Drugs, Health Technologies, Health Systems
Reimbursement Recommendation
Toripalimab (Loqtorzi)
Indication: In combination with cisplatin and gemcitabine, for the first-line treatment of adults with metastatic or with recurrent, locally advanced nasopharyngeal carcinoma (NPC)
Sponsor: Apotex Inc.
Recommendation: Reimburse with conditions
Summary
What Is the Reimbursement Recommendation for Loqtorzi?
Canada’s Drug Agency (CDA-AMC) recommends that Loqtorzi be reimbursed by public drug plans in combination with gemcitabine plus platinum chemotherapy for the first-line treatment of adults with metastatic or with recurrent, locally advanced nasopharyngeal carcinoma (NPC) if certain conditions are met.
Why Did CDA-AMC Recommend Reimbursement?
The pan-Canadian Oncology Drug Review Expert Review Committee (pERC) determined that Loqtorzi demonstrates acceptable clinical value versus gemcitabine plus cisplatin in patients with metastatic or recurrent, locally advanced NPC. This determination was enough for pERC to recommend that Loqtorzi be reimbursed. Given that Loqtorzi is expected to be an additive treatment to gemcitabine plus platinum chemotherapy, acceptable clinical value refers to added value versus gemcitabine plus platinum chemotherapy.
Evidence from a clinical trial (JUPITER-02; N = 289) demonstrated that, when compared to gemcitabine and cisplatin, treatment with Loqtorzi plus gemcitabine and cisplatin likely results in added clinical benefit in delayed disease progression and in patients living longer (improved overall survival [OS]) in patients with recurrent or metastatic NPC.
Loqtorzi plus gemcitabine and cisplatin was considered an additive therapy to gemcitabine plus platinum chemotherapy, and there was a higher incidence of immune-mediated adverse events (AEs) associated with Loqtorzi plus gemcitabine and cisplatin. Additionally, there was a large amount of missing data for health-related quality of life (HRQoL) outcomes.
Which Patients Are Eligible for Coverage?
Loqtorzi should only be covered for adult patients with recurrent, locally advanced NPC (i.e., NPC that cannot be controlled with local treatments such as surgery or radiation) or NPC that has spread to other parts of the body, in line with the sponsor’s reimbursement request. Patients should also have good performance status and must not have received prior anticancer therapy for recurrent or metastatic NPC.
What Are the Conditions for Reimbursement?
Loqtorzi should only be reimbursed if prescribed by clinicians with expertise in treating NPC and the cost of Loqtorzi is reduced. Reimbursement should be for a maximum of 2 years of treatment, and Loqtorzi should also be discontinued if the cancer worsens or there are unacceptable side effects.
Important budget impact considerations and organizational implications must be addressed for health systems to be able to adopt Loqtorzi.
Review Background
Disease background: NPC is a cancer that arises from the lining of the nasopharynx that causes a range of symptoms and can significantly impact HRQoL. NPC is rare in North America but occurs more frequently in Southern China, Southeast Asia, North Africa, and the Arctic. In Canada (excluding Quebec), the 5-year prevalence was 840 cases in 2018, equivalent to approximately 3 per 100,000 people.
Indication and reimbursement request: Toripalimab (Loqtorzi) has been approved by Health Canada in combination with cisplatin and gemcitabine, for the first-line treatment of adults with metastatic or with recurrent, locally advanced NPC. The sponsor is seeking reimbursement for this patient population.
Drug under review: Toripalimab is a PD-1 inhibitor. It is available as a concentrate for solution for administration by IV infusion and the dosage recommended in the product monograph is 240 mg intravenously every 3 weeks for up to 6 cycles, followed by 240 mg every 3 weeks until disease progression, unacceptable toxicity, or up to 24 months.
Treatment costs: At the submitted price of $8,800 per vial, the 21-day cycle cost of toripalimab is expected to be $8,800 per patient, based on the Health Canada–recommended dosage. When used in combination with cisplatin and gemcitabine, the total cost of treatment is expected to be $10,285 per patient per 21-day cycle. When considering a 28-day cost, the cost for toripalimab is expected to be $11,733 per patient or $13,713 per patient when used in combination with cisplatin and gemcitabine.
Highlights of Input From Interested Parties
Patient groups (Canadian Organization for Rare Disorders, the Canadian Cancer Survivor Network, and the Canadian Cancer Society) noted the following regarding impacts of the disease, unmet needs, and important outcomes:
Symptoms of NPC, and the current standard of care (radiation and chemotherapy) can cause discomfort and serious side effects that impact quality of life (QoL) during or after treatment. Additionally, patients cite long travel times to and from appointments.
Patient groups highlighted improved QoL, delayed disease progression, and improved survival as important goals of treatment. Additionally, they noted that minimizing side effects and reducing radiation and chemotherapy are important.
The clinician group (Ontario Health [Cancer Care Ontario] Head and Neck Cancer Drug Advisory Committee) and the clinical experts consulted by CDA-AMC noted the following regarding unmet needs arising from the disease and place in therapy for the drug under review:
Current therapies are inadequate and are associated with poor OS. Despite multiple rounds of chemotherapy, patients with disease relapse or metastatic disease will ultimately progress. There is a need for additional, more effective treatment options that delay disease progression, improve survival, and have manageable side effects.
Clinical experts anticipate that toripalimab in combination with gemcitabine and platinum chemotherapy could establish a new standard of care for first-line treatment of patients with recurrent or metastatic NPC, representing a shift in the current treatment paradigm.
The participating public drug programs raised potential implementation issues related to considerations for initiation, discontinuation, and prescribing of therapy; generalizability of trial populations to broader populations; care provision issues; system and economic issues; and potential need for a provisional funding algorithm.
Disclaimer: The perspectives shared by people with lived experience who present to the committee reflect their individual experiences and are not necessarily representative of all people with the same condition or course of treatment. Their insights provide valuable context about what a patient, support person, or caregiver might go through with this condition or treatment, helping to inform the committee’s deliberations. These narratives complement other forms of evidence and input and should be considered as 1 element contributing to a broader understanding of the condition and treatment under review.
Recommendation
With a vote of 15 in favour to 0 against, pERC recommends that toripalimab be reimbursed, in combination with gemcitabine plus platinum chemotherapy, for the first-line treatment of adults with metastatic or with recurrent, locally advanced NPC only if the conditions listed in Table 1 are met.
Table 1: Reimbursement Conditions and Reasons
Reimbursement condition | Reason | Implementation guidance |
|---|---|---|
Initiation | ||
1. Treatment with toripalimab plus gemcitabine and platinum chemotherapy should be reimbursed when initiated in adult patients with recurrent (not amenable to local regional or curative treatment) or metastatic NPC. | Evidence from the JUPITER-02 trial demonstrated that treatment with toripalimab plus gemcitabine and cisplatin resulted in a clinically meaningful benefit in patients with these characteristics. | pERC noted that, for patients with prior exposure to platinum-based chemotherapy in a nonmetastatic setting (e.g., neoadjuvant or adjuvant therapy), a minimum interval of 6 months between the completion of the last platinum-based chemotherapy and the onset of disease relapse is required to ensure that the disease remains “platinum-sensitive.” pERC agreed that, for a limited time following implementation, patients who have already initiated first-line treatment with gemcitabine and platinum chemotherapy for recurrent or metastatic, locally advanced NPC, who have no evidence of progressive disease and are still receiving chemotherapy, and otherwise meet the eligibility criteria for toripalimab, may be eligible to receive toripalimab added to their chemotherapy. |
2. Patients should have good performance status. | Patients with an ECOG PS score of 0 or 1 were included in the in the JUPITER-02 trial. | pERC agreed with the clinical experts that patients with an ECOG PS score of greater than 1 may be treated at the discretion of the treating clinician. |
3. Treatment with toripalimab plus gemcitabine and platinum chemotherapy should not be used in patients with any of the following: 3.1. prior systemic therapy for recurrent or metastatic NPC 3.2. active or uncontrolled CNS metastases 3.3. significant autoimmune disease. | The JUPITER-02 trial excluded such patients, and there is no evidence regarding the efficacy and safety of treatment with toripalimab plus gemcitabine and platinum chemotherapy in patients with these characteristics. | — |
Discontinuation | ||
4. Treatment with toripalimab in combination with gemcitabine and platinum chemotherapy should be discontinued upon the occurrence of any of the following: 4.1. disease progression 4.2. unacceptable toxicity 4.3. completion of 24 months of treatment. | In the JUPITER-02 trial, treatment with toripalimab was discontinued upon disease progression, unacceptable toxicity, or patient request. These criteria for discontinuation are aligned with clinical practice, as described by clinical experts consulted by CDA-AMC. In the JUPITER-02 trial, after the initial 6 cycles of therapy, patients continued treatment with toripalimab or placebo as monotherapy every 3 weeks until unacceptable toxicity, progressive disease, or a maximum of 2 years. | During combination therapy, gemcitabine and platinum chemotherapy should be administered for up to 6 cycles (with a minimum of 1 cycle) or until disease progression or unacceptable toxicity. Subsequently, toripalimab can be continued as a monotherapy until the discontinuation criteria in this condition are met. If 1 component of the combination therapy with toripalimab plus gemcitabine and platinum chemotherapy is discontinued permanently because of tolerability concerns, the patient may continue to receive the other components at the discretion of the treating clinician, until the discontinuation criteria are met. pERC agreed with the clinical experts consulted by CDA-AMC that patients who stop treatment with toripalimab for reasons other than disease progression or toxicity may be considered eligible to restart treatment upon disease progression at the discretion of the treating clinician. pERC noted that the JUPITER-02 trial did not provide evidence about re-treatment with toripalimab as patients received treatment for a maximum of 2 years. However, pERC agreed with the clinical experts and advised that if treatment with toripalimab was discontinued before the completion of 2 years of therapy for reasons other than progression or after the completion of 2 years of therapy, patients may receive an additional year of treatment with toripalimab if progression occurs more than 6 months after stopping treatment. pERC also highlighted that the decision to restart treatment as monotherapy or in combination with gemcitabine plus platinum chemotherapy should be left up to clinician discretion. |
Prescribing | ||
5. Toripalimab should be prescribed under the care of clinicians with expertise in managing NPC and immunotherapy toxicity profiles. | This is meant to ensure that toripalimab is prescribed for appropriate patients and that adverse effects are managed in an optimized and timely manner. | pERC noted that there is currently no evidence to support weight-based dosing of toripalimab in the first-line metastatic or recurrent NPC setting. |
Pricing | ||
6. A reduction in price. | Using the CDA-AMC base-case analysis, the ICER for toripalimab plus chemotherapy was $189,118 per QALY gained when compared with chemotherapy alone in the indicated population. A band 4 price reduction would be required to achieve cost-effectiveness at a $50,000 per QALY threshold.a A band 3 price reduction would be required to achieve cost-effectiveness at a $100,000 per QALY threshold.a Price reductions for any given willingness-to-pay threshold are available in the CDA-AMC Main Report and Supplemental Material documents. | The CDA-AMC analysis is based on public list prices for all treatments. Further price reductions may be required if there are price arrangements (discounts) currently in place for any treatment included in the economic analysis. Likewise, further price reductions may be required to address economic feasibility of adoption. |
Feasibility of adoption | ||
7. The economic feasibility of adoption of toripalimab plus chemotherapy must be addressed. | At the submitted price, the magnitude of uncertainty in the budget impact must be addressed to ensure the feasibility of adoption, given the difference between the sponsor’s estimate and the CDA-AMC estimate. | The 3-year budget impact may be 2 or more times that of the sponsor BIA estimates if duration of toripalimab is assumed as 24 months. |
8. The organizational feasibility of adoption of toripalimab must be addressed. | pERC acknowledged that the addition of toripalimab to chemotherapy adds to treatment chair time per cycle and may introduce additional treatment appointments for patients proceeding with toripalimab monotherapy after completion of chemotherapy. | Jurisdictions should assess the financial implications of covering additional resource use and care-related expenses (e.g., travel and accommodations) for patients receiving toripalimab to reduce financial burden on patients and maintain their quality of life during treatment, particularly given the higher incidence of NPC among Inuit who may reside in remote areas, and those who have immigrated from countries with higher risk of disease who may face financial, language, and cultural barriers to care. |
BIA = budget impact analysis; CDA-AMC = Canada’s Drug Agency; CNS = central nervous system; ECOG PS = Eastern Cooperative Oncology Group Performance Status; ICER = incremental cost-effectiveness ratio; NPC = nasopharyngeal carcinoma; pERC = pan-Canadian Oncology Drug Review Expert Review Committee; QALY = quality-adjusted life-year.
aFor the size of the price reduction required, band 1 = 1% to 24%, band 2 = 25% to 49%, band 3 = 50% to 74%, and band 4 = 75% or greater.
Rationale for the Recommendation
Clinical Value
Based on the totality of the clinical evidence, pERC concluded that toripalimab demonstrates acceptable clinical value compared with gemcitabine plus platinum chemotherapy alone in the first-line treatment of adults with metastatic or with recurrent, locally advanced NPC. Given that toripalimab is expected to be an additive treatment to gemcitabine plus platinum chemotherapy, acceptable clinical value refers to added value versus gemcitabine plus platinum chemotherapy.
Evidence from 1 placebo-controlled, phase III randomized controlled trial (JUPITER-02; N = 289) demonstrated that toripalimab in combination with gemcitabine and cisplatin resulted in added clinical value in progression-free survival (PFS) and OS for patients with recurrent or metastatic NPC compared with placebo in combination with gemcitabine and cisplatin. Treatment with toripalimab plus gemcitabine and cisplatin resulted in a statistically significant and clinically meaningful improvement in PFS compared to gemcitabine and cisplatin alone (hazard ratio [HR] = 0.52; 95% confidence interval [CI], 0.37 to 0.73) with a median PFS of 21.40 months (95% CI, 11.73 months to not estimable [NE]) in the toripalimab arm and 8.20 months (95% CI, 7.03 months to 9.79 months) in the placebo arm. Additional analyses of PFS at the landmark time points of 1 and 2 years (59.0% [95% CI, 49.7% to 67.16%] versus 32.9% [95% CI, 24.9% to 41.5%] and 44.8% [95% CI, 34.4% to 54.1%] versus 25.4% [95% CI, 17.0% to 34.8%]) were supportive of the progression-free advantage of toripalimab. Kaplan-Meier estimates of the probability of OS also suggested that toripalimab likely results in improved survival at 2 and 3 years (78.0% [95% CI, 70.2% to 84.0%] versus 65.1% [95% CI, 56.5% to 72.4%] and 64.5% [95% CI, 55.9% to 71.9%] versus 49.2% [95% CI, 40.5% to 57.3%]), with between-group differences of 12.9% (95% CI, 2.3% to 23.4%) and 15.3% (95% CI, 3.6% to 26.9%), respectively.
Patient groups, clinician groups, and clinical experts consulted by CDA-AMC identified the need for new, effective treatments in the first-line setting that delay disease progression, extend survival, and reduce tumour burden and maintain QoL, with minimal adverse side effects. pERC concluded that toripalimab plus gemcitabine and platinum chemotherapy met some patient needs because it is an additional treatment option that delays disease progression and improves survival compared to gemcitabine and cisplatin alone. However, pERC was unable to draw definitive conclusions on the effect of toripalimab on patients’ QoL due to limitations of the evidence. pERC also noted that toripalimab plus gemcitabine and cisplatin group results in more immune-mediated AEs than gemcitabine and cisplatin alone, although the committee agreed with the clinical experts that the types of AEs in the trial were as expected for immunotherapy combined with platinum chemotherapy.
Further information on the committee’s discussion around clinical value is provided in the Summary of Deliberation section.
Developing the Recommendation
The determination of acceptable clinical value was sufficient for pERC to recommend reimbursement of toripalimab. As part of the deliberation on whether to recommend reimbursement, the committee also considered unmet clinical need, unmet nonclinical need, and health inequity. Information on this discussion is provided in the Unmet Clinical Need and Distinct Social and Ethical Considerations domains in the Summary of Deliberation section.
Because pERC recommended that toripalimab be reimbursed, the committee also deliberated on whether reimbursement conditions should be added to address important economic considerations, health system impacts, or social and ethical considerations, or to ensure clinical value is realized. The resulting reimbursement conditions, with accompanying reasons and implementation guidance, are stated in Table 1.
Summary of Deliberation
pERC considered all domains of value of the deliberative framework before developing its recommendation: clinical value, unmet clinical need, distinct social and ethical considerations, economic considerations, and impacts on health systems. For further information on the domains of value, refer to Expert Committee Deliberation at CDA-AMC.
The committee considered the following key discussion points, organized by the 5 domains of value.
Clinical Value
Appropriate comparators: pERC considered the combination of gemcitabine and platinum chemotherapy (i.e., cisplatin or carboplatin) to be an appropriate comparator, as gemcitabine plus platinum chemotherapy is the current standard first-line treatment for patients with recurrent or metastatic NPC.
Efficacy versus gemcitabine plus cisplatin: The phase III JUPITER-02 trial demonstrated that first-line treatment with toripalimab plus gemcitabine and cisplatin resulted in a statistically significant and clinically meaningful improvement in the primary end point of median PFS compared to placebo plus gemcitabine and cisplatin (HR = 0.52; 95% CI, 0.37 to 0.73). The median OS could not be estimated in the toripalimab arm (95% CI, 38.7 months to NE), and was 33.7 months (95% CI, 27.0 months to NE) in the placebo arm, corresponding to a stratified HR of 0.63 (95% CI, 0.45 to 0.89; P = 0.0083) in favour of toripalimab. Conclusions regarding HRQoL outcomes could not be drawn from the JUPITER-02 trial due to imprecision and higher dropout rates at later time points.
Clinical importance of treatment effects: pERC considered outcomes of importance identified by patient groups and clinicians, which include prolonging life, delaying cancer progression, relieving symptoms, improving QoL, and avoiding treatments with severe side effects. Thresholds for clinically meaningful between-group differences were suggested by the clinical experts consulted by CDA-AMC for the probability of PFS (8% to 10%) and OS (5%) at each time point. Despite the 95% CIs for each outcome suggesting both the potential for clinically meaningful benefit as well as no benefit, pERC considered the results for these outcomes to be clinically meaningful in consultation with the clinical experts.
Certainty of the evidence: Results for the proportion of patients who are progression-free (PFS) at 1 year and 2 years were associated with a high and low level of certainty respectively, while the proportion of patients alive (OS) at 1 year, 2 years, and 3 years were associated with a moderate level of certainty per the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) assessment. These were primarily driven by serious study limitations and imprecision, where there was a low number of events and potential for an effect that is not clinically meaningful. For QoL outcomes, pERC noted that there is a very low certainty of evidence due to serious study limitations (unblinding, knowledge of treatment assignment, and missing data) and serious imprecision (little to no clinically important difference and CIs include the potential for harm).
Clinical value: Based on the preceding considerations, pERC determined that there was added clinical value for toripalimab in combination with gemcitabine and platinum chemotherapy versus gemcitabine plus platinum chemotherapy alone. Although the chemotherapy regimen used in the JUPITER-02 trial included cisplatin, pERC agreed with the clinical experts that carboplatin would be a reasonable alternative to cisplatin and is already used in combination with gemcitabine for the treatment of recurrent or metastatic NPC in many jurisdictions.
Unmet Clinical Need
Input on unmet clinical need: Patient groups, clinician groups, and clinical experts consulted by CDA-AMC identified an unmet need for treatments that are more effective in prolonging life and delaying disease progression, while controlling symptoms, improving QoL, and minimizing treatment-related AEs.
Severity of the disease: pERC discussed input from patient groups indicating that recurrent or metastatic NPC is associated with serious symptoms and imposes substantial burden on multiple aspects of life including physical health, emotional well-being and mental health, social interactions, work or daily activities, sleep, nutrition, and pain. The committee also acknowledged that the disease prognosis for recurrent or metastatic NPC is poor and is associated with significant mortality.
Availability of treatment options: Currently, the standard first-line treatment for recurrent or metastatic NPC is gemcitabine plus platinum chemotherapy, which is publicly funded in Canada. Other chemotherapy drugs may be considered for patients who are not candidates for this regimen. Palliative radiation therapy may also be used. The patient group input also highlighted that radiation therapy often involves burdensome treatment schedules and side effects, including localized pain and discomfort in the treated area. Patients expressed hope that adding toripalimab to chemotherapy as a first-line treatment for recurrent or metastatic NPC could help patients who were eligible to reduce radiation and chemotherapy which are associated with significant side effects. pERC additionally considered input from clinical experts consulted by CDA-AMC and clinician groups who emphasized that, although NPC is initially chemotherapy-sensitive, not all patients experience a response to treatment, and that responses are not durable. Clinical experts also noted that toxicity from gemcitabine plus platinum chemotherapy can include both short-term and long-term effects, is often cumulative, and may negatively impact QoL.
Distinct Social and Ethical Considerations
Input on unmet nonclinical need: Input from patient groups highlighted that current treatments are associated with severe side effects (e.g., changes in smell or taste, loss of appetite, fatigue, neuropathy, hearing loss, radiation burns, weight loss) that significantly impact QoL. The committee also recognized the financial burden of treatment for NPC on patients and caregivers, including costs related to travel, meal replacements, medications to manage AEs, and loss of income due to work absenteeism. Individuals with lower household incomes experienced the greatest financial hardship.
Equity considerations: pERC noted that NPC disproportionately affects Inuit who may reside in remote areas, and some people who have immigrated from regions with higher risk of the disease (namely East Asia and Southeast Asia, North Africa, or the Arctic) who may already face barriers to diagnosis, access to care, and equitable outcomes due to financial, language, or cultural challenges. Given the higher incidence of NPC among Inuit who may reside in remote areas, significant travel may be required for these patients to receive care (including diagnosis, imaging, and systemic therapy). pERC acknowledged that these factors could introduce additional barriers and burden (e.g., travel and related expenses) for patients and caregivers. The committee emphasized that resources to support patient travel and accommodations would be necessary to ensure equitable access and continuity of treatment. pERC considered the unmet nonclinical needs and health inequities for patients with recurrent or metastatic NPC and determined that these are not necessarily addressed by toripalimab.
Economic Considerations
The following guidance has been provided to align with the deliberative framework domains and considerations:
Health impacts of toripalimab plus chemotherapy versus relevant comparators: Toripalimab plus chemotherapy compared to chemotherapy alone is predicted to be associated with a gain of 1.56 life-years and may result in a gain of 1.16 quality-adjusted life-years (QALY), over a lifetime horizon (15 years).
Cost of toripalimab plus chemotherapy versus relevant comparators: Toripalimab plus chemotherapy compared to chemotherapy alone is predicted to be associated with higher costs to health care systems (incremental costs = $219,624), primarily driven by increased costs associated with drugs costs (incremental = $201,226) and health care resource use, over a lifetime horizon (15 years).
Key findings of the economic evaluation: Based on the submitted evidence using the sponsor’s cost-utility analysis, the CDA-AMC base-case analysis estimates that the incremental cost-effectiveness ratio (ICER) of toripalimab plus chemotherapy for the first-line treatment of patients with metastatic or recurrent NPC was $189,118 per QALY gained when compared to chemotherapy alone. (Figure 1).
Figure 1: Estimate of the ICER Used by pERC to Inform the Price Condition
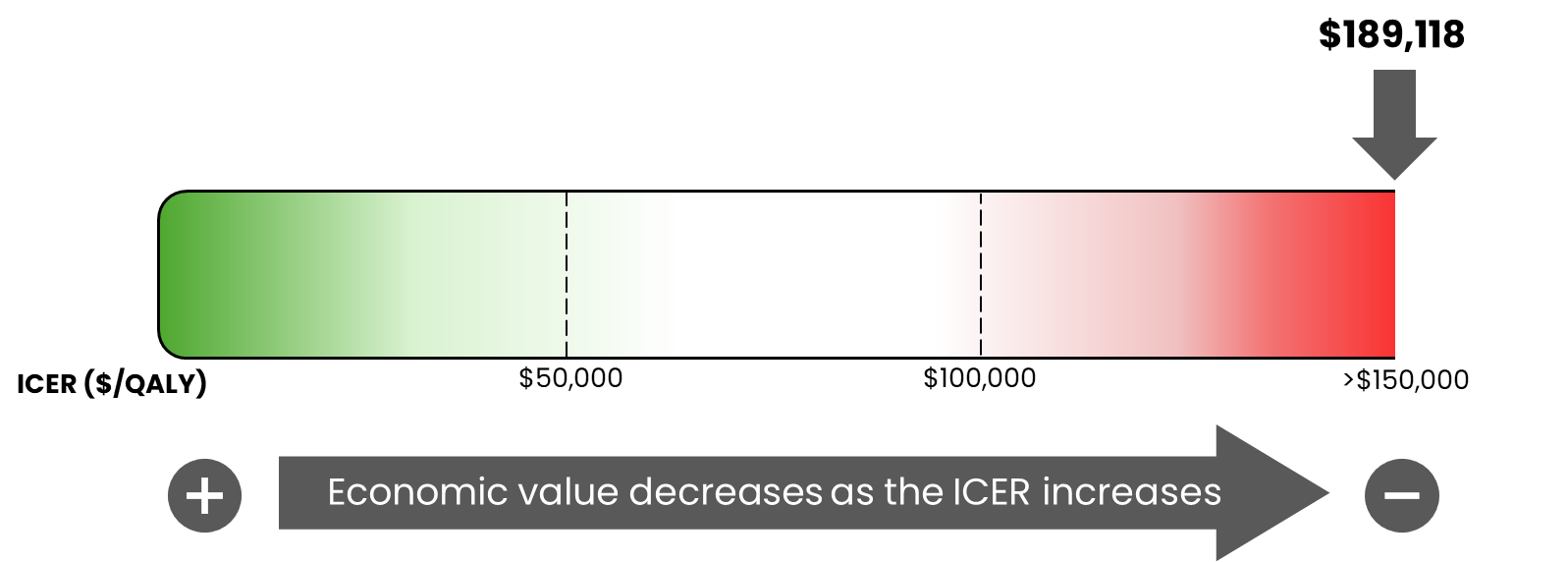
ICER = incremental cost-effectiveness ratio; pERC = pan-Canadian Oncology Drug Review Expert Review Committee; QALY = quality-adjusted life-year.
Certainty of the evidence: The estimated ICER is uncertain due to uncertainty in the comparative efficacy data informing the model, long-term survival estimates, and the economic model structure. As a result, the economic analysis may not accurately assess the true impact of toripalimab plus chemotherapy on patient health and health care resources. Thus, the cost-effectiveness of Loqtorzi plus chemotherapy remains uncertain and higher price reductions may be required to achieve a given willingness-to-pay threshold.
Other considerations: The committee discussed that NPC may disproportionately impact Inuit who may reside in remote areas and some people who have immigrated from regions with higher risk of the disease and those living in rural and remote settings. Given that this treatment is likely to be administered only in cancer centres with a compounding pharmacy, the committee noted that this may introduce additional costs to patients and the public health system (e.g., travel and accommodation, preparation of the product for administration). The economic analysis did not incorporate these costs incurred by patients or the public health system. The cost-effectiveness of toripalimab when considering these additional costs is unknown.
The committee noted that tislelizumab in combination with gemcitabine and cisplatin was recently reviewed by CDA-AMC and received a positive recommendation for the first-line treatment of patients with recurrent or metastatic NPC, and then as a single drug after up to 6 cycles of combination therapy. Price negotiations for toripalimab for the same indication may need to account for the different duration of therapy between toripalimab (up to 24 months) and tislelizumab (until disease progression) in the same indication.
Impacts on Health Systems
Anticipated budget impact: CDA-AMC estimated 647 patients would be eligible for treatment with toripalimab in combination with gemcitabine and cisplatin over a 3-year period, of whom 473 are expected to receive toripalimab in combination with gemcitabine and cisplatin. CDA-AMC estimates that the budget impact of reimbursing toripalimab for use in combination with gemcitabine and cisplatin for the first-line treatment of NPC will be approximately $52 million for the first 3 years of reimbursement compared to the amount currently spent on comparators. The expenditure on toripalimab for this period is predicted to be $52 million (toripalimab plus gemcitabine and cisplatin as a regimen = $55 million). The actual budget impact of reimbursing toripalimab will depend on the number of people eligible for treatment that will receive treatment, the duration of treatments, and toripalimab uptake.
Feasibility of adoption: pERC noted that the feasibility of adoption must be addressed. The 3-year budget impact may be greater than 2 times what was predicted by the sponsor if duration of toripalimab is assumed as 24 months. This approach may provide a more approximate estimate of the budget impact by accounting for scenarios such as re-treatment with toripalimab, or an extension of eligibility criteria to include patients who have already initiated first-line treatment with gemcitabine and platinum chemotherapy for recurrent or metastatic, locally advanced NPC; remain free of progressive disease; and are still receiving chemotherapy.
Equity considerations: pERC noted that NPC disproportionately affects Indigenous populations (including Inuit), populations who do not speak English, and those who have immigrated (particularly of South Asian descent). pERC acknowledged that these patients may also reside in remote settings, significant travel may be required to receive care (including diagnosis, imaging, and systemic therapy). The committee stated that resources to support patient travel and accommodations would need to be addressed to ensure equitable access for the intended duration of treatment.
Sources of Information Used by the Committee
To make its recommendation, the committee considered the following information (links to the full documents for the review can be found on the project webpage):
the CDA-AMC review of the clinical and pharmacoeconomic evidence submitted by the sponsor, as well as relevant ethical issues related to toripalimab (refer to the Main Report and Supplemental Material documents)
the sponsor’s comments on the draft report and the responses by CDA-AMC
patients' perspectives gathered by 3 patient groups, the Canadian Organization for Rare Disorders, the Canadian Cancer Survivor Network, and the Canadian Cancer Society (refer to the Patient and Clinician Group Input document)
input from a person with lived experience who delivered a brief presentation and answered questions from the committee (refer to the Person with Lived Experience section)
input from 1 clinician group, Ontario Health (Cancer Care Ontario) Head and Neck Cancer Drug Advisory Committee (refer to the Patient and Clinician Group Input document)
input from public drug programs that participate in the reimbursement review process (refer to the Supplemental Material document)
input from 3 clinical experts with expertise in the management of NPC consulted by CDA-AMC.
Special thanks: CDA-AMC extends our special thanks to the individual who presented directly to pERC, and to the patient organizations representing the community of those living with NPC, including the Canadian Cancer Society, the Canadian Organization for Rare Disorders, and the Canadian Cancer Survivor Network.
General note: CDA-AMC makes every attempt to engage with people with lived experience as closely to the indication under review as possible; however, at times, CDA-AMC is unable to do so and instead engages with individuals with similar treatment journeys to ensure lived experience perspectives are included and considered in Reimbursement Reviews. CDA-AMC is fortunate to be able to engage with individuals who are willing to share their treatment journeys with pERC.
pERC Information
Members of the Committee
Dr. Catherine Moltzan (Chair), Dr. Kelvin Chan (Vice-Chair), Paul Agbulu, Dr. Phillip Blanchette, Dr. Matthew Cheung, Dr. Michael Crump, Annette Cyr, Dr. Jennifer Fishman, Dr. Jason Hart, Terry Hawrysh, Dr. Yoo-Joung Ko, Dr. Aly-Khan Lalani, Amy Peasgood, Dr. Anca Prica, Dr. Michael Raphael, Dr. Adam Raymakers, Dr. Patricia Tang, Dr. Pierre Villeneuve, and Danica Wasney.
Meeting date: December 3, 2025
Regrets: Two expert committee members did not attend.
Conflicts of interest: One expert committee member did not participate due to considerations of conflict of interest.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make
any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca