Drugs, Health Technologies, Health Systems
Reimbursement Recommendation
Avapritinib (Ayvakyt)
Indication: For the treatment of adult patients with indolent systemic mastocytosis (ISM) with moderate to severe symptoms inadequately controlled on symptomatic treatment
Sponsor: Medison Pharma Canada Inc.
Final Recommendation: Reimburse with conditions
Summary
What Is the Reimbursement Recommendation for Ayvakyt?
Canada’s Drug Agency (CDA-AMC) recommends that Ayvakyt be reimbursed by public drug plans for adult patients with indolent systemic mastocytosis (ISM) with moderate to severe symptoms inadequately controlled on symptomatic treatment, if certain conditions are met.
Why Did CDA-AMC Recommend Reimbursement?
The pan-Canadian Oncology Drug Review Expert Review Committee (pERC) determined that it is uncertain whether Ayvakyt demonstrates acceptable clinical value versus symptomatic treatments in adult patients with ISM who have moderate to severe symptoms inadequately controlled on symptomatic treatment. Therefore, the committee also considered whether Ayvakyt addresses a significant unmet clinical need.
Evidence from 1 clinical trial showed that Ayvakyt in combination with symptomatic treatment may result in added clinical benefit, compared with placebo in combination with symptomatic treatment, as per the Indolent Systemic Mastocytosis Symptom Assessment Form (ISM-SAF) total symptom score (TSS). However, the evidence for Ayvakyt is uncertain because there were differences between groups in terms of prognostic factors as well as in the occurrence of edema, which might have allowed patients to infer treatment allocation. The effect of Ayvakyt to reduce anaphylaxis was also uncertain due to the small number of events.
ISM is a rare disease that can cause life-threatening anaphylaxis. Current treatment options available to patients with ISM in Canada only palliate the symptoms. pERC determined that Ayvakyt may meet some of the unmet clinical need in terms of improving disease symptoms with an acceptable safety profile.
Based on all of the preceding considerations, pERC recommended that Ayvakyt be reimbursed.
Which Patients Are Eligible for Coverage?
Ayvakyt should only be covered when used in conjunction with symptomatic treatments in adult patients with a confirmed diagnosis of ISM with a KIT D816V mutation, and who have moderate to severe disease based on the clinician’s assessment, with no clinical improvement in at least 1 type of symptom after receiving at least 2 prior symptomatic treatments, as determined by the clinician.
What Are the Conditions for Reimbursement?
Ayvakyt should only be reimbursed if the treatment is initiated by a hematologist, allergist, or immunologist with expertise in the diagnosis, treatment, and response evaluation of patients with ISM, and if the cost of Ayvakyt is reduced. Reimbursement of Ayvakyt may be continued for patients with disease response to treatment, as assessed by the treating clinician every 24 weeks. Reimbursement of Ayvakyt should be discontinued in cases of unacceptable toxicity, failure to meet follow-up requirements, or lack of clinical benefit as determined by the treating clinician.
Review Background
Disease background:
ISM is a condition in which abnormal immune cells called mast cells build up in the body. ISM can cause long-lasting and often severe symptoms affecting the skin, the stomach and intestines, brain function, muscles and bones, the whole body and, in some cases, it can lead to life-threatening anaphylaxis.
The incidence of ISM was estimated to be 0.4 cases per 100,000 people per year in a population-based matched cohort, which included 1,275 patients with mastocytosis identified between 1977 and 2014 from the Danish National Health Registries.
The median overall survival in patients with ISM was estimated to be 28.4 years (95% CI, 24.1 to 32.7), based on a study published in 2020 and analyzing a dataset of 1,993 patients from the registry of the European Competence Network on Mastocytosis.
Disease progression of ISM to a more advanced form of systemic mastocytosis (e.g., aggressive systemic mastocytosis, systemic mastocytosis with an associated hematological neoplasm, or mast cell leukemia) is not common. A natural history study in patients with ISM showed a 4.9% progression rate to a more advanced form of systemic mastocytosis.
Indication and reimbursement request: Avapritinib (Avvakyt) has been approved by Health Canada for the treatment of adult patients with ISM with moderate to severe symptoms inadequately controlled on symptomatic treatment.
Drug under review: Avapritinib is a tyrosine kinase inhibitor available as an oral tablet. The dosage recommended in the draft product monograph is 25 mg orally once daily, to be continued until disease progression or unacceptable toxicity.
Treatment costs: At the submitted price of $1,343.26 per 25 mg tablet, the per 28-day cost of Ayvakyt is expected to be $37,614 per patient, based on the Health Canada–recommended dosage.
Highlights of Input From Interested Parties
The patient group (Leukemia & Lymphoma Society of Canada [LLSC]) noted the following regarding impacts of the disease, unmet needs, and important outcomes:
ISM significantly impacts every aspect of a patient’s daily life due to the highly unpredictable occurrences of mast cell mediator-related symptoms (even life-threatening anaphylaxis) and the fear of this unpredictability.
The treatment goals for ISM include adequate symptom relief, fewer side effects from medications, and quality of life improvement.
There is an unmet need for accessible treatments that target the root cause of ISM, reduce the mast cell burden, restore a sense of safety and stability in patients’ daily lives, and have tolerable side effects.
The clinician groups (LLSC Clinician Network and Canadian Myeloproliferative Neoplasm Group, and the Ontario Health (Cancer Care Ontario) Hematology Cancer Drug Advisory Committee) and the clinical experts consulted by CDA-AMC noted the following regarding unmet needs arising from the disease and the place in therapy for the drug under review:
There is a need for effective and accessible treatments with fewer side effects that can modify the disease course, prevent the life-threatening symptoms of ISM (e.g., recurrent anaphylaxis), treat patients with ISM who become refractory to current symptomatic treatments, and improve patients’ quality of life.
Avapritinib should be used as the first choice in the indicated patient population, along with symptomatic treatments.
The participating public drug programs raised potential implementation issues related to considerations for initiation, renewal, discontinuation, and prescribing of therapy; generalizability of trial populations to broader populations; care provision issues; system and economic issues; and potential need for a provisional funding algorithm.
Disclaimer: The perspectives shared by people with lived experience who present to the committee reflect their individual experiences and are not necessarily representative of all people with the same condition or course of treatment. Their insights provide valuable context about what a patient, support person, or caregiver might go through with this condition or treatment, helping to inform the committee’s deliberations. These narratives complement other forms of evidence and input and should be considered as 1 element contributing to a broader understanding of the condition and treatment under review.
Recommendation
With a vote of 11 in favour to 5 against, the pan-Canadian Oncology Drug Review Expert Review Committee (pERC) recommends that avapritinib be reimbursed for the treatment of adult patients with ISM with moderate to severe symptoms inadequately controlled on symptomatic treatment only if the conditions listed in Table 1 are met.
Table 1: Reimbursement Conditions and Reasons
Reimbursement condition | Reason | Implementation guidance |
|---|---|---|
Initiation | ||
1.Treatment with avapritinib should be reimbursed when initiated in adult patients (aged 18 years or older) who meet all of the following: 1.1. have confirmed diagnosis of ISM with a KIT D816V mutation 1.2. present with moderate to severe disease, as determined based on clinician assessment 1.3. showed no clinical improvement in at least 1 type of symptom after having received at least 2 symptomatic treatments, as determined based on clinician assessment. | Avapritinib is a selective KIT D816V-targeting agent. According to clinical experts’ opinion, KIT wildtype disease may not respond to avapritinib therapy. Evidence from the PIONEER part 2 trial demonstrated that avapritinib in combination with BSC resulted in an added clinical benefit, compared to placebo in combination with BSC, in patients with a confirmed diagnosis of ISM who had moderate to severe symptoms and had failed to achieve adequate symptom control for 1 or more baseline symptoms with at least 2 symptomatic therapies, as determined by investigators. In PIONEER part 2, moderate to severe symptoms were based on a minimum mean ISM-SAF TSS ≥ 28 over the 14-day eligibility screening period for assessment of TSS. The ISM-SAF measurement instrument is a proprietary tool developed by the sponsor and not freely available for routine clinical use. According to clinical experts’ input, clinicians in Canada have little experience with the ISM-SAF tool in clinical practice and routinely determine patients’ symptom severity based on clinical judgment. | Condition 1.1: Based on clinical experts’ input, pERC noted that a diagnosis of ISM should be based on the current WHO or ICC diagnostic criteria. pERC also noted that both the WHO and ICC diagnostic criteria recognize the KIT D816V mutation as 1 of the minor criteria for diagnosing systemic mastocytosis. Condition 1.2: pERC recognized the challenges with using the ISM-SAF measurement tool to determine a patient’s disease severity, as discussed in the Summary of Deliberation section. Input from clinical experts suggests that disease severity should be determined based on clinician judgment and on a case-by-case basis, though pERC advised that, in alignment with what was measured in the PIONEER trial using the ISM-SAF tool, symptoms to consider in the assessment of severity may include bone pain, joint pain, abdominal pain, nausea, skin lesions, itching, flushing, fatigue, dizziness, brain fog, headache, and diarrhea. Condition 1.3: pERC recommends that avapritinib be initiated after optimal management with concurrent symptomatic treatments due to the uncertainty surrounding the risks and toxicities of long-term treatment with avapritinib. pERC noted that in the PIONEER trial, BSC (i.e., symptomatic treatments) mainly referred to drugs from the following drug classes:
|
2. Avapritinib should only be reimbursed when used in conjunction with symptomatic treatments. | There is no evidence to support the combination of avapritinib with any other mastocytosis therapy other than best supportive care. | — |
Renewal | ||
3.Patients should be assessed for disease response to avapritinib by the treating clinician every 24 weeks to determine whether reimbursement should continue. | This is to allow sufficient time for patients and clinicians to assess response to treatment. Evidence from the PIONEER part 2 trial was derived from assessment of end points at cycle 7, day 1 (i.e., 24 weeks post treatment with avapritinib). This timing was also agreed upon by the clinical experts consulted by CDA-AMC. | — |
Discontinuation | ||
4.Reimbursement of avapritinib should be discontinued upon occurrence of any of the following: 4.1. Unacceptable toxicity 4.2. Patients not fulfilling follow-up requirements 4.3. Lack of clinical benefit as determined by the treating clinician. | In the PIONEER part 2 trial, treatment with avapritinib was discontinued upon disease progression, unacceptable toxicity, loss to follow-up, and patient request. According to clinical experts, treatment with avapritinib should also be discontinued if there is a lack of clinical benefit based on clinician assessment. | pERC noted that there is currently no evidence that avapritinib delays progression to advanced systemic mastocytosis, given that the PIONEER part 2 trial did not investigate such outcomes. In line with input from clinical experts, pERC acknowledged that ISM is a chronic condition; disease progression to a more advanced form of systemic mastocytosis is uncommon and slow. pERC acknowledged that avapritinib has been approved by Health Canada at a higher dose (i.e., 200 mg daily) for patients with advanced forms of systemic mastocytosis. Therefore, the decision to discontinue treatment upon occurrence of disease progression should be made on a case-by-case basis by the treating clinician. Condition 4.1: In line with input from clinical experts, pERC noted that patients may or may not be rechallenged with avapritinib depending on the reasons for discontinuation. Avapritinib may be discontinued temporarily for mild side effects, cognitive changes, blood count abnormalities, or drug interaction and rechallenged after the resolution of these issues. However, patients may not be re-treated with avapritinib if they experienced intracranial bleeding. Condition 4.2: For follow-up requirements, pERC referred to the requirements for condition 3 (renewal), as well as any additional follow-up deemed appropriate by the treating clinician. Condition 4.3: Based on clinical experts’ input, pERC recognized that there are no standardized criteria for defining treatment response, given the heterogeneous and nonspecific nature of ISM symptoms and interpatient subjectivity in symptom assessment. In clinical practice, HRQoL, symptom burden, and mast cell burden are usually assessed to determine whether treatments provide clinical benefit. pERC noted that subjective concerns may weigh more on patient outcomes than objective markers, given that objective measures do not always correlate with clinical manifestations of the disease in patients with ISM. Altogether, pERC noted that the determination of clinical benefit or treatment response should be based on clinician judgment, taking into consideration of improvements in symptoms and quality of life. |
Prescribing | ||
5.Avapritinib should be initiated by a hematologist, allergist, or immunologist with expertise in the diagnosis, treatment, and response evaluation of patients with ISM, including managing the toxicities associated with avapritinib. | This is meant to ensure that avapritinib is prescribed for appropriate patients and that adverse effects are managed in an optimized and timely manner. | pERC noted that once avapritinib is initiated, subsequent management and follow-up care, including drug renewal, may involve different specialists with relevant expertise in ISM, who could be an oncologist, allergist, immunologist, or internal medicine specialist. |
Pricing | ||
6. A reduction in price | Using the CDA-AMC base-case analysis, the ICER for avapritinib plus BSC was $1,871,956 per QALY gained when compared with BSC alone in the indicated population. A band 4a price reduction would be required to achieve cost-effectiveness at a $50,000 per QALY threshold. A band 4a price reduction would be required to achieve cost-effectiveness at a $100,000 per QALY threshold. Price reductions for any given willingness-to-pay threshold are available in the CDA-AMC main report and Supplemental Material document. | The CDA-AMC analysis is based on public list prices for all treatments. Further price reductions may be required if there are price arrangements (discounts) currently in place for any treatment included in the economic analysis. Likewise, further price reductions may be required to address the economic feasibility of adoption. |
Feasibility of adoption | ||
7. The economic feasibility of adoption of avapritinib must be addressed. | At the submitted price, the incremental budget impact of avapritinib plus BSC is expected to be greater than $40 million in year 1, year 2, and year 3. | — |
BSC = best supportive care; CDA-AMC = Canada’s Drug Agency; HRQoL = health-related quality of life; ICC = International Consensus Classification; ICER = incremental cost-effectiveness ratio; ISM = indolent systemic mastocytosis; ISM-SAF = Indolent Systemic Mastocytosis Symptom Assessment Form; pERC = pan-Canadian Oncology Drug Review Expert Review Committee; QALY = quality-adjusted life-year; TSS = total symptom score.
aFor the statement regarding the size of the price reduction required, band 1 = 1% to 24%, band 2 = 25% to 49%, band 3 = 50% to 74%, and band 4 = 75% or greater.
Rationale for the Recommendation
Due to the uncertainty in clinical value, pERC could not recommend whether to reimburse avapritinib or not based on clinical value alone. Therefore, they also considered whether avapritinib addresses a significant unmet clinical need. pERC concluded that avapritinib addresses a significant unmet clinical need with an acceptable level of certainty. Based on these considerations, pERC recommended that avapritinib be reimbursed.
Clinical Value
Based on the totality of the clinical evidence, pERC concluded that it is uncertain whether avapritinib demonstrates acceptable clinical value, compared with best supportive care (BSC), in patients with ISM who have moderate to severe symptoms inadequately controlled on symptomatic treatment. Given that avapritinib is expected to be an additive treatment to BSC treatments, acceptable clinical value refers to added value versus BSC alone (i.e., symptomatic treatments).
Evidence from 1 phase II, double-blind, randomized controlled trial (PIONEER part 2; N = 212) showed that avapritinib in combination with BSC may result in added clinical benefit, compared with placebo in combination with BSC, for adults with ISM who had moderate to severe symptoms and had not achieved adequate symptom control for 1 or more baseline symptoms, as per the ISM-SAF TSS, with at least 2 of the symptom-directed treatments in BSC. Results from the PIONEER trial part 2 showed that avapritinib in combination with BSC, compared to placebo in combination of BSC, may lead to a statistically significant improvement in the ISM-SAF TSS from baseline to 24 weeks post treatment (i.e., at cycle 7, day 1), with a between-group difference of −6.43 (95% confidence interval [CI], −10.90 to −1.96; P = 0.003). The proportion of patients with a 50% reduction or greater in the ISM-SAF TSS was 24.8% (95% CI, 17.9 to 32.8) for the avapritinib plus BSC group and 9.9% (95% CI, 4.1 to 19.3) for the placebo plus BSC group, with a between-group difference of 14.96 (95% CI, 5.02 to 24.91) in favour of avapritinib in combination with BSC. The proportion of patients with a 30% reduction or greater in the ISM-SAF TSS was 45.4% (95% CI, 37.0 to 54.0) for the avapritinib plus BSC group and 29.6% (95% CI, 19.3 to 41.6) for the placebo plus BSC group, with a between-group difference of 15.81 (95% CI, 2.39 to 29.24) in favour of avapritinib in combination with BSC. Evidence on the proportion of patients who had anaphylaxis treated with epinephrine post baseline was of high uncertainty due to the small number of events (i.e., 2 patients in the avapritinib in combination with BSC group and 3 patients in the placebo in combination with BSC group).
Further information on the committee’s discussion around clinical value is provided in the Summary of Deliberation section.
Considering Significant Unmet Clinical Need
ISM is a rare disease that can cause life-threatening anaphylaxis. Current treatment options available to patients with ISM in Canada include various BSC options, which only palliate the symptoms. According to the clinical experts consulted by CDA-AMC, currently available treatments are associated with significant patient and caregiver burden. Input from clinician groups noted that many patients experience either minimal benefit or intolerable side effects with currently available treatments, resulting in poor adherence and frequent medication changes.
Patient groups, clinician groups, and clinical experts consulted by CDA-AMC identified a need for effective and accessible treatments with minimal side effects that can modify the disease course, improve symptoms, prevent life-threatening anaphylaxis, and improve patients’ quality of life. pERC concluded that avapritinib in combination with BSC treatments may meet some of the needs, notably improving disease symptoms as measured by the ISM-SAF, with an acceptable safety profile. However, pERC was unable to draw any conclusions on whether avapritinib could modify the disease, given that the PIONEER part 2 trial did not provide any evidence that the underlying disease was cured, reversed, or that the disease progression was slowed by avapritinib.
pERC concluded that avapritinib addresses a significant unmet clinical need with an acceptable level of certainty in clinical value.
Further information on the committee’s discussion around unmet clinical need is provided in the Summary of Deliberation section.
Developing the Recommendation
As part of the deliberation on whether to recommend reimbursement or not, the committee also considered unmet nonclinical need and health inequity. Information on this discussion is provided in the Distinct Social and Ethical Considerations domain in the Summary of Deliberation section.
Because pERC recommended that avapritinib be reimbursed, the committee also deliberated on whether reimbursement conditions should be added to address important economic considerations, health system impacts, or social and ethical considerations, or to ensure clinical value is realized. The resulting reimbursement conditions, with accompanying reasons and implementation guidance, are stated in Table 1.
Summary of Deliberation
pERC considered all domains of value of the deliberative framework before developing its recommendation: clinical value, unmet clinical need, distinct social and ethical considerations, economic considerations, and impacts on health systems. For further information on the domains of value, refer to Expert Committee Deliberation at Canada’s Drug Agency.
The committee considered the following key discussion points, organized by the 5 domains of value.
Clinical Value
Request for minor revisions: During the feedback period on the draft recommendation, the sponsor requested that the prescribing condition be modified so that avapritinib may be initiated by a hematologist, allergist, or immunologist with expertise in the diagnosis, treatment, and response evaluation of patients with ISM, rather than by a hematologist only. The pERC subpanel committee considered the sponsor’s request and acknowledged that expanding the list of prescribers may improve timely access to treatment, reflect real-world clinical practice, and address geographic and specialist access barriers.
Appropriate comparators: According to clinical experts, pERC recognized that the BSC treatments used in the PIONEER part 2 trial as comparators to avapritinib were appropriate and generally reflective of the symptomatic treatments commonly used in Canada. pERC also noted that optimizing BSC treatments is highly individualized, with therapy tailored to patient needs, symptom severity, and tolerability. pERC noted that there were no specified trial criteria in PIONEER part 2 regarding optimization of BSC treatments before the first dose of avapritinib and concomitant BSC treatments over the course of the trial, which were managed based on investigator’s discretion. Given the heterogeneous nature of symptoms and symptom severity for ISM, as well as the interpatient subjectivity in symptom evaluation, pERC agreed with the clinical experts that relying on investigator discretion to determine the optimal use of BSC on a case-by-case basis increases the trial’s pragmatic relevance and reflects clinical practice in Canada.
Efficacy versus BSC treatments: One phase II, double-blind randomized controlled trial (PIONEER part 2; N = 212) showed that avapritinib in combination with BSC may result in a statistically significant improvement in the ISM-SAF TSS at 24 weeks, compared to placebo in combination with BSC, with a between-group difference of −6.43 (95% CI, −10.90 to −1.96; P = 0.003). Results for the proportions of patients with at least a 50% or 30% reduction in the ISM-SAF TSS at 24 weeks reached statistical significance in favour of avapritinib in combination with BSC. Only 2 patients in the avapritinib in combination with BSC group and 3 patients in the placebo in combination with BSC group experienced anaphylaxis during the trial. At cycle 7, day 1, the mean change from baseline in the Mastocytosis Quality of Life Questionnaire (MC-QoL) total score was −19.2 (standard deviation [SD] = 18.191) for the avapritinib plus BSC group and −9.55 (SD = 14.933) for the placebo plus BSC group, with a between-group difference of −9.65 (95% CI, −15.01 to −4.30) in favour of the avapritinib group. pERC was unable to draw any conclusion on the comparative efficacy of avapritinib in the long-term based on the PIONEER part 3 study, an ongoing, long-term extension study with a median duration of treatment of about 35 months (data cut-off date: September 20, 2024), considering the single-arm study design.
Clinical importance of treatment effects: pERC noted that anaphylaxis was considered by clinical experts as 1 of the most clinically relevant outcomes; however, pERC was unable to determine the clinical meaningfulness of the outcome due to the very small number of events that occurred. pERC noted that the primary end point of PIONEER part 2, ISM-SAF TSS at 24 weeks, was assessed using the ISM-SAF measurement instrument, developed and validated by the sponsor. A range between 6 and 10 points was reported as the minimal important difference (MID) for the ISM-SAF TSS, based on a study carried out by the sponsor using blinded, pooled data from patients enrolled in PIONEER. Based on the smallest MID (i.e., 6 points), pERC determined that the between-group difference in ISM-SAF at 24 weeks in favour of the avapritinib group may be clinically important. However, pERC agreed with the clinical experts that the ISM-SAF TSS, a total score calculated by adding each of the 11 item scores, may not account for interpatient subjectivity, given that there is high heterogeneity in the value patients place on different disease symptoms and their severity. Patients may consider 1 specific symptom as most burdensome, and improvement in that symptom as most meaningful; however, an improvement in the total score may not necessarily reflect the improvement in the specific symptom. The improvement favouring avapritinib in the proportion of patients with a greater than 30% or 50% reduction in ISM-SAF TSS at 24 weeks was considered by pERC as clinically meaningful based on the smallest value from the MID range provided by the clinical experts (i.e., 5% to 20%). However, uncertainty remains, given that these 2 outcomes were based on the scores obtained from the ISM-SAF measurement instrument. pERC noted that no between-group MIDs were identified for MC-QoL. The MID provided by the clinical experts ranged from 5 to 10 points. The 95% CI of the between-group difference (i.e., −15.01 to −4.30 points) in MC-QoL total score crossed the smallest MID of 5 points, suggesting uncertainty in clinical meaningfulness.
Safety versus BSC treatments: Overall, pERC agreed with the clinical experts that the safety profile of avapritinib was acceptable. In the PIONEER part 2 trial, the median treatment duration at a dose of 25 mg once daily was about 5.55 months. The proportion of patients who had at least 1 serious adverse event was 5.0% in the avapritinib in combination with BSC group and 11.3% in the placebo in combination with BSC group. A higher proportion of patients in the avapritinib plus BSC group had at least 1 adverse event (AE) of edema than the patients in the placebo plus BSC group (25.5% versus 11.3%), but none of the edema events were of grade 3 or higher. No intracranial bleeding events occurred. Four patients (2.8%) in the avapritinib in combination with BSC group and 3 patients (4.2%) in the placebo in combination with BSC group had 1 or more AEs of cognitive effect, none of which were AEs of grade 3 or higher. No additional safety concerns were identified with longer-term treatment with avapritinib in the PIONEER part 3 trial (i.e., 35 months). Due to the single-arm design of PIONEER part 3, pERC could not make any conclusions on the comparative longer-term safety of avapritinib. pERC noted that the safety profile and toxicities of avapritinib beyond 35 months of treatment are currently unknown. Based on current input and evidence, pERC recognized that long-term, continuous use of avapritinib is expected. However, pERC could not draw any definitive conclusions on the long-term safety of avapritinib beyond the time frame of the evidence reviewed. Longer-term safety data are needed.
Certainty of the evidence: The assessment of certainty of evidence using the GRADE (Grading of Recommendations Assessment, Development and Evaluation) approach was rated as very low for the proportion of patients who had anaphylaxis post baseline; low for the ISM-SAF TSS at 24 weeks, the proportion of patients with a greater than 30% reduction in ISM-SAF TSS at 24 weeks, and the MC-QoL total score at 24 weeks; and moderate for the proportion of patients with a greater than 50% reduction in ISM-SAF TSS at 24 weeks. One of the major sources of uncertainty was the serious risk of bias at the study level, given that the estimated treatment effects may have been influenced, at least in part, by prognostic differences between groups. In addition, treatment effect estimates on patient-reported end points (e.g., ISM-SAF TSS, proportion of patients with ≥ 30% or ≥ 50% reduction in ISM-SAF TSS) and HRQoL end points (e.g., MC-QoL) might have been biased due to the differential occurrence of AEs of edema between groups (25.5% versus 11.3%), which might have caused patients, clinicians, and/or investigators to be able to infer treatment assignments.
Place in therapy: pERC noted that avapritinib should be used along with BSC treatments in the indicated patient population. Avapritinib is expected to complement the use of existing treatments, which are primarily directed at symptom control. pERC noted the importance of optimal ISM management with symptomatic treatments before initiation of avapritinib, considering the uncertainty surrounding the risks and toxicities of long-term treatment. pERC agreed with the clinical experts and emphasized that it would be premature to characterize avapritinib as “disease-modifying,” although avapritinib showed improvements in measures of mast cell burden. According to the clinical experts, it is currently unclear whether, and to what extent, changes in these measures influence the natural history of ISM. The PIONEER trial did not provide any evidence that the underlying disease was cured, reversed, or that disease progression was slowed by avapritinib.
Adopting the ISM-SAF measurement instrument in clinical practice: According to information provided by the sponsor, pERC noted several potential challenges of adopting ISM-SAF in clinical practice. First, ISM-SAF requires daily patient input over 14 days, which may increase the burden for both patients and clinicians. Second, clinicians must obtain a licence from the sponsor to use ISM-SAF in clinical practice. Third, patient-reported symptom scores may not reliably reflect disease severity due to adaptation over time and individual interpretation. Fourth, ISM-SAF focuses on symptom burden, while clinicians in practice may focus on quality of life through direct patient interaction. According to the clinical experts consulted by the CDA-AMC, pERC acknowledged clinicians’ limited experience with ISM-SAF in clinical practice and noted that the clinical experts anticipated that the assessment of symptom severity based on the ISM-SAF TSS would generally align with clinicians’ own evaluations. pERC further noted the clinical experts’ concerns that some patients who may benefit from avapritinib (e.g., patients with ISM who have predominant and severe anaphylaxis or skin symptoms but a low ISM-SAF TSS) may not be eligible for avapritinib using the ISM-SAF TSS to determine symptom severity.
Clinical value: Based on all of the preceding considerations, the committee determined that the clinical value of avapritinib versus appropriate comparators (BSC treatments) was uncertain.
Unmet Clinical Need
Input on unmet clinical need: Patient groups, clinician groups, and clinical experts consulted by CDA-AMC identified an unmet need for effective treatment options that are safe and accessible, and can modify the disease course, prevent life-threatening anaphylaxis, improve symptoms, can be used to treat patients with ISM who become refractory to current BSC options, and improve patients’ quality of life.
Severity of the disease: Based on published data, pERC recognized that the incidence of ISM is low; that is, it was estimated to be 0.4 cases per 100,000 people per year in a population-based matched cohort including 1,275 patients with mastocytosis identified between 1977 and 2014 from the Danish National Health Registries. pERC also noted that the median overall survival of patients with ISM was 28.4 years (95% CI, 24.1 to 32.7), according to published data from 1,993 patients from the registry of the European Competence Network on Mastocytosis. Based on input from patient groups, clinician groups, and clinical experts, pERC acknowledged that ISM significantly impacts every aspect of a patient’s daily life due to the highly unpredictable occurrences of mast cell mediator-related symptoms, and that the anaphylactic reactions are life-threatening.
Availability of treatment options: According to the clinical experts, pERC noted that the treatment of ISM mainly focuses on symptom management. Current symptomatic treatment options that are readily available for the indicated patient population include various BSC treatments used concurrently (e.g., H1 antihistamines, H2 antihistamines, proton pump inhibitors, leukotriene inhibitors, corticosteroids, anti-IgE antibodies, and cromolyn sodium; bisphosphonates for osteoporosis; and other drugs for osteoporosis). Based on input from clinician groups, pERC noted that many patients with ISM experience either minimal benefit or intolerable side effects with currently available treatments, resulting in poor adherence and frequent medication changes.
Disease diagnosis: Based on patient input, pERC noted that 1 of the most significant challenges for patients with ISM is obtaining an accurate diagnosis without delay. Many patients surveyed by the patient group described years of unexplained symptoms, misdiagnoses, and repeated visits to various specialists (e.g., dermatologists, allergists, rheumatologists, cardiologists, and even psychiatrists) before finally receiving a diagnosis of ISM. pERC recognized that delay in diagnosis or misdiagnosis for years both prevents patients from benefiting from appropriate treatments and causes harm if patients receive inappropriate treatments without an accurate diagnosis or based on an inaccurate diagnosis. pERC noted, however, the lack of evidence to address this challenge, given that the PIONEER trial included patients who had confirmed ISM.
Significant unmet clinical need: Based on the preceding considerations, the committee determined that avapritinib may meet some of the unmet clinical need in terms of improving disease symptoms with an acceptable safety profile.
Distinct Social and Ethical Considerations
Input on unmet nonclinical need: According to input from patients, ISM affects patients’ sense of safety and autonomy as well as their ability to work, parent, and participate in everyday life due to the unpredictable nature of disease symptoms. Patients with ISM usually live in fear of eating, not knowing which foods might trigger a reaction. To prevent a reaction or when a reaction happens, patients and caregivers must take an unexpected leave of absence from work, which makes it difficult to maintain employment or care for children.
Equity considerations: According to the input from the clinical experts, pERC acknowledged that ISM disproportionately impacts groups experiencing systemic marginalization, equity-deserving populations, and people living in remote or rural areas. pERC noted that individuals experiencing marginalization may not be able to avoid triggers at work, may only be able to work in places that have environmental allergens, and may be unable to afford the cost of epinephrine (EpiPens), which is essential to treat life-threatening anaphylaxis. pERC acknowledged that patients who live in remote or rural areas might not have specialists available in their area who can provide them with a diagnosis, treatment, or monitoring. Even those in remote or rural areas who have access to specialists in their communities often have to wait a long time before seeing a specialist.
Ethical implications: Based on input from clinical experts, pERC recognized that current treatment options for the management of ISM are not easily accessed by all patients with ISM. pERC noted that patients with ISM also experience challenges due to the cost of current treatments and barriers to accessing specialists, particularly hematologists and allergists with expertise in mast cell diseases. Furthermore, a patient may need to visit different specialists or travel to specialized centres for access to some treatments, which involves additional appointments and increases the burden to patients and caregivers in terms of time absent from work and costs related to travel.
Economic Considerations
Health impacts of avapritinib plus BSC versus relevant comparators: Avapritinib plus BSC is predicted to be associated with a gain of 0.05 life-years compared to BSC alone and may result in a gain of 0.71 quality-adjusted life-years (QALYs) compared to BSC alone over a lifetime time horizon.
Cost of avapritinib plus BSC versus relevant comparators: Avapritinib plus BSC is predicted to be associated with higher costs to the health care system than BSC alone (incremental costs = $1,324,561), primarily driven by increased costs associated with drug acquisition.
Key findings of the economic evaluation: Based on the submitted evidence using the sponsor’s cost-utility analysis, the CDA-AMC base-case analysis estimated that the incremental cost-effectiveness ratio (ICER) for avapritinib plus BSC in patients with moderate to severe ISM was $1,871,956 per QALY gained when compared with BSC alone (Figure 1).
Figure 1: Estimate of the ICER Used by pERC to Inform the Price Condition
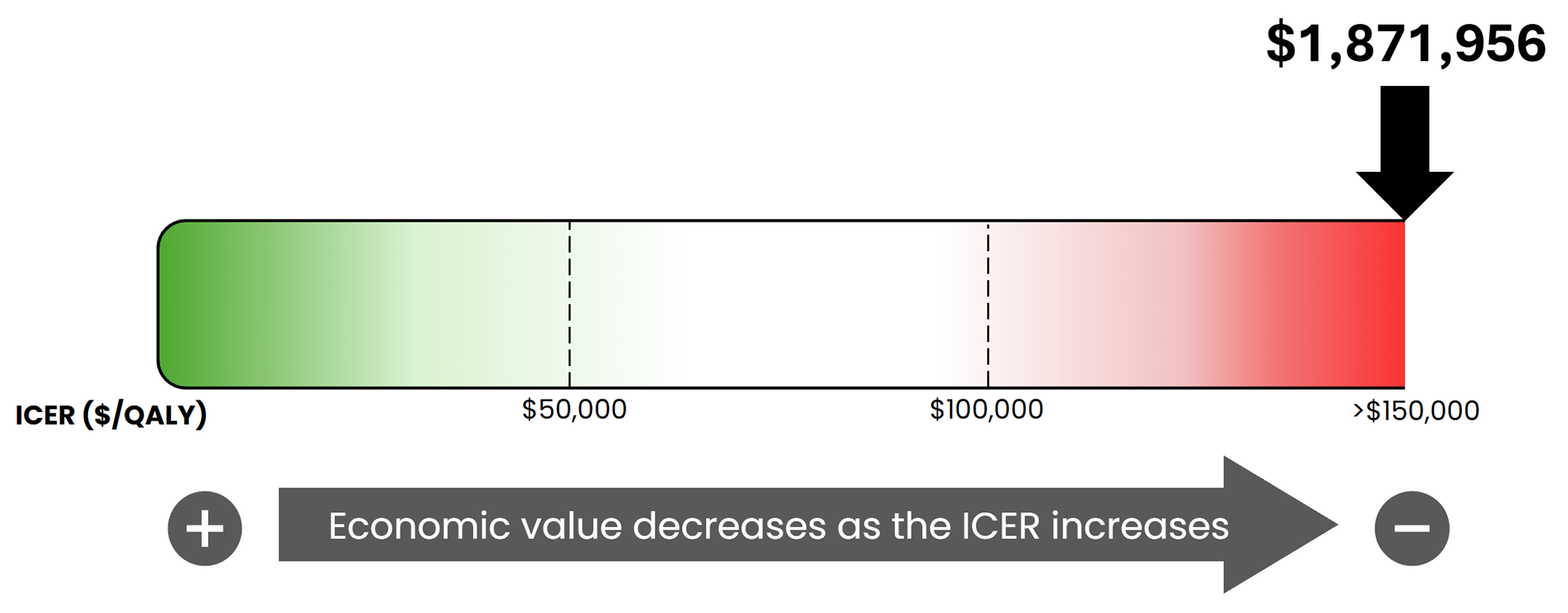
ICER = incremental cost-effectiveness ratio; PERC = pan-Canadian Oncology Drug Review Expert Review Committee; QALY = quality-adjusted life-year.
Certainty of the evidence: pERC noted that the certainty of the evidence supporting the reimbursement of avapritinib is limited because the cost-effectiveness results hinge on key assumptions that are not well supported by available data, particularly the durability of benefit after treatment discontinuation and extrapolation of outcomes beyond the observed evidence base. At the submitted price, avapritinib plus BSC was associated with a very high incremental cost ($1.3 million per patient) for a relatively modest incremental benefit (0.7 QALYs and 0.05 life-years), yielding an ICER of approximately $1.87 million per QALY. These results are highly sensitive to the postdiscontinuation benefit trajectory in that there is insufficient evidence to justify a long-term carryover effect, and substantial uncertainty remains regarding the appropriate duration and magnitude of treatment waning. Uncertainty in the cost-effectiveness results is accompanied by uncertainty in the projected budget impact (approximately $407 million over 3 years under high-uptake assumptions), which could be higher if the eligible population is larger than estimated.
Impact of response criteria on cost-effectiveness: The cost-effectiveness results are highly sensitive to how response is defined at 24 weeks and how that definition triggers treatment discontinuation. In the CDA-AMC base case, using the failure to achieve a 30% or greater improvement in TSS as the criteria for discontinuing treatment produced an ICER of approximately $1.87 million per QALY; when the response threshold was tightened to 50% or greater improvement (CDA-AMC scenario analysis), the ICER decreased to approximately $1.47 million per QALY, largely driven by lower drug costs ($1.60 million versus $1.15 million total costs for avapritinib plus BSC) with only a small reduction in total QALYs (14.28 versus 14.17). While this demonstrates that the model’s results change materially with alternative response thresholds, it also underscores a larger limitation: because TSS-based response assessment and discontinuation is not currently used in clinical practice in Canada, avapritinib may be continued in patients who would have been classified as not responding to treatment in the trial-based algorithm, increasing costs with smaller incremental quality-of-life gains than assumed and likely worsening cost-effectiveness relative to the base case.
Impact of treatment duration on cost-effectiveness: pERC noted that the submitted model assumes patients receive avapritinib for 5.5 years, based on modelling that draws on US real-world data to simulate individual patient trajectories and extrapolate long-term time on treatment. This treatment duration is highly uncertain and may not reflect real-world use in Canada. Based on input from clinical experts, pERC acknowledged that patients will likely receive avapritinib indefinitely if there is clinical benefit and acceptable toxicity. If patients remain on avapritinib for longer than assumed, cumulative drug acquisition and administration-related costs (including for ongoing monitoring and the management of adverse events over a longer exposure period) would increase materially. This concern is amplified if treatment discontinuation in practice in Canada is not closely tied to trial-based response rules (e.g., formal TSS-based stopping criteria at 24 weeks), such that some patients with smaller-than-assumed symptom improvement continue treatment. Consequently, the CDA-AMC base case ICER is underestimated if the real-world duration of therapy exceeds 5.5 years and/or if treatment is continued in patients who derive less benefit than assumed in the model.
Other considerations: The sponsor submitted an additional cost-effectiveness analysis adopting a societal perspective. In this analysis, the sponsor’s approach to estimating costs associated with productivity loss, travel, and informal care were uncertain due to a lack of empirical evidence. As a result of the lack of evidence relating to the impact of treatment for patients with ISM on these outcomes, CDA-AMC was unable to present an analysis from the societal perspective.
Impacts on Health Systems
Anticipated budget impact: The sponsor estimated that by year 3 of reimbursement, 455 patients would be eligible for avapritinib plus BSC; of these, 387 are expected to receive avapritinib plus BSC. The estimated incremental budget impact of reimbursing avapritinib plus BSC is predicted to be approximately $407 million over the first 3 years, all of which reflects the expected expenditure on avapritinib as an add-on treatment to BSC. The actual budget impact will depend on the number of patients eligible for treatment. pERC noted that the feasibility of adoption must be addressed.
Testing procedure considerations: pERC acknowledged that evaluating KIT D618V mutation status before the initiation of avapritinib would be required. Based on the input of clinical experts, pERC also noted that KIT mutation testing is broadly available across Canada and part of the diagnostic criteria for ISM, and therefore, is not anticipated to be an implementation or access barrier.
Sources of Information Used by the Committee
To make its recommendation, the committee considered the following information (links to the full documents for the review can be found on the project webpage):
the CDA-AMC review of the clinical and pharmacoeconomic evidence submitted by the sponsor, as well as relevant ethical issues related to avapritinib (refer to the main report and Supplemental Material document)
the sponsor’s comments on the draft report and the CDA-AMC responses
patients' perspectives gathered by 1 patient group, LLSC (refer to the Patient and Clinician Group Input document)
input from a person with lived experience who delivered a brief presentation and answered questions from the committee (refer to the Person With Lived Experience section earlier in this document)
input from 2 clinician groups, the LLSC Clinician Network and Canadian Myeloproliferative Neoplasm Group and the Ontario Health (Cancer Care Ontario) Hematology Cancer Drug Advisory Committee (refer to the Patient and Clinician Group Input document)
input from public drug programs that participate in the reimbursement review process (refer to the Supplemental Material document)
input from 3 clinical experts with expertise in the management of ISM consulted by CDA-AMC.
Special thanks: CDA-AMC extends our special thanks to the individual who presented directly to pERC and to the patient organizations supporting the community of those living with ISM, including LLSC.
General note: CDA-AMC makes every attempt to engage with people with lived experience as closely to the indication under review as possible; however, at times, CDA-AMC is unable to do so and instead engages with individuals with similar treatment journeys to ensure lived experience perspectives are included and considered in reimbursement reviews. CDA-AMC is fortunate to be able to engage with individuals who are willing to share their treatment journeys with pERC.
Request for Reconsideration
The sponsor filed a request for reconsideration of the draft recommendation for avapritinib for the treatment of adult patients with ISM with moderate to severe symptoms inadequately controlled on symptomatic treatment. In their request, the sponsor identified the following issues:
The sponsor requested that the prescribing condition be modified so that avapritinib may be initiated by a hematologist, allergist, or immunologist with expertise in the diagnosis, treatment, and response evaluation of patients with ISM.
To address the sponsor’s request for reconsideration, pERC considered the following information:
information submitted as part of the sponsor’s request for reconsideration and feedback on the draft recommendation
information from the initial submission related to the issues identified by the sponsor
feedback from 3 clinical specialists with expertise in diagnosing and treating patients with ISM
feedback on the draft recommendation from 1 patient group, LLSC
feedback on the draft recommendation from 1 clinician group, the Ontario Health (Cancer Care Ontario) Hematology Cancer Drug Advisory Committee
feedback on the draft recommendation from the public drug programs that participate in the reimbursement review process.
All feedback received in response to the draft recommendation is available on the CDA-AMC project webpage.
pERC Information
Members of the Committee
Dr. Catherine Moltzan (Chair), Dr. Kelvin Chan (Vice-Chair), Paul Agbulu, Dr. Phillip Blanchette, Dr. Matthew Cheung, Dr. Michael Crump, Annette Cyr, Dr. Jennifer Fishman, Dr. Jason Hart, Terry Hawrysh, Dr. Yoo-Joung Ko, Dr. Aly-Khan Lalani, Amy Peasgood, Dr. Anca Prica, Dr. Michael Raphael, Dr. Adam Raymakers, Dr. Patricia Tang, Dr. Pierre Villeneuve, and Danica Wasney.
Meeting date: February 11, 2026
Regrets: Two expert committee members did not attend.
Conflicts of interest: None
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.