Drugs, Health Technologies, Health Systems
Health Technology Review
Cost-Effectiveness of Antiviral Drugs to Prevent or Treat Influenza A, Influenza B, or Zoonotic Influenza
Authors: Ilke Akpinar, Dagmara Chojecki
This rapid review was conducted by the Alberta Drug and Therapeutic Evaluation Consortium (ADTEC) through the Post-Market Drug Evaluation CoLab Network.
Key Messages
What Is the Issue?
Influenza is a major public health concern, causing significant illness, death, economic challenges, and pandemic potential. This underscores the need for effective prevention (also known as prophylaxis), treatment, and pandemic preparedness strategies.
Antiviral medications such as baloxavir marboxil, oseltamivir, peramivir, zanamivir are recommended for the treatment of influenza; however, their economic value remains unclear.
What Did We Do?
We conducted a rapid review to identify and summarize evidence on the cost-effectiveness of antivirals for preventing and treating influenza A, influenza B, and zoonotic influenza, as well as the cost-effectiveness of antiviral stockpiling.
We searched electronic databases and key online sources for economic evaluation studies published in English from January 1, 2019, to December 13, 2024. Additionally, we examined the cost-effectiveness of stockpiling from studies published from January 1, 2020, to April 4, 2025.
One researcher screened citations, selected studies, and narratively summarized the study findings.
What Did We Find?
We identified 9 economic evaluations: 8 examining the treatment of influenza and 1 examining both post-exposure prophylaxis and treatment.
We did not identify any studies on the cost-effectiveness of antivirals for the prophylaxis or treatment of zoonotic influenza or any studies that evaluated the cost-effectiveness of stockpiling antiviral drugs.
Economic studies suggest that certain antivirals may be cost-effective for treating influenza compared to standard of care, particularly in high-risk populations. However, it is unclear how cost-effective antivirals are for post-exposure prophylaxis, as there is limited evidence from just 1 study.
What Does It Mean?
Economic evaluations suggest that oseltamivir or baloxavir marboxil are cost-effective treatments for influenza, particularly in high-risk populations.
Baloxavir marboxil may be a valuable alternative in cases of oseltamivir resistance to ensure optimal resource allocation and long-term sustainability of antiviral treatments. However, its higher cost requires careful consideration.
The generalizability of existing economic evaluations may be limited due to variability in influenza strains, health care systems, and cost structures that differ from Canada.
Abbreviations
CEA
cost-effectiveness analysis
CUA
cost-utility analysis
ICER
incremental cost-effectiveness ratio
ICU
intensive care unit
INMB
incremental net monetary benefit
NAI
neuraminidase inhibitor
NMB
net monetary benefit
PSA
probabilistic sensitivity analysis
RCT
randomized controlled trial
SEIR
Susceptible-Exposed-Infected-Recovered model
QALY
quality-adjusted life-year
QoL
quality of life
WTP
willingness to pay
Introduction and Rationale
Background
Influenza is a viral infection of the respiratory system that carries a significant risk of morbidity and mortality. It is among the top 10 leading causes of death in Canada.1 The severity of the disease can vary, from asymptomatic cases to severe complications. Common symptoms of influenza usually start suddenly and include fever, cough, and myalgias. Other frequently reported symptoms include chills, fatigue, headache, sore throat, loss of appetite, and nasal congestion.1 Uncomplicated influenza typically resolves within 3 to 8 days.2 However, influenza infection can lead to severe complications, particularly among high-risk groups. These include individuals over 65 years of age, pregnant people, children under 6 years old, and people with underlying health conditions such as heart, kidney, or liver disease; obesity; diabetes; or weakened immune systems.1,2 The 3 primary types of influenza viruses that infect humans are A, B, and C. Among these, influenza A has the broadest host range, affecting humans, swine, equines, and birds. Its high susceptibility to antigenic variations makes it the leading cause of pandemics.1 Influenza B primarily infects humans and can lead to seasonal influenza outbreaks.1 Influenza C causes mild respiratory illness and is generally not associated with epidemics or pandemics.2 Zoonotic influenza refers to strains of the virus that are transmitted from animals to humans, which can result in severe illness and even death, especially when the virus undergoes mutations that allow efficient human-to-human transmission.2
In Canada, influenza represents a major economic burden, affecting both the health care system and broader economic productivity. Before the COVID-19 pandemic, influenza caused an estimated 12,200 hospitalizations and 3,500 deaths annually.3 Each hospitalization was estimated to cost between CA$14,000 and CA$20,000, contributing to an annual economic burden of CA$168 million to CA$240 million.3,4 Beyond health care, influenza also has a significant impact on workplace productivity. For example, during the H1N1 pandemic in November 2009, approximately 1.5 million employed people living in Canada who were aged 15 to 69 reported absences from work due to influenza, resulting in a loss of 29.5 million work hours.5 These figures underscore the widespread economic consequences of influenza, highlighting the critical need for effective prevention and control measures to mitigate its impact on both public health and the economy.6
Prevention and Treatment of Influenza
The National Advisory Committee on Immunization of the Public Health Agency of Canada recommends annual seasonal influenza vaccination for all individuals aged 6 months and older, unless contraindicated, regardless of prior vaccination history.6 Antiviral drug prophylaxis is recommended for both pre-exposure and post-exposure in various scenarios by the Association for Medical Microbiology and Infectious Disease Canada.7
As of January 2025, 3 antiviral drugs are available in Canada for the prophylaxis and treatment of influenza: oseltamivir (Tamiflu), zanamivir (Relenza), and peramivir (Rapivab).8,9 Additionally, baloxavir marboxil (Xofluza) was approved by Health Canada in 2020 for the treatment of uncomplicated influenza in individuals aged 12 years and older.9 Only Health Canada–approved antivirals are considered in this review.
When given before or shortly after exposure, oseltamivir and zanamivir have been reported to be 68% to 92% and 69% to 81% effective, respectively, in preventing influenza in general adult populations.10 Early antiviral treatment, especially within 24 to 36 hours of symptom onset, can reduce the severity and duration of influenza. Neuraminidase inhibitors (NAIs), like oseltamivir, zanamivir, and peramivir, can shorten symptom duration by 30% to 40% and reduce the severity of the illness.11 These treatments also help reduce the risk of complications such as pneumonia and sinusitis.11 Additionally, antiviral treatments can decrease viral transmission within households, contributing to controlling the spread of influenza.12
The cost-effectiveness of antiviral drugs for outpatient influenza, including prophylaxis and treatment of seasonal, pandemic, and zoonotic strains, remains unclear.
Policy Issue
This rapid review is part of a broader project examining antiviral drugs for influenza. Evidence from this review, along with other components, including safety, effectiveness, and cost-effectiveness, will inform multijurisdictional decisions on the appropriate use of these drugs for the prophylaxis and treatment of influenza A, influenza B, and zoonotic influenza for pandemic preparedness.
Policy Questions
Is there a need to stockpile antiviral drugs for prepandemic or pandemic preparedness for treatment and prophylaxis of influenza A or B or zoonotic influenza strains?
What are the priorities for use of influenza antivirals by risk group, and high-risk setting including treatment and for pre-exposure and post-exposure prophylaxis?
1.1 Which influenza antivirals should be stockpiled for prepandemic or pandemic preparedness for treatment and prophylaxis?
1.2 What does each influenza antiviral offer in the prepandemic or pandemic context, considering relevant outcomes for specific populations?
Purpose
The purpose of this report is to summarize the evidence on the cost-effectiveness of antiviral drugs for the pre-exposure prophylaxis, post-exposure prophylaxis, and treatment of influenza A, B, and zoonotic influenza in individuals who are not hospitalized.
The scope of this project does not include evaluating the availability of antiviral drugs for influenza A and B, specifically addressing potential shortages that may require stockpiling. It also excludes the assessment of the accessibility and feasibility of these drugs for Canadians, including the availability of medications and the timeliness of health care access for diagnosis and prescription during a pandemic. Additionally, this project does not examine primary health care providers’ hesitancy to prescribe antiviral drugs for the prophylaxis and treatment of influenza or exploring the underlying reasons for such hesitancy. Lastly, the creation of a mathematical model and conducting a pharmacoeconomic analysis to assist decision-making on stockpiling strategies for both prepandemic and pandemic preparedness fall outside the scope of this work.
Research Question
What is the cost-effectiveness of antiviral drugs administered to individuals who are not hospitalized for the prophylaxis and treatment of influenza A or B or zoonotic influenza?
Methods
Literature Search Methods
An information specialist conducted searches in the electronic databases Ovid MEDLINE, Ovid Embase, and Web of Science for English-language literature published from January 1, 2019, to December 13, 2024. Articles were identified using a combination of controlled vocabulary, for example, MeSH and Embase subject heading terms, and relevant keywords surrounding the topics of antivirals and influenza. A cost analysis filter developed by Canada’s Drug Agency was also used to limit the search to economic analyses. Grey literature searching was conducted in ChatGPT, Perplexity AI, Google Scholar, Google Advanced, The National Institute for Health and Care Research website, the International Network of Agencies for Health Technology Assessment database, and Research Papers in Economics (RePEc). Reference lists of included articles were scanned, to help identify additional relevant evidence. An additional search was conducted on April 5, 2025, within the same databases to gather studies published from January 1, 2020, to April 4, 2025, focusing on the cost-effectiveness of stockpiling antivirals for influenza. This search employed MeSH terms and keywords related to stockpiles and stockpiling, as well as antivirals and influenza.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the selection criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Individuals who were not hospitalized requiring antiviral drugs for PrEP, PEP, or treatment for influenza A, influenza B, or zoonotic influenza. |
Interventionsa | Baloxavir marboxil, oseltamivir, peramivir, zanamivir, combination therapyb |
Comparators | Active control(s) approved in Canada, placebo, no treatment, or standard of care |
Outcomes |
|
Settings |
|
Study designs | Pharmacoeconomic studies (e.g., cost-effectiveness studies, cost-utility studies) |
PEP = post-exposure prophylaxis; PrEP = pre-exposure prophylaxis; QALY = quality-adjusted life-year.
Notes: PrEP is an antiviral drug taken before any exposure to virus or pathogen (likely in the context of at-risk workers e.g., occupational exposure, high-risk individuals) to reduce or prevent the risk of developing an infection. PEP is an antiviral drug given after exposure to virus or pathogen (e.g., after exposure to an infectious case) before the presence of symptoms and/or a positive test result to prevent or control the spread of disease. Treatment is with an antiviral drug to treat signs and symptoms. Prepandemic is the period before a widespread outbreak and seasonal flu is categorized within the prepandemic context.
aIncluding comparing different doses of the same intervention.
bCombination treatment includes a neuraminidase inhibitor with another neuraminidase inhibitor or a neuraminidase inhibitor with baloxavir marboxil.
cFor example, unvaccinated population (i.e., before a vaccine is available).
Exclusion Criteria
Studies were excluded if they did not meet Table 1 criteria, they were duplicate publications, or they were published before 2019. Costing studies, which focus solely on the costs associated with a particular intervention or program without considering the outcomes or effectiveness, are often categorized as partial economic evaluations. As they do not involve a full comparison of both costs and outcomes, they were excluded. Additionally, studies on the cost-effectiveness of drugs not approved in Canada (e.g., laninamivir) were excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the Drummond checklist.13 Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Data Extraction
One reviewer extracted information from each article using a standardized data extraction form. During data extraction, the following were collected: author, publication year, country, source of funding, study design, modelling approach, study perspective, population characteristics, intervention(s), and comparator(s), discounting, time horizon, outcomes, source of clinical efficacy, cost and utility data, and results.
Summary of Evidence
Quantity of Research Available
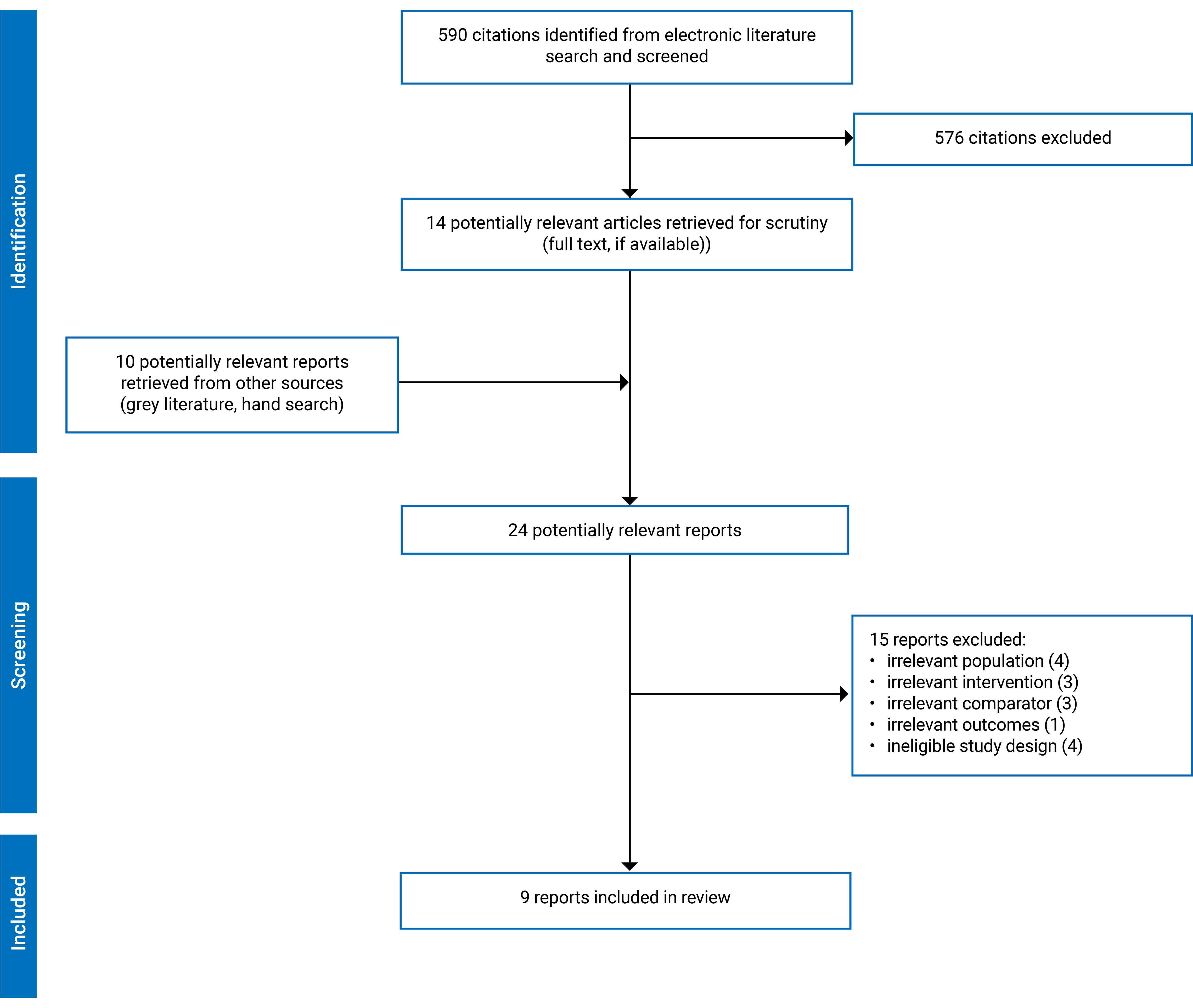
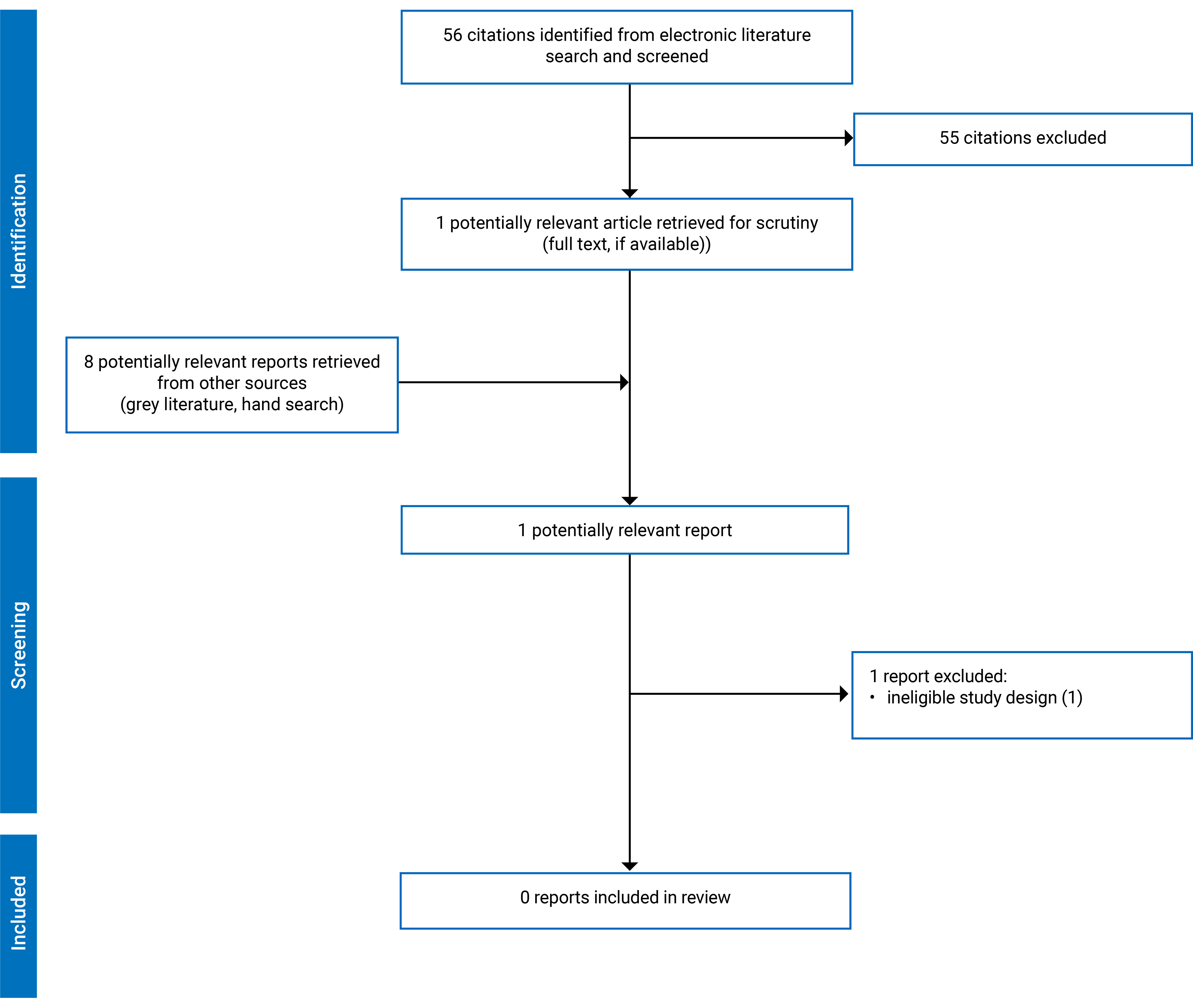
Of the 590 citations identified in the economic evaluation literature search, 14 were potentially relevant based on title and abstract screening and were retrieved for full-text review. The full-text articles of an additional 10 potentially relevant publications identified through the grey literature search were similarly retrieved. Of these 24 articles, 15 were excluded, and 8 peer-reviewed articles and 1 paper identified through grey literature met the inclusion criteria and were included in this report. These comprised 9 economic evaluations.14-22 An additional search on economic evaluation of stockpiling antiviral drugs identified 88 citations. After removing duplicates, 56 citations from databases and 8 from the grey literature were included for the title and abstract screening. One study was potentially relevant based on title and abstract, it was retrieved for full-text review but was not included. While this study incorporates cost considerations, it does not constitute a full economic evaluation. Rather, it provides insights into the trade-offs between antiviral effectiveness and cost, making it a cost-effectiveness–informed modelling study rather than a comprehensive economic analysis. Appendix 2 presents the PRISMA23 flow chart of the study selection. A list of the excluded studies with reasons for exclusion are available in Appendix 3.
Study Characteristics
Nine economic evaluations14-22 were identified and included in this rapid review, all of which were peer-reviewed except 1.13 Of the 9 studies identified, 8 focused on the treatment of influenza,14-18,20-22 while 1 examined post-exposure prophylaxis and treatment.19 No economic evaluations were found for zoonotic influenza. The settings of the included studies were as follows: 7 focused on seasonal influenza,14,16,18-22 1 on pandemic influenza,15 and 1 addressed both seasonal and pandemic influenza.17 Table 2 presents the studies on the post-exposure prophylaxis and treatment of influenza, organized by interventions, comparators, and respective settings, including both seasonal and pandemic influenza contexts, along with the number of studies under each category. Additional details regarding the characteristics of included publications are provided in Appendix 4.
Table 2: Studies on Post-Exposure Prophylaxis and the Treatment of Influenza
Description (interventions and comparators) | Number of studies | Reference | Setting |
|---|---|---|---|
Post-exposure prophylaxis and treatment | |||
8 Prophylaxis (first antiviral) and treatment (second antiviral) strategies:b
| 1 | Nakagawa et al. (2024)19 | Seasonal influenza |
Treatment | |||
Baloxavir marboxil vs. oseltamivir vs. baseline. | 1 | Chen et al. (2025)14 | Seasonal influenza |
Baloxavir marboxil vs. oseltamivir vs. no treatment. | 2 | Kommandantvold et al. (2024)16 | Seasonal influenza |
Kommandantvold et al. (2024)17 | Seasonal and pandemic influenza | ||
Baloxavir marboxil vs. oseltamivir. | 1 | Jiang et al. (2024)15 | Pandemic influenza |
Baloxavir marboxil vs. standard of care (symptomatic treatment, primarily with paracetamol). | 1 | van der Pol et al. (2024)20 | Seasonal influenza |
Standard of care + oseltamivir vs. standard of care (NOS). | 1 | Li et al. (2023)21 | Seasonal influenza |
Oseltamivir vs. zanamivir vs. peramivir vs. laninamivir.a | 2 | Nakagawa et al. (2024)18 | Seasonal influenza |
Nakagawa et al. (2021)22 | Seasonal influenza | ||
NOS = not otherwise specified; vs. = versus.
aLaninamivir is not approved in Canada.
bIn the study, the first drug was used for prophylaxis, followed by the second drug for treatment.
Study Design
All economic evaluations identified14-22 were cost-utility analysis (CUA).
Six economic evaluations adopted a health care payer’s perspective.14,15,17-19,22 One study16 used a US commercial payer perspective. van der Pol et al.20 employed a societal perspective for the CUA. Similarly, Li et al.21 adopted both societal and health care payer perspectives to provide a comprehensive evaluation of the economic impact of interventions.
Six studies14,16,18-20,22 employed decision-tree models. The assumptions included in the reviewed studies are as follows: fixed infection rates,15 one-time infection scenarios,15 and the exclusion of long-term health consequences of influenza.18,19,21,22 Additionally, it was assumed that patients tested positive for influenza before receiving antiviral therapy,14 with an antiviral drug uptake rate of 35% among infected patients, and only 1 complication was considered in the analysis.15 A zero-mortality rate was assumed for exposed and infected individuals before becoming infectious.17 Furthermore, baloxavir marboxil was assumed to be effective only for the “true influenza” group, and outcomes were assumed to be the same for both baloxavir marboxil and the current standard of care arms.20 Two studies15,17 used linked dynamic transmission-economic models.21 All decision-tree models incorporated key health states such as infection onset, treatment, complications, and recovery, while dynamic models captured population-level transmission and mitigation effects. Sensitivity analyses, including probabilistic and scenario-based approaches, were conducted in all studies to evaluate the robustness of results.
The time horizons varied across the included studies, reflecting differences in the scope and objectives of the analyses. Eight studies employed relatively short time frames, with 4 studies using a 14-day horizon18,19,21,22 and 2 studies adopting a 1-year horizon.14,15 In contrast, 3 studies used a lifetime horizon.16,17,20 These variations highlight the diversity in methodological approaches tailored to specific research questions and health care contexts.
Setting
Three economic evaluations were conducted based on country-specific data and costs from Japan,18,19,22 and 1 study each for the following jurisdictions: Hong Kong,14 China,15 the US,16 the UK,17 and the Netherlands.20 One economic evaluation used country-specific costs and drug prices for 15 different European countries.21
Patient Population
The studies investigated diverse populations that varied by age, risk profile, time since exposure or symptom onset (within 48 hours of symptom onset14 or at least 24 hours after onset15) and influenza symptoms. Nakagawa et al.18,22 examined adults aged 18 and older diagnosed with influenza. Symptomatic individuals aged 12 and older were evaluated by Kommandantvold et al. in both the US16 and the UK,17 including a mix of healthy and high-risk groups. Nakagawa et al.19 focused on prophylaxis and treatment strategies in healthy adults while Li et al.21 investigated influenza-like illness among adults/adolescents (aged 13 and over), and children (≥ 1 year and < 13 years), including subgroups with and without comorbidities. van der Pol et al.20 examined at-risk groups, such as older individuals and those with comorbidities.
Interventions and Comparators
The included studies evaluated cost-effectiveness of various antiviral interventions for influenza management, addressing both post-exposure prophylaxis and treatment. Nakagawa et al.19 focused on the cost-effectiveness of 8 antiviral post-exposure prophylaxis and treatment combinations, with the first drug administered for prophylaxis and the second for treatment.
For treatment, Chen et al.14 examined baloxavir marboxil for oseltamivir-resistant seasonal influenza and compared baloxavir marboxil to oseltamivir or baseline. Kommandantvold et al.16,17 compared baloxavir marboxil to oseltamivir or no antiviral treatment in both seasonal16,17and pandemic influenza.17 Jiang et al.15 compared baloxavir marboxil to oseltamivir for influenza pandemics.
Additionally, van der Pol et al.20 evaluated baloxavir marboxil against the current standard of care, which included symptomatic treatment with paracetamol. Li et al.21 focused on comparing oseltamivir to standard care, specifically examining the addition of oseltamivir to usual care. Finally, Nakagawa et al.18,22 compared oseltamivir, zanamivir, laninamivir, and peramivir for the treatment of seasonal influenza.
As laninamivir is not available in Canada, the results of from the laninamivir arms will not be discussed further.18,19,22
Outcomes
The included studies14-22 evaluated the cost-effectiveness of antiviral treatments for influenza using a variety of clinical and economic outcomes. Common economic outcomes included incremental cost-effectiveness ratios (ICERs) and net monetary benefit (NMB) at specified willingness-to-pay (WTP) thresholds. QALYs were derived from clinical trial data, network meta-analyses, and utility instruments like EQ-5D, a standardized instrument used to measure and assess the health-related quality of life (QoL) of individuals. Cost data encompassed drug acquisition costs, health care resource utilization (e.g., outpatient visits, hospitalization), and, where applicable, indirect costs, including productivity loss for studies adopting a societal perspective.
Funding
Industry funding played a dominant role in supporting economic evaluations of influenza interventions, with additional contributions from government and academic sources. Four studies reported industry funding,15-17,20 while 2 studies received support from government funding,14,21 and 1 received funding from a university.18 Two studies reported receiving no funding.19,22
Characteristics of Individual Studies
None of the studies included in this report were conducted in Canada, which makes it uncertain how well their findings apply to context in Canada. Differences in population demographics, disease prevalence, and WTP thresholds can affect the relevance of these results. However, 2 studies17,21 provide the most directly applicable insights for policy in Canada. While studies from Japan and China are of high quality, their direct relevance to cost structures in Canada is limited due to significant differences in health care financing systems. Given these considerations regarding the applicability of the findings to the context in Canada, the studies in this report are listed in order of recency and are organized based on the specific interventions (e.g., antiviral drugs) they compare. This structure allows for a clear comparison of the studies, while acknowledging the varying degrees of relevance to Canadian policy.
Cost-Effectiveness of Influenza Post-Exposure Prophylaxis and Treatment
Nakagawa et al.19 conducted a CUA in Japan to evaluate the cost-effectiveness of post-exposure prophylaxis followed by treatment strategies for seasonal influenza. The study focused on healthy adults aged 18 and older and employed a decision-tree model with a 14-day time horizon from a health care payer's perspective. The following 8 prophylaxis-treatment antiviral combination strategies (the first drug was used for prophylaxis, followed by the second drug for treatment) were examined in the study: oseltamivir with zanamivir, oseltamivir with laninamivir, oseltamivir with baloxavir marboxil, zanamivir with baloxavir marboxil, laninamivir with baloxavir marboxil, baloxavir marboxil with oseltamivir, baloxavir marboxil with zanamivir, and baloxavir marboxil with laninamivir. Effectiveness probabilities were obtained from clinical trials, while cost data were sourced from the 2020 Japanese Medical Fee Index. Utility values were derived from EQ-5D-5L questionnaires. The decision tree categorized patients into 8 health statuses based on prophylaxis effectiveness, treatment outcomes, side effects, and pneumonia-related hospitalizations. The study defined antiviral dosages for post-exposure prophylaxis as follows: oseltamivir was administered orally at a dose of 75 mg once daily for 10 days, while zanamivir was given as an inhaled dose of 10 mg once daily for the same duration. Laninamivir was prescribed as a 20 mg inhaled dose once daily for 2 days. Baloxavir marboxil was dosed based on body weight, with patients weighing less than 80 kg receiving 40 mg and those weighing 80 kg or more receiving 80 mg once orally. If post-exposure prophylaxis failed, patients were assumed to receive an alternative influenza treatment with 1 of these drugs, with its effectiveness incorporated into the analysis.
Cost-Effectiveness of Influenza Treatment
Cost-Effectiveness of Baloxavir Marboxil Versus Oseltamivir Versus Baseline
Chen et al.14 conducted a CUA comparing baloxavir marboxil, oseltamivir, or no treatment for treating seasonal influenza in adult outpatients in Hong Kong. The study used a decision-tree model with a 1-year time horizon from a health care payer’s perspective. The analysis accounted for key clinical events among patients with confirmed influenza receiving antiviral treatment, including treatment-related adverse events, the development of antiviral resistance, influenza-related complications, hospitalization due to complications, and mortality from complications or other causes. Both otherwise healthy and high-risk adult populations were considered. Clinical data were sourced from 2 Phase III clinical trials, while cost estimates were derived from Hong Kong-specific health care data, including outpatient consultations, diagnostic tests, medications, hospitalizations, and intensive care unit (ICU) costs. Utility values were adjusted to reflect the impact of treatment-related adverse events, the duration of influenza symptoms, and influenza-related complications, based on data from health technology assessments. A key assumption in the model was that all patients were tested for influenza before treatment initiation.
Cost-Effectiveness of Baloxavir Marboxil Versus Oseltamivir
Jiang et al.15 evaluated the public health and economic impacts of adding baloxavir marboxil as a treatment option, in addition to oseltamivir for influenza pandemic control in China. The study employed a linked dynamic transmission-economic evaluation model over a one-year time horizon from the perspective of the Chinese health care system. Health state utilities for the baseline healthy state, influenza-infected state, and complication-related states were sourced from the literature, while clinical data were drawn from existing studies. Cost estimates, including treatment costs, were derived from 2021 CN¥ values and economic evaluations specific to China. The decision-tree model compared 2 strategies— access to only oseltamivir and - access to baloxavir marboxil or oseltamivir—with patient numbers estimated based on cumulative infection incidence from the Susceptible-Exposed-Infected-Recovered model (SEIR) model. Outpatients were categorized into 5 groups according to complication status: uncomplicated influenza, pneumonia, bronchitis, middle ear infection, and sinus infection. Treatment pathways included outpatient care or hospitalization, with hospital cases further classified into general ward or ICU admissions. The model assumed that each patient could only experience 1 influenza infection per year and develop a single complication. Sensitivity analyses confirmed the robustness of the results across a range of parameter variations.
Cost-Effectiveness of Baloxavir Marboxil Versus Oseltamivir Versus no Treatment
Kommandantvold et al.16 conducted a cost-effectiveness analysis (CEA) comparing baloxavir marboxil, oseltamivir, and no antiviral treatment for seasonal influenza management in the US. The study employed a decision-tree model with a lifetime horizon from the perspective of a US payer. The analysis included individuals aged 12 and older with influenza, with 56% classified as otherwise healthy and 44% as high risk, based on a real-world study with a mean age of 32 years. The decision-tree model incorporated mutually exclusive pathways, where each individual could experience infection, receive treatment, develop complications, and either recover or die. In cases of complications, individuals could receive outpatient or inpatient care, including ICU admission. Clinical and cost data were obtained from the Merative™ MarketScan® Research Databases. The study applied a 3.0% annual discount rate and conducted sensitivity analyses, including scenarios assessing the impact of transmission reduction.
Kommandantvold et al.17 evaluated the cost-effectiveness of baloxavir marboxil for managing seasonal and pandemic influenza in the UK. The study employed a SEIR model alongside a cost-effectiveness model from the perspective of the UK National Health Service. It compared baloxavir marboxil to oseltamivir or to no antiviral treatment in individuals aged 12 and older, categorized as otherwise healthy or high-risk. The analysis used a lifetime horizon with a 3.5% annual discount rate, assessing key outcomes such as attack rates (proportions of the population infected), QALYs, and ICERs. Utility values for various health states, including healthy, influenza-infected, and complication-related states, were derived from the literature. Cost data were obtained from the NHS 2021/2022 National Cost Collection, while information on influenza-related complications and their likelihood in the otherwise healthy and high-risk populations was obtained from existing studies. The cost-effectiveness model analyzed the otherwise healthy and high-risk populations separately, incorporating data from the SEIR model under seasonal, pandemic, and high-treatment pandemic scenarios. The decision-tree model structured disease progression through mutually exclusive pathways: individuals could be infected or not, receive antiviral treatment or not, experience 1 complication at a time or none, and either recover or die. Those with complications could receive outpatient care, general inpatient care, or ICU admission.
Cost-Effectiveness of Baloxavir Marboxil Versus Standard of Care
van der Pol et al.20 conducted a CUA to evaluate the cost-effectiveness of baloxavir marboxil for treating seasonal influenza in the Netherlands. The CUA employed a lifetime horizon. The study adopted a societal perspective for the CUA. The base-case CUA included a cohort of 1,000 individuals aged 52 and at risk for influenza-related complications. Scenario analysis considered other age groups. The study applied a 4% discount rate to costs and 1.5% to outcomes. A decision-tree model was used, with clinical data sourced from the CAPSTONE-2 trial and cost data obtained from Dutch reference prices and existing literature. Sensitivity analyses, including deterministic sensitivity analysis, probabilistic sensitivity analysis (PSA), and scenario analysis, were conducted to assess the robustness of the findings. Baloxavir marboxil was compared to the current standard of care, which consists of symptomatic treatment with paracetamol.
Cost-Effectiveness of Oseltamivir Plus Standard of Care Versus Standard of Care
Li et al.21 conducted a CUA to evaluate the economic impact of adding oseltamivir to the usual care for managing influenza-like illness across 15 European countries. This study, part of the European Commission’s Seventh Framework Programme, adopted both health care payer and societal perspectives. The analysis used data from the ALIC4E randomized controlled trial (RCT) and assessed outcomes in terms of QALYs and associated health care costs. The study population included adults/adolescents (aged 13 years and older), and children (≥ 1 year and < 13 years) diagnosed with influenza-like illness. A 14-day time horizon was applied, and cost estimates were derived from patient-reported resource use and country-specific unit costs. The analysis did not capture long-term health consequences from influenza-like illness.
Cost-Effectiveness of Oseltamivir Versus Zanamivir Versus Peramivir Versus Laninamivir
Nakagawa et al.18 conducted a CEA of anti-influenza drugs for adult patients in outpatient settings in Japan. The study employed a decision-tree model with 7 disease states, which were evaluated under both the base-case scenario and various sensitivity analyses. The model utilized a 14-day time horizon, and the cost-effectiveness evaluation focused on multiple NAIs, including oseltamivir, zanamivir, laninamivir, and peramivir. The study population comprised patients aged 18 and older, all diagnosed with seasonal influenza virus infection in Japan. Sensitivity analyses were performed using deterministic sensitivity analysis, Monte Carlo simulations, and PSA with 10,000 iterations to evaluate the results robustness. Cost data were sourced from the 2020 Japanese Medical Fee Index, and utility values were derived from EQ-5D-5L questionnaires.
Nakagawa et al.22 conducted a CEA to assess the economic value of NAIs for treating seasonal influenza virus infections in adult outpatients in Japan. The analysis adopted a health care payer perspective and employed a decision-tree model with a 14-day time horizon. Clinical inputs were derived from RCTs, while cost data were sourced from the 2016 Japanese medical fee schedule. Utility values were obtained using EQ-5D-3L questionnaires. The study compared 4 NAIs: oseltamivir, zanamivir, laninamivir, and peramivir. The decision-tree model categorized disease progression into 3 states: effective treatment within 5 days using NAIs, ineffective treatment leading to hospitalization and pneumonia, and ineffective treatment requiring more than 5 days of therapy with persistent fever. Medical costs, including physician fees, hospital admission costs, and drug prices, were evaluated from the health care payer's perspective. Community pharmacy costs, covering dispensing fees, pharmaceutical management fees, and drug costs were also considered. One-way sensitivity analyses were conducted to assess the impact of variations in factors such as treatment duration, QoL values, drug prices, and the costs associated with physician and community pharmacy visits, as well as hospital admission.
Critical Appraisal
The included economic evaluations had several strengths as assessed using the Drummond checklist.14-22 The objectives and economic importance of the studies were described, the interventions and comparators of interest were clearly reported, and the form of analysis and perspectives were described. The sources of input parameters in the analysis were mentioned,14-22 and currency, conversion rates, and price data were described. One of the studies21 used a trial-based analysis, and other 8 studies14-20,22 used modelling with parameters obtained from other sources to conduct analysis. All studies conducted sensitivity analyses and incremental effectiveness results were reported. Conclusions were consistent with the data reported and were accompanied by the appropriate caveats.14-22
In the study by Chen et al.14 the input parameters were sourced from local data (Hong Kong-specific costs, and epidemiological inputs) enhancing the validity of the results. Subgroup analyses (healthy versus high-risk adults) improved the generalizability of the findings. A decision-tree model was employed, and the rates were not discounted, given the shorter time horizon of 1 year. Sensitivity analyses (both one-way and probabilistic) confirmed the cost-effectiveness of baloxavir marboxil across plausible scenarios. While the funding sources were disclosed, a conflict of interest (author ties to Roche) introduces potential bias. Overall, the analysis is robust for short-term decision-making.
The Jiang et al.15 study adopted a Chinese health care system perspective and employed a linked SEIR and decision-tree model, incorporating both transmission dynamics and individual patient outcomes. Local data from China, including data from the 2009 H1N1 pandemic, inform key parameters. The one-year time horizon limits the ability to assess long-term consequences. Sensitivity analyses confirm the robustness of the findings. However, uncertainties remain regarding key parameters, particularly the transmission coefficient and vaccination assumptions, and the model does not explicitly account for viral evolution. The study clearly articulates its assumptions and limitations. Additionally, funding from Hoffmann-La Roche introduces a potential source of bias. Overall, while the analysis provides valuable insights for short-term pandemic planning, it warrants cautious interpretation due to the limitations of scope and parameter uncertainty.
In the study by Kommandantvold et al.16 use of a decision-tree model is appropriate for the clinical pathway being examined, and a lifetime time horizon with discounting is employed to capture long-term effects. US administrative claims data inform key model parameters, enhancing the validity and relevance to the US health care setting. Scenario analysis explores the potential impact of baloxavir marboxil on viral transmission. The study includes sensitivity analysis, examining a range of transmission reduction scenarios. The authors disclosed funding from Hoffmann-La Roche and Genentech, manufacturers of baloxavir marboxil, which introduces a potential for bias. Overall, the study provides useful information for decision-makers in the US health care system, although the generalizability of the findings may be limited to Canada.
In the study by Kommandantvold et al.,17 the use of a linked SEIR and decision-tree model is a strength as it captures both the transmission dynamics and individual patient outcomes. UK-specific data are used, including population size, health care costs, and estimates of influenza burden. The SEIR model allows for estimating the population attack rates under different treatment strategies, while the decision-tree model captures short-term costs and outcomes. Scenario analyses explored different settings (seasonal, pandemic, high-treatment pandemic) and the impact of asymptomatic patients and self-isolation. However, the study has limitations. The time horizon for the SEIR model is limited to 1 influenza season, potentially missing longer-term effects. The study discloses funding from Hoffmann-La Roche, which introduces a potential bias. Overall, the study provides useful information for decision-makers in the UK, particularly regarding the potential benefits of baloxavir marboxil in reducing influenza transmission, but the limitations related to model assumptions and potential bias should be considered.
In the study by Nakagawa et al.,18 the objective is clearly defined: to re-evaluate the cost-effectiveness of NAIs (oseltamivir, laninamivir, zanamivir, and peramivir) for influenza treatment in Japan from a health care payer perspective. This study addresses limitations in a prior study22 by incorporating network meta-analysis (NMA) data, a more detailed decision tree, and EQ-5D-5L-derived QoL scores. Both studies use Japanese medical costs. Deterministic and probabilistic sensitivity analyses were performed. However, the study has limitations. The time horizon is limited to 14 days, which may not capture all relevant long-term outcomes. The QoL scores are based on a relatively small sample (n = 50). While the study uses NMA data, the validity of the overall analysis depends on the quality and assumptions within that NMA. The reliance on the EQ-5D-5L, although an improvement over the EQ-5D-3L, introduces potential biases inherent in utility elicitation methods. Additionally, the study does not evaluate baloxavir marboxil, which could be a relevant comparator. Finally, the study was publicly funded, and none of the authors disclosed any financial relationship with drug manufacturers. Overall, the study provides useful information for decision-makers in Japan, but the limitations related to the short time horizon, sample size for QoL scores, and the exclusion of baloxavir marboxil may be a consideration.
In the study by Nakagawa et al.,19 a decision-tree model is employed to simulate 8 combination treatment strategies for prophylaxis, with a time horizon of 14 days, which may limit the capture of long-term effects. The study uses Japanese cost data from the 2020 Medical Fee Index and utility values derived from EQ-5D-5L questionnaires administered to healthy university students. Deterministic and probabilistic sensitivity analyses are conducted to assess the robustness of the results. A key limitation is that utility values from healthy individuals may not accurately reflect the QoL impact on those who develop influenza. The study identifies and values all relevant inputs, but the reliance on a short time horizon for influenza treatment warrants caution. Overall, the study provides useful information for formulary management in Japan, suggesting the potential cost-effectiveness of baloxavir marboxil and oseltamivir as prophylactic drugs. However, its limitations related to the short time horizon and the use of utility values from healthy individuals should be considered when interpreting the results.
In the study by van der Pol et al.,20 a decision-tree model is used for the CUA, and a lifetime horizon allows for capturing long-term QALY effects, with appropriate discounting. The study incorporates Dutch-specific data, and productivity losses are included. However, the study has limitations: the modelled results are uncertain due to variability in key outcomes, particularly the hospitalization rate. The reliance on data from the CAPSTONE-2 trial may not fully reflect real-world effectiveness in the Netherlands. Although baloxavir marboxil has been shown to reduce the viral load of influenza and shorten the time to cessation of viral shedding, which may impact transmission, these effects were not included in the CEA. Additionally, the study discloses funding from Roche Netherlands B.V. which introduces the potential for bias. Overall, the study provides useful information for health care decision-makers in the Netherlands, but limitations related to model structure, data sources, and sensitivity analysis should be considered.
In the study by Li et al.,21 the analysis is conducted from both health care payers’ and societal perspectives. The study leverages patient-level data on resource use, costs, and health-related QoL, collected prospectively in the ALIC4E trial, which enhances validity and reduces reliance on modelling assumptions. Country-specific unit costs and purchasing power parity conversions are used, increasing the relevance and comparability of the findings. However, the 14-day time horizon is a limitation, potentially missing the longer-term sequelae of influenza-like illness. The study appropriately addresses uncertainty through PSA and also conducts an expected value for perfect information analysis. Nonetheless, important methodological details are lacking, such as the translation of EQ-5D-Y (a generic self-report instrument designed to measure health-related QoL in children and adolescents aged 8 to 15) results. Finally, the study was publicly funded, and none of the authors disclosed any financial relationships with drug manufacturers. It provides valuable evidence on the cost-effectiveness of oseltamivir for influenza-like illness in Europe. The limitations related to the short time horizon and methodological transparency should be considered when interpreting the results.
In the study by Nakagawa et al.,22 a decision-tree model used is appropriate for this clinical context. The study employs Japanese cost data from the 2016 medical fee schedule as well as effectiveness probabilities derived from RCTs. QoL values are elicited using EQ-5D-3L questionnaires administered to patients who had previously experienced influenza. One-way sensitivity analyses are conducted. The study identifies and values most relevant inputs, but there are several limitations. The time horizon is limited to 14 days, which may not capture all relevant costs or long-term effects. The reliance on the EQ-5D-3L for QoL assessment may introduce biases, and the sample of patients used to derive the EQ-5D-3L values is not described in detail beyond being collected from a community pharmacy. Additionally, the study does not appear to conduct PSA. The base-case analysis found oseltamivir to be the most cost-effective NAI. Overall, the study provides useful information for decision-makers in Japan, but the limitations related to the short time horizon, the QoL data collection, and the lack of PSA should be considered when interpreting the results.
Although the included studies discussed the results and acknowledged limitations, several assumptions made it difficult to assess the reliability of the results and the model’s robustness to changes. Finally, none of the studies were conducted in Canada, making the generalizability of the findings to settings in Canada uncertain due to differences in population, differences in health care financing systems, and WTP thresholds.
Additional details regarding the strengths and limitations of included publications are provided in Appendix 4.
Findings
Nine economic evaluations were included in this rapid review. The cost-effectiveness of antivirals for post-exposure prophylaxis and treatment was examined in 1 study,19 and the cost-effectiveness of antivirals for the treatment of influenza was examined in all 9 studies.14-22
No relevant evidence was identified on the cost-effectiveness of antivirals for pre-exposure prophylaxis, zoonotic influenza post-exposure prophylaxis, or treatment of zoonotic influenza; therefore, a summary of the evidence could not be provided.
Cost-Effectiveness of Influenza Post-Exposure Prophylaxis and Treatment
Nakagawa et al.19 conducted a pharmacoeconomic study in Japan to assess the cost-effectiveness of 8 prophylaxis-treatment antiviral combination strategies (the first drug was used for prophylaxis, followed by the second drug for treatment) for seasonal influenza: oseltamivir with zanamivir, oseltamivir with laninamivir, oseltamivir with baloxavir marboxil, zanamivir with baloxavir marboxil, laninamivir with baloxavir marboxil, baloxavir marboxil with oseltamivir, baloxavir marboxil with zanamivir, and baloxavir marboxil with laninamivir.
The results indicated that the most cost-effective approach was using baloxavir marboxil for post-exposure prophylaxis and laninamivir for treatment, yielding a NMB of ¥179,952 at the WTP level of ¥5,000,000 per QALY. The second most cost-effective strategy involved oseltamivir for post-exposure prophylaxis and zanamivir for treatment, with an NMB of ¥180,148 at the WTP level of ¥5,000,000 per QALY. The authors concluded that baloxavir marboxil and oseltamivir are the most cost-effective treatments for post-exposure prophylaxis in Japan from the perspective of health care payers.
Cost-Effectiveness of Influenza Treatment
Cost-Effectiveness of Baloxavir Marboxil Versus Oseltamivir Versus Baseline
Chen et al.14 conducted a CUA comparing baloxavir marboxil to oseltamivir or to no treatment for the treatment of seasonal influenza in adult outpatients in Hong Kong. In the general population, baloxavir marboxil demonstrated an ICER of US$66,856 per QALY gained compared to no treatment and US$29,660 per QALY gained compared to oseltamivir, both of which were lower than the WTP threshold of US$152,667. In otherwise healthy adults, the ICERs were US$122,767 compared to baseline and US$75,800 compared to oseltamivir. In the high-risk population, baloxavir marboxil was dominant (more effective and less costly), with ICERs of US$20,222 compared to baseline and US$–1,813 compared to oseltamivir. At the baseline, sensitivity analysis indicated a 78% probability of baloxavir marboxil being cost-effective at the specified WTP threshold ($152,667 per QALY). In the otherwise healthy subpopulation, baloxavir marboxil is cost-effective in 72% of scenarios, while in the high-risk population, it is cost-effective in 99% of scenarios. The study concluded that baloxavir marboxil is a cost-effective alternative to oseltamivir and effective against resistant strains with a single-dose regimen.
Cost-Effectiveness of Baloxavir Marboxil Versus Oseltamivir
Jiang et al.15 evaluated the public health and economic impacts of adding baloxavir marboxil to oseltamivir for influenza pandemic control in China. The addition of baloxavir marboxil reduced the cumulative infection incidence from 49.5% to 43.3% and increased QALYs by 0.00021 per person. At a WTP threshold of CN¥80,976 per QALY, the NMB was CN¥77.85 per person. The authors concluded that, in the context of an influenza pandemic, adding baloxavir marboxil to oseltamivir is a cost-effective strategy in China.
Cost-Effectiveness of Baloxavir Marboxil Versus Oseltamivir Versus No Treatment
Kommandantvold et al.16 evaluated the cost-effectiveness of baloxavir marboxil compared to oseltamivir or no treatment for seasonal influenza management in the US. The study found that baloxavir marboxil was cost-effective in all scenarios. In the base-case analysis, the ICER for baloxavir marboxil was US$6,813 per QALY gained compared to oseltamivir and US$669 per QALY gained compared to no treatment, both well lower than the WTP (US$100,000 per QALY) threshold. In the high-risk subpopulation, baloxavir marboxil was dominant compared to no treatment, and had an ICER of US$8,597 per QALY compared to oseltamivir. In the otherwise healthy subpopulation, the ICER for baloxavir marboxil was US$5,861 per QALY gained compared to oseltamivir and US$2,037 per QALY gained compared to no treatment. The NMB of baloxavir marboxil in the base case was US$1,180 compared to oseltamivir and US$6,208 compared to no treatment. A scenario analysis showed that a 5% reduction in viral transmission increased baloxavir marboxil’s NMB compared to oseltamivir from US$1,180 in the base case to US$2,592. Each additional 5% reduction further increased baloxavir marboxil’s incremental NMB by approximately US$1,413 relative to oseltamivir or no treatment. Baloxavir marboxil became cost-dominant when it decreased viral transmission by 12% compared to oseltamivir and by 6% compared to no treatment. The authors concluded that baloxavir marboxil is a cost-effective alternative to oseltamivir or no treatment, with its potential to reduce viral transmission providing economic benefits from a US payer perspective.
Kommandantvold et al.17 evaluated the cost-effectiveness of baloxavir marboxil for treating seasonal and pandemic influenza in the UK. The SEIR model predicted greater reductions in infections with baloxavir marboxil compared to oseltamivir or no treatment. In the seasonal influenza setting, the ICER for baloxavir marboxil compared to oseltamivir was £1,884 per QALY gained, and baloxavir marboxil was dominant (more effective and less costly) compared to no treatment. Among high-risk individuals in the seasonal influenza setting, baloxavir marboxil had an ICER of £2,574 per QALY gained compared to oseltamivir and £128 per QALY gained compared to no treatment. In the pandemic influenza setting, the ICER for baloxavir marboxil compared to oseltamivir was £11,693 per QALY gained, and in a high-treatment scenario, this decreased slightly to £10,186 per QALY gained. For high-risk individuals during a pandemic, baloxavir marboxil had an ICER of £12,802 per QALY gained compared to oseltamivir and £1,401 per QALY gained compared to no treatment. Overall, the study highlighted baloxavir marboxil as a cost-effective treatment option at the WTP threshold of £20,000 per QALY for both seasonal and pandemic influenza from the UK National Health Service perspective.
Cost-Effectiveness of Baloxavir Marboxil Versus Standard of Care
van der Pol et al.20 conducted a CUA to assess the cost-effectiveness of baloxavir marboxil for treating seasonal influenza in the Netherlands. The economic evaluation showed that the base-case ICER for baloxavir marboxil was €8,300 per QALY gained compared to the current standard of care. At a WTP threshold of €20,000 per QALY, baloxavir marboxil had a 58% probability of being cost-effective. Baloxavir marboxil remained cost-effective across various scenarios, particularly for older adults and individuals at high risk of influenza-related complications. The primary drivers of cost-effectiveness were reduced illness duration and productivity gains in the working population. Overall, the study concluded that baloxavir marboxil is a cost-effective treatment for seasonal influenza in the Netherlands, particularly for individuals aged 60 years and older or those at high-risk for severe influenza outcomes.
Cost-Effectiveness of Oseltamivir Plus Standard of Care Versus Standard of Care
Li et al.21 conducted a CUA to evaluate the economic value of adding oseltamivir to usual care for managing influenza-like illness across 15 European countries. From a health care payer perspective, the ICER for oseltamivir was €22,445 per QALY gained for adults and adolescents and €13,006 per QALY gained for children. From a societal perspective that accounted for productivity losses, oseltamivir was cost-saving for adults and adolescents and had an ICER of €8,347 per QALY for children. The cost-effectiveness of oseltamivir varied by country. Sensitivity analyses confirmed the robustness of the findings across various parameters, though uncertainties remained in subgroups with comorbidities, particularly among children. These uncertainties were primarily due to the small sample sizes, greater variability in treatment outcomes and costs, and the impact of hospitalization events in the usual care group, which introduced additional variability in cost-effectiveness estimates. At a WTP threshold of €20,000 per QALY, oseltamivir had a 45% probability of being cost-effective. The expected value of perfect information (the value of conducting additional research to reduce uncertainty in estimating incremental costs and effects of oseltamivir vs. usual care) ranged from €1 to €35 per patient. The study concluded that adding oseltamivir to usual care is likely cost-effective for the treatment of influenza-like illness in Europe from a health care payer perspective when the WTP exceeds €22,445 per QALY and cost-saving (WTP > €8,347) from a societal perspective for adults and adolescents. These findings support oseltamivir as a feasible treatment option in primary care settings across Europe, particularly during seasonal influenza epidemics.
Cost-Effectiveness Comparing Oseltamivir, Zanamivir, Peramivir, and Laninamivir
Nakagawa et al.18 performed a CEA of anti-influenza drugs for adult patients in outpatient settings in Japan and found oseltamivir to be the most cost-effective NAI for treating seasonal influenza in Japan. In the initial analysis, the authors re-examined the most cost-effective anti-influenza drug by using a decision tree from the previously referenced study,22 while also incorporating data from the NMA. The analysis found that oseltamivir outperformed zanamivir, laninamivir, and peramivir. Sensitivity analyses revealed that zanamivir had a negative INMB of ¥−38,470 (US$ −384) compared to oseltamivir, while laninamivir and peramivir had INMBs of ¥−1,836 (US$ −18) and ¥−6,178 (US$ −61) compared to oseltamivir, respectively. PSA showed that oseltamivir was the most cost-effective option in 32.3% of iterations at a WTP threshold of ¥5,000,000 per QALY. In the second analysis, the authors used a more detailed decision tree (comprising 7 disease states) along with the NMA data. Oseltamivir consistently yielded the highest INMB, while laninamivir and peramivir remained less cost-effective. Two-way sensitivity analyses focused on comparing the probability of effectiveness of laninamivir and oseltamivir indicated that oseltamivir covered the largest cost-effectiveness area, with acceptability curves reinforcing its preferred status across a broad range of WTP thresholds (¥ 0 to ¥10,000,000 per QALY). The authors concluded that oseltamivir is the most cost-effective NAI for treating influenza in Japan.
Nakagawa et al.22 conducted a CEA to evaluate the economic value of NAIs for treating seasonal influenza in adult outpatients in Japan. The analysis identified oseltamivir as the most cost-effective NAI, with an incremental cost-effectiveness ratio of ¥393,674 per QALY (US$3,883.41 per QALY) at a WTP threshold of ¥5,000,000 per QALY. In comparison, the cost-effectiveness ratios for zanamivir, laninamivir, and peramivir were ¥ 408,241 per QALY (US$4,027.10 per QALY), 407,980 yen per QALY (US$4,024.53 per QALY), and 444,264 yen per QALY (US$4,382.45 per QALY), respectively. Zanamivir was dominated, as it was both less effective and more costly than oseltamivir. Compared to oseltamivir, laninamivir and peramivir were less cost-effective, with ICERs of 1,129,459 yen per QALY (US$11,141.58 per QALY) and 1,287,118 yen per QALY (US$12,696.81 per QALY), respectively. One-way sensitivity analyses on various parameters (duration of treatment, QoL values, drug prices, costs of physician visits, costs of community pharmacy visits, costs of hospital admission and effectiveness to high-risk patients) confirmed the robustness of the results, with laninamivir showing a minimum ICER of −596,850 yen per QALY (US$ −5,887.64 per QALY) and peramivir a maximum ICER of 14,717,518 yen per QALY (US$145,181.32 per QALY). The study concluded that oseltamivir is the most cost-effective NAI for treating influenza in adult outpatients in Japan.
Cost-Effectiveness of Stockpiling
A comprehensive economic evaluation of antiviral stockpiling is lacking in the literature. The study “Estimation of Optimal Antiviral Stockpile for a Novel Influenza Pandemic”24 employs epidemiological modelling to assess antiviral stockpile composition, comparing NAIs and cap-dependent endonuclease inhibitors using data from South Korea’s 2009 H1N1 pandemic. The results show that cap-dependent endonuclease inhibitors, despite their higher cost, could reduce infections from 30% to 25% when administered to 10% of cases. When the cost of cap-dependent endonuclease inhibitors is 3 times that of NAIs, no additional expenditures beyond the current budget are needed; however, if the cost of cap-dependent endonuclease inhibitors is 5 times that of NAIs, expenditures increase by 17%. The authors concluded that stockpiling cap-dependent endonuclease inhibitors reduces patient numbers by shortening the infectious period, but the government must consider the cost-effectiveness of the stockpile, factoring in the drug’s cost, virus transmissibility, vaccine development time, and the potential for resistance. While this study incorporates cost considerations, it does not provide a full economic evaluation but offers insights into the trade-offs between antiviral effectiveness and cost, making it a cost-effectiveness–informed modelling study rather than a comprehensive economic analysis.
Appendix 5 presents the main study findings, antiviral drug costs reported in included studies, and opportunity cost information.
Limitations
No pharmacoeconomic studies evaluating the cost-effectiveness of antivirals for pre-exposure prophylaxis, zoonotic influenza post-exposure prophylaxis, or treatment for zoonotic influenza were identified. Additionally, there is no evidence on the cost-effectiveness of stockpiling antiviral drugs.
The cost-effectiveness of post-exposure prophylaxis remains uncertain, as only 1 study was identified.19 This study primarily focused on Japanese populations and used utility values derived from a young, healthy cohort, which may limit its generalizability to broader age populations and to the population in Canada.
The cost-effectiveness of antiviral treatments for influenza varies depending on the drug, population, and implementation strategy. While antiviral drugs can be cost-effective, particularly for high-risk groups and during severe seasons, the generalizability of the identified studies to Canada is limited due to differences across jurisdictions and study settings. These include variations in health care systems, population characteristics, epidemiological contexts, and treatment costs, all of which can have an impact on the cost-effectiveness of antiviral treatments.
While the 5 studies14-17,20 offer valuable insights into the potential cost-effectiveness of baloxavir marboxil, the direct industry funding and authors’ affiliations with the industry raise significant concerns regarding potential bias. Therefore, the findings should be interpreted with caution.
Conclusions and Implications for Decision- or Policy-Making
Economic Findings
Oseltamivir was most consistently reported to be a cost-effective option, especially when considering broader health care system and societal costs.
Baloxavir marboxil was also reported to be a cost-effective treatment, particularly for high-risk populations, for reducing viral transmission or in cases of oseltamivir resistance.
The cost-effectiveness of antiviral treatments depends on factors such as drug choice, target population, and implementation strategies. While newer treatments like baloxavir marboxil may be more expensive, their cost-effectiveness in high-risk groups may justify the investment, particularly when considering potential savings from reduced transmission, hospitalizations, and complications.
Implications for the Health Care Systems in Canada
The use of antiviral treatments for post-exposure prophylaxis and influenza treatment may reduce overall health care costs by preventing transmission, hospitalizations, and alleviating the economic burden associated with severe influenza cases.
Given the potential for oseltamivir resistance, evaluating the cost-effectiveness of alternative antivirals like baloxavir marboxil is crucial to ensure optimal resource allocation and the long-term sustainability of antiviral strategies.
While thresholds like £30,000 per QALY (UK) and $100,000 per QALY (US) reflect the health system’s opportunity cost of care, few studies explicitly discussed antiviral use in the context of constrained health care resources. Although many studies applied WTP thresholds or NMB frameworks, most did not examine the trade-offs between antiviral investment and other potentially cost-effective interventions.
Limitations of the Assessment or Evidence
Economic analyses were based on modelled data and assumptions, which may not fully capture the complexities of real-world implementation and costs.
Not all studies considered the transmission dynamics of influenza.
A key limitation across the existing economic evaluations is the use of region-specific data, such as country-specific costs, utility values, and WTP thresholds, combined with assumptions (e.g, treatment adherence, transmission dynamics) that may not reflect the context in Canada.
Conclusions
The available evidence suggests that antiviral drugs are cost-effective for both post-exposure prophylaxis and the treatment of influenza, particularly in high-risk groups. However, cost-effectiveness of specific antivirals could vary based on population characteristics, differences in influenza strain, health care delivery systems, and resource availability. It is important to note that much of the current evidence is not based on settings in Canada, which may limit its direct applicability to the health care systems in Canada.
Given the higher cost of newer treatments such as baloxavir marboxil, careful consideration is warranted related to their potential cost-effectiveness to better understand how overall population health is improved through efficient use of resources.
There is no evidence on the cost-effectiveness of antivirals for pre-exposure prophylaxis of seasonal influenza, and pre-exposure prophylaxis of zoonotic influenza, post-exposure prophylaxis, or the treatment for zoonotic influenza. Additionally, there is no evidence on the cost-effectiveness of antiviral stockpiling.
The generalizability of these findings to the population in Canada is limited due to differences in study settings.
Authors
Ilke Akpinar led the rapid review, conducted title and abstract screening, study selection, and data extraction, and authored the report.
Dagmara Chojecki developed search strategies and conducted the literature searches.
Conflicts of Interest
No conflicts of interest were declared.
References
1.Public Health Agency of Canada. Flu (influenza): For health professionals. 2024; https://www.canada.ca/en/public-health/services/diseases/flu-influenza/health-professionals.html. Accessed January 20, 2025.
2.Paules C, Ubbarao K. Influenza. Lancet. 2017;390(10095):697-708. doi:10.1016/S0140-6736(17)30129-0 PubMed
3.Canadian Public Health Association. The cost of influenza is nothing to sneeze at. 2019; https://cpha.ca/cost-influenza-nothing-sneeze. Accessed January 20, 2025.
4.Ng C, Ye L, Noorduyn S, et al. Resource utilization and cost of influenza requiring hospitalization in Canadian adults: A study from the serious outcomes surveillance network of the Canadian Immunization Research Network. Influenza Other Respir Viruses. 2018;12(2):232-240. doi:10.1111/irv.12521 PubMed
5.Statistics Canada. H1N1 flu pandemic: Impact on Canadian workers. 2010; https://www150.statcan.gc.ca/n1/daily-quotidien/100115/dq100115c-eng.htm. Accessed January 20, 2025.
6.Public Health Agency of Canada. Summary of National Advisory Committee on Immunization statement: Recommendation on repeated seasonal influenza vaccination. Ottawa: PHAC;2023. https://www.canada.ca/en/public-health/services/immunization/national-advisory-committee-on-immunization-naci/recommendation-repeated-seasonal-influenza-vaccination/summary.html. Accessed January 20, 2025.
7.Aoki F, Allen U, Mubareka S, Papenburg J, Stiver H, Evans G. Use of antiviral drugs for seasonal influenza: Foundation document for practitioners-update J Assoc Med Microbiol Infect Dis Can 2019. doi:10.3138/jammi.2019.02.08 PubMed
8.Canadian Paediatric Society. Antiviral drugs for influenza. 2023; https://cps.ca/en/documents/position/antiviral-drugs-for-influenza. Accessed January 20, 2025.
9.Public Health Ontario. Antiviral medications for seasonal influenza in 2024-25: Public health considerations 2024; https://www.publichealthontario.ca/-/media/Documents/A/2023/antiviral-medications-seasonal-influenza.pdf?rev=58d2f4ec01574efe813fc6e0dceb3f13&sc_lang=en&hash=07F15DFB2FD3901AFED1EDB640416650. Accessed January 20, 2025.
10.Ison M. Clinical use of approved influenza antivirals: Therapy and prophylaxis. Influenza Other Respir Viruses. 2013;7:7-13. doi: 10.1111/irv.12046 PubMed
11.Treanor J, Hayden F, Vrooman P. Efficacy and safety of the oral neuraminidase inhibitor oseltamivir in treating acute influenza: A randomized controlled trial. US Oral Neuraminidase Study Group. JAMA. 2000;283(8):1016-1024. doi:10.1001/jama.283.8.1016. PubMed
12.Hayden FG, Asher J, Cowling BJ, et al. Reducing influenza virus transmission: The potential value of antiviral treatment. Clin Infect Dis. 2022;74(3):532-540. doi:10.1093/cid/ciab625 PubMed
13.Drummond MF, Jefferson TO. Guidelines for authors and peer reviewers of economic submissions to the BMJ. The BMJ economic evaluation working party. BMJ. 1996;313(7052):275-283. doi:10.1136/bmj.313.7052.275 PubMed
14.Chen R, Shao Z, Bi K, Cowling B, Du Z. Evaluating the health economic impacts of baloxavir marboxil and oseltamivir for the treatment of influenza in adult outpatients in Hong Kong: A cost-effectiveness analysis. 2025. doi:/10.2139/ssrn.5085546
15.Jiang Y, Wen J, Sun J, Shu Y. Evaluating the public health and health economic impacts of baloxavir marboxil and oseltamivir for influenza pandemic control in China: A cost-effectiveness analysis using a linked dynamic transmission-economic evaluation model. Pharmacoeconomics. 2024;42(10):1111-1125. doi:10.1007/s40273-024-01412-9 PubMed
16.Kommandantvold SA, Chang SC, Surinach A, et al. Cost-effectiveness of baloxavir marboxil versus oseltamivir or no treatment for the management of influenza in the United States. Infect. 2024;13(9):2071-2087. doi:10.1007/s40121-024-01027-9 PubMed
17.Kommandantvold SA, Lemenuel-Diot A, Skedgel C, et al. A cost-effectiveness analysis of reduced viral transmission with baloxavir marboxil versus oseltamivir or no treatment for seasonal and pandemic influenza management in the United Kingdom. Expert rev. 2024;24(8):953-966. doi:10.1080/14737167.2024.2365421
18.Nakagawa N, Kanazawa Y, Morikawa A, Lai L. Pharmacoeconomic study of anti-influenza virus drugs in Japan based on a network meta-analysis. J Antimicrob Chemother. 2024;79(7):1590-1596. doi:10.1093/jac/dkae141 PubMed
19.Nakagawa N, Ono R, Odanaka K, Ohara H, Kisara S, Ito K. A pharmacoeconomic study of post-exposure prophylaxis strategies for influenza virus infections in Japan. Adv Ther. 2024;05:05. doi:10.1007/s12325-024-02988-6
20.van der Pol S, Postma MJ, Boersma C. Antivirals to prepare for surges in influenza cases: An economic evaluation of baloxavir marboxil for the Netherlands. Eur J Health Econ. 2024;25(9):1557-1567. doi:10.1007/s10198-024-01683-1 PubMed
21.Li X, Bilcke J, van der Velden AW, et al. Cost-effectiveness of adding oseltamivir to primary care for influenza-like-illness: Economic evaluation alongside the randomised controlled ALIC4E trial in 15 European countries. Eur J Health Econ. 2023;24(6):909-922. doi:10.1007/s10198-022-01521-2 PubMed
22.Nakagawa N, Morikawa A, Kanazawa Y, Lai L. A cost-effectiveness analysis of Neuraminidase inhibitors for influenza virus infections in an adult-outpatient setting in Japan. Value Health Reg Issues. 2021;24:117-122. doi:10.1016/j.vhri.2020.07.579 PubMed
23.Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71 PubMed
24.Kim S, Bin Seo Y, Lee J, Kim YS, Jung E. Estimation of optimal antiviral stockpile for a novel influenza pandemic. J Infect Public Health. 2022;15(7):720-725. doi:10.1016/j.jiph.2022.05.012 PubMed
Appendix 1: Selection of Included Studies
Please note that this appendix has not been copy-edited.
Appendix 2: List of Excluded Studies by Reason for Exclusion
Please note that this appendix has not been copy-edited.
Cost-Effectiveness of Antivirals
Irrelevant Population (n = 4)
Benlloch J-M, Cortés J-C, Martínez-Rodríguez D, Julián R-S, Villanueva R-J. Effect of the early use of antivirals on the COVID-19 pandemic. A computational network modeling approach. Chaos, Solitons & Fractals. 2020;140:110168. PubMed
Jo Y, Kim SB, Radnaabaatar M, et al. Model-based cost-effectiveness analysis of oral antivirals against SARS-CoV-2 in Korea. Epidemiol Health. 2022;44:e2022034. PubMed
Le Rutte EA, Shattock AJ, Marcelino I, Goldenberg S, Penny MA. Efficacy thresholds and target populations for antiviral COVID-19 treatments to save lives and costs: a modelling study. eClinicalMedicine. 2024;73. PubMed
Metry A, Pandor A, Ren S, et al. Cost-effectiveness of therapeutics for COVID-19 patients: a rapid review and economic analysis. Health Technol Assess. 2023;27(14):1-92. PubMed
Irrelevant Intervention (n = 3)
Dawoud DM, Soliman KY. Cost-Effectiveness of Antiviral Treatments for Pandemics and Outbreaks of Respiratory Illnesses, Including COVID-19: A Systematic Review of Published Economic Evaluations. Value Health. 2020;23(11):1409-1422. PubMed
Newall AT, Wood JG, Oudin N, MacIntyre CR. Cost-effectiveness of pharmaceutical-based pandemic influenza mitigation strategies. Emerg Infect Dis. 2010;16(2):224-230. PubMed
Rasmussen MK, Kronborg C, Fasterholdt I, Kidholm K. Economic evaluations of interventions against viral pandemics: a scoping review. Public Health. 2022;208:72-79. PubMed
Irrelevant Comparator (n = 3)
Dronova M, Ikeoka H, Itsumura N, et al. Cost-effectiveness of baloxavir marboxil compared with laninamivir for the treatment of influenza in patients at high-risk for complications in Japan. Curr Med Res Opin. 2021;37(7):1135-1148. PubMed
Huang G, Tian Y, Cui W, Zhang X, Zhao Y, Liu X. Rapid health technology assessment of the novel endonuclease inhibitor baloxavir for the treatment of influenza. J Chemother. 2024;36(4):267-282. PubMed
Skrzeczek A, Ikeoka H, Hirotsu N, et al. Cost-effectiveness of baloxavir marboxil compared to laninamivir for the treatment of influenza in Japan. J Infect Chemother. 2021;27(2):296-305. PubMed
Irrelevant Outcome(s) (n = 1)
Panovska-Griffiths J, Grieco L, van Leeuwen E, Grove P, Utley M. A method for evaluating the cost-benefit of different preparedness planning policies against pandemic influenza. MethodsX. 2020;7(no pagination). PubMed
Ineligible Study Design (n = 4)
National Institute for Health and Care Excellence (NICE). Baloxavir marboxil for treating acute uncomplicated influenza (terminated appraisal). 2021; https://www.nice.org.uk/guidance/ta732/.Accessed January 20, 2025.
Suslo R, Pobrotyn P, Brydak L, Rypicz L, Grata-Borkowska U, Drobnik J. Seasonal Influenza and Low Flu Vaccination Coverage as Important Factors Modifying the Costs and Availability of Hospital Services in Poland: A Retrospective Comparative Study. Int J Environ Res Public Health. 2021;18(10). PubMed
van der Pol S, Postma MJ, Boersma C. Cost-effectiveness and Budget Impact of Baloxavir Marboxil in the Netherlands based on Post-COVID Seasonal Influenza Scenario. Poster presented at ISPOR 2022; 2022 Nov 6-9, 2022; Vienna, Austria. https://www.ispor.org/docs/default-source/euro2022/isporxofluzadef-pdf.pdf?sfvrsn=799e0269. Accessed January 20, 2025.
Yechezkel M, Ndeffo Mbah ML, Yamin D. Optimizing antiviral treatment for seasonal influenza in the USA: a mathematical modeling analysis. BMC Med. 2021;19(1):54. PubMed
Cost-Effectiveness of Stockpiling
Ineligible Study Design (n = 1)
Kim S, Bin Seo Y, Lee J, Kim YS, Jung E. Estimation of optimal antiviral stockpile for a novel influenza pandemic. J Infect Public Health. 2022;15(7):720-725. PubMed
Appendix 3: Characteristics of Included Publications
Table 3: Characteristics of Included Economic Evaluations
Study citation, country, funding source | Type of analysis, time horizon, perspective | Population characteristics and setting | Intervention and comparator(s) | Approach | Source of clinical, cost, and utility data used in analysis | Main assumptions |
|---|---|---|---|---|---|---|
Chen et al. (2025)14 Hong KongFood and Health Bureau of the Government of Hong Kong | CUA Time horizon: 1 year Perspective: Health care payer Discount rate: NA | Adult outpatients, not adequately protected by vaccination, consulting within 48 hours of symptom onset, and with a positive rapid influenza test in Hong Kong (otherwise healthy and high risk) Seasonal influenza | Intervention: baloxavir marboxil Comparator: oseltamivir or baseline | Decision-tree model DSA, PSA, scenario analyses | Clinical data were from 2 Phase III clinical trials and utility data were from HTAs. All cost data were from Hong Kong- based sources. Total cost for each treatment included outpatient consultation, influenza diagnostic tests, medication, hospitalization care, and ICU care. | Assumed that the patient has tested positive for influenza before receiving antiviral therapy. |
Jiang et al. (2024)15 China Guangdong Basic and Applied Basic Research Foundation and F. Hoffmann-La Roche Ltd. | CUA Time horizon: 1 year Perspective: Chinese health care system Discount rate: NA | Outpatient presenting ≥ 24 hours since symptom onset Pandemic influenza | Intervention: baloxavir marboxil Comparator: oseltamivir | Linked dynamic transmission-economic evaluation model (SEIR + decision tree) DSA, PSA | Clinical data were from clinical trials and observational studies from literature. Utility values obtained from literature. Cost data were extracted from economic evaluation studies in the Chinese setting. Total cost for each treatment included drug acquisition costs, the costs of treating complications, and the costs of hospitalization. | Assumed an antiviral drug uptake rate of 35% among infected patients, that each patient could only be infected with influenza once a year, and that only 1 complication needed to be considered. |
Kommandantvold et al. (2024)16 US F. Hoffmann-La Roche, Ltd. | CUA Time horizon: Lifetime Perspective: US commercial payer Discount rate: 3% (cost and outcomes) | Symptomatic individuals ≥ 12 years of age (56% otherwise healthy, 44% high risk) with influenza in an insured US population (mean age = 32) Seasonal influenza | Intervention: baloxavir marboxil Comparators: oseltamivir or no antiviral treatment | Decision-tree model DSA, PSA, scenario analyses | Clinical data were from Merative MarketScan Research Databases including US commercial claims and Medicare and Medicaid Supplemental databases. Total cost for each treatment included GP visit costs, drug costs, adverse events, and costs of complications. | Assumed that there is no reduction in viral transmission with antiviral treatment in base-case analysis. |
Kommandantvold et al. (2024)17 UK F. Hoffmann-La Roche, Ltd. | CUA Time horizon: Lifetime Perspective: UK National Health Service Discount rate: 3.5% (cost and outcomes) | Otherwise, healthy and individuals aged ≥ 12 years at high risk. Seasonal and pandemic influenza | Intervention: baloxavir marboxil Comparators: oseltamivir or no antiviral treatment | Linked dynamic transmission-economic evaluation model (SEIR + decision tree) DSA, PSA, scenario analysis | Clinical data were from the literature and from clinical trials (CAPSTONE-1 and CAPSTONE-2). Cost data were extracted from the 2021/2022 National Health Service England National Cost Collection data. Total cost for each treatment included GP visit costs, drug costs, adverse event, and costs of complications. | Assumed a proportion of the total population would receive antiviral treatment and assumed a zero-mortality rate among exposed and infected individuals before becoming infectious. |
Nakagawa et al. (2024)18 Japan Individual research fund from the university | CUA Time horizon: 14 days Perspective: health care payer Discount rate: NR | Outpatient adults aged 18 years and older are diagnosed with influenza virus infection Seasonal influenza | Intervention: oseltamivir Comparators: zanamivir, laninamivir, peramivir | Decision-tree model DSA, PSA | Clinical data were from a NMA, and utility data were from EQ-5D-5L questionnaires. Cost data were extracted from 2020 Japanese medical fee index. Total cost for each treatment included medical costs, drug prices, hospital admission costs. | Assumed 3 days for prolonged symptoms for the disease state 1. |
Nakagawa et al. (2024)19 Japan Funding source: None | CUA Time horizon: 14 days Perspective: health care payer Discount rate: NR | Healthy adults (≥ 18 years) Seasonal influenza | Interventions: (post-exposure prophylaxis then treatment)
Comparator: direct comparison | Decision-tree model DSA, PSA Post-exposure prophylaxis and treatment | Clinical data were from clinical trials and utility data were from EQ-5D-5L questionnaires. Cost data were extracted from 2000 Japanese medical fee index. Total cost for each treatment included second physician visit, pharmacy, and hospital admission expenses, and drug prices. | Assumed that when people who received post-exposure prophylaxis were infected, all of them received treatment with the other drug therapy. |
van der Pol et al. (2024)20 Netherlands Roche Netherlands B.V. | CUA and BIA Time horizon: Lifetime (CUA), 5 years (BIA) Perspective: societal (CUA), health care (BIA) Discount rate: 4% (costs), 1.5% (outcomes) | Patients (cohort of 52-year-olds) are at risk of influenza-related complications, including patients with comorbidities and older individuals (CUA) Whole eligible population (around 5.6 million individuals), covering both vaccinated and unvaccinated people (BIA) Seasonal influenza | Intervention: baloxavir marboxil Comparator: current standard of care (symptomatic treatment with paracetamol) | Decision-tree model DSA, PSA, scenario analysis | Clinical data were from clinical trials (CAPSTONE-2 trial). Cost data were extracted from Dutch reference prices and literature. Total cost for each treatment included drug costs, GP consult, hospitalization, outpatient pneumonia, productivity loss, indirect medical costs. | Assumed that baloxavir marboxil was only effective for the “true influenza” group and mortality only occurred in the hospital. The outcomes were assumed to be the same for the baloxavir marboxil and current standard of care arms in the model. |
Li et al. (2023)21 15 European Countries European Commission’s Seventh Framework Programme: Platform for European Preparedness Against (Re-) emerging Epidemics Grant | CUA Time horizon: 14 days Perspective: Both health care and societal Discount rate: NA | Adults/adolescents (13 years +) and children (≥ 1 year and < 13 years) with ILI Subgroup: patients with and without comorbidity Seasonal influenza | Intervention: usual care + oseltamivir Comparator: usual care | Economic evaluation alongside an RCT Compare the direct medical costs and health outcomes (in terms of number of days where ILI limits usual activities and in terms of QALYs gained) between the different arms. PSA, EVPI analysis, scenario, and subgroup analyses | Clinical data were from a ALIC4E trial (did not capture any ILI-associated intensive care admissions or death) Cost data were extracted from the patient-reported resource use and official country-specific unit costs (2018). Total cost for each treatment included direct and indirect costs. | Long-term health consequences of ILI would not be fully captured in the 14-day time horizon. |
Nakagawa et al. (2021)22 Japan Funding source: None | CUA Time horizon: 14 days Perspective: health care payer Discount rate: NR | Adult outpatients Seasonal influenza | Intervention: oseltamivir, zanamivir, laninamivir, and peramivir Comparator: direct comparison | Decision-tree model DSA | Clinical data were from relevant RCTs. Effectiveness outcomes were measured using EQ-5D-3L questionnaires administered to adult patients who had previously experienced influenza virus infections. Cost data were extracted from the 2016 medical fee schedule table. Costs included medical costs and drug prices. | Long-term health consequences of ILI would not be fully captured in the 14-day time horizon. |
BIA = budget impact analysis; CUA = cost-utility analysis; DSA = deterministic sensitivity analysis; EVIP = expected value for perfect information; GP = general practitioner; HTA = health technology assessment; ICU = intensive care unit; ILI = influenza-like illness; NA = not applicable; NR = not reported; NMA = network meta-analysis; PSA = probabilistic sensitivity analysis; QALY = quality-adjusted life-year; RCT = randomized controlled trial; SEIR = Susceptible-Exposed-Infected-Recovered model.
Note: This table has not been copy-edited.
Appendix 4: Critical Appraisal of Included Publications
Please note that this appendix has not been copy-edited.
Table 4: Strengths and Limitations of Economic Evaluations Using the Drummond Checklist13
Strengths | Limitations |
|---|---|
Chen et al. (2025)14 | |
Local Relevance: Hong Kong-specific cost and resistance data improve regional applicability. Subgroup Analysis: Separate evaluations for OwH and HR populations provide nuanced insights. Dynamic Resistance Consideration: Addressed how rising oseltamivir resistance impacts cost-effectiveness, a critical real-world factor. Transparency in Funding: Supported by non-industry grants (e.g., Hong Kong government funds), reducing industry bias risk. | Time Horizon: A one-year horizon may overlook long-term outcomes or rare complications. Adherence Assumptions: Assumed perfect medication adherence, which may overestimate real-world effectiveness. Societal Costs: Excluded indirect costs (e.g., productivity loss), potentially underestimating economic impact. Conflict of Interest: One author disclosed consulting fees from pharmaceutical companies, including Roche (baloxavir marboxil manufacturer). |
Jiang et al. (2024)15 | |
Comprehensive Modelling Approach: Uses a linked dynamic transmission-economic evaluation model (SEIR + decision tree) capturing both transmission dynamics and individual-level disease progression. Data-Driven Parameterization: Uses data from clinical trials, observational studies, and the 2009 H1N1 pandemic in China to parameterize the models, enhancing validity. Sensitivity Analyses: Employs one-way, two-way, and probabilistic sensitivity analyses to assess the robustness of findings across various assumptions. Clear Presentation: Article’s compliance with CHEERS 2022 reporting standards, promoting transparency. | Short Time Horizon: A one-year time horizon may not capture long-term effects or potential resurgence of the virus. Limited Perspective: The study is conducted from the Chinese health care system perspective, which may not capture broader societal costs (e.g., productivity losses). Parameter Uncertainty: The transmission coefficient is based on the 2009 pandemic, which may not be representative of future pandemics. Vaccination Assumption: Assumes 0% overall effectiveness of vaccination which is not realistic in a real pandemic scenario. Uptake Rate Assumption: Assumes antiviral drug uptake rate of 35%, which is a conservative assumption. Limited Consideration of Viral Evolution: Does not explicitly model the potential for rapid viral evolution and resistance to antivirals over the pandemic period. Funding Source: Discloses funding from Hoffmann-La Roche, which introduces potential for bias. |
Kommandantvold et al. (2024)16 | |
Robust Modelling Approach: The use of a decision-analytic model is justified, and the model structure appears appropriate for the research question. Comprehensive Sensitivity Analysis: The study includes thorough sensitivity analyses (one-way, two-way, probabilistic) to assess the impact of parameter uncertainty on the results. Transparent Reporting: The study generally provides transparent reporting of methods, assumptions, and results, enhancing its credibility. | Limited Details on Effectiveness Data: The study does not provide comprehensive details on the design and results of the effectiveness studies used to inform the model, which may limit the ability to fully assess the validity of the effectiveness inputs. Lack of Subject Valuation Details: Details about the subjects from whom valuations were obtained are not comprehensively discussed, impacting the generalizability and transferability of the results. Exclusion of Productivity Changes: The study does not include productivity changes, which may underestimate the true economic benefits of baloxavir marboxil, especially from a societal perspective. Lack of Separate Reporting of Resource Use and Costs: Not reporting quantities of resource use separately from their unit costs reduces transparency and reproducibility. Limited External Validity: The results may have limited external validity to other health care settings or populations due to differences in treatment patterns, health care costs, and influenza epidemiology. Funding Source: Discloses funding from Hoffmann-La Roche, which introduces potential for bias. |
Kommandantvold et al. (2024)17 | |
Pandemic and Seasonal Scenarios: Addresses both seasonal and pandemic influenza, which is important for comprehensive planning. Transmission Dynamics: Uses a SEIR model to capture the impact of reduced viral shedding with baloxavir marboxil on transmission dynamics. Subgroup Analysis: Considers both OwH and HR populations. UK-Specific Context: The study is set in the UK and uses data relevant to the UK health care system. | Model Assumptions: The SEIR model relies on several assumptions, including the basic reproduction number, susceptibility rates, and treatment rates, which are subject to uncertainty. Time Horizon: The SEIR model has a time horizon of 1 influenza season, which may not capture longer-term effects. Data Sources: The SEIR model relies on several data sources, which may not be fully representative of the UK population. Simplified Representation: The SEIR model simplifies complex real-world dynamics, such as individual behaviour and adherence to treatment. Limited Perspective: Although mentioned health care resource utilization, other economic perspectives such as patients or societal may not be captured. Funding Source: Discloses funding from Hoffmann-La Roche, which introduces potential for bias. |
Nakagawa et al. (2024)18 | |
Addresses Prior Limitations: The study explicitly addresses the shortcomings of a previous analysis by incorporating PSA and using EQ-5D-5L for QoL assessment. NMA: It uses data from a NMA to derive effectiveness probabilities, strengthening the evidence. Improved Decision-Tree Model: A more detailed decision tree with 7 health states, compared to the original 3 health states. Japanese Data: Uses Japanese medical costs and tariffs Sensitivity Analyses: DSA and PSA, addressing parameter uncertainty. | Limited Scope: It only evaluates neuraminidase inhibitors (oseltamivir, laninamivir, zanamivir, and peramivir) and does not include baloxavir marboxil, which is a relevant alternative. Short Time Horizon: The 14-day time horizon may not capture all relevant costs or long-term consequences of influenza. QoL Data: The QoL scores are derived from a relatively small sample (n = 50) of patients with a history of influenza virus infections. The study does not describe the 50 patients, and they may not be representative of the target population. Model assumptions: The study assumes that the drug adverse event and pneumonia is 4.4% and 0.5% for baloxavir marboxil, respectively. It is assumed that baloxavir marboxil causes the pneumonia, but the relationship is not clear. NMA Limitations: The validity of the study is dependent on the quality of the NMA used to derive effectiveness estimates. The NMA is accepted without validation or verification. |
Nakagawa et al. (2024)19 | |
Relevant Perspective: The study is conducted from the perspective of the health care payer in Japan, making it directly relevant to decision-making within the Japanese health care system. Considers Multiple Strategies: The study compares a range of PEP and treatment combinations, providing a more comprehensive analysis than studies that focus on single interventions. Japanese Data: The study uses Japanese cost data from the 2020 Medical Fee Index, enhancing the relevance of the findings to the Japanese context. Addresses Uncertainty: The study uses both DSA and PSA to address uncertainty in the model parameters. Accessibility: Datasets used in the study are available on Dryad platform. | Exclusion of Initial Doctor Visit Costs: Due to Japanese policy on out-of-pocket expenses for PEP, the analysis excludes the costs of the initial doctor and pharmacy visits. This may underestimate the true cost of PEP strategies. Short Time Horizon: The 14-day time horizon may not capture all relevant costs or long-term effects of influenza and its treatment. Drug cost DSA: Limited variation in the drug cost DSA to just 10%. Utility data source: Utility data were measured using EQ-5D-5L questionnaires administered to healthy university students and may not be representative of actual patients. |
van der Pol et al. (2024)20 | |
Relevant Population: The focus on at-risk patients (those eligible for annual influenza vaccination) is appropriate for the Netherlands, where antiviral use is uncommon. Societal Perspective: The adoption of a societal perspective, including productivity losses, provides a more comprehensive assessment of economic impact. Dutch-Specific Data: The study incorporates Dutch-specific data on costs, epidemiology, health care resource utilization, and vaccination coverage, enhancing the relevance of the results to the Netherlands. Budget Impact Analysis: The inclusion of a budget impact analysis provides valuable information for decision-makers regarding the potential financial implications of adopting baloxavir marboxil. Considers Uncertainty: The use of PSA allows for the assessment of uncertainty in the model parameters and their impact on the results. Mortality Consideration: Incorporates a lifetime horizon to capture the QALYs lost in case of mortality. | Model Description Detail: The description of the model in the methods section could be more detailed, particularly regarding the specific assumptions and calculations used. CAPSTONE-2 Trial Data: The reliance on data from the CAPSTONE-2 trial may not fully reflect real-world effectiveness in the Netherlands, as trial populations and settings can differ from routine clinical practice. Scenario Details: The different scenarios that were analyzed were not well described in the results. PSA Description Clarity: While a probabilistic sensitivity analysis is performed, the specific parameters varied and the rationale for their ranges could be clearer. Dutch context: The Dutch context for influenza vaccination is a specific one, as the government aims at good communication about the national vaccination program for influenza, rather than implementing performance indicators such as vaccination coverage. This context should be considered for the interpretation of the model. Funding Source: Discloses funding from Roche Netherlands B.V., which introduces potential for bias. |
Li et al. (2023)21 | |
Relevant Perspectives: The analysis is conducted from both health care payers’ and societal perspectives, providing a more comprehensive assessment. Patient-Level Data: The use of patient-level data on resource use, costs, and HRQoL, collected prospectively in the ALIC4E trial, enhances the validity of the results. Multi-Country Design: The study's multi-country design increases its generalizability to other European settings. Country-Specific Costs: The use of country-specific unit costs and PPP conversions makes the results more relevant to individual countries. Addresses Uncertainty: The study addresses uncertainty through PSA and EVPI analysis. Real-World Setting: The study was conducted in a real-world primary care setting, which increases its relevance to clinical practice. | Short Time Horizon: The 14-day time horizon is a limitation, as it may miss longer-term sequelae of ILI. Generalizability to Specific Subgroups: The study may not be generalizable to specific subgroups of patients, such as those with severe ILI or those at high risk of complications. Data Quality: The reliance on patient-reported data may be subject to recall bias. Lack of Methodological Details: Important methodological details are lacking, for example around the approach for dealing with missing data and translation of EQ-5D-Y results. |
Nakagawa et al. (2021)22 | |
Relevant Perspective: The analysis is conducted from the health care payer's perspective in Japan, which is relevant for local decision-making. Appropriate Model: A decision-tree model is used, which is a reasonable approach for analyzing the short-term treatment of influenza. Japanese Data: The study uses Japanese cost data from the 2016 medical fee schedule, enhancing its relevance to the Japanese health care system. One-Way Sensitivity Analysis: This helps to understand the impact of changing key parameters on the results. | Short Time Horizon: The 14-day time horizon is a major limitation, as it may not capture all relevant costs or long-term effects of influenza and its treatment. QoL Data Concerns: The use of the EQ-5D-3L may not be as sensitive as newer versions (e.g., EQ-5D-5L). Small Sample Size and Description: The patient number is only 41 patients, and their description is only “patients who had experienced influenza virus infections previously.” Lack of PSA: The absence of PSA means that the uncertainty in the parameters is not fully explored, and the robustness of the conclusions cannot be fully assessed. Limited Scope: The study does not consider other potentially relevant comparators. |
DSA = deterministic sensitivity analysis; EVPI = expected value of perfect information; HR = high risk; HRQoL = health-related quality of life; ILI = influenza-like illness; NAIs = neuraminidase inhibitors; NMA = network meta-analysis; OwH = otherwise healthy; PEP = post-exposure prophylaxis; PPP = purchasing power parity; PSA = probabilistic sensitivity analysis; QALY = quality-adjusted-life-year; QoL = quality of life.
Appendix 5: Main Study Findings
Please note that this appendix has not been copy-edited.
Table 5: Summary of Findings of Included Economic Evaluations
Main study findings | Authors’ conclusion |
|---|---|
Chen et al. (2025)14 | |
General population results:
Otherwise, healthy population:
High-risk population:
Oseltamivir resistance:
| “Baloxavir is more effective and economical compared to oseltamivir, thereby optimizing healthcare delivery and improving patient outcomes (p.2).”14 |
Jiang et al. (2024)15 | |
Infection reduction:
QALY gain:
Economic benefit:
| “Adding baloxavir marboxil to treatment choices instead of only treating with oseltamivir for influenza pandemic control in China appears to be cost-effective compared with oseltamivir alone. The dual-agent strategy not only enhances population health outcomes and conserves resources but also mitigates influenza transmission and alleviates healthcare burden (p.1111).”15 |
Kommandantvold et al. (2024)16 | |
Base-case analysis (total population):
High-risk population:
Otherwise, healthy population:
Scenario analysis:
| “This model estimated a meaningful health economic benefit of baloxavir treatment compared with oseltamivir or no antiviral treatment from a US payer perspective. Findings were robust in favour of baloxavir being cost-effective in the total insured US population as well as in the high-risk and otherwise healthy subpopulation analyses. Baloxavir provided a meaningful improvement in NMB compared with oseltamivir or no treatment when hypotheticala rates of reduced viral transmission were explored in a scenario analysis. The ability of baloxavir to reduce viral transmission appeared to offer a substantial additional economic benefit (p. 2084).”16 |
Kommandantvold et al. (2024)17 | |
Infection reduction:
Seasonal setting -total population:
Seasonal setting - high-risk population:
Pandemic scenario:
Transmission reduction impact:
| “Antiviral treatment with baloxavir is cost-effective compared with oseltamivir or no antiviral treatment from a UK NHS perspective. Cost- effectiveness findings were driven by a greater estimated relative reduction in infections across the population, which was associated with greater reduced onward transmission when infected individuals were treated with baloxavir compared with oseltamivir or no antiviral treatment in the SEIR model. Findings in favour of baloxavir were substantial when treatment was targeted to the high-risk subset of the population only and in pandemic settings in which viral transmission is greater and downstream outcomes are likely to be the worst (p.964).”17 |
Nakagawa et al. (2024)18 | |
Expected value of INMB:
Base case:
PSA:
| “This study thus reaffirms oseltamivir’s position as the most cost-effective NAI for the treatment of influenza virus infections in Japan from the perspective of healthcare payment p. (1590).”18 |
Nakagawa et al. (2024)19 | |
QALY values:
Patients with body weight < 80 kg, 4 dominant strategies:
Patients with body weight ≥ 80 kg, 3 dominant strategies:
PSA results at a WTP threshold of 5,000,000 yen per QALY: Most cost-effective:
Second most cost-effective:
| “In conclusion, this study confirms that baloxavir marboxil and oseltamivir are cost-effective drugs for post-exposure prophylaxis in Japan from the health care payer perspective. The strategy of baloxavir marboxil as the post-exposure prophylaxis drug and laninamivir as the treatment drug is the most cost-effective in Japan (p.14).”19 |
van der Pol et al. (2024)20 | |
Base-case:
BIA:
PSA:
| “In the Netherlands, baloxavir is a cost-effective treatment option for seasonal influenza, with a base-case ICER of €8,300 per QALY for the population aged 60 years and over and patients at high risk of influenza-related complications (p.1565)”20 |
Li et al. (2023)21 | |
Health care payer perspective:
Societal perspective:
EVPI:
| “Adding oseltamivir to primary usual care in Europe is likely to be cost-effective for treating adults/adolescents and children with ILI from the healthcare payers’ perspective (if WTP per QALY gained > €22,459) and cost-saving in adults/adolescents from a societal perspective (p.909).”21 |
Nakagawa et al. (2021)22 | |
Cost-effectiveness ratios:
ICERs:
Sensitivity analyses:
| “Using a decision-tree model, a CEA was built to elucidate which NAI medication is most cost-effective for use in an adult outpatient setting, and to measure QoL values with EQ-5D-3L from the healthcare payer’s perspective in Japan. Oseltamivir was concluded to be the most cost-effective NAI for the treatment of influenza virus infection in an adult outpatient setting (p.121).”22 |
BIA = budget impact analysis; CEA = cost-effectiveness analysis; CN¥: Chinese yuan; EQ-5D: EuroQol – 5 Dimension; EVPI = expected value of perfect information; ICER = incremental cost-effectiveness ratio; ILI = influenza like illness; INMB = incremental net monetary benefit; NAI = neuraminidase inhibitor; NHS = National Health Service; NMB = net monetary benefit; SEIR = Susceptible-Exposed-Infected-Recovered model; QALY = quality-adjusted life-year; QoL = quality of life; WTP = willingness to pay.
aConsidering various potential level.
Table 6: Antiviral Drug Costs Reported in Included Studies
Study citation | Antiviral | Drug cost | Currency | Year |
|---|---|---|---|---|
Chen et al. (2025)14 | Baloxavir marboxil | Per course Base case (min-max): 123.50 (117.00 to 130.00) | US$ | 2024 |
Oseltamivir | Per course Base case (min-max): 91.00 (56.00 to 117.00) | US$ | 2024 | |
Jiang et al. (2024)15 | Baloxavir marboxil | Drug acquisition cost Baseline (SE): 189.00 (18.90) | CN¥ | 2021 |
Oseltamivir | Drug acquisition cost Baseline (SE): 123 (12.30) | CN¥ | 2021 | |
Kommandantvold et al. (2024)16 | Baloxavir marboxil | Drug cost (per episode of care): 159.14 | US$ | 2022 |
Oseltamivir | Drug cost (per episode of care): 50.40 | US$ | 2022 | |
Kommandantvold et al. (2024)17 | Baloxavir marboxil | Drug cost: 100.00 | £ | 2021 |
Oseltamivir | Drug cost: 12.33 | £ | 2021 | |
Nakagawa et al. (2024)18 | Oseltamivir 75 mg capsule | Authorized drug price: 3.00 | US$ | 2020 |
Zanamivir 5 mg blister | Authorized drug price: 1.00 | US$ | 2020 | |
Peramivir 300 mg bag | Authorized drug price: 63.00 | US$ | 2020 | |
Nakagawa et al. (2024)19 | Oseltamivir 75 mg capsule | Authorized drug price: 3.00 | US$ | 2020 |
Zanamivir 5 mg blister | Authorized drug price: 1.00 | US$ | 2020 | |
Baloxavir marboxil 20 mg | Authorized drug price: 24.00 | US$ | 2020 | |
van der Pol et al. (2024)20 | Baloxavir marboxil | Drug cost including pharmacy fee: 133.00 | € | 2021 |
Li et al. (2023)21 | Oseltamivir 30 mg | List price range: 7.00 to 19.00 | € PPP | 2018 |
Oseltamivir 45 mg | List price range: 14.00 to 32.00 | € PPP | 2018 | |
Oseltamivir 60 mg | List price range: 14.00 to 37.00 | € PPP | 2018 | |
Oseltamivir 75 mg | List price range: 15.00 to 50.00 | € PPP | 2018 | |
Nakagawa et al. (2021)22 | Oseltamivir 75 mg capsule | Authorized drug price: 2.79 | US$ | 2018 |
Zanamivir 5 mg blister | Authorized drug price: 1.51 | US$ | 2018 | |
Peramivir 300 mg bag | Authorized drug price: 61.32 | US$ | 2018 |
NR = not reported; PPP = purchasing power parity.
Table 7: Consideration of Opportunity Cost Across Included Studies
Study citation | Opportunity cost considered | Details |
|---|---|---|
Chen et al. (2025)14 | Partial | Uses ICER, but no broader discussion of what resources are replaced. |
Jiang et al. (2024)15 | Yes (at system level) | Compares influenza control strategies (quarantine, antivirals); implicitly addresses opportunity cost through competing interventions. |
Kommandantvold et al. (2024)16 | Yes (implicitly via WTP) | Opportunity cost is built into the threshold; no separate analysis but implies that antivirals must displace interventions < $100K/QALY. |
Kommandantvold et al. (2024)17 | Yes (implicitly via WTP) | Used UK’s threshold of £30,000/QALY, which reflects the health opportunity cost in the NHS (i.e., displaced QALYs elsewhere). |
Nakagawa et al. (2024)18 | Indirectly | Uses a NMB approach, which can imply opportunity cost, but no explicit discussion. |
Nakagawa et al. (2024)19 | Indirectly | NMB is used clearly but is not discussed in terms of forgone health gains. |
van der Pol et al. (2024)20 | Partial | Includes budget impact analysis, which is relevant to opportunity cost, but does not link to QALY displacement. |
Li et al. (2023)21 | Not explicitly addressed | Focus is on cost-effectiveness within trial—not broader budget or displacement effects. |
Nakagawa et al. (2021)22 | Indirectly | NMB used to compare treatments, but no context on thresholds or displacement. |
NMB = net monetary benefit; NHS = National Health Service; QALY = quality-adjusted life-year; WTP = willingness to pay.
ISSN: 2563-6596
This work was conducted by the Alberta Drug and Therapeutic Evaluation Consortium (ADTEC) through the Post-Market Drug Evaluation CoLab Network. It was supported by Canada’s Drug Agency (CDA-AMC) and its Post-Market Drug Evaluation Program through funding provided by Health Canada.
CDA-AMC is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we are responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
CoLab is a pan-Canadian network of experts in applied research, scientific methods, and data analysis. CoLab members work with the Post-Market Drug Evaluation Program to produce credible and timely evidence on post-market drug safety and effectiveness.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
This document is the property of ADTEC. CDA-AMC has a nonexclusive, limited, royalty-free, worldwide, nontransferable, fully paid-up, and irrevocable licence to use the report in support of its objects, mission, and reasonable operational requirements.