Drugs, Health Technologies, Health Systems
Reimbursement Review
Polatuzumab Vedotin (Polivy)
Sponsor: BC Cancer Lymphoma and Myeloma Tumour Group
Therapeutic area: Large B-cell lymphoma
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
TPA Review
Clinical Review
Abbreviations
AE
adverse event
ABC
activated B cell–like
CAR
chimeric antigen receptor
CDA-AMC
Canada’s Drug Agency
CI
confidence interval
COO
cell of origin
CNS
central nervous system
DAC
Drug Advisory Committee
DLBCL
diffuse large B-cell lymphoma
EBV
Epstein-Barr virus
ECOG PS
Eastern Cooperative Oncology Group Performance Status
EPOCH-R
etoposide, doxorubicin, vincristine, cyclophosphamide, prednisone, and rituximab
G-CSF
granulocyte colony-stimulating factor
GCB
germinal centre B cell
GEP
gene expression profiling
HR
hazard ratio
HRQoL
health-related quality of life
IHC
immunohistochemistry
IPI
International Prognostic Index
ITT
intention to treat
LBCL
large B-cell lymphoma
LC-SAB
Lymphoma Canada Scientific Advisory Board
MMAE
monomethyl auristatin E
NHL
non-Hodgkin lymphoma
NOS
not otherwise specified
OS
overall survival
PFS
progression-free survival
pola-R-CHP
polatuzumab vedotin, rituximab, cyclophosphamide, doxorubicin, and prednisone
QoL
quality of life
R-CHP
rituximab, cyclophosphamide, doxorubicin, and prednisone
R-CHOP
rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone
SOC
standard of care
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Table 1: Background Information of Application Submitted for Review
Item | Description |
|---|---|
Drug product | Polatuzumab vedotin (Polivy), 30 mg or 140 mg single-use vial, lyophilized powder for solution for IV infusion |
Sponsor | BC Cancer Lymphoma and Myeloma Tumour Group; Hoffmann-La Roche Ltd. (submitting consultant) |
Indication | Polivy (polatuzumab vedotin) in combination with R-CHP, indicated for the treatment of adult patients with previously untreated LBCL, including DLBCL NOS, high grade B-cell lymphoma, EBV-positive DLBCL NOS, and T-cell/histiocyte rich LBCL |
Reimbursement request | Polivy (polatuzumab vedotin) in combination with R-CHP, indicated for the treatment of adult patients with previously untreated LBCL, including DLBCL NOS, high-grade B-cell lymphoma, EBV-positive DLBCL NOS, and T-cell/histiocyte-rich LBCL that are classified as activated B-cell–like (ABC) lymphoma subtype |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | November 14, 2022 |
Recommended dose | Patients with previously untreated LBCL: Polivy 1.8 mg/kg given as an IV infusion every 21 days for 6 cycles in combination with R-CHP. Polivy, rituximab, cyclophosphamide, and doxorubicin can be administered in any order on day 1 after administration of prednisone. Prednisone is administered on days 1 to 5 of each cycle. Cycles 7 and 8 consist of rituximab as monotherapy. |
DLBCL = diffuse large B-cell lymphoma; EBV = Epstein-Barr virus; NOC = Notice of Compliance; NOS = not otherwise specified; LBCL = large B-cell lymphoma; R-CHP = rituximab, cyclophosphamide, doxorubicin, and prednisone.
Introduction
An estimated 11,700 people in Canada were expected to be diagnosed with non-Hodgkin lymphoma (NHL) and 3,100 people were expected to die from it in 2024.1 Large B-cell lymphoma (LBCL) is a type of NHL that has histologic, proteomic, and molecular subsets with distinctive prognostic profiles, including cell of origin (COO) activated B-cell–like (ABC) and germinal centre B-cell–like (GCB) subtypes, elevated protein expression of MYC and BCL2 seen in double-expressor lymphoma, and gene rearrangements involving MYC and BCL2 and/or BCL6 (double-hit lymphoma or triple-hit lymphoma).2-6 Diffuse large B-cell lymphoma (DLBCL), not otherwise specified (NOS), is the most common subtype of LBCL, accounting for 35% of NHL cases and 80% of aggressive lymphomas.7,8 DLBCL may be classified as a limited-stage disease (stage I or II) or advanced-stage disease (stage III or IV); approximately two-thirds of patients with DLBCL present with stage III or IV disease.9 Patients with LBCL experience debilitating symptoms and psychosocial impacts (e.g., fatigue, drenching night sweats, loss of appetite, anxiety, and depression) that negatively affect their health-related quality of life (HRQoL). Evaluations of patients with newly diagnosed DLBCL to determine treatment options include assessment of disease stage, comorbid conditions and performance status, cytogenetic or molecular features, risk of central nervous system (CNS) involvement, and International Prognostic Index (IPI) score.9 First-line treatment of DLBCL is 6 cycles of rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP) for those with high-risk and advanced-stage disease and for a proportion of those with limited-stage disease (e.g., aged younger than 60 years, bulky disease and an Eastern Cooperative Oncology Group Performance Status [ECOG PS] score of 2 to 4).9-11 While treatment with R-CHOP can be curative in approximately 60% of patients with DLBCL,10,12,13 about 40% of patients relapse or experience disease progression.8,14,15 The clinical experts consulted for this review noted that patients with refractory disease or early relapse may proceed to salvage therapy (e.g., stem-cell transplant or chimeric antigen receptor [CAR] T-cell therapy), which is associated with increased toxicity, poor outcomes, and increased costs.
Health care centres across Canada do not have routine access to COO-based molecular testing with gene expression profiling (GEP) to determine ABC lymphoma subtype,16-18 and instead rely on immunohistochemistry (IHC) with the Hans algorithm as a surrogate to dichotomize LBCL into GCB and non-GCB subtypes, with the latter representing primarily the ABC subtype.19,20 However, the limited diagnostic accuracy of immunostaining algorithms warrant caution when using it to guide treatment.21 The clinical experts consulted for the review emphasized that non-GCB subtypes of LBCL are more likely to have high-risk disease features (e.g., advanced-stage disease at diagnosis or an IPI score of 3 to 5) that is associated with higher rates of relapse and less-favourable prognosis compared to those with the GCB subtype.9 Patients with the ABC subtype of LBCL experience significantly poorer outcomes with standard upfront chemoimmunotherapy.22-29 Because there is no specific approach to treating patients with the ABC lymphoma subtype, the current treatment paradigm for patients with LBCL, regardless of COO classification, is R-CHOP for 6 cycles.11 According to the clinical experts, the goals of treatment for DLBCL are cure or prolonging survival, minimizing treatment-related toxicities, alleviating disease-related symptom burdens, and maintaining HRQoL; patients with high-risk disease (e.g., those with an IPI score of 3 to 5 or an ABC subtype) need improved front-line treatment options to achieve cure and avoid the need for toxic salvage therapies.
Basis of Resubmission
A previous review by Canada’s Drug Agency (CDA-AMC) of polatuzumab vedotin, rituximab, cyclophosphamide, doxorubicin, and prednisone (pola-R-CHP) for the treatment of adult patients with previously untreated LBCL, including DLBCL NOS, high-grade B-cell lymphoma, Epstein-Barr virus (EBV)-positive DLBCL NOS, and T-cell/histiocyte-rich LBCL, received a recommendation not to reimburse in December 2023.30 Key reasons for the recommendation included uncertainty in whether the between-group difference in progression-free survival (PFS) at 24 months was clinically meaningful and a lack of demonstrated benefit in overall survival (OS) based on evidence from the POLARIX trial. Additionally, the pan-Canadian Oncology Drug Review Expert Review Committee could not conclude that treatment with pola-R-CHP would meaningfully prolong remission compared with standard of care (SOC) R-CHOP. The committee also could not reach conclusions regarding the effects of pola-R-CHP compared to R-CHOP on disease symptoms, normalized blood counts, or HRQoL.
The sponsor’s rationale for the resubmission of polatuzumab vedotin pointed out that patients with the ABC subtype of LBCL experience poorer outcomes with SOC R-CHOP and would therefore benefit from treatment with pola-R-CHP. The sponsor submitted an exploratory subgroup analysis of the POLARIX trial according to COO status, including a cohort of patients with the ABC lymphoma subtype. The sponsor also indicated that, because the ABC subtype of LBCL is more common in older adults who may not be candidates for second- or later-line treatment options, the potential for curative first-line treatment is important in this patient population. While the sponsor included a subgroup analysis of COO status for PFS at the 2-year follow-up (unstratified results with a forest plot) in the original polatuzumab vedotin submission, new evidence provided in the resubmission pertaining to the ABC lymphoma subtype included the following: patient information (study disposition, baseline characteristics, treatment exposure, concomitant treatments, and new antilymphoma treatments), efficacy results (PFS at 2 years and 5 years [stratified results with a Kaplan-Meier plot] and OS at 2 years [stratified results] and at 5 years [stratified results with a Kaplan-Meier plot]), and harms.
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of pola-R-CHP for the treatment of adult patients with previously untreated LBCL, including DLBCL NOS, high-grade B-cell lymphoma, EBV-positive DLBCL NOS, and T-cell/histiocyte-rich LBCL that are classified as the ABC lymphoma subtype. The focus of the review of the resubmission is to appraise the evidence for the subgroup of patients with the ABC subtype of LBCL. Clinical evidence from the original review of polatuzumab vedotin that focused on the overall LBCL population is discussed in this Clinical Review Report to provide context for the new clinical evidence that was reviewed and appraised as part of the resubmission (refer to the Discussion section).
Perspectives of Patient, Clinicians, and Drug Programs
The information in this section is a summary of input provided by the patient and clinician groups who responded to our call for input and from 2 clinical experts consulted for this review.
Patient Input
Lymphoma Canada provided input from an online survey of patients with LBCL (n = 89). Lymphoma Canada is a national registered charity that empowers the lymphoma community through education, support, advocacy, and research. Information from the survey was used to identify the main areas of concern for patients with LBCL. Subtype of LBCL according to COO status was not identified for the respondents. Most patients lived in Canada (94%) and were aged 55 years to 74 years (64%). The breakdown by sex was 58% female and 42% male. Most (61%) were diagnosed with DLBCL (89%) 1 year to 5 years ago.
Symptoms that affected quality of life (QoL) among patients with LBCL included fatigue, bodily aches and pain, night sweats, enlarged lymph nodes, reduced appetite, and headaches. Patients experienced mental health challenges, including fear of progression or relapse, stress of having cancer, and anxiety or worry. Patients also identified activities that affected their daily life, such as their ability to exercise, travel, spend time with family, volunteer, and attend work or school.
More survey respondents indicated that they received 2 or more lines of therapy compared with those who received first-line therapy. In the first-line setting, 48% of patients received chemoimmunotherapy with R-CHOP, while others received rituximab, cyclophosphamide, doxorubicin, and prednisone (R-CHP) or etoposide, doxorubicin, vincristine, cyclophosphamide, prednisone, and rituximab (EPOCH-R). While 28% of patients were satisfied with their first-line treatment options and 57% were very satisfied with the number of available treatment options, 15% expressed dissatisfaction with the available options. Many patients reported no difficulty accessing treatment for their lymphoma in Canada; however, many other patients reported having challenges such as delays, cost of travelling long distances for treatment, absence from work, and the financial burden of drugs for treatment and supplementary drugs for managing side effects.
Of the 4 individuals with experience with pola-R-CHP treatment, 2 patients reported a good overall experience and 3 patients indicated that they would recommend the treatment to other individuals with LCBL. Side effects of pola-R-CHP treatment reported by at least 2 patients included fatigue, neutropenia, thrombocytopenia, decreased appetite, and diarrhea.
Most patients agreed that there was a need for more treatment options for those with LBCL. Many patients were willing to tolerate side effects to access new treatment and sought a choice in their selection of treatment. Factors important to LBCL patients when considering new treatments included longer disease remission, controlled disease symptoms, longer survival, normalized blood counts, and improved QoL to enable activities of daily living.
Clinician Input
Input From Clinical Experts Consulted for This Review
Two clinical specialists provided input on the diagnosis and management of LBCL. The clinical experts noted that, although many patients with LBCL experience cure with R-CHOP as a first-line SOC treatment, many patients with high-risk disease (i.e., an IPI score of 3 to 5 or the ABC lymphoma subtype) experience poor outcomes with SOC. The clinical experts reported that patients with the non-GCB lymphoma subtype (mostly the ABC lymphoma subtype) commonly exhibit high-risk disease features (e.g., a high IPI score) and, compared with the GCB subtype, high-risk molecular features are associated with poorer outcomes using SOC treatment for LBCL.22-29 Furthermore, patients with refractory disease or early relapse require salvage therapy (e.g., stem-cell transplant, CAR T-cell therapy, or bispecific T-cell engager therapy), which is intensive, toxic, costly, and has limited curative potential. The experts indicated that patients with high-risk LBCL, regardless of subtype, would benefit from more efficacious first-line treatments that avoid the need for toxic salvage therapies. The current treatment in the first-line setting for patients with ABC lymphoma, 6 cycles of R-CHOP, is the same as for patients with LBCL regardless of subtype. The experts anticipated that, if approved, pola-R-CHP would supplant R-CHOP as the SOC, resulting in a shift in the current treatment paradigm for patients with ABC COO. The clinical experts indicated that all patients who are eligible for treatment with R-CHOP (those who are generally fit and without significant comorbidities), including patients with ABC lymphoma, would be suited for treatment with pola-R-CHP. Individuals considered ineligible for treatment with pola-R-CHP due to its toxicity include those with reduced cardiac function (e.g., a smaller ejection fraction) and/or significant comorbidities, and those for whom other treatments are more appropriate (e.g., more intensive treatments for patients with double-hit or double-expressor lymphoma).
According to the clinical experts, eligibility for treatment with pola-R-CHP according to the proposed reimbursement population requires COO determination to ascertain ABC subtype. In Canada, COO testing is routinely conducted using IHC-based testing with the Hans algorithm. IHC testing distinguishes GCB from non-GCB subtypes and, while it has demonstrated high concordance with GEP (the gold standard for COO diagnostic testing), it is regarded as a proxy for identifying the ABC lymphoma subtype. However, misclassification can occur in approximately 10% to 15% of patients.31
According to the experts, treatment response is assessed radiographically at 2 time points: after 3 or 4 cycles of treatment (with a CT scan) and at the end of treatment (with a PET scan). Upon attaining remission at end of treatment, patients are monitored every 3 months clinically (e.g., physical examination, symptom assessment, laboratory testing) to screen for relapses, with any additional imaging assessments guided by the clinical assessment. The experts reported that, because of the low likelihood of disease relapse 2 years after completing treatment, patients are generally followed up for at least 2 years (or up to 5 years after completing treatment). Most patients who have not experienced disease progression or relapse for 2 years are considered to be cured of their disease. Routine patient imaging is not typically conducted after complete disease remission. The experts noted that, because the goal of treatment for DLBCL is cure, OS is the most important outcome for patients, although PFS is also a critical outcome to assess given that disease progression or relapse is common within the first 2 years of treatment. According to the clinical experts, treatment would be discontinued in patients with the ABC subtype of LBCL due to lack of efficacy or unacceptable toxicity. The clinical experts indicated that it would be appropriate for any hematologist or oncologist who treats DLBCL in a community or tertiary care centre to manage patients with ABC lymphoma using pola-R-CHP. The clinical experts reiterated that restricting polatuzumab vedotin treatment to those with ABC lymphoma would be impractical based on current diagnostic testing practices in Canada (IHC with the Hans algorithm) and potentially inequitable due to the exclusion of eligible patients who would otherwise benefit from this treatment (e.g., patients with high-risk LBCL, including those with non-GCB lymphoma and/or an IPI score of 3 to 5).
Clinician Group Input
Two clinician groups provided input for this submission: the Lymphoma Canada Scientific Advisory Board (LC-SAB) comprising 9 clinicians with expertise in lymphoid cancer and the Ontario Health (Cancer Care Ontario) (OH [CCO]) Hematology Cancer Drug Advisory Committee (DAC) comprising 7 clinicians. The clinician groups were aligned with the clinical experts in identifying patients at high risk of poor response to SOC R-CHOP chemoimmunotherapy (e.g., advanced disease stage, IPI score of 2 to 5, relapsed or refractory disease), including patients with the ABC lymphoma subtype, as individuals who would benefit from treatment with pola-R-CHP. Both the LC-SAB and OH-CCO Hematology Cancer DAC agreed with the clinical experts that pola-R-CHP would replace R-CHOP in the first-line setting for treatment of patients with ABC lymphoma subtype. Whereas OH-CCO Hematology Cancer DAC reported that an outpatient setting would be most appropriate for treatment administration, the LC-SAB agreed with the clinical experts that any site that currently administers R-CHOP would be appropriate for managing patients with pola-R-CHP. The LC-SAB emphasized that, because polatuzumab vedotin has been approved in combination with bendamustine and rituximab for the treatment of relapsed or refractory DLBCL, there is broad experience with the drug and in a combination chemotherapy regimen.
Drug Program Input
Input was obtained from the drug programs that participate in the CDA-AMC reimbursement review process on relevant comparators, considerations for initiation and for prescribing of therapy, generalizability, funding algorithm, care provision issues, and system and economic issues (refer to Table 4).
Clinical Evidence
Systematic Review
Description of Study
One phase III, multicentre, randomized, double-blind, placebo-controlled trial (POLARIX) assessed the efficacy and safety of pola-R-CHP compared with SOC R-CHOP in the first-line treatment of adults with previously untreated LBCL, including DLBCL NOS, high-grade B-cell lymphoma, EBV-positive DLBCL NOS, and T-cell/histiocyte-rich LBCL. The focus of this resubmission of polatuzumab vedotin was a subgroup of patients in the POLARIX trial who have the ABC lymphoma subtype. In the POLARIX trial, investigator-assessed PFS was the primary outcome, and OS was a key secondary outcome. OS and PFS were exploratory outcomes in the subgroup analyses of patients with ABC lymphoma subtype. Treatment-emergent adverse events (AEs), serious AEs, including AEs of grade 3 or higher, withdrawals due to AEs, deaths, and AEs of special interest were reported for the ABC subpopulation.
Patients with the ABC lymphoma subtype (N = ███) accounted for █████ of the overall population in the POLARIX trial. The median age of patients with ABC lymphoma was ██ years (range, ██ █████ ██ ██ █████). At baseline, patients had an ECOG PS of 0 (█████), 1 (█████), and 2 (█████). Patients had disease designated as Ann Arbor stage I (████), II (█████), III (█████), or IV (█████). At screening, more patients had an IPI score of 3 to 5 (█████) than 1 to 2 (█████). Bulky disease was present at baseline in █████ of patients but absent in █████ of patients. Most patients were negative for double-hit or triple-hit lymphoma (█████). In addition to stratified randomization factors (IPI score, bulky disease, and geographical location), the treatment groups were generally similar in demographics and disease characteristics. However, more patients had disease designated as Ann Arbor stage III in the pola-R-CHP group (█████) compared with the R-CHOP group (█████) whereas fewer patients had Ann Arbor stage IV disease in the pola-R-CHP group (█████) compared with the R-CHOP group (█████). Additionally, fewer patients had 2 or more extranodal disease sites in the pola-R-CHP group (█████) compared with the R-CHOP group (█████).
Efficacy Results
Key efficacy results for patients with the ABC lymphoma subtype in the POLARIX trial are summarized in Table 2. The analysis population for OS and PFS included randomized patients regardless of treatment received (the intention to treat [ITT] population) who had an evaluable COO status at baseline. Patients with ABC lymphoma were included as a subgroup for analysis by COO status and followed to the clinical cut-off date of June 15, 2022, for PFS (included as a forest plot in the original submission for polatuzumab vedotin). The sponsor supplemented its resubmission with Kaplan-Meier estimates of OS and PFS at this follow-up. The resubmission also provided OS and PFS data for long-term follow-ups of patients with the ABC lymphoma subtype at the clinical cut-off date of July 5, 2024, and these data were included in this report.
Overall Survival
██ ██████ █████████ █████ ███████ ██ ████ ███ ██████ ███ ██████ ██ ███ ███ ████ ███████ ██ ██████ ███ ██████████ █████ ██ ███ ██████ ██████. The 2-year OS was 91.4% in the pola-R-CHP group versus 87.11% in the R-CHOP group, with a difference of 4.3% (stratified hazard ratio [HR] = 0.46; 95% confidence interval [CI], 0.23 to 0.92). At the 5-year follow-up (data cut-off of July 5, 2024), the median duration of follow-up was 63.9 months (range, 0 months to 73 months) in the pola-R-CHP group and 64.2 months (range, 1 month to 78 months) in the R-CHOP group. Median OS had not been reached in the pola-R-CHP group or the R-CHOP group. The 5-year OS was 84.6% in the pola-R-CHP group versus 69.9% in the R-CHOP group, with a difference of 14.7% (stratified HR = 0.49; 95% CI, 0.27 to 0.90). Analyses of OS were uncontrolled for multiplicity and considered supportive.
Investigator-Assessed Progression-Free Survival
██ ██████ ██████████ ███ ██████ ████████ ██ █████████ ███ ████ ██████ ███████ █ ██████ ██ ██ ███████ ██ ███ ██████████ █████ ███ ██████ ████ ██████ ███████ █ ██████ ██ ██ ███████ ██ ███ ██████ ███████████ █████████████████████ ███ ███ ███ ████ ███████ ██ ███ ██████████ ██████ ███ ███ ██████ ███ ███ ████ ██████ ████ ███ ████ ██████ ██ ███ ██████████ ██ ███ ██████ ██████. The 2-year investigator-assessed PFS was 84.7% in the pola-R-CHP group versus 55.7% in the R-CHOP group, with a difference of 29.0% (stratified HR = 0.31; 95% CI, 0.18 to 0.52). At 5-year follow-up, the median duration of follow-up was 55.0 months (range, 0 to 71 months) in the pola-R-CHP group and median 56.1 months (range, 0 to 68 months) in the R-CHOP group. Median investigator-assessed PFS was 70.5 months (95% CI not estimable) in the pola-R-CHP group, compared with 33.2 months (95% CI, 18.9 months to 66.7 months) in the R-CHOP group. The 5-year investigator-assessed PFS was 72.5% in the pola-R-CHP group versus 45.8% in the R-CHOP group, with a difference of 26.7% (stratified HR = 0.33; 95% CI, 0.21 to 0.53). Analyses of investigator-assessed PFS were uncontrolled for multiplicity and considered supportive.
Harms Results
Key harms data for patients with the ABC lymphoma subtype in the POLARIX trial are summarized in Table 2. The analysis population for harms included all patients who received at least 1 dose of study treatment, with patients grouped according to the treatment received. Safety data were from the 5-year follow-up data.
In the ABC subpopulation, the numbers of patients who experienced at least 1 treatment-emergent AE were 105 of 106 patients (99.1%) in the pola-R-CHP group and 127 of 129 patients (98.4%) in the R-CHOP group. Of the patients who experienced at least 1 grade 3 to 5 AE, 70 (66.0%) were in the pola-R-CHP group and 81 (62.8%) were in the R-CHOP group. Of the patients who experienced serious AEs, 34 (32.1%) were in the pola-R-CHP group and 38 (29.5%) were in the R-CHOP group. Of the patients who stopped treatment due to AEs, 7 (6.6%) were in the pola-R-CHP group and 11 (8.5%) were in the R-CHOP group. Types of treatment-emergent AEs, serious AEs, and the reasons for treatment discontinuation due to AEs were not specified. Of the patients who died, 17 (16.0%) were in the pola-R-CHP group and 39 (30.2%) were in the R-CHOP group. Reasons for deaths in the pola-R-CHP and R-CHOP groups were progressive disease (7.5% and 17.1%, respectively), an AE (4.7% and 6.2%, respectively), and unspecified (3.8% and 7.0%, respectively).
Table 2: Summary of Key Results in the POLARIX Study
Outcome measure | POLARIX ABC subpopulation | |
|---|---|---|
Pola-R-CHP (N = 106) | R-CHOP (N = 129) | |
OS (global ITT analysis set) | ||
Data cut-off date | June 15, 2022 | |
Median follow-up duration, months (range) | ██ | ██ |
Patients with events, n (%) | ██ ██████ | ██ ██████ |
Censored, n (%) | ██ ██████ | ██ ██████ |
Time to OS (months), median (95% CI) | ██ ████ | ██ ████ |
Unstratified HR (95% CI)a | ████ █████ | █████████ |
P valueb | ██████ | █████████ |
Stratified HR (95% Cl)c | ████ ████ | █████████ |
P valued | ██████ | █████████ |
OS at 24 months | ||
Patients remaining at risk at 24 months, n (%) | ██ ██████ | ███ ██████ |
24-month OS rate (95% CI) | █████ ████ | ███ ██ ██████ |
Difference in OS rate at 24 months (95% CI) | ███ ████████ | █████████ |
Data cut-off date | July 5, 2024 | |
Median follow-up duration, months (range) | 63.9 (0 to 73) | 64.2 (1 to 78) |
Patients with events, n (%) | 17 (16.0) | 38 (29.5) |
Censored, n (%) | 89 (84.0) | 91 (70.5) |
Time to OS (months), median (95% CI) | NE (NE) | NE (NE) |
Unstratified HR (95% CI)a | 0.49 (0.28 to 0.88) | Reference |
P valueb | 0.0136 | Reference |
Stratified HR (95% Cl)c | 0.49 (0.27 to 0.90) | Reference |
P valued | 0.0190 | Reference |
OS at 60 months | ||
Patients remaining at risk at 60 months, n (%) | 81 (76.4) | 82 (63.6) |
60-month OS rate (95% CI) | 84.59 (77.64 to 91.54) | 69.89 (61.76 to 78.02) |
Difference in OS rate at 60 months (95% CI) | 14.70 (4.00 to 25.39) | Reference |
Investigator-assessed PFS (global ITT analysis set) | ||
Data cut-off date | June 15, 2022 | |
Median follow-up duration, months (range) | ████ ██ ██ | ████ ██ ██ |
Patients with investigator-assessed PFS events, n (%) | ██ ██████ | ██ ██████ |
Disease progression, n (%) | ██ ██████ | ██ ██████ |
Death, n (%) | █████ | █████ |
Censored, n (%) | ██ ██████ | ██ ██████ |
Time to investigator-assessed PFS (months), median (95% CI) | ██ █████ ██ ███ | ████ █████ |
Unstratified HR (95% CI)a | ███████ █████ | █████████ |
P valueb | ██████ | █████████ |
Stratified HR (95% CI)c | ████ █████ | █████████ |
P valued | ██████ | █████████ |
PFS at 24 months | ||
Patients remaining at risk at 24 months, n (%) | ██ ██████ | ██ ██████ |
24-month PFS rate (95% CI) | ███ ██ ██████ | ██ ██ ██████ |
Difference in PFS rate at 24 months (95% CI)e | ███ ██ ██████ | █████████ |
Data cut-off date | July 5, 2024 | |
Median follow-up duration, months (range) | 55.0 (0 to 71) | 56.1 (0 to 68) |
Patients with investigator-assessed PFS events, n (%) | 28 (26.4) | 69 (53.5) |
Disease progression, n (%) | 17 (16.0) | 58 (45.0) |
Death, n (%) | 11 (10.4) | 11 (8.5) |
Censored, n (%) | 78 (73.6) | 60 (46.5) |
Time to investigator-assessed PFS (months), median (95% CI) | 70.5 (NE) | 33.2 (18.9 to 66.7) |
Unstratified HR (95% CI)a | 0.38 (0.24 to 0.59) | Reference |
P valueb | < 0.0001 | Reference |
Stratified HR (95% CI)c | 0.33 (0.21 to 0.53) | Reference |
P valued | < 0.0001 | Reference |
PFS at 60 months | ||
Patients remaining at risk at 60 months, n (%) | 28 (26.4) | 26 (20.2) |
60-month PFS rate (95% CI) | 72.46 (62.82 to 82.10) | 45.78 (36.47 to 55.08) |
Difference in PFS rate at 60 months (95% CI)e | 26.69 (13.29 to 40.09) | Reference |
Harms (safety analysis set) | ||
Data cut-off date | July 5, 2024 | |
N | 106 | 129 |
Treatment-emergent AEs, n (%) | 105 (99.1) | 127 (98.4) |
Serious AEs, n (%) | 34 (32.1) | 38 (29.5) |
Treatment discontinuations due to AEs, n (%) | 7 (6.6) | 11 (8.5) |
Deaths, n (%) | 17 (16.0) | 39 (30.2) |
Notable harms, n (%) | ||
Peripheral neuropathy | 56 (52.8) | 65 (50.4) |
Neutropenia | 56 (52.8) | 60 (46.5) |
Febrile neutropenia | 20 (18.9) | 7 (5.4) |
Infections | 58 (54.7) | 54 (41.9) |
Anemia | 30 (28.3) | 33 (25.6) |
Infusion-related reactions | 13 (12.3) | 25 (19.4) |
Thrombocytopenia | 16 (15.1) | 16 (12.4) |
Hepatic toxicity | 13 (12.3) | 10 (7.8) |
Tumour lysis syndrome | 1 (0.9) | 2 (1.6) |
Progressive multifocal leukoencephalopathy | 0 | 0 |
ABC = activated B cell–like; AE = adverse event; CI = confidence interval; HR = hazard ratio; ITT = intention to treat; NE = not estimable; NR = not reported; OS = overall survival; PFS = progression-free survival; pola-R-CHP = polatuzumab vedotin, rituximab, cyclophosphamide, doxorubicin, and prednisone; R-CHOP = rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone.
aBased on Kaplan-Meier estimates with 95% CI for median computed using the Brookmeyer and Crowley method.
bBased on an unstratified Cox regression model.
cOne-sided P value based on an unstratified log-rank test. P value has not been adjusted for multiplicity.
dBased on a stratified Cox regression model with stratification factors for geographical region and IPI score, and bulky disease defined as 1 lesion of 7.5 cm or larger.
eOne-sided P value based on a stratified log-rank test. P value has not been adjusted for multiplicity.
Sources: POLARIX Clinical Study Report.32 Details included in the table were additional data provided from the sponsor.33
Notable Harms
Of the patients in the ABC subpopulation who experienced peripheral neuropathy, 56 (52.8%) were in the pola-R-CHP group and 65 (50.4%) were in the R-CHOP group. Of the patients who experienced neutropenia, including febrile neutropenia, 56 (52.8%) were in the pola-R-CHP group and 60 (46.5%) were in the R-CHOP group. Of the patients who experienced infections, 58 (54.7%) were in the pola-R-CHP group and 54 (41.9%) were in the R-CHOP group. Of the patients who experienced anemia, 30 (28.3%) were in the pola-R-CHP group and 33 (25.6%) were in the R-CHOP group.
Critical Appraisal
Findings for PFS and OS for the ABC subpopulation were based solely on exploratory subgroup analyses that, in principle, should be interpreted as hypothesis-generating; a well-designed and adequately powered trial would be required to confirm these findings. Although patients in the overall global ITT population were allocated to treatment groups by stratified randomization (for IPI score, bulky disease, and geographical location), the randomization principle may not have been preserved for patients with ABC lymphoma who were not randomized by the stratification factors. There were between-group differences in the proportion of patients with Ann Arbor stage III lymphoma (█████ versus █████ in the pola-R-CHP versus R-CHOP groups, respectively) and stage IV lymphoma (█████ versus █████ in the pola-R-CHP versus R-CHOP groups, respectively). However, it was unclear whether these imbalances had any impact on patient prognoses or treatment effects. Median OS had not been reached despite prolonged follow-up, with few events at 2 years (approximately 40 deaths) and 5 years (approximately 60 deaths), and any beneficial effect on difference in prolonged survival time and reduced risk of death remains unknown. Despite the adjustment of stratified factors, it is unknown if additional covariates (e.g., disease status) may have biased the findings. Multiplicity is a concern, as it could result in inflated type I error, leading to inappropriate conclusions of statistical inference, given that the observed P values for both stratified and unstratified OS were just below the significance level of 0.05. Although both investigator and independent review assessments of PFS would be preferred, the double-blinded study design may limit potential bias (e.g., more frequent assessments, subjective interpretation of radiographic images and clinical assessments) arising from assessment by investigator. ████████ ██ ████████ ███ ███ ███ ████████ ████████ ███████ ██ ██ ██ █ █████ ███ █████ ████████ ████████ ████ █████████████ ███████ ██ █████████ ██████████ ███ ███ ████████ ███████ ███ █ ███████ ███ ████████████ ████ ██ ███ ███████ ███ ████████████ ██ ██████ ███ ███████ ██ ████████████ █████ ██ ██ ██ █ █████ ██ ██████████. The findings should be interpreted cautiously given the small sample sizes.
The clinical experts indicated that patients with the ABC lymphoma subtype enrolled in the POLARIX trial were representative of patients in clinical practice, and 65% of the patients had an IPI score of 3 to 5, which aligned with the experts’ expectation of high-risk disease among individuals in the ABC subpopulation. Overall, the experts agreed with the inclusion criteria of the POLARIX study, although excluding patients with some comorbidity conditions as well as patients with poorer performance status at presentation (i.e., those with an ECOG PS of 3 or 4) may have resulted in a selected population that is healthier.
Long-Term Extension Studies
No long-term extension studies were submitted in the systematic review evidence.
Indirect Comparisons
No indirect treatment comparisons studies were submitted in the systematic review evidence.
Studies Addressing Gaps in the Evidence From the Systematic Review
No additional studies addressing important gaps in the systematic review evidence were identified.
Conclusions
This report is based on evidence from a phase III, double-blind, randomized trial (POLARIX). In contrast to the previous CDA-AMC review of polatuzumab vedotin that used the same study to evaluate the effects of the drug on the overall LBCL population,30 the current report focuses on a subpopulation of 235 previously untreated adult patients identified as having the ABC lymphoma subtype of LBCL. Patients and clinicians identified a need for new treatments for LBCL that prolong disease remission and survival, control symptoms, normalize blood counts, improve HRQoL, and have tolerable side effects. Evidence from the POLARIX trial demonstrated that, compared with SOC R-CHOP, treatment with pola-R-CHP may provide a clinically important increase in PFS at 2 years and at 5 years in patients with the ABC subtype of LBCL. There was uncertainty in the estimated magnitude of the PFS benefit due to a small population sample size with few events. A definitive conclusion could not be drawn about the comparative OS benefit of pola-R-CHP versus R-CHOP in patients with the ABC subtype of LBCL because the OS data were immature at the 5-year follow-up analysis. However, the percentage of reported deaths among patients treated with R-CHOP was nearly twice that of patients receiving pola-R-CHP. No evidence regarding the comparative efficacy of pola-R-CHP on HRQoL in patients with the ABC lymphoma subtype was available. Overall, treatment-emergent AEs, serious AEs, and withdrawals due to AEs were comparable between the pola-R-CHP and R-CHOP groups. The safety profile of pola-R-CHP treatment in patients with ABC lymphoma subtype was similar to that observed in the LBCL population, and no new safety signals were identified. For notable harms, the evidence suggested a higher incidence of infections and neutropenia (and febrile neutropenia in particular) but a lower incidence of infusion-related reactions with pola-R-CHP compared with R-CHOP. However, the clinical importance of the differences was unclear.
In most centres in Canada, testing to determine COO status is based on IHC with the Hans algorithm. This diagnostic test has limited ability to distinguish among patients with ABC lymphoma and those with other subtypes of lymphoma. The POLARIX study produced no evidence supporting a benefit from pola-R-CHP in patients with non-ABC lymphoma subtypes. Given the limited accuracy of the IHC with the Hans algorithm to correctly identify patients with non-ABC lymphoma subtypes and the lack of supporting evidence of clinical effect, it is therefore unknown if the PFS benefit of pola-R-CHP in patients with ABC lymphoma will be replicated in patients with non-ABC lymphoma subtypes.
Introduction
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of polatuzumab vedotin 1.8 mg/kg in combination with R-CHP for previously untreated LBCL, including DLBCL NOS, high-grade B-cell lymphoma, EBV-positive DLBCL NOS, and T-cell/histiocyte-rich LBCL that are classified as the ABC lymphoma subtype in adults.
Disease Background
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following have been summarized and validated by the review team.
Lymphomas are cancers that grow in lymph nodes and can affect other organs, such as the spleen, liver, and bone marrow. Lymphomas are divided into Hodgkin and NHL based on histology, with the latter comprising 85% of cases. An estimated 11,700 people in Canada were expected to be diagnosed with NHL and 3,100 to die from it in 2024.1 LBCL is a type of NHL that has a number of histologic, proteomic, and molecular subsets with distinctive prognostic profiles, including COO ABC and GCB subtypes, elevated protein expression of MYC and BCL2 seen in double-expressor lymphoma, and gene rearrangements involving MYC and BCL2 and/or BCL6 (double-hit lymphoma or triple-hit lymphoma).2-6 DLBCL NOS is the most common subtype of LBCL, accounting for 35% of NHL cases and 80% of aggressive lymphomas.7,8 DLBCL may be classified as limited-stage disease (stage I or II) or advanced-stage disease (stage III or IV); approximately two-thirds of patients with DLBCL present with stage III or IV disease.9
The most debilitating physical symptoms associated with DLBCL and treatment include fatigue, enlarged lymph nodes, drenching night sweats, weight loss, loss of appetite, flu-like symptoms, and persistent cough. Aside from the physical effects of the disease and treatment, patients with LBCL also experience mental and emotional stress, including fear of disease recurrence, memory loss, anxiety, problems concentrating, difficulty sleeping, loss of sexual desire, stress of diagnosis, and depression. Most patients reported that the symptoms negatively affect their QoL.34 Patients with the ABC subtype of LBCL experience significantly poorer outcomes with standard upfront chemoimmunotherapy compared to those with the GCB subtype.22-29 The ABC subtype of LBCL is more common in older patients who may not be candidates for downstream intensive treatment options.35,36
Molecular classification based on COO plays a key role in the prognosis of DLBCL as it defines higher- and lower-risk subtypes. WHO has recognized COO-based molecular classification of DLBCL as the global standard for patient stratification in medical practice.23,37 The COO status of an ABC lymphoma subtype can be determined by GEP; approximately 30% (range, 25% to 36%) of DLBCL cases are estimated to comprise the ABC subtype.16-18 GEP is conducted mainly in clinical trials and not routinely in clinics.10 IHC with the Hans algorithm can also be used to determine COO status by dichotomizing DLBCL into GCB and non-GCB subtypes, with the latter primarily representing the ABC subtype.19,20 Because health care centres across Canada do not have routine access to GEP, the clinical experts consulted for the review reported that IHC as a surrogate for GEP is a more readily available and practical diagnostic test to distinguish GCB from non-GCB subtypes, thereby indirectly identifying the ABC lymphoma subtype. However, the immunostaining algorithms have limited diagnostic accuracy (sensitivity of 85% to 90% and specificity of 52% to 82% for a positive predictive value of 55% to 82% and a negative predictive value of 83% to 90%) and caution is warranted when using them to guide treatment.21
Standards of Therapy
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following have been summarized and validated by the review team.
Evaluations of patients with newly diagnosed DLBCL to determine treatment options include assessment of disease stage, comorbid conditions and performance status, cytogenetic or molecular features, risk of CNS involvement, and IPI score.9 IPI scores are used to identify specific groups of patients who are more or less likely to be cured with standard therapy,10,38,39 based on patient age, number of extranodal disease sites, stage of disease, serum lactate dehydrogenase level, and ECOG PS; an age-adjusted IPI includes the latter 3 prognostic factors for patients aged 60 years and younger.10,40
Treatment of advanced-stage DLBCL is curative in intent using rituximab-based chemotherapy.9 The preferred choice of regimen for first-line treatment of DLBCL is 6 cycles of R-CHOP.9-11 Based on clinical practice across Canada, approximately 85% to 90% of patients in Canada with DLBCL receive R-CHOP as first-line therapy.41 There are exceptions to SOC first-line therapy for LBCL when accounting for patient factors (e.g., age, risk factors, stage of disease, comorbidities, and molecular features). For patients with high-grade B-cell lymphoma and rearrangements of MYC plus BCL2 and/or BCL6 (double- or triple-hit lymphoma), treatment is usually with dose-adjusted EPOCH-R or another regimen more intensive than R-CHOP, such as rituximab, cyclophosphamide, doxorubicin, vincristine, and high-dose methotrexate alternating with ifosfamide, etoposide, and cytarabine (also referred to as the Magrath regimen).9 For patients with heart disease (e.g., poor left ventricular function such as a baseline ejection fraction < 30%), treatment options can include nonanthracycline (e.g., excluding doxorubicin) regimens: rituximab, cyclophosphamide, etoposide, vincristine, and prednisone; cyclophosphamide, gemcitabine, prednisolone, rituximab, and vincristine; cyclophosphamide, etoposide, prednisolone, rituximab, and vincristine; or rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisolone.9,10 According to the clinical experts consulted for this review, there is no specific treatment approach for patients with the ABC subtype of LBCL. The current treatment paradigm for patients with LBCL, regardless of COO classification, is 6 cycles of chemoimmunotherapy with R-CHOP for those with high-risk and advanced-stage disease and for a proportion of those with limited-stage disease (e.g., age > 60 years, bulky disease, ECOG PS of 2 to 4).11 According to the clinical experts, goals of treatment for DLBCL are cure or prolonging survival, minimizing treatment-related toxicities, alleviating disease-related symptom burden, and maintaining HRQoL.
While treatment with R-CHOP achieves cure in approximately 60% of patients with DLBCL,10,12,13 about 40% of patients experience a relapse or disease progression (approximately 10% to 15% of patients experience primary refractory disease and 20% to 30% of patients experience relapse after achieving complete remission).8,14,15 The clinical experts noted that patients with refractory disease or early relapse have very poor outcomes and, if adequately fit, may proceed to salvage therapy (e.g., stem-cell transplant or CAR T-cell therapy), but remain at high risk for disease relapse or refractory disease. Moreover, the clinical experts added that salvage therapies are associated with increased toxicity and costs.
Although COO status does not influence the choice of initial treatment for advanced DLBCL, GCB status is generally associated with a favourable prognosis compared with non-GCB status, which is associated with higher rates of relapse and less-favourable prognoses.9 The clinical experts emphasized that patients with the non-GCB subtype of LBCL (ABC) are more likely to have high-risk disease features (e.g., advanced-stage disease at diagnosis and an IPI score of 3 to 5), which are associated with poorer outcomes among patients treated with SOC R-CHOP. The clinical experts identified patients with high-risk disease (e.g., an IPI score of 3 to 5 or an ABC subtype of lymphoma) as having a clear unmet need in LBCL, and they advocated for improved front-line treatment options to achieve cure and avoid the need for toxic salvage therapies.
Drug Under Review
Polatuzumab vedotin is administered by IV infusion. The Health Canada–recommended dose is 1.8 mg/kg every 21 days for 6 cycles in combination with R-CHP. Polatuzumab vedotin, rituximab, cyclophosphamide, and doxorubicin can be administered in any order on day 1 after the administration of prednisone. Prednisone is administered on days 1 to 5 of each cycle. Cycles 7 and 8 consist of rituximab as monotherapy.
Polatuzumab vedotin is a CD79b-targeted antibody-drug conjugate that delivers an antimitotic drug, monomethyl auristatin E (MMAE) to B-cells, which results in the killing of malignant B-cells. MMAE is covalently attached via a cleavable linker to a humanized immunoglobulin G1 monoclonal antibody, which binds with nanomolar affinity and selectivity to CD79b, a cell-surface component of the B-cell receptor. CD79b expression is restricted to normal cells within the B-cell lineage (with the exception of plasma cells) and malignant B cells; it is expressed in more than 95% of cases of DLBCL. Upon binding to CD79b, polatuzumab vedotin is rapidly internalized and the linker is cleaved by lysosomal proteases to enable intracellular delivery of MMAE. MMAE binds to microtubules and kills dividing cells by inhibiting cell division and inducing apoptosis.
Pola-R-CHP was previously reviewed by CDA-AMC for the treatment of adult patients with previously untreated LBCL, including DLBCL NOS, high-grade B-cell lymphoma, EBV-positive DLBCL NOS, and T-cell/histiocyte-rich LBCL; a recommendation of “do not reimburse” was issued in December 2023.42 In May 2022, the European Medicines Agency approved pola-R-CHP for the treatment of adult patients with previously untreated DLBCL.43 In April 2023, the US FDA approved pola-R-CHP for adult patients who have previously untreated DLBCL NOS or high-grade B-cell lymphoma and who have an IPI score of 2 or greater.
Key characteristics of pola-R-CHP are summarized in Table 3 with other treatments available for the treatment of adult patients with previously untreated LBCL, including DLBCL NOS, high-grade B-cell lymphoma, EBV-positive DLBCL NOS, and T-cell/histiocyte-rich LBCL that are classified as ABC lymphoma subtype.
Table 3: Key Characteristics of Polatuzumab Vedotin and R-CHOP
Characteristic | Polatuzumab vedotin | Rituximab | Cyclophosphamide | Doxorubicin | Vincristine | Prednisone |
|---|---|---|---|---|---|---|
Mechanism of action | CD79b-targeted antibody-drug conjugate; delivers an antimitotic drug to B cells | — | Alkylating drug; cytotoxic action due to cross-linking of strands of DNA and RNA and inhibiting DNA synthesis | Anthracycline antibiotic; binds to DNA and inhibits nucleic acid synthesis | Vinca alkaloid; binds with tubulin and disrupts progression of mitosis | Synthetic corticosteroid; associated with anti-inflammatory and immune-modulating effects |
Indicationa | In combination with R-CHP, is indicated for the treatment of adult patients with previously untreated LBCL, including DLBCL NOS, high-grade B-cell lymphoma, Epstein-Barr virus–positive DLBCL NOS, and T-cell/histiocyte-rich LBCL | Non-Hodgkin lymphoma | Non-Hodgkin lymphoma | Neoplastic diseases (adjunct treatment); non-Hodgkin lymphoma | Neoplastic diseases (adjunct treatment); non-Hodgkin lymphoma | Neoplastic diseases (adjunct treatment); non-Hodgkin lymphoma |
Route of administration | IV infusion | IV infusion, SC injection | IV infusion | IV infusion | IV infusion | Oral |
Recommended doseb | 1.8 mg/kg every 21 days for 6 cycles in combination with R-CHP | 375 mg/m2 (IV) on day 1 of each cycle, or 1,400 mg (SC) on second or subsequent cycles, and only after at least 1 full rituximab IV dose, day 1 | 750 mg/m2 on day 1 of each cycle | 50 mg/m2 on day 1 of each cycle | 1.4 mg/m2 on day 1 of each cycle | 100 mg or 45 mg/m2 daily (round off dose to nearest 25 mg) on days 1 to 5 of each cycle |
Serious adverse effects or safety issues | Infusion-related reactions, peripheral neuropathy, tumour lysis syndrome, myelosuppression, hepatic toxicity, infections, progressive multifocal leukoencephalopathy | Infections, neutropenia, hypotension, tumour lysis syndrome, infusion-related reactions | Secondary malignancy, cardiac toxicity, lung and liver injury, severe QT prolongation, serious allergic reaction | Cardiomyopathy, secondary malignancies, extravasation and tissue necrosis, myelosuppression and sequelae, hepatic impairment | Uric acid nephropathy, shortness of breath, severe bronchospasm, constipation, hair loss | Osteoporosis, infections, cataracts, hypertension, Cushing syndrome, hyperglycemia, delayed wound healing |
LBCL = large B-cell lymphoma; NOS = not otherwise specified; R-CHP = rituximab, cyclophosphamide, doxorubicin, and prednisone; R-CHOP = rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone; SC = subcutaneous.
aHealth Canada–approved indication.
bR-CHOP–recommended doses based on BC Cancer and Cancer Care Ontario treatment guidelines.44,45
Sources: Product monographs for Polivy,46 Riabni,47 cyclophosphamide,48 doxorubicin,49 and prednisone.50
Perspectives of Patients, Clinicians, and Drug Programs
The full patient and clinician group submissions received are available in the consolidated patient and clinician group input document for this review on the project website.
Patient Group Input
This section was prepared by the review team based on the input provided by patient groups.
One patient group, Lymphoma Canada, submitted input for this review. Lymphoma Canada is a national registered charity whose mission is to empower patients and the lymphoma community in Canada through education, support, advocacy, and research. The input was based on an online anonymous patient survey among patients with a subtype of LBCL, created and promoted by Lymphoma Canada, available from February 2 to March 13, 2023. Information from the survey was used to identify the main areas of concern for patients with LBCL (n = 89). Subtype of LBCL according to COO status was not identified for the respondents. Most patients lived in Canada (94%) and were aged 55 years to 74 years (64%). The sex breakdown was 58% female and 42% male, and most (61%) were diagnosed 1 year to 5 years ago with DLBCL (89%). Four patients (3 from Canada and 1 from Italy) confirmed that they had experience with polatuzumab vedotin.
The most common physical symptoms reported by patients upon diagnosis included fatigue (59%), bodily aches and pain (42%), night sweats (42%), enlarged lymph nodes (41%), and a reduced appetite (33%). Sixty-nine patients reported experiencing psychosocial impacts upon being diagnosed with LCBL, including stress of diagnosis (81%), anxiety or worry (79%), fear of progression (60%), inability to continue daily activities (51%), and difficulty sleeping (47%). Additional details regarding challenges that patients experienced during diagnosis included feeling isolated with minimal support during the COVID-19 pandemic. Factors affecting patients’ QoL (rated as ≥ 3 on a scale of 1 = no impact to 5 = significant impact) included fatigue (42%), bodily aches (25%), and headaches (17%). Mental health challenges experienced by patients included fear of progression or relapse (66%), stress of having cancer (56%), and anxiety or worry (42%). Factors affecting patients’ daily activities (59 patients gave them a rating of ≥ 3 on a scale of 1 = no impact to 5 = very significant impact) included the ability to exercise (41%) or travel (39%), spend time with family and friends (36%), and to work, attend school, or volunteer (34%).
Among survey respondents (n = 56), more received 2 or more lines of therapy (53%) compared with those who received first-line therapy (41%). In the first-line setting, 48% of patients received chemoimmunotherapy with R-CHOP, while others received R-CHP or EPOCH-R. Overall, 28% of patients were satisfied with their first-line treatment options and 57% were very satisfied with the number of available treatment options; 15% of patients expressed dissatisfaction with the available treatment options. While many patients (n = 35 of 52; 67%) indicated no difficulty accessing treatment for their lymphoma in Canada, others reported having challenges such as delays, cost of travelling long distances for treatment, absence from work, and the financial burden of drugs for treatment and supplementary drugs for managing side effects.
Four individuals had experience with pola-R-CHP treatment, of whom 2 patients indicated a good overall experience and 3 patients indicated that they would recommend the treatment to other individuals with LCBL. Side effects of pola-R-CHP treatment experienced by at least 2 patients included fatigue, neutropenia, thrombocytopenia, decreased appetite, and diarrhea.
Most patients (9 of 11 respondents) expressed a desire for more treatment options for LBCL. Patients were willing to tolerate side effects to access new treatments (n = 8) and sought choices in their selection of treatment (n = 7). When considering new treatments, factors that were important to patients with LBCL included longer disease remission and survival, controlled disease symptoms, normalized blood counts, and improved QoL to enable activities of daily living.
Clinician Input
Input From Clinical Experts Consulted for This Review
All CDA-AMC review teams include at least 1 clinical specialist with expertise in the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of LBCL.
Unmet Needs
The clinical experts stated that, although many patients with LBCL experience cure with R-CHOP as a first-line SOC treatment, many patients with high-risk disease (i.e., those with an IPI score of 3 to 5 and the ABC lymphoma subtype) experience poor outcomes with R-CHOP. Treatment cure may be possible in 50% to 60% of patients with high IPI scores compared with 80% to 90% of patients with low IPI scores.51 The clinical experts reported that patients with a non-GCB lymphoma subtype (comprising primarily the ABC lymphoma subtype) commonly exhibit high-risk disease features (e.g., a high IPI score), and, compared with the GCB subtype, high-risk molecular features are associated with poorer outcomes using SOC treatment for LBCL. OS has been estimated to be inferior, ranging from 45% to 56% for the ABC subtype compared with 78% to 80% for the GCB subtype.6,21 Patients with ABC lymphoma are often underrepresented in clinical trials due to a poor presentation at diagnosis that precludes enrolment eligibility. Furthermore, patients with refractory disease or early relapse require salvage therapy (e.g., stem-cell transplant, CAR T-cell therapy, or bispecific T-cell engager therapy) which can be intensive, toxic, and costly, with limited curative potential. The experts agreed that patients with high-risk LBCL, regardless of subtype, would benefit from more efficacious first-line treatments that avoid the need for toxic salvage therapies. The most important goals of treatment for DLBCL are cure or improved survival while minimizing treatment-related toxicities and alleviating disease-related symptom burden.
Place in Therapy
The clinical experts noted that there is no specific treatment approach for the ABC lymphoma subtype in Canada. Therefore, the current first-line setting treatment paradigm for patients with ABC lymphoma subtype is the same 6 cycles of R-CHOP as in patients with LBCL (regardless of subtype). The experts added that the 6 cycles of R-CHOP treatment for de novo DLBCL is also generally applied to patients with indolent lymphoma that has transformed into DLBCL, including grade 3B follicular lymphoma, and high-grade B-cell lymphoma NOS (i.e., without both MYC and BCL2 rearrangements).11,52 According to the clinical experts, the goal of adding polatuzumab vedotin to front-line treatment for DLBCL is to maximize the impact on improving outcomes. The experts anticipated that, if approved, pola-R-CHP would supplant the current SOC, R-CHOP, resulting in a shift in the current treatment paradigm for patients with ABC COO.
Patient Population
The clinical experts indicated that all patients eligible for treatment with R-CHOP (generally fit and without significant comorbidities), including patients with ABC lymphoma, would be best suited for treatment with pola-R-CHP. In particular, patients with high-risk disease have the potential to benefit from pola-R-CHP, particularly in the first-line setting, where it may improve cure rates and decrease treatment needs in second- or later-line settings. In addition to considerations of patient preferences, individuals considered as ineligible for R-CHOP — and therefore ineligible for treatment with pola-R-CHP due to its toxicity — include those with reduced cardiac function (e.g., a smaller ejection fraction) and/or significant comorbidities, and those for whom other treatments are more appropriate (e.g., more intensive treatments for patients with double-hit or double-expressor lymphoma).
According to the clinical experts, eligibility for treatment with pola-R-CHP in the proposed reimbursement population requires COO testing to determine the ABC subtype. In Canada, COO testing is routinely based on IHC and the Hans algorithm. GEP to determine COO is the gold standard for diagnostic testing but it is not readily available at most centres. The IHC testing method distinguishes GCB from non-GCB subtypes and, while it has demonstrated high concordance with GEP, it is nevertheless considered a proxy for identifying ABC lymphoma subtype. However, misclassification can occur in approximately 10% to 15% of patients.31
Assessing the Response Treatment
According to the experts consulted for this review, treatment response is assessed radiographically at 2 time points: after 3 or 4 cycles of treatment (with a CT scan) and at the end of treatment (with a PET scan). Upon attaining remission at end of treatment, patients are monitored every 3 months clinically (physical examinations, symptom assessment, and laboratory testing) to screen for relapses, with any additional imaging assessments guided by the clinical assessment. The experts reported that, because of the low likelihood of disease relapse occurring 2 years after completing treatment, patients are generally followed up for at least 2 years (or up to 5 years after completing treatment). Most patients who have not experienced disease progression or relapse for 2 years are considered to be cured. Routine patient imaging is not typically conducted after complete disease remission. The experts noted that, because the goal of treatment for DLBCL is curative in intent, OS is the most important outcome for patients, although PFS is also a critical outcome to assess, given that disease progression or relapse is common within the first 2 years of treatment.
Discontinuing Treatment
According to the clinical experts, treatment for patients with the ABC subtype of LBCL would be discontinued due to a lack of efficacy or unacceptable toxicity. The experts added that dose reductions of polatuzumab vedotin or other components of the pola-R-CHP regimen may be warranted for patients who experience AEs (e.g., infections, neutropenia, and/or thrombocytopenia).
Prescribing Considerations
The clinical experts indicated that it would be appropriate for any hematologist or oncologist who treats DLBCL in a community or tertiary care centre to manage patients with ABC lymphoma using pola-R-CHP, adding that many centres are familiar with the use of polatuzumab vedotin in combination with bendamustine and rituximab for patients with relapsed or refractory DLBCL.
Additional Considerations
The clinical experts reiterated that restricting polatuzumab vedotin treatment to those with the ABC lymphoma subtype based on current diagnostic testing practice in Canada (IHC with the Hans algorithm) would be impractical and potentially inequitable because eligible patient populations that would otherwise benefit from this treatment (e.g., patients with high-risk LBCL including those with a non-GCB lymphoma subtype and/or an IPI score of 3 to 5) could be excluded.
Clinician Group Input
This section was prepared by the review team based on the input provided by clinician groups.
Two clinician groups provided input for this submission. The LC-SAB is a volunteer group of scientists and clinicians distinguished in fields related to lymphoid cancer research and clinical care. The LC-SAB is an integral part of Lymphoma Canada that provides advice and guidance on clinical care and research related programs, patient education activities and resources, public policy and advocacy activities, and research grants and programs. The OH-CCO Hematology Cancer DAC provides evidence-based clinical and health system guidance on drug-related issues in support of OH-CCO mandate, including the Provincial Drug Reimbursement Programs and the Systemic Treatment Program. Input from the LC-SAB was provided by 9 clinicians and included information from the previous CDA-AMC review, the randomized POLARIX trial, and published abstracts and articles pertaining to pola-R-CHP in patients with LBCL. Information from the OH-CCO Hematology Cancer DAC was provided by 7 clinicians and was gathered via video conferencing and emails.
The LC-SAB noted that a significant portion of patients may not achieve a complete remission or can develop disease progression after an initial response of remission with current therapy (R-CHOP). They indicated that patients with the ABC subtype of lymphoma are particularly at high risk of relapsing or developing refractory disease following R-CHOP treatment. The OH-CCO Hematology Cancer DAC noted that treatment goals should focus on a cure and preventing the need for salvage treatment (e.g., transplant and CAR T-cell therapy). The LC-SAB pointed out that the main treatment goal that current therapy does not meet is minimizing the number of patients who relapse or experience disease progression after initial therapy. The OH-CCO Hematology Cancer DAC agreed that a large proportion of patients still fail first-line therapy. Both clinician groups agreed that pola-R-CHP would replace R-CHOP in the first-line setting for the ABC subtype.
The LC-SAB noted that adult patients with advanced-stage LBCL and an IPI score of 2 to 5 that have not yet been treated and those eligible for multidrug chemoimmunotherapy would be suitable for treatment with pola-R-CHP if they are classified as having the ABC subtype. The OH-CCO Hematology Cancer DAC noted that patients best suited for treatment would be those described by the inclusion criteria for the ABC subtype. Both clinician groups emphasized that the classification of subtype in Canada is usually done via standard IHC algorithms. The LC-SAB further noted that this classification system has an approximately 80% to 90% agreement with GEP; however, patients may be misclassified by IHC. They noted that a misclassified patient with GCB DLBCL would not be harmed by receiving pola-R-CHP as the POLARIX trial demonstrated an overall benefit. The OH-CCO Hematology Cancer DAC suggested that there should be allowance for time-limited switching by patients being treated with R-CHOP at the time of implementation and for re-treatment with polatuzumab in combination with bendamustine and rituximab, as long as the patient is not refractory to polatuzumab vedotin.
The LC-SAB noted that repeat imaging would be used to determine response following the Lugano criteria using CT after 3 to 4 cycles of therapy and with standard PET and/or CT at end of treatment. They added that a switch to pola-R-CHP would not affect response assessments as the SOC procedures would be the same as for R-CHOP, and therefore no additional tests would be implemented. The OH-CCO Hematology Cancer DAC noted that responses to treatment would be assessed according to standard lymphoma response criteria and testing.
Both clinician groups noted that disease progression would lead to discontinuation of treatment. The LC-SAB further noted that a lack of response to treatment and development of peripheral neuropathy, if severe, would lead to treatment discontinuation. In addition, the OH-CCO Hematology Cancer DAC noted that AEs would lead to treatment discontinuation.
According to the LC-SAB, the regimen could be administered at any site or by any practitioner that currently gives R-CHOP chemotherapy due to similar toxicity profiles. The clinician group pointed out that polatuzumab vedotin has been approved in combination with bendamustine and rituximab for the treatment of relapsed or refractory DLBCL, and that there is broad experience with the drug and in a combination chemotherapy regimen. The OH-CCO noted that an outpatient setting would be most appropriate for treatment administration.
Drug Program Input
The drug programs provide input on each drug being reviewed through the reimbursement review processes by identifying issues that may affect their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by for this review are summarized in Table 4.
Table 4: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Relevant comparators | |
R-CHOP, R-CEOP, and R-mini-CHOP are funded as first-line treatment options for patients with DLBCL. Some jurisdictions fund DA-EPOCH-R for first-line treatment of aggressive lymphomas with high-risk features (i.e., double-hit, triple-hit). | The clinical experts agreed that the available first-line treatments for patients with DLBCL are relevant comparators for pola-R-CHP, with most (> 75%) patients treated with R-CHOP. R-mini-CHOP incorporates a dose reduction in some of its components and may be most appropriate for patients with frailty or significant comorbidities, but this is not a clinically unique population that would warrant precluding them from being eligible for treatment with pola-R-CHP. There is some uncertainty regarding the optimal therapy for patients with double-hit or triple-hit lymphoma, for whom alternatives to R-CHOP that are more intensive may be prescribed (e.g., DA-EPOCH-R and the McGrath regimen). Patients with significant cardiac dysfunction may be more appropriately treated with R-CEOP, and removing anthracycline from their treatment regimen. Altogether, R-CEOP and DA-EPOCH-R were not considered by the experts to be appropriate comparators for pola-R-CHP. |
Considerations for initiation of therapy | |
The POLARIX trial included patients with an IPI score of 2 to 5. Should patients with the ABC subtype have an IPI score of 2 to 5 to be eligible for pola-R-CHP? | The clinical experts felt that patients with ABC lymphoma subtype with an IPI score of 2 to 5 should be eligible for treatment with pola-R-CHP, given that they are reflective of patients who were included in the POLARIX trial. The experts added that patients with LBCL who have IPI scores of 0 or 1 have better prognoses compared with those who have higher IPI scores and experience favourable outcomes with R-CHOP. It is unknown whether patients with the ABC lymphoma subtype who have an IPI score of 0 or 1 would experience a meaningful benefit from pola-R-CHP treatment because of an absence of evidence. |
The POLARIX trial included patients aged 18 to 80 years. Would patients older than 80 years who have the ABC subtype be eligible for pola-R-CHP? | The clinical experts expressed that any patient treated with R-CHOP–like therapy for curative intent should be eligible for treatment with pola-R-CHP, including those older than 80 years who may currently be treated with dose-reduced R-CHOP (i.e., R-mini-CHOP) for improved tolerance. |
The POLARIX trial excluded patients with indolent lymphoma. PAG would like to confirm the following 2 questions: 1. Would patients with follicular lymphoma grade 3B (also called follicular large B-cell lymphoma) be eligible for pola-R-CHP provided all other criteria are met? 2. Would patients who received treatment for indolent follicular lymphoma (i.e., bendamustine-rituximab) and then transform to DLBCL be eligible for treatment with pola-R-CHP? | 1. According to the clinical experts, follicular lymphoma of grade 3B (neither an indolent nor transformed lymphoma) is categorized as a GCB lymphoma subtype. Patients with grade 3B follicular lymphoma are treated the same way as those with de novo DLBCL (with SOC R-CHOP chemotherapy) and therefore would be eligible for treatment with pola-R-CHP, However, the current resubmission of polatuzumab vedotin does not include this population as it is focused on patients with the ABC lymphoma subtype. 2. Although the experts felt that patients with indolent lymphoma whose disease transforms to DLBCL should be treated as having de novo DLBCL, most follicular lymphomas that transform to DLBCL are of the GCB subtype. Few patients would be eligible for treatment with polatuzumab vedotin based on the requested reimbursement population of those with the ABC subtype. |
Considerations for prescribing of therapy | |
Cycles 1 to 6: pola-R-CHP every 21 days for 6 cycles; cycles 7 and 8: rituximab only. The drug plans note that polatuzumab vedotin is available in 30 mg and 140 mg vials that require reconstitution. The dose is 1.8 mg/kg IV every 21 days for 6 cycles. Polatuzumab vedotin, rituximab, cyclophosphamide, and doxorubicin can be administered in any order on day 1 after the administration of prednisone. Prednisone is administered on days 1 to 5 of each cycle. Cycles 7 and 8 consist of rituximab as monotherapy, which is an additional 2 cycles of therapy compared to the standard 6 cycles of R-CHOP that is usually administered, adding additional pharmacy workload and chair time visits. The drug plans would like to know if cycles 7 and 8 of single-drug rituximab would be recommended, as R-CHOP is normally given every 21 days for 6 cycles (and no cycles 7 and 8) in most jurisdictions. | According to the clinical experts, since rituximab monotherapy is administered in current practice for 6 cycles, and there is an absence of evidence to support an additional 2 cycles of treatment (e.g., patients were not randomized to receive rituximab monotherapy 6 cycles vs. 8 cycles), rituximab monotherapy in cycles 7 and 8 of treatment may be safely omitted. |
The dose of CHOP in R-CHOP is sometimes reduced in older patients (mini-R-CHOP). 1. Is it appropriate to reduce the dose of CHP when used in the pola-R-CHP regimen in elderly or frail patients, or to substitute etoposide for doxorubicin in patients who may not be able to receive doxorubicin? 2. Can polatuzumab vedotin be used with rituximab SC or rituximab biosimilar as part of the pola-R-CHP regimen? | 1. The clinical experts indicated that if an R-CHOP-like regimen is administered at a reduced dose to improve intolerance with curative intent, it would be reasonable to consider treatment with pola-R-CHP. Moreover, because R-CEOP is a treatment option with curative intent in patients who cannot tolerate doxorubicin (e.g., due to issues with cardiac function such as low ejection fraction), it would be appropriate to consider treatment with pola-RCEP for those with such contraindications. 2. The experts had no concerns about using polatuzumab vedotin with rituximab SC or a rituximab biosimilar as part of the pola-R-CHP regimen, as rituximab SC is used in current practice in combination with either R-CHOP (from cycle 2 onward) or pola-BR. |
For cycle 1, it may be difficult for treatment rooms to accommodate the time of administration for slow-infusion rituximab, 90 minutes for polatuzumab vedotin infusion, and 90 minutes for observation and cyclophosphamide infusion and doxorubicin IV. For treatment rooms that are only open for 8 hours, would it be advisable to administer R-CHP on day 1 and then polatuzumab vedotin on day 2 or is there a preference of which drugs should be split? Acknowledging that there may be no answer to this question, this will be an implementation issue for many treatment rooms that are only open for 8 hours. This would only be for cycle 1. | According to the clinical experts, it would be reasonable to divide cycle 1 of the pola-R-CHP regimen components as necessary for ease of administration (e.g., administer rituximab and polatuzumab vedotin on same day, followed by CHP on the next day) and as logistically feasible at each institution. |
Generalizability | |
The POLARIX trial enrolled patients with an ECOG PS of 0, 1, or 2. If a patient has an ECOG PS of 3 because of their aggressive lymphoma, would they be recommended to use pola-R-CHP? | The clinical experts expressed that a patient with an ECOG PS of 3, while typically excluded from clinical trials due to significant disease or symptom burden at presentation, would likely improve with their first cycle of treatment (e.g., to achieve ECOG PS of 2 or better) such that they should be considered eligible for treatment with pola-R-CHP. |
Would patients with the ABC subtype DLBCL who are currently on treatment with R-CHOP be switched to pola-R-CHP? If so, is there a maximum number of cycles of R-CHOP that would be recommended before allowing treatment to be switched to pola-R-CHP? | The experts indicated that patients with the ABC lymphoma subtype who have proceeded further along in therapy with R-CHOP (e.g., 2 cycles or more of treatment) should continue with R-CHOP. Because there may be delays in receiving results of GEP testing (if GEP diagnostic testing becomes available), initiation of urgent therapy may be warranted; that is, patients could receive 1 cycle of R-CHOP while awaiting diagnostic testing and then be allowed to switch to pola-R-CHP for cycle 2 and onward, as long as the total duration of treatment is not more than 6 cycles. However, the experts acknowledge that there is a lack of evidence to suggest that switching regimens part-way through treatment improves outcomes. |
Funding algorithm | |
Request an initiation of a rapid provisional funding algorithm. | This is a comment from the drug plans to inform pERC deliberations. |
Drug may change place in therapy of drugs reimbursed in subsequent lines. | This is a comment from the drug plans to inform pERC deliberations. |
Complex therapeutic space with multiple lines of therapy, subpopulations, or competing products. | This is a comment from the drug plans to inform pERC deliberations. |
If a patient receives pola-R-CHP as first-line treatment and relapses, would pola-BR be an option for second-line treatment? If so, what would be the minimum time from the last polatuzumab vedotin treatment to new initiation of polatuzumab vedotin in the relapsed setting? | Both clinical experts felt that patients who experienced relapse after first-line treatment with pola-R-CHP should be eligible for second-line treatment with pola-BR. One of the experts noted that, because pola-BR is a palliative regimen, it may be considered in the second-line setting for patients ineligible for aggressive salvage therapy (e.g., R-GDP, CAR T-cell therapy, ASCT) and who have not experienced refractory disease (i.e., did not progress on treatment, or experience relapse > 3 months from last treatment dose). According to the other expert, their jurisdiction requires 6 months to have elapsed since the last rituximab dose for a patient to be eligible for re-treatment with rituximab. As such, patients who experience relapse within 1 year are more likely to proceed to CAR T-cell therapy than to receive pola-BR. Nevertheless, the second expert pointed out that, because patients with LBCL need bridging therapy to keep their disease under reasonable control before having to escalate to CAR T-cell therapy, pola-BR should be available to patients who relapse at 6 to 12 months. |
Care provision issues | |
Jurisdictions are familiar with the preparation of rituximab, polatuzumab vedotin, cyclophosphamide, and doxorubicin. This is an enabler to preparation. From a pharmacy point of view, polatuzumab vedotin requires more compounding time than does vincristine. From a nursing point of view, extra chair time is required with the use of polatuzumab vedotin. | This is a comment from the drug plans to inform pERC deliberations. |
Growth factor support was mandated for patients in the POLARIX trial for the use of pola-R-CHP and will be required upon implementation of pola-R-CHP. Growth factor support is funded differently across jurisdictions. | The clinical experts indicated that growth factor support should be mandated with pola-R-CHP treatment, based on the use of G-CSF as primary prophylaxis during cycles 1 to 6 of treatment in the POLARIX trial. The experts highlighted that there was a relatively high rate of infectious toxicities among patients in the trial despite G-CSF prophylaxis, particularly in the pola-R-CHP group. |
Because ABC testing may not be available across all jurisdictions, this is an implementation issue that will need to be addressed by the jurisdictions. What is the turnaround time for ABC testing in lymphoma? | The experts reported that GEP testing to determine ABC lymphoma subtype is not performed across most centres in Canada. IHC testing is required for the diagnosis of LBCL in current practice. Diagnostic testing using the IHC method can differentiate GCB from non-GCB subtypes (the non-GCB subtype includes the ABC subtype and unclassified COO). |
If a patient experiences neuropathies despite dose reductions on polatuzumab vedotin, and polatuzumab vedotin needs to be discontinued, is it advisable to continue only with R-CHP? | The experts agreed that a patient may be continued on treatment with R-CHP alone if they experienced serious neuropathies with polatuzumab vedotin (as part of pola-R-CHP) or with vincristine (as part of R-CHOP). |
System and economic issues | |
There is concern regarding the substantial budget impact of addition of polatuzumab vedotin as it will replace vincristine (vincristine is generic and the incremental cost of 6 cycles of polatuzumab vedotin per patient is substantial). | This is a comment from the drug plans to inform pERC deliberations. |
There are large incremental budget impacts for polatuzumab vedotin. | This is a comment from the drug plans to inform pERC deliberations. |
ABC = activated B cell–like; ASCT = autologous stem cell therapy; CAR = chimeric antigen receptor; COO = cell of origin; DA-EPOCH-R = dose-adjusted etoposide, prednisone, vincristine, cyclophosphamide, doxorubicin, and rituximab; DLBCL = diffuse large B-cell lymphoma; ECOG PS = Eastern Cooperative Oncology Group Performance Status; GCB = germinal centre B cell; GEP = gene expression profiling; G-CSF = granulocyte colony-stimulating factor; IHC = immunohistochemistry; IPI = International Prognostic Index; PAG = Provincial Advisory Group; pERC = pan-Canadian Oncology Drug Review Expert Review Committee; pola-BR = polatuzumab vedotin, bendamustine, and rituximab; pola-R-CHP = polatuzumab vedotin, rituximab, cyclophosphamide, doxorubicin, and prednisone; R-CEOP = rituximab ,cyclophosphamide, etoposide, vincristine, and prednisone; R-GDP = rituximab, gemcitabine, doxorubicin, and prednisone; R-CHOP = rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone; R-mini-CHOP = rituximab and reduced-dose cyclophosphamide, doxorubicin, vincristine, and prednisone; SOC = standard of care; SC = subcutaneous.
Clinical Evidence
The objective of this Clinical Review report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of polatuzumab vedotin in combination with R-CHP for the treatment of adult patients with previously untreated LBCL, including DLBCL NOS, high-grade B-cell lymphoma, EBV-positive DLBCL NOS, and T-cell/histiocyte-rich LBCL that are classified as the ABC lymphoma subtype. The focus is on comparing pola-R-CHP to relevant comparators and identifying gaps in the current evidence.
A summary of the clinical evidence included by the sponsor in the review of pola-R-CHP is presented in 4 sections, with our critical appraisal of the evidence included at the end of each section. The first section, the systematic review, includes pivotal studies and randomized controlled trials that were selected according to the sponsor’s systematic review protocol, followed by a critical appraisal of the evidence. No long-term extension studies, indirect evidence, or additional studies addressing important gaps in the systematic review evidence were submitted by the sponsor.
Included Studies
Clinical evidence from 1 randomized controlled trial (POLARIX) is included in the review and appraised in this document.
Systematic Review
Contents within this section have been informed by materials submitted by the sponsor. The following have been summarized and validated by the review team.
Description of Studies
Characteristics of the included studies are summarized in Table 5.
Table 5: Details of Studies Included in the Systematic Review
Detail | POLARIX |
|---|---|
Design and populations | |
Study design | Phase III, multicentre, double-blind, placebo-controlled, randomized controlled trial |
Locations | 211 sites in 22 countries, in 3 regions:
|
Patient enrolment dates | Start date: November 15, 2017 End date: June 27, 2019 Primary analysis: clinical cut-off date of June 28, 2021 Updated analysis: clinical cut-off date of June 15, 2022 Longest available follow-up: clinical cut-off date of July 5, 2024 |
Randomized (N) | Global population: N = 879 (440 in pola-R-CHP, 439 in R-CHOP) Global population, ABC lymphoma subtype = 235 (106 in pola-R-CHP, 129 in R-CHOP) Expanded population: N = 1,000 (500 in pola-R-CHP, 500 in R-CHOP) |
Inclusion criteria | Previously untreated patients with CD20-positive DLBCL, included 1 of the following diagnoses by 2016 WHO classification of lymphoid neoplasms:
For females and males: agreed to remain abstinent |
Exclusion criteria |
|
Drugs | |
Intervention | Polatuzumab vedotin 1.8 mg/kg IV, rituximab 375 mg/m2 IV, cyclophosphamide 750 mg/m2 IV, doxorubicin 50 mg/m2 IV, placebo for vincristine, each on day 1; and prednisone 100 mg/day orally on days 1 to 5 of every 21-day cycle for 6 cycles; rituximab 375 mg/m2 IV monotherapy in cycles 7 and 8 |
Comparator(s) | Placebo for polatuzumab vedotin, rituximab 375 mg/m2 IV, cyclophosphamide 750 mg/m2 IV, doxorubicin 50 mg/m2 IV, vincristine 1.4 mg/m2 IV (maximum 2 mg/dose), each on day 1; and prednisone 100 mg/day orally on days 1 to 5 of every 21-day cycle for 6 cycles; rituximab 375 mg/m2 IV monotherapy in cycles 7 and 8 |
Study duration | |
Screening phase | 28 days before randomization to day 1 (randomization) |
Treatment phase | Polatuzumab vedotin in pola-R-CHP and vincristine in R-CHOP: median of 3.5 months Rituximab in both pola-R-CHP and R-CHOP: median of 4.9 months |
Follow-up phase | Primary analysis: median 28.2 months (range, 0 to 43 months) Updated analysis: median 40.2 months (range not reported) Post-treatment follow-up visit: up to approximately 65 months |
Outcomes | |
Primary end point | PFS (investigator)a |
Secondary and exploratory end points | Key secondaryb
Secondaryc
Exploratory
|
Publication status | |
Publications | ClinicalTrials.gov Identifier: NCT03274492 Tilly et al. (2022)53 Morschhauser et al. (2023)54 Salles et al. (2024)55 |
ABC = activated B cell–like; ALK = anaplastic lymphoma kinase; BICR = blinded independent central review; BOR = best overall response; CNS = central nervous system; CR = complete response; DFS = disease-free survival; DLBCL = diffuse large B-cell lymphoma; DOR = duration of response; EFSall = event-free survival from all causes; EFSeff = event-free survival efficacy; ECOG PS = Eastern Cooperative Oncology Group Performance Status; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; FACT/GOG-Ntx = Functional Assessment of Cancer Therapy/Gynecologic Oncology Group – Neurotoxicity; FACT-Lym = Functional Assessment of Cancer Therapy – Lymphoma; FDG-PET = fluorodeoxyglucose PET; HTLV-1 = human T-lymphotrophic 1 virus; ORR = objective response rate; NOS = not otherwise specified; OS = overall survival; PFS = progression-free survival; PFS24 = progression-free survival at 24 months; pola-R-CHP = polatuzumab vedotin, rituximab, cyclophosphamide, doxorubicin, and prednisone; R-CHOP = rituximab, cyclophosphamide, doxorubicin, vincristine, prednisone; ULN = upper limit of normal.
aPFS (investigator-assessed) and OS were included as outcomes based on subgroup analyses for patients with the ABC lymphoma subtype.
bKey secondary end points were included in the hierarchical testing procedure.
cSecondary end points were not adjusted for multiple testing and there is an increased risk of type I error.
Source: POLARIX Clinical Study Report.32
POLARIX was a phase III, global, multicentre (211 sites with 7 in Canada), randomized, double-blind, trial that compared the efficacy and safety of pola-R-CHP versus SOC R-CHOP in patients with previously untreated CD20-positive DLBCL with an IPI score of 2 to 5. Eligible patients were randomized in permuted blocks stratified by IPI score (2 versus 3 to 5), bulky disease defined as at least 1 lesion 7.5 cm or greater (presence versus absence), and geographical region (Western Europe, US, Canada and Australia versus Asia versus remaining countries). Patients were randomized in a 1:1 ratio to pola-R-CHP or R-CHOP. Crossover of patients from the R-CHOP group to the pola-R-CHP group was not allowed.
In the POLARIX study, 879 patients were enrolled and randomized from November 2017 to June 2019 to form the global ITT population. Recruitment was expanded to include an additional 121 patients from a China extension cohort from July 2019 to December 2020 to form the expanded population of 1,000 patients. In the global ITT population, the primary analysis was the 2-year follow-up based on the clinical cut-off date of June 28, 2021, with an updated analysis for a 3-year follow-up based on a clinical cut-off date of June 15, 2022, to provide the results of the prespecified final OS analysis. The current review is a resubmission of polatuzumab vedotin that focuses on patients with the ABC subtype of LBCL, which was included as a subgroup analysis in the POLARIX trial. This report summarizes results for the ABC subpopulation from the global ITT population for the 3-year analysis (median of 40.2 months of follow-up) and for the 5-year follow-up (median follow-up duration not reported).
Figure 1: Schematic of the POLARIX Study Design
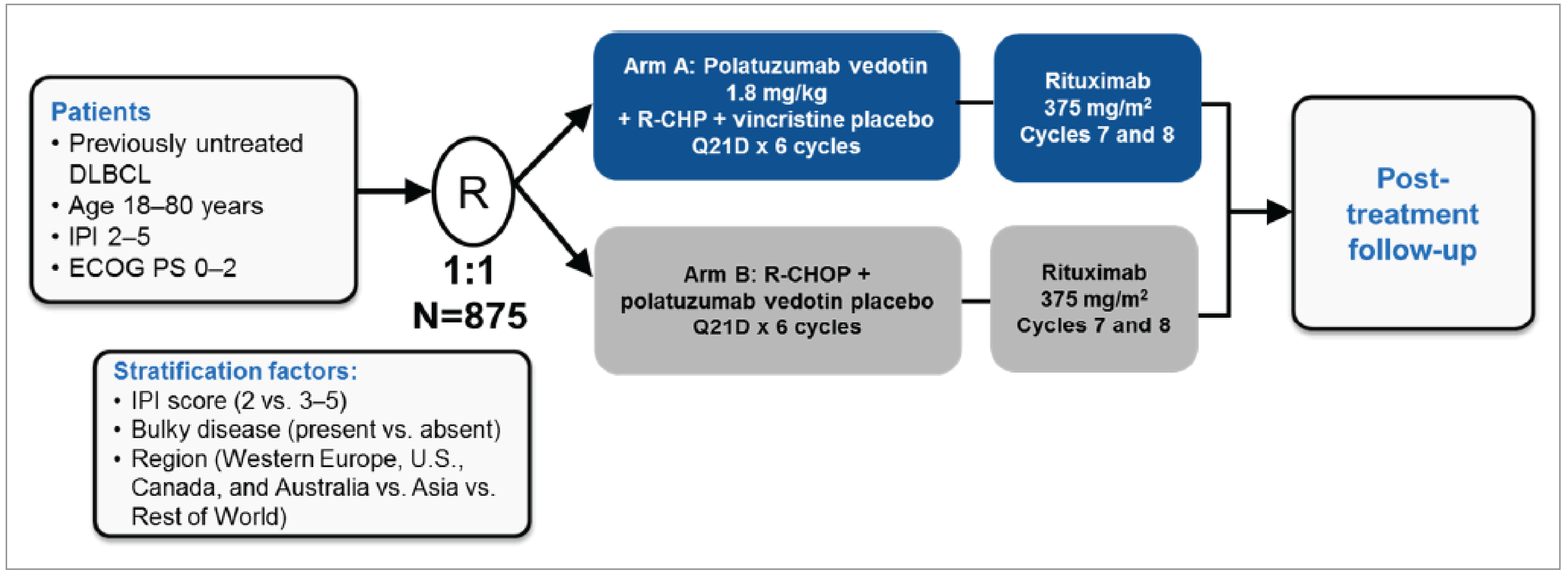
DLBCL = diffuse large B-cell lymphoma; ECOG PS = Eastern Cooperative Oncology Group Performance Status; IPI = International Prognostic Index; Q21D = every 21 days; R = randomization; R-CHOP = rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone; R-CHP = rituximab, cyclophosphamide, doxorubicin, and prednisone; vs. = versus.
Source: POLARIX Clinical Study Report.32
Populations
Inclusion and Exclusion Criteria
The POLARIX trial included adults (aged 18 years to 80 years) with previously untreated CD20-positive DLBCL, including the following WHO 2016 classification of lymphoid neoplasms:
DLBCL NOS, including germinal centre B-cell (GCB) type, and ABC
T-cell/histiocyte-rich LBCL
EBV-positive DLBCL, NOS
anaplastic lymphoma kinase–positive LBCL
human herpes virus 8–positive DLBCL, NOS
high-grade B-cell lymphoma with MYC and BCL2 and/or BCL6 rearrangements (double-hit or triple-hit lymphoma)
high-grade B-cell lymphoma, NOS.
Key eligibility criteria for enrolment in the POLARIX study included patients with an IPI score of 2 to 5, an ECOG PS of 0 to 2, and a life expectancy of 12 months or greater. Patients were excluded from the study if they had a diagnosis of grade 3B follicular lymphoma, B-cell lymphoma unclassifiable with features intermediate between DLBCL and classical Hodgkin lymphoma (grey-zone lymphoma), primary mediastinal (thymic) LBCL, Burkitt lymphoma, CNS lymphoma (primary or secondary involvement), primary effusion DLBCL, and primary cutaneous DLBCL.
Interventions
Patients were randomly assigned to the treatment groups using an interactive voice or web response system. Patients in the POLARIX study received 6 cycles of either pola-R-CHP or standard R-CHOP chemoimmunotherapy regimens. In the pola-R-CHP intervention group, the components of chemoimmunotherapy comprised polatuzumab vedotin, rituximab, cyclophosphamide, doxorubicin, placebo for vincristine, and prednisone. Infusions of each component were administered on day 1 (except for prednisone on day 1 to day 5) of every 21-day cycle for 6 cycles in the following order: prednisone, rituximab, and polatuzumab vedotin. Infusions for placebo for vincristine, cyclophosphamide, and doxorubicin were administered thereafter according to institutional preference. In the R-CHOP comparator group, the chemoimmunotherapy regimen mirrored that of the intervention group, except for placebo for polatuzumab vedotin and treatment with vincristine. In both groups, rituximab was administered as monotherapy in cycle 7 and cycle 8.
Before study treatment initiation (i.e., prephase treatment), steroids were permitted to prevent tumour lysis syndrome in patients with extensive disease and to reduce toxicity of the first cycle of the study treatment (e.g., cytokine release syndrome) . Premedication with antihistamines, antipyretics, and/or analgesics could be administered at the discretion of the investigator. Other than the prednisone given as study treatment and prednisone that could be given as prephase treatment at the discretion of the treating investigator physician, corticosteroids could be used only for the treatment of conditions other than lymphoma (e.g., asthma). In general, investigators were to manage a patient’s care with supportive therapies as clinically indicated, following local standard practices. Vitamin D substitution was encouraged for patients with vitamin D deficiency. All rituximab infusions were to be administered to patients after premedication.
Polatuzumab vedotin and placebo for polatuzumab vedotin was identical in dosage, preparation, and administration. Vincristine (1.4 mg/m2; maximum dose 2 mg) or placebo for vincristine (i.e., normal saline) were identical in dosage and administration. Vincristine was typically administered as an IV infusion via a minibag over approximately 10 minutes to 30 minutes through a dedicated line. Rituximab was administered as 375 mg/m2 IV infusion on day 1 of each cycle; no dose modifications were permitted. Rituximab was administered after the prednisone dosing, and before the cyclophosphamide, doxorubicin, polatuzumab vedotin (or placebo for polatuzumab vedotin), and vincristine (or placebo for vincristine) infusions. Cyclophosphamide (750 mg/m2) and doxorubicin (50 mg/m2) were administered as IV infusions after both rituximab and polatuzumab vedotin or its placebo. Oral prednisone (100 mg per day) was administered on day 1 to day 5 of each of 6 cycles, with prednisolone (100 mg/day) or IV methylprednisolone (80 mg per day) as substitutes; hydrocortisone was not permitted as a substitute.
Prophylaxis for CNS (with intrathecal chemotherapy), hemorrhagic cystitis (with mesna), neutropenia (with granulocyte colony-stimulating factor [G-CSF]), and infection (with anti-infectives) were documented. G-CSF was required as primary prophylaxis for neutropenia in each cycle of therapy during cycles 1 through 6, typically starting 1 to 3 days after administration of myelotoxic chemotherapy (doxorubicin, cyclophosphamide, and polatuzumab vedotin); dosing of G-CSF was according to institutional practice or at the investigator’s discretion. G-CSF may also be considered in patients with fever and neutropenia who are at high risk for infection-associated complications or who have prognostic factors predictive of poor clinical outcomes.
Concomitant therapies that were permitted beginning 7 days before study drug initiation to study completion or discontinuation included prescription drugs, over-the-counter drugs, nonlive vaccines, herbal or homeopathic remedies, nutritional supplements, and treatments for an infusion-related reaction or an AE. Other therapies permitted during the study included hormone replacement therapy, oral contraceptives, antihistamines, antipyretics, and analgesics.
New antilymphoma treatment, including unplanned radiotherapy or systemically administered therapies, could be administered after the patient had completed study treatment. New antilymphoma treatment was allowed with or without disease progression.
Outcomes
A list of efficacy end points assessed in this Clinical Review Report (Table 6) is followed by descriptions of the outcome measures. Summarized end points are based on outcomes included in the sponsor’s Summary of Clinical Evidence as well as any outcomes identified as important to this review by the clinical experts consulted for this review and input from patient and clinician groups and public drug plans. Using the same considerations, we selected end points that were considered to be most relevant to inform expert committee deliberations and finalized this list of end points in consultation with members of the expert committee. The included end points were specific to patients with the ABC lymphoma subtype who were the focus of this review. For consistency with the original reimbursement review of polatuzumab vedotin30 and following CDA-AMC resubmission policies, summarized efficacy end points and notable harms were not assessed using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach.
Table 6: Outcomes Summarized From the Studies Included in the Systematic Review
Outcome measure | Time point | POLARIX |
|---|---|---|
OS | Date of death from any cause | Key secondarya |
PFS | First occurrence of disease progression or relapse, or death from any cause, whichever occurs earlier | Primarya |
Biomarker analyses | On day 1 of cycle 1 and 5, and at treatment completion | Exploratory |
Safety | On day 1 of cycle 1 until 90 days after the last dose of study treatment. AEs of special interest were monitored from day 1 of cycle 1 until 12 months after the last dose of study treatment | Safety |
ABC = activated B cell–like; AE = adverse event; OS = overall survival; PFS = progression-free survival.
aStatistical testing for these end points was adjusted for multiple comparisons (e.g., hierarchical testing) in the overall population. Preplanned biomarker analyses included PFS at the 2-year follow-up in the ABC subpopulation. PFS at the 5-year follow-up and OS at the 2-year and 5-year follow-ups were exploratory end points in the POLARIX study.
Source: POLARIX Clinical Study Report.32
The primary end point in the POLARIX study was investigator-assessed PFS. PFS was defined as the time from randomization to the first occurrence of disease progression or relapse as assessed by the investigator, using the Lugano response criteria for malignant lymphoma, or death from any cause, whichever occurred earlier. OS was a key secondary end point and defined as time from randomization to date of death from any cause. Prespecified exploratory analyses of unstratified investigator-assessed PFS and OS were conducted for subgroups by baseline molecular DLBCL subtypes.
Safety was evaluated by monitoring all AEs, serious AEs, abnormalities identified through physical examinations, vital signs, and laboratory assessments. AEs included treatment-emergent AEs during the AE reporting period only, and were defined as a new or worsening AE from the first dose of any study drug through to 90 days after the last dose of any study drug or before new antilymphoma treatment. Such events were graded using the National Cancer Institute Common Terminology Criteria for Adverse Events, version 4.0. An independent data monitoring committee reviewed safety data during the study. AEs of special interest for the review included peripheral neuropathy, neutropenia (including febrile neutropenia), anemia, thrombocytopenia, infections, hepatic toxicity, tumour lysis syndrome, progressive multifocal leukoencephalopathy, and infusion-related reactions.46 Treatment-emergent notable harms of interest prespecified in the POLARIX trial for neutropenia included febrile neutropenia, peripheral neuropathy, infections, and hepatic toxicity.
Assessment
Response was evaluated at the end of study treatment, or sooner in the event a patient discontinued early. After completion of therapy, all patients were followed at clinic visits conducted every 3 months for 2 years, and then every 6 months until month 60. Assessments at each visit up to the month 60 assessment of year 5 (or until disease progression if it occurred before 5 years) included physical examinations, standard hematologic and biochemistry assessments, vital signs, and “B” symptoms of lymphoma (i.e., weight loss, night sweats, or fever). After 5 years, patients were followed only for survival and initiation of a new antilymphoma treatment by telephone contact approximately every 6 months until study termination, patient withdrawal of consent, or death. After disease progression, patients were followed by telephone contact for survival, applicable AE reporting, and initiation of a new antilymphoma treatment. Patients who terminated study treatment early without progressive disease completed their early study treatment termination visit and then were followed for progression, new antilymphoma treatment, and OS. Patients who initiated new antilymphoma treatment in the absence of progressive disease also continued to be followed for progression, additional new antilymphoma treatment, and OS. Patients who discontinued the protocol-defined treatment and needed to start a new antilymphoma treatment in the absence of documented disease progression (e.g., if wrong diagnosis at screening and new diagnosis required a change of treatment) were followed for disease progression and survival. Patients who terminated study treatment early because of disease progression were followed for new antilymphoma treatment and OS.
Statistical Analysis
Sample Size and Power Calculation
Sample-size calculations for the primary end point of investigator-assessed PFS were based on assumptions for the overall population (adults with untreated CD20-positive DLBCL, including prespecified WHO 2016 classification of lymphoid neoplasms according to the POLARIX study’s eligibility criteria). A separate sample-size calculation was not conducted for efficacy end points among the subgroup of patients with the ABC subtype of LBCL who form the population of interest to this review.
Sample-size calculations for the primary end point of PFS was based on the following assumptions, for approximately 228 investigator-assessed PFS events needed to detect a HR of 0.69 in PFS:
a randomization ratio of 1:1 in pola-R-CHP versus R-CHOP
one-sided log-rank test
an 80% power at the 2.5% significance level
PFS in the control group was assumed to follow a piece-wise exponential distribution, and estimated using the historical data obtained from the GOYA study56 among patients with an IPI score of 2 to 5 who received R-CHOP; the hazard rate over time [h (t)] was estimated as follows: h (t = 1 month and 6 months) = 0.018217; h (6 months and 9 months) = 0.031606; h (9 months and 12 months) = 0.018519; h (12 months and 24 months) = 0.11737; h (24 months and 36 months) = 0.005636; and h (greater than 36 months) = 0.005958
using the hazard rate assumption for the control group and an HR of 0.69 for pola-R-CHP over R-CHOP (i.e., 31% reduction in the risk of disease progression, relapse, or death), the 3-year PFS rate is expected to improve from 62% to 72%
an annual dropout rate of 5% for each treatment group.
The minimal detectable difference for PFS HR at the final PFS analysis was 0.771 (i.e., 22.9% reduction in the risk of disease progression, relapse, or death). The 3-year PFS was expected to improve from 62% to 70% under the minimal detectable difference. No interim analyses were planned for the primary end point of PFS. The PFS primary analysis was conducted after approximately 228 PFS events occurred in the ITT population and at least 24 months after enrolling the last patient (clinical cut-off date of June 2021).
Sample-size considerations for OS were based on the following assumptions:
a randomization ratio of 1:1 in pola-R-CHP versus R-CHOP
a 1-sided log-rank test
a 27% reduction in the risk of death (i.e., OS HR = 0.73 for pola-R-CHP over R-CHOP)
OS in the control group followed an exponential distribution with a hazard rate of 0.006923
an annual dropout rate of 5% for each treatment group.
Based on these assumptions, approximately 134, 164, and 178 OS events were expected to be observed at the 2 interim analyses and the final analysis, respectively. The minimal detectable difference for the OS HR at the final OS analysis was 0.75. Overall power for detecting an OS HR of 0.73 was 52%, tested at a 1-sided alpha of 0.02.
Efficacy Analyses
To control the overall type I error rate at a 1-sided level of significance of 0.025, a hierarchical testing procedure, including possible alpha recycling, was used to adjust for multiple statistical testing of the primary and key secondary efficacy end points. The POLARIX statistical analysis plan is depicted in Figure 2. Relevant to the population of interest for this review, the subgroup of patients with ABC lymphoma subtype were not included in the testing procedure.
Figure 2: Statistical Analysis Plan in POLARIX Study
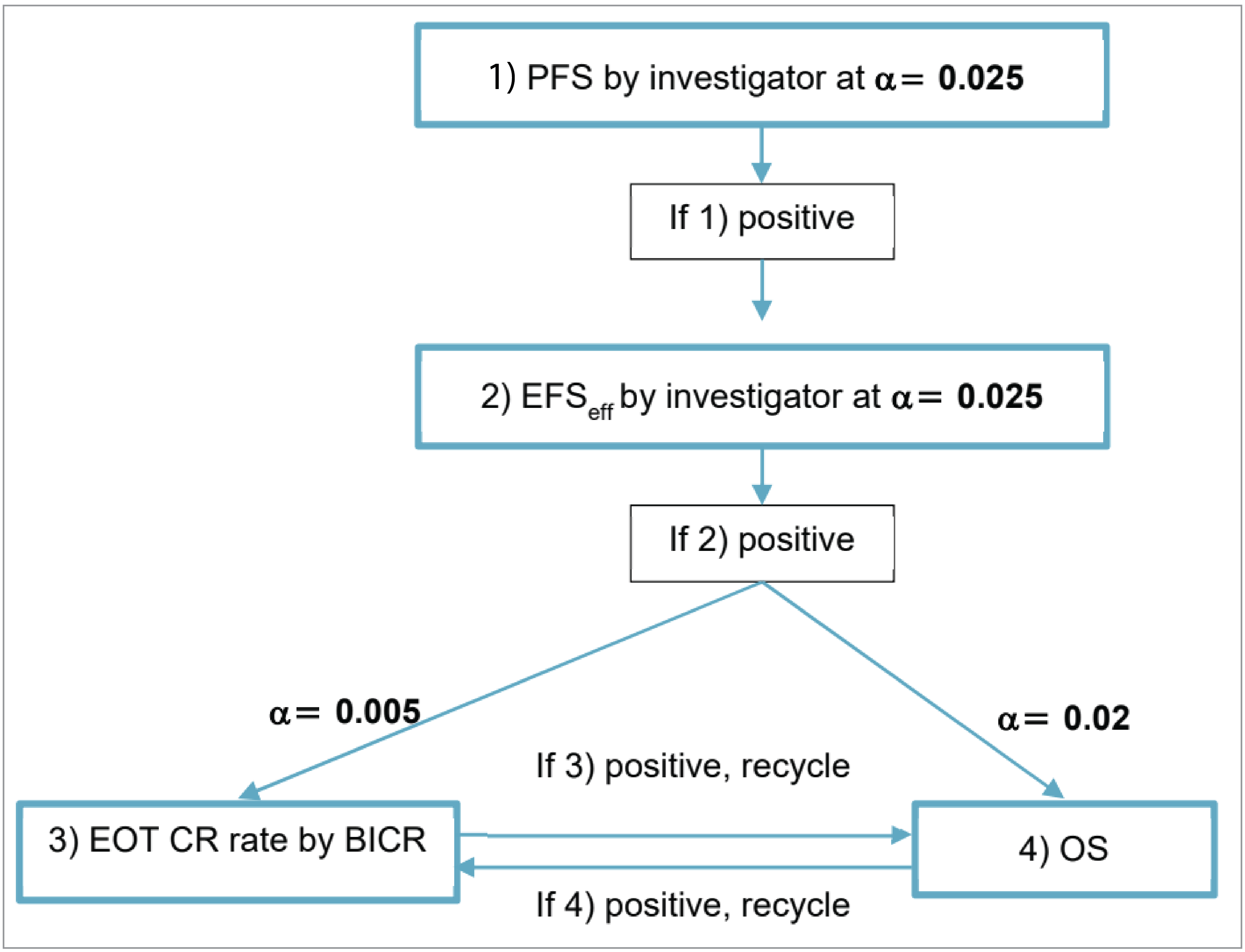
α = alpha significance level; BICR = blinded independent central review; CR = complete response; EFSeff = event-free survival efficacy; EOT = end of treatment; OS = overall survival; PFS = progression-free survival.
Source: POLARIX Clinical Study Report.32
Censoring
For the primary efficacy end point of investigator-assessed PFS, patients who did not experience disease progression, a relapse, or death at the data cut-off for analysis were censored on the date of last disease assessment when the patient was known to be progression-free. If no tumour assessments were performed after the baseline visit or postbaseline tumour assessment results were not evaluable, PFS was censored on the date of randomization. For OS, patients who had not died at the clinical data cut-off for analysis were censored on the last date when the patients were known to be alive, as documented by the investigator.
Biomarker and Statistical Analyses
Planned exploratory analyses of biomarkers related to tumour biology and the mechanisms of action of polatuzumab vedotin and rituximab were conducted to assess the prognostic and/or predictive value of candidate markers. The effects of baseline prognostic characteristics, including molecular DLBCL subtypes (i.e., COO status) on selected efficacy end points (e.g., investigator-assessed PFS, OS) were evaluated using subgroup analysis. COO status was centrally assessed at Q2 Solutions by RNA expression using the NanoString Lymph2Cx assay. The RUO version of the NanoString Lymphoma Subtyping Test algorithm was used to determine the COO molecular subtype of each sample. Sample quality control, data generation, and analysis were performed at Q2 Solutions, and the final COO status of sample were reported to the sponsor (Roche).
Patients with the ABC lymphoma subtype, the population of interest for this review, were included in an exploratory COO subgroup analysis. Prespecified summaries of PFS, including unstratified HRs estimated from Cox proportional hazards models and Kaplan-Meier estimates of 1-year and 2-year PFS rates, and median PFS (if reached), were produced separately for each level of the categorical variables for the comparisons between treatments arms displayed in a forest plot. Unstratified HRs estimated from Cox proportional hazards models and Kaplan-Meier estimates of 1-year OS and median OS (if reached), were also prespecified. No tests for interaction to evaluate differences in effects between COO subgroups were conducted. Compared to the primary analysis for the overall population, the subgroup analyses of PFS and OS for patients with ABC lymphoma subtype used the same statistical model (Kaplan-Meier) and adjustment factors that were used in randomization (geographical region, IPI score, and bulky disease). In contrast to stratified estimates of treatment effects that were prespecified in the overall population, stratified estimates of treatment effects for ABC lymphoma subtype were post hoc analyses. Statistical analyses of OS and investigator-assessed PFS for patients with ABC lymphoma subtype are summarized in Table 7.
Safety Analyses
Descriptive statistics (i.e., frequencies) were summarized for each treatment group for AEs, serious AEs, AEs of special interest, AEs leading to study drug discontinuation, and deaths.
Table 7: Statistical Analysis of Efficacy End Points
End point | Statistical model | Adjustment factors | Handling of missing data | Sensitivity analyses |
|---|---|---|---|---|
OS |
| Stratified by the same stratification factors employed in randomization:
| For patients who had not died at the clinical cut-off date for analysis, OS was censored on the last date when the patient was known to be alive, as documented by investigator | None |
Investigator-assessed PFS |
| Stratified by the same stratification factors employed in randomization:
| PFS was censored on the date of last disease assessment when the patient is known to be progression-free; if no tumour assessments were performed after the baseline visit or postbaseline tumour assessment results were not evaluable, PFS was censored on the date or randomization | None |
IPI = International Prognostic Index; OS = overall survival; PFS = progression-free survival; vs. = versus.
Source: POLARIX Clinical Study Report.32
Analysis Populations
The analysis population for the primary and secondary efficacy analyses consisted of all randomized patients, with patients grouped according to their assigned treatment (Table 8). The ITT population included all patients randomized during the global enrolment phase (including patients enrolled in China during that phase), regardless of the treatment received. The global study included 879 patients randomized on or before June 27, 2019; this (global ITT) population is the population for which the primary analysis was performed. The safety population included all patients in the global study who received at least 1 dose of study treatment (any of the treatment components), with patients grouped according to the treatment regimen they actually received. The China extension cohort included patients from mainland China who were randomized after June 27, 2019; this cohort was excluded from the ITT and the safety populations. Patients with the ABC lymphoma subtype were included as a preplanned subgroup analysis of the global ITT population.
Table 8: Analysis Populations of POLARIX Study
Population | Definition | Application |
|---|---|---|
ITT population | The ITT population is defined as all patients randomized during the global enrolment phase (i.e., the global study, whether or not the patients received the assigned treatment); subgroup analysis by baseline molecular DLBCL subtypes using centrally tested COO was conducted in the ITT population for patients who had baseline tumour biopsies | Efficacy analyses (PFS and OS) |
Safety population | The safety analysis population includes all patients in the global study who received at least 1 dose of study treatment (polatuzumab vedotin, rituximab, cyclophosphamide, doxorubicin, vincristine, or prednisone), with patients grouped according to the treatment regimen actually received | Safety analyses |
COO = cell of origin; DLBCL = diffuse large B-cell lymphoma; ITT = intention to treat; OS = overall survival; PFS = progression-free survival.
Source: POLARIX Clinical Study Report.32
Results
Patient Disposition
In the POLARIX study, COO status in the biomarker evaluable population (central review by NanoString) was available for ███ patients (███ patients in the pola-R-CHP group and ███ patients in the R-CHOP group) as follows: ABC (n = ███), GCB (n = ███), and unclassified (n = ██). COO status was unknown for ███ of ███ patients (█████) in the POLARIX study.
At the data cut-off on July 5, 2024, of ███ patients in the ABC subpopulation, █████ of patients had completed treatment, █████ of patients had discontinued treatment, and █████ of patients had discontinued the study (Table 9). In the pola-R-CHP group (n = ███) and the R-CHOP group (n = ███), the numbers of patients who discontinued treatment and reasons for discontinuing treatment were similar between groups. Study discontinuations were lower in the pola-R-CHP group (█████) compared to the R-CHOP group (█████). Reasons for study discontinuations were similar between groups, except for fewer deaths occurring in the pola-R-CHP group (█████) than the R-CHOP group (█████).
Table 9: Summary of Patient Disposition From the POLARIX Study (Global ITT Analysis Set)
Patient disposition | POLARIX ABC subpopulation | |
|---|---|---|
Pola-R-CHP (N = 106) | R-CHOP (N = 129) | |
Screened, N | ██ ██████ | |
Not meeting eligibility, n (%) | ██ ██████ | |
Randomized, n (%) | ██ ██████ | ██ ██████ |
Discontinued treatment, n (%) | ██ ██████ | ██ ██████ |
Reason for treatment discontinuation, n (%) | ||
Adverse events | ██ ██████ | ██ ██████ |
Death | ██ ██████ | ██ ██████ |
Physician decision | ██ ██████ | ██ ██████ |
Withdrawal by patient | ██ ██████ | ██ ██████ |
Progressive disease | ██ ██████ | ██ ██████ |
Other | ██ ██████ | ██ ██████ |
Completed treatment, n (%) | ██ ██████ | ██ ██████ |
Discontinued study, n (%) | ██ ██████ | ██ ██████ |
Reason for study discontinuation, n (%) | ||
Death | ██ ██████ | ██ ██████ |
Withdrawal by patient | ██ ██████ | ██ ██████ |
Physician decision | ██ ██████ | ██ ██████ |
Lost to follow-up | ██ ██████ | ██ ██████ |
ITT, N | ██ ██████ | ██ ██████ |
Subgroup analysis, N | ██ ██████ | ██ ██████ |
Safety, N | ██ ██████ | ██ ██████ |
ABC = activated B cell–like; ITT = intention to treat; pola-R-CHP = polatuzumab vedotin, rituximab, cyclophosphamide, doxorubicin, and prednisone; R-CHOP = rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone.
Source: From sponsor in response to additional data requests.33,57
Baseline Characteristics
Baseline characteristics of patients in the POLARIX trial among the patient subpopulation with the ABC lymphoma subtype (N = 235) are summarized (refer to Table 10).
Patients were aged a median of ██ years (range, ██ █████ ██ ██ █████), and female (█████) and male (█████). Patient race included American Indian or Alaska Native (████), Asian (█████), Black or African American (████), white (from original source; █████), other (unspecified, from original source; ████), and unknown (█████). Patients (n = ███) had an ECOG PS of 0 (█████), 1 (█████), or 2 (█████). More patient IPI scores at screening were 3 to 5 (█████) than 2 (█████). Bulky disease, defined as at least 1 lesion of 7.5 cm, was present at baseline in █████ of patients but absent in █████ of patients. Most patients were categorized as DLBCL NOS, ABC, or GCB (combined; █████) and were negative for double-hit or triple-hit lymphoma (█████). Demographic and clinical characteristics of patients with ABC lymphoma subtype were generally similar between treatment groups. However, more patients had disease designated as Ann Arbor stage III in the pola-R-CHP group (█████) than the R-CHOP group (█████) whereas fewer patients had Ann Arbor stage IV disease in the pola-R-CHP group (█████) compared with the R-CHOP group (█████). Additionally, fewer patients had 2 or more extranodal disease sites in the pola-R-CHP group (█████) than in the R-CHOP group (█████).
Table 10: Summary of Baseline Characteristics in POLARIX Study (Global ITT Analysis Set)
Characteristic | POLARIX ABC subpopulation; Pola-R-CHP (N = 106) | R-CHOP (N = 129) | Total (N = 235) |
|---|---|---|---|
Age (years), median (range) | ██ ██████ | ██ ██ | ██ ██ |
≥ 65 years, n (%) | ██ ██████ | ██ ██ | ██ ██ |
Sex, n (%) | |||
Female | ██ ██████ | ██ ██ | ██ ██ |
Male | ██ ██████ | ██ ██ | ██ ██ |
Race, n (%) | |||
American Indian or Alaska Native | ██ ██████ | ██ ██ | ██ ██ |
Asian | ██ ██████ | ██ ██ | ██ ██ |
Black or African American | ██ ██████ | ██ ██ | ██ ██ |
White | ██ ██████ | ██ ██ | ██ ██ |
Other | ██ ██████ | ██ ██ | ██ ██ |
Unknown | ██ ██████ | ██ ██ | ██ ██ |
Ethnicity, n (%) | |||
Hispanic or Latino | ██ ██████ | ██ ██ | ██ ██ |
Not Hispanic or Latino | ██ ██████ | ██ ██ | ██ ██ |
Not stated | ██ ██████ | ██ ██ | ██ ██ |
Unknown | ██ ██████ | ██ ██ | ██ ██ |
ECOG PS score, n (%) | |||
0 | ██ ██████ | ██ ██ | ██ ██ |
1 | ██ ██████ | ██ ██ | ██ ██ |
2 | ██ ██████ | ██ ██ | ██ ██ |
Baseline bulky disease (eCRF), n (%) | |||
Absent | ██ ██████ | ██ ██ | ██ ██ |
Present | ██ ██████ | ██ ██ | ██ ██ |
Stratification: IPI score (IxRS), n (%) | |||
2 | ██ ██████ | ██ ██ | ██ ██ |
3 to 5 | ██ ██████ | ██ ██ | ██ ██ |
Stratification: bulky disease (IxRS), n (%) | |||
Absent | ██ ██████ | ██ ██ | ██ ██ |
Present | ██ ██████ | ██ ██ | ██ ██ |
Stratification: geographic region (IxRS), n (%) | |||
Asia | ██ ██████ | ██ ██ | ██ ██ |
Australia, Canada, US, Western Europe | ██ ██████ | ██ ██ | ██ ██ |
Rest of world | ██ ██████ | ██ ██ | ██ ██ |
Ann Arbor stage, n (%) | |||
I | ██ ██████ | ██ ██ | ██ ██ |
II | ██ ██████ | ██ ██ | ██ ██ |
III | ██ ██████ | ██ ██ | ██ ██ |
IV | ██ ██████ | ██ ██ | ██ ██ |
Baseline lactate dehydrogenase > 1 × ULN, n (%) | ██ ██████ | ██ ██ | ██ ██ |
Bone marrow involvement at diagnosis, n (%) | ██ ██████ | ██ ██ | ██ ██ |
Number of extranodal sites, n (%) | |||
0 to 1 | ██ ██████ | ██ ██ | ██ ██ |
≥ 2 | ██ ██████ | ██ ██ | ██ ██ |
NHL histologic diagnosis according to investigator | |||
DLBCL NOS, ABC, GCB | ██ ██████ | ██ ██ | ██ ██ |
HGBCL, double-hit lymphoma, or triple-hit lymphoma | ██ ██████ | ██ ██ | ██ ██ |
Other LBCL | ██ ██████ | ██ ██ | ██ ██ |
Double-expressor lymphoma by IHC (central review), n (%) | |||
Double-expressor lymphoma | ██ ██████ | ██ ██ | ██ ██ |
Non–double-expressor lymphoma | ██ ██████ | ██ ██ | ██ ██ |
Unknown | ██ ██████ | ██ ██ | ██ ██ |
Double-hit lymphoma or triple-hit lymphoma (central review), n (%) | |||
Double-hit positive or triple-hit positive | ██ ██████ | ██ ██ | ██ ██ |
Double-hit negative or triple-hit negative | ██ ██████ | ██ ██ | ██ ██ |
Unknown | ██ ██████ | ██ ██ | ██ ██ |
Time from diagnosis to study dose, days | |||
Mean (SD) | ██ ██████ | ██ ██ | ██ ██ |
Median (range) | ██ ██████ | ██ ██ | ██ ██ |
≤ 30 days, n (%) | ██ ██████ | ██ ██ | ██ ██ |
> 30 days, n (%) | ██ ██████ | ██ ██ | ██ ██ |
ABC = activated B cell–like; DLBCL = diffuse large B-cell lymphoma; ECOG PS = Eastern Cooperative Oncology Group Performance Status; eCRF = electronic case report form; GBC = germinal centre B cell; HGBCL = high-grade B-cell lymphoma; IHC = immunohistochemistry; IPI = International Prognostic Index; ITT = intention to treat; IxRS = interactive voice or web-based response system; LBCL = large B-cell lymphoma; NOS = not otherwise specified; pola-R-CHP = polatuzumab vedotin, rituximab, cyclophosphamide, doxorubicin, and prednisone; R-CHOP = rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone; SD = standard deviation; ULN = upper limit of normal.
aECOG PS score was not reported for 1 patient in the R-CHOP group, making the denominator for calculating percent 128 patients.
bBaseline lactate dehydrogenase was not reported for 1 patient in the pola-R-CHP group, making the denominator for calculating percent 125 patients.
cBone marrow involvement at diagnosis was not available for 3 patients in the R-CHOP group, making the denominator for calculating percent 126 patients.
Source: From sponsor in response to additional data request.33
Exposure to Study Treatments
At the data cut-off on July 5, 2024, mean treatment durations in the ABC subpopulation were similar between the pola-R-CHP and R-CHOP groups for rituximab (4.7 months and 4.5 months, respectively), cyclophosphamide (3.4 months and 3.3 months, respectively), doxorubicin (3.4 months and 3.3 months, respectively), and prednisone (3.5 months in both groups) (Table 11). The median relative dose intensity was greater than 97% for all components of treatment in each treatment group.
Table 11: Summary of Patient Exposure in the POLARIX Study (Safety Analysis Set)
Treatment exposure | POLARIX ABC subpopulation | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
Pola-R-CHP (N = 106) | R-CHOP (N = 129) | |||||||||
Pola n = 106 | RTX n = 106 | CYC n = 106 | DOX n = 106 | PRED n = 106 | RTX n = 129 | CYC n = 129 | DOX n = 129 | VIN n = 129 | PRED n = 129 | |
Treatment duration, months | ||||||||||
Mean (SD) | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ███ |
Median (range) | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ███ |
Number of cycles | ||||||||||
Mean (SD) | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ███ |
Median (range) | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ███ |
Relative dose intensity, % | ||||||||||
n | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ███ |
Mean (SD) | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ███ |
Median (range) | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ███ |
Total cumulative dose, mg | ||||||||||
Mean (SD) | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ███ |
Median (range) | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ███ | ███ |
ABC = activated B cell–like; CYC = cyclophosphamide; DOX = doxorubicin; Pola = polatuzumab vedotin; PRED = prednisone (includes prednisone, prednisolone, and methylprednisone); RTX = rituximab; SD = standard deviation; VIN = vincristine.
Source: From sponsor in response to additional data request.33
Concomitant Treatments
At the data cut-off on July 5, 2024, ███ patients in the ABC subpopulation received at least 1 concomitant treatment during the study (Table 12). The numbers of patients who received concomitant treatment were generally similar between groups for anti-infective prophylaxis, and prephase steroid treatment. While concomitant G-CSF use for prophylaxis was similar between groups, concomitant G-CSF use for nonprophylaxis was ██████ in the pola-R-CHP group (█████) compared to the R-CHOP group (█████).
Table 12: Concomitant Treatments in the POLARIX Study (Safety Analysis Set)
Exposure | POLARIX ABC subpopulation | |
|---|---|---|
Pola-R-CHP (N = 106) | R-CHOP (N = 129) | |
Patients with ≥ 1 concomitant medication, n (%) | ███ █████ | ███ █████ |
Anti-infective prophylaxis, n (%) | ██ ██████ | ██ ██████ |
Patients who received ≥ 1 prephase steroid treatment, n (%) | ██ ██████ | ██ ██████ |
Patients who received concomitant G-CSF, n (%) | ███ ██████ | ███ ██████ |
Concomitant G-CSF for prophylaxis, n (%) | ██ ██████ | ███ ██████ |
Concomitant G-CSF for nonprophylaxis, n (%) | ██ ██████ | ██ ██████ |
ABC = activated B cell–like; G-CSF = granulocyte colony-stimulating factor; pola-R-CHP = polatuzumab vedotin, rituximab, cyclophosphamide, doxorubicin, and prednisone; R-CHOP = rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone.
Source: From sponsor in response to additional data request.57
New Antilymphoma Treatment
At the data cut-off on July 5, 2024, the numbers of patients in the ABC subpopulation with subsequent new antilymphoma treatment were ██ patients (█████) in the pola-R-CHP group versus ██ patients (█████) in the R-CHOP group (Table 13). Compared to the pola-R-CHP group, ████ patients in the R-CHOP group received radiotherapy, systemic therapy, stem-cell transplant, CAR T-cell therapy, platinum-based therapy, and bispecifics.
Table 13: New Antilymphoma Treatments in the POLARIX Study (Global ITT Analysis Set)
Exposure | POLARIX ABC subpopulation | |
|---|---|---|
Pola-R-CHP N = 106 | R-CHOP N = 129 | |
Patients with ≥ 1 subsequent antilymphoma treatment, n (%) | ██ ██████ | ██ ██████ |
Patients with ≥ 1 new antilymphoma treatment before PFS event, n (%) | ██ ██████ | ██ ██████ |
Patients with ≥ 1 new antilymphoma treatment after PFS event, n (%) | ██ ██████ | ██ ██████ |
Patients with ≥ 1 new antilymphoma treatment and without PFS event, n (%) | ██ ██████ | ██ ██████ |
Patients with ≥ 1 radiotherapy treatment, n (%) | ██ ██████ | ██ ██████ |
Preplanned radiotherapy, n (%) | ██ ██████ | ██ ██████ |
Unplanned radiotherapy, n (%) | ██ ██████ | ██ ██████ |
Patients who received ≥ 1 systemic therapy, n (%) | ██ ██████ | ██ ██████ |
Patients who received stem-cell transplant, n (%) | ██ ██████ | ██ ██████ |
Autologous transplant, n (%) | ██ ██████ | ██ ██████ |
Allogeneic transplant, n (%) | ██ ██████ | ██ ██████ |
Patients who received CAR T-cell therapy, n (%) | ██ ██████ | ██ ██████ |
Patients who received platinum-based therapy, n (%) | ██ ██████ | ██ ██████ |
Patients who received bispecifics, n (%) | ██ ██████ | ██ ██████ |
ABC = activated B cell–like; CAR = chimeric antigen receptor; ITT = intention to treat; PFS = progression-free survival; pola-R-CHP = polatuzumab vedotin, rituximab, cyclophosphamide, doxorubicin, and prednisone; R-CHOP = rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone.
Source: From sponsor in response to additional data request.33
Efficacy
Findings for key efficacy outcomes in the POLARIX study for patients with ABC lymphoma subtype are summarized in Table 14.
Overall Survival
At the 3-year follow-up, ███ ██████ ██ ███ ███ ████ ███████ ██ ██████ ███ ██████████ █████ ██ ███ ██████ █████. ████████ patients (█████) in the pola-R-CHP group and ██ patients (█████) in the R-CHOP group had died. The differences in OS probability were ████ at 12 months and ████ at 24 months. The 2-year OS was █████ in the pola-R-CHP group versus ██████ in the R-CHOP group (stratified HR = ████; 95% CI, ████ ██ ████; P value = ██████).
At the 5-year follow-up, the median duration of follow-up was 63.9 months (range, 0 to 73) in the pola-R-CHP group and 64.2 months (range, 1 to 78) in the R-CHOP group. Median OS had not been reached in the pola-R-CHP group or the R-CHOP group. Seventeen patients (16.0%) in the pola-R-CHP group and 38 patients (29.5%) in the R-CHOP group had died. The differences in OS probability were 9.5%, 13.4%, and 14.7% at 36 months, 48 months, and 60 months, respectively. The 5-year OS was 84.6% in the pola-R-CHP group versus 69.9% in the R-CHOP group (stratified HR = 0.49; 95% CI, 0.27 to 0.90; P value = 0.0190).
Results of the unstratified analysis were consistent with the results of the stratified analysis for OS at 2 years (unstratified HR = 0.49; 95% CI, 0.25 to 0.94; P value = 0.0273) and at 5 years (unstratified HR = 0.49; 95% CI, 0.28 to 0.88; P value = 0.0136) (Figure 3).
Results of OS at 2 years for GCB lymphoma subtype and unclassified COO were not reported. Results of OS at 5 years for GCB lymphoma subtype (n = 357; unstratified HR = 0.99; 95% CI, 0.60 to 1.61) and for unclassified COO (n = 97; unstratified HR = 4.46; 95% CI, 1.23 to 16.21) were not consistent with findings for the ABC lymphoma subtype.
Figure 3: Kaplan-Meier Estimate of OS by COO Subgroup (Global ITT Analysis Set) — Data Cut-Off Date July 5, 2024
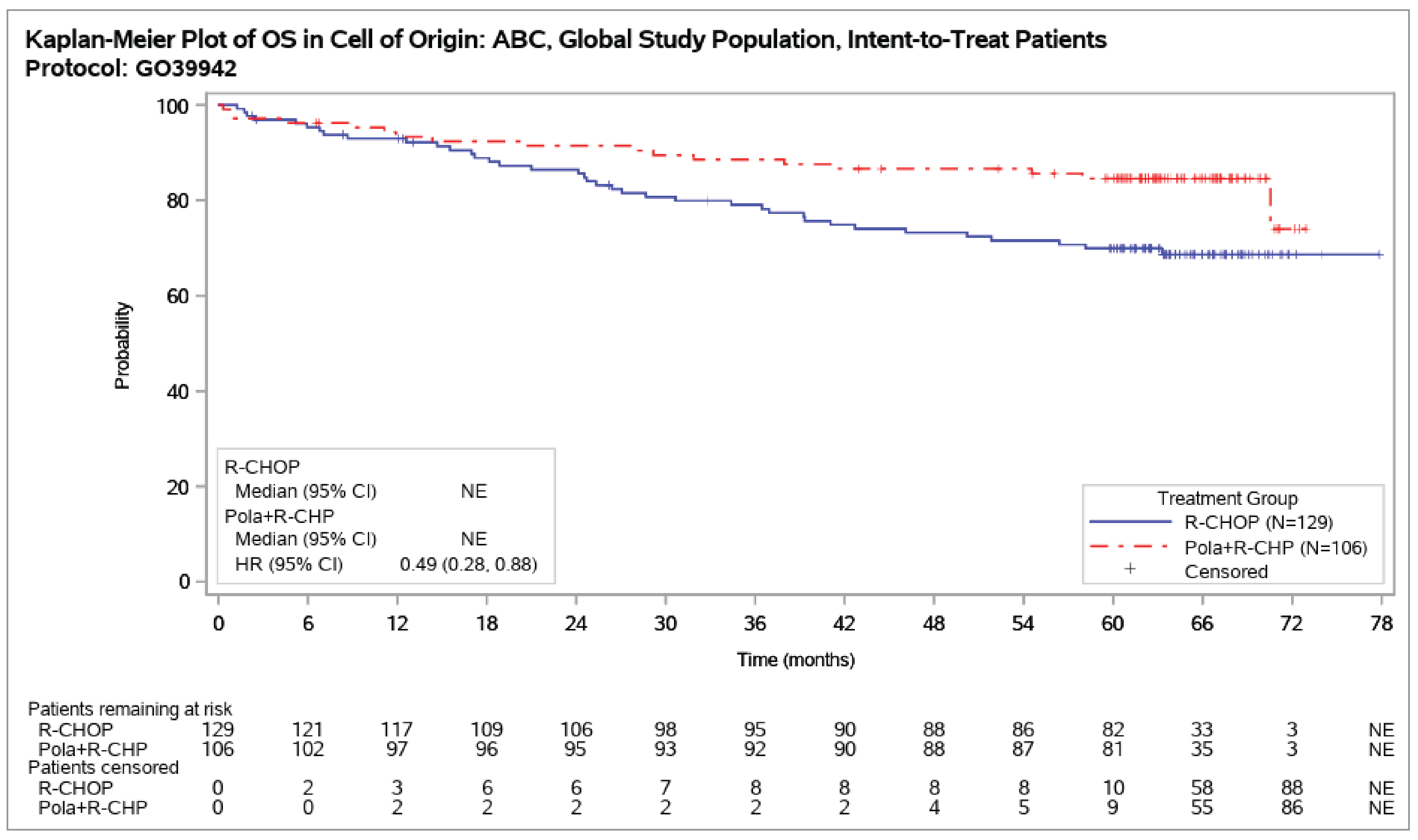
CI = confidence interval; COO = cell of origin; HR = hazard ratio; ITT = intention to treat; OS = overall survival; pola+R-CHP = polatuzumab vedotin, rituximab, cyclophosphamide, doxorubicin, and prednisone; R-CHOP = rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone.
Source: From sponsor in response to additional data request.57
Progression-Free Survival
At the 3-year follow-up, the median durations of follow-up were ████ months (range, █████ ██ ██ ██████) in the pola-R-CHP group and ████ months (range, █████ ██ ██ ██████) in the R-CHOP group. ██████ █████████████████████ ███ ███ ███ ████ ███████ in the pola-R-CHP group compared with ████ months (95% CI, ████ ██████ ██ ███ █████████) in the R-CHOP group. ██████████ of ███ patients (█████) in the pola-R-CHP group and ██ of ███ patients (█████) in the R-CHOP group experienced an event, of which █████ in the pola-R-CHP group and █████ in the R-CHOP group were due to disease progression and ████ in the pola-R-CHP group and ████ in the R-CHOP group were due to death. The differences in investigator-assessed PFS probability were █████ at 12 months and █████ at 24 months. The 2-year investigator-assessed PFS was 84.7% in the pola-R-CHP group versus 56.1% in the R-CHOP group (stratified HR = 0.31; 95% CI, 0.18 to 0.52; P < 0.0001).
At the 5-year follow-up, the median durations of follow-up were 55.0 months (range, 0 to 71) in the pola-R-CHP group and 56.1 months (range, 0 to 68) in the R-CHOP group. The median investigator-assessed PFS was 70.5 months (95% CI, not estimable) in the pola-R-CHP group, compared with 33.2 months (95% CI, 18.9 to 66.7) in the R-CHOP group. Twenty-eight patients (26.4%) in the pola-R-CHP group and 69 patients (53.5%) in the R-CHOP group experienced an event, of which 16.0% in the pola-R-CHP group and 45.0% in the R-CHOP group were due to disease progression and 10.4% in the pola-R-CHP group and 8.5% in the R-CHOP group were due to death. The differences in investigator-assessed PFS probability were 29.7%, 27.5%, and 26.7% at 36 months, 48 months, and 60 months, respectively. The 5-year investigator-assessed PFS was 72.5% in the pola-R-CHP group versus 45.8% in the R-CHOP group (stratified HR = 0.33; 95% CI, 0.21 to 0.53; P < 0.0001).
Results of the unstratified analysis were consistent with the those of the stratified analysis for investigator-assessed PFS at 2 years (unstratified HR = 0.34; 95% CI, 0.21 to 0.56; P < 0.0001) (Figure 4 and Figure 5) and at 5 years (unstratified HR = 0.38; 95% CI, 0.24 to 0.59; P < 0.0001) (Figure 6).
Compared to the findings for the ABC lymphoma subtype, there were no differences between pola-R-CHP and R-CHOP in investigator-assessed PFS at 2 years or at 5 years for the GCB lymphoma subtype (n = 357; unstratified HR = 1.07; 95% CI, 0.74 to 1.56) or for unclassified COO (n = 97; unstratified HR = 1.60; 95% CI, 0.79 to 3.25).
Table 14: Summary of Key Efficacy Results in the POLARIX Study (Global ITT Analysis Set)
Outcome measure | POLARIX ABC subpopulation | |
|---|---|---|
Pola-R-CHP N = 106 | R-CHOP N = 129 | |
OS | ||
Data cut-off date | June 15, 2022 | |
Median follow-up duration, months (range) | ██ | ██ |
Patients with events, n (%) | ██ ██████ | ██ ██████ |
Censored, n (%) | ██ ██████ | ██ ██████ |
Time to OS (months), median (95% CI) | ██ ████ | ██ ████ |
Unstratified HR (95% CI)a | ████ ██████ ██ | █████████ |
P valueb | ██████ | █████████ |
Stratified HR (95% Cl)c | ████ ██████ ██ | █████████ |
P valued | ██████ | █████████ |
Data cut-off date | July 5, 2024 | |
Median follow-up duration, months (range) | 63.9 (0 to 73) | 64.2 (1 to 78) |
Patients who died, n (%) | 17 (16.0) | 38 (29.5) |
Censored, n (%) | 89 (84.0) | 91 (70.5) |
Time to OS (months), median (95% CI) | NE (NE) | NE (NE) |
Unstratified HR (95% CI)a | 0.49 (0.28 to 0.88) | Reference |
P valueb | 0.0136 | Reference |
Stratified HR (95% Cl)c | 0.49 (0.27 to 0.90) | Reference |
P valued | 0.0190 | Reference |
12 months | ||
Patients remaining at risk at 12 months, n (%) | 97 (91.5) | 117 (90.7) |
12-month OS rate (95% CI) | 93.34 (88.57 to 98.11) | 92.95 (88.50 to 97.39) |
Difference in OS rate at 12 months (95% CI) | 0.39 (−6.13 to 6.91) | Reference |
24 months | ||
Patients remaining at risk at 24 months, n (%) | 95 (89.6) | 106 (82.2) |
24-month OS rate (95% CI) | 91.42 (86.05 to 96.78) | 86.43 (80.43 to 92.43) |
Difference in OS rate at 24 months (95% CI) | 4.98 (−3.07 to 13.03) | Reference |
36 months | ||
Patients remaining at risk at 36 months, n (%) | 92 (86.8) | 95 (73.6) |
36-month OS rate (95% CI) | 88.53 (82.42 to 94.64) | 79.04 (71.87 to 86.22) |
Difference in OS rate at 36 months (95% CI) | 9.48 (0.06 to 18.91) | Reference |
48 months | ||
Patients remaining at risk at 48 months, n (%) | 88 (83.0) | 88 (68.2) |
48-month OS rate (95% CI) | 86.60 (80.07 to 93.14) | 73.22 (65.38 to 81.05) |
Difference in OS rate at 48 months (95% CI) | 13.38 (3.18 to 23.58) | Reference |
60 months | ||
Patients remaining at risk at 60 months, n (%) | 81 (76.4) | 82 (63.6) |
60-month OS rate (95% CI) | 84.59 (77.64 to 91.54) | 69.89 (61.76 to 78.02) |
Difference in OS rate at 60 months (95% CI) | 14.70 (4.00 to 25.39) | Reference |
Investigator-assessed PFS | ||
Data cut-off date | June 15, 2022 | |
Median follow-up duration, months (range) | ████ ██ ██ ███ | ████ ██ ██ ███ |
Patients with investigator-assessed PFS events, n (%) | ██ ██████ | ██ ██████ |
Disease progression, n (%) | ██ ██████ | ██ ██████ |
Death, n (%) | █████ | █████ |
Censored, n (%) | ██ ██████ | ██ ██████ |
Time to investigator-assessed PFS (months), median (95% CI) | ██ █████ ██ ███ | ████ █████ |
Unstratified HR (95% CI)a | ██████████ █ | █████████ |
P valueb | ██████ | █████████ |
Stratified HR (95% CI)c | ██████████ ██ | █████████ |
P valued | ██████ | █████████ |
Data cut-off date | July 5, 2024 | |
Median follow-up duration, months (range) | 55.0 (0 to 71) | 56.1 (0 to 68) |
Patients with investigator-assessed PFS events, n (%) | 28 (26.4) | 69 (53.5) |
Disease progression, n (%) | 17 (16.0) | 58 (45.0) |
Death, n (%) | 11 (10.4) | 11 (8.5) |
Censored, n (%) | 78 (73.6) | 60 (46.5) |
Time to investigator-assessed PFS (months), median (95% CI) | 70.5 (NE) | 33.2 (18.9 to 66.7) |
Unstratified HR (95% CI)a | 0.38 (0.24 to 0.59) | Reference |
P valueb | < 0.0001 | Reference |
Stratified HR (95% CI)c | 0.33 (0.21 to 0.53) | Reference |
P valued | < 0.0001 | Reference |
12 months | ||
Patients remaining at risk at 12 months, n (%) | 94 (88.7) | 90 (69.8) |
12-month PFS rate (95% CI) | 90.50 (84.89 to 96.10) | 70.88 (62.98 to 78.78) |
Difference in PFS rate at 12 months (95% CI)e | 19.61 (9.93 to 29.30) | Reference |
24 months | ||
Patients remaining at risk at 24 months, n (%) | 86 (81.1) | 68 (52.7) |
24-month PFS rate (95% CI) | 84.71 (77.81 to 91.61) | 55.70 (47.03 to 64.37) |
Difference in PFS rate at 24 months (95% CI)e | 29.01 (17.93 to 40.09) | Reference |
36 months | ||
Patients remaining at risk at 36 months, n (%) | 78 (73.6) | 60 (46.5) |
36-month PFS rate (95% CI) | 79.65 (64.98 to 85.70) | 49.92 (41.15 to 58.68) |
Difference in PFS rate at 36 months (95% CI)e | 29.74 (18.02 to 41.46) | Reference |
48 months | ||
Patients remaining at risk at 48 months, n (%) | 70 (66.0) | 58 (45.0) |
48-month PFS rate (95% CI) | 76.59 (68.37 to 84.81) | 49.07 (40.29 to 57.84) |
Difference in PFS rate at 48 months (95% CI)e | 27.52 (15.50 to 39.54) | Reference |
60 months | ||
Patients remaining at risk at 60 months, n (%) | 28 (26.4) | 26 (20.2) |
60-month PFS rate (95% CI) | 72.46 (62.82 to 82.10) | 45.78 (36.47 to 55.08) |
Difference in PFS rate at 60 months (95% CI)e | 26.69 (13.29 to 40.09) | Reference |
ABC = activated B cell–like; CI = confidence interval; HR = hazard ratio; ITT = intention to treat; NE = not estimable; NR = not reported; OS = overall survival; PFS = progression-free survival; pola-R-CHP = polatuzumab vedotin, rituximab, cyclophosphamide, doxorubicin, and prednisone; R-CHOP = rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone.
aBased on Kaplan-Meier estimates with 95% CI for median computed using the Brookmeyer and Crowley method.
bBased on an unstratified Cox regression model.
cOne-sided P value based on an unstratified log-rank test. P value has not been adjusted for multiplicity.
dBased on a stratified Cox regression model with stratification factors for geographical region, IPI score, and bulky disease defined as 1 lesion of 7.5 cm or larger.
eOne-sided P value based on a stratified log-rank test. P value has not been adjusted for multiplicity.
Sources: POLARIX Clinical Study Report,32 Salles et al. (2024),55 and additional data provided by the sponsor.33
Figure 4: Forest Plot of Investigator-Assessed PFS by Molecular DLBCL Subtypes (Global ITT Analysis Set) — Data Cut-Off Date June 15, 2022
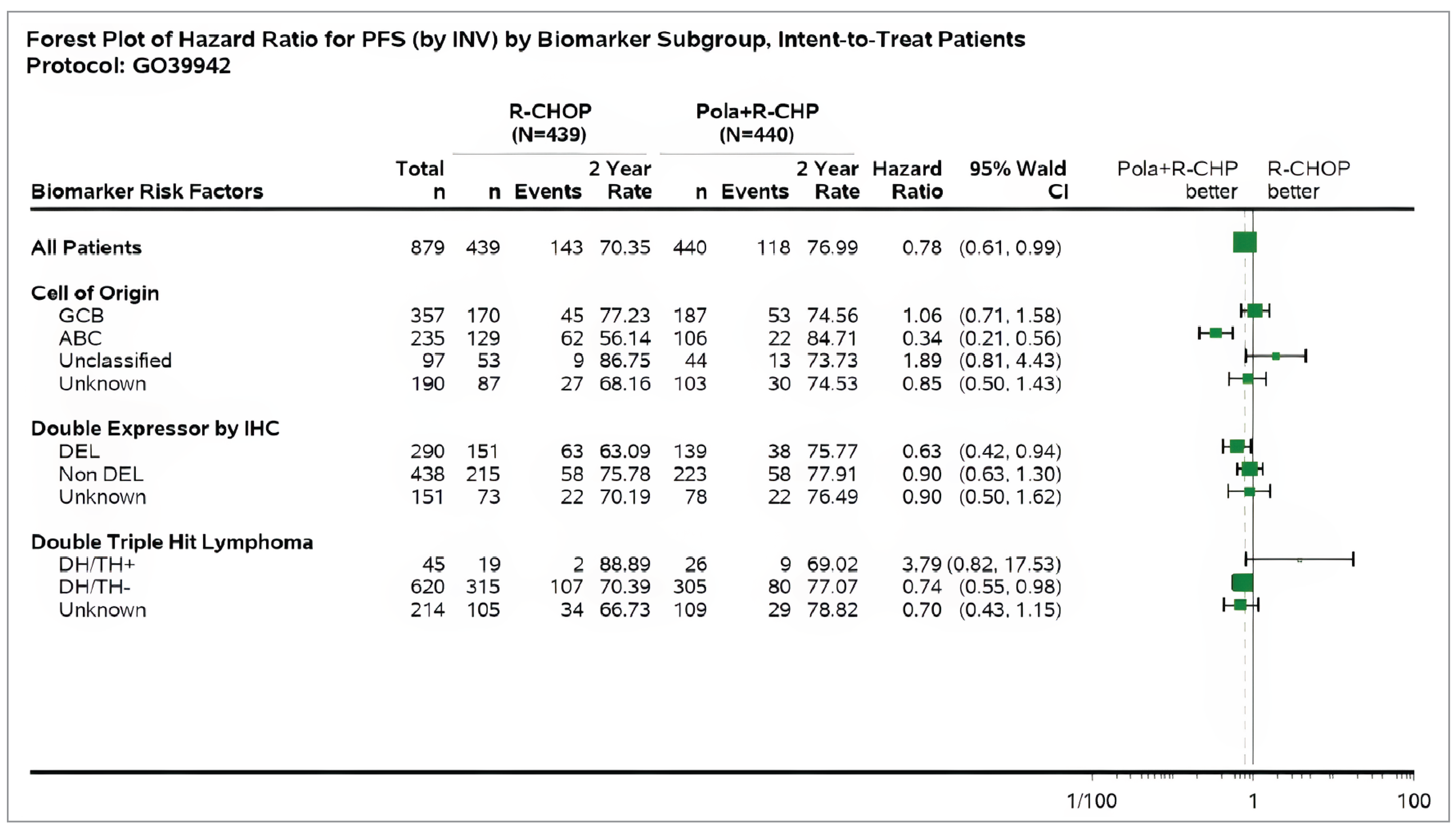
ABC = activated B cell–like; CI = confidence interval; DEL = double-expressor lymphoma; DH = double-hit; DLBCL = diffuse large B-cell lymphoma; GCB = germinal centre B cell; ITT = intention to treat; pola-R-CHP = polatuzumab vedotin, rituximab, cyclophosphamide, doxorubicin, and prednisone; R-CHOP = rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone; TH+ = triple-hit–positive; TH- = triple-hit–negative.
Source: POLARIX Clinical Study Report.32
Figure 5: Kaplan-Meier Estimate of Investigator-Assessed PFS by COO Subgroup (Global ITT Analysis Set) — Data Cut-Off Date June 15, 2022
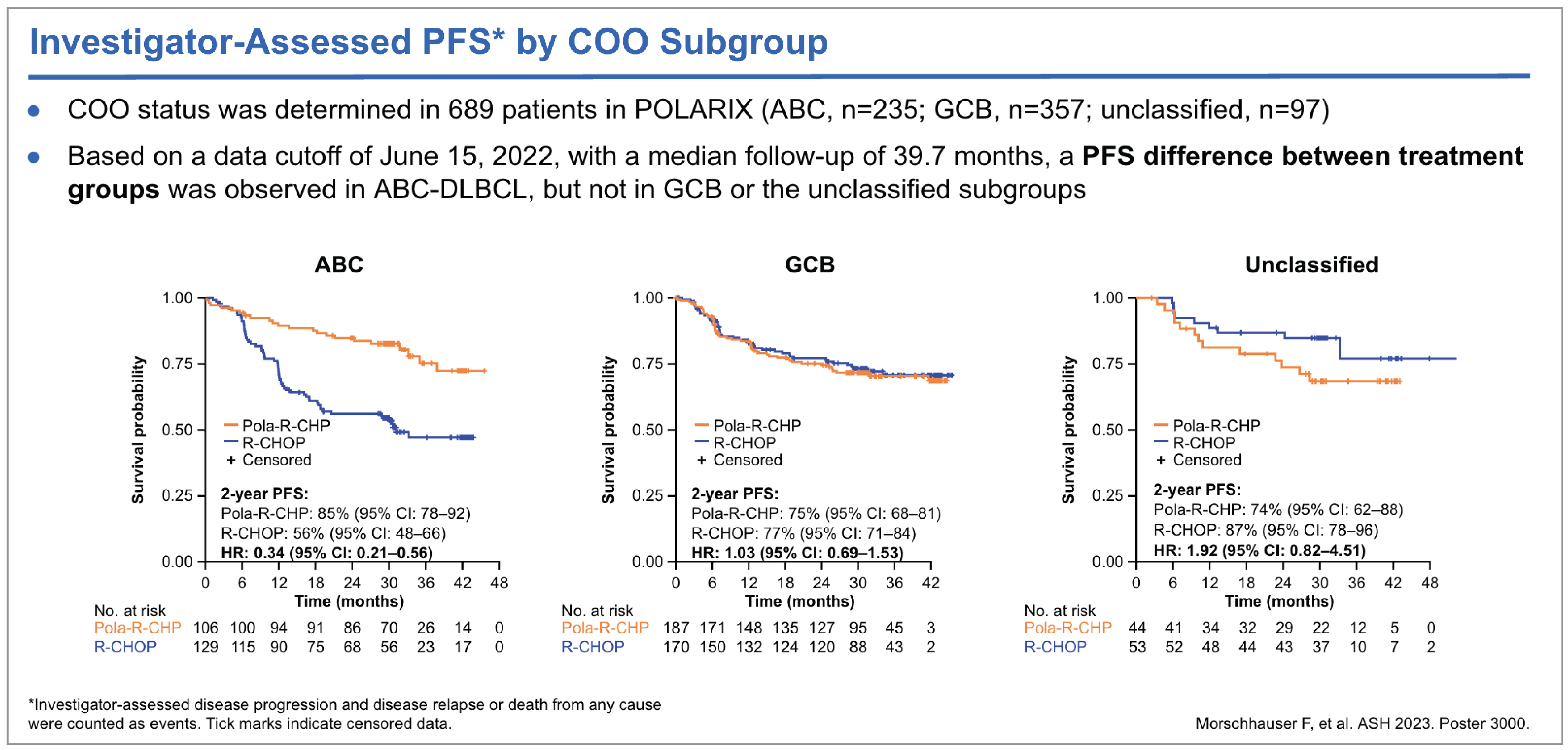
ABC = activated B cell–like; CI = confidence interval; COO = cell of origin; GCB = germinal centre B cell; HR = hazard ratio; ITT = intention to treat; PFS = progression-free survival; pola-R-CHP = polatuzumab vedotin, rituximab, cyclophosphamide, doxorubicin, and prednisone; R-CHOP = rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone.
Source: Morschbauser et al. (2023).54
Harms
Data for harms among patients with ABC lymphoma subtype at the data cut-off on July 5, 2024, are summarized in Table 15. The harms analyses were conducted in 106 patients in the pola-R-CHP group and 129 patients in the R-CHOP group.
Adverse Events
The number of patients who experienced at least 1 treatment-emergent AE was 105 patients (99.1%) in the pola-R-CHP group and 127 (98.4%) in the R-CHOP group. Types of treatment-emergent AEs were not specified.
Adverse Event of Grade 3 or Higher
The numbers of patients who experienced at least 1 AE of grade 3 to 5 were 70 (66.0%) in the pola-R-CHP group and 81 (62.8%) in the R-CHOP group. AEs of grade 3 to 4 occurred in 69 patients (65.1%) in the pola-R-CHP group and 79 patients (61.2%) in the R-CHOP group. AEs of grade 5 occurred in 4 patients (3.8%) in the pola-R-CHP group and 7 patients (5.4%) in the R-CHOP group.
Serious Adverse Events
The numbers of patients who experienced serious AEs were 34 (32.1%) in the pola-R-CHP group and 38 (29.5%) in the R-CHOP group; types of serious AEs were not specified.
Figure 6: Kaplan-Meier Estimate of Investigator-Assessed PFS by COO Subgroup (Global ITT Population) — Data Cut-Off Date July 5, 2024
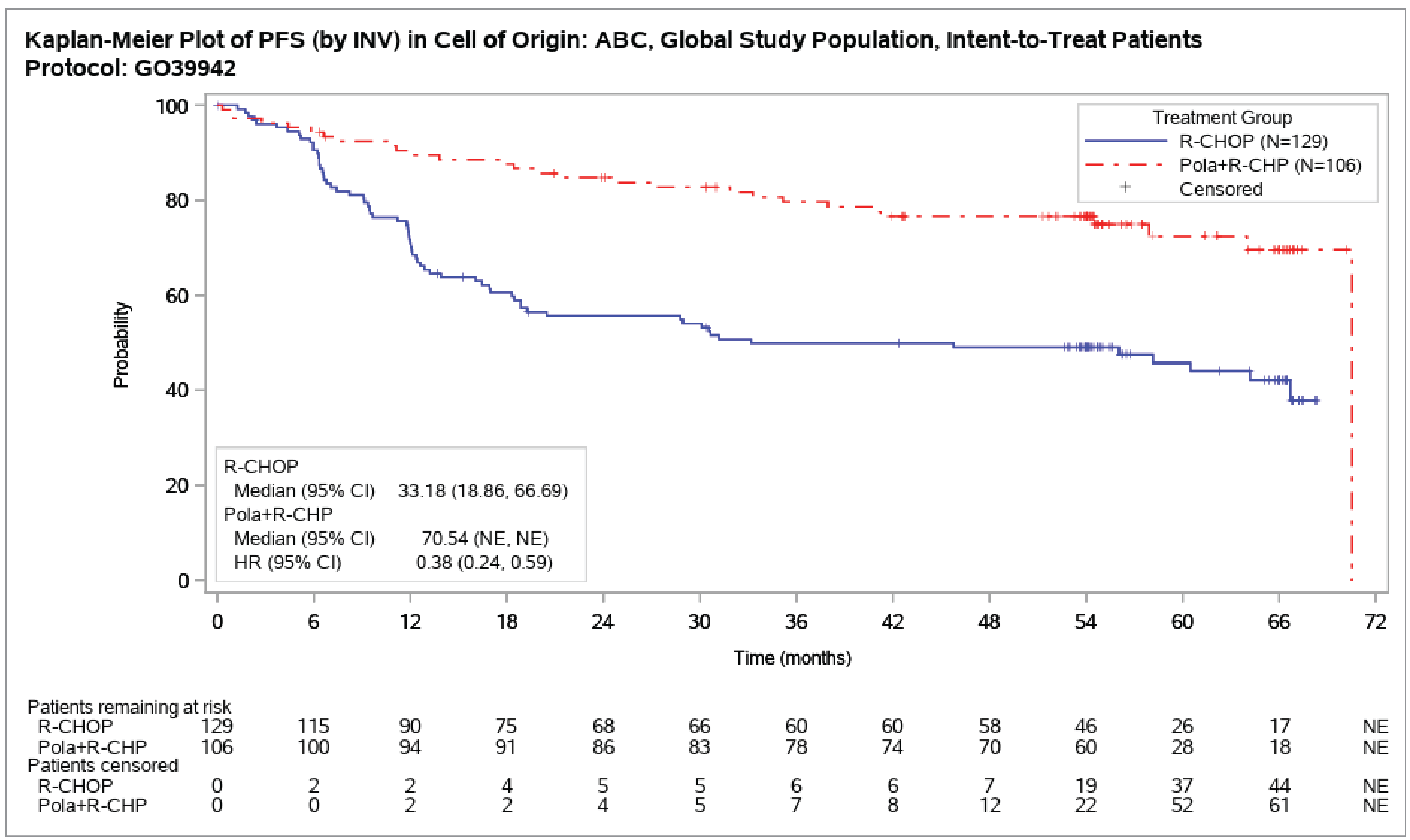
CI = confidence interval; COO = cell of origin; HR = hazard ratio; ITT = intention to treat; NE = not estimable; PFS = progression-free survival; pola+R-CHP = polatuzumab vedotin, rituximab, cyclophosphamide, doxorubicin, and prednisone; R-CHOP = rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone.
Source: From sponsor in response to additional data request.57
Table 15: Summary of Harms Results From POLARIX Study (Safety Analysis Set)
Adverse events | POLARIX ABC subpopulation | |
|---|---|---|
Pola-R-CHP N = 106 | R-CHOP N = 129 | |
Data cut-off date | July 5, 2024 | |
Patients with ≥ 1 treatment-emergent adverse event, n (%) | 105 (99.1) | 127 (98.4) |
Treatment-emergent adverse events occurring in ≥ 10% of patients in any group, n (%) | ||
Patients with ≥ 1 adverse event of grade 3 to 5, n (%) | 70 (66.0) | 81 (62.8) |
Adverse event of grade 3 to 4 | 69 (65.1) | 79 (61.2) |
Adverse event of grade 5 | 4 (3.8) | 7 (5.4) |
Patients with ≥ 1 serious adverse event, n (%) | 34 (32.1) | 38 (29.5) |
Patients who stopped treatment due to adverse events, n (%) | 7 (6.6) | 11 (8.5) |
Patients who died, n (%) | 17 (16.0) | 39 (30.2) |
Progressive disease | 8 (7.5) | 22 (17.1) |
Adverse event | 5 (4.7) | 8 (6.2) |
Othera | 4 (3.8) | 9 (7.0) |
Adverse events of special interest, n (%) | ||
Peripheral neuropathy | 56 (52.8) | 65 (50.4) |
Grade 3 to 4 | 0 | 1 (0.8) |
Neutropenia | 56 (52.8) | 60 (46.5) |
Grade 3 to 4 | 53 (50.0) | 54 (41.9) |
Febrile neutropenia | 20 (18.9) | 7 (5.4) |
Febrile neutropenia, grade 3 to 4 | 19 (17.9) | 7 (5.4) |
Infections | 58 (54.7) | 54 (41.9) |
Grade 3 to 4 | 10 (9.4) | 15 (11.6) |
Anemia | 30 (28.3) | 33 (25.6) |
Grade 3 to 4 | 10 (9.4) | 7 (5.4) |
Infusion-related reactions | 13 (12.3) | 25 (19.4) |
Grade 3 to 4 | 1 (0.9) | 2 (1.6) |
Thrombocytopenia | 16 (15.1) | 16 (12.4) |
Grade 3 to 4 | 6 (5.7) | 7 (5.4) |
Hepatic toxicity | 13 (12.3) | 10 (7.8) |
Grade 3 to 4 | 3 (2.8) | 3 (2.3) |
Tumour lysis syndrome | 1 (0.9) | 2 (1.6) |
Grade 3 to 4 | 1 (0.9) | 1 (0.8) |
Progressive multifocal leukoencephalopathy | 0 | 0 |
ABC = activated B cell–like; pola-R-CHP = polatuzumab vedotin, rituximab, cyclophosphamide, doxorubicin, and prednisone; R-CHOP = rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone.
aDeaths due to other reasons were not specified in the pola-R-CHP or R-CHOP groups; diffuse large B-cell lymphoma was not known to be a contributing factor in these deaths.
Source: From sponsor in response to additional data request.33
Withdrawals due to Adverse Events
Of the patients who stopped treatment due to AEs, 7 (6.6%) were in the pola-R-CHP group and 11 (8.5%) were in the R-CHOP group. Reasons for treatment discontinuation due to AEs were not specified.
Mortality
Of the patients who died, 17 (16.0%) were in the pola-R-CHP group and 39 (30.2%) were in the R-CHOP group. The reasons for deaths in the pola-R-CHP and R-CHOP groups were progressive disease (7.5% and 17.1%, respectively), an AE (4.7% and 6.2%, respectively), and unspecified (3.8% and 7.0%, respectively).
Notable Harms
Peripheral Neuropathy
Of the patients who experienced peripheral neuropathy, 56 (52.8%) were in the pola-R-CHP group and 65 (50.4%) were in the R-CHOP group; peripheral neuropathy of grade 3 or 4 occurred in 50.0% of patients in the pola-R-CHP group and 41.9% of patients in the R-CHOP group.
Neutropenia Including Febrile Neutropenia
Of the patients who experienced neutropenia, 56 (52.8%) were in the pola-R-CHP group and 60 (46.5%) were in the R-CHOP group; neutropenia of grade 3 or 4 occurred in 50.0% of patients in the pola-R-CHP group and 41.9% of patients in the R-CHOP group. Febrile neutropenia occurred in 20 patients (18.9%) in the pola-R-CHP group and 7 patients (5.4%) in the R-CHOP group, including febrile neutropenia of grade 3 or 4 in 17.9% of patients in the pola-R-CHP group and 5.4% of patients in the R-CHOP group.
Infections
Of the patients who experienced infections, 58 (54.7%) were in the pola-R-CHP group and 54 (41.9%) were in the R-CHOP group; infections of grade 3 or 4 occurred in 9.4% of patients in the pola-R-CHP group and 11.6% of patients in the R-CHOP group.
Anemia
Of the patients who experienced anemia, 30 (28.3%) were in the pola-R-CHP group and 33 (25.6%) were in the R-CHOP group; anemia of grade 3 or 4 occurred in 9.4% of patients in the pola-R-CHP group and 5.4% of patients in the R-CHOP group.
Infusion-Related Reactions
Of the patients who experienced infusion-related reactions, 13 (12.3%) were in the pola-R-CHP group and 25 (19.4%) were in the R-CHOP group; infusion-related reactions of grade 3 or 4 occurred in 1 patient (0.9%) in the pola-R-CHP group and in 2 patients (1.6%) in the R-CHOP group.
Thrombocytopenia
Of the patients who experienced thrombocytopenia, 16 (15.1%) were in the pola-R-CHP group and 16 (12.4%) were in the R-CHOP group; thrombocytopenia of grade 3 or 4 occurred in 5.7% of patients in the pola-R-CHP group and 5.4% of patients in the R-CHOP group.
Hepatic Toxicity
Of the patients who experienced hepatic toxicity, 13 (12.3%) were in the pola-R-CHP group and 10 (7.8%) were in the R-CHOP group; hepatic toxicity of grade 3 or 4 occurred in 3 patients (2.8%) in the pola-R-CHP group and in 3 patients (2.3%) in the R-CHOP group.
Tumour Lysis Syndrome
Of the patients who experienced tumour lysis syndrome, 1 (0.9%) was in the pola-R-CHP group and 2 (1.6%) were in the R-CHOP group. Tumour lysis syndrome of grade 3 or 4 occurred in 1 patient in each treatment group.
Progressive Multifocal Leukoencephalopathy
No patient experienced progressive multifocal leukoencephalopathy.
Critical Appraisal
Internal Validity
Findings for PFS and OS for the ABC subpopulation were based solely on exploratory subgroup analyses. The subgroup results were highly promising. However, in principle, they should be interpreted as hypothesis-generating, and a well-designed and adequately powered study is required to confirm them. Other key limitations are worthy of highlighting when interpreting the findings, particularly with respect to OS.
Although patients in the overall global ITT population were allocated to treatment groups by stratified randomization (for IPI score, bulky disease, and geographical location), patients with the ABC lymphoma subtype were not randomized by stratification factors, and the randomization principle may not have been preserved in the ABC subpopulation. There were differences between pola-R-CHP and R-CHOP in the proportion of patients with Ann Arbor stage III disease (34.9% versus 19.4% in the pola-R-CHP versus R-CHOP groups, respectively) and stage IV disease (51.9% versus 69.0% in the pola-R-CHP versus R-CHOP groups, respectively) and the proportion of patients with 2 or more extranodal disease sites (37.7% versus 46.5% in the pola-R-CHP versus R-CHOP groups, respectively). Whether these imbalances had any effect on patient prognoses or treatment effects is unclear.
Median OS had not been reached despite prolonged follow-up, with few events at 2 years (approximately 40 deaths) and 5 years (approximately 60 deaths). The beneficial effect in terms of difference in prolonged survival time, although likely to be a reduced risk of death, is therefore unknown. Despite the adjustment of stratified factors, the subgroup analyses did not or was unable to account for the imbalance of other factors, and it is also unknown if additional covariates (i.e., disease status) biased the findings. Finally, multiplicity is a concern because it could result in inflated type I error, leading to an inappropriate conclusion of statistical inference, given that the observed P values for both stratified and unstratified OS were just below the significance level of 0.05.
PFS was based on assessment by investigator rather than a blinded independent central review. Although both investigator and independent review assessments of PFS would be preferred, the double-blinded study design may limit potential bias (e.g., more frequent assessments, subjective interpretation of radiographic images and clinical assessments) arising from assessment by investigator.
████████ ██ ████████ ███ ███ ███ ████████ ████████ ███████ ██ ██ ██ █ █████ ███ ████████ ████████ █████ ████ ███ ████ █████████████ ███████ ██ █████████ ██████████ ███ ███ ████████ ███████ ███ █ ███████ ███ ████████████ ████ ██ ███ ███████ ███ ████████████ ██ ██████ ███ ███████ ██ ████████████ █████ ██ ██ ██ █ █████ ██ ██████████. These findings should be interpreted cautiously given the small sample sizes.
External Validity
Overall, the clinical experts indicated that patients with the ABC lymphoma subtype enrolled in the POLARIX trial were representative of patients in clinical practice. Combined, patients with an NHL histology of DLBCL NOS, ABC, and GCB accounted for nearly 90% of the population, with 34% of patients identified as having the ABC lymphoma subtype. Sixty-five percent of patients had an IPI score of 3 to 5, which aligned with the experts’ expectation of high-risk disease among individuals in the ABC subpopulation. Overall, the experts agreed with the inclusion criteria of the POLARIX study, although the trial eligibility criteria excluded some comorbidity conditions as well as patients with poorer performance status at presentation (i.e., an ECOG PS of 3 or 4), potentially resulting in a selected population that is healthier.
Long-Term Extension Studies
No long-term extension studies were submitted by the sponsor.
Indirect Evidence
No indirect treatment comparisons were submitted by the sponsor.
Studies Addressing Gaps in the Systematic Review Evidence
No additional studies addressing important gaps in the systematic review evidence were submitted by the sponsor.
Discussion
Summary of Available Evidence
One phase III, multicentre, double-blind, randomized trial assessed the efficacy and safety of pola-R-CHP compared with R-CHOP for the treatment of adults with previously untreated LBCL, including DLBCL NOS, high-grade B-cell lymphoma, EBV-positive DLBCL NOS, and T-cell/histiocyte-rich LBCL. Patients with ABC lymphoma subtype (n = 235) were included as a subgroup of the POLARIX trial. Based on a subgroup analysis, exploratory efficacy end points included OS and investigator-assessed PFS. Treatment-emergent AEs were reported for the ABC subpopulation.
The number of sites or patients in Canada with the ABC lymphoma subtype were not reported. All patients enrolled in the POLARIX study had CD20-positive LBCL, an IPI score of 2 to 5, an ECOG PS of 0 to 2, and a life expectancy of 12 months or greater. ████████ ███ █ ██████ █████ ██████████ ███ ██ ██ ██████ ████████ ███ ██ ███ █████ ██ █ ██ █ ██████ ██ ███████ ██ █████ ███████ ██████ ███ ███████ ██████████ ██ ███ █████ █████ ██ ██████.
Interpretation of Results
Efficacy
The original review of pola-R-CHP for the treatment of adult patients with previously untreated LBCL, including DLBCL NOS, high-grade B-cell lymphoma, EBV-positive DLBCL NOS, and T-cell/histiocyte-rich LBCL, resulted in a recommendation of “do not reimburse.”42 As such, the resubmission of polatuzumab vedotin was put forth to focus on the proposed subgroup of patients with ABC lymphoma with unmet needs and observed benefits with pola-R-CHP treatment. ██ ██████ ██████████ ████████ ████ ███ ████████ ███████ ███ █ ███ █████████ ██ ███████ ████████████ ████████ ██ █████ █████████████ ██ █ █████ ███ ███ ████ ██ ██████ ███████ ████████ ████ ████ ███ █ ███ █████████ ██ ███████ ████████████ ████████ ██ █████ █████████████ ██ █ █████ ███ ███ ████ ██ ██████. At 2 years, patients with ABC lymphoma had a 51% reduction in mortality (unstratified HR = 0.49; 95% CI, 0.25 to 0.94), whereas patients with LBCL had a 6% reduced risk of mortality (unstratified HR = 0.94; 95% CI, 0.67 to 1.33).
To address the uncertainty in PFS findings and lack of OS benefit at the updated analysis in the overall population of the POLARIX trial, the sponsor submitted results for the 5-year follow-up (data cut-off on July 5, 2024).55 At 5 years, patients with the ABC lymphoma subtype had a 62% reduction in disease progression, relapse, or death (unstratified HR = 0.38; 95% CI, 0.24 to 0.59), whereas patients with LBCL had a 22% reduced risk of disease progression, relapse, or death (unstratified HR = 0.78; 95% CI, 0.62 to 0.97). At 5 years, patients with ABC lymphoma had a 51% reduction in mortality (unstratified HR = 0.49; 95% CI, 0.28 to 0.88), whereas patients with LBCL had a 15% reduction in mortality (unstratified HR = 0.85; 95% CI, 0.63 to 1.16). Notwithstanding the limitations of subgroup analyses, relative to the overall population with LBCL, treatment with pola-R-CHP had a greater magnitude of benefit for patients with ABC lymphoma subtype.
Patient input identified longer disease remission and survival, along with controlled disease symptoms and improved HRQoL, as important outcomes of new treatment for LBCL. Clinicians also identified OS and PFS as important outcomes for patients with LBCL. For the ABC subpopulation, the POLARIX trial prespecified PFS and OS as exploratory end points in subgroup analyses.
In the ABC subpopulation, the estimated OS at 24 months (between-group difference in OS probability of 5.0%; 95% CI, −3.1% to 13.0%) was just below the 5% threshold, and the wide 95% CI included the null value, suggesting little to no difference in clinically important benefits. One of the clinical experts consulted for this review identified PFS at 12 months as important for those patients who experience early disease progression and may be offered CAR T-cell therapy. Based on a minimum 10% threshold that the clinical experts suggested was clinically important, the estimated PFS in the ABC subpopulation at 24 months (between-group difference in PFS probability of 29.0%; 95% CI, 17.9% to 40.1%) demonstrated that treatment with pola-R-CHP made an appreciably clinically meaningful improvement over SOC with R-CHOP. While there was a clear improvement in PFS with pola-R-CHP over R-CHOP, the translation of PFS benefits did not appear to translate to improved OS over the same treatment duration.
Findings with prolonged follow-up suggested a sustained benefit of treatment with pola-R-CHP compared with SOC R-CHOP among patients with ABC lymphoma subtype. At 60 months, the point estimate for OS was clinically meaningful (between-group difference in OS probability of 14.7%), but the wide 95% CI suggested uncertainty regarding a clinically important benefit. Similar to OS, the probability of PFS at 60 months demonstrated a sustained benefit of pola-R-CHP treatment over R-CHOP based on the point estimate (between-group difference in PFS probability of 26.7%) but with wide 95% CIs that made the clinically important benefit uncertain. The clinical experts noted that, because very few patients are likely to experience a relapse after 2 years of treatment, findings from prolonged follow-ups aligned with the expected maintenance of PFS improvement observed at 24 months. Given that OS had not been reached for patients in the POLARIX trial after a median of 63.9 months, and that the 60-month estimates of both OS and PFS were imprecise, the review team interpreted this as indicative of a low to moderate certainty of the benefit of pola-R-CHP compared with R-CHOP at 60 months. Further limitations to interpreting OS in the context of PFS arise from some controversy regarding the use of PFS as a surrogate outcome for OS in patients with LBCL because enrolment criteria used in clinical trials tend to result in a more selective population than that of patients in real-world settings.58
While the subgroup analyses were prespecified, they were exploratory, not adjusted for multiplicity, and therefore considered to be supportive evidence. The clinical experts remarked that any statistically significant OS benefit would be considered clinically meaningful for patients with DLBCL. The subgroup analysis was not designed or powered to demonstrate OS or PFS given the reduced sample size when compared with the overall LBCL population in the POLARIX trial. The small sample size likely contributed to imprecision in findings, particularly for OS and PFS at longer follow-ups. Altogether, findings for the ABC subpopulation were limited by evidence from a subgroup analysis and challenging to interpret.
The clinical experts indicated that the finding that subsequent antilymphoma treatment was higher in the R-CHOP group (46%) compared with the pola-R-CHP group (20%) was unsurprising and likely indicative of poor efficacy with SOC treatment. Radiotherapy that was preplanned (planned before randomization to be given at end of study treatment to initial sites of bulky or extranodal disease following institutional practices) was permitted, and unplanned radiotherapy was treated as new antilymphoma treatment. According to the clinical experts, the reason for unplanned radiotherapy is not always due to progressive disease and radiotherapy is not routinely preplanned (e.g., radiotherapy may be offered in the event of persistent disease based on end-of-treatment PET, which is considered in the palliative setting). In the ABC subpopulation, more patients who were receiving R-CHOP had radiotherapy (among the 14% of patients who had radiotherapy, 12% received unplanned treatment) compared with those receiving pola-R-CHP (among the 7% of patients who had radiotherapy, 3% received unplanned treatment). According to the experts, new antilymphoma treatments in the context of treatment efficacy were challenging to interpret in the absence of information on timing of the treatments.
The clinical experts indicated that there is no standard treatment for patients with the ABC lymphoma subtype, and that the current SOC for all patients with LBCL in the first-line setting is chemoimmunotherapy with R-CHOP. R-CHOP is therefore an appropriate comparator in the POLARIX trial for the ABC subpopulation. The experts noted that, because polatuzumab vedotin is an antibody-drug conjugate that targets CD79a expression on the surface of B-cells, its mechanism of action, targeting CD20, is independent of the components of R-CHOP, including rituximab. The experts anticipated that, if approved, pola-R-CHP would result in a shift in the current treatment paradigm for patients with ABC lymphoma. Overall, the clinical experts agreed that patients with LBCL classifications who would be treated similarly to those with DLBCL using R-CHOP (e.g., non-GCB lymphomas including the ABC subtype) should be eligible for treatment with pola-R-CHP. Patients with high-grade B-cell lymphoma who have dual translocations (i.e., BCL2 and MYC) and those with double-hit or triple-hit lymphomas require a treatment regimen that is more intensive than R-CHOP and they would not be considered eligible for pola-R-CHP treatment.
Important outcomes of treatment identified by the patient groups included longer disease remission, longer survival, controlled disease symptoms, normalized blood counts, and improved HRQoL to enable activities of daily living. Patient-reported outcomes were not included as end points in the subgroup analyses. In the overall LBCL population of the POLARIX trial, there were no differences between treatment groups on the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 physical functioning and fatigue components at the primary analysis (data cut-off on June 28, 2021); longer follow-up of patient-reported outcomes would provide context for interpreting efficacy and inform risk-benefit of pola-R-CHP treatment. While survival estimates suggested a benefit from treatment with pola-R-CHP in patients with ABC lymphoma, how this may translate to patients’ HRQoL is unknown in the absence of evidence.
Results for the ABC subpopulation were based on a subgroup analysis reported in a sponsor-submitted Clinical Study Report for the 2-year follow-up, but no similar summary was provided for results of the 5-year follow-up, with key data from the sponsor in response to additional information requests by the review team supplementing Kaplan-Meier plots, estimates from a conference abstract, and a presentation. In the resubmission, efficacy end points for the ABC subpopulation focused on OS and PFS. In addition to HRQoL, other outcomes that were provided for the overall population with LBCL (e.g., complete response) were not reported for the subgroup of patients with ABC lymphoma subtype.
Harms
While there were no notable differences in the incidence of treatment-emergent AEs, serious AEs, and AEs of grade 3 to 5, no details were provided on specific AEs in the ABC subpopulation. The number of patients with the ABC lymphoma subtype who discontinued study treatment due to AEs were also similar between pola-R-CHP and R-CHOP, but the specific AEs that contributed to the treatment discontinuations were not reported. AEs of special interest for this review were identified based on the product monograph for polatuzumab vedotin, which included infections and myelosuppression (i.e., neutropenia, febrile neutropenia, thrombocytopenia, and anemia) as “Serious Warnings and Precautions,” hepatic toxicity, infusion-related reactions, peripheral neuropathy, progressive multifocal leukoencephalopathy, and tumour lysis syndrome.46
At the 5-year follow-up, patients with ABC lymphoma in the pola-R-CHP and R-CHOP groups had similar rates of peripheral neuropathy (53% and 50%, respectively), anemia (28% and 26%, respectively), thrombocytopenia (15% and 13%, respectively), infusion-related reactions (12% and 19%, respectively), hepatic toxicity (12% and 8%, respectively), and tumour lysis syndrome (0.9% and 1.6%, respectively); no patient in the ABC subpopulation experienced progressive multifocal leukoencephalopathy. However, more patients in the pola-R-CHP group compared with the R-CHOP group experienced infections (55% and 42%, respectively) and neutropenia, including febrile neutropenia (53% and 47%, respectively). According to the clinical experts, this was indicative of greater toxicity associated with pola-R-CHP treatment, as premedication with anti-infectives were allowed and prophylactic G-CSF was required in the trial.
The clinical experts described pola-R-CHP as generally well tolerated based on the AE profile of patients with ABC lymphoma subtype in the POLARIX trial. Dose modifications and reductions during the trial would have contributed to the overall comparable safety profile between pola-R-CHP and R-CHOP group.
Other Considerations
Diagnostic testing to determine COO status provides context that is important for interpreting the evidence base and implications in real-world settings. In the POLARIX study, GEP using a NanoString Lymph2Cx assay identified the proportions of patients as 51.8% for the GCB subtype, 34% for the ABC subtype, and 14.1% for unclassified subtypes. When evaluating the available findings for PFS at up to 5-year follow-up, the benefit of treatment with pola-R-CHP that was demonstrated in the ABC subpopulation was not demonstrated in patients with non-ABC subtypes. While GEP is the gold and reference standard diagnostic test for determining COO molecular subtypes, IHC with the Hans algorithm is the method that is currently used at most centres in Canada; the latter can only distinguish GCB from non-GCB lymphoma subtypes. A meta-analysis of newly diagnosed DLBCL patients treated with R-CHOP (N = 712) found that the non-GCB profile (N = 333) was associated with reduced OS and PFS compared with the GCB profile; however, these findings were not retained in a multivariate survival analysis.59 The study suggests that the Hans algorithm may not have prognostic value in stratifying patients by DLBCL subtype, particularly in the context of modern practice and treatment (e.g., rituximab therapy).59 It is challenging to interpret these findings, given that patients were identified from retrospective studies (with available patient-level data) based on a literature search from 2004 to 2010 (patient study enrolment dates were not reported) and medical records of 2 hospitals in the US from 2002 to 2008. In the POLARIX study, more than 20% of patients had an unknown COO status, and reasons for this categorization were not available for all patients; as such, it was unclear whether these cases may be captured within the non-GCB subtype or were missing data.
The clinical experts indicated that a diagnostic biopsy to determine COO status is part of standard clinical practice, with no additional risks to the patient, and that this is commonly done using IHC with the Hans algorithm at time of diagnosis. IHC-based testing is not carried out during treatment, although it may be conducted at the time of relapse, in which case it does not usually alter treatment management. Potential exceptions to identification of COO in a patient can include issues such as insufficient size of the biopsy sample for staining or problems with the IHC stain. Acknowledging the limitations of IHC testing to accurately identify patients with ABC lymphoma subtype who may be eligible for pola-R-CHP treatment and the likely delay and costs of potential GEP implementation, the clinical experts advocated for polatuzumab vedotin to be offered to all patients with non-GCB lymphomas.
Conclusion
This report is based on evidence from a phase III, double-blind, randomized trial (POLARIX). In contrast to the previous CDA-AMC review of polatuzumab vedotin that evaluated the effects of the drug on the overall LBCL population of the same study,30 the current report focuses on a subpopulation of 235 previously untreated adult patients identified as having the ABC subtype of LBCL. Patients and clinicians identified a need for new treatments for LBCL that prolong disease remission and survival, control symptoms, normalize blood counts, improve HRQoL, and have tolerable side effects. Evidence from the POLARIX trial demonstrated that, compared with SOC R-CHOP, treatment with pola-R-CHP may provide a clinically important increase in PFS at 2 years and at 5 years in patients with the ABC lymphoma subtype of LBCL. There was uncertainty in the estimated magnitude of the PFS benefit due to the small population sample size and few events. A definitive conclusion could not be drawn about the comparative OS benefit of pola-R-CHP versus R-CHOP in patients with ABC subtype LBCL because the OS data were immature at the 5-year follow-up analysis. However, the percentage of reported deaths was nearly twice as high with R-CHOP compared with pola-R-CHP. Evidence about the comparative efficacy of pola-R-CHP on HRQoL in patients with the ABC subtype of lymphoma was not available. Overall, treatment-emergent AEs, serious AEs, and withdrawals due to AEs were comparable between the pola-R-CHP and R-CHOP groups. The safety profile of pola-R-CHP treatment in patients with ABC lymphoma was similar to that observed in the LBCL population, and no new safety signals were identified. For notable harms, the evidence suggested a higher incidence of infections and neutropenia (and febrile neutropenia in particular) but a lower incidence of infusion-related reactions with pola-R-CHP compared with R-CHOP. However, the clinical importance of the differences was unclear.
In most centres in Canada, testing to determine COO status is based on IHC with the Hans algorithm. This diagnostic test has limited ability to distinguish between patients with ABC lymphoma and those with other subtypes of lymphoma. The POLARIX study provided no evidence supporting a benefit of pola-R-CHP in patients with other lymphoma subtypes apart from the ABC subtype. Given the limited accuracy of the IHC with the Hans algorithm to correctly identify patients with non-ABC type lymphoma and the lack of supporting evidence of clinical effect, it is therefore unknown if the PFS benefit of pola-R-CHP in patients with ABC lymphoma will be replicated in patients with non-ABC lymphoma.
References
1.Canadian Cancer Society. Non-Hodgkin lymphoma statistics. May 2024. Accessed March 12, 2025. https://cancer.ca/en/cancer-information/cancer-types/non-hodgkin-lymphoma/statistics
2.Johnson NA, Boyle M, Bashashati A, et al. Diffuse large B-cell lymphoma: reduced CD20 expression is associated with an inferior survival. Blood. 2009;113(16):3773-3780. doi:10.1182/blood-2008-09-177469 PubMed
3.Johnson NA, Slack GW, Savage KJ, et al. Concurrent expression of MYC and BCL2 in diffuse large B-cell lymphoma treated with rituximab plus cyclophosphamide, doxorubicin, vincristine, and prednisone. J Clin Oncol. 2012;30(28):3452-9. doi:10.1200/JCO.2011.41.0985 PubMed
4.Lenz G, Wright GW, Emre NC, et al. Molecular subtypes of diffuse large B-cell lymphoma arise by distinct genetic pathways. Proc Natl Acad Sci U S A. 2008;105(36):13520-5. doi:10.1073/pnas.0804295105 PubMed
5.Schmitz R, Wright GW, Huang DW, et al. Genetics and Pathogenesis of Diffuse Large B-Cell Lymphoma. N Engl J Med. 2018;378(15):1396-1407. doi:10.1056/NEJMoa1801445 PubMed
6.Scott DW, Mottok A, Ennishi D, et al. Prognostic Significance of Diffuse Large B-Cell Lymphoma Cell of Origin Determined by Digital Gene Expression in Formalin-Fixed Paraffin-Embedded Tissue Biopsies. J Clin Oncol. 2015;33(26):2848-56. doi:10.1200/JCO.2014.60.2383 PubMed
7.Armitage JO, Weisenburger DD. New approach to classifying non-Hodgkin's lymphomas: clinical features of the major histologic subtypes. Non-Hodgkin's Lymphoma Classification Project. J Clin Oncol. 1998;16(8):2780-95. doi:10.1200/JCO.1998.16.8.2780 PubMed
8.Sehn LH, Gascoyne RD. Diffuse large B-cell lymphoma: optimizing outcome in the context of clinical and biologic heterogeneity. Blood. 2015;125(1):22-32. doi:10.1182/blood-2014-05-577189 PubMed
9.Freedman AS, Friedberg JW. Post TW, ed. Initial treatment of advanced-stage diffuse large B cell lymphoma. UpToDate; 2024. Accessed March 12, 2025. http://www.uptodate.com
10.National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: B-Cell Lymphomas. V 3.2024. August 26, 2024. Accessed March 12, 2025. https://www.nccn.org/
11.Shafey M, Savage KJ, Skrabek P, et al. Canadian Evidence-Based Guideline for the Frontline Treatment of Diffuse Large B-Cell Lymphoma [sponsor supplied reference]. Lymphoma Canada; 2021. https://www.lymphoma.ca/wp-content/uploads/2021/09/LymphomaCanada_Guideline_Frontline_DLBCL_VF_Digital.pdf
12.Coiffier B, Lepage E, Briere J, et al. CHOP chemotherapy plus rituximab compared with CHOP alone in elderly patients with diffuse large-B-cell lymphoma. N Engl J Med. 2002;346(4):235-42. doi:10.1056/NEJMoa011795 PubMed
13.Pfreundschuh M, Kuhnt E, Trümper L, et al. CHOP-like chemotherapy with or without rituximab in young patients with good-prognosis diffuse large-B-cell lymphoma: 6-year results of an open-label randomised study of the MabThera International Trial (MInT) Group. Lancet Oncol. 2011;12(11):1013-22. doi:10.1016/s1470-2045(11)70235-2 PubMed
14.Crump M, Neelapu SS, Farooq U, et al. Outcomes in refractory diffuse large B-cell lymphoma: results from the international SCHOLAR-1 study. Blood. 2017;130(16):1800-1808. doi:10.1182/blood-2017-03-769620 PubMed
15.Zhou Z, Sehn LH, Rademaker AW, et al. An enhanced International Prognostic Index (NCCN-IPI) for patients with diffuse large B-cell lymphoma treated in the rituximab era. Blood. 2014;123(6):837-42. doi:10.1182/blood-2013-09-524108 PubMed
16.Lacy SE, Barrans SL, Beer PA, et al. Targeted sequencing in DLBCL, molecular subtypes, and outcomes: a Haematological Malignancy Research Network report. Blood. 2020;135(20):1759-1771. doi:10.1182/blood.2019003535 PubMed
17.Nowakowski GS, Chiappella A, Witzig TE, et al. Variable global distribution of cell-of-origin from the ROBUST phase III study in diffuse large B-cell lymphoma. Haematologica. 2020;105(2):e72-e75. doi:10.3324/haematol.2019.220475 PubMed
18.Alduaij W, Collinge B, Ben-Neriah S, et al. Molecular determinants of clinical outcomes in a real-world diffuse large B-cell lymphoma population. Blood. 2023;141(20):2493-2507. doi:10.1182/blood.2022018248 PubMed
19.Balasubramanian S, Wang S, Major C, et al. Comparison of immunohistochemistry and gene expression profiling subtyping for diffuse large B‐cell lymphoma in the phase III clinical trial of R‐CHOP ± ibrutinib. Br J Haematol. 2021;194(1):83-91. doi:10.1111/bjh.17450 PubMed
20.Sehn LH, Salles G. Diffuse Large B-Cell Lymphoma. N Engl J Med. 2021;384(9):842-858. doi:10.1056/nejmra2027612 PubMed
21.Gutiérrez-García G, Cardesa-Salzmann T, Climent F, et al. Gene-expression profiling and not immunophenotypic algorithms predicts prognosis in patients with diffuse large B-cell lymphoma treated with immunochemotherapy. Blood. 2011;117(18):4836-43. doi:10.1182/blood-2010-12-322362 PubMed
22.Rho H, Jeong IJ, Prica A. Ibrutinib Plus RCHOP versus RCHOP Only in Young Patients with Activated B-Cell-like Diffuse Large B-Cell Lymphoma (ABC-DLBCL): A Cost-Effectiveness Analysis. Curr Oncol. 2023;30(12):10488-10500. doi:10.3390/curroncol30120764 PubMed
23.Masir N, Akhter A, Roshan TM, et al. Diffuse large B-cell lymphoma in Southeast Asian cohort: expression patterns of B-cell receptor (BCR) repertoire and its linkage with molecular subtypes and response to R-CHOP therapy. J Clin Pathol. 2019;72(9):630-635. doi:10.1136/jclinpath-2019-205837 PubMed
24.Liu Y, Barta SK. Diffuse large B‐cell lymphoma: 2019 update on diagnosis, risk stratification, and treatment. Am J Hematol. 2019;94(5):604-616. doi:10.1002/ajh.25460 PubMed
25.Wilson WH, Young RM, Schmitz R, et al. Targeting B cell receptor signaling with ibrutinib in diffuse large B cell lymphoma. Nat Med. 2015;21(8):922-926. doi:10.1038/nm.3884 PubMed
26.Nowakowski GS, Czuczman MS. ABC, GCB, and Double-Hit Diffuse Large B-Cell Lymphoma: Does Subtype Make a Difference in Therapy Selection? Am Soc Clin Oncol Educ Book. 2015;(35):e449-e457. doi:10.14694/edbook_am.2015.35.e449 PubMed
27.Roschewski M, Staudt LM, Wilson WH. Diffuse large B-cell lymphoma-treatment approaches in the molecular era. Nat Rev Clin Oncol. 2014;11(1):12-23. doi:10.1038/nrclinonc.2013.197 PubMed
28.Barton S, Hawkes EA, Wotherspoon A, Cunningham D. Are We Ready To Stratify Treatment for Diffuse Large B‐Cell Lymphoma Using Molecular Hallmarks? Oncol. 2012;17(12):1562-1573. doi:10.1634/theoncologist.2012-0218 PubMed
29.Thieblemont C, Briere J, Mounier N, et al. The Germinal Center/Activated B-Cell Subclassification Has a Prognostic Impact for Response to Salvage Therapy in Relapsed/Refractory Diffuse Large B-Cell Lymphoma: A Bio-CORAL Study. J Clin Oncol. 2011;29(31):4079-4087. doi:10.1200/jco.2011.35.4423 PubMed
30.CADTH. Drug Reimbursement Review clinical guidance report: polatuzumab vedotin (Polivy) for the treatment of adult patients with previously untreated large B-cell lymphoma (LBCL), including diffuse large B-cell lymphoma (DLBCL) not otherwise specified (NOS), high grade B-cell lymphoma, Epstein-Barr virus-positive (EBV+) DLBCL NOS, and T-cell/histiocyte rich LBCL. Can J Health Technol. 2024;4(2):1-170. doi:10.51731/cjht.2024.842
31.Scott DW. Cell-of-Origin in Diffuse Large B-Cell Lymphoma: Are the Assays Ready for the Clinic? Am Soc Clin Oncol Educ Book. 2015:e458-66. doi:10.14694/EdBook_AM.2015.35.e458 PubMed
32.F. Hoffman-La Roche Ltd. Clinical Study Report: Study GO39942. A phase III, multicenter, randomized, double-blind, placebo-controlled trial comparing the efficacy and safety of polatuzumab vedotin in combination with rituximab and CHP (R-CHP) versus rituximab and CHOP (R-CHOP) in previously untreated patients with diffuse large B-cell lymphoma [internal sponsor's report]. September 2022.
33.BC Cancer Lymphoma and Myeloma Tumour Group. BC Cancer Lymphoma and Myeloma Tumour Group response to January 10, 2025 CDA-AMC request for additional information regarding Polivy CDA-AMC review [internal additional sponsor's information]. 2025.
34.Tholstrup D, brown PDn, Jurlander J, jeppesen PB, Groenvold M. Quality of life in patients with diffuse large B-cell lymphoma treated with dose-dense chemotherapy is only affected temporarily. Leuk Lymphoma. 2011;52(3):400-408. doi:10.3109/10428194.2010.541310 PubMed
35.Mareschal S, Lanic H, Ruminy P, Bastard C, Tilly H, Jardin F. The proportion of activated B-cell like subtype among de novo diffuse large B-cell lymphoma increases with age. Haematologica. 2011;96(12):1888-1890. doi:10.3324/haematol.2011.050617 PubMed
36.Urata T, Naoi Y, Jiang A, et al. Distribution and clinical impact of molecular subtypes with dark zone signature of DLBCL in a Japanese real-world study. Blood Adv. 2023;7(24):7459-7470. doi:10.1182/bloodadvances.2023010402 PubMed
37.Swerdlow SH, Campo E, Harris NL, et al. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues [sponsor supplied reference]. 4th ed. vol 2. IARC Publications; 2017.
38.International Non-Hodgkin's Lymphoma Prognostic Factors Project. A predictive model for aggressive non-Hodgkin's lymphoma. N Engl J Med. 1993;329(14):987-94. doi:10.1056/NEJM199309303291402 PubMed
39.Sehn LH, Berry B, Chhanabhai M, et al. The revised International Prognostic Index (R-IPI) is a better predictor of outcome than the standard IPI for patients with diffuse large B-cell lymphoma treated with R-CHOP. Blood. 2007;109(5):1857-61. doi:10.1182/blood-2006-08-038257 PubMed
40.Meyer PN, Fu K, Greiner TC, et al. Immunohistochemical methods for predicting cell of origin and survival in patients with diffuse large B-cell lymphoma treated with rituximab. J Clin Oncol. 2011;29(2):200-7. doi:10.1200/jco.2010.30.0368 PubMed
41.Roche. Hematology National Consultancy Meeting [sponsor supplied reference]. 2024. https://app.readcube.com/library/516efe2e-6cb6-4217-9499-6c51218c7daa/item/c1afe810-31c2-40de-a18d-e8b1076fd42d
42.CADTH. CADTH Drug Reimbursement Expert Review Committee final recommendation: polatuzumab vedotin (Polivy - Hoffman-La Roche Ltd.). Can J Health Technol. January 2024;4(1):1-18. doi:10.51731/cjht.2024.813
43.Committee for Medicinal Products for Human Use. Assessment report: Polivy (polatuzumab vedotin). European Medicines Agency; May 2022. Accessed March 12, 2025. https://www.ema.europa.eu/en/documents/overview/polivy-epar-medicine-overview_en.pdf
44.Cancer Care Ontario. Cancer Care Ontario Drug Formulary CHOP+R. November 2023. Accessed March 12, 2025. https://www.cancercareontario.ca/en/drugformulary/regimens/monograph/45801
45.BC Cancer. BC Cancer Protocol Summary for Treatment of Lymphoma with DOXOrubicin, Cyclophosphamide, vinCRIStine, predniSONE and riTUXimab (CHOP-R). 2024. Accessed March 12, 2025. http://www.bccancer.bc.ca/chemotherapy-protocols-site/Documents/Lymphoma-Myeloma/LYCHOPR_Protocol.pdf
46.Hoffman-La Roche Limited. Polivy (polatuzumab vedotin): 30 mg or 140 mg single-use vial lyophilized powder for solution for intravenous infusion [product monograph]. January 20, 2023.
47.Amgen Canada Inc. Riabni (rituximab): 10 mg/mL intravenous infusion [product monograph]. March 11, 2021. Accessed March 12, 2025. https://pdf.hres.ca/dpd_pm/00060341.PDF
48.Accord Healthcare Inc. Cyclophosphamide: 500 mg, 1000 mg and 2000 mg per vial, lyophilized powder for injection [product monograph]. September 14, 2022. Accessed March 12, 2025. https://pdf.hres.ca/dpd_pm/00067461.PDF
49.Pfizer Canda ULC. Doxorubicin: solution, 2 mg/mL, for intravenous and intravesical use [product monograph]. November 25, 2022. Accessed March 12, 2025. https://pdf.hres.ca/dpd_pm/00068415.PDF
50.Teva Canada Ltd. Teva-Prednisone (prednisone): 5 mg and 50 mg tablets [product monograph]. December 07, 2020. Accessed March 12, 2025. https://pdf.hres.ca/dpd_pm/00059252.PDF
51.Ziepert M, Hasenclever D, Kuhnt E, et al. Standard International prognostic index remains a valid predictor of outcome for patients with aggressive CD20+ B-cell lymphoma in the rituximab era. J Clin Oncol. 2010;28(14):2373-80. doi:10.1200/jco.2009.26.2493 PubMed
52.CADTH. CADTH Reimbursement Review: Provisional Funding Algorithm for Indication - Large B-cell lymphoma [sponsor supplied reference]. 2024. https://www.cda-amc.ca/sites/default/files/DRR/2024/PH0048_Rapid_Algorithm_Report_LBCL_Final.pdf
53.Tilly H, Morschhauser F, Sehn LH, et al. Polatuzumab Vedotin in Previously Untreated Diffuse Large B-Cell Lymphoma. N Engl J Med. 2022;386(4):351-363. doi:10.1056/NEJMoa2115304 PubMed
54.Morschhauser F, Leung W, Raghavan V, et al. Deciphering the Clinical Benefit of Pola-R-CHP versus R-CHOP in Different Genetic Subtypes Beyond Cell of Origin in the POLARIX Study. Blood. 2023;142(Supplement 1):3000. doi:10.1182/blood-2023-178623
55.Salles G, Morschhauser F, Sehn LH, et al. Five-Year Analysis of the POLARIX Study: Prolonged Follow-up Confirms Positive Impact of Polatuzumab Vedotin Plus Rituximab, Cyclophosphamide, Doxorubicin, and Prednisone (Pola-R-CHP) on Outcomes. Blood. 2024;144(Supplement 1):469-469. doi:10.1182/blood-2024-197938
56.Sehn LH, Martelli M, Trneny M, et al. A randomized, open-label, Phase III study of obinutuzumab or rituximab plus CHOP in patients with previously untreated diffuse large B-Cell lymphoma: final analysis of GOYA. J Hematol Oncol. 2020;13(1):71. doi:10.1186/s13045-020-00900-7 PubMed
57.BC Cancer Lymphoma and Myeloma Tumour Group. BC Cancer Lymphoma and Myeloma Tumour Group response to February 14, 2025 CDA-AMC request for additional information regarding Polivy CDA-AMC review [internal additional sponsor's information]. 2025.
58.van der Galien HT, Hoogendoorn M, Kibbelaar RE, van Meerten T, van Rijn RS. Progression-free survival at 24 months (PFS24) and subsequent outcome for patients with diffuse large B-cell lymphoma (DLBCL) in the real-world setting. Ann Oncol. 2019;30(1):151-152. doi:10.1093/annonc/mdy482 PubMed
59.Castillo JJ, Beltran BE, Song MK, et al. The Hans algorithm is not prognostic in patients with diffuse large B-cell lymphoma treated with R-CHOP. Leuk Res. 2012;36(4):413-7. doi:10.1016/j.leukres.2011.12.012 PubMed
Pharmacoeconomic Review
Abbreviations
ABC
activated B cell–like
AE
adverse event
ASCT
autologous stem cell transplant
BIA
budget impact analysis
CAR
chimeric antigen receptor
CDA-AMC
Canada’s Drug Agency
CI
confidence interval
DLBCL
diffuse large B-cell lymphoma
EFS
event-free survival
ECOG PS
Eastern Cooperative Oncology Group Performance Status
GCB
germinal centre B cell–like
GemOx
gemcitabine plus oxaliplatin
HRQoL
health-related quality of life
ICER
incremental cost-effectiveness ratio
IHC
immunohistochemistry
LBCL
large B-cell lymphoma
NOS
not otherwise specified
OS
overall survival
PFS
progression-free survival
pola-BR
polatuzumab vedotin, bendamustine, and rituximab
pola-R-CHP
polatuzumab vedotin, rituximab, cyclophosphamide, doxorubicin, and prednisone
QALY
quality-adjusted life-year
R-chemo
rituximab-based chemotherapy
R-CHOP
rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone
R-CHP
rituximab, cyclophosphamide, doxorubicin, and prednisone
R-GemOx
rituximab, gemcitabine, and oxaliplatin
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Polatuzumab vedotin (Polivy), 30 mg or 140 mg single-use vial, lyophilized powder for solution for IV infusion |
Indication | In combination with R-CHP for the treatment of adult patients with previously untreated LBCL, including DLBCL NOS, high grade B-cell lymphoma, Epstein-Barr virus positive DLBCL NOS, and T-cell/histiocyte rich LBCL |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | November 22, 2022a |
Reimbursement request | In combination with R-CHP for the treatment of adult patients with previously untreated LBCL, including DLBCL NOS, high-grade B-cell lymphoma, Epstein-Barr virus–positive DLBCL NOS, and T-cell/histiocyte-rich LBCL that are classified as activated B-cell–like lymphoma subtype |
Sponsor | BC Cancer Lymphoma and Myeloma Tumour Group; Hoffmann-La Roche Ltd. (submitting consultant) |
Submission history | Previously reviewed: Yes Indication: In combination with R-CHP for the treatment of adult patients with previously untreated LBCL, including DLBCL NOS, high-grade B-cell lymphoma, Epstein-Barr virus–positive DLBCL NOS, and T-cell/histiocyte-rich LBCL Recommendation date: December 20, 2023 Recommendation: Do not reimburse Indication: In combination with bendamustine and rituximab for the treatment of adult patients with relapsed or refractory DLBCL NOS who are not eligible for autologous stem cell transplant and have received at least 1 prior therapy Recommendation date: April 21, 2021 Recommendation: Reimburse with clinical criteria and/or conditions |
DLBCL = diffuse large B-cell lymphoma; LBCL = large B-cell lymphoma; NOC = Notice of Compliance; NOS = not otherwise specified; R-CHP = rituximab, cyclophosphamide, doxorubicin, and prednisone.
aBased on the Sponsor’s Application Overview. Canada’s Drug Agency noted that the previous review reported that the NOC date was November 13, 2022.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Markov Model |
Target population | Adult patients with previously untreated LBCL, including DLBCL NOS, high-grade B-cell lymphoma, EBV-positive DLBCL NOS, and T-cell/histiocyte-rich LBCL that are classified as having the ABC lymphoma subtype |
Treatments | Pola-R-CHP: Polatuzumab vedotin in combination with rituximab, cyclophosphamide, doxorubicin, and prednisone |
Dose regimen |
|
Submitted price | Polatuzumab vedotin: $3,160.71 per 30 mg vial or $14,750.00 per 140 mg vial |
Submitted treatment cost | Pola-R-CHP: $18,289 ($15,247 for polatuzumab vedotin) per 21-day cycle |
Comparator | R-CHOP |
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | Lifetime (35 years) |
Key data source | POLARIX trial |
Submitted results | Pola-R-CHP was less costly (incremental costs: −$32,350) and more effective (incremental QALYs: 2.43) than R-CHOP (i.e., pola-R-CHP is dominant) |
Key limitations |
|
CDA-AMC reanalysis results |
|
ABC = activated B cell–like; CDA-AMC = Canada’s Drug Agency; DLBCL = diffuse large B-cell lymphoma; EBV = Epstein-Barr virus; GCB = germinal centre B cell–like; GEP = gene expression profiling; HRQoL = quality of life; ICER = incremental cost-effectiveness ratio; IHC = immunohistochemistry; LBCL = large B-cell lymphoma; LY = life-year; NOS = not otherwise specified; OS = overall survival; PFS = progression-free survival; QALY = quality-adjusted life-year; pola-BR = polatuzumab vedotin, bendamustine, and rituximab; pola-R-CHP = polatuzumab vedotin, rituximab, cyclophosphamide, doxorubicin, and prednisone; R-CHOP = rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone.
Conclusions
Evidence from a randomized phase III, double-blind trial (POLARIX) that enrolled a subpopulation of 235 adult patients identified as activated B-cell-like (ABC) lymphoma subtype of large B-cell lymphoma (LBCL) who had been previously untreated for the disease demonstrated that compared with standard of care treatment in the form of rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP), treatment with polatuzumab vedotin in combination with rituximab, cyclophosphamide, doxorubicin, and prednisone (pola-R-CHP) may provide a clinically important increase in progression-free survival (PFS) at 2 years and 5 years. There was uncertainty in the estimated magnitude of PFS benefit due to a small population sample size with few events. Because data for overall survival (OS) were immature at 2 years and at 5 years, a definitive conclusion could not be drawn about the OS benefit of pola-R-CHP in patients with ABC lymphoma subtype LBCL. The comparative efficacy of pola-R-CHP on health-related quality of life (HRQoL) was not available.
CDA-AMC notes that it is unknown whether the PFS benefit of pola-R-CHP observed in patients with the ABC lymphoma subtype will be replicated in patients with non-ABC lymphoma. Current testing in clinical practice across most jurisdictions uses immunohistochemistry (IHC) testing via the Hans algorithm for detecting the germinal centre B-cell–like (GCB) and non-GCB lymphoma subtypes (ABC is captured within the non-GCB lymphoma subtype). However, published literature indicates that specificity ranges from 52% to 82% for identification of the ABC lymphoma subtype with this testing method. As such, there is a large range in the number of patients who may be misclassified as having the ABC subtype, and this would therefore result in overuse of pola-R-CHP in patients for whom treatment would not be advised, as it is unclear whether they would benefit from pola-R-CHP, experience little to no benefit from treatment, or potentially experience harms. All testing costs associated with identifying patients with the ABC subtype were excluded from the analysis by the sponsor and could not adequately be incorporated into a reanalysis by CDA-AMC.
CDA-AMC identified several limitations in the sponsor’s pharmacoeconomic analysis that have notable implications on the cost-effectiveness of pola-R-CHP. In a base-case reanalysis, CDA-AMC incorporated the cost impact of the overestimation of individuals with the ABC subtype by IHC genetic testing to reflect clinical practice. CDA-AMC reanalyses assessed the impact of including a 52% (lower bound) and 82% (upper bound) specificity value for detecting the ABC subtype. The patients who test positive but do not actually have the ABC subtype (false-positives) are assumed to incur treatment costs of pola-R-CHP. In line with the subgroup data from the trial, there is no robust evidence of an incremental treatment benefit with pola-R-CHP in other subtypes of diffuse large B-cell lymphoma (DLBCL). The CDA-AMC base-case analysis resulted in an incremental cost-effectiveness ratio (ICER) of $25,952 per quality of life-year (QALY) gained (2.42 incremental QALYs; $62,825 in incremental costs) for pola-R-CHP versus R-CHOP when assuming a 52% testing specificity for the ABC subtype. When assuming an 82% testing specificity for the ABC subtype, the resulting ICER was estimated to be $1,616 per QALY gained (2.42 incremental QALYs; $3,911 in incremental costs) for pola-R-CHP versus R-CHOP. CDA-AMC was unable to address concerns surrounding the face validity of cure assumptions and uncertainty in the clinical evidence. The CDA-AMC Clinical Review of the POLARIX trial concluded that it was uncertain if pola-R-CHP was associated with an OS benefit. The sponsor’s model predicts that pola-R-CHP is associated with 3 additional life-years compared with R-CHOP. CDA-AMC could not address issues related to the predicted magnitude of the treatment benefit, and assumed that patients receiving pola-R-CHP will live for 17 years after treatment, largely due to the sponsor’s modelling of cure assumptions, the assumption that the PFS benefit will translate to an OS benefit, the assumption that treatment effect will be maintained over the duration of the model, and uncertainty in the long-term efficacy (i.e., 91% of the incremental benefit was predicted to occur after the trial period of 46 months). For the ICER to be realized, a gain of 3 years of life on pola-R-CHP and a reduction in subsequent treatments to the level estimated by sponsor would be required. CDA-AMC undertook a scenario analysis assessing the impact of alternative assumptions regarding subsequent therapies that resulted in an increase in the ICER.
The analysis includes additional drug acquisition costs of pola-R-CHP due to treating the false-positive patients identified with IHC testing, but the additional costs associated with health care resource utilization and any potential harms with overtreatment could not be assessed in this analysis. Testing costs could not be included in the CDA-AMC reanalyses. If gene expression profiling (GEP) tests were to be implemented and proved accurate, pola-R-CHP under GEP testing may be cost-effective in treating adult patients identified as having ABC lymphoma subtype LBCL who had been previously untreated for the disease. However, the analysis does not incorporate the additional costs required to implement GEP testing to more accurately identify patients with DLBCL with the ABC subtype. Based on the sponsor’s estimated number of patients with confirmed DLBCL across all CDA-AMC–participating jurisdictions from the budget impact analysis (BIA), funding GEP testing to identify patients with the ABC subtype would result in additional testing costs of more than $1,761,300 per year to jurisdictions. This estimate does not incorporate costs related to assay development and validation, staff training, and equipment procurement and maintenance.
A price reduction may be required to ensure that pola-R-CHP is a cost-effective regimen for patients with ABC lymphoma subtype LBCL who had been previously untreated for the disease due to the uncertainty associated with the magnitude of the clinical benefit, inability of the sponsor’s model to adequately assess the impact of testing implications, limitations with the sponsor’s economic model, concerns regarding the generalizability of the trial population to the population in Canada, and presence of negotiated prices for subsequent therapies (e.g., chimeric antigen receptor [CAR] T cells).
Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, clinician groups, and drug plans that participated in the CDA-AMC review process.
Patient group input was received from Lymphoma Canada. This submission collected information from 89 patients diagnosed with LBCL, the majority of whom were in Canada, using an anonymous online survey. The proportion of patients classified as having the ABC lymphoma subtype was not reported. Patients reported that at the time of diagnosis they experienced several physical and psychosocial struggles affecting their quality of life. It was also reported that patients experience mental health challenges associated with the fear that their cancer may progress or relapse. Respondents indicated that they were satisfied with first-line treatment options, which included some form of chemotherapy or chemoimmunotherapy. However, some respondents reported that they faced challenges and delays accessing treatment due to long travel times to hospital, an unsatisfactory number of available treatment options, and waitlists. The patient responses identified a gap in treatment for therapies that lead to longer disease remission, controlled symptoms, longer survival, normalized blood counts, and improved quality of life. Four respondents had experience with pola-R-CHP as a first-line therapy. Three of these patients would recommend the treatment to other patients, and 2 patients reported that their overall experience was very good. The most common side effects included fatigue, neutropenia, thrombocytopenia, and diarrhea.
Clinician group input was received from the Lymphoma Canada Scientific Advisory Board and Ontario Health (Cancer Care Ontario) Hematology Cancer Drug Advisory Committee. There was consensus that the goal of first-line treatment was to cure LBCL and prevent the need for salvage treatment. Both submissions indicated that patients classified as having the ABC lymphoma subtype and receiving current treatment options are at high risk of relapsing or experiencing refractory disease following initial first-line therapy (R-CHOP). Compared to the current standard of care, it is expected that pola-R-CHP will reduce the need for subsequent therapies. Regarding safety, it was noted that pola-R-CHP has a safety profile similar to that of the current standard of care. As a result, pola-R-CHP would replace R-CHOP as first-line therapy for the indicated population of patients who are classified as having the ABC lymphoma subtype. The clinician group input noted that classification of subtypes in Canada is usually carried out via standard IHC algorithms, and that it has 80% to 90% agreement with GEP testing, but the group acknowledged that patients may be misclassified by IHC. The clinician group input noted that a misclassified patient is not expected to be harmed by receiving pola-R-CHP as an overall benefit was reported in the POLARIX trial.
Drug plan input raised concerns about the impact that pola-R-CHP would have on resource use compared to existing first-line treatment options. This was attributed to the 2 additional cycles of rituximab monotherapy, which would increase pharmacy workloads and chair-time visits if these additional cycles are required. A second concern related to the implementation of ABC testing, which may not be available across all jurisdictions in Canada. The drug plans also cited concerns relating to the presence of confidentially negotiated prices for rituximab, cyclophosphamide, and doxorubicin. Finally, a substantial budget impact was anticipated as a result of the introduction of polatuzumab vedotin as a first-line regimen.
Two of these concerns were addressed in the sponsor’s model:
Rituximab, cyclophosphamide, and doxorubicin are constituent treatments of both first-line regimens considered in the economic evaluation. It was acknowledged that cost differences will emerge as a result of differences in the recommended doses between the first-line regimens. However, the impact of confidentially negotiated prices is mitigated by the fact that the cost differences will be driven by the uncommon treatments (polatuzumab vedotin and vincristine) in each regimen.
Inclusion of additional chair time associated with pola-R-CHP.
In addition, CDA-AMC addressed the following concern:
The impact of overtreatment of patients was assessed by applying lowered specificity rates (52% and 82%) for detecting the ABC subtype associated with the IHC testing currently available in jurisdictions.
CDA-AMC was unable to address the following concerns:
The implementation of ABC testing costs was not considered in the economic evaluation.
The impact of subtype misclassification on treatment outcomes could not be considered in the economic evaluation.
Economic Review
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted an economic evaluation comparing costs and outcomes for pola-R-CHP with the current standard of care, R-CHOP. The model population comprised adult patients with previously untreated LBCL, including DLBCL, not otherwise specified (NOS); high-grade B-cell lymphoma; Epstein-Barr virus–positive DLBCL NOS; and T-cell/histiocyte-rich LBCL, which are classified as the ABC lymphoma subtype. This was aligned with the sponsor’s reimbursement request and agreed to by CDA-AMC, but was narrower than the Health Canada indication.
Polatuzumab vedotin is administered intravenously, with the initial dose administered as a 90-minute infusion followed by 90 minutes of observation. Subsequent doses may be administered as 30-minute infusions with a 30-minute observation period. The recommended dose of polatuzumab vedotin is 1.80 mg/kg every 21 days for a maximum of 6 cycles, in combination with rituximab, cyclophosphamide, doxorubicin, and prednisone (R-CHP). Polatuzumab vedotin is available in either 30 mg or 140 mg vials, at a submitted price of $3,160.71 and $14,750 per vial, respectively. Using a range of patient weights from the POLARIX trial to determine the dose used, the sponsor estimated the cost of polatuzumab vedotin to be $15,247 per 21-day cycle. When used over the maximum of 6 cycles, the treatment cost of polatuzumab vedotin was estimated to be $91,484. The sponsor determined the cost of R-CHP to be approximately $3,041 per 21-day cycle. The sponsor therefore estimated the 21-day cycle cost of pola-R-CHP was $18,289, resulting in a 6-cycle cost of $109,732. According to the product monograph, 2 additional cycles of rituximab may be administered as needed. The sponsor’s economic submission assumed that no patients received additional cycles of rituximab.
The sponsor considered R-CHOP the only relevant comparator. The dosing schedule for R-CHOP is identical to that of R-CHP used in the pola-R-CHP regimen, with the addition of vincristine administered 1.4 mg/m2 on day 1 every 21 days for up to 6 cycles. The sponsor estimated the cost per 21-day cycle of R-CHOP to be $3,136, resulting in a 6-cycle cost of $18,816.
Modelled outcomes included life-years and QALYs. Costs were estimated from the perspective of the Canadian public health care payer. Model outputs were generated over a lifetime horizon of 35 years, with a cycle length of 1 week. Costs and outcomes were discounted annually at 1.5%.
Model Structure
The sponsor submitted a Markov model that sought to track progression through a sequence of treatment regimens (first-line through third-line) culminating in a cure or death (Figure 1). At model entry patients entered the first-line state where pola-R-CHP or R-CHOP was initiated. After each cycle, patients could remain in their current state, switch to a later line of therapy (if permitted), or transition to either the cure or death state. Movements between the discrete states were dependent on the specific state occupied by the patient and the amount of time spent in that state. For example, patients could only transition to the cure state from the first-line state if they had occupied the first-line state for 2 years following completion of their treatment. In addition, patients could transition to the cure state if they had received CAR T-cell therapy or autologous stem cell transplant (ASCT) as second-line or third-line therapy.
Patients were assumed to initiate second- or third-line therapy upon entry to the respective states. For the second-line state, the eligible regimens were dependent on the amount of time spent in the first-line state. If progression occurred within the first 12 months after the completion of first-line therapy, a patient was considered refractory. Eligible second-line treatments for this subgroup included CAR T-cell therapy, rituximab-based chemotherapy (R-chemo), or polatuzumab vedotin, bendamustine, and rituximab (pola-BR). If progression occurred more than 12 months after the completion of first-line therapy, a patient was considered relapsed. In this subgroup, eligible second-line treatments included salvage therapy followed by ASCT, R-chemo, or pola-BR. In third-line therapy, the treatment options included salvage therapy plus ASCT, glofitamab, epcoritamab, pola-BR, R-chemo, and CAR T-cell therapy.
Model Inputs
All data summarizing baseline characteristics were obtained from the POLARIX trial and were specific to the ABC subpopulation. Baseline characteristics of interest included age (mean = 65 years; range, 23 to 79 years), weight (mean = 74.45; standard deviation = 19.90), and body surface area (mean = 1.83 m2).1,2
Transitions from the first-line state were influenced by the time-varying risk of disease progression and the risk of death. Estimates of the risk of disease progression (defined as progression or death events) were obtained from the parametric analysis of time-to-progression data of the ABC subpopulation of patients from the POLARIX trial. Treatment-independent parametric models were fitted for PFS using the exponential, log-logistic, log-normal, Weibull, Gompertz, gamma, and generalized gamma distributions for pola-R-CHP or R-CHOP. Selection of the base-case configuration was informed by visual inspection of the Kaplan-Meier curve, assessment of model-fit statistics, and clinical plausibility. In the base case, the sponsor selected PFS models that followed the generalized gamma distribution. The effect of treatment waning was explored in a scenario analysis, in which the benefit of pola-R-CHP began to decline at month 30 until no incremental benefit compared with R-CHOP was observed at month 60. The probability of remaining in the first-line state reflected the product of the probability of remaining progression-free and remaining alive (the complement of the mortality risk). Meanwhile, the probability of transitioning to the second-line state reflected the probability of experiencing progression and remaining alive. Finally, patients could only transition to the cure state if they remained alive 2 years after completing their first-line regimen.1
The sponsor made several assumptions regarding treatment use in the second-line health state, specifically that all patients who are refractory to first-line treatment, are alive, and discontinue first-line treatment receive a second-line treatment. If the relapse occurs within 12 months, 70% are transplant-eligible and 30% are transplant-ineligible. For patients who are transplant-eligible, 95% receive CAR T-cell therapy and 5% receive rituximab plus gemcitabine and oxaliplatin (R-GemOx); for patients who are transplant-ineligible receiving R-CHOP, 70% would receive pola-BR and 30% would receive R-GemOx, while for patients who are transplant-ineligible receiving pola-R-CHP, all patients would receive R-GemOx. If relapse occurs beyond 12 months, 50% are transplant-eligible and 50% are transplant-ineligible. For patients who are transplant-eligible, 80% receive salvage chemotherapy then ASCT, and 20% receive R-GemOx; for patients who are transplant-ineligible, 70% would receive pola-BR and 30% would receive R-GemOx. Some treatment-use assumptions were informed by prior CDA-AMC reviews, although most were stated as assumptions or based on expert opinion. Transitions from the second-line state were influenced by competing risks related to a cure, progression, and death. Patients were only eligible to transition to the cure state if their second-line treatment involved CAR T-cell therapy or salvage therapy plus ASCT. The sponsor assumed that the weekly probability of a cure would be 47% for CAR T-cell therapy and 53% for salvage therapy plus ASCT. These estimates reflected the unadjusted Kaplan-Meier event-free survival (EFS) estimate at 12 or 15 months.1,3,4 The progression risks for CAR T-cell therapy and salvage therapy plus ASCT were assumed to be 89% and 96%, respectively. These estimates were obtained from published probabilities of second-line EFS in the ZUMA-7 trial, in which the events of interest included progression, death, or a new antilymphoma treatment.1,3 Meanwhile, the progression risk for the noncurative treatments (pola-BR and R-GemOx) reflected univariate Kaplan-Meier estimates from patient-level data.1,5,6 The probability of remaining in the second-line state reflected the product of remaining progression-free, no cure (if eligible), and remaining alive. Transitions to the second-line state reflected the product of the progression risk and remaining alive.
The sponsor made several assumptions regarding treatment use in the third-line health state, assuming all patients who discontinue second-line treatment and are alive are treated. For patients who were refractory to first-line treatment, the sponsor assumed 10% are transplant-eligible and 90% are transplant-ineligible. All patients who are transplant-eligible receive salvage chemotherapy then ASCT. For patients who are transplant-ineligible, 65% would receive R-GemOx and 35% would receive a bispecific (evenly split between glofitamab and epcoritamab at 17.5% each). For patients who relapse after first-line treatment, 45% are assumed to be eligible for CAR T-cell therapy and 55% are ineligible. For patients eligible for CAR T-cell therapy, 80% receive CAR T-cell therapy, 5% receive R-GemOx, and 15% receive a bispecific (evenly split between glofitamab and epcoritamab). For patients ineligible for CAR T-cell therapy, 80% receive a bispecific (evenly split between glofitamab and epcoritamab), 15% receive pola-BR and 5% receive R-GemOx. Some treatment-use assumptions were informed by prior CDA-AMC reviews, although most were stated as assumptions or based on expert opinion. Transitions from the third-line state were influenced by competing risks relating to a cure and death. Patients were only eligible to transition to the cure state if their third-line therapy involved CAR T-cell therapy or salvage therapy plus ASCT. It was assumed that the weekly probability of cure would be 53% for CAR T-cell therapy and 18% for salvage therapy plus ASCT. These estimates reflected the Kaplan-Meier 16-month OS estimate from the ZUMA-1 trial and the 12-month EFS estimate from the ZUMA-7 trial.1,3,7 For the noncurative third-line treatments (pola-BR, R-GemOx, and glofitamab), the risks of death were obtained using univariate Kaplan-Meier estimates from patient-level data.1,5,6,8
Throughout the specified time horizon, patients were subject to a risk of death that varied with age or state occupancy. The all-cause mortality risk was assumed to follow age- and sex-specific mortality risks reflecting the general population of patients in Canada. Data for this input were obtained from life tables published by Statistics Canada. Patients also faced a risk of death because of adverse events (AEs) or a cause other than progression. In the first-line state, these inputs (0.05% for pola-R-CHP; 0.07% for R-CHOP) were obtained using data specific to the ABC subpopulation in the POLARIX trial. The sponsor divided the number of deaths that occurred before disease progression (7 and 9 for pola-R-CHP and R-CHOP, respectively) by the cumulative PFS months (3,127 for pola-R-CHP; 2,941 for R-CHOP) and then converted the time scale of the risk of death risk from monthly to weekly. In the second-line state, the corresponding death risks for CAR T-cell therapy and salvage therapy plus ASCT were assumed to be 11% and 4%, respectively. These were estimated from published probabilities of second-line EFS in the ZUMA-7 trial.1,3 For R-GemOx and pola-BR, the weekly risk of death was assumed to be 0.16%. These inputs were calculated from patient-level data, in which the number of deaths (3 for R-GemOx: 5 for pola-BR) was divided by the cumulative number of EFS months (286 for R-GemOx; 723 for pola-BR).1,5,6 In each cycle, the mortality risk from the first-, second-, or third-line states reflected the higher value between the mortality risk of the general population and the risk calculated from the POLARIX trial.1
In addition to tracking the proportion of the cohort in each state, the model also tracked the occurrence of AEs. This was restricted to grade 3 to 5 AEs occurring in more than 2% of ABC patients in any arm of the POLARIX trial. The identified AEs included anemia, febrile neutropenia (grade 3 or 4), neutropenia, pneumonia, and vomiting. Each event was assumed to occur in the first cycle of the model.1
HRQoL was captured in the model using utility values specific to each health state and subgroup, where relevant. Data from the intention-to-treat population of the POLARIX trial were used to obtain the utility values specific to the first-line state (0.85; 95% confidence interval [CI], 0.84 to 0.86), second-line state (refractory = 0.83; 95% CI, 0.80 to 0.85; relapsed = 0.81; 95% CI, 0.78 to 0.84).1,2 Meanwhile, utility values for the third-line state were obtained from the ZUMA-1 trial for axicabtagene ciloleucel (0.720; standard error = 0.03).1,7 These values were adjusted using age- and sex-specific utility norms for the population in Canada.1,9
Costs in the model included those for acquisition and administration, health-state monitoring, management of AEs, and end-of-life care. Treatment acquisition costs were calculated from the price per unit consumed following the recommended dosage for each regimen.1,10,11 The sponsor’s submitted price was used for polatuzumab vedotin, while wholesale list prices in the IQVIA DeltaPA database were used for all other drugs.1,12 Treatment administration costs were applied for any treatment that required IV administration. These were estimated using the assumed chair time for each regimen (pola-R-CHP: 7.92 hours in the first cycle, 3.17 hours in subsequent cycles; R-CHOP: 5.09 hours in the first cycle, 2.34 hours in subsequent cycles), and the cost per hour of chair time.1,13 Costs also reflected the physician billing code for IV administration ($75) from the Ontario Schedule of Benefits for Physician Services.1,14 Costs related to the management of AEs, except for vomiting, reflected inpatient and outpatient costs estimated from the Ontario Case Costing Initiative.1,15 Meanwhile, vomiting costs were sourced from a patient cost calculator and a physician billing code.1,14,16 Monitoring costs included the costs for resource utilization associated with routine patient monitoring, such as clinician assessments, laboratory testing, and imaging. Unit prices were obtained from the Ontario Schedule of Benefits for Physician and Laboratory Services, the Ontario Case Costing Initiative, and other relevant literature. The frequency of resource utilization was assumed to be consistent with the assumptions used in a National Institute for Health and Care Excellence technology appraisal for pola-R-CHP.1,17 The cost of end-of-life care ($43,112.18) was assumed to represent the average direct medical cost per patient associated with the last 6 months of life for patients with lymphoma or leukemia in a study of patients in Canada from 2002 to 2003.1,18 This estimate was inflated to a 2023 price and applied as a one-time cost upon entry to the death state.1
CDA-AMC requested an updated model due to concerns regarding several calculations, inadequate parameterization of uncertainty, and exclusion of the impact of testing for ABC subtype. Although the sponsor provided an updated model clarifying some of these issues (e.g., inadequate parameterization of uncertainty), it declined to address issues regarding a cure upon entry to the third-line state of the model and the implications of testing for the ABC subtype. The sponsor used the unadjusted EFS survival probabilities described previously without further transformation to obtain probability of the event over 1 week (i.e., the cycle length).
Summary of Sponsor’s Economic Evaluation Results
In the submitted base case, costs and QALYs for each alternative were generated in a Monte Carlo simulation of 1,000 iterations. Meanwhile, the scenario analyses were conducted deterministically. The deterministic and probabilistic base-case results were similar. The probabilistic findings are presented in the following section.
Base-Case Results
The submitted analysis was based on publicly available prices of the comparator treatments. Results from the base case of the submitted economic evaluation are presented in Table 3. Pola-R-CHP was less costly (−$32,350 in incremental costs) and more effective (2.43 incremental QALYs) compared with R-CHOP. This means that pola-R-CHP is cost-effective because a lower cost is required to obtain more QALYs. As a result, pola-R-CHP had a 100% probability of being cost-effective at a willingness-to-pay threshold of $50,000 per QALY gained. In the deterministic base case, approximately 91% of the incremental QALYs for pola-R-CHP were gained beyond 46 months, the maximum follow-up of pola-R-CHP in the POLARIX trial.
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER ($ per QALY) |
|---|---|---|---|---|---|
Pola-R-CHP | 185,373 | Reference | 11.78 | Reference | Reference |
R-CHOP | 217,723 | 32,350 | 9.34 | −2.43 | Dominated |
ICER = incremental cost-effectiveness ratio; pola = polatuzumab vedotin; QALY = quality-adjusted life-year; R-CHP = rituximab, cyclophosphamide, doxorubicin, and prednisone; R-CHOP = rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone.
Note: Additional results from the sponsor’s submitted economic evaluation base case are presented in Appendix 3.
Source: Sponsor’s pharmacoeconomic submission.1
Sensitivity and Scenario Analysis Results
In addition to the submitted base case, the sponsor considered 14 scenario analyses. These scenarios explored alternate inputs or assumptions relating to the time horizon, discount rate, duration of PFS treatment effect, survival distribution, use of subcutaneous rituximab, proportion of eligible patients receiving CAR T cells as second-line therapy, and the population used for the utility values. While each scenario had a slight impact on the expected costs and benefits, none had a meaningful effect on the conclusion of the economic evaluation. No scenario analysis was conducted using a perspective other than that of the health care payer.
CDA-AMC Appraisal of the Sponsor’s Economic Evaluation
CDA-AMC identified several key limitations to the sponsor’s analysis that have notable implications on the economic analysis:
The IHC testing method to identify patients with LBCL classified as having the ABC subtype lacks accuracy and likely misclassifies patients: Based on the POLARIX trial results, pola-R-CHP is expected to result in a clinically meaningful PFS benefit relative to R-CHOP in patients with the ABC subtype of LBCL. However, these findings were based on subgroup analyses and are associated with various limitations identified in the CDA-AMC Clinical Review that affect the interpretability and certainty of the trial results. The POLARIX trial results indicate that any clinical benefit in terms of PFS or OS is anticipated to occur in patients who are classified as having the ABC subtype, although the magnitude of this benefit is unknown given the limitations with the available data. In Canada, testing to identify subtype is predominantly undertaken via IHC testing using the Hans algorithm, which can only identify 2 categories: GCB and non-GCB. Non-GCB includes the ABC and unclassified subtypes. IHC therefore cannot accurately identify the patients with the ABC subtype who would most benefit from pola-R-CHP. Ideally, GEP would be used to identify patients with the ABC subtype; however, this is not widely available in Canada and it is available and funded only in British Columbia. If patients who are incorrectly identified as having the ABC subtype receive pola-R-CHP, it is highly uncertain that they would benefit from treatment, and they may potentially experience harms due to exposure to pola-R-CHP. The clinical experts consulted by CDA-AMC agreed that, based on the current testing methods for the ABC subtype in practice, a proportion of patients will be overtreated because they do not require treatment. However, the experts also indicated that the potential benefit would be great enough to warrant the risk. CDA-AMC notes that the sponsor’s submitted analysis assumes the IHC testing method using the Hans algorithm provides 100% specificity and sensitivity for detecting the ABC subtype. However, published literature indicates that the specificity of this testing method ranges from 52% to 82%, and the sensitivity ranges from 85% to 90%.19 As such, there is a large range in the number of patients that may be misclassified as having the ABC subtype, as highlighted in the CDA-AMC Testing Procedure Assessment and the CDA-AMC Clinical Review. Based on this range of specificity values, for every 1.50 to 2.31 patients classified as having non-GCB disease by the Hans algorithm, only 1 would have the ABC subtype. The remaining patients would therefore be misclassified and may not have the ABC subtype.
Clinical expert feedback obtained by CDA-AMC indicated that the availability of pola-R-CHP would change the treatment paradigm, which currently does not factor in disease subtype when determining treatments. The clinical experts noted that patients with LBCL who were classified as having high-risk disease (e.g., an IPI score of 3 to 5 and the ABC subtype) are more likely to experience poor outcomes with R-CHOP treatment. The availability of pola-R-CHP for use in patients with the ABC subtype of LBCL is likely to increase subtype testing. The clinical experts indicated that considerable costs would be associated with implementing GEP testing to more accurately identify patients with LBCL classified as the ABC subtype. Feedback indicated that additional resources will be required, as GEP testing is not available in most jurisdictions, and additional funding would be required to allow its use in provinces other than British Columbia. Clinical experts indicated that sending tests to British Columbia is associated with challenges, and patients would experience delays in receiving tests results in exterior provinces. Experts further emphasized that, because LBCL is the most common type of lymphoma seen in practice, testing costs would increase considerably across all jurisdictions other than British Columbia to accommodate GEP testing, as would costs related to assay development and validation, staff training, and equipment procurement and maintenance. CDA-AMC notes that the sponsor’s submission does not include testing costs for identifying patients with LBCL presenting with the ABC subtype. Based on the CDA-AMC Testing Procedures Assessment, the cost in British Columbia of GEP using the Lymph2Cx assay on the NanoString platform to identify patients is about $570 per tumour.
CDA-AMC included specificity rates of 52% and 82% to test the impact of overtreatment of patients with LBCL who would be misclassified as having the ABC subtype.
While drug acquisition costs due to overtreatment are captured in this reanalysis, CDA-AMC notes that potential harms due to overtreatment could not be accounted for.
Because the cost of testing is not captured within the economic analysis, the total incremental cost of pola-R-CHP is underestimated.
The modelling assumptions surrounding a cure lacked face validity and likely did not capture the clinical pathway of disease: The treatment effect of pola-R-CHP was captured through PFS data from the POLARIX trial and various cure assumptions implemented by the sponsor. For example, the sponsor assumes that cured patients who remain progression-free for 2 years after treatment discontinuation are considered functionally cured. Clinical expert feedback obtained by CDA-AMC indicated that, while this assumption is reasonable, patients considered to be cured are expected to remain at risk of relapse or disease progression for the remainder of their lifetime. Feedback indicated that 20 years between relapses is possible. CDA-AMC notes that the sponsor included a 5% risk of relapse for up to up to 3 years for patients after being considered functionally cured, which may slightly overestimate the stability of disease in these patients.
However, once patients are considered cured, the sponsor assumed that their risk of mortality is equivalent to that of the general population. Clinical expert feedback obtained by CADTH indicated that this assumption does not meet face validity, as most long-term survival studies report an increase in mortality from nonrelapse causes in patients treated for DLBCL.20-22 Furthermore, the sponsor assumed that the quality of life for patients who are progression-free was equivalent to that of the general population; clinical expert feedback obtained by CDA-AMC indicated that this assumption was likely optimistic and that patients would be expected to experience some long-term effects from treatment and likely require additional resources. The assumption that patients who are progression-free experience the same quality of life as the general population likely biases the results in favour of pola-R-CHP.
Clinical expert feedback obtained by CDA-AMC indicated that long-term follow-up is ideal for all patients who are assumed to be cured after remaining progression-free for 2 years after treatment discontinuation. However, resource and capacity restraints may result in earlier discharge of patients to primary care. Clinical experts indicated that follow-ups should occur every 3 months for the first year and every 6 months thereafter until year 5. Their feedback also indicated that follow-ups should occur for at least 2 years, and monitoring can vary but should consist primarily of clinical visits, imaging, and bloodwork. However, the sponsor assumes that patients who are considered cured no longer receive active monitoring and therefore no longer incur costs to the health system after 2 years post–treatment discontinuation, which likely underestimates costs associated with managing patients who are treated with pola-R-CHP and therefore biases cost-effectiveness in favour of pola-R-CHP.
Overall, the sponsor’s model and various assumptions regarding a cure and the clinical pathway of disease likely bias the results in favour of pola-R-CHP. CDA-AMC could not address these concerns in reanalysis due to limitations with the model structure and issues with face validity of results as outlined in the following section.
CDA-AMC could not address this limitation in its reanalysis due to the submitted model structure.
The long-term benefit of pola-R-CHP and predicted impact on long-term OS are uncertain: The sponsor predicted that pola-R-CHP would be associated with approximately 3 additional years of life compared with R-CHOP based on PFS data from the POLARIX trial and other modelling assumptions that extrapolate the impacts of pola-R-CHP. According to the CDA-AMC Clinical Review of the POLARIX trial, the estimated PFS in the ABC subpopulation showed a clinically meaningful improvement from pola-R-CHP versus R-CHOP, but no definitive conclusion could be drawn for OS due to immature data. Based on the subgroup analysis reported in Salles et al.,23 the treatment benefit with pola-R-CHP demonstrated in the ABC subpopulation was not demonstrated in other subtypes of LBCL for either PFS or OS. For 5-year PFS, the hazard ratio point estimates for GCB, unclassified and unknown, ranged from 0.83 to 1.60, although estimates for all 3 groups spanned the null. For 5-year OS, the hazard ratio point estimates for GCB, unclassified and unknown, ranged from 0.80 to 4.46; estimates for GCB and unknown spanned the null, although the results for the unclassified subgroup did not. However, the data were based on exploratory subgroup analyses that were not adjusted for multiplicity, nor were they designed or powered to demonstrate OS or PFS given the reduced sample size compared to the overall LBCL population from the pivotal trial. The small sample size likely contributed to imprecision in findings, particularly for OS and PFS at longer follow-ups, leading to wide 95% CIs. The interpretation of OS results was limited given that OS had not been reached after a median of 63.9 months (for pola-R-CHP) and the 60-month estimates for PFS and OS were imprecise. The use of PFS as a surrogate outcome for OS is also problematic because enrolment criteria used in clinical trials tend to result in a more selective population than that of patients in real-world settings. Altogether, findings for the ABC subpopulation were limited by evidence from a subgroup analysis and challenging to interpret, and it was therefore uncertain if pola-R-CHP was associated with an OS benefit.
The reason for all “unknown” classifications was not provided to CDA-AMC, making it unclear whether these patients would be captured within the non-GCB subtype or all “unknown” classifications were a result of missing data. The CDA-AMC Clinical Review and clinical experts consulted for this review noted that pola-R-CHP is expected to result in a survival benefit only in patients with the ABC subtype, although the magnitude of the benefit is uncertain. There is no robust evidence that pola-R-CHP is associated with a survival benefit compared to R-CHOP in other (non-ABC) subgroups, although the interpretability of the results remains highly uncertain.
Notably, a high degree of censoring was observed in the pola-R-CHP group relative to the R-CHOP group (84% versus 71% for OS; 74% versus 47% for PFS). Despite patients being lost to follow-up, the PFS estimates remained similar after 40 months. Because the reasons for patients in the ABC subpopulation being censored at follow-up time points were not provided, it was not possible for the review team to assess the appropriateness of the censoring (e.g., informative censoring such as loss to follow-up to due AEs, poor prognosis) and any between-group differences that could affect the efficacy in magnitude and direction. The lack of information regarding censoring introduces further uncertainty to the cost-effectiveness estimates for pola-R-CHP. The concerns with the available clinical evidence informing the efficacy of pola-R-CHP in patients with LBCL classified as the ABC subtype result in high uncertainty surrounding the model’s predicted OS benefit. In the model, patients treated with pola-R-CHP are expected to experience a median OS of approximately 17 years compared to the 10 years predicted for R-CHOP. The sponsor assumed that treatment benefit with pola-R-CHP would be maintained indefinitely with no treatment-waning effect modelled. According to clinical expert feedback, the model results lacked face validity as it is unlikely that patients would survive an additional 17 years after treatment with pola-R-CHP, and these estimates were likely overestimated. Clinical expert feedback indicated that the predicted PFS associated with R-CHOP appeared to be reasonable, particularly between year 2 and year 5, with uncertainty in the long term noted after the trial period. CDA-AMC notes that the majority of the predicted OS benefit occurs after the trial period, with up to 91% of the incremental benefit predicted to occur in the extrapolated period. The analysis submitted by the sponsor is therefore subject to a high degree of uncertainty.
CDA-AMC could not address issues with the face validity of the results predicted by the sponsor’s model or the limitations with the available clinical evidence.
Subsequent therapy assumptions were not reflective of clinical practice in Canada: In the submitted model, the sponsor applies various assumptions regarding the proportion of patients who receive subsequent therapies in second- and third-line treatment, which is dependent on the treatment arm and whether second-line relapse is less than or greater than 12 months. The sponsor assumes that 100% of patients who relapse would go on to receive subsequent therapy. However, clinical expert feedback indicated that this number is likely overestimated and that some patients (approximately 1 in 20) who are frail and/or do not tolerate first-line treatment well would opt to not receive further therapy. As such, the sponsor likely overestimates subsequent treatment costs. The experts also indicated that, in Canadian clinical practice, the approach to subsequent therapy would not differ between first-line therapy (i.e., whether a patient receives pola-R-CHP or R-CHOP) and that they expected the distribution and number of subsequent therapies would be nearly equivalent between groups, with exception of pola-BR, which would be used more frequently in patients who receive R-CHOP in first-line treatment, which aligns with the sponsor’s approach. For relapses in the second line occurring after less than 12 months, the clinical experts also indicated that the proportion of patients receiving CAR T-cell therapy is likely overestimated at 67% because of various barriers to access, including the limited number of CAR T-cell therapy centres and the need to travel to these centres. According to the clinical experts, even 50% may be an overestimate of the proportion of individuals who actually receive CAR T-cell therapy. For relapses occurring after 12 months, clinical expert feedback indicated that the proportion of those receiving salvage therapy plus ASCT was also likely overestimated; while 40% may go on that treatment pathway, it is more likely that 20% would ultimately receive ASCT. Last, third-line chemotherapy appeared to be overestimated at 42.5% given new treatment options; the clinical experts indicated that this value would likely be closer to 20%, and the use of glofitamab and epcoritamab would likely be 28.6% instead of 18.6%.
CDA-AMC assessed the impact of alternate distribution of subsequent treatments aligned with clinical expert feedback in a scenario analysis.
A price reduction of 45% for CAR T-cell therapy was also applied in this scenario analysis to reflect the CDA-AMC review of axicabtagene ciloleucel.24
Poor modelling practices were employed: The sponsor’s submitted model included numerous IFERROR statements, which lead to situations in which the parameter value is overwritten with an alternative value without alerting the user to the automated overwriting. The systematic use of IFERROR statements makes thorough auditing of the sponsor’s model impractical and it remains unclear whether the model is running inappropriately by overriding errors.
CDA-AMC could not address this limitation. Due to the sponsor’s approach, a thorough validation of the sponsor’s model was not possible.
The trial population does not reflect the population likely to be treated in clinical practice in Canada: Clinical expert feedback indicated that the proportions of patients with an Eastern Cooperative Oncology Group Performance Status (ECOG PS) of 0 to 1 were 81.1% in the pola-R-CHP arm and 82.8% in the R-CHOP arm, indicating that patients from the trial were healthier than those in practice. In practice, a large proportion would be expected to have an ECOG PS of 3, and some would be hospitalized. However, clinical expert feedback also indicated that patients with an ECOG PS of 3 would not be excluded from treatment in clinical practice. In clinical practice, performance status is not a criterion for treatment for R-CHOP and poor performance status does not exclude these patients from treatment. Clinical expert feedback noted that the trial is biased toward patients who are more fit, and patients with more severe disease are not included in the trial population. The proportion of patients who received CAR T-cell therapy was also much lower than expected, largely due to the availability of CAR T-cell therapy at the time of the trial.
CDA-AMC could not address this limitation in its reanalysis but notes that this limitation increases the uncertainty of the cost-effectiveness of pola-R-CHP in the requested population.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CDA‑AMC (refer to Table 4).
Table 4: Key Assumptions of the Submitted Economic Evaluation (Not Noted as Limitations to the Submission)
Sponsor’s key assumption | CDA-AMC comment |
|---|---|
The price of a rituximab biosimilar is used, as opposed to the brand price. | Acceptable. The biosimilar rituximab product is available and widely used in Canadian jurisdictions. |
Rituximab was assumed to be administered intravenously rather than subcutaneously in subsequent cycles. | Acceptable. This assumption was applied for both pola-R-CHP and R-CHOP. |
Health resource utilization for patients was derived from the NICE technology appraisal for pola-R-CHP. | Ideally, Canadian resource use estimates would be used, however, the impact of these estimates on the model results is small. |
CDA-AMC = Canada’s Drug Agency; NICE = National Institute for Health and Care Excellence; pola-R-CHP = polatuzumab vedotin, rituximab, cyclophosphamide, doxorubicin, and prednisone; R-CHOP = rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone.
CDA-AMC Reanalyses of the Economic Evaluation
Base-Case Results
The CDA-AMC reanalyses were derived by incorporating the cost impact of the overestimation of individuals with ABC subtype by IHC genetic testing to reflect clinical practice (Table 5). CDA-AMC undertook these reanalyses after confirming with the clinical experts consulted by CDA-AMC that patients who were considered to have the non-GCB subtype would be treated with pola-R-CHP in practice in Canada. Reanalyses tested the impact of including a 52% (lower bound) and 82% (upper bound) specificity value for detecting the ABC subtype. The Scenario Analysis subsection of Appendix 4 and Table 13 describe how these values were derived.
Table 5: CDA-AMC Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
Changes to derive the CDA-AMC base case | ||
1. Overestimation of individuals with ABC subtype included to reflect clinical practice | 100% testing accuracy with IHC for detecting ABC subtype | Base case 1: 52% specificity value for detecting ABC subtype Base case 2: 82% specificity value for detecting ABC subtype |
CDA-AMC base case | ― | Reanalysis 1 |
ABC = activated B cell–like; CDA-AMC = Canada’s Drug Agency; IHC = immunohistochemistry.
In the CDA-AMC base case, pola-R-CHP was associated with an estimated cost of $292,436 and 11.75 QALYs over a lifetime horizon when adopting a specificity rate of 52% for detecting the ABC subtype. When adopting a specificity rate of 82%, pola-R-CHP was associated with an estimated cost of $225,883 and 11.75 QALYs over a lifetime horizon (Table 6).
The key driver of the analysis among patients receiving pola-R-CHP is the estimated PFS benefit and impact of cure assumptions. CDA-AMC notes that the reanalysis was unable to address issues concerning uncertainty in the clinical evidence and lack of face validity surrounding the submitted model. Approximately 91% of the incremental QALYs for pola-R-CHP were gained beyond 46 months (i.e., the maximum follow-up of pola-R-CHP in the POLARIX trial), which aligns with the sponsor’s base-case analysis.
Table 6: Summary of the CDA-AMC Reanalysis Results
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($ per QALY) |
|---|---|---|---|---|
Sponsor’s base case | Pola-R-CHP | 184,780 | 11.75 | Reference |
R-CHOP | 217,233 | 9.32 | Dominant | |
CDA-AMC base case: 52% specificity (reanalysis 1) | R-CHOP | 229,611 | 9.32 | Reference |
Pola-R-CHP | 292,436 | 11.75 | 25,952 | |
CDA-AMC base case: 82% specificity (reanalysis 1) | R-CHOP | 221,972 | 9.32 | Reference |
Pola-R-CHP | 225,883 | 11.75 | 1,616 |
CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; pola-R-CHP = polatuzumab vedotin, rituximab, cyclophosphamide, doxorubicin, and prednisone; R-CHOP = rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone.
Notes: The CDA-AMC reanalysis is based on publicly available prices of the comparator treatments. The results of the CDA-AMC reanalysis are presented deterministically.
Scenario Analysis Results
CDA-AMC conducted scenario analyses to evaluate the impact of alternate distributions across subsequent treatment options to reflect clinical expert feedback obtained for this review. In this scenario analysis, a price reduction of 45% for CAR T-cell therapy was also applied to reflect the CDA-AMC review of axicabtagene ciloleucel.24 When adopting a specificity rate of 82% for detecting the ABC subtype in this scenario analysis, the ICER increased to $26,600 per QALY gained versus R-CHOP. When adopting a specificity rate of 52% for detecting the ABC subtype in this scenario analysis, the ICER increased to $57,344 per QALY gained versus R-CHOP.
In the scenario analysis including alternate distributions for subsequent treatment and a 45% price reduction for CAR T-cell therapy in which the specificity rate for detecting the ABC subtype is 52%, a price reduction of at least 8% is required for pola-R-CHP to be considered cost-effective at a willingness-to-pay threshold of $50,000 per QALY gained relative to R-CHOP.
Issues for Consideration
The pan-Canadian Pharmaceutical Alliance concluded negotiations with a letter of intent for pola-BR for the treatment of relapsed or refractory DLBCL. As such, a confidential negotiated price exists for polatuzumab vedotin, while the sponsor’s base case and all CDA-AMC reanalyses rely on the price submitted by the sponsor.25
The pan-Canadian Oncology Drug Review Expert Review Committee recommended that pola-R-CHP not be reimbursed for adult patients with previously untreated LBCL, including DLBCL NOS, high-grade B-cell lymphoma, Epstein-Barr virus–positive DLBCL NOS, and T-cell/ histiocyte-rich LBCL (i.e., the POLARIX trial population not restricted to the ABC subtype). The committee made this recommendation as the evidence for the full POLARIX trial population showed that, while 6.6% more patients with newly diagnosed moderate- to high-risk LBCL were alive without their disease progressing 2 years after treatment with pola-R-CHP compared to those treated with R-CHOP, whether the difference observed in the clinical trial translates to a meaningful difference in the real world is uncertain. The evidence from the trial did not show that pola-R-CHP prolonged survival compared to R-CHOP. It is also unknown if pola-R-CHP would reduce disease symptoms or improve functioning compared to R-CHOP because there were no differences between the 2 groups, and it was not clear that pola-R-CHP would provide a meaningful benefit in prolonging remission or meet the other important patient-identified needs. In this prior review, CDA-AMC estimated that the ICER for pola-R-CHP compared with R-CHOP would be $394,163 per QALY gained (0.19 incremental QALYs and $76,379 in incremental costs).
The sponsor estimated that pola-R-CHP is associated with additional chair time compared with R-CHOP (based on the sponsor’s assumptions of approximately 2.8 additional hours in cycle 1 and 0.8 additional hours in subsequent cycles).
The sponsor reported GEP is the most accurate way to identify patients with the ABC lymphoma subtype. The CDA-AMC Testing Procedure Assessment reported that GEP using the Lymph2Cx assay had a lower misclassification rate compared with IHC via the Hans algorithm. No published evidence regarding the sensitivity and specificity of GEP-based testing was identified.
Input received by CDA-AMC indicated that there are implementation considerations that are likely to have an economic impact that could not be addressed in the pharmacoeconomic submission. Issues around the centralized locations in some jurisdictions where polatuzumab vedotin would be reconstituted and need to be transported to treatment facilities were noted. Economic impacts of this may include increased administrative costs associated with coordinating the timely and temperature-controlled transportation of the reconstituted product and potential for drug wastage due to product aggregation. Additionally, there are treatment centres that may not be able to accommodate the length of the regimen infusion for pola-R-CHP (infusion time for cycle 1 of the regimen may be 8 hours). Accommodating this regimen may result in increased costs as a result of extended operating hours and staffing requirements. However, because pola-BR is approved for use, physicians and treatment centres have experience implementing a regimen that includes this treatment.
Overall Conclusions
Evidence from a randomized phase III, double-blind trial (POLARIX) that enrolled a subpopulation of 235 adult patients identified as having the ABC lymphoma subtype of LBCL who had been previously untreated for the disease demonstrated that, compared with standard of care (R-CHOP), treatment with pola-R-CHP may provide a clinically important increase in PFS at 2 years and 5 years. There was uncertainty in the estimated magnitude of the PFS benefit due to a small population sample size with few events. Data for OS were immature at 2 years and at 5 years, and a definitive conclusion could not be drawn about the OS benefit of pola-R-CHP in patients with the ABC lymphoma subtype. The comparative efficacy of pola-R-CHP on HRQoL was not available.
It is unknown whether the PFS benefit of pola-R-CHP observed in patients with the ABC lymphoma subtype will be replicated in patients with non-ABC lymphoma. Current testing in clinical practice across most jurisdictions uses the IHC testing via the Hans algorithm for detecting GCB and non-GCB lymphoma subtypes (ABC is captured within the non-GCB lymphoma subtype). However, published literature indicates that the specificity ranges from 52% to 82% for identification of the ABC lymphoma subtype with this testing method. As such, there is a large range in the number of patients that may be misclassified as having the ABC subtype and would therefore result in overuse of pola-R-CHP in patients for whom treatment would not be advised, as it is unclear whether they would benefit from pola-R-CHP, experience little to no benefit from treatment, or potentially experience harms. All testing costs associated with identifying patients with the ABC subtype were excluded from the analysis by the sponsor and could not adequately be incorporated into a reanalysis by CDA-AMC.
CDA-AMC identified several limitations in the sponsor’s pharmacoeconomic analysis that have notable implications on the cost-effectiveness of pola-R-CHP. In its base-case reanalysis, CDA-AMC incorporated the cost impact of the overestimation of individuals with the ABC subtype by IHC genetic testing to reflect clinical practice. CDA-AMC reanalyses assessed the impact of including a 52% (lower bound) and 82% (upper bound) specificity value for detecting the ABC subtype. The patients who test positive but do not actually have the ABC subtype (false-positives) are assumed to incur treatment costs of pola-R-CHP. In line with the subgroup data from the trial, there is no robust evidence of an incremental treatment benefit with pola-R-CHP in other DLBCL subtypes. The CDA-AMC base-case analysis resulted in an ICER of $25,952 per QALY gained (2.42 incremental QALYs and $62,825 in incremental costs) for pola-R-CHP versus R-CHOP when assuming a 52% testing specificity for the ABC subtype. When assuming an 82% testing specificity for the ABC subtype, the resulting ICER was estimated to be $1,616 per QALY gained (2.42 incremental QALYs and $3,911 in incremental costs) for pola-R-CHP versus R-CHOP. CDA-AMC was unable to address issues related to the concerns surrounding the face validity of the cure assumptions and uncertainty in the clinical evidence. The CDA-AMC Clinical Review of the POLARIX trial concluded that it was uncertain if pola-R-CHP was associated with an OS benefit. The sponsor’s model predicts that pola-R-CHP is associated with 3 additional life-years compared with R-CHOP. CDA-AMC could not address issues related to the predicted magnitude of treatment benefit, and assumes that patients receiving pola-R-CHP will live for 17 years after treatment, largely due to the sponsor’s modelling of cure assumptions, the assumption that the PFS benefit will translate to an OS benefit, the assumption that treatment effects will be maintained over the duration of the model, and uncertainty in the long-term efficacy (i.e., 91% of the incremental benefit was predicted to occur after the trial period of 46 months). For the ICER to be realized, a gain of 3 years of life on pola-R-CHP and a reduction in subsequent treatments to the level estimated by the sponsor would be required. A CDA-AMC scenario analysis assessing the impact of alternate assumptions regarding subsequent therapies resulted in an increased the ICER.
The analysis includes additional drug acquisition costs of pola-R-CHP due to treating the false-positive patients identified with IHC testing; the additional costs associated with health care resource utilization and any potential harms with overtreatment could not be assessed in this analysis. Testing costs could not be included in the CDA-AMC reanalyses. If GEP testing were to be implemented and is accurate, pola-R-CHP under GEP testing may be cost-effective in treating adult patients identified as having the ABC lymphoma subtype of LBCL who had been previously untreated for the disease. However, the analysis does not incorporate the additional costs required to implement GEP testing to more accurately identify patients with DLBCL with the ABC subtype. Based on the sponsor’s estimated number of patients with confirmed DLBCL across all CDA-AMC–participating jurisdictions from the BIA, funding GEP testing to identify patients with ABC subtype would result in additional costs of more than $1,761,300 per year in testing costs to jurisdictions. This estimate does not incorporate costs related to assay development and validation, staff training, and equipment procurement and maintenance.
A price reduction may be required to ensure that pola-R-CHP is a cost-effective regimen for patients with the ABC lymphoma subtype of LBCL who had been previously untreated for the disease due to the uncertainty associated with the magnitude of the clinical benefit, inability of the sponsor’s model to adequately assess the impact of testing implications, limitations with the sponsor’s economic model, concerns regarding the generalizability of the trial population to the population in Canada, and presence of negotiated prices for subsequent therapies (e.g., CAR T cells).
References
1.Hoffmann-La Roche Ltd. Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Polivy (polatuzumab vedotin), 30 mg or 140 mg single-use vial, lyophilized powder for solution for intravenous infusion only. November 27, 2024.
2.Hoffmann-La Roche Ltd. Clinical Study Report: Study GO39942 (POLARIX). A Phase III, multicenter, randomized, double-blind, placebo-controlled trial comparing the efficacy and safety of polatuzumab vedotin in combination with rituximab and CHP (R-CHP) versus rituximab and CHOP (R-CHOP) in previously untreated patients with diffuse large B-cell lymphoma. [internal sponsor's report]. October 2021.
3.Locke FL, Miklos DB, Jacobson CA, et al. Axicabtagene Ciloleucel as Second-Line Therapy for Large B-Cell Lymphoma. N Engl J Med. 2022;386(7):640-654. doi:10.1056/NEJMoa2116133 PubMed
4.Gisselbrecht C, Glass B, Mounier N, et al. Salvage regimens with autologous transplantation for relapsed large B-cell lymphoma in the rituximab era. J Clin Oncol. 2010;28(27):4184-90. doi:10.1200/JCO.2010.28.1618 PubMed
5.Sehn LH, Herrera AF, Flowers CR, et al. Polatuzumab Vedotin in Relapsed or Refractory Diffuse Large B-Cell Lymphoma. J Clin Oncol. 2020;38(2):155-165. doi:10.1200/JCO.19.00172 PubMed
6.Hertzberg M, Ku M, Catalani O, Althaus B, Simko S, Gregory GP. A Phase III Trial of Glofitamab Plus Gemcitabine and Oxaliplatin (Gemox) Vs Rituximab Plus Gemox for Relapsed/Refractory Diffuse Large B‐Cell Lymphoma. Hematol Oncol. 2021;39(S2):344-345. doi:10.1002/hon.165_2880
7.Neelapu SS, Jacobson CA, Ghobadi A, et al. Five-year follow-up of ZUMA-1 supports the curative potential of axicabtagene ciloleucel in refractory large B-cell lymphoma. Blood. 2023;141(19):2307-2315. doi:10.1182/blood.2022018893 PubMed
8.Dickinson MJ, Carlo-Stella C, Morschhauser F, et al. Glofitamab for Relapsed or Refractory Diffuse Large B-Cell Lymphoma. N Engl J Med. 2022;387(24):2220-2231. doi:10.1056/NEJMoa2206913 PubMed
9.Guertin JR, Feeny D, Tarride JE. Age- and sex-specific Canadian utility norms, based on the 2013-2014 Canadian Community Health Survey. CMAJ. 2018;190(6):E155-E161. doi:10.1503/cmaj.170317 PubMed
10.Cancer Care Ontario. Rituximab [sponsor supplied reference]. 2020. https://www.cancercareontario.ca/en/drugformulary/drugs/monograph/44031
11.Cancer Care Ontario. CHOP+R [sponsor supplied reference]. 2020. https://www.cancercareontario.ca/en/drugformulary/regimens/monograph/45801
12.IQVIA. Delta PA Database [sponsor supplied reference]. 2024.
13.Tam VC, Ko YJ, Mittmann N, et al. Cost-effectiveness of systemic therapies for metastatic pancreatic cancer. Curr Oncol. 2013;20(2):e90-e106. doi:10.3747/co.20.1223 PubMed
14.Ontario Ministry of Health. Schedule of benefits for physician services under the Health Insurance Act: (June 29, 2023 (effective July 24, 2023)) [sponsor supplied reference]. 2023.
15.Ontario Case Costing Initiative. Costing Analysis Tool [sponsor supplied reference]. 2017. Updated 2018.
16.Canadian Institute for Health Information. CIHI Patient Cost Estimator [sponsor supplied reference]. 2024.
17.National Institute for Health and Care Excellence. Final appraisal document - Polatuzumab vedotin in combination for untreated diffuse large B-cell lymphoma [sponsor supplied reference]. 2023.
18.Walker H, Anderson M, Farahati F, et al. Resource use and costs of end-of-Life/palliative care: Ontario adult cancer patients dying during 2002 and 2003. J Palliat Care. 2011;27(2):79-88. PubMed
19.Scott DW. Cell-of-Origin in Diffuse Large B-Cell Lymphoma: Are the Assays Ready for the Clinic? Am Soc Clin Oncol Educ Book. 2015:e458-66. doi:10.14694/EdBook_AM.2015.35.e458 PubMed
20.Lemoine J, Bachy E, Cartron G, et al. Causes and Risk Factors of Early and Late Non-Relapse Mortality after CD19 CAR T-Cell Therapy for Diffuse Large B-Cell Lymphoma (DLBCL): A Lysa Study from the Descar-T Registry. Blood. 2022;140(Supplement 1):1859-1861. doi:10.1182/blood-2022-167840
21.Hill BT, Rybicki L, Bolwell BJ, et al. The non-relapse mortality rate for patients with diffuse large B-cell lymphoma is greater than relapse mortality 8 years after autologous stem cell transplantation and is significantly higher than mortality rates of population controls. Br J Haematol. 2011;152(5):561-9. doi:10.1111/j.1365-2141.2010.08549.x PubMed
22.Cordas Dos Santos DM, Tix T, Shouval R, et al. A systematic review and meta-analysis of nonrelapse mortality after CAR T cell therapy. Nat Med. 2024;30(9):2667-2678. doi:10.1038/s41591-024-03084-6 PubMed
23.Salles G, Morschhauser F, Sehn LH, et al. Five-year analysis of the POLARIX study: Prolonged follow-up confirms positive impact of polatuzumab vedotin plus rituximab, cyclophosphamide, doxorubicin, and prednisone (Pola-R-CHP) on outcomes [conference slides]. 66th ASH Annual Meeting; December 7–10, 2024; San Diego, CA.
24.CADTH. CADTH Canadian Drug Expert Committee (CDEC) final recommendation: Yescarta. Can J Health Technol. 2023;3:2. doi:10.51731/cjht.2023.578
25.pan-Canadian Pharmaceutical Alliance. Polivy (polatuzumab vedotin). 2021. Updated December 1, 2021. Accessed January 9, 2025. https://www.pcpacanada.ca/negotiation/21471
26.IQVIA. DeltaPA. 2023. Accessed February 25, 2025. https://www.iqvia.com/
27.Ontario Ministry of Health, Ontario Ministry of Long-Term Care. Ontario drug benefit formulary/comparative drug index. 2023. Accessed March 1, 2025. https://www.formulary.health.gov.on.ca/formulary/
28.Lacy SE, Barrans SL, Beer PA, et al. Targeted sequencing in DLBCL, molecular subtypes, and outcomes: a Haematological Malignancy Research Network report. Blood. 2020;135(20):1759-1771. doi:10.1182/blood.2019003535 PubMed
29.Kotlov N, Bagaev A, Revuelta MV, et al. Clinical and Biological Subtypes of B-cell Lymphoma Revealed by Microenvironmental Signatures. Cancer Discov. 2021;11(6):1468-1489. doi:10.1158/2159-8290.CD-20-0839 PubMed
30.Alduaij W, Collinge B, Ben-Neriah S, et al. Molecular determinants of clinical outcomes in a real-world diffuse large B-cell lymphoma population. Blood. 2023;141(20):2493-2507. doi:10.1182/blood.2022018248 PubMed
31.Shafey M, Savage KJ, Skrabek P, et al. Canadian Evidence-Based Guideline for the Frontline Treatment of Diffuse Large B-Cell Lymphoma [sponsor supplied reference]. Lymphoma Canada.
32.Government of Canada. Canadian Cancer Statistics 2023. Table 1.5 Projected for new cases for selected cancers, by sex and province, Canada, 2023 [sponsor supplied reference]. 2023.
33.Statistics Canada. Table: 13-10-0747-01 (formerly CANSIM 103-0554) [sponsor supplied reference]. 2024. https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310074701&pickMembers%5B0%5D=2.1&pickMembers%5B1%5D=3.48&cubeTimeFrame.startYear=2014&cubeTimeFrame.endYear=2018&referencePeriods=20140101%2C20180101
34.Institut national d'excellence en santé et en services sociaux (INESSS). Minjuvi (Diffuse Large B-Cell Lymphoma). Excerpt from the notice to the Minister on Minjuvi [sponsor supplied reference]. 2022.
Appendix 1: Cost-Comparison Table
Please note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical expert(s). Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 7: CDA-AMC Cost Comparison Table for First-Line Treatment of DLBCL
Treatment | Strength / concentration | Form | Price | Recommended dosage | Daily cost ($) | Average 28-day cost ($) |
|---|---|---|---|---|---|---|
Polatuzumab vedotin (Polivy) | 20 mg/mL | 30 mg vial | 3,160.7143a | 1.8 mg/kg on day 1 every 21 days for up to 6 cycles | 702.38 | 19,667 |
Cyclophosphamide (Procytox) | 20 mg/mL | 500 mg vial | 107.8100 195.4200 | 750 mg/m2 on day 1 every 21 days for up to 6 cycles | 14.44 | 404 |
Doxorubicin (generic) | 2 mg/mL | 10 mg vial | 50.4500 285.0000 | 50 mg/m2 on day 1 every 21 days for up to 6 cycles | 27.14 | 760 |
Prednisone (generic) | 5 mg | Tablet | 0.0220 | 100 mg on days 1 to 5 every 21 days for up to 6 cycles | 0.08 | 2 |
Rituximab (biosimilar) | 10 mg/m | 100 mg vial | 297.0000 | 375 mg/m2 on day 1 every 21 days for up to 6 cycles, with option for 2 additional cycles | 99.00 | 2,772 |
Pola plus R-CHP | 843.05 | 23,605 | ||||
R-CHOP | ||||||
Cyclophosphamide (Procytox) | 20 mg/mL | 500 mg vial | 107.8100 195.4200 | 750 mg/m2 on day 1 every 21 days for up to 6 cycles | 14.44 | 404 |
Doxorubicin (generic) | 2 mg/mL | 10 mg vial | 50.4500 285.0000 | 50 mg/m2 on day 1 every 21 days for up to 6 cycles | 27.14 | 760 |
Prednisone (generic) | 5 mg | Tablet | 0.0220 | 100 mg on days 1 to 5 every 21 days for up to 6 cycles | 0.08 | 2 |
Rituximab (biosimilar) | 10 mg/mL | 100 mg vial | 297.0000 | 375 mg/m2 on day 1 every 21 days for up to 6 cycles | 99.00 | 2,772 |
Vincristine (generic) | 1 mg/mL | 1 mL vial | 30.6000 | 1.4 mg per m2 on day 1 every 21 days for up to 6 cycles | 4.37 | 122 |
R-CHOP | 140.58 | 3,936 | ||||
DLBCL = diffuse large B-cell lymphoma.
Note: All prices are from the DeltaPA database (accessed March 2025) using the Ontario Drug Benefit Formulary price unless otherwise indicated, and do not include dispensing fees.26,27 Calculations assume mean patient weight of 75 kg and BSA of 1.85.2 Daily and cycle costs assume wastage of excess medication. 28-day costs are rounded to the nearest dollar.
aSponsor’s submitted price.1
Appendix 2: Submission Quality
Please note that this appendix has not been copy-edited.
Description | Yes or No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | Yes | No comment. |
Model has been adequately programmed and has sufficient face validity | No | Refer to CDA-AMC appraisal regarding the face validity of the model structure and various issues surrounding testing costs and overestimation of the ABC subtype that was not included in the submitted model. |
Model structure is adequate for decision problem | Yes | No comment. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | No | Refer to CDA-AMC appraisal regarding poor modelling practices. Note that CDA-AMC sent an additional information request regarding the transition of patients into third-line state of the model that the sponsor declined to correct. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | Yes | No comment. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | No | Technical documentation was not available in adequate detail regarding several issues such as the definition of multiple cure parameters and parameterization of uncertainty for PFS. The organization of model worksheets was poor and prevented full validation by CDA-AMC reviewers. The pharmacoeconomic report had several errors that were identified by CDA-AMC reviewers and acknowledged by the sponsor. |
CDA-AMC = Canada’s Drug Agency; PFS = progression-free survival.
Appendix 3: Additional Information on the Submitted Economic Evaluation
Please note that this appendix has not been copy-edited.
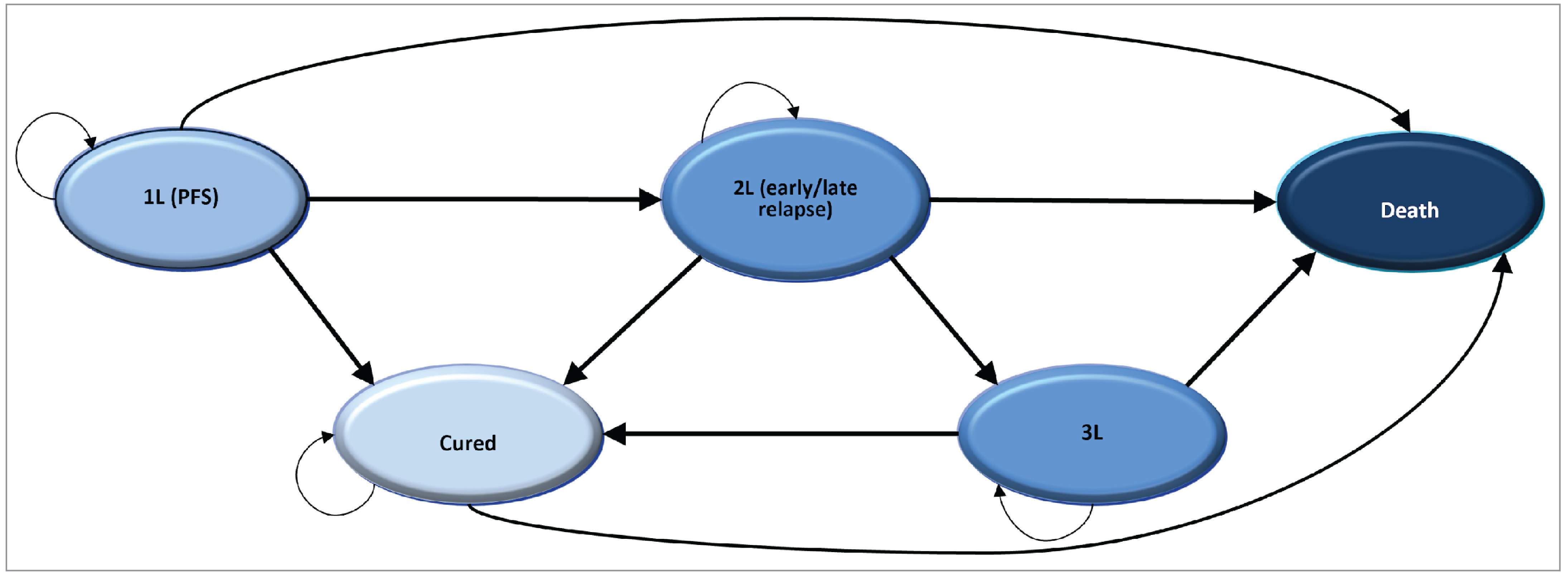
1L = first-line treatment; 2L = second-line treatment; 3L = third-line treatment; PFS = progression-free survival.
Source: Sponsor’s pharmacoeconomic submission.1
Detailed Results of the Sponsor’s Base Case
Table 9: Disaggregated Summary of the Sponsor’s Economic Evaluation Results
Parameter | pola-R-CHP | R-CHOP |
|---|---|---|
Discounted LYs | ||
Total | 14.85 | 11.79 |
By health state | ||
First-line treatment | 13.43 | 8.25 |
Second-line treatment | 0.15 | 0.40 |
Third-line treatment | 0.20 | 0.46 |
Cured | 1.07 | 2.68 |
Discounted QALYs | ||
Total | 11.78 | 9.34 |
By health state | ||
First-line treatment | 10.67 | 6.58 |
Second-line treatment | 0.12 | 0.32 |
Third-line treatment | 0.15 | 0.33 |
Cured | 0.84 | 2.11 |
Discounted costs ($) | ||
Total | 185,373 | 217,723 |
By health statea | ||
First-line treatment | 111,426 | 29,893 |
Second- and third-line treatment | 63,179 | 172,430 |
End of Life cost | 10,768 | 15,400 |
Genetic testing cost | 0 | 0 |
LY = life-year; POLA = polatuzumab vedotin; QALY = quality-adjusted life-year; R-CHP = rituximab, cyclophosphamide, doxorubicin, and prednisone; R-CHOP = rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone.
aDisaggregated results were only available as the total acquisition, administration, and monitoring costs for the first line of therapy as well as the combined second and third lines of therapy.
Source: Sponsor’s pharmacoeconomic submission.1
Appendix 4: Additional Details on the CDA-AMC Reanalyses and Sensitivity Analyses of the Economic Evaluation
Please note that this appendix has not been copy-edited.
Detailed Results of CDA-AMC Base Case
Table 10: Disaggregated Summary of the CDA-AMC Economic Evaluation Results (52% Specificity Rate)
Parameter | pola-R-CHP | R-CHOP |
|---|---|---|
Discounted LYs | ||
Total | 14.80 | 11.75 |
Discounted QALYs | ||
Total | 11.74 | 9.32 |
Discounted costs ($) | ||
Total | 292,436 | 229,611 |
Drug acquisition | 206,945 | 24,292 |
Administration | 4,189 | 2,741 |
AE management | 1,347 | 386 |
Supportive care | 8,196 | 16,349 |
Subsequent therapy | 60,952 | 170,486 |
End of life | 10,807 | 15,357 |
Genetic testing | 0 | 0 |
LY = life-year; POLA = polatuzumab vedotin; QALY = quality-adjusted life-year; R-CHP = rituximab, cyclophosphamide, doxorubicin, and prednisone; R-CHOP = rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone.
Table 11: Disaggregated Summary of the CDA-AMC Economic Evaluation Results (82% Specificity Rate)
Parameter | pola-R-CHP | R-CHOP |
|---|---|---|
Discounted LYs | ||
Total | 14.80 | 11.75 |
Discounted QALYs | ||
Total | 11.75 | 9.32 |
Discounted costs ($) | ||
Total | 225,883 | 221,972 |
Drug acquisition | 142,979 | 24,292 |
Administration | 4,189 | 2,741 |
AE management | 1,347 | 386 |
Supportive care | 8,196 | 16,349 |
Subsequent therapy | 58,365 | 162,846 |
End of life | 10,807 | 15,357 |
Genetic testing | 0 | 0 |
LY = life-year; POLA = polatuzumab vedotin; QALY = quality-adjusted life-year; R-CHP = rituximab, cyclophosphamide, doxorubicin, and prednisone; R-CHOP = rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone.
Scenario Analyses
As noted in the Testing Procedure Assessment, when compared with the gene expression panel (GEP), IHC using the Hans algorithm showed 65% to 86% concordance, with sensitivity ranging from 85% to 90% and specificity from 52% to 82%, all for detecting the ABC subtype.19 The sponsor reported that the ABC subtype is present of the 30% of individuals in the indicated population,28 which was based on trial population including patients with DLBCL NOS. CDA-AMC noted that there was a recent large cohort study reported that reported ABC subtype was present in 41% of individuals with DLBCL,29 however the sponsor and clinical experts also indicated that smaller proportions of ABC cases occur in rare LBCL entities which may conversely suggest the proportion of individuals with ABC subtype in the indicated population is overestimated. Refer to Table 12 for relevant testing inputs.
Based on these sources of information, there is a large range in the number of patients that may be misclassified with having the ABC subtype. Based on the range of specificity values, for every 1.50 to 2.31 patients classified as non-GCB by the Hans algorithm, only 1 has the ABC subtype. The remaining 0.50 (or of 1.50) to 1.31 patients (out of 2.31) are misclassified and may not actually have the ABC subtype (Table 13). CDA-AMC considered additional analyses which adjusted for unclassified subtypes and for GCB misclassification, but the results of these additional analyses were generally aligned with aforementioned estimates.
Table 12: Flow of Calculations for Detecting ABC Subtype
Category | Inputs |
|---|---|
Total patients | 100a |
Proportion of individuals with ABC subtype via GEP | 30%28 |
Sensitivity (true positive rate) | 87.5%b |
Specificity (true negative rate lower bound) | 52%19 |
Specificity (true negative rate upper bound) | 82%19 |
aAssumption to inform the calculation of number of patients tested to identify one patient with ABC subtype.
bMidpoint between 85% to 90%19
Table 13: Results for the Different Specificity for Detecting ABC Subtype
Categories | ABC by GEP | GCB+UNC by GEP | Total |
|---|---|---|---|
Lower boundary specificity value (52%) for detecting ABC subtype | |||
Total | 30 (100 × 0.30) | 70 (100 x [1 to 0.30]) | 100 |
Non-GCB (ABC+UNC) by Hans | 26 (30 × 0.875) | 34 (70 x [1 to 0.52]) | 60 |
GCB by Hans | 4 (30 x [1 to 0.875]) | 36 (70 × 0.52) | 40 |
Total non-GCB by IHC/True ABC cases in non-GCB by IHC | 2.31 (60/26) | ||
Upper boundary specificity value (82%) for detecting ABC subtype | |||
Total | 30 (100 × 0.30) | 70 (100 x [1 to 0.30]) | 100 |
Non-GCB (ABC+UNC) by Hans | 26 (30 × 0.875) | 13 (70 x [1 to 0.82]) | 39 |
GCB by Hans | 4 (30 x [1 to 0.875]) | 57 (70 × 0.82) | 61 |
Total non-GCB by IHC/True ABC cases in non-GCB by IHC | 1.50 (39/26) | ||
UNC = unclassified.
Note: Numbers are rounded to the nearest whole number.
The sponsor provided additional information during the review in which they indicated that they performed GEP and Hans IHC on tumours from a population-based cohort of DLBCL NOS. Based on this analysis, they reported that 88% of tumours that were assessed as ABC tumours by GEP were identified as non-GCB by Hans IHC, and that 75% of tumours that were assessed as non-GCB by Hans IHC were ABC by GEP. While the sponsor provided information suggests a lower misclassification rate based on the IHC by Hans Algorithm (the sponsor reports specificity of 84%), the CDA-AMC Testing Procedure Assessment team reviewed the publication30 and could not validate the information provided by the sponsor. As a result, no reanalyses were undertaken based on the sponsor-provided estimates. The sponsor’s specificity estimate was similar to the 82% specificity estimate tested by CDA-AMC in 1 of its reanalyses.
Appendix 5: Submitted Budget Impact Analysis and CDA‑AMC Appraisal
Please note that this appendix has not been copy-edited.
Table 14: Summary of Key Take-Aways
Key take-aways of the budget impact analysis |
|---|
|
Summary of Sponsor’s Budget Impact Analysis
The sponsor submitted a BIA for the introduction of pola-R-CHP for the treatment of adult patients with previously untreated LBCL, including DLBCL NOS, high-grade B-cell lymphoma, Epstein-Barr virus–positive DLBCL NOS, and T-cell/histiocyte-rich LBCL, that are classified as ABC lymphoma subtype. Estimates were generated from the perspective of CDA-AMC-participating drug plans (all but Quebec) and the results were aggregated into pan-Canadian totals over a three-year time horizon (2025 to 2027). Key inputs to the BIA are documented in Table 16.
In the reference scenario, it was assumed that patients eligible for treatment would receive R-CHOP. In the new drug scenario, it was assumed that pola-R-CHP would displace market share from R-CHOP in the reference scenario.
The sponsor’s BIA included the following key assumptions:
Beginning with an estimate of Canadian incident non-Hodgkin lymphoma cases, the sponsor narrowed the population using estimates of those that are DLBCL. DLBL was assumed to reflect all untreated LBCL in the eligible population.31,32 The model accounted for incident DLBCL cases only, as prevalent cases were assumed to have received prior treatment and would not be eligible for pola-R-CHP.
The annual growth rate for non-Hodgkin lymphoma cases was estimated as the average growth rate (1.63%) of incident cases from 2014 to 2018 reported by Statistics Canada.33
It was assumed that 35% of Non-Hodgkin lymphoma cases in Canada were DLBCL. This parameter was obtained as the average of a range (30% to 40%) reported by Lymphoma Canada.31
Consistent with an assumption used by INESSS, it was assumed that 85% of patients would be deemed fit to receive R-CHOP or pola-R-CHP as first-line treatment.34
The distribution of subsequent therapies used in the BIA were derived from the POLARIX trial and reflected what was used in the sponsor’s submitted BIA.
Justification for the market share gains from pola-R-CHP was not provided.
Table 15: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (year 1 / year 2 / year 3) |
|---|---|
Target population | |
Incident Non-Hodgkin lymphoma cases in Canada | |
Proportion that are DLBCL cases | 35%31 |
Percent eligible for public coverage | 100% |
Percent eligible for first-line treatment | 85%34 |
Percent that are in ABC subgroup | 30%28 |
Number of patients eligible for drug under review | 801 / 814 / 827 |
Market uptake (3 years) | |
Uptake (reference scenario) R-CHOP | 100% / 100% / 100% |
Uptake (new drug scenario) pola-R-CHP R-CHOP | 85% / 90% / 95% 15% / 10% / 5% |
Cost of treatment (per patient, per 21 days) | |
pola-R-CHP | $18,339.24 |
R-CHOP | $3,650.44 |
ABC = activated B cell–like; DLBCL = diffuse large B-cell lymphoma; POLA = polatuzumab vedotin; R-CHOP = rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone; R-CHP = rituximab, cyclophosphamide, doxorubicin, and prednisone.
Summary of the Sponsor’s BIA Results
The sponsor estimated that the 3-year budget impact of pola-R-CHP would be $46,361,549 (Year 1: $18,961,969; Year 2: $ 14,606,278; Year 3: $12,793,302). The sponsor estimated that currently, the 3-year budget impact of first-line R-CHOP would be $53,480,802, with subsequent treatment costs of $253,065,549 over that 3-year period, resulting in a total spend of $306,546,352. The sponsor estimated that if pola-R-CHP is reimbursed, over the first 3 years of reimbursement, the cost of first-line pola-R-CHP would be $241,956,008, the cost of first-line R-CHOP would be $5,319,271, and treatment costs in subsequent lines totalling $105,632,621 for a total spend of $352,907,901 over 3 years. Thus, the 3-year upfront cost of first-line treatment will increase by $193,794,477, but result in downstream savings that reduce the 3-year budget impact.
CDA-AMC Appraisal of the Sponsor’s BIA
CDA-AMC identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
IHC testing method to identify patients with LBCL classified as ABC subtype lacks accuracy and likely misclassifies patients which introduces uncertainty into the number of eligible patients: Based on the POLARIX trial results, pola-R-CHP is expected to result in a clinically meaningful benefit relative to R-CHOP. However, these findings were based on subgroup analyses and are associated with various limitations as described in the CUA limitations section. Notably, however, the observed benefit from pola-R-CHP was present only in the ABC subgroup. However, with current IHC testing using the Hans algorithm only GCB and non-GCB (including ABC and unclassified) can be identified. Therefore, IHC cannot accurately identify only the patients as ABC subtype that would most benefit from pola-R-CHP. Ideally, GEP would be used to identify these patients most accurately however this is not widely available in Canada and it is available and funded in British Columbia only.
If patients who are incorrectly identified as ABC subtype receive pola-R-CHP, it is highly uncertain whether they would benefit from treatment and potentially experience harms due to exposure to pola-R-CHP. Clinical expert feedback obtained by CDA-AMC agreed that based on the current testing methods for the ABC subtype in practice, there is a proportion of patients that will be overtreated due to not requiring treatment, however this feedback also indicated that they believed the potential benefit is deemed to be great enough to warrant the risk. CDA-AMC notes that the sponsor’s submitted analysis assumes 100% specificity with the IHC testing method using the Hans algorithm for detecting the ABC subtype. However, published literature indicates that specificity ranges from 52% to 82% with this testing method.19 As such, there is a large range in the number of patients that may be misclassified with having the ABC subtype based on published literature, as highlighted in the CDA-AMC Testing Procedures Assessment and the CDA-AMC Clinical Review. Based on the range of specificity values cited previously for every 1.50 to 2.31 patients classified as non-GCB by the Hans algorithm, only 1 patient would have the ABC subtype. The remaining patients would therefore be misclassified and may not have the ABC subtype. Treating these patients would result in additional budget impact considerations to jurisdictions and was not incorporated by the sponsor in their submitted analysis.
CDA-AMC notes that the sponsor included a scenario analysis that increased the proportion of patients that are identified as ABC subtype to 45%, although limitations were identified with this approach. For example, the sponsor’s scenario analysis was not based on published specificity data for IHC testing, and this approach maintains the proposed benefit of reductions in subsequent treatment costs for patients treated with pola-R-CHP that is not supported by the clinical evidence. In this approach, the subsequent treatment costs are likely underestimated in the new drug scenario for pola-R-CHP and thus the estimated budget impact is underestimated.
CDA-AMC included a specificity rate of 52% and 82% to test the impact of overtreatment of patients with LBCL who would be misclassified as having the ABC subtype. The budget impact of treating patients who are incorrectly identified as ABC subtype will present considerable costs to public payers.
Testing costs associated with GEP testing to accurately identify the ABC subtype was not incorporated in the analysis: which currently does not factor in disease subtype when determining treatments. This feedback further indicated that the identification of patients with LBCL classified as ABC subtype would impact practice, as these specific patients would be expected to receive pola-R-CHP as frontline treatment where possible due to the severity of their disease and poor response to other treatments. Clinical expert feedback obtained by CDA-AMC indicated that considerable costs would be associated with implementing GEP testing to accurately identify patients with LBCL classified as ABC subtype in lieu of current methods using IHC. Feedback indicated that additional resources will be required, because tests required outside of British Columbiawould need to be sent to British Columbia and therefore patients would experience delays in receiving tests results in exterior provinces. Experts further emphasized that since LBCL is the most common lymphoma type seen in practice, testing costs would be considerably increased across all jurisdictions other than British Columbia to accommodate GEP testing as well as costs related to assay development and validation, staff training, and equipment procurement and maintenance. CDA-AMC notes that the sponsor’s submission does not include testing costs for identifying patients with LBCL presenting with the ABC subtype.
Based on the CDA-AMC Testing Procedures Assessment, the cost of GEP using the Lymph2Cx assay on the NanoString platform to identify patients is about $570 per tumour in British Columbia. According to the sponsor’s submitted model, it assumed that 35% of Non-Hodgkin lymphoma cases in Canada were DLBCL based on a range of inputs derived from Lymphoma Canada which resulted in an estimated 3,090 patients across jurisdictions in the base year of the analysis.31 Based on this estimate, the approximate total costs required to test all DLBCL (n = 3,090) to identify those with the ABC subtype would be at least $1,761,300. CDA-AMC notes that this sum includes the costs of GEP testing in British Columbia where it is currently implemented and also additional costs required to test those outside of British Columbia (i.e., the costs for GEP testing for the 1,749 patients residing outside of British Columbia). This estimate does not incorporate costs related to assay development and validation, staff training, equipment procurement and maintenance.
Based on the cost of GEP submitted by the sponsor, the additional costs of implementing GEP testing in jurisdictions other than British Columbia to accurately identify patients with LBCL with the ABC subtype would result in additional costs of $570 per tumour. This translates to additional testing costs for 1,749 patients who have confirmed DLBCL outside of British Columbia, estimated to be approximately $996,930.
Subsequent therapy assumptions were not reflective of Canadian clinical practice: In the submitted model, the sponsor applies various assumptions regarding the proportion of patients who receive subsequent therapies in second and third-line treatment, which is dependent on treatment arm and whether second-line relapse is less than or greater than 12 months. As noted in the CUA limitations section, feedback from clinical experts consulted by CDA-AMC indicated that in Canadian clinical practice, the approach to subsequent therapy would not differ between first-line therapy (i.e., whether a patient receives pola-R-CHP or R-CHOP) and that they expected the distribution and number of subsequent therapies would be nearly equivalent between groups with exception of pola-BR which would be used more frequently in patients who receive R-CHOP in first-line treatment. Aligned with the feedback described in the CUA limitations section, the proportion of patients receiving CAR T-cell therapy likely overestimated. This overestimation was found to not meet face validity due to the limited CAR T-cell therapy centres, various limitations with patients not willing to travel and other treatment barriers. For relapse occurring after 12 months, clinical expert feedback indicated that the proportion of those receiving salvage therapy plus ASCT was also likely overestimated; while 40% may go on that treatment pathway, it is more likely that 20% would actually receive ASCT. Lastly, third-line chemotherapy appeared to be overestimated given new treatment options; clinical expert feedback indicated that this estimate would likely halved and the use of glofitamab and epcoritamab would likely be higher instead.
CDA-AMC assessed the impact of alternate distribution of subsequent treatments aligned with clinical expert feedback in a scenario analysis. The alternate distribution is aligned with the CUA scenario analysis.
A price reduction of 45% for CAR T-cell therapy was also applied in this scenario analysis to reflect the CDA-AMC review of axicabtagene ciloleucel24 aligned with the CUA scenario analysis.
An additional scenario analysis was undertaken that excluded subsequent treatment from the analysis due to uncertainty.
Drug prices paid by public drug plans are uncertain: Both the sponsor’s and the CDA-AMC analyses are based on publicly available list prices for all comparators. Actual costs paid by public drug plans are unknown.
CDA-AMC could not address this limitation in reanalysis.
CDA-AMC Reanalyses of the BIA
Table 16: CDA-AMC Revisions to the Submitted Budget Impact Analysis
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
Changes to derive the CDA-AMC base case | ||
1. Overestimation of individuals with ABC subtype included to reflect clinical practice | 100% testing accuracy with IHC for detecting ABC subtype | Base case 1: 52% specificity value for detecting ABC subtype Base case 2: 82% specificity value for detecting ABC subtype |
CDA-AMC base case | Reanalysis 1 | |
IHC = immunohistochemistry.
The results of the CDA-AMC step-wise reanalysis are presented in summary format in Table 17 and a more detailed breakdown is presented in Table 18.
In the CDA-AMC reanalysis, the estimated 3-year budget impact of reimbursing pola-R-CHP would be $107,095,178 if assuming 52% specificity for IHC testing used to detect patients with DLBCL for the ABC subtype (Year 1: $43,802,149; Year 2: $33,740,502; Year 3: $29,552,527). This increase in costs is due to an increase in the size of the eligible population (those who test to have the ABC subtype) from 801 patients in year 1 (sponsor’s base case) to 1,201 patients in year 1 in this scenario. When assuming a rate of 82% specificity for IHC testing, the estimated 3-year budget impact of reimbursing pola-R-CHP would be $69,542,323 (Year 1: $28,442,954; Year 2: $21,909,417; Year 3: $19,189,953). This increase in costs is due to an increase in the size of the eligible population (those who test to have the ABC subtype) from 801 patients in year 1 (sponsor’s base case) to 1,842 patients in year 1 in this scenario.
In these analyses, the incremental cost reimbursing pola-R-CHP as a first-line regimen is greater than $200M but offset by estimated cost offsets based on subsequent treatment usage (Table 18). Subsequent treatment use is associated with uncertainty, thus the cost offsets are associated with uncertainty.
Notably, the current submitted analysis does not incorporate the additional costs required to implement GEP testing in jurisdictions other than British Columbia to accurately identify patients with DLBCL with the ABC subtype. Based on the sponsor’s estimated number of patients with confirmed DLBCL across all CDA-AMC-participating jurisdictions, funding GEP testing to identify patients with ABC subtype would result in additional costs of more than $1,761,300 per year to jurisdictions.
Table 17: Summary of the CDA-AMC Reanalyses of the Budget Impact Analysis
Stepped analysis | Three-year total ($) |
|---|---|
Submitted base case | 46,361,549 |
CDA-AMC base case (52% specificity) | 107,095,178 |
CDA-AMC base case (82% specificity) | 69,542,323 |
BIA = budget impact analysis.
CDA-AMC conducted the following scenario analyses to address remaining uncertainty, using the CDA-AMC base case (results are provided in Table 19).
Assuming an alternate distribution of subsequent therapy aligned with the CUA according to clinical expert feedback received by CDA-AMC for this review, and applying a 45% price reduction to CAR T-cell therapy
Excluding subsequent treatment from the analysis.
Table 18: Detailed Breakdown of the CDA-AMC Reanalyses of the BIA
Stepped analysis | Scenario | Year 0 (current situation) ($) | Year 1 ($) | Year 2 ($) | Year 3 ($) | Three-year total ($) |
|---|---|---|---|---|---|---|
Submitted base case | Reference | 84,446,070 | 95,522,026 | 102,826,782 | 108,197,544 | 306,546,352 |
1L treatment | — | 17,539,614 | 17,825,382 | 18,115,807 | 53,480,802 | |
Subsequent treatment | — | 77,982,412 | 85,001,400 | 90,081,737.32 | 253,065,549 | |
New drug | 84,446,070 | 114,483,995 | 117,433,060 | 120,990,846 | 352,907,901 | |
1L treatment | — | 77,529,778 | 82,379,279 | 87,366,222 | 247,275,279 | |
Subsequent treatment | — | 36,954,217 | 35,053,781 | 33,624,623.42 | 105,632,622 | |
Budget impact | 0 | 18,961,969 | 14,606,278 | 12,793,302 | 46,361,549 | |
1L treatment | — | 59,990,164 | 64,553,897 | 69,250,416 | 193,794,477 | |
Subsequent treatment | — | −41,028,195 | −49,947,619 | −56,457,114 | −147,432,928 | |
CDA-AMC base case: 52% specificity | Reference | 195,070,422 | 220,655,880 | 237,529,866 | 249,936,327 | 708,122,073 |
1L treatment | — | 40,516,507 | 41,176,633 | 41,847,513 | 123,540,654 | |
Subsequent treatment | — | 180,139,373 | 196,353,233 | 208,088,813 | 584,581,419 | |
New drug | 195,070,422 | 264,458,029 | 271,270,368 | 279,488,854 | 815,217,251 | |
1L treatment | — | 179,093,787 | 190,296,134 | 201,815,974 | 571,205,895 | |
Subsequent treatment | — | 85,364,242 | 80,974,234 | 77,672,880 | 244,011,356 | |
Budget impact | 0 | 43,802,149 | 33,740,502 | 29,552,527 | 107,095,178 | |
1L treatment | — | 138,577,279 | 149,119,501 | 159,968,461 | 447,665,241 | |
Subsequent treatment | — | −94,775,131 | −115,378,999 | −130,415,933 | −340,570,063 | |
CDA-AMC base case: 82% specificity | Reference | 126,669,105 | 143,283,039 | 154,240,173 | 162,296,316 | 459,819,528 |
1L treatment | — | 26,309,420 | 26,738,073 | 27,173,710 | 80,221,204 | |
Subsequent treatment | — | 116,973,619 | 127,502,100 | 135,122,606 | 379,598,324 | |
New drug | 126,669,105 | 171,725,993 | 176,149,590 | 181,486,269 | 529,361,851 | |
1L treatment | — | 116,294,667 | 123,568,918 | 131,049,334 | 370,912,919 | |
Subsequent treatment | — | 55,431,326 | 52,580,672 | 50,436,935 | 158,448,933 | |
Budget impact | 0 | 28,442,954 | 21,909,417 | 19,189,953 | 69,542,323 | |
1L treatment | — | 89,985,246 | 96,830,845 | 103,875,624 | 290,691,715 | |
Subsequent treatment | — | −61,542,293 | −74,921,428 | −84,685,671 | −221,149,392 |
BIA = budget impact analysis.
Note: The submitted analysis is based on the publicly available prices of the comparator treatments.
Table 19: Detailed Breakdown of the CDA-AMC Scenario Analyses of the BIA
Stepped analysis | Scenario | Year 0 (current situation) ($) | Year 1 ($) | Year 2 ($) | Year 3 ($) | 3-year total ($) |
|---|---|---|---|---|---|---|
CDA-AMC scenario analysis 1: Alternate distribution of subsequent treatment and 45% price reduction on CAR T-cell therapy (52% specificity) | Reference | 116,473,985 | 140,573,796 | 155,801,322 | 166,591,428 | 462,966,546 |
New drug | 116,473,985 | 231,404,735 | 240,295,411 | 250,895,130 | 722,595,276 | |
Budget impact | 0 | 90,830,939 | 84,494,089 | 84,303,701 | 259,628,730 | |
CDA-AMC scenario analysis 1: Alternate distribution of subsequent treatment and 45% price reduction on CAR T-cell therapy (82% specificity) | Reference | 75,632,458 | 91,281,686 | 101,169,690 | 108,176,252 | 300,627,627 |
New drug | 75,632,458 | 150,262,815 | 156,035,981 | 162,918,915 | 469,217,712 | |
Budget impact | 0 | 58,981,129 | 54,866,292 | 54,742,663 | 168,590,084 | |
CDA-AMC scenario analysis 2: Subsequent treatment removed (52% specificity) | Reference | 50,696,981 | 65,870,391 | 76,158,069 | 83,533,024 | 225,561,485 |
New drug | 50,696,981 | 198,954,096 | 210,710,695 | 222,831,502 | 632,496,293 | |
Budget impact | 0 | 133,083,705 | 134,552,626 | 139,298,477 | 406,934,808 | |
CDA-AMC scenario analysis 2: Subsequent treatment removed (82% specificity) | Reference | 32,920,117 | 42,772,981 | 49,453,292 | 54,242,224 | 146,468,497 |
New drug | 32,920,117 | 129,190,972 | 136,825,127 | 144,695,780 | 410,711,879 | |
Budget impact | 0 | 86,417,990 | 87,371,835 | 90,453,557 | 264,243,382 |
BIA = budget impact analysis.
Note: The submitted analysis is based on the publicly available prices of the comparator treatments.
TPA Review
Abbreviations
ABC
activated B cell–like
COO
cell of origin
DLBCL
diffuse large B-cell lymphoma
FFPE
formalin-fixed paraffin-embedded
GCB
germinal centre B cell–like
GEP
gene expression profiling
HGBCL
high-grade B-cell lymphoma
IHC
immunohistochemistry
LBCL
large B-cell lymphoma
NHL
non-Hodgkin lymphoma
NOS
not otherwise specified
pola-R-CHP
polatuzumab vedotin, rituximab, cyclophosphamide, doxorubicin, and prednisone
Objective
The objective of this Testing Procedure Assessment is to identify and describe important health system implications of cell of origin (COO) testing for the activated B-cell–like (ABC) subtype of lymphoma in adult patients with previously untreated large B-cell lymphoma (LBCL), including diffuse large B-cell lymphoma (DLBCL) not otherwise specified (NOS), high-grade B-cell lymphoma (HGBCL), Epstein-Barr virus–positive DLBCL NOS, and T-cell/histiocyte-rich LBCL, to determine eligibility for treatment with polatuzumab vedotin, rituximab, cyclophosphamide, doxorubicin, and prednisone (pola-R-CHP).
Methods
The contents within this section have been informed by materials submitted by the sponsor, a literature search, and clinical expert input, as well as input from clinician groups collected as part of the review.
Materials submitted by the sponsor related to COO testing were validated when possible and summarized by the review team.
An information specialist conducted a literature search on key resources, including MEDLINE, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of health technology assessment agencies in Canada and major international health technology assessment agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were COO testing, including gene expression profiling (GEP) and immunohistochemistry (IHC), and LBCL. Search filters were applied to limit retrieval to health technology assessments, systematic reviews, meta-analyses, or indirect treatment comparisons. The search was completed on December 23, 2024, and limited to English-language documents.
Clinical expert input was provided by 2 clinical specialists with expertise in hematology. Input from 2 clinician groups — the Lymphoma Canada Scientific Advisory Board and Ontario Health (Cancer Care Ontario) Cancer Drug Advisory Committee — was used to inform current practices of COO testing methods and their utility for identifying potentially eligible patients for pola-R-CHP.
Context
What Is LBCL With the ABC Subtype?
Under the current review, pola-R-CHP is intended for adult patients with previously untreated LBCL classified as the ABC lymphoma subtype. LBCL is a group of morphologically and molecularly heterogeneous B-cell neoplasms, accounting for about 30% of non-Hodgkin lymphoma (NHL) cases.1 According to sponsor-submitted materials, COO can be used to categorize LBCL into 2 main subtypes: ABC and germinal centre B cell–like (GCB), with a small proportion of cases remaining unclassified.2 The ABC subtype reflects the gene expression profile of activated peripheral B cells.3 It is characterized by constitutive activation of the antiapoptotic nuclear factor kappa B pathway.3
According to the sponsor and clinical experts consulted for this review, most LBCL patients with the ABC subtype have DLBCL NOS. DLBCL NOS is the most common entity of LBCL, accounting for more than 80% of LBCL cases.1 About 30% of DLBCL NOS cases are classified as the ABC subtype, and about 10% to 15% are categorized as unclassified (i.e., neither ABC nor GCB) based on COO testing using GEP.2 The sponsor and clinical experts also indicated that smaller proportions of ABC cases occur in rare LBCL entities, such as HGBCL NOS, which represents 1% to 2% of LBCL cases, with about 20% being ABC subtype, and Epstein-Barr virus–positive DLBCL NOS, the prevalence of which is unknown. The LBCL subtype classification and COO testing workflow are shown in Figure 1.
Figure 1: LBCL Subtype Classification and COO Testing by GEP and IHC
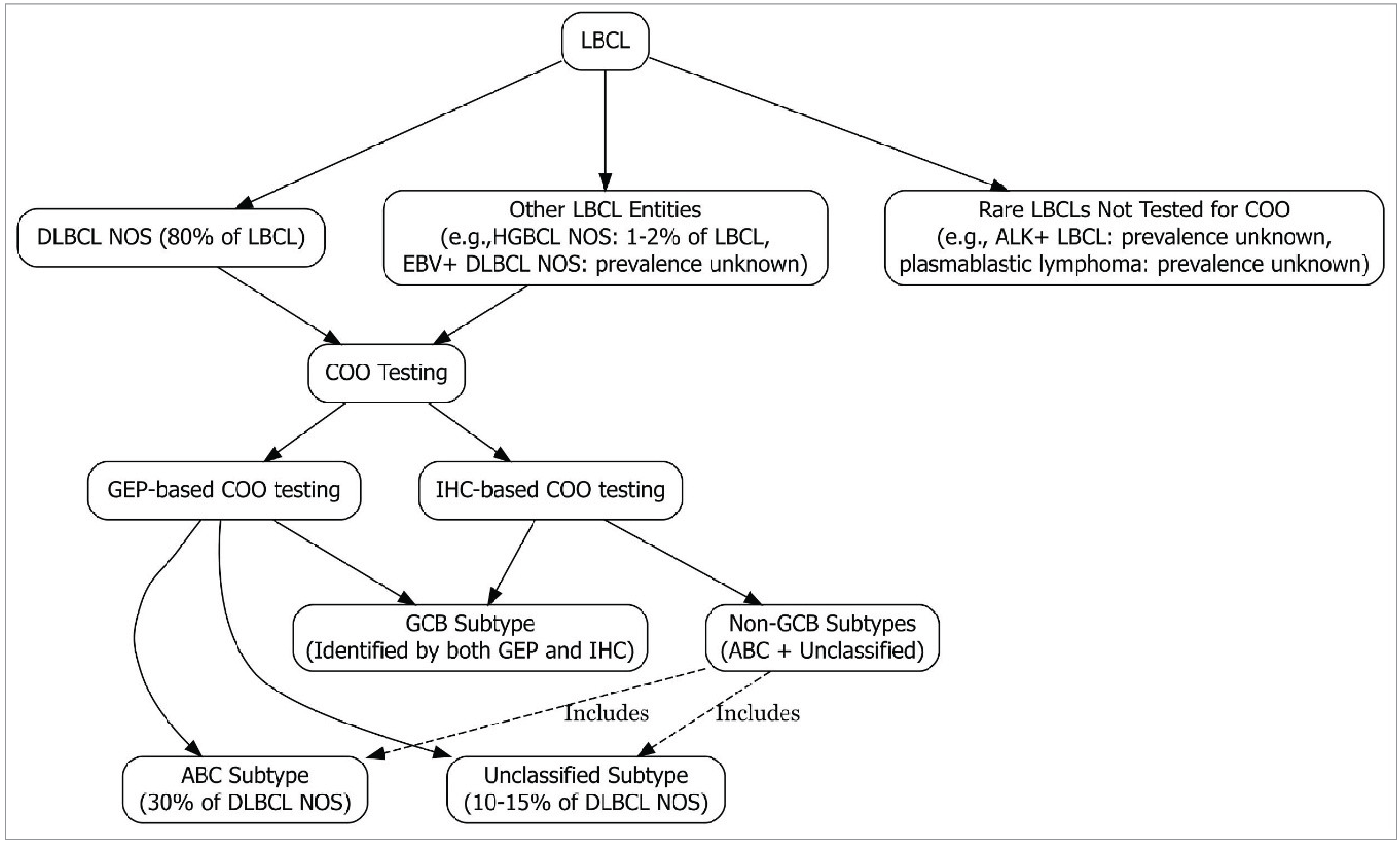
ABC = activated B cell–like; ALK = anaplastic lymphoma kinase; COO = cell of origin; DLBCL = diffuse large B-cell lymphoma; EBV+ = Epstein-Barr virus–positive; GCB = germinal centre B cell–like; GEP = gene expression profiling; HGBCL = high-grade B-cell lymphoma; IHC = immunohistochemistry; LBCL = large B-cell lymphoma; NOS = not otherwise specified.
How Is the ABC Subtype of LBCL Identified?
The ABC subtype of LBCL is identified by 1 of 2 COO testing methods: GEP or IHC.
Gene Expression Profiling
GEP is the gold standard method for determining the COO subtype. Using the microarray technology, it compares ribonucleic acid (RNA) expression levels of genes that are differentially expressed in, and therefore distinguishable between, the GCB and ABC subtypes of lymphoid tumours and produces a linear predictor score that estimates the probability of being the ABC subtype.2 Cases with scores exceeding 90% are classified as ABC, while those below 10% are classified as GCB.4 Cases that do not meet these criteria are identified as “unclassifiable.”2
The traditional GEP method requires RNA from fresh frozen tissues, which limits its use in clinical settings.2 New methods, such as NanoString’s Lymph2Cx assay used in the sponsor-submitted pivotal POLARIX trial, have been developed to use degraded RNA extracted from formalin-fixed paraffin-embedded (FFPE) tissue samples for GEP testing.2,5 Published evidence suggests that GEP using the Lymph2Cx assay and FFPE tissues can be incorporated into routine diagnostic work-ups for DLBCL cases.6
Immunohistochemistry
According to the sponsor and clinical experts consulted for this review, IHC is a widely used alternative COO testing method in Canada. It is performed using FFPE tissue samples collected during tumour biopsy as part of standard diagnostic care of patients suspected of having LBCL. This method provides an approximation of gene expression by dichotomizing LBCL classifications into GCB and non-GCB subtypes, with the latter including the ABC and unclassified subtypes, as identified by GEP.7
The clinical experts noted that the Hans algorithm is the most commonly used IHC-based COO testing method. The algorithm assesses expression levels of CD10, BCL6, and MUM1 proteins using specific antibodies to classify samples into GCB and non-GCB subtypes.7 The non-GCB subtype requires a negative stain for both CD10 and BCL6 or a positive stain for both BCL6 and MUM1 when CD10 is negative.7 According to sponsor-submitted information, patients who are categorized by the Hans algorithm as having the non-GCB subtype are likely to be considered to have the ABC subtype in clinical practices where GEP is not available.
What Is the Current Testing Practice for Diagnosing LBCL in Canada?
The diagnosis of LBCL generally begins with a morphological assessment of tumour tissues obtained from an excisional or incisional biopsy.8 Subsequent diagnostic testing typically includes IHC and other tests, such as flow cytometry, fluorescence in situ hybridization, and molecular testing, to ensure accurate classification.8 WHO classification of lymphoid neoplasms recommends categorizing DLBCL NOS into the GCB or ABC subtype using GEP, with a small subset of cases remaining unclassifiable.9 When GEP is unavailable, IHC can be used to categorize DLBCL NOS into GCB or non-GCB.9 According to the clinical experts consulted for this review, hematopathology laboratories across Canada routinely incorporate the Hans algorithm (assessing CD10, BCL6, and MUM1) into the diagnostic work-up involving IHC panels for most cases of LBCL. For example, Alberta Health Services recommends the Hans algorithm for IHC-based COO testing to dichotomize DLBCL NOS classifications into GCB and non-GCB subtypes.10 The clinical experts indicated that the markers used in the Hans algorithm for DLBCL subclassification are also routinely included in IHC panels for the HGBCL subclassification.
Clinical practices for determining COO in certain rare LBCL subtypes may vary across jurisdictions. According to the literature, T-cell/histiocyte-rich LBCL is mainly diagnosed by morphology.11 While the sponsor and 1 clinical expert indicated that COO testing for this subtype is generally not performed in Alberta and British Columbia, the other clinical expert and 1 provincial lead noted that it is routinely performed in Manitoba and some centres in Ontario. In addition, the clinical experts noted that COO testing is generally not performed for certain rare LBCLs, such as anaplastic lymphoma kinase–positive LBCL and plasmablastic lymphoma.
Testing Procedure Considerations
What Are Some Health System–Related Considerations?
How Many Individuals in Canada Would Be Expected to Require COO Testing for LBCL Subclassification?
Based on sponsor-provided estimates confirmed by the clinical experts consulted for this review, about 8,973 new cases of NHL are expected to be diagnosed across Canada (excluding Quebec) in 2025. Published evidence indicated that about 30% of NHL cases are classified as LBCL,1 resulting in an estimated 2,692 LBCL diagnoses. According to the clinical experts, COO testing is routinely performed for most LBCL cases as part of the standard of care during the diagnostic work-ups, except for certain rare subtypes, such as anaplastic lymphoma kinase–positive LBCL (representing less than 1% of LBCL cases)12 and plasmablastic lymphoma (prevalence unclear). No new impact on the volume of COO testing is therefore anticipated if pola-R-CHP were to be funded.
Availability and Reimbursement Status of COO Testing in Jurisdictions Across Canada
According to the sponsor and clinical experts, IHC-based COO testing is readily available in jurisdictions across Canada through hematopathology or cancer centres. This testing is generally funded without requiring additional reimbursement approvals across Canada.
The clinical experts indicated that GEP is not available in jurisdictions outside of British Columbia. According to sponsor-submitted information, GEP-based COO testing — specifically, the Lymph2Cx assay performed on the NanoString platform using FFPE tissues — is available and funded in British Columbia as part of the routine pathology work-up of aggressive B-cell lymphoma. The sponsor indicated that the same assay has been validated at the Princess Margaret Cancer Centre in Toronto, but that it is not used as part of routine pathology.
Expected Timing and Frequency of COO Testing
The clinical experts confirmed that COO testing is typically performed once at the time of diagnosis, as repeating the test after relapse would not affect the clinical management of LBCL.
Expected Impacts of COO Testing on Human and Other Health Care Resources
According to the sponsor and clinical experts, IHC-based COO testing is currently a routine diagnostic procedure for most patients with LBCL. The clinical experts confirmed that no additional impact on human and other health care resources is anticipated if IHC-based COO testing is used to establish eligibility for pola-R-CHP.
However, there could be several impacts if GEP testing is required to determine treatment eligibility, particularly in jurisdictions that do not currently use GEP. For example, incorporating GEP into routine diagnostic practice may require upscaling current COO testing infrastructure with additional laboratory equipment and resources, and training for laboratory staff.2 The sponsor indicated that, for GEP to be used more widely across Canada, it is anticipated that the Lymph2Cx or a similar assay would be performed on FFPE tissues rather than traditional GEP on fresh frozen tissues. Because FFPE tissues are obtained during routine biopsies,6 adopting the new GEP method would not impose additional procedures or testing-related burdens on patients.
What Are Some Patient-Related Considerations?
Accessibility of COO Testing in Jurisdictions Across Canada
IHC-based COO testing is widely accessible across Canada as a routine diagnostic procedure for patients with LBCL. The test is typically conducted in a hematopathology laboratory. According to the clinical experts consulted for this review, laboratories in small community centres lacking testing facilities for the required biomarkers generally refer tests to facilities with such capacity. The experts confirmed that no barriers to accessing IHC-based COO testing are anticipated if pola-R-CHP were to be funded.
Access to GEP testing via traditional means using fresh frozen tissues or a new assay performed on FFPE tissues is limited in Canada. The sponsor indicated that GEP using the Lymph2Cx assay performed on FFPE tissues is currently included in routine diagnostic procedures in British Columbia. However, whether the assay is consistently available across all centres within the jurisdiction is unclear. According to the clinical experts, this GEP method remains unavailable in jurisdictions outside of British Columbia.
Expected Turnaround Times for COO Testing
According to the clinical experts, IHC-based COO testing results are generally available concurrently with the LBCL diagnostic report and would not delay a clinical diagnosis, including subtype identification or treatment initiation. However, in smaller community laboratories without the capacity to test for CD10, BCL6, and MUM1 markers using the Hans algorithm, delays may occur due to the need to refer the test to laboratories that have the capacity to test for these markers.
For GEP using the NanoString platform (e.g., Lymph2Cx assay) and FFPE tissues, the workflow typically requires about 15 minutes of hands-on time and produces data within 24 hours,5 although the total turnaround time may be longer depending on the entire clinical workflow.
Burden Associated With COO Testing for Patients, Families, and/or Care Partners
While a tissue biopsy is invasive, it is the gold standard for acquiring molecular data and categorizing lymphoma patients into genetic subtypes.13 Because COO testing, whether by IHC or GEP, is performed on tissue samples already collected during routine biopsy, no additional burden associated with COO testing is anticipated for patients, families, or care partners.
What Are Some Clinical Considerations?
Clinical Utility of COO Testing
COO testing is needed to identify LBCL patients with the ABC subtype. According to the clinical experts consulted for this review, IHC-based COO testing is widely used across Canada due to its availability and accessibility in clinical practice, although evidence suggests that it is less accurate than GEP, as it simply enriches the non-GCB population by identifying the GCB subtype instead of specifically identifying ABC cases.2 New GEP-based methods performed on FFPE tissues, which specifically identify the ABC subtype, can provide more accurate COO classification than IHC-based methods can.2 New GEP methods are also more practical than traditional GEP methods that require fresh and unfixed tissues.2 While sponsor-submitted information indicated the potential for a broader use of the Lymph2Cx or similar assay across Canada in the future, according to the clinical experts, GEP performed on FFPE tissues is currently not available in most jurisdictions except British Columbia. If pola-R-CHP were to be funded, and COO testing were to be performed using IHC, the patient population would therefore include both those with the ABC subtype, who are eligible for treatment, and those with the unclassified subtypes, who are ineligible for treatment.
Diagnostic Accuracy of COO Testing
IHC-Based COO Testing Using the Hans Algorithm
Compared with GEP, IHC-based COO testing using the Hans algorithm showed 65% to 86% concordance for classifying the ABC subtype, along with 85% to 90% sensitivity and 52% to 82% specificity for detecting the ABC subtype.2,7 Accordingly, the Hans algorithm can correctly identify most patients with the ABC subtype but also includes unclassified cases within the non-GCB category, as well as some true GCB cases who may be misclassified. For the GCB subgroup, sensitivity of IHC by the Hans algorithm ranges from 52% to 82%,2,14,15 suggesting that this method may miss about 18% to 48% of true GCB cases. Additional information from the supplementary material of a cohort study suggesting higher sensitivity (88%) and specificity (84%) values for identifying the ABC subtype using IHC-based testing and the Hans algorithm was provided by the sponsor; however, these values were not explicitly reported in the main publication.9 The review team was unable to fully validate the evidence.
GEP Using the Lymph2Cx Assay
The Lymph2Cx assay demonstrated 92% to 95% concordance for classifying the ABC subtype, compared with traditional GEP.16-18 This suggests that the assay can classify the ABC subtype of LBCL based on COO status with high accuracy. Although the sensitivity and specificity data of this method were not found, 1 study reported that the Lymph2Cx assay had a lower COO misclassification rate in patients with DLBCL, compared to IHC-based COO testing using the Hans algorithm (2% versus 9%, respectively).19
Limitations and Risks of Harm Associated With COO Testing
Regarding IHC-based COO testing by the Hans algorithm, its high sensitivity and moderate specificity for detecting ABC cases, along with the moderate sensitivity for detecting GCB cases and inability to specifically identify ABC cases within the non-GCB subtype, would likely result in overestimating eligible patients by including unclassified cases and misclassified GCB cases of LBCL.2 The clinical experts and 1 clinician group confirmed the risk of misclassifying some LBCL cases as the ABC subtype using IHC-based COO testing, which may lead to overtreating patients who in fact have a GCB or unclassified COO status.
Despite these limitations, the clinical experts and clinician groups confirmed that IHC-based COO testing by the Hans algorithm could be used to establish treatment eligibility if pola-R-CHP were to be funded, particularly given the lack of GEP in clinical practice. The WHO classification of lymphoid neoplasms also acknowledges that using IHC algorithms for COO testing is acceptable when GEP is unavailable.20 The clinical experts confirmed that IHC-based COO testing can identify most patients with the ABC subtype of LBCL. According to 1 clinician group, even in cases of potential misclassification, patients with the GCB subtype are unlikely to be harmed by receiving pola-R-CHP.
What Are Some Cost Considerations?
Projected Cost of COO Testing
Depending on the size and number of slides, the cost of IHC may range from $30 to $550 in Canada.21 No information regarding the cost of IHC-based COO testing could be obtained.
According to sponsor-submitted materials, the cost of GEP using the Lymph2Cx assay on the NanoString platform is about $570 per tumour in British Columbia. This cost includes RNA extraction, machine maintenance, and all related components.
Expected Impacts of Cost of COO Testing to Health Systems
Because IHC-based COO testing is already part of the standard of care for patients with LBCL across Canada, no additional cost for COO testing is anticipated if pola-R-CHP were to be funded for the proposed indication.
Regarding GEP using an assay performed on FFPE tissues, no additional cost is anticipated for health care systems in British Columbia as GEP using the Lymph2Cx assay is already part of the standard of care. However, in jurisdictions where this method is currently not available, upfront costs may be required to support its development and establishment. These costs would include assay development and validation, staff training, and equipment procurement and maintenance.
References
1.Sehn LH, Salles G. Diffuse Large B-Cell Lymphoma. N Engl J Med. 2021;384(9):842-858. doi:10.1056/NEJMra2027612 PubMed
2.Scott DW. Cell-of-Origin in Diffuse Large B-Cell Lymphoma: Are the Assays Ready for the Clinic? Am Soc Clin Oncol Educ Book. 2015:e458-66. doi:10.14694/EdBook_AM.2015.35.e458 PubMed
3.Roschewski M, Phelan JD, Wilson WH. Molecular Classification and Treatment of Diffuse Large B-Cell Lymphoma and Primary Mediastinal B-Cell Lymphoma. Cancer J. 2020;26(3):195-205. doi:10.1097/ppo.0000000000000450 PubMed
4.Wright G, Tan B, Rosenwald A, Hurt EH, Wiestner A, Staudt LM. A gene expression-based method to diagnose clinically distinct subgroups of diffuse large B cell lymphoma. Proc Natl Acad Sci U S A. 2003;100(17):9991-6. doi:10.1073/pnas.1732008100 PubMed
5.NanoString. nCounter® Analysis Systems for Biomarker Validation and Biomarker Development: Accelerate Your Insights Today. Accessed February 05, 2025. https://nanostring.com/products/ncounter-analysis-system/ncounter-systems-overview/
6.Robetorye RS, Ramsower CA, Rosenthal AC, et al. Incorporation of Digital Gene Expression Profiling for Cell-of-Origin Determination (Lymph2Cx Testing) into the Routine Work-Up of Diffuse Large B-Cell Lymphoma. J Hematop. 2019;12(1):3-10. doi:10.1007/s12308-019-00344-0 PubMed
7.Balasubramanian S, Wang S, Major C, et al. Comparison of immunohistochemistry and gene expression profiling subtyping for diffuse large B-cell lymphoma in the phase III clinical trial of R-CHOP ± ibrutinib. Br J Haematol. 2021;194(1):83-91. doi:10.1111/bjh.17450 PubMed
8.Cheson BD, Fisher RI, Barrington SF, et al. Recommendations for initial evaluation, staging, and response assessment of Hodgkin and non-Hodgkin lymphoma: the Lugano classification. J Clin Oncol. 2014;32(27):3059-68. doi:10.1200/jco.2013.54.8800 PubMed
9.Alaggio R, Amador C, Anagnostopoulos I, et al. The 5th edition of the World Health Organization Classification of Haematolymphoid Tumours: Lymphoid Neoplasms. Leukemia. 2022;36(7):1720-1748. doi:10.1038/s41375-022-01620-2
10.Cancer Care Alberta. Clinical Practice Guideline LYHE-002: Lymphoma. Alberta Health Services; 2024. Accessed January 27, 2025. https://www.albertahealthservices.ca/assets/info/hp/cancer/if-hp-cancer-guide-lyhe002-lymphoma.pdf
11.Nair R, Deen N, Ahmed S, et al. Outcome of Patients with T- Cell Histiocyte Rich B Cell Lymphoma: Single Institution Series. Blood. 2021;138(Supplement 1):1448-1448. doi:10.1182/blood-2021-154035
12.Wei P, Jin M, Jiang L, Wang Y, Xie J, Hu X. Anaplastic lymphoma kinase-positive large B-cell lymphoma with a diagnostic pitfall of carcinoma: a case report. Int J Clin Exp Pathol. 2017;10(11):11219-11224. Accessed February 20, 2025. https://e-century.us/files/ijcep/10/11/ijcep0052864.pdf PubMed
13.Huang Z, Fu Y, Yang H, et al. Liquid biopsy in T-cell lymphoma: biomarker detection techniques and clinical application. Mol Cancer. 2024;23(1):36. doi:10.1186/s12943-024-01947-7 PubMed
14.Hans CP, Weisenburger DD, Greiner TC, et al. Confirmation of the molecular classification of diffuse large B-cell lymphoma by immunohistochemistry using a tissue microarray. Blood. 2004;103(1):275-82. doi:10.1182/blood-2003-05-1545 PubMed
15.Gutierrez-Garcia G, Cardesa-Salzmann T, Climent F, et al. Gene-expression profiling and not immunophenotypic algorithms predicts prognosis in patients with diffuse large B-cell lymphoma treated with immunochemotherapy. Blood. 2011;117(18):4836-43. doi:10.1182/blood-2010-12-322362 PubMed
16.Read JA, Koff JL, Nastoupil LJ, Williams JN, Cohen JB, Flowers CR. Evaluating cell-of-origin subtype methods for predicting diffuse large B-cell lymphoma survival: a meta-analysis of gene expression profiling and immunohistochemistry algorithms. Clin Lymphoma Myeloma Leuk. 2014;14(6):460-467.e2. doi:10.1016/j.clml.2014.05.002 PubMed
17.Xu-Monette ZY, Zhang H, Zhu F, et al. A refined cell-of-origin classifier with targeted NGS and artificial intelligence shows robust predictive value in DLBCL. Blood Adv. 2020;4(14):3391-3404. doi:10.1182/bloodadvances.2020001949 PubMed
18.Zamò A, Gerhard-Hartmann E, Ott G, et al. Routine application of the Lymph2Cx assay for the subclassification of aggressive B-cell lymphoma: report of a prospective real-world series. Virchows Arch. 2022;481(6):935-943. doi:10.1007/s00428-022-03420-6 PubMed
19.Scott DW, Wright GW, Williams PM, et al. Determining cell-of-origin subtypes of diffuse large B-cell lymphoma using gene expression in formalin-fixed paraffin-embedded tissue. Blood. 2014;123(8):1214-7. doi:10.1182/blood-2013-11-536433 PubMed
20.Swerdlow SH, Campo E, Pileri SA, et al. The 2016 revision of the World Health Organization classification of lymphoid neoplasms. Blood. 2016;127(20):2375-90. doi:10.1182/blood-2016-01-643569 PubMed
21.Sunnybrook Research Institute. Biomarker Imaging Research Laboratory: Recovery Fees. Accessed July 16, 2025. https://research.sunnybrook.ca/facilities-and-research-groups/biomarker-imaging-research-laboratory/
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.