Drugs, Health Technologies, Health Systems
Reimbursement Review
Trastuzumab Deruxtecan (Enhertu)
Sponsor: AstraZeneca Canada Inc.
Therapeutic area: Gastric or gastroesophageal junction (GEJ) adenocarcinoma
Summary
What Is Gastric or Gastroesophageal Junction Cancer?
Gastric or gastroesophageal junction (GEJ) cancer can develop in the stomach or at the connection between the stomach and the esophagus; it is life-threatening and is associated with significant gastrointestinal symptoms, including nausea, vomiting, pain, and difficulty eating.
The projected incidence rate of gastric cancer in Canada is 8.3 per 100,000 adults in 2024, with an estimated 1,400 cases in females and 2,600 cases in males.1
What Are the Treatment Goals and Current Treatment Options for Gastric or GEJ Cancer?
Clinical experts consulted for this review agreed that the goal of treatment is palliative and focuses on extending survival and improving disease control with manageable toxicity and maintenance of patients’ quality of life. Patients and caregivers prioritized effective cancer control with prolonged survival, delayed disease progression, relief of cancer-related symptoms, minimal side effects, treatment convenience and ease of access, improved quality of life, and additional treatment choice. Clinician groups providing input agreed that important outcomes included prolonged survival (overall survival [OS] and progression-free survival [PFS]), reduced tumour burden and improved response, improved health-related quality of life, and minimal treatment toxicity. Most patients whose disease has progressed on or after first-line trastuzumab-containing chemotherapy receive ramucirumab plus paclitaxel. There are limited chemotherapy treatment options for patients who may not be eligible for ramucirumab plus paclitaxel.
What Is Enhertu and Why Did Canada’s Drug Agency Conduct This Review?
Enhertu is a drug that is administered by IV infusion. Health Canada has approved Enhertu “for the treatment of adult patients with unresectable, locally advanced or metastatic HER2-positive gastric or gastroesophageal junction (GEJ) adenocarcinoma who have received a prior trastuzumab-based regimen.”
Canada’s Drug Agency (CDA-AMC) reviewed Enhertu to inform a recommendation to the participating public drug programs on whether it should be reimbursed for the second-line treatment of adult patients with unresectable, locally advanced, or metastatic HER2-positive gastric or GEJ adenocarcinoma who have received a prior anti–HER2-based regimen. The sponsor is seeking reimbursement for this patient population.
CDA-AMC previously reviewed Enhertu and issued a conditional positive time-limited reimbursement (TLR) recommendation for the second-line treatment of adult patients with unresectable, locally advanced, or metastatic HER2-positive gastric or GEJ adenocarcinoma who have received a prior anti–HER2-based regimen for a time-limited period while additional evidence is generated. Subsequently, new phase III study evidence has become available, allowing the sponsor to fulfill its commitment to file a reassessment to address uncertainty in the original evidence as is required under the TLR category.
How Did CDA-AMC Evaluate Enhertu?
CDA-AMC reviewed the clinical evidence on the beneficial and harmful effects, as well as the economic evidence, of Enhertu versus other treatments used in Canada for the treatment of adult patients with unresectable, locally advanced, or metastatic HER2-positive gastric or GEJ adenocarcinoma who have received a prior trastuzumab-based regimen. Ramucirumab plus paclitaxel was considered as the most relevant comparator treatment; however, less commonly used treatments (folinic acid, fluorouracil, and irinotecan [FOLFIRI]) or single-agent chemotherapies (paclitaxel or irinotecan) were also considered relevant comparators.
CDA-AMC identified equity and ethical considerations relevant to Enhertu and gastric or GEJ adenocarcinoma.
The review was informed by materials submitted by the sponsor, which included clinical and economic evidence as well as literature searches.
The review was also informed by 1 patient group submission, 2 clinician group submissions, and 1 industry submission in response to our call for input, and by input from the participating public drug programs regarding issues that may impact their ability to implement a recommendation.
Two oncologists with representation from Ontario and British Columbia were consulted as part of the review process.
What Were the Findings?
Clinical Evidence
CDA-AMC reviewed the following clinical evidence:
One randomized controlled phase III trial (the DESTINY-Gastric04 trial) was included, comparing Enhertu with ramucirumab plus paclitaxel in 494 patients with unresectable locally advanced or metastatic HER2-positive gastric or GEJ adenocarcinoma who have received a first-line trastuzumab-based regimen in the advanced or metastatic setting. The previous TLR recommendation for Enhertu included 1 single-arm study (the DESTINY-Gastric02 trial; N = 79) assessing the same patient population and intervention as being reviewed for this reassessment.
One network meta-analysis of Enhertu versus comparators (listed in the Indirect Evidence section) was also included.
For the comparison of Enhertu versus ramucirumab plus paclitaxel:
OS is likely improved with Enhertu versus ramucirumab plus paclitaxel, although the certainty of this finding diminishes with longer follow-up. PFS may be improved with Enhertu versus ramucirumab plus paclitaxel after 6 and 9 months of follow-up; however, there is less certainty in these findings because of the lack of blinding in this study. The impact of Enhertu on health-related quality of life is very uncertain because of the lack of blinding in the study and because of missing data. Enhertu likely increases the risk of patients developing interstitial lung disease, which can have a serious impact on their ability to breathe.
Based on the results of a sponsor-submitted network meta-analysis, the evidence is insufficient to draw definitive conclusions on the relative efficacy of trastuzumab deruxtecan compared to chemotherapy options, including FOLFIRI and single-agent chemotherapy (paclitaxel, irinotecan, or docetaxel). There were no long-term extensions and no studies addressing gaps in the literature.
This reassessment fulfills the requirements under the TLR category to address the uncertainty in the original evidence for the TLR recommendation for Enhertu in April 2025. As per the TLR process requirements, this reassessment was based on a confirmatory phase III trial (the DESTINY-Gastric04 trial). The DESTINY-Gastric04 trial addressed evidence gaps from the previous TLR recommendation by including a relevant randomized comparator, clinically relevant survival outcomes, and comparative safety data.
Economic Evidence
Enhertu is available as a powder for concentrate for solution (100 mg vial). At the submitted price of $2,440.00 per 100 mg vial, the 28-day cycle cost of Enhertu is expected to be $16,267 per patient, based on the Health Canada–recommended dosage.
Key clinical efficacy in the economic analysis (PFS and OS) for Enhertu versus ramucirumab plus paclitaxel was derived from the DESTINY-Gastric04 trial. Evidence submitted by the sponsor indicates that Enhertu likely improves OS versus ramucirumab plus paclitaxel; however, the certainty associated with this finding diminishes with longer follow-up (18 months or longer). Enhertu may improve PFS compared to ramucirumab plus paclitaxel after 6 and 9 months of follow-up; however, the lack of blinding introduces uncertainty into the assessment of progression. Clinical efficacy in the economic analysis for Enhertu versus FOLFIRI was informed by a sponsor-submitted indirect treatment comparison. Because of limitations with the indirect treatment comparison, the evidence is insufficient to draw definitive conclusions on the relative efficacy of trastuzumab deruxtecan compared to chemotherapy options such as FOLFIRI.
The results of the CDA-AMC base-case analysis suggest the following:
Enhertu is predicted to be associated with higher costs to the health care system than ramucirumab plus paclitaxel (incremental costs = $34,953), primarily driven by increased drug acquisition costs associated with Enhertu.
Enhertu is predicted to be associated with a gain of 0.41 life-years compared to ramucirumab plus paclitaxel and may result in a gain of 0.27 quality-adjusted life-years compared to ramucirumab plus paclitaxel.
The incremental cost-effectiveness ratio of Enhertu compared to ramucirumab plus paclitaxel was $130,777 per quality-adjusted life-year gained in the CDA-AMC base-case analysis. The estimated incremental cost-effectiveness ratio was highly sensitive to assumptions with clinical efficacy and remains uncertain due to limitations with the available clinical evidence and the sponsor’s modelling approach. Additional price reductions to those presented in this report may therefore be required to achieve cost-effectiveness at a given willingness-to-pay threshold.
The sponsor indicated that Enhertu was already funded and being used in CDA-AMC–participating jurisdictions, given that it was previously reviewed and recommended as a TLR recommendation (PC0367). Therefore, the sponsor assumed that Enhertu would not result in any incremental budget impact for the second-line treatment of patients with HER2-positive gastric or GEJ adenocarcinoma over the first 3 years of reimbursement. Over this time period, CDA-AMC estimated expenditure of $77.9 million on Enhertu. The actual budget impact of maintaining reimbursement of Enhertu will depend on the current funding agreements for Enhertu, the number of patients who are eligible for treatment, and the market share of Enhertu.
Abbreviations
AE
adverse event
BIA
budget impact analysis
BSC
best supportive care
CDA-AMC
Canada’s Drug Agency
CGOEN
Canadian Gastrointestinal Oncology Evidence Network
CI
confidence interval
ECOG PS
Eastern Cooperative Oncology Group Performance Status
ESMO
European Society for Medical Oncology
FACT-Ga
Functional Assessment of Cancer Therapy–Gastric
FE
fixed effect
FOLFIRI
folinic acid, fluorouracil, and irinotecan
GC
gastric cancer
GEJ
gastroesophageal junction
GI DAC
Gastrointestinal Cancer Drug Advisory Committee
GRADE
Grading of Recommendations Assessment, Development and Evaluation
HR
hazard ratio
HRQoL
health-related quality of life
ICER
incremental cost-effectiveness ratio
IHC
immunohistochemistry
ILD
interstitial lung disease
ISH
in situ hybridization
ITC
indirect treatment comparison
KM
Kaplan-Meier
MAB
medical advisory board
MID
minimal important difference
NMA
network meta-analysis
OH (CCO)
Ontario Health (Cancer Care Ontario)
ORR
objective response rate
OS
overall survival
PFS
progression-free survival
PH
proportional hazards
RCT
randomized controlled trial
RECIST 1.1
Response Evaluation Criteria in Solid Tumours Version 1.1
RPSFTM
rank-preserving structural failure time model
SAE
serious adverse event
SLR
systematic literature review
TEAE
treatment-emergent adverse event
TLR
time-limited reimbursement
QALY
quality-adjusted life-year
Background
Introduction
The objectives of this report are as follows:
This report will review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of trastuzumab deruxtecan, at a dose of 6.4 mg/kg given as an IV infusion in the second-line treatment of adult patients with unresectable locally advanced or metastatic HER2-positive gastric or gastroesophageal junction (GEJ) adenocarcinoma who have received a prior anti–HER2-based regimen. The focus will be placed on comparing trastuzumab deruxtecan to relevant comparators in clinical practice in Canada and identifying gaps in the current evidence; this focus is outlined in Table 1.
This report will review and critically appraise the economic information submitted by the sponsor, including a cost-effectiveness analysis and budget impact analysis (BIA). The focus of the Economic Review is aligned with the scope of the Clinical Review, unless otherwise stated. For most reviews, a Canada’s Drug Agency (CDA-AMC) base case is developed, informed by clinical expert input, the available clinical evidence, and the best interpretation of the economic evidence based on the information provided by the sponsor.
In April 2025, CDA-AMC issued a conditional positive time-limited reimbursement (TLR) recommendation for trastuzumab deruxtecan as monotherapy for the second-line treatment of adult patients with unresectable locally advanced or metastatic HER2-positive gastric or GEJ adenocarcinoma who had received a prior anti–HER2-based regimen. The TLR recommendation was issued for a time-limited period contingent on a future reassessment of additional evidence to address the uncertainties in the original data. The TLR decision was based on evidence from the phase II, single-arm DESTINY-Gastric02 trial, which suggested that treatment with trastuzumab deruxtecan may result in added clinical benefit in terms of objective response rate (ORR), with the potential to improve overall survival (OS) and progression-free survival (PFS). There was an absence of direct comparative data between trastuzumab deruxtecan and currently available comparator treatments and limited comparative evidence from the sponsor-submitted indirect treatment comparison (ITC). The pan-Canadian Oncology Drug Review Expert Review Committee concluded that a reassessment based on a properly designed and executed phase III confirmatory clinical trial would be required to establish whether trastuzumab deruxtecan provides a clinically meaningful survival benefit relative to comparator treatments and has an acceptable safety profile.
In September 2025, the sponsor filed this reassessment, as required under the TLR category, to address the uncertainty in the original evidence. The data from the phase III DESTINY-Gastric04 trial provide the required confirmatory evidence under the TLR process, and its patient population aligns with the sponsor’s requested reimbursement request. This current review will assess whether the data from the DESTINIY-Gastric04 trial address the evidence gaps identified by the pan-Canadian Oncology Drug Review Expert Review Committee in the TLR recommendation for trastuzumab deruxtecan in April 2025.
Table 1: Information on the Application Submitted for Review and on the CDA-AMC Review
Item | Description |
|---|---|
Information on the application submitted for review | |
Drug | Trastuzumab deruxtecan (Enhertu), powder for concentrate for solution for IV infusion (100 mg vial) |
Sponsor | AstraZeneca Canada Inc. |
Health Canada indication | For the treatment of adult patients with unresectable, locally advanced or metastatic HER2-positive gastric or gastroesophageal junction (GEJ) adenocarcinoma who have received a prior trastuzumab-based regimen |
Health Canada approval status | NOC/c |
Health Canada review pathway | Standard review pathway (in fulfillment of NOC/c) |
NOC date | Original NOC/c: January 17, 2025 |
Mechanism of action | Targets HER2-positive cells and releases topoisomerase I inhibitor to induce DNA damage and cell death |
Recommended dosage | 6.4 mg/kg administered as an IV infusion once every 3 weeks, until disease progression or unacceptable toxicity |
Submission type | Reassessment (in fulfillment of requirements under the TLR process) |
Submission history for the indication | Previously reviewed for: as monotherapy for the treatment of adult patients with unresectable, locally advanced, or metastatic HER2-positive gastric or GEJ adenocarcinoma who had received a prior trastuzumab-based regimen for a time-limited period while additional evidence is generated Recommendation category: TLR Recommendation date: April 03, 2025 |
Sponsor’s reimbursement request | For the second-line treatment of adult patients with unresectable, locally advanced, or metastatic HER2-positive gastric or GEJ adenocarcinoma who have received a prior anti–HER2-based regimen |
Submitted price | $2,440.000 per 100 mg vial |
Information on the CDA-AMC review | |
Review type | Standard |
Clinical review focusa | Population: as defined in the reimbursement request Subgroups: none Intervention: trastuzumab deruxtecan, 6.4 mg/kg q.3.w., IV infusion Comparators: ramucirumab plus paclitaxel, FOLFIRI, paclitaxel, irinotecan, or docetaxel Outcomes: OS, PFS, ORR, DOR, HRQoL (FACT-Ga), harms (AEs, grade 3 or greater AEs, SAEs, treatment discontinuations due to AEs, deaths due to AEs, and notable harms [ILD]) |
AE = adverse event; CDA-AMC = Canada’s Drug Agency; DOR = duration of response; FACT-Ga = Functional Assessment of Cancer Therapy–Gastric; FOLFIRI = folinic acid, fluorouracil, and irinotecan; GEJ = gastroesophageal junction; HRQoL = health-related quality of life; ILD = interstitial lung disease; NOC/c = Notice of Compliance with Conditions; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; q.3.w. = every 3 weeks; SAE = serious adverse event; TLR = time-limited reimbursement.
aThe Economic Review aligns with the scope of the Clinical Review, unless otherwise stated.
Submission History for the Drug Under Review
CDA-AMC previously reviewed trastuzumab deruxtecan through the reimbursement review process for the following indications: A conditional positive TLR recommendation was issued for trastuzumab deruxtecan as monotherapy for the treatment of adult patients with unresectable locally advanced or metastatic HER2-positive gastric or GEJ adenocarcinoma who have received a prior trastuzumab-based regimen for a time-limited period while additional evidence is generated.
A conditional positive recommendation was issued for trastuzumab deruxtecan as monotherapy for the treatment of adult patients with unresectable or metastatic HER2-low (immunohistochemistry [IHC] 1+ or IHC 2+ or in situ hybridization [ISH] negative) breast cancer who have received at least 1 prior line of chemotherapy in the metastatic setting or developed disease recurrence during or within 6 months of completing adjuvant chemotherapy. Patients with hormone receptor–positive breast cancer should have received at least 1 prior line of therapy and no longer be considered eligible for endocrine therapy.
A conditional positive recommendation was issued for trastuzumab deruxtecan for the treatment of adult patients with unresectable or metastatic HER2-positive breast cancer who have received prior treatment with an anti–HER2-based regimen in the metastatic setting or developed disease recurrence during or within 6 months of completing neoadjuvant or adjuvant therapy.
Sources of Information
The contents of the Reimbursement Review report are informed by materials submitted by the sponsor, input received from interested parties (patient groups, clinician groups, and drug programs), and input from clinical experts consulted for this review.
Calls for patient group and clinician group input are issued for each Reimbursement Review report. One patient group submission from My Gut Feeling–Stomach Cancer Foundation of Canada (hereafter referred to as My Gut Feeling) and 2 clinician group submissions — 1 joined submission from the Canadian Gastrointestinal Oncology Evidence Network (CGOEN) and the My Gut Feeling Medical Advisory Board (My Gut Feeling MAB), and 1 submission from the Ontario Health (Cancer Care Ontario) (OH [CCO]) Gastrointestinal Cancer Drug Advisory Committee (GI DAC) — were received.
My Gut Feeling distributed an international electronic survey to patients and caregivers affected by gastric, GEJ, and esophageal cancer between September 9 and 25, 2025, posted via social media and the group’s email list; 30 respondents completed the survey (75% patients; 25% caregivers). Data were primarily received from people living in Canada (95%), with most respondents living in Ontario. Three respondents reported experience with trastuzumab deruxtecan.
The clinician group submissions gathered information through virtual discussion, meetings, email exchange, clinical experience, and a targeted literature review. In total, 14 clinicians contributed to the clinician group inputs: 10 clinicians from CGOEN and My Gut Feeling MAB, and 4 clinicians from OH (CCO) GI DAC.
The full submissions received are available on the CDA-AMC project landing page in the consolidated Patient and Clinician Group Input document. The drug programs provide input on each drug being reviewed through the reimbursement review process by identifying issues that may impact their ability to implement a recommendation.
Input from patient and clinician groups is considered throughout the review, including in the selection of outcomes to include in the clinical review and in the interpretation of the clinical and economic evidence. Relevant patient and clinician group input is summarized in the Disease Background, Current Management, and Unmet Needs and Existing Challenges sections.
Each review team includes at least 1 clinical expert with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process. Two medical oncologists with expertise in the diagnosis and management of gastric or GEJ adenocarcinoma participated as part of the review team, with representation from Ontario and British Columbia.
Disease Background
Gastric cancer (GC) is a malignant tumour that arises from the cells within the inner lining of the stomach. Approximately 95% of GCs are adenocarcinomas.2 GEJ adenocarcinoma is a specific type of adenocarcinoma that develops at the junction where the esophagus meets the stomach. Gastric and GEJ adenocarcinoma have often been reviewed, investigated, or presented together in literature reviews, clinical trials, and clinical management guidelines because of the similarities in the tumour growth and patterns of disease spread between the 2 patient populations.3 The symptoms of GC generally present late in disease progression and can be nonspecific; consequently, almost half of patients with GC in Canada are diagnosed with stage IV or metastatic disease.4-6 Signs and symptoms of GC include abdominal pain, heartburn, loss of appetite, bloating, nausea, vomiting, difficulty swallowing, blood in the stool, anemia, fatigue, ascites, and jaundice.7
In a population-based study conducted in Canada, an estimated 21% of all GCs and GEJ cancers show an overexpression of HER2.8 The prognostic role of HER2 in GC remains uncertain because of conflicting evidence.9-13 GC is the fifth most common cancer and the fifth leading cause of cancer mortality worldwide, with approximately 968,000 incidence cases and 659,853 associated deaths in 2022 (equating to 6.8% of all cancer-related deaths).3 The projected incidence rate of GC in Canada is 8.3 per 100,000 adults in 2024, with an estimated 1,400 cases in females and 2,600 cases in males.1 There are some data suggesting a higher risk of GC in racialized populations.14 It is unknown whether any equity-deserving groups experience worse outcomes from GC. The overall 5-year survival for all patients with GC is estimated to be 29%,15 and patients with distant metastasis experience worse outcomes, with an estimated 5-year survival rate of 7%, compared to individuals without GC.16
Patient group input: Patients and caregivers described a substantial multidomain burden, including physical difficulties (e.g., eating problems, reflux, weight loss, pain, fatigue, and nausea or vomiting), mental health impacts (anxiety, depression, and trauma), and financial hardship, contributing to a reduced quality of life. Caregivers indicated the significant difficulties associated with watching their family members experience illness, with some describing the experience as “traumatic.”
Current Management
Treatment Goals
Patient group input: Patients and caregivers prioritized effective cancer control with prolonged survival, delayed disease progression, relief of cancer-related symptoms, minimal side effects, treatment convenience and access, improved quality of life, and additional treatment choice. Participants frequently emphasized the financial and time burdens of care as important factors when weighing benefits and harms.
Clinician input: Clinical experts consulted by CDA-AMC agreed that the goal of treatment is palliative and focuses on extending survival and improving disease control with manageable toxicity and maintenance of patients’ quality of life. Across both clinician group inputs, key goals for a treatment for second-line HER2-positive GC were to prolong survival (OS and PFS), reduce tumour burden and improve response, improve health-related quality of life (HRQoL), and minimize treatment toxicity.
Current Treatment Options
The standard of care first-line treatment for advanced HER2-positive gastric or GEJ adenocarcinoma is a trastuzumab-based regimen, consisting of trastuzumab with or without pembrolizumab (if the patient has PD-L1–positive disease) in combination with fluoropyrimidine-based chemotherapy (e.g., FOLFOX), and platinum-based chemotherapy (e.g., capecitabine plus oxaliplatin or cisplatin plus capecitabine).17-19 Despite the efficacy of trastuzumab-based therapy in the first-line treatment, the disease ultimately progresses in most patients.
Before the recent Health Canada approval of trastuzumab deruxtecan for the indication to be reviewed by CDA-AMC, there were no HER2-targeted treatment options available to patients beyond trastuzumab-based regimens in the first-line treatment setting.20 Thus, following progression on first-line therapy, the majority of patients with gastric or GEJ adenocarcinoma, regardless of HER2 status, would receive ramucirumab plus paclitaxel, or less commonly, an alternative chemotherapy (folinic acid, fluorouracil, and irinotecan [FOLFIRI]), or single-agent chemotherapy (paclitaxel or irinotecan).19,21,22 According to the clinical experts consulted by CDA-AMC, approximately one-third of patients may not be eligible for ramucirumab plus paclitaxel, including patients at risk of bleeding or neuropathy. Based on the recent conditional positive TLR recommendation issued by CDA-AMC, trastuzumab deruxtecan is now a funded second-line treatment option for patients with HER2-positive gastric or GEJ adenocarcinoma in most Atlantic provinces (except Prince Edward Island), Quebec, Ontario, Saskatchewan, Alberta, and British Columbia at the time of writing this document.23,24
In the third-line setting, trifluridine tipiracil is available for patients who received ramucirumab plus paclitaxel or an alternative chemotherapy in the second-line setting.17-19 For patients who receive trastuzumab deruxtecan in the second-line setting, third-line options include ramucirumab plus paclitaxel or an alternative chemotherapy, in which trifluridine tipiracil may be considered as a fourth-line treatment option.17-19
Key characteristics of trastuzumab deruxtecan and relevant comparator treatments for the current target patient population are summarized in the Key Characteristics table in Appendix 1 in the Supplemental Material document (available on the CDA-AMC project landing page).
Unmet Needs and Existing Challenges
Patient group input: Patients and caregivers reported that current second-line options often provide limited cancer control with considerable adverse effects, leaving a need for treatments that more reliably prolong survival, delay progression, relieve symptoms, and are better tolerated. According to the patient group input, patients seek to eat and maintain weight with less reflux, nausea, pain, and fatigue, and to reduce the psychological toll of ongoing care and uncertainty. Patient and caregivers described persistent access and equity challenges. Specialized services and trials are located in large centres. Therefore, while most patients will incur costs related to travel, parking, and time away from work or caregiving responsibilities, individuals from rural or remote areas will be disproportionately affected because of the need for long-distance travel. System delays at referral and treatment initiation and inconsistent access to supportive services further strain patients and families. Patients have had to declare bankruptcy because of the combination of loss of employment and costs of care, and those of lower baseline socioeconomic status or single parents are particularly vulnerable to these financial concerns. Patients in rural and remote areas may face even higher expenses related to time or travel required for care of their disease. Caregivers face a practical and emotional load, and respondents asked for clearer information early in the pathway, simpler logistics (fewer or shorter visits where feasible), and more equitable, timely access to effective additional treatment options, enabling patients to make more informed decisions aligned with their values.
Clinician input: There is a need for treatments that achieve higher response rates and extend PFS and OS while maintaining or improving quality of life. Additionally, toxicity with existing options constrains tolerability and adherence. Implementation challenges include establishing routine, reliable monitoring and explicit stopping rules (e.g., imaging approximately every 3 months; discontinuation for radiologic or clinical progression, unacceptable toxicity, or patient preference). Programs require protocols for recognition and management of interstitial lung disease (ILD) or pneumonitis, readiness for dose holds or reductions, consideration of cardiac risk in susceptible patients, and clinic capacity for periodic imaging and follow-up. Eligibility and delivery considerations include use in appropriate patients with HER2-positive disease in the second-line setting, with adequate performance status and organ function, delivered in outpatient oncology settings with confirmed HER2 testing. The clinical experts consulted for this review noted that the majority of centres (community and academic) have access to HER2 testing. Sometimes testing may be done at central laboratories, depending on the province. Because HER2 testing is considered standard of care and the tissue gets sent to the central laboratory for testing, the experts did not anticipate specific barriers.
Considerations for Using the Drug Under Review
Contents within this section have been informed by input from the clinical experts consulted for the purpose of this review and from clinician groups, as well as the reimbursement conditions proposed by the sponsor (refer to the Initiation, Renewal, Discontinuation, and Prescribing Conditions Proposed by the Sponsor table in Appendix 1 in the Supplemental Material document available on the CDA-AMC project landing page). The implementation questions from the public drug programs and corresponding responses from the clinical experts consulted for this review are summarized in the Summary of Drug Program Input and Clinical Expert Responses table in Appendix 1 in the Supplemental Material document. The following has been summarized by the review team.
Place in Therapy
Based on clinician group inputs and clinical experts consulted for this review, trastuzumab deruxtecan would be used as second-line monotherapy for adults with HER2-positive gastric or GEJ adenocarcinoma whose disease progresses after first-line trastuzumab-based chemotherapy (with or without pembrolizumab when indicated). Clinicians expect this to shift the current treatment paradigm by making trastuzumab deruxtecan the preferred second-line option in patients who are eligible, in place of ramucirumab plus paclitaxel or less commonly, FOLFIRI or single-agent chemotherapy.
Clinician groups specified that trastuzumab deruxtecan should not replace established first-line trastuzumab-based regimens. Its role is after exposure to trastuzumab at progression. If trastuzumab deruxtecan is contraindicated, not available, or not tolerated, clinicians would continue to use currently available options (e.g., ramucirumab plus paclitaxel or irinotecan-based therapy), and clinical trial enrolment remains appropriate.
Patient Population
According to the OH (CCO) GI DAC and the clinical experts consulted by CDA-AMC, trastuzumab deruxtecan is intended for adults with HER2-positive gastric or GEJ adenocarcinoma whose disease progresses after first-line trastuzumab-based chemotherapy (with or without pembrolizumab). Treatment would begin at progression in the second-line setting. Patients who are eligible should have confirmed HER2 positivity and prior trastuzumab exposure, with adequate performance status and organ function for outpatient infusion and routine monitoring.
According to the CGOEN and My Gut Feeling MAB, patient identification relies on standard local HER2 testing (IHC with reflex ISH per institutional practice) and baseline clinical and imaging assessment. Patients with current or prior ILD or pneumonitis or who are at high risk for ILD are not appropriate candidates; grade 2 or greater ILD requires permanent discontinuation. Caution is advised in those with cardiac risk, and cardiology involvement is recommended when left ventricular ejection fraction is reduced; dose interruptions or reductions may be used to manage adverse effects.
Safety and implementation considerations highlighted by clinician groups include the need for program-level protocols for ILD or pneumonitis (patient education on respiratory symptoms; prompt evaluation of suspected cases; treatment interruption with corticosteroids as indicated; and permanent discontinuation for clinically significant ILD) and attention to cardiac risk in susceptible patients with cardiology involvement when needed. Dose interruptions and reductions may be required to maintain treatment while managing adverse effects.
All patients with advanced or metastatic GC or GEJ cancer, including patients with both gastric and gastroesophageal adenocarcinomas, should undergo HER2 testing. HER2 testing is typically conducted at the time of diagnosis or at the onset of advanced or metastatic disease. Additionally, HER2 testing may be repeated if there is a need for revaluation because of disease progression or development of metastases. HER2-positive status is confirmed when the test results show IHC 3+ or IHC 2+ followed by ISH.25
Assessing the Response to Treatment
According to clinician group inputs and clinical experts consulted for this review, response to trastuzumab deruxtecan should be assessed using routine clinical practice tools with timing aligned to workflows in Canada. Tumour response is evaluated radiographically by Response Evaluation Criteria in Solid Tumours Version 1.1 (RECIST 1.1) (using CT scans of the chest, abdomen, or pelvis), with scans obtained approximately every 9 to 12 weeks. Clinical benefit is judged on overall disease control and patient status: continuation is appropriate for partial response or stable disease with acceptable toxicity and maintained or improved symptoms or function; treatment should be discontinued if the disease progresses radiologically or clinically, for unacceptable toxicity, or because of patient preference.
Clinician groups and clinical experts consulted for this review recommend standard clinical assessments at each visit (history, physical exam, Eastern Cooperative Oncology Group Performance Status [ECOG PS], weight, and symptom review, including dyspnea or cough), with laboratory testing as per local practice. Because ILD or pneumonitis is a known risk, programs should incorporate ongoing ILD surveillance into routine follow-up (patient education regarding respiratory symptoms, a low threshold for evaluation, and CT review for pneumonitis features). When cardiotoxicity risk is present, clinicians may obtain cardiac assessments based on clinical judgment. Overall, the proposed instruments and timing are feasible within outpatient oncology in Canada and mirror current monitoring cadence for second-line systemic therapy. Patients from smaller, rural communities may be required to travel to their appointments, which would be an additional burden for them with respect to time and travel.
Discontinuing Treatment
According to clinician group inputs and clinical experts consulted for this review, trastuzumab deruxtecan should be discontinued if the disease progresses radiographically or clinically or for unacceptable treatment-related toxicity. In routine practice, continuation is appropriate only while there is disease control (partial response or stable disease by RECIST 1.1) with acceptable tolerability and maintained clinical status. Treatment should stop for symptomatic deterioration, patient preference, or when a new systemic therapy is initiated. Specific safety rules include permanent discontinuation for grade 2 or greater ILD or pneumonitis; interruption with evaluation and management is required for suspected cases. Clinicians may also discontinue for clinically significant cardiac dysfunction or other serious adverse events (SAEs) despite dose modifications and supportive care. These criteria align with practice in Canada and are feasible to implement in outpatient oncology settings.
Prescribing Considerations
According to clinician group inputs and clinical experts consulted for this review, trastuzumab deruxtecan should be prescribed by medical oncologists within hospital-based outpatient cancer centres that can provide infusion services, timely cross-sectional imaging, and coordinated toxicity monitoring. Programs should have access to pathology services for accurate HER2 testing (IHC with reflex ISH per local practice) and to specialty support for managing pulmonary and cardiac adverse effects (e.g., rapid assessment of suspected ILD or pneumonitis and cardiology consultation when left ventricular ejection fraction is reduced).
Safety and implementation considerations highlighted by clinician groups include the need for program-level protocols for ILD or pneumonitis, such as patient education on respiratory symptoms, prompt evaluation of suspected cases, treatment interruption with corticosteroids as indicated, and permanent discontinuation for clinically significant ILD, as well as attention to cardiac risk in patients who are at a high risk of cardiovascular disease. Standard dosing is used with allowance for dose interruptions and reductions to maintain treatment while managing adverse effects. Ongoing monitoring should include symptom review (notably dyspnea or cough), examination, laboratory testing per local practice, and CT imaging approximately every 9 to 12 weeks. Programs should implement explicit stopping rules (progression, unacceptable toxicity, or patient preference) and address regional variation in infusion capacity or timely imaging with referral to centres with the required infrastructure as necessary. The clinical experts consulted for this review noted that the majority of centres (community and academic) have access to HER2 testing. Sometimes testing may be done at central laboratories depending on the province. Because HER2 testing is considered standard of care and the tissue gets sent to the central laboratory for testing, the experts did not anticipate specific barriers.
Clinical Review
Methods
The review team considered studies in the sponsor’s systematic review (pivotal studies and randomized controlled trials [RCTs]), and sponsor-submitted ITCs. The sponsor did not submit long-term extensions or studies addressing gaps in the evidence for inclusion. Eligible studies for the systematic review included published and unpublished pivotal studies and phase III and IV RCTs. Relevant patients and interventions were defined as relevant by the reimbursement request and the recommended dosage in the product monograph. Relevant comparators were drugs used in clinical practice in Canada to treat patients described in the indication under review. These included ramucirumab plus paclitaxel and, less commonly, alternative chemotherapy (FOLFIRI) or single agents (paclitaxel, irinotecan, or docetaxel).19,21,22 Sponsor-submitted ITCs were included when they filled an identified gap in the systematic review evidence (e.g., missing comparator).
The review team selected outcomes (and follow-up times) for review considering the sponsor’s Summary of Clinical Evidence, clinical expert input, and patient group and clinician group input. Included outcomes are those considered relevant to expert committee deliberations, and they were selected in consultation with committee members. Evidence from the systematic review for the most important outcomes was assessed using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach. The following outcomes were assessed with GRADE because they are efficacy or safety measures that address 1 of the main treatment goals for gastric or GEJ adenocarcinoma and were considered important to patients and their clinicians according to patient and clinician group inputs as well as the clinical experts consulted by CDA-AMC: OS (6, 12, and 18 months), PFS (6 and 9 months), HRQoL (measured via the Functional Assessment of Cancer Therapy–Gastric [FACT-Ga] total score), and ILD. Although response outcomes were considered important for GC, the clinical experts consulted by CDA-AMC considered them supportive to OS and PFS. Thus, ORR and duration of response were not formally included in the GRADE assessment, but their results are discussed in this review. All relevant harms (adverse events [AEs], grade 3 or greater AEs, SAEs, treatment discontinuation because of AE, and death because of AE) were also summarized.
Methods for data extraction, risk-of-bias appraisal, and certainty of evidence assessment are in Appendix 2 in the Supplemental Material document.
Clinical Evidence
In this report, the following sources of evidence submitted by the sponsor are reviewed and appraised:
1 pivotal RCT included in the systematic review, the DESTINY-Gastric04 trial
1 ITC.
Systematic Review
Description of Study
Study Characteristics
Characteristics of the included study are summarized in Table 2. Details pertaining to the comparators and relevant outcome measures are in Appendix 3 in the Supplemental Material document.
DESTINY-Gastric04 was a global, multicentre, open-label, randomized, active-controlled, phase III trial evaluating trastuzumab deruxtecan versus ramucirumab plus paclitaxel in adults with HER2-positive locally advanced unresectable or metastatic gastric or GEJ adenocarcinoma whose disease had progressed on or after first-line trastuzumab-containing chemotherapy. HER2-positive status was defined as IHC 3+, IHC 2+, or ISH-positive per the American Society of Clinical Oncology clinical practice guideline.26 It could be confirmed locally or centrally on tumour tissue after progression on first-line trastuzumab-containing therapy.
A total of 494 patients were randomized 1:1 through an interactive response technology system to receive either trastuzumab deruxtecan 6.4 mg/kg by IV infusion once every 3 weeks (n = 246) or ramucirumab 8 mg/kg by IV on day 1 and day 15 plus paclitaxel 80 mg/m2 by IV on day 1, day 8, and day 15 of each 28-day cycle (n = 248). Randomization was stratified by HER2 status (IHC 3+ versus IHC 2+ or ISH-positive), geographic region (Asia excluding mainland China versus Western Europe versus mainland China and the rest of world), and time to progression on first-line therapy (less than 6 months versus 6 months or longer). Treatment continued until radiologic progression per RECIST 1.1, unacceptable toxicity, withdrawal of consent, or investigator decision. Crossover between treatment arms was not permitted, although subsequent anticancer therapies, including trastuzumab deruxtecan, in jurisdictions in which available, were allowed after study treatment discontinuation.
Efficacy evaluations were performed every 6 weeks (plus or minus 7 days) during the first year and every 12 weeks thereafter until disease progression, the start of new anticancer therapy, or withdrawal. Safety assessments were conducted at each treatment visit and at a follow-up visit approximately 40 days (plus or minus 7 days) after the last dose. Long-term follow-up for survival occurred every 2 months (plus or minus 2 weeks) until death or study completion.
The trial enrolled patients at 156 sites across 24 countries throughout Asia-Pacific, Europe, and South America. There were no trial sites in Canada. The first patient was enrolled on May 21, 2021, and the estimated study completion date is February 1, 2026. The data supporting this review are from the prespecified interim analysis (data cut-off: October 24, 2024), which served as the primary analysis for OS. Based on the statistical analysis plan, no further formal hypothesis testing will be conducted, given that the OS superiority boundary was met at this interim analysis.
Table 2: Characteristics of Studies Included in the Systematic Review
Study name, design, and sample size | Key inclusion criteria | Key exclusion criteria | Intervention and comparator | Relevant end points |
|---|---|---|---|---|
DESTINY-Gastric04 study Multicentre, open-label, active-controlled, phase III RCT Total N = 494 |
|
| Intervention:
Comparators:
| Primary:
Secondary:
Exploratory: HRQoL, assessed via FACT-Ga Harms:
|
AE = adverse event; ASCO = American Society of Clinical Oncology; CAP = College of American Pathologists; DOR = duration of response; ECG = electrocardiogram; ECOG PS = Eastern Cooperative Oncology Group Performance Status; FACT-Ga = Functional Assessment of Cancer Therapy–Gastric; GEJ = gastroesophageal junction; HRQoL = health-related quality of life; IHC = immunohistochemistry; ILD = interstitial lung disease; ISH = in situ hybridization; ORR = overall response rate; OS = overall survival; PFS = progression-free survival; q.3.w. = every 3 weeks; QTcF = QT interval corrected with Fridericia formula; RCT = randomized controlled trial; RECIST 1.1 = Response Evaluation Criteria in Solid Tumours Version 1.1; SAE = serious adverse event.
Sources: Details included in the table are from the sponsor’s Summary of Clinical Evidence and the DESTINY-Gastric04 trial Clinical Study Report.27 The DESTINY-Gastric04 Study Protocol.28
Statistical Testing and Analysis Populations
The DESTINY-Gastric04 study was designed to randomize approximately 490 patients (245 per treatment arm) to evaluate the efficacy and safety of trastuzumab deruxtecan compared with ramucirumab plus paclitaxel in patients with previously treated HER2-positive gastric or GEJ adenocarcinoma.
The study was event-driven and intended to be powered to detect a statistically significant difference in OS between treatment arms. Assuming a median OS of 10.8 months in the control arm (based on the RAINBOW29 trial) and a hazard ratio (HR) of 0.70, corresponding to an approximate 43% improvement in median OS (to 15.4 months) in the trastuzumab deruxtecan arm, the trial would have 90% power at a 2-sided significance level of 5% using a log-rank test.
A group-sequential design was implemented, with 1 planned interim analysis using a Lan-DeMets alpha-spending function (O’Brien-Fleming boundary) to preserve the overall type I error rate. The interim analysis was planned after approximately 237 deaths (about 70% of the 339 events targeted for the final analysis). If superiority in OS was established at the interim analysis, no further confirmatory testing was to be conducted. Otherwise, a final analysis was planned after 339 deaths were observed.
Multiplicity control was managed using a hierarchical testing procedure, with formal testing conducted in the following sequence: OS (primary end point), PFS (secondary end point), and ORR (secondary end point).
Once statistical significance was reached for OS, the subsequent secondary end points were to be tested sequentially at the same overall 2-sided 5% significance level.
Efficacy analyses were performed in the full analysis set, which included all randomized patients. The safety analysis set included all patients who received at least 1 dose of study drug, analyzed according to the actual treatment received. The per-protocol set included patients in the full analysis set without major protocol deviations likely to affect efficacy outcomes.
Patient Disposition
Patient disposition for the included study is summarized in Appendix 4 in the Supplemental Material document.
A total of 494 patients were randomized at 117 sites across the Asia-Pacific (58 sites), Europe (53 sites), and Latin America (7 sites). There were 638 patients who entered main screening and 144 for whom screening was not successful. The reasons for 90% of the screen failures was not meeting eligibility requirements.
Most randomized patients received study drug; 2 of 246 patients (0.8%) in the trastuzumab deruxtecan arm and 15 of 248 patients (6.0%) in the ramucirumab plus paclitaxel arm were randomized but did not receive treatment.
A similar proportion of patients discontinued the study drug across both study groups (i.e., 198 of 244 patients [81.1%] received trastuzumab deruxtecan and 190 of 233 patients [81.5%] received ramucirumab plus paclitaxel). The most common reason for study drug discontinuation was progressive disease, reported in 139 patients (57.0%) in the trastuzumab deruxtecan arm and 125 patients (53.6%) in the ramucirumab plus paclitaxel arm. Overall study discontinuation occurred in 129 patients (52.4%) in the trastuzumab deruxtecan arm and 155 patients (62.5%) in the ramucirumab plus paclitaxel arm. The most common reason for study discontinuation was death (119 patients [48.4%] versus 131 patients [52.8%]).
Baseline Characteristics
Baseline demographic and disease characteristics for patients enrolled in the DESTINY-Gastric04 trial are summarized in Table 3. Characteristics were generally similar between treatment arms. The median age was 63.2 years (range, 21.1 years to 84.1 years) in the trastuzumab deruxtecan arm and 64.3 years (range, 31.9 years to 87.0 years) in the ramucirumab plus paclitaxel arm; most patients were male (trastuzumab deruxtecan, 76.0%; ramucirumab plus paclitaxel 82.7%). HER2 status at baseline was predominantly IHC 3+ (trastuzumab deruxtecan, 84.1%; ramucirumab plus paclitaxel 83.9%). Most patients had an ECOG PS score of 1 (trastuzumab deruxtecan, 60.2% and ramucirumab plus paclitaxel 63.7%).
Table 3: Summary of Baseline Characteristics From the DESTINY-Gastric04 Study (ITT Population)
Characteristic | DESTINY-Gastric04 study | |
|---|---|---|
Trastuzumab deruxtecan (N = 246) | Ramucirumab + paclitaxel (N = 248) | |
Age (years)a | ||
Mean (SD) | 61.6 (10.97) | 63.4 (10.98) |
Median (range) | 63.2 (21.1 to 84.1) | 64.3 (31.9 to 87.0) |
Sex, n (%) | ||
Female | 59 (24.0) | 43 (17.3) |
Male | 187 (76.0) | 205 (82.7) |
Race and Ethnicity, n (%) | ||
Asian | 101 (41.1) | 97 (39.1) |
Black or African American | 0 | 2 (0.8) |
Multiple | 1 (0.4) | 0 |
White | 116 (47.2) | 130 (52.4) |
Other | 28 (11.4) | 19 (7.7) |
Stratification factor 1 (HER-2 status) – IRT | ||
IHC 2+ and ISH-positive | 39 (15.9) | 40 (16.1) |
IHC 3+ | 207 (84.1) | 208 (83.9) |
Stratification factor 2 (geography) – IRT | ||
Asia (excluding mainland China) | 57 (23.2) | 60 (24.2) |
Mainland China and RoW | 49 (19.9) | 49 (19.8) |
Western Europe | 140 (56.9) | 139 (56.0) |
Stratification factor 3 (time to progression on first-line therapy) – IRT | ||
< 6 months | 61 (24.8) | 61 (24.6) |
≥ 6 months | 185 (75.2) | 187 (75.4) |
ECOG PS | ||
0 | 97 (39.4) | 88 (35.5) |
1 | 148 (60.2) | 158 (63.7) |
2 | 1 (0.4) | 1 (0.4) |
Missing | 0 | 1 (0.4) |
Number of metastatic sites | ||
< 2 | 73 (29.7) | 75 (30.2) |
≥ 2 | 173 (70.3) | 173 (69.8) |
History of liver metastasis | ||
Yes | 147 (59.8) | 158 (63.7) |
No | 99 (40.2) | 90 (36.3) |
Cancer type, n (%) | ||
Gastric | 153 (62.2) | 149 (60.1) |
GEJ | 93 (37.8) | 99 (39.9) |
Disease presentation at study entry, n (%) | ||
Metastatic disease | 230 (93.5) | 228 (91.9) |
Locally advanced | 13 (5.3) | 16 (6.5) |
Localized | 2 (0.8) | 3 (1.2) |
Unknown | 1 (0.4) | 0 |
Missing | 0 | 1 (0.4) |
Prior cancer systemic therapy of trastuzumab (first-line) for: | ||
Neoadjuvant and/or adjuvant | 0 | 2 (0.8) |
Locally advanced | 38 (15.4) | 23 (9.3) |
Metastatic | 205 (83.3) | 223 (89.9) |
Maintenance | 1 (0.4) | 0 |
Any prior systemic cancer therapy (≥ 30% of patients in either group) | ||
Trastuzumab (Herceptin or approved biosimilar) | 244 (99.2) | 248 (100) |
Trastuzumab (Herceptin) | 215 (87.4) | 221 (89.1) |
Trastuzumab (approved biosimilar) | 31 (12.6) | 28 (11.3) |
Oxaliplatin | 177 (72.0) | 157 (63.3) |
Fluorouracil | 120 (48.8) | 123 (49.6) |
Capecitabine | 110 (44.7) | 103 (41.5) |
Cisplatin | 77 (31.3) | 85 (34.3) |
ECOG PS = Eastern Cooperative Oncology Group Performance Status; GEJ = gastroesophageal junction; IHC = immunohistochemistry; IRT = interactive response technology; ISH = in situ hybridization; ITT = intention to treat; RoW = rest of world; SD = standard deviation.
Note: Racial categories used in the table are as reported in the source and may not align with Canada's Drug Agency inclusive language guidelines.
Sources: Details included in the table are from the sponsor’s Summary of Clinical Evidence, and the DESTINY-Gastric04 trial Clinical Study Report.27
Treatment Exposure and Concomitant Medications
Full details on exposure, concomitant medications, and subsequent therapies are provided in Appendix 4 in the Supplemental Material document.
At the time of the data cut-off, the median duration of study treatment was 5.4 months (range, 0.7 months to 30.3 months) with trastuzumab deruxtecan and 4.6 months (range: 0.9 months to 34.9 months) with ramucirumab plus paclitaxel. The median duration of exposure to the individual treatment components (i.e., ramucirumab, paclitaxel) ranged from 4.34 months to 4.6 months.
Concomitant medications were used by nearly all patients (trastuzumab deruxtecan, 99.6%; ramucirumab plus paclitaxel 99.1%). Common classes (used in more than 30% of patients) included antiemetics or antinauseants, corticosteroids for systemic use, drugs for acid-related disorders, antibacterials for systemic use, and blood substitutes or perfusion solutions.
Subsequent systemic anticancer therapy was received by approximately half of patients (trastuzumab deruxtecan, 126 of 246 patients [51.2% of patients]; ramucirumab plus paclitaxel 118 of 248 patients [47.6%]). After trastuzumab deruxtecan, the most frequent poststudy drug was paclitaxel (63 of 246 patients [25.6%]). After ramucirumab plus paclitaxel, trastuzumab deruxtecan was the most common subsequent therapy (52 of 248 patients [21.0%]). Ramucirumab was used postdiscontinuation in 43 of 246 patients (17.5% of patients) who had received trastuzumab deruxtecan. Most subsequent therapy occurred in the third-line setting (122 of 246 patients [49.6% of patients] versus 111 of 248 patients [44.8%]), and the majority was systemic (126 of 246 patients [51.2%] versus 118 of 248 patients [47.6%]).
Critical Appraisal
Internal Validity
The randomization and allocation methods were appropriate, and patients’ demographic and disease characteristics were balanced across treatment groups at baseline; therefore, there is a low risk of bias in the randomization process. The open-label design increases the risk of bias in the assessment of patient-reported outcomes such as HRQoL, and potentially even for more objective outcomes (but for which there is some subjectivity), such as ORR and PFS, particularly because these were measured by the investigators (without central review).30,31 The direction of bias cannot be definitively ascertained but would likely favour the intervention group. It is possible that patients assigned to trastuzumab deruxtecan will have greater expectations regarding treatment success. Assessment of subjective harms may also be biased. If a drug is associated with specific known harms, it is possible that patients may be more inclined to report them. This tendency would be more impactful for subjective harms, such as nausea or headache, and less likely to influence reporting of more objective harms, such as ILD.
The open-label design also introduces the potential for bias in the assessment of disease progression, which is a key component of the PFS and ORR outcomes. This potential for bias can be offset by the use of blinded independent review; however, this does not appear to have been done in the DESTINY trial. With no blinding and no blinded independent review, the results for PFS and ORR are at risk of being biased by investigators’ knowledge of treatment assignment.
There were fewer patients who discontinued the study in the trastuzumab deruxtecan group than in control group (52.4% versus 62.5%); however, the number of patients who discontinued study drug was similar between groups (81.1% versus 81.5%). There was an imbalance between the trastuzumab deruxtecan and ramucirumab plus paclitaxel groups in the proportion of patients who were randomized but never received treatment (0.8% versus 6.0%). Furthermore, fewer patients in the trastuzumab deruxtecan group than in the ramucirumab plus paclitaxel group discontinued the study drug because of the reasons of “withdrawal by patient” (2.0% versus 6.9%) and “physician decision” (0.8% versus 1.7%). Particularly in an open-label trial, these imbalances raise concerns for risk of bias because of deviations from the intended interventions. In the absence of additional details, it is not possible to ascertain whether the reasons for early discontinuation of the study drugs were related to the outcomes, and the magnitude and direction of potential bias are uncertain.
There was a large amount of missing data for the assessment of HRQoL. Much of these missing data may be accounted for by patients having discontinued the study; however, there appears to have been data missing among patients who were still in the trial as well. For example, at day 190 (the latest time point for which data were available), 135 of 494 patients (27%) reported data. The sponsor used the mixed effects model for repeated measures to account for missing data; however, the flaw with this approach is that it assumes data are missing at random. This assumption may not hold in this case, as it would be reasonable to assume that those who remain in the trial are those whose disease is responding and who therefore may also have better quality of life. In the analysis of OS, fewer patients were censored due to “withdrawal by patient” in the trastuzumab deruxtecan group compared with the ramucirumab plus paclitaxel group (1.6% versus 4.8%). In the analysis of PFS, fewer patients were censored because of “no postbaseline tumour assessment” in the trastuzumab deruxtecan group compared with the ramucirumab plus paclitaxel group (4.9% versus 10.9%). No sensitivity analyses testing different assumptions about these censoring reasons were planned or reported. Without additional details, it is uncertain whether these imbalances would result in a risk of bias because of informative censoring. There were notably fewer patients with trastuzumab deruxtecan compared to ramucirumab plus paclitaxel (3% versus 15%) who were reported as “not evaluable” for the assessment of ORR. It is not clear why so many patients were not evaluable, as the reasons were not elaborated within the submitted documents. As such, there are some concerns about risk of bias because of missing outcome data for this end point.
The primary outcome, OS, and secondary outcomes, PFS and ORR, were formally assessed for statistical significance. No methods were reported by the sponsor to test the validity of the proportional hazards (PH) assumption underlying the Cox PH model (for OS and PFS). Visual inspections of the Kaplan-Meier (KM) curves by the CDA-AMC review team identified no major violations of the assumption for OS. However, for PFS, the curves converged a number of times during the first 6 months of treatment, suggesting a violation of the PH assumption. As such, the HR for PFS may be misleading. The KM-estimated probabilities of PFS are not affected by this limitation. Sensitivity analyses were performed, including the use of a rank-preserving structural failure time model (RPSFTM) to attempt to account for postprogression trastuzumab deruxtecan or disitamab vedotin use among 26% of patients in the ramucirumab plus paclitaxel group, which could have attenuated the OS benefit of trastuzumab deruxtecan. This analysis yielded a very similar result to the primary analysis, suggesting no attenuation of the treatment effect. However, it should be noted that the RPSFTM analysis is subject to assumptions that may not be plausible and cannot be verified via the observed data. Briefly, the assumption is that the treatments have the same efficacy, regardless of the line of treatment in which they are used. This is unlikely to be clinically plausible.32 Therefore, the presence and/or degree of any attenuation of the treatment effect is uncertain. Multiplicity control was managed using a hierarchical testing procedure, with testing proceeding in that order (OS, then PFS, then ORR). There were subgroups specified a priori, and OS results for the Western Europe subgroup were overall aligned with those for the overall study population. However, no tests for subgroup-by-treatment interaction were planned or performed, and the trial was unlikely powered to detect a subgroup difference if one were to exist.
No notable, systematic protocol deviations were identified in the Clinical Study Report that would be expected to materially affect interpretation of the results. Because the results are based on an interim analysis, there is the potential that beneficial effects on survival end points (i.e., HRs for OS and PFS) are overestimated.33 At the time of the interim analysis, the information fraction (number of observed events divided by the total events planned for the final analysis) was 79% for OS and 74% for PFS. The sponsor confirmed that because the criteria for superiority were met in the interim OS analysis, this was considered the final analysis. Regarding the KM-estimated probabilities of OS and PFS, estimates at later time points (e.g., beyond 18 months for OS and 9 months for PFS) are of lower certainty because of the few patients at risk at these follow-up times.33
The FACT-Ga is an established instrument used to assess HRQoL in GCs. A within-group minimal important difference (MID) has been reported in the literature; however, evidence for a between-group MID was not supplied by the sponsor. The absence of an estimated between-groups MID challenged the interpretation of the clinical meaningfulness of the between-group difference in HRQoL at day 190. However, because the point estimate for the between-group difference was far smaller than the within-group MID estimate (15.1 points; 95% confidence interval [CI], 10.4 to 19.5), the CDA-AMC review team judged that the difference was unlikely to be clinically meaningful.
External Validity
The clinical experts consulted by CDA-AMC believed that results for the population enrolled in the DESTINY-Gastric04 trial were generalizable to the patients who would be expected to receive the drug. The CDA-AMC review team noted that population groups that are African American or Black or that comprise multiple racial or ethnic groups were underrepresented in the trial, which limits the generalizability of the results to these population groups. There was a relatively large proportion of patients (approximately 40%) who identified as Asian in the DESTINY-Gastric04 trial. The clinical experts consulted by CDA-AMC agreed that the condition under review is common in populations in Asia; however, certain locations of practice may have higher percentages of population groups of Asian descent, though likely not as high as 40%. The clinical experts agreed that the DESTINY-Gastric04 trial was a global study and considered its findings generalizable to clinical practice in Canada, including patients from diverse ethnic backgrounds.
The experts noted that while differences in practice patterns across geographic regions (e.g., Asia versus Europe) may exist in earlier stages of disease detection and surgical management, as well as in subsequent lines of therapy beyond the second-line setting, they agreed that there is insufficient evidence to determine the potential impact of these differences on treatment outcomes in the current second-line metastatic setting. The clinical experts also believed that the dosing regimen used for trastuzumab deruxtecan was reasonable. The comparator, ramucirumab plus paclitaxel, was considered the most appropriate choice in this setting according to the clinical experts. Furthermore, approximately one-third of patients may not be eligible for ramucirumab plus paclitaxel and may receive alternative chemotherapy (e.g., FOLFIRI or single agents like, paclitaxel, irinotecan, or docetaxel). Based on their clinical experience, the experts anticipated that these comparator treatments offer broadly similar efficacy. The outcomes investigated in the trial were aligned with those that are considered important by interested parties, including patients and clinicians. Although HRQoL was measured in the trial, definitive conclusions could not be drawn because of serious risks of bias in outcome measurement (because of the open-label design and subjective nature of the assessment) and missing outcome data (because of lower completion rates at clinically relevant follow-up times).
Results
The key efficacy and harms results and findings from the GRADE assessment are presented in this section. Detailed efficacy and harms results can be found in Appendix 4 in the Supplemental Material document.
Efficacy
OS: Median OS was 14.7 months (95% CI, 12.1 months to 16.6 months) with trastuzumab deruxtecan versus 11.4 months (95% CI, 9.9 months to 15.5 months) with ramucirumab plus paclitaxel. The stratified HR was 0.70 (95% CI, 0.55 to 0.90; P = 0.0044). The probabilities of OS were 83.5% (95% CI, 78.0% to 87.7%) versus 74.4% (95% CI, 68.0% to 79.7%) at 6 months (difference, 9.1%; 95% CI, ███ ██ ████), and 39.7% (95% CI, 32.0% to 47.3%) versus 34.1% (95% CI, 26.6% to 41.8%) at 18 months (difference, 5.6%; 95% CI, ████ ██ ████). Results for the Western Europe subgroup were overall aligned with those for the primary analysis (HR = 0.62; 95% CI, 0.45 to 0.86).
PFS: Median PFS was 6.7 months (95% CI, 5.6 months to 7.1 months) with trastuzumab deruxtecan versus 5.6 months (95% CI, 4.9 months to 5.8 months) with ramucirumab plus paclitaxel; HR was 0.74 (95% CI, 0.59 to 0.92; P = 0.0074). The probabilities of PFS were 52.6% (95% CI, 45.7% to 59.1%) versus 41.5% (95% CI, 34.3% to 48.7%) at 6 months (difference, 11.1%; 95% CI, ███ ██ ████), and 33.4% (95% CI, 26.7% to 40.1%) versus 20.4% (95% CI, 14.3% to 27.2%) at 9 months (difference, 13.0%; 95% CI, ███ ██ ████).
ORR: Confirmed ORR among patients who were response-evaluable was 44.3% (95% CI, 37.8% to 50.9%) with trastuzumab deruxtecan and 29.1% (95% CI, 23.4% to 35.3%) with ramucirumab plus paclitaxel (difference, 15.1%; 95% CI, 6.1% to 24.2%; P = 0.0006, nominal). Complete response was observed in 3.0% of patients in the trastuzumab deruxtecan group and 1.3% of patients in the ramucirumab plus paclitaxel group, and partial response was observed in 41.3% of patients in the trastuzumab deruxtecan group and 27.8% in the ramucirumab plus paclitaxel group. The median duration of response among patients with a confirmed complete or partial response was 7.4 months (95% CI, 5.7 months to 10.1 months) with trastuzumab deruxtecan and 5.3 months (95% CI, 4.1 months to 5.7 months) with ramucirumab plus paclitaxel.
HRQoL (measured via the FACT-Ga): In both groups, FACT-Ga total scores declined over time, although the declines did not reach clinical significance in either group (based on an estimated within-group MID of 15.1 points). Least squares mean changes from baseline in FACT-Ga total score were small (never exceeding 2.7 points at all reported follow-up time points) and unlikely to be clinically meaningful.
Harms
Key results for the overall safety analysis set at the October 24, 2024, data cut-off date include the following:
AEs: At least 1 treatment-emergent adverse event (TEAE) was reported for all 244 of 244 patients (100%) in the intervention group and 228 of 233 patients (98%) in the comparison group. TEAEs that occurred in at least 30% of patients in either the intervention group or comparison group, respectively, were fatigue (58% and 49%), nausea (53% and 20%), neutropenia (50% in each group), anemia (49% and 45%), decreased appetite (40% and 30%), diarrhea (35% and 28%).
Grade 3 or greater AEs: These occurred in 166 of 244 patients (68%) in the trastuzumab deruxtecan group and 172 of 233 patients (74%) in the ramucirumab plus paclitaxel group. Grade 3 or greater AEs that occurred in at least 10% of patients in either the trastuzumab deruxtecan group or the ramucirumab plus paclitaxel group, respectively, were neutropenia (72 of 244 patients [30%] and 84 of 233 patients [36%]), anemia (56 of 244 patients [23%] and 48 of 233 patients [21%]), leukopenia (19 of 244 patients [8%] and 29 of 233 patients [12%]), and hypertension (1 of 244 patients [0.4%] and 25 of 233 patients [10.7%]).
SAEs: SAEs were reported in 100 of 244 patients (41%) in the trastuzumab deruxtecan arm and 101 of 233 patients (43%) in the ramucirumab plus paclitaxel arm. The most common SAEs (intervention versus control) included anemia (12 of 244 patients [4.9%] and 8 of 233 patients [3.4%]), pneumonia (10 of 244 patients [4.1%] and 8 of 233 patients [3.4%]), vomiting (9 of 244 patients [3.7%] and 2 of 233 patients [0.9%]), disease progression (8 of 244 patients [3.3%] and 18 of 233 patients [7.7%]), and dysphagia (7 of 244 patients [2.9%] and 4 of 233 patients [1.7%]).
AEs leading to treatment discontinuation: AEs were reported in 35 of 244 patients (14.3%) in the trastuzumab deruxtecan arm and 40 of 233 patients (17.2%) in the ramucirumab plus paclitaxel arm. The most common reason, intervention and control, was adjudicated drug-related ILD (16 of 244 patients [6.6%] and 3 of 233 patients [1.3%]).
Deaths because of AEs: AEs associated with an outcome of death occurred in 22 of 244 patients (9.0% of patients) in the trastuzumab deruxtecan arm and in 35 of 233 patients (15.0%) in the ramucirumab plus paclitaxel arm.
AEs of special interest — ILD or pneumonitis (adjudicated): These occurred in 34 of 244 patients (13.9%) in the trastuzumab deruxtecan arm and 4 of 233 patients (1.7%) in the ramucirumab plus paclitaxel arm.
Summary of Findings and Certainty of the Evidence
Literature-based MID estimates were used as the thresholds for the following outcomes: FACT-Ga (MID = 15 points). Note that this MID was for within-group differences; uncertainty with respect to the MID for a between-group difference was considered when rating the certainty of evidence and drawing conclusions about the clinical importance of the observed effects, in collaboration with the clinical experts consulted for the review. Refer to the summary of outcome measures in Appendix 3 in the Supplemental Material document. In the absence of literature-based MID estimates, thresholds suggested by the clinical experts were used for the following outcomes: OS (threshold = 5% to 10% at 6, 12, and 18 months), PFS (threshold = 10% at 6 and 9 months), and adjudicated ILD AE (threshold = 10% at the latest time point reported).
Table 4: Summary of Findings for Trastuzumab Deruxtecan vs. Ramucirumab Plus Paclitaxel for Patients With Gastric or GEJ Adenocarcinoma
Outcome and follow-up | Patients (studies), N | Relative effect (95% CI) | Absolute effects (95% CI) | Certainty | What happens | ||
|---|---|---|---|---|---|---|---|
RAM plus PTX | Trastuzumab deruxtecan | Difference | |||||
Overall survival | |||||||
Probability of being alive at 6 months Median follow-up: 16.8 months (TDXD), 14.4 months (RAM plus PTX) | 494 (1 RCT) | NR | 744 per 1,000 | 835 per 1,000 (780 to 877 per 1,000) | 91 more per 1,000 ███ ██ ███ ████ ███ █████ | Moderatea | Trastuzumab deruxtecan likely results in a clinically important increase in the probability of being alive at 6 months compared to RAM plus PTX. |
Probability of being alive at 12 months Median follow-up: 16.8 months (TDXD), 14.4 months (RAM plus PTX) | 494 (1 RCT) | NR | 489 per 1,000 | 576 per 1,000 (503 to 642 per 1,000) | 87 more per 1,000 ███ ████ ██ ███ ████ ███ █████ | Moderatea | Trastuzumab deruxtecan likely results in a clinically important increase in the probability of being alive at 12 months compared to RAM plus PTX. |
Probability of being alive at 18 months Median follow-up: 16.8 months (TDXD), 14.4 months (RAM plus PTX) | 494 (1 RCT) | NR | 341 per 1,000 | 397 per 1,000 (320 to 473 per 1,000) | 56 more per 1,000 ███ ████ ██ ███ ████ ███ █████ | Lowb | Trastuzumab deruxtecan may result in a clinically important increase in the probability of being alive at 18 months compared to RAM plus PTX. |
Progression-free survival | |||||||
Probability of being alive and with PFS at 6 months Median follow-up: 13.7 months (TDXD), 8.5 months (RAM plus PTX) | 494 (1 RCT) | NR | 415 per 1,000 | 526 per 1,000 (457 to 591 per 1,000) | 111 more per 1,000 ███ ██ ███ ████ ███ █████ | Lowc | Trastuzumab deruxtecan may result in a clinically important increase in the probability of being alive and with progression-free survival at 6 months compared to RAM plus PTX. |
Probability of being alive and with PFS at 9 months Median follow-up: 13.7 months (TDXD), 8.5 months (RAM plus PTX) | 494 (1 RCT) | NR | 204 per 1,000 | 334 per 1,000 (267 to 401 per 1,000) | 130 more per 1,000 ███ ██ ███ ████ ███ █████ | Lowc | Trastuzumab deruxtecan may result in a clinically important increase in the probability of being alive and with progression-free survival at 9 months compared to RAM plus PTX. |
Health-related quality of life | |||||||
FACT-Ga, LS mean total score change from baseline to day 190 (total scores range from 0 [worst] to 184 [best QoL]) | 135 (1 RCT) | NA | −6.5 | −3.8 (−7.9 to 0.3) | 2.7 (−3.0 to 8.4) | Very lowd | The evidence is very uncertain about the effects of trastuzumab deruxtecan compared to RAM plus PTX on HRQoL assessed by FACT-Ga. |
Harms | |||||||
Patients with ILD, adjudicated Follow-up: latest time point | 477 (1 RCT) | RR = ████ █████ ██ ██████ | 17 per 1,000 | 139 per 1,000 ███ ██ ███ ███ █████ | ███ more per 1,000 ███ ██ ███ ████ ███ █████ | Moderatee | Trastuzumab deruxtecan likely results in a clinically important increase in the risk of ILD compared to RAM plus PTX. |
CI = confidence interval; FACT-Ga = Functional Assessment of Cancer Therapy–Gastric; GEJ = gastroesophageal junction; HRQoL = health-related quality of life; ILD = interstitial lung disease; LS = least squares; NA = not applicable; OS = overall survival; PFS = progression-free survival; PTX = paclitaxel; QoL = quality of life; RAM = ramucirumab; RCT = randomized controlled trial; RR = risk ratio; TDXD = trastuzumab deruxtecan; vs. = versus.
Note: Study limitations (which refer to internal validity or risk of bias), indirectness, imprecision of effects, and publication bias were considered when assessing the certainty of the evidence. All serious concerns in these domains that led to the rating down of the level of certainty are documented in the table footnotes. Between-group differences in the proportion of patients with adjudicated ILD events were not defined in the statistical analysis plan, but were requested from the sponsor for the purpose of the certainty of evidence appraisal.
aThe level of evidence was rated down 1 level for serious imprecision. The clinical experts consulted for this review identified a between-group MID at this time point for this outcome as 5% to 10%; therefore, the lower bound of the 95% CI did not meet this threshold.
bThe level of evidence was rated down 2 levels for very serious imprecision. The clinical experts consulted for this review identified a between-group MID at this time point for this outcome as 5% to 10%; therefore, the lower bound of the 95% CI did not meet this threshold and may also suggest potential harm.
cThe level of evidence was rated down 1 level for serious imprecision. The clinical experts consulted on this review identified a between-group MID at this time point for this outcome as 10%; therefore, the lower bound of the 95% CI did not meet this threshold. The level of evidence was also rated down 1 level for serious concerns over risk of bias because of a lack of blinding. The assessment of PFS was not performed using a blinded independent review committee, which may have resulted in bias.
dThe level of evidence was rated down 3 levels for critical concerns over risk of bias because of a lack of blinding and the potential for bias in this patient-reported outcome, as well as for missing data.
eThe level of evidence was rated down 1 level for serious imprecision. The clinical experts consulted for this review suggested that a 10% difference between groups would be clinically meaningful. Considering this threshold, the 95% CI includes the potential for little to no clinically meaningful difference.
Source: Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Long-Term Extension Studies
No long-term extension studies were submitted.
Indirect Evidence
The indirect evidence was considered to address relative efficacy estimates of comparators not investigated by the DESTINY-Gastric04 phase III head-to-head trial. This involved looking at how trastuzumab deruxtecan compares with a larger set of guideline-recommended second-line treatments for advanced GC or GEJ adenocarcinoma. The comparators considered relevant to the context in Canada were:
ramucirumab plus paclitaxel
paclitaxel
FOLFIRI
irinotecan
docetaxel.
Description of the ITC
The ITC is a Bayesian network meta-analysis (NMA) using the DESTINY-Gastric04 trial as the trastuzumab deruxtecan source trial and incorporating RCTs of the identified comparators. The objective was to estimate relative efficacy of trastuzumab deruxtecan versus these comparators for OS and PFS in adults with advanced or metastatic GC or GEJ adenocarcinoma after 1 prior line of therapy. Outcomes were assessed in terms of HR for trastuzumab deruxtecan versus other comparators.
Study Selection and Review Methods
The sponsor conducted a systematic literature review (SLR) to identify published literatures of RCTs relevant to second-line or later treatment of advanced GC or GEJ adenocarcinoma. Published literature was identified by searching electronic databases (including MEDLINE and Embase), grey literature (conference proceedings, trial registries, and relevant submissions to multiple health technology assessment bodies), and handsearching reference lists of included studies and relevant SLRs and NMAs. Studies were eligible for inclusion in the SLR based on the Population, Intervention, Comparator, Outcomes, and Study Design criteria. Study selection and data extraction were conducted by 2 independent reviewers with the risk of bias of the selected studies assessed by 2 independent reviewers using the Cochrane risk-of-bias version 2 tool. Any disputes between reviewers were resolved by a third independent reviewer. This SLR was conducted in May 2020 with a first update in September 2021 and the second update in January 2025.
The RCTs included in the NMA are trials with adult patients with advanced or metastatic GC or GEJ adenocarcinoma who experienced disease progression after at least 1 prior line of therapy. Study populations were not required to have HER2-positive disease for inclusion in the NMAs. The intervention was trastuzumab deruxtecan by IV at a dose of 6.4mg/kg every 3 weeks until disease progression. Comparators for the NMA (ramucirumab plus paclitaxel, ramucirumab plus FOLFIRI, ramucirumab monotherapy, FOLFIRI, paclitaxel, irinotecan, docetaxel, cisplatin plus irinotecan, and best supportive care [BSC]) were selected based on international guidelines from the National Comprehensive Cancer Network and European Society for Medical Oncology (ESMO). The outcomes included primarily OS and PFS. Only peer-reviewed full-text publications of phase II or III RCTs were included in the NMA.
ITC Analysis Methods
For additional information on the analysis methods for the ITC, refer to Table 12 in Appendix 6 in the Supplemental Material document.
A Bayesian NMA was conducted to compare trastuzumab deruxtecan with guideline-recommended second-line therapies for the advanced GC or GEJ adenocarcinoma network. Both fixed-effect (FE) and random-effect (RE) Bayesian models were built to estimate HRs with 95% credible intervals (CrIs). The treatment effect modifiers were identified through available subgroup analyses from studies included in the NMA, with any characteristics that resulted in a change of greater than or equal to 0.2 in the estimated HR between subgroups being considered as a potential treatment effect modifier. Treatment effect modifiers found in a previously published SLR and NMA conducted in advanced gastroesophageal cancers treated with checkpoint inhibitors (Da Silva et al. [2021] 34) and an RCT evaluating trastuzumab in combination with chemotherapy as first-line treatment for HER2-positive advanced GC or GEJ adenocarcinoma (Bang et al. [2010]35) were also consulted in identifying effect modifiers. The treatment effect modifiers identified by the sponsor included geographic region, time to progression on first-line therapy, disease measurability, primary tumour location, previous weight loss, sex, ECOG PS score, histological subtype, presence of peritoneal metastases, PD-L1 combined positive score, HER2 expression, presence of target lesion, and number of metastases. The FE model assumed a common treatment effect across studies, while the RE model allowed between-study heterogeneity. A feasibility assessment for the NMA was conducted to assess heterogeneity in study design, outcome definitions, and patient characteristics to evaluate potential treatment effect modifiers and prognostic factors. There was no preliminary preference for either model because according to the sponsor, the feasibility assessment showed some, but not substantial, heterogeneity between trials. The lowest deviance information criterion was used to compare the FE and RE models for model selection.
The nodes of the NMA were constructed by treatment regimen (monotherapy and combined). Different doses, routes of administration, or schedules of the same drug (e.g., paclitaxel or irinotecan) were pooled into a single node. The NMA considered both OS and PFS in separate networks. Subgroup analyses were conducted to explore heterogeneity and improve comparability of the studies included in the NMA. The most clinically relevant was the analysis of the RAINBOW trial subgroup of patients who previously received trastuzumab, used as a proxy for HER2-positive disease. Additional subgroup analyses restricted the network to Western populations, and sensitivity analyses excluded small, high-risk-of-bias trials (Thuss-Patience et al. [2011]36).
Summary of Included Studies
The SLR identified 39 RCT studies, of which 12 RCTs (including the DESTINY-Gastric04 trial) were eligible for inclusion in the NMA. The 12 RCTs included had study sample sizes ranging from 40 to 665 participants. Most included RCTs were assessed by the sponsor as having low risk of bias or some concerns based on the Cochrane risk-of-bias version 2 tool, with 1 study (Thuss-Patience et al. [2011]36; irinotecan versus BSC) assessed as high risk because of early termination and evaluated in a sensitivity analysis. Several studies did not meet the non-PH assumption tests (e.g., the RAINBOW study, the WJOG 4007 study, and the study by Roy et al. [2013]39, as well as others); however, according to the sponsor, visual checks suggested only modest deviations; OS and PFS were nevertheless both meta-analyzed as HRs, with this limitation noted. Across studies, all RCTs enrolled adults (≥ 18 years) with advanced or metastatic GC or GEJ adenocarcinoma whose disease had progressed after 1 prior line of therapy. All studies reported OS, with some also reporting PFS.
There were several important cross-study differences relevant to critical appraisal:
The DESTINY-Gastric04 trial enrolled only patients with HER2-positive disease, whereas none of the other comparator trials had this requirement.
There were differences in required prior treatment (e.g., trastuzumab or platinum and fluoropyrimidine).
Some studies limited ECOG PS scores to 0 or 1, while others allowed a score of 2.
All studies included GC as a tumour location, while 3 studies did not include GEJ adenocarcinoma.
The studies were conducted in different geographic regions, with 3 studies conducted in Western countries and 5 studies conducted in Asian countries.
Ethnicity is a potentially important treatment effect modifier but was reported in only 3 studies.
There were differences in life expectancy as an inclusion criterion (e.g., ≥ 12 weeks, ≥ 3 weeks, or not stated).
Follow-up time differed (the median ranged from 7 months to 18 months or was not reported).
Two studies were blinded, whereas the remainder were open-label studies.
Outside of the cross-study differences listed, there were additional potential sources of heterogeneity within the NMA:
There were differences in treatment interventions (e.g., dose and dosing frequency, allowance of crossover in multiple studies, and the possibility of differences in standard supportive care).
There were no descriptions of censoring rules for OS and PFS, and there were differences in assessment intervals and handling of postprogression therapy.
Three comparators in the NMA had dosages that differ from real-world clinical practice (paclitaxel, docetaxel, irinotecan plus cisplatin).
Of the 12 RCTs in the NMA, there was 1 direct head-to-head trastuzumab deruxtecan comparison (the DESTINY-Gastric04 trial). All other trastuzumab deruxtecan comparisons involved indirect evidence via the ramucirumab plus paclitaxel to paclitaxel pathway. Subnetworks were created for sensitivity analyses to test the robustness of the NMA. These included restricting comparators to those recommended by ESMO guidelines, constructing Western-only networks, using subgroups who received prior treatment with trastuzumab as a proxy for a population with HER2-positive disease, excluding high-risk-of-bias trials, and adjusting for crossover in the DESTINY-Gastric04 trial OS estimates.
Critical Appraisal of ITCs
Overall Strengths
Strengths of the SLR and ITCs include the following:
An appropriate NMA framework was used.
The network was built with appropriate guideline-listed post–first-line treatments with a direct head-to-head anchor that connected new therapy (trastuzumab deruxtecan) to other options.
Strong robustness checks were employed to test the strength of the networks.
There was a clear focus on the OS and PFS end points, which are important to interested parties, such as patients and clinicians.
Further, the SLR searches were adequately comprehensive and the methods for study selection and data extraction were adequate to limit the risks in these processes. The Bayesian NMA framework is advantageous to this ITC because it is capable of handling small and unbalanced networks because of its ability to incorporate priors for between-study variance (an informed assumption about how much the study results are expected to differ from one another). All comparators for this ITC were selected from international treatment guidelines, which ensures clinical relevance to current practice (though not all are relevant to clinical practice in Canada).
Limitations
Although this ITC has several strengths, there are some limitations to consider. The SLR used to identify studies for inclusion in the NMA had limitations. There were no clearly defined research questions and target questions, only inclusion and exclusion criteria, which made it difficult to determine whether they were aligned. In addition, no registered, prespecified protocol was identified for either the SLR or the NMA, increasing the risk that the reported results were selected from multiple analyses of the data based on their magnitude and/or direction. Publication bias was not assessed and therefore cannot be ruled out. Of the 39 studies identified in the SLR, 27 studies were not included in the NMA because the comparators did not permit them to form a part of the connected network. Despite a Bayesian NMA framework being used, the network was overall sparse. The sponsors claimed that the 12 RCTs included were of acceptable quality, although multiple studies showed quality and/or risk of bias issues. For 5 of the 12 studies, there was no evidence of risk-of-bias appraisal, making the quality and/or risk-of-bias claim uncertain. The risk-of-bias assessments were conducted at the study level rather than at the outcome level (i.e., for OS and PFS individually). This method does not account for the fact that risk of bias can differ depending on the effect estimate being evaluated, particularly for such domains as performance, detection, attrition, and reporting bias. As such, the reported risk of bias may not universally apply to OS and PFS. Among the studies that received a risk-of-bias appraisal, Roy et al. contributed HR values for OS and PFS estimated from digitized KM curves rather than direct values. This could have introduced uncertainty into the network because of imprecise measurement and may have weakened the internal validity of the NMA. Another risk to internal validity is the difference in study design, because 2 of the 12 studies were blinded while the remaining 10 studies were open label. The difference in the patients’ and investigators’ knowledge of the study drug could have influenced the duration of patients’ participation in the studies and introduced bias in the measurement of efficacy end points (particularly PFS, if measured by investigators), which in turn could affect the consistency and validity of the efficacy estimates for both direct and indirect comparisons across studies. The pivotal study, the DESTINY-Gastric04 trial, enrolled only patients with HER2-positive disease who received prior treatment with trastuzumab, whereas the other 11 RCTs did not strictly follow these criteria. This poses a transitivity risk because HER2-positive status and trastuzumab-pretreatment could both influence treatment effects, making it difficult to draw indirect comparisons between treatments from different studies. In addition, there were baseline heterogeneities that could also lead to transitivity risks, including differences in geographic location, ECOG PS score (0 to 1 versus 2), number of metastatic sites, tumour site (GC only versus GC and GEJ adenocarcinoma), and life expectancy (≥ 3 weeks or ≥ 12 weeks). For some treatment effect modifiers identified by the sponsor, including ethnicity, primary tumour at entry, previous surgery, PD-L1 status, peritoneal metastases and ascites, and number of metastatic sites, reporting was insufficient to inform a robust appraisal of the similarity across trials, further limiting the CDA-AMC review team’s certainty of the plausibility of the transitivity assumption.
For OS and PFS, although the FE and RE models produced similar point estimates, several studies included in the NMA had a failed PH assumption for OS or PFS, which could have led to misleading pooled HRs. There were also differences in follow-up durations between studies (median follow-up times ranging from 7 to 18 months), which could have led to undercapturing late OS effects and exacerbated concerns regarding PH assumptions. In the results presented for FE and RE models, the results of the RE models were imprecise, with 95% CrIs frequently including the value 1. Compared to the FE model (which assumes a single true treatment effect across studies), the RE model is more appropriate because it accounts for the existing heterogeneity (previously stated) in this NMA. Sensitivity analyses were performed to test the robustness of the main analysis, including restricting regimen comparators to those recommended by ESMO, constructing Western-only networks, using subgroups who received prior treatment with trastuzumab as a proxy for a population with HER-positive disease, excluding the high-risk-of-bias trial (Thuss-Patience et al. [2011]36), and adjusting for crossover in the DESTINY-Gastric04 trial OS analysis using the RPSFTM with and without recensoring. However, the results were statistically imprecise, with most 95% CrIs including 1 for the RE models.
The heterogeneities could have led to a decrease in the external validity (generalizability) of the ITC because most trials enrolled predominantly healthier patients (ECOG PS score of 0 to 1; ≥ 12 weeks life expectancy) and combined GC and GEJ adenocarcinoma populations. Consequently, the network’s findings may be less generalizable to patients with poorer performance status or those with disease limited to a specific tumour site. The NMA may have further generalization issues because of the trial locations and real-world clinical practice. Of the 12 included studies, 5 were conducted in Asia, 3 were conducted in Western countries, and 4 were global. The higher number of studies conducted in specific geographic regions and the high correlation of ethnicity with region (confirmed in the NMA technical report) weakens the generalizability of the results of this NMA to the setting in Canada. In addition, the NMA focused on survival end points (OS and PFS) but did not analyze HRQoL or harms. As a result, conclusions about trastuzumab deruxtecan’s comparative efficacy and safety relative to other active treatments used in Canada cannot be drawn from the NMA.
Efficacy Results of ITCs
Key results of the ITCs are in Table 5 and Table 6.
The Bayesian FE model is presented as the base case because it showed a slightly better fit than the RE model, based on a lower deviance information criterion, and produced very similar point estimates. The FE and RE models produced directionally consistent results, with HRs of trastuzumab deruxtecan versus other comparators generally less than 1 (i.e., favouring trastuzumab deruxtecan) and overlapping CrIs. However, the RE model (more suitable for this NMA because of heterogeneity) had wider CrIs (reflecting between-study heterogeneity), with most including 1 for OS, whereas the FE model did not. Sensitivity analysis results were directionally consistent with the base case when restricting comparators to those recommended by the ESMO, constructing Western-only networks, using trastuzumab-pretreated data from the RAINBOW study as a proxy for a HER2-positive population, excluding the high-risk-of-bias irinotecan versus BSC trial, and adjusting OS for crossover in the DESTINY-Gastric04 trial.
Table 5: Summary of NMA Results for Trastuzumab Deruxtecan vs. Comparators (OS)
Comparator | FE model | RE model |
|---|---|---|
HR (95% CrI), trastuzumab deruxtecan vs. comparator | HR (95% CrI), trastuzumab deruxtecan vs. comparator | |
RAM + PTX | ████ ██████ █████ | ████ ██████ █████ |
PTX | ████ ██████ █████ | ████ ██████ █████ |
Irinotecan | ████ ██████ █████ | ████ ██████ █████ |
FOLFIRI | ████ ██████ █████ | ████ ██████ █████ |
Docetaxel | ████ ██████ █████ | ████ ██████ █████ |
CrI = credibility interval; FE = fixed effects; FOLFIRI = folinic acid, fluorouracil, and irinotecan; HR = hazard ratio; NMA = network meta-analysis; OS = overall survival; PTX = paclitaxel; RAM = ramucirumab; RE = random effects; vs. = versus.
Source: Details included in the table are from the sponsor’s NMA technical report.
Table 6: Summary of NMA Results for Trastuzumab Deruxtecan vs. Comparators (PFS)
Comparator | FE model | RE model |
|---|---|---|
HR (95% CrI), trastuzumab deruxtecan vs. comparator | HR (95% CrI), trastuzumab deruxtecan vs. comparator | |
RAM + PTX | ████ ██████ █████ | ████ ██████ █████ |
PTX | ████ ██████ █████ | ████ ██████ █████ |
FOLFIRI | ████ ██████ █████ | ████ ██████ █████ |
Irinotecan | ████ ██████ █████ | ████ ██████ █████ |
Docetaxel | ████ ██████ █████ | ████ ██████ █████ |
CrI = credibility interval; FE = fixed effects; FOLFIRI = folinic acid, fluorouracil, and irinotecan; HR = hazard ratio; NMA = network meta-analysis; PFS = progression-free survival; PTX = paclitaxel; RAM = ramucirumab; RE = random effects; vs. = versus.
Source: Details included in the table are from the sponsor’s NMA technical report.
Studies Addressing Gaps in the Systematic Review Evidence
No studies addressing gaps in the systematic review were submitted.
Discussion
Efficacy
The conditional positive TLR recommendation was issued contingent on a future reassessment of additional evidence to address the uncertainties in the original data. The TLR recommendation was based on data from the phase II, single-arm DESTINY-Gastric02 trial, which randomized 79 patients with unresectable or metastatic centrally confirmed HER2-positive gastric or GEJ cancer who experienced disease progression during or after first-line therapy with a trastuzumab-containing regimen. The primary outcome was ORR assessed by an independent committee review; 42% of patients achieved either a complete (5%) or partial (37%) response. The median OS was 12.1 months (95% CI, 9.4 months to 15.4 months) and the median PFS was 5.6 months (95% CI, 4.2 months to 8.3 months) (key results for the DESTINY-Gastric02 trial are summarized in Appendix 8 in the Supplemental Material document).
The committee identified the following key limitations in the original evidence based on the DESTINY-Gastric02 trial:
Uncertainty in current phase II evidence must be adequately addressed in the upcoming confirmatory phase III DESTINY-Gastric04 randomized trial.
Evidence from the DESTINY-Gastric04 trial needs to ascertain a clinically meaningful survival benefit of trastuzumab deruxtecan relative to the comparator treatment.
Trastuzumab deruxtecan needs to present an acceptable safety profile relative to the comparator treatment.
Interpretation of the results is organized according to these points described in the following paragraphs.
The reassessment was based on the confirmatory phase III trial. In fulfillment of the requirements under the TLR process, the sponsor filed this reassessment based on data from the phase III DESTINY-Gastric04 trial, and its patient population aligns with the sponsor’s reimbursement request: “trastuzumab deruxtecan for the second-line treatment of adult patients with unresectable, locally advanced, or metastatic HER2-positive gastric or GEJ adenocarcinoma who have received a prior anti–HER2-based regimen.” The phase III DESTINY-Gastric04 trial was a global, multicentre, open-label RCT that randomized 494 patients. The study was designed to evaluate the efficacy and safety of trastuzumab deruxtecan compared with ramucirumab plus paclitaxel. The data provided to CDA-AMC reflected results at the October 24, 2025, data cut-off date, aligned with the primary analysis for the primary end point, OS. Sample size calculation and randomization methods appeared appropriate. The study recruited the intended number of patients.
Evidence from the DESTINY-Gastric04 trial needs to ascertain a clinically meaningful survival benefit of trastuzumab deruxtecan relative to the comparator treatment. The DESTINY-Gastric04 trial met its primary end point, OS, at the interim analysis. Based on the clinical expert-identified threshold of 5% to 10%, trastuzumab deruxtecan likely results in a clinically important increase in the probability of patients being alive at 6 and 12 months and may also improve survival at 18 months compared with ramucirumab plus paclitaxel. The estimates were limited by serious imprecision at 6 and 12 months, with CIs encompassing small effects near the null, and by very serious imprecision at 18 months, with CIs including the possibility of both important harm and benefit. Beyond 18 months, the number of patients remaining at risk was very low, and interpretation of long-term survival was very uncertain. More patients in the ramucirumab plus paclitaxel group received trastuzumab deruxtecan or disitamab vedotin postprogression, which could have attenuated the OS benefit of trastuzumab deruxtecan. Sensitivity analyses undertaken by the sponsor to adjust for these imbalances in postprogression treatment yielded similar results to the primary analysis; however, these analyses were limited by implausible assumptions that cannot be verified with the observed data.
The secondary end point, PFS, was also met at the interim analysis. Based on the threshold of 10% identified by the clinical experts, trastuzumab deruxtecan likely results in a clinically important increase in the probability of PFS at 6 and 9 months compared with ramucirumab plus paclitaxel. The estimates were limited by serious imprecision at 6 and 9 months, with CIs encompassing small effects near the null, and by the risk of bias stemming from the lack of blinding for this investigator-assessed outcome. Beyond 9 months, the number of patients remaining at risk was very low, and interpretation was very uncertain.
The secondary outcome of ORR was also met at the interim analysis. The results of this analysis showed that patients who received trastuzumab deruxtecan experienced an increased ORR compared with those receiving ramucirumab plus paclitaxel. ORR was not formally included in the GRADE assessment because it was considered a supportive outcome to OS and PFS by the clinical experts consulted by CDA-AMC. However, the clinical experts agreed that the benefit in ORR observed with trastuzumab deruxtecan was clinically meaningful. The lack of blinding and independent review introduces a risk of bias for ORR. Additionally, a higher proportion of patients in the comparator arm were reported as “not evaluable” for ORR (15% versus 3%), with unclear reasons. This raises concerns about potential bias from missing outcome data.
The assessment of HRQoL was very uncertain because of risks of bias owing to the lack of blinding in the study and a sizable amount of missing outcome data at all clinically relevant follow-up times.
According to the clinical experts, most patients with gastric or GEJ carcinoma receive ramucirumab plus paclitaxel. About one-third of patients may be ineligible for ramucirumab plus paclitaxel and may receive chemotherapy (e.g., FOLFIRI or single agents such as paclitaxel, irinotecan, or docetaxel). Comparative evidence of trastuzumab deruxtecan versus chemotherapy for the target patient population was available through a sponsor-submitted NMA. Based on the results of the NMA, the evidence is insufficient to draw definitive conclusions on the relative efficacy (OS and PFS) of trastuzumab deruxtecan compared to FOLFIRI or single-agent chemotherapy (e.g., paclitaxel, irinotecan, or docetaxel). The uncertainty in the study results from the NMAs mainly resulted from the heterogeneity across study designs and populations (e.g., eligibility criteria, lengths of follow-up time, blinding), a sparse network, and imprecision of the effect estimates. HRQoL and AEs were not assessed in the NMA.
Trastuzumab deruxtecan needs to present an acceptable safety profile relative to the comparator treatment. There were no unexpected AEs reported with trastuzumab deruxtecan, according to the clinical experts consulted on this review. Fatigue, gastric AEs (e.g., nausea, decreased appetite, and diarrhea), and anemia were among the most common events that occurred more frequently with trastuzumab deruxtecan than with ramucirumab plus paclitaxel. Serious TEAEs and TEAEs associated with study drug modification, including discontinuation, dose reduction, and interruption, were similar between the trastuzumab deruxtecan and the ramucirumab plus paclitaxel arms.
Based on results from the DESTINY-Gastric04 trial, the most common safety issue associated with trastuzumab deruxtecan is ILD. The clinical experts were aware of this safety issue, which has been described previously in the literature with trastuzumab. The product monograph for trastuzumab deruxtecan highlights ILD under the Warnings and Precautions section, noting that it appeared to occur more frequently in patients with moderate renal impairment. The product monograph also notes the pulmonary symptoms associated with ILD, and the clinical experts consulted for this review agreed that it is a serious issue but one that can be diagnosed and addressed by discontinuing the drug, as recommended in the product monograph. Cardiotoxicity, another notable harm associated with trastuzumab deruxtecan, occurred in a similar proportion of patients between groups. For example, there were 12 patients (6.3%) with a worst left ventricular ejection fraction grade of 2 in the trastuzumab deruxtecan group compared to 7 patients (4.5%) in the ramucirumab plus paclitaxel group. There were 2 patients (1.1%) in the trastuzumab deruxtecan group and 1 patient (0.6%) in the ramucirumab plus paclitaxel group with a worst left ventricular ejection fraction grade of 3.
Other Considerations
The conditional positive TLR recommendation for trastuzumab deruxtecan was informed by the DESTINY-Gastric02 trial, whose study population was predominantly white (87.3%) and located in North America and Western Europe. The pharmacoeconomic submission included an analysis based on the Western Europe patient subgroup from the DESTINY-Gastric04 trial, comprising patients located in Belgium, France, Germany, Ireland, Italy, Portugal, Spain, Türkiye, and the UK. The sponsor noted that because prognosis may vary by geographic region, the Western Europe cohort may be considered the most representative of clinical practice in Canada.
The preplanned subgroup analyses in the DESTINY-Gastric04 trial were not designed to detect treatment effect differences between study groups, and the study was unlikely powered to detect subgroup differences if they were to exist. Patients from Western Europe made up more than half of the population enrolled in the DESTINY-Gastric04 trial (279 of 494 patients [56%]), and the additional subgroups reported were fairly evenly split between Asia (117 patients [24%]) and mainland China and the rest of the world (98 patients [20%]). Potentially, because of the smaller sample sizes, regions outside Western Europe showed wider CIs and higher HRs (with values less than 1 favouring trastuzumab deruxtecan and values greater than 1 favouring the control). The OS HRs were 0.82 (95% CI, 0.50 to 1.34) for Asia, 0.78 (95% CI, 0.46 to 1.33) for mainland China and the rest of the world, and 0.62 (95% CI, 0.45 to 0.86) for Western Europe. In studies comparing survival outcomes between patients in Asia and Western Europe, numerous limitations, including interregional differences in clinicopathological features, tumour biology, dietary patterns, baseline performance status, and the generally higher use of cytotoxic therapies and palliative care after progression in clinical settings in Asia, limit the ability to draw firm prognostic conclusions.37 The clinical experts consulted by CDA-AMC agreed that at present, there is no conclusive evidence that regional or ethnic differences function as independent prognostic factors in adults in Asia versus in Western Europe with unresectable locally advanced or metastatic HER2-positive gastric or GEJ adenocarcinoma previously treated with trastuzumab-based therapy.
Ethics and Equity Considerations
There is evidence in the literature that the risk of being diagnosed with GC is higher in racialized populations, including people of Asian descent; however, whether prognosis is also impacted is less well-known.14 In the DESTINY-Gastric04 trial, populations of people who are African American or Black and populations of multiple races or ethnicities were underrepresented. In Canada, patients who identify as Black often face barriers to several aspects of cancer care, including screening, access to targeted therapies, and enrolment in clinical trials.38The clinical experts considered the findings from the DESTINY-Gastric04 trial generalizable to the clinical practice setting in Canada, including in patients from diverse ethnic backgrounds. Limited representation in certain groups in the trial may lead to decisional uncertainties for these groups.
According to the patient group input received, caregivers often carry significant practical and emotional burdens, and respondents emphasized the need for clearer information earlier in the care pathway; simpler logistics, such as fewer or shorter visits when feasible; and more equitable and timely access to effective therapies. They also emphasized the need for a broader range of effective treatment options to support informed, values-aligned decision-making. Patient input and the clinical experts consulted for this review noted that shared decision-making is essential to ensure treatment choices appropriately reflect each patient’s comorbidities, preferences, and values.
Patients in rural and remote regions of the country are less likely to have local access to infusion centres where trastuzumab deruxtecan can be administered or to specialist care to manage their condition. This means that these patients will need to travel, sometimes long distances, to receive their treatment (every 3 weeks) and to consult their specialist.
Conclusion
The findings from 1 open-label, phase III RCT, the DESTINY-Gastric04 trial, suggest that trastuzumab deruxtecan likely improves OS compared with ramucirumab plus paclitaxel; however, the certainty associated with this finding diminishes with longer follow-up (18 months or longer) because of the smaller number of patients at risk at this time and imprecision in the effect estimates. Trastuzumab deruxtecan may improve PFS compared to ramucirumab plus paclitaxel after 6 and 9 months of follow-up; however, the lack of blinding introduces uncertainty into the assessment of progression. The assessment of HRQoL was also limited by risks of bias because of the lack of blinding in the study and a sizable amount of missing outcome data at all clinically relevant follow-up times. Trastuzumab deruxtecan likely increases the risk of developing ILD, which is a known safety issue associated with trastuzumab. There were no unexpected AEs reported with trastuzumab deruxtecan, according to the clinical experts consulted for this review.
Based on the results of a sponsor-submitted NMA, the evidence is insufficient to draw definitive conclusions on the relative efficacy of trastuzumab deruxtecan compared to chemotherapy options, such as FOLFIRI, or single-agent chemotherapy (paclitaxel, irinotecan, or docetaxel).
The DESTINY-Gastric04 trial addressed evidence gaps from the previously issued TLR recommendation by including a relevant randomized comparator, clinically relevant survival outcomes, and comparative safety data.
Economic Review
Methods
CDA-AMC previously reviewed trastuzumab deruxtecan (PC0367) and issued a conditional positive TLR recommendation for the second-line treatment of adult patients with unresectable locally advanced or metastatic HER2-positive gastric or GEJ adenocarcinoma who have received a prior anti–HER2-based regimen for a time-limited period while additional evidence is generated. Subsequently, new phase III study evidence has become available, allowing the sponsor to fulfill its commitment to file a reassessment to address uncertainty in the original evidence, as required under the TLR category. Data from this new study have been incorporated into an updated economic evaluation. The primary comparator in the initial submission was ramucirumab plus paclitaxel, with additional comparisons against FOLFIRI and single-agent chemotherapies.
The objective of the Economic Review is to review and critically appraise the submitted pharmacoeconomic evidence, which included an economic evaluation comparing the cost-effectiveness of trastuzumab deruxtecan to ramucirumab plus paclitaxel and FOLFIRI for the requested reimbursement population (i.e., the second-line treatment of adult patients with unresectable locally advanced or metastatic HER2-positive gastric or GEJ adenocarcinoma who have received a prior anti-HER2-based regimen), which is narrower than the Health Canada indication that does not restrict use to the second-line setting. The sponsor additionally submitted a BIA assessing the budgetary impact of reimbursing trastuzumab deruxtecan for the requested reimbursement population. CDA-AMC accepted 2 deviation requests regarding the narrowing of the requested reimbursement population and limiting the comparators included in the economic analysis.
Summary of the Submitted Economic Evaluation
The sponsor submitted a cost-utility analysis to estimate the cost-effectiveness of trastuzumab deruxtecan from the perspective of a public health care payer in Canada over a lifetime horizon (5 years). The modelled population was composed of adults with HER2-positive locally advanced or metastatic GC or GEJ carcinoma who have experienced disease progression on or after receiving a trastuzumab-containing regimen, which is aligned with the Health Canada indication and was based on the participants in the Western Europe cohort subgroup in the DESTINY-Gastric04 trial. The sponsor’s base-case analysis included costs related to drug acquisition, administration, disease management, AEs, and end-of-life costs.
In the sponsor’s base case, trastuzumab deruxtecan was associated with incremental costs of $98,151 and 0.66 incremental quality-adjusted life-years (QALYs) relative to FOLFIRI. This resulted in an incremental cost-effectiveness ratio (ICER) of $148,923 per QALY gained. Ramucirumab plus paclitaxel was extendedly dominated through FOLFIRI and trastuzumab deruxtecan. Of the incremental benefit compared to ramucirumab plus paclitaxel (0.66 incremental QALYs), approximately 51% of benefit was predicted to be accrued after the observation period of the DESTINY-Gastric04 trial (trial median follow-up was 16.8 months). Additional information about the sponsor’s submission is summarized in Appendix 11 in the Supplemental Material document.
CDA-AMC identified several key issues with the sponsor’s analysis (e.g., refer to Table 7; full details are provided in Appendix 12 in the Supplemental Material document).
Table 7: Key Issues With the Sponsor’s Economic Submission
Issue | What evidence is there to inform this issue? | How was this issue addressed by CDA-AMC? | Did CDA-AMC explore uncertainty in a scenario analysis? |
|---|---|---|---|
The long-term comparative efficacy of trastuzumab deruxtecan to comparators is uncertain. | Comparative efficacy in the model was informed by the DESTINY-Gastric04 trial or sponsor-submitted ITC. While results from the DESTINY-Gastric04 trial suggest that trastuzumab deruxtecan likely improves OS and may improve PFS compared with ramucirumab plus paclitaxel, the certainty around the long-term efficacy diminishes over longer follow-up. Second, the sponsor only analyzed a subset of the DESTINY-Gastric04 trial, focusing on participants from Western Europe. Third, the sponsor also assumed proportional hazards, meaning that the treatment effect is constant over time; however, this assumption could not be verified. Finally, limitations with the sponsor-submitted ITC used to inform comparative efficacy to FOLFIRI suggest that the magnitude and duration of benefit associated with trastuzumab deruxtecan relative to comparators is highly uncertain. | The base-case analysis conducted by CDA-AMC was on the ITT population and focused on the comparison of trastuzumab deruxtecan vs. ramucirumab plus paclitaxel because the trial evidence was associated with fewer limitations than the ITC. | CDA-AMC conducted a scenario analysis assuming equal efficacy between ramucirumab plus paclitaxel and FOLFIRI. |
The model fails to capture the causal disease pathway appropriately. | The sponsor’s use of a PSM introduces structural assumptions about the relationship between PFS and OS that may not accurately reflect the causal disease pathway. This approach could introduce postprogression survival bias, potentially biasing results in favour of trastuzumab deruxtecan. | This issue could not be addressed. | CDA-AMC conducted a scenario analysis that removed any postprogression survival benefit. |
Subsequent therapy costs are uncertain. | The sponsor considered only subsequent therapy costs because the survival benefits were assumed to be captured within the OS curve. However, limitations with the PSM model structure and sponsor assumptions around the proportion of patients receiving subsequent treatment and lack of subsequent treatment with trastuzumab deruxtecan make subsequent therapies in the model uncertain. | CDA-AMC excluded subsequent therapy. | CDA-AMC conducted a scenario analysis where subsequent therapy was included and assumed 30% of patients receive a subsequent line of therapy. |
Health state utility values are uncertain. | Health state utility values in the model were derived from the DESTINY-Gastric04 trial. However, clinical expert feedback noted that the reported values did not meet clinical expectations as the preprogression (2L) utility value was similar to or higher than the quality of life of an average person living in Canada aged 50 to 60 years old. | CDA-AMC used health state utility values derived from the RAINBOW trial. | No scenario analysis was conducted. |
TTD may underestimate treatment costs in the model. | Treatment duration was informed by the DESTINY-Gastric04 trial for trastuzumab deruxtecan and adjusted with PFS HR for comparators. TTD occurred before PFS in the trial. The respective product monographs and clinical expert feedback received by CDA-AMC noted that most patients would receive treatment until disease progression, and in some cases, beyond disease progression; therefore, the use of TTD may underestimate total costs, biasing results in favour of trastuzumab deruxtecan. | CDA-AMC set TTD equal to PFS for all comparators. | No scenario analysis was conducted. |
Treatment costs estimated by the sponsor are uncertain. | RDI for trastuzumab deruxtecan, ramucirumab, and paclitaxel were informed by the RDI observed in the DESTINY-Gastric04 trial. However, no information was provided to indicate why RDI was less than 100%. There is not a perfect correlation between RDI and cost, and without a further breakdown, this may underestimate drug costs. Additionally, the sponsor assumed wastage for fluorouracil and leucovorin despite using bulk pharmacy vials. This may overestimate the cost associated with FOLFIRI. | CDA-AMC assumed 100% RDI for all treatments and incorporated vial sharing for fluorouracil and leucovorin. | No scenario analysis was conducted. |
2L = second line; CDA-AMC = Canada’s Drug Agency; FOLFIRI = folinic acid, fluorouracil, and irinotecan; HR = hazard ratio; ITC = indirect treatment comparison; ITT = intention to treat; OS = overall survival; PFS = progression-free survival; PSM = partitioned survival model; RDI = relative dose intensity; TTD = time to treatment discontinuation; vs. = versus.
Note: Full details of the issues identified by CDA-AMC are provided in Appendix 12 in the Supplemental Material document.
CDA-AMC Assessment of Cost-Effectiveness
The CDA-AMC base case was derived by making changes to model parameter values and assumptions (refer to Appendix 12 in the Supplemental Material document for further information), in consultation with clinical experts. Due to clinical expert feedback which noted that ramucirumab plus paclitaxel is the primary comparator, along with limitations in the comparative clinical efficacy of trastuzumab deruxtecan versus FOLFIRI that precluded any conclusions regarding the relative efficacy, the CDA-AMC analysis focuses primarily on the comparison of trastuzumab deruxtecan versus ramucirumab plus paclitaxel. Detailed information about the CDA-AMC base case is provided in Appendix 12 in the Supplemental Material document.
Impact on Health Care Costs
Trastuzumab deruxtecan is predicted to be associated with additional health care costs compared to ramucirumab plus paclitaxel (incremental costs = $34,953). This increase in health care spending results from drug acquisition costs associated with associated with trastuzumab deruxtecan (refer to Figure 1).
Figure 1: Impact of Trastuzumab Deruxtecan vs. Ramucirumab Plus Paclitaxel on Health Care Costs
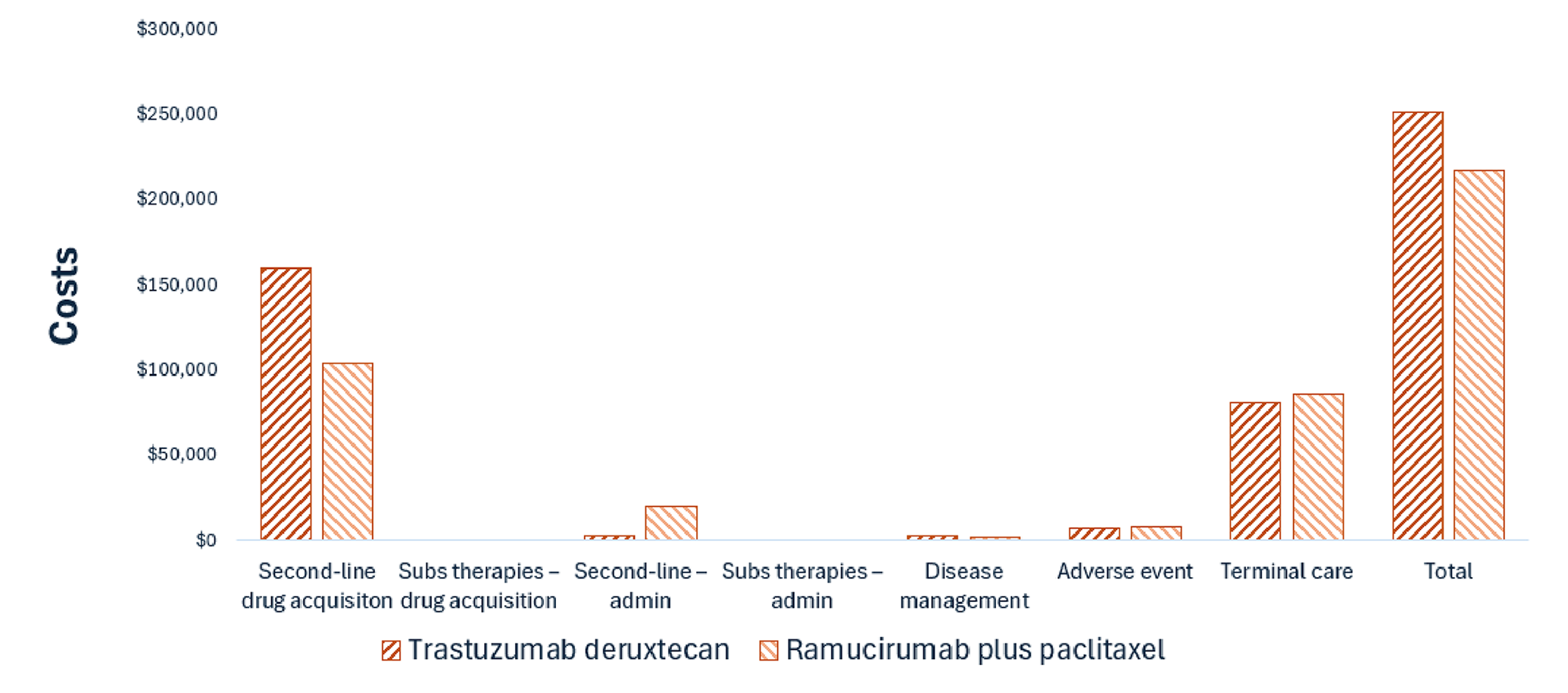
admin = administration; subs = subsequent; vs. = versus.
Notes: Results for FOLFIRI are not presented in this figure. Refer to Appendix 12 in the Supplemental Material document for full results. Trastuzumab deruxtecan is associated with an incremental cost of approximately $126,000 relative to FOLFIRI over the modelled time horizon.
Impact on Health
Relative to ramucirumab plus paclitaxel, trastuzumab deruxtecan is predicted to increase the amount of time a patient remains in both the preprogression and postprogression health states by approximately 0.13 and 0.14 years (refer to Figure 2). Considering the impact of treatment on both quality and length of life, trastuzumab deruxtecan is predicted to result in 0.27 additional QALYs per patient compared to ramucirumab plus paclitaxel. Approximately 53% of the incremental QALYs were obtained in the postprogression period, meaning that a large portion of the benefit is derived after the patient discontinues trastuzumab deruxtecan. Clinical experts noted that there are no robust data to support this model output.
Figure 2: Impact of Trastuzumab Deruxtecan vs. Ramucirumab Plus Paclitaxel on Patient Health
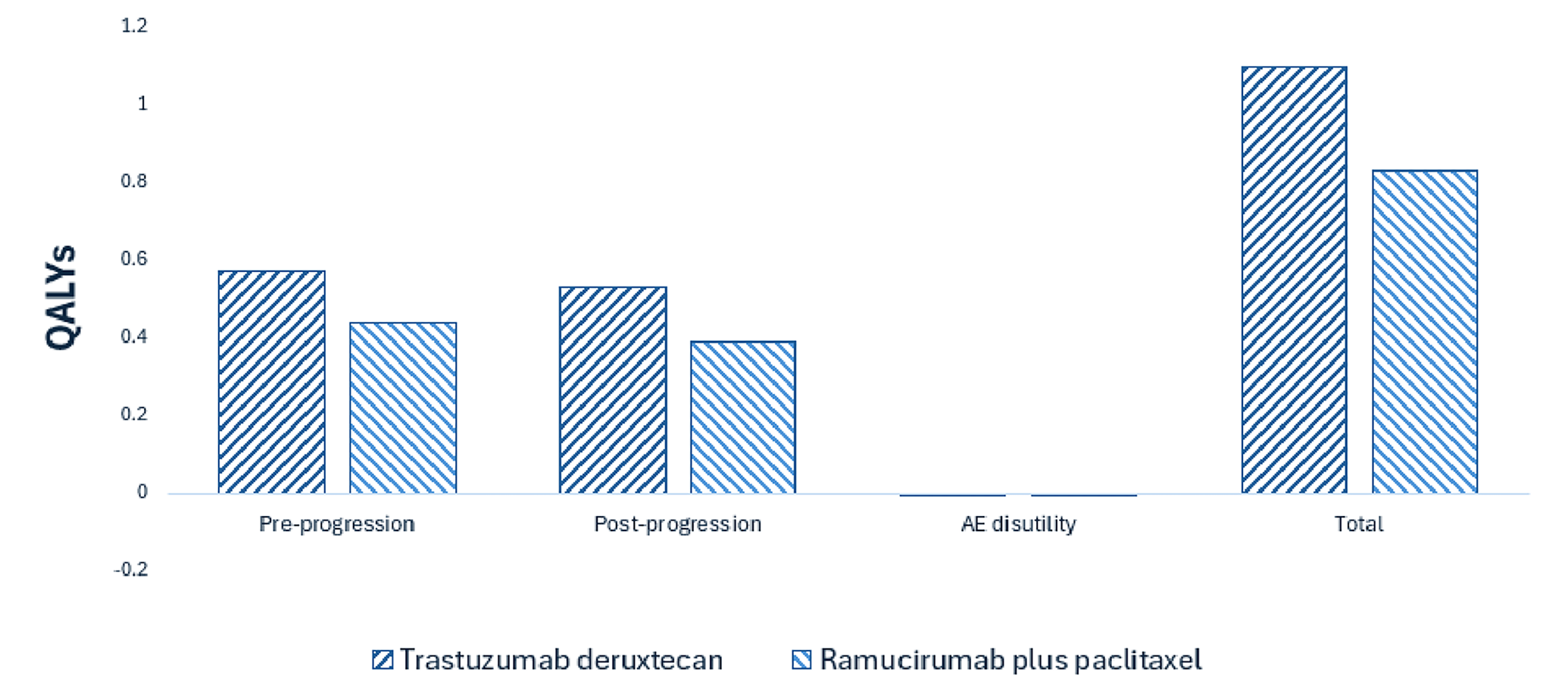
AE = adverse event; QALY = quality-adjusted life-year; vs. = versus.
Notes: Results for FOLFIRI are not presented in this figure. Refer to Appendix 12 in the Supplemental Material document for full results.
Overall Results
Based on the CDA-AMC analysis, the following treatments are on the cost-effectiveness frontier: FOLFIRI and trastuzumab deruxtecan. However, because of the limitations with the indirect comparative clinical efficacy of trastuzumab deruxtecan versus FOLFIRI, the results were considered highly uncertain. The CDA-AMC analysis focuses on the comparison of trastuzumab deruxtecan versus ramucirumab plus paclitaxel. The results of the CDA-AMC base case suggest an ICER of $130,777 per QALY gained for trastuzumab deruxtecan compared to ramucirumab plus paclitaxel (refer to Table 8). Detailed information about the CDA-AMC base case is provided in Appendix 12 in the Supplemental Material document. The results from the CDA-AMC reanalysis of the initial submission reported an ICER of $242,356 per QALY gained for trastuzumab deruxtecan compared to ramucirumab plus paclitaxel (deterministic analysis).
Table 8: Summary of CDA-AMC Economic Evaluation Results
Drug | Total costs ($) | Total QALYs | ICER vs. ramucirumab plus paclitaxel ($ per QALY) |
|---|---|---|---|
Ramucirumab plus paclitaxel | 216,357 | 0.83 | Reference |
Trastuzumab deruxtecan | 251,310 | 1.10 | 130,777 |
CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus.
Note: Publicly available list prices were used for all comparators.
Uncertainty and Sensitivity
Uncertainty was explored in the scenario analyses. Uncertainty around comparative efficacy of trastuzumab deruxtecan versus FOLFIRI had the largest impact on cost-effectiveness in addition to the removal of a postprogression benefit for trastuzumab deruxtecan. Based on the results of these analyses, the ICER for trastuzumab deruxtecan may range from $150,144 per QALY gained to $279,196 per QALY gained when compared to ramucirumab plus paclitaxel. When considering FOLFIRI as a relevant comparator under an assumption of equal efficacy between ramucirumab plus paclitaxel and FOLFIRI based on clinical expert opinion, the ICER for trastuzumab deruxtecan was estimated to be $376,214 per QALY gained versus FOLFIRI.
Summary of the Budget Impact
The sponsor submitted a BIA to estimate the 3-year (2026 to 2028) budget impact of trastuzumab deruxtecan for the second-line treatment for adult patients with HER2-positive GC or GEJ adenocarcinoma. The sponsor assumed that the payer would be CDA-AMC–participating public drug plans and derived the size of the eligible population using an epidemiologic approach. The price of trastuzumab deruxtecan was aligned with the price included in the sponsor’s economic evaluation, while the prices of comparators were based on the publicly available list prices. Additional information pertaining to the sponsor’s submission is provided in Appendix 11 in the Supplemental Material document.
CDA-AMC identified a number of issues with the sponsor’s estimated budget impact and made changes to model parameters and assumptions in consultation with clinical experts to derive the CDA-AMC base case (refer to Appendix 12 in the Supplemental Material document for further details). CDA-AMC estimated that by year 3 of reimbursement, 648 patients would be eligible for trastuzumab deruxtecan; of these, 453 patients are expected to receive trastuzumab deruxtecan. The estimated expenditure on trastuzumab deruxtecan is $77,916,780.
Conclusion
Based on the CDA-AMC base case, trastuzumab deruxtecan would be considered cost-effective at the submitted price if the public health care system was willing to pay at least $130,777 for each additional QALY gained. If the public health care system is not willing to pay that amount, a price reduction should be considered (refer to Figure 3; full details of the impact of price reductions on cost-effectiveness are presented in Appendix 12 in the Supplemental Material document). The estimated cost-effectiveness of trastuzumab deruxtecan compared to comparators is uncertain because of limitations in the comparative efficacy, assumptions around the cohort used in the analysis, and the removal of a postprogression benefit for trastuzumab deruxtecan.
Figure 3: Summary of the CDA-AMC Economic Analysis and Price Reduction

CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Notes: Expenditure includes only the drug cost of trastuzumab deruxtecan. The term dominant indicates that a drug costs less and provides more QALYs than the comparator.
References
1.Brenner DR, Gillis J, Demers AA, et al. Projected estimates of cancer in Canada in 2024. CMAJ. 2024;196(18):E615-E623. doi:10.1503/cmaj.240095 PubMed
2.Society AC. What Is Stomach Cancer? 2021. https://www.cancer.org/cancer/types/stomach-cancer/about/what-is-stomach-cancer.html#:~:text=Most%20cancers%20of%20the%20stomach,almost%20always%20be%20an%20adenocarcinoma
3.Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229-263. doi:10.3322/caac.21834 PubMed
4.Canadian Cancer Society. Stomach Cancer. Available from: https://cancer.ca/en/cancer-information/cancer-types/stomach [sponsor supplied reference].
5.Mahar AL, Zagorski B, Kagedan D, et al. Evaluating TNM stage prognostic ability in a population-based cohort of gastric adenocarcinoma patients in a low-incidence country. Can J Public Health. 2018;109(4):480-488. doi:10.17269/s41997-018-0102-1 PubMed
6.Canadian Cancer Statistics Advisory Committee. Canadian Cancer Statistics: a 2018 special report on cancer incidence by stage. Canadian Cancer Society; 2018. Accessed January 1, 1800. https://cdn.cancer.ca/-/media/files/research/cancer-statistics/2018-statistics/canadian-cancer-statistics-2018-en.pdf
7.Symptoms of stomach cancer. Canadian Cancer Society; 2019. Accessed 2024 Oct 14. https://cancer.ca/en/cancer-information/cancer-types/stomach/signs-and-symptoms
8.Holland P, Rafiq R, Matheson K, et al. Population based assessment of HER-2 and PD-L1 positivity in gastric and gastroesophageal junction adenocarcinomas in a Canadian population. J Clin Oncol. 2024;42(16_suppl):e16038-e16038. doi:10.1200/JCO.2024.42.16_suppl.e16038
9.Zhou F, Li N, Jiang W, et al. Prognosis significance of HER-2/neu overexpression/amplification in Chinese patients with curatively resected gastric cancer after the ToGA clinical trial. World J Surg Oncol. 2012;10:274. doi:10.1186/1477-7819-10-274 PubMed
10.Roviello G, Catalano M, Iannone LF, et al. Current status and future perspectives in HER2 positive advanced gastric cancer. Clin Transl Oncol. 2022;24(6):981-996. doi:10.1007/s12094-021-02760-0 PubMed
11.Ma C, Wang X, Guo J, Yang B, Li Y. Challenges and future of HER2-positive gastric cancer therapy. Front Oncol. 2023;13:1080990. doi:10.3389/fonc.2023.1080990 PubMed
12.Jorgensen JT, Hersom M. HER2 as a Prognostic Marker in Gastric Cancer - A Systematic Analysis of Data from the Literature. J Cancer. 2012;3:137-44. doi:10.7150/jca.4090 PubMed
13.Barros-Silva JD, Leitao D, Afonso L, et al. Association of ERBB2 gene status with histopathological parameters and disease-specific survival in gastric carcinoma patients. Br J Cancer. 2009;100(3):487-93. doi:10.1038/sj.bjc.6604885 PubMed
14.Shah SC, McKinley M, Gupta S, Peek RM, Jr., Martinez ME, Gomez SL. Population-Based Analysis of Differences in Gastric Cancer Incidence Among Races and Ethnicities in Individuals Age 50 Years and Older. Gastroenterology. 2020;159(5):1705-1714 e2. doi:10.1053/j.gastro.2020.07.049 PubMed
15.Canadian Cancer Society, Canadian Cancer Statistics Advisory Committee. Canadian Cancer Statistics 2023. Government of Canada; 2023. Accessed 2024 Jun 25. https://cdn.cancer.ca/-/media/files/research/cancer-statistics/2023-statistics/2023_pdf_en.pdf
16.Stomach (Gastric) Cancer Survival Rates. American Cancer Society; 2024. Accessed 2024 Jan 17. https://www.cancer.org/cancer/types/stomach-cancer/detection-diagnosis-staging/survival-rates.html
17.National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology. Gastric Cancer. Version 2.2025 — April 4, 2025.
18.National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology. Esophageal and Esophagogastric Junction Cancers. Version 3.2025 — April 22, 2025.
19.Canada's Drug Agency. Provisional Funding Algorithm: Advanced or metastatic gastric, gastroesophageal junction, or esophageal cancer. 2025. https://www.cda-amc.ca/sites/default/files/DRR/2025/PH0061-Gastric_Cancer.pdf
20.AstraZeneca Canada Inc. ENHERTU® (Trastuzumab deruxtecan) Product Monograph. 2025.
21.National Comprehensive Cancer Network. Gastric Cancer, Version 2.2025, NCCN Clinical Practice Guidelines In Oncology. 2025.
22.National Comprehensive Cancer Network. Esophageal and Esophagogastric Junction Cancers, Version 3.2025, NCCN Clinical Practice Guidelines In Oncology. 2025.
23.Canada's Drug Agency. Time-limited Reimbursement Recommendation: Trastuzumab Deruxtecan (Enhertu). 2025. https://cda-amc.ca/sites/default/files/DRR/2025/PC0367_Enhertu_FINAL_Recommendation.pdf
24.pan-Canadian Pharmaceutical Alliance. Enhertu (trastuzumab deruxtecan) pCPA negotiation. 2025. https://www.pcpacanada.ca/negotiation/23037
25.Candia L, Cervantes A, Martinelli E, clinicalguidelines@esmo.org EGCEa. Updated treatment recommendations for third and further lines of treatment in advanced colorectal cancer: from the ESMO Metastatic Colorectal Cancer Living Guideline. Ann Oncol. 2025;36(3):342-344. doi:10.1016/j.annonc.2024.11.015 PubMed
26.Bartley AN, Washington MK, Colasacco C, et al. HER2 Testing and Clinical Decision Making in Gastroesophageal Adenocarcinoma: Guideline From the College of American Pathologists, American Society for Clinical Pathology, and the American Society of Clinical Oncology. J Clin Oncol. 2017;35(4):446-464. doi:10.1200/JCO.2016.69.4836 PubMed
27.AstraZeneca Canada Inc. DESTINY-Gastric04 Clinical Study Report [sponsor supplied reference]. 2025.
28.Daiichi Sankyo Inc. Clinical Study Protocol: DS8201-A-U306, version 5. A Phase 3, Multicenter, 2-Arm Randomized, Open-Label Study of Trastuzumab Deruxtecan in Subjects with HER2-Positive Metastatic and/or Unresectable Gastric or Gastro-Esophageal Junction (GEJ) Adenocarcinoma Subjects who have Progressed on or After a Trastuzumab Containing Regimen (DESTINY-Gastric04) [internal sponsor's report]. September 30, 2024.
29.Wilke H, Muro K, Van Cutsem E, et al. Ramucirumab plus paclitaxel versus placebo plus paclitaxel in patients with previously treated advanced gastric or gastro-oesophageal junction adenocarcinoma (RAINBOW): a double-blind, randomised phase 3 trial. The Lancet Oncology. 2014;15(11):1224-1235. doi:10.1016/S1470-2045(14)70420-6 PubMed
30.US Food and Drug Administration (FDA). Clinical trial endpoints for the approval of cancer drugs and biologics guidance for industry. 2018. Available at: https://www.fda.gov/media/71195/download. April 2015 [sponsor supplied reference].
31.European Medicines Agency (EMA). Guideline on the evaluation of anticancer medicinal products in man. 2017. Available at: https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-evaluation-anticancer-medicinal-products-man-revision-5_en.pdf. Last accessed: March 2024 [sponsor supplied reference].
32.Latimer NR, Abrams KR. NICE DSU Technical Support Document 16: Adjusting Survival Time Estimates in the Presence of Treatment Switching. 2014. NICE Decision Support Unit Technical Support Documents.
33.Bassler D, Briel M, Montori VM, et al. Stopping randomized trials early for benefit and estimation of treatment effects: systematic review and meta-regression analysis. JAMA. 2010;303(12):1180-7. doi:10.1001/jama.2010.310 PubMed
34.da Silva LL, Aguiar PN, Jr., Park R, Edelman Saul E, Haaland B, de Lima Lopes G. Comparative Efficacy and Safety of Programmed Death-1 Pathway Inhibitors in Advanced Gastroesophageal Cancers: A Systematic Review and Network Meta-Analysis of Phase III Clinical Trials. Cancers (Basel). 2021;13(11):2614. doi:10.3390/cancers13112614 PubMed
35.Bang YJ, Van Cutsem E, Feyereislova A, et al. Trastuzumab in combination with chemotherapy versus chemotherapy alone for treatment of HER2-positive advanced gastric or gastro-oesophageal junction cancer (ToGA): a phase 3, open-label, randomised controlled trial. Lancet. 2010;376(9742):687-97. doi:10.1016/S0140-6736(10)61121-X PubMed
36.Thuss-Patience PC, Kretzschmar A, Bichev D, et al. Survival advantage for irinotecan versus best supportive care as second-line chemotherapy in gastric cancer--a randomised phase III study of the Arbeitsgemeinschaft Internistische Onkologie (AIO). Eur J Cancer. 2011;47(15):2306-14. doi:10.1016/j.ejca.2011.06.002 PubMed
37.Zhang Z, Liu Z, Chen Z. Comparison of Treatment Efficacy and Survival Outcomes Between Asian and Western Patients With Unresectable Gastric or Gastro-Esophageal Adenocarcinoma: A Systematic Review and Meta-Analysis. Front Oncol. 2022;12:831207. doi:10.3389/fonc.2022.831207 PubMed
38.Ezeife DA, Padmore G, Vaska M, Truong TH. Ensuring equitable access to cancer care for Black patients in Canada. CMAJ. 2022;194(41):E1416-E1419. doi:10.1503/cmaj.212076 PubMed
39.Roy AC, Park SR, Cunningham D, et al. A randomized phase II study of PEP02 (MM-398), irinotecan or docetaxel as a second-line therapy in patients with locally advanced or metastatic gastric or gastro-oesophageal junction adenocarcinoma. Ann Oncol. 2013;24(6):1567-1573. doi:10.1093/annonc/mdt002 Medline PubMed
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.