Drugs, Health Technologies, Health Systems
Health Technology Review
Flexible Dentures for Edentulism
Key Messages
What Is the Issue?
Partial and complete edentulism, or tooth loss, affects millions of people in Canada. It can influence the ability to chew and speak, change facial structure and appearance, and affect physical and mental health. Treatment options for edentulism include removable partial and complete dentures.
Removable denture bases are conventionally made with acrylic or cast metal. Newer materials, including thermoplastics, are of more interest as they create more flexible dentures and may provide better function, aesthetics, and comfort. However, they may be more expensive than conventional dentures.
The relative clinical and cost-effectiveness of removable flexible thermoplastic dentures compared to conventional dentures is unclear. The need for this review was identified by a policy decision-maker, and this review is a response to that request.
What Did We Do?
We conducted a Rapid Review to summarize evidence comparing the clinical effectiveness and cost-effectiveness of removable partial or complete flexible dentures to removable conventional (acrylic or metal) partial or complete dentures. We also sought to identify evidence-based guidelines regarding the use of removable partial or complete flexible dentures for this patient population.
We searched key resources, including journal citation databases, and conducted a focused internet search for relevant evidence published since 2019. We also screened literature included in a previous Canada’s Drug Agency (formerly CADTH) report.
What Did We Find?
We identified 7 randomized controlled trials and 1 nonrandomized controlled study evaluating the clinical effectiveness of removable flexible partial or complete dentures compared to removable conventional partial or complete dentures. No cost-effectiveness evaluations or evidence-based guidelines that met our inclusion criteria were identified.
No identified studies were conducted in Canada; studies were conducted in Africa, Asia, and Europe and included diverse participants in terms of number and locations of missing teeth, and diverse denture materials.
Findings from the included studies suggest that, compared to removable conventional dentures, removable flexible dentures may improve several clinical outcomes (e.g., aesthetics and overall satisfaction), may be comparable for others (e.g., speech, pain while eating, and prosthesis fractures or discoloration), and may be inferior for others (e.g., denture retention). The comparative clinical effectiveness between these devices for other outcomes (e.g., chewing ability, oral health-related quality of life, and effort for maintenance) was inconsistent across studies and measurement methods.
The included clinical studies may be at risk of bias given that many outcomes were measured subjectively with methods of unknown validity, and patients and outcome assessors were aware of the treatments received. We did not identify studies with sufficient follow-up to inform the relative durability of these devices over a denture’s lifespan, and there is uncertain generalizability of the evidence to the context in Canada.
What Does This Mean?
The evidence informing the comparative clinical effectiveness of removable partial or complete flexible dentures and removable partial or complete conventional dentures is inconsistent across the outcomes of primary interest to patients, clinicians, and payers. While there is evidence that removable flexible dentures may be similar or superior to removable conventional dentures for some outcomes, they may be inferior for others. Due to their relative cost, comparative cost-effectiveness research would help inform the potential role of these denture options in Canada.
Future research should focus on large, well-designed clinical trials and cost-effectiveness research in health systems within Canada with validated outcome measurement tools, clear reporting, and longer follow-up. Additionally, it is important to explore the relative value placed on outcomes for different groups, including patients, clinicians, and payers and how these may differ by factors such as age, degree of edentulism, access to technology and materials, and access to oral health care services and insurance.
Abbreviations
Cr-Co
cobalt-chromium (alloy)
OHIP
Oral Health Impact Profile
OHRQoL
oral health-related quality of life
PMMA
polymethyl methacrylate (acrylic)
RCD
removable complete denture
RCT
randomized controlled trial
RPD
removable partial denture
SES
socioeconomic status
VAS
visual analogue scale
Key Terminology
Health equity: Equity is the absence of unfair, avoidable, or remediable differences among groups of people, whether those groups are defined socially, economically, demographically, or geographically or by other dimensions of inequality (e.g., sex, gender, ethnicity, disability, or sexual orientation). Health is a fundamental human right. Health equity is achieved when everyone can attain their full potential for health and well-being. Health and health equity are determined by the conditions in which people are born, grow, live, work, play, and age, as well as biological determinants. Structural determinants (political, legal, and economic) with social norms and institutional processes shape the distribution of power and resources determined by the conditions in which people are born, grow, live, work, play, and age.1
PROGRESS-Plus: An acronym used to identify characteristics that stratify health opportunities and outcomes. PROGRESS refers to place of residence, race/ethnicity/culture/language, occupation, gender/sex, religion, education, socioeconomic status, and social capital. Plus refers to personal characteristics associated with discrimination (e.g., age, disability), features of relationships (e.g., smoking parents, excluded from school), and time-dependent relationships (e.g., leaving the hospital, respite care, other instances in which a person may be temporarily at a disadvantage).2
Racialized: A person or group of people categorized according to ethnic or racial characteristics and subjected to discrimination on that basis.3
Research Questions
What is the clinical effectiveness of removable partial or complete flexible dentures compared to removable partial or complete conventional dentures for edentulism?
What is the cost-effectiveness of removable partial and complete flexible dentures compared to removable partial or complete conventional dentures for edentulism?
What are the evidence-based guidelines on the use of removable partial or complete flexible dentures?
Context and Policy Issues
What Is Edentulism?
The term edentulism refers to both the loss of all natural teeth (complete edentulism) and the irreversible loss of 1 or more natural teeth (partial edentulism).4-6 Complete edentulism affects approximately 4% to 8% of adults in Canada;7,8 worldwide, it affects an estimated 350 million people,4 and there is substantial global variation in prevalence.8,9 Causes of tooth loss include trauma, genetic diseases, oral cancer, and periodontal disease, the last of these being the most common. Prevention of periodontal disease includes ensuring equitable access to oral health care services and promoting personal oral hygiene.
Prevalence of edentulism increases with age4,5,7 and global rates of edentulism are projected to increase with aging populations and population growth.4,10 Other factors associated with edentulism include a history of smoking,5,7 engagement in high-risk activities such as contact sports or working in high-risk environments (e.g., military), being female (although associations are inconsistent),4,5,7 having a lower socioeconomic status (SES) or level of education,4,5 and race or ethnicity.5,7 Reported disparities for the latter are inconsistent between countries and may reflect social and health inequities, including inequitable access to health insurance or oral health care services, rather than differential biological risk.11 While Canada has 1 of the highest per capita expenditures for oral health globally,12 it has high rates for both absolute and relative inequality for edentulism compared to some other high-income countries.13 Those seeking care for oral health problems are also more likely to have higher income levels and access to dental insurance, most often covered by private insurance plans.14,15
Tooth loss can affect overall health, quality of life, and mental health.4,16 Whether partial or complete, it can affect chewing ability and the ability to speak clearly; these, in turn, can affect food choices, nutritional intake, social engagement, and well-being. Tooth loss can also change facial shape, through anatomic changes to the jaw bones, tissues, or position of the remaining natural teeth, and this may impact self-esteem. A qualitative systematic review examined, in part, the experiences of those with tooth loss, and key themes were its perceived effect on chewing, speaking, appearance, social position, and confidence.17
Removable Dentures for Edentulism
Dentures are devices used to replace missing teeth. They may replace a few teeth (partial dentures), an entire arch of missing teeth on either mandibular or maxillary arches, or all teeth (complete or full dentures). Available denture options include fixed or removable prostheses and those with and without implants. Removable, non-implant-supported dentures, whether removable partial dentures (RPDs) or removable complete dentures (RCDs) are popular as they typically cost less than implant-supported dentures, do not require surgery, and are less dependent on the health of bones and gums.18-21 Dentures may increase the ability to chew and speak; decrease changes to facial shape; and improve health, social, and mental well-being compared to no intervention. The authors of a qualitative systematic review17 reported that users of RPDs often viewed their dentures as a “gift” and that it helped achieve “an ideal.”
Different materials may be used to manufacture removable dentures and acrylic or cast metal are common options. Acrylic dentures, frequently manufactured using polymethyl methacrylate (PMMA), typically cost less, whereas cast metal dentures, frequently manufactured using chromium-cobalt (Cr-Co) or nickel-chromium alloys, are typically stronger and less bulky than acrylic options.22,23 However, both options can cause discomfort and irritate the gums or oral tissues; they may require professional adjustments, care, and maintenance, and can be prone to damage or loss of retention over time. They also often use metal clasps to anchor the denture in the mouth, which may be perceived as aesthetically disadvantageous.
More recently, removable dentures made with thermoplastics are of interest; these include thermoplastic nylons, polyamides, and acrylics.22,23 Examples of commercial options for thermoplastic dentures available in Canada include Valplast, Duraflex, and TCS.24 These materials are attractive alternatives to acrylic and cast metal because they are more flexible, allowing them to adapt more easily to changes in the mouth shape, such as when chewing.23 Literature reviews typically also cite them as being more compatible with living tissue (e.g., less toxic or reactive), resistant to water absorption, and durable than conventional options, although the conclusions of literature overviews are inconsistent.22,23 The denture base and clasps are also translucent, appearing more natural, and the absence of metal elements provides options in the case of allergies or sensitivity. However, thermoplastic dentures tend to be more expensive than conventional options such as acrylic or metal, and some sources suggest that they may not be suitable for people with more extensive tooth loss.22,23,25 Additionally, the relative durability of removable flexible dentures in terms of risk of fractures, retention, and maintenance of colour compared to removable conventional dentures is unclear.22,25
Why Is It Important to Do This Review?
Thermoplastic resin removable dentures may offer advantages to people with edentulism in terms of aesthetics or comfort, but they typically cost more than removable dentures made from acrylic or metal, and their comparative long-term durability is unclear. As the various options may not all be equally accessible due to cost or insurance coverage, understanding their relative clinical effectiveness and cost-effectiveness informs decision-making. We previously published a Rapid Response (summary of abstracts) in 2019 reviewing the clinical effectiveness, cost-effectiveness, and guideline recommendations on the use of removable partial or complete flexible dentures for edentulism.26 This was a summary of abstracts with no critical appraisal of the evidence and identified no economic evaluations or evidence-based guidelines with which to inform practice or policy. A policy decision-maker indicated a need for an update of the previous review to support evidence-informed decision-making regarding the available options, including newer technologies, if relevant. This review is a response to that request.
Objectives
To support decision-making, we prepared this Rapid Review to identify, summarize, and critically appraise available evidence regarding the clinical effectiveness and cost-effectiveness of flexible RPDs and RCDs compared to conventional RPDs or RCDs for edentulism. This review also aimed to summarize the related guideline recommendations available for this patient population.
Methods
Included studies from a previous Canada’s Drug Agency (CDA-AMC) (formerly CADTH) report26 were screened for eligibility. In addition, an information specialist conducted a customized literature search, balancing comprehensiveness with relevance, of multiple sources and grey literature on August 1, 2025. One reviewer screened citations and selected studies based on the inclusion criteria presented in Table 1. Included studies were critically appraised by 1 reviewer using established critical appraisal tools. Appendix 1 presents a detailed description of methods and selection criteria for included studies.
Criteria | Description |
|---|---|
Population | People of all ages, in any setting, with partial or complete edentulism |
Intervention | Flexible nonacrylic, nonmetal partial or complete dentures, using thermoplastic materials, including:
|
Comparator | Q1 and Q2: Conventional partial or complete dentures, using acrylic or acrylic with metala Q3: Not applicable |
Outcomes | Q1: Clinical effectiveness (e.g., wear resistance and longevity, masticatory function, fit and comfort, quality of life, side effects, adverse events) Q2: Cost-effectiveness (e.g., incremental cost per health benefit gained, cost per patient adverse events avoided, cost-minimization) Q3: Guidelines on appropriate use and recommendations regarding best practices (e.g., appropriate patient populations, contraindications) |
Study designs | Q1: Health technology assessments, systematic reviews, randomized controlled trials, nonrandomized controlled studiesb Q2: Economic evaluations Q3: Evidence-based guidelines |
Publication date | 2009 to present |
aImplant-supported removable dentures (i.e., snap on) and thermoplastic resin dentures incorporating metal elements (e.g., for framework or clasps) were not eligible for this review.
bLimited to interventional studies.
Summary of Evidence
Quantity of Research Available
This report includes 9 publications27-35 of 8 studies meeting our inclusion criteria, comprising 5 studies29,31,33-35 identified from the previous CDA-AMC report,26 2 from our current updated search27,28 and 2 reports30,32 (1 companion to an existing included study30) from a systematic review36 identified during screening. We excluded 3 studies from the current Rapid Review that had been included in the previous CDA-AMC report:26 2 due to updated study eligibility criteria for the current Rapid Review37,38 and 1 due to an ineligible intervention.39
Nine publications were included for question 1: 7 randomized controlled trials (RCTs)27-30,32-35 and 1 study for which the reporting on study group allocation methods was unclear.31 We have included this as a nonrandomized controlled trial because study authors briefly refer to “experimental groups,” although it is possible that it is an observational study. We discuss the potential implications of this decision in the Limitations section of this review.
We did not identify relevant evidence regarding the cost-effectiveness of removable flexible dentures compared to removable conventional dentures that addressed question 2. We excluded 1 economic evaluation40 from this analysis, conducted in an educational institution in India, which compared the cost-effectiveness of thermoplastic resin RPDs with metal clasp–retained and cast metal RPDs because it was not considered generalizable or transferable to the health care context in Canada.
We did not identify any evidence-based clinical practice guidelines providing recommendations on the use of removable partial or complete flexible dentures for edentulism (question 3) that met the inclusion criteria for this report; therefore, no summary is provided.
Appendix 2 presents the PRISMA41 flow chart of the study selection.
Summary of Study Characteristics
Appendix 3 provides details regarding the characteristics of included publications.
Included Studies for Question 1: Clinical Effectiveness of Removable Flexible Dentures Compared to Removable Conventional Dentures
We identified 9 publications, including 4 parallel-group RCTs,28,32,33,35 4 publications of 3 crossover RCTs,27,29,30,34 and 1 nonrandomized controlled study31 addressing this research question. Two reports29,30 corresponded to 1 study, and the report authors reported different outcome measures (patient satisfaction,30 oral health-related quality of life29) at the same time point in the same study population. The included studies were published between 2015 and 2022, were conducted in Egypt,32 India,28,35 Italy,31 Nigeria,27,29,30 Poland,34 and Saudi Arabia,33 and were most often conducted within outpatient clinics and in university hospital settings. Study sample sizes ranged between 10 and 120 participants, and the longest follow-up for each study was as follows: 1 month,29,30 3 months,27,34 6 months,33 1 year,28,31 1.5 years35 (with unclear timing for outcome assessments), and 24 months32 (this study assessed most outcomes after 3 months).
Dentition status varied across the studies in both the number and location of missing teeth (e.g., Kennedy classification) with 6 studies limited to participants with partial tooth loss on a single dental arch (maxillary,31 mandibular,28,32 or either arch29,30,34,35), 1 study limited to those with complete loss on 1 arch (maxillary27), and 1 study limited to those with complete loss on both arches.33 Two studies28-30 excluded individuals with a previous history of denture use, whereas eligibility based on previous denture use was not explicitly stated in the other reports.
When reported, studies limited participants to those aged at least 16 years,29,30 between 30 and 70 years,28 and 65 years and older,31 and the mean participant age (based on reported means or ranges) was younger than 60 years in 6 studies.28-30,32-35 Sex or gender was reported in 5 studies: the authors of 3 studies reported the proportion of females (ranging from 50% to 60%);27,28,31 the authors of 1 study reported the proportion of males (50%);29,30 the authors of 1 study reported the number of men and women;34 and the authors of 3 studies did not report sex or gender distributions.32,33,35 No other sex or genders were reported, and no report defined these terms. While not frequently reported, diversity in participant race or ethnicity may be present across studies due to the studies’ country settings. Akinyamoju et al.29,30 reported participants’ place of residence (urban or suburban), proportions of participants from select Nigerian tribes, and the level of completed education, marital status, and SES. Hundal and Madan35 also reported SES. The authors of 6 studies did not report other factors associated with health equity, and no report authors reported other PROGRESS-Plus criteria,2 including occupation or religion. Most studies included only participants with good overall health status, with some excluding participants based on specific health conditions (chemotherapy,27,31 temporomandibular disorders,34 movement disorders,33 diabetes,31 psychiatric disease,33 or systemic medical conditions28).
The types of removable dentures evaluated and compared also varied. Two studies compared flexible RCDs to conventional heat-cured acrylic resin RCDs27,33 and 3 studies compared flexible RPDs (including thermoplastic polyamide, thermoplastic acetyl) to either acrylic RPDs,29,30 cast metal RPDs (e.g., Cr-Co alloy),28 or both.31 Macura-Karbownik et al.34 compared flexible RPDs to both acrylic RPDs and RPDs with acetal frameworks and clasps and an acrylic base. Sadek and Elawady32 compared Thermopress RPDs (specific thermoplastic material not stated) to cast metal RPDs with and without a surveyed bridge. The reports often described the denture design and manufacturing process in detail or provided references to design methodology, although this has not been extracted for this report.
The authors of the included studies reported a wide range of outcomes and, in the absence of a known core outcome set for nonimplant dentures, we categorized them using a subset of consensus core outcome domains from implant dentistry.42 The following clinical outcomes were extracted:
pathophysiology
masticatory function — up to 3 months,32,34 6 months,33 and 1 year31
aesthetics — up to 1 month,29,30 1 year,31 and 1 study with unclear timing of outcome assessment35
complications (e.g., injuries to adjacent structures, infection, pain, and plaque on teeth or prosthesis) — up to 1 month,29,30 1 year,31 and 24 months32
tissue health (e.g., health of mucosa or gingival tissue) — up to 1 year31 and 1 study with unclear timing of outcome assessment35
prosthesis lifespan
life impacts
overall satisfaction with treatment (e.g., visual analogue scale [VAS], Likert scale) — up to 1 month30 and 1 study with unclear timing of outcome assessment35
oral health-related quality of life (OHRQoL) — up to 1 month,29 3 months,32 and 1 year28
effort for maintenance (e.g., outcomes related to self-performed or professional visits for oral hygiene) — up to 1 month30 and 1 year.31
Summary of Critical Appraisal
Appendix 4 provides additional details about the strengths and limitations of the included publications.
Included Studies for Question 1: Clinical Effectiveness of Removable Flexible Dentures Compared to Removable Conventional Dentures
We identified 4 parallel-group design RCTs,28,32,33,35 3 crossover RCTs,27,29,30,34 and 1 nonrandomized controlled study31 that met the eligibility criteria for this research question. A detailed review of the critical appraisal is provided in Appendix 4.
The reporting quality of these studies varied. All reports clearly described the objectives, the main outcomes, and the study findings. No report referenced protocols or registration records, and to what extent results or analyses were prespecified is unclear. Seven studies27-32,34,35 clearly described the eligibility criteria and the details of the interventions (or provided a supplementary reference), whereas 1 report did not describe either.33 Estimates of random variability for the main outcomes were provided in reports of 6 studies27-30,33-35 but not in 2.31,32 The authors of 4 reports included some adverse events or reported no losses due to harms,28,31,32,35 and 4 did not mention adverse events.27,29,30,33,34 P values were reported for the main outcomes in reports of 6 studies27-31,33,34 but not in 2.32,35
The risk of selection bias in these studies is unclear. The authors of all studies reported recruiting participants in each arm from the same population over the same time period, except for Hundal and Mudan,35 who did not report the time frame of recruitment. The authors of all studies except 131 described randomly allocating participants to intervention groups, but the authors of only 3 studies27-30 described randomization procedures, of which the authors of only 1 study28 described a concealed randomized sequence. When reported, the studies appeared balanced for key variables at baseline, although the authors of 4 studies, all of which were parallel-group RCTs, reported few baseline characteristics31-33,35 and did not adjust for potential confounders (e.g., age, gender, race); whether these factors were balanced or could have a potential impact on the main findings is unclear.
All studies were at risk for performance bias, and 6 studies were at risk for measurement bias.27-32,35 Although masking participants and outcome assessors to the interventions received is difficult or not possible between the comparisons of interest, none of the studies’ authors reported that they attempted to conceal interventions or study objectives from participants or outcome assessors, and this may have impacted the use of, or perceptions related to, the devices. Although contamination across study arms was not expected, none of the studies’ authors reported how often participants used their prosthesis(es) or if they followed cleaning and maintenance instructions, where relevant. Carryover effects were not a primary concern for crossover studies27,29,30,34 and there were no washout periods. Measurement bias was primarily a concern for subjective outcomes, such as participant self-perceived quality of life or satisfaction. While the main outcome measures appear to be valid and reliable (e.g., measuring what they intend to measure with reproducible results) in 4 studies,28-30,33,34 those in the other 4 pose some concern. For example, Hundal and Madan35 did not report the time point of outcome measurement (or the period of recall required), and most outcomes were assessed using single questions with qualitative responses that were converted to scores, the validity of which is unclear. Others posed questions from seemingly unvalidated instruments31 or selected questions from multiple validated instruments.32
Seven studies had similar lengths of follow-up across study arms27-34 or adjusted for differences in the analysis.32 One study35 did not report the follow-up and outcome assessment timing clearly. The authors of 1 study reported no losses to follow-up,28 the authors of another study (2 reports) reported few losses, which were unlikely to impact the results,29,30 and the authors of 6 studies did not report whether there were losses to follow-up.27,31-35 The authors of 2 studies29,30,33 reported conducting power or sample size calculations for the primary outcomes, although neither reported the minimum clinical difference used in this calculation; the power of other studies to detect clinically meaningful differences is unclear. In 2 studies,32,34 an adjustment was made for multiplicity in analyses.
Studies were primarily conducted in university hospital or military settings in Africa, Asia, Europe, in countries with racial distributions and social and health inequalities that may differ from the context in Canada. Their generalizability (external validity) to other populations and dental care settings, including to those in Canada, is unclear. The authors of 2 studies27,29,30 reported recruiting consecutive patients over a set period of time; the authors of 2 studies33,35 reported recruiting a random sample of individuals presenting to their institution, but neither mentioned the selection method; and, for the remainder,28,31,32,34 reports did not describe participant selection or the representativeness of the study population to the source populations. The authors of all but 1 study34 reported seeking consent, but no report described the numbers or characteristics of those declining consent, if relevant.
The authors of 4 studies29,30,32,33,35 declared they had no conflicts of interest relevant to the research, and the authors of 4 studies made no statement related to conflict of interest.27,28,31,34 The authors of 4 studies declared the absence of study-specific funding28-30,32,33, and authors of the other 4 studies27,31,34,35 did not disclose receipt of funding or, if relevant, the source.
Summary of Findings
Appendix 5 presents additional details regarding the main study findings.
Question 1: Clinical Effectiveness of Removable Flexible Dentures Compared to Removable Conventional Dentures
Pathophysiology
Masticatory Function
Masticatory function was reported in publications of 2 parallel-group RCTs,32,33 1 crossover RCT,34 and 1 nonrandomized controlled study31 and included both objective and subjective outcome measures (Table 4). Overall, the evidence of the effectiveness of removable flexible dentures compared to conventional dentures for outcomes of masticatory function was inconsistent across studies, including between different objective measures.
Occlusal force, measured by dynamometer, was significantly lower after 3 months with flexible RPDs compared to conventional RPDs (acetal or PMMA).33,34
Maximum bite force, measured by occlusal force metre, was significantly higher after 6 months with flexible RCDs compared to conventional RCDs (acrylic).33
Chewing efficiency, defined based on the mass of particles of various sizes remaining after chewing 3 g of peanuts for 40 chewing cycles, was significantly lower after 7 days with flexible RPDs compared to conventional RPDs (acetal or PMMA RPDs).34 Results were also presented for this outcome at 1 month and 3 months and remained in favour of conventional RPDs, although the authors do not present the results of statistical comparisons between groups at these time points.
Chewing function, measured subjectively by study participants in 2 studies using different tools, showed variable results.31,32 The authors of 1 study reported statistically significantly better perceived chewing function based on a Chewing Function Quality questionnaire with flexible RPDs over cast metal RPDs after 3 months.32 The authors of the other study reported no statistically significant difference in satisfaction with chewing ability between flexible RPDs and either PMMA or Cr-Co RPDs (1 question with 2 response options) after 1 year.31
Aesthetics
Aesthetics were reported in publications of 1 parallel-group RCT,35 1 crossover RCT,30 and 1 nonrandomized controlled study31 based on subjective outcome measures (Table 5), all with different methods of measurement. Overall, removable flexible dentures may lead to higher perceived aesthetic satisfaction compared to removable conventional dentures, but our confidence in this evidence is low.
Patient satisfaction with appearance (or aesthetic satisfaction) was assessed in 3 studies with varied results. The authors of 1 study found no statistically significant difference in patient satisfaction between flexible and acrylic RPDs after 1 month (1 crossover RCT).30 Two studies reported statistically significantly higher patient-reported aesthetic satisfaction with flexible RPDs (after 1 year31 and unclear follow-up35) compared to conventional RPDs (PMMA or Cr-Co).
Clinician-assessed aesthetics were significantly more likely to be rated higher for flexible RPDs compared to conventional RPDs (time point of assessment is unclear).35
One study30 reported subgroup summary data and analyses based on participant age, gender, and SES; no significant differences were reported based on a P value of 0.05 or less, but the sufficiency of study power to detect such differences is not clear.
Phonetics or Speech
Phonetics or speech were reported in publications of 1 crossover RCT29,30 and 1 nonrandomized controlled study31 limited to participant-reported subjective outcome measures (Table 6). Overall, the evidence of the comparative effectiveness of removable flexible dentures compared to conventional dentures for outcomes of speech or phonetics was inconsistent across studies.
Satisfaction with the ability to speak was not significantly different between flexible and acrylic RPDs after 1 month, measured with a VAS of 100 mm converted into 4 categories (1 crossover RCT).30
Speech defects or difficulties were reported in 1 crossover RCT29 and 1 nonrandomized controlled study.31 The authors of 1 study found that speech difficulties were less prevalent (no significance testing) for participants wearing flexible RPDs compared to acrylic RPDs after 1 month.29 The other found speech difficulties were statistically significantly less prevalent for participants wearing flexible or Cr-Co RPDs compared to PMMA RPDs after 1 year and found no statistically significant difference between participants wearing flexible RPDs compared to Cr-Co RPDs.31
The authors of 1 study30 also reported summary data and analyses based on participant age, gender, and SES; no significant differences were reported based on a P value of 0.05 or less, but the sufficiency of the power of the study to detect such differences is not clear.
Denture Retention
Denture retention was reported in publications of 1 crossover RCT27 and 1 nonrandomized controlled study,31 and included both objective and subjective outcome measures (Table 7). Both were conducted in older adult populations (mean age older than 65 years). Overall, the evidence of the effectiveness of removable flexible dentures compared to conventional dentures for objective and subjective outcomes of denture retention was inconsistent across and within studies.
Retention, measured objectively using a pull digital force gauge, was found to be significantly lower for flexible RCDs compared to acrylic RCDs after 1 week, 1 month, and 3 months in 1 crossover RCT.27
Retention, measured subjectively using various methods, found inconsistent results. Kapur’s retention score,43 which was categorized, was lower (no statistical comparison) for flexible RCDs compared to acrylic RCDs after 1 week, 1 month, and 3 months in 1 study.27 In the same study, participant-reported satisfaction with retention, measured with a 100 mm VAS, which was categorized, was not statistically significantly different between groups after 3 months.27 Participant-reported retention, measured in 1 study by a single question (with response options of “decreased” retention or “same as before,” with no definition for “before”), found significantly more participants perceiving “decreased” retention with flexible RPDs compared to those with conventional RPDs (Cr-Co or PMMA) after 1 year.31
Complications
Complications with dentures were reported in publications of 1 crossover RCT,29,30 1 parallel-group RCT,32 and 1 nonrandomized controlled study.31
The authors of 1 crossover RCT29,30 and 1 nonrandomized controlled study31 reported pain or comfort while eating (Table 8). Overall, the evidence of the effectiveness of removable flexible dentures compared to conventional dentures for comfort or pain while chewing suggests there is little or no difference between these interventions.
Patient-reported satisfaction with comfort while chewing was not statistically significantly different between flexible and acrylic RPDs after 1 month in 1 study.29,30 The authors of this study also reported the scores from the Oral Health Impact Profile (OHIP)-14 items “found it uncomfortable to eat” and “painful aching in mouth.” Response groupings and results make it difficult to make inferences from this information, although there were little to no differences between these outcomes at follow-up compared to baseline. In this study, subgroup analyses were reported based on participant age, gender, and SES; no significant differences were reported based on a P value of 0.05 or less, but the sufficiency of study power to detect such differences is not clear.
Patient-reported pain during chewing was not statistically significantly different between flexible and conventional (Cr-Co or PMMA) RPDs after 1 year.31
Manzon et al.31 reported other complications, all based on patient- or clinician-reported observations, comparing flexible RPDs to Cr-Co RPDs and PMMA RPDs (Table 9). The results, after 1 year, are summarized in the following bullets:
“Feeling of encumbrance” (not otherwise described) was significantly different across the groups and lower for flexible RPDs.
Prevalence of the following complications was similar between the groups: calculus on the prosthesis, plaque presence on abutment teeth, abutment teeth health, and change in occlusal position.
Roughness perceived by the tongue was statistically significantly different across the groups and higher for flexible RPDs.
Survival of abutment teeth was not statistically significantly different with the use of flexible compared to conventional RPDs (Vitallium with or without surveyed bridge) at 24 months in 1 study.32
Tissue or Periodontal Health
Outcomes associated with tissue or periodontal health were reported in the publications of 1 parallel-group RCT35 and 1 nonrandomized controlled study,31 and included both objective and subjective outcome measures (Table 10). Overall, the evidence of the comparative effectiveness of removable flexible dentures compared to conventional dentures for outcomes of tissue and periodontal health showed similar prevalence of complications for most outcomes. However, in 1 study, it was found that mucosa redness around the abutment teeth may be statistically more likely with flexible compared to conventional RPDs.
The prevalence of mucosa redness around the edentulous area was not statistically significantly different for flexible compared to conventional RPDs (Cr-Co or PMMA) after 1 year.31
The prevalence of mucosa redness around the abutment teeth was statistically significantly different between flexible, Cr-Co, and PMMA RPDs and lowest with Cr-Co RPDs after 1 year.31
Oral tissue tolerance (measured both subjectively and objectively), gingival and periodontal health (both measured using existing indices), and the need for a block in areas with undercut were “statistically on par” (as reported by authors) for flexible compared to Cr-Co RPDs after an unclear follow-up period (follow-up was reported to be 1.5 years in the study, but the timing of outcome assessment is not clear; no P values were presented).35 The method of analysis poses concerns; individual patient data are provided.35
Prosthesis Lifespan
Technical Complications (Prosthesis)
Technical complications related to the prostheses were reported in publications of 1 parallel-group RCT35 and 1 nonrandomized controlled study,31 and were limited to objective outcome measures (Table 11). Overall, the evidence of the effectiveness of removable flexible dentures compared to conventional dentures for prosthesis lifespan varied across the outcomes assessed.
The authors of 2 studies reported the frequency of fractures of prostheses — in 1 study no fractures for flexible, Cr-Co, or PMMA-based RPDs were reported after 1 year,31 and in the other study no difference between frequencies of fractures in flexible RPDs and Cr-Co alloy RPDs (no statistical testing) were reported after an unclear follow-up period (in the study, follow-up to 1.5 years is reported, but the timing of the outcome assessment is not clear).35
The frequency of prosthesis discoloration and loss of artificial teeth was also assessed in 1 study,31 which reported no statistically significant difference in prevalence of prosthesis discoloration between flexible, Cr-Co, and PMMA-based RPDs after 1 year and a significantly higher frequency of artificial tooth loss with flexible compared to conventional RPDs after 1 year.
Life Impacts
The terms “patient satisfaction” and OHRQoL were used inconsistently across studies, and scales designed and validated to measure the latter are sometimes described as measuring satisfaction. We reported these outcomes based on the purpose of the scales or questionnaires (i.e., if an OHRQoL scale is used but is reported to measure patient satisfaction, we report this with other OHRQoL results).
Overall Satisfaction With Treatment
Overall satisfaction with prostheses was reported in publications of 1 crossover RCT29,30 and 1 parallel-group RCT,35 limited to subjective outcome measures (Table 12). Overall, the evidence of the comparative effectiveness of removable flexible dentures compared to conventional dentures for patient satisfaction with treatment showed statistically higher patient satisfaction with flexible dentures. However, there are considerable concerns with the methodology and analysis for this outcome.
Patient satisfaction was measured with a single-question 100 mm VAS regrouped into 4 categories in 1 study,30 and with a single question with 4 response options to which numerical values were assigned in another study.35 Both studies reported a statistically significantly higher overall satisfaction with the use of flexible compared to conventional RPDs (acrylic in 1 study and Cr-Co alloy with PMMA base in the other), after 1 year and unclear follow-up (follow-up to 1.5 years is reported in the study, but the timing of the outcome assessment is not clear), although the latter does not report the results of statistical analyses.
Oral Health-Related Quality of Life
OHRQoL was reported in publications of 1 crossover RCT29,30 and 2 parallel-group RCTs35 (Table 13). Overall, the evidence of the comparative effectiveness of removable flexible dentures versus conventional dentures for overall OHRQoL is inconsistent.
Overall OHRQoL using the OHIP-14 questionnaire was reported in 2 studies.44-46 The authors of 1 study found that, compared to baseline, OHRQoL was statistically significantly increased (decreased OHIP-14 summary scores) for both flexible and acrylic RPDs after 1 month. They did not report statistical analyses between groups but, at 1 month, 95% confidence intervals of OHIP-14 scores overlap substantially between groups (i.e., scores are likely to be similar). The authors of another study28 also reported statistically significantly increased OHRQoL between baseline and 1 year for both flexible and cast metal RPDs. They found that OHRQoL was statistically significantly higher for flexible RPDs compared to cast metal RPDs at 1 year; however, the differences between groups at follow-up range from not clinically meaningful to clinically meaningful.47
OHRQoL, measured with a 100 mm VAS for 12 questions derived from other tools (e.g., OHIP-49,48 the Geriatric Oral Health Assessment Index49), was reported to be significantly higher overall for flexible compared to conventional RPDs at the 3-month follow-up in 1 study.32
Domain-specific OHIP-14 scores44-46 were reported in 2 studies.28,29 These domains included Functional Limitation, Physical Pain, Psychological Discomfort, Physical Disability, Social Disability, and Handicap. They were assessed at 1 month in 1 study18 (compared to baseline only, with no between-group analysis), and 1 year in another study22 (comparing both within-group changes from baseline and between-group analyses at follow-up). Although the results for the domain-specific changes from baseline were inconsistent between studies, in 1 study it was reported that flexible dentures were associated with a statistically significantly increased OHIP-14 Functional Limitation score compared to cast metal RPDs at 1 year; no other significant differences were found between all other domain-specific between-group comparisons.
The authors of 1 study29 reported results for all individual questions on OHIP-14. They also presented mean OHIP-14 scores by age, gender, and SES. They compared within-group differences, noting no significant within-group differences for these factors at follow-up. Differences between groups were not assessed, but descriptive results were presented in the publication (not extracted for the current review).
Effort for Maintenance
Satisfaction or perceived experience for prosthesis cleaning was reported in publications of 1 crossover RCT29,30 and 1 nonrandomized controlled study31 (Table 14). Overall, the evidence of the comparative effectiveness of removable flexible dentures versus conventional dentures for maintenance is inconsistent.
Satisfaction with ease of cleaning, measured using a 100 mm VAS converted to categories, was not statistically significantly different for flexible compared to acrylic RPDs after 1 month in 1 crossover RCT.29,30 The authors of this study also reported subgroup analyses based on participant age, gender, and SES; no significant differences were reported based on a P value of 0.05 or less, but the sufficiency of study power to detect such differences is not clear.
The perception of difficulty with prosthesis care, measured using 1 question with 2 response options, was statistically significantly more likely to be rated as “difficult” by participants using flexible RPDs compared to those using conventional RPDs (Cr-Co or PMMA) after 1 year in 1 study.31
Limitations
Current Evidence and Gaps
We identified studies providing inconsistent evidence overall, and often for specific outcomes, for the relative clinical effectiveness of removable flexible dentures compared to removable conventional dentures. Limitations with the body of evidence decrease our confidence in drawing conclusions from the effects and comparisons reported.
All the studies are at some risk of bias, primarily due to the risk of performance and measurement bias. Masking participants and outcome assessors to the interventions received is difficult or not possible when comparing removable dentures because they may look and feel different. However, within the context of a clinical trial, knowing the intervention received can affect subsequent behaviours through the trial, such as frequency of denture use and cleaning, due to conscious or unconscious biases. It can also affect subjectively assessed outcomes (e.g., satisfaction and preferences), although it may be less of a concern for objectively measured outcomes (e.g., masticatory function using occlusal force metres) or, possibly, subjectively measured outcomes using validated scales (such as the OHIP-14 scale). None of the included studies masked subjects or outcome assessors to the interventions received, and subjective, nonvalidated measurement tools (or tools with unclear validity) were common. We also noted inconsistent conclusions between objective and subjective tools (e.g., for denture retention27) or lack of correlation between 2 objective measures intended to measure the same outcomes (e.g., masticatory function34), highlighting the need for a better understanding of the validity of measurement tools and for the use of consistent measurement tools to enable comparison between studies. Finally, most studies did not report sample size (power) calculations or minimally important differences for the main outcomes. Some studies identified no statistically significant differences between interventions but may have been underpowered to detect true differences (e.g., subgroup analyses in 1 study29,30), whereas some studies identified statistically significant differences between interventions but had 95% confidence intervals that ranged from not clinically meaningful to clinically meaningful (e.g., OHRQoL in 1 study31).
There are gaps in the evidence for some outcomes of potential interest, long-term follow-up, reliable and transferable estimates of relative cost-effectiveness of removable flexible and conventional dentures, and evidence-based guideline recommendations. For example, no studies included in this review assessed duration or frequency of professional treatments (e.g., repairs, adjustments), and this can impact perceived satisfaction with care and perceived burden. Studies were also often limited by duration, both for assessment of some pathophysiological outcomes and relative to expected denture lifespans, with most outcomes measured after 1 year or less. Patient satisfaction and functional outcomes have been associated with length of previous denture use36 and, while some studies suggest that people may adjust to new dentures within 3 months or less, others suggest that sufficiently longer (e.g., greater than 10 months) is required to accurately compare longer-term function and satisfaction.50 Longer-term studies are also required to understand the comparative durability (e.g., retention or fractures) and acceptability (e.g., tissue health or aesthetics) of the denture base materials.38 We identified no cost-effectiveness research conducted in Canada and no evidence-based clinical practice guideline recommendations for this population.
Heterogeneity
Across the 8 included studies, substantial heterogeneity in terms of the target population, the comparisons of interest, and the methods and timing of outcome assessment limited our ability to assess the consistency of the evidence within or across populations. For example, every study targeted a population with different numbers and locations, or patterns, of missing teeth (e.g., partial or complete, mandibular or maxillary jaw, Kennedy class), and this may be a factor in describing differences in conclusions across studies. Patient satisfaction, for instance, has been shown to vary across denture types by the number and location of missing teeth.36 Studies also measured or analyzed outcomes in different ways, sometimes with questionable validity.
Generalizability
We identified no studies conducted in Canada, and most studies were conducted in settings with low generalizability to oral care settings in Canada, both generally or across factors that may be associated with inequity in Canada, such as place of residence, race, and socioeconomic status. While reports described the study target populations, they typically excluded participants based on health status, so these results may not be generalizable to all, including those with neurological conditions or those having received chemotherapy. All studies were also limited to adults or older adults, and these results may not represent the experiences of younger people with tooth loss. Few studies reported health equity–focused2 population characteristics other than age and gender or sex. Akinyamoju et al.29,30 reported subgroup summary data and noted no significant differences across outcomes of satisfaction and OHRQoL by age, sex, or SES; however, this study included 30 participants and may be underpowered to detect such differences, if they exist. While the included studies were conducted in countries that are ethnically and racially diverse by the nature of their location (i.e., within Africa and Asia), the racial distributions and social and health inequalities within these countries may differ from the context in Canada. Therefore, with limited information across studies, drawing conclusions regarding how these results might reflect the experiences of diverse populations within Canada is not possible.
Other uncertainties regarding the generalizability of this evidence are the study settings and denture manufacturing practices. Studies were conducted in university hospitals or military settings in Africa, Asia, or Europe, and it is unclear how these settings and the care offered might compare to dental care in Canada, where most people receive dental care in outpatient, private clinic settings. Valplast, a thermoplastic denture that is available in Canada, was investigated in 4 studies; we were unable to confirm the availability of the other investigated interventions in Canada. The materials for comparators of interest, although not necessarily the specific manufacturers, appear similar to those available in Canada. We did not extract or compare the denture manufacturing techniques described, so we are not able to comment on how these may compare or how results might differ based on these variables.
Limitations of Our Approach
We limited our search to studies published in English for feasibility, and whether the findings from studies in other languages might influence the conclusions of our Rapid Review is unclear. We also did not compare the design and manufacturing details of dentures explored across these studies (e.g., techniques or machines, whether any used computer-aided design) and whether these variables might impact outcomes, or the generalizability of the studies to technologies available in Canada.
We also limited the evidence summarized in this report to experimental studies for feasibility within a Rapid Review context, given the volume of available interventional trials that addressed relevant outcomes for this review. Two observational studies included in the previous CDA-AMC summary of abstracts26 were therefore excluded from this review (1 reported patient satisfaction37 and 1 reported multiple relevant outcomes [e.g., mastication, aesthetics, retention, comfort] with 24-month follow-up38). Due to the conduct and reporting of these studies, they would be unlikely to change our conclusions. We also included 1 study for which the reporting on study group allocation methods was unclear, and although there were some indications that it was an experimental study, it is also possible that it is an observational study.31 Our overall assessment of the comparative effectiveness of these devices would not change if this study had been excluded, and our assessment by outcome would change for only 1 domain, “effort for maintenance.” The authors of this study reported a statistically significantly lower perceived ease of cleaning for dentures at 1 year compared to conventional dentures, whereas the authors of the other included study reported no statistically significant difference for satisfaction with ease of cleaning at 1 month between denture types. However, this study included some unique outcomes (tissue health, periodontal health, and technical complications) and longer-term follow-up for all outcomes (1 year) than other included studies. With these considerations, the inclusion of this study does not appear to drive our conclusions about the comparative effectiveness of these devices but may add perspective for longer-term follow-up and for outcomes not otherwise reported.
As the nature and scope of the request were focused on reviewing published clinical data, we did not conduct direct engagement with patients, caregivers, or providers. We also did not search for or include literature on perspectives, experiences, or other evidence that is relevant to underserved groups. Despite the inclusion of clinical studies conducted in a variety of countries with ethnic and racial diversity, sampling methods and patient characteristics were often poorly reported. With this limited scope, we have missed including the lived and living experience of individuals with disproportionate rates of tooth loss (e.g., racialized individuals living in Canada7) or those with inequitable access to oral health care.14 We acknowledge this as a limitation of our work, and that this Rapid Review may not highlight or identify perspectives and evidence of relevance to these underserved groups in Canada. Of note, as part of the CDA-AMC organizational commitment to reconciliation and inclusion, diversity, equity, and accessibility, we know it is important to consider and learn from First Nations, Inuit, and Métis and other diverse perspectives in our work. We also recognize that the research team consists of settler researchers, and we come to this work with our individual privileges and biases. Understanding the perspectives and priorities of First Nations, Inuit, and Métis Peoples and other underserved groups as they relate to tooth loss and prostheses can support informed health care decision-making.
Conclusions and Implications for Decision- or Policy-Making
This Rapid Review evaluated the literature regarding the clinical effectiveness and cost-effectiveness of removable partial or complete flexible dentures compared to removable partial or complete conventional dentures (e.g., acrylic or metal) for people with missing teeth, as well as guidelines related to the use of removable partial or complete flexible dentures. This report includes 8 publications of 7 RCTs27-30,32-35 (including 3 crossover trials27,29,30,34) and 1 nonrandomized controlled study31 addressing question 1. We did not identify any relevant economic evaluations addressing question 2 or evidence-based clinical practice guidelines addressing question 3.
Summary of Evidence
The evidence comparing removable flexible and conventional dentures provides inconsistent support for the relative clinical effectiveness of these interventions across pathophysiological, prosthesis-related, and life impact-related outcomes. No cost-effectiveness information was identified that may be relevant to Canada. Notwithstanding the concerns about study and outcome-specific risk of bias, the included studies suggest that flexible dentures may lead to improved aesthetics and overall patient satisfaction, lower levels of denture retention (when measured objectively, but inconsistent results dependent on measurement methods), and higher rates of some complications (perceived roughness on the tongue and loss of artificial teeth); the latter were often limited to results from single studies. Studies also showed that flexible and conventional removable dentures may be comparable for speech difficulties, complications such as pain while eating, plaque on the prosthesis or abutment teeth, discoloration of the prosthesis, frequencies of fractures, change in occlusal position, and abutment survival; again, each was often limited to results from single studies. For some indices, such as masticatory function, tissue and periodontal health, overall OHRQoL, and effort for maintenance, inconsistent conclusions were reported across studies. Due to risk of bias and validity concerns, small sample sizes in many studies, and short timelines relative to expected prosthesis lifespan, substantial uncertainty exists around the strength of these findings to inform decision-making.
We also identified 1 additional systematic review51 after the literature search and screening was complete that met our eligibility criteria and was not identified in our search (not indexed in MEDLINE and published the day of our literature search). It included more interventions than those relevant to the current Rapid Review and examined a subset of outcomes. One additional study52 of potential relevance to this Rapid Review was included in this systematic review, of which the findings seem consistent with the current review.
We identified no cost-effectiveness studies comparing removable flexible dentures to removable conventional dentures deemed generalizable or transferable to the oral health care context in Canada. We excluded 1 economic evaluation40 from this analysis comparing flexible RPDs to conventional RPDs that was conducted in India at 1 university-based institution. The authors of this study concluded that the cost-effectiveness of flexible dentures varies depending on the number of teeth being replaced; however, there are concerns with the validity of the estimates of clinical effect used in the analysis. A brief summary of this excluded economic evaluation can be found in Appendix 6. We identified 1 other cost-effectiveness study that was based on an RCT39 included in the previous CDA-AMC summary of abstracts26 but was excluded from the current Rapid Review because the flexible RPD incorporated metal elements for rests and connectors (not clear from the abstract); these types of rigid removable thermoplastic dentures were not of interest for the current review.
We identified no evidence-based clinical practice guideline recommendations for this population that met our eligibility criteria. One position paper from Japan53 does not recommend flexible non-metal-clasp dentures as definitive dentures and recommends them only in limited scenarios such as in the presence of metal allergies. Instead, they recommend flexible RPDs with metal elements or rigid thermoplastic dentures, as previously described. However, this recommendation, published in 2014, is based primarily on expert opinion, and they acknowledge the need to assess assumptions in well-designed clinical trials.
The current Rapid Review built upon a previous CDA-AMC report published in 2019. We excluded 3 studies from the previous report, 2 due to study design (observational studies)37,38 and 1 due to an ineligible intervention (rigid thermoplastic denture).39 We also identified 3 new studies and 1 companion report for a study included in the previous review. The previous review summarized abstracts only and did not critically appraise the evidence, so comparing findings between reviews, beyond the numbers and types of studies identified, is not possible.
Considerations for Future Research
Future clinical research should ideally focus on improving key elements of design and reporting of clinical trials (e.g., CONSORT statement54), including using randomized allocation, concealing allocation from participants before enrolment, and recording the numbers and characteristics of eligible and consenting participants compared to their source population. While edentulism is less common in younger age groups, children and adolescents may place differential value on the various outcomes; research in this population is warranted. Reports should also include study population characteristics associated with potential health inequities (e.g., place of residence, race or ethnicity, socioeconomic status),2 so readers may better understand the generalizability of the results to their specific settings as well as to systemically marginalized populations. We also recommend that researchers consider employing standardized and validated outcome assessment tools to increase confidence in the results of individual studies and comparability across studies. Longer-term studies with large sample sizes are also required; the first to capture comparative durability and satisfaction across the expected denture lifespan, and the second to ensure studies are adequately powered to detect important differences, should they exist, between interventions and to enable comparisons between participant characteristics (e.g., by age, gender).
Although we did not identify a core outcome set specific to studies of removable dentures, a consensus statement (based on methodological best practices and including engagement with people with lived experience) provided a list of core outcomes for implant dentistry that is informative for the current review.42 Our included studies addressed many of the core outcomes included in this set (i.e., masticatory function, aesthetics, speech difficulties, denture retention, complications, tissue health, technical complications, patient satisfaction, OHRQoL, and effort for daily maintenance). However, we did not identify evidence to inform perspectives for some outcomes in this set that may be relevant to removable dentures, including duration of treatment (e.g., visits for initial denture fabrication and fitting, repairs, and adjustments) and domains of access to care, cost-effectiveness, and level of professional competence or experience necessary to ensure a good outcome.
Finally, we identified no economic evidence conducted within Canada or from transferable cost-effectiveness studies. As patient preferences and costs may play a key role in differentiating the relative benefits and risks of these devices, and these may both be highly context specific (e.g., patient satisfaction may vary based on a number of factors36 and costs will vary based on materials used and access to these materials), conducting research within populations and settings in Canada is important.
Considerations for Decision- or Policy-Making
The findings of this report suggest that flexible removable dentures may improve clinical outcomes such as aesthetics and satisfaction for adults with edentulism compared to conventional removable dentures, and they may be comparable for prosthesis-related factors such as frequency of fractures. The studies showed inconsistent results for many outcomes, including masticatory function, indices of tissue health, and OHRQoL and suggested, for some outcomes, such as retention, these devices may be inferior to removable prostheses made with acrylic or metal. However, because the current body of evidence has substantial methodological limitations, most follow-up is 1 year or less, and the relative cost-effectiveness, long-term durability, and lifespan of removable flexible compared to conventional dentures are unknown, the potential role of removable flexible dentures compared to removable conventional dentures for edentulism remains to be clearly defined. We identified no economic evidence generalizable or transferable to Canada to inform a decision based on cost-effectiveness, and this is important for future research.
Therefore, deciding which devices might be best may require a better understanding of the relative value of these outcomes to patients, clinicians, and payers. Both cost and clinical effectiveness determine the optimal choice in specific clinical scenarios and patient needs. From a clinician’s perspective, outcomes such as relative function, durability, and rates of oral health complications (e.g., to tissues, teeth, or prostheses) may be priorities. However, patient choice and access to care typically influence tooth replacement. From a patient perspective, key factors may include aspects of the design, look, long-term maintenance, costs or insurance coverage, and experience with their prosthesis. Important drivers may include lifestyle, social factors, allergies, expectations, available options, and budget; for some, appearance may surpass function in terms of importance.17 Age, gender, and the number or location of missing teeth have also been shown to impact OHRQoL and patient satisfaction scores.36,40
Decision-makers considering these interventions may also wish to reflect on other factors, including barriers and potential solutions to barriers to achieving equitable access to oral health care in Canada. This may include equitable access to qualified professionals and equipment and access to oral health services or coverage across insurance plans.14 In Canada, dentures may be paid for by patients, private insurance, or public insurance such as the Canadian Dental Care Plan55 and the Non-Insured Health Benefits program for First Nations and Inuit.56 Differences in coverage, or access to coverage, for removable dentures and eligibility criteria for frequency of replacements could affect health and social outcomes, potentially disproportionately affecting vulnerable groups.
Finally, many current advancements in denture manufacturing, such as more advanced thermoplastics, 3D printing technology, and digital dentistry, may impact outcomes; for example, computer-aided design and manufacturing may create precise dentures with superior function and comfort. These variables will be important to consider in future primary research and evidence summaries.
References
1.World Health Organization. Health Equity. https://www.who.int/health-topics/health-equity#tab=tab_1
2.O'Neill J, Tabish H, Welch V, et al. Applying an equity lens to interventions: using PROGRESS ensures consideration of socially stratifying factors to illuminate inequities in health. J Clin Epidemiol. 2014;67(1):56-64. doi: 10.1016/j.jclinepi.2013.08.005 PubMed
3.Government of Canada. IRCC Anti-Racism Strategy 2.0 (2021-2024) – Glossary. 2022. Updated 2022-07-18. Accessed September 2, 2025. https://www.canada.ca/en/immigration-refugees-citizenship/corporate/mandate/anti-racism-strategy/glossary.html
4.World Health Organization. Global oral health status report: towards universal health coverage for oral health by 2030. Geneva; Licence: CC BY-NC-SA 3.0 IGO. 2022. Accessed August 27, 2025. file:///C:/Users/Jennifer.Tetzlaff/Downloads/9789240061484-eng.pdf.
5.Centers for Disease Control and Prevention. Oral Health Surveillance Report: Dental Caries, Tooth Retention, and Edentulism, United States, 2017–March 2020. U.S. Dept of Health and Human Services; 2024. Accessed August 28, 2025. https://www.cdc.gov/oral-health/php/2024-oral-health-surveillance-report/index.html
6.edentulism. (n.d.) Medical Dictionary for the Dental Professions. (2012). Retrieved August 29 2025 from https://medical-dictionary.thefreedictionary.com/edentulism.
7.The Daily: Self-reported oral health problems in the Canadian population living in the provinces, November 2023 to March 2024. 2024. Accessed August 15, 2025. https://www150.statcan.gc.ca/n1/daily-quotidien/241023/dq241023b-eng.htm
8.World Health Organization. The Global Health Observatory - Oral health: edentulism in people 20+ years, prevalence (%). 2019. Accessed August 22, 2025. https://www.who.int/data/gho/data/indicators/indicator-details/GHO/prevalence-of-edentulism-in-people-20--years
9.Guan W, Li J, Liang Q, et al. Disease burden and health inequality of older adults with edentulism and the projected trend until 2040: based on the global burden of disease study 2021. Clin Oral Investig. 2024;29(1):22. doi: 10.1007/s00784-024-06111-5 PubMed
10.Jiang H, Yin L, Hu Z, Chen Z, Yue H, Qin Z. Global, regional, and national temporal trends of edentulism burden from 1990to 2021 and predictions to 2050: an age-period-cohort analysis, decomposition analysis and frontier analysis. J Stomatol Oral Maxillofac Surg. 2025:102374. doi: 10.1016/j.jormas.2025.102374 PubMed
11.Roberto LL, Crespo TS, Monteiro-Junior RS, et al. Sociodemographic determinants of edentulism in the elderly population: A systematic review and meta-analysis. Gerodontology. 2019;36(4):325-337. doi: 10.1111/ger.12430 PubMed
12.World Health Organization. The Global Health Observatory - Oral health: dental healthcare expenditure, per capita (US$). 2019. Accessed August 22, 2025. https://www.who.int/data/gho/data/indicators/indicator-details/GHO/per-capita-expenditure-on-dental-healthcare-(us-dollar)
13.Chari M, Ravaghi V, Sabbah W, Gomaa N, Singhal S, Quiñonez C. Oral health inequality in Canada, the United States and United Kingdom. PLoS ONE. 2022;17(5):e0268006. doi: 10.1371/journal.pone.0268006 PubMed
14.Moharrami M, Sano S, Murphy K, et al. Health Reports: Assessing the role of dental insurance in oral health care disparities in Canadian adults. Statistics Canada; 2024. Accessed August 27, 2025. https://www150.statcan.gc.ca/n1/pub/82-003-x/2024004/article/00001-eng.htm
15.Statistics Canada. Table 13-10-0877-01 Dental insurance coverage and dental visits, by age group and gender. Accessed September 15, 2025. https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310087701&pickMembers%5B0%5D=1.1&pickMembers%5B1%5D=2.1&pickMembers%5B2%5D=5.4
16.Hunter E, De Moura Brito L, Piyasena P, et al. Impact of edentulism on community-dwelling adults in low-income, middle-income and high-income countries: a systematic review. BMJ Open. 2024;14(12):e085479. doi: 10.1136/bmjopen-2024-085479 PubMed
17.Broomhead T, Baker SR, Martin N, et al. Exploring experiences of living with removable dentures-A scoping review of qualitative literature. Gerodontology. 2024;41(3):314-327. doi: 10.1111/ger.12735 PubMed
18.Park Meadows Blog: Dental Implants vs Dentures: Making the Right Choice for Your Smile. Updated February 19, 2025. Accessed September 23, 2025. https://parkmeadowsdental.ca/blog/dental-implants-vs-dentures/
19.hellodent - Canadian Dental Health Guide: How much do dentures cost in Canada? Accessed September 23, 2025. https://www.hellodent.com/site/blog/2023/12/22/dentures-cost
20.hellodent editorial team. hellodent - Canadian Dental Health Guide: How much do dental implants cost in Canada? Updated January 25, 2024. Accessed September 23, 2025. https://www.hellodent.com/site/blog/2024/01/25/dental-implants-cost
21.Mesiels D. Dental Implants, Dental Service: Full Mouth Dental Implants Cost in Canada (2025 Guide). Updated September 10, 2025. Accessed September 23, 2025. https://thedentalteam.ca/full-mouth-dental-implants-cost-in-canada/
22.Binaljadm TM. Flexible Denture: A Literature Review. Cureus. 2024;16(3):e55425. doi: 10.7759/cureus.55425 PubMed
23.Binhuraib H, Alhajrassi S, Bukhari H, et al. Flexible Dentures: Materials, Properties, and Patients Satisfaction. Journal of Healthcare Sciences. 2023;3(12):554-560. doi: http://dx.doi.org/10.52533/JOHS.2023.31201
24.Government of Canada. Medical devices active licences search. 2025. https://health-products.canada.ca/mdall-limh/prepareSearch?type=active
25.Mendoza-Carrasco I, Hotta J, Sugio CYC, et al. Nonmetal clasp dentures: What is the evidence about their use? J. 2020;20(3):278-284. doi: 10.4103/jips.jips_459_19
26.Hill S, Wright M. Flexible dentures for edentulism: Clinical effectiveness, cost-effectiveness, and guidelines (CADTH rapid response report: Summary of abstracts). CADTH; 2019.
27.Olawale OF, Ogunrinde TJ, Dosumu OO, Ajayi DM. The Effect of Ridge Height on Retention of Acrylic and Flexible Dentures in Patients with Complete Edentulous Maxillary Arch: A Pilot Study. Ann Ib Postgrad Med. 2022;20(2):151-159. PubMed
28.Kumar N, Koli DK, Jain V, Nanda A. Stress distribution and patient satisfaction in flexible and cast metal removable partial dentures: Finite element analysis and randomized pilot study. J Oral Biol Craniofac Res. 2021;11(4):478-485. doi: 10.1016/j.jobcr.2021.06.004 PubMed
29.Akinyamoju CA, Dosumu OO, Taiwo JO, Ogunrinde TJ, Akinyamoju AO. Oral health-related quality of life: acrylic versus flexible partial dentures. Ghana Med J. 2019;53(2):163-169. doi: 10.4314/gmj.v53i2.12 PubMed
30.Akinyamoju CA, Ogunrinde TJ, Taiwo JO, Dosumu OO. Comparison of patient satisfaction with acrylic and flexible partial dentures. Niger Postgrad Med J. 2017;24(3):143-149. doi: 10.4103/npmj.npmj_54_17 PubMed
31.Manzon L, Fratto G, Poli O, Infusino E. Patient and Clinical Evaluation of Traditional Metal and Polyamide Removable Partial Dentures in an Elderly Cohort. J Prosthodont. 2019;28(8):868-875. doi: 10.1111/jopr.13102 PubMed
32.Sadek SA, Elawady D. Impact of Removable Partial Denture Type on Patient Satisfaction and Abutment Survival Rate-RCT. Open Access Maced J Med Sci. 2019;7(15):2513-2519. doi: 10.3889/oamjms.2019.668 PubMed
33.Fayad MI, Alruwaili HHT, Khan MS, Baig MN. Bite Force Evaluation in Complete Denture Wearer with Different Denture Base Materials: A Randomized Controlled Clinical Trial. J Int Soc Prev Community Dent. 2018;8(5):416-419. doi: 10.4103/jispcd.JISPCD_2_18 PubMed
34.Macura-Karbownik A, Chladek G, Żmudzki J, Kasperski J. Chewing efficiency and occlusal forces in PMMA, acetal and polyamide removable partial denture wearers. Acta Bioeng Biomech. 2016;18(1):137-44. PubMed
35.Hundal M, Madan R. Comparative clinical evaluation of removable partial dentures made of two different materials in Kennedy Applegate class II partially edentulous situation. Med J Armed Forces India. 2015;71(Suppl 2):S306-12. doi: 10.1016/j.mjafi.2012.08.020 PubMed
36.Awawdeh M, Alotaibi MB, Alharbi AH, Alnafisah SA, Alasiri TS, Alrashidi NI. A Systematic Review of Patient Satisfaction With Removable Partial Dentures (RPDs). Cureus. 2024;16(1):e51793. doi: 10.7759/cureus.51793 PubMed
37.Aljabri MK, Ibrahim TO, Sharka RM. Removable partial dentures: Patient satisfaction and complaints in Makkah City, KSA. J Taibah Univ Med Sci. 2017;12(6):561-564. doi: 10.1016/j.jtumed.2017.03.002 PubMed
38.Dhiman RK, Chowdhury SR. Midline Fractures in Single Maxillary Complete Acrylic vs Flexible Dentures. Med J Armed Forces India. 2009;65(2):141-5. doi: 10.1016/s0377-1237(09)80128-7 PubMed
39.Fueki K, Yoshida-Kohno E, Inamochi Y, Wakabayashi N. Patient satisfaction and preference with thermoplastic resin removable partial dentures: a randomised cross-over trial. J Prosthodont Res. 2020;64(1):20-25. doi: 10.1016/j.jpor.2019.05.003 PubMed
40.Subash S, Kumar KA, Karuveettil V. Evaluating the cost-effectiveness of prosthetic rehabilitation for partially edentulous teeth in India: A comparative study of Clasp-Retained RPDs, Thermoplastic Resin RPDs, and Cast Partial Dentures. J Oral Biol Craniofac Res. 2025;15(2):240-245. doi: 10.1016/j.jobcr.2025.01.014 PubMed
41.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. doi: 10.1016/j.jclinepi.2009.06.006 PubMed
42.Tonetti MS, Sanz M, Avila-Ortiz G, et al. Relevant domains, core outcome sets and measurements for implant dentistry clinical trials: The Implant Dentistry Core Outcome Set and Measurement (ID-COSM) international consensus report. Clin Oral Implants Res. 2023;34 Suppl 25:4-21. doi: 10.1111/clr.14074 PubMed
43.Kapur KK. A clinical evaluation of denture adhesives. J Prosthet Dent. 1967;18(6):550-8. doi: 10.1016/0022-3913(67)90221-1 PubMed
44.Slade GD. Derivation and validation of a short-form oral health impact profile. Community Dent Oral Epidemiol. 1997;25(4):284-90. doi: 10.1111/j.1600-0528.1997.tb00941.x PubMed
45.Verma S, Sharma H. Translation and validation of hindi version of oral health impact profile-14, a measure of oral health-related quality of life of geriatrics. Indian J Dent Res. 2019;30(2):180-184. doi: 10.4103/ijdr.IJDR_729_17 PubMed
46.Lawal FB, Taiwo JO, Arowojolu MO. How valid are the psychometric properties of the oral health impact profile-14 measure in adult dental patients in Ibadan, Nigeria? Ethiop J Health Sci. 2014;24(3):235-42. doi: 10.4314/ejhs.v24i3.7 PubMed
47.Myint Oo KZ, Fueki K, Yoshida-Kohno E, Hayashi Y, Inamochi Y, Wakabayashi N. Minimal clinically important differences of oral health-related quality of life after removable partial denture treatments. J Dent. 2020;92:103246. doi: 10.1016/j.jdent.2019.103246 PubMed
48.Slade GD, Spencer AJ. Development and evaluation of the Oral Health Impact Profile. Community Dent Health. 1994;11(1):3-11. PubMed
49.Atchison KA, Dolan TA. Development of the Geriatric Oral Health Assessment Index. J Dent Educ. 1990;54(11):680-7. PubMed
50.Goiato MC, Garcia AR, Dos Santos DM, Zuim PR. Analysis of masticatory cycle efficiency in complete denture wearers. J Prosthodont. 2010;19(1):10-3. doi: 10.1111/j.1532-849X.2009.00520.x PubMed
51.Mendes Senna P, Mourão CF, Teixeira Rodrigues CR, et al. Clinical Assessment of Flexible and Non-Metal Clasp Dentures: A Systematic Review. Prosthesis. 2025;7(4). doi: https://doi.org/10.3390/prosthesis7040091
52.Saad E, Harby N, Baraka O. Clinical and Radiographic Comparison between Acetal Resin and Cobalt-Chromium Partial Dentures in Kennedy’s Class I Situations. J Dent Med Sci. 2021;20:20–25.
53.Fueki K, Ohkubo C, Yatabe M, et al. Clinical application of removable partial dentures using thermoplastic resin-part I: definition and indication of non-metal clasp dentures. J Prosthodont Res. 2014;58(1):3-10. doi: 10.1016/j.jpor.2013.12.002 PubMed
54.Hopewell S, Chan AW, Collins GS, et al. CONSORT 2025 explanation and elaboration: updated guideline for reporting randomised trials. Bmj. 2025;389:e081124. doi: 10.1136/bmj-2024-081124 PubMed
55.Government of Canada. Canadian Dental Care Plan: What is covered [Internet]. Ottawa (ON): Government of Canada. 2025. Updated August 27, 2025. https://www.canada.ca/en/services/benefits/dental/dental-care-plan/coverage.html#wb-cont
56.Government of Canada. Non-Insured Health Benefits program for First Nations and Inuit: Dental Benefits Guide. 2025. Updated August 20, 2025. https://sac-isc.gc.ca/eng/1579538771806/1579538804799
57.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. doi: 10.1136/jech.52.6.377 PubMed
58.Canada’s Drug Agency. Canada's Drug Agency Style: A Guide for Authors and Editors. 2025. Accessed September 16, 2025. https://www.cda-amc.ca/sites/default/files/pdf/style_guide_2025_digital.pdf
Appendix 1: Detailed Methods and Selection of Included Studies
Please note that this appendix has not been copy-edited.
What Is a Rapid Review?
Rapid reviews are based on accelerated and abbreviated systematic review methods, balancing timeliness with rigour, to allow for timely decision-making. Due to these abbreviated methods, rapid reviews have some limitations. For example, our electronic literature search was limited to studies published from 2019 to present, and older studies were identified from a previous CDA-AMC (formerly CADTH) review.26 We attempted to mitigate this potential limitation by searching for and including relevant systematic reviews published in the past 5 years to identify other relevant studies, 1 of which36 was identified through this process. Focusing on more recently published articles may also be more reflective of current practices. Finally, screening, critical appraisal, and data extraction were conducted by 1 reviewer.
Literature Search Methods
The literature search strategy used in this report is an update of 1 developed for a previous CDA-AMC (formerly CADTH) report.26 For the current report, an information specialist conducted a literature search on key resources including MEDLINE, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of health technology assessment agencies in Canada and major international HTA agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevance. The initial search was limited to English-language documents published between January 1, 2009 and August 29, 2019. For the current report, database searches were rerun on August 1, 2025 to capture any articles published or made available since the initial search date. The search of major HTA agencies was also updated to include documents published since January 2019.
Selection Criteria and Methods
One reviewer screened citations and selected studies. Titles and abstracts were reviewed, and potentially relevant articles were retrieved and assessed for inclusion. As an update to a previous CDA-AMC (formerly CADTH) report, articles were screened for eligibility if they were published and indexed over the current search period or were included in the 2019 CDA-AMC report.26 In addition, we identified 1 eligible systematic review36 from the current search that had broader eligibility criteria than, but focused on only 1 outcome domain of relevance (patient satisfaction) to, the current review. Given that some of the included studies included other outcomes of relevance to our review, it was deemed important to review the primary study records to capture additional relevant outcomes. Therefore, this systematic review was excluded from the current review, and its included studies were screened for relevance; most of those of relevance to the current Rapid Review were previously identified in the 2019 report, and we included 1 additional study.32
Economic studies conducted in health care systems outside of Canada were not eligible for this review due to their uncertain or limited transferability to Canada. In the absence of economic studies conducted in health care systems within Canada, economic studies conducted outside of Canada are provided in Appendix 6 and briefly discussed.
The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Exclusion Criteria
Articles were excluded for the following reasons:
did not meet the selection criteria outlined in Table 1
were duplicate publications or were published before 2019, unless included in the previous CDA-AMC (formerly CADTH) report26 or a relevant systematic review
were systematic reviews in which all relevant studies were captured in other more recent or more comprehensive systematic reviews
were primary studies captured in 1 or more included systematic reviews, unless the systematic review was deemed to provide insufficient information (e.g., limited outcomes)
were in vitro studies, simulation or lab-based studies, case reports, or case series
were guidelines with unclear methodology
economic studies conducted in health care systems outside of Canada.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the Downs and Black checklist57 for randomized and nonrandomized studies. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Data Extraction
One reviewer extracted data directly into tables created in Microsoft Word, modifying them as necessary. The extracted information included study characteristics, methodology (e.g., study design), and characteristics of the population (including information on factors associated with health equity), intervention, comparator, and results regarding the outcomes of interest. Details are reported in Appendix 3. The PROGRESS-Plus2 framework guided equity considerations and includes place of residence, race (or ethnicity, culture), occupation, gender or sex, religion, education, SES, and social capital. These characteristics are discussed across the evidence, when available.
When reporting on sex, gender, race, or ethnicity in this Rapid Review, we retained the language used by the original study authors, and, whenever possible, we referred to these groups based on guidance from the CDA-AMC style guide58 at the time of this Rapid Review, with an understanding that language is constantly evolving.
Appendix 2: Selection of Included Studies
Please note that this appendix has not been copy-edited.
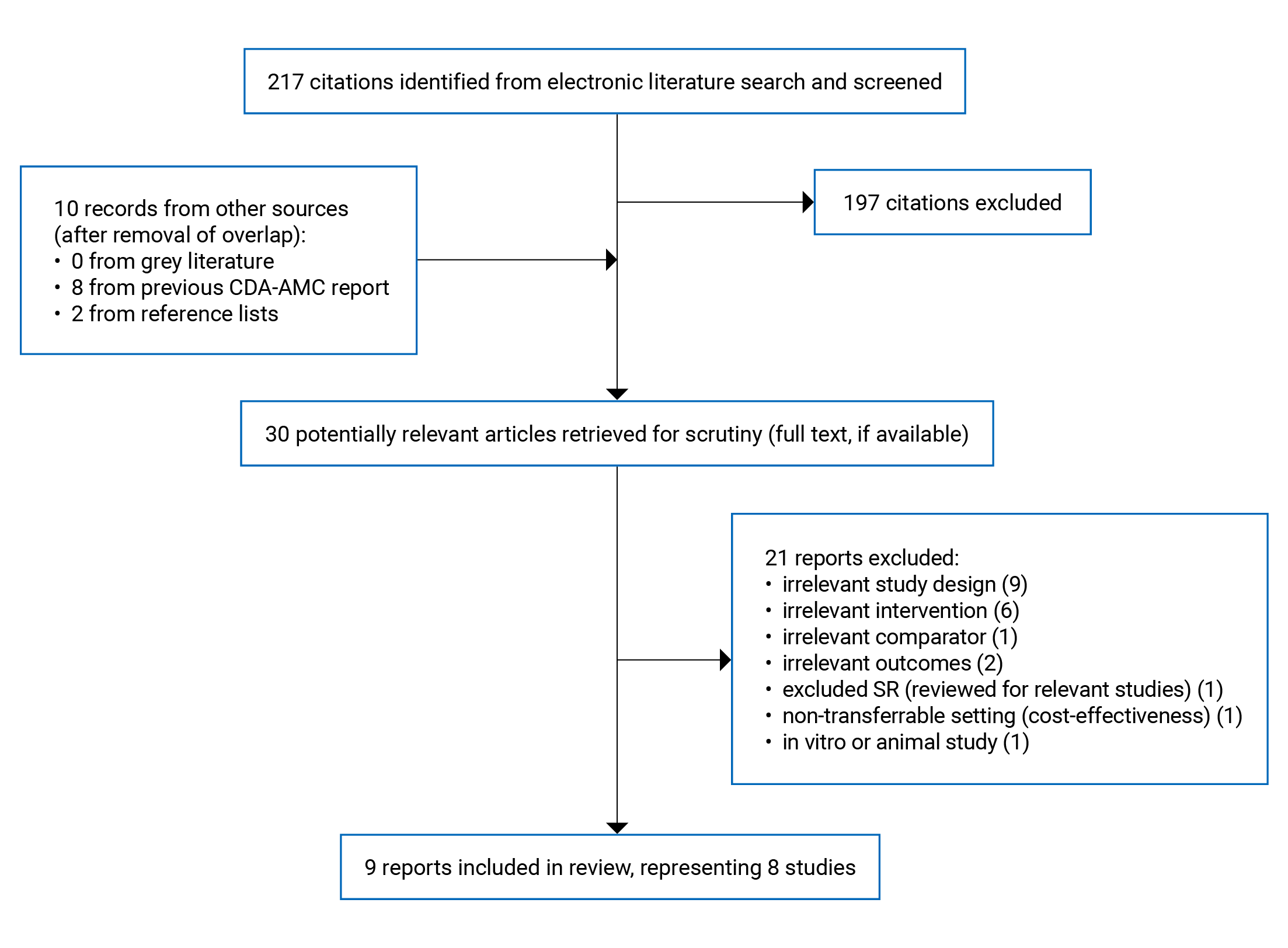
Appendix 3: Characteristics of Included Publications
Please note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Primary Clinical Studies
Study citation, country, funding source | Study design and setting | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Olawale et al. (2022)27 Country: Nigeria Funding source: NR | Crossover RCT; additional details, including the number of centres, were not specified Consecutive individuals consenting to participate Recruitment and treatment between March 2019 and February 2020 | Summary eligibility criteria: Patients with complete edentulous maxillary arch for at least 6 months, any dentition on lower arch Exclusions: Bruxism, previous chemotherapy or radiotherapy, allergy to acrylic resin, abnormal tongue movement or size, xerostomia or excessive salivation, unfavourable ridge undercut Number of participants: 10 Age (years), mean (SD): 66.5 (9.7); 80% 60 years and older Sex or gender: 50% female, 50% male Cause of edentulism: NR Missing teeth: 100% completely edentulous upper jaw (eligibility); 70% completely edentulous lower jaw; 30% partial edentulous lower jaw Other PROGRESS-Plus criteria: NRa | Intervention: Flexite plus (thermoplastic acrylic) RCD (n = 10) Comparator: Acrylic RCD (pink shade, heat cure acrylic resin, company NR) (n = 10) Other select details: Identical cast was made for each denture and data collected by 1 researcher | Relevant outcomes:
Follow-up: Up to 3 months after using each denture |
Kumar et al. (2021)28 Country: India Funding source: Authors reported that no specific funding was received for this research | A single-centre, prospective, concurrent, parallel-arm RCT Prosthodontics, tertiary care, metropolitan city Patients were recruited between December 2016 to October 2017 | Summary eligibility criteria: Aged 30 to 70 years, with Kennedy Class I, partially edentulous mandibular arch, completely dentate maxillary arch. No previous denture use, healthy mucosa and periodontal status. Exclusions: Systemic medical conditions and previous denture use Number of participants: 22 Age (years), mean (SD): Intervention: 42.92 (8.15) Comparator: 42.50 (7.49) Sex or gender: 54.54% females and 45.45% males; authors reported as “gender” Cause of edentulism: NR Missing teeth: Refer to eligibility, no other details reported Other PROGRESS-Plus criteria: NRa | Intervention: Thermoplastic polyacetyl based flexible RPD (company NR) (n = 11) Comparator: Cast metal RPD (company NR) (n = 11) Other select details: All patients were treated by the same single operator | Relevant outcomes:
Follow-up: 1 year |
Akinyamoju et al. (2019)29 and Akinyamoju et al. (2017)30 Country: Nigeria Funding source: Authors reported that no specific funding was received for this research | Single-centre crossover RCT Prosthetics clinic at a tertiary university hospital Patients were recruited between November 2014 and April 2015 | Summary eligibility criteria: age ≥ 16 years, with 1 to 3 missing teeth in the anterior region of the maxillary or mandibular arch (Kennedy class IV and anterior class III edentulous spaces) for at least 3 months, good periodontal health or mild periodontal disease, mild to moderate Seibert’s classes I and II edentulous ridge, no previous denture use. Number of participants: 32 recruited, 2 lost to follow-up after delivery of the initial denture (1 flexible, 1 acrylic), 30 analyzed Age (years), mean (SD): 33.8 (10.01), range: 16 to 51 Sex or gender: 50% reported as male (sex); other sexes or genders NR Cause of edentulism: 90% trauma (e.g., road traffic accident, falls, assault, sports); 10% periodontal disease Missing teeth: All patients were partially dentate, and 91% were replacing maxillary teeth. The mean (SD) duration of edentulism was 11.37 (10.52) years Race or ethnicity (Tribe): 90% Yoruba, 6.7% Igbo, 3.3% Ibibio Place of residence: 90% urban, 10% suburban SES: Reported as 60% lower class; 30% lower middle class; 10% upper middle class Education: 6.7% completed up to primary school; 33.3% completed up to secondary school; 16.7% completed postsecondary (technical); 43.3% completed tertiary Marital status: 56.7% married, 43.3% single Other PROGRESS-Plus criteria: NRa | Intervention: Valplast flexible RPD (Dentiflex-Roko) (n = 30) Comparator: All-acrylic RPD (Trevalon) (n = 30) Other select details: All laboratory procedures were done by 1 dental technologist. Oral prophylaxis was done for all patients before denture fitting was complete. Postinsertion instructions were given to patients in oral and written forms. | Relevant outcomes:
Follow-up: up to 1 month of denture use |
Manzon et al. (2019)31 Country: Not stated; author affiliation is in Italy Funding source: NR | Nonrandomized controlled study, allocation method unclearc; details regarding the number of centres and recruitment dates were not reported | Summary eligibility criteria: ≥ 65 years, requiring removable partial dentures of maxillary arch, missing no more than 4 contiguous teeth and alveolar bone retraction < 4.5 mm as measured by OPT Exclusion: Poor oral hygiene, periodontitis, dental mobility, diabetes, ongoing chemotherapy Number of participants: 120 Age (years), mean (range): 73 (65 to 84) Sex or gender: 60% were female and 40% were male (sex or gender not specified) Cause of edentulism: NR Missing teeth: Refer to eligibility, no other details reported Other PROGRESS-Plus criteria: NRa | Intervention:
Comparators:
Other select details: Patients received detailed information as recommended by manufacturers. Patients with Valplast RPD were advised to only brush manually with a soft brush. Patients with Cr-Co RPD were furnished with a denture brush and nonabrasive paste. | Relevant outcomes:
Follow-up: 1 year |
Sadek and Elawady (2019)32 Country: Egypt Funding source: Authors reported that no specific funding was received for this research | Single-centre parallel-group randomized study Outpatient clinic of a removable prosthodontics university department Details regarding recruitment dates were not reported | Summary eligibility criteria: Kennedy Class II modification 1, partially edentulous mandible, opposing maxillary teeth, periodontally healthy remaining teeth, “medically free” Number of participants: 42 Age (years), range: 45 to 60 Sex or gender: NR Cause of edentulism: NR Missing teeth: Refer to eligibility, no other detail reported Other PROGRESS-Plus criteria: NRa | Intervention:
Comparators:
Other select details: Participants were instructed to maintain proper denture hygiene: remove dentures for sleeping hours, keep it in tap water, clean the dentures after each meal under tap water only, not to use any mouthwashes or denture cleansers during the study period and not to use any denture adhesives | Relevant outcomes:
Follow-up: Up to 24 months; most data collection at 3 months |
Fayad et al. (2018)33 Country: Saudi Arabia Funding source: Authors reported that no specific funding was received for this research | Single-centre, prospective, parallel-arm randomized trial Outpatient clinic, university Recruitment between June 2016 to June 2017 | Summary eligibility criteria: Completely edentulous patients, no psychiatric disease or movement disorders Number of participants: 100 Age (years), mean: 52 Sex or gender: NR Cause of edentulism: NR Missing teeth: Refer to eligibility, no other details reported Other PROGRESS-Plus criteria: NRa | Intervention: Vertex ThermoSens thermoplastic RCD (Vertex-Dental B.V.) (n = 50) Comparator: Conventional heat-cured acrylic RCD (Vertex Regular, Vertex-Dental B.V.) (n = 50) Other select information: NR | Relevant outcomes:
Follow-up: 6 months |
Macura-Karbownik et al. (2016)34 Country: Not stated; all authors cite affiliations from Poland Funding source: NR | Randomized, crossover study; 3 dentures were tested in all patients Other details, including the number of centres and dates of recruitment, were NR | Summary eligibility criteria: Patients with unilateral or bilateral loss of 3 to 6 teeth from 1 dental arch (Kennedy class III) and natural teeth in the opposing dental arch, at least 2 years since the last episode of tooth loss, no pain or temporomandibular abnormalities Number of participants: 30 Age (years), mean (range): 49.6 (35 to 60 years) Sex or gender: 12 men and 18 women; NR how sex or gender was defined Cause of edentulism: NR Missing teeth: 16 patients with bilateral teeth loss, 14 with unilateral teeth loss Other PROGRESS-Plus criteria: NRa | Intervention:
Comparators:
Other select details: NR | Relevant outcomes:
Follow-up: 90 days |
Hundal and Madan (2015)35 Country: India Funding source: NR | Single-centre parallel-group RCT Outpatient department of a military dental centre Participants were randomly selected from those who reported to the centre. Dates of recruitment were not reported. | Summary eligibility criteria: Kennedy Applegate class II partially edentulous, medically fit with average oral health status Number of participants: 30 Age (years), range: 25 to 45 years Sex or gender: NR Cause of edentulism: NR Missing teeth: NR SES: Patients were reported to be from middle-income group or socioeconomic strata Other PROGRESS-Plus criteria: NRa | Intervention: Valplast flexible RPD made of nylon-based super polyamide resin (n = 15) Comparator: conventional cast Cr-Co alloy (clasps with occlusal rests) and PMMA denture base RPD (ProBase Hot, Ivoclar Vivadent) (n = 15) Other select details: NR | Relevant outcomes:
Follow-up: 1.5 years, outcome measurement timing is unclear |
Cr-Co = chromium-cobalt; NR = not reported; OHIP-14 = Oral Health Impact Profile−14; OHRQoL = Oral Health-Related Quality of Life; OPT = orthopantomography; PMMA = polymethyl methacrylate; RCD = removable complete denture; RCT = randomized controlled trial; RPD = removable partial denture; SD = standard deviation; SES = socioeconomic status.
aThe main PROGRESS-Plus criteria include place of residence, race, ethnicity, culture, language, occupation, gender, sex, religion, education, SES, social capital, personal characteristics associated with discrimination (e.g., age, disability), features of relationships, and time-dependent relationships.2
bThis study stated they measured patient satisfaction but used a tool typically described to measure OHRQoL (Oral Health Impact Profile−14).
cThis study was included although there is uncertainty regarding its study design due to lack of clear reporting on study group allocation methods and may be an observational study.
Appendix 4: Critical Appraisal of Included Publications
Please note that this appendix has not been copy-edited.
Table 3: Clinical Effectiveness of Flexible Dentures: Strengths and Limitations of Clinical Studies Using the Downs and Black Checklist57
Strengths | Limitations |
|---|---|
Olawale et al. (2022)27 | |
|
|
Kumar et al. (2021)28 | |
|
|
|
|
Manzon et al. (2019)31 | |
|
|
Sadek and Elawady (2019)32 | |
|
|
Fayad et al. (2018)33 | |
|
|
Macura-Karbownik et al. (2016)34 | |
|
|
Hundal and Madan (2015)35 | |
|
|
AE = adverse event.
Appendix 5: Main Study Findings
Please note that this appendix has not been copy-edited.
Table 4: Summary of Findings by Outcome — Masticatory Function
Citation and study design Outcome name and measurement method | Time points | Intervention groups and number of participants (n) | Outcome result | Within-group difference from baseline (P value) | Between-group difference (P value) |
|---|---|---|---|---|---|
Follow-up: Up to 3 months | |||||
Sadek and Elawady (2019)32 Parallel-group RCT Outcome: Chewing Function Measurement: Chewing Function Quality questionnairea (lower is better) | Baseline and 3-month follow-up | Thermopress RPD (n = 14) | Results shared in figures and not extracted – groups similar at baseline | NR | One-way ANOVA, Tukey’s post hoc test: Thermopress significantly lower than other groups (P value < 0.05) |
Vitallium RPD (n = 14) | NR | ||||
Vitallium RPD with surveyed bridge (n = 14) | NR | ||||
Macura-Karbownik et al. (2016)34 RCT-CO Outcome: Chewing efficiency Measurement: Chewing efficiency coefficientb | Baselinec | Total sample – without denture (n = 30) | Median (IQR): 0.77 (0.12) Range: 0.63 to 0.97 | NA | NR |
7 days | Valplast polyamide RPDs (n = 30) | Median (IQR): 0.79 (0.06) Range: 0.69 to 0.95 | P = 1.000 | Flexible vs. acetal: P < 0.001 Flexible vs. PMMA: P < 0.001 PMMA vs. acetal: P = 0.005 | |
Acetal RPDsd (n = 30) | Median (IQR): 0.89 (0.06) Range: 0.81 to 1.09 | P < 0.001 | |||
PMMA RPDs (n = 30) | Median (IQR): 1.02 (0.13) Range: 0.90 to 1.29 | P < 0.001 | |||
1 month | Valplast polyamide RPDs (n = 30) | Median (IQR): 0.81 (0.09) Range: 0.73 to 0.96 | NR | NR | |
Acetal RPDsd (n = 30) | Median (IQR): 0.94 (0.11) Range: 0.82 to 1.15 | NR | |||
PMMA RPDs (n = 30) | Median (IQR): 1.07 (0.17) Range: 0.93 to 1.32 | NR | |||
3 months | Valplast polyamide RPDs (n = 30) | Median (IQR): 0.80 (0.11) Range: 0.68 to 0.96 | NR | NR | |
Acetal RPDsd (n = 30) | Median (IQR): 0.93 (0.13) Range: 0.77 to 1.16 | NR | |||
PMMA RPDs (n = 30) | Median (IQR): 1.10 (0.17) Range: 0.87 to 1.34 | NR | |||
Macura-Karbownik et al. (2016)34 RCT-CO Outcome: Occlusal force Measurement: Measured using a dynamometere (unit: Newtons) | Baselinee | Valplast polyamide RPDs (n = 30) | Median (IQR): 48 (44) Range: 10 to 220 | NA | NR |
Acetal RPDsd (n = 30) | Median (IQR): 81 (59) Range: 29 to 263 | NA | |||
PMMA RPDs (n = 30) | Median (IQR): 100 (71) Range: 38 to 272 | NA | |||
7 days | Valplast polyamide RPDs (n = 30) | Median (IQR): 50 (47) Range: 10 to 208 | NR | NR | |
Acetal RPDsd (n = 30) | Median (IQR): 81 (64) Range: 30 to 260 | NR | |||
PMMA RPDs (n = 30) | Median (IQR): 90 (83) Range: 38 to 250 | NR | |||
1 month | Valplast polyamide RPDs (n = 30) | Median (IQR): 48 (50) Range: 10 to 220 | NR | NR | |
Acetal RPDsd (n = 30) | Median (IQR): 85 (59) Range: 34 to 263 | NR | |||
PMMA RPDs (n = 30) | Median (IQR): 106 (71) Range: 50 to 269 | NR | |||
3 months | Valplast polyamide RPDs (n = 30) | Median (IQR): 39 (42) Range: 14 to 178 | NR | P < 0.001 Post hoc test: Flexible vs. acetal: P < 0.001 Flexible vs. PMMA: P < 0.001 PMMA vs. acetal: P = 0.048 | |
Acetal RPDsd (n = 30) | Median (IQR): 71 (41) Range: 29 to 250 | NR | |||
PMMA RPDs (n = 30) | Median (IQR): 99 (64) Range: 45 to 272 | NR | |||
Follow-up: Up to 6 months | |||||
Fayad et al. (2018)33 Parallel-group RCT Outcome: Maximum bite force Measurement: Occlusal force metref | Baseline | Vertex ThermoSens thermoplastic RCD (n = 50) | Mean (SD): 34.37 (12.25), SE: 1.93 | NA | 0.819 |
Vertex Regular, conventional heat-cured acrylic RCD (n = 50) | Mean (SD): 33.75 (12.07), SE: 1.90 | NA | |||
6 months | Vertex ThermoSens thermoplastic RCD (n = 50) | Mean (SD): 47.50 (11.30), SE: 1.74 | NR | 0.007 | |
Vertex Regular, conventional heat-cured acrylic RCD (n = 50) | Mean (SD): 39.37 (14.85), SE: 2.34 | NR | |||
Follow-up: Up to 1 year | |||||
Manzon et al. (2019)31 Nonrandomized controlled study Outcome: Chewing ability Measurement: Subjective response to 1 question (2 response options) | 1 year | Valplast flexible RPD (n = 40) | 0.27 | ||
Kennedy Class I or II | Not satisfied: 6 (30%) Satisfied: 14 (70%) | NA | |||
Kennedy Class III or IV | Not satisfied 2 (10%) Satisfied: 18 (90%) | NA | |||
Cr-Co RPD (n = 40) | |||||
Kennedy Class I or II | Not satisfied: 4 (20%) Satisfied: 16 (80%) | NA | |||
Kennedy Class III or IV | Not satisfied 2 (10%) Satisfied: 18 (90%) | NA | |||
PMMA-RPD (n = 40) | |||||
Kennedy Class I or II | Not satisfied: 7 (35%) Satisfied: 13 (65%) | NA | |||
Kennedy Class III or IV | Not satisfied 5 (25%) Satisfied: 15 (75%) | NA | |||
CO = crossover; IQR = interquartile range; NA = not applicable; NR = not reported; PMMA = polymethyl methacrylate; RCD = removable complete denture; RCT = randomized controlled trial; RPD = removable partial denture; SD = standard deviation; vs. = versus.
aPatient or caregiver reported 10 questions about potential difficulties, 5-point Likert scale with scores 0 (Never) to 4 (Very often).
bDefined based on the mass of particles of various sizes remaining after chewing 3 g of peanuts for 40 chewing cycles. Theoretical values of the chewing efficiency coefficient could range between 1.5 and 4.5. More details and calculations are provided in the publication.34
cIt was unclear from this report if baseline measurements were conducted with or without dentures inserted.
dAcetal-based framework and clasps, PMMA base, and teeth.
eDetails in publication.34
fPatients were instructed to bite as powerfully as possible 3 times per side with a rest time of 2 minutes in between. The highest of the 3 records was the patient’s maximum bite force.
Table 5: Summary of Findings by Outcome — Aesthetics
Citation and study design Outcome name and measurement method | Intervention and comparator group(s) and number of participants (n) | Outcome label | Outcome result n (%) | Between-group difference (as reported) | P value for between-group difference |
|---|---|---|---|---|---|
Follow-up: 1 month | |||||
Akinyamoju et al. (2019)29 and Akinyamoju et al. (2017)30 CO-RCT Outcome: Satisfaction with appearance Measurement: Interviewer-administered 100 mm VAS, reclassified into 4 categoriesa | Valplast flexible RPDs (n = 30) | Totally dissatisfied | 0 (0%) | More satisfied with: flexible RPD: n = 16 acrylic RPD: n = 4 Similarly satisfied with both: n = 10 | P value for Wilcoxon signed rank test: 0.06b |
Slightly dissatisfied | 1 (3.3%) | ||||
Slightly satisfied | 2 (6.7%) | ||||
Satisfied | 27 (90%) | ||||
Acrylic RPDs (n = 30) | Totally dissatisfied | 1 (3.3%) | |||
Slightly dissatisfied | 1 (3.3%) | ||||
Slightly satisfied | 5 (16.7%) | ||||
Satisfied | 23 (76.7%) | ||||
Follow-up: 1 year | |||||
Manzon et al. (2019)31 Nonrandomized controlled study Outcome: Aesthetic satisfaction Measurement: 1 question (3 response options) | Valplast flexible RPD (n = 40) | NR | P < 0.001 (Chi-square) | ||
Kennedy Class I or II | Not satisfied | 1 (5%) | |||
Satisfied | 18 (90%) | ||||
Very satisfied | 1 (5%) | ||||
Kennedy Class III or IV | Not satisfied | 0 (0%) | |||
Satisfied | 15 (75%) | ||||
Very satisfied | 5 (25%) | ||||
Cr-Co RPD (n = 40) | |||||
Kennedy Class I or II | Not satisfied | 12 (60%) | |||
Satisfied | 8 (40%) | ||||
Very satisfied | 0 (0%) | ||||
Kennedy Class III or IV | Not satisfied | 13 (65%) | |||
Satisfied | 7 (35%) | ||||
Very satisfied | 0 (0%) | ||||
PMMA-RPD (n = 40) | |||||
Kennedy Class I or II | Not satisfied | 14 (70%) | |||
Satisfied | 6 (30%) | ||||
Very satisfied | 0 (0%) | ||||
Kennedy Class III or IV | Not satisfied | 5 (25%) | |||
Satisfied | 15 (75%) | ||||
Very satisfied | 0 (0%) | ||||
Follow-up: Unclearc | |||||
Hundal and Madan (2015)35 Parallel-group RCT Outcome: Aesthetics, subjective assessment Measurement: 1 question (3 response options converted to scores 0 to 2 — higher is better) | Valplast RPD (n = 15) | NA | Mean (SD): 1.67 (0.488) Range: 1 to 2 Median: 2 | NR | Uncleard |
Cr-Co alloy with PMMA base RPD (n = 15) | NA | Mean (SD): 0.67 (0.488) Range: 0 to 1 Median: 1 | NR | ||
Hundal and Madan (2015)35 Parallel-group RCT Outcome: Aesthetics, objective assessment Measurement: Clinician assessment with extraoral and intraoral photographs (3 response scores 0 to 2 — higher is better) | Valplast RPD (n = 15) | NA | Mean (SD): 1.4 (0.507) Range: 1 to 2 Median: 1 | NR | Uncleard |
Cr-Co alloy with PMMA base RPD (n = 15) | NA | Mean (SD): 0 (0) Range: 0 to 0 Median: 0 | NR | ||
CO = crossover; Cr-Co = chromium-cobalt; NA = not applicable; NR = not reported; PMMA = polymethyl methacrylate (acrylic); RCT = randomized controlled trial; RPD = removable partial denture; SD = standard deviation; VAS = visual analogue scale.
aThe scores from the VAS, a continuous graphical rating scale from 0 to 100 were classified as totally dissatisfied (0 to 31), slightly dissatisfied (> 31 to 50), slightly satisfied (> 50 to 79), and satisfied (80 to 100).
bSubgroup analyses were also conducted for age, gender, and socioeconomic status; no significant differences reported based on P ≤ 0.05 (unclear power to detect differences)
CTiming of outcome assessment is unclear for this study. After insertion of the prosthesis, the “clinical performances were reviewed periodically during one and half years for the nine parameters as listed in Table 1. The periodicity of recall was twenty-four hours, one week, one month, three months and six months after insertion of prostheses.”
dAbstract states: “statistically significant results were obtained in favor of flexible RPDs, in the parameters of ‘aesthetics’.” No other details are provided.
Table 6: Summary of Findings by Outcome — Speech or Phonetics
Citation and study design | Outcome name and measurement method | Intervention and comparator groups and number of participants (n) | Outcome label | Outcome result n (%) | Difference from baseline | Between-group difference (as reported) | P value for between-group difference |
|---|---|---|---|---|---|---|---|
Follow-up: 1 month | |||||||
Akinyamoju et al. (2019)29 and Akinyamoju et al. (2017)30 CO-RCT | Outcome: Satisfaction with ability to speak Measurement: 100 mm VAS, categorized into 1 of 4 groupsa | Valplast flexible RPDs (n = 30) | Totally dissatisfied | 0 (0%) | NR | More satisfied with: flexible RPD: n = 19 acrylic RPD: n = 6 Similarly satisfied with both: n = 11 | P value for Wilcoxon signed rank test: 0.20b |
Slightly dissatisfied | 2 (6.7%) | NR | |||||
Slightly satisfied | 3 (10.0%) | NR | |||||
Satisfied | 25 (83.3%) | NR | |||||
Acrylic RPDs (n = 30) | Totally dissatisfied | 0 (0%) | NR | ||||
Slightly dissatisfied | 2 (6.7%) | NR | |||||
Slightly satisfied | 5 (16.7%) | NR | |||||
Satisfied | 23 (76.7%) | NR | |||||
Outcome: Trouble pronouncing words Measurement: Question on OHIP-14 questionnaire | Valplast flexible RPDs (n = 30) | Prevalence of grouped responses (occasionally, fairly often and very often)c | 6 (20.0%) | MD (SD): 0.7 (2.2) CI: - 0.1 to 1.5 P = 0.08 | NR | NR | |
Acrylic RPDs (n = 30) | 11 (36.6%) | MD (SD): 0.5 (2.4) CI: - 0.4 to 1.4 P = 0.29 | |||||
Follow-up: 1 year | |||||||
Manzon et al. (2019)31 Nonrandomized controlled study | Outcome: Speech defects/difficulties Measurement: Question with 2 response options | Valplast flexible RPD (n = 40) | P < 0.002 (Chi-square) | ||||
Kennedy Class I or II | Yes | 0 (0%) | NR | NR | |||
No | 20 (100%) | NR | NR | ||||
Kennedy Class III or IV | Yes | 0 (0%) | NR | NR | |||
No | 20 (100%) | NR | NR | ||||
Cr-Co RPD (n = 40) | |||||||
Kennedy Class I or II | Yes | 0 (0%) | NR | NR | |||
No | 20 (100%) | NR | NR | ||||
Kennedy Class III or IV | Yes | 0 (0%) | NR | NR | |||
No | 20 (100%) | NR | NR | ||||
PMMA-RPD (n = 40) | |||||||
Kennedy Class I or II | Yes | 5 (25%) | NR | NR | |||
No | 15 (75%) | NR | NR | ||||
Kennedy Class III or IV | Yes | 2 (10%) | NR | NR | |||
No | 18 (90%) | NR | NR | ||||
CI = confidence interval; CO = crossover; MD = mean difference; NR = not reported; OHIP-14 = Oral Health Impact Profile-14; RCT = randomized controlled trial; RPD = removable partial denture; SD = standard deviation; VAS = visual analogue scale.
aThe scores from the VAS, a continuous graphical rating scale from 0 to 100 were classified as totally dissatisfied (0 to 31), slightly dissatisfied (> 31 to 50), slightly satisfied (> 50 to 79), and satisfied (80 to 100).
bSubgroup analyses were conducted for age, gender, and socioeconomic status; no significant differences reported based on P ≤ 0.05 (unclear power to detect differences).
cBaseline prevalence (total sample, n = 30) of grouped responses (occasionally, fairly often, or very often) 14 (46.7%).
Table 7: Summary of Findings by Outcome — Denture Retention
Citation and study design Outcome name and measurement method | Time points | Intervention and comparison groups and number of participants (n) | Outcome label | Outcome result | Between-group difference (P value) |
|---|---|---|---|---|---|
Follow-up: Up to 3 months | |||||
Olawale et al. (2022)27 RCT-CO Outcome: Retention Measurement: Kapur’s retention score, categorizeda | 7 days | Flexite plus RCDs (n = 10) | No retention | 0 (0%) | NR |
Minimum retention | 1 (10%) | ||||
Moderate retention | 6 (60%) | ||||
Good retention | 3 (30%) | ||||
Acrylic RCDs (n = 10) | No retention | 0 (0%) | |||
Minimum retention | 0 (0%) | ||||
Moderate retention | 3 (30%) | ||||
Good retention | 7 (70%) | ||||
1 month | Flexite plus RCDs (n = 10) | No retention | 0 (0%) | ||
Minimum retention | 0 (0%) | ||||
Moderate retention | 5 (50%) | ||||
Good retention | 5 (50%) | ||||
Acrylic RCDs (n = 10) | No retention | 0 (0%) | |||
Minimum retention | 0 (0%) | ||||
Moderate retention | 1 (10%) | ||||
Good retention | 9 (90%) | ||||
3 months | Flexite plus RCDs (n = 10) | No retention | 0 (0%) | ||
Minimum retention | 0 (0%) | ||||
Moderate retention | 7 (70%) | ||||
Good retention | 3 (30%) | ||||
Acrylic RCDs (n = 10) | No retention | 0 (0%) | |||
Minimum retention | 0 (0%) | ||||
Moderate retention | 0 (0%) | ||||
Good retention | 10 (100%) | ||||
Olawale et al. (2022)27 RCT-CO Outcome: Retention Measurement: 100 mm VAS, categorized into 4 groupsb | 3 months | Flexite plus RCDs (n = 10) | Totally dissatisfied | 0 (0%) | 0.157 |
Dissatisfied | 2 (20%) | ||||
Satisfied | 3 (30%) | ||||
Totally satisfied | 5 (50%) | ||||
Mean VAS score (SD) | 73.0 (15.67) | ||||
Acrylic RCDs (n = 10) | Totally dissatisfied | 0 (0%) | |||
Dissatisfied | 1 (10%) | ||||
Satisfied | 1 (10%) | ||||
Totally satisfied | 8 (80%) | ||||
Mean VAS score (SD) | 84.6 (16.88) | ||||
Olawale et al. (2022)27 RCT-CO Outcome: Retention Measurement: Pull digital force gauge (units: Newtons) | 1 week | Flexite plus RCDs (n = 10) | NA | Mean (SD): 27.39 (14.50) | 0.050 |
Acrylic RCDs (n = 10) | NA | Mean (SD): 34.17 (17.76) | |||
1 month | Flexite plus RCDs (n = 10) | NA | Mean (SD): 28.64 (13.34) | 0.016 | |
Acrylic RCDs (n = 10) | NA | Mean (SD): 37.24 (18.16) | |||
3 months | Flexite plus RCDs (n = 10) | NA | Mean (SD): 29.88 (14.36) | 0.002 | |
Acrylic RCDs (n = 10) | NA | Mean (SD): 39.70 (17.09) | |||
Follow-up: Up to 1 year | |||||
Manzon et al. (2019)31 Nonrandomized controlled study Outcome: Retention of the prosthesis Measurement: Patient-reported, subjective response 1 question (2 response options) | 1 year | Valplast flexible RPD (n = 40) | < 0.001 | ||
Kennedy Class I or II | Same as before | 11 (55%) | |||
Decreased | 9 (45%) | ||||
Kennedy Class III or IV | Same as before | 13 (65%) | |||
Decreased | 7 (35%) | ||||
Cr-Co RPD (n = 40) | |||||
Kennedy Class I or II | Same as before | 20 (100%) | |||
Decreased | (0%) | ||||
Kennedy Class III or IV | Same as before | 20 (100%) | |||
Decreased | (0%) | ||||
PMMA-RPD (n = 40) | |||||
Kennedy Class I or II | Same as before | 20 (100%) | |||
Decreased | (0%) | ||||
Kennedy Class III or IV | Same as before | 20 (100%) | |||
Decreased | (0%) | ||||
CO = crossover; Cr-Co = chromium-cobalt; NA = not applicable; NR = not reported; PMMA = polymethyl methacrylate; RCD = removable complete denture; RCT = randomized controlled trial; RPD = removable partial denture; SD = standard deviation; VAS = visual analogue scale.
aKapur’s score is calculated based on a standard questionnaire;43 and was graded. Grade 0 = No retention (the denture displaces itself when patient talks); 1 = Minimum retention (denture offers slight resistance to vertical pull and no resistance to lateral pull); 2 = Moderate retention (denture offers slight resistance to lateral pull); and 3 = Good retention (denture offers maximum resistance to vertical and lateral forces).
bThe scores from the VAS, a continuous graphical rating scale from 0 to 100 were classified as: totally dissatisfied (0 to 30), dissatisfied (> 31 to 50), satisfied (> 50 to 79) and totally satisfied (80 to 100).
Table 8: Summary of Findings by Outcome — Comfort or Pain While Eating or Chewing
Citation and study design Outcome name and measurement method | Intervention group(s) and number of participants (n) | Outcome label | Outcome result | Difference from baseline | Between-group difference (as reported) | P value for between-group difference |
|---|---|---|---|---|---|---|
Follow-up: 1 month | ||||||
Akinyamoju et al. (2019)29 and Akinyamoju et al. (2017)30 CO- RCT Outcome: Satisfaction with comfort while eating Measurement: 100 mm VAS, categorized into 4 groupsa | Valplast flexible RPDs (n = 30) | Totally dissatisfied | 2 (6.7%) | NR | More satisfied with: flexible RPD: n = 19 acrylic RPD: n = 6 Similarly satisfied with both: n = 5 | P value for Wilcoxon signed rank test: 0.06b |
Slightly dissatisfied | 0 (0%) | |||||
Slightly satisfied | 3 (10.0%) | |||||
Satisfied | 25 (83.3%) | |||||
Acrylic RPDs (n = 30) | Totally dissatisfied | 1 (3.3%) | NR | |||
Slightly dissatisfied | 1 (3.3%) | |||||
Slightly satisfied | 8 (26.7%) | |||||
Satisfied | 20 (66.7%) | |||||
Akinyamoju et al. (2019)29 and Akinyamoju et al. (2017)30 CO-RCT Outcome: Found it uncomfortable to eat Measurement: Question on OHIP-14 questionnaire | Valplast flexible RPDs (n = 30) | Prevalence of grouped responses (occasionally, fairly often, and very often)c | 9 (30.0%) | MD (SD) = 0.2 (2.3) CI = –0.1 to 0.7 P = 0.69 | NR | NR |
Acrylic RPDs (n = 30) | 9 (30.0%) | MD (SD) = 0.1 (2.0) CI = –0.9 to 0.7 P = 0.86 | ||||
Akinyamoju et al. (2019)29 and Akinyamoju et al. (2017)30 CO- RCT Outcome: Painful aching in mouth Measurement: Question on OHIP-14 questionnaire | Valplast flexible RPDs (n = 30) | Prevalence of grouped responses (occasionally, fairly often and very often)c | 4 (13.3%) | MD (SD) = 0.1 (1.4) CI = –0.4 to 0.6 P = 0.69 | NR | NR |
Acrylic RPDs (n = 30) | 2 (6.7%) | MD (SD) = 0.5 (1.3) CI = 0.0 to 1.0 P = 0.04 | ||||
Follow-up: 1 year | ||||||
Manzon et al. (2019)31 Nonrandomized controlled study Outcome: Discomfort/pain during mastication Measurement: Patient-reported, subjective response 1 question (2 response options) | Valplast flexible RPD (n = 40) | NA | NR | 0.10 | ||
Kennedy Class I or II | Yes | 11 (55%) | ||||
No | 9 (45%) | |||||
Kennedy Class III or IV | Yes | 6 (30%) | ||||
No | 14 (70%) | |||||
Cr-Co RPD (n = 40) | NA | |||||
Kennedy Class I or II | Yes | 5 (25%) | ||||
No | 15 (75%) | |||||
Kennedy Class III or IV | Yes | 3 (15%) | ||||
No | 17 (85%) | |||||
PMMA-RPD (n = 40) | NA | |||||
Kennedy Class I or II | Yes | 8 (40%) | ||||
No | 12 (60%) | |||||
Kennedy Class III or IV | Yes | 5 (25%) | ||||
No | 15 (75%) | |||||
CI = confidence interval; CO = crossover; Cr-Co = chromium-cobalt; MD = mean difference; NA = not applicable; NR = not reported, OHIP-14 = Oral Health Impact Profie-14; PMMA = polymethyl methacrylate; RCT = randomized controlled trial; RPD = removable partial denture; SD = standard deviation; VAS = visual analogue scale.
aThe scores from the VAS, a continuous graphical rating scale from 0 to 100 were classified as: totally dissatisfied (0 to 31), slightly dissatisfied (> 31 to 50), slightly satisfied (> 50 to 79), and satisfied (80 to 100).
bSubgroup analyses were conducted for age, gender, and socioeconomic status; no significant differences reported based on P ≤ 0.05 (unclear power to detect differences).
cBaseline prevalence (total sample, n = 30) of grouped responses (occasionally, fairly often, or very often). Found it uncomfortable to eat: 8 (26.7%); painful aching in mouth: 9 (30%).
Table 9: Summary of Findings by Outcome — Other Complications
Citation and study design Outcome name and measurement method | Intervention and control groups and number of participants (n) | Outcome label | Outcome result | P value for between-group difference |
|---|---|---|---|---|
Follow-up: 1 year | ||||
Manzon et al. (2019)31 Nonrandomized controlled study Outcome: Roughness perceived by the tongue Measurement: Patient-reported, subjective response 1 question (2 response options) | Valplast flexible RPD (n = 40) | Chi-square P value < 0.001 | ||
Kennedy Class I or II | Smooth prothesis | 12 (60%) | ||
Wrinkled prothesis | 8 (40%) | |||
Kennedy Class III or IV | Smooth prothesis | 10 (50%) | ||
Wrinkled prothesis | 10 (50%) | |||
Cr-Co RPD (n = 40) | ||||
Kennedy Class I or II | Smooth prothesis | 20 (100%) | ||
Wrinkled prothesis | 0 (0%) | |||
Kennedy Class III or IV | Smooth prothesis | 20 (100%) | ||
Wrinkled prothesis | 0 (0%) | |||
PMMA-RPD (n = 40) | ||||
Kennedy Class I or II | Smooth prothesis | 20 (100%) | ||
Wrinkled prothesis | 0 (0%) | |||
Kennedy Class III or IV | Smooth prothesis | 20 (100%) | ||
Wrinkled prothesis | 0 (0%) | |||
Manzon et al. (2019)31 Nonrandomized controlled study Outcome: Feeling of encumbrance Measurement: Patient-reported, subjective response 1 question (3 response options) | Valplast flexible RPD (n = 40) | Chi-square P value < 0.001 | ||
Kennedy Class I or II | No encumbrance | 18 (90%) | ||
Little encumbrance | 2 (10%) | |||
Very cumbersome | 0 (0%) | |||
Kennedy Class III or IV | No encumbrance | 17 (65%) | ||
Little encumbrance | 3 (15%) | |||
Very cumbersome | 0 (0%) | |||
Cr-Co RPD (n = 40) | ||||
Kennedy Class I or II | No encumbrance | 12 (60%) | ||
Little encumbrance | 8 (40%) | |||
Very cumbersome | 0 (0%) | |||
Kennedy Class III or IV | No encumbrance | 13 (65%) | ||
Little encumbrance | 7 (35%) | |||
Very cumbersome | 0 (0%) | |||
PMMA-RPD (n = 40) | ||||
Kennedy Class I or II | No encumbrance | 3 (15%) | ||
Little encumbrance | 5 (25%) | |||
Very cumbersome | 12 (60%) | |||
Kennedy Class III or IV | No encumbrance | 3 (15%) | ||
Little encumbrance | 6 (30%) | |||
Very cumbersome | 11 (55%) | |||
Manzon et al. (2019)31 Nonrandomized controlled study Outcome: Calculus presence on prothesis Measurement: Clinician-assessed (3 response options) | Valplast flexible RPD (n = 40) | Chi-square P value = 0.23 | ||
Kennedy Class I or II | Calculus free | 17 (85%) | ||
Covering < 1/3 of prothesis | 3 (15%) | |||
Covering > 1/3 of prothesis | 0 (0%) | |||
Kennedy Class III or IV | Calculus free | 20 (100%) | ||
Covering < 1/3 of prothesis | 0 (0%) | |||
Covering > 1/3 of prothesis | 0 (0%) | |||
Cr-Co RPD (n = 40) | ||||
Kennedy Class I or II | Calculus free | 20 (100%) | ||
Covering < 1/3 of prothesis | 0 (0%) | |||
Covering > 1/3 of prothesis | 0 (0%) | |||
Kennedy Class III or IV | Calculus free | 20 (100%) | ||
Covering < 1/3 of prothesis | 0 (0%) | |||
Covering > 1/3 of prothesis | 0 (0%) | |||
PMMA-RPD (n = 40) | ||||
Kennedy Class I or II | Calculus free | 19 (95%) | ||
Covering < 1/3 of prothesis | 1 (5%) | |||
Covering > 1/3 of prothesis | 0 (0%) | |||
Kennedy Class III or IV | Calculus free | 17 (65%) | ||
Covering < 1/3 of prothesis | 3 (15%) | |||
Covering > 1/3 of prothesis | 0 (0%) | |||
Manzon et al. (2019)31 Nonrandomized controlled study Outcome: Plaque presence on abutment teeth Measurement: Clinician-assessed (2 response options) | Valplast flexible RPD (n = 40) | Chi-square P value 0.37 | ||
Kennedy Class I or II | Yes | 13 (65%) | ||
No | 7 (35%) | |||
Kennedy Class III or IV | Yes | 12 (60%) | ||
No | 8 (40%) | |||
Cr-Co RPD (n = 40) | ||||
Kennedy Class I or II | Yes | 7 (35%) | ||
No | 13 (65%) | |||
Kennedy Class III or IV | Yes | 8 (40%) | ||
No | 12 (60%) | |||
PMMA-RPD (n = 40) | ||||
Kennedy Class I or II | Yes | 10 (50%) | ||
No | 10 (50%) | |||
Kennedy Class III or IV | Yes | 9 (45%) | ||
No | 11 (55%) | |||
Manzon et al. (2019)31 Nonrandomized controlled study Outcome: Abutment teeth health Measurement: Clinician-assessed (3 response options) | Valplast flexible RPD (n = 40) | Chi-square P value: 0.28 | ||
Kennedy Class I or II | Same as before | 17 (85%) | ||
Decay | 3 (15%) | |||
Dental mobility | 0 (0%) | |||
Kennedy Class III or IV | Same as before | 19 (95%) | ||
Decay | 1 (5%) | |||
Dental mobility | 0 (0%) | |||
Cr-Co RPD (n = 40) | ||||
Kennedy Class I or II | Same as before | 19 (95%) | ||
Decay | 1 (5%) | |||
Dental mobility | 0 (0%) | |||
Kennedy Class III or IV | Same as before | 20 (100%) | ||
Decay | 0 (0%) | |||
Dental mobility | 0 (0%) | |||
PMMA-RPD (n = 40) | ||||
Kennedy Class I or II | Same as before | 20 (100%) | ||
Decay | 0 (0%) | |||
Dental mobility | 0 (0%) | |||
Kennedy Class III or IV | Same as before | 18 (90%) | ||
Decay | 2 (10%) | |||
Dental mobility | 0 (0%) | |||
Manzon et al. (2019)31 Nonrandomized controlled study Outcome: Change in occlusal position Measurement: Clinician-assessed (2 response options) | Valplast flexible RPD (n = 40) | Chi-square P value 0.07 | ||
Kennedy Class I or II | Yes | 2 (10%) | ||
No | 18 (90%) | |||
Kennedy Class III or IV | Yes | 0 (0%) | ||
No | 20 (100%) | |||
Cr-Co RPD (n = 40) | ||||
Kennedy Class I or II | Yes | 0 (0%) | ||
No | 20 (100%) | |||
Kennedy Class III or IV | Yes | 0 (0%) | ||
No | 20 (100%) | |||
PMMA-RPD (n = 40) | ||||
Kennedy Class I or II | Yes | 0 (0%) | ||
No | 20 (100%) | |||
Kennedy Class III or IV | Yes | 0 (0%) | ||
No | 20 (100%) | |||
Follow-up: 24 months | ||||
Sadek and Elawady (2019)32 Parallel-group RCT Outcome: Survival rate of abutment teeth Measurement: Clinically stable, functioning abutments without any mobility | Thermopress RPD (n = 14) | 100% | Kaplan Maier - P value = 0.104 | |
Vitallium RPD (n = 14) | 10 (71.4%) | |||
Vitallium RPD with surveyed bridge (n = 14) | 12 (85.7%) | |||
Cr-Co = chromium-cobalt; PMMA = polymethyl methacrylate; RCT = randomized controlled trial; RPD = removable partial denture.
Table 10: Summary of Findings by Outcome — Tissue and Periodontal Health
Citation and study design Outcome name and measurement method | Intervention groups and number of participants (n) | Outcome label | Outcome result | P value for between-group difference |
|---|---|---|---|---|
Follow-up: 1 year | ||||
Manzon et al. (2019)31 Nonrandomized controlled study Outcome: Mucosa redness of edentulous areas Measurement: Clinician-assessed (2 response options) | Valplast flexible RPD (n = 40) | Chi-square P value = 0.13 | ||
Kennedy Class I or II | Yes | 12 (60%) | ||
No | 8 (40%) | |||
Kennedy Class III or IV | Yes | 9 (45%) | ||
No | 11 (55%) | |||
Cr-Co RPD (n = 40) | ||||
Kennedy Class I or II | Yes | 6 (30%) | ||
No | 14 (70%) | |||
Kennedy Class III or IV | Yes | 4 (20%) | ||
No | 16 (80%) | |||
PMMA-RPD (n = 40) | ||||
Kennedy Class I or II | Yes | 10 (50%) | ||
No | 10 (50%) | |||
Kennedy Class III or IV | Yes | 8 (40%) | ||
No | 12 (60%) | |||
Manzon et al. (2019)31 Nonrandomized controlled study Outcome: Mucosa redness around abutment teeth Measurement: Clinician-assessed (2 response options) | Valplast flexible RPD (n = 40) | Chi-square P value < 0.001 | ||
Kennedy Class I or II | Yes | 18 (90%) | ||
No | 2 (10%) | |||
Kennedy Class III or IV | Yes | 15 (75%) | ||
No | 5 (25%) | |||
Cr-Co RPD (n = 40) | ||||
Kennedy Class I or II | Yes | 8 (40%) | ||
No | 12 (60%) | |||
Kennedy Class III or IV | Yes | 4 (20%) | ||
No | 16 (80%) | |||
PMMA-RPD (n = 40) | ||||
Kennedy Class I or II | Yes | 14 (70%) | ||
No | 6 (30%) | |||
Kennedy Class III or IV | Yes | 12 (60%) | ||
No | 8 (40%) | |||
Follow-up: Uncleara | ||||
Hundal and Madan (2015)35 Parallel-group RCT Outcome: Oral soft tissue tolerance, subjective assessment Measurement: Participant responses to 1 question (3 response options with scores 0 to 3 — lower scores are better) | Valplast RPD (n = 15) | NA | Mean (SD): 0.27 (0.458) Range: 0 to 1 Median: 0 | Unclearb |
Cr-Co alloy with PMMA base RPD (n = 15) | NA | Mean (SD): 0.13 (0.352) Range: 0 to 1 Median: 0 | ||
Hundal and Madan (2015)35 Parallel-group RCT Outcome: Oral soft tissue tolerance, objective assessment Measurement: Clinician responses to 1 question (2 response options with scores 0 to 1 — lower is better) | Valplast RPD (n = 15) | NA | Mean (SD): 0 (0) Range: 0 to 0 Median: 0 | Unclearb |
Cr-Co alloy with PMMA base RPD (n = 15) | NA | Mean (SD): 0 (0) Range: 0 to 0 Median: 0 | ||
Hundal and Madan (2015)35 Parallel-group RCT Outcome: Gingival health Measurement: Clinician-assessed using Gingival index of Loe H and Sillness J (1963) (scores 0 to 3, lower is better) | Valplast RPD (n = 15) | NA | Mean (SD): 0 (0) Range: 0 to 0 Median: 0 | Unclearb |
Cr-Co alloy with PMMA base RPD (n = 15) | NA | Mean (SD): 0 (0) Range: 0 to 0 Median: 0 | ||
Hundal and Madan (2015)35 Parallel-group RCT Outcome: Periodontal health Measurement: Clinician-assessed using Periodontal index of AL Russell (1967) (range 0 to 8, lower is better) | Valplast RPD (n = 15) | NA | Mean (SD): 0 (0) Range: 0 to 0 Median: 0 | Unclearb |
Cr-Co alloy with PMMA base RPD (n = 15) | NA | Mean (SD): 0 (0) Range: 0 to 0 Median: 0 | ||
Hundal and Madan (2015)35 Parallel-group RCT Outcome: Adaptability in areas with undercut Measurement: Clinician-assessed — whether a block out is required — score 0 to 1, lower is better | Valplast RPD (n = 15) | NA | Mean (SD): 0.73 (0.458) Range: 0 to 1 Median: 1 | Unclearb |
Cr-Co alloy with PMMA base RPD (n = 15) | NA | Mean (SD): 0.87 (0.352) Range: 0 to 1 Median: 1 | ||
Cr-Co = chromium-cobalt; NA = not applicable; PMMA = polymethyl methacrylate; RCT = randomized controlled trial; RPD = removable partial denture; SD = standard deviation.
aAfter insertion of the prosthesis, their clinical performances were reviewed periodically during one and half years for the 9 parameters as listed in Table 1. The periodicity of recall was 24 hours, 1 week, 1 month, 3 months and 6 months after insertion of prostheses.”
bFrom abstract: “The clinical parameters of ‘oral soft tissue tolerance,’ ‘gingival health’, ‘periodontal health’ and ‘adaptability in areas with undercut’ were statistically at par for all the 30 patients thus suggesting the comparable biocompatibility of the two materials.” No other details are provided.
Table 11: Summary of Findings by Outcome — Technical Complications
Citation and study design Outcome name and measurement method | Intervention group and number of participants (n) | Outcome label | Outcome result | P value for between-group difference |
|---|---|---|---|---|
Follow-up: 1 year | ||||
Manzon et al. (2019)31 Nonrandomized controlled study Outcome: Prosthesis fractures Measurement: Clinician-assessed (2 response options) | Valplast flexible RPD (n = 40) | NA | ||
Kennedy Class I or II | Yes | 0 (0%) dentures with clasp fractures or denture base fractures for any Kennedy classification | ||
No | ||||
Kennedy Class III or IV | Yes | |||
No | ||||
Cr-Co RPD (n = 40) | ||||
Kennedy Class I or II | Yes | 0 (0%) dentures with clasps factures or denture base fractures for any Kennedy classification | ||
No | ||||
Kennedy Class III or IV | Yes | |||
No | ||||
PMMA-RPD (n = 40) | ||||
Kennedy Class I or II | Yes | 0 (0%) dentures with clasps factures or denture base fractures for any Kennedy classification | ||
No | ||||
Kennedy Class III or IV | Yes | |||
No | ||||
Manzon et al. (2019)31 Nonrandomized controlled study Outcome: Discoloration of prosthesis Measurement: Clinician-assessed (2 response options) | Valplast flexible RPD (n = 40) | Chi-square P value = 0.54 | ||
Kennedy Class I or II | Yes | 1 (5%) | ||
No | 19 (95%) | |||
Kennedy Class III or IV | Yes | 1 (5%) | ||
No | 19 (95%) | |||
Cr-Co RPD (n = 40) | ||||
Kennedy Class I or II | Yes | 0 (0%) | ||
No | 20 (100%) | |||
Kennedy Class III or IV | Yes | 0 (0%) | ||
No | 20 (100%) | |||
PMMA-RPD (n = 40) | ||||
Kennedy Class I or II | Yes | 0 (0%) | ||
No | 20 (100%) | |||
Kennedy Class III or IV | Yes | 0 (0%) | ||
No | 20 (100%) | |||
Manzon et al. (2019)31 Nonrandomized controlled study Outcome: Loss of artificial teeth Measurement: Clinician-assessed (2 response options) | Valplast flexible RPD (n = 40) | Chi-square P value = 0.04 | ||
Kennedy Class I or II | Yes | 3 (15%) | ||
No | 17 (85%) | |||
Kennedy Class III or IV | Yes | 1 (5%) | ||
No | 19 (95%) | |||
Cr-Co RPD (n = 40) | ||||
Kennedy Class I or II | Yes | 0 (0%) | ||
No | 20 (100%) | |||
Kennedy Class III or IV | Yes | 0 (0%) | ||
No | 20 (100%) | |||
PMMA-RPD (n = 40) | ||||
Kennedy Class I or II | Yes | 0 (0%) | ||
No | 20 (100%) | |||
Kennedy Class III or IV | Yes | 0 (0%) | ||
No | 20 (100%) | |||
Follow-up: Uncleara | ||||
Hundal and Madan (2015)35 Parallel-group RCT Outcome: Frequency of fracture/repair of RPD, objective Measurement: Clinician-assessed (2 response options converted to scores of 0 or 1 — higher scores are better) | Valplast RPD (n = 15) | NA | Mean (SD): 0.67 (0.488) Range: 0 to 1 Median: 1 | NR |
Cr-Co alloy with PMMA-RPD base | NA | Mean (SD): 0.8 (0.414) Range: 0 to 1 Median: 1 | ||
Cr-Co = chromium-cobalt; NR = not reported; PMMA = polymethyl methacrylate; RCT = randomized controlled trial; RPD = removable partial denture; SD = standard deviation.
aFrom report: “After insertion of the prosthesis, their clinical performances were reviewed periodically during one and half years for the nine parameters as listed in Table 1. The periodicity of recall was 24 hours, 1 week, 1 month, 3 months, and 6 months after insertion of prostheses.”
Table 12: Summary of Findings by Outcome — Overall Patient Satisfaction
Citation and study design Outcome name and measurement method | Intervention and comparator group and number of participants (n) | Outcome result n (%) | Between-group difference (as reported) | P value for between-group difference |
|---|---|---|---|---|
Follow-up: 1 month | ||||
Akinyamoju et al. (2019)29 and Akinyamoju et al. (2017)30 CO-RCT Outcome: Overall satisfaction Measurement: 100 mm VAS, categorized into 4 groupsa | Valplast flexible RPDs (n = 30) | NR | More satisfied with: flexible RPD: n = 21 acrylic RPD: n = 6 Similarly satisfied with both: n = 3 | P value for Wilcoxon signed rank test: 0.04b |
Acrylic RPDs (n = 30) | NR | |||
Follow-up: Unclearc | ||||
Hundal and Madan (2015)35 Parallel-group RCT Outcome: Overall patient satisfaction, subjective assessment Measurement: Participant responses to 1 question (4 response options with scores 0 to 3, higher is better) | Valplast RPD (n = 15) | Mean (SD): 2.07 (0.594) Range: 1 to 3 Median: 2 | NR | Uncleard |
Cr-Co alloy with PMMA base RPD (n = 15) | Mean (SD): 1.47 (0.516) Range: 1 to 2 Median: 1 | |||
CO = crossover; Cr-Co = chromium-cobalt; PMMA = polymethyl methacrylate; RCT = randomized controlled trial; RPD = removable partial denture; SD = standard deviation; VAS = visual analogue scale.
aThe scores from the VAS, a continuous graphical rating scale from 0 to 100 were classified as totally dissatisfied (0 to 31), slightly dissatisfied (> 31 to 50), slightly satisfied (> 50 to 79), and satisfied (80 to 100).
bSubgroup analyses were conducted for age, gender, and socioeconomic status; no significant differences reported based on P ≤ 0.05 (unclear power to detect differences).
cFrom report: “After insertion of the prosthesis, their clinical performances were reviewed periodically during one and half years for the nine parameters as listed in Table 1. The periodicity of recall was 24 hours, 1 week, 1 month, 3 months, and 6 months after insertion of prostheses.”
dFrom abstract: “Statistically significant results were obtained in favor of flexible RPDs, in the parameters of ‘overall patient satisfaction’.”
Table 13: Summary of Findings by Outcome — OHRQoL (Overall and Domain-Specific)
Citation and study design | Outcome name and measurement method | Interventions and number of participants (n) | Baseline | Follow-up | Within-group difference between baseline and follow-up (as reported) | P value for within-group change from baseline | Between-group difference (as reported) and P value |
|---|---|---|---|---|---|---|---|
Follow-up: 1 month | |||||||
Akinyamoju et al. (2019)29 and Akinyamoju et al. (2017)30 CO- RCTa | Summary OHIP-14 score (lower is better) | Valplast flexible RPDs (n = 30) | Mean (SD): 12.4 (9.8) | Mean (SD): 3.8 (5.6) | MD (SD): 8.6 (11.7) 95% CI, 4.3 to 13.0 | < 0.001 | NR |
Acrylic RPDs (n = 30) | Mean (SD): 4.8 (5.3) | MD (SD): 7.7 (11.6) 95% CI, 3.3 to 12.0 | 0.001 | ||||
OHIP-14 domain score: Functional Limitation | Valplast flexible RPDs (n = 30) | NR | NR | MD (SD): 0.7 (2.6) 95% CI, −0.3 to 1.6 | 0.16 | NR | |
Acrylic RPDs (n = 30) | NR | NR | MD (SD): 0.3 (2.4) 95% CI, −0.6 to 1.2 | 0.49 | |||
OHIP-14 domain score: Physical Pain | Valplast flexible RPDs (n = 30) | NR | NR | MD (SD): −0.1 (3.3) 95% CI, −1.4 to 1.1 | 0.83 | NR | |
Acrylic RPDs (n = 30) | NR | NR | MD (SD): 0.4 (2.9) 95% CI, −0.6 to 1.5 | 0.42 | |||
OHIP-14 domain score: Psychological Discomfort | Valplast flexible RPDs (n = 30) | NR | NR | MD (SD): 2.7 (2.5) 95% CI, 1.8 to 3.7 | < 0.001 | NR | |
Acrylic RPDs (n = 30) | NR | NR | MD (SD): 2.6 (2.7) 95% CI, 1.6 to 3.6 | < 0.001 | |||
OHIP-14 domain score: Physical Disability | Valplast flexible RPDs (n = 30) | NR | NR | MD (SD): 0.4 (1.9) 95% CI, −0.3 to 1.1 | 0.22 | NR | |
Acrylic RPDs (n = 30) | NR | NR | MD (SD): −0.1 (2.3) 95% CI, −1.0 to 0.7 | 0.76 | |||
OHIP-14 domain score: Social Disability | Valplast flexible RPDs (n = 30) | NR | NR | MD (SD): 1.2 (1.7) 95% CI, 0.6 to 1.9 | < 0.001 | NR | |
Acrylic RPDs (n = 30) | NR | NR | MD (SD): −1.2 (1.7) 95% CI, 1.9 to 4.1 | < 0.001 | |||
OHIP-14 domain score: Handicap | Valplast flexible RPDs (n = 30) | NR | NR | MD (SD): 1.0 (2.1) 95% CI, 0.3 to 1.8 | 0.01 | NR | |
Acrylic RPDs (n = 30) | NR | NR | MD (SD): 1.0 (1.8) 95% CI, 0.3 to 1.7 | 0.005 | |||
Sadek and Elawady (2019)32 Parallel-group RCT | Oral Health-Related Quality of Life questionnaire (patient or caregiver reported, 12 closed-ended questions; lower is better)b | Thermopress RPD (n = 14) | Results shared in figure and not extracted | Results shared in figure and not extracted | NR | NR | Significantly lower for Thermopressc P value < 0.05 |
Vitallium RPD (n = 14) | NR | NR | |||||
Vitallium RPD with surveyed bridge (n = 14) | NR | NR | |||||
Follow-up: 1 year | |||||||
Kumar (2021)28 Parallel-group RCT | Summary OHIP-14 | Polyacetyl RPD (n = 11) | Meanc,d: 33.27 (6.37) | Meand: 13.63 (2.37) | CI = 15.94 to 23.33 | < 0.001 | CI = 0.68 to 5.86 P = 0.015 |
Cast metal RPD (n = 11) | Meand: 37.81 (8.80) | Meand: 16.90 (3.36) | CI = 16.14 to 25.67 | < 0.001 | |||
OHIP-14 domain score: Functional Limitation | Polyacetyl RPD (n = 11) | Meand: 4.90 (1.97) | Meand: 1.09 (0.53) | NR | 0.003 | P = 0.048 | |
Cast metal RPD (n = 11) | Meand: 5.63 (2.46) | Meand: 1.63 (0.80) | NR | 0.003 | |||
OHIP-14 domain score: Physical Pain | Polyacetyl RPD (n = 11) | Meand: 4.81 (1.83) | Meand: 2.09 (0.53) | NR | 0.008 | P = 0.429 | |
Cast metal RPD (n = 11) | Meand: 5.90 (2.50) | Meand: 2.54 (0.93) | NR | 0.007 | |||
OHIP-14 domain score: Physical Disability | Polyacetyl RPD (n = 11) | Meand: 5.54 (1.29) | Meand: 2.18 (0.98) | NR | 0.003 | P = 0.211 | |
Cast metal RPD (n = 11) | Meand: 6.18 (1.72) | Meand: 2.72 (0.78) | NR | 0.005 | |||
OHIP-14 domain score: Physical Discomfort | Polyacetyl RPD (n = 11) | Meand: 5.90 (1.57) | Meand: 2.54 (0.82) | NR | 0.005 | P = 0.490 | |
Cast metal RPD (n = 11) | Meand: 6.36 (1.74) | Meand: 2.90 (1.13) | NR | 0.004 | |||
OHIP-14 domain score: Psychological Disability | Polyacetyl RPD (n = 11) | Meand: 4.63 (1.12) | Meand: 2.45 (0.68) | NR | 0.005 | P = 0.373 | |
Cast metal RPD (n = 11) | Meand: 5.09 (1.75) | Meand: 2.81 (0.98) | NR | 0.007 | |||
OHIP-14 domain score: Social Disability | Polyacetyl RPD (n = 11) | Meand: 3.72 (1.10) | Meand: 1.63 (0.50) | NR | 0.005 | P = 0.357 | |
Cast metal RPD (n = 11) | Meand: 4.54 (1.29) | Meand: 2.09 (1.04) | NR | 0.005 | |||
OHIP-14 domain score: Handicap | Polyacetyl RPD (n = 11) | Meand: 4.27 (1.19) | Meand: 1.63 (0.50) | NR | 0.003 | P = 0.061 | |
Cast metal RPD (n = 11) | Meand: 4.81 (1.66) | Meand: 2.18 (0.40) | NR | 0.005 | |||
CI = confidence interval; CO = crossover; MD = mean difference; NR = not reported; OHIP-14 = Oral Health Impact Profile; OHRQoL = Oral Health-Related Quality of Life; RCT = randomized controlled trial; RPD = removable partial denture; SD = standard deviation.
aSubgroup analyses were conducted for age, gender, and socioeconomic status; no significant differences reported based on P ≤ 0.05 (unclear power to detect differences).
bQuestions from other tools such as OHIP-49 and GOHAI; 5-point Likert scale with scores 0 (Never) to 4 (Very often).
cThe time point for the “baseline” measurement for this study is after 1 week follow-up.
dUnclear if study is reporting standard deviations or standard errors.
Table 14: Summary of Findings by Outcome — Effort for Maintenance in Daily Care
Citation and study design Outcome name and measurement method | Interventions and number of participants (n) | Outcome label | Outcome result n (%) | Between-group difference (as reported) | P value for between-group difference |
|---|---|---|---|---|---|
Follow-up: 1 month | |||||
Akinyamoju et al. (2019)29 and Akinyamoju et al. (2017)30 CO-RCT Outcome: Satisfaction with ease of cleaning/cleanliness Measurement: 100 mm VAS, categorized into 4 groupsa | Valplast flexible RPDs (n = 30) | Totally dissatisfied | 0 (0%) | More satisfied with: flexible RPD: n = 5 acrylic RPD: n = 5 Similarly satisfied with both: n = 20 | P value for Wilcoxon signed rank test: 1.00b |
Slightly dissatisfied | 0 (0%) | ||||
Slightly satisfied | 0 (0%) | ||||
Satisfied | 30 (100%) | ||||
Acrylic RPDs (n = 30) | Totally dissatisfied | 0.0% | |||
Slightly dissatisfied | 1 (3.3%) | ||||
Slightly satisfied | 0.0% | ||||
Satisfied | 29 (96.7%) | ||||
Follow-up: 1 year | |||||
Manzon et al. (2019)31 Unclear design Outcome: Prosthesis care Measurement: Patient subjective — 1 question (2 response options) | Valplast flexible RPD (n = 40) | NR | Chi-square P value < 0.001 | ||
Kennedy Class I or II | Difficult | 10 (50%) | |||
Not difficult | 10 (50%) | ||||
Kennedy Class III or IV | Difficult | 13 (65%) | |||
Not difficult | 7 (35%) | ||||
Cr-Co RPD (n = 40) | |||||
Kennedy Class I or II | Difficult | 1 (5%) | |||
Not difficult | 19 (95%) | ||||
Kennedy Class III or IV | Difficult | 0 (0%) | |||
Not difficult | 20 (100%) | ||||
PMMA-RPD (n = 40) | |||||
Kennedy Class I or II | Difficult | 2 (10%) | |||
Not difficult | 18 (90%) | ||||
Kennedy Class III or IV | Difficult | 1 (5%) | |||
Not difficult | 19 (95%) | ||||
CO = crossover; Cr-Co = chromium-cobalt; NR = not reported; PMMA = polymethyl methacrylate; RCT = randomized controlled trial; RPD = removable partial denture; VAS = visual analogue scale.
aThe scores from the VAS, a continuous graphical rating scale from 0 to 100 were classified as: totally dissatisfied (0 to 31), slightly dissatisfied (> 31 to 50), slightly satisfied (> 50 to 79), and satisfied (80 to 100).
bSubgroup analyses were conducted for age, gender, and socioeconomic status; no significant differences reported based on P ≤ 0.05 (unclear power to detect differences).
Appendix 6: Excluded Economic Evaluation
Please note that this appendix has not been copy-edited.
Table 15: Summary of Excluded Economic Evaluations
Study citation, setting, funding source cost year | Population characteristics Type of analysis, time horizon, perspective | Analytic technique, study design, perspective, time horizon | Intervention and comparator(s) | Outcomes | Summary of outcomes | Main assumptions |
|---|---|---|---|---|---|---|
Subash et al. (2025)40 Country: India Funding source: Authors reported no funding sources Cost year: 2021 / 2022 (assumed, NR), Indian Rupeea | Participants recruited from a single tertiary care centre in India between January 2021 and January 2022 Summary eligibility criteria: Partial edentulism (any Kennedy class), aged 50 to 65 years, unsuitable for, or facing financial constraints for implants or fixed partial dentures. Most lower dentures were the participants’ first denture (not stated for upper dentures) and most participants had them for less than a year Number of participants: 42 Cause of edentulism and PROGRESS-Plus criteria: NRb | Analytic Technique: not stated (seems to be deterministic analysis) Study design: Clinical evidence based on cross-sectional study; Cost-effective analysis Perspective: NR but health care payer perspective (educational institution in India) Time horizon: 3 months | Intervention:
Comparators:
| Cost estimates: Based on the subsidized cost for patients at the educational institution. Included lab charge (base cost) plus a 35% markup to account for overhead costs Outcome: ICER per improvement in OHIP-14 summary scores and patient satisfaction scoresc | Authors concluded that: “The cost-effectiveness of prosthetic rehabilitation options varies depending on the number of teeth being replaced. [thermoplastic RPDs] are generally more cost-effective for fewer teeth scenarios, whereas [metal clasp– retained RPDs] and [cast partial dentures] tend to be more cost-effective for scenarios involving more teeth”d | The ICER was calculated based on the ratio of the difference in cost between interventions and the difference in change of OHIP and patient satisfaction scoresb |
ICER = incremental cost-effectiveness ratio; NR = not reported; OHIP-14 = Oral Health Impact Profile-14; RPD = removable partial denture.
Note: Lower OHIP-14 scores indicate a higher quality of life, whereas higher patient satisfaction scores indicate higher satisfaction.
aCost-year not reported. Assumption made based on the clinical study recruitment timing on which the clinical effectiveness data are based.
bThe main PROGRESS-Plus criteria include place of residence, race, ethnicity, culture, language, occupation, gender, sex, religion, education, socioeconomic status, social capital, personal characteristics associated with discrimination (e.g., age, disability), features of relationships, and time-dependent relationships.2
cThe authors also report the calculation of the direct cost of achieving the clinically minimally important difference in OHIP-14 summary score with each RPD treatment but do not report either the minimally important difference or the results of the direct cost to achieve this.
dEdited to more clearly references relevant intervention groups (study report used inconsistent terminology throughout).
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.