Drugs, Health Technologies, Health Systems
Health Technology Review
Quetiapine for Insomnia
Summary
Main Take-Aways
Evidence-based guidelines recommend against the use of quetiapine for the treatment of insomnia.
The findings of this review suggest that antipsychotics such as quetiapine should not be used in the treatment of insomnia.
Key Messages
What Is the Issue?
Quetiapine is an atypical or second-generation antipsychotic drug that is primarily used for treating schizophrenia and bipolar disorder. Quetiapine extended-release is also indicated by Health Canada for the symptomatic relief of major depressive disorder when currently available approved antidepressant drugs have failed.
Decision-makers are interested in evidence on the clinical effectiveness, safety, and place in therapy of quetiapine relative to other medications for the treatment of insomnia.
What Did We Do?
We searched key resources, including journal citation databases, and conducted a focused internet search for relevant evidence published since 2020.
What Did We Find?
Evidence-based guidelines recommend against the use of quetiapine for the treatment of insomnia due to potential concerns about safety and lack of evidence of clinical benefit.
What Does It Mean?
Current evidence-based guidelines advise against prescribing quetiapine for the treatment of insomnia due to safety concerns and a lack of demonstrated clinical benefit.
The findings of this review suggest that antipsychotics such as quetiapine should not be used in the treatment of insomnia.
Abbreviations
DoD
US Department of Defense
OSA
obstructive sleep apnea
RCT
randomized controlled trial
SR
systematic review
VA
US Department of Veterans Affairs
Context and Policy Issues
What Is Insomnia?
Insomnia is a common sleep disorder. People with insomnia experience dissatisfaction with the quantity or quality of their sleep, have difficulty initiating or maintaining sleep, and/or wake up early in the morning without the ability to return to sleep.1 For a diagnosis of insomnia disorder, the symptoms must occur at least 3 nights per week for at least 3 months and cause significant distress or impairment in daily functioning.1 Sleep difficulty must be present despite adequate opportunity for sleep, ruling out of other sleep disorders, and exclude the possibility of being better explained by coexisting mental disorders or other medical conditions.1 Approximately 10% of the adult population has an insomnia disorder.2 In 2021, 20.4% of adults aged 18 to 64 years in Canada experienced insomnia symptoms.3
Insomnia is a significant health problem that negatively impacts a person’s daytime function, safety, and quality of life.1 It is associated with a range of adverse outcomes, including accidents and injuries, cognitive impairment, cardiovascular disease, diabetes, psychiatric disorders, neurodegenerative disorders, suicide, and self-medication with alcohol and other substances.1 Insomnia also carries a substantial economic burden for patients, society, and the health system due to the direct costs of treatment and the indirect costs of high rates of absenteeism and lack of work productivity.4
What Are Current Treatment Options for Insomnia?
The main interventions for insomnia are cognitive behavioural therapy and pharmacotherapy, including over-the-counter medications, prescription hypnotic drugs, and other nonspecific prescription medications. Cognitive behavioural therapy for insomnia is recommended as the first-line treatment for insomnia in adults; however, there is limited access to this therapy and pharmacotherapy remains the most frequently used treatment in clinical practice.
What Is Quetiapine?
Quetiapine is available in 2 oral formulations — immediate-release tablets in 25 mg, 100 mg, 200 mg, and 300 mg doses of quetiapine fumarate5 and extended-release tablets in 50 mg, 150 mg, 200 mg, 300 mg, and 400 mg doses of quetiapine fumarate.6 Quetiapine is an atypical or second-generation antipsychotic drug that is primarily used for treating schizophrenia and bipolar disorder.5 Additionally, the extended-release formulation is also indicated as an adjunct or augmentation treatment for adults with major depressive disorder when currently available antidepressant drugs have failed due to lack of efficacy and/or lack of tolerability.6 Off-label use of quetiapine for several conditions, such as agitation, delirium, delusional infestation, posttraumatic stress disorder, and sleep problems, has been documented.7 The side effects of quetiapine include somnolence, dizziness, dry mouth, withdrawal (discontinuation) symptoms, elevations in serum triglyceride levels, elevations in total cholesterol (predominantly low-density lipoprotein cholesterol), decreases in high-density lipoprotein cholesterol, weight gain, decreased hemoglobin, and extrapyramidal symptoms (involuntary movements induced by medications).5,6
Why Is It Important to Do This Review?
Higher doses of quetiapine and concomitant use with central nervous system drugs are associated with an increased risk of adverse effects.8,9 Given the frequent off-label use and potential for harm associated with quetiapine, it is important to review the current evidence on the efficacy, safety, and place in therapy of quetiapine for the treatment of people with insomnia. An overview of the evidence may aid decision-making with respect to prescribing and recommended use of quetiapine for adults with insomnia.
Research Questions
What is the clinical effectiveness and safety of quetiapine versus other drug interventions for adults with insomnia?
What are the evidence-based guidelines regarding the use and administration of quetiapine for adults with insomnia?
Methods
Literature Search Methods
An information specialist conducted a literature search on key resources, including MEDLINE, Embase, the Cochrane Database of Systematic Reviews, the International HTA Database, and the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concepts were quetiapine and insomnia. Search filters were applied to limit retrieval to health technology assessments, systematic reviews (SRs), meta-analyses, indirect treatment comparisons, randomized controlled trials (RCTs), controlled clinical trials, and guidelines. The search was completed on April 29, 2025, and limited to English-language documents published since January 1, 2020.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Adults aged ≥ 18 years with insomnia |
Intervention | Quetiapine fumarate immediate-release tablets, quetiapine fumarate extended-release tablets |
Comparator | Other drug interventions: other second-generation atypical antipsychotics, mood stabilizers, antidepressants (e.g., mirtazapine), nonbenzodiazepine medications (e.g., zolpidem), melatonin, antihistamines, orexin inhibitors, antinauseants (e.g., dimenhydrinate), herbal supplements (e.g., valerian root), magnesium |
Outcomes |
|
Study designs | RCTs, systematic reviews, (including MAs and NMAs), evidence-based guidelines,a and published HTAs |
HTA = health technology assessment; MA = meta-analysis; NMA = network meta-analysis; RCT = randomized controlled trial.
aA guideline is defined as a systematically developed statement or set of statements to assist practitioner and patient decisions about appropriate health care for specific clinical circumstances. A guideline is considered evidence-based if a systematic search of the literature was undertaken to inform the recommendations.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1 or they were duplicate publications. SRs in which all relevant studies were captured in other more recent or more comprehensive SRs were excluded. Primary studies retrieved by the search were excluded if they were captured in 1 or more included SRs. Guidelines with an unclear methodology were also excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument as a guide.10 Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
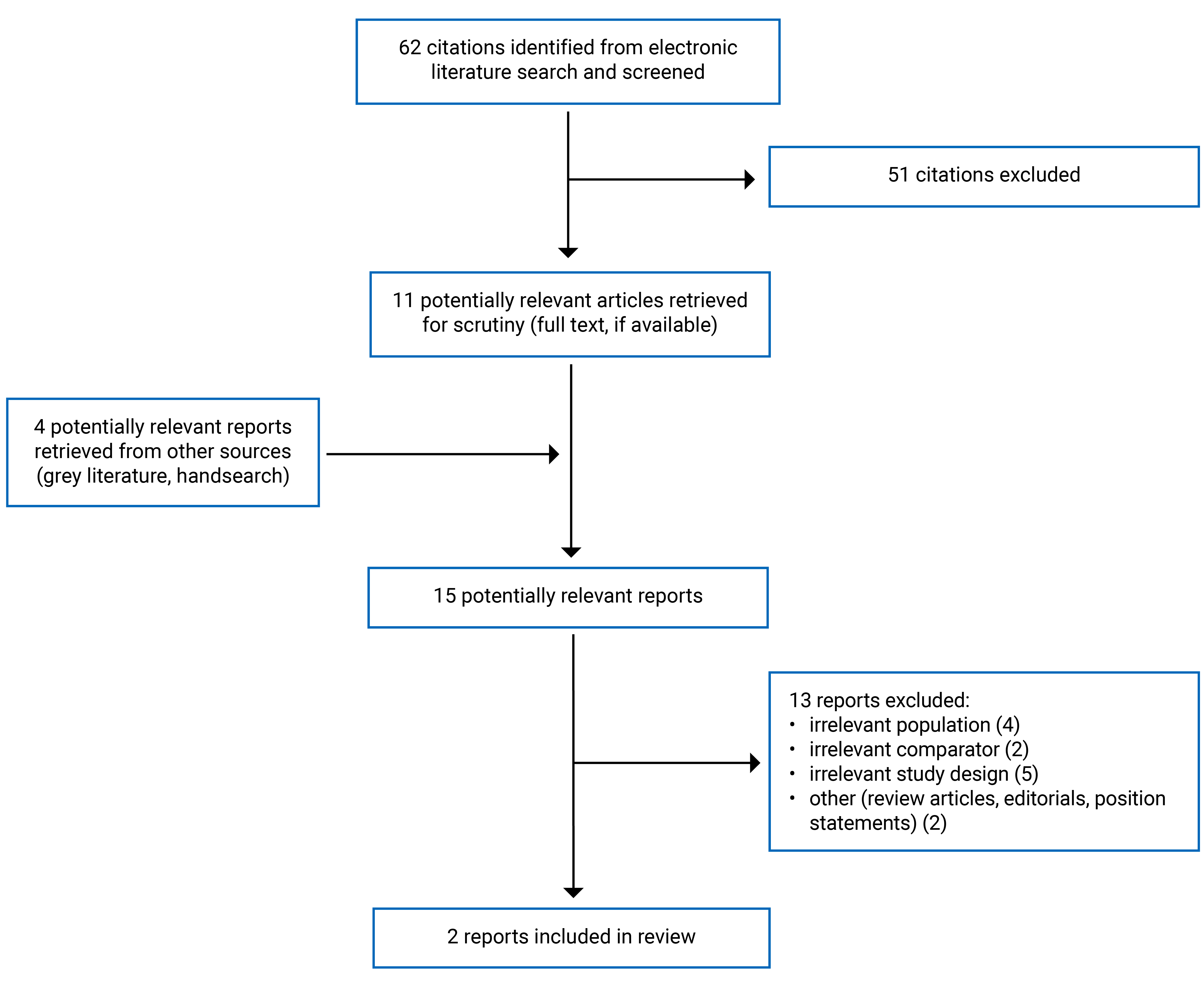
A total of 62 citations were identified in the literature search. Following screening of titles and abstracts, 51 citations were excluded and 11 potentially relevant reports from the electronic search were retrieved for full-text review. Four potentially relevant publications were retrieved from the grey literature search for full-text review. Of these 15 potentially relevant articles, 13 publications were excluded for various reasons and 2 publications met the inclusion criteria and were included in this report. The included publications were 2 evidence-based guidelines.11,12 Appendix 1 presents the PRISMA13 flow chart of the study selection.
Summary of Study Characteristics
Appendix 2 provides details regarding the characteristics of the included publications.
Included Studies for Research Question 1: What Is the Clinical Effectiveness and Safety of Quetiapine Versus Other Drug Interventions for Adults With Insomnia?
We did not identify any studies that evaluated the clinical efficacy and/or safety of quetiapine versus other drug interventions for the treatment of insomnia that met the inclusion criteria for this review.
Included Studies for Research Question 2: What Are the Evidence-Based Guidelines Regarding the Use and Administration of Quetiapine for Adults With Insomnia?
Study Design
Two evidence-based guidelines were included to answer research question 2. The guidelines are the 2023 European Insomnia Guideline11 and the 2025 VA/DoD Clinical Practice Guidelines, from the US Department of Veterans Affairs (VA) and US Department of Defense (DoD),12 for chronic insomnia disorder and/or obstructive sleep apnea (OSA).
The systematic literature search for the 2023 European Insomnia Guideline11 primarily focused on meta-analyses on the diagnosis and treatment of insomnia. The guideline was developed by a task force comprised of researchers and clinicians in the European Sleep Research Society and the European Insomnia Network. The evidence was reported as graded using the hierarchy of evidence from level 1a, representing highest quality (SRs and meta-analyses of RCTs), to level 5, representing expert opinion. The translation of levels of evidence into grades of recommendation was based on the hierarchy of evidence and consensus among the guideline authors. Four steps of recommendations were used: A (very strong recommendation), B (strong), C (weak), and D (very weak recommendation).
To develop the 2025 VA/DoD guideline12 for chronic insomnia disorder and/or OSA, an SR of both clinical and epidemiological evidence was conducted. A working group of multidisciplinary experts interpreted the systematic evidence review’s findings and rated both the quality of the evidence and the strength of the recommendation. The evidence was assessed using the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) methodology and assigned a rating of very low, low, moderate, or high.
Country of Origin
The European Insomnia Guideline11 is an international guide developed for multiple European countries. The VA/DoD guideline12 was developed in the US.
Guideline Population and Audience
The target patient population in the VA/DoD guideline12 is adult beneficiaries of VA or DoD health care delivery systems with chronic insomnia disorder and/or OSA who are eligible for care in VA, DoD, or community-based locations. Though OSA was included in the guideline, only the recommendations for patients with insomnia are discussed in this report. The European Insomnia Guideline11 focuses on adults with chronic insomnia.
The 2025 VA/DoD guideline12 is intended for use by VA, DoD, community-based, and other health care providers who are involved in evaluating and managing adults with chronic insomnia disorder and/or OSA. The 2023 European Insomnia Guideline11 is meant for health professionals, including general practitioners, specialists, and sleep medicine experts, who diagnose and treat insomnia in various clinical settings, especially where advanced expertise or facilities may be limited.
Interventions and Practice Considered
Both guidelines have a broad scope and included recommendations for pharmacological and nonpharmacological treatments. The 2023 European Insomnia Guideline11 includes recommendations for cognitive behavioural therapy and pharmacological treatments (e.g., herbal, other forms of psychotherapy, exercise, light therapy, music, and noninvasive brain stimulation). Only the recommendations relevant to quetiapine (or antipsychotics as a therapeutic class) will be discussed in this report.
Outcomes
Both guidelines11,12 considered a range of outcomes relevant to this review, including insomnia severity, sleepiness, daytime functioning, fatigue, sleep efficiency, sleep onset latency, wake after sleep onset, sleep quality, total sleep time, quality of life, and harms.
Summary of Critical Appraisal
Both guidelines11,12 provided a description of their scope and purpose, in terms of the objectives, guideline questions, intended users, and target populations. The VA/DoD guideline12 clearly reported comprehensive evidence synthesis methods, including the key research questions, search strategy, criteria for selection based on population, intervention, comparison, outcome, timing, and setting (i.e., PICOTS framework), and methods for assessing quality and synthesizing the evidence. The European Insomnia Guideline11 reported the electronic databases, search date limits, study designs, and keywords that were used for the literature search but detailed information on a comprehensive literature search strategy, selection criteria, process for study selection, and synthesis methods was missing. The systemic reviews conducted for each guideline did not identify evidence from SRs and RCTs; as such, the quality of evidence was not reported.
The VA/DoD guideline12 engaged multidisciplinary parties, including clinicians and patients living with insomnia and/or OSA, which ensured a broad spectrum of perspectives were represented in the process of the guidelines’ development. Although the European Insomnia Guideline11 states that an update will occur when new important evidence is available in the future, no dates were indicated. The VA/DoD guideline12 indicates it aims to review the evidence at least every 5 years for an update and/or reaffirmation of recommendations in the emergence of new evidence. Both guidelines11,12 were reviewed independently by relevant professional experts, professional colleges and societies, or a guideline committee. Funding sources and competing interests of authors were reported in the guidelines.11,12
Additional details on the critical appraisal of the included guidelines are provided in Appendix 3.
Summary of Findings
Guidelines Regarding the Use of Quetiapine
The study findings from all included publications are provided in Appendix 4.
The VA/DoD guideline12 made a weak recommendation against using antipsychotic drugs, including quetiapine, for the treatment of chronic insomnia disorder due to lack of clinical effectiveness evidence and potential safety concerns. Regarding safety, the guideline indicated harms associated with antipsychotics, including low-dose quetiapine (e.g., sedation, hypotension, hyperglycemia, dyslipidemia, and weight gain). The quality of evidence was not reported as no evidence was identified that met the guideline’s inclusion criteria.
The 2023 European Insomnia Guideline11 does not recommend quetiapine and other antipsychotics for the treatment of insomnia due to lack of clinical effectiveness evidence and potential safety concerns. The recommendation was rated as very strong (A) while the quality of evidence was not reported as no evidence was identified.
Limitations
This report is limited by the lack of available evidence on the clinical effectiveness and safety of quetiapine for the treatment of insomnia in adults. Evidence from published SRs and RCTs to evaluate the clinical effectiveness and safety of quetiapine versus other drug interventions was not identified in our literature search spanning the previous 5 years (i.e., from 2020 to 2025). The European Insomnia Guideline11 did not provide a detailed description of the SR that informed the recommendations. Although the recommendation against antipsychotics was rated as very strong (A), the quality of evidence was not reported as no evidence was identified. None of the guidelines were specifically developed for Canada; however, the VA/DoD guideline12 recommendations may be applicable to the health care systems in Canada as the quetiapine formulations included in the guideline are available in Canada.
Conclusions and Implications for Decision- or Policy-Making
Two evidence-based guidelines were identified that reviewed the use of antipsychotics, including quetiapine, for insomnia. Both the 2023 European Insomnia Guideline11 and the 2025 VA/DoD guideline12 for chronic insomnia disorder recommend against using antipsychotic drugs, including quetiapine, for the treatment of insomnia due to concerns about safety and lack of evidence on clinical benefit.s
Implications for Clinical Practice
The findings of this review suggest that antipsychotics such as quetiapine should not be used in the treatment of insomnia.
Acknowledgement
Clinical Expert
This individual has kindly provided comments on the report:
Diane McIntosh, BSc Pharmacy, MD, FRCPC
Psychiatrist
References
1.American Psychiatric Association. Sleep-Wake disorders. Diagnostic and Statistical Manual of Mental Disorders, 5th ed, Text Revision (DSM-5-TR). American Psychiatric Association; 2022.
2.Morin CM, Jarrin DC. Epidemiology of Insomnia: Prevalence, Course, Risk Factors, and Public Health Burden. Sleep Med Clin. 2013;8(3):281-297. doi: 10.1016/j.jsmc.2013.05.002 PubMed
3.Chaput J-P, Morin CM, Robillard R, et al. Trends in nighttime insomnia symptoms in Canada from 2007 to 2021. Sleep Med. 2025;125:21-26. doi: https://doi.org/10.1016/j.sleep.2024.11.025 PubMed
4.Chaput J-P, Janssen I, Sampasa-Kanyinga H, et al. Economic burden of insomnia symptoms in Canada. Sleep Health. 2023;9(2):185-189. PubMed
5.Seroquel (quetiapine fumarate): tablets, 25 mg, 100 mg, 200 mg and 300 mg, oral Use [product monograph]. CheplaPharm Arzneimittel GmbH; 2025. Accessed 2025 May 10. https://pdf.hres.ca/dpd_pm/00078929.PDF
6.Seroquel XR (quetiapine fumarate); extended-release tablets, 50 mg, 150 mg, 200 mg, 300 mg and 400 mg, oral use [product monograph]. CheplaPharm Arzneimittel GmbH; 2025. Accessed 2025 May 10. https://pdf.hres.ca/dpd_pm/00080013.PDF
7.Quetiapine: Drug information. UpToDate. Accessed 2025 April 11.
8.Peridy E, Hamel J-F, Rolland A-L, Gohier B, Boels D. Quetiapine Poisoning and Factors Influencing Severity. J Clin Psychopharmacol. 2019;39(4). PubMed
9.Curry DE, Richards BL. A Brief Review of Quetiapine. American Journal of Psychiatry Residents' Journal. 2022;18(2):20-22. doi: 10.1176/appi.ajp-rj.2022.180207
10.Agree Next Steps C. The AGREE II Instrument. AGREE Enterprise; 2017. Accessed January 1, 1800. https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf
11.Riemann D, Espie CA, Altena E, et al. The European Insomnia Guideline: An update on the diagnosis and treatment of insomnia 2023. J Sleep Res. 2023;32(6):e14035. doi: 10.1111/jsr.14035 PubMed
12.VA/DOD Clinical Practice Guideline. Management of Chronic Insomnia Disorder and Obstructive Sleep Apnea. 2025.
13.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. doi: 10.1016/j.jclinepi.2009.06.006 PubMed
Appendix 1: Selection of Included Studies
Figure 1: PRISMA13 Flow Chart of Study Selection
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of Included Guidelines
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality assessment | Recommendations development and evaluation | Guideline validation |
|---|---|---|---|---|---|---|
2025 VA/DoD | ||||||
Intended Users: VA, DoD, community providers, and others involved in the health care team evaluating and managing adults with chronic insomnia disorder Target Population: adults of VA or DoD with chronic insomnia disorder eligible for care in the VA, DoD or community-based care |
| Benefits and harms of interventions | Systematic evidence review, guided by 12 clinically relevant key questions of high priority for the VA and DoD populations. | The GRADE approach was used to assess the overall quality of the body of evidence for each outcome and rated as high, moderate, low or very low. GRADE was applied in a more rigorous way than previous iterations of the guideline. | To develop recommendations, the Work Group of multidisciplinary experts interpreted the systematic evidence review’s findings. Each recommendation’s strength (strong/weak) and direction (for/against/neither for or against) was determined based on 4 domains as per GRADE: confidence in the quality of evidence, balance of desirable and undesirable outcomes, patient values and preferences, and other implications (e.g., resource use, equity, feasibility, patient subgroup considerations). Recommendations were categorized The Work Group used an iterative review process to solicit feedback on 3 drafts of the CPG and made revisions. |
|
2023 European Insomnia Guideline | ||||||
Intended Users: general practitioners, specialists, and sleep medicine experts who diagnose and treat insomnia in various clinical settings Target Population: adult patients with chronic insomnia |
| Sleep quality, insomnia symptoms, daytime functioning | Systematic literature search focused on meta-analyses on the diagnosis and treatment of insomnia | The evidence was graded according to the hierarchy of evidence. The grading scheme ranged from 1 to 5 with level 1a representing the highest quality of evidence (systematic review and meta-analysis of RCTs) to level 5 representing expert opinion | The guideline was developed by a task force comprised of researchers and clinicians in the ESRS, and the EIN. The transformation of grades of evidence into grades of recommendations was performed according to this grading scheme and through consensus decision between all involved authors |
|
CPG = clinical practice guideline; DoD = US Department of Defense; EIN = European Insomnia Network; ESRS = European Sleep Research Society; GRADE = Grading of Recommendations Assessment, Development, and Evaluation; VA = US Department of Veterans Affairs
Note: This table has not been copy-edited.
Appendix 3: Critical Appraisal of Included Publications
Please note that this appendix has not been copy-edited.
Table 3: Strengths and Limitations of Guidelines Using AGREE II10
Item | 2025 VA/DoD | 2023 European Insomnia guideline |
|---|---|---|
Domain 1: scope and purpose | ||
1. The overall objective(s) of the guideline is (are) specifically described. | Yes | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes | Yes |
3. The population (patients, public, etc.) to whom the guideline is meant to apply is specifically described. | Yes | Yes |
Domain 2: stakeholder involvement | ||
4. The guideline development group includes individuals from all relevant professional groups. | Yes | Yes |
5. The views and preferences of the target population (patients, public, etc.) have been sought. | Yes | No |
6. The target users of the guideline are clearly defined. | Yes | Yes |
Domain 3: rigour of development | ||
7. Systematic methods were used to search for evidence. | Yes | Yes |
8. The criteria for selecting the evidence are clearly described. | Yes | Partial |
9. The strengths and limitations of the body of evidence are clearly described. | Yes | Yes |
10. The methods for formulating the recommendations are clearly described. | Yes | Partial |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes | Yes |
12. There is an explicit link between the recommendations and the supporting evidence. | Yes | Yes |
13. The guideline has been externally reviewed by experts prior to its publication. | Yes | Yes |
14. A procedure for updating the guideline is provided. | Yes | Partial |
Domain 4: clarity of presentation | ||
15. The recommendations are specific and unambiguous. | Yes | Yes |
16. The different options for management of the condition or health issue are clearly presented. | Yes | Yes |
17. Key recommendations are easily identifiable. | Yes | Partial |
Domain 5: applicability | ||
18. The guideline describes facilitators and barriers to its application. | Yes | Yes |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | Partial | Partial |
20. The potential resource implications of applying the recommendations have been considered. | Yes | Yes |
21. The guideline presents monitoring and/or auditing criteria. | Yes | Partial |
Domain 6: editorial independence | ||
22. The views of the funding body have not influenced the content of the guideline. | Yes | Yes |
23. Competing interests of guideline development group members have been recorded and addressed. | Yes | Yes |
AGREE II = Appraisal of Guidelines for Research and Evaluation II; DoD = US Department of Defense; GRADE = Grading of Recommendations Assessment, Development, and Evaluation; VA = US Department of Veterans Affairs.
Appendix 4: Main Study Findings
Please note that this appendix has not been copy-edited.
Table 4: Summary of Recommendations in Included Guidelines
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
|---|---|
2025 VA/DoD12 | |
Antipsychotic drugs (including quetiapine), benzodiazepines, diphenhydramine and trazodone are not recommended for treatment of chronic insomnia disorder. Supporting evidence: “Evidence on using low-dose quetiapine for the treatment of chronic insomnia disorder is limited to a few studies and case series with short duration, small sample sizes, and vague and incomplete details, thus making any determination regarding efficacy inconclusive….Quetiapine has a black box warning indicating a 1.6 to 1.7 fold increase in mortality in elderly populations with dementia-related psychosis.” p.157 | Quality of evidence: NR Strength of recommendation: Weak against |
2023 European Insomnia Guideline11 | |
Quetiapine and other antipsychotics are not recommended for the treatment of insomnia Supporting evidence: “no randomized controlled clinical studies on these substances (antipsychotics) concerning insomnia disorder either with or without comorbidities. Therefore, at present the scientific evidence does not recommend the use of antipsychotics (including quetiapine) in the treatment of insomnia without comorbidities, in either the short or long term.” p.17 “Because of insufficient evidence and in light of their side-effects, antipsychotics are not recommended for insomnia treatment” p.23 | Quality of evidence: NR Strength of recommendation: Very strong (A) |
NR = not reported in guideline publication.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@cda-amc.ca.