Drugs, Health Technologies, Health Systems
Health Technology Review
Attention-Deficit/Hyperactivity Disorder Medications for Adults
Key Messages
What Is the Issue?
Pharmacological treatment for attention-deficit/hyperactivity disorder (ADHD) focuses on medications that elevate the levels of certain neurotransmitters in the brain such dopamine and norepinephrine to target ADHD symptoms of impulsivity, inattention, and hyperactivity.
The medications are classified as stimulants and nonstimulants. Stimulants are drugs with a rapid effect, but they also have the potential for dependence, misuse, and diversion; nonstimulants may take longer to have an effect, but they do not have the same potential for drug misuse.
Decision-makers are interested in understanding how medications are chosen to treat ADHD in the general adult population as well as in the correctional setting.
What Did We Do?
We identified and summarized the literature on the evidence of the clinical effectiveness, safety, and cost-effectiveness of stimulants and nonstimulants for the treatment of ADHD in adults. We also searched for evidence-based guidelines that provide recommendations on the use of stimulants and nonstimulants for the management of ADHD in adults.
We searched key resources, including journal citation databases, and conducted a focused internet search for relevant evidence published since 2019. One reviewer screened citations for inclusion based on predefined criteria, critically appraised the included studies, and narratively summarized the findings.
What Did We Find?
We identified an Australian evidence-based guideline for ADHD. The aim of the guideline is to promote the timely identification, diagnosis, and treatment of ADHD across the lifespan of patients.
With respect to medication choice for the treatment of ADHD in adults (aged 18 years and older), the guideline recommends that stimulants — such as methylphenidate, dexamfetamine, or lisdexamfetamine — be offered as first-line treatment for people living with ADHD whose symptoms cause significant impairment.
The guideline recommends that nonstimulants, such as atomoxetine or guanfacine, be offered as second-line treatment if stimulants are contraindicated, not tolerated, or ineffective. Concurrent treatment with both stimulants and nonstimulants is also recommended to increase the benefit of treatment. Other drugs such as bupropion, clonidine, modafinil, reboxetine, and venlafaxine may be offered as third-line treatments. Regarding fourth-line treatments for adults with ADHD, based on expert opinion and clinical experience of the guideline development group members, a clinical practice point was made to include lamotrigine, aripiprazole, agomelatine, armodafinil, and desvenlafaxine.
Although we found no evidence on the optimal medication choice for specific populations, such as people in the correctional system or people with co-occurring substance use disorder, the guideline recommends exercising caution when prescribing stimulants as first-line therapy to people who have a risk of misuse or diversion.
We did not find any studies on the clinical effectiveness, safety, and cost-effectiveness of stimulants compared to nonstimulants for the management of adult ADHD.
What Does This Mean?
Recommendations from the identified guideline suggest that stimulants are commonly prescribed as first-line treatment for adult ADHD because of their rapid effect.
However, for people living with ADHD who have a risk of misuse or diversion, prescribing nonstimulants as first-line therapy may be a better option.
Abbreviations
AADPA
Australian ADHD Professionals Association
ADHD
attention-deficit/hyperactivity disorder
CPP
clinical practice point
EBR
evidence-based recommendation
GDG
guideline development group
GRADE
Grading of Recommendations, Assessment, Development and Evaluation
Context and Policy Issues
What Is ADHD in Adults?
ADHD is a neurologic and neurodevelopmental disorder, affecting 4% to 6% adults and 5% to 7% children in Canada.1 ADHD begins in childhood and, for up to 50% of these people, continues into adulthood.2 People living with ADHD experience 1 or a combination of 3 main types of symptoms such as inattention (having difficulty paying attention), hyperactivity (having too much energy), and impulsivity (acting without proper thinking or having difficulty with self-control).3 Adults with ADHD experience various complications such as problems at work, in life, and with relationships.4
Often, people with ADHD have difficulty regulating their emotions and are unaware of their ADHD symptoms.1 Moreover, adult ADHD is usually comorbid with other psychiatric disorders that mask ADHD symptoms and make receiving a correct diagnosis even more difficult.5 There is no single “gold standard” tool for diagnosing ADHD. Therefore, in adults, a thorough evaluation using a differential diagnosis for ADHD requires a range of data including history of childhood behaviour and school performance, self-reported symptoms, and mental health status testing.2,3 Some risk factors that may play a role in developing ADHD include genetics, brain injury, nutrition, exposure to toxic substances, and alcohol and/or substance abuse during pregnancy.4
Treatment of ADHD usually requires a multimodal approach, which includes medications, nonpharmacological interventions (such as cognitive behavioural therapy), and self-management strategies.2,5
What Are the Medication Options for ADHD in Adults?
ADHD is associated with a deficiency of some neurotransmitters, which are chemicals that transmit signals between nerve cells in specific areas of the brain.6 ADHD medications can be classified into 3 main types: stimulants, nonstimulants, and antidepressants; antidepressants are sometimes grouped into the nonstimulant class.7 Irrespective of the types of ADHD medications, they primarily act by increasing levels of neurotransmitters in the brain through different mechanisms.6,8 Increasing levels of these chemicals help to reduce ADHD symptoms such as hyperactivity and impulsivity, improve attention span, and regulate emotions.8
Stimulants, also called psychostimulants, have been considered the primary pharmacologic therapy for ADHD.8,9 They stimulate specific cells in the brain to produce more neurotransmitters, like dopamine and norepinephrine.8 Two common types of stimulants that are prescribed for adult ADHD are amphetamine and methylphenidate and their derivatives.8,9 They can be short-acting or long-acting.8 These drugs have a rapid effect, which can be seen in about 30 to 45 minutes. The effect lasts for 3 to 6 hours for short-acting stimulants and 8 to 16 hours for long-acting stimulants.8 The most common side effects of stimulant medications for ADHD are increased heart rate, increased blood pressure, reduced appetite, and difficulty sleeping, among others.8,9 Stimulants have the potential for dependence, misuse, and diversion.8
There are 2 classes of nonstimulant medications for ADHD.8,10 These are the selective norepinephrine reuptake inhibitors (atomoxetine and viloxazine) and the apha-2 adrenergic agonists (clonidine and guanfacine).8,10 Atomoxetine and viloxazine increase concentrations of norepinephrine and dopamine by inhibiting the reuptake of those chemicals, while clonidine and guanfacine act as receptor modulators by mimicking the effects of norepinephrine in the brain receptors.6,7 Compared to stimulants, nonstimulant medications take longer to start working, and ADHD symptoms begin to improve after about 4 to 8 weeks.11 Nonstimulant medications are not considered to be first-line treatment for ADHD, but they may be suitable for patients who cannot tolerate the side effects of stimulants, have no improvement in symptoms with stimulants, cannot take stimulants because of another health condition, have a history of substance abuse, or could benefit from a combination of stimulant and nonstimulant medications.7 Some side effects associated with nonstimulants include fatigue, insomnia, nausea, loss of appetite, and stomach pain.8,9 Unlike stimulants, nonstimulant drugs do not have the same potential for drug misuse.9
Antidepressants that increase the levels of norepinephrine have been used as off-label medications to treat ADHD in adults.8,9 These include venlafaxine (a serotonin and norepinephrine reuptake inhibitor), bupropion (a norepinephrine and dopamine reuptake inhibitor), and tricyclic antidepressants (e.g., nortriptyline, imipramine, desipramine), which block the reabsorption of serotonin and norepinephrine in different neurotransmitter pathways.8,9 These antidepressant medications are also considered to be nonstimulants and are usually used as second- or third-line treatment for ADHD, or they are prescribed to people with mild symptoms of ADHD and depression.8,9 Side effects of venlafaxine include diarrhea, dry mouth, feeling nervous, insomnia, restlessness, fatigue, increased blood pressure, and sexual difficulties.8,9 Side effects of bupropion include headache, weight loss, nausea, dizziness, dry mouth, irregular heartbeats, trouble sleeping, and constipation.8,9 Side effects of tricyclic antidepressants include constipation, dizziness, dry mouth, blurred vision, confusion, urinary retention, and increased heart rate.8,9
Why Is It Important to Do This Review?
Because evidence of the efficacy and safety of stimulant and nonstimulant medications for the treatment of ADHD in adults was mostly derived from randomized placebo-controlled trials,12 it is unclear if there are any head-to-head comparisons of the clinical efficacy and safety of stimulants versus nonstimulants. In addition, decision-makers want to know whether nonstimulants could be used as first-line treatment for ADHD in adults, especially for people in correctional settings, since these medications have a lower potential to be misused compared to stimulants.
Objective
To support decision-making about the relative effects of pharmacologic treatments (stimulants versus nonstimulants), we prepared this Rapid Review to summarize and critically appraise the available studies on the clinical effectiveness and cost-effectiveness of stimulants compared to nonstimulants for the management ADHD in adults. We also sought to summarize recommendations from evidence-based guidelines on the pharmaceutical options for the management of ADHD in adults.
Research Questions
What is the clinical effectiveness and safety of stimulants compared to nonstimulants for the management of ADHD in adults?
What is the cost-effectiveness of stimulants compared to nonstimulants for the management of ADHD in adults?
What are the evidence-based guidelines for the use of stimulants compared to nonstimulants for the management of ADHD in adults?
Methods
Literature Search Methods
An information specialist conducted a literature search on key resources including MEDLINE, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concepts were stimulants and ADHD. Search filters were applied to limit retrieval to health technology assessments, systematic reviews, meta-analyses, indirect treatment comparisons, randomized controlled trials or controlled clinical trials, guidelines, and economic studies. The search was completed on August 20, 2024, and limited to English-language documents published since January 01, 2019.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Adults (≥ 18 years) with a diagnosis of ADHD Subgroup of interest: people incarcerated in correctional facilities/engaged in criminal activity |
Intervention | Stimulants Psychostimulant drugs (short-acting or extended-release)
|
Comparator | Nonstimulants Nonpsychostimulant drugs (with or without adjunctive psychostimulants)
Antidepressant drugs (e.g., bupropion, venlafaxine) Second-generation atypical antipsychotics (e.g., aripiprazole, clozapine, ziprasidone, risperidone, quetiapine, olanzapine, asenapine, and paliperidone) |
Outcomes | Clinical effectiveness (e.g., behavioural, functional, developmental, or cognitive outcomes assessed by validated scales [e.g., BRIEF-P, ADHD-RS IV, CGI-S, and CGI-I]) Patient-reported outcomes (e.g., health-related quality of life) Safety outcomes (e.g., harms, AEs including AEs of particular interest [e.g., hypotension and cardiovascular AEs], SAEs, discontinuations due to TEAEs, mortality) Cost-effectiveness Guidelines recommendations |
Study designs | RCTs, published HTAs, systematic reviews (including NMAs and MAs), published economic evaluations, evidence-based guidelines |
ADHD = attention-deficit/hyperactivity disorder; AE = adverse event; HTA = health technology assessment; MA = meta-analysis; NMA = network meta-analysis; RCT = randomized controlled trial; SAE = serious adverse event; TEAE = treatment-emergent adverse event.
Exclusion Criteria
We excluded articles that did not meet the selection criteria outlined in Table 1 and articles published before 2019. Guidelines with unclear methodology were excluded. Some of the guidance reports, which are not evidence-based guidelines, are presented in Appendix 5 as references of potential interest. Appendix 6 presents the summary of recommendations from 2 non-evidence-based clinical guidance reports that did not meet selection criteria.
Critical Appraisal of Individual Studies
One reviewer critically appraised the included evidence-based guideline using the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument.13 Summary scores were not calculated; rather, the strengths and weaknesses of the guideline were described narratively.
Summary of Evidence
Quantity of Research Available
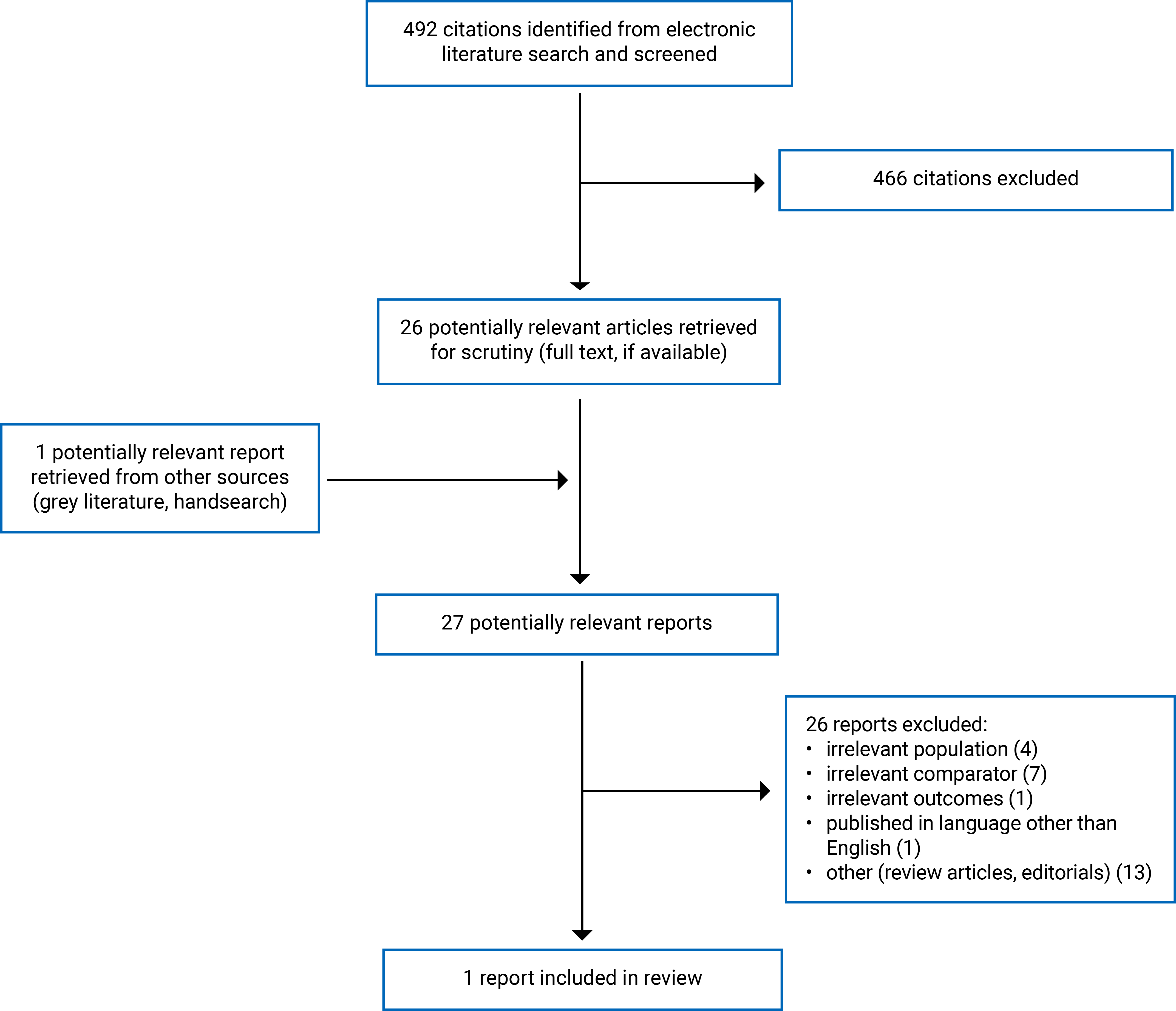
We identified a total of 492 citations from the literature search. Following screening of titles and abstracts, we excluded 466 citations and retrieved 26 potentially relevant reports from the electronic search for full-text review. We also retrieved 1 potentially relevant publication from the grey literature search. Of these potentially relevant articles, we excluded 26 publications for various reasons and included 1 publication (an evidence-based guideline) that met the inclusion criteria. Appendix 1 presents the PRISMA14 flow chart of the study selection.
Summary of Study Characteristics
Included Studies for Question 1: What Is the Clinical Effectiveness and Safety of Stimulants Compared to Nonstimulants for the Management of ADHD in Adults?
We did not identify any studies on the comparative clinical effectiveness and safety of stimulants versus nonstimulants for the management of ADHD in adults.
Included Studies for Question 2: What Is the Cost-Effectiveness of Stimulants Compared to Nonstimulants for the Management of ADHD in Adults?
We did not identify any economic evaluations on the cost-effectiveness of stimulants compared to nonstimulants for the management of ADHD in adults.
Included Studies for Question 3: What Are the Evidence-Based Guidelines for the Use of Stimulants Compared to Nonstimulants for the Management of ADHD in Adults?
Appendix 2 provides details regarding the characteristics of the included evidence-based guideline.15
Study Design
The identified guideline15 was developed by the Australian ADHD Professionals Association (AADPA) to update the evidence-based UK National Institute for Health and Care Excellence (NICE) guideline on the diagnosis and management of ADHD.16 Evidence supporting the recommendations of the AADPA guideline15 was derived, in part, from the NICE guideline.16 A systematic search for new evidence, study selection, data extraction, and data synthesis were also performed for the AADPA guideline.15
The guideline development group (GDG) consisted of 23 members, including psychiatrists, pediatricians, general practitioners, psychologists, speech pathologists, occupational therapists, educators, Indigenous psychologists, and people with a lived experience of ADHD, with 2 independent chairs and a methodologist. The methods used to develop the guideline were aligned with the AGREE II and the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) approach to meet the criteria for approval of an evidence-based guideline.
Each recommendation was rated and classified by 4 key elements: type, wording, strength, and certainty.
Recommendation type was either evidence-based recommendation (EBR) (a systematic evidence review) or clinical consensus recommendation (a narrative review). In addition, clinical practice points (CPPs) (guidance based on expert opinion) were included for implementation issues such as safety, side effects, and risks.
Recommendation wording reflects the GDG’s overall interpretation of the evidence and other considerations. The word should indicates the GDG’s judgment that the benefits of the recommended action exceed the harms. Could indicates that the quality of evidence was limited, the available studies did not clearly demonstrate the advantage of 1 approach over another, or the balance of benefits to harm was unclear. Should not indicates either a lack of appropriate evidence or that the harms were judged to outweigh the benefits.
The grade (or strength) of EBRs (e.g., strong recommendation or conditional recommendation) was determined by the GDG based on a comprehensive consideration of all elements of the evidence-to-decision framework, including desirable and undesirable effects, balance of effects, resource requirements, equity, acceptability, and feasibility.
Certainty of evidence (very low to high) for EBRs reflects the quality and relevance of the evidence, based on information about the number and design of studies addressing the outcome; judgments about the quality of the studies and/or synthesized evidence across risk of bias, inconsistency, indirectness, imprecision, and any other quality considerations; key statistical data; and classification of the importance of outcomes. Certainty was graded using GRADE.
Country of Origin
The authors of the AADPA guideline15 were from Australia.
Patient Population
The target populations of the AADPA guideline15 were children, adolescents, and adults with ADHD and their families, parents and carers, and partners. The intended users included clinicians, nurses, pharmacists, and other people involved in supporting people living with ADHD, such as educators.
Interventions and Practice Considered
The AADPA guideline15 provides guidance on identification, diagnosis, and multimodal treatment and support of people with ADHD by addressing 50 prioritized clinical questions. Treatments included pharmacological and nonpharmacological interventions.
Outcomes
The AADPA guideline15 considered all relevant outcomes related to the clinical questions.
Summary of Critical Appraisal
The AADPA guideline15 had several strengths related to reporting. It was explicit in terms of scope and purpose (i.e., objectives, health questions, and populations) and clearly presented the recommendations (i.e., specific, unambiguous, and easy-to-find key recommendations, with options for managing the different conditions or health issues). In terms of the involvement of interested parties, the authors of the guideline clearly defined target users and the development groups, and they reported that they sought the views and preferences of patients. The methodology for the development of the guideline was robust. The authors of the guideline clearly reported methods for evidence collection, criteria for selection, and methods for evidence synthesis. There were explicit links between recommendations and the supporting evidence and methods of formulating the recommendations. Also, the authors of the guideline considered the health benefits and risks of side effects when formulating the recommendations. The authors reported that the guideline will be updated in the next 5 years. The guideline was reviewed independently by relevant professional experts, by professional colleges and societies, and through public consultation. However, there were some limitations related to guideline implementation and applicability. Specifically, facilitators and barriers to application, advice and/or tools on how the recommendations can be put into practice, and monitoring or auditing criteria were unclear. For editorial independence, the authors of the guideline declared the competing interests of all GDG members and disclosed that the views of the funding body (i.e., the Australian Government’s Department of Health) had no influence on the content of the guidelines.
Overall, the included guideline was robust in terms of scope and purpose, the involvement of interested parties, rigour of development, clarity of presentation, and editorial independence.
Summary of Findings
Appendix 4 presents the recommendations of the AADPA guideline15 on the choice of medications for the treatment of ADHD in adults (aged 18 years and older) (Table 4). We also referred to the first edition of the guideline published online for additional CPP recommendations.17
The AADPA guideline15 recommends prescribing stimulants such as methylphenidate, dexamfetamine, or lisdexamfetamine as first-line treatment for people living with ADHD. The recommendation was supported by evidence provided from the previous NICE guideline,16 with no new studies identified. This recommendation was an EBR, which was rated as a strong recommendation but with very low certainty.
The AADPA guideline15 recommends prescribing nonstimulants, such as atomoxetine or guanfacine, as second-line treatment of ADHD in adults if stimulants are contraindicated or if patients experience negative side effects from stimulants, have no improvement in symptoms from stimulants, or could benefit from a combination of stimulants and nonstimulants. For atomoxetine versus placebo, the recommendation was supported by evidence provided from the previous NICE guideline,16 with no new studies identified. For guanfacine versus placebo, the recommendation was supported by evidence from the NICE guideline16 and 1 new randomized controlled trial. No new evidence was found for guanfacine versus dexamfetamine. This recommendation was an EBR, which was rated as a strong recommendation but with very low certainty.
The AADPA guideline15 also recommends further medication choices as a subsequent line of treatment for ADHD in adults. These medications include antidepressants (e.g., venlafaxine, desvenlafaxine, bupropion, reboxetine, and agomelatine), blood pressure medications (e.g., clonidine), atypical antipsychotics (e.g., aripiprazole), a mood stabilizer (e.g., lamotrigine), and other stimulants (e.g., modafinil and armodafinil). The recommendation on the use of bupropion, clonidine, modafinil, reboxetine, and venlafaxine was an EBR, and these drugs were recommended as third-line treatments with very low certainty of evidence based on the evidence review. The recommendation on the use of the remaining medications as fourth-line treatments (i.e., lamotrigine, aripiprazole, agomelatine, armodafinil, and desvenlafaxine) was a CPP, of which guidance was based on expert opinion and clinical experience of the GDG members. There is no particular order for using these medications. However, the guideline suggests that side effects of these medications should be carefully monitored.
The AADPA guideline15 also narratively reviewed the identification and treatment of ADHD in 3 subgroups: people in the correctional system, Aboriginal and Torres Strait Islander peoples, and people with co-occurring substance use disorder. With respect to pharmacological interventions, the guideline warns that stimulants should be offered with caution if there is a risk of diversion for cognitive enhancement. The guideline also recommends against prescribing immediate-release stimulants or modified-release stimulants that can be easily injected or inhaled if there is a risk of stimulant misuse or diversion. These recommendations are CPPs.
Limitations
Evidence Gaps
No evidence was found, therefore no conclusions can be formed, on the research questions related to:
the clinical effectiveness and safety of stimulants compared to nonstimulants for the management of ADHD in adults
the cost-effectiveness of stimulants compared to nonstimulants for the management of ADHD in adults.
Generalizability
Although we did not identify any Canadian guidelines regarding pharmacological interventions for ADHD in adults in this review, the recommendations in the AADPA guideline15 may be applicable to the adult population with ADHD living in Canada.
Certainty of Evidence
A limitation in the AADPA guideline15 was that most of the recommendations on the use of stimulants and nonstimulants for treatment of ADHD in adults were supported by evidence from the 2019 NICE guideline,16 without identifying any new evidence thereafter. Evidence on the efficacy and safety of stimulants and nonstimulants was derived mostly from placebo-controlled trials, without head-to-head trials. Although the strength of the EBRs for stimulants and nonstimulants was strong, the certainty of the evidence supporting the recommendation was low or very low, which impacts the confidence, as the true effect may be or is likely to be substantially different from the estimate of the effect.
Conclusions and Implications for Decision- or Policy-Making
This review included 1 Australian guideline15 that recommends stimulants (i.e., methylphenidate, dexamfetamine, or lisdexamfetamine) as first-line pharmacological treatment of ADHD in adults. If stimulants are not tolerated or ineffective, nonstimulants, such as atomoxetine or guanfacine, should be offered as a second-line treatment. A combination of stimulants and nonstimulants may be prescribed to increase the benefit of the treatment. Other drugs such as bupropion, clonidine, modafinil, reboxetine, and venlafaxine could be offered as third-line treatments. A CPP based on GDG clinical expertise was made regarding fourth-line treatments for adults with ADHD that included lamotrigine, aripiprazole, agomelatine, armodafinil, and desvenlafaxine.
These recommendations were made for the general population of adults living with ADHD. There was no evidence on medication options specifically for treating ADHD in people in the correctional system. The AADPA guideline15 recommends against prescribing stimulants as first-line therapy to people who have a risk of misuse or diversion.
Considerations for Future Research
Future research with head-to-head trials is needed to compare the clinical efficacy, safety, and cost-effectiveness of stimulants and nonstimulants for the treatment of ADHD in the general adult population as well as in the subpopulation of people in the correctional setting.
Implications for Clinical Practice
The findings of this report suggest that stimulants are commonly prescribed as first-line treatment for adult ADHD because of their rapid effect. However, prescribing nonstimulants as first-line therapy for ADHD to people who have a risk of misuse or diversion may be a better or more favourable option. Thus, the choice of medications used in the management of adult ADHD should be based on local resources and individual patients, who may or may not have a risk of abuse and diversion.
References
1.Centre for ADHD Awareness, Canada (CADDAC). About ADHD. 2024; https://caddac.ca/about-adhd/. Accessed 2024 Aug 22.
2.Searight HR, Burke JM, Rottnek F. Adult ADHD: evaluation and treatment in family medicine. Am Fam Physician. 2000;62(9):2077-2086. https://www.aafp.org/pubs/afp/issues/2000/1101/p2077.html. Accessed 2024 Aug 22. PubMed
3.ADHD in adults: 4 things to know. Bethesda (MD): National Institute of Mental Health; 2024: https://www.nimh.nih.gov/health/publications/adhd-what-you-need-to-know. Accessed 2024 Aug 22.
4.WebMD Editorial Contributor. Adult ADHD: symptoms, causes, treatments. New York (NY): WebMD LLC; 2023: https://www.webmd.com/add-adhd/adhd-adults. Accessed 2024 Aug 22.
5.Attention-deficit/hyperactivity disorder in adults: what you need to know. Bethesda (MD): National Institute of Mental Health; 2021: https://infocenter.nimh.nih.gov/sites/default/files/2021-12/attention-deficit-hyperactivity-disorder-in-adults-what-you-need-to-know_0.pdf. Accessed 2024 Aug 22.
6.Silver L. ADHD medication: stimulants, non-stimulants & more. New York (NY): ADDitude; 2024: https://www.additudemag.com/adhd-medication-for-adults-and-children/. Accessed 2024 Aug 22.
7.McMillen M, Walker-Journey J, King LM. ADHD Medication. New York (NY): WebMD LLC; 2024: https://www.webmd.com/add-adhd/adhd-medication-chart. Accessed 2024 Aug 22.
8.Frida. A complete guide to ADHD medications for adults. 2023; https://www.talkwithfrida.com/learn/a-complete-guide-to-adhd-medications-for-adults/. Accessed 2024 Aug 22.
9.Tee-Melegrito RA. Which medication is best for adult ADHD? Brighton (UK): Healthline Media UK Ltd; 2023: https://www.medicalnewstoday.com/articles/best-medication-for-adult-adhd. Accessed 2024 Aug 22.
10.Cleveland Clinic. ADHD medications: how they work & side effects. 2022; https://my.clevelandclinic.org/health/treatments/11766-adhd-medication. Accessed 2024 Aug 22.
11.Caporuscio J. List of ADHD medications: comparing types. Brighton (UK): Healthline Media UK Ltd; 2024: https://www.medicalnewstoday.com/articles/325201. Accessed 2024 Aug 22.
12.Veronesi GF, Gabellone A, Tomlinson A, Solmi M, Correll CU, Cortese S. Treatments in the pipeline for attention-deficit/hyperactivity disorder (ADHD) in adults. Neurosci Biobehav Rev. 2024;163:105774. PubMed
13.Agree Next Steps Consortium. The AGREE II Instrument. Hamilton (ON): AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf. Accessed 2024 Aug 20.
14.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
15.May T, Birch E, Chaves K, et al. The Australian evidence-based clinical practice guideline for attention deficit hyperactivity disorder. Aust N Z J Psychiatry. 2023;57(8):1101-1116. PubMed
16.National Institute for Health and Care Excellence. Attention deficit hyperactivity disorder: diagnosis and management. (NICE guideline NG87) 2019; https://www.nice.org.uk/guidance/ng87. Accessed 2024 Sep 09.
17.ADHD Guideline Development Group. Australian evidence-based clinical practice guideline for Attention Deficit Hyperactivity. 1st ed. Melbourne (AU): Australasian ADHD Professionals Association; 2022: https://adhdguideline.aadpa.com.au/. Accessed 2024 Aug 29.
18.ADHD and the justice system: the benefits of recognizing and treating ADHD in Canadian justice and correction systems. Toronto (ON): CADDAC; 2016: https://caddac.ca/wp-content/uploads/ADHD-and-the-Justice-system_-the-benefits-of-recognizing-and-treating-ADHD-EN.pdf. Accessed 2024 Aug 27.
19.Adult attention deficit/hyperactivity disorder (ADHD) - clinical guidance. Washington (DC): Federal Bureau of Prisons; 2021: https://www.bop.gov/resources/pdfs/adult_adhd_cd.pdf. Accessed 2024 Aug 26.
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publication
Please note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Guideline
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality assessment | Recommendations development and evaluation | Guideline validation |
|---|---|---|---|---|---|---|
AADPA, May et al. (2023)15 | ||||||
Intended users: Clinicians, nurses, pharmacists, and other people involved in the support of people with ADHD, such as educators Target population: People with ADHD and their families, parents and carers, and partners | Identification, diagnosis, and treatment of people with ADHD by addressing 50 prioritized clinical questions | All relevant outcomes | The guideline was based, in part, on the evidence-based NICE UK guidance on the diagnosis and management of ADHD. Systematic search for evidence, study selection, data extraction, and data synthesis were performed. | There are 4 key elements of each recommendation:
| The GDG consisted of professionals having backgrounds including, but not limited to, psychiatry, pediatrics, psychology, allied health, and ADHD coaching, as well as research into the causes and treatments of ADHD. | The guideline was reviewed independently by relevant professional experts, professional colleges and societies, and through public consultation. The guideline was published online and in a peer-reviewed journal. |
AADPA = Australian ADHD Professionals Association; ADHD = attention-deficit/hyperactivity disorder; GDG = guideline development group; GRADE = Grading of Recommendations, Assessment, Development and Evaluation; NICE = National Institute for Health and Care Excellence.
aRecommendation is either an evidence-based recommendation or a clinical consensus recommendation. In addition, clinical practice points were included for implementation issues such as safety, side effects, and risks.
bRecommendation wording reflects the GDG’s overall interpretation of the evidence and other considerations. The word should indicates the GDG’s judgment that the benefits of the recommended action exceed the harms. Could indicates that the quality of evidence was limited, or the available studies did not clearly demonstrate advantage of one approach over another, or the balance of benefits to harm was unclear. Should not indicates either a lack of appropriate evidence or that the harms were judged to outweigh the benefits.
cThe grade (strength) of evidence-based recommendations (strong recommendation or conditional recommendation) was determined by the GDG based on comprehensive consideration of all elements of the evidence-to-decision framework including desirable and undesirable effects, balance of effects, resource requirements, equity, acceptability, and feasibility. These include: strong recommendation for the option, conditional recommendation for the option, conditional recommendation for either the option or the comparator, and conditional recommendation against the option.
dCertainty of evidence (very low to high) for evidence-based recommendations reflects the quality and relevance of the evidence, based on information about the number and design of studies addressing the outcome, judgments about the quality of the studies and/or synthesized evidence across risk of bias, inconsistency, indirectness, imprecision, and any other quality considerations; key statistical data; and classification of importance of outcomes. High means we are very confident that the true effect lies close to that of the estimate of the effect. Moderate means we are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low means our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect. Very low means we have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect.
Appendix 3: Critical Appraisal of Included Publication
Please note that this appendix has not been copy-edited.
Table 3: Strengths and Limitations of Guideline Using AGREE II13
Item | AADPA, May et al. (2023)15 |
|---|---|
Domain 1: Scope and purpose | |
1. The overall objective(s) of the guideline is (are) specifically described. | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes |
3. The population (patients, public, etc.) to whom the guideline is meant to apply is specifically described. | Yes |
Domain 2: Involvement of interested parties | |
4. The guideline development group includes individuals from all relevant professional groups. | Yes |
5. The views and preferences of the target population (patients, public, etc.) have been sought. | Yes |
6. The target users of the guideline are clearly defined. | Yes |
Domain 3: Rigour of development | |
7. Systematic methods were used to search for evidence. | Yes |
8. The criteria for selecting the evidence are clearly described. | Yes |
9. The strengths and limitations of the body of evidence are clearly described. | Yes |
10. The methods for formulating the recommendations are clearly described. | Yes |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes |
12. There is an explicit link between the recommendations and the supporting evidence. | Yes |
13. The guideline has been externally reviewed by experts before its publication. | Yes |
14. A procedure for updating the guideline is provided. | Yes (after 5 years) |
Domain 4: Clarity of presentation | |
15. The recommendations are specific and unambiguous. | Yes |
16. The different options for management of the condition or health issue are clearly presented. | Yes |
17. Key recommendations are easily identifiable. | Yes |
Domain 5: Applicability | |
18. The guideline describes facilitators and barriers to its application. | Unclear |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | Unclear |
20. The potential resource implications of applying the recommendations have been considered. | Unclear |
21. The guideline presents monitoring and/or auditing criteria. | Unclear |
Domain 6: Editorial independence | |
22. The views of the funding body have not influenced the content of the guideline. | Yes |
23. Competing interests of guideline development group members have been recorded and addressed. | Yes |
AADPA = Australian ADHD Professionals Association; AGREE II = Appraisal of Guidelines for Research and Evaluation II.
Appendix 4: Main Study Findings
Please note that this appendix has not been copy-edited.
Table 4: Summary of Recommendations in Included Guideline15,17
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
|---|---|
Medication choice for adults (aged 18 years and older) | |
“Methylphenidate or dexamfetamine or lisdexamfetamine should be offered as the first-line pharmacological treatment for people with ADHD, where ADHD symptoms are causing significant impairment.”15 (p. 1107) | Type: EBR Strength: Strong Certainty: Low |
Supporting evidence: No new evidence was found. Evidence was from previous NICE guideline.16 | — |
“Atomoxetine or guanfacine should be offered to adults with ADHD if any of the following apply:
Due consideration of risks and safety is required, especially if medications are used in combination.”15 (p. 1107) | Type: EBR Strength: Strong Certainty: Very low |
Supporting evidence:
| |
Further medication choices | |
“The following could be offered to adults with ADHD, in no particular order:
Careful monitoring of adverse side effects is required.”15 (p. 1107) | Type: EBR Strength: Strong Certainty: Very low |
Supporting evidence: NR | — |
“The following could also be offered to adults with ADHD, in no particular order:
Careful monitoring of adverse side effects is required.”17 (p. 139) | Type: CPP Strength: NA Certainty: NA |
Supporting evidence: NA | — |
Factors influencing medication choices | |
“Clinicians should exercise caution when prescribing stimulants if there is a risk of diversion for cognitive enhancement.”17 (p. 140) | Type: CPP Strength: NA Certainty: NA |
“Clinicians should not offer immediate-release stimulants or modified-release stimulants that can be easily injected or inhaled if there is a risk of stimulant misuse or diversion.”17 (p. 140) | Type: CPP Strength: NA Certainty: NA |
Supporting evidence: NA | — |
AADPA = Australian ADHD Professionals Association; ADHD = attention-deficit/hyperactivity disorder; CPP = clinical practice point; EBR = evidence-based recommendation; NA = not applicable; NICE = National Institute for Health and Care Excellence; NR = not reported; RCT = randomized controlled trial; vs. = versus.
Appendix 5: References of Potential Interest
Please note that this appendix has not been copy-edited.
Randomized Controlled Trials
Asherson PJ, Johansson L, Holland R, et al. Randomised controlled trial of the short-term effects of osmotic-release oral system methylphenidate on symptoms and behavioural outcomes in young male prisoners with attention deficit hyperactivity disorder: CIAO-II study. Br J Psychiatry. 2023 01;222(1):7-17. PubMed
Clinical Practice Guidelines
Adult attention deficit/hyperactivity disorder (ADHD) - clinical guidance. Washington (DC): Federal Bureau of Prisons; 2021: https://www.bop.gov/resources/pdfs/adult_adhd_cd.pdf. Accessed 2024 Aug 26.
Canadian ADHD Resource Alliance. Canadian ADHD practice guidelines. 4.1 ed. Toronto (ON): CADDRA; 2020: https://adhdlearn.caddra.ca/wp-content/uploads/2022/08/Canadian-ADHD-Practice-Guidelines-4.1-January-6-2021.pdf. Accessed 2024 Oct 07.
Additional References
Tully J. Management of ADHD in prisoners-evidence gaps and reasons for caution. Front Psychiatry. 2022;13:771525. PubMed
Grimley A, Bartels L. The need for speed? Exploring the risks and benefits of pharmacological treatment for adult ADHD in prisons. Psychiatr Psychol Law. 2024:1-21.
ADHD and the justice system: the benefits of recognizing and treating ADHD in Canadian justice and correction systems. Toronto (ON): CADDAC; 2016: https://caddac.ca/wp-content/uploads/ADHD-and-the-Justice-system_-the-benefits-of-recognizing-and-treating-ADHD-EN.pdf. Accessed 2024 Aug 27.
Appendix 6: Summary of Recommendations From Non-Evidence-Based Clinical Guidance Reports
Given the fact that there is interest in the choice of medication for treatment of ADHD in people in correctional systems, it is noteworthy to highlight the pharmacological treatment protocols from the 2 papers,18,19 which were initially excluded from the review as they are not evidence-based guidelines. The first paper was developed by the Centre for ADHD Awareness, Canada (CADDAC) for recognizing and treating ADHD within Canadian justice and correction systems.18 The second paper was a US Federal Bureau of Prisons (BOP) Clinical Guidance,19 which provides recommendations for diagnosis and management of ADHD in adult patients in BOP custody.
The CADDAC paper18 recommends:
Nonstimulants such as atomoxetine, venlafaxine, or bupropion should be used as first-line treatment for people with ADHD in correction systems.
Stimulants such as lisdexamfetamine or osmotic-release oral system methylphenidate should be used as second-line if they are included in the Corrections Canada formulary, and they should be taken under supervision.
Stimulants should be given as liquid or soluble formulations to reduce the risk of diversion.
The Federal BOP clinical guidance19 recommends:
Concurrent treatment of ADHD with both medication therapy and psychotherapy should be prescribed, rather than sequential treatment, for adult patients in prisons.
As stimulants present many difficulties in the correctional setting because of the risk of abuse and diversion, nonstimulants (e.g., atomoxetine, guanfacine, clonidine, desipramine, bupropion) should be prescribed as first-line treatment for adults with ADHD in BOP facilities, while prescribing a stimulant should be withheld until failure with a nonstimulant.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.