Drugs, Health Technologies, Health Systems
Reimbursement Recommendation
Durvalumab (Imfinzi)
Indication: Durvalumab in combination with fluorouracil, leucovorin, oxaliplatin, and docetaxel (FLOT) chemotherapy as neoadjuvant and adjuvant treatment, followed by adjuvant durvalumab monotherapy, is indicated for the treatment of adult patients with resectable gastric or gastroesophageal junction adenocarcinoma (GC/GEJC) (Stage II to IVA)
Sponsor: AstraZeneca Canada Inc.
Final recommendation: Reimburse with conditions
Summary
What Is the Reimbursement Recommendation for Imfinzi?
Canada’s Drug Agency (CDA-AMC) recommends that Imfinzi in combination with fluorouracil, leucovorin, oxaliplatin, and docetaxel (FLOT) chemotherapy as neoadjuvant and adjuvant treatment, followed by adjuvant durvalumab monotherapy, be reimbursed by public drug plans for the treatment of adult patients with resectable gastric or gastroesophageal junction (GEJ) adenocarcinoma (stages II to IVA) if certain conditions are met.
Why Did CDA-AMC Recommend Reimbursement?
The pan-Canadian Oncology Drug Review Expert Review Committee (pERC) determined that Imfinzi in combination with FLOT demonstrates acceptable clinical value compared with perioperative placebo in combination with FLOT in patients with resectable gastric or GEJ adenocarcinoma (stages II to IVA).
Evidence from a clinical trial (the MATTERHORN trial) showed that treatment with Imfinzi in combination with FLOT likely results in delayed disease recurrence or death compared with placebo plus FLOT. The results for the other secondary outcomes, including pathologic complete response rate and disease-free survival, further supported the findings. The safety profile of Imfinzi is considered generally predictable and manageable in adult patients with resectable gastric or GEJ adenocarcinoma. The comparative evidence of Imfinzi in combination with FLOT against other relevant therapies for GEJ cancer, particularly neoadjuvant chemoradiotherapy followed by adjuvant nivolumab, remains unknown.
Which Patients Are Eligible for Coverage?
Imfinzi in combination with FLOT should only be covered for the treatment of adults with documented stage II to IVA gastric or GEJ adenocarcinoma who have good performance status, are eligible for radical surgery, and have not received anticancer therapy for treatment of gastric or GEJ adenocarcinoma. Imfinzi in combination with FLOT should not be covered for patients with peritoneal dissemination or distant metastases, adenosquamous or squamous cell carcinoma, or uncontrolled autoimmune or inflammatory disorders.
What Are the Conditions for Reimbursement?
Imfinzi in combination with FLOT should be initiated by clinicians with expertise and experience in treating gastric or GEJ adenocarcinoma. Following initiation, ongoing treatment can be delivered at a site closer to home (e.g., local clinic).
Imfinzi in combination with FLOT should only be reimbursed if the cost of Imfinzi is reduced. Important budget impact considerations must be addressed for health systems to be able to adopt Imfinzi in combination with FLOT.
Review Background
Disease background: Gastric or GEJ adenocarcinomas are serious cancers that start in the stomach or where the stomach meets the esophagus (the tube that connects the throat to the stomach). These cancers can grow quickly and spread to nearby lymph nodes. In 2024, approximately 4,000 people living in Canada were diagnosed with gastric cancer, and approximately 2,000 people died from the disease.
Indication and reimbursement request: Durvalumab (Imfinzi) in combination with FLOT chemotherapy as neoadjuvant and adjuvant treatment, followed by adjuvant durvalumab monotherapy, has been approved by Health Canada for the treatment of adult patients with resectable gastric or GEJ adenocarcinoma (stage II to IVA). The sponsor is seeking reimbursement for this patient population.
Drug under review: Durvalumab is a PD-L1 inhibitor. It is administered by IV infusion. The recommended dosage of durvalumab is 1,500 mg every 4 weeks for up to 4 cycles in combination with FLOT chemotherapy (2 cycles before surgery and 2 cycles after surgery), followed by adjuvant durvalumab monotherapy at 1,500 mg for up to 10 additional cycles. Patients with a body weight of 30 kg or less must receive weight-based dosing of durvalumab at 20 mg/kg every 4 weeks in combination with FLOT chemotherapy for 2 cycles before surgery and 2 cycles postsurgery, followed by durvalumab 20 mg/kg every 4 weeks as monotherapy until weight increases to greater than 30 kg.
Treatment costs: At the submitted price of $938.67 per 2.4 mL vial and $3,911.11 per 10 mL vial, the cost of durvalumab per 28-day cycle is expected to be $11,733 per patient based on the Health Canada–recommended dosage. Durvalumab is indicated for use in combination with FLOT; the cost of the regimen is expected to be $15,588 per patient per 28-day cycle.
Highlights of Input From Interested Parties
The patient group (My Gut Feeling–Stomach Cancer Foundation of Canada) noted the following regarding impacts of the disease, unmet needs, and important outcomes:
As gastric or GEJ cancer progress, symptoms may include abdominal pain, fatigue, poor appetite, trouble eating, weight loss, nausea, bleeding, and anemia.
The negative impacts of gastric or GEJ cancer are emotional distress, loss of independence, financial burdens from treatment and travel, and changes in identity and personal relationships.
Important treatment outcomes for patients include living longer, delaying disease from getting worse, managing disease symptoms, having fewer side effects, maintaining or improving quality of life, and lowering the financial burden of care.
The clinician groups (the Canadian GI Oncology Evidence Network [CGOEN] and the Ontario Health [Cancer Care Ontario] Gastrointestinal Cancer Drug Advisory Committee [GI DAC]) and the clinical experts consulted by CDA-AMC noted the following regarding unmet needs arising from the disease and place in therapy for the drug under review:
There is a need for curative treatments that help to achieve durable cure, improve overall survival (OS), prevent or delay relapse, maintain quality of life, minimize long-term toxicity, and maximize the likelihood of achieving a complete surgical resection.
Durvalumab in combination with FLOT is anticipated to serve as an alternative perioperative treatment option for patients with resectable gastric or GEJ adenocarcinoma, leveraging both cytotoxic and immune-mediated antitumour mechanisms.
The participating public drug programs raised potential implementation issues related to considerations for initiation and renewal of therapy, generalizability of trial populations to broader populations, and the potential need for a provisional funding algorithm.
Recommendation
With a vote of 17 in favour to 0 against, pERC recommends that durvalumab be reimbursed for the treatment of resectable gastric or GEJ adenocarcinoma (stage II to IVA) in combination with FLOT chemotherapy as neoadjuvant and adjuvant treatment followed by adjuvant durvalumab monotherapy only if the conditions listed in Table 1 are met.
Table 1: Reimbursement Conditions and Reasons
Reimbursement condition | Reason | Implementation guidance |
|---|---|---|
Initiation | ||
1. Treatment with durvalumab in combination with FLOT chemotherapy as neoadjuvant and adjuvant treatment, followed by adjuvant durvalumab monotherapy in adult patients who meet all the following criteria: 1.1. have histologically documented stage II to IVA gastric or GEJ adenocarcinoma (AJCC manual, 8th edition) of either: 1.1.1. > T2, N0 to N3, M0 1.1.2. T0 to T4, N1 to N3, M0 1.2. are eligible for radical surgery 1.3. have not received anticancer therapy (e.g., chemotherapy, chemoradiation) for treatment of gastric or GEJ cancer. | Evidence from the MATTERHORN trial demonstrated that treatment with durvalumab in combination with FLOT chemotherapy resulted in a clinical benefit compared with placebo plus FLOT chemotherapy in patients with these characteristics. In the MATTERHORN trial, surgery was recommended to be performed within 4 to 8 weeks following completion of neoadjuvant treatment with durvalumab in combination with FLOT. | pERC noted that patients with esophageal adenocarcinoma should be eligible for treatment with durvalumab in combination with FLOT. Although the MATTERHORN trial did not include patients with esophageal adenocarcinoma, the clinical experts noted that it is biologically similar to gastric and GEJ adenocarcinoma and is treated similarly in clinical practice in Canada. pERC agreed with the clinical experts that an interval of 4 to 12 weeks between completion of neoadjuvant durvalumab plus FLOT and surgery is appropriate. Extending the interval to up to 16 weeks may be considered in certain cases, such as when patients need additional time to recover from treatment-related adverse effects. pERC agreed with the clinical experts that durvalumab may be added for patients already receiving neoadjuvant FLOT chemotherapy. The clinical experts noted that adding durvalumab during the adjuvant phase is not recommended because current evidence suggests that the primary benefit of durvalumab plus FLOT is primarily achieved during the neoadjuvant phase rather than in the postoperative setting. |
2. Patients should have good performance status. | Patients with an ECOG Performance Status score of 0 or 1 were included in the MATTERHORN trial. | pERC agreed with the clinical experts that patients considered eligible for FLOT chemotherapy before surgery can also be considered eligible for treatment with durvalumab in combination with FLOT. Patients with an ECOG Performance Status score greater than 1 may be considered for treatment at the clinician’s discretion. |
3. Patients must not have any of the following: 3.1. peritoneal dissemination or distant metastasis 3.2. adenosquamous cell carcinoma, squamous cell carcinoma, or gastrointestinal stromal tumours 3.3. uncontrolled autoimmune or inflammatory disorders. | No evidence was identified to demonstrate a benefit of durvalumab in combination with FLOT in patients who have peritoneal dissemination or distant metastasis, adenosquamous cell carcinoma, squamous cell carcinoma, gastrointestinal stromal tumours, or autoimmune disorders in the MATTERHORN trial. | — |
Renewal (continuation with adjuvant therapy) | ||
4. Continued reimbursement of durvalumab adjuvant therapy should be based on meeting all the following criteria: 4.1. completion of neoadjuvant durvalumab in combination with FLOT 4.2. completion of a surgical procedure 4.3. initiation of adjuvant durvalumab in combination with FLOT no more than 12 weeks after surgery with no evidence of disease progression (refer to the implementation guidance for exceptions) 4.4. initiation of adjuvant durvalumab monotherapy after completion of combination therapy. | In the MATTERHORN trial, patients were required to undergo a radical surgery to continue with adjuvant treatment with durvalumab in combination with FLOT and as monotherapy. In the MATTERHORN trial, adjuvant combination therapy was initiated no earlier than 4 weeks and within 12 weeks following radical surgery. | pERC noted that for patients who receive neoadjuvant durvalumab plus FLOT but do not proceed to, or choose to forgo, surgery for reasons other than disease progression, there is insufficient evidence to guide subsequent treatment. pERC agreed with the clinical experts that a time interval of up to 16 weeks between surgery and the initiation of adjuvant treatment would be reasonable for most patients, but longer delays may be necessary in some cases (e.g., postoperative complications, prolonged recovery). Patients will be eligible for treatment with PD-1 inhibitors in the metastatic setting if there is a disease-free interval of 6 months or more. |
Discontinuation | ||
5. Treatment with durvalumab in combination with FLOT should be discontinued in the neoadjuvant phase upon the occurrence of any of the following: 5.1. disease progression 5.2. unacceptable toxicity. | Patients in the MATTERHORN trial received 2 cycles of durvalumab in combination with FLOT before surgery. | pERC agreed with the clinical experts that if neoadjuvant FLOT is discontinued due to toxicity, patients should proceed to radical surgery when clinically feasible. Adjuvant durvalumab either in combination or as monotherapy may be continued after surgery. Patients will be eligible for treatment with PD-1 inhibitors in the metastatic setting if there is a disease-free interval of 6 months or more. |
6. Treatment with durvalumab, whether in combination with FLOT or as monotherapy, should be discontinued in the adjuvant phase upon the occurrence of any of the following: 6.1. disease progression 6.2. unacceptable toxicity 6.3. the maximum number of 12 cycles of durvalumab after surgery. | Patients in the MATTERHORN trial received a maximum of 12 cycles of durvalumab after surgery: durvalumab in combination with FLOT for 2 cycles followed by durvalumab monotherapy for up to 10 cycles. | pERC agreed with the clinical experts that if adjuvant FLOT chemotherapy is discontinued due to toxicity, adjuvant durvalumab may be continued. |
Prescribing | ||
7. Treatment with durvalumab in combination with FLOT chemotherapy should be initiated by clinicians with expertise and experience in treating gastric or GEJ adenocarcinoma. After specialized initiation, ongoing treatment can be delivered at a site closer to home. | This is meant to ensure that durvalumab is prescribed for appropriate patients and that adverse effects are managed in an optimized and timely manner. | pERC noted that jurisdictions may consider implementing weight-based dosing as per their jurisdictional policies. |
Pricing | ||
8. A reduction in price. | Using the CDA-AMC base-case analysis, the ICER for durvalumab in combination with FLOT was $67,176 per QALY gained when compared with FLOT alone in the indicated population. A band 1 price reductiona would be required to achieve cost-effectiveness at a $50,000 per QALY threshold. No price reduction would be required to achieve cost-effectiveness at a $100,000 per QALY threshold. Price reductions for any given willingness-to-pay threshold are available in the CDA-AMC Main Report and the Supplemental Material document. | The CDA-AMC analysis is based on public list prices for all treatments. Further price reductions may be required if there are price arrangements (discounts) currently in place for any treatment included in the economic analysis. Likewise, further price reductions may be required to address economic feasibility of adoption. |
Feasibility of adoption | ||
9. The economic feasibility of adoption of durvalumab in combination with FLOT must be addressed. | At the submitted price, the incremental budget impact of durvalumab in combination with FLOT is expected to be greater than $40 million in years 2 and 3. | — |
AJCC = American Joint Committee on Cancer; CDA-AMC = Canda’s Drug Agency; ECOG = Eastern Cooperative Oncology Group; FLOT = fluorouracil, leucovorin, oxaliplatin, and docetaxel; GEJ = gastroesophageal junction; ICER = incremental cost-effectiveness ratio; pERC = pan-Canadian Oncology Drug Review Expert Review Committee; QALY = quality-adjusted life-year, T,N, M = tumour, node, metastasis.
aFor the statement regarding the size of the price reduction required, band 1 = 1% to 24%, band 2 = 25% to 49%, band 3 = 50% to 74%, and band 4 = 75% or greater.
Rationale for the Recommendation
Clinical Value
Based on the totality of the clinical evidence, pERC concluded that durvalumab in combination with FLOT as neoadjuvant and adjuvant treatment followed by adjuvant durvalumab monotherapy demonstrates acceptable clinical value compared with perioperative placebo in combination with FLOT in patients with resectable gastric or GEJ adenocarcinoma (stages II to IVA).
Evidence from 1 randomized controlled trial (the MATTERHORN trial; N = 948) demonstrated that perioperative treatment with durvalumab plus FLOT likely results in added clinical benefit for patients with resectable gastric or GEJ adenocarcinoma compared with perioperative placebo plus FLOT in event-free survival (EFS) at 36 months and OS at 36 months. Treatment with durvalumab plus FLOT was associated with statistically significant and clinically meaningful improvements in EFS compared with placebo plus FLOT. At a median follow-up time of approximately 31 months, the median EFS for the durvalumab plus FLOT group was not reached, compared with 32.8 months in the placebo plus FLOT group. The Kaplan-Meier estimated between-group difference in EFS rates at 36 months was 14.7% (95% confidence interval [CI], █████ to ██████) in favour of durvalumab plus FLOT. At the time of the final analysis, the median OS was not reached in either group. Treatment with durvalumab plus FLOT was associated with statistically significant improvements in OS compared with placebo plus FLOT. At a median follow-up time of approximately 43 months, the 36-month between-group difference in OS rates was 6.7% (95% CI, █████ to ██████) in favour of durvalumab plus FLOT. The outcomes of other secondary end points, including pathologic complete response rate and disease-free survival, were supportive of the OS and EFS results.
pERC considered clinician input indicating that the safety profile of durvalumab plus FLOT observed in the MATTERHORN trial appeared consistent with the established safety profiles of FLOT chemotherapy and PD-L1 inhibitors, which are regarded as generally predictable and manageable.
Patients and clinicians identified the need for effective treatment options that delay disease progression, extend survival, improve disease and symptom control, minimize side effects, and improve quality of life. pERC concluded that, compared to placebo plus FLOT, durvalumab in combination with FLOT addresses some of the identified unmet needs by likely delaying disease recurrence, improving survival outcomes, and demonstrating a manageable safety profile. The impact of durvalumab plus FLOT on health-related quality of life (HRQoL) compared to placebo plus FLOT was uncertain due to a large amount of missing data.
The comparative evidence of durvalumab plus FLOT against other relevant therapies for GEJ cancer, particularly neoadjuvant chemoradiotherapy followed by adjuvant nivolumab, remains unknown.
Further information on the committee’s discussion around clinical value is provided in the Summary of Deliberation section.
Developing the Recommendation
The determination of acceptable clinical value was sufficient for pERC to recommend reimbursement of durvalumab. As part of the deliberation on whether to recommend reimbursement, the committee also considered unmet clinical need, unmet nonclinical need, and health inequity. Information on this discussion is provided in the Unmet Clinical Need and Distinct Social and Ethical Considerations domains in the Summary of Deliberation section.
Because pERC recommended that durvalumab be reimbursed, the committee also deliberated on whether reimbursement conditions should be added to address important economic considerations, health system impacts, or social and ethical considerations or to ensure clinical value is realized. The resulting reimbursement conditions, with accompanying reasons and implementation guidance, are stated in Table 1.
Summary of Deliberation
pERC considered all domains of value of the deliberative framework before developing its recommendation: clinical value, unmet clinical need, distinct social and ethical considerations, economic considerations, and impacts on health systems. For further information on the domains of value, refer to Expert Committee Deliberation at Canada’s Drug Agency.
The committee considered the following key discussion points, organized by the 5 domains of value.
Clinical Value
Appropriate comparators: The committee determined that appropriate comparators for perioperative durvalumab in combination with FLOT include perioperative FLOT chemotherapy, doublet fluoropyrimidine-platinum regimens with cisplatin or oxaliplatin, and neoadjuvant chemoradiation followed by adjuvant nivolumab in patients with GEJ cancer.
Efficacy versus placebo plus FLOT: One phase III randomized controlled trial (the MATTERHORN trial; N = 948) demonstrated that treatment with durvalumab plus FLOT resulted in improvement in EFS at 36 months at the second interim analysis (hazard ratio = 0.71; 95% CI, 0.58 to 0.86), and OS at 36 months at the final analysis (hazard ratio = 0.78; 95% CI, 0.63 to 0.96) compared with placebo plus FLOT in adults with gastric or GEJ cancer (stages II to IVA). These results were statistically significant and were considered clinically meaningful by the clinical experts. Although interim analyses carry some risk of overestimating treatment effects, the extent of any potential overestimation in the EFS benefit is uncertain. Although OS reached statistical significance at the final analysis, the median OS had not been reached in either group. OS data remain relatively immature, limiting the precision of the estimated long-term OS benefit.
Clinical importance of treatment effects: The committee considered the improvements in EFS and OS to be clinically meaningful based on patient and clinical expert input. Patients prioritized disease control, prolonged survival, and tolerability as key priorities. pERC concurred with the clinical experts that, in the current therapeutic setting, clinically meaningful benefit corresponds to an absolute improvement of at least 10% in 36-month EFS rates and at least 7% in 36-month OS rates. Perioperative durvalumab in combination with FLOT likely meets the EFS threshold and appears borderline for the OS threshold.
Certainty of the evidence: The certainty of evidence for EFS at 36 months was rated as moderate (downgraded 1 level for imprecision). Although the point estimate met the clinically important threshold suggested by the clinical experts, the lower bound of the CI crossed this threshold. There is low level of certainty that durvalumab plus FLOT may result in a clinically meaningful increase in the probability of being alive at 36 months when compared with placebo plus FLOT. The point estimate was borderline relative to the clinically important threshold suggested by the clinical experts, and the lower bound of the CI crossed this threshold. Additionally, the subsequent anticancer treatments were not balanced between groups. At the end of treatment, the assessment of HRQoL (European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 [EORTC QLQ-C30] Global Health Status score) was rated as low certainty of evidence due to missing data and imprecision. Results for serious adverse events were associated with low certainty of evidence, suggesting that durvalumab in combination with FLOT may result in an increase in serious adverse events.
Indirect treatment comparison and gaps in the evidence: The sponsor-submitted indirect treatment comparison feasibility assessment found that valid treatment comparisons between perioperative durvalumab plus FLOT and neoadjuvant chemoradiation followed by adjuvant nivolumab in esophageal and GEJ cancer were not feasible due to substantial methodological limitations, baseline heterogeneity, and nonaligned outcome reporting. Nonetheless, comparative evidence for perioperative durvalumab plus FLOT versus adjuvant nivolumab in patients with GEJ cancer remain an important evidence gap.
Harms: Durvalumab was generally considered tolerable in the MATTERHORN trial. Comparative safety showed that the occurrences of adverse events of any grade, serious adverse events, and treatment discontinuations due to adverse events were similar between the groups treated with durvalumab plus FLOT and placebo plus FLOT. pERC noted that pulmonary embolism and septic shock were reported at higher rates with durvalumab plus FLOT than with placebo plus FLOT. The clinical experts highlighted that several immune-related adverse events associated with immunotherapy (including durvalumab), particularly adrenal insufficiency, hypophysitis, and myocarditis, are permanent and life-altering conditions rather than transient toxicities. The clinical experts noted that treatment discontinuation in the study was expected given the intensity and toxicity burden of FLOT chemotherapy, noting that a substantial proportion of patients discontinue perioperative chemotherapy in routine clinical practice. Overall, the committee indicated that the safety profile of durvalumab plus FLOT was acceptable.
Generalizability: pERC discussed the use of durvalumab in combination with FLOT in patients with esophageal adenocarcinoma. Patients with esophageal adenocarcinoma were not included in the MATTERHORN trial. pERC heard from the clinical experts that esophageal adenocarcinoma is biologically similar to gastric and GEJ adenocarcinoma and is treated similarly in clinical practice in Canada. pERC agreed with the clinical experts that it would be reasonable to generalize the results of the MATTERHORN trial to patients with esophageal adenocarcinoma.
Primary prophylaxis with growth factors: Because FLOT carries a high risk of febrile neutropenia, primary prophylaxis with growth factors (granulocyte-colony stimulating factor [G-CSF], such as filgrastim or pegfilgrastim) is strongly recommended particularly in the perioperative, curative-intent setting. In the MATTERHORN trial, growth factor support was used in approximately three-quarters of patients in both groups (74.5% in the durvalumab plus FLOT group and 73.8% in the placebo plus FLOT group). pERC noted that, in clinical practice, most patients receiving FLOT would be expected to receive primary G-CSF prophylaxis and that institutional protocols are already in place to guide neutropenia prevention.
PD-L1 expression: pERC discussed PD-L1 expression in relation to the efficacy of the durvalumab and FLOT treatment. pERC noted from the clinical experts that testing has not been routinely performed in Canada to guide treatment options. In the MATTERHORN trial, patients were enrolled irrespective of PD-L1 expression level and the clinical benefit of treatment with durvalumab in combination with FLOT was observed in the overall randomized population. The PD-L1 subgroup analysis was not powered to detect differences in efficacy between patients with PD-L1 expression of at least 1% and those with PD-L1 expression less than 1%. The clinical experts indicated that there is no strong evidence at present to suggest that those with PD-L1 less than 1% would not benefit from treatment with durvalumab. pERC agreed with the clinical experts that eligibility for treatment with durvalumab in combination with FLOT chemotherapy should not be restricted by a minimum PD-L1 expression.
Clinical value: Based on the totality of evidence, the committee determined that neoadjuvant and adjuvant durvalumab in combination with FLOT followed by adjuvant durvalumab monotherapy provides added clinical value compared with perioperative FLOT alone in resectable gastric or GEJ cancer stages II to IVA.
Unmet Clinical Need
Input on unmet clinical need: Patients identified a need for new treatments for resectable gastric or GEJ cancer that prolong survival, delay remission, have fewer side effects, and improve HRQoL. The clinical experts consulted for this review and input received from clinician groups highlighted the need for curative-intent treatments that are safer, reduce risk of recurrence, and improve OS. Patient and clinician group submissions also indicated that, despite the availability of treatment options, important unmet needs persist, including high relapse rates, treatment-related toxicity, limited curative options after recurrence, and a need for therapies that provide durable benefit in the curative intent setting for patients with resectable gastric or GEJ cancer.
Severity of the disease: Adenocarcinoma is the most common type of gastric cancer, accounting for approximately 95% of all gastric cancer cases. The committee considered gastric or GEJ adenocarcinoma to be a serious and life-threatening condition that is associated with a high risk of progression and mortality. The overall 5-year net survival rate for gastric or GEJ cancer is estimated at approximately 40% to 50% for stage II disease, declining further to 20% to 30% for stage III disease.
Availability of treatment options: In Canada, the standard treatment for resectable gastric or GEJ adenocarcinoma involves perioperative FLOT chemotherapy along with radical gastrectomy and lymphadenectomy. For patients who are unable to receive FLOT, doublet regimens combining fluoropyrimidine-platinum with cisplatin or oxaliplatin are appropriate alternatives. The curative strategy for patients with esophageal or GEJ cancer includes neoadjuvant chemoradiation followed by surgical resection and adjuvant nivolumab for 1 year.
Distinct Social and Ethical Considerations
Input on unmet nonclinical need: Patients and clinicians emphasized the need for effective treatments that are feasible to deliver and minimize travel-related burden and costs, particularly for those in rural or remote areas. The committee also identified a nonclinical unmet need for standardized access to perioperative chemotherapy across Canada. The clinical experts noted that, in Canada, PD-L1 combined positive score (CPS) testing is used to guide immunotherapy decisions in gastric or GEJ adenocarcinoma. However, it has not been routinely performed across jurisdictions, limiting the ability to accurately determine the prevalence of PD-L1-expressing tumours in the treatment-eligible population. pERC noted that the PD-L1 tumour area positivity (TAP) score, which was used in the MATTERHORN trial, is not currently available in Canada.
Equity considerations: Equity concerns were identified for patients experiencing barriers, including those in remote or under-resourced settings. Evidence suggests that equity-deserving groups, particularly Indigenous peoples, face higher rates of late-stage diagnosis and poorer survival due to longstanding barriers to timely detection and treatment. Consistent with this evidence, the clinical experts noted reduced access to diagnostic imaging, specialist care, and supportive services for those living in Indigenous communities, living in rural or remote areas, or experiencing homelessness. These geographic and system-level barriers may limit the feasibility of completing complex perioperative regimens and could contribute to poorer clinical outcomes.
Ethical implications: pERC discussed the potential challenges associated with the management of perioperative treatment with durvalumab in combination with FLOT. Patient group input highlighted substantial physical, psychosocial, and financial burden throughout the perioperative treatment course. Patients and caregivers reported significant mental health impacts, including anxiety and emotional distress associated with prolonged treatment. The clinical experts noted that perioperative therapy is often poorly tolerated and requires substantial supportive care (e.g., nutritional support and symptom management). Limitations in supportive infrastructure at many rural sites, such as access to dietitian services, rapid access clinics, and symptom management programs, may increase reliance on caregivers, thereby compounding caregiver burden.
Economic Considerations
Health impacts of durvalumab plus FLOT versus relevant comparators: Durvalumab plus FLOT is predicted to be associated with a gain of 1.63 life-years compared to FLOT alone and may result in a gain of 1.44 quality-adjusted life-years (QALYs) compared to FLOT alone over a lifetime time horizon (39 years).
Cost of durvalumab plus FLOT versus relevant comparators: Durvalumab plus FLOT is predicted to be associated with higher costs to the health care system than FLOT alone (incremental costs = $96,818) over a lifetime time horizon, primarily driven by increased costs associated with drug acquisition.
Key findings of the economic evaluation: Based on the submitted evidence using the sponsor’s cost-utility analysis, the CDA-AMC base-case analysis estimated that the incremental cost-effectiveness ratio for durvalumab in combination with FLOT in patients with resectable gastric or GEJ cancer was $67,176 per QALY gained when compared with FLOT alone (Figure 1).
Figure 1: Estimate of the ICER Used by pERC to Inform the Price Condition
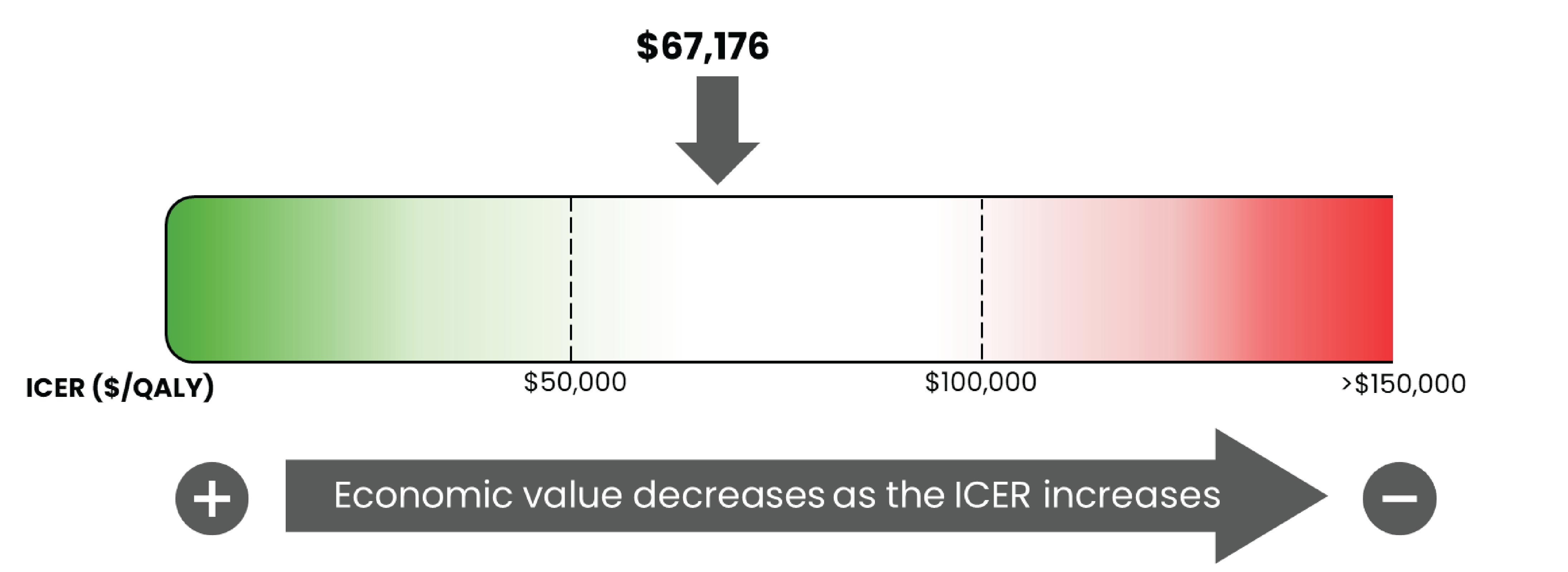
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Certainty of the evidence: Due to the lack of long-term evidence, extrapolation of both time to first recurrence and survival outcomes are subject to considerable uncertainty, and approximately 89% of the predicted incremental benefit was accrued on the basis of extrapolation. Higher price reductions than those presented may therefore be required to achieve cost-effectiveness at a given willingness-to-pay threshold.
Impacts on Health Systems
Anticipated budget impact: The estimated budget impact of reimbursing durvalumab for use in combination with FLOT for the treatment of resectable gastric or GEJ cancer will be approximately $113 million over the first 3 years of reimbursement compared to the amount currently spent on comparators. The expenditure on durvalumab over this period is predicted to be $114 million. pERC noted that the feasibility of adoption must be addressed because the incremental budget impact of reimbursing durvalumab is predicted to be greater than $40 million in year 2 and year 3. The committee additionally noted that if patients with esophageal adenocarcinoma are treated with durvalumab in combination with FLOT the anticipated budget impact would increase.
Sources of Information Used by the Committee
To make its recommendation, the committee considered the following information (links to the full documents for the review can be found on the project webpage:
the CDA-AMC review of the clinical and pharmacoeconomic evidence submitted by the sponsor related to durvalumab (refer to the Main Report and Supplemental Material document)
the sponsor’s comments on the draft report and the CDA-AMC responses
patients' perspectives gathered by 1 patient group, My Gut Feeling–Stomach Cancer Foundation of Canada (refer to the Patient and Clinician Group Input document)
input from 2 clinician groups, CGOEN and the Ontario Health (Cancer Care Ontario) GI DAC (refer to the Patient and Clinician Group Input document)
input from public drug programs that participate in the reimbursement review process (refer to the Supplemental Material document)
input from 2 clinical experts with expertise in the management of gastric or GEJ cancer consulted by CDA-AMC.
All feedback received in response to the draft recommendation is available on the CDA-AMC project webpage.
pERC Information
Members of the Committee
Dr. Catherine Moltzan (Chair), Dr. Kelvin Chan (Vice-Chair), Paul Agbulu, Dr. Phillip Blanchette, Dr. Matthew Cheung, Dr. Michael Crump, Annette Cyr, Dr. Jennifer Fishman, Dr. Jason Hart, Terry Hawrysh, Dr. Yoo-Joung Ko, Dr. Aly-Khan Lalani, Amy Peasgood, Dr. Anca Prica, Dr. Michael Raphael, Dr. Adam Raymakers, Dr. Patricia Tang, Dr. Pierre Villeneuve, and Danica Wasney.
Meeting date: February 11, 2026
Regrets: One member was absent.
Conflicts of interest: None
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@cda-amc.ca.