2024. Accessed November 25, 2024. https://www.cda-amc.ca/pembrolizumab-13
42.CADTH Reimbursement Review: Keytruda (Pembrolizumab) for Non-Small Cell Lung Cancer (Second Line or Beyond). 2016. Accessed November 25, 2024. https://www.cda-amc.ca/keytruda-non-small-cell-lung-cancer-second-line-or-beyond-details
43.CADTH Reimbursement Review: Keytruda (Pembrolizumab) for Squamous NSCLC. 2020. Accessed November 25, 2024. https://www.cda-amc.ca/keytruda-squamous-nsclc-details
44.CADTH Reimbursement Review: Keytruda (Pembrolizumab) for Advanced Non-Small Cell Lung Carcinoma (First Line). 2017. Accessed November 25, 2024. https://www.cda-amc.ca/keytruda-advanced-non-small-cell-lung-carcinoma-first-line-details
45.CADTH Reimbursement Review: Keytruda (Pembrolizumab) for Non-Squamous Non-Small Cell Lung Cancer. 2019. Accessed November 25, 2024. https://www.cda-amc.ca/keytruda-non-squamous-nsclc-details
46.pan-Canadian Pharmaceutical Alliance. Keytruda (pembrolizumab). 2020. Accessed November 25, 2024. https://www.pcpacanada.ca/negotiation/21137
47.pan-Canadian Pharmaceutical Alliance. Keytruda (pembrolizumab). 2017. Accessed November 25, 2024. https://www.pcpacanada.ca/negotiation/20928
48.Cancer Care Ontario. Drug Formulary: CISPGEMC+NIVL. 2024. Accessed October 17, 2024. https://www.cancercareontario.ca/en/drugformulary/regimens/72886
49.Cancer Care Ontario. Drug Formulary: CISPPEME+NIVL. 2024. Accessed October 17 2024. https://www.cancercareontario.ca/en/drugformulary/regimens/72876
50.Cancer Care Ontario. Drug Formulary: CISPVINO+NIVL. 2024. Accessed October 17, 2024. https://www.cancercareontario.ca/en/drugformulary/regimens/72881
51.Cancer Care Ontario. Drug Formulary: CRBPGEMC+NIVL. 2024. Accessed October 17, 2024. https://www.cancercareontario.ca/en/drugformulary/regimens/76456
52.Cancer Care Ontario. Drug Formulary: CRBPPACL+NIVL. 2024. Accessed October 17, 2024. https://www.cancercareontario.ca/en/drugformulary/regimens/71631
53.Calvert AH, Newell DR, Gumbrell LA, et al. Carboplatin dosage: Prospective evaluation of a simple formula based on renal function. J Clin Oncol. 1989;7(11):1748-56. doi: 10.1200/JCO.1989.7.11.1748 PubMed
54.Merck Canada Inc. Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Keytruda (pembrolizumab), solution for infusion 100 mg/4 mL vial. September 7, 2024.
55.Canadian Cancer Statistics Advisory Committee in collaboration with the Canadian Cancer Society, Statistics Canada, and the Public Health Agency of Canada. Canadian Cancer Statistics 2023. Canadian Cancer Society; 2023. Accessed July 17, 2024. https://cdn.cancer.ca/-/media/files/research/cancer-statistics/2023-statistics/2023_pdf_en
56.Canadian Cancer Statistics Advisory Committee in collaboration with the Canadian Cancer Society, Statistics Canada, and the Public Health Agency of Canada. Canadian Cancer Statistics 2024. Canadian Cancer Society; 2024. Accessed July 17, 2024. https://cdn.cancer.ca/-/media/files/research/cancer-statistics/2024-statistics/2024-cmaj/2024_cancer-specific-stats.pdf
57.Brenner DR, Poirier A, Woods RR, et al. Projected estimates of cancer in Canada in 2022. CMAJ. 2022;194(17):E601-E607. doi: 10.1503/cmaj.212097 PubMed
58.Canadian Statistics Advisory Committee. Canadian Cancer Statistics. A 2020 Special Report on Lung Cancer. Canadian Cancer Society; 2020. Accessed June 12, 2024. https://cdn.cancer.ca/-/media/files/research/cancer-statistics/2020-statistics/canadian-cancer-statistics/2020-special-report/res-cancerstatistics-canadiancancerstatistics-2020_special-report_en.pdf
59.EpicOncology. Incidence (AJCC 8th Edition) by Stage (Lung, Non-Small Cell (NSCLC)) [accessed by sponsor]. 2022. https://epic.time4epi.com/
60.Goldstraw P, Chansky K, Crowley J, et al. The IASLC Lung Cancer Staging Project: Proposals for Revision of the TNM Stage Groupings in the Forthcoming (Eighth) Edition of the TNM Classification for Lung Cancer. J Thorac Oncol. 2016;11(1):39-51. doi: 10.1016/j.jtho.2015.09.009 PubMed
61.CADTH Reimbursement Review: Atezolizumab (Tecentriq). Can J Health Technol. 2022;2(12). doi:10.51731/cjht.2022.526
62.Drug Intelligence. ONCO-CAPPS: NSCLC Market Sizing & Treatment Rate Audit, Q42023 [sponsor supplied reference]. 2024.
Appendix 1: Cost Comparison Table
Please note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical expert(s). Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans. Additional details are presented in Table 5.
Table 5: CDA-AMC Cost Comparison Table for Resectable Stage II, Stage IIIA, or Stage IIIB NSCLC
Treatment | Concentration | Form | Price ($) | Recommended dosage | Daily cost ($) | Cost for 21 days ($) |
|---|---|---|---|---|---|---|
Pembrolizumab (Keytruda) | 25 mg/mL | 4 mL solution | 4,400.0000a | 200 mg every 3 weeks for a maximum of 4 cycles in the neoadjuvant setting or 13 cycles in the adjuvant setting | 419.05 | 8,800 |
Cisplatin (Generic) | 1 mg/mL | 50 mL solution 100 mL solution | 135.0000 270.0000 | 75 mg/m2 every 3 weeks for a maximum of 4 cycles in the neoadjuvant setting | 19.29 | 405 |
Gemcitabine | 38 mg/mL | 26. 3mL solution 52.6 mL solution | 270.0000 540.0000 | 1,000 mg/m2 (day 1 and day 8) every 3 weeks for a maximum of 4 cycles in the neoadjuvant setting | 25.71 | 540 |
Pemetrexed | 10 mg/mL | 10 mL vial 50 mL vial | 429.0000 2,145.0000 | 500 mg/m2 every 3 weeks for a maximum of 4 cycles in the neoadjuvant setting | 204.29 | 4,290 |
Neoadjuvant pembrolizumab + cisplatin + pemetrexed + adjuvant pembrolizumab | Neoadjuvant: 642.62 Adjuvant: 419.05 | Neoadjuvant: 13,495 Adjuvant: 8,800 | ||||
Neoadjuvant pembrolizumab + cisplatin + gemcitabine + adjuvant pembrolizumab | Neoadjuvant: 464.05 Adjuvant: 419.05 | Neoadjuvant: 9,745 Adjuvant: 8,800 | ||||
Neoadjuvant chemotherapy | ||||||
Cisplatin | 1 mg/mL | 50 mL solution 100 mL solution | 135.0000 270.0000 | 75 mg/m2 every 3 weeks for a maximum of 4 cycles | 19.29 | 405 |
Gemcitabine (Generic) | 38 mg/mL | 26.3 mL solution 52.6 mL solution | 270.0000 540.0000 | 1,000 mg/m2 every 3 weeks for a maximum of 4 cycles | 21.71 | 540 |
Pemetrexed | 10 mg/mL | 10 mL vial 50 mL vial | 429.0000 2,145.0000 | 500 mg/m2 every 3 weeks for a maximum of 4 cycles | 204.29 | 4,290 |
Neoadjuvant cisplatin + gemcitabine | 45.00 | 945 | ||||
Neoadjuvant cisplatin + pemetrexed | 223.57 | 4,695 | ||||
Neoadjuvant nivolumab + chemotherapy | ||||||
Neoadjuvant nivolumab + cisplatin + gemcitabineb | ||||||
Nivolumab (Opdivo) | 10 mg/mL | 4 mL vial 10 mL vial | 782.2200 1,955.5600 | 4.5 mg/kg every 3 weeks for a maximum of 3 cycles | 316.62 | 6,649 |
Cisplatin (Generic) | 1 mg/mL | 50 mL solution 100 mL solution | 135.0000 270.0000 | 75 mg/m2 every 3 weeks for a maximum of 3 cycles | 19.29 | 405 |
Gemcitabine (Generic) | 38 mg/mL | 26.3 mL solution 52.6 mL solution | 270.0000 540.0000 | 1,000 mg/m2 to 1,250 mg/m2 on day 1 and day 8 for three 21-day cycles | 25.71 | 540 |
Neoadjuvant nivolumab + cisplatin + gemcitabine | 361.61 | 7,594 | ||||
Neoadjuvant nivolumab + pemetrexed + cisplatinb | ||||||
Nivolumab (Opdivo) | 10 mg/mL | 4 mL vial 10 mL vial | 782.2200 1,955.5600 | 4.5 mg/kg every 3 weeks for a maximum of 3 cycles | 316.62 | 6,649 |
Cisplatin | 1 mg/mL | 50 mL solution 100 mL solution | 135.0000 270.0000 | 75 mg/m2 every 3 weeks for a maximum of 3 cycles | 19.29 | 405 |
Pemetrexed | 10 mg/mL | 10 mL vial 50 mL vial | 429.0000 2,145.0000 | 500 mg/m2 every 3 weeks for a maximum of 3 cycles | 204.29 | 4,290 |
Neoadjuvant nivolumab + pemetrexed + cisplatin | 540.18 | 11,344 | ||||
Neoadjuvant nivolumab + cisplatin + vinorelbineb | ||||||
Nivolumab (Opdivo) | 10 mg/mL | 4 mL vial 10 mL vial | 782.2200 1,955.5600 | 4.5 mg/kg every 3 weeks for a maximum of 3 cycles | 316.62 | 6,649 |
Cisplatin | 1 mg/mL | 50 mL solution 100 mL solution | 135.0000 270.0000 | 75 mg/m2 every 3 weeks for a maximum of 3 cycles | 19.29 | 405 |
Vinorelbine | 10 mg/mL | 1 mL vial 5 mL vial | 68.0000 340.0000 | 25 mg/m2 on day 1 and day 8 for three 21-day cycles | 32.38 | 680 |
Neoadjuvant nivolumab + cisplatin + vinorelbine | 368.28 | 7,734 | ||||
Neoadjuvant nivolumab + gemcitabine + carboplatinb | ||||||
Nivolumab (Opdivo) | 10 mg/mL | 4 mL vial 10 mL vial | 782.2200 1,955.5600 | 4.5 mg/kg every 3 weeks for a maximum of 3 cycles | 316.62 | 6,649 |
Carboplatin | 10 mg/mL | 5 mL vial 15 mL vial 45 mL vial 60 mL vial | 70.0000 210.0000 599.9850 775.0020 | AUC 5 to 6 every 3 weeks for a maximum of 3 cyclesc | 31.90 | 670 |
Gemcitabine (Generic) | 38 mg/mL | 26.3 mL solution 52.6 mL solution | 270.0000 | 1,000 mg/m2 on day 1 and day 8 for three 21-day cycles | 25.71 | 540 |
Neoadjuvant nivolumab + gemcitabine + carboplatin | 374.23 | 7,859 | ||||
Neoadjuvant nivolumab + paclitaxel + carboplatinb | ||||||
Nivolumab (Opdivo) | 10 mg/mL | 4 mL vial 10 mL vial | 782.2200 1,955.5600 | 4.5 mg/kg every 3 weeks for a maximum of 3 cycles | 316.62 | 6,649 |
Carboplatin (Generic) | 10 mg/mL | 5 mL vial 15 mL vial 45 mL vial 60 mL vial | 70.0000 210.0000 599.9850 775.0020 | AUC 5 to 6 every 3 weeks for a maximum of 3 cyclesc | 31.90 | 670 |
Paclitaxel | 6 mg/mL | 5 mL vial 16.7 mL vial 50 mL vial | 300.0000 1,196.8000 971.0000 | 175 mg/m2 to 200 mg/m2 every 3 weeks for a maximum of 3 cycles | 74.81 | 1,571 |
Neoadjuvant nivolumab + paclitaxel + carboplatin | 423.33 | 8,890 | ||||
Neoadjuvant nivolumab + pemetrexed + carboplatinb | ||||||
Nivolumab (Opdivo) | 10 mg/mL | 4 mL vial 10 mL vial | 782.2200 1,955.5600 | 4.5 mg/kg every 3 weeks for a maximum of 3 cycles | 316.61 | 6,649 |
Carboplatin | 10 mg/mL | 5 mL vial 15 mL vial 45 mL vial 60 mL vial | 70.0000 210.0000 599.9850 775.0020 | AUC 5 to 6 every 3 weeks for a maximum of 3 cyclesc | 31.90 | 670 |
Pemetrexed | 10 mg/mL | 10 mL vial 50 mL vial | 429.0000 2,145.0000 | 500 mg/m2 every 3 weeks for a maximum of 3 cycles | 204.29 | 4,290 |
Neoadjuvant nivolumab + pemetrexed + carboplatin | 552.80 | 11,609 | ||||
AUC = product of serum concentration (mg/mL) and time (min); CDA-AMC = Canada’s Drug Agency; NSCLC = non–small cell lung cancer.
Note: All prices are IQVIA DeltaPA wholesale list prices (accessed October 2024), unless otherwise indicated, and do not include dispensing fees or markups.29 Costs were calculated assuming a hypothetical patient weighing 73.7 kg with a body surface area of 1.9m2 and a glomerular filtration rate of 75.
aSponsor’s submitted price.1
bRecommended dose obtained from multiple Cancer Care Ontario Regimens:.48-52
cRecommended dose calculated using Calvert Formula: Dose (mg) = Target AUC x (glomerular filtration rate + 25).53
Appendix 2: Submission Quality
Please note that this appendix has not been copy-edited.
Description | Yes or no | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | Yes | No comment |
Model has been adequately programmed and has sufficient face validity | No | Refer to limitation regarding model transparency |
Model structure is adequate for decision problem | Yes | No comment |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | Yes | No comment |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | Yes | No comment |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | Yes | No comment |
Appendix 3: Additional Information on the Submitted Economic Evaluation
Please note that this appendix has not been copy-edited.

Detailed Results of the Sponsor’s Base Case
Table 7: Disaggregated Summary of the Sponsor’s Economic Evaluation Results
Parameter | Neoadjuvant pembrolizumab + chemotherapy and adjuvant pembrolizumab | Neoadjuvant chemotherapy | Neoadjuvant nivolumab + chemotherapy | Surgery only |
|---|---|---|---|---|
Discounted LYs | ||||
Total | 9.53 | 6.29 | 8.97 | 5.61 |
By health state or data source | ||||
Event free | 8.31 | 4.52 | 7.63 | 4.05 |
Local-regional recurrence or progression | 0.51 | 0.66 | 0.54 | 0.59 |
Distant metastasis | 0.72 | 1.10 | 0.80 | 0.97 |
Discounted QALYs | ||||
Total | 8.12 | 5.25 | 7.62 | 4.69 |
By health state or data source | ||||
Event free | 7.18 | 3.91 | 6.60 | 3.51 |
Local-regional recurrence or progression | 0.43 | 0.55 | 0.45 | 0.49 |
Distant metastasis | 0.51 | 0.79 | 0.57 | 0.69 |
AE-related disutility | –0.0040 | –0.0033 | –0.0016 | 0.00 |
Discounted costs ($) | ||||
Total | 268,346 | 254,323 | 208,689 | 227,767 |
Acquisition | 155,729 | 127,061 | 93,230 | 101,817 |
Administration | 756 | 807 | 746 | 517 |
Surgical care | 12,460 | 12,367 | 12,738 | 15,197 |
Radiotherapy | 5,301 | 7,949 | 5,359 | 7,318 |
Disease management | 24,624 | 32,377 | 26,182 | 28,579 |
Terminal care | 69,184 | 73,529 | 69,936 | 74,340 |
Adverse events | 291 | 234 | 497 | 0 |
LYs = life years; QALYs = quality-adjusted life-years
Source: Sponsor’s pharmacoeconomic submission.1
Appendix 4: Additional Details on the CDA-AMC Reanalyses and Sensitivity Analyses of the Economic Evaluation
Please note that this appendix has not been copy-edited.
CDA-AMC did not identify any key limitations which could be addressed by modifying the submitted economic evaluation. As a result, CDA-AMC did not conduct any additional analyses to assess the relative cost-effectiveness of neoadjuvant pembrolizumab in combination with platinum-based chemotherapy followed by adjuvant pembrolizumab for the treatment of adult patients with resectable stage II, IIIA, or IIIB (T3-4N2) NSCLC.
Appendix 5: Submitted BIA and CDA-AMC Appraisal
Please note that this appendix has not been copy-edited.
Table 8: Summary of Key Take-Aways
Key take-aways of the budget impact analysis |
|---|
|
CDA-AMC = Canada’s Drug Agency.
Summary of Sponsor’s BIA
The sponsor submitted a BIA estimating the budget impact of reimbursing pembrolizumab as neoadjuvant therapy in combination with platinum-containing chemotherapy followed by adjuvant pembrolizumab for the treatment of adult patients with resectable stage II, IIIA, or IIIB NSCLC. The BIA was undertaken from the perspective of Canadian public drug plans (excluding Quebec) and the Non-Insured Health Benefits program over a 3-year time horizon (2025 to 2027). An epidemiological approach was used to estimate the eligible number of patients in each year of the analysis.54 Key inputs to the BIA are documented in Table 9.
In the reference scenario, it was assumed that patients would receive 1 of the existing neoadjuvant regimens. This included neoadjuvant nivolumab or neoadjuvant chemotherapy. In the new drug scenario, it was assumed that perioperative pembrolizumab would slowly gain market share over the forecasted time horizon.54
Key assumptions:
Incident cases of lung cancer (by province) were obtained from the 2022, 2023, and 2024 versions of the Canadian Cancer Statistics report published by the Canadian Cancer Society.55-57 These were used to estimate an annual growth rate of 3.2% and predict the size of the starting population in 2025.
It was assumed that 88% of all lung cancer cases can be classified as NSCLC.58 Incidence estimates in Canada from 2023 were used to determine the proportion that were stage II (8.6%) or stage III (20.5%) at diagnosis.59 Among patients in stage III, 76.2% were assumed to be stage IIIA and 21.7% were assumed to be stage IIIB.60
Consistent with a prior review for adjuvant treatment of NSCLC, it was assumed that 60% of patients with NSCLC will be eligible for resection.61
Based on market research data in Canada, it was assumed that 43.8% of patients will be referred to a medical oncologist for neoadjuvant or perioperative treatment by a thoracic surgeon. This was calculated as the weighted average between the stage-specific referral rates (stage II = 39%, stage IIIA = 55%, stage IIIB = 14%) and the number of patients estimated to be in each stage.54,62
Based on market research data in Canada, it was assumed that 66.4% of patients referred to a medical oncologist will initiate neoadjuvant therapy. This was calculated as the weighted average between the proportion of patients, by stage, that begin neoadjuvant treatment (stage II = 79.5%, stage IIIA = 61.8%, stage IIIB = 57.1%) and the number of patients estimated to be in each stage.54,62
Table 9: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (year 1/year 2/year 3) |
|---|---|
Target population | |
Projected lung cancer cases | 22,110 |
Proportion of patients with NSCLC | 88% |
NSCLC stage at diagnosis | 8.6% (stage II); 20.5% (stage III) |
Stage III substage at diagnosis | 76.2% (stage IIIA); 21.7% (stage IIIB) |
Proportion that is resectable | 60% |
Referred for neoadjuvant-perioperative treatment | 43.8% |
Proportion eligible for treatment | 66.4% |
Number of patients eligible for drug under review | 1,030/1,062/1,096 |
Market uptake (3 years) | |
Uptake (reference scenario) | |
Neoadjuvant nivolumab | 80%/80%/80% |
Neoadjuvant chemotherapy | 20%/20%/20% |
Uptake (new drug scenario) | |
Perioperative pembrolizumab | ███████████ |
Neoadjuvant nivolumab | ███████████ |
Neoadjuvant chemotherapy | ███████████ |
Cost of treatment (per patient, per 21-day cycle) | |
Perioperative pembrolizumaba | $11,919 (neoadjuvant); $8,800 (adjuvant) |
Neoadjuvant nivolumabb | $10,669 |
Neoadjuvant chemotherapyc | $3,118 |
NSCLC = non–small cell lung cancer.
aNeoadjuvant pembrolizumab calculated as a weighted sum with the following treatment combinations: cisplatin (100%); gemcitabine (44%) or pemetrexed (56%).
bNeoadjuvant nivolumab calculated as a weighted sum with the following treatment combinations: cisplatin (58%) or carboplatin (42%); gemcitabine (27.3%), pemetrexed (45.4%) or paclitaxel (27.3%). Costs for optional adjuvant therapy are not reported.
cNeoadjuvant chemotherapy calculated as a weighted sum with the following treatment combinations: cisplatin (100%); gemcitabine (44%) or pemetrexed (56%).
Source: Sponsor’s budget impact analysis.54
Summary of the Sponsor’s BIA Results
The net budget impact of pembrolizumab for the neoadjuvant treatment of adults with resectable stage II, IIIA, or IIIB NSCLC was $931,612 in year 1, $6,329,996 in year 2, and $10,092,729 in year 3. The 3-year net budget impact was estimated to be $17,354,337.
CDA-AMC Appraisal of the Sponsor’s BIA
CDA-AMC identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
Market uptake of pembrolizumab is underestimated: In the new drug scenario, the sponsor assumed that the market share of neoadjuvant pembrolizumab would be ███ in year 1, ███ in year 2, and ███ in year 3. Clinical experts consulted by CDA-AMC anticipated that perioperative pembrolizumab would obtain a much larger market share in the short-term. The underestimation of the market update may have meaningful impacts on the BIA, as a higher market share would correspond to a larger budget impact for perioperative pembrolizumab.
CDA-AMC conducted a scenario analysis which explored the impact of a larger market share for perioperative pembrolizumab. It was assumed that a market share of 33% would be reached for all 3 years of the BIA.
CDA-AMC Reanalyses of the BIA
In the absence of more reliable estimates to inform the parameters of the BIA, the sponsor’s base case was maintained. CDA-AMC expects that the budget impact of perioperative pembrolizumab will be sensitive to the inputs and assumptions that affect the market size calculated or anticipated market uptake. This is reflected in a scenario analysis conducted by CDA-AMC which explored how a larger market uptake would affect the budget impact. In this scenario, a 33% market share was assumed for perioperative pembrolizumab in all 3 years of the BIA.
Table 10: CDA-AMC Revisions to the Submitted BIA
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
1. Pembrolizumab market share | ██ (year 1); ███ (year 2); ███ (year 3) | 33% |
2. Pembrolizumab unit price | $4,400 | 30% reduction ($3,080) |
BIA = budget impact analysis; CDA-AMC = Canada’s Drug Agency.
The results of the CDA-AMC stepwise reanalysis are presented in summary format in Table 11 and a more detailed breakdown is presented in Table 12. All analyses were based on publicly available prices of the comparator treatments. In the market share scenario analysis, the 3-year net budget impact of perioperative pembrolizumab was estimated to be $71,873,074. This increase illustrates how the budget impact is sensitive to market share assumptions.
An additional scenario analysis was conducted to explore how the budget impact would be affected by the price reduction identified in the economic evaluation. Assuming a 30% price reduction for pembrolizumab, the net budget impact of perioperative pembrolizumab was estimated to be $10,665,174.
Table 11: Summary of the CDA-AMC Reanalyses of the BIA
Stepped analysis | Three-year total ($) |
|---|---|
Submitted base case | 17,354,337 |
CDA-AMC scenario 1: Pembrolizumab market share | 71,873,074 |
CDA-AMC scenario 2: 30% price reduction | 10,665,174 |
BIA = budget impact analysis; CDA-AMC = Canada’s Drug Agency.
Table 12: Detailed Breakdown of the CDA-AMC Reanalyses of the BIA
Stepped analysis | Scenario | 2024 (current situation) ($) | 2025 ($) | 2026 ($) | 2027 ($) | Three-year total ($) |
|---|---|---|---|---|---|---|
Submitted base case | Reference | 30,800,054 | 49,056,471 | 66,450,801 | 82,743,636 | 198,250,908 |
New drug | 30,800,054 | 49,988,083 | 72,780,797 | 92,836,365 | 215,605,245 | |
Budget impact | 0 | 931,612 | 6,329,996 | 10,092,729 | $17,354,337 | |
CDA-AMC scenario analysis 1: 33% market share | Reference | 30,800,054 | 49,056,471 | 66,450,801 | 82,743,636 | 198,250,908 |
New drug | 30,800,054 | 61,662,331 | 97,582,208 | 110,879,443 | 270,123,982 | |
Budget impact | 0 | 12,605,861 | 31,131,407 | 28,135,807 | 71,873,074 | |
CDA-AMC scenario analysis 2: 30% price reduction | Reference | 30,646,433 | 47,331,430 | 61,754,607 | 74,512,253 | 183,598,291 |
New drug | 30,646,433 | 47,845,806 | 65,630,268 | 80,787,390 | 194,263,464 | |
Budget impact | 0 | 514,376 | 3,875,661 | 6,275,137 | 10,665,174 |
BIA = budget impact analysis; CDA-AMC = Canada’s Drug Agency.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@cda-amc.ca.