CADTH Health Technology Review
Renal Denervation for Uncontrolled Hypertension
Rapid Review
Key Messages
What Is the Issue?
It is estimated that 23% of adults in Canada have hypertension. About 1/3 of this population have uncontrolled hypertension, a condition in which (BP) blood pressure levels continue to remain high despite treatment. People with high BP despite being prescribed 3 or more blood pressure-lowering (antihypertensive) medicines are considered to have uncontrolled resistant hypertension.
Renal denervation is a therapy that involves disrupting activity in the sympathetic nerves in the renal artery using a minimally invasive catheter-based procedure to treat high BP.
We wanted to know if renal denervation would effectively and safely reduce BP in people with uncontrolled hypertension.
What Did We Do?
We identified and summarized the literature comparing the clinical effectiveness and safety of renal denervation in individuals with uncontrolled hypertension to help guide decisions on the use of this intervention.
An information specialist searched for peer-reviewed and grey literature sources published between January 1, 2019, and February 5, 2024. The search was limited to English-language documents. One reviewer screened articles for inclusion based on predefined criteria, critically appraised the included studies, and narratively summarized the findings.
What Did We Find?
The evidence for this report was based on 2 systematic reviews and 3 randomized controlled trials (RCTs).
Renal denervation could lead to a reduction in BP compared to sham in adults with uncontrolled nonresistant hypertension.
It is uncertain if renal denervation is an effective treatment for resistant hypertension and suspected hypertensive heart disease due to the methodological limitations of the included studies.
Serious side effects of renal denervation were rare.
What Does This Mean?
Our findings agree with evidence-based guidelines and real-world evidence that suggest renal denervation can be considered a treatment option for patients with uncontrolled nonresistant hypertension. Other factors, including costs and resources, equity, acceptability, and patient selection, should be considered when implementing renal denervation in Canada, where it remains an emerging medical technology.
Future research should assess important patient outcomes, such as quality of life.
Abbreviations
BP
blood pressure
eGFR
estimated glomerular filtration rate
RCT
randomized controlled trial
RDN
renal denervation
SR
systematic review
Context and Policy Issues
What Is Uncontrolled Hypertension?
In Canada, approximately 5.8 million people, or 23% of adults had hypertension in the 2016 to 2017 Canadian Health Measures Survey.1 Currently, 1/3 of people in Canada living with hypertension have uncontrolled hypertension,1,2 most commonly defined as office systolic BP between 150 mm Hg and 180 mm Hg, mean 24-hour ambulatory systolic BP between 140 mm Hg and 170 mm Hg, and taking 3 or less antihypertensive medications.3 The terms “uncontrolled hypertension” and “resistant hypertension” are often used interchangeably but are not synonymous. Resistant hypertension, typically defined as office systolic BP over 140 mm Hg despite taking 3 or more BP-lowering drugs at optimal doses (with 1 being a diuretic),3-6 is 1 of the causes of uncontrolled hypertension.4 Other causes include patient nonadherence to antihypertensive medications, adverse effects of medications, socioeconomic factors (e.g., medication costs), inadequate treatment regimens, lack of patient education, physician inertia to initiate or intensify therapy, and white coat effect (when office BP is above the threshold, but out-of-office BP is below threshold).1,2 Patients with uncontrolled hypertension are at greater risk of cardiovascular disease and kidney disease.7
What Is the Current Practice?
The current approach to managing hypertension consists of lifestyle and diet modifications and pharmacological interventions. Hypertension Canada’s 2020 guidelines8 recommend weight reduction, physical exercise, and decreasing alcohol and sodium intake as first-line interventions for hypertension. Medications such as angiotensin-converting enzyme inhibitors, angiotensin receptor blockers, calcium channel blockers, and longer-acting thiazide-like diuretics are considered for adults with uncontrolled hypertension.8 Hypertension Canada8 recommends drugs such as spironolactone, bisoprolol, doxazosin, amiloride, eplerenone, or clonidine as an adjunct treatment for patients with resistant hypertension.
What Is Renal Denervation?
Renal denervation (RDN) is a minimally invasive procedure that reverses the activation of sympathetic nerves in the renal artery using a catheter that releases energy (typically low-dose radiofrequency or focused ultrasound) to disrupt their activity, which can lower BP.9,10 The renal sympathetic nervous system innervates several organ systems, including major structural components of the kidneys. Increased activity of the renal sympathetic nervous system, through a chain of pathophysiological changes, results in an increased volume of blood in the circulatory system as well as increased resistance of blood vessels, and subsequently increased BP.9
Why Is It Important to Do This Review?
Large observational studies have shown that roughly half of participants stop taking their antihypertensive drugs within a year for various reasons, including poor patient adherence, adverse effects of drug therapy, and socioeconomic factors.9 A systematic review (SR)11 published in 2020 reported that the prevalence of medication nonadherence was 35% in patients with resistant hypertension. Therefore, additional or alternative therapy is required for patients who cannot take medication or do not adhere to their prescribed regimen.9 RDN could be a complementary or alternative device-based BP-lowering therapy for those patients.9
Early research demonstrated that RDN reduced BP at 6 months in patients with persistent hypertension without major complications.12 However, this evidence came from observational, uncontrolled studies with short-term follow-up, small sample sizes, and high heterogeneity in BP measurement.13 RCTs did not find statistically significant benefits of RDN compared to placebo or standard therapy for uncontrolled hypertension.13 Initial and subsequent RCTs evaluating RDN compared to sham reported varying results.14 In 2022, CADTH produced a Horizon Scan15 that summarized the available information on Symplicity Spyral, a second-generation RDN system that uses multi-electrode catheter and radiofrequency generator to treat uncontrolled hypertension. In recent years, new RCTs and SRs evaluating the clinical effectiveness of different RDN systems compared to sham procedures have been published. Therefore, a review of the most current evidence is warranted.
Objective
To support decision-making about RDN for individuals with uncontrolled hypertension, we prepared this Rapid Review to summarize and critically appraise the available evidence regarding the clinical effectiveness of RDN versus sham.
Research Question
What is the clinical effectiveness of renal denervation in individuals with uncontrolled hypertension?
Methods
Literature Search Methods
An information specialist conducted a literature search on key resources including MEDLINE, Embase, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concepts were renal denervation and hypertension. CADTH-developed search filters were applied to limit retrieval to health technology assessments, systematic reviews, meta-analyses, or indirect treatment comparisons, and RCT or controlled clinical trials. The search was completed on February 5, 2024 and limited to English-language documents published since January 1, 2019.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Adult individuals with uncontrolled hypertension |
Intervention | Renal denervation |
Comparator | Sham device |
Outcomes | Clinical effectiveness (e.g., reduction in blood pressure, reduction in office systolic blood pressure, reduction in 24-hour ambulatory systolic blood pressure, time spent in therapeutic range) and safety |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials. |
Exclusion Criteria
The following were excluded:
articles that did not meet the selection criteria outlined in Table 1
duplicate publications
articles published before 2019
RCTs that were captured in an included SR
SRs in which all relevant studies were captured in other more recent or more comprehensive SRs.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)16 for SRs and the Downs and Black checklist17 for RCTs. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
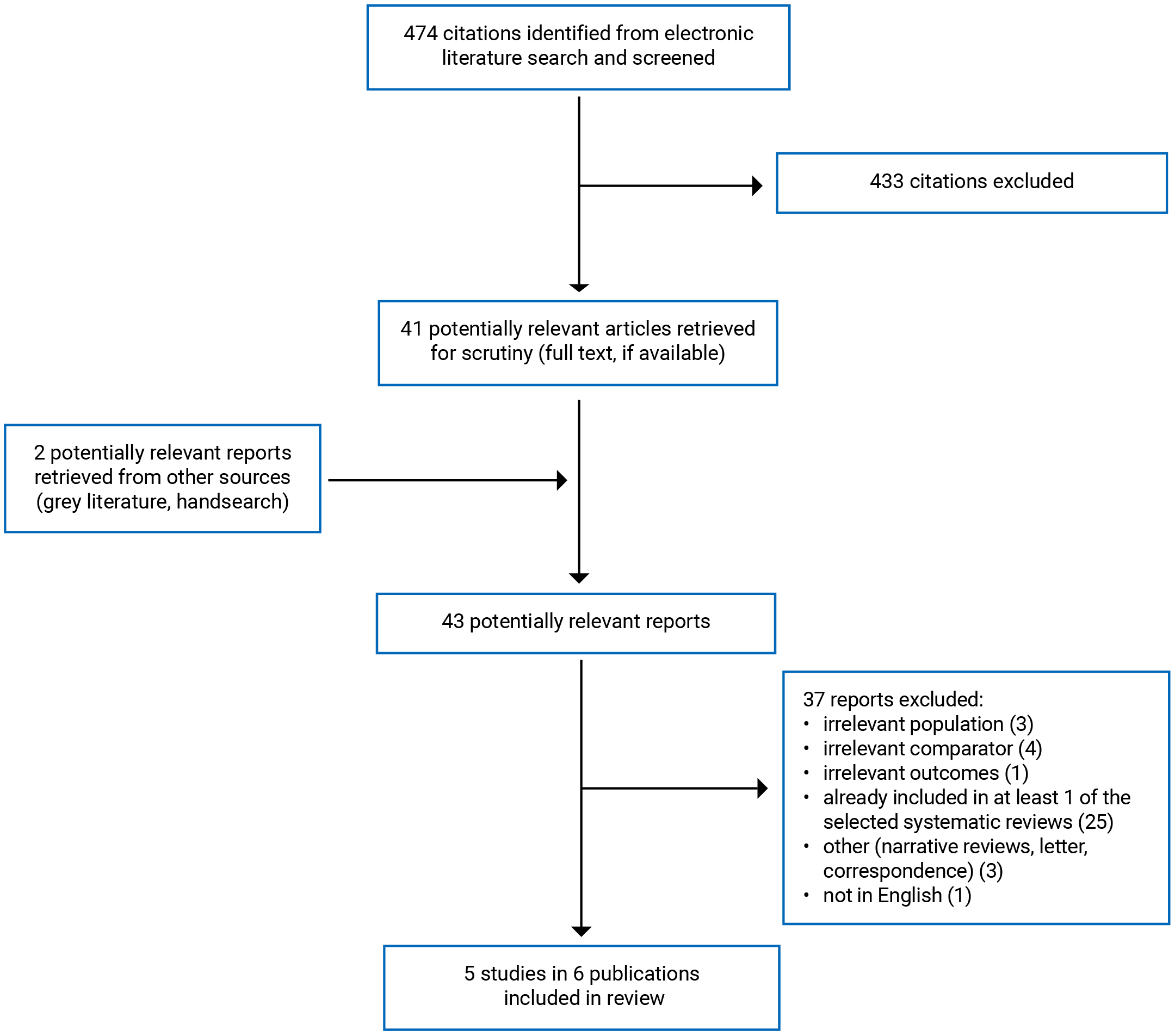
This report includes 5 studies presented in 6 publications.14,18-22 These were 2 SRs14,18,19 (there were 2 publications14,18 of 1 SR) and 3 RCTs.20-22 Study selection details are presented in Appendix 1.
Appendix 6 presents additional references of potential interest related to RDN for uncontrolled hypertension. These included SRs in which all relevant primary studies were captured in at least 1 of the 2 included SRs14,18,19 and 2 cost-effectiveness studies.
Summary of Study Characteristics
Detailed characteristics of included publications are provided in Appendix 2.
Study Design
One SR19 queried the electronic databases from inception to March 2023 and the other SR14,18 from January 2000 to October 2021. There were 11 RCTs published between 2014 and 2023 identified across both SRs.14,18,19 The 2 SRs14,18,19 included overlapping primary studies, with 8 RCTs included in both SRs18,19 (refer to Appendix 6 for details regarding overlap). To avoid duplication of results, outcome data from the individual RCTs is only reported once.
The RCT by Heradien et al.22 published in 2022 was a single-centre patient- and assessor-blinded trial. The other 2 RCTs20,21 were published in 2023 and used an international, multicentre, patient- and assessor-blinded design. One of them, the SPYRAL HTN-ON MED trial was reported by Kandzari et al.20 and included the findings from both the pilot trial (n = 80) and the extension trial (n = 257). The SPYRAL HTN-ON MED pilot trial was also included in the 2 SRs.14,18,19 To avoid duplication of results, outcome data on the SPYRAL HTN-ON MED pilot trial is reported only once in the current report.
The RCTs were carried out in Australia,20 Austria,20 Belgium,21 Canada,20 France,20,21 Germany,20,21 Greece,20 Ireland,20 Japan,20 South Africa,22 UK,20,21 and US.21 The 2 SRs14,18,19 (both by authors in the US) did not report the countries in which the included trials were carried out.
Population
The population in the included studies14,18-22 were adults with uncontrolled hypertension. The 2 SRs14,18,19 categorized participants as having resistant hypertension (defined as uncontrolled BP despite being on 3 or more antihypertensive medications) and nonresistant hypertension (or essential hypertension, defined as BP above the goal while taking less than 3 antihypertensive medications). The participants in the RCT by Heradien et al.22 were also at high risk of experiencing subclinical atrial fibrillation (suspected hypertensive heart disease). The number of participants across primary studies in the 2 SRs14,18,19 ranged from 51 to 535, and mean ages ranged from 53 to 62 years. The number of participants in the 3 RCTs20-22 ranged from 8122 to 257,20 and mean ages ranged from 5421 to 6422 years.
Intervention and Comparators
The interventions in the included studies were RDN using radiofrequency,14,18-20,22 ultrasound ablation14,18,19 or alcohol-mediated;21 and included both first-generation14,18,19 and second-generation RDN.14,18-22 First-generation RDN used a single-tip radiofrequency catheter, made fewer lesions that were placed randomly in the main renal artery, while second-generation systems used multi-electrode catheters and newer ablation techniques, and placed lesions in the distal segments of the renal arteries, achieving a greater degree of RDN.5 The types of RDN systems used in the studies included Kona Surround Sound,14 Paradise,14 Peregrine,21 Simplicity Flex,14 Simplicity G3,14,20 Symplicity Spyral,14,20,22 and Vessex.14
The sham comparator was renal angiography alone in 2 RCTs20,21 and prerecorded renal denervation generator sounds to simulate the RDN procedure in the other RCT.22 The 2 SRs14,18,19 did not report any details about the sham comparisons in their included studies.
Two RCTs20,22 assessed the effectiveness of RDN in the presence of antihypertensive medications, as an adjunct therapy, while the other RCT21 assess the effectiveness of RDN in the absence of antihypertensive medications, as a pharmacotherapy replacement (following a medication washout period).
Outcomes
Clinical effectiveness outcomes assessed in the studies included 24-hour ambulatory systolic and diastolic BP;18-22 office systolic and diastolic BP;14,19-22 daytime systolic and diastolic BP (measured 7:00 to 21:59);14,19 nighttime systolic and diastolic BP (measured 22:00 to 6:59),14,23,24 estimated glomerular filtration rate (eGFR, to measure level of kidney function),21 antihypertensive medication utilization (measured by the mean number of prescribed antihypertensive medications),20,21 and antihypertensive medication burden.20,21 Safety was assessed by adverse events.19-22
Across the studies, the follow-up period ranged from 2 months14,18,19 to 2 years.22
Summary of Critical Appraisal
Systematic Reviews
The 2 SRs14,18,19 clearly stated their review objective and inclusion criteria. The authors of the 2 SRs14,18,19 performed literature searches in 2 or more electronic databases and provided the search strategies18,19 or key search terms.19 This increases the transparency and reproducibility of the literature searches and article selection process. Both SRs18,19 presented a flow chart illustrating the study selection process. Data extraction was performed in duplicate; thus, decreasing the possibility of errors in the 2 SRs14,18,19 In both SRs,14,18,19 the authors used the Cochrane tool to assess the risk of bias of the included studies. The 2 SRs14,18,19 performed random-effects meta-analysis using the inverse variance method to estimate mean difference with a 95% confidence interval. Both SRs18,19 conducted sensitivity analyses by systematically excluding 1 RCT at a time to investigate the effect on the results. The authors of both SRs14,18,19 reported no conflicts of interest and no funding was received for the review.
There were limitations in the 2 SRs.18,19 Both SRs14,18,19 did not report the establishment of an a priori method or development of a review protocol. A preestablished review method is important for informing the conduct of reviews and allows readers to assess any protocol deviations that could introduce potential risk of bias to the review's findings. Neither SR14,18,19 reported whether there were publication restrictions in their searches, nor did they incorporate searches of the grey literature or trial registries, nor did they provide a list of excluded studies. One publication18 on the SR by Ahmed et al. did not report the I-squared statistic (estimate of heterogeneity between studies) in their meta-analyses. Publication bias might account for some of the effects observed in the 2 SRs; 14,18,19 however, this was not investigated in either SR.14,18,19
Randomized Controlled Trials
The 3 RCTs20-22 clearly reported the study objective, inclusion and exclusion criteria, intervention, and demographics of included participants. Because RDN and sham were administered by study personnel, it was assumed that adherence to the intervention or comparator was reliable for each RCT.20-22 The methods of randomization and allocation concealment were appropriate, reducing the risk of selection bias. The participants and outcome assessors were blinded to the interventions, reducing the risk of performance and detection bias. There were no significant losses to follow-up of randomized patients in the 3 RCTs.20-22 All the predefined outcomes were relevant and valid, and adequately reported. All RCTs20-22 were analyzed on an intention-to-treat basis. The 3 RCTs20-22 reported adverse events or complications associated with the intervention.
The RCTs20-22 had overall low risk of bias. However, it was uncertain if the participants were representative of the entire population from which they were recruited in all RCTs.20-22 For example, in the TARGET BP OFF-MED trial, 70% of patients who consented to participation in the trial were not randomized because they did not meet inclusion criteria before or after the run-in period, were excluded during run-in period for other reasons, were lost or withdrawn before randomization, or were not willing to stop antihypertensive medications. The authors did not report any baseline characteristics for this group compared to those who were randomized.21 Two RCTs21,22 were not powered for statistical comparisons of clinical effectiveness outcomes. Two RCTs20,21 were fully funded by the manufacturer of the RDN device being investigated and the other RCT22 was partially funded by the device manufacturer. In 1 RCT,20 the funding body identified clinical sites in collaboration with the executive committee and was responsible for data collection, monitoring, and data analysis. The funder also assisted in generating the figures and tables, copyediting, and formatting.20 In another RCT,22 the funder had no role in writing the protocol, executing the trial, handling the data or statistical analysis, and had no veto power over the manuscript’s content. In the third RCT,21, the role of the funder was not described. The statement of conflicts of interest also helps readers to understand the potential bias from study funders. Most of the authors of each RCT20-22 disclosed potential conflicts of interest, specifically ties with the device manufacturer or other industries (e.g., speaker honorariums, consulting fees, institutional grants, study fees to enrol patients). Direct funding from industry for the 3 RCTs20-22 and potential conflicts of interest with RDN manufacturers20-22 could potentially have led to publication, performance, or other bias in favour of the intervention.
Additional details regarding the strengths and limitations of the included publications are provided in Appendix 3.
Summary of Findings
The main study findings are provided in Appendix 4.
24-Hour Ambulatory BP
There were statistically significant reductions in 24-hour ambulatory systolic and diastolic BP with RDN compared to sham procedure in:
patients with nonresistant hypertension (uncontrolled hypertension on less than 3 antihypertensive medications) at 2 to 6 months (meta-analyses in 1 SR)18
patients with uncontrolled hypertension not taking any hypertensive medications at 2 months (1 RCT in 1 SR).19
Based on a clinically important difference of 2.0 mm Hg,23-25 these reductions appear to be clinically significant.
There were no statistically significant differences between RDN and sham in 24-hour ambulatory systolic and diastolic BP in:
patients with resistant hypertension (uncontrolled hypertension despite taking 3 or more hypertensive medications at 2 to 6 months; meta-analyses in 1 SR)18
patients with uncontrolled hypertension taking 1 to 3 hypertensive medications at 6 months (for 24-hour ambulatory systolic BP only since 24-hour ambulatory diastolic BP was not reported, 1 RCT)20
patients with suspected hypertensive heart disease on 3 or more hypertensive medications at 6 months (1 RCT).22.
At 1 year, RDN statistically and clinically significantly increased 24-hour ambulatory diastolic BP compared to sham, but had no statistically significant effect on 24-hour ambulatory systolic BP in patients with uncontrolled hypertension not taking any hypertensive medications (1 RCT).21 The authors suggested that these results may have been effected by COVID-19 pandemic; i.e., BP outcomes may have been sensitive to COVID-19 stressors and public health measures which also impacts lifestyle and social living.21
Office BP
There were statistically significant reductions in office systolic BP with RDN compared to sham procedure in:
patients with uncontrolled nonresistant hypertension at 2 to 12 months (meta-analyses in 1 SR)19
patients with uncontrolled hypertension on 1 to 3 hypertensive medications at 6 months (1 RCT).20
Based on a clinically important difference of 5 mm Hg,25 these reductions in office systolic BP appear to be clinically significant.
There was a statistically significant reduction in office diastolic BP with RDN compared to sham procedure in patients with uncontrolled nonresistant hypertension at 2 to 12 months, but this effect was not clinically significant (meta-analyses in 1 SR).19
A statistically significant, but not clinically important (< 5 mm Hg), reduction in office diastolic BP at 2 to 12 months was found with RDN versus sham in patients with resistant hypertension; and the reduction in office systolic BP was not statistically or clinically significant (meta-analyses in 1 SR).19
There were no statistically significant differences between RDN and sham in office systolic and diastolic BP in:
patients with resistant hypertension at 3 and 6 months (2 RCTs in 1 SR)14
patients with suspected hypertensive heart disease at 6 months (1 RCT)22
patients with uncontrolled hypertension off hypertensive medications at 1 year (1 RCT).21
Daytime BP
There were statistically and clinically significant reductions in daytime ambulatory systolic and diastolic BP with RDN compared to sham in patients with uncontrolled nonresistant hypertension at 2 to 12 months (meta-analysis in 1 SR).19
In patients with resistant hypertension, a meta-analysis in 1 SR19 found that RDN statistically and clinically significantly reduced daytime ambulatory systolic BP, but had no effect on daytime ambulatory diastolic BP, compared to sham at 2 to 12 months (meta-analysis in 1 SR).19 However, 1 RCT in another 1 SR18 reported no statistically or clinically significant differences between RDN and sham in daytime systolic and diastolic BP in patients with resistant hypertension at 3 months. It is possible that the difference in findings is because meta-analyses have higher statistical power and are likely able to detect between-group differences more precisely.
Nighttime BP
In patients with uncontrolled hypertension (regardless of antihypertensive medication usage), there was no statistically significant difference in change from baseline of nighttime ambulatory systolic and diastolic BP between RDN and sham at 2 to 6 months (meta-analysis in 1 SR).14
Estimated Glomerular Filtration Rate
There was a statistically significant difference in change from baseline of eGFR between RDN and sham at 12 months; eGFR remained stable in the RDN group but decreased in the sham group (1 RCT).21 However, the clinical importance of this finding is unclear.
Antihypertensive Medication Utilization
Patients taking antihypertensive medications at baseline who received RDN compared to sham were prescribed statistically significantly fewer antihypertensive medications at 6 months (1 RCT). 20 Patients who received RDN in the absence of antihypertensives (at baseline) were also prescribed statistically significantly fewer antihypertensive medications at 12 months compared to the sham group (1 RCT).21
In patients taking antihypertensive medications at baseline, medication burden was statistically significantly lower in the RDN group compared to the sham group at 6 months (1 RCT).20 In patients not taking antihypertensives at baseline, medical burden was statistically significantly lower with RDN compared to sham at 12 months (1 RCT).21
Adverse Events
In patients with uncontrolled hypertension, there were no significant differences in major adverse events with RDN versus sham procedure (1 RCT included in 1 SR,19 2 RCTs).20,21 In patients with suspected hypertensive heart disease, there was a statistically significant reduction in subclinical atrial fibrillation with RDN compared to sham at 2-year follow-up (1 RCT).22
Limitations
Certainty of the Evidence
Risk of Bias of Included Studies in SRs
Of the 8 included trials in both SRs,14,18,19 the review authors of 1 SR19 assessed the 8 trials as high risk of bias related to allocation concealment; whereas, the authors of the other SR18 assessed 7 trials as having some concerns about allocation concealment, 2 studies had some concerns related to blinding, 1 with some concerns with incomplete outcome data, and all 8 studies as having some concerns related to industry funding. Of the 3 trials included in either 1 of the SRs (i.e., non-overlapping studies),14,18,19 as assessed by the review authors, 1 study had high risk of bias related to allocation concealment; another study had some concerns regarding allocation concealment, blinding of patients and personnel, and industry funding, and high risk of bias related to incomplete outcome data; and the third study had some concerns regarding blinding and industry funding. Therefore, there is some uncertainty in the evidence from the SRs14,18,19 due to risk of bias.
Generalizability
Of the included primary studies, only the RCT evaluating the Symplicity Spyral RDN system20 had a study site in Canada. Thus, the generalizability of the effectiveness of other RDN systems (not yet available in Canada) may not be generalizable to the health care context in Canada. The 2 SRs14,18,19 did not identify the countries in which their included studies were conducted; therefore, the generalizability (or directness) of their findings is unknown.
Heterogeneity
There was variability in patient populations (e.g., different inclusion criteria, number of comorbidities, types of hypertensives taken), interventions (e.g., first- or second-generation device, energy source, expertise of physicians performing RDN), and time periods (e.g., length of follow-up, during or not during the COVID-19 pandemic) across included studies. Patient adherence to antihypertensive medications was monitored in some included studies (e.g., with urine and plasma testing)14,18-21 but not others,14,18,19,22 which may have led to inconsistencies in categorizing patients as having resistant or nonresistant hypertension.14,18,19
Imprecision
Two RCTs21,22 had small sample sizes. Effect estimates for several outcomes had wide confidence intervals.18,19 One RCT20 did not report the confidence intervals for the effect estimates.
Conclusions and Implications for Decision- or Policy-Making
This report comprises 2 SRs14,18,19 and 3 RCTs20-22 on the clinical effectiveness of RDN compared to sham for uncontrolled hypertension.
Clinical Effectiveness of Renal Denervation Compared to Sham
In adults with uncontrolled nonresistant hypertension, RDN compared to sham may have a favourable effect on 24-hour ambulatory BP, office systolic BP, and daytime BP at 2 to 12 months following treatment, but these findings are uncertain due to risk of bias, imprecision and potential indirectness.18,19 In adults with resistant hypertension, RDN compared to sham had no effect on 24-hour ambulatory BP, office systolic BP, and daytime diastolic BP at 2 to 12 months following treatment, but these findings have some uncertainty due to risk of bias and potential indirectness.18,19 The effect of RDN compared to sham on office diastolic BP and daytime systolic BP is uncertain due to conflicting findings across studies.18,19
In adults with uncontrolled hypertension on antihypertensive medications, RDN compared to sham may have no effect on 24-hour systolic ambulatory BP, but a favourable effect on office systolic BP and medication burden, at 6 months following treatment, but these findings are uncertain due to unknown precision.20
In adults with uncontrolled hypertension not taking antihypertensive medications, RDN compared to sham may have a favourable effect on 24-hour ambulatory BP at 2 months19 and following treatment and no effect on office BP at 12 months (despite statistically significantly lower medication burden in the RDN group),21 but these findings are uncertain due to risk of bias, imprecision, and potential indirectness.19,21 In patients with suspected hypertensive heart disease, RDN compared to sham may a favourable impact on subclinical atrial fibrillation but no effect on 24-hour ambulatory BP and office BP, at 6 months following treatment, but these findings are uncertain due to imprecision and indirectness.22
Major adverse events (including cardiovascular events) following treatment with RDN were rare.19-22
Clinical Effectiveness of Renal Denervation at Longer Follow-Up
All included studies investigated short-term effects of RDN, with follow-up periods ranging from 2 to 12 months for clinical effectiveness outcomes14,18-22 and up to 2 years for safety outcomes.22 Three publications of 2 RCTs26-28 included in the 2 SRs14,18,19 reported longer-term effects of RDN versus sham on BP outcomes, time in therapeutic BP range, and safety in patients with treatment-resistant hypertension. While we did not critically appraise these primary studies, we present a summary of their findings in Table 10. The authors of these publications26,27 concluded that patients in the RDN group had statistically significantly larger reductions from baseline to 3-year follow-up in 24-hour ambulatory, office, morning, and nighttime BP compared with the sham control group.26,27 The RDN group spent approximately twice as much time in a therapeutic BP range compared with the sham control group.27 Additionally, there were no late-emerging complications with RDN at 3-27 and 4-year follow-up.28
Guidelines and Real-World Evidence on the Use of Renal Denervation for Uncontrolled Hypertension
Findings of this review appear to be generally consistent with that of guidelines and real-world evidence regarding RDN for uncontrolled hypertension. Although we did not formally review and appraise the real-world evidence and evidence-based guidelines, a brief summary is provided in this section. Additional details are presented in Appendix 5.
While Hypertension Canada’s 2020 guidelines8 do not include recommendations about the use of RDN, we identified 3 evidence-based guidelines29-31 that include recommendations about the use of RDN for uncontrolled hypertension. The European Society of Hypertension,29 the National Institute for Health and Care Excellence (NICE),30and the Taiwan Hypertension Guidelines29 recommend that RDN can be considered as a treatment option for patients with uncontrolled hypertension. The European Society of Hypertension29 and NICE30 provide further recommendations regarding patient selection and RDN performance. A summary of the guideline recommendations is presented in Table 11.
The Medtronic-funded Global SYMPLICITY registry is an international, multicentre, prospective, open-label, observational study to evaluate real-world effectiveness and safety after treatment with the Symplicity RDN system using either the single-electrode Symplicity Flex or the multi-electrode Symplicity Spyral radiofrequency catheter systems.32,33 As of March 2023, over 3,000 patients from 45 countries have been enrolled.33 According to the published results, there was a statistically significant decrease from baseline in 24-hour and office systolic BP at 3 years in patients with uncontrolled hypertension and with resistant hypertension.32,33 The authors concluded that radiofrequency RDN reduced BP consistently up to 36 months independent of the number of baseline antihypertensive medications33 and that RDN-induced reductions in BP were associated with fewer strokes and other adverse cardiovascular events within 3 years.32 Recent real-world studies with smaller populations have also demonstrated decreases in 24-hour ambulatory and office BP values with RDN in patients with resistant hypertension over 12 months10 and 9 years without adverse renal function effects.2 While we did not critically appraise these primary studies, we present a summary of their findings, a summary of the findings of real-world studies is presented in Table 12.
Considerations for Future Research
As the findings of ongoing sham-controlled RCTs on RDN using newer ablation techniques34 and alcohol-based methods35 become available, they should be combined with the evidence in this Rapid Review. Future RCTs should measure patient-important outcomes, such as quality of life and patient preferences, with longer follow-up periods, larger sample sizes, and more standardized procedural methods. The finding that RDN compared to sham may reduce atrial fibrillation independent of its effect on BP22 should be confirmed in trials with a larger population. Future work should also focus on the development of a periprocedural marker for successful renal nerve ablation,36 common to all RDN methods, and predictors of significant response to RDN to identify patient populations who will benefit most from treatment, factors leading to improved procedural efficacy, and direct comparison of different RDN techniques.37
To help address health equity concerns in future studies, researchers should consider collecting equity-relevant population characteristics (e.g., gender, education, socioeconomic status, place of residence) to assess potential health inequities related to RDN for uncontrolled hypertension.
Implications for Clinical Practice
Although the findings of this report are not conclusive, they do suggest a potential short-term benefit of RDN for uncontrolled nonresistant hypertension without negative major adverse events. RDN remains an emerging technology in Canada, with approval from Health Canada pending at the time of authoring this report. Decision-makers should consider factors such as cost of RDN, potential health care resource need required for the procedure,38 possible long wait times, and concerns related to equity of access. In addition, as per the NICE guidelines,30 patients who receive RDN should be selected by a multidisciplinary team and health care providers should audit and review clinical outcomes for all RDN procedures. The evidence does not support decision-making in favour of the use of RDN for resistant hypertension and suspected hypertensive heart disease currently.
References
1.Leung AA, Williams JVA, McAlister FA, et al. Worsening hypertension awareness, treatment, and control rates in Canadian women between 2007 and 2017. Can J Cardiol. 2020;36(5):732-739. PubMed
2.Sesa-Ashton G, Nolde JM, Muente I, et al. Catheter-based renal denervation: 9-year follow-up data on safety and blood pressure reduction in patients with resistant hypertension. Hypertension. 2023;80(4):811-819. PubMed
3.Silverwatch J, Marti KE, Phan MT, et al. Renal denervation for uncontrolled and resistant hypertension: Systematic review and network meta-analysis of randomized trials. J Clin Med. 2021;10(4):16. PubMed
4.Townsend RR. Definition, risk factors, and evaluation of resistant hypertension. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2023: http://www.uptodate.com. Accessed 2024 Feb 29.
5.Stavropoulos K, Patoulias D, Imprialos K, et al. Efficacy and safety of renal denervation for the management of arterial hypertension: A systematic review and meta-analysis of randomized, sham-controlled, catheter-based trials. J Clin Hypertens (Greenwich). 2020;22(4):572-584. PubMed
6.Filippone EJ, Naccarelli GV, Foy AJ. Controversies in hypertension IV: Renal denervation. Am J Med. 2023;136(9):857-868. PubMed
7.Hiremath S, Sapir-Pichhadze R, Nakhla M, et al. Hypertension Canada's 2020 evidence review and guidelines for the management of resistant hypertension. Can J Cardiol. 2020;36(5):625-634. PubMed
8.Rabi DM, McBrien KA, Sapir-Pichhadze R, et al. Hypertension Canada's 2020 comprehensive guidelines for the prevention, diagnosis, risk assessment, and treatment of hypertension in adults and children. Can J Cardiol. 2020;36(5):596-624. PubMed
9.Choi KH, Choi SH. Current status and future perspectives of renal denervation. Korean Circ J. 2021;51(9):717-732. PubMed
10.Rodriguez-Leor O, Segura J, Garcia Donaire JA, et al. Renal denervation for the treatment of resistant hypertension in Spain. The Flex-Spyral Registry. Rev Esp Cardiol (Engl Ed). 2020;73(8):615-622. PubMed
11.Bourque G, Ilin JV, Ruzicka M, Davis A, Hundemer G, Hiremath S. The prevalence of non-adherence in patients with resistant hypertension: A systematic review and meta-analysis [non peer-reviewed preprint]. medRxiv. 2020. https://www.medrxiv.org/content/10.1101/2020.08.14.20175125v1. Accessed 2024 Feb 29.
12.Davis MI, Filion KB, Zhang D, et al. Effectiveness of renal denervation therapy for resistant hypertension: A systematic review and meta-analysis. J Am Coll Cardiol. 2013;62(3):231-241. PubMed
13.Pisano A, Iannone LF, Leo A, Russo E, Coppolino G, Bolignano D. Renal denervation for resistant hypertension. Cochrane Database Syst Rev. 2021;11:CD011499. PubMed
14.Ahmed M, Nudy M, Bussa R, et al. A systematic review, meta-analysis, and meta regression of the sham controlled renal denervation randomized controlled trials. Trends Cardiovasc Med. 2023;33(8):490-498. PubMed
15.Kumar D, Loshak H. CADTH horizon scan: Renal denervation for people with hypertension. Can J Health Technol. 2022;2(1). https://canjhealthtechnol.ca/index.php/cjht/article/view/en0038/en0038. Accessed 2024 Feb 29. PubMed
16.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
17.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
18.Ahmed M, Nudy M, Bussa R, Naccarelli GV, Filippone EJ, Foy AJ. A subgroup meta-analysis comparing the renal denervation sham-controlled randomized trials among those with resistant and nonresistant hypertension. Am J Cardiol. 2023;191:119-124. PubMed
19.Singh S, Rout A, Garg A. Renal denervation in hypertension: An updated meta-analysis of the randomized controlled trials. Catheter Cardiovasc Interv. 2023;102(4):663-671. PubMed
20.Kandzari DE, Townsend RR, Kario K, et al. Safety and efficacy of renal denervation in patients taking antihypertensive medications. J Am Coll Cardiol. 2023;82(19):1809-1823. PubMed
21.Pathak A, Rudolph UM, Saxena M, et al. Alcohol-mediated renal denervation in patients with hypertension in the absence of antihypertensive medications. EuroIntervention. 2023;19(7):602-611. PubMed
22.Heradien M, Mahfoud F, Greyling C, et al. Renal denervation prevents subclinical atrial fibrillation in patients with hypertensive heart disease: Randomized, sham-controlled trial. Heart Rhythm. 2022;19(11):1765-1773. PubMed
23.Whelton PK, He J, Appel LJ, et al. Primary prevention of hypertension: clinical and public health advisory from The National High Blood Pressure Education Program. JAMA. 2002;288(15):1882-1888. PubMed
24.Makai P, IntHout J, Deinum J, Jenniskens K, Wilt GJV. A network meta-analysis of clinical management strategies for treatment-resistant hypertension: Making optimal use of the evidence. J Gen Intern Med. 2017;32(8):921-930. PubMed
25.Bhatt DL, Kandzari DE, O'Neill WW, et al. A controlled trial of renal denervation for resistant hypertension. N Engl J Med. 2014;370(15):1393-1401. PubMed
26.Kario K, Mahfoud F, Kandzari DE, et al. Long-term reduction in morning and nighttime blood pressure after renal denervation: 36-month results from SPYRAL HTN-ON MED trial. Hypertens Res. 2023;46(1):280-288. PubMed
27.Bhatt DL, Vaduganathan M, Kandzari DE, et al. Long-term outcomes after catheter-based renal artery denervation for resistant hypertension: Final follow-up of the randomised SYMPLICITY HTN-3 Trial. Lancet. 2022;400(10361):1405-1416. PubMed
28.Mahfoud F, Kandzari DE, Kario K, et al. Long-term efficacy and safety of renal denervation in the presence of antihypertensive drugs (SPYRAL HTN-ON MED): A randomised, sham-controlled trial. Lancet. 2022;399(10333):1401-1410. PubMed
29.Mancia G, Kreutz R, Brunstrom M, et al. 2023 ESH Guidelines for the management of arterial hypertension The Task Force for the management of arterial hypertension of the European Society of Hypertension: Endorsed by the International Society of Hypertension (ISH) and the European Renal Association (ERA). J Hypertens. 2023;41(12):1874-2071. PubMed
30.National Institute for Health and Care Excellence. Percutaneous transluminal renal sympathetic denervation for resistant hypertension (NICE interventional procedures guidance IPG754). 2023; https://www.nice.org.uk/guidance/ipg754/. Accessed 2024 Feb 13.
31.Wang TD, Chiang CE, Chao TH, et al. 2022 Guidelines of the Taiwan Society of Cardiology and the Taiwan Hypertension Society for the Management of Hypertension. Acta Cardiologica Sin. 2022;38(3):225-325. PubMed
32.Schmieder RE, Mahfoud F, Mancia G, et al. Clinical event reductions in high-risk patients after renal denervation projected from the global SYMPLICITY registry. Eur Heart J Qual Care Clin Outcomes. 2023;9(6):575-582. PubMed
33.Mahfoud F, Mancia G, Schmieder RE, et al. Outcomes following radiofrequency renal denervation according to antihypertensive medications: Subgroup analysis of the Global SYMPLICITY Registry DEFINE. Hypertension. 2023;80(8):1759-1770. PubMed
34.Otsuka Medical Devices Co., Ltd. Japan. A Clinical Study of the Paradise™ Renal Denervation System in Patients With Hypertension (RADIANCE‐HTN DUO). ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine: https://clinicaltrials.gov/study/NCT05326230. Accessed 2024 Feb 28.
35.Ablative Solutions, Inc. TARGET BP I Clinical Trial (TARGET BP I). ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2023: https://clinicaltrials.gov/study/NCT02910414. Accessed 2024 Feb 28.
36.Azizi M, Schmieder RE, Mahfoud F, et al. Six-month results of treatment-blinded medication titration for hypertension control after randomization to endovascular ultrasound renal denervation or a sham procedure in the RADIANCE-HTN SOLO trial. Circulation. 2019;139(22):2542-2553. PubMed
37.Shah RT, Wang BX. Effectiveness of renal denervation in the treatment of hypertension: A literature review. Clin Hypertens. 2022;28(1):11. PubMed
38.Marcusohn E, Tobe SW, Dueck A, Madan M. Renal denervation for uncontrolled hypertension. CMAJ. 2023;195(43):E1475-E1480. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Systematic Reviews
Study citation, country, funding source | Study design, review objective, search dates, numbers of primary studies included | Population characteristics | Relevant intervention and comparator | Relevant clinical outcomes, length of follow-up |
|---|---|---|---|---|
US Funding source: No funding received | Study design: SR with MA of RCTs Review objective: To assess BP-lowering effect of RDN compared to sham control. Search dates: January 2000 to October 2021. Number of included primary studies: 10 RCTs | Adults with uncontrolled resistant and unresistant HTN. N: total 1,544, range 51 to 535 Sex: female 35%, male NR Age: mean 56 years, range 53 to 62 years Baseline SBP: mean 140 to162 mm Hg Baseline DBP: mean 78 to 99 mm Hg Comorbidities: NR | Intervention: RDN procedure using radiofrequency or ultrasound ablation Comparator: Sham control. | Outcomes:
Follow-up: 2 to 12 months (mean 4.2 months) |
Singh et al. 202319 US Funding source: No funding received | Study design: SR with MA of RCTs Review objective: To understand the role of RDN in patients with HTN. Search dates: Electronic database inception to March 2023. Number of included studies: 9 RCTs. | Adults with uncontrolled resistant HTN or unable to tolerate AH medications. N: total 1,643, range 51 to 535 Sex: female NR, male 70% Age: mean 56 years, range 53 to 61 years Baseline BP: NR Comorbidities: DM 25%, history of CAD 21% | Intervention: RDN procedure using radiofrequency or ultrasound ablation Comparator: Sham control. | Outcomes:
Follow-up: 2 to 12 months (mean 5 months) |
ABP = ambulatory blood pressure; AH = antihypertensive; BP = blood pressure; CAD = coronary artery disease; DBP = diastolic blood pressure; DM = diabetes mellitus; HTN = hypertension; MA = meta-analyses; NR = not reported; RCT = randomized controlled trial; RDN = renal denervation; SBP = systolic blood pressure.
Table 3: Characteristics of Included Randomized Controlled Trials
Study citation, country, funding source | Trial name, study design, setting | Inclusion criteria | Population characteristics | Intervention and comparator | Clinical outcomes, length of follow-up |
|---|---|---|---|---|---|
Kandzari et al. 202320 US Funding source: Medtronic. | SPYRAL-HTN-ON MED Expansion trial Patient- and assessor-blinded RCT 56 clinical centres in Australia, Austria, Canada, France, Germany, Greece, Ireland, Japan, UK, and US. | Patients (20 to 80 years old) with uncontrolled HTN, defined as office SBP ≥ 150 mm Hg and < 180 mm Hg, office DBP ≥ 90 mm Hg, mean 24 hour SBP ≥ 140 mm Hg and < 170 mm Hg. | N randomized: RDN: n = 168 Sham: n = 89 Sex: female 21%, male NR Age, mean years (SD): 55.5 (8.9) Baseline office SBP, mean mm hg (SD): 162.7 (7.9) Baseline office DBP, mean mm hg (SD): 101.3 (6.9) Comorbidities: DM 13%, CAD 7%, obstructive sleep apnea 13%. | Intervention: RDN procedure using Symplicity Spyral multielectrode RDN catheter and Symplicity G3 RDN radiofrequency generator Comparator: Sham procedure with renal angiogram only | Outcomes:
Follow-up: 6 months |
Pathak et al. 202321 Monaco Funding source: Ablative Solutions, Inc. | TARGET BP OFF-MED trial Patient- and assessor-blinded RCT 25 centres in Belgium, France, Germany, US, and UK. | Patients (18 to 80 years old) with a mean office SBP between 140 and 180 mm Hg and a mean DBP ≥ 90 mm Hg who were taking 0 to 2 AH medications. | N randomized: RDN: n = 50 Sham: n = 56 Sex: RDN: female NR, male 80% Sham: female NR, male 67.9% Age, mean years (SD): RDN: 53.8 (11.0) Sham: 54.4 (11.5) Baseline office SBP, mean mm hg (SD): RDN: 159.4 (10.9) Sham: 160.1 (11.0) Baseline office DBP, mean mm hg (SD): RDN: 100.4 (7.0) Sham: 98.3 (6.1) Comorbidities: RDN: DM 4%, CCS 4.0% Sham: DM 8.9%, CCS 1.8% | Intervention: Alcohol-mediated RDN using Peregrine Catheter Comparator: Sham control with diagnostic renal angiography only | Outcomes:
Follow-up: 12 months |
Heradien et al. 202222 South Africa Funding sources: Hamilton Naki Trust; Medronic. | Patient- and assessor-blinded RCT 1 hospital in Cape Town, South Africa. | Patients (≥ 55 years old) with uncontrolled HTN despite treatment with ≥ 3 AH drugs of different classes (including a diuretic), sinus rhythm, and high risk of experiencing subclinical atrial fibrillation (suspected coronary artery disease). | N randomized: RDN: n = 43 Sham: n = 38 Sex: RDN: female 31%, male NR Sham: female 21%, male NR Age, mean years (range): RDN: 66.5 (59 to 71) Sham: 63.0 (59 to 72) Baseline Office SBP, mean mm hg (SD): RDN: 149.1 (20.3) Sham:146.1 (22.5) Baseline Office DBP, mean mm hg (SD): RDN: 85.2 (11.8) Sham: 83.6 (16.0) Comorbidities: RDN: DM 60%, CAD 67% Sham: DM 47%, CAD 68% | Intervention: RDN procedure using Symplicity Flex and Symplicity Spyral radiofrequency catheter systems Comparator: Sham with prerecorded RDN generated sounds. | Outcomes:
Follow-up: 6 months (BP outcomes) and 12 months (adverse events) |
ABP = ambulatory blood pressure; BP = blood pressure; CAD = coronary artery disease; CCS = chronic coronary syndrome; DBP = diastolic blood pressure; eGFR = estimated glomerular filtration rate; HTN = hypertension; NR = not reported; RDN = renal denervation; RCT = randomized controlled trial; SBP = systolic blood pressure; SD = standard deviation.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 4: Strengths and Limitations of Systematic Reviews Using AMSTAR 216
Strengths | Limitations |
|---|---|
The objective of the review was clearly stated. The authors search 2 electronic databases and provided the search strategies. The inclusion criteria included the population, intervention, comparators, and outcomes. Two reviewers independently performed data extraction. A flow chart of study selection was provided. An appropriate tool (Cochrane RoB tool) was used to assess risk of bias of included studies. The authors used appropriate statistical methods for the meta-analyses. The authors reported that all included RCTs received industry funding. The authors discussed the heterogeneity observed in the review. The authors declared no disclosures of competing interest. The authors reported that they received no funding for the review. | There was no explicit statement that review methods were established before the conduct of the review. The authors did not provide a justification for eligible study designs. It was unclear if there were publication restrictions. The authors did not search the reference lists of selected papers, grey literature, or trial registries. It was unclear if study selection was conducted in duplicate. While the authors provided the number of excluded studies and reasons for their exclusion, they did not provide references for the excluded studies. The authors did not investigate publication bias. The authors did not discuss the potential impact of risk of bias on the results of the review. |
Singh 202319 | |
The objective of the review was clearly stated. The authors search 4 electronic databases and provided the search terms. The inclusion criteria included the population, intervention, comparators, and outcomes. Two reviewers independently performed study selection, data extraction and risk of bias assessment. A flow chart of study selection was provided. An appropriate tool (Cochrane ROB tool) was used to assess risk of bias of included studies. The authors used appropriate statistical methods for the meta-analyses. The authors discussed the potential impact of risk of bias on the results of the review. The authors discussed the heterogeneity observed in the review. The authors declared no conflicts of interest. The authors reported that they received no funding for the review. | There was no explicit statement that review methods were established before the conduct of the review. The authors did not provide a justification for eligible study designs. It was unclear if there were publication restrictions. The authors did not search the reference lists of selected papers, grey literature, or trial registries. The authors report adverse events in the most recent trial in the Discussion section and do not report adverse events in the other included RCTs. The authors did not report the sources of funding for each study. While the authors provided the number of excluded studies and reasons for their exclusion, they did not provide references for the excluded studies. The authors did not investigate publication bias. |
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; RCT = randomized controlled trial; ROB = risk of bias.
Table 5: Strengths and Limitations of Randomized Controlled Trials Using the Downs and Black Checklist17
Strengths | Limitations |
|---|---|
Kandzari et al. 202320 | |
Reporting:
External validity:
Internal validity – bias:
Internal validity – confounding:
Power:
| Reporting:
External validity:
|
Pathak et al. 202321 | |
Reporting:
External validity:
Internal validity – bias:
Internal validity – confounding:
| External validity:
Power:
|
Heradien et al. 202222 | |
Reporting:
External validity:
Internal validity – bias:
Internal validity – confounding:
| External validity:
Power:
|
Appendix 1: Main Study Findings
Table 6: Summary of Findings by Outcome — Blood Pressure Outcomes
Study citation | Study design, trial name | Outcome | No. AH medications | Outcome result, sample size | Effect estimate (95% CI) | P value | |
|---|---|---|---|---|---|---|---|
RDN | Sham | ||||||
24-Hour ambulatory BP | |||||||
Ahmed et al. 202318 | SR and MA (4 RCTs) | 24-hour ambulatory SBP at 2 to 6 months [mm hg] | < 3a | N = 543 | MD −4.19 (−6.07 to −2.30) | 0.000 | |
24-hour ambulatory DBP at 2 to 6 months [mm hg] | MD −2.60 (−3.79 to −1.42) | 0.000 | |||||
SR and MA (6 RCTs) | 24-hour ambulatory SBP at 2 to 6 months [mm hg] | ≥ 3b | N = 1,001 | MD −1.87 (−3.89 to 0.16) | 0.071 | ||
24-hour ambulatory DBP at 2 to 6 months [mm hg] | MD −0.67 (−1.84 to 0.50) | 0.263 | |||||
Singh et al. 202319 | SR (1 RCT)c RADIANCE II | 24-hour ambulatory DBP at 2 months [mm hg] | 0 | N = 150 | N = 74 | MD −6.20 (−9.00 to −3.40) | NR |
24-hour ambulatory DBP at 2 months [mm hg] | MD −4.1 (−5.67 to −2.53) | NR | |||||
Kandzari et al. 202320 | RCT SPYRAL-HTN-ON MED Expansion trial | 24-hour ambulatory SBP at 6 months, mean change from baseline [mm hg] | 1 to 3 | −5.9 N = 168 | −5.8 N = 89 | MD 0.0 | 0.97 |
Patak et al. 202321 | RCT TARGET BP OFF-MED trial | 24-hour ambulatory SBP at 12 months, mean (SD) [mm hg] | 0 | 137.6 (11.4) N = 41 | 133.7 (11.3) N = 44 | Difference 5.3 (−0.1 to 10.7) | 0.0775 |
24-hour ambulatory SBP at 12 months, mean change from baseline (SD) [mm hg] | −10.6 (11.5) N = 41 | −15.9 (13.1) N = 43 | |||||
24-hour ambulatory DBP at 12 months, mean (SD) [mm hg] | 85.6 (8.7) N 41 | 81.0 (7.9) N = 44 | Difference 2.5 (−0.9 to 6.0) | 0.0341 | |||
24-hour ambulatory DBP at 12 months, mean change from baseline (SD) [mm hg] | −7.3 (7.5) N = 41 | −9.8 (8.3) N = 43 | |||||
Heradien et al. 202222 | RCT | 24-hour ambulatory SBP at 6 months, mean (SD) [mm hg] | ≥ 3 | 138.1 (14.6) N = 38 | 136.0 (18.4) N = 30 | Adjusted MDd −2.7 (−3.7 to 9.2) | 0.392 |
24-hour ambulatory SBP at 6 months, mean change from baseline (SD) [mm hg] | −0.1 (15.8) N = 38 | −3.4 (16.3) N = 30 | |||||
24-hour ambulatory DBP at 6 months, mean (SD) [mm hg] | 78.6 (9.2) N = 38 | 78.3 (7.5) N = 30 | Adjusted MDd 1.2 (−2.1 to 4.5) | 0.473 | |||
24-hour ambulatory DBP at 6 months, mean change from baseline (SD) [mm hg] | 0.2 (7.9) N = 38 | −1.6 (7.1) N = 30 | |||||
Office BP | |||||||
Ahmed et al. 202314 | SR (1 RCT)e WAVE IV | Office SBP at 6 months [mm hg] | ≥ 3 | N = 55 | MD 12.5 (−3.17 to 28.17) | 0.118 | |
Office DBP at 6 months [mm hg] | MD 5.4 (−6.03 to 16.83) | 0.36 | |||||
SR (1 RCT)e REQUIRE | Office SBP at 3 months [mm hg] | ≥ 3 | N = 136 | MD −2.0 (−7.81 to 3.81) | 0.50 | ||
Office DBP at 3 months [mm hg] | MD 0.10 (−4.20 to 4.40) | 0.97 | |||||
Singh et al. 202319 | SR and MA (5 RCTs) | Office SBP at 2 to 12 months [mm hg] | < 3 | NR | NR | MD −5.84 (−7.71 to −3.98) I2 = 0% | < 0.00001 |
Office DBP at 2 to 12 months [mm hg] | MD −3.38 (−4.57 to −2.19) I2 = 0% | < 0.00001 | |||||
SR and MA (2 RCTs) | Office SBP at 2 to 12 months [mm hg] | ≥ 3 | NR | NR | MD −4.23 (−8.65 to 0.20) I2 = 30% | 0.06 | |
Office DBP at 2 to 12 months [mm hg] | MD −2.40 (−4.68 to 0.12) I2 = 0% | 0.04 | |||||
Kandzari et al. 202320 | RCT SPYRAL-HTN-ON MED Expansion trial | Office SBP at 6 months, mean change from baseline [mm hg] | 1 to 3 | −10.1 N = 168 | −6.2 N = 89 | MD −4.0 | 0.03 |
Pathak et al. 202321 | RCT TARGET BP OFF-MED trial | Office SBP at 12 months, mean (SD) [mm hg] | 0 | 147.9 (18.5) N = 41 | 147.8 (15.1) N = 50 | Difference 2.2 (−4.5 to 8.9) | 0.6823 |
Office SBP at 12 months, mean change from baseline (SD) [mm hg] | −11.0 (15.3) N = 41 | −13.2 (16.6) N = 50 | |||||
Office DBP at 12 months, mean (SD) [mm hg] | 91.0 (11.0) N = 41 | 88.5 (11.5) N = 50 | Difference −1.6 (−5.4 to 2.1) | 0.6375 | |||
Office DBP at 12 months, mean change from baseline (SD) [mm hg] | −9.4 (9.4) N = 41 | −9.6 (11.0) N = 50 | |||||
Heradien et al. 202222 | RCT | Office SBP at 6 months, mean (SD) [mm hg] | ≥ 3 | 136.7 (16.9) N = 41 | 136.8 (23.9) N = 35 | Adjusted MDd −1.3 (−9.9 to 7.3) | 0.762 |
Office SBP at 6 months, mean change from baseline (SD) [mm hg] | −12.4 (21.2) N = 41 | −9.3 (23.9) N = 35 | |||||
Office DBP at 6 months, mean (SD) [mm hg] | 79.3 (9.9) N = 41 | 80.3 (14.6) N = 35 | Adjusted MDd −1.5 (−6.8 to 3.7) | 0.561 | |||
Office DBP at 6 months, mean change from baseline (SD) [mm hg] | −5.9 (12.9) N = 41 | −3.3 (16.4) N = 35 | |||||
Daytime BP | |||||||
Ahmed et al. 202314 | SR (1 RCT)f | Daytime SBP at 3 months [mm hg] | ≥ 3 REQUIRE | N = 136 | MD −1.2 (−6.6 to 4.2) | NR | |
Daytime DBP at 3 months [mm hg] | MD −0.8 (−3.7 to 2.1) | NR | |||||
Singh et al. 202319 | SR and MA (4 RCTs) | Daytime ambulatory SBP at 2 to 12 months [mm hg] | < 3 | NR | NR | MD −5.52 (−7.52 to −3.52) I2 = 0% | < 0.00001 |
Daytime ambulatory DBP at 2 to 12 months [mm hg] | MD −3.64 (−4.90 to −2.38) I2 = 0% | < 0.00001 | |||||
SR and MA (3 RCTs) | Daytime ambulatory SBP at 2 to 12 months [mm hg] | ≥ 3 | NR | NR | MD −4.26 (−7.12 to −1.40) I2 = 0% | 0.004 | |
Daytime ambulatory DBP at 2 to 12 months [mm hg] | MD −1.37 (−3.15 to 0.41) I2 = 0% | 0.13 | |||||
Nighttime BP | |||||||
Ahmed et al. 202314 | SR and MA (8 RCTs) | Nighttime ambulatory SBP at 2 to 6 months [mm hg] | 0 to 4 | NR | NR | MD −2.64 (−5.84 to 0.56) I2 = 44.72% | 0.106 |
Nighttime ambulatory DBP at 2 to 6 months [mm hg] | MD −1.21 (−3.17 to 0.75) I2 = 40.01% | 0.226 | |||||
AH = antihypertensive; CI = confidence interval; DBP = diastolic blood pressure; MA = meta-analysis; MD = mean difference; NA = not applicable; NR = not reported; RCT = randomized controlled trial; RDN = renal denervation; SD = standard deviation; SR = systematic review; SBP = systolic blood pressure.
aPatients whose BP remains above the goal and are taking < 3 AH medications were described as having nonresistant uncontrolled HTN.14,18,20
bPatients whose BP remains above the goal and are taking ≥ 3 AH medications were described as having resistant HTN.14,18,20
cOne RCT (RADIANCE II trial) was not reported in the SR by Ahmed et al.14,18 Therefore, data from this trial is presented separately, rather than the MA reported in this SR to avoid duplicate reporting.19
dAdjusted for baseline values.22
eTwo RCTs (REQUIRE and WAVE IV trials) were not reported in the SR by Singh et al.19 Therefore, data from these trials is presented separately, rather than the MA reported in this SR to avoid duplicate reporting.
fOne RCT (REQUIRE trial) was not reported in the SR by Singh et al.19 Therefore, data from this is presented separately, rather than the MA reported in this SR to avoid duplicate reporting.14
Note that this appendix has not been copy-edited.
Table 7: Summary of Findings by Outcome — Estimated glomerular filtration rate
Study citation | Study design, trial name | Outcome | Outcome result, sample size | P value | |
|---|---|---|---|---|---|
RDN | Sham | ||||
Patak et al. 202321 | RCT TARGET BP OFF-MED trial | eGFR at 12 months, mean (SD) [mm hg] | 83.5 (13.8) N = 48 | 79.6 (15.8) N = 53 | 0.0224 |
eGFR at 12 months, mean change from baseline (SD) [mm hg] | −2.1 (8.9) N = 48 | −6.4 (10.0) N = 53 | |||
AH = antihypertensive; CI = confidence interval; eGFR = estimated glomerular filtration rate; NR = not reported; RCT = randomized controlled trial; RDN = renal denervation; SD = standard deviation.
Table 8: Summary of Findings by Outcome — Antihypertension Medication Utilization
Study citation | Study design, trial name | Outcome | Outcome result, sample size | P value | |
|---|---|---|---|---|---|
RDN | Sham | ||||
Kandari et al. 202320 | RCT SPYRAL-HTN-ON MED Expansion trial | Number of AH medications at 6 months, mean (SD) | 1.9 (0.9) N = 204 | 2.1 (0.9) N = 130 | 0.0085a |
Patak et al. 202321 | RCT TARGET BP OFF-MED trial | Number of AH medications (for safety reasons, per the discretion of the treating investigator) at 12 months, mean | 1.10 | 1.60 | 0.0081 |
Proportion of patients on ≥ 2 AH medications at 12 months | 29% | 57% | 0.005 | ||
AH medication burden | |||||
Kandari et al. 202320 | RCT SPYRAL-HTN-ON MED Expansion trial | AH medication burdenb at 6 months, mean (SD) | 2.9 (2.7) N = 204 | 3.5 (3.2) N = 130 | 0.043a |
Patak et al. 202321 | RCT TARGET BP OFF-MED trial | AH medication burdenc at 12 months | 0.66 | 0.85 | 0.088 |
AH = antihypertensive; CI = confidence interval; NA = not applicable; RCT = randomized controlled trial; RDN = renal denervation; SD = standard deviation.
aP values used ANCOVA adjusted for baseline values.
bComposite index based on the doses of medications but multiplies this result by the number of prescribed medications. AH medication burden was calculated for all AH medication prescribed at study specified follow-up visits for each patient and added to yield a single, summative score.20
cComposite index based on the doses of medications and is a proportional measure of prescribed to maximum daily dose, as recommended by the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure, calculated for each antihypertensive medication.21
Table 9: Summary of Findings by Outcome — Adverse Events
Study citation | Study design, trial name | Outcome | Outcome result | Effect estimate (95% CI) | P value | |
|---|---|---|---|---|---|---|
RDN | Sham | |||||
Mortality | ||||||
Kandzari et al. 202320 | RCT SPYRAL-HTN-ON MED Expansion trial | All-cause mortality at 6 months, n of N | 0 of 168 | 0 of 89 | NR | NR |
Pathak et al. 202321 | RCT TARGET BP OFF-MED trial | All-cause death at 30 days, n of N | 0 of 50 | 0 of 56 | NR | NR |
Nonfatal cardiovascular events | ||||||
Kandzari et al. 202320 | RCT SPYRAL-HTN-ON MED Expansion trial | New myocardial infarction at 6 months, n of N | 0 of 168 | 0 of 89 | NR | NR |
New stroke at 6 months, n of N (%) | 0 of 206 | 1 of 131 (0.7%) | NR | NR | ||
Heradien et al. 202222 | RCT | Subclinical atrial fibrillation at 2 years, n of N (%) | 8 of 42 (19%) | 15 of 38 (39.5%) | HR 0.40 (0.17 to 0.96) | 0.031 |
Major adverse events | ||||||
Singh et al. 202319 | SR (1 RCT) | Any major adverse events, n of N | 0 of 150 | 0 of 74 | NR | NR |
Kandzari et al. 202320 | RCT SPYRAL-HTN-ON MED Expansion trial | Significant embolic event resulting in end-organ damage, n of N | 0 of 168 | 0 of 89 | NR | NR |
Major bleeding at 6 months, n of N | 0 of 206 | 0 of 131 | NR | NR | ||
Vascular complicationsa at 6 months, n of N (%) | 2 of 206 (1.0%) | 2 of 131 (0.7%) | NR | NR | ||
Renal function eventsb at 6 months, n of N | 0 of 206 | 0 of 131 | NR | NR | ||
Pathak et al. 202321 | RCT TARGET BP OFF-MED trial | Any major adverse event at 30 days, n (%) | 1 (2.0)c | 1 (1.8)d | RR 1.12 (0.07 to 17.44) | 1.0 |
Any major adverse event at 12 months, n (%) | 1 (2.0) | 2 (3.8) | RR 0.54 (0.05 to 5.78) | 1.0 | ||
Heradien et al. 202222 | RCT | Periprocedural complications, n of N | 0 of 42 | 0 of 38 | NR | NR |
CI = confidence interval; HR = hazard ratio; NR = not applicable; RR = relative risk; RCT = randomized controlled trial; RDN = renal denervation.
aVascular complications included requiring surgical repair, intervention procedure, thrombin injection, or blood transfusion.
bRenal function complications included renal artery stenosis, renal artery perforation or dissection requiring intervention, serum creatinine elevation > 50%, or new-onset end-stage renal disease.
cHypertensive crisis.
dVascular complication (the patient developed a small subcutaneous hematoma; aneurysma spurium was subsequently diagnosed).
Appendix 5: Summary of Findings from Other Publications of Interest
Note that this appendix has not been copy-edited.
Table 10: Summary of Findings — Longer Follow-Up Periods
Trial name, study citation | Study design | Outcome | Outcome result, sample size | Effect estimate (95% CI) | P value | |
|---|---|---|---|---|---|---|
RDN | Sham | |||||
24-Hour ambulatory BP | ||||||
SPYRAL HTN-ON MED Pilot, Kario 202326 | RCT | 24-hour ambulatory SBP at 36 months, mean change from baseline [mm hg] | −20.2 N = 20 | −10.2 N = 18 | MD −10.5 (−18.2 to −2.8) | 0.0087 |
24-hour ambulatory DBP at 36 months, mean change from baseline [mm hg] | −13.2 N = 20 | −6.5 N = 18 | MD −7.4 (−11.8 to −3.1) | 0.0014 | ||
SYMPLICITY HTN-3, Bhatt 202227 | RCT | 24-hour ambulatory SBP at 36 months, mean change from baseline (SD) [mm hg] | −15.6 (20.8) N = 152 | −0.3 (15.1) N = 119 | MD −16.5 (−20.5 to −12.5) | < 0.0001 |
24-hour ambulatory DBP at 36 months, mean change from baseline [mm hg] | −9.9 N = 152 | −0.5 N = 119 | MD −11.2 (−13.6 to −8.7) | < 0.0001 | ||
Office BP | ||||||
SYMPLICITY HTN-3, Bhatt 202227 | RCT | Office SBP at 36 months, mean change from baseline (SD) [mm hg] | −26.4 (25.9) N = 219 | −5.7 (24.4) N = 134 | MD −22.1 (−27.2 to −17.0) | < 0.0001 |
Office DBP at 36 months, mean change from baseline [mm hg] | −12.2 N = 152 | −2.0 N = 119 | MD −12.0 (−14.6 to −9.3) | < 0.0001 | ||
Morning BPa | ||||||
SPYRAL HTN-ON MED Pilot, Kario 202326 | RCT | Morning SBP at 36 months, mean change from baseline [mm hg] | −23.9 N = 20 | −8.0 N = 18 | MD −12.3 (−23.2 to −1.3) | 0.0029 |
Morning DBP at 36 months, mean change from baseline [mm hg] | −17.0 N = 20 | −1.8 N = 18 | MD −13.3 (−20.9 to −5.8) | 0.0010 | ||
SYMPLICITY HTN-3, Bhatt 202227 | RCT | Morning SBP at 36 months, mean change from baseline [mm hg] | −13.9 N = 152 | 0.7 N = 119 | MD −15.1 (−19.6 to −10.4) | < 0.0001 |
Morning DBP at 36 months, mean change from baseline [mm hg] | −8.8 N = 152 | −0.8 N = 119 | MD −10.4 (−13.6 to −7.3) | < 0.0001 | ||
Nighttime BPb | ||||||
SPYRAL HTN-ON MED Pilot, Kario 202326 | RCT | Nighttime SBP at 36 months, mean change from baseline [mm hg] | −20.8 N = 20 | −7.2 N = 18 | MD −15.0 (−23.7 to −6.4) | 0.0011 |
Nighttime DBP at 36 months, mean change from baseline [mm hg] | −15.0 N = 20 | −4.7 N = 18 | MD −11.8 (−17.8 to −5.9) | 0.0003 | ||
SYMPLICITY HTN-3, Bhatt 202227 | RCT | Nighttime SBP at 36 months, mean change from baseline [mm hg] | −14.5 N = 152 | 2.0 N = 119 | MD −15.9 (−20.4 to −11.5) | < 0.0001 |
Nighttime DBP at 36 months, mean change from baseline [mm hg] | −9.4 N = 152 | −0.8 N = 119 | MD −11.2 (−14.0 to −8.4) | < 0.0001 | ||
TTR | ||||||
SYMPLICITY HTN-3, Bhatt 202227 | RCT | TTR % at 36 months, mean (SD) | 18 (25) N = 357 | 9 (19) N = 171 | NR | < 0.0001 |
Adverse events | ||||||
SPYRAL HTN-ON MED Pilot, Mahfoud 202328 | RCT | Composite safety end pointc at 36 months, n of N | 1d | 1e | NR | NR |
SYMPLICITY HTN-3, Bhatt 202227 | RCT | Composite safety end pointc at 48 months, n of N (%) | 54 of 352 (15%) | Crossoverf 13 of 96 (14%) Noncrossoverg 10 of 69 (14%) | NR | NR |
AH = antihypertensive; CI = confidence interval; DBP = diastolic blood pressure; MD = mean difference; RCT = randomized controlled trial; RDN = renal denervation; SD = standard deviation; SBP = systolic blood pressure; TTR = time in therapeutic range.
aMorning is defined as 7:00 a.m. to 9:00 a.m.
bNighttime is defined as 1:00 a.m. to 6:00 a.m.
cDefined as a composite of all-cause mortality, end-stage renal disease, embolic event resulting in end-organ damage, renal artery perforation requiring reintervention, renal artery dissection requiring reintervention, vascular complications, hospitalization for hypertensive crisis or emergency, or new renal artery stenosis > 70%.
dOne patient had a hypertension crisis and stroke at 427 days after the procedure; the patient presented to the emergency department with weakness on the left side and elevated BP (193 mm Hg over 123 mm Hg), received inpatient treatment, and was discharged in a stable condition.
eOne cardiovascular death occurred 693 days after the procedure; the patient was found unconscious at home, and an autopsy was not performed; therefore, cause of death is unknown.
f Crossover group included patients randomized to sham, who underwent RDN after 6 months.
gNoncrossover group included patients randomized to sham, who did not receive RDN.
Table 11: Summary of Recommendations in Guidelines
Recommendations |
|---|
ESH (2023)29 |
RDN can be considered as a treatment option in patients with an eGFR > 40 mL/min/1.73m2 who have uncontrolled BP despite the use of antihypertensive drug combination therapy, or if drug treatment elicits serious side effects and poor quality of life. |
RDN can be considered as an additional treatment option in patients with true resistant hypertension if eGFR is > 40 mL/min/1.73m2. |
Selection of patients to whom RDN is offered should be done in a shared decision-making process after objective and complete patient’s information. |
RDN should only be performed in experienced specialized centres to guarantee appropriate selection of eligible patients and completeness of the denervation procedure. |
NICE (2023)30 |
1.1 Percutaneous transluminal renal sympathetic denervation for resistant hypertension should only be used with special arrangements for clinical governance, consent, and audit or research. |
1.2 Clinicians wanting to do percutaneous transluminal renal sympathetic denervation for resistant hypertension should:
|
1.3 Health care organizations should:
|
1.4 Further research should include randomized controlled trials or analysis of registry data. It should report details of patient selection, technique used and long-term outcomes. |
1.5 Patient selection should be done by a multidisciplinary team including experts in managing hypertension and potential complications, and clinicians with specific training in this procedure. |
Taiwan Hypertension Guidelines 202231 |
9. Renal denervation can be considered as a BP-lowering strategy in hypertensive patients with high CV risk, such as resistant or masked uncontrolled hypertension, established ASCVD, intolerant or nonadherent to antihypertensive drugs, or features indicative of neurogenic hypertension after careful clinical and imaging evaluation. |
ASCVD = atherosclerotic cardiovascular diseases; BP = blood pressure; CV = cardiovascular; eGFR = estimated glomerular filtration rate; ESH = European Society of Hypertension; RDN = renal denervation; NICE = National Institute for Health and Care Excellence.
Table 12: Summary of Findings — Real-World Evidence
Study citation | Study design | Outcomes | No. AH medications | Outcome result, sample size | Effect estimate (SD or 95% CI) | P value | |
|---|---|---|---|---|---|---|---|
Baseline (pre-RDN) | Follow-up (post-RDN) | ||||||
24-Hour BP | |||||||
Global SYMPLICITY registry DEFINE33 | Multicentre, prospective, open-label, observational studya | Change in 24-hour SBP from baseline at 36 months, mean (SD) [mm hg] | 0 to 3 | N = 70 | MD −10.7 (19.7) | < 0.0001 | |
≥ 4 | N = 420 | MD −8.9 (20.5) | < 0.0001 | ||||
Flex-Sypral Registry10 | Multicentre registry in Spainb | 24-hour ambulatory SBP at baseline and 12 months, mean (SD) [mm hg] | ≥ 3 | 151 (20) N = 68 | 136 (22) N = 53 | NR | < 0.0001 |
24-hour ambulatory DBP at baseline and 12 months, mean (SD) [mm hg] | 89 (16) N = 68 | 82 (16) N = 53 | NR | < 0.0001 | |||
Sea Ashton et al. 20232 | Prospective observational studyc | 24-hour ambulatory SBP at baseline and 8.8 mean (SD 1.2) years, mean (SD) [mm hg] | ≥ 3 | 145.2 (17.3) N = 61 | 133.1 (18.3) N = 61 | MD −12.1 (−17.78 to −6.32) | < 0.0001 |
24-hour ambulatory DBP at baseline and 8.8 mean (SD 1.2) years, mean (SD) [mm hg] | 81.2 (12.2) N = 61 | 72.7 (10.4) N = 61 | MD −8.8 (−12.12 to −5.48) | < 0.0001 | |||
Office BP | |||||||
SYMPLICITY registry33 | Multicentre, prospective, open-label, observational studya | Office SBP at 36 months, mean change from baseline [mm hg] | 0 to 3 | N = 223 | MD −19.0 (28.3) | < 0.0001 | |
≥ 4 | N = 1,008 | MD −16.2 (28.6) | < 0.0001 | ||||
Flex-Sypral Registry10 | Multicentre registry in Spainb | Office SBP at baseline and 12 months, mean (SD) [mm hg] | ≥ 3 | 166 (20) N = 110 | 146 (22) N = 99 | NR | < 0.0001 |
Office SBP at baseline and 12 months, mean (SD) [mm hg] | 95 (16) N = 110 | 87 (16) N = 99 | NR | < 0.0001 | |||
Sea Ashton et al. 20232 | Prospective observational studyc | 24-hour ambulatory SBP at baseline and 8.8 mean (SD 1.2) years, mean (SD) [mm hg] | ≥ 3 | 151.5 (22.1) | 138.8 (21.0) | NR | < 0.01 |
24-hour ambulatory DBP at baseline and 8.8 mean (SD 1.2) years, mean (SD) [mm hg] | 79.4 (16.0) | 75.9 (14.6) | NR | NSS | |||
Adverse events | |||||||
SYMPLICITY registry33 | Multicentre, prospective, open-label, observational studya | Composite major cardiovascular adverse eventsd at 36 months | 0 to 3 | N = 310 | 10.6% | NR | |
≥ 4 | N = 1,465 | 11.1% | NR | ||||
Sea Ashton et al. 20232 | Prospective observational studyc | Nonfatal major adverse cardiovascular events at 8.8 mean (SD 1.2) years, mean (SD) [mm hg] | ≥ 3 | N = 66 | 6.0%e | < 0.0001 | |
AH = antihypertensive; DBP = diastolic blood pressure; MD = mean difference; NS = not statistically significant; RDN = renal denervation; SD = standard deviation; SBP = systolic blood pressure.
aFull population included patients with a mean age of 61 years, 42% female gender, 47% with a history of cardiovascular disease, and mean 4.6 prescribed AH medications.33
bPopulation included patients with a mean age of 56 years, 41% female gender, and 12% with previous ischemic heart disease and mean 4.9 prescribed AH medications.10
cPopulation included patients with a mean age of 61 years, 16% female gender, and mean 4.2 prescribed AH medications.2
dIncluded myocardial infarction, cardiovascular deaths, all-cause deaths, and hospitalization for heart disease.33
eThe 4 events were 3 nonfatal strokes and 1 nonfatal myocardial infarction. Sixty-two participants reported no adverse major cardiovascular events; however, 3 additional patients received coronary artery stents following the discovery of notable coronary stenosis. One participant noted they had begun dialysis treatment on a background of significant preexisting chronic kidney disease before RDN.
Appendix 6: Overlap Between Included SRs
Note that this appendix has not been copy-edited.
Table 13: Overlap in Relevant Primary Studies Between Included Systematic Reviews
Trial name, primary study citation | Singh 202319 | |
|---|---|---|
Desch S, et al. Hypertension. 2015; 65(6):1202 to 8. | Yes | Yes |
RADIANCE-HTN SOLO. Azizi M, et al. Lancet. 2018;391(10137):2235 to 2345. | Yes | Yes |
RADIANCE HTN TRIO Azizi M, et al. Lancet. 2021;397(10293):2476 to 86. | Yes | Yes |
RADIANCE II. Azizi M, et al. JAMA. 2023;329(8):651 to 61. | — | Yes |
REDUCE HTN: REINFORCE. Weber MA, et al. JACC: Cardiovasc Interven. 2020;13(4):461 to 70. | Yes | Yes |
REQUIRE. Kario K, et al. Hypertens Res. 2022;45(2):221 to 31. | Yes | — |
ReSET. Mathiassen ON, et al. J Hypertens. 2016;34(8):1639 to 47. | Yes | Yes |
SPYRAL HTN-OFF MED Pivotal. Böhm M, et al. Lancet. 2020;395(10234):1444 to 51. | Yes | Yes |
SPYRAL HTN-ON MED Pilot. Kandzari DE, et al. Lancet. 2018;391(10137):2346 to 55. | Yes | Yes |
SYMPLICITY HTN 3. Bhatt DL, et al. N Engl J Med. 2014;370(15):1393 to 1401. | Yes | Yes |
WAVE IV. Schmeider RE, et al. J Hypertens. 2018;36(3):680 to 9. | Yes | — |
Appendix 7: References of Potential Interest
Previous CADTH Reports
Kumar D, Loshak H. CADTH horizon scan: Renal denervation for people with hypertension. Can J Health Technol. 2022;2(1). https://canjhealthtechnol.ca/index.php/cjht/article/view/en0038/en0038. PubMed
Systematic Reviews
Systematic Reviews in Which All Relevant Studies Were Captured in Systematic Reviews Included in the Report
Ahmed M, Nudy M, Bussa R, Filippone EJ, Foy AJ. A systematic review and meta-analysis of all sham and placebo controlled trials for resistant hypertension. Eur J Intern Med. 2023;113:83-90. PubMed
Agasthi P, Shipman J, Arsanjani R, et al. Renal denervation for resistant hypertension in the contemporary era: A systematic review and meta-analysis. Sci Rep. 2019;9(1):6200. PubMed
Cheng X, Zhang D, Luo S, Qin S. Effect of catheter-based renal denervation on uncontrolled hypertension: A systematic review and meta-analysis. Mayo Clin Proc. 2019;94(9):1695-1706. PubMed
Dahal K, Khan M, Siddiqui N, et al. Renal denervation in the management of hypertension: A meta-analysis of sham-controlled trials. Cardiovasc Revasc Med. 2020;21(4):532-537. PubMed
Clinical evidence assessment: Paradise Renal Denervation System (ReCor Medical, Inc.) for treatment-resistant hypertension. Plymouth Meeting (PA): ECRI Institute; 2024: www.ecri.org. Accessed 2024 Feb 5.
Maqsood MH, Rubab K, Anwar F, et al. A systematic review of randomized controlled trials comparing renal sympathetic denervation versus sham procedure for the management of uncontrolled hypertension. J Cardiovasc Pharmacol. 2021;77(2):153-158. PubMed
Pisano A, Iannone LF, Leo A, Russo E, Coppolino G, Bolignano D. Renal denervation for resistant hypertension. Cochrane Database Syst Rev. 2021;11():CD011499.
Silverwatch J, Marti KE, Phan MT, et al. Renal denervation for uncontrolled and resistant hypertension: Systematic review and network meta-analysis of randomized trials. J Clin Med. 2021;10(4):782. PubMed
Sardar P, Bhatt DL, Kirtane AJ, et al. Sham-controlled randomized trials of catheter-based renal denervation in patients with hypertension. J Am Coll Cardiol. 2019;73(13):1633-1642. PubMed
Stavropoulos K, Patoulias D, Imprialos K, et al. Efficacy and safety of renal denervation for the management of arterial hypertension: A systematic review and meta-analysis of randomized, sham-controlled, catheter-based trials. J Clin Hypertens (Greenwich). 2020;22(4):572-584. PubMed
Syed M, Osman M, Alhamoud H, et al. The state of renal sympathetic denervation for the management of patients with hypertension: A systematic review and meta-analysis. Catheter Cardiovasc Interv. 2021;97(4):E438-E445. PubMed
Tian Z, Vollmer Barbosa C, Lang H, Bauersachs J, Melk A, Schmidt BMW. Efficacy of pharmacological and interventional treatment for resistant hypertension-a network meta-analysis. Cardiovasc Res. 2023;27():27.
Wales Health Technology. Renal denervation to treat people with resistant hypertension [Evidence Appraisal Report]. 2023: https://healthtechnology.wales/wp-content/uploads/2022/02/EAR042-Renal-Denervation-WEB.pdf Accessed 2024 Feb 13.
Yang X, Liu H, Chen S, Dong P, Zhao D. Intravascular renal denervation reduces ambulatory and office blood pressure in patients with essential hypertension: A meta-analysis of randomized sham-controlled trials. Kidney Blood Press Res. 2022;47(6):363-374. PubMed
Economic Evaluations
Sharp ASP, Cao KN, Esler MD, et al. Cost-effectiveness of catheter-based radiofrequency renal denervation for the treatment of uncontrolled hypertension: An analysis for the UK based on recent clinical evidence. Eur Heart J Qual Care Clin Outcomes. 2024; 09:qcae001. PubMed
Taylor RS, Bentley A, Metcalfe K, et al. Cost effectiveness of endovascular ultrasound renal denervation in patients with resistant hypertension. Pharmacoeconom Open. 2024;30:30. PubMed
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for noncommercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca