Drugs, Health Technologies, Health Systems
Health Technology Review
Quetiapine for Bipolar Disorder
Summary
Main Take-Away
Quetiapine, among other antipsychotics, could be used as a first-line treatment option for the management of bipolar disorder in adults.
Key Messages
What Is the Issue?
Pharmacological treatments used for bipolar disorder include mood stabilizers (e.g., lithium, valproate), atypical (second generation) antipsychotics (e.g., quetiapine, lurasidone, cariprazine, olanzapine, aripiprazole, ziprasidone), either alone or in combination, as well as the occasional addition of antidepressants or benzodiazepines.
Decision-makers are interested in understanding quetiapine’s place in therapy compared with other medications for the treatment of bipolar disorder in adults.
What Did We Do?
We searched key resources, including journal citation databases, and conducted a focused internet search for relevant evidence published since 2020.
What Did We Find?
Clinical evidence suggests that quetiapine and lithium have similar efficacy and safety for the treatment of bipolar depression in adults. Quetiapine appears to be efficacious for the treatment of bipolar depression in adults despite its adverse effects, such as somnolence and weight gain.
Evidence-based guidelines recommend the use of antipsychotics (including quetiapine), either as monotherapy or in combination with a mood stabilizer, for both the treatment and maintenance of mania (or hypomania) and bipolar depression. The choice of antipsychotic should be guided by patient preference and past response to therapy.
What Does This Mean?
Quetiapine, among other antipsychotics, could be used as first-line treatment option for the management of bipolar disorder in adults.
The prescribing of antipsychotics (either alone or in combination with a mood stabilizer) for the management of bipolar disorder should be guided by patient characteristics, patient tolerability, patient values, side effect profiles of individual antipsychotic medications, and clinician expertise.
Abbreviations
AE
adverse event
CANMAT
Canadian Network for Mood and Anxiety Treatments
CI
confidence interval
CGI-BP-S
Clinical Global Impressions-Bipolar-Severity
CrI
credible interval
GRADE
Grading of Recommendations Assessment, Development and Evaluation
HAM-D17
17-item Hamilton Depression Rating Scale
ISBD
International Society for Bipolar Disorders
MA
meta-analysis
MADRS
Montgomery-Åsberg Depression Rating Scale
MD
mean difference
NICE
National Institute for Health and Care Excellence
NMA
network meta-analysis
OR
odds ratio
RCT
randomized controlled trial
RR
relative risk
SMD
standardized mean difference
SR
systematic review
VA/DoD
Department of Veterans Affairs/Department of Defense
Context and Policy Issues
What Is Bipolar Disorder?
Bipolar disorder is a chronic mental illness that affects up to 3% of people in Canada over their lifetime.1 The disorder is characterized by cyclical periods of mania (excessive excitement, energy, or euphoria) or hypomania (a milder form of mania) and usually depression.2 The onset of bipolar disorder commonly occurs during late adolescence or early adulthood.3 Although both environmental and genetic factors contribute to the development of bipolar disorder,2 it is highly heritable, with approximately 85% of the risk attributable to genetics.4 Environmental factors include a history of childhood trauma, substance use (especially high-potency tetrahydrocannabinol [THC]), and maternal and childhood infection exposure, among others.2
There are several types of bipolar disorder, including bipolar I disorder, bipolar II disorder, and cyclothymic disorder. Patients diagnosed with specified or unspecified bipolar disorder do not meet the full bipolar diagnostic criteria but have symptoms characteristic of the disorder and experience distress or functional impairment.5 To be diagnosed with bipolar I disorder, an individual must have experienced at least 1 manic episode, with or without depressive episodes. Bipolar II disorder is characterized by at least 1 hypomanic episode and 1 or more major depressive episodes.5 A cyclothymic disorder diagnosis requires at least 2 years of recurrent hypomania and depression symptoms; however, the full criteria for a hypomanic or depressive episode are not met.5
What Are the Medications for Treatment of Bipolar Disorder?
Both acute and maintenance treatment are required for optimal management of bipolar disorder. For decades, lithium has been used as a long-term mood stabilizer.6,7 Many antipsychotics are effective for short-term treatment of bipolar disorder mania and may have more rapid antimanic effects than lithium.8 Some atypical antipsychotics — including quetiapine, lurasidone, cariprazine, and olanzapine — can be used alone or in combination with mood stabilizers for the treatment of acute episodes or the prevention of recurrence of both mania and bipolar depression.9 The anticonvulsants divalproate and carbamazepine have also been approved for treatment of acute maniac episodes.8 Antidepressant monotherapy is not recommended for the treatment of bipolar depression.10
Immediate-release quetiapine tablets are available as 25 mg, 100 mg, 200 mg, and 300 mg of quetiapine fumarate,11 while extended-release quetiapine (quetiapine XR) tablets are available as 50 mg, 150 mg, 200 mg, 300 mg, and 400 mg of quetiapine fumarate.12
Why Is It Important to Do This Review?
Quetiapine is approved for the treatment of bipolar disorder based on short-term (12 weeks) efficacy trials.11,12 Data on the long-term efficacy and safety of quetiapine in clinical trials has not been systematically evaluated.11 In addition, there have not been systematic evaluations of the relative clinical efficacy and safety of quetiapine with other relevant comparators for the treatment of bipolar disorder.
Objective
To support decision-making about the relative effects of quetiapine for treatment of bipolar disorder, we prepared this Rapid Review to summarize and critically appraise the available studies on the clinical effectiveness and safety of quetiapine compared with other drug interventions for treatment of adults with bipolar disorder. We also sought to summarize recommendations from evidence-based guidelines on the use of quetiapine for the management of adults with bipolar disorder.
Research Questions
What is the clinical effectiveness and safety of quetiapine versus other drug interventions for adults with bipolar disorder?
What are the evidence-based guidelines regarding the use and administration of quetiapine for adults with bipolar disorder?
Methods
Literature Search Methods
An information specialist conducted a literature search on key resources, including MEDLINE, Embase, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concepts were quetiapine and bipolar disorder. Search filters were applied to limit retrieval to health technology assessments, systematic reviews (SRs), meta-analyses (MAs), or indirect treatment comparisons, randomized controlled trials (RCTs), controlled clinical trials, or guidelines. The search was completed on March 27, 2025, and was limited to English-language documents published since January 1, 2020.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Adults aged 18 years or older with bipolar disorder |
Intervention | Quetiapine fumarate immediate-release tablets, quetiapine fumarate extended-release tablets |
Comparator | Other drug interventions (e.g., other second-generation atypical antipsychotics, mood stabilizers, antidepressants) |
Outcomes |
|
Study designs | RCTs, systematic reviews (including NMAs and MAs), evidence-based guidelines,a published HTAs |
HTA = health technology assessment; MA = meta-analysis; NMA = network meta-analysis; RCT = randomized controlled trial.
aA guideline is defined as a systematically developed statement or set of statements to assist practitioner and patient decisions about appropriate health care for specific clinical circumstances. A guideline is considered evidence-based if a systematic search of the literature was undertaken to inform the recommendations.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1 or they were published before 2020. SRs in which all relevant studies were captured in other more recent or more comprehensive SRs were excluded. Primary studies retrieved by the search were excluded if they were captured in 1 or more included SRs. Guidelines with unclear methodology were also excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A Measurement Tool to Assess Systematic Reviews 2 (AMSTAR 2)13 for SRs, the International Society for Pharmacoeconomics and Outcomes Research (ISPOR) questionnaire to assess the relevance and credibility of a network meta-analysis14 for network meta-analyses (NMAs), and the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument15 for guidelines. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
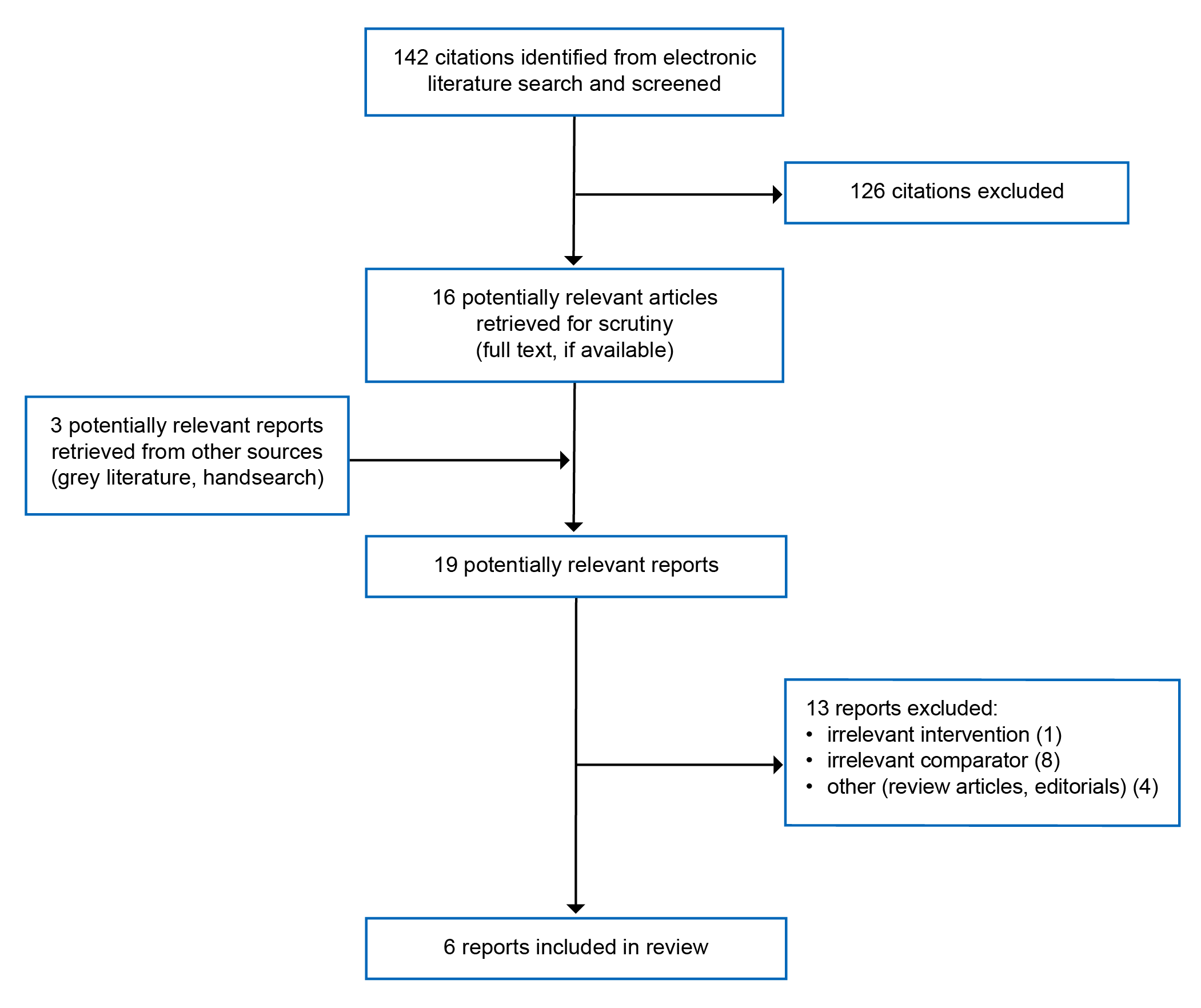
A total of 142 citations were identified in the literature search. Following screening of titles and abstracts, 126 citations were excluded and 16 potentially relevant reports from the electronic search were retrieved for full-text review. Three potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 13 publications were excluded for various reasons, and 6 publications met the inclusion criteria and were included in this report. These comprised 3 SRs and 3 evidence-based guidelines. Appendix 1 presents the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)16 flow chart of the study selection.
Summary of Study Characteristics
Appendix 2 provides details regarding the characteristics of the included SRs17-19 and guidelines.20-22
Included Studies for Research Question 1: What Is the Clinical Effectiveness and Safety of Quetiapine Versus Other Drug Interventions for Adults With Bipolar Disorder?
Study Design
Three SRs17-19 were included to answer research question 1.
The SR by Ogasawara et al. (2022)17 included 3 RCTs and used MA to compare the efficacy and safety of quetiapine and lithium for bipolar depression. The literature search was conducted until March 2021. Continuous outcome data were summarized using effect size, with standardized mean difference (SMD) and 95% confidence interval (CI); for dichotomous outcome (having 2 possible values) data, relative risk (RR) with 95% CI were used. A random-effects model was used for outcome data analyses. For rare dichotomous outcomes, odds ratios (ORs) with 95% CI were used for analyses.
The SR by Tao et al. (2022)23 included 17 studies. The study designs of the included primary studies were not described. The SR used MA to compare the efficacy and safety of quetiapine and aripiprazole for bipolar depression. The literature search covered the period of 2000 to 2021. The pooled effect size with a 95% CI was obtained using a random- or fixed-effects model based on the I2 value, which describes the percentage of total variation across trials that is due to heterogeneity rather than chance or sampling errors. The dichotomous outcomes were reported as RRs or ORs with 95% CIs.
The SR by Kadakia et al. (2021)19 included 18 RCTs and used Bayesian NMA to compare the relative efficacy and tolerability of atypical antipsychotic monotherapy in adults with bipolar depression. The authors included studies identified up to May 2015 in a recent NMA examining bipolar depression and conducted an updated search to identify studies published between May 2015 and May 2020. The authors initially performed a pairwise MA using a random-effects model. NMA was conducted with a Bayesian framework, and the methodology followed guidance from the ISPOR Task Force on Indirect Treatment Comparisons. The relative effect estimates were described as SMDs or mean differences (MDs) for efficacy-related continuous outcomes and as ORs for binary outcomes with 95% credible intervals (CrIs). All identified trials were placebo-controlled RCTs, leading to star-shaped networks.
Country of Origin
The 3 SRs were conducted by authors in Japan,17 China,23 and the US.19
Patient Population
The interested patient populations included in all 3 SRs17-19 were patients diagnosed with bipolar I or II depression. Two SRs17,19 reported a higher proportion of female patients, while the SR by Tao et al. (2022)23 did not report details of patient demographics and characteristics.
Interventions and Comparators
The SR by Ogasawara et al. (2022)17 compared quetiapine with lithium, while the SR by Tao et al. (2022)18 compared aripiprazole with quetiapine. The interventions investigated in the SR by Kadakia et al. (2021)19 were atypical antipsychotics (i.e., aripiprazole, cariprazine, olanzapine, quetiapine, ziprasidone, and lurasidone).
Outcomes
Outcomes assessed in the included SRs included remission rates, response rates, dropout rates, metabolic outcomes, and adverse events (AEs). Patient-reported outcomes, such as health-related quality of life (HRQoL), were not reported in any of the included SRs.
Remission rate was assessed using the either Montgomery-Åsberg Depression Rating Scale (MADRS) or the 17-item Hamilton Depression Rating Scale (HAM-D17). Remission was defined as a score of less than or equal to 12 on the on the MADRS or less than or equal to 7 on the HAM-D17 at the study end point.
Response rate was also assessed using the MADRS and was defined as greater than or equal to 50% improvement in MADRS score.
The Clinical Global Impressions-Bipolar-Severity (CGI-BP-S) Scale was used to assess depression, mania, and overall illness, for which a higher score is associated with greater illness severity.
Included Studies for Research Question 2: What Are the Evidence-Based Guidelines Regarding the Use and Administration of Quetiapine for Adults With Bipolar Disorder?
Study Design
Three evidence-based guidelines20-22 were included to answer research question 2.
The National Institute for Health and Care Excellence (NICE) guideline20 was developed by a panel of health care professionals involved in the care of people with bipolar disorder. Committee members developed review questions, reviewed research evidence, incorporated an economic evaluation and other guidance, and wrote recommendations. Systematic methods were used to search for evidence. The quality of evidence was rated using the Grading of Recommendations Assessment, Development and Evaluation (GRADE). However, this guideline did not report the strength of the recommendations and the level of evidence.
The US Department of Veterans Affairs (VA)/Department of Defence (DoD) clinical practice guideline21 was developed by a panel of multidisciplinary experts in psychiatry, psychology, internal medicine, nursing, primary care, pharmacy, mental health counselling, and social work. The working group determined the scope of the guideline, crafted key questions to guide the systematic evidence review, identified discussion topics, provided direction on inclusion and exclusion criteria, developed evidence-based recommendations, and determined the strength and category of each recommendation. The working group used the GRADE approach to craft each recommendation and determined its strength (i.e., strong or weak) based on 4 domains:
confidence in the quality of the evidence
balance of desirable and undesirable outcomes
patient values and preferences
other considerations (e.g., resource use, equity, acceptability, feasibility, subgroup considerations).
The strength of recommendation was described by the working group with the following general corresponding text:
Strong for (“We recommend…”)
Weak for (“We suggest…”)
Neither for nor against (“There is insufficient evidence to recommend for or against…”)
Weak against (“We suggest against…”)
The Canadian Network for Mood and Anxiety Treatments (CANMAT) and the International Society for Bipolar Disorders (ISBD) guidelines published in 202322 provide a summary and updates of the 2018 CANMAT and ISBD guideline recommendations for the treatment of bipolar disorder.24 The treatment recommendations were ranked as first, second, and third line, taking into consideration safety, tolerability, and risk of treatment-emergent affective switch. The definitions of the level of evidence and the strength of recommendations are as follows.
Level of evidence:
Level 1: MA with narrow CI or replicated double-blind RCT that includes a placebo or active control comparison (N ≥ 30 in each active treatment arm)
Level 2: MA with wide CI or 1 double-blind RCT with placebo or active control comparison condition (N ≥ 30 in each active treatment arm)
Level 3: At least 1 double-blind RCT with placebo or active control comparison condition (N = 10 to 29 in each active treatment arm) or health system administrative data
Level 4: Uncontrolled trial, anecdotal reports, or expert opinion
Strength of recommendation
First line: Level 1 or level 2 evidence for efficacy plus clinical support for safety and/or tolerability as well as no risk of treatment-emergent switch
Second line: Level 3 or higher evidence for efficacy plus clinical support for safety and/or tolerability and low risk of treatment-emergent switch
Third line: Level 4 evidence or higher for efficacy plus clinical support for safety and/or tolerability
Not recommended: Level 1 evidence for lack of efficacy or level 2 evidence for lack of efficacy plus expert opinion
Country of Origin
The authors of the NICE guideline, the VA/DoD guideline, and the CANMAT and ISBD guideline were from the UK,20 the US,21 and Canada22 (with the participation of authors from various countries in the original publication24), respectively.
Patient Population
The patient population in the NICE guideline20 and the CANMAT and ISBD guideline22 includes adults, adolescents, and children with bipolar disorder, while the target population in the VA/DoD guideline21 is adults with bipolar and related disorders. The intended users of all 3 guidelines include health care professionals, patients, and patients’ family members caring for individuals with bipolar disorder.
Interventions and Practice Considered
The NICE guideline20 provides clinical practice recommendations for recognizing, assessing, and treating bipolar disorder, including bipolar I, bipolar II, and related disorders.
The VA/DoD guideline21 provides clinical practice recommendations for the management of bipolar disorder with various treatments, including screening and evaluation, pharmacotherapy, other somatic therapies, psychosocial and recovery-oriented therapy, and supportive care.
The CANMAT and ISBD guideline22 provides recommendations on the pharmacological and psychological treatments of various phases of bipolar disorder throughout the patient’s lifespan.
Outcomes
The included guidelines20-22 considered all relevant outcomes related to the clinical questions crafted in the guidelines, including short-, intermediate-, and long-term outcomes.
Summary of Critical Appraisal
The SRs17,18 with MA were explicit in their respective objectives and inclusion criteria for the review. One SR17 had published the study protocol before the conduct of the review, whereas the other SR18 did not. The lack of a published protocol increased the risk of modifying the methods after the completion of the review. The literature search strategy was comprehensive and clearly described in both SRs. Both SRs partially described the characteristics of the included studies but did not provide a list of excluded studies and the reasons for exclusion. Therefore, it was not possible to assess whether any relevant articles were excluded and, if they were, for what reasons. The methodological quality of the included studies in both SRs was assessed using the Cochrane Risk of Bias tool. In both SRs, the review authors provided a discussion of the heterogeneity observed in the results. The review authors for both SRs reported the source of funding and declared potential conflicts of interest. Overall, both SRs17,18 had several limitations in reporting.
The SR with NMA by Kadakia et al. (2021)19 included relevant populations, interventions, and outcomes. This NMA also had several strengths contributing to its credibility related to the quality and comprehensiveness of the evidence base, appropriate analysis methods, and the reporting and interpretation of results. Specifically, the rationale for the study and the study objectives were clearly stated. The authors clearly presented the literature search methods, search terms, search dates, search strategy, and criteria for the SR, with an attempt to identify and include all relevant RCTs. All included RCTs were assessed for risk of bias using the Cochrane Risk of Bias tool, with the results presented and discussed in the context of both risk of bias and heterogeneity. Study selection, appraisal, and data extraction were performed in duplicate. The primary outcome (i.e., change in the MADRS total score) was clearly defined. The authors provided a description of the analysis methods and models, and a description and justification for the statistics used. The analysis in the primary model was well-conducted using appropriate methodology. For instance, random-effect Bayesian NMA was used to combine evidence from RCTs that formed a connected network of intervention comparisons. This methodology combines both direct and indirect evidence and allows for comparison of interventions not directly compared in head-to-head RCTs as long as the interventions form part of a connected network. Vague priors were assumed for all parameters. The model was implemented in the Bayesian OpenBUGS software. Studies were assessed for heterogeneity using the I2 measure before inclusion in the analysis. The methodology followed guidance from the ISPOR Task Force on Indirect Treatment Comparisons. Sensitivity analyses were conducted to examine the impact of pooled versus stratified doses of each of the included atypical antipsychotics, and the results were largely similar to the base-case findings. Network diagrams of connected interventions were presented. Study characteristics and patient characteristics of the included RCTs were presented. Heterogeneity observed in the results was discussed. The authors presented direct estimates and network estimates with 95% CIs and 95% CrIs, respectively. The authors provided a clear summary of main findings and discussed the strengths and limitations at the study and outcome level. Overall, this SR19 with NMA was conducted with relatively good methodology.
For reporting, the NICE and VA/DoD guidelines20,21 were explicit in terms of scope and purpose (i.e., objectives, health questions, and populations), and had a clear presentation of recommendations (i.e., specific, unambiguous, easy-to-find key recommendations, options for managing the different conditions or health issues). In terms of interested party involvement, the authors of these 2 guidelines20,21 clearly defined target users and the guideline development groups and reported that the views and preferences of the patients were sought. The methodology for the development of both guidelines20,21 was robust. The authors of these guidelines20,21 clearly reported methods for evidence collection, criteria for selection, and methods for evidence synthesis. There were explicit links between recommendations and the supporting evidence, and methods of formulating the recommendations. Also, the authors of both guidelines20,21 considered the clinical benefits and risks of side effects in formulating the recommendations. Both guidelines20,21 will be updated when new important information and appropriate comments are received. However, specific dates are not indicated. Both guidelines20,21 were reviewed independently by relevant professional experts as well as professional colleges and societies through public consultation. However, there are some limitations related to guideline implementation and applicability. Specifically, facilitators and barriers to application, and the monitoring or auditing criteria were unclear. Both guidelines20,21 provide advice and/or tools on how the recommendations can be put into practice. For editorial independence, the authors of both guidelines20,21 declared competing interests of all guideline development group members and disclosed that the views of the funding body had no influence on the content of the guidelines. Overall, the included guidelines20,21 were robust in terms of scope and purpose, interested party involvement, rigour of development, clarity of presentation, and editorial independence.
The methodology of the CANMAT and ISBD guideline22 was similarly as robust as the other 2 guidelines,20,21 with the exception that details about interested party involvement and some items in the rigour of development could not be found in the original 2018 publication.24
Additional details regarding the strengths and limitations of the included SRs17-19 are provided in Table 4 and the guidelines20-22 are presented in Table 5 of Appendix 3.
Summary of Findings
Appendix 4 presents the main study findings, which are summarized by outcome. Only comparisons of quetiapine with other antipsychotics are presented.
Clinical Effectiveness and Safety of Quetiapine Versus Other Drug Interventions for Adults With Bipolar Disorder
Remission Rates From Bipolar Depressive Episodes
All included SRs17-19 reported remission rates from bipolar depressive episodes (Table 6). There were no statistically significant differences in the remission rates from depressive episodes between quetiapine and lithium, between quetiapine and aripiprazole, and between quetiapine and lurasidone. However, quetiapine was found to be more efficacious than olanzapine (OR = 1.45; 95% CrI, 1.07 to 1.92) and ziprasidone (OR = 1.96; 95% CrI, 1.45 to 2.78) for remission from depressive episodes.
Change in Scores for Bipolar Depressive Symptoms
All included SRs17-19 reported change in scores for bipolar depressive symptoms (Table 7). No statistically significant differences in the change scores for depressive symptoms were observed between quetiapine and lithium, between quetiapine and olanzapine, and between quetiapine and lurasidone. However, quetiapine was associated with statistically significantly higher reduction in scores for depressive symptoms compared with cariprazine (MD = −2.52; 95% CrI, −4.11 to −0.92), aripiprazole (MD = −3.72; 95% CrI, −6.21 to −1.28), and ziprasidone (MD = −3.46; 95% CrI, −5.76 to −1.24).
Response Rates
Two included SRs18,19 reported response rates (Table 8). Similar to the change scores for depressive symptoms, there were no statistically significant differences in response rates between quetiapine and olanzapine and between quetiapine and lurasidone. However, quetiapine was associated with statistically significantly greater odds of response compared with cariprazine (OR = 1.44; 95% CrI, 1.08 to 1.91), aripiprazole (OR = 1.92; 95% CrI, 1.32 to 2.71), and ziprasidone (OR = 1.92; 95% CrI, 1.35 to 2.86).
Change in Social Functioning
One SR17 reported change in social functioning (Table 9). No statistically significant difference was observed in the changes in social functioning between quetiapine and lithium.
All-Cause Discontinuations
All included SRs17-19 reported all-cause discontinuations (Table 10). No statistically significant differences were observed in all-cause discontinuations when comparing quetiapine with lithium, aripiprazole, cariprazine, or lurasidone. However, the odds of all-cause discontinuation for quetiapine was statistically significantly higher than olanzapine (OR = 1.46; 95% CrI, 1.08 to 1.94) and statistically significantly lower than aripiprazole (OR = 0.61; 95% CrI, 0.43 to 0.85).
Discontinuations Due to AEs
Two included SRs17,19 reported discontinuations due to AEs (Table 11). No statistically significant differences were observed in discontinuations due to AEs when comparing quetiapine with lithium, olanzapine, cariprazine, aripiprazole, or ziprasidone. However, quetiapine was associated with higher odds of discontinuation due to AEs than lurasidone (OR = 2.22; 95% CrI, 1.03 to 5.56).
Discontinuation Due to Lack of Efficacy
One SR19 reported discontinuations due to lack of efficacy (Table 12). Quetiapine had similar odds of discontinuation due to lack of efficacy compared with cariprazine, but lower odds compared with aripiprazole, ziprasidone, or lurasidone.
Suicide-Related Events
One SR17 reported on suicide-related events (Table 13). No statistically significant difference was observed in the risk of suicide in participants who were prescribed quetiapine compared with those who were prescribed lithium.
Serious AEs
One SR17 reported serious AEs (Table 14). No statistically significant difference was observed in the odds of serious AEs between quetiapine and lithium.
Metabolic Outcomes
One SR19 reported on the following outcomes.
Weight gain (Table 15): Quetiapine was associated with statistically significantly less weight gain compared with olanzapine (MD = −1.74; 95% CrI, −2.17 to −1.31), but statistically significantly more weight gain compared with cariprazine (MD = 0.53; 95% CrI, 0.18 to 0.87), aripiprazole (MD = 0.98; 95% CrI, 0.21 to 1.74), and lurasidone (MD = 0.82; 95% CrI, 0.36 to 1.27).
Triglycerides (Table 16): There were no statistically significant differences for change in triglyceride levels between quetiapine and other antipsychotics (i.e., olanzapine, cariprazine, aripiprazole, and lurasidone).
Cholesterol (Table 17): There were no statistically significant differences for change in total cholesterol levels between quetiapine and other antipsychotics (i.e., olanzapine, cariprazine, aripiprazole, and lurasidone).
Low-density lipoprotein (Table 18): There were no statistically significant differences for change in low-density lipoprotein levels between quetiapine and other antipsychotics (i.e., olanzapine, cariprazine, aripiprazole, and lurasidone).
Glucose (Table 19): There were no statistically significant differences for change in glucose levels between quetiapine and other antipsychotics (i.e., olanzapine, cariprazine, aripiprazole, and lurasidone).
Prolactin (Table 20): Quetiapine was associated with a lower change in prolactin levels compared with lurasidone (MD = −6.35; 95% CrI, −11.87 to −0.80). Similar changes in prolactin levels were observed between quetiapine and cariprazine and between quetiapine and aripiprazole.
Other Tolerability Measures
One SR19 reported on the following outcomes.
Somnolence (excessive sleepiness) (Table 21): Quetiapine was associated with higher odds of somnolence compared with the antipsychotics investigated (i.e., olanzapine [OR = 1.75; 95% CrI, 1.09 to 2.66], cariprazine [OR = 2.93; CrI, 1.16 to 5.86], aripiprazole [OR = 2.69; 95% CrI, 1.21 to 5.14], and lurasidone [OR = 2.94; 95% CrI, 1.12 to 10.00]), with the exception of ziprasidone (no difference).
Switch to mania (a depressive episode followed by a manic or hypomanic episode, often within the following 12 weeks) (Table 22): Treatment with quetiapine had statistically significantly lower odds of switch to mania compared with aripiprazole (OR = 0.32; 95% CI, 0.12 to 0.67). However, no statistically significant differences were observed between quetiapine and other antipsychotics, such as olanzapine, cariprazine, and lurasidone.
Extrapyramidal symptoms (involuntary movements induced by certain medications) (Table 23): There were no statistically significant differences in odds of extrapyramidal symptoms occurring between quetiapine and other antipsychotics (i.e., cariprazine, aripiprazole, and lurasidone).
Evidence-Based Guidelines Regarding the Use and Administration of Quetiapine for Adults With Bipolar Disorder
A summary of recommendations from the included guidelines is presented in Table 24 in Appendix 4.
Of note, the NICE guideline and the VA/DoD guideline21 state that the choice of antipsychotic depends on the person’s preference and previous response to treatment. The CANMAT and ISBD guideline22 use the hierarchical ranking approach, in which treatments listed higher up need to be considered first, unless other factors (e.g., history of previous nonresponse or patient preference) dictate otherwise.
Treatment of Mania or Hypomania
The NICE guideline20
recommends the use of quetiapine, haloperidol, olanzapine, or risperidone for people who develop mania or hypomania and who are not taking an antipsychotic or mood stabilizer (strength of recommendation: not reported)
recommends the use of quetiapine, haloperidol, olanzapine, or risperidone for people who are already taking lithium (strength of recommendation: not reported)
recommends adding quetiapine, haloperidol, olanzapine, or risperidone for people who are already taking a mood stabilizer as prophylactic treatment and if there is no improvement after increasing the dose of the mood stabilizer (strength of recommendation: not reported).
The VA/DoD guideline21
suggests using quetiapine or lithium as monotherapy for people with acute mania (weak recommendation, categorized as reviewed, new-added)
suggests adding lithium or valproate in combination with quetiapine, haloperidol, olanzapine, or risperidone for people with acute mania who have an unsatisfactory response with antipsychotic monotherapy (weak recommendation, categorized as reviewed, new-added).
The CANMAT and ISBD guideline22
recommends lithium, quetiapine, divalproex, asenapine, aripiprazole, paliperidone, risperidone, or cariprazine monotherapy options for the treatment of acute mania (strength of recommendation: first line)
recommends a combination of quetiapine, aripiprazole, risperidone, or asenapine with lithium or divalproex as combination therapy options for the treatment of acute mania (strength of recommendation: first line)
does not have specific recommendations for the treatment of hypomania due to lack of clinical trial evidence.
Treatment of Bipolar Depression
The NICE guideline20
recommends the use of combination therapy of fluoxetine with olanzapine or quetiapine for people with moderate or severe bipolar depression (strength of recommendation: not reported)
recommends the use of combination therapy of fluoxetine with olanzapine or quetiapine for people with moderate or severe bipolar depression who are taking lithium and have an inadequate response with an increasing dose of lithium (strength of recommendation: not reported)
recommends the use of combination therapy of fluoxetine with olanzapine or quetiapine for people with moderate or severe bipolar depression who are taking valproate and have an inadequate response with the maximum tolerated dose of valproate (strength of recommendation: not reported).
The VA/DoD guideline21
recommends quetiapine as monotherapy for acute bipolar depression (strong recommendation, categorized as reviewed, new-added).
The CANMAT and ISBD guideline22
recommends quetiapine, lithium, lamotrigine, and lurasidone as monotherapy options; lurasidone and lamotrigine are also recommended as adjunctive treatments for acute bipolar I depression (strength of recommendation: first line)
recommends quetiapine (only drug) as treatment for bipolar II depression (strength of recommendation: first line).
Maintenance (Prevention of Recurrence) Therapy
The VA/DoD guideline21
recommends lithium or quetiapine as monotherapy for the prevention of recurrence of mania (strong recommendation, categorized as reviewed, new-added)
suggests the combination therapy of lithium or valproate with aripiprazole, olanzapine, quetiapine, or ziprasidone for the prevention of recurrence of mania (weak recommendation, categorized as reviewed, new-added)
suggests lithium or quetiapine as monotherapy for the prevention of recurrence of bipolar depressive episodes (weak recommendation, categorized as reviewed, new-added)
suggests combination therapy of lithium or valproate with antipsychotics such as olanzapine, lurasidone, or quetiapine for the prevention of recurrence of bipolar depressive episodes (weak recommendation, categorized as reviewed, new-added).
The CANMAT and ISBD guideline22
recommends lithium, quetiapine, divalproex, lamotrigine, asenapine, or aripiprazole (oral or once-monthly injection) monotherapies as options for maintenance therapy in bipolar I (strength of recommendation: first line)
recommends combination therapies of quetiapine or aripiprazole combined with lithium or divalproex as options for maintenance therapy in bipolar I (strength of recommendation: first line)
recommends quetiapine, lithium, and lamotrigine monotherapies as options for maintenance therapy in bipolar II (strength of recommendation: first line).
Limitations
Evidence Gaps
Clinical evidence on the use of quetiapine for managing mania or hypomania in people with bipolar disorder was not identified. Also, evidence on the use of combination therapy with quetiapine and mood stabilizers was not identified. It is possible that these issues have been addressed before and were not captured in this literature search. Evidence on the effect of quetiapine treatment for bipolar disorder on HRQoL was not identified.
Generalizability
The findings of all included clinical studies, with the exception of the study by Tao et al. (2022),18 could be generalizable to the adult population with bipolar disorder living in Canada. The CANMAT and ISBD guideline22 provides recommendations for the Canadian population with bipolar disorder. Recommendations of the other 2 guidelines20,21 may also be applicable to the Canadian context.
Certainty of Evidence
The included SRs17-19 may have been well conducted, but they may have limitations with respect to their included primary studies. The SR by Ogasawara et al. (2022)17 included only 3 RCTs, leading to a relatively low statistical power. The SR by Tao et al. (2022)18 included only studies from China, with unclear study designs and characteristics, limiting the generalizability of its findings to other populations. The SR by Kadakia et al. (2021)19 included only placebo-controlled RCTs leading to star-shaped networks, and therefore indirect evidence among antipsychotics should be interpreted with caution. The presence of heterogeneity among the primary studies in the included SRs17-19 in terms of patients and study characteristics, inconsistency in reported outcomes, and study quality should be acknowledged when interpreting the findings.
Although the NICE guideline20 and the VA/DoD guideline21 were generally of high methodological quality, the strengths of some relevant recommendations were weak based on low-quality evidence. The CANMAT and ISBD guideline22 used the hierarchical ranking approach based on the levels of evidence to rank the recommendations as first, second, or third line.
Conclusions and Implications for Decision- or Policy-Making
This review included 3 SRs17-19 and 3 evidence-based guidelines,20-22 all of which were relevant to the research questions.
Clinical Efficacy and Safety of Treatment With Quetiapine
There were no differences in the efficacy and safety of quetiapine and lithium for treatment of bipolar depression in terms of remission rate, response rate, discontinuation rate, suicide-related events, and serious AEs.
Quetiapine was found to be more efficacious than olanzapine and ziprasidone for remission from depressive episodes.
Quetiapine had similar rates of discontinuation due to AEs compared to other antipsychotics, except lurasidone (which had a lower rate).
Quetiapine had better response rates compared with cariprazine, aripiprazole, and ziprasidone. There were no differences in response rates between quetiapine and olanzapine or lurasidone.
Quetiapine had lower rates of discontinuation due to lack of efficacy compared with most antipsychotics (i.e., olanzapine, aripiprazole, ziprasidone, lurasidone), except cariprazine (no difference).
Quetiapine was associated with more weight gain compared with most antipsychotics (i.e., cariprazine, aripiprazole, lurasidone), except olanzapine (which had more weight gain).
There were no differences between quetiapine and other antipsychotics in metabolic parameters, such as triglycerides, total cholesterol, low-density lipoprotein cholesterol, glucose, and prolactin, except lurasidone (which had higher increased prolactin).
Quetiapine was associated with higher odds of somnolence compared with other antipsychotics, except ziprasidone (no difference).
There were no differences between quetiapine and other antipsychotics in terms of extrapyramidal symptoms or switch to mania.
Summary
Quetiapine and lithium were similar in efficacy and safety for treatment of bipolar depression. Compared with olanzapine and ziprasidone, quetiapine was found to be more efficacious for remission from depressive episodes. With respect to response rates, quetiapine was better than cariprazine, aripiprazole, and ziprasidone, and showed no differences compared with olanzapine and lurasidone. Quetiapine had a similar discontinuation rate due to AEs compared with other antipsychotics, except lurasidone. Compared with other antipsychotics, quetiapine had lower rates of discontinuation due to lack of efficacy, higher chance of somnolence, and more weight gain, but had no differences in metabolic parameters, extrapyramidal symptoms, or switch to mania. However, most studies were short term (2 to 3 months). Longer-term side effects, such as weight gain and other metabolic indices, are likely to negatively impact discontinuation rates.
Recommendations From Included Evidence-Based Guidelines
For Treatment of Mania or Hypomania
The NICE guideline20 recommends the use of quetiapine, haloperidol, olanzapine, or risperidone in people with acute mania or hypomania who have not been previously treated with lithium, are already taking lithium, or are already taking a mood stabilizer.
The VA/DoD guideline21 suggests using quetiapine or lithium as monotherapy for people with acute mania or adding lithium or valproate in combination with quetiapine, haloperidol, olanzapine, or risperidone for people with an unsatisfactory response on monotherapy of antipsychotics (weak recommendation).
The CANMAT and ISBD guideline22 recommends both monotherapy and combination therapy with an atypical antipsychotic and a mood stabilizer as first-line treatment for acute mania. Specifically, quetiapine monotherapy or combination therapy of quetiapine plus lithium or divalproex is recommended as 1 of the options for first-line therapy. There were no specific recommendations for treatment of hypomania.
For Treatment of Bipolar Depression
The NICE guideline20 recommends the combination of fluoxetine with olanzapine or quetiapine in people who have not been previously treated with lithium, are already taking lithium, or are already taking valproate.
The VA/DoD guideline21 recommends quetiapine as monotherapy (strong recommendation).
The CANMAT and ISBD guideline22 recommends quetiapine, lithium, lamotrigine, or lurasidone as first-line monotherapy options for acute bipolar I depression, and quetiapine as the only drug for acute bipolar II depression.
For Maintenance (Prevention of Recurrence) Therapy
The VA/DoD guideline recommends21 quetiapine or lithium as monotherapy for the prevention of recurrence of mania (strong recommendation). It also suggests using lithium or valproate in combination with aripiprazole, olanzapine, quetiapine, or ziprasidone (weak recommendation).
The VA/DoD guideline21 suggests lithium or quetiapine as monotherapy (weak recommendation) or combination therapy of lithium or valproate with antipsychotics, such as olanzapine, lurasidone, or quetiapine, for prevention of recurrence of bipolar depressive episodes (weak recommendation).
The CANMAT and ISBD guideline22 recommends monotherapies of lithium, quetiapine, divalproex, lamotrigine, asenapine, or aripiprazole as first-line options for maintenance therapy in bipolar I. It also recommends combination therapies of quetiapine or aripiprazole combined with lithium or divalproex as first-line options for maintenance therapy in bipolar I. For maintenance therapy in bipolar II, quetiapine, lithium, and lamotrigine monotherapies are first-line options.
Considerations for Future Research
Future clinical research is needed in the areas where recommendations of the included guidelines were based on low-level evidence, particularly in the treatment and maintenance of mania and bipolar depression. Clinical evidence on long-term treatment of mania and bipolar depression as well as treatment-resistant bipolar disorder remains unclear. Research investigating the effect of antipsychotics in patient-reported outcomes, such as HRQoL, is also warranted.
Implications for Clinical Practice
The findings of this review suggest that monotherapy with quetiapine, among other antipsychotics, could be used as first-line treatment for the management and prevention of recurrence of mania and bipolar depression. Combination therapy of mood stabilizers with certain antipsychotics, including quetiapine, could be used in persons who have no improvement with monotherapy. The prescribing of antipsychotics for the treatment or prevention of mania and bipolar depression should be based on patient characteristics, patient tolerability, patient values and preferences, side effect profiles of different antipsychotic medications, and clinician expertise. Of note, clinical evidence on long-term treatment of mania and bipolar depression as well as treatment-resistant bipolar disorder remains unclear.
Acknowledgement
Clinical Expert
This individual has kindly provided comments on the report:
Diane McIntosh, BSc Pharmacy, MD, FRCPC
Psychiatrist
References
1.Message from the Minister of Mental Health and Addictions and Associate Minister of Health – World Bipolar Day. 2024; https://www.canada.ca/en/health-canada/news/2024/03/message-from-the-minister-of-mental-health-and-addictions-and-associate-minister-of-health--world-bipolar-day.html. Accessed 16 April, 2025.
2.Anderson IM, Haddad PM, Scott J. Bipolar disorder. BMJ. 2012;345:e8508. PubMed
3.Miller S, Dell'Osso B, Ketter TA. The prevalence and burden of bipolar depression. J Affect Disord. 2014;169 Suppl 1:S3-11. PubMed
4.Stahl EA, Breen G, Forstner AJ, et al. Genome-wide association study identifies 30 loci associated with bipolar disorder. Nat Genet. 2019;51(5):793-803. PubMed
5.Bipolar Disorder. 2024; https://www.mayoclinic.org/diseases-conditions/bipolar-disorder/symptoms-causes/syc-20355955. Accessed 01 May, 2025.
6.Cipriani A, Hawton K, Stockton S, Geddes JR. Lithium in the prevention of suicide in mood disorders: updated systematic review and meta-analysis. BMJ. 2013;346:f3646. PubMed
7.Chiu CT, Wang Z, Hunsberger JG, Chuang DM. Therapeutic potential of mood stabilizers lithium and valproic acid: beyond bipolar disorder. Pharmacol Rev. 2013;65(1):105-142. PubMed
8.Baldessarini RJ, Tondo L, Vázquez GH. Pharmacological treatment of adult bipolar disorder. Mol Psychiatry. 2019;24(2):198-217. PubMed
9.Yatham LN, Chakrabarty T, Bond DJ, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) and International Society for Bipolar Disorders (ISBD) recommendations for the management of patients with bipolar disorder with mixed presentations. Bipolar Disord. 2021;23(8):767-788. PubMed
10.Goodwin FK, Ghaemi SN. Bipolar disorder. Dialogues Clin Neurosci. 1999;1(1):41-51. PubMed
11.SEROQUEL® (quetiapine fumarate). 2021; https://www.astrazeneca.ca/content/dam/az-ca/downloads/productinformation/seroquel-product-monograph-en.pdf. Accessed 16 April, 2025.
12.QUETIAPINE FUMARATE XR. 2021; https://pdf.hres.ca/dpd_pm/00061368.PDF. Accessed 24 April, 2025.
13.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
14.Jansen JP, Trikalinos T, Cappelleri JC, et al. Indirect treatment comparison/network meta-analysis study questionnaire to assess relevance and credibility to inform health care decision making: an ISPOR-AMCP-NPC Good Practice Task Force report. Value Health. 2014;17(2):157-173. PubMed
15.Agree Next Steps C. The AGREE II Instrument. Hamilton (ON): AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf. Accessed January 1, 1800.
16.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
17.Ogasawara M, Takeshima M, Esaki Y, et al. Comparison of the efficacy and safety of quetiapine and lithium for bipolar depression: A systematic review and meta-analysis of randomized controlled trials. Neuropsychopharmacol. 2022;42(4):410-420. PubMed
18.Tao H, Wang J, Shen D, Sun F, Jin W. Is aripiprazole similar to quetiapine for treatment of bipolar depression? Results from meta-analysis of Chinese data. Front Psychiatr. 2022;13:850021. PubMed
19.Kadakia A, Dembek C, Heller V, et al. Efficacy and tolerability of atypical antipsychotics for acute bipolar depression: a network meta-analysis. BMC Psychiatry. 2021;21(1):249. PubMed
20.NICE. Bipolar disorder: assessment and management. 2023; https://www.nice.org.uk/guidance/cg185/resources/bipolar-disorder-assessment-and-management-pdf-35109814379461. Accessed 04 April, 2025.
21.VA/DoD. VA/DoD CLINICAL PRACTICE GUIDELINE FOR MANAGEMENT OF BIPOLAR DISORDER. 2023; https://www.healthquality.va.gov/guidelines/MH/bd/VA-DoD-CPG-BD-Full-CPGFinal508.pdf. Accessed 04 April, 2025.
22.Keramatian K, Chithra NK, Yatham LN. The CANMAT and ISBD Guidelines for the Treatment of Bipolar Disorder: Summary and a 2023 Update of Evidence. Focus (Am Psychiatr Publ). 2023;21(4):344-353. PubMed
23.Tao H, Shen D, Zhou Y, Sun F, Li G, Jin W. A Systematic Review and Meta-Analysis of Metabolic Syndrome Prevalence in Chinese Inpatients with Bipolar Disorder. Horm Metab Res. 2022;54(9):587-592. PubMed
24.Yatham LN, Kennedy SH, Parikh SV, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) and International Society for Bipolar Disorders (ISBD) 2018 guidelines for the management of patients with bipolar disorder. Bipolar Disord. 2018;20(2):97-170. PubMed
25.Jansen JP, Trikalinos T, Cappelleri JC, et al. Supplementary material to: Indirect treatment comparison/network meta-analysis study questionnaire to assess relevance and credibility to inform health care decision making: an ISPOR-AMCP-NPC Good Practice Task Force report. Value Health. 2014;17(2):157-173. PubMed
Appendix 1: Selection of Included Studies
Figure 1: PRISMA16 Flow Chart of Study Selection
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of Included Systematic Reviews
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Ogasawara et al. (2022)17 Japan Funding source: The authors declared that this research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors | SR with MA 3 RCTs | Patients diagnosed with a depressive episode of bipolar spectrum disorder, and at least 90% of the participants were diagnosed with bipolar I or II depression (N = 740; range: 35 to 669) Sex:
Mean age: 42.1 years | Intervention: Quetiapine (300 mg/day or 600 mg/day) Comparator: Lithium (300 mg/day or 600 mg/day to maintain a serum level between 0.6 and 1.2 mEq/L Treatment duration: 8 weeks or 16 weeks | Outcomes: Primary:
Secondary:
Follow-up: NR |
Tao et al. (2022)18 China Funding source: Peak Subject of Psychiatry, Zhejiang Province Tongde Hospital | SR with MA 17 studies Study design: NR | Patients with bipolar depression (N = 1,546) Details of patient characteristics: NR | Intervention: Aripiprazole Comparator: Quetiapine Details of study characteristics: NR | Outcomes:
Follow-up: NR |
Kadakia et al. (2021)19 US Funding source: Sunovion Pharmaceuticals Inc. | SR with NMA 18 RCTs | Adults with bipolar depression, and at least 50% of the population were diagnosed with bipolar I disorder (N = 7,969) Sex:
Mean age: 33.1 years to 43.6 years Bipolar I: 50.9% to 100% Mean MADRS: 28.2 to 32.0 | Intervention: Atypical antipsychotic monotherapy Comparator: Any atypical antipsychotics or placebo Treatment duration: 6 weeks or 8 weeks | Outcomes:
Follow-up: NR |
SGI-BP-S = Clinical Global Impressions – Bipolar Disorder – Severity; HAM-D17 = 17-item Hamilton Depression Rating Scale; MA = meta-analysis; MADRS = Montgomery-Åsberg Depression Rating Scale; NMA = network meta-analysis; NR = not reported; RCT = randomized controlled trial; SR = systematic review.
Note: This table has not been copy-edited.
aRemission was defied as scores on the MADRS ≤ 12 or the HAM-D17 ≤ 7 at end point. Remission rates from depressive episodes were calculated by dividing the number of participants who achieved remission in a group by the total number of participants in that group.
bRemission rate was defined as the proportion of subjects achieving HAMD of 7 at an end point. HAMD (Hamilton Depression Rating Scale) scoring is based on 17-item rating scale. Scores of 0 to 7: normal; 8 to 16: mild depression; 17 to 23: moderate depression; > 24: severe depression.
cResponse was defined as ≥ 50% improvement in MADRS score. MADRS is a 10-item clinician-rated assessment used to measure the severity of depressive episodes in patients with mood disorders, with higher scores indicating more severe depression.
dCGI-BP-S is a clinician-rated scale that measures the patient's current illness state on a 21-point scale that assesses depression, mania, and overall illness, where a higher score is associated with greater illness severity.
Table 3: Characteristics of Included Guidelines
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality assessment | Recommendations development and evaluation | Guideline validation |
|---|---|---|---|---|---|---|
NICE (2023)20 | ||||||
Intended users: Health care professionals Target population: People with bipolar disorder and their family members | Recognizing, assessing, and treating bipolar disorder (formerly known as manic depression) | All relevant outcomes | Systematic methods were used to search for evidence. | GRADE approach was used for assessing and rating the quality of evidence. | Committee members developed review questions, reviewed research evidence, incorporated economic evaluation, incorporated other guidance, and wrote recommendations. | The draft version of the guideline was posted on the NICE website for consultation with registered stakeholders. |
VA/DoD (2023)21 | ||||||
Intended users: Primary care providers, mental health providers, and others involved in the health care team caring for individuals with bipolar disorder Target population: Adults (age 18 years and older) treated with any diagnosis covered within “bipolar and related disorders” | This guideline provides recommendations for providers on identifying and treating individuals with bipolar disorders. | All relevant health outcomes including clinical and health-related quality of life outcomes. | Systematic search for evidence, study selection, data extraction, and data synthesis were performed. | The WG used the GRADE approach to craft each recommendation and determined its strengtha (strong, weak) based on 4 domains: 1. Confidence in the quality of the evidence 2. Balance of desirable and undesirable outcomes 3. Patient values and preferences 4. Other considerations (e.g., resource use, equity, acceptability, feasibility, subgroup considerations) | The CPG WG comprised experts in psychiatry, psychology, internal medicine, nursing, primary care, pharmacy, mental health counselling, and social work. Tasks of the WG:
Determine the strength and category of each recommendation | The CPG was reviewed by experts outside the organization |
CANMAT/ISBD (2023)22 | ||||||
Intended users: Physicians, patients, and family Target population: Adults, children, adolescents, and older adults | This guideline provides recommendations for the treatment of bipolar disorder across the lifespan. | All relevant outcomes | Methods: Not reported Guideline was regularly updated with new evidence | The recommendations were graded into first, second, or third lineb considering the levels of evidencec for efficacy, safety, tolerability, and risk of treatment-emergent switch. | Not reported in the original 2018 CAMAT/ISBD publication24 | Published in peer-reviewed journal |
CANMAT = Canadian Network for Mood and Anxiety Treatments; CPG = clinical practice guideline; ISBD = International Society of Bipolar Disorders; GRADE = Grading of Recommendations Assessment, Development and Evaluation; NICE = National Institute for Health and Care Excellence; VA/DoD = Veteran Affairs/Department of Defense; WG = working group.
Note: This table has not been copy-edited.
aRecommendation strength (General corresponding text):
Strong for (We recommend . . .)
Weak for (We suggest . . .)
Neither for nor against (There is insufficient evidence to recommend for or against . . .)
Weak against (We suggest against . . .)
Strong against (We recommend against . . .)
bRecommendation strength:
First line: Level 1 or Level 2 evidence for efficacy plus clinical support for safety/tolerability and no risk of treatment-emergent switch
Second line: Level 3 or higher evidence for efficacy plus clinical support for safety and/or tolerability and low risk of treatment-emergent switch
Third line: Level 4 evidence or higher for efficacy plus clinical support for safety/tolerability
Not recommended: Level 1 evidence for lack of efficacy, or Level 2 evidence for lack of efficacy plus expert opinion
cLevel of evidence:
Level 1: Meta-analysis with narrow confidence interval or replicated double-blind, randomized controlled trial that includes a placebo or active control comparison (N ≥ 30 in each active treatment arm)
Level 2: Meta-analysis with wide confidence interval or one DB RCT with placebo or active control comparison condition (N ≥ 30 in each active treatment arm)
Level 3: At least one DB RCT with placebo or active control comparison condition (N = 10 to 29 in each active treatment arm) or health system administrative data
Level 4: Uncontrolled trial, anecdotal reports, or expert opinion
Appendix 3: Critical Appraisal of Included Publications
Please note that this appendix has not been copy-edited.
Table 4: Strengths and Limitations of Systematic Reviews and Network Meta-Analyses Using AMSTAR 213 and the ISPOR Questionnaire25
Strengths | Limitations |
|---|---|
Ogasawara et al. (2022)17 | |
|
|
Tao et al. (2022)18 | |
|
|
Kadakia et al. (2021)19 | |
Objectives:
Search strategies:
Data collection:
Methods for analysis/synthesis of evidence:
Reporting:
Discussion:
| Methods for analysis/synthesis of evidence:
Reporting:
|
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; CI = confidence interval; CrI = credible interval; GRADE = Grading of Recommendations Assessment, Development and Evaluation; ISPOR = International Society for Pharmacoeconomics and Outcomes Research; MD = mean difference; NA = not applicable; NMA = network meta-analysis; NR = not reported; RCT = randomized controlled trial; RoB = risk of bias; OR = odds ratio; SMD = standardized mean difference.
Table 5: Strengths and Limitations of Guidelines Using AGREE II15
Item | NICE (2023)20 | VA/DoD (2023)21 | CANMAT/ISBD22 |
|---|---|---|---|
Domain 1: scope and purpose | |||
1. The overall objective(s) of the guideline is (are) specifically described. | Yes | Yes | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes | Yes | Yes |
3. The population (patients, public, etc.) to whom the guideline is meant to apply is specifically described. | Yes | Yes | Yes |
Domain 2: stakeholder involvement | |||
4. The guideline development group includes individuals from all relevant professional groups. | Yes | Yes | NR |
5. The views and preferences of the target population (patients, public, etc.) have been sought. | Yes | Yes | NR |
6. The target users of the guideline are clearly defined. | Yes | Yes | NR |
Domain 3: rigour of development | |||
7. Systematic methods were used to search for evidence. | Yes | Yes | NR |
8. The criteria for selecting the evidence are clearly described. | Yes | Yes | NR |
9. The strengths and limitations of the body of evidence are clearly described. | Yes | Yes | Yes |
10. The methods for formulating the recommendations are clearly described. | Yes | Yes | Yes |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes | Yes | Yes |
12. There is an explicit link between the recommendations and the supporting evidence. | Yes | Yes | Yes |
13. The guideline has been externally reviewed by experts before its publication. | Yes | Yes | Yes |
14. A procedure for updating the guideline is provided. | Yes | Yes | Yes |
Domain 4: clarity of presentation | |||
15. The recommendations are specific and unambiguous. | Yes | Yes | Yes |
16. The different options for management of the condition or health issue are clearly presented. | Yes | Yes | Yes |
17. Key recommendations are easily identifiable. | Yes | Yes | Yes |
Domain 5: applicability | |||
18. The guideline describes facilitators and barriers to its application. | Unclear | Unclear | Unclear |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | Yes | Yes | Yes |
20. The potential resource implications of applying the recommendations have been considered. | Yes | Yes | Yes |
21. The guideline presents monitoring and/or auditing criteria. | Unclear | Unclear | Unclear |
Domain 6: editorial independence | |||
22. The views of the funding body have not influenced the content of the guideline. | Yes | Yes | Yes |
23. Competing interests of guideline development group members have been recorded and addressed. | Yes | Yes | Yes |
AGREE II = Appraisal of Guidelines for Research and Evaluation II; CANMAT = Canadian Network for Mood and Anxiety Treatments; ISBD = International Society of Bipolar Disorders; NICE = National Institute for Health and Care Excellence; VA/DoD = Veteran Affairs/Department of Defense.
Appendix 4: Main Study Findings
Please note that this appendix has not been copy-edited.
Table 6: Summary of Findings by Outcome — Remission Rate From Depressive Episodes
Study citation and study design | Interventions vs. comparators | Results, RR (95% CI) or OR (95% CrI) | Notes |
|---|---|---|---|
Ogasawara et al. (2022)17 SR with MA | Quetiapine vs. Lithium | 1.80 (0.51 to 6.40) | 2 RCTs (N = 683); NS |
Tao et al. (2022)18 SR with MA | Aripiprazole vs. Quetiapine | 1.23 (0.86 to 1.77) | 10 studies (N = 1,002); NS |
Kadakia et al. (2021)19 SR with NMA | Quetiapine vs. Olanzapine | 1.45 (1.07 to 1.92) | Favours quetiapine |
Ziprasidone vs. Quetiapine | 0.51 (0.36 to 0.69) | Favours quetiapine | |
Lurasidone vs. Quetiapine | 1.08 (0.67 to 1.66) | Uncertain |
CI = confidence interval; CrI = credible interval; MA = meta-analysis; NMA = network meta-analysis; NS = not statistically significant; OR = odds ratio; RCT = randomized controlled trial; RR = relative risk; SR = systematic review.
Table 7: Summary of Findings by Outcome — Change Scores for Depressive Symptoms
Study citation and study design | Interventions vs. comparators | Results, SMD (95% CI) or MD (95% CrI) | Notes |
|---|---|---|---|
Ogasawara et al. (2022)17 SR with MA | Quetiapine vs. Lithium | −0.22 (−0.52 to 0.08) | 2 RCTs (N = 718); NS |
Tao et al. (2022)18 SR with MA | Aripiprazole vs. Quetiapine | 0.26 (−0.33 to 0.85); P = 0.39 | 9 studies (N = 794); NS |
Kadakia et al. (2021)19 SR with NMA | Quetiapine vs. Olanzapine | −0.23 (−2.05 to 1.53) | Uncertain |
Quetiapine vs. Cariprazine | –2.52 (−4.11 to −0.92) | Favours quetiapine | |
Quetiapine vs. Aripiprazole | –3.72 (−6.21 to −1.28) | Favours quetiapine | |
Ziprasidone vs. Quetiapine | 3.46 (1.24 to 5.76) | Favours quetiapine | |
Lurasidone vs. Quetiapine | 0.10 (−2.44 to 2.61) | Uncertain |
CI = confidence interval; CrI = credible interval; MA = meta-analysis; MD = mean difference NMA = network meta-analysis; NS = not statistically significant; OR = odds ratio; RCT = randomized controlled trial; RR = relative risk; SMD = standardized mean difference; SR = systematic review.
Table 8: Summary of Findings by Outcome — Response Rate
Study citation and study design | Interventions vs. comparators | Results, RR (95% CI) or OR (95% CrI) | Notes |
|---|---|---|---|
Tao et al. (2022)18 SR with MA | Aripiprazole vs. Quetiapine | 1.11 (0.98 to 1.25) | 12 studies (N = 1,144); NS |
Kadakia et al. (2021)19 SR with NMA | Quetiapine vs. Olanzapine | 1.36 (0.98 to 1.84) | Uncertain |
Quetiapine vs. Cariprazine | 1.44 (1.08 to 1.91) | Favours quetiapine | |
Quetiapine vs. Aripiprazole | 1.92 (1.32 to 2.71) | Favours quetiapine | |
Ziprasidone vs. Quetiapine | 0.52 (0.35 to 0.74) | Favours quetiapine | |
Lurasidone vs. Quetiapine | 1.25 (0.78 to 1.90) | Uncertain |
CI = confidence interval; CrI = credible interval; MA = meta-analysis; MD = mean difference; NMA = network meta-analysis; NS = not statistically significant; OR = odds ratio; RR = relative risk; SR = systematic review.
Table 9: Summary of Findings by Outcome — Change in Social Functioning
Study citation and study design | Interventions vs. comparators | Results, SMD (95% CI) | Notes |
|---|---|---|---|
Ogasawara et al. (2022)17 SR with MA | Quetiapine vs. Lithium | −0.00 (−0.19 to 0.18) | 2 RCTs (N = 658); NS |
CI = confidence interval; MA = meta-analysis; NS = not statistically significant; RCT = randomized controlled trial; SMD = standardized mean difference; SR = systematic review.
Table 10: Summary of Findings by Outcome — All-Cause Discontinuation
Study citation and study design | Interventions vs. comparators | Results RR (95% CI) or OR (95% CrI) | Notes |
|---|---|---|---|
Ogasawara et al. (2022)17 SR with MA | Quetiapine vs. Lithium | 0.95 (0.74 to 1.22) | 3 RCTs (N = 740); NS |
Tao et al. (2022)18 SR with MA | Aripiprazole vs. Quetiapine | 0.53 (0.26 to 1.06) | 10 studies (N = 1,002); NS |
Kadakia et al. (2021)19 SR with NMA | Quetiapine vs. Olanzapine | 1.46 (1.08 to 1.94) | Higher odds with quetiapine |
Quetiapine vs. Cariprazine | 0.96 (0.70 to 1.28) | Uncertain | |
Quetiapine vs. Aripiprazole | 0.61 (0.43 to 0.85) | Lower odds with quetiapine | |
Ziprasidone vs. Quetiapine | 1.39 (0.98 to 1.9) | Uncertain | |
Lurasidone vs. Quetiapine | 1.10 (0.68 to 1.70) | Uncertain |
CI = confidence interval; CrI = credible interval; MA = meta-analysis; NMA = network meta-analysis; NS = not statistically significant; OR = odds ratio; RCT = randomized controlled trial; RR = relative risk; SR = systematic review.
Table 11: Summary of Findings by Outcome — Discontinuation Due to Adverse Events
Study citation and study design | Interventions vs. comparators | Results RR (95% CI) or OR (95% CrI) | Notes |
|---|---|---|---|
Ogasawara et al. (2022)17 SR with MA | Quetiapine vs. Lithium | 1.19 (0.76 to 1.87) | 3 RCTs (N = 734); NS |
Kadakia et al. (2021)19 SR with NMA | Quetiapine vs. Olanzapine | 1.68 (0.94 to 2.78) | Uncertain |
Quetiapine vs. Cariprazine | 1.81 (0.98 to 3.05) | Uncertain | |
Quetiapine vs. Aripiprazole | 1.08 (0.56 to 1.89) | Uncertain | |
Ziprasidone vs. Quetiapine | 0.64 (0.36 to 1.05) | Uncertain | |
Lurasidone vs. Quetiapine | 0.45 (0.18 to 0.97) | Lower odds with lurasidone |
CI = confidence interval; CrI = credible interval; MA = meta-analysis; NMA = network meta-analysis; NS = not statistically significant; OR = odds ratio; RCT = randomized controlled trial; RR = relative risk; SR = systematic review.
Table 12: Summary of Findings by Outcome — Discontinuation Due to Lack of Efficacy
Study citation and study design | Interventions vs. comparators | Results OR (95% CrI) | Notes |
|---|---|---|---|
Kadakia et al. (2021)19 SR with NMA | Quetiapine vs. Olanzapine | 0.50 (0.28 to 0.81) | Lower odds with quetiapine |
Quetiapine vs. Cariprazine | 0.51 (0.22 to 1.01) | Uncertain | |
Quetiapine vs. Aripiprazole | 0.43 (0.18 to 0.86) | Lower odds with quetiapine | |
Ziprasidone vs. Quetiapine | 7.26 (2.79 to 16.04) | Higher odds with ziprasidone | |
Lurasidone vs. Quetiapine | 3.18 (1.23 to 6.92) | Higher odds with lurasidone |
CrI = credible interval; MA = meta-analysis; NMA = network meta-analysis; OR = odds ratio; RCT = randomized controlled trial; SR = systematic review.
Table 13: Summary of Findings by Outcome — Suicidal-Related Events
Study citation and study design | Interventions vs. comparators | Results OR (95% CI) | Notes |
|---|---|---|---|
Ogasawara et al. (2022)17 SR with MA | Quetiapine vs. Lithium | 2.35 (0.40 to 13.65) | 2 RCTs (N = 699); NS |
CI = confidence interval; MA = meta-analysis; NS = not statistically significant; OR = odds ratio; RCT = randomized controlled trial; SR = systematic review.
Table 14: Summary of Findings by Outcome — Serious Adverse Events
Study citation and study design | Interventions vs. comparators | Results OR (95% CrI) | Notes |
|---|---|---|---|
Ogasawara et al. (2022)17 SR with MA | Quetiapine vs. Lithium | 1.63 (0.51 to 5.20) | 2 RCTs (N = 699); NS |
CI = confidence interval; MA = meta-analysis; NS = not statistically significant; OR = odds ratio; RCT = randomized controlled trial; SR = systematic review.
Table 15: Summary of Findings by Outcome — Weight Gain
Study citation and study design | Interventions vs. comparators | Results MD (95% CrI) | Notes |
|---|---|---|---|
Kadakia et al. (2021)19 SR with NMA | Quetiapine vs. Olanzapine | –1.74 (−2.17 to −1.31) | Less weight gain with quetiapine |
Quetiapine vs. Cariprazine | 0.53 (0.18 to 0.87) | More weight gain with quetiapine | |
Quetiapine vs. Aripiprazole | 0.98 (0.21 to 1.74) | More weight gain with quetiapine | |
Lurasidone vs. Quetiapine | –0.82 (−1.27 to −0.36) | More weight gain with quetiapine |
CrI = credible interval; MD = mean difference NMA = network meta-analysis; SR = systematic review.
Table 16: Summary of Findings by Outcome — Triglycerides
Study citation and study design | Interventions vs. comparators | Results MD (95% CrI) | Notes |
|---|---|---|---|
Kadakia et al. (2021)19 SR with NMA | Quetiapine vs. Olanzapine | 10.12 (−3.84 to 24.07) | Uncertain |
Quetiapine vs. Cariprazine | 10.66 (−3.29 to 24.59) | Uncertain | |
Quetiapine vs. Aripiprazole | 9.83 (−8.07 to 27.81) | Uncertain | |
Lurasidone vs. Quetiapine | −13.83 (−32.08 to 4.36) | Uncertain |
CrI = credible interval; MD = mean difference NMA = network meta-analysis; SR = systematic review.
Table 17: Summary of Findings by Outcome — Cholesterol
Study citation and study design | Interventions vs. comparators | Results MD (95% CrI) | Notes |
|---|---|---|---|
Kadakia et al. (2021)19 SR with NMA | Quetiapine vs. Olanzapine | −0.86 (−4.81 to 3.08) | Uncertain |
Quetiapine vs. Cariprazine | 0.40 (−3.48 to 4.29) | Uncertain | |
Quetiapine vs. Aripiprazole | 0.13 (−5.10 to 5.32) | Uncertain | |
Lurasidone vs. Quetiapine | 1.52 (−5.14 to 8.18) | Uncertain |
CrI = credible interval; MD = mean difference NMA = network meta-analysis; SR = systematic review.
Table 18: Summary of Findings by Outcome — Low-Density Lipoprotein Cholesterol
Study citation and study design | Interventions vs. comparators | Results MD (95% CrI) | Notes |
|---|---|---|---|
Kadakia et al. (2021)19 SR with NMA | Quetiapine vs. Olanzapine | −0.85 (−4.21 to 2.50) | Uncertain |
Quetiapine vs. Cariprazine | −0.51 (−3.87 to 2.85) | Uncertain | |
Quetiapine vs. Aripiprazole | −0.08 (−4.74 to 4.58) | Uncertain | |
Lurasidone vs. Quetiapine | 1.70 (−4.07 to 7.46) | Uncertain |
CrI = credible interval; MD = mean difference NMA = network meta-analysis; SR = systematic review.
Table 19: Summary of Findings by Outcome — Glucose
Study citation and study design | Interventions vs. comparators | Results MD (95% CrI) | Notes |
|---|---|---|---|
Kadakia et al. (2021)19 SR with NMA | Quetiapine vs. Olanzapine | 1.18 (−1.35 to 3.73) | Uncertain |
Quetiapine vs. Cariprazine | 1.23 (−0.49 to 2.96) | Uncertain | |
Quetiapine vs. Aripiprazole | 0.38 (−2.77 to 3.52) | Uncertain | |
Lurasidone vs. Quetiapine | −2.66 (−6.56 to 1.24) | Uncertain |
CrI = credible interval; MD = mean difference NMA = network meta-analysis; SR = systematic review.
Table 20: Summary of Findings by Outcome — Prolactin
Study citation and study design | Interventions vs. comparators | Results MD (95% CrI) | Notes |
|---|---|---|---|
Kadakia et al. (2021)19 SR with NMA | Quetiapine vs. Olanzapine | — | Data not available |
Quetiapine vs. Cariprazine | −1.32 (−3.82 to 1.19) | Uncertain | |
Quetiapine vs. Aripiprazole | 0.57 (−2.34 to 3.49) | Uncertain | |
Lurasidone vs. Quetiapine | 6.35 (0.80 to 11.87) | Higher increased prolactin with lurasidone |
CrI = credible interval; MD = mean difference NMA = network meta-analysis; SR = systematic review.
Table 21: Summary of Findings by Outcome — Somnolence
Study citation and study design | Interventions vs. comparators | Results OR (95% CrI) | Notes |
|---|---|---|---|
Kadakia et al. (2021)19 SR with NMA | Quetiapine vs. Olanzapine | 1.75 (1.09 to 2.66) | Higher odds with quetiapine |
Quetiapine vs. Cariprazine | 2.93 (1.16 to 5.86) | Higher odds with quetiapine | |
Quetiapine vs. Aripiprazole | 2.69 (1.21 to 5.14) | Higher odds with quetiapine | |
Ziprasidone vs. Quetiapine | 1.06 (0.51 to 2.02) | Uncertain | |
Lurasidone vs. Quetiapine | 0.34 (0.10 to 0.89) | Higher odds with quetiapine |
CrI = credible interval; NMA = network meta-analysis; OR = odds ratio; RCT = randomized controlled trial; SR = systematic review.
Table 22: Summary of Findings by Outcome — Switch to Mania
Study citation and study design | Interventions vs. comparators | Results OR (95% CrI) | Notes |
|---|---|---|---|
Kadakia et al. (2021)19 SR with NMA | Quetiapine vs. Olanzapine | 0.82 (0.37 to 1.59) | Uncertain |
Quetiapine vs. Cariprazine | 0.70 (0.31 to 1.35) | Uncertain | |
Quetiapine vs. Aripiprazole | 0.32 (0.12 to 0.67) | Lower odds with quetiapine | |
Lurasidone vs. Quetiapine | 4.07 (0.75 to 14.64) | Uncertain |
CrI = credible interval; NMA = network meta-analysis; OR = odds ratio; RCT = randomized controlled trial; SR = systematic review.
Table 23: Summary of Findings by Outcome — Extrapyramidal Symptoms
Study citation and study design | Interventions vs. comparators | Results OR (95% CrI) | Notes |
|---|---|---|---|
Kadakia et al. (2021)19 SR with NMA | Quetiapine vs. Cariprazine | 1.25 (0.63 to 2.27) | Uncertain |
Quetiapine vs. Aripiprazole | 1.48 (0.70 to 2.77) | Uncertain | |
Lurasidone vs. Quetiapine | 1.62 (0.43 to 4.84) | Uncertain |
CrI = credible interval; NMA = network meta-analysis; OR = odds ratio; RCT = randomized controlled trial; SR = systematic review.
Table 24: Summary of Recommendations in Included Guidelines for Bipolar Disorder
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
|---|---|
NICE (2023)20 | |
Managing mania or hypomania in adults in secondary care | |
“If a person develops mania or hypomania and is not taking an antipsychotic or mood stabiliser, offer haloperidol, olanzapine, quetiapine or risperidone, taking into account any advance statements, the person's preference and clinical context (including physical comorbidity, previous response to treatment and side effects).” p. 14 Supporting evidence: NR | NR |
“If the person is already taking lithium, check plasma lithium levels to optimise treatment. Consider adding haloperidol, olanzapine, quetiapine or risperidone, depending on the person's preference and previous response to treatment.” p. 15 Supporting evidence: NR | NR |
“If the person is already taking a mood stabiliser as prophylactic treatment, consider increasing the dose, up to the maximum level in the BNF if necessary, depending on clinical response. If there is no improvement, consider adding haloperidol, olanzapine, quetiapine or risperidone, depending on the person's preference and previous response to treatment.” p. 16 Supporting evidence: NR | NR |
Managing bipolar depression in adults in secondary care | |
“If a person develops moderate or severe bipolar depression and is not taking a drug to treat their bipolar disorder, offer fluoxetine combined with olanzapine, or quetiapine on its own, depending on the person's preference and previous response to treatment.” p. 18 Supporting evidence: NR | NR |
“If a person develops moderate or severe bipolar depression and is already taking lithium, check their plasma lithium level. If it is inadequate, increase the dose of lithium; if it is at maximum level, add either fluoxetine combined with olanzapine or add quetiapine.” p. 18 Supporting evidence: NR | NR |
“If the maximum tolerated dose, or the top of the therapeutic range for valproate, has been reached and there is a limited response, add either of the following options, depending on the person's preference and previous response to treatment:
Supporting evidence: NR | NR |
Managing bipolar disorder in adults in the longer term in secondary care | |
“If lithium is ineffective, poorly tolerated, or is not suitable (for example, because the person does not agree to routine blood monitoring), consider an antipsychotic (for example asenapine, aripiprazole, olanzapine, quetiapine or risperidone).” P. 24 Supporting evidence: NR | NR |
VA/DoD (2023)21 | |
Acute mania (bipolar I disorder) | |
“We suggest lithium or quetiapine as monotherapy for acute mania.” p. 33 Supporting evidence: 2 SRs, 1 cross-sectional study, and a narrative review Lithium and quetiapine have demonstrated efficacy for acute mania, prevention of recurrence of episodes of mania, and prevention of recurrence of depression (with quetiapine additionally having efficacy for acute depression). | Strength: Weak for Category: Reviewed, New-added |
“We suggest lithium or valproate in combination with haloperidol, asenapine, quetiapine, olanzapine, or risperidone for acute mania symptoms in individuals who had an unsatisfactory response or a breakthrough episode on monotherapy.” P. 34 Supporting evidence: 1 SR Evidence from a SR suggests that treatment with lithium or valproate in combination with either haloperidol, asenapine, quetiapine, olanzapine, or risperidone improves mania symptom severity in individuals with BD who had an unsatisfactory response or a breakthrough episode on monotherapy. | Strength: Weak for Category: Reviewed, New-added |
Acute bipolar depression (bipolar I disorder and bipolar II disorder) | |
“We recommend quetiapine as monotherapy for acute bipolar depression.” p. 34 Supporting evidence: 2 SRs and 2 RCTs The benefits of quetiapine for the treatment of bipolar depression outweighed the potential harms. | Strength: Strong for Category: Reviewed, New-added |
Prevention of recurrence of mania (bipolar I disorder) | |
“We recommend lithium or quetiapine for the prevention of recurrence of mania.” p. 34 Supporting evidence: 7 SRs, 1 cohort study, 1 narrative review, and 1 review of case reports Evidence from recent SRs suggests that lithium and quetiapine are the most effective medications for maintenance treatment to prevent recurrence of mania. Lithium had lower all-cause discontinuation rates compared with placebo, and no difference in all-cause discontinuation rates with lithium was found when compared with quetiapine. Overall, the benefits of both lithium and quetiapine as maintenance treatments for mania outweighed the potential harms from adverse effects. | Strength: Strong for Category: Reviewed, New-added |
“We suggest aripiprazole, olanzapine, quetiapine, or ziprasidone in combination with lithium or valproate for the prevention of recurrence of mania.” p.34 Supporting evidence: 2 SRs, 2 RCTs, and a post hoc analysis Evidence from SRs and RCTs suggests using antipsychotics (e.g., aripiprazole, olanzapine, quetiapine, and ziprasidone) in combination with lithium or valproate as maintenance medication for the prevention of recurrence of mania. The benefits of adding 1 of these atypical antipsychotics slightly outweighed the potential harm from adverse effects. | Strength: Weak for Category: Reviewed, New-added |
Prevention of recurrence of bipolar depression (bipolar I disorder and bipolar II disorder) | |
“We suggest lithium or quetiapine as monotherapy for the prevention of recurrence of bipolar depressive episodes.” p. 35 Supporting evidence: 2 SRs, and 1 RCT Evidence from SRs and RCT suggests that treatment with lithium, quetiapine, or olanzapine can help prevent the recurrence of depressive episodes in individuals with bipolar disorder. | Strength: Weak for Category: Reviewed, New-added |
“We suggest olanzapine, lurasidone, or quetiapine in combination with lithium or valproate for the prevention of recurrence of bipolar depressive episodes.” p. 35 Supporting evidence: 2 SRs, and 1 RCT Evidence from SRs and RCT suggests that treatment with olanzapine, lurasidone, or quetiapine with lithium or valproate can help prevent the recurrence of depressive episodes in individuals with bipolar disorder. | Strength: Weak for Category: Reviewed, New-added |
CANMAT/ISBD22 | |
Acute mania | |
“Both monotherapy and the combination of a mood stabilizer and an atypical antipsychotic are appropriate first-line treatments for acute mania. Specific medications include lithium, quetiapine, divalproex, asenapine, aripiprazole, paliperidone, risperidone, and cariprazine as first-line monotherapy options and a combination of quetiapine, aripiprazole, risperidone, or asenapine with lithium or divalproex as first-line combination therapy options.” p. 346 to 347 Hierarchical ranking: “The 2018 CANMAT/ISBD guideline recommends that treatments listed higher up in the Box need to be considered first, unless other factors such as history of previous nonresponse or patient’s preferences dictate otherwise” The ranking applied for all of the following recommendations. Supporting evidence: 3 SRs, 1 RCT, and 3 narrative reviews | Level of evidence: 1 or 2 Strength of recommendation: First line |
Acute bipolar I depression | |
“Quetiapine, lithium, lamotrigine, and lurasidone are recommended as first-line monotherapy options; lurasidone and lamotrigine are also recommended as first-line adjunctive treatments.” p. 348 Supporting evidence: 3 meta-analyses of RCTs (for quetiapine) | Level of evidence: 1 or 2 Strength of recommendation: First line |
Maintenance therapy in bipolar I | |
“Lithium, quetiapine, divalproex, lamotrigine, asenapine, and aripiprazole (oral or once-monthly injection) monotherapies are recommended as first-line maintenance treatments. Combination therapies recommended as first-line include quetiapine or aripiprazole combined with lithium or divalproex.” p. 349 Supporting evidence: 1 SR with NMA and 1 RCT (for quetiapine) | Level of evidence: 1 or 2 Strength of recommendation: First line |
Acute hypomania | |
No specific recommendations for treatment of hypomania due to lack of clinical evidence. | NA |
Acute bipolar II depression | |
“Quetiapine is the only recommended first-line treatment for bipolar II depression.” p. 350 Supporting evidence: 1 RCT and 1 meta-analysis of 4 large RCTs | Level of evidence: 1 or 2 Strength of recommendation: First line |
Maintenance therapy in bipolar II | |
“Quetiapine, lithium, and lamotrigine monotherapies are first-line options.” p. 350 Supporting evidence: 2 RCTs (for quetiapine) | Level of evidence: 1 or 2 Strength of recommendation: First line |
CANMAT = Canadian Network for Mood and Anxiety Treatments; BNF = British National Formulary; ISBD = International Society of Bipolar Disorders; NMA = network meta-analysis; NA = not applicable; NR = not reported; RCT = randomized controlled trial; SR = systematic review.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to requests@CDA-AMC.ca.