Drugs, Health Technologies, Health Systems
Reimbursement Review
Nivolumab
Requester: Public drug programs
Therapeutic Area: Hodgkin lymphoma
Summary
What Is Classic Hodgkin Lymphoma?
Classic Hodgkin lymphoma (cHL) is a relatively rare cancer of the immune system that contains abnormal B lymphocytes called Reed-Sternberg cells in the lymph nodes. cHL is the most common type of Hodgkin lymphoma, accounting for 95% of all Hodgkin lymphoma cases. The other 5% of Hodgkin lymphoma cases are nodular lymphocyte-predominant Hodgkin lymphoma.
In Canada, about 1,000 people are diagnosed with Hodgkin lymphoma each year, which occurs more frequently in males than females.
What Are the Treatment Goals and Current Treatment Options for Hodgkin Lymphoma?
The treatment goal for patients with advanced-stage cHL is to achieve cure, delay progression, prevent refractory or relapsed disease, decrease radiation use, reduce late toxic effects, and improve health-related quality of life (HRQoL).
Combination chemotherapy has been the first-line treatment for advanced-stage Hodgkin lymphoma.
Combination chemotherapy regimens for adults include:
brentuximab vedotin plus doxorubicin (Adriamycin), vinblastine, and dacarbazine (BV + AVD)
doxorubicin (Adriamycin), bleomycin, vinblastine, and dacarbazine (ABVD)
bleomycin, etoposide, doxorubicin (Adriamycin), cyclophosphamide, vincristine (Oncovin), procarbazine, and prednisone (BEACOPP).
Pediatric combination chemotherapy regimens include:
brentuximab vedotin plus doxorubicin (Adriamycin), vincristine, etoposide, prednisone, and cyclophosphamide (BV + AVEPC)
doxorubicin (Adriamycin), bleomycin, vincristine, etoposide, prednisone, and cyclophosphamide (ABVE-PC).
What Is Nivolumab Plus AVD and Why Did We Conduct This Review?
The PD-1 ligand is ubiquitously expressed in Hodgkin Reed-Sternberg cells. PD-1 blockade by the PD-1 inhibitor nivolumab has been approved by Health Canada for the treatment of adult patients with cHL that has relapsed or progressed after autologous stem cell transplant (ASCT) and brentuximab vedotin (BV), or 3 or more lines of systemic therapy including ASCT.
At the request of the participating public drug programs, we reviewed nivolumab combined with AVD (nivolumab + AVD) to inform a recommendation on whether it should be reimbursed for adolescents and adults with previously untreated stage III or IV cHL.
How Did We Evaluate Nivolumab Plus AVD?
We reviewed the clinical evidence on the beneficial and harmful effects and compared costs of nivolumab + AVD versus BV + AVD, ABVD, or BEACOPP in adults with untreated stage III or IV cHL. Other specific comparators for the pediatric population include BV + AVEPC and ABVE-PC.
The clinical evidence was identified through systematic searches for available studies.
The review was also informed by 2 clinician group submissions, 1 patient group submission, and 1 industry submission in response to our call for input and by input from the participating public drug programs around issues that may impact their ability to implement a recommendation. We consulted 2 clinical experts in hematology (adult and pediatric) as part of the review process.
What Did We Find?
Clinical Evidence
We reviewed a phase III, multicentre, open-label, randomized trial (the S1826 trial) comparing the efficacy and safety of nivolumab + AVD with BV + AVD in adolescent and adult patients with newly diagnosed stage III or IV cHL.
The combination of nivolumab + AVD was associated with a clinically important improvement in progression-free survival (PFS) compared to BV + AVD. Event-free survival was also improved. Sources of uncertainty included the interim nature of the findings (potential for overestimation of the magnitude of effect), open-label assessment of PFS by the investigator, lack of confidence intervals for the absolute between-group differences, and relatively short follow-up.
There were too few events and inadequate follow-up to form a conclusion on the comparative efficacy in overall survival (OS). HRQoL is important to patients and was collected but not reported in the study publication.
Nivolumab + AVD had a better side-effect profile than BV + AVD. Use of radiotherapy after treatment was low in both groups.
Evidence on the clinical benefit of nivolumab + AVD compared with other relevant comparators is unavailable.
Economic Evidence
Reimbursing nivolumab + AVD for the treatment of patients with previously untreated stage III or IV classic Hodgkin lymphoma is expected to result in lower overall drug acquisition costs compared with BV + AVD in adult patients and BV + AVEPC in pediatric patients and to result in higher overall drug acquisition costs compared with ABVD and BEACOPP in adult patients and ABVE-PC in pediatric patients, at public list prices.
Abbreviations
ABVD
doxorubicin (Adriamycin), bleomycin, vinblastine, and dacarbazine
ABVE-PC
doxorubicin (Adriamycin), bleomycin, vincristine, etoposide, prednisone, and cyclophosphamide
AE
adverse event
AVD
doxorubicin (Adriamycin), vinblastine, and dacarbazine
AVEPC
doxorubicin (Adriamycin), vincristine, etoposide, prednisone, and cyclophosphamide
BEACOPP
bleomycin, etoposide, doxorubicin (Adriamycin), cyclophosphamide, vincristine (Oncovin), procarbazine, and prednisone
BV
brentuximab vedotin
cHL
classic Hodgkin lymphoma
CI
confidence interval
EFS
event-free survival
G-CSF
granulocyte colony-stimulating factor
HRQoL
health-related quality of life
IPS
international prognostic score
ITC
indirect treatment comparison
mITT
modified intention-to-treat
OS
overall survival
PFS
progression-free survival
Background
Introduction
The objective of the Clinical Review is to review and critically appraise the evidence on the beneficial and harmful effects of nivolumab + AVD in the treatment of newly diagnosed stage III or IV cHL in adolescents and adults. The focus will be placed on comparing nivolumab + AVD to relevant comparators and identifying gaps in the current evidence. The economic review consists of a cost comparison for nivolumab + AVD compared with relevant comparators. The comparators for the adult population considered relevant to the reviews were BV + AVD, ABVD, and BEACOPP. Specific comparators for the pediatric population include BV + AVEPC and ABVE-PC. The information on the drug under review is presented in Table 1.
Table 1: Information on the Drug Under Review and on the Canada’s Drug Agency Review
Item | Description |
|---|---|
Information on the drug under review | |
Drug (product) | Nivolumab, 10 mg nivolumab/mL, 40 mg and 100 mg single-use vials, IV infusion with:
|
Relevant Health Canada indication | Not applicable |
Mechanism of action | Nivolumab is a PD-1 inhibitor. Doxorubicin, vinblastine, and dacarbazine are chemotherapeutic agents:
|
Data protection status | Data protection expired in March 2024. |
Status of generic drugs/biosimilarsa | Drug Name: Biosimilar nivolumab (Biocad) Other names: nivolumab, Biocad, BCD263, BCD 263 Indication: Melanoma |
Drug Name: Biosimilar nivolumab (Mabpharm) Other names: CMAB819, CMAB-819, CMAB 819, biosimilar Opdivo (Mabpharm) Indication: Solid tumours | |
Drug Name: Biosimilar Opdivo (NeuClone) Other names: Biosimilar Opdivo (NeuClone) Indication: Cancer | |
Drug Name: BA1104 Other names: LY 01015, LY-01015, LY01015, Biosimilar Nivolumab (Luye Pharma), BA 1104, BA-1104, Biosimilar Opdivo (Luye Pharma) Indication: Cancer | |
Drug Name: Xdivane Other names: Biosimilar nivolumab (Xbrane/STADA), biosimilar Opdivo (Xbrane/STADA), nivolumab, Xbrane Biopharma, Opdivo, Xbrane Biopharma Indication: Melanoma | |
Information on the Canada’s Drug Agency review | |
Requestor | Provincial Advisory Group |
Indication under consideration for reimbursement | Nivolumab in combination with AVD for the first-line treatment of stage III and stage IV cHL in patients aged 12 years and older |
AVD = doxorubicin (Adriamycin), vinblastine, and dacarbazine; cHL = classic Hodgkin lymphoma; RNA = ribonucleic acid.
aAll these biosimilars have not yet been reviewed or approved by Health Canada.
Sources of Information
The contents of the Clinical Review report are informed by studies identified through systematic literature searches and input received from interested parties.
Calls for patient group, clinician group, and industry input are issued for each Nonsponsored Reimbursement Review. We received 1 patient group input submission (Lymphoma Canada), 2 clinician group submissions from the Ontario Health (Cancer Care Ontario) Hematology Cancer Drug Advisory Committee and the Lymphoma Canada Scientific Advisory Board, and 1 submission from industry (Bristol Myers Squibb). The full submissions received are available in the consolidated input document on the project landing page.
Input from patient and clinician groups is considered throughout the review, including in the selection of outcomes to include in the Clinical Review and in the interpretation of the clinical evidence. Relevant patient and clinician group input and industry input is summarized in the Disease Background, Current Management, and Unmet Needs and Existing Challenges sections.
The drug programs provide input on each drug being reviewed through the Reimbursement Review process by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted for this review are summarized and provided to the expert committee in a separate document.
Each review team includes at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process. Two clinical specialists with expertise in the diagnosis and management of lymphoma with hematologic malignancies in adolescents and adults participated as part of the review team, with representation from Ontario and British Columbia.
Disease Background
There are 2 main types of lymphocytes in the lymphatic system (B cells and T cells) that can develop into lymphomas.1 B cells are the type of cells that become cancerous in Hodgkin lymphoma, characterized by the presence of large and abnormal B cells called Reed-Sternberg cells.1
There are 2 main types of Hodgkin lymphoma: cHL and nodular lymphocyte-predominant Hodgkin lymphoma. cHL is the most common type of Hodgkin lymphoma, accounting for about 95% of all Hodgkin lymphoma cases.1 About 5% of patients diagnosed with Hodgkin lymphoma have nodular lymphocyte-predominant Hodgkin lymphoma.1
cHL is further subdivided into 4 subtypes:1
Nodular sclerosis: This is the most common subtype of cHL (60% to 70% of all Hodgkin lymphoma cases), which mostly develops in young people aged 15 to 35 years. It affects lymph nodes of the neck and chest.
Mixed cellularity: Occurs in approximately 25% of all Hodgkin lymphoma cases and mostly develops in people older than 55 years who have existing infections. It affects the lymph nodes within the abdomen that contain a mixture of Reed-Sternberg cells and other cell types.
Lymphocyte-rich: Occurs in about 4% of all Hodgkin lymphoma cases and is usually found at an early stage in adults aged 40 to 50 years. It mainly affects lymph nodes of the neck and armpits. There are few Reed-Sternberg cells with abundant normal lymphocytes.
Lymphocyte-depleted: Occurs in about 1% of all Hodgkin lymphoma cases, mostly in older adults or patients living with HIV/AIDS. It is a more aggressive subtype and mainly affects lymph nodes in the abdomen. There are many Reed-Sternberg cells with few normal lymphocytes.
There are 4 main stages of Hodgkin lymphoma based on the findings from clinical examinations:1
Stage I: The lymphoma is confined in 1 group of lymph nodes.
Stage II: The lymphoma is found in 2 or more groups of lymph nodes on the same side of the diaphragm.
Stage III: The lymphoma is found in lymph nodes on both sides of the diaphragm.
Stage IV: The lymphocyte spreads to multiple areas throughout the body.
Stage I and II are considered early stages, whereas stage III and IV are advanced stages.1
The common sign of Hodgkin lymphoma is painless swelling of lymph nodes in the neck, armpit, chest, abdomen, or groin regions.1 Patients may experience a group of symptoms called B symptoms, which are fever (temperature of more than 38°C with no sign of an infection), drenching night sweats, weight loss with unknown reason (at least 10% of body weight over 6 months), and pruritus.1
In Canada, about 1,000 people are diagnosed with Hodgkin lymphoma each year.1 It more commonly occurs in males than females, primarily in younger patients (aged 15 to 39 years) and in older adults (aged 55 years and older).1 In 2024, it was estimated that 110 people would die from Hodgkin lymphoma.2 The 5-year survival rate for Hodgkin lymphoma in Canada is 85%. Based on race or ethnicity in the US, cHL is more common in people who identify as non-Hispanic white, followed by people who identify as Hispanic, Black, and Asian/Pacific Islander.3
Current Management
Treatment Goals
According to clinical experts consulted for this review, the treatment goal for patients with advanced-stage cHL is to achieve cure, delay progression, prevent refractory or relapsed disease, decrease radiation use, reduce late toxic effects, and improve HRQoL.
Current Treatment Options
The main current treatment options for stage III and IV cHL are chemotherapy, targeted therapy, and radiation therapy.1 The 2 most common chemotherapy combinations used to treat stage III and IV adult patients with cHL are ABVD and BEACOPP, depending on patients’ risk and the results of PET-directed therapy.4 A clinician group and the clinical expert consulted for this review indicated that targeted therapy using BV in combination with chemotherapy AVD is the standard of care for advanced-stage cHL patients. This treatment has been shown to improve outcomes compared with ABVD.5,6 Nevertheless, in adults, the incorporation of BV into the treatment of advanced-stage cHL has led to a higher incidence of toxic effects compared to ABVD, and 53% of pediatric patients still receive radiotherapy with BV-based therapy.7 BEACOPP is associated with a higher incidence of acute and chronic toxicities.8
The clinical expert consulted for this review noted that the standard treatment in the pediatric population has been a combined modality of chemotherapy plus radiation. The Canadian standard for treatment of advanced-stage disease in the pediatric population has been BV + AVEPC or ABVE-PC. The alternative approach is a EuroNet-based chemotherapy (vincristine [Oncovin], etoposide, prednisone, and doxorubicin plus cyclophosphamide, vincristine [Oncovin], prednisone, and dacarbazine).
The drug program input and clinician group inputs noted that BV + AVD is currently funded and used as the standard of care for the treatment of stage IV cHL. ABVD is the current standard of care for stage III cHL. Recently, CDA has recommended BV + AVD as standard treatment for advanced-stage (including stage III) cHL. BV + AVD is currently under review by the federal, provincial, and territorial drug programs. A clinician group noted that BV +AVD is associated with significant peripheral neuropathy, neutropenia, and febrile neutropenia. A clinician group also highlighted that, in patients aged 60 years and older, no benefit was observed with BV + AVD over ABVD, and there was a higher incidence of toxicity, even death.
Key characteristics of nivolumab + AVD are summarized with other treatments available for cHL in the Supplemental Material, in the Key Characteristics table in Appendix 1.
Unmet Needs and Existing Challenges
According to clinical expert input submissions and clinician group submissions, there are remaining unmet clinical needs for more effective therapies that cure the disease, prolong survival, prevent relapse and refractory disease, reduce toxic effects, and improve HRQoL.
The clinical expert consulted for this review noted that more than 50% of pediatric patients still receive radiotherapy with BV-based therapy. The approach has been to try to limit radiation fields and doses over time to reduce the risk of late toxicities. There is an unmet clinical need for therapies that will reduce the need for radiotherapy in this population.
Considerations for Using the Drug Under Review
Contents within this section have been informed by input from the clinical expert(s) consulted for the purpose of this review and from clinician groups. The following has been summarized by the review team.
Place in Therapy
The clinical expert suggested that many Canadian centres would move to nivolumab + AVD as first-line therapy for advanced-stage (stage III and IV) cHL in patients aged 12 years and older.
Clinician group input submissions suggest that nivolumab + AVD will be the standard of care for first-line stage III and IV cHL because, in their opinion, it is associated with low toxicity and better tolerance compared to BV + AVD, especially in those aged 60 years and older.
Patient Population
The best-suited patients for treatment with nivolumab + AVD are those who fit the eligibility criteria of the S1826 trial, described in Herrera et al. (2024),9 according to the clinician group input submissions. The clinical expert noted that patients with pre-existing autoimmune disease that is active are not eligible for nivolumab therapy.
A clinician group highlighted that the recently updated National Comprehensive Cancer Network guidelines not only included nivolumab + AVD as the preferred regimen for stage III and IV cHL but also for unfavourable stage I and II cHL (i.e., with bulky disease or B symptoms).
Assessing the Response to Treatment
A clinician group explained that a PET scan with or without CT is used to assess response to treatment, usually midtreatment and at the end of treatment. The clinical expert listed a number of outcomes to be assessed, including event-free survival (EFS), disease-free survival, and OS. In the pediatric population, school attendance and performance are also outcomes of interest to be monitored when assessing the response to treatment.
Discontinuing Treatment
Nivolumab should be discontinued when there is evidence of disease progression or significant toxicities, according to clinical expert input and clinician group input.
Prescribing Considerations
The clinical expert indicated that patients are primarily followed by hematologists or oncologists who would prescribe the regimen. A clinical group said that this regimen can be given in both outpatient academic and community-based settings, and that physicians should be familiar with the management of immune-related adverse events (AEs) from using single-agent PD-1 inhibitor therapy.
Additional Considerations
The clinical expert mentioned that this treatment regimen was currently available through a compassionate program offered by the drug company. The industry (Bristol Myers Squibb) input indicated that the cost of treatment with nivolumab + AVD is significantly lower than the cost of the standard treatment (BV + AVD) currently administered to patients in Canada. The industry also explained that the addition of granulocyte colony-stimulating factor (G-CSF) for prophylaxis and extra supportive care due to toxicities in the current standard of care would further increase the cost of treatment with BV + AVD.
Clinical Review
Methods
We conducted a systematic review to identify randomized controlled trial evidence for nivolumab + AVD for the treatment of cHL. Studies were selected according to the eligibility criteria in Table 2. We also included long-term extension studies of included randomized controlled trials, indirect treatment comparisons (ITCs) that adhered to the eligibility criteria except for the study design criteria, and studies addressing gaps that did not meet the eligibility criteria but were considered to address important gaps in the systematic review evidence.
Relevant comparators included treatments used in clinical practice in Canada in the patient population under review. We selected outcomes (and follow-up times) for review, considering clinical expert input, patient input, and clinician group input. Selected outcomes are those considered relevant to expert committee deliberations. Detailed methods for literature search(es), study selection, data extraction, and risk of bias appraisal are in Appendix 2 in the Supplemental Material.
Table 2: Systematic Review Eligibility Criteria
Criteria | Description |
|---|---|
Population | Adolescent and adult patients with previously untreated stage III or IV classic Hodgkin lymphoma Subgroups:
|
Intervention | Nivolumab with doxorubicin, vinblastine and dacarbazine (nivolumab + AVD) |
Comparator | Comparators for the adult population:
Comparators for the pediatric population:
|
Outcomes | Efficacy outcomes:
Harms outcomes: AEs, SAEs, WDAEs, death due to AE, immune-mediated AEs |
Study design | Published phase III and IV RCTs |
AE = adverse event; BV = brentuximab vedotin; HRQoL = health-related quality of life; RCT = randomized controlled trial; SAE = serious adverse event; WDAE = withdrawal due to adverse event; vs. = versus.
Clinical Evidence
From the search for primary studies, we identified 383 unique records via the searches of databases and registers, of which we excluded 367 by title and abstract. We screened 16 records by full text and included 1 report of 1 study. No long-term extensions of the included study were identified.
From the search for ITCs, we identified 64 unique records via the searches of databases, of which we did not identify any relevant ITCs.
Lists of included and excluded studies, including reasons for exclusion, are in Table 3 and Table 4 of Appendix 3 in the Supplemental Material, respectively.
Systematic Review
Description of Studies
Characteristics of the included study9 are summarized in Table 3. Additional details of eligible criteria are presented in Table 5 of Appendix 3 in the Supplemental Material.
Table 3: Characteristics of the Included Study
Detail | S1826 trial |
|---|---|
Study design | Ongoing, multicentre (256 sites across the US and Canada), open-label, phase III randomized trial |
Patient enrolment dates | Between July 19, 2019, and October 5, 2022 |
Study dates |
|
Key inclusion criteria |
|
Key exclusion criteria |
|
Intervention | Nivolumab IV, doxorubicin IV, vinblastine IV, and dacarbazine IV over 30 minutes on days 1 and 15 of each 28-day cycle for 6 cycles
|
Comparator | Brentuximab vedotin IV, doxorubicin IV, vinblastine IV, and dacarbazine IV over 30 minutes on days 1 and 15 of each 28-day cycle for 6 cycles.
|
Primary end point | PFS |
Secondary end points | OS, EFS, CRR, and AEs Assessment of patient-reported fatigue, neuropathy, and HRQoL using the Patient-Reported Outcomes Measurement Information System (PROMIS) Fatigue, the Functional Assessment of Cancer Therapy/Gynecologic Oncology Group — Neurotoxicity (FACT/GOG-NTX), and the PROMIS Global, respectively, was mentioned in the study protocol, but the results have not yet been made available. |
AE = adverse event; CRR = complete response rate; EFS = event-free survival; HRQoL = health-related quality of life; OS = overall survival; PFS = progression-free survival.
aStaging was assessed using the Ann Arbor staging criteria: Stage III — involvement of lymph node regions on both sides of the diaphragm (III), which may be accompanied by localized involvement of an associated extralymphatic organ or site (IIIE) or spleen (IIIS) or both (IIISE); stage IV — diffuse or disseminated involvement of 1 or more extra lymphatic organs with or without associated lymph node involvement, or isolated extralymphatic organ involvement with distant (nonregional) nodal involvement.
bZubrod performance status is measured on a 5-point scale, with higher number reflecting greater disability.
cLansky performance status is measured on a scale ranging from 0 to 100, with higher numbers indicating better performance on play and activity.
Source: Herrera et al. (2024);9 ClinicalTrials.gov (NCT03907488).10
The S1826 trial described in Herrera et al. (2024)9 is an ongoing, multicentre, open-label, randomized phase III trial. There were multiple sources of support for the study, including the manufacturer, Bristol Myers Squibb. The study had 256 sites across the US and Canada. The number of sites in Canada was unclear. A total of 994 adolescent (12 to < 18 years) and adult (≥ 18 years) patients with newly diagnosed stage III or IV cHL were assigned in a 1:1 ratio to receive either nivolumab + AVD or BV + AVD. The combination therapy was given to patients on days 1 and 15 of each 28-day cycle for 6 cycles. Full details of the treatment plan, including premedication, concomitant therapy, and supportive care guidelines; PET-CT response assessment; radiotherapy indications; and dose modifications due to toxicities related to therapy are presented in Appendix 4 in the Supplemental Material.
The randomization was dynamically balanced across 3 stratification factors (i.e., age [years]: 12 to 17 versus 18 to 60 versus > 60; international prognostic score (IPS): 0 to 3 versus 4 to 7; and prespecified plan to use residual PET radiation: yes versus no). After completion of cycle 6, patients might receive radiation therapy 5 days per week for approximately 4 weeks at the discretion of the treating physician. Patients also underwent peripheral blood specimen collection and CT, PET/CT, and/or MRI in the study.
Disease assessments occurred at baseline and at 4 to 8 weeks after completion of the study treatment. After completion of the study treatment and before disease progression, patients are followed up every 3 months for the first year, every 6 months for years 2 and 3, then annually until 10 years after registration. Following disease progression, patients are followed up annually until 10 years after registration. Patients who receive radiation therapy are followed up at 8 to 12 weeks after completion of radiation therapy.
The primary end point was PFS (defined as the time from randomization to the first observation of disease progression or death from any cause). Key secondary end points were OS (defined as the time from randomization to death from any cause), EFS (defined as the time from randomization to the date of progression or relapse, death from any cause, or administration of non–protocol-specified antilymphoma therapy in the absence of progression), and incidence of AEs. Assessment of patient-reported outcomes, including HRQoL, was mentioned in the protocol, but the results have not yet been made available. Response to treatment was assessed by PET-CT, the preferred imaging method. CT or MRI was acceptable if PET-CT was contraindicated. Responses were assessed based on the local radiology review according to the 2014 Lugano classification using the 5-point Deauville score. Toxicity was evaluated using Common Terminology Criteria for Adverse Events (CTCAE) version 5.
Statistical Testing and Analysis Population
Based on previous data and an exponential cure-rate model, the trial9 was anticipated to have 86% power to detect a between-group difference of 6 percentage points in PFS (i.e., 2-year PFS of 90%). A total of 940 eligible patients were expected to be accrued over 4 years, with a total of 987 patients assuming an expected ineligible rate of 5%. The final analysis was to be conducted when 179 events of disease progression or death occurred across both groups. Interim analyses were planned when 25%, 50%, and 75% of the anticipated PFS events in both groups had been observed. The type I error was controlled across interim analyses of PFS at a 1-sided alpha of less 0.025. P values for superiority were calculated based on simulation studies using the information times in the interim analysis schedule. There was no type I error control for other end points.
The modified intention-to-treat (mITT) population consisted of all the patients who underwent randomization except for those who were deemed to be ineligible by pathology review or owing to violation of the eligibility criteria. All analyses of the primary and secondary end points were conducted with the mITT population.
Patient Disposition
Table 4 presents patient disposition of the S1826 trial reported in Herrera et al. (2024).9
Between July 19, 2019, and October 5, 2022, 496 patients were assigned to receive nivolumab + AVD and 498 patients were assigned to receive BV + AVD. Eligible patients included in the mITT cohort consisted of 487 patients in the nivolumab + AVD group and 483 patients in the BV + AVD group. Any discontinuation of nivolumab occurred in 9.4% of patients in the nivolumab + AVD group, and any discontinuation of BV occurred in 22.2% in the BV + AVD group. Major protocol deviation, loss to follow-up, and consent withdrawal after treatment initiation were low and similar between groups.
Table 4: Patient Disposition in the mITT Analysis Set
Category | Total n (%) | Nivolumab + AVD n (%) | BV + AVD n (%) |
|---|---|---|---|
Eligible patients | 970 (100) | 487 (100) | 483 (100) |
Completed treatment | 875 (90.2) | 450 (92.4) | 425 (88.0) |
Early discontinuation of all treatment | 95 (9.8) | 37 (7.6) | 58 (12.0) |
Reason for discontinuation | |||
AE | 40 (4.1) | 20 (4.1) | 20 (4.1) |
Refuse treatment (unrelated to AE) | 22 (2.3) | 9 (1.8) | 13 (2.7) |
Progression or relapse | 9 (0.9) | 0 | 9 (1.9) |
Death | 11 (1.1) | 3 (0.6) | 8 (1.7) |
Other (not protocol-specified) | 13 (1.3) | 5 (1.0) | 8 (1.7) |
Any discontinuation of nivolumab or BV | 153 (15.8) | 46 (9.4) | 107 (22.2) |
Discontinued nivolumab or BV, but continued other agents | 78 (8.0) | 19 (3.9) | 59 (12.2) |
Major protocol deviation | 11 (1.1) | 5 (1.0) | 6 (1.2) |
Withdrawal from the study | |||
Loss to follow-up | 4 (0.4) | 3 (0.6) | 1 (0.2) |
Consent withdrawal after treatment initiation | 35 (3.6) | 15 (3.1) | 20 (4.1) |
AE = adverse event; AVD = doxorubicin (Adriamycin), vinblastine, and dacarbazine; BV = brentuximab vedotin; mITT = modified intention-to-treat.
Source: Supplementary Appendix of Herrera et al. (2024).9 From The New England Journal of Medicine, Herrera AF, LeBlanc M, Castellino SM, et al., Nivolumab+AVD in Advanced-Stage Classic Hodgkin's Lymphoma, Volume No. 391, Page No. 1379–1389. Copyright © 2024 Massachusetts Medical Society. Reprinted with permission from Massachusetts Medical Society.
Baseline Characteristics
Baseline demographics and disease characteristics of the S1826 trial reported in Herrera et al. (2024)9 are presented in Table 5.
The characteristics of patients in the mITT population at baseline were balanced between groups. The median ages were 27.6 years and 26.8 years in the nivolumab + AVD group and BV + AVD group, respectively. For age distribution, most patients in both groups were adults (18 to 60 years; 66%), followed by children and adolescents (12 to 17 years; 24%), and older adults (> 60 years; 10%). There were more males (56%) than females (44%), and most patients were white (76%). Patients were at disease stage III (36%) and IV (64%), and 58% of patients had B symptoms. Most patients (68%) had low risk of poor prognostic factor (IPS of 0 to 3).
Table 5: Baseline Characteristics of Patients in the mITT Population
Characteristics | Nivolumab + AVD (487 patients) | BV + AVD (483 patients) |
|---|---|---|
Age | ||
Median (range), years | 27.6 (12.0 to 83.7) | 26.8 (12.0 to 81.7) |
Distribution, n (%) | ||
12 to 17 years | 118 (24) | 118 (24) |
18 to 60 years | 321 (66) | 318 (66) |
> 60 years | 48 (10) | 47 (10) |
Sex, n (%) | ||
Female | 216 (44) | 210 (43) |
Male | 271 (56) | 273 (57) |
Race, n (%) | ||
White | 372 (76) | 361 (75) |
Black | 58 (12) | 56 (12) |
Asian | 11 (2) | 17 (4) |
Hispanic | 66 (14) | 58 (12) |
Other or unknown | 46 (9) | 49 (10) |
Disease stage, n (%) | ||
III | 185 (38) | 168 (35) |
IV | 302 (62) | 315 (65) |
B symptoms, n (%) | 288 (59) | 273 (57) |
IPS,a n (%) | ||
0 to 3 | 332 (68) | 328 (68) |
4 to 7 | 155 (32) | 155 (32) |
Bulky disease, n (%) | 156 (32) | 127 (26) |
HIV-positive status, n (%) | 11 (2) | 5 (1) |
AVD = doxorubicin (Adriamycin), vinblastine, and dacarbazine; BV = brentuximab vedotin; IPS = international prognostic score; mITT = modified intention-to-treat.
aIPS is a 7-point scoring system in which 1 point is scored for the presence of each poor prognostic factor and higher scores indicate a poorer prognosis (higher risk).
Source: Herrera et al. (2024).9 From The New England Journal of Medicine, Herrera AF, LeBlanc M, Castellino SM, et al., Nivolumab+AVD in Advanced-Stage Classic Hodgkin's Lymphoma, Volume No. 391, Page No. 1379–1389. Copyright © 2024 Massachusetts Medical Society. Reprinted with permission from Massachusetts Medical Society.
Treatment Exposure and Concomitant Medications
Dose reduction of nivolumab was not permitted in the nivolumab +AVD group, whereas the dose of BV was reduced in 26.7% of patients in the BV + AVD group.
G-CSF, used as primary prophylaxis to prevent neutropenia, was administered in 56.3% of patients in the nivolumab + AVD group and in 96.7% of patients in the BV + AVD group. The use of G-CSF was required for patients receiving BV + AVD but was optional for patients receiving nivolumab + AVD.
The use of dexrazoxane, concomitantly used with doxorubicin as a cardiac protectant, was similar between nivolumab + AVD and BV + AVD groups (29.2% versus 27.1%).
The end-of-treatment radiotherapy was administered in 3 patients (0.6%) in the nivolumab + AVD group and 4 patients (0.8%) in the BV + AVD group (Table 7 of Appendix 6 in the Supplemental Material).
Critical Appraisal
Table 6 of Appendix 5 in the Supplemental Material presents the results of the risk of bias appraisal of the included study.9
Internal Validity
The S1826 trial9 was a phase III, multicentre, open-label, randomized trial. The risk of bias was low regarding the randomization process. Despite the fact that allocation concealment was not clearly described, the characteristics of the patients at baseline were balanced between the 2 treatment groups. The trial was open-label, but there was low risk of bias regarding deviations from the intended interventions. According to the clinical experts, any discontinuation rates of both treatments (i.e., 9.4% in nivolumab + AVD and 22.2% in BV + AVD) are consistent with what has been seen in clinical practice for both adult and pediatric populations. Major protocol deviation was balanced between intervention groups, and all prespecified outcomes were analyzed using the mITT population. While this mITT excluded some randomized participants, the proportion of patients excluded was low and based on violations of the eligibility criteria and, therefore, would not introduce bias. The trial followed a prespecified analysis plan; in time-to-event analyses, patients without an event were censored at the date of last contact. A detailed description of the handling of intercurrent events (e.g., dropouts, missed assessments, subsequent antilymphoma treatment) was not reported, nor were particular censoring reasons. However, there were few losses to follow-up, with losses balanced across groups. Thus, there was a low risk of bias due to missing outcome data, and there is no clear evidence of any bias resulting from informative censoring.
Interim analyses were planned when 25%, 50%, and 75% of the anticipated PFS events had been observed. At the second interim analysis, the testing for PFS crossed the protocol-specified efficacy threshold for a 1-sided P value of less than 0.005. The absolute rates of PFS at 2 years were provided for each group, but the between-group differences with a 95% confidence interval (CI) were not provided, which hindered, to an extent, a full appraisal of the clinical importance of effects within the CI. A later analysis was performed at the 70% information fraction. These findings supported the primary analysis, but interim analyses are at risk of overestimating the magnitude of treatment effects.11 The median was not reached in either group, with more than 80% of patients remaining event-free at the time of the data cut-off and many patients being censored while remaining in follow-up beyond 24 months. The trial did not conduct an adjustment for multiplicity for all secondary analyses and subgroup analyses that could lead to potential inflation of type I error for statistically significant findings (i.e., EFS). Thus, the findings for those outcomes and subgroups should be treated as exploratory results. The validity of the proportional hazards assumption underlying the hazard ratios from time-to-event analyses could not be determined because results of the testing were not reported. Visual inspection of the Kaplan-Meier plots did not appear to suggest large departures from this assumption for the overall population analysis. Kaplan-Meier plots for OS did not separate at any time during follow-up.
All patients registered to the trial underwent retrospective pathology review, radiology review, and radiation therapy review. The review was coordinated by SWOG Cancer Research Network. All the data were maintained by the SWOG Statistics and Data Management Center, and the trial was monitored by the SWOG Data and Safety Monitoring Committee. The evaluation of progression was semiobjective in that it was evaluated using the revised international working group guidelines (Lugano classification), requiring interpretation of PET-CT scans. The measurements or ascertainment of the outcomes did not differ between intervention groups. Given that this was an open-label trial, central adjudication of PFS and EFS events would have been preferred, and there is some possibility for bias to be introduced via unblinded investigator assessment. However, the clinical experts indicated that any suspicion for relapse on imaging would be confirmed by biopsy given that this was strongly recommended in the trial. Data were analyzed in accordance with a prespecified plan, and the results being assessed were unlikely to have been selected. Therefore, risk of bias in measurement of outcomes and in selection of reported results was low. Sensitivity analyses of PFS with and without censoring for nonprotocol subsequent treatments were planned but not reported. The full impact cannot be ascertained, but the use of nonprotocol treatments appeared to be infrequent.
To date, the trial is still ongoing, and the follow-up time is short. The results of HRQoL have not yet been reported, and few OS events have accrued. The final analysis for OS is planned after 61 events have accrued. Although PFS can be a surrogate outcome for OS, particularly in oncology, it was used as a primary outcome in this trial, A 2024 analysis of 9 randomized trials of 16 treatment regimens for previously untreated Hodgkin lymphoma suggested a strong trial-level correlation between PFS and OS, but heterogeneity was observed and the magnitude of effect on PFS to predict a clinically important benefit on OS was not estimated.12 Nivolumab was not 1 of the treatments included in the analysis, so generalizability of the findings to this regimen is a source of uncertainty. The clinical expert noted that it would take a longer period of follow-up (up to 6 years) to be able to identify a between-group difference in OS, particularly in cHL under treatment with the study interventions. The progression and response results, therefore, needed to be validated with a longer follow-up to understand whether OS will demonstrate a difference between groups.
External Validity
The S1826 trial9 enrolled patients who were representative of patients in Canada regarding sex, age, race or ethnicity, and geography. The proportion of males and females in the S1826 trial matched the incidence rates of cHL, with more male patients (56% male versus 44% female). The trial enrolled patients across age groups: 66% of patients aged 18 to 60 years, 24% of patients aged 12 to 17 years, and 10% of patients aged 65 years and older. Patients in the S1826 trial also demonstrated the expected proportion of white, Black, Hispanic, and Asian populations based on the reported incidence rates in the US. The S1826 trial was conducted at 256 sites that were geographically diverse across the US and Canada. The clinical experts indicated that the patient characteristics in the S1826 trial are similar to what they observe in practice. In terms of the exclusion criteria in the S1826 trial, the clinical experts think that patients with some neuropathy should not be excluded from the nivolumab treatment as long as it was known that neuropathy was not caused by receiving nivolumab + AVD. Pediatric patients with a Lansky score less than 50 should be considered for treatment based on clinical judgment. In general, the clinical experts emphasized that if they feel that the patients can safely receive nivolumab + AVD, then they should receive the medication, irrespective of some of the exclusion criteria listed in the S1826 trial.
Therefore, the inclusion criteria of the S1826 trial were clinically relevant, and the results were generalizable to the patient population in Canada. According to the clinical experts, the trial regimens (i.e., dose and treatment duration) were also generalizable to the clinical setting in Canada. The comparator of the trial, which was BV + AVD, is 1 of the treatment options for cHL in Canada. Studies comparing nivolumab + AVD with BV-AVEPC or ABVE-PC for the pediatric population were not identified.
Results
Efficacy
Results important for this review are presented in Table 6. The Kaplan-Meier plots for PFS, OS, and EFS are presented in Figure 1 and Figure 2, respectively.
Key results included the following for nivolumab + AVD versus BV + AVD:
The median follow-up was 2.1 years (range 0 to 4.2 years).
Median time to event was not reached for PFS, EFS, or OS.
For PFS, the hazard ratio was 0.45 (95% CI, 0.30 to 0.65), favouring nivolumab + AVD. The 2-year PFS rate was 92% (95% CI, 89 to 94) in the nivolumab + AVD group compared with 83% (95% CI, 79 to 86) in the BV +AVD group. A between-group difference was not reported.
The results for PFS were consistent across prespecified patient subgroups according to age, IPS, and disease stage (Figure 1 and Figure 2 of Appendix 6 in the Supplemental Material).
The result was similar for the secondary outcome EFS, with a stratified hazard ratio of 0.50 (95% CI, 0.36 to 0.71) favouring the nivolumab + AVD group. The 2-year EFS rates were 90% after nivolumab + AVD and 81% after BV + AVD treatment. A between-group difference was not reported. The types of EFS events are presented in Table 8 of Appendix 6 in the Supplemental Material.
The evidence was insufficient to show a difference in OS between groups; few events had accrued.
Although HRQoL outcomes were preplanned in the trial and have been considered important to this review, they have not been reported in the included study.
Table 6: Summary of Key Efficacy Results
Variable | Nivolumab + AVD (487 patients) | BV + AVD (483 patients) |
|---|---|---|
PFSa | ||
Patients with disease progression or death, n (%) | 41 (8) | 81 (17) |
Median (95% CI) time to event | Not reached | Not reached |
Hazard ratio (95% CI) | 0.45 (0.30 to 0.65) | Reference |
P value | NR | Reference |
2-year event-free rates (95% CI) | 92 (89 to 94) | 83 (79 to 86) |
Subgroups by age, hazard ratio (95% CI) | ||
12 to 17 years | 0.31 (0.13 to 0.74) | Reference |
18 to 60 years | 0.59 (0.36 to 0.95) | Reference |
> 60 years | 0.30 (0.12 to 0.72) | Reference |
EFSa,b | ||
Patients with disease progression, nonprotocol antilymphoma therapy, or death | 52 (11) | 91 (19) |
Median (95% CI) time to event | Not reached | Not reached |
Hazard ratio (95% CI) | 0.50 (0.36 to 0.71) | Reference |
P value | NR | Reference |
2-year event-free rates (95% CI), % | 90 (86 to 92) | 81 (77 to 84) |
OSa | ||
Patients who died, n (%) | 7 (1) | 14 (3) |
Median (95% CI) time to event | Not reached | Not reached |
Hazard ratio (95% CI) | 0.39 (0.15 to 1.03) | Reference |
P value | NR | Reference |
2-year event-free rates (95% CI), % | 99 (97 to 100) | 98 (96 to 99) |
AVD = doxorubicin (Adriamycin), vinblastine, and dacarbazine; BV = brentuximab vedotin; CI = confidence interval; EFS = event-free survival; NR = not reported; OS = overall survival; PFS = progression-free survival.
Notes: PFS is the time from randomization to the first observation of progressive disease or death from any cause; EFS is the time from randomization to the date of progression or relapse, death from any cause, or administration of non–protocol-specified antilymphoma therapy in the absence of progression; and OS is defined as time from randomization to death from any cause.
aAll these end points, including those of the subgroups, were analyzed in mITT analysis set at median follow-up of 2.1 years (range, 0 to 4.2), with absolute event-free probabilities at 2 years.
bAnalysis of these end points was not adjusted for multiplicity; there is an increased risk of erroneously rejecting the null hypothesis.
Source: Herrera et al. (2024)9 and its supplementary appendix.
Figure 1: PFS and OS (mITT Population)
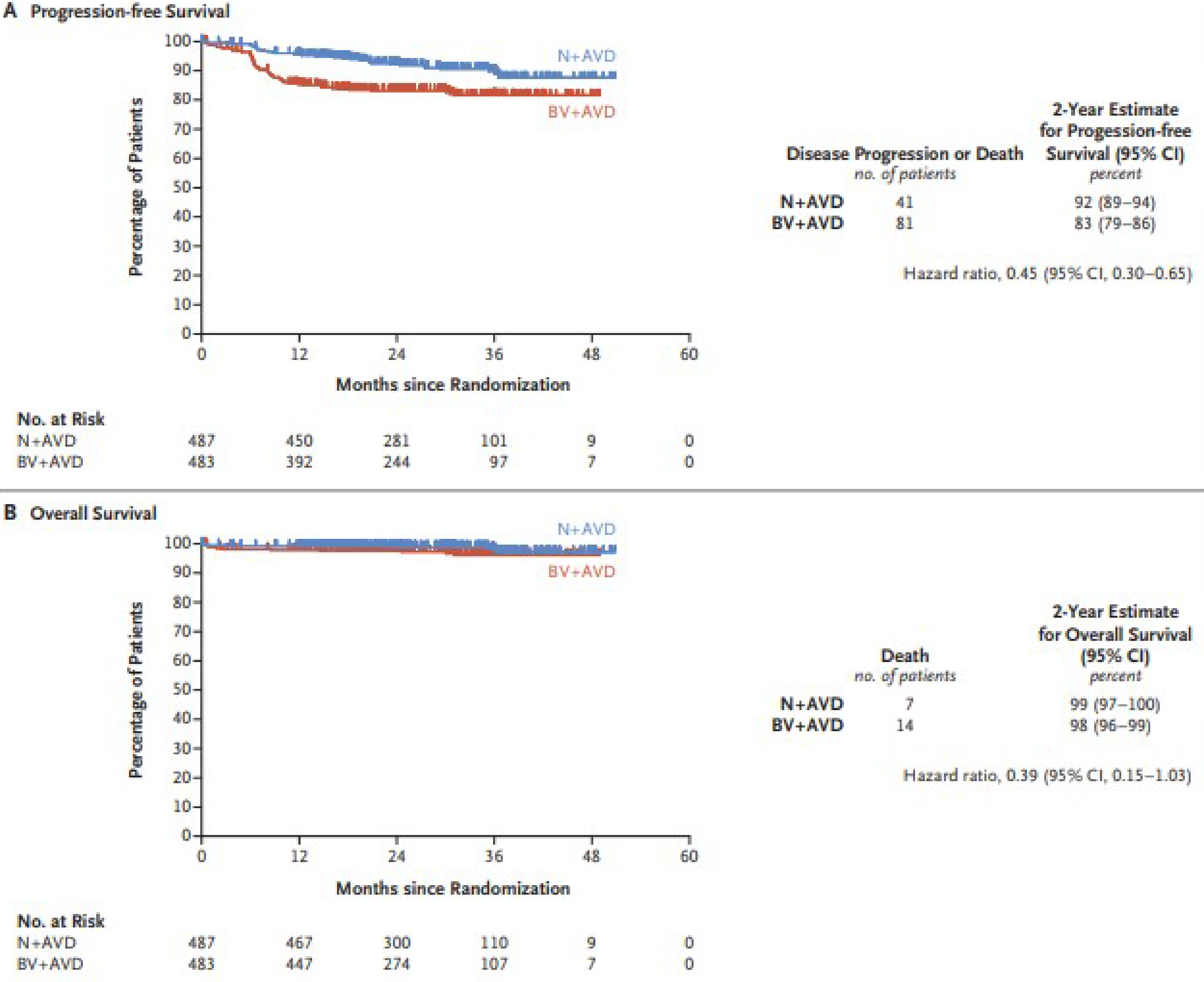
AVD = doxorubicin (Adriamycin), vinblastine, and dacarbazine; BV = brentuximab vedotin; CI = confidence interval; mITT = modified intention-to-treat; N = nivolumab; OS = overall survival; PFS = progression-free survival.
Source: Herrera et al. (2024).9 From The New England Journal of Medicine, Herrera AF, LeBlanc M, Castellino SM, et al., Nivolumab+AVD in Advanced-Stage Classic Hodgkin's Lymphoma, Volume No. 391, Page No. 1379–1389. Copyright © 2024 Massachusetts Medical Society. Reprinted with permission from Massachusetts Medical Society.
Figure 2: EFS in the mITT Analysis Set
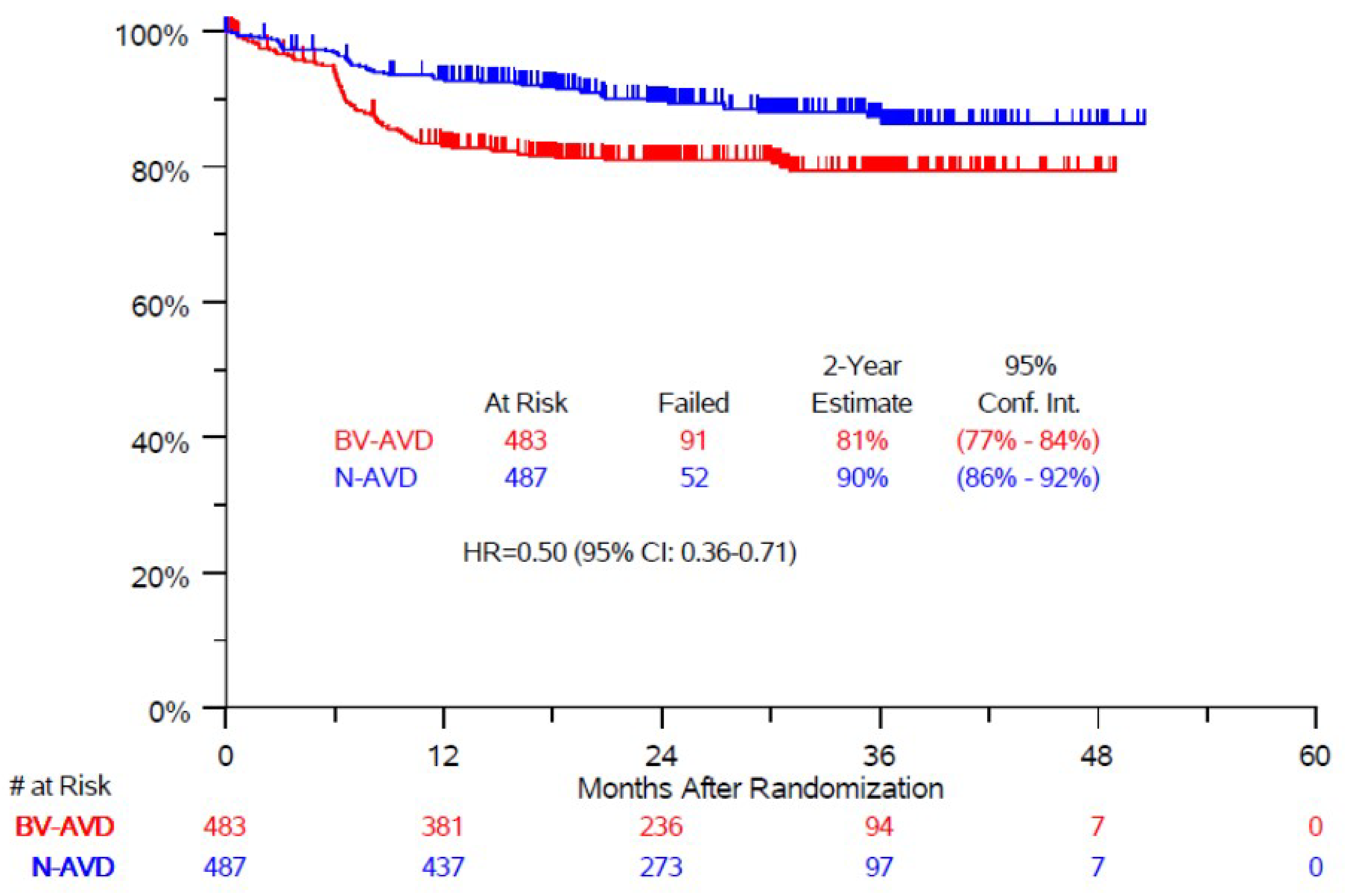
AVD = doxorubicin (Adriamycin), vinblastine, and dacarbazine; BV = brentuximab vedotin; CI = confidence interval; Conf. Int. = confidence interval; EFS = event-free survival; HR = hazard ratio; mITT = modified intention-to-treat; N = nivolumab; OS = overall survival; PFS = progression-free survival.
Source: Supplementary Appendix of Herrera et al. (2024).9 From The New England Journal of Medicine, Herrera AF, LeBlanc M, Castellino SM, et al., Nivolumab+AVD in Advanced-Stage Classic Hodgkin's Lymphoma, Volume No. 391, Page No. 1379–1389. Copyright © 2024 Massachusetts Medical Society. Reprinted with permission from Massachusetts Medical Society.
Harms
AEs of any grade, AEs of grade 3 or higher, and possible immune-related AEs are listed in Table 9, Table 10, and Table 11 of Appendix 7 in the Supplemental Material, respectively. A complete list of all AEs from grade 1 to 5 of both groups can be found in the supplementary appendix of Herrera et al. (2024).9
The proportion of patients with 1 or more AEs was not reported. All AEs, except neutropenia, occurred with a similar or greater frequency in the BV + AVD group compared with the nivolumab + AVD group.
Neutropenia of any grade occurred in 272 patients (56%) in the nivolumab + AVD group compared with 160 patients (34%) in the BV + AVD group. The reason there was a higher incidence of neutropenia in the nivolumab + AVD group was that the use of G-CSF was required for patients receiving BV + AVD but was optional in patients receiving nivolumab + AVD.
AEs of grade 3 or higher, except neutropenia, occurred with a similar or greater frequency in the BV + AVD group compared to the nivolumab + AVD group.
Neutropenia of grade 3 or higher occurred in 232 patients (48%) in the nivolumab + AVD group compared with 126 patients (26%) in the BV + AVD group.
The incidences of febrile neutropenia (5.8% versus 6.9%), sepsis (1.7% versus 3.4%), and infection and infestation (3.7% versus 2.5%) were similar in both groups, but these events occurred more frequently in older adults (18% in the group of patients aged 12 to 17 years; 20% in the group aged 18 to 60 years; and 33% in the group older than 60 years). The authors of the study noted that these events occurred more often in patients who received BV + AVD; however, data for each group were not reported.
Peripheral sensory neuropathy of any grade occurred in 139 patients (29%) in the nivolumab + AVD group and 266 patients (56%) in the BV + AVD group; 1% of those in the nivolumab + AVD group and 8% of those in the BV + AVD group had peripheral sensory neuropathy of grade 3 or higher.
The most common immune-related AEs that occurred more frequently in the BV + AVD group were increased alanine aminotransferase (33% versus 42%), increased aspartate aminotransferase (26% versus 34%), and diarrhea (21% versus 27%). Those that occurred more frequently in the nivolumab + AVD group were hypothyroidism (3% versus 0%) and hyperthyroidism (7% versus 0.6%). Occurrences of arthralgia (13% versus 12%), pneumonitis (2% versus 3%), and rash (15% versus 15%) were similar in both groups.
Death due to infection or sepsis occurred in 4 patients (0.8%) in the nivolumab + AVD group and 6 patients (1.2%) in the BV + AVD group.
Serious AEs and withdrawal due to AEs were not reported.
Discussion
Efficacy
A patient group (Lymphoma Canada) highlighted that the majority of patients surveyed believe it is very important to have a choice in their treatment decision and a variety of treatment options to choose from. According to those patients, important factors for novel treatments include longer life span, longer remission, better quality of life, and fewer side effects. Side effects of the currently available treatments and their impacts on patient quality of life remain a significant issue.
The S1826 trial9 demonstrated that nivolumab + AVD improved PFS compared with BV + AVD in adolescent and adult patients with advanced-stage cHL. EFS, which was defined similarly to PFS but included nonprotocol antilymphoma therapy as an event, was also higher in patients receiving nivolumab + AVD compared with those receiving BV + AVD. The improvement of PFS with nivolumab + AVD was consistent across subgroups (i.e., age, IPS group, stage of disease, and symptoms). The clinical experts and the clinician group input submissions indicated that the magnitude of the absolute between-group difference at 2 years was clinically meaningful. No CIs for the between-group differences were reported, so it is not possible to ascertain whether all values within the CI would be clinically important. Some sources of uncertainty included the interim nature of the findings (potential for overestimation of the magnitude of effect), open-label assessment of PFS by the investigator, and relatively short follow-up. A difference between groups in OS was not observed in the current findings of the trial due to the short time of follow-up during which very few events accrued, as noted by the clinical expert. However, the clinical experts considered that the PFS benefit was meaningful on its own and noted that it might be difficult to show an OS benefit given that several salvage therapies are available. The trial is ongoing, and the reported findings were based on preplanned interim analyses. The final OS analysis is planned after 61 events have accrued. HRQoL, an important patient-reported outcome when comparing treatments, was preplanned, but it has not yet been reported.
Harms
In the S1826 trial,9 the nivolumab + AVD regimen had a better side-effect profile compared with BV + AVD. In the nivolumab + AVD group, fewer patients discontinued treatment early and fewer deaths and lower immune-related toxic effects occurred during treatment. Death due to infection or sepsis were similar in both groups. The clinician group input noted that the toxicity of the nivolumab + AVD regimen was low, which resulted in better tolerance in the older age group. Very few patients (< 1%) in both groups received end-of-treatment radiation therapy, a significant reduction in the use of radiation compared with other contemporary regimens. The clinical experts explained that it had been recognized up front in the study that radiation therapy was not going to be required in either the pediatric or adult groups unless there was PET residual positive disease at the end of the 6 cycles, which was rarely seen in the trial. Most AEs, except neutropenia, more frequently occurred in BV + AVD. The reason for the lower frequency of neutropenia observed in the BV + AVD group might be due to the prophylactic use of G-CSF required for patients receiving BV + AVD compared with the optional use of G-CSF for patients receiving nivolumab + AVD. However, the higher frequency of neutropenia in the nivolumab + AVD was not associated with a higher incidence of infection, sepsis, and febrile neutropenia compared with BV + AVD. The clinical experts explained that G-CSF was mandated in BV + AVD because BV is known to be myelosuppressive and the higher rates of infection with BV treatment are not insignificant. Nivolumab is not expected to be myelosuppressive.
It appears that the treatment regimen under review (i.e., nivolumab + AVD) satisfies the unmet need in terms of lower toxic effects compared to BV + AVD and results in improved 2-year PFS and EFS due to lower rates of relapsed or refractory disease in the nivolumab + AVD group compared with the BV + AVD group. However, it remains unclear to what extent the nivolumab + AVD regimen could prolong survival, prevent relapse and refractory disease, and improve HRQoL compared with other comparators, including BV + AVD, because these outcomes have not been either studied or reported. Evidence regarding the clinical efficacy and safety of nivolumab + AVD compared with other comparators of interest, especially those currently used in the pediatric population, was not identified.
The patient group input from Lymphoma Canada surveyed 2 patients, both male, who were treated with nivolumab + AVD. One patient had stage III cHL, and the other had stage IV cHL. One patient had been in remission, while the other had relapsed. The main side effects reported by these patients included decreased appetite, nausea and/or vomiting, headache, and fatigue. Both patients indicated that fatigue was the most challenging symptom. Both patients indicated that fear of progression or relapse, anxiety, and worry were major psychological impacts. Despite those concerns, both patients indicated that the therapy was very tolerable with fewer side effects, primarily fatigue, and that they would recommend the therapy to other patients with advanced cHL, despite 1 patient having a relapse. The patient group highlighted that there is a need to have more treatment options so that patients can choose a therapy that aligns with their personal goals in collaboration with their medical care team.
Conclusion
The evidence from a randomized phase III trial (S1826)9 assessing the efficacy and safety of nivolumab + AVD compared with BV + AVD in adolescents and adults with previously untreated stage III or IV cHL suggests that nivolumab + AVD improved PFS and had a better side-effect profile. The duration of follow-up in this trial was relatively short, and secondary analyses and subgroup analyses did not have adequate statistical power. Longer follow-up would provide a more definitive conclusion regarding the long-term relative clinical efficacy and safety of the regimen. The clinical experts highlighted that the greatest risk for relapse is within the first 2 years post-therapy (75% to 80%). Therefore, although further follow-up is warranted, the clinical experts indicated that the 2-year follow-up in the trial is relevant for the majority of patients, and the significant differences in PFS and EFS between groups were clinically meaningful. Results of OS were uncertain due to short follow-up during which few events accrued; it will take several years for OS data to mature. While HRQoL was measured and the outcome is important to patients, the results were not reported. Based on the evidence from the S1826 trial, the clinical expert input and clinician group input suggests that nivolumab + AVD will become the standard of care for untreated stage III and IV cHL. However, evidence on the clinical benefit and harm of nivolumab + AVD compared with other comparators is still unavailable.
Economic Review
The economic review consisted of a cost comparison of nivolumab + AVD for the treatment of patients with previously untreated stage III or IV classic Hodgkin lymphoma. In adults, comparators included BV + AVD, ABVD, and BEACOPP, and in pediatric patients, comparators were BV + AVEPC and ABVE-PC.
Based on the price of nivolumab from a previous CADTH review,13 in the adult patient population, nivolumab is expected to have a per-patient cost of $9,387 per 28-day cycle (Supplemental Material, Appendix 8, Table 12). In the adult patient population, nivolumab + AVD is expected to have a per-patient cost of $11,611 per 28-day cycle (Supplemental Material, Appendix 8 Table 12). In the adult population, BV + AVD, ABVD, and BEACOPP are expected to have per-patient costs of $21,584, $3,902, and $7,653 per 28-day cycle, respectively (Supplemental Material, Appendix 8, Table 12). Therefore, at public list prices, nivolumab + AVD is associated with incremental savings of $9,973 per patient per 28-day cycle compared with BV + AVD. Compared with ABVD and BEACOPP, at public list prices, nivolumab + AVD is associated with incremental costs of $7,709 and $3,956 per patient per 28-day cycle, respectively. As such, in the adult patient population, the reimbursement of nivolumab + AVD for the treatment of previously untreated stage III or IV classic Hodgkin lymphoma is expected to result in lower overall drug acquisition costs compared with BV + AVD and to result in higher overall drug acquisition costs compared with ABVD and BEACOPP.
Based on the price of nivolumab from a previous CADTH review13 in the pediatric patient population, nivolumab is expected to have a per-patient cost of $7,822 per 28-day cycle (Supplemental Material, Appendix 8, Table 13). In the pediatric patient population, nivolumab + AVD is expected to have a per-patient cost of $9,189 per 28-day cycle (Supplemental Material, Appendix 8, Table 13). In the pediatric population, BV + AVEPC and ABVE-PC are expected to have per-patient costs of $21,140 and $3,021 per 28-day cycle, respectively (Supplemental Material, Appendix 8, Table 13). Therefore, at public list prices, nivolumab + AVD is associated with incremental savings of $11,950 per patient per 28-day cycle compared with BV + AVEPC. Compared with ABVE-PC, at public list prices, nivolumab + AVD is associated with incremental costs of $6,169 per patient per 28-day cycle. As such, in the pediatric patient population, the reimbursement of nivolumab plus AVD for the treatment of previously untreated stage III or IV classic Hodgkin lymphoma is expected to result in lower overall drug acquisition costs compared with BV + AVEPC and result in higher overall drug acquisition costs compared with ABVE-PC.
Additional items for consideration are provided in the following bullets:
According to the CDA-AMC Clinical Review, evidence from a randomized phase III trial (S1826)9 assessing the efficacy and safety of nivolumab + AVD compared with BV + AVD in adolescents and adults with previously untreated stage III or IV cHL suggested that nivolumab + AVD improved PFS and had a better side-effect profile. Results of OS were uncertain due to the short follow-up during which few events occurred. No evidence was identified regarding the comparative efficacy and safety of nivolumab + AVD versus other available comparators.
No health care resource use outcomes were reported in the clinical trial.9
As of March 2025, nivolumab is only available as a brand-name product in Canada.
According to clinical expert feedback received by Canada’s Drug Agency for this review, use of concurrent G-CSF is optional for nivolumab + AVD. Expert feedback noted that some use of G-CSF with nivolumab + AVD occurred in the clinical trial9 and that concurrent use of G-CSF may occur in pediatric practice. Expert feedback noted that, in adult clinical practice, G-CSF would only be used with nivolumab + AVD in instances of neutropenia before subsequent cycles or if patients are experiencing fevers or infections. However, G-CSF is expected to be used concurrently with BV + AVD (it was required for use with BV + AVD in the clinical trial).9 Not routinely requiring G-CSF administration for nivolumab + AVD would result in lower drug acquisition costs for nivolumab + AVD compared with BV + AVD.
No Canadian cost-effectiveness studies were identified based on a literature search conducted on March 26, 2025.
Conclusion
The reimbursement of nivolumab + AVD for the treatment of patients with previously untreated stage III or IV classic Hodgkin’s lymphoma is expected to result in both lower overall drug acquisition costs (compared with BV + AVD in adult patients and BV + AVEPC in pediatric patients) and higher overall drug acquisition costs (compared with ABVD and BEACOPP in adult patients and ABVE-PC in pediatric patients) at publicly available list prices. Based on the Clinical Review conclusions, compared with BV + AVD, nivolumab + AVD is expected to result in improved PFS and safety. However, no conclusions could be made regarding OS, and HRQoL outcomes were not reported. No evidence was identified regarding the comparative efficacy and safety of nivolumab + AVD versus other available comparators.
Given that nivolumab + AVD is associated with lower drug acquisition costs compared with BV + AVD at public list prices and incremental benefit in terms of PFS and safety, compared with BV + AVD, nivolumab + AVD may represent a cost-effective treatment option. If, based on confidential prices, nivolumab + AVD has a higher cost relative to BV + AVD, then a cost-effectiveness analysis would be required to determine whether a price premium is justified.
In the comparison of nivolumab + AVD with BV + AVEPC, nivolumab + AVD is associated with lower drug acquisition costs and unknown clinical benefit. To ensure cost-effectiveness, the price of nivolumab + AVD should be priced no higher than that of BV + AVEPC.
In comparison to other available regimens (i.e., ABVD and BEACOPP in adult patients and ABVE-PC in pediatric patients), reimbursing nivolumab + AVD is associated with higher drug acquisition costs and unknown clinical benefit. Similar to the clinical evidence base, no economic evidence was identified regarding the comparative cost-effectiveness of nivolumab + AVD versus other available comparators. Based on clinical expert feedback for this review, these other available regimens are less commonly used in clinical practice in Canada compared with BV-based regimens; however, it is expected that if nivolumab + AVD is reimbursed, it may still displace some use of non–BV-based regimens.
References
1.Lymphoma Canada. Understanding Hodgkin lymphoma: a patient's guide to Hodgkin lymphoma. 2020. Accessed January 21, 2025. https://www.lymphoma.ca/wp-content/uploads/2020/05/20200430-HL-WEB.pdf
2.Canadian Cancer Society. Hodgkin lymphoma statistics. 2024. Accessed January 21, 2025. https://cancer.ca/en/cancer-information/cancer-types/hodgkin-lymphoma/statistics
3.Evens AM, Antillón M, Aschebrook-Kilfoy B, Chiu BC. Racial disparities in Hodgkin's lymphoma: a comprehensive population-based analysis. Ann Oncol. 2012;23(8):2128-2137. doi: 10.1093/annonc/mdr578 PubMed
4.Canadian Cancer Society. Treatments for classical Hodgkin lymphoma. Accessed January 21, 2025. https://cancer.ca/en/cancer-information/cancer-types/hodgkin-lymphoma/treatment/classical
5.Ansell SM, Radford J, Connors JM, et al. Overall Survival with Brentuximab Vedotin in Stage III or IV Hodgkin's Lymphoma. N Engl J Med. 2022;387(4):310-320. doi: 10.1056/NEJMoa2206125 PubMed
6.Connors JM, Jurczak W, Straus DJ, et al. Brentuximab Vedotin with Chemotherapy for Stage III or IV Hodgkin's Lymphoma. N Engl J Med. 2018;378(4):331-344. doi: 10.1056/NEJMoa1708984 PubMed
7.Kelly KM, Friedberg JW. Classic Hodgkin Lymphoma in Adolescents and Young Adults. J Clin Oncol. 2024;42(6):653-664. doi: 10.1200/jco.23.01799 PubMed
8.Borchmann P, Ferdinandus J, Schneider G, et al. Assessing the efficacy and tolerability of PET-guided BrECADD versus eBEACOPP in advanced-stage, classical Hodgkin lymphoma (HD21): a randomised, multicentre, parallel, open-label, phase 3 trial. Lancet. 2024;404(10450):341-352. doi: 10.1016/s0140-6736(24)01315-1 PubMed
9.Herrera AF, LeBlanc M, Castellino SM, et al. Nivolumab+AVD in Advanced-Stage Classic Hodgkin's Lymphoma. N Engl J Med. 2024;391(15):1379-1389. doi: 10.1056/NEJMoa2405888 PubMed
10.National Cancer Institute (NCI). NCT03907488: Immunotherapy (Nivolumab or Brentuximab Vedotin) Plus Combination Chemotherapy in Treating Patients With Newly Diagnosed Stage III-IV Classic Hodgkin Lymphoma. ClinicalTrials.gov; 2019. Updated March 25, 2025. Accessed March 31, 2025. https://www.clinicaltrials.gov/study/NCT03907488
11.Bassler D, Briel M, Montori VM, et al. Stopping randomized trials early for benefit and estimation of treatment effects: systematic review and meta-regression analysis. JAMA. 2010;303(12):1180-7. doi: 10.1001/jama.2010.310 PubMed
12.Bröckelmann PJ, Muller H, Fuchs M, et al. Correlation between progression-free and overall survival in patients with Hodgkin lymphoma: a comprehensive analysis of individual patient data from randomized German Hodgkin Study Group (GHSG) trials. Ann Oncol. 2025;36(4):393-402. doi: 10.1016/j.annonc.2024.12.009 PubMed
13.CADTH. Reimbursement Review: nivolumab (Opdivo) in combination with ipilimumab (Yervoy). Can J Health Technol. 2021;1(9). doi: 10.51731/cjht.2021.168
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.