CADTH Health Technology Review
Liraglutide for Pediatric Patients With Type 2 Diabetes
Rapid Review
Authors: Kellee Kaulback, Melissa Walter
Abbreviations
BMI
body mass index
CI
confidence interval
FPG
fasting plasma glucose
GLP-1
glucagon-like peptide-1
A1C
hemoglobin A1C
SD
standard deviation
T2D
type 2 diabetes
Key Messages
While metformin is the treatment of choice for most children and adolescents with type 2 diabetes, along with lifestyle interventions such as diet and exercise, approximately half of youth with type 2 diabetes fail to maintain glycemic control when treated with metformin, either alone or in conjunction with lifestyle interventions.
Basal insulin can be used in children and adolescents with type 2 diabetes who do not have an adequate response to metformin monotherapy; however, basal insulin therapy has been associated with weight gain and hypoglycemia.
There is very limited evidence of moderate to moderately high-quality to support the effectiveness of liraglutide (Victoza) in attaining glycemic control when added to treatment with metformin, with or without basal insulin, in children and adolescents with type 2 diabetes.
Adverse events, such as hypoglycemia and gastrointestinal issues, are reportedly higher in patients receiving liraglutide (Victoza) than in those receiving placebo.
There is a lack of long-term safety data evaluating the use of liraglutide (Victoza) in children and adolescents with type 2 diabetes.
Context and Policy Issues
The incidence of type 2 diabetes (T2D) in children and adolescents is increasing worldwide, with a reported incidence in Canada estimated at 1.54 per 100,000 per year.1 T2D onset in youth can result in earlier and more serious long-term complications than T2D in adulthood, including macrovascular complications such as myocardial infarction, cerebral stroke, and other conditions such as amputation and end-stage renal disease.2
Along with lifestyle interventions, such as diet and exercise, metformin is the treatment of choice for most children and adolescents with T2D.3 However, approximately half of youth with T2D fail to maintain glycemic control when treated with metformin alone or in conjunction with lifestyle interventions.4 Basal insulin can be used in youth who do not have an adequate response to metformin monotherapy; however, insulin therapy has been associated with weight gain and hypoglycemia.4,5
In cases where metformin monotherapy fails to maintain glycemic control, glucagon-like peptide-1 (GLP-1) agonists can be added to ongoing treatment. Liraglutide (Victoza) is a GLP-1 agonist indicated in adults, adolescents, and children aged 10 years and older with T2D, as an adjunct to metformin with or without basal insulin, when diet and exercise plus the maximal tolerated dose of metformin do not achieve adequate glycemic control.6 There are no alternative metformin adjuncts to liraglutide for glucose control in children and adolescents currently approved in Canada.7 Liraglutide is also available under the brand name Saxenda, but this is a higher dose indicated for weight management in adults and certain youth aged 12 to younger than 18.8 Saxenda is not indicated for glycemic control and hence is out of scope for this review.
CADTH previously reviewed Liraglutide in 2011 for adults, where it received a do not list recommendation, and in 2016, a manufacturer resubmission for a reimbursement review was withdrawn.9,10 Since then, data on pediatric populations has become available, and Heath Canada has studied and approved liraglutide for pediatric use.
The objective of this review is to evaluate the clinical effectiveness of liraglutide (Victoza) for pediatric patients with T2D, alone or in combination with metformin, with or without basal insulin, as compared with standard of care (i.e., basal insulin, metformin, diet and exercise, alone or in combination) or placebo with or without standard of care.
Research Question
What is the clinical effectiveness of liraglutide for pediatric patients with type 2 diabetes?
Methods
Literature Search Methods
An information specialist conducted a literature search on key resources including MEDLINE, Embase, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concepts were liraglutide, type 2 diabetes, and children/pediatrics. Conference abstracts were excluded. The search was completed on June 12, 2023 and limited to English-language documents published since January 1, 2013.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Pediatric patients with type 2 diabetes |
Intervention | Liraglutide up to 1.8 mg per day, alone or in combination with metformin, with or without basal insulin |
Comparator | Standard of care (i.e., insulin, metformin, diet and exercise, alone or in combination) or placebo with or without standard of care |
Outcomes | Clinical benefits (e.g., glycemic control, health-related quality of life, changes in insulin requirements, change in weight, treatment duration) and harms (e.g., hypoglycemic events, adverse events, pancreatitis) |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, nonrandomized studies |
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications or were published before 2013. Systematic reviews/meta-analyses without separate presentations of liraglutide outcomes were excluded, as were systematic reviews that included partial results from just 1 liraglutide study (the individual study, Tamborlane et al.,3 was included in this report). Liraglutide (Saxenda) studies were excluded, as were studies that evaluated liraglutide against other GLP-1 agents. Case reports, in vitro and animal studies, and narrative reviews were also excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the Downs and Black checklist11 for measuring study quality as a guide. Summary scores were not calculated for the included studies; rather, each publication's strengths and limitations were described narratively.
Summary of Evidence
Quantity of Research Available
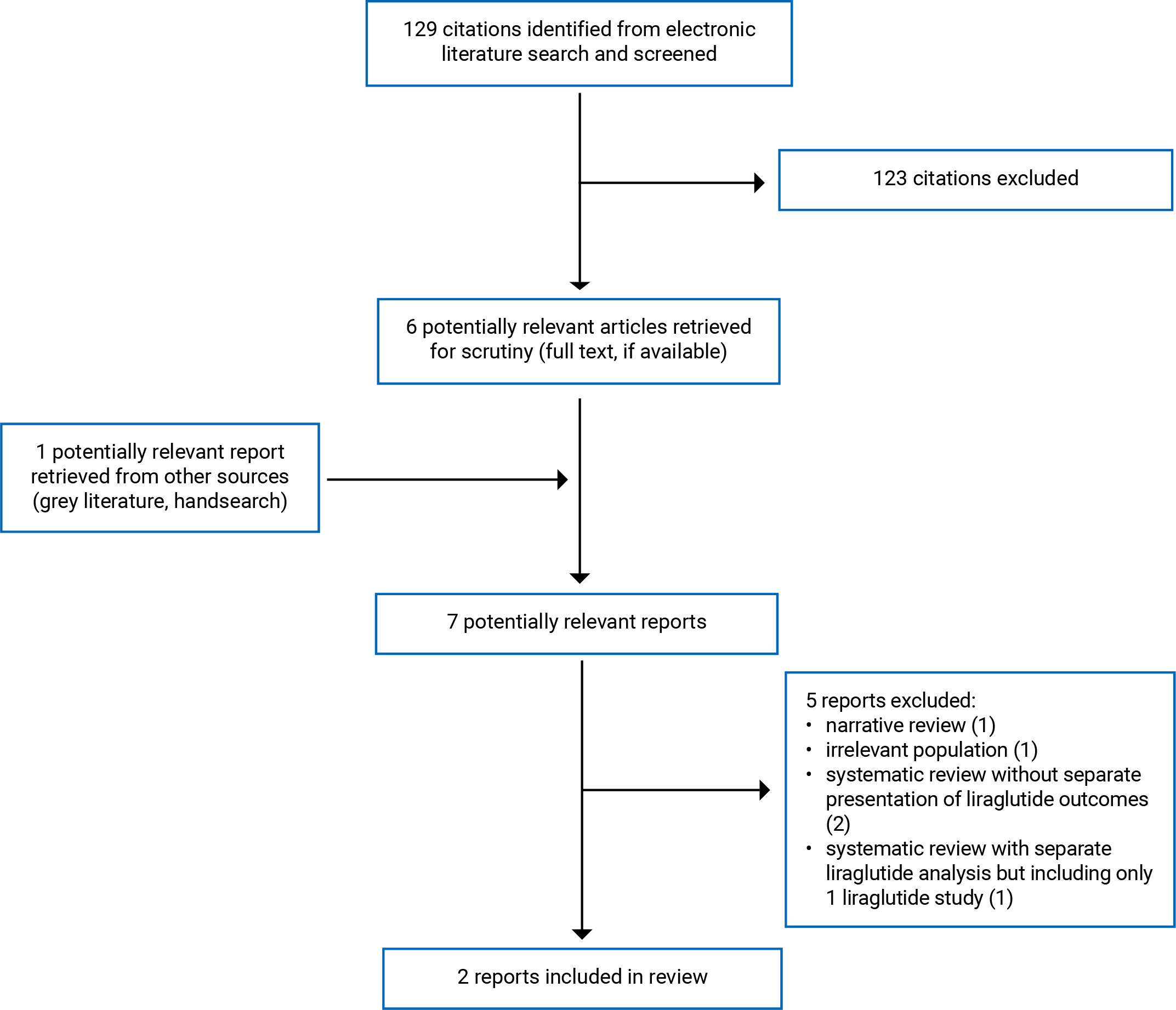
A total of 129 citations were identified in the literature search. Following the screening of titles and abstracts, 123 citations were excluded and 6 potentially relevant reports from the electronic search were retrieved for full-text review. One potentially relevant publication was retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 5 publications were excluded for various reasons, and 2 publications met the inclusion criteria and were included in this report. These comprised 2 randomized controlled trials (RCTs).3,4 Appendix 1 presents the PRISMA12 flow chart of the study selection.
Additional references of potential interest are provided in Appendix 5.
Summary of Study Characteristics
Additional details regarding the characteristics of included publications are provided in Appendix 2.
Two RCTs were identified that met the inclusion criteria.3,4 One systematic review which included liraglutide along with several other glucose-lowering agents, was excluded because it reported partial results of 1 of the RCTs3 that met our inclusion criteria.5 One meta-analysis13 and 1 network meta-analysis14 were excluded because they made additional comparisons of glucose-lowering medications beyond those of interest in the current report.
Study Design
There were 2 RCTs identified that evaluated liraglutide compared with placebo, 1 published in 20144 and 1 published in 2019.3 Both were randomized, parallel-group, placebo-controlled trials, with 1 of the RCTs3 having a 26-week double-blind period followed by a 26-week open-label extension period. The other RCT had a 5-week follow-up.4
Country of Origin
One RCT with a US-based lead author was conducted across 84 sites in 25 countries, with the majority of participants coming from the US, Mexico, Russia, and Israel.3 The other RCT also had a US-based lead author, and was conducted across 16 sites in 4 countries (the US, UK, Slovenia, and Belgium).4
Patient Population
The RCT by Tamborlane et al3 included youth with T2D between 10 and 17 years of age (at randomization), with a hemoglobin A1C (A1C) of 7% to 11% if treated with diet and exercise only or A1C of 6.5% to 11% if treated with metformin with or without basal insulin, with a BMI greater than the 85th percentile (age- and sex-matched population as reference). Eligible patients entered an 11-to-12-week pretrial run-in period during which metformin was increased to the maximum tolerated dose between 1,000 mg and 2,000 mg per day, for at least 8 weeks for all participants. Of the 134 study participants (liraglutide: n = 66, placebo: n = 68) the mean age was 14.6 years (standard deviation [SD] 1.7), with a mean BMI z score of 2.9 (SD 1.3). As per the study details, mean weight was 91.5 kg (SD 26.8), and 83 were classified as female (61.9%). Within the RCT, it was noted that 3 of the participants were American Indian or Alaska Native (2.2%), 39 (29.1%) were Hispanic or Latino, 18 were Asian (13.4%), 16 were Black (11.9%), 87 were white (64.9%), and 10 (7.5%) were classified as other. The mean duration of T2D was 1.9 years (SD 1.5). The mean A1C was 7.8% (SD 1.3), and the mean fasting plasma glucose (FPG) was 8.4 mmol/L (SD 2.5). The mean systolic and diastolic blood pressure (mmHg) was 116.8 (SD 11.8) and 72.2 (SD 8.1), respectively. Mean metformin use at baseline was 1,894 mg/day (SD 339), and insulin was used at baseline by 25 (18.7%) participants. No significant differences between intervention and control groups were reported at baseline.
The RCT by Klein et al4 included participants with T2D who were 10 to 17 years of age, with a BMI of more than the 85th percentile for age and gender, treated with diet and exercise alone or in combination with a stable dose of metformin for at least 4 weeks before screening. At baseline, metformin was being used by 11 participants in the liraglutide arm and by 5 participants in the placebo arm. The mean age of the 21 included study participants (liraglutide: n = 14, placebo: n = 7) was 14.8 (SD 2.2) years, with 3 participants under 12 years of age. The majority of participants were white, female, and postpubertal. The mean baseline body weight was 113.2 kg (SD 35.6, range 57 to 214), body mass index (BMI) was 40 kg/m2 (range 29.2 to 71.6 kg/ m2), and the mean BMI z scores were 3.41 for liraglutide and 3.38 in the placebo group at baseline. The mean duration of T2D was 1.7 years (SD 1.4). The mean A1C level was 8.1% (SD 1.2%), and 76% of participants had been previously treated with metformin and continued the regimen unchanged during the trial. Demographic and baseline characteristics were generally similar between groups except for baseline mean A1C, which was slightly higher (8.3%) in the liraglutide group compared with the placebo group (7.8%). In terms of ethnicity/race, 3 participants (14.3%) were Hispanic or Latino, 16 were described as not being Hispanic or Latino, 14 (67%) were described as white, and 7 (33.3%) were described as Black or African American. Patients treated with basal insulin at baseline were excluded from participation in the study.
Interventions and Comparators
The RCT by Tamborlane et al3 evaluated metformin combination therapy with subcutaneous liraglutide (≤ 1.8 mg per day) compared to metformin with placebo (in a visually identical prefilled pen injector with the same procedure as the liraglutide group).3 The liraglutide was administered subcutaneously at 0.6 mg/day, escalated in approximately 0.6 mg/week increments over 2 to 3 weeks, followed by a maintenance period to a maximum of 1.8 mg/day. Dose adjustment was made based on side effects and the efficacy of low doses. Most patients did not receive the maximum dose of liraglutide or placebo because the FPG level was less than 6.1 mmol/L (110 mg/dL). At the end of week 3, a total of 55.6% of the patients in the liraglutide group and 72.7% in the placebo group reached the 1.8-mg dose equivalent. Throughout the remainder of the trial, doses in both groups remained relatively stable. After 26 weeks, there was a further 26-week open-label extension period with participants in the liraglutide group continuing assignment and participants in the placebo group remaining on metformin/insulin only. Diet and exercise counselling was provided at several visits.
The RCT by Klein et al4 randomized eligible participants in a 2:1 ratio to once-daily subcutaneous injections of either liraglutide or placebo., either as monotherapy (n = 5), or in combination with metformin (n = 16). Liraglutide treatment was initiated with 0.3 mg daily during the first week and increased weekly to 0.6 mg, 0.9 mg, 1.2 mg, and 1.8 mg, for a total of 5 weeks of treatment. Drug dose was not increased if FPG (average of measurements on 3 consecutive days) was less than 6.1 mmol/L, and participants whose dose was not escalated to the next higher 1 continued on the highest dose attained for the remainder of the trial. Nine of the 14 participants receiving liraglutide reached the highest dose (1.8 mg), and doses were not escalated for 4 participants who did not meet the FPG-based dose escalation criterion. These 4 participants received either liraglutide 0.3 mg (n = 1) or 0.6 mg (n = 3) for the remainder of the trial. The liraglutide dose was not escalated in 1 other participant because of early withdrawal. All participants in the placebo group were escalated to the 1.8 mg dose equivalent.
Outcomes
Indicators of Glycemic Control
A1C Levels
The A1C levels, as well as the estimated mean treatment difference between liraglutide and placebo groups, was reported for both RCTs.3,4 The Tamborlane et al3 RCT also reported the number of participants who attained A1C levels of less than 7%.
FPG Levels
The estimated mean treatment difference between the liraglutide and placebo groups for FPG levels was reported in both RCTs.
Rescue Insulin Requirement
One RCT reported the need for insulin administration to maintain acceptable glycemic control.3
BMI Z Score and/or Weight Gain or Loss
Mean body weight was reported for both RCTs,3,4 and BMI z scores were reported for 1 RCT.3
Adverse Events, Including Hypoglycemic Episodes
For both RCTs, adverse events, including serious adverse events, were assessed throughout the trial, and hypoglycemic episodes were classified according to the Novo Nordisk and American Diabetes Association definitions.
Safety and Tolerability Parameters
Both RCTs evaluated safety and tolerability parameters.3,4 Tamborlane et al3 evaluated fasting lipid levels, systolic and diastolic, blood pressure, lipase, amylase, and calcitonin levels, at baseline and during the trial with standard laboratory tests. Klein et al4 conducted laboratory tests, including biochemistry, hematology, urinalysis, calcitonin, amylase, lipase, fasting lipids, vital signs, physical examination, electrocardiogram, fundoscopy, and antiliraglutide antibodies), along with a range of biomarkers and hormones.
Summary of Critical Appraisal
One of the included RCTs3 was of moderately high quality when appraised using the domains detailed in the Downs and Black checklist.11 The other RCT by Klein et al4 was of moderate quality. In the domain of Reporting, both RCTs were well reported, including a clearly stated objective and outcomes; the characteristics of the included participants were clearly described, as was the distribution of potential confounders, and the treatment and placebo were described (Klein et al4 did not describe the placebo in detail but did mention dose escalation of the placebo). The main findings are clearly described, and the investigators have presented SDs and confidence intervals where required. Adverse events were comprehensively measured and reported, characteristics of patients lost to follow-up were reported where it occurred, and actual P values were reported.
In the domain of External Validity, neither RCTs described the source population for the included participants, nor described whether the subjects who were prepared to participate were representative of the entire population from which they were recruited, nor did they describe whether the staff, places, and facilities where the patients were treated, representative of the treatment the majority of patients receive. However, the RCTs were both multicentre from multiple countries, suggesting considerable variation in populations and processes, which would, therefore, likely capture a more real-world variability in treatment, increasing the generalizability of the findings. A detailed list of exclusion criteria was presented in the Tamborlane et al3 RCT, potentially limiting generalizability of findings to the general T2D population, and the Klein et al4 group excluded potential participants that were using basal insulin at baseline. The Klein et al4 authors also included 5 participants not using metformin at baseline. Due to external validity issues for both RCTs, there may be some concerns regarding the generalizability of findings.
Both RCTs performed well in the Internal Validity (Bias) domain. Study participants were blinded to the intervention, outcome assessors were blinded (assumed as the 2 RCTs are described as double-blind), there were no unplanned subgroup analyses, and follow-up was described as being at the same time point for all participants in both RCTs. Statistical tests used to evaluate outcomes were appropriate in both RCTs, and the outcome measures used are clearly described and considered valid. One RCT4 reported a suspected (but not confirmed) case of noncompliance, while the other RCT3 reported equal noncompliance in both treatment arms (n = 4 in each group).
In the domain of Internal Validity (Confounding), neither of the included RCTs provided information concerning the source of patients included in the study, but they did appear to be recruited over the same period of time. In both RCTs, study participants were randomized to treatment groups, but concealment allocation was not described. There appeared to be adequate adjustment for confounding in both RCTs, and loss to follow-up was addressed.
In the Power domain, only Tamborlane et al.3 provided a power calculation, suggesting that the RCT had sufficient power to detect a clinically important effect not due to chance alone. A power calculation was not performed in the Klein et al.4 RCT, which had a relatively small study population, N = 21, allowing for the possibility that any observed clinical effect may have been due to chance.
Both RCTs were at least partially funded by the manufacturer of liraglutide. Also, due to recruitment challenges, both RCTs made amendments to the protocols after the study started.
Overall, there were just 2 RCTs evaluating liraglutide in the pediatric and adolescent population, and the quality of the 2 RCTs was assessed to be of moderate4 to moderately high3 quality, with external validity concerns potentially affecting the generalizability to the general population of children and adolescents with T2D.
Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
Summary of Findings
Appendix 4 presents the main study findings.
A1C and FPG
Two RCTs were identified that evaluated the effectiveness of liraglutide as compared with placebo in children and adolescents with T2D, with 1 RCT reporting follow-up at 5 weeks (N = 19),4 and the other RCT3 (N = 135) reporting follow-up at 26 weeks, and then again at 52 weeks (open-label for the second half of study). Both authors reported on indicators of glycemic control, such as A1C and FPG. Both RCTS reported statistically significant reductions in A1C levels in the liraglutide group compared to the group receiving placebo, with A1C levels either remaining stable or increasing in the placebo group. One RCT reported that participants attained statistically significant A1C levels of less than 7% compared to the placebo group.3 For FPG, 1 RCT reported a statistically insignificant improvement from baseline in the liraglutide group compared to the placebo group.4 The second RCT reported statistically significant reductions in FPG levels in the liraglutide group and increases in FPG levels in the placebo group.3 One RCT reported that a greater number of participants in the liraglutide group were able to finish the study without the use of rescue insulin to ensure acceptable glycemic control as compared with the placebo group at both 26 weeks (86.4% versus 66.7%) and 52 (71.2% vs. 50.7%) weeks (statistical significance not reported).3
BMI Z Score and Weight
The included RCTs3,4 reported minor reductions in mean body weight in both the liraglutide and placebo groups. The weight loss was maintained in the liraglutide group only (at week 52) as compared with the placebo group in 1 RCT (statistical significance not reported), and the same RCT reported an insignificant reduction in BMI z scores at 26 weeks, which subsequently increased at week 52.3
Adverse Events
Adverse events were reportedly higher in the liraglutide group in both of the included RCTs,3,4 with Tamborlane et al3 reporting a relative risk for all adverse events of 1.05. The majority of adverse events reported in both RCTs were gastrointestinal, including nausea, vomiting, and diarrhea. They were mild in severity and resolved quickly. One RCT4 did not report any serious adverse events during the trial, while the Tamborlane et al.3 RCT reported an RR of 2.32 in the liraglutide group for serious adverse events (9 serious events reported in the liraglutide group versus 4 in the placebo group). The serious adverse events in the liraglutide participants were described as follows: neck abscess, viral infection, hyperglycemia, abdominal pain, diarrhea, vertigo, scoliosis, A1C increase.
Hypoglycemic events were reportedly higher in the liraglutide arm than in the placebo arm for both of the included RCTs using either the Novo Nordisk classification or the American Diabetes Association classification (note Tamborlane et al3 did not report separate values for the Novo Nordisk classifications). The RR of a hypoglycemic event (both documented symptomatic and asymptomatic) in the liraglutide group was 1.82 in 1 RCT which reported an RR.3
Safety and Tolerability Parameters (Laboratory Tests to Evaluate Thyroid and Pancreatic Function)
Both RCTs reported no statistically significant changes in safety parameters. While amylase and calcitonin remained within the normal range for the study populations in both RCTs, and the majority of patients did not have elevated lipase levels, there were higher lipase levels reported in both RCTs for the liraglutide group as compared with the placebo group. The authors of the Klein et al4 RCT reported that the clinical significance of the elevated lipase levels observed in some participants was unknown. No significant changes were reported in either RCT for other safety and tolerability parameters and tests, such as very-low-density lipoprotein cholesterol levels, triglyceride levels, and systolic and diastolic blood pressure.
Limitations
There is a limited amount of evidence evaluating liraglutide in children and adolescents. There are 2 RCTs3,4 evaluating liraglutide for glycemic control in the pediatric population, and the study participant numbers for both RCTs are relatively small, particularly in the Klein et al4 RCT that had 14 participants in the liraglutide arm. The small study populations also contribute to the observed wider confidence intervals, leading to less confidence in the observed treatment effects. However, the available research is limited because there is a relatively low prevalence of pediatric T2D patients, which impedes recruitment into clinical trials.4,5 The Klein et al4 RCT had a 5-week follow-up period, which brings into question the usefulness of measuring A1C levels, given that A1C reflects average plasma glucose over the previous 8 to 12 weeks.14,15
There is limited data generalizable to Canadian populations. There were 3 patients from 1 Canadian centre included in 1 RCT.3 Most patients included in both RCTs were described as white and female, which means that the data may also not be generalizable to non-white populations and males.
Another limitation is the lack of safety data in children, particularly in the long term since children would be taking medication for a long time. Klein et al.4 had a 5-week follow-up, and the Tamborlane et al.3 RCT had a 52-week follow-up. The authors of both RCTs reported that not all study participants had received the highest dose of liraglutide (1.8 mg), limiting data collection regarding the safety profile of liraglutide. Approximately half the patients in 1 RCT did not receive the highest dose.3 In the other RCT, 9 of 14 participants received the highest dose.4 Karavanaki et al.2 have indicated uncertainties regarding the potential long-term effects of liraglutide on brain and body growth, given a lack of long-term studies in children and adolescents. There are also concerns about the potential for pancreatitis and even pancreatic cancer associated with liraglutide.4,16
The Klein et al4 study did not include participants who were receiving basal insulin at baseline, while the Tamborlane et al3 study included a total of 25 (out of 134) participants who were receiving insulin at baseline. Klein et al4 also included 5 participants who were not receiving metformin therapy at baseline. Hence there is limited evidence for the effectiveness and safety of liraglutide in patients receiving therapy that includes basal insulin and for liraglutide monotherapy (i.e., without metformin).
Conclusions and Implications for Decision- or Policy-Making
While metformin is the treatment of choice for most children and adolescents with T2D, along with lifestyle interventions such as diet and exercise, approximately half of youth with T2D fail to maintain glycemic control when treated with metformin, either alone or in conjunction with lifestyle interventions.3,4 Basal insulin can be used in children and youth who do not respond adequately to metformin monotherapy; however, insulin therapy has been associated with weight gain and hypoglycemia. In cases where metformin monotherapy fails to maintain glycemic control, glucagon-like peptide-1 (GLP-1) agonists can be added. Liraglutide (Victoza) is a GLP-1 agonist indicated in adolescents and children aged 10 years and older with T2D as an adjunct to metformin with or without basal insulin when diet and exercise plus a maximally tolerated dose of metformin do not achieve adequate glycemic control. There are no metformin adjunct alternatives to liraglutide for glucose control in children and adolescents currently approved in Canada.7
There is limited evidence to evaluate the effectiveness of liraglutide alone or when added to treatment with metformin, with or without basal insulin, in children and adolescents. There were 2 RCTs published that evaluated the effectiveness of liraglutide in children and adolescents, 1 of moderate quality with a relatively short follow-up of 5 weeks and a limited number of participants (n = 14 in the liraglutide group),4 and 1 of moderately high quality with follow-up at 26 and at 52 weeks (n = 66 patients in the liraglutide arm).3 Both RCTs reported statistically significant improvements in indicators of glycemic control. In the liraglutide group, both RCTs reported statistically significant improvements in A1C, and 1 RCT3 reported that significantly more patients in the liraglutide arm were able to attain A1C levels of less than 7%. One RCT3 reported significant improvements in FPG levels, while the other RCT4 showed an insignificant trend toward improvement of FPG levels. Neither RCT showed significant improvements in weight loss, and the RCT that reported BMI z scores also reported no significant improvements. However, liraglutide (Victoza) is not indicated for weight loss. One RCT reported that a greater percentage of participants were able to complete the trial without using insulin to attain optimal glycemic control in the liraglutide group (71.2%) than in the placebo group (50.7%).3
Adverse events were higher in the liraglutide group in both of the included RCTs.3,4 The majority of adverse events reported in both RCTs were gastrointestinal, including nausea, vomiting, and diarrhea. They were considered mild in severity and resolved quickly. More serious adverse events were reported in the liraglutide group in 1 RCT,3 and no serious events were reported in the other RCT.4 The percentage of patients who had hypoglycemic episodes and the incidence of hypoglycemia were higher with liraglutide than with placebo in both RCTs. It is widely accepted that GLP-1 receptor agonists do not cause hypoglycemia,17 and Tamborlane et al.18 felt that the observed hypoglycemic events could only be partially explained by the use of insulin during the trial.
There have been postmarketing reports of pancreatitis during T2D treatment with liraglutide, and it is not known whether patients with a history of pancreatitis are at higher risk for developing pancreatitis with liraglutide treatment.4,6 The Tamborlane et al.3 RCT excluded children with a history of pancreatitis; it is unknown if the Klein et al. RCT4 excluded children with a history of pancreatitis. It is worth noting that lipase levels were reportedly higher with liraglutide than with placebo at follow-up for both RCTs, though most participants did not have elevated lipase levels, and no events meeting the diagnostic criteria for pancreatitis occurred. The clinical significance of the elevated lipase levels is unknown.4 There appears to be no evidence for or against the use of liraglutide in children with a history of pancreatitis, and the product monograph cautions that patients given liraglutide be observed carefully for signs and symptoms of pancreatitis. Overall, there is a lack of long-term safety data for using liraglutide in children, and children could be more at risk as they grow and use liraglutide over a long period.16 In the largest RCT to date with the longest follow-up duration of 1 year, only approximately half of the study participants received the maximum dose of liraglutide, limiting data collection relating to the safety profile of liraglutide.3
The available research may not be generalizable to the Canadian population due to a paucity of data in Canadians and limited data for males and non-white individuals. Of the 2 included RCTs, 14 excluded participants receiving basal insulin at baseline, limiting the amount of evidence available to evaluate the effectiveness and safety profile of liraglutide in children and adolescents currently receiving insulin therapy. Finally, 1 of the included RCTs included 5 participants who were not receiving metformin at baseline, which may have affected the trial results and limited the generalizability in patients receiving metformin.
References
1.Spurr S, Bally J, Bullin C, Allan D, McNair E. The prevalence of undiagnosed Prediabetes/type 2 diabetes, prehypertension/hypertension and obesity among ethnic groups of adolescents in Western Canada. BMC Pediatr. 2020;20(1):31. PubMed
2.Karavanaki K, Paschou SA, Tentolouris N, Karachaliou F, Soldatou A. Type 2 diabetes in children and adolescents: distinct characteristics and evidence-based management. Endocrine. 2022;78(2):280-295. PubMed
3.Tamborlane WV, Barrientos-Perez M, Fainberg U, et al. Liraglutide in Children and Adolescents with Type 2 Diabetes. N Engl J Med. 2019;381(7):637-646. PubMed
4.Klein DJ, Battelino T, Chatterjee DJ, et al. Liraglutide's safety, tolerability, pharmacokinetics, and pharmacodynamics in pediatric type 2 diabetes: a randomized, double-blind, placebo-controlled trial. Diabetes Technol Ther. 2014;16(10):679-687. PubMed
5.Diabetes (type 1 and 2) in children and young people: diagnosis and management. [D] Evidence review for glucose-lowering agents for managing blood glucose levels in children and young people with type 2 diabetes. (NICE guideline NG18). London (GB): National Institute for Health and Care Excellence (NICE); 2023: https://www.nice.org.uk/guidance/ng18/evidence/d-glucoselowering-agents-for-managing-blood-glucose-levels-in-children-and-young-people-with-type-2-diabetes-pdf-13060839133. Accessed 2023 Jun 16.
6.Victoza (liraglutide): 6 mg/mL solution for injection in a pre-filled pen [product monograph]. Mississauga (ON): Novo Nordisk Canada Inc.; 2022: https://www.novonordisk.ca/content/dam/nncorp/ca/en/products/victoza-product-monograph.pdf. Accessed 2023 Jun 25.
7.Health Canada. Drug Product Database online query. 2023; https://www.canada.ca/en/health-canada/services/drugs-health-products/drug-products/drug-product-database.html. Accessed 2023 Jul 4.
8.Saxenda (liraglutide): 6 mg/mL solution for injection in a pre-filled pen [product monograph]. Mississauga (ON): Novo Nordisk Canada Inc.; 2022: https://www.novonordisk.ca/content/dam/nncorp/ca/en/products/saxenda-product-monograph.pdf. Accessed 2023 Jun 25.
9.CADTH. CADTH Reimbursement Review: Liraglutide [withdrawn]. 2016; https://www.cadth.ca/liraglutide-0. Accessed 2023 Jul 12.
10.CADTH. CADTH Reimbursement Review: Liraglutide. 2011; https://www.cadth.ca/liraglutide. Accessed 2023 Jul 13.
11.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
12.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
13.Carydias E, Tasho A, Kani C, Bacopoulou F, Stefanaki C, Markantonis SL. Systematic Review and Meta-Analysis of the Efficacy and Safety of Metformin and GLP-1 Analogues in Children and Adolescents with Diabetes Mellitus Type 2. Children. 2022;9(10):18. PubMed
14.Wu S, He Y, Wu Y, et al. Comparative efficacy and safety of glucose-lowering drugs in children and adolescents with type 2 diabetes: A systematic review and network meta-analysis. Front Endocrinol (Lausanne). 2022;13:897776. PubMed
15.Use of Glycated Haemoglobin (HbA1c) in the Diagnosis of Diabetes Mellitus: Abbreviated Report of a WHO Consultation. Geneva (CH): World Health Organization; 2011: https://www.ncbi.nlm.nih.gov/books/NBK304271/. Accessed 2023 Jun 29.
16.Anonymous. Liraglutide (victozadegree) and type 2 diabetes in children aged 10 years and above. Prescrire Int. 2021;30(222):38.
17.Javor E, Skelin M, Lucijanic M. Liraglutide in Children and Teens with Type 2 Diabetes. N Engl J Med. 2019;381(18):1786-1787. PubMed
18.Tamborlane WV, Fainberg U, Barrett T. Liraglutide in Children and Teens with Type 2 Diabetes. Reply. N Engl J Med. 2019;381(18):1787. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Primary Clinical Studies
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Tamborlane et al. (2019)3 Multicentre (US lead author) Funding source: Novo Nordisk; UK Medical Research Council; National Institutes of Health Research (NIHR); Translational Research Collaboration for Rare Diseases; NIHR Wellcome Clinical Research Facility | Double-blind RCT for 26 weeks, followed by a 26-week open-label extension | Mean Age: 14.6 years (SD 1.7) Mean BMI z score: 2.9 (SD 1.3) Mean weight: 91.5 kg (SD 26.8) Gender: 83 (61.9%) were classified as female Ethnicity/Race American Indian or Alaska Native: 3 (2.2%) Hispanic or Latino: 39 (29.1%) Asian: 18 (13.4%) Black: 16 (11.9%) White: 87 (64.9%) Other: 10 (7.5%) Mean duration of T2D: 1.9 years (SD 1.5). Mean A1C: 7.8% (SD 1.3) Mean FPG: 8.4 mmol/L (SD 2.5). Mean systolic and diastolic blood pressure (mmHg): 116.8 (SD 11.8) and 72.2 (SD 8.1) respectively Mean metformin use at baseline: 1,894 mg/day (SD 339) Basal insulin use at baseline: n = 25 (18.7%) | Intervention: liraglutide (n = 66) Comparator: a placebo (n = 68) Dose escalation: Administration of liraglutide was initiated at a dose of 0.6 mg per day, and increased in increments of 0.6 mg per week to a max of 1.8 mgs, based on side effects and efficacy. Doses were not increased if FPG levels were < 6.1 mmol/L. | Outcomes A1C ETD Attainment of A1C levels of < 7%FPG Requirement for insulin rescue Weight BMI z scores Adverse events Safety and tolerability parameters (lipase, amylase and calcitonin, etc.) Follow-up 26 weeks (RCT) 52 weeks (open label) |
Klein et al. (2014)4 Multicentre (US lead author) Funding source: Novo Nordisk | Double-blind RCT | Mean age: 14.8 years (SD 2.2) Gender: 67% female Ethnicity/Race Hispanic or Latino: 3 (14.3%) White 14 (67%) Black or African American: 7 (33.3%) Mean baseline body weight: 113.2 kg (SD 35.6, range 57 to 214) Mean BMI: 40 kg/m2, (range from 29.2 to 71.6 kg/ m2) Mean BMI z scores for liraglutide group: 3.41; placebo: 3.38. Mean duration of T2D: 1.7 years (SD 1.4, range 0.12 to 5.45 years) Mean hemoglobin A1C level: 8.1% (SD 1.2%) Previously treated with metformin: 76% Basal insulin use at baseline: 0 | Intervention: Liraglutide (n = 14) Comparator: Placebo (n = 7) Dose Escalation: Liraglutide treatment was initiated with 0.3 mg daily during the first week and increased weekly to 0.6 mg, 0.9 mg, 1.2 mg, and 1.8 mg unless FPG levels were < 6.1 mmol/L. | Outcomes Adverse events Safety and tolerability parameters A1C ETD FPG Weight Follow-up 5 weeks |
A1C = hemoglobin A1Cl; BMI = body mass index; ETD = estimated treatment difference; FPG = fasting plasma glucose; NR = not reported; RCT = randomized controlled trial; SD = standard deviation; T2D = type 2 diabetes.
aPlacebo in visually identical pen injector.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 3: Strengths and Limitations of Clinical Studies Using the Downs and Black Checklist)11
Strengths | Limitations |
|---|---|
Tamborlane et al. (2019)3 | |
The authors clearly stated the objectives, main outcomes, patient characteristics, distribution of potential confounders, and interventions (treatment and placebo). The main findings were clearly described, with SD, CI and P values provided. Adverse events were comprehensively measured and reported, and characteristics of patients lost to follow-up were reported. Study participants were blinded to intervention. There were no unplanned subgroup analyses, and follow-up was described as being at 26 and 52 weeks for all participants. Statistical tests used to evaluate outcomes seemed to be appropriate and the outcome measures utilized are widely used and considered valid (not described in the RCT). Participants were recruited over the same time period and were randomized to treatment groups. There appeared to be adequate adjustment for confounding, and loss to follow-up was described. Nonadherence was the same in both treatment arms. A power calculation was performed, suggesting that the RCT had sufficient power to detect a clinically important effect not due to chance alone. | It is unclear whether the patients recruited, patients prepared to participate, or the staff, places, and facilities where patients were treated, were representative of the source population. Concealment allocation was not reported. It is not known if outcome assessors were blinded. Partial funding from liraglutide manufacturer Protocol amendment due to recruitment challenges and resulting long recruitment period. |
Klein (2014)4 | |
The authors clearly stated the objectives, main outcomes, patient characteristics, distribution of potential confounders, and interventions (treatment but not placebo). The main findings were clearly described, with SD, CI and p values provided. Adverse events were comprehensively measured and reported, and characteristics of patients lost to follow-up were reported. Study participants were blinded to intervention. There were no unplanned subgroup analyses, and follow-up was described as being at 26 and 52 weeks for all participants. Statistical tests used to evaluate outcomes seemed to be appropriate and the outcome measures utilized are widely used and considered valid (not described in the RCT). There was equal nonadherence in both treatment arms. Participants were recruited over the same time-period and were randomized to treatment groups. There appeared to be adequate adjustment for confounding, and withdrawal from the study was the same in both arms. | It is unclear whether the patients recruited, patients prepared to participate, or the staff, places, and facilities where patients were treated, were representative of the source population. Concealment allocation was not reported. It is not known if outcome assessors were blinded. The placebo was not described. Relatively small sample size No power calculation was performed. Relatively short follow-up period which may not have captured changes in hemoglobin A1C levels in response to treatment (hemoglobin A1C reflects average plasma glucose over the previous 8 to 12 weeks) Protocol amendment due recruitment challenges due to small pool of participants |
CI = confidence interval; SD = standard deviation; RCT = randomized controlled trial.
Appendix 4: Main Study Findings
Note that this appendix has not been copy-edited.
Table 4: Summary of Findings by Outcome — Glycemic Control Parameters, BMI Z Score, and Weight Change
Outcome | Tamborlane et al. (2019)3RCT | Klein et al. (2014)4RCT | |
|---|---|---|---|
26-week follow-up | 52-week follow-up (open label between 26 and 52 weeks) | 5-week follow-up | |
Glycemic control parameters | |||
A1C (mean ETD mmol/mol) | −1.06 (95% CI, −1.65 to −0.46; P < 0.001) | –1.30 (95% CI, –1.89 to –0.70) a | –0.90 (95% CI, –1.36 to –0.45; P = 0.0007) |
Attainment of A1C levels of < 7% | Liraglutide: 63.7% Placebo: 36.5% OR 5.35 (95% CI, 2.10 to 13.61, P < 0.001) | NR | NR |
FPG (mean ETD mmol/mol) | –1.88 (95% CI, –3.09 to –0.66; 0.66; P = 0.002) | –1.81 (95% CI, –3.17 to –0.44) a | –1.44 (95% CI, –3.61 to 0.73; P = 0.1797) |
BMI z score (mean ETD) | –0.05 (95% CI, –0.15 to 0.06; P = 0.39) | –0.18 (95% CI, –0.33 to –0.03) a | NR |
Mean body weight a | Liraglutide: −2.3 kg Placebo: −0.99 kg | Liraglutide: −1.91 kg Placebo: 0.87 kg | Liraglutide: - 0.5 kg Placebo: - 0.5 kg |
Insulin rescue requirement (% completed without need for insulin rescue) | Liraglutide: 86.4% Placebo: 66.7% | Liraglutide: 71.2% Placebo: 50.7% | NR |
CI = confidence interval; ETD = estimated treatment difference; NR = not reported; OR = odds ratio.
Note: ETD is mean change from baseline in the liraglutide group compared to placebo in percentage points.
aSignificance not reported.
Table 5: Summary of Findings by Outcome —Adverse Events, Safety and Tolerability Parameters
Outcome | Tamborlane et al3 | Klein et al4 | ||
|---|---|---|---|---|
Liraglutide (N = 66) | Placebo (n = 68) | Liraglutide (n = 14) | Placebo (n = 7) | |
Adverse events | ||||
Total adverse events | n = 56 (84.8%) 426 events Event rate: 7.144 RR: 1.05 (0.90, 1.22) | n = 55 (80.9%) 321 events Event rate: 5.425 | n = 10 (71.4%) 38 events | n = 3 (42.9%) 18 events |
Serious adverse events | n = 9 (13.6%) experienced 10 events Event rate: 0.168 RR: 2.32 (0.75, 7.16) | n = 4 (5.9%) experienced 5 events Event rate: 0.085 | 0 | 0 |
Hypoglycemiaa | n = 30 (45.5%) 160 events RR: 1.82 (1.11 to 2.97) | n = 17 (25%) 63 events | n = 5 (35.7%) 11 events | n = 1 (14.3%) 1 event |
Gastrointestinal eventsb | ||||
Diarrhea | N = 15 (22.7%) 22 events 1.40 (0.70 to 2.83) | n = 11 (16.2%) 13 events | N = 6 (42.9%) 7 events | n = 1 (14.3%) 1 event |
Nausea | n = 19 (28.8%) 25 events RR: 2.18 (1.06 to 4.46) | n = 9 (13.2%) 12 events | n = 3 (21.4%) 4 events | n = 1 (14.3%) 1 event |
Vomiting | 17 (25.8%) 46 events RR: 2.92 (1.23 to 6.95) | 6 (8.8%) 8 events | 2 (14.3%) 2 events | 2 (28.6%) 3 events |
Safety and tolerability parametersc | ||||
Lipase levels | Treatment ratio in liraglutide vs placebo group: 1.20 (95% CI, 1.08 to 1.32) | Treatment ratio in liraglutide vs placebo group: 1.11 (95% CI, 1.01 to 1.23) | Liraglutided Screening: 25.5 +/− 7.1 U/L Follow-up: 37.5 +/− 18.4U/L | Placebod Screening: 27.1 +/− 12.0 Follow-up: 33.2 +/− 18.5 U/L |
CI = confidence interval; RR = relative risk.
aUsing American Diabetes Association definition.
bTop 3 most frequently reported events.
cAmylase, calcitonin levels, blood pressure and more are not reported here because they were in low to normal range for all participants with no significant differences between groups.
dNormal lipase levels range from: < / = 13 years, < / = 37 U/L; > 13 to 18 years, < / = 46 U/L).
Appendix 5: References of Potential Interest
Systematic Reviews
Diabetes (type 1 and 2) in children and young people: diagnosis and management. [D] Evidence review for glucose-lowering agents for managing blood glucose levels in children and young people with type 2 diabetes. (NICE guideline NG18). London (GB): National Institute for Health and Care Excellence (NICE); 2023: https://www.nice.org.uk/guidance/ng18/evidence/d-glucoselowering-agents-for-managing-blood-glucose-levels-in-children-and-young-people-with-type-2-diabetes-pdf-13060839133
Carydias E, Tasho A, Kani C, Bacopoulou F, Stefanaki C, Markantonis SL. Systematic Review and Meta-Analysis of the Efficacy and Safety of Metformin and GLP-1 Analogues in Children and Adolescents with Diabetes Mellitus Type 2. Children. 2022 Oct 18;9(10):18. PubMed
Wu S, He Y, Wu Y, et al. Comparative efficacy and safety of glucose-lowering drugs in children and adolescents with type 2 diabetes: A systematic review and network meta-analysis. Front Endocrinol (Lausanne). 2022;13:897776. PubMed
Contributors: Chris Kamel
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for noncommercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca