Drugs, Health Technologies, Health Systems
Health Technology Review
Automated Chest Compression Devices
Key Messages
What Is the Issue?
People who experience cardiac arrest need immediate care. Cardiopulmonary resuscitation (CPR), performed manually by a human rescuer, is a first line of treatment.
Automated chest compression devices, also known as mechanical CPR devices, are designed to deliver high-quality, consistent compressions and may be of particular interest in settings with limited human rescuers or long travel times in emergency vehicles. However, whether these devices are more clinically or cost-effective than manual chest compressions is unclear.
What Did We Do?
To inform decisions about the use of automated chest compression devices for chest compressions (described as “automated chest compressions” in this report) compared to manual chest compressions, Canada’s Drug Agency (CDA-AMC) conducted a Rapid Review to identify and summarize the literature about the clinical and cost-effectiveness of automated chest compression devices in people of any age. We also aimed to identify evidence-based recommendations for the use of automated chest compression devices.
We searched key resources, including journal citation databases, and conducted a focused internet search for relevant evidence published since 2020. Two reviewers screened articles for inclusion based on predefined criteria, and 1 reviewer critically appraised the included studies and narratively summarized the findings.
What Did We Find?
We identified 4 systematic reviews (SRs) that examined the clinical effectiveness or safety of automated chest compressions via AutoPulse or Lund University Cardiopulmonary Assist System (LUCAS) devices compared to manual chest compressions, and 2 guidelines with recommendations for the use of automated chest compression devices overall. We did not find information for other devices licensed for sale in Canada. We did not find economic evaluations on the cost-effectiveness of automated chest compression devices.
Clinical evidence showed mixed results on survival, neurologic outcomes, and return to spontaneous circulation between automated chest compressions and manual chest compressions, and a potential increase in harms with the use of these devices. However, these findings are based on heterogeneous evidence of variable quality and should be interpreted with caution.
Evidence-based guidelines do not recommend the routine use of automated chest compression devices. They indicate that these devices could be applied under specific circumstances, such as when high-quality compressions are impractical or a danger to health care workers, provided professionals are trained and have experience with the device.
Evidence was largely based on studies conducted outside of Canada, making the generalizability of the evidence unclear. One primary study found in 3 of the 4 SRs had a population from Canada, and no other clinical evidence was from Canada. No evidence-based guidelines were found from Canadian organizations.
Most of the evidence did not include details about study participant demographics or dimensions of diversity or information specifically for rural, remote, territorial hospital, nurse-led hospital, small community, or tertiary care settings. The applicability of the evidence is unknown, including the potential benefits or harms in people with different sexes or genders; different ethnic, religious, educational, socioeconomic, or cultural backgrounds; or with limited access to health care services or in resource-limited settings.
What Does This Mean?
Health care professionals can consider following the recommendations from evidence-based guidelines, which do not encourage the routine use of automated chest compression devices, except under specific circumstances. This aligns with the heterogeneous clinical evidence identified from the included SR.
Because there was no evidence found on cost-effectiveness or information on the clinical effectiveness for people with different sexes or genders; people from different ethnic, religious, educational, socioeconomic, or cultural backgrounds in Canada, or contexts such as rural, remote, or low-staff settings, decision-makers may wish to consider whether the potential benefits and harms from the evidence in this report are applicable to their local context before more high-quality evidence for Canadian settings is available.
Abbreviations
AE
adverse event
CI
confidence interval
CPR
cardiopulmonary resuscitation
IHCA
in-hospital cardiac arrest
ILCOR
International Liaison Committee on Resuscitation
LUCAS
Lund University Cardiopulmonary Assist System
MA
meta-analysis
OHCA
out-of-hospital cardiac arrest
RCT
randomized controlled trial
ROSC
return of spontaneous circulation
SES
socioeconomic status
SR
systematic review
Key Terminology
Ethnicity: “A socially defined category or membership of people who may share a nationality, heritage, language, culture, and/or religion.”1
Equity-deserving: “Groups of people who have been historically disadvantaged and under-represented. These groups include but are not limited to the 4 designated groups in Canada – women, racialized groups, Indigenous Peoples, and people with disabilities — and people in the 2SLGTBQ+ community/people with diverse gender identities and sexual orientations.”2
Gender: “Gender can refer to the individual and/or social experience of being a man, a woman, or neither. Social norms, expectations and roles related to gender vary across time, space, culture, and individuals.”3
Health equity: “Equity is the absence of unfair, avoidable or remediable differences among groups of people, whether those groups are defined socially, economically, demographically, or geographically or by other dimensions of inequality (e.g., sex, gender, ethnicity, disability, or sexual orientation). Health is a fundamental human right. Health equity is achieved when everyone can attain their full potential for health and well-being. Health and health equity are determined by the conditions in which people are born, grow, live, work, play and age, as well as biological determinants. Structural determinants (political, legal, and economic) with social norms and institutional processes shape the distribution of power and resources determined by the conditions in which people are born, grow, live, work, play and age.”4
Indigenous: The term “Indigenous” is used to describe people and communities who identify with and have historical claim as “First Peoples” who have been on these lands (colonially known as Canada and the US) since time immemorial. Indigenous Peoples within Canada often refers to people who belong to First Nations, Inuit, and Métis communities; however, we acknowledge that all Indigenous communities are widely heterogenous having distinct social, economic, and political systems, as well as distinct language(s), cultures, and beliefs. In addition, we acknowledge that the term “Indigenous” may also not align with how community members self-identify and that their multilayered identities may include (but are not limited to) “nation,” “territory,” “family,” “band,” or “Native.” The term “Indigenous” is commonly used within the context of Canada, but some of the identified literature uses a variety of terms commonly accepted within their jurisdiction (i.e., the US, Australia).5,6
PROGRESS-Plus: “An acronym used to identify characteristics that stratify health opportunities and outcomes. PROGRESS refers to: place of residence, race/ethnicity/culture/language, occupation, gender/sex, religion, education, socioeconomic status, social capital. Plus refers to: (1) personal characteristics associated with discrimination (e.g., age, disability), (2): features of relationships (e.g., smoking parents, excluded from school), (3) time-dependent relationships (e.g., leaving the hospital, respite care, other instances where a person may be temporarily at a disadvantage).”7
Racialized: “A person or group of people categorized according to ethnic or racial characteristics and subjected to discrimination on that basis.”8
Racism: “Racism is the belief that a group of people are inferior based on the colour of their skin or due to the inferiority of their culture or spirituality. It leads to discriminatory behaviours and policies that oppress, ignore or treat racialized groups as ‘less than’ non-racialized groups. One result of racism is substantive inequity — a state in which racialized groups do not have equitable outcomes, or equitable opportunities, to non-racialized groups. This is systemic racism — where acceptance of these discriminatory and prejudicial practices has become normalized across our society and institutions.”9
Remote: “Statistics Canada has developed an index of remoteness that ranges from 0 (least remote) to 1 (most remote) for every municipality (census subdivision) in Canada.… The index of remoteness assigns a value to each municipality based on geographic proximity to urban areas (service and population centres) and on the population size of those urban areas. Remoteness is an important determinant of socioeconomic and health outcomes and is consequently an essential indicator for delivery of policies and programs.… Although most municipalities in the three territories are classified as remote, they are also home to urban centres, which are concentrated in 12 municipalities: Whitehorse in Yukon; Yellowknife, Hay River, Inuvik and Fort Smith in Northwest Territories; and Iqaluit, Rankin Inlet, Arviat, Baker Lake, Cambridge Bay, Kugluktuk and Gjoa Haven in Nunavut.”10
Rural: “The rural area of Canada is the area that remains after the delineation of population centres using current census population data. Within rural areas, population densities and living conditions can vary greatly. Included in rural areas are: small towns, villages, and other populated places with less than 1,000 population according to the current census; rural areas of census metropolitan areas and census agglomerations that may contain estate lots, as well as agricultural, undeveloped and non-developable lands; agricultural lands; remote and wilderness areas.”11
Sex: “The classification of people as male, female, or intersex. Sex is typically assigned at birth and is based on an assessment of one’s reproductive systems, hormones, chromosomes, and other physical characteristics.”1,3
Research Questions
What is the clinical effectiveness and safety of automated chest compressions compared to manual chest compression for people of any age requiring chest compressions?
What is the cost-effectiveness of automated chest compressions compared to manual chest compression for people of any age requiring chest compressions?
What are the evidence-based guidelines regarding the use of automated chest compression devices for people of any age requiring chest compressions?
Context and Policy Issues
What Is Cardiac Arrest?
Cardiac arrest is when cardiac activity stops suddenly in a person who then loses circulation, stops breathing, and becomes unresponsive.12 There are several causes of cardiac arrest, such as coronary artery disease, heart failure, a heart attack, hypertrophic cardiomyopathy (i.e., heart enlargement), blood clots in the lungs, injuries, drowning, or poisoning, including poisoning related to the ongoing drug poisoning crisis.13-15 Cardiac arrest can be fatal if care is not provided immediately by, for example, administering CPR, cardiac pacing (i.e., using a pacemaker to stimulate electric heart activity), defibrillation (i.e., sending shocks to the heart to restore regular rhythm), or cardioversion (i.e., electrical treatment for irregular heartbeats [arrythmias]).12,13,16,17 CPR is a first line of treatment performed manually by a human rescuer who compresses the patient’s chest to help blood flow to their organs.12,18
A 2024 report by the Heart and Stroke Foundation of Canada revealed that there are 60,000 cardiac arrests in Canada per year, that 10% of people survive out-of-hospital cardiac arrest (OHCA), and that doing CPR and using an automated external defibrillator can double a patient’s chance of survival.14 This report also indicated that remote, rural, and Indigenous communities in Canada have challenges accessing emergency and other medical services for cardiac arrest.14
Several health inequities exist for those who need cardiac arrest treatment, and this can depend on their geographic location, gender, race, perceived socioeconomic status (SES), body size, and education. For example, there may be fewer resources for those living in rural and remote areas, including Indigenous communities in northern Canada, where there may be no access to emergency services, fewer staff and equipment, and larger distances to travel to access health care services.19
A 2024 scoping review20 of global data (which did not clearly distinguish between sex and gender) showed that, in 59% of studies, women were less likely to receive bystander CPR in public compared to men, and more or equally likely to receive bystander CPR in residential settings; there was a reluctance to assist women in Western countries because of gender stereotypes, perceived frailty of women, pregnancy, chest exposure of women, oversexualization of women’s bodies, or assumptions that women are unlikely to have cardiac arrest.
Other studies have shown that racialized people and those with lower SES are more likely to experience OHCA and less likely to survive after being discharged from hospitals, compared to people who are white and who have higher incomes.21 Data from the US has shown that bystander CPR is less likely to be performed for those who are racialized or perceived to have lower income or education, which may in part be related to structural racism, implicit bias, cultural barriers, a lack of CPR training, poor defibrillator access, or fear of financial or legal ramifications.21,22
What Are Automated Chest Compression Devices?
First developed in the 1960s, automated chest compression devices, also referred to as mechanical chest compression devices or mechanical CPR devices, were designed to deliver high-quality chest compressions to those experiencing cardiac arrest as an alternative to receiving chest compressions from a human rescuer.23,24 This may be needed if there is a lack of human personnel, human rescuers become fatigued or experience challenges in moving emergency vehicles, prolonged CPR is required, or rescuers have other tasks to perform.23 There are now devices that not only assist with chest compressions but can also monitor physiological data from patients and combine this with algorithmic artificial intelligence to make adjustments or provide feedback, and there are robots that can conduct chest compressions while also checking vital signs.25,26
The automated chest compression devices currently used in the health care system are generally categorized as load distributing band devices, which have a wide band that encircles the patient’s chest and constricts to deliver compressions, or piston devices that use a plunger to depress the sternum and in some cases include a suction cup to recoil the chest to its original position.27,28 Most of these devices are for use in adults or people who the device can fit around.29,30
As of February 2025, we identified the following automated chest compression devices that are licensed for sale in Canada as Class II medical devices:31
AutoPulse, load distributing (ZOLL Medical Corporation)32
EASY PULSE, combination of load distributing and piston33 (SCHILLER Americas Inc.)34
the Lifeline ARM, piston (Defibtech LLC)35
LUCAS devices such as LUCAS 2 and LUCAS 3, piston (Stryker Medical)36
Other devices might be licensed in Canada but were not identified.
Why Is It Important to Do This Review?
Given that cardiac arrest is a concern in Canada with a 10th of patients surviving it out of hospital, and that there are challenges in access to emergency services for people living in rural, remote, and/or northern communities or where there is limited staff, health care workers are interested in understanding whether automated chest compression devices can provide an alternative clinical and cost-effective solution when manual CPR is difficult. A previous CDA-AMC report published in 2008 concluded that there was no evidence of benefit from the use of mechanical devices, and they did not find cost-effectiveness evidence or evidence-based guidelines.37 SRs and meta-analyses (MAs) published by others have suggested that these devices may not provide any benefit compared to manual compressions, and there is concern that their use may be associated with increased compression-induced injuries.38,39 There is substantial research on the use of these devices, but it is unclear whether this previous literature contains information specifically for rural, remote, and limited-staff settings and whether there has been new evidence published about cost-effectiveness or evidence-based guidelines released. Therefore, the current report aims to review the clinical and cost-effectiveness evidence on automated chest compression devices and summarize any recommendations on automated chest compression devices for people of any age.
Objective
To support decision-making on the use of automated chest compression devices, we conducted a Rapid Review to identify, summarize, and critically appraise available evidence on the clinical effectiveness and cost-effectiveness of automated chest compressions compared to manual compressions for people of any age. We also summarized the related guideline recommendations available for this patient population.
Methods
An information specialist conducted a customized literature search, balancing comprehensiveness with relevancy, of multiple sources and grey literature on February 5, 2025. Two reviewers screened citations and selected studies based on the inclusion criteria presented in Table 1, and 1 reviewer critically appraised and narratively summarized the included studies. Appendix 1 presents a detailed description of methods and selection criteria for included studies.
Criteria | Description |
|---|---|
Population | People (all ages) requiring chest compressions |
Intervention | Chest compression using automated chest compression devices (described as “automated chest compressions” in this report), specifically those licensed for sale in Canada, such as AutoPulse, EASY PULSE, Lifeline ARM, and LUCAS |
Comparator | Q1 to Q2: Manual chest compressions Q3: Not applicable |
Outcomes | Q1: Clinical benefits (e.g., survival, ROSC, neurologic recovery) and harms (e.g., AEs) Q2: Cost-effectiveness (e.g., cost per quality-adjusted life-year gained) Q3: Recommendations regarding best practices for automated chest compression devices (e.g., appropriate indication, longevity of use) |
Study designs | Health technology assessments, systematic reviews, economic evaluations, evidence-based guidelines |
Publication date | Since January 1, 2020 |
AE = adverse event; LUCAS = Lund University Cardiopulmonary Assist System; ROSC = return of spontaneous circulation.
Summary of Evidence
Quantity of Research Available
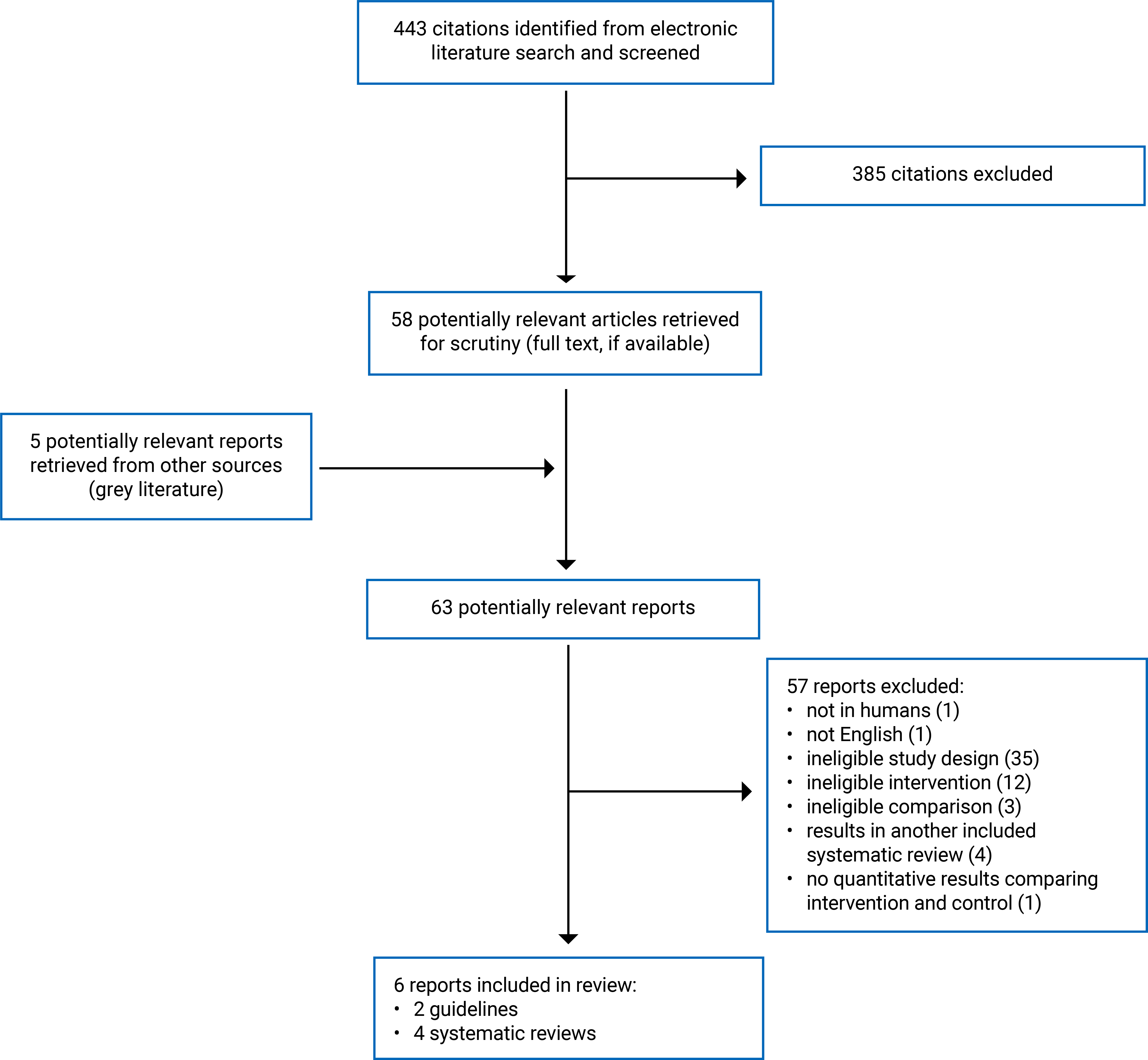
This report includes 4 SRs40-43 with clinical effectiveness information, and 2 guidelines44,45 with recommendations for the use of automated chest compression devices. No studies were found for cost-effectiveness. The authors of 1 SR40 planned to synthesize evidence on cost-effectiveness. However, no cost-effectiveness results were presented, and the authors did not disclose the reasons (i.e., lack of identified evidence or other factors).
Appendix 1 presents the PRISMA46 flow chart of study selection. Appendix 6 includes additional references of potential interest, including an SR with insufficient quantitative information for data extraction and guidance documents (not evidence-based).
Summary of Study Characteristics
Appendix 2 contains detailed characteristics of included studies.
Included Studies for Question 1: Clinical Effectiveness and Safety of Automated Chest Compression Devices
We identified 4 relevant SRs40-43 with MAs. Each SR searched at least 3 electronic literature databases from database inception to December 2023 in 2 SRs,40,43 to May 2023 in 1 SR,42 and to May 2020 in 1 SR41 (i.e., clinical evidence informing this report is based on evidence published before 2024). The SRs40-43 included data from 58 studies with substantial overlap of included primary studies across the SRs. One SR43 uniquely contributed approximately one-third of the included studies (21 unique studies) and 1 SR,41 which focused exclusively on safety outcomes (i.e., injuries), had very little overlap with the other SRs (10 unique studies). The remaining 2 SRs40,42 have substantial overlap with Zhu and Fu43 but have been included in this Rapid Review because they contributed unique studies and outcomes. A citation matrix illustrating the degree of primary study overlap is presented in Appendix 5.
Two SRs40,43 focused on adult patients experiencing OHCA, 1 of which was limited to nontraumatic cardiac arrest and also included 1 study with patients experiencing in-hospital cardiac arrest (IHCA).40 Another SR42 was also limited to OHCA and did not specify study eligibility limits based on participant age. The final included SR41 was limited to adult patients with cardiac arrest and no stated limits on the setting of that arrest. The studies included in this SR41 differed from those in other SRs: 9 of 11 included studies were in populations of nonsurvivors of cardiac arrest (compared to other SRs that included both survivors and nonsurvivors of cardiac arrest), and the outcomes were measured by autopsy or postmortem CT. Two SRs included studies comparing any automated chest compressions to manual chest compressions40,41 and 2 SRs were limited to specific devices: LUCAS41 and AutoPulse.40,41 All SRs40-43 included interventional studies (e.g., randomized controlled trials [RCTs]) and both prospective and retrospective observational studies. One SR43 presented subgroup analyses for different versions of LUCAS (i.e., LUCAS, LUCAS 2, LUCAS 3); the other SRs did not provide information regarding device versions.
The 58 relevant studies included in the 4 SRs40-43 were conducted in more than 20 countries across Asia, Oceania, Europe, and North America, were published between 2005 and 2023, and included from 30 to more than 30,000 participants. Three of the SRs40,42,43 included 1 primary study with participants from Canada and the US; when reported, all other studies were in populations outside of Canada. The populations reflected the review eligibility criteria, with the caveat that the 2 SRs included patients experiencing IHCA as a population of interest yet identified limited studies with this population (n = 2).40,41 No SR reported, for all included studies, the settings where automated devices were used for patients experiencing OHCA but, when reported, they included emergency departments and paramedic services (ambulance, helicopter transport). Twenty relevant included studies focused on AutoPulse, 31 focused on LUCAS, and 7 focused on both AutoPulse and LUCAS. No SRs had results for Lifeline ARM, and 1 SR43 included a primary study with EASY PULSE but did not provide device-specific outcomes.
Larik et al.42 reported the following participant characteristics, presenting this by study arm: mean age (ranging from 63 to 80 years), sex or gender (ranging from 54% to 83% males, where “males” was not specified as referring to sex or gender), patients with shockable cardiac rhythm (ranging from 7% to 64%), patients with witnessed cardiac arrest (ranging from 34% to 96%) and patients receiving bystander CPR (ranging from 0% to 57%). The other 3 SRs40,41,43 did not report these characteristics, and none of the SRs provided participant information for other PROGRESS-Plus7 criteria such as place of residence, disability, race, ethnicity, culture, language, occupation, religion, education, SES, or social capital.
No SRs40-43 extracted information on who administered the devices or conducted CPR, or the methods used to train staff for these procedures.
No SRs reported funding sources of included primary studies.
Clinical outcomes to address the research questions across the 4 SRs40-43 included:
Survival40,42,43 (limited in 2 reviews to specific time points)
Adverse events (AEs) including rate of overall compression-induced injuries,40,41 life-threatening injuries,41 skeletal fractures,41 visceral injuries (lung, heart, spleen, and kidney lesions),41 and other soft tissue injuries.41
Included Studies for Question 2: Guidelines for Automated Chest Compression Devices
The 2 guidelines provided recommendations for automated chest compression device use on adults.44,45 Both44,45 were from groups under the International Liaison Committee on Resuscitation (ILCOR) and had similar processes for guideline development and the involvement of ILCOR; these guidelines were for both IHCA and OHCA.
No guidelines had recommendations for rural settings, remote settings, territorial hospitals, nurse-led hospitals, small communities, or tertiary care.
Summary of Critical Appraisal
Appendix 3 contains details about the strengths and limitations of the included SRs and guidelines.
Included Studies for Question 1: Clinical Effectiveness and Safety of Automated Chest Compression Devices
We noted several strengths. SRs40-43 had clearly defined objectives, eligibility criteria, and search methods. All SRs40-43 searched at least 3 major databases, 2 SRs41,43 reported additional search methods, and all SRs provided keywords or full search strategies in the report or supplementary materials. At least 2 reviewers were involved in the study selection in all SRs, 1 SR40 reported duplicate data extraction, and another43 reported single data extraction with verification. Gao et al.41 reported funding by various grants, 3 SRs40,42,43 reported no funding for the research, and all SRs40-43 stated that the authors declared no financial or other conflicts of interest related to the research. While no SR included a list of excluded studies along with reasons for exclusion, all provided the number of studies excluded at full-text screening and broad reasons for exclusions. All SRs40-43 reported satisfactory techniques for assessing risk of bias in individual studies; this was completed by at least 2 reviewers in 2 SRs.42,43
Possible concerns were also noted across SRs. Authors of 2 SRs42,43 did not mention a review protocol and while the authors of the others40,41 mentioned registering a review protocol, in both cases the protocol was registered after review conduct began, making it difficult to confirm the degree to which methods were prespecified. Additionally, the comprehensiveness of the search strategies and search methods were unclear because SRs with similar eligibility criteria had incomplete overlap of their included primary studies. At least 2 SRs41,42 also included outcomes in their electronic search strategies, which may have limited their ability to identify relevant studies, especially for AEs, because these are inconsistently reported in titles and abstracts.
The degree, or lack of clarity about the degree, of consistency across study populations and the potential effect of heterogeneity is a primary concern across these SRs. The authors of each SR extracted and presented key variables, including study design, numbers of participants, and broad settings. However, other than 1 SR,42 reviews did not report important variables of included primary studies such as age, gender or sex distributions, or the proportion of patients with a witnessed cardiac arrest or shockable rhythm. Authors also presented little information on health equity variables, including the settings (e.g., urban or rural) or participants’ dimensions of diversity based on PROGRESS-Plus criteria.7 This lack of information makes it difficult to assess the internal validity of the MA results and the applicability of the results to varied populations. No SR presented the sources of funding for included primary studies, inhibiting the ability to assess the risk of sponsorship bias across the evidence base.
Importantly, MAs frequently combined controlled trials and observational studies, had studies that were deemed to be at a low and high risk of bias, and had inconsistent outcome definitions across studies (i.e., outcome definitions for complications and neurological outcomes were not provided for each included study). As evidenced by the study-level data from Larik et al.,42 imbalances in key factors often existed between study arms, and no SR with MAs reported using adjusted effect measures from observational studies to account for imbalances. Furthermore, many of the MAs noted high levels of heterogeneity across their included studies (both clinical and statistical). While subgroup and sensitivity analyses were conducted (by device, study design, risk of bias), statistical heterogeneity often remained moderate or high and largely unexplained. Finally, 3 of the SRs40,41,43 investigated the potential presence and impact of publication bias, but concerns exist with some of these assessments. Overall, while there appear to be strengths in the conduct of these SRs, the validity and applicability of their MA results is unclear.
Included Studies for Question 2: Guidelines For Automated Chest Compression Devices
Both guidelines44,45 clearly outlined their scope and purpose, indicated who the target users and intended population were, sought the views of the target population, explained how SRs were conducted to inform the guideline, described how the guideline was validated, provided the methods for forming recommendations, provided specific recommendations that were easy to identify with options for managing the health issue, provided explicit links between the recommendations and the supporting evidence, noted resource implications of applying the recommendations, described facilitators and barriers to its application, and addressed conflicts of interest of the guideline development group members.
One guideline45 clearly described the criteria for selecting evidence, and 1 guideline44 did not report this information. One guideline44 clearly described the strengths and limitations of the body of evidence that linked to the strength of the recommendations, and the other45 did not. A procedure for updating the guideline or monitoring the criteria was provided for 1 guideline44 and was unclear for the other.44
Neither of the guidelines provided tools to support the application of recommendations in practice. It was unclear whether any of the guideline funding bodies influenced its content.
Summary of Findings
Appendix 4 presents the main study findings.
Clinical Effectiveness and Safety of Chest Compression Devices
Four SRs40-43 provided information on the clinical effectiveness and safety of automated chest compressions versus manual compression. There was considerable overlap in the primary studies that were included in these SRs; the pooled estimates from separate reviews thus contain much of the same data (refer to Appendix 5 for details regarding overlap).
Survival
Three SRs40,42,43 compared survival outcomes between people who experienced cardiac arrest and received automated chest compressions with those who received manual compressions. MAs, often with a high degree of unexplained heterogeneity and including studies at both a high and low risk of bias, provided mixed results across survival outcomes but suggested that AutoPulse may be associated with similar survival at discharge and potentially increased survival at other time points whereas LUCAS may be associated with a similar or decreased survival at discharge compared to manual compressions. The following outcomes were reported:
Survival to hospital admission: Two SRs40,43 examined device-specific survival to hospital admission — 1 SR43 with MAs and 1 SR40 with primary study results. All but 1 relevant primary study focused on adults with OHCA (in the other, adolescents were eligible for inclusion, but study participant age ranges were not reported), using manual chest compression as the comparator. The overview of the results follows and should be interpreted with consideration of the limitations:
Automated chest compression devices (mix of AutoPulse and LUCAS within the studies):
There was no statistically significant difference in the odds of survival to admission (1 SR with MA of 2 studies).43
AutoPulse:
LUCAS:
Survival to hospital discharge: Three SRs,40,42,43 2 with MAs,42,43 included evidence for this outcome.
Automated chest compression devices (mix of AutoPulse and LUCAS within the studies):
There was no statistically significant difference in the odds of survival to discharge (1 SR with MA of 4 studies).43
AutoPulse:
LUCAS:
There were mixed results for odds of survival to discharge with LUCAS — lower odds (1 SR with MA of 9 studies)43 and no statistically significant difference (1 SR with MA of 7 studies).42
There was no statistically significant difference in the odds of survival to discharge with the use of LUCAS 2 (1 SR with 1 primary study).43
There was no statistically significant difference in the odds of survival to discharge with the use of LUCAS 3 (1 SR with MA of 2 studies).43
30-day survival:
Automated chest compression devices:
No SRs included results for this outcome for studies of mixed devices.
AutoPulse
There were higher odds of survival to 30 days with the use of AutoPulse (1 SR with results from 1 retrospective observational study deemed to be at a high risk of bias).40
LUCAS
No SRs included results for this outcome.
Other survival outcomes:
One SR40 reported data from single studies, including adjusted analyses from primary studies that were in other MAs for 4-hour and 24-hour survival with the use of AutoPulse; there were conflicting results across the outcomes.40,42,43
Neurologic Outcomes
Two SRs40,42 compared neurologic outcomes between people who experienced cardiac arrest and received automated chest compressions with those who received manual compressions. Results from 1 MA in 1 SR42 were not extracted because it included 1 large ineligible study; thus, the results of the 12 relevant primary studies from that SR are discussed. The SRs defined this outcome as a “favourable neurologic outcome” in 1 SR42 and survivors with “cerebral performance category 1” and “overall performance category 1” in the other SR40 (specific scale is not referenced in the SR) based on results from 1 relevant primary study. Neither SR presented the time points for outcome measurements.40,42 Given the variability of the study designs, outcome measurements, and risk of bias, it is difficult to draw conclusions regarding neurologic outcomes. The following is a summary:
Automated chest compression devices (AutoPulse, LUCAS, or mixed):
AutoPulse:
There were mixed results, ranging from increased to decreased odds of a favourable neurologic outcome with the use of AutoPulse (4 primary studies reported in 1 of 2 SRs).40,42 One of these primary studies (included in 1 SR42) was an RCT with 4,231 participants and was rated at a low risk of bias: it reported no statistically significant difference in the odds of a favourable neurologic outcome with AutoPulse in adults experiencing OHCA.
LUCAS:
Return of Spontaneous Circulation
Three SRs40,42,43 with MAs compared the odds of ROSC with automated chest compressions with that of manual chest compressions for patients experiencing cardiac arrest; due to variable risk of bias across included studies and high statistical heterogeneity, the MA results should be interpreted with caution.
Automated chest compression devices (AutoPulse, LUCAS, or mixed):
AutoPulse:
LUCAS:
There was no statistically significant difference in the odds of ROSC with the use of LUCAS (2 SRs with MAs of 13 studies in which the device version is not defined,42 and 1543 in which results for LUCAS 2 and LUCAS 3 are considered separately).
There was no statistically significant difference in the odds of ROSC with the use of LUCAS 2 (1 SR with 1 retrospective observational study).43
There was no statistically significant difference in the odds of ROSC with the use of LUCAS 3 (1 SR with MA of 2 studies).43
Adverse Events
Two SRs40,41 compared the compression-induced injuries of people who experienced cardiac arrest and received automated chest compressions with those who received manual compressions. One SR41 contributed most of the results for safety outcomes; it was limited to primary studies that compared AutoPulse or LUCAS to manual compressions, and 9 out of 11 included studies were conducted in populations of nonsurvivors of cardiac arrest. The safety outcomes included:
Life-threatening compression-induced injuries41
Skeletal fractures41
Visceral injuries41
Other soft tissue injuries.41
Overall and life-threatening compression-related injuries: Both SRs40,41 included an MA of the odds of compression-related injuries, and Gao et al.41 included an MA of the odds of all life-threatening injuries (not otherwise defined).
Automated chest compression devices (AutoPulse, LUCAS, or mixed):
There were higher odds of any compression-related injury with the use of automated chest compression devices (1 SR with MA of 4 studies).41
There was no statistically significant difference in the odds of a life-threatening injury with the use of automated chest compression devices, but there was high imprecision in the odds ratio estimate (95% confidence interval [CI], 0.53 to 53.16) (1 SR with MA of 3 studies).41
AutoPulse:
There was no statistically significant difference in the odds of any compression-related injury with the use of AutoPulse (1 SR with MA of 4 RCTs).40
LUCAS:
There were no results included in the SR for this outcome for LUCAS.
Skeletal fractures: One SR41 reported outcomes of skeletal fractures.
Automated chest compression devices (AutoPulse, LUCAS, or mixed):
There was no statistically significant difference in the odds of sternal fractures (MA of 11 studies; high statistical heterogeneity) or vertebral fractures (MA of 4 studies; wide CIs) with the use of automated chest compression devices.41
There was a higher odds of posterior rib fractures with the use of automated chest compression devices (MA of 5 studies).41
AutoPulse:
There were no statistically significant differences in the odds of sternal fractures (MA of 4 studies), anterolateral fractures (MA of 3 studies), or vertebral fractures (MA of 2 studies; wide 95% CI) with the use of AutoPulse.41
There were higher odds of posterior rib fractures with the use of AutoPulse (MA of 3 studies).41
LUCAS:
There was no statistically significant difference in the odds of vertebral fractures with the use of LUCAS (MA with 2 studies; wide 95% CI).41
There were higher odds of sternal fractures (MA of 8 studies), rib fractures (MA of 7 studies), and multiple (≥ 3) rib fractures (MA of 3 studies) with the use of LUCAS.41
Visceral injuries: One SR41 with MAs reported outcomes of visceral injuries. As with other analyses, 95% CIs were often wide and the heterogeneity high, even within subgroup analyses.
Automated chest compression devices (AutoPulse, LUCAS, or mixed):
There were no statistically significant differences in the odds of visceral injuries (MA of 3 studies), lung lesions (MA of 8 studies), spleen lesions (MA of 3 studies), or kidney and perirenal lesions (MA of 4 studies) with the use of automated compression devices.41
There were higher odds of heart lesions (MA of 8 studies), liver lesions (MA of 8 studies), and pneumothorax (MA of 9 studies) with the use of automated chest compression devices.41
AutoPulse:
There were no statistically significant differences in the odds of heart lesions (MA of 2 studies), liver lesions (MA of 2 studies), spleen lesions (1 retrospective cohort study), or kidney and perirenal lesions (1 retrospective cohort study; wide CI) with the use of AutoPulse.41
There were higher odds of pneumothorax with the use of AutoPulse (MA of 3 studies).41
LUCAS:
There were no statistically significant differences in the odds of lung lesions (MA of 7 studies), spleen lesions (MA of 2 studies), kidney and perirenal lesions (MA of 3 studies), or pneumothorax (MA of 7 studies) with the use of LUCAS.41
There were higher odds of heart lesions (MA of 6 studies), liver lesions (MA of 7 studies), and lesions of major vessels (MA of 4 studies) with the use of LUCAS.41
Other soft tissue injuries: Gao et al.41 also reported the odds of other soft tissue injuries.
Automated chest compression devices (AutoPulse, LUCAS, or mixed):
There were no statistically significant differences in the odds of hemothorax (MA of 6 studies; high heterogeneity) or retrosternal bleeding (MA of 5 studies) with the use of automated chest compression devices.41
There were higher odds of hemoperitoneum (MA of 3 studies) and skin lesions (MA of 5 studies) with automated chest compression devices.41
AutoPulse:
There were no statistically significant differences in the odds of hemothorax (1 retrospective cohort study) or retrosternal bleeding (1 retrospective study) with the use of AutoPulse.41
There were higher odds of hemoperitoneum (1 retrospective study) and skin lesions (1 retrospective study) with the use of AutoPulse.41
LUCAS:
There were no statistically significant differences in the odds of retrosternal bleeding (MA of 4 studies) or mediastinal hemorrhage (MA of 4 studies) with the use of LUCAS.41
There were higher odds of hemothorax (MA of 5 studies), hemoperitoneum (MA of 2 studies), and skin lesions (MA of 4 studies) with the use of LUCAS.41
Guidelines for Automated Chest Compression Devices
In general, both guidelines,44,45 which were based on evidence that was reported as weak44 or for which the overall quality of the evidence was not clearly reported,45 did not recommend the routine use of automated chest compressions, and advised considering using these devices under specific circumstances, such as:
When high-quality manual chest compression is not practical or can be dangerous for the provider44,45
When prolonged CPR is needed for patients in cardiac arrest who have hyperkalemia45
When a patient has coronary thrombosis and no sustained ROSC, and resuscitation is not futile45
When resuscitating and treating possible causes in a catheterization laboratory.45
In special circumstances for which automated chest compression devices were warranted, the guidelines recommended the following considerations for staff:
Using only trained teams who are familiar with the device to minimize interruptions while the device is being used45
Having the provider limit CPR interruptions while using and removing the device.44
These recommendations for automated chest compression devices were often considered in parallel with other health technologies or guidance not relevant for this report; the complete guidance with recommendations for all devices, settings, and circumstances can be found in the guideline publications.44,45
Neither of the guidelines had specific information for rural settings, remote settings, territorial hospitals, nurse-led hospitals, small communities, or tertiary care. However, 1 guideline44 used information from supporting evidence that listed situations with limited personnel or moving ambulances as a risk to providers.
Neither of the guidelines had specific recommendations for different sexes or genders or people with different ethnic, religious, educational, socioeconomic, or cultural backgrounds.
Limitations
Gaps in Evidence
In this Rapid Review, we found evidence on clinical effectiveness and recommendations from evidence-based guidelines; however, we did not find evidence published since 2020 on the cost-effectiveness of automated chest compression devices, representing a gap in knowledge on the value of these devices for the health care system in the current economic climate. The clinical evidence we found focused on AutoPulse and LUCAS devices; there is a gap in SR evidence for other devices such as EASY PULSE and Lifeline ARM. The included guidelines had recommendations for automated chest compression devices overall rather than specific recommendations about individual devices; it is unclear whether recommendations could differ by device type.
Within the clinical evidence, the MAs within the SRs combined primary studies that had diverse study designs, that had a range of low to high risk of bias in the primary studies, and whose effect estimates lacked adjustments for key confounders. The MAs often had high heterogeneity that could not be explained after the SR authors conducted various sensitivity analyses. The SRs primarily focused on effectiveness outcomes, and the AEs reported in the SRs were primarily based on primary studies with nonsurvivors of cardiac arrest; therefore, the risk of AEs in a population of both survivors and nonsurvivors is unclear. Across the 4 SRs,40-43 there was also limited or no information on 2 outcomes that the Core Outcome Set for Cardiac Arrest initiative47 recommends reporting for adults: health-related quality of life or survival status after 30 days. Overall, the lack of high-quality evidence and heterogeneity across primary studies make the findings difficult to interpret conclusively.
Most included SRs did not report information for various PROGRESS-Plus7 criteria (e.g., age, sex, gender, race, ethnicity, culture, language, occupation, religion, education, SES, social capital, discrimination [e.g., disability-based], or relationships), specific settings (e.g., rural settings, remote settings, territorial hospitals, nurse-led hospitals, small communities, tertiary care) or on variables that could have affected the results (e.g., patients with shockable cardiac rhythm; events during which cardiac arrest was witnessed, patients who received bystander CPR). The included guidelines44,45 also did not have recommendations that considered PROGRESS-Plus criteria. No SRs extracted information on who administered the devices or conducted CPR or the methods used to train staff for these procedures. Altogether, it is unclear whether any of these contextual factors could have explained any effects of the interventions on health outcomes or provided additional knowledge about unique settings. For example, it is unclear whether automated chest compressions could be used on people who experience frailty because of their age or disability status. Similarly, it is unclear from the evidence found in this Rapid Review whether people with different body sizes may experience automated chest compression devices differently. Because previous research20-22 has shown that whether a bystander chooses to perform CPR can be biased against a patient’s gender, race, perceived income, or educational status or a bystander’s culture, training, or fear of consequences, it is unknown whether these factors could have played a role in the research studies and understanding of the evidence.
Further, having information on the use of automated devices in settings that are remote or where there are fewer health care providers would be important for understanding if there are unique scenarios that may require training for health care providers on device use (e.g., if there are longer travel times for emergency medical services, if the division of tasks with fewer personnel is challenging, in rural or remote areas where there are potentially greater risks of AEs because of difficult terrain or smaller hospitals with fewer resources to address AEs). The lack of cost-effectiveness information for the devices overall and for specific settings also makes it difficult to know whether there may be value in providing access to these devices in low-resource settings and whether the additional costs of the devices could be worth the potential benefits to patients.
Generalizability
The SRs40-43 in this Rapid Review included evidence from more than 20 countries across Asia, Oceania, Europe, and North America, with 1 primary study reported by SRs as including participants from Canada; the generalizability of the findings to settings in Canada is unknown. Three40,41,43 of the 4 SRs and the 2 guidelines44,45 focused on adults with cardiac arrest; 1 SR42 did not specify eligibility based on participant age.42 Thus, it is unclear whether the evidence found in this Rapid Review could apply to other age groups.
Because no SRs reported on rural settings, remote settings, territorial hospitals, nurse-led hospitals, small communities, or tertiary care; on how health care teams were trained on device use; or on patient race, ethnicity, culture, language, occupation, religion, education, SES, or social capital, it is unclear what the effect of using automated chest compression devices is in these contexts and in the context of potential health inequities.
Conclusions and Implications for Decision- or Policy-Making
We conducted a Rapid Review of the evidence on the clinical effectiveness and cost-effectiveness of automated chest compressions for people of any age; we also searched for guidelines with recommendations for these populations. We found 4 SRs40-43 published between 2021 and 2024 with global evidence for automated chest compression compared to manual chest compression, and 2 evidence-based guidelines44,45 published between 2020 and 2021, from American and European organizations, with recommendations for any automated chest compression device. We did not find any eligible economic evaluations with cost-effectiveness information.
Automated Chest Compression Device Evidence
This Rapid Review found heterogeneous evidence based on studies with varying risk of bias (from low to high) for the clinical effectiveness of automated chest compressions compared to manual compressions. The identified clinical evidence on survival, neurologic outcomes, and ROSC is mixed and suggests a potential increase in compression-induced injuries.
Survival: Based on heterogeneous evidence40,42,43 that includes studies with a high risk of bias, AutoPulse may be beneficial or have no effect on survival, whereas LUCAS may be harmful or have no effect on survival.
Neurologic outcomes: There is mixed evidence40,42 on the effect of relevant devices (i.e., AutoPulse, LUCAS) on neurologic outcomes. Given the variability of the study designs, outcome measurements, and risk of bias, it is difficult to draw conclusions for this outcome.
ROSC: Based on heterogeneous evidence40,42 that includes studies with a high risk of bias, AutoPulse may be beneficial or have no effect on ROSC, whereas LUCAS may have no effect on ROSC.
AEs: Based on evidence on nonsurvivors of cardiac arrest, the use of AutoPulse or LUCAS devices may increase the risk of overall and specific compression-induced injuries and may have no effect on the risk of life-threatening injuries, and complication-induced injuries may vary by specific device type.
The evidence-based guidelines44,45 did not recommend the routine use of automated chest compression devices. They indicated that the use of these devices, often alongside other health technologies or guidance, could be considered in specific circumstances such as when high-quality chest compressions are impractical or dangerous for the rescuer; when prolonged CPR is needed for patients in cardiac arrest who have hyperkalemia; if a patient has coronary thrombosis, no sustained ROSC, and resuscitation is not futile; or in a catheterization laboratory when resuscitating and treating possible causes. Under these circumstances, guidelines recommend having trained professionals familiar with the device to limit CPR interruptions when using and removing the device. Although we did not include consensus statements in this Rapid Review, we found 148 published by the Australasian College for Emergency Medicine that had similar recommendations, namely that automated CPR devices should only be used if staff are trained and if the devices are available so that fewer staff need to be present during compressions.
This Rapid Review compares to the previous CDA-AMC report in the following ways:
Similar to previous SRs and MAs,38,39 we found evidence of harms with the use of these devices, including AEs such as compression-induced injuries.
Different from the previous CDA-AMC report,37 which did not find evidence-based guidelines, we found guidelines that recommend not using these devices routinely.
Different from previous SRs and MAs and the previous CDA-AMC report,37-39 which suggested no evidence of benefits, we found mixed and heterogenous evidence of the clinical effectiveness of these devices.
Similar to the previous CDA-AMC report,37 we found no cost-effectiveness information.
Across the included evidence in this Rapid Review, there was evidence from 1 primary study across 3 included SRs40,42,43 that had participants in Canada; however, generalizability of the evidence to the context in Canada is unclear. Most SRs did not report age, sex, or gender, and it is unclear whether the findings can be extrapolated to different populations without this information. Similarly, because there was limited information on other PROGRESS-Plus criteria,7 it is unclear whether the results are applicable to different settings (e.g., urban, rural, remote, under-staffed, and territorial hospital settings and other settings in Canada) or for equity-deserving groups based on dimensions of diversity such as age, gender, SES, education, or ethnic, religious, or cultural backgrounds.
Considerations for Future Research
To address the identified issues, further studies are needed that include the following: improvements on risk-of-bias issues reported in current primary literature (e.g., robust prospective studies); measurement of outcomes such as 30-day survival and quality of life, which are important considerations in cardiac arrest studies;47 and evidence for populations in different settings (e.g., urban, rural, remote, and under-staffed, and territorial hospital settings and other settings in Canada) or for equity-deserving groups based on dimensions of diversity such as age, gender, SES, education, or ethnic, religious, or cultural backgrounds. Previous research suggests that the longer distances that rural and remote patients need to travel results in greater travel times and potential delays in receiving the care that they need, in addition to the disparities in survival between urban and rural settings in Canada;49,50 thus, understanding the effectiveness of mechanical CPR devices in rural and remote transport contexts is important. Another research consideration in rural and remote settings in Canada, including in northern Canada, is how colder temperatures can affect automated chest compression devices and battery performance.51 Battery life may have unique considerations in this context because, for longer travel times, longer-lasting batteries or a greater supply of batteries may be needed.
Because most of the identified literature was for AutoPulse and LUCAS devices, future primary research could also address the clinical effectiveness of other devices, such as EASY PULSE and Lifeline ARM.
Although there is a large body of evidence on automated chest compression devices, including published overviews of reviews, the included SRs in this Rapid Review had substantial heterogeneity within their MAs. There is a need to reanalyze the existing literature to explore reasons for this heterogeneity and consider using adjusted analyses or subgroup analyses from existing primary data (e.g., considering variables such as whether cardiac arrest was witnessed, the proportion of patients with shockable cardiac rhythm, results by age or gender). Future SRs should be high-quality and report the funding sources of primary studies, include the rationale for how the MAs are conducted (e.g., how primary study results are combined), provide separate results for RCTs and observational studies, and extract variables that may give insights on health equity such as place of residence (e.g., urban, rural, or remote), race, ethnicity, occupation, religion, education, SES, social capital, or disability.
Although we found 2 guidelines44,45 that provided recommendations for chest compression devices overall, it is unclear whether different devices require different recommendations. Future guideline developers could consider providing recommendations for different devices, if appropriate.
Because we did not find economic evaluations published since 2020, research on cost-effectiveness is needed, taking the current economic climate into consideration.
Implications for Clinical Practice
Based on this Rapid Review, evidence-based guidelines do not recommend the routine use of automated chest compression devices except in specific scenarios. The heterogeneous clinical evidence does not provide sufficient information about patient demographics or for certain settings, there are risks of AEs from these devices, and information about the cost-effectiveness of the devices was not found. Decision-makers can use this evidence to help understand whether using automated chest compression devices provides potential clinical benefits or harms in their local context.
Clinicians and researchers may also wish to consider the following in practice: whether there are certain populations that have limited access to emergency services overall or limited access to automated devices; how health care staff can get additional specialized training on using automated devices, especially in settings with long distances and difficult terrain; how participants are selected into primary research studies and which population types are included in research based on dimensions of diversity (e.g., including women, people of different ethnic and socioeconomic backgrounds); how patient quality of life and experience outcomes are collected; and the balance of any potential benefits to patients and providers given known safety risks.
Acknowledgement
This document was externally reviewed by the following content expert, who has granted permission to be cited:
Dr. Brodie Nolan, MD, MSc, FRCPC; Emergency Physician and Trauma Team Leader (St. Michael’s Hospital), Scientist (Li Ka Shing Knowledge Institute), Assistant Professor (University of Toronto), Transport Medicine Physician and Chair, Research (Ornge)
References
1.Rainbow Health Ontario. Glossary. Accessed March 7, 2025. https://www.rainbowhealthontario.ca/news-publications/glossary/
2.Canadian Centre for Diversity and Inclusion. Glossary of IDEA terms. 2023. Accessed March 7, 2025. https://ccdi.ca/media/4005/20230509-glossary-of-idea-terms-en.pdf
3.The 519. The 519 Glossary of Terms. 2020. Accessed March 7, 2025. https://www.the519.org/education-training/glossary/
4.World Health Organization. Health equity. Accessed March 7, 2025. https://www.who.int/health-topics/health-equity#tab=tab_1
5.Public Health Ontario. Rapid review: Substance use services with, and for, Indigenous communities. 2023. Accessed March 20, 2025. https://www.publichealthontario.ca/-/media/Documents/S/2023/substance-use-services-indigenous-communities.pdf?rev=c50da5f26fea491caf6bfc937a0d9060&sc_lang=en
6.Health Standards Organization. British Columbia Cultural Safety and Humility standard (HSO 75000:2022). 2022. Accessed March 20, 2025. https://healthstandards.org/standard/cultural-safety-and-humility-standard/
7.O'Neill J, Tabish H, Welch V, et al. Applying an equity lens to interventions: using PROGRESS ensures consideration of socially stratifying factors to illuminate inequities in health. J Clin Epidemiol. 2014;67(1):56-64. doi:10.1016/j.jclinepi.2013.08.005 PubMed
8.Cochrane Methods Equity. PROGRESS-Plus. Accessed March 7, 2025. https://methods.cochrane.org/equity/projects/evidence-equity/progress-plus
9.Turpel Lafond ME. In Plain Sight: Addressing Indigenous-specific Racism and Discrimination in B.C. Health Care. 2020. Accessed March 7, 2025. https://engage.gov.bc.ca/app/uploads/sites/613/2020/11/In-Plain-Sight-Summary-Report.pdf
10.Statistics Canada. Population growth in Canada’s rural areas, 2016 to 2021. 2022. Accessed March 27, 2025. https://www12.statcan.gc.ca/census-recensement/2021/as-sa/98-200-x/2021002/98-200-x2021002-eng.cfm
11.Statistics Canada. Rural area (RA). 2021. Accessed March 7, 2025. https://www12.statcan.gc.ca/census-recensement/2021/ref/dict/az/Definition-eng.cfm?ID=geo042
12.Patel K, Hipskind J. Cardiac Arrest. 2023. Accessed February 27, 2025. https://www.ncbi.nlm.nih.gov/books/NBK534866/
13.MyHealth.Alberta.Ca. Cardiac Arrest. Government of Alberta; 2023. Accessed February 27, 2025. https://myhealth.alberta.ca/Health/pages/conditions.aspx?hwid=abh2047
14.Heart and Stroke Foundation of Canada. Every second counts: Transforming resuscitation to restart more hearts. 2024. Accessed February 27, 2025. https://issuu.com/heartandstroke/docs/cardiac_arrest_report_feb_2024?fr=sYWQ2NjY0NDEzNjI
15.Health Canada. Canada’s overdose crisis and the toxic illegal drug supply. 2024. Accessed April 8, 2025. https://www.canada.ca/en/health-canada/services/opioids/overdose-crisis-toxic-illegal-drug-supply.html
16.Fraser Health Authority. Cardioversion. 2022. Accessed February 27, 2025. https://www.fraserhealth.ca/health-topics-a-to-z/heart-health/heart-surgery-and-procedures/arrhythmia-procedures/cardioversion
17.Tarun D, Bashar S.A. Pacemaker Indications. StatPearls Publishing; 2023. Accessed February 27, 2025. https://www.ncbi.nlm.nih.gov/books/NBK507823/
18.Chrispin J. Cardiac Arrest. The Johns Hopkins University; 2025. Accessed February 27, 2025. https://www.hopkinsmedicine.org/health/conditions-and-diseases/cardiac-arrest#:~:text=Cardiac%20arrest%2C%20also%20known%20as,cardiac%20arrest%2C%20call%20911%20immediately
19.Heart and Stroke Foundation of Canada. Addressing Cardiac Arrest in Canada. 2019. Accessed February 28, 2025. https://www.heartandstroke.ca/-/media/pdf-files/canada/2020-position-statement/en-addressingcardiacarreststatement-feb-2020.ashx?rev=26387381b3b5407d9d98a543ed1ff1ed&hash=B3345326DD44FB0B6DF990D3E8DA1BC2
20.Chen C, Lo CYZ, Ho MJC, et al. Global Sex Disparities in Bystander Cardiopulmonary Resuscitation After Out-of-Hospital Cardiac Arrest: A Scoping Review. J Am Heart Assoc. 2024;13(18):e035794. doi:10.1161/JAHA.124.035794 PubMed
21.Mehta NK, Allam S, Mazimba S, Karim S. Racial, ethnic, and socioeconomic disparities in out-of-hospital cardiac arrest within the United States: Now is the time for change. Heart Rhythm O2. 2022;3(6Part B):857-863. doi:10.1016/j.hroo.2022.07.009 PubMed
22.Zahra SA, Choudhury RY, Naqvi R, et al. Health inequalities in cardiopulmonary resuscitation and use of automated electrical defibrillators in out-of-hospital cardiac arrest. Curr Probl Cardiol. 2024;49(5):102484. doi:10.1016/j.cpcardiol.2024.102484 PubMed
23.Sheraton M, Columbus J, Surani S, Chopra R, Kashyap R. Effectiveness of Mechanical Chest Compression Devices over Manual Cardiopulmonary Resuscitation: A Systematic Review with Meta-analysis and Trial Sequential Analysis. West J Emerg Med. 2021;22(4):810-819. doi:10.5811/westjem.2021.3.50932 PubMed
24.Harrison-Paul R. Resuscitation great. A history of mechanical devices for providing external chest compressions. Resuscitation. 2007;73(3):330-6. doi:10.1016/j.resuscitation.2007.01.002 PubMed
25.MyCPR NOW. Can Robots Learn CPR? Exploring the Future of Resuscitation. 2025. Accessed March 10, 2025. https://cprcertificationnow.com/blogs/mycpr-now-blog/can-robots-learn-cpr-exploring-the-future-of-resuscitation
26.Kim T, Suh GJ, Kim KS, et al. Development of artificial intelligence-driven biosignal-sensitive cardiopulmonary resuscitation robot. Resuscitation. 2024;202:110354. doi:10.1016/j.resuscitation.2024.110354 PubMed
27.Cave DM, Gazmuri RJ, Otto CW, et al. Part 7: CPR techniques and devices: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2010;122(18 Suppl 3):S720-8. doi:10.1161/CIRCULATIONAHA.110.970970 PubMed
28.Poole K, Couper K, Smyth MA, Yeung J, Perkins GD. Mechanical CPR: Who? When? How? Crit Care. 2018;22(1):140. doi:10.1186/s13054-018-2059-0 PubMed
29.Sugarman L, Hedley D, Crowe S. Mechanical CPR in a child: can one size fit all? BMJ Case Rep. 2017;2017doi:10.1136/bcr-2017-219728 PubMed
30.National Institute of Health and Care Excellence. The AutoPulse non-invasive cardiac support pump for cardiopulmonary resuscitation (MedTech Innovation Briefing MIB18). 2015. Accessed March 10, 2025. https://www.nice.org.uk/advice/mib18/resources/the-autopulse-noninvasive-cardiac-support-pump-for-cardiopulmonary-resuscitation-pdf-63498991381189
31.Government of Canada. Medical Devices Active Licence Listing (MDALL). 2024. Accessed February 28, 2025. https://health-products.canada.ca/mdall-limh/
32.ZOLL Medical Corporation. The ZOLL AutoPulse® Resuscitation System. 2025. Accessed March 20, 2025. https://www.zoll.com/en-GB/Products/Emergency-Care/Automated-CPR/Autopulse-Resuscitation-System
33.Primi R, Bendotti S, Currao A, et al. Use of Mechanical Chest Compression for Resuscitation in Out-Of-Hospital Cardiac Arrest-Device Matters: A Propensity-Score-Based Match Analysis. J Clin Med. 2023;12(13)4429. doi:10.3390/jcm12134429 PubMed
34.SCHILLER Americas Inc. EASY PULSE. 2025. Accessed March 20, 2025. https://www.schiller.ch/en-ca/products/easy-pulse-p49
35.Defibtech LLC. Lifeline ARM ACC. 2025. Accessed March 20, 2025. https://www.defibtech.com/products/lifeline-arm-acc/
36.Jolife AB. LUCAS - Chest Compression System. 2025. Accessed March 20, 2025. https://www.lucas-cpr.com/
37.Canadian Agency for Drugs and Technologies in Health. Mechanical Cardiopulmonary Resuscitation Versus Manual Cardiopulmonary Resuscitation for Cardiac Arrest in Pre-Hospital and Hospital Settings. Health Technology Inquiry Service (HTIS). 2008. Accessed February 25, 2025. https://www.cda-amc.ca/sites/default/files/pdf/htis/Mechanical%20CPR%20versus%20Manual%20CPR%20for%20Cardiac%20Arrest%20in%20Pre-Hospital%20and%20Hospital%20Settings%20Clinical%20.pdf
38.Wang PL, Brooks SC. Mechanical versus manual chest compressions for cardiac arrest. Cochrane Database Syst Rev. 2018;8(8):CD007260. doi:10.1002/14651858.CD007260.pub4 PubMed
39.Khan SU, Lone AN, Talluri S, Khan MZ, Khan MU, Kaluski E. Efficacy and safety of mechanical versus manual compression in cardiac arrest - A Bayesian network meta-analysis. Resuscitation. 2018;130:182-188. doi:10.1016/j.resuscitation.2018.05.005 PubMed
40.Almulihi QA, Shujaa AS, Aldossary BJ, et al. Does Autopulse Mechanical chest compression improve outcomes after cardiac arrest? A systemic review and meta-analysis. Saudi Journal of Emergency Medicine. 2024;5(1):030 - 041. doi:10.24911/SJEMed/72-1704226267
41.Gao Y, Sun T, Yuan D, et al. Safety of mechanical and manual chest compressions in cardiac arrest patients: A systematic review and meta-analysis. Resuscitation. 2021;169:124-135. doi:10.1016/j.resuscitation.2021.10.028 PubMed
42.Larik MO, Ahmed A, Shiraz MI, Shiraz SA, Anjum MU, Bhattarai P. Comparison of manual chest compression versus mechanical chest compression for out-of-hospital cardiac arrest: A systematic review and meta-analysis. Medicine (Baltimore). 2024;103(8):e37294. doi:10.1097/MD.0000000000037294 PubMed
43.Zhu X, Fu J. Efficacy of mechanical against manual method in cardiopulmonary resuscitation for out-of-hospital cardiac arrest: A meta-analysis. Exp Ther Med. 2024;28(6):458. doi:10.3892/etm.2024.12748 PubMed
44.American Heart Association. 2020 American Heart Association (AHA) Guidelines for Cardiopulmonary Resuscitation (CPR) and Emergency Cardiovascular Care. 2020. Accessed February 24, 2025. https://cpr.heart.org/en/resuscitation-science/cpr-and-ecc-guidelines/executive-summary
45.Perkins GD, Graesner JT, Semeraro F, et al. European Resuscitation Council Guidelines 2021: Executive summary. Resuscitation. 2021;161:1-60. doi:10.1016/j.resuscitation.2021.02.003 PubMed
46.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. Journal of Clinical Epidemiology. 2009;62(10):e1-e34. PubMed
47.Haywood K, Whitehead L, Nadkarni VM, et al. COSCA (Core Outcome Set for Cardiac Arrest) in Adults: An Advisory Statement From the International Liaison Committee on Resuscitation. Circulation. 2018;137(22):e783-e801. doi:10.1161/CIR.0000000000000562 PubMed
48.Craig S, Cubitt M, Jaison A, et al. Management of adult cardiac arrest in the COVID-19 era: consensus statement from the Australasian College for Emergency Medicine. Med J Aust. 2020;213(3):126-133. doi:10.5694/mja2.50699 PubMed
49.Connolly MS, Goldstein Pcp JP, Currie M, et al. Urban-Rural Differences in Cardiac Arrest Outcomes: A Retrospective Population-Based Cohort Study. CJC Open. 2022;4(4):383-389. doi:10.1016/j.cjco.2021.12.010 PubMed
50.Mseke EP, Jessup B, Barnett T. Impact of distance and/or travel time on healthcare service access in rural and remote areas: A scoping review. Journal of Transport & Health. 2024;37:101819. doi:10.1016/j.jth.2024.101819
51.Canadian Centre for Occupational Health and Safety. Climate Change: Extreme Weather - Cold. 2024. Accessed April 8, 2025. https://www.ccohs.ca/oshanswers/safety_haz/climate/climate-change-extreme-weather-cold.html
52.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. doi:10.1136/bmj.j4008 PubMed
53.Agree Next Steps C. The AGREE II Instrument. AGREE Enterprise; 2017. Accessed March 21, 2025. https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf
54.CDA-AMC. CDA-AMC style guide, 2025 edition. 2025. Accessed February 24, 2025. https://www.cda-amc.ca/style-guide
Appendix 1: Detailed Methods and Selection of Included Studies
Please note that this appendix has not been copy-edited.
Literature Search Methods
An information specialist conducted a literature search on key resources including MEDLINE via Ovid, Scopus, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of health technology assessment agencies in Canada and major international HTA agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevance. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concept was automated chest compression devices. The search was completed on February 5, 2025 and limited to English-language documents published since January 1, 2020. Search strategies available on request.
Selection Criteria and Methods
Two reviewers screened citations and selected studies. In the first level of screening, they independently screened titles and abstracts of all retrieved citations for relevance following a liberal-accelerated approach, whereby a single reviewer was required to include a study and exclusion by both reviewers was needed to exclude a study. Full texts of titles and abstracts that were judged to be potentially relevant by at least 1 reviewer were retrieved and independently assessed by 2 reviewers for inclusion based on the inclusion criteria presented in Table 1. Discrepancies between reviewers at the full-text level were discussed until consensus was reached. Figure 1 presents the PRISMA flow chart of the study selection.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1 or were duplicate studies. Studies were also excluded if they were not published in English, simulations in mannequins, the intervention of interest was aimed at elevating the human body during chest compressions, the intervention was an audiovisual feedback device to help with performing chest compressions, the study results were included in an already included SR, the study did not have quantitative results comparing intervention and control, or the study was withdrawn from a journal. Guidelines with unclear methodology were also excluded.
Critical Appraisal of Individual Studies
One reviewer critically appraised the included studies using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)52 for SRs and the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument53 for guidelines. Summary scores for the included studies were not calculated; rather, the strengths and limitations of each included study were described narratively in this report.
Data Extraction and Reporting
One reviewer extracted data directly into standardized tables created in Microsoft Word, which were modified as necessary. The extracted information included study characteristics, methodology (e.g., study design), population, intervention, comparator, and results regarding the outcomes of interest. One reviewer extracted information from the included studies using the PROGRESS-Plus7 tool to describe different population groups. Each included study was checked to determine if PROGRESS-Plus7 criteria were reported by study authors to describe the participants. Detailed characteristics, if available, were then extracted and reported in tables in Appendix 2. The main PROGRESS-Plus7 criteria include place of residence, race/ethnicity/culture/language, occupation, gender/sex, religion, education, SES, and social capital. As part of report writing, we discuss these characteristics across the evidence, if they are available, when presenting results within the text.
When reporting on sex, gender, race, or ethnicity in this Rapid Review, we planned to retain the language used by the original study authors, and, whenever possible, we referred to these groups based on guidance from the CDA-AMC Style Guide54 at the time this Rapid Review was conducted, with an understanding that language is constantly evolving.
Appendix 2: Characteristics of Included Studies
Table 2: Characteristics of Included Systematic Reviews
Study citation, country, countries of included studies, funding source | Study design, number of primary studies included | Population characteristicsa | Intervention and comparator | Outcomes, length of follow-up |
|---|---|---|---|---|
Almulihi et al. (2024)40 Saudi Arabia Countries of included studies eligible for the current review: Australia (1), Austria (1), China (1), Denmark (1), Italy (1), Japan (2), Netherlands (1), Norway (1), Singapore (1), UK (1), US (1), and 1 conducted in the US and Canada Funding source: Authors reported no funding was received for this study | Study design: Systematic review and meta-analysis of literature published up to December 2023 Number of included studies: A total of 16 included studies, of which 13 are relevant to the present review
| Eligibility: Adults (> 18 years old), nontraumatic cause of cardiac arrest; both IHCA and OHCA N per study = 82 to 4,292 participantsa Age (years): NR Sex or gender: NR % Shockable rhythm: NR % Witnessed arrest: NR Time from arrest to start of compression: NR % Bystander CPR: NR Other PROGRESS-Plus criteria: NRc | Intervention: AutoPulse automated chest compression device Comparator: Manual CPR | Outcomes:
Follow-up: NR |
Larik et al. (2024)42 Nepal, Pakistan, United Arab Emirates Countries of included studies eligible for the current review: NR in review (based on overlap with other reviews): Australia (1), Austria (1), China (1), Italy (1), Japan (1), Norway (1), Singapore (1), Sweden (3), Netherlands (1), Taiwan (1), Thailand (1), UK (2), US (5), 1 conducted in US and Canada, and 2 NR. Funding source: Authors declared no funding was received for this study | Study design: Systematic review and meta-analysis of literature published up to May 2023 Number of included studies: A total of 24 included studies, of which 21 are relevant to the present review
| Eligibility: OHCA N per study = 30 to > 30,000 participantsa Age (years): means per study arm range from 63 to 80 years. Sex or gender:e Number (%) male reported. % male across studies arms ranges from 54 to 83%. % Shockable rhythm: range across study arms is 7 to 64% % Witnessed arrest: range across study arms is 34 to 96% Time from arrest to start of compression: NR % Bystander CPR: range across study arms is 0 to 57% Other PROGRESS-Plus criteria: NRc | Relevant Interventionf: AutoPulse and LUCAS chest compression devices Comparator: Manual chest compressions | Outcomes:
Follow-up: NR Subgroup or sensitivity analyses
|
Zhu and Fu (2024)43 China Countries of included studies eligible for the current review: Australia (1), Austria (1), Belgium (1), China (2), Czech Republic (2), Denmark (1), Germany (2), Hungary (1), Israel (1), Italy (2), Japan (2), South Korea (1), Netherlands (1), Norway (1), Russia (1), Singapore (2), Sweden (6), Taiwan (1), Thailand (1), Turkey (1), UK (2), US (9), 1 conducted in US and Canada, and 1 NR. Funding source: Authors reported that they received no funding for the study | Study design: Systematic review with meta-analysis of literature published up to December 2023 Number of included studies: A total of 50 included studies, of which 43 are relevant to the present review
| Eligibility: Adults (> 18 years old) who had OHCA N per study = 30 to > 30,000 participantsa Age (years): NR Sex or gender: NR % Shockable rhythm: NR % Witnessed arrest: NR Time from arrest to start of compression: NR % Bystander CPR: NR Other PROGRESS-Plus criteria: NRc | Relevant interventionf: AutoPulse and LUCAS chest compression devices Comparator: Manual CPR | Outcomes:
Follow-up: NR Subgroup and sensitivity analyses
|
Gao et al. (2021)41 China Countries of included studies eligible for the current review: Denmark (1), Germany (1), Japan (1), Netherlands (2), Sweden (2), Switzerland (2), and US (1) Funding source: The authors disclosed that the research was supported by grants and specified these in their publication. | Study design: Systematic review with meta-analysis of literature published up to May 2020 11 included studies, all relevant to the present review
| Eligibility: Adults with cardiac arrest; no stated limits on setting. Outcomes determined by autopsy, postmortem CT, or dedicated imaging. N per study = 44 to 427 participants Age (years): NR Sex or gender: NR % Shockable rhythm: NR % Witnessed arrest: NR Time from arrest to start of compression: NR % Bystander CPR: NR Other PROGRESS-Plus criteria: NRc | Intervention: LUCAS or AutoPulse chest compression devices Comparator: Manual chest compressions | Outcomes
|
CPR = cardiopulmonary resuscitation; IHCA = in-hospital cardiac arrest; LUCAS = Lund University Cardiopulmonary Assist System; NR = not reported; OHCA = out-of-hospital cardiac arrest; RCT = randomized controlled trial; ROSC = return of spontaneous circulation; SES = socioeconomic status.
Note: information regarding studies included in SRs is extracted across reviews and may not be reported in each SR
aFor SRs with broader inclusion criteria than this report, participant characteristic data (e.g., age, sex) from the subset of studies relevant to the current report were summarized.
bWhere discrepancies were noted in extracted information across reviews, study abstract was consulted, if available, and study authors’ terms recorded.
cThe main PROGRESS-Plus criteria7 include place of residence, race, ethnicity, culture, language, occupation, gender, sex, religion, education, SES, and social capital, personal characteristics associated with discrimination (e.g., age, disability), features of relationships, and time-dependent relationships.
dCost-effectiveness was a relevant outcome for this Rapid Review. This SR aimed to review evidence on cost-effectiveness. However, no information was reported regarding cost-effectiveness, and the study authors did not disclose the reason (i.e., lack of identified evidence or other factor). The same is true for quality of CPR and duration of resuscitation outcomes: no information reports and no reason disclosed.
eThe SR did not indicate whether they were reporting sex or gender, or how “male” data were measured.
fThe scope of this SR was broader than this Rapid Review and included additional interventions. The interventions relevant to this report are included in this table.
Note: This table has not been copy-edited.
Table 3: Characteristics of Included Guidelines
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality assessment | Recommendations development and evaluation | Guideline validation |
|---|---|---|---|---|---|---|
European Resuscitation Council (2021)45 | ||||||
Intended users: First responders, first aiders, community health care staff, ambulance staff, hospital staff, trainers, and instructors, people responsible for health care policy and practice, and the public Target population: Adults requiring ALS treatments for IHCA and OHCA | ALS treatments for IHCA and OHCA (i.e., community); automated chest compression devices are relevant to the present review | Survival, neurologic outcomes | SRs conducted according to methods from the Institute of Medicine, Cochrane Collaboration, and GRADE. Scoping review methods followed the ILCOR framework and reporting followed the PRISMA extension for scoping reviews. Evidence updates from ILCOR 2020 CoSTR for ALS | Evidence evaluation using GRADE and strength of recommendations using Evidence to Decision Framework by GRADE | ERC guideline development committee was formed to review the literature, form recommendations, and provide expertise. Evidence was reviewed and discussed until consensus was achieved | The original scope of the guidelines and the draft underwent public consultation followed by peer review and approval by the ERC general assembly |
American Heart Association (2020)44 | ||||||
Intended users: North American health care providers, rescuers from the public, people with advanced resuscitation training with or without access to resuscitation drugs and devices, within or outside a hospital Target population: Adults requiring BLS or ALS treatments for IHCA and OHCA | CPR and ECC, including adult BLS and ALS for IHCA and OHCA; automated chest compression devices are relevant to the present review | NR | SR conducted according to methods from the National Academy of Medicine and GRADE Scoping review methods based on PRISMA extension for scoping reviews Evidence updates by AHA or ILCORO | GRADE | Evidence evaluation conducted by AHA guideline writing groups, ILCOR task forces (2020 CoSTR methods) and ILCOR SAC. Recommendations made based on consensus | Public input during scope development and for draft statements. Peer review by subject matter experts, AHA SACC, and AHA Executive Committee. Final endorsement from ILCOR board |
AHA = American Heart Association; ALS = advanced life support; BLS = basic life support; CoSTR = Consensus on Science and Treatment Recommendations; CPR = cardiopulmonary resuscitation; ECC = emergency cardiovascular care; ERC = European Resuscitation Council; GRADE = Grading of Recommendations Assessment, Development and Evaluation; IHCA = in-hospital cardiac arrest; ILCOR = International Liaison Committee on Resuscitation; NR = not reported; OHCA = out-of-hospital cardiac arrest; SAC = Scientific Advisory Committee; SACC = Science Advisory and Coordinating Committee; SR = systematic review.
Note: This table has not been copy-edited.
Appendix 3: Critical Appraisal of Included Publications
Please note that this appendix has not been copy-edited.
Table 4: Strengths and Limitations of Systematic Reviews Using AMSTAR 252
Strengths | Limitations |
|---|---|
Almulihi et al. (2024)40 | |
|
|
Larik et al. (2024)42 | |
|
|
Zhu and Fu (2024)43 | |
|
|
Gao et al. (2021)41 | |
|
|
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; CINAHL = Cumulative Index to Nursing and Allied Health Literature; CPR = cardiopulmonary resuscitation; MA = meta-analysis; NRS = nonrandomized studies; RCT = randomized controlled trial; RoB = risk of bias; ROBINS-I = Risk Of Bias In Nonrandomized Studies - of Interventions (tool for risk of bias assessment); vs. = versus.
Table 5: Strengths and Limitations of Guidelines Using AGREE II53
Item | European Resuscitation Council (2021)45 | American Heart Association (2020)44 |
|---|---|---|
Domain 1: Scope and purpose | ||
1. The overall objective(s) of the guideline is (are) specifically described. | Yes | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes | Yes |
3. The population (patients, public, etc.) to whom the guideline is meant to apply is specifically described. | Yes | Yes |
Domain 2: Stakeholdera involvement | ||
4. The guideline development group includes individuals from all relevant professional groups. | Yes | Yes |
5. The views and preferences of the target population (patients, public, etc.) have been sought. | Yes | Yes |
6. The target users of the guideline are clearly defined. | Yes | Yes |
Domain 3: Rigour of development | ||
7. Systematic methods were used to search for evidence. | Yes | Yes |
8. The criteria for selecting the evidence are clearly described. | Yes | No |
9. The strengths and limitations of the body of evidence are clearly described. | No | Yes |
10. The methods for formulating the recommendations are clearly described. | Yes | Yes |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes | Yes |
12. There is an explicit link between the recommendations and the supporting evidence. | Yes | Yes |
13. The guideline has been externally reviewed by experts before its publication. | Yes | Yes |
14. A procedure for updating the guideline is provided. | Yes | Unclear |
Domain 4: Clarity of presentation | ||
15. The recommendations are specific and unambiguous. | Yes | Yes |
16. The different options for management of the condition or health issue are clearly presented. | Yes | Yes |
17. Key recommendations are easily identifiable. | Yes | Yes |
Domain 5: Applicability | ||
18. The guideline describes facilitators and barriers to its application. | Yes | Yes |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | No | No |
20. The potential resource implications of applying the recommendations have been considered. | Yes | Yes |
21. The guideline presents monitoring and/or auditing criteria. | Yes | Unclear |
Domain 6: Editorial independence | ||
22. The views of the funding body have not influenced the content of the guideline. | Unclear | Unclear |
23. Competing interests of guideline development group members have been recorded and addressed. | Yes | Yes |
AGREE II = Appraisal of Guidelines for Research and Evaluation II.
aWe retained the domain names that are included in the original AGREE II checklist, which includes the term “stakeholder” (i.e., in Domain 2), to be clear that we assessed the strengths and limitations of guidelines using AGREE II. However, the CDA-AMC understands that language is constantly evolving and the word “stakeholder” has an association with colonialism; whenever possible, CDA-AMC does not use this word in our reports.
Appendix 4: Main Study Findings
Please note that this appendix has not been copy-edited.
Table 6: Summary of Findings by Outcomes — Survival
Citation, Outcome | Evidence source, characteristics of participants | Outcome result | Relative effect (95% CI) | P value | |
|---|---|---|---|---|---|
Automated chest compressions | Manual chest compressions | ||||
AutoPulse vs. manual compressions | |||||
Almulihi et al. (2024)40 Survival to hospital admission | 1 retrospective case-control studya; Jennings et al. (2012) 286 participants; adults; OHCA | 17/66 (26%) | 43/220 (20%) | Propensity score AOR = 1.69 (0.79 to 3.63) | NR |
Almulihi et al. (2024)40 4-hour survival | 1 RCT; Hallstrom et al. (2006) 1,071 participants, OHCA, EMS | 28.5% | 29.5% | NR | P = 0.74 |
Almulihi et al. (2024)40 24-hour survival | 1 Cluster RCTa; Gao et al. (2016) 133 participants; adults and adolescents eligible; OHCA | 39.1% | 21.9% | NR | P = 0.03 |
1 RCT; Wik et al. (2014) 4,231 participants, missing outcome data for 12 participants; OHCA, nontrauma | 456 (21.8%) | 532 (25%) | NR | NR | |
Almulihi et al. (2024)40 Survival to hospital discharge | 1 RCT; Omori et al. (2013) 92 participants; OHCA, using helicopter transport | 6.1% | 2.3% | NR | NR |
1 cohort study; Spiro et al. (2015) 285 participants; IHCA | 7/25 (28%) | 28/260 (11%) | NR | NR | |
1 RCT; Wik et al. (2014) 4,231 participants, missing outcome data for 12 participants; OHCA, nontrauma | 196 (9.4%) | 233 (11%) | AOR = 1.06 (0.83 to 1.37) | NR | |
Almulihi et al. (2024)40 30-day survival | 1 retrospective cohort; Primi et al. (2023) 4,292 participantsa; OHCA | 6% | 14% | After correction for confounding: HR = 0.9 (0.8 to 0.9) | P = 0.005c |
Larik et al. (2024)42 Survival to hospital discharge | SR with MA (6 studies including RCTs, prospective and retrospective observational studies) 7,568 participants; OHCA | 284/3,134 | 386/4,434 | OR = 1.25 (0.70 to 2.17)b I2 = 83% | P = 0.45 |
Zhu and Fu (2024)43 Survival to hospital admission | SR with MA (11 studies including RCTs, prospective and retrospective observational studies) # participants NR; OHCA | NR | NR | OR = 1.70 (1.21 to 2.37) I2 = 86.5% | NR |
Zhu and Fu (2024)43 Survival to hospital discharge | SR with MA (10 studies including RCTs, prospective and retrospective observational studies) # participants NR; OHCA | NR | NR | OR = 0.99 (0.60 to 1.66) I2 = 80.8% | NR |
LUCAS vs. manual compressionsd | |||||
Larik et al. (2024)42 Survival to discharge | SR with MA (7 studies including RCTs, prospective and retrospective observational studies) 7,834 participants; OHCA | 208/2,809 | 411/5,025 | OR = 0.84 (0.66 to 1.08)b I2 = 23% | P = 0.17 |
Zhu and Fu (2024)43 Survival to hospital admission | SR with MA (10 studies including RCTs, prospective and retrospective observational studies) # participants NR; OHCA | NR | NR | OR = 1.00 (0.89 to 1.13) I2 = 37.3% | NR |
Zhu and Fu (2024)43 Survival to discharge | SR with MA (9 studies including RCTs, prospective and retrospective observational studies) # participants NR; OHCA | NR | NR | OR = 0.78 (0.61 to 0.99) I2 = 77.1% | NR |
LUCAS 2 vs. manual compressions | |||||
Zhu and Fu (2024)43 Survival to discharge | 1 nonrandomized controlled trial; Canakci et al. (2021) 178 participants; OHCA | NR | NR | OR = 2.25 (0.74 to 6.87) I2 = 0.0% | NR |
LUCAS 3 vs. manual compressions | |||||
Zhu and Fu (2024)43 Survival to hospital admission | 1 Retrospective cohort/chart reviewa; Tantarattanapong and Chantaramanee (2022) 168 participants; OHCA | NR | NR | OR = 0.20 (0.05 to 0.89) I2 = 0.0% | NR |
Zhu and Fu (2024)43 Survival to hospital discharge | SR with MA (2 studies, both retrospective observational studies) # participants NR (> 1,500); OHCA | NR | NR | OR = 0.75 (0.11 to 5.08) I2 = 53.8% | NR |
Mix of AutoPulse and LUCAS vs. manual compressions | |||||
Zhu and Fu (2024)43 Survival to hospital admission | SR with MA (2 studies including 1 prospective and 1 retrospective observational study) # participants NR; OHCA | NR | NR | OR = 1.16 (0.75 to 1.78) I2 = 92.9% | NR |
Zhu and Fu (2024)43 Survival to hospital discharge | SR with MA (4 prospective observational studies) # participants NR (> 31,000); OHCA | NR | NR | OR = 0.84 (0.65 to 1.10) I2 = 33.7% | NR |
AOR = adjusted odds ratio; CI = confidence interval; EMS = emergency medical services; HR = hazard ratio; IHCA = in-hospital cardiac arrest; LUCAS = Lund University Cardiac Assist System; MA = meta-analyses; NR = not reported; OHCA = out-of-hospital cardiac arrest; OR = odds ratio; RCT = randomized controlled trial; RoB = risk of bias; SR = systematic review; vs. = versus.
Note: The pooled estimates from separate reviews presented in this table include many of the same studies. Refer to Appendix 5 for a citation matrix illustrating the degree of overlap between SRs
aDifferences/errors were present between data extracted across SRs for the same studies (e.g., study design classification. number of participants). Where possible, we resolved discrepancies from original study record.
bThe findings from Larik et al. (2024)42 were calculated using automated chest compressions as the comparator, rather than the intervention. To align with the direction of this review (i.e., automated chest compression devices compared to manual compressions) the effect estimates were inverted by taking the reciprocal of the odds ratio and the bounds of the CI. The survival outcomes as reported in the SR were: AutoPulse vs. manual compressions, OR = 0.80 (95% CI, 0.46 to 1.42); LUCAS vs. manual compressions, OR = 1.19 (95% CI, 0.93 to 1.52).
cResults reported by Almulihi et al. (2024)40 SR for Primi et al. (2023) may be limited to those with significant results.
dOriginal LUCAS device or not specified.
Table 7: Summary of Findings by Outcomes — Neurologic Outcomes
Citation, outcome definition/time point | Evidence source, characteristics of participants | Outcome result | Odds ratio (95% CI) | P value | |
|---|---|---|---|---|---|
Automated chest compressions | Manual chest compressions | ||||
AutoPulse vs. manual compressions | |||||
Larik et al. (2024)42 Favourable neurologic outcome; not otherwise defined in SRa | 1 cluster RCTb; Gao et al. (2016) 133 participants with 46 contributing to this analysis; OHCA | 5/31 | 2/15 | 1.25 (0.21 to 7.14)d | NR |
1 cluster RCT with crossoverb; (Hallstrom et al. 2006) 767 participantsb; OHCA, EMS | 12/394 | 28/373 | 0.39 (0.19 to 0.78)d | NR | |
1 RCT; Wik et al. (2014) 4,231 participantsb; OHCA | 87/2,099 | 112/2,132 | 0.78 (0.58 to 1.04)d | NR | |
Almulihi et al. (2024)40 Survivors with CPC 1 (good); Time point unclear | 1 prospective cohort study; Ong et al. (2012) 1,011 participantsb; OHCA | 12/552 | 1/459 | NR | P = 0.01 |
Almulihi et al. (2024)40 Overall performance category 1 (good) | 10/552 | 1/459 | NR | P = 0.06 | |
LUCAS vs. manual compressionsc | |||||
Larik et al. (2024)42 Favourable neurologic outcome; not otherwise defined in SRa | 1 non-RCT/prospective cohortb; Axelsson et al. (2006) 328 participantsb; OHCA | 14/159 | 9/169 | 1.72 (0.72 to 4.17)d | NR |
1 retrospective cohort; Chen et al. (2021) 552 participantsb; OHCA | 15/279 | 12/273 | 1.23 (0.57 to 2.70)d | NR | |
1 retrospective; Gonzales (2019) 352 participants; OHCA | 10/176 | 21/176 | 0.44 (0.20 to 0.97)d | NR | |
1 retrospective cohort; Mistraletti et al. (2023) 1,366 participants; OHCA | 33/305 | 72/1,061 | 1.67 (1.08 to 2.56)d | NR | |
1 retrospective cohort; Newberry et al. (2018) 2,999 participants; 1,783 in this analysis; OHCA | 29/763 | 129/1,020 | 0.27 (0.18 to 0.41)d | NR | |
1 cluster RCT; Perkins et al. (2015) 4,471 participants; OHCA | 77/1,652 | 168/2,819 | 0.77 (0.58 to 1.02)d | NR | |
1 RCT; Rubertsson et al. (2014) 2,589 participants; OHCA | 108/1,300 | 100/1,289 | 1.08 (0.81 to 1.43)d | NR | |
LUCAS 3 vs. manual compressions | |||||
Larik et al. (2024)42 Favourable neurologic outcome; not otherwise defined in SRa | 1 retrospective cohort/chart reviewb; Tantarattanapong and Chantaramanee (2022) 227 participants; OHCA | 0/34 | 19/193 | 0.13 (0.01 to 2.22)d | NR |
Mix of AutoPulse and LUCAS vs. manual compressions | |||||
Larik et al. (2024)42 Favourable neurologic outcome; not otherwise defined in SRa | 1 prospective cohortb; Zeiner et al. (2015) 938 participantsb; OHCA | 21/283 | 92/655 | 0.49 (0.30 to 0.81)d | NR |
Almulihi et al. (2024)40 ‘Neurologic outcome measured by CPC’: where % seems to be % with positive outcome | 56.8% | 78.6% | NR | P = 0.009 | |
CI = confidence interval; CPC = cerebral performance category; EMS = emergency medical services; LUCAS = Lund University Cardiac Assist System; NR = not reported; OHCA: out-of-hospital cardiac arrest; RCT = randomized controlled trial; RoB = risk of bias; SR = systematic review; vs. = versus.
aSR included a meta-analysis that included 1 study that was not eligible for the current review. The study-level estimates for the remaining studies are included here.
bNumbers/study design descriptions varied between SRs.
cOriginal LUCAS device or specific version of LUCAS device (i.e., LUCAS 2, LUCAS 3) not specified.
dThe findings from Larik et al. (2024)33 were calculated using automated chest compressions as the comparator, rather than the intervention. To align with the direction of this review (i.e., automated chest compression devices compared to manual compressions) the effect estimates were inverted by taking the reciprocal of the odds ratio and the bounds of the CI. The neurologic outcomes for AutoPulse vs. manual compressions as reported in the SR were: Gao et al. (2016), OR = 0.80 (95% CI, 0.14 to 4.70); Hallstrom et al. (2006), OR = 2.58 (95% CI, 1.29 to 5.16); Wik et al. (2014), OR = 1.28 (95% CI, 0.96 to 1.71). The neurologic outcomes for LUCAS vs. manual compressions as reported in the SR were: Axelsson et al. (2006), OR = 0.58 (95% CI, 0.24 to 1.39); Chen et al. (2021), OR = 0.81 (95% CI, 0.37 to 1.76); Gonzales et al. (2019), OR = 2.25 (95% CI, 1.03 to 4.93); Mistraletti et al. (2023), OR = 0.60 (95% CI, 0.39 to 0.93); Newberry et al. (2018), OR = 3.66 (95% CI, 2.42 to 5.55); Perkins et al. (2015), OR = 1.30 (95% CI, 0.98 to 1.71); Rubertsson et al. (2014), OR = 0.93 (95% CI, 0.70 to 1.23). The neurologic outcomes for LUCAS 3 vs. manual compressions as reported in the SR were: Tantarattanapong and Chantaramanee (2022), OR = 7.71 (95% CI, 0.45 to 130.76). The neurologic outcomes for a mix of AutoPulse and LUCAS vs. manual compressions as reported in the SR were: Zeiner et al. (2015), OR = 2.04 (95% CI, 1.24 to 3.35).
Table 8: Summary of Findings by Outcomes — ROSC
Citation | Evidence source, characteristics of participants | Outcome result | Odds ratio (95% CI) | P value | |
|---|---|---|---|---|---|
Automated chest compressions | Manual chest compressions | ||||
AutoPulse vs. manual compressions | |||||
Almulihi et al. (2024)40 | SR with MA (7 studies including RCTs, prospective and retrospective observational) # participants NR (> 8,000); OHCA | NR | NR | 1.43 (1.07 to 1.92) I2 = 88% | P = 0.02 |
1 RCT; Omori et al. (2013) 92 participants; OHCA, using helicopter transport | 15 (30.6%) | 3 (7.0%) | Factors associated with ROSC, multivariate analysis OR = 7.22 (NR) | P = 0.005 | |
Larik et al. (2024)42 | SR with MA (5 studies including RCTs, prospective and retrospective observational studies) 6,810 participants; OHCA | 856/2,811 | 954/3,999 | 1.67 (0.96 to 2.94)c I2 = 93% | P = 0.07 |
Zhu and Fu (2024)43 | SR with MA (12 studies including RCTs, prospective and retrospective observational studies) # participants NR (> 11,000); OHCA | NR | NR | 1.63 (1.20 to 2.22) I2 = 89.4% | NR |
LUCAS vs. manual compressionsa | |||||
Larik et al. (2024)42 | SR with MA (13 studies including RCTs, non-RCT/ prospective observational and retrospective observational studies)b 32,942 participants; OHCA | 1,864/6,058 | 5,020/26,884 | 1.03 (0.88 to 1.19)c I2 = 68% | P = 0.73 |
Zhu and Fu (2024)43 | SR with MA (15 studies including RCTs non-RCT/prospective observational and retrospective observational studies) # participants NR (> 15,000); OHCA | NR | NR | 1.07 (0.92 to 1.25) I2 = 67.1%, | NR |
LUCAS 2 vs. manual compressions | |||||
Zhu and Fu (2024)43 | 1 retrospective observational; Mastenbrook et al. (2022) 264 participants; OHCA | NR | NR | 0.99 (0.55 to 1.78) | NR |
LUCAS 3 vs. manual compressions | |||||
Zhu and Fu (2024)43 | SR with MA (2 retrospective observational studies) # participants NR (> 1,000); OHCA | NR | NR | 0.61 (0.12 to 3.01) I2 = 84.3% | NR |
Mix of AutoPulse and LUCAS vs. manual compressions | |||||
Zhu and Fu (2024)43 | SR with MA (4 studies including prospective and retrospective observational studies) # participants NR (> 25,000); OHCA | NR | NR | 0.91 (0.58 to 1.43) I2 = 96.3% | NR |
AutoPulse, LUCAS, or mix of AutoPulse and LUCAS across studies vs. manual compressionsa | |||||
Zhu and Fu (2024)43 | SR with MA (34 studies including RCTs, prospective and retrospective observational studies) # participants NR; OHCA | NR | NR | 1.20 (1.04 to 1.38) I2 = 87.2% | NR |
CI = confidence interval; LUCAS = Lund University Cardiac Assist System; MA = meta-analyses; NR = not reported; OHCA = out-of-hospital cardiac arrest; OR = odds ratio; RCT = randomized controlled trial; RoB = risk of bias; ROSC = return of spontaneous circulation; SR = systematic review; vs. = versus.
Note: The pooled estimates from separate reviews presented in this table include many of the same studies. Refer to Appendix 5 for a citation matrix illustrating the degree of overlap between SRs.
aOriginal LUCAS device or specific LUCAS device not specified.
bIncludes 1 large study (> 17,000 participants) at a high risk of bias that is not listed in included studies list for this SR.
cThe findings from Larik et al. (2024)33 were calculated using automated chest compressions as the comparator, rather than the intervention. To align with the direction of this review (i.e., automated chest compression devices compared to manual compressions) the effect estimates were inverted by taking the reciprocal of the odds ratio and the bounds of the CI. The ROSC outcome as reported in the SR were: AutoPulse vs. manual compressions, OR = 0.60 (95% CI, 0.34 to 1.04); LUCAS vs. manual compressions, OR = 0.97 (95% CI, 0.84 to 1.13).
Table 9: Summary of Findings by Outcomes — Overall Rate of Compression-Induced Injuries
Citation | Outcome definition, method of detection | Evidence source, characteristics of participants | Outcome result | Odds ratio (95% CI) | P value | |
|---|---|---|---|---|---|---|
Automated chest compressions | Manual chest compressions | |||||
AutoPulse vs. manual compressions | ||||||
Almulihi et al. (2024)40 | Definition: “Complications and adverse events’ (‘complications in terms of rib breakage and chest complications’)” Method of detection: NR | SR with MA (4 RCTs) 4,675 participants Mixed settings: IHCA and OHCA, including helicopter transport | 294/2,311 | 282/2,364 | 1.11 (0.93 to 1.33) I2 = 0% | P = 0.24 |
AutoPulse, LUCAS, or mix of AutoPulse and LUCAS vs. manual compressions | ||||||
Gao et al. (2021)41 | Definition: Rate of overall compression-induced injuries (not otherwise defined) b Method of detection: Autopsy | SR with MA (4 studies including prospective and retrospective observational studies) # participants NR; all nonsurvivors of cardiac arrest; Setting(s): NR | NR | NR | 1.29 (1.19 to 1.41) I2 = 21.83% | P = 0.00 |
CI = confidence interval; IHCA = in-hospital cardiac arrest; LUCAS = Lund University Cardiac Assist System; MA = meta-analyses; NR = not reported; OHCA = out-of-hospital cardiac arrest; RCT = randomized controlled trial; RoB = risk of bias; SR = systematic review; vs. = versus.
Table 10: Summary of Findings by Outcomes — Life-Threatening Injuries
Citation | Outcome definition, method of detection | Evidence source, characteristics of participants | Outcome result | Odds ratio (95% CI) | P value | |
|---|---|---|---|---|---|---|
Automated chest compressions | Manual chest compressions | |||||
AutoPulse, LUCAS, or mix of AutoPulse and LUCAS vs. manual compressions | ||||||
Gao et al. (2021)41 | Definition: Incidence of life-threatening injuries (not otherwise defined) Method of detection: autopsy, PMCT, diagnostic imaging, medical records, or clinical follow-up | SR with MA (3 studies including 1 RCT, 1 prospective observational study, 1 retrospective observational study) # participants NR; IHCA, OHCA, and unclear | NR | NR | 5.30 (0.53 to 53.16) I2 = 71.62% | P = 0.16 |
CI = confidence interval; IHCA = in-hospital cardiac arrest; LUCAS = Lund University Cardiac Assist System; MA = meta-analyses; NR = not reported; OHCA = out-of-hospital cardiac arrest; PMCT = postmortem CT; RCT = randomized controlled trial; RoB = risk of bias; SR = systematic review; vs. = versus.
Table 11: Summary of Findings by Outcomes — Skeletal Fractures
Citation | Outcome definition, method of detection | Evidence source, characteristics of participants | Outcome result | Odds ratio (95% CI) | P value | |
|---|---|---|---|---|---|---|
Automated chest compressions | Manual chest compressions | |||||
AutoPulse vs. manual compressions | ||||||
Gao et al. (2021)41 | Definition: Sternal fractures (all) Method of detection: autopsy, PMCT, or clinical follow-up | SR with MA (4 studies including 1 RCT and retrospective observational studies) # participants NR; IHCA, OHCA, unclear; 3 studies with nonsurvivors of cardiac arrest | NR | NR | OR = 0.69 (0.30 to 1.57) I2 = 81.82% | NR |
Gao et al. (2021)41 | Definition: Rib fractures - anterolateral Method of detection: autopsy, PMCT | SR with MA (3 retrospective observational studies) # participants NR; all nonsurvivors of cardiac arrest | NR | NR | 1.05 (0.94 to 1.17) I2 = 0.00 | NR |
Gao et al. (2021)41 | Definition: Rib fractures - posterior Method of detection: autopsy, PMCT | SR with MA (3 retrospective observational studies) # participants NR; all nonsurvivors of cardiac arrest | NR | NR | 9.94 (2.02 to 48.86) I2 = 67.85% | NR |
Gao et al. (2021)41 | Definition: Vertebral fractures Method of detection: autopsy, PMCT | SR with MA (including 2 retrospective observational studies) # participants NR; all nonsurvivors of cardiac arrest | NR | NR | 6.53 (0.83 to 51.36) I2 = 0.00% | NR |
LUCAS vs. manual compressions | ||||||
Gao et al. (2021)41 | Definition: Sternal fractures (any) Method of detection: autopsy, PMCT, or clinical follow-up | SR with MA (8 studies including 1 RCT, prospective and retrospective observational studies) # participants NR; IHCA, OHCA, unclear; 9 of 11 studies from nonsurvivors of cardiac arrest | NR | NR | 1.63 (1.23 to 2.15) I2 = 67.63% | NR |
Gao et al. (2021)41 | Definition: Rib fractures (incidence) Method of detection: autopsy, PMCT, or clinical follow-up | SR with MA (7 studies including 1 RCT, prospective and retrospective observational studies) # participants NR; IHCA, OHCA, unclear; 9 of 11 studies from nonsurvivors of cardiac arrest | NR | NR | 1.23 (1.12 to 1.35) I2 = 22.35% | NR |
Gao et al. (2021)41 | Definition: incidence of < 3 rib fractures Method of detection: autopsy, diagnostic imaging, or medical records | SR with MA (3 studies including prospective and retrospective observational studies) # participants NR; OHCA or unclear setting; 9 of 11 studies from nonsurvivors of cardiac arrest | NR | NR | 0.97 (0.26 to 3.61) I2 = 35.56% | NR |
Gao et al. (2021)41 | Definition: incidence of ≥ 3 rib fractures Method of detection: autopsy, diagnostic imaging, or medical records | SR with MA (3 studies including prospective and retrospective observational studies) # participants NR; OHCA, unclear; 9 of 11 studies from nonsurvivors of cardiac arrest | NR | NR | 1.45 (1.13 to 1.87) I2 = 62.36% | NR |
Gao et al. (2021)41 | Definition: Vertebral fractures Method of detection: autopsy, diagnostic imaging, or medical records | SR with MA (2 studies including prospective and retrospective observational studies) # participants NR; OHCA or all nonsurvivors of cardiac arrest | NR | NR | 2.08 (0.23 to 18.72) I2 = 0.00% | NR |
AutoPulse, LUCAS, or mix of AutoPulse and LUCAS vs. manual compressions | ||||||
Gao et al. (2021)41 | Definition: Sternal fractures (any) Method of detection: autopsy, PMCT, or clinical follow-up | SR with MA (11 studies including 1 RCT, prospective and retrospective observational studies) # participants NR; IHCA, OHCA, unclear; 9 of 11 studies from nonsurvivors of cardiac arrest | NR | NR | 1.28 (0.92 to 1.78) I2 = 81.85% | P = 0.14 |
Gao et al. (2021)41 | Definition: Rib fractures - posterior Method of detection: autopsy, PMCT | SR with MA (5 studies, all retrospective observational studies) # participants NR; IHCA, OHCA, unclear; 9 of 11 studies from nonsurvivors of cardiac arrest | NR | NR | 7.28 (2.47 to 21.49) I2 = 37.96% | P = 0.00 |
Gao et al. (2021)41 | Definition: Vertebral fractures Method of detection: autopsy, PMCT, diagnostic imaging, or medical records | SR with MA (4 studies including prospective and retrospective observational studies) # participants NR; OHCA or nonsurvivors of cardiac arrest | NR | NR | 3.82 (0.85 to 17.19) I2 = 0.00% | NR |
CI = confidence interval; IHCA = in-hospital cardiac arrest; LUCAS = Lund University Cardiac Assist System; MA = meta-analyses; NR = not reported; OHCA = out-of-hospital cardiac arrest; OR = odds ratio; PMCT = postmortem; RCT = randomized controlled trial; RoB = risk of bias; SR = systematic review; vs = versus.
Table 12: Summary of Findings by Outcomes — Visceral Injuries
Citation | Outcome definition, method of detection | Evidence source, characteristics of participants | Outcome result | Odds ratio (95% CI) | P value | |
|---|---|---|---|---|---|---|
Automated chest compressions | Manual chest compressions | |||||
AutoPulse vs. manual compressions | ||||||
Gao et al. (2021)41 | Definition: Heart lesions Method of detection: PMCT | SR with MA (2 retrospective observational studies) # participants NR; nonsurvivors of cardiac arrest | NR | NR | 2.08 (0.81 to 5.36) I2 = 0.00% | NR |
Gao et al. (2021)41 | Definition: Liver lesions Method of detection: autopsy, PMCT, or clinical follow-up | SR with MA (2 studies including 1 RCT and 1 retrospective observational studies) # participants NR; IHCA, OHCA, or all nonsurvivors of cardiac arrest | NR | NR | 0.80 (0.16 to 4.07) I2 = 19.02% | NR |
Gao et al. (2021)41 | Definition: Spleen lesions Method of detection: PMCT | 1 retrospective cohort study: Sonnemans et al. (2020) 72 participants; nonsurvivors of cardiac arrest | 2/43 | 4/29 | 0.34 (0.07 to 1.72) | NR |
Gao et al. (2021)41 | Definition: Kidney and perirenal lesions Method of detection: PMCT | 1 retrospective cohort study: Sonnemans et al. (2020) 71 participants; nonsurvivors of cardiac arrest | 1/42 | 0/29 | 3.09 (0.72 to 13.35) | NR |
Gao et al. (2021)41 | Definition: Pneumothorax Method of detection: autopsy, PMCT, or clinical follow-up | SR with MA (3 studies with 1 RCT and 2 retrospective observational studies) # participants NR; IHCA, OHCA, or nonsurvivors of cardiac arrest | NR | NR | 2.25 (1.17 to 4.31) I2 = 0.00% | NR |
LUCAS vs. manual compressions | ||||||
Gao et al. (2021)41 | Definition: Heart lesions Method of detection: autopsy, diagnostic imaging, or medical records | SR with MA (6 studies including prospective and retrospective observational studies) # participants NR; OHCA or all nonsurvivors of cardiac arrest | NR | NR | 2.17 (1.07 to 4.39) I2 = 57.31% | NR |
Gao et al. (2021)41 | Definition: Lung lesions Method of detection: autopsy, PMCT, diagnostic imaging, medical records, or clinical follow-up | SR with MA (7 included studies with 1 RCT, prospective and retrospective observational studies) # participants NR; OHCA or all nonsurvivors of cardiac arrest | NR | NR | 1.91 (0.80 to 4.56) I2 = 69.30% | P = 0.14 |
Gao et al. (2021)41 | Definition: Liver lesions Method of detection: autopsy, PMCT, diagnostic imaging, medical records, or clinical follow-up | SR with MA (7 studies including 1 RCT, prospective and retrospective observational studies) # participants NR; IHCA, OHCA, or all nonsurvivors of cardiac arrest | NR | NR | 4.10 (2.27 to 7.40) I2 = 0.0% | NR |
Gao et al. (2021)41 | Definition: Spleen lesions Method of detection: autopsy, diagnostic imaging, or medical records | SR with MA (2 studies including 1 prospective and 1 retrospective observational study) # participants NR; OHCA or nonsurvivors of cardiac arrest | NR | NR | 2.24 (0.17 to 30.05) I2 = 53.93% | NR |
Gao et al. (2021)41 | Definition: Kidney and perirenal lesions Method of detection: autopsy, diagnostic imaging, or medical records | SR with MA (3 studies including prospective and retrospective observational studies) # participants NR; OHCA or nonsurvivors of cardiac arrest | NR | NR | 3.46 (0.66 to 18.05) I2 = 0.15% | NR |
Gao et al. (2021)41 | Definition: lesions to major vessels Method of detection: autopsy | SR with MA (4 studies including prospective and observational studies) # participants NR; nonsurvivors of cardiac arrest | NR | NR | 2.93 (1.01 to 8.46) I2 = 0.0% | P = 0.05 |
Gao et al. (2021)41 | Definition: pneumothorax Method of detection: autopsy, PMCT, diagnostic imaging, medical records, or clinical follow-up | SR with MA (7 studies including 1 RCT, prospective and retrospective observational studies) # participants NR; IHCA, OHCA or nonsurvivors of cardiac arrest | NR | NR | 1.64 (0.72 to 3.76) I2 = 39.73% | NR |
AutoPulse, LUCAS, or mix of AutoPulse and LUCAS vs. manual compressions | ||||||
Gao et al. (2021)41 | Definition: Visceral injuries Method of detection: autopsy, diagnostic imaging, or medical records | SR with MA (3 retrospective observational studies) # participants NR; OHCA or nonsurvivors of cardiac arrest | NR | NR | 3.04 (0.41 to 22.54) I2 = 85.33% | P = 0.28 |
Gao et al. (2021)41 | Definition: Heart lesions Method of detection: autopsy, PMCT, diagnostic imaging, or medical records | SR with MA (8 studies including prospective and retrospective observational studies) # participants NR; OHCA or nonsurvivors of cardiac arrest | NR | NR | 2.10 (1.25 to 3.55) I2 = 40.96% | NR |
Gao et al. (2021)41 | Definition: Lung lesions Method of detection: autopsy, PMCT, diagnostic imaging, medical records, or clinical follow-up | SR with MA (8 studies including 1 RCT, prospective and retrospective observational studies) # participants NR; OHCA or all nonsurvivors of cardiac arrest | NR | NR | 1.94 (0.83 to 4.56) I2 = 68.94% | P = 0.13 |
Gao et al. (2021)41 | Definition: Liver lesions Method of detection: autopsy, PMCT, diagnostic imaging, medical records, or clinical follow-up | SR with MA (8 studies including 1 RCT, prospective and retrospective observational studies) # participants NR; IHCA, OHCA, or all nonsurvivors of cardiac arrest | NR | NR | 2.75 (1.22 to 6.20) I2 = 44.92% | P = 0.01 |
Gao et al. (2021)41 | Definition: Spleen lesions Method of detection: autopsy, PMCT, diagnostic imaging, or medical records | SR with MA (3 studies including prospective and retrospective observational studies) # participants NR; OHCA or nonsurvivors of cardiac arrest | NR | NR | 1.06 (0.13 to 8.63) I2 = 67.28% | NR |
Gao et al. (2021)41 | Definition: Kidney and perirenal lesions Method of detection: autopsy, PMCT, diagnostic imaging, or medical records | SR with MA (4 studies including prospective and retrospective observational studies) # participants NR; OHCA or nonsurvivors of cardiac arrest | NR | NR | 3.09 (0.72 to 13.36) I2 = 0.0% | NR |
Gao et al. (2021)41 | Definition: Pneumothorax Method of detection: autopsy, PMCT, diagnostic imaging, medical records, or clinical follow-up | SR with MA (9 studies including 1 RCT, prospective and retrospective observational studies) # participants NR; IHCA, OHCA, or nonsurvivors of cardiac arrest | NR | NR | 2.05 (1.19 to 3.54) I2 = 21.1% | P = 0.01 |
CI = confidence interval; IHCA = in-hospital cardiac arrest; LUCAS = Lund University Cardiac Assist System; MA = meta-analyses; NR = not reported; OHCA = out-of-hospital cardiac arrest; PMCT = postmortem; RCT = randomized controlled trial; RoB = risk of bias; SR = systematic review; vs. = versus.
Table 13: Summary of Findings by Outcomes — Other Soft Tissue Injuries
Citation | Outcome definition, method of detection | Evidence source, characteristics of participants | Outcome result | Odds ratio (95% CI) | P value | |
|---|---|---|---|---|---|---|
Automated chest compressions | Manual chest compressions | |||||
AutoPulse vs. manual compressions | ||||||
Gao et al. (2021)41 | Definition: Hemothorax Method of detection: PMCT | 1 retrospective cohort study: Sonnemans et al. (2020) 72 participants; nonsurvivors of cardiac arrest | 16/43 | 14/29 | 0.77 (0.45 to 1.32) | NR |
Gao et al. (2021)41 | Definition: Hemoperitoneum Method of detection: PMCT | 1 retrospective observational study; Koga et al. (2015) 323 participants; nonsurvivors of cardiac arrest | 40/241 | 4/82 | 3.40 (1.36 to 9.22) | NR |
Gao et al. (2021)41 | Definition: retrosternal bleeding Method of detection: PMCT | 1 retrospective observational study; Koga et al. (2015) 323 participants; nonsurvivors of cardiac arrest | 55/241 | 16/82 | 1.17 (0.71 to 1.92) | NR |
Gao et al. (2021)41 | Definition: Skin lesion Method of detection: autopsy | 1 retrospective observational study; Pinto et al. (2013) 175 participants; nonsurvivors of cardiac arrest | 84/88 | 21/87 | 3.95 (2.72 to 5.76) | NR |
LUCAS vs. manual compressions | ||||||
Gao et al. (2021)41 | Definition: Hemoperitoneum Method of detection: autopsy, diagnostic imaging, or medical records | SR with MA (2 retrospective observational studies) # participants NR; OHCA or nonsurvivors of cardiac arrest | NR | NR | 5.44 (1.31 to 22.55) I2 = 0.00 | NR |
Gao et al. (2021)41 | Definition: Skin lesion Method of detection: autopsy, diagnostic imaging, or medical records | SR with MA (4 studies including prospective and retrospective observational studies) # participants NR; OHCA or nonsurvivors of cardiac arrest | NR | NR | 3.80 (1.87 to 7.70) I2 = 56.85% | NR |
Gao et al. (2021)41 | Definition: Hemothorax Method of detection: autopsy, PMCT, diagnostic imaging, or medical records | SR with MA (5 studies including prospective and retrospective observational studies) # participants NR; OHCA or nonsurvivors of cardiac arrest | NR | NR | 3.62 (1.92 to 6.83) I2 = 0.00% | NR |
Gao et al. (2021)41 | Definition: retrosternal bleeding Method of detection: autopsy, PMCT | SR with MA (4 studies including prospective and retrospective observational studies) # participants NR; nonsurvivors of cardiac arrest | NR | NR | 1.39 (0.97 to 1.98) I2 = 0.00% | NR |
Gao et al. (2021)41 | Definition: mediastinal hemorrhage Method of detection: autopsy | SR with MA (4 studies including prospective and retrospective observational studies) # participants NR; nonsurvivors of cardiac arrest | NR | NR | 1.87 (0.96 to 3.63) I2 = 21.58% | NR |
AutoPulse, LUCAS, or mix of AutoPulse and LUCAS vs. manual compressions | ||||||
Gao et al. (2021)41 | Definition: Hemoperitoneum Method of detection: autopsy, PMCT, diagnostic imaging, or medical records | SR with MA (3 retrospective observational studies) # participants NR; OHCA or nonsurvivors of cardiac arrest | NR | NR | 3.97 (1.76 to 8.99) I2 = 0.00% | NR |
Gao et al. (2021)41 | Definition: Skin lesion Method of detection: autopsy, diagnostic imaging, or medical records | SR with MA (5 studies including prospective and retrospective observational studies) # participants NR; OHCA or nonsurvivors of cardiac arrest | NR | NR | 3.53 (2.34 to 5.33) I2 = 58.79% | NR |
Gao et al. (2021)41 | Definition: Hemothorax Method of detection: autopsy, PMCT, diagnostic imaging, or medical records | SR with MA (6 studies including prospective and retrospective observational studies) # participants NR; OHCA or nonsurvivors of cardiac arrest | NR | NR | 2.24 (0.87 to 5.79) I2 = 70.80% | NR |
Gao et al. (2021)41 | Definition: retrosternal bleeding Method of detection: autopsy, PMCT | SR with MA (5 studies including prospective and retrospective observational studies) # participants NR; nonsurvivors of cardiac arrest | NR | NR | 1.31 (0.98 to 1.75) I2 = 0.00 | NR |
CI = confidence interval; IHCA = in-hospital cardiac arrest; LUCAS = Lund University Cardiac Assist System; MA = meta-analyses; NR = not reported; OHCA = out-of-hospital cardiac arrest; PMCT = postmortem; RCT = randomized controlled trial; RoB = risk of bias; SR = systematic review; vs. = versus.
Table 14: Summary of Recommendations in Included Guidelines
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
|---|---|
European Resuscitation Council (2021)45 | |
Recommendations for mechanical [automated] chest compression devices:
Supporting evidence: Based on 8 RCTs in ILCOR 2015 CoSTR, 2 new RCTs, 6 SRs and MAs. | Quality of evidence: Quality of evidence reported for 1 of the new SRs as very-low certainty evidence. Strength of recommendation: NR |
Special cause recommendations:a
Supporting evidence: Based on 8 RCTs in ILCOR 2015 CoSTR, 2 new RCTs, 6 SRs and MAs. | |
Special setting recommendations:a
Supporting evidence: Based on 8 RCTs in ILCOR 2015 CoSTR, 2 new RCTs, 6 SRs and MAs. | |
American Heart Association (2020)44 | |
Adult BLS and ALS: Alternative CPR techniques and devicesb Recommendation: “The use of mechanical [automated] CPR devices may be considered in specific settings where the delivery of high-quality manual compressions may be challenging or dangerous for the provider, as long as rescuers strictly limit interruptions in CPR during deployment and removal of the device.” Supporting evidence: Based on limited data. “Acknowledging these data, the use of mechanical [automated] CPR devices by trained personnel may be beneficial in settings where reliable, high-quality manual compressions are not possible or may cause risk to personnel (i.e., limited personnel, moving ambulance, angiography suite, prolonged resuscitation, or with concerns for infectious disease exposure).” | Level of evidence: NR Class of recommendation: Weak evidence where benefits may be greater than risks |
Adult BLS and ALS: Alternative CPR techniques and devicesb Recommendation: “The routine use of mechanical [automated] CPR devices is not recommended.” Supporting evidence: Based on limited data. “Acknowledging these data, the use of mechanical [automated] CPR devices by trained personnel may be beneficial in settings where reliable, high-quality manual compressions are not possible or may cause risk to personnel (i.e., limited personnel, moving ambulance, angiography suite, prolonged resuscitation, or with concerns for infectious disease exposure).” | Level of evidence: NR Class of recommendation: Weak evidence where benefits may be equal to risks |
ALS = advanced life support; BLS = basic life support; CoSTR = Consensus on Science and Treatment Recommendations; CPR = cardiopulmonary resuscitation; ECPR = extracorporeal cardiopulmonary resuscitation; ILCOR = International Liaison Committee on Resuscitation; MA = meta-analysis; NR = not reported; RCT = randomized controlled trial; ROSC = return of spontaneous circulation; SR = systematic review.
aFor this guideline,45 we limited our data extraction to mechanical devices for “compression” and not for other types of mechanical devices (e.g., extracorporeal membrane oxygenation); the complete guidance with recommendations for all devices, settings, and circumstances can be found in the guideline publication
bThis guideline44 referred to “mechanical CPR devices” as those that “deliver automated chest compressions,” and the recommendations for these devices were considered relevant for data extraction.
Appendix 5: Overlap Between Included SRs
Please note that this appendix has not been copy-edited.
Table 15: Overlap in Relevant Primary Studies Between Included SRs
Primary study citation | Almulihi et al. (2024)40 | Larik et al. (2024)42 | Zhu and Fu (2024)43 | Gao et al. (2021)41 |
|---|---|---|---|---|
Anantharaman et al. Singapore Med J. 2017;58:424 to 431. | — | Yes | Yes | — |
Axelsson et al. Resuscitation. 2006;71:47 to 55. | — | Yes | Yes | — |
Axelsson et al. Am J Emerg Med. 2013;31:1196 to 1200. | — | — | Yes | — |
Baumeister et al. J Forensic Radiol Imaging. 2015;3(3):167 to 173. | — | — | — | Yes |
Canakci et al. Cureus. 2021;13(5):e15131. | — | — | Yes | — |
Casner et al. Prehosp Emerg Care. 2005;9:61 to 67. | — | Yes | Yes | — |
Chen et al. Int J Environ Res Public Health. 2021;18:3636. | — | Yes | Yes | — |
de Wilde et al. Resuscitation. 2008;77:S49. | — | — | Yes | — |
Friberg et al. Eur Heart J Qual Care Clin Outcomes. 2019;5(3):259 to 265. | — | — | — | Yes |
Gao et al. Arch Med Sci. 2016;12:563 to 570. | Yes | Yes | Yes | — |
Gonzales et al. Am J Emerg Med. 2019;37:913 to 920. | — | Yes | — | — |
Halhalli et al. J Emerg Med. 2020;59:680 to 686. | — | — | Yes | — |
Hallstrom et al. JAMA. 2006;295:2620 to 2628. | Yes | Yes | Yes | — |
Hardig et al. Resuscitation. 2017;115:155 to 162. | — | — | Yes | — |
Hayashida et al. J Am Heart Assoc. 2017;6:e007420. | Yes | Yes | Yes | — |
Hock Ong et al. Crit Care. 2012;16:R144. | Yes | — | Yes | — |
Jennings et al. BMC Emerg Med. 2012;12:8. | Yes | Yes | Yes | — |
Jung et al. J Emerg Med. 2020;58:424 to 431. | — | — | Yes | — |
Karasek et al. J Emerg Med. 2020;59:673 to 679. | — | — | Yes | — |
Koga et al. Resuscitation. 2015;96:226 to 231. | — | — | — | Yes |
Koster et al. Eur Heart J. 2017;38(40):3006 to 3013. | Yes | — | — | Yes |
Lairet and Lee. Ann Emerg Med. 2005;46:S114. | — | — | Yes | — |
Lardi et al. Int J Legal Med. 2015;129(5):1035 to 1042. | — | — | — | Yes |
Liu. Chin J Emerg Disaster. 2016;10:657 to 659. | — | — | Yes | — |
Mastenbrook et al. Cureus. 2022;14:e26131. | — | Yes | Yes | — |
Maule. Urgences Accueil. 2007;7:4 to 7. | — | — | Yes | — |
Milling et al. Acta Anaesthesiol Scand. 2019;63(6):789 to 795. | — | — | — | Yes |
Mistraletti et al. Resuscitation. 2023;182:109659. | — | Yes | — | — |
Morozov et al. Eur Heart J. 2012;3:S702. | — | — | Yes | — |
Newberry et al. Prehosp Emerg Care. 2018;22:338 to 434. | — | Yes | Yes | — |
Omori et al. Resuscitation. 2013;84(8):1045 to 1050. | Yes | — | — | — |
Ondruschka et al. Forensic Sci Med Pathol. 2018;14(4):515 to 525. | — | — | — | Yes |
Ong et al. JAMA. 2006;295:2629 to 2637. | Yes | Yes | Yes | — |
Ornato et al. Prehosp Emerg Care 2005;9:104. | — | — | Yes | — |
Paradis et al. Circulation. 2009;120:S1457. | — | — | Yes | — |
Perkins et al. Lancet. 2015;385:947 to 955. | — | Yes | Yes | — |
Pinto et al. J Forensic Sci. 2013;58(4):904 to 905. | — | — | — | Yes |
Primi et al. J Clin Med. 2023;12:4429. | Yes | — | Yes | — |
Rubertsson et al. JAMA. 2014;311:53 to 61. | — | Yes | Yes | — |
Saleem et al. Emerg Med. 2022;14:557 to 562. | — | — | Yes | — |
Satterlee et al. J Emerg Med. 2013;45:562 to 569. | — | Yes | Yes | — |
Savastano et al. Int J Cardiol. 2019;287:81 to 85. | — | Yes | Yes | — |
Schmidbauer et al. Resuscitation. 2017;120:95 to 102. | — | — | Yes | — |
Seewald et al. PloS One. 2019;14:e0208113. | — | — | Yes | — |
Smekal et al. Resuscitation. 2009;80(10):1104 to 1107. | — | — | — | Yes |
Smekal et al. Resuscitation. 2011;82:702 to 706. | — | Yes | Yes | — |
Smekal et al. Resuscitation. 2014;85(12):1708 to 1712. | — | — | — | Yes |
Sonnemans et al. Eur J Emerg Med. 2020;27(3):197 to 201. | — | — | — | Yes |
Spiro et al. Int J Cardiol. 2015;180:7 to 14. | Yes | — | — | — |
Steinmetz et al. Acta Anaesthesiol Scand. 2008;52:908 to 913. | Yes | — | Yes | — |
Swanson et al. Circulation. 2006;114:554. | — | — | Yes | — |
Takayama et al. J Pers Med. 2023;13:1202. | — | — | Yes | — |
Tantarattanapong and Chantaramanee. Emerg Med. 2022;14:599 to 608. | — | Yes | Yes | — |
Truhlar et al. Resuscitation. 2010;81:S62. | — | — | Yes | — |
Ujvárosy et al. BMC Cardiovasc Disord. 2018;18:227. | — | — | Yes | — |
Viniol et al. Eur J Radiol. 2020;131:109244. | — | — | Yes | — |
Wik et al. Resuscitation. 2014;85:741 to 748. | Yes | Yes | Yes | — |
Zeiner et al. Resuscitation. 2015;96:220 to 225. | Yes | Yes | Yes | — |
Appendix 6: References of Potential Interest
Please note that this appendix has not been copy-edited.
Guidance Documents
BC Emergency Health Services. PR31: Automated CPR Devices. [date not specified] Accessed February 25, 2025. https://handbook.bcehs.ca/clinical-practice-guidelines/pr-clinical-procedure-guide/pr31-automated-cpr-devices/
Craig S, Cubitt M, Jaison A, et al. Management of adult cardiac arrest in the COVID-19 era: consensus statement from the Australasian College for Emergency Medicine. Med J Aust. 2020;213(3):126-133. doi:10.5694/mja2.50699 PubMed
Agency for Clinical Innovation. NSW automated cardiopulmonary resuscitation (mCPR). 2021. Accessed February 25, 2025. https://aci.health.nsw.gov.au/__data/assets/pdf_file/0003/645078/ACI-NSW-automated-cardiopulmonary-resuscitation-mCPR.pdf
Systematic Review With Insufficient Quantitative Information
El-Menyar A, Naduvilekandy M, Rizoli S, et al. Automated versus manual cardiopulmonary resuscitation (CPR): an umbrella review of contemporary systematic reviews and more. Crit Care. 2024;28(1):259. doi:10.1186/s13054-024-05037-4 PubMed
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.