Drugs, Health Technologies, Health Systems
Health Technology Review
Nabilone for Behavioural and Psychological Symptoms of Dementia
Summary
Main Take-Away
Nabilone, a synthetic cannabinoid, may be an effective treatment for agitation in some patients with Alzheimer disease, based on 1 small trial. However, the evidence is uncertain, and it is unclear whether the effects of nabilone are meaningful to patients.
Key Messages
What Is the Issue?
Nabilone may have neuroprotective effects that could reduce the behavioural and psychological symptoms of dementia (BPSD).
Decision-makers are interested in understanding whether nabilone could be used as a potential alternative to antipsychotics for the treatment of BPSD in people with dementia.
What Did We Do?
We conducted a focused literature search and issued a targeted call for input from interested parties to inform our understanding of the current treatment landscape for BPSD, interpretation of the literature, and outcomes that are important to patients and clinicians.
We engaged 2 clinical experts in the management and treatment of certain health conditions in older adults to provide input on the project protocol and peer review the draft report.
What Did We Find?
A small placebo-controlled trial, in which patients with moderate-to-severe Alzheimer disease received both nabilone and placebo at different times, showed that compared to placebo, nabilone:
moderately decreased agitation; however, it is unclear whether this effect is meaningful to patients
improved neuropsychiatric symptoms and overall behavioural symptoms; however, the clinical meaningfulness of this is unknown
resulted in small improvements in cognition, nutritional status, and caregiver burden, though the clinical meaningfulness of these observations remains to be determined
resulted in a higher clinically meaningful frequency of sedation.
We found an evidence-based guideline that suggests that synthetic cannabinoids, including nabilone, may be used for severe agitation in people living with Alzheimer disease or related dementia if other pharmacological treatments have been unsuccessful.
We did not find any studies on the cost-effectiveness of nabilone or data on potential cost offsets associated with nabilone use in long-term care settings.
What Does This Mean?
The effects of nabilone on agitation in patients with moderate-to-severe Alzheimer disease were moderate, and it is unclear whether this improvement is meaningful to patients.
Evidence from larger studies with robust methodology and a longer follow-up period is needed to validate these observations.
Abbreviations
ADAS-Cog
Alzheimer Disease Assessment Scale–Cognitive Subscale
AE
adverse event
BMI
body mass index
BPSD
behavioural and psychological symptoms of dementia
CGI
Clinical Global Impression
CGIC
Clinical Global Impression of Change
CMAI
Cohen-Mansfield Agitation Inventory
IPA
International Psychogeriatric Association
MNA-SF
Mini Nutritional Assessment Short-Form
NPI-NH
Neuropsychiatric Inventory–Nursing Home version
PAINAD
Pain Assessment in Advanced Dementia
RCT
randomized controlled trial
SAE
serious adverse event
SIB
Severe Impairment Battery
SMMSE
Standardized Mini-Mental State Examination
TEAE
treatment-emergent adverse event
Context and Policy Issues
What Are Dementia and Behavioural and Psychological Symptoms of Dementia?
In the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, dementia is formally classified as a major neurocognitive disorder that is characterized by a decline in cognition (e.g., memory, executive function, language) and loss of function (e.g., ability to perform daily tasks).1 Many diseases, injuries, and conditions that affect different parts of the brain can cause dementia, with Alzheimer disease being the most common cause, accounting for up to 70% of cases.2 The other types of dementia include vascular dementia, Lewy body disease, mixed dementia, frontotemporal dementia, Parkinson disease, and Korsakoff dementia, among others.3
Between April 2022 and March 2023 in Canada, approximately 99,000 people aged 65 and older were newly diagnosed with dementia, and 487,000 people aged 65 and older were living with diagnosed dementia.4 The number of people living with dementia in Canada may be higher if it also includes those who have not been formally diagnosed by a health care provider.4 Approximately 3% of all people living with dementia are younger than 65 years.4
Behavioural and psychological symptoms of dementia (BPSD), also known as responsive behaviours, are noncognitive, neuropsychiatric, and behavioural disturbances.5 In Canada, BPSD affects up to 75% of community-dwelling people living with dementia6 and more than 80% of people living with dementia who reside in long-term care facilities.7 Common symptoms of BPSD include agitation, aggression, mood disorders (e.g., depression, apathy, anxiety), psychosis (e.g., hallucinations, delusions), sleep disturbances, and changes in appetite.6,8 These symptoms are more frequent and worsen as dementia progresses, and are associated with poor mental health outcomes and decreased quality of life for people living with dementia as well as caregivers.8
What Are the Treatment Options for BPSD?
BPSD is usually managed by nonpharmacological and pharmacological interventions to improve the symptoms and quality of life.5 Nonpharmacological interventions include sensory and cognitive stimulation, psychological approaches, environmental modifications, and caregiver education.9 Pharmacological interventions sometimes used for BPSD can include antipsychotic agents, antidepressants, sedative and hypnotic agents, mood stabilizers, and cholinesterase inhibitors, although the evidence for many of these medications is limited outside of specific situations.10
First-line treatment of BPSD involves a range of non-pharmacological interventions, which have limited adverse effects, and are more effective than pharmacological interventions for managing less severe symptoms.5,10 Pharmacological interventions may be required to manage more severe symptoms, particularly for agitation, or when nonpharmacological interventions have been unsuccessful.10
Despite their moderate efficacy in improving BPSD, the side effects of antipsychotics are substantial, including excessive sedation, orthostatic hypotension (increasing the risk of falls), and cerebrovascular accidents (increasing the risk of stroke and death).10
Why Is It Important to Do This Review?
There is an unmet need to find an alternative therapy that is as effective as antipsychotics but with less severe side effects for specific BPSD such as agitation. More recently, cannabinoids have been investigated for the treatment of multiple medical conditions, including chronic pain and psychiatric disorders.11
Cannabinoids consist of 3 general classes, including herbal cannabinoids (from the cannabis plant), endogenous cannabinoids (produced in the bodies of humans and animals), and synthetic cannabinoids (e.g., dronabinol, nabilone).12 In Canada, nabilone is approved for the treatment of severe nausea and vomiting associated with cancer chemotherapy due to its antiemetic properties.13 However, a recent database study showed that prescriptions of nabilone for long-term care residents in Canada increased following the legalization of recreational cannabis. Most of the nabilone prescriptions were off-label, particularly for non–cancer-related pain, depression, or anxiety disorders.14
As potential treatments for dementia, the safety and efficacy of cannabinoids in the management of BPSD have been investigated in preclinical studies and in several small clinical trials.12 Although findings from preclinical studies were promising for BPSD-like behaviours, such as agitation, aggression, and apathy, the findings from the clinical studies were mixed due to small sample size, lack of an adequate control, short trial duration, and low quality, which limit the ability to draw informed, evidence-based conclusions.12
With the need to identify alternative treatment options for BPSD, such as agitation, that may reduce health care-related costs associated with antipsychotic drug use in long-term care settings, a review of the efficacy, safety, and cost-effectiveness of nabilone was undertaken to help inform decision-makers. In addition, this review also aimed to identify recommendations from evidence-based guidelines regarding the use of nabilone for the treatment of BPSD.
Research Questions
What is the clinical efficacy and safety of nabilone compared with pharmacological treatments, nonpharmacological treatments, or no treatment for patients with specific BPSD?
What is the cost-effectiveness of nabilone compared with pharmacological treatments, nonpharmacological treatments, or no treatment for patients with BPSD?
What are the evidence-based guideline recommendations on the use of nabilone for the treatment of patients with BPSD?
Methods
Literature Search Methods
An information specialist conducted a literature search on key resources including MEDLINE, Embase, PsycINFO, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of health technology assessment agencies in Canada and major international HTA agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevance. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concepts were nabilone and dementia. An additional search was conducted using the search concepts dementia and behavioural and psychological symptoms; search filters were applied to this search to limit retrieval to guidelines. Conference abstracts and clinical trial registry records were excluded from both searches. The searches were completed on March 2, 2026, and were limited to English-language documents published since January 1, 2016. The search strategies are available on request.
Selection Criteria and Methods
Two reviewers independently selected relevant studies for inclusion in 2 stages, first by titles and abstracts and then by full texts based on the inclusion criteria presented in Table 1. Any record considered relevant by either reviewer at the title and abstract stage was reviewed by full text. Both reviewers agreed on the studies included in the report.
Criteria | Description |
|---|---|
Population | Adults with BPSD |
Intervention | Nabilone |
Comparator |
|
Outcome | Question 1:
Question 2:
Question 3:
|
Study designa | RCTs, systematic reviews (including NMAs and MAs), evidence-based guidelinesb |
AE = adverse event; BPSD = behavioural and psychological symptoms of dementia; MA = meta-analysis; NMA = network meta-analysis; NPI = Neuropsychiatric Inventory; PICO = population, intervention, comparison, and outcome; QALY = quality-adjusted life-year; RCT = randomized controlled trial.
aThis review employed a hierarchical approach to evidence inclusion, prioritizing the most robust and current evidence. We first sought recent, comprehensive, and high-quality systematic reviews, MAs, or NMAs. If we did not identify suitable systematic reviews for the PICO question, or if supplementation is needed, we included RCTs.
bA guideline is considered evidence-based if a systematic search of the literature was undertaken and a guideline panel was involved in informing the recommendations.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1 or if they were published before 2016. Systematic reviews were excluded if the included studies evaluating natural cannabinoids and synthetic cannabinoids were combined in a meta-analysis. Guidelines with unclear methodology were also excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer and checked by a second reviewer using the following tools as a guide: the revised Cochrane Risk of Bias Tool for Randomized Controlled Trials (RoB 2)15 and the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument16 for guidelines. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Engagement
A call for input on the project protocol from interested parties was issued at project initiation through the Canada’s Drug Agency weekly newsletter and on our website. Patient and clinician groups with whom we have previously engaged were proactively notified of the opportunity to provide input. Two clinicians from Western and Central Canada with expertise in geriatric psychiatry provided input on the project scope. Their input provided important contextual insights that helped inform the research team’s understanding of the current treatment landscape, unmet needs, priority outcomes, search strategy, and interpretation of evidence. The clinicians highlighted ongoing challenges in the management of BPSD, noting that many affected patients reside in long-term care settings, where care needs are often complex. Key issues raised included limitations associated with current treatment options in terms of efficacy and safety, and workforce constraints that impact the ability to deliver care. Collectively, the input highlighted that there may be a need for additional therapeutic options that are feasible to implement in long-term care settings across Canada. It was also noted that there is an ongoing phase III clinical trial evaluating nabilone for the treatment of agitation in patients with Alzheimer disease (NCT04516057).
Clinical Expert Engagement
Two clinical experts with expertise in the management and treatment of certain health conditions in older adults, as well as the appropriate use of drugs in this population, were consulted during the review. Both experts provided input on the project protocol, including the proposed scope and refinement of the review. The experts also reviewed and provided feedback on the draft report, offering clinical context and interpretation of the evidence. Their input was used to help inform the interpretation of findings and the identification of key limitations and considerations for future research.
Summary of Evidence
Quantity of Research Available
A total of 189 citations were identified in the literature search. Following screening of titles and abstracts, 176 citations were excluded, and 13 potentially relevant reports from the electronic search were retrieved for full-text review. One potentially relevant publication was retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 12 publications were excluded for various reasons, and 2 publications met the inclusion criteria and were included in this report. These included 1 randomized controlled trial (RCT) and 1 evidence-based guideline. Appendix 1 presents the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA)17 flow chart of the study selection. The lists of included studies (Table 2) and excluded studies (Table 3), with the inputs from the clinical experts, are provided in Appendix 2.
Summary of Study Characteristics
Appendix 3 provides details regarding the characteristics of the included primary study (Table 4) and the included evidence-based guideline (Table 5).
Included Studies for Research Question 1: What Is the Clinical Efficacy and Safety of Nabilone Compared With Pharmacological Treatments, Nonpharmacological Treatments, or No Treatment for Patients With BPSD?
Study Design
The included primary study was a randomized, placebo-controlled, double-blind crossover trial.
Country of Origin
The crossover RCT by Herrmann et al. (2019)18 was conducted by authors in Canada.
Patient Population
Patients in the RCT by Herrmann et al. (2019)18 were adults with moderate-to-severe Alzheimer disease, who had a score of less than or equal to 24 on the Standardized Mini-Mental State Examination (SMMSE) and clinically substantial agitation/aggression (Neuropsychiatric Inventory–Nursing Home version [NPI-NH]-agitation/aggression subscore ≥ 3). All but 1 participant (97%) met the International Psychogeriatric Association (IPA) research diagnostic criteria for agitation. The mean age of participants was 87 years, with fewer female (23%) than male (77%) participants. Most of the participants were patients from the Sunnybrook Health Sciences Centre long-term care facility (72%), whereas the remaining were outpatients (18%) from geriatric psychiatry clinics across the Greater Toronto Area.
Patients had to be on a stable dose of a cognitive enhancer (cholinesterase inhibitors or memantine) for 3 months or more and psychotropics for more than 1 month before randomization. Patients were excluded if they had contraindications to nabilone, unstable cardiovascular disease, or the presence or history of other neurologic conditions or other psychiatric disorders, including delusions or hallucinations.
Interventions and Comparators
The crossover RCT by Herrmann et al. (2019)18 compared the efficacy and safety of nabilone versus placebo in patients living in long-term care settings and outpatients with moderate-to-severe Alzheimer disease and agitation. The study was a 14-week crossover trial that compared nabilone (1 mg to 2 mg per day) to placebo (6 weeks each) with a 1-week washout between phases. During the nabilone phase, participants initially received 0.25 mg/day, which was slowly titrated up to a maximum target dose of 2 mg/day. In case of an intolerable adverse event (AE) potentially related to the study medication, the dose was decreased by 0.5 mg increments until resolution. The study medication was discontinued if side effects were still intolerable at 1 mg/day. The maintenance dose was down-titrated at week 6 to reduce the risk of potential withdrawal. The same dosing structure was applied during the placebo phase. The mean tolerated dose of nabilone per day was 1.6 mg (± 0.5 mg).
Outcomes
The efficacy outcomes in the crossover RCT by Herrmann et al. (2019)18 were agitation assessed by the Cohen-Mansfield Agitation Inventory (CMAI); cognition assessed by the SMMSE, the Severe Impairment Battery (SIB), and the Alzheimer Disease Assessment Scale–Cognitive Subscale (ADAS-Cog); neuropsychiatric symptoms assessed by the NPI-NH; caregiver burden assessed by the NPI-NH caregiver distress score; behaviour assessed by taking the sum of 3 CMAI subscales (CMAI-IPA score) (physical aggression, verbal aggression, and physical nonaggression) and the Clinical Global Impression of Change (CGIC); nutritional status assessed by the Mini Nutritional Assessment Short-Form (MNA-SF), weight, and body mass index (BMI); and pain assessed by the Pain Assessment in Advanced Dementia (PAINAD).
Brief descriptions of the efficacy outcome measures are as follows:
CMAI: a 29-item scale that measures 4 domains of agitation — physical/aggressive (questions 1 to 11), physical/nonaggressive (questions 12 to 21), verbal/aggressive (questions 22 to 24), and verbal nonaggressive (questions 25 to 29).19 Each item is rated on a scale from 1 (never) to 7 (several times an hour). The overall CMAI total score (29 items) ranges from 29 to 203, with higher scores indicating greater agitation severity. The minimal important difference (MID) for CMAI total score ranges from –4 points (up to a month) to –11 points (more than 1 to 3 months).20
SMMSE: an 11-question measure that tests 5 areas of cognitive function — orientation, registration, attention and calculation, recall, and language.21 The maximum score is 30. A score of 23 or lower is indicative of cognitive impairment. The MID for SMMSE is 1.4 points.22
SIB: used to assess cognition in patients with SMMSE less than or equal to 15.23 The SIB contains 6 major subscales to assess mild-to-moderate dementia: attention, orientation, language, memory, visuospatial ability, and construction. All but 2 of the SIB items are scored on a 3-point scale: 2 = correct; 1 = partially correct, and appropriate or closely related answer; and 0 = incorrect. The other 2 questions only have a 0 or a 1 point answer. Lower scores indicate greater impairment. Specific numerical MID for SIB is not available.
ADAS-Cog: an 11-task neuropsychological assessment (0 to 70 scale) measuring dementia severity, memory, language, and praxis (motor tasks).24 Higher scores indicate greater impairment. The MID for ADAS-Cog is 2 points.25
NPI-NH: a carer-based tool that assesses the possible presence of 12 symptoms in dementia cases, including delusions, hallucinations, apathy, depression, agitation, euphoria, aberrant motor behaviour, irritability, disinhibition, anxiety, sleeping, and eating.26 The greater the score, the more severe and frequent the behavioural disturbances. The MID for NPI-NH severity ranges from –3.2 to –2.8 points.27
NPI-NH caregiver distress score: a tool that measures the emotional burden and work disruption of caregiver caused by dementia-related behaviours by using a 6-point scale (0 to 5) per symptom listed in NPI-NH (e.g., agitation, delusions, or apathy) with 0 being “not at all” and 5 being “extremely” distressing.28 Higher scores indicate higher levels of stress and burden on caregiver. The MID for NPI-NH caregiver distress ranges from –3.95 to –3.10 points.27
CMAI-IPA: derived from the 29-item questionnaire of CMAI by selecting items that align with the 3 main IPA Provisional Research Criteria for Agitation (i.e., physical aggression, verbal aggression, and physical nonaggression/restlessness).29 Higher scores indicate more severe, frequent agitation. The MID for CMAI-IPA ranges from –2 (at 1 month) to –5 (at 3 months) points.30
CGI: a 3-item clinician-rated assessment tool that measures psychiatric illness severity (CGI-S), global improvement (CGI-I) and efficacy (CGI-E).31 The scale is often used as an anchor to define the MID for other instruments (such as the CMAI, rather than having a single fixed MID value itself). CGI-S rates the current state of the illness from 1 (normal, not at all ill) to 7 (among the most extremely ill). CGI-I rates the change in the patient's condition compared to baseline, ranging from 1 (very much improved) to 7 (very much worse).CGI-E is an efficacy index integrating the treatment effect with its side effects on a 4-point matrix (ranging from no side effects to significant side effects that outweigh the treatment benefits.
CGIC: a 7-point scale used in clinical trials and practice to measure a patient’s improvement or decline after treatment. It assesses the overall effectiveness of the treatment, typically ranging from "very much improved" to "very much worse." Usually, the scale is 1 to 7 — 1) Very much improved, 2) Much improved, 3) Minimally improved, 4) No change, 5) Minimally worse, 6) Much worse, 7) Very much worse.
MNA-SF: a screening tool used to categorize patients as malnourished or at risk of malnutrition. It contains 6 questions (maximum 14 points) assessing recent changes in appetite, weight loss, mobility, psychological stress/acute disease, current neuropsychological problems, and BMI.32 A score of 11 or less is considered a threshold that requires assessment and intervention.33 A specific numerical MID for MNA-SF is not available. A score of 12 to 14 points indicates normal nutritional status, a score of 8 to 11 points indicates that the patient is at risk of malnutrition, and a score of 0 to 7 points indicates that the patient is malnourished.
PAINAD: a tool used to evaluate pain in individuals with dementia or cognitive impairment who cannot verbally communicate their pain. It assesses 5 behaviours: breathing, negative vocalization, facial expression, body language, and consolability, with total scores ranging from 0 (no pain) to 10 (severe pain).34 A score of 2 or more is considered a threshold for indicating “probable pain.”35
Safety outcomes reported in the included RCT18 were treatment-emergent AEs (TEAEs) and serious adverse events (SAEs).
Included Studies for Research Question 2: What Is the Cost-Effectiveness of Nabilone Compared With Pharmacological Treatments, Nonpharmacological Treatments, or No Treatment for Patients With BPSD?
We did not identify any economic evaluation studies on the cost-effectiveness of nabilone compared with pharmacological treatments, non-pharmacological treatments, or no treatment for patients with BPSD.
Included Studies for Research Question 3: What Are the Evidence-Based Guideline Recommendations on the Use of Nabilone for the Treatment of Patients With BPSD?
Study Design
The Canadian Coalition for Seniors’ Mental Health (CCSMH)36,37 developed an evidence-based clinical practice guideline to provide good practice statements and recommendations on assessing and managing specific BPSD among people living with dementia. The guideline development group consisted of 15 members and included representatives from geriatric psychiatry, geriatric medicine, family medicine, pharmacy, psychology, neurology, nursing, and pharmacology. Guideline panel members were involved in the development of topics and in reviewing the evidence by conducting a systematic review of existing guidelines on BPSD, a rapid overview of systematic reviews on BPSD assessment and management, and a rapid review of nonpharmacological and pharmacological interventions. The quality of evidence was rated per GRADE (Grading of Recommendations Assessment, Development and Evaluation) methodology as very low, low, moderate, or high. Each recommendation was rated as either strong or conditional, based on the level of evidence and the confidence that the benefits of each recommendation outweighed the risks.
Country of Origin
The authors of the CCSMH guideline36,37 were from Canada.
Target Population and Intended Users
The patient population of the CCSMH guideline36,37 was people with lived experience of dementia. The guideline may be applied in community, outpatient, inpatient, and long-term care and other residential care settings.
The intended users of the guideline include health care providers, people living with dementia, and caregivers of people living with dementia.
Interventions and Practice Considered
The CCSMH guideline36,37 provides guidance on assessing and managing BPSD in the care of people living with dementia within a Canadian context, using nonpharmacological and pharmacological approaches.
Outcomes
The CCSMH guideline36,37 considered all relevant outcomes related to the clinical effectiveness, health-related quality of life, and safety of nonpharmacological and pharmacological interventions.
Summary of Critical Appraisal
Randomized Controlled Trial
Table 6 of Appendix 4 presents the risk of bias assessment of the included RCT by Herrmann et al. (2019)18 using the RoB 2 tool.15
Internal Validity
Randomization was conducted using a block randomization code that was independently computer-generated by the institutional pharmacy department. The methods of randomization and allocation concealment were reported. There were no imbalances in patient baseline characteristics because all participants received the first treatment (nabilone) for 6 weeks, followed by a 1-week washout, then crossed over to a second treatment (placebo) for another 6 weeks. The 1-week washout period appeared to be sufficient to clear any carryover effects, given that the plasma half-life values for nabilone and its metabolites are approximately 2 and 35 hours, respectively.
Of the 38 patients who underwent treatment with nabilone in the first phase, 5 terminated treatment early due to a SAE. Of the remaining 33 patients who then underwent treatment with placebo in the second phase, 4 patients terminated treatment early due to an SAE. Thus, it appears that the number of participants who underwent each treatment was not equal. However, data from all participants were included in the analyses, and paired data from all participants were used without imputation. All prespecified outcomes were analyzed using the intention-to-treat population, meaning that all patients who were randomized to receive at least 1 dose of the study medication and completed at least 1 nonbaseline questionnaire were included.
The study reported that patients, family members, nurses, clinicians, outcome assessors, and investigators were blinded to treatment allocation and block size. However, clinicians and outcome assessors could be considered unblinded due to the specific AE of nabilone (i.e., sedation).
Methods of measuring the outcomes were appropriate, similar between intervention groups, and clearly described in the published protocol38 of the trial and in ClinicalTrials.gov (NCT02351882). The data were analyzed in accordance with a prespecified plan, and therefore, the results being assessed were unlikely to have been selected. However, measurement of outcomes could have been influenced by the knowledge of the intervention due to the presence of the specific AE of nabilone (i.e., sedation).
There was no adjustment for multiple testing of the secondary outcomes, which means that there is a higher probability of statistical significance by chance alone, increasing the risk a false-positive result (type I error).
Overall, the study had a low risk of bias in terms of the randomization process, carryover effects, missing outcome data, and selection of the reported results. However, the study might have a high risk of bias in the measurement of outcomes and had some limitations in the statistical analyses.
External Validity
The inclusion and exclusion criteria of the study limit the ability to generalize the findings to all patients with dementia in Canada. Participants in this study were mostly male, limiting its generalizability to female patients with dementia. Patients were recruited from a single centre (i.e., Sunnybrook Health Sciences Centre long-term care facility) and outpatient geriatric psychiatry clinics across the Greater Toronto Area, which may limit broad generalization of the results to patients across Canada.
Guideline
Table 7 of Appendix 4 presents the strengths and limitations of the included guideline.36,37
The CCSMH guideline36,37 had several strengths related to reporting. It was explicit in terms of scope and purpose (i.e., objectives, health questions and populations) and had a clear presentation of recommendations (i.e., specific, unambiguous, and easy-to-find key recommendations, with options for managing the different conditions or health issues). In terms of interest-holder involvement, the authors of the guideline clearly defined target users and the development groups, and reported that the views and preferences of patients were sought. The methodology for the development of the guideline was robust. The authors of the guideline clearly reported methods for evidence collection, criteria for selection, and methods for evidence synthesis. There were explicit links between recommendations and the supporting evidence and methods of formulating the recommendations. The authors of the guideline considered the health benefits and risks of side effects in formulating the recommendations. The guideline was explicit in terms of implementation and applicability, despite unclear resource implications. The authors reported that the guideline will be updated in the next 3 to 4 years. The guideline was reviewed independently by relevant professional experts and through public consultation. For editorial independence, the authors of the guideline declared the competing interests of all members in the guideline development group and disclosed that the views of the funding bodies (i.e., the Public Health Agency of Canada) had no influence on the content of the guidelines.
Overall, the included guideline36,37 was robust in terms of scope and purpose, involvement from interested parties, rigour of development, clarity of presentation, and editorial independence.
Summary of Findings
Appendix 5 presents the main study findings.
Clinical Efficacy and Safety of Nabilone Compared With Placebo for Patients With BPSD
Key results of the clinical efficacy outcomes are outlined in Table 8, and safety outcomes are included in Table 9.
Multiple outcome measures used to assess the efficacy of nabilone included CMAI, SMMSE, SIB, NPI-NH, CMAI-IPA, and CGI. In the included RCT,18 differences in outcome measures between treatment phases were analyzed using a statistical approach that estimates how outcomes changed over time while patients were receiving treatment (a linear mixed model). Results were reported as a value (b value or beta coefficient) representing the average change in outcome scores associated with each treatment phase. The mean differences in the b values between treatment phases were then compared with corresponding MIDs to assess whether the observed effects were clinically relevant.25
Agitation
The change in CMAI scores from the start of the study to week 6 was better with nabilone than with placebo, and this difference was unlikely to be due to chance. On average, scores were reduced by about 4 points more with nabilone than with placebo. This represents a moderate effect.
It is unclear whether this improvement is meaningful for patients. A 4-point change may be clinically meaningful over a short period (1 month), but a larger change (about 11 points) may be needed over longer periods (1 to 3 months). However, the change of nabilone in CMAI scores was greater than that of atypical antipsychotics, such as risperidone (1 mg/day),39 or antidepressants, such as citalopram (30 mg/day),40 which have reported improvements in CMAI scores of −1.17 points and −2.38 points compared to placebo, respectively.
Cognition
SMMSE: The difference in SMMSE scores was statistically significant; on average, scores were about 1 point higher with nabilone compared with placebo. This improvement may be clinically meaningful, given that the range of possible effects (from 0.1 to 2.0) includes 1.4, which is considered clinically important.
SIB: The difference in SIB scores was statistically significant; on average, scores were about 4.6 points lower with nabilone compared with placebo. However, the clinical meaningfulness of the difference was unclear due to the lack of a specific numerical MID.
ADAS-Cog: This outcome measure was not analyzed, given that only 3 patients completed this scale, and only 1 patient had scores for both treatment phases.
Neuropsychiatric Symptoms
The difference in NPI-NH scores was statistically significant; on average, scores were about 4.6 points lower with nabilone compared with placebo. This improvement may be clinically meaningful as the MID for NPI-NH severity ranges from −3.2 to −2.8.
Caregiver Burden
The difference in NPI-NH caregiver distress scores was statistically significant; on average, scores were about 1.7 lower with nabilone compared with placebo. However, the improvement may not be clinically meaningful, given that the MID for NPI-NH caregiver distress ranges from −3.95 to −3.10.
Behaviour
The difference in behaviour assessed by CMAI-IPA subdomain scores was statistically significant; on average, scores were about 3.8 points lower with nabilone compared with placebo. A 2-point change may be clinically meaningful over a short period (at 1 month), but a larger change (about 5 points) may be needed over longer periods (at 3 months).
Global Status
On the CGIC scale, 47% of patients in the nabilone phase experienced improvement compared to 23% of patients in the placebo phase (P = 0.09).
Nutritional Status
The difference in MNA-SF scores was statistically significant; on average, scores were about 0.2 higher with nabilone compared with placebo. However, the clinical meaningfulness of the difference was unclear due to the lack of a specific numerical MID.
There were no differences between treatment phases in weight or BMI.
Pain
There were no differences between treatment phases on the PAINAD scale.
Safety
More patients in the nabilone phase experienced TEAEs compared to the placebo phase (81.6% versus 36.8%; P = 0.05).
More patients in the nabilone phase experienced sedation compared to the placebo phase (44.7% versus 15.8%; P = 0.02).
There were no differences between treatment phases in other TEAEs or in SAEs.
Guidelines Regarding the Use of Nabilone for the Treatment of Patients With BPSD
Table 10 presents the recommendations of the included guideline.36,37
Due to limited and low-quality evidence, the CCSMH guideline36,37 conditionally recommends synthetic cannabinoids, including nabilone, for the treatment of severe agitation in patients with Alzheimer disease and related dementias if the symptoms do not respond to other pharmacological treatments.
Limitations
Evidence Gaps
No conclusions can be formed on the following research questions, given that no evidence was found:
the clinical efficacy and safety of nabilone compared with other pharmacological treatments or nonpharmacological treatments for patients with BPSD
the cost-effectiveness of nabilone compared with pharmacological treatments, nonpharmacological treatments, or no treatment for patients with BPSD
the impact of nabilone on health care-related costs due to antipsychotic drug utilization in the long-term care setting.
Generalizability
The findings of the RCT18 and the recommendations of the CCSMH guideline36,37 may be applicable to patients with dementia living in Canada, given that they were both conducted by authors in Canada.
Certainty of Evidence
Major limitations of the RCT18 included the crossover design and relatively small sample size. The results of the included RCT should be carefully interpreted, given the study limitations. Given the limited and low-quality evidence on the use of synthetic cannabinoids (including nabilone) for treatment of agitation in people with Alzheimer disease, the CCSMH guideline36,37 recommends that synthetic cannabinoids should be reserved for severe agitation in cases in which other medications have been trialled and found to be ineffective.
Conclusions and Implications for Decision- or Policy-Making
This review included 1 RCT18 and 1 evidence-based guideline.36,37
Clinical Efficacy and Safety of Nabilone for Treatment of BPSD
The crossover RCT by Herrmann et al. (2019)18 showed that nabilone resulted in a moderate reduction in agitation and a greater frequency of sedation compared to placebo. The trial also showed that nabilone resulted in an improvement in neuropsychiatric symptoms and overall behaviour, and had small benefits in caregiver burden, cognition, and nutrition, with no differences in weight and pain. However, the clinical meaningfulness of these observations remains to be determined.
Recommendations From the Included Evidence-Based Guideline
The 2025 CCSMH Canadian guideline36,37 conditionally recommends synthetic cannabinoids, including nabilone, for the treatment of severe agitation in people with Alzheimer disease and related dementias if other pharmacological treatments have been trialled and found to be ineffective.
Considerations for Future Research
Clinical evidence from well-controlled studies is needed to inform decision-making with respect to the use of nabilone for the treatment of BPSD. A large, parallel, placebo-controlled trial of nabilone with longer follow-up is ongoing (NCT04516057).
Implications for Decision-Making
The evidence presented in this review is insufficient to form a strong conclusion on the use of nabilone for the treatment of BPSD. Given the limited evidence base, nabilone or other synthetic cannabinoids are currently recommended for the treatment of severe agitation in people with Alzheimer disease if symptoms remain resistant to other pharmacological treatments.
Acknowledgement
Clinical Experts
The following individuals have kindly provided comments on the report:
Shanna C. Trenaman, BScPharm, ACPR, PhD
Assistant Professor, College of Pharmacy, Faculty of Health, Dalhousie University
Affiliated Scientist, Geriatric Medicine Research, Nova Scotia Health
Dallas Seitz, MD, PhD
Chief, Division of Geriatric Psychiatry, Centre for Addiction and Mental Health
Professor, Department of Psychiatry, Temerty Faculty of Medicine, University of Toronto
References
1.Hugo J, Ganguli M. Dementia and cognitive impairment: epidemiology, diagnosis, and treatment. Clin Geriatr Med. 2014;30(3):421-42. doi: 10.1016/j.cger.2014.04.001 PubMed
2.Reitz C, Mayeux R. Alzheimer disease: epidemiology, diagnostic criteria, risk factors and biomarkers. Biochem Pharmacol. 2014;88(4):640-51. doi: 10.1016/j.bcp.2013.12.024 PubMed
3.Emmady PD, Schoo C, Tadi P. Major Neurocognitive Disorder (Dementia). StatPearls. StatPearls Publishing Copyright © 2026, StatPearls Publishing LLC.; 2026.
4.Dementia: Overview. 2025. Accessed 10 March https://www.canada.ca/en/public-health/services/diseases/dementia.html
5.Cloak N, Schoo C, Al Khalili Y. Behavioral and Psychological Symptoms in Dementia. StatPearls. StatPearls Publishing Copyright © 2026, StatPearls Publishing LLC.; 2026.
6.Lyketsos CG, Lopez O, Jones B, Fitzpatrick AL, Breitner J, DeKosky S. Prevalence of neuropsychiatric symptoms in dementia and mild cognitive impairment: results from the cardiovascular health study. JAMA. 2002;288(12):1475-83. doi: 10.1001/jama.288.12.1475 PubMed
7.Selbæk G, Engedal K, Bergh S. The prevalence and course of neuropsychiatric symptoms in nursing home patients with dementia: a systematic review. J Am Med Dir Assoc. 2013;14(3):161-9. doi: 10.1016/j.jamda.2012.09.027 PubMed
8.Cerejeira J, Lagarto L, Mukaetova-Ladinska EB. Behavioral and psychological symptoms of dementia. Front Neurol. 2012;3:73. doi: 10.3389/fneur.2012.00073 PubMed
9.Brath H, Wiesenfeld L, Stall NM. Nonpharmacologic management of the behavioural and psychological symptoms of dementia. CMAJ. 2025;197(11):E298-e299. doi: 10.1503/cmaj.241076 PubMed
10.Wang F, Feng TY, Yang S, Preter M, Zhou JN, Wang XP. Drug Therapy for Behavioral and Psychological Symptoms of Dementia. Curr Neuropharmacol. 2016;14(4):307-13. doi: 10.2174/1570159x14666151208114232 PubMed
11.Hillen JB, Soulsby N, Alderman C, Caughey GE. Safety and effectiveness of cannabinoids for the treatment of neuropsychiatric symptoms in dementia: a systematic review. Ther Adv Drug Saf. 2019;10:2042098619846993. doi: 10.1177/2042098619846993 PubMed
12.Bosnjak Kuharic D, Markovic D, Brkovic T, et al. Cannabinoids for the treatment of dementia. Cochrane Database Syst Rev. 2021;9(9):CD012820. doi: 10.1002/14651858.CD012820.pub2 PubMed
13.TEVA-NABILONE (Nabilone) 0.25 mg Capsules. 2012. Accessed 10 March. https://pdf.hres.ca/dpd_pm/00020321.PDF
14.Winters EM, Gordon JL, Hadjistavropoulos T. Patterns of Nabilone Prescriptions in Canadian Long-Term Care Facilities. Can J Aging. 2025;44(2):235-242. doi: 10.1017/S0714980824000448 PubMed
15.RoB2 Development Group. PT Higgins JPT, Savović J, Page MJ, Sterne JAC, eds. Revised Cochrane risk-of-bias tool for randomized trials (RoB 2). 2019. Accessed January 1, 1800. https://sites.google.com/site/riskofbiastool/welcome/rob-2-0-tool/current-version-of-rob-2
16.Agree Next Steps Consortium. The AGREE II Instrument. AGREE Enterprise; 2017. Accessed January 1, 1800. https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf
17.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-34. doi: 10.1016/j.jclinepi.2009.06.006 PubMed
18.Herrmann N, Ruthirakuhan M, Gallagher D, et al. Randomized Placebo-Controlled Trial of Nabilone for Agitation in Alzheimer's Disease. Am J Geriatr Psychiatry. 2019;27(11):1161-1173. doi: 10.1016/j.jagp.2019.05.002 PubMed
19.Cohen-Mansfield J. Agitation in the elderly. Adv Psychosom Med. 1989;19:101-13. doi: 10.1159/000417403 PubMed
20.Liu KY, Ivenso C, Howard R, et al. Three approaches to determining clinically meaningful benefit on the Cohen-Mansfield Agitation Inventory in dementia clinical trials for agitation. Alzheimers Dement (N Y). 2025;11(2):e70099. doi: 10.1002/trc2.70099 PubMed
21.Molloy DW, Standish TI. A guide to the standardized Mini-Mental State Examination. Int Psychogeriatr. 1997;9 Suppl 1:87-94; discussion 143-50. doi: 10.1017/s1041610297004754 PubMed
22.Howard R, Phillips P, Johnson T, et al. Determining the minimum clinically important differences for outcomes in the DOMINO trial. Int J Geriatr Psychiatry. 2011;26(8):812-7. doi: 10.1002/gps.2607 PubMed
23.Panisset M, Roudier M, Saxton J, Boller F. Severe impairment battery. A neuropsychological test for severely demented patients. Arch Neurol. 1994;51(1):41-5. doi: 10.1001/archneur.1994.00540130067012 PubMed
24.Weyer G, Erzigkeit H, Kanowski S, Ihl R, Hadler D. Alzheimer's Disease Assessment Scale: reliability and validity in a multicenter clinical trial. Int Psychogeriatr. 1997;9(2):123-38. doi: 10.1017/s1041610297004298 PubMed
25.Hamilton JL, Fuller RLM, Modi N, Sampaio C. Utilizing MCID for evaluating clinical relevance of AD therapeutic interventions. Alzheimers Dement (N Y). 2025;11(3):e70138. doi: 10.1002/trc2.70138 PubMed
26.Cummings JL, Mega M, Gray K, Rosenberg-Thompson S, Carusi DA, Gornbein J. The Neuropsychiatric Inventory: comprehensive assessment of psychopathology in dementia. Neurology. 1994;44(12):2308-14. doi: 10.1212/wnl.44.12.2308 PubMed
27.Mao HF, Kuo CA, Huang WN, Cummings JL, Hwang TJ. Values of the Minimal Clinically Important Difference for the Neuropsychiatric Inventory Questionnaire in Individuals with Dementia. J Am Geriatr Soc. 2015;63(7):1448-52. doi: 10.1111/jgs.13473 PubMed
28.Cummings JL. Neuropsychiatric Inventory Nursing Home Version (NPI-NH) Comprehensive Assessment of Psychopathology in Patients with Dementia Residing in Nursing Homes. 1994. Accessed 10 March. www.dementiaresearch.org.au/wp-content/uploads/2016/01/NPI-NH_cr.pdf
29.Cummings J, Mintzer J, Brodaty H, et al. Agitation in cognitive disorders: International Psychogeriatric Association provisional consensus clinical and research definition. Int Psychogeriatr. 2015;27(1):7-17. doi: 10.1017/s1041610214001963 PubMed
30.De Mauleon A, Ismail Z, Rosenberg P, et al. Agitation in Alzheimer's disease: Novel outcome measures reflecting the International Psychogeriatric Association (IPA) agitation criteria. Alzheimers Dement. 2021;17(10):1687-1697. doi: 10.1002/alz.12335 PubMed
31.Guy W. ECDEU assessment manual for psychopharmacology, William Guy. Rockville, Md.: U. S. Dept. of Health, Education, and Welfare, Public Health Service, Alcohol, Drug Abuse, and Mental Health Administration, National Institute of Mental Health, Psychopharmacology Research Branch, Division of Extramural Research Programs; 1976.
32.Rubenstein LZ, Harker JO, Salvà A, Guigoz Y, Vellas B. Screening for undernutrition in geriatric practice: developing the short-form mini-nutritional assessment (MNA-SF). J Gerontol A Biol Sci Med Sci. 2001;56(6):M366-72. doi: 10.1093/gerona/56.6.m366 PubMed
33.A guide to completing the Mini Nutritional Assessment – Short Form (MNA®-SF) 2021. Accessed 10 March. https://www.mna-elderly.com/sites/default/files/2021-10/mna-guide-english-sf.pdf
34.Warden V, Hurley AC, Volicer L. Development and psychometric evaluation of the Pain Assessment in Advanced Dementia (PAINAD) scale. J Am Med Dir Assoc. 2003;4(1):9-15. doi: 10.1097/01.Jam.0000043422.31640.F7 PubMed
35.Zwakhalen SM, van der Steen JT, Najim MD. Which score most likely represents pain on the observational PAINAD pain scale for patients with dementia? J Am Med Dir Assoc. 2012;13(4):384-9. doi: 10.1016/j.jamda.2011.04.002 PubMed
36.Hatch S, Seitz DP, Bruneau MA, et al. The Canadian Coalition for Seniors' Mental Health Canadian Clinical Practice Guidelines for Assessing and Managing Behavioural and Psychological Symptoms of Dementia (BPSD). Can Geriatr J. 2025;28(1):91-102. doi: 10.5770/cgj.28.820 PubMed
37.Canadian Clinical Practice Guidelines for Assessing and Managing Behavioural and Psychological Symptoms of Dementia (BPSD). 2024. Accessed 13 March. https://ccsmh.ca/wp-content/uploads/2024/03/V4-CCSMH-BPSD-Clinical-Guidelines_Final-for-webinar.pdf
38.Ruthirakuhan MT, Herrmann N, Gallagher D, et al. Investigating the safety and efficacy of nabilone for the treatment of agitation in patients with moderate-to-severe Alzheimer's disease: Study protocol for a cross-over randomized controlled trial. Contemp Clin Trials Commun. 2019;15:100385. doi: 10.1016/j.conctc.2019.100385 PubMed
39.Ballard C, Waite J. The effectiveness of atypical antipsychotics for the treatment of aggression and psychosis in Alzheimer's disease. Cochrane Database Syst Rev. 2006;2006(1):Cd003476. doi: 10.1002/14651858.CD003476.pub2 PubMed
40.Porsteinsson AP, Drye LT, Pollock BG, et al. Effect of citalopram on agitation in Alzheimer disease: the CitAD randomized clinical trial. JAMA. 2014;311(7):682-91. doi: 10.1001/jama.2014.93 PubMed
Appendix 1: Selection of Included Studies
Note that this appendix has not been copy-edited.
Figure 1: PRISMA Flow Chart of Study Selection
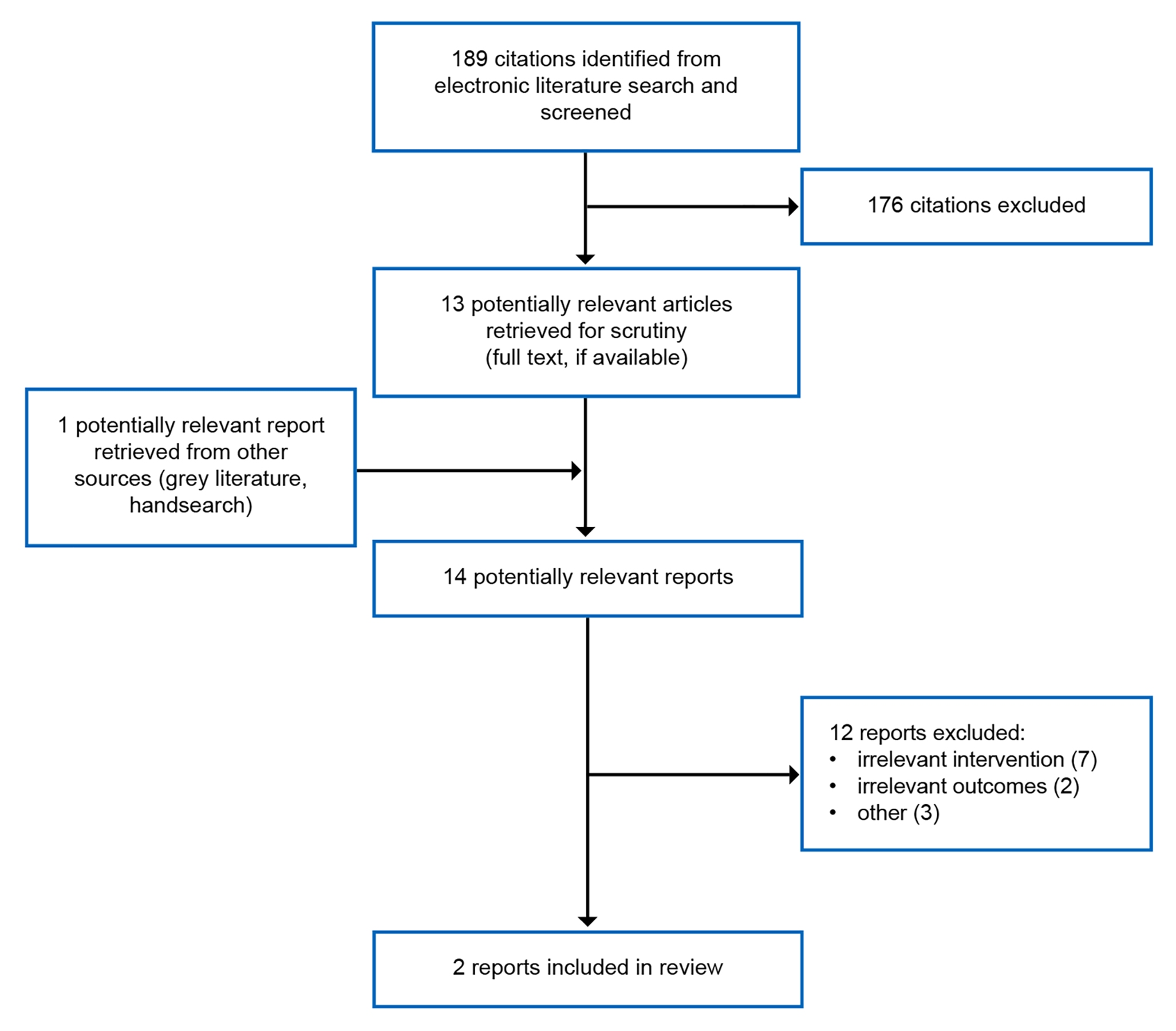
PRISMA = Preferred Reporting Items for Systematic reviews and Meta-Analyses.17
Appendix 2: Lists of Included and Excluded Studies
Note that this appendix has not been copy-edited.
Study | Title |
|---|---|
Herrmann et al. (2019)18 Phase II/III, multicentre, double-blind, placebo-controlled, crossover RCT | Randomized Placebo-Controlled Trial of Nabilone for Agitation in Alzheimer Disease. Am J Geriatr Psychiatry. 2019;27(11):1161 to 1173 |
Evidence-based guideline | The Canadian Coalition for Seniors' Mental Health Canadian Clinical Practice Guidelines for Assessing and Managing Behavioural and Psychological Symptoms of Dementia (BPSD). Can Geriatr J. 2025;28(1):91 to 102. |
RCT = randomized controlled trial.
Study | Reasons for exclusion |
|---|---|
Bahji A, Meyyappan AC, Hawken ER. Cannabinoids for the Neuropsychiatric Symptoms of Dementia: A Systematic Review and Meta-Analysis. Can J Psychiatry. 2020;65(6):365 to 376. | Only 1 relevant contributing study (Herrmann et al.), already included |
Bosnjak Kuharic D, Markovic D, Brkovic T, et al. Cannabinoids for the treatment of dementia. Cochrane Database Syst Rev. 2021;9(9):CD012820. | Only 1 relevant contributing study (Herrmann et al.), already included |
Charernboon T, Lerthattasilp T, Supasitthumrong T. Effectiveness of Cannabinoids for Treatment of Dementia: A Systematic Review of Randomized Controlled Trials. | Just included a nabilone study by Herrmann |
Feldman OJ, Herrmann N, Ruthirakuhan M, et al. Assessment of clinical factors that predict response to nabilone for agitation in Alzheimer disease: A post hoc analysis of a randomized placebo-controlled trial. Int Psychogeriatr. 2026:100183 | Post hoc analysis |
Wang HJ, Ruthirakuhan M, Andreazza AC, Beroncal EL, Black SE, Gallagher D, Herrmann N, Kiss A, Verhoeff NPLG, Lanctôt KL. Identifying a combination of biomarkers to predict treatment response to nabilone for agitation in Alzheimer disease - an exploratory post hoc analysis. Neurodegener Dis Manag. 2025 Nov 11:1 to 10. | Post hoc analysis |
Grossberg GT, Sanford A, Montano CB, et al. A US-based practitioner's guide to diagnosis, evaluation, and evidence-based treatment of agitation in Alzheimer dementia - recommendations of an expert, multispecialty advisory panel. Postgrad Med. 2025;137(6):469 to 485. | Not an evidence-based guideline |
Hillen JB, Soulsby N, Alderman C, Caughey GE. Safety and effectiveness of cannabinoids for the treatment of neuropsychiatric symptoms in dementia: a systematic review. Therapeutic Advances in Drug Safety. 2019;10:2042098619846993. | Did not include nabilone |
Pan TJ, Wang HJ, Siddiqui A, et al. Efficacy and Safety of Cannabinoids for Neuropsychiatric Symptoms of Dementia: A Systematic Review with Meta-analysis. CNS Drugs. 2026;26:26. | Only 1 relevant contributing study (Herrmann et al.), already included |
Paunescu H, Dima L, Ghita I, et al. A Systematic Review of Clinical Studies on the Effect of Psychoactive Cannabinoids in Psychiatric Conditions in Alzheimer Dementia. Am J Ther. 2020;27(3):e249-e269. | Only 1 relevant contributing study (Herrmann et al.), already included |
Ravelli A, Ceolin C, Papa MV, et al. Can cannabinoids alleviate behavioural symptoms in older adults with dementia? A systematic review. J Psychopharmacol. 2025:2698811251375895. | Only 1 relevant contributing study (Herrmann et al.), already included |
Ruthirakuhan M, Lanctôt KL, Vieira D, Herrmann N. Natural and Synthetic Cannabinoids for Agitation and Aggression in Alzheimer Disease: A Meta-Analysis. J Clin Psychiatry. 2019;80(2):29. | No eligible studies identified; only an abstract of NCT04516057 |
Watt JA, Porter J, Tavilsup P, et al. Guideline Recommendations on Behavioural and Psychological Symptoms of Dementia: A Systematic Review. J Am Med Dir Assoc. 2024;25(5):837 to 846.e21. | Systematic review of guidelines |
Appendix 3: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 4: Characteristics of Included Primary Clinical Study
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Herrmann et al. (2019)18 Canada Funding source: ASC and ADDF | Randomized, double-blind, placebo-controlled crossover trial | Adults with moderate-to-severe Alzheimer disease Mean age (SD): 87 (10) years Sex Female: 23% Male: 77% Inpatient: 72% Met IPA criteria for agitation/aggression: 97% Mean CMAI (SD): 67.9 (17.6) Mean NPI-NH total (SD): 34.3 (15.8) Mean NPI-NH agitation/aggression (SD): 7.1 (3.3) Mean NPI-NH total caregiver distress score (SD): 12.7 (7.9) Mean SMMSE (SD): 6.5 (6.8) Mean SIB (SMMSE ≤ 15) (n = 28) (SD): 36.5 (3.0) Mean ADAS-Cog (SMMSE > 15) (n = 3) (SD): 22.7 (3.1) Mean MNA-SF (SD): 8.7 (2.9) Mean PAINAD (SD): 2.6 (1.4) CGI severity, % Moderate: 50 Marked: 29 Severe: 18 Extreme: 3 Mean BMI (SD): 24.5 (3.9) Mean weight (SD): 67.9 (14.1) kg | Intervention: Nabilone (target 1 to 2 mg per day) (N = 38) Comparator: Placebo (N = 38) | Outcomes: Primary:
Secondary:
Exploratory:
Safety:
Follow-up:
|
ADAS-Cog = Alzheimer Disease Assessment Scale–Cognitive Subscale; ADDF = Alzheimer Drug discovery foundation; BMI = body mass index; CGIC = Clinical Global Impression–clinician-rated; CMAI = Cohen-Mansfield Agitation Inventory; IPA = International Psychogeriatric Association; MNA-SF = Mini Nutritional Assessment Short-Form; NPI-NH = Neuropsychiatric Inventory–Nursing Home version; PAINAD = Pain Assessment in Advanced Dementia; SAE = serious adverse event; SD = standard deviation; SIB = Severe Impairment Battery; SMMSE = Standardized Mini-Mental State Examination, TEAE = treatment-emergent adverse event.
aCMAI: a 29-item scale that measures 4 domains of agitation: physical/aggressive (Questions 1 − 11), physical/nonaggressive (Questions 12 − 21), verbal/aggressive (Questions 22 − 24), and verbal nonaggressive (Questions 25 − 29). Each item is rated on a scale from 1 (never) to 7 (several times an hour). The overall CMAI total score (29 items) ranges from 29 to 203, with higher scores indicate greater agitation severity.
bSMMSE: an 11-question measure that tests 5 areas of cognitive function: orientation, registration, attention and calculation, recall, and language. The maximum score is 30. A score of 23 or lower is indicative of cognitive impairment.
cSIB: cognition is also assessed using SIB in patients with SMMSE less than or equal to 15. It contains 6 major subscales to assess mild-to-moderate dementia; attention, orientation, language, memory, visuospatial ability, and construction. All but 2 of the SIB items are scored on a 3-point scale: 2 = correct; 1 = partially correct, and appropriate or closely related answer; and 0 = incorrect. The other 2 questions only have a 0 or a 1 point answer. Lower scores indicate greater impairment.
dADAS-Cog: an 11-task neuropsychological assessment (0 to 70 scale) measuring dementia severity, memory, language, and praxis (motor tasks). Higher scores indicate greater impairment.
eNPI-NH: a carer-based tool that assesses the possible presence of 12 symptoms in dementia cases, including delusions, hallucinations, apathy, depression, agitation, euphoria, aberrant motor behaviour, irritability, disinhibition, anxiety, sleeping, and eating. The greater the score, the more severe and frequent the behavioural disturbances.
fNPI-NH caregiver distress score: a tool that measures the emotional burden and work disruption of caregiver caused by dementia-related behaviours by using a 6-point scale (0 to 5) per symptom listed in NPI-NH (e.g., agitation, delusions, or apathy) with 0 being “not at all” and 5 being “extremely” distressing. Higher scores indicate higher levels of stress and burden on caregiver.
gCMAI IPA: derived from the 29-item questionnaire of CMAI by selecting items that align with the 3 main IPA Provisional Research Criteria for Agitation (i.e., physical aggression, verbal aggression, and physical nonaggression/restlessness). Higher scores indicate more severe, frequent agitation.
hCGIC: a 7-point scale used in clinical trials and practice to measure a patient’s improvement or decline after treatment. It assesses overall effectiveness of the treatment, typically ranging from "very much improved" to "very much worse." Usually, the scale is 1-7: 1) Very much improved, 2) Much improved, 3) Minimally improved, 4) No change, 5) Minimally worse, 6) Much worse, 7) Very much worse.
IMNA-SF: a screening tool used to categorize patients as malnourished or at risk of malnutrition. It contains 6 questions accessing recent changes in appetite, weight loss, mobility, psychological stress/ acute disease, current neuropsychological problems, and BMI.
jPAINAD: a tool used to evaluate pain in individuals with dementia or cognitive impairment who cannot verbally communicate their pain. It assesses 5 behaviours: breathing, negative vocalization, facial expression, body language, and consolability, with total scores ranging from 0 (no pain) to 10 (severe pain).
Table 5: Characteristics of the Included Guideline
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality assessment | Recommendations development and evaluation | Guideline validation |
|---|---|---|---|---|---|---|
Intended users: Health care providers, people living with dementia, and caregivers of people living with dementia Target population: People with lived experience of dementia | Provide guidance on assessing and managing BPSD in the care of people living with dementia within a Canadian context, using nonpharmacological and pharmacological approaches. | Relevant outcomes related to the clinical effectiveness, health-related quality of life, and safety of nonpharmacological and pharmacological interventions. | The guideline panel conducted
|
|
|
|
BPSD = behavioural and psychological symptoms of dementia; CCSMH = Canadian Coalition for Seniors’ Mental Health; GRADE = Grading of Recommendations Assessment, Development and Evaluation.
Appendix 4: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 6: Risk of Bias Assessment of the Included Study Using the Revised Cochrane Risk of Bias Tool for Randomized Trials (RoB 2)
Questions | Comments | Response |
|---|---|---|
Domain 1: Risk of bias arising from randomization process | ||
1.1. Was the allocation sequence random? | The study was a 14-week randomized double-blind crossover trial comparing nabilone to placebo. A block randomization code was independently computer-generated by the institutional Pharmacy Department. | Y |
1.2. Was the allocation sequence concealed until participants were enrolled and assigned to interventions? | Method of allocation concealment was reported in published article. | Y |
1.3. Did baseline differences between intervention groups at the start of the first period suggest a problem with the randomization process? | No imbalances in patient baseline characteristics as all participants received first treatment (nabilone) for 6 weeks, followed by 1-week washout, then crossed over to a second treatment (placebo) for another 6 weeks. | N |
Risk-of-bias judgment | There were no apparent differences in characteristics of the patients at baseline in both intervention groups. The methods of randomization and allocation concealment were reported. | Low risk of bias |
Domain S: Risk of bias arising from period and carryover effects | ||
S.1. Was the number of participants allocated to each of the 2 sequences equal or nearly equal? | 38 patients underwent treatment with nabilone, 5 terminated early due a SAE; 33 then underwent treatment with placebo, 4 terminated early due a SAE. Thus, it appears that the number of participants underwent each treatment was not equal. | N |
S.2 If N/PN/NI to S.1: Were period effects accounted for in the analysis? | All 38 participants were included in the analyses. | Y |
S.3 Was there sufficient time for any carryover effects to have disappeared before outcome assessment in the second period? | The plasma half-life (T1/2) values for nabilone and total radioactivity of identified and unidentified metabolites are about 2 and 35 hours, respectively. Thus, 1-week washout appeared to be sufficient to clear any carryover effects. | PY |
Risk-of-bias judgment | Despite there was potential imbalance in the number of participants in both period of treatments, all participants were included in the analyses. There were potentially no carryover effects. | Low risk of bias |
Domain 2: Risk of bias due to deviations from the intended interventions (effect of assignment to intervention) | ||
2.1. Were participants aware of their assigned intervention during the trial? | Patients were blinded to treatment allocation and block size. | N |
2.2. Were carers and people delivering the interventions aware of participants' assigned intervention during the trial? | Family members, nurses, clinicians, outcome assessors, and investigators were blinded to treatment allocation and block size. However, clinicians and outcome assessors could be unblinded due to specific AE of nabilone (i.e., sedation) | PY |
2.3. If Y/PY/NI to 2.1 or 2.2: Were there deviations from the intended intervention that arose because of the trial context? | Not detected | NA |
2.4. If Y/PY to 2.3: Were these deviations likely to have affected the outcome? | NA | NA |
2.5. If Y/PY/NI to 2.4: Were these deviations from intended intervention balanced between groups? | NA | NA |
2.6. Was an appropriate analysis used to estimate the effect of assignment to intervention? | All prespecified outcomes were analyzed using the intention-to-treat population, meaning that all patients who were randomized received at least 1 dose of the study medication and completed at least 1 nonbaseline questionnaire were included. | Y |
2.7. If N/PN/NI to 2.6: Was there potential for a substantial impact (on the result) of the failure to analyze participants in the group to which they were randomized? | NA | NA |
Risk-of-bias judgment | Unblinding may occur due to specific AE of nabilone (i.e., sedation). Appropriate analysis was used to estimate the effect of the assignment to intervention. | Some concerns |
Domain 3: Risk of bias due to missing outcome data | ||
3.1. Were data for this outcome available for all, or nearly all, participants randomized? | All analyses were performed on a modified intention-to-treat population using data from participants who took at least 1 dose of study medication after randomization. | Y |
3.2. If N/PN/NI to 3.1: Is there evidence that the result was not biased by missing outcome data? | Paired data from all participants were used without imputation. | Y |
3.3. If N/PN to 3.2: Could missingness in the outcome depend on its true value? | NA | NA |
3.4. If Y/PY/NI to 3.3: Is it likely that missingness in the outcome depended on its true value? | NA | NA |
Risk-of-bias judgment | Outcome data were available for all randomized participants. | Low risk of bias |
Domain 4: Risk of bias in measurement of the outcome | ||
4.1. Was the method of measuring the outcome inappropriate? | The methods of measuring the outcomes were appropriate and clearly described in the protocol of the trial. | N |
4.2. Could measurement or ascertainment of the outcome have differed between intervention groups? | Methods of outcome measurement were similar between intervention groups. | N |
4.3. If N/PN/NI to 4.1 and 4.2: Were outcome assessors aware of the intervention received by study participants? | The study reported that outcomes were assessed by the investigators, who were blinded to the treatment allocation and block size. However, blinding may be broken due to specific AE of nabilone (i.e., sedation) | PY |
4.4. If Y/PY/NI to 4.3: Could assessment of the outcome have been influenced by knowledge of intervention received? | Probably yes | PY |
4.5. If Y/PY/NI to 4.4: Is it likely that assessment of the outcome was influenced by knowledge of intervention received? | Probably yes | PY |
Risk-of-bias judgment | The methods of measuring the outcomes were appropriate and the measurements or ascertainment of the outcomes did not differ between intervention groups. However, measurement of outcomes could have been influenced by the knowledge of the intervention due to the presence of specific AE of nabilone (i.e., sedation). | High risk of bias |
Domain 5: Risk of bias in selection of the reported result | ||
5.1. Were the data that produced this result analyzed in accordance with a prespecified analysis plan that was finalized before unblinded outcome data were available for analysis? | Data that produced the results in the published report were analyzed in accordance with a prespecified analysis plan reported in detail in the protocol of the trial. | Y |
Is the numerical result being assessed likely to have been selected, on the basis of the results, from... | ||
5.2. multiple eligible outcome measurements (e.g., scales, definitions, time points) within the outcome domain? | Efficacy outcomes were assessed followed their predefined analyses and performed interim analyses as described in the protocol. | N |
5.3. multiple eligible analyses of the data? | The protocol was generally followed. | N |
Risk-of-bias judgment | The data were analyzed in accordance with a prespecified plan. The results being assessed were unlikely to have been selected. | Low risk of bias |
AE = adverse event; N = no; NA = not applicable; PLB = placebo; PN = probably no; PY = probably yes; SAE = serious adverse event; Y = yes.
Source: The Revised Cochrane Risk of Bias Tool for Randomized Trials (RoB 2)15
Table 7: Strengths and Limitations of Guideline Using AGREE II
Item | |
|---|---|
Domain 1: scope and purpose | |
1. The overall objective(s) of the guideline is (are) specifically described. | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes |
3. The population (patients, public, and so forth) to whom the guideline is meant to apply is specifically described. | Yes |
Domain 2: stakeholdera involvement | |
4. The guideline development group includes individuals from all relevant professional groups. | Yes |
5. The views and preferences of the target population (patients, public, and so forth) have been sought. | Yes |
6. The target users of the guideline are clearly defined. | Yes |
Domain 3: rigour of development | |
7. Systematic methods were used to search for evidence. | Yes |
8. The criteria for selecting the evidence are clearly described. | Yes |
9. The strengths and limitations of the body of evidence are clearly described. | Yes |
10. The methods for formulating the recommendations are clearly described. | Yes |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes |
12. There is an explicit link between the recommendations and the supporting evidence. | Yes |
13. The guideline has been externally reviewed by experts before its publication. | Yes |
14. A procedure for updating the guideline is provided. | Yes |
Domain 4: clarity of presentation | |
15. The recommendations are specific and unambiguous. | Yes |
16. The different options for management of the condition or health issue are clearly presented. | Yes |
17. Key recommendations are easily identifiable. | Yes |
Domain 5: applicability | |
18. The guideline describes facilitators and barriers to its application. | Yes |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | Yes |
20. The potential resource implications of applying the recommendations have been considered. | Unclear |
21. The guideline presents monitoring and/or auditing criteria. | Yes |
Domain 6: editorial independence | |
22. The views of the funding body have not influenced the content of the guideline. | No |
23. Competing interests of guideline development group members have been recorded and addressed. | Yes |
AGREE II = Appraisal of Guidelines for Research and Evaluation II.16
aWherever possible, Canada’s Drug Agency no longer uses the term stakeholder because of its harmful association with colonialism; in this case, the word appears in the original phrasing of AGREE II.
Appendix 5: Main Study Findings
Note that this appendix has not been copy-edited.
Table 8: Summary of Comparative Clinical Efficacy Findings
Study citation, study design, intervention vs. comparator | Outcomes | Outcome measures | Results b value (95% CI), P value |
|---|---|---|---|
Herrmann et al. (2019)18 Randomized double-blind crossover trial Nabilone vs. placebo | Agitation | CMAI | −4.0 (−6.5 to −1.5), 0.003 |
Cognition | SMMSE | 1.1 (0.1 to 2.0), 0.026 | |
SIB | −4.6 (−7.3 to −1.8), 0.003 | ||
ADAS-Cog | Not analyzed as only 3 patients completed this scale | ||
Neuropsychiatric symptoms | NPI-NH | −4.6 (−7.5 to −1.6), 0.004 | |
Caregiver burden | NPI-NH caregiver distress score | −1.7 (−3.4 to −0.7), 0.041 | |
Behaviour | CMAI-IPA | −3.8 (−5.8 to −1.7), 0.001 | |
Global status | CGIC | “minimal” to “marked” improvement:
| |
Nutritional status | MNA-SF | 0.2 (0.02 to 0.4), 0.03 | |
Weight | 0.01 (−0.69 to 0.71), 0.97 | ||
BMI | −0.14 (−0.35 to 0.07), > 0.05 | ||
Pain | PAINAD | 0.03 (−0.22 to 0.27), 0.82 |
ADAS-Cog = Alzheimer Disease Assessment Scale–Cognitive Subscale; BMI = body mass index; CGI-I = Clinical Global Impression–Improvement; CI = confidence interval; CMAI = Cohen-Mansfield Agitation Inventory; IPA = International Psychogeriatric Association; MNA-SF = Mini Nutritional Assessment Short-Form; NPI-NH = Neuropsychiatric Inventory–Nursing Home version; PAINAD = Pain Assessment in Advanced Dementia; SIB = Severe Impairment Battery; SMMSE = Standardized Mini-Mental State Examination; vs. = versus.
Table 9: Summary of Comparative Safety Findings
Study citation, study design, intervention vs. comparator | Outcomes | Results % (n/N) |
|---|---|---|
Herrmann et al. (2019)18 Randomized double-blind crossover trial Nabilone vs. placebo | Total TEAEs | 81.6 (31/38) vs. 36.8 (14/38) |
Sedation (including lethargy) | 44.7 (17/38) vs. 15.8 (6/38); P = 0.02 | |
Treatment limiting sedation (by reduction in nabilone dose) | 13.2 (5/38) vs. 2.6 (1/38); P = 0.22 | |
Falls | 21.1 (8/38) vs. 18.4 (7/38) | |
Bradycardia | 2.6 (1/38) vs. 0 | |
Myoclonic jerk | 2.6 (1/38) vs. 0 | |
Elevated urea levels | 2.6 (1/38) vs. 0 | |
Rash | 2.6 (1/38) vs. 0 | |
Significant increase in NPS | 2.6 (1/38) vs. 5.3 (2/38) | |
Dizziness | 2.6 (1/38) vs. 0 | |
Shakiness | 0 vs. 2.6 (1/38) | |
Total SAEs | 13.2 (5/38) vs. 10.5(4/38) | |
Lethargy | 5.3 (2/38) vs. 0 | |
Death | 2.6 (1/38) vs. 2.6 (1/38) | |
Myocardial infarction | 2.6 (1/38) vs. 0 | |
Cancer diagnosis | 0 vs. 2.6 (1/38) | |
Pneumothorax | 0 vs. 2.6 (1/38) | |
Sepsis due to UTI | 0 vs. 2.6 (1/38) |
NPS = neuropsychiatric symptoms; SAE = serious adverse event; TEAE = treatment-emergent adverse event; UTI = urinary tract infection; vs. = versus.
Table 10: Summary of Recommendations in the Included Guideline
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
|---|---|
“We suggest synthetic cannabinoids for the treatment of severe agitation in Alzheimer’s disease and related dementias if symptoms are refractory to other pharmacological treatments.” (p. 17 in the document published on the CCHMS website)37 Supporting evidence:
| Quality of evidence: Low Strength of recommendation: Conditional |
CCSMH = Canadian Coalition for Seniors’ Mental Health; RCT = randomized controlled trial; vs. = versus.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.