Drugs, Health Technologies, Health Systems
Reimbursement Recommendation
Cabozantinib
Reimbursement request: For the treatment of adults with locally advanced or metastatic extrapancreatic or pancreatic neuroendocrine tumours who have received at least 1 prior therapy
Requester: Public drug programs
Final recommendation: Reimburse with conditions
Summary
What Is the Reimbursement Recommendation for Cabozantinib?
The Formulary Management Expert Committee (FMEC) recommends that cabozantinib be reimbursed for adult patients with locally advanced or metastatic extrapancreatic or pancreatic neuroendocrine tumours who have received at least 1 prior therapy, provided certain conditions are met.
What Are the Conditions for Reimbursement?
Cabozantinib may be initiated in patients for the treatment of metastatic extrapancreatic or pancreatic neuroendocrine tumours if the following conditions are met: the tumour grade is consistent with WHO tumour grade 1 to 3; there is histological documentation of neuroendocrine tumour of pancreatic, gastrointestinal, lung, thymus, other, or unknown primary site; there is disease progression or unacceptable side effects after at least 1 prior therapy other than somatostatin analogue; and there is good performance status. A price reduction for cabozantinib may be required.
Why Did CDA-AMC Make This Recommendation?
FMEC reviewed the Canada’s Drug Agency (CDA-AMC) report, which included a review of the clinical evidence, specifically the CABINET trial, and a cost comparison of cabozantinib versus other treatments used in Canada. Cabozantinib improved progression-free survival compared to placebo. FMEC also considered input received from 1 patient group, the Canadian Neuroendocrine Tumour Society, and 1 clinician group, the Commonwealth Neuroendocrine Tumour Research Collaborative.
Based on the CDA-AMC assessment of the health economic evidence, which consisted of a cost comparison table, reimbursement of cabozantinib is associated with higher drug acquisition costs to publicly funded drug programs than best supportive care, everolimus, sunitinib, and capecitabine in combination with temozolomide, based on publicly available list prices; cabozantinib is associated with lower drug acquisition costs to publicly funded drug programs than lutetium (177Lu) dotatate. The cost-effectiveness of cabozantinib compared to relevant comparators is unknown. A price reduction may therefore be required.
FMEC concluded that cabozantinib demonstrates acceptable clinical value. FMEC also considered unmet clinical needs, distinct social and ethical considerations, economic considerations, and the impact on health systems.
Therapeutic Landscape
What Are Neuroendocrine Tumours?
Neuroendocrine tumours (NETs), including extrapancreatic (epNETs) and pancreatic (pNETs) types, originate from secretory cells and can occur in various organs. These tumours can be functional, causing various symptoms, or nonfunctional, presenting with nonspecific symptoms and leading to delays in diagnosis. These tumours significantly impact individuals’ quality of life and functional performance. In Canada, an Ontario-based study (2015) reported an increase in incidence from 2.46 per 100,000 to 5.86 per 100,000 over 15 years, with pNETs accounting for approximately 10% of cases. The estimated overall survival rates for patients with NETs are 68.3% at 3 years, 61.0% at 5 years, and 46.5% at 10 years.
What Are the Current Treatment Options?
For locally advanced or metastatic epNET or pNET, treatment approaches vary based on tumour grade, differentiation, functionality, and the extent and location of the disease. For localized solid tumours, surgery is typically the first-line treatment. For patients with metastatic disease, systemic drug therapies are used. Somatostatin analogues (SSAs) are generally the initial therapy for patients with unresectable metastatic disease or hormonal overproduction syndromes. For those whose disease has progressed while on SSAs, treatment options include targeted agents like everolimus, sunitinib, and cabozantinib; chemotherapy such as capecitabine plus temozolomide; lutetium (177Lu) dotatate; and peptide receptor radionuclide therapy (PRRT).
What Is the Treatment Under Review?
Cabozantinib is a small molecule that inhibits multiple receptor tyrosine kinases, which are involved in tumour cell proliferation and angiogenesis. Cabozantinib is approved by Health Canada for the following indications: renal cell carcinoma, hepatocellular carcinoma, and differentiated thyroid carcinoma. This review of cabozantinib is for off-label use in NETs. Cabozantinib is available as an oral tablet in doses of 60 mg, 40 mg, or 20 mg.
Why Did We Conduct This Review?
As identified by clinicians, cabozantinib offers a novel mechanism of action and potential to fulfill an unmet need in adult patients with locally advanced or metastatic epNET or pNET. Given that the active pharmaceutical ingredient patent of cabozantinib has expired, this drug is eligible for a nonsponsored reimbursement review, per the Procedures for Reimbursement Reviews. Of note, cabozantinib has 2 generics under review by Health Canada.
At the request of the public drug programs, we initiated a review to inform a recommendation on whether cabozantinib should be reimbursed for adults with locally advanced or metastatic epNET or pNET who have received at least 1 prior therapy.
Input From Interested Parties
The Canadian Neuroendocrine Tumour Society, as a patient group, provided input summarizing patient experiences and perspectives on living with NETs, drawing from multiple sources, including the Global NET Patient Survey (2017), the NET Patient Experiences and Perspectives Survey (2022), and qualitative interviews with patients and caregivers who have experience with cabozantinib. Patients reported that NETs significantly reduce quality of life (QoL), with symptoms such as fatigue, diarrhea, and pain, which affect daily activities, emotional well-being, social interactions, and the ability to work.
The Commonwealth Neuroendocrine Tumour Research Collaborative, as a clinician group, noted that NETs are among the fastest-growing classes of cancers in Canada and globally. Treatment goals for patients with locally advanced or metastatic epNET or pNET include prolonging survival, delaying disease progression, managing symptoms, preventing treatment-related complications, and maintaining or improving QoL and functional status. Available systemic treatment options include SSAs, targeted agents, PRRT, and other chemotherapy when appropriate.
Disclaimer: The perspectives shared by people with lived experience who present to the committee reflect their individual experiences and are not necessarily representative of all people with the same condition or course of treatment. Their insights provide valuable context about what a patient, support person, or caregiver might go through when facing this condition or treatment, helping to inform the committee’s deliberations. These narratives complement other forms of evidence and input and should be considered as part of a broader understanding of the condition and treatment under review. Where gender or gendered pronouns are used in these narratives, they are included with the permission of the individual.
Summary of Deliberation
FMEC deliberated on all domains of value of the deliberative framework before developing their recommendation: clinical value, unmet clinical need, distinct social and ethical considerations, economic considerations, and impacts on health systems. For further information on the domains of value, please refer to the Expert Committee Deliberation at Canada’s Drug Agency document.
FMEC considered the following key discussion points, organized by the 5 domains of value.
Clinical Value
FMEC concluded that cabozantinib demonstrates acceptable clinical value versus appropriate comparators in the setting in Canada.
Through reflection on the input from 1 patient group or insights shared by the person with lived experience, FMEC members noted the following important patient values or perspectives: patients value progression-free survival as an outcome. However, patients also value symptom control and would like there to be more treatment options available to address drug resistance and to improve their overall outcomes and their QoL.
FMEC members highlighted the following discussion points:
FMEC noted that NETs encompass many different types of cancers with both endocrine and neural characteristics. Depending on the tumour site(s), the treatment options and management can vary. However, guest specialists have shared that most patients would begin with a treatment with an SSA, which has both antiproliferative properties and the ability to manage symptoms related to secretory tumours. As per the guest specialists, most patients would typically remain on an SSA, whereas additional treatments are needed when there is disease progression. FMEC noted there is some variation in practice in terms of how long patients remain on SSAs.
In the CABINET study, in which cabozantinib was compared to placebo, cabozantinib was associated with a hazard ratio of 0.38 (95% CI, 0.25 to 0.59) for disease progression or death in the epNET cohort and a hazard ratio of 0.23 (95% CI, 0.12 to 0.42) in the pNET cohort. Nearly all participants had received prior SSA therapy, with most continuing SSAs as background treatment during the CABINET trial. FMEC noted that progression-free survival is an important outcome for patients, and the committee is satisfied, overall, with the level of evidence on this outcome.
FMEC also discussed the concern for potential toxicity with cabozantinib. In the CABINET study, in which cabozantinib was compared to placebo, patients in the cabozantinib group had higher proportions of any-grade treatment-related adverse events, serious adverse events, and withdrawals due to adverse events. In the epNET cohort, the most common (10% or more) treatment-related grade 3 or 4 adverse events were hypertension (21%), fatigue (13%), and diarrhea (11%). In the pNET cohort, the most common (10% or more) treatment-related grade 3 or 4 adverse events were hypertension (22%), fatigue (11%), and thromboembolic events (11%).
FMEC discussed whether cabozantinib was compared and assessed against an appropriate comparator, which was placebo. FMEC discussed that cabozantinib may address the need to delay progression in NETs. However, there were some dissenting opinions on whether we need more treatment options for NETs and whether the comparative evidence against placebo is clinically relevant. FMEC heard from the clinician experts that at the time the CABINET trial was conducted, placebo as the comparator in the trial was a reasonable approach, given that other treatment options were not funded or available at that time. 177Lu dotatate, for example, was not standard of care at the time the trial was initiated. In essence, the trial evaluated cabozantinib as compared to the standard of care at the time, when no other treatments were funded or available. In the current context in Canada, for patients with lung NETs, who make up the highest proportion of neuroendocrine cancers, placebo (reflecting the standard of care) is an appropriate comparator, given that everolimus is currently the only funded treatment available in first line for these patients. FMEC agreed with the guest specialists that for some patients, a placebo would be an appropriate comparator, especially if they had already exhausted multiple lines of therapy and had no other treatment options available.
FMEC acknowledged that there is evidence for comparing cabozantinib to placebo, but there is a lack of comparative evidence with other treatment options available for NETs. FMEC noted that, given that the trial design included NET patients with variable and heterogeneous disease characteristics for which treatment options are also variable, some patients, such as those with lung NETs, would have limited options, in which case the use of a placebo as a comparator in the trial would be reasonable. However, in patients with pNETs, for which there are more options, including chemotherapies, sunitinib, and everolimus, the comparative evidence between cabozantinib and these treatment options is lacking.
Unmet Clinical Need
FMEC concluded that there is a significant clinical need arising from NETs despite available treatments.
Through reflection on the input from 1 patient group or insights shared by the person with lived experience, FMEC members noted the following important patient values or perspectives: patients have noted that resistance to current therapies is concerning and that treatment options with intolerable side effects (e.g., everolimus) are problematic; patients are interested to have more effective and better tolerated treatment options for NETs.
FMEC members highlighted the following discussion points:
FMEC discussed and agreed that there are other treatment options available for patients with NETs. These include SSAs, PRRT, and other tyrosine kinase inhibitors. However, not all these options are available or acceptable to patients.
FMEC also highlighted that NETs are incurable; patients with these tumours experience symptoms such as fatigue and diarrhea. These symptoms may affect their daily activities and emotional health.
FMEC also discussed the unmet needs related to the condition; these include the need to prolong survival, delay progression, reduce symptoms, prevent treatment complications, and improve and maintain QoL.
FMEC noted that NETs are relatively rare; hence, there are challenges with evidence generation to support treatment in this therapeutic area.
FMEC heard from the guest specialists who underscored the opportunity for patients with lung NETs, who make up the highest proportion of neuroendocrine cancers. Given that everolimus is currently the only funded first-line treatment available for these patients, cabozantinib, if reimbursed, would be the second drug approved for lung NETs. The guest specialists also shared their concern that everolimus is associated with unfavourable side effects such as profound hyperglycemia, pneumonitis, and interstitial lung disease. Other commonly reported adverse effects include fatigue, stomatitis, and leukopenia. As such, the guest specialists also indicated that cabozantinib will be preferred over everolimus if funded in this setting.
Distinct Social and Ethical Considerations
FMEC concluded that cabozantinib would potentially address a significant nonclinical need arising from NETs despite available treatments. FMEC did not identify any important measures that should be implemented to ensure that the use of cabozantinib addresses relevant social and ethical implications.
Through reflection on the input from 1 patient group or insights shared by the person with lived experience, FMEC members noted the following important patient values or perspectives: patients value the oral route of treatment administration. This has important mental health benefits for both the patient and the family when the patient can remain at home to receive this treatment.
FMEC members highlighted the following discussion points:
FMEC discussed that, as an oral treatment, cabozantinib offers the benefits of receiving treatment at home, especially for patients who live far from a cancer treatment centre.
One FMEC member noted that patients with NETs who are of a lower socioeconomic status and those living in rural areas may be at a disadvantage, and an oral treatment may help address this.
Economic Considerations
FMEC concluded that there are economic considerations that are important to address when implementing the reimbursement of cabozantinib.
FMEC members highlighted the following discussion points:
For patients who have no other treatment options available, the drug acquisition costs of cabozantinib per patient per 28 days are higher than best supportive care.
The committee noted there are potentially relevant comparators for patients with NETs who have not yet exhausted multiple lines of therapy. These comparators include everolimus, sunitinib, capecitabine in combination with temozolomide, and 177Lu dotatate.
The drug acquisition costs per patient per 28 days of cabozantinib are higher than those of everolimus, sunitinib, and capecitabine in combination with temozolomide, and lower than those of 177Lu dotatate.
The comparative effectiveness relative to any of the active comparators is unknown due to a lack of data. Existing evidence from a randomized study comparing cabozantinib against placebo demonstrated a meaningful progression-free survival benefit.
No Canadian cost-effectiveness or cost-utility studies were available.
There is no evidence of clinical effectiveness against active comparators to justify a greater cost for cabozantinib relative to current treatments for this population.
Two generic formulations are under review by Health Canada. Currently, only a branded version of cabozantinib (Cabometyx) is available in Canada.
Cabozantinib is expected to have similar treatment-related health care resource use as other treatments, except for 177Lu dotatate, which has administration costs due to specialized infrastructure needs.
Given the incremental costs and potential clinical benefit of cabozantinib, especially for patients with no other treatments available, a price reduction may be warranted.
Impacts on Health Systems
FMEC did not identify any impacts on health systems that are important to address when implementing cabozantinib.
FMEC members highlighted the following discussion points:
FMEC discussed and agreed that there are no impacts on the health care system that need to be addressed to implement cabozantinib.
FMEC highlighted that the cost of oral medications is variable across jurisdictions and presents a concern for inequity. These treatments should be available for all patients regardless of where they reside within Canada.
Figure 1: Recommendation Pathway
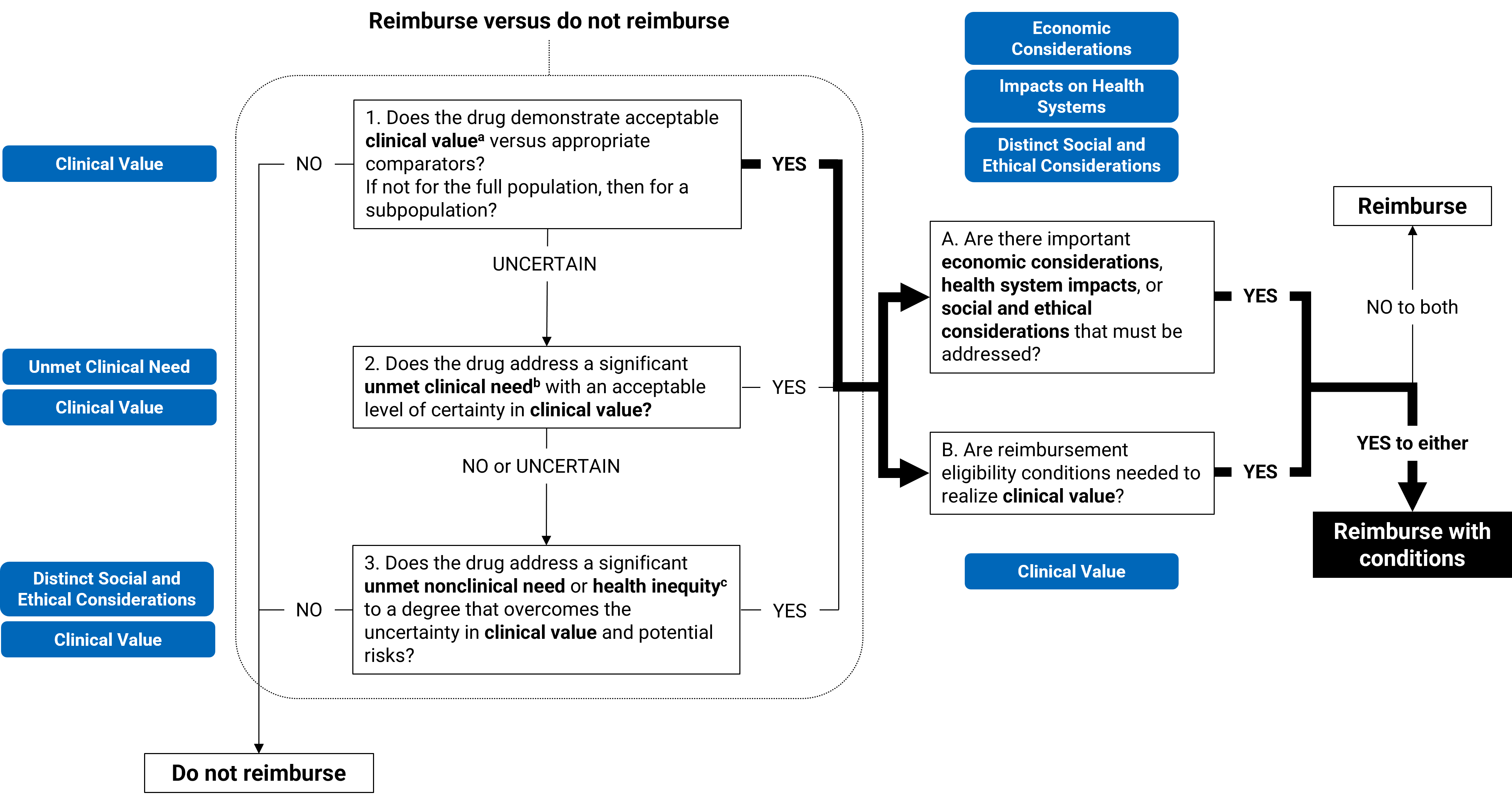
aAcceptable clinical value refers to at least comparable clinical value (if the drug is expected to be substitutive treatment) or added clinical value (if the drug is expected to be additive treatment) versus appropriate comparators.
bSignificant unmet clinical need depends on all of the following: severity of the condition, availability of effective treatments, and challenges in evidence generation due to the rarity of the condition or ethical issues.
cUnmet nonclinical need and health inequity are key components within the distinct and social ethical considerations domain of value.
Full Recommendation
With a vote of 7 to 0, FMEC recommends that cabozantinib, for the treatment of adults with locally advanced or metastatic extrapancreatic or pancreatic neuroendocrine tumours, be reimbursed if the conditions presented in Table 1 are met.
Table 1: Conditions, Reasons, and Guidance
Reimbursement condition | Reason | Implementation guidance |
|---|---|---|
Initiation | ||
1. Cabozantinib may be initiated in patients for the treatment of metastatic epNETs or pNETs if the following conditions are met: 1.1. the tumour grade is consistent with WHO tumour grades 1 to 3 1.2. there is histological documentation of NETs of pancreatic, gastrointestinal, lung, thymus, other, or unknown primary site 1.3. there is disease progression or unacceptable side effects after at least 1 prior therapy other than an SSA 1.4. there is good performance status. | There is evidence from the CABINET trial that cabozantinib improved progression-free survival when compared to placebo in adults with locally advanced or metastatic epNETs or pNETs who have at least 1 prior therapy, not including SSAs. | — |
Discontinuation and renewal | ||
2. Cabozantinib should be discontinued if there is any of the following: 2.1. disease progression 2.2. unacceptable toxicities. | Consistent with clinical practice, patients in the CABINET trial discontinued treatment upon disease progression or treatment intolerance. | — |
Prescribing | ||
3. Prescribing should be limited to clinicians with expertise in the diagnosis and management of NETs. | This will ensure that appropriate treatment is prescribed for patients and adverse events are optimally managed. | In CABINET trial, cabozantinib was prescribed as a single-drug regimen. Note that in remote and rural settings, it may be necessary for the prescribing and management to be done in partnership with community physicians and specialists of NETs. |
Pricing | ||
4. A price reduction may be required. | Based on publicly available pricing information, cabozantinib is more costly than best supportive care and other active comparators, leading to incremental costs to the health care system. The cost-effectiveness of cabozantinib relative to best supportive care and other active comparators is currently unknown; thus, a price reduction may be required. | — |
epNET = extrapancreatic neuroendocrine tumour; NET = neuroendocrine tumour; pNET = pancreatic neuroendocrine tumour; SSA = somatostatin analogue.
Feedback on Draft Recommendation
Canada’s Drug Agency (CDA-AMC) received feedback from 1 clinician group (the Ontario Health [Cancer Care Ontario] Gastrointestinal Cancer Drug Advisory Committee), 1 patient group (the Canadian Neuroendocrine Tumour Society), and the public drug programs. Both the clinician group and the patient group have expressed support for the draft recommendation. The patient group advocated for equitable access to treatment. As such, this consideration has been incorporated in the prescribing guidance. The public drug programs have provided feedback on editorial revisions, which has been incorporated.
FMEC Information
Members of the committee: Dr. Emily Reynen (Chair), Dr. Zaina Albalawi, Dr. Hardit Khuman, Ms. Valerie McDonald, Dr. Bill Semchuk, Dr. Marianne Taylor, Dr. Maureen Trudeau, Dr. Dominika Wranik. Two guest specialists from Ontario and the Prairies participated in this review.
Meeting date: July 17, 2025
Regrets: One expert committee member did not attend the meeting.
Conflicts of interest: None
Special thanks: CDA-AMC extends our special thanks to the individuals who presented directly to FMEC and to patient organizations representing the community of those living with NETs, particularly the Canadian Neuroendocrine Tumour Society, which includes Jackie Herman and Patricia Graefer.
Note: CDA-AMC makes every attempt to engage with people with lived experience as closely to the indication and treatments under review as possible; however, at times, CDA-AMC is unable to do so and instead engages with individuals with similar treatment journeys or experience with comparators under review to ensure lived experience perspectives are included and considered in Reimbursement Reviews. CDA-AMC is fortunate to be able to engage with individuals who are willing to share their treatment journey with FMEC.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.