CADTH Health Technology Review
Virtual Care Use in Primary Care or Specialty Care Settings
Rapid Review
Authors: Ransi Nayakarathna, Heather Neilson, Danielle MacDougall, Tara Cowling
Abbreviations
APLAR
Asia Pacific League of Associations for Rheumatology
ArLAR
Arab League of Associations for Rheumatology
ASCO
American Society of Clinical Oncology
GRADE
Grading of Recommendations, Assessment, Development and Evaluations
LOE
level of evidence
Key Messages
Five evidence-based guidelines met the eligibility criteria for this report. Of the 5 guidelines, 2 provided recommendations on rheumatology practice, 1 on stroke, 1 on oncology, and 1 on digital innovations for all areas of health; none of them focused on primary care specifically. Three were developed in the context of COVID-19.
While all 5 guidelines were informed by a systematic literature search, some specific recommendations were based on expert consensus, given the absence of literature on the respective topics. The quality of evidence and strength of recommendations, where available, were generally assessed to be low across the guidelines.
The evidence-based guidelines provided recommendations across various aspects of virtual care delivery including population considerations, patient conditions, and the types of care that can be offered virtually. They also provided recommendations on when to offer or discontinue virtual care, on patient privacy, and on staff training. One guideline provided a recommendation on fees and reimbursement.
Multiple evidence-based guidelines stated that virtual care should complement rather than replace in-person care, and that virtual care should only be implemented when adequate resources and personnel are available and patient privacy can be secured.
Context and Policy Issues
Virtual care has been defined as any interaction between patients and members of their circle of care that occurs remotely, using any form of communication or information technologies, with the aim of facilitating or maximizing the quality or effectiveness of patient care.1 Also known as direct-to-patient virtual care or e-visits, virtual care may be synchronous (i.e., happening in real-time) or asynchronous (i.e., not happening in concurrent time) in nature.2 Included in this definition are telehealth services, audio conferencing (e.g., telephone), video conferencing (e.g., Zoom), secure messaging (e.g., text), and patient monitoring systems. The term telehealth refers to the remote delivery of health care and related clinical or non-clinical services such as patient-to-provider interactions, provider-to-provider interactions, health care education, self-care, and health information services using telecommunication technologies such as computers, mobile devices, or wearable devices.3 Telemedicine refers to a practice of medicine involving the use of information and communication technologies by a health care provider to administer health care to patients.3 Of note, there is variability in how virtual care and other terms in this space such as telehealth and telemedicine are defined across settings and regions.
The COVID-19 pandemic led to an unprecedented rapid increase in the use of virtual care across multiple specialties and settings in Canada. For example, during the first wave, telemedicine was responsible for an estimated 77% of all ambulatory visits in Ontario.4 At the time, the aim of virtual care in Canada was to maintain health care delivery to the population while physically distancing to reduce the spread of COVID-19. Guidance for health care providers quickly emerged, such as the Canadian Medical Association’s Virtual Care Playbook for Canadian physicians.5 An early analysis of Canada’s pandemic response by Health Canada suggested that virtual care should remain a publicly funded service, and “while change was forced upon us by the pandemic it was, in many cases, long overdue”.6 Even before the COVID-19 pandemic, Canada’s experience and interest in virtual care had been growing. Guidance for health care professionals on the use virtual care had already been published,7 evaluation studies had been done,8 and strategic planning (e.g., in oncology) had already included virtual care.9
Yet issues and uncertainties remain regarding the appropriateness of virtual care for long-term implementation. For various reasons, some patients prefer not to receive virtual care,2 and for many, certain care modalities are unavailable or not easily accessible. For example, patients living in rural areas with limited internet access, older adults, and patients living with disabilities may face challenges engaging with technology, and out-of-pocket expenses may be relatively high for patients with a lower household budget.10 There may also be implications for clinical processes and for clinical quality and safety; for example, health care providers may be concerned about the inability to conduct in-person physical examinations.11 Clinicians’ experiences with technology and its effects on their work, as well as the financial and operational impact of virtual care including costs and payment issues, medical education, and licensure, also need to be considered.10
To effectively integrate virtual care into the health care delivery continuum, there is a need to first understand what is and what is not an appropriate use of virtual care. Evidence syntheses based on the peer-reviewed literature could inform future decisions about which virtual services should be maintained, either through continual or increased funding, and which virtual services should be stopped. It is possible that the quantity and quality of existing evidence varies by health care setting (e.g., primary versus specialty care) and by health condition (e.g., diabetes versus oncology).
The objective of this report is to summarize recent evidence-based guidelines regarding the appropriate use of virtual care for individuals using primary care or specialty care services.
Research Question
What are the evidence-based guidelines regarding the appropriate use of virtual care for individuals using primary care or specialty care services?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concept was virtual care. CADTH-developed search filters were applied to limit retrieval to guidelines. Where possible, retrieval was limited to the human population. The search was completed on June 14, 2022 and limited to English-language documents published since January 1, 2017.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Individuals using primary care or specialty care services |
Intervention | Virtual care |
Comparator | Not applicable |
Outcomes | Recommendations regarding the appropriate use of virtual care services (e.g., population considerations, patient conditions that may be prioritized by virtual care services, type of virtual care that may be offered, when virtual care should be offered or discontinued) |
Study designs | Evidence-based guidelines |
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, if they were duplicate publications, or if they were published before 2017. Guidelines with unclear methodology (e.g., systematic literature review not reported) were also excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument12 for guidelines. Summary scores were not calculated for the included publications; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
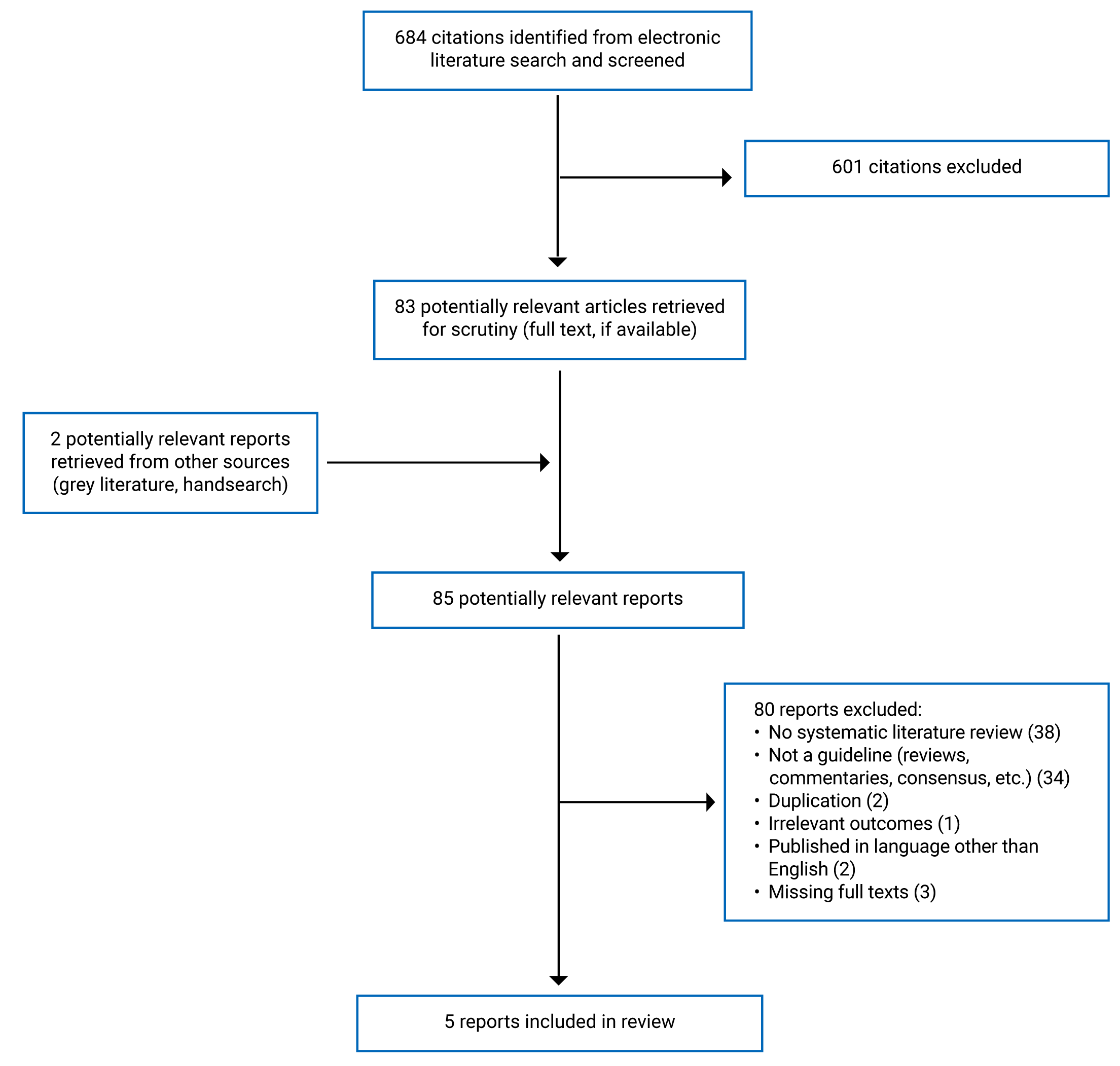
A total of 684 citations were identified in the literature search. Following screening of titles and abstracts, 601 citations were excluded, and 83 potentially relevant reports from the electronic search were retrieved for full-text review. Two potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 80 publications were excluded for various reasons, and 5 publications met the inclusion criteria and were included in this report. Appendix 1 presents the PRISMA13 flow chart of the study selection.
Additional references of potential interest, including additional publications that did not meet our eligibility criteria, are provided in Appendix 5. The majority of the additional references were practice guidelines developed by various organizations that did not use or report using an evidence-based approach. An Executive Summary of the recommendations from these practice guidelines is provided for primary care and musculoskeletal care, along with a list of the publications and their recommendations (Table 5). A list of citations for other areas of health care, where virtual care has been reported, is also included in Appendix 5.
Summary of Study Characteristics
Overall, 5 evidence-based guidelines met the eligibility criteria and were included in this report.14-18 Additional details regarding the characteristics of included publications are provided in Appendix 2.
Study Design
Five guidelines were eligible for inclusion in this report. The first guideline, published in 2022 by the Asia Pacific League of Associations for Rheumatology (APLAR), provided evidence-based recommendations for telemedicine in rheumatology.14 The second guideline, published in 2022 by a committee from the Arab League of Associations for Rheumatology (ArLAR),16 provided general principals and best practice guidelines for telehealth in rheumatology. The third guideline, published in 2021 by the American Society of Clinical Oncology (ASCO), provided standards for telehealth in oncology.17 The fourth guideline, first published in 2019 by the WHO,18 provided 9 priority emergent digital innovation recommendations intended for health system strengthening. The fifth guideline, published in 2017 by the Heart and Stroke Foundation for Canadian Stroke Best Practices, provided evidence related to the establishment of Telestroke systems and the use of Telestroke.15 The methods used to develop the guidelines are described below.
The APLAR guidelines14 focused on the practice of telemedicine in rheumatology. A systematic literature review was conducted, and evidence from randomized controlled trials and observational studies was considered. The quality of evidence was appraised using GRADE (ranging from A [highest] to D [very low]), and the level of evidence was indicated according to the Oxford Levels of Evidence (ranging from 1 [systematic review of randomized trials] to 5 [mechanism-based reasoning]). Recommendations were developed using a modified Delphi technique to establish consensus. When evidence was limited, recommendations were created based on clinical expertise and practical experience of working group members, to provide practical guidance in the areas of telemedicine that are most relevant to rheumatology practice. Guideline validation was not reported. Strength of the recommendations was not reported.
The ArLAR Best Practice Guidelines,16 for telehealth in rheumatology, were based on a systematic literature review of available guidelines and studies. Levels of evidence (LOEs) were indicated according to the Oxford Centre for Evidence Based Medicine (ranging from 1 [highest] to 5 [lowest]). Based on the available literature, general principles and best practice statements were drafted by 2 authors. A multidisciplinary task force then assessed the guidelines using a modified Delphi process. The final draft was validated by a core steering committee and subsequently reviewed by another committee, advisor, and expert. Strength of the recommendations was not reported.
The ASCO Standards and Practice Recommendations,17 for telehealth in oncology, were based on a systematic literature search combined with an expert panel consensus. Following an initial scoping review and consensus on oncology-specific topics to be included, a systematic literature search was conducted for relevant systematic reviews or primary studies. The quality of included studies was assessed using a variety of instruments (e.g., adaptation of Critical Appraisal Skill Program checklist for qualitative research, modified Hawker et al. tool, adapted Cochrane Collaboration Back Review Group Checklist, GRADE, Cochrane risk of bias tool, Downs and Black checklist). Literature search results were combined with an expert panel consensus to develop the standards, followed by a 2-week period allowing the public to review and comment. The quality of evidence and strength of the recommendations were not reported. Standards were subsequently reviewed by an expert panel and ASCO Quality of Care Council and the ASCO Board of Directors.
The WHO Digital Health Guidelines were based on evidence from a systematic literature review.18 The 2 main types of evidence considered were: evidence on the effectiveness of digital health interventions, based on randomized controlled trials, non-randomized studies, controlled before-and-after studies, and interrupted time series studies; and evidence on the factors affecting the acceptability, feasibility, and implementation of digital health interventions, based on qualitative studies. The certainty of the quantitative evidence was classified using GRADE criteria (ranging from high to very low), and confidence in the qualitative evidence was assessed using Confidence in the Evidence from Reviews of Qualitative Research (GRADE-CERQual; ranging from high to very low). Both evidence and expert opinions were used to develop the recommendations and, when minimal evidence existed, a post-deliberation consensus position of the Guidelines Development Group was considered. An external review group peer-reviewed the final guideline document. Strength of the recommendations was not reported.
The Canadian Stroke Best Practice Recommendations consisted of evidence-based recommendations for Telestroke systems.15 An interprofessional writing group developed the recommendations based on a systematic literature search. Systematic reviews, meta-analyses, randomized controlled trials, and observational studies were included, where available. Recommendations based on the evidence identified were formulated by the working group through discussion and debate, and additional research of value that was identified through these discussions. Evidence supporting each recommendation was assigned a level (ranging from A [highest] to C [lowest]), according to a table of criteria defined by the working group. Recommendations were subsequently reviewed internally by the Canadian Stroke Best Practices Advisory Committee, as well as externally. Strength of the recommendations was not reported.
Country of Origin
The APLAR guidelines are intended for clinical practice in the Asia Pacific region; the ArLAR guidelines are intended for use in the Arab region; the ASCO recommendations are intended for use in the US; the WHO guidelines are intended for global use; and the Telestroke recommendations are intended for use in Canada.
Patient Population
The target population for the APLAR recommendations14 are rheumatology patients and clinicians in the Asia Pacific region, and the intended users are clinicians in that region.
The ArLAR guidelines16 target patient populations with rheumatology conditions in the Arab region, and the intended users are rheumatologists in that region.
The ASCO recommendations17 are intended for oncologists, nurses, advanced practice providers, allied health professionals, and administrators involved in cancer care delivery. The target population for these standards include individuals undergoing diagnosis, treatment, survivorship, or palliative care for cancer.
The WHO guidelines18 are intended for health system decision-makers and public health practitioners, to help them develop a better understanding of digital health interventions with an evidence base, to support health system needs. These guidelines are also beneficial to investors who resource digital health systems, as implementation and development partners. The guidelines are aimed at strengthening the health system for the general patient population and all health conditions.
The Canadian Stroke Best Practice Recommendations15 are intended for use by health care professionals across all disciplines who treat patients not living close to a specialized stroke centre. The recommendations are intended to support decision-making for patients who are potential candidates for acute endovascular treatment and to support the use of Telestroke in stroke prevention and rehabilitation services. These recommendations also provide guidance for health system decision-makers and planners.
Interventions
The interventions considered within the APLAR guidelines14 were for telemedicine in rheumatology practice, where telemedicine was defined as “the delivery of health care services, where distance is a critical factor, by all health care professionals using information and communication technologies for the exchange of valid information for diagnosis, treatment and prevention of disease and injuries, research and evaluation, and for the continuing education of health care providers, all in the interests of advancing the health of individuals and their communities” (p.248).14 The ArLAR guidelines16 considered best practice interventions for teleconsultation in rheumatology, where teleconsultation was defined as the “synchronous exchange of medical information between a patient and a rheumatologist via audio or audiovisual electronic communication, to improve the patient's health status” (p.381).16 The ASCO recommendations17 considered interventions for telehealth in oncology; the definition of telehealth was not reported. The WHO guidelines18 examined 9 priority emergent digital innovations that target health system strengthening, including the use of telemedicine, targeted client communication, health worker decision support, digital tracking, and training. The Canadian Stroke Best Practice Recommendations15 considered interventions related to forming Telestroke systems and the use of Telestroke, which was defined as the use of remote telecommunications in stroke care.
Outcomes
The primary outcomes considered within the APLAR guidelines14 were disease remission, disease activity indices, and patient-reported outcomes. Secondary outcomes included adverse events, patient satisfaction, drug compliance, drug dosage optimization, improvement in knowledge, attitude, practices, and cost-effectiveness. Additional outcomes considered were latency to diagnosis and latency to rheumatology referral.19
The outcomes considered within the ArLAR guidelines16 included the main barriers and facilitators to telehealth in the Arab region, general principles, best practice guidelines, and a practical toolkit for implementing telehealth services in rheumatology clinics.
The ASCO recommendations17 considered the outcomes of in-person versus telehealth visits on patient outcomes, workflow and implementation considerations for telehealth applications, patient selection, standards, establishing physician patient relationship, role of advanced practice providers and allied health professionals in oncology telehealth interventions, virtual multidisciplinary cancer conferences, and teletrials and/or virtual participation in oncology clinical trials.
The outcomes of relevance to this report that were considered in the WHO guidelines18 were health system improvements, including an assessment of the benefits, harms, acceptability, feasibility, resource use, and equity considerations.
The Canadian Stroke Best Practices Recommendations15 considered the organization of Telestroke systems for the hyperacute phase of stroke and for ongoing stroke assessment and management. Staff training, ongoing education, barriers to Telestroke, and updated versions of a previously developed set of clinical practice recommendations on equipment accessibility and data privacy considerations were also considered.
Summary of Critical Appraisal
All 5 articles reported on the evidence-based methodology that was applied when deriving recommendations. In all 5 guidelines, the objectives and population of interest were noted, and all 5 guidelines clearly described the health questions of interest. Additionally, 4 guidelines15-18 clearly defined the target users of the guideline and included views of the target population and relevant professionals in the guideline development process. The remaining guideline (i.e., APLAR14) did not provide explicit details on these areas. The recommendations provided by all guidelines were specific and clearly identifiable. The methods of guideline development (e.g., selection criteria and process for consensus) were consistently reported in all 5 guidelines. Although 4 out of 5 guidelines stated the need or intention to update guidelines periodically,14,15,17,18 none of them except the WHO guidelines18 explicitly described the process for updating. All guidelines lacked monitoring and/or auditing criteria. Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
Summary of Findings
Three of the 5 guidelines (i.e., APLAR,14 ASCO,17 and ArLAR16) were published in the context of the COVID-19 pandemic. Two guidelines provided recommendations for rheumatology practice,14,16 1 for oncology,17 1 for digital innovations in all areas of health,18 and 1 for stroke.15 Summaries of recommendations in each area are provided below according to the main outcomes of interest to this report. Appendix 4 presents the specific recommendations along with the quality of the supporting evidence, where available.
Recommendations for Rheumatology Practice
Two guidelines provided recommendations or standards for rheumatologists on different aspects of virtual care. The 2022 APLAR guidelines14 included 13 recommendations and the 2022 ArLAR guidelines16 included 3 general principles and 12 best practice standards.
Population considerations: The APLAR guidelines14 recommend that in new patients without a diagnosis, telemedicine should be limited to early guidance (GRADE C); that all patients can be assessed for eligibility for telemedicine follow-up for up to 12 months (GRADE B); that having a pre-teleconsultation triage system may help to identify patients that would not benefit from telemedicine (GRADE C); and that teleconsultations with a health care professional, co-located with the patient, is preferred (GRADE C). The ArLAR guidelines16 report that teleconsultation can be used for patients who are home-bound, live in remote areas or underserved communities, or who need to adhere to social distancing restrictions (LOE-3).
Patient conditions: Both guidelines provide recommendations or standards for access and continuity of care for patients with rheumatic diseases. The ArLAR guidelines report that telehealth can help some patients adhere to the management plan, and this is likely to improve disease outcomes in some selected disease states (LOE 2).16
Types of virtual care: The APLAR guidelines conditionally recommend the adoption of video consultation over other forms such as telephone or asynchronous messaging via email, short message services, and other internet-based services (GRADE C).14
When to offer: The APLAR guidelines recommend telemedicine consultations over unsupervised medication changes when normal health services are disrupted (GRADE B).14
When to discontinue: The APLAR guidelines conditionally recommend scheduling an in-person consultation when a rheumatologist encounters unexplained symptoms or has difficulty in assessing the patient, or if the rheumatologist or patient perceives a gap in communication during the telemedicine consultation (GRADE C).14
Apart from these main outcomes of interest, both guidelines provide recommendations on protection of data privacy/confidentiality (APLAR GRADE B, ArLAR LOE 5), on the importance of using patient-reported outcomes (APLAR GRADE B, ArLAR LOE 3), and on staff training (APLAR no evidence, ArLAR LOE 5). Further the APLAR guidelines recommend that if for in-person care a treat-to-target approach is practiced, a similar approach should be practiced for telemedicine (GRADE C). The ArLAR guidelines provide standards on informed consent (LOE 5), shared decision or choice between care provider and patient (LOE 5), documentation (LOE 5), safe prescription (LOE 5), teleconsultation fees and reimbursement being similar to in-person visits (LOE 5), ethical considerations similar to in-person care (LOE 5), and the improvement of infrastructure (LOE 5). Further the ArLAR guidelines encourage research projects to assess the implementation of telehealth and the resulting disease outcomes in the Arab region (LOE 5).
Recommendations for Oncology Practice
The 2021 ASCO recommendations17 provided 15 standards for oncology practice. The quality of evidence was not reported.
Population considerations: The standards were developed for use across the spectrum of care delivery in individuals with cancer.
Types of virtual care: Telehealth via telephone or videoconferencing is recommended when infrastructure and personnel are available. Diagnosis (skin lesions) via asynchronous transmission of images can be done. Individualized orientation should be provided to both parties for the specific type of technology that will be used (e.g., mobile phone, web-based). Asynchronously delivered interventions, such as automated reminders delivered via text message, can be used. Patients and caregivers should be involved in user testing of new interventions (e.g., apps) whenever possible.17
When to offer: Telehealth is recommended for treatment or long-term management of various conditions including new patient consultations (followed by in-patient care), prescribing and management, prechemotherapy evaluations, and follow-up. It is also recommended when care access issues exist for family conferences, genetic counselling, and second opinions.17 An extensive list of services that are reasonable to offer via telehealth versus those that may be preferred in person is provided in Appendix 4.
Apart from the above standards, guidance is also included on when to offer in-person consultation, documentation, policies and standard operation procedures; the importance of technology support during the consultation; evaluations of key performance indicators; establishment of the doctor-patient relationship; use of advanced practice providers and allied health professionals; virtual multidisciplinary cancer conferences; and teletrials and/or virtual participation in oncology clinical trials.
Recommendations for Digital Interventions
The 2019 WHO guidelines18 provided evidence on 9 priority emergent digital innovations. Six of the 9 recommendations are relevant to this report.
Population considerations: The recommendations were developed for use by policy-makers and investors to strengthen the health systems for all populations.18
Patient conditions: The 6 recommendations of relevance to this report are for all health conditions. One recommendation that targeted 5 specific areas of health (i.e., sexual, reproductive, newborn, child, and adolescent health) recommended the use of digital interventions only when potential concerns about sensitive content and data privacy can be addressed.18
Types of virtual care: Telemedicine and mobile devices are the types of interventions included in the guideline.18
When to offer: Telemedicine (both client-provider and provider-provider interactions) is only recommended to complement, rather than replace, in-person care, in settings where patient safety, privacy, traceability, accountability, and security can be monitored. Health worker decision support tools through mobile devices are recommended only for tasks that are defined within the scope of practice for the health worker. Digital tracking of patients’ or clients’ health status and services through mobile devices is recommended only when the health system can support the implementation of these intervention components in an integrated manner and when potential concerns about data privacy and transmitting sensitive content can be addressed. The provision of training to health workers via mobile devices is recommended as a complement, rather than a replacement, for traditional methods of delivering continued health education and post-certification training.18
Recommendations for Stroke Practice
One guideline (i.e., Canadian Stroke Best Practice Guideline)15 provided recommendations for stroke practice. This 2017 guideline includes 23 main recommendations with several subcategories.
Population considerations: The Canadian Stroke Best Practice Guidelines recommend that Telestroke services should be encompassed in a combined stroke services delivery plan to address hyperacute stroke care, acute stroke care, stroke prevention, rehabilitation, home-based care, and ambulatory care to support optimal patient recovery and family support in all geographic locations in Canada (LOE C).15
Patient conditions: Telestroke can be used for hyperacute and acute stroke assessment, diagnosis, and treatment, including acute thrombolytic therapy and decision-making for endovascular therapy (LOE B). Protocols should be available for patient transfer criteria to advanced care facilities (e.g., endovascular [if available] and neurosurgical intervention) (LOE C).15
Types of virtual care: Videoconferencing and teleradiology systems can be used to support screening and decision-making regarding eligibility for endovascular therapy (LOE B). The guidelines also include the importance of real-time 2-way audiovisual communication (LOE B). The benefits of telephone consultation without video are not well-established (LOE C).15
Additional recommendations are that consultation should be performed by a physician with specialized training in hyperacute stroke management and must have timely access to diagnostic-quality images (e.g., brain CT, CTA; LOE A). Also, referring physicians should follow an established protocol with major steps for recanalization therapies (LOE A). Apart from this, there are recommendations regarding the importance of processes, protocols, and referral systems available for Telestroke consultation (LOE B); for staff training and continuing education (LOE C); for shared decision-making (LOE C); for access for follow-up guidance to referring site (LOE C); and for documentation (LOE C).
Limitations
There are several limitations to this body of evidence. First it should be noted that among the recommendations, a wide variety of clinical areas are addressed (2 guidelines were intended for virtual care in rheumatology, 1 for oncology, 1 for stroke, and 1 for general health systems). The limited volume in each category and diversity in the recommendations identified limited the synthesis across the guidelines included in this report. Further, as no guidelines in primary care were identified, it was not possible to summarize recommendations for virtual care in primary care. It should also be noted that, while all 5 guidelines were informed by a systematic literature search, some specific recommendations were based on expert consensus only, given the absence of literature on the respective topics. Further, where available, quality of evidence and strength of recommendations were generally assessed to be low across the guidelines. Finally, while the included guidelines were evidence-based, these were primarily intended for non-Canadian populations (except for the WHO guidelines18 and Canadian Stroke Best Practice Recommendations15). Thus, they may not be generalizable to the Canadian population. Due to the limited volume of evidence, some consensus-based recommendations, and limited generalizability, caution should be used when translating the findings of this report into Canadian clinical practice.
Conclusions and Implications for Decision or Policy-Making
Five guidelines met the inclusion criteria for this rapid review and were included in this report. The included evidence comprised 2 sets of evidence-based guidelines on virtual care in rheumatology,14,16 1 on Telestroke,15 1 on telehealth for oncology,17 and 1 for digital interventions for all areas of health.18 None specifically focused on virtual care for primary care settings. The recommendations are wide-ranging, addressing various aspects of virtual care, including when to offer or discontinue virtual care, patient privacy, and staff training. The guidelines addressed the utilization of virtual care across multiple geographic locations, patient conditions, and virtual care modalities. One guideline provided a recommendation on fees and reimbursement.
Three out of the 5 guidelines were developed in the context of COVID-19, after the demand and usage of virtual care had increased.4 These guidelines reported on various types of virtual care, including but not limited to video, telephone, and mobile devices. All 5 guidelines provided recommendations on when and how to use virtual care, on privacy and confidentiality, on staff training, and on education or research of relevance to virtual care. The WHO guidelines on digital interventions18 specifically addressed investors and policy-makers, offering key considerations for acceptability and feasibility.
The recurring themes among the guidelines were that virtual care should be a complement rather than a replacement to in-person care, and that virtual care should only be implemented when adequate resources and personnel are available and patient privacy and confidentiality can be secured. While the guidelines identified the convenience, flexibility, and potential time and cost savings associated with virtual care, there was limited evidence describing the potential barriers or limitations to virtual care, such as issues with internet access, technical support and infrastructure, and the appropriate use of virtual care in underserved populations.
CADTH has published many reports on various topics within virtual care, including virtual care evaluation approaches,10 enablers for virtual visits,20 effectiveness of and guidelines for telehealth-delivered supervised consumption services,21 virtual care for patients with schizophrenia/psychosis,22 perspectives and experiences of virtual care,23 virtual waiting rooms,24 and remote presence versus videoconference.25 CADTH’s evidence bundle on Digital Health contains additional reports on telehealth and telemedicine.26 More recently, CADTH published 2 reports on evidence-based guidelines relevant to specific clinical areas: 1 was on virtual clinical assessments for adults with back pain, which identified no relevant guidelines27; the other was on virtual oncology visits, which identified 4 relevant guidelines.28 Notably, guidelines from the Clinical Oncology Society of Australia29 and the National Institute for Health and Care Excellence in the UK,30 included in the latter report,28 are not in the current report on account of different literature searches conducted (i.e., the previous CADTH report28 specific to oncology was able to conduct more focused literature searches). Finally, also of note, a previous CADTH report10 identified no evidence discussing approaches to evaluating virtual care in primary care from Indigenous Peoples’ perspectives in Canada or in other countries, in line with the current report.
The findings of this review should be interpreted with caution, given that: the quality of evidence, where available, was generally assessed to be low; the strength of the recommendations was not reported; and consensus-based recommendations were made when evidence was lacking. Future guidelines on virtual care that are supported by high-quality evidence are needed in both primary care and specialty care settings and for all populations and conditions. As new evidence becomes rapidly available in this highly evolving field, living guidelines may prove useful. In fact, the WHO proposed updating its guidelines as a living document.18
Virtual care is expected to continue to play a significant role in Canada’s health care system and will likely evolve over time. Additional studies and guidelines of high quality and strength will help in guiding its appropriate use.
References
1.Shaw J, Jamieson T, Agarwal P, Griffin B, Wong I, Bhatia RS. Virtual care policy recommendations for patient-centred primary care: findings of a consensus policy dialogue using a nominal group technique. J Telemed Telecare. 2018;24(9):608-615. PubMed
2.Analysis of the current and potential benefits of virtual care in Canada. Toronto (ON): Canada Health Infoway; 2020: https://www.infoway-inforoute.ca/en/component/edocman/3819-analysis-of-the-current-and-potential-benefits-of-virtual-care-in-canada/view-document?Itemid=101. Accessed 2022 Jul 19.
3.CHIEF Executive Forum Virtual Care Working Group. Virtual care in Canada: lexicon. (CHIEF Executive Forum Resource). Toronto (ON): Digital Health Canada; 2022: https://digitalhealthcanada.com/wp-content/uploads/2022/06/Virtual-Care-National-Lexicon-v-JAN2521.pdf. Accessed 2022 Jul 28.
4.Mehrotra A, Bhatia RS, Snoswell CL. Paying for Telemedicine After the Pandemic. JAMA. 2021;325(5):431-432. PubMed
5.Virtual care playbook for Canadian physicians. Ottawa (ON): Canadian Medical Association (CMA); 2020: https://www.cma.ca/sites/default/files/pdf/Virtual-Care-Playbook_mar2020_E.pdf. Accessed 2022 Jul 18.
6.Falk W. The state of virtual care in Canada as of wave three of the COVID-19 pandemic: an early diagnostique and policy recommendations. Ottawa (ON): Health Canada; 2021: https://www.canada.ca/content/dam/hc-sc/documents/corporate/transparency_229055456/health-agreements/bilateral-agreement-pan-canadian-virtual-care-priorities-covid-19/template-wf-report-eng.pdf. Accessed 2022 Jul 06.
7.The College of Physicians and Surgeons of Ontario (CPSO). Virtual Care. 2022; https://www.cpso.on.ca/en/Physicians/Policies-Guidance/Policies/Virtual-Care. Accessed 2022 Jul 18.
8.Home health monitoring common evaluation framework: an integrated approach to assessing value. Victoria (BC): Ministry of Health, Virtual Care Strategy Branch; 2018: https://ehealthresearch.no/files/documents/FINAL-HHM-Common-Evaluation-Framework-v.10.pdf. Accessed 2022 Jul 18.
9.Canadian Partnership Against Cancer. Canadian Strategy for Cancer Control 2019–2029: doing together what cannot be done alone. Toronto (ON): Canadian Partnership Against Cancer; 2019: https://s22457.pcdn.co/wp-content/uploads/2019/06/Canadian-Strategy-Cancer-Control-2019-2029-EN.pdf. Accessed 2022 Jul 18.
10.Hui D, Dolcine B, Loshak H. Approaches to evaluations of virtual care in primary care. Can J Health Technol. 2022;2(1). https://www.cadth.ca/sites/default/files/ES/ES0358%20Evaluations%20of%20virtual%20care-Final.pdf. Accessed 2022 Jul 06.
11.Ong MK, Pfeffer M, Mullur RS. Telemedicine for adults. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2022: www.uptodate.com. Accessed 2022 Jun 13.
12.Agree Next Steps Consortium. The AGREE II Instrument. Hamilton (ON): AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf. Accessed 2022 Jul 28.
13.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
14.Ahmed S, Grainger R, Santosa A, et al. APLAR recommendations on the practice of telemedicine in rheumatology. Int J Rheum Dis. 2022;25(3):247-258. PubMed
15.Blacquiere D, Lindsay MP, Foley N, et al. Canadian Stroke Best Practice Recommendations: Telestroke Best Practice Guidelines Update 2017. Int J Stroke. 2017;12(8):886-895. PubMed
16.Ziade N, Hmamouchi I, El Kibbi L, et al. Telehealth in rheumatology: the 2021 Arab League of Rheumatology Best Practice Guidelines. Rheumatol Int. 2022;42(3):379-390. PubMed
17.Zon RT, Kennedy EB, Adelson K, et al. Telehealth in Oncology: ASCO Standards and Practice Recommendations. JCO Oncology Practice. 2021;17(9):546-564. PubMed
18.WHO guideline: recommendations on digital interventions for health system strengthening. Geneva (CH): World Health Organization; 2019: https://www.who.int/publications/i/item/9789241550505. Accessed 2022 Jul 19.
19.Adnan A, Alnaqbi K, Chen Y, et al. Systematic review informing the APLAR recommendations on the practice, approach and use of telemedicine for rheumatology (CRD42021258712). PROSPERO: International prospective register of systematic reviews. York (GB): University of York Centre for Reviews and Dissemination; 2021: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42021258712. Accessed 2022 Jul 29.
20.Enablers for virtual visits. (CADTH policy insights). Ottawa (ON): CADTH; 2020: https://www.cadth.ca/sites/default/files/covid-19/cy0006-enablers-for-virtual-visits.pdf. Accessed 2022 Jul 06.
21.Gunn H, Wright MD. Telehealth-delivered supervised consumption services: clinical effectiveness, cost-effectiveness, and guidelines. (CADTH reference list). Ottawa (ON): CADTH; 2020: https://www.cadth.ca/sites/default/files/pdf/htis/2020/RA1131%20Telehealth%20Consumption%20Services%20Final.pdf. Accessed 2022 Jul 06.
22.Gunn H, Argάez C, Walter M, Loshak H. Virtual health care for adults with schizophrenia and/or psychosis: clinical effectiveness and guidelines. (CADTH reference list). Ottawa (ON): CADTH; 2020: https://www.cadth.ca/sites/default/files/pdf/htis/2020/RA1136%20Virtual%20Care%20for%20Schizophrenia%20and%20Psychosis%20Final.pdf. Accessed 2022 Jul 06.
23.Gray C, Mason J, Loshak H. An overview of direct-to-patient virtual visits in Canada. Can J Health Technol. 2021;1(6). https://www.cadth.ca/sites/default/files/hs-eh/EH0091%20Virtual%20Visits%20Final.pdf. Accessed 2022 Jul 06.
24.Jones S. A virtual waiting room? Technologies that limit contact while maintaining patient flow in medical practice settings. (CADTH health technology update). Ottawa (ON): CADTH; 2020: https://www.cadth.ca/sites/default/files/hs-eh/en0019-topic1.pdf. Accessed 2022 Jul 06.
25.Marchand DK, Visintini S. Remote presence versus videoconference technologies for the delivery of health services: clinical effectiveness, cost-effectiveness, and guidelines. (CADTH reference list). Ottawa (ON): CADTH; 2018: https://www.cadth.ca/sites/default/files/pdf/htis/2018/RA0969%20Remote%20Presence%20Technologies%20Final.pdf. Accessed 2022 Jul 06.
26.Evidence on digital health. (CADTH evidence bundles). Ottawa (ON): CADTH: https://www.cadth.ca/digital-health. Accessed 2022 Jul 06.
27.Santos C, Ryce A. Virtual clinical assessments for adults with back pain. (CADTH reference list). Ottawa (ON): CADTH; 2022: https://www.cadth.ca/sites/default/files/pdf/htis/2022/RA1219%20Virtual%20Assessments%20for%20Back%20pain%20Final.pdf. Accessed 2022 Jul 29.
28.Khangura SD, Severn M. Virtual oncology visits. (CADTH reference list: summary of abstracts). Ottawa (ON): CADTH; 2022: https://www.cadth.ca/sites/default/files/pdf/htis/2022/RB1618Virtual-Oncology-Visits-Final.pdf. Accessed 2022 Jul 29.
29.COSA Teleoncology Guidelines Working Group. Clinical practice guidelines for teleoncology. Sydney (AU): Clinical Oncological Society of Australia; 2016: https://wiki.cancer.org.au/australia/COSA:Teleoncology. Accessed 2022 Jul 29.
30.National Institute for Health and Care Excellence. COVID-19 rapid guideline: delivery of systemic anticancer treatments. (NICE guideline NG161) 2021; https://www.nice.org.uk/guidance/ng161. Accessed 2022 Jul 29.
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of Included Guidelines
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality assessment | Recommendations development and evaluation | Guideline validation |
|---|---|---|---|---|---|---|
APLAR, 202214 | ||||||
Intended Users: Rheumatology clinicians in the Asia Pacific region Target Population: Rheumatology patients and clinicians in the Asia Pacific region | Evidence-based recommendations for telemedicine* in rheumatology practice *Defined as “the delivery of health care services, where distance is a critical factor, by all health care professionals using information and communication technologies for the exchange of valid information for diagnosis, treatment and prevention of disease and injuries, research and evaluation, and for the continuing education of health care providers, all in the interests of advancing the health of individuals and their communities” (p.248).14 | Primary outcomes: disease remission determined by physician global assessment, disease activity indices, and patient-reported outcomes Secondary outcomes: adverse events, patient satisfaction, drug compliance, drug dosage optimization, improvement in knowledge, attitude, practices, and cost-effectiveness Additional outcomes: latency to diagnosis and latency to rheumatology referral. | Research questions were identified by the working group. A systematic literature search for RCTs and observational studies was conducted across 3 databases: MEDLINE / PubMed, Web of Science and Scopus. The search was limited to English-language articles (including conference abstracts) published from inception to May 2021. Articles were matched according to relevance with each clinical question. Four sub-working groups were assigned with different research questions. Relevant study types included clinical trials: (phase I to IV), observational / real-world studies, noncontrolled trials, cohort and other comparative studies, case series, and case reports. | The quality of evidence was appraised using GRADE (ranging from A [highest] to D [very low]), and the level of evidence was indicated according to the Oxford Levels of Evidence (ranging from 1 [systematic review of randomized trials] to 5 [mechanism-based reasoning]). | Sub-working groups drafted preliminary guidance statements. One member from each subgroup presented draft recommendations and tables of supporting evidence. After grading evidence, the full working group reviewed and generated recommendations. A voting process was conducted using a modified Delphi method by a voting group (working group members and APLAR representatives from the executive and scientific committees). A consensus was reached for ≥70% agreement. After further editing, a second vote took place for recommendation statements that did not reach a consensus in the first round or that had been significantly re-worded. Strength of recommendations: NR. | NR |
ArLAR, 202216 | ||||||
Intended Users: Rheumatologists in the Arab region Target Population: Population with rheumatology conditions in the Arab region | Best practices for the use of teleconsultation* in rheumatology *Defined as the “synchronous exchange of medical information between a patient and a rheumatologist via audio or audiovisual electronic communication, to improve the patient’s health status” (p.381).17 | General principals, best practices guidelines, barriers / facilitators to telehealth in rheumatology, and practical toolkit for the implementation of telehealth. | A systematic literature review was performed using PubMED and websites of American College of Rheumatology, American Telemedicine Association, and World Health Organization to identify available guidelines and studies. Articles published in English between 2001 and 2020 were included. | Levels of evidence were indicated according to the Oxford Centre for Evidence Based Medicine (ranging from 1 [highest] to 5 [lowest]). | Based on the available published guidelines, general principles and best practice statements were drafted by 2 authors. After validation, a multidisciplinary task force convened to assess the Best Practice Guidelines using 3 rounds of voting by a modified Delphi process. Strength of recommendations: NR. | The draft was validated by the core steering committee and reviewed and edited by the ArLAR scientific committee, a law firm advisor, and an American College of Rheumatology telemedicine expert. |
ASCO, 202117 | ||||||
Intended Users: oncologists, nurses, advanced practice providers, allied health professionals, and administrators involved in the delivery of cancer care Target Population: Individuals undergoing diagnosis, treatment, survivorship, or palliative care for cancer | Standards for telehealth* in oncology *Definition: NR | Patient outcomes for in-person versus telehealth visits, workflow and implementation considerations for telehealth applications, patient selection, standards, establishing physician patient relationship, role of advanced practice providers and allied health professionals in oncology telehealth interventions, virtual multidisciplinary cancer conferences, teletrials and/or virtual participation in oncology clinical trials. | Following an initial scoping review and consensus on oncology-specific topics to be included, a systematic literature search was conducted for systematic reviews or primary studies using PubMed and Cochrane Database of Systematic Reviews from 2016 to December 2020. Article screening and data extraction was done by 1 researcher and reviewed by a second researcher. | The included studies were assessed with a variety of instruments, including adaptation of Critical Appraisal Skill Programme checklist for qualitative research, modified Hawker et al tool, adapted Cochrane Collaboration Back Review Group Checklist, GRADE, Cochrane risk of bias tool, Downs and Black checklist. However, the quality of evidence was not reported. | The results of the literature search were combined with expert panel consensus to develop standards. Strength of recommendations: NR. | After development, the standards underwent 2 weeks of an open-comment period, which allowed public to review and comment, and were subsequently reviewed by expert panel and the ASCO quality of care council and approved by the ASCO board of directors. |
WHO, 201918 | ||||||
Intended Users: Policy-makers, donors, and implementers Target Population: Health systems | Nine priority emergent digital innovations* targeting health system strengthening; 6 of 9 recommendations were relevant to the current report. *Including use of telemedicine, targeted client communication, health worker decision support, digital tracking, and training. | Health system improvements, including an assessment of the benefits, harms, acceptability, feasibility, resource use, and equity considerations. | Systematic literature review for: 1. evidence on the effectiveness digital health interventions based on RCTs, non-randomized studies, controlled before-and-after studies, and interrupted time series studies; and 2. evidence on factors affecting the acceptability, feasibility and implementation of digital health interventions based on qualitative studies. For systematic reviews of the effects of interventions, meta-analyses were conducted, or a structured narrative summary was provided. For qualitative evidence, data were analyzed to identify themes. | Using GRADE, the certainty of quantitative evidence for each outcome was rated as “high”, “moderate”, “low” or “very low”. Confidence in qualitative evidence was assessed using Confidence in the Evidence from Reviews of Qualitative Research (GRADE-CERQual; ranging from “high” to “very low”). | Existing evidence and expert opinions were used for the development of recommendations. In the presence of minimal evidence, a post-deliberation consensus position of the members of the Guidelines Development Group was considered. | An external review group of 6 additional expert stakeholders peer-reviewed the final guideline document to identify any factual errors, and commented on the clarity of the language, contextual issues, and implications for implementation. They were not responsible for changing of any recommendations. |
Canadian Stroke, 201715 | ||||||
Intended Users: Health care professionals across all disciplines that provide care to patients and health system planners and decision-makers Target population: Patients not living close to a specialized stroke centre, potential acute endovascular treatment candidates, and the use of Telestroke to support stroke prevention and rehabilitation services | The evidence related to the establishment of Telestroke* systems and the use of Telestroke *Defined as the use of remote telecommunications in stroke care. | Organization of Telestroke systems for both the hyperacute phase of stroke and for ongoing stroke assessment and management, staff training, ongoing education, and updated versions of a previously developed set of clinical practice recommendations on equipment accessibility and data privacy considerations. | Literature searches were conducted by an author with expertise performing systematic literature reviews. The databases searched and keywords used were not provided. The literature published until August 2016 was included. Systematic reviews, meta-analyses, RCTs, and observational studies were included, where available. | Evidence supporting each recommendation was assigned a level from A (highest) to C (lowest), defined by the working group as follows: A: Evidence from a meta-analysis of RCTs or consistent findings from 2 or more RCTs. B: Evidence from a single RCT or consistent findings from 2 or more well-designed non-randomized and/or noncontrolled trials, and large observational studies C: Writing group consensus and/or supported by limited research evidence. When developing ‘‘C-Level’’ recommendations, consensus was obtained within the group and validated through the internal and external review process. | Due to lack of evidence on many of the topics under consideration, there was reliance on expert opinion and the consensus of the writing group and external reviewers. In some areas, added information was included as “clinical considerations”, even though it did not meet the evidence criteria for a ‘‘recommendation.’’. | After the recommendations were drafted, the module underwent an internal review by the Canadian Stroke Best Practices Advisory Committee and an external review. |
APLAR = Asia Pacific League of Associations for Rheumatology; ArLAR = Arab League of Associations for Rheumatology; ASCO = American Society of Clinical Oncology; Canadian Stroke = Canadian Stroke Best Practice Recommendations; EPOC = Effective Practice and Organization of Care; GRADE = Grading of Recommendations, Assessment, Development and Evaluations; NR = Not reported; RCT = randomized controlled trial.
Note that this table has not been copy-edited.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 3: Strengths and Limitations of Guidelines Using AGREE II12
Item | APLAR, 202214 | ArLAR, 202216 | ASCO, 202117 | WHO, 201918 | Canadian Stroke, 201715 |
|---|---|---|---|---|---|
Domain 1: Scope and Purpose | |||||
1. The overall objective(s) of the guideline is (are) specifically described. | Yes | Yes | Yes | Yes | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes | Yes | Yes | Yes | Yes |
3. The population (patients, public, etc.) to whom the guideline is meant to apply is specifically described. | Yes | Yes | Yes | Yes | Yes |
Domain 2: Stakeholder Involvement | |||||
4. The guideline development group includes individuals from all relevant professional groups. | Unclear | Yes | Yes | Yes | Yes |
5. The views and preferences of the target population (patients, public, etc.) have been sought. | No | Yes | Yes | Yes | Yes |
6. The target users of the guideline are clearly defined. | Yes | Yes | Yes | Yes | Yes |
Domain 3: Rigour of Development | |||||
7. Systematic methods were used to search for evidence. | Yes | Yes | Yes | Yes | Yes |
8. The criteria for selecting the evidence are clearly described. | Yes | Yes | Yes | Yes | Yes |
9. The strengths and limitations of the body of evidence are clearly described. | Yes | Yes | Yes | Yes | Yes |
10. The methods for formulating the recommendations are clearly described. | Yes | Yes | Yes | Yes | Yes |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes | Yes | Yes | Yes | Yes |
12. There is an explicit link between the recommendations and the supporting evidence. | Yes | Yes | Yes | Yes | Yes |
13. The guideline has been externally reviewed by experts prior to its publication. | No | Yes | No | Yes | Yes |
14. A procedure for updating the guideline is provided. | Yes | Unclear | Yes | Yes | Yes |
Domain 4: Clarity of Presentation | |||||
15. The recommendations are specific and unambiguous. | Yes | Yes | Yes | Yes | Yes |
16. The different options for management of the condition or health issue are clearly presented. | Yes | Yes | Yes | Yes | Yes |
17. Key recommendations are easily identifiable. | Yes | Yes | Yes | Yes | Yes |
Domain 5: Applicability | |||||
18. The guideline describes facilitators and barriers to its application. | Yes | Yes | Yes | Yes | Yes |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | Yes | Yes | Yes | Yes | Yes |
20. The potential resource implications of applying the recommendations have been considered. | No | Yes | Yes | Yes | Yes |
21. The guideline presents monitoring and/or auditing criteria. | No | No | No | No | No |
Domain 6: Editorial Independence | |||||
22. The views of the funding body have not influenced the content of the guideline. | Yes | Yes | Yes | Yes | Yes |
23. Competing interests of guideline development group members have been recorded and addressed. | Yes | Yes | Yes | Yes | Yes |
AGREE II = Appraisal of Guidelines for Research and Evaluation II; APLAR = Asia Pacific League of Associations for Rheumatology; ArLAR = Arab League of Associations for Rheumatology; ASCO = American Society of Clinical Oncology; Canadian Stroke = Canadian Stroke Best Practice Recommendations.
Appendix 4: Main Study Findings and Authors’ Conclusions
Note that this appendix has not been copy-edited.
Table 4: Summary of Recommendations in Included Guidelines
Recommendations | Quality of evidence and strength of recommendationsa |
|---|---|
APLAR, 202214 | |
1. All patients can be assessed for suitability of telemedicine follow-up and, if suitable, offered teleconsultations over a period not exceeding 12 months. | GRADE of Evidence: B; Level of Evidence: 3 Strength of Recommendation: NR |
2. In a new patient without a confirmed rheumatic disease diagnosis, telemedicine consultation should be limited to early guidance to a healthcare practitioner treating the patient regarding diagnostic work-up, interim management and appropriate timing of an in-person assessment by a rheumatologist. | GRADE of Evidence: C; Level of Evidence: 4 Strength of Recommendation: NR |
3. Having a pre-teleconsultation triage system may help in scheduling in-person visits earlier for patients unlikely to benefit from teleconsultation alone. | GRADE of Evidence: C; Level of Evidence: 4 Strength of Recommendation: NR |
4. When normal health services are disrupted, scheduled telemedicine consultations are recommended over unsupervised medication changes. | GRADE of Evidence: B; Level of Evidence: 3 Strength of Recommendation: NR |
5. The adoption of video consultation over other forms of teleconsultation such as telephone or asynchronous messaging via email, short message services and other internet-based services, is conditionally recommended. | GRADE of Evidence: C; Level of Evidence: 4 Strength of Recommendation: NR |
6. Scheduling of an in-person consultation with the patient at an earliest possible date if the consulting rheumatologist comes across unexplained symptoms or has difficulty in assessing the patient or if the rheumatologist or the patient perceives a gap in communication during the telemedicine consultation, is conditionally recommended. | GRADE of Evidence: C; Level of Evidence: 4 Strength of Recommendation: NR |
7. Teleconsultations with a healthcare professional adequately trained in rheumatology examination, co-located with the patient, is preferred when and if feasible. | GRADE of Evidence: C; Level of Evidence: 4 Strength of Recommendation: NR |
8. Patient data privacy, integrity and security should be protected according to local expectations and regulations. | GRADE of Evidence: B; Level of Evidence: 3 Strength of Recommendation: NR |
9. Routine patient-reported outcome collection is suggested to ensure the quality of care and may be used for pre-consultation triage. | GRADE of Evidence: B; Level of Evidence: 3 Strength of Recommendation: NR |
10. In rheumatic diseases where a treat-to-target approach is recommended for in-person care, a similar approach for telemedicine should be practiced. | GRADE of Evidence: C; Level of Evidence: 2 Strength of Recommendation: NR |
11. Rheumatologists practicing telemedicine should be acquainted with the process and technology used. Training of rheumatologists in telemedicine is conditionally recommended. | GRADE of Evidence: N/A (no published evidence) Level of Evidence: 5 Strength of Recommendation: NR |
12. Beyond patient care, telemedicine may also include training of healthcare workers (general practitioners or nurse practitioners). | GRADE of Evidence: N/A (no published evidence) Level of Evidence: 4 Strength of Recommendation: NR |
13. The potential of telemedicine platforms may be developed to provide patient education and other activities to benefit patients.” (p. 250-251)14 | GRADE of Evidence: N/A (no published evidence) Level of Evidence: 5 Strength of Recommendation: NR |
ArLAR, 202216 | |
General Principles | |
1. Definition of a teleconsultation: A rheumatology teleconsultation is a synchronous exchange of medical information betw een a patient and a rheumatologist via audio or audiovisual electronic communication, to improve the patient's health status | Level of Evidence: 5 Strength of Recommendation: NR |
2. Access and Continuity of Care: Telehealth may improve the access and continuity of care for patients with rheumatic diseases who are home-bound, live in remote areas or underserved communities, or who need to adhere to social distancing restrictions. | Level of Evidence: 3 Strength of Recommendation: NR |
3. Improving disease outcomes: Telehealth can help some patients adhere to the management plan, and this is likely to improve disease outcomes in some selected disease states. | Level of Evidence: 2 Strength of Recommendation: NR |
4. Quality of medical care: Rheumatologists need to use professional experience and judgment to assess whether telehealth is suitable in each situation. | Level of Evidence: 5 Strength of Recommendation: NR |
Best Practice Statements | |
1. Informed consent: Before the teleconsultation visit, an informed consent should be obtained from the patient, in writing or verbally; it should include an explanation, in a simple language, of the benefits and risks of telehealth encounters, as well as the conditions under which telehealth services may be terminated and a referral made to in-person care | Level of Evidence: 5 Strength of Recommendation: NR |
2. Confidentiality: The use of telehealth services must ensure the patient's information security and confidentiality | Level of Evidence: 5 Strength of Recommendation: NR |
3. Documentation: The provision of telehealth services should be well documented in the patient's file, similarly to any in-person medical visit. The decision to assess the patient remotely should be justified and recorded in the patient's file | Level of Evidence: 5 Strength of Recommendation: NR |
4. Shared decision and choice: The choice of using telehealth services should be based on a shared decision between the patient and the physician. Patients should have a choice of their provider of medical teleconsultation | Level of Evidence: 5 Strength of Recommendation: NR |
5. Patient's physical examination: Some parts of the physical exam might be performed remotely, e.g., inspection and evaluation of the range of motion. The patient should be instructed on how to be prepared for a remote physical exam, using appropriate educational material | Level of Evidence: 2 Strength of Recommendation: NR |
6. Patient-reported outcomes: In some chronic rheumatic diseases, the use of patient-reported outcomes by means of self-completed questionnaires adapted for telehealth can help the physician make informed clinical decisions and improve the quality of care | Level of Evidence: 3 Strength of Recommendation: NR |
7. Safe Prescription: The prescription should be transmitted in a safe and confidential manner to the patient with a particular attention to avoiding abuse (of opioids and narcotics' prescriptions in particular) | Level of Evidence: 5 Strength of Recommendation: NR |
8. Fees and reimbursement: The teleconsultation is subject to medical fees and reimbursement similar to an in-person visit. Fees should be set before the teleconsultation | Level of Evidence: 5 Strength of Recommendation: NR |
9. Ethical considerations: Telehealth practice should conform to the same professional ethics that govern in-person care and comply with local jurisdictional laws and regulations of the physician's location | Level of Evidence: 5 Strength of Recommendation: NR |
10. Rheumatologist training: The rheumatologists are encouraged to receive proper training through seminars, workshops, and conferences to familiarize with the advantages and disadvantages of telehealth and to acquire strategies about the most productive approach to remote medical care | Level of Evidence: 5 Strength of Recommendation: NR |
11. Technical infrastructure and equity: The technical infrastructure should be improved for patients and physicians, to enable efficient and equitable access to telehealth services across the countries and in vulnerable populations | Level of Evidence: 5 Strength of Recommendation: NR |
12. Research: Local and regional research projects to assess the implementation of telehealth and the resulting disease outcomes in the Arab region are strongly encouraged.” (p. 382)16 | Level of Evidence: 5 Strength of Recommendation: NR |
ASCO, 202117 | |
1. Patient selection and implementation of telehealth in oncology Standard 1.1 Where appropriate infrastructure and personnel are available, telehealth via telephone or videoconferencing, delivered by health professionals who are certified and participating in routine maintenance of certification activities, is a reasonable option for: Treatment or long-term management:
Others:
In-person consultations may be preferred by clinicians and/or patients for:
Standard 1.2 Diagnosis via asynchronous transmission of images:
Standard 1.3 Practices should develop policies and procedures that outline preferred frequency of telehealth versus in-person visits during the cancer care continuum and consider patient preferences. Frequency of telehealth versus in-person visits may evolve as outcome or impact data become available. Standard 1.4 All clinical visits conducted via telehealth should be documented, including but not limited to the following information:
Standard 1.5 Before participation in telehealth visits, individualized orientation should be provided to patients and health care professionals for the specific type of technology that will be used to deliver the intervention (e.g., mobile phone, web-based, etc.) on topics including but not limited to instructions to access the platform, navigation of the platform, and provider-specific instructions on the video if needed to physically assess an area of the body. Note: Although orientation is required, there is no formal telehealth certification required on the part of health care professionals before engaging in telehealth clinical visits with patients. The Expert Panel does not suggest or endorse formal certification for telehealth competencies. Standard 1.6 For clinical visits conducted via synchronous videoconferencing, a staff member or external technology support person should be available to troubleshoot technology issues, potentially via telephone, and to facilitate workflow. Standard 1.7 Practices should evaluate key performance indicators for oncology telehealth initiatives and quality of care. Standard 1.8 For interventions delivered asynchronously, for example, online patient symptom reporting systems, standard operating procedures should be in place that outline appropriate and timely responses to patient-reported outcomes. Standard 1.9 To optimize adherence to and minimize discontinuation of treatment regimens, asynchronously delivered interventions, such as automated reminders delivered via text message, should be tailored to the individual patient. Standard 1.10 Where possible, patients and caregivers should be involved in user testing of new interventions (e.g., apps) 2. Establishment of the doctor-patient relationship Standard 2.1 State and federal policies permitting telemedicine to cross state lines should include a provision requiring that the doctor-patient relationship is established before provision of any telemedicine service 3. Advanced practice providers (APPs) Standard 3.1 Practices should develop standards, algorithms, or policies that govern when patients may see an advanced practice provider or require a physician telehealth visit on the basis of disease, treatment, or decision inflection points. 4. Allied health professionals Standard 4.1
5. Virtual multidisciplinary cancer conferences (MCCs) Standard 5.1 Where appropriate technology and supports are in place, such as those outlined below, virtual MCCs via videoconferencing are recommended. The Expert Panel endorses the following recommendations from Dharmarajan et al for implementation of a virtual MCC meeting:
6. Teletrials and/or virtual participation in oncology clinical trials Standard 6.1 Teletrials and/or virtual participation in oncology clinical trials are recommended as a method of increasing recruitment and reducing the burden of trial participation on patients. To facilitate the conduct of teletrials, the following are recommended:
| NR |
WHO, 201918 | |
Six of the 9 recommendations were relevant to the current report. These 6 recommendations are as follows: | |
1. Client-to-provider telemedicine: recommended only in specific contexts or conditions: To complement, rather than replace, the delivery of health services and in settings where patient safety, privacy, traceability, accountability, and security can be monitored. | Certainty of evidence: Very low to moderate Strength of Recommendation: NR |
2. Provider-to-provider telemedicine: recommended only in specific contexts or conditions: Where: patient safety, privacy, traceability, accountability, and security can be monitored | Certainty of evidence: Very low to low Strength of Recommendation: NR |
3. Targeted client communication (TCC) across 5 population groups (sexual, reproductive, newborn, child, and adolescent health): recommended only in specific contexts or conditions: Under the condition that potential concerns about sensitive content and data privacy can be addressed. | Certainty of evidence:
|
4. Health worker decision support via mobile devices (CDSS): recommended only in specific contexts or conditions; For tasks that are already defined within the scope of practice for the health worker | Certainty of evidence: Very low to moderate Strength of Recommendation: NR |
5. Digital tracking of patients’ / clients’ health status and services via mobile devices: recommended only in specific contexts or conditions: Where the health system can support the implementation of these intervention components in an integrated manner; For tasks that are already defined as within the scope of practice for the health worker; and where potential concerns about data privacy and transmitting sensitive content to clients can be addressed. | Certainty of evidence:
|
6. Provision of training to health workers via mobile devices (mLearning): recommended; To complement, rather than replace, traditional methods of delivering continued health education and post-certification training.” (p.2)18 | Certainty of evidence: Very low to low Strength of Recommendation: NR |
Canadian Stroke, 201715 | |
Section 1: Organization of Telestroke services for hyperacute stroke management | |
Telestroke care delivery modalities should be integrated into stroke care planning and service delivery across the continuum to ensure equitable access to care across geographic regions in Canada | Evidence Level: C Strength of Recommendation: NR |
1. Telestroke networks should be implemented to provide access to stroke expert consultations for hyperacute and acute stroke assessment, diagnosis, and treatment, including acute thrombolytic therapy with tissue plasminogen activator (tPA) and decision-making for endovascular therapy | Evidence Level: B Strength of Recommendation: NR |
| Evidence Level: B Strength of Recommendation: NR |
2. Standardized, time-driven protocols are required for a coordinated and efficient approach to Telestroke service delivery in the hyperacute phase of stroke to facilitate delivery of advanced stroke therapies in referring sites. | Evidence Level: B Strength of Recommendation: NR |
3. Clearly defined criteria and protocols are required at referring sites to guide the Telestroke consultation process. This referral system should be part of a coordinated system of stroke care. | Evidence Level: B Strength of Recommendation: NR |
4. The consultant should be a physician with specialized training in hyperacute stroke management, and must have timely access to diagnostic-quality neurovascular (e.g., brain CT, CTA) images during the Telestroke consultation. Note: The decision to use acute stroke therapies in emergency management requires imaging to rule out hemorrhage. | Evidence Level: A Strength of Recommendation: NR |
5. Real-time two-way audiovisual communication should be in place to enable remote clinical assessment of the patient by the consulting stroke expert. | Evidence Level: B Strength of Recommendation: NR |
| Evidence Level: C Strength of Recommendation: NR |
6. All laboratory and diagnostic results required by the consultant should be made readily available during the Telestroke consultation. | Evidence Level: B Strength of Recommendation: NR |
7. Referring physicians should follow an established protocol or algorithm which describes the critical steps and inclusion/exclusion criteria for recanalization therapies, which are agreed upon by both referring and consulting sites. | Evidence Level: A Strength of Recommendation: NR |
8. Referring physician and nursing staff who may be involved in acute Telestroke consultations should ideally be trained in administration of the National Institute of Health Stroke Scale (NIHSS), to efficiently and competently assist the Telestroke consultant with the remote video neurological examination. | Evidence Level: B Strength of Recommendation: NR |
9. The most responsible physician remains the attending physician at the referring site. Decision-making is a consensus process that is achieved in consultation with the attending medical staff at the referring site, the patient and family, and the consulting physician with stroke expertise. | Evidence Level: C Strength of Recommendation: NR |
10. A consulting physician may be required to provide ongoing guidance to the referring site following initial consultation and should be accessible. | Evidence Level: C Strength of Recommendation: NR |
11. Protocols should be in place to define patient transfer criteria to a more advanced stroke care facility when clinically indicated (e.g., endovascular (if available) and neurosurgical intervention) | Evidence Level: C Strength of Recommendation: NR |
| Evidence Level: C Strength of Recommendation: NR |
| Evidence Level: C Strength of Recommendation: NR |
12. Standardized documentation should be considered for both the referring site and the consulting site (in accordance to hospital processes, jurisdictional legislation, and regulatory bodies) This may include: | Evidence Level: C Strength of Recommendation: NR |
| Evidence Level: C Strength of Recommendation: NR |
| Evidence Level: C Strength of Recommendation: NR |
| Evidence Level: C Strength of Recommendation: NR |
| Evidence Level: C Strength of Recommendation: NR |
Section 2: Organization of Telestroke services for ongoing stroke assessment and management | |
1. Telestroke services should be part of an integrated stroke services delivery plan that addresses hyperacute stroke care, acute stroke care, stroke prevention, rehabilitation, home-based, and ambulatory care to support optimal patient recovery and family support regardless of geographic location. | Evidence Level: C Strength of Recommendation: NR |
2. Telehealth enabling technologies, including real-time two-way videoconferencing with or without medical peripheral devices and potentially asynchronous (store-forward) tools, such as an e-referral system for non-urgent consultations and remote patient monitoring devices, can be used to enable consultations and/or service delivery regarding: | Evidence Level: C Strength of Recommendation: NR |
| Evidence Level: C Strength of Recommendation: NR |
| Evidence Level: A Strength of Recommendation: NR |
| Evidence Level: C Strength of Recommendation: NR |
| Evidence Level: C Strength of Recommendation: NR |
| Evidence Level: B Strength of Recommendation: NR |
3. Clearly defined criteria and protocols or algorithms should be available for referring sites to determine when and how to access these rehabilitation, prevention, and ambulatory services for stroke patients. | Evidence Level: C Strength of Recommendation: NR |
4. The consulting healthcare provider may provide documentation to the referring site to be included in the patient medical record, regarding patient progress, treatment plans, plans for ongoing follow-up, and discharge recommendations (in accordance with clinical care processes, organizational requirements, jurisdictional legislation, and regulatory bodies).” (p. 891-892)15 | Evidence Level: C Strength of Recommendation: NR |
Section 3: Staff training and ongoing education | |
1. It is recommended that Telestroke care providers attain and maintain the necessary competencies required in telemedicine in order to provide safe, competent care and to create a satisfactory telehealth encounter for both the patient and the healthcare provider. | Evidence Level: C Strength of Recommendation: NR |
2. Referring and consulting service providers should be trained in using the Telestroke system and understand their roles and responsibilities for technical and clinical aspects of a Telestroke consultation. | Evidence Level: C Strength of Recommendation: NR |
3. Training should include physicians, nurses, therapists, and any support staff (such as members of technology department), who may be involved in any Telestroke consultation or therapy appointment. | Evidence Level: C Strength of Recommendation: NR |
4. Ongoing Telestroke training and education with a regular update cycle is useful to ensure competency of providers. | Evidence Level: C Strength of Recommendation: NR |
5. Consulting physicians and other healthcare professionals involved in Telestroke consults should have expertise and experience in managing stroke patients. | Evidence Level: C Strength of Recommendation: NR |
6. Continuing education in online and face-to-face formats is useful to ensure remote-based practitioners have access to Ongoing education. | Evidence Level: C Strength of Recommendation: NR |
7. Mock patients simulations may be helpful, especially for hyperacute Telestroke care for new sites, and where the ongoing number of cases is low.” (p. 892)15 | Evidence Level: C Strength of Recommendation: NR |
APLAR = Asia Pacific League of Associations for Rheumatology; APP = advanced practice providers; ArLAR = Arab League of Associations for Rheumatology; ASCO = American Society of Clinical Oncology; Canadian Stroke = Canadian Stroke Best Practice Recommendations; CDSS = clinical decision support system; CT = computed tomography; CTA = computed tomography angiography; MCC = multidisciplinary cancer conferences; MDT = multidisciplinary team; N/A = not applicable; NIHSS = National Institute of Health Stroke Scale; NR = not reported; TCC = targeted client communication; tPA = tissue plasminogen activator.
aGrading of evidence: For APLAR,14 the quality of evidence was assessed using GRADE, ranging from A (high quality of evidence) to D (very low quality of evidence). For APLAR14 and ArLAR,16 the levels of evidence were assessed using the Oxford Centre for Evidence-Based Medicine scale from 1 (systematic review of randomized trials) to 5 (mechanism-based reasoning). For WHO,18 authors assessed the certainty of evidence using GRADE, ranging from “very low” to “low” to “moderate” to “high”. For Canadian Stroke,15 authors assessed the level of evidence as A, B, or C where A = Evidence from a meta-analysis of randomized controlled trials or consistent findings from 2 or more randomized controlled trials; B = Evidence from a single randomized controlled trial or consistent findings from 2 or more well-designed non-randomized and/or noncontrolled trials and large observational studies; and C = Writing group consensus and/or supported by limited research evidence.
Appendix 5: References of Potential Interest
Note that this appendix has not been copy-edited.
Previous CADTH Reports
Khangura SD, Severn M. Virtual oncology visits. (CADTH reference list: summary of abstracts). Ottawa (ON): CADTH; 2022: https://www.cadth.ca/sites/default/files/pdf/htis/2022/RB1618Virtual-Oncology-Visits-Final.pdf. Accessed 2022 Jul 28.
Santos C, Ryce A. Virtual clinical assessments for adults with back pain. (CADTH reference list). Ottawa (ON): CADTH; 2022: https://www.cadth.ca/sites/default/files/pdf/htis/2022/RA1219%20Virtual%20Assessments%20for%20Back%20pain%20Final.pdf. Accessed 2022 Jul 28.
Hui D, Dolcine B, Loshak H. Approaches to evaluations of virtual care in primary care. Can J Health Technol. 2022;2(1). https://www.cadth.ca/sites/default/files/ES/ES0358%20Evaluations%20of%20virtual%20care-Final.pdf. Accessed 2022 Jul 06.
Gray C, Mason J, Loshak H. An overview of direct-to-patient virtual visits in Canada. Can J Health Technol. 2021;1(6). https://www.cadth.ca/sites/default/files/hs-eh/EH0091%20Virtual%20Visits%20Final.pdf. Accessed 2022 Jul 06.
Enablers for virtual visits. (CADTH policy insights). Ottawa (ON): CADTH; 2020: https://www.cadth.ca/sites/default/files/covid-19/cy0006-enablers-for-virtual-visits.pdf. Accessed 2022 Jul 06.
Evidence on digital health. (CADTH evidence bundles). Ottawa (ON): CADTH: https://www.cadth.ca/digital-health. Accessed 2022 Jul 06.
Review Articles
Primary Care
Omboni S Omboni S, Padwal RS, Alessa T, et al. The worldwide impact of telemedicine during COVID-19: current evidence and recommendations for the future. Connect Health. Jan 4 2022;1:7-35. PubMed
Musculoskeletal Specialties
Gottlieb AB, Wells AF, Merola JF. Telemedicine and psoriatic arthritis: best practices and considerations for dermatologists and rheumatologists. Clin Rheumatol. May 2022;41(5):1271-1283. PubMed
Other
Anvari S, Neumark S, Jangra R, Sandre A, Pasumarthi K, Xenodemetropoulos T. Best Practices for the Provision of Virtual Care: A Systematic Review of Current Guidelines. Telemed J E Health. May 9 2022. PubMed
Additional Publications That Did Not Meet Eligibility Criteria of This Report
Additional references of interest, for guidelines without a systematic literature review or for best practice guidelines and consensus statements, are provided below. Separate lists are provided for primary care (including a summary and table of recommendations), musculoskeletal specialties (including a summary and table of recommendations), and other specialities (a reference list only).
Primary Care
The study designs included in these articles were practice guidelines and consensus-based guidelines. In total, 12 articles covered topics regarding the use of telemedicine in primary care. The majority of them were best practice guidelines developed by different organizations. Eleven out of 12 articles were published in the context of the COVID-19 pandemic. Nine articles were developed by Canadian researchers/organizations, thereby increasing the relevance and generalizability to the Canadian population. Common themes included: the potential for virtual visits and different forms of telemedicine to be appropriate for a variety of medical visits; the need for adequate patient and physician preparation to ensure the virtual visit is optimized; ensuring that regular medical compliances such as privacy to information is adhered to; the potential for virtual visits to reach more patients than possible with physical visits; patient consent; and documentation. Each article is listed below, with corresponding recommendations in Table 5.
Furlepa K, Tenderenda A, Kozlowski R, Marczak M, Wierzba W, Sliwczynski A. Recommendations for the Development of Telemedicine in Poland Based on the Analysis of Barriers and Selected Telemedicine Solutions. Int J Environ Res Public Health. Jan 22 2022;19(3):1221. PubMed
Virtual health handbook for PHSA staff. Vancouver (BC): Provincial Health Services Authority; 2022: http://www.phsa.ca/health-professionals-site/Documents/Office%20of%20Virtual%20Health/Virtual%20Health%20Handbook.pdf. Accessed 2022 Jul 17.
Telemedicine and virtual care guidelines (and other clinical resources for COVID-19). Ottawa (ON): Royal College of Physicians and Surgeons of Canada; 2020: https://www.royalcollege.ca/rcsite/documents/about/covid-19-resources-telemedicine-virtual-care-e. Accessed 2022 Jul 17.
UHN Virtual Care Clinical Advisory Panel. Clinical Guiding Principles for Virtual Care. (Virtual care: a healthier world is within our reach). Toronto (ON): University Health Network (UHN); 2022: https://www.uhn.ca/corporate/AboutUHN/Virtual_Care/Documents/Clinical-Guiding-Principles-Virtual-Care.pdf. Accessed 2022 Jul 17.
Ong MK, Pfeffer M, Mullur RS. Telemedicine for adults. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2022: www.uptodate.com. Accessed 2022 Jun 13.
COVID-19 toolkit: virtual care. Considerations for patients, health professionals and digital teams involved in Virtual Health. Ottawa (ON): Accreditation Canada; 2020: https://sharedhealthmb.ca/files/covid-19-virtual-care-toolkit.pdf. Accessed 2022 Jul 17
Virtual care best practices guide. Ottawa (ON): University of Ottawa; 2020: https://med.uottawa.ca/family/sites/med.uottawa.ca.family/files/virtual_care_best_practices_guide_-_en_-_april_3_2020.pdf. Accessed 2022 Jul 18.
Getting started with virtual care. Everything you need to know to provide synchronous virtual care. Dartmouth (NS): Doctors Nova Scotia; 2020: https://doctorsns.com/sites/default/files/2020-06/toolkit-virtual-care-v2.pdf. Accessed 2022 Jul 17.
Adopting and integrating virtual visits into care: draft clinical guidance for health care providers in Ontario. Toronto (ON): Ontario Health; 2020: https://quorum.hqontario.ca/Portals/0/Users/170/54/10154/Draft%20Clinical%20Guidance_Adopting%20and%20integrating%20virtual%20visits%20into%20care_V1.pdf?ver=2020-03-13-091936-370. Accessed 2022 Jul 17.
Prasad A, Brewster R, Rajasekaran D, Rajasekaran K. Preparing for telemedicine visits: guidelines and setup. Front Med (Lausanne). 2020;7:600794. PubMed
Providing geriatric virtual care across the South West: guidance document for health care and community support services providers. London (ON): South West Frail Senior Strategy; 2020: https://www.sjhc.london.on.ca/sites/default/files/documents/2020-12/guidance_document_-_providing_geriatric_virtual_care_across_the_sw-12.15.20.pdf. Accessed 2022 Jul 18.
Advice to the profession: virtual care. Toronto (ON): College of Physicians and Surgeons of Ontario: https://www.cpso.on.ca/en/Physicians/Policies-Guidance/Policies/Virtual-Care/Advice-to-the-Profession-Virtual-Care. Accessed 2022 Jul 17.
Musculoskeletal Specialties
Two articles were found covering musculoskeletal topics: 1 consensus-based guideline and 1 practice guideline. Wahezi et al., 2020 reported on a reference guide for musculoskeletal and neurologic examination that can be used in telemedicine practice. Barber et al., 2022, who included a rapid literature review and a subsequent Delphi process, reported on quality and patient safety considerations when developing the best practice statements for rheumatology virtual care. The common themes identified in both articles were that virtual care can be appropriate to assess certain musculoskeletal conditions; physicians/clinicians should adhere to national recommendations on best practices, provincial standards, and regulations for virtual care; and, where appropriate, patient-reported outcomes that help direct approaches for care should be used during virtual encounters. Each article is listed below, with corresponding recommendations listed in Table 5 in Appendix 6.
Barber CEH, Levy DM, Ahluwalia V, et al. Best practices for virtual care: a consensus statement from the Canadian Rheumatology Association. J Rheumatol. Apr 2022;49(4):408-418. PubMed
Wahezi SE, Duarte RA, Yerra S, et al. Telemedicine during COVID-19 and beyond: a practical guide and best practices multidisciplinary approach for the orthopedic and neurologic pain physical examination. Pain Physician. Aug 2020;23(4S):S205-S238. PubMed
Other Specialties: Consensus Statements and Guidelines
Marino LV, Collaco NC, Ashton JJ, et al. Pedi-R-MAPP: The development of a nutritional awareness tool for use in remote paediatric consultations using a modified Delphi consensus. Clin Nutr. Mar 2022;41(3):661-672. PubMed
Puts M, Papadopoulos E, Brennenstuhl S, et al. The development of geriatric assessment and intervention guidelines for an online geriatric assessment tool: a Canadian modified Delphi panel study. Curr Oncol. Feb 4 2022;29(2):853-868. PubMed
Ben-Arye E, Paller CJ, Lopez AM, et al. The Society for Integrative Oncology Practice recommendations for online consultation and treatment during the COVID-19 pandemic. Support Care Cancer. Oct 2021;29(10):6155-6165. PubMed
Couturier J, Pellegrini D, Miller C, et al. The COVID-19 pandemic and eating disorders in children, adolescents, and emerging adults: virtual care recommendations from the Canadian consensus panel during COVID-19 and beyond. J Eat Disord. Apr 16 2021;9(1):46. PubMed
Cremers HP, Theunissen L, Hiddink J, et al. Successful implementation of ehealth interventions in healthcare: Development of an ehealth implementation guideline. Health Serv Manage Res. Nov 2021;34(4):269-278. PubMed
Qureshi AZ, Ullah S, Aldajani AA, et al. Telerehabilitation guidelines in Saudi Arabia. Telemed J E Health. Oct 2021;27(10):1087-1098. PubMed
Stipa G, Gabbrielli F, Rabbito C, et al. The Italian technical/administrative recommendations for telemedicine in clinical neurophysiology. Neurol Sci. May 2021;42(5):1923-1931. PubMed
Other Specialties: Practice Guidelines and Recommendations
Virtual care in Canada: strengthening data and information. Ottawa (ON): Canadian Institute for Health Information; 2022: https://www.cihi.ca/sites/default/files/document/virtual-care-in-canada-strengthening-data-information-report-en.pdf. Accessed 2022 Jul 19.
Deda LC, Goldberg RH, Jamerson TA, Lee I, Tejasvi T. Dermoscopy practice guidelines for use in telemedicine. NPJ Digit Med. Apr 27 2022;5(1):55. PubMed
Cancer Care Ontario. Person-centred virtual cancer care clinical guidance. 2022; https://www.cancercareontario.ca/en/guidelines-advice/types-of-cancer/69581. Accessed 2022 Jul 19.
Adopting e-health solutions: implementation strategies. Best practice guidelines. Toronto (ON): Registered Nurses' Association of Ontario; 2017: https://rnao.ca/sites/rnao-ca/files/bpg/Adopting_eHealth_Solutions_WEB_FINAL.pdf. Accessed 2022 Jul 19.
Venkatesh U, Aravind GP, Velmurugan AA. Telemedicine practice guidelines in India: Global implications in the wake of the COVID-19 pandemic. World Med Health Policy. 2022. PubMed
Privacy and security considerations for virtual health care visits. Guidelines for the health sector. Toronto (ON): Information and Privacy Commissioner of Ontario; 2021: https://www.ipc.on.ca/wp-content/uploads/2021/02/virtual-health-care-visits.pdf. Accessed 2022 Jul 19.
Sarveswaran G, Rangamani S, Ghosh A, et al. Management of diabetes mellitus through teleconsultation during COVID-19 and similar scenarios - Guidelines from Indian Council of Medical Research (ICMR) expert group. Diabetes Metab Syndr. 2021;15(5):102242. PubMed
Sharma VD, Safarpour D, Mehta SH, et al. Telemedicine and deep brain stimulation - current practices and recommendations. Parkinsonism Relat Disord. 2021;89:199-205. PubMed
Thai-Van H, Bakhos D, Bouccara D, et al. Telemedicine in audiology. Best practice recommendations from the French Society of Audiology (SFA) and the French Society of Otorhinolaryngology-Head and Neck Surgery (SFORL). Eur Ann Otorhinolaryngol Head Neck Dis. 2021;138(5):363-375. PubMed
Gómez Rivas J, Rodríguez-Serrano A, Loeb S, et al. Telemedicine and smart working: Spanish adaptation of the European Association of Urology recommendations. Actas Urol Esp (Engl Ed). 2020;44(10):644-652. PubMed
Horton MB, Brady CJ, Cavallerano J, et al. Practice guidelines for ocular telehealth-diabetic retinopathy, third edition. Telemed J E Health. 2020;26(4):495-543. PubMed: PM32209018
Rodriguez Socarrás M, Loeb S, Teoh JY, et al. Telemedicine and smart working: recommendations of the European Association of Urology. Eur Urol. 2020;78(6):812-819. PubMed
Virtual care guidelines for clinicians. Toronto (ON): Holland Bloorview Kids Rehabilitation Hospital; 2020: https://hollandbloorview.ca/sites/default/files/2020-05/HB-VirtualCareGuidelines-May20.pdf. Accessed 2022 Jul 19.
Virtual visit guide for midwives. Toronto (ON): Association of Ontario Midwives; 2020: https://www.ontariomidwives.ca/sites/default/files/2020%2004%2006%20Virtual%20Visits%20Guidance%20for%20Midwives%20-%202020.pdf. Accessed 2022 Jul 19.
Lopes M, Oliveira GMM, Ribeiro ALP, et al. Guideline of the Brazilian Society of Cardiology on Telemedicine in Cardiology - 2019. Arq Bras Cardiol. 2019;113(5):1006-1056. PubMed
Myers K, Nelson EL, Rabinowitz T, et al. American Telemedicine Association practice guidelines for telemental health with children and adolescents. Telemed J E Health. 2017;23(10):779-804. PubMed
Appendix 6: Recommendations Related to Musculoskeletal Topics
Two articles were found covering musculoskeletal topics: 1 consensus-based guideline and 1 practice guideline. Wahezi et al., 2020 reported on a reference guide for musculoskeletal and neurologic examination that can be used in telemedicine practice. Barber et al., 2022, who included a rapid literature review and a subsequent Delphi process, reported on quality and patient safety considerations when developing the best practice statements for rheumatology virtual care. The recommendations from those articles are listed in Table 5.
Table 5: Summary of Recommendations in Documents of Potential Interest
Guideline development group (year) | Recommendations, standards, guidelines |
|---|---|
Primary care | |
Furlepa et al. (2022) | Recommendation themes:
|
Provincial Health Services Authority, British Columbia (2022) | Key messages were as follows:
|
Royal College of Physicians (2022) |
|
University Health Network (2022) |
|
UpToDate (2022) |
|
Accreditation Canada and Health Standards Organization (2020) |
|
Department of Family Medicine, University of Ottawa (2020) |
|
Doctors of Nova Scotia (2020) |
|
Ontario Health (2020) |
|
Prasad et al. (2020) |
|
South West Frail Senior Strategy (2020) |
|
College of Physicians and Surgeons of Ontario (2014) |
|
Musculoskeletal specialties | |
Barber et al. (2022) |
|
Wahezi et al. (2020) |
|
ID = identity; OTN = Ontario Telemedicine Network.
Acknowledgment: Nikolay Alabi
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca