CADTH Health Technology Review
Alternative Therapies to Immunoglobulin for Idiopathic Inflammatory Myopathies
Rapid Review
Authors: Anusree Subramonian, Kendra Brett, Melissa Severn
Abbreviations
GRADE
Grading of Recommendations Assessment, Development, and Evaluation
IIM
idiopathic inflammatory myopathies
ILD
interstitial lung disease
IVIG
IV immunoglobulin
MDA-5
melanoma differentiation-association protein 5
OSTEBA
Basque Office for Health Technology Assessment
SER
Sociedad Espanola de Reumatología
SIGN
Scottish Intercollegiate Guidelines Network
SR
systematic review
Key Messages
We did not find any evidence regarding the clinical effectiveness and safety of alternative treatments to IV Immunoglobulin (IVIG) compared to IVIG or placebo for idiopathic inflammatory myopathies (IIM) that met our inclusion criteria for this review.
Three evidence-based guidelines provide recommendations regarding IVIG and other drugs to manage IIM. However, we did not find any recommendations regarding alternative treatments to IVIG specifically.
Rituximab may be considered as another option to IVIG to treat IIM-related skeletal muscle inflammation (1 guideline) or skin manifestations (1 guideline) resistant to treatment with steroids.
In juvenile IIM, rituximab or IVIG can be used as adjunct care in case of treatment failure.
Context and Policy Issues
Idiopathic inflammatory myopathies (IIM) are a group of autoimmune diseases characterized by immune-mediated muscle inflammation along with the involvement of other organs and organ systems.1 They are rare disorders2,3 with an estimated incidence rate of 11 cases per million person-years, and a prevalence of 14 per 100,000 people based on a Swedish population-based study2-4 The main clinical presentation of IIM is the subacute progressive weakness of the proximal muscles (e.g., hips, upper thighs, shoulders, and upper arms), along with muscle pain and tenderness. If the muscles of the esophagus are affected, there may be difficulty swallowing, and if the respiratory muscles are affected, there may be shortness of breath.1
IIM are classified into various subtypes based on clinical and histopathologic features. Major subtypes include dermatomyositis, polymyositis, and inclusion body myositis – however, classification and subtypes of IIM remains disputed in the literature.1,5-7 Polymyositis presents with predominantly muscle involvement. Dermatomyositis is associated with characteristic skin rashes such as Grotton’s papules and heliotrope rash.6 It can occur in children (juvenile dermatomyositis) and adults with a mean age of onset of 7.3 years and 42 years respectively.8 In sporadic inclusion body myositis, both proximal and distal musculature is involved, often presented in individuals aged 50 or more.6 Extramuscular involvement of IIM includes interstitial lung disease (ILD), increased risk of cancers, and cardiac involvement, depending on the type of myositis-specific antibodies produced in the body.2,5 For example, antimelanoma differentiation-association protein (antiMDA-5) antibodies in dermatomyositis are associated with rapidly progressing ILD, a distinctive condition with a poor prognosis and around 50% mortality rate.9
Management of IIM aims to improve muscle weakness and functional ability, and enabling activities of daily living.6 The main treatment strategy is immunosuppression. Glucocorticoids (e.g., prednisolone) with or without disease-modifying antirheumatic drugs (e.g., methotrexate) are typically the first-line treatment.1,10 Steroid-sparing therapy using azathioprine, mycophenolate mofetil, or methotrexate may be considered in mild or moderate IIM after initial treatment.2 Patients with severe and/or refractory disease may require IV immunoglobulin (IVIG)1,11 Biologic drugs such as rituximab are often considered treatment of IIM refractory to first-line treatment. Other immunosuppressants, including azathioprine, mycophenolate mofetil, and tacrolimus have also been explored for their role in the treatment of refractory IIM.8 Due to increased demand, and due to the COVID-19 pandemic, there is a global shortage of immunoglobulin products.12,13 An evaluation of alternative treatment options to IVIG has been of interest.
The purpose of this report is to summarize the evidence regarding clinical effectiveness and guidelines regarding alternative treatments to IVIG, specifically, methotrexate, azathioprine, tacrolimus, rituximab, and mycophenolate mofetil for severe and/or refractory IIM. This report is part of a series of CADTH reports examining the alternatives to IVIG for various conditions.
Research Questions
What is the clinical effectiveness of alternative treatments to IV Immunoglobulin (IVIG) compared to IVIG or placebo for idiopathic inflammatory myopathies?
What is the safety of alternative treatments to IVIG compared to IVIG or placebo for idiopathic inflammatory myopathies?
What are the evidence-based guidelines regarding alternative treatments to IVIG for idiopathic inflammatory myopathies?
Methods
Literature Search Methods
An information specialist conducted a literature search on key resources, including MEDLINE, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of Canadian and major international health technology agencies, and a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategy comprised controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concepts were inflammatory myopathies, polymyositis, dermatomyositis, and inclusion body myositis. CADTH-developed search filters were applied to limit retrieval to health technology assessments, systematic reviews, meta-analyses, or indirect treatment comparisons. The search was completed on April 26, 2023, and was limited to English-language documents published since January 1, 2018.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Patients with severe or refractory IIM (i.e., polymyositis, dermatomyositis, and inclusion body myositis) |
Intervention | Methotrexate, Azathioprine, Tacrolimus, Rituximab, Mycophenolate mofetil |
Comparator | Q1 to 2: IV Immunoglobulin, placebo Q3: NA |
Outcomes | Q1: Clinical effectiveness (e.g., total improvement score, muscle strength, disability, HRQoL) Q2: Safety (e.g., adverse events, severe adverse events) Q3: Recommendations regarding best practices (e.g., which alternative to use, dose and timing of treatment, indications) |
Study designs | Health technology assessments, systematic reviews, evidence-based guidelines |
HRQoL = health-related quality of life; IIM = idiopathic inflammatory myopathies; NA = not applicable.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, were duplicate publications, or were published before 2018. SRs in which all relevant studies were captured in other more recent or more comprehensive SRs were excluded. Guidelines with unclear methodology were also excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)14 for SRs and the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument15 for guidelines. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
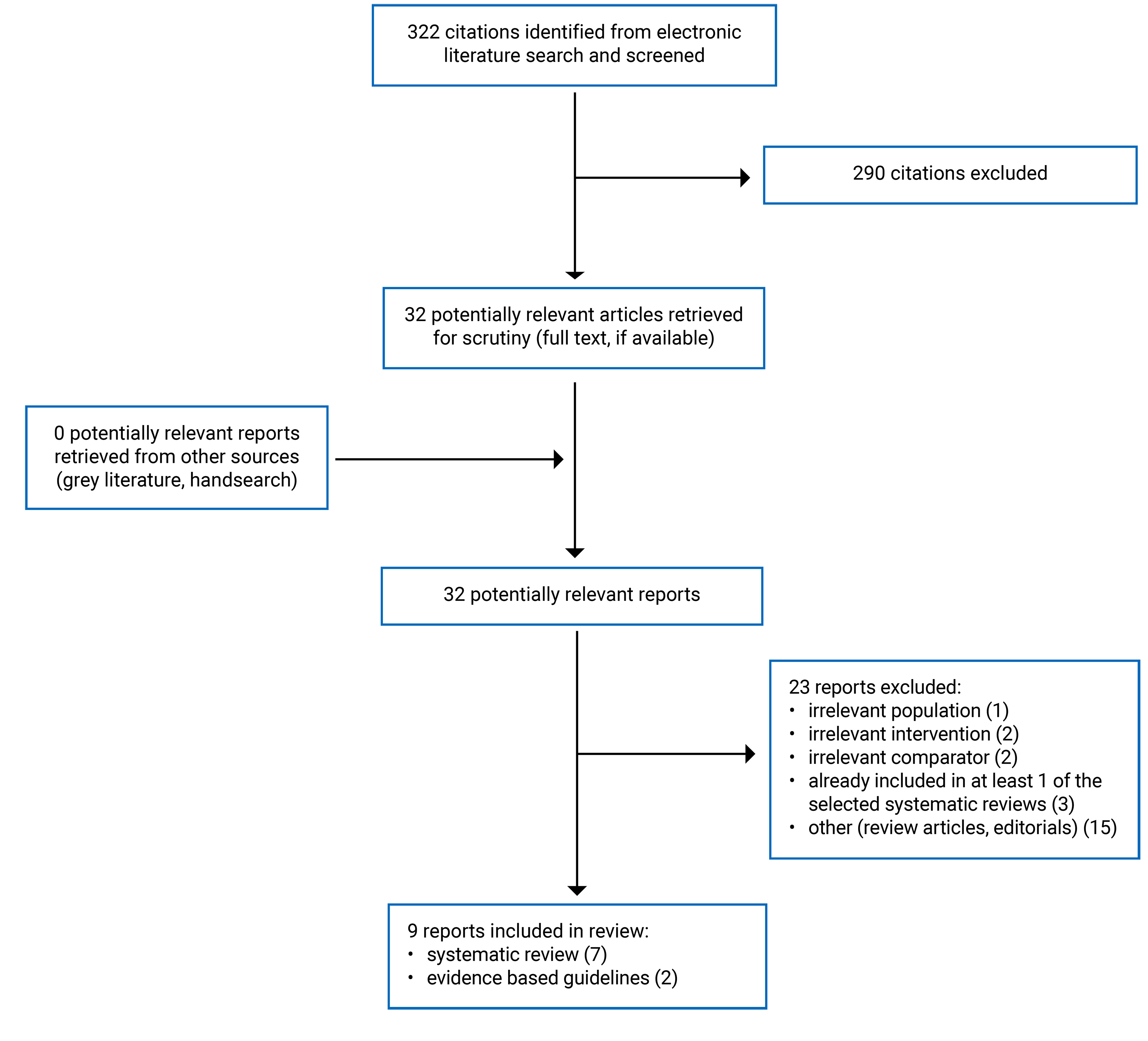
A total of 322 citations were identified in the literature search. Following screening of titles and abstracts, 290 citations were excluded and 32 potentially relevant reports from the electronic search were retrieved for full-text review. No potentially relevant publications were retrieved from the grey literature search for full-text reviews. Of these potentially relevant articles, 23 publications were excluded for various reasons, and 9 publications met the inclusion criteria and were included in this report. These comprised 7 SRs16-22 and 2 evidence-based guidelines.10,23 Appendix 1 presents the PRISMA24 flow chart of the study selection. Additional references of potential interest are provided in Appendix 5.
Summary of Study Characteristics
Seven SRs16-22 and 2 evidence-based guidelines10,23 were included in this report. Among the included publications, 1 was an SR of guidelines.22 The other 6 SRs16-21 included clinical studies, and searched for randomized or nonrandomized trials, and case series with or without including case reports.
The included clinical SRs16-21 evaluated various treatment options for different subtypes of IIM. Liao et al. (2023)16 examined the effectiveness of tacrolimus in patients with polymyositis or dermatomyositis. Zhen et al. (2022)20 included patients with IIM (all subtypes) and examined the effectiveness of rituximab. Xu et al. (2022)19 included studies in patients with ILD due to any type of connective tissue disorder and evaluated the effectiveness of treatment with rituximab. The SR by McPherson et al. (2022)18 considered studies about all treatment options in patients with dermatomyositis. The SR by Barba and colleagues (2019) examined the effectiveness of corticosteroids or immunosuppressive therapies in adult patients presenting with IIM-associated ILD.21 Lastly, Marrani et al. (2022)17 evaluated the effectiveness of all biologic agents in juvenile IIM where the disease onset was before 16 years of age. The search date of SRs ranged from July 201721 to October 2022.16 However, none of the included studies from any SRs evaluated the comparison of interest for this report, namely the clinical effectiveness and safety of specific alternative treatments to IVIG (i.e., methotrexate, azathioprine, tacrolimus, rituximab, mycophenolate mofetil) compared to IVIG or placebo for IIM Most of the included primary studies included in all SRs were single-arm observational studies, case series and/or case reports, and thus did not provide any relevant comparative evidence.
The guideline SR22 was published in 2018 and had broader inclusion criteria than our review. Guidelines regarding all appropriate health care (e.g., treatment, cancer screening, pregnancy planning and management, treatment of ILD, outcome assessment) for children and adults with IIM were considered in the SR. Only the characteristics and results of the subset of relevant guidelines will be described in this report.
Additional details regarding the characteristics of all included publications are provided in Appendix 2. Detailed study characteristics for the relevant included guidelines are described narratively in the following sections.
Study Design
The guideline SR by Meyer et al.22 aimed to identify available clinical practice guidelines for IIM. They searched multiple electronic databases to identify eligible guidelines published until February 2018. The authors defined ‘clinical practice guidelines’ as statements informed by a systematic literature review of evidence and including an assessment of the benefit and harms of alternative care options. However, guidelines with unclear methods of evidence search that did not meet the definition of clinical practice guidelines were also included in the SR. Among the 14 included guidelines in this SR, 1 guideline produced by Rheumatology specialists and focused on juvenile IIM was relevant to the current report. The level of evidence was assessed based on the Grading of Recommendations Assessment, Development, and Evaluation framework (GRADE).
Two other guidelines were included in the current report.10,23 The British Society for Rheumatology guideline (2022),10 produced recommendations regarding all treatment options for pediatric, adolescent, and adult IIM. Relevant evidence for each key question was identified through systematic literature searches of multiple databases published until October 2020. The quality of included studies was assessed using the GRADE framework and was categorized as high (A), moderate (B), or low or very low (C) quality. Recommendations were developed using the methodology from the Scottish Intercollegiate Guidelines Network (SIGN) and were classified as strong or weak based on the level of supporting evidence. Draft recommendations were finalized through a consensus-building process. The guideline development committee was multidisciplinary and included a patient partner.
The guideline by Sociedad Espanola de Reumatología (SER),23 published in 2020, was regarding the treatment of rapidly progressing ILD associated with anti-MDA 5 positive dermatomyositis. Relevant evidence for each key question was identified through systematic literature searches of multiple databases published until July 2019. The quality of evidence was assessed using a tool developed by the Basque Office for Health Technology Assessment (OSTEBA, reported in the publication as Agency for Health care Technology Assessment of the Basque Country)). Evidence was ranked from 1++ (evidence from high-quality meta-analysis, or high-quality randomized studies) to 4 (expert opinion). Recommendations were developed using SIGN methodology and were classified as A (strongest) to D (weakest), based on the rank of associated evidence. Draft recommendations were finalized through a consensus-building process. The guideline development committee consisted of health care professionals and method experts.
Country of Origin
The guideline SR was conducted in the European Union.22 The guideline development group and country of the relevant guideline were unclear.
The 2 included guidelines were developed for Spain23 and the UK.10
Patient Population
In the guideline SR,22 the target population for the relevant included guideline was patients with juvenile IIM. Intended users were unclear from the SR.22
The target populations for the British Society for Rheumatology guideline 10 were pediatric, adolescent, and adult populations with IIM. The intended users of the guideline were health care professionals (e.g., clinicians, occupational therapists, pharmacists, and nurses). In the SER guidelines,23 the primary target population was patients with rapidly progressing ILD associated with anti-MDA5 positive dermatomyositis. To secure more evidence, a broader population of rapidly progressive ILD with negative or unknown anti-MDA5 status, or that not associated with dermatomyositis, and anti-MDA5 positive nonrapidly progressing ILD were also considered. The intended users of the guideline were not explicitly mentioned but were likely clinicians.
Only the recommendations regarding treatment using IVIG alternatives for either severe or refractory IIM are summarized in this review.
Interventions and Comparators
The interventions considered in the relevant recommendations were rituximab,10,22,23 mycophenolate mofetil,22,23 methotrexate,23 and azathioprine.23
Outcomes
The outcomes considered by the guidelines10,22,23 were clinical benefits in myositis, skin disease, and ILD in patients with refractory IIM.
Summary of Critical Appraisal
Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
Systematic Reviews of Clinical Studies
A high-level summary of strengths and weaknesses of the 616-21 clinical SRs is provided in this section. As there were no relevant primary studies included in any of them, the critical appraisal is focused on methodology related to objectives, inclusion criteria, literature search, and study selection.
The aim of the review was clearly stated in all 6 SRs.16-21 The research questions and inclusion criteria included components of population, intervention, comparator (if any), and outcomes. They were appropriate for the review objectives. Review methods were established and published before the conduct of 2 SRs16,19 The literature search and selection methods were generally comprehensive across SRs, and therefore expected to identify relevant existing evidence. Specifically, authors of all SRs searched multiple electronic databases within 24 months of SR publication, and the search strategy or keywords were provided in 5 SRs.16-20 In all SRs, randomized and nonrandomized studies were considered eligible. While 1 SR17 excluded case reports with appropriate reasoning, the other SRs16,18-21 included all study designs. In 5 SRs,16-20 study selection was made in duplicate (triplicate in 1 SR18) by 2 or more reviewers independently. Authors declared that there were no conflicts of interest for 4 SRs.16,18-20
The included SRs also presented some methodological limitations. For example, 3 of the included SRs did not state whether review methods were established before the conduct of the review.17,18,20 While inclusion criteria were established a priori in the SR by Barba et al.,21 it was unclear whether additional methods were established and published. None of the included SRs provided a list of excluded studies and reasons for excluding them. Without this information, it is challenging to verify if any potentially relevant articles were missed. Lastly, in 2 SRs, information on funding sources and possible conflicts of interest (if any) were not reported.
Systematic Review of Guidelines
The guideline SR22 had several strengths, mostly related to clear reporting of objectives and inclusion criteria, and comprehensive literature search and selection methods. Specifically, a clear and appropriate definition of clinical practice guidelines eligible for inclusion was provided. Multiple electronic databases were searched, and a search strategy was reported. The search was conducted within 24 months of publication. Article selection was performed by 2 reviewers independently, and disagreements were resolved with discussion. The authors reported their funding source and declared no conflicts of interest. Recommendation statements from the included guidelines were clearly and unambiguously described and was easy to identify. A narrative summary of recommendations from all, including guidelines, was also provided.
However, some of the methods of reporting were unclear or conflicting throughout the guideline. It was unclear whether the review methods were established before the conduct of the SR. Even though a clear definition of clinical practice guidelines was provided, the authors reported that in half of the included guidelines, the evidence search methodology was unclear. Although clearly denoted as ‘eminence-based guidelines’, the rationale for including them was not provided. Detailed characteristics of the included guidelines, such as guideline development organization, country, or the methodology framework used (e.g., GRADE, SIGN) were not reported. This could affect the generalizability of the recommendations. A quality assessment of the included guidelines was not conducted. Without this detail, the rigour of development, applicability, and editorial independence of the individual guidelines could not be evaluated. The strength of each recommendation statement from included guidelines and the supporting evidence were not reported. Overall, the guideline SR was likely able to identify clinical practice guidelines for treating IIM. However, a lack of quality assessment and limitations in reporting lowered the quality of the SR.
Evidence-Based Guidelines
Both guidelines were generally well conducted, using robust and inclusive development methods, and clear reporting. The scope and purpose of the included guidelines10,23 were clearly stated. The target population was clear, and the intended users were clear or implied. The British Society for Rheumatology guideline10 was developed by a multidisciplinary committee that included a patient and caregiver partner along with clinical and methodological experts. Both guidelines were developed using a rigorous methodology detailed in the publication. The authors used systematic literature searches to inform evidence and used appropriate methods for appraising the quality of evidence (GRADE or OSTEBA) and for formulating recommendations (SIGN). The level of evidence and strength of recommendations were clearly denoted in both guidelines. The SER guideline23 was externally reviewed by experts before publication. The British guideline reported procedures for updating the guideline.10 In both guidelines, the recommendations were clear and easily identifiable. Different options for the management of the target condition were presented. The authors of the British guideline were clear about the possible facilitators and barriers to the application of the guidelines and provided tools for implementation and auditing. They also reported possible conflicts of interest of the guideline authors.10
However, the included guidelines had some limitations, mostly involving stakeholder involvement and implementation. In the SER guideline,23 the stakeholder involvement was limited. The development committee was not multidisciplinary and did not include patient partners. While the guideline followed a rigorous development process, there were no reported procedures for updates or tools for implementation and auditing. Barriers to the application of guidelines, and resource implications were unclear. Lastly, it was unclear whether the authors had possible conflicts of interest.23 The British guideline authors reported receiving funding from various sources, and it was unclear whether the views of the funding body have not influenced the content. It was also unclear whether external stakeholders reviewed the guideline before publication.10
Summary of Findings
Appendix 4 presents the main study findings.
Clinical Effectiveness and Safety of Alternative Treatments to IV Immunoglobulin Compared to IVIG or Placebo
No relevant evidence regarding methotrexate, azathioprine, tacrolimus, rituximab, or mycophenolate mofetil versus IVIG or placebo for IIM was identified; therefore, no summary can be provided.
Evidence-Based Guidelines
We identified 3 evidence-based guidelines10,22,23 (one identified in a guideline SR22) that made recommendations relevant to the current report for managing refractory IIM. We did not identify any specific formal recommendation statements regarding which drugs to use as IVIG alternatives for refractory IIM. Clinical conditions where IVIG and other therapeutic options (relevant to this report) were recommended are summarized herein. Detailed recommendation statements and supporting evidence are provided in Tables 6 and 7.
Myositis
The British Society for Rheumatology guideline (2022)10 recommend that rituximab can be used as a treatment option in refractory myositis, especially in patients with juvenile onset disease, with a positive myositis autoantibody profile, or with a lower disease burden (conditional recommendation based on high-quality evidence). For severe and/or refractory muscle inflammation, IVIG can also be considered as a treatment option (strong recommendation based on moderate quality evidence).
Skin Manifestations
The British Society for Rheumatology guideline (2022)10 recommend that rituximab should be an option for the treatment of IIM-related skin disease refractory to glucocorticoids or disease-modifying antirheumatic drugs (conditional recommendation based on moderate quality evidence). Supporting evidence was from 1 randomized trial; however, additional details were not reported. IVIG was also recommended as a treatment option for skin disease refractory to glucocorticoids or disease-modifying antirheumatic drugs (strong recommendation based on moderate quality evidence). The authors noted the limited evidence base available for the treatment of IIM-related skin manifestations.
Interstitial Lung Disease
Two guidelines10,23 provided recommendations regarding the management of ILD associated with IIM. In patients with rapidly progressive ILD associated with anti-MDA-5 antibodies, who are refractory to treatment with glucocorticoids and immunosuppressants, the SER guideline23 recommends adding cyclophosphamide, mycophenolate mofetil, rituximab, basiliximab, or tofacitinib to the existing treatment regimen (combination therapy). IVIG is recommended in patients who are not responding to this combination therapy. Azathioprine and methotrexate are not recommended for treating these patients (based on clinical experience and consensus of the guideline authors).23 These recommendations were based on evidence from case series, case reports, and /or expert opinion. The British guideline10 did not make recommendations for or against the use of IVIG in rapidly progressing ILD. They recommend using tacrolimus (or ciclosporin) along with steroids, as well as rituximab (or cyclophosphamide) early on as part of induction (conditional recommendation based on low-quality evidence)10
In patients with chronic IIM-associated ILD who are treatment-resistant, the British Society for Rheumatology guideline10 recommends rituximab (or cyclophosphamide) (conditional recommendation based on low-quality evidence). The authors did not make any recommendation for or against IVIG for the management of Chronic ILD associated with IIM. Therefore, it is unclear whether rituximab is a possible IVIG alternative for this patient population.
Juvenile IIM
One guideline included in the guideline SR22 provided recommendations specific to juvenile IIM. Corticosteroids and methotrexate are the recommended first-line treatment options. In case of failure of first-line treatment, mycophenolate mofetil is recommended (if methotrexate is not tolerated). Rituximab can be considered as an alternative to IVIG as an adjunct treatment. Cyclophosphamide or anti tumour necrosis factor therapies are also recommended. The strength of recommendations and the evidence supporting these recommendations were unclear from the SR.22
Limitations
The main limitation of this report is the lack of identified clinical evidence. Even though the included clinical SRs conducted comprehensive searches for evidence, they did not identify any relevant primary studies eligible for inclusion. Without comparative evidence of IVIG alternatives versus IVIG or placebo, we could not provide meaningful answers to the research questions on clinical effectiveness and safety. Among the identified evidence-based guidelines, recommendations were mostly made based on weak evidence (case series or reports) and expert opinion due to the rarity of the disease and the limited availability of evidence. The authors of the guidelines highlighted a lack of clinical evidence. No specific recommendations related to alternative treatment options to IVIG were made in the guidelines; instead, several therapeutic options for refractory IIM were provided with no recommended order of preference. Therefore, 1 may assume that these options are equivalent in efficacy and safety; however, there was no evidence identified regarding the comparative effectiveness of IVIG and its alternatives. None of the recommendations addressed possible adverse events of IVIG or IVIG alternatives. Lastly, as no guidelines from Canada were identified, the applicability of recommendations regarding IVIG alternatives in settings across Canada is unclear.
Conclusions and Implications for Decision- or Policy-Making
Six clinical SRs,16-21 1 guideline SR,22 and 2 evidence-based guidelines10,23 were included in this report. No relevant primary studies comparing rituximab, azathioprine, methotrexate, tacrolimus, or methotrexate to IVIG or placebo were identified in the 6 SRs. Therefore, no summary regarding the comparative clinical effectiveness or safety of alternatives to IVIG are provided in this report. This highlights the gap in our knowledge regarding whether IVIG alternatives are as effective and safe as IVIG for IIM. However, 3 evidence-based guidelines10,22,23 were identified recommending IVIG and other therapies for treating IIM.
To treat muscle inflammation in refractory IIM, rituximab, cyclophosphamide, and abatacept are recommended as treatment options along with IVIG.10 For IIM-associated skin manifestations, rituximab is recommended as a treatment option in addition to IVIG.10 These recommendations were based on moderate to high-quality evidence from observational studies. In patients with treatment-resistant juvenile IIM, IVIG or rituximab are recommended as adjunct therapeutic options. In patients with rapidly progressing ILD associated with IIM, IVIG is recommended when there is no response to treatment with immunosuppressants (e.g., rituximab, mycophenolate mofetil).23 It should be noted that the comparative clinical effectiveness of IVIG and these alternative options is unclear. Most recommendations were based on case series, reports, and expert opinions. Therefore, any consideration of these therapeutics as IVIG alternatives in refractory IIM should be made with caution. Overall, the guidelines were developed with methodological rigour, highlighting the lack of conclusive evidence for treatment of refractory IIM.
In a qualitative study of patient perspectives,25 individuals living with IIM have pointed out the limitations of current disease activity measurement methods, and the need for researchers and clinicians to prioritize outcomes perceived to be important by the patients (e.g., pain, fatigue). IIMs were felt as “invisible” diseases by the patients, and because of low awareness among friends, families, and even clinicians, patients often feel isolated and lonely in their journey. The guideline SR included in this report emphasized the unmet needs of patients, and a lack of patient involvement in developing their care pathways.22
Considering the decrease in the availability of IVIG globally,12 interest exists in exploring alternative treatment options for various conditions. Evidence from real-world settings focusing on patient-important outcomes is warranted to examine the effectiveness and safety of IVIG alternatives for patients with IIM, given the paucity of existing clinical trial evidence and the rarity of this class of diseases. Thorough and robust evidence-based recommendations that also consider facilitators and barriers to equitable access to care, as well as patient perspectives, would support clinicians and other care providers.
References
1.Ashton C, Paramalingam S, Stevenson B, Brusch A, Needham M. Idiopathic inflammatory myopathies: a review. Intern Med J. 2021;51(6):845-852. PubMed
2.Gazeley DJ, Cronin ME. Diagnosis and treatment of the idiopathic inflammatory myopathies. Ther Adv Musculoskelet Dis. 2011;3(6):315-324. PubMed
3.Oldroyd A, Lilleker J, Chinoy H. Idiopathic inflammatory myopathies – a guide to subtypes, diagnostic approach and treatment. Clin Med (Northfield Il). 2017;17(4):322-328. PubMed
4.Svensson J, Arkema EV, Lundberg IE, Holmqvist M. Incidence and prevalence of idiopathic inflammatory myopathies in Sweden: a nationwide population-based study. Rheumatology (Oxford). 2017;56(5):802-810. PubMed
5.Sabouri AH, Christopher-Stine L, Kafaie J. Inflammatory Myopathies. Pract Neurol. 2021 July/August. https://practicalneurology.com/articles/2021-july-aug/inflammatory-myopathies. Accessed 22 May 2023.
6.Malik A, Hayat G, Kalia JS, Guzman MA. Idiopathic Inflammatory Myopathies: Clinical Approach and Management. Front Neurol. 2016;7:64. PubMed
7.Benveniste O, Stenzel W, Hilton-Jones D, Sandri M, Boyer O, van Engelen BGM. Amyloid deposits and inflammatory infiltrates in sporadic inclusion body myositis: the inflammatory egg comes before the degenerative chicken. Acta Neuropathol. 2015;129(5):611-624. PubMed
8.Patil A, Lu J, Kassir M, Babaei M, Goldust M. Adult and juvenile dermatomyositis treatment. J Cosmet Dermatol. 2023;22(2):395-401. PubMed
9.Nombel A, Fabien N, Coutant F. Dermatomyositis With Anti-MDA5 Antibodies: Bioclinical Features, Pathogenesis and Emerging Therapies. Front Immunol. 2021;12. https://www.frontiersin.org/articles/10.3389/fimmu.2021.773352. Accessed 22 May 2023. PubMed
10.Oldroyd AGS, Lilleker JB, Amin T, et al. British Society for Rheumatology guideline on management of paediatric, adolescent and adult patients with idiopathic inflammatory myopathy. Rheumatology. 2022;61(5):1760-1768. PubMed
11.Patwardhan A. The Value of Intravenous Immunoglobulin Therapy in Idiopathic Inflammatory Myositis in the Current Transformed Era of Biologics. Cureus. 2020;12(2):e7049. PubMed
12.U.S. Food and Drug Administration. CBER-Regulated Products: Current Shortages. 2023; https://www.fda.gov/vaccines-blood-biologics/safety-availability-biologics/cber-regulated-products-current-shortages. Accessed 22 May 2023.
13.N'Kaoua E, Attarian S, Delmont E, et al. Immunoglobulin shortage: Practice modifications and clinical outcomes in a reference centre. Rev Neurol (Paris). 2022;178(6):616-623. PubMed
14.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
15.Agree Next Steps C. The AGREE II Instrument. [Hamilton, ON]: AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf. Accessed 22 May 2023.
16.Liao J, Peng X, Liu J, Xie X, Wang J. The efficacy and safety of tacrolimus in patients with dermatomyositis/polymyositis: A meta-analysis and systematic review. Eur J Intern Med. 2023;110:35-40. PubMed
17.Marrani E, Abu-Rumeileh S, Mastrolia MV, Maccora I, Pagnini I, Simonini G. A systematic review on biological therapies in juvenile idiopathic inflammatory myopathies: an evidence gap in precision medicine. Clin Exp Rheumatol. 2022;40(2):457-470. PubMed
18.McPherson M, Economidou S, Liampas A, Zis P, Parperis K. Management of MDA-5 antibody positive clinically amyopathic dermatomyositis associated interstitial lung disease: A systematic review. Semin Arthritis Rheum. 2022;53:151959. PubMed
19.Xu L, Wang F, Luo F. Rituximab for the treatment of connective tissue disease-associated interstitial lung disease: A systematic review and meta-analysis. Front Pharmacol. 2022;13:1019915. PubMed
20.Zhen C, Hou Y, Zhao B, Ma X, Dai T, Yan C. Efficacy and safety of rituximab treatment in patients with idiopathic inflammatory myopathies: A systematic review and meta-analysis. Front Immunol. 2022;13:1051609. PubMed
21.Barba T, Fort R, Cottin V, et al. Treatment of idiopathic inflammatory myositis associated interstitial lung disease: A systematic review and meta-analysis. Autoimmun Rev. 2019;18(2):113-122. PubMed
22.Meyer A, Scire CA, Talarico R, et al. Idiopathic inflammatory myopathies: state of the art on clinical practice guidelines [corrected]. RMD Open. 2018;4(Suppl 1):e000784. PubMed
23.Romero-Bueno F, Diaz Del Campo P, Trallero-Araguas E, et al. Recommendations for the treatment of anti-melanoma differentiation-associated gene 5-positive dermatomyositis-associated rapidly progressive interstitial lung disease. Semin Arthritis Rheum. 2020;50(4):776-790. PubMed
24.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
25.Oldroyd A, Dixon W, Chinoy H, Howells K. Patient insights on living with idiopathic inflammatory myopathy and the limitations of disease activity measurement methods – a qualitative study. BMC Rheumatol. 2020;4(1):47. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of Included Systematic Reviews
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes |
|---|---|---|---|---|
Systematic reviews of clinical studies | ||||
Liao et al. (2023)16 China Funding source: The National Natural Science Foundation of China (No. 81601435), the Human Province Clinical Medical Technology Innovation Guiding Project (No. 2020SK53409), and the Human Province Natural Science Foundation for Youths (No. 2021JJ40841) | SR with MA Number of included primary studies: 9 Number of relevant primary studies: none | Patients diagnosed with polymyositis or dermatomyositis based on Bohan and Peter criteria or 2017 ACR/EULAR. | Intervention: tacrolimus Comparator: any or none | Outcomes: overall survival, progression free survival, muscle damage, pulmonary function, adverse events. |
Marrani et al. (2022)17 Italy Funding source: NR | SR with MA Number of included primary studies: 18. Number of relevant primary studies: none | Pediatric patients with JIIM (disease onset before 16 years of age, and treatment initiation before 18 years of age); persistent muscle inflammation and/or skin involvement; biologic treatment naive. | Intervention: All biologic agents Comparator: any or none | Outcomes: complete clinical response for muscle and/or skin involvement. |
McPherson et al. (2022)18 US Funding source: No funding received. | SR Number of included primary studies: 15. Number of relevant primary studies: none | Patients with dermatomyositis or clinically amyopathic dermatomyositis with antimelanoma differentiation-associated gene 5 antibodies and interstitial lung disease. | Intervention: any treatment for ILD or for rapidly progressive ILD Comparator: any or none | Outcomes: respiratory status, mortality, remissions, relapses, adverse events. |
Xu et al. (2022)19 China Funding source: Sichuan Science and Technology Program (No.2021YFQ0030); Tibet Science and Technology Program (XZ202201ZY0002G); West China Hospital, Sichuan University (ZYJC18021); Post-Doctor Research Project, West China Hospital (2021HXBH074) and the National Natural Science Foundation of China (No. 82100075). | SR with MA Number of included primary studies: 13. Number of relevant primary studies: none | Patients diagnosed with connective tissue disease who met the international criteria for ILD based on chest high-resolution CT and/or lung biopsy. | Intervention: rituximab Comparator: any or none | Outcomes: pulmonary function, adverse events. |
Zhen et al. (2022)20 China Funding source: National Natural Science Foundation of China (Grant No. 82171395), Natural Science Foundation of Shandong Province (Grant No. ZR2021QH120), Key Research and Development Project of Shandong Province (2019GXRC050), and Qingdao Technology Program for Health and Welfare (20 to 3-3 to 42-nsh). | SR with MA Number of included primary studies: 26 Number of relevant primary studies: none | Patients diagnosed with IIM based on Bohan and Peter criteria or 2017 ACR/EULAR. | Intervention: Rituximab Comparator: Any or none | Outcomes: Complete response rate, partial response rate, overall effective rate, adverse vents. |
Barba et al. (2019)21 France Funding source: Not reported | SR with MA Number of included primary studies: 27 Number of relevant primary studies: none | Adults presenting with ILD related to IIM. | Intervention: corticosteroids or immunosuppressive therapies Relevant interventions: Azathioprine, rituximab Comparator: any or none | Outcomes: survival rates, pulmonary function. |
Systematic review of guidelines | ||||
Meyer et al. (2018)22 France (and other EU countries) Funding source: European Union’s Health Programme (2014 to 2020), Framework Partnership Agreement Number 739531- ERN ReCONNECT | SR of clinical practice guidelines Number of included guidelines: 14 Number of relevant guidelines: 1 | Children and adults with IIM Target population of the relevant guideline: children with IIM. | Intervention: Appropriate health care (e.g., treatment, cancer screening, pregnancy planning and management, treatment of ILD, outcome assessment) Relevant interventions: Tacrolimus, mycophenolate mofetil, rituximab, ciclosporin Comparator: NA | Outcomes: Recommendations regarding best practices. |
ACR = American College of Rheumatology; EULAR = European League Against Rheumatism; ILD = interstitial lung disease; IIM = idiopathic inflammatory myopathies; MA = meta-analysis; NA = not applicable; NR = not reported; SR = systematic review; IVIG = IV immunoglobulin.
Note that this appendix has not been copy-edited.
Table 3: Characteristics of Included Guidelines
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality assessment | Recommendations development and evaluation | Guideline validation |
|---|---|---|---|---|---|---|
British Society for Rheumatology Guideline (2022)10 | ||||||
Intended users: Health care professionals such as clinicians (e.g., rheumatologists., dermatologists, respirologists) nurses, physiotherapists, pharmacists, occupational therapists. Target population: Pediatric, adolescent, and adult patients with IIM. Note: Inclusion body myositis was excluded. | All treatment options for the management of IIM were considered. Relevant interventions: Alternative to immunoglobulins. | Outcomes related to skeletal muscle inflammation, skin manifestations, and ILD | Key questions prepared by the guideline committee. Studies identified through systematic literature search of multiple databases. Included studies published until October 2020. 213 studies were selected to inform the recommendations. | Quality of included studies assessed using GRADE framework as high (A), moderate (B), or low or very low (C) quality. | Guidelines was developed suing the AGREEII methodology. Recommendations were developed using SIGN methodology. Strength of recommendations were classified as strong (1) or weak (2). Draft recommendations were finalized through a consensus process building process. Only recommendations with > 80% agreement were included. | The guideline development committee was multidisciplinary and included a patient partner in addition to clinical experts. A methodologist participated in the literature searches. |
Sociedad Espanola de Reumatología, SER (2020)23 | ||||||
Intended Users: Clinicians (unclear but implied) Target Population: Patients with anti-MDA 5 positive DM-RPILD, anti-MDA 5 positive non-RPILD, RPILD with negative or unknown anti MDA5 status, RPILD with systemic autoimmune diseases other than DM. Relevant target population: Patients with anti-MDA 5 positive DM-RPILD, patients with DM -RPILD with negative or unknown anti MDA5 status. | All treatment options for the management of anti-MDA 5 positive dermatomyositis-RPILD considered. Relevant interventions: Alternative to immunoglobulins. | Lung improvement in ILD | Key questions prepared by the guideline committee. Studies identified through systematic literature search of multiple databases. Included studies published until July 2019. 57 and 30 studies were selected to inform recommendations for each of the relevant populations. | Quality of included studies assessed and classified using a tool by the OSTEBA toola. | Recommendations were developed using SIGN methodology based on ‘formal evaluation’ or ‘justified opinion.’ The statements were finalized using a consensus approach. Grades of recommendation were ranked from A (strongest) to D (weakest)b. | Guideline development committee consisted of 7 health care professionals, method experts and scientific societies. Draft guidelines were reviewed externally. Feedback from other external stakeholders were sought. |
AGREE II = Appraisal of Guidelines for Research and Evaluation II; DM = dermatomyositis; GRADE = Grading of Recommendations Assessment, Development and Evaluation; ILD = interstitial lung disease; IIM = idiopathic inflammatory myopathies; MA = meta-analysis; MDA-5 = antimelanoma differentiation-associated gene 5; NRS = nonrandomized study; OSTEBA = Basque Office for Health Technology Assessment ; RCT = randomized controlled trial; RPILD = rapidly progressing interstitial lung disease; SIGN = Scottish Intercollegiate Guidelines Network; SR = systematic review. ‘
a1++ - High-quality meta-analyses (MA), systematic reviews (SR) of clinical trials or high-quality clinical trials with low risk of bias.
1+ Well-conducted MA, SR of clinical trials, or well-conducted clinical trials with little risk of bias.
1-MA, SR of clinical trials, or clinical trials with high risk of bias.
2++ High-quality SRs of cohort or case-control studies; cohort or case-control studies with very low risk of bias and high probability of establishing a causal relationship.
2+ Well-conducted cohort or case-control studies with low risk of bias and moderate probability of establishing a causal relationship.
2- Cohort or case-control studies with high risk of bias 3 case reports and significant risk that the relationship is not causal.
3 Nonanalytical studies such as case series and case reports.
4 Expert opinion.
bA- at least 1 MA, SR or clinical trial rated ad 1++ and directly applicable to the target population, or a body of evidence consisting of studies rated as1+ showing overall consistency of results.
B- Body of evidence rated as 2++ directly applicable to the target population, and showing overall consistency of results; or evidence extrapolated form studies rated 1++ or 1+.
c- Body of evidence rated 2+ directly applicable to the target population, and showing overall consistency of results, or extrapolated from evidence rated 2++.
D- Evidence rated 3 or 4; or extrapolated from evidence rated 2+.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 4: Strengths and Limitations of Systematic Reviews Using AMSTAR 214
Strengths | Limitations |
|---|---|
Systematic reviews of clinical studies | |
Liao et al. (2023)16 | |
The aim of the review was clearly stated. The population, intervention, and outcomes of interest were clearly stated. An explicit statement was provided that the review methods were established before the conduct of the review (registered in PROSPERO). The search was conducted in multiple databases and trial registries, key search terms were provided, and reference lists of selected systematic reviews were hand-searched for additional relevant studies. Search was conducted within 24 months of publication. Two authors independently selected studies for inclusion and disagreements were resolved by the whole authorship group. The authors reported their funding source and declared that there were no conflicts of interest. | The comparator was not clearly stated. The authors did not describe which study designs were eligible. Authors did not provide justification for restricting to studies published in English. Grey literature was not searched. A list of excluded studies with justifications for exclusion was not provided. |
Marrani et al. (2022)17 | |
The aim of the review was clearly stated. The population, intervention, and outcomes of interest were clearly stated. Outcome measures were well defined. The search was conducted in multiple databases, key search terms were provided, and reference lists of selected publications were hand-searched for additional relevant studies. Search was conducted within 24 months of publication. Case reports and were excluded with appropriate reasoning. Eligible study designs were described. Study selection was performed by 2 reviewers independently and disagreements were resolved with consensus during a meeting. Data extraction was also performed by 2 reviewers independently, and cross verified by a third reviewer. | It is unclear if the review methods were established before the conduct of the review. The comparator was not clearly stated. A list of excluded studies with justifications for exclusion was not provided. Authors did not report whether they received funding for the systematic review. The authors did not declare whether they had potential conflicts of interest. |
McPherson et al. (2022)18 | |
The aim of the review was clearly stated. The population, intervention, and outcomes of interest were clearly stated. The search was conducted in multiple databases, key search terms were provided, and reference lists of selected publications were hand-searched for additional relevant studies. Search was conducted within 24 months of publication. Study selection was performed by 3 reviewers independently and disagreements were resolved with consensus during a meeting. Authors declared that they did not receive funding for this work and that there were no conflicts of interest. | The comparator was not clearly stated. It is unclear if the review methods were established before the conduct of the review. Authors did not provide justification for eligible study designs. Trial registries and grey literature were not searched. Authors did not provide justification for restricting to studies published in English. A list of excluded studies with justifications for exclusion was not provided. |
Xu et al. (2022)19 | |
The aim of the review was clearly stated. The population, intervention, and outcomes of interest were clearly stated. An explicit statement was provided that the review methods were established before the conduct of the review (registered in PROSPERO). The search was conducted in multiple databases, the search strategy was provided. The search was conducted within 24 months of publication. Study selection was performed by 2 reviewers independently, and any disagreements were resolved through a consensus-based discussion between 2 reviewers. The authors reported their funding source and declared that there were no conflicts of interest. | The comparator was not clearly stated. The authors did not provide justification for having no restriction on eligible study designs. Authors did not provide justification for restricting to studies published in English. Trial registries and grey literature were not searched. A list of excluded studies with justifications for exclusion was not provided. |
Zhen et al. (2022)20 | |
The aim of the review was clearly stated. The population, intervention, and outcomes of interest were clearly stated. The inclusion and exclusion criteria for study eligibility were appropriate for the research question. The search was conducted in multiple databases and trial registries, and key search terms were provided. Search was conducted within 24 months of publication. Two authors independently selected studies for inclusion and extracted the data from included studies. The authors reported their funding source and declared that there were no conflicts of interest. | It is unclear if the review methods were established before the conduct of the review. The comparators of interest was not clearly stated. Trial registries and grey literature were not searched. A bibliographic search for additional relevant literature was not done. A list of excluded studies with justifications for exclusion was not provided. |
Barba et al. (2019)21 | |
The aim of the review was clearly stated. The population, intervention, and outcomes of interest were clearly stated. Authors reported that the inclusion criteria were established a priori. Authors provide the full search strategy in a supplemental appendix. Search was conducted within 24 months of publication. | The comparator was not clearly stated. It was unclear all review methods were established before the conduct of the review (e.g., review questions, search strategy). Authors did not provide justification for eligible study designs. The search was conducted in only 1 database. Trial registries and grey literature were not searched. Authors did not provide justification for restricting to studies published in English and French. It was unclear if study selection was performed by a sole reviewer or in duplicate. A list of excluded studies with justifications for exclusion was not provided. Authors did not report whether they received funding for the systematic review. The authors did not declare whether they had potential conflicts of interest. |
Systematic reviews of guidelines | |
Meyer et al. (2018)22 | |
The aim of the review was clearly stated. The research questions and inclusion criteria for the review included components of population, intervention, and outcomes of interest. They were appropriate for the review objective. The “clinical practice guidelines” were defined clearly as on in which systematic review of evidence and assessment of benefits and harm was conducted. Where methods of evidence search were unclear, it was clearly noted in the review. The search was conducted in multiple databases, key search terms were provided, and reference lists of selected publications were hand-searched for additional relevant studies. Search was conducted within 24 months of publication. Study selection was performed by 2 reviewers independently and disagreements were resolved with discussion. The authors reported their funding source and declared that there were no conflicts of interest. | It was unclear all review methods were established before the conduct of the review. Detailed characteristics of the included guidelines, such as guideline development organization, country, or the guideline development methodology used were not reported. It was unclear whether a quality assessment of the include guidelines were conducted. Strength of each recommendation statement from included guidelines and the supporting evidence were not reported. |
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2.
Table 5: Strengths and Limitations of Guidelines Using AGREE II15
Item | British Society for Rheumatology Guideline (2022)10 | Romero-Bueno et al. (2020)23 |
|---|---|---|
Domain 1: Scope and purpose | ||
1.The overall objective(s) of the guideline is (are) specifically described. | Yes | Yes |
2.The health question(s) covered by the guideline is (are) specifically described. | Yes | Yes |
3.The population (patients, public, etc.) to whom the guideline is meant to apply is specifically described. | Yes | Yes |
Domain 2: Stakeholder involvement | ||
4.The guideline development group includes individuals from all relevant professional groups. | Yes | No |
5.The views and preferences of the target population (patients, public, etc.) have been sought. | Yes, patient and caregiver input were sought | No |
6.The target users of the guideline are clearly defined. | Yes | No, but implied |
Domain 3: Rigour of development | ||
7.Systematic methods were used to search for evidence. | Yes | Yes |
8.The criteria for selecting the evidence are clearly described. | No | Yes |
9.The strengths and limitations of the body of evidence are clearly described. | Quality of evidence was assessed, but not reported in the publication | Yes |
10.The methods for formulating the recommendations are clearly described. | Yes | Yes |
11.The health benefits, side effects, and risks have been considered in formulating the recommendations. | Partially | Yes |
12.There is an explicit link between the recommendations and the supporting evidence. | Partially | Partially |
13.The guideline has been externally reviewed by experts before its publication. | Unclear | Yes |
14.A procedure for updating the guideline is provided. | Yes | No |
Domain 4: Clarity of presentation | ||
15.The recommendations are specific and unambiguous. | Yes | Yes |
16.The different options for management of the condition or health issue are clearly presented. | Yes | Yes |
17.Key recommendations are easily identifiable. | Yes | Yes |
Domain 5: Applicability | ||
18.The guideline describes facilitators and barriers to its application. | Yes, no barriers were identified | No |
19.The guideline provides advice and/or tools on how the recommendations can be put into practice. | Yes | No |
20.The potential resource implications of applying the recommendations have been considered. | No | No |
21.The guideline presents monitoring and/or auditing criteria. | Yes | No |
Domain 6: Editorial independence | ||
22.The views of the funding body have not influenced the content of the guideline. | Unclear | Unclear |
23.Competing interests of guideline development group members have been recorded and addressed. | Yes | No |
AGREE II = Appraisal of Guidelines for Research and Evaluation II.
Appendix 4: Main Study Findings
Note that this appendix has not been copy-edited.
Table 6: Summary of Recommendations in Included Guidelines
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
|---|---|
British Society for Rheumatology Guideline, (2022) 10 | |
Severe and/or refractory muscle inflammation (myositis) | |
IVIGa | Strong recommendation based on moderate (B) quality evidence. Strength of agreement: 100% |
Rituximabb (particularly in juvenile-onset disease, patients with a positive myositis autoantibody profile, or patients with lower burden of disease damage) Note: The guideline authors noted that rituximab and IVIG are options for the management of active IIM (e.g., myositis, dysphagia, refractory skin disease) resistant to glucocorticoid or csDMARD based immunosuppression. In England, rituximab and IVIG can only be prescribed in conjunction with a specialist centre. | Conditional recommendation based on high (A) quality evidence. Strength of agreement: 100% |
Cyclophosphamidec | Strong recommendation based on moderate (B) quality evidence. Strength of agreement: 100% |
Abataceptd (for refractory adult IIM) | Conditional recommendation based on moderate (B) quality evidence. Strength of agreement: 100% |
Refractory skin manifestations | |
Rituximabe | Conditional recommendation based on moderate (B) quality evidence. Strength of agreement: 100% |
IVIGf Authors’ note: Evidence is limited in terms of treatment of IIM related skin manifestations. However, studies indicate the effectiveness of both IVIG and rituximab in treating skin manifestations refractory to steroids or csDMARDS. (details of studies NR) Nailfold capillary abnormalities in pediatric patients with IIM can reflect systemic disease activity. This should be considered in management. | Strong recommendation based on moderate (B) quality evidence. Strength of agreement: 100% |
Chronic ILD associated with IIM | |
Note: Authors did not make a recommendation for or against IVIG for the management of Chronic ILD associated with IIM. | Conditional recommendation based on low quality (C) evidence. Strength of agreement: 100% |
Romero-Bueno et al. (2020)23 | |
For refractory patients with IIM associated RP-ILD | — |
In patients with CADM-associated RPILD anti-MDA5 (+) who do not respond to combination therapy with glucocorticoids plus immunosuppressive drugs, consider adding cyclophosphamidei, mycophenolate mofetilj, rituximabk, basiliximabl, or tofacitinibm to the current therapy. | Level of evidence: 3 Grade of recommendation: D (based on non-analytical studies and expert opinion) |
Change one immunosuppressant for anothern | Level of evidence: NA Grade of recommendation: Based on expert opinion and consensus of the editorial team. |
In patients who are not responding to combined immunosuppressive drugs, use of alternate rescue therapies (either separate or sequential), consider | — |
Polymyxin B hemoperfusiono | Level of evidence: 3 Grade of recommendation: D (based on non-analytical studies and expert opinion) |
Plasmapheresisp | Level of evidence: 3 Grade of recommendation: D (based on non-analytical studies and expert opinion) |
IVIGq | Level of evidence: NA Grade of recommendation: Based on expert opinion and consensus of the editorial team. |
“Azathioprine, methotrexate and leflunomide are not recommended for the treatment of RPILD associated to anti- MDA5.”23 (p.778)r | Level of evidence: NA Grade of recommendation: Based on expert opinion and consensus. |
CADM = clinically amyopathic dermatomyositis; CsDMARDS = Conventional synthetic disease-modifying antirheumatic drugs; DMARD = disease-modifying antirheumatic drugs; IIM = idiopathic inflammatory myopathies; IVIG = IV immunoglobulin; MDA-5 = antimelanoma differentiation-associated gene 5; NA = not applicable; NRS = nonrandomized study; RCT = randomized controlled trial; RPILD = rapidly progressing ILD.
aEvidence from 4 studies. Additionally, findings from an RCT showed that IVIG is effective in patients with treatment resistant IIM. Additional details NR.
bEvidence from 1 RCT (2 publications) and 2 NRS. Additional details NR
cEvidence from 4 studies. Additional details NR. IV cyclophosphamide has fewer side effect compared to oral route, with lower risks of leucopenia, hemorrhagic cystitis, and gonadal toxicity.
dEvidence from one prospective delayed-start study. Additional details NR.
eEvidence from 1 RCT. Additional details NR.
fEvidence from 3 studies. Additional details NR.
gAzathioprine- 4 studies, tacrolimus or ciclosporin - 12 studies, mycophenolate – 2 studies
hRituximab – 3 studies, cyclophosphamide – 11 studies; Additional details NR.
iNR
jevidence from 1 case report, in which patient improved after adding mycophenolate.
kAcross 9 case reports or case series, 5 out of 13 refractory patients improved after adding rituximab to standard immunosuppression, although in one case there was no lung improvement.
lEvidence from 1 case series (4 patients who were resistant to prednisone, cyclosporine, and IVIG. 3 out of 4 patients improved with adding basiliximab.
mEvidence from 1 case report (responsive to add-on tofacitinib) and 1 case series (3 out of 5 patients survived after adding tofacitinib. Adverse events: infections.
nsupporting evidence NR. One patient (case report) died despite switching from cyclosporine to tacrolimus (additional details NR)
oEvidence from NRS, case series and case reports showed that 5 out of 14 anti MDA5 RPILD patients who received polymyxin B hemoperfusion survived.
pEvidence from 10 patients who received plasmapheresis in addition to immunosuppressive therapy or polymyxin hemoperfusion. 2 of those 10 patients survived.
qAuthors noted that there is insufficient data to support IVIGs as a direct therapy for anti MDA5 positive RP-ILD associated with DM, expert panel agreed on considering IVIG as an adjuvant treatment.
rEvidence from case reports and case series informed this recommendation. In all identified studies, azathioprine was given with or without other immunosuppressants with inconsistent results. Methotrexate were given to less than 7 patients and were given in combination with other immunosuppressants. Therefore, the authors noted that even though all 7 patients had a “good clinical course”, an evaluation of the effect of methotrexate was difficult. Evidence for leflunomide was from a case series of 7 patients, in all of whom concurrent immunosuppressants and Chinese herbs, and IVIG were given. Authors also noted that the role of leflunomide was difficult to evaluate.
Table 7: Summary of Recommendations in Included Systematic Review of Guidelines
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
|---|---|
Meyer et al. (2018)22 | |
Systematic review of clinical practice guidelines on the management of IIM. One relevant evidence-based guideline, Enders et al., (2017), on the treatment of juvenile IIM was identified. Relevant recommendation “Juvenile IIMs treatment includes:
Summary of evidence: NR | Evidence grade: NR Strength of recommendation: NR |
CS = corticosteroids; CsA = ciclosporin; CYC = cyclophosphamide; IIM = idiopathic inflammatory myopathies; IVIG = IV immunoglobulin; MMF = mycophenolate mofetil; MTX = methotrexate; NR = not reported; RTX = rituximab.
Appendix 5: References of Potential Interest
Note that this appendix has not been copy-edited.
Additional CADTH Reports
CADTH. Alternative Therapies to Immunoglobulin for Guillain-Barré Syndrome. Ottawa: CADTH; 2023. https://www.cadth.ca/alternative-therapies-immunoglobulin-guillain-barre-syndrome Accessed 22 May 2023.
CADTH. Alternative Therapies to Immunoglobulin for Multifocal Motor Neuropathy. Ottawa: CADTH; 2023. https://www.cadth.ca/alternative-therapies-immunoglobulin-multifocal-motor-neuropathy Accessed 22 May 2023.
Guidelines and Recommendations
Hinze CH, Oommen PT, Dressler F, et al. Development of practice and consensus-based strategies including a treat-to-target approach for the management of moderate and severe juvenile dermatomyositis in Germany and Austria. Pediatr Rheumatol Online J. 2018;16(1):40. PubMed
Koo SM, Kim SY, Choi SM, Lee HK. Korean Guidelines for Diagnosis and Management of Interstitial Lung Diseases: Part 5. Connective Tissue Disease Associated Interstitial Lung Disease. Tuberc Respir Dis (Seoul). 2019;82(4):285-297. PubMed
Systematic Review – Irrelevant Outcomes
Tang K, Zhou J, Lan Y, Zhang H, Jin H. Pregnancy in adult-onset dermatomyositis/polymyositis: A systematic review. Am J Reprod Immunol. 2022;88(5):e13603. PubMed
Protocol
Raaphorst J, Gullick NJ, Pipitone N, Shokraneh F, Brassington R, Ali SSasha, Gordon PA. Immunosuppressive and immunomodulatory therapies for idiopathic inflammatory myopathies (Protocol). Cochrane Database of Systematic Reviews 2023, Issue 1. Art. No.: CD014510.
Review Articles
Pipitone N, Salvarani C. Up-to-date treatment and management of myositis. Curr Opin Rheumatol. 2020;32(6):523-527. PubMed
Chen KL, Zeidi M, Werth VP. Recent Advances in Pharmacological Treatments of Adult Dermatomyositis. Curr Rheumatol Rep. 2019;21(10):53. PubMed
Natour AEH, Kivity S. Biological Therapies in Inflammatory Myopathies. Rambam Maimonides Med J 2023;14 (2):e0008. PubMed
Contributors: Elizabeth Carson, Farhana Shivji
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for noncommercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca