Drugs, Health Technologies, Health Systems
Health Technology Review
Quetiapine for Major Depressive Disorder
Summary
Main Take-Aways
Quetiapine could be used as second-line augmentation treatment for major depressive disorder in patients who had partial or no response to an adequate dose and duration of 2 or more antidepressants.
Second-line antipsychotics, such as quetiapine, in combination with an antidepressant, may be used as a first-line treatment for major depressive disorder that is very severe or has associated psychotic features.
Quetiapine may reduce symptoms of depression and improve social functioning compared with lithium.
Key Messages
What Is the Issue?
Quetiapine is a second-generation antipsychotic (SGA) or atypical antipsychotic drug primarily used for treating schizophrenia and bipolar disorder. Quetiapine extended-release is also indicated by Health Canada for the symptomatic relief of major depressive disorder (MDD) when currently available approved antidepressant drugs have failed.
Decision-makers are interested in understanding the evidence regarding quetiapine’s clinical effectiveness, safety, and place in therapy relative to other medications for the treatment of MDD.
What Did We Do?
We searched key resources, including journal citation databases, and conducted a focused internet search for relevant evidence published since 2020.
What Did We Find?
The evidence suggests that quetiapine and other SGAs (particularly aripiprazole, brexpiprazole, cariprazine, olanzapine, risperidone, and ziprasidone) have similar efficacy but have unique safety profiles when used for the treatment of adults with treatment-resistant MDD.
The evidence also suggests that treatment with quetiapine reduced symptoms of treatment-resistant depression compared to treatment with lithium.
Evidence-based guidelines recommend using quetiapine as a second-line augmentation treatment option for MDD in patients whose disease had partial or no response to an adequate dose of initial pharmacotherapy.
The Canadian Network for Mood and Anxiety Treatments (CANMAT) guideline recommends atypical antipsychotics such as quetiapine in combination with an antidepressant as the first-line treatment for MDD with psychotic features. The Royal Australian and New Zealand College of Psychiatrists (RANZCP) guideline suggests using quetiapine as monotherapy or adjunct therapy for patients with major depression.
What Does It Mean?
Quetiapine could be used as second-line augmentation treatment for MDD in patients whose disease had partial or no response to an adequate dose and duration of 2 or more antidepressants (i.e., those with treatment-resistant depression or difficult to treat depression). SGAs such as quetiapine, in combination with an antidepressant, may be used as a first-line treatment for MDD that is very severe or has associated psychotic features.
Quetiapine may reduce symptoms of depression and improve social functioning compared with lithium. However, patients reported more side effects with quetiapine than lithium and viewed the side effects of lithium as more manageable.
Factors such as patient characteristics, patient tolerability, patient values, side effect profiles of different treatment options, and clinician expertise may also be important to guide choice of treatment for MDD.
Abbreviations
ACP
American College of Physicians
AE
adverse event
CANMAT
Canadian Network for Mood and Anxiety Treatments
CDA-AMC
Canada’s Drug Agency
CI
confidence interval
CGI-S
Clinical Global Impression-Severity
LQD
Lithium Versus Quetiapine in Depression
MADRS
Montgomery-Asberg Depression Rating Scale
MDD
major depressive disorder
NICE
National Institute for Health and Care Excellence
NMA
network meta-analysis
PRISE
Patient-Rated Inventory of Side Effects
QIDS-SR
Quick Inventory of Depressive Symptomatology via Self-Report
RCT
randomized controlled trial
RANZCP
Royal Australian and New Zealand College of Psychiatrists
SD
standard deviation
SGA
second-generation antipsychotic
SR
systematic review
VA/DoD
US Department of Veterans Affairs and Department of Defense
WSAS
Work and Social Adjustment Scale
Context and Policy Issues
What Is Major Depressive Disorder?
Major depressive disorder (MDD) is a mental illness defined by a depressed mood or loss of interest or pleasure in doing activities that were previously enjoyed (i.e., anhedonia) that lasts most of the day for at least 2 consecutive weeks, without a history of mania or hypomania.1 In 2022, 7.6% of people aged 15 and older in Canada had had at least 1 major depressive episode in the previous 12 months.2 Treatment-resistant depression is a subset of MDD in which a patient’s disease does not respond to 2 or more adequate trials of antidepressant medications.3 “Difficult to treat” deрrеsѕiοn has also been used to describe patients whose disease does not respond sufficiently to antidepressants.3
MDD involves more than having decreased interest or depressed mood.4 Individuals diagnosed with MDD typically experience 4 or more of the following symptoms along with either depressed mood or anhedonia: insomnia or hypersomnia, unintended change in appetite or weight, increased restlessness or slowing down, fatigue or low energy, poor concentration or memory, feelings of worthlessness or guilt, or recurrent suicidal thoughts and behaviours.4
The symptoms of MDD can impair an individual’s ability to function at home, at work, or in social settings.4,5 People with MDD are at a higher risk of developing and experiencing poorer health outcomes from a range of comorbid medical conditions such as diabetes, metabolic syndrome, obesity, and cardiovascular disease.6 Thus, treatments that improve symptoms of depression and functional outcomes are a priority for MDD treatment.7
What Are Current Treatment Options for MDD?
The treatment goals for MDD are to achieve symptom remission, restore baseline functioning, and prevent relapse.4 Remission refers to resolution of symptoms. Evidence suggests that a delay in treatment is associated with poorer clinical outcomes,7 so early diagnosis and treatment is critical to achieving remission of symptoms and functional recovery.7
Standard treatment approaches for MDD include the use of antidepressant medications, psychotherapy, or a combination of both.4 Exercise and other supplemental interventions can be used as an alternative to standard treatment in some individuals with mild MDD and as an adjunct to standard treatment for all individuals with MDD.4 The choice of treatment strategies is primarily based on depression severity, though other factors such as patient preference, treatment availability, cost, and ease of use should be considered. The severity of depression depends on the degree of functional impairment and the number, frequency, intensity, and duration of an individual’s symptoms.4
What Is Quetiapine?
Quetiapine is available in 2 oral formulations — immediate-release tablets in 25 mg, 100 mg, 200 mg, and 300 mg doses of quetiapine fumarate8 and extended-release tablets in 50 mg, 150 mg, 200 mg, 300 mg, and 400 mg doses of quetiapine fumarate.9 Quetiapine is an atypical or second-generation antipsychotic (SGA) drug primarily used for treating schizophrenia and bipolar disorder.8 Additionally, the extended-release formulation is also indicated as an adjunct or augmentation treatment for adults with MDD when currently available antidepressant drugs have failed either due to lack of efficacy and/or lack of tolerability.9 Off-label use of quetiapine has been documented for several conditions such as agitation, delirium, delusional infestation, posttraumatic stress disorder, and insomnia.10 The side effects of quetiapine include somnolence, dizziness, dry mouth, withdrawal (discontinuation) symptoms, elevations in serum triglyceride levels, elevations in total cholesterol (predominantly low-density lipoprotein cholesterol), decreases in high-density lipoprotein cholesterol, weight gain, decreased hemoglobin, and extrapyramidal symptoms (involuntary movements induced by medications).8,9
Why Is It Important to Do This Review?
Higher doses of quetiapine and concomitant use with central nervous system drugs are associated with an increased risk of adverse effects.11,12 There are many available treatment options for depression but limited direct comparative trials of quetiapine versus relevant comparators. Findings from a previous Canada’s Drug Agency (CDA-AMC) report published in 2020 indicated that while quetiapine monotherapy may be more efficacious than some antidepressants in older adults, and some guidelines have recommended quetiapine as add-on therapy in treatment-resistant depression, its comparative efficacy remains uncertain, and it is associated with higher rates of adverse events (AEs) relative to its alternatives. These findings, which were limited by lack of direct comparative trials, underscore the need for an updated review of the current evidence on the efficacy and safety of quetiapine for treatment of people with MDD.
Research Questions
What is the clinical effectiveness and safety of quetiapine versus other drug interventions for adults with MDD?
What are the evidence-based guidelines regarding the use and administration of quetiapine for adults with MDD?
Methods
Literature Search Methods
An information specialist conducted a literature search on key resources including MEDLINE, Embase, the Cochrane Database of Systematic Reviews, the International HTA Database, and the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concepts were quetiapine and depression. Search filters were applied to limit retrieval to health technology assessments, systematic reviews (SRs), meta-analyses, indirect treatment comparisons, randomized controlled trials (RCTs), controlled clinical trials, and guidelines. The search was completed on April 11, 2025, and limited to English-language documents published since January 1, 2020.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. As an update to a previous CDA-AMC report on quetiapine for MDD, articles were included if they were made available since the previous search date and were not included in the 2020 CDA-AMC report. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Adults aged ≥ 18 years with major depressive disorder and/or treatment-resistant depression |
Intervention | Quetiapine fumarate immediate-release tablets, quetiapine fumarate extended-release tablets |
Comparator | Other drug interventions (e.g., other second-generation atypical antipsychotics, mood stabilizers, antidepressants) |
Outcomes |
|
Study designs | RCTs, systematic reviews, (including MAs and NMAs), evidence-based guidelines,a and published HTAs |
HTA = health technology assessment; MA = meta-analysis; NMA = network meta-analysis; RCT = randomized controlled trial.
aA guideline is defined as a systematically developed statement or set of statements to assist practitioner and patient decisions about appropriate health care for specific clinical circumstances. A guideline is considered evidence-based if a systematic search of the literature was undertaken to inform the recommendations.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1 or they were duplicate publications. SRs in which all relevant studies were captured in other more recent or more comprehensive SRs were excluded. Primary studies retrieved by the search were excluded if they were captured in 1 or more included SRs. Guidelines with an unclear methodology were also excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess Systematic Reviews 2 (AMSTAR 2)13 for SRs, the ISPOR (the Professional Society for Health Economics and Outcomes Research) questionnaire to assess the relevance and credibility of a network meta-analysis14 for network meta-analyses (NMAs), the Standards for Reporting Qualitative Research (SRQR)15 for qualitative research, and the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument for guidelines.16 Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
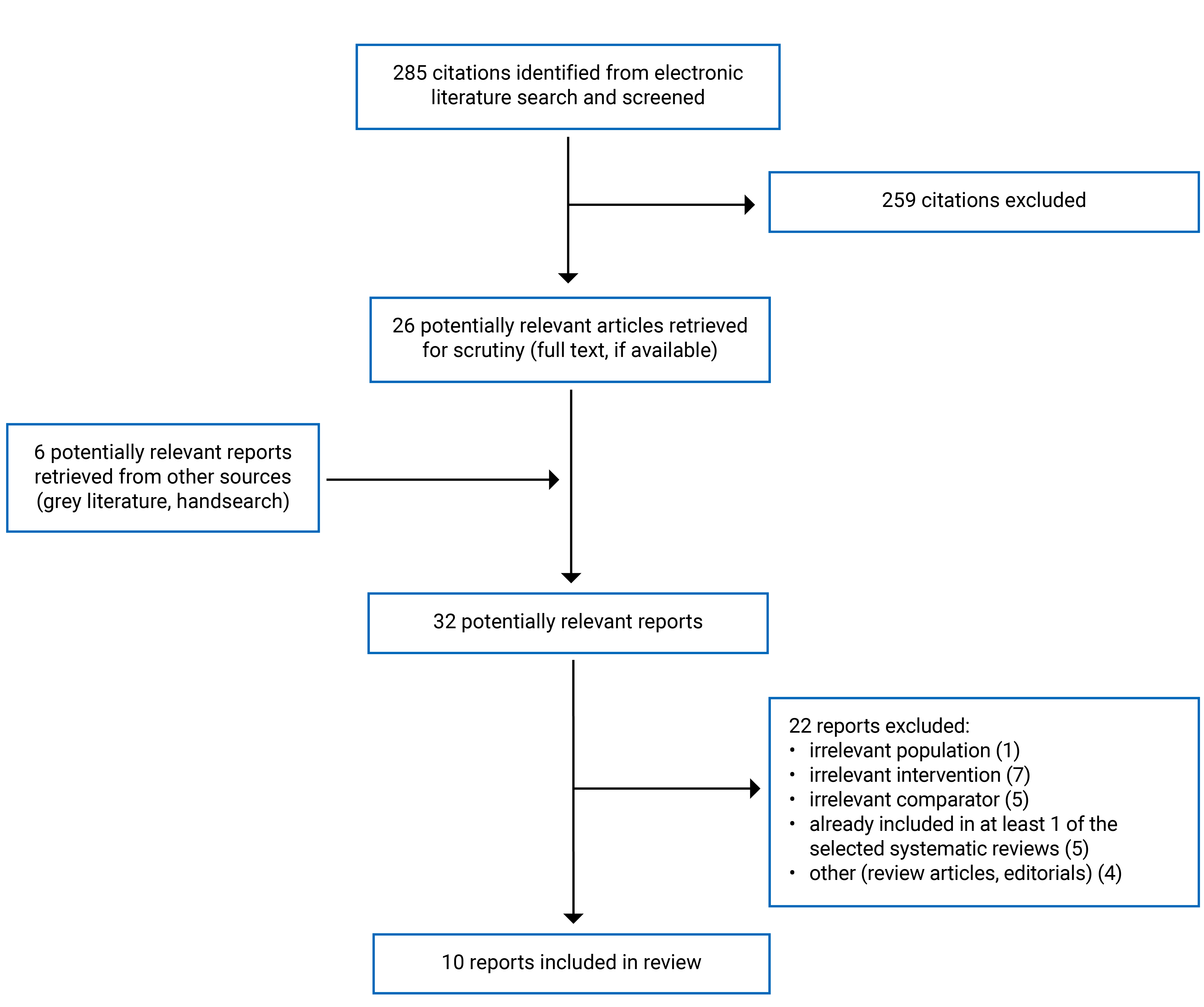
A total of 285 citations were identified in the literature search. Following screening of titles and abstracts, 259 citations were excluded and 26 potentially relevant reports from the electronic search were retrieved for full-text review. Six potentially relevant publications were retrieved from the grey literature search for full-text review. Of these 32 potentially relevant articles, 22 publications were excluded for various reasons, and 10 publications met the inclusion criteria and were included in this report. The included publications were 3 SRs,17-19 1 RCT,20 1 qualitative study,21 and 5 evidence-based guidelines.22-26 Appendix 1 presents the PRISMA27 flow chart of the study selection.
Summary of Study Characteristics
Appendix 2 provides details regarding the characteristics of the included publications.
Included Studies for Research Question 1: What Is the Clinical Effectiveness and Safety of Quetiapine Versus Other Drug Interventions for Adults With MDD?
Study Design
Three SRs,17-19 1 RCT,20 and 1 qualitative study21 were included to answer research question 1. The SRs were authored by Bai et al. (2025),17 Guo et al. (2024),18 and Yan et al. (2022).19 The 2 primary studies included an RCT by Cleare et al. (2025)20 and a qualitative study by McKeown et al. (2022).21
The SR by Bai et al. (2025)17 included 23 RCTs in total and used Bayesian network meta-regression to compare the efficacy of SGA augmentation (including quetiapine) to antidepressants in the treatment of treatment-resistant depression. The literature search covered available literature from electronic database inception to May 15, 2024. The follow-up duration of the included trials ranged from 6 weeks to 16 weeks. The effect size was obtained using a fixed-effects model or random-effects model based on the I2 value, which describes the percentage of total variation across trials that is due to heterogeneity rather than chance or sampling error.
The SR by Guo et al. (2024)18 included 72 RCTs and used NMAs to assess the efficacy and safety of 2 SGAs (brexpiprazole and quetiapine), physical therapies (electroconvulsive therapy and transcranial magnetic stimulation) and novel medications (i.e., esketamine, ketamine, psilocybin) for treatment-resistant depression. The literature search dates covered available literature from electronic database inception to January 28, 2024. The median duration of treatment was 8 weeks (range, 2 to 12 weeks). The SR by Guo et al. (2024)18 was broader in scope as it included additional network comparisons beyond those of interest for the current review (i.e., different types of physical therapies and placebo). Only the relevant comparisons of quetiapine versus other drug interventions will be described further in this report.
The SR by Yan et al. (2022)19 included 33 RCTs and used NMAs to evaluate the comparative efficacy and acceptability of SGAs (including quetiapine) as adjunctive therapy in combination with antidepressants in patients with suboptimal antidepressant responses. The literature search covered available literature from electronic database inception to May 25, 2021. A frequentist random-effects NMA using multivariate meta-analysis was performed. Dichotomous outcomes were reported as odds ratios with 95% credible intervals.
The 2 primary studies were the RCT by Cleare et al. (2025)20 and the qualitative study by McKeown et al. (2022).21 The RCT by Cleare et al. (2025), referred to as the “Lithium Versus Quetiapine in Depression” (LQD). study was a phase IV, head-to-head. Pragmatic. open-label superiority trial that compared the clinical effectiveness and cost-effectiveness of quetiapine and lithium augmentation for adults with treatment-resistant depression. The study was conducted between December 5, 2016, and July 26, 2021. Patients were randomized using a 1:1 ratio to lithium or quetiapine and followed up for 12 months or 52 weeks. Only the clinical effectiveness component is relevant to this rapid review.
The qualitative study by McKeown et al. (2022)21 was conducted to explore patient perspectives and experiences of augmentation treatment with quetiapine versus lithium in treatment-resistant depression. It was an optional add-on to the LQD trial, conducted with a subset of participants. Between November 2018 and February 2020, LQD study participants were invited to participate in semistructured interviews at their week 52 study assessments after randomization to treatment arms.
Country of Origin
All 3 SRs were conducted in China.17-19 The RCT20 and the qualitative study21 were conducted in the UK.
Patient Population
The patient population in the 5 studies (SRs,17-19 the RCT,20 and the qualitative study21) were adults with treatment-resistant depression.
The SR by Bai et al. (2025)17 included 10,679 patients across 23 RCTs. The average age of the participants varied between 38.1 to 46.6 years. The proportion of females ranged from 35.5% to 78.0%.17
The SR by Guo et al. (2024)18 included 12,105 patients across 72 RCTs. The mean age of the participants was 46.6 years (standard deviation [SD] = 11.9 years) and 69.3% of the participants on average were female across the included studies.
The SR by Yan et al. (2022)19 consisted of 4,543 and 6,059 patients across 33 RCTs randomized to the placebo and antipsychotics groups, respectively. The mean age of the participants was 44.5 years (SD = 11.5 years). The majority of the participants (65%) in the included studies were female.
A total of 212 patients were enrolled in the RCT by Cleare et al. (2025). 20 The mean age of the participants was 42.4 years (SD = 14 years), and there were more female (54%) than male (46%) participants.
The qualitative study by McKeown et al. (2022)21 consisted of 32 patients with a mean age of 43.1 years (15 years). The proportion of female participants (59.4%) was higher than male participants (40.6%).
Interventions and Comparators
In the SR by Bai et al. (2025),17 quetiapine as augmentative therapy was compared with antidepressant therapy and other SGAs of varying dosing regimens. Eight SGAs with up to 24 dosing regimens were compared: aripiprazole, brexpiprazole, cariprazine, olanzapine, combination olanzapine and fluoxetine, quetiapine, risperidone, and ziprasidone. Similarly, the SR by Yan et al. (2022)19 compared the same SGAs as the Bai et al. (2025) SR, except the olanzapine-fluoxetine combination. Unlike the Bai et al. (2025) SR, multiple dosing regimens of the SGAs were not accounted for in the Yan et al. (2022) NMA. In the SR by Guo et al. (2024),18 5 drug interventions were compared which included 2 SGAs (i.e., brexpiprazole, quetiapine), esketamine, ketamine and psilocybin. The SR by Guo et al. (2024)18 also compared physical interventions to these drugs, which were out of scope and excluded in this review.
The intervention examined in the Cleare et al. (2025) RCT20 was quetiapine and the comparator was lithium. The McKeown et al. (2022) qualitative study21 investigated patient experiences with quetiapine and lithium.
Outcomes
One or more of the following outcomes were assessed across the 3 SRs17-19 and 1 RCT:20 response rate, remission rate, illness severity, symptom severity, medication adherence, and AEs. Patient-reported outcome measures were captured in the RCT20 by Cleare et al. (2025), and included Quick Inventory of Depressive Symptomatology via Self-Report (QIDS-SR), Medication Adherence Report Scale (MARS), Patient-Rated Inventory of Side Effects (PRISE), and Work and Social Adjustment Scale (WSAS) scores.
Brief descriptions of the outcomes measured in the included SRs and RCT are as follows:
Response rate: Defined as the proportion of patients achieving a 50% or greater reduction in total score on standardized depression observer rating scales from baseline. The scales used were the Montgomery-Asberg Depression Rating Scale (MADRS) or the Hamilton Depression Rating Scale.
Remission rate: Defined as the total number of patients whose standardized depression scale score was less than a predefined threshold or specific cut-off. The SR by Guo et al. (2024)18 defined remission as a MADRS score 10 or lower or a Hamilton Depression Rating Scale score of 8 or lower for at least 2 subsequent treatments or at least 5 days.
Clinical Global Impression-Severity (CGI-S): A Clinician-rated scale for assessing overall illness severity in terms of subjective well-being, problems or symptoms, life functioning, and risk and/or harm.
QIDS-SR: A self-report scale that measures the burden of depressive symptom severity over the past 7 days.
MARS score: A self-report questionnaire that assesses participant adherence to the trial medication.
PRISE: Used to assess the presence and severity of side effects.
WSAS: A self-report tool to assess functional impairment due to mental health in 5 key domains: work, home, social leisure activities, private leisure activities, and personal or family relationships. A higher score is associated with greater illness severity.
Discontinuation due to an AE: Defined as the proportion of patients withdrawing from the trial due to any AE.
All-cause dropout rate: Defined as the percentage of participants withdrawing from the trial for whatever reason.
In the SR by Bai et al. (2025),17 the primary outcome was change in MADRS score, the secondary outcome was MADRS response rate, and the tertiary outcomes were CGI-S score and remission rates. The SR by Guo et al. (2024)18 examined response rate, remission rate, tolerability, and safety as primary outcomes. The SR by Yan et al. (2022)19 examined response rate and all-cause dropout rate or discontinuation as primary outcomes, while remission rates and discontinuation due to an AE were secondary outcomes. The primary outcomes in the RCT20 were QIDS-SR score and time to all-cause treatment discontinuation. Multiple secondary outcomes were measured in the RCT, including disease severity (MADRS score), EQ-5D (used for economic analysis in the trial and out of scope for this review), social functioning (WSAS score), adherence (MARS score), weight, diastolic BP and systolic BP, CGI-S score, and PRISE score.
Included Studies for Research Question 2: What Are the Evidence-Based Guidelines Regarding the Use and Administration of Quetiapine for Adults With MDD?
Study Design
Five evidence-based guidelines22-26 were included to answer the research question 2. The guidelines are the 2023 American College of Physicians (ACP) guideline,22 the 2023 Canadian Network for Mood and Anxiety Treatments (CANMAT) guideline,23 the 2022 National Institute for Health and Care Excellence (NICE) guideline,24 the 2022 US Department of Veterans Affairs and Department of Defense (VA/DoD) guideline,25 and the 2020 Royal Australian and New Zealand College of Psychiatrists (RANZCP) guideline.26
All guidelines were broad in scope and included recommendations for nonpharmacological treatments beyond those relevant to this review, such as psychotherapy, complementary and alternative medicine, and lifestyle (e.g., exercise) models of care delivery. Only the recommendations relevant to quetiapine (or SGAs as a therapeutic class) will be discussed in this report.
All the guidelines reported that systematic literature reviews were conducted to inform the recommendations. The systematic review for the 2023 ACP guideline22 focused on RCTs and nonrandomized studies to synthesize the comparative effectiveness and safety of treatments. Additionally, 2 rapid reviews informed the ACP guideline: 1 rapid review informed on patient values and preferences, and 1 rapid review informed on cost-effectiveness. The review for the 2023 CANMAT guideline23 prioritized SRs and meta-analyses and used RCTs where SRs were unavailable.
To develop the 2022 NICE guideline,24 the committee focused on evidence gathered through a systematic literature review. The quality of evidence was rated using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) system. However, this guideline did not report the strength of the recommendation and quality of the evidence that informed the recommendation in the main guideline publication; rather, it was reported in separate evidence review documents.
The systematic literature review for the 2022 VA/DoD guideline25 included SRs and RCTs. The literature review for the 2020 RANZCP guideline26 focused on SRs and meta-analyses. Evidence-based recommendations were developed using the Australian National Health and Medical Research Council levels of evidence for treatment studies. Where evidence was insufficient, absent, or its clinical impact and relevance uncertain, the Mood Disorders Committee developed expert consensus-based recommendations after extensive deliberations.
Country of Origin
The ACP22 and VA/DoD25 guideline applies to the US. The CANMAT guideline applies to Canada.23 The NICE guideline applies to the UK24 and the RANZCP guideline26 applies to Australia and New Zealand.26
Patient Population
The target patient population in the ACP22 guideline includes adults in the acute phase of MDD. The CANMAT23 and VA/DoD25 guidelines are intended for adults with MDD. The intended population of the NICE guidleine24 is adults with depression, while the target population for the RANZCP guideline26 are people of any age with mood disorders, mainly depression and bipolar disorder.
The intended users of the ACP22 guideline include ambulatory care clinicians caring for adults in the acute phase of MDD. The CANMAT23 is intended for community-based psychiatrists and mental health providers, similar to the VA/DoD25 guideline, which is intended for primary care providers and mental health providers caring for patients with MDD. The NICE guideline24 has a broader and more inclusive scope and is meant for health care professionals, commissioners, providers of health and public services for people with depression, individuals with depression, and their families and carers. The RANZCP guideline26 is intended for clinicians (psychiatrists and psychologists), primary care physicians, clinicians, and carers involved in managing patients with mood disorders.
Interventions and Practice Considered
All 5 guidelines22-26 covered multiple types of interventions and practices for the management of depression — pharmacological treatments and at least 1 type of nonpharmacological treatment. Nonpharmacological treatments included psychotherapy,22-26 complementary and alternative treatments, lifestyle interventions22-26 (e.g., physical activity or exercise, sleep, diet), and models of care24,25 (e.g., team-based interdisciplinary or collaborative care model, telehealth visits, in-person treatments).
Outcomes
Guidelines considered a range of outcomes relevant to this review, including symptom remission, treatment response, functional improvement, functional restoration, quality of life, recurrence rate, recurrence prevention, AEs, and suicidal behaviour.
Summary of Critical Appraisal
Critical Appraisal of SRs and Primary Studies
The study rationale and objectives for the 3 SRs,17-19 Bai et al. (2025),17 Guo et al. (2024),18 and Yan et al. (2022),19 were clearly stated. The literature search methods, search strategy, and criteria for the SRs were clearly presented. The comprehensiveness of the literature search of multiple databases and 2 or more reviewers involved in study screening, selection, data extraction, and risk of bias evaluation contributed to the validity of the 3 SRs.17-19 NMA are based on the integration of direct and indirect comparisons, which allows for the comparison of interventions not directly compared in head-to-head trials. Some methods were applied to make the results more reliable, such as the evaluations of heterogeneity and inconsistency in each of the 3 SRs,17-19 and sensitivity analysis in 2 SRs.18,19 Risk of bias assessment was conducted for individual articles using validated tools such as the Cochrane Risk of Bias tool.17-19 Additionally, the certainty of evidence in the Guo et al. (2024)18 SR was assessed using the Confidence in Network Meta-Analysis (CINeMA) framework. Funding sources and competing interests of authors were reported for all 3 SRs. Overall, the SRs were conducted with a relatively good methodology and presented a transparent, robust synthesis of the evidence.
In the RCT by Cleare et al. (2025),20 the authors described the objective, patient characteristics, intervention, outcome, and findings. The clinical effectiveness analyses were conducted using the intention-to-treat population and per-protocol populations. Sample size and statistical methods appeared appropriate. The long follow-up duration of 52 weeks provides a more relevant duration to compare treatment effectiveness in clinical practice as patients with treatment-resistant depression have chronic symptoms that fluctuate in severity. Blinded assessment of some outcome measures (MADRS and CGI-S) resulted in reduced measurement bias and added to the validity of the study. However, there were limitations. Not all outcomes were assessed by blinded raters and patient responses on the QIDS-SR questionnaire were self-rated and may be affected by patient’s subjectivity, recall bias, or social desirability. In addition, the higher rate of treatment discontinuation and withdrawal from the study before 12 months in the lithium group compared to the quetiapine group may have differential effects on outcomes.
In the qualitative study by McKeown et al. (2022),21 the authors described the significance of the study, purpose, and objectives. The type of qualitative approach, research paradigm, researchers’ characteristics, and reflexivity were not reported. The context and setting of the research, particularly as a part of an ongoing RCT, were described. The methods for data collection and analysis appear appropriate; however, the process of data management and security, verification of data integrity, and anonymization and/pr deidentification of excerpts were not described. The report did not include the techniques used to ensure the trustworthiness of the findings, such as an audit trail and concurrent data collection and analysis. Evidence (e.g., quotes from participants) was reported to substantiate analytic findings.
Critical Appraisal of Guidelines
All the guidelines clearly stated their scope and purpose, in terms of the objectives, guideline questions, intended users, and target population. While 4 of the 5 guidelines (ACP,22 CANMAT,23 NICE,24 and VA/DoD25) sought to gather the views and perspectives of people with depression, the RANZCP guideline26 did not state that they sought the views and preferences of the target population and therefore the recommendations may not be reflective of the views of people with mood disorders.
Four of the guidelines, ACP,22 CANMAT,23 NICE,24 and VA/DoD,25 used comprehensive methods to search for evidence and reported on their search strategy. The RANZCP guideline26 did not report on the search strategy or key search terms used, search dates, or inclusion or exclusion criteria. Including details on these elements of the search strategy increases its reproducibility and helps the reader determine if the search was comprehensive or if important evidence may have been missed. Four of the guidelines, ACP,22 CANMAT,23 NICE,24 and VA/DoD,25 included an explicit link between the recommendations and supporting evidence or rationale. The RANZCP guideline26 reported on the evidence supporting some of the recommendations for depression management; however, limited details of specific evidence supporting the quetiapine recommendation for the treatment of MDD were provided. The RANZCP guideline appears to have given significant weight to the consensus-driven process for developing the recommendations. It also focused more on recommendations for bipolar disorder than depression. All 5 guidelines were validated through an external review by relevant experts, public panels, or interest groups before publication. Funding sources and competing interests of authors were reported in all guidelines.
Additional details regarding the strengths and limitations of the included publications are provided in Appendix 3.
Summary of Findings
Clinical Effectiveness of Quetiapine Versus Other Drug Interventions for Adults With MDD
In the SR by Bai et al. (2025),17 brexpiprazole 2 mg to 3 mg (standardized mean difference = 0.155; 95% confidence interval [CI], 0.042 to 0.268) and combination olanzapine plus fluoxetine (standardized mean difference = 0.141; 95% CI, 0.019 to 0.264) were more effective as adjuvant treatment of treatment-resistant depression than quetiapine. No treatment was favoured between quetiapine and other antipsychotics or between quetiapine and antidepressant treatment.
In the Cleare et al. (2025)20 RCT, statistically significant differences in MADRS score were found between quetiapine and lithium, with results favouring quetiapine (adjusted mean difference = −2.98; 95% CI −5.87 to −0.09).
In the SR by Guo et al. (2024),18 no treatment was favoured for response rates between quetiapine and the other medications — brexpiprazole, esketamine, ketamine, and psilocybin.
Evidence from the Bai et al. (2025) SR17 found that quetiapine was associated with higher remission rates than risperidone 0.5 mg to 2 mg (hazard ratio = 0.17; 95% CI, 0.047 to 0.632) and ziprasidone 160 mg (hazard ratio = 0.091; 95% CI, 0.01 to 0.816). Evidence did not show statistically significant differences between quetiapine and the other drug interventions (i.e., other SGAs and antidepressants).
Psilocybin was associated with higher odds of remission from depression compared with quetiapine in the Guo et al. (2024) SR18 (odds ratio = 3.07; 95% CI, 1.21 to 7.82). No statistically significant differences were observed between quetiapine and other medications, including brexpiprazole, esketamine, and ketamine.
In the SR by Yan et al. (2022),19 no significant differences in response and remission rates were found in comparisons of quetiapine and other SGAs.
QIDS-SR scores measured in the Cleare et al. (2025)20 RCT showed a greater improvement in symptoms of depression in the quetiapine group compared with the lithium group (adjusted mean difference = −68.36; 95% CI −129.95 to −6.76).
Safety Outcomes
No significant differences in tolerability were found in the comparison of quetiapine with other SGAs in the SR by Yan et al. (2022).19
No significant differences in tolerability and safety were observed for quetiapine compared with other medications such as brexpiprazole, esketamine, ketamine, and psilocybin in the Guo et al. (2024)18 SR.
Time to all-cause discontinuation did not significantly differ between the quetiapine and lithium groups in the RCT by Cleare et al. (2025).20
In the RCT by Cleare et al. (2025), 20 15 serious AEs were reported in 7 of 107 patients (7%) in the quetiapine group and 17 serious AEs were reported in 11 of 105 patients (11%) in the lithium group. One patient in the lithium group had acute renal failure.
The results from the RCT by Cleare et al. (2025)20 demonstrated that side effects, as measured by the PRISE, and physical parameters (weight and blood pressure) were similar between the quetiapine and lithium groups.
No safety data regarding misuse or diversion of quetiapine were found in the included studies.
Social Functioning
Social functioning was reported in the RCT by Cleare et al. (2025).20 Quetiapine resulted in a significant improvement in social functioning compared with lithium (adjusted mean difference = −3.64; 95% CI −6.28 to −0.99). Social functioning was not reported in the SRs or qualitative study.
Patient Experience and Perspectives
The qualitative study by McKeown et al. (2022)21 reported on patient experiences and perspectives of quetiapine and lithium augmentation medications, such as initial concerns, experience of side effects, perception of treatment efficacy, and positive perception of treatment monitoring. Patients expressed greater apprehension toward lithium over quetiapine before treatment initiation. By contrast, patients reported side effects to a greater extent for quetiapine compared to lithium during treatment (e.g., sedation, weight gain, and appetite changes). They viewed the side effects of lithium to be more manageable.
While most patients perceived treatment with either medication (quetiapine or lithium) as beneficial, some patients perceived treatment to be ineffective. Clinical monitoring was perceived positively in terms of regular appointments, reassurance regarding the ease and speed of communication with study team and clinicians, and acceptance of blood monitoring for patients treated with lithium.
Guidelines Regarding the Use of Quetiapine
The 2023 ACP guideline22 recommends switching to a different second-generation antidepressant or augmenting with a second pharmacologic treatment such as quetiapine for patients in the acute phase of moderate to severe MDD whose disease does not respond to initial treatment with an adequate dose of a second-generation antidepressant.
The 2023 CANMAT guideline23 recommends quetiapine in combination with a first-line antidepressant for MDD with psychotic features. The guideline recommends quetiapine as a second-line treatment option for adults with MDD. The guideline also recommends quetiapine as a second-line adjunctive treatment option for adults with difficult to treat depression. Atypical psychotics such as quetiapine in combination with an antidepressant may be used as a first-line treatment for MDD with psychotic features.
The NICE guideline24 recommends combination treatment for people with depression with psychotic symptoms that includes an antidepressant medication and an antipsychotic medication (for example, olanzapine or quetiapine).
The VA/DoD guideline25 provides recommendations for patients with MDD who have demonstrated partial or no response to an adequate trial of initial pharmacotherapy. One of the recommendations is augmenting with an SGA such as aripiprazole, brexpiprazole, cariprazine, olanzapine, quetiapine, or risperidone.
The RANZCP guideline26 recommends that SGAs such as lurasidone, quetiapine, and olanzapine be used either as monotherapy or adjunctively in the treatment of major depression. New drugs such as aripiprazole and brexpiprazole are indicated for adjunctive treatment of major depression.
The study findings from all included publications are provided in Appendix 4.
Limitations
The evidence base for the SRs17-19 was drawn from clinical trials and thus may not be reflective of real-world practice with respect to the use of quetiapine. Important factors such as concurrent treatments and comorbidities were not explored. Many patients with depression have coexisting mental health and chronic medical conditions; however, patients with these conditions were excluded from participation in the trials, which may limit the generalizability of the evidence. There was heterogeneity among the primary studies included in the SRs in terms of patient and study characteristics, and inconsistency in the reported outcomes. The influence of these factors on the SR findings is unknown. The SR by Yan et al. (2022)19 did not consider drug doses in the analysis due to the unavailability of this information in the original articles.
In the RCT by Cleare et al. (2025),20 not all outcomes were assessed by blinded raters; patient responses on the QIDS-SR questionnaire were self-rated and may have been affected by patients’ subjectivity, recall bias, or social desirability. The higher rate of treatment discontinuation and withdrawal from the trial before 12 months in the lithium group compared to the quetiapine group may have had differential effects on outcomes. In the qualitative study by McKeown et al. (2022),21 recall bias is a limitation as interviews were conducted 52 weeks after the patients were first enrolled in the trial.
No safety data regarding misuse or diversion of quetiapine were found in the included studies. The lack of data may be due to the type of study designs specified in the eligibility criteria for the current review rather than absence of misuse in the existing literature.
This report is limited by the quantity and the quality of available evidence. Five evidence-based guidelines were identified that included recommendations on the use of quetiapine specifically or the therapeutic class of SGAs more broadly for MDD. Additionally, the quality of evidence supporting the recommendations was rated as low for 2 guidelines (ACP22 and VA/DoD25) and was not reported for 2 guidelines, NICE24 and RANZCP.26 Only the recommendations included in the 2023 CANMAT guideline23 were based on evidence that was rated as high quality by the authors.
Conclusions and Implications for Decision- or Policy-Making
We identified 3 SRs,17-19 1 RCT,20 1 qualitative study,21 and 5 evidence-based guidelines22-26 relevant to the research questions.
Evidence from the SRs included in this review suggests that quetiapine and other SGAs (particularly aripiprazole, brexpiprazole, cariprazine, olanzapine, risperidone, and ziprasidone) have similar efficacy and safety for the treatment of adults with treatment-resistant MDD. Evidence from the included RCT suggests that quetiapine reduced depression symptoms and improved social functioning compared with lithium. While not an approved indication by the FDA or Health Canada, lithium has long been used as an augmentation treatment for MDD. In the qualitative study by McKeown et al. (2022),21 patients perceived both quetiapine and lithium to improve depression. However, they reported more side effects with quetiapine than lithium and viewed the side effects of lithium to be more manageable.
The included guidelines suggest using quetiapine as a second-line augmentation treatment option for MDD in patients whose disease had partial or no response to an adequate dose of 2 or more antidepressant medications (i.e., those with difficult to treat depression). In addition, the CANMAT guideline recommends a combination of an antidepressant and antipsychotic as a first-line treatment for MDD with psychotic features. The RANZCP guideline suggests using quetiapine as monotherapy or adjunct therapy for patients with major depression.
Implications for Clinical Practice
The findings of this review suggest that antipsychotics such as quetiapine could be used as a second-line augmentation treatment option for MDD in patients whose disease had partial or no response to an adequate dose of 2 or more antidepressants (i.e., those with treatment-resistant depression or difficult to treat depression). The findings of this review also suggest that SGAs such as quetiapine, in combination with an antidepressant, may be used as a first-line treatment for MDD that is very severe or has associated psychotic features. According to the included RCT, quetiapine is more beneficial than lithium in reducing depressive symptoms and improving functioning in treatment-resistant depression. Factors such as patient characteristics, patient tolerability, patient values, side effect profiles of different treatment options, and clinician expertise may also be important to guide treatment choice for people with MDD. The findings of this review should be interpreted in conjunction with the previous 2020 CDA-AMC report, which provides additional context and evidence on the use of quetiapine for MDD.
Acknowledgement
Clinical Expert
This individual has kindly provided comments on the report:
Diane McIntosh, BSc Pharmacy, MD, FRCP
Psychiatrist
References
1.American Psychiatric Association. Depressive disorders. Diagnostic and Statistical Manual of Mental Disorders, 5th ed, Text Revision (DSM-5-TR). American Psychiatric Association; 2022.
2.Statistics Canada. Insights on Canadian Society: Mental disorders and access to mental health care. Statistics Canada; 2023. Accessed 2025 May 2. https://www150.statcan.gc.ca/n1/pub/75-006-x/2023001/article/00011-eng.htm
3.Thase M, Connolly KR. Roy-Byrne PP, ed. Unipolar treatment-resistant depression in adults: Epidemiology, risk factors, assessment, and prognosis. UpToDate; 2025. Accessed 2025 April 11. https://www.uptodate.com/
4.Rush AJ. Roy-Byrne PPM, Robert ed. Major depressive disorder in adults: Approach to initial management. UpToDate; 2025. Accessed 2025 April 11. https://www.uptodate.com/
5.CAMH. Depression. 2024. Accessed 2025 May 10. https://www.camh.ca/en/health-info/mental-illness-and-addiction-index/depression
6.Arnaud AM, Brister TS, Duckworth K, et al. Impact of Major Depressive Disorder on Comorbidities: A Systematic Literature Review. J Clin Psychiatry. 2022;83(6). doi: 10.4088/JCP.21r14328 PubMed
7.Oluboka OJ, Katzman MA, Habert J, et al. Functional Recovery in Major Depressive Disorder: Providing Early Optimal Treatment for the Individual Patient. Int J Neuropsychopharmacol. 2018;21(2):128-144. doi: 10.1093/ijnp/pyx081 PubMed
8.Seroquel (quetiapine fumarate): tablets, 25 mg, 100 mg, 200 mg and 300 mg, oral Use [product monograph]. CheplaPharm Arzneimittel GmbH; 2025. Accessed 2025 May 10. https://pdf.hres.ca/dpd_pm/00078929.PDF
9.Seroquel XR (quetiapine fumarate); extended-release tablets, 50 mg, 150 mg, 200 mg, 300 mg and 400 mg, oral use [product monograph]. CheplaPharm Arzneimittel GmbH; 2025. Accessed 2025 May 10. https://pdf.hres.ca/dpd_pm/00080013.PDF
10.Quetiapine: Drug information. UpToDate. Accessed 2025 April 11.
11.Peridy E, Hamel J-F, Rolland A-L, Gohier B, Boels D. Quetiapine Poisoning and Factors Influencing Severity. J Clin Psychopharmacol. 2019;39(4). PubMed
12.Curry DE, Richards BL. A Brief Review of Quetiapine. American Journal of Psychiatry Residents' Journal. 2022;18(2):20-22. doi: 10.1176/appi.ajp-rj.2022.180207
13.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. doi: 10.1136/bmj.j4008 PubMed
14.Jansen JP, Trikalinos T, Cappelleri JC, et al. Indirect treatment comparison/network meta-analysis study questionnaire to assess relevance and credibility to inform health care decision making: an ISPOR-AMCP-NPC Good Practice Task Force report. Value Health. 2014;17(2):157-73. doi: 10.1016/j.jval.2014.01.004 PubMed
15.O’Brien BC, Harris IB, Beckman TJ, Reed DA, Cook DA. Standards for Reporting Qualitative Research: A Synthesis of Recommendations. Acad Med. 2014;89(9):1245-1251. doi: 10.1097/acm.0000000000000388 PubMed
16.Agree Next Steps C. The AGREE II Instrument. AGREE Enterprise; 2017. Accessed January 1, 1800. https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf
17.Bai B, Li Y, Chen X, et al. The augmentative efficacy of second-generation anti-psychotics (SGA) to anti-depressants in treating treatment-resistant depression: a network meta-regression analysis. BMC Psychiatry. 2025;25(1):338. doi: 10.1186/s12888-025-06783-7 PubMed
18.Guo Q, Guo L, Wang Y, Shang S. Efficacy and safety of eight enhanced therapies for treatment-resistant depression: A systematic review and network meta-analysis of RCTs. Psychiatry Res. 2024;339:116018. doi: 10.1016/j.psychres.2024.116018 PubMed
19.Yan Y, Yang X, Wang M, Chen B, Yin L, Ma X. Efficacy and acceptability of second-generation antipsychotics with antidepressants in unipolar depression augmentation: a systematic review and network meta-analysis. Psychol Med. 2022;52(12):2224-2231. doi: 10.1017/s0033291722001246 PubMed
20.Cleare AJ, Kerr-Gaffney J, Goldsmith K, et al. Clinical and cost-effectiveness of lithium versus quetiapine augmentation for treatment-resistant depression: a pragmatic, open-label, parallel-group, randomised controlled superiority trial in the UK. Lancet Psychiatry. 2025;12(4):276-288. doi: 10.1016/s2215-0366(25)00028-8 PubMed
21.McKeown L, Taylor RW, Day E, et al. Patient perspectives of lithium and quetiapine augmentation treatment in treatment-resistant depression: A qualitative assessment. Journal of Psychopharmacology. 2022;36(5):557-565. doi: 10.1177/02698811221089042 PubMed
22.Qaseem A, Owens DK, Etxeandia-Ikobaltzeta I, et al. Nonpharmacologic and Pharmacologic Treatments of Adults in the Acute Phase of Major Depressive Disorder: A Living Clinical Guideline From the American College of Physicians. Ann Intern Med. 2023;176(2):239-252. doi: 10.7326/M22-2056 PubMed
23.Lam RW, Kennedy SH, Adams C, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) 2023 Update on Clinical Guidelines for Management of Major Depressive Disorder in Adults: Réseau canadien pour les traitements de l'humeur et de l'anxiété (CANMAT) 2023: Mise à jour des lignes directrices cliniques pour la prise en charge du trouble dépressif majeur chez les adultes. The Canadian Journal of Psychiatry. 2024;69(9):641-687. PubMed
24.National Institute for Health and Care Excellence. Depression in adults treatment and management. 2022. Accessed 2025 May 15. https://www.nice.org.uk/guidance/ng222
25.US Department of Veterans Affairs and the Department of Defense. VA/DoD Clinical Practice Guideline: The Management of Major Depressive Disorder (MDD) Version 4.0 – (2022). U.S. Department of Veterans Affairs; 2022.
26.Malhi GS, Bell E, Bassett D, et al. The 2020 Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for mood disorders. Aust N Z J Psychiatry. 2021;55(1):7-117. doi: 10.1177/0004867420979353 PubMed
27.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. doi: 10.1016/j.jclinepi.2009.06.006 PubMed
28.Gedikli C, Miraglia M, Connolly S, Bryan M, Watson D. The relationship between unemployment and wellbeing: an updated meta-analysis of longitudinal evidence. European Journal of Work and Organizational Psychology. 2022;32(1):128-144. doi: 10.1080/1359432x.2022.2106855
Appendix 1: Selection of Included Studies
Figure 1: PRISMA27 Flow Chart of Study Selection
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of Included Systematic Reviews
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Bai et al. (2025)17 China Funding source: Zhejiang Medical and Health Science and Technology Project and the Science and Technology Department of Zhejiang Province Foundation | SR and NMR 23 RCTs in total | Adult patients with treatment-resistant depression (TRD). TRD was defined as minimum of 2 prior treatment failures at adequate dose and duration) Diagnostic criteria: DSM-IV or DSM IV-TR or DSM V N = 10,679 patients Mean age: 38.1 to 46.6 years Sex: Female 35.5% to 78.0% | Interventions: SGAs as augmentative therapy 24 dosing regimens for SGAs – quetiapine (XR 150mg/d, XR 300mg/d), aripiprazole, brexpiprazole, cariprazine, olanzapine, olanzapine-fluoxetine combination, risperidone, ziprasidone Comparators: Antidepressant therapy or mutual comparison among the SGA dosing regimens | Primary outcomes: Change in MADRS score (assessed for 16 regimens) Secondary outcome: MADRS response rate (assessed for 16 regimens) Tertiary outcome:
Follow-up duration: 6 weeks to 16 weeks |
Guo et al. (2024)18 China Funding source: Not reported | SR and NMA 72 RCTs in total | Adult patients with treatment-resistant depression (TRD) Diagnostic criteria: ICD-10, ICD-11, DSM-3, DSM-4, DSM-5 N = 12,105 patients Mean age: 46.6 years (SD 11.9 years) Sex: Female 69.3% | Interventions: 7 therapies — Atypical antipsychotics (Brexpiprazole, Quetiapine), Physical therapies (ECT, TMS), and Novel medications (Esketamine, Ketamine, Psilocybin) Comparators: Placebo or mutual comparison among the 7 therapies | Outcomes:
Follow-up duration: Acute treatment for 8 weeks |
Yan et al. (2022)19 China Funding source: Key Research and Development Program of the Science and Technology Department of Sichuan Province, Program of Chengdu Science and Technology, National Natural Science Foundation of China, China Postdoctoral Science Foundation, Open Project Program of the National Laboratory of Pattern Recognition, and West China Hospital Postdoctoral Science Foundation. | SR and NMA 33 RCTs in total | Adult patients with treatment-resistant depression 4,543 and 6,059 patients randomized to the placebo and antipsychotics groups respectively Patients Mean age: 44.5 years (SD 11.5 years) Sex: Female 65% Length of trials was 7.24 weeks (SD 3.42), ranging from 4 to 24 weeks | Interventions: Seven SGAs — aripiprazole, brexpiprazole, cariprazine, olanzapine, quetiapine, risperidone, and ziprasidone. Comparators: SGAs or placebo | Primary Outcomes:
Secondary outcomes:
|
CGI-S = Clinical Global Impression-severity; ECT = electroconvulsive therapy; HAM-D17 = Hamilton Rating Scale for Depression, 17 item version; MADRS = Montgomery-Asberg Depression Scale; MDD = major depressive disorder; NMR = Network meta-regression; RCT = randomized controlled trials; TMS = transcranial magnetic stimulation; TRD = treatment-resistant depression.
Note: This table has not been copy-edited.
Table 3: Characteristics of Included Randomized Controlled Trial
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Cleare et al. (2025)20 UK Funding source: NIHR Health Technology Assessment Programme | Phase IV, pragmatic, open-label, parallel-group 1:1 RCT Lithium vs quetiapine in depression (LQD) trial | Adult patients with treatment-resistant depression (TRD) Diagnostic criteria: DSM-V N = 212 patients Mean age: 42.4 years (SD 14 years) Sex:
Ethnicity:
| Intervention: Quetiapine Comparator: Lithium | Primary outcomes:
Secondary outcomes:
Trial duration/Follow-up: 52 weeks in total (12 months). Assessments at baseline, 8, 26 and 52 weeks with weekly online assessments for primary outcomes. |
CGI-S = Clinical Global Impression-Severity; MADRS = Montgomery-Asberg Depression Rating Scale; MARS-5 = five‐item Medication Adherence Report Scale; MDD = major depressive disorder; PRISE = Patient-Rated Inventory of Side Effects; QIDS-SR = self-rated Quick Inventory of Depressive Symptomatology; RCT = randomized controlled trials; TRD = treatment-resistant depression; WSAS = Work and Social Adjustment Scale.
Note: This table has not been copy-edited.
Table 4: Characteristics of Included Qualitative Study
Study citation, country, funding source | Study objectives | Study design | Sample description | Data collection and analysis |
|---|---|---|---|---|
McKeown et al. (2022)21 UK Funding source: NIHR HTA Programme | To describe patient experiences and perspectives of quetiapine and lithium augmentation for TRD | Qualitative study embedded within the larger ongoing LQD trial | 32 adult patients with TRD Mean age: 43.1 years (15 years) Sex:
| Data collection: semistructured audio-recorded interviews. Data analysis: thematic analysis |
HTA = health technology assessment; LQD = Lithium vs quetiapine in depression study; TRD = treatment-resistant depression.
Note: This table has not been copy-edited.
Table 5: Characteristics of Included Guidelines
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality assessment | Recommendations development and evaluation | Guideline validation |
|---|---|---|---|---|---|---|
2023 ACP22 | ||||||
Intended Users: ambulatory care clinicians caring for adult patients in the acute phase of MDD Target Population: adults in the acute phase of MDD. |
| Clinical outcomes: suicidal ideas or behaviours, symptom remission, treatment response, functional capacity, quality of life, mental suffering, serious adverse events Cost outcomes: cost-effectiveness | The Clinical Guidelines Committee reviewed evidence derived from several sources: SR and NMA on comparative effectiveness and safety of treatments (completed by ACP), 2 rapid reviews (1 on patient values and preferences, 1 on cost-effectiveness), cost data from the validated US Centers for Medicare and Medicaid Services databases and mental health billing services. Evidence-to-decision tables were used for evidence reporting | The GRADE approach was used to grade the certainty of evidence and strength of recommendations. Two types of rating were assigned to each recommendation:
| CGC and CGC Public Panel contributed to developing guidelines. The Public Panel informed patient values and preferences by independent outcome rating, participation in various stages of guideline development, and thorough review of the guideline. CGC graded the strength of each recommendation, the evidence quality, patient preferences and values, and considerations about cost or resource allocation CGC members independently evaluated the guidelines using the AGREE II guidelines |
|
2023 CANMAT23 | ||||||
Intended users: community-based psychiatrists and mental health providers Target population: adults with MDD |
| Symptom remission, functional improvement, functional restoration, QoL, recurrence prevention, adverse events | Systematic literature review focused on SRs and meta-analyses (and RCTs and other studies where SRs were unavailable). Included studies since the previous 2016 guidelines. Relevant studies were selected by 2 independent reviewers. | Quality of evidence was assessed using the modified global ratings from GRADE methodology. Evidence was assigned a level from 1 to 4 (highest to lowest):
| Recommendations were developed and reviewed through a formal iterative consensus process among the CANMAT authors. Treatment recommendations were organized by the lines of treatment, based on both the level of evidence and clinical support. CANMAT criteria of evidence for lines of treatment:
|
|
2022 NICE24 | ||||||
Intended Users: HCPs, Commissioners, providers of health and public services for people with depression, people with depression, their families and carers Target Population: adults with depression |
| Benefits and harms of interventions | Systematic evidence reviews to identify published evidence relevant to review questions. The review questions were based on key areas identified in the scope of the guideline. Intervention reviews and qualitative reviews were conducted to inform guideline development | The quality of evidence was appraised using GRADE methodology for intervention reviews and GRADE-CERQual methodology for qualitative reviews | Recommendations were drafted on the basis of the committee’s interpretation of the available evidence, taking account of the balance of benefits, harms and costs between different courses of action. When effectiveness and economic evidence was of poor quality, conflicting or absent, the committee drafted recommendations based on their expert opinion. | Public consultation and feedback process with registered partiesz. |
2022 VA/DoD25 | ||||||
Intended Users: primary care providers (PCPs) and mental health providers caring for patients with MDD Target Population: adults who have MDD diagnosis eligible for care in the VA or DoD health care delivery systems |
| Symptom improvement, remission rate, functional status measures, QoL, relapse or recurrence rate, treatment adherence/ retention, adverse events, suicidal behaviour, mortality | Systematic evidence review, guided by 12 clinically relevant key questions of high priority for the VA and DoD populations. Patient perspectives were collected through a virtual focus group | The methodological risk of bias of included individual studies was assessed using the USPSTF method. Each study is assigned a rating (good, fair or poor) based on a set of criteria that vary according to study design. The GRADE approach was used to assess the overall quality of the body of evidence for each outcome and rated as high, moderate, low or very low. GRADE was applied in a more rigorous way than previous iterations of the guideline. | To develop recommendations, the Work Group of multidisciplinary experts interpreted the systematic evidence review’s findings and considered patient perspectives. The recommendations built on the previous 2016 CPG, to modify, replace, amend, and craft new recommendations not included in the 2016 update. Each recommendation’s strength (strong/weak) and direction (for/against/neither for or against) was determined based on 4 domains as per GRADE: confidence in the quality of evidence, balance of benefits and harms outcomes, patient values and preferences, and other implications (e.g., resource use, equity, feasibility, patient subgroup considerations). The Work Group used an iterative review process to solicit feedback on 3 drafts of the CPG and made revisions. |
|
2020 RANZCP | ||||||
Intended Users: Specialist clinicians (psychiatrists and psychologists), primary care physicians, clinicians and carers involved in the management of patients with mood disorders Target population: people with mood disorders — depression and bipolar disorders |
| Target Outcomes organized by phase of treatment (initial to maintenance):
| Evidence was sourced from published depression guidelines, systematic search of electronic databases. Recent systematic reviews and meta-analyses were prioritized. MDC identified areas where significant changes had occurred (e.g., new therapies, practice changes, concept and changes to conceptual models relevant to condition and its management). | Evidence used to formulate recommendations were assigned levels of evidence and graded as 1 of 4 levels - EBR level I (highest quality), II, III or IV (lowest quality). | Evidence-based recommendations (EBR) were developed using the Australian National Health and Medical Research Council (NHMRC) levels of evidence for treatment studies. Where evidence was insufficient, absent or its clinical impact and relevance uncertain, expert consensus-based recommendations (CBR) were developed after extensive deliberations of the committee. Interventions were classified as actions, choices, or alternatives.
|
|
ACP = American College of Physicians; CAM = complementary and alternative medicine; CANMAT = Canadian Network for Mood and Anxiety Treatments; CPG = clinical practice guideline; DBS = deep brain stimulation; DoD = US Department of Defense; ECT = electroconvulsive therapy; GRADE = Grading of Recommendations Assessment, Development, and Evaluation; MDD = major depressive disorder; QoL = quality of life; RANZCP = Royal Australian and New Zealand College of Psychiatrists; RCT = randomized controlled trial; SR = systematic review; TRD = treatment-resistant depression; USPSTF = US Preventive Services Task Force; VA = US Department of Veterans Affairs.
Note: This table has not been copy-edited.
Appendix 3: Critical Appraisal of Included Publications
Please note that this appendix has not been copy-edited.
Table 6: Strengths and Limitations of Clinical Studies
Strengths | Limitations |
|---|---|
Cleare et al. (2025)20 | |
Internal validity:
External validity:
| Internal validity:
External validity:
|
Table 7: Strengths and Limitations of Qualitative Study Using SRQR Checklist15
Item | Description | Reported |
|---|---|---|
McKeown et al. (2022)21 | ||
1. Title | Concise description of the nature and topic of the study. Identifying the study as qualitative or indicating the approach (e.g., ethnography, grounded theory) or data collection methods (e.g., interview, focus group) is recommended | Partial |
2. Abstract | Abstract - Summary of key elements of the study using the abstract format of the intended publication; typically includes background, purpose, methods, results, and conclusions | Yes |
Introduction | ||
3. Problem formulation | Description and significance of the problem/phenomenon studied; review of relevant theory and empirical work; problem statement | Yes |
4. Purpose | Purpose of the study and specific objectives or questions | Yes |
Methods | ||
5. Qualitative approach and research paradigm | Qualitative approach (e.g., ethnography, grounded theory, case study, phenomenology, narrative research) and guiding theory if appropriate; identifying the research paradigm (e.g., postpositivist, constructivist/ interpretivist) is also recommended; rationale | No |
6. Researcher characteristics and reflexivity | Researchers’ characteristics that may influence the research, including personal attributes, qualifications/experience, relationship with participants, assumptions, and/or presuppositions; potential or actual interaction between researchers’ characteristics and the research questions, approach, methods, results, and/or transferability | No |
7. Context | Setting/site and salient contextual factors; rationale | Yes |
8. Sampling strategy | How and why research participants, documents, or events were selected; criteria for deciding when no further sampling was necessary (e.g., sampling saturation); rationale | Partial |
9. Ethics | Documentation of approval by an appropriate ethics review board and participant consent, or explanation for lack thereof; other confidentiality and data security issues | Yes |
10. Data collection methods | Types of data collected; details of data collection procedures including (as appropriate) start and stop dates of data collection and analysis, iterative process, triangulation of sources/methods, and modification of procedures in response to evolving study findings; rationale | Yes |
11. Data collection instruments and technologies | Description of instruments (e.g., interview guides, questionnaires) and devices (e.g., audio recorders) used for data collection; if/how the instrument(s) changed over the course of the study | Yes |
12. Units of study | Number and relevant characteristics of participants, documents, or events included in the study; level of participation (could be reported in results) | Yes |
13. Data processing | Methods for processing data before and during analysis, including transcription, data entry, data management and security, verification of data integrity, data coding, and anonymization/de-identification of excerpts | Partial |
14. Data analysis | Process by which inferences, themes, etc., were identified and developed, including the researchers involved in data analysis; usually references a specific paradigm or approach; rationale | Yes |
15. Techniques to enhance trustworthiness | Techniques to enhance trustworthiness and credibility of data analysis (e.g., member checking, audit trail, triangulation); rationale | Partial |
Results | ||
16. Synthesis and interpretation | Main findings (e.g., interpretations, inferences, and themes); might include development of a theory or model, or integration with prior research or theory | Yes |
17. Links to empirical data | Evidence (e.g., quotes, field notes, text excerpts, photographs) to substantiate analytic findings | Yes |
Discussion | ||
18. Integration with prior work, implications, transferability, and contribution(s) to the field | Integration with prior work, implications, transferability, and contribution(s) to the field - Short summary of main findings; explanation of how findings and conclusions connect to, support, elaborate on, or challenge conclusions of earlier scholarship; discussion of scope of application/generalizability; identification of unique contribution(s) to scholarship in a discipline or field | Yes |
19. Limitations | Trustworthiness and limitations of findings | Yes |
Other | ||
20. Conflicts of interest | Potential sources of influence or perceived influence on study conduct and conclusions; how these were managed | Yes |
21. Funding | Sources of funding and other support; role of funders in data collection, interpretation, and reporting | Yes |
SRQR = Standards for Reporting Qualitative Research.
Table 8: Strengths and Limitations of Guidelines Using AGREE II16
Item | 2023 ACP | 2023 CANMAT | 2022 NICE | 2022 VA/DoD | 2020 RANZCP |
|---|---|---|---|---|---|
Domain 1: Scope and purpose | |||||
1. The overall objective(s) of the guideline is (are) specifically described. | Yes | Yes | Yes | Yes | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes | Yes | Yes | Yes | Yes |
3. The population (patients, public, etc.) to whom the guideline is meant to apply is specifically described. | Yes | Yes | Yes | Yes | Yes |
Domain 2: Stakeholder involvement | |||||
4. The guideline development group includes individuals from all relevant professional groups. | Yes | Yes | Yes | Yes | Yes |
5. The views and preferences of the target population (patients, public, etc.) have been sought. | Yes | Yes | Yes | Yes | No |
6. The target users of the guideline are clearly defined. | Yes | Yes | Yes | Yes | Yes |
Domain 3: Rigour of development | |||||
7. Systematic methods were used to search for evidence. | Yes | Yes | Yes | Yes | Partial |
8. The criteria for selecting the evidence are clearly described. | Yes | Yes | Yes | Yes | No |
9. The strengths and limitations of the body of evidence are clearly described. | Yes | Yes | Yes | Yes | Partial |
10. The methods for formulating the recommendations are clearly described. | Yes | Yes | Yes | Yes | Yes |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes | Yes | Yes | Yes | Yes |
12. There is an explicit link between the recommendations and the supporting evidence. | Yes | Yes | Yes | Yes | Partial |
13. The guideline has been externally reviewed by experts before its publication. | Yes | Yes | Yes | Yes | Yes |
14. A procedure for updating the guideline is provided. | Yes | Partial | Partial | Yes | No |
Domain 4: Clarity of presentation | |||||
15. The recommendations are specific and unambiguous. | Yes | Yes | Yes | Yes | Yes |
16. The different options for management of the condition or health issue are clearly presented. | Yes | Yes | Yes | Yes | Yes |
17. Key recommendations are easily identifiable. | Yes | Yes | Yes | Yes | Partial |
Domain 5: Applicability | |||||
18. The guideline describes facilitators and barriers to its application. | Yes | Yes | Yes | Partial | Yes |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | Partial | Yes | Yes | Yes | Partial |
20. The potential resource implications of applying the recommendations have been considered. | Yes | Yes | Yes | Yes | Yes |
21. The guideline presents monitoring and/or auditing criteria. | Yes | Yes | Unclear | Partial | No |
Domain 6: Editorial independence | |||||
22. The views of the funding body have not influenced the content of the guideline. | Yes | Yes | Yes | Yes | Yes |
23. Competing interests of guideline development group members have been recorded and addressed. | Yes | Yes | Yes | Yes | Yes |
AGREE II = Appraisal of Guidelines for Research and Evaluation II; CANMAT = Canadian Network for Mood and Anxiety Treatments; DoD = US Department of Defense; ECT = electroconvulsive therapy; GRADE = Grading of Recommendations Assessment, Development, and Evaluation; MDD = major depressive disorder; RANZCP = Royal Australian and New Zealand College of Psychiatrists; USPSTF = US Preventive Services Task Force; VA = US Department of Veterans Affairs.
Appendix 4: Main Study Findings
Please note that this appendix has not been copy-edited.
Table 9: Summary of Findings by Outcome — MADRS Score
Study citation and study design | Interventions vs comparators | Results SMD or MD (95% CI) | Notes |
|---|---|---|---|
Bai et al. (2025)17 SR and NMR | Quetiapine vs ADT | −0.1 (−0.212, 0.014) | No treatment is favoured |
Quetiapine vs Aripiprazole 3 to 12 mg | 0.214 (−0.019, 0.448) | No treatment is favoured | |
Quetiapine vs Brexpiprazole 1 mg | 0.096 (−0.031, 0.224) | No treatment is favoured | |
Quetiapine vs Brexpiprazole 2 to 3 mg | 0.155 (0.042, 0.268) | Favours brexpiprazole | |
Quetiapine vs Brexpiprazole 2 mg | 0.109 (−0.043, 0.261) | No treatment is favoured | |
Quetiapine vs Brexpiprazole 3 mg | 0.039 (−0.091, 0.167) | No treatment is favoured | |
Quetiapine vs Cariprazine 1 to 2 mg | 0.001 (−0.176, 0.177) | No treatment is favoured | |
Quetiapine vs Cariprazine 2 to 4.5 mg | 0.011 (−0.179, 0.199) | No treatment is favoured | |
Quetiapine vs Cariprazine 0.1 to 0.3 mg | −0.042 (−0.308, 0.222) | No treatment is favoured | |
Quetiapine vs Cariprazine 1.5 mg | 0.068 (−0.087, 0.226) | No treatment is favoured | |
Quetiapine vs Cariprazine 3 mg | 0.068 (−0.084, 0.225) | No treatment is favoured | |
Quetiapine vs Olanzapine 6 to 12 mg plus fluoxetine | 0.141 (0.019, 0.264) | Favours olanzapine plus fluoxetine | |
Quetiapine vs Olanzapine 6 to 12 mg | −0.071 (−0.191, 0.054) | No treatment is favoured | |
Quetiapine vs Ziprasidone 160 mg | 0.161 (−0.337, 0.666) | No treatment is favoured | |
Quetiapine vs Ziprasidone 80 mg | 0.05 (−0.466, 0.548) | No treatment is favoured | |
Cleare et al. (2025)20 RCT | Quetiapine vs Lithium | At 52 weeks MD −2.98 (−5.87 to −0.09) P value = 0.0435 | Favours quetiapine |
Table 10: Summary of Findings by Outcome — MADRS Response Rate
Study citation and study design | Interventions vs comparators | Results HR (95% CI) | Notes |
|---|---|---|---|
Bai et al. (2025)17 SR and NMR | Quetiapine vs ADT | 1.182 (0.581, 2.42) | No treatment is favoured |
Quetiapine vs Aripiprazole 3 to 12 mg | 0.485 (0.219, 1.086) | No treatment is favoured | |
Quetiapine vs Brexpiprazole 1 mg | 0.695 (0.319, 1.509) | No treatment is favoured | |
Quetiapine vs Brexpiprazole 2 to 3 mg | 0.753 (0.372, 1.51) | No treatment is favoured | |
Quetiapine vs Brexpiprazole 2 mg | 0.798 (0.37, 1.716) | No treatment is favoured | |
Quetiapine vs Brexpiprazole 3 mg | 0.666 (0.291, 1.506) | No treatment is favoured | |
Quetiapine vs Cariprazine 0.1 to 0.3 mg | 0.921 (0.362, 2.322) | No treatment is favoured | |
Quetiapine vs Cariprazine 1 to 2 mg | 0.697 (0.308, 1.558) | No treatment is favoured | |
Quetiapine vs Cariprazine 1.5 to 4.5 mg | 0.688 (0.309, 1.523) | No treatment is favoured | |
Quetiapine vs Cariprazine 1.5 mg | 0.963 (0.44, 2.102) | No treatment is favoured | |
Quetiapine vs Cariprazine 3 mg | 0.881 (0.404, 1.938) | No treatment is favoured | |
Quetiapine vs Risperidone 0.5 to 3 mg | 0.485 (0.147, 1.65) | No treatment is favoured | |
Quetiapine vs Risperidone 1 to 2 mg | 0.576 (0.247, 1.349) | No treatment is favoured | |
Quetiapine vs Ziprasidone 160 mg | 0.212 (0.026, 1.736) | No treatment is favoured | |
Quetiapine vs Ziprasidone 80 mg | 1.143 (0.125, 10.872) | No treatment is favoured | |
Cleare et al. (2025)20 RCT | Quetiapine vs Lithium | Odds ratio 3.67 (95% CI 0.94 to 14.25) | No treatment is favoured |
Guo et al. (2024)18 SR and NMA | Brexpiprazole vs Quetiapine | Odds ratio 0.80 (95% CI 0.31, 2.11) | No treatment is favoured |
Esketamine vs Quetiapine | Odds ratio 1.39 (95% CI 0.64, 3.01) | No treatment is favoured | |
Ketamine vs Quetiapine | Odds ratio 2.60 (95% CI 0.95, 7.20) | No treatment is favoured | |
Psilocybin vs Quetiapine | Odds ratio 1.31 (95% CI 0.49, 3.52) | No treatment is favoured | |
Yan et al. (2022)19 SR and NMA | Quetiapine vs Aripiprazole | Odds ratio 0.86 (95% CrI 0.64 to 1.17) | No treatment is favoured |
Quetiapine vs Olanzapine | Odds ratio 1.18 (95% CrI 0.83 to 1.67) | No treatment is favoured | |
Quetiapine vs Brexpiprazole | Odds ratio 1.11 (95% CrI 0.83 to 1.48) | No treatment is favoured | |
Quetiapine vs Cariprazine | Odds ratio 1.18 (95% CrI 0.85 to 1.64) | No treatment is favoured | |
Quetiapine vs Ziprasidone | Odds ratio 0.76 (95% CrI 0.34 to 1.68) | No treatment is favoured | |
Quetiapine vs Risperidone | Odds ratio 0.73 (95% CrI 0.44 to 1.22) | No treatment is favoured |
Table 11: Summary of Findings by Outcome — CGI-S Score
Study citation and study design | Interventions vs comparators | Results SMD (95% CI) | ||
|---|---|---|---|---|
Quetiapine XR 150 to 300mg/d | Quetiapine XR 150mg/d | Quetiapine XR 300mg/d | ||
Bai et al. (2025)17 SR and NMR | Quetiapine vs ADT | 0.001 (−0.198, 0.192) | −0.003 (−0.187, 0.179) | 0.135 (−0.048, 0.317) |
Quetiapine vs Aripiprazole 2 to 20mg/d | 0.338 (0.101, 0.568) | 0.333 (0.113, 0.555) | 0.472 (0.252, 0.695) | |
Quetiapine vs Aripiprazole 3 to 12mg/d | 0.141 (−0.138, 0.423) | 0.136 (−0.135, 0.412) | 0.275 (0.005, 0.548) | |
Quetiapine vs Aripiprazole 3 to 15mg/d | 0.145 (−0.116, 0.4) | 0.142 (−0.111, 0.39) | 0.279 (0.029, 0.531) | |
Quetiapine vs Aripiprazole 3mg/d | 0.218 (−0.044, 0.474) | 0.213 (−0.038, 0.458) | 0.352 (0.103, 0.601) | |
Quetiapine vs Brexpiprazole 1mg/d | 0.169 (−0.042, 0.372) | 0.164 (−0.03, 0.361) | 0.304 (0.108, 0.497) | |
Quetiapine vs Brexpiprazole 2 to 3mg/d | 0.076 (−0.121, 0.271) | 0.073 (−0.183, 0.327) | 0.211 (−0.04, 0.463) | |
Quetiapine vs Brexpiprazole 2mg/d | 0.242 (0.021, 0.457) | 0.237 (0.026, 0.446) | 0.376 (0.166, 0.584) | |
Quetiapine vs Brexpiprazole 3mg/d | 0.137 (−0.077, 0.342) | 0.134 (−0.064, 0.331) | 0.273 (0.075, 0.47) | |
Quetiapine vs Cariprazine 1 to 2mg/d | 0.023 (−0.289, 0.331) | 0.019 (−0.283, 0.316) | 0.157 (−0.144, 0.457) | |
Quetiapine vs Cariprazine 1 to 2mg/d | 0.023 (−0.214, 0.256) | 0.02 (−0.211, 0.241) | 0.157 (−0.071, 0.381) | |
Quetiapine vs Cariprazine 1.5 to 4.5mg/d | 0.023 (−0.225, 0.264) | 0.019 (−0.219, 0.253) | 0.157 (−0.077, 0.389) | |
Quetiapine vs Cariprazine 1.5mg/d | 0.097 (−0.127, 0.317) | 0.093 (−0.118, 0.307) | 0.23 (0.021, 0.443) | |
Quetiapine vs Cariprazine 2 to 4.5mg/d | 0.024 (−0.219, 0.265) | 0.02 (−0.214, 0.253) | 0.158 (−0.076, 0.395) | |
Quetiapine vs Cariprazine 3mg/d | 0.128 (−0.093, 0.346) | 0.124 (−0.088, 0.336) | 0.262 (0.052, 0.475) | |
Quetiapine vs Olanzapine 6 to 12mg/d | 0.108 (−0.155, 0.368) | 0.105 (−0.15, 0.356) | 0.243 (−0.013, 0.492) | |
Quetiapine vs Quetiapine XR 150 to 300mg/d | 0 | −0.003 (−0.269, 0.261) | 0.134 (−0.131, 0.402) | |
Quetiapine vs Quetiapine XR 150mg/d | 0.003 (−0.261, 0.269) | 0 | 0.138 (−0.047, 0.322) | |
Quetiapine vs Quetiapine XR 300mg/d | −0.134 (−0.402, 0.131) | −0.138 (−0.322, 0.047) | 0 | |
Quetiapine vs Risperidone 0.5 to 3mg/d | 0.427 (−0.052, 0.887) | 0.424 (−0.049, 0.88) | 0.561 (0.098, 1.018) | |
Quetiapine vs Ziprasidone 160mg/d | 0.102 (−0.446, 0.649) | 0.096 (−0.457, 0.646) | 0.234 (−0.314, 0.785) | |
Quetiapine vs Ziprasidone 80mg/d | 0.054 (−0.487, 0.589) | 0.052 (−0.488, 0.574) | 0.191 (−0.345, 0.71) | |
Quetiapine vs Olanzapine 6 to 12mg/d and Fluoxetine 25 to 50mg/d combination | 0.337 (0.075, 0.6) | 0.333 (0.081, 0.589) | 0.472 (0.219, 0.725) | |
Cleare et al. (2025)20 RCT | Quetiapine vs Lithium | Odds ratio 1.12 (95% CI, 0.32 to 3.92) | ||
Table 12: Summary of Findings by Outcome — MADRS Remission Rate
Study citation and study design | Comparisons | Results HR (95% CI) | Notes |
|---|---|---|---|
Bai et al. (2025)17 SR and NMR | Quetiapine vs ADT | 0.447 (0.139, 1.428) | No treatment is favoured |
Quetiapine vs Aripiprazole 3 to 12 mg | 0.176 (0.053, 0.569) | No treatment is favoured | |
Quetiapine vs Brexpiprazole 1 mg | 0.389 (0.117, 1.286) | No treatment is favoured | |
Quetiapine vs Brexpiprazole 2 to 3 mg | 0.28 (0.089, 0.892) | No treatment is favoured | |
Quetiapine vs Brexpiprazole 2 mg | 0.347 (0.104, 1.141) | No treatment is favoured | |
Quetiapine vs Brexpiprazole 3 mg | 0.285 (0.082, 0.989) | Favours quetiapine | |
Quetiapine vs Cariprazine 1.5 to 4.5mg/d | 0.334 (0.098, 1.111) | No treatment is favoured | |
Quetiapine vs Cariprazine 2 to 4.5mg/d | 0.388 (0.117, 1.293) | No treatment is favoured | |
Quetiapine vs Cariprazine 0.1 to 0.3mg/d | 0.438 (0.121, 1.544) | No treatment is favoured | |
Quetiapine vs Cariprazine 1 to 2mg/d | 0.379 (0.114, 1.248) | No treatment is favoured | |
Quetiapine vs Cariprazine 1.5mg/d | 0.373 (0.109, 1.256) | No treatment is favoured | |
Quetiapine vs Cariprazine 3mg/d | 0.302 (0.089, 1.032) | No treatment is favoured | |
Quetiapine vs Risperidone 0.5 to 2mg/d | 0.17 (0.047, 0.632) | Favours quetiapine | |
Quetiapine vs Risperidone 0.5 to 3mg/d | 0.134 (0.034, 0.516) | Favours quetiapine | |
Quetiapine vs Ziprasidone 160mg/d | 0.091 (0.01, 0.816) | Favours quetiapine | |
Quetiapine vs Ziprasidone 80mg/d | 0.475 (0.044, 5.398) | No treatment is favoured | |
Cleare et al. (2025)20 RCT | Quetiapine vs Lithium | Remission: defined as a MADRS total score of no greater than 10 points Odds ratio 1.38 (95% CI 0.29 to 6.60) | No treatment is favoured |
Guo et al. (2024)18 SR and NMA | Brexpiprazole vs Quetiapine | Odds ratio 1.52 (95% CI 0.69, 3.54) | No treatment is favoured |
Esketamine vs Quetiapine | Odds ratio 1.38 (95% CI 0.75, 2.62) | No treatment is favoured | |
Ketamine vs Quetiapine | Odds ratio 0.87 (95% CI 0.32, 2.57) | No treatment is favoured | |
Psilocybin vs Quetiapine | Odds ratio 3.07 (95% CI 1.21, 7.82) | Psilocybin is favoured | |
Yan et al. (2022) SR and NMA | Quetiapine vs Aripiprazole | Odds ratio 0.93 (95% CrI 0.66 to 1.31) | No treatment is favoured |
Quetiapine vs Olanzapine | Odds ratio 1.16 (95% CrI 0.77 to 1.74) | No treatment is favoured | |
Quetiapine vs Brexpiprazole | Odds ratio 1.20 (95% CrI 0.86 to 1.69) | No treatment is favoured | |
Quetiapine vs Cariprazine | Odds ratio 1.42 (95% CrI 0.99 to 2.05) | No treatment is favoured | |
Quetiapine vs Ziprasidone | Odds ratio 1.26 (95% CrI 0.59 to 2.67) | No treatment is favoured | |
Quetiapine vs Risperidone | Odds ratio 0.59 (95% CrI 0.31 to 1.12) | No treatment is favoured |
Table 13: Summary of Findings by Outcome — Additional Efficacy Outcomes
Study citation and study design | Outcome | Interventions vs. Comparators | Results | Notes |
|---|---|---|---|---|
Cleare et al. (2025)20 RCT | QIDS-SR | Quetiapine vs Lithium | – 68.36 (95% CI –129.95 to –6.76) P value = 0.0296 | Favours quetiapine |
WSAS score | Quetiapine vs Lithium | Adjusted mean difference −3.64 (−6.28 to −0.99) P = 0.0071 | Favours quetiapine | |
MARS-5 score | Quetiapine vs Lithium | Adjusted mean difference −0.44 (−1.04 to 0.17) P = 0.1563 | No treatment is favoured |
MARS-5 = five‐item Medication Adherence Report Scale; QIDS-SR = self-rated Quick Inventory of Depressive Symptomatology; RCT = randomized controlled trials; WSAS = Work and Social Adjustment Scale
Table 14: Summary of Findings by Outcome — Safety Outcomes
Study citation and study design | Outcome | Interventions vs. comparators | Results | Notes |
|---|---|---|---|---|
Cleare et al. (2025)20 RCT | Time to all-cause discontinuation | Quetiapine vs Lithium | Median time for QTP 365 days (IQR 57 to 365) Median time for Lithium 212 (IQR 21 to 365) Hazard ratio: 0.72 (95% CI 0.47 to 1.09) P value = 0.1196 | No treatment is favoured |
PRISE total score | Quetiapine vs Lithium | Adjusted mean difference −0.89 (−2.03 to 0.25) P = 0.1265 | No treatment is favoured | |
Body Weight (kg) | Quetiapine vs Lithium | Adjusted mean difference 1.33 (−1.82 to 4.48) P = 0.4075 | No treatment is favoured | |
Guo et al. (2024)18 SR and NMA | Tolerability | Brexpiprazole vs Quetiapine | Odds ratio 1.00 (95% CI; 0.85, 3.37) | No treatment is favoured |
Esketamine vs Quetiapine | Odds ratio 0.39 (95% CI; 0.09, 3.00) | No treatment is favoured | ||
Ketamine vs Quetiapine | Odds ratio 0.02 (95% CI; 0.02, 164.38) | No treatment is favoured | ||
Psilocybin vs Quetiapine | Odds ratio 0.87 (95% CI; 0.33, 2.31) | No treatment is favoured | ||
Guo et al. (2024)18 SR and NMA | Safety | Brexpiprazole vs Quetiapine | Odds ratio 0.89 (95% CI; 0.36, 2.18) | No treatment is favoured |
Esketamine vs Quetiapine | Odds ratio 2.05 (95% CI; 0.97, 4.57) | No treatment is favoured | ||
Ketamine vs Quetiapine | Odds ratio 6.84 (95% CI; 0.33, 274.53) | No treatment is favoured | ||
Psilocybin vs Quetiapine | Odds ratio 1.45 (95% CI; 0.55, 4.04) | No treatment is favoured | ||
Yan et al. (2022)19 SR and NMA | All-cause dropout rate | Quetiapine vs Aripiprazole | Odds ratio 1.32 (95% CrI 0.88 to 1.97) | No treatment is favoured |
Quetiapine vs Olanzapine | Odds ratio 1.35 (95% CrI 0.89 to 2.03) | No treatment is favoured | ||
Brexpiprazole vs Quetiapine | Odds ratio 0.98 (95% CrI 0.69 to 1.40) | No treatment is favoured | ||
Cariprazine vs Quetiapine | Odds ratio 1.10 (95% CrI 0.72 to 1.67) | No treatment is favoured | ||
Ziprasidone vs Quetiapine | Odds ratio 1.07 (95% CrI 0.47 to 2.43) | No treatment is favoured | ||
Risperidone vs Quetiapine | Odds ratio 0.74 (95% CrI 0.39 to 1.41) | No treatment is favoured | ||
Yan et al. (2022)19 SR and NMA | Drop out due to AE | Quetiapine vs Aripiprazole | Odds ratio 1.70 (95% CrI 0.62 to 4.66) | No treatment is favoured |
Quetiapine vs Olanzapine | Odds ratio 2.03 (95% CrI 0.69 to 5.93) | No treatment is favoured | ||
Brexpiprazole vs Quetiapine | Odds ratio (95% CrI) 0.63 (0.24 to 1.67) | No treatment is favoured | ||
Cariprazine vs Quetiapine | Odds ratio (95% CrI) 0.89 (0.28 to 2.86) | No treatment is favoured | ||
Ziprasidone vs Quetiapine | Odds ratio (95% CrI) 5.93 (0.26 to 133.00) | No treatment is favoured | ||
Risperidone vs Quetiapine | Odds ratio (95% CrI) 0.53 (0.10 to 2.97) | No treatment is favoured |
Table 15: Summary of Findings by Outcome — Patient Experience
Study citation and study design | Results | Notes |
|---|---|---|
McKeown et al. (2022)21 Qualitative study | Four main themes and 11 subthemes were generated about patient experiences and perspectives of augmentation medications: ‘Initial concerns’, ‘Experience of side effects’, ‘Perception of treatment efficacy’ and ‘Positive perception of treatment monitoring.’ Patients expressed greater apprehension toward lithium and less fear over quetiapine before treatment initiation. By contrast, they reported negative side effects to a greater extent for quetiapine during the actual treatment (sedation, weight gain and appetite). Despite being largely positive, some patients perceived treatment to be ineffective. Clinical monitoring was perceived positively in terms of regular appointments, reassurance regarding the ease and speed of communication with study team and clinicians, and acceptance of blood monitoring for patients treated with lithium. | Treatment augmentation for TRD with lithium and quetiapine was viewed beneficial and acceptable by most patients |
Table 16: Summary of Recommendations in Included Guidelines
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
|---|---|
2023 ACP22 | |
Switching to a different second-generation antidepressant or augmenting with a second pharmacologic treatment is recommended for patients in the acute phase of moderate to severe major depressive disorder who did not respond to initial treatment with an adequate dose of a second-generation antidepressant. Recommended pharmacologic augmentation addition of a non- second-generation antidepressant medication (i.e., atypical antipsychotics, psychostimulants, buspirone, L-thyroxine, triiodothyronine, lithium) for second-line treatment Supporting evidence: Second-line treatment strategies showed similar efficacy when compared with each other in a systematic review | Conditional recommendation; low-certainty evidence |
2023 CANMAT23 | |
Quetiapine or other SGA is recommended as a second-line treatment option for adults with MDD Supporting evidence: NMA demonstrated that quetiapine is more effective than placebo. Evidence from meta-analyses for comparable response of quetiapine vs. active comparator medications including, trazodone, nefazodone and tricyclic antidepressants (e.g., amitriptyline, clomipramine, desipramine, nortriptyline) | Quality of evidence: Level 1 (high quality) Line of treatment: Second line |
Quetiapine XR is recommended as a second-line adjunctive treatment option for adults with difficult to treat depression (DTD) Supporting evidence: Adjunctive treatment with atypical antipsychotic agents (serotonin-dopamine activity modulators) such as aripiprazole, brexpiprazole, quetiapine have the most consistent evidence for efficacy in DTD and shorter time to response or remission, but they generally have a greater side effect burden than antidepressant monotherapy. RCTs directly comparing switching to adjunctive strategies have shown that adjunctive strategies have superior outcomes and often have similar tolerability. Typically, lower doses of these medications are used for adjunctive treatment in MDD compared to other conditions such as bipolar disorder or schizophrenia. Quetiapine has Level 1 evidence for efficacy are recommended as second-line treatment because of the increased risk of sedation and metabolic side effects | Quality of evidence: Level 1 (high quality) Line of treatment: Second line |
A combination of antidepressant and atypical antipsychotic treatment such as quetiapine for first line treatment of MDE with psychotic features Supporting evidence: NR | Quality of evidence: Level 1 (high quality) Line of treatment: First line |
2022 NICE24 | |
“Combination treatment for people with depression with psychotic symptoms with antidepressant medication and antipsychotic medication (for example, olanzapine or quetiapine).” Rationale: Quetiapine showed clinical benefits for acute treatment of psychotic depression. Clinical knowledge is that it has both antidepressant and antipsychotic effects | Quality of evidence: NR Strength of recommendation: NR |
Combined therapy of second-generation antipsychotic (e.g., aripiprazole, olanzapine, quetiapine or risperidone) or lithium with antidepressant medication is 1 of the treatment options if a person who has not responded to antidepressants wants to try combination treatment Supporting evidence: NR | Quality of evidence: NR Strength of recommendation: NR |
2022 VA/DoD25 | |
“For patients with MDD who have demonstrated partial or no response to an adequate trial of initial pharmacotherapy, we suggest (not rank ordered):
Supporting evidence: Three SRs showed the significant benefit of SGAs (alone or augmentation) for remission in MDD. The SGAs included aripiprazole, brexpiprazole, cariprazine, olanzapine, quetiapine, risperidone. | Quality of evidence: Low Strength of recommendation: Weak for |
SGAs require appropriate monitoring (e.g., glucose, complete blood count, hepatic panel, lipid panel, body mass index, waist circumference, blood pressure, involuntary movements/tardive dyskinesia, slit lamp exam [for quetiapine only]) due to the potential for significant side effects, drug-drug interactions Supporting evidence: Systematic review showed significantly greater weight gain and sedation with quetiapine. | |
2020 RANZCP26 | |
“SGAs such as lurasidone, quetiapine and olanzapine may be used either as monotherapy or adjunctively in the treatment of major depression and comparatively new agents such as aripiprazole and brexpiprazole have formal indications for adjunctive treatment of major depression.” (p.54) | Quality of evidence: NR Strength of recommendation: NR |
MDD = major depressive disorder; MDE = major depressive episode; NR = not reported in guideline publication; SGA = second-generation antipsychotic.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@cda-amc.ca.