Drugs, Health Technologies, Health Systems
Reimbursement Review
Asciminib (Scemblix)
Sponsor: Novartis Pharmaceuticals Canada Inc.
Therapeutic area: Philadelphia chromosome–positive chronic myeloid leukemia
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Clinical Review
Abbreviations
AE
adverse event
CDA-AMC
Canada’s Drug Agency
CI
confidence interval
CML
chronic myelogenous leukemia
CML-CP
chronic myelogenous leukemia in chronic phase
CNS
central nervous system
ELTS
European Treatment and Outcome Study long-term survival
EORTC QLQ-C30
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30
EORTC QLQ-CML24
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire – Chronic Myeloid Leukemia 24
FAS
full analysis set
GHS
global health status
GRADE
Grading of Recommendations Assessment, Development and Evaluation
HRQoL
health-related quality of life
IS-TKI
investigator-selected tyrosine kinase inhibitor
MMR
major molecular response
MR
molecular response
MR2
2-log or greater reduction in BCR::ABL1 transcripts
MR4
4-log or greater reduction in BCR::ABL1 transcripts
MR4.5
4.5-log or greater reduction in BCR::ABL1 transcripts
OS
overall survival
PCR
polymerase chain reaction
Ph+
Philadelphia chromosome positive
RCT
randomized controlled trial
TKI
tyrosine kinase inhibitor
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Table 1: Background Information of Application Submitted for Review
Item | Description |
|---|---|
Drug product | Asciminib (Scemblix), 20 mg and 40 mg, film-coated tablets, oral |
Sponsor | Novartis Pharmaceuticals Canada Inc. |
Indication | For the treatment of adult patients with Philadelphia chromosome-positive chronic myeloid leukemia (Ph+ CML) in chronic phase (CP) who are newly diagnosed or who have previously received 1 or more tyrosine kinase inhibitors |
Reimbursement request | First-line: For adult patients with newly diagnosed Ph+ CML in CP |
Health Canada approval status | NOC |
Health Canada review pathway | Project Orbis |
NOC date | July 25, 2025 |
Recommended dose | Asciminib 80 mg daily, orally, either as a single dose or 40 mg twice daily |
CP = chronic phase; NOC = Notice of Compliance; Ph+ CML = Philadelphia chromosome–positive chronic myeloid leukemia.
Source: Details included in the table are from the sponsor’s summary of clinical evidence.
Introduction
Chronic myeloid leukemia (CML) is a type of blood cancer in which certain white blood cells (granulocytes) grow and multiply in an uncontrolled way (proliferation).1 This happens because of a change in the genes in which parts of 2 chromosomes (9 and 22) swap places (reciprocal translocation), creating the Philadelphia chromosome.1 This leads to the formation of the BCR::ABL1 fusion gene, which produces an enzyme (tyrosine kinase) that is constantly active. This abnormal enzyme continuously sends signals (cell cycle pathways) that push bone marrow cells to keep dividing, leading to excessive growth (myeloid cell proliferation).2
CML accounts for approximately 15% to 20% of all adult cases of leukemia.12 The incidence rate of CML across all ages and sexes in Canada, excluding Quebec, ranged from 400 to 665 cases from 2009 to 2019, respectively.3 This corresponds to an incidence rate of 2.3 per 100,000 population in 2019.3 The 20-year prevalence rate in 2018 in Canada (excluding Quebec) was higher in males (17.1 per 100,000) than in females (13.3 per 100,000).4 The 20-year prevalence of CML across all ages and sexes in Canada, excluding Quebec, ranged from 3,785 cases in 2015 to 4,325 cases in 2018. This corresponds to a 20-year prevalence rate of 15.2 per 100,000 population in 2018.4 It is estimated that about 90% to 95% of patients with CML have disease that is in the chronic phase (CML-CP) at diagnosis, which usually manifests as leukocytosis and immature myeloid cells in the blood.1,2
Treatments have a variety of goals, and these can vary depending on the experts asked and the patients themselves, according to the clinical experts. They include survival, molecular response (MR) of varying depths, symptom control and quality of life (QoL), treatment-free remission, and freedom from side effects. The mainstay of treatment for CML-CP are the tyrosine kinase inhibitors (TKIs) that target abnormal BCR::ABL1 kinase: imatinib (first generation); dasatinib, nilotinib, and bosutinib (second generation); and ponatinib (third generation). Presently, first- and second-generation TKIs are recommended for first-line therapy of CML-CP. In the case of treatment failure, warning (previously called suboptimal response), or intolerance, the recommendation is to switch to a previously unused first- or second-generation TKI or to a third-generation TKI.5 Asciminib inhibits the ABL1 kinase activity of the BCR::ABL1 fusion protein by specifically targeting the ABL myristoyl pocket. Asciminib has been previously reviewed by Canada’s Drug Agency (CDA-AMC) and received a positive recommendation on August 5, 2022, for the treatment of adult patients with Philadelphia chromosome–positive (Ph+) CML-CP previously treated with 2 or more TKIs.
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of asciminib 20 mg and 40 mg film-coated oral tablets in the treatment of adult patients with newly diagnosed Ph+ CML-CP.
Perspectives of Patients, Clinicians, and Drug Programs
The information in this section is a summary of input provided by the patient and clinician groups that responded to the CDA-AMC call for input and from the clinical experts consulted for the purpose of this review.
Patient Input
Four organizations provided input: CML Society of Canada, Heal Canada, and a joint submission from the Canadian CML Network and the Leukemia & Lymphoma Society of Canada. Input was gathered using surveys and interviews from a total of 126 patients.
Patients described the significant physical and emotional burden of CML, including stress, fatigue, pain, and sleep disturbances, which impact their daily activities, work, and social life. The patients also added the challenges in finding an effective treatment with minimal side effects, and expressed a desire to someday be able to discontinue their treatment while maintaining remission.
With respect to outcomes of importance, patients prioritized symptom control, reduced side effects, and enhanced QoL, as well as treatment convenience.
Clinician Input
Input From the Clinical Experts Consulted for This Review
The clinical experts noted that newer drugs have not been able to improve survival. Although the vast majority of patients who are managed properly and are adherent to therapy do well, there are patients whose disease does not respond or becomes refractory to therapy, according to the clinical experts. Nonadherence occurs due to a variety of reasons, including side effects that are not being addressed, patient age, and beliefs. The clinical experts also added that although newer drugs may not have the same side effects as older drugs, they come with their own set of unique side effects. The experts note that the more advanced the disease is, or the more advanced the disease becomes, the harder it is to control. They emphasized the importance of having many treatment options available to patients, with the ultimate goal of having the best response possible with the fewest side effects possible.
One clinical expert noted that asciminib and other second-generation drugs may have better efficacy in patients with high Sokal risk scores (a score to assess prognosis and severity of disease); other considerations that determine choice of treatment include comorbidities.33 This clinical expert noted that some clinicians may use asciminib in the first line in patients with multiple comorbidities and in patients with high-risk features (i.e., high-risk group on any prognostic score model; the most commonly used tools being the European Treatment and Outcome Study long-term survival [ELTS] score and Sokal). The experts noted that if treatment-free remission is not the goal, it is unclear how aggressive one needs to be, considering that survival is more or less the same with all TKIs. In situations in which treatment-free remission is the goal, it is typically achieved with faster-acting or more potent drugs, and this in turn could lead to cost savings. The experts noted that if patients are to be on a treatment for the rest of their life, they likely prefer the treatment with the fewest side effects.
The clinical experts note that, at this time, there is insufficient evidence to conclusively predict which patients may experience a better response to asciminib than to the other available TKIs, adding that the patients most in need of intervention are those with multiple comorbidities that can make it difficult to use another TKI.
One clinical expert emphasized that patients do not need to meet all their milestones to have a normal survival, adding that how a patient functions is often a mental state, influenced by their own psyche, coping skills, support structures, and philosophy of life. The other clinical expert noted that the objective outcome is reduction of the mutated BCR::ABL1 gene, and that improvement in these molecular markers can have an important impact on a patient’s mental health, and noted that MR has been used as an end point in clinical trials, in addition to QoL and freedom from symptoms, which for some patients is a very important outcome.
The clinical expert noted that reasons for discontinuation would include disease progression or resistance, serious adverse effects that cannot be controlled, or if treatment-free remission data become available. Other reasons for discontinuation could include a switch in drug therapy or a stem cell transplant (if necessary).
The clinical expert highlighted the importance of having CML experts, or hematologists in consultation with CML experts, diagnosing and monitoring the disease due to its rarity and the expense of the drugs involved.
Clinician Group Input
Two clinician groups (Canadian CML Physicians Interest Group and Ontario Health (Cancer Care Ontario) Hematology Cancer Drug Advisory Committee), including 43 physicians, provided input.
There were no obvious areas of disagreement between the clinical experts and the clinician groups.
The clinician groups agreed with the clinical experts that improving survival and MRs, maintaining or improving health-related quality of life (HRQoL), providing the opportunity for treatment-free remission, and minimizing harms are all treatment goals in CML.
The clinician groups did not specifically identify whether they had experience with asciminib in clinical practice.
Drug Program Input
Input was obtained from the drug programs that participate in the CDA-AMC Reimbursement Review process. Key factors identified in the context of the asciminib in the present target population included comparator treatments, considerations for initiation of therapy, considerations for prescribing of therapy, generalizability, funding algorithm, care provision issues, and system and economic issues (refer to Table 5).
Clinical Evidence
Systematic Review
Description of Studies
The available evidence for this review of asciminib includes 1 ongoing open-label randomized controlled trial (RCT) (ASC4FIRST) that compares asciminib with imatinib and 3 second-generation TKIs (dasatinib, bosutinib, and nilotinib). There were 405 patients with CML-CP who were randomized 1:1 to asciminib or 1 of the other investigator-selected TKIs (IS-TKIs), with imatinib making up half of the patients in this control group. Randomization was stratified by ELTS category (low, intermediate, or high risk) and by the TKI selected by investigators before randomization (including imatinib and second-generation TKIs). The ASC4FIRST trial is ongoing, with an expected follow-up of 5 years, and the latest report submitted by the sponsor provided results up to 96 weeks. The coprimary outcome was the comparison of asciminib versus IS-TKI for major molecular response (MMR) rate at 48 weeks, and the other coprimary outcome compared asciminib with imatinib, in what was referred to as the imatinib stratum. The study was to be declared positive if it met either of the 2 primary objectives. Key secondary end points compared the efficacy of asciminib versus IS-TKI and imatinib based on the proportion of participants with an MMR at week 96. Time to discontinuation of study treatment due to adverse events (AEs) for asciminib versus second-generation TKIs was designated a secondary outcome. The overall safety objective was to characterize the safety and tolerability profile of asciminib compared with IS-TKIs and second-generation TKIs.
There was no indirect treatment comparison or studies addressing gaps submitted for this review.
Patients in the imatinib stratum were older than patients in the second-generation stratum. The median age of patients in the imatinib stratum was 56 years (range, 21 to 79 years) in the asciminib group and 54.5 years (range, 20 to 86 years) in the control group, and in the second-generation stratum was 43 years (range, 18 to 76 years) in the asciminib group and 43 years (range, 19 to 83 years) in the control group. The majority of patients (55%) had a Framingham risk score of “low” across all groups; however, the percentage of patients who were low risk was lower in the imatinib stratum (40%) than in the second-generation TKI stratum (69%). The majority of patients (61%) had an ELTS score of “low,” and this was consistent across strata.
Efficacy Results
Overall Survival
At the week 96 analysis, at a median follow-up time of ████ months, █patients (█████ died during the survival follow-up in the asciminib group versus █patients (████) in the IS-TKI group. No on-treatment deaths were reported. The █ deaths in the asciminib group were due to ██████████ █████████ █████████ and complications from a █████████████ ████ ████ ██████████. In the IS-TKI group, deaths occurred due to ███ ██████████ ██████████ ███████ ███████ █████ ███████████ ███ ███████ ██████..
Major Molecular Response
The ASC4FIRST trial met both primary end points. At 48 weeks, within the full analysis set (FAS), there were 136 patients (67.7%) in the asciminib group and 100 patients (49.0%) in the IS-TKI group who experienced an MMR, for a between-group difference of 18.88% (95% confidence interval [CI], 9.59% to 28.17%; P < 0.001). In the imatinib stratum, there were 70 patients (69.3%) in the asciminib group who experienced an MMR and 41 patients (40.2%) in the imatinib group, for a between-group difference of 29.55% (95% CI, 16.91% to 42.18%; P < 0.001). The results of the other secondary end point, MMR at week 48 in the second-generation TKI FAS, showed that 66 patients (66%) in the asciminib group and 59 patients (58%) in the second-generation TKI group experienced an MMR, for a between-group difference of 8.17% (95% CI, −5.14% to 21.47%).
The ASC4FIRST trial met both key secondary end points (refer to Table 15). At 96 weeks, 149 patients (74.1%) in the asciminib group and 106 patients (52.0%) in the IS-TKI group had experienced an MMR, for a between-group difference of 22.42% (95% CI, 13.55% to 31.29%; P < 0.001). In the imatinib stratum, 77 patients (76.2%) in the asciminib group and 48 patients (47.1%) in the imatinib group had experienced an MMR, for a between-group difference of 29.68% (95% CI, 17.57% to 41.79%; P < 0.001). The results of the other secondary end point, MMR at week 48 in the second-generation TKI FAS, showed that 72 patients (72.0%) in the asciminib group and 58 patients (56.9%) in the second-generation TKI group had experienced an MMR, for a between-group difference of 15.14% (95% CI, 2.32% to 27.95%).
Sensitivity Analysis
Within the FAS, the sensitivity analysis (in which patients with missing polymerase chain reaction [PCR] evaluations were considered nonresponders) conducted in the ASC4FIRST trial for the rate of MMR at week 48 showed consistency with the primary results, and this was also the case within the imatinib stratum and within the second-generation TKI stratum. There were no participants missing an MMR assessment at week 96. Therefore, the results of the sensitivity analysis of the MMR rate at week 96, without imputation of data for participants who had missing BCR::ABL1 transcript evaluations, were identical to the main analysis results. Within the imatinib stratum, there were no participants missing a week 96 MMR assessment. Therefore, the results of the sensitivity analyses of MMR rate at week 96 without imputation (treatment difference of ██████) were identical to the main analysis.
Subgroup Analysis
Subgroup analyses for the primary end point in the FAS were performed based on demographics as well as ELTS scores. At 96 weeks, results for the number of patients experiencing an MMR were reported for patients according to their ELTS scores at randomization, with a risk difference between groups of 15.5% for low scores (95% CI, 4.6% to 26.5%; N = 247), 31.0% for intermediate scores (95% CI, 13.5% to 48.5%; N = 113), and 38.1% for high scores (95% CI, 11.6% to 64.7%; N = 45). Results were similar when ELTS scores were based on case report form data. There were no tests for interaction reported.
Duration of MMR
By the week 96 assessment, ███ patients in the asciminib group and ███ patients in the IS-TKI group had experienced an MMR at least once, and █████ patients (██) in the asciminib group and █████ patients (██) in the IS-TKI group had subsequently experienced the loss of an MMR. Among the █ patients who experienced the loss of an MMR in the asciminib group, █ had confirmed loss of MMR and subsequently discontinued treatment, while █ patient interrupted their dose (patient decision) and subsequently discontinued treatment due to a protocol deviation. Among the █ patients who experienced the loss of response to an IS-TKI, █ had a confirmed loss of MMR and subsequently discontinued treatment while █ patient discontinued treatment due to an AE and had a BCR::ABL1 transcript level greater than 1% at week 48 at the early discontinuation visit. The estimated Kaplan-Meier probability of patients continuing to experience an MMR for at least 96 weeks was █████ ████ ███ █████ █████ in the asciminib group and █████ ████ ███ █████ █████ in the IS-TKI group.
MR With a 2-Log or Greater Reduction in BCR::ABL1 Transcripts
At 48 weeks, 175 patients (87.1%) in the asciminib group and 148 patients (72.5%) in the IS-TKI group had experienced an MR with a 2-log or greater reduction in BCR::ABL1 transcripts (MR2), for a between-group difference of █████ ████ ███ █████ ███████. In the stratum of patients who received imatinib, 85 patients (84.2%) in the asciminib group and 63 patients (61.7%) in the imatinib group had experienced an MR2, for a between-group difference of ██████ ████ ███ ███████ ████████. In the second-generation TKI stratum, 90 patients (90.0%) in the asciminib group and 85 patients (83.3%) in the IS-TKI group had experienced an MR2, for a between-group difference of █████ ████ ███ ██████ ████████.
At 96 weeks, ███ patients ███████ ██ ███ █████████ █████ ███ ███ patients ███████ in the IS-TKI group had experienced an ████ ███ █ █████████████ ██████████ ██ ██████ ████ ███ ███████ ████████ ██ ███ ████████ ████████ █████ ████ ██ ████████ ███████ ██ ███ █████████ █████ ███ ██ ████████ ███████ ██ ███ ████████ █████ ███ ████████ ████ ███ █ █████████████ ██████████ ██ ██████ ████ ███ ███████ ████████ ██ ███ ██████ ██████████ ███ ████████ █████ ████ ██ ████████ ███████ ██ ███ █████████ █████ ███ ██ ████████ ███████ ██ ███ █████████████████ ███ █████ ███ ████████ ████ ███ █ █████████████ ██████████ ██ ██████ ████ ███ ██████ ████████.
MR With a 4-Log or Greater Reduction in BCR::ABL1 Transcripts
At 48 weeks, 78 patients (38.8%) in the asciminib group and 40 patients (20.6%) in the IS-TKI group had experienced an MR with a 4-log or greater reduction in BCR::ABL1 transcripts (MR4), for a between-group difference of 18.38% ████ ███ ██████ ████████. In the imatinib stratum, 43 patients (42.6%) in the asciminib group and 15 patients (14.7%) in the imatinib group had experienced an MR4, for a between-group difference of 28.22% ████ ███ ███████ ████████. In the second-generation TKI stratum, 35 patients (35.0%) in the asciminib group and 27 patients (26.5%) in the second-generation TKI group had experienced an MR4, for a between-group difference of 7.54% ████ ███ ███████ █████████.
At 96 weeks, there were 98 patients (48.8%) in the asciminib group and 56 patients (27.5%) in the IS-TKI group who experienced an MR4, for a between-group difference of ██████ ████ ███ ███████ ████████. In the imatinib stratum, 53 patients (52.5%) in the asciminib group and 24 patients (23.5%) in the IS-TKI group experienced an MR4, for a between-group difference of ██████ ████ ███ ███████ ████████. In the second-generation stratum, 45 patients (45.0%) in the asciminib group and 32 patients (31.4%) in the second-generation TKI group experienced an MR4, for a between-group difference of ██████ ████ ███ ██████ █████████.
MR With a 4.5-Log or Greater Reduction in BCR::ABL1 Transcripts
At 48 weeks, 34 patients (16.9%) in the asciminib group and 18 patients (8.8%) in the IS-TKI group had experienced an MR with a 4.5-log or greater reduction in BCR::ABL1 transcripts (MR4.5), for a between-group difference of 8.20% (95% CI, 1.78% to 14.62%). In the imatinib stratum, 18 patients (17.8%) in the asciminib group and 5 patients (4.9%) in the imatinib group had experienced an MR4.5, for a between-group difference of 13.13% (95% CI, 4.69% to 21.56%). In the second-generation TKI stratum, 16 patients (16.0%) in the asciminib group and 13 patients (12.7%) in the IS-TKI group had experienced an MR4.5, for a between-group difference of 3.24% (95% CI, −6.34% to 12.83%).
At 96 weeks, 62 patients (30.9%) in the asciminib group and 36 patients (17.7%) in the IS-TKI group had experienced an MR4.5, for a between-group difference of ██████ ███████ ████████. In the imatinib stratum, 36 patients (35.6%) in the asciminib group and 12 patients (11.8%) in the imatinib group had experienced an MR4.5, for a between-group difference of ██████ ████ ███ ███████ ████████. In the second-generation TKI stratum, 26 patients (26.0%) in the asciminib group and 24 patients (23.5%) in the IS-TKI group had experienced an MR4.5, for a between-group difference of █████ ████ ███ ███████ ████████.
Time to First MMR
Within the FAS, the probability of a patient experiencing an MMR by week 48 was numerically higher in the asciminib arm (66.5%; 95% CI, 59.5 to 72.6) compared with the IS-TKI arm (46.3%; 95% CI, 39.2 to 53.0) (refer to Table 15). Within the imatinib stratum, the probability of experiencing an MMR by week 48 was numerically higher in the asciminib arm (69.1%; 95% CI to 58.8 to 77.2) compared with the IS-TKI arm (38.0%; 95% CI, 28.5 to 47.5). Within the second-generation TKI stratum, the probability of experiencing an MMR by week 48 was numerically higher in the asciminib arm (64.0%; 95% CI, 53.7 to 72.6) compared with the IS-TKI arm (54.5; 95% CI, 44.2 to 63.6).
In the FAS, the time to first MMR was numerically higher in the asciminib arm compared with the IS-TKI arm (median time to first MMR: 24.3 versus 36.4 weeks). In the imatinib stratum, an MMR was achieved numerically faster in the asciminib arm compared with the IS-TKI arm (median time to first MMR: 24.1 weeks versus 48.6 weeks). In the second-generation TKI stratum, an MMR was achieved numerically faster in the asciminib arm compared with the IS-TKI arm (median time to first MMR: 24.3 weeks versus 36.1 weeks).
Health-Related Quality of Life
HRQoL was reported as ordinal categorical data for the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC QLQ-C30) global health status (GHS) score and the EORTC Quality of Life Questionnaire – Chronic Myeloid Leukemia 24 (QLQ-CML24) symptom burden. A large number of participants (approximately ███) in both groups had missing baseline assessments. There was a large amount of missing data in the asciminib (███ ███ ███ with missing data at week 48 and week 96, respectively) and IS-TKI groups (███ ███ ███ with missing data at week 48 and week 96, respectively) for the EORTC QLQ-C30 GHS. There was a similar amount of missing data for the EORTC-CML24 symptom burden (██████████ ████ ███████ ███ ████ ███████ ████ ██ ████ ██). At week 96, for EORTC QLQ-C30 GHS, the number of patients who indicated they were “very much better” was ██ patients (███) versus █ patients ██████ in the asciminib versus IS-TKI groups, respectively, while the number who indicated they were “very much worse” was █ patients (███ versus █ patients (███), respectively. At week 96, for EORTC QLQ-C30 GHS, ██ ██ ██ ███████ patients in the asciminib group and ██ ██ ██ ███████ in the IS-TKI group had a moderate to high worsening, defined as a score that decreased by more than 10 points from baseline. For EORTC-CML24 symptom burden, the number of patients in the asciminib group versus the IS-TKI group who were “very much better,” was █ patients (███) versus 0, respectively, and the number of patients in the asciminib group versus the IS-TKI group who were “very much worse,” was █ patients (██) versus ██ patients (███), respectively.
Health Care Resource Utilization
After 96 weeks, ██ patients (███) in the asciminib group and ██ patients (███) in the IS-TKI group had used at least 1 health care resource. The most common resource used was hospitalization (██ patients [███] in the asciminib group and ██ patients [███] in the IS-TKI group).
Harms Results
Adverse Events
AEs were reported in 191 patients (96%) in the asciminib group and 197 patients (98%) in the IS-TKI group at 96 weeks. AEs of grade 3 or higher occurred in 89 patients (45%) in the asciminib group compared with 110 patients (55%) in the IS-TKI group at 96 weeks. ███ ████ ██████ ███ ████ █████████ █████████ ██ ██ ████████ █████ ██ █████████ ███ ██ ████████ █████ ██ ███ ██████ ██████ ███ █████████ █████████ ██ ██ ████████ █████ ██ ███ █████████ █████ ███ ██ ████████ █████ ██ ███████.
Serious Adverse Events
Serious AEs occurred in ██ ████████ █████ in the asciminib group and ██ patients █████ ██ ███ ██████ ██████ after 96 weeks of treatment| ███ ████ ███ ████ ████████ ██ ████ ████ █ ████████ ███ ███████ █████████ █████ ████████ ██ ██ ████████ ██ ███ █████████ █████ ███ █ ████████ ████ ██ ███ ██████ █████.
Withdrawals Due to Adverse Events
AEs leading to treatment discontinuation occurred in 10 patients (5%) in the asciminib group and 26 patients (13%) in the IS-TKI group after 96 weeks of treatment.
The secondary end point, time to discontinuation of study treatment due to AEs for asciminib versus second-generation TKIs, was tested at week 96 and was met. Results of the cause-specific hazard analysis showed that the risk of study treatment discontinuation due to AEs was lower in the asciminib group compared with the second-generation TKI group (HR = 0.463; 95% CI, 0.215 to 0.997; P = 0.0246).
Mortality
After 96 weeks, there were ████████ ██████ ███ ████ ██ ███ █████████ █████ ███ █ ████████ ████ ███ ████ ██ ███ ██████ ██████ ███ ██████ ████████ ██████ ███ ████████ ██████████ ███ █ ██████ ██ ███ █████████ █████ ████ ███ ██ █████████████ ████ █████████████ ████ ████ ██████████ ███ ███ ██ ██████████ █████████ ██████████ ██ ███ █ ██████ ██ ███ ██████ ██████ ███ ████ ██ ███ ████████ █████ ████ ██████████ ██████████ ███████ ███████ █████ ██████████ ███ ███████ ███████.
Notable Harms
The notable harms prioritized by the clinical experts were acute pancreatitis, and the category of ischemic cardiac and central nervous system (CNS) events. After 96 weeks, there were █ patients ████ in each of the asciminib and IS-TKI groups who had an event of acute pancreatitis and there were ██ patients ██████ in the asciminib group and ██ patients ████ in the IS-TKI group who had an AE that fell under the broad category of ischemic heart and CNS conditions.
Other notable harms included myelosuppression, which occurred in ██ patients █████ in the asciminib group and ███ patients █████ in the IS-TKI group; gastrointestinal toxicity, which occurred in ██ patients █████ in the asciminib group and ██ patients █████ in the IS-TKI group; and clinical hepatotoxicity, occurring in █ patients (██) in the asciminib group and █ patients ████ in the IS-TKI group. Other notable harms are summarized in Table 18.
Critical Appraisal
The open-label design of the ASC4FIRST trial may bias the assessment of outcomes, particularly patient-reported outcomes such as HRQoL. The evidence was very uncertain about the effect of asciminib on HRQoL compared with IS-TKIs due to the open-label design and the large amount of missing data. Fewer patients in the asciminib group discontinued treatment early compared with the IS-TKI group, and this may have biased the assessment of outcomes, most notably, harms outcomes due to the differences in exposure. MMR (48 and 96 weeks) and time to discontinuation of study treatment due to an AE were adjusted for multiple testing; however, several other important outcomes such as HRQoL and other MRs were not adjusted for multiplicity and are considered to provide supportive evidence.
ASC4FIRST is an ongoing trial, and the current follow-up of 96 weeks is not of sufficient duration to assess key clinical outcomes such as overall survival (OS), long-term MRs, and harms.
The clinical experts noted that the dosing of the comparators may not reflect dosing in routine clinical practice, within which patients would be carefully up-titrated to minimize the risk of side effects, which, according to the clinical experts, may have inflated the occurrence of harms in the IS-TKI group. Results from the ASC4FIRST trial were not stratified by second-generation TKI, though the clinical experts noted that the occurrence and specific harms of interest are different among the second-generation TKIs.
GRADE Summary of Findings and Certainty of the Evidence
For pivotal studies and RCTs identified in the sponsor’s systematic review, Grading of Recommendations Assessment, Development and Evaluation (GRADE) was used to assess the certainty of the evidence for outcomes considered most relevant to inform expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group.10,11 Following the GRADE approach, evidence from RCTs started as high-certainty evidence and could be rated down for concerns related to study limitations (which refers to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias.
When possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect; if this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., the clinical importance is unclear). In all cases, the target of the certainty-of-evidence assessment was based on the point estimate and where it was located relative to the threshold for a clinically important effect (when a threshold was available) or to the null. For the MMR outcome, the threshold for a clinically important between-group effect was estimated by the clinical experts to be 10% to 15%; for MR2, it was estimated to be 5% to 10%. Due to the significant amount of missing baseline data (about 40%) for patient-reported outcomes, change from baseline data were not interpretable. The 95% CIs for the change from baseline scores in each group as well as the between-group difference with its associated 95% CI were lacking. For harms outcomes, the clinical experts estimated that a 10% between-group difference would be clinically meaningful.
The selection of outcomes for GRADE assessment was based on the sponsor’s summary of clinical evidence, consultation with clinical experts, and input received from patient and clinician groups and public drug plans. The following list of outcomes was finalized in consultation with expert committee members:
patients experiencing an MMR at week 48
patients experiencing an MR2 at week 48
change in EORTC QLQ-C30 GHS score from baseline
harms: patients experiencing acute pancreatitis (clinical), ischemia (cardiac and/or CNS).
Table 2 presents the GRADE summary of findings for asciminib versus IS-TKIs for patients with newly diagnosed or previously treated Ph+ CML-CP.
Table 2: Summary of Findings for Asciminib vs. IS-TKI for Patients With CML-CP
Outcome and follow-up | Patients (studies), N | Relative effect (95% CI) | Absolute effects (95% CI) | Certainty | What happens | ||
|---|---|---|---|---|---|---|---|
IS-TKI | Asciminib 80mg | Difference | |||||
Major molecular response | |||||||
Proportion of patients who experienced an MMR at week 48 (primary outcome) | N = 405 (1 RCT) | NR | 49 per 100 | 68 per 100 (61 to 74 per 100) | 19 more per 100 (10 more to 28 more) | Higha | Asciminib results in a clinically important increase in the proportion of patients experiencing an MMR compared with an IS-TKI. |
Molecular responseb | |||||||
MR2 rate at scheduled data collection time points at week 48 | N = 405 (1 RCT) | NR | 73 per 100 | ████ ████ | ████ ████ ████ ████ | Higha | Asciminib results in a clinically important increase in the number of patients experiencing an MR2 when compared with an IS-TKI. |
Health-related quality of lifeb | |||||||
Change in EORTC QLQ-C30 GHS score from baseline Follow-up: 96 weeks | N = 123 (1 RCT) | NR | ██ ██ ██ ███████ patients in the asciminib group and ██ ██ ██ ███████ in the IS-TKI group had a moderate to high worsening, defined as a score that decreased by more than 10 points from baseline. | Very lowc | The evidence is very uncertain about the effect of asciminib on HRQoL when compared with an IS-TKI. | ||
Harms (safety setd) | |||||||
Acute pancreatitis Follow-up: 96 weeks | N = 401 (1 RCT) | NR | ████ ████ | ████ ████ | ████ ████ | Lowe | Asciminib may result in little to no difference in acute pancreatitis compared with an IS-TKI. The clinical importance of the effect is unclear. |
Ischemic heart and CNS conditions Follow-up: 96 weeks | N = 401 (1 RCT) | NR | ████ ████ | ████ ████ | ████ ████ ████ ████ | Lowe | Asciminib may result in little to no difference in acute ischemic heart and CNS conditions compared with IS-TKI after 96 weeks of treatment. The clinical importance of the effect is unclear. |
CDA-AMC = Canada’s Drug Agency; CI = confidence interval; CML-CP = chronic myelogenous leukemia in chronic phase; CNS = central nervous system; EORTC QLQ-C30 = European Organisation for the Research and Treatment of Cancer Quality of Life Questionnaire Core 30; GHS = global health status; IS-TKI = investigator-selected tyrosine kinase inhibitor; MMR = major molecular response; MR2 = molecular response with a 2-log or greater reduction in BCR::ABL1 transcripts; NR = not reported; RCT = randomized controlled trial; TKI = tyrosine kinase inhibitor; vs. = versus.
Notes: Study limitations (which refer to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias were considered when assessing the certainty of the evidence. All serious concerns in these domains that led to the rating down of the level of certainty are documented in the table footnotes.
aThe clinical experts consulted by CDA-AMC identified a clinically meaningful between-group difference of 10% to 15% for MMR and of 5% to 10% for MR2.
bThese outcomes were not adjusted for multiplicity.
cThe level of evidence was rated down 3 levels for extremely serious risk of bias due to the open-label nature of the study and the subjective nature of the outcome (rated down once), as well as the missing outcome data (65% missing outcome data in the asciminib group and 74% missing outcome data in the IS-TKI group) (rated down twice). The level of evidence was rated down 1 level for serious imprecision. As a large proportion of participants were missing baseline data (about 40% in both arms), the changes from baseline EORTC QLQ-C30 GHS scores are not interpretable. The 95% CIs for the change from baseline scores in each group as well as the between-group difference with its associated 95% CI were lacking.
dThe safety set comprises all participants who receive at least 1 dose of any study treatment. Participants were analyzed according to the actual study treatment received; actual treatment received is defined as the randomized treatment if the participant took at least 1 dose of that treatment, or the first treatment received if the randomized treatment was never received.
eThe CDA-AMC review team did not rate down for risk of bias because, according to the team’s judgment, the potential risk of bias arising from the open-label study design was unlikely to impact AEs such as acute pancreatitis and ischemic heart and CNS conditions. The clinical experts suggested a minimal important difference of 10%, which was used to assess certainty. The level of evidence was rated down 2 levels for very serious imprecision due to the low number of events in each group.
Source: Details included in the table are from the sponsor’s summary of clinical evidence.
Long-Term Extension Studies
No long-term extension study was submitted by the sponsor.
Studies Addressing Gaps in the Evidence From the Systematic Review
No studies addressing gaps were submitted by the sponsor.
Conclusion
The ASC4FIRST trial met both its primary outcomes and showed statistically significant and clinically meaningful increases in the proportion of patients experiencing an MMR at 48 weeks in the asciminib versus IS-TKI stratum and the asciminib versus imatinib stratum. The certainty of the evidence for these outcomes was rated as “high,” based on the GRADE approach. Likewise, the study met both key secondary efficacy end points, with asciminib showing statically significant and clinically meaningful benefit versus IS-TKIs and versus imatinib at week 96. The clinical significance of this finding with respect to OS are uncertain because data were immature at the time of analysis at 96 weeks in the ASC4FIRST trial. Although there is some evidence in the literature that early MMR may predict long-term survival, no TKI has demonstrated a survival benefit over another TKI in long-term studies. The clinical experts consulted on this review noted that treatment-free remission is among the key treatment goals; however, it was not assessed in the ASC4FIRST trial. HRQoL is an important outcome in CML; however, the evidence was very uncertain about the effect of asciminib on HRQoL compared with IS-TKIs. In the ASC4FIRST trial, fewer patients discontinued treatment due to an AE in the asciminib group (6%) compared with the IS-TKI group (13%); however, comparisons with other TKIs in this study are limited by the variation in the side effect profiles of these drugs and lack of stratification by each TKI. Results from the ASC4FIRST trial suggest that asciminib results in little to no difference in the notable harms, acute pancreatitis, and ischemic heart and CNS conditions compared with IS-TKIs; however, the certainty of evidence was rated as low using the GRADE approach.
Introduction
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of asciminib, 20 mg and 40 mg oral film-coated tablets in the treatment of treatment of adult patients with newly diagnosed or previously treated Ph+ CML-CP.
Disease Background
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following has been summarized and validated by the review team.
CML is a type of blood cancer in which certain white blood cells (granulocytes) grow and multiply in an uncontrolled way (proliferation).1 This happens because of a change in the genes, when parts of 2 chromosomes (9 and 22) swap places (reciprocal translocation), creating the Philadelphia chromosome.1 This leads to the formation of the BCR::ABL1 fusion gene, which produces an enzyme (tyrosine kinase) that is constantly active. This abnormal enzyme continuously sends signals (cell cycle pathways) that push bone marrow cells to keep dividing, leading to excessive growth (myeloid cell proliferation).2
CML accounts for approximately 15% to 20% of all adult cases of leukemia.12 CML can occur in all age groups; however, most cases are diagnosed in patients aged 60 or older, with a median age at presentation of 66 years in the US.1,13 Primary risk factors for CML include high-dose radiation exposure, increasing age, and male gender.14,15 It is estimated that about 90% to 95% of patients with CML are in the chronic phase at diagnosis, which usually manifests as leukocytosis (high white blood cell count) and immature myeloid cells in the blood. These manifestations appear because CML disrupts normal cell development, resulting in immature forms of granulocytes being released.1,2 About 50% of patients with CML-CP are asymptomatic at presentation and are often diagnosed upon receiving reports of laboratory abnormalities following a routine examination.1 Patients with symptoms most commonly present with anemia, fatigue, splenomegaly, and weight loss. Infrequently, patients are initially diagnosed in advanced CML stages: accelerated phase or blast phase.1 These stages show more immature blood cells in the blood and bone marrow. They also involve worsening symptoms and additional cytogenetic abnormalities.
CML diagnoses are confirmed by identification of the Philadelphia chromosome, the BCR::ABL1 fusion gene, or BCR::ABL1 fusion mRNA using conventional cytogenetics, fluorescence in situ hybridization analysis, or reverse transcriptase PCR.16 The incidence rate of CML across all ages and sexes in Canada, excluding Quebec, ranged from 400 to 665 incident cases from 2009 to 2019, respectively.3 This corresponds to an incidence rate of 2.3 per 100,000 population in 2019.3 The 20-year prevalence rate in 2018 in Canada (excluding Quebec) was higher in males (17.1 per 100,000) than in females (13.3 per 100,000).4 The 20-year prevalence of CML across all ages and sexes in Canada, excluding Quebec, ranged from 3,785 cases in 2015 to 4,325 cases in 2018. This corresponds to a 20-year prevalence rate of 15.2 per 100,000 population in 2018.4
The average age at diagnosis is 64 years of age; CML is rarely diagnosed in children.17
Before the use of modern treatments, OS was approximately 3 to 5 years. The blast phase is usually fatal, with a median survival of 3 to 6 months. The median duration of the accelerated phase ranges from 6 to 9 months, although up to 40% of patients may progress from the chronic phase to blast phase without a clear, defined intervening accelerated phase.5
In the past, an allogeneic stem cell transplant from a sibling or matched unrelated donor resulted in the cure of 70% to 80% of patients treated in the chronic phase but was limited to younger patients and those with available donors, representing less than 25% of the patient population. Hence, CML was previously fatal for 80% to 90% of patients before the introduction of specific inhibitors of the BCR::ABL1 kinase. For those who were not candidates for allogeneic stem cell transplant, or for whom a donor could not be found, interferon alpha was effective in producing hematologic and occasional cytogenetic responses, but side effects limited its use to those younger than 50 years of age.18 Following the development of the first TKIs in 2001, survival on therapy is roughly that of age-matched controls for chronic-phase disease, according to the clinical experts consulted for this review.
Standards of Therapy
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following has been summarized and validated by the review team.
CML is relatively unique among cancers in having 1 specific molecular target, the BCR::ABL1 tyrosine kinase receptor, and TKIs are the mainstay of treatment for CML since the discovery of imatinib at the turn of this century. Imatinib was the first TKI to be approved for CML, and reports of improvements in population-based CML outcomes can largely be attributed to the use of this drug.19
Imatinib was joined by second-generation TKIs like dasatinib, nilotinib, and bosutinib within 15 years of its approval, followed by a third-generation TKI, ponatinib. Presently, first- and second-generation TKIs are recommended for first-line therapy of CML-CP. In the case of treatment failure, warning (previously called suboptimal response), or intolerance, the recommendation is to switch to a previously unused first- or second-generation TKI or to a third-generation TKI.5 According to the clinical experts consulted by CDA-AMC, patients most commonly receive either imatinib or dasatinib as first-line treatments in Canadian clinical practice. The 2025 National Comprehensive Cancer Network guidelines emphasize individualized treatment selection in the first-line setting based on individual treatment goals, risk scores (e.g., Sokal, ELTS), and comorbidities (e.g., cardiovascular risk).20 For example, a younger patient’s goal may be to achieve a deep and rapid MR and eventual discontinuation of TKI therapy for family planning purposes. Imatinib may be preferred for patients who are older with comorbidities such as cardiovascular disease. The trial evidence compares second-generation TKIs in the first line versus first-line imatinib rather than versus each other.20
Mutations to the adenosine triphosphate (ATP) binding site of the BCR::ABL1 gene are associated with drug resistance and a high risk of progression, with about 10% to 15% of patients with CML-CP developing resistance to imatinib within 18 months to 2 years of treatment.1,21 According to the European LeukemiaNet guidelines, there is no clear recommendation for selecting 1 second-generation TKI (dasatinib, nilotinib, and bosutinib) over another in second-line treatment; all second-line TKIs are effective and there are no studies comparing the TKIs with each other.22 Ponatinib is a third-generation TKI that is used in patients with CML in all phases who have a BCR::ABL1 T315I mutation and in patients when no other TKI is indicated.22,23
Evidence suggests that approximately one-third of patients have switched to an alternative TKI in randomized studies of CML-CP, mainly due to toxicity or suboptimal response.24
Guidelines on monitoring molecular milestones in patients with CML have been outlined by the 2020 European LeukemiaNet and suggest that this monitoring should be done using reverse transcriptase PCR testing at the time of diagnosis and quantitative reverse transcriptase PCR every 3 months after beginning treatment, regardless of previous results.22 The guidelines further outline early treatment molecular milestones and provide accompanying management recommendations for each response level. The monitoring milestones of BCR::ABL1 transcript levels according to the International Scale at 3, 6, and 12 months determine whether the current treatment should be continued (optimal response), changed (failure or resistance), or carefully considered for continuation or change, depending on patients’ characteristics, comorbidities, and tolerance (warning). Additional quantitative PCR testing may be indicated if the kinetics of the response are not clear, or if toxicity or intolerance cause dose interruptions or reductions. The International Scale defines the standard baseline as a BCR::ABL1 transcript level of 100%. Any log reduction indicates the BCR::ABL1 transcript level has decreased by a certain amount from the standard baseline. For example, a 3-log reduction means the BCR::ABL1 transcript level has decreased to 1,000 times below the standardized baseline, meaning that 0.1% of cells (1 out of every 1,000 cells) has the BCR::ABL1 gene. A BCR::ABL1 transcript level of 0.1% or less is defined as an MMR or MR.3,22,25 A BCR::ABL1 transcript level of greater than 10% at 3 months indicates treatment failure when confirmed.22 The clinical experts noted that most provinces in Canada, except Quebec, use the 2020 European LeukemiaNet guidelines.
Table 3: Molecular Milestones in the Treatment of CML-CP Over Time According to the 2020 ELN Guidelines
Time category | Optimal response | Warning | Failure to respond |
|---|---|---|---|
Baseline | NA | High-risk ACA, high-risk ELTS score | NA |
3 months | ≤ 10% | > 10% | > 10%, if confirmed within 1 to 3 months |
6 months | ≤ 1% | > 1% to 10% | > 10% |
12 months | ≤ 0.1% | > 0.1% to 1% | > 1% |
Any time | ≤ 0.1%a | > 0.1% to 1%, loss of MMR | > 1%, resistance mutations, high-risk ACA |
ACA = additional chromosomal aberration; CML-CP = chronic myeloid leukemia in chronic phase; ELN = European LeukemiaNet; ELTS = European Treatment and Outcome Study long-term survival; MMR = major molecular response; NA = not applicable.
aA change of treatment may be considered if an MMR is not reached by 36 to 48 months.
Source: Hehlmann (2020).26
According to the clinical experts consulted by CDA-AMC, treatment goals can vary depending on the perspectives of clinicians and their patients. They include survival, achieving an MR, symptom management, improved QoL, treatment-free remission, and minimizing side effects. According to the European LeukemiaNet recommendation (2020),22 the selection of therapies for a patient include considerations of efficacy, tolerability, and early and late toxicity. Increasing focus is on QoL, preventing long-term organ toxicities, and identifying strategies to maximize the possibility of stopping TKI therapy resulting in treatment-free remission. However, the accessibility of effective drugs and requirements for monitoring may be limited, in which case the goal of treatment remains survival.22 According to the European LeukemiaNet guidance, 80% of patients will never achieve a treatment-free remission.22
Drug Under Review
Key characteristics of asciminib are summarized in Table 4 with other treatments available for Ph+ CML-CP in the second-line setting.
Asciminib can be taken orally either as 80 mg once daily at approximately the same time each day, or as 40 mg twice daily at approximately 12-hour intervals. Asciminib has been previously reviewed by CDA-AMC and received a positive recommendation on August 5, 2022, for the treatment of adult patients with Ph+ CML-CP previously treated with 2 or more TKIs.18
Asciminib is an oral, third-generation TKI that selectively targets the ABL myristoyl pocket of the BCR::ABL1 fusion protein. This results in blocked kinase activity, preventing tumour cell proliferation.
The sponsor’s reimbursement request is for asciminib for the first line for adult patients with newly diagnosed Ph+ CML-CP. A concurrent CDA-AMC submission by the same sponsor is requesting reimbursement for asciminib for the second line for adult patients with Ph+ CML-CP previously treated with 1 TKI. The Health Canada indication is for the treatment of adult patients with newly diagnosed or previously treated Ph+ CML-CP.
Asciminib was reviewed by Health Canada through an expedited pathway (Project Orbis). The Notice of Compliance was issued on July 25, 2025. Asciminib was also approved by the FDA for newly diagnosed Ph+ CML-CP. This FDA indication was approved under accelerated approval based on the MMR rate. Continued approval for this FDA indication may be contingent upon verification of clinical benefit in confirmatory trial(s).27 Scemblix has not been filed for review by the European Medicines Agency for newly diagnosed Ph+ CML-CP.
Table 4: Key Characteristics of Asciminib, Bosutinib, Nilotinib, Dasatinib, and Ponatinib
Characteristic | Asciminib | Bosutinib | Nilotinib | Dasatinib | Ponatinib |
|---|---|---|---|---|---|
Mechanism of action | Asciminib is a potent inhibitor of BCR::ABL1 tyrosine kinase; it inhibits the ABL1 kinase activity of the BCR::ABL1 fusion protein by specifically targeting the ABL myristoyl pocket. | Bosutinib inhibits the activity of the oncogenic BCR::ABL1 kinase that promotes CML through binding of the ATP binding site of the BCR::ABL1 oncoprotein. | Nilotinib inhibits the activity of the oncogenic BCR::ABL1 kinase that promotes CML through binding of the ATP binding site of the BCR::ABL1 oncoprotein. | Dasatinib inhibits the activity of the oncogenic BCR::ABL1 kinase that promotes CML, binding both the inactive and active conformations of the enzyme. | Ponatinib is a potent pan-BCR::ABL1 inhibitor with structural elements, including a carbon–carbon triple bond that enables high-affinity binding to native BCR::ABL1 and mutant forms of the ABL kinase. |
Indicationa | For the treatment of adult patients with newly diagnosed or previously treated Ph+ CML-CP. | For the treatment of newly diagnosed Ph+ CML-CP. For the treatment of adult patients with AP, BP, or CP Ph+ CML with resistance or intolerance to prior TKI therapy. | For the treatment of newly diagnosed Ph+ CML-CP For the treatment of adult patients with CP and AP Ph+ CML resistant to or intolerant of at least 1 prior therapy including imatinib. | For the treatment of newly diagnosed Ph+ CML-CP For the treatment of adult patients with Ph+ CP, AP, or BP CML with resistance or intolerance to prior therapy, including imatinib. | For the treatment of adult patients with AP, BP, or CP CML, or Ph+ ALL for whom other TKI therapy is not appropriate, including CML or Ph+ ALL that is T315I mutation–positive or when there is prior TKI resistance or intolerance. |
Route of administration | Oral | Oral | Oral | Oral | Oral |
Recommended dose | 80 mg q.d. or 40 mg b.i.d. at 12-hour intervals | 500 mg b.i.d. with food | 400 mg b.i.d. | 100 mg q.d. | Starting dosage: 45 mg q.d. |
Serious adverse effects or safety issues | QT interval prolongation, hypertension, embryo-fetal toxicity, myelosuppression, pancreatic toxicity, hepatitis B reactivation | Gastrointestinal toxicity, hepatic toxicity, cardiac toxicity, pancreatic toxicity, fluid retention, hemorrhage, QT interval prolongation, myelosuppression, tumour lysis syndrome, hepatitis B reactivation, second primary malignancies | Cardiac deaths, QT interval prolongation, ischemic heart disease, ischemic cerebrovascular events, peripheral arterial occlusive disease, hepatoxicity, pancreatitis, myelosuppression | Myelosuppression, hemorrhage, fluid retention, congestive heart failure, and pulmonary arterial hypertension | Arterial occlusions, venous thromboembolism, heart failure, hemorrhage events, hepatotoxicity, myelosuppression, and pancreatitis |
ALL = acute lymphoblastic leukemia; AP = accelerated phase; ATP = adenosine triphosphate; b.i.d. = twice daily; BP = blast phase; CML = chronic myelogenous leukemia; CML-CP = chronic myelogenous leukemia in chronic phase; CP = chronic phase; Ph+ = Philadelphia chromosome–positive; q.d. = once daily; TKI = tyrosine kinase inhibitor.
aHealth Canada–approved indication.
Sources: Product monograph for asciminib (draft),28 bosutinib,29 nilotinib,30 dasatinib,31 and ponatinib.32
Perspectives of Patients, Clinicians, and Drug Programs
The full patient and clinician group submissions received are available in the consolidated patient and clinician group input document for this review on the project website.
Patient Group Input
This section was prepared by the review team based on the input provided by patient groups.
CDA-AMC received 3 submissions for this review, including inputs from the CML Society of Canada, Heal Canada, and a joint submission from the Canadian CML Network and the Leukemia & Lymphoma Society of Canada. The CML Society of Canada collected insights through surveys and phone interviews with more than 20 patients from Canada, France, the US, and the UK who had experience with asciminib after at least 1 prior therapy. Heal Canada conducted a survey of 15 patients in Canada living with CML and interviewed 16 patients from other countries who have had experience with asciminib, most of whom accessed the treatment upon TKI failure. The joint submission gathered responses from an online survey of 80 patients in Canada with CML; 52 patients had been diagnosed with Ph+ CML, and all had been treated with at least 1 prior therapy. Twenty patient respondents provided details of their experience with asciminib treatment. Additional input from the Leukemia & Lymphoma Society of Canada included in-person interviews with 2 patients living with CML and a round table discussion with 3 patients receiving treatment with asciminib. Across submissions, details on the proportion of patients with Ph+ CML-CP were not identified consistently.
The CML Society of Canada highlighted the significant physical and emotional burden of CML, including stress, fatigue, pain, and sleep disturbances, which affect daily activities, work, and social life. Heal Canada noted that most patients were asymptomatic before diagnosis and that lifelong medication is often undesirable because many patients hope to discontinue treatment while maintaining remission. The joint submission emphasized the emotional toll of CML and the challenge of finding an effective treatment with manageable side effects. According to the patient group inputs, patients reported experience with various TKIs (e.g., bosutinib, dasatinib, imatinib), as well as other treatments such as allopurinol, bone marrow or stem cell transplant, chemotherapy, hydroxyurea, and radiation. Many patients undergo a trial-and-error process with their health care providers to identify the most suitable therapy. Commonly reported side effects of currently available treatments across submissions included fatigue; bone, joint, or muscle pain; diarrhea; headache; nausea; vomiting; sleep issues; reduced functional capabilities; emotional and mental health issues; reduced social relationships; reduced sexuality; and impacted cognitive functioning. The CML Society of Canada noted that patients who live in Ontario, Quebec, New Brunswick, Nova Scotia, Prince Edward Island, or Newfoundland and Labrador have challenges with treatment costs and must access their provincial reimbursement programs and/or access employer drug benefit plans.
Side effects experienced by patients treated with asciminib across submissions included cold-like symptoms; bone, joint, and muscle pain; brain fog; fatigue; headache; low blood cell count; and skin rash. Across submissions, patients who had experience with asciminib reported improved blood counts, reduced fatigue, and enhanced QoL, with milder side effects compared with other TKIs. Patients found asciminib easy to use, with fewer disruptions to their daily lives; those whose disease was resistant to or who were intolerant to other TKIs experiencing notable benefits. The CML Society of Canada highlighted the ability of asciminib to target a broader range of mutations, increasing the likelihood of achieving deep MR and improving patients’ QoL. The joint submission reported that more than half of respondents on asciminib experienced moderate to significant improvements in daily routines, half of the respondents experienced moderate to significant improvements in mental health, and nearly half noted benefits in personal and work life compared with other treatments.
Patients and caregivers prioritize treatments that improve symptom control, reduce side effects, and enhance QoL, even if some side effects must be managed. The joint submission emphasized the importance of having multiple treatment options, having data on long-term effects, and improved coordination of care because disconnection between different health care providers can lead to confusion about treatment options and the stress of navigating their health care by patients themselves. Key considerations when evaluating new therapies included QoL during treatment, the number and severity of side effects, and treatment convenience.
Heal Canada noted that with asciminib in the first line, treatment-free remission will be an option for more patients and significantly shorten the treatment duration; a shorter treatment duration means a lower treatment cost per patient, including a shorter TKI intake and fewer adverse reaction management costs. Fewer patients will have to switch to the second and third lines of treatment or receive a transplant, which can be costly, health care resource–intensive, and less efficient.
Clinician Input
Input From Clinical Experts Consulted for This Review
All CDA-AMC review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of CML.
Unmet Needs
The clinical experts noted that newer drugs have not been able to improve survival. Although the vast majority of patients who are managed properly and are adherent to therapy do well, there are patients whose disease does not respond or becomes refractory to therapy, according to the clinical experts. Nonadherence occurs due to a variety of reasons, including side effects that are not being addressed, patient age, and beliefs. The clinical experts also added that although newer drugs may not have the same side effects as older drugs, they come with their own set of unique side effects. The experts note that the more advanced the disease is, or the more advanced the disease becomes, the harder it is to control. They emphasized the importance of having many treatment options available to patients, with the ultimate goal of having the best response possible with the fewest side effects possible.
Place in Therapy
The CDA-AMC review team notes that the reimbursement request for this present file targets the newly diagnosed setting. One clinical expert noted that asciminib and other second-generation drugs may have better efficacy in patients with high Sokal risk scores (a score to assess prognosis and severity of disease); other considerations that determine choice of treatment include comorbidities.33 This clinical expert noted that some clinicians may use asciminib in the first line in patients with multiple comorbidities and in patients with high-risk features (i.e., high-risk group on any prognostic score model; the most commonly used tools being the ELTS and Sokal). The experts noted that if treatment-free remission is not the goal, it is unclear how aggressive one needs to be, considering that survival is more or less the same with all TKIs. In situations in which treatment-free remission is the goal, it is typically achieved with faster-acting or more potent drugs, and this in turn could lead to cost savings. The experts noted that if patients are to be on a treatment for the rest of their life, they likely prefer the treatment with the fewest side effects.
Patient Population
The clinical experts note that, at this time, there is insufficient evidence to conclusively predict which patients may experience a better response to asciminib than to the other available TKIs, adding that the patients most in need of intervention are those with multiple comorbidities that can make it difficult to use another TKI. One clinical expert noted that asciminib and other second-generation drugs may have better efficacy in patients with high Sokal risk scores (a score to assess prognosis and severity of disease); other considerations that determine choice of treatment include comorbidities.33
Assessing the Response to Treatment
One clinical expert emphasized that patients do not need to meet all their milestones to have a normal survival, adding that how a patient functions is often a mental state, influenced by their own psyche, coping skills, support structures, and philosophy of life. The other clinical expert noted that the objective outcome is reduction of the mutated BCR::ABL1 gene, and that improvement in these molecular markers can have an important impact on a patient’s mental health, and noted that MR has been used as an end point in clinical trials, in addition to QoL and freedom from symptoms, which for some patients is a very important outcome.
Discontinuing Treatment
The clinical expert noted that reasons for discontinuation would include disease progression or resistance, serious adverse effects that cannot be controlled, or if treatment-free remission data become available. The clinical expert added that other reasons for discontinuation could include a switch in drug therapy or a stem cell transplant (if necessary), as would cases in which the patient develops a separate terminal illness, making aggressive treatment of CML unnecessary.
Prescribing Considerations
The clinical expert highlighted the importance of having CML experts, or hematologists in consultation with CML experts, diagnosing and monitoring the disease due to its rarity and the expense of the drugs involved.
Clinician Group Input
This section was prepared by the review team based on the input provided by clinician groups.
Two clinician groups consisting of a total of 43 clinicians provided input for this review, including the Canadian CML Physicians Interest Group and the Ontario Health (Cancer Care Ontario) Hematology Cancer Drug Advisory Committee.
The Canadian CML Physicians Interest Group noted that the introduction of TKIs transformed CML from a fatal disease into a manageable chronic condition. Both submissions noted that in Canada, standard first-line treatment for CML-CP includes imatinib, dasatinib, nilotinib, and bosutinib, though access varies by province and territory. Additional TKIs like asciminib and ponatinib are approved for later lines of therapy, including for patients with the T315I mutation, which presents resistance to first-line options. The FDA has approved asciminib’s use in first-line therapy in the US while, in Canada, asciminib is indicated and funded only for patients with multiple TKI failures. Across the submissions, the main treatment goals for patients with CML-CP included prolonging survival, preventing disease progression to accelerated or blast phase CML, achieving response milestones (i.e., complete molecular remission, MMR, and deep MR), improving or maintaining QoL, improving blood counts, minimizing treatment-related toxicities, reducing splenomegaly and other disease symptoms, and offering eligible patients the opportunity to attempt treatment-free remission. For individual patients, treatment goals evolve over time and across lines of therapy but are based on patient- and disease-specific characteristics and preferences. The Canadian CML Physicians Interest Group noted that despite the transformative impact of TKI therapy in CML, treatment failure remains a persistent issue across all lines of therapy, leading to continued CML-related mortality. As such, the clinician groups noted there is a need for TKIs that are better tolerated, have superior efficacy, improved tolerability, and a more favourable toxicity profile. The Ontario Health (Cancer Care Ontario) Hematology Cancer Drug Advisory Committee noted that asciminib could be an option for first-line therapy and could become the standard of care for patients with CML. The Canadian CML Physicians Interest Group stated that recent studies on asciminib have proven its efficacy, safety, and tolerability beyond simply the third-line setting and recommended that asciminib be made available as a first-line and second-line treatment option for patients with CML-CP.
The Canadian CML Physicians Interest Group added that all CML-CP patients who fit the criteria for the ASC4FIRST trial in the first line and the ASC2ESCALATE trial in the second line are best suited for treatment with asciminib, and this is regardless of whether progression was caused by resistance, intolerance, or lack of response.
The Canadian CML Physicians Interest Group stated that most physicians in Canada follow the European LeukemiaNet guidelines for treatment decisions. Response assessment begins with baseline quantitative PCR and mutation testing if resistance is suspected. During the first 12 months of treatment, quantitative PCR is performed every 3 months, with treatment changes recommended for intolerance or unmet molecular milestones. After 12 months, BCR::ABL1 transcript levels are monitored every 3 to 6 months, with increased monitoring and mutation testing if response is lost. The input noted that BCR::ABL1 transcript levels serve as a surrogate marker for treatment efficacy and long-term survival, with lower levels linked to reduced progression risk and improved outcomes. Patients who experience a sustained MR4 or a deeper MR for at least 2 years may be eligible for treatment-free remission. Both inputs agreed that asciminib should be discontinued in cases of response failure (BCR::ABL1 transcript level > 10% at 3 or 6 months or > 1% at 12 months or later), persistent toxicity despite dose adjustments, or intolerance. Experienced hematologists should oversee initial treatment and early monitoring, while pharmacy and nursing teams can support oral medication management, AE monitoring, and treatment adherence. According to the clinical experts consulted by CDA-AMC, the use of asciminib should be restricted to settings in which all the required diagnostic tests have been performed and molecular monitoring is available.
Drug Program Input
The drug programs provide input on each drug being reviewed through the Reimbursement Review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by for this review are summarized in Table 5.
Table 5: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Relevant comparators | |
The ASC4FIRST trial compared asciminib with standard of care TKIs (i.e., imatinib, nilotinib, dasatinib, or bosutinib). Bosutinib is currently funded only in patients previously treated with TKI. Imatinib is a full benefit in some jurisdictions. Ponatinib is available after 2 or more TKIs or for T315i mutation–positive disease. | This is a comment from the drug programs to inform pERC deliberations. |
Considerations for initiation of therapy | |
The funding request and Health Canada–approved indication for asciminib is specifically for patients with CML-CP. Imatinib, nilotinib, dasatinib, and bosutinib are funded for CML in CP, AP, or BC. Should patients in AP or BC be eligible for asciminib? | The clinical experts noted that asciminib should be considered a viable treatment option for these patients when it is deemed the most appropriate choice for an individual patient, particularly given the precedent of using other drugs in this setting. However, the experts also note it is unclear whether asciminib would be more effective than any other treatment currently used for this patient population due to the lack of evidence in this specific population. The CDA-AMC review team notes that the Health Canada indication for the present file is limited to patients with Ph+ CML-CP. |
Patients were older than 18 years and had an ECOG score 0 to 1. Can patients with an ECOG score of 2 or greater receive treatment with asciminib? | The clinical experts agreed it would be reasonable to generalize the results of the ASC4FIRST trial to patients with an ECOG score of 2 or greater. |
Can asciminib be given again to patients who relapsed while off therapy? | In the absence of data to guide a firm recommendation, the clinical experts stated it may be reasonable to expect that asciminib could be given again to patients who relapsed while off therapy, based on data from other TKIs in comparable treatment settings. |
Ponatinib is considered for patients that are T315i mutation positive. Should patients with a T315i mutation be eligible for asciminib? | The ASC4FIRST trial excluded patients with T315i mutations. The clinical experts noted that patients with a T315i mutation should not be excluded from receiving asciminib. The clinical experts noted there is evidence (a phase I study34) to support asciminib’s activity in advanced lines in patients with T315i mutations; the experts felt there is no biological rationale to assume that asciminib in the first line in patients with T315i mutations would not have similar activity. One clinical expert added that having an alternative to ponatinib would be welcomed because it has some concerning long-term side effects (vascular and metabolic toxicities), and patients with T315i mutations have a poor prognosis. |
Considerations for prescribing of therapy | |
The recommended total daily dose is 80 mg, which can be taken orally either as 80 mg once daily at approximately the same time each day, or as 40 mg twice daily at approximately 12-hour intervals. | This is a comment from the drug programs to inform pERC deliberations. |
Generalizability | |
In the event of a positive funding recommendation, should patients receiving an alternative TKI be eligible to switch to asciminib when funding becomes available? | According to the clinical experts, for patients to be switched from 1 therapy to another, a valid clinical reason should be present, such as either treatment intolerance or treatment failure. |
Funding algorithm | |
Asciminib may change the place in therapy of comparator drugs. | This is a comment from the drug programs to inform pERC deliberations. |
This is a complex therapeutic space with multiple lines of therapy, subpopulations, and competing products. Under what clinical circumstances would asciminib be used over existing first-line drugs? | The clinical experts consulted by CDA-AMC agreed that asciminib constitutes another effective treatment option for patients in the first line. However, while it showed benefit compared with imatinib, comparison with 2G-TKIs was less certain; no head-to-head comparison against individual 2G-TKIs was available and the comparison against the mix of 2G-TKIs in the ASC4FIRST trial was not adjusted for multiple comparisons. The ASC4FIRST trial compared asciminib against a basket of 2G-TKIs with heterogenous adverse event profiles and treatment doses that were in line with the product monograph but likely higher than commonly used in clinical practice. It was unclear whether the safety differences between asciminib and 2G-TKIs were driven by a specific TKI within that group. The clinicians noted that while asciminib’s adverse events profile appeared manageable overall, its long-term safety was unknown. The choice to use asciminib in the first line would be a patient-centred choice based on patient- and disease-specific characteristics and preferences. One clinical expert noted that, based on the available evidence, asciminib may not meet any unmet needs when compared with existing treatments. The other clinical expert noted that asciminib may be a preferred option in the first line in patients with multiple comorbidities (e.g., pulmonary hypertension, cardiovascular disease, bleeding) who cannot tolerate other TKIs. This expert also noted that asciminib’s safety profile (less pulmonary and vascular toxicity) may make it a preferable option for patients with high-risk features (i.e., in a high-risk group within a prognostic score model, the most commonly used tools being the ELTS and Sokal). |
Care provision issues | |
Asciminib is associated with potential drug–drug, drug–food, and drug–herb interactions. | This is a comment from the drug programs to inform pERC deliberations. |
System and economic issues | |
There is confidential pricing for bosutinib, and nilotinib, dasatinib, and imatinib, which are available as generics. | This is a comment from the drug programs to inform pERC deliberations. |
2G-TKI = second-generation tyrosine kinase inhibitor; AP = accelerated phase; BC = blast crisis; CDA-AMC = Canada’s Drug Agency; CML = chronic myeloid leukemia; CML-CP = chronic myeloid leukemia in chronic phase; CP = chronic phase; ECOG = Eastern Cooperative Oncology Group; ELTS = European Treatment and Outcome Study long-term survival; pERC = pan-Canadian Oncology Drug Review Expert Review Committee; TKI = tyrosine kinase inhibitor.
Clinical Evidence
The objective of this Clinical Review report is to review and critically appraise the clinical evidence submitted by the sponsor on the beneficial and harmful effects of asciminib (20 mg and 40 mg oral film-coated tablets) in the treatment of adults with newly diagnosed Ph+ CML-CP. The focus will be placed on comparing asciminib to relevant comparators and identifying gaps in the current evidence.
A summary of the clinical evidence included by the sponsor in the review of asciminib is presented in 4 sections with the CDA-AMC critical appraisal of the evidence included at the end of each section. The first section, the systematic review, includes pivotal studies and RCTs that were selected according to the sponsor’s systematic review protocol. The CDA-AMC assessment of the certainty of the evidence in this first section using the GRADE approach follows the critical appraisal of the evidence. The sponsor did not submit long-term extension studies, indirect evidence, or additional studied addressing important gaps in the systematic review evidence.
Included Studies
Clinical evidence from the following are included in the review and appraised in this document:
1 pivotal study identified in systematic review.
Systematic Review
Contents within this section have been informed by materials submitted by the sponsor. The following has been summarized and validated by the review team.
Description of Studies
ASC4FIRST is an ongoing multicentre, open-label, randomized, phase III study. The primary end points of the ASC4FIRST trial were to compare the efficacy of asciminib with IS-TKIs and imatinib (selected prerandomization), in terms of the proportion of patients experiencing an MMR at week 48. The study was to be declared positive if it met either of the 2 primary objectives. Key secondary end points compared the efficacy of asciminib versus IS-TKIs and imatinib based on the proportion of participants with an MMR at week 96. Time to discontinuation of study treatment due to AEs for asciminib versus second-generation TKIs was designated a secondary outcome. The overall safety objective was to characterize the safety and tolerability profile of asciminib compared with IS-TKIs and second-generation TKIs.
The study consisted of a 21-day screening period followed by a treatment duration of 5 years with end points assessed at 48 weeks (analysis of primary outcomes), 96 weeks (analysis of key secondary outcomes), and after 5 years (final analysis). Participants who discontinued study treatment prematurely due to any reason were followed up for survival and progression (to the accelerated phase or a blast crisis) until the end of study. A total of 475 patients were screened and 405 males and females aged 18 years or older diagnosed with CML-CP within 3 months were enrolled in 116 sites across 29 countries, including 4 sites in Canada. Eligible patients were randomized 1:1 to receive either asciminib 80 mg or an IS-TKI (imatinib 400 mg, nilotinib 300 mg, dasatinib 100 mg, or bosutinib 400 mg). Randomization was stratified into 6 groups based on 2 stratification factors at screening: ELTS score (low versus intermediate versus high) and prerandomization selection of TKI (imatinib versus second-generation TKIs). No crossover of patients between study groups and no change of study treatment within an IS-TKI group were permitted. The data cut-off dates were November 28, 2023, and October 22, 2024, for the 48-week and 96-week analyses, respectively. The study is still ongoing, and a final analysis will be performed once the end of the study (i.e., 5 years from the last patient's first treatment date in the study) is reached. This CDA-AMC Clinical Review report presents data based on the week 48 and week 96 assessments.
Study details and the study design of the ASC4FIRST trial are described in Table 6 and Figure 1.
Table 6: Details of Studies Included in the Systematic Review
Detail | ASC4FIRST trial |
|---|---|
Designs and populations | |
Study design | Phase III, multicentre, open-label, randomized trial |
Locations | Number of sites: 116 in 29 countries Countries and regions where the trial was conducted: Australia, Austria, Belgium, Bulgaria, Canada, China, Czechia, Denmark, Finland, France, Germany, Hungary, India, Israel, Italy, Japan, Republic of Korea, Malaysia, Netherlands, Norway, Portugal, Singapore, Slovakia, Spain, Sweden, Switzerland, Taiwan, UK, US |
Patient enrolment dates | Start date: November 5, 2021 End date: December 5, 2022 |
Randomized (N) | N = 405:
|
Inclusion criteria |
|
Exclusion criteria |
|
Drugs | |
Intervention | Asciminib 80 mg orally, once daily administered under fasting conditions |
Comparators |
|
Study duration | |
Screening phase | 21 days |
Treatment phase | Last patient, first treatment plus 5 years |
Follow-up phase | 5-year planned follow-up |
Outcomes | |
Primary end point |
|
Secondary and exploratory end points | Secondary:
Exploratory:
|
Publication status | |
Publications | Publications:
WHO ICRTP entries:
Health Canada's Clinical Trials Database entry: Novartis Pharmaceuticals Canada Inc. A Phase III, Multi-Center, Open-Label, Randomized Study of Oral Asciminib versus Investigator Selected TKI in Patients with Newly Diagnosed Philadelphia Chromosome Positive Chronic Myelogenous Leukemia in Chronic Phase. [Internet] Available from: https://health-products.canada.ca/ctdb-bdec/brand/?submissionNo=255554 ClinicalTrials.gov entry: Novartis Pharmaceuticals. A Study of Oral Asciminib versus Other TKIs in Adult Patients with Newly Diagnosed Ph+ CML-CP. [Internet]. ClinicalTrials.gov. 2024. Available from: https://clinicaltrials.gov/study/NCT04971226 Novartis internal sources:
|
AUClast = area under the curve to the last measurable concentration; AUCtau = area under the curve over the dosing interval; AV = atrioventricular; CCyR = complete cytogenetic response; CHR = complete hematologic response; CL/F = clearance/fraction bioavailable; Cmax = maximum concentration; CML = chronic myeloid leukemia; CML-CP = chronic myeloid leukemia in chronic phase; CTCAE = Common Terminology Criteria for Adverse Events; ECG = electrocardiogram; ECOG = Eastern Cooperative Oncology Group; ELN = European LeukemiaNet; ELTS = European Treatment and Outcome Study long-term survival; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; FACIT-GP5 = Functional Assessment of Chronic Illness Therapy–General Population item 5; IS-TKI = investigator-selected tyrosine kinase inhibitor; MMR = major molecular response; MR4 = molecular response with a 4-log or greater reduction in BCR::ABL1 transcripts; MR4.5 = molecular response with a 4.5-log or greater reduction in BCR::ABL1 transcripts; PK = pharmacokinetic; PRO = patient-reported outcome; QTc = corrected QT interval; QTcF = Fridericia corrected QT interval formula; TKI = tyrosine kinase inhibitor; Tmax = time to maximum concentration; TTDAE = time to treatment discontinuation due to adverse event.
Source: Details included in the table are from the sponsor’s summary of clinical evidence.
Figure 1: Study Design of the Phase III ASC4FIRST Trial
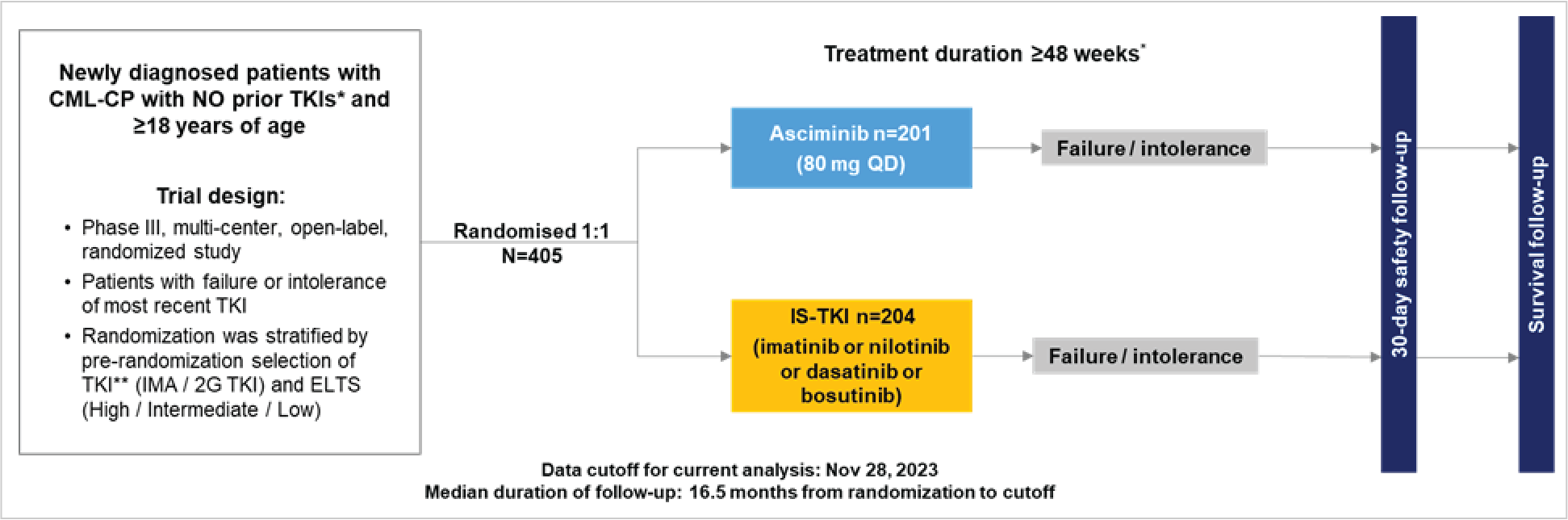
2G TKI = second-generation tyrosine kinase inhibitor; CML = chronic myeloid leukemia; CML-CP = chronic myeloid leukemia in chronic phase; ELTS = European Treatment and Outcome Study long-term survival score; IMA = imatinib; IS-TKI = investigator-selected tyrosine kinase inhibitor; TKI = tyrosine kinase inhibitor.
Note: The analysis data cut-off dates for the planned analyses were week 48 for the primary analysis, a week 96 analysis, and the final analysis.
* Imatinib, nilotinib, dasatinib, or bosutinib for ≤ 2 weeks was allowed. No other treatment with TKIs before randomization was permitted.
** Before randomization, the investigator, in consultation with the patient, and considering the current treatment paradigm and patient characteristics and comorbidities, made a preference selection for imatinib or a second-generation TKI if the patient had been randomized to the comparator arm. The selection was to be made as close as possible to the randomization date once all relevant clinical information became available.
Source: Novartis (2022) Clinical Study Report.35
Populations
Inclusion and Exclusion Criteria
Key inclusion and exclusion criteria are summarized in Table 6. Adult patients with a new diagnosis of Ph+ CML-CP within 3 months before enrolment according to ELN 2020 criteria were eligible for inclusion. Previous treatment with hydroxyurea, anagrelide, or both was permitted. Treatment with imatinib, nilotinib, dasatinib, or bosutinib for 2 weeks or less before randomization was also permitted. Evidence of BCR::ABL1 transcript was required at time of screening. Eligible patients were required to have a European Cooperative Oncology Group Performance Status of 0 to 1. Patients were excluded if they had received treatment with any other anticancer drug for disease control before randomization, including chemotherapy and/or biological drugs or a prior stem cell transplant.
Interventions
In the ASC4FIRST trial, treatment will be administered for 5 years. Treatment with asciminib 80 mg is administered to patients orally once daily under fasting conditions. Imatinib 400 mg and bosutinib 400 mg are administered orally once daily with food. Dasatinib 100 mg is administered orally once daily with or without food. Nilotinib 300 mg is administered orally twice daily under fasting conditions. For participants who did not tolerate the protocol-specified asciminib dosing schedule, dose interruptions, and/or reductions were either recommended or mandated to allow participants to continue the study treatment. Dose modifications of the IS-TKI were at the investigator's discretion and in accordance with institutional practice and local labels.
Concomitant medications and therapies deemed necessary for the supportive care and safety of the participants were allowed. Concomitant use of hydroxyurea for urgent control of high cell counts during the first 2 weeks of study treatments was allowed. The use of bisphosphonates, regardless of indication, and anticancer treatments of newly diagnosed solid cancers that would not impact the level of minimal residual disease of participants was allowed. Use of cytochrome P (CYP) 3A4/5 and CYP2C9 substrates with narrow therapeutic index, strong CYP3A4 inducers, substrates of organic anion transporter polypeptide (OATP)1B, breast cancer resistant protein (BCRP) or both transporters, and drugs with “known risk,” “possible risk,” or “conditional risk of Torsades de pointes” were allowed with caution and with close monitoring to ensure participants’ safety.
Treatment is to be discontinued when the trial participant (or their guardian) asks to discontinue treatment or has used a prohibited treatment, or in any situation in which continued study participation might result in a safety risk to the participant. In addition to the general discontinuation criteria, the following study-specific criteria also required discontinuation of study treatment:
detection of a T315I mutation at any time
confirmed loss of MMR (in 2 consecutive tests) at any time during the study treatment
treatment failure, which was defined as per Hochhaus A. et al. (2020)22 (i.e., a BCR::ABL1 transcript level greater than 10% at 3 months)
disease progression
pregnancy during the study; if a participant wanted to pursue the pregnancy, then they were to discontinue from the study treatment; however, in the event of a spontaneous miscarriage or an elective abortion, the participant was permitted to continue study treatment.
Discontinuation from study occurred when the participant permanently stopped receiving the study treatment and further protocol-required assessments or follow-up, for any reason. If the participant agreed, a final evaluation at the time of the participant’s study discontinuation was made.
Outcomes
A list of efficacy end points assessed in this Clinical Review report is provided in Table 7, followed by descriptions of the outcome measures. Summarized end points are based on outcomes included in the sponsor’s summary of clinical evidence as well as any outcomes identified as important to this review according to the clinical experts consulted for this review and input from patient and clinician groups and public drug plans. Using the same considerations, CDA-AMC selected end points that were considered to be most relevant to inform expert committee deliberations and finalized this list of end points in consultation with members of the expert committee. The outcomes rated most important by the clinical experts consulted for this review, patient and clinical group input, and public drug plan input were assessed using GRADE.
The following outcomes were assessed using GRADE: Proportion of patients experiencing an MMR at 48 weeks, proportion of patients experiencing an MR2 at 48 weeks, and the change from baseline to 96 weeks in the EORTC QLQ-C30 GHS. Select notable harms outcomes considered important for informing expert committee deliberations were also assessed using GRADE, specifically, patients with acute clinical pancreatitis and patients with an ischemic event (acute cardiac or CNS). These outcomes were deemed the most important for determining the comparative efficacy and safety of asciminib compared with the currently available therapies. Molecular outcomes are important for the assessment of treatment response and in CML, as per the clinical experts consulted for this review as well as treatment guidelines.22 MMR at 48 weeks was chosen as an outcome for GRADE because it was the primary outcome of the ASC4FIRST trial. MR2 was chosen because of its relevance in achieving treatment outcomes, as noted by the clinical experts consulted for this review. The 48-week time point for MR2 was chosen for the GRADE assessment to be consistent with the time point for the primary outcome. The clinical experts agreed that the most important harms to assess were acute pancreatitis (clinical) and ischemic events (cardiac and/or CNS).
Other outcomes are summarized in the CDA-AMC Clinical Review report to provide further context but were not appraised using GRADE (refer to Table 7). The EORTC QLQ-C30 was appraised using GRADE because it is a generic measure that provides a comprehensive picture of a patient’s HRQoL. The EORTC QLQ-CML24 focuses on CML cancer–specific symptoms and results are reported in the main section of this report. Health care resource utilization was used in the submitted economic model and has been summarized in the main section of this report.
Table 7: Efficacy Outcomes Summarized From the Studies Included in the Systematic Review
Outcome measure | Time point | ASC4FIRST trial | Assessed with GRADE |
|---|---|---|---|
Proportion of the patients with MMR; versus IS-TKIs | Week 48 | Coprimary | Yes |
Proportion of patients with MMR versus imatinib | Week 48 | Coprimary | Yes |
Proportion of patients who are in MMR versus IS-TKIs | Week 96 | Key secondary | No |
Proportion of patients with MMR versus imatinib | Week 96 | Key secondary | No |
Proportion of patients with MMR versus second-generation TKIs | Weeks 48 and 96 | Other secondary | No |
Proportion of patients experiencing MR2 at scheduled data collection time points (week 4, 8, 12, 24, 36, 48, 96) | Week 48 | Other secondary | Yes |
Week 96 | No | ||
Proportion of patients who experienced MR4 at scheduled time points (week 4, 8, 12, 24, 36, 48, 96) | Weeks 48 and 96 | Other secondary | No |
Proportion of patients who experienced MR4.5 at scheduled time points (week 4, 8, 12, 24, 36, 48, 96) | Weeks 48 and 96 | Other secondary | No |
Duration of MMR | Week 96 | Other secondary | No |
Time to first MMR | Week 12 and 48 | Other secondary | No |
Overall survival | Week 96 | Other secondary | No |
EORTC QLQ C30 global health status | Week 48 | Other secondary | No |
Week 96 | Yes | ||
EORTC QLQ-CML24 | Week 48 Week 96 | Other secondary | No |
EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EORTC QLQ-CML24 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire – Chronic Myeloid Leukemia 24; GRADE = Grading of Recommendations Assessment, Development and Evaluation; IS-TKI = investigator-selected tyrosine kinase inhibitor; MMR = major molecular response; MR2 = molecular response with a 2-log or greater reduction in BCR::ABL1 transcripts; MR4 = molecular response with a 4-log or greater reduction in BCR::ABL1 transcripts; MR4.5 = molecular response with a 4.5-log or greater reduction in BCR::ABL1 transcripts; TKI = tyrosine kinase inhibitor.
Source: Details included in the table are from the sponsor’s summary of clinical evidence.
Molecular Response
MMR was defined as a 3.0-log or greater reduction in BCR::ABL1 transcripts compared with the standardized baseline equivalent to a 0.1% or less BCR::ABL1 to ABL1 ratio percentage according to the International Scale as measured by reverse transcriptase quantitative PCR and confirmed by a duplicate analysis of the same sample.
MR2 was defined as a 2-log or greater reduction in BCR::ABL1 transcripts compared with the standardized baseline equivalent to a BCR::ABL1 to ABL1 ratio percentage of 1% or less according to the International Scale.
MR4 was defined as a 4-log or greater reduction in BCR::ABL1 transcripts compared with the standardized baseline equivalent to a 0.01% or less BCR::ABL1 to ABL1 ratio percentage according to the International Scale.
MR4.5 was defined as a 4.5-log or greater reduction in BCR::ABL1 transcripts compared with the standardized baseline equivalent to a 0.0032% or less BCR::ABL1 to ABL1 ratio percentage according to the International Scale.
Duration of MMR
Defined as the time from the date of first documented MMR to the earliest date of loss of MMR, treatment failure per ELN criteria, progression to accelerated phase, blast phase, or CML-related death.
Time to First MMR
Defined as the time from the date of randomization to the date of the first documented MMR.
Overall Survival
OS was defined as the time from the date of randomization to the date of death from any cause (including deaths observed during the survival follow-up period). For patients that had not experienced an event before or at the analysis cut-off date, the time was censored at the date of last contact before the cut-off date.
EORTC QLQ-C30 and QLQ-CML24
The EORTC QLQ-C30 is a validated questionnaire developed to assess the QoL of cancer patients and used frequently in cancer clinical trials.36 The questionnaire contains 30 items and is composed of both multi-item scales and single-item measures based on the participant's experience over the past week. These include 5 functional scales (physical, role, emotional, cognitive, and social functioning), 3 symptom scales (fatigue, nausea/vomiting, and pain), 6 single items (dyspnea, insomnia, appetite loss, constipation, diarrhea, and financial impact) and a GHS or QoL scale. All of the scales and single-item measures are standardized to range in score from 0 to 100. A higher score represents a higher response level. Thus, a high score for a functional scale represents a high or healthy level of functioning; a high score for GHS or QoL represents a high QoL, but a high score for a symptom scale or item represents a high level of symptomatology or problems. All scoring follows the scoring procedures defined by the EORTC scoring manual. The EORTC QLQ-CML24 assesses specific concepts relevant to the experience of patients with CML. The QLQ-CML24 has 24 items that assess symptom burden and impact on daily life and on worry or mood, body image problems, and satisfaction with care and social life based on the participant’s experience over the past week. The QLQ-CML24 items are scored on a 4-point Likert scale, with a range of “not at all” to “very much.”
Table 8: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
EORTC QLQ-C30 | A multidimensional, cancer-specific, patient-reported measure used to assess HRQoL in response to treatment in clinical trials.36 The core questionnaire consists of 30 items that make 5 multi-item functional scales: physical (5 items), role (2 items), emotional (4 items), cognitive (2 items), and social functioning (2 items); 3 multi-item symptom scales: fatigue (3 items), nausea/vomiting (2 items), and pain (2 items); 6 single-item symptom scales (dyspnea, insomnia, appetite loss, constipation, diarrhea, and financial impact), and a 2-item global QoL scale. Patients complete the questionnaire based on a 1-week recall period by rating most items on a 4-point Likert-type scale (1 = not at all, 2 = a little, 3 = quite a bit, 4 = very much). For the 2 items in the global QoL scale, the response format is a 7-point Likert-type scale (1 = very poor; 7 = excellent).37 Raw scores for each scale are computed as the average of the items that contribute to a particular scale. Each raw scale score is converted to a standardized score that ranges from 0 to 100 using a linear transformation. A decline in the symptom scale score reflects an improvement, whereas an increase in the function and QoL scale scores reflect an improvement.37 According to the EORTC QLQ-C30 scoring algorithm, if there are missing items for a scale, the score for that scale can still be computed if there are responses for at least one-half of the items. In calculating the scale score, missing items are ignored.37 | The psychometric properties of the EORTC QLQ-C30 were evaluated in the validation study in which patients with cholangiocarcinoma and gallbladder cancer were enrolled.38 Validity: All items demonstrated item-scale convergence (construct) validity (Pearson r > 0.4, prespecified). Although the study authors stated that a known-group comparison was performed for the EORTC QLQ-C30, the results were not reported. Reliability: Internal consistency was acceptable (alpha ≥ 0.70) for all scales, except for the physical function (alpha = 0.47), cognitive function (alpha = 0.65), and nausea/vomiting (alpha = 0.67) scales at baseline. Test–retest reliability was demonstrated by the ICCs that ranged from 0.52 to 0.92 in 67 patients with clinically stable disease across all intervention groups over 2 weeks.a Responsiveness: Although the study stated that responsiveness of the EORTC QLQ-30 to clinical change over time was measured, results were not reported. | MIDs for other types of cancers:39 The between-group MID for improvement and deterioration ranged from 5 to 10 points across most scales:
|
EORTC QLQ-CML24 | To assess QoL in adults with CML. Designed to be used in conjunction with the EORTC QLQ-C30. A 24-item questionnaire with the following domains:
Scored on a 4-point Likert or Likert-type scale ranging from 1 (not at all) to 4 (very much). Higher scores indicate worse outcomes (i.e., high symptom burden, high impact on worry/mood, high impact on daily life, and higher problems with body image). Higher scores indicate better outcomes (i.e., higher levels of satisfaction with care and information and with social life).40 | The psychometric properties of the EORTC QLQ-CML24 were evaluated in the validation study in which patients with CML patients were enrolled40,41 In general, convergent validity was demonstrated with item scales correlations between −0.34 and 0.6241 and −0.69 to 0.65.40 Known-group comparison: Patients without comorbidities and better ECOG Performance Status (ECOG = 0), and patients treated with imatinib (second or third generation) compared with first generation reported better quality of life.41 Reliability: Internal consistency ranged from a Cronbach alpha of 0.66 to 0.83.41 Test–retest reliability was demonstrated by the ICCs, which ranged from 0.66 to 0.83.41 Changes in scores indicate that the instrument is responsive to clinically meaningful deterioration and improvement, respectively, in the EORTC QLQ-C30 global health status (quality of life) scale. There was no statistical difference in scores based on CCyR achievement.41 | MID not identified for EORTC QLQ-CML24 |
CCyR = complete cytogenetic response; CML = chronic myeloid leukemia; ECOG = Eastern Cooperative Oncology Group; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; QLQ-CML24 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire – Chronic Myeloid Leukemia 24; HRQoL = health-related quality of life; ICC = intraclass correlation coefficient; MID = minimal important difference; QoL = quality of life.
aPatients who received IV chemotherapy at the time were excluded from the test–retest assessment.
Statistical Analysis
Sample Size and Power Calculation
Based on a 1-sided 2.5% level of significance, with 402 participants and a 1:1 randomization ratio between arms, and with 50% in the imatinib stratum (i.e., 201 participants in the asciminib arm and 201 participants in the IS-TKI arm), there is 94.6% power to reject at least 1 of the null hypotheses from the coprimary outcomes. For the overall population, the null hypothesis was that the proportion of participants who experienced an MMR at week 48 in the asciminib arm is less than or equal to the proportion of participants who experienced an MMR at week 48 in the IS-TKI arm. Within the stratum of participants who have imatinib as their prerandomization selection of TKI, the null hypothesis was that the proportion of participants who experience an MMR at week 48 in the asciminib arm is less than or equal to the proportion of participants who experience an MMR at week 48 in the IS-TKI arm. At this sample size, the local power to reject the null hypothesis for the overall population is 88.5% and local power to reject the null hypothesis for the imatinib stratum is 92.7%.
Statistical Test or Model
The primary efficacy analysis was performed using the FAS. Following the intent-to-treat principle, participants were analyzed according to the treatment arm and stratum they were assigned to at randomization. The null hypothesis was tested using a 1-sided Cochrane-Mantel-Haenszel (CMH) chi-square test stratified by both randomization stratification factors, the ELTS risk score and pretreatment risk score for the TKI. The secondary efficacy analysis was performed using the FAS imatinib stratum, in which the null hypothesis was tested using a 1-sided CMH chi-square test stratified by the randomization stratification factor ELTS risk score.
Multiple Testing Procedure
The familywise type I error rate was controlled at a 2.5% level via the graphical gatekeeping procedure. The null hypothesis was rejected if the 1-sided P value was less than the nominal alpha level as specified. The point estimates and their corresponding 95% CIs were calculated using the Clopper-Pearson method.
The key secondary end points for the 2 key secondary objectives of the study were defined as the binary outcome (yes or no) of whether a participant is in MMR at week 96. The testing of the key secondary end points was conducted only if the null hypothesis associated with the second primary objective was rejected.
The secondary safety end point, time to discontinuation of study treatment due to AEs for asciminib versus second-generation TKIs, was planned to be tested at week 96 if the null hypotheses for both secondary objectives are rejected.
Data Imputation Methods
Data imputation methods are described in Table 9.
Subgroup Analyses
Prespecified subgroup analyses were to be conducted for the primary and key secondary efficacy end points, MMR at week 48 and MMR at week 96, based on the FAS, imatinib stratum FAS, and second-generation TKI FAS, to examine the homogeneity of treatment effect, provided that the respective primary or key secondary efficacy analysis based on the FAS or imatinib stratum FAS was statistically significant.
Subgroup analyses were conducted by ELTS (low versus intermediate versus high) based on randomization data from interactive response technology, ELTS based on data collected on the electronic case report form, sex, race (Asian, white, or other), and age groups (18 years to younger than 65 years, 65 years to younger than 75 years, and 75 years or older).
No formal statistical test of hypotheses was performed for the subgroups.
Sensitivity Analyses
A description of the sensitivity analyses is provided in Table 9.
Table 9: Statistical Analysis of Efficacy End Points in the ASC4FIRST Trial
End point | Statistical model | Adjustment factors | Handling of missing data | Sensitivity analyses |
|---|---|---|---|---|
Proportion of patients in MMR at week 48 (yes or no) | A 1-sided CMH chi-square test | Stratified by ELTS risk score and PRS-TKI | Participants with missing PCR evaluation at week 48 visit will be imputed as MMR responders if they have nonmissing PCR evaluations at both the week 36 and week 60 visits, and both meet the MMR criteria, assuming that MMR is maintained between week 36 and week 60. If PCR evaluations are performed at unscheduled visits closer to the week 48 visit (before or after), these will be taken into account for the imputation; otherwise, participants with missing PCR evaluations at week 48 will be considered nonresponders. | The CMH chi-square test of MMR rate at 48 weeks was repeated without the imputation rule used in the main primary analyses for participants who have missing PCR evaluations at 48 weeks. In such cases, these participants are considered nonresponders for the end point MMR at week 48. |
Proportion of patients in MMR at week 96 (yes or no) | Similar to the model used for the primary outcome (i.e., the proportion of patients in MMR at week 48) | Similar to the factors used for the primary outcome (i.e., the proportion of patients in MMR at week 48) | Similar to how data were handled for the primary outcome (i.e., the proportion of patients in MMR at week 48) | Similar to the sensitivity analyses for the primary outcome (i.e., the proportion of patients in MMR at week 48) |
The time from the date of FD to the date of discontinuation of study treatment due to AE, including death due to AE (TTDAE) | The stratified log-rank test | The stratification factor is the ELTS category | NR | NR |
AE = adverse event; CMH = Cochran-Mantel-Haenszel; ELTS = European Treatment and Outcome Study long-term survival; FD = first dose; MMR = major molecular response; NR = not reported; PCR = polymerase chain reaction; PRS-TKI = pretreatment risk score for tyrosine kinase inhibitor; TTDAE = time to treatment discontinuation due to adverse event.
Source: Details included in the table are from the sponsor’s summary of clinical evidence.
Analysis Populations
The analysis populations of the ASC4FIRST study are summarized in Table 10.
Table 10: Analysis Populations
Population | Definition | Application |
|---|---|---|
FAS (N = 405) | The FAS includes all participants whose study treatment was assigned by randomization. | All efficacy analyses |
Imatinib FAS (N = 203) | Includes all participants from the FAS whose prerandomization TKI selection was imatinib. | Efficacy analyses |
2G-TKI FAS (N = 202) | Includes all participants from the FAS whose prerandomization TKI selection was a 2G-TKI (nilotinib, dasatinib, or bosutinib). | Efficacy analyses |
Safety set (N = 401) | The safety set comprises all participants who receive at least 1 dose of any study treatment. Participants were analyzed according to the actual study treatment received. Actual treatment received was defined as the randomized treatment if the participant took at least 1 dose of that treatment, or the first treatment received if the randomized treatment was never received. | All safety analyses |
2G-TKI = second-generation tyrosine kinase inhibitor; FAS = full analysis set; TKI = tyrosine kinase inhibitor.
Source: Details included in the table are from the sponsor’s summary of clinical evidence.
Results
Patient Disposition
A summary of patient disposition in the ASC4FIRST study is provided in Table 11.
There were 36 patients (18%) in the asciminib group and 78 patients (38%) in the IS-TKI group who discontinued the study drug. There were differences in the proportion of patients who discontinued treatment in the imatinib stratum compared with the second-generation TKI stratum. In the imatinib stratum, 17 patients (17%) discontinued treatment in the asciminib group compared with 47 patients (46%) in the IS-TKI group; in the second-generation stratum, the proportions were 19 (19%) and 31 (30%), respectively. The most common reasons for discontinuation of the study drug were unsatisfactory therapeutic effect, reported in 19 patients (10%) in the asciminib group and 42 patients (21%) in the IS-TKI group, followed by treatment failure, reported in 10 patients (5%) in the asciminib group and 28 patients (14%) in the IS-TKI group. There were 12 patients (6%) who discontinued the study in the asciminib group and 19 patients (9%) who discontinued the study in the IS-TKI group. The difference between the asciminib group and the IS-TKI group was more pronounced in the imatinib stratum, with 8 patients (8%) discontinuing versus 29 patients (28%), respectively. In the second-generation stratum, 11 patients (11%) in the asciminib group versus 13 patients (3%) in the IS-TKI group discontinued for unsatisfactory therapeutic effect.
Table 11: Summary of Patient Disposition From the ASC4FIRST Trial
Patient disposition | Asciminib | IS-TKIs | ||||
|---|---|---|---|---|---|---|
Imatinib stratum (N = 101) | 2G-TKI stratum (N = 100) | All asciminib 80 mg (N = 201) | Imatinib stratum (N = 102) | 2G-TKI stratum (N = 102) | IS-TKIs (N = 204) | |
Screened, N | 475 | |||||
Completed screening phase, randomized, n (%) | 405 (85) | |||||
Did not complete screening, n (%) | 70 (15) | |||||
Randomized, N (%) | 101 (100) | 100 (100) | 201 (100) | 102 (100) | 102 (100) | 204 (100) |
Randomized and treated | ||||||
Number (%) | 100 (99) | 100 (100) | 200 (99.5) | 100 (98) | 101 (99) | 201 (99) |
Randomized and not treated | ||||||
Number (%) | 1 (1.0) | 0 | 1 (0.5) | 2 (2.0) | 1 (1.0) | 3 (2) |
Reason for not being treated, n (%) | ||||||
Patient decision | ████ | ████ | ████ | ████ | ████ | ████ |
Adverse event | ████ | ████ | ████ | ████ | ████ | ████ |
Screen failure | ████ | ████ | ████ | ████ | ████ | ████ |
Treatment ongoing | ████ | ████ | ████ | ████ | ████ | ████ |
Discontinued from treatment | ||||||
Number, (%) | ████ | ████ | ████ | ████ | ████ | ████ |
< week 48 | ████ | ████ | ████ | ████ | ████ | ████ |
≥ week 48 and < week 96 | ████ | ████ | ████ | ████ | ████ | ████ |
≥ week 96 | ████ | ████ | ████ | ████ | ████ | ████ |
Reason for discontinuation, n (%) | ||||||
Unsatisfactory therapeutic effect | 8 (8) | 11 (11) | 19 (10) | 29 (28) | 13 (13) | 42 (21) |
Treatment failure per ELN | 6 (6) | 4 (4) | 10 (5) | 19 (19) | 9 (9) | 28 (14) |
Confirmed loss of MMR | 2 (2) | 2 (2) | 4 (2) | 2 (2) | 1 (1.0) | 3 (2) |
Other | 0 | 5 (5) | 5 (3) | 8 (8) | 3 (3) | 11 (5) |
Adverse event | 6 (6) | 6 (6) | 12 (6) | 13 (13) | 13 (13) | 26 (13) |
Progressive disease | 2 (2) | 0 | 2 (1.0) | 3 (3) | 1 (1.0) | 4 (2) |
Protocol deviation | 0 | 1 (1.0) | 1 (0.5) | 1 (1.0) | 1 (1.0) | 2 (1.0) |
Patient decision | 1 (1.0) | 0 | 1 (0.5) | 1 (1.0) | 1 (1.0) | 2 (1.0) |
Pregnancy | 0 | 1 (1.0) | 1 (0.5) | 1 (1.0) | 2 (2.0) | 3 (2) |
Discontinued from study | ||||||
Number (%) | ████ | ████ | ████ | ████ | ████ | ████ |
Reason for discontinuation, n (%) | ████ | ████ | ████ | ████ | ████ | ████ |
FAS, N | 101 | 100 | 201 | 102 | 102 | 204 |
Imatinib FAS, N | 101 | 0 | 101 | 102 | 0 | 102 |
2G-TKI FAS, N | 0 | 100 | 100 | 0 | 102 | 102 |
PP, N | NR | NR | NR | NR | NR | NR |
Safety, N | 100 | 100 | 200 | 99 | 102 | 201 |
2G-TKI = second-generation tyrosine kinase inhibitor; ELN = European Leukemia Network; FAS = full analysis set; IS-TKI = investigator-selected tyrosine kinase inhibitor; MMR = major molecular response; NR = not reported; PP = per protocol.
Source: Details included in the table are from the sponsor’s summary of clinical evidence.
Baseline Characteristics
The baseline characteristics outlined in Table 12 are limited to those that are most relevant to this review or were noted by the clinical experts to affect the outcomes or interpretation of the study results.
Patients in the imatinib stratum were older than patients in the second-generation stratum. The median age of patients in the imatinib stratum was 56 years (range, 21 to 79 years) in the asciminib group and 54.5 years (range, 20 to 86 years) in the control group, and in the second-generation stratum was 43 years (range, 18 to 76 years) in the asciminib group and 43 years (range, 19 to 83 years) in the control group. The majority of patient s (54%) had a Framingham risk score of “low” across all groups; however, the percentage of patients who were low risk was lower in the imatinib stratum (40%) than in the second-generation TKI stratum (68%). The majority of patients (61%) had an ELTS score of “low,” and this was consistent across strata.
Table 12: Summary of Baseline Characteristics From the ASC4FIRST Trial
Characteristic | Asciminib group | IS-TKI group | ||||
|---|---|---|---|---|---|---|
Imatinib stratum (n = 101) | 2G-TKI stratum (n = 100) | Asciminib 80mg (N = 201) | Imatinib stratum (n = 102) | 2G-TKI stratum (n = 102) | IS-TKIs (N = 04) | |
Age, median (range), years | 56.0 (21.0 to 79.0) | 43.0 (18.0 to 76.0) | 52.0 (18.0 to 79.0) | 54.5 (20.0 to 86.0) | 43.0 (19.0 to 83.0) | 50.5 (19.0 to 86.0) |
Age group, n (%) | ||||||
18 to < 65 years | 69 (68) | 86 (86) | 155 (77) | 70 (69) | 85 (83) | 155 (76) |
65 to < 75 years | 24 (24) | 12 (12) | 36 (18) | 22 (22) | 12 (12) | 34 (17) |
≥ 75 years | 8 (8) | 2 (2) | 10 (5) | 10 (10) | 5 (5) | 15 (7) |
< 65 years | 69 (68) | 86 (86) | 155 (77) | 70 (69) | 85 (83) | 155 (76) |
≥ 65 years | 32 (32) | 14 (14) | 46 (23) | 32 (31) | 17 (17) | 49 (24) |
Sex, n (%) | ||||||
Female | 39 (39) | 31 (31) | 70 (35) | 37 (36) | 42 (41) | 79 (39) |
Male | 62 (61) | 69 (69) | 131 (65) | 65 (64) | 60 (59) | 125 (61) |
Race, n (%) | ||||||
Asian | 37 (37) | 53 (53) | 90 (45) | 34 (33) | 56 (55) | 90 (44) |
Black or African American | 1 (1.0) | 1 (1.0) | 2 (1.0) | 1 (1.0) | 1 (1.0) | 2 (1.0) |
White | 63 (62) | 45 (45) | 108 (54) | 66 (65) | 44 (43) | 110 (54) |
Unknown | 0 | 1 (1.0) | 1 (0.5) | 1 (1.0) | 1 (1.0) | 2 (1.0) |
BMI, median (range), kg/m2 | 25.4 (13.6, 51.2) | 24.5 (16.8, 42.9) | 24.9 (13.6, 51.2) | 26.1 (17.5, 38.6) | 22.9 (16.6, 40.1) | 24.9 (16.6, 40.1) |
Estimated 10-year cardiovascular disease risk by Framingham risk category, n (%) | ||||||
Low (< 10%) | 41 (41) | 68 (68) | 109 (54) | 40 (39) | 72 (71) | 112 (55) |
Intermediate (10% to 20%) | 21 (21) | 11 (11) | 32 (16) | 29 (28) | 15 (15) | 44 (22) |
High (≥ 20%) | 39 (39) | 21 (21) | 60 (30) | 33 (32) | 15 (15) | 48 (24) |
Charlson comorbidity index score, n (%) | ||||||
2 | ████ | ████ | ████ | ████ | ████ | ████ |
3 | ████ | ████ | ████ | ████ | ████ | ████ |
4 | ████ | ████ | ████ | ████ | ████ | ████ |
5 | ████ | ████ | ████ | ████ | ████ | ████ |
6 | ████ | ████ | ████ | ████ | ████ | ████ |
7 | ████ | ████ | ████ | ████ | ████ | ████ |
8 | ████ | ████ | ████ | ████ | ████ | ████ |
9 | ████ | ████ | ████ | ████ | ████ | ████ |
Information missing | ████ | ████ | ████ | ████ | ████ | ████ |
10-year probability of survival estimated from the median Charlson comorbidity index, median (Q1 to Q3) | ████ | ████ | ████ | ████ | ████ | ████ |
ECOG Performance Status, n (%) | ||||||
0 | 85 (84) | 85 (85) | 170 (85) | 83 (81) | 87 (85) | 170 (83) |
1 | 16 (16) | 15 (15) | 31 (15) | 18 (18) | 15 (15) | 33 (16) |
Information missing | 0 | 0 | 0 | 1 (1.0) | 0 | 1 (0.5) |
ELTS score (randomization data), n (%) | ||||||
Low | 62 (61) | 60 (60) | 122 (61) | 64 (63) | 61 (60) | 125 (61) |
Intermediate | 30 (30) | 26 (26) | 56 (28) | 30 (29) | 27 (27) | 57 (28) |
High | 9 (9) | 14 (14) | 23 (11) | 8 (8) | 14 (14) | 22 (11) |
ACAs in Ph+ metaphases, n (%)a | ||||||
Patient with ACAs | ████ | ████ | ████ | ████ | ████ | ████ |
High-riskb | ████ | ████ | ████ | ████ | ████ | ████ |
Patients without ACAs | ████ | ████ | ████ | ████ | ████ | ████ |
Missing | ████ | ████ | ████ | ████ | ████ | ████ |
Predominant reason for TKI selection, n (%) | ||||||
Age | 13 (13) | 16 (16) | 29 (14) | 16 (16) | 15 (15) | 31 (15) |
Comorbidities | 9 (9) | 1 (1) | 10 (5) | 6 (6) | 6 (6) | 12 (6) |
Local practice, guidelines, clinical experience | 33 (33) | 42 (42) | 75 (37) | 29 (28) | 46 (45) | 75 (37) |
Other | 14 (14) | 13 (13) | 27 (13) | 20 (20) | 11 (11) | 31 (15) |
Risk category | 23 (23) | 13 (13) | 36 (18) | 24 (24) | 18 (18) | 42 (21) |
Treatment objective | 9 (9) | 15 (15) | 24 (12) | 6 (6) | 6 (6) | 12 (6) |
Information missing | 0 | 0 | 0 | 1 (1.0) | 0 | 1 (0.5) |
2G-TKI = second-generation tyrosine kinase inhibitor; ACA = additional chromosomal abnormality; BMI = body mass index; ECOG = Eastern Cooperative Oncology Group; ELTS = European Treatment and Outcome Study long-term survival; IS-TKI = investigator-selected tyrosine kinase inhibitor; MMR = major molecular response; Ph+ = Philadelphia chromosome–positive; Q1 = first quartile; Q3 = third quartile; TKI = tyrosine kinase inhibitor; TTDAE = time to treatment discontinuation due to adverse event.
aOne patient stratified to imatinib as their prerandomization TKI selection received nilotinib as actual treatment. Hence, this patient is considered to be in the imatinib stratum for the efficacy analysis and considered to have been treated with a 2G-TKI for the safety analysis.
bOngoing at the time of the October 22, 2024, data cut-off date.
Source: Details included in the table are from the sponsor’s summary of clinical evidence.
Exposure to Study Treatments
In the ASC4FIRST trial, the median duration of exposure to the study drug was longer in the asciminib group (26.6 months) compared with the IS-TKI group (25.0 months) (Table 13). When stratifying patients based on duration of exposure, more patients in the asciminib group were exposed to therapy for at least 24 weeks compared with the IS-TKI group. However, at less than 24 weeks, fewer patients in the asciminib group (7%) were exposed to therapy compared with IS-TKIs (12%). In total, the duration of exposure was 410.63 patient-years (i.e., the sum of all patients’ treatment exposure in years) in the asciminib group compared with 353.62 patient-years in the IS-TKIs group.
Table 13: Summary of Patient Exposure From the ASC4FIRST Trial [Redacted]
████ ██████ | ████ ██████ | ████ ██████ | ████ ██████ |
|---|---|---|---|
████ ██████ | ████ ██████ | ████ ██████ | ████ ██████ |
████ ██████ | ████ ██████ | ████ ██████ | ████ ██████ |
Source: Details included in the table are from the sponsor’s summary of clinical evidence.
Concomitant Medications
A summary of the concomitant medications used by patients in the safety set is provided in Table 14. In the ASC4FIRST trial, at 48 weeks, 94.0% of participants in the asciminib arm compared with 95.5% of participants in the IS-TKI arm required concomitant medications. At 96 weeks, █████ of participants in the asciminib arm compared with █████ of participants in the IS-TKI arm required concomitant medications. The nature of concomitant medications was similar in patients across the 2 treatment arms at both time points. The most frequently reported concomitant medications (reported in at least 20% of patients in any treatment group) included drugs in the following Anatomical Therapeutic Chemical classes: alimentary tract and metabolism, musculoskeletal system, nervous system, cardiovascular system, anti-infectives for systemic use, blood and blood-forming organs, respiratory system, and dermatologicals. Of note, statins were the most frequently reported concomitant medications across all treatment groups.
Table 14: Concomitant Treatment in the ASC4FIRST Trial (Safety Set) at 48 Weeks [Redacted]
███ ████ | ███ █████ | ███ █████ | ███ █████ |
|---|---|---|---|
███ █████ | ███ █████ | ███ █████ | ███ █████ |
███ █████ | ███ █████ | ███ █████ | ███ █████ |
Source: Details included in the table are from the sponsor’s summary of clinical evidence.
Efficacy
Overall Survival
At the week 96 analysis, at a median follow-up time of ████ months, there were █ patients ██████ who died during the survival follow-up in the asciminib group and █ patients ██████ in the IS-TKI group. No on-treatment deaths were reported. The █ deaths in the asciminib group were due to ██████████ █████████ █████████ and complications from █████████████ ████ ████ ███████████In the IS-TKI group, deaths occurred due to ███ ██████████ ██████████ ███████ ███████ █████ ███████████ ███ ███████ █████.
Major Molecular Response
The ASC4FIRST trial met both primary end points (refer to Table 15). At 48 weeks, within the FAS, 136 patients (67.7%) in the asciminib group and 100 patients (49.0%) in the IS-TKI group experienced an MMR, for a between-group difference of 18.88% (95% CI, 9.59% to 28.17%; P < 0.001). In the imatinib stratum, 70 patients (69.3%) in the asciminib group and 41 patients (40.2%) in the imatinib group experienced an MMR, for a between-group difference of 29.55% (95% CI, 16.91% to 42.18%; P < 0.001). The results of the other secondary end point, MMR at week 48 in the second-generation TKI FAS, showed that 66 patients (66%) in the asciminib group and 59 patients (58%) in the second-generation TKI group experienced an MMR, for a between-group difference of 8.17% (95% CI, −5.14% to 21.47%).
The ASC4FIRST trial met both key secondary end points (refer to Table 15). At 96 weeks, there were 149 patients (74.1%) in the asciminib group and 106 patients (52.0%) in the IS-TKI group who experienced an MMR, for a between-group difference of 22.42% (95% CI,13.55% to 31.29%; P < 0.001). In the imatinib stratum, 77 patients (76.2%) in the asciminib group and 48 patients (47.1%) in the imatinib group experienced MMR, for a between-group difference of 29.68% (95% CI, 17.57% to 41.79% P < 0.001). The results of the other secondary end point, MMR at week 48 in the second-generation TKI FAS, showed that 72 patients (72.0%) in the asciminib group and 58 patients (56.9%) in the second-generation TKI group experienced an MMR, for a between-group difference of 15.14% (95% CI, 2.32% to 27.95%).
Sensitivity Analysis
Within the FAS, the sensitivity analysis (in which patients missing PCR evaluations were considered nonresponders) conducted in the ASC4FIRST trial for the rate of MMR at week 48 showed consistency with the primary results, and this was also the case within the imatinib stratum and within the second-generation TKI stratum. There were no participants with missing week 96 assessments. Therefore, the results of the sensitivity analysis of the MMR rate at week 96, without imputation of data for participants who had missing BCR::ABL1 transcript evaluations, were identical to the main analysis results. Within the imatinib stratum, there were no participants with missing week 96 assessments. Therefore, the results of the sensitivity analyses of MMR rate at week 96 without imputation (treatment difference of ███████) were identical to the main analysis.
Subgroup Analysis
Subgroup analyses for the primary end point in the FAS were performed based on demographics as well as ELTS scores. At 96 weeks, the results for the number of patients experiencing an MMR were reported for patients according to their ELTS scores at randomization, with a risk difference between groups of 15.5% for low scores (95% CI, 4.6% to 26.5%; N = 247), 31.0% for intermediate scores (95% CI, 13.5% to 48.5%; N = 113), and 38.1% for high scores (95% CI, 11.6% to 64.7%; N = 45). Results were similar when ELTS scores were based on case report form data. There were no tests for interaction reported.
Duration of MMR
By the week 96 assessment, ███ patients in the asciminib group and ███ patients in the IS-TKI group had experienced an MMR at least once, and █████ patients ████ in the asciminib group and █████ patients ████ in the IS-TKI group had subsequently experienced the loss of an MMR (refer to Table 15). Among the █ patients who experienced the loss of an MMR in the asciminib group, █ had a confirmed loss of an MMR and subsequently discontinued treatment, while █ patient interrupted their dose (patient decision) and subsequently discontinued treatment due to a protocol deviation. Among the █ patients who experienced the loss of response in an IS-TKI, █ had a confirmed loss of an MMR and subsequently discontinued treatment, while █ patient discontinued treatment due to an AE and had a BCR::ABL1 transcript level greater than 1% at week 48 at the early discontinuation visit. The Kaplan-Meier estimated probability of an MMR being maintained for at least 96 weeks was █████ ████ ███ █████ █████ in the asciminib group and █████ ████ ███ █████ █████ in the IS-TKI group.
Molecular Response 2
At 48 weeks, 175 patients (87.1%) in the asciminib group and 148 patients (72.5%) in the IS-TKI group experienced an MR2, for a between-group difference of █████ ████ ███ █████ ███████ (refer to Table 15). In the stratum of patients who received imatinib, 85 patients (84.2%) in the asciminib group and 63 patients (61.7%) in the imatinib group experienced an MR2, for a between-group difference of ██████ ████ ███ ███████ ███████. In the second-generation TKI stratum, 90 patients (90.0%) in the asciminib group and 85 patients (83.3%) in the second-generation TKI group experienced an MR2, for a between-group difference of █████ ████ ███ ██████ ███████..
At 96 weeks, ███ patients ███████ in the asciminib group and ███ patients ███████ in the IS-TKI group experienced an ████ ███ █ █████████████ ██████████ ██ ██████ ████ ███ ███████ ████████ refer to Table 15. ██ ███ ████████ ████████ █████ ████ ██ ████████ ███████ ██ ███ █████████ █████ ███ ██ ████████ ███████ ██ ███ ████████ █████ ███ ████████ ████ ███ █ █████████████ ██████████ ██ ██████ ████ ███ ███████ ████████ ██ ███ ██████ ██████████ ███ ████████ █████ ████ ██ ████████ ███████ ██ ███ █████████ █████ ███ ██ ████████ ███████ ██ ███ █████████████████ ███ █████ ███ ████████ ████ ███ █ █████████████ ██████████ ██ ██████ ████ ███ ██████ ████████..
Molecular Response 4
At 48 weeks, 78 patients (38.8%) in the asciminib group and 40 patients (20.6%) in the IS-TKI group experienced an MR4, for a between-group difference of 18.38% ████ ███ ██████ ████████ (refer to Table 15). In the imatinib stratum, 43 patients (42.6%) in the asciminib group and 15 patients (14.7%) in the imatinib group experienced an MR4, for a between-group difference of 28.22% ████ ███ ███████ ███████. In the second-generation TKI stratum, 35 patients (35.0%) in the asciminib group and 27 patients (26.5%) in the second-generation TKI group experienced an MR4, for a between-group difference of 7.54% ████ ███ ███████ ████████x..
At 96 weeks, 98 patients (48.8%) in the asciminib group and 56 patients (27.5%) in the IS-TKI group experienced an MR4, for a between-group difference of ██████ ████ ███ ███████ ████████ (refer to Table 15). In the imatinib stratum, 53 patients (52.5%) in the asciminib group and 24 patients (23.5%) in the IS-TKI group experienced an MR4, for a between-group difference of ██████ ████ ███ ███████ ████████ . In the second-generation stratum, 45 patients (45.0%) in the asciminib group and 32 patients (31.4%) in the second-generation TKI group experienced an MR4, for a between-group difference of ██████ ████ ███ ██████ ███████.
Molecular Response 4.5
At 48 weeks, 34 patients (16.9%) in the asciminib group and 18 patients (8.8%) in the IS-TKI group experienced an MR4.5, for a between-group difference of 8.20% (95% CI, 1.78% to 14.62%) (refer to Table 15). In the imatinib stratum, 18 patients (17.8%) in the asciminib group and 5 patients (4.9%) in the imatinib group experienced an MR4.5, for a between-group difference of 13.13% (95% CI, 4.69% to 21.56%). In the second-generation TKI stratum, 16 patients (16.0%) in the asciminib group and 13 patients (12.7%) in the second-generation TKI group experienced an MR4.5, for a between-group difference of 3.24% (95% CI, −6.34% to 12.83%).
At 96 weeks, 62 patients (30.9%) in the asciminib group and 36 patients (17.7%) in the IS-TKI group experienced an MR4.5, for a between-group difference of ██████ ███████ ████████ (refer to Table 15). In the imatinib stratum, 36 patients (35.6%) in the asciminib group and 12 patients (11.8%) in the imatinib group experienced an MR4.5, for a between-group difference of ██████ ████ ███ ███████ ███████. In the second-generation TKI stratum, 26 patients (26.0%) in the asciminib group and 24 patients (23.5%) in the second-generation TKI group experienced an MR4.5, for a between-group difference of █████ ████ ███ ███████ ████████.
Time to First MMR
Within the FAS, the probability of achieving an MMR by week 48 was numerically higher in the asciminib arm (66.5%; 95% CI, 59.5 to 72.6) compared with the IS-TKI arm (46.3%; 95% CI, 39.2 to 53.0) (refer to Table 15). Within the imatinib stratum, the probability of experiencing an MMR by week 48 was numerically higher in the asciminib arm (69.1%; 95% CI, 58.8 to 77.2) compared with the IS-TKI arm (38.0%; 95% CI, 28.5 to 47.5). Within the second-generation TKI stratum, the probability of achieving an MMR by week 48 was numerically higher in the asciminib arm (64.0%; 95% CI, 53.7 to 72.6) compared with the IS-TKI arm (54.5; 95% CI, 44.2 to 63.6).
In the FAS, the time to first MMR was numerically higher in the asciminib arm compared with the IS-TKI arm (median time to first MMR: 24.3 versus 36.4 weeks). In the imatinib stratum, MMR was achieved numerically faster in the asciminib arm compared with the IS-TKI arm (median time to first MMR: 24.1 versus 48.6 weeks). In the second-generation TKI stratum, MMR was achieved numerically faster in the asciminib arm compared with the IS-TKI arm (median time to first MMR: 24.3 versus 36.1 weeks).
Health-Related Quality of Life
HRQoL was reported as ordinal categorical data for the EORTC QLQ-C30 GHS and EORTC QLQ-CML24 symptom burden (Table 16). A large number of participants (approximately ███) in both groups had missing baseline assessments. There was a large amount of missing data in the asciminib (███ ███ ███ with missing data at week 48 and week 96, respectively) and IS-TKI groups (███ ███ ███ with missing data at week 48 and week 96, respectively) for the EORTC QLQ-C30 GHS. There was a similar amount of missing data for the EORTC-CML24 symptom burden (██████████ ████ ███████ ███ ██ ████████ ████ ███████ ████ ██ ████ ██). At week 96, for EORTC QLQ-C30 GHS, the number of patients who indicated they were “very much better” was ██ patients █████ versus █ patients ██████ in the asciminib versus IS-TKI groups, respectively, while the number who indicated they were “very much worse” was █ patients ████ versus █ patients ██████ respectively. At week 96, for EORTC QLQ-C30 GHS, ██ ██ ██ ███████ patients in the asciminib group and ██ ██ ██ ███████ in the IS-TKI group had a moderate to high worsening, defined as a score that decreased by more than 10 points from baseline. For EORTC-CML24 symptom burden, the number of patients in the asciminib group versus the IS-TKI group who were “very much better” was █ patients ████ versus 0, respectively, and the number of patients in the asciminib group versus the IS-TKI group who were “very much worse” was █ patients ████ versus ██ patients █████, respectively.
Health Care Resource Utilization
After 96 weeks, ██ patients █████ in the asciminib group and ██ patients █████ in the IS-TKI group had used at least 1 health care resource (Table 17). The most common resource used was hospitalization (██ patients █████ in the asciminib group and ██ patients █████ in the IS-TKI group).
Table 15: Summary of Key Efficacy Results (FAS)
Variable | ASC4FIRST trial | |||||
|---|---|---|---|---|---|---|
FAS | Imatinib stratum | 2G-TKI stratum | ||||
Asciminib 80 mg N = 201 | IS-TKI N = 204 | Asciminib 80 mg N = 101 | IS-TKI N = 102 | Asciminib 80 mg N = 100 | IS-TKI N = 102 | |
MMR at 48 weeksa | ||||||
Response, n (%) | 136 (67.66) | 100 (49.02) | 70 (69.31) | 41 (40.20) | 66 (66.00) | 59 (57.84) |
Response, 95% CI | 60.72 to 74.07 | 41.97 to 56.10 | 59.3 to 78.10 | 30.61 to 50.37 | 55.85 to 75.18 | 47.66 to 67.56 |
Unstratified difference in response rates versus comparator, % | 18.64 | NR | NR | |||
Unstratified difference in response rates versus comparator, 95% CI | 9.21 to 28.07 | NR | NR | |||
Common treatment difference (%) | 18.88 | 29.55 | 8.17 | |||
Common treatment difference, 95% CI | 9.59 to 28.17 | 16.91 to 42.18 | −5.14 to 21.47 | |||
CMH 1-sided test P value | < 0.001 | < 0.001 | 0.116 | |||
CMH 1-sided test-adjusted P value | < 0.001 | < 0.001 | — | |||
MMR at 96 weeksb | ||||||
Response, n (%) | 149 (74.13) | 106 (51.96) | 77 (76.24) | 48 (47.06) | 72 (72.00) | 58 (56.86) |
Response, 95% CI | ███ | ███ | ███ | ███ | ███ | ███ |
Unstratified difference in response rates versus comparator, % | ██████ | ██████ | ██████ | |||
Unstratified difference in response rates versus comparator, 95% CI | ██████ | ██████ | ██████ | |||
Common risk difference, % | ██████ | ██████ | ██████ | |||
Common risk difference, 95% CI | 13.55 to 31.29 | 17.57 to 41.79 | 2.32 to 27.95 | |||
CMH 1-sided test P value | < 0.001 | < 0.001 | 0.011 | |||
CMH 1-sided test-adjusted P value | < 0.001 | < 0.001 | — | |||
MR2 at 48 weeks | ||||||
MR2 response, n (%) | 175 (87.06) | 148 (72.55) | 85 (84.16) | 63 (61.76) | 90 (90.00) | 85 (83.33) |
Common treatment difference, % | ██████ | ██████ | ██████ | |||
Common treatment difference, 95% CI | ██████ | ██████ | ██████ | |||
MR2 at 96 weeks | ||||||
MR2 response, n (%) | ███ | ███ | ███ | ███ | ███ | ███ |
Common treatment difference, % | ██████ | ██████ | ██████ | |||
Common treatment difference, 95% CI | ██████ | ██████ | ██████ | |||
MR4 at 48 weeks | ||||||
MR4 response, n (%) | 78 (38.81) | 42 (20.59) | 43 (42.57) | 15 (14.71) | 35 (35.0) | 27 (26.47) |
Common treatment difference, % | 18.38 | 28.22 | 8.49 | |||
Common treatment difference, 95% CI | 9.96 to 26.79 | 16.81 to 39.63 | −3.58 to 20.56 | |||
MR4 at 96 weeks | ||||||
MR4 response, n (%) | 98 (48.76) | 56 (27.45) | 53 (52.48) | 24 (23.53) | 45 (45.00) | 32 (31.37) |
Common treatment difference, % | ██████ | ██████ | ██████ | |||
Common treatment difference, 95% CI | ██████ | ██████ | ██████ | |||
MR4.5 at 48 weeks | ||||||
MR4.5 response, n (%) | 34 (16.92) | 18 (8.82) | 18 (17.82) | 5 (4.90) | 16 (16.00) | 13 (12.75) |
Common treatment difference, % | ██████ | ██████ | ██████ | |||
Common treatment difference, 95% CI | ██████ | ██████ | ██████ | |||
MR4.5 at 96 weeks | ||||||
MR4.5 response, n (%) | 62 (30.85) | 36 (17.65) | 36 (35.64) | 12 (11.76) | 26 (26.00) | 24 (23.53) |
Common treatment difference, % | ██████ | ██████ | ██████ | |||
Common treatment difference, 95% CI | ██████ | ██████ | ██████ | |||
Cumulative incidence function of time to first MMR at 12 weeks since randomizationc | ||||||
Estimated cumulative incidence rate, % | ███ | ███ | ███ | ███ | ███ | ███ |
Estimated cumulative incidence rate, 95% CI | ███ | ███ | ███ | ███ | ███ | ███ |
Cumulative incidence function of time to first MMR at 48 weeks since randomizationc | ||||||
Estimated cumulative incidence rate, % | 66.5 | 46.3 | 69.1 | 38.0 | 64.0 | 54.5 |
Estimated cumulative incidence rate, 95% CI | 59.5 to 72.6 | 39.2 to 53.0 | 58.8 to 77.2 | 28.5 to 47.5 | 53.7 to 2.6 | 44.2 to 63.6 |
2G-TKI = second-generation tyrosine kinase inhibitor; CI = confidence interval; CMH = Cochran-Mantel-Haenszel; FAS = full analysis set; IS-TKI = investigator-selected tyrosine kinase inhibitor; MMR = major molecular response; MR = molecular response; MR2 = molecular response with a 2-log or greater reduction in BCR::ABL1 transcripts; MR4 = molecular response with a 4-log or greater reduction in BCR::ABL1 transcripts; MR4.5 = molecular response with a 4.5-log or greater reduction in BCR::ABL1 transcripts; NA = not available; NR = not reported; PCR = polymerase chain reaction.
aParticipants without a PCR assessment at week 48 were considered nonresponders unless their disease was in the MMR state at both week 36 and week 60. One participant in the asciminib arm and 2 participants in the IS-TKI arm were imputed as responders. Common treatment difference and common risk difference are synonymous.
bPatients without a PCR assessment at week 96 are considered nonresponders unless their disease was in the MMR state at both week 84 and week 108. Zero patients in the asciminib arm and 0 patients in the IS-TKI arm are imputed as responders.
cAll patients who had experienced an MMR at any time on or before the data cut-off date were included.
Source: Details included in the table are from the sponsor’s summary of clinical evidence.
Table 16: HRQoL Data at Week 96 [Redacted]
███ █████ | ███ █████ | ███ █████ | ███ █████ |
|---|---|---|---|
███ █████ | ███ █████ | ███ █████ | ███ █████ |
███ █████ | ███ █████ | ███ █████ | ███ █████ |
Source: Details included in the table are from the sponsor’s summary of clinical evidence.
Table 17: Health Care Resource Utilization [Redacted]
███ █████ | ███ █████ | ███ █████ | ███ █████ |
|---|---|---|---|
███ █████ | ███ █████ | ███ █████ | ███ █████ |
███ █████ | ███ █████ | ███ █████ | ███ █████ |
Source: Details included in the table are from the Clinical Study Report for the ASC4FIRST trial.42
Harms
Refer to Table 18 for harms data.
Adverse Events
AEs were reported in 191 patients (96%) in the asciminib group and 197 patients (98%) in the IS-TKI group at 96 weeks. ███ ████ ██████ ███ ████ █████████ █████████ ██ ██ ████████ █████ ██ █████████ ███ ██ ████████ █████ ██ ███ ██████ ██████ ███ █████████ █████████ ██ ██ ████████ █████ ██ ███ █████████ █████ ███ ██ ████████ █████ ██ ███ ██████ ██████.
Serious Adverse Events
Serious AEs occurred in ██ ████████ █████ █ the asciminib group and ██ patients █████ in the IS-TKI group, after 96 weeks of treatment ████ ███ ████ ████████ ██ ████ ████ █ ████████ ███ ███████ █████████ █████ ████████ ██ ██ ████████ ██ ███ █████████ █████ ███ █ ████████ ████ ██ ███ ██████ ██████.
Grade 3 or Higher Adverse Events
AEs of grade 3 or higher occurred in 89 patients (45%) in the asciminib group compared with ███ ████████ █████ in the IS-TKI group at 96 weeks. The most common grade 3 or higher AEs were ███████████, occurring in ████ patients in the asciminib and ██ █████ patients in the IS-TKI group; ██████████ █████ █████████, occurring in ██ ████ patients in the asciminib group and ██ ████ patients in the IS-TKI group; and ████████████████ occurring in ██ ████ patients in the asciminib group and ██ ████ patients in the IS-TKI group.
Withdrawals Due to Adverse Events
AEs leading to treatment discontinuation occurred in 12 patients (6%) in the asciminib group and 26 patients (13%) in the IS-TKI group after 96 weeks of treatment.
The secondary end point, time to discontinuation of study treatment due to AEs for asciminib versus second-generation TKIs was formally tested at week 96 and was met. Results of the cause-specific hazard analysis showed that the risk of study treatment discontinuation due to AEs was lower in the asciminib group compared with the second-generation TKI group (HR = 0.463; 95% CI, 0.215 to 0.997; P = 0.0246).
Mortality
After 96 weeks, there were ████████ ██████ ███ ████ ██ ███ █████████ █████ ███ █ ████████ ████ ███ ████ ██ ███ ██████ ██████ ███ ██████ ████████ ██████ ███ ████████ ██████████ ███ █ ██████ ██ ███ █████████ █████ ████ ███ ██ █████████████ ████ █████████████ ████ ████ ██████████ ███ ███ ██ ██████████ █████████ ██████████ ██ ███ █ ██████ ██ ███ ██████ ██████ ███ ████ ██ ███ ████████ █████ ████ ██████████ ██████████ ███████ ███████ █████ ██████████ ███ ███████ ███████.
Notable Harms
The notable harms prioritized by the clinical experts were acute clinical pancreatitis and the category of ischemic cardiac and CNS events. After 96 weeks, there were ████████ ████ in each of the asciminib and IS-TKI groups who had an event of acute pancreatitis and there were ██ ████████ ██████ in the asciminib group and ██ ████████ ████ in the IS-TKI group who had an AE that fell under the broad category of ischemic heart and CNS conditions.
Other notable harms included myelosuppression, which occurred in ██ patients █████ in the asciminib group and ███ patients █████ in the IS-TKI group; gastrointestinal toxicity, which occurred in ██ patients █████ in the asciminib group and ██ patients █████ in the IS-TKI group; and clinical hepatotoxicity, which occurred in █ patients ████ in the asciminib group and █ patients ████ in the IS-TKI group. Other notable harms are summarized in Table 18.
Table 18: Summary of Harms Results From ASC4FIRST (96 Weeks, Safety Set) [Redacted]
███ █████ | ███ █████ | ███ █████ | ███ █████ |
|---|---|---|---|
███ █████ | ███ █████ | ███ █████ | ███ █████ |
███ █████ | ███ █████ | ███ █████ | ███ █████ |
Source: Details included in the table are from the sponsor’s summary of clinical evidence.
Critical Appraisal
Internal Validity
The ASC4FIRST trial was a phase III, open-label RCT that evaluated asciminib in comparison to IS-TKI in patients with newly diagnosed Ph+ CML. The lack of blinding in the ASC4FIRST trial may influence AE reporting, discontinuation rates between treatment groups, and patient-reported outcomes such as HRQoL, potentially leading to a more favourable assessment for asciminib due to expectation bias; the magnitude of this bias is uncertain. Patients’ knowledge of their assigned treatment may impact their willingness to adhere to and persist with therapy, potentially impacting the assessment of outcomes such as time to discontinuation of study treatment due to an AE. However, the primary and key secondary end points of MR are objective outcomes that are less likely to be subject to bias.
More than twice as many patients in the control group discontinued study treatment compared with the asciminib group (38% versus 18%). In the asciminib group, 9.5% discontinued due to an unsatisfactory treatment effect and 6% due to an AE. In the IS-TKI group, 21% discontinued due to an unsatisfactory treatment effect and 13% due to an AE. This imbalance suggests that the reasons for discontinuation may be related to treatment response and tolerability, which suggests that the missing data may not be missing at random. If patients with worse outcomes are dropping out at higher rates, which is more common in the IS-TKI group, the remaining sample is biased toward better outcomes. The sponsor included a sensitivity analysis in which all patients without outcome data were classified as nonresponders, which is an appropriate and conservative “worst-case” imputation strategy that reduces the chance of falsely inflating efficacy. However, given that the IS-TKI control group has a higher discontinuation rate (38% versus 18% in the asciminib group), and all dropouts are labelled as nonresponders, it may bias the results in favour of the asciminib group, given that more patients in the IS-TKI group were considered “nonresponders,” which may overestimate the treatment effect. On the other hand, the assessment of harms may have been biased against asciminib because patients in the asciminib group were exposed to treatment for a longer duration than those in the control group (mean and standard deviation exposure of ████ ████ months versus ████ ████ months). This increases the time at risk for harms in the treatment group, potentially inflating the occurrence of harms.
The statistical analysis was appropriate; the primary end points of MMR at week 48 and key secondary end points of MMR at week 96 and time to treatment discontinuation due to AEs were formally tested for statistical significance. No other outcomes assessed in the ASC4FIRST trial were adjusted for multiplicity and are considered to provide supportive evidence. This includes potentially important outcomes such as MR2, MR4, and MR4.5, outcomes that may be used to assess the impact of treatment on future survival, and also to assess the depth of response to predict future treatment-free remission. Subgroup analyses were preplanned but were exploratory assessments.
Because HRQoL was reported as ordinal categorical data and there was a high proportion of missing outcome data █████), the between-group HRQoL difference for asciminib compared with IS-TKI is not interpretable. At 96 weeks, results were available for ██ ██ ███ ████████ █████ in the asciminib group and ██ ██ ███ ████████ █████ in the IS-TKI group for the EORTC QLQ-C30 GHS. The sponsor noted that approximately ███ of patients were missing an HRQoL assessment at baseline because their baseline assessments were conducted either after randomization or after initiating treatment. The sponsor reported that HRQoL data were excluded for █ patients at a site in Singapore because these patients reported data using a paper form rather than an electronic form, as specified in the protocol.
The duration of follow-up was sufficient for the assessment of the primary outcome of MMR at 48 weeks; however, conclusions regarding longer-term survival outcomes like OS are uncertain, given the immaturity of the data. In addition, the long-term magnitude of response (e.g., deep MR, eligibility for attempts at treatment-free remission), durability of response, and long-term safety outcomes, particularly for harms with lower event rates such as arterial occlusive events, pancreatic toxicity, and QTc prolongation, remain uncertain.
External Validity
According to the clinical experts consulted by CDA-AMC, the demographic and disease characteristics of the ASC4FIRST trial population were overall reflective of the patients living in Canada newly diagnosed with CML-CP. The majority of patients (61%) had an ELTS score of “low,” and this was consistent across strata. The majority of patients (54%) had a Framingham risk score of “low” across all groups; however, the percentage of patients who were low risk was lower in the imatinib stratum (40%) than in the second-generation TKI stratum (68%). These baseline characteristics are expected, given that patients in the imatinib group would be expected to be older and have a higher cardiovascular risk, according to the clinical experts. In the ASC4FIRST trial, patients were discontinued from study treatment if a T315I mutation was detected, which may have reduced the generalizability of the study findings; however, the clinical experts noted that similar results would be expected if patients with a T315I mutation were included in the study.
The current analysis includes a follow-up to 96 weeks, which was sufficient to assess MMR. Although biochemical responses are important for monitoring progress with respect to treatment and can impact a patient’s mental outlook, patient and clinician group inputs have highlighted the importance of long-term outcomes and survival end points in managing Ph+ CML. It needs to be acknowledged, however, that the success of TKI therapy in managing CML means that patients are surviving much longer; therefore, collecting reliable OS data, even after 5 years of follow-up (the end of the ASC4FIRST trial will occur 5 years from the last participant's first treatment in the study), may be challenging. This lack of long-term data also precludes the assessment of the durability of the reported responses and the assessment of longer-term harms. The lack of long-term harms data may be particularly important for this therapeutic class; as 1 of the clinical experts pointed out, the harms related to cardiovascular safety for another TKI, nilotinib, were not detected until it had been on the market for a decade. The clinical experts also noted the importance of treatment-free remission as an outcome in CML, and this outcome was not assessed in the ASC4FIRST trial.
The ASC4FIRST trial is the first head-to-head trial comparing a TKI with a basket of other available TKI therapies (first-generation TKI imatinib and second-generation TKIs nilotinib, dasatinib, or bosutinib). The clinical experts consulted by CDA-AMC noted that second-generation TKIs are more potent than imatinib and it is expected that they lead to faster and higher MRs. Second-generation TKIs were approved for first-line treatment based on phase III RCTs46-49 comparing each of them with imatinib. While these studies demonstrated superior MRs over imatinib, this came at the cost of higher rates of AEs, according to the clinical experts consulted for this review. The clinical experts emphasized that survival with imatinib therapy is roughly that of age-matched controls for chronic-phase disease, and there is no evidence to suggest that second-generation TKIs demonstrate superior OS. In the absence of direct head-to-head comparisons of data between individual second-generation TKIs in the first line, the clinical experts noted that while second-generation TKIs appear to have similar MRs based on how these drugs perform in clinical practice, their safety profiles appear more distinct. The experts estimated that most patients would receive either imatinib or dasatinib (broadly 50% each) in the first line in Canadian clinical practice, with jurisdictional variations. According to the clinical experts, the frequency of dasatinib use was lower in the ASC4FIRST trial than anticipated in clinical practice. The experts noted that this may limit the applicability of the safety results in the ASC4FIRST trial to clinical practice in Canada. However, because second-generation TKIs were not individually stratified in the trial, it remained unclear whether the safety differences between asciminib and second-generation TKIs were driven by a specific TKI within that group.
The clinical experts noted that the dosing for the IS-TKIs in the trial was based on the product monographs and not titrated, as it would be in clinical practice in Canada (e.g., dasatinib is commonly used at 50 mg to 70 mg, bosutinib at 200 mg to 400 mg, and imatinib at 300 mg to 400 mg). In clinical practice, IS-TKI comparators would likely be used at lower doses and subsequently increased as tolerated by the patient. This may reduce the generalizability of study results, particularly for harms. For example, the experts noted this may have inflated the occurrence of AEs in the trial control group. Furthermore, although results were presented separately for a first-generation TKI (imatinib) and second-generation TKIs, there was no further stratification within the second-generation TKIs. The clinical experts noted this stratification was important because there is variability among these second-generation TKIs; for example, the occurrence and specific harms of interest are different among the second-generation TKIs.
The dosage of asciminib in the ASC4FIRST trial (80 mg once daily) represents only 1 of the Health Canada–approved dosages (40 mg twice daily and 80 mg once daily). It is unclear whether the ASC4FIRST trial evidence is generalizable to a 40 mg twice-daily dosage; however, the clinical experts cited evidence in the literature that suggests there is no reason to expect a clear difference in efficacy between the 2 dose regimens.43
GRADE Summary of Findings and Certainty of the Evidence
Methods for Assessing the Certainty of the Evidence
For pivotal studies and RCTs identified in the sponsor’s systematic review, GRADE was used to assess the certainty of the evidence for outcomes considered most relevant to inform expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group:10,11
High certainty: We are very confident that the true effect lies close to that of the estimate of the effect.
Moderate certainty: We are moderately confident in the effect estimate — The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. We use the word “likely” for evidence of moderate certainty (e.g., “X intervention likely results in Y outcome”).
Low certainty: Our confidence in the effect estimate is limited — The true effect may be substantially different from the estimate of the effect. We use the word “may” for evidence of low certainty (e.g., “X intervention may result in Y outcome”).
Very low certainty: We have very little confidence in the effect estimate — The true effect is likely to be substantially different from the estimate of effect. We describe evidence of very low certainty as “very uncertain.”
Following the GRADE approach, evidence from RCTs started as high-certainty evidence and could be rated down for concerns related to study limitations (which refer to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias.
When possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect; if this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., the clinical importance is unclear). In all cases, the target of the certainty-of-evidence assessment was based on the point estimate and where it was located relative to the threshold for a clinically important effect (when a threshold was available) or to the null. For the MMR outcome, the threshold for a clinically important between-group effect was estimated by the clinical experts to be 10% to 15%; for MR2, it was estimated to be 5% to 10%. Due to the significant amount of missing baseline data (about 40%) for patient-reported outcomes, change from baseline data were not interpretable. The 95% CIs for the change from baseline scores in each group as well as the between-group difference with its associated 95% CI were lacking. For harms outcomes, the clinical experts estimated that a 10% between-group difference would be clinically meaningful.
Results of GRADE Assessments
Table 2 presents the GRADE summary of findings for asciminib versus IS-TKI.
Long-Term Extension Studies
No long-term extension study was submitted by the sponsor.
Indirect Evidence
No indirect evidence was submitted by the sponsor.
Studies Addressing Gaps in the Systematic Review Evidence
No studies for addressing gaps were submitted by the sponsor.
Discussion
Summary of Available Evidence
The available evidence for this review of asciminib includes 1 ongoing open-label RCT (ASC4FIRST) that compares asciminib to imatinib and 3 second-generation TKIs (dasatinib, bosutinib, and nilotinib). There were 405 patients with CML-CP who were randomized, 1:1, to asciminib or 1 of the other IS-TKIs, with imatinib making up half of the patients in this control group. The ASC4FIRST trial is ongoing, with an expected follow-up of 5 years, and the latest report submitted by the sponsor provided results up to 96 weeks. The coprimary outcomes were the comparison of asciminib versus IS-TKIs and asciminib versus imatinib for MMR rate at 48 weeks. Key secondary end points compared the efficacy of asciminib versus IS-TKIs and imatinib based on the proportion of participants with an MMR at week 96. Time to discontinuation of study treatment due to AEs for asciminib versus second-generation TKIs was designated a secondary outcome that was also adjusted for multiple comparisons, as were the coprimary and secondary outcomes. There was no indirect treatment comparison submitted for this review, and no studies addressing gaps were submitted.
Patients in the imatinib stratum were older than patients in the second-generation stratum. The median age of patients in the imatinib stratum was 56 years (range, 21 to 79 years) in the asciminib group and 54.5 years (range, 20 to 86 years) in the control group; in the second-generation stratum, the median age was 43 years (range, 18 to 76 years) in the asciminib group and 43 years (range, 19 to 83 years) in the control group.
No evidence addressing gaps, long-term extensions, or indirect treatment comparisons was submitted.
Interpretation of Results
Efficacy
Treatment goals for patients with Ph+ CML include survival, achieving an MR, symptom management, improved QoL, treatment-free remission, and minimizing side effects.
The ASC4FIRST trial met both its primary outcomes and showed statistically significant and clinically meaningful increases in the proportion of patients experiencing an MMR at 48 weeks in the asciminib versus IS-TKI stratum and the asciminib versus imatinib stratum. The certainty of the evidence for these outcomes was rated as “high,” based on the GRADE approach. Likewise, the study met both key secondary efficacy end points with asciminib showing a statistically significant and clinically meaningful benefit versus IS-TKIs and versus imatinib at week 96. Results for other MRs (other secondary outcomes), including MR2, MR4, and MR4.5, were supportive of the results observed in the primary and key secondary analyses, showing clinically meaningful benefits of asciminib versus IS-TKIs and versus imatinib through to week 96. The comparison of asciminib versus second-generation TKIs was not adjusted for multiple testing and were considered supportive evidence. The MR outcomes for asciminib versus second-generation TKIs showed uncertainty due to imprecision in the between-group differences (wide 95% CIs that were close to or crossed the null) as well as inconsistency in the direction of results. While the data appear to suggest a trend in favour of asciminib versus second-generation TKI treatments for some MRs (though less pronounced than for asciminib compared with imatinib), there appeared to be little to no difference between groups for other MRs (i.e., MMR response at week 48) (based on a 10% threshold suggested by the clinical experts), and MR4.5 responses at weeks 48 and 96 (based on the 5% threshold suggested by the clinical experts). The ASC4FIRST trial suggested there was little to no difference in notable harms, including acute pancreatitis, ischemic heart, and CNS conditions in the asciminib group compared with IS-TKIs; however, the certainty of evidence was rated as low using the GRADE approach. Results for HRQoL were rated as “very low” based on GRADE, due to several limitations in the analyses of the EORTC QLQ-C30 GHS outcome.
Treatment guidelines22 and inputs from patients and clinicians highlight OS as a key treatment goal for patients with Ph+ CML. In the ASC4FIRST trial, the final assessment of OS is planned at 5 years of follow-up. However, given the success of treatment for CML,44 the clinical experts were of the opinion that there are unlikely to be many more events after 5 years; therefore, it may be unrealistic to expect asciminib to demonstrate a survival benefit over other TKIs in the typical follow-up for a clinical trial. The clinical experts noted that no TKI has demonstrated a survival benefit over another TKI, including imatinib.45 This means that in the typical follow-up of a clinical trial for a TKI, surrogate markers such as an MR must be relied on to assess the potential long-term benefit of asciminib over another TKI therapy. For example, the phase III RCTs for the TKIs dasatinib, bosutinib, nilotinib, and imatinib in the first-line setting used MMR or complete cytogenetic response at 12 months as primary end points.46-49 The clinical experts consulted for this review noted that molecular outcomes are important outcomes of treatment in clinical practice. The 2020 European LeukemiaNet guidelines suggest that reaching an MMR is associated with a near-100% CML-specific survival rate because disease progression is rare once this level of molecular remission is attained.22 The FDA supports the use of molecular outcomes as a surrogate end point for traditional approval for therapies in CML.50 The IRIS study, an open-label multicentre trial with a crossover design that included patients with newly diagnosed CML-CP that randomly assigned patients to receive either imatinib or interferon alfa plus cytarabine, estimated the 10-year OS according to MMR levels at 18 months.51 In the IRIS study, among patients treated with first-line imatinib therapy, the estimated 10-year OS was 93% (95% CI, 89% to 97%) among patients experiencing an MMR and 86% (95% CI, 78% to 93%; P = 0.04) among patients without an MMR.51 The IRIS study also found that 100% of patients who experienced an MMR at 18 months were “free from CML-related death” at 10 years; in patients who did not experience an MMR at 18 months, 91% were free from CML-related death (95% CI, 84% to 97%; P < 0.001).51 An important limitation of this analysis was that survival status was missing for 20% of patients in the original imatinib group; however, this is not unexpected with such a long-term follow-up, and data from the IRIS study suggest that MMR may play a role in predicting OS in the long-term. The clinical experts also noted the importance of MR2 in attaining OS goals. MR2 is considered equivalent to complete cytogenetic remission in which no detectable Ph+ cells are present in the bone marrow sample; the absence of detectable Ph+ cells has, historically, been considered to have one of the clearest associations with long-term OS, according to the clinical experts, citing retrospective studies such as Bidikian et al. (2023).52
The clinical experts consulted for this review agreed that treatment-free remission has become a key outcome in assessing response to a TKI in CML, and an important goal from a patient perspective. The clinical experts asserted that the depth and duration of an MR are important success criteria for achieving treatment-free remission. Treatment-free remission was not assessed in the ASC4FIRST trial. Guidelines suggest that the presence of a sustained MR (MR4 for more than 3 years or MR4.5 for more than 2 years) is optimal to attempt to discontinue treatment.22 There were numerically more patients who experienced an MR4 or MR4.5 in the asciminib group compared with the IS-TKI group at week 96; however, because treatment-free remission was not assessed, no firm conclusions can be drawn about this outcome. The clinical experts noted that, in their experience, approximately half of patients treated with a TKI are ultimately able to achieve a treatment-free remission.
The evidence was very uncertain about the effect of asciminib on HRQoL compared with IS-TKIs due to the open-label design of the trial and the large amount of missing data. With the advent of TKI therapy, CML has become a readily treatable disease with which patients can expect to live a relatively normal lifespan; however, the trade-off is that these patients must continue to be adherent to and persist with their TKI treatment. As described in the next section, each TKI has its own side effects profile, which can impact QoL. The clinical experts emphasized that CML is still cancer and while some patients are satisfied with experiencing an MR2, others aim for the deepest possible response, such as an MR4 or beyond, as quickly as possible. If a TKI does not meet these expectations, it can negatively impact the patient’s QoL. Therefore, QoL is important in CML and the limitations in these data from the ASC4FIRST trial should be considered an important gap in knowledge about asciminib.
Harms
The lack of long-term safety data is a limitation when assessing asciminib, according to the clinical experts consulted for this review. One of the clinical experts cited the case of nilotinib, for which cardiovascular safety harms did not become evident until nearly a decade after its initial approval. A long-term follow-up of the ENESTnd study found that after 10 years, cardiovascular events were more common with nilotinib (300 mg dose: 16.5% of patients; 400 mg dose: 23.5%) compared with imatinib (3.6%).53 After 96 weeks of follow-up, the ASC4FIRST trial suggested there was little to no difference in the number of ischemic events in the asciminib group compared with other TKIs; however, the absolute number of events was low, and no conclusions can be drawn about the cardiovascular safety of asciminib compared with baseline because a placebo group was not included in the trial. Given the experience with nilotinib, 96 weeks may be a sufficient follow-up time to assess the safety of asciminib. These long-term harms are particularly relevant in CML because, unlike many cancers, patients may be on the same TKI for many years.
To date, a unifying feature of second-generation TKIs has been an increased risk of various cardiopulmonary harms. Well-summarized in reviews like Kaddoura et al. (2023),54 each TKI seems to have its own cardiopulmonary issues, all of which seem more common than with imatinib. For example, vascular AEs appear more common with nilotinib compared with other TKIs, as well as cardiomyopathy and fluid retention, while dasatinib is associated with pleural effusion (as is bosutinib) and pulmonary hypertension.54
In the ASC4FIRST trial, fewer patients discontinued treatment due to an AE in the asciminib group (6%) compared with the IS-TKI group (13%). This may be an important finding because patient adherence and/or persistence with therapy is one of the main reasons for treatment failure. The difference in treatment discontinuation between the asciminib group and the IS-TKI group did not appear to be related to any specific AE, which may reflect the lack of stratification for each comparator TKI because the clinical experts noted that the occurrence of specific AEs varies by TKI. Because the second-generation TKIs were not stratified, it is not clear whether the differences in AEs between asciminib and second-generation TKIs are driven by a specific TKI within that group.
Conclusion
The ASC4FIRST trial met both its primary outcomes and showed statistically significant and clinically meaningful increases in the proportion of patients experiencing an MMR at 48 weeks in the asciminib versus IS-TKI stratum and the asciminib versus imatinib stratum. The certainty of the evidence for these outcomes was rated as “high,” based on the GRADE approach. Likewise, the study met both key secondary efficacy end points with asciminib showing statistically significant and clinically meaningful benefit versus IS-TKI and versus imatinib at week 96. The clinical significance of this finding with respect to OS is uncertain because data were immature at the time of analysis at 96 weeks in the ASC4FIRST trial. Although there is some evidence in the literature that early MMR may predict long-term survival, no TKI has demonstrated a survival benefit over another TKI in long-term studies. The clinical experts consulted for this review noted that treatment-free remission is among the key treatment goals; however, it was not assessed in the ASC4FIRST trial. HRQoL is an important outcome in CML; however, the evidence was very uncertain about the effect of asciminib on HRQoL compared with IS-TKIs. In the ASC4FIRST trial, fewer patients discontinued treatment due to an AE in the asciminib group (6%) compared with the IS-TKI group (13%); however, comparisons with other TKIs in this study are limited by the variation in the side effect profiles of these drugs and the lack of stratification by each TKI. Results from the ASC4FIRST trial suggest that asciminib results in little to no difference in the notable harms, acute pancreatitis, and ischemic heart and CNS conditions compared with IS-TKIs; however, the certainty of evidence was rated as low using the GRADE approach.
References
1.Van Etten RA, Atallah E. Larson RA, Rosmarin AG, eds. Chronic myeloid leukemia: Pathogenesis, clinical manifestations, and diagnosis. UpToDate; 2025. Accessed March 15, 2025. https://www.uptodate.com/contents/chronic-myeloid-leukemia-pathogenesis-clinical-manifestations-and-diagnosis
2.Jabbour E, Kantarjian H. Chronic myeloid leukemia: 2022 update on diagnosis, therapy, and monitoring. Am J Hematol. 2022;97(9):1236-1256. doi: 10.1002/ajh.26642 PubMed
3.Table 13-10-0747-01. Number of new cases and age-standardized rates of primary cancer, by cancer type and sex. Statistics Canada; 2025. Accessed 2025 Mar 24. https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310074701&pickMembers%5B0%5D=2.1&pickMembers%5B1%5D=3.53&cubeTimeFrame.startYear=2009&cubeTimeFrame.endYear=2022&referencePeriods=20090101%2C20220101
4.Table 13-10-0751-01. Number of prevalent cases and prevalence proportions of primary cancer by prevalence duration, cancer type, attained age group and sex. Statistics Canada; 2022. Accessed April 16, 2025. https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310075101&pickMembers%5B0%5D=2.1&pickMembers%5B1%5D=3.2&pickMembers%5B2%5D=4.53&pickMembers%5B3%5D=5.4&cubeTimeFrame.startYear=2015&cubeTimeFrame.endYear=2018&referencePeriods=20150101%2C20180101
5.CDA-AMC Sponsor Summary of Clinical Evidence Template [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Scemblix (asciminib): 20 mg and 40 mg, oral tablets. Novartis Pharmaceuticals Canada; 2025.
6.Novartis Pharmaceuticals Canada I. Patient medication information: Gleevec®. Novartis Pharmaceuticals Canada Inc.; 2015.
7.Bristol-Myers Squibb C. Product monograph including patient medication information: Sprycel®. 2007.
8.Novartis Pharmaceuticals Canada I. Product monograph: PrTasigna®. Novartis Pharmaceuticals Canada Inc.; 2016.
9.Pfizer C. Product monograph: PrBOSULIF®. 2024.
10.Balshem H, Helfand M, Schünemann HJ, et al. GRADE guidelines: 3. Rating the quality of evidence. Journal of clinical epidemiology. 2011;64(4):401-6. doi: 10.1016/j.jclinepi.2010.07.015 PubMed
11.Santesso N, Glenton C, Dahm P, et al. GRADE guidelines 26: informative statements to communicate the findings of systematic reviews of interventions. Journal of clinical epidemiology. 2020;119:126-135. doi: 10.1016/j.jclinepi.2019.10.014 PubMed
12.Flis S, Chojnacki T. Chronic myelogenous leukemia, a still unsolved problem: pitfalls and n ew therapeutic possibilities. Drug Des Devel Ther. 2019;Volume 13:825-843. doi: 10.2147/DDDT.S191303 PubMed
13.Hoffmann VS, Baccarani M, Hasford J, et al. The EUTOS population-based registry: incidence and clinical characteri stics of 2904 CML patients in 20 European Countries. Leukemia. 2015;29(6):1336-1343. doi: 10.1038/leu.2015.73 PubMed
14.Canadian Cancer Society. Risk for chronic leukemia. 2024.
15.Hehlmann R. Chronic Myeloid Leukemia in 2020. HemaSphere. 2020;4(5):e468. doi: 10.1097/HS9.0000000000000468 PubMed
16.Arber DA, Orazi A, Hasserjian R, et al. The 2016 revision to the World Health Organization classification of m yeloid neoplasms and acute leukemia. Blood. 2016;127(20):2391-2405. doi: 10.1182/blood-2016-03-643544 PubMed
17.American Cancer Society. Key Statistics for Chronic Myeloid Leukemia. 2025. Accessed June 2025. https://www.cancer.org/content/dam/CRC/PDF/Public/8684.00.pdf
18.Agency CsD. asciminib reimbursement review. 2022. https://www.cda-amc.ca/asciminib
19.Höglund M, Sandin F, Hellström K, et al. Tyrosine kinase inhibitor usage, treatment outcome, and prognostic scores in CML: report from the population-based Swedish CML registry. Blood. 2013;122(7):1284-92. doi: 10.1182/blood-2013-04-495598 PubMed
20.National Comprehensive Cancer N. National Comprehensive Cancer Network. NCCN Clinical Practice Guidelin es in Oncology (NCCN Guidelines®) Chronic Myeloid Leukemia Version 2. 2025.
21.Statistics C. Data from: Number of new cases and age-standardized rates of primary cancer, by cancer type and sex. 2025. Table: 13-10-0747-01 (formerly CANSIM 103-0554). doi:10.25318/1310075101-ENG
22.Hochhaus A, Baccarani M, Silver RT, et al. European LeukemiaNet 2020 recommendations for treating chronic myeloid leukemia. Leukemia. 2020;34(4):966-984. doi: 10.1038/s41375-020-0776-2 PubMed
23.Schiffer C, Atallah E. Larson RA, Rosmarin AG, eds. Overview of the treatment of chronic myeloid leukemia. UpToDate; 2022. Accessed 2025 Mar 15. http://www.uptodate.com
24.Schiffer C, Atallah E. Larson RA, Rosmarin AG, eds. Chronic myeloid leukemia in chronic phase: Initial treatment. UpToDate; 2025. Accessed 2025 Mar 18. http://www.uptodate.com
25.Society TLL. Chronic myeloid leukemia-Treatment Outomes. Accessed June 2025. https://www.lls.org/leukemia/chronic-myeloid-leukemia/treatment/treatment-outcomes
26.Hehlmann R. The New ELN Recommendations for Treating CML. Journal of Clinical Medicine. 2020;9(11):3671. doi: 10.3390/jcm9113671 PubMed
27.FDA. HIGHLIGHTS OF PRESCRIBING INFORMATION, SCEMBLIX® (asciminib). 2024. https://www.accessdata.fda.gov/drugsatfda_docs/label/2024/215358s009lbl.pdf
28.Scemblix (asciminib): 20 mg and 40 mg, oral tablets [product monograph]. 2025.
29.PrBosulif® (bosutinib): 100 mg, 400 mg, 500 mg, oral tablets [product monograph]. Pfizer Canada; 2021.
30.PrTasinga® (nilotinib): 150 mg, 200 mg, oral capsules [product monograph]. Novartis Pharmaceuticals Canada; 2015.
31.PrSprycel® (dasatinib): 20 mg, 50 mg, 70 mg, 80 mg, 100 mg, 140 mg, oral tablets [product monograph]. Bristol-Myers Squibb Canada; 2021.
32.PrIclusig® (ponatinib): 15 mg, 45 mg, oral tablets [product monograph]. ARIAD Pharmaceuticals; 2019.
33.Laneuville P, Barnett MJ, Bélanger R, et al. Recommendations of the Canadian Consensus Group on the Management of C hronic Myeloid Leukemia. Current Oncology. 2006;13(6):201-221. PubMed
34.Cortes JE, Sasaki K, Kim DW, et al. Asciminib monotherapy in patients with chronic-phase chronic myeloid leukemia with the T315I mutation after ≥1 prior tyrosine kinase inhibitor: 2-year follow-up results. Leukemia. 2024;38(7):1522-1533. doi: 10.1038/s41375-024-02278-8 PubMed
35.Novartis P. Clinical Study Report: A phase III, multi-center, open-label, randomiz ed study of oral asciminib versus Investigator selected TKI in patien ts with newly diagnosed Philadelphia Chromosome Positive Chronic Mye logenous Leukemia in Chronic Phase. 2022. 2022/11/22/. Accessed 2024/11/26/.
36.Giesinger JM, Kieffer JM, Fayers PM, et al. Replication and validation of higher order models demonstrated that a summary score for the EORTC QLQ-C30 is robust. J Clin Epidemiol. 2016;69:79-88. doi: 10.1016/j.jclinepi.2015.08.007 PubMed
37.Fayers PM, Aaronson NK, Bjordal K. The EORTC QLC-C30 scoring manual (3rd Edition). EORTC; 2001. Accessed 2024 May 25. https://www.eortc.org/app/uploads/sites/2/2018/02/SCmanual.pdf
38.Kaupp-Roberts SD, Yadegarfar G, Friend E, et al. Validation of the EORTC QLQ-BIL21 questionnaire for measuring quality of life in patients with cholangiocarcinoma and cancer of the gallbladder. Br J Cancer. 2016;115(9):1032-1038. doi: 10.1038/bjc.2016.284 PubMed
39.Musoro JZ, Coens C, Sprangers MAG, et al. Minimally important differences for interpreting EORTC QLQ-C30 change scores over time: A synthesis across 21 clinical trials involving nine different cancer types. Eur J Cancer. 2023;188:171-182. doi: 10.1016/j.ejca.2023.04.027 PubMed
40.Efficace F, Baccarani M, Breccia M, et al. International development of an EORTC questionnaire for assessing health-related quality of life in chronic myeloid leukemia patients: the EORTC QLQ-CML24. Qual Life Res. 2014;23(3):825-36. doi: 10.1007/s11136-013-0523-5 PubMed
41.Efficace F, Iurlo A, Patriarca A, et al. Validation and reference values of the EORTC QLQ-CML24 questionnaire to assess health-related quality of life in patients with chronic myeloid leukemia. Leuk Lymphoma. 2021;62(3):669-678. doi: 10.1080/10428194.2020.1838509 PubMed
42.Novartis. CSR cabl001j12301oct2024-Novartis response to Canada's Drug Agency request for additional information regarding DRUG NAME review on April 11 2025. 2025.
43.Hoch M, Huth F, Manley PW, et al. Clinical Pharmacology of Asciminib: A Review. Clin Pharmacokinet. 2024;63(11):1513-1528. doi: 10.1007/s40262-024-01428-6 PubMed
44.Bower H, Björkholm M, Dickman PW, Höglund M, Lambert PC, Andersson TM-L. Life Expectancy of Patients With Chronic Myeloid Leukemia Approaches the Life Expectancy of the General Population. J Clin Oncol. 2016;34(24):2851-2857. doi: 10.1200/jco.2015.66.2866 PubMed
45.Sasaki K, Strom SS, O'Brien S, et al. Relative survival in patients with chronic-phase chronic myeloid leukaemia in the tyrosine-kinase inhibitor era: analysis of patient data from six prospective clinical trials. Lancet Haematol. 2015;2(5):e186-93. doi: 10.1016/s2352-3026(15)00048-4 PubMed
46.O'Brien SG, Guilhot F, Larson RA, et al. Imatinib compared with interferon and low-dose cytarabine for newly diagnosed chronic-phase chronic myeloid leukemia. N Engl J Med. 2003;348(11):994-1004. doi: 10.1056/NEJMoa022457 PubMed
47.Kantarjian H, Shah Neil P, Hochhaus A, et al. Dasatinib versus Imatinib in Newly Diagnosed Chronic-Phase Chronic Myeloid Leukemia. N Engl J Med. 2010;362(24):2260-2270. doi: 10.1056/NEJMoa1002315 PubMed
48.Brümmendorf TH, Cortes JE, Milojkovic D, et al. Bosutinib versus imatinib for newly diagnosed chronic phase chronic my eloid leukemia: final results from the BFORE trial. Leukemia. 2022;36(7):1825-1833. doi: 10.1038/s41375-022-01589-y PubMed
49.Saglio G, Kim D-W, Issaragrisil S, et al. Nilotinib versus Imatinib for Newly Diagnosed Chronic Myeloid Leukemia. N Engl J Med. 2010;362(24):2251-2259. doi: doi:10.1056/NEJMoa0912614 PubMed
50.FDA. Clinical Trial Endpoints for the Approval of Cancer Drugs and Biologics Guidance for Industry. 2025. Accessed May 12, 2025. https://www.fda.gov/media/71195/download
51.Hochhaus A, Larson RA, Guilhot F, et al. Long-Term Outcomes of Imatinib Treatment for Chronic Myeloid Leukemia. N Engl J Med. 2017;376(10):917-927. doi: doi:10.1056/NEJMoa1609324 PubMed
52.Bidikian A, Jabbour E, Issa GC, Short NJ, Sasaki K, Kantarjian H. Chronic myeloid leukemia without major molecular response after 2 years of treatment with tyrosine kinase inhibitor. Am J Hematol. 2023;98(4):639-644. doi: 10.1002/ajh.26836 PubMed
53.Kantarjian HM, Hughes TP, Larson RA, et al. Long-term outcomes with frontline nilotinib versus imatinib in newly diagnosed chronic myeloid leukemia in chronic phase: ENESTnd 10-year analysis. Leukemia. 2021;35(2):440-453. doi: 10.1038/s41375-020-01111-2 PubMed
54.Kaddoura R, Dabdoob WA, Ahmed K, Yassin MA. A practical guide to managing cardiopulmonary toxicities of tyrosine kinase inhibitors in chronic myeloid leukemia. Front Med (Lausanne). 2023;10:1163137. doi: 10.3389/fmed.2023.1163137 PubMed
Pharmacoeconomic Review
Abbreviations
AE
adverse event
AP
accelerated phase
BIA
budget impact analysis
BC
blast crisis
CDA-AMC
Canada’s Drug Agency
CML
chronic myeloid leukemia
CP
chronic phase
DMR
deep molecular response
ICER
incremental cost-effectiveness ratio
LY
life-year
MMR
major molecular response
OS
overall survival
Ph+
Philadelphia chromosome positive
QALY
quality-adjusted life-year
TKI
tyrosine kinase inhibitor
TFR
treatment-free remission
Economic Review
The objective of the economic review undertaken by Canada’s Drug Agency (CDA-AMC) is to review and critically appraise the pharmacoeconomic evidence submitted by the sponsor on the cost-effectiveness and budget impact of asciminib compared to a pooled comparator of tyrosine kinase inhibitors (TKIs) (henceforth referred to as “All TKIs”) for the requested reimbursement population of adult patients with newly diagnosed Philadelphia chromosome–positive (PH+) chronic myeloid leukemia (CML) in chronic phase (CP). The reimbursement request is narrower than the Health Canada indication.
Item | Description |
|---|---|
Drug product | Asciminib (Scemblix), 20 mg and 40 mg tablets |
Indication | Adult patients with Ph+ CML in CP who are newly diagnosed or who have previously received 1 or more TKIs |
Submitted price | Asciminib: $63.00 per 20 mg tablet Asciminib: $85.00 per 40 mg tablet |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | July 25, 2025 |
Reimbursement request | For the treatment of adult patients with newly diagnosed Ph+ CML in CP |
Sponsor | Novartis Pharmaceuticals Canada |
Submission history | Previously reviewed: Yes Indication: For the treatment of adult patients with Ph+ CML in CP previously treated with 2 or more TKIs Recommendation date: August 5, 2022 Recommendation: Reimburse with clinical criteria and/or conditions |
CP = chronic phase; NOC = Notice of Compliance; CML =chronic myeloid leukemia; Ph+ = Philadelphia chromosome positive; TKI = tyrosine kinase inhibitor.
Key Messages
Asciminib is available as 20 mg and 40 mg tablets. At the submitted prices of $63.00 per 20 mg and $85.00 per 40 mg, the 28-day cost of asciminib is expected to be $4,760 per patient, based on the Health Canada–recommended dosage.
Clinical efficacy in the economic analysis was derived from the ASC4FIRST trial, which compared asciminib with All TKIs. Evidence submitted by the sponsor indicates that asciminib is likely to increase the number of patients experiencing a major molecular response (MMR) and deep molecular response (DMR) compared with All TKIs among patients with Ph+ CML in CP who are newly diagnosed. The impact of asciminib on overall survival (OS) could not be assessed because of immature data.
The results of the CDA-AMC base case suggest:
Asciminib is predicted to be associated with higher costs to the health care system than All TKIs (incremental costs = $273,995), primarily driven by increased costs associated with drug acquisition.
Asciminib is predicted to be associated with a gain of 3.48 life-years (LYs) compared to All TKIs and may result in a gain of 2.91 quality-adjusted life-years (QALYs) compared to All TKIs.
The incremental cost-effectiveness ratio (ICER) of asciminib compared to All TKIs was $94,270 per QALY gained. The estimated ICER for asciminib versus All TKIs was highly sensitive to assumptions about long-term efficacy and OS. Approximately 99% of the incremental health benefit of asciminib compared to All TKIs was gained in the extrapolated period. In the absence of long-term comparative evidence, the predicted QALY gain for patients receiving asciminib is highly uncertain and may be overestimated.
Results of the CDA-AMC base case are highly uncertain and likely overestimate the benefit of asciminib. The model contains structural design choices that could not be modified and bias the results in favour of asciminib. Moreover, there is no long-term evidence to support the magnitude of OS benefit assumed by the sponsor. As such, the cost-effectiveness of asciminib is expected to lie between the CDA-AMC base case (ICER = $94,270 per QALY gained) and the scenario assuming a shorter time horizon (ICER = 276,985 per QALY gained).
CDA-AMC estimates that the budget impact of reimbursing asciminib for the treatment of adult patients with newly diagnosed Ph+ CML in CP when asciminib is initiated as first-line therapy will be approximately $18 million over the first 3 years of reimbursement compared to the amount currently spent on comparators, with an estimated expenditure of $43 million on asciminib over this period. The actual budget impact of reimbursing asciminib will depend on the percentage of patients covered by public drug plans and subsequent therapies.
Summary of the Submitted Economic Evaluation
The sponsor submitted a cost-utility analysis to estimate the cost-effectiveness of asciminib from the perspective of a public health care payer in Canada over a lifetime horizon (40 years). The modelled population comprised patients with newly diagnosed Ph+ CML in CP which is aligned with the reimbursement request and was based on participants in the ASC4FIRST trial. The sponsor’s base-case analysis included costs related to drug acquisition, health care resource use, adverse events (AEs), and terminal care.
In the sponsor’s base case, asciminib was associated with incremental costs of $177,775 and 2.94 incremental QALYs relative to All TKIs. This resulted in an ICER of $60,469 per QALY gained. Approximately 99% of the incremental benefit (2.94 incremental QALYs) of asciminib compared to All TKIs was predicted to be accrued after the ASC4FIRST trial’s observation period (96 weeks). Additional information about the sponsor’s submission is summarized in Appendix 3.
CDA-AMC identified several key issues with the sponsor’s analysis (refer to Table 2; full details are provided in Appendix 4).
Table 2: Key Issues With the Sponsor’s Economic Submission
Issue | What evidence is there to inform this issue? | How was this issue addressed by CDA-AMC? | Did CDA-AMC explore uncertainty in a scenario analysis? |
|---|---|---|---|
The model structure does not accurately reflect the clinical course of CML as observed in real-world practice. | The sponsor assumed no transitions from 2L treatment to MMR, DMR, or TFR. However, literature and clinical experts confirm TFR is possible in 2L. The model also omitted transitions from 2L to AP and CML-related death, despite expert input that progression and CML-related mortality can occur in 2L. The model’s definition of CML-related death differed from that used in the ASC4FIRST trial. | CDA-AMC could not address this issue in the base case due to the structure of the sponsor’s model. | No scenario analysis was conducted. |
The model structure and input assumptions obscure meaningful differences in comparative effectiveness. | Asciminib was compared to a pooled comparator (All TKIs), preventing direct comparison with second-generation TKIs. This is problematic, as the ASC4FIRST trial’s data at 96 weeks showed ██ ███████████ ██████████ in MMR to DMR transitions between asciminib and second-generation TKIs. Additionally, the model used different TKI distributions for efficacy and cost inputs, introducing inconsistency. | CDA-AMC could not address the first issue due to structural limitations in the submitted model, which did not allow for a direct comparison between asciminib and second-generation TKIs. | CDA-AMC aligned the modelled TKI treatment distribution with that observed in the ASC4FIRST trial in a scenario analysis. |
The long-term OS benefit predicted for asciminib relative to All TKIs is highly uncertain. | The model predicts a 3.07 LY survival benefit for asciminib over All TKIs, driven by structural and transition probability assumptions. The near entirety of this benefit (99.9%) is derived through extrapolation when there is no long-term evidence. | CDA-AMC did not address this issue in the base case due to remaining uncertainty. | CDA-AMC conducted a 10-year time horizon scenario to reduce the influence of unsupported long-term OS gains embedded in the model structure. |
The efficacy assumptions in the model were biased in favour of asciminib. | In the absence of supporting trial data and evidence, the sponsor made transition probability assumptions that favoured asciminib. | CDA-AMC applied the same transition probabilities to asciminib and All TKIs when differences were not statistically significant or based on assumptions. | No scenario analysis was conducted. |
The long-term OS benefit is likely underestimated for All TKIs. | The model likely underestimates long-term OS for All TKIs, projecting a 10-year OS of 65% — lower than asciminib (75%) and external data like the IRIS trial (83%). This reflects structural and methodological limitations that bias results in favour of asciminib. | CDA-AMC could not address this issue in the base case because it is driven by fixed structural features and assumptions embedded in the sponsor’s model. | No scenario analysis was conducted. |
The sponsor did not apply age- or sex-specific adjustments to health state utility values. | The model does not account for natural declines or demographic differences in quality of life over time. | CDA-AMC adjusted health state utility values by age and sex. | No scenario analysis was conducted; best available evidence was used in the CDA-AMC base case. |
The costs and LYs accrued in the long-term DMR health state did not align. | The sponsor assumed 5 years of treatment costs in the long-term DMR state, despite the model projecting 10.9 years for asciminib and 6.9 years for All TKIs, underestimating asciminib’s costs. | CDA-AMC adjusted drug costs to reflect the full duration patients remained in the long-term DMR health state. | No scenario analysis was conducted; best available evidence was used in the CDA-AMC base case. |
The dosages modelled for All TKIs may not align with clinical practice. | The sponsor used dosing consistent with the ASC4FIRST clinical trial; however, in clinical practice, lower dosages are often used to reduce side effects and manage AEs. | CDA-AMC did not address this issue because the dosages used in the base case were consistent with those specified in the respective Health Canada product monographs. | No scenario analysis was conducted; best available evidence was used in the CDA-AMC base case. |
2L = second-line treatment; AE = adverse event; AP = accelerated phase; CDA-AMC = Canada’s Drug Agency; DMR = deep molecular response; CML = chronic myeloid leukemia; LY = life-year; MMR = major molecular response; OS = overall survival; TFR = treatment-free remission; TKI = tyrosine kinase inhibitor.
Note: Full details of the issues identified by CDA-AMC are provided in Appendix 3.
CDA-AMC Assessment of Cost-Effectiveness
The CDA-AMC base case was derived by making changes to model parameter values and assumptions (refer to Table 6), in consultation with clinical experts. Detailed information about the CDA-AMC base case is provided in Appendix 4.
Impact on Health Care Costs
Asciminib is predicted to be associated with additional health care costs compared to All TKIs (incremental costs = $265,680). This increase in health care spending results from increased drug acquisition costs associated with asciminib (refer to Figure 1). All other health care costs are expected to be similar between asciminib and All TKIs.
Figure 1: Impact of Asciminib vs. All TKIs on Health Care Costs
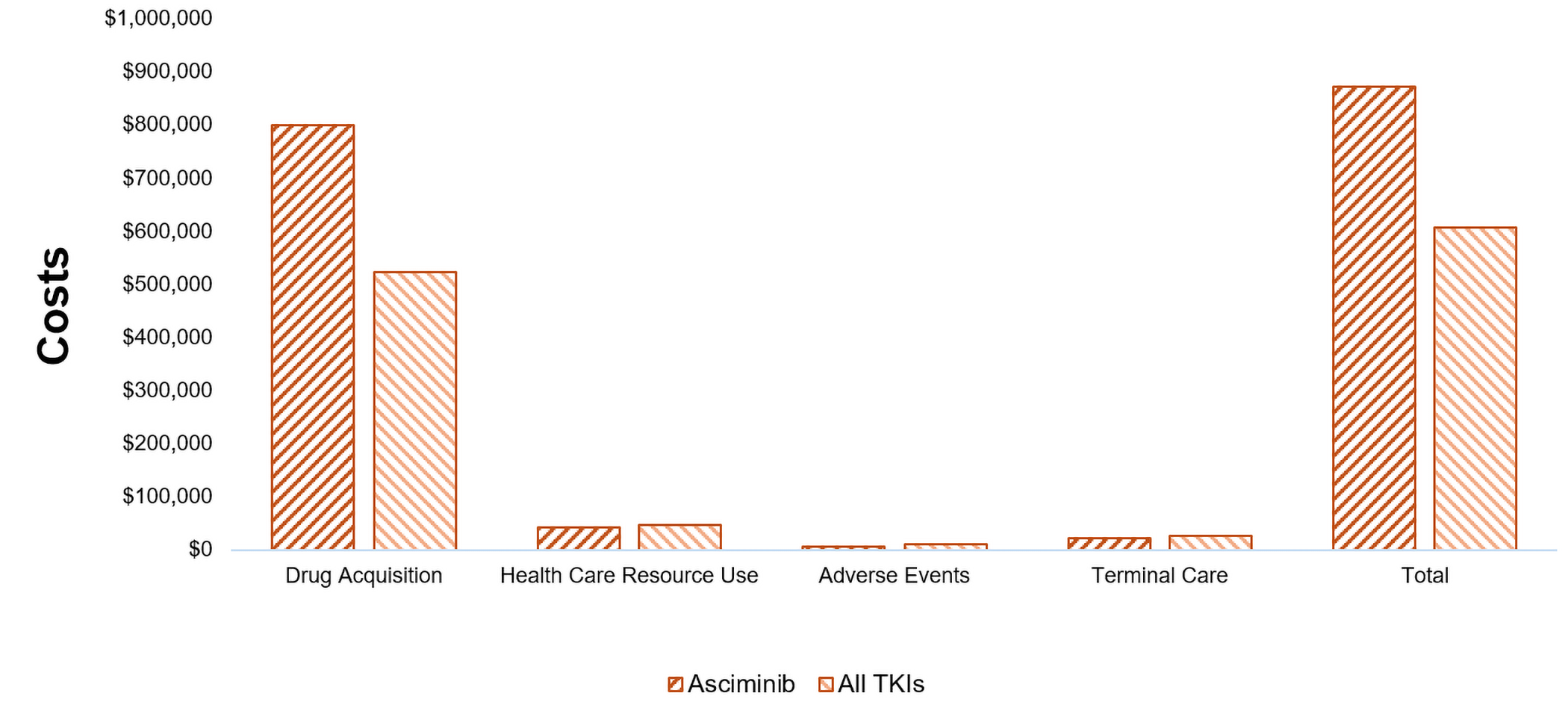
TKI = tyrosine kinase inhibitor; vs. = versus.
Impact on Health
Relative to All TKIs, asciminib is predicted to increase the amount of time a patient remains in the long-term DMR health state by approximately 4 years (refer to Table 8) and to extend OS by 3.37 years. The impact this has on QALYs is shown in Figure 2. Considering the impact of treatment on both quality and length of life, asciminib is predicted to result in 2.82 additional QALYs per patient compared to All TKIs. Approximately 99% of the predicted incremental benefit was accrued on the basis of extrapolation.
Figure 2: Impact of Asciminib vs. All TKIs on Patient Health
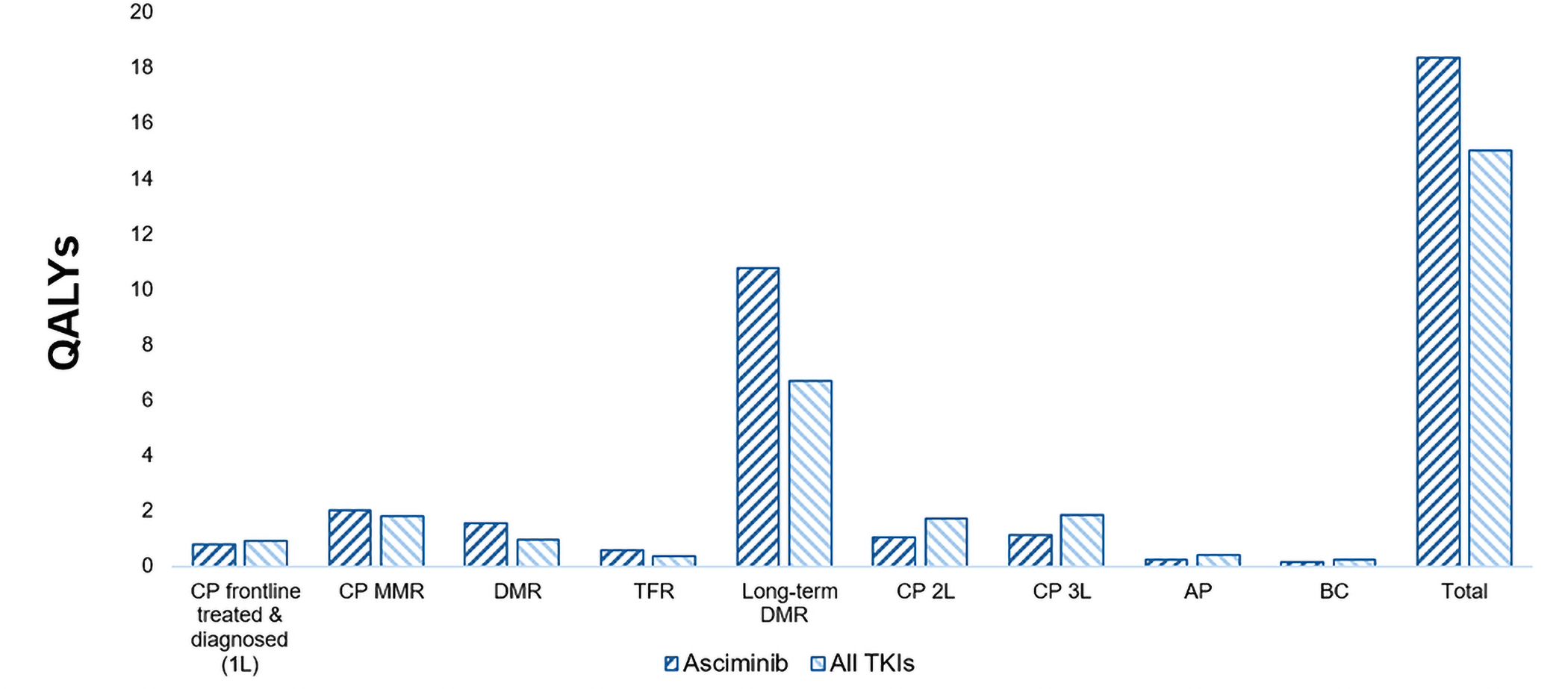
1L = first line; 2L = second line; 3L = third line; AP = accelerated phase; BC = blast crisis; CP = chronic phase; DMR = deep molecular response; MMR = major molecular response; QALY = quality-adjusted life-year; TFR = treatment-free remission; TKI = tyrosine kinase inhibitor; vs. = versus.
Overall Results
The results of the CDA-AMC base case suggest an ICER of $94,270 per QALY gained for asciminib compared to all TKIs (refer to Table 3). Additional details of the CDA-AMC base case are available in Appendix 4.
Table 3: Summary of CDA-AMC Economic Evaluation Results
Drug | Total costs ($) | Total LYs | Total QALYs | ICER vs. All TKIs ($/QALY) |
|---|---|---|---|---|
All TKIs | 607,504 | 15.02 | 10.59 | Reference |
Asciminib | 873,183 | 18.39 | 13.41 | 94,270 |
CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year; TKI = tyrosine kinase inhibitor; vs. = versus.
Note: Publicly available list prices were used for all comparators.
Uncertainty and Sensitivity
Due to immature data and the lack of long-term evidence, the OS benefit associated with asciminib was uncertain. The OS benefit was informed by 96-week trial outcomes extrapolated over a 40-year time horizon (refer to Table 2). Based on the results of a scenario analysis assuming a shorter time horizon, the ICER for asciminib increased to $276,985 per QALY gained compared to All TKIs (refer to Table 10).
CDA-AMC conducted a scenario to explore the impact of aligning the TKI treatment distribution with that observed in the ASC4FIRST trial. Based on the results of this analysis, the ICER for asciminib increased to $112,673 per QALY gained compared to All TKIs (refer to Table 10).
Summary of the Budget Impact
The sponsor submitted a budget impact analysis (BIA) to estimate the 3-year (2026 to 2028) budget impact of reimbursing asciminib for the treatment of adult patients with newly diagnosed Ph+ CML in CP when asciminib is initiated as a first-line therapy.1 The sponsor assumed that the payer would be CDA-AMC–participating public drug plans and derived the size of the eligible population using an epidemiologic approach.2 The price of asciminib was aligned with the price included in the sponsor’s economic evaluation, while the prices of comparators were based on the publicly available list prices.3-5 Additional information pertaining to the sponsor’s submission is provided in Appendix 5. CDA-AMC identified a number of issues with the sponsor’s estimated budget impact and made changes to model parameters and assumptions in consultation with clinical experts to derive the CDA-AMC base case (Appendix 5). CDA-AMC estimated that 3,807 patients would be eligible for treatment with asciminib over a 3-year period (year 1 = 913; year 2 = 1,252; year 3 = 1,642), of whom 693 are expected to receive asciminib (year 1 = 76; year 2 = 199; year 3 = 418). The estimated incremental budget impact of reimbursing asciminib is predicted to be approximately $18 million over the first 3 years, with an expected expenditure of $43 million on asciminib. The actual budget impact of reimbursing asciminib will depend on the percentage of patients covered by public drug plans and subsequent therapies.
Conclusion
Based on the CDA-AMC base case, asciminib would be considered cost-effective at the submitted price if the public health care system were willing to pay at least $94,270 for each additional QALY gained. If the public health care system is not willing to pay that amount, a price reduction should be considered (refer to Figure 3; full details of the impact of price reductions on cost-effectiveness are presented in Table 9). The estimated cost-effectiveness of asciminib compared to All TKIs is highly uncertain because it relies on a predicted OS benefit of 3.37 LYs that is not supported by available clinical evidence. More than 99% of this predicted benefit is derived from extrapolation. When a shorter time horizon is used to mitigate the influence of long-term survival gains that are unsupported by evidence, the ICER of asciminib compared to All TKIs increases to $276,985 per QALY gained.
The budget impact of reimbursing asciminib on the public drug plans in the first 3 years is estimated to be approximately $18 million. The 3-year expenditure on asciminib (i.e., not accounting for current expenditure on comparators) is estimated to be $43 million. The estimated budget impact is uncertain due to assumptions related to public coverage, access to care, and subsequent therapy use.
Figure 3: Summary of the CDA-AMC Economic Analysis and Price Reduction
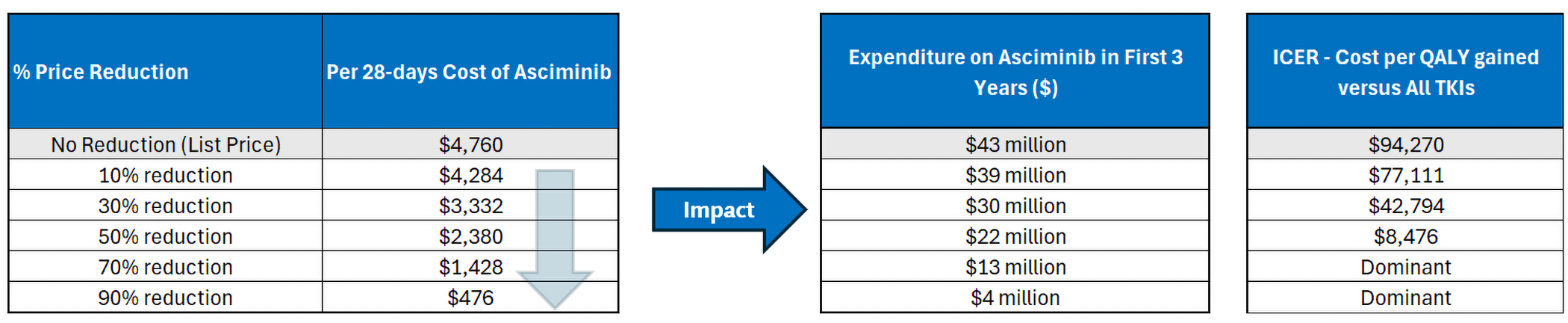
CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; TKI = tyrosine kinase inhibitor.
Note: Expenditure includes only the drug cost of asciminib in first-line treatment. The term dominant indicates that a drug costs less and provides more QALYs than the comparator.
References
1.Novartis Pharmaceuticals Canada Inc. Scemblix (asciminib): tablets, 20 mg and 40 mg (as asciminib hydrochloride), oral [product monograph]. June 21, 2022. Updated July 25, 2024.
2.Novartis Pharmaceuticals Canada Inc. Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Scemblix (asciminib) tablets, 20 mg and 40 mg (as asciminib hydrochloride), oral. March 10, 2025.
3.Novartis Pharmaceuticals Canada Inc. Drug Reimbursement Review sponsor submission: Scemblix (asciminib) tablets, 20 mg and 40 mg (as asciminib hydrochloride), oral [internal sponsor's package]. March 10, 2025.
4.Ontario Ministry of Health. Exceptional Access Program (EAP). Accessed May 26, 2025. http://www.health.gov.on.ca/en/pro/programs/drugs/odbf/odbf_except_access.aspx
5.Ontario Ministry of Health. Ontario drug benefit formulary/comparative drug index. Accessed May 26, 2025. https://www.formulary.health.gov.on.ca/formulary/
6.Hochhaus A, Wang J, Kim DW, et al. Asciminib in Newly Diagnosed Chronic Myeloid Leukemia. N Engl J Med. 2024;391(10):885-898. doi: 10.1056/NEJMoa2400858 PubMed
7.Radich JP, Hochhaus A, Masszi T, et al. Treatment-free remission following frontline nilotinib in patients with chronic phase chronic myeloid leukemia: 5-year update of the ENESTfreedom trial. Leukemia. 2021;35(5):1344-1355. doi: 10.1038/s41375-021-01205-5 PubMed
8.Lefkowitz RJ. The beta-adrenergic receptor. Life Sci. 1976;18(5):461-72. doi: 10.1016/0024-3205(76)90323-4 PubMed
9.Clifford JM, Cookson JH, Wickham PE. A comparative study of the disposition of quinalbarbitone, heptabarbitone and methaqualone in the rhesus monkey (Macaca mulatta) and the beagle dog (Canis familiaris). Comp Biochem Physiol C Comp Pharmacol. 1977;56(2):147-53. doi: 10.1016/0306-4492(77)90030-2 PubMed
10.Kantarjian HM, Giles FJ, Bhalla KN, et al. Nilotinib is effective in patients with chronic myeloid leukemia in chronic phase after imatinib resistance or intolerance: 24-month follow-up results. Blood. 2011;117(4):1141-5. doi: 10.1182/blood-2010-03-277152 PubMed
11.Cortes JE, Kantarjian HM, Brummendorf TH, et al. Safety and efficacy of bosutinib (SKI-606) in chronic phase Philadelphia chromosome-positive chronic myeloid leukemia patients with resistance or intolerance to imatinib. Blood. 2011;118(17):4567-76. doi: 10.1182/blood-2011-05-355594 PubMed
12.Shah NP, Kim DW, Kantarjian H, et al. Potent, transient inhibition of BCR-ABL with dasatinib 100 mg daily achieves rapid and durable cytogenetic responses and high transformation-free survival rates in chronic phase chronic myeloid leukemia patients with resistance, suboptimal response or intolerance to imatinib. Haematologica. 2010;95(2):232-40. doi: 10.3324/haematol.2009.011452 PubMed
13.Cortes JE, Kim DW, Pinilla-Ibarz J, et al. Ponatinib efficacy and safety in Philadelphia chromosome-positive leukemia: final 5-year results of the phase 2 PACE trial. Blood. 2018;132(4):393-404. doi: 10.1182/blood-2016-09-739086 PubMed
14.Rea D, Mauro MJ, Boquimpani C, et al. A phase 3, open-label, randomized study of asciminib, a STAMP inhibitor, vs bosutinib in CML after 2 or more prior TKIs. Blood. 2021;138(21):2031-2041. doi: 10.1182/blood.2020009984 PubMed
15.Garg RJ, Kantarjian H, O'Brien S, et al. The use of nilotinib or dasatinib after failure to 2 prior tyrosine kinase inhibitors: long-term follow-up. Blood. 2009;114(20):4361-8. doi: 10.1182/blood-2009-05-221531 PubMed
16.Statistics Canada. Life Tables, Canada, Provinces and Territories. 2024. Accessed May 28, 2025. https://www150.statcan.gc.ca/n1/pub/84-537-x/84-537-x2024001-eng.htm
17.Foulon S, Cony-Makhoul P, Guerci-Bresler A, et al. Health state utility and quality of life measures in patients with chronic myeloid leukemia in France. Qual Life Res. 2021;30(7):2021-2032. doi: 10.1007/s11136-021-02794-5 PubMed
18.Szabo SM, Levy AR, Davis C, Holyoake TL, Cortes J. A multinational study of health state preference values associated with chronic myelogenous leukemia. Value Health. 2010;13(1):103-11. doi: 10.1111/j.1524-4733.2009.00573.x PubMed
19.National Institute for Health and Care Excellence. Asciminib for treating chronic myeloid leukaemia after 2 or more tyrosine kinase inhibitors (NICE Technology appraisal guidance TA813). 2022. Accessed March 11, 2025. https://www.nice.org.uk/guidance/ta813
20.National Institute for Health and Care Excellence. Dasatinib, nilotinib and imatinib for untreated chronic myeloid leukaemia (NICE Technology appraisal guidance TA426). 2016. Accessed February 27, 2025. https://www.nice.org.uk/guidance/ta426
21.IQVIA. DeltaPA [sponsor supplied reference]. 2022. https://www.iqvia.com/locations/canada/library/fact-sheets/iqvia-deltapa
22.Ontario Ministry of Health. Ontario Case Costing Initiative (OCCI). Accessed March 26, 2025. https://data.ontario.ca/dataset/ontario-case-costing-initiative-occi
23.Walker H, Anderson M, Farahati F, et al. Resource use and costs of end-of-Life/palliative care: Ontario adult cancer patients dying during 2002 and 2003. J Palliat Care. 2011;27(2):79-88. PubMed
24.Novartis Pharmaceuticals Canada Inc. Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Scemblix (asciminib) tablets, 20 mg and 40 mg (as asciminib hydrochloride), oral. March 10, 2025.
25.Mahon FX, Boquimpani C, Kim DW, et al. Treatment-Free Remission After Second-Line Nilotinib Treatment in Patients With Chronic Myeloid Leukemia in Chronic Phase: Results From a Single-Group, Phase 2, Open-Label Study. Ann Intern Med. 2018;168(7):461-470. doi: 10.7326/M17-1094 PubMed
26.CADTH. Guidelines for the economic evaluation of health technologies: Canada. 4th ed. 2017. Accessed May 22, 2025. https://www.cadth.ca/dv/guidelines-economic-evaluation-health-technologies-canada-4th-edition
27.Oriana C, Martin H, Toby P, et al. Complete cytogenetic response and major molecular response as surrogate outcomes for overall survival in first-line treatment of chronic myelogenous leukemia: a case study for technology appraisal on the basis of surrogate outcomes evidence. Value Health. 2013;16(6):1081-90. doi: 10.1016/j.jval.2013.07.004 PubMed
28.Hochhaus A, Larson RA, Guilhot F, et al. Long-Term Outcomes of Imatinib Treatment for Chronic Myeloid Leukemia. N Engl J Med. 2017;376(10):917-927. doi: 10.1056/NEJMoa1609324 PubMed
29.Ara R, Brazier JE. Populating an economic model with health state utility values: moving toward better practice. Value Health. 2010;13(5):509-18. doi: 10.1111/j.1524-4733.2010.00700.x PubMed
30.Maas C, van Klaveren D, Ector G, et al. The evolution of the loss of life expectancy in patients with chronic myeloid leukaemia: a population-based study in the Netherlands, 1989-2018. Br J Haematol. 2022;196(5):1219-1224. doi: 10.1111/bjh.17989 PubMed
31.Bottomley A. The cancer patient and quality of life. Oncologist. 2002;7(2):120-5. doi: 10.1634/theoncologist.7-2-120 PubMed
32.Gandhi M, Tan RS, Ng R, et al. Comparison of health state values derived from patients and individuals from the general population. Qual Life Res. 2017;26(12):3353-3363. doi: 10.1007/s11136-017-1683-5 PubMed
33.Copland M. Is There a Role for Dose Modification of TKI Therapy in CML? Curr Hematol Malig Rep. 2019;14(4):337-345. doi: 10.1007/s11899-019-00524-w PubMed
34.CADTH Reimbursement Recommendation: Asciminib (Scemblix). Can J Health Technol. 2022;2(8). doi:10.51731/cjht.2022.422
35.pan-Canadian Pharmaceutical Alliance. Scemblix (asciminib). Accessed May 30, 2025. https://www.pcpacanada.ca/negotiation/21956
36.pan-Canadian Pharmaceutical Alliance. Bosulif (bosutinib). Accessed May 30, 2025. https://www.pcpacanada.ca/negotiation/21160
37.Alberta Health Services. Outpatient Cancer Drug Benefit Program. Accessed May 30, 2025. https://www.bccancer.bc.ca/systemic-therapy-site/Documents/Policy%20and%20Forms/Benefit%20Drug%20List.pdf
38.B. C. Government. BC Cancer Benefit Drug List. Accessed May 30, 2025. https://www.bccancer.bc.ca/systemic-therapy-site/Documents/Policy%20and%20Forms/Benefit%20Drug%20List.pdf
39.Cancer Care Ontario. Funded evidence-informed regimens. Accessed May 30, 2025. https://www.cancercareontario.ca/en/drugformulary/regimens
40.Statistics Canada. Canada's population estimates: Strong population growth in 2023 [sponsor supplied reference]. 2024. Updated March 27, 2024. https://www150.statcan.gc.ca/n1/daily-quotidien/240327/dq240327c-eng.htm
41.Canadian Cancer Society. Chronic myeloid leukemia statistics [sponsor supplied reference]. 2024. https://cancer.ca/en/cancer-information/cancer-types/chronic-myeloid-leukemia-cml/statistics
42.Eden RE, Coviello JM. Chronic Myelogenous Leukemia [sponsor supplied reference]. StatPearls Publishing; 2023. https://www.ncbi.nlm.nih.gov/books/NBK531459/
43.Perah G, Feldman M. In vitro activation of the in vivo colony-forming units of the mouse yolk sac. J Cell Physiol. 1977;91(2):193-9. doi: 10.1002/jcp.1040910205 PubMed
44.Gerson DF, Burton AC. The relation of cycling of intracellular pH to mitosis in the acellular slime mould Physarum polycephalum. J Cell Physiol. 1977;91(2):297-303. doi: 10.1002/jcp.1040910214 PubMed
45.IQVIA. PharmaStat. 2023. Accessed April 11, 2025. https://www.iqvia.com/
46.Novartis Pharmaceuticals Canada Inc. Novartis Market Research (Data on file) [sponsor supplied reference]. 2025.
47.Sutherland G, Dihn T. Understanding the gap: a pan-Canadian analysis of prescription drug insurance coverage. The Conference Board of Canada; 2017. Accessed May 30, 2025. https://www.conferenceboard.ca/e-library/abstract.aspx?did=9326
48.Isabelle G-A, Wanlin C, Chad L. Understanding the gap 2.0: A pan-Canadian analysis of prescription drug insurance coverage. The Conference Board of Canada; 2022. Accessed May 26, 2025. https://www.conferenceboard.ca/product/understanding-the-gap-2-0-a-pan-canadian-analysis-of-prescription-drug-insurance-coverage-2/
Appendix 1: Cost Comparison Table
Please note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical experts and CDA-AMC–participating public drug plans. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 4: Cost Comparison for Newly Diagnosed Ph+ CML in CP
Treatment | Strength | Form | Price ($) | Recommended dosage | Daily cost ($) | 28-day cost ($) |
|---|---|---|---|---|---|---|
Asciminib | 20 mg 40 mg | Tablet | 63.0000a 85.0000a | 40 mg twice daily or 80 mg once daily | 170.00 | 4,760 |
Tyrosine kinase inhibitors | ||||||
Bosutinib | 100 mg 500 mg | Tablet | 38.9787b 152.2403b | 400 mg once daily | 155.91 | 4,366 |
Dasatinib | 20 mg 50 mg 70 mg 80 mg 100 mg | Tablet | 32.8823c 66.1782c 72.9337c 117.3255c 132.2671c | 100 mg once daily | 132.27 | 3,703 |
Imatinib | 100 mg 400 mg | Tablet | 5.2079c 20.8314c | 400 once mg daily | 20.83 | 583.28 |
Nilotinib | 150 mg 200 mg | Tablet | 24.8355c 34.5709c | 300 mg twice daily | 99.34 | 2,782 |
CML = Philadelphia chromosome positive; CP = chronic phase; Ph+ = chronic myeloid leukemia.
aSponsor’s submitted price.3
bOntario Exceptional Access Program (accessed May 2025).4
cOntario Drug Benefit Formulary (accessed May 2025).5
Appendix 2: Input Relevant to the Economic Review
Please note that this appendix has not been copy-edited.
This section is a summary of the input received from the patient groups, clinician groups, and drug plans that participated in the CDA-AMC review process.
Patient input was received from Heal Canada, from the Chronic Myelogenous Leukemia Society of Canada, and from the Leukemia & Lymphoma Society of Canada and Canadian CML Network. Heal Canada surveyed 31 patients. The Chronic Myelogenous Leukemia Society of Canada conducted a survey of more than 20 patients with CML who were treated with asciminib in Canada, the US, and other countries between January 2024 and March 2025. The Leukemia and Lymphoma Society of Canada and the Canadian CML Network conducted an online survey in February and March 2025 of 80 patients with lived experience with CML, of which 70 identified a Canadian province or territory as their primary residence. They also conducted 2 one-on-one interviews and a round table with 3 patients living with CML. The most important outcomes for patients included delaying disease progression and experiencing durable remission, with the ultimate objective of improving survival; reducing side effects from treatments; and maintaining quality of life. Overall, patients’ disease experience was influenced by the physical symptoms associated with CML and the psychosocial effects associated with the disease (i.e., anxiety associated with disease progression and the interruption of life goals due to absence from work). Patients emphasized the need for front-line therapies that could help them experience treatment-free remission (TFR) and significantly shorten treatment duration. Patients noted that a shorter duration of therapy not only reduces time on TKIs but also lowers overall treatment costs per patient, including those related to drug use and management of AEs. Patients who had been on imatinib for more than 5 years commonly reported fatigue, pain, sleep disturbances, and reduced functional capacity as ongoing side effects. In contrast, those with experience using other therapies, including asciminib, noted milder side effects and an overall improvement in quality of life while on asciminib.
Clinician input was provided by the Canadian CML Physicians Interest Group and the Ontario Health (Cancer Care Ontario) Hematology Cancer Drug Advisory Committee. Experts confirmed that first-line treatment for CML typically involves TKIs. They noted that asciminib may be a suitable first-line option for patients who do not respond well to, or cannot tolerate, existing TKIs, due to its distinct mechanism of action. For disease monitoring, clinicians recommended real-time polymerase chain reaction (RT-PCR) every 3 months during the first year of treatment, and BCR::ABL1 level monitoring every 3 to 6 months thereafter. They also indicated that asciminib could be prescribed in an outpatient setting by hematologists experienced in CML management.
Input from CDA-AMC–participating drug plans highlighted that not all of the TKIs included in the ASC4FIRST trial are currently funded across jurisdictions. The drug plans also raised questions about whether patients already receiving a TKI would be eligible to switch to asciminib if it were publicly funded. Additionally, the drug plans sought clarification on whether asciminib could be re-administered to patients who relapse after stopping therapy.
Several of these concerns were addressed in the sponsor’s model:
The impact of disease and treatment on patient’s quality of life was captured with health state utilities values.
AEs, including decreased neutrophil count, decreased platelet count, and thrombocytopenia, were incorporated as disutilities.
CDA-AMC addressed some of these concerns as follows:
Health state utility values were adjusted to account for natural declines and demographic differences in quality of life over time.
Drug costs were adjusted to reflect the full duration that patients spend in long-term DMR.
CDA-AMC was unable to address the following concerns:
The model does not compare asciminib directly to second-generation TKIs. Hence, the cost-effectiveness of asciminib relative to second-generation TKIs (e.g., nilotinib, dasatinib, bosutinib) is unknown.
Patients value the potential to stop treatment, but the model did not allow second-line therapies to achieve TFR.
Appendix 3: Summary of the Sponsor’s Submission
Please note that this appendix has not been copy-edited.
Summary of the Sponsor’s Economic Evaluation
For the pharmaceutical reviews program, clinical and economic information is submitted to CDA-AMC by the sponsor. The CDA-AMC health economics team reviews the submitted economic information and appraises the information in collaboration with clinical experts and the clinical review team to evaluate key assumptions, influential parameters, and the overall rigour of the economic submission. Based on what the team learns through this process, adjustments may be made to the sponsor’s model to produce the CDA-AMC base case. The CDA-AMC base case represents the team’s current understanding of the clinical condition, clinical evidence currently available, and best interpretation of the economic evidence based on the information provided.
For the review of asciminib the sponsor provided a cost-utility analysis and a BIA. The sponsor’s economic submission is summarized in Table 5.
Table 5: Key Components of the Sponsor’s Economic Evaluation
Component | Description |
|---|---|
Treatment information | |
Drug under review | Asciminib (Scemblix), 20 mg and 40 mg tablets |
Submitted price of drug under review | Asciminib: $63.000 per 20 mg tablet Asciminib: $85.000 per 40 mg tablet |
Regimen | 40 mg twice daily or 80 mg once daily. Treatment should be continued as long as clinical benefit is observed or until unacceptable toxicity occurs. |
Per-cycle cost of drug under review | $4,760 per patient per 28-day cycle |
Model information | |
Type of economic evaluation | CUA Markov model |
Treatment | Asciminib |
Included comparators | All TKIs Note: the comparator is a basket of TKIs, including imatinib, nilotinib, dasatinib, and bosutinib |
Perspective | Publicly funded health care payer perspective |
Time horizon | Lifetime (40 years) |
Cycle length | 1 month |
Modelled population | Adult patients with naive Ph+ CML in CP who did not receive any treatment |
Characteristics of modelled population | Derived from the ASC4FIRST trial (mean age = 51 years; sex = 63% male, 37% female)6 |
Model health states |
For additional information, refer to Model Structure |
Data sources | |
Comparative efficacy |
|
Natural history and/or clinical pathway |
|
Health-related utilities and disutilities | |
Costs included in the model |
|
Summary of the submitted results | |
Base-case results | ICER = $60,469 per QALY gained (incremental costs = $177,775; incremental QALYs = 2.94) |
Scenario-analysis results |
|
1L = first line; 2L = second line; 3L = third line; AE = adverse event; AP = accelerated phase; BC = blast crisis; CCI = Case Costing Initiative; CML = chronic myeloid leukemia; CP = chronic phase; CUA = cost-utility analysis; DMR = deep molecular response; ICER = incremental cost-effectiveness ratio; MMR = major molecular response; ODB = Ontario Drug Benefit; Ph+ = Philadelphia chromosome positive; QALY = quality-adjusted life-year; TFR = treatment-free remission; TKI = tyrosine kinase inhibitor.
Model Structure
The sponsor submitted a Markov model with 11 health states to reflect the clinical pathway of patients with CML. The model includes 5 health states related to first-line treatment in CP: CP front-line diagnosed and treated, CP with MMR, CP with DMR, TFR, and long-term DMR. It also includes 2 subsequent treatment states — second-line treatment and third-line treatment — as well as 2 disease-progression states: accelerated phase (AP) and blast crisis (BC). Finally, the model includes 2 terminal states: CML-related death and non–CML-related death.24 Patients enter the model in CP front-line diagnosed and receive first-line treatment. From this state, patients may transition to CP MMR, second-line treatment, or AP, based on fixed treatment-specific transition probabilities derived from the 96-week outcomes of the ASC4FIRST trial. Patients experiencing MMR may progress to CP DMR or transition to a second-line treatment at fixed treatment-specific probabilities derived from the 96-week outcomes of the ASC4FIRST trial. Those who continue responding to first-line treatment may sequentially transition from CP DMR to TFR, and ultimately, to long-term DMR. Patients who discontinue first-line treatment for reasons other than disease progression move to a second-line treatment, and potentially to third-line treatment if further discontinuation occurs. Patients who experience disease progression from either the CP or third line states enter the AP state, followed by BC, and ultimately progress to CML-related death. At any point in the model, patients may transition to non–CML-related death. A figure of the sponsor’s model is available in Figure 4.
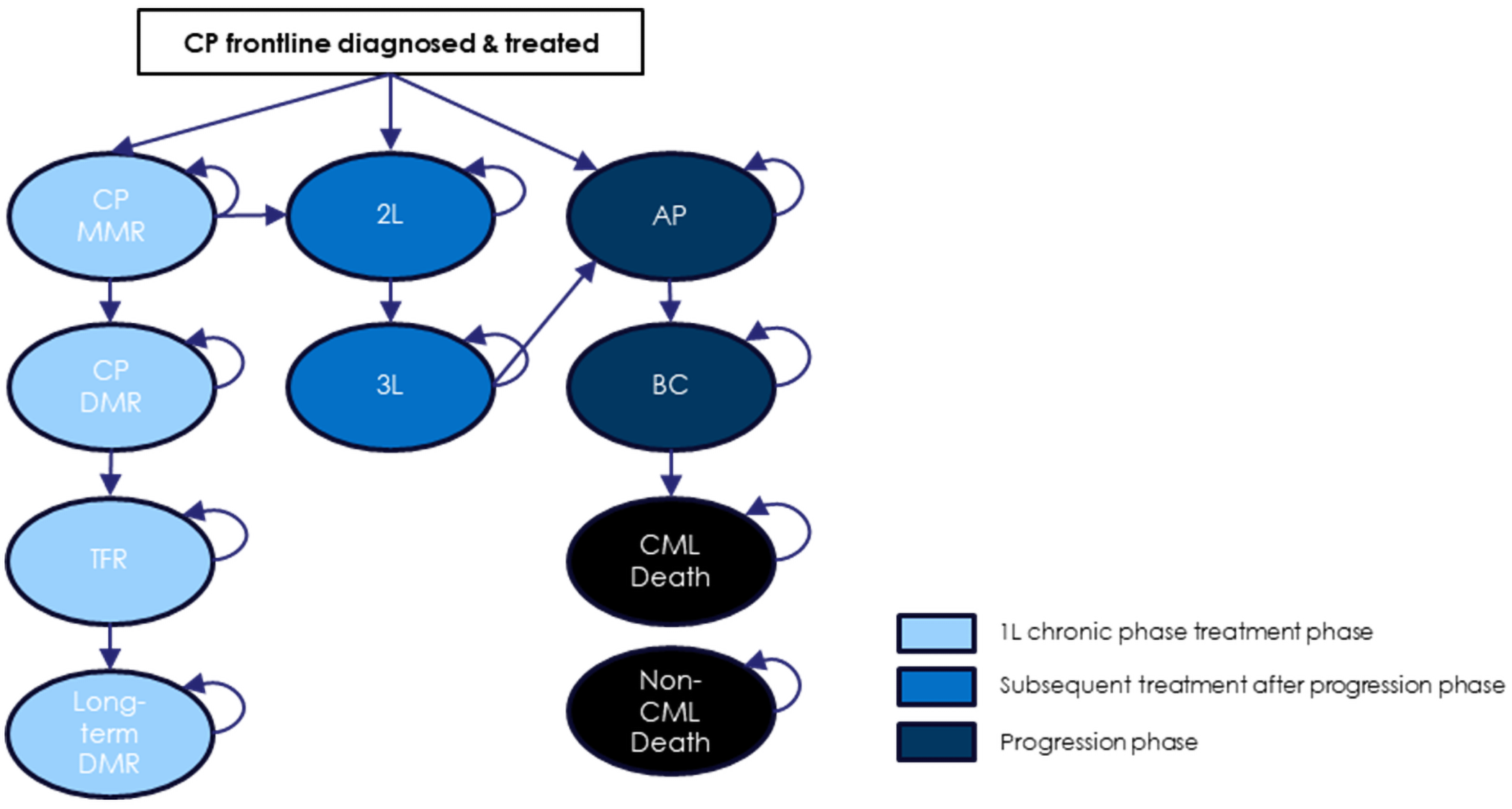
2L = second line; 3L = third line; AP = accelerated phase; BC = blast crisis; CML = chronic myeloid leukemia; CP = chronic phase; DMR = deep molecular response; MMR = major molecular response; TFR = treatment-free remission.
Source: Sponsor’s pharmacoeconomic submission.24
Appendix 4: Additional Details of CDA-AMC Reanalyses
Please note that this appendix has not been copy-edited.
Clinical Data in the Economic Model
The CDA-AMC clinical review found that asciminib increases the proportion of patients who experience an MMR or DMR (molecular response4.5) compared to the All TKIs at 48 weeks and 96 weeks, based on findings from the ASC4FIRST trial. Evidence from the ASC4FIRST stratum that compared asciminib to second-generation TKIs suggest that asciminib increases the proportion of patients who experience an MMR at 48 weeks and 96 weeks but does not increase the proportion of patients who experience a DMR (molecular response4.5). Data from the ASC4FIRST trial include follow-up to 96 weeks, with OS to be formally assessed only after 5 years. The CDA-AMC clinical review noted that the impact of achieving MMR at 96 weeks on OS remains unclear. Additionally, conclusions about differences in health-related quality of life between asciminib and All TKIs could not be drawn due to limitations in how data were collected in the trial.
In the economic model submitted by the sponsor, OS for asciminib was extrapolated beyond the ASC4FIRST trial period based on structural modelling assumptions. Notably, 99.9% of the survival benefit associated with asciminib in the sponsor’s model was accrued in the observed trial follow-up, contributing to additional uncertainty in the projected LYs and QALYs gained. Consequently, the CDA-AMC reanalysis is subject to a high degree of uncertainty due to the assumptions underpinning long-term survival benefit for asciminib. Due to uncertainty in the clinical effectiveness data — particularly the immature long-term survival data — the model’s predicted gains in LYs, QALYs, and overall cost-effectiveness are highly uncertain.
Key Issues of the Submitted Economic Evaluation
CDA-AMC identified the following key issues with the sponsor’s analysis:
The model structure does not adequately reflect CML in clinical practice. The sponsor submitted a Markov model with 11 health states (Figure 4), through which patients transition over time in alignment with CML treatment and disease progression. However, the model excluded key transitions from the second-line treatment state. In clinical practice, patients receiving second-line therapy can achieve MMR, DMR, and even TFR — a possibility supported by evidence showing that 41% of patients switching from imatinib to nilotinib maintained TFR at 96 weeks.25 Patients in the TFR health state do not accrue treatment costs, and omitting this transition underestimates potential cost savings and clinical benefits accrued by patients receiving a second-line therapy. The model also failed to capture disease progression accurately. According to clinical experts consulted by CDA-AMC, patients may develop accelerated phase disease from any treatment line, but the sponsor’s model restricted AP transitions to later stages. Moreover, the model’s definition of CML-related death — only occurring after blast crisis24 — differs from the ASC4FIRST trial, where CML deaths could occur at any stage.6 As noted in the CDA-AMC guidelines for economic evaluation, model health states should be based on the clinical or care pathway for the condition of interest.26 Movement between states in a Markov model structure should represent patient progression through the disease course. The sponsor’s model does not meet this standard, limiting its ability to accurately capture differences in costs and health outcomes between asciminib and All TKIs.
CDA-AMC was unable to address this limitation owing to the structure of the submitted model. Without addressing this, the underlying model structure biases in favour of asciminib.
The model structure and input assumptions obscure meaningful differences in comparative effectiveness. The sponsor’s model used a pooled comparator group (All TKIs) that combined first-generation (imatinib) and second-generation TKIs (nilotinib, dasatinib, bosutinib), despite clear differences in their clinical efficacy6 and drug acquisition costs. While such pooling may be justifiable in some contexts, it is problematic in this case for 2 reasons. First, the estimated clinical benefit of asciminib is influenced by the inclusion of imatinib in the comparator group, which has lower efficacy than second-generation TKIs.6 In the ASC4FIRST trial, asciminib demonstrated █████████████ ███████████ ███████████ in DMR at 96 weeks compared to the pooled All TKIs comparator. However, this difference was not observed when asciminib was compared directly to second-generation TKIs. As a result, the relative effectiveness of asciminib in the model reflects comparisons with a less effective treatment mix, rather than with the second-generation TKIs more commonly used in current practice. Second, the model applies different treatment distributions for cost and efficacy inputs, introducing a structural inconsistency. In the ASC4FIRST trial, 50% of patients in the comparator arm received imatinib. However, the sponsor’s model assumed that only 30% of patients received imatinib, while assigning disproportionately high use to more costly second-generation TKIs — e.g., dasatinib at 55% (compared to ███ in the trial). This mismatch creates a structural inconsistency: efficacy results reflect a less costly, more imatinib-heavy population, while costs are calculated as if most patients received higher-cost therapies. The combined effect of these choices is to favour asciminib in the economic analysis by aligning its benefits with a less effective comparator and its costs with a more costly one, making asciminib appear more cost-effective than it likely would be if costs and effectiveness were derived from the same distribution.
CDA-AMC was unable to address the first issue due to structural limitations in the submitted model, which did not allow for a direct comparison between asciminib and second-generation TKIs. This reduces the internal validity of the economic evaluation and limits its relevance for real-world reimbursement decisions — particularly in jurisdictions where imatinib use is limited or where second-generation TKIs are the preferred first-line therapy.
CDA-AMC conducted a scenario analysis aligning the TKI treatment distribution in the model with that observed in the ASC4FIRST trial to address the second issue.
The impact of asciminib on long-term OS is highly uncertain. The sponsor estimated a 3.07 LY gain for asciminib compared to All TKIs based on 96-week outcomes from the ASC4FIRST trial and modelling assumptions informing long-term extrapolations (Figure 5). However, the trial reported only 5 deaths and does not provide robust OS evidence. In the model, patients treated with asciminib were more likely to achieve MMR (███ versus ███) and DMR (███ versus ███) by 96 weeks compared to patients receiving All TKIs, making them more likely to enter TFR and long-term DMR health states. Conversely, patients treated with All TKIs were more likely to require multiple lines of therapy, resulting in higher projected CML-related mortality and a modelled survival advantage for asciminib. While statistically significant differences between asciminib and All TKIs were observed for earlier end points such as MMR and DMR, the sponsor did not establish or validate a surrogacy relationship between these intermediate outcomes and long-term OS. In response to a request from CDA-AMC, the sponsor provided additional information suggesting a potential surrogacy relationship between MMR and OS. However, evidence from the cited observational studies does not demonstrate a consistent or statistically significant association between MMR at 12 months and mean OS up to 84 months.27 Clinical experts consulted by CDA-AMC indicated that they would not expect asciminib to yield a 3-year survival advantage over other TKIs. CDA-AMC notes that the near entirety of the modelled OS benefit occurs beyond the trial follow-up period (99.9%), highlighting the extent to which survival gains are driven by structural assumptions rather than demonstrated survival differences. Hence, the estimated cost-effectiveness of asciminib compared to All TKIs is highly uncertain as it relies on an extrapolated OS benefit that is not supported by clinical evidence.
To mitigate this uncertainty, CDA-AMC conducted a scenario analysis that shortened the model’s time horizon to 10 years. This approach reduced the influence of long-term survival gains that are unsupported by evidence and structurally embedded in the model. As expected, the longer the time horizon, the greater the impact of these uncertain assumptions on the cost-effectiveness of asciminib.
The efficacy assumptions in the model were inconsistently justified and biased in favour of asciminib. The sponsor used point estimates from the ASC4FIRST trial at 96 weeks to inform several transitions in the model, including: from first-line therapy to MMR, from MMR to DMR, from MMR to second-line therapy, from first-line therapy to second-line therapy, and from first-line therapy to AP.6 However, at this time point, the rates of progressed disease and loss of MMR among patients receiving first-line treatment were not statistically different between asciminib and All TKIs, indicating similar efficacy. Despite this, the sponsor made favourable assumptions for asciminib where trial data or supporting evidence were lacking. For example, in the absence of evidence, asciminib was assumed to behave like the best performing TKI (nilotinib) for some transitions (e.g., from TFR to long-term DMR). Conversely, other TKIs were assumed to perform like the worst alternative (e.g., nilotinib for imatinib in the transition from third-line treatment to AP). These assumptions systematically biased the model in favour of asciminib by inflating its long-term benefits and worsening outcomes for comparators.
To address this, CDA-AMC applied more balanced and evidence-aligned assumptions. Where available, CDA-AMC used averages of trial estimates from ASC4FIRST (e.g., for transitions from first-line therapy to AP and from MMR to second-line therapy).
In cases lacking evidence (e.g., from TFR to long-term DMR and from third-line therapy to AP), CDA-AMC applied the same transition probabilities across treatments, calculated by averaging values from TKIs supported by evidence.
The model likely underestimates long-term OS for All TKIs. The model projects a 10-year OS of 65% for patients receiving All TKIs, compared to 75% for asciminib (Figure 5). These projections appear inconsistent with external clinical evidence. For example, the IRIS trial reported a 10-year OS of 83% among patients who received first-line treatment with imatinib,28 which is notable given that 50% of patients receiving All TKIs in the ASC4FIRST trial also received imatinib.6 Clinical experts consulted by CDA-AMC expressed concerns that the sponsor’s model substantially underestimated survival outcomes for patients receiving All TKIs, particularly in the context of modern treatment patterns and long-term outcomes observed in practice. This underestimation is not an isolated issue — it is the cumulative result of the modelling limitations highlighted in the preceding appraisal points: a constrained model structure that omits clinically plausible transitions; a pooled comparator group that masks differences in efficacy; an overreliance on unvalidated surrogate outcomes to project long-term OS; and inconsistent, selectively favourable efficacy assumptions for asciminib. Together, these limitations distort the survival estimates for All TKIs and inflate the incremental survival — and therefore the cost-effectiveness — of asciminib.
CDA-AMC was unable to address this limitation given that the survival projections are driven by fixed structural features and assumptions embedded in the sponsor’s model. However, the impact of these modelling choices is clear: the sponsor’s analysis does not provide a reliable estimate of the OS benefit of asciminib relative to All TKIs.
Health state utility values are inappropriately modelled. The sponsor did not adjust health state utility values by age and sex. If a baseline value of perfect health is assumed, natural declines in quality of life as patients age are not considered. This leads to an overestimate in the value of treatment.29 In addition, the health state utility values in the sponsor’s model for earlier disease states and advanced disease states were sourced from 2 different studies with different populations at different time points. Utilities for CP first line, CP MMR, TFR, second line, and third line were sourced from a cross-sectional study in 2018 of patients with CML living in France.17 Utilities for AP and BC were sourced from interviews conducted in 2006 and 2007 of individuals without CML living in Canada, the US, the UK, and Australia.18 Between 2006 and 2018 the life expectancy of patients with CML increased,30 likely leading to increases in quality of life among patients with CML. In addition, the utilities for the advanced disease states (AP and BC) were sourced from individuals without CML. The assessment of quality of life among patients with cancer should be from patients themselves.31 Furthermore, utility values derived from members of the general population may not accurately reflect the lived experience of patients with CML, particularly in advanced disease states. Individuals without the disease tend to assign lower values to hypothetical health states than patients living with the condition, potentially underestimating the true quality of life in these states.32 As such, caution is warranted when interpreting modelled outcomes based on these general population-derived utilities.
In the CDA-AMC base case, utilities were adjusted by age and sex.
CDA-AMC was unable to address the limitations related to the literature used to inform the health state utility values.
The LYs and costs accrued in the long-term DMR health state are not aligned: In the sponsor’s model, patients entering the long-term DMR health state were assumed patients to remain on treatment for 4.7 years, with drug costs applied as a 1-time lump sum. However, in the probabilistic results, patients accrued substantially more LYs in this state: 10.88 LYs for patients who received asciminib as a first-line treatment and 6.85 LYs for those who received All TKIs. This mismatch between time spent in the health state and the associated treatment costs leads to an undercounting of costs for both treatment groups. The implications are 2-fold. First, the model underrepresents the total cost of therapy, particularly for asciminib, which is associated with longer time in the long-term DMR state. Second, by underestimating costs while maintaining LYs, the model artificially improves the cost-effectiveness profile of asciminib. This results in an ICER that is more favourable than would be expected if costs and LYs were aligned.
In the CDA-AMC base case, this issue was corrected by adjusting drug costs to align with the LYs accumulated in the long-term DMR health state, ensuring consistency between clinical outcomes and associated resource use.
The dosages modelled for All TKIs may not align with clinical practice. In clinical practice, TKI doses are frequently individualized to manage AEs and improve tolerability while maintaining therapeutic efficacy.33 For example, for imatinib, a lower dose (300 mg once daily) can be used if 400 mg once daily is not tolerated.9 Similarly, for dasatinib, a 50 mg once daily dose can be used instead of 100 mg, leading to fewer side effects and similar response rates.9 In the ASC4FIRST clinical trial, patients discontinued first-line treatment due primarily to unsatisfactory therapeutic effect or AEs.6 However, clinical experts consulted by CDA-AMC indicated that in routine care, many patients would not discontinue therapy under these circumstances. Instead, physicians would often adjust the dose to manage side effects and support long-term adherence. This practice is not reflected in the sponsor’s model, which assumes fixed-dose treatment and does not account for dose modifications. By not accounting for these real-world adjustments, the sponsor’s model likely overestimates the transition from first-line to second-line therapy among patients receiving All TKIs. This, in turn, underestimates the clinical benefits of existing TKIs. The resulting structural bias favours asciminib by exaggerating its relative durability and cost-effectiveness compared to standard treatments.
CDA-AMC did not address this issue, as the dosages used in the base case were consistent with those specified in the respective Health Canada product monographs. However, the exclusion of dose adjustment practices limits the generalizability of the model results to real-world Canadian clinical settings, where individualized dosing is a standard part of care.
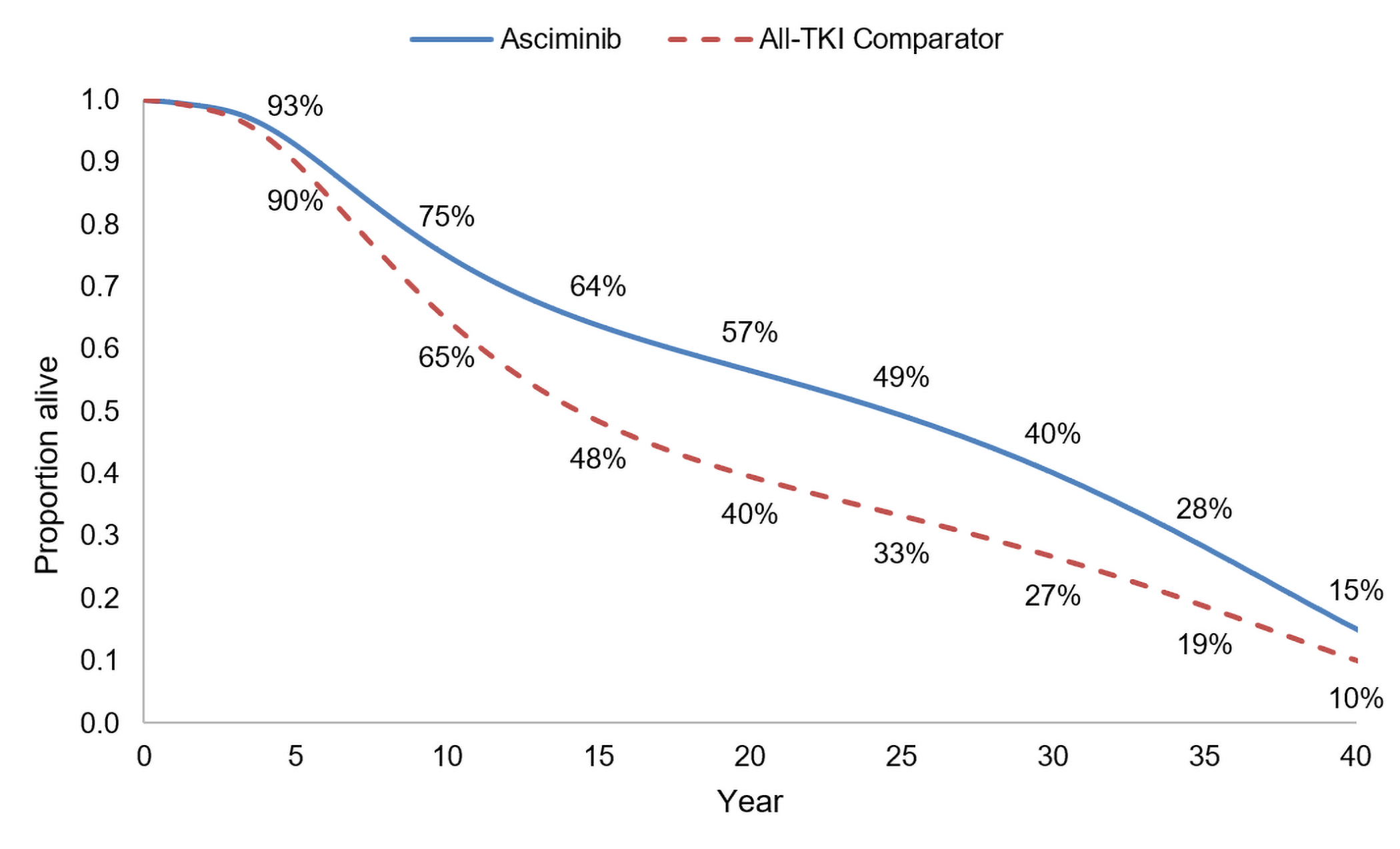
CDA-AMC Reanalysis of the Economic Evaluation
The CDA-AMC base case was derived by making changes in model parameter values and assumptions, in consultation with clinical experts (refer to Table 6). The impact of these changes, individually and collectively, is presented in Table 7.
Table 6: Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
1. Equate nonstatistically significant transition probabilities informed by ASC4FIRST trial | 1L to AP
MMR to 2L
| 1L to AP
MMR to 2L
|
2. Equate transition probabilities informed by assumption | TFR to long-term DMR
3L to AP
| TFR to long-term DMR
3L to AP
|
3. Use age- and sex-adjusted utility values | No adjustment for age and sex | Adjustment for age and sex |
4. Align time on treatment and associated drug costs in the long-term DMR state with LYs | Asciminib
All TKIs
| Asciminib
All TKIs
|
CDA-AMC base case (health care payer perspective) | ― | Reanalysis 1 + 2 + 3 + 4 |
1L = first line; 2L = second line; 3L = third line; AP = accelerated phase; CDA-AMC = Canada’s Drug Agency; CML = chronic myeloid leukemia; DMR = deep molecular response; LY = life-year; MMR = major molecular response; TFR = treatment-free remission; TKI = tyrosine kinase inhibitor.
Note: CDA-AMC was unable to resolve the issues with the sponsor’s model structure.
Table 7: Summary of the Stepped Analysis
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|---|
Sponsor’s base case | All TKIs | 605,035 | 11.82 | Reference |
Asciminib | 782,326 | 14.84 | 58,841 | |
CDA-AMC reanalysis 1: Transitions informed by numerical differences | All TKIs | 605,998 | 11.84 | Reference |
Asciminib | 781,349 | 14.82 | 58,924 | |
CDA-AMC reanalysis 2: Transitions informed by assumption | All TKIs | 588,057 | 11.63 | Reference |
Asciminib | 787,250 | 14.90 | 61,021 | |
CDA-AMC reanalysis 3: Utilities adjusted by age and sex | All TKIs | 605,035 | 10.99 | Reference |
Asciminib | 782,326 | 13.71 | 65,394 | |
CDA-AMC reanalysis 4: Align costs and LYs in long-term DMR | All TKIs | 626,583 | 11.82 | Reference |
Asciminib | 880,258 | 14.84 | 84,192 | |
CDA-AMC base case: Reanalysis 1 + 2 + 3 + 4 (deterministic) | All TKIs | 610,535 | 10.84 | Reference |
Asciminib | 884,530 | 13.74 | 94,212 | |
CDA-AMC base case: Reanalysis 1 + 2 + 3 + 4 (probabilistic) | All TKIs | 607,504 | 10.59 | Reference |
Asciminib | 873,183 | 13.41 | 94,270 |
CDA-AMC = Canada’s Drug Agency; DMR = deep molecular response; ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year; TKI = tyrosine kinase inhibitor.
Note: The CDA-AMC reanalysis is based on the publicly available prices of the comparator treatments. Deterministic results are presented, unless otherwise indicated.
Table 8: Disaggregated Results of the CDA-AMC Base Case
Parameter | Asciminib | All TKIs |
|---|---|---|
Discounted LYs | ||
Total | 18.39 | 15.02 |
CP front-line treated and diagnosed (1L) | 0.81 | 0.94 |
CP MMR | 2.04 | 1.80 |
DMR | 1.58 | 0.95 |
TFR | 0.59 | 0.37 |
Long-term DMR | 10.76 | 6.70 |
CP 2L | 1.06 | 1.73 |
CP 3L | 1.13 | 1.86 |
AP | 0.25 | 0.41 |
BC | 0.16 | 0.26 |
Discounted QALYs | ||
Total | 13.41 | 10.59 |
CP front-line treated and diagnosed (1L) | 0.58 | 0.67 |
CP MMR | 1.53 | 1.33 |
DMR | 1.29 | 0.77 |
TFR | 0.47 | 0.29 |
Long-term DMR | 7.98 | 4.96 |
CP 2L | 0.70 | 1.15 |
CP 3L | 0.73 | 1.21 |
AP | 0.10 | 0.17 |
BC | 0.03 | 0.04 |
Discounted costs ($) | ||
Total | 873,183 | 607,504 |
Drug acquisition | 799,869 | 523,338 |
Health care resource use | 42,286 | 47,356 |
AEs | 7,323 | 10,180 |
Terminal care | 23,706 | 26,630 |
1L = first line; 2L = second line; 3L = third line; AE = adverse event; AP = accelerated phase; BC = blast crisis; CDA-AMC = Canada’s Drug Agency; CML = chronic myeloid leukemia; CP = chronic phase; DMR = deep molecular response; LY = life-year; MMR = major molecular response; QALY = quality-adjusted life-year; TFR = treatment-free remission; TKI = tyrosine kinase inhibitor.
Price Reduction Analysis
CDA-AMC conducted price reduction analyses using the sponsor’s base case and the CDA-AMC base case (refer to Table 9).
Table 9: Results of the Price Reduction Analysis
Price reduction | Unit drug cost ($) | Cost per 28 days ($) | ICERs for asciminib vs. All TKIs ($/QALY) | |
|---|---|---|---|---|
Sponsor base case | CDA-AMC base case | |||
No price reduction | 85.00a | 4,760 | 60,469 | 94,270 |
10% | 76.50 | 4,284 | 43,957 | 77,111 |
20% | 68.00 | 3,808 | 27,447 | 59,952 |
30% | 59.50 | 3,332 | 10,937 | 42,794 |
40% | 51.00 | 2,856 | Dominant | 25,635 |
50% | 42.50 | 2,380 | Dominant | 8,476 |
60% | 34.00 | 1,904 | Dominant | Dominant |
70% | 25.50 | 1,428 | Dominant | Dominant |
80% | 17.00 | 952 | Dominant | Dominant |
90% | 8.50 | 476 | Dominant | Dominant |
CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; TKI = tyrosine kinase inhibitor; vs. = versus.
Note: The term dominant indicates that a drug costs less and provides more QALYs than the comparator.
aSponsor’s submitted price for asciminib, 40 mg tablets.24
Assessment of Uncertainty
CDA-AMC used the CDA-AMC base case to conduct scenario analyses that address uncertainty within the economic evaluation. The results are provided in Table 10.
Aligning the first-line treatment distribution of TKIs with that observed in the ASC4FIRST trial.
Applying a 10-year time horizon to reduce the influence of long-term survival gains that are unsupported by evidence and structurally embedded in the model.
Table 10: Results of CDA-AMC Scenario Analyses
Analysisa | Drug | Total costs ($) | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|
CDA-AMC base casea | All TKIs | 607,504 | 10.59 | Reference |
Asciminib | 873,183 | 13.41 | 94,270 | |
CDA-AMC scenario 1: Treatment distribution from ASC4FIRST trial | All TKIs | 561,545 | 10.60 | Reference |
Asciminib | 873,583 | 13.37 | 112,673 | |
CDA-AMC scenario 2: 10-year time horizon | All TKIs | 439,385 | 5.68 | Reference |
Asciminib | 608,822 | 6.29 | 276,985 |
CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; OS = overall survival; QALY = quality-adjusted life-year; TKI = tyrosine kinase inhibitor.
Issues for Consideration
CDA-AMC has reviewed asciminib for the treatment of adult patients with Ph+ CML in CP previously treated with 2 or more TKIs. The pan-Canadian Oncology Drug Review Expert Review Committee recommended that asciminib be reimbursed for this indication with clinical criteria and conditions on August 5, 2022.34 The pan-Canadian Pharmaceutical Alliance (pCPA) concluded negotiations with a letter of intent for asciminib.35 As such, the negotiated price of asciminib is confidential, and it is currently funded by jurisdictional cancer formularies.
Asciminib is currently under review at CDA-AMC for the treatment of adult patients with Ph+ CML in CP previously treated with 1 TKI. The cost-effectiveness of asciminib in the first-line setting compared to the second-line setting remains unknown. In addition, it is unclear how reimbursement of asciminib in the second-line setting may influence future market share projections for its use in the first-line setting, and how this, in turn, could affect the overall budget impact.
The pCPA concluded negotiations with a letter of intent for bosutinib for CML.36 As such bosutinib has a confidential negotiated price and is currently funded by jurisdictional cancer formularies.37-39 The CDA-AMC reanalyses are based on the publicly available price of bosutinib, which may be different from the confidential price and may influence the results of the cost-effectiveness and budget impact analyses.
Appendix 5: Budget Impact Analysis
Please note that this appendix has not been copy-edited.
Summary of the Submitted BIA
The sponsor submitted a BIA that estimated the expected incremental budgetary impact of reimbursing asciminib for the treatment of adult patients with newly diagnosed Ph+ CML in CP initiating first-line therapy.2
The BIA was conducted from the perspective of public drug plan payers over a 3-year time horizon (2026 to 2028), with 2025 as the base year. The sponsor’s estimate reflects the aggregated results from the jurisdictional provincial budgets (excluding Quebec) as well as the Non-Insured Health Benefits Program. The sponsor estimated the eligible population using an epidemiological approach.2 The market uptake for asciminib was estimated using the sponsor’s market research analysis.2 The key inputs to the BIA are documented in Table 11.
The sponsor estimated the 3-year incremental budget impact associated with reimbursing asciminib would be $10,415,670 (year 1 = $1,208,902; year 2 = $2,949,460; year 3 = $6,257,307).
Table 11: Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1 / year 2 / year 3, if appropriate) |
|---|---|
Target population | |
Starting number of people | 34,187,229 / 35,281,220 / 36,410,21940 |
Annual population growth rate | 3.20%40 |
Percentage of the adult population | 81.60%40 |
Percentage receiving public payer reimbursement | 65.00%2 |
Incidence of newly diagnosed CML patients | 2.19 per 100,00041 |
Percentage of Ph+ | 92.50%42 |
Percentage in CP | 95.00%43 |
Percentage of adults with health access | 85.00%2 |
Percentage of patients initiating a first treatment | 97.29%44 |
Number of patients eligible for the drug under review | 519 / 712 / 933 |
Market shares (reference scenario) | |
Asciminib | ███ / ███ / ███ |
Imatinib | ███ / ███ / ███ |
Nilotinib | ███ / ███ / ███ |
Dasatinib | ███ / ███ / ███ |
Bosutinib | ███ / ███ / ███ |
Market shares (new drug scenario) | |
Asciminib | ███ / ███ / ███ |
Imatinib | ███ / ███ / ███ |
Nilotinib | ███ / ███ / ███ |
Dasatinib | ███ / ███ / ███ |
Bosutinib | ███ / ███ / ███ |
Cost of treatment (per patient per 28 days) | |
Asciminib | $5,174 |
Imatinib | $634 |
Nilotinib | $3,786 |
Dasatinib | $4,026 |
Bosutinib | $4,634 |
CML = chronic myeloid leukemia; CP = chronic phase; Ph+ = Philadelphia chromosome positive.
Key Issues of the Submitted BIA
CDA-AMC identified several key issues to the sponsor’s analysis that have notable implications on the results of the BIA:
The percentage of public payer reimbursement is uncertain. The sponsor assumed that only 65% of Canadians would receive public payer reimbursement.45 The sponsor assumed 60% of adult patients in Ontario and the Atlantic provinces (i.e., New Brunswick, Nova Scotia, Prince Edward Island, and Newfoundland) would receive public coverage, whereas 100% of adult patients in the remaining provinces, except Quebec, would be publicly reimbursed.46 Given the younger age at diagnosis according to the ASC4FIRST trial, the sponsor increased private coverage to 35%. Therefore, 65% of adult patients in Canada were assumed to receive public payer reimbursement at baseline year. This approach is subject to uncertainty for several reasons. First, while the resulting estimate is used to refine the eligible population for asciminib under public drug plans, it is based on private claims data from IQVIA and reflects a subset of comparator drug claims selected by the sponsor. The extent to which this data accurately represents the proportion of public versus private claims is unclear, limiting its validity as a proxy for public drug plan eligibility. Second, the approach does not account for age-based differences in public coverage, which are recognized as key determinants of eligibility.47 Third, it does not consider jurisdictional variation in public drug plan eligibility, which further limits the generalizability of the estimate across Canadian provinces. As such, the estimated eligible population may not reflect actual reimbursement contexts at the jurisdictional level.47 Overall, CDA-AMC was unable to validate the sponsor’s approach, as the specific years of claims data and the list of drugs used for validation were not disclosed.
CDA-AMC conducted a base-case reanalysis in which public payer reimbursement was 97.2% across jurisdictions.48
The estimation of the proportion of newly diagnosed adult patients with access to health care is inappropriate. Specifically, the sponsor assumed that 85% of adult patients with newly diagnosed Ph+ CML in CP would have general access to health care across Canada.2 While access-related challenges may exist, this assumption does not reflect an epidemiological criterion and is not appropriate for determining eligibility for asciminib. Moreover, because public payer reimbursement is already incorporated as an access-related parameter, the inclusion of this additional assumption is redundant. It would be more appropriate to apply disease-related criteria that directly influence treatment eligibility.
CDA-AMC excluded this parameter due to its lack of disease specificity. In the revised base case, CDA-AMC assumed that 100% of patients with Ph+ CML in CP would have access to public health care.
The impact of subsequent therapy was excluded from the BIA. The sponsor did not include the cost of subsequent therapies in the budget impact model.24 The sponsor only included the drug acquisition costs for asciminib and comparators in the first-line setting. This is especially relevant because asciminib is indicated for patients with CML in the third-line setting. While the current reimbursement request is for first-line use, subsequent therapy costs remain relevant, as differences in treatment sequences could lead to downstream cost implications. The exclusion of subsequent therapy costs prevents a complete estimation of the budgetary impact associated with asciminb’s adoption in clinical practice.
CDA-AMC was unable to address this limitation owing to the submitted model structure.
CDA-AMC Reanalyses of the BIA
CDA-AMC revised the sponsor’s submitted analyses by making changes in model parameter values and assumptions, in consultation with clinical experts, as outlined in Table 11.
Table 12: Revisions to the Submitted BIA
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
1. Adult population in Canada receiving public payer reimbursement | 65% | 97% |
2. Percentage of adult patients with Ph+ CML in CP with health access | 85% | 100% |
CDA-AMC base case | ― | Reanalysis 1 + 2 |
BIA = budget impact analysis; CDA-AMC = Canada’s Drug Agency; CML = chronic myeloid leukemia; CP = chronic phase; Ph+ = Philadelphia chromosome positive.
Note: CDA-AMC was unable to resolve the issues with subsequent therapy.
The results of the CDA-AMC stepwise reanalysis are presented in summary format in Table 13, and a more detailed breakdown is presented in Table 14. In the CDA-AMC base case, the 3-year budget impact of reimbursing asciminib for the treatment of adult patients with newly diagnosed Ph+ CML in CP when asciminib is initiated as first-line therapy was $18,324,038 (year 1 = $2,126,793; year 2 = $5,188,915; year 3 = $11,008,331).
Table 13: Summary of the Stepped Analysis of the CDA-AMC Base Case
Stepped analysis | Three-year total ($) |
|---|---|
Submitted base case | 10,415,670 |
CDA-AMC reanalysis 1 | 15,575,432 |
CDA-AMC reanalysis 2 | 12,253,729 |
CDA-AMC base case: (reanalysis 1 + 2) | 18,324,038 |
CDA-AMC = Canada’s Drug Agency.
Note: The CDA-AMC reanalysis is based on publicly available prices of the comparator treatments.
Table 14: Disaggregated Summary of the BIA
Stepped analysis | Scenario | Year 0 (current situation) ($) | Year 1 ($) | Year 2 ($) | Year 3 ($) | Three-year total ($) |
|---|---|---|---|---|---|---|
Submitted base case | Reference total | 10,031,264 | 19,069,656 | 26,720,537 | 34,318,271 | 80,108,464 |
Asciminib | 0 | 0 | 0 | 0 | 0 | |
All other comparators | 10,031,264 | 19,069,656 | 26,720,537 | 34,318,271 | 80,108,464 | |
New drug total | 10,031,264 | 20,278,558 | 29,669,997 | 40,575,579 | 90,524,134 | |
Asciminib | 0 | 2,687,956 | 7,029,004 | 14,764,273 | 24,481,233 | |
All other comparators | 10,031,264 | 17,590,602 | 22,640,993 | 25,811,306 | 66,042,901 | |
Budget Impact | $0 | 1,208,902 | 2,949,460 | 6,257,307 | 10,415,670 | |
CDA-AMC base case | Reference total | 17,647,763 | 33,548,788 | 47,008,800 | 60,375,311 | 140,932,900 |
Asciminib | 0 | 0 | 0 | 0 | 0 | |
All other comparators | 17,647,763 | 33,548,788 | 47,008,800 | 60,375,311 | 140,932,900 | |
New drug total | 17,647,763 | 35,675,580 | 52,197,715 | 71,383,642 | 159,256,938 | |
Asciminib | 0 | 4,728,856 | 12,365,959 | 25,974,431 | 43,069,246 | |
All other comparators | 17,647,763 | 30,946,724 | 39,831,756 | 45,409,211 | 116,187,692 | |
Budget impact | 0 | 2,126,793 | 5,188,915 | 11,008,331 | 18,324,038 |
BIA = budget impact analysis; CDA-AMC = Canada’s Drug Agency.
Note: The CDA-AMC reanalysis is based on the publicly available prices of the comparator treatments.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.