Drugs, Health Technologies, Health Systems
Reimbursement Recommendation
Pertuzumab
Reimbursement request: In combination with trastuzumab and chemotherapy for early-stage HER2-positive breast cancer in the neoadjuvant setting
Requester: Public drug programs
Final recommendation: Reimburse with conditions
Summary
What Is the Reimbursement Recommendation for Pertuzumab?
The Formulary Management Expert Committee (FMEC) recommends that pertuzumab in combination with trastuzumab and chemotherapy be reimbursed for the treatment of adults with early-stage HER2-positive breast cancer in the neoadjuvant setting, provided certain conditions are met.
What Are the Conditions for Reimbursement?
Pertuzumab in combination with trastuzumab and chemotherapy may be initiated in adult patients for the neoadjuvant treatment of early-stage HER2-positive breast cancer if all of the following conditions are met: it is locally advanced, inflammatory or early-stage breast cancer (> 2 cm or node positive) and there is no evidence of metastasis. A price reduction for pertuzumab may be required.
Why Did CDA-AMC Make This Recommendation?
FMEC reviewed the Canada’s Drug Agency (CDA-AMC) report, which included a review of the clinical evidence, specifically 2 randomized controlled trials (PEONY and NeoSphere) and 5 real-world evidence (RWE) studies, and a cost comparison of pertuzumab in combination of trastuzumab and chemotherapy versus other treatments used in Canada. FMEC also considered input received from 4 patient groups (Breast Cancer Canada, the Inflammatory Breast Cancer Network Foundation Canada, the Canadian Breast Cancer Network, and Rethink Breast Cancer), 4 clinician groups (Ontario Health [Cancer Care Ontario] Breast Cancer Drug Advisory Committee; the Breast Medical Oncology Group at the Juravinski Cancer Centre in Hamilton, Ontario; the Research Excellence, Active Leadership [REAL] Canadian Breast Cancer Alliance; and Sunnybrook Odette Cancer Centre), and 1 industry group (Hoffmann-La Roche Limited).
Based on the CDA-AMC assessment of the health economic evidence, which consisted of a cost comparison table, the reimbursement of pertuzumab in combination with trastuzumab and chemotherapy is associated with higher drug acquisition costs to publicly funded drug programs than relevant comparators based on publicly available list prices.
FMEC concluded there was uncertainty in the clinical value demonstrated by pertuzumab in combination with trastuzumab and chemotherapy; however, pertuzumab in combination with trastuzumab and chemotherapy was considered to fill a significant unmet clinical need to minimize the risk of residual disease following resection, thereby avoiding exposure to adjuvant treatment with trastuzumab emtansine (T-DM1), which is associated with more toxicities and monitoring requirements. The reimbursement conditions were further developed based on distinct social and ethical considerations, economic considerations, and impacts on health systems.
Therapeutic Landscape
What Is Early-Stage HER2-Positive Breast Cancer?
HER2-positive breast cancer is a subtype of breast cancer characterized by overexpression of the HER2 protein, which is associated with more aggressive disease and a higher risk of recurrence. In Canada, breast cancer is the second most common cancer. An estimated 30,800 new cases of breast cancer were diagnosed in 2024, of which approximately 15% to 20% were HER2-positive.
What Are the Current Treatment Options?
In patients with HER2-positive breast tumours, the availability of HER2-targeted therapy has changed the natural history of the disease. Most patients with a tumour larger than 2 cm or with at least 1 positive lymph node should receive neoadjuvant HER2-targeted therapy in addition to taxane-based chemotherapy with or without anthracyclines. The standard of care in other international jurisdictions is to offer dual HER2-targeted therapies (e.g., pertuzumab in combination with trastuzumab) together with chemotherapy in the neoadjuvant setting. The rationale for this treatment strategy is to offer synergy, whereby the responses to this combination therapy are expected to be greater than sum of responses to individual therapy. Trastuzumab and pertuzumab have been reported to enhance apoptosis.
What Is the Treatment Under Review?
The treatment under review is a dual HER2 blockade (pertuzumab-trastuzumab) plus taxane-based chemotherapy with or without anthracycline-based chemotherapy (with variable dosing and treatment frequencies) as a neoadjuvant regimen.
Pertuzumab is a monoclonal antibody that targets the extracellular dimerization domain of HER2 and blocks ligand-dependent heterodimerization of HER2 with other HER family members. This inhibits intracellular signalling, resulting in cell growth arrest and apoptosis. Health Canada recommends initial pertuzumab treatment with 840 mg as a 60-minute IV infusion and maintenance treatment with 420 mg ever 3 weeks as a 30- to 60-minute IV infusion.
Why Did We Conduct This Review?
Data protection for pertuzumab ended in April 2021. As such, this drug is eligible for a nonsponsored reimbursement review, per the Procedures for Reimbursement Reviews.
Pertuzumab, in combination with trastuzumab and chemotherapy, has previously been reviewed twice by CADTH for the neoadjuvant treatment of patients with HER2-positive locally advanced, inflammatory or early-stage breast cancer (> 2 cm in diameter or node positive) in 2015 and 2022. Both reviews resulted in a do not reimburse recommendation. In 2015, a negative recommendation was issued because there was no demonstrated progression-free survival benefit, and it was unclear whether pathologic complete response (pCR) correlated with survival outcomes. In 2022, a negative recommendation was issued again because the available evidence did not show significant differences in progression-free survival and disease-free survival, and other survival outcomes were either immature or not reported.
At the request of the public drug programs, a new review of the evidence for pertuzumab in the neoadjuvant setting was conducted. The request was prompted by emerging evidence suggesting potential efficacy and safety benefits and opportunities for cost minimization, particularly by reducing reliance on adjuvant T-DM1, which has notable toxicity concerns.
Input From Interested Parties
Breast Cancer Canada shared patient group input in support of the reimbursement review, citing that the use of pertuzumab in combination with trastuzumab and chemotherapy is supported by published guidance by Manna et al. in 2024 in Canada. Results of a survey conducted with individuals diagnosed with stage II or III HER2-positive breast cancer were also submitted, which highlighted their treatment experiences, their perspectives of benefits and side effects of treatment, as well as insights on treatment burden and financial impacts.
The Inflammatory Breast Cancer Network Foundation Canada submitted detailed patient group feedback. The group shared members’ concerns about inequitable access to neoadjuvant treatment with pertuzumab in Canada, citing that this treatment is readily accessible in other countries. The input also highlighted that diarrhea is a common adverse event of pertuzumab treatment and also highlighted other side effects (e.g., febrile neutropenia leading to hospitalization) related to other chemotherapies. In addition, this patient group highlighted the importance of having access to a treatment that reduces the risk of recurrence. Doing so also helps to avoid subsequent treatment, such as T-DM1 which is more toxic and difficult for patients to tolerate. The financial impact of treatment was shared by some members as well. Overall, this group advocated for the reimbursement of neoadjuvant pertuzumab in early HER2-positive breast cancer.
The Canadian Breast Cancer Network submitted detailed patient group input. In particular, survey results of patients with HER2-positive breast cancer were provided to highlight important considerations in treatment decision-making. In particular, the patients highlighted that key considerations include the efficacy of treatment and impact on quality of life. Respondents’ survey results also indicated that as many as 18% of all prescribed treatments are not publicly funded; among these unfunded treatments, pertuzumab is a treatment commonly prescribed by oncologists.
Rethink Breast Cancer shared insights as a patient group about the disease, current available treatment options, and survey results of outcomes important to patients diagnosed with breast cancer. These results indicate a high proportion of respondents rate maintaining quality of life and managing side effects as important outcomes. Two detailed testimonies were also submitted, highlighting the patients’ experiences and challenges with treatment access for pertuzumab due to cost or lack of public funding for this treatment in early HER2-positive breast cancer treatment.
The Ontario Health (Cancer Care Ontario) Breast Cancer Drug Advisory Committee provided clinician group input on the current treatments and treatment goals for early HER2-positive breast cancer. This clinician group highlighted important treatment gaps and unmet needs, specifically that dual HER2-directed therapy with neoadjuvant pertuzumab with trastuzumab is a standard of care in other jurisdictions. The input also shared the potential benefits of this treatment regimen in avoiding the use of T-DM1 in the adjuvant setting. The clinician group also highlighted the challenge of prescribing and supporting a combination treatment for which some treatments are administered and provided in publicly funded clinics and others (e.g., pertuzumab) are supported by private infusion clinics.
The Breast Medical Oncology Group at the Juravinski Cancer Centre in Hamilton, Ontario, submitted clinician group input, sharing various clinical evidence in support of the treatment of pertuzumab in combination with trastuzumab and chemotherapy in early HER2-positive breast cancer. This clinician group also discussed the value of patients achieving pCR and how it affects treatment decisions in the adjuvant setting (e.g., treatment options to lower the risk of toxicity). The clinician group also highlighted that the most important goals for patients are to increase their ability to achieve the best response and remain cancer-free.
The REAL Canadian Alliance shared clinician group input for the review by referencing a recent publication on expertise guidance. The group highlighted the following recommendation: “For patients with HER2 early breast cancer with ≥ cT2 or those with nodal disease (cN+), the standard of care is neoadjuvant therapy with trastuzumab plus pertuzumab plus chemotherapy.” The group also provided clinical evidence in support of this treatment. The group also highlighted other benefits, such as reducing the adjuvant use of T-DM1 by supporting more patients to achieve pCR.
Sunnybrook Breast Medical Oncology Team submitted a letter of support to advocate for the optimization of neoadjuvant therapy for patients with HER2-positive early breast cancer. Specifically, the group strongly supports CDA-AMC to recommend funding for this treatment. The group also shared key benefits of this treatment for patients, including improved breast cancer outcomes and the potential to avoid adjuvant T-DM1.
Hoffmann-La Roche Limited provided input to highlight the inequity of treatment access for neoadjuvant treatment in breast cancer. The industry group also provided information related to the latest treatment guidelines and evidence in support of the use of pertuzumab in combination with trastuzumab and chemotherapy in early breast cancer.
Disclaimer: The perspectives shared by people with lived experience who present to the committee reflect their individual experiences and are not necessarily representative of all people with the same condition or course of treatment. Their insights provide valuable context about what a patient, support person, or caregiver might go through when facing this condition or treatment, helping to inform the committee’s deliberations. These narratives complement other forms of evidence and input and should be considered as part of a broader understanding of the condition and treatment under review. Where gender or gendered pronouns are used in these narratives, they are included with the permission of the individual.
Summary of Deliberation
FMEC deliberated on all domains of value of the deliberative framework prior to developing their recommendation: clinical value, unmet clinical need, distinct social and ethical considerations, economic considerations, and impacts on health systems. For further information on the domains of value, please refer to the Expert Committee Deliberation at Canada’s Drug Agency document.
FMEC considered the following key discussion points, organized by the 5 domains of value.
Clinical Value
FMEC concluded that it is uncertain whether pertuzumab in combination with trastuzumab and chemotherapy demonstrates acceptable clinical value versus appropriate comparators in the Canadian setting.
Through reflection on the input from patient groups or insights shared by the person with lived experience, FMEC members noted the following important patient value or perspective: patients acknowledge the importance of total pCR as an outcome. In addition, survival outcomes, safety outcomes related to treatments, and quality of life are all important outcomes to patients.
FMEC members highlighted the following discussion points:
FMEC discussed that the PEONY trial plus all 5 RWE studies included total pCR as an outcome, whereas the NeoSphere trial considered breast pCR. pCR is an important patient outcome because it helps to determine the adjuvant treatment options. FMEC noted that pertuzumab resulted in clinically important and statistically significant improvements in pCR compared to no pertuzumab based on results from the PEONY trial (odds ratio [OR] = 0.43; 95% confidence interval [CI], 0.25 to 0.73), the NeoSphere trial (absolute between-group difference = 16.82%; 95% CI, 3.5% to 30.1%; P = 0.0141), and 4 RWE studies. As such, FMEC discussed that, because there were higher portions of patients achieving pCR with the addition of pertuzumab to trastuzumab in the neoadjuvant setting, this led to a decrease in residual disease and resulted in less utilization of adjuvant therapy with T-DM1, which is associated with high rates of toxicity relative to adjuvant trastuzumab monotherapy.
FMEC noted that, based on the body of evidence from the PEONY and NeoSphere trials and the included RWE studies, there is support that the addition of neoadjuvant pertuzumab may lead to increased total pCR rates. This is an important outcome to patients, and adding pertuzumab to trastuzumab and chemotherapy in the neoadjuvant setting offers overall benefits to them.
FMEC further discussed the additional benefits of achieving total pCR. Patients with total pCR tend to also benefit from other improved outcomes, such as improved quality of life, avoiding more toxic downstream treatments (e.g., T-DM1), and returning to work sooner. These benefits are different and separate from the overall survival outcomes measured in clinical trials. Further, patients have voiced that they value these benefits and outcomes in the treatment journey.
FMEC noted that the 3-year and 5-year between-group difference in overall survival (OS) (6.0% and 3.9%, respectively) and the 5-year hazard ratio (HR) of 0.53 were not statistically significant in the PEONY trial. However, the guest specialists noted that a 4% absolute between-group difference in OS and the estimated HR were clinically meaningful. However, the evidence was very uncertain due to imprecision because the number of events was low, the CIs were wide, and the lower bound of the 95% CI for the difference in OS included the possibility of little to no clinically significant benefit. In contrast, the RWE study by van der Voort et al. (2022) reported an adjusted HR of 0.51 for 5-year OS, which was both statistically significant and clinically meaningful. However, this finding also has some uncertainty due to residual confounding and imprecision. FMEC also discussed some emerging evidence from a meta-analysis that suggests pCR is an informative surrogate outcome for survival benefits, although a comprehensive appraisal of this topic is outside the scope of this review.
Unmet Clinical Need
FMEC concluded there is a significant clinical need arising from early breast cancer despite available treatments.
Through reflection on the input from patient groups and the insights shared by the person with lived experience, FMEC members noted the following important patient values or perspectives: patients want treatments that offer a better chance of cure and OS. Their treatment goals include pCR, reduced risk of recurrence, and minimized toxicity of and need for additional treatments with additional adverse events. They would also like to maintain their quality of life.
FMEC members highlighted the following discussion points:
FMEC noted that the alternative treatment options for HER2-positive breast cancer (> 2 cm or node positive) include chemotherapy in combination with trastuzumab followed by adjuvant T-DM1 if total pCR is not achieved with surgery; otherwise, the adjuvant treatment is trastuzumab for patients with total pCR.
FMEC discussed that T-DM1 is associated with more toxicities, as shared by guest specialists, the patient groups, and the person with lived experience. As such, it would be preferable to achieve a total pCR and avoid T-DM1, if possible. Toxicities with T-DM1 are manageable; however, in the adjuvant setting in the Katherine trial, 18% (n = 133) of patients from the T-DM1 group developed adverse events leading to discontinuation of treatment versus 2.1% (n = 15) of patients from the trastuzumab monotherapy group. One guest specialist estimated a lower rate of discontinuation of T-DM1 in their clinical practice.
Distinct Social and Ethical Considerations
FMEC concluded that pertuzumab in combination with trastuzumab and chemotherapy would potentially address a significant nonclinical need arising from early breast cancer despite available treatments.
FMEC did not identify any important measures that would need to be implemented to ensure the use of pertuzumab in combination with trastuzumab and chemotherapy addresses relevant social and ethical implications.
Through reflection on the input from patient groups or insights shared by the person with lived experience, FMEC members noted the following important patient values or perspectives: The current access to neoadjuvant treatment of pertuzumab is inequitable due to its high cost. Additional treatment requirements include the administrative burden associated with applying for financial assistance and the need to navigate and access private infusion clinics. Many patients face additional challenges due to potential concerns for fertility, childcare coordination, financial burden, and implications on career development.
FMEC members highlighted the following discussion points:
FMEC discussed that many breast cancer oncologists value the benefits of neoadjuvant pertuzumab in combination with trastuzumab and chemotherapy and they also shared concerns about the toxicity and additional monitoring requirements associated with adjuvant treatment of T-DM1.
FMEC noted that, based on published guidelines, input from external partners, and discussion with guest specialists, the use of neoadjuvant pertuzumab in combination with trastuzumab and chemotherapy has become a standard of care in early HER2-positive breast cancer management, both within Canada and outside of Canada. However, the lack of public funding of this treatment regimen has created inequity, in which only a subset of patients can access the treatment if it is affordable through private insurance or by paying out-of-pocket. The patients also need to have the means to coordinate the treatment and monitoring from multiple treatment centres because neoadjuvant pertuzumab is administered in private infusion clinics.
Economic Considerations
FMEC concluded there are economic considerations that are important to address when implementing the reimbursement of pertuzumab
FMEC members highlighted the following discussion points:
The reimbursement of pertuzumab is expected to increase drug acquisition costs and total treatment costs because it is always added to other current treatments for this patient population.
The total treatment cost calculation accounts for the known clinical benefit of increased pCR. Other clinical benefits (e.g., improved survival) remain uncertain, although evidence from observational studies suggests that event-free survival and OS are at least similar compared to regimens without pertuzumab.
A price reduction is warranted given the higher drug acquisition costs of pertuzumab coupled with uncertainty in outcomes.
There are currently no generic pertuzumab formulations under review by Health Canada.
No Canadian cost-effectiveness studies have been published since 2020.
Cost-effectiveness assessments from the 2022 CADTH review showed some scenarios in which pertuzumab in combination with trastuzumab and chemotherapy may be cost-effective compared to trastuzumab in combination with chemotherapy at an incremental cost-effectiveness ratio threshold of $50,000 per quality-adjusted life-year gained, but this result was dependent on how pCR outcomes were assumed to translate into survival outcomes. Under the assumption of equivalent impact on event-free survival (HR = 1), the economic model showed that pertuzumab in combination with trastuzumab and chemotherapy was more costly and less effective than trastuzumab in combination with chemotherapy.
Impacts on Health Systems
FMEC concluded that there are impacts on health systems that are important to address when implementing pertuzumab in combination with trastuzumab and chemotherapy.
FMEC members highlighted the following discussion points:
FMEC discussed that the use of neoadjuvant pertuzumab would increase the nursing and pharmacy resources required to prepare and administer this treatment for an additional 3 to 6 cycles.
FMEC also discussed that the subsequent resources required in the adjuvant setting differ depending on if pCR was reached or if the patient has residual disease. For patients with pCR, the adjuvant treatment of trastuzumab monotherapy is typically well tolerated for 14 cycles. For patients who continue to have residual disease after neoadjuvant treatment, the use of adjuvant T-DM1 is associated with more toxicities, frequent bloodwork investigations, and clinic visits. FMEC noted that it is generally preferred for pCR to occur so patients can receive adjuvant treatment with trastuzumab, which is perceived to be better tolerated than adjuvant T-DM1 in patients with residual disease.
Figure 1: Recommendation Pathway
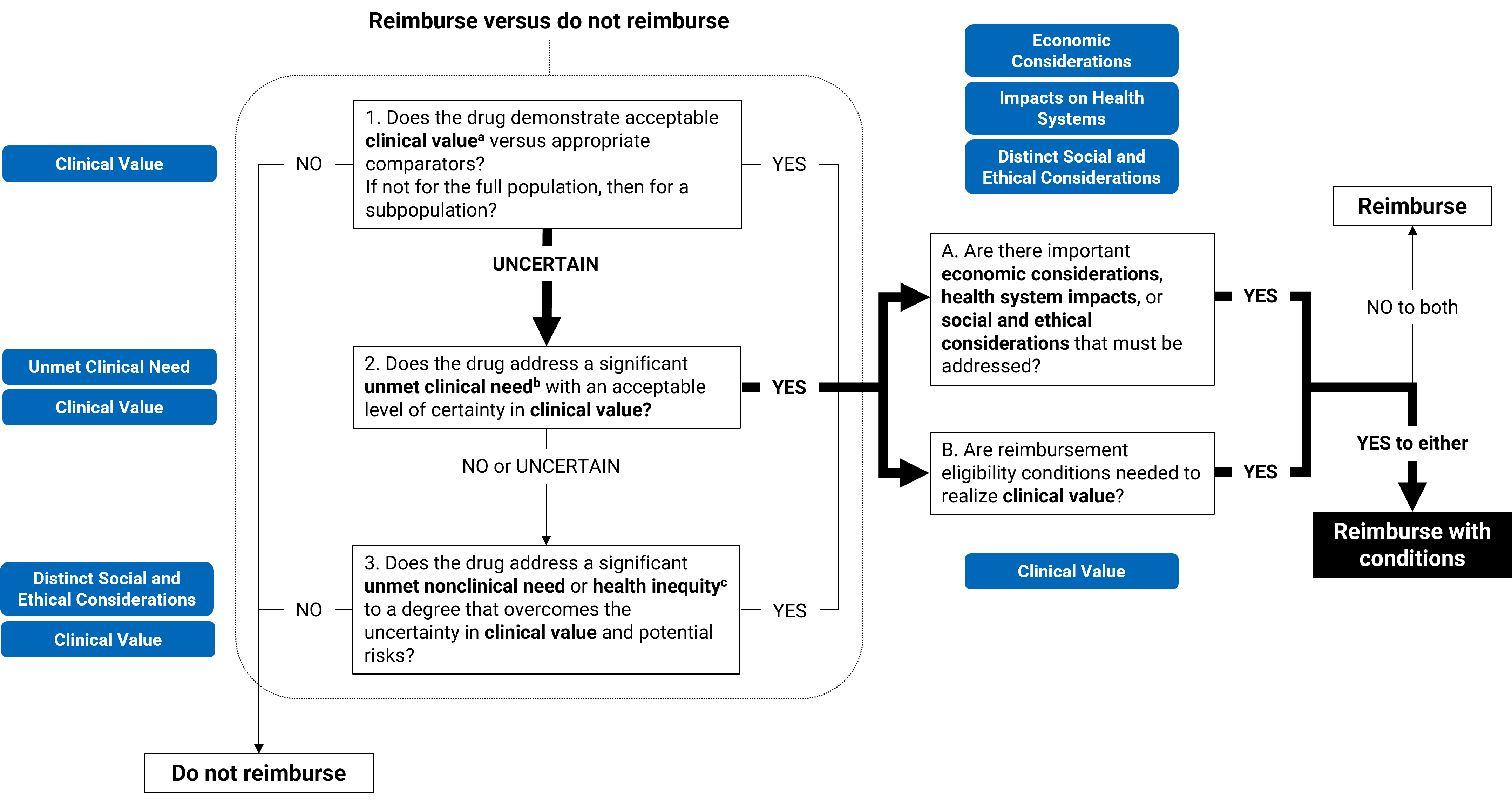
aAcceptable clinical value refers to at least comparable clinical value (if the drug is expected to be a substitutive treatment) or added clinical value (if the drug is expected to be an additive treatment) versus appropriate comparators.
bSignificant unmet clinical need depends on all the following: severity of the condition, availability of effective treatments, and challenges in evidence generation due to the rarity of the condition or ethical issues.
cUnmet nonclinical need and health inequity are key components within the distinct and social ethical considerations domain of value.
Full Recommendation
With a vote of 7 to 0, FMEC recommends that pertuzumab in combination with trastuzumab and chemotherapy for the treatment of early-stage HER2-positive breast cancer in the neoadjuvant setting be reimbursed if the conditions presented in Table 1 are met.
Table 1: Conditions, Reasons, and Guidance
Reimbursement condition | Reason | Implementation guidance |
|---|---|---|
Initiation | ||
1. Pertuzumab in combination with trastuzumab and chemotherapy may be initiated in adult patients for the neoadjuvant treatment of early-stage HER2-positive breast cancer if all the following conditions are met: 1.1. there is locally advanced, inflammatory or early-stage breast cancer (> 2 cm or node positive) 1.2. there is no evidence of metastasis 1.3. treatment of pertuzumab is limited to a maximum of 6 cycles in the neoadjuvant setting. | The evidence suggests pertuzumab in combination with trastuzumab and chemotherapy results in a clinically important improvement in pCR compared to placebo in combination with trastuzumab and chemotherapy. Further, patients with pCR can avoid adjuvant treatment with T-DM1, which is associated with higher rates of toxicity relative to trastuzumab monotherapy in the adjuvant setting. FMEC also noted that pertuzumab in combination with trastuzumab and chemotherapy is considered a standard of care in the management of early HER2-positive breast cancer based on published guidelinesa-c and input from the clinician groups and guest specialists consulted for this review. | The exact number of cycles of pertuzumab neoadjuvant treatment depends on the chemotherapy backbone and may range from 3 to 6 cycles. |
Discontinuation and renewal | ||
2. Treatment should be discontinued if there is any of the following: 2.1. disease progression 2.2. unacceptable toxicities. | Consistent with clinical practice, patients discontinued treatment upon disease progression or unacceptable toxicities. | — |
Prescribing | ||
3. Prescribing should be limited to clinicians with expertise in the diagnosis and management of breast cancer. | This will ensure that appropriate treatment is prescribed for patients, and adverse events are optimally managed. | — |
Pricing | ||
4. A price reduction may be required. | The reimbursement of pertuzumab is expected to increase overall drug acquisition costs. No recent evidence was identified regarding the cost-effectiveness of pertuzumab relative to relevant comparators. A cost-effectiveness analysis would be needed to determine whether pertuzumab is cost-effective. Price reductions may be required, because pertuzumab is associated with increased drug acquisition costs and likely clinical benefit. | — |
LVEF = left ventricular ejection fraction; pCR = pathologic complete response; T-DM1 = trastuzumab emtansine.
aLoibl S, Andre F, Bachelot T, et al. Early breast cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann Oncol. 2024;35(2):159182. doi.org/10.1016/j.annonc.2023.11.016
bGradishar WJ, Moran MS, Abraham J, et al. Breast Cancer, Version 3.2024, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2024;22(5):331-357. doi.org/10.6004/jnccn.2024.0035
cManna M, Gelmon KA, Boileau J-F, et al. Guidance for Canadian Breast Cancer Practice: National Consensus Recommendations for the Systemic Treatment of Patients with HER2-POSITIVE Breast Cancer in Both the Early and Metastatic Setting. Current Oncology. 2024;31(11):6536-6567.
Feedback on Draft Recommendation
CDA-AMC received feedback from 3 clinician groups (Ontario Health [Cancer Care Ontario] Breast Cancer Drug Advisory Committee, REAL Canadian Breast Cancer Alliance, London Health Sciences Centre), 2 patient groups (Canadian Breast Cancer Network, Breast Cancer Canada), and the public drug programs. All groups were in support of the draft recommendation and acknowledged the committee for considering the input from external partners and alignment of recommendation with current standard of care. Both REAL Canadian Breast Cancer Alliance and Breast Cancer Canada have shared comments on economic considerations related to the pertuzumab neoadjuvant treatment regimen. CDA-AMC may work with jurisdictions, if requested, to provide additional implementation support (e.g., budget impact analysis modelling).
FMEC Information
Members of the committee: Dr. Emily Reynen (Chair), Dr. Zaina Albalawi, Dr. Hardit Khuman, Ms. Valerie McDonald, Dr. Bill Semchuk, Dr. Jim Silvius, Dr. Marianne Taylor, Dr. Maureen Trudeau, Dr. Dominika Wranik. Two guest specialists from British Columbia and Ontario participated in this review.
Regrets: One expert committee member did not attend the meeting.
Meeting date: July 17, 2025
Conflicts of interest: None
Special thanks: CDA-AMC extends our special thanks to the individuals who presented directly to FMEC and to the patient organizations representing the community of those with or having had breast cancer, including the Canadian Breast Cancer Network, J. K. Miller, and Bukun Adegbembo.
Note: CDA-AMC makes every attempt to engage with people with lived experience as closely to the indication and treatments under review as possible. However, at times, CDA-AMC is unable to do so and instead engages with individuals who have similar treatment journeys or experience with the comparators under review to ensure that lived experience perspectives are included and considered in Reimbursement Reviews. CDA-AMC is fortunate to be able to engage with individuals who are willing to share their treatment journey with FMEC.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.