Drugs, Health Technologies, Health Systems
Health Technology Review
Antiviral Drugs for Post-Exposure Prophylaxis Against Influenza A or Influenza B
Authors: Michael Law
This rapid review was conducted by Michael Law through the Post-Market Drug Evaluation CoLab Network.
Key Messages
What Is the Issue?
Antiviral medications for influenza can be used after exposure but before symptom onset to reduce the occurrence of symptomatic and asymptomatic influenza.
There are several different antiviral medications available for preventing influenza after exposure (also known as post-exposure prophylaxis). It is important to understand their overall and comparative efficacy for treatment and stockpiling decisions.
What Did We Do?
We conducted a rapid review of the recent evidence on the clinical efficacy and safety of different antiviral medications available in Canada for post-exposure prophylaxis.
We searched key resources, including journal citation databases, and conducted a focused internet search for relevant evidence published since 2020.
What Did We Find?
We identified 2 systematic reviews (SRs) of 12 randomized studies published in 2024. The included studies examined the efficacy of 3 antiviral medications (baloxavir, oseltamivir, and zanamivir) in preventing influenza infection. The reviews were generally well conducted.
The findings show that these 3 antiviral medications are effective in reducing symptomatic influenza infection; however, the evidence on their impact on overall influenza and asymptomatic influenza infections is less clear.
The evidence on the impact of these medicines on hospitalization and mortality was generally weak, with no strong conclusions. There is also little evidence of any additional adverse events (side effects) from these medicines.
We found no evidence on peramivir for any of the outcomes.
What Does It Mean?
The included studies support the efficacy and safety of 3 antiviral medications in post-exposure settings for influenza prevention. More evidence is needed to understand their impact on hospitalization and mortality.
Abbreviations
CI
confidence interval
HA
hemagglutinin
NA
neuraminidase
NMA
network meta-analysis
OR
odds ratio
RCT
randomized controlled trial
RR
rate ratio
SR
systematic review
Introduction and Rationale
Background
Disease Background
Influenza is an acute viral respiratory infection that can cause significant morbidity and mortality.1 There are 3 distinct types of influenza viruses that infect humans, including influenza A, B, and C.1 Influenza A infects multiple species, including humans, swine, equines, birds, and some marine mammals.1 It is more susceptible to antigenic mutations, which makes it a major cause of pandemics.1 In influenza A, the surface of the virion envelope is covered with the hemagglutinin (HA), neuraminidase (NA), and matrix 2 proteins.1 Each influenza A subtype is characterized by numbering both the HA and NA proteins (e.g., H3N2, H5N1).1 Antigenic mutations are associated with changes in the HA or NA surface proteins and are generally classified as antigenic drift or shift.1 Antigenic drift involves small, gradual amino acid substitutions of the HA or NA proteins that can result in smaller outbreaks.1 Antigenic shift occurs when there are significant changes in the HA or NA proteins that create novel influenza subtypes with the potential to cause widespread pandemics.1
Influenza is highly contagious and the primary symptoms are abrupt onset of fever, cough, chills or sweats, muscle aches, and malaise.2 Its onset is typically rapid and symptoms can persist for 2 to 8 days.2 Gastrointestinal symptoms, such as vomiting and diarrhea, can occur in children.1 A minority of patients, especially older adults, children, and those with comorbidities, can experience severe disease from viral or secondary bacterial pneumonia with respiratory and multiorgan failure.1 There are many complications of influenza, including cardiovascular, hematologic, musculoskeletal, neurologic, ocular, pulmonary, and renal.1 Patients can have an increased risk of complications from influenza because of having coexisting medical conditions, being aged 65 years or older, being aged 5 years or younger, residing in a long-term care facility, or being pregnant or postpartum.1
Influenza is ranked among the top 10 leading causes of death in Canada.1 According to data from before the COVID-19 pandemic, each year in Canada, it was estimated that influenza causes approximately 12,200 hospitalizations and 3,500 deaths.3 This resulted in each hospitalization for influenza costing between $14,000 to $20,000 for the Canadian health care system.3,4 Given the estimated number of hospitalizations each year, the cost to the Canadian economy is between $168 to $240 million.3
In clinical practice, influenza diagnosis is based on presenting signs and symptoms, or if the patient has a suspected influenza-associated complication, such as exacerbation of a chronic disease, concomitant pneumonia, or rhabdomyolysis (i.e., muscle breakdown).2 In outpatient and emergency department settings, influenza testing is not necessary to start antiviral treatment in a patient with suspected influenza, especially during seasons when influenza A or B viruses are circulating in the local community.2 According to the Centers for Disease Control, influenza testing can be considered when the results will modify treatment or when a patient with signs or symptoms is hospitalized.2 There are several point of care diagnostic test types for influenza.2
Prevention of Influenza
The Public Health Agency of Canada National Advisory Committee on Immunization recommends that the seasonal influenza vaccine be offered annually to everyone aged 6 months and older who does not have contraindications to the vaccine, regardless of whether they received the seasonal influenza vaccine in previous seasons.5 Influenza immunization is particularly important for high-risk groups.5 In addition, prophylaxis with antiviral medication can be used in either a pre-exposure or post-exposure approach. In a post-exposure setting, this involves the administration of an antiviral medication after exposure to an infectious case but before the presence of symptoms or a positive test result. Antiviral drugs are recommended under various scenarios for pre-exposure or post-exposure prevention.6
Treatment of Influenza
The Public Health Agency of Canada recommends treatment with antiviral drugs in persons with influenza symptoms who are considered high risk for severe influenza or who are severely ill.1 Early treatment with an antiviral drug has been shown to lead to shorter duration of symptoms and fewer complications.7 The Centers for Disease Control recommends antiviral therapy for patients with severe or progressive illness who are at risk of influenza-associated complications or who are hospitalized.2 It is also recommended that antiviral treatment be considered for household contacts of people at high risk of influenza-associated complications.2
In Canada, 4 antiviral drugs are available to treat influenza (details on these drugs are presented in Appendix 6).1 Oseltamivir and zanamivir are both approved and marketed. They are available by prescription and are stockpiled as part of the National Antiviral Stockpile. Peramivir and baloxavir marboxil are approved for use but not marketed, although the latter is available for hospital formularies. These drugs can also be obtained for individual patient use through Health Canada’s Special Access Program. Refer to Appendix 6 for additional information on the drugs of interest, including their dosing and administration.
Pagebreak
Policy Issue
As a shared responsibility between federal, provincial, and territorial jurisdictions, Canada maintains reserves of influenza antiviral drugs within the National Antiviral Stockpile to ensure timely and equitable access to effective drugs during a pandemic and/or potential global shortage until such time a vaccine is available. Recommendations for composition of the antiviral stockpiles were last updated in 2017. Uncertainties related to effectiveness, efficacy, and the extent of antiviral resistance were identified as key concerns during pandemics. Assessing the current evidence on antiviral use is necessary to inform multijurisdictional decisions related to the safe and appropriate use of antiviral drugs for influenza A and B for pandemic preparedness. This rapid review examines the evidence on the safety and efficacy of antiviral drugs for post-exposure prophylaxis against influenza.
Policy Questions
What does each influenza antiviral offer in the prepandemic or pandemic context, considering relevant outcomes for specific populations?
What are the priorities for use of influenza antivirals by risk group, and in the high-risk setting for post-exposure prophylaxis?
Purpose
To synthesize the relevant literature published within the past 5 years to assess the efficacy and safety of antiviral drugs for post-exposure prophylaxis of influenza.
Research Questions
What is the efficacy of antiviral drugs for post-exposure prophylaxis in nonhospitalized individuals exposed to influenza A or B?
What is the safety of antiviral drugs for post-exposure prophylaxis in nonhospitalized individuals exposed to influenza A or B?
Methods
Literature Search Methods
An information specialist conducted a literature search on key resources including MEDLINE, Embase, the Cochrane Database of Systematic Reviews, the International HTA Database, and the websites of health technology assessment agencies in Canada and major international HTA agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevance. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concepts were antivirals (including oseltamivir, peramivir, zanamivir, and baloxavir marboxil) and influenza. Search filters were applied to limit retrieval to health technology assessments, SRs, meta-analyses, indirect treatment comparisons, randomized controlled trials (RCTs), or controlled clinical trials. The search was completed on January 8, 2025, and limited to English-language documents published since January 1, 2020.
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Nonhospitalized individuals exposed to influenza A or B |
Subgroups and priority populations | 1. Health care workers 2. Populations in congregate living settings (e.g., long-term care homes, correctional facilities) |
Interventions | 1. Baloxavir 2. Oseltamivir 3. Peramivir 4. Zanamivir 5. Combination therapy with baloxavir, oseltamivir, peramivir, or zanamivir |
Comparators | 1. Active control(s) that are approved in Canada 2. Placebo 3. No treatment or standard of care |
Outcomes | Primary Outcomes 1. Influenza diagnosis (symptomatic or asymptomatic infection) 2. Any hospitalization 3. Mortality Secondary Outcomes 1. Withdrawal due to adverse events 2. Emergence of antiviral resistance 3. Patient acceptance |
Settings | 1. Prepandemic (during seasonal flu) 2. Pandemic |
Study designs | 1. SRs, meta-analyses, and NMAs 2. RCTs after the last search date of the included systematic reviews |
NMA = network meta-analysis; RCT = randomized controlled trial; SR = systematic review.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications, or were published before 2020. SRs in which all relevant studies were captured in other more recent or more comprehensive SRs were excluded. Primary studies retrieved by the search were excluded if they were captured in 1 or more included SRs. Observational studies, economic evaluations, clinical guidelines, and open-label studies were also excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)8 for SRs and the Questionnaire to assess the relevance and credibility of a network meta-analysis9 for network meta-analyses (NMAs). No RCTs published after the SRs were found, so no tool was required. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were assessed and described narratively.
Summary of Evidence
Quantity of Research Available
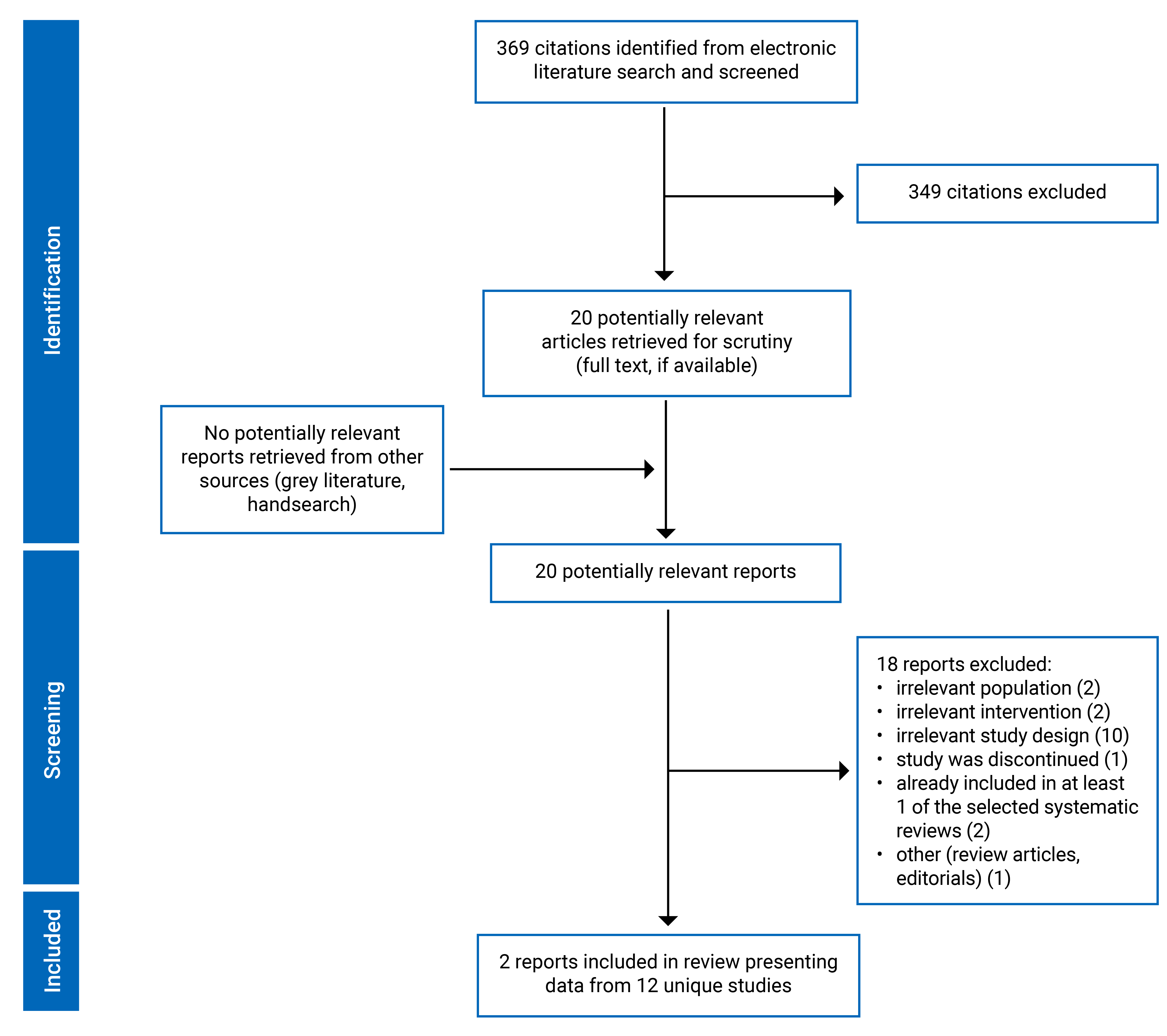
A total of 369 citations were identified in the literature search. Following screening of titles and abstracts, 349 citations were excluded and 20 potentially relevant reports from the electronic search were retrieved for full-text review. No potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 18 publications were excluded for various reasons and 2 publications met the inclusion criteria and were included in this report. These comprised 2 SRs and no RCTs that were not captured in the SRs. Appendix 1 presents the PRISMA flow chart of the study selection.
Additional references of potential interest but not meeting the inclusion criteria are provided in Appendix 5.
Study Characteristics
Additional details regarding the characteristics of included publications are provided in Appendix 2.
Summary of Study Characteristics
Both10,11 of the SRs had broader inclusion criteria than the present review. Specifically, the first SR10 included both pharmacological and nonpharmacological interventions for influenza prevention in care home settings. Only the characteristics and results of the subset of relevant studies will be described in this report. The second SR11 included an NMA that had additional network comparisons beyond those of interest to the present review. Specifically, it included comparisons between the interventions of interest and other drugs that are not approved in Canada (e.g., laninamivir). Only the relevant comparisons (i.e., the study drugs versus placebo) will be described further in this report.
In addition, it is important to note that 13 of 33 studies included in the second SR had post-exposure prophylaxis treatment, while for the remaining 20 studies, exposure treatment models were not necessarily limited to post-exposure; any evidence noted in the following should be interpreted with this caveat in mind. It was beyond the scope of this rapid review to re-estimate the parameters from the NMA conducted as part of this study by including only the studies that focused exclusively on post-exposure prophylaxis. Wherever estimates are pooled, this is noted in the text and appendices.
Study Design
The 2 SRs were both published in 2024. The first, by Willcox et al.,10 reviewed interventions for the prevention of influenza transmission in care home settings. The date range for their search was any randomized study published through April 2023. As the scope of their review included nonpharmacological interventions, we focused on the 6 RCTs that were relevant to the present review. The second SR and NMA conducted by Zhao et al.11 focused on studies published up to September 20, 2023. The scope of their review included several drugs that are not in the patient or population, intervention, comparison, and outcomes (PICO) for this rapid response report. Therefore, we focused on results derived from the 17 relevant studies that focused on our drugs of interest. As previously noted, this included studies focused on all types of influenza prophylaxis. Post-exposure prophylaxis was the exclusive focus of 7 of these studies, but estimates were unavailable for just these studies alone. The authors conducted an NMA using frequentist random-effects NMAs with 6 comparator drugs versus placebo, 3 of which are relevant to the current report. One study12 was included in both SRs.
Study Setting
The relevant RCTs in the first SR10 were conducted in the US (2 studies), Australia (1 study), the Netherlands (1 study), and across 3 or more countries (2 studies). In the second SR,11 the 7 studies relevant to this report were conducted in the US (2 studies), Japan (1 study), Canada and the US (1 study each), and across 3 or more countries in Europe and North America (3 studies).
Patient Population
The first SR10 focused on the residents and staff of care facilities, including nursing homes, residential homes, and sheltered accommodations. The number of participants in the original studies relevant to this report ranged from 140 to 548. Further demographic information on the study participants, including age and sex or gender, was not reported. The second SR11 included studies enrolling study participants from multiple settings. In the studies that were relevant to this report, the average age ranged from 26.2 to 35.5, and the percentage of male participants ranged from 21.6% to 56.7%. Information on the gender of study participants was not reported in either SR.
Interventions and Comparators
Both SRs focused on the use of several specific drugs that were the subject of this review. The first SR10 included 2 RCTs that compared zanamivir (10 mg inhaled) to both rimantadine and placebo (3 arms), 1 RCT that compared zanamivir (10 mg inhaled) to placebo, and 3 RCTs that compared oseltamivir (75 mg once daily) to placebo. These treatments were commenced when an outbreak was detected in the facility and were continued for a duration of 10 to 42 days. The second SR11 included 4 RCTs that compared zanamivir (10 mg or 3.2 mg) for between 5 and 21 days to placebo, 1 study that compared zanamivir to rimantadine or placebo for 14 days, 1 study that compared oseltamivir 75 mg for 7 days versus placebo, and 1 study that compared a one-time dose of baloxavir (based on weight up to 40 mg) to placebo. No studies were found that assessed the use of peramivir for prophylaxis.
Outcomes
Data were sought in both SRs for several of the PICO outcomes in this review, including laboratory-confirmed influenza, symptomatic laboratory-confirmed influenza, asymptomatic laboratory-confirmed influenza, and incidence of adverse drug reactions. In addition, 1 SR11 sought information on hospitalization, mortality, and serious adverse events. All outcomes were reported as odds ratios, rate ratios, or risk differences in both SRs.
Pagebreak
Critical Appraisal
Overall, the critical appraisal noted similar strengths and weaknesses for the 2 SRs.10,11 For example, both had very clear research questions, inclusion criteria, search strategies, and review approaches. Both used appropriate tools to assess the risk of bias and conflicts of interest were disclosed. They also shared some weaknesses, such as not reporting a list of excluded studies and not providing a justification for only including RCTs. In addition to these weaknesses, the first SR10 did not assess heterogeneity in reporting or publication bias. The second SR11 was very comprehensive and was judged to be high quality based on the questions in the ISPOR questionnaire.
Additional details regarding the strengths and limitations of the included publications are provided in Appendix 3.
Findings
Appendix 4 presents the main study findings, which are summarized in the following by outcome.
Clinical Efficacy of Antiviral Drugs for Post-Exposure Prophylaxis
There were 5 clinical outcomes that met the PICO criteria of this review that were assessed by 1 or both of the included SRs. These included 3 outcomes of laboratory-confirmed influenza (overall,10,11 symptomatic,10,11 and asymptomatic11), admission to hospital,11 and all-cause mortality.11 The results for each therapy compared to placebo are presented in the following. As previously noted, results for 1 of the SRs11 pooled both post-exposure and other prophylaxis in their estimates, so these should be interpreted with that caveat in mind.
Laboratory-Confirmed Influenza
The summary of findings for laboratory-confirmed influenza is shown in Table 4. Both SRs assessed oseltamivir versus placebo in preventing laboratory-confirmed influenza. In the first SR,10 the estimated odds ratio (OR) for infection was negative but not statistically different from the null at 0.59 (95% confidence interval [CI], 0.32 to 1.08). The second SR11 found a lower rate in drug recipients, with a rate ratio (RR) of 0.58 (95% CI, 0.39 to 0.86). This SR found a similar effect for zanamivir, with an RR of 0.57 (95% CI, 0.43 to 0.76). Finally, the point estimate in this SR for baloxavir was similar, with a RR of 0.50, but was not statistically different from the null (95% CI, 0.24 to 1.05).
Laboratory-Confirmed Symptomatic Influenza
The findings from the SRs for laboratory-confirmed symptomatic influenza are shown in Table 5. Both SRs found a lower risk of symptomatic influenza infection with oseltamivir prophylaxis, with an OR of 0.39 (95% CI, 0.16 to 0.95) in the first SR and an RR of 0.40 (95% CI, 0.26 to 0.62) in the second. The estimates for zanamivir were mixed, with an estimated OR that was 0.66 but not statistically different from the null in the first SR (95% CI, 0.33 to 1.29) and an RR that was statistically different at 0.35 (95% CI, 0.25 to 0.50) in the second SR. Finally, 1 SR assessed baloxavir and found a lower risk versus placebo with an estimated RR of 0.43 (95% CI, 0.23 to 0.79).
Laboratory-Confirmed Asymptomatic Influenza
The effect of antiviral prophylaxis on asymptomatic influenza was assessed in 1 SR.11 The results were consistently null for all 3 antivirals that were assessed, including oseltamivir, zanamivir, and baloxavir.
Admission to Hospital
One SR11 estimated the effect of oseltamivir prophylaxis on hospital admission rates, with an estimated RR of 1.11 that was not statistically different from the null (95% CI, 0.81 to 1.52). Neither SR reported data for the other drugs on this outcome.
All-Cause Mortality
In terms of the final clinical outcome of all-cause mortality, 1 SR11 reported estimates for 3 different antivirals. Across all 3 drugs (oseltamivir, zanamivir, and baloxavir), none of the point estimates were either clinically or significantly different than no change in the risk difference.
Safety of Antiviral Drugs for Post-Exposure Prophylaxis
Two broad areas of adverse events were reported in the SRs:10,11 drug-related adverse events and serious adverse events.
Drug-Related Adverse Events
While both SRs collected data on drug-related adverse events, only 111 presented specific estimates. This included results that were not statistically different for both zanamivir and baloxavir versus placebo. No data were presented on this outcome for oseltamivir versus placebo. The other SR10 did not provide specific figures, but noted that there were no significant differences found between the intervention and control groups in any of the included studies.
Serious Adverse Events
Similar to drug-related adverse events, the SR that assessed serious adverse events11 found no statistically significant differences in the risk difference between placebo and oseltamivir, zanamivir, or baloxavir.
Limitations
While the SRs in this review were generally well conducted, there were significant limitations to the literature base that should be noted. First, while the key question for this report was related to post-exposure prophylaxis, neither of the reviews were limited to examining that or examined it separately. This resulted in the reporting and discussion of evidence on potentially heterogenous models of prophylaxis for 1 of the SRs.11 A separate analysis, if feasible, might confirm these results; however, this is beyond the scope of this rapid review. Second, while the SRs were all published in 2024, the primary studies they relied on were not particularly recent. Despite our review including RCTs, there was only 1 study published in the past 5 years13 that would have been included in this review had it not already been summarized in 1 of the SRs. Finally, neither of the included SRs contained information on the emergence of antiviral resistance or patient acceptance of the different antivirals in question. In addition, neither contained information on 1 of the study interventions of interest, peramivir. In terms of generalizability, the studies came from a broad range of countries and at least 1 included study sites in Canada, so it is likely that the results would be relevant in this setting.
Conclusions and Implications for Decision- or Policy-Making
We identified 2 SRs published within the past 5 years10,11 that included 12 relevant randomized studies examining the clinical efficacy and safety of antiviral medicines for use in post-exposure prophylaxis for influenza. Overall, these studies found consistent evidence supporting the efficacy of oseltamivir, zanamivir, and baloxavir in preventing infection when used as post-exposure prophylaxis in the general population. The scale of these effects was relatively large, with ORs and RRs that were regularly half of those in the placebo arms of the included studies. In addition, the evidence supported the use of oseltamivir to prevent symptomatic infection in care home settings. There was also evidence supporting the use of oseltamivir and zanamivir in preventing any infection in the general population. In contrast, we found no evidence that any of these therapies are effective at preventing asymptomatic infection, admission to hospital, or all-cause mortality when used for post-exposure prophylaxis. With respect to safety, we found no evidence that drug-related or overall serious adverse events were higher in the intervention groups than the comparators for all 3 of the medications.
Given the strength of the reviews that were included, these findings likely represent the most current evidence on the efficacy and safety of these medications. Notably, some of the outcomes that would be of highest clinical interest, such as hospitalization and mortality, remained the areas in which the SRs concluded the evidence base was weakest. Additional research on the effectiveness of these therapies in preventing these outcomes would be valuable for planning and reducing clinical uncertainty.
Pagebreak
Authors and Contributors
Author
Michael Law designed the study, acquired data, analyzed, and interpreted the results. He also drafted the report.
Conflicts of Interest
Michael Law disclosed the following:
Employment
University of British Columbia
Travel or Other Expense Payments
University of British Columbia
Payment as Advisor or Consultant
CDA-AMC CGRP inhibitors buprenorphine
Durham Police Association — Private Benefits (expert witness testimony)
Society of United Professionals — Private Benefits (expert witness testimony)
Orr Taylor LLP — generic drugs (expert witness testimony)
Research Funding or Grants Paid to My Institution
CIHR — access to medicines
BC Ministry of Health — Pharmacy Reimbursement
Involvement With Projects or Scientific Advice
CDA-AMC Bulk Purchasing Advisory Panel
No other conflicts of interest were declared.
References
1.Public Health Agency of Canada. Flu (influenza): For health professionals. October 19, 2018. Accessed March 25, 2025. https://www.canada.ca/en/public-health/services/diseases/flu-influenza/health-professionals.html
2.Gaitonde DY, Moore FC, Morgan MK. Influenza: Diagnosis and Treatment. Am Fam Physician. 2019;100(12):751-758. Accessed March 25, 2025. https://www.aafp.org/pubs/afp/issues/2019/1215/p751.html PubMed
3.Culbert I. The Cost of Influenza Is Nothing to Sneeze At. Canadian Public Health Association; 2019. Accessed March 25, 2025. https://cpha.ca/cost-influenza-nothing-sneeze
4.Ng C, Ye L, Noorduyn SG, et al. Resource utilization and cost of influenza requiring hospitalization in Canadian adults: A study from the serious outcomes surveillance network of the Canadian Immunization Research Network. Influenza Other Respir Viruses. 2018;12(2):232-240. doi:10.1111/irv.12521 PubMed
5.Sinilaite A, Young K, Papenburg J. Summary of the National Advisory Committee on Immunization (NACI) Statement—Recommendation on Repeated Seasonal Influenza Vaccination. Can Commun Dis Rep. 49(4):99-102. doi:10.14745/ccdr.v49i04a02 PubMed
6.Aoki FY, Allen UD, Mubareka S, Papenburg J, Stiver HG, Evans GA. Use of antiviral drugs for seasonal influenza: Foundation document for practitioners—Update 2019. J Assoc Med Microbiol Infect Dis Can. 4(2):60-82. doi:10.3138/jammi.2019.02.08
7.Harrison R, Mubareka S, Papenburg J, et al. AMMI Canada 2023 update on influenza: Management and emerging issues. J Assoc Med Microbiol Infect Dis Can. 8(3):176-185. doi:10.3138/jammi-2023-07-12
8.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. doi:10.1136/bmj.j4008 PubMed
9.Jaime Caro J, Eddy DM, Kan H, et al. Questionnaire to Assess Relevance and Credibility of Modeling Studies for Informing Health Care Decision Making: An ISPOR-AMCP-NPC Good Practice Task Force Report. Value in Health. 2014;17(2):174-182. doi:10.1016/j.jval.2014.01.003 PubMed
10.Willcox ML, Lavu D, Yousaf U, Dalton S, Roberts N, Pluddemann A. The effectiveness of interventions to reduce the transmission of acute respiratory infections in care homes: a systematic review. J Public Health (Oxf). 2024;46(4):551-563. doi:10.1093/pubmed/fdae178 PubMed
11.Zhao Y, Gao Y, Guyatt G, et al. Antivirals for post-exposure prophylaxis of influenza: a systematic review and network meta-analysis. Lancet. 2024;404(10454):764-772. doi:10.1016/S0140-6736(24)01357-6 PubMed
12.Schilling M, Povinelli L, Krause P, et al. Efficacy of zanamivir for chemoprophylaxis of nursing home influenza outbreaks. Vaccine. 1998;16(18):1771-1774. doi:10.1016/s0264-410x(98)00141-8 PubMed
13.Ikematsu H, Hayden FG, Kawaguchi K, et al. Baloxavir Marboxil for Prophylaxis against Influenza in Household Contacts. N Engl J Med. 07 23;383(4):309-320. doi:10.1056/NEJMoa1915341
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Please note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Systematic Reviews
Study citation, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Willcox, M et al. (2024)10 Funding source: National Institute for Health Research (NIHR) School for Primary Care Research, Project 569 | 21 RCTs in total; 6 RCTs relevant to present review | People in nursing homes/long-term care/residential homes 5 RCTs included residents only, 1 RCT included Staff and residents Percentage of participants vaccinated ranged from 9% to 100%. One study did not report the percent vaccinated | Interventions:
| Outcomes: Symptomatic laboratory-confirmed influenza Follow-up: Ranged from 10 to 42 days |
Zhao et al. (2024)11 Funding source: WHO | 33 RCTs in total; 17 RCTs relevant to the present review, 7 of which focused on post-exposure prophylaxis | All populations Average age ranged from 26 to 36, percent male from 22% to 57% | Intervention:
Comparator: Placebo | Outcomes: Symptomatic or asymptomatic infection, admission to hospital, all-cause mortality, adverse events related to antivirals, and serious adverse events. Follow-up: NR |
NR = not reported.
Appendix 3: Critical Appraisal of Included Publications
Please note that this appendix has not been copy-edited.
Table 3: Strengths and Limitations of Systematic Reviews and Network Meta-Analyses Using AMSTAR 28 and the ISPOR Questionnaire9
Strengths | Limitations |
|---|---|
Willcox et al. (2024)10 | |
AMSTAR 2
| AMSTAR 2
|
Zhao et al. (2024)11 | |
AMSTAR 2
ISPOR Questionnaire
| AMSTAR 2
|
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; ISPOR = International Society for Pharmacoeconomics and Outcomes Research.
Appendix 4: Main Study Findings
Please note that this appendix has not been copy-edited.
Table 4: Summary of Findings by Outcome — Laboratory-Confirmed Influenza
Comparisons | Willcox (2024)10 Systematic Review | Zhao (2024)11 Systematic Review |
|---|---|---|
Oseltamivir Compared to Placebo | Meta-analysis of 2 studies (total N = 648) OR: 0.59 (0.32 to 1.08) demonstrating no change in laboratory-confirmed influenza with Oseltamivir compared to placebo | Meta-analysis of 6 studies (total N = 3,821) RR: 0.58 (0.39 to 0.86) |
Zanamivir Compared to Placebo | NA | Meta-analysis of 10 studies (total N = 8,156) RR: 0.57 (0.43 to 0.76) |
Baloxavir Compared to Placebo | NA | 1 study (total N = 749) RR: 0.50 (0.24 to 1.05) |
NA = not applicable; NR = not reported.
Note: The definition of symptomatic varied by primary study. In addition, the study by Zhao et al. included other interventions that were not in the criteria for this report, including other drugs not approved in Canada and the use of these drugs for general antiviral prophylaxis (as opposed to just post-exposure prophylaxis).
Table 5: Summary of Findings by Outcome — Laboratory-Confirmed Symptomatic Influenza
Comparisons | Willcox (2024)10 Systematic Review | Zhao (2024)11 Systematic Review |
|---|---|---|
Oseltamivir Compared to Placebo | Meta-analysis of 3 studies (total N = 1299) OR: 0.39 (0.16 to 0.94) demonstrating a statistically significant reduction in symptomatic laboratory-confirmed influenza with Oseltamivir compared to placebo | Meta-analysis of 5 studies (total N = 3,742) RR: 0.40 (0.26 to 0.62) |
Zanamivir Compared to Placebo | 1 study (N = 489) OR: 0.66 (0.33 to 1.29) demonstrating no change in symptomatic laboratory-confirmed influenza with Zanamivir compared to placebo | Meta-analysis of 9 studies (total N = 8,104) RR: 0.35 (0.25 to 0.50) |
Baloxavir Compared to Placebo | NA | 1 study (total N = 749) RR: 0.43 (0.23 to 0.79) |
NA = not applicable; NR = not reported.
Note: The definition of symptomatic varied by primary study. In addition, the study by Zhao et al. included other interventions that were not in the criteria for this report, including other drugs not approved in Canada and the use of these drugs for general antiviral prophylaxis (as opposed to just post-exposure prophylaxis).
Table 6: Summary of Findings by Outcome — Laboratory-Confirmed Asymptomatic Influenza
Comparisons | Willcox (2024)10 Systematic Review | Zhao (2024)11 Systematic Review |
|---|---|---|
Oseltamivir Compared to Placebo | NA | Meta-analysis of 5 studies (N = 3,742) RR: 0.86 (0.60 to 1.23) |
Zanamivir Compared to Placebo | NA | Meta-analysis of 9 studies (total N = 8,104) RR: 0.91 (0.76 to 1.10) |
Baloxavir Compared to Placebo | NA | 1 study (total N = 749) RR: 1.08 (0.51 to 2.27) |
NA = not applicable; NR = not reported.
Note: The definition of symptomatic varied by primary study. In addition, the study by Zhao et al. included other interventions that were not in the criteria for this report, including other drugs not approved in Canada and the use of these drugs for general antiviral prophylaxis (as opposed to just post-exposure prophylaxis).
Table 7: Summary of Findings by Outcome — Admission to Hospital
Comparisons | Willcox (2024)10 Systematic Review | Zhao (2024)11 Systematic Review |
|---|---|---|
Oseltamivir Compared to Placebo | NA | Meta-analysis of 4 studies (N = 3,434) RR: 1.11 (0.81 to 1.52) |
Zanamivir Compared to Placebo | NA | NA |
Baloxavir Compared to Placebo | NA | NA |
NA = not applicable; NR = not reported.
Note: The definition of symptomatic varied by primary study. In addition, the study by Zhao et al. included other interventions that were not in the criteria for this report, including other drugs not approved in Canada and the use of these drugs for general antiviral prophylaxis (as opposed to just post-exposure prophylaxis).
Table 8: Summary of Findings by Outcome — All-Cause Mortality
Comparisons | Willcox (2024)10 Systematic Review | Zhao (2024)11 Systematic Review |
|---|---|---|
Oseltamivir Compared to Placebo | NA | Network meta-analysis of 5 studies (N = 3,507) RD: 0 (−0.002 to 0.002) |
Zanamivir Compared to Placebo | NA | Meta-analysis of 5 studies (total N = 4,295) RD: 0.001 (−0.001 to 0.002) |
Baloxavir Compared to Placebo | NA | 1 study (total N = 749) RD: 0.0 (−0.005 to 0.005) |
NA = not applicable; NR = not reported.
Note: The definition of symptomatic varied by primary study. In addition, the study by Zhao et al. included other interventions that were not in the criteria for this report, including other drugs not approved in Canada and the use of these drugs for general antiviral prophylaxis (as opposed to just post-exposure prophylaxis).
Table 9: Summary of Findings by Outcome — Drug-Related Adverse Events
Comparisons | Willcox (2024)10 Systematic Review | Zhao (2024)11 Systematic Review |
|---|---|---|
Oseltamivir Compared to Placebo | The report noted that incidence of adverse events varied widely between trials but there were not significant differences between treatment and control groups in any of the studies. | NA |
Zanamivir Compared to Placebo | Meta-analysis of 8 studies (total N = 6,814) RR: 1.07 (0.83 to 1.38) | |
Baloxavir Compared to Placebo | 1 study (total N = 749) RR: 1.17 (0.4 to 3.45) |
NA = not applicable; NR = not reported.
Note: The definition of symptomatic varied by primary study. In addition, the study by Zhao et al. included other interventions that were not in the criteria for this report, including other drugs not approved in Canada and the use of these drugs for general antiviral prophylaxis (as opposed to just post-exposure prophylaxis).
Table 10: Summary of Findings by Outcome — Serious Adverse Events
Comparisons | Willcox (2024)10 Systematic Review | Zhao (2024)11 Systematic Review |
|---|---|---|
Oseltamivir Compared to Placebo | NA | Meta-analysis of 5 studies (n = 3,742) RD: 0.0 (−0.002 to 0.007) |
Zanamivir Compared to Placebo | NA | Meta-analysis of 7 studies (total N = 6,239) RD: 0.0 (−0.003 to 0.004) |
Baloxavir Compared to Placebo | NA | 1 study (total N = 749) RD: 3.0 (−0.010 to 0.005) |
NA = not applicable; NR = not reported.
Note: The definition of symptomatic varied by primary study. In addition, the study by Zhao et al. included other interventions that were not in the criteria for this report, including other drugs not approved in Canada and the use of these drugs for general antiviral prophylaxis (as opposed to just post-exposure prophylaxis).
Appendix 5: References of Potential Interest
Please note that this appendix has not been copy-edited.
This appendix includes references that were part of the full-text review that are of potential interest, but which did not meet the inclusion criteria and were not assessed for quality.
Previous CDA-AMC Reports
Subramonian A, Horton J. Oseltamivir for the Prevention of Influenza in Residents of Long-Term Care Facilities. Can J Health Technol. 2022;2(11). doi:10.51731/cjht.2022.511 PubMed
Chao YS, Spry C. The Use of Antivirals for Influenza Prophylaxis: A Review of the Clinical Effectiveness (Rapid Response Report: Summary with Critical Appraisal). CADTH; 2017. Accessed February 5, 2025. https://www.ncbi.nlm.nih.gov/books/NBK519835/
Systematic Reviews
Tadount F, Laghdir Z, Quach C. Antiviral use in healthcare workers-A systematic review. Infect Control Hosp Epidemiol. 2022;43(4):518-523. doi:10.1017/ice.2021.79 PubMed
Boikos C, Caya C, Doll MK, et al. Safety and effectiveness of neuraminidase inhibitors in situations of pandemic and/or novel/variant influenza: a systematic review of the literature, 2009-15. J Antimicrob Chemother. 2017;72(6):1556-1573. doi:10.1093/jac/dkx013 PubMed
Doll MK, Winters N, Boikos C, Kraicer-Melamed H, Gore G, Quach C. Safety and effectiveness of neuraminidase inhibitors for influenza treatment, prophylaxis, and outbreak control: a systematic review of systematic reviews and/or meta-analyses. J Antimicrob Chemother. 2017;72(11):2990-3007. doi:10.1093/jac/dkx271 PubMed
Review Articles
Institut national d’excellence en santé et en services sociaux (INESSS). Use of Antivirals for the Treatment and Prophylaxis of Influenza in Children and Adults in the Context of COVID-19: Report in Support of the Optimal Use Guide. INESSS; 2020. Accessed March 25, 2025. https://www.inesss.qc.ca/publications/repertoire-des-publications/publication/utilisation-des-antiviraux-pour-le-traitement-et-la-prophylaxie-de-linfluenza-chez-lenfant-et-ladulte-dans-le-contexte-de-la-covid-19.html
Baloxavir (Xofluza) for post-exposure prophylaxis of influenza. Med Lett Drugs Ther. 2021;63(1615):2-3. Accessed March 25, 2025. https://secure.medicalletter.org/TML-article-1615b PubMed
Health Canada. Guidance on human health issues related to avian influenza in Canada. February 11, 2025. Accessed April 15, 2025. https://www.canada.ca/en/public-health/services/publications/diseases-conditions/guidance-human-health-issues-avian-influenza.html
Appendix 6: Drug Information
Please note that this appendix has not been copy-edited.
Table 11 outlines the indications for antiviral drugs approved in Canada for influenza.
Table 11: Approved Indications for Antiviral Drugs
Approved Indications | Formulation and Administration |
|---|---|
baloxavir marboxila (Xofluza) NOC February 2020 | |
Treatment of uncomplicated influenza in patients 12 years of age and older who have been symptomatic for no more than 48 hours and who are otherwise healthy or at high risk of developing influenza complications. | Formulation:
Administration:
|
oseltamivir (Tamiflu and generics) NOC December 1999 | |
Treatment of uncomplicated acute illness due to influenza infection in adults and adolescents (≥ 13 years) who have been symptomatic for no more than 2 days. Treatment of uncomplicated acute illness due to influenza in pediatric patients 1 year and older who have been symptomatic for no more than 2 days. | Formulation:
Administration:
|
peramivir (Rapivab) NOC January 2018 | |
Treatment of acute uncomplicated influenza in patients 18 years and older, who have been symptomatic for no more than 2 days. | Formulation:
Administration:
|
zanamivir (Relenza) NOC July 2018 | |
Treatment of uncomplicated acute illness due to influenza A and B virus in adults and pediatric patients 7 years of age and older, who have been symptomatic for no more than 2 days. | Formulation:
Administration:
|
NOC = notice of compliance.
aIn the US, approved for post-exposure prophylaxis in persons 5 years and older.
ISSN: 2563-6596
This work was conducted by Michael Law through the Post-Market Drug Evaluation CoLab Network. It was supported by Canada’s Drug Agency (CDA-AMC) and its Post-Market Drug Evaluation Program through funding provided by Health Canada.
CDA-AMC is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
CoLab is a pan-Canadian network of experts in applied research, scientific methods, and data analysis. CoLab members work with the Post-Market Drug Evaluation Program to produce credible and timely evidence on postmarket drug safety and effectiveness.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
This document is the property of Michael Law. CDA-AMC has a nonexclusive, limited, royalty-free, worldwide, nontransferable, fully paid-up, and irrevocable license to use the report in support of its objects, mission, and reasonable operational requirements.