Drugs, Health Technologies, Health Systems
Reimbursement Review
Ibrutinib
Requester: Public drug programs
Therapeutic area: Mantle cell lymphoma
Summary
What Is Mantle Cell Lymphoma?
Mantle cell lymphoma (MCL) is a rare subtype of B-cell non-Hodgkin lymphoma (NHL) that develops from malignant B lymphocytes within the outer region of a lymph node (i.e., mantle zone).
MCL accounts for 5% to 10% of all new NHL diagnoses in Canada.
What Are the Treatment Goals and Current Treatment Options for MCL?
The main goals of treatment are to achieve a durable remission, improve progression-free survival (PFS), and improve overall survival (OS). Minimizing potential toxicities from treatments is important. Given that there is no curative therapy for MCL, a critical treatment goal is to prolong the time to subsequent lines of therapy.
The current treatment approaches for first-line therapy for MCL (for patients who are previously untreated) are primarily based on patient’s age, fitness for intensive chemotherapy and potential autologous stem cell transplant (ASCT), and disease biology. Observation (known as a “watch and wait” strategy) is a suitable option for patients with asymptomatic MCL with a low tumour burden, leukemic non-nodal presentation, and nonbulky disease.
The standard of care in Canada for fit and newly diagnosed younger patients (aged up to 65 years, approximately) consists of an alternating schedule of immunochemotherapy induction using R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone) and R-DHAP (rituximab, dexamethasone, high-dose cytarabine, and cisplatin) followed by ASCT and then 2 years of rituximab maintenance. Some treatment institutions administer bendamustine and rituximab (BR) for induction therapy before ASCT.
What Is Ibrutinib and Why Did Canada’s Drug Agency Conduct This Review?
Ibrutinib is an oral drug that blocks specific molecules involved in cancer cell growth and survival. Health Canada has approved ibrutinib for patients with relapsed or refractory MCL.
At the request of the participating public drug programs, Canada’s Drug Agency (CDA-AMC) reviewed ibrutinib to inform a recommendation on whether it should be reimbursed in combination with immunochemotherapy for the first-line treatment of MCL in adult patients who are previously untreated and eligible for ASCT.
How Did CDA-AMC Evaluate Ibrutinib?
CDA-AMC reviewed the clinical evidence on the beneficial and harmful effects and compared costs of ibrutinib in combination with immunochemotherapy versus other treatments used in Canada for first-line treatment of MCL in adult patients who are previously untreated and eligible for ASCT. The comparators considered relevant to the reviews were an alternating R-CHOP and R-DHAP regimen and a BR regimen.
The clinical evidence was identified through systematic searches for available studies.
The review was also informed by 3 clinician group submission(s) in response to our call for input, and by input from the participating public drug programs around issues that may impact their ability to implement a recommendation. Two hematologists with representation from Ontario and the Prairies were consulted as part of the review process.
What Were the Findings?
Clinical Evidence
CDA-AMC reviewed the following clinical evidence:
One randomized controlled, 3-arm, open-label phase III trial (the TRIANGLE study) was reviewed comparing the addition of ibrutinib to alternating R-CHOP and R-DHAP cycles with ASCT (group A plus I) versus a regimen of alternating R-CHOP and R-DHAP cycles with ASCT (group A), and versus a regimen of ibrutinib plus alternating R-CHOP and R-DHAP cycles without ASCT (group I) for patients with previously untreated MCL.
For the comparison of group A plus I versus group A: Ibrutinib combined with alternating R-CHOP and R-DHAP cycles with ASCT (group A plus I) may improve PFS, failure-free survival (FFS), and duration of remission (DOR) compared with alternating R-CHOP and R-DHAP cycles with ASCT (group A).
For the comparison of pooled groups receiving ibrutinib (group A plus I and group I) versus group A: Complete remission rates and overall response rates (ORR) were higher in groups receiving ibrutinib.
For the comparison of group I versus A: Evidence suggests that results achieved by combining ibrutinib with alternating R-CHOP and R-DHAP cycles were similar to those achieved with alternating R-CHOP and R-DHAP cycles and ASCT in terms of PFS, FFS, and DOR outcomes.
For the comparison of group A plus I versus group I: Results comparing the efficacy in group A plus I versus group I were not yet reported; as such, the effect of adding ibrutinib and ASCT to treatment compared to adding ibrutinib only without ASCT is unknown.
The safety profile of ibrutinib combined with an R-CHOP and R-DHAP regimen was as expected, and no new safety outcomes were identified. However, the long-term safety and effectiveness of the combined therapy remain unknown.
No evidence was identified to inform how ibrutinib combined with immunochemotherapy compares with BR.
No evidence was identified to inform how ibrutinib combined with immunochemotherapy affects patients’ health-related quality of life (HRQoL).
Economic Evidence
Reimbursing ibrutinib for patients with previously untreated MCL is expected to increase costs to public drug programs.
Abbreviations
AE
adverse event
ASCT
autologous stem cell transplant
BR
bendamustine and rituximab
BTK
Bruton tyrosine kinase
CDA-AMC
Canada’s Drug Agency
CI
confidence interval
DOR
duration of remission
ECOG
Eastern Cooperative Oncology Group
FFS
failure-free survival
HR
hazard ratio
HRQoL
health-related quality of life
IQR
interquartile range
ITT
intention to treat
MCL
mantle cell lymphoma
MIPI
Mantle Cell Lymphoma Prognostic Index
NHL
non-Hodgkin lymphoma
ORR
overall response rate
OS
overall survival
PFS
progression-free survival
R-CHOP
rituximab, cyclophosphamide, doxorubicin, vincristine, prednisone
R-DHAP
rituximab, dexamethasone, cytarabine, cisplatin
SAE
serious adverse event
Background
Introduction
The objective of the Clinical Review is to review and critically appraise the evidence on the beneficial and harmful effects of ibrutinib in combination with immunochemotherapy with or without ASCT in the treatment of adults with previously untreated MCL who are transplant eligible. The focus will be placed on comparing the addition of ibrutinib to relevant comparators in clinical practice in Canada. The Economic Review consists of a cost comparison for the addition of ibrutinib compared with relevant comparators for the same population. The comparators considered relevant to the reviews were an alternating R-CHOP and R-DHAP regimen and a BR regimen. The R-CHOP and R-DHAP regimen and the BR regimen are immunochemotherapies that combine CD20 antibody therapy with chemotherapy.
Table 1: Information on the Drug Under Review and on the CDA-AMC Review
Item | Description |
|---|---|
Information on the drug under review | |
Drug | Ibrutinib (Imbruvica) |
Relevant Health Canada indication | Not yet approved as first-line therapy for MCL; approved for relapsed or refractory MCL |
Mechanism of action | Small-molecule, targeted inhibitor of Bruton tyrosine kinase |
Recommended dosage | 560 mg daily |
Data protection status | May 17, 2023 |
Status of generic drugs or biosimilars | At least 4 generic drugs have been accepted into review by Health Canada, with the earliest submission in 2021 |
Information on the CDA-AMC review | |
Requester | Oncology Working Group |
Indication under consideration for reimbursement | In combination with immunochemotherapy with or without ASCT in the treatment of previously untreated transplant-eligible patients with MCL |
ASCT = autologous stem cell transplant; CDA-AMC = Canada’s Drug Agency; MCL = mantle cell lymphoma.
Sources of Information
The contents of the Clinical Review are informed by studies identified through systematic literature searches, input received from interested parties (patient groups, clinician groups, drug programs, and industry), and input from clinical experts consulted for this review.
Calls for patient group, clinician group, and industry input are issued for each Non-Sponsored Reimbursement Review. The following submissions were received: 3 clinician group submission(s) from the Alberta Provincial Lymphoma Group, the Leukemia and Lymphoma Society of Canada Pharmacist Network, and the Ontario Health (Cancer Care Ontario) Hematology Cancer Drug Advisory Committee. Clinician groups gathered input through various ways: a literature search of PubMed for published clinical trials of first-line treatment for adult patients with MCL, a targeted interview with an experienced oncology pharmacist in Canada, and a video conference meeting with Ontario Health (Cancer Care Ontario) Hematology Cancer Drug Advisory Committee members. The full submissions received are available on the project landing page in the consolidated input document. Input from patient and clinician groups is considered throughout the review, including in the selection of outcomes to include in the Clinical Review and in the interpretation of the clinical evidence.
The drug programs provide input on each drug being reviewed through the Reimbursement Review process by identifying issues that may affect their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted for this review are summarized and provided to the expert committee in a separate document.
Each review team includes at least 1 clinical expert with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process. Two oncologists with expertise in the diagnosis and management of MCL participated as part of the review team, with representation from Ontario and the Prairies. Relevant input is summarized in the Disease Background, Current Management, and Unmet Needs and Existing Challenges sections.
Disease Background
MCL is a rare subtype of B-cell NHL that develops from malignant B lymphocytes within the outer region of a lymph node (i.e., mantle zone).1 MCL can involve lymph nodes and often non–lymph node sites, such as the blood, bone marrow, spleen, liver, and gastrointestinal tract.2 MCL accounts for 5% to 10% of all new NHL diagnoses in Canada. In 2022, NHL incidence was estimated as 11,400 cases per year in Canada.3 About 75% of patients with MCL are male.2 MCL is twice as common in white individuals as it is in Black individuals.2 It is usually diagnosed in people aged older than 65 years.4
There are 2 major subtypes of MCL, which present differently.2 Most people with MCL have an aggressive form, also known as nodal or classic MCL, with involvement of multiple lymph nodes, with or without spreading to other tissues outside of the lymph nodes, as described in the previous paragraph.2 Less commonly, one-fifth of patients have the indolent form of non-nodal MCL that may not need immediate treatment, despite presenting with blood and bone marrow involvement.5 Individuals are usually diagnosed at advanced stage II to IV and rarely at limited stages (stage I).5
The symptoms individuals experience depend on the extent of the disease and the affected region of the body. Examples of symptoms include swollen painless lymph nodes, headache, weakness, decreased appetite, and indigestion. Other nonspecific symptoms may include unexplained fever, weight loss, sweating at night (“night sweats”), fatigue, reduced energy, and easy bruising or bleeding.2
Current Management
Treatment Goals
The main goals of treatment are to achieve a durable remission, improve PFS, and improve OS. Minimizing potential toxicities from treatments is important. Given that there is no curative therapy for MCL, a critical treatment goal is to prolong the time to subsequent lines of therapy being required. Overall, an optimal therapeutic regimen would effectively balance efficacy with tolerability, reduce the need for intensive interventions such as ASCT, and maintain the patient’s HRQoL.
Current Treatment Options
The current treatment approaches for first-line therapy for MCL (for patients who are previously untreated) are primarily based on a patient’s age, fitness for intensive chemotherapy, fitness for potential ASCT, and disease biology. Observation (known as a “watch and wait” strategy) is a suitable option for patients with asymptomatic MCL with a low tumour burden, leukemic non-nodal presentation, and nonbulky disease.
The standard of care in Canada for fit and newly diagnosed younger patients (aged up to 65 years, approximately) consists of an alternating schedule of immunochemotherapy induction using R-CHOP and R-DHAP followed by high-dose chemotherapy and ASCT, and then 2 years of rituximab maintenance. Some treatment institutions administer BR for induction therapy before ASCT.
Clinician groups acknowledged that due to improved response rates and PFS outcomes, Bruton tyrosine kinase (BTK) inhibitors (e.g., ibrutinib) may be added to the upfront rituximab with chemotherapy regimen and rituximab maintenance. However, ibrutinib and other BTK inhibitors are not yet provincially funded for previously untreated patients with MCL and may be available via compassionate access programs.
Older and less fit patients might not be able to tolerate the intensive strategies recommended for younger patients. They could be treated with chemoimmunotherapy using BR followed by rituximab maintenance. As with younger patients, there may be opportunities to add in BTK inhibitors, if available.
Unmet Needs and Existing Challenges
The following is based on input provided by 3 clinician groups and clinical experts consulted for this review.
There are substantial unmet needs and limitations associated with current treatment approaches. One key challenge is variability in treatment response. Not all patients achieve an adequate response to standard therapies, such as immunochemotherapy or ASCT. Patients with high-risk disease features, such as tumours with TP53 mutations, blastoid or pleomorphic disease, and/or high Ki-67 index scores may have a lower likelihood of response to induction treatment and shorter DOR following high-dose therapy and ASCT. Patients with MCL whose tumours that have TP53 mutations tend to have poorer outcomes; median PFS has been estimated at less than 1 year after intensive chemotherapy with or without ASCT.
Another limitation is that ASCT is an intensive therapy that requires prolonged hospitalization and carries risks of severe adverse events (AEs), including myelosuppression, infections, organ injury, transplant-related mortality, and late secondary malignancies. Total body irradiation-based induction before ASCT adds additional toxicity for younger patients, so an effective alternative that would reduce or eliminate the need for this procedure is a critical unmet need. Additionally, the availability of oral or less-intensive formulations may potentially improve patient adherence.
Furthermore, current therapies are often associated with complex administration schedules, frequent hospital visits, and poor treatment adherence, especially in older patients or those with comorbidities. Current therapies primarily aim to manage the disease rather than reverse its course, which is particularly concerning in advanced stages of MCL and highlights the lack of curative therapies and the difficulty in sustaining long-term remission.
For these reasons, there is a need for more effective and better tolerated first-line treatments for MCL that are capable of providing durable responses, reduce reliance on intensive interventions such as ASCT, reduce toxicity, improve survival, and promote quality of life.
Considerations for Using the Drug Under Review
Contents within this section have been informed by input from the clinical experts consulted for the purpose of this review and from clinician groups. The following has been summarized by the review team.
Place in Therapy
Ibrutinib is a drug that targets the underlying disease biology by inhibiting BTK, which is a crucial part of the B-cell receptor signalling pathway associated with the growth and survival of malignant B cells, including MCL. This mechanism of action complements conventional treatments, such as chemotherapy, which primarily work through cytotoxic effects on cancer cells but often result in collateral damage to healthy cells. Therefore, ibrutinib offers a potential new approach to the current treatment paradigm for MCL. Ibrutinib is expected to be added to front-line immunochemotherapy for more effective induction and maintenance treatment for select patients. Addition of ibrutinib may defer or eliminate the need for ASCT and its toxicity and enhance the efficacy of chemoimmunotherapy.
Patient Population
The clinical experts and clinician groups identified individuals with newly diagnosed symptomatic or progressive MCL, adequate performance status, and adequate organ function who are fit enough for intensive therapy with ASCT, without significant comorbidities (e.g., significant cardiac disease), and without contraindications to BTK inhibitors. Most patients respond adequately to ibrutinib, even those with central nervous system lymphoma and other high-risk features (e.g., blastoid or pleomorphic disease, tumours with high Ki-67 index scores, p53 genetic mutations), and could be candidates for this regimen. The clinical experts indicated that diagnostic accuracy is considered excellent using immunohistochemistry testing (immunophenotype; expression of CD5, p53, or cyclin D1 proteins), flow cytometry, and molecular or genetic assessment by experienced hematopathologists, so misdiagnosing MCL is very rare. In addition, companion testing is not required. It is expected that the number of patients potentially eligible for ibrutinib would be small because MCL is a rare subtype of lymphoma and is primarily diagnosed in older individuals who do not proceed to ASCT.
Patients least suited for ibrutinib include those who are unlikely to tolerate the regimen due to old age, poor performance status, inadequate organ function, or active uncontrolled infections. Ibrutinib would not be suitable for patients at high risk for bleeding or bleeding disorders, patients requiring anticoagulation with warfarin or treatment with strong CYP3A4 inducers or inhibitors, or those who have significant cardiac disease, especially cardiac arrhythmias.
Assessing the Response to Treatment
In clinical practice, treatment response in patients with MCL is assessed using laboratory testing, clinical assessments, and imaging. Laboratory testing is done every 3 weeks before each cycle if the patient is receiving the R-CHOP and R-DHAP regimen or every 4 weeks if receiving the BR regimen to determine if blood count levels have improved (i.e., lymphocytosis, cytopenia, hemoglobin, platelets, neutrophils). Clinical assessments are completed before each cycle. In terms of imaging, PET or CT scans (depending on local diagnostic imaging resources) are performed after cycle 3 or 4 of induction immunochemotherapy and then after cycle 6, before transplant (if planned). PET or CT scans are repeated posttransplant (if performed) before maintenance treatment. While receiving maintenance treatment, patients are clinically examined every 3 months. Imaging during maintenance therapy is not performed routinely, is based on physician discretion, and is only done if there is a clinical need to assess symptoms suggesting lymphoma recurrence or late toxicities.
The experts indicated that indicators of clinically meaningful response to treatment include resolution of symptoms such as constitutional symptoms and lymphadenopathy, improvement in laboratory test parameters that were abnormal at baseline, improvement in performance status, and improvement in their ability to return to independence in activities of daily living, work, or previous level of functioning.
Discontinuing Treatment
The most common factors in deciding to discontinue treatment with ibrutinib is if there is objective evidence of disease progression, lack of response, or side effects of treatment (low blood counts, skin rash, gastrointestinal symptoms, joint pain) that cannot be resolved with dose reduction or a delay in ibrutinib treatment. Other less common reasons for discontinuation of ibrutinib include life-threatening cardiac complications (e.g., cardiac arrhythmia or new onset atrial fibrillation warranting ablation), life-threatening bleeding (e.g., intracranial bleed), recurrent or severe infections, or other persistent intolerances.
Prescribing Considerations
Ibrutinib should be prescribed by a hematologist or medical oncologist with experience in managing patients with MCL from diagnosis to treatment and monitoring. Experience with chemoimmunotherapy, maintenance rituximab, and use of BTK inhibitors is required.
Clinicians should be familiar with managing potential AEs of ibrutinib (e.g., cardiac toxicities, bleeding, rash, arthralgia) and intensive chemotherapy (e.g., cytopenia, infections, gastrointestinal toxicities, and other organ toxicities). Regarding the setting, ibrutinib is an oral therapy regimen and is given on an outpatient basis at tertiary care and community hospitals with experience treating patients with MCL. This regimen would permit many patients with MCL to avoid being referred to a transplant centre, thereby improving convenience and quality of life by allowing patients to receive treatment closer to home.
Clinical Review
Methods
The review team conducted a systematic review to identify evidence for ibrutinib for the first-line treatment of MCL in adult patients who are previously untreated and transplant eligible. Studies were selected according to the eligibility criteria in Table 2.
Relevant comparators included treatments used in clinical practice in Canada in the patient population under review. Clinical expert input, patient group input, and clinician group input were considered when selecting outcomes (and follow-up times) for review. Selected outcomes are those considered relevant to expert committee deliberations. Detailed methods for the literature searches, study selection, and data extraction are provided in Appendix 1 in the Supplemental Material document.
Table 2: Systematic Review Eligibility Criteria
Criteria | Description |
|---|---|
Population | Adult patients with previously untreated MCL (first-line treatment) who are eligible for ASCT |
Intervention | Ibrutinib in combination with immunochemotherapy with or without ASCT |
Comparator |
|
Outcomes | Efficacy outcomes:
Safety:
AEs of special interest — bleeding, cardiac-related toxicity, infection, prolonged cytopenia, gastrointestinal side effects, rash, arthralgia |
Study design | Published phase II, III, and IV clinical trials |
AE = adverse event; ASCT = autologous stem cell transplant; BR = bendamustine and rituximab; HRQoL = health-related quality of life; MCL = mantle cell lymphoma; OS = overall survival; PFS = progression-free survival; R-CHOP = rituximab, cyclophosphamide, doxorubicin, vincristine, prednisone; R-DHAP = rituximab, dexamethasone, cytarabine, cisplatin; SAE = serious adverse event.
Clinical Evidence
From the search for primary studies, the review team identified 235 unique records via the searches of databases and registries, of which 225 were excluded by title and abstract. The review team screened 10 records by full text and included 1 report of 1 study. No potentially relevant records were identified from other sources.
A list of excluded studies, including reasons for exclusion, is provided in Appendix 1 in the Supplemental Material document.
Systematic Review
Description of Study
Study Characteristics
Characteristics of the included study are summarized in Table 3. Details pertaining to the eligibility criteria are provided in the Dreyling et al. study.6
Table 3: Characteristics of the Study Included in the Systematic Review
Study name, design, and sample size | Key inclusion criteria | Key exclusion criteria | Intervention and comparator | Relevant end points |
|---|---|---|---|---|
TRIANGLE study Phase III open-label, 3-arm, multicentre superiority trial N = 870 |
|
| Three treatment arms: Group A (standard of care): Immunochemotherapy with ASCT Six alternating cycles of R-CHOP (cycles 1, 3, 5) and R-DHAP induction (cycles 2, 4, 6) followed by ASCT Group A plus I: Ibrutinib plus immunochemotherapy with ASCT Six alternating cycles of R-CHOP induction plus ibrutinib on days 1 to 19 (cycles 1, 3, 5) and R-DHAP induction (cycles 2, 4, 6). Followed by ASCT and 2 years ibrutinib maintenancea Group I: Ibrutinib plus immunochemotherapy without ASCT Six alternating cycles of R-CHOP induction plus ibrutinib on days 1 to 19 (cycles 1, 3, 5) and R-DHAP induction (cycles 2, 4, 6). Followed by 2 years ibrutinib maintenancea | Primary end point: Investigator-assessed FFS Secondary end points:
|
ASCT = autologous stem cell transplant; DOR = duration of remission; ECOG = Eastern Cooperative Oncology Group; FFS = failure-free survival; MCL = mantle cell lymphoma; ORR = overall response rate; OS = overall survival; PFS = progression-free survival; R-CHOP = rituximab, cyclophosphamide, doxorubicin, vincristine, prednisone; R-DHAP = rituximab, dexamethasone, cytarabine, cisplatin; ULN = upper limit of normal.
aMaintenance therapy was given in all study arms if considered standard; as such, not all patients received it.
bThe primary end point is FFS, defined as time from randomization to stable disease at the end of immunochemotherapy, progressive disease, or death from any cause, whichever comes first. FFS is used as the primary end point instead of PFS, because FFS is more suitable for assessment of treatment efficacy than PFS in this setting, where at least partial response is a prerequisite to proceeding to ASCT.
Source: Dreyling et al.6
Statistical Testing and Analysis Populations
A sample size of 870 patients was calculated for the trial to be 90% powered to detect superiority of group A plus I versus group A and of group A plus I versus group I of 12 percentage points in FFS at 5 years (77.1% versus 64.8%; hazard ratio [HR] = 0.60) and superiority of group A versus group I of 16 percentage points in FFS at 5 years (64.8% versus 48.5%; HR = 0.60) with a statistical power of 95%. Three pairwise 1-sided hypothesis tests using log-rank statistics for FFS were planned: group A plus I versus group A, group A plus I versus group I, and group A versus group I. For each pairwise comparison, interim analyses were planned to be performed twice yearly to allow early stopping for efficacy or futility with truncated sequential probability ratio tests correcting for multiple testing. The significance level of each pairwise comparison is 1-sided, at 0.01666 (0.05 ÷ 3; Bonferroni correction) to maintain a global 1-sided significance level of 5%.
Kaplan-Meier methods uncorrected for the sequential design were used to estimate FFS, OS, PFS, and DOR. Time-to-event outcomes were censored at the last date showing absence of any event. One-sided 98.3% confidence intervals (CIs) for HRs were calculated based on Cox regression with Bonferroni correction for the 3 pairwise tests. For sensitivity analyses, the models adjusted for Mantle Cell Lymphoma Prognostic Index (MIPI) score without and with Ki-67 index scores and stratified for the randomization factors study group and MIPI risk group. Complete remission rates and ORRs were compared between group A and pooled A plus I and I induction groups using Fisher’s exact test.
An intention-to-treat (ITT) population of all randomized patients was used for efficacy analysis. The modified ITT population analysis, defined as all randomly assigned patients with confirmed MCL who started induction immunochemotherapy according to the randomly assigned arm, was used for sensitivity analysis. AEs were evaluated according to treatment periods (induction, ASCT, and maintenance or follow-up) and analyzed in groups according to the treatment actually given. Safety analysis during induction treatment compared group A with pooled ibrutinib A plus I and I induction groups. An exploratory analysis was done using Cox regression with 2-sided 95% CIs for HRs to compare the DOR in group I between patients with and without rituximab maintenance. The frequency of AEs during maintenance or follow-up was compared between patients with ibrutinib maintenance without rituximab maintenance and patients with both ibrutinib and rituximab maintenance.
Patient Disposition
Between July 29, 2016, and December 28, 2020, a total of 907 patients were screened for eligibility and 870 patients were randomized in a 1:1:1 ratio to group A (n = 288), group A plus I (n = 292), or group I (n = 290). Before receiving treatment, 2 patients assigned to group A and 2 patients assigned to group I withdrew from the study due to patient decision. Table 4 presents patient disposition of the TRIANGLE trial.
Table 4: Patient Disposition in the TRIANGLE Trial
Patient disposition | Group A (R-CHOP and R-DHAP with ASCT) | Group A plus I (R‑CHOP and R-DHAP with ASCT plus ibrutinib) | Group I (ibrutinib plus R-CHOP and R-DHAP without ASCT) |
|---|---|---|---|
Enrolled, n | 288 | 292 | 290 |
Did not start induction therapy due to patient decision, n | 2 | 0 | 2 |
Started induction therapy, n | 286 | 292 | 288 |
Completed induction therapy, n | 261 | 275 | 272 |
Did not complete induction therapy, n | 25 | 17 | 16 |
Reasons for noncompletion | |||
Progression | 8 | 2 | 2 |
Adverse events | 4 | 5 | 10 |
MCL diagnosis rejected | 2 | 4 | 1 |
Patient decision | 5 | 4 | 2 |
Physician decision | 4 | 0 | 0 |
Death | 1 | 2 | 1 |
COVID-19 death | 1 | 1 | 1 |
Suicide | 0 | 1 | 0 |
Treatment of other malignancy | 0 | 0 | 0 |
Insufficient documentation | 0 | 0 | 0 |
Started high-dose treatment, n | 244 | 252 | 3 |
Did not start high-dose treatment, n | 42 | 40 | 285 |
Started maintenance therapy, n | 168 | 238 | 260 |
Ibrutinib plus rituximab maintenance | 0 | 152 | 151 |
Ibrutinib maintenance | 0 | 86 | 109 |
Rituximab maintenance only | 168 | 13 | 7 |
Did not start maintenance therapy or progressed or died during maintenance, n | 141 | 41 | 24 |
Ongoing maintenance therapy, n | 78 | 124 | 122 |
MCL = mantle cell lymphoma.
Baseline Characteristics
Patients’ baseline characteristics from the included study are detailed in the Dreyling et al. study.6
Table 5: Summary of Baseline Characteristics From the Study Included in the Systematic Review
Characteristic | Group A (R-CHOP and R-DHAP with ASCT) N = 288 | Group A plus I (R-CHOP and R-DHAP with ASCT plus ibrutinib) N = 292 | Group I (ibrutinib plus R-CHOP and R-DHAP without ASCT) N = 290 |
|---|---|---|---|
Age (years),a median (IQR) | 57 (52 to 61) | 57 (52 to 61) | 57.5 (52 to 61) |
Sex, n (%) | |||
Female | 70 (24) | 76 (26) | 62 (21) |
Male | 218 (76) | 216 (74) | 228 (79) |
Race, n (%) | |||
White | 283 (98) | 283 (97) | 290 (100) |
Other [wording from original source] | 5 (2) | 9 (3) | 0 (0) |
ECOG Performance Status score, n (%) | |||
0 | 213 (74) | 213 (73) | 208 (72) |
1 | 70 (24) | 77 (26) | 77 (27) |
2 | 5 (2) | 2 (1) | 5 (2) |
Histologyb | |||
Mantle cell lymphoma, n (%) | 286 (99) | 288 (99) | 288 (99) |
Ann Arbor stage, n (%) | N = 285 | N = 290 | N = 289 |
I | 0 (0) | 0 (0) | 0 (0) |
II | 11 (4) | 12 (4) | 18 (6) |
III | 24 (8) | 21 (7) | 29 (10) |
IV | 250 (88) | 257 (89) | 242 (84) |
B symptoms, n of N (%) | 72 of 285 (25) | 78 of 290 (27) | 87 of 285 (31) |
LDH:ULN ratio, median (IQR) | 0.94 (0.78 to 1.20) | 0.94 (0.77 to 1.18) | 0.87 (0.74 to 1.12) |
LDH > ULN, n (%) | 123 (43) | 120 (41) | 105 (36) |
Leukocytes (white blood cells, G/L), median (IQR) | 7.34 (5.50 to 10.91) | 7.09 (5.28 to 11.11) | 7.4 (5.77 to 11.92) |
MIPI score, median (IQR) | 5.62 (5.40 to 5.91) | 5.64 (5.35 to 5.95) | 5.61 (5.39 to 5.92) |
Low < 5.7, n (%) | 168 (58) | 168 (58) | 168 (58) |
Intermediate ≥ 5.7 and < 6.2, n (%) | 79 (27) | 80 (27) | 77 (27) |
High ≥ 6.2, n (%) | 41 (14) | 44 (15) | 45 (16) |
Ki-67 index, n | 249 | 262 | 259 |
Ki-67 index, median (IQR) | 18 (10 to 38) | 18 (12 to 40) | 18.5 (10 to 35) |
Ki-67 index ≥ 30%, n (%) | 81 (33) | 81 (31) | 82 (32) |
Cytology blastoid, n of N (%) | 28 of 253 (11) | 34 of 261 (13) | 31 of 265 (12) |
p53 expression > 50%, n of N (%) | 21 of 183 (11) | 25 of 175 (14) | 31 of 189 (16) |
High-risk biology, n of N (%) | 31 of 185 (17) | 37 of 179 (21) | 44 of 192 (23) |
ASCT = autologous stem cell transplant; ECOG = Eastern Cooperative Oncology Group; IQR = interquartile range; LDH = lactate dehydrogenase; MIPI = Mantle Cell Lymphoma International Prognostic Index; ULN = upper limit of normal.
aOne patient aged 68 years and 1 patient aged 66 years were randomly assigned to group A plus I.
bHistology of patients without MCL: 1 follicular lymphoma and 1 chronic lymphocytic leukemia were diagnosed in group A; 1 lymphoma not otherwise specified, 1 non-Hodgkin lymphoma not otherwise specified, 1 splenic marginal zone lymphoma, and 1 marginal zone lymphoma were diagnosed in group A plus I, and 1 diffuse large B-cell lymphoma and 1 hairy cell leukemia were diagnosed in group I.
Source: Dreyling M, Doorduijn J, Gine E, et al. Ibrutinib combined with immunochemotherapy with or without autologous stem-cell transplantation versus immunochemotherapy and autologous stem-cell transplantation in previously untreated patients with mantle cell lymphoma (TRIANGLE): a three-arm, randomised, open-label, phase 3 superiority trial of the European Mantle Cell Lymphoma Network. Lancet. 2024;403(10441):2293-2306. doi: 10.1016/S0140-6736(24)00184-3. Copyright 2024 by the authors. Available from: https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(24)00184-3/fulltext. Adapted in accordance with Creative Commons Attribution 4.0 International Deed (CC-BY 4.0): https://creativecommons.org/licenses/by/4.0/.
Treatment Exposure and Concomitant Medications
At the data cut-off on May 22, 2022, a total of 808 patients had completed 6 cycles of induction treatment (261 in group A treated with R-CHOP and R-DHAP; 275 in group A plus I treated with R-CHOP with ibrutinib and R-DHAP; and 272 in group I treated with R-CHOP with ibrutinib and R-DHAP). ASCT was completed in 242 patients from group A and 250 patients from group A plus I, and, deviating from the designated study group, in 3 patients from group I.
Median duration of completed ibrutinib maintenance was 22.3 months (interquartile range [IQR], 7.4 months to 24.0 months) for group A plus I (n = 168) and 23.9 months (IQR, 15.4 months to 24.0 months) for group I (n = 181). The median time between end of ASCT (stem cell re-transfusion) and start of ibrutinib maintenance was 49 days (range 20 days to 351 days; IQR, 39 days to 75 days).
Ibrutinib maintenance was started in 238 patients in group A plus I and 260 patients in group I, among whom 98 (41%) of 238 patients in group A plus I and 82 (32%) of 260 patients in group I stopped ibrutinib maintenance more than 2 weeks before the completion of 2 years. Seventy patients in group A plus I and 78 patients in group I were still receiving ibrutinib maintenance by the data cut-off date. Rituximab maintenance was added for 168 (58%) of 288 patients in group A, 165 (57%) of 292 patients in group A plus I, and 158 (54%) of 290 patients in group I. Treatment had ended in 546 patients (210 in group A, 168 in group A plus I, and 168 in group I), among whom 340 (69 in group A, 127 in group A plus I, and 144 in group I) ended ibrutinib or rituximab maintenance, and 206 (141 in group A, 41 in group A plus I, and 24 in group I) either did not start maintenance therapy, experienced disease progression, or died during the maintenance therapy period. At the data cut-off on May 22, 2022, 324 patients (78 in group A, 124 in group A plus I, and 122 in group I) were still receiving ibrutinib or rituximab maintenance without documentation of end of maintenance, disease progression, or death.
Concomitant medication use was not specifically reported in the trial. Six patients without treatment failure had new treatments initiated (2 in group A, 1 in group A plus I, and 3 in group I).
Critical Appraisal
Internal Validity
Randomization was achieved through blocking and stratification by study groups and MIPI risk groups. The randomization process used computer-generated random numbers to ensure treatment allocation could not be predicted. The risk of selection bias can be considered low because baseline characteristics were generally balanced across the 3 groups. Slight imbalances between groups were noted in the prevalence of B symptoms and in lactate dehydrogenase levels. However, these imbalances were not considered to be important by the clinical experts.
The trial followed a predefined statistical analysis plan. An ITT population of all randomized patients was used for efficacy analysis of primary end points, which ensures that the effect of deviations from the protocol is minimized. The modified ITT population excluded a similar number of patients in each treatment group (4 in group A, 5 in group A plus I, and 5 in group I) so any effect on study results is likely minimal.
In the analysis of this trial, multiple pairwise comparisons of the primary outcome were made between treatment groups, which may increase the chance of false-positive statistically significant results. Bonferroni correction was applied to multiple group comparisons. Therefore, multiplicity is appropriately considered in the statistical analysis given that more stringent statistical significance levels are applied, largely reducing the likelihood of type I error.
The open-label design may introduce potential bias in the subjectivity in efficacy (investigator-assessed FFS) and safety assessment. The investigator’s assessment of FFS, especially in counting patients with stable disease, could involve a degree of subjectivity in determining whether there is a change of disease status (e.g., stable disease with symptoms such as headache, fatigue, loss of appetite). Such subjectivity may be less likely a concern in assessing disease progression.
Subgroup analyses for FFS were prespecified and based on stratification for randomization. A key limitation is that FFS was used as the primary end point, and it has not been validated as a surrogate for OS.
HRQoL was considered important in this review but it was not assessed.
Statistical evaluation of OS was not reported. It is uncertain if the benefits observed with FFS and PFS will translate to similar benefits in OS.
External Validity
According to the clinical experts, the key demographic and disease characteristics at baseline were considered to be representative of patients with untreated MCL in Canada. For example, most patients were male and had stage III or IV MCL, which was consistent with clinical experience. Although the TRIANGLE trial was conducted in European centres, the clinical experts did not raise concerns about the applicability of the results to Canadian practices.
The clinical experts indicated that ibrutinib combined with immunochemotherapy is being used in the first-line treatment of patients with MCL in clinical practice, usually accessed through compassionate access programs. In practice, the dosage of ibrutinib combined with immunochemotherapy is in line with details reported in the TRIANGLE study.
The experts identified immunochemotherapy, R-CHOP and R-DHAP, as the main comparator because it is the current standard of care for the first-line treatment of patients with MCL across Canada. The use of BR combination therapy in transplant-eligible patients with newly diagnosed MCL is limited to a few jurisdictions in Canada (e.g., British Columbia), and this regimen was included as a relevant comparator in the review. No studies were found that compared ibrutinib in combination with immunochemotherapy versus the BR regimen for the population of interest, transplant-eligible adult patients with previously untreated MCL. The inclusion of rituximab also reflects real-world practice and improves the relevance of findings.
Results
Efficacy
Results for efficacy outcomes important to this review are presented in Table 6 and Table 7. The Kaplan-Meier curves for the primary end point FFS are displayed in Figure 1. Kaplan-Meier curves for OS are displayed in Figure 2.
Key results include the following:
As of the data cut-off date of May 22, 2022, for primary analysis, the median follow-up in the overall population was 31 months (95% CI, 30.1 months to 33.0 months).
Comparative efficacy results, where available, are presented are for group A plus I versus group A and for group I versus group A.
Comparisons between group A plus I versus group I were ongoing and planned to be done with prolonged follow-up at the end of the trial.
Overall Survival
OS at 3 years was similar in group A plus I (91%; 95% CI, 88% to 95%) and group I (92%; 95% CI, 88% to 95%). OS was slightly lower in group A (86%; 95% CI, 82% to 91%). However, no statistical testing for between-group differences for OS estimates was reported. The study investigators noted that formal statistical tests for OS (reported CIs and P values) were planned for the final analysis to allow full power at the end of the trial.
Progression-Free Survival
The Kaplan-Meier probability of PFS was higher in group A plus I (88%; 95% CI, 84% to 93%) than in group A (73%; 95% CI, 67% to 79%). The HR for PFS favoured group A plus I over group A (HR = 0.46; 1-sided 98.33% CI, 0.00 to 0.72).
In a comparison of group I and group A, PFS was not statistically significant (HR = 0.48; 1-sided 98.33% CI, 0.31 to undefined).
Failure-Free Survival
FFS was higher in group A plus I (88%; 95% CI, 84% to 92%) compared with group A (72%; 95% CI, 67% to 79%). The HR was 0.52 (1-sided 98.33% CI, 0 to 0.86).
Differences in FFS between group I and group A did not reach statistical significance (HR = 0.56; 1-sided 98.33% CI, 0.27 to undefined).
ORR and Complete Remission Rates
At the end of induction, ORRs were 94% (95% CI, 91% to 97%) in group A and 98% (95% CI, 97% to 99%) in the pooled groups receiving ibrutinib (group A plus I and group I).
At the end of induction, complete remission rates were 36% (95% CI, 30% to 42%) in group A and 45% (95% CI, 41% to 49%) in the pooled groups receiving ibrutinib (group A plus I and group I).
Duration of Remission
The proportion of patients with DOR at least 3 years or longer was 76% in group A, 88% in group A plus I, and 87% in group I (HR = 0.52; 1-sided 98.33% CI, 0.00 to 0.84).
DOR did not differ significantly between group I and group A (HR = 0.56; 1-sided 98.33% CI, 0.34 to undefined)
Table 6: Summary of Key Efficacy Results — Overall Survival, Progression-Free Survival, Failure-Free Survival, and Duration of Remission
Outcome | Group A (R-CHOP and R-DHAP with ASCT) N = 288 | Group A plus I (R‑CHOP and R‑DHAP with ASCT plus ibrutinib) N = 292 | Group I (ibrutinib plus R-CHOP and R-DHAP without ASCT) N = 290 | P value |
|---|---|---|---|---|
Overall survival | ||||
OS, % (95% CI) | 86 (82 to 91) | 91 (88 to 95) | 92 (88 to 95) | — |
Number of patients who died, n (%) | 39 (13.5) | 25 (8.6) | 23 (7.9) | — |
Cause of death | ||||
Disease progression (lymphoma), n (%) | 16 (6) | 4 (1) | 11 (4) | — |
Concomitant disease, n (%) | 11 (4) | 7 (2) | 5 (2) | — |
Lymphoma and concomitant disease, n (%) | 0 (0) | 1 (0.3) | 1 (0.3) | — |
Secondary malignancy, n (%) | 1 (0.3) | 2 (1) | 0 (0) | — |
Therapy, n (%) | 4 (1) | 3 (1) | 0 (0) | — |
Therapy and concomitant disease, n (%) | 1 (0.3) | 0 (0) | 0 (0) | — |
Unknown, n (%) | 6 (2) | 8 (3) | 6 (2) | — |
Progression-free survival | ||||
Number of patients with PFS events, n | 67 | 34 | 35 | — |
PFS, % (95% CI) | 73 (67 to 79) | 88 (84 to 93) | 87 (83 to 92) | — |
Comparison of group A plus I vs. group A, HR (1-sided 98.33% CI) | Reference group A | 0.46 (0.00 to 0.72) | NA | 0.00012 |
Comparison of group A vs. group I, HR (1-sided 98.33% CI) | 2.10 (0.00 to 3.28) | NA | Reference group I | > 0.99 |
Comparison of group I vs. group A,a HR (1-sided 98.33% CI) | Reference group A | NA | 0.48 (0.31 to undefined) | > 0.99 |
Failure-free survivala | ||||
FFS, % (95% CI) | 72 (67 to 79) | 88 (84 to 92) | 86 (82 to 91) | — |
Comparison of group A plus I vs. group A, HR (1-sided 98.33% CI) | Reference group A | 0.52 (0 to 0.86) | NA | 0.0008 |
Comparison of group A vs. group I, HR (1-sided 98.33% CI) | 1.77 (0 to 3.76) | NA | Reference group I | 0.9979 |
Comparison of group I vs. group A,b HR (1-sided 98.33% CI) | Reference group A | NA | 0.56 (0.27 to undefined) | 0.9979 |
Duration of remission | ||||
Disease progression or death in patients with response, n | 52 | 30 | 32 | — |
3-year DOR, % (95% CI) | 76 (70 to 83) | 88 (84 to 93) | 87 (82 to 92) | — |
Comparison of group A plus I vs. group A, HR (1-sided 98.33% CI) | Reference group A | 0.52 (0.00 to 0.84) | NA | 0.0021 |
Comparison of group A vs. group I, HR (1-sided 98.33% CI) | 1.80 (0.00 to 2.91) | NA | Reference group I | > 0.99 |
Comparison of group I vs. group A,a HR (1-sided 98.33% CI) | Reference group A | NA | 0.56 (0.34 to undefined) | > 0.99 |
ASCT = autologous stem cell transplant; CI = confidence interval; DOR = duration of remission; FFS = failure-free survival; HR = hazard ratio; NA = not applicable; ORR = overall response rate; PFS = progression-free survival; R-CHOP = rituximab, cyclophosphamide, doxorubicin, vincristine, prednisone; R-DHAP = rituximab, dexamethasone, cytarabine, cisplatin; vs. = versus.
aThe median follow-up duration for FFS was 31 months (95% CI, 30.1 months to 33.0 months).
bCalculations for estimated HRs and CIs for the comparison of group I vs. group A (reference group A) were performed by inverting HRs and CIs for group A vs. group I (reference group I) reported in the published TRIANGLE trial. The review team used a published method for estimating hazard from reported summary statistics.7
Source: Dreyling et al.6
Table 7: Summary of Key Efficacy Results — Response Rates
Characteristic | Group A (R-CHOP and N = 288 | Pooled ibrutinib groups (group A plus I N=559 | P value |
|---|---|---|---|
Response rates | |||
At midterm | |||
Complete remission rate, % (n of N) | 26 (66 of 250) | 29 (148 of 514) | 0.55 |
ORR, % (n of N) | 98 (244 of 250) | 98 (504 of 514) | 0.79 |
At the end of induction | |||
Complete remission rate, % (n of N) | 36 (98 of 272) | 45 (249 of 559) | 0.020 |
95% CI | 30 to 42 | 41 to 49 | — |
ORR, % (n of N) | 94 (256 of 272) | 98 (549 of 559) | 0.0025 |
95% CI | 91 to 97 | 97 to 99 | — |
ASCT = autologous stem cell transplant; CI = confidence interval; DOR = duration of remission; FFS = failure-free survival; HR = hazard ratio; NA = not applicable; ORR = overall response rate; PFS = progression-free survival; R-CHOP = rituximab, cyclophosphamide, doxorubicin, vincristine, prednisone; R-DHAP = rituximab, dexamethasone, cytarabine, cisplatin; vs. = versus.
Figure 1: Kaplan-Meier Estimates of Failure-Free Survival for Group A Plus I vs. Group A
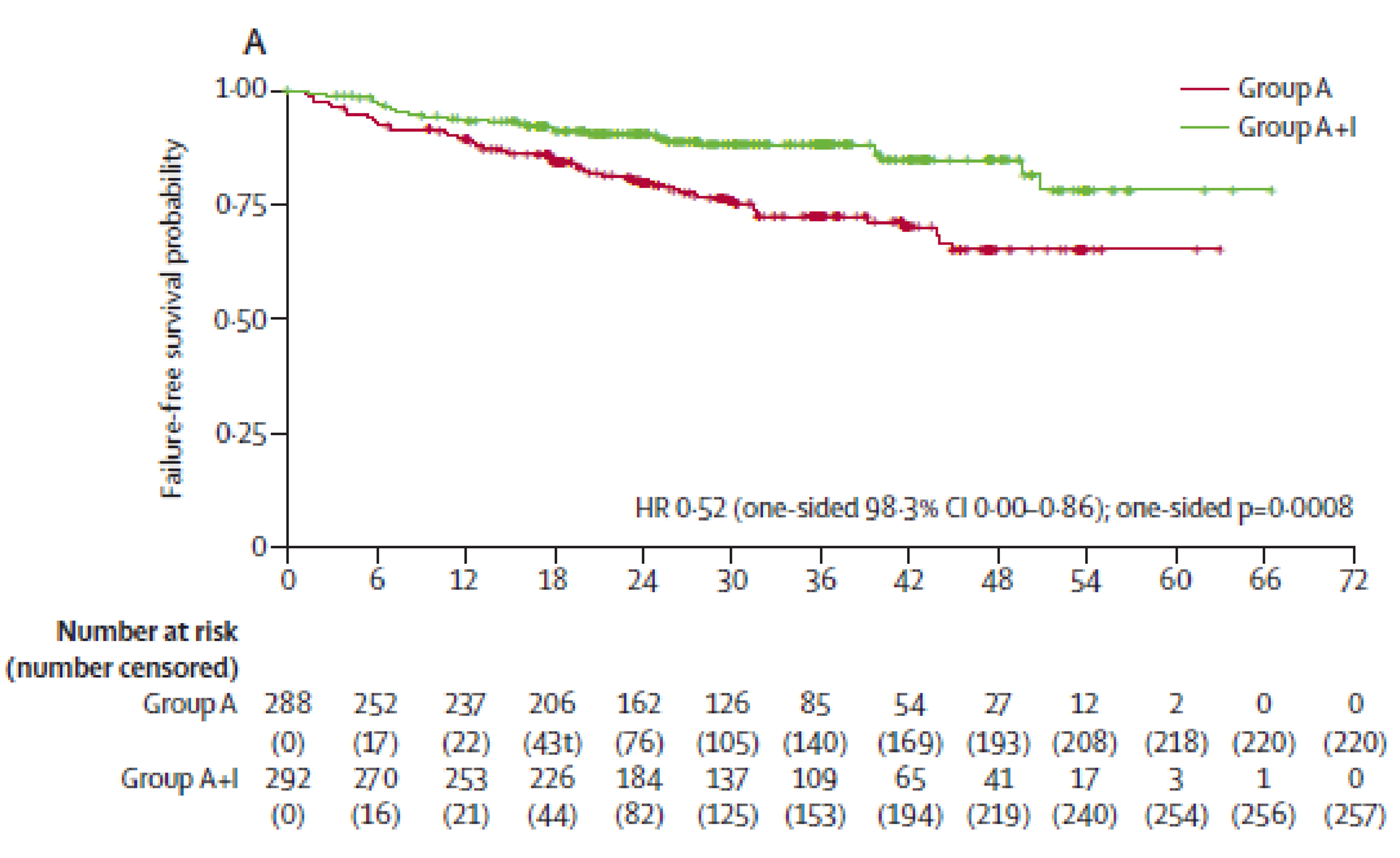
CI = confidence interval, HR = hazard ratio; vs. = versus.
Source: Dreyling M, Doorduijn J, Gine E, et al. Ibrutinib combined with immunochemotherapy with or without autologous stem-cell transplantation versus immunochemotherapy and autologous stem-cell transplantation in previously untreated patients with mantle cell lymphoma (TRIANGLE): a three-arm, randomised, open-label, phase 3 superiority trial of the European Mantle Cell Lymphoma Network. Lancet. 2024;403(10441):2293-2306. doi: 10.1016/S0140-6736(24)00184-3. Copyright 2024 by the authors. Available from: https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(24)00184-3/fulltext. Reprinted in accordance with Creative Commons Attribution 4.0 International Deed (CC-BY 4.0): https://creativecommons.org/licenses/by/4.0/.
Figure 2: Kaplan-Meier Estimates of Overall Survival for All Treatment Groups
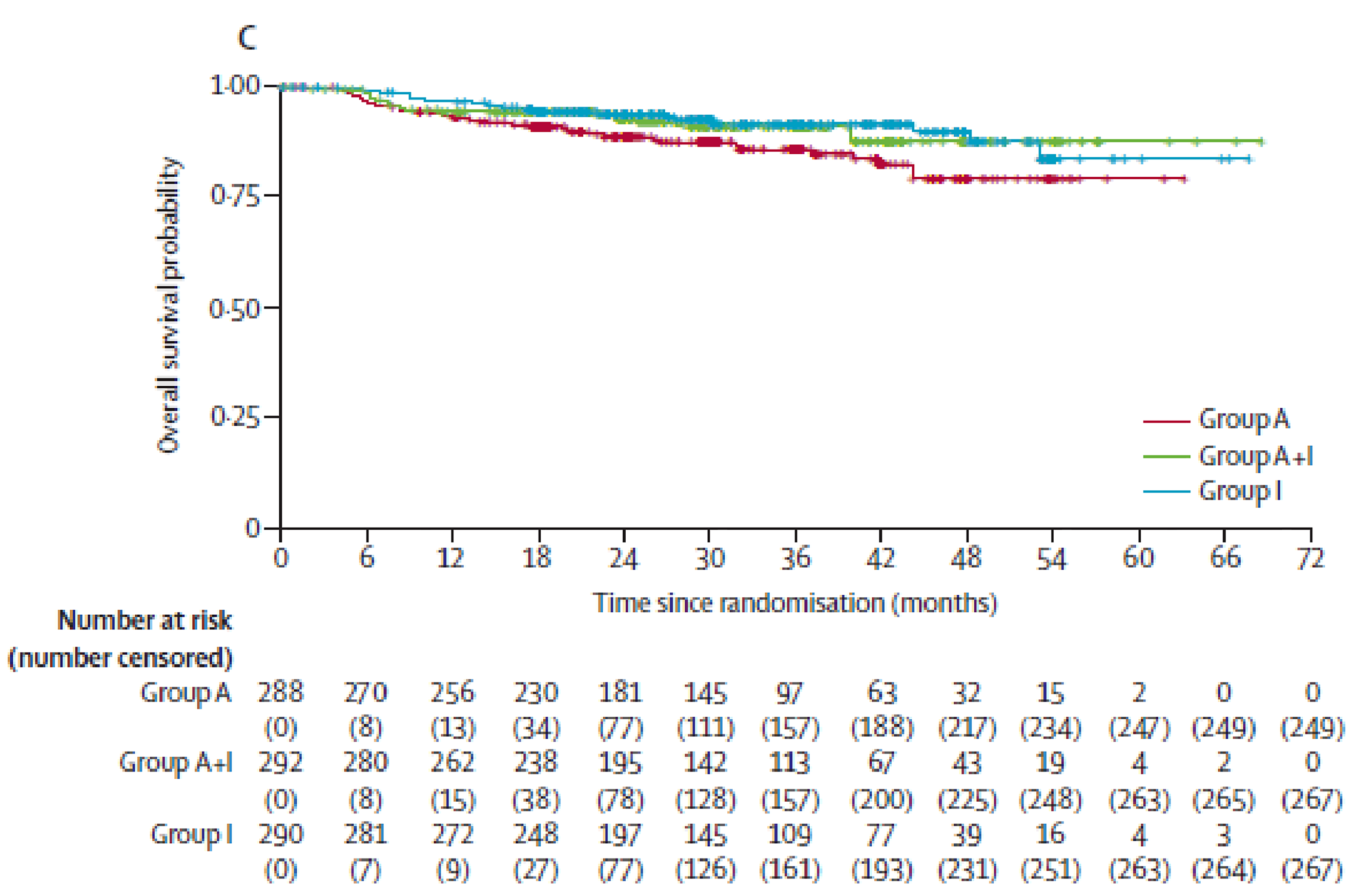
Source: Dreyling M, Doorduijn J, Gine E, et al. Ibrutinib combined with immunochemotherapy with or without autologous stem-cell transplantation versus immunochemotherapy and autologous stem-cell transplantation in previously untreated patients with mantle cell lymphoma (TRIANGLE): a three-arm, randomised, open-label, phase 3 superiority trial of the European Mantle Cell Lymphoma Network. Lancet. 2024;403(10441):2293-2306. doi: 10.1016/S0140-6736(24)00184-3. Copyright 2024 by the authors. Available from: https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(24)00184-3/fulltext. Reprinted in accordance with Creative Commons Attribution 4.0 International Deed (CC-BY 4.0): https://creativecommons.org/licenses/by/4.0/.
Harms
Detailed results for harms for the included study are provided in the Dreyling et al. study.6
Key harms results from the TRIANGLE study include the following:
During induction treatment, the most common grade 3 or higher AEs were blood and lymphatic system disorders, including decreased platelet and neutrophil counts. There was no evidence of differences between patients treated with R-CHOP and R-DHAP or with ibrutinib combined with R-CHOP and R-DHAP.
During ASCT, the most common grade 3 or higher AEs were blood and lymphatic system disorders. There was no evidence of differences between the 2 treatment groups (patients who received R-CHOP and R-DHAP or ibrutinib combined with R-CHOP and R-DHAP for induction).
During maintenance or follow-up, grade 3 or higher AEs were more frequent in patients receiving ibrutinib either after ASCT (group A plus I) or without preceding ASCT (group I), compared with patients without ibrutinib maintenance (group A). For the groups who received ibrutinib, the toxicity profile for ibrutinib-only treatment (group I) appeared to be more favourable compared to ibrutinib after ASCT (group A plus I). For example, hematologic toxicity and infections occurred twice as frequently in the ibrutinib maintenance group treated with prior ASCT consolidation compared to the group with prior ASCT but without ibrutinib maintenance.
The total numbers of patients with any AEs in each of the treatment groups were not reported.
Serious AEs and discontinuations due to AEs were not reported.
Hemorrhagic events were one of the AEs of special interest, and there were no reported hemorrhagic events of grade 3 or higher that occurred during induction, ASCT, or maintenance therapy.
Table 8: Summary of Key Harms During Induction and ASCT
Outcome | R-CHOP and N = 287 | Ibrutinib plus N = 579 | R-CHOP and N = 245 | Ibrutinib plus R-CHOP and N = 254 |
|---|---|---|---|---|
Grade ≥ 3 AE, n (%) | During induction treatment | During ASCT | ||
Hematologic AEs (blood and lymphatic system disorders) | 203 (71) | 438 (76) | 145 (59) | 150 (59) |
Platelet count decreased | 169 (59) | 351 (61) | 119 (49) | 111 (44) |
Neutrophil count decreased | 135 (47) | 288 (50) | 89 (36) | 85 (33) |
Anemia | 62 (22) | 140 (24) | 50 (20) | 56 (22) |
White blood cell count decreased | 44 (15) | 88 (15) | 42 (17) | 42 (17) |
Febrile neutropenia | 25 (9) | 70 (12) | 49 (20) | 56 (22) |
Lymphocyte count decreased | 15 (5) | 38 (7) | 9 (4) | 7 (3) |
Infections and infestations | 26 (9) | 72 (12) | 41 (17) | 52 (20) |
Gastrointestinal disorders | 36 (13) | 70 (12) | 51 (21) | 51 (20) |
Cardiac disorders | 6 (2) | 19 (3) | 6 (2) | 2 (1) |
Skin and subcutaneous tissue disorders | NR | NR | 3 (1%) | 10 (4) |
Metabolism and nutrition disorders | 19 (7) | 75 (13) | 27 (11) | 21 (8) |
General disorders and administration site conditions | 16 (6) | 37 (6) | 49 (20) | 54 (21) |
Investigations | 11 (4) | 42 (7) | 12 (5) | 13 (5) |
Renal and urinary disorders | 14 (5) | 38 (7) | NR | NR |
Vascular disorders | 13 (5) | 32 (6) | 7 (3) | 9 (4) |
Nervous system disorders | 9 (3) | 28 (5) | NR | NR |
Respiratory, thoracic, and mediastinal disorders | 8 (3) | 17 (3) | 9 (4) | 12 (5) |
AE = adverse event; ASCT = autologous stem cell transplant; NR = not reported; R-CHOP = rituximab, cyclophosphamide, doxorubicin, vincristine, prednisone; R-DHAP = rituximab, dexamethasone, cytarabine, cisplatin.
Source: Dreyling M, Doorduijn J, Gine E, et al. Ibrutinib combined with immunochemotherapy with or without autologous stem-cell transplantation versus immunochemotherapy and autologous stem-cell transplantation in previously untreated patients with mantle cell lymphoma (TRIANGLE): a three-arm, randomised, open-label, phase 3 superiority trial of the European Mantle Cell Lymphoma Network. Lancet. 2024;403(10441):2293-2306. doi: 10.1016/S0140-6736(24)00184-3. Copyright 2024 by the authors. Available from: https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(24)00184-3/fulltext. Adapted in accordance with Creative Commons Attribution 4.0 International Deed (CC-BY 4.0): https://creativecommons.org/licenses/by/4.0/.
Table 9: Summary of Key Harms During Maintenance or Follow-up
Outcome | Group A (ASCT) N = 238 | Group A plus I (ibrutinib after ASCT) N = 231 | Group I (ibrutinib without ASCT) (N = 269) |
|---|---|---|---|
Grade ≥ 3 AE, n (%) | |||
Hematologic AEs (blood and lymphatic system disorders) | 51 (21) | 114 (50) | 74 (28) |
Platelet count decreased | 5 (2) | 13 (6) | 8 (3) |
Neutrophil count decreased | 40 (17) | 101 (44) | 62 (23) |
Anemia | 4 (2) | 6 (3) | 4 (1) |
White blood cell count decreased | 4 (2) | 10 (4) | 6 (2) |
Febrile neutropenia | 6 (3) | 14 (6) | 7 (3) |
Infections and infestations | 32 (13) | 58 (25) | 52 (19) |
Gastrointestinal disorders | 7 (3) | 14 (6) | 12 (4) |
Cardiac disorders | 3 (1) | 7 (3) | 12 (4) |
Skin and subcutaneous tissue disorders | 1 (< 1) | 8 (3) | 1 (< 1) |
Metabolism and nutrition disorders | 0 | 4 (2) | 7 (3) |
General disorders and administration site conditions | 5 (2) | 6 (3) | 11 (4) |
Investigations | 2 (1) | 12 (5) | 2 (1) |
Vascular disorders | 2 (1) | 3 (1) | 7 (3) |
Nervous system disorders | 3 (1) | 12 (5) | 12 (4) |
Respiratory, thoracic, and mediastinal disorders | 2 (1) | 7 (3) | 4 (1) |
AE = adverse event; ASCT = autologous stem cell transplant.
Source: Dreyling M, Doorduijn J, Gine E, et al. Ibrutinib combined with immunochemotherapy with or without autologous stem-cell transplantation versus immunochemotherapy and autologous stem-cell transplantation in previously untreated patients with mantle cell lymphoma (TRIANGLE): a three-arm, randomised, open-label, phase 3 superiority trial of the European Mantle Cell Lymphoma Network. Lancet. 2024;403(10441):2293-2306. doi: 10.1016/S0140-6736(24)00184-3. Copyright 2024 by the authors. Available from: https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(24)00184-3/fulltext. Adapted in accordance with Creative Commons Attribution 4.0 International Deed (CC-BY 4.0): https://creativecommons.org/licenses/by/4.0/.
Discussion
Efficacy
The results of the TRIANGLE trial at the cut-off date with the median follow-up of 31 months have demonstrated that treatment with ibrutinib plus alternating R-CHOP and R-DHAP cycles with or without ASCT may result in increases in FFS and PFS when compared with alternating R-CHOP and R-DHAP cycles with ASCT. Treatment with ibrutinib plus R-CHOP and R-DHAP with ASCT improved 3-year FFS by 16 percentage points compared to R-CHOP and R-DHAP with ASCT (88% vs 72%). Ibrutinib combined with R-CHOP and R-DHAP (group I) compared with R-CHOP and R-DHAP plus ASCT (group A) resulted in a 3-year FFS difference of 14 percentage points that was not statistically significant, so there is no evidence from the trial that the addition of ibrutinib to the current standard of care can replace transplant.
Similar improvements were documented in terms of PFS. In fact, the percentages of PFS were close to that of FFS, indicating the percentage of patients with stable disease was low, indicating the improvements in FFS were mostly driven by the reduction in progressive disease. The between-group differences as estimated by HRs and 95% CIs under Kaplan-Meier curves were statistically significant. The study involved multiple comparisons; therefore, Bonferroni methodology was applied to the 3 treatment groups. Multiplicity is appropriately adjusted when more stringent statistical significance levels (0.01666 1-sided significance level) are applied to claim statistical significance of the findings. The results of investigator-assessed FFS and PFS were unlikely to have been affected by the nature of the open-label study design given that the differences between comparison arms were deemed to have been most likely driven by disease progression.
However, it is uncertain if the benefits observed with FFS and PFS could translate to similar benefits in OS. There were insufficient data to demonstrate that adding ibrutinib improved OS, as the final analysis was not yet available. The clinical experts emphasized that the more important outcomes for MCL are PFS and OS. Moreover, there was no assessment of HRQoL, which is also a clinically important outcome.
As to other outcome measures, such as ORR, complete remission rates, and DOR, the study consistently showed improvements in favour of ibrutinib combination therapy. In particular, the complete remission rate was higher in the group A plus I and group I pooled results than in results for group A (45% versus 36%, respectively). The proportion of patients with DOR at least 3 years or longer was also higher (88% versus 76%), which is in line with the improvement of FFS and PFS.
Although exploratory in nature, subgroup analysis showed the FFS for group A plus I versus group A was similar within MIPI risk groups and rituximab maintenance subgroups (i.e., whether or not rituximab maintenance was started). The results showed greater benefit for group A plus I versus group A in patients with high p53 expression (HR = 0.14; 1-sided 98.3% CI, 0.00 to 0.57) and high-risk biology (HR = 0.31; 1-sided 98.3% CI, 0.00 to 0.78). Whether a subgroup of patients would have received a differential treatment benefit from ibrutinib might be worthy of further investigation.
No comparative evidence was identified to assess the relative treatment effect of ibrutinib combined with immunochemotherapy versus BR for this review.
Harms
In the TRIANGLE trial, patients treated with combination ibrutinib with R-CHOP and R-DHAP had a higher rate of AEs compared to patients treated with R-CHOP and R-DHAP during induction therapy. Rates of AEs were similarly higher during the ASCT and maintenance treatment period. The most common grade 3 or higher AEs were hematologic toxicity followed by infections. For groups treated with ibrutinib, the toxicity profile for ibrutinib-only treatment (group I) was more favourable compared to ibrutinib after ASCT (group A plus I). The clinical experts explained that the AEs observed across the treatment groups are known and the harms results showed no surprising or new safety concerns. Serious AEs and discontinuations due to AEs were not reported.
Conclusion
The evidence from a randomized, 3-arm, open-label phase III trial (TRIANGLE) that included patients with previously untreated MCL demonstrated that ibrutinib combined with alternating R-CHOP and R-DHAP with ASCT (group A plus I) for first-line treatment may improve FFS, PFS, ORR, complete remission rates, and DOR compared with alternating R-CHOP and R-DHAP with ASCT (group A). A comparison of ibrutinib combined with R-CHOP and R-DHAP (group I) compared with R-CHOP and R-DHAP plus ASCT (group A) did not show statistically significant differences, so there is no evidence from the trial that the addition of ibrutinib to the current standard of care can replace transplant. The safety profile of ibrutinib combined with alternating R-CHOP and R-DHAP treatment was as expected, and no new important safety outcomes were identified. However, the long-term safety and effectiveness of the combined therapy, specifically in relation to OS, remain unknown.
No comparative evidence was identified on the relative treatment effect of ibrutinib combined with immunochemotherapy versus BR. There was no evidence to inform how ibrutinib combined with immunochemotherapy affects patients’ HRQoL.
Economic Review
CDA-AMC Assessment of Costs
The Economic Review consisted of a cost comparison of ibrutinib in combination with the alternating R-CHOP and R-DHAP regimen versus the BR regimen for first-line treatment of MCL in adult patients who are previously untreated and eligible for ASCT.
Based on public list prices, ibrutinib during induction therapy is expected to have an incremental cost of $5,058 per patient per 28 days when added to alternating R-CHOP and R-DHAP cycles, increasing the average cost of the regimen from $5,290 to $10,348 (refer to Supplemental Material). When combined with other regimens such as BR, ibrutinib is expected to have an incremental cost of $11,182 per patient per 28 days, which increases the average cost of the BR regimen from $8,435 to $19,617. The costs of adding ibrutinib to alternating R-CHOP and R-DHAP cycles are lower as it is administered only during 19 days of each R-CHOP cycle of the regimen, whereas for other regimens ibrutinib is administered daily. As such, the reimbursement of ibrutinib for the indication of this review is expected to increase overall drug acquisition costs based on the costs associated with ibrutinib added on to each regimen. The following are additional items for consideration:
According to the Clinical Review, evidence from the TRIANGLE trial suggests that ibrutinib combined with alternating R-CHOP and R-DHAP cycles and ASCT may improve PFS, FFS, and DOR compared with alternating R-CHOP and R-DHAP cycles with ASCT. The effect of adding ibrutinib with ASCT compared to ibrutinib only without ASCT is unknown. No new important safety outcomes were identified in the trial, and no evidence was identified regarding the comparative efficacy and safety of ibrutinib versus BR.
As of July 2025, ibrutinib is only available as a brand name product in Canada (Imbruvica). There are at least 4 generic formulations currently under review by Health Canada. As such, 1 or more generic versions of ibrutinib may become available. According to the pan-Canadian Pharmaceutical Alliance Tiered Pricing Framework, after 3 months of funding, a single-source generic reduces to 55% of the brand reference price.8 Assuming a price consistent with 55% of the price of the reference brand, the cost of generic ibrutinib would be $2,782 per 28-day cycle. If more than 1 generic product becomes available, the cost of ibrutinib would be further reduced.
No health care resource use outcomes were reported in the clinical trial.
According to the clinical experts consulted for this review, ibrutinib is not expected to increase treatment-related health care resource use as it is an oral therapy regimen given on an outpatient basis. They noted that given that the TRIANGLE trial indicated no difference in clinical outcomes between the 2 groups receiving ibrutinib with or without ASCT, the addition of ibrutinib may eliminate the need for ASCT and therefore decrease the use of health care-system resources associated with the procedure.
Ibrutinib was not previously reviewed by CDA-AMC for this indication. As of August 2025, there are no drugs under review for first-line treatment of MCL in previously untreated adult patients eligible for ASCT.
No cost-effectiveness studies conducted in Canada were identified based on a literature search conducted on August 5, 2025, with alerts maintained until the Formulary Management Expert Committee meeting on September 18, 2025.
Conclusion
The reimbursement of ibrutinib for first-line treatment of MCL in adult patients who are previously untreated and eligible for ASCT is expected to increase overall drug acquisition costs. Based on the Clinical Review conclusions, ibrutinib combined with the alternating R-CHOP and R-DHAP regimen and ASCT may improve FFS, PFS, ORR, complete remission rates, and DOR compared with the alternating R-CHOP and R-DHAP regimen and ASCT. The comparative efficacy of ibrutinib when combined with the BR regimen is unknown, as no published literature was identified that had undertaken this assessment.
Given that ibrutinib combined with alternating R-CHOP and R-DHAP cycles is associated with higher drug acquisition costs and incremental benefits in terms of clinical outcomes, a cost-effectiveness analysis would be required to determine its cost-effectiveness relative to alternating R-CHOP and R-DHAP cycles. As this was not available, the cost-effectiveness of ibrutinib could not be determined. Given that ibrutinib combined with BR is associated with higher drug acquisition costs and uncertain clinical benefit, reimbursement of ibrutinib with this regimen will add costs to the public health care system with uncertain benefit.
References
1.Canadian Cancer Society. Mantle cell lymphoma. 2023. Accessed 2025 June 20. https://cancer.ca/en/cancer-information/cancer-types/non-hodgkin-lymphoma/treatment/treatment-by-type/mantle-cell-lymphoma
2.Freedman AS, Aster JC. Lister AL, Ann, ed. Mantle cell lymphoma: Epidemiology, pathobiology, clinical manifestations, diagnosis, and prognosis. UpToDate; 2024. Accessed 2025 April 4. https://www.uptodate.com/
3.Villa D, Kansara R, Lemieux C, Kuruvilla J. Updates in the treatment of mantle cell lymphoma: A Canadian expert framework. Can Hematol Today. 2022;1(S12):2-11.
4.Cancer Care Alberta. Lymphoma: Clinical Practice Guideline. 2025. Accessed 2025 June 12. https://www.albertahealthservices.ca/assets/info/hp/cancer/if-hpcancer-guide-lyhe002-lymphoma.pdf
5.Herrera AF. LaCasce A, ed. Mantle cell lymphoma: Initial management. UpToDate; 2025. Accessed 2025 April 4. https://www.uptodate.com/
6.Dreyling M, Doorduijn J, Gine E, et al. Ibrutinib combined with immunochemotherapy with or without autologous stem-cell transplantation versus immunochemotherapy and autologous stem-cell transplantation in previously untreated patients with mantle cell lymphoma (TRIANGLE): a three-arm, randomised, open-label, phase 3 superiority trial of the European Mantle Cell Lymphoma Network. Lancet. 2024;403(10441):2293-2306. doi: 10.1016/S0140-6736(24)00184-3 PubMed
7.Hebert AE, Kreaden US, Yankovsky A, et al. Methodology to standardize heterogeneous statistical data presentations for combining time-to-event oncologic outcomes. PLoS One. 2022;17(2):e0263661. doi: 10.1371/journal.pone.0263661 PubMed
8.Pan-Canadian Pharmaceutical Alliance. Pan-Canadian Tiered Pricing Framework. Accessed July 29, 2025. https://www.pcpacanada.ca/generic-drug-framework
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.