Drugs, Health Technologies, Health Systems
Health Technology Review
Quetiapine for Schizophrenia
Summary
Main Take-Aways
Evidence-based guidelines recommend second-generation antipsychotics over first-generation antipsychotics for the management of first-episode schizophrenia.
Clinical evidence did not clearly indicate which antipsychotics, including quetiapine, are the better choice for treatment of schizophrenia.
Key Messages
What Is the Issue?
Antipsychotic medications are the mainstay of treatment and the most prescribed drugs for the treatment of schizophrenia. There are 2 classes of antipsychotics — first-generation antipsychotics (FGAs) and second-generation antipsychotics (SGAs). Quetiapine is an SGA drug. Decision-makers are interested in understanding the clinical efficacy, safety, and place in therapy of quetiapine compared to other medications for the treatment of schizophrenia in adults.
What Did We Do?
We searched key resources, including journal citation databases, and conducted a focused internet search for relevant evidence published since 2020.
What Did We Find?
The clinical evidence did not clearly indicate which antipsychotics, including quetiapine, are the better choice for the treatment of schizophrenia.
Evidence-based guidelines recommend SGAs over FGAs for the management of first-episode psychosis and schizophrenia, as well as for maintenance treatment of schizophrenia. For the treatment of recurrent or relapsing schizophrenia, the guidelines provided diverging recommendations.
What Does This Mean?
Prescribing antipsychotics for the treatment of schizophrenia should be based on patient characteristics, patient tolerability, patient values, side effect profiles of different antipsychotic medications, and clinician expertise.
Abbreviations
AE
adverse event
BPRS
Brief Psychiatric Rating Scale
CDSS
Calgary Depression Scale for Schizophrenia
CGI
Clinical Global Impression
CI
confidence interval
FGA
first-generation antipsychotic
JSNPP
Japanese Society of Neuropsychopharmacology
LAI
long-acting injection
LS
least squares
MA
meta-analysis
MD
mean difference
NMA
network meta-analysis
PANSS
Positive and Negative Symptom Scale
RCT
randomized controlled trial
RR
relative risk
SANS
Scale for Assessment of Negative Symptoms
SAPS
Scale for Assessment of Positive Symptoms
SE
standard error
SGA
second-generation antipsychotic
SMD
standardized mean difference
SR
systematic review
VA/DoD
Veterans Affairs/Department of Defense
XR
extended release
YMRS
Young Mania Rating Scale
Context and Policy Issues
What Is Schizophrenia?
Schizophrenia is a mental health condition that involves cognitive, behavioural, and emotional dysfunctions and mood-related symptoms.1,2 The symptoms are usually classified into positive symptoms (e.g., hallucination and delusion), negative symptoms (e.g., social withdrawal, appearing emotionless, and self-neglect), disorganized speech and/or behaviour, and cognitive symptoms (e.g., difficulties with attention, processing speed, and executive function).1,3 It affects approximately 1% of people living in Canada, with a slightly higher proportion in males than females (56% males and 44% females).4
What Are the Medications for the Treatment of Schizophrenia?
There is no cure for schizophrenia. However, the symptoms associated with schizophrenia can be managed by medication. Other modes of management include brain stimulation therapies, psychosocial therapies and supports, physical activity, and diet.3
Antipsychotic medications are the most commonly prescribed drugs for the treatment of schizophrenia.5 Antipsychotics are broadly classified into 2 classes — first-generation antipsychotics (FGAs) and second-generation antipsychotics (SGAs) — based on the time of their development.5 FGAs, which are also called conventional or typical antipsychotics, are associated with extrapyramidal side effects that include Parkinson-like symptoms (e.g., stiffness, dry mouth, sedation), akathisia (inability to remain still), and dyskinesia (e.g., involuntary, erratic, writhing movements of the face, arms, legs, or trunk).6 SGAs, which are also called atypical antipsychotics, appear to be associated with a lower risk of the extrapyramidal side effects associated with FGAs. However, overall, SGAs have more metabolic side effects (e.g., weight gain, risk of diabetes, high cholesterol) than FGAs.6
Examples of FGAs include chlorpromazine, levomepromazine, fluphenazine, haloperidol, thioridazine, perphenazine, pipotiazine, thiothixene, and trifluoperazine. Examples of SGAs include quetiapine, sertindole, zotepine, aripiprazole, asenapine, clozapine, lurasidone, olanzapine, risperidone, amisulpride, sulpiride, and ziprasidone. Immediate-release quetiapine is available as 25 mg, 100 mg, 200 mg, and 300 mg quetiapine fumarate tablets, whereas extended-release quetiapine (quetiapine XR) is available as 50 mg, 150 mg, 200 mg, 300 mg, and 400 mg quetiapine fumarate tablets.
Why Is It Important to Do This Review?
Quetiapine is approved for the treatment of schizophrenia based on short-term (6 weeks) efficacy trials.7 Data on the long-term efficacy of quetiapine in clinical trials are still limited.7 In addition, there have not been systematic evaluations of the clinical efficacy and safety of quetiapine with other relevant comparators for the treatment of schizophrenia.
Objective
To support decision-making on quetiapine for the treatment of schizophrenia, we prepared this Rapid Review report to summarize and critically appraise the available studies on the clinical effectiveness and safety of quetiapine compared with other drug interventions for the treatment of adults with schizophrenia. We also sought to summarize recommendations from evidence-based guidelines on the use of quetiapine for the treatment of adults with schizophrenia.
Research Questions
What is the clinical effectiveness and safety of quetiapine versus other drug interventions for adults with schizophrenia?
What are the evidence-based guidelines regarding the use and administration of quetiapine for adults with schizophrenia?
Methods
Literature Search Methods
An information specialist conducted a literature search of key resources, including MEDLINE, Embase, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concepts were quetiapine and schizophrenia. Search filters were applied to limit retrieval to health technology assessments, systematic reviews (SRs), meta-analyses (MAs), or indirect treatment comparisons, randomized controlled trials (RCTs), controlled clinical trials, or guidelines. The search was completed on March 20, 2025, and was limited to English-language documents published since January 1, 2020.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Adults aged 18 years or older with schizophrenia |
Intervention | Quetiapine fumarate immediate-release tablets, quetiapine fumarate extended-release tablets |
Comparator | Other drug interventions (e.g., other first- or second-generation antipsychotics, placebo) |
Outcomes |
|
Study designs | RCTs, SRs (including NMAs and MAs), evidence-based guidelines,a published HTAs |
HTA = health technology assessment; MA = meta-analysis; NMA = network meta-analysis; RCT = randomized controlled trial; SR = systematic review.
aA guideline is defined as a systematically developed statement or set of statements to help practitioners and patients make decisions about appropriate health care for specific clinical circumstances. A guideline is considered evidence-based if a systematic search of the literature was undertaken to inform the recommendations.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1 or if they were published before 2020. SRs in which all relevant studies were captured in other more recent or more comprehensive SRs were excluded. Primary studies retrieved by the search were excluded if they were captured in 1 or more included SRs. Guidelines with unclear methodology were also excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)8 for SRs, the “Questionnaire to assess the relevance and credibility of a network meta-analysis”9 for network meta-analyses (NMA), the Downs and Black checklist10 for RCTs, and the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument11 for guidelines. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
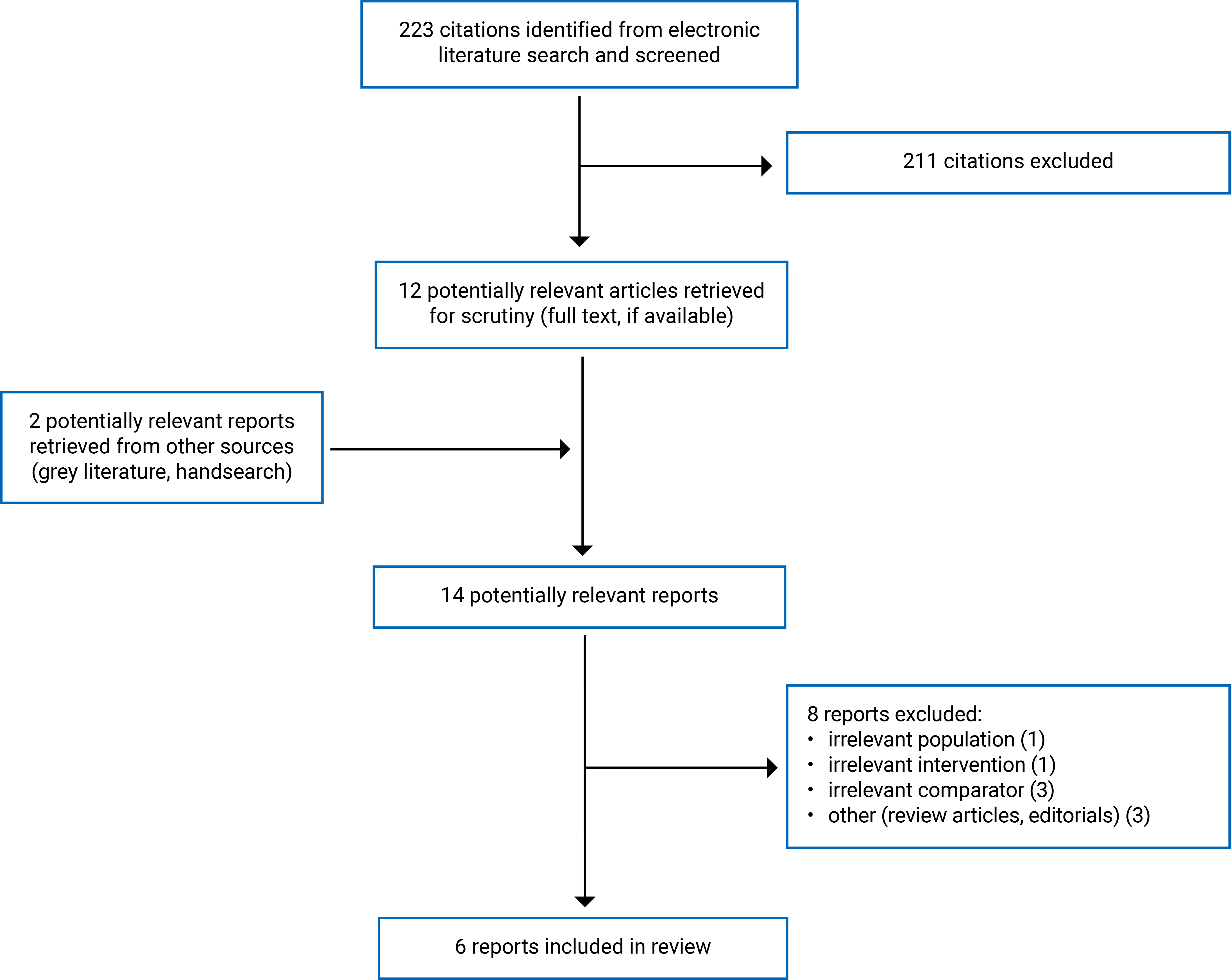
A total of 223 citations were identified in the literature search. Following screening of titles and abstracts, 211 citations were excluded and 12 potentially relevant reports from the electronic search were retrieved for full-text review. Two potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 8 publications were excluded for various reasons, and 6 publications met the inclusion criteria and were included in this report. These comprised 3 SRs, 1 RCT, and 2 evidence-based guidelines. Appendix 1 presents the PRISMA12 flow chart of the study selection.
Summary of Study Characteristics
Appendix 2 provides details regarding the characteristics of the included SRs13-15 (Table 2), the included RCT16 (Table 3), and the included evidence-based guidelines17,18 (Table 4).
Included Studies for Research Question 1: What Is the Clinical Effectiveness and Safety of Quetiapine Versus Other Drug Interventions for Adults With Schizophrenia?
Study Design
Three SRs13-15 and 1 RCT16 were included to answer research question 1.
The SR by Dong et al. (2024)13 included 60 RCTs and used an NMA to examine the efficacy and adverse events (AEs) of different antipsychotics in the treatment-resistant schizophrenia. The literature search was conducted on April 27, 2020, and updated 3 times, with the last update on January 20, 2023. The median duration of the included trials was 12 weeks (range: 4 weeks to 52 weeks).
The SR by Leucht et al. (2023)14 included 45 RCTs and used NMA to assess the long-term efficacy and tolerability of antipsychotics in patients with an acute episode of schizophrenia. The literature search was conducted on June 14, 2021, and updated twice, with the last update on March 6, 2022. The included RCTs had at least a 24-week duration (range: 24 weeks to 156 weeks).
The authors of both SRs13,14 conducted a random-effects pairwise MA and NMA in a frequentist framework. In the primary outcome (i.e., change in overall symptoms), there were 12 network comparators included in the NMA by Dong et al. (2024)13 and 13 network comparators included in the NMA by Leucht et al. (2023).14 Both NMAs13,14 included comparisons of different types of antipsychotics (both FGAs and SGAs) and placebo. Only the relevant comparisons of quetiapine with other antipsychotics are described throughout this report.
The SR by Sherzad Qadir et al. (2023)15 included 21 RCTs and used an MA to compare the efficacy and tolerability of oral antipsychotics used for the treatment of patients newly diagnosed with schizophrenia. The literature search was restricted to the period from 2000 to 2021. The pooled effect size with a 95% confidence interval (CI) was obtained using a random-effects model or fixed-effects model based the I2 value, which describes the percentage of total variation across trials that is due to heterogeneity rather than chance or sampling errors. When the I2 value was 30% or less, the fixed-effects model was used for reporting, and when it was more than 30%, the random-effects model was used for more precise findings. The follow-up period of the included RCTs ranged from 8 weeks to 9 years.
The included RCT by Kim et al. (2024)16 compared the efficacy and safety of lurasidone, an SGA, with quetiapine XR in acutely psychotic patients with schizophrenia. The study was a randomized, parallel (1:1 ratio), double-blind, active-controlled trial over a 6-week period. The follow-up (week 7) visit took place 1 week after patients’ last dose of the study medication. The trial was published in 2024.
Country of Origin
The 3 SRs were conducted by authors in Germany;13 in Germany, Switzerland, and the US;14 and in Australia.15
The included RCT was conducted by authors in the Republic of Korea.16
Patient Population
The patient population included in the SR by Dong et al. (2024)13 were those with treatment-resistant schizophrenia and a mean age of 38 years, and there were more male (71.5%) than female (28.5%) participants. The mean duration of illness was 14.5 years.
The patient population in the SR by Leucht et al. (2023)14 consisted of acutely ill adults with schizophrenia and a mean age of 37 years, and there were more male (60%) than female (40%) participants. The mean study duration of the studies included in the SR was 42 weeks.
The SR by Sherzad Qadir et al. (2023)15 included studies with patients aged 15 years or older (mostly adults) who were newly diagnosed with schizophrenia. Details of the study characteristics and patient characteristics of each primary study were not summarized in the SR but were presented in its supplementary appendix.
The RCT by Kim et al. (2024)16 recruited adult patients with a diagnosis of schizophrenia who were in a state of acute exacerbation of psychosis symptoms lasting 2 months or less. The mean age of participants was 41.7 years, with more female (63%) than male (37%) participants. The duration of illness ranged from 1 year to ≥ 10 years.
Interventions and Comparators
Both SRs — Dong et al. (2024)13 and Leucht et al. (2023)14 — included all SGAs available in Europe or the US, and a selection of FGAs informed by a survey of international schizophrenia experts.19
The interventions included in the SR by Sherzad Qadir et al. (2023)15 were quetiapine, aripiprazole, ziprasidone, risperidone, olanzapine, and haloperidol.
The RCT by Kim et al. (2024)16 compared the efficacy and safety of lurasidone versus quetiapine XR.
Outcomes
The primary outcome in all included studies (i.e., 3 SRs13-15 and 1 RCT16) was the overall symptoms of schizophrenia as measured by various rating scales such as the Positive and Negative Syndrome Scale (PANSS), the Brief Psychiatric Rating Scale (BPRS), or any other validated scales. Brief Descriptions of the scales used in the included SRs and RCT are as follows:
PANSS: A 30-item clinician-rated instrument to assess schizophrenia psychopathology, including positive (e.g., hallucinations, delusions) and negative (e.g., blunted effect, social withdrawal) symptoms, as well as general psychopathology (range: 30 to 210 points, lower score is favourable).
BPRS: Measures psychiatric symptoms such as depression, anxiety, hallucinations, psychosis, and unusual behaviour (range: 18 to 126 points, lower score is favourable).
Scale for the Assessment of Negative Symptoms (SANS): Measures the levels of negative symptoms of schizophrenia (affective flattening or blunting, alogia [speaking with fewer words], avolition-apathy [lack of motivation and/or lack of interest], anhedonia-asociality [diminished ability to experience pleasure or enjoyment and/or lack of interest in social interaction, attention]) (range: 0 to 125, lower score is favourable).
Scale for the Assessment of Positive Symptoms (SAPS): Measures levels of positive symptoms of schizophrenia (delusions, hallucinations, and thought disorder) (range: 0 to 170, lower score is favourable).
Calgary Depression Scale for Schizophrenia (CDSS): Measures the level of depression in people with schizophrenia (range: 0 to 27, lower score is favourable).
Young Mania Rating Scale (YMRS): Measures manic symptoms (elevated mood, increased motor activity and/or energy, sexual interest, sleep, irritability, speech, language-thought disorder, content, disruptive-aggressive behaviour, appearance, insight) (range: 0 to 60, lower score is favourable).
The secondary outcomes reported in the included studies were positive symptoms; negative symptoms; response to treatment; social functioning; study discontinuation; use of antiparkinsonian medication; and AEs such as sedation, akathisia, increased prolactin level, weight gain, corrected QT interval (QTc) prolongation (longer-than-normal time for the heart's electrical system to recharge between beats), depressive symptoms, and other metabolic parameters. The authors of 2 SRs13,14 reported health-related quality of life (HRQoL) as a patient-reported outcome.
Included Studies for Research Question 2: What Are the Evidence-Based Guidelines Regarding the Use and Administration of Quetiapine for Adults With Schizophrenia?
Study Design
The Veterans Affairs/Department of Defense (VA/DoD) clinical practice guideline17 was developed by a panel of multidisciplinary experts in psychiatry, psychology, internal medicine, nursing, primary care, pharmacy, mental health counselling, and social work. The working group determined the scope of the guideline, crafted key questions to guide the systematic evidence review, identified discussion topics, provided direction on inclusion and exclusion criteria, developed evidence-based recommendations, and determined the strength and category of each recommendation. The working group used the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach to craft each recommendation and determined its strength (i.e., strong or weak) based on 4 domains:
confidence in the quality of the evidence
balance of desirable and undesirable outcomes
patient values and preferences
other considerations (e.g., resource use, equity, acceptability, feasibility, subgroup considerations).
The strength of recommendation was described with the general corresponding text as follows:
Strong for (We recommend…)
Weak for (We suggest…)
Neither for nor against (There is insufficient evidence to recommend for or against…)
Weak against (We suggest against…).
The Japanese Society of Neuropsychopharmacology (JSNPP) clinical practice guideline18 was developed by a panel of multidisciplinary experts in the treatment and management of schizophrenia. The society’s task force determined the scope of the guideline and determined clinical questions based on the scope. Each working group of the task force conducted an SR for each question, evaluated the body of evidence, and crafted the recommendation drafts for each clinical question. The level of evidence was assessed as strong, moderate, weak, and very weak, based on the degree of certainty of the true effect:
Strong (A): It is almost certain that the true effect is close to the estimated effect.
Moderate (B): The true effect is thought to be close to the estimated effect, but the possibility that results may be different remains.
Weak (C): The true effect is thought to be close to the estimated effect, but the results may be different.
Very weak (D): The estimated effect is very unclear and is often very different from the true effect.
The strength of recommendation was described with the general corresponding text as follows:
Action is recommended (labelled as 1)
Action is not recommended (1)
Action is suggested or desirable (labelled as 2)
Action is not suggested or desirable (2).
Country of Origin
The authors of the VA/DoD guideline and of the JSNPP guideline were from the US17 and Japan,18 respectively.
Patient Population
The patient population for the VA/DoD guideline17 consists of adults with schizophrenia, schizophrenia spectrum disorders, schizoaffective disorder, schizophreniform disorder, or first-episode of psychosis being treated in any setting. The intended users of this guideline include primary care providers, mental health providers, and others involved in the health care team for this patient population.
The patient population of the JSNPP guideline18 is patients with first-episode psychosis and schizophrenia. The intended users of this guideline include specialists in the treatment of schizophrenia and patients, their families, and their supporters.
Interventions and Practice Considered
The VA/DoD guideline17 provides clinical practice recommendations for the care of patients with schizophrenia using various treatments (e.g., drugs, surgery, lifestyle changes) and approaches (e.g., doses, frequency, methods of administering treatments).
The JSNPP guideline18 provides recommendations on comprehensive treatments such as pharmacological therapy and psychosocial therapy in collaboration with medical welfare.
Outcomes
Both included guidelines17,18 considered all relevant outcomes related to the clinical questions outlined in the guidelines, including short, intermediate, and long-term outcomes.
Summary of Critical Appraisal
The SRs with NMA by Dong et al. (2024)13 and by Leucht et al. (2023)14 included relevant populations, interventions, and outcomes. Both SRs13,14 used the same NMA method and approach. This NMA had several strengths contributing to its credibility related to the quality and comprehensiveness of the evidence base, appropriate analysis methods, and reporting and interpretation of results. Specifically, the rationale for the study and the study objectives were clearly stated. The authors of both SRs13,14 clearly presented the literature search methods, search terms, search dates, search strategy, and criteria for the SRs, with an attempt to identify and include all relevant RCTs. All included RCTs were assessed for risk of bias using the Cochrane Risk of Bias tool, the results of which were presented and discussed in terms of risk of bias and heterogeneity. The authors of both SRs13,14 conducted sensitivity analyses to exclude studies that were not double-blind, studies that presented completer analyses only, studies that did not use operationalized criteria to diagnose schizophrenia, studies with a high risk of bias, and studies that only included children and/or adolescents. Based on the results of the sensitivity analyses, the authors found that the results of the primary analyses were not altered. Study selection, appraisal, and data extraction were performed in duplicate. The primary outcome (i.e., overall symptoms of schizophrenia) was clearly defined. The authors provided a description of analysis methods and models, a description of statistics used, and justification for the statistics. The analysis in the primary model was well-conducted using appropriate methodology. The authors initially performed a pairwise MA using a random-effects model. The statistical heterogeneity among trials was assessed using a visual inspection of forest plots, I2 statistics, and the Chi-square test. The authors then evaluated the feasibility of conducting an NMA by checking the availability of evidence, transitivity assumption (assessing transitivity involves evaluating the similarity of study characteristics across different comparisons), connectivity (all treatments in the network must be linked together, either directly or indirectly through a shared comparator), and coherence or consistency (level of statistical agreement between direct and indirect evidence) in the network. The authors performed a frequentist random-effects NMA using a multivariate MA. The relative effect estimates were described as standardized mean differences (SMDs) for efficacy-related continuous outcomes and odds ratios for binary outcomes, with their 95% CIs. The presence of incoherence between direct and indirect estimates of the effect was investigated on possible sources of incoherence (e.g., mistakes in data entry, clear differences in study characteristics) and used analytical approaches. The confidence in the relative treatment effects for the primary outcome was evaluated using the Confidence in Network Meta-Analysis framework, which evaluated the credibility of the findings across the domains of within-study bias, across-study bias, indirectness, imprecision, heterogeneity, and incoherence. The authors performed subgroup or subset analysis, and explored the potential sources of heterogeneity or inconsistency using a priori planned subgroup analyses. Network diagrams of connected interventions were presented. Study characteristics and patient characteristics of the included RCTs were presented in an appendix to the SRs. Forest plots were provided summarizing the results for each intervention. Heterogeneity observed in the results was discussed. The authors noted that the robustness of the analysis may be limited due to a high risk of bias from the individual studies and heterogeneity. Thus, the effect estimates may not be driven solely by the assessed interventions.
The SR with MA by Sherzad Qadir et al. (2023)15 was explicit in its objective, inclusion criteria for the review, and selection of the study designs for inclusion. A study protocol had been published before conducting the review, preventing bias in modifying the methods after the review had been conducted. The literature search strategy was comprehensive and clearly described. The review authors performed study selection in duplicate. This reduced the risk of missing relevant studies and making errors in data extraction. The characteristics of the included studies were described in adequate detail, including objective, design, setting, population, follow-up time, interventions, outcomes, and the source of funding. However, a list of excluded studies and the reasons for exclusion were not provided. Therefore, it was not possible to assess whether any relevant articles were excluded and, if so, for what reasons. The methodological quality of the included studies was assessed using the Cochrane Risk of Bias tool. A MA was conducted for both continuous and dichotomous outcomes, which were reported as a mean difference (MD) and relative risk (RR), respectively, with a 95% CI. A subgroup analysis was performed to explore diverse outcomes or to address particular inquiries concerning specific categories of interventions. The review authors provided a discussion of the heterogeneity observed in the results. The review authors declared that this research received no external funding and that there were no potential conflicts of interest.
For reporting, the authors of the included RCT by Kim et al. (2024)16 clearly described the objective of the study, the intervention of interest, the main outcomes, and the main findings of the study. The authors clearly described the patient characteristics at baseline, and there were no group differences in the demographics of the randomized participants. The existence of potential confounders was low. Actual P values and AEs of the intervention were reported. In terms of external validity, the patients included in the RCT may represent the entire eligible population, given that they were recruited from multiple centres. The treatment settings (i.e., hospitals) appeared to be representative of the treatment received by most of the patients in Korea. However, the generalizability of the patient population and treatment settings to the context in Canada remains questionable. For internal validity related to bias, the study was a randomized, double-blind, active-controlled study that took place over a 6-week period in which all patients were followed up for the same period of time, which took place 1 week after the patients’ last dose of the study medication. Statistical tests were used appropriately, and the main outcome measures were accurate and reliable. Compliance with the intervention was reliable, give that 95% of the patients completed the study. The primary end point, which was the overall symptoms of schizophrenia, was accurately measured using PANNS. For internal validity related to confounding, patients in both intervention groups appeared to be recruited from the same population and over the same period of time, and methods of randomization and allocation concealment were described. However, about one-third of the intention-to-treat population was excluded, and the reasons for exclusion were not reported. Those patients were not taken into account in the analysis, and the primary analysis was based on the per-protocol set, leading to a potentially high risk of reporting bias. Because a sample size calculation was not performed, real effects may not be detected due to a lack of power.
For reporting, both included guidelines17,18 were explicit in terms of scope and purpose (i.e., objectives, health questions and populations) and had a clear presentation of recommendations (i.e., specific, unambiguous, and easy to find key recommendations, with options for managing the different conditions or health issues). In terms of the involvement of interested parties, the authors of both guidelines17,18 clearly defined target users and the development groups, and reported that the views and preferences of the patients were sought. The methodology for the development of the guidelines was robust. The authors of both guidelines17,18 clearly reported methods for evidence collection, criteria for selection, and methods for evidence synthesis. There were explicit links between recommendations and the supporting evidence and the methods for formulating the recommendations. Also, the authors of both guidelines17,18 considered health benefits and risks of side effects when formulating the recommendations. Both guidelines17,18 will be updated when new important information and appropriate comments are received, though specific dates were not indicated. Both guidelines17,18 were reviewed independently by relevant professional experts, professional colleges, and societies and through public consultation. However, there were some limitations related to guideline implementation and applicability. Specifically, facilitators and barriers to application and monitoring or auditing criteria were unclear. Both guidelines17,18 provide advice and/or tools on how the recommendations can be put into practice. For editorial independence, the authors of the guidelines17,18 declared the competing interests of all guideline development group members and disclosed that the views of the funding body had no influence on the content of the guidelines. Overall, the included guidelines17,18 were robust in terms of scope and purpose, involvement of interested parties, rigour of development, clarity of presentation, and editorial independence.
Additional details regarding the strengths and limitations of the included SRs13-15 are provided in Table 5, the RCT16 in Table 6, and the guidelines17,18 in Table 7 of Appendix 3.
Summary of Findings
Appendix 4 presents the main study findings, which are summarized by outcome. Only comparisons of quetiapine with other antipsychotics are presented.
Clinical Effectiveness and Safety of Quetiapine Versus Other Drug Interventions for Adults With Schizophrenia
Overall Symptoms of Schizophrenia
The authors of 3 included SRs13-15 and 1 RCT16 reported on overall symptoms of schizophrenia (Table 8). In the SRs, the results were reported as an SMD with a 95% CI of the changes from baseline. In the included RCT, the changes from baseline were presented as least squares (LS) mean plus or minus the standard error (SE) of the mean.
Efficacy and safety of antipsychotics in treatment-resistant schizophrenia: In the SR with NMA by Dong et al. (2024),13 clozapine (SMD = −0.44; 95% CI, −0.66 to −0.22) and olanzapine (SMD = −0.40; 95% CI, −0.67 to −0.13) were more effective than quetiapine. There were no clear differences between quetiapine and other antipsychotics (i.e., levomepromazine, amisulpride, zotepine, risperidone, ziprasidone, haloperidol, fluphenazine, chlorpromazine, and sertindole) according to the 95% CI. The results were based on 45 studies with 12 interventions involving 5,303 patients.
Long-term efficacy and safety of antipsychotics in acutely ill adults with schizophrenia: In the SR with NMA by Leucht et al. (2023),14 lurasidone (SMD = −0.42; 95% CI, −0.71 to −0.13) and olanzapine (SMD = −0.25; 95% CI, −0.38 to −0.12) appeared to be more effective than quetiapine. The differences between quetiapine and other antipsychotics (i.e., amisulpride, perphenazine, clozapine, risperidone, aripiprazole, zotepine, haloperidol, paliperidone, iloperidone, asenapine, and ziprasidone) were uncertain. The results were based on 23 studies with 9,814 patients.
Efficacy and safety of antipsychotics for treatment of newly diagnosed patients with schizophrenia: The SR with MA by Sherzad Qadir et al. (2023)15 presented 2 sets of comparisons using different rating scales to measure symptoms of schizophrenia:
Aripiprazole versus quetiapine (3 studies): Aripiprazole appeared to be more effective than quetiapine under BPRS (MD = −4.77; 95% CI, −7.83 to −1.71), but the differences between quetiapine and aripiprazole were not statistically significant according to other rating scales (i.e., Clinical Global Impression [CGI], SANS, SAPS, CDSS, and YMRS).
Ziprasidone versus quetiapine (3 studies): There were no statistically significant differences between quetiapine and ziprasidone assessed by various rating scales (i.e., CGI, BPRS, SANS, SAPS, CDSS, and YMRS).
The RCT by Kim et al. (2024)16 verified the noninferiority of lurasidone to quetiapine XR, given that the lower limit of the 95% 2-sided CI for the difference in score change did not exceed the predefined noninferiority margin of −8.99. The difference in PANSS total score between groups was −0.91 (95% CI, −6.31 to 4.53). Thus, the noninferiority of lurasidone compared to quetiapine XR was verified, given that the lower limit of the CI did not exceed the noninferiority margin. Under CGI scores, the results showed statistically significant differences between groups, which were observed at 4 weeks and 6 weeks of treatment, favouring lurasidone.
Positive Symptoms
The authors of 1 included SR13 and 1 RCT16 reported on positive symptoms (Table 9). In the SR, the results were reported as SMD with 95% CI of the changes from baseline. In the included RCT, the changes from baseline were presented as LS means plus or minus the SE of the mean.
Efficacy of antipsychotics in treatment-resistant schizophrenia: In the SR with NMA by Dong et al. (2024),13 amisulpride (SMD = −1.48; 95% CI, −0.16 to −0.22), clozapine (SMD = −0.61; 95% CI, −0.90 to −0.32), risperidone (SMD = −0.51; 95% CI, −0.82 to −0.20), and olanzapine (SMD = −0.49; 95% CI, −0.78 to −0.19) were found to be more effective than quetiapine for treatment of positive symptoms. Quetiapine showed no clear difference from levomepromazine, ziprasidone, haloperidol, sertindole, chlorpromazine, and fluphenazine. The results were based on 39 studies with 4,649 patients.
Efficacy and safety of antipsychotics for the treatment of newly diagnosed patients with schizophrenia: The results from the RCT by Kim et al. (2024)16 showed no statistically significant difference between lurasidone and quetiapine in terms of PANSS positive subscale scores.
Negative Symptoms
The authors of 1 included SR13 and 1 RCT16 reported on negative symptoms (Table 10). In the SR, the results were reported as SMD with 95% CI of the changes from baseline. In the included RCT, the changes from baseline were presented as LS mean plus or minus the SE of the mean.
Efficacy and safety of antipsychotics in treatment-resistant schizophrenia: In the SR with NMA by Dong et al. (2024),13 the differences in negative symptoms between quetiapine and most antipsychotics (i.e., amisulpride, clozapine, zotepine, olanzapine, fluphenazine, levomepromazine, ziprasidone, risperidone, haloperidol, and sertindole) were uncertain, except that chlorpromazine was less effective than quetiapine (SMD = −0.66; 95% CI, −1.28 to −0.05). The results were based on 42 studies with 4,863 patients.
Efficacy and safety of antipsychotics for the treatment of newly diagnosed patients with schizophrenia: The results from the RCT by Kim et al. (2024)16 showed no statistically significant difference between lurasidone and quetiapine in terms of PANSS negative subscale scores. The study included 210 patients.
Response to Treatment
The authors of 1 included SR13 reported on response to treatment (Table 11). The results were reported as RR with 95% CI.
Efficacy and safety of antipsychotics in treatment-resistant schizophrenia: The differences in response to treatment between quetiapine and all other antipsychotics under investigation (i.e., sulpiride, levomepromazine, aripiprazole, trifluoperazine, perphenazine, clozapine, thioridazine, olanzapine, ziprasidone, amisulpride, risperidone, chlorpromazine, haloperidol, fluphenazine, sertindole, thiothixene, fluphenazine long-acting injection [LAI], and pipotiazine LAI) were uncertain. The results were based on 46 studies with 6,043 patients.
Social Functioning
The authors of 1 included SR14 reported on social functioning (Table 12). The results were reported as SMD with 95% CI of the changes from baseline.
Long-term efficacy and safety of antipsychotics in initially acutely ill adults with schizophrenia: In 5 studies with 1,390 patients, there were no clear differences in social functioning between quetiapine and other antipsychotics (i.e., olanzapine, amisulpride, risperidone, and paliperidone).
Quality of Life
The authors of 2 SRs13,14 reported on quality of life (Table 13). The results were reported as SMD with 95% CI of the changes from baseline.
Efficacy and safety of antipsychotics in treatment-resistant schizophrenia: In the SR by Dong et al. (2024),13 8 studies with 1,159 patients provided data on QoL. Because conducting an NMA was not feasible given that there were no closed loops in the network, pairwise MA results were presented instead. The results showed no statistically significant differences between quetiapine and fluphenazine, between quetiapine and risperidone, and between quetiapine and chlorpromazine.
Long-term efficacy and safety of antipsychotics in initially acutely ill adults with schizophrenia: In the SR by Leucht et al. (2023), there were no clear differences in QoL between quetiapine and other antipsychotics (i.e., zotepine, amisulpride, olanzapine, asenapine, ziprasidone, perphenazine, haloperidol, and risperidone). The results were based on 8 studies with 2,949 patients.
All-Cause Discontinuation
The authors of 2 SRs13,14 reported on all-cause discontinuation (Table 14). The results were reported as RR with 95% CI.
Efficacy and safety of antipsychotics in treatment-resistant schizophrenia: In the SR by Dong et al. (2024),13 quetiapine showed no clear difference in all-cause discontinuation compared to other antipsychotics (i.e., sulpiride, levomepromazine, olanzapine, clozapine, ziprasidone, risperidone, sertindole, chlorpromazine, zotepine, haloperidol, fluphenazine LAI, pipotiazine LAI). The results were based on 54 studies with 6,228 patients.
Long-term efficacy and safety of antipsychotics in initially acutely ill adults with schizophrenia: In the SR by Leucht et al. (2023),14 long-term treatment with quetiapine resulted in a higher frequency of all-cause discontinuation compared with amisulpride (RR = 0.70; 95% CI, 0.54 to 0.88), aripiprazole (RR = 0.73; 95% CI, 0.57 to 0.89), risperidone (RR = 0.82; 95% CI, 0.68 to 0.95), and perphenazine (RR = 0.82; 95% CI, 0.67 to 0.97). The differences in all-cause discontinuation between quetiapine and other antipsychotics (i.e., lurasidone, zotepine, haloperidol, ziprasidone, asenapine, paliperidone, thiothixene, fluspirilene, pimozide, fluphenazine, olanzapine) were uncertain. The results were based on 41 studies with 8,882 patients.
Discontinuation Due to Lack of Efficacy
The authors of 2 included SRs13,15 reported on discontinuation due to lack of efficacy (Table 15). The results were reported as RR with 95% CI.
Efficacy and safety of antipsychotics in treatment-resistant schizophrenia: In the SR by Dong et al. (2024),13 treatment with quetiapine resulted in no clear differences in discontinuation due to lack of efficacy compared to other antipsychotics (i.e., fluphenazine LAI, ziprasidone, pipotiazine LAI, sulpiride, amisulpride, chlorpromazine, risperidone, sertindole, haloperidol, zotepine, trifluoperazine, thioridazine, and fluphenazine), with the exception of clozapine (RR = 0.28; 95% CI, 0.14 to 0.53) and olanzapine (RR = 0.52; 95% CI, 0.27 to 0.95), which were superior than quetiapine. The results were based on 48 studies with 5,142 patients.
Efficacy and safety of antipsychotics for treatment of newly diagnosed patients with schizophrenia: The SR by Sherzad Qadir et al. (2023)15 with pairwise MA showed that discontinuation due to lack of efficacy was statistically significantly more frequent with quetiapine compared to olanzapine (RR = 3.48; 95% CI, 3.05 to 5.91), ziprasidone (RR = 2.05; 95% CI, 1.57 to 2.68), and aripiprazole (RR = 3.69; 95% CI, 2.56 to 5.32). Discontinuation due to lack of efficacy was not statistically significant between quetiapine and risperidone.
Discontinuation Due to AEs
The authors of 2 included SRs13,15 reported on discontinuation due to AEs (Table 16). The results were reported as RR with 95% CI.
Efficacy and safety of antipsychotics in treatment-resistant schizophrenia: In the SR by Dong et al. (2024),13 there were no clear differences in treatment discontinuation due to AEs between quetiapine and most antipsychotics (i.e., fluphenazine, olanzapine, risperidone, haloperidol, clozapine, sertindole, zotepine, ziprasidone, thioridazine, sulpiride, levomepromazine, trifluoperazine, thiothixene, amisulpride, pipotiazine LAI, and fluphenazine LAI), with the exception being that chlorpromazine (RR = 0.51; 95% CI, 0.26 to 0.95) was less tolerable than quetiapine. The results were based on 50 studies with 5,103 patients.
Efficacy and safety of antipsychotics for treatment of newly diagnosed patients with schizophrenia: The SR by Sherzad Qadir et al. (2023)15 with pairwise MA showed that discontinuation due to AEs was statistically significantly less frequent with quetiapine compared with risperidone (RR = 0.44; 95% CI, 0.21 to 0.89), ziprasidone (RR = 0.34; 95% CI, 0.22 to 0.51), and haloperidol (RR = 0.43; 95% CI, 0.22 to 0.84).
Use of Antiparkinsonian Medication
The authors of 2 SRs13,14 reported on use of antiparkinsonian medication (Table 17). The results were reported as RR with 95% CI.
Efficacy and safety of antipsychotics in treatment-resistant schizophrenia: In the SR by Dong et al. (2024),13 quetiapine showed no clear difference in the use of antiparkinsonian medication compared to most antipsychotics (i.e., levomepromazine, thioridazine, sulpiride, clozapine, amisulpride, olanzapine, ziprasidone, pipotiazine LAI, chlorpromazine, fluphenazine LAI, risperidone, and trifluoperazine), with the exception that quetiapine was associated with less use of antiparkinsonian medication compared with fluphenazine (RR = 0.37; 95% CI, 0.11 to 0.99) and haloperidol (RR = 0.34; 95% CI, 0.13 to 0.77). The results were based on 24 studies with 2,061 patients.
Long-term efficacy and safety of antipsychotics in initially acutely ill adults with schizophrenia: In the SR by Leucht et al. (2023),14 long-term treatment with quetiapine was associated with less use of antiparkinsonian medication compared with a number of antipsychotics, including amisulpride (RR = 0.43; 95% CI, 0.20 to 0.86), risperidone (RR = 0.35; 95% CI, 0.19 to 0.65), paliperidone (RR = 0.35; 95% CI, 0.18 to 0.69), ziprasidone (RR = 0.35; 95% CI, 0.183 to 0.68), perphenazine (RR = 0.34; 95% CI, 0.17 to 0.67), haloperidol (RR = 0.24; 95% CI, 0.12 to 0.46), and asenapine (RR = 0.18; 95% CI, 0.06 to 0.51). The differences between quetiapine and other antipsychotics such as aripiprazole, zotepine, and olanzapine were uncertain. The results were based on 14 studies with 7,794 patients.
Sedation
The authors of 2 SRs13,14 reported sedation (Table 18). The results were reported as RR with 95% CI.
Efficacy and safety of antipsychotics in treatment-resistant schizophrenia: In the SR by Dong et al. (2024),13 quetiapine showed no clear differences in sedation compared with other antipsychotics (i.e., thiothixene, ziprasidone, sertindole, sulpiride, olanzapine, fluphenazine, haloperidol, risperidone, trifluoperazine, chlorpromazine, thioridazine, and levomepromazine), with the exception that quetiapine was associated with higher risk of sedation than amisulpride (RR = 1.72; 95% CI, 1.01 to 3.85) and lower risk of sedation than clozapine (RR = 0.82; 95% CI, 0.65 to 0.96). The results were based on 30 studies with 4,079 patients.
Long-term efficacy and safety of antipsychotics in initially acutely ill adults with schizophrenia: In the SR by Leucht et al. (2023),14 there were no clear differences in sedation between quetiapine and other antipsychotics (i.e., lurasidone, ziprasidone, haloperidol, amisulpride, asenapine, perphenazine, risperidone, paliperidone, zotepine, and olanzapine), with the exception that quetiapine had a higher risk of sedation compared to aripiprazole (RR = 1.89; 95% CI, 1.08 to 3.03). The results were based on 16 studies with 8,096 patients.
Akathisia (Inability to Remain Still)
The authors of 1 SR14 reported on akathisia (Table 19). The results were reported as RR with 95% CI.
Long-term efficacy and safety of antipsychotics in initially acutely ill adults with schizophrenia: In the SR by Leucht et al. (2023),14 there were no clear differences in the risk of akathisia between quetiapine and other antipsychotics such as paliperidone, amisulpride, aripiprazole, risperidone, perphenazine, ziprasidone, and olanzapine. Quetiapine had a lower risk of akathisia compared with haloperidol (RR = 0.43; 95% CI, 0.23 to 0.81), asenapine (RR = 0.40; 95% CI, 0.17 to 0.86), and lurasidone (RR = 0.22; 95% CI, 0.05 to 0.80). The results were based on 16 studies with 7,916 patients.
Increased Prolactin Levels
The authors of 2 SRs13,14 reported on increased prolactin levels (Table 20). The results were reported as an MD with 95% CI.
Efficacy and safety of antipsychotics in treatment-resistant schizophrenia: In the SR by Dong et al. (2024),13 quetiapine was associated with less of an effect on prolactin levels than olanzapine (MD = −13.19; 95% CI, −21.95 to −4.43), chlorpromazine (MD = −20.57; 95% CI, −32.74 to −8.39), haloperidol (MD = −23.96; 95% CI, −35.92 to −12.00), and risperidone (MD = −34.24; 95% CI, −43.51 to −24.96). The differences in increased prolactin levels between quetiapine and other antipsychotics such as ziprasidone, clozapine, and fluphenazine were uncertain. The results were based on 18 studies with 1,533 patients.
Long-term efficacy and safety of antipsychotics in initially acutely ill adults with schizophrenia: In the SR by Leucht et al. (2023),14 the data of direct and indirect evidence for this outcome were inconsistent. The results were therefore focused on pairwise MA. Quetiapine was associated with higher average prolactin levels than risperidone (MD = −24.70; 95% CI, −37.41 to −11.99), but there were no statistically significant differences between quetiapine and other antipsychotics such as olanzapine, lurasidone, ziprasidone, and perphenazine.
Weight Gain
The authors of 2 SRs13,14 reported on weight gain (Table 21). The results were reported as a MD with 95% CI.
Efficacy and safety of antipsychotics in treatment-resistant schizophrenia: In the SR by Dong et al. (2024),13 quetiapine was associated with less weight gain compared to olanzapine (MD = −2.86; 95% CI, −4.14 to −1.21) and clozapine (MD = −2.70; 95% CI, −4.17 to −1.23). There were no clear differences in weight gain between quetiapine and other antipsychotics (i.e., haloperidol, fluphenazine, chlorpromazine, levomepromazine, amisulpride, risperidone, and sertindole). The results were based on 20 studies with 3,393 patients.
Long-term efficacy and safety of antipsychotics in initially acutely ill adults with schizophrenia: In the SR by Leucht et al. (2023),14 the network for this outcome was inconsistent. The results of the pairwise MA showed that quetiapine was associated with less weight gain compared to olanzapine (MD = −3.76; 95% CI, −6.10 to −1.42). There were no statistically significant differences in weight gain between quetiapine and other antipsychotics such as ziprasidone, perphenazine, lurasidone, and risperidone.
QTc Prolongation
The authors of 2 SRs13,14 reported on QTc prolongation (Table 22). The results were reported as MD with 95% CI.
Efficacy and safety of antipsychotics in treatment-resistant schizophrenia: In the SR by Dong et al. (2024),13 data on QTc prolongation were scarce and the network was disconnected. Pairwise MA showed that chlorpromazine was associated with more QTc prolongation than quetiapine (MD = 19.80; 95% CI, 12.10 to 27.50).
Long-term efficacy and safety of antipsychotics in initially acutely ill adults with schizophrenia: In the SR by Leucht et al. (2023),14 quetiapine was associated with larger average QTc prolongation than paliperidone (MD = −7.40; 95% CI, −13.19 to −1.62), risperidone (MD = −5.30; 95% CI, −10.21 to −0.40), and olanzapine (MD = −5.18; 95% CI, −9.81 to −0.55). The differences in QTc prolongation between quetiapine and other antipsychotics (i.e., asenapine, perphenazine, ziprasidone amisulpride, and lurasidone) were uncertain. The results were based on 7 studies with 4,060 patients.
Depressive Symptoms
The authors of 1 SR14 reported on depressive symptoms (Table 23). The results were reported as SMD with 95% CI.
Long-term efficacy and safety of antipsychotics in initially acutely ill adults with schizophrenia: In the SR by Leucht et al. (2023),14 most results of quetiapine compared with other antipsychotics (i.e., lurasidone, olanzapine, perphenazine, aripiprazole, risperidone, amisulpride, ziprasidone, asenapine, haloperidol, and paliperidone) were uncertain. The results were based on 11 studies with 6,686 patients.
Other Side Effects
One included SR15 and 1 RCT16 presented the results of different AEs in the comparisons of aripiprazole versus quetiapine, quetiapine versus ziprasidone, olanzapine versus quetiapine, risperidone versus quetiapine, and lurasidone versus quetiapine (Table 24).
Aripiprazole versus quetiapine:
Sleepiness (RR = 0.58; 95% CI, 0.45 to 0.75), increased duration of sleep (RR = 0.53; 95% CI, 0.36 to 0.78), galactorrhea (milk production from the breast unrelated to pregnancy or lactation) (RR = 0.10; 95% CI, 0.01 to 0.78), and erectile dysfunction (RR = 0.20; 95% CI, 0.07 to 0.56) occurred less frequently with aripiprazole than with quetiapine.
Aripiprazole was associated with a higher incidence of tremors compared to quetiapine (RR = 3.07; 95% CI, 1.07 to 8.77).
There were no clear differences between quetiapine and aripiprazole for other AEs such as concentration difficulties, increased fatigability, depression, restlessness, rigidity, increased salivation, constipation, vertigo, amenorrhea, diminished sexual desire, orgasmic dysfunction, ejaculatory dysfunction, weight gain, and memory impairment.
Quetiapine versus ziprasidone:
There were no clear differences in most AEs (i.e., concentration difficulties, increased fatigability, sleepiness, memory impairment, depression, restlessness, increased duration of sleep, rigidity, tremors, increased salivation, constipation, diminished sexual desire, orgasmic dysfunction, ejaculatory dysfunction, and weight gain) between quetiapine and ziprasidone.
Vertigo (RR = 0.13; 95% CI, 0.02 to 0.99) and amenorrhea (RR = 0.11; 95% CI, 0.02 to 0.50) occurred more frequently with ziprasidone than with quetiapine.
Olanzapine versus quetiapine:
There were no clear differences in most AEs (i.e., sleepiness, increased duration of sleep, akinesia, constipation, galactorrhea, diminished sexual desire, and orgasmic dysfunction) between olanzapine and quetiapine.
Weight gain (RR = 1.34; 95% CI, 1.15 to 1.56) occurred more frequently with olanzapine than with quetiapine.
Risperidone versus quetiapine:
There were no clear differences between risperidone and quetiapine in weight gain, sleepiness, akinesia, constipation, galactorrhea, and orgasmic dysfunction.
Quetiapine was associated with a higher incidence of increased duration of sleep (RR = 0.54; 95% CI, 0.32 to 0.91) compared to risperidone.
Lurasidone versus quetiapine:
Quetiapine was associated with higher risk of weight gain (1.65 kg versus −0.24 kg), elevation of serum glucose levels (2.77 mg/dL versus 1.69 mg/dL), increased total cholesterol levels (11.13 mg/dL versus −3.92 mg/dL), increased LDL-cholesterol levels (5.32 mg/dL versus −4.84 mg/dL), and increased triglyceride levels (24.21 mg/dL versus 0.63 mg/dL) compared with lurasidone.
Lurasidone was associated with a higher incidence of nausea (16.7% versus 2.9%) and increased blood prolactin (7.8% versus 1.9%) compared with quetiapine.
There were no clear differences between lurasidone and quetiapine in akathisia, dizziness, somnolence, tremor, constipation, anxiety, muscle rigidity, HDL-cholesterol, electrocardiography, extrapyramidal side effects (involuntary movements induced by medications), and suicidal ideation and behaviour.
Evidence-Based Guidelines Regarding the Use and Administration of Quetiapine for Adults With Schizophrenia
A summary of recommendations from the included guidelines is presented in Table 25 of Appendix 4.
Management of First-Episode Psychosis and Schizophrenia
The VA/DoD guideline17 recommends the use of an antipsychotic medication other than clozapine (strong recommendation, categorized as reviewed, newly added).
Similarly, the JSNPP guideline18 recommends SGAs over FGAs (degree 2 recommendation based on strong-quality evidence).
The JSNPP guideline18 presents optimal doses of various antipsychotics, including quetiapine, which has been reported to be effective at 311.4 mg/day to 506 mg/day. However, the guideline noted that treatment discontinuation rates of quetiapine were higher than other antipsychotics in long-term trials (recommendation with no reported degree based on moderate- to weak-quality evidence).
The JSNPP guideline18 suggests an optimal period of 2 to 4 weeks of treatment for determining the therapeutic response of antipsychotics in first-episode psychosis (degree 2 recommendation based on very weak-quality evidence).
Both guidelines17,18 indicated that the choice of antipsychotic medication should be based on patient characteristics and side effect profiles of different antipsychotic medications.
Maintenance Treatment of Schizophrenia
The VA/DoD guideline17 recommends the use of antipsychotic medication for the maintenance treatment of schizophrenia to prevent relapse and hospitalization (strong recommendation, categorized as reviewed, newly added).
The JSNPP guideline18 recommends SGAs over FGAs for reducing the relapse rate (recurrence of a psychotic episode after a period of response to treatment) or for continuing treatment in the maintenance phase (degree 2 recommendation based on moderate-quality evidence).
The JSNPP guideline18 recommends continuing the administration of antipsychotics for at least 1 year to prevent the recurrence of first-episode psychosis (degree 1 recommendation based on strong-quality evidence).
Both guidelines17,18 indicated that the choice of antipsychotic medication should be based on patient characteristics and side effect profiles of different antipsychotic medications.
Treatment of Recurrence or Relapse of Schizophrenia
The VA/DoD guideline17 suggests switching to another antipsychotic medication for patients who do not respond to (or tolerate) the current medication (weak recommendation, categorized as reviewed, newly added).
In contrast, the JSNPP guideline18 suggests increasing the dose rather than switching the antipsychotic (Degree 2 recommendation based on weak-quality evidence).
The JSNPP guideline18 noted that, among antipsychotics, quetiapine is effective at doses of more than 150 mg/day, or of more than 250 mg/day at the time of recurrence or relapse of schizophrenia (recommendation with no reported degree based on moderate- to weak-quality evidence).
Limitations
Evidence Gaps
The included clinical studies (i.e., 2 SRs13,14 with NMA, 1 SR15 with MA, and 1 RCT16) on antipsychotic drugs covered different areas of treatment of adults with schizophrenia, including treatment of patients newly diagnosed with schizophrenia, long-term maintenance treatment, and treatment-resistant schizophrenia. Most of the outcomes assessed by the included studies focused mainly on clinical efficacy and safety outcomes. However, the evidence on HRQoL and social functioning, which are outcomes important to patients, is too scarce to make any conclusions.
Generalizability
The findings of the included clinical studies and the recommendations of the guidelines could be generalizable to the adult population with schizophrenia living in Canada.
Certainty of Evidence
The 2 SRs13,14 with NMA had several limitations. First, there were some inconsistencies in the analyses of certain outcomes, which was mainly due to disagreement between direct and indirect evidence. To find the reason for inconsistency, the authors of the SRs13,14 performed a sensitivity analysis by excluding some studies. Second, there was substantial heterogeneity in patient characteristics and in the definition of treatment-resistant schizophrenia, which varied from partial to substantial treatment resistance. However, subgroup analyses performed across different criteria of definitions did not reveal significant differences from the main analysis. Third, although the search was comprehensive, there was potential publication bias as indicated by the pairwise MA funnel plot. Fourth, the scarcity of available evidence with several comparisons lay outside the networks, resulting in thinly connected networks and low statistical power to detect possible differences. Finally, the confidence in the evidence was generally moderate to low, meaning the results could potentially change if more evidence becomes available.
The SR15 with MA had several limitations. First, heterogeneity existed among studies with respect to patient characteristics, reported numerical data, number of outcome measures, and rating scales used to measure the outcomes. Second, the scarcity of evidence in some subgroups meant that it was not possible to generalize the findings to a wider population. Third, the SR did not consider confounding factors such as age, gender, or ethnicity, which may impact the outcome measures such as response to treatment and side effects. Fourth, the findings are not applicable to patients with chronic psychosis, because the included patients were either antipsychotic-naive or exposed to short-term antipsychotic use (0 to 16 weeks).
The included RCT16 had several limitations. First, treatment duration was short (i.e., 6 weeks), so the findings could not be extrapolated to a longer time period. Second, the study had a mixed population that may have included patients with treatment-resistant schizophrenia. Patients included in the study had an illness duration of at least 1 year, and more than one-third had the disease for more than 10 years.
Although the guidelines17,18 included in this report were generally of high methodological quality, the strength of some relevant recommendations was weak due to low-quality evidence.
Taken together, despite several limitations of the included SRs13-15 and RCT,16 the findings were derived from a collective large body of evidence that aligned with the included guidelines,17,18 which provided comprehensive recommendations and supporting evidence.
Conclusions and Implications for Decision- or Policy-Making
This review included 3 SRs,13-15 1 RCT,16 and 2 evidence-based guidelines,17,18 all of which were relevant to the research questions.
Clinical Efficacy and Safety of Treatment With Quetiapine
Quetiapine demonstrated moderate efficacy for schizophrenia symptoms, showing that it was less effective than olanzapine and lurasidone (in acutely ill adults with schizophrenia) and less effective than clozapine and olanzapine (in patients with treatment-resistant schizophrenia) for overall symptoms, but comparable to most other antipsychotics (e.g., risperidone, ziprasidone). It showed no clear benefit for negative symptoms, social functioning, or quality of life compared to other antipsychotics. Among newly diagnosed patients with schizophrenia, quetiapine had higher discontinuation rates due to lack of efficacy compared to olanzapine, aripiprazole, and ziprasidone, but lower discontinuation due to AEs compared to risperidone, ziprasidone, and haloperidol. Quetiapine was associated with less use of antiparkinsonian medication and lower prolactin increases than several antipsychotics; comparable sedation risk to other antipsychotics (with the exception of amisulpride and aripiprazole); comparable weight gain to other antipsychotics; and more QTc prolongation than paliperidone, risperidone, and olanzapine.
In newly diagnosed patients with schizophrenia (evidence from 1 SR with MA15 and 1 RCT16):
There were no clear differences in overall symptoms (including positive and negative symptoms) assessed by various rating scales between quetiapine and other antipsychotics such as aripiprazole, ziprasidone, and lurasidone.
Treatment with quetiapine was associated with higher rates of discontinuation due to lack of efficacy compared to olanzapine, ziprasidone, and aripiprazole.
Discontinuation due to AEs was less frequent with quetiapine than with risperidone, ziprasidone, and haloperidol.
For AEs, quetiapine was associated with high rates of sleepiness compared with aripiprazole and risperidone, and higher rates of weight gain and metabolic outcomes compared to lurasidone. Quetiapine was associated with a lower incidence of tremors compared to aripiprazole, less frequent incidence of vertigo and amenorrhea compared to ziprasidone, and lower rates of nausea and blood prolactin increases compared to lurasidone.
In long-term treatment (at least 6-month duration) (evidence from 1 SR with NMA14):
Quetiapine was less effective than lurasidone and olanzapine in overall symptoms, but the differences between quetiapine and other antipsychotics were uncertain.
There were no clear differences in social functioning and QoL between quetiapine and other antipsychotics.
Long-term treatment with quetiapine resulted in higher rates of all-cause discontinuation compared with amisulpride, aripiprazole, risperidone, and perphenazine. Discontinuation due to lack of efficacy and due to AEs was not reported.
Long-term treatment with quetiapine was associated with less use of antiparkinsonian medication compared with a number of antipsychotics.
For AEs, long-term treatment of quetiapine was associated with a higher risk of sedation compared to aripiprazole, higher average prolactin levels than risperidone, and higher average QTc prolongation than paliperidone, risperidone, and olanzapine. In contrast, long-term treatment with quetiapine was associated with less weight gain compared with olanzapine and clozapine. There were no clear differences in depressive symptoms between quetiapine and other antipsychotics.
In treatment-resistant schizophrenia (evidence from 1 SR with NMA13):
Quetiapine was less effective than clozapine and olanzapine in terms of managing overall symptoms. For positive symptoms, quetiapine was less effective than amisulpride, clozapine, risperidone, and olanzapine. For negative symptoms, quetiapine was less effective than chlorpromazine. The differences in response to treatment between quetiapine and all other antipsychotics investigated were uncertain.
Studies on QoL were scarce and not feasible for NMA. The pairwise MA results showed no statistically significant differences between quetiapine and other antipsychotics such as fluphenazine, risperidone, and chlorpromazine.
There were no clear differences in all-cause discontinuation and discontinuation due to lack of efficacy for treatment-resistant schizophrenia between quetiapine and other antipsychotics. Similarly, there were no clear differences in treatment discontinuation due to AEs between quetiapine and most antipsychotics, except that chlorpromazine was less tolerable than quetiapine.
Treatment with quetiapine in treatment-resistant schizophrenia was associated with less use of antiparkinsonian medication compared with fluphenazine and haloperidol. There were no clear differences between quetiapine and other antipsychotics.
For AEs, quetiapine was associated with a higher risk of sedation than amisulpride, and a lower risk of sedation than clozapine. Quetiapine was associated with less prolactin increase than olanzapine, chlorpromazine, haloperidol, and risperidone. Quetiapine was also associated with less weight gain compared with olanzapine and clozapine, and shorter QTc prolongation than chlorpromazine. There were no clear differences for the reported AEs between quetiapine and other antipsychotics.
Recommendations From Included Evidence-Based Guidelines
For the management of first-episode psychosis and schizophrenia, both guidelines17,18 recommend the use of antipsychotic medication, particularly SGAs over FGAs, except clozapine. The JSNPP guideline18 suggests an optimal period of 2 to 4 weeks of treatment for determining the therapeutic response of antipsychotics. The choice of antipsychotic medication should be based on patient characteristics and side effect profiles of different antipsychotic medications.17,18
For maintenance treatment of schizophrenia, both guidelines17,18 recommend the use of antipsychotic medication, particularly SGAs over FGAs, to prevent relapse and hospitalization. The JSNPP guideline18 recommends continuing the administration of antipsychotics for at least 1 year. The choice of antipsychotic medication should be based on patient characteristics and side effect profiles of different antipsychotic medications.17,18
For the treatment of recurring or relapsing schizophrenia, the VA/DoD guideline17 suggests switching to another antipsychotic medication, while the JSNPP guideline18 suggests increasing the dose rather than switching the antipsychotic.
Considerations for Future Research
The guideline recommendations included in this review that were based on a low level of evidence, particularly in the treatment of recurrent or relapsing schizophrenia, indicate areas for which future clinical research is needed. More research investigating the effect of antipsychotics on patient-reported outcomes such as QoL is also warranted.
Implications for Clinical Practice
The findings of this review suggest that antipsychotics have different efficacy and safety profiles in the treatment of schizophrenia. The evidence was insufficient for an accurate comparison of antipsychotics, which cannot be ranked relative to each other. Prescribing antipsychotics for the treatment of newly diagnosed patients, for maintenance treatment, and for the treatment of recurring or relapsing schizophrenia should be based on patient characteristics, patient tolerability, patient values and preferences, the side effect profiles of different antipsychotic medications, and clinician expertise.
Acknowledgement
Clinical Expert
This individual has kindly provided comments on the report:
Naista Zhand, MD, FRCPC
Psychiatrist, Integrated Schizophrenia Recovery Program
Assistant Professor, University of Ottawa
Tier 2 Clinical Research Chair in Schizophrenia, University of Ottawa
References
1.American Psychiatric Association. Schizophrenia spectrum and other psychotic disorders. In Diagnostic and statistical manual of mental disorders (5th ed.). 2013; https://dsm.psychiatryonline.org/doi/full/10.1176/appi.books.9780890425596.dsm02. Accessed 07 April, 2025.
2.American Psychiatric Association. (1994). Diagnostic and statistical manual of mental disorders (4th ed.). American Psychiatric Publishing, Inc. 1994; https://psycnet.apa.org/record/1994-97698-000. Accessed 12 May, 2025.
3.Schizophrenia. 2017; https://www.camh.ca/en/health-info/mental-illness-and-addiction-index/schizophrenia. Accessed 08 April, 2025.
4.Schizophrenia in Canada. 2020; https://www.canada.ca/en/public-health/services/publications/diseases-conditions/schizophrenia-canada.html. Accessed 07 April, 2025.
5.Schizophrenia. 2024; https://www.mayoclinic.org/diseases-conditions/schizophrenia/diagnosis-treatment/drc-20354449. Accessed 07 April, 2025.
6.Schizophrenia Society of Canada - Education. 2025; https://schizophrenia.ca/about-schizophrenia/. Accessed 08 April, 2025.
7.SEROQUEL - (quetiapine fumarate tablets). 2006; https://pdf.hres.ca/dpd_pm/00001972.PDF. Accessed 08 April, 2025.
8.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
9.Jansen JP, Trikalinos T, Cappelleri JC, et al. Indirect treatment comparison/network meta-analysis study questionnaire to assess relevance and credibility to inform health care decision making: an ISPOR-AMCP-NPC Good Practice Task Force report. Value Health. 2014;17(2):157-173. PubMed
10.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
11.Agree Next Steps C. The AGREE II Instrument. Hamilton (ON): AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf. Accessed January 1, 1800.
12.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
13.Dong S, Schneider-Thoma J, Bighelli I, et al. A network meta-analysis of efficacy, acceptability, and tolerability of antipsychotics in treatment-resistant schizophrenia. Eur Arch Psychiatry Clin Neurosci. 2024;274(4):917-928. PubMed
14.Leucht S, Schneider-Thoma J, Burschinski A, et al. Long-term efficacy of antipsychotic drugs in initially acutely ill adults with schizophrenia: systematic review and network meta-analysis. World Psychiatry. 2023;22(2):315-324. PubMed
15.Sherzad Qadir Z, Ball PA, Morrissey H. Efficacy and Tolerance of Antipsychotics Used for the Treatment of Patients Newly Diagnosed with Schizophrenia: A Systematic Review and Meta-Analysis. Pharmacy (Basel). 2023;11(6):10. PubMed
16.Kim SH, Jung DU, Kim DH, et al. Efficacy and Safety of Lurasidone vs. Quetiapine XR in Acutely Psychotic Patients With Schizophrenia in Korea: A Randomized, Double-Blind, Active-Controlled Trial. Psychiatry Investig. 2024;21(7):762-771. PubMed
17.VA/DoD clinical practice guideline for the management of first-episode psychosis and schizophrenia. 2023; https://www.healthquality.va.gov/guidelines/MH/scz/VADoDCPGSchizophreniaCPG_Final_508.pdf. Accessed 27 March, 2025.
18.Japanese Society of Neuropsychopharmacology: “Guideline for Pharmacological Therapy of Schizophrenia”. 2021; https://onlinelibrary.wiley.com/doi/10.1002/npr2.12193. Accessed 27 March, 2025.
19.Leucht S, Davis JM. Which first-generation antipsychotics should be “repurposed” for the treatment of schizophrenia. Eur Arch Psychiatry Clin Neurosci. 2022;272(1):1-3. PubMed
Appendix 1: Selection of Included Studies
Figure 1: PRISMA12 Flow Chart of Study Selection
Appendix 2: Characteristics of Included Publications
Please note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Systematic Reviews
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Interventions | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Dong et al. (2024)13 Germany Funding source: Projekt DEAL and China Scholarship Council | SR with NMA 60 RCTs | Patients with treatment-resistant schizophrenia (N = 6,838 patients) Sex: Female: 28.5% Male: 71.5% Mean (SD) age: 38.07 (6.98) years Mean (SD) duration of illness: 14.53 (5.56) years Mean (SD) number of previous episodes: 6.97 (3.41) | SGAs available in Europe or the US, and a selection of FGAs based on a survey of international schizophrenia experts. (i.e., sulpiride, levomepromazine, aripiprazole, trifluoperazine, perphenazine, clozapine, thioridazine, olanzapine, ziprasidone, quetiapine, amisulpride, risperidone, chlorpromazine, haloperidol, fluphenazine, sertindole, thiothixene, fluphenazine LAI, pipotiazine LAI, and placebo) | Outcomes: Primary:
Secondary:
Follow-up: Median trial duration: 12 weeks (range, 4 to 52) |
Leucht et al. (2023)14 Germany, Switzerland, US Funding source: German Ministry of Education and Research | SR with NMA 45 RCTs | Acutely ill adult patients with schizophrenia Sex: Female: 40% Male: 60% Mean (IQR) age: 37.2 (IQR: 35.2 to 39.1) years Mean (IQR) study duration: 42 (IQR: 26 to 52) weeks | SGAs available in Europe or the US, and a selection of FGAs based on a survey of international schizophrenia experts. (i.e., amisulpride, aripiprazole, asenapine, chlorpromazine, clozapine, fluphenazine, fluspirilene, haloperidol, iloperidone, loxapine, lurasidone, olanzapine, paliperidone, penfluridol, perphenazine, pimozide, quetiapine, risperidone, thioridazine, tiotixene, trifluoperazine, ziprasidone, zotepine, and placebo) | Outcomes: Primary:
Secondary:
Follow-up: Trial duration: at least 24 weeks (range, 24 to 156) |
Sherzad Qadir et al. (2023)15 Australia Funding source: The authors declared that the study received no external funding | SR with MA 21 RCTs | Patients newly diagnosed with schizophrenia (N = 3,911 reported in 19 studies) Details of study characteristics and patient characteristics of individual studies were presented in the supplementary appendix of the study. | Quetiapine Aripiprazole Ziprasidone Risperidone Olanzapine Haloperidol | Outcomes:
Follow-up: 8 weeks to 9 years |
AE = adverse event; BPRS = Brief Psychiatric Rating Scale; CDSS = Calgary Depression Scale for Schizophrenia; FGA = first-generation antipsychotic; IQR = interquartile range; LAI = long-acting injectable; MA = meta-analysis; NMA = network meta-analysis; PANSS = Positive and Negative Syndrome Scale; RCT = randomized controlled trial; SANS = Scale for the Assessment of Negative Symptoms; SAPS = Scale for the Assessment of Positive Symptoms; SD = standard deviation; SGA = second-generation antipsychotic; SR = systematic review; YMRS = Young Mania Rating Scale.
aPANSS is a 30-item clinician-rated instrument to assess schizophrenia psychopathology, including positive (e.g., hallucinations, delusions) and negative (e.g., blunted effect, social withdrawal) symptoms, as well as general psychopathology. Of the 30 items, each is rated on a 7-point scale (1 = absent to 7 = extreme). The items are divided into 3 subscales: positive symptoms — 7 items focusing on hallucinations, delusions, and other positive symptoms; negative symptoms — 7 items assessing negative symptoms such as blunted affect and social withdrawal; general psychopathology — 16 items covering a broader range of symptoms, including somatic concern, anxiety, and depression.
bBPRS is a rating scale used to measure psychiatric symptoms such as depression, anxiety, hallucinations, psychosis, and unusual behaviour. Total scores range from 18 to 126, whereas higher scores indicate stronger psychotic symptoms.
cSANS: Measures the levels of negative symptoms of schizophrenia (affective flattening or blunting, alogia, avolition-apathy, anhedonia-asociality, attention). 0 to 125, a lower score is favourable.
dSAPS: Measures levels of positive symptoms of schizophrenia (delusions, hallucination, and thought disorder). 0 to 170, lower score is favourable.
eCDSS: Measures the level of depression in people with schizophrenia. 0 to 27, lower score is favourable.
fYMRS: Measures manic symptoms (elevated mood, increased motor activity/energy, sexual interest, sleep, irritability, speech, language-thought disorder, content, disruptive-aggressive behaviour, appearance, insight). 0 to 60, lower score is favourable.
Table 3: Characteristics of Included Primary Clinical Study
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Kim et al. (2024)16 Republic of Korea Funding source: Bukwang Pharmaceuticals | Parallel, 1:1 ratio, double-blind, active-controlled trial (RCT) Predefined noninferiority margin: −8.99 | Adult patients with a diagnosis of schizophrenia, being at a state of acute exacerbation of psychosis symptoms, lasting ≤ 2 months. Mean (SD) age: 41.74 (14.81) years Sex, %: Female: 63% Male: 37% Duration of illness: 1 year to ≥ 10 years | Intervention: Lurasidone (N = 102) Comparator: Quetiapine XR (N = 104) | Outcomes: Primary:
Secondary:
Treatment duration: 6 weeks Follow-up: 1 week after last dose of study medication |
AE = adverse event; CGI-S = Clinical Global Impression–Severity of Illness; PANSS = Positive and Negative Syndrome Scale; RCT = randomized controlled trial; SD = standard deviation; XR = extended release.
aPANSS is a 30-item clinician-rated instrument to assess schizophrenia psychopathology, including positive (e.g., hallucinations, delusions) and negative (e.g., blunted effect, social withdrawal) symptoms, as well as general psychopathology. 30 to 210, lower score is favourable.
bCGI-S is a 7-point scale ranging from 1 (normal, not at all ill) to 7 (among the most extremely ill patients) used by clinicians to rate the current severity of a patient's mental illness.
Table 4: Characteristics of Included Guidelines
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality assessment | Recommendations development and evaluation | Guideline validation |
|---|---|---|---|---|---|---|
VA/DoD (2023)17 | ||||||
Intended users: Primary care providers, mental health providers, and others involved in the health care team Target population: Patients with schizophrenia and their caregivers | Treatment (e.g., drug, surgery, lifestyle changes), approach (e.g., doses, frequency, methods of administering treatments), or diagnostic or screening test or both used with the patient or population Management of first-episode psychosis and schizophrenia | Outcomes of interest (e.g., mortality, morbidity, QoL, complications). Outcomes can include short, intermediate, and long-term outcomes. | Systematic search for evidence, study selection, data extraction, and data synthesis were performed. | The WG used the GRADE approach to craft each recommendation and determined its strengtha (strong, weak) based on 4 domains:
| The CPG WG comprised experts in psychiatry, psychology, internal medicine, nursing, primary care, pharmacy, mental health counselling, and social work. Tasks of the WG:
| The CPG was reviewed by experts outside the organization. |
JSNPP (2021)18 | ||||||
Intended users: Specialists in the treatment of schizophrenia, patients, and their families and supporters Target population: Patients with first-episode psychosis and schizophrenia | Pharmacological therapy and psychosocial therapy in collaboration with medical welfare Management of schizophrenia | All relevant outcomes | Systematic search for evidence, study selection, data extraction, and data synthesis were performed. | Level of evidence was assessed as strong, moderate, weak, and very weak.b The strength of recommendation was described with the general corresponding text.c | The Task Force determined the scope of the guideline and determined clinical questions based on scope. Each WG conducted a systematic review and evaluated the body of evidence. Each WG crafted the recommendation drafts for each clinical question. | The guideline was reviewed by internal and external experts. |
CPG = clinical practice guideline; GRADE = Grading of Recommendations Assessment, Development and Evaluation; JSNPP = Japanese Society of Neuropsychopharmacology; QoL = quality of life; VA/DoD = Veterans Affairs/Department of Defense; WG = working group.
aRecommendation strength (General corresponding text): Strong for (We recommend…), Weak for (We suggest…), Neither for nor against (There is insufficient evidence to recommend for or against…), Weak against (We suggest against…), Strong against (We recommend against…).
bLevel of evidence: Strong (A): It is almost certain that the true effect is close to the estimated effect; Moderate (B): The true effect is thought to be close to the estimated effect, but the possibility that results may be different remains; Weak (C): The true effect is thought to be close to the estimated effect, but the results may be different; Very weak (D): The estimated effect is very unclear and is often very different from the true effect.
cStrength of recommendation: Action is recommended (1), Action is not recommended (1), Action is suggested/desirable (2), Action is not suggested/desirable (2).
Appendix 3: Critical Appraisal of Included Publications
Please note that this appendix has not been copy-edited.
Table 5: Strengths and Limitations of the SRs and NMAs Using AMSTAR 28 and the ISPOR Questionnaire9
Strengths | Limitations |
|---|---|
Dong et al. (2024)13 | |
Objectives:
Search strategies:
Data collection:
Methods for analysis/synthesis of evidence:
Reporting:
Discussion:
| Search strategies:
Methods for analysis/synthesis of evidence:
Reporting:
|
Leucht et al. (2023)14 | |
Objectives:
Search strategies:
Data collection:
Methods for analysis/synthesis of evidence:
Reporting:
Discussion:
| Search strategies:
Methods for analysis/synthesis of evidence:
Reporting:
|
Sherzad Qadir et al. (2023)15 | |
|
|
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; CI = confidence interval; ISPOR = International Society for Pharmacoeconomics and Outcomes Research; MA = meta-analysis; NMA = network meta-analysis; OR = odds ratio; PICO = population, intervention, comparator, and outcome; RCT = randomized controlled trial; SMD = standardized mean difference.
Table 6: Strengths and Limitations of Clinical Studies Using the Downs and Black Checklist10
Strengths | Limitations |
|---|---|
Kim et al. (2024)16 | |
Reporting:
External validity:
Internal validity — bias:
Internal validity — confounding:
| Internal validity — confounding:
|
ITT = intention-to-treat; PANSS = Positive and Negative Syndrome Scale; PP = per-protocol.
Table 7: Strengths and Limitations of Guidelines Using AGREE II11
Item | VA/DoD (2023)17 | JSNPP (2021)18 |
|---|---|---|
Domain 1: Scope and purpose | ||
1. The overall objective(s) of the guideline is (are) specifically described. | Yes | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes | Yes |
3. The population (patients, public, and so forth) to whom the guideline is meant to apply is specifically described. | Yes | Yes |
Domain 2: Stakeholder involvement [wording from original source] | ||
4. The guideline development group includes individuals from all relevant professional groups. | Yes | Yes |
5. The views and preferences of the target population (patients, public, and so forth) have been sought. | Yes | Yes |
6. The target users of the guideline are clearly defined. | Yes | Yes |
Domain 3: Rigour of development | ||
7. Systematic methods were used to search for evidence. | Yes | Yes |
8. The criteria for selecting the evidence are clearly described. | Yes | Yes |
9. The strengths and limitations of the body of evidence are clearly described. | Yes | Yes |
10. The methods for formulating the recommendations are clearly described. | Yes | Yes |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes | Yes |
12. There is an explicit link between the recommendations and the supporting evidence. | Yes | Yes |
13. The guideline has been externally reviewed by experts before its publication. | Yes | Yes |
14. A procedure for updating the guideline is provided. | Yes | Yes |
Domain 4: Clarity of presentation | ||
15. The recommendations are specific and unambiguous. | Yes | Yes |
16. The different options for management of the condition or health issue are clearly presented. | Yes | Yes |
17. Key recommendations are easily identifiable. | Yes | Yes |
Domain 5: Applicability | ||
18. The guideline describes facilitators and barriers to its application. | Unclear | Unclear |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | Yes | Yes |
20. The potential resource implications of applying the recommendations have been considered. | Yes | Yes |
21. The guideline presents monitoring and/or auditing criteria. | Unclear | Unclear |
Domain 6: Editorial independence | ||
22. The views of the funding body have not influenced the content of the guideline. | Yes | Yes |
23. Competing interests of guideline development group members have been recorded and addressed. | Yes | Yes |
AGREE II = Appraisal of Guidelines for Research and Evaluation II; JSNPP = Japanese Society of Neuropsychopharmacology; VA/DoD = Veterans Affairs/Department of Defense.
Appendix 4: Main Study Findings
Please note that this appendix has not been copy-edited.
Table 8: Summary of Findings by Outcome — Overall Symptoms of Schizophrenia
Study citation and study design | Interventions vs. comparators | Results SMD or MD (95% CI) | Notes |
|---|---|---|---|
Dong et al. (2024)13 SR with NMA | Levomepromazine vs. quetiapine | −0.71 (−1.49 to 0.07) | Uncertain |
Amisulpride vs. quetiapine | −0.64 (−1.28 to 0.01) | Uncertain | |
Clozapine vs. quetiapine | −0.44 (−0.66 to −0.22) | Favours clozapine | |
Olanzapine vs. quetiapine | −0.40 (−0.67 to −0.13) | Favours olanzapine | |
Zotepine vs. quetiapine | −0.37 (−1.08 to 0.33) | Uncertain | |
Risperidone vs. quetiapine | −0.29 (−0.57 to 0.00) | Uncertain | |
Ziprasidone vs. quetiapine | −0.25 (−0.64 to 0.14) | Uncertain | |
Haloperidol vs. quetiapine | −0.14 (−0.40 to 0.13) | Uncertain | |
Fluphenazine vs. quetiapine | −0.04 (−0.51 to 0.42) | Uncertain | |
Chlorpromazine vs. quetiapine | −0.01 (−0.25 to 0.24) | Uncertain | |
Quetiapine vs. sertindole | −0.03 (−0.55 to 0.48) | Uncertain | |
Leucht et al. (2023)14 SR with NMA | Lurasidone vs. quetiapine | −0.42 (−0.71 to −0.13) | Favours lurasidone |
Olanzapine vs. quetiapine | −0.25 (−0.38 to −0.12) | Favours olanzapine | |
Amisulpride vs. quetiapine | −0.19 (−0.38 to 0.01) | Uncertain | |
Perphenazine vs. quetiapine | −0.16 (−0.32 to 0.00) | Uncertain | |
Clozapine vs. quetiapine | −0.14 (−0.55 to 0.27) | Uncertain | |
Risperidone vs. quetiapine | −0.13 (−0.27 to 0.01) | Uncertain | |
Aripiprazole vs. quetiapine | −0.09 (−0.27 to 0.08) | Uncertain | |
Zotepine vs. quetiapine | −0.09 (−0.49 to 0.31) | Uncertain | |
Quetiapine vs. haloperidol | −0.02 (−0.19 to 0.16) | Uncertain | |
Quetiapine vs. paliperidone | −0.03 (−0.22 to 0.17) | Uncertain | |
Quetiapine vs. Iloperidone | −0.07 (−0.28 to 0.14) | Uncertain | |
Quetiapine vs. asenapine | −0.08 (−0.26 to 0.10) | Uncertain | |
Quetiapine vs. ziprasidone | −0.12 (−0.28 to 0.03) | Uncertain | |
Sherzad Qadir et al. (2023)15 SR with MA | Aripiprazole vs. quetiapine | CGI: −0.32 (−0.71 to 0.07) | NS |
BPRS: −4.77 (−7.83 to −1.71) | P = 0.002; favours aripiprazole | ||
SANS: −1.06 (−2.43 to 0.32) | NS | ||
SAPS: −0.32 (−0.93 to 0.30) | NS | ||
CDSS: 0.25 (−0.56 to 1.06) | NS | ||
YMRS: −0.43 (−1.78 to 0.91) | NS | ||
Ziprasidone vs. quetiapine | CGI: −0.21 (−0.60 to 0.17) | NS | |
BPRS: 1.07 (−2.60 to 4.93) | NS | ||
SANS: −0.20 (−1.55 to 1.14) | NS | ||
SAPS: −0.33 (−1.49 to 0.82) | NS | ||
CDSS: 0.73 (−0.04 to 1.49) | NS | ||
YMRS: 0.27 (−1.10 to 1.63) | NS | ||
Kim et al. (2024)16 RCT | Lurasidone vs. quetiapine | MD (95% CI) PANNS: −0.91 (−6.35 to 4.53) | NS |
CGI: Results were presented in a graphical manner. | Statistically significant differences observed at 4-week and 6-week treatments, favouring lurasidone |
BPRS = Brief Psychiatric Rating Scale; CDSS = Calgary Depression Scale for Schizophrenia; CGI = Clinical Global Impression; CI = confidence interval; MA = meta-analysis; MD = mean difference; NMA = network meta-analysis; NS = not statistically significant; PANSS = Positive and Negative Syndrome Scale; RCT = randomized controlled trial; SANS = Scale for the Assessment of Negative Symptoms; SAPS = Scale for the Assessment of Positive Symptoms; SMD = standardized mean difference; SR = systematic review; vs. = versus; YMRS = Young Mania Rating Scale.
Table 9: Summary of Findings by Outcome — Positive Symptoms
Study citation and study design | Interventions vs. comparators | Results SMD (95% CI) | Notes |
|---|---|---|---|
Dong et al. (2024)13 SR with NMA | Amisulpride vs. quetiapine | –0.82 (−1.48 to −0.16) | Favours amisulpride |
Levomepromazine vs. quetiapine | −0.81 (−1.62 to 0.00) | Uncertain | |
Clozapine vs. quetiapine | −0.61 (−0.90 to −0.32) | Favours clozapine | |
Risperidone vs. quetiapine | −0.51 (−0.82 to −0.20) | Favours risperidone | |
Olanzapine vs. quetiapine | −0.49 (−0.78 to −0.19) | Favours olanzapine | |
Ziprasidone vs. quetiapine | −0.33 (−0.75 to 0.10) | Uncertain | |
Haloperidol vs. quetiapine | −0.26 (−0.55 to 0.03) | Uncertain | |
Sertindole vs. quetiapine | −0.13 (−0.67 to 0.40) | Uncertain | |
Chlorpromazine vs. quetiapine | −0.12 (−0.43 to 0.19) | Uncertain | |
Fluphenazine vs. quetiapine | 0.02 (−0.74 to 0.78) | Uncertain | |
Leucht et al. (2023)14 SR with NMA | Quetiapine was not part of the NMA | — | — |
Kim et al. (2024)16 RCT | Lurasidone vs. quetiapine | PANSS positive subscores: Results were presented in a graphical manner. | No statistically significant difference was found between groups in terms of PANSS positive subscale scores. |
CI = confidence interval; NMA = network meta-analysis; PANSS = Positive and Negative Syndrome Scale; RCT = randomized controlled trial; SMD = standardized mean difference; SR = systematic review; vs. = versus.
Table 10: Summary of Findings by Outcome — Negative Symptoms
Study citation and study design | Interventions vs. comparators | Results SMD (95% CI) | Notes |
|---|---|---|---|
Dong et al. (2024)13 SR with NMA | Amisulpride vs. quetiapine | −0.46 (−1.68 to 0.75) | Uncertain |
Clozapine vs. quetiapine | −0.22 (−0.76 to 0.31) | Uncertain | |
Zotepine vs. quetiapine | −0.36 (−1.61 to 0.89) | Uncertain | |
Olanzapine vs. quetiapine | −0.14 (−0.68 to 0.40) | Uncertain | |
Fluphenazine vs. quetiapine | −0.10 (−0.98 to 0.78) | Uncertain | |
Levomepromazine vs. quetiapine | −0.11 (−1.44 to 1.22) | Uncertain | |
Ziprasidone vs. quetiapine | −0.01 (−0.90 to 0.89) | Uncertain | |
Quetiapine vs. risperidone | 0.02 (−0.54 to 0.57) | Uncertain | |
Quetiapine vs. haloperidol | 0.01 (−0.54 to 0.56) | Uncertain | |
quetiapine vs. sertindole | −0.17 (−1.33 to 0.98) | Uncertain | |
Quetiapine vs. chlorpromazine | −0.66 (−1.28 to −0.05) | Favours quetiapine | |
Leucht et al. (2023)14 SR with NMA | Quetiapine was not part of the NMA | — | — |
Kim et al. (2024)16 RCT | Lurasidone vs. quetiapine | PANSS negative subscores: Results were presented in a graphical manner. | No statistically significant difference was found between groups in terms of PANSS negative subscale scores. |
CI = confidence interval; NMA = network meta-analysis; PANSS = Positive and Negative Syndrome Scale; SMD = standardized mean difference; SR = systematic review; vs. = versus.
Table 11: Summary of Findings by Outcome — Response to Treatment
Study citation and study design | Interventions vs. comparators | Results RR (95% CI) | Notes |
|---|---|---|---|
Dong et al. (2024)13 SR with NMA | Sulpiride vs. quetiapine | 1.67 (0.75 to 2.24) | Uncertain |
Levomepromazine vs. quetiapine | 1.43 (0.72 to 2.02) | Uncertain | |
Aripiprazole vs. quetiapine | 1.33 (0.41 to 2.15) | Uncertain | |
Trifluoperazine vs. quetiapine | 1.32 (0.45 to 0.11) | Uncertain | |
Perphenazine vs. quetiapine | 1.29 (0.48 to 2.05) | Uncertain | |
Clozapine vs. quetiapine | 1.16 (0.79 to 1.55) | Uncertain | |
Thioridazine vs. quetiapine | 1.15 (0.37 to 1.99) | Uncertain | |
Olanzapine vs. quetiapine | 1.11 (0.73 to 1.51) | Uncertain | |
Ziprasidone vs. quetiapine | 1.10 (0.63 to 1.61) | Uncertain | |
Quetiapine vs. amisulpride | 1.03 (0.39 to 1.82) | Uncertain | |
Quetiapine vs. Risperidone | 1.13 (0.73 to 1.58) | Uncertain | |
Quetiapine vs. Chlorpromazine | 1.30 (0.87 to 1.77) | Uncertain | |
Quetiapine vs. Haloperidol | 1.33 (0.89 to 1.82) | Uncertain | |
Quetiapine vs. Fluphenazine | 1.36 (0.61 to 2.28) | Uncertain | |
Quetiapine vs. Sertindole | 1.56 (0.71 to 2.59) | Uncertain | |
Quetiapine vs. Thiothixene | 2.96 (0.87 to 5.64) | Uncertain | |
Quetiapine vs. Fluphenazine LAI | 3.52 (0.59 to 7.50) | Uncertain | |
Quetiapine vs. Pipotiazine LAI | 3.52 (0.59 to 7.50) | Uncertain | |
Leucht et al. (2023)14 SR with NMA | No NMA for this outcome | — | — |
CI = confidence interval; LAI = long-acting injectable; NMA = network meta-analysis; RR = relative risk; SR = systematic review; vs. = versus.
Table 12: Summary of Findings by Outcome — Social Functioning
Study citation and study design | Interventions vs. comparators | Results SMD (95% CI) | Notes |
|---|---|---|---|
Dong et al. (2024)13 SR with NMA | No NMA for this outcome | — | — |
Leucht et al. (2023)14 SR with NMA | Quetiapine vs. olanzapine | −0.17 (−0.60 to 0.25) | Uncertain |
Quetiapine vs. amisulpride | −0.18 (−0.65 to 0.29) | Uncertain | |
Quetiapine vs. risperidone | −0.37 (−0.88 to 0.13) | Uncertain | |
Quetiapine vs. paliperidone | −0.47 (−1.00 to 0.06) | Uncertain |
CI = confidence interval; NMA = network meta-analysis; SMD = standardized mean difference; SR = systematic review; vs. = versus.
Table 13: Summary of Findings by Outcome — Quality of Life
Study citation and study design | Interventions vs. comparators | Results SMD (95% CI) | Notes |
|---|---|---|---|
Dong et al. (2024)13 SR with NMA | Fluphenazine vs. quetiapine | 0.18 (−0.68 to 1.03) | Pairwise MA; NS |
Quetiapine vs. risperidone | 0.03 (−0.81 to 0.86) | Pairwise MA; NS | |
Chlorpromazine vs. quetiapine | −0.21 (−0.46 to 0.04) | Pairwise MA; NS | |
Leucht et al. (2023)14 SR with NMA | Zotepine vs. quetiapine | −0.44 (−1.12 to 0.23) | Uncertain |
Amisulpride vs. quetiapine | −0.33 (−0.83 to 0.16) | Uncertain | |
Olanzapine vs. quetiapine | −0.33 (−0.69 to 0.03) | Uncertain | |
Asenapine vs. quetiapine | −0.30 (−0.76 to 0.17) | Uncertain | |
Ziprasidone vs. quetiapine | −0.26 (−0.67 to 0.14) | Uncertain | |
Perphenazine vs. quetiapine | −0.19 (−0.60 to 0.23) | Uncertain | |
Haloperidol vs. quetiapine | −0.17 (−0.69 to 0.34) | Uncertain | |
Risperidone vs. quetiapine | −0.16 (−0.53 to 0.22) | Uncertain |
CI = confidence interval; MA = meta-analysis; NMA = network meta-analysis; NS = not statistically significant; SMD = standardized mean difference; SR = systematic review; vs. = versus.
Table 14: Summary of Findings by Outcome — All-Cause Discontinuation
Study citation and study design | Interventions vs. comparators | Results RR (95% CI) | Notes |
|---|---|---|---|
Dong et al. (2024)13 SR with NMA | Sulpiride vs. quetiapine | 0.42 (0.02 to 2.21) | Uncertain |
Levomepromazine vs. quetiapine | 0.43 (0.08 to 1.51) | Uncertain | |
Olanzapine vs. quetiapine | 0.75 (0.52 to 1.05) | Uncertain | |
Clozapine vs. quetiapine | 0.77 (0.53 to 1.05) | Uncertain | |
Ziprasidone vs. quetiapine | 0.81 (0.46 to 1.17) | Uncertain | |
Risperidone vs. quetiapine | 0.83 (0.57 to 1.16) | Uncertain | |
Sertindole vs. quetiapine | 0.99 (0.52 to 1.57) | Uncertain | |
Chlorpromazine vs. quetiapine | 0.99 (0.73 to 1.27) | Uncertain | |
Quetiapine vs. zotepine | 0.93 (0.32 to 1.72) | Uncertain | |
Quetiapine vs. haloperidol | 0.90 (0.64 to 1.18) | Uncertain | |
Quetiapine vs. fluphenazine LAI | 0.87 (0.08 to 2.09) | Uncertain | |
Quetiapine vs. pipotiazine LAI | 0.87 (0.08 to 2.09) | Uncertain | |
Quetiapine vs. amisulpride | 0.78 (0.31 to 1.40) | Uncertain | |
Quetiapine vs. Fluphenazine | 0.69 (0.30 to 1.18) | Uncertain | |
Quetiapine vs. thioridazine | 0.52 (0.07 to 1.25) | Uncertain | |
Quetiapine vs. trifluoperazine | 0.49 (0.09 to 1.11) | Uncertain | |
Leucht et al. (2023)14 SR with NMA | Amisulpride vs. quetiapine | 0.70 (0.54 to 0.88) | Favours amisulpride |
Aripiprazole vs. quetiapine | 0.73 (0.57 to 0.89) | Favours aripiprazole | |
Lurasidone vs. quetiapine | 0.80 (0.60 to 1.01) | Uncertain | |
Risperidone vs. quetiapine | 0.82 (0.68 to 0.95) | Favours risperidone | |
Perphenazine vs. quetiapine | 0.82 (0.67 to 0.97) | Favours perphenazine | |
Zotepine vs. quetiapine | 0.91 (0.60 to 1.20) | Uncertain | |
Haloperidol vs. quetiapine | 0.93 (0.78 to 1.08) | Uncertain | |
Ziprasidone vs. quetiapine | 0.93 (0.78 to 1.07) | Uncertain | |
Asenapine vs. quetiapine | 0.94 (0.78 to 1.09) | Uncertain | |
Paliperidone vs. quetiapine | 0.95 (0.79 to 1.10) | Uncertain | |
Thiothixene vs. quetiapine | 0.98 (0.66 to 1.24) | Uncertain | |
Fluspirilene vs. quetiapine | 0.99 (0.23 to 1.49) | Uncertain | |
Quetiapine vs. pimozide | 0.80 (0.30 to 1.14) | Uncertain | |
Quetiapine vs. fluphenazine | 0.77 (0.41 to 1.04) | Uncertain | |
Quetiapine vs. olanzapine | 1.55 (1.35 to 1.72) | Favours olanzapine |
CI = confidence interval; LAI = long-acting injectable; NMA = network meta-analysis; RR = relative risk; SR = systematic review; vs. = versus.
Table 15: Summary of Findings by Outcome — Discontinuation Due to Lack of Efficacy
Study citation and study design | Interventions vs. comparators | Results RR (95% CI) | Notes |
|---|---|---|---|
Dong et al. (2024)13 SR with NMA | Clozapine vs. quetiapine | 0.28 (0.14 to 0.53) | Favours clozapine |
Fluphenazine LAI vs. quetiapine | 0.32 (0.03 to 2.27) | Uncertain | |
Ziprasidone vs. quetiapine | 0.43 (0.08 to 1.73) | Uncertain | |
Pipotiazine LAI vs. quetiapine | 0.48 (0.04 to 2.71) | Uncertain | |
Sulpiride vs. quetiapine | 0.51 (0.01 to 3.78) | Uncertain | |
Amisulpride vs. quetiapine | 0.51 (0.03 to 3.02) | Uncertain | |
Chlorpromazine vs. quetiapine | 0.52 (0.19 to 1.25) | Uncertain | |
Olanzapine vs. quetiapine | 0.52 (0.27 to 0.95) | Favours olanzapine | |
Risperidone vs. quetiapine | 0.63 (0.32 to 1.17) | Uncertain | |
Sertindole vs. quetiapine | 0.81 (0.33 to 1.69) | Uncertain | |
Quetiapine vs. haloperidol | 0.98 (0.56 to 1.57) | Uncertain | |
Quetiapine vs. zotepine | 0.86 (0.04 to 3.21) | Uncertain | |
Quetiapine vs. trifluoperazine | 0.73 (0.06 to 2.60) | Uncertain | |
Quetiapine vs. thioridazine | 0.54 (0.03 to 1.91) | Uncertain | |
Quetiapine vs. fluphenazine | 0.51 (0.17 to 1.12) | Uncertain | |
Leucht et al. (2023)14 SR with NMA | No NMA for this outcome | — | — |
Sherzad Qadir et al. (2023)15 SR with MA | Quetiapine vs. olanzapine | 3.48 (3.05 to 5.91) | P < 0.001; more frequent with quetiapine |
Quetiapine vs. risperidone | 0.68 (0.01 to 33.70) | NS | |
Quetiapine vs. ziprasidone | 2.05 (1.57 to 2.68) | P < 0.001; more frequent with quetiapine | |
Quetiapine vs. haloperidol | 1.14 (0.41 to 3.16) | NS | |
Quetiapine vs. aripiprazole | 3.69 (2.56 to 5.32) | P < 0.001; more frequent with quetiapine |
CI = confidence interval; LAI = long-acting injectable; MA = meta-analysis; NMA = network meta-analysis; NS = not statistically significant; RR = relative risk; SR = systematic review; vs. = versus.
Table 16: Summary of Findings by Outcome — Discontinuation Due to AEs
Study citation and study design | Interventions vs. comparators | Results RR (95% CI) | Notes |
|---|---|---|---|
Dong et al. (2024)13 SR with NMA | Fluphenazine vs. quetiapine | 0.36 (0.04 to 2.65) | Uncertain |
Olanzapine vs. quetiapine | 0.47 (0.22 to 1.00) | Uncertain | |
Risperidone vs. quetiapine | 0.52 (0.24 to 1.11) | Uncertain | |
Haloperidol vs. quetiapine | 0.57 (0.29 to 1.12) | Uncertain | |
Clozapine vs. quetiapine | 0.74 (0.38 to 1.40) | Uncertain | |
Sertindole vs. quetiapine | 0.89 (0.25 to 2.86) | Uncertain | |
Zotepine vs. quetiapine | 0.92 (0.21 to 3.55) | Uncertain | |
Quetiapine vs. ziprasidone | 0.99 (0.42 to 2.23) | Uncertain | |
Quetiapine vs. thioridazine | 0.55 (0.01 to 7.15) | Uncertain | |
Quetiapine vs. sulpiride | 0.52 (0.01 to 7.56) | Uncertain | |
Quetiapine vs. chlorpromazine | 0.51 (0.26 to 0.95) | Favours quetiapine | |
Quetiapine vs. levomepromazine | 0.51 (0.03 to 4.94) | Uncertain | |
Quetiapine vs. trifluoperazine | 0.45 (0.03 to 4.17) | Uncertain | |
Quetiapine vs. thiothixene | 0.41 (0.03 to 3.29) | Uncertain | |
Quetiapine vs. amisulpride | 0.37 (0.03 to 2.45) | Uncertain | |
Quetiapine vs. pipotiazine LAI | 0.30 (0.02 to 2.69) | Uncertain | |
Quetiapine vs. fluphenazine LAI | 0.22 (0.01 to 1.85) | Uncertain | |
Leucht et al. (2023)14 SR with NMA | No NMA for this outcome | — | — |
Qadir et al. (2023) SR with MA | Quetiapine vs. olanzapine | 0.81 (0.49 to 1.37) | NS |
Quetiapine vs. risperidone | 0.44 (0.21 to 0.89) | P = 0.02; more frequent with risperidone | |
Quetiapine vs. ziprasidone | 0.34 (0.22 to 0.51) | P < 0.001; more frequent with ziprasidone | |
Quetiapine vs. haloperidol | 0.43 (0.22 to 0.84) | P = 0.01; more frequent with haloperidol | |
Quetiapine vs. aripiprazole | 1.03 (0.62 to 1.73) | NS |
AE = adverse event; CI = confidence interval; LAI = long-acting injectable; MA = meta-analysis; NMA = network meta-analysis; NS = not statistically significant; RR = relative risk; SR = systematic review; vs. = versus.
Table 17: Summary of Findings by Outcome — Use of Antiparkinsonian Medication
Study citation and study design | Interventions vs. comparators | Results RR (95% CI) | Notes |
|---|---|---|---|
Dong et al. (2024)13 SR with NMA | Levomepromazine vs. quetiapine | 0.30 (0.01 to 3.92) | Uncertain |
Thioridazine vs. quetiapine | 0.38 (0.01 to 4.70) | Uncertain | |
Sulpiride vs. quetiapine | 0.57 (0.03 to 4.84) | Uncertain | |
Clozapine vs. quetiapine | 0.68 (0.23 to 1.81) | Uncertain | |
Amisulpride vs. quetiapine | 0.77 (0.15 to 3.01) | Uncertain | |
Olanzapine vs. quetiapine | 0.79 (0.29 to 1.94) | Uncertain | |
Ziprasidone vs. quetiapine | 0.92 (0.23 to 2.87) | Uncertain | |
Pipotiazine LAI vs. quetiapine | 0.97 (0.01 to 7.53) | Uncertain | |
Quetiapine vs. chlorpromazine | 0.96 (0.07 to 5.37) | Uncertain | |
Quetiapine vs. fluphenazine LAI | 0.80 (0.01 to 6.08) | Uncertain | |
Quetiapine vs. risperidone | 0.59 (0.22 to 1.36) | Uncertain | |
Quetiapine vs. trifluoperazine | 0.41 (0.03 to 2.57) | Uncertain | |
Quetiapine vs. fluphenazine | 0.37 (0.11 to 0.99) | Favours quetiapine | |
Quetiapine vs. haloperidol | 0.34 (0.13 to 0.77) | Favours quetiapine | |
Leucht et al. (2023)14 SR with NMA | Quetiapine vs. aripiprazole | 0.78 (0.73 to 1.53) | Uncertain |
Quetiapine vs. zotepine | 0.62 (0.22 to 1.57) | Uncertain | |
Quetiapine vs. amisulpride | 0.43 (0.20 to 0.86) | Favours quetiapine | |
Quetiapine vs. risperidone | 0.35 (0.19 to 0.65) | Favours quetiapine | |
Quetiapine vs. paliperidone | 0.35 (0.18 to 0.69) | Favours quetiapine | |
Quetiapine vs. ziprasidone | 0.35 (0.18 to 0.68) | Favours quetiapine | |
Quetiapine vs. perphenazine | 0.34 (0.17 to 0.67) | Favours quetiapine | |
Quetiapine vs. haloperidol | 0.24 (0.12 to 0.46) | Favours quetiapine | |
Quetiapine vs. asenapine | 0.18 (0.06 to 0.51) | Favours quetiapine | |
Quetiapine vs. olanzapine | 0.56 (0.29 to 1.04) | Uncertain |
CI = confidence interval; LAI = long-acting injectable; NMA = network meta-analysis; RR = relative risk; SR = systematic review; vs. = versus.
Table 18: Summary of Findings by Outcome — Sedation
Study citation and study design | Interventions vs. comparators | Results RR (95% CI) | Notes |
|---|---|---|---|
Dong et al. (2024)13 SR with NMA | Thiothixene vs. quetiapine | 0.37 (0.03 to 1.29) | Uncertain |
Amisulpride vs. quetiapine | 0.58 (0.26 to 0.99) | Favours amisulpride | |
Ziprasidone vs. quetiapine | 0.89 (0.63 to 1.12) | Uncertain | |
Sertindole vs. quetiapine | 0.96 (0.62 to 1.22) | Uncertain | |
Sulpiride vs. quetiapine | 0.99 (0.56 to 1.28) | Uncertain | |
Olanzapine vs. quetiapine | 0.99 (0.77 to 1.17) | Uncertain | |
Fluphenazine vs. quetiapine | 1.00 (0.47 to 1.33) | Uncertain | |
Quetiapine vs. haloperidol | 0.98 (0.73 to 1.18) | Uncertain | |
Quetiapine vs. risperidone | 0.97 (0.74 to 1.14) | Uncertain | |
Quetiapine vs. trifluoperazine | 0.95 (0.44 to 1.27) | Uncertain | |
Quetiapine vs. chlorpromazine | 0.92 (0.74 to 1.06) | Uncertain | |
Quetiapine vs. thioridazine | 0.89 (0.41 to 1.18) | Uncertain | |
Quetiapine vs. clozapine | 0.82 (0.65 to 0.96) | Favours quetiapine | |
Quetiapine vs. levomepromazine | 0.81 (0.33 to 1.09) | Uncertain | |
Leucht et al. (2023)14 SR with NMA | Aripiprazole vs. quetiapine | 0.53 (0.33 to 0.93) | Favours aripiprazole |
Lurasidone vs. quetiapine | 0.73 (0.21 to 2.09) | Uncertain | |
Ziprasidone vs. quetiapine | 0.78 (0.54 to 1.12) | Uncertain | |
Haloperidol vs. quetiapine | 0.78 (0.47 to 1.27) | Uncertain | |
Amisulpride vs. quetiapine | 0.82 (0.43 to 1.48) | Uncertain | |
Asenapine vs. quetiapine | 0.85 (0.50 to 1.37) | Uncertain | |
Perphenazine vs. quetiapine | 0.92 (0.64 to 1.29) | Uncertain | |
Risperidone vs. quetiapine | 0.93 (0.67 to 1.26) | Uncertain | |
Quetiapine vs. paliperidone | 0.88 (0.33 to 1.99) | Uncertain | |
Quetiapine vs. zotepine | 0.69 (0.24 to 1.61) | Uncertain | |
Quetiapine vs. olanzapine | 1.02 (0.75 to 1.36) | Uncertain |
CI = confidence interval; NMA = network meta-analysis; RR = relative risk; SR = systematic review; vs. = versus.
Table 19: Summary of Findings by Outcome — Akathisia
Study citation and study design | Interventions vs. comparators | Results RR (95% CI) | Notes |
|---|---|---|---|
Dong et al. (2024)13 SR with NMA | No NMA for this outcome | — | — |
Leucht et al. (2023)14 SR with NMA | Paliperidone vs. quetiapine | 0.85 (0.40 to 1.75) | Uncertain |
Amisulpride vs. quetiapine | 0.93 (0.44 to 1.94) | Uncertain | |
Quetiapine vs. aripiprazole | 0.93 (0.49 to 1.75) | Uncertain | |
Quetiapine vs. risperidone | 0.77 (0.43 to 1.37) | Uncertain | |
Quetiapine vs. perphenazine | 0.77 (0.39 to 1.46) | Uncertain | |
Quetiapine vs. ziprasidone | 0.72 (0.38 to 1.31) | Uncertain | |
Quetiapine vs. haloperidol | 0.43 (0.23 to 0.81) | Favours quetiapine | |
Quetiapine vs. asenapine | 0.40 (0.17 to 0.86) | Favours quetiapine | |
Quetiapine vs. lurasidone | 0.22 (0.05 to 0.80) | Favours quetiapine | |
Quetiapine vs. olanzapine | 1.03 (0.58 to 1.79) | Uncertain |
CI = confidence interval; NMA = network meta-analysis; RR = relative risk; SR = systematic review; vs. = versus.
Table 20: Summary of Findings by Outcome — Increased Prolactin Levels
Study citation and study design | Interventions vs. comparators | Results MD (95% CI) | Notes |
|---|---|---|---|
Dong et al. (2024)13 SR with NMA | Quetiapine vs. ziprasidone | −5.90 (−20.63 to 8.83) | Uncertain |
Quetiapine vs. clozapine | −6.82 (−15.48 to 1.83) | Uncertain | |
Quetiapine vs. fluphenazine | −10.76 (−29.29 to 7.78) | Uncertain | |
Quetiapine vs. olanzapine | −13.19 (−21.95 to −4.43) | Favours quetiapine | |
Quetiapine vs. chlorpromazine | −20.57 (−32.74 to −8.39) | Favours quetiapine | |
Quetiapine vs. haloperidol | −23.96 (−35.92 to −12.00) | Favours quetiapine | |
Quetiapine vs. risperidone | −34.24 (−43.51 to −24.96) | Favours quetiapine | |
Leucht et al. (2023)14 SR with NMA | Olanzapine vs. quetiapine | 3.20 (−9.39 to 15.79) | Pairwise MA; NS |
Quetiapine vs. lurasidone | −1.30 (−19.41 to 16.81) | Pairwise MA; NS | |
Quetiapine vs. ziprasidone | −4.80 (−17.56 to 7.96) | Pairwise MA; NS | |
Quetiapine vs. perphenazine | −9.70 (−22.51 to 3.11) | Pairwise MA; NS | |
Quetiapine vs. risperidone | −24.70 (−37.41 to −11.99) | Pairwise MA; favours quetiapine |
CI = confidence interval; MA = meta-analysis; MD = mean difference; NMA = network meta-analysis; NS = not statistically significant; QTc = QT interval; SR = systematic review; vs. = versus.
Table 21: Summary of Findings by Outcome — Weight Gain
Study citation and study design | Interventions vs. comparators | Results MD (95% CI) | Notes |
|---|---|---|---|
Dong et al. (2024)13 SR with NMA | Ziprasidone vs. quetiapine | −1.21 (−3.05 to 0.63) | Uncertain |
Haloperidol vs. quetiapine | −0.93 (−2.33 to 0.46) | Uncertain | |
Fluphenazine vs. quetiapine | −0.71 (−4.57 to 3.15) | Uncertain | |
Chlorpromazine vs. quetiapine | −0.50 (−2.13 to 1.13) | Uncertain | |
Quetiapine vs. levomepromazine | 0.30 (−11.96 to 12.56) | Uncertain | |
Quetiapine vs. amisulpride | −1.18 (−3.64 to 1.29) | Uncertain | |
Quetiapine vs. risperidone | −1.28 (−2.79 to 0.23) | Uncertain | |
Quetiapine vs. sertindole | −1.88 (−4.10 to 0.34) | Uncertain | |
Quetiapine vs. olanzapine | −2.68 (−4.14 to −1.21) | Favours quetiapine | |
Quetiapine vs. clozapine | −2.70 (−4.17 to −1.23) | Favours quetiapine | |
Leucht et al. (2023)14 SR with pairwise NMA | Ziprasidone vs. quetiapine | −1.23 (−3.64 to 1.18) | Pairwise MA; NS |
Perphenazine vs. quetiapine | −1.41 (−3.82 to 1.00) | Pairwise MA; NS | |
Lurasidone vs. quetiapine | −0.50 (−3.19 to 2.19) | Pairwise MA; NS | |
Quetiapine vs. risperidone | 0.14 (−2.20 to 2.48) | Pairwise MA; NS | |
Quetiapine vs. olanzapine | −3.76 (−6.10 to −1.42) | Pairwise MA; favours quetiapine |
CI = confidence interval; MA = meta-analysis; MD = mean difference; NMA = network meta-analysis; NS = not statistically significant; SR = systematic review; vs. = versus.
Table 22: Summary of Findings by Outcome — QTc Prolongation
Study citation and study design | Interventions vs. comparators | Results MD (95% CI) | Notes |
|---|---|---|---|
Dong et al. (2024)13 SR with NMA | Chlorpromazine vs. quetiapine (1 RCT) | 19.80 (12.10 to 27.50) | Pairwise MA; More frequent with chlorpromazine |
Leucht et al. (2023)14 SR with NMA | Paliperidone vs. quetiapine | −7.40 (−13.19 to −1.62) | More frequent with quetiapine |
Risperidone vs. quetiapine | −5.30 (−10.21 to −0.40) | More frequent with quetiapine | |
Olanzapine vs. quetiapine | −5.18 (−9.81 to −0.55) | More frequent with quetiapine | |
Asenapine vs. quetiapine | −4.78 (−9.92 to 0.36) | Uncertain | |
Perphenazine vs. quetiapine | −4.50 (−9.90 to 0.90) | Uncertain | |
Ziprasidone vs. quetiapine | −4.47 (−9.32 to 0.37) | Uncertain | |
Amisulpride vs. quetiapine | −0.18 (−8.41 to 8.05) | Uncertain | |
Quetiapine vs. lurasidone | −3.20 (−10.22 to 3.82) | Uncertain |
CI = confidence interval; MA = meta-analysis; NMA = network meta-analysis; RCT = randomized controlled trial; RR = relative risk; SR = systematic review; vs. = versus.
Table 23: Summary of Findings by Outcome — Depressive Symptoms
Study citation and study design | Interventions vs. comparators | Results SMD (95% CI) | Notes |
|---|---|---|---|
Dong et al. (2024)13 SR with NMA | No NMA for this outcome | — | — |
Leucht et al. (2023)14 SR with NMA | Lurasidone vs. quetiapine | −0.31 (−0.61 to 0.00) | Uncertain |
Olanzapine vs. quetiapine | −0.01 (−0.18 to 0.16) | Uncertain | |
Quetiapine vs. perphenazine | −0.03 (−0.22 to 0.17) | Uncertain | |
Quetiapine vs. aripiprazole | −0.03 (−0.28 to 0.22) | Uncertain | |
Quetiapine vs. risperidone | −0.09 (−0.26 to 0.09) | Uncertain | |
Quetiapine vs. amisulpride | −0.10 (−0.34 to 0.13) | Uncertain | |
Quetiapine vs. ziprasidone | −0.13 (−0.32 to 0.06) | Uncertain | |
Quetiapine vs. asenapine | −0.15 (−0.38 to 0.08) | Uncertain | |
Quetiapine vs. haloperidol | −0.15 (−0.40 to 0.10) | Uncertain | |
Quetiapine vs. paliperidone | −0.24 (−0.49 to 0.01) | Uncertain |
CI = confidence interval; NMA = network meta-analysis; SMD = standardized mean difference; SR = systematic review; vs. = versus.
Table 24: Summary of Findings by Outcome — Other Side Effects
Study citation and study design | Interventions vs. comparators | Results RR (95% CI) or % or mean change from baseline | Notes |
|---|---|---|---|
Sherzad Qadir et al. (2023)15 SR with MA | Aripiprazole vs. quetiapine | Concentration difficulties: 1.10 (0.49 to 2.48) | NS |
Increased fatigability: 0.76 (0.58 to 1.01) | NS | ||
Sleepiness: 0.58 (0.45 to 0.75) | P < 0.001; more frequent with quetiapine | ||
Depression: 2.11 (0.58 to 7.66) | NS | ||
Restlessness: 2.05 (0.42 to 9.91) | NS | ||
Increased duration of sleep: 0.53 (0.36 to 0.78) | P = 0.001; more frequent with quetiapine | ||
Rigidity: 1.36 (0.60 to 7.29) | NS | ||
Tremors: 3.07 (1.07 to 8.77) | P = 0.04; more frequent with aripiprazole | ||
Increased salivation: 0.72 (0.35 to 1.47) | NS | ||
Constipation: 0.60 (0.31 to 1.17) | NS | ||
Vertigo: 4.81 (0.60 to 38.41) | NS | ||
Amenorrhea: 5.33 (0.96 to 29.48) | NS | ||
Galactorrhea: 0.10 (0.01 to 0.78) | P = 0.03; more frequent with quetiapine | ||
Diminished sexual desire: 0.62 (0.30 to 1.26) | NS | ||
Orgasmic dysfunction: 0.34 (0.06 to 1.82) | NS | ||
Erectile dysfunction: 0.20 (0.07 to 0.56) | P = 0.002; more frequent with quetiapine | ||
Ejaculatory dysfunction: 0.52 (0.10 to 2.58) | NS | ||
Weight gain: 1.10 (0.84 to 1.44) | NS | ||
Memory impairment: 2.05 (0.42 to 9.91) | NS | ||
Quetiapine vs. ziprasidone | Concentration difficulties:0.62 (0.35 to 1.11) | NS | |
Increased fatigability: 1.14 (0.86 to 1.50) | NS | ||
Sleepiness: 1.22 (0.98 to 1.52) | NS | ||
Memory impairment: 0.39 (0.81 to 1.86) | NS | ||
Depression: 0.38 (0.10 to 1.37) | NS | ||
Restlessness: 0.39 (0.08 to 1.86) | NS | ||
Increased duration of sleep: 1.05 (0.71 to 1.56) | NS | ||
Rigidity: 0.19 (0.04 to 0.84) | NS | ||
Tremors: 0.77 (0.22 to 2.64) | NS | ||
Increased salivation: 2.21 (0.29 to 16.63) | NS | ||
Constipation: 1.81 (0.58 to 3.70) | NS | ||
Vertigo: 0.13 (0.02 to 0.99) | P = 0.05; more frequent with ziprasidone | ||
Amenorrhea: 0.11 (0.02 to 0.50) | P = 0.006; more frequent with ziprasidone | ||
Galactorrhea: 1.16 (0.34 to 4.02) | NS | ||
Diminished sexual desire: 1.56 (0.74 to 3.29) | NS | ||
Orgasmic dysfunction: 0.77 (0.22 to 2.64) | NS | ||
Erectile dysfunction: 1.17 (0.45 to 3.00) | NS | ||
Ejaculatory dysfunction: 0.91 (0.35 to 2.35) | NS | ||
Weight gain: 1.49 (1.15 to 1.94) | NS | ||
Olanzapine vs. quetiapine | Weight gain: 1.34 (1.15 to 1.56) | P < 0.001; more frequent with olanzapine | |
Sleepiness: 0.90 (0.75 to 1.08) | NS | ||
Increased duration of sleep: 0.80 (0.61 to 1.05) | NS | ||
Akinesia: 0.62 (0.18 to 2.14) | NS | ||
Constipation: 0.71 (0.39 to 1.30) | NS | ||
Galactorrhea: 4.84 (0.56 to 42.07) | NS | ||
Diminished sexual desire: 1.02 (0.70 to 1.49) | NS | ||
Orgasmic dysfunction: 1.05 (0.62 to 1.79) | NS | ||
Risperidone vs. quetiapine | Weight gain: 1.11 (0.88 to 1.41) | NS | |
Sleepiness: 0.76 (0.55 to 1.05) | NS | ||
Increased duration of sleep: 0.54 (0.32 to 0.91) | P = 0.02; more frequent with quetiapine | ||
Akinesia: 1.06 (0.73 to 1.54) | NS | ||
Constipation: 0.86 (0.50 to 1.46) | NS | ||
Galactorrhea: 5.96 (0.72 to 49.02) | NS | ||
Orgasmic dysfunction: 1.22 (0.74 to 2.03) | NS | ||
Kim et al. (2024)16 RCT | Lurasidone vs. quetiapine | Akathisia: 22.6% vs. 15.4% | NS |
Dizziness: 2.9% vs. 8.7% | NS | ||
Somnolence: 2.0% vs. 7.7% | NS | ||
Tremor: 6.9% vs. 2.9% | NS | ||
Nausea: 16.7% vs. 2.9% | P = 0.001; more frequent with lurasidone | ||
Constipation: 4.9% vs. 9.6% | NS | ||
Anxiety: 6.9% vs. 2.9% | NS | ||
Blood prolactin increased: 7.8% vs. 1.9% | P = 0.048; more frequent with lurasidone | ||
Muscle rigidity: 5.9% vs. 1% | NS | ||
Weight: –0.24 kg vs. 1.65 kg | P < 0.001; significant increase with quetiapine | ||
Serum glucose levels: 1.69 mg/dL vs. 2.77 mg/dL | P < 0.001; significant higher with quetiapine | ||
Total cholesterol: –3.92 mg/dL vs. 11.13 mg/dL | P = 0.040; significant higher with quetiapine | ||
HDL-C: 0.06 mg/dL vs. −0.68 mg/dL | NS | ||
LDL-C: –4.84 mg/dL vs. 5.32 mg/dL | P = 0.032; significant higher with quetiapine | ||
Triglyceride: 0.63 mg/dL vs. 24.21 mg/dL | P = 0.033; significant higher with quetiapine | ||
ECG; EPS; Suicidal ideation and behaviour | NS |
CI = confidence interval; ECG = electrocardiography; EPS = extrapyramidal side effects; HDL-C = high-density lipoprotein-cholesterol; LDL-C = low-density lipoprotein; MA = meta-analysis; NS = not statistically significant; RR = relative risk; SMD = standardized mean difference; RCT = randomized controlled trial; SR = systematic review; vs. = versus.
Table 25: Summary of Recommendations in Included Guidelines for Schizophrenia
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
|---|---|
VA/DoD (2023)17 | |
Management of first-episode psychosis and schizophrenia — Pharmacological interventions for psychosis | |
“We recommend the use of an antipsychotic medication other than clozapine for the treatment of an acute episode in individuals with schizophrenia or first-episode psychosis who have previously responded to antipsychotic medications. The choice of antipsychotic medication should be based on an individualized evaluation that considers patient characteristics and side effect profiles of the different antipsychotic medications.” p. 35 Supporting evidence: 3 RCTs, 14 SRs and MAs, and a review of guidelines. The Working Group considered antipsychotic medications as a class rather than individually when formulating the recommendation. FGAs are more prone to produce persistent EPS, while SGAs are less likely than FGAs to cause EPS but might be associated with increased risk of weight gain and other metabolic abnormalities, including hyperlipidemias and type 2 diabetes mellitus. Therefore, the choice of antipsychotic medication should be based on an individualized evaluation that considers patient-specific characteristics and preferences and the side effect profiles of the medications. | Strength: Strong for Category: Reviewed, newly added |
“We recommend the use of an antipsychotic medication for the maintenance treatment of schizophrenia to prevent relapse and hospitalization in individuals with schizophrenia who have responded to treatment. Choice of antipsychotic medication should be based on an individualized evaluation that considers patient-specific characteristics and side effect profiles of the different antipsychotic medications.” p. 35 Supporting evidence: 8 SRs, 3 RCTs The Working Group considered antipsychotic medications as a class, rather than considering each medication individually. The choice of antipsychotic medication should be based on an individualized evaluation that considers individual characteristics, including culturally influenced beliefs about mental illness and medication, and preferences and the side effect profiles of the different antipsychotic medications. | Strength: Strong for Category: Reviewed, newly added |
“We suggest a trial of another antipsychotic medication for individuals with schizophrenia who do not respond to (or tolerate) an adequate trial of an antipsychotic medication. Choice of antipsychotic medication should be based on an individualized evaluation that considers patient-specific characteristics and side effect profiles of the different antipsychotic medications.” p. 36 Supporting evidence: 13 SRs, 2 RCTs, 1 case-control study, and 1 cohort study The Working Group’s confidence in the quality of the evidence was very low. However, the benefits of monotherapy outweighed the potential harm of no medication, polypharmacy, or continuing a medication with significant adverse events. Choice of antipsychotic medication should be based on an individualized evaluation that considers patient-specific characteristics and side effect profiles of the different antipsychotic medications. | Strength: Weak for Category: Reviewed, newly added |
JSNPP (2021)18 | |
Which antipsychotics are recommended for the treatment of first-episode psychosis? | |
“SGAs are recommended over FGAs.” p. 276 “SGAs are the better choice for treatment of first-episode psychosis.” p. 277 Supporting evidence: 2 SRs, 10 RCTs, 1 guideline, 1 cohort study Both short-term and long-term studies showed that SGAs had a low discontinuation rate due to side effects and tended to have a lower all-cause of discontinuation. | Degree of recommendation: 2 Strength of evidence: A |
“No specific drugs are recommended when selecting SGAs.” p. 276 “It is recommended to choose the specific SGA after considering the individual factors in each case.” p. 277 Supporting evidence: 2 SRs, 9 RCTs, and 1 cohort study There are no MAs that directly compare SGAs, and it was not possible to strictly define a drug’s relative superiority or inferiority. There are RCTs and open-label trials of SGAs for first-episode psychosis, but it is difficult to establish a ranking among drugs because there are no RCTs or network meta-analyses which directly compared all SGAs. However, meta-analyses which examine the efficacy and safety of SGAs and FGAs suggest that SGAs should be prioritized for first-episode psychosis. | Degree of recommendation: 2 Strength of evidence: D |
What is the optimal dose of antipsychotics for first-episode psychosis? | |
“Quetiapine has been shown to be effective at 311.4-506 mg/d.” p. 278 Supporting evidence: 5 RCTs The average dose in 2 trials, which showed efficacy with short-term (6 to 12 weeks) administration, was 358.3 to 413.8 mg/d. The average dose in 3 trials, which showed efficacy with long-term (1 year) administration, was 311.4 to 506 mg/d. | Degree of recommendation: NR Strength of evidence: C |
“Treatment discontinuation rates (of quetiapine) tended to be higher than with other antipsychotics in long-term administration trials.” p. 278 Supporting evidence: 3 RCTs The all-cause of treatment discontinuation rate of quetiapine in long-term trials was 53% to 82.3% and tended to be higher than for other antipsychotics. | Degree of recommendation: NR Strength of evidence: B |
What is the optimal period for determining the therapeutic response of antipsychotics in first-episode psychosis? | |
“Approximately 60%-70% of patients may respond to treatment by 2-4 weeks after starting treatment with antipsychotics for first-episode psychosis, but patients may respond after this period as well. Therefore, it is desirable to wait at least 2-4 weeks after the start of treatment to determine the response to treatment. However, increasing the dose while paying attention to side effects may be considered before the 2 to 4-week period if the response to treatment is insufficient at low doses.” p. 280 Supporting evidence: 2 guidelines, 1 review, 4 observational studies Many treatment guidelines for acute schizophrenia with multiple episodes recommend an effect decision period of 4 to 6 weeks. However, treatment response by 2 to 4 weeks after starting treatment has been suggested in different studies, which showed that about 60% to 705 of patients with first-episode psychosis may have a treatment response by 2 to 4 weeks. | Degree of recommendation: 2 Strength of evidence: D |
What is the optimal treatment duration for antipsychotics for preventing the recurrence of first-episode psychosis? | |
“Continuing the administration of antipsychotics for at least one year is recommended for preventing the recurrence of first-episode psychosis.” p. 281 Supporting evidence: SR, 3 RCTs The SR reported that antipsychotics had a significant recurrence prevention effect relative to placebos over a half-year to 1-year timespan. Evidence from additional RCTs also supported continued antipsychotic treatment for as long as possible when remission of symptoms is first seen in first-episode psychosis. | Degree of recommendation: 1 Strength of evidence: A |
Which is more appropriate, increasing the dose of the current antipsychotic or switching to another one? | |
“It is desirable to attempt to increase the dose rather than switching the antipsychotic during at the time of the recurrence/relapse of schizophrenia.” p. 282 Supporting evidence: 4 guidelines Many guidelines recommend increasing doses to the maximum level while confirming adherence and side effects and observing for a sufficient period before switching. | Degree of recommendation: 2 Strength of evidence: D |
Which antipsychotics have evidence of usefulness and recommended dose at the time of recurrence/relapse of schizophrenia? | |
“Quetiapine is effective at over 250 mg/d and may be effective even at over 150 mg/d. Certainty of evidence for efficacy is weak to moderate, but tolerability is high” p. 284 Supporting evidence: 4 RCTs One RCT showed a higher efficacy than placebo at doses of more than 150 mg/d, and 1 RCT showed a higher efficacy than placebo at doses of more than 250 mg/d. However, the remaining 2 RCTs did not show any differences from placebo at doses of 300 mg/d to 800 mg/d. | Degree of recommendation: NR Strength of evidence: B, C, A |
Which antipsychotics are favourable for reducing the relapse rate or for continuing treatment in the maintenance phase? | |
“It is desirable to select SGAs over FGAs. There is insufficient evidence regarding comparisons between SGAs. No recommendations are made for drug selection since factors of each case need to be considered.” P. 289 Supporting evidence: 1 SR, 2 RCTs A meta-analysis that compared the relapse prevention effects of FGAs and SGAs. There were no significant differences between the 2 groups for discontinuation due to all reasons, discontinuation due to side effects, and adherence. However, SGAs tended to show superior values for discontinuation due to all reasons and discontinuations due to side effects. There are only a few RCTs that directly compared individual SGAs, and there is little evidence on which drug is superior. | Degree of recommendation: 2 Strength of evidence: B |
EPS = extrapyramidal symptoms; FGA = first-generation antipsychotics; JSNPP = Japanese Society of Neuropsychopharmacology; MA = meta-analysis; NR = not reported; RCT = randomized controlled trial; SGAs = second-generation antipsychotics; SR = systematic review; VA/DoD = Veterans Affairs/Department of Defense.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.