Drugs, Health Technologies, Health Systems
Health Technology Review
Longevity of Relined or Rebased Dentures
Key Messages
What Is the Issue?
Tooth loss is a common condition that can affect speech, nutrition, mental health, and quality of life. Dentures are prosthetic devices used to replace missing teeth and restore oral function and aesthetics.
Dentures require regular care and maintenance — including relining and rebasing procedures, which can restore denture fit, function, and comfort in individuals with tooth loss.
There is uncertainty regarding the longevity of complete or partial removable dentures following relining or rebasing, as well as the appropriate timing of providing these procedures. This Rapid Review was prepared in response to a request from decision-makers.
What Did We Do?
We conducted a rapid review to summarize evidence on the longevity of relined and rebased dentures. We searched key resources, including journal citation databases, and conducted a focused internet search for relevant evidence published since 2001.
What Did We Find?
We did not find any clinical evidence on the longevity of rebased dentures that met our selection criteria for this review. We did not find any evidence-based guidelines that provide recommendations on how often dentures should be relined or rebased.
We identified 1 prospective single-arm cohort study that evaluated the longevity of relined dentures.
Of the 50 participants evaluated at 1-year follow-up, 47 (94%) were assessed as having well-fitted dentures with no need for adjustment or additional relining, while 3 (6%) were assessed as having a slight change in adaptation that remained within the normal range and was clinically acceptable. No participants were assessed as having an ill-fitted denture that required additional relining or fabrication of a new denture. The authors did not report the types of dentures or denture materials eligible for inclusion in the study.
These findings have a risk of bias due to several methodological and reporting issues, including concerns related to how the need for additional denture relining was assessed. The findings have limited applicability to clinical settings in Canada.
What Does This Mean?
Published evidence on the longevity of relined and rebased dentures and the appropriate timing of these procedures is limited.
Decision-making regarding the appropriate timing of relining and rebasing procedures could draw on clinical expertise and other sources of information (e.g., dental service utilization data, patient preferences).
Research Questions
What is the clinical evidence on the longevity of removable complete or partial dentures following a relining procedure?
What is the clinical evidence on the longevity of removable complete or partial dentures following a rebasing procedure?
What are the evidence-based guidelines regarding the timing of relining or rebasing procedures for removable complete or partial dentures?
Context and Policy Issues
What Is Tooth Loss?
Tooth loss is a condition in which natural teeth are missing from the mouth. It can be classified as partial tooth loss, in which 1 or more teeth are missing, or complete tooth loss (i.e., edentulism), in which all teeth are missing.
Tooth loss can have a range of effects on individuals. It can lead to psychological stress, changes in eating patterns, nutrient deficiencies, and difficulty speaking.1,2 It may also affect an individual’s appearance and negatively affect quality of life.3
Several factors can contribute to tooth loss, including oral health conditions and social and behavioural factors. Common causes of tooth loss include dental caries (i.e., tooth decay or cavities), periodontal disease, injury or trauma, systemic diseases, and congenital conditions.4-8
In Canada, tooth loss disproportionately affects certain population groups. Across the adult population, complete tooth loss affects about 4% of individuals aged 18 years or older.1 The prevalence is higher among older adults, affecting about 11% of those aged 60 years or older.1 Tooth loss also disproportionately affects individuals living with disabilities, those with lower socioeconomic status or education levels, and individuals who experience barriers to accessing dental care.1,9-11
What Are Dentures?
Dentures are prosthetic devices used to replace missing teeth and restore oral function and aesthetics.12 The 2 main components of dentures are the artificial teeth and the denture base. Artificial denture teeth are commonly made from acrylic resin, although porcelain had been used for many years.13 The denture base, which supports the appliance in the oral cavity, is typically made of materials such as acrylic resin, metal alloys (e.g., cobalt-chromium), or thermoplastic polymers.14
Dentures can be classified in several ways according to their design and properties. For example, they can be classified as:
partial (i.e., replaces some missing teeth) or complete (i.e., replaces all teeth in an arch)15
removable (i.e., can be removed by the patient) or fixed (i.e., secured in place and not removable by the patient)16
tissue supported (i.e., rests on the gums) or implant supported (i.e., supported by dental implants)17
maxillary (i.e., located in or on the upper jaw) or mandibular (i.e., located in or on the lower jaw)
immediate (i.e., inserted immediately after tooth extraction) or conventional (i.e., inserted after a healing period, which allows the surrounding tissue to adjust following tooth extraction).15
What Are Relining and Rebasing Procedures?
Dentures require regular care and maintenance to maintain oral health and the longevity of the prosthesis.18 For removable dentures, daily cleaning by brushing and soaking can remove plaque and tartar and reduce levels of microbial biofilms.19-21 In addition to needing routine cleaning and disinfecting, dentures may require professional dental procedures to ensure proper fit, function, and comfort, including relining and rebasing.22
Relining procedures are used to resurface the tissue-facing side of a denture with new material to improve its fit and adaptation to the supporting tissue.23 They can be performed using a direct chairside technique or an indirect laboratory technique.24 For the direct chairside technique, self-curing soft relining materials are added to the tissue side of the denture, which is then placed in the patient’s mouth. The new material will conform to the oral tissue, and after a short setting time, the denture is available for use.23 With the indirect laboratory technique, an impression is taken and the denture is sent to a dental laboratory, where a dental technician resurfaces the denture to adjust its shape.25
Rebasing is a laboratory process in which the entire denture base material of an existing prosthesis is replaced. It is indicated in cases of severe bone loss that affects denture fit; when the denture base is cracked or damaged; or when a more durable, longer-term solution than relining is needed.26 Both relining and rebasing procedures retain the denture’s original artificial teeth.22
Why Is It Important to Do This Review?
Denture relining and rebasing are important maintenance procedures that can restore denture fit, function, comfort, and quality of life in individuals with tooth loss, particularly as the structure of the underlying oral tissue changes over time (e.g., due to residual ridge resorption).22,23,27,28 However, there is uncertainty regarding the longevity of removable dentures following relining or rebasing, as well as uncertainty regarding the appropriate timing of these procedures, including the timing of:
initial relining or rebasing after denture provision
additional relining or rebasing of dentures on which these procedures have been performed previously.
This review builds on a previously published Rapid Review29 that evaluated the clinical evidence on the longevity of removable dentures by focusing on removable dentures that have undergone relining or rebasing procedures.
Objectives
To inform decision-making, we prepared this Rapid Review to summarize and critically appraise available clinical evidence on the longevity of removable dentures following relining or rebasing procedures in people with tooth loss. This report also aimed to review evidence-based guideline recommendations on the appropriate timing of denture relining and rebasing procedures.
Methods
An information specialist conducted a customized literature search, balancing comprehensiveness with relevance, of multiple sources and grey literature on March 19, 2026.
One reviewer screened citations and selected studies based on the inclusion criteria presented in Table 1, and they critically appraised the included publication using an established critical appraisal tool. Appendix 1 presents a detailed description of methods and selection criteria for included studies.
Criteria | Description |
|---|---|
Population | People with tooth loss |
Intervention |
|
Comparator |
|
Outcomes |
|
Study designs |
|
Publication date | January 1, 2001, to March 19, 2026 |
HTA = health technology assessment; RCT = randomized controlled trial; SR = systematic review.
aBoth tissue-supported dentures and implant-supported dentures were eligible.
Summary of Evidence
Quantity of Research Available
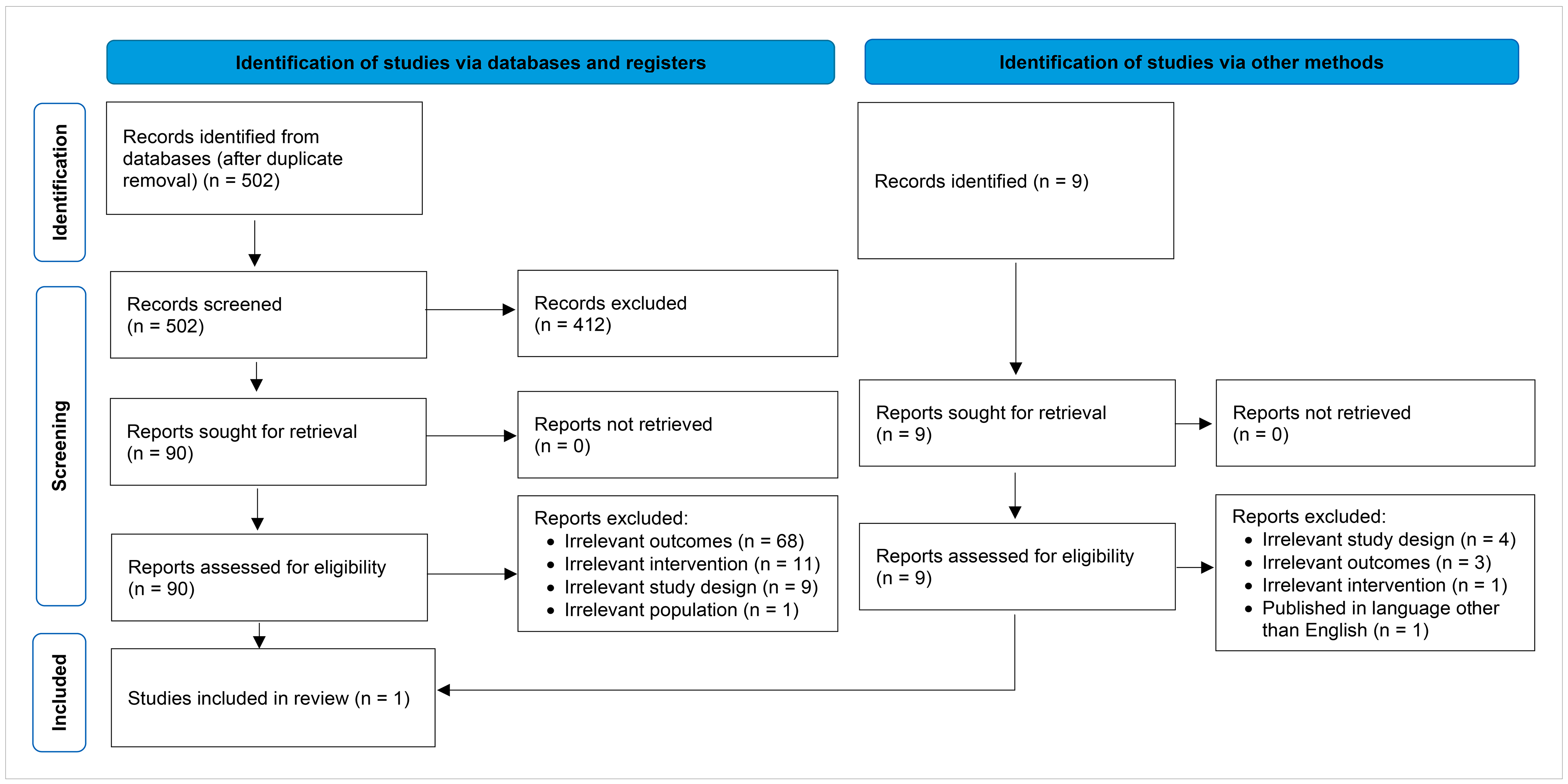
This report includes 1 publication30 that met our inclusion criteria. The included publication is a nonrandomized study30 that provides clinical evidence on the longevity of dentures following a relining procedure (research question 1). We did not identify any publications that provided clinical evidence on the longevity of dentures following a rebasing procedure (research question 2) or any evidence-based guidelines providing recommendations on how often dentures should be relined or rebased after a new denture is inserted or after an initial relining or rebasing procedure (research question 3) that met the inclusion criteria for this report.
Appendix 2 presents the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA)31 flow diagram of the study selection.
Appendix 6 (Table 6) summarizes additional references of potential interest, including clinical studies that did not meet the inclusion criteria but provide indirect evidence on the longevity of relined or rebased dentures.
Summary of Study Characteristics
Summaries of study characteristics are organized by research question. Appendix 3 (Table 3) provides details regarding the characteristics of the included publication.
Included Studies for Question 1: Clinical Evidence on the Longevity of Relined Dentures
We identified 1 clinical study30 addressing this question. This prospective single-arm cohort study30 included 50 adult participants who required denture relining. The study30 was conducted at the Nagasaki University School of Dentistry in Japan. The authors did not report the participant recruitment or observation periods. All participants used dentures made of heat-polymerized polymethyl methacrylate-based acrylic. The authors did not explicitly report the types of dentures eligible for inclusion in the study. However, based on the information provided, the dentures included in the study appear to have been complete, removable, and tissue supported.
All participants received a denture base relining using a self-curing powder-liquid material (Tokuso Rebase Normal-set). The publication30 provides details on the relining protocol, which was consistently used for all dentures. The authors did not provide information on the age, sex, or gender of participants. The included study30 did not provide any participant information for other PROGRESS-Plus criteria,32 such as place of residence, race, ethnicity, culture, language, occupation, religion, education, socioeconomic status, or social capital.
The included single-arm cohort study30 evaluated 1 outcome relevant to longevity. Adaptation was assessed based on US Public Health Service criteria33 for direct evaluation of restorative materials. The authors modified the US Public Health Service criteria33 to rate denture adaptation on a 3‑point scale:
1 (Alfa) — well-fitted and no need of adjustment or re-relining
2 (Bravo) — slight change in adaptation, but within the normal range, and clinically acceptable
3 (Charlie) — ill-fitted, need of additional relining, or need of fabrication of a new denture.
Outcomes were evaluated at baseline (i.e., immediately after relining) and at 1-year follow-up (i.e., after participants had used their relined dentures for 1 year).
Included Studies for Question 2: Clinical Evidence on the Longevity of Rebased Dentures
The rapid review did not identify relevant studies that addressed research question 2; therefore, no summary can be provided.
Included Studies for Question 3: Guidelines on the Timing of Relining or Rebasing Procedures for Dentures
The rapid review did not identify any relevant evidence-based guidelines that addressed research question 3; therefore, no summary can be provided.
Summary of Critical Appraisal
Appendix 4 (Table 4) provides additional details about the critical appraisal of the included publication.
Included Studies for Question 1: Clinical Evidence on the Longevity of Relined Dentures
The included cohort study30 used a single-arm design in which participants were not allocated into intervention and comparator groups. As a result, we considered the risk of bias related to the selection and allocation of participants to different treatment groups to be not relevant. Similarly, we considered the risk of bias related to confounding factors to be not relevant, as the study only included 1 group and the authors did not investigate the effects of participant- or intervention-related factors (e.g., participant age, denture type, denture material) on outcomes. The Limitations section of this report discusses the appropriateness of participant selection and its impact on the external validity of the study.
The cohort study30 had a low risk of bias related to classification of the exposure. This was a prospective study in which all participants were provided with a denture relining shortly after enrolment in the study. Although there may have been minor differences in denture relining procedures, as multiple clinicians were involved in the study, the denture relining procedure followed a standardized approach that was reported in detail.
The risk of bias related to temporal precedence was low. Following initial denture relining, clinicians evaluated denture adaptation for all participants and determined that dentures were well-fitted and did not require adjustment or additional relining. This suggests that all dentures were free of the outcome of interest (i.e., the need for additional relining) at the start of the observation period.
The study had a high risk of bias related to the assessment, detection, and measurement of the outcome. Denture adaptation was evaluated using modified criteria for the evaluation of relined dentures, which was based on the US Public Health Service criteria for direct evaluation of restorative materials.33 Although this appears to be an established method, it was unclear how the authors modified the criteria and who was responsible for assessing participants. The authors provided limited information on how the need for additional relining was assessed (e.g., whether it was determined using inspection of the oral cavity, functional tests, or participant feedback). This creates uncertainty as to whether the outcome was assessed using a reliable and valid method.
Risk of bias related to participant retention was low, as all 50 participants enrolled in the study completed the 1-year follow-up. This eliminates the risk that missing data could have influenced the results.
The study had a high risk of reporting bias, as the authors did not report whether the study followed a prespecified protocol. It is unclear to what extent participant eligibility, outcomes, and analyses were established before initiating the study.
The authors did not report their potential conflicts of interest or sources of funding for this study, which introduces uncertainty regarding whether financial or other interests may have influenced the study’s design and conduct.
Table 2 presents a summary of the risk of bias assessment for the included cohort study.30
Table 2: Summary of Risk of Bias in the Included Cohort Study Using the Revised JBI Cohort Studies Critical Appraisal Tool34
Study citation | Risk of bias | |||||
|---|---|---|---|---|---|---|
Selection and allocation | Classification of the exposure | Confounding factors | Temporal precedence | Assessment, detection, and measurement of the outcome | Participant retention | |
Matsumura et al. (2001)30 | NAa | Low | NAa | Low | High | Low |
NA = not applicable.
Note: We assessed all risk of bias domains appraised at the outcome level for the adaptation outcome, which is the only reported outcome relevant to this rapid review.
aBecause the study evaluated a descriptive outcome (i.e., denture longevity) using a single-arm design, we considered bias related to participant selection between groups and bias due to confounding factors to be not applicable. The representativeness of the study population was assessed in relation to external validity (generalizability).
Included Studies for Question 2: Clinical Evidence on the Longevity of Rebased Dentures
This rapid review did not identify relevant studies that addressed research question 2; therefore, no appraisal can be provided.
Included Studies for Question 3: Guidelines on the Timing of Relining or Rebasing Procedures for Dentures
We did not identify any relevant evidence-based guidelines that addressed research question 3; therefore, no appraisal can be provided.
Summary of Findings
Appendix 5 (Table 5) presents additional details regarding the main study findings.
Question 1: Clinical Evidence on the Longevity of Relined Dentures
Clinical evidence on the longevity of removable complete or partial dentures following a relining procedure was available from 1 single-arm cohort study.30
Longevity of Relined Dentures
Adaptation
The authors of the single-arm cohort study30 reported that no participants were assessed as needing additional denture relining or fabrication of a new denture after the 1-year observation period (i.e., following use of a relined denture for 1 year). Of the 50 participants evaluated at 1-year follow-up, 47 (94%) were assessed as having well-fitted dentures with no need for adjustment or re-relining, while 3 (6%) were assessed as having a slight change in adaptation that remained within the normal range and was clinically acceptable.
There were no statistically significant differences in the distribution of adaptation ratings between baseline (i.e., immediately following denture relining, when all 50 participants were rated as having well-fitted dentures) and 1-year follow-up (P = 0.0833).
Question 2: Clinical Evidence on the Longevity of Rebased Dentures
This rapid review did not identify any publications that provided clinical evidence on the longevity of removable complete or partial dentures following a rebasing procedure for people with tooth loss. Therefore, we could not provide a summary.
Question 3: Guidelines on the Timing of Relining or Rebasing Procedures for Dentures
This rapid review did not identify any evidence-based guidelines that provide recommendations on how often dentures should be relined or rebased after a new denture is inserted or after an initial reline or rebase procedure. Therefore, we could not provide a summary.
Limitations
Evidence Gaps
A major limitation of the current evidence base is the lack of data on denture longevity and maintenance timelines.
We found no clinical evidence on the longevity of rebased dentures; therefore, no conclusions can be drawn regarding the longevity of rebased dentures. Furthermore, no evidence-based guidelines providing recommendations on the timing of denture relining or rebasing after a new denture is inserted or after an initial reline or rebase procedure were identified.
The 1 included cohort study30 conducted a final follow-up at 1 year. This follow-up may have been appropriate for many outcomes evaluated in the study, including denture staining, discoloration, peeling or detachment of material, and irritation to oral tissue (not relevant to this report); however, no participants required denture relining during the study period, so the follow-up was too short to provide estimates on the longevity of relined dentures. As a result, the findings of the included cohort study30 have limited usefulness for informing decisions on the appropriate timing of denture relining procedures.
Generalizability
We used PROGRESS-Plus32 criteria to guide data extraction and provide insights into whether the population in the included cohort study30 may be representative of populations in Canada. In addition to PROGRESS-Plus32 criteria, denture longevity following a relining or rebasing procedure may be influenced by many factors, including:
denture characteristics (e.g., implant supported or tissue supported, mandibular or maxillary, complete or partial)
timing of denture provision (e.g., immediately following tooth extraction or following a healing period)
denture relining materials
relining and rebasing protocols and manufacturing practices
clinician experience
treatment setting (e.g., public or private clinic)
The included cohort study30 reported little to no information on key participant characteristics and intervention-related factors such as denture design and materials. This limited reporting prevents a meaningful assessment of whether the study population is representative of the target population. In addition, the cohort study30 included only 50 participants, and larger sample sizes may better reflect the full range of denture longevity (e.g., in a larger sample, some individuals may have required relining within 1 year).
Overall, we judged the generalizability of the findings summarized in this report to clinical settings in Canada to be low. This judgment was due to the sample size and lack of detailed reporting in the included study,30 as well as potential differences in population characteristics and standards of care, especially given that the included cohort study30 was conducted at least 25 years ago in Japan.
Conclusions and Implications for Decision- or Policy-Making
We identified 1 prospective single-arm cohort study30 that provided clinical evidence on the longevity of relined dentures. We did not identify any publications that provided clinical evidence on the longevity of rebased dentures or any evidence-based guidelines providing recommendations on how often dentures should be relined or rebased.
Summary of Evidence
The included cohort study30 conducted a final follow-up 1 year after denture relining. At the 1-year follow-up, none of the 50 participants required additional denture relining. Although the findings suggest that the longevity of all relined dentures in the study population exceeded 1 year, they do not provide information on when relining would be required over a longer observation period. Additionally, methodological limitations may affect the internal validity of the study, and the findings have low generalizability to clinical settings in Canada. As a result, the findings of the cohort study30 have limited usefulness for informing decisions on the appropriate timing of denture relining procedures, and additional evidence that provides more precise estimates of the longevity of denture relining is needed.
We identified no clinical evidence on the longevity of rebased dentures and no evidence-based guidelines that provide recommendations on how often dentures should be relined or rebased after a new denture is inserted and after an initial reline or rebase procedure that met our eligibility criteria.
Considerations for Future Research
Future research is needed to strengthen the evidence base on the longevity of relined and rebased dentures and to better inform policy and clinical decision-making. Well-designed studies that evaluate key outcomes (e.g., denture survival rates and the mean time to relining, rebasing, or replacement) would provide more meaningful evidence to inform decision-making. Studies should include large sample sizes, assess outcomes (e.g., the need to additional relining or rebasing) using validated methods, and conduct long-term follow-up assessments that are sufficient for a meaningful number of outcomes to occur. Reporting results according to denture or relining materials and other important factors, such as denture characteristics, relining or rebasing protocols, and treatment settings, could provide insights into how these variables may influence longevity.
To support assessments of generalizability, future studies should report key participant characteristics. These include race, ethnicity, age, sex, gender, place of residence, disability status, education levels, socioeconomic status, and other characteristics associated with potential health inequities.1,9-11 Findings from studies that include participants with a diversity of these characteristics would have increased applicability across different populations and care contexts.
As more robust clinical evidence becomes available, it may support the development of evidence-based guidelines that provide recommendations on the appropriate timing of denture relining and rebasing procedures. Such guidelines would be useful for informing clinical practice and policy decision-making.
Considerations for Clinical Practice or Considerations for Decision- or Policy-Making
The limited evidence base on this topic has been described in the broader literature. In 2011, the American College of Prosthodontists published evidence-based guidelines22 on the care and maintenance of complete dentures. These guidelines22 state that there were no published clinical guidelines to assist clinicians in determining how frequently to reline or rebase dentures. Additionally, evidence-based guidelines39 published in 2007 by the Japan Prosthodontic Society recommend relining dentures when the mandibular position and occlusal relationship are appropriate but the fit of the denture base to the mucosa is poor. However, they do not provide recommendations on the timing of relining or rebasing procedures.39
In addition to these guidelines,22,39 we also identified a systematic review40 that described the availability of evidence-based recommendations on the frequency of denture relining. Although it did not meet the inclusion criteria for our rapid review, the authors of this systematic review40 stated there are no evidence-based recommendations on the frequency of denture relining, but regular intervals are recommended. While the statements made in these sources22,39,40 are consistent with the findings of this report, the methods used to inform statements made in these evidence-based guidelines and by the authors of the systematic review were not assessed as part of this report.
In the absence of robust direct evidence and evidence-based guidelines, decisions regarding denture relining and rebasing may be informed by indirect clinical evidence, clinical expertise, and context-specific factors such as dental service utilization data and patient preferences.
References
1.Statistics Canada. Self-reported oral health problems in the Canadian population living in the provinces, November 2023 to March 2024. Accessed April 7, 2026. https://www150.statcan.gc.ca/n1/daily-quotidien/241023/dq241023b-eng.htm
2.Hao Y, Yuan Z, Zhu Y, et al. Association between tooth loss and depression mediated by lifestyle and Inflammation- a cross-sectional investigation. BMC Public Health. 2024;24(1):2627. doi:10.1186/s12889-024-20065-z PubMed
3.Al-Rafee MA. The epidemiology of edentulism and the associated factors: A literature Review. J Family Med Prim Care. 2020;9(4):1841-1843. doi:10.4103/jfmpc.jfmpc_1181_19 PubMed
4.Giacaman RA, Fernández CE, Muñoz-Sandoval C, et al. Understanding dental caries as a non-communicable and behavioral disease: Management implications. Front Oral Health. 2022;3:764479. doi:10.3389/froh.2022.764479 PubMed
5.Hashim NT, Babiker R, Padmanabhan V, et al. The global burden of periodontal disease: A narrative review on unveiling socioeconomic and health challenges. Int J Environ Res Public Health. 2025;22(4)doi:10.3390/ijerph22040624 PubMed
6.Juneja P, Kulkarni S, Raje S. Prevalence of traumatic dental injuries and their relation with predisposing factors among 8-15 years old school children of Indore city, India. Clujul Med. 2018;91(3):328-335. doi:10.15386/cjmed-898 PubMed
7.Chatzopoulos GS, Jiang Z, Marka N, Wolff LF. Periodontal disease, tooth loss, and systemic conditions: An exploratory study. Int Dent J. 2024;74(2):207-215. doi:10.1016/j.identj.2023.08.002 PubMed
8.Rakhshan V. Congenitally missing teeth (hypodontia): A review of the literature concerning the etiology, prevalence, risk factors, patterns and treatment. Dent Res J (Isfahan). 2015;12(1):1-13. doi:10.4103/1735-3327.150286 PubMed
9.Gabiec K, Bagińska J, Łaguna W, et al. Factors associated with tooth loss in general population of Bialystok, Poland. Int J Environ Res Public Health. 2022;19(4)doi:10.3390/ijerph19042369 PubMed
10.De Rubeis V, Jiang Y, de Groh M, et al. Oral health problems among Canadians aged 45 to 85: Data from the Canadian Longitudinal Study on Aging Baseline Survey (2011-2015). Int J Environ Res Public Health. 2023;20(8)doi:10.3390/ijerph20085533 PubMed
11.Kim JK, Baker LA, Seirawan H, Crimmins EM. Prevalence of oral health problems in U.S. adults, NHANES 1999-2004: exploring differences by age, education, and race/ethnicity. Spec Care Dentist. 2012;32(6):234-41. doi:10.1111/j.1754-4505.2012.00280.x PubMed
12.Sailasri K, Kar AK, Shujaulla S, et al. Patient Satisfaction and Oral Health-Related Quality of Life with Complete Dentures. J Pharm Bioallied Sci. 2025;17(Suppl 3):S2289-S2891. doi:10.4103/jpbs.jpbs_674_24 PubMed
13.Muhammad N, Sarfraz Z, Zafar MS, et al. Characterization of various acrylate based artificial teeth for denture fabrication. J Mater Sci Mater Med. 2022;33(2):17. doi:10.1007/s10856-022-06645-8 PubMed
14.Sadek SA, Dehis WM, Hassan H. Different materials used as denture retainers and their colour stability. Open Access Maced J Med Sci. 2018;6(11):2173-2179. doi:10.3889/oamjms.2018.415 PubMed
15.Canadian Dental Association. Dentures. Accessed April 7, 2026. https://www.cda-adc.ca/en/oral_health/procedures/bridges_dentures/dentures.asp
16.Ali Hassan MA, Elhadi RM, Osman M, Mohammed Abdalrahman SA, Elzibair Eltahir MA, Nureldinn S. Choosing between fixed and removable prosthetic modalities for completely edentulous patients: A systematic review of evidence-based outcomes. Cureus. 2026;18(1):e101213. doi:10.7759/cureus.101213 PubMed
17.Bandiaky ON, Lokossou DL, Soueidan A, et al. Implant-supported removable partial dentures compared to conventional dentures: A systematic review and meta-analysis of quality of life, patient satisfaction, and biomechanical complications. Clin Exp Dent Res. 2022;8(1):294-312. doi:10.1002/cre2.521 PubMed
18.Mylonas P, Milward P, McAndrew R. Denture cleanliness and hygiene: an overview. Br Dent J. 2022;233(1):20-26. doi:10.1038/s41415-022-4397-1 PubMed
19.Brown JL, Young T, McKloud E, et al. An in vitro evaluation of denture cleansing regimens against a polymicrobial denture biofilm model. Antibiotics (Basel). 2022;11(1)doi:10.3390/antibiotics11010113 PubMed
20.Nishi Y, Seto K, Murakami M, et al. Effects of denture cleaning regimens on the quantity of Candida on dentures: A cross-sectional survey on nursing home residents. Int J Environ Res Public Health. 2022;19(23)doi:10.3390/ijerph192315805 PubMed
21.Berteretche MV, Mastari F, Nicolas E, Hüe O. The needs of denture-brushing in geriatrics: clinical aspects and perspectives. Gerodontology. 2012;29(2):e768-71. doi:10.1111/j.1741-2358.2011.00557.x PubMed
22.Felton D, Cooper L, Duqum I, et al. Evidence-based guidelines for the care and maintenance of complete dentures: a publication of the American College of Prosthodontists. J Prosthodont. 2011;20 Suppl 1:S1-S12. doi:10.1111/j.1532-849X.2010.00683.x PubMed
23.Rathi A, Banerjee R, Radke U, Lahoti S, Sahni S. Knowledge and attitude about relining of complete dentures in clinical practice: A cross-sectional study. J Indian Prosthodont Soc. 2018;18(2):174-180. doi:10.4103/jips.jips_302_17 PubMed
24.Duran İ, Yilmaz B, Ural Ç. A technique for removing implant-retained denture: Direct relining complication. Case Rep Dent. 2015;2015:126257. doi:10.1155/2015/126257 PubMed
25.Hill EE, Rubel B. Direct chairside hard reline at delivery of a newly fabricated distal extension removable partial denture: considerations and techniques. J Can Dent Assoc. 2011;77:b84. PubMed
26.Bansal M, Kumar S, Kumar R. Clinical perspectives on denture relining: A review of literature and current best practices. IOSR-JDMS. 2025;24(6):50-53. doi:10.9790/0853-2406015053
27.Krunić N, Kostić M, Petrović M, Igić M. Oral health-related quality of life of edentulous patients after complete dentures relining. Vojnosanit Pregl. 2015;72(4):307-11. doi:10.2298/vsp1504307k PubMed
28.Haywood J, Basker RM, Watson CJ, Wood DJ. A comparison of three hard chairside denture reline materials. Part I. Clinical evaluation. Eur J Prosthodont Restor Dent. 2003;11(4):157-63. PubMed
29.Khangura SD, Grobelna A, Haas R, Subramonian A. Longevity of removable prosthodontics: a review of the clinical evidence. Can J Health Technol. 2023;3(3):1-33. doi:10.51731/cjht.2022.595
30.Matsumura H, Tanoue N, Kawasaki K, Atsuta M. Clinical evaluation of a chemically cured hard denture relining material. J Oral Rehabil. 2001;28(7):640-4. doi:10.1046/j.1365-2842.2001.00701.x PubMed
31.Page MJ, Moher D, Bossuyt PM, et al. PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. BMJ. 2021;372:n160. doi:10.1136/bmj.n160 PubMed
32.O'Neill J, Tabish H, Welch V, et al. Applying an equity lens to interventions: using PROGRESS ensures consideration of socially stratifying factors to illuminate inequities in health. J Clin Epidemiol. 2014;67(1):56-64. doi:10.1016/j.jclinepi.2013.08.005 PubMed
33.Cvar JF, Ryge G. Reprint of criteria for the clinical evaluation of dental restorative materials. 1971. Clin Oral Investig. 2005;9(4):215-32. doi:10.1007/s00784-005-0018-z PubMed
34.Barker TH, Hasanoff S, Aromataris E, et al. The revised JBI critical appraisal tool for the assessment of risk of bias for cohort studies. JBI Evid Synth. 2025;23(3):441-453. doi:10.11124/jbies-24-00103 PubMed
35.Hinz S, Bomicke W, Schweyen R, Bensel T. Ten-year clinical performance of non-precious metal double crowns with friction pins in severely reduced dentitions-a retrospective study. Clin Oral Investig. 2023;27(4):1623-1635. doi:10.1007/s00784-022-04788-0 PubMed
36.Taylor M, Masood M, Mnatzaganian G. Longevity of complete dentures after relines: A 20-year population based retrospective study of 187,227 publicly insured adults. J Dent. 2022;121:104073. doi:10.1016/j.jdent.2022.104073 PubMed
37.Kimoto S, Kimoto K, Kitamura A, Saita M, Iijima M, Kawai Y. Effect of dentist's clinical experience on treatment satisfaction of a complete denture. J Oral Rehabil. 2013;40(12):940-7. doi:10.1111/joor.12108 PubMed
38.Dinu RC, Comanescu CL, Drafta S, Petre AE. Clinical performance and longevity of implant-assisted removable partial dentures compared to other removable prosthesis types: A systematic review. Dent J (Basel). 2025;13(9)doi:10.3390/dj13090389 PubMed
39.Shiga H, Terada Y, Ikebe K, Akagawa Y, Hirai T, Inoue H. Guideline for Denture Relining. Prosthodont Res Pract. 2007;6:209-216. doi:10.2186/prp.6.209
40.Dawid M-T, Moldovan O, Rudolph H, Kuhn K, Luthardt RG. Technical complications of removable partial dentures in the moderately reduced dentition: A systematic review. Dent J (Basel). 2023;11(2)doi:10.3390/dj11020055 PubMed
41.Japan Prosthodontic Society. Clinical guidelines for denture relining with soft relining materials. Accessed April 7, 2026. https://www.hotetsu.com/files/files_865.pdf
42.Canada’s Drug Agency. Canada's Drug Agency Style: A Guide for Authors and Editors. 2025. Accessed March 30, 2026. https://www.cda-amc.ca/sites/default/files/pdf/style_guide_2025_digital.pdf
43.Ettinger RL, Qian F. Longitudinal assessment of denture maintenance needs in an overdenture population. J Prosthodont. 2019;28(1):22-29. doi:10.1111/jopr.12735 PubMed
44.Fernandez-Estevan L, Montero J, Selva Otaolaurruchi EJ, Sola Ruiz MF. Interventions to maintain locator-retained mandibular overdentures on both external hex and internal connection implants: A retrospective study. Int J Oral Maxillofac Implants. 2018;33(16):838-846. doi:10.11607/jomi.6182 PubMed
45.Attard NJ, Zarb GA. Long-term treatment outcomes in edentulous patients with implant overdentures: the Toronto study. Int J Prosthodont. 2004;17(4):425-33. doi:10.1016/j.prosdent.2004.09.017 PubMed
Appendix 1: Detailed Methods and Selection of Included Studies
Please note that this appendix has not been copy-edited.
What Is a Rapid Review?
Rapid reviews are based on accelerated and abbreviated systematic review methods, balancing timeliness with rigour, to allow for timely decision-making. Due to these abbreviated methods, rapid reviews have some limitations. For example, we included studies published from 2001, excluding older studies. We attempted to mitigate this by searching for and including relevant systematic reviews published in the past 25 years that included older studies. Focusing on more recently published articles may also be more reflective of current practices. Additionally, we limited study eligibility to those that were published in English for feasibility reasons. As a result, 1 potentially relevant citation41 identified in the search was excluded.
Our rapid review intends to summarize the available evidence, rather than provide recommendations. These findings should not be interpreted as prescriptive guidance.
Literature Search Methods
An information specialist conducted a literature search on key resources including MEDLINE, Embase, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of health technology assessment agencies in Canada and major international health technology assessment agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevance. The search strategy comprised both controlled vocabulary, such as the US National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concepts were denture relining procedures, denture rebasing procedures, and longevity or timing of procedures. The search was completed on March 19, 2026, and limited to English-language documents published since January 1, 2001. The search strategy is available on request.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Exclusion Criteria
Articles were excluded if they:
did not meet the selection criteria outlined in Table 1
were duplicate publications or were published before 2001
were guidelines with unclear methodology
were case series or case reports
were published in languages other than English (for feasibility reasons).
Critical Appraisal of Individual Studies
The included publication was critically appraised by 1 reviewer using the revised JBI critical appraisal tool for the assessment of risk of bias for cohort studies.34 Following published guidance34 for this tool, the reviewer provided responses to each signalling question, rationale for responses, and domain level risk of bias judgments. Summary scores were not calculated for the included study; rather, the strengths and limitations of each included publication were described narratively.
Data Extraction
One reviewer extracted data directly into standardized tables created in Microsoft Word, which were modified as necessary. The extracted information included study characteristics, methodology (e.g., study design), population, intervention, comparator, and results regarding the outcomes of interest.
One reviewer extracted information from the included study using the PROGRESS-Plus framework32 to describe different population groups. Each included study was checked to determine if PROGRESS-Plus32 criteria were reported by study authors to describe the participants; detailed characteristics, if available, were then extracted and reported in Table 3 (Appendix 3). The main PROGRESS-Plus32 criteria include place of residence, race, ethnicity, culture, language, occupation, gender, sex, religion, education, socioeconomic status, social capital, personal characteristics associated with discrimination (e.g., age, disability), features of relationships, and time-dependent relationships. As part of report writing, we discuss these characteristics across the evidence, where available, when presenting results within the text.
When reporting on sex, gender, race, or ethnicity in this Rapid Review, we planned to retain the language used by the original study authors, and, whenever possible, we referred to these groups based on guidance from Canada’s Drug Agency Style: A Guide for Authors and Editors42 at the time this rapid review was conducted, with an understanding that language is constantly evolving.
Appendix 2: Selection of Included Studies
Please note that this appendix has not been copy-edited.
Appendix 3: Characteristics of Included Publication
Please note that this appendix has not been copy-edited.
Table 3: Characteristics of Included Nonrandomized Study
Study citation, country, funding source | Study design and setting | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Matsumura et al. (2001)30 Japan Funding source: NR | Single-centre, single-arm, prospective cohort study conducted at Nagasaki University School of Dentistry in Nagasaki, Japan. The participant recruitment period was NR. | Adults with dentures made of heat-polymerized PMMA-based acrylic resin. The type of denture (i.e., partial or complete) was NR. Number of participants: 50 Age: NR Sex or gender: NR Other PROGRESS-Plus criteria: NRa | Intervention: Denture relining performed with a hard denture relining agent (Tokuso Rebase Normal-set). Comparator: No control group; within-group comparisons were made from immediately after relining to follow-up at 1 year. | Relevant outcomes:
Follow-up: 1 year |
NR = not reported; PMMA = polymethyl methacrylate.
aThe main PROGRESS-Plus32 criteria include place of residence, race, ethnicity, culture, language, occupation, gender, sex, religion, education, socioeconomic status, social capital, personal characteristics associated with discrimination (e.g., age, disability), features of relationships, and time-dependent relationships.
Appendix 4: Critical Appraisal of Included Publication
Please note that this appendix has not been copy-edited.
Table 4: Risk of Bias Assessment of the Matsumura et al. (2001) Study30 — Revised JBI Cohort Studies Critical Appraisal Tool34
Item | Judgment | Support for judgment |
|---|---|---|
Bias related to selection and allocation | ||
Q1: Were the 2 groups similar and recruited from the same population? | Not applicable | This was a single-arm study with no comparison group. |
Bias related to classification of the exposure | ||
Q2: Were the exposures measured similarly to assign people to both the exposed and unexposed groups? | Not applicable | This was a single-arm study with no comparison group. All participants had the same exposure (i.e., a denture relining procedure). |
Q3: Was the exposure measured in a valid and reliable way? | Yes | This was a prospective study in which all participants received the exposure (i.e., a denture relining procedure) following enrolment. |
Bias related to confounding factors | ||
Q4: Were confounding factors identified? | Not applicable | This was a single-arm study with no comparison group. Confounding was considered not appliable because the outcome of interest was descriptive, and the study did not evaluate factors that could influence denture longevity. |
Q5: Were strategies to deal with confounding factors stated? | Not applicable | This was a single-arm study with no comparison group. Confounding was considered not appliable because the outcome of interest was descriptive, and the study did not evaluate factors that could influence denture longevity. |
Bias related to temporal precedence | ||
Q6: Were the groups/participants free of the outcome at the start of the study (or at the moment of the exposure)? | Yes | Following denture relining (i.e., at baseline), all participants were assessed for denture adaptation. In all cases, dentures were rated as well-fitted with no need for adjustment or re-relining. |
Bias related to assessment, detection, and measurement of the outcome | ||
Q7: Were the outcomes measured in a valid and reliable way? | Unclear | Denture adaptation, including the need for additional relining, was evaluated using modified criteria for the evaluation of relined dentures, which was based on the US Public Health Service criteria for direct evaluation of restorative materials.33 Specific details on how the need for additional relining was assessed were not reported, so the validity of this approach is unclear. |
Q8: Was the follow-up time reported and sufficient to be long enough for outcomes to occur? | No | The final follow-up for the study was performed after 1 year of relined denture service. A longer follow-up period would be needed to appropriately evaluate the need for additional relining (i.e., denture adaptation). |
Bias related to participant retention | ||
Q9: Was follow-up complete, and if not, were the reasons to loss to follow-up described and explored? | Yes | All 50 participants were evaluated at final follow-up. |
Q10: Were strategies to address incomplete follow-up utilized? | Not applicable | Strategies to address incomplete follow-up were not relevant because all participants were available at final follow-up. |
Statistical conclusion validity | ||
Q11: Was appropriate statistical analysis used? | Yes | The authors used Wilcoxon signed-ranks tests to determine whether there was a statistically significant difference in denture adaptation between baseline and final follow-up. |
Note: All items appraised at the outcome level (i.e., Q5 to Q11) were assessed for the adaptation outcome, which is the only reported outcome relevant to this rapid review. For items appraised at the level of the result (i.e., Q9 to Q11), the 1-year results were used, as this was the only follow-up time point reported.
Appendix 5: Main Study Findings
Please note that this appendix has not been copy-edited.
Table 5: Summary of Findings by Outcome — Need for Additional Relining
Study citation | Denture type | Outcome | Outcome result | P value | |
|---|---|---|---|---|---|
Baseline | Follow-up | ||||
Follow-up: 1 year | |||||
Matsumura et al. (2001)30 | Conventional dentures relined with self-curing powder-liquid material | Participants with Adaptation score, n/N (%)a | — | — | 0.1573b |
1 (Alfa) | 50/50 (100%) | 48/50 (96%) | — | ||
2 (Bravo) | 0/50 (0%) | 2/50 (4%) | — | ||
3 (Charlie) | 0/50 (0%) | 0/50 (0%) | — | ||
aDenture adaptation was rated on a 3-point scale: 1 (Alfa) indicates a well-fitted denture with no need of adjustment or relining; 2 (Bravo) indicates slight change in denture adaptation but within the normal range and is clinically acceptable; and 3 (Charlie) indicates an ill-fitted denture with need for additional relining or fabrication of a new denture. The authors modified this evaluation method based on the US Public Health Service criteria for direct evaluation of restorative materials.33
bResults of a Wilcoxon signed-ranks test comparing results at baseline (immediately following denture relining) and follow-up.
Appendix 6: Additional References of Potential Interest
Please note that this appendix has not been copy-edited.
Table 6: Summary of Additional Clinical Studies of Potential Interest
Study citation, country, funding course | Study design and setting | Population characteristics | Intervention and comparator(s) | Key findings and author’s conclusions |
|---|---|---|---|---|
Hinz et al. (2023)35 Germany Funding source: NR. | Single-centre, retrospective cohort study with an observation period between January 2006 and January 2022. The study took place at the Martin-Luther-University Halle-Wittenberg in Germany. | Adults with partial tooth loss. Individuals with temporomandibular disorders or who were undergoing radiotherapy due to head and neck cancer were excluded. Number of participants: 158 Age (years), mean (SD): 62.6 (12.7) Sex or gender: 44.9% women. Other genders or sexes were NR. Other PROGRESS-Plus criteria: NRa | Intervention: Removable partial dentures retained by double crowns with spark-eroded friction pins Comparator: No control group | Over a mean observation period of 67.2 (SD = 39.7) months, 26.08% (48/182) of dentures were relined. The denture survival rate was 54.6% (95% CI, 33.4% to 75.8%) for relined dentures and 70.1% (95% CI, 56.7% to 83.5%) for nonrelined dentures (P = 0.052). The authors did not provide any information on the timing of relining procedures. |
Taylor et al. (2022)36 Australia Funding source: The authors reported that they received no funding for this work. | Multicentre, retrospective cohort study with an observation period between January 2000 and December 2019. The study included data from participants who received treatment from public or private clinics located in metropolitan, regional, and rural areas of Victoria, Australia. | Adults (aged 18 years or older) who received complete dentures for tooth loss. Number of participants: 187,227 Age (years), mean (SD): 67.4 (12.9) vs. 63.9 (14.2)b Sex or gender: 55.1% female and 43.9% male vs. 50.5% female and 48.2% male.b Other sexes or genders were NR. Indigeneity: 0.93% Aboriginal and 97.6% non-Aboriginal vs.1.3% Aboriginal and 97.4% non-Aboriginalb Geographic location: The geographic location of participants was reported as major city (54.3% vs. 42.4%), inner regional (30.7% vs. 31.0%), or outer regional and remote (14.8% vs. 26.4%).b SES: Reported using IRSAD quintiles. In the no reline group, the distribution of participants across quintiles was:
In the reline group, the distribution of participants across quintiles was:
Other PROGRESS-Plus criteria: NRa | Intervention: Removable complete dentures. Participants were stratified by reline status. Comparator: No control group | Across the 20-year observation period, 5.9% (10,961/187,227) of participants received a reline of their complete denture. Of the relined dentures, 50.4% were performed within 12 months of denture issue (i.e., early reline), and 49.6% were performed more than 12 months after denture issue (i.e., late reline). Dentures receiving an early reline had a mean longevity of 5.03 (SD = 3.76) years. Dentures which received a late reline had a mean longevity of 7.12 (SD = 3.32) years. An early reline was associated with a 2% reduction in denture longevity in comparison to those who did not receive a reline (IRR = 0.98; 95% CI, 0.97 to 0.99; P < 0.001), while a late reline was associated with a 15% increase in longevity in comparison to dentures which received no reline (IRR = 1.15; 95% CI, 1.13 to 1.16; P < 0.001). “Almost 6% of participants who received a complete denture during the 20-year observation period also received a reline of that denture. The incidence of relining was lower than previous findings, and the rate of relining decreased with each year of denture life. The results show that the timing of a reline during a denture’s life modulates its effect on denture longevity. Denture longevity was reduced in those receiving an early reline and was prolonged in those receiving a late reline” (p. 5).36 |
Ettinger and Qian (2019)43 US Funding source: NR | Single-centre, prospective cohort study conducted at the Department of Prosthodontics, University of Iowa in Iowa City, US. Participant enrolment occurred between 1974 and 1994. | Participants who received complete mandibular overdentures supported by natural teeth. Number of participants: 91 Age (years), mean (SD): 59.5 (10.1) Sex or gender: 36.3% female and 63.7% male. Other sexes or genders were NR. Other PROGRESS-Plus criteria: NRa | Intervention: Complete maxillary dentures and complete mandibular overdentures supported by natural teeth numbers #22 and #27 Comparator: No control group | The proportions of participants who underwent 0, 1, 2, 3, or 4 or more relines were 23.1%, 27.5%, 27.5%, 8.8%, and 13.1%, respectively. The average number of relines per participant was 1.8 (SD = 1.6). The proportions of participants who underwent 0, 1, or 2 or more repairs to the denture base were 78.0%, 11.0%, and 11.0%, respectively. The average number of repairs to the denture base per participant was 0.5 (SD = 1.6). The mean follow-up period during which these outcomes were assessed was NR, though each participant must have remained in the study for at least 2 years and returned for at least 2 recalls in that period. The maximum follow-up duration was 53 months. “The three most common denture treatment needs in this study were adjustment of the denture bases, denture relines, or denture remakes” (p.29).43 |
Fernandez-Estevan et al. (2018)44 Spain Funding source: NR | Single-centre, retrospective cohort study conducted at the University of Valencia in Valencia, Spain. The study analyzed data collected between 2000 and the final assessment in July 2012. | Participants who received prosthetic treatment for complete tooth loss of the mandible. Number of participants: 136 Age: Mean age of 73.5 (SD = 9.1) years in the overdentures on externally hexed implants group, 67.2 (SD = 8.3) years in the overdentures on internally hexed implants group, and 69.5 (SD = 12.9) years in the complete dentures group. Sex or gender: 61.3% female and 38.7% male in the overdentures on externally hexed implants group, 59.2% female and 40.8% male in the overdentures on internally hexed implants group, and 57.1% female and 42.9% male in the complete dentures group. Other sexes or genders were NR. Education level: Participants were categorized as illiterate (48.4% vs. 28.6% vs. 39.3%) or as having primary education (32.2% vs. 34.3% vs. 35.7%), high school (12.9% vs. 28.5% vs. 21.5%), or university degrees (3.2% vs. 8.2% vs. 3.6%).c Smoking status: Participants reported no history of smoking (54.8% vs. 40.8% vs. 38.2%), previous use of smoking (29.0% vs. 36.7% vs. 30.9%), or current use of smoking (16.1% vs. 22.4% vs. 30.9%).c Coexisting conditions: Participants were categorized as having no systemic disease (32.3% vs. 30.6% vs. 32.1%), diabetes (12.9% vs. 16.3% vs. 14.3%), osteoporosis (25.8% vs. 8.2% vs. 16.1%), heart disease (9.7% vs. 12.2% vs. 19.6%), or other (19.4% vs. 32.7% vs. 17.9%).c Other PROGRESS-Plus criteria: NRa | Participants were divided into 3 groups based on the type of prosthesis received: implant-retained overdentures on externally hexed implants, implant-retained overdentures on internally hexed implants, and conventional complete dentures. | Over a mean follow-up time of 60 months (range, 2 months to 144 months), 61.3% of participants in the overdentures on externally hexed implants group, 44.9% of participants in the overdentures on internally hexed implants group, and 25.0% of participants in the complete denture group required relining. The denture relining rate (the mean number of relining events per participant per year) was 0.13 (SD = 0.13) in the overdentures on externally hexed implants group, 0.14 (SD = 0.28) in the overdentures on internally hexed implants group, and 0.22 (SD = 1.10) in the complete denture group. “Relining was also frequently required, occurring on average every 4 years in the control group and every 7 years in the overdenture groups” (p. 838).44 |
Attard et al. (2004)45 Canada Funding source: NR | Single-centre, prospective cohort study conducted at the Implant Prosthodontic Unit, University of Toronto, in Toronto, Canada. Participant enrolment occurred between early 1982 and 1992. The final recall visit was in 2002. | Participants who received implant-supported removable dentures for tooth loss. Number of participants: 45 (15 were lost to follow-up due to death or migration and were not included in the analysis) Age (years), mean (SD): 57.27 (11.18) Sex or gender: 80% women and 20% men. Other genders or sexes were NR. Coexisting conditions: 69% reported a chronic medical condition managed with medications. Smoking status: 78% reported no current use of smoking and 22% reported current use of smoking. Other PROGRESS-Plus criteria: NRa | Intervention: Removable overdentures supported by Brånemark implants Comparator: No control group | Over a mean follow-up time of 15.53 (SD = 2.39) years, participants received an average of 1.6 (SD = 1.3) relines to the overdenture. The average time to the first relining procedure was 4.41 (SD = 2.75) years. Relines occurred on average every 4.40 (SD = 2.81) years (including the initial reline). In participants who had overdentures opposed by complete dentures, the average time before the first reline of opposing dentures was 2.82 (SD = 1.25) years. Relining procedures on the opposing complete denture occurred on average every 3.89 (SD = 2.57) years (including the initial reline). “Relines were required on average every 4 to 5 years for both overdentures and opposing complete dentures” (p. 431 to 432).45 |
CI = confidence interval; IRR = incidence rate ratio; IRSAD = Index of Relative Socio-Economic Advantage and Disadvantage; NR = not reported; SD = standard deviation; SES = socioeconomic status; vs. = versus.
Notes: The studies summarized in this table were not critically appraised and their findings may be affected by methodological limitations that could affect their reliability. For example, Taylor and colleagues36 indicated that the early reline group in their study may have had a higher proportion of participants with immediate dentures (i.e., dentures provided immediately following tooth extraction) than the no reline or late reline groups. As a result, their findings may be at risk of bias related to confounding factors, as immediate dentures are likely to have shorter lifespans because of the increased rate of residual ridge resorption following tooth extraction.
Racial categories used in the table are as reported in the source and may not align with Canada's Drug Agency inclusive language guidelines.
aThe main PROGRESS-Plus32 criteria include place of residence, race, ethnicity, culture, language, occupation, gender, sex, religion, education, socioeconomic status, social capital, personal characteristics associated with discrimination (e.g., age, disability), features of relationships, and time-dependent relationships.
bParticipants with no denture reline vs. participants with a denture reline.
cParticipants in the overdenture on externally hexed implants group vs. overdenture on internally hexed implants group vs. complete denture group.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.