CADTH Health Technology Review
Intravenous Iron Preparations for Patients Undergoing Elective Surgery: A 2022 Update
Rapid Review
Authors: Shannon Hill, Melissa Severn
Abbreviations
AGREE
Appraisal of Guidelines for Research and Evaluation
AMSTAR 2
A MeaSurement Tool to Assess systematic Reviews 2
CI
confidence interval
EQ-5D
European Quality of Life – 5 Dimension Questionnaire
GRADE
Grading of Recommendations Assessment, Development and Evaluation
ICU
intensive care unit
MA
meta-analysis
NICE
National Institute for Health and Care Excellence
PRISMA
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
PROSPERO
Prospective Register of Systematic Reviews
RCT
randomized controlled trial
SR
systematic review
Key Messages
For adults who are iron deficient before elective surgery, patients who received IV iron supplementation may have greater increases in hemoglobin and ferritin concentrations, similar or lower lengths of stay in hospital, and similar quality of life measures, functional outcomes, and rates of adverse events, compared to patients who did not receive IV supplementation. The findings were mixed for the rate of blood transfusions.
For adults who are iron deficient before elective surgery, patients who received IV iron supplementation may experience similar changes in hemoglobin levels, quality of life scores, or number of adverse events when compared to patients who received oral iron supplementation. The findings were mixed regarding the risk of blood transfusions.
No studies were found on the cost-effectiveness of IV iron preparation therapy for patients who are iron deficient undergoing elective surgery that met the criteria for this review.
One guideline recommends the use of IV iron supplementation for patients with iron deficient anemia when surgery is less than 8 weeks away, patients are unable to tolerate or absorb oral iron supplementation, or for patient with suboptimal hemoglobin levels.
Context and Policy Issues
Pre-operative anemia is a common problem and can impact as much as 30% to 50% of patients presenting for surgery.1,2 The WHO defines anemia as a hemoglobin level of less than 130 mg/mL in men and 120 mg/mL in non-pregnant women.1 It is estimated that approximately 3% of Canadians have anemia and is most prevalent for people age 65 to 79.3 The most common form of anemia is iron deficiency anemia, which can be acute or chronic, but becomes problematic when there are insufficient number of red blood cells to maintain oxygen demand.1 This can be detrimental during surgery where blood loss may be high and may result in peri-operative blood transfusions and adverse post-operative outcomes such as inpatient complications, delayed hospital discharge, or mortality.1,2
A 2015 National Institute for Health and Care Excellence (NICE) guideline recommends that oral iron supplementation should be the first-line treatment option for patients with anemia undergoing surgery.2,4 Oral iron supplementation is common and inexpensive, and can be an effective method of iron supplementation; however, oral iron can be poorly absorbed by the body and compliance with oral iron treatment is often low with only 20% to 40% of patients completing a full course of treatment.2 Another common treatment option is peri-operative blood transfusion, but this can be associated with increased patient length of stay, morbidity, and mortality, and may be effected by a limited supply and increase demand of donated blood.1 IV iron preparation (or supplementation) is an alternative treatment option for patients with iron deficiency undergoing elective surgery. IV iron is a method of iron supplementation administered directly to the patient and is often given to patients to correct anemia before surgery.2 IV iron can be administered closer to the time of surgery because iron absorption is often more rapid compared to oral iron supplementation.2 There are a number of common IV iron supplementations available to treat pre-operative anemia including ferric carboxymaltose, ferric derisomaltose (also known as iron isomaltoside), ferric gluconate, ferumoxytol, iron dextran, and iron sucrose.5 The recommended doses for each type of IV iron supplementation varies, but can range from multiple doses at 125 mg to single doses at 2,000 mg.5 IV iron supplementations approved for use in Canada include ferric derisomaltose,6 ferric gluconate,7 ferumoxytol,8 iron dextran,9 and iron sucrose.10
The purpose of this report is to summarize the evidence related to clinical effectiveness, cost-effectiveness, and recommendations regarding IV iron preparations to support decisions involved in the use of this treatment for patients identified as iron deficient undergoing elective surgery. This report is an update to a previous CADTH report from 2019 that evaluated the use of IV iron preparations for the same population.11
Research Questions
What is the clinical effectiveness of IV iron preparations for patients identified as iron deficient undergoing elective surgery, including high blood loss surgery?
What is the cost-effectiveness of IV iron preparations for patients identified as iron deficient undergoing elective surgery, including high blood loss surgery?
What are the evidence-based guidelines regarding the use of IV iron preparations for patients identified as iron deficient undergoing elective surgery, including high blood loss surgery?
Methods
Literature Search Methods
The literature search strategy used in this report is an update of 1 developed for a previous CADTH report.11 For the current report, a limited literature search was conducted by an information specialist on key resources including MEDLINE, the Cochrane Database of Systematic Reviews, the International HTA Database, Canadian and major international health technology agencies, as well as a focused internet search. No filters were applied to limit the retrieval by study type. The initial search was limited to English-language documents published between January 1, 2014 and February 28, 2019. For the current report, database searches were rerun on September 13, 2022 to capture any articles added to the databases since the initial search date. The search of major health technology agencies was also updated to include documents published since February 2019.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. As an update to a previous CADTH report, articles were reviewed if they were made available since the previous search date and were not included in the 2019 CADTH report.11 The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
The terms IV iron, IV iron preparation, IV iron supplementation are all used in the literature to describe the intervention of interest, but for the purpose of this report the term IV iron supplementation will be used consistently to summarize the findings from the literature.
Criteria | Description |
|---|---|
Population | Adult patients identified as iron deficient undergoing elective surgery (i.e., any surgery scheduled in advance of the operation) |
Intervention | IV iron preparations (e.g., iron isomaltoside, ferric carboxymaltose, iron sucrose, ferumoxytol, iron dextran, sodium ferric gluconate) |
Comparator | Q1 to Q2: Blood transfusion, standard of care, saline, no treatment, no IV iron, placebo Q3: No comparator |
Outcomes | Q1: Clinical Effectiveness (e.g., mortality and morbidity, length of hospital stay, comorbidities, need for blood transfusion, hemoglobin level, hemoglobin change, patient quality of life), safety (e.g., hypersensitivity, allergic reaction, rate of adverse events) Q2: Cost-effectiveness (e.g., cost per quality-adjusted life-years gained, incremental cost. cost per adverse event avoided) Q3: Recommendations related to the use of IV iron preparations for adult patients identified as iron deficient undergoing elective surgery |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, non-randomized studies, economic evaluations, evidence-based guidelines |
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, or they were duplicate publications. Economic evaluations and evidence-based guidelines were excluded if they were published before 2019, and health technology assessments, systematic reviews, RCTs, and non-randomized studies were excluded if they were published before 2021. Systematic reviews in which all relevant studies were captured in other more recent or more comprehensive systematic reviews were excluded. Primary studies retrieved by the search were excluded if they were captured in 1 or more included systematic reviews. Guidelines with unclear methodology were also excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)12 for systematic reviews, the Downs and Black checklist13 for randomized and non-randomized studies, and the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument14 for guidelines. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
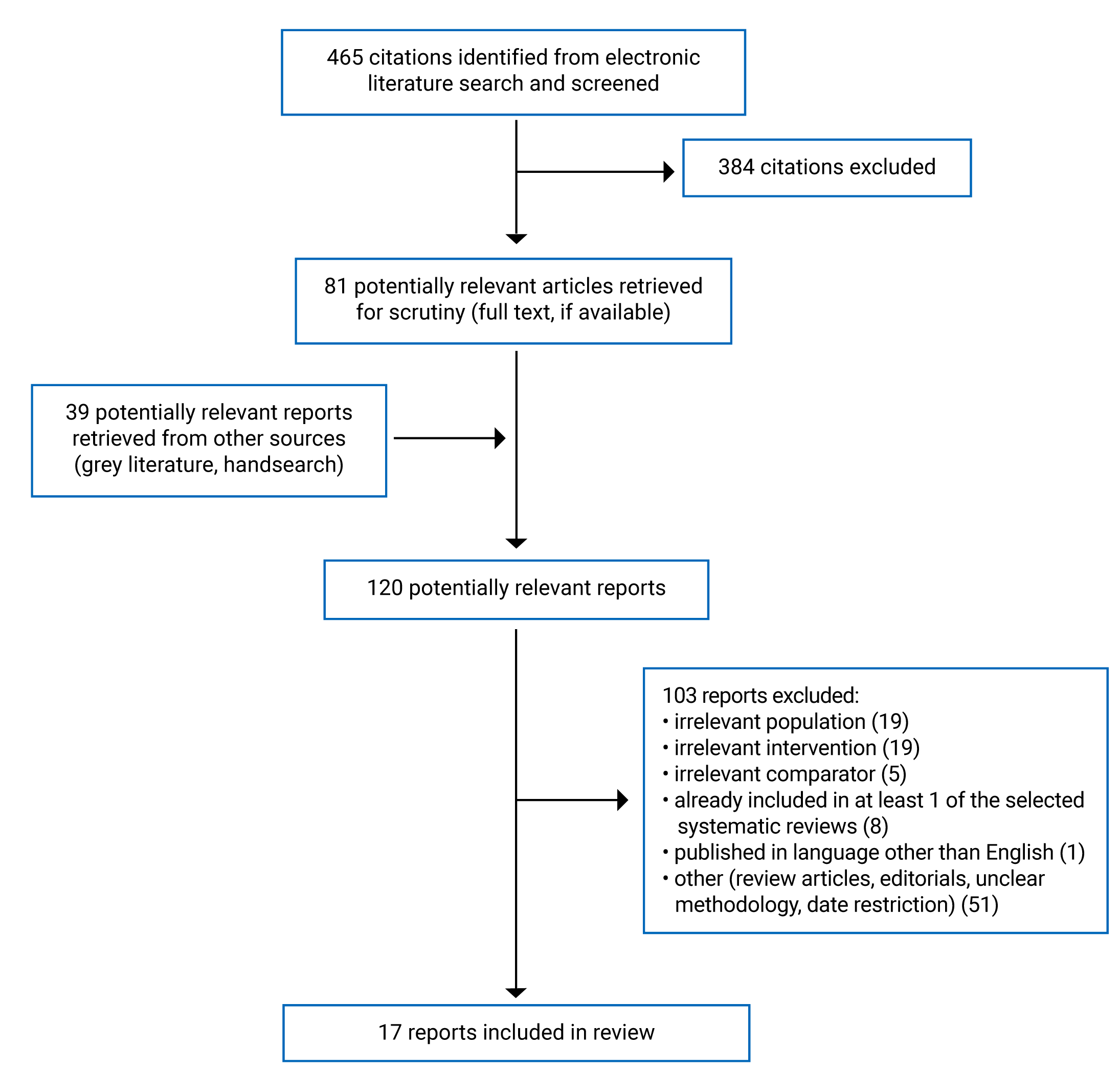
A total of 465 citations were identified in the literature search. Following screening of titles and abstracts, 384 citations were excluded and 81 potentially relevant reports from the electronic search were retrieved for full-text review. Thirty-nine potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 103 publications were excluded for various reasons, and 17 publications met the inclusion criteria and were included in this report, with 1 additional report included through a bibliographical hand-search. These comprised 6 systematic reviews (SRs), 4 randomized controlled trials (RCTs), 6 non-randomized studies, and 1 evidence-based guideline. Appendix 1 presents the PRISMA15 flow chart of the study selection.
Summary of Study Characteristics
Six SRs16-21 including 3 with meta-analysis (MA),16,17,19 4 RCTs,22-25 6 non-randomized studies,26-31 and 1 evidence-based guideline32 was included in this report.
Four SRs16-18,20 had broader inclusion criteria than this report: 3 SRs16-18 including 2 with MA16,17 included a range of interventions related to iron supplementation including the use of oral iron supplementation. One SR included a study with an irrelevant comparator.20 Only studies that fit the inclusion criteria for this report will be reported on.
Additional details regarding the characteristics of included publications are provided in Appendix 2, Tables 2 to 4. There was some overlap of studies included in the SRs, and the degree of overlap is summarized in Appendix 5, Table 15.
Study Design
All 6 SRs were published in 202118-21 or 2022.16,17The authors of 1 SR and MA included 10 RCTs published up to December 2020.16 The authors of 1 SR and MA included 7 primary studies comprised of 2 RCTs and 5 non-randomized studies published up to February 2021.17 The authors of 1 SR included 7 RCTs published up to December 2019.18 The authors of 1 SR and MA included 10 RCTs published up to February 2019.19 The authors of 1 SR included 10 RCTs published up to January 2021.20 The authors of 1 SR included 9 primary studies comprised of 5 RCTs and 4 non-randomized studies published up to November 2020.21 The primary study overlap between these SR is summarized in Appendix 5, Table 15. Eleven of the 30 primary studies were included in 2 or more SRs.
Three RCTs were published in 2022,22-24 while 1 RCT was published in 2021.25 One non-randomized study was published in 2022,26 while 5 non-randomized studies were published in 2021.27-31 Five of the non-randomized studies were retrospective cohort studies that used historical patient data in their analysis.26-30 One non-randomized study was a multicenter prospective cohort study that used prospectively collected patient data.31 When reported, patient follow-up time varied across studies depending on the outcome being reported, but ranged from 21 days to 3 months.
One evidence-based guideline32 was identified that presented recommendations that were broader in scope than this report; however, recommendations related to the management of pre-operative anemia were presented. Recommendations were developed by 2 reviewers based on a systematic review of evidence.32 In addition, 1 evidence-based guideline from NICE33 was identified from the literature search but did not provide any specific recommendations related to the use of IV iron supplementation for patients identified as iron deficient undergoing elective surgery; therefore, no summary of can be provided. This evidence-based guideline did reference a recommendation from an evidence-based guideline from 20154 that was captured in the 2019 CADTH report.11
Country of Origin
The included SRs were conducted in the UK,16 China,17 the US,18,20,21 and Canada.19
The included RCTs were conducted in Hong Kong,22 Norway,23 Egypt,24 and Singapore.25 The included non-randomized studies were conducted in Denmark,26 Singapore,27 the UK,28,30 Canada,29 and Germany.31
The included evidence-based guideline was conducted in Canada.32
Patient Population
Two SRs16,21 included primary studies of adult patients undergoing elective abdominal surgery receiving pre-operative iron supplementation; however, 1 of these SRs16 did not restrict on the type of iron supplementation, while the other SR specified including studies that focused on IV iron supplementation.21 One SR included primary studies of patients who received iron supplementation undergoing surgery for colorectal cancer.17 One SR included primary studies of adult patients who receive intra-operative or post-operative iron supplementation for elective total joint arthroplasty surgery.18 Two SRs19,20 included primary studies of adult patients who received IV iron supplementation and underwent any elective surgery. One of these SRs focused on pre-operative IV iron supplementation,19 while the other did not specify.20
One RCT included adults with colorectal cancer undergoing elective curative tumour resection operation and anemia or iron deficiency.22 One RCT included patients who severe aortic stenosis and iron deficiency.23 One RCT included patients aged 52 to 67 with anemia scheduled for elective coronary artery bypass grafting.24 One RCT included adult patients with iron deficiency or anemia scheduled for elective major abdominal surgery.25
Four non-randomized studies (3 retrospective cohort studies27-29 and 1 prospective cohort study)31 included adult patients undergoing any elective surgery but did specify that patients included in the study were either iron deficient and/or anemic. One non-randomized study included adult patients undergoing colorectal cancer surgery with iron deficiency anemia.26 One non-randomized study included adult elective cardiac and aortic surgical patients with iron deficiency and anemia.30
The target population for the included evidence-based guideline was patients with comorbid condition, specifically anemia, hyperglycemia, and smoking, undergoing major surgery.32 The authors did not specify a type of major surgery for the recommendations.
Interventions and Comparators
Consistent with the inclusion criteria for the current report, the identified SRs included primary studies examined the effectiveness of IV iron supplementation for patients identified as iron deficient undergoing elective surgery.16-21 The type of IV iron supplementation included IV ferric carboxymaltose,16-21 IV iron sucrose,16,17,19,21 IV isomaltoside,17,18 and unspecified IV iron.16,19 IV iron supplementation was administered pre-operatively,16,17,19-21 intra-operatively,18 and/or post-operatively17,18,20 at varied doses ranging from 100 mg to 2,000 mg. The comparators for the identified SRs included oral iron supplementation (usual care),16-21 placebo,16-21 and no treatment.17,18,20,21
Similarly, the identified RCTs examined to effectiveness various IV supplementation including IV iron isomaltoside or ferric derisomlatose,22,23 and IV ferric carboxymaltose.24,25 IV supplementation for each RCT was given pre-operatively at various doses ranging from 1,000 mg to 2,000 mg.22-25 The comparators for the identified RCTs included no treatment,22 placebo,23,24 or oral iron supplementation.25 The non-randomized studies examined the effectiveness of various IV supplementation including IV ferric carboxymaltose,26,27,31 IV iron isomaltoside,28,30 and IV iron sucrose.29 Each non-randomized study administer the IV iron supplementation pre-operatively at various doses ranging from 200 mg to 1,000 mg.26-31 The comparators for the identified non-randomized studies included no treatment26,28-31 and oral iron supplementation.27,29
The identified evidence-based guideline presented diagnostic and treatment algorithms for the management of pre-operative anemia which included a recommendation related to IV iron supplementation specifically.32
Outcomes
The identified SRs reported outcomes related to the clinical effectiveness of IV iron supplementation for patients identified as iron deficient undergoing elective surgery. Each SR reported outcomes related to patient hemoglobin levels, and safety and adverse events including mortality and infection.16-21 Five SRs reported outcomes related to the incidence of blood transfusion.16,17,19-21 Three SRs reported on patient quality of life outcomes,18-20 and 2 of these SRs reported on hospital length of stay.19,20 Additional clinical effectiveness outcomes were captured in the SRs, which included incidence of anemia,18,19 measures of ferritin level,19,20 and various measures of functional outcomes.18
Similarly, the identified RCTs and non-randomized studies reported outcomes related to the clinical effectiveness of IV supplementation for patients identified as iron deficient undergoing elective surgery. Each RCT22-25 and 3 non-randomized studies reported outcomes related to patient hemoglobin levels.26,28,29 Two RCTs22,25 and 6 non-randomized studies26-31 reported outcomes related to the incidence of blood transfusion. Each RCT22-25 and 2 non-randomized studies26,30 reported various outcomes related to safety and adverse events. In relations to safety and adverse event outcomes, 2 of the RCTs23,24 and 4 non-randomized studies26,28,30,31 reported mortality outcomes, while 3 RCTs22-24 and 2 non-randomized studies reported infection related outcomes.26,30 Three RCTs22,23,25 reported outcomes related to quality of life measured by quality of recovery22 and the European Quality of Life – 5 Dimensions questionnaire.23,25 Three RCTs22,24,25 and 4 non-randomized studies26-28,31 reported outcomes related to length of patient recovery measured by length of hospital stay22,24,26-28,31 or days alive at home.22,25,26 Additional clinical effectiveness outcomes were captured from the identified RCTs and non-randomized studies including measures of ferritin level,22,23,28 and measures of functional outcomes.23
The identified evidence-based guideline provided recommendations related to the use of IV iron supplementation for the management of pre-operative anemia for patients undergoing surgery.32 The strength of recommendation and quality of evidence supporting the recommendation was assessed using Grading of Recommendations Assessment, Development and Evaluation (GRADE).32
Summary of Critical Appraisal
An overview of the critical appraisal of the included studies is summarized below. Additional details regarding the strengths and limitations of included publications are provided in Appendix 3, Tables 5 to 7.
Systematic Reviews
All 6 included SRs provided clearly defined research questions and inclusion criteria, included multiple databases in the literature searches, and provided adequate details of the included primary studies.16-21 Four SRs stated that review methods were established before the review was conducted,16,19-21 with 3 of the SRs providing PROSPERO registration numbers.16,19,21 Each SR also indicated that literature search screening and study inclusion was conducted in duplicate,16-21 but only 4 SRs indicated that additional handsearching of included or relevant studies was done.16,17,19,20 Two SR indicated that no restrictions were included in the search methods,17,19 while 3 SRs indicated that no restrictions on search time frame was included in their search.16,18,20 Two SRs indicated that data extraction of primary studies was performed in duplicate,17,19 while 1 study indicated that data extraction was performed by 1 author and checked by another author21; thus minimizing potential errors in data collection. Each SR assessed the risk of bias of the included primary studies using appropriate techniques,16-21 while 4 SRs used appropriate techniques for assessing publication bias.16,17,19,20 SRs with MA included appropriate methods of statistical combination and measurement of heterogeneity (e.g., Cochrane’s Q-test and I2 statistics).16,17,19 Two SRs indicated that risk of bias was accounted for in the analysis,19,20 while all 3 of the SRs with MA indicated that heterogeneity was accounted for and discussed in their findings.16,17,19 Three SRs disclosed if any funding was received for the review,17,20,21 and 5 SRs disclosed any potential conflict of interest implications for the review.17-21
Overall, none of the SRs provided justification for their exclusion criteria or a list of excluded studies,16-21 while 5 of the SRs did not adequately justify the included study designs for the review.16-19,21 SRs that included publication restrictions did not provided adequate details or justifications for restricting publication in their search.16,18,20,21 This lack of detail may present issues in determining if bias may have impacted the authors selection of primary studies. Two SRs did not indicate if the review protocol was established in advance of conducting the review, presenting challenges in determining if there had been any post hoc deviations to the findings.17,18 None of the SRs reported sources of funding for the included primary studies.16-21 Three SRs did not provide adequate information related to the statistical analysis, presenting challenges in determining if appropriate statistical analyses were conducted for primary study outcomes.18,20,21 Three SRs did not indicate if risk of bias was accounted for in their findings.16,18,21 Finally, 3 SRs did not report if any funding was received for the review,16,18,19 while 1 of these SRs did not report if there was any potential conflicts of interest which may impact the ability to determine if these review may have been impacted by any external influence.16
Randomized Controlled Trials
All 4 RCTs clearly defined the objective, outcomes, inclusion and exclusion criteria, interventions used, and characteristics of included patients.22-25 Three of the RCTs indicated that the trial protocol had been registered before conducting the trial.22,24,25 Each RCT clearly described the main findings and included appropriate measures of variability (standard deviation, mean difference, 95% confidence intervals[CI]) and exact P values when needed.22-25 Each RCT used appropriate statistical tests to assess main outcomes and outcome measures were valid and reliable.22-25 The patients who were recruited in each RCT and who participated in the trials were likely representative of the entire population from which they were recruited.22-25 For 2 of the RCTs,22,24 it is likely that the staff, places, and facilities used in the trial may have been representative of the treatment that majority of patients would likely receive; the level of detail related to staff, places, and facilities was insufficient and therefore unclear for 2 RCTs.23,25 Three RCTs reported that no patients were lost to follow-up,22,24,25 and 1 RCT provided characteristics of any patients that were lost to follow-up.23 Only 1 RCT blinded the patients, investigators, and data collectors to the treatment received,23 while 2 RCT indicated that only those providing the treatment, the investigators, and data collectors were blinded to the treatment received by the patient.22,24 One RCT indicated that patients were not blinded to the treatment for safety considerations.22 One RCT did not provide details of patient blinding,24 while another RCT indicated that neither the patients, investigators, or data collectors were blinded to treatment allocation.25 Each RCT clearly described the randomization process,22-25 while 3 studies clearly described randomization concealment strategies.22-24 Because of the nature of the intervention, it was assumed that compliance to the intervention was reliable for each RCT.22-25 Sufficient power calculations were used to determine adequate sample sizes for 3 RCT,22-24 while 1 RCT did not provide details related to determining adequate sample size.25 Each RCT provided information related to any funding received for the trial, and any potential conflicts of interest implications.22-25
Non-Randomized Studies
All 6 non-randomized studies clearly defined the objectives, outcomes, inclusion criteria, interventions used, and characteristics of included patients.26-31 Four of the non-randomized studies received ethical approval,26,27,29,30 while 1 non-randomized study registered the protocol before conducting their study.31 Each non-randomized study clearly described the main findings including appropriate measures of variability (interquartile range, standard deviation, 95% CI) and exact P values when needed.26-31 Each non-randomized study used appropriate statistical tests to assess main outcomes and outcome measures used were valid and reliable.26-31 Five non-randomized studies used patient data from the same population over the same period of time for both intervention and comparator groups, and patient data was likely representative of the population from which they were recruited.26-29,31 One non-randomized study identified principle confounders and accounted for possible confounding factors in the analysis using regression models.29 Five non-randomized studies did not adequately identify principle confounders and it was not clear if confounding factors were accounted for in the analysis.26-31 One non-randomized study indicated that sufficient power calculations were used to determine adequate sample size.27 It is unclear if all important adverse events were captured in any of the non-randomized studies.26-31 Due to the retrospective cohort study design of 5 non-randomized studies, it is unlikely that follow-up information was captured.26-30 One non-randomized study that used a prospective cohort study design did not provide sufficient detail related to patient loss to follow up, and it was unclear if loss to follow-up was accounted for in the analysis.31 Three non-randomized studies provided information related to any funding received for the study,26,27,29 while 5 non-randomized studies declared any potential conflict of interest implications.27-31
Evidence-Based Guideline
The identified evidence-based guideline clearly described the overall objective and population to which the guideline is meant to apply, its target users, the systematic methods used to collect evidence, and the link between the recommendations and supporting evidence using GRADE.32 The recommendations are easily identifiable, specific and unambiguous, and provide different options for conditions or health issues.32 The evidence-based guideline, however, did not clearly describe the health questions covered in the guideline, did not clearly indicate if relevant professionals or the views and preferences of the target population were included in the guideline development, did not clearly indicate if additional health benefits were considered in the formulation of the recommendations, and did not clearly indicate if the guideline had been externally reviewed before its publication.32 In addition, the evidence-based guideline did not provide criteria for evidence selection, the strengths and limitations of the body of evidence, the methods formulating the evidence, or a procedure for updating the guideline.32 This evidence-based guideline did not provide consideration for external applicability, and it is unclear if the guideline had been influenced by funding of competing interests.32
Summary of Findings
Clinical Effectiveness of IV Iron Preparations for Patients Identified as Iron Deficient Undergoing Elective Surgery
Six SRs16-21 (3 with MA),16,17,19 4 RCTs,22-25 and 6 non-randomized studies26-31 were identified regarding the clinical effectiveness of IV iron preparations for patients identified as iron deficient undergoing elective surgery, including high blood loss surgery. Additional details are available in Appendix 4 by outcome: patient hemoglobin level (Table 8), blood transfusion occurrence (Table 9), quality of life (Table 10), days in hospital or recovery (Table 11), safety and adverse events (Table 12), and additional clinical outcomes (Table 13).
Three SRs with MA16,17,19 were found to have some overlap between studies included in their analysis. A summary table outlining the degree of overlap between the SRs is included in Appendix 5. One SR with MA16 in which each primary study was captured in another SR was included in this report because the MA presented a combined synthesis of outcomes not captured in other SRs included in this report. Similarly, findings from other SRs are presented for uniquely reported outcomes or primary studies that are not captured in any other included SR. Findings from included SRs with MA16,17,19 are presented as combined measures of effects, and no attempt was made to present findings from individual studies included in each MA, thus the pooled estimates from separate SRs contain some of the same data. When applicable, findings are presented in relation to comparator as patients who did not receive IV iron supplementation or patients who received oral iron supplementation.
Patient Hemoglobin Level
When Compared to No Treatment or Placebo
Two SRs with MA found that patients who received IV iron supplementation showed statistically significantly higher concentrations of hemoglobin compared to those who did not receive IV iron supplementation.16,17 Similarly, the third SR with MA found that patients who received IV iron supplementation showed a statistically significantly greater increase in hemoglobin concentrations compared to those who did not receive IV iron supplementation at post-treatment and over 4 weeks post-operatively.19 One SR18 included 4 primary RCT studies that reported on mean hemoglobin concentrations at various time points between patients who received IV iron supplementation and patients who did not; however, numerical findings and P values were not presented among studies for these outcomes. One included RCT reported that mean post-operative hemoglobin levels significantly favoured those who received IV iron supplementation.18 One included RCTs reported that the change in pre-operative to post-operative hemoglobin levels was not significant for all patients, but 2 included RCTs reported that change in hemoglobin levels at post-operative day 30 significantly favoured those who received IV iron supplementation.18 Two included RCTs reported the rate of anemia at post-operative day 30 was significantly lower for those who received IV iron supplementation.18
One SR20 included 3 primary RCT studies not captured in a SR with MA that reported on measured of hemoglobin concentration at various time points between patients who received IV iron supplementation and patients who did not; however, statistical comparisons were not presented for the studies. Two included RCTs consistently showed higher levels of hemoglobin concentrations for patients who received IV iron supplementation compared to patients who did not, however it is unclear whether these findings are statistically different.20 One SR21 included 3 primary studies (3 non-randomized studies) that reported on the mean change in hemoglobin concentration from iron deficiency diagnosis to surgical admission for patients who received IV iron supplementation compared to patients who did not. Three included primary studies showed that the change in hemoglobin concentration was statistically significantly larger for patients who received IV iron supplementation.21
Two RCTs reported the mean change in hemoglobin from baseline to before the time of surgery22 or follow-up,23 and reported that patients who received IV iron supplementation showed a statistically significantly greater change in hemoglobin compared to patients who did not receive IV iron supplementation.22,23 One RCT reported the comparison of mean hemoglobin concentrations at various time points, including on admission, pre-operatively, post-operatively, 1 week after surgical discharge, and 4 weeks after surgical discharge for patients who received IV iron supplementation compared to placebo.24 The RCT reported that patients who received IV iron supplementation showed statistically significantly higher hemoglobin concentrations pre-operatively and 4 weeks after surgical discharge, while a statistically significantly lower hemoglobin concentration was shown post-operatively.24 The findings should be interpreted with caution because these only give a comparison of hemoglobin level at certain time points rather than comparing a change in hemoglobin levels over time. In addition, the RCT reported that patients who received IV iron supplementation had a statistically significantly lower incidence of anemia 4 weeks after surgical discharge compared to placebo.24
One retrospective cohort study reported that the mean change between baseline and pre-operative hemoglobin concentrations were higher for patients who received IV iron supplementation compared to patients who did not, but this change was not statistically significantly different.26
One retrospective cohort study compared mean hemoglobin levels at various time points across different patients groups, which included patients who were responsive to IV iron supplementation, patients who were unresponsive to IV iron supplementation, patients who did not received treatment, and patients who were not anemic.28 The authors of this retrospective cohort study found that the change in mean hemoglobin concentrations were statistically significantly different from pre-assessment to pre-operative phase, while the change in mean hemoglobin concentrations were lowest among patients who did not received treatment from pre-operative to post-operative phase but the measure of statistical significance was not reported.28
When Compared to Oral Iron
One SR included 1 RCT that reported a lower level of hemoglobin concentration for patients who received IV iron supplementation compared to patients who received oral iron supplementation; however, it is unclear whether these findings are statistically different.20
One RCT reported that the mean rise in hemoglobin levels was not statistically significantly different between patients who received IV iron supplementation and those who received oral iron supplementation.25
One retrospective cohort study reported the change in hemoglobin concentration from referral to pre-operative for patients who received IV iron supplementation at 3 different doses (1 to 300 mg, 301 mg to 600 mg, and > 600 mg), and patients who received oral iron supplementation.29 The authors reported that patients who received IV iron supplementation at more than 600 mg showed a statistically significant increase in hemoglobin concentration from referral to pre-operative, while each other group showed an increase but was reported to be not significant.29
Blood Transfusion Occurrence
When Compared to No Treatment or Placebo
Three SRs with MA with some overlapping primary studies reported findings on the combined total number of blood transfusions received between patients who received IV iron supplementation and patients who did not.16,17,19 A non-statistically significant finding from 1 SR with MA suggest that for patients who received pre-operative IV iron supplementation there may be little-to-no difference in risk of receiving a pre-operative blood transfusion when compared to patients who received no treatment [i.e., risk ratio (95% CI), 0.57 (0.30 to 1.09); P = 0.09].16 However, this finding was based on a MA of 4 studies and there was a moderately high level of statistical heterogeneity (i.e., I2 = 64%), and it is unclear whether this had an impact on the precision of this effect estimate.
One SR with MA reported that the risk of receiving a blood transfusion was statistically significantly lower for patients who received IV iron supplementation compared to patients who did not [i.e., 35% lower risk (95% CI, 52% to 12%); P = 0.005].17 One SR with MA reported the risk of receiving a blood transfusion was statistically significantly lower for patients who did not receive IV iron supplementation in both a random and fixed effects model, respectively [i.e., 16% lower risk (95% CI, 29% to 1%); P = 0.04; 17% lower risk (95% CI, 30% to 2%); P = 0.03].19
One SR20 included 5 primary RCT studies that reported the proportion of patients who received an allogenic blood transfusion for patients who received IV iron supplementation compared to patients who did not; however, statistical comparisons were not presented among studies. The proportion of patients who received an allogenic blood transfusion varied across individual studies, with 3 RCTs reporting a lower proportion of blood transfusions for patients who received IV iron supplementation while 2 RCTs reported higher proportions of blood transfusions for patients who received IV iron supplementation; however, it is unknown whether these difference are statistically significant.20 One SR21 included 3 non-randomized studies that reported the proportion of patients who received a blood transfusion and the amount of blood transfused between patients who received IV iron supplementation and those who did not. The proportion of patients who received a blood transfusion was not statistically, significantly different for 2 non-randomized studies, while 1 retrospective cohort study showed that a the proportion of patients who received a blood transfusion was statistically significantly lower for patients who received IV iron supplementation compared to patients who did not.21 Similarly, the amount of blood transfused was not statistically significantly different for 1 retrospective cohort study, while 1 retrospective cohort study showed that the amount of blood transfused was statistically, significantly lower for patients who received IV iron supplementation compared to patients who did not.21
Two RCTs reported on the number of patients who received a red blood cell transfusion at various time points for patients who received IV iron supplementation compared to patients who did not.22,25 One RCT found that the proportion of patients who received a red blood cell transfusion pre-operatively and post-operatively was lower for patients who received IV iron supplementation but was not shown to be statistically significant.22
One retrospective cohort study reported the median number of blood transfusion at various time points, and found that the group of patients who received IV iron supplementation had a higher proportion of blood transfusions at the pre-operative, day of surgery, and post-operative time points compared to the group of patients who did not receive IV iron; however, no statistical comparisons were reported, thus limiting the interpretation of these findings.26 One retrospective cohort study found that the median number of red blood cell units transfused perioperatively was statistically significantly lower for patients who were responsive to IV iron supplementation compared to patients who received IV iron supplementation and were unresponsive or patients who were untreated.28 One retrospective cohort study found that anemic patients who received IV iron supplementation had a statistically significantly higher number of blood transfusion events and median number of blood cell units transfused compared to patients who were not anemic and did not receive treatment; however, no statistically significant difference was found between anemic patients who received IV iron supplementation and anemic patients who did not receive IV iron supplmentation.30 One prospective cohort study found that the mean total blood cell units transfused was highest among patients who are anemic and did not receive treatment compared to patients who are anemic, iron deficient, and received IV iron supplementation or patients who are not anemic and did not receive treatment; however, statistical comparisons were not presented among patient groups, thus limiting the interpretation of these findings.31
One retrospective cohort study showed that patients who received IV iron supplementation at the lowest dose (1 mg to 300 mg) had statistically significantly greater odds of receiving a blood transfusion compared to no treatment.29 Patients who received IV supplementation at larger doses (301 mg to 600 mg, and > 600 mg) and oral iron supplementation reported that the odds of receiving a blood transfusion compared to no treatment was not statistically significantly different.29
When Compared to Oral Iron
One SR with MA also reported that the risk of blood transfusion between patients who received IV iron supplementation and patients who received oral iron supplementation was not statistically significantly different [i.e., risk ratio (95% CI), 0.88 (0.51 to 1.51); P = 0.63].19
One RCT that compared patients who received IV iron supplementation to oral iron supplementation found no statistically significant difference in the number of patients who received a blood transfusion from recruitment to discharge, pre-operatively, or post-operatively.25 The RCT found a statistically significantly larger number of patients who received IV iron supplementation had blood transfusions intra-operative [i.e., 6 (46.2%) versus 1 (7.7%) respectively; P = 0.03].25
One retrospective cohort study reported the number of blood transfusions at various time points for patients who received IV iron supplementation compared to oral supplementation, and found that patients who received IV iron supplementation had a significantly lower number of intra-operative blood transfusions.27 The authors found that number of transfusions received over the entire peri-operative period was not statistically significantly different between IV iron and oral iron supplementation.27
Quality of Life
When Compared to No Treatment or Placebo
One SR included 1 primary RCTs that reported quality of life outcomes using the European Quality of Life – 5 Dimension Questionnaire (EQ-5D).18 The SR authors reported that for the included RCT that the difference in EQ-5D scores between patients who receive IV iron supplementation and patients who did not was not significant, however, no numerical or statistical values were reported.18 One SR with MA reported quality of life outcomes from 2 included RCTs, and the SR authors reported that the changes in quality of life outcomes were not statistically significant at 60-days post-hospital discharge and 4 weeks post-surgery for patients who received IV supplementation and patients who did not; however, the measurements were not reported.19
One SR included 3 primary RCTs that reported on various quality of life outcomes for patients who received IV iron supplementation compared to patients who did not; however, statistical significance findings were not presented among studies.20 One included RCT reported that quality of life, physical, and mental scores from post-operative day 1 to week 12 were higher for patients who received IV iron supplementation compared to patients who did not.20 One included RCT reported that mean fatigue and dyspnea scores were lower for patients who received IV iron supplementation compared to placebo.20 One included RCT reported similar mean EQ-5D 5 level utility and health scores at 10 days, 8 weeks, and 6 months post-operative and similar multi-dimensional fatigue inventory scores for patients who receive IV iron supplementation compared to placebo.20
One RCT reported a lower median quality of recover score for patients who received IV iron supplementation compared to patients who did not; however, this was not statistically significantly different.22 One RCT reported EQ-5D 3 level index and visual analogue scale scores at baseline and follow up and found no statistically, significant difference between patients who received IV iron supplementation and placebo.23
When Compared to Oral Iron
One SR included 1 RCT that reported quality of life outcomes using the EQ-5D and independence index score outcomes.18 The SR authors reported that the difference in EQ-5D scores and independence index scores between patients who received IV iron supplementation and oral iron supplementation was not significant; however, no numerical or statistical values were reported.
One RCT reported no statistically significant difference in EQ-5D 3 level scores at baseline, 1 month, and 3-month follow-up for patients who received IV iron supplementation compared to oral iron supplementation.25
Days in Hospital or Recovery
When Compared to No Treatment or Placebo
One SR included 8 primary RCTs that reported mean or median length of stay in hospital for patients who received IV iron supplementation compared to patients who did not; however, statistical comparisons were not presented for the studies.20 Each included RCT reported the same or a lower number of days spent in hospital for patients who received IV iron supplementation compared to patients who did not, but the lack of statistical comparisons limits the certainty in these findings.20 One SR included 3 non-randomized studies (1 retrospective cohort studies, 1 retrospective and prospective cohort study, and 1 prospective cohort study) that reported the mean length of hospital stay for patients who receive IV iron supplementation compared to patients who did not.21 Two included non-randomized studies reported no statistically significant difference in mean length of hospital stay between groups, while 1 retrospective and prospective cohort study reported a statistically significant lower number of days spent in hospital for patients who received IV iron supplementation.21
One RCT reported no statistically significant difference in median post-operative length of stay days and days at home within 30 days of surgery for patients who received IV iron supplementation compared to patients who did not.22 One RCT reported that patients who received IV iron supplementation showed a statistically significantly lower length of hospital and ICU stay compared to placebo.24
One retrospective cohort study reported no statistically significant difference in median length of hospital stay days and days alive and out of hospital at 30 days and 90 days between patients who receive IV iron supplementation and those who did not.26 One retrospective cohort study reported that the mean length of stay in days was statistically significantly higher among patients who received IV iron supplementation but were unresponsive to treatment compared to patients who were not anemic and did not receive treatment.28 One prospective cohort study found that the mean length of hospital stay in days was lowest among patients who were not anemic and received no treatment compared to patients who were anemic, iron deficient and received IV iron supplementation, patients who were just iron deficient and received IV iron supplementation, and patients who were anemic and did not receive treatment; however, statistical comparisons were not presented among patient groups, thus limiting the interpretation of these findings.31
When Compared to Oral Iron
One RCT reported that patients who received IV iron supplementation compared to oral supplementation showed no statistically significant difference in mean days alive and out of hospital at 30 days, 3 months, and 6 months.25
One retrospective cohort study reported a statistically significantly lower mean length of hospital stay for patients who received IV iron supplementation compared to oral supplementation.27
Safety and Adverse Events
When Compared to No Treatment or Placebo
One SR included 2 primary RCTs that reported the rates of adverse events for patients who received IV iron supplementation compared to patients who did not; however, no statistical comparisons were presented among studies.18 The rates of adverse events was similar for patients who received IV iron supplementation compared to patients who did not for both included RCTs, with 1 RCT reporting no adverse events for both groups.18
One SR with MA reported on the occurrence of serious adverse effects based on findings from 2 included primary studies, and the occurrence non-serious adverse effects based on the findings from 7 included primary studies.19 The findings suggest that patients who received IV iron supplementation had no difference in risk of serious adverse effects compared to patients who did not receive IV iron supplementation [i.e., risk ratio (95% CI), 0.96 (0.44 to 2.10); P = 0.92].19 The findings also suggested that patients who received IV iron supplementation had little-to-no difference in risk of non-serious adverse effects compared to patients who did not receive IV iron supplementation [i.e., risk ratio (95% CI), 1.13 (0.78 to 1.65); P = 0.52].19
One SR included 4 primary RCTs that reported the proportion of patients who experienced adverse events for patients who receive IV iron supplementation and patients who did not; however, no statistical comparisons were presented among studies.20 Two included RCTs reported that a higher proportion of patients who received IV iron supplementation experienced adverse events compared to placebo, while 2 included RCT reported that 0 patients who received IV iron supplementation experience adverse events.20
One RCT reported the number of patients who experienced any surgical complications, the grade of surgical complication, and hospital readmissions within 30 days and found no statistically significant difference in each outcome for patients who received IV iron supplementation compared to patients who did not.22 One RCT reported that patients who received IV iron supplementation had a lower number of serious and non-serious adverse events compared to patients who received placebo.23 One RCT reported the incidence of adverse cardiovascular events, prolonged ventilation, heart failure, and stroke for patient who receive IV iron supplementation compared to placebo.24 Patients who received IV iron supplementation reported lower numbers for each outcome compared to placebo; however, the incidence for each outcomes was not significantly different.24
One retrospective cohort study reported the proportion of patients experiencing any complication, surgical complications, and medical complications for patient who received IV iron supplementation compared to patients who did not.26 The authors found that the number of all complications and surgical complications was significantly higher for patients who received IV iron supplementation, and that the number of medical complications was higher for patients who received IV iron supplementation but was shown to be not statistically significant.26
One retrospective cohort study reported the number of cerebrovascular accidents, renal replacement procedures, and re-operations for patients who are anemic and received IV iron supplementation, patients who are anemic and did not receive IV supplementation, and patient who are not anemic.30 Overall, patients who are anemic and received IV iron supplementation reported the highest relative proportion for each outcome across groups.30
One SR with MA,19 and 1 SR20 with 2 included primary RCTs not captured in a SR with MA reported the difference in risk and proportion of patients who died for patients who received IV iron supplementation compared to those who did not. The authors of the SR and MA reported little-to-no difference in the risk of mortality at 30-days post-operatively and more than 2 months post-hospital discharge.19 The SR reported similar proportions of post-operative mortality across both included RCT for patients who received IV iron supplementation compared to patients who did not.20 In addition, 2 RCTs,23,24 3 retrospective cohort studies,26,28,30 and 1 prospective cohort study reported the number of deaths or mortality rate for patients who received IV iron supplementation compared to patients who did not. Generally, the number or rate of mortality was similar for each included primary study23,24,26,28,30,31; however, 1 retrospective cohort study found that the number of in-hospital mortality was statistically significantly lower for patient who were anemic and received IV iron supplementation compared to patients who were anemic and did not receive IV iron supplementation.30
One SR with MA19 reported little-to-no difference in the risk of post-operative infection for patients who received IV iron supplementation compared to patients who did not.19 Three RCTs22-24 and 2 retrospective cohort studies26,30 reported number or incidence of infections between patients who received IV iron supplementation and patients who did not. Generally, the number or incidence of infections were similar between groups and no statistically significant difference was found in any of the included primary studies.22-24,26,30
When Compared to Oral Iron
One RCT reported the number patients readmitted to hospital for 6 months follow-up was not statistically significantly different between patients who received IV iron supplementation and oral iron supplementation.25
Additional Clinical Outcomes
Functional Outcomes
One SR included 2 primary RCTs that reported functional outcomes for 6-Minute Walk Test scores and Functional Assessment of Cancer Therapy for patients with Anemia/Fatigue scores and the SR authors reported that the difference in both functional outcomes was not significant for patients who received IV iron supplementation and patients who did not, however, numerical findings were not reported.18 One RCT reported the mean 6-Minute Walk Test distance between patients who received IV iron supplementation and placebo at baseline and follow-up and found the mean difference in distance between the groups was not statistically significantly different.23
Ferritin Levels
One SR and MA reported mean ferritin level differences at various time points.19 The authors found that mean ferritin levels were significantly higher at post-treatment and pre-surgery, hospital discharge, and at 4 or more weeks post-operative for patients who received IV iron supplementation compared to patients who did not.19 Two RCTs reported a significantly greater mean change in ferritin concentration from baseline to before surgery or follow-up for patients who received IV iron supplementation compared to patients who did not.22,23,28
Cost-Effectiveness of IV Iron Preparations for Patients Identified as Iron Deficient Undergoing Elective Surgery
No evidence was identified regarding the cost-effectiveness of IV iron preparations for patients identified as iron deficient undergoing elective surgery; therefore, no summary can be provided.
Guidelines Regarding the Use of IV Iron Preparations for Patients Identified as Iron Deficient Undergoing Elective Surgery
One evidence-based guideline was identified regarding the use of IV iron preparations for patients identified as iron deficient undergoing elective surgery, including high blood loss surgery.32 Additional details are available in Appendix 4, Table 14.
The guideline recommends that IV iron supplementation may be appropriate for patients with iron deficient anemia in certain circumstances which includes less than 8 weeks until surgery, unable to tolerate or absorb oral iron supplementation, or hemoglobin levels under 100 g/L.32 Evidence supporting this recommendation was from 1 SR, 4 RCTS, 1 prospective cohort study, and 2 retrospective cohort studies.32 The strength of recommendation was considered strong and the quality of evidence was considered high.32
Limitations
The primary studies summarized in the 6 included SRs were of variable quality.16-21 Three of the 4 RCTs included in 1 SR with MA were shown to have high risk of bias.16 One SR with MA reported that each primary study (2 RCTs and 5 non-randomized studies) had low risk of bias.17 The risk of bias for the 7 RCTs included in 1 SR were reported to be varied, with 4 RCTs having low risk of bias, 1 RCT having high risk of bias, and 2 RCTs having unclear risk of bias.18 Six of the 10 included RCTs for 1 SR with MA were reported to have unclear of high risk of bias.19 One SR reported that each of the 10 included RCTs were considered to have high risk of bias largely due to a lack of blinding.20 All 9 included studies for 1 SR were reported to have low risk of bias due to blinding and randomization in the RCTs and good comparability of cohorts in the non-randomized studies.21 In addition, 3 included SR with MA reported a large degree of heterogeneity across primary studies for major outcomes related to hemoglobin concentration16,17,19 and risk of blood transfusion.16 There was also a large degree of overlap in primary studies included in the SRs, and this overlap should be considered when interpreting findings from SRs with MA.16,17,19
The evidence in this report may be limited by the clinical heterogeneity of the included publications. The type of IV iron supplementation, the time of administration, and the dose of supplementation varied across each included SR and primary study included in this report. In addition, the type of comparator varied across each study and some included studies described the comparator as a control, which may include more than 1 relevant comparator. The populations varied across each study, specifically in relation to the type of surgery that was provided which can be challenging to compare outcomes between surgery type. Because of the heterogeneity across each study in terms of intervention used and comparator, it may be challenging to determine the generalizability of the overall findings for outcomes related to clinical effectiveness of IV iron use in patients identified as iron deficient. The recommendation from the included evidence-based guideline did not specify the type, administration, or dose of IV iron supplementation; however, this may be dependent on the patient and type of surgery.
No evidence was identified regarding the cost-effectiveness of IV iron preparations for patients identified as iron deficient undergoing elective surgery, and no conclusion can be drawn related to funding considerations for this treatment.
One non-randomized study29 and the included evidence-based guideline32 was conducted in Canada. One SR and MA was conducted in Canada but included primary studies from a variety of countries.19 Majority of the included evidence related to the clinical effectiveness of IV iron use for patients identified as iron deficient undergoing elective surgery were conducted in a variety of countries. Thus, it is unclear how generalizable the findings are to the Canadian context. This should be considered because the prevalence of iron deficiency, access to elective surgeries, and availability or type of IV iron supplementation may vary between countries, and therefore may have different implications depending on the population and cultural context.
Conclusions and Implications for Decision- or Policy-Making
This report included 6 SRs (3 with MA),16-21 4 RCTs,22-25 6 non-randomized studies,26-31 and 1 evidence-based guideline related to the use of IV iron preparations for patients identified with iron deficiency undergoing elective surgery, including high blood loss surgery. No evidence was identified regarding the cost-effectiveness of IV iron preparations for patients identified as iron deficient undergoing elective surgery.
Each of the included studies and evidence-based guideline specified that the population of interest included adult patients identified as anemic and/or iron deficient undergoing elective surgery.16-32 Most of the included studies specified that IV iron treatment was administer pre-operatively,16,19,21,22,24-30 while some studies indicated that IV iron was administered intra-operatively, post-operatively, or did not specify.17,18,20,23,31,32 Each study indicated the specific type and dose of IV iron supplementation used, but this varied among studies. The type of IV iron supplementation included IV ferric carboxymaltose, iron sucrose, iron isomaltoside, or unspecified IV iron and doses ranged from 100 mg to 2,000 mg.
Based on the evidence summarized within this report, patients who received IV iron supplementation were reported to generally have greater increases in the change of hemoglobin levels at various time points of the surgical care compared to patients who did not receive IV iron supplementation.16-24,26,28 Similar findings were present for patient ferritin levels.19,22,23 The evidence also showed that patients who received IV iron supplementation had similar or lower lengths of hospital stay or days in recovery compared to patients who did not receive IV iron supplementation.20-22,24,26,28,31 The evidence related to the number of patients who received a blood transfusion was mixed, with some studies reporting fewer blood transfusion occurrences while some studies reported no difference or more blood transfusion occurrences for patient who received IV iron supplementation compared to patients who did not.16,17,19-22,26,28,30,31 Findings related to blood transfusion occurrences should be interpreted with caution due to measurements of imprecision and heterogeneity within studies, and a lack of statistical tests reported for some results. Because of these variations in findings, it is challenging to accurately draw conclusion on the impact of IV iron supplementation for blood transfusion occurrences. The evidence related to patient quality of life generally found outcomes for patients who received IV iron supplementation and patients who did not were similar for various quality of life measures.18-20,22,23 Similarly, the evidence that reported on outcomes related to adverse events and safety was mixed but generally found no differences between patients who received IV iron supplementation and patients who did not for various outcomes.18-20,22-24,26,30 In addition, evidence related to the number or rate of mortality19,20,23,24,26,28,30,31 and the number or incidence of infection19,22-24,26,30 generally found similar or no difference in patients who received IV iron supplementation compared to patients who did not. Outcomes related to patient function also showed no difference in patients who receive IV iron supplementation and patients who did not.18,23
In general, the studies summarized in this report suggest that when compared to oral iron supplementation, those who were treated with IV iron supplementation had no difference in hemoglobin levels,20,25,29 quality of life scores,18,25 or the number of adverse events.25 The findings related to mean length of stay were mixed with 1 study reporting no difference,25 or lower lengths of stay when comparing IV iron to oral iron supplementation.27 The findings were mixed regarding the risk of blood transfusions at various time points, with studies reporting no differences,19,25,27 increases,25 and decreases27 when comparing IV iron to oral iron supplementation,
The evidence-based guideline was conducted in Canada for patients with comorbid condition, specifically anemia, hyperglycemia, and smoking, undergoing major surgery.32 This guideline provided a strong recommendation for the use of IV iron supplementation for patients with iron deficient anemia in circumstances where surgery is less than 8 weeks away, patients are unable to tolerate or absorb oral iron supplementation, or for patient with hemoglobin levels under 100 g/L.32
The previous 2019 CADTH report reported on similar outcomes related to hemoglobin concentration, blood transfusion occurrences, and adverse events including infections and mortality.11 The findings from this report are generally consistent with those outlined in the previous CADTH report, with IV iron supplementation being favoured for hemoglobin concentration control and mixed results found for the need for blood transfusion and mortality between IV iron supplementation compared to no treatment.11 These clinical findings may be challenging to compare between reports due to the volume and level of evidence that informed the findings in the 2019 CADTH report, which included 1 SR and 3 non-randomized studies, while the clinical evidence in this report is informed by 6 SRs (3 with MA), 4 RCTs and 6 non-randomized studies. The 2019 CADTH report also included 1 economic evaluation and an evidence-based guideline, which was used to inform an updated guideline identified (but not included) in this report.11
The limitations for the included literature (e.g., variable quality of primary studies included in the SRs, clinical heterogeneity of the included studies, the overall quality of the included studies, lack of cost-effectiveness literature, and limited Canadian context) should be considered when interpreting the findings of this report. The evidence from this report is meant to build from the literature that was identified in the 2019 CADTH report,11 and provide decision-makers with the updated and relevant evidence related to the use of IV iron preparations for patients identified as iron deficient undergoing elective surgery. Further research that is specific to the Canadian context is needed to adequately assess the clinical effectiveness and cost-effectiveness of IV iron preparation and inform recommendations that are relevant to Canadian users.
References
1.Patel N, Evans CR. Pre-oeprative Intravenous Iron to Optimise Patients Before Cardiac Surgery. J Clin Haematol. 2021;2(1):24-35. https://www.scientificarchives.com/admin/assets/articles/pdf/pre-operative-intravenous-iron-to-optimise-patients-before-cardiac-surgery-20210506050541.pdf. Accessed September 22, 2022.
2.Richards T, Baikady RR, Clevenger B, et al. Preoperative intravenous iron for anaemia in elective major open abdominal surgery: the PREVENTT RCT. Health Technology Assessment (Winchester, England). 2021;25(11):1-58. PubMed
3.Statistics Canada. Iron Sufficiency of Canadians. 2015; https://www150.statcan.gc.ca/n1/pub/82-003-x/2012004/article/11742-eng.htm#:~:text=2009%20to%202011-,Anemia,iron%2C%20but%20by%20other%20factors. Accessed October 7, 2022.
4.National Institute for Health and Care Excellence. Blood Transfusion. NICE Guideline NG24. 2015: https://www.nice.org.uk/guidance/ng24/resources/blood-transfusion-pdf-1837331897029. Accessed October 7, 2022.
5.Intravenous (IV) iron products (use in adults). Waltham (MA): UpToDate; 2022: https://www.uptodate.com/contents/image?imageKey=HEME%2F106130. Accessed October 11, 2022.
6.Monoferric. Monoferric: Ferric Derisomaltose for Injection [product monograph]. Kirkland (QC): Pfizer Canada ULC; 2021: https://pdf.hres.ca/dpd_pm/00062976.PDF. Accessed October 11, 2022.
7.Ferrlecit: Sodium Ferric Gluconate Complex in Sucrose Injection [product monograph]. Laval (QC): sanofi-aventis Canada Inc.; 2022:. Accessed October 11, 2022.
8.Feraheme: ferumoxytol for injection [product monograph]. Waltham (MA): AMAG Pharmaceuticals, Inc; 2015: https://pdf.hres.ca/dpd_pm/00031146.PDF. Accessed October 11, 2022.
9.Dexiron: Iron Dextran Injection, USP [product monograph]. Richmond Hill (ON): Fresenius Medical Care Canada Inc.; 2019: https://pdf.hres.ca/dpd_pm/00049568.PDF. Accessed October 11, 2022.
10.Venofer: Iron Sucrose Injection, USP [product monograph]. Richmond Hill (ON): Fresenius Medical Care Canada Inc.; 2019: https://pdf.hres.ca/dpd_pm/00049389.PDF. Accessed October 11, 2022.
11.Banerjee S, McCormack S. Intravenous Iron Preparations for Patients Undergoing Elective Surgery: A Review of Clinical Effectiveness, Cost-Effectiveness, and Guidelines CADTH Rapid Response Report: Summary with Critical Appraisal. Ottawa: CADTH; 2019: https://www.ncbi.nlm.nih.gov/books/NBK545893/.
12.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
13.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
14.Agree Next Steps C. The AGREE II Instrument. [Hamilton, ON]: AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf.
15.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
16.Meyer J, Cirocchi R, Di Saverio S, Ris F, Wheeler J, Davies RJ. Pre-operative iron increases haemoglobin concentration before abdominal surgery: a systematic review and meta-analysis of randomized controlled trials. Sci Rep. 2022;12(1):2158. PubMed
17.Tang G, Zhang L, Huang W, Wei Z. Iron Supplementation Effectively Ameliorates Anemia and Reduces the Need for Blood Transfusion in Patients Undergoing Colorectal Cancer Surgery: A Meta-Analysis. Nutr Cancer. 2022;74(7):2303-2312. PubMed
18.Chaudhry YP, MacMahon A, Hasan SA, et al. Intraoperative and Postoperative Iron Supplementation in Elective Total Joint Arthroplasty: A Systematic Review. J Am Acad Orthop Surg. 2021;29(23):e1200-e1207. PubMed
19.Elhenawy AM, Meyer SR, Bagshaw SM, MacArthur RG, Carroll LJ. Role of preoperative intravenous iron therapy to correct anemia before major surgery: a systematic review and meta-analysis. Syst Rev. 2021;10(1):36. PubMed
20.Jones JJ, Mundy LM, Blackman N, Shwarz M. Ferric Carboxymaltose for Anemic Perioperative Populations: A Systematic Literature Review of Randomized Controlled Trials. J Blood Med. 2021;12:337-359. PubMed
21.Moon T, Smith A, Pak T, et al. Preoperative Anemia Treatment with Intravenous Iron Therapy in Patients Undergoing Abdominal Surgery: A Systematic Review. Adv Ther. 2021;38(3):1447-1469. PubMed
22.Fung PLP, Lau VNM, Ng FF, Leung WW, Mak TWC, Lee A. Perioperative changes in haemoglobin and ferritin concentrations from preoperative intravenous iron isomaltoside for iron deficiency anaemia in patients with colorectal cancer: A pilot randomised controlled trial. PLoS One. 2022;17(6):e0270640. PubMed
23.Kvaslerud AB, Bardan S, Andresen K, et al. Intravenous iron supplement for iron deficiency in patients with severe aortic stenosis scheduled for transcatheter aortic valve implantation: results of the IIISAS randomised trial. Eur J Heart Fail. 2022;24(7):1269-1279. PubMed
24.Shokri H, Ali I. Intravenous iron supplementation treats anemia and reduces blood transfusion requirements in patients undergoing coronary artery bypass grafting-A prospective randomized trial. Ann Card Anaesth. 2022;25(2):141-147. PubMed
25.Thin TN, Tan BPY, Sim EY, Shum KL, Chan HSP, Abdullah HR. Preoperative Single-Dose Intravenous Iron Formulation to Reduce Postsurgical Complications in Patients Undergoing Major Abdominal Surgery: A Randomized Control Trial Feasibility Study (PIRCAS Trial Pilot). Cureus. 2021;13(8):e17357. PubMed
26.Ploug M, Kroijer R, Qvist N, Knudsen T. Preoperative Intravenous Iron Treatment in Colorectal Cancer: Experience From Clinical Practice. J Surg Res. 2022;277:37-43. PubMed
27.Abdullah HR, Thamnachit T, Hao Y, Lim WY, Teo LM, Sim YE. Real-world results of the implementation of preoperative anaemia clinic with intravenous iron therapy for treating iron-deficiency anaemia: a propensity-matched case-control study. Ann Transl Med. 2021;9(1):6. PubMed
28.Evans CR, Jones R, Phillips G, Greene G, Phillips M, Morris-Clarke R. Observational study of pre-operative intravenous iron given to anaemic patients before elective cardiac surgery. Anaesthesia. 2021;76(5):639-646. PubMed
29.Peel JK, Trudeau J, Tano R, et al. Determining Optimal Treatment to Correct Preoperative Anemia and Reduce Perioperative Allogeneic Blood Transfusions in Cardiac Surgery: A Retrospective Cohort Study. J Cardiothorac Vasc Anesth. 2021;35(9):2631-2639. PubMed
30.Quarterman C, Shaw M, Hughes S, Wallace V, Agarwal S. Anaemia in cardiac surgery - a retrospective review of a centre's experience with a pre-operative intravenous iron clinic. Anaesthesia. 2021;76(5):629-638. PubMed
31.Triphaus C, Judd L, Glaser P, et al. Effectiveness of Preoperative Iron Supplementation in Major Surgical Patients With Iron Deficiency: A Prospective Observational Study. Ann Surg. 2021;274(3):e212-e219. PubMed
32.Greenberg JA, Zwiep TM, Sadek J, et al. Clinical practice guideline: evidence, recommendations and algorithm for the preoperative optimization of anemia, hyperglycemia and smoking. Can J Surg. 2021;64(5):E491-E509. PubMed
33.National Institute for Health and Care Excellence. Perioperative care in adults. NICE guideline [NG180]. 2020: https://www.nice.org.uk/guidance/ng180. Accessed September 22, 2022.
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of Included Systematic Reviews
Study citation, country, funding source | Study design, last search date and numbers of relevant primary studies included | Population characteristics | Relevant intervention(s) and comparator(s) | Relevant clinical outcomes, length of follow-up |
|---|---|---|---|---|
Meyer et al. (2022)16 UK Funding source: NR | Study design: SR with MA Last search date: December 2020 Number of included studies: 4 RCTs | Eligibility criteria: Studies that included patients who received pre-operative iron supplementation undergoing abdominal surgery Total number of patients included: 312 Sample size (range): 45 to 135 | Interventions (dose):
Comparators: Placebo or usual care (undefined) | Outcomes:
Follow-up: NR |
Tang et al. (2022)17 China Funding source: No funding | Study design: SR with MA Last search date: February 2021 Number of included studies: 7 (2 RCTs and 5 non-randomized studies) | Eligibility criteria: Studies that included patients who received iron supplementation undergoing surgery for colorectal cancer Total number of patients included: 879 Sample size (range): 45 to 318 | Interventions (dose):
Comparators: No treatment; IV placebo; usual care (undefined) | Outcomes:
Follow-up: NR |
Chaudhry et al. (2021)18 US Funding source: NR | Study design: SR Last search date: December 2019 Number of included studies: 7 RCTs | Eligibility criteria: Studies that included patients aged 18 years or older who received intra-operative or post-operative iron supplementation for elective TJA surgery Total number of patients included: 646 Sample size (range): 58 to 122 | Interventions (dose):
Comparators: Oral iron supplementation; placebo; no treatment | Outcomes:
Follow-up: Varied by individual study or was NR |
Elhenawy et al. (2021)19 Canada Funding source: NR | Study design: SR with MA Last search date: February 2019 Number of included studies: 10 RCTs | Eligibility criteria: Studies that included adult patients who received pre-operative IV iron supplementation for elective surgery Total number of patients included: 1039 Sample size (range): 56 to 203 | Interventions (dose):
Comparators: Placebo; usual care (undefined); oral iron supplementation | Outcomes:
Follow-up: Varied by study but ranged from hospital discharge to 3 months post-hospital discharge |
Jones et al. (2021)20 US Funding source: Peloton Advantage, LLC funded by American Regent, Inc. | Study design: SR Last search date: January 2021 Number of included studies: 10 RCTs | Eligibility criteria: Studies that included adult patients who underwent elective surgery and received IV iron supplementation Total number of patients included: 1975 Sample size (range): 44 to 481 | Interventions (dose):
Comparators: Placebo; usual care, oral iron supplementation; no treatment | Outcomes:
Follow-up: Varied by individual study or was NR |
Moon et al. (2021)21 US Funding source: No funding | Study design: SR Last search date: November 2020 Number of included studies: 9 (5 RCTs and 4 non-randomized studies) | Eligibility criteria: Studies that included adult patients who underwent elective abdominal surgery and received pre-operative IV iron supplementation Total number of patients included: 1817 Sample size (range): 60 to 487 | Interventions (dose):
Comparators: Placebo; oral iron supplementation; no treatment | Outcomes:
Follow-up: Varied by individual study or was NR |
IV = intravenous; kg = kilogram; MA = meta-analyses; mg = milligram; ml = milliliter; NR = not reported; QoL = quality of life; RCT = randomized controlled trial; SR = systematic review; TJA = total joint arthroplasty.
Note: This table has not been copy-edited.
Table 3: Characteristics of Included Primary Clinical Studies
Study citation, country, funding source | Study design and objective | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Randomized Controlled Trials | ||||
Fung et al. (2022)22 Hong Kong Funding source: No funding | Study design: RCT Objective: To determine the effects of IV iron isomaltoside for iron deficiency treatment in individuals scheduled for colorectal surgery | Eligibility criteria: Adults diagnosed with colorectal cancer listed for elective curative tumour resection operation with anemia or iron deficiency Number of participants: 40 (20 in iron therapy group and 20 in control group) Mean age (SD): 68.4 (6.8) iron therapy group; 69.8 (12.6) control group Number of males (%): 15 (75%) iron therapy group; 9 (45%) control group | Intervention (dose): IV iron isomaltoside (20 mg/kg up to 1,000 mg infused for 30 minutes) 3 weeks before surgery Comparator: No treatment | Outcomes:
Follow-up: 30 days after surgery for quality of recovery measurement |
Kvaslerud et al. (2022)23 Norway Funding source: Pharmacosmos provided medication and the study grant | Study design: RCT Objective: To evaluate whether IV iron could provide benefits for iron deficient patients with severe aortic stenosis after TAVI | Eligibility criteria: Patients who had severe aortic stenosis and iron deficiency Number of participants: 104 (51 received intervention and 53 received a placebo) Mean age, years (SD): 80 (7.8) intervention group; 79.2 (6.5) control group Number of males (%): 28 (55%) intervention group; 32 (60%) control group | Intervention (dose): IV ferric derisomaltose (20 mg/kg or maximum dose of 2,000 mg) Comparator: Placebo (IV saline solution) | Outcomes:
Follow-up: 3 months post-operative |
Shokri et al. (2022)24 Egypt Funding source: No funding | Study design: RCT Objective: To evaluate the effects of pre-operative IV iron use in patients undergoing elective coronary artery bypass grafting | Eligibility criteria: Patients aged 52 to 67 with anemia scheduled for elective coronary artery bypass grafting and eligible to receive IV iron Number of participants: 80 (40 received intervention and 40 received a placebo) Mean age, years (SD): 58.35 (4.44) intervention group; 60.8 (4.79) control group Number of female (%): 22 (55%) intervention group; 15 (37.5%) control group | Intervention (dose): IV ferric carboxymaltose (single dose of 1,000 mg) 7 days before surgery Comparator: Placebo (100 ml of saline solution) 7 days before surgery | Outcomes:
Follow-up: 4 weeks post discharge |
Thin et al. (2021)25 Singapore Funding source: Khoo Pilot Award from Duke-NUS Medical School. Vifor Pharma provided the investigational product medication doses. | Study design: RCT Objective: To determine the feasibility to compare the pre-operative treatment of iron deficiency with IV iron therapy versus oral iron therapy in patients undergoing elective major abdominal surgery | Eligibility criteria: Patients adults aged 21 years and older with iron-deficiency anemia, scheduled for elective major abdominal surgery, presenting between one and 4 weeks of their planned surgery, and who can receive the study intervention at least 7 days before the date of surgery Number of participants: 26 (13 received intervention and 13 received a placebo) Mean age, years (SD): 59.2 (12.4) intervention group; 55.2 (23.3) control group Number of female (%): 10 (76.9%) intervention group; 8 (61.5%) control group | Intervention (dose): IV ferric carboxymaltose (single dose of 15 mg/kg up to 1,000 mg) Comparator (dose): Oral iron (ferrous fumarate 200 mg twice daily until 1 day before surgery) | Outcomes:
Follow-up: 30 days for complications and mortality outcomes |
Non-randomized Studies | ||||
Ploug et al. (2022)26 Denmark Funding source: Supported by grants from “The region of Southern Denmark”, “The University of Southern Denmark, SDU” and from Pharmacosmos. | Study design: Retrospective cohort study Objective: To investigate the efficacy of pre-operative IV iron treatment in everyday clinical practice in a series of consecutive iron deficient anemic patients undergoing elective surgery for colorectal cancer | Eligibility criteria: Patients undergoing colorectal cancer surgery and who were diagnosed with iron deficiency anemia at the time of the colorectal cancer diagnosis. Number of participants: 170 (122 received iron therapy and 48 did not receive iron therapy) Mean age, years (range): 75 (70 to 82) treatment group; 74.5 (63.5 to 82.5) no treatment group Number of female (%): 54 (44.3%) treatment group; 26 (54.2%) no treatment group | Intervention (dose): IV ferric derisomaltose (20 mg/kg) Comparator: No treatment | Outcomes:
Follow-up:
|
Abdullah et al. (2021)27 Singapore Funding source: Funded by department funds from the Department of Anaesthesiology, Singapore General Hospital | Study design: Retrospective cohort study Objective: To compare the incidence of blood transfusion and hospital length of stay between anemic patients who received IV iron pre-operatively to undergoing elective surgery versus standard care | Eligibility criteria: Patients who had undergone elective surgeries requiring general anesthesia or regional anesthesia, except for transplant, burns and cardiac surgery, and who were diagnosed with iron deficiency anemia and were prescribed pre-operative IV iron therapy Number of participants: 7696 (89 received IV iron therapy and 7607 received oral iron therapy) Mean age, years (SD): 55.2 (15.3) in IV iron therapy group; 58 (16.2) in oral iron therapy group Number of female (%): 68 (76.4%) in IV iron therapy group; 5483 (72.1%) in oral iron therapy group | Intervention (dose): IV ferric carboxymaltose (15 mg/kg up to 1,000 mg Comparator: Oral iron therapy (dose not specified) | Outcomes:
Follow-up: NA (chart review) |
Evans et al. (2021)28 UK Funding source: NR | Study design: Retrospective cohort study Objective: To analyze data from patients undergoing elective cardiac surgery to assess the impact of intravenous iron on pre-operative hemoglobin and transfusion | Eligibility criteria: Patients with iron deficiency anemia at surgical pre-assessment were considered for intravenous iron as an outpatient Number of participants: 447 (75 were anemic and received treatment; 72 were anemic and did not receive treatment; and 300 were not anemic) Mean age, years (SD): 71 (11) in the treated anemic group; 72 (8) in the anemic untreated group; 68 (11) in the non-anemic group Number of male (%): 48 (64%) in the treated anemic group; 32 (44%) in the anemic untreated group; 228 (76%) in the non-anemic group | Intervention (dose): IV iron isomaltoside (20 mg/kg) Comparator: No treatment | Outcomes:
Follow-up: 30-day mortality |
Peel et al. (2021)29 Canada Funding Source: The University of Toronto Quality in Utilization, Education and Safety Research Program as part of a Canadian Blood Services Project Grant | Study design: Retrospective cohort study Objective: To determine optimal treatment strategies for using iron therapy for pre-operative anemia in adults undergoing cardiac surgery | Eligibility criteria: Patients with anemia schedules for a procedure with a high transfusion rate, all major high blood loss surgeries, and bleeding disorder or signed refusal of blood products Number of participants: 532 (84 IV iron therapy; 207 oral iron therapy; 71 epoetin therapy; 92 dual therapies; 78 no treatment) Mean age, years (SD): 68 (13) IV iron therapy; 67 (12) oral iron therapy; 71 (8) epoetin therapy; 70 (12) dual therapy; 68 (10) no treatment Number of female (%): 41 (48%) IV iron therapy; 77 (68%) oral therapy; 34 (48%) epoetin therapy; 53 (58%) dual therapy; 24 (31%) no treatment | Intervention (dose): IV iron sucrose (200 to 300 mg) Comparator: Oral iron (ferrous fumarate), epoetin alfa, no treatment | Outcomes:
Follow-up: NA (chart review) |
Quarterman et al. (2021)30 UK Funding source: NR | Study design: Retrospective cohort study Objective: To evaluate outcomes of patients undergoing elective cardiac surgery who attended a pre-operative anemia clinic for the diagnosis and treatment of iron deficiency anemia | Eligibility criteria: Elective cardiac and aortic surgical patients with proven iron deficiency and anemia Number of participants: 2864 (190 received treatment; 581 did not receive treatment; 2093 not anemic) Mean age, years (range): 71 (63 to 77) received treatment; 73 (67 to 78) did not receive treatment; 69 (61 to 75) not anemic Number of female (%): 104 (54.7%) received treatment; 280 (48.2%) did not receive treatment; 409 (19.5%) not anemic | Intervention (dose): Iv iron isomaltoside (single dose of 1,000 mg or 20 mg/kg) Comparator: No treatment | Outcomes:
Follow-up: NA (chart review) |
Triphaus et al. (2021)31 Germany Funding source: NR | Study design: Prospective cohort study Objective: To evaluate the outcomes of iron deficient anemic patients with and without iron supplementation compared to non-anemic patients | Eligibility criteria: Adults undergoing major surgery were screened for iron deficiency anemia between 2015 and 2018 and grouped based on anemia and treatment status Number of participants: 1728 (184 patients with iron deficiency anemia and received treatment; 55 patients without anemia but iron deficiency and received treatment; 461 with anemia and no treatment; 1028 without anemia and no treatment) Mean age, years (SD): 63.3 (16.1) iron deficient anemic who received treatment; 59.5 (15.7) not anemic but iron deficient and received treatment; 65.6 (14.2) anemic with no treatment; 63.6 (13.2) not anemic and no treatment Number of female (%): 73 (39.5%) iron deficient anemic who received treatment; 29 (52.7%) not anemic but iron deficient and received treatment; 111 (24.1%) anemic with no treatment; 307 (29.9%) not anemic and no treatment | Intervention (dose): IV ferric carboxymaltose (500 mg or 1,000 mg) Comparator: No treatment | Outcomes:
Follow-up: 21-day postoperative follow-up for hemoglobin level analysis |
IV = intravenous; kg = kilogram; mg = milligram; ml = milliliter; NA = not applicable; NR = not reported; QoL = quality of life; RCT = randomized controlled trial; SD = standard deviation; TAVI = transcatheter aortic valve implementation.
Note: This table has not been copy-edited.
Table 4: Characteristics of Included Guidelines
Intended users, target population | Relevant intervention and practice considered | Major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality assessment | Recommendations development and evaluation | Guideline validation |
|---|---|---|---|---|---|---|
Greenberg et al. (2021)32 | ||||||
Intended users: Surgeons caring for patients scheduled to undergo major elective surgery Target population: Patients with comorbid conditions (specifically anemia, hyperglycemia, and smoking) undergoing major surgery | Present diagnostic and treatment algorithms for the management of pre-operative anemia including iron supplementation |
| A systematic review was undertaken which included multiple database searches (Ovid MEDLINE[R] Epub Ahead of Print, In-Process & Other Non-Indexed Citations, Ovid MEDLINE[R] Daily and Ovid MEDLINE[R]) from 1946 to time of review | Strength of recommendationa and quality of evidenceb was assessed using GRADE | Recommendations were developed by 2 reviewers | NR |
GRADE = Grading of Recommendations Assessment, Development and Evaluation; NR = not reported.
aStrength of recommendation was assessed using a combination of quality of supporting evidence described as a “balance between desired and undesired effects, how wise the proposed use of resources is, and variability of individual preferences and values.”32 Strength of recommendation was “strong” or “weak”.
bQuality of evidence was based on how likely further research is to change confidence in the estimate of effect. Classified in 4 levels: “high”, “moderate”, “low”, or “very low”.
Note: This table has not been copy-edited.
Appendix 3: Critical Appraisal of Included Publications
Note that this table has not been copy-edited.
Table 5: Strengths and Limitations of Systematic Reviews Using AMSTAR 212
Strengths | Limitations |
|---|---|
Meyer et al. (2022)16 | |
|
|
Tang et al. (2022)17 | |
|
|
Chaudhry et al. (2021)18 | |
|
|
Elhenawy et al. (2021)19 | |
|
|
Jones et al. (2021)20 | |
|
|
Moon et al. (2021)21 | |
|
|
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; GRADE = Grading of Recommendations Assessment, Development, and Evaluation; RCT = randomized controlled trial; RoB = risk of bias.
Table 6: Strengths and Limitations of Clinical Studies Using the Downs and Black Checklist13
Strengths | Limitations |
|---|---|
Randomized Controlled Trials | |
Fung et al. (2022)22 | |
|
|
Kvaslerud et al. (2022)23 | |
|
|
Shokri et al. (2022)24 | |
|
|
Thin et al. (2021)25 | |
|
|
Non-Randomized Studies | |
Ploug et al. (2022)26 | |
|
|
Abdullah et al. (2021)27 | |
|
|
Evans et al. (2021)28 | |
|
|
Peel et al. (2021)29 | |
|
|
Quarterman et al. (2021)30 | |
|
|
Triphaus et al. (2021)31 | |
|
|
Table 7: Strengths and Limitations of Guidelines Using AGREE II14
Item | Greenberg et al. (2021)32 |
|---|---|
Domain 1: scope and purpose | |
1. The overall objective(s) of the guideline is (are) specifically described. | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Unclear |
3. The population (patients, public, etc.) to whom the guideline is meant to apply is specifically described. | Yes |
Domain 2: stakeholder involvement | |
4. The guideline development group includes individuals from all relevant professional groups. | Unclear |
5. The views and preferences of the target population (patients, public, etc.) have been sought. | Unclear |
6. The target users of the guideline are clearly defined. | Yes |
Domain 3: rigour of development | |
7. Systematic methods were used to search for evidence. | Yes |
8. The criteria for selecting the evidence are clearly described. | No |
9. The strengths and limitations of the body of evidence are clearly described. | No |
10. The methods for formulating the recommendations are clearly described. | No |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Unclear |
12. There is an explicit link between the recommendations and the supporting evidence. | Yes |
13. The guideline has been externally reviewed by experts prior to its publication. | Unclear |
14. A procedure for updating the guideline is provided. | No |
Domain 4: clarity of presentation | |
15. The recommendations are specific and unambiguous. | Yes |
16. The different options for management of the condition or health issue are clearly presented. | Yes |
17. Key recommendations are easily identifiable. | Yes |
Domain 5: applicability | |
18. The guideline describes facilitators and barriers to its application. | No |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | No |
20. The potential resource implications of applying the recommendations have been considered. | No |
21. The guideline presents monitoring and/or auditing criteria. | No |
Domain 6: editorial independence | |
22. The views of the funding body have not influenced the content of the guideline. | Unclear |
23. Competing interests of guideline development group members have been recorded and addressed. | No |
AGREE II = Appraisal of Guidelines for Research and Evaluation II.
Appendix 4: Main Study Findings
Note that this table has not been copy-edited.
Table 8: Summary of Findings by Outcome — Patient Hemoglobin Level
Study citation and design | Study findings |
|---|---|
Meyer et al. (2022)16 SR and MA (Based on 3 included studies) | Hemoglobin concentration at time of admission Combined total concentration for patients who received pre-operative IV iron = 258 g/dl Combined total concentration for no treatment = 256 g/dl Mean difference (95% CI) = 0.81 (0.30 to 1.33); P = 0.002; I2 = 60% |
Tang et al. (2022)17 SR and MA (Based on 3 included studies) | Effect of iron therapy on hemoglobin concentrations (units not specified) Combined total concentration for patients who received IV iron therapy = 123 Combined total concentration for control group = 213 Mean difference (95% CI) = 0.29 (0.02 to 0.56); P = 0.04; I2 = 77% |
Chaudhry et al. (2021)18 SR (1 RCT, Na et al. 2011) | Mean pre-operative hemoglobin levels IV iron therapy group = 12 g/dl Control group = 12 g/dl Mean postoperative hemoglobin levels POD 1, 2, 3, 2 week and 6-week follow-up significantly favours the intervention; POD 5 was not significant |
Chaudhry et al. (2021)18 SR (1 RCT, Bisbe et al. 2014) | Mean pre-operative hemoglobin levels IV iron group = 14 g/dl Oral iron group = 14 g/dl Mean follow-up hemoglobin levels (SD) IV iron group = 12 g/dl (1.2) Oral iron group = 11 g/dl (1.1) Pre- to postoperative change in hemoglobin POD 30 change was not significant for all patients; Subset analysis of pre-operative low iron or severe postoperative anemia was significant favouring IV iron therapy (1.9 g/dl vs 1.2 g/dl pre-operative low iron subset; 2.4 g/dl vs 1.1 g/dl severe postoperative anemia subset) Mean postoperative hemoglobin levels POD 1, 4 and 30 was not significant for all patients; Subset analysis of pre-operative low iron or severe postoperative anemia was significant favouring IV iron therapy Rate of anemia at final follow-up POD 30 significantly favours IV iron therapy group (58% IV iron vs 76% oral iron) |
Chaudhry et al. (2021)18 SR (1 RCT, Park et al. 2019) | Mean pre-operative hemoglobin levels IV iron group = 12 g/dl Placebo group = 13 g/dl Mean follow-up hemoglobin levels (SD) IV iron group = 13 g/dl (1.3) Placebo group = 13 g/dl (1.1) Pre- to postoperative change in hemoglobin POD 1 and 5 change was not significant for all patients; POD 30 change was significant favouring IV iron group (0.3 g/dl vs -0.8 g/dl) Mean postoperative hemoglobin levels POD 1, 5 and 30 was not significant between groups |
Chaudhry et al. (2021)18 SR (1 RCT, Yoo et al. 2019) | Mean pre-operative hemoglobin levels IV iron group = 14 g/dl Control group = 13 g/dl Mean follow-up hemoglobin levels (SD) IV iron group = 13 g/dl (0.9) Control group = 12 g/dl (1.0) Mean postoperative hemoglobin levels POD 1 and 7 was not significant for all patients; POD 30 was significant favouring the IV iron group Rate of anemia at final follow-up POD 30 significantly favours IV iron therapy group (34% IV iron vs 62% control group) |
Elhenawy et al. (2021)19 SR and MA | Change in hemoglobin levels at post-treatment (random effects model based on 7 included studies) Combined total hemoglobin level for patients who received IV iron therapy = 298 g/L Combined total hemoglobin level for placebo or standard of care group = 282 g/L Mean difference (95% CI) = 7.15 (2.26 to 12.04); P = 0.004; I2 = 79% Direct comparison between IV iron and oral iron therapy for change in hemoglobin levels at post-treatment (random effects model based on 5 included studies) Combined total hemoglobin level for patients who received IV iron therapy = 224 g/L Combined total hemoglobin level for patients who received oral iron therapy = 225 g/L Mean difference (95% CI) = 7.63 (1.41 to 13.86); P = 0.02; I2 = 87% Change in hemoglobin levels at > 4 weeks postoperative follow-up (random effects model based on 4 included studies) Combined total hemoglobin level for patients who received IV iron therapy = 227 g/L Combined total hemoglobin level for placebo or standard of care group = 282 g/L Mean difference (95% CI) = 6.46 (3.10 to 9.81); P = 0.0002; I2 = 33% |
Jones et al. (2021)20 SR (1 RCT, Khalafallah et al. 2016) | Mean change in hemoglobin from postoperative day 1 to postoperative week 12 (SD)a IV iron group = 3.2 g/dl (0.16) Standard of care group = 2.81 g/dl (0.18) |
Jones et al. (2021)20 SR (1 RCT, Kim et al. 2017) | Increase in hemoglobin level from baseline to postoperative week 12a IV iron group = 3.3 g/dl Placebo = 1.6 g/dl |
Jones et al. (2021)20 SR (1 RCT, Padmanabhan et al. 2019) | Change in mean hemoglobin level between enrollment and surgical admission (SD)a IV iron group = 1.3 g/dl (0.9) Oral iron group = 4.4 g/dl (0.9) |
Moon et al. (2021)21 SR (1 retrospective cohort study, Wilson et al. 2018) | Mean change in hemoglobin from iron deficiency anemia diagnosis to admission IV iron group = 1.05 g/dl Control group = 0.16 g/dl P < 0.0001 |
Moon et al. (2021)21 SR (1 retrospective and prospective cohort study, Calleja et al. 2015) | Mean change in hemoglobin from iron deficiency anemia diagnosis to admission IV iron group = 1.5 g/dl Control group = 0.5 g/dl P < 0.0001 |
Moon et al. (2021)21 SR (1 prospective cohort study, Kam et al. 2020) | Mean change in hemoglobin from iron deficiency anemia diagnosis to admission IV iron group = 1.9 g/dl Control group = 0.6 g/dl P < 0.001 |
Fung et al. (2022)22 RCT | Mean change in hemoglobin from baseline to before surgery (95% CI) IV iron group = 7.9 g/L (3.2 to 12.3) Control group = 1.7 g/L (-1.9 to 5.3) P = 0.040 |
Kvaslerud et al. (2022)23 RCT | Mean hemoglobin from baseline to follow-up (SD) Mean IV iron group hemoglobin at baseline = 13.3 g/L (1.2); Mean IV iron group hemoglobin at follow-up = 13.7 g/L (1.4) Mean placebo group hemoglobin at baseline = 13.3 g/L (1.3); Mean placebo group hemoglobin at follow-up = 13.1 g/L (1.5) Mean difference (95% CI) = 0.6 g/L (0.1 to 1.0); P = 0.015 |
Shokri et al. (2022)24 RCT | Mean hemoglobin levels on admission between IV iron group and placebo group (SD) IV iron group = 9.53 g/dl (0.84) Placebo group = 9.77 g/dl (0.74) P = 0.103 Mean pre-operative hemoglobin levels between IV iron group and placebo group (SD) IV iron group = 12.76 g/dl (0.88) Placebo group = 10.03 g/dl (0.83) P < 0.001 Mean postoperative hemoglobin levels between IV iron group and placebo group (SD) IV iron group = 9.1 g/dl (0.63) Placebo group = 7.55 g/dl (0.6) P < 0.001 Mean hemoglobin levels 1 week after discharge between IV iron group and placebo group (SD) IV iron group = 10.35 g/dl (0.89) Placebo group = 10.18 g/dl (0.85) P = 0.397 Mean hemoglobin levels 4 weeks after discharge between IV iron group and placebo group (SD) IV iron group = 12.44 g/dl (0.71) Placebo group = 11.26 g/dl (1.13) P < 0.001 Incidence of anemia 4 weeks after discharge between IV iron group (N = 40) and placebo group (N = 40), n (%) IV iron group = 13 (32%) Placebo group = 32 (80%) P < 0.001 |
Thin et al. (2021)25 RCT | Mean rise in hemoglobin level between IV iron group and oral iron group (SD) IV iron group = 0.2 g/dl (1.6) Oral iron group = 0.8 g/dl (0.7) P = 0.3 |
Ploug et al. (2022)26 Retrospective cohort study | Change between baseline and pre-operative hemoglobin levels for IV iron group and control group (range) IV iron group = 0.64 g/dl (0.32 to 1.61) Control group = 0.48 g/dl (0.81 to 2.09) P = 0.94 |
Evans et al. (2021)28 Retrospective cohort study | Comparison of mean hemoglobin levels at pre-assessment phase (SD) IV treatment responsive group = 120 g/l-1 (7) IV treatment unresponsive group = 114 g/l-1 (9) Untreated anemic group = 121 g/l-1 (7) Non-anemic group = 146 g/l-1 (10) P < 0.001 Comparison of mean hemoglobin levels at pre-surgery phase (SD) IV treatment responsive group = 137 g/l-1 (8) IV treatment unresponsive group = 120 g/l-1 (7) Untreated anemic group = 119 g/l-1 (10) Non-anemic group = 143 g/l-1 (11) P < 0.001 Comparison of mean hemoglobin levels at post-surgery phase (SD) IV treatment responsive group = 111 g/l-1 (17) IV treatment unresponsive group = 104 g/l-1 (11) Untreated anemic group = 106 g/l-1 (15) Non-anemic group = 115 g/l-1 (16) P < 0.001 Change in mean hemoglobin levels from pre-assessment to pre-operative phase (95% CI) IV treatment responsive group = 17 g/l-1 (13 to 21) IV treatment unresponsive group = 6 g/l-1 (3 to 8) Untreated anemic group = -2 g/l-1 (-4 to 0) Non-anemic group = -2 g/l-1 (-3 to -1) P < 0.001 Change in mean hemoglobin levels from pre-operative to postoperative phase (95% CI) IV treatment responsive group = -26 g/l-1 (-31 to -19) IV treatment unresponsive group = -16 g/l-1 (-20 to -12) Untreated anemic group = -13 g/l-1 (-16 to -9) Non-anemic group = -29 g/l-1 (-31 to -27) P = NR |
Peel et al. (2021)29 Retrospective cohort study | Change in hemoglobin level between referral and pre-operative level for each relevant group (95% CI) IV iron 1 to 300 mg group = 2.49 g/L (-0.68 to 5.66); P = 0.1238 IV iron 301 to 600 mg group = 1.48 g/L (-1.73 to 4.69); P = 0.3646 IV iron > 600 mg group = 9.80 g/L (6.17 to 13.42); P < 0.0001 Oral iron group = 1.62 g/L (-0.85 to 4.08); P = 0.1974 |
CI = confidence interval; dl = deciliter; EPO = erythropoietin; g = grams; L = liter; MA = meta-analysis; mg = milligram; NR = not reported; POD = postoperative day; SD = standard deviation; SR = systematic review; vs = versus.
aStatistical significance between groups was not provided by Jones et al. (2021)
Table 9: Summary of Findings by Outcome — Blood Transfusion Occurrence
Study citation and design | Study findings |
|---|---|
Meyer et al. (2022)16 SR and MA (Based on 4 included studies) | Pre-operative allogenic blood transfusion Combined total number of transfusion events for patients who received pre-operative IV iron = 334 Combined total number of transfusion events for no treatment = 317 Risk difference (95% CI) = -0.13 (-0.27 to 0.01); P = 0.07; I2 = 65% Risk ratio (95% CI) = 0.57 (0.30 to 1.09); P = 0.09; I2 = 64% |
Tang et al. (2022)17 SR and MA (Based on 5 included studies) | Number of patients receiving blood transfusion Combined number of transfusion events for patients who received IV iron therapy = 289 Combined number of transfusion events for control group = 429 Risk ratio (95% CI) = 0.65 (0.48 to 0.88); P = 0.005; I2 = 0% |
Elhenawy et al. (2021)19 SR and MA | Number of patients receiving blood transfusion (random effects model based on 8 studies) Combined number of transfusion events for patients who received IV iron therapy = 445 Combined number of transfusion events for placebo or standard of care group = 428 Risk ratio (95% CI) = 0.84 (0.71 to 0.99); P = 0.04; I2 = 0% Number of patients receiving blood transfusion (fixed effects model based on 8 studies) Combined number of transfusion events for patients who received IV iron therapy = 445 Combined number of transfusion events for placebo or standard of care group = 428 Risk ratio (95% CI) = 0.83 (0.70 to 0.98); P = 0.03; I2 = 0% Direct comparison between IV iron and oral iron therapy for number of blood transfusions (random effects model based on 3 studies) Combined number of transfusion events for patients who received IV iron therapy = 139 Combined number of transfusion events for patients who received oral iron therapy = 144 Risk ratio (95% CI) = 0.88 (0.51 to 1.51); P = 0.63; I2 = 37% |
Jones et al. (2021)20 SR (1 RCT, Brisbe et al. 2014) | Proportion of patients receiving an allogenic blood transfusion, n/N (%)a IV iron group = 3/59 (5.1%) Oral iron group = 2/62 (3.2%) |
Jones et al. (2021)20 SR (1 RCT, Khalafallah et al. 2016) | Proportion of patients receiving an allogenic blood transfusion, n/N (%)a IV iron group = 1/103 (0.1%) Standard of care group = 5/98 (5.1%) |
Jones et al. (2021)20 SR (1 RCT, Kim et al. 2017) | Proportion of patients receiving an allogenic blood transfusion, n/N (%)a IV iron group = 3/218 (1.4%) Placebo group = 4/219 (1.8%) |
Jones et al. (2021)20 SR (1 RCT, Padmanabhan et al. 2019) | Proportion of patients receiving an allogenic blood transfusion, n/N (%)a IV iron group = 16/20 (80%) Oral iron group = 12/20 (60%) |
Jones et al. (2021)20 SR (1 RCT, Park et al. 2019) | Proportion of patients receiving an allogenic blood transfusion, n/N (%)a IV iron group = 2/29 (6.9%) Placebo group = 4/29 (12.8%) |
Moon et al. (2021)21 SR (1 retrospective cohort study, Laso-Morales et al. 2017) | Proportion of patients receiving a transfusion (%) IV iron group = 17% Control group = 16% P = NS Mean amount of blood transfused per patient (unit not specified) IV iron group = 0.4 Control group = 0.3 P = NS |
Moon et al. (2021)21 SR (1 retrospective and prospective cohort study, Calleja et al. 2015) | Proportion of patients receiving a transfusion (%) IV iron group = 9.9% Control group = 38.7% P < 0.001 Mean amount of blood transfused per patient (unit not specified) IV iron group = 0.2 Control group = 0.8 P < 0.001 |
Moon et al. (2021)21 SR (1 prospective cohort study, Kam et al. 2020) | Proportion of patients receiving a transfusion (%) IV iron group = 1.42% Control group = 0.55% P = 0.076 |
Fung et al. (2022)22 RCT | Number of patients receiving pre-operative red blood cell transfusion, n (%) IV iron group = 1 (5%) Control group = 3 (15%) P = 0.605 Number of patients receiving postoperative red blood cell transfusion, n (%) IV iron group = 1 (5%) Control group = 4 (20) P = 0.342 |
Thin et al. (2021)25 RCT | Number of patients who received red blood cell transfusion from recruitment to discharge, n (%) IV iron group = 6 (46.2%) Oral iron group = 6 (46.2%) P = 1.0 Number of patients who received red blood cell transfusion pre-operatively, n (%) IV iron group = 0 Oral iron group = 3 (23.1%) P = 0.07 Number of patients who received red blood cell transfusion intra-operatively, n (%) IV iron group = 6 (46.2%) Oral iron group = 1 (7.7%) P = 0.03 Number of patients who received red blood cell transfusion post-operatively, n (%) IV iron group = 2 (15.4%) Oral iron group = 4 (30.8%) P = 0.4 |
Ploug et al. (2022)26 Retrospective cohort study | Median number of red blood cell transfusions between IV iron group (N = 122) and control group (N = 48), n (%) IV iron group = 55 (45%) Control group = 19 (40%) Median number of pre-operative red blood cell transfusions between IV iron group (N = 122) and control group (N = 48), n (%) IV iron group = 29 (24%) Control group = 16 (33%) Median number of the day of surgery red blood cell transfusions between IV iron group (N = 122) and control group (N = 48), n (%) IV iron group = 13 (11%) Control group = 2 (4%) Median number of postoperative day 1 to 30 red blood cell transfusions between IV iron group (N = 122) and control group (N = 48), n (%) IV iron group = 24 (20%) Control group = 8 (17%) |
Abdullah et al. (2021)27 Retrospective cohort study | Number of pre-operative transfusions received for 1:1 propensity matched IV iron group (N = 89) and oral iron group (N = 89), n (%) IV iron group = 10 (11.2%) Oral iron group = 16 (18%) P = 0.289 Number of pre-operative transfusions received for 1:2 propensity matched IV iron group (N = 89) and oral iron group (N = 178), n (%) IV iron group = 10 (11.2%) Oral iron group = 30 (16.9%) P = 0.303 Number of intra-operative transfusions received for 1:1 propensity matched IV iron group (N = 89) and oral iron group (N = 89), n (%) IV iron group = 18 (20.2%) Oral iron group = 33 (37.1%) P = 0.02 Number of intra-operative transfusions received for 1:2 propensity matched IV iron group (N = 89) and oral iron group (N = 178), n (%) IV iron group = 18 (20.2%) Oral iron group = 72 (40.4%) P = 0.002 Number of post-operative transfusions received for 1:1 propensity matched IV iron group (N = 89) and oral iron group (N = 89),n (%) IV iron group = 20 (22.5%) Oral iron group = 15 (16.9%) P = 0.451 Number of post-operative transfusions received for 1:2 propensity matched IV iron group (N = 89) and oral iron group (N = 178), n (%) IV iron group = 20 (22.5%) Oral iron group = 28 (15.7%) P = 0.237 Number of transfusions received over entire peri-operative period for 1:1 propensity matched IV iron group (N = 89) and oral iron group (N = 89), n (%) IV iron group = 37 (41.6%) Oral iron group = 34 (38.2%) P = 0.759 Number of transfusions received over entire peri-operative period for 1:2 propensity matched IV iron group (N = 89) and oral iron group (N = 178), n (%) IV iron group = 37 (41.6%) Oral iron group = 73 (41%) P = 1.00 |
Evans et al. (2021)28 Retrospective cohort study | Median number of red blood cell units transfused perioperatively by group (range) IV treatment responsive group = 0 (0 to 15) IV treatment unresponsive group = 2 (0 to 13); P < 0.001 vs non-anemic group; P = 0.013 vs treatment responsive group Untreated anemic group = 2 (0 to 16); P < 0.001 vs non-anemic group; P = 0.038 vs treatment responsive group Non-anemic group = 0 (0 to 17) |
Peel et al. (2021)29 Retrospective cohort study | Odds of receiving a transfusion for each relevant group compared to no treatment, OR (95% CI) IV iron 1 to 300 mg group = 2.32 (1.10 to 4.93); P = 0.0280 IV iron 301 to 600 mg group = 0.77 (0.39 to 1.50); P = 0.4422 IV iron > 600 mg group = 0.97 (0.49 to 1.95); P = 0.9401 Oral iron group = 0.84 (0.49 to 1.45); P = 0.5317 Count of red blood cell units transfused for each relevant group, count ratiob (95% CI) IV iron 1 to 300 mg group = 1.36 (0.91 to 2.03); P = 0.1305 IV iron 301 to 600 mg group = 0.84 (0.54 to 1.31); P = 0.4414 IV iron > 600 mg group = 0.66 (0.40 to 1.10); P = 0.1151 Oral iron group = 0.66 (0.47 to 0.94); P = 0.0196 |
Quarterman et al. (2021)30 Retrospective cohort study | Number of patients receiving red blood cell transfusion from each group, n (%) Anemic and received IV iron treatment group (N = 190) = 114 (60%) Anemic and did not receive IV iron treatment or not iron deficient group (N = 581) = 368 (63.3%); P = 0.41 vs IV iron treatment group Not anemic group (N = 2093) = 548 (26.2%); P < 0.001 vs IV iron treatment group Median number of red blood cell units received for each group (range) Anemic and received IV iron treatment group (N = 190) = 1 (0 to 17) Anemic and did not receive IV iron treatment or not iron deficient group (N = 581) = 1 (0 to 13); P = 0.29 vs IV iron treatment group Not anemic group (N = 2093) = 0 (0 to 31); P < 0.001 vs IV iron treatment group |
Triphaus et al. (2021)31 Prospective cohort study | Mean total red blood cell units transfused for each group (SEM) Anemic, iron deficient and IV iron treatment group = 2 (0.3) Iron deficient and IV iron treatment group = 1.4 (0.4) Anemic and no treatment group = 2.5 (0.2) Not anemic and no treatment group = 1 (0.1) |
CI = confidence interval; EPO = erythropoietin; IV = intravenous; MA = meta-analysis; N = number; NR = not reported; NS = not significant; OR = odds ratio; SEM = standard error mean; SR = systematic review; vs = versus.
aStatistical significance between groups was not provided by Jones et al. (2021)
bCount ratio represents how many times more red blood cell units are transfused for each variable group.
Table 10: Summary of Findings by Outcome — Quality of Life
Study citation and design | Study findings |
|---|---|
Chaudhry et al. (2021)18 SR (1 RCT, Brisbe et al. 2014) | EQ-5D score Difference in EQ-5D score between IV iron group and oral iron group was not significant Independence index score Difference in independence index score between IV iron group and oral iron group was not significant |
Chaudhry et al. (2021)18 SR (1RCT, Yoo et al. 2019) | EQ-5D score Difference in EQ-5D score between IV iron group and control group was not significant |
Elhenawy et al. (2021)19 SR with MA (1 RCT, Bernabeu-Wittel et al. 2016) | SF36v2 at 60 days post-hospital discharge reassessment for IV iron therapy versus control Results showed statistically non-significant changes between groups (measurements NR) |
Elhenawy et al. (2021)19 SR with MA (1 RCT, Froessler et al. 2016) | SF36 at 4 weeks post-surgery reassessment for IV iron therapy versus control Results showed statistically non-significant changes between groups (measurements NR) |
Jones et al. (2021)20 SR (1 RCT, Khalafallah et al. 2016) | SF36 scores from postoperative day 1 to postoperative week 12a IV iron group = 13.4 Standard of care group = 9.1 Physical scores from postoperative day 1 to postoperative week 12a IV iron group = 13.4 Standard of care group = 7.9 Mental scores from postoperative day 1 to postoperative week 12a IV iron group = 13.3 Standard of care group = 9.9 |
Jones et al. (2021)20 SR (1 RCT, Kim et al. 2017) | Mean fatigue scores at week 3 (95% CI)a IV iron group = 30 (26.8 to 33.1) Placebo = 34.6 (31.3 to 37.9) Mean dyspnea scores at week 12 (95% CI)a IV iron group = 9.5 (7.2 to 11.8) Placebo = 14.2 (11.3 to 17.1) |
Jones et al. (2021)20 SR (1 RCT, Richards et al. 2019) | Mean EQ-5D-5L Utility scores at 10 days, 8 weeks, and 6 months postoperative (SD)a IV iron group = 0.80 (0.20); 0.79 (0.20); 0.82 (0.22) Placebo group = 0.81 (0.21); 0.77 (0.21); 0.82 (0.21) Mean EQ-5D-5L Health scores at 10 days, 8 weeks, and 6 months postoperative (SD)a IV iron group = 70.6 (20.5); 70.7 (19.4); 75.0 (18.4) Placebo group = 73.8 (19.6); 71.1 (19.5); 76.2 (19.2) Mean MFI scores at 10 days, 8 weeks, and 6 months postoperative (SD)a IV iron group = 53.2 (18.4); 52.9 (17.1); 48.8 (18.9) Placebo group = 50.5 (18.9); 53.9 (17.7); 47.4 (19.1) |
Fung et al. (2022)22 RCT | Median QOR-15 score (range) IV iron group = 107 (100 to 124) Control group = 115 (103 to 125) P = 0.547 |
Kvaslerud et al. (2022)23 RCT | Mean EQ-5D3L index scores between IV iron group and placebo group at baseline and follow-up (range) Mean IV iron group scores at baseline = 0.83 (0.77 to 0.93); Mean IV iron group scores at follow-up = 0.91 (0.82 to 0.97) Mean placebo group scores at baseline = 0.81 (0.74 to 0.93); Mean placebo group scores at follow-up = 0.91 (0.78 to 0.97) Mean difference (95% CI) = -0.001 (-0.4 to 0.4); P = 0.97 Mean EQ-5D VAS scores between IV iron group and placebo group at baseline and follow-up (range) Mean IV iron group scores at baseline = 67 (50 to 80); Mean IV iron group scores at follow-up = 70 (48 to 84) Mean placebo group scores at baseline = 50 (40 to 73); Mean placebo group scores at follow-up = 75 (60 to 85) Mean difference (95% CI) = -7.8 (-16.5 to 0.86); P = 0.077 |
Thin et al. (2021)25 RCT | Mean EQ-5D-3L score at baseline between IV iron group (N = 15) and oral iron group (N = 15) (SD) IV iron group = 70.3 (22) Oral iron group = 73 (8) P = 0.6 Mean EQ-5D-3L score at 1 month follow-up between IV iron group (N = 13) and oral iron group (N = 11) (SD) IV iron group = 70.4 (21.8) Oral iron group = 84.5 (12.1) P = 0.07 Mean EQ-5D-3L score at 3-month follow-up between IV iron group (N = 13) and oral iron group (N = 11) (SD) IV iron group = 80 (18.4) Oral iron group = 85.9 (10.7) P = 0.4 |
CI = confidence interval; EQ-5D = European Quality of Life – 5 Dimensions Questionnaire; EQ-5D-3L = European Quality of Life – 5 Dimension – 3 Levels; EQ-5D-5L = European Quality of Life – 5 Dimension – 5 Levels; IV = intravenous; MA = meta-analysis; MFI = Multidimensional Fatigue Inventory; NR = not reported; QOR-15 = 15-iten Quality of Recovery; RCT = randomized controlled trial; SD = standard deviation; SF36 = short form-36; SR = systematic review; VAS = visual analogue scale.
aStatistical significance between groups was not provided by Jones et al. (2021)
Table 11: Summary of Findings by Outcome — Days in Hospital or Recovery
Study citation and design | Study findings |
|---|---|
Jones et al. (2021)20 SR (1 RCT, Brisbe et al. 2014) | Mean length of hospital stay, days (SD)a IV iron group = 7.9 (1.7) Oral iron group = 7.6 (0.9) |
Jones et al. (2021)20 SR (1 RCT, Bernabeu-Wittel et al. 2016) | Median length of hospital stay, days (range)a IV iron group = 8 (6 to 11) IV iron + EPO group = 7 (5 to 10) Placebo group = 8 (6 to 10) |
Jones et al. (2021)20 SR (1 RCT, Froessler et al. 2016) | Median length of hospital stay, days (range)a IV iron group = 6 (1 to 19) No treatment group = 9 (1 to 23) |
Jones et al. (2021)20 SR (1 RCT, Khalafallah et al. 2016) | Mean length of hospital stay, days (SD)a IV iron group = 7.8 (10.3) Standard of care group = 11.6 (15.6) |
Jones et al. (2021)20 SR (1 RCT, Keeler et al. 2017) | Median length of hospital stay, days (range)a IV iron group = 6 (5 to 10) Oral iron group = 6 (4 to 9) |
Jones et al. (2021)20 SR (1 RCT, Kim et al. 2017) | Mean length of hospital stay, days (SD)a IV iron group = 10.7 (7.9) Placebo = 10.9 (13.8) |
Jones et al. (2021)20 SR (1 RCT, Padmanabhan et al. 2019) | Median length of hospital stay, days (range)a IV iron group = 7 (6 to 12) Oral iron group = 9 (6 to 14) |
Jones et al. (2021)20 SR (1 RCT, Richards et al. 2019) | Median length of hospital stay, days (range)a IV iron group = 9 (7 to 14) Placebo group = 9 (5 to 14) |
Moon et al. (2021)21 SR (1 retrospective cohort study, Laso-Morales et al. 2018) | Mean length of stay (days) IV iron group = 9 Control group = 9 P = NS |
Moon et al. (2021)21 SR (1 retrospective and prospective cohort study, Calleja et al. 2015) | Mean length of stay (days) IV iron group = 8.4 Control group = 10.9 P < 0.001 |
Moon et al. (2021)21 SR (1 prospective cohort study, Kam et al. 2020) | Mean length of stay (days) IV iron group = 9 Control group = 8.5 P = NS |
Fung et al. (2022)22 RCT | Median postoperative length of stay days (range) IV iron group = 10 (5 to 19) Control group = 7 (5 to 10) P = 0.289 Days at home within 30 days of surgery (range) IV iron group = 20 (10 to 15) Control group = 23 (20 to 25) P = 0.461 |
Shokri et al. (2022)24 RCT | Length of hospital stay days between IV iron group and placebo group (SD) IV iron group = 4.33 (1) Placebo group = 8.68 (1.1) P < 0.001 ICU stay days between IV iron group and placebo group (SD) IV iron group = 1.28 (0.45) Placebo group = 2.23 (0.95) P < 0.001 |
Thin et al. (2021)25 RCT | Mean total DAOH within 30 days between IV iron group and oral iron group (SD) IV iron group = 19.3 (8.9) Oral iron group = 18.6 (10.2) P = 0.9 Mean total DAOH within 3 months between IV iron group and oral iron group (SD) IV iron group = 75.2 (16.1) Oral iron group = 68.8 (26.9) P = 0.5 Mean total DAOH within 6 months between IV iron group and oral iron group (SD) IV iron group = 166.8 (14.5) Oral iron group = 270.7 (442) P = 0.4 |
Ploug et al. (2022)26 Retrospective cohort study | Median length of stay days between IV group and control group (range) IV iron group = 4 (3 to 5) Control group = 3.5 (3 to 5.5) P = 0.74 Median DAOH 30-day follow-up between IV iron group and control group (range) IV iron group = 26 (23 to 27) Control group = 26 (24 to 27) P = 0.997 Median DAOH 90-day follow-up between IV iron group and control group (range) IV iron group = 86 (83 to 87) Control group = 86 (82 to 87) P = 0.79 |
Abdullah et al. (2021)27 Retrospective cohort study | Mean length of stay days for 1:1 propensity matched IV iron group (N = 89) and oral iron group (N = 89) (SD) IV iron group = 8 (12.5) Oral iron group = 15.1 (23.6) P = 0.013 Mean length of stay days for 1:2 propensity matched IV iron group (N = 89) and oral iron group (N = 178) (SD) IV iron group = 8 (12.5) Oral iron group = 14.1 (23.3) P = 0.006 |
Evans et al. (2021)28 Retrospective cohort study | Median length of stay days for each group (range) IV treatment responsive group = 9 (6 to 41) IV treatment unresponsive group = 11 (5 to 182); P < 0.001 vs non-anemic group Untreated anemic group = 10 (3 to 53) Non-anemic group = 8 (4 to 49) |
Triphaus et al. (2021)31 Prospective cohort study | Mean length of hospital stay days for each group (SEM) Anemic, iron deficient and IV iron treatment group = 13.9 (0.8) Iron deficient and IV iron treatment group = 14.9 (1.8) Anemic and no treatment group = 16.7 (0.7) Not anemic and no treatment group = 11.8 (0.3) |
DAOH = days alive and out of hospital; EPO = erythropoietin; ICU = intensive care unit; IV = intravenous; MA = meta-analysis; NS = not significant; RCT = randomized controlled trial; SD = standard deviation; SR = systematic review.
aStatistical significance between groups was not provided by Jones et al. (2021)
Table 12: Summary of Findings by Outcome — Safety and Adverse Events
Study citation and design | Study findings |
|---|---|
Chaudhry et al. (2021)18 SR (1 RCT, Brisbe et al. 2014) | Rate of adverse events IV iron group = 33% Oral iron group = 32% |
Chaudhry et al. (2021)18 SR (1RCT, Yoo et al. 2019) | Rate of adverse events IV iron group = 0% Control group = 0% |
Elhenawy et al. (2021)19 SR with MA (Based on 2 included study) | Effects of IV iron therapy versus placebo or standard of care on the occurrence of associated serious adverse effects Total IV iron group events = 85 Total placebo or standard of care group events = 91 Risk ratio (95% CI) = 0.96 (0.44 to 2.10); P = 0.92; I2 = 0% |
Elhenawy et al. (2021)19 SR with MA (Based on 7 included studies) | Effect of IV iron therapy versus placebo or standard of care on the occurrence of non-serious adverse effects (random effects model) Total IV iron group events = 412 Total placebo or standard of care group events = 401 Risk ratio (95% CI) = 1.13 (0.78 to 1.65); P = 0.52; I2 = 0% |
Jones et al. (2021)20 SR (1 RCT, Kim et al. 2017) | Proportion of patients experiencing adverse events, n/N (%)a IV iron group = 15/222 (6.8%) Placebo = 1/223 (0.4) |
Jones et al. (2021)20 SR (1 RCT, Padmanabhan et al. 2019) | Proportion of patients experiencing adverse events, n/N (%)a IV iron group = 0/20 Oral iron group = 3/20 (15%) |
Jones et al. (2021)20 SR (1 RCT, Park et al. 2019) | Proportion of patients experiencing adverse events, n/N (%)a IV iron group = 0/29 Placebo group = NR |
Jones et al. (2021)20 SR (1 RCT, Richards et al. 2019) | Proportion of patients experiencing adverse events, n/N (%)a IV iron group = 11/237 (5%) Placebo group = 5/237 (5%) |
Fung et al. (2022)22 RCT | Number of patients experiencing any surgical complications, n (%) IV iron group = 11 (55%) Control group = 8 (40%) P = 0.342 Number of patients experiencing surgical complication grade 0, 1, 2, or 3 IV iron group = 9;7;3;1 Control group = 12;6;2;0 P = 0.636 Hospital readmission within 30 days, n (%) IV iron group = 1 (5%) Control group = 1 (5%) P = 1.00 |
Kvaslerud et al. (2022)23 RCT | Number of adverse events between IV iron group (N = 73) and Placebo group (N = 75) IV iron group = 53 Placebo group = 66 Number of serious adverse events between IV iron group (N = 73) and Placebo group (N = 75) IV iron group = 37 Placebo group = 49 |
Shokri et al. (2022)24 RCT | Incidence of adverse cardiovascular events between IV iron group (N = 40) and placebo group (N = 40), n (%) IV iron group = 5 (12.5%) Placebo group = 7 (17.5%) P = 0.531 Incidence of prolonged ventilation between IV iron group (N = 40) and placebo group (N = 40), n (%) IV iron group = 2 (5%) Placebo group = 6 (15%) P = 0.136 Incidence of heart failure between IV iron group (N = 40) and placebo group (N = 40), n (%) IV iron group = 1 (2.5%) Placebo group = 3 (7.5%) P = 0.305 Incidence of stroke between IV iron group (N = 40) and placebo group (N = 40), n (%) IV iron group = 0 Placebo group = 1 (2.5%) P = 0.314 |
Thin et al. (2021)25 RCT | Number of patients readmitted during 6-month follow-up between IV iron group (N = 13) and oral iron group (N = 12), n (%) IV iron group = 4 (30.8%) Oral iron group = 4 (33.3%) P = 0.9 |
Ploug et al. (2022)26 Retrospective cohort study | All complications rate between IV iron group (N = 122) and control group (N = 48), n (%) IV iron group = 31 (25%) Control group = 4 (8%) P = 0.01 All surgical complications rate between IV iron group (N = 122) and control group (N = 48), n (%) IV iron group = 24 (20%) Control group = 4 (8%) P = 0.05 All medical complications rate between IV iron group (N = 122) and control group (N = 48), n (%) IV iron group = 10 (8%) Control group = 1 (2%) P = 0.13 |
Quarterman et al. (2021)30 Retrospective cohort study | Number of cerebrovascular accidents from each group, n (%) Anemic and received IV iron treatment group (N = 190) = 7 (3.7%) Anemic and did not receive IV iron treatment or not iron deficient group (N = 581) = 11 (1.9%); P = 0.17 vs IV iron treatment group Not anemic group (N = 2093) = 24 (1.2%); P = 0.01 vs IV iron treatment group Number of renal replacement therapy procedures from each group, n (%) Anemic and received IV iron treatment group (N = 190) = 7 (6.7%) Anemic and did not receive IV iron treatment or not iron deficient group (N = 581) = 9 (1.6%); P = 0.08 vs IV iron treatment group Not anemic group (N = 2093) = 13 (0.6%); P < 0.001 vs IV iron treatment group Number of re-operations from each group, n (%) Anemic and received IV iron treatment group (N = 190) = 9 (4.7%) Anemic and did not receive IV iron treatment or not iron deficient group (N = 581) = 24 (4.1%); P = 0.72 vs IV iron treatment group Not anemic group (N = 2093) = 73 (3.5%); P = 0.36 vs IV iron treatment group |
Mortality | |
Elhenawy et al. (2021)19 SR with MA | Effect of IV iron therapy versus placebo or standard of care on 30-day mortality (random effects model based on 4 included studies) Total IV iron group events = 303 Total placebo or standard of care group events = 284 Risk ratio (95%CI) = 1.10 (0.60 to 2.00); P = 0.76; I2 = 0% Effect of IV iron therapy versus placebo or standard of care on mortality ≥ 2 months post-hospital discharge (based on 2 studies) Total IV iron group events = 164 Total placebo or standard of care group events = 155 Risk ratio (95% CI) = 1.18 (0.63 to 2.19); P = 0.60; I2 = 0% |
Jones et al. (2021)20 SR (1 RCT, Padmanabhan et al. 2019) | Proportion of postoperative mortality, n/N (%)a IV iron group = 1/20 (5%)b Oral iron group = 0/29 |
Jones et al. (2021)20 SR (1 RCT, Richards et al. 2019) | Proportion of postoperative mortality, n/N (%)a IV iron group = 12/238 (5%) Placebo group = 10/236 (4%) |
Kvaslerud et al. (2022)23 RCT | Number of deaths between IV iron group (N = 73) and Placebo group (N = 75) IV iron group = 2 Placebo group = 5 |
Shokri et al. (2022)24 RCT | Mortality rate between IV iron group (N = 40) and placebo group (N = 40), n (%) IV iron group = 2 (5%) Placebo group = 3 (7.5%) P = 0.644 |
Ploug et al. (2022)26 Retrospective cohort study | 30-day mortality rate between IV iron group (N = 122) and control group (N = 48), n (%) IV iron group = 1 (1%) Control group = 0 P = 0.72 90-day mortality rate between IV iron group (N = 122) and control group (N = 48), n (%) IV iron group = 2 (2%) Control group = 3 (6%) P = 0.14 |
Evans et al. (2021)28 Retrospective cohort study | Number of deaths for each group, n (%) IV treatment responsive group (N = 24) = 0 IV treatment unresponsive group (N = 51) = 1 (2%) Untreated anemic group (N = 72) = 3 (6%); P = 0.012 vs non-anemic group Non-anemic group (N = 300) = 3 (1%) |
Quarterman et al. (2021)30 Retrospective cohort study | Number of in-hospital mortality from each group, n (%) Anemic and received IV iron treatment group (N = 190) = 3 (1.6%) Anemic and did not receive IV iron treatment or not iron deficient group (N = 581) = 14 (2.4%); P = 0.78 vs IV iron treatment group Not anemic group (N = 2093) = 17 (0.8%); P = 0.23 vs IV iron treatment group |
Triphaus et al. (2021)31 Prospective cohort study | Mortality rate for each group, n (%) Anemic, iron deficient and IV iron treatment group (N = 184) = 7 (3.8%) Iron deficient and IV iron treatment group (N = 55) = 3 (5.5%) Anemic and no treatment group (N = 461) = 27 (5.9%) Not anemic and no treatment group (N = 1028) = 31 (3%) |
Infection | |
Elhenawy et al. (2021)19 SR with MA (Based on 2 included studies) | Effect of IV iron therapy versus placebo or standard of care on postoperative infection occurrence (random effects model) Total IV iron group events = 143 Total placebo or standard of care group events = 132 Risk ratio (95% CI) = 0.64 (0.30 to 1.40); P = 0.27; I2 = 0% |
Fung et al. (2022)22 RCT | Number of patients experiencing infection, n (%) IV iron group = 6 (30%) Control group = 4 (20%) P = 0.465 |
Kvaslerud et al. (2022)23 RCT | Number of infections during IV treatment between IV iron group (N = 73) and Placebo group (N = 75) IV iron group = 5 Placebo group = 6 |
Shokri et al. (2022)24 RCT | Incidence of infection between IV iron group (N = 40) and placebo group (N = 40), n (%) IV iron group = 3 (7.5%) Placebo group = 5 (12.5%) P = 0.456 |
Ploug et al. (2022)26 Retrospective cohort study | All infectious complications rate between IV iron group (N = 122) and control group (N = 48), n (%) IV iron group = 10 (8%) Control group = 1 (2%) P = 0.14 |
Quarterman et al. (2021)30 Retrospective cohort study | Number of sternal wound infections from each group, n (%) Anemic and received IV iron treatment group (N = 190) = 7 (3.7%) Anemic and did not receive IV iron treatment or not iron deficient group (N = 581) = 16 (2.8%); P = 0.51 vs IV iron treatment group Not anemic group (N = 2093) = 42 (2%); P = 0.12 vs IV iron treatment group |
CI = confidence interval; EPO = erythropoietin; IV = intravenous; MA = meta-analysis; N = number; NR = not reported; RCT = randomized controlled trial; SR = systematic review; vs = versus.
aStatistical significance between groups was not provided by Jones et al. (2021)
bMortality in this population was due to unrelated causes.
Table 13: Summary of Findings by Outcome — Additional Clinical Outcomes
Study citation and design | Study findings |
|---|---|
Functional outcomes | |
Chaudhry et al. (2021)18 SR (1 RCT, Brisbe et al. 2014) | 6MWT score Difference in 6MWT score between IV iron group and oral iron group was not significant |
Chaudhry et al. (2021)18 SR (1RCT, Yoo et al. 2019) | FACT-An score Difference in FACT-An score between IV iron group and control iron group was not significant |
Kvaslerud et al. (2022)23 RCT | Mean 6MWT distance between IV iron group and placebo group at baseline and follow-up (SD) Mean IV iron group baseline distance = 355 m (113); Mean IV iron group follow-up distance = 375 m (132) Mean placebo group baseline distance = 367 m (129); Mean placebo group follow-up distance = 384 m (128) Mean difference (95% CI) = 2 m (-21 to 25); P = 0.86 |
Ferritin Levels | |
Elhenawy et al. (2021)19 SR with MA (Based on 3 included studies) | Ferritin level comparison at post-treatment and pre-surgery between IV iron and placebo or standard of care Mean difference (95% CI) = 94.09 ng/ml (51.57 to 136.61); P < 0.0001 Ferritin level comparison at hospital discharge between IV iron and placebo or standard of care Mean difference (95% CI) = 547.77 ng/ml (36.61 to 1058.94); P = 0.04 Ferritin level comparison > 4 weeks postoperative between IV iron and placebo or standard of care Mean difference (95% CI) = 347.57 ng/ml (290.92 to 404.21); P < 0.0001 Ferritin level comparison at post-treatment and pre-surgery between IV iron and oral iron therapy Mean difference (95% CI) = 106.12 ng/ml (32.46 to 179.78); P = 0.005 |
Fung et al. (2022)22 RCT | Mean change in ferritin concentration from baseline to before surgery between IV iron therapy and control Mean difference (95% CI) = 296.8 ng/L (200.6 to 393.2); P < 0.001 |
Kvaslerud et al. (2022)23 RCT | Mean ferritin level from baseline to follow-up (SD) Mean IV iron group ferritin level at baseline = 74.3 μg/L (57); Mean IV iron group ferritin level at follow-up = 361 μg/L (221) Mean placebo group ferritin level at baseline = 69 μg/L (52); Mean placebo group ferritin level at follow-up = 79 μg/L (86) Mean difference (95% CI) = 276 μg/L (216 to 336); P < 0.001 |
6MWT = 6-minute walk test; CI = confidence interval; FACT-An = Functional Assessment of Cancer Therapy for patients with Anemia/Fatigue; IV = intravenous; l = liter; m = meters; MA = meta-analysis; ml = milliliter; μg = microgram; ng = nanogram; NR = not reported; RCT = randomized controlled trial; SR = systematic review.
Table 14: Summary of Recommendations in Included Guidelines
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
|---|---|
Greenberg et al. (2021)32 | |
“Intravenous iron infusions may be appropriate for patients with IDA in certain circumstances (i.e., < 8 wk until surgery, unable to tolerate/absorb oral iron formulation, hemoglobin level < 100 g/L).”[ref] Evidence supporting this recommendation was from 1 SR, 4 RCTs, 1 prospective cohort study, and 2 retrospective cohort studies. | Strength of recommendation: Strong Quality of evidence: High |
IDA = iron deficient anemia; RCT = randomized controlled trial; SR = systematic review.
Appendix 5: Overlap Between Included Systematic Reviews
Note that this table has not been copy-edited.
Table 15: Overlap in Relevant Primary Studies Between Included Systematic Reviews
Primary study citation | Meyer (2022)16 | Tang (2022)17 | Chaudhry (2021)18 | Elhenawy (2021)19 | Jones (2021)20 | Moon (2021)21 |
|---|---|---|---|---|---|---|
Kam et al. Int J Colorectal Dis. 2020; 35(3): 521-527 | — | Yes | — | — | — | Yes |
Richards et al. Lancet 2020; 396: 1353-1361 | Yes | — | — | — | Yes | — |
Lee et al. J Obstet Gynaecol Res. 2019; 45 (4): 858-864 | — | — | — | — | Yes | — |
Padmanabhan et al. Interact Cardiovasc Thorac Surg. 2019; 28 (3): 447-454 | — | — | — | — | Yes | — |
Park et al. J Clin Med 2019; 8:1674 | — | — | Yes | — | Yes | — |
Yoo et al. SSRN 2019 | — | — | Yes | — | — | — |
Wilson et al. Transfusion 2018; 58 (3): 795-803 | — | Yes | — | — | — | Yes |
Keeler et al. Br J Surg 2017; 104 (3): 214-21 | — | — | — | Yes | Yes | Yes |
Kim et al. JAMA 2017; 317 (20): 2097-2104 | — | — | — | — | Yes | — |
Laso-Morales et al. Transfusion 2017; 57 (12): 3040-8 | — | — | — | — | — | Yes |
Wilson et al. Surg Oncol. 2018; 27 (2): 192-199 | — | Yes | — | — | — | — |
Bernabeu-Wittel et al. Transfusion 2016; 56 (9): 2199-211 | — | — | — | Yes | Yes | — |
Calleja et al. Int J Colorectal Dis. 2016; 31 (3): 543-51 | — | — | — | — | — | Yes |
Froessler et al. Ann. Surg. 2016; 264 (1): 41-46 | Yes | — | Yes | Yes | Yes | Yes |
Khalafallah et al. Lancet Haematol. 2016; 3 (9): e415-425 | — | — | — | — | Yes | — |
Shah et al. Natl J Commun Med. 2016; 7(1): 60-3 | — | — | — | Yes | — | — |
Johansson et al. Vox Sang 2015; 109 (3): 257-66 | — | — | — | Yes | — | — |
Bisbe et al. Br J Anaesth 2014; 113: 402-409 | — | — | Yes | — | Yes | — |
Garrido-Martin et al. Interact Cardiovasc Thoracic Surg. 2012; 15 (6): 1013-8 | — | — | — | Yes | — | — |
Titos-Acros et al. World J Surg. 2012; 36 (8): 1893-1897 | — | Yes | — | — | — | — |
Na et al. Transfusion (Paris) 2011; 51: 118-124 | — | — | Yes | — | — | — |
Serrano-Trenas et al. Transfusion 2011; 51 (1): 97-104 | — | — | — | Yes | — | — |
Edwards et al. Br. J. Surg 2009; 96 (10): 1122-1128 | Yes | Yes | — | Yes | — | Yes |
Kim et al. Acta Haemotal 2009; 121 (1): 37-41 | — | — | — | Yes | — | Yes |
Lidder et al. Ann. R Coll. 2007; 89 (4): 418-421 | Yes | Yes | — | — | — | — |
Mundy et al. J Bone Joint Surg Br 2005; 87: 213-217 | — | — | Yes | — | — | — |
Okuyama et al. Surg today. 2005; 35 (1): 36-40 | — | Yes | — | — | — | — |
Sutton et al. J Bone Joint Surg Br 2004; 113: 402-409 | — | — | Yes | — | — | — |
Weatherall et al. ANZ J Surg 2004; 74: 1049-1051 | — | — | Yes | — | — | — |
Weisbach et al. Transfusion 1999; 39 (5): 465-72 | — | — | — | Yes | — | — |
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca