Drugs, Health Technologies, Health Systems
Reimbursement Review
Trabectedin
Requester: Public drug programs
Therapeutic area: Soft tissue and uterine leiomyosarcoma
Summary
What Is Soft Tissue and Uterine Leiomyosarcoma?
Soft tissue sarcomas are a heterogeneous group of rare tumours in muscle, adipose, fibrous, cartilage, nerve, and vascular tissue. Leiomyosarcoma is the most frequent subtype of soft tissue sarcoma that originates in smooth muscle, such as the gastrointestinal tract, large blood vessels, or the uterus, and it commonly spreads to the liver, lung, upper abdomen, and pelvis. The rarity and heterogeneity of leiomyosarcoma impact patients’ ability to receive timely and accurate diagnoses; access support services, including specialized health care providers; and receive timely and appropriate treatment. Patients with soft tissue sarcoma commonly present with a gradually enlarging, painless mass and may develop pain or symptoms due to compression by the mass. Patients with uterine leiomyosarcoma present with a uterine mass and can experience no symptoms to abnormal uterine bleeding, abdominal distension or pain, and pelvic pain or pressure.
In 2024, it was estimated that 1,700 people in Canada would be diagnosed with soft tissue sarcoma and 360 people would die from it. The incidence of uterine leiomyosarcoma was estimated to be 0.86 per 100,000 people based on data from Norway collected between 2000 and 2012.
What Are the Treatment Goals and Current Treatment Options for Advanced Unresectable or Metastatic Uterine or Soft Tissue Leiomyosarcoma?
Patients and clinicians identified a need for treatments for leiomyosarcoma that prolong survival and time to remission, reduce the likelihood of recurrence, and improve health-related quality of life. Other important outcomes identified through clinician input were decreasing disease burden and improving patient symptoms.
Current treatment options for advanced unresectable or metastatic uterine or soft tissue leiomyosarcoma include doxorubicin monotherapy, gemcitabine-docetaxel, and doxorubicin-ifosfamide.
What Is Trabectedin and Why Did We Conduct This Review?
Trabectedin is a drug that is administered by IV infusion. Health Canada has approved trabectedin in combination with pegylated liposomal doxorubicin for the treatment of patients with platinum-sensitive ovarian cancer for whom 1 first-line platinum-based chemotherapy regimen, including adjuvant therapy, has failed, and who are not expected to benefit, are ineligible or not willing to receive retreatment with platinum-based chemotherapy. Health Canada has also approved trabectedin for the treatment of patients with metastatic liposarcoma or leiomyosarcoma after failure of prior anthracycline and ifosfamide chemotherapy.
At the request of the participating public drug programs, we reviewed trabectedin in combination with doxorubicin to inform a recommendation on whether it should be reimbursed for adult patients with advanced unresectable or metastatic uterine or soft tissue leiomyosarcoma.
How Did We Evaluate Trabectedin?
We reviewed the clinical evidence on the beneficial and harmful effects and compared the costs of trabectedin-doxorubicin versus other treatments used in Canada for advanced unresectable or metastatic uterine or soft tissue leiomyosarcoma in adults.
The clinical evidence was identified through systematic searches for available studies.
The review was also informed by 1 patient group submission and 1 clinician group submission in response to our call for input and by input from the participating public drug programs around issues that may impact their ability to implement a recommendation. We consulted 2 medical oncologists as part of the review process.
What Did We Find?
Clinical Evidence
We reviewed the following clinical evidence:
One randomized controlled phase III open-label trial (LMS04) comparing trabectedin-doxorubicin with doxorubicin in 150 patients with previously untreated advanced or metastatic uterine or soft tissue leiomyosarcoma.
When comparing the use of trabectedin-doxorubicin versus doxorubicin:
Trabectedin-doxorubicin demonstrated an improved progression-free survival by blinded independent central review and likely had superior effectiveness to doxorubicin in the median time to overall survival and improved survival at 24 months. The magnitude of effects is uncertain due to missing data for calculating group differences for key estimands, and the confidence interval for overall survival indicated the possibility of no difference between treatment groups.
The evidence was insufficient to demonstrate a difference in objective response rate (ORR) between the treatment groups. The number of patients with complete response, the number of patients with ORR, and the absolute between-group difference in ORR were not reported.
There was no evidence to inform how trabectedin-doxorubicin compares with gemcitabine-docetaxel or doxorubicin-ifosfamide.
There was no evidence to inform how trabectedin-doxorubicin impacts patients’ health-related quality of life.
The safety profile of trabectedin-doxorubicin was as expected, with no new safety signals.
Economic Evidence
Reimbursing trabectedin-doxorubicin for advanced unresectable or metastatic uterine or soft tissue leiomyosarcoma in adults is expected to increase costs to the public drug programs.
Abbreviations
AE
adverse event
BICR
blinded independent central review
CDA-AMC
Canada’s Drug Agency
CI
confidence interval
DAC
Drug Advisory Committee
ECOG
Eastern Cooperative Oncology Group
G-CSF
granulocyte colony-stimulating factor
HR
hazard ratio
HRQoL
health-related quality of life
IQR
interquartile range
OH (CCO)
Ontario Health (Cancer Care Ontario)
ORR
objective response rate
OS
overall survival
PFS
progression-free survival
RECIST
Response Evaluation Criteria in Solid Tumours
Background
Introduction
The objective of the clinical review is to review and critically appraise the evidence on the beneficial and harmful effects of trabectedin 1.1 mg/m2 in combination with doxorubicin (trabectedin-doxorubicin henceforth) for the first-line treatment of advanced unresectable or metastatic uterine or soft tissue leiomyosarcoma in adults. The focus will be placed on comparing trabectedin-doxorubicin to relevant comparators and identifying gaps in the current evidence. The economic review consists of a cost comparison for trabectedin-doxorubicin compared with relevant comparators for the same population. The comparators considered relevant to the reviews were doxorubicin monotherapy, gemcitabine-docetaxel, and doxorubicin-ifosfamide.
Trabectedin was previously reviewed by Canada’s Drug Agency (CDA-AMC) for the treatment of patients with liposarcoma or leiomyosarcoma after failure of prior anthracycline and ifosfamide chemotherapy. A recommendation to not reimburse trabectedin was issued in August 2016 due to the pan-Canadian Expert Review Committee conclusion that, compared with dacarbazine, there was no net clinical benefit of trabectedin based on a very modest progression-free survival benefit, no detectable overall survival benefit, moderate but not insignificant toxicities, and limited quality of life data; the pan-Canadian Expert Review Committee also noted that, compared with dacarbazine, trabectedin was not cost-effective in the indicated population.1
Health Canada has approved trabectedin in combination with pegylated liposomal doxorubicin for the treatment of patients with platinum-sensitive ovarian cancer for whom 1 first-line platinum-based chemotherapy regimen, including adjuvant therapy, has failed, and who are not expected to benefit, are ineligible or not willing to receive retreatment with platinum-based chemotherapy.2 Trabectedin has also been approved for the treatment of patients with metastatic liposarcoma or leiomyosarcoma after failure of prior anthracycline and ifosfamide chemotherapy.2
This review focuses on trabectedin-doxorubicin as first-line treatment for the advanced unresectable or metastatic uterine or soft tissue leiomyosarcoma.
Table 1: Information on the Drug Under Review and on the CDA-AMC Review
Item | Description |
|---|---|
Information on the drug under review | |
Drug (product) | Trabectedin, 1 mg per vial, sterile lyophilized powder for IV injection through a central line |
Relevant Health Canada indication | Not applicable |
Mechanism of action | Antineoplastic agent that binds to DNA and interferes with DNA transcription and repair, disrupting cell cycle processes and inducing apoptosis |
Recommended dosage |
|
Data protection status | Data protection end date: May 13, 2018 |
Status of generic drugs or biosimilars | No generics on the market; 1 generic application under review by Health Canada (submission accepted: April 2021) No current biosimilar on the market |
Information on the CDA-AMC review | |
Requester | Oncology Working Group |
Indication under consideration for reimbursement | Trabectedin in combination with doxorubicin for the first-line treatment of advanced unresectable or metastatic uterine or soft tissue leiomyosarcoma in adults |
CDA-AMC = Canada’s Drug Agency.
Sources of Information
The contents of the clinical review report are informed by studies identified through systematic literature searches and input received from interested parties.
Calls for patient group, clinician group, and industry input are issued for each Non-Sponsored Reimbursement Review. We received 1 patient group submission from the Canadian Cancer Society and 1 clinician group submission from Ontario Health (Cancer Care Ontario) (OH [CCO]) Gynecological Cancer Drug Advisory Committee (DAC). The Canadian Cancer Society gathered input via interviews with 6 patients and 3 caregivers. OH (CCO) Gynecological Cancer DAC gathered input via conference call and emails (number of clinicians was not specified). The full submissions received are available on the project landing page in the consolidated input document.
Input from patient and clinician groups is considered throughout the review, including in the selection of outcomes to include in the clinical review and in the interpretation of the clinical evidence. Relevant patient and clinician group input and industry input are summarized in the Disease Background, Current Management, and Unmet Needs and Existing Challenges sections.
The drug programs provide input on each drug being reviewed through the Reimbursement Review process by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted for this review are summarized and provided to the expert committee in a separate document.
Each review team includes at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process. Two medical oncologists with expertise in the diagnosis and management of leiomyosarcoma participated as part of the review team, with representation from Calgary and Winnipeg.
Disease Background
Soft tissue sarcomas are a heterogeneous group of rare tumours in muscle, adipose, fibrous, cartilage, nerve, and vascular tissue.3 Leiomyosarcoma is the most frequent subtype of soft tissue sarcoma.4 It starts in smooth muscle such as the gastrointestinal tract, large blood vessels, or the uterus.5 Common sites of metastases include the liver, lung, upper abdomen, and pelvis; less common sites of involvement include bone and the brain.5 Unresectable tumours are those involving vital structures or tumours whose removal would cause unacceptable morbidity.4 In 2024, it was estimated that 1,700 people in Canada would be diagnosed with soft tissue sarcoma and 660 people would die from it.6 The incidence of leiomyosarcoma increases with age, except for uterine leiomyosarcoma, which occurs most commonly in perimenopausal individuals. The incidence of uterine leiomyosarcoma, based on a population in Norway from 2000 to 2012, was estimated as 0.86 per 100,000 people.7
Patients with soft tissue sarcoma commonly present with a gradually enlarging, painless mass and may develop pain or symptoms due to compression by the mass, such as paresthesia or edema.5 In patients with suspected soft tissue sarcoma, evaluation involves a physical examination to determine clinical signs and symptoms; radiographic imaging to determine tumour etiology, extent, and metastatic disease; and biopsy for histologic diagnosis and treatment planning.5 Prognostic factors associated with improved outcomes in metastatic soft tissue sarcoma include female sex, younger age, good performance status, lack of bone or liver metastases, low-grade histology, and longer disease-free interval between initial diagnosis and metastatic disease.3 The 5-year overall survival (OS) of metastatic soft tissue sarcoma is estimated to range from 15% to 25% and the median survival time is 12 to 24 months.3,8
Uterine leiomyosarcoma is a rare uterine malignancy arising from smooth muscle of the uterus wall; they are typically large (> 10 cm) masses with soft, fleshy cut surfaces that have areas of hemorrhage and necrosis.9,10 Symptoms of uterine sarcomas (e.g., leiomyosarcoma) include a uterine mass, abnormal uterine bleeding, abdominal distension or pain, and/or pelvic pain or pressure, although some patients may be asymptomatic.10 Diagnosis of uterine leiomyosarcoma is made following hysterectomy or myomectomy for presumed benign uterine leiomyomas;9 the prevalence of unexpected leiomyosarcoma at the time of surgery for presumed symptomatic leiomyomas ranges from fewer than 1 to 13 per 10,000 surgeries.10 The clinical experts consulted for this review noted that inadequate surgery (e.g., morcellation) should be avoided as it is detrimental to patient care. However, because the differential diagnosis of benign conditions (e.g., distinguishing smooth muscle tumour of uncertain malignant potential [STUMP] benign leiomyoma from uterine leiomyosarcoma) is challenging despite biopsy with CT or MRI, consultation with a multidisciplinary care team is warranted, according to the clinical experts. Because approximately 30% of patients with newly diagnosed uterine leiomyosarcoma present with distant metastatic disease, it is recommended that all patients undergo imaging (with CT, MRI, or PET scan) to evaluate for metastatic disease.9 Uterine leiomyosarcoma is an aggressive tumour with a high risk of relapse and a poor prognosis, regardless of disease stage at presentation.9 Prognostic factors associated with OS for patients with uterine leiomyosarcoma include patient age, tumour size, grade, local extension, distant metastasis, and mitotic rate.9 The 5-year disease-specific survival of patients with uterine leiomyosarcoma is approximately 66%; it was estimated to be 76%, 60%, 45%, and 29% for stage I, II, III, and IV, respectively.9
Patients with leiomyosarcoma and their caregivers expressed that the rarity and heterogeneity of the disease have impacted their ability to receive timely and accurate diagnosis; access support services, including specialized health care providers; and receive timely and appropriate treatment. In addition to delayed diagnoses spanning years leading to advanced disease at detection, the variability in tumour presentation and behaviour can additionally complicate the diagnosis process by requiring multiple tests and biopsies, delaying treatment initiation, and requiring frequent adjustment to treatment plans and ongoing monitoring. The disease itself and the debilitating effects of available treatments impact patients’ physical health, mental health, ability to work, ability to participate in activities of daily living, relationships with family and friends, overall quality of life, and financial stability.
Current Management
Treatment Goals
Patients seek more effective treatments that improve survival, prolong remission, and improve health-related quality of life (HRQoL) while having minimal side effects. Patients and their caregivers also desire treatments that are widely accessible, can be administered locally, and are affordable.
The clinical experts consulted for this review and clinician groups echoed that patients with advanced unresectable or metastatic uterine or soft tissue leiomyosarcoma need treatments that decrease disease burden, improve symptoms, improve quality of life, and prolong survival.
Current Treatment Options
The decision to initiate therapy in patients with advanced unresectable metastatic soft tissue sarcoma is based on pace of disease progression and patient symptoms.3 Selection of initial therapy may be based on tumour histology and sensitivity to specific therapies, patient characteristics, toxicity profiles, and clinician or institutional preferences.3 Patients with unresectable tumours can be treated primarily with radiation therapy, chemoradiation, chemotherapy, or regional limb therapy.4 Tumours that become resectable with acceptable functional outcomes following primary treatment can be treated with surgery followed by radiation therapy with or without postoperative chemotherapy.4 There is no evidence to support optimal management of patients with metastatic disease, so treatment may be based on factors including performance status, patient preferences, location and volume of metastatic disease, and treatment availability.4 Patients with limited metastasis confined to a single organ and limited tumour bulk amenable to local therapy should receive primary tumour management.4 For patients with disseminated metastases, disease of small volume and slow growth may be managed using a “watchful waiting” approach, whereas symptomatic disease may be treated with palliative radiation therapy, surgery, or chemotherapy.4 Patients with uterine leiomyosarcoma who have intra-abdominal involvement of disease (stage III) or distant metastases (stage IV) are at high risk of disease progression following surgery alone; both surveillance and adjuvant chemotherapy are reasonable options because improved survival has not been established with the latter,9 and primary tumour removal should be considered for metastatic uterine leiomyosarcoma that is symptomatic.
For patients with advanced, unresectable, or metastatic soft tissue sarcoma, treatment is based on palliative intent.3,9 Chemotherapy options include single drugs (e.g., commonly pegylated liposomal doxorubicin or gemcitabine) or combination anthracycline-based regimens (e.g., doxorubicin plus ifosfamide, gemcitabine plus docetaxel, or doxorubicin plus dacarbazine).3,4 Other drugs, including docetaxel, vinorelbine, and temozolomide, have also been evaluated in clinical trials.4 After consideration for potential resection, anthracycline-based regimens may be an option for patients with metastatic soft tissue sarcomas and symptomatic or rapidly progressive disease.3 Single-drug anthracycline may be an alternative for those who cannot tolerate combination therapy (e.g., patients with advanced age, poor Eastern Cooperative Oncology Group [ECOG] performance status, or comorbidities) or have indolent disease that does not require a rapid reduction in tumour burden.3
The same therapies are used for leiomyosarcomas, regardless of primary site.5 Doxorubicin may be an option for individuals who are asymptomatic or have slowly changing metastatic disease, or those who cannot tolerate combination therapy.3 Based on the GeDDis trial, doxorubicin or gemcitabine-docetaxel are both reasonable first-line treatment options with similar efficacy; treatment selection may be dependent on patient factors and preferences.11 According to the clinical experts consulted, doxorubicin, gemcitabine-docetaxel, and doxorubicin-ifosfamide are available and funded in Canada as first-line treatment for leiomyosarcoma.
Unmet Needs and Existing Challenges
Patient Input
The Canadian Cancer Society interviewed 6 patients and 3 caregivers of patients with uterine (n = 5) and soft tissue (n = 2) leiomyosarcoma across Canada (Nova Scotia, Ontario, Alberta, British Columbia) in February 2025. All but 1 patient had metastatic disease. The patient group input detailed the diagnosis journeys of patients and their caregivers, highlighting the challenges of a relatively rare form of cancer. Due to the rarity and complexity of leiomyosarcoma, patients faced challenges including a lack of familiarity and clinical knowledge, delays and difficulties in obtaining a diagnosis, advanced disease at presentation or detection, delays in treatment, lack of standardized treatment protocols and treatment options, and debilitating effects of available treatments. Driven by limited awareness of or experience with leiomyosarcoma among health care providers, patients versed themselves in disease education and research. Patients often struggled with a lack of support services (e.g., patient groups) and specialized health care providers, particularly for those living in rural areas or smaller provinces who needed to consult knowledgeable specialists in other provinces. Moreover, patients commonly found themselves in a role of self-advocacy in all areas, including access to testing, frequency of CT scans, treatments, and referrals. Due to its rarity and variability in initial symptoms, patients experienced challenges in receiving a diagnosis, such as dismissal of symptoms, undergoing multiple tests before a diagnosis of leiomyosarcoma, and misdiagnoses. Once diagnosed, patients faced lengthy wait times or prolonged intervals between scans during which time the tumour may continue to grow. These delays resulted in a more advanced stage of disease, worsening symptoms, poor or worsened prognosis, unnecessary or hazardous procedures, and inadequate treatment. Due to the variability in the type of leiomyosarcoma across individuals and genetic differences within the same type of leiomyosarcoma, sensitivity to specific treatments (e.g., hormone therapy) and response to treatment may vary. Furthermore, within patients, the tumour may change over time (e.g., genetic mutations) and progress or become more aggressive, such that previously effective treatments no longer work. Overall, the variability in tumour presentation and behaviour can complicate the diagnosis process and require multiple tests and biopsies, delay treatment initiation, and require frequent adjustment to treatment plans and ongoing monitoring.
There were significant and multifaceted impacts of leiomyosarcoma on patients’ health, including anxiety (e.g., hypervigilance to new tumours, wait times for procedures, risks and impacts of treatment, duration of treatment effectiveness, or availability of treatment options), reduced ability to participate in physical or mental tasks (e.g., taking care of the home or engaging in previously enjoyable activities), impacted relationships with family and friends, and reduced overall quality of life. Patients’ inability to work (e.g., short-term leave, permanent disability leave, or early retirement) was commonly identified as imposing the heaviest financial burden in addition to the costs of diagnostic procedures (e.g., genomic testing or surgery), chemotherapies, alternative treatments (e.g., naturopathy), travel for treatment, and health insurance. Many patients relied heavily on the health system for resources, and some required government assistance for income. The disease-related costs impacted patients’ ability to maintain financial stability.
Although none of the patients have had experience with trabectedin-doxorubicin due to the absence of clinical trials conducted in Canada, patients shared their experiences of treatments to date and their expectations for this treatment regimen. Over their cancer journey, patients reported having undergone multiple surgeries, chemotherapy (e.g., doxorubicin, gemcitabine-docetaxel, or letrozole), and sometimes radiation treatment, with a high physical burden of disease. Importantly, all patients indicated there was inequitable access to trabectedin-doxorubicin, which is available in the US but not in Canada except potentially in private clinics, and which is not affordable or accessible to most patients. One patient had participated in clinical trials in the US for doxorubicin, 2 types of checkpoint inhibitor, and an antibody-drug conjugate. Side effects of treatments experienced by patients included nerve damage leading to loss of sensation, bodily deformation, neuropathy, constipation, bowel problems, edema, brain fog, and exhaustion. Given the scarcity of treatment options for leiomyosarcoma in Canada and the possibility of exhausting available treatments (e.g., lifetime dose limit of doxorubicin), patients expressed their willingness to tolerate drugs with higher side effect profiles if they offered a significant improvement in survival or quality of life. Importantly, nearly all patients expressed a desire to have access to treatment with trabectedin.
Clinician Input
The clinical experts indicated that currently available treatments for patients with leiomyosarcoma do not significantly modify the disease. Therefore, most patients are exposed to standard of care chemotherapy that is toxic and experience low objective response rates (range of 10% to 40% response rate, with single-drug or doublet therapy, for uterine or soft tissue leiomyosarcoma) and short duration of response. The experts highlighted that patients with advanced or metastatic leiomyosarcoma need treatments that improve response rates, thereby potentially prolonging survival and increasing access to localized therapies such as surgery or radiation. The clinician group echoed the clinical experts in advocating for access to new treatments for leiomyosarcoma that can delay disease progression and reduce treatment intolerance and toxicity in patients with this disease.
Considerations for Using the Drug Under Review
Contents within this section have been informed by input from the clinical experts consulted for the purpose of this review and from clinician groups. The following has been summarized by the review team.
Place in Therapy
According to the clinical experts consulted, trabectedin has a long history in the treatment of sarcomas; in addition to some soft tissue sarcomas (e.g., myxoid liposarcoma or synovial sarcoma), leiomyosarcoma has a demonstrated sensitivity to trabectedin. A key feature of trabectedin is its ability to bind to DNA, kill tumour cells directly, and modulate the tumour microenvironment. Trabectedin’s unique mechanism of action differs from that of first-line cytotoxic chemotherapies such as doxorubicin, gemcitabine, or docetaxel. When used in combination with doxorubicin, trabectedin appears to work synergistically. While not considered to be a curative treatment for leiomyosarcoma, the experts felt that trabectedin would provide an additional treatment option for both combination treatment in the first-line setting and as single-drug treatment in second- or later-line settings. Patients with leiomyosarcoma who are sufficiently fit to receive doublet chemotherapy and who are candidates for surgical resection should be eligible for first-line treatment with trabectedin-doxorubicin; in contrast, those who are not considered eligible for treatment with trabectedin-doxorubicin should be considered for second- or later-line treatment with trabectedin alone. The clinical experts expressed that trabectedin-doxorubicin would be used as a first-line treatment for locally advanced or metastatic leiomyosarcoma, representing a moderate but important shift in the current treatment paradigm.
Patient Population
The clinical experts indicated that any patient who is eligible for treatment with doxorubicin should be eligible for treatment with trabectedin-doxorubicin; generally, this includes those who are deemed fit (e.g., based on adequate baseline organ function and clinician judgment), including those who seek a good response from systemic treatment and who are potential candidates for surgery to resect primary or metastatic disease. Patients who are not considered fit would not be eligible for treatment with trabectedin-doxorubicin. Patients who may be unable to tolerate combination treatment with trabectedin-doxorubicin include those with advanced age, frailty, or comorbidities. The experts remarked that there is difficulty predicting which patients would respond to treatment with trabectedin-doxorubicin; anecdotally, patients with uterine leiomyosarcoma (commonly with homologous recombination deficiency) may experience better response rates compared to patients with soft tissue leiomyosarcoma.
According to the clinical experts, leiomyosarcoma is 1 of the most frequent soft tissue sarcomas (only outnumbered by liposarcoma), making up an estimated 10% to 20% of all soft tissue sarcomas.
Assessing the Response to Treatment
According to the clinical experts, it is standard of care for patients with leiomyosarcoma to be assessed at every clinic visit before each treatment cycle (to evaluate eligibility for treatment or ascertain adverse effects of recent treatment before proceeding with the next cycle) and every 2 to 3 months with imaging (e.g., CT) for response per Response Evaluation Criteria in Solid Tumours (RECIST) criteria, clinical response (i.e., symptoms improvement), quality of life, and OS. The experts emphasize that OS, objective response rate (ORR), and progression-free survival (PFS) were key outcomes to be assessed with leiomyosarcoma treatment.
Discontinuing Treatment
The clinical experts indicated that treatment with trabectedin-doxorubicin should be discontinued in the event of disease progression (both radiographically and clinically) or upon significant treatment intolerance, adding that systemic treatment could also be stopped if local therapy (e.g., surgery or radiation therapy) was successful in eliminating gross disease.
Prescribing Considerations
The clinical experts expressed that patients with leiomyosarcoma should be treated with trabectedin-doxorubicin in a sarcoma-specialized centre with a multidisciplinary group practice by medical oncologists and/or gynecologic oncologists, noting that a community oncology setting may be appropriate for supervising chemotherapy and monitoring adverse events (AEs).
Input from OH (CCO) Gynecological Cancer DAC agreed with the clinical experts that trabectedin-doxorubicin would be an additional option for first-line treatment of patients with leiomyosarcoma (current available treatments include doxorubicin and gemcitabine-docetaxel), particularly for individuals with uterine leiomyosarcoma (due to its associated resistance to chemotherapy and poor disease prognosis) and those with metastatic disease. The clinician group further expressed that if trabectedin were approved, patients currently undergoing treatment for leiomyosarcoma should be able to access trabectedin on a time-limited basis.
Clinical Review
Methods
We conducted a systematic review to identify evidence for trabectedin in combination with doxorubicin as first-line treatment for the treatment of adults with advanced unresectable or metastatic uterine or soft tissue leiomyosarcoma. Studies were selected according to the eligibility criteria in Table 2. Long-term extension studies of included randomized controlled trials, indirect treatment comparisons that adhered to the eligibility criteria except for the study design criteria, and studies that did not meet the eligibility criteria but addressed important gaps were also eligible for inclusion in the systematic review evidence.
Relevant comparators included treatments used in clinical practice in Canada in the patient population under review. We selected outcomes (and follow-up times) for review, considering clinical expert input and patient and clinician group inputs. Selected outcomes are those considered relevant to expert committee deliberations. Detailed methods for literature searches, study selection, data extraction, and risk of bias appraisal are in Appendix 1 of the Supplemental Material (available on the project landing page).
Table 2: Systematic Review Eligibility Criteria
Criteria | Description |
|---|---|
Population | Adults with advanced unresectable or metastatic uterine or soft tissue leiomyosarcoma |
Intervention | Trabectedin-doxorubicin |
Comparator |
|
Outcomes | Efficacy outcomes:
Harms outcomes:
|
Study design | Published phase III and IV RCTs |
AE = adverse event; HRQoL = health-related quality of life; RCT = randomized controlled trial; TEAE = treatment-emergent adverse event.
Clinical Evidence
From the search for primary studies, we identified 750 unique records via the searches of databases and registers, of which we excluded 748 by title and abstract. We screened 2 records by full text and included 2 reports of 1 study. We did not identify reports of long-term extensions of the included study, indirect treatment comparisons, studies addressing gaps (e.g., patient-reported outcomes), or potentially relevant records via other sources.
From the search for indirect treatment comparisons, we identified 68 unique records via the searches of databases and registers, of which none were eligible by title and abstract. No potentially relevant records were identified via other sources.
Systematic Review
Description of LMS04 Study
Study Characteristics
The LMS04 study12,13 was a multicentre (20 sites in France), phase III, open-label randomized controlled trial that enrolled 150 patients from January 18, 2017, to March 21, 2019. Sources of funding for the trial included the manufacturer (PharmaMar). Eligible patients were those with locally advanced or metastatic uterine or soft tissue leiomyosarcoma who were previously untreated with chemotherapy. Patients were randomized in a 1:1 ratio to trabectedin-doxorubicin (n = 74) or doxorubicin alone (n = 76), for up to 6 cycles. Randomization was stratified by tumour site origin (uterine versus soft tissue) and disease stage (locally advanced versus metastatic). Patients without disease progression in the trabectedin-doxorubicin group received trabectedin monotherapy for up to 17 cycles. The primary end point was PFS, defined as the time from randomization to date of progression, or the date of death due to any cause, whichever occurred first; PFS was assessed by blinded independent central review (BICR). Secondary end points included ORR, OS, and safety. ORR was defined as the proportion of patients with complete or partial responses; tumour response was assessed by an investigator. OS was defined as the time from randomization to the date of death from any cause. Safety outcomes included all AEs occurring from the time of randomization until the date of first progression, death, or withdrawal from the trial.
Key inclusion criteria were as follows: adult patients (≥ 18 years) with at least 1 measurable lesion according to RECIST version 1.1 criteria; with an ECOG performance status of 0 or 1 (a 5-point scale; 0 = fully active to 5 = death); and with adequate hematological, liver, and cardiac functions. Patients with a history of malignancy and who were in complete remission for less than 3 years, who had used chemotherapy, or who had central nervous system metastases were excluded. Prior surgery, radiotherapy, and other systemic therapies — including treatments for other malignancies (e.g., hormone therapy for breast cancer) — were permitted.
The study design of LMS04 is depicted in Figure 1. In the trabectedin-doxorubicin group, patients received doxorubicin (60 mg/m2) as a 10- to 15-minute central venous perfusion followed by trabectedin (1.1 mg/m2) as a 3-hour central venous perfusion on day 1. Pretreatment with IV dexamethasone (20 mg) was administered 30 minutes before trabectedin. Pegfilgrastim (6 mg) as a subcutaneous injection was administered on day 2. Trabectedin-doxorubicin was administered every 3 weeks for a maximum of 6 cycles. Those without disease progression after 6 cycles of trabectedin-doxorubicin, with or without surgery, received maintenance treatment with trabectedin alone. Maintenance trabectedin (1.1 mg/m2) was administered every 3 weeks until disease progression or for a maximum treatment duration of 12 months (maximum 17 cycles in maintenance therapy), whichever occurred first. In the doxorubicin group, patients received doxorubicin (75 mg/m2) as a 10- to 15-minute central venous perfusion every 3 weeks for up to 6 cycles. Lenograstim (150 mcg/m2/day) was administered as a subcutaneous injection from day 3 to day 9. Post-treatment (after 6 cycles) surgery to resect residual disease (primary tumour, metastasis, or both primary tumour and metastasis) was permitted in both treatment groups among patients without progressive disease. Dose reductions for hematologic toxicity were permitted for trabectedin and doxorubicin. For trabectedin, a maximum of 2 dose reductions was permitted (from 1.1 mg/m2 to 0.9 mg/m2 or to 0.7 mg/m2) during induction or maintenance treatment. For doxorubicin, a maximum of 2 dose reductions were permitted in the trabectedin-doxorubicin group (from 60 mg/m2 to 50 mg/m2 or to 45 mg/m2) and in the doxorubicin group (from 75 mg/m2 to 60 mg/m2 or to 50 mg/m2). Treatment delays of more than 3 weeks’ duration due to AEs resulted in a withdrawal of the patient from the study. Concomitant treatments (e.g., diphosphonates for bone metastasis, transfusions, hematopoietic growth factors, erythropoietin, analgesics, antibiotics, and antidiarrheals) were permitted. Concomitant treatment with trabectedin was not permitted for potent CYP34A inhibitors (e.g., aprepitant) due to the potential for metabolism of trabectedin to be modified, and for dexrazoxane due to the risk of myelosuppression.
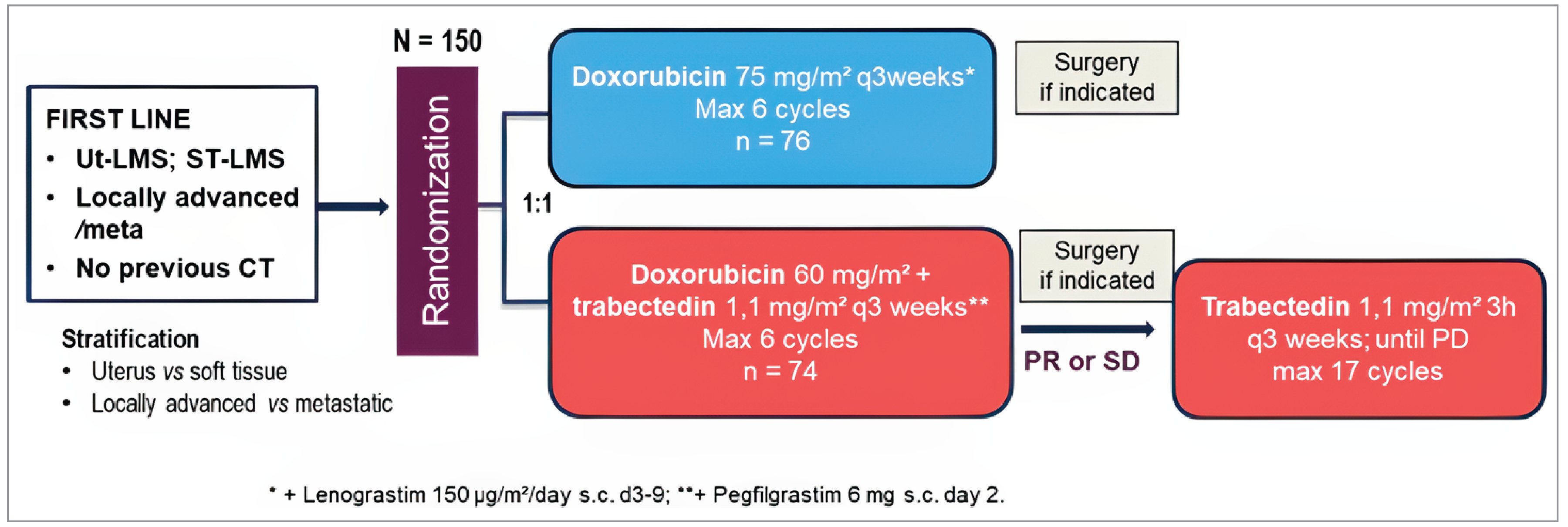
CT = computed tomography; h = hour; max = maximum; PD = progressive disease; PR = partial response; q3 = every 3; SD = stable disease; ST-LMS = soft tissue leiomyosarcoma; Ut-LMS = uterine leiomyosarcoma; vs = versus.
Source: New England Journal of Medicine, Pautier P, Italiano A, Piperno-Neumann S, et al. for the French Sarcoma Group. Doxorubicin-trabectedin with trabectedin maintenance in leiomyosarcoma, 391(9), 789 to 799. Copyright © 2024 Massachusetts Medical Society. Reprinted with permission from Massachusetts Medical Society.
Tumour imaging (thoracic and abdominal-pelvic CT scans or MRI) was performed every 6 weeks during treatment and at 3 weeks after the last cycle. During maintenance, imaging was conducted every 9 weeks until progression or for up to 12 months. During the follow-up period, patients without disease progression had tumour evaluations with physical examination every 9 weeks until disease progression or a maximum of 2 years from randomization. During long-term follow-up of patients without progression, a CT scan and physical examination were performed every 3 months for 12 months and, thereafter, every 6 months until disease progression or the last follow-up visit, approximately 2 years after the last patient was enrolled. ORR included complete response and partial response, taking into consideration the best response until the end of 6 induction cycles (approximately week 18) (details of ORR are in Supplemental Material, Appendix 2). PFS and ORR were evaluated using the RECIST version 1.1 criteria. Patients without follow-up or RECIST evaluation were censored on the date of randomization. Patients who had not experienced an event (disease progression or death) were censored at the last date of data collection. AEs were graded (intensity was scored as toxicity grade of 1 to 5) using the National Cancer Institute’s Common Terminology Criteria for Adverse Events version 4.0 at each cycle (every 3 weeks).
Statistical Testing and Analysis Populations
Sample size calculations for the LMS04 trial were based on the following assumptions to achieve 80% power at a 0.05 alpha level: the PFS event times were assumed to follow an exponential distribution specified with a hazard ratio (HR) of 0.62 and a corresponding 3.7-month difference in median PFS and an assumed dropout rate of 3% over a total study duration of 48 months. A sample size of 150 patients (75 patients per group, 136 events over the follow-up time) was calculated to be sufficient to achieve the desired power.
A stratified Cox proportional hazards model, adjusted for the stratification factors used in randomization, was used to quantify treatment effect on PFS. HRs with corresponding Wald 95% confidence intervals (CIs) and P values were reported. Survival curves were estimated using the Kaplan-Meier, with median survival times presented as a summary statistic. The proportional hazards assumption was graphically assessed based on complementary log-log survival curves visual diagnostics. Subgroup analyses of PFS were conducted to assess treatment effect within groups defined by the randomization factors (i.e., tumour location [uterus or soft tissue] and advanced disease [locally advanced or metastatic]).
Sensitivity analyses of PFS were performed to evaluate the impact of investigator-assessed progression and the impact of missing dates (progression or death) by imputing date of loss to follow-up. OS was analyzed using the same methods as the primary end point, including the treatment arm, and adjusted for stratification variables. Results of secondary end points (median time to event for OS and proportion for response rate) were reported as point estimates with 95% CIs. Toxicities were grouped according to the following major types: myelosuppression (neutropenia, thrombocytopenia, and anemia), liver, cardiac, and nausea or vomiting. AEs of grade 3 or higher were compared with those of grade 0 to 1 or 2.
All randomized patients were included in the intention-to-treat analysis for the efficacy end points. Patients who received at least 1 cycle of the assigned study treatment were included in the safety analysis. No interim analysis was planned. The primary efficacy analyses were conducted at the data cut-off date of August 30, 2021, with updated analyses conducted at the final data cut-off date of January 2023.
Patient Disposition
In the LMS04 trial, information on the number of patients screened for eligibility, including those deemed ineligible, and the reasons for exclusion were not reported. A total of 150 patients were enrolled and randomized to trabectedin-doxorubicin (n = 74) and doxorubicin (n = 76). Sixty-seven patients (45%) had uterine leiomyosarcoma and 83 patients (55%) had soft tissue leiomyosarcoma. Sixty patients (81%) in the trabectedin-doxorubicin group and 54 patients (71%) in the doxorubicin group completed induction therapy for 6 cycles. In the trabectedin-doxorubicin group, 21 patients (28%) completed maintenance treatment with trabectedin. Seventeen patients (23%) did not proceed to maintenance therapy due to disease progression (n = 5), AEs (n = 5), or patient decision (n = 2); reasons were not reported for 5 patients (6.8%). Data on treatment or study discontinuation, including reasons for discontinuation, were not provided.
Baseline Characteristics
At baseline, the median patient age was 61 years (interquartile range [IQR], 52 to 68), with 75% identifying as female and 25% as male. Among patients with available data on ECOG performance status (n = 70 in the trabectedin-doxorubicin group and n = 74 in the doxorubicin group), 67% and 61% respectively, had a score of 0, while 33% and 39% had a score of 1. Disease grade at baseline was reported as grade 1 in 27% and 19% of patients in the trabectedin-doxorubicin and doxorubicin groups, respectively; grade 2 in 27% and 38%; and grade 3 in 29% and 24%. Data on disease grade were missing for 17% and 19% of patients in the respective groups. Most patients had metastatic disease (90%), with 80% presenting with 2 or more sites of metastases. The primary tumour site was in soft tissue in 55% of patient and uterine in 45%. Patients in the trabectedin-doxorubicin and doxorubicin groups had extrauterine disease located in the wall (7% and 10%, respectively), viscera (20% and 21%, respectively), limb (15% and 19%, respectively), retroperitoneum (44% and 24%, respectively), and “other” (unspecified; 15% and 26%, respectively). Patients in the trabectedin-doxorubicin and doxorubicin groups had metastatic disease in the lung (73% and 71%, respectively), liver (32% and 30%, respectively), bone (9% and 22%, respectively), cutaneous site (5% and 1%, respectively), and “other” (not specified; 43% and 34%, respectively).
Treatment Exposure, Concomitant Medications, and Subsequent Treatments
During induction therapy, the median number of treatment cycles in the trabectedin-doxorubicin group (n = 74) was 6 (IQR, 6 to 6), and in the doxorubicin group (n = 76), the median number was also 6 (IQR, 4 to 6). During maintenance therapy in the trabectedin-doxorubicin group, the median number of treatment cycles was 10.5 (IQR, 4 to 17). Thirty-two patients (43%) in the trabectedin-doxorubicin group and 17 patients (22%) in the doxorubicin group required dose reductions during induction therapy. Sixteen patients (22%) in the trabectedin-doxorubicin group required dose reductions during maintenance therapy.
Concomitant medications were not reported in the LMS04 trial.
Fifteen patients (20%) in the trabectedin-doxorubicin group and 6 patients (8%) in the doxorubicin group underwent surgery after 6 cycles of treatment. A total of 15 patients with nonuterine sarcomas and 6 patients with uterine sarcomas underwent surgery (data by treatment group were not reported). Two patients (3%) in the trabectedin-doxorubicin group and 28 patients (38%) in the doxorubicin group received trabectedin as second-line treatment after the trial. Seventeen patients (23%) in the doxorubicin group received trabectedin as a subsequent line of treatment after the trial. The number of patients in the trabectedin-doxorubicin group who received trabectedin as a subsequent line of treatment after the trial was not available.
Critical Appraisal
Internal Validity
The risk of bias in the randomization process was considered low because allocation used central randomization (by interactive web response system) and was stratified by tumour location and disease stage. While baseline characteristics were generally balanced, between-group imbalances were observed in the distribution of extrauterine disease located in the retroperitoneum (44% in the trabectedin-doxorubicin group versus 24% in the doxorubicin group) and the location designated as “other” (15% in the trabectedin-doxorubicin group versus 26% in the doxorubicin group). Additionally, the prevalence of metastatic disease in the lung, liver, and cutaneous site was similar between groups, and imbalances were noted between the trabectedin-doxorubicin group and the doxorubicin group on metastatic disease in bone (9% and 22%, respectively) and other sites (43% and 34%, respectively). However, these imbalances did not appear to systematically favour 1 treatment group over another. A post hoc multivariate analysis adjusting for bone localized disease — due to their known association with poor prognosis — resulted in an HR of 0.42 for PFS (95% CI, 0.3 to 0.6; P < 0.0001), which was consistent with the primary analysis for PFS.12
Due to the open-label trial design, the response outcome measures (e.g., PFS, ORR) and subjective harms were at risk of measurement or reporting bias. However, the potential risk of biased assessments for PFS may be minimal due to the use of the RECIST criteria and BICR. For ORR, there was a risk of subjectivity in radiological assessments and the clinical review, which were assessed by the investigator. No external data monitoring committee was used to assess AEs in the LMS04 study, based on the author’s rationale that no indications of toxicity were found in 10 patients who were monitored during maintenance treatment with trabectedin and that there was prior experience based on patients in the preceding LMS02 trial. There is a risk of biased reporting of subjective AEs (e.g., febrile neutropenia reported by patients); however, the magnitude of bias is unknown.
The primary end point was PFS, and the treatment effect was assessed using the Cox proportional hazards model with adjustment for stratification factors that were used in randomization. Although reasons for censoring were not reported, there is a low risk of bias for informative censoring (reasons for patients lost to follow-up related to prognosis) or biased treatment effects due to censoring. Subgroup analyses for PFS were prespecified and based on stratification variables, thereby preserving randomization. A key limitation of the results is that PFS was used as the primary end point and may be a poor surrogate for OS or HRQoL in this indication.14 The evidence of a treatment correlation between PFS and OS is limited to a specific disease and drug class, and there is generally a weak association between PFS and HRQoL.15 The appropriateness of PFS as a surrogate for OS in the indicated population has not been validated by the FDA, EMA, or the LMS04 study authors. Therefore, a benefit in PFS may not result in direct patient benefits (e.g., improved duration or quality of survival) and may be potentially harmful when toxicities are factored in the weighing of benefits versus risks of treatment.
No imputation of missing data was performed. However, no information was reported for the number of patients who discontinued their assigned treatment or the study, so how this may impact treatment effects is unknown.
External Validity
According to clinical experts, key demographics and disease characteristics at baseline in the LSM04 trial were considered to be representative of patients with advanced unresectable or metastatic uterine and soft tissue leiomyosarcoma in Canada. For example, most patients in the LMS04 trial had good ECOG performance status (score of 0 or 1), and the low prevalence of bone metastasis was consistent with clinical experience. Due to randomization being stratified by factors including disease site (uterine versus soft tissue), the proportion of patients with uterine leiomyosarcoma (45%) was higher than expected by the experts in clinical practice. No information on race distribution was available due to the prohibition of such data collection in France.
According to the clinical experts, patients in clinical practice would be administered trabectedin-doxorubicin in line with the LMS04 trial (i.e., trabectedin 1.1 mg/m2 and doxorubicin 60 mg/m2), including dose modifications as warranted. For doxorubicin, the experts indicated that patients currently receive doxorubicin 75 mg/m2 as monotherapy. Although pegylated liposomal doxorubicin is approved in combination with trabectedin for ovarian cancer,2 experts noted that this formulation is not used — either as monotherapy or in combination — for leiomyosarcoma. While the LMS04 protocol transitioned patients without disease progression to trabectedin monotherapy after 6 cycles, experts stated that in clinical practice, combination therapy may be continued beyond 6 cycles if there is evidence of ongoing response and clinical benefit. Finally, the experts indicated that the timing and frequency of assessments in clinical practice (e.g., approximately every 3 months [4 cycles] during treatment) would be less frequent than those in the trial (e.g., every 6 weeks during induction treatment and every 9 weeks during maintenance and follow-up).
The experts identified doxorubicin, gemcitabine-docetaxel, and doxorubicin-ifosfamide as relevant currently available treatment comparators for trabectedin-doxorubicin, and they estimated that these treatments are used to treat 45%, 45%, and 10%, respectively, of patients with leiomyosarcoma. Therefore, doxorubicin as the comparator in the trial is representative of approximately half of the available treatments for leiomyosarcoma in Canada.
In current practice, patients who are treated with doxorubicin-ifosfamide are given granulocyte colony-stimulating factor (G-CSF) as primary prophylaxis and those treated with doxorubicin monotherapy or gemcitabine-docetaxel are given G-CSF as secondary prophylaxis. Therefore, patients treated with trabectedin-doxorubicin would be given G-CSF as primary prophylaxis per the LMS04 trial, representing a change in prophylactic practices among those currently treated with doxorubicin or gemcitabine-docetaxel. It is unknown whether concomitant treatments are aligned with clinical practice in Canada due to the absence of this information.
Results
Efficacy
Results for outcomes important to this review are presented in Table 3. In the overall population, the follow-up duration was a median 37 months (IQR, 31 to 44) at the primary analysis and a median 55 months (IQR, 49 to 63) at the updated analysis. Key results at the updated analysis include the following:
Trabectedin-doxorubicin is likely to improve PFS by BICR over doxorubicin (Figure 2). Median time to PFS was 12 months (95% CI, 10 to 16) for trabectedin-doxorubicin compared to 6 months (95% CI, 4 to 7) for doxorubicin.
Trabectedin-doxorubicin may improve OS (Figure 3); however, there is uncertainty in the magnitude of the benefit.
Between-group differences in probabilities of PFS and OS at clinically relevant follow-up time points were not reported.
The evidence was insufficient to demonstrate a difference in ORR between the treatment groups. The number of patients with complete response and the number of patients with ORR were not reported. An absolute between-group difference with CI for ORR was not reported.
Although HRQoL was considered important to this review, it was not assessed in the LMS04 study.
Figure 2: Kaplan-Meier Estimate of Progression-Free Survival (ITT Population)
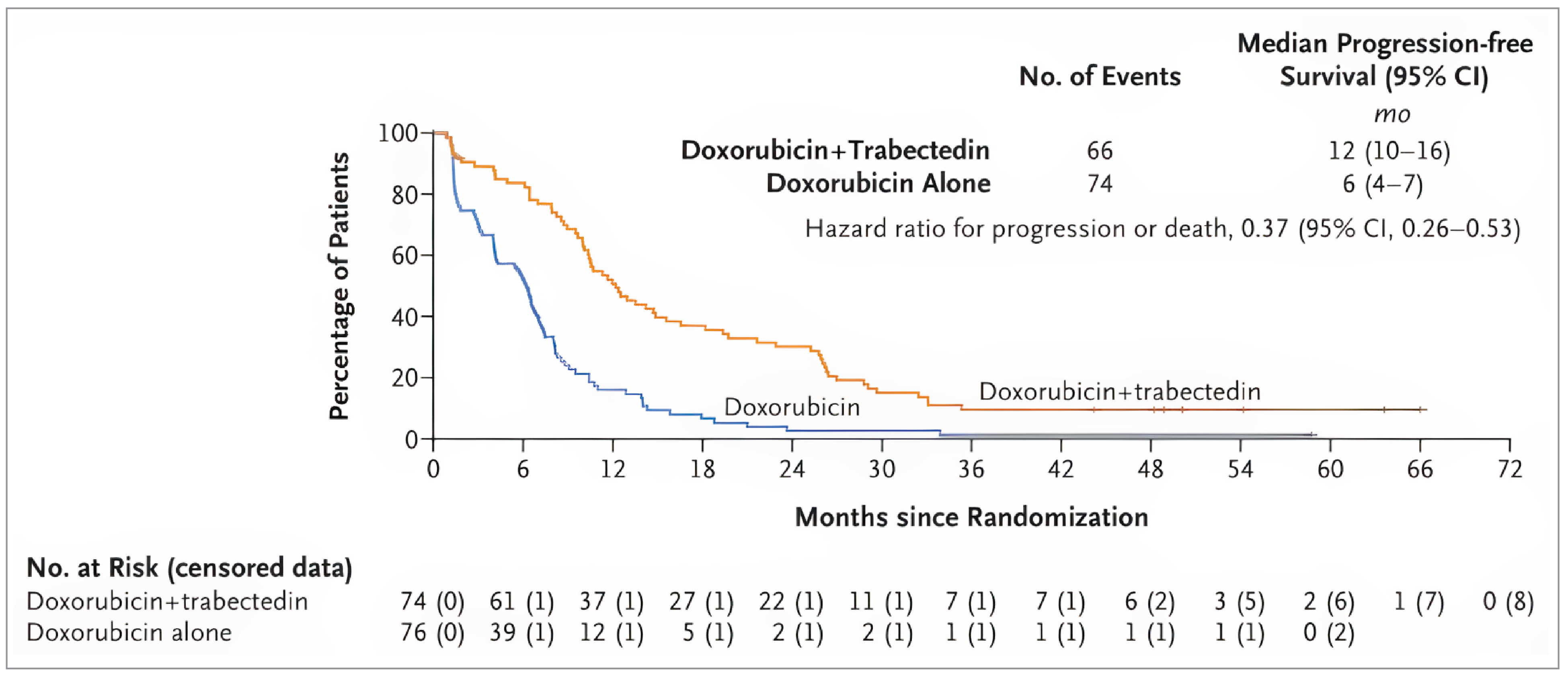
CI = confidence interval; ITT = intention to treat; mo = month; no. = number.
Note: Data were from updated analyses (data cut-off of January 2023).
Source: New England Journal of Medicine, Pautier P, Italiano A, Piperno-Neumann S, et al. for the French Sarcoma Group. Doxorubicin-trabectedin with trabectedin maintenance in leiomyosarcoma, 391(9), 789 to 799. Copyright © 2024 Massachusetts Medical Society. Reprinted with permission from Massachusetts Medical Society.
Figure 3: Kaplan-Meier Estimate of Overall Survival (ITT Population)
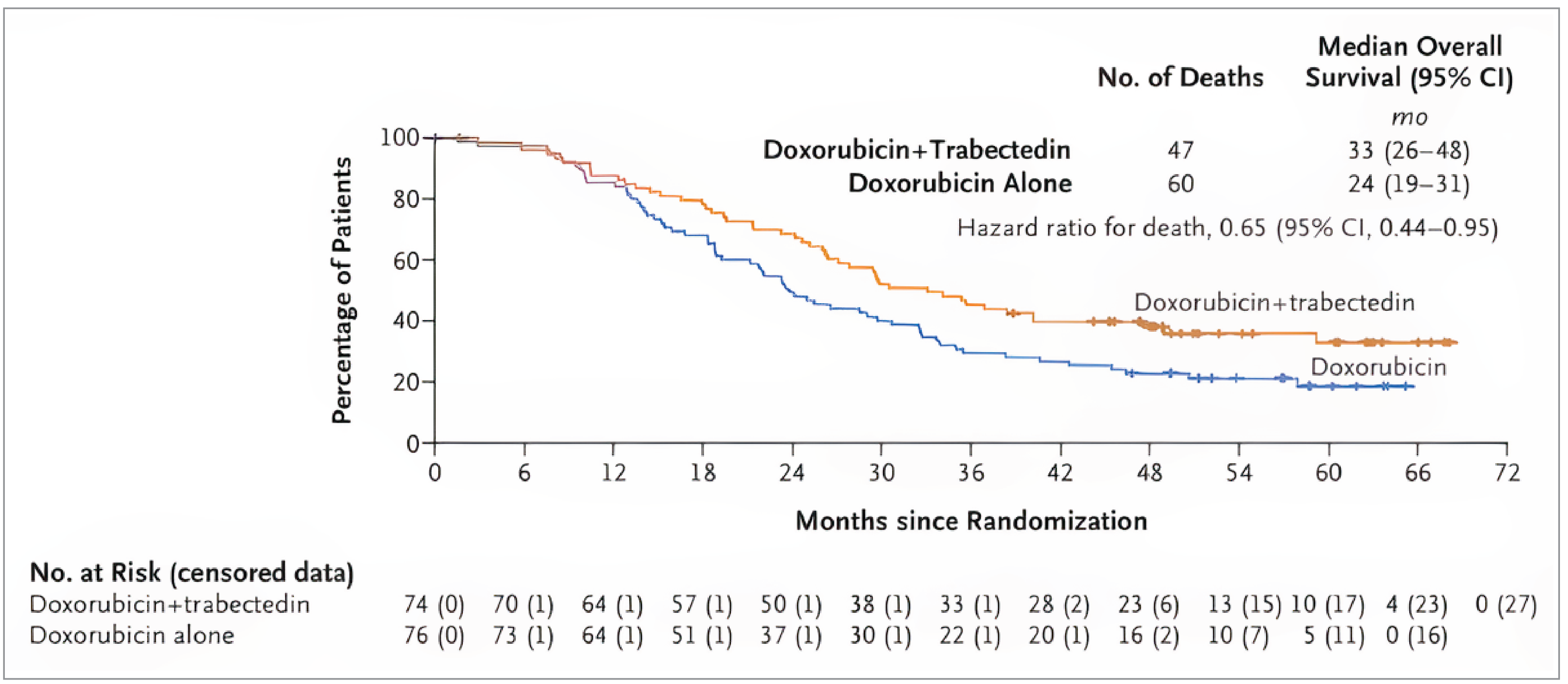
CI = confidence interval; ITT = intention to treat; mo = month; no. = number.
Note: Data were from updated analyses (data cut-off of January 2023).
Source: New England Journal of Medicine, Pautier P, Italiano A, Piperno-Neumann S, et al. for the French Sarcoma Group. Doxorubicin-trabectedin with trabectedin maintenance in leiomyosarcoma, 391(9), 789 to 799. Copyright © 2024 Massachusetts Medical Society. Reprinted with permission from Massachusetts Medical Society.
Table 3: Summary of Key Efficacy Results
Variable | LMS04 | |
|---|---|---|
Trabectedin-doxorubicin N = 74 | Doxorubicin N = 76 | |
Primary end point: PFSa | ||
Median follow-up duration, months (IQR) | 55 (49 to 63) | |
Number of patients with PFS events, n (%) | 66 (89.2) | 74 (97.4) |
Disease progression, n (%) | NR | NR |
Death, n (%) | NR | NR |
Patients censored,b n (%) | 8 (10.8) | 2 (2.6) |
Time to PFS (months), median (95% CI) | 12 (10 to 16) | 6 (4 to 7) |
HR (95% CI)c | 0.37 (0.26 to 0.53) | Reference |
P valued | NR | Reference |
Probability of PFS at 12 months, % (95% CI) | 50.7 (39.5 to 61.9) | 16.0 (9.4 to 25.9) |
Probability of PFS at 24 months, % (95% CI) | 30.2 (20.9 to 41.5) | 3 (1 to 9) |
Difference in PFS probability at 24 months, % (95% CI) | NR | Reference |
Secondary end points | ||
Overall survivala | ||
Median follow-up duration, months (range) | NR | NR |
Patients with events, n (%) | 47 (63.5) | 60 (78.9) |
Patients censored,e n (%) | 27 (36.5) | 16 (21.1) |
Time to OS (months), median (95% CI) | 33 (26 to 48) | 24 (19 to 31) |
HR (95% CI)c | 0.65 (0.44 to 0.95) | Reference |
P valuef | NR | Reference |
Probability of OS at 24 months, % (95% CI) | 68 (57 to 78) | 49 (38 to 60) |
Difference in OS probability at 24 months, % (95% CI) | NR | Reference |
Objective response ratea | ||
Complete response, n (%) | NR | NR |
Partial response, n (%) | 27 (36.5) | 10 (13.2) |
Patients with ORR, n (%) | NR | NR |
Risk difference, % (95% CI) | NR | Reference |
P valuef | NR | Reference |
CI = confidence interval; HR = hazard ratio; IQR = interquartile range; NR = not reported; ORR = objective response rate; OS = overall survival; PFS = progression-free survival.
Note: Data were from the clinical data cut-off date of January 2023.
aThis analysis was conducted in the intention-to-treat population (74 patients in the trabectedin-doxorubicin group and 76 patients in the doxorubicin group).
bPatients who were alive and disease-free at the last follow-up visit were censored on the date of their last CT scan.
cBased on a Cox proportional hazards model that adjusted for stratification factors used in randomization (tumour site, disease stage).
dP value based on a log-rank test and stratified by tumour site (uterine or soft tissue) and disease stage (locally advanced or metastatic).
ePatients who were alive at the last follow-up visit were censored on the last date of data collection.
fNo adjustment was conducted for multiple testing and there is a higher risk of type I error.
Source: Pautier et al. (2022)12 and Pautier et al. (2024).13
Harms
Detailed results for harms in the included study are in the Supplemental Material, Appendix 3.
Data for harms in the updated analysis are summarized for 74 patients in the trabectedin-doxorubicin group and 75 patients in the doxorubicin group. Key results include the following:
The overall numbers of patients with treatment-emergent AEs and commonly occurring AEs were not reported.
Serious AEs occurred in 37 patients (50%) in the trabectedin-doxorubicin group and 20 patients (27%) in the doxorubicin group. Commonly occurring serious AEs were not reported.
Grade 3 or 4 AEs occurred in 97% of patients in the trabectedin-doxorubicin group and 56% of patients in the doxorubicin group. Commonly occurring AEs of grade 3 or higher were not reported.
Withdrawals due to AEs occurred in 7 patients (9%) in the trabectedin-doxorubicin group and 3 patients (4%) in the doxorubicin group.
Data for deaths in the updated analysis were not reported. At the primary analysis,12 42 patients (57%) in the trabectedin-doxorubicin group had died and 50 patients (67%) in the doxorubicin group had died. Deaths in the trabectedin-doxorubicin and doxorubicin groups were due to progressive disease (54% and 62%, respectively), calcium-channel antagonist overdose (1.4% and 0%), toxic death (0% and 1.3%), septic shock (0% and 1.3%), and suicide (reported as per study) (1.4% and 0%). The cause of death was missing for 1 patient in the doxorubicin group.
Notable harms of neutropenia and liver toxicity were prespecified in the included study. Numerical data on notable harms (hepatotoxicity, rhabdomyolysis, febrile neutropenia, sepsis, pulmonary embolism, and injection site reactions) in the updated analysis in the supplement13 were reported according to grade of AE (i.e., 1, 2, 3, and 4) in both treatment groups and stratified by treatment in the trabectedin-doxorubicin group (induction treatment from cycle 1 to cycle 6 versus maintenance treatment from cycle 6 to progression). In the updated analysis:
Grade 3 or 4 cytolysis occurred in 34 patients (46%) in the trabectedin-doxorubicin group and 2 patients (3%) in the doxorubicin group. Grade 1 hepatic cytolysis occurred in 4 patients (5.4%) in the trabectedin-doxorubicin group and 0 patients in the doxorubicin group during cycle 1 until disease progression. Grade 2 hepatic cytolysis occurred in 1 patient (1.4%) in the trabectedin-doxorubicin during induction (from cycle 1 to cycle 6) and 1 patient (1.3%) in the doxorubicin group from cycle 1 until disease progression. Grade 3 hepatic cytolysis occurred in 1 patient (1.4%) during induction and in 1 patient (1.4%) during maintenance (from cycle 6 until disease progression) in the trabectedin-doxorubicin. No patient in the doxorubicin group had hepatic cytolysis from cycle 1 until disease progression. During induction treatment in the trabectedin-doxorubicin group, grade 1 cholestasis occurred in 1 patient (1.4%) and grade 2 cholestasis occurred in 2 patients (2.7%). One patient (1.4%) each experienced grade 2 and grade 3 cholestasis during maintenance treatment with trabectedin. No patient in the doxorubicin group experienced cholestasis from cycle 1 to disease progression.
Grade 3 rhabdomyolysis occurred in 1 patient (1.4%) in the trabectedin-doxorubicin group during maintenance treatment with trabectedin. No patient in the doxorubicin group experienced rhabdomyolysis from cycle 1 to disease progression.
Grade 1 febrile neutropenia occurred in 1 patient (1.4%) during induction treatment and in 1 patient (1.4%) during maintenance treatment in the trabectedin-doxorubicin group. Two patients (2.7%) in the doxorubicin group experienced grade 1 febrile neutropenia from cycle 1 to disease progression. Grade 2 febrile neutropenia occurred in 4 patients (5.4%) during induction treatment and in 1 patient (1.4%) during maintenance treatment in the trabectedin-doxorubicin group. One patient (1.3%) in the doxorubicin group experienced grade 2 febrile neutropenia from cycle 1 to disease progression. Grade 3 febrile neutropenia occurred in 10 patients (13.4%) during induction treatment and in 2 patients (2.7%) during maintenance treatment in the trabectedin-doxorubicin group. Six patients (8.0%) in the doxorubicin group experienced grade 3 febrile neutropenia from cycle 1 to disease progression. Grade 4 febrile neutropenia occurred in 4 patients (5.4%) during induction treatment in the trabectedin-doxorubicin group and in 1 patient (1.3%) from cycle 1 to disease progression in the doxorubicin group.
Grade 4 septic shock 4 occurred in 2 patients (2.7%) in the trabectedin-doxorubicin group during induction treatment. No patients in the doxorubicin group experienced septic shock from cycle 1 to disease progression.
Grade 1 pulmonary embolism occurred in 0 patients in the trabectedin-doxorubicin and in 1 patient (1.3%) in the doxorubicin group from cycle 1 until disease progression.
Grade 1 catheter site edema or inflammation occurred in 2 patients (2.7%) in the trabectedin-doxorubicin group during induction treatment. No patient in the doxorubicin group experienced grade 1 catheter site edema or inflammation. Grade 2 catheter site edema or inflammation occurred in 0 patients in the trabectedin-doxorubicin group and 1 patient (1.3%) in the doxorubicin group from cycle 1 to disease progression. Medical device site thrombosis occurred in 1 patient (1.4%) during induction treatment and in 1 patient (1.4%) during maintenance treatment in the trabectedin-doxorubicin group. No patient in the doxorubicin group experienced medical device site thrombosis from cycle 1 to disease progression.
Discussion
Efficacy
The results of the LMS04 trial demonstrated that treatment with trabectedin-doxorubicin may result in an increase in PFS when compared with doxorubicin monotherapy. Relative to doxorubicin, treatment with trabectedin-doxorubicin improved the probability of PFS by approximately 35% at 12 months and 25% at 24 months; these were clinically meaningful to the clinical experts based on a between-group difference of approximately 10% as being important for making decisions regarding treatment. Considering the consensus among clinicians treating sarcomas that an improvement in median OS time of 11 months (with an associated HR of 0.60 or 0.70) is a clinically important difference, and an improvement in the median time to PFS (median 12 months for trabectedin-doxorubicin versus median 6 months for doxorubicin; an HR of 0.37 [95% CI, 0.26 to 0.53]) suggests a meaningful benefit of treatment with trabectedin-doxorubicin. Although exploratory in nature, a subgroup analysis of PFS showed that results for uterine and soft tissue leiomyosarcoma were similar to the primary analysis findings, such that a differential benefit in PFS by disease site may be considered unlikely.
There was insufficient evidence to demonstrate that treatment with trabectedin-doxorubicin increased ORR when compared with doxorubicin. In the absence of information on the number of patients with ORR (including the number of patients with complete response) and absolute differences for ORR, the CDA-AMC review team was unable to evaluate the effects of treatment on ORR based solely on partial response. Specifically, evidence of tumour shrinkage is typically used to ascertain an objective response; however, response to treatment in leiomyosarcoma is more likely to be demonstrated by fibrosis such that measurable lesion(s) may not reduce in size or meet the threshold for reduction. Because more patients in the trabectedin-doxorubicin group (20%) than the doxorubicin group (8%) were able to undergo surgery after induction treatment, this signalled to the experts that treatment with trabectedin-doxorubicin was associated with tumour stability and delayed progression.
There were several missing outcome data in the publications. For PFS, the number of patients with disease progression as distinct from those who die, and between-group differences in probabilities of PFS at reported follow-up time points (12 months and 24 months) were not provided. For OS, the probability of OS at follow-up time points other than 24 months (e.g., 12 months) and the between-group difference in probability of OS at the reported time point were not reported. A gap in the evidence was the absence of information on HRQoL, given that it was not evaluated in the trial. Therefore, it is unknown how treatment with trabectedin-doxorubicin may impact patient-reported outcomes in the LMS04 study. The comparative efficacy and harms of trabectedin-doxorubicin relative to other currently available treatments (e.g., gemcitabine-docetaxel, and doxorubicin-ifosfamide) are unknown in the absence of evidence. Overall, the interpretation of findings was challenged by the open-label study design and missing outcome data.
Harms
In the LMS04 trial, a greater number of patients in the trabectedin-doxorubicin group experienced serious AEs, grade 3 AEs, or grade 4 AEs (including grade 3 or 4 cytolysis and grade 3 or 4 febrile neutropenia). However, the number of patients who experienced the notable harms was small. The interpretation of harms was challenged by missing information and reporting of available data. The total number of patients with treatment-emergent AEs, commonly occurring treatment-emergent AEs, and types of serious AEs were not provided. Furthermore, the trial protocol and publications did not clearly distinguish between treatment withdrawals and study withdrawals due to AEs. Although there were fewer deaths among patients treated with trabectedin-doxorubicin compared with doxorubicin at the primary analysis, data on deaths at the updated analysis were not reported. Finally, no details were provided on the inclusion of AE data for cycle 6 (to confirm or rule out the possibility of overlapping counts), which was included in both the induction phase and the maintenance phase of the trabectedin-doxorubicin group.
According to the clinical experts, the observed higher frequency of liver-related AEs in the trabectedin-doxorubicin group was not indicative of compromised liver function and was considered manageable (e.g., by adjusting the treatment dose or schedule). The experts acknowledged the higher frequencies of febrile neutropenia despite the administration of prophylactic G-CSF among patients treated with trabectedin-doxorubicin. Because patients currently treated with combination chemotherapy are given G-CSF as primary or secondary prophylaxis, clinicians are familiar with monitoring and managing patients during combination treatment. Additionally, the experts had no concerns with the number of patients in the trabectedin-doxorubicin group who required dose reductions during treatment, remarking that this was aligned with good clinical practice and there was evidence of improved efficacy despite necessary dose reductions.
Conclusion
Patients with leiomyosarcoma seek more efficacious treatment options to decrease disease burden, improve symptoms, improve quality of life, and prolong survival. The clinical experts consulted for this review expressed that doublet chemotherapy with trabectedin-doxorubicin would provide an additional first-line treatment option for locally advanced or metastatic leiomyosarcoma. Evidence from a randomized, phase III, open-label trial (LMS04) that included 150 patients with locally advanced or metastatic uterine or soft tissue leiomyosarcoma who were previously untreated with chemotherapy demonstrated that compared with doxorubicin, treatment with trabectedin-doxorubicin likely results in a clinically important improvement in PFS and OS. The evidence was insufficient to demonstrate a difference between trabectedin-doxorubicin and doxorubicin in ORR. The safety profile of trabectedin-doxorubicin was as expected with no new safety signals. The efficacy and safety of trabectedin-doxorubicin compared with other available treatments are unknown in the absence of evidence.
The reimbursement of trabectedin-doxorubicin for the treatment of advanced unresectable or metastatic uterine or soft tissue leiomyosarcoma is expected to increase overall drug acquisition costs. Based on the clinical review conclusions, compared to doxorubicin, trabectedin-doxorubicin likely extends PFS and OS. The comparative efficacy of trabectedin-doxorubicin with other comparators is unknown because it has not yet been assessed in the published literature.
Given that trabectedin-doxorubicin is associated with higher drug acquisition costs and incremental benefits in terms of PFS and OS, a cost-effectiveness analysis would be required to determine the cost-effectiveness of trabectedin-doxorubicin relative to doxorubicin, docetaxel + gemcitabine (DOCEGEMC), and doxorubicin + ifosfamide (DOXOIFOS). As this was not available, the cost-effectiveness of trabectedin-doxorubicin for the treatment of advanced unresectable or metastatic uterine or soft tissue leiomyosarcoma could not be determined.
Economic Review
The economic review consisted of a cost comparison for trabectedin 1.1 mg/m2 in combination with doxorubicin 60 mg/m2 (trabectedin-doxorubicin henceforth) compared with doxorubicin 75 mg/m2, DOCEGEMC, and DOXOIFOS for the treatment of advanced unresectable or metastatic uterine or soft tissue leiomyosarcoma in adults.
Based on public list prices, trabectedin-doxorubicin is expected to have a per-patient cost of $9,559 per 28-day cycle (Supplemental Material, Appendix 4, Table 3). Doxorubicin, DOCEGEMC, and DOXOIFOS are expected to have per-patient costs of $1,297, $3,442, and $7,126 per 28-day cycle, respectively. The incremental costs of trabectedin-doxorubicin compared with doxorubicin, DOCEGEMC, and DOXOIFOS are $8,262, $6,116, and $2,433 per patient per 28 days, respectively. After the 6 initial cycles of trabectedin-doxorubicin, patients can continue on maintenance therapy with trabectedin alone at the same dosage for up to 17 cycles (or 12 months) based on the LMS04 trial protocol.12 In the LMS04 trial, patients in this regimen received a median of 10.5 cycles of maintenance therapy. The 28-day cost of maintenance therapy (trabectedin monotherapy) is $8,164. As such, the reimbursement of trabectedin-doxorubicin for the treatment of advanced unresectable or metastatic uterine or soft tissue leiomyosarcoma is expected to increase overall drug acquisition costs on a per-cycle basis. Additional items for consideration are provided in the following bullets:
According to the clinical review, the main source of evidence is the LMS04 trial, which compared trabectedin-doxorubicin with doxorubicin in 150 patients with previously untreated advanced or metastatic uterine or soft tissue leiomyosarcoma.13 The study results suggest that trabectedin-doxorubicin is likely to improve PFS by BICR, and may improve OS compared to doxorubicin; however, the magnitude of effect is uncertain. The evidence is insufficient to demonstrate a difference in ORR between the treatment groups. No evidence was identified regarding the comparative efficacy and safety of trabectedin-doxorubicin versus other active comparators.
As of June 10, 2025, trabectedin is only available as a brand name product in Canada (Yondelis). There is 1 generic currently under review by Health Canada (submission accepted in April 2021). There are no active negotiations with the pan-Canadian Pharmaceutical Alliance.
No health care resource use outcomes were reported in the LMS04 clinical trial. However, when compared with doxorubicin, higher rates of grade 3 or 4 cytolysis and of febrile neutropenia were observed in the trabectedin-doxorubicin group. These AEs may increase costs due to additional unplanned hospitalizations and outpatient visits.
According to the clinical experts consulted for this review, when compared with doxorubicin and DOCEGEMC, trabectedin-doxorubicin is expected to increase treatment-related health care resource use due to the administration of G-CSF for primary prophylaxis of febrile neutropenia. They noted that the administration of G-CSF is already part of the clinical protocols for the DOXOIFOS regimen, and that in certain jurisdictions, this regimen is administered in hospitals, and therefore the reimbursement of trabectedin-doxorubicin may decrease costs because it can be administered in lower complexity settings. Additionally, when compared to DOXOIFOS, the clinical experts expect that trabectedin-doxorubicin is better tolerated by patients, and therefore it may decrease health care costs due to unplanned hospitalizations and outpatient visits.
Trabectedin monotherapy was previously reviewed by CDA-AMC in 2016 for the treatment of patients with metastatic liposarcoma or leiomyosarcoma and received a “do not reimburse” recommendation.1
No cost-effectiveness studies conducted in Canada were identified based on a literature search conducted on June 10, 2025.
References
1.pCODR Expert Review Committee (pERC) final recommendation: Trabectedin (Yondelis). 2016. Accessed May 26, 2025. https://www.cda-amc.ca/sites/default/files/pcodr/pcodr_trabectedin_yondelis_lile_scarcoma_fn_rec.pdf
2.Valeo Pharma Inc. Yondelis (trabectedin): 1 mg/vial for injection [product monograph]. March 2020. Updated May 28, 2020. Accessed May 26, 2025. https://pdf.hres.ca/dpd_pm/00056559.PDF
3.George S, Abdul Razak AR. Post TW, ed. Overview of the initial treatment of metastatic soft tissue sarcoma. UpToDate; 2024. Accessed January 23, 2025. http://www.uptodate.com
4.National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines) Soft Tissue Sarcoma, Version 4.2024. November 21, 2024. Accessed February 10, 2025. https://www.nccn.org/
5.Ryan CW, Meyer J. Post TW, ed. Clinical presentation, diagnostic evaluation, and staging of soft tissue sarcoma. UpToDate; 2024. Accessed January 23, 2025. http://www.uptodate.com
6.Brenner DR, Gillis J, Demers AA, et al. Projected estimates of cancer in Canada in 2024. CMAJ. 2024;196(18):E615-E623. doi: 10.1503/cmaj.240095 PubMed
7.Skorstad M, Kent A, Lieng M. Uterine leiomyosarcoma - incidence, treatment, and the impact of morcellation. A nationwide cohort study. Acta Obstet Gynecol Scand. 2016;95(9):984-90. doi: 10.1111/aogs.12930 PubMed
8.Canadian Cancer Society. Survival statistics for soft tissue sarcoma. Accessed May 26, 2025. https://cancer.ca/en/cancer-information/cancer-types/soft-tissue-sarcoma/prognosis-and-survival/survival-statistics
9.Hensley ML, Leitao MM, Jr. Post TW, ed. Treatment and prognosis of uterine leiomyosarcoma. UpToDate; 2024. Accessed January 23, 2025. http://www.uptodate.com
10.Memarzadeh S, Berek JS. Post TW, ed. Uterine sarcoma: Classification, epidemiology, clinical manifestations, and diagnosis. UpToDate; 2024. Accessed January 23, 2025. http://www.uptodate.com
11.Seddon B, Strauss SJ, Whelan J, et al. Gemcitabine and docetaxel versus doxorubicin as first-line treatment in previously untreated advanced unresectable or metastatic soft-tissue sarcomas (GeDDiS): A randomised controlled phase 3 trial. Lancet Oncol. 2017;18(10):1397-1410. doi: 10.1016/S1470-2045(17)30622-8 PubMed
12.Pautier P, Italiano A, Piperno-Neumann S, et al. Doxorubicin alone versus doxorubicin with trabectedin followed by trabectedin alone as first-line therapy for metastatic or unresectable leiomyosarcoma (LMS-04): A randomised, multicentre, open-label phase 3 trial. Lancet Oncol. 2022;23(8):1044-1054. doi: 10.1016/S1470-2045(22)00380-1 PubMed
13.Pautier P, Italiano A, Piperno-Neumann S, et al. Doxorubicin-trabectedin with trabectedin maintenance in leiomyosarcoma. N Engl J Med. 2024;391(9):789-799. doi: 10.1056/NEJMoa2403394 PubMed
14.U.S. Food and Drug Administration (FDA). Guidance for industry clinical trial endpoints for the approval of cancer drugs and biologics. 2007. Accessed May 26, 2025. https://www.fda.gov/regulatory-information/search-fda-guidance-documents/clinical-trial-endpoints-approval-cancer-drugs-and-biologics
15.Booth CM, Eisenhauer EA, Gyawali B, Tannock IF. Progression-free survival should not be used as a primary end point for registration of anticancer drugs. J Clin Oncol. 2023;41(32):4968-4972. doi: 10.1200/JCO.23.01423 PubMed
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.