Drugs, Health Technologies, Health Systems
Reimbursement Review
Exagamglogene Autotemcel (Casgevy)
Vertex Pharmaceuticals (Canada) Incorporated
Therapeutic area: Transfusion-dependent beta thalassemia
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Ethics Review
Clinical Review
Abbreviations
AE
adverse event
ATC
authorized treatment centre
CanHaem
Canadian Hemoglobinopathy Association / L’Association canadienne d’hémoglobinopathie
Cas9
CRISPR-associated protein 9
CDA-AMC
Canada’s Drug Agency
CI
confidence interval
CRISPR
clustered regularly interspaced short palindromic repeats
EMA
European Medicines Agency
EOS
end of study
EQ VAS
EQ visual analogue scale
ESS
effective sample size
FACT-BMT
Functional Assessment of Cancer Therapy–Bone Marrow Transplantation
FAS
full analysis set
GANSID
Global Action Network for Sickle Cell and Other Inherited Blood Disorders
GRADE
Grading of Recommendations Assessment, Development and Evaluation
hemoglobin A
adult hemoglobin
hemoglobin F
fetal hemoglobin
HLA
human leukocyte antigen
HRQoL
health-related quality of life
HSCT
hematopoietic stem cell transplant
HSPC
hematopoietic stem and progenitor cell
HTA
health technology assessment
IA
interim analysis
ICT
iron chelation therapy
LTE
long-term extension
M24
month 24
MAIC
matching-adjusted indirect comparison
MID
minimal important difference
NBS
newborn screening
PedsQL
Pediatric Quality of Life Inventory
PES
primary efficacy set
PRO
patient-reported outcome
RBC
red blood cell
RCT
randomized controlled trial
RR
rate ratio
SAE
serious adverse event
SD
standard deviation
SES
socioeconomic status
SLR
systematic literature review
SOC
standard of care
TDT
transfusion-dependent beta thalassemia
TFC
Thalassemia Foundation of Canada
TI
transfusion independence
TI3
transfusion independence for 3 consecutive months
TI6
transfusion independence for 6 consecutive months
TI12
transfusion independence for 12 consecutive months
VAS
visual analogue scale
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Table 1: Background Information of Application Submitted for Review
Item | Description |
|---|---|
Drug product | Exagamglogene autotemcel cell suspension in patient-specific vials, 4 × 106 cells/mL to 13 × 106 cells/mL, for IV infusion |
Sponsor | Vertex Pharmaceuticals (Canada) Inc. |
Indication | For the treatment of patients 12 years of age and older with TDT |
Reimbursement request | As per indication |
Health Canada approval status | NOC |
Health Canada review pathway | Priority review |
NOC date | September 23, 2024 |
Recommended dose | The minimum recommended dose of exagamglogene autotemcel is 3 × 106 viable CD34+ cells/kg |
NOC = Notice of Compliance; TDT = transfusion-dependent beta thalassemia.
Introduction
Transfusion-dependent beta thalassemia (TDT) is a rare, autosomal recessive genetic hemoglobinopathy and the more severe form of beta thalassemia. Without the support of red blood cell (RBC) transfusions, patients with TDT develop severe anemia due to ineffective erythropoiesis, as well as comorbidities such as splenomegaly, bone marrow expansion with accompanying bone pain, progressive bone deformities, extramedullary erythropoiesis, and iron overload.1,2 Without regular transfusions, 85% of patients with TDT would die in the first 5 years of life due to severe anemia.3 Furthermore, the consequences of inadequate oxygen delivery, including cerebral ischemia and myocardial ischemia, can be life-threatening.4 Patients with TDT also have poorer health-related quality of life (HRQoL) compared with the general population, with disease-related impacts affecting physical and mental well-being.5-7
Early diagnosis as soon as possible after birth is essential for patients with TDT. Newborn screening (NBS) initiatives help in identifying affected individuals before symptom onset and allow access to specialty care and initiation of RBC transfusions before development of severe complications. High performance liquid chromatography, capillary electrophoresis, and isoelectric focusing are the most common methods of detection used during NBS.8 Screening and confirmatory tests for patients with a clinical suspicion of beta thalassemia can also be performed as well as preconception screening and prenatal testing for parents known to be at risk of having a child with TDT.8
Although a rare disease in Canada, the number of individuals with beta thalassemia is evolving.8,9 It may also continue to rise in the Western world due to continued immigration from endemic regions including the Mediterranean, Asian, Indian, and Middle Eastern regions.8,10-13 Of patients with beta thalassemia, the submission noted an estimated 70% are thought to have TDT.14,15 Within the jurisdictions relevant to the submission to Canada’s Drug Agency (CDA-AMC), there were an estimated 1,900 patients with TDT.9
In general, patients with TDT require lifelong care and routine monitoring which ideally is performed in specialized centres by a team of multidisciplinary experts.8,15,16 The main goals of managing TDT in Canada include ameliorating the negative effects of anemia through regular packed RBC transfusions and reducing iron overload with iron chelation therapy (ICT), both of which represent the standard of care (SOC).8,17 Lifelong regular RBC transfusions (typically every 2 weeks to 4 weeks, beginning in infancy) aim to maintain a pretransfusion hemoglobin between 90 g/L to 100 g/L.8,17 Iron chelation is also required to manage the iron overload which results from both transfusion and TDT. Other potential treatment options to accompany transfusion for adult patients with TDT include luspatercept, an erythroid maturation drug approved for the treatment of anemia in adults with TDT which stimulates erythroid response.18 The clinical experts consulted by CDA-AMC noted that if transfusion and iron chelation are optimized, with newer iron chelation therapies available patients with TDT can have life expectancy beyond the mean ages of death that have been previously reported for this disease.19,20
Allogenic hematopoietic stem cell transplant (HSCT) is the only curative treatment available for patients with TDT. HSCT with a human leukocyte antigen (HLA)-matched sibling donor is considered the SOC for children with TDT and is recommended to be discussed as a treatment option before puberty; HSCT for adult patients with thalassemia is associated with increased morbidity and not generally available in most centres.21 The best outcomes of HSCT are when it is performed with HLA-matched sibling donors and among patients of younger ages before TDT-related end-organ damage has accumulated.22,23 Per the clinical experts consulted by CDA-AMC, HSCT with an HLA-matched donor is an option for approximately 20% of patients.
Exagamglogene autotemcel is a cellular therapy consisting of autologous CD34+ human hematopoietic stem and progenitor cells (HSPCs) edited by clustered regularly interspaced short palindromic repeats (CRISPR)/CRISPR-associated protein 9 (Cas9) technology; the editing is intended to correct the alpha-like and beta-like globin imbalance inherent to TDT through the production of fetal hemoglobin (hemoglobin F). Exagamglogene autotemcel is approved by Health Canada for the treatment of patients aged 12 years and older with TDT. The reimbursement request is aligned with the Health Canada–approved indication. Exagamglogene autotemcel is provided as a single dose for infusion containing a suspension of CD34+ cells in 1 or more vials; the minimum recommended dose is 3 × 106 viable CD34+ cells/kg.
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of exagamglogene autotemcel cell suspension in patient-specific vials, 4 × 106 cells/mL to 13 × 106 cells/mL IV infusion, for the treatment of patients aged 12 years and older with TDT.
Perspectives of Patients, Clinicians, and Drug Programs
The information in this section is a summary of input provided by the patient and clinician groups who responded to the call for input from the CDA-AMC and from clinical experts consulted by CDA-AMC for the purpose of this review.
Patient Input
CDA-AMC received 2 patient group submissions, from the Thalassemia Foundation of Canada (TFC) as well as the Global Action Network for Sickle Cell & Other Inherited Blood Disorders (GANSID), a global organization with 4 member organizations: TFC, Sickle Cell Awareness Group of Ontario, Sickle Cell Awareness Network of Saskatchewan, and Sickle Cell Disease Association of Atlantic Provinces. TFC collected information via prior surveys conducted in 2022 and a new survey launched across Canada in April 2024, collecting responses from 80 respondents across 5 provinces (Quebec, Ontario, Manitoba, Alberta, and British Columbia). GANSID’s submission was based on the TFC survey and comments from peers living with thalassemia disorders outside of Canada.
Common patient symptoms noted in the inputs were severe anemia, lethargy, tiredness, feeling short of breath, and feeling weak. The input noted that thalassemia can also cause other health issues including loss of bone density (e.g., osteopenia or osteoporosis), a higher risk of liver cancers, and so forth. Many patients experience growth delays, bone deformities, and other physical changes due to anemia, iron chelation side effects, and hormone insufficiency. Furthermore, the chronic nature of thalassemia, with its lifelong treatment requirements and potential complications, can lead to emotional distress in patients, and patients may experience feelings of anxiety, depression, or fear about their health and future. Due to misconceptions about the condition, patients with thalassemia may also face stigma and discrimination in various aspects of their lives, such as education, employment, and social interactions.
Patients with thalassemia and their caregivers face various challenges in managing the illness, but with currently available treatments, many are able to effectively control symptoms and improve quality of life and life expectancy. When asked about their main expectations for gene therapy, patient expectations included transfusion independence (TI), maintaining hemoglobin at a high enough level to function daily, safety and efficacy, and improved HRQoL including freedom to travel, work, and spend time where they wished.
There were 2 patients who had experience with exagamglogene autotemcel in the US through clinical trials, and their family members shared their experiences with TFC. Both patients had discontinued blood products, and their blood parameters were normal, which according to family members, was life-changing. TFC asked the respondents to identify as many concerns regarding gene therapy as they wanted, and patients and caregivers responded with concerns around cost and affordability of treatment (75%), length of treatment and/or recovery (71%), chemotherapy (61%), as well as eligibility due to older age.
Clinician Input
Input From Clinical Experts Consulted by CDA-AMC
The information in this section is based on input received from a panel of 3 clinical specialists consulted by CDA-AMC for the purpose of this review.
According to the expert panel, the major goals of therapy in TDT are to prolong life, reduce severity of symptoms, and improve HRQoL. The curative SOC for TDT is HSCT; therefore, patients with an available HLA-matched sibling donor (approximately 20% of patients) are recommended for this treatment. The experts noted that most patients in this situation will be recommended to undergo transplant as early as possible if there is an HLA-matched sibling, as outcomes are generally better for patients younger than 17 years old and there is less risk of organ damage from iron overload in younger patients. Patients without an HLA-matched donor or who decide not to undergo HSCT would receive lifelong blood transfusions on an approximately monthly basis, with iron chelation to address iron overload. The experts noted that other risks of transfusion include developing allogenic antibodies to transfusion, transfusion reactions, transfusion-transmitted infections, and the potential for vascular access issues. Current treatment goals for transfusion focus on maintaining a hemoglobin level of 9.5 g/dL to 10.5 g/dL and maintaining liver iron, measured by FerriScan, of 2 mg/g to 3 mg/g or 2 mg/g to 5 mg/g. Luspatercept is used in adult patients; however, the experts noted that a minority of patients (20%) respond to it and if they do, treatment would reduce, but not eliminate, the need for transfusion. The longitudinal nature of therapy and commitments associated with travelling to receive transfusion therefore remains an unmet need for patients. The experts noted that removing the need for transfusions would likely allow for considerable improvement in HRQoL, particularly as the life expectancy for patients with TDT can be beyond the mean ages of death that have been previously reported for this disease,19,20 with optimized transfusion and iron chelation. They noted that the majority of organ damage due to TDT comes from end-organ damage and toxicity associated with iron overload; adherence to iron chelation can be difficult for some patients, and also becomes difficult to deliver as patients age, requiring a combination of drugs. In addition, adult patients who may not have had newer iron chelation drugs available earlier in their lives may have accrued end-organ damage from iron overload. Therefore, there also remains an unmet need in some patients if there are challenges in optimizing chelation either due to patient age, clinical characteristics, or adherence concerns.
The expert panel noted that exagamglogene autotemcel would potentially change the treatment paradigm as it may modify the disease course to provide TI for patients for whom HSCT is not a treatment option. The experts felt that patients should have tried transfusion and iron chelation before exagamglogene autotemcel, but patients should not need to try luspatercept before exagamglogene autotemcel because not all patients respond to this treatment and the expected results from treatment are different (i.e., luspatercept does not eliminate the need for transfusion). Families who are eligible but who do not opt for HSCT may be considered for exagamglogene autotemcel; however, the experts noted these patients may also not choose exagamglogene autotemcel due to concerns around myeloablative conditioning. The experts felt that discussions for exagamglogene autotemcel would likely be approached similarly, and involve similar specialists, as discussions about HSCT.
The expert panel noted that TDT diagnosis is generally done to the molecular level for patients at most centres; therefore, patients who might be candidates for exagamglogene autotemcel would be readily identifiable. The experts felt that the patient population they would consider for exagamglogene autotemcel therapy would align with the lower age range and the inclusion criteria for the pivotal trial. They felt strongly that there should not be an upper age limit for therapy, but suitability and choice for exagamglogene autotemcel should be determined on a case-by-case basis. Patients they might consider prioritizing for therapy would be those who are not responding to their current therapy or whose HRQoL is impacted by their current therapy. It would also need to be established that such patients did not have end-organ damage severe enough to negatively affect the safety of myeloablative therapy. The experts noted that patient and family preference would likely be the biggest determinant to identify those patients who would not be suitable candidates for exagamglogene autotemcel.
The experts stated they typically meet with their patients every 3 months to 6 months and assessments include whether they are meeting transfusion targets (i.e., sufficient transfusion to suppress endogenous RBC production) and whether iron overload is a concern (typically assessed using MRI). For the experts, a clinically meaningful response would be whether patients were transfusion independent with a hemoglobin level of 9 g/dL or more. Another potentially important outcome would be if patients need less than 6 transfusions per year (decreased from approximately 12 per year), as well as any changes in HRQoL and decreases in iron overload or need for chelation from that patient’s baseline. They noted that these changes would be meaningful even if patients had not reached TI.
Because exagamglogene autotemcel is a one-time treatment, criteria for discontinuation would be less applicable; however, the experts noted that patients may choose to stop the exagamglogene autotemcel process after mobilization but before myeloablative conditioning. When asked whether another treatment of exagamglogene autotemcel might be given if its efficacy were to wane in the future, the experts felt that a second round of myeloablative conditioning would be challenging for patients, although not impossible for pediatric patients if there was a strong reason.
The experts noted that the management of TDT in general requires a hematologist and they emphasized that the mobilization, myeloablative conditioning, and exagamglogene autotemcel infusion would need to be undertaken at an accredited transplant facility. Following this, patients could be transferred back to their hemoglobinopathy care provider and be followed by a specialist at a centre of excellence (i.e., a clinic with a hematology specialist in thalassemia as well as trained nurses); the experts estimated there were approximately 17 such centres across Canada. A hematologist who has an understanding of the disease would be important for ongoing care. They also noted that patients undergoing transplant use an autologous transplant centre and their follow-up consists of appointments with both the transplant hematologist and their TDT hematologist, so it was likely that the patients receiving exagamglogene autotemcel could be followed in a similar manner. They emphasized that patients receiving exagamglogene autotemcel should receive long-term follow-up.
Clinician Group Input
CDA-AMC received 1 clinician group submission from the Canadian Hemoglobinopathy Association/L’Association canadienne d’hémoglobinopathie (CanHaem). CanHaem is a not-for-profit organization that was established in 2013 and is composed of health care providers of individuals in Canada with hemoglobinopathies. CanHaem’s proposed submission was drafted by a CanHaem physician member and then shared among other members (including the CanHaem chair) for review.
The clinician group agreed with the expert panel on the need for lifelong, multidisciplinary care for patients with TDT and the general impact of the disease on patients’ lives and HRQoL, and that with optimized care, patients with TDT may have a near-normal life expectancy. In addition to the limitations of SOC therapies noted by the clinical expert panel, they also highlighted that emerging disease-related complications are now appreciated in the aging thalassemia population including increased risk of hepatocellular carcinoma, as well as renal, cardiac, and hepatic failure, all of which are related to the chronic toxicity of iron. The clinical group agreed with the clinical experts regarding the patients who might be considered candidates for exagamglogene autotemcel and also agreed that there should not be an upper age limit for eligibility. The clinician group input noted that outcomes for efficacy should be the same as those in the pivotal clinical trial, including HRQoL measures. They agreed with the clinical expert panel that patients should receive long-term follow-up and their care for the exagamglogene autotemcel treatment process should be handled by a facility experienced with stem cell collection, administration of myeloablative chemotherapy, and specialized hematologic care. The clinician group emphasized the need for equity in the availability of exagamglogene autotemcel, particularly for patients living in geographically remote areas, as well as the need to offer fertility preservation as part of the treatment process.
Drug Program Input
Input was obtained from the drug programs that participate in the CDA-AMC reimbursement review process. The following were identified as key factors that could potentially impact the implementation of a CDA-AMC recommendation for exagamglogene autotemcel:
considerations for initiation of therapy
considerations for continuation or renewal of therapy
generalizability
care provision issues.
The clinical expert panel convened by CDA-AMC provided advice on the potential implementation issues raised by the drug program. Refer to Table 5 for more details.
Clinical Evidence
Systematic Review
Description of Studies
The CLIMB-111 study is an ongoing phase I, II, and III single-arm, multisite, single-dose trial which enrolled a total of 59 patients aged 12 to 35 years who had TDT.2 Transfusion dependence was defined as a history of at least 100 mL/kg per year or 10 units/year of packed RBC transfusions in the past 2 years before enrolment. The primary objective of the CLIMB-111 study was to evaluate the safety and efficacy of a single dose of autologous CRISPR/Cas9-modified CD34+ human HSPCs, otherwise known as exagamglogene autotemcel. The CLIMB-111 study contained 3 prespecified interim analysis (IA) points — IA1, IA2, and IA3 — and data from IA3 were submitted based on a data cut-off of January 16, 2023. Additional supplemental data from a further data cut-off on April 16, 2023, was also supplied by the sponsor and used in the report where available.24 The study took place at 13 sites in 5 countries including 2 sites in Canada.
Key inclusion criteria required patients to be between the ages of 12 and 35 years, inclusive; have a diagnosis of TDT; be eligible for autologous stem cell transplant; and have a functional status greater than specific thresholds for 2 different scales, depending on patient age. Key exclusion criteria included patients who had a willing and healthy 10/10 HLA-matched donor per investigator judgment; patients with any illness or clinical condition that, in the opinion of the investigator, might confound the results of the study or pose an additional risk to the patient; and prior recipients of allogenic HSCT.
The primary outcome was the proportion of patients with TI for at least 12 consecutive months (TI12), and the key secondary outcome was the proportion of patients with TI for at least 6 consecutive months (TI6). TI was defined as maintaining a weighted average hemoglobin of 9 g/dL or greater without RBC transfusions. The evaluation of TI12 and TI6 commenced 60 days after the last RBC transfusion for post–exagamglogene autotemcel infusion support or TDT disease management. Secondary outcomes were total hemoglobin and hemoglobin F concentrations, the proportion of alleles with the intended genetic modification in the CD34+ cells of the bone marrow and the peripheral blood, and changes from baseline in HRQoL assessed by the Functional Assessment of Cancer Therapy–Bone Marrow Transplantation (FACT-BMT) and EQ-5D-5L in adults, as well as the Pediatric Quality of Life Inventory (PedsQL) and EQ-5D-Y measures in pediatric patients. Additional secondary outcomes included the duration of TI with weighted average hemoglobin of 9 g/dL or greater in patients with TI12, and the time to the last RBC transfusion for patients with TI12.
As of the data cut-off on April 16, 2023, a total of 59 patients were enrolled, 54 had received an infusion of exagamglogene autotemcel, and 42 patients were included in the primary efficacy set (PES). A total of 23 (39.0%) patients had completed the CLIMB-111 study; the mean duration of follow-up was 19.2 months (standard deviation [SD] = 6.97 months). Baseline characteristics were broadly similar between the PES and the full analysis set (FAS). The majority of patients (59.5% in the PES) expressed a beta0/beta0-like genotype of TDT. In the PES, the average age was 21.6 years; 31.0% of patients were pediatric patients (12 years or older and younger than 18 years), and 69.0% were adult patients between the ages of 18 and 35 years. Of note, the study did not enrol any Black or African American, ████████ ██████ ██ ██████ ███████ ███ ██████ ████████ ██ ███████ ████████ patients. In addition, the study did not enrol any patients with the █████ █████ thalassemia genotypes.
Efficacy Results
Proportion of Patients With TI12
The proportion of patients who achieved TI12 following infusion of exagamglogene autotemcel and as of the April 16, 2023, data cut-off was 92.9% (95% confidence interval [CI], 80.5% to 98.5%) in the PES. Among patients with TI12, the time from the exagamglogene autotemcel infusion to the last RBC transfusion was 28.0 days (range, 11.0 to 91.0 days). The mean duration of TI to date was 23.6 months (SD = 7.8 months).
Proportion of Patients With TI6
Following infusion with exagamglogene autotemcel, the proportion of patients in the PES who achieved TI6 as of the data cut-off was 92.9% (95% CI, 80.5% to 98.5%).
Hemoglobin F Levels
Clinical experts consulted by CDA-AMC note that in patients with TDT, almost all the total hemoglobin is expected to be hemoglobin F after exagamglogene autotemcel infusion, and total hemoglobin should be maintained at greater than 9 g/dL. Total hemoglobin F concentrations at 6 months post-exagamglogene autotemcel infusion were a mean of 10.8 g/dL (SD = 2.8 g/dL). At 12 months post-exagamglogene autotemcel infusion, the observed mean concentration of hemoglobin F was 11.5 g/dL (SD = 2.5 g/dL), and at 24 months post-exagamglogene autotemcel infusion, the observed mean concentration of hemoglobin F was 11.5 g/dL (SD = 2.7 g/dL).
Total Hemoglobin Concentration
The total hemoglobin concentrations targeted by SOC are 9 g/dL to 10 g/dL.1 At 6 months post-exagamglogene autotemcel infusion, the observed mean hemoglobin concentration was 12.1 g/dL (SD = 2.0 g/dL). At 12 months post-exagamglogene autotemcel infusion, the observed mean hemoglobin concentration was 12.8 g/dL (SD = 2.1 g/dL). At 24 months post-exagamglogene autotemcel infusion, the observed mean hemoglobin concentration was 12.9 g/dL (SD = 2.4 g/dL).
Proportion of Alleles With the Intended Genetic Modification in the CD34+ Cells of the Bone Marrow
At 6 months post-exagamglogene autotemcel infusion, the observed mean proportion of CD34+ cells with the intended genetic modification was 78.48% (SD = 11.39%). At 12 months post-exagamglogene autotemcel infusion, the observed mean proportion was █████ ████████. At 24 months post-exagamglogene autotemcel infusion, the observed mean proportion was █████ █████████
Proportion of Alleles With the Intended Genetic Modification in the Peripheral Blood
At 6 months post-exagamglogene autotemcel infusion, the observed mean proportion of CD34+ cells with the intended genetic modification was █████ ████████. At 12 months post-exagamglogene autotemcel infusion, the observed mean proportion was █████ ████████. At 24 months post-exagamglogene autotemcel infusion, the observed mean proportion was █████ ████████.
Functional Assessment of Cancer Therapy–Bone Marrow Transplantation
FACT-BMT is a quality-of-life measure for patients with cancer aged 18 years or older undergoing bone marrow transplant.25 Total scores range from 0 to 164,26 with higher scores indicating greater quality of life. Results were not reported at 6 months post-exagamglogene autotemcel infusion. At 12 months post-exagamglogene autotemcel infusion, the observed mean change in scores from baseline was 7.4 points (SD = 23.0 points). At 24 months post-exagamglogene autotemcel infusion, the observed mean change in scores from baseline was 13.9 points (SD = 21.4 points).
Pediatric Quality of Life Inventory
PedsQL scores range from 0 to 100 and describe general quality of life in children; the total score is the mean of all items and higher scores represent greater quality of life.27,28 At 6 months post-exagamglogene autotemcel infusion, the observed mean change from baseline in scores was 10.8 points (SD = 10.2 points). At 12 months post-exagamglogene autotemcel infusion, the observed mean change from baseline in scores was 12.0 points (SD = 10.3 points). At 24 months post-exagamglogene autotemcel infusion, the observed mean change from baseline in scores was 12.3 points (SD = 17.4 points).
EQ Visual Analogue Scale
The EQ visual analogue scale (EQ VAS) is a self-reported health rating using a 20 cm visual analogue scale (VAS) that ranged from 0 (worst imaginable health state) to 100 (best imaginable health state) points with higher scores indicating better HRQoL. At 9 months post-exagamglogene autotemcel infusion, the observed mean change from baseline was ███ ██████ points. At 12 months post-exagamglogene autotemcel infusion, the observed mean change from baseline was 7.9 points (SD = 16.7 points). At 24 months post-exagamglogene autotemcel infusion, the observed mean change from baseline was 10.7 points (SD = 18.6 points).
Nonadult EQ VAS
The EQ VAS used for pediatric patients was identical to that used in adults in the trial. Based on the January 16, 2023, data cut-off, at 6 months post-exagamglogene autotemcel infusion, the observed mean change from baseline was ███ ██████ points. At 12 months post-exagamglogene autotemcel infusion, the observed mean change from baseline was ███ ██████ points. At 18 months post-exagamglogene autotemcel infusion, the observed mean change from baseline was ███ █████ points.
Harms Results
During the course of the entire study to date, a total of 58 (98.3%) patients had any adverse events (AEs). A total of 56 (94.9%) patients had any AE during the time from enrolment until the day before exagamglogene autotemcel infusion, which included myeloablative conditioning. A total of 100% of patients had any AE during the time period from the day of exagamglogene autotemcel infusion to either the month 24 (M24) visit or the end-of-study (EOS) visit. The most common AEs from the time of enrolment to the day before exagamglogene autotemcel infusion were nausea (44.1% of patients), headache (39.0% of patients), bone pain (33.9% of patients), vascular site access pain (28.8% of patients), and vomiting (20.3% of patients). The most common AEs to date from the day of exagamglogene autotemcel infusion to the M24 or EOS study visit were febrile neutropenia (61.1% of patients), headache (55.6% of patients), stomatitis (51.9% of patients), thrombocytopenia (46.3% of patients), anemia (44.4% of patients), mucosal inflammation (42.6% of patients), nausea (42.6% of patients), and vomiting (40.7% of patients).
A total of 9 (15.3%) patients had any serious AE (SAE) during the time from enrolment until the day before exagamglogene autotemcel infusion, which included myeloablative conditioning. A total of 26 (44.1%) patients had any SAE during the time period from the day of enrolment to either their M24 or EOS visit. The SAEs that occurred in 2 or more patients during the study to date were veno-occlusive liver disease, pneumonia, COVID-19, hypoxia, thrombocytopenia, upper respiratory tract infection, nausea, vomiting, and bacteremia.
To date, no patients withdrew from the study drug or withdrew from the study due to AEs after exagamglogene autotemcel infusion. A total of 3 withdrawals before exagamglogene autotemcel infusion were reported; reasons included █████████ █ ██████ █████████ █████████ ██ ████████ ████████ ████ █████████ █████ █████████████ ██ ████████ ███ ███████████ ███████ ██ ███████. To date, no deaths had been reported in the study.
To date, all 54 (100.0%) patients had achieved neutrophil engraftment. The median time to neutrophil engraftment was 29.0 days (range, 12 to 56 days). A total of 53 patients achieved platelet engraftment; the median time to engraftment was 44.0 days (range, 20 to 200 days). Engraftment syndrome was not reported. Delayed engraftment was reported as a SAE in 1 patient during the time between exagamglogene autotemcel infusion and M24 or EOS visit.
Other AEs of special interest included 41 (69.5%) patients who reported AEs of infection or infestation and 33 (55.9%) patients who experienced febrile neutropenia. A total of | types of bleeding AEs were reported: gingival bleeding in 6 (10.2%) patients, ██████████████ ████████ ██ █ ██████ patients and █████ █████████ ████████ ██ █ ██████ patients. Veno-occlusive liver disease SAEs occurred in 5 (8.5%) patients. ████████████████ ████████ ███ ████████ ██ █ ██████ ████████. No information was reported regarding hemophagocytic lymphohistiocytosis, engraftment syndrome, infections and infestations classified as SAEs, bleeding classified as SAEs, or anaphylaxis. The submission noted that no malignancies had been reported in patients after exagamglogene autotemcel infusion in the study to date. No information was provided on off-target editing.
Critical Appraisal
There are several internal validity limitations to note. First, the CLIMB-111 study is a single-arm trial with no blinding, randomization, or allocation concealment, and therefore the study population may have unknown confounders and the results observed may not be able to be entirely attributable to the study drug. While a well-designed randomized controlled trial (RCT) that allows for causal inferences to be drawn with greater certainty than a single-arm treatment design is preferred, especially for decisions in health technology assessment (HTA) and reimbursement, the use of a single-arm study in this scenario is understandable. Nevertheless, it results in the Grading of Recommendations Assessment, Development and Evaluation (GRADE) assessment of certainty being very low, without evidence for grading up as is typical for single-arm studies. The CLIMB-111 study underwent several protocol changes including conversion to a phase I, II, and III trial, which has implications for the sample size and measurement of outcomes that may increase the heterogeneity of the results because of the confirmatory expectations of the phase III designation. The European Medicines Agency (EMA) review of exagamglogene autotemcel for TDT highlighted that 1 patient in the CLIMB-111 study had achieved the primary outcome at the time some of these key amendments were made.29 The EMA accepted that, while not ideal for internal validity, this likely had little effect on the overall validity or results of the study.29 Nonetheless, the number of important protocol and statistical analysis revisions for a study that does not have a true confirmatory phase III design adds to the very low certainty of the evidence. The results submitted from the CLIMB-111 study are an IA based on the PES; IAs may overestimate the true effect of treatment. Furthermore, the PES is potentially a select population because it reflects only those patients who completed the exagamglogene autotemcel treatment process in the time since the study began. Reporting all the study results to date based only on the PES could bias the effect estimate against a null hypothesis, favouring the intervention. In addition, the alpha spending methods used patient denominators to derive the alpha values for the IA1, IA2 and IA3, an approach which is considered more data-driven and there is potential to adjust for and not adjust for type I error based on the fluctuating thresholds. The first and second IAs were not done; the statistical analysis for IA3 recycled the alpha from the previous unused alpha spends but the appropriateness of this is questionable and would not necessarily result in a sufficiently conservative threshold. Furthermore, a response rate of 50% was used as the null threshold for the primary testing hypothesis, which was considered by the clinical experts consulted by CDA-AMC to be low. There are also no adjustments for multiplicity in the secondary and exploratory outcomes, and this reduces the ability to draw firm conclusions on the results from these analyses. There are also limitations regarding outcome ascertainment. The HRQoL measures are subjective and the single-arm, open-label nature of the study may bias the reporting of these results. There is also no rationale provided for the flexibility of the potential start and finish of the TI monitoring period within the 2 years of follow-up, and the clinical relevance of the TI6 outcome is somewhat uncertain especially whether it represents TI12 and longer-term outcomes. The use of a flexible outcome window increases the risk of overestimating the true effect. Furthermore, the analysis noted that the efficacy analyses were based on patients’ available data before death or loss to follow-up. As the submission did not describe whether any patient results were carried forward, there is a risk of additional uncertainty in the results. With regards to the duration of TI reported for those patients with TI12 (a secondary outcome), patients were required to maintain a weighted average hemoglobin of 9 g/dL or greater; however no rationale was provided for choosing a weighted average and there is a possibility that absolute hemoglobin values less than this would erroneously contribute to the proportion of TI responders.
There are some external validity limitations to note. The transfusion criteria used in the inclusion criteria were an internationally accepted cut-off for severe transfusion dependence; the study results are therefore only generalizable to patients with this degree of transfusion dependence. In addition, the clinical experts felt the age range was narrow and felt strongly that there should not be an upper age limit, but rather the suitability of patients for the therapy should be determined on a case-by-case basis as is done for HSCT. However, the age cut-off in the trial means the results are not necessarily generalizable outside of these age ranges. In addition, the exclusion criteria for any comorbidity which may impact outcomes or suitability for therapy does not specify comorbidities, and the available evidence was insufficient to assess with certainty whether patients in the CLIMB-111 study were on optimal SOC before initiating exagamglogene autotemcel. This may reduce the generalizability of these study results to all patients with TDT who may be considered for exagamglogene autotemcel therapy. In addition, the exclusion criteria for alpha thalassemia, multiple alpha deletions, and sickle cell thalassemia mean that results of the study do not apply to situations of co-inheritance of multiple types of thalassemia. Furthermore, the frequency of follow-up visits and laboratory measures undertaken in the trial may not reflect those in clinical practice, and therefore the results may not be wholly extrapolatable to clinical settings. In addition, the relatively short follow-up duration of patients in the trial is a concern for both efficacy and safety assessments; the mean follow-up after exagamglogene autotemcel infusion of 19 months (SD = 7 months) was not sufficient so far as to inform the issues of potential waning of effect over time, as well as longer-term toxicities such as the potential occurrence of malignancies. Lastly, the clinical experts noted that while SOC is generally similar across countries with higher socioeconomic status (SES), the CLIMB-111 study did not take place in any lower SES countries where thalassemias are endemic, and patient outcomes in these settings or the clinical status of patients who have recently immigrated to Canada from these countries may be different than those observed in the trial.
GRADE Summary of Findings and Certainty of the Evidence
For pivotal studies and RCTs identified in the sponsor’s systematic review, GRADE was used to assess the certainty of the evidence for outcomes considered most relevant to inform CDA-AMC expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group.30,31
Although GRADE guidance is not available for noncomparative studies, the CDA-AMC review team assessed pivotal single-arm trials for study limitations (which refers to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias to present these important considerations. Because the lack of a comparator arm in the CLIMB-111 study does not allow for a conclusion to be drawn on the effect of the intervention versus any comparator, the certainty of evidence for this GRADE assessment started at very low certainty with no opportunity for rating up.
When possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect; if this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., the clinical importance is unclear). In all cases, the target of the certainty of evidence assessment was based on the point estimate and where it was located relative to the threshold for a clinically important effect (when a threshold was available) or to the null.
The following list of outcomes was finalized in consultation with expert committee members.
Clinical outcomes:
proportion of patients with TI12
proportion of patients with TI6
total hemoglobin F
total hemoglobin concentration
HRQoL outcomes:
change from baseline to 24 months in FACT-BMT scores
change from baseline to 24 months in PedsQL scores
Harms:
all-cause mortality
proportion of patients with engraftment (platelet and neutrophil)
time to engraftment (platelet and neutrophil)
AEs in 25% or more patients and SAEs in 2 or more patients
Table 2: Summary of Findings for Exagamglogene Autotemcel for Patients With Transfusion-Dependent Beta Thalassemia
Outcome and follow-up | Patients (studies), N | Effect | Certaintya | What happens |
|---|---|---|---|---|
Transfusion and hematologic outcomes | ||||
Patients achieving TI12 Follow-up: any 12-month period 60 days after last RBC transfusion up to 2 years after exagamglogene autotemcel infusion | 42 (1 single-arm study) | Patients with TI12 (n = 39; 929 per 1,000 patients): 92.9% (95% CI, 80.5% to 98.5%) | Very lowb,c,d | The evidence is very uncertain about the effect of exagamglogene autotemcel on the proportion of patients achieving TI12 when compared with any comparator. |
Patients achieving TI6 Follow-up: any 12-month period 60 days after last RBC transfusion up to 2 years after exagamglogene autotemcel infusion | 42 (1 single-arm study) | Patients with TI6 (n = 39; 929 per 1,000 patients): 92.9% (95% CI, 80.5% to 98.5%) | Very lowb,c,d | The evidence is very uncertain about the effect of exagamglogene autotemcel on the proportion of patients achieving TI6 when compared with any comparator. |
Total hemoglobin F (g/dL) Follow-up: 24 months | 42 (1 single-arm study) | Mean total hemoglobin F = 11.5 g/dL (SD = 2.7 g/dL) Change from baseline: NR | Very lowc,d | The evidence is very uncertain about the effect of exagamglogene autotemcel on the total hemoglobin F when compared with any comparator. |
Total hemoglobin concentration (g/dL) Follow-up: 24 months | 42 (1 single-arm study) | Mean total hemoglobin = 12.9 g/dL (SD = 2.4 g/dL) Change from baseline: NR, (95% CI, NR to NR) | Very lowc,d | The evidence is very uncertain about the effect of exagamglogene autotemcel on the total hemoglobin concentration when compared with any comparator. |
HRQoL and symptom outcomes | ||||
Change in FACT-BMT scores from baseline Follow-up: 24 months | 29 (1 single-arm study) | Mean = 13.9 (SD = 21.4) | Very lowc,d | The evidence is very uncertain about the effect of exagamglogene autotemcel on the change from baseline in FACT-BMT scores when compared with any comparator. |
Changes in PedsQL scores from baseline Follow-up: 24 months | 12 (1 single-arm study) | Mean = 12.3 (SD = 17.4) | Very lowc,d | The evidence is very uncertain about the effect of exagamglogene autotemcel on change from baseline in PedsQL scores when compared with any comparator. |
Harms | ||||
All-cause mortality Follow-up: 24 months | 59 (1 single-arm study) | Patients who died: n = 0 (95% CI, NR) | Very lowd, e | The evidence is very uncertain about the effect of exagamglogene autotemcel on all-cause mortality when compared with any comparator. |
Patients with engraftment (neutrophil and platelet) | 54 (patients who had undergone myeloablative conditioning in 1 single-arm study) | Patients with neutrophil engraftment: n = 54 (1,000 per 1,000 patients) Patients with platelet engraftment: n = 53 (981 per 1,000 patients) | Very lowd,e | The evidence is very uncertain about the effect of exagamglogene autotemcel on the proportion of patients with engraftment when compared with any comparator. |
Time to engraftment (neutrophil and platelet) | 54 (patients who had undergone myeloablative conditioning in 1 single-arm study) | Median time to neutrophil engraftment = 29 days (range, 12 to 56 days) Median time to platelet engraftment = 44 days (range, 20 to 200 days) | Very lowd,e | The evidence is very uncertain about the effect of exagamglogene autotemcel on the time to neutrophil or platelet engraftment when compared with any comparator. |
AEs (in ≥ 25% of patients) and SAEs (in ≥ 2 patients) | 59 (1 single-arm study) | AEs: n = 58 (983 per 1,000 patients) SAEs: n = 26 (441 per 1,000 patients) | Very lowd,e | The evidence is very uncertain about the effect of exagamglogene autotemcel on AEs, SAEs, and AEs of special interest when compared with any comparator. |
AE = adverse event; CI = confidence interval; FACT-BMT = Functional Assessment of Cancer Therapy–Bone Marrow Transplantation; hemoglobin F = fetal hemoglobin; HRQoL = health-related quality of life; NR = not reported; PedsQL = Pediatric Quality of Life Inventory; RBC = red blood cell; SAE = serious adverse event; SD = standard deviation; TI = transfusion independence; TI6 = transfusion independence for 6 consecutive months; TI12 = transfusion independence for 12 consecutive months.
Note: All serious concerns with study limitations (which refers to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias are documented in the table footnotes.
aIn the absence of a comparator arm, conclusions about efficacy relative to any comparator cannot be drawn and certainty of evidence started at very low. None of the outcomes were rated up because of serious study limitations (refer to specific footnotes).
bSerious study limitations. The flexibility of the start and finish dates of the TI monitoring period during the 2-year follow-up risks overestimating the treatment effect. Updates to the outcomes made to the study protocol after enrolment with no rationale provided cause an unknown risk of bias.
cSerious indirectness. According to clinical experts consulted by CDA-AMC, the age limit in the trial is not likely to represent all patients with TDT who may be considered for exagamglogene autotemcel therapy, and the list of comorbidities in the exclusion criteria is not known.
dSerious study limitations. The interim analysis provided results only for the primary efficacy set, which is potentially a select sample as it represents those patients who have completed the study to date, as opposed to the full enrolled sample. Information on the outcomes based on the full treatment experience is therefore lacking.
eSerious imprecision. The study captured a very small number of events, and the study duration is unlikely to be long enough to fully capture the outcome.
Sources: Details included in the table are from the sponsor’s Summary of Clinical Evidence,2 Clinical Addendum Update24 and additional information provided by the sponsor.32-34
Long-Term Extension Studies
The sponsor submitted 1 long-term extension (LTE) study for this review. The CLIMB-131 study is an ongoing, multisite, open-label, rollover study designed to evaluate the long-term safety and efficacy of exagamglogene autotemcel in patients who received treatment in the CLIMB-111 study and who completed or discontinued the study.24,35 The primary objective was to evaluate the long-term safety of exagamglogene autotemcel.
Description of Studies
All patients who completed or discontinued the CLIMB-111 study after exagamglogene autotemcel infusion and signed and dated the informed consent form were invited to participate in the CLIMB-131 study, with no exclusion criteria. Patients did not receive any study drug. All medication taken from the signing of the consent form for the CLIMB-131 study through the data cut-off date (April 16, 2023) were recorded. The CLIMB-131 study is planned to provide an additional 13 years of follow-up, totalling 15 years of follow-up after exagamglogene autotemcel infusion.
The primary safety end points for the CLIMB-131 study included new malignancies, new or worsening hematologic disorders, all-cause mortality, all SAEs (to be recorded up to 5 years after infusion) and exagamglogene autotemcel-related AEs and SAEs. The secondary end points summarized in this section for the CLIMB-131 study included the same outcomes that were assessed in the CLIMB-111 study, with the exception of TI6 and TI12. Of note, HRQoL results were not reported past 24 months in the submission.
Analysis sets for patients with TDT in the CLIMB-131 study were the same as for the CLIMB-111 study. All data from the extension studies were analyzed descriptively using summary statistics. Continuous variables were summarized using the following descriptive number of patients (n), mean, SD, median, minimum, and maximum values. For certain continuous variables, such as hemoglobin and hemoglobin F, additional summary statistics including the first and third quartiles were presented. Categorical variables were summarized using counts and percentages. Baseline value, unless specified otherwise, was defined as the baseline in the CLIMB-111 study.
Missing data were not imputed, and all data were evaluated as observed. Patients who discontinued the study were listed with the reasons for withdrawal. The submission noted that starting after the M24 visit, only AEs related or possibly related to exagamglogene autotemcel, SAEs, new malignancies, and new or worsening hematologic disorders were recorded.
Efficacy Results
A total of 23 patients had completed the 2-year follow-up after exagamglogene autotemcel in the CLIMB-111 study and rolled over into the CLIMB-131 study. To date, no patient had discontinued from the CLIMB-131 study.
Total Hemoglobin and Hemoglobin F
At 36 months post-exagamglogene autotemcel infusion, the observed mean concentration of hemoglobin F was ████ █████ g/dL and ████ █████ █ ██ █████ ██ ██ █ ██. At 48 months post-exagamglogene autotemcel infusion, the observed mean concentration of hemoglobin F was ████ ████ g/dL and ████ ████ █ ██ █████ ██ ██ █ ██.
Proportion of Alleles With the Intended Genetic Modification in the CD34+ Cells of the Bone Marrow
At 36 months post-exagamglogene autotemcel infusion, the observed mean proportion of CD34+ cells with the intended genetic modification was █████ ████ █ ██ █ ██. At 48 months post-exagamglogene autotemcel infusion, the observed mean proportion was █████ █████ ██ █ ██.
Proportion of Alleles With the Intended Genetic Modification in the Peripheral Blood
At 36 months post-exagamglogene autotemcel infusion, the observed mean proportion of CD34+ cells with the intended genetic modification was █████ ████████ ██ █ ██. At 48 months post-exagamglogene autotemcel infusion, the observed mean proportion was █████ █████ ██ █ ██.
Health-Related Quality of Life
HRQoL assessments were conducted for patients with TDT included EQ-5D-5L, EQ-5D-Y, FACT-BMT, and PedsQL. Due to a paucity of long-term patient-reported outcome (PRO) data collected as of the January 12, 2023, data cut-off, PRO data for the CLIMB-131 study are not reported herein.
Transfusion Independence
All patients who achieved TI12 continued to remain transfusion independent in the CLIMB-111 study. These benefits were sustained through the CLIMB-131 study. The mean duration of TI to date was 23.6 months (SD = 7.8 months) with a range of 13.5 months to 48.1 months, starting 60 days after the last RBC transfusion for posttransplant support or TDT disease management.
Harms Results
As of April 16, 2023, a total of 23 patients with TDT were rolled over in the CLIMB-131 study after completion of the M24 visit. The overall duration of follow-up (including follow-up in the CLIMB-131 study) for these patients ranged from 25.2 months to 51.1 months after exagamglogene autotemcel infusion. No deaths have occurred during the CLIMB-131 study. ███ ███████ ████ ███ ███ ██ ███ ██ █████████ ██ █████ ███ █████ █████ ███ ████████ ██████ █ ████. No new safety findings were observed for 23 patients enrolled in the CLIMB-131 study including no evidence of new malignancies or new or worsening hematologic disorders long-term after exagamglogene autotemcel infusion.
Critical Appraisal
The CLIMB-131 study was an open-label extension designed to evaluate the long-term efficacy and safety of exagamglogene autotemcel in treating patients with TDT. However, the same study design, study population, and outcome ascertainment limitations noted in the critical appraisal for the CLIMB-111 study also apply to the LTE. In addition, the available data for the CLIMB-131 study are limited to a greater extent due to the fact that it is an IA which only a fraction of patients have completed at the time of the submission, which hampers the ability to draw definitive long-term conclusions until the follow-up is complete. The same limitations regarding external validity of the LTE (including the age and comorbidity exclusion criteria) which were identified in the CLIMB-111 study also apply to the LTE. Additionally, the study did not report HRQoL results for the CLIMB-131 study period as of the data cut-off date; therefore, long-term data on HRQoL are lacking. Another important limitation is the fact that no harms were reported after M24 unless they were judged related to the study drug, which is an important limitation as relation to the study drug can be a subjective measure, and therefore complete harms reporting in the LTE is lacking.
Indirect Comparisons
Description of Studies
The sponsor submitted a matching-adjusted indirect comparison (MAIC) based on the data cut-off up to January 16, 2023, to assess the relative safety and efficacy of exagamglogene autotemcel and luspatercept as well as SOC, defined as RBC transfusions and ICT.36 The objective of the indirect comparisons were to provide comparative efficacy data for exagamglogene autotemcel versus appropriate comparators (luspatercept and SOC).
The feasibility of conducting an indirect comparison against the comparators of interest was considered separately for each comparator. Relevant baseline covariates identified as the key effect modifiers and/or prognostic factors were selected using a targeted literature review and clinical expert consultation (N = 7 clinical experts). Variables were ranked in order of importance and were confirmed by clinical consensus. A maximum of 3 adjustment variables were used at 1 time. The adjustment variables were as follows:
genotype (proportions of patients with beta0/beta0 versus non-beta0/beta0 genotype)
baseline annualized units or volume (mL/kg) of transfusions
age
sex
race and/or ethnicity (white versus nonwhite [only categories used in source]).
Patients from the CLIMB-111 study were re-weighted according to the methodology proposed by the Signorovitch et al. study.37 The outcome assessed in the MAICs was the proportion of patients TI6 (for the CLIMB-111 study) and transfusion independent after 3 consecutive months (TI3) (for the BELIEVE study).
Efficacy Results
The report identified that there were qualitative differences between the 2 studies in several areas including study design, inclusion and exclusion criteria, and the timing of outcome ascertainment. The results of the quality assessment for the BELIEVE study reported that 2 domains were assessed as “no,” suggesting that the evidence was a low to moderate rating overall on the basis of the National Institute for Health and Care Excellence quality appraisal checklist.
Exagamglogene Autotemcel Versus SOC
The individual patient data from the CLIMB-111 study were statistically adjusted to match the aggregate population characteristics of the BELIEVE study using genotype, baseline units of RBC transfusions, and age. The results showed a numeric difference in the proportion of patients with TI6 in the CLIMB-111 study (proportion = 90.0; 95% CI, 64.7 to 97.8) relative to the proportion of patients with TI3 on SOC (proportion = 0; 95% CI, not reported).
Exagamglogene Autotemcel Versus Luspatercept
Adjustment was performed on genotype, baseline units of RBC transfusions, and age. A total of 4.0% patients in the luspatercept arm of the BELIEVE study had TI3, and 93.2% of patients in the adjusted CLIMB-111 study arm had TI6. The rate ratio (RR) for the proportion of patients with TI was 23.3 (95% CI, 12.2 to 44.7).
Harms Results
Harms were not analyzed in the indirect comparison.
Critical Appraisal
The systematic literature review (SLR) which informed the indirect treatment comparisons is subject to some limitations, including that the results of the quality assessment were not provided for the CLIMB-111 study and therefore the risk of bias is not known.
There are several important limitations in the MAIC analysis to note. The MAICs were unanchored, which requires the assumption that all possible treatment effect modifiers and prognostic factors are controlled for, which is an assumption largely considered impossible to achieve and therefore adds uncertainty to the results.38 The analysis solicited expert input to help provide a list of possible factors to include in the weighting, but limited weighting on 3 of them; a clear rationale for this was not given. Furthermore, the submission did not include details on the baseline characteristics that were not included in matching; therefore, it is unknown whether there are other sources of heterogeneity in the patient population. In addition, the homogeneity assessment identified several potentially important differences between the CLIMB-111 and BELIEVE studies which remain even after excluding patients from the CLIMB-111 study who would not match the BELIEVE study population. First, the 2 studies had a different study design (the BELIEVE study was a double-blind RCT while the CLIMB-111 study was a single-arm phase I, II, and III study) and weighting would not account for this difference. Second, different timing of outcome evaluation would not be controlled by weighting. The CLIMB-111 study was evaluated over a longer time frame than the BELIEVE study, with 2 years follow-up, while the BELIEVE study lasted for 48 weeks. This suggests that the study populations and the results as reported are likely not able to satisfy the comparability assumptions required for an unanchored MAIC. An additional limitation to the MAIC methodology is a small effective sample size (ESS) after matching which imparts instability to the results. In addition, there is no summary provided of the distribution of weights from the matching, so it is unknown whether there were extreme weights applied to any of the patient data in the CLIMB-111 study. Overall, these limitations impact a high degree of uncertainty in the results, and it is challenging to draw firm conclusions on the basis of the analysis.
There are additional limitations to the generalizability of the MAIC and the similarity of the comparator treatments which are important to note. First, the clinical expert panel highlighted that luspatercept does not generally lead to TI, and approximately 20% of patients respond to it; it is not known whether the subgroup within the BELIEVE trial who reached TI differs from the main study population in meaningful ways. Furthermore, patients randomized to the SOC arm of the BELIEVE study would, by definition, be unable to reach TI as transfusions are an integral part of the SOC for TDT. Other generalizability limitations include that the comparative results cannot be generalized to pediatric patients. Lastly, the MAIC did not analyze harms outcomes; therefore, comparative data on the safety of treatments remains unknown. Overall, this suggests that the comparators used in the MAIC may not be wholly similar to one another and makes it challenging to make meaningful conclusions about the comparative efficacy of luspatercept, SOC, and exagamglogene autotemcel for the outcomes that were measured in the indirect comparison.
Studies Addressing Gaps in the Evidence From the Systematic Review
No additional studies were submitted by the sponsor addressing gaps in the systematic review evidence.
Conclusions
In the absence of direct comparative data, evidence from the IA of the CLIMB-111 study, a phase I, II, and III multisite, single-arm, single-dose trial in the PES of 42 patients aged 12 years to 35 years with TDT is very uncertain about the effect of exagamglogene autotemcel on clinical efficacy and harms outcomes in patients with TDT when compared with any comparator. Findings from the trial are consistent with a clinically meaningful reduction in transfusion leading to TI, according to clinical expert input. While improvements in HRQoL scores from baseline were reported, it is uncertain if the changes are clinically meaningful due to the lack of estimated minimal important differences (MIDs) in TDT. The available results from the trial are subject to important potential biases in outcome ascertainment, study population, and statistical analysis plan changes which impact the certainty that the observed effect is truly attributable to the study drug. Results from the LTE portion were only available from a fraction of patients for all outcomes and therefore remain highly uncertain; in general, a relatively short time period after infusion is included in the submission. With regards to safety, most AEs and SAEs reported in the pivotal trial could be considered attributable to the myeloablative conditioning; however, the clinical experts noted that a longer time to engraftment was noted for patients after exagamglogene autotemcel infusion which may impart additional harms such as reduced engraftment potential, higher risks of infection, bleeding, and longer stays in hospital which would have resource use implications. The submission did not report details on off-target editing or fertility to date. Conclusions around long-term harms results are generally limited by the ongoing nature of the trial and the short follow-up to date. The indirect evidence submitted by the sponsor, consisting of 2 MAICs comparing exagamglogene autotemcel to SOC (transfusions and chelation) and luspatercept, respectively, were considerably limited by differences in the study design, outcome ascertainment, and concerns around the validity of the comparators in terms of their potential for attaining the outcome of TI. Therefore, information on the comparative nature of exagamglogene autotemcel to other treatment options remains lacking due to limitations with the indirect evidence as well as the use of a single-arm trial. Overall, the evidence is highly uncertain about the impact of exagamglogene autotemcel on clinical efficacy and harms when compared with any comparator.
However, the treatment landscape for TDT, a rare, severe disease in which optimized transfusion and ICT can provide life expectancy beyond the mean ages of death that have been previously reported in patients with TDT but which provides few treatment options that achieve TI, is also a consideration. The clinical experts noted that they would likely prioritize patients who are struggling on SOC for exagamglogene autotemcel therapy, and HSCT would remain a first-line consideration for patients who were eligible for it and have a matched donor. The potential resource and personal impact of averting transfusions in patients who have lifelong requirements was also highlighted, although additional resources will also be required for offering exagamglogene autotemcel and ensuring equity in access, particularly to transplant centres. However, clinicians also emphasized that patient preference and the weighting of risks versus benefits would be of great importance in identifying candidates for therapy.
Introduction
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of exagamglogene autotemcel cell suspension in patient-specific vials, 4 × 106 cells/mL to 13 × 106 cells/mL IV infusion, in the treatment of TDT in patients aged 12 years or older.
Disease Background
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following have been summarized and validated by the CDA-AMC review team.
Thalassemias are a group of hemoglobinopathies where the normal ratio of alpha-globin to beta-like globin production is disrupted due to genetic mutations in the alpha-like or beta-like globin genes, which result in reduced or absent synthesis of the corresponding chain in hemoglobin, the oxygen-carrying protein in RBCs. The resulting abnormal alpha to beta chain ratio leads to precipitation in the unpaired chains, destroying RBC precursors in the bone marrow and in the circulation.39 The 2 main clinical phenotypes are alpha thalassemia and beta thalassemia.
In beta thalassemia, limited or absent beta-like globin drives the imbalance between alpha-globin and beta-like globin chains, which comprise the subunits of adult hemoglobin (hemoglobin A).40 Beta thalassemia is caused by mutations in the HBB gene and is characterized by ineffective erythropoiesis and hemolysis, which leads to chronic severe anemia with inadequate oxygen delivery to organs and tissues.41 It is classified into 2 subtypes: transfusion dependent (i.e., TDT) and non–transfusion dependent. The HBB gene variants, or mutations, are classified according to the degree of reduction in beta-like globin production. Beta0 refers to pathogenic gene variants that completely abolish beta-like globin production, while beta+ refers to variants that cause decreased, but not absent, beta-like globin production.42 Patients who are homozygous or compound heterozygous for beta0 thalassemia mutations are more likely to have TDT, while individuals homozygous for beta+ thalassemia mutations can make some hemoglobin A and may be less severely affected.42 TDT and non–transfusion dependent are fluid categorizations based on clinical parameters and variations, and patients may shift from one to the other during their lives.43
Different combinations of the globin subunits give rise to multiple types of hemoglobin, which predominate at different stages of life,44 with hemoglobin F as the predominant hemoglobin type before birth and during the newborn phase.40 Hemoglobin F does not contain any beta-like globin chains and as a result, individuals with beta thalassemia are asymptomatic at birth. Disease pathology arises as hemoglobin F switches to hemoglobin A, with the onset of symptoms typically occurring a few months after birth when hemoglobin A replaces hemoglobin F as the predominant type of hemoglobin.40,45
TDT is a rare, autosomal, recessive genetic hemoglobinopathy and the more severe form of beta thalassemia. Without the support of RBC transfusions, patients with TDT develop severe anemia due to ineffective erythropoiesis, as well as comorbidities such as splenomegaly, bone marrow expansion with accompanying bone pain, progressive bone deformities, extramedullary erythropoiesis, and iron overload.1,2 High plasma iron levels result in oversaturation of transferrin (an iron transport protein) and intracellular accumulation of free unbound iron causing cellular dysfunction, apoptosis, necrosis, and end-organ damage, with the liver and the heart being most severely affected.3 High cardiac iron levels have been identified as the strongest predictor of cardiac iron-related comorbidities and mortality among patients with TDT.46 Patients with TDT typically require lifelong regular packed RBC transfusions (typically administered every 2 weeks to 4 weeks)16 which can further exacerbate iron overload.47 Without regular transfusions, 85% of patients with TDT would die in the first 5 years of life due to severe anemia.3 Furthermore, the consequences of inadequate oxygen delivery, including cerebral ischemia and myocardial ischemia, can be life-threatening.4 Patients with TDT also have worse HRQoL compared with the general population, with disease-related impacts affecting physical and mental well-being.5-7
Early diagnosis as soon as possible after birth is essential for patients with TDT. NBS initiatives allow identification of affected individuals before symptom onset and allow access to specialty care and initiation of RBC transfusions before development of severe complications. Canadian guidelines (CanHaem and TFC) recommend NBS should include testing for thalassemia syndromes.8,17 High performance liquid chromatography, capillary electrophoresis, and isoelectric focusing are the most common methods of detection used during NBS.8 Screening and confirmatory tests for patients with a clinical suspicion of beta thalassemia can also be performed as well as preconception screening and prenatal testing for parents known to be at risk of having a child with TDT.8
Although a rare disease in Canada, the number of individuals with beta thalassemia is evolving.8 It may continue to rise in the Western world due to continued immigration from endemic regions including the Mediterranean, Asian, Indian, and Middle Eastern regions.8,10-13 Of patients with beta thalassemia, an estimated 70% are thought to have TDT.14,15 Within the jurisdictions relevant to the CDA-AMC submission, there were an estimated 1,900 patients with TDT, with the majority residing in Ontario (approximately 1,100), British Columbia (approximately 370), and Alberta (approximately 250) in 2022.14 The estimated prevalence of beta thalassemia by region is presented in Table 3.
Table 3: Estimated Prevalence of Beta Thalassemia by Region (2022)
Region | Estimated prevalence | ||
|---|---|---|---|
Lower estimate | Best estimate | Upper estimate | |
Newfoundland and Labrador | 2 | 4 | 4 |
Prince Edward Island | 2 | 3 | 3 |
Nova Scotia | 10 | 19 | 19 |
New Brunswick | 6 | 11 | 11 |
Ontario | 616 | 1,099 | 1,099 |
Manitoba | 38 | 67 | 67 |
Saskatchewan | 20 | 36 | 36 |
Alberta | 143 | 256 | 256 |
British Columbia | 210 | 374 | 374 |
Yukon | 1 | 1 | 1 |
Northwest Territories | 1 | 1 | 1 |
Nunavut | 0 | 0 | 0 |
Non-Insured Health Benefits | 2 | 2 | 2 |
Pan-Canadian (excluding Quebec)a | 1,049 | 1,872 | 1,872 |
TDT = transfusion-dependent beta thalassemia.
Note: This table provides an estimate of all patients with TDT covered by each of the participating drug plans. Exagamglogene autotemcel is only indicated for patients aged ≥ 12 years.
aValues may differ slightly from the sum of the preceding rows due to rounding.
Source: Details included in the table are from the sponsor’s Summary of Clinical Evidence.14
Standards of Therapy
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following have been summarized and validated by the CDA-AMC review team.
In general, patients with TDT require lifelong care and routine monitoring which ideally is performed in specialized centres by a team of multidisciplinary experts.8,15,16 The main goals of managing TDT in Canada include ameliorating the negative effects of anemia through regular packed RBC transfusions and reducing iron overload with ICT, both of which represent the SOC.8,17
Lifelong transfusion support both prevents life-threatening anemia and suppresses the endogenous erythropoiesis and the accompanying hypertrophy of myeloid bone marrow; to this end, transfusion support targets the maintenance of hemoglobin between 90 g/L to 100 g/L, as this maintains erythroid mass at 1 to 4 times normal and is generally adequate to prevent other comorbidities such as growth retardation, extramedullary hematopoiesis, and dysmorphic bone changes.1 Clinical experts consulted by CDA-AMC noted that current treatment goals for transfusion focus on maintaining a hemoglobin level of 9.5 g/dL to 10.5 g/dL and maintaining liver iron, measured by FerriScan, of 2 mg/g to 3 mg/g or 2 mg/g to 5 mg/g. Regular RBC transfusions (typically every 2 weeks to 4 weeks, beginning in infancy) aim to maintain this pretransfusion level.8,17 For patients with TDT, regular RBC transfusions are usually initiated within the first 2 years of life in response to severe anemia and other factors such as poor growth or facial changes (e.g., enlargement of the jaw, bulging cheekbone).16 ICT is also required to manage the iron overload which results from both transfusion as well as TDT; the main mechanism of iron chelation drugs is to penetrate organs to varying extents and remove intracellular iron. Newer iron chelation options deferiprone and deferasirox are oral medications and there is 1 parenteral infusion drug, deferoxamine; patients take iron chelation drugs daily either alone or in combination if additional chelation is needed. Deferasirox is the preferred chelator for most patients, and the chelating drug(s) used should be tolerable and effective; intolerance to ICTs can impact adherence and result in increased iron overload and comorbidities.48 Other potential treatment options to accompany transfusion for adult patients with TDT include luspatercept, an erythroid maturation drug approved for the treatment of anemia in adults with TDT.18 Luspatercept stimulates erythroid response and in clinical trials was shown to reduce transfusion burden by approximately 33% in more patients compared to placebo.49 Folic acid supplementation is also a possible concomitant medication option if there is evidence of ongoing hemolysis.50
Routine disease monitoring is focused mainly on monitoring for iron overload and associated complications and includes assessment of serum ferritin (every 1 month to 3 months), liver iron concentration via MRI (every 6 months to 24 months), and myocardial iron via cardiac MRI (every 6 months to 24 months).8,15,16 Target organ function should also be assessed regularly with clinical exams, electrocardiograms, chest radiograms, and echocardiography performed every 6 months to 12 months and bone mineral density testing occurs every 12 months to 24 months.16 Complete blood count is recommended at every RBC transfusion (i.e., every 2 weeks to 4 weeks).8 The clinical experts consulted by CDA-AMC noted that if transfusion and ICT are optimized, with newer iron chelation therapies available, patients with TDT can have life expectancy beyond the mean ages of death that have been previously reported for this disease.19,20
Allogenic HSCT is the only curative treatment available for patients with TDT. HSCT with an HLA-matched sibling donor is considered the SOC for children with TDT; discussion of HSCT as a treatment option for children is recommended to be undertaken with families before the patient reaches puberty, to maximize the likelihood of preserving fertility.21 HSCT for adult patients with thalassemia is associated with increased morbidity and not generally available in most centres.21 Per the clinical experts consulted by CDA-AMC, HSCT with an HLA-matched donor is an option in approximately 20% of patients, and if available is one they discuss with patients. The experts also noted that patient preference and detailed discussions around the risks and benefits is important before undertaking HSCT, as not all families eligible will decide to undertake it. The best outcomes of HSCT are when it is performed with HLA-matched sibling donors and among patients of younger ages before TDT-related end-organ damage has accumulated.22,23 Patients undergoing HSCT with an HLA-matched sibling donor have overall survival rates of 91% to 98% and disease-free survival rates from 83% to 95%.21 The main complications from HSCT are acute and chronic graft versus host disease, engraftment failure (secondary bone marrow rejection), hypofertility, and sterility, and the main causes of death are infectious complications after HSCT rejection.21 The entire procedure requires several weeks of hospitalization and several months of close follow-up after transplant.
Drug Under Review
Key characteristics of exagamglogene autotemcel are summarized in Table 4 with other treatments available for the treatment of patients aged 12 years and older with TDT.
Health Canada Indication
Exagamglogene autotemcel is approved by Health Canada for the treatment of patients aged 12 years and older with TDT.51 The sponsor reimbursement request is as per the approved indication.
Dosing and Administration
The minimum recommended dose of exagamglogene autotemcel is 3 × 106 viable CD34+ cells/kg.51 Exagamglogene autotemcel is provided as a one-time, patient-specific single dose for IV infusion containing a suspension of CD34+ cells in 1 or more vials. All vials of exagamglogene autotemcel provided for the patient must be administered. Exagamglogene autotemcel’s proposed administration would take place only in a treatment centre with experience in stem cell transplant.51
Administration of exagamglogene autotemcel would require patients to undergo CD34+ HSPC mobilization followed by apheresis to isolate the CD34+ cells for medicinal product manufacturing. Before transplant of the edited cells, full myeloablative conditioning would be required. Following the last dose of myeloablation, the patient would receive a single exagamglogene autotemcel infusion. Details of the proposed treatment process are in Figure 1.
Mechanism of Action
Exagamglogene autotemcel is a cellular therapy consisting of autologous CD34+ HSPCs edited by CRISPR/Cas9 technology. The guide ribonucleic acid enables CRISPR/Cas9 to make a precise DNA double-strand break at the critical transcription factor binding site (GATA1) in the erythroid-specific enhancer region of the BCL11A gene.51 The editing is specific. As a result of the editing, GATA1 binding is irreversibly disrupted and BCL11A expression reduced. Reduced BCL11A expression results in an increase in gamma-globin expression and hemoglobin F protein production in erythroid cells. As hemoglobin F does not contain any beta-globin chains, in patients with TDT, the production of hemoglobin F is intended to correct the alpha-globin to beta-globin imbalance which would reduce ineffective erythropoiesis and hemolysis. Following successful engraftment, the effects of exagamglogene autotemcel are proposed to be lifelong.51 The submission noted that no off-target editing has been observed based on in vitro studies with exagamglogene autotemcel manufactured using either healthy donor or patient cells, but did not provide any details on the known prevalence of off-target effects in vivo in patients to date.
Prescribing
The submission noted that exagamglogene autotemcel can only be administered at an authorized treatment centre (ATC) with experience in stem cell transplant and in the treatment of patients with TDT. Exagamglogene autotemcel treatment requires both hematology and transplant expertise; hematologists will need to have expertise and capacity to discuss treatment options, refer the appropriate patients for treatment, and inform follow-up care while transplant physicians will need to have the capacity and expertise to finalize patient treatment plans, administer exagamglogene autotemcel treatment, and advise on patients’ follow-up care.
Given that access to these clinical specialists may differ across provinces and territories, the submission suggested that a referral network could be established similar to networks which currently exist for other complex treatments such as HSCT and chimeric antigen receptor T-cell therapy. The submission noted that it is highly unlikely that a suitable ATC would be situated in every province or territory; therefore, interprovincial and territorial collaboration would be necessary to ensure equitable access to exagamglogene autotemcel for all eligible patients with TDT. There is uncertainty regarding the current number, location, and specific bed capacity of ATCs, as well as the timing of when such ATCs could be ready to provide exagamglogene autotemcel treatment.
Details of exagamglogene autotemcel and relevant comparators are presented in Table 4.
Figure 1: Proposed Exagamglogene Autotemcel Treatment Process
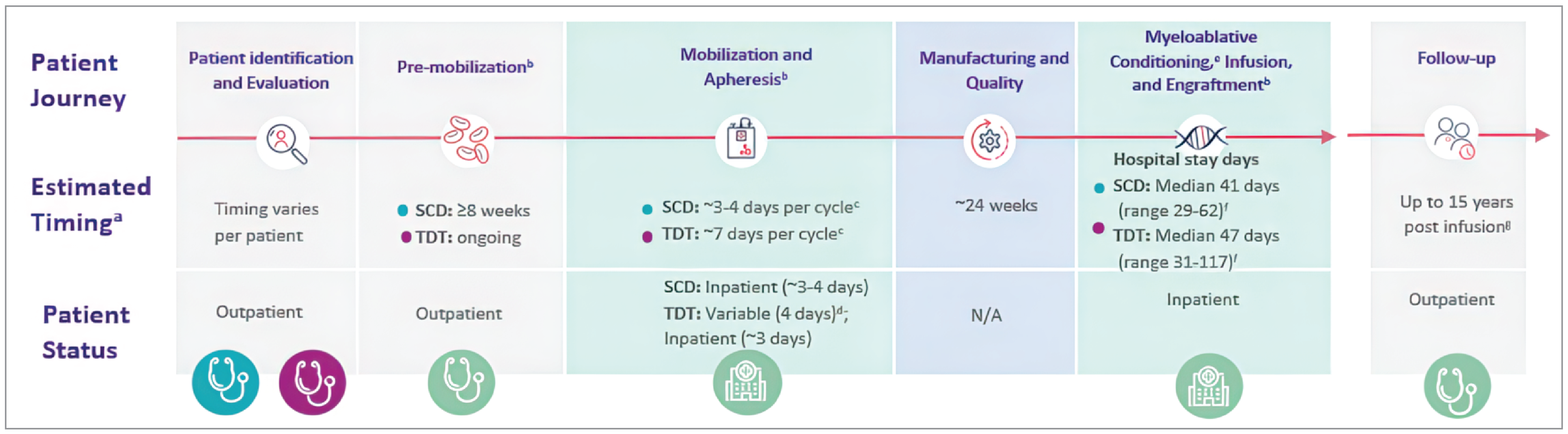
N/A = not applicable; SC = subcutaneous; SCD = sickle cell disease; TDT = transfusion-dependent beta thalassemia; VOC = vaso-occlusive crisis.
Note: This figure represents both patients with TDT and SCD (exagamglogene autotemcel is also approved by Health Canada for the treatment of patients with SCD with recurrent VOCs).
aThe submission noted that the time frame for each step of exagamglogene autotemcel administration is approximate and could vary per patient; the entire exagamglogene autotemcel procedure could take up to a year.
bTiming and patient status are based on clinical trials; the submission did not specify which trials.
cThe median number of collection cycles for SCD and TDT was 2 (range, 1 to 6) and 1 (range, 1 to 4), respectively. Timing is reflective of a hospital admission on day 0 for SCD and day 4 for TDT.
dThe submission noted that SC-administered mobilizing drugs can be self-administered at home, but inpatient administration of the injection may be required.
eThe median total length of hospitalization for myeloablative conditioning and exagamglogene autotemcel infusion through discharge for SCD and TDT was approximately 6 weeks and 7 weeks, respectively.
fHospital stay days. It is recommended that patients with SCD or TDT be transfused for at least 8 weeks or for 60 days, respectively, before the initiation of myeloablative conditioning.
gTo be confirmed following Health Canada review.
Source: Details included in the figure are from the sponsor’s Summary of Clinical Evidence.52
Table 4: Key Characteristics of Exagamglogene Autotemcel, Luspatercept, and SOC
Characteristic | Exagamglogene autotemcel | Luspatercept | Transfusion and ICT |
|---|---|---|---|
Mechanism of action | Cellular therapy consisting of autologous CD34+ HSPCs edited by CRISPR/Cas9 technology. As a result of the editing, GATA1 binding is irreversibly disrupted and BCL11A expression reduced. Reduced BCL11A expression results in an increase in gamma-globin expression and hemoglobin F protein production in erythroid cells. In patients with TDT, gamma-globin production corrects the alpha-globin to non–alpha-globin imbalance. | Recombinant fusion protein derived from human activin receptor type IIb linked to a protein derived from immunoglobulin G. It binds TGF superfamily ligands to reduce SMAD signalling. The reduction in SMAD signalling leads to enhanced erythroid maturation. | Transfusion: Type-matched RBC transfusions directly supply blood to patients and are intended to address TDT-related anemia as well as suppress endogenous erythropoiesis ICT: ICTs penetrate organs to varying extents and remove intracellular iron; ICT products have varying affinities for different forms of iron and varying degrees of organ penetration |
Indicationa | Treatment of patients aged ≥ 12 years with TDT. | Treatment of adult patients with RBC transfusion-dependent anemia associated with beta thalassemia. | RBC transfusions: SOC for patients with TDT Deferasirox:
Deferiprone: Treatment of patients with transfusion-related iron overload due to thalassemia syndromes when current chelation therapy is inadequate Deferoxamine:
|
Recommended dose | Single-dose IV infusion of a minimum dose of 3 × 106 viable CD34+ cells/kg. Administer all vials. | 1.0 mg/kg once every 3 weeks by SC injection. | RBC transfusions: IV, typically every 2 weeks to 4 weeks beginning in infancy, targeting hemoglobin levels of 90 g/L to 100 g/L8,17 Deferasirox (dispersible tablets): Recommended initial daily dose is 10 mg/kg per day, 20 mg/kg per day, or 30 mg/kg per day body weight, depending on the patient’s transfusion rate and the goal of treatment Deferasirox (Type J tablets): Recommended initial daily dose of 7 mg/kg per day, 14 mg/kg per day, or 21 mg/kg per day body weight, depending on the patient’s transfusion rate and the goal of treatment Deferiprone (tablets and oral solution): Recommended dose is 25 mg/kg to 33 mg/kg body weight orally t.i.d. for a total daily dose of 75 mg/kg to 100 mg/kg body weight Deferoxamine:
|
Serious AEs or safety issues |
|
| Deferasirox:
Deferiprone: Agranulocytosis/severe neutropenia that may lead to serious and life-threatening infections Deferoxamine: Rapid IV injection exceeding 15 mg/kg per hour has produced flushing, urticaria, hypotension, and shock |
AE = adverse event; Cas9 = CRISPR-associated protein 9; CRISPR = clustered regularly interspaced short palindromic repeats; hemoglobin F = fetal hemoglobin; HSPC = hematopoietic stem and progenitor cell; ICT = iron chelation therapy; IM = intramuscular; RBC = red blood cell; SC = subcutaneous; SOC = standard of care; TDT = transfusion-dependent beta thalassemia; TGF = transforming growth factor; t.i.d. = 3 times a day.
aHealth Canada–approved indication.
Sources: Approved product monographs for exagamglogene autotemcel,51 product monographs for Apo-Deferasirox,53 Apo-Deferasirox (Type J),54 Ferriprox,55 deferoxamine mesylate for injection,56 and Reblozyl.57
Perspectives of Patients, Clinicians, and Drug Programs
The full patient and clinician group submissions received by CDA-AMC are available in the consolidated patient and clinician group input document for this review on the project website.
Patient Group Input
This section was prepared by the CDA-AMC review team based on the input provided by patient groups.
CDA-AMC received 2 patient groups submission, from the TFC and GANSID. TFC is a volunteer-run charitable organization established in 1982 as a support group and eventually incorporated as a Canadian charity in 1988. The GANSID is a global organization registered in the US as a charitable organization and in Canada as a not-for-profit entity with 4 member organizations, TFC, Sickle Cell Awareness Group of Ontario, Sickle Cell Awareness Network of Saskatchewan, and Sickle Cell Disease Association of Atlantic Provinces.
TFC collected information via prior surveys conducted in 2022 and a new survey launched across Canada in April 2024 resulting 80 respondents across 5 provinces (Quebec [13.75%], Ontario [45.00%], Manitoba [1.25%], Alberta [6.25%], and British Columbia [33.75%]) to focus on the responses of patients with TDT (> 90% of response). Patients of different genotypes were also welcome to respond, and GANSID’s submission was based on the TFC survey and comments from peers living with thalassemia disorders outside of Canada.
The input noted that patients with TDT are severely anemic, lethargic, tired, feel short of breath, and feel weak. Symptoms, if they are not treated, cause a patient to deteriorate and affect their whole body; ultimately an untreated patient with TDT would die before the age of 5 years due to severe anemia causing heart failure. Thalassemia can also cause other health issues including loss of bone density (e.g., osteopenia or osteoporosis) and higher risk of liver cancers, and so forth, and many patients experience growth delays, bone deformities, and other physical changes due to anemia, iron chelation side effects, and hormone insufficiency. In addition, many patients have had their spleens removed (i.e., splenectomy), to effectively manage ongoing blood requirements. Furthermore, the input noted that the chronic nature of thalassemia, with its lifelong treatment requirements and potential complications, can lead to emotional distress in patients, and patients may experience feelings of anxiety, depression, or fear about their health and future. In addition, due to misconceptions about the condition, the input reported that patients with thalassemia may face stigma and discrimination in various aspects of their lives, such as education, employment, and social interactions.
The patient input noted that living with TDT requires lifelong management, including regular blood transfusions, chelation therapy to prevent iron overload, and comprehensive monitoring of various parameters to detect and manage complications, which are normally arranged at a comprehensive care centre only located in Canada’s major city centres. Adherence to treatment and regular follow-up with health care providers are essential for maintaining quality of life and reducing the risk of long-term complications. The most serious and common side effect is overload of iron (secondary hemochromatosis), which is responsible for most of the complications patients face in TDT. There are 3 common iron chelators (deferoxamine, deferasirox, and deferiprone), and all 3 medications were described as “intense” and need regular monitoring for side effects. The input stated that patients with thalassemia and their caregivers face various challenges in managing the illness, including the time commitment for treatments, cost, administration issues, and disjointed access to health care, but with currently available treatments, many are able to effectively control symptoms and improve quality of life and life expectancy. When asked about their main expectations for gene therapy, patient expectations included TI, maintaining hemoglobin at a high enough level to function daily, safety and efficacy, and improved HRQoL including freedom to travel, work, and spend time where they wished.
There were 2 patients who had experience with exagamglogene autotemcel in the US through clinical trials, and their family members shared their experiences with TFC. Both patients had discontinued blood products, and their blood cell levels returned to normal, which according to the family’s comments, was life-changing. Furthermore, some patient respondents to the 2024 survey informed TFC they had considered or undergone either a stem cell transplant (which involves preconditioning) or a gene therapy treatment via a clinical trial. The feedback was mixed with failure, disappointment, success, and relief. Finally, TFC asked respondents to identify as many concerns as they would like regarding gene therapy. Patients and caregivers responded with concerns around cost and affordability of treatment (75%), length of treatment/recovery (71%), chemotherapy (61%), as well as eligibility due to older age.
Clinician Input
Input From Clinical Experts Consulted by CDA-AMC
All CDA-AMC review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). In addition, as part of the review of exagamglogene autotemcel, a panel of 3 clinical experts from across Canada was convened to characterize unmet therapeutic needs, assist in identifying and communicating situations where there are gaps in the evidence that could be addressed through the collection of additional data, promote the early identification of potential implementation challenges, gain further insight into the clinical management of patients living with a condition, and explore the potential place in therapy of the drug (e.g., potential reimbursement conditions). A summary of this panel discussion follows.
Unmet Needs
According to the expert panel, the major goals of therapy in TDT are to prolong life, reduce severity of symptoms, and improve HRQoL. The curative SOC for TDT is allogeneic HSCT and therefore patients with an available HLA-matched sibling donor are recommended for this treatment. The experts noted that most patients in this situation will be recommended to undergo transplant as early as possible if there is an HLA-matched sibling, as outcomes are generally better for patients younger than 17 years and there is less risk of organ damage from iron overload in younger patients. HSCT is not routinely done for adult patients with beta thalassemia. Approximately 20% of patients who would be candidates for allogeneic HSCT have an HLA-matched donor; therefore, the remaining majority of patients do not have a potentially curative treatment.
Patients without an HLA-matched donor or who decide not to undergo HSCT would receive lifelong blood transfusions on an approximately monthly basis, with iron chelation to address the iron overload which accompanies transfusion. The experts noted that other risks of transfusion include developing allogenic antibodies to transfusion, transfusion reactions, transfusion-transmitted infections, and the potential for vascular access issues. The longitudinal nature of therapy and commitments associated with travelling to receive transfusion therefore remain an unmet need for patients which impacts their HRQoL. The experts noted that removing the need for transfusions would likely allow for substantial improvement in HRQoL, particularly as life expectancy can be beyond the mean ages of death that have been previously reported in patients with TDT19,20 if they have optimized transfusion and iron chelation.
Luspatercept is another treatment option, but it is approved for use in adult patients only. The experts noted that a minority of patients (20%) respond to it and if they do, treatment reduces transfusion burden but does not eliminate the need entirely (e.g., it may lower by approximately 30% in a patient receiving 100 units/year).
According to the experts, the majority of organ damage due to TDT comes from end-organ damage and toxicity associated with iron overload, and if iron chelation is optimized, patients may receive regular transfusions and have life expectancy beyond the mean ages of death that have been previously reported for this disease.19,20 They noted that newer iron chelation therapies are oral rather than subcutaneous; however, adherence to iron chelation can be difficult for some patients, potentially due to the frequency, time required for administration, or side effects, which vary by product. As patients age, they often require a combination of iron chelation drugs to achieve iron chelation. In addition, adult patients who may not have had newer iron chelation drugs available earlier in their lives may have accrued end-organ damage from iron overload. Therefore, there remains an unmet need in some patients if there are challenges in optimizing chelation either due to patient age, clinical characteristics, or adherence concerns.
Place in Therapy
According to the clinical experts, exagamglogene autotemcel would potentially change the treatment paradigm as it may modify the disease course to provide TI for patients for whom HSCT is not a treatment option. The experts felt that patients should have tried transfusion and iron chelation before exagamglogene autotemcel. While the current age limit for the indication of exagamglogene autotemcel would generally mean eligible patients would already be receiving transfusions with chelation, in situations where both treatments are an option, the experts would not go directly to exagamglogene autotemcel therapy without a trial (approximately 6 months) of transfusions to ensure patients truly are transfusion dependent; they noted that receiving a volume of RBCs greater than 100 mL/kg per year is a generally accepted definition of transfusion dependence. The clinical experts recommended that patients should not need to try luspatercept before exagamglogene autotemcel because, as mentioned, a small percentage of patients respond to this treatment and the expected results from treatment are variable but typically only result in a 30% reduction in transfusion burden (i.e., luspatercept does not eliminate the need for transfusion). Families who are eligible but who do not opt for HSCT may be considered for exagamglogene autotemcel; however, the experts noted that considerations around myeloablative conditioning, which is common to both procedures, may mean these patients do not choose exagamglogene autotemcel either. The experts felt that discussions with patients for exagamglogene autotemcel would likely be approached similarly, and involving similar specialists and allied health providers, to discussions around treatment with HSCT.
Patient Population
The experts noted that TDT diagnosis is generally done to the molecular level for patients at most centres; therefore, patients who might be candidates for exagamglogene autotemcel would be readily identifiable. The experts felt that the patient population they would consider for exagamglogene autotemcel therapy would align with the lower age range and the inclusion criteria for the pivotal trial; they were not convinced that all patients with an HLA-matched donor would have received a transplant by the time they reached the age of eligibility for exagamglogene autotemcel (12 years of age), citing patients newly immigrated to Canada who may not have been followed since birth. They felt strongly that there should not be an upper age limit for therapy, but suitability and choice for exagamglogene autotemcel should be determined on a case-by-case basis. Patients they might consider prioritizing for therapy would be those who are not responding to their current therapy or whose HRQoL is impacted by their current therapy. Examples given by the experts included patients with multiple allogenic antibodies, significant iron overload (liver iron > 7 mg/g) despite chelation, or serious adverse effects from iron overload such as cardiac, endocrine, or liver complications. It would also need to be established that such patients did not have end-organ damage severe enough to negatively affect the safety of myeloablative therapy.
The experts noted that patient and family preference would likely be the biggest determinant to identify those patients who would not be suitable candidates for exagamglogene autotemcel, as generally the considerations around the burden of myeloablative conditioning play a role in patients deciding for or against the therapy. They emphasized that patient involvement in the decision-making process would be very important.
Assessing the Response Treatment
The experts stated they typically meet with their patients every 3 months to 6 months and assessments include whether they are meeting transfusion targets (i.e., sufficient transfusion to suppress endogenous RBC production — a hemoglobin target of ≥ 9.5 g/dL)8,12 and whether iron overload is a concern. Assessments include regular laboratory assessments, physical exam, and an MRI for iron overload assessment; if there are abnormalities, a bone marrow biopsy would be considered. MRIs may be spaced out longer over time if transfusion needs decrease.
For the experts, a clinically meaningful response would be whether patients were transfusion independent with a hemoglobin level of 9 g/dL or more. Another potentially important outcome would be if patients need less than 6 transfusions per year (decreased from approximately 12 per year), as well as any changes in HRQoL and decreases in iron overload or need for chelation from that patient’s baseline. They noted that these changes would be meaningful even if patients had not reached TI.
Discontinuing Treatment
As exagamglogene autotemcel is a one-time treatment, criteria for discontinuation would be less applicable; however, the experts noted that patients may choose to stop the exagamglogene autotemcel process after mobilization but before myeloablative conditioning.
When asked whether a second treatment of exagamglogene autotemcel might be given if its efficacy were to wane in the future, the experts felt that a second round of myeloablative conditioning would be challenging for patients, although not impossible for pediatric patients if there was a strong reason.
Prescribing Considerations
The experts noted that the management of TDT in general requires a hematologist and they emphasized that the mobilization, myeloablative conditioning, and exagamglogene autotemcel infusion would need to be undertaken at an accredited transplant facility. Following this, patients could be transferred back to their hemoglobinopathy care provider. Being followed by specialist at a centre of excellence (i.e., a clinic with a hematology specialist in thalassemia as well as trained nurses) was important to the experts; the experts estimated there were approximately 17 such centres across Canada. A hematologist who has an understanding of the disease would be important for ongoing care. They also noted that patients undergoing transplant use an autologous transplant centre and their follow-up consists of appointments with both the transplant hematologist and their TDT hematologist, so it was likely that patients receiving exagamglogene autotemcel could be followed in a similar manner. They emphasized that patients receiving exagamglogene autotemcel should receive long-term follow-up.
Clinician Group Input
This section was prepared by the CDA-AMC review team based on the input provided by clinician groups.
CDA-AMC received 1 clinician group submission from CanHaem. CanHaem is a not-for-profit organization that was established in 2013 and is composed of health care providers dedicated to the care of individuals in Canada with hemoglobinopathies.
CanHaem’s proposed submission was drafted by a CanHaem physician member and then shared among other members (including the CanHaem chair) for review.
CanHaem stated that thalassemias are a heterogeneous group of disorders resulting from defects in hemoglobin production, and migration patterns are such that the number of people affected with thalassemias in Canada has substantially increased over time. CanHaem further commented that TDT is a severe, autosomal, recessive disorder due to pathogenic variants in the beta-globin gene, HBB, resulting in absent or greatly reduced beta-globin production and consequent ineffective erythropoiesis and chronic hemolysis; therefore, patients with thalassemia require subspecialty multidisciplinary care throughout their lives.
In terms of current treatment options, CanHaem stated that currently, ICT options include oral drugs deferasirox and deferiprone as well as subcutaneous or IV deferoxamine, either used as single drugs or employed as dual chelation therapy in patients with dose-limiting toxicities or severe iron overload. Luspatercept is now approved for use in patients with TDT aged 18 years or older in Canada, but the majority of patients with TDT do not respond to luspatercept and postmarketing surveillance has identified paraspinal extramedullary hematopoiesis as a complication limiting therapy in some patients. CanHaem also indicated that in patients seeking curative therapy, HSCT can be considered for pediatric patients with an HLA-matched sibling donor, and who do not have evidence of hepatic fibrosis or significant hepatic iron overload; however, only 10% to 15% of patients will have one and the optimal age for transplant is less than 14 years. As of the date of submission, there are no other commercially available gene therapy products in Canada.
Regarding the unmet needs, CanHaem said that with improvement in transfusion safety, monitoring for iron overload, and chelation, patients with thalassemia may have near-normal life expectancy. However, emerging disease-related complications are now appreciated in the aging thalassemia population including increased risk of hepatocellular carcinoma, as well as renal, cardiac, and hepatic failure, all of which are related to the chronic toxicity of iron. Furthermore, CanHaem also mentioned that the impact of this chronic disorder on HRQoL as well as increased risk for mental health issues like anxiety and depression are well described.
CanHaem stated that exagamglogene autotemcel represents a significant shift in the current treatment landscape by providing a highly efficacious, one-time, disease-modifying therapy, in contrast to decades of transfusion and iron chelation. CanHaem stated that potentially eligible patients with TDT would be identified by their hemoglobinopathy team. At this time, CanHaem believed that patients with TDT could be offered exagamglogene autotemcel if they do not have an available HLA-matched sibling donor, meet age requirements, and are otherwise felt to be eligible for this therapy. CanHaem noted that the FDA did not cite an upper age limit for receipt of this therapy and CanHaem believed that age older than 35 years should not be an absolute exclusion criteria; they noted that patients up to 50 years were included in the betibeglogene autotemcel trial. CanHaem considered that outcomes used to determine response would include the same end points as the clinical trial: transfusion reduction or independence, increase in total hemoglobin, decrease in serum ferritin and tissue-specific iron overload, and discontinuation of chelation over time; also, HRQoL outcomes should be monitored in alignment with clinical trials. CanHaem also stated that treatment with exagamglogene autotemcel would ideally occur at a facility experienced with stem cell collection, administration of myeloablative chemotherapy, and specialized hematologic care because patients will need to be admitted to hospital for approximately 35 days to facilitate neutrophil engraftment and will require long-term follow-up with their hemoglobinopathy providers to ensure there are no long-term complications of thalassemia, iron overload, conditioning chemotherapy, or the exagamglogene autotemcel product, in addition to follow-up with their transplant centre.
Last but not least, CanHaem highlighted the need for equitable access for this therapy to eligible patients, so that patients, regardless of their geographic distance from treatment centres are able to access this therapy. In addition, CanHaem recognized that this treatment is associated with a high risk of infertility and that the cost of fertility preservation should be included in price negotiations.
Drug Program Input
The drug programs provide input on each drug being reviewed through the CDA-AMC reimbursement review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CDA-AMC are summarized in Table 5.
Table 5: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Considerations for initiation of therapy | |
Patients were eligible for the pivotal trial if they had:
Question for the clinical experts: Would these criteria from the pivotal trial be appropriate for reimbursement purposes? | The clinical experts indicated that diagnosis of TDT would be sufficient for a patient to be eligible for exagamglogene autotemcel, but a patient who is struggling with response to their current therapy, having challenges to the chelation therapy, or whose HRQoL is impacted would be more likely to be prioritized for exagamglogene autotemcel. |
Would any additional laboratory tests be required for reimbursement purposes based on the pivotal trial inclusion or exclusion criteria? | The clinical experts indicated that testing for associated alpha thalassemia including > 1 alpha deletion or alpha multiplications, which was done in the pivotal trial, would be additional testing. The clinical experts also noted that the percentage of cells with edited alleles would be additional testing after treatment. |
Eligibility criteria for the pivotal trial required patients to be 12 to 35 years of age. The submission notes that “if patients with TDT who are older than 35 years of age are deemed fit for treatment with exagamglogene autotemcel, there is no plausible biologic mechanism to limit access to exagamglogene autotemcel to those no older than 35 years.” Question for the clinical experts: Should patients older than 35 years be eligible to receive exagamglogene autotemcel? | The clinical experts indicated that there should not be a hard upper age limit for exagamglogene autotemcel therapy as patients with TDT who are well-chelated and well-transfused have increased life expectancy compared to those who are not and may tend to reach the higher percentiles of the general population. Patients’ ability to tolerate myeloablative conditioning should be assessed and their eligibility for treatment should be at the discretion of the treating physician. |
Exagamglogene autotemcel is proposed as a one-time treatment. Are there any instances where a second dose would be considered appropriate? | The clinical experts indicated that at this time a second dose of exagamglogene autotemcel would not be considered appropriate. |
Considerations for continuation or renewal of therapy | |
The submission notes that “patients with TDT who participated in CLIMB-111 were asked to enrol in the long-term follow-up study CLIMB-131, where they will be followed for up to 15 years postinfusion. The primary and key secondary end points evaluated in CLIMB-111 will continue to be evaluated in CLIMB-131.” Question for the clinical experts: How should clinically meaningful response be defined using objective parameters? | The clinical experts indicated that the only indicator of a clinically meaningful response would be transfusion independence, that is, with a hemoglobin level of ≥ 9 g/dL. They indicated that response should be assessed at the standard care assessments which are usually every 3 months to 6 months. |
How long should follow-up last to confirm a clinically meaningful response is maintained? | The clinical experts indicated that these patients should receive lifelong follow-up; 5 years follow-up would be ideal to confirm clinical response, but 2 years is a reasonable surrogate to suggest a sustained response. |
Generalizability | |
The pivotal trial listed numerous exclusion criteria, but there are no related contraindications or warnings or precautions to therapy listed in the product monograph for most of these. The submission notes that “patients with an available HLA-matched related donor were excluded from the pivotal clinical trials due to ethical concerns around including patients with a viable treatment option in a trial for a treatment without proven efficacy or safety at the time. However, based on the results of CLIMB-111 this may no longer be a valid concern.” Question for the clinical experts: Which, if any, of the pivotal trial exclusion criteria should be used to determine eligibility for treatment? | The clinical experts indicated that excluding patients with an available HLA-matched donor sibling is reasonable, but based on the science, any patient who is older than the lower limit of the age range used in the pivotal trial, who can safely undergo the autologous transplant as per their clinical team, should be eligible for exagamglogene autotemcel. |
Eligibility criteria for the pivotal trial required patients to be 12 to 35 years of age, and the product monograph states, “No data in patients less than 12 years of age are available to Health Canada; therefore, Health Canada has not authorized an indication of pediatric use in patients less than 12 years of age.” Question for the clinical experts: Will there be interest in using exagamglogene autotemcel in those younger than 12 years? If so, should such patients be considered for reimbursement? | The clinical experts indicated that given the lack of safety data in patients who are younger than 12 years, exagamglogene autotemcel should not be considered in these patients. |
Care provision issues | |
The sponsor notes the following.
Question for the clinical experts: Is this accurate from a diagnostic standpoint? | The clinical experts agreed with the sponsor’s comments. |
Is the blood spot screening test referenced by the sponsor widely available, in use in Canada, and most importantly, reliable and accurate? | The clinical experts indicated that blood spot screening is widely used although not universal, and it is reliable. |
The sponsor notes the following.
Question for the clinical experts: Is this information accurate from an implementation and resources standpoint? | The clinical experts indicated that in general, transplant centres are operating a their maximum capacity and this would be an added service, so the impact will not be minimal as an added number of patients will become eligible for services that these centres offer, and many transplant centres in the country are funded exclusively for patients with malignancies. In particular, it would lead to increased work for the transplant teams. Regarding hemoglobinopathy, the process would be similar for exagamglogene autotemcel as what is currently done for HSCT; however, there would be additional discussion and education required for families which will require additional resources, and which would ideally be built into the process. Overall, there would need to be dedicated resources to the transplant teams, thalassemia teams, and for patients with TDT so they do not compete with other patients (e.g., patients with cancer who may have time-sensitive transplant requirements) so that the treatment may be available and patients will have access to it. |
ATC = authorized treatment centre; HRQoL = health-related quality of life; HSCT = hematopoietic stem cell transplant; NBS = newborn screening; TDT = transfusion-dependent beta thalassemia.
Clinical Evidence
The objective of the CDA-AMC Clinical Review Report is to review and critically appraise the clinical evidence submitted by the sponsor on the beneficial and harmful effects of exagamglogene autotemcel, an autologous genome-edited hematopoietic stem cell suspension in patient-specific vials for IV infusion (4 × 106 cells/mL to 13 × 106 cells/mL; 1.5 mL to 20 mL per vial; 1 vial to 9 vials per carton) in the treatment of TDT in patients aged 12 years and older. The focus will be placed on comparing exagamglogene autotemcel to relevant comparators and identifying gaps in the current evidence.
A summary of the clinical evidence included by the sponsor in the review of exagamglogene autotemcel is presented in 4 sections with the CDA-AMC critical appraisal of the evidence included at the end of each section. The first section, the systematic review, includes pivotal studies and RCTs that were selected according to the sponsor’s systematic review protocol. The CDA-AMC assessment of the certainty of the evidence in this first section using the GRADE approach follows the critical appraisal of the evidence. The second section includes sponsor-submitted LTE studies. The third section includes indirect evidence from the sponsor.
Included Studies
Clinical evidence from the following is included in the CDA-AMC review and appraised in this document:
one pivotal study identified in systematic review
one LTE study
one indirect treatment comparison.
Systematic Review
Contents within this section have been informed by materials submitted by the sponsor. The following have been summarized and validated by the CDA-AMC review team.
Description of Studies
Characteristics of the included studies are summarized in Table 6.
Table 6: Details of Studies Included in the Systematic Review
Detail | CLIMB-111 |
|---|---|
Designs and populations | |
Study design | Phase I, II, and III single-arm, open-label, multisite, single-dose study |
Locations | 13 sites in 5 countries: Canada (2 sites), Germany, Italy, UK, US |
Patient enrolment dates | Start date: September 10, 2018 Data cut-off (interim analysis): January 16, 2023; updated April 16, 2023 (second data cut-off appraised by CDA-AMC) |
Enrolled (N) | 59 |
Inclusion criteria |
|
Exclusion criteria |
|
Drugs | |
Intervention | Single IV infusion of exagamglogene autotemcel at minimum recommended dose of 3.0 × 106 CD34+ cells/kg, administered in hospital a minimum of 48 hours and maximum of 7 days following myeloablative conditioning |
Comparator(s) | None |
Study duration | |
Patient identification and evaluation | Varies per patient |
Premobilization phase | Ongoing |
Mobilization | Approximately 7 days per cycle |
Manufacturing and quality control | Approximately 24 weeks |
Myeloablative conditioning, infusion, and engraftment | Median = 47 days (range, 31 to 117 days) |
Follow-up | 24 months, followed by entry into LTE for a total anticipated follow-up of 15 years after infusion (ongoing) |
Outcomes | |
Primary end point | Proportion of patients achieving TI12 from 60 days after last RBC transfusion to up to 24 months post-exagamglogene autotemcel infusion. |
Secondary and exploratory end points | Key secondary end point:
Secondary end points:
|
Publication status | |
Publications | Frangoul et al.58 Locatelli et al.59 NCT0365567860 |
CDA-AMC = Canada’s Drug Agency; DLCO = diffusing capacity for carbon monoxide; FACT-BMT = Functional Assessment of Cancer Therapy–Bone Marrow Transplantation; G-CSF = granulocyte colony-stimulating factor; hemoglobin F = fetal hemoglobin; HLA = human leukocyte antigen; HSCT = hematopoietic stem cell; LTE = long-term extension; LVEF = left ventricular ejection fraction; PedsQL = Pediatric Quality of Life Inventory; PRO = patient-reported outcome; RBC = red blood cell; TI6 = transfusion independence for 6 consecutive months; TI12 = transfusion independence for 12 consecutive months; WBC = white blood cell.
Source: Details included in the table are from the sponsor’s Summary of Clinical Evidence.52
The CLIMB-111 study is an ongoing phase I, II, and III single-arm, multisite, single-dose trial which enrolled a total of 59 patients aged 12 years to 35 years who had TDT.2 Transfusion dependence was defined as a history of at least 100 mL/kg per year or 10 units/year of packed RBC transfusions in the past 2 years before enrolment. The primary objective of the CLIMB-111 study was to evaluate the safety and efficacy of a single dose of autologous CRISPR/Cas9-modified CD34+ human HSPCs, otherwise known as exagamglogene autotemcel.
The study was revised after the January 2018 start at several time points. Of note, a long-term follow-up of 15 years was added (July 2018); the statistical analyses including efficacy boundaries for the expanded study were updated (December 2018); patients with the beta0/beta0 genotype were added to the eligible study population as well as a note that at least 2 patients with the non-beta0/beta0 genotype will be enrolled before any patients with the beta0/beta0 genotype (August 2019); the study was expanded to include patients aged 12 years to less than 18 years, based on a data monitoring committee review of 3 months of efficacy and safety data in at least 2 patients older than 18 years who had received exagamglogene autotemcel (February 2020); the primary, key secondary, and secondary end points were updated in response to scientific advice, and the statistical analyses and IAs were updated (January 2021); the safety end point for successful neutrophil engraftment was updated to remove the specification of 42 days (May 2021); a secondary end point for the duration of transfusion-free period in patients reaching the primary outcome (TI12) was added (June 2021); and the study was updated to phase I, II, and III (August 2021).
The CLIMB-111 study contained 3 prespecified IA points — IA1, IA2, and IA3 — and data from IA3 was submitted based on a data cut-off of January 16, 2023 (IA1 and IA2 were not conducted, and the submission did not provide a rationale for skipping these analyses). Additional supplemental data from a further data cut-off on April 16, 2023, was also supplied by the sponsor. The updated data cut-off was provided by the sponsor in response to regulatory authority request and was not prespecified in the statistical analysis plan. The study took place at 13 sites in 5 countries; 2 study sites were in Canada in Vancouver and Toronto. A summary of the data cut-offs available for the CLIMB-111 study (pivotal trial) and the CLIMB-131 study (LTE) is presented in Table 7.
Table 7: Summary of Available Data Cut-Offs for CLIMB-111 and CLIMB-131
Data cut-off date | Description |
|---|---|
January 16, 2023 |
|
April 16, 2023 |
|
CDA-AMC = Canada’s Drug Agency; PE = pharmacoeconomic.
Source: Details included in the table are from the sponsor’s Summary of Clinical Evidence.52
The study design consisted of several stages as detailed in the CLIMB-111 study design in Figure 2. The overall length of time from stages 1 to 3 varied per patient; mobilization lasted approximately 7 days per cycle, product manufacturing took approximately 24 weeks, and myeloablative conditioning ranged from 31 days to 177 days. After exagamglogene autotemcel infusion, which was carried out in 1 day, patients were followed for 24 months. All patients who received exagamglogene autotemcel were asked to enrol in the LTE, the CLIMB-131 study, after either completion or withdrawal from CLIMB-111. A range of the total length of time in the study from stage 1 (screening) to stage 4B for the patients who had completed it was not provided in the submission.
Figure 2: CLIMB-111 Study Design
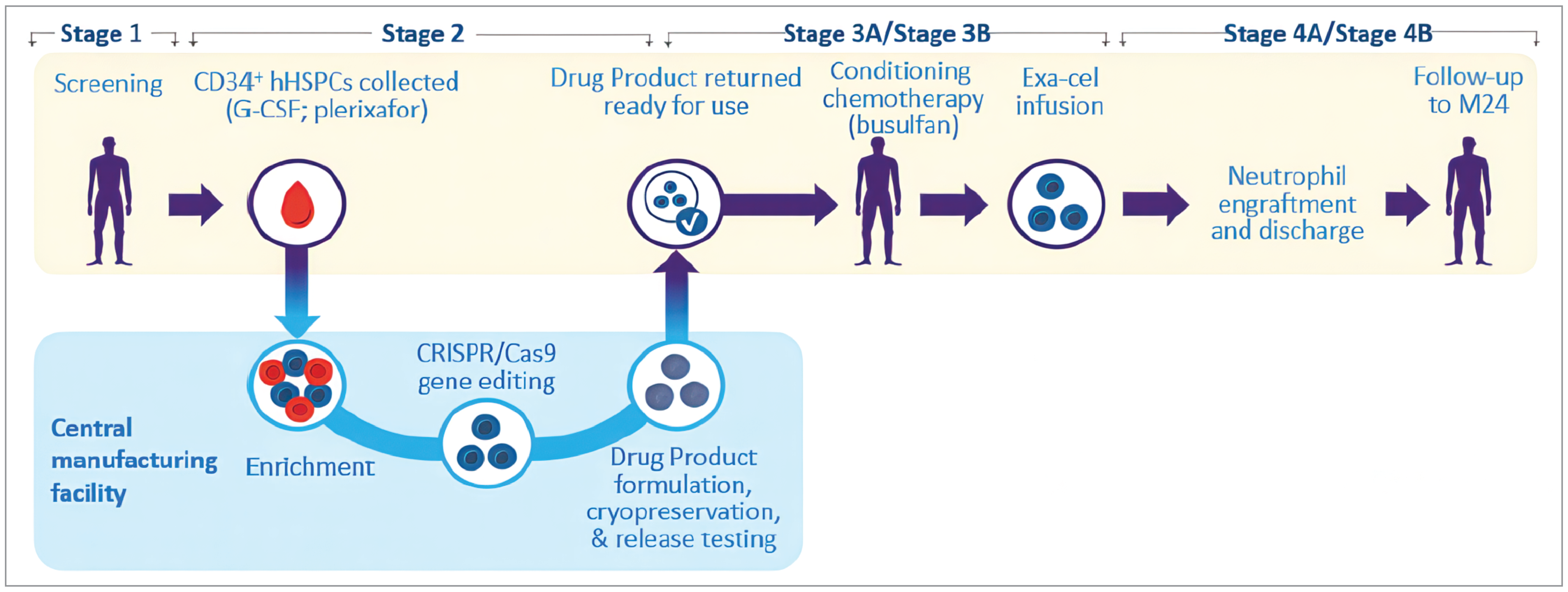
CRISPR/Cas9 = clustered regularly interspaced short palindromic repeats and CRISPR-associated 9 nuclease; exa-cel = exagamglogene autotemcel; G-CSF = granulocyte colony-stimulating factor; hHSPC = human hematopoietic stem and progenitor cell; M24 = month 24.
Source: Details included in the figure are from the CLIMB-111 Clinical Study Report.2
Populations
Inclusion and Exclusion Criteria
Key inclusion criteria required patients to be aged between 12 and 35 years, inclusive; have a diagnosis of TDT; be eligible for autologous stem cell transplant; and have good performance status based on specific thresholds for 2 different scales, depending on patient age. The diagnosis of TDT was defined by documented homozygous beta thalassemia or compound heterozygous beta thalassemia including beta thalassemia and hemoglobin E, as well as a history of at least 100 mL/kg per year or 10 units/year of packed RBC transfusions in the 2 years before consent. Patients could be enrolled based on historical data, but a confirmation of genotype was required before busulfan conditioning; beta0 and non-beta0 genotypes were confirmed using the HbVar Database. The full list of inclusion criteria is available in Table 6.
Key exclusion criteria included patients who had an HLA-matched donor per investigator judgment; the rationale for this was that there were ethical concerns around including patients with a viable treatment option in a trial for an unproven treatment. Prior recipients of allogenic HSCT were also excluded, with the rationale that most patients with a matched donor available and willing to donate would have received this treatment before they reached the age of eligibility for exagamglogene autotemcel. Canadian treatment guidelines for TDT suggest that HSCT is best undertaken at a very young age.8 Prior allogenic HSCT was also a criterion for exclusion as the submission noted it would not be recommended to undergo a subsequent round of myeloablative conditioning following the one that would have been required for HSCT.15 In addition to these, exclusion criteria also included other forms of thalassemia (alpha thalassemia, > 1 alpha deletion or alpha multiplications, sickle cell beta thalassemia variant); clinically significant infections, specific liver, lung, or cardiac conditions; white blood cell count less than 3 × 109/L or platelet count less than 50 × 109/L not related to hypersplenism; or history of any illness or clinical condition which, in the opinion of the investigator, might confound the study results or pose an additional risk in administering treatment. The full list of key exclusion criteria is available in Table 6.
Interventions
Screening and Mobilization
In stage 1, before the start of apheresis and at least 60 days before the planned initiation of myeloablative conditioning, it was recommended that patients undergo transfusion to achieve a goal of pretransfusion hemoglobin of 11 g/dL or greater; the submission did not provide details on how many patients undertook this transfusion. Patients could also undergo fertility preservation or gonadal tissue banking as appropriate per patient age and local practice; the submission did not provide further details on the numbers of patients who opted for this.
Stage 2 corresponded to the first day of mobilization, and patients received a combination of granulocyte colony-stimulating factor products (either subcutaneous or IV 5 mcg/kg/dose approximately every 12 hours for 5 days to 6 days) and plerixafor subcutaneously. Patients underwent apheresis for up to 3 consecutive days to collect CD34+ human HSPCs, targeting CD34+ cell collection at least 15 × 106 cells/kg; an additional 2 × 106 cells/kg were collected as back-up and cryopreserved. If sufficient numbers of cells were not available, up to 2 additional mobilization and apheresis cycles were allowed. The collected CD34+ cells were sent to the manufacturer for enrichment, CRISPR/Cas9 editing, formulation, and quality control.
Myeloablative Conditioning and Exagamglogene Autotemcel Infusion
Patients were hospitalized and underwent stage 3A (myeloablative conditioning) with busulfan. Per the submission, the target cumulative area under the curve for the busulfan exposure as part of the myeloablative conditioning was 74 mg × hours/L (range, 59 mg × hours/L to 89 mg × hours/L ) for the regimen dosed every 6 hours and 82 mg × hours/L (range, 74 mg × hours/L to 90 mg × hours/L ) for the regimen dosed once a day. The target busulfan cumulative area under the curve was the same across all age groups. During conditioning, antiseizure prophylaxis (except for phenytoin) and other supportive measures were initiated as per hospital guidelines.
In stage 3B, all patients received exagamglogene autotemcel infusion as an entire dose unfiltered through a central venous catheter as an IV bolus at a minimum recommended dose of 3 × 106 CD34+ cells/kg. Just before the scheduled infusion, exagamglogene autotemcel vials were thawed per local site standard operating procedures and infused within 20 minutes of the end of thaw of each vial. Exagamglogene autotemcel was administered by trained personnel and as per standard practice at the ATC, between 48 hours and 7 days after the last busulfan dose. If the exagamglogene autotemcel infusion did not occur within this time frame, patients were to receive their back-up CD34+ stem cells.
Monitoring and Follow-Up
In stage 4A, patients underwent surveillance and infection prophylaxis according to local guidelines and investigator judgment. Patients received supportive care (e.g., packed RBC and platelet transfusions) according to standard practices for undergoing HSCT. Patients were discharged from the medical unit upon neutrophil engraftment and stabilization of major medical issues per local guidelines. If engraftment did not occur by day 21 postinfusion, granulocyte colony-stimulating factor could have been administered following discussion with the medical monitor. If engraftment had not occurred within 42 days of infusion (i.e., after study day 43) the investigator determined whether or not the patient should receive their back-up CD34+ stem cells based on clinical assessment.
Following successful engraftment and when patients were clinically stable, patients progressed to stage 4B (discharge from the transplant unit follow-up) for approximately 2 years. Patients were recommended not to restart iron chelation (if required) until at least 3 months after the exagamglogene autotemcel dose, and transfusions were avoided for hemoglobin greater than or equal to 9 g/dL, unless medically indicated.
Outcomes
A list of efficacy end points assessed in this Clinical Review Report is provided in Table 8, followed by descriptions of the outcome measures. Summarized end points are based on outcomes included in the sponsor’s Summary of Clinical Evidence as well as any outcomes identified as important to this review according to the clinical expert(s) consulted by CDA-AMC and input from patient and clinician groups and public drug plans. Using the same considerations, the CDA-AMC review team selected end points that were considered to be most relevant to inform the expert committee deliberations and finalized this list of end points in consultation with members of the expert committee. All summarized efficacy end points were assessed using GRADE. Select notable harms outcomes considered important for informing the expert committee’s deliberations were also assessed using GRADE.
Outcomes included in the GRADE assessment were related to transfusions (TI12 and TI6), hematologic outcomes (hemoglobin F, total hemoglobin concentration) and HRQoL (FACT-BMT and PedsQL). Per the submission, FACT-BMT was selected for its specificity to HSCT and PedsQL was selected for its focus on pediatric patients. To capture additional potential HRQoL aspects, EQ-5D-5L and EQ-5D-Y changes from baseline were included in the report but not in the GRADE assessment. In addition, all-cause mortality, proportion of patients with engraftment (neutrophil and platelet), time to engraftment (neutrophil and platelet), AEs in 25% or more patients, and SAEs in 2 or more patients were included in the GRADE assessment. To provide additional context on efficacy, the proportion of alleles with the intended modification in the CD34+ cells of the bone marrow and the peripheral blood, as well as duration of TI for patients with TI12 and time to last RBC transfusion for patients with TI12 were included in the report, but not in the GRADE assessment. Apart from TI12 and TI6, all other outcomes assessed in GRADE were assessed at the end of follow-up (M24). A list of all outcomes included in the clinical report is presented in Table 8.
Table 8: Outcomes Summarized From CLIMB-111
Outcome measure | CLIMB-111 | Time point |
|---|---|---|
Proportion of patients achieving TI12 | Primarya | Any 12-month period starting from 60 days after last RBC transfusion up to 2 years after exagamglogene autotemcel infusion |
Proportion of patients achieving TI6 | Key secondarya | Any 6-month period starting from 60 days after last RBC transfusion up to 2 years after exagamglogene autotemcel infusion |
Total fetal hemoglobin concentration | Secondary | Baseline to months 3, 6, 9, 12, 18, and 24 |
Total hemoglobin concentration | Secondary | Baseline to months 3, 6, 9, 12, 18, and 24 |
Proportion of alleles with intended genetic modification in the CD34+ cells of the bone marrow | Secondary | Baseline to months 1, 3, 6, 12, and 24 |
Proportion of alleles with intended genetic modification in the peripheral blood | Secondary | Baseline to months 1, 3, 6, 12, and 24 |
Change from baseline in PROs over time assessed using EQ-5D-5L (patients aged ≥ 18 years) | Secondary | Baseline to months 3, 4, 5, 6, 9, 12, 15, 18, 21, and 24 |
Change from baseline in PROs over time assessed using FACT-BMT (patients aged ≥ 18 years) | Secondary | Baseline to months 3, 4, 5, 6, 9, 12, 15, 18, 21, and 24 |
Change from baseline in PROs over time assessed using EQ-5D-Y (patients aged < 18 years) | Secondary | Baseline to months 3, 4, 5, 6, 9, 12, 15, 18, 21, and 24 |
Change from baseline in PROs over time assessed using PedsQL (patients aged < 18 years) | Secondary | Baseline to months 3, 4, 5, 6, 9, 12, 15, 18, 21, and 24 |
Time to engraftment | Safety | Time to event |
All-cause mortality | Safety | Continuous from ICF and assent signing |
AEs, SAEs, and AESIs (malignancies and engraftment) | Safety | Continuous from ICF and assent signing |
AE = adverse event; AESI = adverse event of special interest; FACT-BMT = Functional Assessment of Cancer Therapy–Bone Marrow Transplantation; ICF = informed consent form; PedsQL = Pediatric Quality of Life Inventory; PRO = patient-reported outcome; RBC = red blood cell; SAE = serious adverse event; TI6 = transfusion independence for 6 consecutive months; TI12 = transfusion independence for 12 consecutive months.
aStatistical testing for these end points was adjusted for multiple comparisons (e.g., hierarchal testing).
bBaseline was defined in the study as the most recent nonmissing measurement collected before the start of mobilization.
Source: Details included in the table are from the sponsor’s Summary of Clinical Evidence.52
TI Efficacy Outcomes
Proportion of Patients Achieving TI6 and TI12
The primary outcome of the CLIMB-111 study was the proportion of patients achieving TI12 and the key secondary outcome was the proportion of patients achieving TI6. TI was defined as maintaining a weighted average hemoglobin of 9 g/dL or greater without RBC transfusions; the submission noted that this threshold was chosen as it is the usual clinical threshold for triggering transfusions in patients with TDT. The weighted averages for hemoglobin were calculated by incorporating the time between consecutive hemoglobin measurements and the hemoglobin concentrations at those time points. The evaluation of TI12 and TI6 commenced 60 days after the last RBC transfusion for post-exagamglogene autotemcel infusion support or TDT disease management. Only RBC transfusions adjudicated by an end point adjudication committee as meeting the purpose of post-exagamglogene autotemcel infusion support or TDT disease management were included.
No specific MID was provided in the submission for these 2 outcomes. Statistical testing used a 1-sided test using a binomial distribution against a 50% response rate. Evidence for 50% as a clinically important threshold was not provided in the submission. The clinical experts consulted by CDA-AMC noted that a response rate similar to HSCT would be a more clinically relevant threshold; depending on the risk profile for exagamglogene autotemcel, a response of 70% may be acceptable.
Hemoglobin F and Total Hemoglobin
Hemoglobin F and hemoglobin levels are related; increases in hemoglobin F lead to increases in total hemoglobin, therefore both outcomes were considered important. Patients with high hemoglobin F are asymptomatic, have no need for RBC transfusions, and are hematologically normal.45 Total hemoglobin and hemoglobin F concentrations were evaluated from baseline, which was defined as the most recent measurement collected before the start of mobilization.
No MID was provided in the submission for these 2 outcomes. The clinical experts consulted by CDA-AMC noted the interrelatedness of the hemoglobin outcomes with TI and highlighted that TI was overall the more clinically important outcome.
Proportion of Alleles With Intended Genetic Modification in the CD34+ Cells of the Bone Marrow and in the Peripheral Blood
The proportion of alleles with the intended genetic modification in the CD34+ cells of the bone marrow and in the peripheral blood reflect the efficiency of the CRISPR/Cas9 editing at modifying the target gene in the bone marrow stem cells, and the progeny of the stem cells in the peripheral blood. Bone marrow aspirate samples and blood samples were collected until 2 years post-exagamglogene autotemcel infusion to evaluate the proportion of alleles with intended genetic modification present.
No MID was provided in the submission for these 2 outcomes.
Patient-Reported Efficacy Outcomes
HRQoL was assessed using 2 measures each in adult (aged 18 to 35 years, inclusive) and pediatric (aged 12 to 17 years, inclusive) patients. Adult patients received the FACT-BMT and EQ-5D-5L measures, while pediatric patients received the PedsQL and EQ-5D-Y measures. Full details of the HRQoL measures are contained in Table 9. The clinical experts agreed that HRQoL was an important outcome for patients with TDT and agreed with the use of multiple HRQoL measures to capture adult and pediatric patients’ HRQoL. However, they noted that these scales are not routinely used in clinical practice.
Functional Assessment of Cancer-Related Therapy–Bone Marrow Transplantation
The FACT-BMT consists of the FACT–General which measures overall quality of life (including subscales for physical, social/family, emotional, and functional well-being) and treatment-specific concerns of bone marrow transplantation subscale.61 Each statement in the FACT-BMT has a 5-point Likert-type response scale ranging from 0 to 4 (0 = “not at all,” 1 = “a little bit,” 2 = “somewhat,” 3 = “quite a bit,” and 4 = “very much”). For each total and subscale score, a higher value is indicative of better quality of life. The total score ranges from 0 to 164.26
The submission did not provide a MID for patients with TDT for the total FACT-BMT score; however, the MID for the total FACT-BMT score among patients with cancer who undergo allogenic HSCT was considered to be 7 or more points.62 The MID for the Functional Assessment of Cancer Therapy–General (minus the Bone Marrow Transplantation subscale) is 3 points to 7 points.63
Pediatric Quality of Life Inventory
The PedsQL scores are linearly transformed onto a scale from 0 to 100 and include domains for physical health and psychosocial health, which includes emotional functioning, social functioning, and school functioning. Each statement in the PedsQL has a 5-point Likert-type response scale ranging from 0 to 4 (0 = “never,” 1 = “almost never,” 2 = “sometimes,” 3 = “often,” and 4 = “almost always”). For each total and subscale score, higher values are indicative of better quality of life. The US population mean is 82.87 for the PedsQL total score, 86.86 for the physical functioning score, and 80.73 for the psychosocial health score.64
A 4.4-point change in the total score for child self-report (or 4.5 in the total score for parent proxy) is considered the MID; these scores were derived from a population with a majority of healthy children.64 No MID was provided for patients with TDT or patients with transplant.
EQ-5D-5L
The EQ-5D-5L descriptive system contains health utility scores which range from 1 (“best possible health”) to 0 (“dead”). Patients in the CLIMB-111 study also rated their health using a 20 cm VAS) that ranged from 0 (worst imaginable health state) to 100 (best imaginable health state) points with higher scores indicating better HRQoL. The average UK general population health utility score is 0.86 and the EQ VAS is 82.8.65 In the US, the average US general population health utility score is 0.87 and the EQ VAS is 79.3.66 Research suggests that the EQ-5D-5L lacks content validity and the derived health utility index score may not fully represent the burden of disease in TDT.67
The population means for the EQ VAS provided by the submission were 82.8 for the UK and 79.3 for the US.65 The MID for EQ VAS is considered to be 7 points to 11.5 points in patients with cancer.68 Utility scores were not available in patients with TDT or in a population of people living in Canada for health utility or for the EQ VAS. Results from the EQ VAS scale instead of health utilities were appraised by CDA-AMC to improve comparability of HRQoL between adult and pediatric patients.
EQ-5D-Y
The EQ-5D-Y consists of 2 parts: the EQ-5D-Y descriptive system and the EQ VAS. The descriptive system comprises the same 5 dimensions as the EQ-5D-5L but uses child-friendly wording and has 3 levels. The EQ VAS used in the youth version is identical to the EQ VAS used in EQ-5D-5L. The submission noted that due to a lack of utility scores in pediatric patients for the EQ-5D-Y, results from the change from baseline in the nonadult EQ VAS score were reported as a secondary outcome for pediatric patients. Results were available from the January data cut-off only.
No MID was provided by the submission for this study population.
Table 9: Summary of HRQoL Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
FACT-BMT | A 47-item questionnaire with 7-day recall period which consists of the FACT-G and treatment-specific concerns of the FACT-BMT subscale.25,61 Each statement in the FACT-BMT has a 5-point Likert-type response scale ranging from 0 to 4 (0 = not at all, 1 = a little bit, 2 = somewhat, 3 = quite a bit, and 4 = very much). For each total and subscale score, a higher value is indicative of better quality of life. Final scores range from 0 to 164.26 The subscale domains are physical well-being, social/family well-being, emotional well-being, functional well-being, and BMT subscale.25 | Validity and reliability: FACT-BMT was validated in a population of 182 transplant patients at hospital admission, 74 patients at hospital discharge (from 18 days to 63 days later), and 64 patients at 100 days posttransplant.61 Sixty patients had data at all 3 time points; 88% had undergone autologous bone marrow transplant and 12% had undergone allogenic bone marrow transplant.61 For measures of internal consistency, Cronbach alpha coefficients range from 0.85 to 0.92 for FACT-BMT in the transplant population.61,62 Responsiveness: Statistically significant changes in the expected direction at 3 time points in 60 patients with data at admission, discharge, and 100 days posttransplant were also observed in 4 subscales of the FACT-BMT and indicated sensitivity to change.61 | The MID among patients with cancer who undergo allogenic HSCT is considered ≥ 7 points in the total score.62 The MID for FACT-G (minus the BMT subscale) is 3 points to 7 points.63 No MID was provided for patients with TDT. |
PedsQL | PedsQL scores include domains for physical health and psychosocial health, which includes physical functioning, emotional functioning, social functioning, and school functioning. Each statement in the PedsQL has a 5-point Likert-type response scale ranging from 0 to 4 (0 = never, 1 = almost never, 2 = sometimes, 3 = often, and 4 = almost always).69 For each total and subscale score, higher values are indicative of better quality of life. PedsQL also has a module for stem cell transplant (composed of 31 to 41 items and 8 dimensions including pain, fatigue, nausea, worry, nutrition, thinking, communication, and other concerns) and transplant (composed of 46 items comprising 8 dimensions including medicines, transplant, pain, worry, anxiety, appearance, and communication), with higher scores representing better HRQoL.70 | Validity and reliability: Consistent with previous research with the PedsQL, healthy children scored significantly higher on the PedsQL than children with a chronic health condition.64 Reliability: The majority of the child self-report scales and parent proxy-report scales exceeded the minimum reliability standard of 0.70 required for group comparisons, while the Total Scale Score across the ages approached or exceeded the reliability criterion of 0.90 recommended for analyzing individual patient scale scores.64 Responsiveness: No evidence on responsiveness was provided. | A 4.4-point change in the total score for child self-report (or 4.5 in the total score for parent proxy) is considered a MID.64 This was derived from a population with a majority of healthy children.64 |
EQ-5D-5L | EQ-5D-5L descriptive system contains health utility scores which range from 1 (“best possible health”) to 0 (“dead”). | Validity and reliability: The EQ-5D-5L has been validated and found to be a reliable measure in various conditions71,72; however, none that are specific to TDT. Research suggests that the EQ-5D-5L lacks content validity and the derived health utility index score may not fully represent the burden of disease in TDT.67 | The general population means provided by the submission for the EQ VAS for patients living in the UK was 82.8 and for patients living in the US was 79.3.65 The MID for EQ VAS is considered to be 7 points to 11.5 points in patients with cancer.68 No MIDs were provided for patients with TDT or patients in a Canadian context. |
EQ-5D-Y | The EQ-5D-Y consists of 2 parts: the EQ-5D-Y descriptive system and the EQ VAS. The descriptive system comprises the same 5 dimensions as the EQ-5D-5L but uses child-friendly wording and has 3 levels. The EQ VAS used in the youth version is identical to the EQ VAS used in EQ-5D-5L. | No evidence on validation, responsiveness, and reliability was provided in the submission. | No MID was provided by the submission for this study population or available in the literature. |
EQ VAS = EQ visual analogue scale; FACT-BMT = Functional Assessment of Cancer Therapy–Bone Marrow Transplantation; FACT-G = Functional Assessment of Cancer Therapy–General; HRQoL = health-related quality of life; HSCT = hematopoietic stem cell transplant; MID = minimal important difference; PedsQL = Pediatric Quality of Life Inventory; TDT = transfusion-dependent beta thalassemia.
Specific Harms Outcomes
The safety analysis included AEs, SAEs, and mortality (all-cause). AEs of special interest in the submission were malignancies and engraftment. All of these were included in the GRADE assessment except for malignancies, of which none were reported in the CLIMB-111 study.
Engraftment
Neutrophil engraftment was defined as the first day of 3 consecutive measurements of absolute neutrophil count of 500/µL or greater on 3 different days, achieved within 42 days after exagamglogene autotemcel infusion (study day 43) without the use of unmodified CD34+ cells after reaching the nadir, defined as an absolute neutrophil count less than 500/µL. Engraftment failure criteria were not achieving neutrophil engraftment by 42 days after exagamglogene autotemcel infusion (study day 43) or receipt of back-up CD34+ stem cells at any time during the period of neutropenia.
Platelet engraftment was defined as the first day of 3 consecutive measurements of unsupported (i.e., no platelet transfusions for the last 7 days) platelet counts of 20 000/µL or greater on 3 different days after exagamglogene autotemcel infusion, after reaching the nadir (i.e., platelets < 20 000/µL) or the first platelet transfusion, whichever was earlier. For patients discharged before platelet engraftment, it was defined as the seventh day after the last platelet transfusion, if there were 3 subsequent and consecutive unsupported measurements of platelets 20 000/µL or greater on 3 different days.
Malignancies
The submission noted that following administration of busulfan conditioning and exagamglogene autotemcel, patients would undergo at least yearly comprehensive physical examinations and receive screening for malignancy based on appropriate country-specific cancer guidelines and patient medical history. Patients would also undergo appropriate malignancy evaluation if they have unexplained symptoms, signs, or laboratory abnormalities that could be related to an underlying malignancy. Examples included unexplained weight loss or fever, lymphadenopathy, and/or abnormal blood counts. The medical monitor would be notified if a patient was diagnosed with a malignancy, and any new malignancy would be reported as a SAE.
Statistical Analysis
General Considerations
Baseline values, unless otherwise specified, were defined as the most recent nonmissing measurement (scheduled or unscheduled) collected before the start of mobilization. Measurements obtained at unscheduled study visits were included in the analyses according to visit windowing rules defined in the study protocol. Hemoglobin assessments from central laboratories were used in efficacy analyses, while the hemoglobin assessments from both local and central laboratories were used for safety analyses.
Baseline annualized volumes of RBC transfusions were calculated using records of all transfusion events in the 2 years before study consent, or at the latest rescreening for patients going through study enrolment. Postbaseline annualized volume and or units of RBC transfusions were calculated using the transfusions that occur post-exagamglogene autotemcel infusion until the end of the study (M24).
Sample Size and Power Calculations
With a total of 45 patients dosed, 3 IAs could be performed following a group sequential testing procedure in the study to allow for early evaluation of efficacy. This sample size provided at least 95% power to rule out a response rate of 50% when the true response rate is 80% for both the primary and key secondary efficacy end points with a 1-sided alpha of 2.5%. The submission did not provide a justification for the selection of a 50% response rate in the power calculations. Details of the efficacy boundary, response rates, and overall power are in Table 10.
Control for Multiplicity
Multiplicity was considered for the primary and key secondary end points. No analyses were adjusted for covariates or baseline values. The family-wise type I error rate was controlled by an alpha spending approach for tests at interim and final analyses and a sequential testing of the primary and key secondary efficacy end points (i.e., the key secondary efficacy end point was to be tested only if the primary efficacy end point crossed an efficacy boundary). The efficacy boundaries for the primary efficacy end point (TI12) and key secondary efficacy end point (TI6) specified to control the type I error at a 1-sided alpha of 2.5% across multiple looks, based on the exact binomial distribution, are summarized in Table 10.
If an IA was not conducted, the alpha planned for this IA would be recovered in the subsequent analysis. Of note, IA1 and IA2 were not conducted according to the submission, and it was noted that the alpha planned for these 2 time points was recovered at IA3. As such, the primary and key secondary outcomes based on the PES were considered statistically significant if the corresponding 1-sided P value was less than 0.01692.
Table 10: Operating Characteristics of Efficacy Boundaries for the Primary and Key Secondary Efficacy Outcomes — PES
Analysis stage | Efficacy boundary | Boundary in response rate (95% CI) | Probability of crossing efficacy boundaries under different true response ratesa | One-sided alpha spending assuming 50% response rate | ||
|---|---|---|---|---|---|---|
Probability1 = 80% | Probability1 = 85% | Probability1 = 90% | ||||
IA1 | █████ | █████ █ | █████ | █████ | █████ | ██████ |
IA2 | █████ | ███████ | █████ | █████ | █████ | ██████ |
IA3 | █████ | ███████ | █████ | █████ | █████ | ██████ |
Final | █████ | ███████ | █████ | █████ | █████ | ██████ |
Overall power | — | █████ | █████ | █████ | ██████ | |
IA = interim analysis; PES = primary efficacy set.
aMarginal probability of crossing the efficacy boundary at a specific IA or final analysis.
Source: Details included in the table are from the CLIMB-111 Clinical Study Report.2
Statistical Analysis Methods
Details of the statistical analysis methods by outcome are presented in Table 11. Briefly, the majority of efficacy and safety outcomes were summarized descriptively, and the primary and key secondary outcomes were modelled.
Primary End Point — TI12
Patients were considered to have met the primary end point (TI12) if they had maintained a weighted average hemoglobin of 9 g/dL or greater without RBC transfusion for at least 12 consecutive months, at any time after the exagamglogene autotemcel infusion. Monitoring started 60 days after the last RBC transfusion for posttransplant support or TDT disease management. A patient was considered a responder if they met the response criteria any time during the response evaluation period. If a patient died or discontinued the study before achieving TI12 starting 60 days after the last RBC transfusion for posttransplant support or TDT management post-exagamglogene autotemcel infusion, due to reasons other than exagamglogene autotemcel-related AEs, the transfusion-free status and weighted average hemoglobin starting from 60 days after the last RBC transfusion of the patient was carried forward up to 24 months postinfusion. Patients who died or discontinued the study due to exagamglogene autotemcel-related AEs before achieving TI12, or who continuously received RBC transfusion for posttransplant support or TDT management after 10 months postinfusion were considered nonresponders for TI12.
The proportion of patients who achieved TI12 over the course of the study to date was provided with 1-sided P value (against a null hypothesis of 50% response rate) and 2-sided 95% exact Clopper-Pearson CI based on the PES. If the prespecified efficacy boundary was crossed at any IA, efficacy was considered established for exagamglogene autotemcel.
Key Secondary End Point — TI6
Patients were considered to have met the key secondary end point (TI6) if they had maintained a weighted average hemoglobin of 9 g/dL or greater without RBC transfusion for at least 6 consecutive months, at any time after the exagamglogene autotemcel infusion; monitoring started 60 days after the last RBC transfusion for posttransplant support or TDT disease management. A patient was a responder if they met the response criteria any time during the response evaluation period. If a patient died or discontinued the study before achieving TI6 starting 60 days after the last RBC transfusion for posttransplant support or TDT management post-exagamglogene autotemcel infusion due to reasons other than exagamglogene autotemcel-related AEs, the transfusion-free status and weighted average hemoglobin starting from 60 days after the last RBC transfusion of the patient was carried forward up to 24 months postinfusion. Patients who died or discontinued the study due to exagamglogene autotemcel-related AEs before achieving TI6 were considered nonresponders for TI6.
The proportion of patients who achieved TI6 over the course of the study to date was provided, with 1-sided P value (against a null hypothesis of 50% response rate) and two-sided 95% exact Clopper-Pearson CI based on the PES, with an alternate analysis done on the early efficacy set (not reported by CDA-AMC). For analysis of TI6 based on the early efficacy set, patients who continuously received RBC transfusions for more than 16 months post-exagamglogene autotemcel infusion were considered nonresponders for TI6.
Other Secondary End Points
The analysis for the other end points was based on the PES. Total hemoglobin and hemoglobin F concentrations were summarized as continuous variables. Changes from baseline in the patient-reported HRQoL measures were summarized as a continuous variable over time including fatigue-related item scores, dimensional score, and total score (if applicable). The derivation of the score was based on each PRO scoring manual.
Table 11: Statistical Analysis of Efficacy End Points for CLIMB-111
End point | Statistical model | Adjustment factors | Handling of missing data | Sensitivity analyses |
|---|---|---|---|---|
Proportion of patients achieving TI12 | 1-sided P value against a 50% response rate and 2-sided 95% exact Clopper-Pearson CI | NR | Incomplete or missing data were not imputed, unless otherwise specified. For patients who were lost to follow-up or died, efficacy analyses were based on their available data before death or loss to follow-up. | NR |
Proportion of patients achieving TI6 | ||||
Absolute and relative monthly change from baseline in volume, units, and episodes of RBC transfusions | Descriptive summary from baseline up to 24 months | |||
Fetal hemoglobin concentration | Summarized as a continuous variable over time | |||
Total hemoglobin concentration | ||||
Change from baseline in PROs over time assessed using EQ VAS (patients aged ≥ 18 years) | Summarized as a continuous variable over time including domain score and total score (if applicable) | |||
Change from baseline in PROs over time assessed using FACT-BMT (patients aged ≥ 18 years) | ||||
Change from baseline in PROs over time assessed using EQ-5D-Y (patients aged < 18 years) | ||||
Change from baseline in PROs over time assessed using PedsQL (patients aged < 18 years) |
CI = confidence interval; EQ VAS = EQ visual analogue scale; FACT-BMT = Functional Assessment of Cancer Therapy–Bone Marrow Transplantation; NR = not reported; PedsQL = Pediatric Quality of Life Inventory; PRO = patient-reported outcome; RBC = red blood cell; TI6 = transfusion independence for 6 consecutive months; TI12 = transfusion independence for 12 consecutive months.
Source: Details included in the table are from the sponsor’s Summary of Clinical Evidence.52
Analysis Populations
Details of all analysis sets in the CLIMB-111 study are in Table 12. Briefly, the results appraised by CDA-AMC for efficacy end points were those from the April 16, 2023, data cut-off in the PES (n = 42 patients). Harms results were reported from the April 16, 2023, data cut-off in the safety analysis set (N = 59). Efficacy results from the January 16, 2023, data cut-off are reported in Appendix 1.
Table 12: Summary of Analysis Sets for CLIMB-111
Population | Definition | Application |
|---|---|---|
Enrolled set (N = 59) | All enrolled patients who signed informed consent and met the eligibility criteria | Listings of the demographics and baseline characteristics. |
FAS (N = 54) | A subset of the enrolled set that included patients who received exagamglogene autotemcel infusion | Summary of the demographics, medical history, and baseline characteristics, and efficacy analyses where applicable; used in supportive analyses. |
PES (N = 42) | A subset of the FAS that included all patients who were followed for at least 16 months after exagamglogene autotemcel infusion and for at least 14 months after completion of the RBC transfusions for posttransplant support or TDT disease management | Summary of the demographics and baseline characteristics and all efficacy analyses. Used in primary data analysis and supportive analyses. |
SAS (N = 59) | A subset of the enrolled set that included patients who started the mobilization regimen | Summary of prior and concomitant medications and safety analyses. |
FAS = full analysis set; PES = primary efficacy set; RBC = red blood cell; SAS = safety analysis set; TDT = transfusion-dependent beta thalassemia.
Source: Details included in the table are from the sponsor’s Summary of Clinical Evidence.52
Subgroup Analyses
Prespecified subgroup analyses were performed for TI12 (primary efficacy end point) and TI6 (key secondary efficacy end point) with point estimate and 95% CI for each of the subgroups during IAs based on the PES. Subgroups were as follows:
age at screening (aged ≥ 12 to < 18 years and ≥ 18 to ≤ 35 years)
genotype (beta0/beta0-like and non-beta0/beta0-like)
sex
race (Asian, white, and other races).
The following subgroup analyses were also carried out for hemoglobin F concentration and total hemoglobin concentration based on the FAS only:
age at screening (aged ≥ 12 to < 18 years and ≥ 18 to ≤ 35 years)
genotype (beta0/beta0-like and non-beta0/beta0-like)
sex
race (Asian, white, and other races).
Subgroups of age and genotype were considered relevant to the review and were appraised by CDA-AMC.
Results
Patient Disposition
As of the data cut-off on April 16, 2023, a total of 59 patients were enrolled, 54 had received an infusion of exagamglogene autotemcel, and 42 patients were included in the PES. The submission did not provide additional details on the numbers of patients screened and the numbers of screening failures. A total of 3 patients discontinued the study to date, all between the start of mobilization and the start of myeloablative conditioning. A total of 2 patients were enrolled in the study but had not yet received exagamglogene autotemcel as of the April 16, 2023, data cut-off. A total of 23 patients had completed the 24-month follow-up and enrolled in the LTE. Full details of the patient disposition are in Table 13.
Table 13: Summary of Patient Disposition From CLIMB-111
Patient disposition | CLIMB-111 N = 59 |
|---|---|
Screened, N | NR |
Reason for screening failure, n (%) | NR |
Enrolled, N (%) | 59 |
Never dosed with any study drug, n (%)a | █████ |
Never dosed with exagamglogene autotemcel, n (%)b | 3 (5.1) |
Started conditioning regimen, n (%) | 54 (91.5) |
Started exagamglogene autotemcel infusion, n (%) | 54 (91.5) |
Completed exagamglogene autotemcel infusion, n (%) | 54 (100.0) |
Did not complete exagamglogene autotemcel infusion, n (%) | 0 |
On study and not yet dosed with exagamglogene autotemcel, n (%) | 2 (3.4) |
On study and dosed with exagamglogene autotemcel | 31 (52.5) |
Completed study, n (%) | 23 (39.0) |
Completed study and enrolled in LTE | 23 (100.0) |
Discontinued from study, n (%)c | 3 (5.1) |
Discontinued study after exagamglogene autotemcel infusion | 0 |
Discontinued study after exagamglogene autotemcel infusion and enrolled in LTE | 0 |
Reason for discontinuation, n (%) | |
███ ███ ████ █ ██████ █████████ █████████ | █████ |
████████ ████ █████████ █████ █████████████ | █████ |
███████████ ███████ | █████ |
FAS, N | 54 |
PES, N | 42 |
SAS, N | 59 |
FAS = full analysis set; LTE = long-term extension; NR = not reported; PES = primary efficacy set; SAS = safety analysis set.
aIncludes all patients who discontinued the study and did not receive any study drugs for mobilization, conditioning, or exagamglogene autotemcel infusion.
bIncludes all patients who discontinued the study and did not receive exagamglogene autotemcel infusion.
cDiscontinuations occurred after the start of mobilization and before myeloablative conditioning.
Sources: Details included in the table are from the sponsor’s Summary of Clinical Evidence52 and the CLIMB-111 Clinical Overview Addendum.24
Baseline Characteristics
The baseline characteristics outlined in Table 14 are limited to those that are most relevant to this review or were felt to affect the outcomes or interpretation of the study results. Briefly, baseline characteristics were broadly similar between the PES and the FAS. The majority of patients (59.5% in the PES) expressed a beta0/beta0-like genotype of TDT. In the PES, the average age was 21.6 years; 31.0% of patients were pediatric patients (aged 12 years or older and less than 18 years), and 69.0% were adult patients were between the ages of 18 years and 35 years. Of note, the study did not enrol any Black or African American, ████████ ██████ ██ ██████ ███████ ███ ██████ ████████ ██ ███████ ████████ patients. In addition, the study did not enrol any patients with the █████ █████ thalassemia genotypes.
The total units of RBC transfusions and the total volume of RBC transfusions were also available for the safety analysis set (N = 59 patients) for the 2 years before the signing of the informed consent or the latest rescreening, for patients undergoing rescreening. Briefly, the mean total volume of RBC transfusions was 403.5 mL/kg (SD = 123.5 mL/kg; range, 96.6 mL/kg to 661.8 mL/kg) and the mean total units of RBC transfusions was 74.9 units (SD = 24.4 units).
Table 14: Summary of Baseline Characteristics From CLIMB-111
Characteristic | CLIMB-111 | |
|---|---|---|
PES (n = 42) | FAS (n = 54) | |
Demographic characteristics | ||
Sex, n (%) | ||
Female | 21 (50.0) | 25 (46.3) |
Female of childbearing potential | 21 (100.0) | 25 (100.0) |
Male | 21 (50.0) | 29 (53.7) |
Age at screening (years), mean (SD) | 21.6 (6.4) | 21.3 (6.6) |
Age category at screening, n (%) | ||
≥ 12 and < 18 years | 13 (31.0) | 19 (35.2) |
≥ 18 and ≤ 35 years | 29 (69.0) | 35 (64.8) |
Race, n (%) | ||
Asian | 16 (38.1) | 23 (42.6) |
Black or African American | 0 | 0 |
White | 17 (40.5) | 18 (33.3) |
████████ ██████ ██ ██████ ██████ | ██████ | ██████ |
██████ ████████ ██ ███████ ████████ | ██████ | ██████ |
Multiracial | 3 (7.1) | 3 (5.6) |
Data not collected per local regulations | 5 (11.9) | 8 (14.8) |
Other | 1 (2.4) | 2 (3.7) |
Ethnicity | ||
Hispanic or Latino | █████ | █████ |
Not Hispanic or Latino | ██ ██████ | ██ ██████ |
Data not collected per local regulations | █████ | ██████ |
Medical characteristics | ||
Genotype, n (%) | ||
Beta0/beta0-like | 25 (59.5) | 33 (61.1) |
Beta0/beta0 | 13 (31.0) | 21 (38.9) |
Beta0/IVS-I-110 | 9 (21.4) | 9 (16.7) |
IVS-I-110/IVS-I-110 | 3 (7.1) | 3 (5.6) |
Non-beta0/beta0-like | 17 (40.5) | 21 (38.9) |
Beta+/beta+ | 4 (9.5) | 4 (7.4) |
Beta+/beta0 | 9 (21.4) | 12 (22.2) |
██ | █████ | █████ |
BetaE/beta0 | 4 (9.5) | 5 (9.3) |
███ | █████ | █████ |
█████ | █████ | █████ |
Spleen intact, n (%) | 30 (71.4) | 38 (70.4) |
Annualized volume of RBC transfusions (mL/kg), mean (SD) | 199.7 (57.2) | 197.6 (62.0) |
Annualized units of RBC transfusions, mean (SD) | 36.5 (10.5) | 36.4 (11.7) |
Annualized number of RBC transfusion episodes, mean (SD)a | 17.0 (5.0) | 16.5 (5.2) |
Total hemoglobin concentration (g/dL), mean (SD) | 10.6 (2.0) | 10.4 (1.9) |
Fetal hemoglobin concentration (%), mean (SD) | 5.1 (5.8) | 6.7 (11.1) |
Fetal hemoglobin concentration (g/dL), mean (SD) | 0.5 (0.6) | 0.7 (0.9)b |
F-cell level (%), mean (SD) | 13.0 (12.0) | 14.2 (14.8) |
Serum ferritin level (pmol/L), mean (SD) | 3,785.4 (2,908.2) | 3,712.4 (2,832.3) |
Cardiac T2* (msec), mean (SD)c | 35.0 (8.9) | 34.2 (9.0) |
Liver iron concentration (mg/g), mean (SD)d | 4.7 (3.2) | 4.5 (3.0) |
Weight (kg), mean (SD) | 54.6 (14.3) | 55.0 (13.9) |
FAS = full analysis set; PES = primary efficacy set; RBC = red blood cell; SD = standard deviation.
aAn RBC transfusion episode was defined as all transfusions within 5 days, starting from the first transfusion in the episode.
bResults available for 53 patients.
cCardiac T2* is the measurement of cardiac iron content.
dLiver iron concentration was derived from liver R2.
Source: Details included in the table are from the sponsor’s CLIMB-111 Clinical Overview Addendum.24
Exposure to Study Treatments
Details of exagamglogene autotemcel dose and the duration of follow-up to date after the exagamglogene autotemcel infusion are presented in Table 15. Briefly, at the time of the April 16, 2023, data cut-off the mean duration of follow-up was 19.2 months (SD = 6.97 months). The median time from the day of exagamglogene autotemcel infusion to neutrophil engraftment was 29 days (range, 12 to 56 days). The median time from the day of exagamglogene autotemcel infusion to platelet engraftment was 44 days (range, 20 to 200 days), as of the January 2023 data cut-off.
Table 15: Summary of Patient Exposure From CLIMB-111 — FAS
Exposure | CLIMB-111 N = 54 |
|---|---|
Exagamglogene autotemcel dose (× 106 cells/kg) | |
N patients receiving exagamglogene autotemcel infusion | 54 |
Mean (SD) | ███ ██████ |
Range | 3.0 to 19.7 |
Follow-up duration after exagamglogene autotemcel infusion (month):a | |
Mean (SD) | 19.2 (6.97) |
Range | 2.1 to 51.1 |
Follow-up duration after exagamglogene autotemcel infusion by interval, n (%)a | |
≤ 3 months | 2 (3.7) |
> 3 months to ≤ 6 months | █████ |
> 6 months to ≤ 12 months | █████ |
> 12 months to ≤ 24 months | ██ ██████ |
> 24 months | ██ ██████ |
FAS = full analysis set; Q6H = every 6 hours; QD = every day; SD = standard deviation.
aFollow-up duration after exagamglogene autotemcel infusion (months) = (data cut-off or end-of-study date, whichever is earlier – exagamglogene autotemcel infusion date + 1)/30.
Source: Details included in the table are from additional information provided by the sponsor.32
Concomitant Medications and Co-Interventions
Information on concomitant medications taken during the 2 years before enrolment in the CLIMB-111 study were not available.
Details on the list of concomitant medications and co-interventions received by more the 25% of patients were available in the submission. Briefly, all patients in the study to date received concomitant medications or co-interventions. The most common medications included antimicrobial medications, pain medications, and medications typically used in the context of myeloablative conditioning.
Efficacy
Detailed results of the primary and key secondary outcomes, as well as the time to last RBC transfusion and the mean duration of TI (secondary outcomes), are presented in Table 16. Detailed results of the secondary outcomes for total hemoglobin, hemoglobin F, and HRQoL measures are presented in Table 17.
Transfusion Independence
Proportion of Patients With TI12
The proportion of patients who achieved TI12 following infusion of exagamglogene autotemcel and as of the April 16, 2023, data cut-off was 92.9% (95% CI, 80.5% to 98.5%) in the PES.
Among patients with TI12, the time from the exagamglogene autotemcel infusion to the last RBC transfusion was 28.0 days (range, 11.0 to 91.0 days). The mean duration of TI to date was 23.6 months (SD = 7.8 months).
Proportion of Patients With TI6
Following infusion with exagamglogene autotemcel, the proportion of patients in the PES who achieved TI6 as of the data cut-off was 92.9% (95% CI, 80.5% to 98.5%).
Patients Not Attaining TI6 or TI12
Out of the 42 patients included in the PES, 3 patients did not attain the TI12 primary outcome. Per the submission, as of the data cut-off, the 3 patients had been transfusion independent for 10.3 months, 7.0 months, and 2.8 months, respectively. ███ ████████ ███ ███ ████ ███████████████████████ ███ ████ ██████ ███ ███ ██████ ████ ███ ███ ████ ███ ████████ ███ ███ ███████ █████ ████████ ██ ███ ███ █████ ██ ███████ ███ █ ███████████ ██████. The 3 patients had total hemoglobin levels of ████████ ███████ ███ ███████, respectively, as well as hemoglobin F levels of █████████ █████████ ███ ████████, respectively, at their last scheduled visits before data cut-off.
Table 16: Summary of Transfusion Results From CLIMB-111 — PES
Outcome | CLIMB-111 N = 42 |
|---|---|
Proportion of patients achieving TI12 (primary end point) | |
Number of patients with TI12, n | 39 |
Proportion of patients with TI12 (95% CI)a | 92.9 (80.5 to 98.5) |
P value (1-sided against 50% response rate)b | < 0.0001 |
Proportion of patients achieving TI6 (key secondary end point) | |
Number of patients with TI6, n | 39 |
Proportion of patients with TI16 (95% CI)a | 92.9 (80.5 to 98.5) |
P value (1-sided against 50% response rate)b | < 0.0001 |
Time to last RBC transfusionc for patients with TI12 (secondary end point) | |
Number of patients with TI12 | 39 |
Time from exagamglogene autotemcel to last RBC transfusion (days), mean (range) | 28.0 (11.0 to 91.0) |
Duration of TI with weighted average hemoglobin ≥ 9 g/dL for patients with TI12 (secondary end point) | |
Number of patients with TI12 | 39 |
Duration of TI (months), mean (SD) | 23.6 (7.8) |
CI = confidence interval; PES = primary efficacy set; RBC = red blood cell; TI = transfusion independence; TI6 = transfusion independence for 6 consecutive months; TI12 = transfusion independence for 12 consecutive months.
aThe 2-sided 95% CI was calculated using the exact Clopper-Pearson method.
bThe 1-sided P value was calculated using the binomial distribution. This outcome was adjusted for multiple comparisons.
cAn RBC transfusion episode was defined as all transfusions within 5 days, starting from the first transfusion in the episode.
Source: Details included in the table are from the sponsor’s CLIMB-111 Clinical Overview Addendum.24
Hemoglobin Outcomes
Hemoglobin F Levels
The mean total hemoglobin F concentrations at 6 months post-exagamglogene autotemcel infusion were 10.8 g/dL (SD = 2.8 g/dL). At 12 months post-exagamglogene autotemcel infusion, the observed mean concentration of hemoglobin F was 11.5 g/dL (SD = 2.5), and at 24 months post-exagamglogene autotemcel infusion, the observed mean concentration of hemoglobin F was 11.5 g/dL (SD = 2.7 g/dL).
Total Hemoglobin Concentration
At 6 months post-exagamglogene autotemcel infusion, the observed mean hemoglobin concentration was 12.1 g/dL (SD = 2.0 g/dL). At 12 months post-exagamglogene autotemcel infusion, the observed mean hemoglobin concentration was 12.8 g/dL (SD = 2.1 g/dL). At 24 months post-exagamglogene autotemcel infusion, the observed mean hemoglobin concentration was 12.9 g/dL (SD = 2.4 g/dL).
Proportion of Alleles With the Intended Genetic Modification in the CD34+ Cells of the Bone Marrow
At 6 months post-exagamglogene autotemcel infusion, the observed mean proportion of CD34+ cells with the intended genetic modification was 78.48% (SD = 11.39%). At 12 months post-exagamglogene autotemcel infusion, the observed mean proportion was █████ ████████. At 24 months post-exagamglogene autotemcel infusion, the observed mean proportion was █████ █████████
Proportion of Alleles With the Intended Genetic Modification in the Peripheral Blood
At 6 months post-exagamglogene autotemcel infusion, the observed mean proportion of CD34+ cells with the intended genetic modification was █████ ████████. At 12 months post-exagamglogene autotemcel infusion, the observed mean proportion was █████ ████████. At 24 months post-exagamglogene autotemcel infusion, the observed mean proportion was █████ ████████.
HRQoL Outcomes
Functional Assessment of Cancer Therapy–Bone Marrow Transplantation
Results were not reported at 6 months post-exagamglogene autotemcel infusion. At 12 months post-exagamglogene autotemcel infusion, the observed mean change in scores from baseline was 7.4 points (SD = 23.0 points). At 24 months post-exagamglogene autotemcel infusion, the observed mean change in scores from baseline was 13.9 points (SD = 21.4 points).
Pediatric Quality of Life Inventory
At 6 months post-exagamglogene autotemcel infusion, the observed mean change from baseline in scores was 10.8 points (SD = 10.2 points). At 12 months post-exagamglogene autotemcel infusion, the observed mean change from baseline in scores was 12.0 points (SD = 10.3 points). At 24 months post-exagamglogene autotemcel infusion, the observed mean change from baseline in scores was 12.3 points (SD = 17.4 points).
EQ VAS
At 9 months post-exagamglogene autotemcel infusion, the observed mean change from baseline was ███ ██████ points. At 12 months post-exagamglogene autotemcel infusion, the observed mean change from baseline was 7.9 points (SD = 16.7 points). At 24 months post-exagamglogene autotemcel infusion, the observed mean change from baseline was 10.7 points (SD = 18.6 points).
Table 17: Summary of Other Secondary Efficacy Results From CLIMB-111 — PES
Outcome | Months after exagamglogene autotemcel | ||
|---|---|---|---|
6 months n = 42 | 12 months n = 42 | 24 months n = 42 | |
Fetal hemoglobin concentration (g/dL) | |||
Baseline, n | 42 | 42 | 42 |
Baseline, mean (SD) | 0.5 (0.6) | 0.5 (0.6) | 0.5 (0.6) |
Patients with data at the time point, n | 42 | 41 | 23 |
Observed, mean (SD) | 10.8 (2.8) | 11.5 (2.5) | 11.5 (2.7) |
Total hemoglobin concentration (g/dL) | |||
Baseline, n | 42 | 42 | 42 |
Baseline, mean (SD) | 10.6 (2.0) | 10.6 (2.0) | 10.6 (2.0) |
Patients with data at the time point, n | 42 | 42 | 23 |
Observed, mean (SD) | 12.1 (2.0) | 12.8 (2.1) | 12.9 (2.4) |
Proportion of alleles with intended genetic modification in CD34+ cells of the bone marrow | |||
Patients with outcome at the time point, n | 44 | ██ | ██ |
Observed proportion (%), mean (SD) | 78.48 (11.39) | █████ ███ | █████ ██ |
Proportion of alleles with intended genetic modification in peripheral blood | |||
Patients with outcome at the time point, n | ██ | ██ | ██ |
Observed proportion (%), mean (SD) | █████ ███ | █████ ███ | █████ ███ |
Change from baseline in EQ VAS (patients aged ≥ 18 years) | |||
Baseline, n | 29 | 29 | 29 |
Baseline, mean (SD) | 81.8 (17.1) | 81.8 (17.1) | 81.8 (17.1) |
Patients with data at the time point, n | 28a | 29 | 19 |
Observed, mean (SD) | 88.5 (10.8)a | 89.7 (11.3) | 90.5 (11.1) |
Change from baseline, mean (SD) | 6.9 (14.8)a | 7.9 (16.7) | 10.7 (18.6) |
Change from baseline in FACT-BMT (patients aged ≥ 18 years) | |||
Baseline, n | 29 | 29 | 29 |
Baseline, mean (SD) | 112.5 (19.5) | 112.5 (19.5) | 112.5 (19.5) |
Patients with data at the time point, n | NR | 29 | 19 |
Observed, mean (SD) | NR | 119.9 (18.6) | 124.4 (18.6) |
Change from baseline, mean (SD) | NR | 7.4 (23.0) | 13.9 (21.4) |
Change from baseline in nonadult EQ VAS (patients aged ≥ 12 and < 18 years)b,c | |||
Baseline, n | ██ | ██ | ██ |
Baseline, mean (SD) | ████ ██ | ████ ██ | ████ ██ |
Patients with data at the time point, n | ██ | ██ | ██ |
Observed, mean (SD) | ████ █████ | ████ █████ | ████ █████ |
Change from baseline, mean (SD) | ███ ██████ | ███ ██████ | ███ █████ |
Change from baseline in PedsQL (aged patients < 18 years) | |||
Baseline, n | 12 | 12 | 12 |
Baseline, mean (SD) | 75.9 (9.6) | 75.9 (9.6) | 75.9 (9.6) |
Patients with data at the time point, n | 13 | 12 | 4 |
Observed, mean (SD) | 87.5 (8.5) | 87.9 (8.9) | 91.3 (10.6) |
Change from baseline, mean (SD) | 10.8 (10.2) | 12.0 (10.3) | 12.3 (17.4) |
EQ VAS = EQ visual analogue scale; FACT-BMT = Functional Assessment of Cancer Therapy–Bone Marrow Transplantation; NR = not reported; PedsQL = Pediatric Quality of Life Inventory; PES = primary efficacy set; SD = standard deviation.
aMeasured at 9 months.
bPer the submission, due to a lack of value sets in the UK or US, index-based summary health scores were not calculated for the EQ-5D-Y. The nonadult EQ VAS, which is identical to the adult EQ VAS, was employed instead.
cResults reported from the January data cut-off (n = 35 patients in the PES).
dMeasured at 18 months.
Sources: Details included in the table are from the sponsor’s CLIMB-111 Clinical Overview Addendum24 and the CLIMB-111 Clinical Study Report.2
Nonadult EQ VAS
At 6 months post-exagamglogene autotemcel infusion, the observed mean change from baseline was ███ ██████ points. At 12 months post-exagamglogene autotemcel infusion, the observed mean change from baseline was ███ ██████ points. At 18 months post-exagamglogene autotemcel infusion, the observed mean change from baseline was ███ █████ points.
Subgroup Analyses
Details of relevant subgroup analyses are presented in Table 29 in Appendix 1 of the report. ████████ ██████ ████ █████████ ███ ██████████ ██ ████████ ████ ███ ███ ████ ████ ██████████ ███ ███████ ███ ████ ███ ███ ████ ███████ ██ ███ ███████ █████ ███████ ██ ███ █████████. The proportion of patients with the TI6 and TI12 outcome in patients with the beta0/beta0 was █████ ████ ███ █████ ██ ██████ and patients with the non-beta0/beta0 genotype was ██████ ████ ███ █████ ██ ███████.
Harms
Refer to Table 18 for harms data, which include data up until the April 16, 2023, data cut-off. AEs and SAEs are reported for the time intervals from enrolment to 1 day before exagamglogene autotemcel infusion, and from exagamglogene autotemcel infusion to the M24 visit or the EOS visit.
Adverse Events
During the course of the entire study to date, a total of 58 (98.3%) patients had any AEs. A total of 56 (94.9%) patients had any AE during the time from enrolment until the day before exagamglogene autotemcel infusion, which included myeloablative conditioning. A total of 100% of patients had any AE during the time period from the day of exagamglogene autotemcel infusion to either M24 visit or the EOS visit.
The most common AEs from the time of enrolment to the day before exagamglogene autotemcel infusion were nausea (44.1% of patients) headache (39.0% of patients), bone pain (33.9% of patients), vascular site access pain (28.8% of patients), and vomiting (20.3% of patients). The most common AEs to date from the day of exagamglogene autotemcel infusion to the M24 or EOS study visit were febrile neutropenia (61.1% of patients), headache (55.6% of patients), stomatitis (51.9% of patients), thrombocytopenia (46.3% of patients), anemia (44.4% of patients), mucosal inflammation (42.6% of patients), nausea (42.6% of patients), and vomiting (40.7% of patients).
Serious Adverse Events
A total of 9 (15.3%) patients had any SAE during the time from enrolment until the day before exagamglogene autotemcel infusion, which included myeloablative conditioning. A total of 26 (44.1%) of patients had any SAE during the time period from enrolment to either their M24 or EOS visit.
The SAEs that occurred in 2 or more patients during the study to date were veno-occlusive liver disease, pneumonia, COVID-19, hypoxia, thrombocytopenia, upper respiratory tract infection, nausea, vomiting, and bacteremia.
Withdrawals Due to AEs
To date, no patients withdrew from the study drug or withdrew from the study due to AEs after exagamglogene autotemcel infusion. A total of 3 withdrawals before exagamglogene autotemcel infusion were reported; reasons included █████████ █ ██████ █████████ █████████ ██ ████████ ████████ ████ █████████ █████ █████████████ ██ ████████ ███ ███████████ ███████ ██ ███████. Further details on patient disposition are presented in Table 13.
Mortality
To date, no deaths had been reported in the study.
Notable Harms
As of the date of the data cut-off, all 54 (100.0%) patients had achieved neutrophil engraftment. The median time to neutrophil engraftment was 29.0 days (range, 12 to 56 days). A total of 53 patients achieved platelet engraftment; the median time to engraftment was 44.0 days (range, 20 to 200 days). Engraftment syndrome was not reported. Delayed engraftment was reported as a SAE in 1 patient during the time between exagamglogene autotemcel infusion and M24 or EOS visit.
In terms of other notable harms, 41 (69.5%) of patients reported AEs of infection or infestation and 33 (55.9%) patients experienced febrile neutropenia from enrolment to the M24 or EOS visit. In terms of bleeding, ██ types of bleeding AEs were reported: gingival bleeding in 6 (10.2%) patients, ██████████████ ████████ ██ █ ██████ patients and █████ █████████ ████████ ██ █ ██████ patients between study enrolment and M24 or EOS visits. Veno-occlusive liver disease SAEs occurred in 5 (8.5%) patients between study enrolment and M24 or EOS visits. ████████████████ ████████ ███ ████████ ██ █ ██████ patients between enrolment and M24 or EOS visits. No information was reported regarding hemophagocytic lymphohistiocytosis, engraftment syndrome, infections and infestations classified as SAEs, bleeding classified as SAEs, or anaphylaxis. No patients received their back-up CD34+ cells to date.
Malignancies
The submission noted that no malignancies had been reported in patients after exagamglogene autotemcel infusion in the study to date. ███ ███████ ██████ ████████ ██ ██ ██ ████ █████████ ███ ████████ █████████████ ██████████ ██████████████ ███ ██████████ ███ ███ ███████ ███████ ████ ███ ███████ █████████ ██ ███████████ ██████████ █████ ███ ████████
Off-Target Editing
The submission did not contain any information related to screening for off-target editing in patients who had received exagamglogene autotemcel.
Table 18: Summary of Harms Results From CLIMB-111 April 2023 Data Cut-Off — FAS
AEs | From enrolment to the day before exagamglogene autotemcel infusion N = 59 | From exagamglogene autotemcel infusion to M24 or EOS visit n = 54 | From enrolment to M24 to EOS visit n = 59 |
|---|---|---|---|
Most common AEs (in ≥ 25% of patients), n (%) | |||
Patients with any AEs | 56 (94.9) | 54 (100.0) | 58 (98.3) |
Febrile neutropenia | 0 | 33 (61.1) | 33 (55.9) |
Headache | 23 (39.0) | 30 (55.6) | 40 (67.8) |
Stomatitis | 2 (3.4) | 28 (51.9) | 28 (47.5) |
Thrombocytopenia | 1 (1.7) | 25 (46.3) | 25 (42.4) |
Anemia | 10 (16.9) | 24 (44.4) | 27 (45.8) |
Mucosal inflammation | 4 (6.8) | 23 (42.6) | 25 (42.4) |
Nausea | 26 (44.1) | 23 (42.6) | 35 (59.3) |
Vomiting | 12 (20.3) | 22 (40.7) | 24 (40.7) |
Hypokalemia | 11 (18.6) | 21 (38.9) | 24 (40.7) |
Platelet count decreased | 2 (3.4) | 21 (38.9) | 22 (37.3) |
Abdominal pain | 10 (16.9) | 20 (37.0) | 23 (39.0) |
Epistaxis | 1 (1.7) | 20 (37.0) | 20 (33.9) |
Arthralgia | 5 (8.5) | 19 (35.2) | 20 (33.9) |
Constipation | 11 (18.6) | 18 (33.3) | 27 (45.8) |
Neutrophil count decreased | 0 | 16 (29.6) | 16 (27.1) |
Diarrhea | 6 (10.2) | 15 (27.8) | 19 (32.2) |
Pruritus | 4 (6.8) | 15 (27.8) | 17 (28.8) |
Pyrexia | 5 (8.5) | 15 (27.8) | 15 (25.4) |
COVID-19 | 4 (6.8) | 14 (25.9) | 18 (30.5) |
Decreased appetite | 0 | 14 (25.9) | 14 (23.7) |
Pain in extremity | 7 (11.9) | 11 (20.4) | 16 (27.1) |
Back pain | 11 (18.6) | 10 (18.5) | 18 (30.5) |
Bone pain | 20 (33.9) | 8 (14.8) | 25 (42.4) |
Vascular access site pain | 17 (28.8) | 3 (5.6) | 19 (32.2) |
Patients with AEs of ≥ grade 3 (in ≥ 10% of patients), n (%) | |||
Patients with any AEs ≥ grade 3 | ██ ██████ | 48 (88.9) | ██ ██████ |
Febrile neutropenia | ██████ | 29 (53.7) | ██ ██████ |
Stomatitis | ██████ | 22 (40.7) | ██ ██████ |
Anemia | ██████ | 21 (38.9) | ██ ██████ |
Platelet count decreased | ██████ | 20 (37.0) | ██ ██████ |
Thrombocytopenia | ██████ | 18 (33.3) | ██ ██████ |
Mucosal inflammation | ██████ | 17 (31.5) | ██ ██████ |
Neutrophil count decreased | ██████ | 16 (29.6) | ██ ██████ |
Decreased appetite | ██████ | 12 (22.2) | ██ ██████ |
Epistaxis | ██████ | 8 (14.8) | ██████ |
White blood cell count decreased | ██████ | 8 (14.8) | ██████ |
Neutropenia | ██████ | 7 (13.0) | ██████ |
Veno-occlusive liver disease | ██████ | 6 (11.1) | ██████ |
Hypophosphatemia | ██████ | 5 (9.3) | ██████ |
Hypokalemia | ██████ | 4 (7.4) | ██████ |
Nausea | ██████ | 4 (7.4) | ██████ |
SAEs (in ≥ 2 patients), n (%) | |||
Patients with any SAEs | 9 (15.3) | 19 (35.2) | 26 (44.1) |
Veno-occlusive liver disease | 0 | 5 (9.3) | 5 (8.5) |
Pneumonia | 0 | 3 (5.6) | 3 (5.1) |
COVID-19 | 0 | 2 (3.7) | 2 (3.4) |
Hypoxia | 0 | 2 (3.7) | 2 (3.4) |
Thrombocytopenia | 0 | 2 (3.7) | 2 (3.4) |
Upper respiratory tract infection | 0 | 2 (3.7) | 2 (3.4) |
Nausea | 1 (1.7) | 1 (1.9) | 2 (3.4) |
Vomiting | 1 (1.7) | 1 (1.9) | 2 (3.4) |
Bacteremia | 2 (3.4) | 0 | 2 (3.4) |
Patients who stopped treatment due to AEs, n (%) | |||
Patients who stopped | NR | 0 | NR |
Deaths, n (%) | |||
Patients who died | NR | 0 | NR |
AEs of special interest, n (%) | |||
Malignancy | NR | 0 | 0 |
Infections and infestations (AEs) | 15 (25.4) | 35 (64.8) | 41 (69.5) |
Febrile neutropenia | 0 | 33 (61.1) | 33 (55.9) |
Gingival bleeding | 0 | 6 (11.1) | 6 (10.2) |
Veno-occlusive liver disease (SAEs) | 0 | 5 (9.3) | 5 (8.5) |
██████████████ | ██████ | ██████ | ██████ |
██████████████ | ██████ | ██████ | ██████ |
█████ █████████ | ██████ | ██████ | ██████ |
Anaphylaxis | NR | NR | NR |
Engraftment syndrome | NR | NR | NR |
Hemophagocytic lymphohistiocytosis | NR | NR | NR |
Infections (SAEs) | NR | NR | NR |
AE = adverse event; EOS = end of study; FAS = full analysis set; M24 = month 24; NR = not reported; SAE = serious adverse event.
Sources: Details included in the table are from the sponsor’s Summary of Clinical Evidence,52 the CLIMB-111 Clinical Study Report,2 the sponsor’s Clinical Addendum Update,24 and additional information provided by the sponsor.33,34
Critical Appraisal
Internal Validity
The CLIMB-111 study is a single-arm phase I, II, and III trial assessing the efficacy and safety of an autologous gene therapy in patients aged 12 years to 35 years with TDT. Included in the submission was an IA (IA3) including data up to January 2023, as well as updated information from an April 2023 data cut-off submitted to Health Canada at their request. The baseline characteristics were assessed before the mobilization phase of therapy, providing a snapshot of the patients’ condition immediately before undertaking the exagamglogene autotemcel treatment process.
There are several limitations to note regarding the study design. First, the CLIMB-111 study is a single-arm trial with no blinding, randomization, or allocation concealment, and therefore the study population may have unknown confounders, and the results observed may not be able to be entirely attributable to the study drug. The clinical experts consulted by CDA-AMC indicated that the sponsor’s decision to perform a noncomparative trial may be reasonable because the SOC treatments of HSCT and RBC transfusions would have limitations as concurrent controls. They also noted that HSCT would remain the preferred treatment in younger patients (aged < 12 years) who have a matched sibling donor who is eligible and willing to donate, and exagamglogene autotemcel treatment would be considered after HSCT in situations where the patient is eligible for both treatments but an HLA-matched sibling donor is available, because of HSCT’s established curative effects. However, a key limitation they identified with HSCT in practice settings is that only approximately 20% of patients have a matched related donor, thus HSCT is not considered widely available or accessible. Independence from transfusion is the primary goal of treatment and the primary outcome of the trial; therefore, it would not be practical to include RBC transfusion as a contemporary comparator. However, using luspatercept as a control would also have limitations because it is only indicated for use in adults with TDT and it is not considered a SOC because only approximately 20% of patients respond to it. Thus, whether there would be equipoise in randomizing patients to exagamglogene autotemcel or luspatercept in a hypothetical RCT is unclear. A placebo-controlled or sham-controlled trial would hold potential ethical considerations because of the need for myeloablative therapy as part of the treatment process. While a well-designed RCT that allows for causal inferences to be drawn with greater certainty than a single-arm treatment design is preferred, especially for decisions in HTA and reimbursement, the use of a single-arm study in this scenario is understandable, but nevertheless results in the GRADE assessment of certainty being very low, without evidence of grading up as is typical for single-arm studies. The submission did not describe whether other study designs using external controls were considered. Of note, the sponsor provided indirect treatment comparisons to support the comparative effectiveness aspects of the review (refer to Indirect Evidence).
An additional limitation impacting the study design is that the CLIMB-111 study underwent several protocol changes including conversion to a phase I, II, and III trial, changes in the primary and secondary outcomes, and addition of the IAs after enrolment began. The change to a mixed phase I, II, and III trial has implications for the sample size and measurement of outcomes that may increase the heterogeneity of the results because of the confirmatory expectations of the phase III designation. The results submitted from the CLIMB-111 study are an IA based on the PES, with 23 (39%) patients providing 2 complete years of follow-up, 3 (5.1%) patients never dosed with exagamglogene autotemcel as they discontinued after enrolment but before exagamglogene autotemcel infusion, and 2 (3.4%) patients on study but not having received exagamglogene autotemcel yet as of the April 2023 data cut-off. IAs may overestimate the true effect of treatment. Furthermore, the timing of the changes in design and primary and key secondary outcomes relative to study participant follow-up status and database analysis is an important consideration. The EMA review of exagamglogene autotemcel for TDT highlighted the various protocol changes in their assessment; according to the EMA, 1 patient in the CLIMB-111 study had achieved the primary outcome at the time some of these key amendments were made.29 The EMA accepted that, while not ideal for internal validity, this likely had little effect on the overall validity or results of the study.29 Nonetheless, the number of important protocol and statistical analysis revisions for a study that does not have a true confirmatory phase III design adds to the very low certainty of the evidence.
In addition, there are limitations in the alpha spending methods described in the study to account for multiplicity over the IAs and control for the family-wise type I error rate. These methods used patient denominators to derive the alpha values for IA1, IA2, and IA3, an approach which is considered more data-driven with varying thresholds of the significance threshold at each analysis point. Thus, there is potential to adjust for and not adjust for type I error based on the fluctuating thresholds. The first and second IAs were not done; the reason for this was not stated in the Clinical Study Report for the CLIMB-111 study. The statistical analysis for IA3 recycled the alpha from the previous unused alpha spends but the appropriateness of this in terms of a planned approach to accounting for multiplicity is questionable and would not necessarily result in a sufficiently conservative threshold. Furthermore, a response rate of 50% was used as the null threshold for the primary testing hypothesis. The clinical relevance of this threshold was not reported in the submission. The EMA and FDA also were concerned with the choice of this threshold as adequate for defining response.29,73 The EMA and FDA used the change from baseline and CIs for the PES instead of the hypothesis test P value to determine treatment effects for their reviews. This response threshold was considered by the clinical experts consulted by CDA-AMC to be low. The clinical experts considered a response of at minimum 70% and more ideally 80% to be of clinical relevance considering the risks associated with myeloablative conditioning and experience with responses to HSCT. Because these statistical threshold points increase the risk of erroneously concluding treatment benefit when one does not exist, CDA-AMC reviewers focused on the point estimate and 95% CIs for the primary outcome, using a threshold of 80% as clinically important. Lastly, there are no adjustments for multiplicity in the secondary and exploratory outcomes, and this reduces the ability to draw firm conclusions on the results from these analyses.
There are also limitations from the study design that impact the interpretation of the results. As mentioned, the results submitted were for the PES, which is a subset of the enrolled patients and therefore is potentially a select population because it reflects only those patients who completed the exagamglogene autotemcel treatment process in the time since the study began. However, all patients in the enrolled population after screening should be considered important in evaluating the effect of assigning patients to exagamglogene autotemcel; analysis of outcomes should include the effects of the full treatment process including the manufacturing process, bridging therapies, and all possible consequences of these steps because all are necessary for the administration of exagamglogene autotemcel. Reporting the study results to date based only on the PES could bias the effect estimate against a null hypothesis, favouring the intervention. It is acknowledged that while that the PES is a relevant analysis population and represents patients who actually received exagamglogene autotemcel, it is difficult to judge the robustness of the observed treatment effect without being able to compare results between the PES and FAS populations.
There are also limitations regarding outcome ascertainment. While the laboratory-based outcomes are likely at low risk of bias due to being measured at a central laboratory, the PROs are subjective measures and the single-arm, open-label nature of the study may bias the reporting of these results. There is also little detail regarding the 6-month and 12-month window used to ascertain the TI primary and key secondary outcomes; specifically, no rationale is provided for the flexibility of the potential start and finish of the 1-year period within the 2 years of follow-up. The use of a flexible outcome window increases the risk of overestimating the true effect. Of note, the sponsor provided details on the time to the last transfusion for patients who attained the TI12 outcome, and also provided details on the changes in transfusions for the 3 patients who did not attain the outcome. However, no information is provided on how long after exagamglogene autotemcel infusion the TI monitoring period started for patients who reached TI6 or TI12, on average. Furthermore, the analysis noted that the efficacy analyses were based on patients’ available data before death or loss to follow-up. As the carrying forward of results was not described as a preplanned analysis, no sensitivity analyses were done testing the rigour of this method, and as the submission did not describe whether any patient results were carried forward, there is a risk of additional uncertainty in the results. With regards to the duration of TI reported for those patients with TI12 (a secondary outcome), patients were required to maintain a weighted average hemoglobin of 9 g/dL or greater; however, no rationale was provided for choosing a weighted average and there is a possibility that absolute hemoglobin values less than this would erroneously contribute to the proportion of TI responders. The EMA reported requesting a sensitivity analysis requiring all hemoglobin measurements to remain at 9 g/dL or higher and that this showed the weighted average approach did not impact the number of responders.29 Lastly, the lack of CIs with wide SDs around the point estimates for the HRQoL measures suggests imprecision in the estimates of the effect and indicate there is a chance of overinterpreting the estimate.
External Validity
Per the clinical experts consulted by CDA-AMC, most of the inclusion and exclusion criteria were similar to those applied in patients with HSCT, and the baseline characteristics broadly represented patients they would treat in their practice. The administration of exagamglogene autotemcel and busulfan myeloablative conditioning chemotherapy in the CLIMB-111 study was in line with the Health Canada–recommended dosages in this indication and with what is expected to be used in the reimbursement population. They noted that the procedure requires collecting “a lot” of stem cells; therefore, the ability of patients to meet this target outside of a trial setting is a consideration. The transfusion criteria used in the inclusion criteria were an internationally accepted cut-off for severe transfusion dependence; the study results are therefore only generalizable to patients with this degree of transfusion dependence. The primary outcome of TI is consistent with the treatment goals of TDT in clinical practice according to the clinical experts and is aligned with expectations from patients for new therapies. Among the secondary outcome measures, the clinical relevance of the TI6 outcome is somewhat uncertain, especially whether it represents TI12 and longer-term outcomes. However, the clinical experts noted that from a patient perspective, 6 months of TI may be important. The HRQoL measurements were considered appropriate by the clinical experts, although they are not used routinely in practice.
There are some important limitations around the generalizability of the results to note. In general, the clinical experts felt the age range was narrow despite there being no biological mechanism to preclude patients aged older than 35 years. They felt strongly that there should not be an upper age limit, but rather the suitability of patients for the therapy should be determined on a case-by-case basis as is done for HSCT. Overall, given the age cut-off, the results are not necessarily generalizable outside of these age ranges. In addition, the exclusion criteria for any comorbidity which may impact outcomes or suitability for therapy does not specify comorbidities, and the available evidence was insufficient to assess with certainty whether patients in the CLIMB-111 study were on optimal SOC before initiating exagamglogene autotemcel. This may reduce the generalizability of these study results to all patients with TDT who may be considered for exagamglogene autotemcel therapy. This is particularly important given the clinical experts consulted by CDA-AMC said they would likely prioritize patients who were not doing as well on SOC, and such patients may have comorbid conditions or be poorly optimized on SOC. In addition, the exclusion criteria for alpha thalassemia, multiple alpha deletions, and sickle cell thalassemia mean that results of the study do not apply to situations of co-inheritance of multiple types of thalassemia. Furthermore, the frequency of follow-up visits and laboratory measures undertaken in the trial may not reflect those in clinical practice, and therefore the results may not be wholly extrapolable to clinical settings. In addition, the relatively short follow-up duration of patients in the trial is a concern for both efficacy and safety assessments, especially in the context of a single-dose drug indicated for the treatment of a lifelong disease. The mean follow-up after exagamglogene autotemcel infusion of 19 months (SD = 7) was not sufficient so far to inform the issues of potential waning of effect over time, as well as longer-term toxicities such as the potential occurrence of malignancies. The clinical experts noted that while SOC is generally similar across higher SES countries, the CLIMB-111 study did not take place in any lower SES countries where thalassemias are endemic, and patient outcomes in these settings or the clinical status of patients who have recently immigrated to Canada from these countries may be different than those observed in the trial. Lastly, the clinical importance of the HRQoL measures is uncertain given that no MIDs were available for patients with TDT.
Certainty of the Evidence
Methods for Assessing the Certainty of the Evidence
For pivotal studies and RCTs identified in the sponsor’s systematic review, GRADE was used to assess the certainty of the evidence for outcomes considered most relevant to inform the expert committee’s deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group.30,31
High certainty: We are very confident that the true effect lies close to that of the estimate of the effect.
Moderate certainty: We are moderately confident in the effect estimate — the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. We use the word “likely” for evidence of moderate certainty (e.g., “X intervention likely results in Y outcome”).
Low certainty: Our confidence in the effect estimate is limited — the true effect may be substantially different from the estimate of the effect. We use the word “may” for evidence of low certainty (e.g., “X intervention may result in Y outcome”).
Very low certainty: We have very little confidence in the effect estimate — the true effect is likely to be substantially different from the estimate of effect. We describe evidence of very low certainty as “very uncertain.”
Although GRADE guidance is not available for noncomparative studies, the CDA-AMC review team assessed pivotal single-arm trials for study limitations (which refers to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias to present these important considerations. Because the lack of a comparator arm does not allow for a conclusion to be drawn on the effect of the intervention versus any comparator, the certainty of evidence for single-arm trials started at very low certainty with no opportunity for rating up.
When possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect; if this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., the clinical importance is unclear). In all cases, the target of the certainty of evidence assessment was based on the point estimate and where it was located relative to the threshold for a clinically important effect (when a threshold was available) or to the null.
Results of GRADE Assessments
Table 2 presents the GRADE summary of findings for exagamglogene autotemcel.
LTE Studies
Contents within this section have been informed by materials submitted by the sponsor. The following have been summarized and validated by the CDA-AMC review team.
Description of Studies
The sponsor submitted 1 LTE study for this review. The CLIMB-131 study is an ongoing, multisite, open-label, rollover study designed to evaluate the long-term safety and efficacy of exagamglogene autotemcel in patients who completed or discontinued the CLIMB-111 study. The study duration is for a total follow-up of 13 additional years.
This section summarizes efficacy and safety data for the CLIMB-131 study as of the data cut-off date (April 16, 2023).
Populations
All patients who completed or discontinued the parent study after exagamglogene autotemcel infusion and signed and dated the informed consent form were invited to participate in the CLIMB-131 study, with no exclusion criteria.
Interventions
Patients did not receive any study drug in the CLIMB-131 study. All medication taken from the signing of the consent form for the CLIMB-131 study through the data cut-off date were recorded.
Outcomes
The primary end points for the CLIMB-131 study included the following safety outcomes:
new malignancies
new or worsening hematologic disorders (e.g., immune-mediated cytopenias, aplastic anemia, primary immunodeficiencies)
all-cause mortality
all SAEs occurring up to 5 years after exagamglogene autotemcel infusion
exagamglogene autotemcel-related AEs and SAEs.
The secondary end points summarized for the CLIMB-131 study included the following efficacy outcomes:
proportion of patients achieving TI12 from 60 days after last RBC transfusion up to 15 years post-exagamglogene autotemcel infusion
proportion of patients achieving TI6 from 60 days after last RBC transfusion up to 15 years post-exagamglogene autotemcel infusion
relative change from baseline in transfusions starting 60 days after exagamglogene autotemcel infusion up to 15 years post-exagamglogene autotemcel infusion
proportion of alleles with intended genetic modification present in peripheral blood over time up to 15 years post-exagamglogene autotemcel infusion
total hemoglobin concentration over time up to 15 years post-exagamglogene autotemcel infusion
hemoglobin F concentration over time up to 15 years post-exagamglogene autotemcel infusion
change in PROs over time from screening for up to 5 years after exagamglogene autotemcel infusion (i.e., EQ-5D-5L and EQ-5D-Y, FACT-BMT, and PedsQL).
Statistical Analysis
Sample size was determined by the total number of patients who were enrolled in the CLIMB-131 study after infusion with exagamglogene autotemcel in the CLIMB-111 study.
Analysis sets for patients with TDT in the CLIMB-131 study were the same as for the CLIMB-111 study, and included the enrolled set, safety analysis set, FAS, and PES. Safety end points were analyzed based on respective safety analysis set, and efficacy end points were analyzed based on respective FAS unless otherwise specified.
All data from the extension studies were analyzed descriptively using summary statistics. Continuous variables were summarized using the following descriptive number of patients (n), mean, SD, median, minimum, and maximum values. For certain continuous variables, such as hemoglobin and hemoglobin F, additional summary statistics including the first and third quartiles were presented. Categorical variables were summarized using counts and percentages. Baseline value, unless specified otherwise, was defined as the baseline in the CLIMB-111 study.
Missing data were not imputed, and all data were evaluated as observed. Patients who discontinued the study were listed with the reasons for withdrawal.
The submission noted that starting after the M24 visit, only AEs related or possibly related to exagamglogene autotemcel, SAEs, new malignancies, and new or worsening hematologic disorders were recorded. Starting after the month 60 visit, only AEs and SAEs related or possibly related to exagamglogene autotemcel, new malignancies, and new or worsening hematologic disorders were to be recorded.
Results
Patient Disposition
As of the data cut-off date (April 16, 2023), 54 patients had received exagamglogene autotemcel infusion and were included in the FAS. Forty-two subjects were included in the PES. A total of 23 patients had completed the 2-year follow-up after exagamglogene autotemcel in the CLIMB-111 study and rolled over into the CLIMB-131 study. To date, no patient had discontinued from the CLIMB-131 study.
Concomitant Medications and Co-Interventions
For patients whose first visit in the CLIMB-131 study did not correspond with their last visit in the parent study, concomitant medications and therapies received after the last visit in the parent study but before the first visit in the CLIMB-131 study were captured as of the data cut-off of January 16, 2023.
Of the 14 patients who rolled over to the CLIMB-131 study from the CLIMB-111 study, ██████ ███████ patients used concomitant medications that were either ongoing at the end of the CLIMB-111 study, received after the last study visit in the CLIMB-111 study, or newly started during the CLIMB-131 study. The most common concomitant medications overall (used by ≥ 2 patients) were ██████████████ ██ ██████████ ███████ █ ███ █████████ █████████ ██ ██████████ ███ ███████████████████████ ██ █████████
Subsequent Treatment
All patients in the CLIMB-131 study received exagamglogene autotemcel infusion in a parent study; as such, no subsequent interventions were administered as part of the CLIMB-131 study.
Efficacy
Updated efficacy data are presented based on the data cut-off date of April 16, 2023 (Table 16).
Hemoglobin Outcomes
Total Hemoglobin and Hemoglobin F
At 36 months post-exagamglogene autotemcel infusion, the observed mean concentration of hemoglobin F was ████ █████ g/dL and ████ █████ █ ██ █████ ██ ██ █ ██. At 48 months post-exagamglogene autotemcel infusion, the observed mean concentration of hemoglobin F was ████ ████ g/dL and ████ ████ █ ██ █████ ██ ██ █ ██.
Proportion of Alleles With the Intended Genetic Modification in the CD34+ Cells of the Bone Marrow
At 36 months post-exagamglogene autotemcel infusion, the observed mean proportion of CD34+ cells with the intended genetic modification was █████ ████ █ ██ █ ██. At 48 months post-exagamglogene autotemcel infusion, the observed mean proportion was █████ █████ ██ █ ██
Proportion of Alleles With the Intended Genetic Modification in the Peripheral Blood
At 36 months post-exagamglogene autotemcel infusion, the observed mean proportion of CD34+ cells with the intended genetic modification was █████ ████████ ██ █ ██. At 48 months post-exagamglogene autotemcel infusion, the observed mean proportion was █████ █████ ██ █ ██.
Health-Related Quality of Life
HRQoL assessments conducted for patients with TDT included EQ-5D-5L or EQ-5D-Y, FACT-BMT, and PedsQL. Due to a paucity of long-term PRO data collected as of the January 12, 2023, data cut-off, PRO data for the CLIMB-131 study is not reported herein.
Transfusion Independence
All patients who achieved TI12 continued to remain transfusion independent in the CLIMB-111 study. These benefits were sustained through the CLIMB-131 study. The mean duration of TI to date was 23.6 months (SD = 7.8) with a range of 13.5 months to 48.1 months, starting 60 days after the last RBC transfusion for posttransplant support or TDT disease management.
Harms
As of April 16, 2023, a total of 23 patients with TDT were rolled over in the CLIMB-131 study after completion of the M24 visit. The overall duration of follow-up (including follow-up in the CLIMB-131 study) for these patients ranged from 25.2 months to 51.1 months after exagamglogene autotemcel infusion.
No deaths have occurred during the CLIMB-131 study. ███ ███████ ████ ███ ███ ██ ███ ██ █████████ ██ █████ ███ █████ █████ ███ ████████ ██████ █ ████.
No new safety findings were observed for 23 patients enrolled in the CLIMB-131 study including no evidence of new malignancies or new or worsening hematologic disorders long-term after exagamglogene autotemcel infusion.
Critical Appraisal
Internal Validity
The CLIMB-131 study was an open-label extension designed to evaluate the long-term efficacy and safety of exagamglogene autotemcel in treating patients with TDT. However, the same study design, study population, and outcome ascertainment limitations noted in the critical appraisal for the CLIMB-111 study also apply to the LTE. In addition, the available data for the CLIMB-131 study is limited to a greater extent due to the fact that it is an IA which only a fraction of patients have completed at the time of the submission, which hampers the ability to draw definitive long-term conclusions until the follow-up is complete.
External Validity
The same limitations regarding external validity of the LTE (including the age and comorbidity exclusion criteria) which were identified in the CLIMB-111 study also apply to the LTE. Additionally, the study did not report HRQoL results for the CLIMB-131 study period as of the data cut-off date; therefore, long-term data on HRQoL is lacking. Another important limitation is the fact that no harms were reported after M24 unless they were judged related to the study drug, which is an important limitation as relation to the study drug can be a subjective measure, and therefore complete harms reporting in the LTE is lacking.
Indirect Evidence
Contents within this section have been informed by materials submitted by the sponsor. The following have been summarized and validated by the CDA-AMC review team.
Objectives for the Summary of Indirect Evidence
A review of the indirect evidence was required as the pivotal trial, CLIMB-111, is a single-arm trial and did not include any comparative arm; therefore, comparisons between exagamglogene autotemcel and placebo or relevant comparators were not done that would inform the comparative effectiveness assessment. An appraisal of the indirect evidence was also necessary as the data from the indirect comparison were used to inform the pharmacoeconomic model.
Description of Indirect Comparison(s)
The submission included a MAIC to assess the relative safety and efficacy of exagamglogene autotemcel and luspatercept as well as SOC, which is defined as RBC transfusions and ICT. These comparators were identified by the submission as relevant to the Canadian context.
Indirect Treatment Comparison Design
Objectives
The objective of the indirect comparisons was to provide comparative efficacy data for exagamglogene autotemcel versus appropriate comparators (luspatercept and SOC).
Study Selection Methods
An SLR was conducted on May 10, 2022, with a search strategy based on a combination of free text words, indexing terms (e.g., Excerpta Medica database [Embase] subject heading [EMTREE] or MESH [Medical Subject Headings] terms) and their relationship using Boolean terms (e.g., “and,” “or,” or “not”). The SLR was conducted including potential comparators available around the world, and then articles were rescreened for inclusion on the basis of whether they included the 2 comparators relevant to the Canadian clinical context (i.e., luspatercept and ICT). Full details of the search; population, intervention, comparators, and outcomes (PICO) criteria; screening; data extraction; and quality assessment are included in Table 19. Of note, the submission did not include details on the dosing of comparators.
Table 19: Study Selection Criteria and Methods for MAICs Included in the Submission
Characteristics | Indirect comparison |
|---|---|
Population | Patients with TDT |
Intervention | Exagamglogene autotemcel (CTX001) |
Comparator | Comparators re-evaluated for inclusion in the Canadian ITC:
|
Outcome | Primary outcome:
Secondary outcomes (not included in submission):
|
Study designs | RCTs and single-arm studies |
Publication characteristics | English language studies only |
Exclusion criteria | Studies were excluded from the SLR if:
Studies were excluded from the ITC feasibility assessment if:
|
Databases searched | Databases searched using the OvidSP platform:
Conference websites searched (the most recent 2 years only as abstracts from prior meetings are indexed in Embase):
|
Selection process | Step 1: Title and abstract review
Step 2: Full-text review
|
Data extraction process |
|
Quality assessment | The quality of included RCTs was assessed using the NICE quality appraisal checklist74 and the quality of single-arm trials were assessed using the Down and Black checklist.75 |
aGvHD = acute graft versus host disease; cGvHD = chronic graft versus host disease; EFS = event-free survival; ICT = iron chelation therapy; ITC = indirect treatment comparison; MAIC = matching-adjusted indirect comparison; NICE = National Institute for Health and Care Excellence; OS = overall survival; PICOTS = Population, Intervention, Comparators, Outcomes, Timing, and Study design; RBC = red blood cell; RCT = randomized controlled trial; SLR = systematic literature review; SOC = standard of care; TDT = transfusion-dependent beta thalassemia; TI = transfusion independence; TRM = transplant-related mortality.
Source: Details included in the table are from the sponsor’s Summary of Clinical Evidence.52
MAIC Analysis Methods
Feasibility Assessment
Studies which met the inclusion criteria after full-text review were prioritized based on their potential relevance of conducting an indirect comparison with exagamglogene autotemcel data from the CLIMB-111 trial (January 16, 2023, data cut-off). Of note, the submission did not provide a comprehensive list for prioritization criteria. To be considered in the indirect comparison, studies were required to have an age range that overlapped with the age range of the CLIMB-111 study (i.e., mean or median age between 12 years and 35 years, inclusive), report on TI (the primary outcome of the CLIMB-111 study), have administered a Health Canada–approved dose, and include 5 or more treated patients. The submission noted that studies in which data on the study population characteristics and/or outcomes were not available were not eligible for the indirect comparison assessment.
The feasibility of conducting an indirect comparison against the comparators of interest was considered separately for each comparator. The information from the SLR, feasibility assessment, and a review of prior HTA submissions was used to inform recommendations for conducting an indirect comparison using a given comparator.
Statistical Analysis Methods
The submission justified the selection of a MAIC by noting that individual patient data for the CLIMB-111 study could be leveraged to correct cross-trial imbalances in patient characteristics. Furthermore, the lack of comparator arm would make a network meta-analysis, anchored MAIC, or Bucher comparison infeasible. Unanchored MAICs were therefore used to assess outcomes.
To identify relevant effect measure modifiers and prognostic factors, the eligibility criteria of the CLIMB-111 study, and comparator studies were first compared, and individuals within the CLIMB-111 study who would not have met any eligibility criteria in the comparator trial were removed. The submission noted that in situations where the comparator trial had a broader study population definition than the CLIMB-111 study, matching was not possible. Relevant baseline covariates identified as the key effect modifiers and/or prognostic factors were selected as adjustment variables; these variables were identified using a targeted literature review and clinical expert consultation (N = 7 clinical experts). Variables were ranked in order of importance and were confirmed by clinical consensus. In the order of importance, the adjustment variables were as follows:
genotype (proportions of patients with beta0/beta0 versus non-beta0/beta0 genotype)
baseline annualized units or volume (mL/kg) of transfusions
age
sex
race and/or ethnicity (white versus nonwhite [only categories used in source]).
No more than 3 variables were used for adjustment based on HTA expert input, starting with the variables ranked as most important and moving onto lower-ranking variables if a match was not possible. The submission did not provide a rationale for adjusting on 3 variables nor what topic the HTA expert input was solicited on.
Patients from the CLIMB-111 study were re-weighted according to the methodology proposed by Signorovitch et al.;37 the weighing methods used propensity score weights to align with the aggregate summary statistics reported for each comparator. The outcome assessed in the MAICs was the proportion of patients who were transfusion-free. For this outcome, a re-weighted proportion of patients who were transfusion-free was calculated for patients in the CLIMB-111 trial. Estimation was done using a generalized linear model with a logit link according to the calculated weights; the submission did not provide details on the assessment of model performance or the number of models run. Indirect comparison methods reported in the technical document provided by the sponsor are in Table 20.
Table 20: MAIC Analysis Methods
Methods | Description |
|---|---|
Analysis methods | Unanchored MAIC |
Priors | NA |
Assessment of model fit | NR |
Outcomes | Proportion of patients achieving TI |
Follow-up time points | Any 12-week interval during the 48-week study (BELIEVE; luspatercept and SOC) versus from 60 days after the last RBC transfusion to up to 2 years post-exagamglogene autotemcel infusion (CLIMB-111; exagamglogene autotemcel) |
Sensitivity analyses | None |
Subgroup analysis | None |
Methods for unanchored MAIC | Using the MAIC methodology proposed by Signorovitch et al.,37 individual patients from the CLIMB-111 trial were re-weighted using the propensity score weight to align with the matching variables’ aggregate summary statistics at baseline as reported for each comparator. For patients treated with exagamglogene autotemcel, descriptive statistics of the matching variables before and after matching were summarized alongside the aggregate summary statistics from the comparator trial. For the binary outcomes of TI3 and TI6, after applying the propensity score weight to each patient treated with exagamglogene autotemcel, a re-weighted percentage of patients achieving TI3 and TI6 was calculated. Standard errors were calculated using a robust sandwich estimator. For the indirect treatment comparisons of re-weighted exagamglogene autotemcel percentage versus comparator’s percentage as extracted from the literature, RRs were calculated, and P values (2-sided) and 95% CI were reported. For all comparisons, if the ESS was < 5 for the exagamglogene autotemcel group after re-weighting, no formal comparisons were made. If the proportion of TI3 and TI6 was 100% or 0% for either exagamglogene autotemcel trial or comparator trial data, no formal statistical comparison was conducted, and 95% CI and P values were not presented for the RR. In addition, a 95% CI was not presented for a value of 100% in the re-weighted analysis. The threshold for statistical significance of a (nominal) P value < 0.05 was used to reject the null hypothesis that there was no difference between the outcomes being compared between exagamglogene autotemcel and comparator’s data. No multiplicity adjustment was applied. |
CI = confidence interval; ESS = effective sample size; MAIC = matching-adjusted indirect comparison; NA = not applicable; NR = not reported; RBC = red blood cell; RR = rate ratio; SOC = standard of care; TI = transfusion independence; TI3 = transfusion independence for 3 consecutive months; TI6 = transfusion independence for 6 consecutive months.
Source: Details included in the table are from the sponsor’s Summary of Clinical Evidence.76
Results
Summary of Included Studies
The SLR identified a total of 2,833 publications, 2,252 of which were screened after de-duplication. A total of 299 texts were retained for full-text screening, and 157 of these were included along with 12 additional records from supplemental conference proceeding searches and bibliography screening. Overall, 169 publications representing 98 unique studies were included in the SLR. Of these, after the feasibility assessment, 1 comparator study was prioritized for the indirect comparison, the BELIEVE trial comparing luspatercept to SOC.77 The submission noted that this study was prioritized based on relevance to the Canadian landscape and initial comparability of study outcomes and patient characteristics with the CLIMB-111 study.
The results of the quality assessment for the BELIEVE study reported that 2 domains were assessed as “no,” suggesting that the evidence was a low to moderate rating overall on the basis of the National Institute for Health and Care Excellence quality appraisal checklist. The submission did not include details on the results of the quality assessment for the CLIMB-111 study using the same checklist. A summary of the studies included in the MAIC is presented in Table 21.
Table 21: Summary of Trial Arms Included in the MAIC
Study | Study design | N or n | Interventions | Follow-up |
|---|---|---|---|---|
CLIMB-111 | Phase I, II, and III single-arm, open-label, multisite, single-dose study | N = 59 (enrolled); n = 35 in the PES (included in MAIC)a | Single infusion of exagamglogene autotemcel after cell mobilization, apheresis, and myeloablative conditioning | 24 months |
BELIEVEb | Phase III, placebo-controlled, double-blind, multisite RCT | N = 336; luspatercept and SOC (n = 224) and placebo and SOC (n = 112) | Luspatercept (1.00 mg/kg to 1.25 mg/kg) and SOC versus placebo and SOC | 48 weeks (double-blind period) |
MAIC = matching-adjusted indirect comparison; PES = primary efficacy set; RCT = randomized controlled trial; SOC = standard of care.
aData from the January 16, 2023, data cut-off were included in the MAIC.
bBoth arms of the BELIEVE trial were analyzed in separate MAICs.
Sources: Details included in the table are from the sponsor’s Summary of Clinical Evidence,52 BELIEVE trial publication,49 and the MAIC technical document.36
Details of the homogeneity assessment reported in the provided technical report are included in Table 22. Briefly, the report identified that there were qualitative differences between the 2 studies in several areas. In terms of study design, the CLIMB-111 study was a single-arm study and the BELIEVE study was placebo-controlled. In terms of trial inclusion criteria, the BELIEVE study enrolled patients aged 18 years and older while the CLIMB-111 study enrolled patients aged between 12 years and 35 years. Functional status was assessed using different scoring tools between the 2 studies and the CLIMB-111 study had the additional inclusion criteria that patients had to be eligible for autologous stem cell transplant. With regards to exclusion criteria, the exclusion criteria for the CLIMB-111 study required specific thresholds for white blood cell counts and platelet counts. With regards to the end point definition, in the BELIEVE trial, TI was not a primary outcome but was measured as an additional efficacy outcome over any 8-week or 12-week interval, whereas the primary and key secondary end point in the CLIMB-111 study was TI for 6 and 12 consecutive months, respectively, with monitoring between 60 days after the last RBC transfusion up to 2 years postinfusion.
Table 22: Assessment of Homogeneity Between CLIMB-111 and BELIEVE
Characteristics | CLIMB-111 | BELIEVE |
|---|---|---|
Disease severity | Not specified | Not specified |
Treatment history | SOC previously; specific thresholds for transfusions in the time before enrolment required | SOC previously; specific thresholds for transfusions in the time before enrolment required |
Trial eligibility criteria | Key inclusion criteria:
Key exclusion criteria:
| Key inclusion criteria:
Key exclusion criteria:
|
Dosing of comparators | IV, single dose of ≥ 3 × 106 modified CD34+ cells/kg |
|
Placebo response | Not applicable; single-arm study | Not reported in submission |
Definitions of end points | Transfusion-free for 6 or 12 consecutive months | Transfusion-free for 12 consecutive weeks |
Timing of end point evaluation | From 60 days after the last RBC transfusion to up to 2 years post-exagamglogene autotemcel infusion | From baseline to weeks 13 through 24 |
Withdrawal frequency | Not reported | 42 discontinued luspatercept; 24 discontinued placebo |
Clinical trial setting | Not reported | Not reported |
DLCO = diffusing capacity of the lungs for carbon monoxide; G-CSF = granulocyte colony-stimulating factor; HLA = human leukocyte antigen; HSCT = hematopoietic stem cell transplant; ICT = iron chelation therapy; LVEF = left ventricular ejection fraction; RBC = red blood cell; q.3.w. = every 3 weeks; SC = subcutaneous; SOC = standard of care; WBC = white blood cell.
Sources: Details included in the table are from the sponsor’s Summary of Clinical Evidence,52 the BELIEVE trial publication,49 and the sponsor’s matching-adjusted indirect comparison technical document.36
Results
Exagamglogene Autotemcel Versus SOC
The feasibility assessment noted some differences between the CLIMB-111 study and the SOC arm of the BELIEVE study in terms of the baseline characteristics to be matched on. More patients in the SOC arm of the BELIEVE trial were genotype beta0/beta0 compared to patients receiving exagamglogene autotemcel; only median age was reported in the BELIEVE trial, and patients in the SOC arm of the BELIEVE trial had a median age of 30 years versus 20 years in the CLIMB-111 study. The individual patient data from the CLIMB-111 study were statistically adjusted to match the aggregate population characteristics of the BELIEVE study using genotype, baseline units of RBC transfusions, and age; sex and race were not used in matching and the submission did not provide a rationale for this; however, imbalances were also noted in these 2 variables before matching. The BELIEVE publication reported the number of RBC unit transfusions in 24 weeks; for adjustment purposes, this was extrapolated to the annualized number of RBC units transfused. Because the BELIEVE study reported median rather than mean age, to match on age, a new intermediate categorical variable was created as patients aged the median age or older versus patients aged less than the median age in the BELIEVE trial. The ESS after matching in the CLIMB-111 study was 16 patients. Details of the baseline characteristics used in matching, prematching, and postmatching are in Table 23. The submission did not include details on baseline characteristics which were not used in matching.
Results of the MAIC are presented in Table 24. Briefly, RRs were not reported, and 0% of patients in the SOC arm of the BELIEVE study had TI. The results showed a large numeric difference in the proportion of patients with TI6 in the CLIMB-111 study (proportion = 90.0; 95% CI, 64.7 to 97.8]) relative to SOC (proportion = 0; 95% CI, not reported).
Table 23: Baseline Characteristics of CLIMB-111 and BELIEVE SOC Prematching and Postmatching
Variable | CLIMB-111 prematching N = 35 | CLIMB-111 postmatching ESS = 16 | BELIEVE SOC arm N = 112 |
|---|---|---|---|
Genotype, n (%) | |||
Beta0/beta0 | 10 (28.6) | 31.3% | 35 (31.3) |
Other | 25 (71.4) | 68.7% | 77 (68.7) |
Baseline unit of RBC transfusion in 24 weeksa | |||
Mean (SD) | 17.1 (5.1) | 16.8 (5.1) | NR |
Median | 16.1 | 14.9 | 15 |
Range | 9.4 to 32.7 | 9.4 to 32.7 | 6 to 26 |
≥ 15, n (%) | 23 (65.7) | 50.0% | NR |
< 15, n (%) | 12 (34.3) | 50.0% | NR |
Age (years) | |||
Mean (SD) | 21.1 (6.1) | 25.3 (5.6) | NR |
Median | 20.0 | 29.0 | 30 |
Range | 12 to 33 | 12 to 33 | 18 to 59 |
≥ 30, n (%) | 5 (14.3) | 50.0% | 50.0% |
< 30, n (%) | 30 (85.7) | 50.0% | 50.0% |
Sex, n (%) | |||
Female | 17 (48.6) | 59.7% | 63 (56.3) |
Male | 18 (51.4) | 40.3% | 49 (43.7) |
Race, n (%)b | |||
Nonwhite | 20 (57.1) | 50.9% | 52 (46.4) |
White | 15 (42.9) | 49.1% | 60 (53.6) |
ESS = effective sample size; max. = maximum; min. = minimum; NR = not reported; RBC = red blood cell; SD = standard deviation; SOC = standard of care.
aBaseline unit of RBC transfusion in 24 weeks was calculated for patients treated with exagamglogene autotemcel and reported for patients treated with SOC in the BELIEVE trial.
bThese were the race categories used in the source documents.
Source: Details included in the table are from the sponsor’s matching-adjusted indirect comparison technical document.36
Table 24: Key Results for CLIMB-111 (TI6) Versus BELIEVE SOC (TI3)
Detail | Unadjusted CLIMB-111 result N = 35 | Adjusted CLIMB-111 result ESS = 16 | BELIEVE SOC result N = 112 |
|---|---|---|---|
Number of patients with outcome | 32 | NR | 0 |
Proportion (95% CI) | 91.4 (76.9 to 98.2) | 90.0 (64.7 to 97.8) | 0.0 (NR to NR) |
Rate ratio (95% CI) | NR | NCa | NR |
P value | NR | NCa | NR |
CI = confidence interval; ESS = effective sample size; NC = not calculated; NR = not reported; SOC = standard of care; TI3 = transfusion independence for 3 consecutive months; TI6 = transfusion independence for 6 consecutive months.
aNo statistical testing was conducted as 0 patients in the SOC arm of the BELIEVE study attained the outcome of interest.
Source: Details included in the table are from the sponsor’s matching-adjusted indirect comparison technical document.36
Exagamglogene Autotemcel Versus Luspatercept
The feasibility assessment noted some differences in the baseline characteristics used in matching. Before adjusting, more patients treated with luspatercept were genotype beta0/beta0 compared to patients receiving exagamglogene autotemcel. Only median age was reported in the BELIEVE trial, and patients treated with luspatercept had a median age of 30 years versus 20 years in the CLIMB-111 study. Adjustment was performed on genotype, baseline units of RBC transfusions, and age. Neither sex nor race were used for adjustment; however, imbalances were noted between the CLIMB-111 study and the BELIEVE luspatercept arm both before and after matching in these characteristics. Similar to weighting for the BELIEVE study’s SOC arm, because the BELIEVE study reported median rather than mean age and to statistically match on age, a new intermediate categorical variable was created for patients aged the median age or older versus patients aged less than the median age in the BELIEVE trial. Matching resulted in an ESS of 12 patients in the CLIMB-111 study. Details of the baseline characteristics used in matching, prematching, and postmatching are in Table 25.
Results of the MAIC are presented in Table 26. Briefly, 4.0% patients in the luspatercept arm of the BELIEVE study had TI3, and 93.2% of patients in the adjusted CLIMB-111 arm had TI6. The RR for the proportion of patients with TI was 23.3 (95% CI, 12.2 to 44.7).
Harms
Safety outcomes were not analyzed in the MAICs provided by the submission.
Table 25: Baseline Characteristics of CLIMB-111 and BELIEVE Luspatercept Arm Prematching and Postmatching
Variable | CLIMB-111 prematching N = 35 | CLIMB-111 postmatching ESS = 12 | BELIEVE luspatercept arm N = 224 |
|---|---|---|---|
Genotype, n (%) | |||
Beta0/beta0 | 10 (28.6) | 30.4% | 68 (30.4) |
Other | 25 (71.4) | 69.6% | 156 (69.6) |
Baseline unit of RBC transfusion in 24 weeks | |||
Mean (SD) | 17.1 (5.1) | 15.1 (4.5) | NR |
Median | 16.1 | 14.0 | 14 |
Range | 9.4 to 32.7 | 9.4 to 32.7 | 6 to 24 |
≥ 14, n (%) | 23 (65.7) | 50.0% | NR |
< 14, n (%) | 12 (34.3) | 50.0% | NR |
Age (years) | |||
Mean (SD) | 21.1 (6.1) | 25.7 (5.1) | NR |
Median | 20.0 | 29.0 | 30 |
Range | 12 to 33 | 12 to 33 | 18 to 66 |
≥ 30, n (%) | 5 (14.3) | 50.0% | NR |
< 30, n (%) | 30 (85.7) | 50.0% | NR |
Sex, n (%) | |||
Female | 17 (48.6) | 64.5% | 132 (58.9) |
Male | 18 (51.4) | 35.5% | 92 (41.1) |
Race, n (%)a | |||
Nonwhite | 20 (57.1) | 61.9% | 102 (45.5) |
White | 15 (42.9) | 38.1% | 122 (54.5) |
ESS = effective sample size; max. = maximum; min. = minimum; NR = not reported; RBC = red blood cell; SD = standard deviation.
aThese groupings were the categories provided by the source documents.
Source: Details included in the table are from the sponsor’s matching-adjusted indirect comparison technical document.36
Table 26: Key Results for CLIMB-111 (TI6) Versus BELIEVE Luspatercept Arm (TI3)
Detail | Unadjusted CLIMB-111 result N = 35 | Adjusted CLIMB-111 result ESS = 16 | BELIEVE luspatercept result N = 112 |
|---|---|---|---|
Number of patients with outcome | 32 | NR | 9 |
Proportion (95% CI) | 91.4 (76.9 to 98.2) | 93.2 (71.8 to 98.7) | 4.0 (NR to NR) |
Rate ratio (95% CI) | NR | 23.3 (12.2 to 44.7) | NR |
P value | NR | < 0.0001 | NR |
CI = confidence interval; ESS = effective sample size; NR = not reported; TI3 = transfusion independence for 3 consecutive months; TI6 = transfusion independence for 6 consecutive months.
Source: Details included in the table are from the sponsor’s matching-adjusted indirect comparison technical document.36
Critical Appraisal
The SLR which informed the indirect treatment comparisons provided a PRISMA diagram as well as a comprehensive search strategy. Comparators chosen were reasonable and relevant to clinical practice according to the clinical experts consulted by CDA-AMC, considering that the majority of patients they treat in their clinical practice do not have a sibling-matched donor for HSCT. However, the experts noted that there may be circumstances where patients who were eligible for HSCT would not have received it by the time they reached the age of eligibility for the CLIMB-111 study (e.g., recent immigrants), and HSCT could be a comparator in those situations, although the experts acknowledged HSCT would likely still be considered before exagamglogene autotemcel.
The SLR is subject to some limitations. First, the SLR did not use a preregistered protocol, and so it is not known whether the search criteria, study selection, or subgroups of interest were prespecified before the search. In addition, the results of the quality assessment were not provided and therefore the risk of bias among the studies is not known. In addition, a list of secondary outcomes was searched in the SLR but not included in the MAIC, and studies were excluded if they did not report a transfusion-independent outcome. This is a possible source of bias as no rationale is provided for why these outcomes were excluded from the indirect evidence analysis despite being included in the SLR, and it is not known whether this exclusion criterion was added after searches had been run.
There are several important limitations in the MAIC analysis to note. The MAICs were unanchored, which requires the assumption that all possible treatment effect modifiers and prognostic factors are controlled for, which is an assumption largely considered impossible to achieve and therefore adds uncertainty to the results.38 The analysis solicited expert input to help provide a list of possible factors to include in the weighting, but limited weighting on 3 of them. A clear rationale for this was not given. Furthermore, the submission did not include details on the baseline characteristics that were not included in matching; therefore, it is unknown whether there are other sources of heterogeneity in the patient population. This is an important source of uncertainty in the results as the unanchored MAIC assumes that all effect measure modifiers and prognostic factors are accounted for. The unanchored comparison should ideally provide sufficient evidence on the likely extent of error due to unaccounted for covariates,38 which this analysis did not do. Cross-validation methods or other sensitivity analyses are also suggested methods to explore the impact of the lack of anchoring.38 However, these were not reported in the current submission. In addition, the homogeneity assessment identified several potentially important differences between the CLIMB-111 and BELIEVE studies which remain even after trimming patients from the CLIMB-111 study who would not match the BELIEVE study population. First, the 2 studies had a different study design (the BELIEVE study was a double-blind RCT while the CLIMB-111 study was a single-arm phase I, II, and III study) and weighting would not account for this difference. Second, different timing of outcome evaluation would not be controlled by weighting. The CLIMB-111 study was evaluated over a longer time frame than the BELIEVE study, with 2 years of follow-up, while the BELIEVE study lasted for 48 weeks. TI during any 8-week and 12-week interval was a secondary efficacy end point. This suggests that the study populations and the results as reported are likely not able to satisfy the comparability assumptions required for an unanchored MAIC. An additional limitation to the MAIC methodology is a small ESS after matching (ESS = 16 in the SOC MAIC and ESS = 12 in the luspatercept MAIC), which imparts instability to the results as the inferences from the MAIC depend on data from a small number of individual patients. In addition, there is no summary provided of the distribution of weights from the matching, so it is unknown whether there were extreme weights applied to any of the patient data in the CLIMB-111 study. Overall, these limitations impact a high degree of uncertainty in the results, and it is challenging to draw firm conclusions on the basis of the analysis.
There are additional limitations to the generalizability of the MAIC and the similarity of the comparator treatments which are important to note. First, the BELIEVE trial’s primary outcome was not TI, but a reduction of at least 33% in transfusion burden. TI, measured over any 8-week or 12-week period during the 48-week study, was an additional end point. The clinical expert panel highlighted that luspatercept does not generally lead to TI, and furthermore a minority of patients (approximately 20%) respond to it. It is not known whether the subgroup within the BELIEVE trial who reached TI differs from the main study population in meaningful ways, and it is therefore possible that the outcome being compared in the MAIC may not have been attainable by all patients randomized to luspatercept in the BELIEVE trial. Furthermore, patients randomized to the SOC arm of the BELIEVE study would, by definition, be unable to reach TI as transfusions are an integral part of the SOC for TDT. Therefore, the similarity of the 3 trial arms for an outcome of TI is questionable. Other generalizability limitations include that the BELIEVE study only randomized adults and luspatercept is not approved for pediatric populations; therefore, the comparative results cannot be generalized to pediatric patients. Furthermore, results were only available for 12 weeks of TI (TI3) in the BELIEVE study, no measures of precision (i.e., CIs) were reported, and only TI6 and TI12 results were reported for exagamglogene autotemcel. Lastly, the MAIC did not analyze harms outcomes; therefore, comparative data on the safety of treatments remain unknown. This is an important consideration given that the CLIMB-111 study also does not have a comparative arm, and so there is no comparison for the harms data in the pivotal trial. Overall, this suggests that the comparators used in the MAIC may not be wholly similar to one another and therefore makes it challenging to make meaningful conclusions about the comparative efficacy of luspatercept, SOC, and exagamglogene autotemcel for the outcomes that were measured in the indirect comparison.
Summary
The body of evidence submitted for the indirect comparison included an SLR, feasibility assessment, and indirect comparison consisting of 2 MAICs, each comparing exagamglogene autotemcel to either SOC or luspatercept. The comparator trial was the BELIEVE trial, a phase III, placebo-controlled, double-blind, multisite RCT with the primary outcome of a reduction of 33% or more in transfusion burden, among patients with TDT randomized either to SOC (transfusions and ICT) or luspatercept. TI for any 8-week or 12-week interval during the study was an additional efficacy outcome. Briefly, the sponsor reduced the CLIMB-111 study population to meet the inclusion criteria for the BELIEVE study, then carried out 2 unanchored MAICs, weighted on 3 effect measure modifiers, which analyzed the outcome of TI for luspatercept versus exagamglogene autotemcel and SOC versus exagamglogene autotemcel. Both MAICs noted a large numeric difference in the proportion of patients with TI6 in the exagamglogene autotemcel treatment arm, relative to the proportion of patients with TI3 in the luspatercept arm. The MAICs are subject to several notable limitations in their methodology, generalizability, and similarity of the comparator treatments. First, the MAICs were unanchored, which requires the assumption that all possible treatment effect modifiers and prognostic factors are controlled for, which is an assumption largely considered impossible to make and therefore adds uncertainty to the results.38 Furthermore, the submission did not include details on the baseline characteristics that were not included in matching; therefore, it is unknown whether there are other sources of heterogeneity in the patient population. This is an important source of uncertainty in the results as the unanchored MAIC assumes that all effect measure modifiers and prognostic factors are accounted for. The homogeneity assessment identified several potentially notable differences between the CLIMB-111 study and the BELIEVE study which remain even after reducing the number of patients in the CLIMB-111 study, including a different study design (the BELIEVE study was a double-blind RCT while the CLIMB-111 study was a single-arm phase I, II, and III study), different study duration, and different timing of outcome evaluation. These would not be controlled by reducing the study population or weighting. This suggests that the study populations and the results as reported are likely not able to satisfy the comparability assumptions required for an unanchored MAIC. There are additional limitations with regards to generalizability and the similarity of the comparators. The clinical expert panel highlighted that luspatercept does not generally lead to TI, and furthermore a minority of patients (approximately 20%) respond to it. It is therefore possible that the outcome being compared in the MAIC may not have been attainable by all patients randomized to luspatercept in the BELIEVE trial. Furthermore, patients randomized to the SOC arm of the BELIEVE study would, by definition, be unable to reach TI as transfusions are an integral part of the SOC for TDT. Therefore, the similarity of the 3 trial arms for an outcome of TI is questionable. Other generalizability limitations include that BELIEVE only randomized adults and luspatercept is not approved for pediatric populations; therefore, the comparative results cannot be generalized to pediatric patients. Furthermore, results were only available for 12 weeks of TI in the BELIEVE study, no measures of precision (i.e., CIs) were reported, and only TI6 and TI12 results were reported for exagamglogene autotemcel. Lastly, no harms were analyzed in the MAICs; therefore, comparative information on harms remains lacking.
Studies Addressing Gaps in the Systematic Review Evidence
There are no additional studies submitted by the sponsor addressing gaps in the systematic review evidence.
Discussion
Summary of Available Evidence
This report summarizes the evidence for exagamglogene autotemcel for the treatment of patients with TDT aged 12 years and older. The evidence appraisal was based on results from an ongoing phase I, II, and III, multisite, single-arm, single-dose trial (CLIMB-111), an LTE extension of the pivotal trial (CLIMB-131), and indirect treatment comparisons consisting of 2 MAICs comparing exagamglogene autotemcel to SOC and luspatercept, respectively.
The CLIMB-111 study was a phase I, II, and III multisite, single-arm, single-dose trial which enrolled a total of 59 patients aged 12 years to 35 years who had TDT. As of the April 16, 2023, data cut-off, 54 patients had received an infusion of exagamglogene autotemcel, and 42 patients were included in the PES. The primary outcome of the CLIMB-111 study was the proportion of patients achieving TI12, and the key secondary outcome was the proportion of patients achieving TI6. TI was defined as maintaining a weighted average hemoglobin of 9 g/dL or more without RBC transfusions. Secondary outcomes were the total hemoglobin concentration, total hemoglobin F, the proportion of alleles with the intended genetic modification in CD34+ cells of the bone marrow and peripheral blood, and changes from baseline in FACT-BMT, EQ-5D-5L, PedsQL, and EQ-5D-Y scores. Additional secondary outcomes were the duration of TI with a weighted average hemoglobin of 9 g/dL or greater, and the time until last RBC transfusion. At the time of the submission, a total of 23 patients had completed the 24-month follow-up and enrolled in the LTE. The 2 MAICS compared patients from the CLIMB-111 study with the BELIEVE trial, a phase III, placebo-controlled, double-blind, multisite RCT comparing luspatercept to SOC. TI6 and TI3 were the outcomes of interest for the MAICs. The clinical experts consulted by CDA-AMC noted that transfusion outcomes are important outcomes, and hemoglobin and hemoglobin F outcomes are highly correlated with transfusion outcomes as well. The proportion of alleles with the intended genetic modification, according to the clinical experts, reflects the magnitude of the genetic changes effected by the therapy and are also important outcomes. While the current SOC, when optimized, was noted by clinicians to provide life expectancy beyond the mean ages of death that have been previously reported in patients with TDT,19,20 both patient groups and clinicians noted the overall impact of TDT on HRQoL. The outcomes in the CLIMB-111 study include transfusion, hematologic, and HRQoL outcomes, and therefore address several outcomes of importance to patients and clinicians.
The baseline characteristics were generally representative of patients with TDT, except the age range was restricted to 12 years to 35 years and the study did not enrol any Black or African American, ████████ ██████ ██ ██████ ███████ ███ ██████ ████████ ██ ███████ ████████ patients. In addition, the study did not enrol any patients with the █████ █████ thalassemia genotypes. According to the clinical experts consulted by CDA-AMC, with the exception of the upper age cap at 35 years, most of the inclusion and exclusion criteria were similar to those as in patients with allogenic HSCT, and the baseline characteristics broadly represented patients they would treat in their practice.
Interpretation of Results
Efficacy
TDT is a rare disease, and although the clinical experts consulted by CDA-AMC noted that patients who are well-transfused and well-chelated can have a good clinical course and may expect almost a full life expectancy, if their care is not optimal, their lifespan can be impacted. In the past 15 years, the development of oral iron chelation drugs has helped improve SOC; however, there remains an unmet need among patients with TDT who are not well-controlled on current therapies or who may have accrued organ damage due to previous therapies. Patient groups highlighted that care coordination is only generally available in Canada’s major cities, and regular follow-up is essential for care. Therefore, there is also an additional unmet need among patients who may not live near a major city to transport themselves for transfusions and for their other TDT care, and a time commitment required among all patients receiving transfusion regardless of location. When asked about identifying candidates for therapy, the clinical expert panel noted that the patients they would prioritize would be those who are struggling on SOC for one reason or another, although they would also have to be considered physically able to undergo the therapy.
TI was the primary and key secondary outcome of the study, and the results, while limited by the study design, suggest that after exagamglogene autotemcel infusion, a high proportion of patients in the PES achieved TI6 and TI12. The proportion of patients with these outcomes was noted by the clinical experts to be clinically meaningful. In addition to the overall study limitations, the TI outcomes are also impacted by potential bias due to the flexibility around the start and end of the TI monitoring period; the study specified that the 6-month or 12-month period could start 60 days after the last RBC infusion and end 6 months (or 12 months) after monitoring began. However, there was no additional information provided on when the monitoring for TI began among patients, on average, or additional context to rule out the possibility that the choice of TI monitoring period could increase the likelihood of observing the outcome in a given patient. Furthermore, the use of a weighted hemoglobin of 9 g/dL or greater, as opposed to raw hemoglobin values, might erroneously contribute to the proportion of TI responders. In addition, the power calculations for these outcomes used a 50% response rate for the null, which was a response that the clinical experts considered to be low. Given the risks inherent to the myeloablative conditioning and the newness of the exagamglogene autotemcel therapy, the clinical experts noted that they would expect a response rate of at least 70% to 80%, closer to that of HSCT. It is important to note, however, that the results to date report that the majority of patients attained the TI12 outcome and using a response rate of 80% as a MID, the point estimates and CIs for TI6 and TI12 meet and surpass this bound over duration of follow-up of up to 2 years post infusion. Despite the potential that treatment with exagamglogene autotemcel has to result in a meaningful effect on a patient-important outcome over the short-term, the evidence is very uncertain about the effect of exagamglogene autotemcel on the proportion of patients achieving TI in the longer term, and the lack of comparative results remain an important limitation to the CLIMB-111 study.
The secondary outcomes pertaining to hematologic outcomes (total hemoglobin concentration, hemoglobin F, the proportion of alleles with the intended modification in the CD34+ cells, and peripheral blood), are all impacted by the overarching study limitations, but their interpretation is also limited by the fact that these results are not reported as changes from baseline, but total values at the time point of interest, and as such the evidence remains uncertain on the impact of exagamglogene autotemcel on these outcomes. It is acknowledged that these outcomes would be difficult to evaluate as changes from baseline because hemoglobin levels were already in normal ranges based on RBC transfusion status at enrolment, and adolescent and adult patients would naturally have very low concentrations of hemoglobin F. The clinical experts consulted by CDA-AMC identified the total hemoglobin levels and the increase in hemoglobin F as supportive of potential benefits from exagamglogene autotemcel. In particular, the elevated hemoglobin F levels were considered positive because of the potential to mitigate some of the complications of TDT. Similarly, the clinical experts identified the proportions of patients with edited alleles in the bone marrow and peripheral blood as a sign of a response to exagamglogene autotemcel treatment.
Patient group input identified the substantial impact that TDT has on patients’ daily living and the expectation that a new treatment such as exagamglogene autotemcel would improve their HRQoL. HRQoL measures were reported as changes from baseline but were only reported descriptively and without CIs. The clinical experts consulted by CDA-AMC noted that the HRQoL measures chosen were all relevant measures of patient outcomes and they agreed with using different tools in different age groups to fully capture HRQoL. However, the subjective reporting inherent to HRQoL measures could be biased by the open-label design of the study. The lack of comparator for these outcomes is particularly notable given that SOC for TDT, when optimized, can provide patients with life expectancy beyond the mean ages of death previously reported in patients with TDT,19,20 and life expectancy may tend to reach the higher percentiles of the general population.78 Of the MIDs available, the results as reported for FACT-BMT and PedsQL surpassed the MIDs provided in the submission, and for EQ VAS, the results as reported surpass the MID provided for adult patients as of 12 months post infusion. However, no TDT-specific MIDs were provided for any of the HRQoL measures and therefore no conclusions can be drawn whether the change is clinically meaningful in this patient population.
The overall interpretation of the efficacy results from the CLIMB-111 study was limited given the internal and external validity issues identified which potentially impact all study outcomes. The main limitation for the CLIMB-111 study was the single-arm, open-label design which precluded the ability to fully attribute the study results to treatment with exagamglogene autotemcel. Similarly, the results are limited by the potential limitations inherent to IA, which carries a risk of overestimating the true treatment effect. More specifically, results are only reported for the PES and not the FAS, which represents only patients who had completed 16 months of follow-up in the CLIMB-111 study to date, and which might be a select population because the PES reflected only those patients who completed the exagamglogene autotemcel treatment process in the time since the study began. Reporting all the study results to date based only on the PES could bias the effect estimate against a null hypothesis, favouring the intervention. Therefore, it is difficult to judge the robustness of the effect without being able to compare observed effects between the PES and FAS populations. These IA limitations were also potentially compounded by several changes to the study protocol which impact the analysis and which took place after study enrolment began, such as unspecified updates to the outcomes, the addition of the 3 IAs (2 of which were not undertaken), and the conversion of the trial to a phase I, II, and III trial. Furthermore, the EMA commented that these changes, particularly the alpha spending methods for the IAs, were undertaken for reasons which could have been data-driven because 1 patient with TDT had reached the primary end point at the time of the revisions and other patients had already been enrolled in the study. The EMA concluded that the overall impact of these changes was not expected to be large,29 but this limitation is important in the context of the other study limitations identified.
The exclusion criteria for the CLIMB-111 study prevented patients aged older than 35 years from participating in the trial, but the submission also noted that there is no plausible biologic mechanism to limit access to exagamglogene autotemcel if patients are older than 35 years, and no upper age limit is specified in the Health Canada–approved indication or in the CDA-AMC reimbursement request. This is an important limitation on the generalizability of the study results, and therefore the population in the trial may not represent all patients who could be considered for exagamglogene autotemcel. The clinical experts agreed with the lower bound of the age range for the time, but felt strongly that there should be no upper age range as patients who are older often have more issues with the typical SOC therapies, including difficulties with adequate iron chelation, and also are not candidates for allogenic HSCT. They noted that considering SOC is lifelong, a disease-modifying therapy such as exagamglogene autotemcel could have a meaningful impact on patients aged older than 35 years because their life expectancy may tend to reach the higher percentiles of the general population78 and a large number of transfusions could be averted. The clinical experts consulted noted that they would need to review data on the efficacy and safety of the treatments before considering them in patients younger than 12 years.
The body of evidence submitted for the LTE consisted of a rollover study to continue the long-term follow-up from the CLIMB-111 study, with no additional interventions or study drug administration anticipated. The results from the LTE to date were available for hemoglobin outcomes (total hemoglobin and hemoglobin F), as well as the proportion of alleles with the desired edit in the CD34+ cells of the bone marrow and the peripheral blood. At the time of the submission, results were only available for a fraction of patients and were not available for HRQoL measures. This is an important limitation for the LTE and makes the efficacy results too uncertain to draw conclusions about the impact of exagamglogene autotemcel after 24 months of follow-up.
Given the lack of a control group in the CLIMB-111 study, the sponsor provided indirect treatment comparisons consisting of 2 unanchored MAICs, each comparing exagamglogene autotemcel to either SOC or luspatercept. The comparator trial had a primary outcome of a reduction of 33% or more in transfusion burden, among patients with TDT randomized either to SOC (transfusions and ICT) or luspatercept. TI for any 8-week or 12-week interval during the study was an additional efficacy outcome. The difference in the outcomes in the BELIEVE and CLIMB-111 trials were a key limitation in the MAICs. In addition to outcome definition and measurement heterogeneity, the assumptions of similarity between the study populations and the inclusion of all relevant effect modifiers and prognostic factors were not fully met. The failure to meet these critical assumptions raises concerns about residual confounding and bias, which likely invalidate the findings. While the unanchored MAICs suggested differences in TI favouring exagamglogene autotemcel versus luspatercept and SOC transfusions, these likely do not accurately reflect the true comparative effectiveness of these treatments based on the aforementioned limitations and no concrete conclusion can be drawn about the comparative effectiveness of exagamglogene autotemcel.
Harms
During the CLIMB-111 study, 100% of patients had any AE during the time period from the day of exagamglogene autotemcel infusion to either the M24 visit or the EOS visit. The proportion of patients with SAEs was 44.1% during the time period starting from the day of exagamglogene autotemcel infusion to the M24 or EOS visit. There were no withdrawals reported after exagamglogene autotemcel infusion (3 withdrawals were reported before myeloablative conditioning), and no deaths had been reported in the study to date. The submission noted that the majority of AEs were related to the myeloablative conditioning, a process which was highlighted by the clinical experts as difficult to undertake for patients. They also noted that the apheresis procedure, which requires a large volume of blood cells be collected, can also be difficult for patients. Overall, the majority of AEs were reported during the time period starting from the day of exagamglogene autotemcel infusion to the M24 or EOS visit, reinforcing that long-term follow-up for harms would continue to be informative.
An additional consideration was the wide range in time to engraftment reported in the study. The clinical experts consulted by CDA-AMC noted that patients who do not achieve engraftment, or for whom time to engraftment is longer than expected are at increased risk of infections and bleeding events in the time period following myeloablative conditioning and exagamglogene autotemcel infusion. Though engraftment is an important milestone, it is unlikely a comprehensive measure of patient harms and overall treatment success. As such, engraftment does not inform on important AEs that could occur before or during the engraftment process and thus the frequency and severity of AEs such as infections (including febrile neutropenia), bleeding, veno-occlusive liver disease, and hemophagocytic lymphohistiocytosis that can occur before engraftment is achieved were also considered in the safety assessment. A total of 61.1% of patients experienced febrile neutropenia during the period from the day of exagamglogene autotemcel infusion to the M24 visit. Infections and infestations were reported by 64.8% of patients from the day of exagamglogene autotemcel infusion to the M24 visit; the most common infection was COVID-19, reported by 25.9% of patients. According to the EMA European public assessment reports, the AEs were consistent with those associated with HSCT;29 therefore, these were not expected to create a greater burden on patients or result in greater resource use to manage AEs for exagamglogene autotemcel compared with what is typical of HSCT.
The clinical experts consulted by CDA-AMC noted that fertility preservation is an important issue for many families, and they felt it should be offered as SOC for this treatment. The CLIMB-111 study included steps for patients to undertake fertility preservation, and the possibility of this harm remains an important consideration. The clinical experts noted that many patients with TDT require fertility aid when trying to conceive children, as the disease itself has an impact on fertility. This reinforces the importance of fertility preservation in this population and may impact considerations around the type of therapies offered as well as the potential necessity of coordinating fertility preservation with fertility treatments.
Per the clinical experts consulted by CDA-AMC, the concern with CRISPR/Cas9 editing, similarly to any gene therapy, is the development of off-target harms due to the editing process. In the long-term, the experts noted that such off-target edits could develop into malignancies, which was their primary concern. They noted that the target for TDT is an erythroid target only expressed by RBCs, but the impacts of this on off-target editing are largely unknown. Early monitoring for these type of harms would involve monitoring the bone marrow for changes using a smear, although the procedure is more invasive and might only be initiated if there were concerns or abnormalities on routine follow-up. A period of 15 years of follow-up is the current regulatory requirement and the experts noted that looking for off-target effects will be important during this time and will likely require follow-up by sophisticated gene analysis. The experts also noted that it was important that the risk of malignancy not be higher than HSCT. HSCT was considered an important reference point for harms as HSCT also has risks, but the level of risk is acceptable in the current clinical setting. They noted that high-dose chemotherapy on its own also has a risk of secondary malignancy and that off-target effects will be an ongoing risk to monitor for separately.
There are important evidence gaps in the safety assessment of exagamglogene autotemcel to date. The short follow-up duration was not sufficient to provide context on longer-term toxicities, particularly because the CLIMB-111 and CLIMB-131 studies remain ongoing. While a 15-year long-term follow-up is scheduled, the clinical experts consulted by CDA-AMC emphasized the importance of continued monitoring. The harms reporting in the LTE to date do not include any additional deaths, discontinuations from the study, new malignancies, or new or worsening hematologic disorders; however, results are only available for a fraction of patients at this time and may change over longer follow-up. Of note, the harms reporting for the CLIMB-131 study after the 24-month follow-up is proposed to only include those harms judged related to exagamglogene autotemcel. Whether this includes harms that can be attributed directly to the exagamglogene autotemcel infusion, or to the entire treatment process including myeloablative conditioning and apheresis, is not clear. Furthermore, harms were not analyzed in the indirect evidence comparison and therefore comparative results remain lacking for exagamglogene autotemcel in patients with TDT.
Other Considerations
There are additional resource considerations for exagamglogene autotemcel treatment. Exagamglogene autotemcel requires the use of ATCs and patients must be hospitalized for lengthy periods in specialized centres, most of which are likely to be located in major cities, which means that equitable access will be a concern between patients living in cities and those in remote areas, for whom transportation and lengthy absences may pose more of a burden. While referral pathways exist for patients with HSCT with TDT, the clinical experts noted that ATC resources are already stretched and adding exagamglogene autotemcel treatment to their services will require an increase in resources as well as a potential separate stream for patients so that they do not compete with patients with malignancy for transplant resources.
Conclusion
In the absence of direct comparative data, evidence from the IA of the CLIMB-111 study, a phase I, II, and III multisite, single-arm, single-dose trial in the PES of 42 patients aged 12 to 35 years with TDT is very uncertain about the effect of exagamglogene autotemcel on clinical efficacy and harms outcomes in patients with TDT when compared with any comparator. Findings from the trial are consistent with a clinically meaningful reduction in transfusion leading to TI, according to clinical expert input. While improvements in HRQoL scores from baseline were reported, it is uncertain if the changes are clinically meaningful due to the lack of estimated MIDs in TDT. The available results from the trial are subject to important potential biases in outcome ascertainment, study population, and statistical analysis plan changes which impact the certainty that the observed effect is truly attributable to the study drug. Results from the LTE portion were only available from a fraction of patients for all outcomes and therefore remain highly uncertain. In general, a relatively short time period after infusion is included in the submission. With regards to safety, most AEs and SAEs reported in the pivotal trial could be considered attributable to the myeloablative conditioning; however, the clinical experts noted that a longer time to engraftment was noted for patients after exagamglogene autotemcel infusion which may impart additional harms such as reduced engraftment potential, higher risks of infection and bleeding, and longer stays in hospital which would have resource use implications. The submission did not report details on off-target editing or fertility to date. Conclusions around long-term harms results are generally limited by the ongoing nature of the trial and the short follow-up to date. The indirect evidence submitted by the sponsor, consisting of 2 MAICs comparing exagamglogene autotemcel to SOC (transfusions and chelation) and luspatercept, respectively, were considerably limited by differences in the study design, outcome ascertainment, and concerns around the validity of the comparators in terms of their potential for attaining the outcome of TI. Therefore, information on the comparative nature of exagamglogene autotemcel to other treatment options remains lacking due to limitations with the indirect evidence as well as the use of a single-arm trial. Overall, the evidence is highly uncertain about the impact of exagamglogene autotemcel on clinical efficacy and harms when compared with any comparator.
However, the treatment landscape for TDT, a rare, severe disease in which optimized transfusion and ICT can provide life expectancy beyond the mean ages of death previously reported in patients with TDT, but which provides few treatment options that achieve TI, is also a consideration. The clinical experts noted that they would likely prioritize patients who are struggling on SOC for exagamglogene autotemcel therapy, and HSCT would remain a first-line consideration for patients who were eligible for it and have a matched donor. The potential resource and personal impact of averting transfusions in patients who have lifelong requirements was also highlighted, although additional resources will also be required for offering exagamglogene autotemcel and ensuring equity in access, particularly to transplant centres. However, clinicians also emphasized that patient preference and the weighting of risks versus benefits would be of great importance in identifying candidates for therapy.
References
1.Consensus Statement of Clinical Care of Patients with Thalassemia in Canada: 2. Transfusion support in thalassemia. The Canadian Hemoglobinopathy Association; 2024: https://canhaem.org/wp-content/uploads/2024/09/Transfusion-Support-in-Thalassemia.pdf Accessed 2024 Aug 6.
2.Interim Clinical Study Report: A Phase 1/2/3 Study of the Safety and Efficacy of a Single Dose of Autologous CRISPR-Cas9 Modified CD34+ Human Hematopoietic Stem and Progenitor Cells (hHSPCs) in Subjects With Transfusion dependent β-Thalassemia [sponsor supplied reference]. Toronto (ON): Vertex Pharmaceuticals, Inc.; 2023.
3.Rachmilewitz EA, Giardina PJ. How I treat thalassemia. Blood. 2011;118(13):3479-3488. PubMed
4.Michiels C. Physiological and pathological responses to hypoxia. Am J Pathol. 2004;164(6):1875-1882. PubMed
5.Arian M, Mirmohammadkhani M, Ghorbani R, Soleimani M. Health-related quality of life (HRQoL) in beta-thalassemia major (beta-TM) patients assessed by 36-item short form health survey (SF-36): a meta-analysis. Qual Life Res. 2019;28(2):321-334. PubMed
6.Knoth RL, Gupta S, Perkowski K, et al. Understanding the Association between Red Blood Cell Transfusion Utilization and Humanistic and Economic Burden in Patients with β-Thalassemia from the Patients' Perspective. J Clin Med. 2023;12(2). PubMed
7.Global PRO survey study: Baseline survey results among adults with TDT and SCD (≥18 years) [sponsor supplied reference]. Toronto (ON): Vertex Pharmaceuticals, Inc.; 2022.
8.Canadian Haemoglobinopathy Association. Consensus Statement of Clinical Care of Patients with Thalassemia in Canada [sponsor supplied reference]. 2018.
9.Data on file. Market research conducted for Vertex [sponsor supplied reference]. Toronto (ON): Vertex Pharmaceuticals, Inc.; 2021.
10.Kattamis A, Forni GL, Aydinok Y, Viprakasit V. Changing patterns in the epidemiology of β-thalassemia. Eur J Haematol. 2020;105(6):692-703. PubMed
11.Taher AT, Weatherall DJ, Cappellini MD. Thalassaemia. Lancet. 2018;391(10116):155-167. PubMed
12.Thalassemia International F. 2021 Guidelines for the Management of Transfusion Dependent Thalassaemia (TDT) [sponsor supplied reference]. 2021; https://www.thalassemia.org/wp-content/uploads/2021/06/TIF-2021-Guidelines-for-Mgmt-of-TDT.pdf.
13.Angastiniotis MCLSS, et al. Global Epidemiology of B-Thalassaemia (TIF report) [sponsor supplied reference]. 2021.
14.Data on File. Epidemiology and Clinical Characteristics of SCD and B-Thal in Canada [sponsor supplied reference]. Toronto (ON): Vertex Pharmaceuticals, Inc.; 2022.
15.Data on File: Canadian clinical advisor interviews for TDT [sponsor supplied reference]. Toronto (ON): Vertex Pharmaceuticals, Inc.; 2023.
16.Cappellini MD, Farmakis D, Porter J, Taher A, et al. 2021 Guidelines for the Management of Transfusion Dependent Thalassaemia (TDT) 4th edition [sponsor supplied reference]. 2021.
17.Thalassemia Foundation of C. Guidelines for the Clinical Care of Patients with Thalassemia in Canada [sponsor supplied reference]. 2009; http://www.thalassemia.ca/wp-content/uploads/Thalassemia-Guidelines_LR.pdf. Accessed 2023 06 09.
18.REBLOZYL (luspatercept-aamt) [sponsor supplied reference]. Cambridge, MA: Celgene Corporation Acceleron Pharma Incorporated; 2020.
19.Baldwin J, Udeze C, Li N, et al. Clinical burden and healthcare resource utilization associated with managing transfusion-dependent beta-thalassemia in France. Curr Med Res Opin. 2024;40(8):1289-1295. PubMed
20.Jobanputra M, Paramore C, Laird SG, McGahan M, Telfer P. Co-morbidities and mortality associated with transfusion-dependent beta-thalassaemia in patients in England: a 10-year retrospective cohort analysis. Br J Haematol. 2020;191(5):897-905. PubMed
21.Consensus Statement of Clinical Care of Patients with Thalassemia in Canada: 4. Hematopoietic Stem Cell Transplantation (HSCT). The Canadian Hemoglobinopathy Association; 2024: https://canhaem.org/wp-content/uploads/2024/09/HSCT-1.pdf. Accessed 2024 Aug 7.
22.Angelucci E, Matthes-Martin S, Baronciani D, et al. Hematopoietic stem cell transplantation in thalassemia major and sickle cell disease: indications and management recommendations from an international expert panel. Haematologica. 2014;99(5):811-820. PubMed
23.Locatelli F, Cavazzana M, Frangoul H, Fuente J, Algeri M, Meisel R. Autologous gene therapy for hemoglobinopathies: From bench to patient's bedside. Mol Ther. 2024. PubMed
24.Exa-Cel TDT Clinical Overview Addendum: Efficacy and Safety Update 16 April 2023 [internal sponsor report]. Toronto (ON): Vertex Pharmaceuticals, Inc.; 2023.
25.FACT-BMT. Chicago (IL): FACIT Group; 2024: https://www.facit.org/measures/fact-bmt. Accessed 2024 Aug 30.
26.Mastropietro AP, Oliveira EA, Santos MA, Voltarelli JC. [Functional Assessment of Cancer Therapy Bone Marrow Transplantation: Portuguese translation and validation]. Rev Saude Publica. 2007;41(2):260-268. PubMed
27.Pediatric Quality of Life (PedsQL) Inventory Generic Core Scales 4.0 Chicago (IL): AbilityLab; 2022: https://www.sralab.org/rehabilitation-measures/pediatric-quality-life-pedsql-inventory-generic-core-scales-40-0#:~:text=A%203%2Dpoint%20scale%20is,higher%20scores%20indicate%20better%20HRQOL. Accessed 2024 Aug 30.
28.Child Outcomes Research Consortium. Paediatric Quality of Life (PedsQL). London (GB): Anna Freud Centre: https://www.corc.uk.net/outcome-experience-measures/paediatric-quality-of-life-pedsql/#:~:text=The%20Pediatric%20Quality%20of%20Life,(the%20Self%2DReport). Accessed 2024 Aug 30.
29.Committee for Medicinal Products for Human Use (CHMP). Assessment report: Casgevy. International non-proprietary name: exagamglogene autotemcel. Procedure No. MEA/H/C/005763/0000. Amsterdam (NL): European Medicines Agency; 2023: https://www.ema.europa.eu/en/documents/assessment-report/casgevy-epar-public-assessment-report_en.pdf. Accessed 2024 Aug 8.
30.Balshem H, Helfand M, Schünemann HJ, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011;64(4):401-406. PubMed
31.Santesso N, Glenton C, Dahm P, et al. GRADE guidelines 26: informative statements to communicate the findings of systematic reviews of interventions. J Clin Epidemiol. 2020;119:126-135. PubMed
32.Vertex Pharmaceuticals response to July 16 2024 CADTH request for additional information regarding exagamglogene autotemcel CADTH review: [internal additional sponsor's information]. Toronto (ON): Vertex Pharmaceuticals, Inc.; 2024.
33.Vertex Pharmaceuticals response to June 28 2024 CADTH request for additional information regarding exagamglogene autotemcel CADTH review: [internal additional sponsor's information]. Toronto (ON): Vertex Pharmaceuticals, Inc.; 2024.
34.Vertex Pharmaceuticals response to August 12, 2024 CADTH request for additional information regarding exagamglogene autotemcel CADTH review: [internal additional sponsor's information]. Toronto (ON): Vertex Pharmaceuticals; 2024.
35.Interim Clinical Study Report: A Long-term Follow-up Study of Subjects With β-thalassemia or Sickle Cell Disease Treated with Autologous CRISPR-Cas9 Modified Hematopoietic Stem Cells (CTX001) [sponsor supplied reference]. Toronto (ON): Vertex Pharmaceuticals, Inc.; 2023.
36.Indirect Treatment Comparison Report: Exagamglogene Autotemcel (exa-cel) for the Treatment of Transfusion-dependent β-thalassemia [sponsor supplied reference]. Toronto (ON): Vertex Pharmaceuticals, Inc.;2023.
37.Signorovitch JE, Wu EQ, Yu AP, et al. Comparative effectiveness without head-to-head trials: a method for matching-adjusted indirect comparisons applied to psoriasis treatment with adalimumab or etanercept. Pharmacoeconomics. 2010;28(10):935-945. PubMed
38.Decision Support Unit, Phillippo DM, \Ades, A.E., Dias S, Palmer S, Abrams KR, Welton NJ. NICE DSU Technical Support Document 18: Methods for population-adjusted indirect comparisons in submissions to NICE. Technical suppor documents. Bristol (GB): University of Bristol; 2016: https://research-information.bris.ac.uk/ws/portalfiles/portal/94868463/Population_adjustment_TSD_FINAL.pdf. Accessed 2024 Aug 29.
39.Benz EJ, Angelucci E. Diagnosis of thalassemia (adults and children). In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2024: http://www.uptodate.com. Accessed 2024 Aug 29.
40.Sankaran VG, Orkin SH. The switch from fetal to adult hemoglobin. Cold Spring Harb Perspect Med. 2013;3(1):a011643. PubMed
41.Dhaliwal G, Cornett PA, Tierney LM, Jr. Hemolytic anemia. Am Fam Physician. 2004;69(11):2599-2606. PubMed
42.Benz EJ. Pathophysiology of thalassemia. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2024: http://www.uptodate.com. Accessed 2024 Aug 29.
43.Thalassaemia. Nicosia (CYP): Thalassaemia International Federation; 2024: https://thalassaemia.org.cy/haemoglobin-disorders/thalassaemia/. Accessed 2024 Aug 6.
44.Kato GJ, Piel FB, Reid CD, et al. Sickle cell disease. Nat Rev Dis Primers. 2018;4:18010. PubMed
45.Musallam KM, Sankaran VG, Cappellini MD, Duca L, Nathan DG, Taher AT. Fetal hemoglobin levels and morbidity in untransfused patients with β-thalassemia intermedia. Blood. 2012;119(2):364-367. PubMed
46.Shah F, Telfer P, Velangi M, et al. Routine management, healthcare resource use and patient and carer-reported outcomes of patients with transfusion-dependent β-thalassaemia in the United Kingdom. eJHaem. 2021(2):738–749. PubMed
47.Taher AT, Musallam KM, Cappellini MD. β-Thalassemias. N Engl J Med. 2021;384(8):727-743. PubMed
48.Consensus Statement of Clinical Care of Patients with Thalassemia in Canada: 3. Iron overload and chelation therapy. The Canadian Hemoglobinopathy Association; 2024: https://canhaem.org/wp-content/uploads/2024/09/Iron-Overload-and-Chelation-Therapy.pdf. Accessed 2024 Aug 7.
49.Cappellini MD, Viprakasit V, Taher AT, et al. A Phase 3 Trial of Luspatercept in Patients with Transfusion-Dependent beta-Thalassemia. N Engl J Med. 2020;382(13):1219-1231. PubMed
50.Benz EJ, Angelucci E. Managment of thalassemia. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2024: http://www.uptodate.com. Accessed 2024 Aug 29.
51.Exa-cel Product Monograph [sponsor supplied reference]. Toronto (ON): Vertex Pharmaceuticals, Inc.; 2024.
52.Exagamglogene Autotemcel (exa-cel) for the Treatment of Transfusion-dependent Beta-thalassemia CDA-AMC Reimbursement Review Sponsor Summary of Clinical Evidence [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Exagamglogene autotemcel, 4-13 x106 cells/mL, for intravenous infusion. Vertex Pharmaceuticals, Incorporated; 2023.
53.PrApo-desferasirox (Deferasirox Dispersible Tablets for Oral Suspension), Dispersible Tablets for Suspension, 125 mg, 250 mg, and 500 mg, Oral [product monograph]. Toronto (ON): Apotex, Inc.; 2023: https://pdf.hres.ca/dpd_pm/00072665.PDF. Accessed 2024 Aug 7.
54.PrApo-desferasirox (Type J). Deferasirox Tablets, 90 mg, 180 mg and 360 mg [product monograph]. Toronto (ON): Apotex, Inc.; 2020: https://pdf.hres.ca/dpd_pm/00055845.PDF. Accessed 2024 Aug 8.
55.PrFerriprox. Deferiprone Tablets, Ph.Eur. 500 mg and 1000 mg. Deferiprone Oral Solution, Ph.Eur. 100 mg/mL [product monograph]. Toronto (ON): Chiesi Canada Corp.; 2020: https://pdf.hres.ca/dpd_pm/00055386.PDF. Accessed 2024 Aug 8.
56.PrDeferoxamine mesylate for injection. 500 mg deferoxamine mesylate /vial, 2 g deferoxamine mesylate /vial [product monograph]. Kirkland (QC): Pfizer Canada, Inc.; 2017: https://pdf.hres.ca/dpd_pm/00040145.PDF. Accessed 2024 Aug 8.
57.PrREBLOZYL® (luspatercept for injection), 25 mg / vial, 75 mg / vial, lyophilized powder for solution for subcutaneous injection [product monograph]. Saint-Laurent (QC): Celgene, Inc.; 2021: https://pdf.hres.ca/dpd_pm/00059994.PDF. Accessed 2024 Sep 27.
58.Frangoul H, Altshuler D, Cappellini MD, et al. CRISPR-Cas9 Gene Editing for Sickle Cell Disease and β-Thalassemia. N Engl J Med. 2021;384(3):252-260. PubMed
59.Locatelli F, Lang P, Wall D, et al. Exagamglogene Autotemcel for Transfusion-Dependent β-Thalassemia. N Engl J Med. 2024;0(0). PubMed
60.Vertex Pharmaceuticals Incorporated. NCT03655678. A Safety and Efficacy Study Evaluating CTX001 in Subjects With Transfusion-Dependent β-Thalassemia. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2024: https://clinicaltrials.gov/study/NCT03655678. Accessed 2024 Aug 29.
61.McQuellon RP, Russell GB, Cella DF, et al. Quality of life measurement in bone marrow transplantation: development of the Functional Assessment of Cancer Therapy-Bone Marrow Transplant (FACT-BMT) scale. Bone Marrow Transplant. 1997;19(4):357-368. PubMed
62.Lin C, Sajeev G, Stiff PJ, et al. Health-Related Quality of Life Following Allogeneic Hematopoietic Cell Transplantation with Omidubicel versus Umbilical Cord Blood. Transplant Cell Ther. 2023;29(1):52 e51-52 e59.
63.Yost KJ, Eton DT. Combining distribution- and anchor-based approaches to determine minimally important differences: the FACIT experience. Eval Health Prof. 2005;28(2):172-191. PubMed
64.Varni JW, Burwinkle TM, Seid M, Skarr D. The PedsQL™* 4.0 as a Pediatric Population Health Measure: Feasibility, Reliability, and Validity. Ambul Pediatr. 2003;3(6):329-341. PubMed
65.Janssen MF, Szende A, Cabases J, Ramos-Goñi JM, Vilagut G, König HH. Population norms for the EQ-5D-3L: a cross-country analysis of population surveys for 20 countries. Eur J Health Econ. 2019;20(2):205-216. PubMed
66.Jiang R, Janssen MFB, Pickard AS. US population norms for the EQ-5D-5L and comparison of norms from face-to-face and online samples. Qual Life Res. 2021;30(3):803-816. PubMed
67.Boateng-Kuffour A, Skrobanski H, Drahos J, et al. Appropriateness of the EQ-5D-5L in capturing health-related quality of life in individuals with transfusion-dependent beta-thalassemia: a mixed methods study. Health Qual Life Outcomes. 2024;22(1):54. PubMed
68.Pickard AS, Neary MP, Cella D. Estimation of minimally important differences in EQ-5D utility and VAS scores in cancer. Health Qual Life Outcomes. 2007;5:70. PubMed
69.Varni JW. The PedsQLTM Scoring Algorithm Lyon (FR): Mapi Research Trust; 2024: https://www.pedsql.org/score.html#:~:text=On%20the%20PedsQL%20Generic%20Core,%3D25%2C%204%3D0. Accessed 2024 Aug 30.
70.Varni JW. Scaling and scoring for the Acute andStandard versions of the Pediatric Quality of Life InventoryTM PedsQLTM. Lyon (FR): Mapi Research Trust; 2023: https://www.pedsql.org/PedsQL-Scoring.pdf. Accessed 2024 Aug 30.
71.EuroQol G. EuroQol--a new facility for the measurement of health-related quality of life. Health Policy. 1990;16(3):199-208. PubMed
72.Brooks R. EuroQol: the current state of play. Health Policy. 1996;37(1):53-72. PubMed
73.Summary basis for regulatory action. Silver Spring (MD): U.S. Food and Drug Administration; 2024: https://www.fda.gov/media/175842/download?attachment. Accessed 2024 Aug 8.
74.Methods for the development of NICE public health guidance (third edition): Appendix F Quality appraisal checklist – quantitative intervention studies [sponsor supplied reference]. London (GB): NICE; 26 September 2012 2012.
75.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
76.Sponsor's clinical summary report [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Exagamglogene autotemcel (CASGEVY). Toronto (ON): Vertex Pharmaceuticals (Canada) Incorporated; 2024 May 27.
77.Cappellini MD, Forni GL, Origa R, et al. A phase 3 trial of luspatercept in patients with transfusion-dependent beta-thalassemia. N Engl J Med. 2020;382(13):1219-1231. PubMed
78.Farmakis D, Giakoumis A, Angastiniotis M, Eleftheriou A. The changing epidemiology of the ageing thalassaemia populations: A position statement of the Thalassaemia International Federation. Eur J Haematol. 2020;105(1):16-23. PubMed
Appendix 1: Additional Outcome Data
Please note that this appendix has not been copy-edited.
Table 27: Summary of Transfusion Results From CLIMB-111 — PES January 16, 2023 Data Cut-Off
Outcome | CLIMB-111 (N = 35) |
|---|---|
Proportion of Patients Achieving TI12 (Primary End point) | |
Number of patients with TI12, n (%) | 32 |
Proportion of patients with TI12 (95% CI)a | 91.4 (76.9, 98.2) |
P value (1-sided against 50% response rate, alpha = 0.01692)b | < 0.0001 |
Proportion of Patients Achieving TI6 (Key Secondary End point) | |
Number of patients with TI6, n (%) | 32 |
Proportion of patients with TI16 (95% CI)a | 91.4 (76.9, 98.2) |
P value (1-sided against 50% response rate, alpha = 0.01692)b | < 0.0001 |
Time to Last RBC Transfusionc for Patients with TI12 (Secondary End point) | |
Number of patients with TI12 | 32 |
Time from exagamglogene autotemcel to last RBC transfusion (days), mean (range) | 35.2 ██████ █████ |
Duration of TI with Weighted Average Hb ≥ 9 g/dL for Patients with TI12 (Secondary End point) | |
Number of patients with TI12 | 32 |
Duration of TI (months), mean (SD) | ████ █████ |
CI = confidence interval; Hb = hemoglobin; PES = primary efficacy set; RBC = red blood cell; SD = standard deviation; TI = transfusion independence; TI6(12) = transfusion independent for 6 (12) consecutive months.
aThe 2-sided 95% CI was calculated using the exact Clopper-Pearson method
bThe 1-sided P value was calculated using the binomial distribution. This outcome was adjusted for multiple comparisons.
cAn RBC transfusion episode was defined as all transfusions within 5 days, starting from the first transfusion in the episode.
Source: details included in the table are from the sponsor’s CLIMB-111 CSR.2
Table 28: Summary of Other Secondary Efficacy Results From CLIMB-111 — PES January 16, 2023, Data Cut-Off
Outcome | 6 months post exagamglogene autotemcel (N = 35) | 12 months post exagamglogene autotemcel (N = 35) | 24 months post exagamglogene autotemcel (N = 35) |
|---|---|---|---|
HbF concentration (g/dL) | |||
Baseline n | 35 | 35 | 35 |
Baseline, mean (SD) | 0.5 (0.6) | 0.5 (0.6) | 0.5 (0.6) |
Patients with data at the time point, n | ██ | ██ | ██ |
Observed, mean (SD) | ████ █████ | ████ █████ | ████ █████ |
HbF concentration (%) | |||
Baseline n | ██ | ██ | ██ |
Baseline, mean (SD) | ███ █████ | ███ █████ | ███ █████ |
Patients with data at the time point, n | ██ | ██ | ██ |
Observed, mean (SD) | ████ ██████ | ████ ██████ | ████ ██████ |
Total Hb concentration (g/dL) | |||
Baseline n | 35 | 35 | 35 |
Baseline, mean (SD) | 10.4 (1.9) | 10.4 (1.9) | 10.4 (1.9) |
Patients with data at the time point, n | ██ | ██ | ██ |
Observed, mean (SD) | ████ █████ | ████ █████ | ████ █████ |
Change from baseline in EQ-5D-5L EQ VAS (patients ≥ 18 and ≤ 35 years) | |||
Baseline n | 24 | 24 | 24 |
Baseline, mean (SD) | 80.8 (18.0) | 80.8 (18.0) | 80.8 (18.0) |
Patients with data at the time point, n | NR | 24 | 15 |
Observed, mean (SD) | NR | ████ ██████ | ████ █████ |
Change from baseline, mean (SD) | NR | 8.6 (17.8) | 10.2 (20.9) |
Change from baseline in FACT-BMT Total Scores (patients ≥ 18 and ≤ 35 years) | |||
Baseline n | 24 | 24 | 24 |
Baseline, mean (SD) | 109.7 (19.8) | 109.7 (19.8) | 109.7 (19.8) |
Patients with data at the time point, n | NR | 24 | 15 |
Observed, mean (SD) | NR | █████ ██████ | █████ ██████ |
Change from baseline, mean (SD) | NR | 9.1 (24.7) | 17.1 (20.8) |
Change from baseline in nonadult EQ VAS (patients ≥ 12 and < 18 years)a | |||
Baseline n | ██ | ██ | ██ |
Baseline, mean (SD) | ████ ██████ | ████ ██████ | ████ ██████ |
Patients with data at the time point, n | ██ | ██ | ██ |
Observed, mean (SD) | ████ █████ | ████ █████ | ████ █████ |
Change from baseline, mean (SD) | ███ ██████ | ███ ██████ | ███ █████ |
Change from baseline in PedsQL Total Score (patients < 18 years) | |||
Baseline n | 10 | 10 | 10 |
Baseline, mean (SD) | 75.1 (6.7) | 75.1 (6.7) | 75.1 (6.7) |
Patients with data at the time point, n | ██ | ██ | ██ |
Observed, mean (SD) | ████ █████ | ████ █████ | ████ █████ |
Change from baseline, mean (SD) | 12.7 (9.9) | 14.7 (9.3) | 14.1 (9.2)b |
EQ VAS = EuroQol Quality of Life Scale – Visual Analogue Scale; EQ-5D-5L = EuroQol Quality of Life Scale-5-dimensions-5 levels of severity; FACT-BMT = Functional Assessment of Cancer Therapy–Bone Marrow Transplantation; Hb = hemoglobin; HbF = fetal hemoglobin; PedsQL = Pediatric Quality of Life Inventory; PES = primary efficacy set; SD = standard deviation.
aPer the submission, due to a lack of value sets in the UK or US, index-based summary health scores were not calculated for the EQ-5D-Y. The nonadult EQ VAS, which is identical to the adult EQ VAS, was employed instead.
bMeasured at 18 months.
Source: details included in the table are from the sponsor’s CLIMB-111 CSR.2
Table 29: Summary of TI12 and TI6 Outcome by Subgroup — PES April 16, 2023, Data Cut-Off
Outcome | CLIMB-111 (N = 42) |
|---|---|
Proportion of Patients Achieving TI12 (Primary End point) | |
Genotype | |
Beta0/beta0 genotype | |
Number of patients in subgroup at screening, n | ██ |
Number of patients with TI12, n | ██ |
Proportion of patients with TI12 (95% CI) | ████ ██████ █████ |
Non-beta0/beta0 genotype | |
Number of patients in subgroup at screening, n | ██ |
Number of patients with TI12, n | ██ |
Proportion of patients with TI12 (95% CI) | █████ ██████ ██████ |
Age | |
Age ≥ 12 and < 18 years at Screening | |
Number of patients in subgroup at screening, n | 13 |
Number of patients with TI12, n | 12 |
Proportion of patients with TI12 (95% CI) | 92.3 ██████ █████ |
Age ≥ 18 and ≤ 35 years at Screening | |
Number of patients in subgroup at screening, n | 29 |
Number of patients with TI12, n | 27 |
Proportion of patients with TI12 (95% CI) | 93.1 ██████ █████ |
Proportion of Patients Achieving TI6 (Key Secondary End point) | |
Genotype | |
Beta0/beta0 genotype | |
Number of patients in subgroup at screening, n | ██ |
Number of patients with TI6, n | ██ |
Proportion of patients with TI6 (95% CI) | ████ ██████ █████ |
Non-beta0/beta0 genotype | |
Number of patients in subgroup at screening, n | ██ |
Number of patients with TI6, n | ██ |
Proportion of patients with TI6 (95% CI) | █████ ██████ ██████ |
Age | |
Age ≥ 12 and < 18 years at Screening | |
Number of patients in subgroup at screening, n | 13 |
Number of patients with TI6, n | 12 |
Proportion of patients with TI6 (95% CI) | 92.3 ██████ █████ |
Age ≥ 18 and ≤ 35 years at Screening | |
Number of patients in subgroup at screening, n | 29 |
Number of patients with TI6, n | 27 |
Proportion of patients with TI6 (95% CI) | 93.1 ██████ █████ |
CI = confidence interval; PES = primary efficacy set; TI6(12) = transfusion independent for 6 (12) consecutive months.
Source: details included in the table are from the sponsor’s Clinical Addendum Update.24
Pharmacoeconomic Review
Abbreviations
AE
adverse event
ATC
authorized treatment centre
BIA
budget impact analysis
CDA-AMC
Canada’s Drug Agency
HSCT
hematopoietic stem cell transplant
ICER
incremental cost-effectiveness ratio
ICT
iron chelation therapy
LY
life-year
MAIC
matching-adjusted indirect comparison
QALY
quality-adjusted life-year
RBC
red blood cell
SOC
standard of care
TDT
transfusion-dependent beta thalassemia
TI
transfusion independence
TR
transfusion reduction
WTP
willingness to pay
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Exagamglogene autotemcel cell suspension in patient-specific vials, 4 × 106 cells/mL to 13 × 106 cells/mL, for IV infusion |
Indication | Proposed: For the treatment of patients aged 12 years and older with transfusion-dependent beta thalassemia |
Health Canada approval status | NOC |
Health Canada review pathway | Priority review |
NOC date | September 23, 2024 |
Reimbursement request | As per indication |
Sponsor | Vertex Pharmaceuticals (Canada) Incorporated |
Submission history | Previously reviewed: No |
NOC = Notice of Compliance.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Markov model |
Target population | Patients aged 12 years and older with TDT |
Treatment | Exagamglogene autotemcel |
Dose regimen | Single infusion of at least 3 × 106 CD34+ cells/kg |
Submitted price | Exagamglogene autotemcel, 4 × 106 cells/mL to 13 × 106 cells/mL: $2,800,000 per administration |
Submitted treatment cost | $2,800,000 per administration |
Comparators |
|
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | Lifetime (79 years) |
Key data sources |
|
Submitted results |
|
Key limitations |
|
CDA-AMC reanalysis results |
|
CDA-AMC = Canada’s Drug Agency; HSCT = hematopoietic stem cell transplant; ICER = incremental cost-effectiveness ratio; ICT = iron chelation therapy; LTE = long-term extension; LY = life-year; MAIC = matching-adjusted indirect comparison; QALY = quality-adjusted life-year; RCT = randomized controlled trial; SOC = standard of care; TDT = transfusion-dependent beta thalassemia.
Conclusions
The clinical review by Canada’s Drug Agency (CDA-AMC) concluded that in the absence of direct comparative data, evidence from the interim analysis of the single-arm CLIMB-111 study is very uncertain regarding the effect of exagamglogene autotemcel on clinical efficacy and harms outcomes in patients with transfusion-dependent beta thalassemia (TDT) when compared with any comparator. Findings from the trial are consistent with a clinically meaningful reduction in transfusion leading to transfusion independence (TI), according to clinical expert input. The available results from the trial are subject to important potential biases in outcome ascertainment, study population, and statistical analysis plan changes which impact the certainty that the observed effect is truly attributable to exagamglogene autotemcel. Results from the long-term extension portion were only available for a fraction of patients for all outcomes and therefore remain highly uncertain; and in general, data were only available for a relatively short time period after infusion. Conclusions around long-term harms results are generally limited by the ongoing nature of the trial and the short follow-up to date. The indirect evidence submitted by the sponsor, consisting of 2 matching-adjusted indirect comparisons (MAICs) comparing exagamglogene autotemcel to standard of care (SOC) transfusions and chelation) and luspatercept, were considerably limited by differences in the study design, outcome ascertainment, and concerns around the validity of the comparators in terms of their potential for attaining the outcome of TI. Overall, information on the comparative nature of exagamglogene autotemcel to SOC and luspatercept remains highly uncertain due to considerable limitations with the indirect evidence as well as the use of a single-arm trial.
The CDA-AMC base case was derived by adjusting the mortality associated with cardiac complications and utility value associated with TI. CDA-AMC was unable to address uncertainty related to comparative clinical data, including the magnitude and duration of benefit for exagamglogene autotemcel and the predicted mortality benefit due to reduced chronic complications. Given the considerable limitations with the sponsor’s MAIC and the CDA-AMC clinical review’s conclusions that no concrete conclusions can be drawn from the indirect evidence about the comparative effectiveness of exagamglogene autotemcel, luspatercept was excluded from the CDA-AMC base case and included as a scenario analysis. The CDA-AMC base-case results align with those of the sponsor’s submitted analysis, indicating that exagamglogene autotemcel is not cost-effective at a willingness-to-pay (WTP) threshold of $50,000 per quality-adjusted life-year (QALY) gained, relative to SOC — CDA-AMC estimates an incremental cost-effectiveness ratio (ICER) of $194,807 per QALY compared to SOC. At the submitted price, exagamglogene autotemcel would require a price reduction of approximately 55% to be considered cost-effective at a WTP threshold of $50,000 per QALY.
Results were largely driven by the acquisition cost of exagamglogene autotemcel as well as the predicted gains in QALYs, life-years (LYs), and cost savings associated with reduced transfusions, iron chelation therapy (ICT) use, and chronic complications (total = $898,371). CDA-AMC notes that these findings are highly uncertain as 95% of the incremental QALYs were accrued in the extrapolation period (i.e., after 20 months). The results are dependent on a survival benefit of approximately 8 years. If the duration and magnitude of benefit associated with exagamglogene autotemcel is less, and/or anticipated cost savings associated with reduced transfusions, ICT use, and chronic complications are lower than estimated, then the ICER may be higher and a higher price reduction may be required.
In the scenario analysis including luspatercept as a comparator, CDA-AMC estimates an ICER of $44,002 per QALY gained compared to luspatercept. Due to the considerable limitations with the indirect evidence, it was not possible to produce a rigorous estimate of incremental benefit for exagamglogene autotemcel compared to luspatercept, and the ICER estimated in the scenario analysis should be interpreted carefully. The estimated ICER compared to luspatercept is still subject to the limitations identified and CDA-AMC notes that several of these limitations implied a directional bias that favoured exagamglogene autotemcel. Given this clinical uncertainty, price reductions may be required to achieve cost-effectiveness compared to luspatercept at a WTP threshold of $50,000 per QALY gained.
Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, clinician groups, and drug plans that participated in the CDA-AMC review process.
Patient input was received from 2 groups including the Thalassemia Foundation of Canada and Global Action Network for Sickle Cell & Other Inherited Blood Disorders (GANSID). Information was gathered via surveys, with 90% of respondents being patients with TDT. Patient input noted that TDT has a significant impact on quality of life due to its chronic nature and complications. In additional to the physical damage, patient input additionally commented on the emotional and financial burden this disease had their lives. All patient group respondents noted that the only treatment options available for the disease are noncurative, being chronic red blood cell (RBC) transfusions and ICT (i.e., deferoxamine, deferasirox, and deferiprone) with need for constant monitoring. The need for additional treatments that could improve clinical outcomes with minimal side effects was emphasized. Two respondents had experience with exagamglogene autotemcel through clinical trials in the US, and both reported successful iron level normalization and discontinuation of current treatments.
Clinician group input was received from the Canadian Hemoglobinopathy Association/ L’Association canadienne d’hémoglobinopathie (CanHaem). Feedback noted that patients with TDT require subspecialty multidisciplinary care throughout their lives and that disease has significant clinical burden due to chronic hemolysis causing renal, cardiac, and hepatic failure. Clinicians noted that despite the availability of allogenic-hematopoietic stem cell transplant (HSCT), blood transfusion, and ICT as treatment options, many patients still experience a lack of effective therapy for their disease, resulting in significant morbidity and early mortality. Clinician input noted that although luspatercept is approved for use in patients with TDT aged 18 years and older, the majority of patients do not respond to luspatercept and postmarketing surveillance identified paraspinal extramedullary hematopoiesis as a complication limiting therapy in some patients. Clinician input noted that exagamglogene autotemcel represents a significant shift in the current treatment paradigm by providing highly efficacious, one-time disease-modifying therapy. However, treatment should occur at a facility experienced with stem cell collection, administration of myeloablative chemotherapy, and specialized hematologic care because patients will need to be admitted to hospital for approximately 35 days to facilitate neutrophil engraftment and will require long-term follow-up by their hemoglobinopathy providers to ensure there are no long-term complications of thalassemia, iron overload, conditioning chemotherapy, or the exagamglogene autotemcel product, in addition to follow-up from their transplant centre.
Drug plan input noted that current public funding for ICTs varies by jurisdiction, although most are covered according to specific criteria for patients with TDT. They further noted that RBC transfusions are provided by Canadian Blood Services. The drug plans questioned if the inclusion criteria from the CLIMB-111 trial are appropriate for reimbursement purposes and if patients younger than 12 years or older than 35 years would be eligible to receive exagamglogene autotemcel. Drug plan feedback flagged that exagamglogene autotemcel needs to be administered by trained personnel at authorized treatment centres (ATCs) and there may be capacity constrains in the initial years postreimbursement. The drug plans additionally inquired about the current screening requirements for a TDT diagnosis and the reliability and accuracy of these tests.
Several of these concerns were addressed in the sponsor’s model:
Health-related quality of life was incorporated in the sponsor’s model based on estimates found in published literature.
Capacity constraints associated with exagamglogene autotemcel administration were considered in the sponsor’s submitted budget impact analysis (BIA).
CDA-AMC was unable to address the following concerns raised from the input:
The uncertainty associated with the long-term efficacy of exagamglogene autotemcel could not be addressed due to a lack of long-term data.
Economic Review
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis to assess the cost-effectiveness of exagamglogene autotemcel for the treatment of patients aged 12 years and older with TDT.1 In the model, the sponsor compared exagamglogene autotemcel to luspatercept and SOC. SOC comprised blood transfusions and ICTs such as deferoxamine, deferasirox, and deferiprone.1 The modelled population is in line with the Health Canada–approved indication and was based on patients enrolled in the CLIMB-111 trial.1
Exagamglogene autotemcel is available as a cell suspension in patient-specific vials, 4 × 106 cells/mL to 13 × 106 cells/mL for IV infusion.2 The minimum recommended dose is 3 × 106 CD34+ cells/kg as a single dose for infusion.2 Exagamglogene autotemcel must be administered between 48 hours and 7 days after the last dose of the myeloablative conditioning drug.2 The submitted price is $2,800,000 per administration per patient, regardless of the number of patient-specific vials required.1 Luspatercept is available as lyophilized powder for solution for subcutaneous injection, with a recommended dose of 1.0 mg/kg once every 21 days. At the publicly available price of $2,189 per 25-mg vial, the sponsor estimated that the 21-day costs of luspatercept would be $4,708.1 For SOC, the sponsor estimated the cost of monthly blood transfusion costs to be $2,048 based on 2.2 units of blood required per transfusion. The sponsor estimated costs of ICT to be $439 per month using a weighted basket of deferoxamine, deferasirox, deferiprone, deferiprone and deferoxamine, deferiprone and deferasirox, and deferasirox and deferoxamine based on published literature.1
The analysis was conducted from the perspective of the Canadian public health care payer. Cost and clinical outcomes (QALYs, LYs) were estimated over a lifetime horizon (79 years; 1-month cycle length). Discounting (1.5% per annum) was applied for both costs and outcomes.
Model Structure
The sponsor submitted a Markov model with 4 health states based on transfusion status: transfusion independent, transfusion reduced, transfusion dependent, and death (Figure 1).1 Transfusion status impacted the frequency of RBC transfusions and determined patient iron levels (normal or nonnormal). Iron level determined the risk of complications that impacted patient mortality, quality of life, and health care resource utilization. It was assumed that patients in the transfusion independent health state achieved normal iron levels and did not require further RBC transfusions after treatment. Patients in the transfusion reduced health state had nonnormal iron levels but experienced a reduction in the frequency of RBC transfusions after treatment, and those in the transfusion dependent health state had nonnormal iron levels and were assumed to have no reduction in RBC transfusions after treatment. All patients were assumed to remain in their posttreatment health state for the remainder of the time horizon, regardless of treatment received. Complications were considered independent and permanent once developed (i.e., the risk of developing chronic complications were independent of each other and were assumed to last until death). All patients could experience death at any point.
Model Inputs
The baseline characteristics used to inform the model were based on the CLIMB-111 trial (mean age = 21.1 years; 48.6% female, 51.4% male).1 In the CLIMB-111 trial, patients aged 12 years and older with TDT were treated with exagamglogene autotemcel. In the pivotal trial, transfusion dependence was defined as having a history of at least 100 mL/kg/year or 10 units/year of packed RBC transfusions in the 2 years preceding trial enrolment.1
Health states were defined by transfusion status, and movement between health states was informed by data from the CLIMB-111 trial using proportion of patients achieving TI and transfusion reduction (TR). Of the patients who received exagamglogene autotemcel, it was assumed that 100% experienced engraftment success. Based on 32 of 35 patients achieving the TI primary end point at 12 months, the sponsor then assumed that 93.2% were assumed to be cured and receive no RBC transfusions after matching and adjusting to the luspatercept arm of the BELIEVE trial.3 The remaining proportion of patients experienced TR, and no patients remained transfusion dependent. Patients receiving exagamglogene autotemcel who were transfusion independent for 12 months were assumed to remain cured of the disease for a lifetime. For patients receiving luspatercept, 21.3% were transfusion reduced and 78.6% remained transfusion dependent.1 It was assumed that patients receiving luspatercept could not become transfusion independent, although 4% achieved TI at 3 months in the BELIEVE trial, and the 12-month adjusted value from the MAIC was 0.1%.1 The sponsor also assumed that patients receiving SOC did not experience any additional clinical benefit (i.e., their frequency of RBC infusions and iron levels were assumed to never change over time).
General population mortality and TDT-related mortality were informed by Statistics Canada and Delea et al. (2007), respectively.4 Additional factors that could impact mortality was exagamglogene autotemcel infusion and occurrence of complications and other infusion-related events. Patients with cured TDT were assumed to experience mortality at a rate based on general population mortality rates adjusted by a hazard ratio of 1.25, based on a National Institute for Health and Care Excellence assessment for TDT.5 The sponsor assumed that patients receiving exagamglogene autotemcel had no risk of infusion-related mortality based on results from the CLIMB-111 trial; however, patients had a 25% mortality risk following exagamglogene autotemcel engraftment failure. Chronic complications (i.e., cardiac complications and diabetes) were assumed to also impact mortality risk as informed by published literature.1
Rates of complications related to cardiac complications, liver complications, osteoporosis, diabetes, and hypogonadism were informed by published literature and differed based on measures of iron levels: serum ferritin, myocardial T2 cardiac iron concentration, and liver iron concentration.1 Iron levels were classified as normal or nonnormal, with nonnormal further categorized as low, moderate, or high based on thresholds aligned with published literature and previous models in TDT.5,6 Infertility inputs in the model were informed by published literature.5,7,8 Treatment-related adverse events (AEs) of grade 3 or higher associated with exagamglogene autotemcel were applied as a one-time event when patients received treatment and were informed by the CLIMB-111 trial. The AEs associated with luspatercept and SOC were assumed to be recurring and informed by the BELIEVE trial.1,9
Health state utility values in the model were informed by a vignette study employing the time trade-off method with respondents in the general UK population to estimate utilities with varying treatment approaches for TDT. The estimated utility value for patients with TI was 0.93, 0.75 for patients with TR, and 0.73 for patients with transfusion dependence.10 Disutilities associated with exagamglogene autotemcel infusion, exagamglogene autotemcel graft failure, ICT use, infertility, and complications were included and informed by published literature.10-12
Costs included in the model consisted of treatment acquisition costs, infusion-related costs, RBC transfusion and ICT costs, chronic complication costs, disease monitoring costs, AE costs, and terminal care costs. Acquisition costs were based on the sponsor’s submitted price for exagamglogene autotemcel. Costs for luspatercept and SOC were informed by either the Ontario or Saskatchewan drug formularies and previous CDA-AMC reimbursement reviews.13,14 The number of RBC units and frequency of transfusions were derived from the CLIMB-111 trial.1 Patients receiving exagamglogene autotemcel additionally incurred infusion-related costs such as preinfusion costs, hospitalization and procedure costs, and postinfusion monitoring costs. Frequency and unit cost of these were informed by data from the CLIMB-111 trial, clinical expert feedback received by the sponsor, and published literature.15,16 Routine disease monitoring costs were included for patients such as inpatient visits, outpatient visits, and emergency department visits where the frequency of each was informed by published literature and clinical expert feedback received by the sponsor.17 Costs for health care resource utilization were informed by the Ontario Schedule of Benefits for physician and laboratory services.1,18 Costs of complications where informed by the Ontario Case Costing Initiative, the Canadian Institute for Health Information patient cost estimator, or Ontario Schedule of Benefits for physician services.19-21 The cost of infertility was assumed to be associated with a one-time retrieval surgery and monthly storage costs.22 Lastly, a one-time cost of terminal care was informed by the average cost for palliative care from the Canadian Institute for Health Information.20
Summary of Sponsor’s Economic Evaluation Results
All analyses were run probabilistically with 1,000 iterations. The deterministic and probabilistic results were similar. The probabilistic findings are presented in the following.
Base-Case Results
In the sponsor’s base case, exagamglogene autotemcel was associated with an incremental cost of $2,002,090 and an incremental QALY gain of 14.10 compared with SOC, resulting in an ICER of $141,962 per QALY gained. Compared with luspatercept, exagamglogene autotemcel was associated with an incremental cost of $256,371 and an incremental QALY gain of 13.70, resulting in an ICER of $18,710 per QALY gained. The absence of direct comparative evidence for exagamglogene autotemcel versus comparators and heterogeneity across trials prevented the implementation of sequential analyses across comparators. Results reflect pairwise comparisons between exagamglogene autotemcel and each comparator.
The sponsor’s model predicted that treatment with exagamglogene autotemcel was associated with an incremental QALY gain of 14.10 and 13.70 compared with SOC and luspatercept, respectively. Given the duration of follow-up in the CLIMB-111 trial (i.e., median follow-up of 23.6 months) in contrast to the model’s lifetime horizon (i.e., 79 years), the majority of the incremental QALYs realized by patients receiving exagamglogene autotemcel was derived from the period beyond which there is observed trial data (i.e., extrapolated period). Furthermore, cost-effectiveness of exagamglogene autotemcel is driven by high drug acquisition costs as well as the assumed reduction in RBC transfusion and ICT costs once patients achieve TI after treatment with exagamglogene autotemcel and remain cured for the remainder of their lifetime.
The probability that exagamglogene autotemcel was cost-effective compared to luspatercept and SOC at a $50,000 per QALY gained threshold was 100% and 0%, respectively. The sponsor’s submitted analysis is based on the publicly available prices for all drug treatments. Additional results from the sponsor’s submitted economic evaluation base case are presented in Appendix 3.
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER ($/QALY)a |
|---|---|---|---|---|---|
Exagamglogene autotemcel versus SOC | |||||
SOC | 1,179,345 | Reference | 13.20 | Reference | Reference |
Exagamglogene autotemcel | 3,181,435 | 2,002,090 | 27.30 | 14.10 | 141,962 |
Exagamglogene autotemcel versus luspatercept | |||||
Luspatercept | 2,925,064 | Reference | 13.60 | Reference | Reference |
Exagamglogene autotemcel | 3,181,435 | 256,371 | 27.30 | 13.70 | 18,710 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; SOC = standard of care.
Note: Submitted analyses are based on the publicly available prices of comparator treatments.
aResults are not presented sequentially due to heterogeneity between comparator trials. ICERs reflect pairwise comparisons between exagamglogene autotemcel and each comparator.
Source: Sponsor’s pharmacoeconomic submission.1
Sensitivity and Scenario Analysis Results
The sponsor conducted several scenario analyses that included adopting alternative modelling assumptions (i.e., alternate data cut-off from April 2023, and different discount rates and time horizons) as well as alternate assumptions related to baseline number of RBC transfusions, efficacy of exagamglogene autotemcel and luspatercept, baseline complications, cardiac mortality, transfusion dependent health state mortality, shorter iron level normalization period, and alternate utility values. The sponsor additionally conducted a distributional cost-effectiveness analysis. The ICERs for exagamglogene autotemcel versus SOC ranged from $72,193 to $228,292 with the scenario assuming a 3% discount rate having the largest ICER. The results for exagamglogene autotemcel versus luspatercept ranged from being dominant to an ICER of $88,304 with the scenario assuming a 3% discount rate having the largest ICER.
The sponsor conducted a scenario analysis from a societal perspective. This analysis included additional costs associated with patient productivity and caregiver burden. In this analysis, relative to SOC, the ICER was $97,826 per QALY gained. Relative to luspatercept, exagamglogene was less costly and more effective. This was lower than the sponsor’s base-case analysis, which used a health care payer perspective.
CDA-AMC Appraisal of the Sponsor’s Economic Evaluation
CDA-AMC identified several key limitations to the sponsor’s analysis that have notable implications on the economic analysis.
The comparative efficacy of exagamglogene autotemcel is highly uncertain. To inform efficacy in the pharmacoeconomic model (i.e., the proportion of patients who achieved TI at 12 months), the sponsor used data from the single-arm CLIMB-111 trial for exagamglogene autotemcel and assumed that patients receiving SOC would experience no change in baseline transfusions required. As noted in the CDA-AMC clinical report, the use of the single-arm treatment design introduces a risk of bias considering the absence of a comparator treatment arm. While clinical expert feedback received by CDA-AMC acknowledges the rationale behind the sponsor’s decision to perform a noncomparative trial, the lack of comparative evidence and lack of details informing the treatments that patients were receiving during the 2 years before the trial makes the evidence very uncertain regarding the true effect of exagamglogene autotemcel compared to any comparator.
To compare the efficacy of exagamglogene autotemcel to luspatercept, the sponsor conducted an unanchored MAIC using data from the BELIEVE trial to inform efficacy for luspatercept. However, the primary outcome of TR measured in the BELIEVE trial was not measured in the CLIMB-111 study; TI during any 8-week or 12-week period in the BELIEVE study was a secondary outcome. Clinical experts consulted by CDA-AMC highlighted that luspatercept does not generally lead to TI, and furthermore a minority of patients (approximately 20%) respond to it. The similarity of exagamglogene autotemcel and luspatercept for an outcome of TI is therefore questionable. The clinical review concluded that the indirect treatment comparison between exagamglogene autotemcel and luspatercept was considerably limited by differences in the study design, outcome ascertainment, and concerns around the validity of the comparators in terms of their potential for attaining the outcome of TI, and concrete conclusions on comparative efficacy could not be drawn. Therefore, information on the comparative nature of exagamglogene autotemcel to other treatment options including luspatercept remains lacking due to considerable limitations with the indirect evidence as well as the use of a single-arm trial.
Given the absence of any direct comparative clinical evidence and limitations with the MAIC, the magnitude of benefit (i.e., the proportion of patients who achieved TI at 12 months) associated with exagamglogene autotemcel versus comparators remains uncertain. CDA-AMC was unable to address this limitation.
Given the considerable limitations with the sponsor’s MAIC and the CDA-AMC clinical review’s conclusions that no concrete conclusions can be drawn from the indirect evidence about the comparative effectiveness of exagamglogene autotemcel, luspatercept was excluded from the CDA-AMC base case and included as a scenario analysis.
The cost-effectiveness of exagamglogene autotemcel versus allogenic-HSCT for young (i.e., aged 16 years and younger) patients with TDT is unknown. The sponsor excluded allogenic-HSCT as a comparator for exagamglogene autotemcel as it was assumed only a small subset of patients would be eligible. Specifically, the Canadian TDT guidelines report that the proposed indication for HSCT is for patients under younger than 16 years. As such, the sponsor speculates that most eligible patients with willing matched sibling donors would likely have received HSCT before reaching the age of eligibility for exagamglogene autotemcel. Clinical expert feedback received by CDA-AMC indicated that most eligible patients with willing matched sibling donors would likely receive HSCT before reaching the age of exagamglogene autotemcel eligibility; however, it was further noted that there may be cases where the age of patients eligible for HSCT overlaps with the eligibility for exagamglogene autotemcel (e.g., patients newly immigrated to Canada). Therefore, allogenic-HSCT remains a relevant comparator for a subset of patients but in the absence of comparative data the cost-effectiveness of exagamglogene autotemcel versus allogenic-HSCT this subpopulation remains unknown.
CDA-AMC was unable to address this limitation in reanalysis.
Evidence to support the duration and magnitude of benefit associated with exagamglogene autotemcel compared to SOC is unavailable. At the time of this review, the CLIMB-111 study is ongoing with the most recent interim analysis based on the data cut-off date of April 16, 2023. Patients who complete the CLIMB-111 study can enrol in the CLIMB-131 study which is an additional ongoing long-term extension study set to assess the long-term safety and efficacy of exagamglogene autotemcel for patients who received exagamglogene autotemcel in the CLIMB-111 and CLIMB-121 studies. Patients in the CLIMB-131 study are to be followed for up to 15 years after exagamglogene autotemcel infusion. As noted in the CDA-AMC clinical review, of the 23 patients who achieved TI for 12 consecutive months in the CLIMB-111 study and rolled over to the CLIMB-131 trial, all remain transfusion independent in the CLIMB-131 study. However, while the proportion of patients who achieved TI for 12 consecutive months in the CLIMB-111 study and the durability for the subset of patients who achieved TI for 12 consecutive months in the CLIMB-131 study seems promising, in the absence of complete long-term data, there remains uncertainty on the long-term efficacy and safety of exagamglogene autotemcel. In the pharmacoeconomic model, the sponsor assumed that patients who achieved TI would sustain their benefit for the duration of the model time horizon (i.e., 79 years), meaning that 93% of patients receiving exagamglogene autotemcel would achieve a “cure” after being transfusion independent and would remain in that state indefinitely. These patients were assumed to have normal iron levels, no longer be at risk of disease-related complications, and not require further transfusions or ICT treatments for their lifetime. Given that approximately 95% of the incremental QALYs predicted to be gained with exagamglogene autotemcel by the sponsor’s model were derived from this assumption, the lack of long-term comparative data introduces considerable uncertainty into this analysis. Lastly, clinical expert feedback received by CDA-AMC for this review indicated that, in the absence of long-term data, the duration of benefit that patients receive from exagamglogene autotemcel is unknown.
CDA-AMC was unable to address this limitation. The CLIMB-111 and CLIMB-131 trials are ongoing. Additional data from longer-duration follow-up may help reduce uncertainty in the duration of effect but will not reduce uncertainty in the direct comparative efficacy or safety data due to lack of head-to-head trial evidence.
The sponsor’s predicted mortality benefit associated with exagamglogene autotemcel is uncertain. In the sponsor’s base-case analysis, patients treated with exagamglogene autotemcel lived approximately 8 years longer (29 years versus 21 years) than patients treated with SOC. Risk of death in the sponsor’s submitted pharmacoeconomic model was dependent on the patient’s transfusion status, occurrence of complications, and other infusion-related events. While clinical expert feedback received by CDA-AMC agreed that there are many factors that contribute to the risk of mortality for a patient with TDT, including complications, they noted that the CLIMB-111 and CLIMB-131 studies did not include survival analysis and therefore the exact mortality benefit associated with exagamglogene autotemcel is uncertain.
The sponsor assumes that chronic complications (i.e., cardiac complications, liver complications, osteoporosis, diabetes, and hypogonadism) will persist until death once they are developed. All complications are modelled individually using data from published literature or assumption, because the pivotal trial did not measure all chronic complications as specific outcomes of interest. Because almost all patients treated with exagamglogene autotemcel achieve TI and are assumed to no longer be at risk of any disease-related chronic complications, the assumed reduction in mortality due to fewer chronic complications is a key driver of cost-effectiveness estimates. The sponsor’s model predicts that the proportion of patients treated with SOC developing complications by the age of 50 years is 24% for cardiac complications, 13% for liver complications, 34% for osteoporosis, 39% for diabetes, and 62% for hypogonadism. Clinical experts consulted by CDA-AMC indicated that these proportions are overestimated and do not accurately reflect current natural history of disease. Furthermore, clinical experts indicated that there have been considerable improvements in management of TDT complications in recent years which is supported by published literature, meaning that the sponsor’s model also likely overestimates mortality associated with complications.
The sponsor’s submitted model lacked the flexibility to fully address issues related to the overestimation of chronic complications occurring in patients treated with SOC and the resulting overestimation of mortality. CDA-AMC was, however, able to address issues specifically related to cardiac mortality in the sponsor’s submitted model. The sponsor assumed an annual probability of cardiac mortality associated with cardiac complications of 13% based on findings from Kremastinos et al. (2001), a study of 52 patients with TDT and heart failure (follow-up duration of 5 years).23 The sponsor’s model assumed that this probability remains constant with a 21-year old patient experiencing the same probability of mortality as a 50-year-old patient, which did not meet face validity according to clinical experts consulted by CDA-AMC. The sponsor includes an option to model cardiac mortality based on Ladis et al. (2011), a historical prospective study of cardiac deaths in 1,044 patients with TDT (median observation time = 28.4 years).24 The latter study also examined deaths over time and concludes that cardiac deaths occurring in patients with TDT have notably improved in the past 20 years, which was supported by clinical experts consulted by CDA-AMC. Results from Ladis et al. (2011) suggest that the standard cardiac mortality rate occurring in patients with TDT is 106.6, which is equivalent to an annual probability of cardiac mortality of 6% at the age of 21 years and 29% at the age of 50 years, which was more reasonable according to clinical experts consulted by CDA-AMC.24 The standard cardiac mortality rate is applied in the model by multiplying against general population mortality risk using Canadian estimates, resulting in annual probabilities of cardiac mortality that are time-varying (i.e., are higher in a 50-year-old patient compared to a 21-year-old patient). Clinical experts consulted by CDA-AMC indicated that using the standard cardiac mortality rate to model cardiac mortality in patients with TDT is more reasonable given the more robust data, higher quality of evidence, and resulting time-varying estimates that allow for annual probabilities that increase with age.
Due to model transparency and inflexibility issues, CDA-AMC was unable to fully address the overestimation of chronic complications and their associated mortality in the submitted model.
CDA-AMC used the standard cardiac mortality rate method to model cardiac mortality in reanalysis.
Modelled population does not fully represent the proposed Health Canada–approved indication. The sponsor’s submitted pharmacoeconomic model was informed by data from the CLIMB-111 trial that enrolled patients aged 12 years to 35 years with TDT. The proposed Health Canada–approved indication of exagamglogene autotemcel is for the treatment of patients with TDT aged 12 years and older. Given the patient population of the CLIMB-111 trial excluded patients aged older than 35 years, the modelled population represents a younger cohort of patients compared to those who may receive exagamglogene autotemcel in clinical practice in Canada. This may bias results in favour of exagamglogene autotemcel as clinical expert feedback received by CDA-AMC noted that older patients with TDT tend have increased likelihood of organ damage and complications due to the disease or its treatments.
CDA-AMC was unable to address the limitation regarding the exclusion of patients aged older than 35 years.
Cost savings due to reduced health care resource utilization and complications are uncertain: The majority of patients treated with exagamglogene autotemcel (93%) are modelled to achieve TI and are assumed to achieve iron level normalization and therefore no longer are at risk of any disease-related chronic complications, essentially being “cured” of the disease. The assumption of cure has considerable implications on the cost-effectiveness of exagamglogene autotemcel. In addition to the limitations described, treatment is also assumed to result in considerable reductions in health care resource utilization and reductions in costs due to avoided RBC transfusions or ICT use.
In the sponsor’s base case, the frequency of resource utilization by health state (i.e., inpatient visits, outpatient visits, and emergency department visits) was informed by a published chart review of National Health Services centres in the UK and clinical expert input. It is uncertain whether these published estimates from the UK are reflective of health care resource utilization in Canada, and clinical experts consulted by CDA-AMC noted that the number of outpatient visits were likely overestimated in those who were transfusion dependent and transfusion reduced. The costs of health care resource utilization for those receiving SOC were therefore likely overestimated, resulting in cost-effectiveness estimates favouring exagamglogene autotemcel.
Furthermore, the cost of complications and health care resource utilization were informed by values obtained from the Canadian Institute for Health Information. CDA-AMC noted that the use of the Canadian Institute for Health Information to inform complication costs implies that all complications are treated in an inpatient setting. Clinical experts consulted by CDA-AMC agreed that while some complications may be severe enough to require inpatient treatment, there are events that occur that are managed at home or in the outpatient setting; therefore, the exclusive use of inpatient costing may further overestimate the cost of complications biasing results in favour of exagamglogene autotemcel. CDA-AMC notes that a key driver of cost-effectiveness estimates is the cost savings associated with avoided RBC transfusions and ICT costs ($809,876), as well as avoided complications ($88,495).
CDA-AMC could not identify alternative sources of cost and resource utilization data during the review period, and was therefore unable to address this limitation.
Health state utility values lacked face validity: The sponsor included utility values for transfusion dependent (0.73), transfusion reduced (0.75), and transfusion independent (0.93) health states in the model based on estimates from published literature. However, the transfusion independent health state utility value does not meet face validity because it suggests that patients who achieve TI have a higher quality of life than the average person living in Canada aged 20 years to 24 years (i.e., utility of 0.892 as reported by the Canadian Community Health Survey). Clinical experts consulted by CDA-AMC indicated that this did not meet face validity and that they did not expect patients with TDT achieving TI would have higher health-related quality of life than the average person living in Canada of a comparable age. Clinical experts consulted by CDA-AMC also noted that the utility value for the transfusion reduced health state also appeared to be underestimated, particularly when considering the incremental difference of 0.02 between the transfusion dependent and transfusion reduced health states. In the absence of more robust data, CDA-AMC was unable to address the uncertainty in the transfusion educed health state utility value.
CDA-AMC reduced the transfusion independent utility value to reflect the utility value of 0.892 for the general population of people living in Canada.
CDA-AMC was unable to address the uncertainty in the transfusion reduced utility value due to lack of data.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CDA-AMC (refer to Table 4).
Table 4: Key Assumptions of the Submitted Economic Evaluation (Not Noted as Limitations to the Submission)
Sponsor’s key assumption | CDA-AMC comment |
|---|---|
Patients receiving SOC would experience no change in transfusion status over the modelled time horizon. | Uncertain. Clinical expert feedback received by CDA-AMC noted that while patients with severe TDT that remain unmanageable with SOC likely experience little change in disease severity over time, there remains a possibility that patients with TDT can experience changes in their transfusion dependence and TDT-related complications. Additionally, in the absence of long-term data to inform if treatment waning for patients treated with exagamglogene autotemcel occurs, there is a possibility that a proportion of patients may transition between transfusion independent and transfusion reduced health states, which is currently not an option in the sponsor’s submitted model structure. The impact of this assumption on the cost-effectiveness of exagamglogene autotemcel is unknown. |
100% of patients receiving exagamglogene autotemcel experience engraftment success. | Uncertain. The proportion of patients experiencing engraftment success after exagamglogene autotemcel administration was based on data from the CLIMB-111 trial. It is unknown if engraftment success will be 100% in the Canadian clinical setting when a larger number of patients are infused. Assuming a proportion of 100% may bias results in favour of exagamglogene autotemcel as a lower engraftment success value would result in more patients being in the transfusion reduced or transfusion dependent health states. |
Annual RBC transfusions (17.2) and units of blood per transfusion (2.2) were informed by baseline utilization data from CLIMB-111 and were assumed to be generalizable to Canadian clinical practice. | Likely reasonable. Clinical experts consulted by CDA-AMC commented that these estimates were likely generalizable to Canadian clinical practice. However, if the frequency of transfusions in those receiving SOC is < 17 per year in clinical practice, the cost-effectiveness of exagamglogene autotemcel could be overly optimistic in the sponsor’s model. |
Distribution of ICT regimen use was parameterized by a chart review study of National Health Services centres in the UK and was assumed to be generalizable to Canadian clinical practice. | Uncertain. Clinical experts consulted by CDA-AMC noted that these proportions seemed relatively reasonable and that most would use deferasirox. However, fewer patients were expected to receive deferoxamine monotherapy in Canada and would more likely receive deferiprone instead. The impact of this assumption is not likely to result in meaningful impact to the cost-effectiveness results. |
CDA-AMC = Canada’s Drug Agency; ICT = iron chelation therapy; RBC = red blood cell; SOC = standard of care; TDT = transfusion-dependent beta thalassemia.
CDA-AMC Reanalyses of the Economic Evaluation
Base-Case Results
The CDA-AMC base case was derived by making changes in model parameter values and assumptions, in consultation with clinical experts. The CDA-AMC base-case reanalysis was derived by adjusting the mortality associated with cardiac complications and utility value associated with TI. CDA-AMC was unable to address uncertainty related to comparative clinical data, including the magnitude and duration of benefit for exagamglogene autotemcel. CDA-AMC was additionally unable to resolve uncertainty related to the predicted mortality benefit associated with exagamglogene autotemcel, the overestimation of TDT-related chronic complications, the modelled population, and complication costs.
Given the considerable limitations with the sponsor’s MAIC and the CDA-AMC clinical review’s conclusions that no concrete conclusions can be drawn from the indirect evidence about the comparative effectiveness of exagamglogene autotemcel, luspatercept was excluded from the CDA-AMC base case and included as a scenario analysis.
Table 5: CDA-AMC Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
Changes to derive the CDA-AMC base case | ||
1. Mortality associated with cardiac complications | Annual probability of 13% derived from a study of 52 patients with TDT (follow-up duration of 5 years) | SMR of 106.6 from historical prospective study of 1,044 patients with TDT (mean observation time of 28.4 years) |
2. Transfusion independent utility value | 0.93 | 0.892 |
CDA-AMC base case | ― | Reanalysis 1 + 2 |
CDA-AMC = Canada’s Drug Agency; SMR = standard mortality ratio; TDT = transfusion-dependent beta thalassemia.
Results of the CDA-AMC base case suggest that exagamglogene autotemcel will be more effective (additional 10.7 QALYs) at an additional cost of $2,078,310 over the lifetime time horizon resulting in an ICER of $194,807 per QALY compared to SOC. Similarly to the sponsor’s submitted results, the CDA-AMC base case further suggests that exagamglogene autotemcel would be associated with increased survival (incremental LYs = 7.98) and have fewer costs associated with RBC transfusions, ICT use, complications, and health care resource utilization. The results also suggest that exagamglogene autotemcel is associated with a reduction in chronic complications over the patient’s lifetime.
Exploration of the CDA-AMC base case shows that approximately 95% of the predicated incremental gain in QALYs with exagamglogene autotemcel is expected to be accrued in the extrapolation period (i.e., after 20 months). CDA-AMC notes that if the magnitude of benefit between exagamglogene autotemcel and SOC is less than estimated by the sponsor (i.e., exagamglogene autotemcel is associated with more RBC transfusions or complications than predicted by the sponsor’s model) then the cost-effectiveness of exagamglogene autotemcel compared to SOC may be higher.
The probability that exagamglogene autotemcel was cost-effective compared to SOC at a WTP threshold of $50,000 per QALY gained was 0% in the CDA-AMC reanalysis. This finding was similar to the sponsor’s submitted results.
Table 6: Summary of the Stepped Analysis of the CDA-AMC Reanalysis Results
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|---|
Sponsor’s base case | SOC | 1,160,001 | 13.08 | Reference |
Exagamglogene autotemcel | 3,179,877 | 27.88 | 136,450 | |
CDA-AMC reanalysis 1: cardiac mortality | SOC | 1,076,037 | 12.58 | Reference |
Exagamglogene autotemcel | 3,164,526 | 24.79 | 170,988 | |
CDA-AMC reanalysis 2: transfusion independent utility value | SOC | 1,160,001 | 13.08 | Reference |
Exagamglogene autotemcel | 3,179,877 | 26.77 | 147,528 | |
CDA-AMC base case (reanalysis 1 + 2) | SOC | 1,076,037 | 12.58 | Reference |
Exagamglogene autotemcel | 3,164,526 | 23.81 | 185,999 | |
CDA-AMC base case (reanalysis 1 + 2; probabilistic) | SOC | 1,087,170 | 12.66 | Reference |
Exagamglogene autotemcel | 3,165,480 | 23.33 | 194,807 |
CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; SOC = standard of care.
Note: The CDA-AMC reanalysis is based on publicly available prices of the comparator treatments. The results of all steps are presented deterministically unless otherwise indicated, while the cumulative CDA-AMC base case is always presented both deterministically and probabilistically.
Scenario Analysis Results
CDA-AMC undertook price reduction analyses based on the sponsor’s results and the CDA-AMC base case. Results of the price reduction analysis suggest that exagamglogene autotemcel would require a price reduction of approximately 55% to be considered cost-effective at a WTP threshold of $50,000 per QALY gained compared to SOC. With this price reduction, the one-time drug acquisition costs for exagamglogene autotemcel would be $1,254,400 per patient.
Table 7: CDA-AMC Price Reduction Analyses
Analysis | Unit drug cost | ICERs for exagamglogene autotemcel versus SOC ($/QALY) | |
|---|---|---|---|
Price reduction | ($) | Sponsor base case | CDA-AMC reanalysis |
No price reduction | 2,800,000 | 141,962 | 194,807 |
10% | 2,520,000 | 122,108 | 168,562 |
20% | 2,240,000 | 102,254 | 142,316 |
30% | 1,960,000 | 82,400 | 116,071 |
40% | 1,680,000 | 62,546 | 89,826 |
50% | 1,400,000 | 42,692 | 63,580 |
60% | 1,120,000 | 22,838 | 37,335 |
70% | 840,000 | 2,984 | 11,090 |
80% | 560,000 | Dominant | Dominant |
90% | 280,000 | Dominant | Dominant |
CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; SOC = standard of care.
CDA-AMC conducted a scenario analysis to evaluate the impact of including luspatercept as a comparator in the cost-effectiveness analysis. Results from the pairwise analysis between exagamglogene autotemcel and luspatercept, which included revisions aligned with the CDA-AMC base-case reanalysis, are presented in Table 14. In this analysis, exagamglogene autotemcel was associated with an incremental cost of $454,980 and an incremental QALY gain of 10.34 compared with luspatercept, resulting in an ICER of $44,002 per QALY gained. Due to the considerable limitations with the indirect evidence, it was not possible to produce a rigorous estimate of incremental benefit for exagamglogene autotemcel compared to luspatercept, and the ICER estimated in the scenario analysis should be interpreted carefully.
The estimated ICER is still subject to the limitations identified, including the considerable limitations with the indirect evidence, potential overestimation of chronic complications and their effect on mortality, the lack of evidence of long-term effectiveness of exagamglogene autotemcel and luspatercept, and concerns about the methods used to estimate costs and resource utilization. Several of these limitations implied a directional bias that favoured exagamglogene autotemcel. Given this clinical uncertainty, price reductions may be required to achieve cost-effectiveness compared to luspatercept at a WTP threshold of $50,000 per QALY gained.
Issues for Consideration
Exagamglogene autotemcel is currently undergoing review by CDA-AMC for the treatment of patients aged 12 years and older with sickle cell disease with recurrent vaso-occlusive crises.
Drug plan feedback and clinical expert feedback indicated there may be issues with access and prolonged stays required near specialized centres, especially for patients from remote areas, and financial support for travel and accommodation would be needed.
To be able to treat patients with exagamglogene autotemcel, specialized centres need to be trained and accredited by the sponsor. Both obtaining and maintaining this accreditation process can result in a high resource burden, including the development of various protocols and supporting yearly audits. In addition, this treatment has the added complexity of needing to coordinate patient care and product preparation with an external manufacturer. Because there will be additional patients with different indications being administered exagamglogene autotemcel by specialized centres, there will be a need to manage various protocols for preparation and delivery of each product type, which can increase the overall administrative burden.
Clinical expert feedback and patient input noted that the risk of infertility associated with myeloablative therapy is of high concern to patients. Patients may opt to plan exagamglogene autotemcel treatment around their family planning which may add additional resource burden due to fertility preservation and emotional support.
Overall Conclusions
The CDA-AMC clinical review concluded that in the absence of direct comparative data, evidence from the interim analysis of the single-arm CLIMB-111 study is very uncertain regarding the effect of exagamglogene autotemcel on clinical efficacy and harms outcomes in patients with TDT when compared with any comparator. Findings from the trial are consistent with a clinically meaningful reduction in transfusion leading to TI, according to clinical expert input. The available results from the trial are subject to important potential biases in outcome ascertainment, study population, and statistical analysis plan changes which impact the certainty that the observed effect is truly attributable to exagamglogene autotemcel. Results from the long-term extension portion were only available from a fraction of patients for all outcomes and therefore remain highly uncertain, and in general, data were only available for a relatively short time period after infusion. Conclusions around long-term harms results are generally limited by the ongoing nature of the trial and the short follow-up to date. The indirect evidence submitted by the sponsor, consisting of 2 MAICs comparing exagamglogene autotemcel to SOC (transfusions and chelation) and luspatercept, were considerably limited by differences in the study design, outcome ascertainment, and concerns around the validity of the comparators in terms of their potential for attaining the outcome of TI. Overall, information on the comparative nature of exagamglogene autotemcel to SOC and luspatercept remains highly uncertain due to considerable limitations with the indirect evidence as well as the use of a single-arm trial.
The CDA-AMC base case was derived by adjusting the mortality associated with cardiac complications and utility value associated with TI. CDA-AMC was unable to address uncertainty related to comparative clinical data, including the magnitude and duration of benefit for exagamglogene autotemcel and the predicted mortality benefit due to reduced chronic complications. Given the considerable limitations with the sponsor’s MAIC and the CDA-AMC clinical review’s conclusions that no concrete conclusions can be drawn from the indirect evidence about the comparative effectiveness of exagamglogene autotemcel, luspatercept was excluded from the CDA-AMC base case and included as a scenario analysis. The CDA-AMC base-case results align with those of the sponsor’s submitted analysis, indicating that exagamglogene autotemcel is not cost-effective at a WTP threshold of $50,000 per QALY gained, relative to SOC — CDA-AMC estimates an ICER of $194,807 per QALY compared to SOC. At the submitted price, exagamglogene autotemcel would require a price reduction of approximately 55% to be considered cost-effective at a WTP threshold of $50,000 per QALY.
Results were largely driven by the acquisition cost of exagamglogene autotemcel as well as the predicted gains in QALYs, LYs, and cost savings associated with reduced transfusions, ICT use, and chronic complications (total = $898,371). CDA-AMC notes that these findings are highly uncertain as 95% of the incremental QALYs were accrued in the extrapolation period (i.e., after 20 months). The results are dependent on a survival benefit of approximately 8 years. If the duration and magnitude of benefit associated with exagamglogene autotemcel is less and/or anticipated cost savings associated with reduced transfusions, ICT use, and chronic complications are lower than estimated, then the ICER may be higher and a higher price reduction may be required.
In the scenario analysis including luspatercept as a comparator, CDA-AMC estimates an ICER of $44,002 per QALY gained compared to luspatercept. Due to the considerable limitations with the indirect evidence, it was not possible to produce a rigorous estimate of incremental benefit for exagamglogene autotemcel compared to luspatercept, and the ICER estimated in the scenario analysis should be interpreted carefully. The estimated ICER compared to luspatercept is still subject to the limitations identified and CDA-AMC notes that several of these limitations implied a directional bias that favoured exagamglogene autotemcel. Given this clinical uncertainty, price reductions may be required to achieve cost-effectiveness compared to luspatercept at a WTP threshold of $50,000 per QALY gained.
References
1.Drug Reimbursement Review sponsor submission: Exagamglogene autotemcel (CASGEVY) [internal sponsor's package]. Toronto (ON): Vertex Pharmaceuticals (Canada), Inc; 2024.
2.Exa-cel Product Monograph (DRAFT) [sponsor supplied reference]. Toronto (ON): Vertex Pharmaceuticals (Canada) Inc; 2024.
3.Exagamglogene Autotemcel (exa-cel) for the Treatment of Transfusion-dependent β-thalassemia: Indirect Treatment Comparison Report [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Exagamglogene autotemcel (CASGEVY). Toronto (ON): Vertex Pharmaceuticals (Canada) Incorporated; 2024.
4.Statistics Canada. Life Tables, Canada, Provinces and Territories 1980/1982 to 2020/2022 (three-year estimates), and 1980 to 2022 (single-year estimates) [sponsor supplied reference]. Ottawa (ON): Government of Canada; 2023: https://www150.statcan.gc.ca/n1/pub/84-537-x/84-537-x2023002-eng.htm.
5.Single Technology Appraisal: Betibeglogene autotemcel for treating transfusion dependent beta-thalassaemia [sponsor supplied reference]. London (GB): National Institute for Health Care Excellence; 2021: https://www.nice.org.uk/guidance/gid-ta10334/documents/committee-papers.
6.Frangoul H, Altshuler D, Cappellini MD, et al. CRISPR-Cas9 Gene Editing for Sickle Cell Disease and β-Thalassemia. N Engl J Med. 2020;384(3):252-260. PubMed
7.Costanian C, McCague H, Tamim H. Age at natural menopause and its associated factors in Canada: cross-sectional analyses from the Canadian Longitudinal Study on Aging. Menopause. 2018;25(3):265-272. PubMed
8.Al-Sahab B, Ardern CI, Hamadeh MJ, Tamim H. Age at menarche in Canada: results from the National Longitudinal Survey of Children & Youth. BMC Public Health. 2010;10:736. PubMed
9.CTX001-121 - Grade 3 or above Adverse Events Related to Busulfan and/or CTX001 by System Organ Class and Preferred Term for the Enroll to M24 Interval. Data on File [sponsor supplied reference]. Toronto (ON): Vertex Pharmaceuticals (Canada) Inc; 2023.
10.Matza LS, Paramore LC, Stewart KD, Karn H, Jobanputra M, Dietz AC. Health state utilities associated with treatment for transfusion-dependent β-thalassemia. Eur J Health Econ. 2020;21(3):397-407. PubMed
11.O'Brien SH, Hankins JS. Decision analysis of treatment strategies in children with severe sickle cell disease. J Pediatr Hematol Oncol. 2009;31(11):873-878. PubMed
12.Krol M, Nap A, Michels R, Veraart C, Goossens L. Health state utilities for infertility and subfertility. Reproductive Health. 2019;16(1):47. PubMed
13.CADTH Reimbursement Recommendation: Luspatercept (Reblozyl) [sponsor supplied reference]. Ottawa (on): CADTH; 2021: https://www.cadth.ca/sites/default/files/attachments/2021-06/CADTH_reimbursement_recommendation_luspatercept_%28reblozyl%29.pdf. Accessed May 19, 2023.
14.Corporation C, Acceleron Pharma Incorporated. REBLOZYL (luspatercept-aamt) [sponsor supplied reference]. Cambridge, MA2020.
15.Data on File: Canadian clinical advisor interviews for TDT [sponsor supplied reference]. Toronto (ON): Vertex Pharmaceuticals (Canada) Incorporated; 2023.
16.Clinical Study Protocol: A Phase 1/2/3 Study to Evaluate the Safety and Efficacy of a Single Dose of Autologous CRISPR-Cas9 Modified CD34+ Human Hematopoietic Stem and Progenitor Cells (CTX001) in Subjects With Severe Sickle Cell Disease. Study Number: CTX001-121 [sponsor supplied reference]. Version 6.10 (CA). Toronto (ON): Vertex Pharmaceuticals (Canada) Inc; 2021.
17.Shah F, Telfer P, Velangi M, et al. Routine management, healthcare resource use and patient and carer-reported outcomes of patients with transfusion-dependent β-thalassaemia in the United Kingdom. eJHaem. 2021(2):738–749. PubMed
18.Ontario Ministry of Health and Long Term Care. Schedule of Benefits, Physician Services Under the Health Insurance Act [sponsor supplied reference]. 2023.
19.Initiative OCC. OCCI database [sponsor supplied reference]. https://data.ontario.ca/en/dataset/ontario-case-costing-initiative-occi. Accessed May 2023.
20.Information CIfH. Pharmaceutical Data Tool [sponsor supplied reference]. https://www.cihi.ca/en/pharmaceutical-data-tool. Accessed April 11, 2024.
21.Ontario Go. Ontario Drug Benefit Formulary [sponsor supplied reference]. 2018; https://www.formulary.health.gov.on.ca/formulary/. Accessed May 2018.
22.Centre OF. Ottawa Fertility Center Fees [sponsor supplied reference]. https://conceive.ca/fees/. Accessed April 2024.
23.Kremastinos DT, Tsetsos GA, Tsiapras DP, Karavolias GK, Ladis VA, Kattamis CA. Heart failure in beta thalassemia: a 5-year follow-up study. Am J Med. 2001;111(5):349-354. PubMed
24.Ladis V, Chouliaras G, Berdoukas V, et al. Survival in a large cohort of Greek patients with transfusion-dependent beta thalassaemia and mortality ratios compared to the general population. Eur J Haematol. 2011;86(4):332-338. PubMed
25.Ontario Go. Ontario Drug Benefit Formulary/Comparative Drug Index [sponsor supplied reference]. https://www.formulary.health.gov.on.ca/formulary/. Accessed February 2024.
26.Saskatchewan Drug Plan: search formulary. 2024; https://formulary.drugplan.ehealthsask.ca/SearchFormulary. Accessed 2024 Jul 15.
27.Rodriguez-Capote K, Higgins TN. Incidence of hemoglobinopathies and thalassemias in Northern Alberta. Establishment of reference intervals for HbF and HbA2. Clin Biochem. 2015;48(10):698-702. PubMed
28.Simpson E, Klaassen RJ, Chakraborty P, et al. Increasing Incidence and Prevalence of Pathologic Hemoglobinopathies Among Children in Ontario, Canada from 1991-2013. Blood. 2018;132(Supplement 1):4698-4698.
29.Simpson E, Laforest I, Barry R, et al. Prevalence of Hemoglobinopathies among Ontario Children after the Implementation of Universal Hemoglobinopathy Screening. Pediatr Blood Cancer. 2017;64(S1):e26591.
30.Epidemiology and Clinical Characteristics of SCD and B-Thal in Canada, Data on File [sponsor supplied reference]. Toronto (ON): Vertex Pharmaceutical (Canada) Inc; 2022.
31.Statistics Canada. Canada's population estimates: Age and sex, July 1, 2022 [sponsor supplied reference]. Ottawa (ON): Government of Canada; 2022: https://www150.statcan.gc.ca/n1/daily-quotidien/220928/dq220928c-eng.htm. Accessed April 13, 2023.
Appendix 1: Cost Comparison Table
Please note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical expert(s) and drug plans. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 8: CDA-AMC Cost Comparison Table for the Treatment of Transfusion-Dependent Beta Thalassemia
Treatment | Strength / concentration | Form | Price ($) | Recommended dosage | Daily cost ($)a | Annual cost ($) |
|---|---|---|---|---|---|---|
Exagamglogene autotemcel | 4 to 13 × 106 cells/mL | Cell suspension for IV infusion | 2,800,000b | Minimum recommended dose of 3 × 106 CD34+ cells/kg as a single dose for infusion | NA | 2,800,000 lifetime cost |
Erythroid Maturation Agent | ||||||
Luspatercept (Reblozyl) | 50 mg/mL | 25 mg powder for SC injection 75 mg powder for SC injection | 2,189.0000 6,567.0000 | 1.0 to 1.75 mg/kg every 3 weeks | 416.95 to 625.43 | 152,188 to 228,281 |
Iron Chelation Therapy | ||||||
Deferasirox | 90 mg 180 mg 360 mg 125 mg 250 mg 500 mg | Tablet | 2.6303 5.261 10.5228 5.2408 10.4820 20.9649 | 7 to 14 mg/kg daily | 15.78 to 31.57 | 5,761 to 13,391 |
Deferiprone | 1,000 mg 100 mg/mL | Tablet Oral solution | 32.7452c 3.2766c | 25 to 33 mg/kg 3 times daily | 196.47 to 294.71 | 71,712 to 107,568 |
Deferoxamine mesylate | 95 mg/mL | 500 mg powder for SC injection 2 g powder for SC injection | 15.1700c 28.3500c | 20 to 60 mg/kg daily 4 to 7 times per week | 28.35 to 87.04 | 5,913 to 31,770 |
SC = subcutaneous.
Note: All prices are from the Ontario Drug Benefit Formulary or Ontario Exceptional Access Program Formulary (accessed July 2024, unless otherwise indicated, and do not include dispensing fees).25 Annual costs are based on 365 days per year.
aRecommended dosages are from the respective product’s monograph. Costs based on a mean weight of 76 kg for an adult in the general population in Canada.
bSponsor submitted price.1
cSaskatchewan drug benefit formulary (accessed July 2024).26
Appendix 2: Submission Quality
Please note that this appendix has not been copy-edited.
Description | Yes or No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | No | Refer to CDA-AMC critical appraisal. |
Model has been adequately programmed and has sufficient face validity | No | Refer to CDA-AMC critical appraisal. |
Model structure is adequate for decision problem | No | Refer to CDA-AMC critical appraisal. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | Yes | No comment. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | Yes | No comment. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | Yes | No comment. |
Appendix 3: Additional Information on the Submitted Economic Evaluation
Please note that this appendix has not been copy-edited.
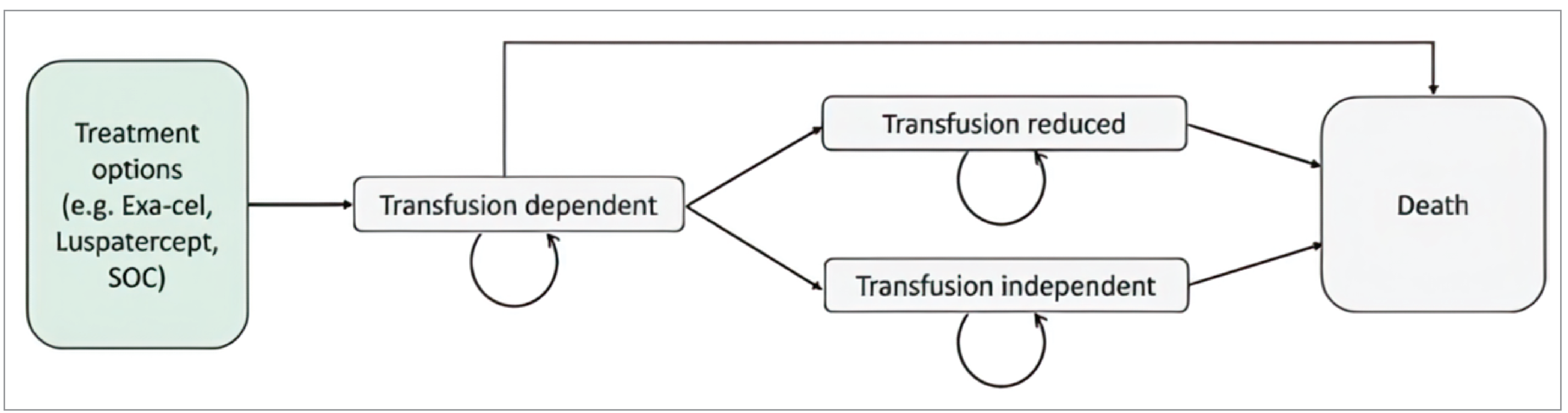
Detailed Results of the Sponsor’s Base Case
Table 10: Disaggregated Summary of the Sponsor’s Economic Evaluation Results
Parameter | Exa-cel | Luspatercept | SOC |
|---|---|---|---|
Discounted LYs | |||
Total | 32.44 | 22.67 | 22.45 |
Discounted QALYs | |||
Total | 27.30 | 13.60 | 13.20 |
Transfusion independent | 27.10 | 0.02 | 0.00 |
Transfusion reduced | 1.55 | 3.41 | 0.00 |
Transfusion dependent | −0.59 | 12.61 | 15.78 |
Complications | −1.19 | −2.31 | −2.45 |
Infertility | −0.21 | −0.13 | −0.13 |
Discounted costs ($) | |||
Total | 3,181,435 | 2,925,064 | 1,179,345 |
Acquisition | 2,800,000 | 1,796,675 | 0 |
Mobilization, apheresis, conditioning, and pre-treatment lab costs | 24,947 | 0 | 0 |
Additional infusion-related costs | 84,914 | 0 | 0 |
Hospitalization costs for procedure | 77,620 | 0 | 0 |
Postinfusion monitoring costs | 7,294 | 0 | 0 |
Blood transfusion costs | 31,939 | 500,362 | 547,347 |
Iron chelation therapy costs | 146,000 | 444,625 | 440,470 |
Phlebotomy costs | 1,317 | 0 | 0 |
Total complication costs | 71,778 | 153,557 | 160,273 |
Cardiac complication costs | 15,178 | 33,936 | 33,666 |
Liver complication costs | 15,266 | 23,109 | 26,551 |
Osteoporosis costs | 7,407 | 11,214 | 11,653 |
Diabetes costs | 7,161 | 14,413 | 16,454 |
Hypogonadism costs | 26,767 | 70,885 | 71,948 |
Splenectomy costs | 0 | 0 | 0 |
Infertility costs | 2,838 | 1,804 | 1,797 |
Disease monitoring costs | 7,368 | 19,853 | 21,485 |
AE management costs | 4,335 | 525 | 272 |
Terminal care costs | 5,999 | 7,664 | 7,702 |
AE = adverse event; exa-cel = exagamglogene autotemcel; LY = life-year; SOC = standard of care; QALY = quality-adjusted life-year.
Source: Sponsor’s pharmacoeconomic submission.1
Table 11: Summary of the Sponsor’s Economic Evaluation Additional Clinical Outcomes
Parameter | Exa-cel | Luspatercept | SOC |
|---|---|---|---|
Proportion of Patients Developing Chronic Complications by Age 100 | |||
Cardiac complication | 6.6% | 27.7% | 27.7% |
Liver complication | 4.2% | 11.3% | 13.4% |
Osteoporosis | 13.7% | 42.2% | 44.3% |
Diabetes | 10.1% | 41.7% | 47.4% |
Hypogonadism | 12.8% | 66.7% | 67.5% |
Splenectomy | 0.0% | 0.0% | 0.0% |
Proportion of Patients Alive at Age 50 | |||
Alive | 78.8% | 47.0% | 46.1% |
Exa-cel = exagamglogene autotemcel; SOC = standard of care.
Appendix 4: Additional Details on the CDA-AMC Reanalyses and Sensitivity Analyses of the Economic Evaluation
Please note that this appendix has not been copy-edited.
Detailed Results of CDA-AMC Base Case
Table 12: Disaggregated Summary of the CDA-AMC Economic Evaluation Results
Parameter | Exa-cel | SOC |
|---|---|---|
Discounted LYs | ||
Total | 29.00 | 21.02 |
Discounted QALYs | ||
Total | 23.33 | 12.66 |
Transfusion independent | 23.15 | 0.00 |
Transfusion reduced | 1.36 | 0.00 |
Transfusion dependent | −0.59 | 14.80 |
Complications | −1.02 | −2.00 |
Infertility | −0.21 | −0.13 |
Discounted costs ($) | ||
Total | 3,165,480 | 1,087,170 |
Acquisition | 2,800,000 | 0 |
Mobilization, apheresis, conditioning, and pre-treatment lab costs | 24,806 | 0 |
Additional infusion-related costs | 84,681 | 0 |
Hospitalization costs for procedure | 77,279 | 0 |
Postinfusion monitoring costs | 7,402 | 0 |
Blood transfusion costs | 31,209 | 513,080 |
Iron chelation therapy costs | 141,202 | 411,313 |
Phlebotomy costs | 1,348 | 0 |
Total complication costs | 61,733 | 132,956 |
Cardiac complication costs | 12,956 | 27,846 |
Liver complication costs | 13,490 | 23,588 |
Osteoporosis costs | 6,349 | 9,328 |
Diabetes costs | 6,131 | 12,991 |
Hypogonadism costs | 22,807 | 59,203 |
Splenectomy costs | 0 | 0 |
Infertility costs | 2,889 | 1,830 |
Disease monitoring costs | 6,621 | 19,724 |
AE management costs | 4,350 | 255 |
Terminal care costs | 6,640 | 8,011 |
AE = adverse event; exa-cel = exagamglogene autotemcel; LY = life-year; SOC = standard of care; QALY = quality-adjusted life-year.
Note: The CDA-AMC reanalysis is based on publicly available prices of the comparator treatments. The results of all steps are presented deterministically unless otherwise indicated, while the cumulative CDA-AMC base case is always presented both deterministically and probabilistically.
Table 13: Summary of the CDA-AMC Base Case Additional Clinical Outcomes
Parameter | Exa-cel | Luspatercept | SOC |
|---|---|---|---|
Proportion of Patients Developing Chronic Complications by Age 100 | |||
Cardiac complication | 6.2% | 25.8% | 26.0% |
Liver complication | 4.2% | 11.4% | 13.5% |
Osteoporosis | 12.7% | 36.3% | 38.7% |
Diabetes | 8.8% | 37.1% | 43.6% |
Hypogonadism | 12.7% | 65.3% | 66.5% |
Splenectomy | 0.0% | 0.0% | 0.0% |
Proportion of Patients Alive at Age 50 | |||
Alive | 78.0% | 42.0% | 41.2% |
Exa-cel = exagamglogene autotemcel; SOC = standard of care.
Scenario Analyses
Table 14: Summary of the CDA-AMC Scenario Analyses
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER ($/QALY)a |
|---|---|---|---|---|---|
Exagamglogene autotemcel versus luspatercept | |||||
Luspatercept | 2,710,500 | Reference | 12.99 | Reference | Reference |
Exagamglogene autotemcel | 3,165,480 | 454,980 | 23.33 | 10.34 | 44,002 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Note: Submitted analyses are based on the publicly available prices of comparator treatments.
Appendix 5: Submitted BIA and CDA-AMC Appraisal
Please note that this appendix has not been copy-edited.
Table 15: Summary of Key Take-Aways
Key take-aways of the budget impact analysis |
|---|
|
Summary of Sponsor’s BIA
The sponsor submitted a BIA to estimate the three-year budget impact of reimbursing exagamglogene autotemcel for the treatment of patients aged 12 years and older with TDT. The analysis was taken from the perspective of the Canadian public drug plan over a 3-year time horizon (2025 to 2027). The target population size was derived using an epidemiological approach and included drug acquisition costs. Province-specific prevalence rates, proportion diagnosed with TDT, and treatment eligibility were estimated using published literature, market research, demographic data, and assumptions. The sponsor compared a reference scenario in which patients received SOC (defined as chronic RBC transfusions every 2 to 4 weeks) and ICT [represented by a weighted basket of treatment options]) or luspatercept to a new drug scenario in which patients could receive exagamglogene autotemcel. Market share was informed by internal market estimates and clinical expert feedback obtained by the sponsor. Wastage and administration costs were not included. Key inputs to the BIA are documented in Table 16.
Table 16: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1 / year 2 / year 3 if appropriate) |
|---|---|
Target population | |
Prevalence of beta thalassemia in adults 18+ Prevalence of beta thalassemia in adolescents ages 12 to 17 % of beta thalassemia patients diagnosed with TDT % of TDT patients (18+) fit for treatment % of TDT patients (12 to 17) fit for treatment Projected annual growth rate of TDT | 70%30 50%30 54%30 1.0%31 |
Number of patients eligible for drug under review | 545 / 550 / 556 |
Market Uptake (3 years) | |
Uptake (reference scenario) SOC Luspatercept | 96% / 95% / 94% 4% / 5% / 6% |
Uptake (new drug scenario) Exagamglogene autotemcel SOC Luspatercept | 0.2% / 1.4% / 4.2% 95.8% / 93.7% / 90.1% 4.0% / 4.9% / 5.7% |
Cost of treatment (per patient, per year) | |
Exagamglogene autotemcel SOC Luspatercept | $2,800,000a $44,229b $156,817 |
SOC = standard of care; TDT = transfusion-dependent beta thalassemia.
aApplied in the model as a one-time cost in the first year for when patients are treated.
bCalculated as a weighted average across all provinces as jurisdiction-specific treatment acquisition costs were used in the pan-Canadian analysis. Annual SOC cost ranged from $11,135 to $46,109 depending on the jurisdiction.
Summary of the Sponsor’s BIA Results
The sponsor estimated the 3-year budget impact of reimbursing exagamglogene autotemcel for the treatment of patients aged 12 years and older with TDT to be $64,585,283 (year 1: $3,052,191; year 2: $18,397,226; year 3: $43,135,865).
CDA-AMC Appraisal of the Sponsor’s BIA
CDA-AMC identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
The market share for exagamglogene autotemcel is uncertain. In the sponsor’s base-case analysis, the anticipated market share of exagamglogene autotemcel was informed by internal market estimates and feedback from clinical experts received by the sponsor. The sponsor noted that exagamglogene autotemcel can only be administered in ATCs and a centre will need 6 to 12 months before it is fully activated. As such, the sponsor assumed that 1 patient will receive exagamglogene autotemcel within the first year of reimbursement, which may be a conservative assumption given that the treatment process could take up to 1 year. CDA-AMC notes that the sponsor’s assumption that it will take a year to set up the ATC centres may be biasing the budget impact in favour of exagamglogene autotemcel especially because the sponsor themselves provide a 6-to-12-month threshold. Should the authorization process it take less than a year, then centres may be able to treat a subset of patients within the first year of reimbursement. As such, the budget impact of exagamglogene autotemcel maybe be larger than the sponsor’s base-case estimate. CDA-AMC notes that the exact number of ATCs that will become online and the number of patients each centre may treat is also associated with significant uncertainty. The exact impact of this on the budget impact of exagamglogene autotemcel is unknown. However, should more centres become available, and more patients are treated, the budget impact will likely be higher.
Lastly the sponsor assumed that of the patients treated with exagamglogene autotemcel, 2/3 of the anticipated patient numbers would be patients with sickle cell disease and 1/3 would be patients with TDT. Clinical expert feedback received by CDA-AMC noted that the exact proportion of patient SCD to TDT is uncertain; however, in the initial years some clinicians may prioritize patients with SCD due to the availability of other therapeutic options for TDT and the large health care resource burden associated with uncontrolled SCD and the other available treatment options for TDT. The specific distribution among the indications remains unknown.
CDA-AMC was unable to address this limitation. CDA-AMC conducted a scenario analysis aligned with expert input obtained by the sponsor representing increased bed capacity with 7 ATCs. This scenario considers the maximum possible anticipated uptake but does not consider the time from listing until treatment (e.g., time from listing until centre “activation,” time from listing to infusion). The scenario with 7 ATCs presumed that 35, 70, and 98 total TDT and SCD patients could be treated in years 1, 2, and 3, respectively. This translates to 12, 23, and 33 TDT patients.
Inclusion of blood product costs is inappropriate. As part of SOC the sponsor included the cost of RBC transfusions using a unit cost obtained from the CDA-AMC reimbursement review of luspatercept. As the budget impact is from the perspective of the Canadian drug plans and RBC transfusions are funded by Canadian Blood Services, the inclusion of RBC transfusion costs is not appropriate biasing BIA results in favour of exagamglogene autotemcel.
In the CDA-AMC base-case analysis, the cost of RBC transfusions was excluded.
CDA-AMC Reanalyses of the BIA
Table 17: CDA-AMC Revisions to the Submitted Budget Impact Analysis
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
Changes to derive the CDA-AMC base case | ||
1. Cost of RBC transfusions | Included | Excluded |
CDA-AMC base case | Reanalysis 1 | |
RBC = red blood cell.
The results of the CDA-AMC step-wise reanalysis are presented in summary format in Table 18 and a more detailed breakdown is presented in Table 19.
In the CDA-AMC base case, the estimated incremental budget impact of reimbursing exagamglogene autotemcel for the treatment of patients aged 12 years and older with TDT to be $64,614,557 (year 1: $3,052,191; year 2: $18,400,764; year 3: $43,161,602).
Table 18: Summary of the CDA-AMC Reanalyses of the Budget Impact Analysis
Stepped analysis | Three-year total ($) |
|---|---|
Submitted base case | 64,585,283 |
CDA-AMC reanalysis 1 | 64,614,557 |
CDA-AMC base case | 64,614,557 |
BIA = budget impact analysis.
CDA-AMC conducted the following scenario analyses to address remaining uncertainty, using the CDA-AMC base case (results are provided in Table 19).
Assuming higher market uptake of exagamglogene autotemcel as per the sponsor provided inputs assuming increased bed capacity with 7 ATCs.
Table 19: Detailed Breakdown of the CDA-AMC Reanalyses of the BIA
Stepped analysis | Scenario | Year 0 (current situation) ($) | Year 1 ($) | Year 2 ($) | Year 3 ($) | Three-year total ($) |
|---|---|---|---|---|---|---|
Submitted base case | Reference | 20,426,704 | 21,235,341 | 22,058,108 | 22,895,207 | 66,188,656 |
New drug | 20,426,704 | 24,287,532 | 40,455,334 | 66,031,072 | 130,773,939 | |
Budget impact | 0 | 3,052,191 | 18,397,226 | 43,135,865 | 64,585,283 | |
CDA-AMC base case | Reference | 18,610,051 | 19,402,298 | 20,208,529 | 21,028,944 | 60,639,770 |
New drug | 18,610,051 | 22,454,489 | 38,609,293 | 64,190,545 | 125,254,327 | |
Budget impact | 0 | 3,052,191 | 18,400,764 | 43,161,602 | 64,614,557 | |
CDA-AMC scenario analysis 1: Increased bed capacity (7 ATCs) | Reference | 18,610,051 | 19,402,298 | 20,208,529 | 21,028,944 | 60,639,770 |
New drug | 18,610,051 | 22,454,489 | 54,022,859 | 84,193,536 | 160,670,884 | |
Budget impact | 0 | 3,052,191 | 33,814,331 | 63,164,592 | 100,031,114 |
ATC = authorized treatment centre; BIA = budget impact analysis.
Ethics Review
Abbreviations
CDA-AMC
Canada’s Drug Agency
HSCT
hematopoietic stem cell transplant
ICT
iron chelation therapy
RBC
red blood cell
SCD
sickle cell disease
TDT
transfusion-dependent beta thalassemia
Summary
Transfusion-dependent beta thalassemia (TDT) is a rare, progressive, autosomal recessive hereditary blood disorder that causes chronic severe anemia. This anemia necessitates lifelong red blood cell (RBC) transfusions, which cause iron overload that must be treated with iron chelation therapy (ICT) to prevent complications leading to morbidity and early mortality.
This report describes ethical considerations regarding the use of exagamglogene autotemcel, a gene therapy for the treatment of patients aged 12 years and older with TDT. Patient group, clinician group, clinical expert, and drug program input, as well as relevant literature, informed this review.
The ethical considerations identified include those related to the following.
Treatment and experiences of TDT: TDT and its treatment are physically and psychosocially burdensome and can adversely impact health-related quality of life. Some people with TDT may fulfill ambitions in education, work, and personal relationships and survive into their 60s when receiving optimal treatment and lifelong, multidisciplinary management. However, existing disease-modifying and curative therapies have limitations in efficacy, present risks, and may be inaccessible or intolerable for some. There is an unmet need for effective treatment for people with TDT who are not eligible for allogenic hemopoietic stem cell transplant (HSCT) that eliminates or reduces burdens associated with lifelong RBC transfusions and ICT. Certain groups including those living far from specialized treatment centres, people experiencing financial hardship, adolescents, older people, and recent immigrants may experience disproportionate difficulty accessing and navigating effective treatment and care and may have higher unmet need for effective, one-time treatment options.
Evidence used in the evaluation of exagamglogene autotemcel: Findings from the ongoing single-arm CLIMB-111 trial are consistent with a clinically meaningful impact on transfusion independence based on clinical expert input. Exagamglogene autotemcel also displays a short-term safety profile consistent with a treatment requiring myeloablative conditioning. However, there is uncertainty in: whether the effect observed is truly attributable to exagamglogene autotemcel because of methodological limitations in the CLIMB-111 trial, the efficacy and safety of exagamglogene autotemcel beyond the current trial follow-up of 24 months, and generalizability beyond the trial population (which excluded people aged ≥ 35 years who the clinical experts noted may benefit from treatment, and people with co-inheritance of multiple types of thalassemia). Additionally, there is considerable uncertainty in indirect evidence comparing exagamglogene autotemcel to luspatercept and standard of care, and a lack of evidence to understand the value of exagamglogene autotemcel versus allogenic HSCT for patients eligible for allogenic HSCT. Given that exagamglogene autotemcel has been proposed as a one-time treatment with potential for lifelong effects, this evidentiary uncertainty highlights the importance of robust consent conversations to support informed, autonomous decision-making and establish reasonable expectations, including for people under-represented in the trial. Evidentiary uncertainty also has implications for health systems decision-making as it presents challenges for assessing the value of exagamglogene autotemcel relative to standard of care and understanding opportunity costs.
Clinical use and implementation of exagamglogene autotemcel: Based on available evidence, the clinical experts would consider exagamglogene autotemcel given high treatment burden and unmet need for effective, one-time treatment options for people with TDT for whom allogenic HSCT is not an option (especially those who do not respond to or have difficulty accessing or tolerating standard care). As a gene therapy, the use of exagamglogene autotemcel is associated with theoretical risks (e.g., genotoxicities) and known risks of myeloablative conditioning (e.g., secondary malignancy and infertility). Understandings of the level of transfusion independence required to deem exagamglogene autotemcel acceptable considering these risks may vary between and among clinicians and patients. This highlights the importance of shared decision-making processes eliciting the values of individual patients. Clinician groups and clinical experts suggested that providing access to fertility preservation (as is common for patients undergoing oncological treatments that present risk of infertility) would help support equitable access and mitigate risks associated with infertility. Providers will need to facilitate thorough consent conversations to ensure patients and their families are aware of the benefits, risks, and evidentiary uncertainty related to exagamglogene autotemcel and have reasonable expectations. Managing expectations will be particularly important to prevent harms related to false hope, as treatment with exagamglogene autotemcel may not cure TDT, may not reverse end-organ damage and related symptoms, and may preclude eligibility for re-treatment and future gene therapies. The clinical experts and literature suggested that equitable access to exagamglogene autotemcel could be supported by addressing barriers to accessing standard TDT care, as well as barriers to accessing specialized treatment centres, undergoing prolonged hospitalization, and receiving long-term follow-up.
Health systems: Uncertainty in evidence regarding the clinical effectiveness and safety of exagamglogene autotemcel and, in turn, cost-effectiveness limits assessments of its value as a one-time therapy. Treatment with exagamglogene autotemcel is resource intensive, requiring pretreatment, month-long hospitalization, and follow-up and administration by experienced personnel in authorized transplant and cell therapy centres. These factors, alongside current health systems capacity constraints, will severely limit the number of eligible patients that can be treated each year and necessitate prioritizing patients for access. To facilitate equitable access to exagamglogene autotemcel and other stem cell transplant-based therapies for people with hemoglobinopathies, the clinical experts proposed reserving a set number of transplant spots annually for people with TDT and sickle cell disease (SCD). Clinical experts reported that, among patients with TDT who are ineligible for allogenic HSCT, they would prioritize those with greatest difficulty responding to, tolerating, or accessing standard care who were still fit and eligible for treatment with exagamglogene autotemcel. As authorized treatment centres may only be situated in certain jurisdictions in Canada, consistent prioritization criteria, intrajurisdictional and interjurisdictional agreements, and patient supports are important for ensuring equitable access to exagamglogene autotemcel.
Objective and Research Questions
The objective of this Ethics Review is to identify and describe ethical considerations associated with the use of exagamglogene autotemcel for the treatment of patients aged 12 years and older with TDT, including considerations related to the disease context, evidentiary basis, the use of exagamglogene autotemcel, and impact on health systems.
To address this objective, this review addresses the following research questions.
What ethical considerations arise in the context of TDT, including considerations related to diagnosis, treatment, and outcomes?
What ethical considerations arise in relation to the evidence (e.g., clinical and economic data) used to evaluate exagamglogene autotemcel?
What ethical considerations arise in relation to the use of exagamglogene autotemcel for patients, their caregivers, and their clinicians?
What are the ethical considerations for health systems related to exagamglogene autotemcel?
Methods
Guiding questions identified in the EUnetHTA Core Model 3.0, Ethics Analysis Domain,1 and supplemented by relevant questions from the Equity Checklist for Health Technology Assessments,2 drive the identification of ethical considerations relevant to the use of exagamglogene autotemcel for the treatment of TDT in this Ethics Review. These guiding questions are organized to respond to the research questions and to investigate ethical considerations related to the following:
patients living with TDT and their caregivers (i.e., disparities in incidence, treatment, or outcomes; challenges or burdens related to diagnosis or clinical care; factors that might prevent patients from gaining access to therapies)
evidence used to demonstrate the benefits, harms, and value of exagamglogene autotemcel (i.e., ethical considerations in relevant clinical trials, including their representativeness, the choice of outcome measures, the appropriateness of the analytical methods and models used to all population groups; ethical considerations related to the data or assumptions in the economic evaluation)
use of exagamglogene autotemcel, including considerations related to benefits and harms to patients, relatives, caregivers, clinicians, and society, as well as considerations related to access to these therapies
uptake of exagamglogene autotemcel in health systems, including considerations related to the distribution of health care resources.
Review of Project Inputs
A single reviewer collected and considered input from 7 main sources of data related to ethical considerations relevant to the research questions guiding this Ethics Review. The reviewer considered the following sources.
The evidence from a search of published literature.
The sponsor submission, including noting relevant information and external references or sources relevant to each of the research questions driving this report.
Clinician group input received from the Canadian Hemoglobinopathy Association.
Patient input received from the Global Action Network for Sickle Cell & Other Inherited Blood Disorders and the Thalassemia Foundation of Canada.
Drug program input received from drug programs participating in the reimbursement review process.
Discussion with the clinical experts (n = 3) directly engaged over the course of this reimbursement review, including through 1 clinical consultation meeting involving 2 experts, and 1 panel meeting involving 3 experts. During each of these meetings, the reviewer asked the clinical experts targeted questions related to ethical considerations corresponding to the research questions driving this report. All the clinical experts are practising hematologists with experience treating pediatric (n = 2) or adult (n = 1) patients with TDT in Canada. One had experience caring for patients who had received exagamglogene autotemcel.
Engagement with clinical and economic reviewers to identify domains of ethical interest arising from their respective reviews and to identify relevant questions and sources to further pursue in this report.
Details on the Published Literature Search
An information specialist conducted a literature search on key resources including MEDLINE via Ovid, Philosopher’s Index via Ovid, and Scopus. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. To address the indication, the main search concept used was “exagamglogene autotemcel.”
A second search was performed to address the population (transfusion-dependent thalassemia), using MEDLINE and Philosopher’s Index. Searches were limited to documents published in the English language and were completed on June 25, 2024.
Search filters were applied to each search to limit retrieval to citations related to ethical concepts or considerations. Duplicates were removed by manual deduplication in EndNote. The search strategy is available on request.
Literature Screening and Selection
A single reviewer screened literature in 2 stages. First, the reviewer screened the titles and abstracts of the retrieved citations and identified and retrieved articles for full-text review if their titles or abstracts identified ethical considerations, or provided normative analyses (i.e., focusing on “what ought to be” through argumentation), or empirical research (i.e., focusing on “what is” through observation) of ethical considerations related to: the experiences, incidence, diagnosis, treatment, or outcomes of TDT; or related to the evidence on, use of, or implications of exagamglogene autotemcel for patients with TDT. In the second stage, the same reviewer reviewed full-text publications categorized as “retrieve.” The reviewer included texts that included substantive information meeting the aforementioned criteria. Additionally, the reviewer retrieved and reviewed select sources drawn from relevant bibliographies, relevant key concepts, and consultation with experts, or other reviewers using the selection criteria listed previously.
Data Analysis
The 4 research questions driving this review guided the collection, coding, and thematic analysis of data. The reviewer conducted 2 iterative cycles of coding and analysis to abstract, identify, and synthesize relevant ethical considerations from the literature and from relevant project inputs. In the initial coding phase, the reviewer read the publications and input sources for ethical content (e.g., claims related to potential harms, benefits, equity, justice, and resource allocation as well as ethical issues in the evidentiary basis). The reviewer coded the identified claims related to ethical content using methods of qualitative description.3 In the second coding phase, the reviewer identified major themes and subcodes through repeated readings of the data,3 and summarized them into thematic categories within each guiding domain or research question. The reviewer noted if the ethical content did not fit into these categories or into the domains outlined in the research questions, or if there were discrepancies or conflicts between the ethical considerations or values identified between project sources or within thematic categories. The data analysis was iterative, and the reviewer used themes identified in the literature, in project inputs, and during consultations with clinical experts to further refine and re-interpret the ethical considerations identified. Finally, the reviewer thematically organized and described the data according to the 4 research questions and domains driving this Ethics Review. The results, limitations, and conclusions of this analysis are described in the following sections.
Results
Key Ethical Considerations
Treatment and Experiences of TDT
TDT is the most severe form of beta thalassemia; a rare, progressive, autosomal recessive hereditary blood disorder characterized by mutations resulting in the reduced or absent synthesis of the beta-globin chain of hemoglobin, the oxygen-carrying protein in RBCs.4-8 This leads to ineffective RBC production, premature RBC destruction, and increased iron absorption leading to iron overload.4,6,9 People with TDT depend on lifelong RBC transfusions to live.10,11 Without RBC transfusions, they develop chronic and severe anemia resulting in reduced oxygen delivery to tissues.10,11 As discussed further in the Clinical Review Report, complications of TDT itself and iron overload from chronic RBC transfusions result in life-altering or life-limiting complications within multiple organs and body systems (including but not limited to the heart, liver, endocrine system, reproductive system, and bones).9,12 Approximately 1,900 people were living with TDT in jurisdictions in Canada as of 2022.13
Psychosocial Burdens of Living With TDT and Caring for Someone With TDT
TDT is a psychosocially burdensome condition.5,7,8,14-16 It can negatively impact health-related quality of life because of associated medical complications, treatment burden, challenges in accessing treatment and care, stigmatization and discrimination associated with having a genetic condition, and lifestyle adjustments.5,7,8,14-16 These factors may negatively impact physical, social, psychological, and emotional functioning and relationships, education, and employment opportunities.5,7,14-16 The patient group input and literature reported that people with TDT may have trauma and anxiety associated with prolonged hospitalizations, medical complications, treatment side effects and invasive procedures, and learning their condition is hereditary5,14 People with TDT have also reported others or themselves as having negative outlooks on their futures because of periods of frequent illness generally increasing with age and because of secondary infertility.5,14 Because of the burden of living with the condition, those who are fertile may choose not to have biological children if their partner is a carrier or may seek reproductive options such as in vitro fertilization with preimplantation genetic testing.5,14 TDT also impacts the mental, physical, social, and financial well-being of families of people with TDT.5,7 Parents and caregivers sometimes feel guilt because of its hereditary nature and devote a large number of hours per week (e.g., > 30 hours) to support its management.5,7
Existing Treatment Options for TDT in Canada
Treatment for TDT in Canada includes disease-modifying therapies (i.e., RBC transfusions and corresponding ICT, luspatercept, and hydroxyurea — described in the following), curative therapy (i.e., allogenic HSCT), and the multidisciplinary monitoring and management of complications of TDT and its treatments.4,8,10,16 However, existing disease-modifying and curative therapies have limitations in efficacy, present risks, and may be inaccessible, burdensome, or intolerable for some people with TDT in Canada.5,7-11,16 The only approved curative therapy for TDT is allogenic HSCT, which involves using chemotherapy to weaken or destroy defective stem cells in the bone marrow (i.e., myeloablative conditioning) and then replacing them with stem cells from a healthy donor.10 However, allogenic HSCT is associated with risks such as organ damage, secondary malignancy, infertility, graft rejection, and life-threatening graft-versus-host disease.8-10 Moreover, as noted by clinical experts and clinician group input, access to allogenic HSCT is limited by donor availability (with only approximately 25% of people with TDT having an appropriately matched donor, ideally a sibling), age (with outcomes being optimal for people before puberty), and health system capacity.10,16
People with TDT require RBC transfusions to live, generally starting within the first 2 years of life and then every 3 weeks to 6 weeks onwards.10 However, chronic RBC transfusions present risks that may limit potential benefits and tolerability, such as iron overload, alloimmunization, blood-borne infections, dangerous hemolytic transfusion reactions, rash or fever, allergic reactions, and pain or bruising at the IV site.5,7,10,11,16 The clinical experts noted that RBC transfusions are generally accessible to people with TDT in Canada, except for people living in rural or remote communities. The literature and patient input also emphasized that chronic RBC transfusions are time-consuming (taking 6 hours to 9 hours) and can interfere with social activities, education, work, and even limit where people with TDT and their families can live, work, and travel.7 Additionally, because transfusion only temporarily corrects anemia, people with TDT may experience increasingly debilitating symptoms such as fatigue, cognitive impairment, and pain in the days and weeks leading up to their next transfusion.5,7
Chronic RBC transfusions result in iron overload, necessitating ICT with drugs administered orally (e.g., deferiprone and deferasirox) or subcutaneously infused over 10 hours to 12 hours a day (i.e., deferoxamine).5,7,14,16 However, the patient group input and the literature reported patients’ concerns regarding commonly reported adverse effects of ICT drugs that can reduce adherence and tolerability (e.g., nausea, diarrhea, abdominal pain, rashes, vision or hearing problems, neutropenia, and toxicity to organs such as the kidneys).7,11 Patient input and clinical experts emphasized that ICT drugs require burdensome monitoring and are associated with access-related issues, including drug shortages and a lack of insurance coverage for infusion supplies. The clinical experts also reported that it can be more challenging to adequately chelate people with TDT as they get older.
Other therapies available in Canada intended to reduce transfusion requirements include luspatercept, hydroxyurea, and thalidomide. However, the clinical experts reported that most people with TDT do not respond to luspatercept. Luspatercept also has uncertain impact on long-term complications, is not approved for pediatric patients in Canada, and may cause serious adverse effects.16 Clinical experts and clinician group input reported that hydroxyurea may be associated with myelosuppression that prevents optimal dosing. Additionally, both hydroxyurea and thalidomide are associated with fertility or teratogenicity concerns that may necessitate reproductive counselling.10 Ultimately, there is an unmet need for effective treatment that eliminates or reduces burdens associated with lifelong RBC transfusions and ICT for people with TDT who are not eligible for allogenic HSCT. This is especially the case for those who have difficulty responding to, tolerating, or accessing standard care.
Inequities and Challenges With Accessing Diagnosis, Care, and Treatment for TDT in Canada
The literature reports that some people with TDT may fulfill ambitions or demonstrate good functioning in education, work, and personal relationships when receiving optimal treatment and lifelong, multidisciplinary management.17,18 The literature and clinical experts reported that optimized transfusion practices and chelation therapy can provide life expectancy beyond the mean ages of death that have been previously reported for this disease,19,20 and life expectancy may tend to reach the higher percentiles of the general population.21 However, patient group input and the literature highlighted challenges related to affording, accessing, navigating, tolerating, and adhering to optimal treatment and care that disproportionally impact certain groups.5,17 These groups include people who live in jurisdictions or rural areas with limited public coverage for treatments and access to providers and centres specializing in TDT management; are experiencing financial hardship, are not eligible for financial supports, or have limited private insurance; experience denial regarding their condition and the need for treatment; are adolescents or young adults first exploring their autonomy to not engage in treatment or who are transitioning from pediatric to adult care contexts (with the availability of transition supports varying between jurisdictions); and older people, who tend to have increased morbidity and treatment-related expenses.5,17 Additionally, the clinical experts noted that while newborn screening to facilitate early diagnosis or treatment of beta thalassemia is readily available in Canada, immigrants born in regions without access to such screening or early treatment may have worse health status upon arrival to the country.12 This is relevant as the population with TDT in Canada is expected to increase because of immigration from Mediterranean, Asian, Indian, and Middle Eastern regions where the condition is endemic.4,6,7,11,17
Ethics of Evidence and Evaluation of Exagamglogene Autotemcel
As detailed in the Clinical Review Report, the clinical evidence for this review is drawn from the ongoing single-arm, phase III, open-label CLIMB-111 trial. The objective of the CLIMB-111 trial is to evaluate the safety and efficacy of exagamglogene autotemcel after single-drug myeloablative conditioning chemotherapy with busulfan for the treatment of TDT in patients between the ages of 12 years and 35 years. Participants in the CLIMB-111 trial comprising the primary efficacy set were those patients followed for at least 16 months after exagamglogene autotemcel infusion and for at least 14 months after completion of RBC transfusion for posttransplant support or TDT management as of the April 15, 2023, data cut-off. Participants who complete the CLIMB-111 trial (with a 2-year follow-up period) are to be enrolled in the CLIMB-131 long-term extension study (with a 13-year follow-up period) for a total of 15 years of follow-up.
The conclusions from the Clinical Review Report were that the interim findings of the CLIMB-111 trial are consistent with a clinically meaningful transfusion independence based on clinical expert input. Thirty-nine of 42 patients (92.9%) in the primary efficacy set experienced transfusion independence for at least 12 consecutive months any time starting 60 days after the last RBC transfusion up to 24 months after exagamglogene autotemcel infusion, the primary efficacy end point in the CLIMB-111 trial. While the proportion of participants experiencing adverse events and serious adverse events was high, the clinical experts and clinician group input noted this finding is generally consistent with harms associated with the underlying disease and myeloablative busulfan conditioning. However, there is uncertainty in whether results from the trial are attributable to the true effect of exagamglogene autotemcel because of factors such as potential biases in outcome ascertainment, study population, and statistical analysis plan changes after enrolment. Additionally, there is uncertainty in the durability and long-term efficacy and safety of exagamglogene autotemcel beyond the current trial follow-up of up to 24 months. The trial also cannot inform on longer-term toxicities, such as the loss of fertility, malignancies, and potential genotoxicities. Of note, neither the CLIMB-111 study nor the CLIMB-131 study include infertility as a safety end point despite this being a known risk of the conditioning required for treatment and a patient-important outcome.15 Indirect evidence consisting of 2 matching-adjusted indirect comparisons noted large numeric differences in the proportion of participants with transfusion independence favouring exagamglogene autotemcel versus luspatercept and standard of care (RBC transfusions and chelation). However, differences in the study design, outcome ascertainment, and concerns around the validity of the comparators in terms of their potential for attaining the outcome of transfusion independence prevent drawing conclusions about the comparative effectiveness of exagamglogene autotemcel. Indirect evidence also did not include allogenic HSCT as a comparator.
There is also uncertainty in the generalizability beyond the trial population. The clinical experts considered the trial population broadly generalizable to the Canadian context with respect to race and ethnicity. However, because of exclusion criteria, the findings may not generalize to people with co-inheritance of multiple types of thalassemia. The clinical experts also noted the exclusion of people older than 35 years, who they anticipated could benefit from exagamglogene autotemcel especially as they often are ineligible for allogenic HSCT and respond less optimally to ICT. For this reason, they recommended accepting usage aligning with the proposed indication without the trial’s upper age limit.
Given that exagamglogene autotemcel has been proposed as a one-time treatment with potential for lifelong effects, evidentiary uncertainty and limitations highlight the importance of robust consent conversations to support informed, autonomous decision-making and establish reasonable expectations, including for people under-represented in the trial.8,9,22,23 Evidentiary uncertainty also has implications for health systems decision-making as it present challenges for assessing the value of exagamglogene autotemcel relative to standard of care and understanding opportunity costs. The clinical experts and published literature emphasized the need for lifelong follow-up of patients who have received exagamglogene autotemcel and the collection and evaluation of long-term safety and efficacy data (e.g., through the CLIMB-131 study and registries, the latter of which are not widely available in Canada).24 This follow-up and data would facilitate timely response to harms and a better understanding of the benefits and risks of treatment. The clinical experts and literature provided insight into how collecting such information may require addressing factors that could contribute to attrition in the CLIMB-131 study, challenges associated with transitioning from pediatric to adult care contexts, and limited epidemiological information and registry data on beta thalassemia in Canada.6,17,24
Ethical Considerations in the Use of Exagamglogene Autotemcel
The use of exagamglogene autotemcel raises ethical considerations regarding balancing benefits and harms, risk of infertility, informed consent, and equitable access.
Balancing Benefits and Harms
The proposed value of exagamglogene autotemcel is its potential to be a one-time therapy to address the unmet need for an effective treatment that meaningfully reduces or eliminates the need for lifelong, chronic RBC transfusions for people with TDT who are ineligible for allogenic HSCT.5,10,16 Of note, the desire for transfusion independence and decreased iron overload and burdens associated with chelation therapy are among factors motivating people with TDT to consider gene therapy.15 The clinical experts and clinician groups perceived that the preliminary results of the CLIMB-111 study were promising.16 Despite evidentiary uncertainty and limitations, the clinical experts would consider exagamglogene autotemcel for patients with TDT who are not eligible for allogenic HSCT (especially those who do not respond to or have difficulty accessing or tolerating standard care) because of high treatment burden and unmet need for effective, one-time treatment in this group. They noted, however, that they would reserve exagamglogene autotemcel for use in patients not eligible for allogenic HSCT for whom they feel clinicians have a better understanding of the benefits and risks at this time. However, they also raised when the evidence base for exagamglogene autotemcel grows, comparative safety and efficacy data between it and allogenic HSCT may be warranted to inform clinical decision-making. Of note, the clinical experts and literature reported that patients and their families may prefer gene therapies like exagamglogene autotemcel over allogenic HSCT because of theoretical safety advantages, including the lack of risk for graft-versus-host disease and graft rejection.8-10,15,16
As a cellular therapy involving ex vivo gene editing using clustered regularly interspaced short palindromic repeats and clustered regularly interspaced short palindromic repeat-associated protein 9 technology, exagamglogene autotemcel is associated with both theoretical and known risks. Theoretical risks include genotoxicities (i.e., unintended on-target and off-target effects), which could cause irreversible, unintended consequences or malignancy.8-10,22,23,25 Known risks include those related to myeloablative conditioning, with common short-term adverse effects (e.g., neutropenia and thrombocytopenia) and long-term risks such as organ damage, secondary malignancy, and infertility, which have been reported as concerning to patients with TDT and their families.9,10,15,26 Of note, the experts and literature raised that clinicians and patients may have varying understandings of the level of transfusion independence required to deem gene therapies like exagamglogene autotemcel acceptable considering these risks.15 According to these sources, some clinicians and patients may understand the risks of gene therapy as being acceptable only with the outcome of transfusion independence.15 In contrast, “over 90%” of parents of children with TDT and adults with TDT interviewed in a qualitative study (N = 25) reported willingness to accept the risks of gene therapy for a 50% to 90% reduction in, rather than total independence from, RBC transfusions.15 It will therefore be important for clinicians to explore treatment values of each patient during shared decision-making processes.
The clinical experts, patient input, and published literature reported that gene therapies offer hope for people with TDT. For this reason, they raised that psychological support may be necessary to minimize harm related to unmet expectations for those who are ineligible for treatment. These include people who have family members eligible for exagamglogene autotemcel but who themselves do not have transfusion dependence despite morbidity related to beta thalassemia and people who are unfit for treatment because of end-organ damage related to iron overload.
Risk of Infertility
While infertility is not included as a safety outcome in the CLIMB-111 trial or CLIMB-131 extension study, it is a known risk of myeloablative conditioning and a patient-important outcome, as per the patient input, clinical experts, and the literature.15,26 The clinical experts and most patients in the literature did not consider infertility a reason to refrain from pursuing exagamglogene autotemcel, with the clinical experts and literature reporting that many people with TDT already experience infertility because of complications of the condition and its treatment.4,7,15 However, the clinical experts and clinician groups suggested that offering and covering fertility preservation for patients receiving exagamglogene autotemcel (as is common for patients undergoing oncological treatments that present risk of infertility) would help support equitable access and mitigate risk of infertility. Of note, the clinical experts reported that people with TDT already experience barriers to accessing fertility preservation in Canada. These include inconsistent coverage across jurisdictions, funding being more widely available to people with oncological rather than hematological conditions, and out-of-pocket costs associated with collection and storage. Costs may be greater for people requiring ovum retrieval and preservation and may prevent some with lower income from being able to afford it. The literature, patient input, and clinician group input also reports that some people with TDT consider infertility an unacceptable risk for gene therapy, even when educated about fertility preservation.15 Some parents reported they would refrain from making decisions about gene therapy for their child until after they are old enough to engage in informed discussions about this risk.15 However, clinician group input noted that optimal timing for transplant may precede that of fertility preservation.
Informed Consent
To facilitate fully informed decision-making, clinical experts and literature emphasized the importance of carefully discussing the benefits, known and theoretical risks, and evidentiary limitations related to all treatment options.25 Of note, people with TDT and their caregivers have reported the lack of long-term efficacy data, the possibility of treatment failure or death, “genetic manipulation,” and trading a known disease (i.e., TDT) with unknown complications of gene therapy as concerns relevant to deciding about gene therapy.15 Given that engraftment time in the CLIMB-111 study was longer than the clinical experts perceived was typical for allogenic HSCT, they emphasized the importance of communicating the need for prolonged and psychosocially burdensome hospitalization under strict isolation precautions required to receive exagamglogene autotemcel. It will also be important for clinicians to establish reasonable long-term expectations as part of informed consent processes to alleviate harms associated with false hope. For example, clinical experts noted it will be important to communicate that while exagamglogene autotemcel may provide a “functional cure” if eliminating transfusion dependence,16 it is not curative (as it stimulates fetal, rather than adult, hemoglobin, and high levels of the former may have variable presentations), will not reverse end-organ damage, and may preclude eligibility for re-treatment and future gene therapies. Promoting informed consent will also require considering peoples’ unique vulnerabilities and decision-making needs. For example, clinicians should consider relational autonomy, or how social status and various forms of oppression influence individuals’ ability to act autonomously in medical decision-making.25 Finally, the clinical experts noted that consent to treatment with exagamglogene autotemcel is an ongoing process and may be withdrawn even after the collection of stem cells.
Equitable Access
The implementation of exagamglogene autotemcel raises challenges regarding meeting patients’ expectations (as per patient group input) for therapy that is equitably accessible and affordable.25 Equitable access will require attention to the previously detailed geographic, psycho-emotional, and age-related barriers to accessing TDT care and effective treatment in Canada. It also requires attention to the need for patients to access specialized treatment centres, to undergo a month-long hospitalization, and to receive long-term follow-up.15 For example, the clinical experts raised that groups experiencing difficulty gaining access to timely optimal TDT care and whose condition may not be as well managed (e.g., recent immigrants or those living far from specialized centres) may also be at a greater risk of not being healthy enough to undergo myeloablative conditioning and thus ineligible for treatment with exagamglogene autotemcel. People with TDT and their caregivers (especially, as per the clinical experts and the literature, those living far from authorized treatment centres, needing childcare, or experiencing financial challenges) may also perceive gene therapies like exagamglogene autotemcel as causing unacceptable burden on their support systems, significant financial strain, and employment risk.15,25 The clinical experts confirmed the importance of patient support programs in mitigating barriers to equitable access. In the implementation plan submitted for this review, the sponsor reported that they are “exploring” funding and implementing such programs, should exagamglogene autotemcel be reimbursed.
Health Systems Considerations
The use of exagamglogene autotemcel for the treatment of TDT raises ethical considerations related to sustainable funding, health system capacity constraints, and prioritization among those eligible for treatment with exagamglogene autotemcel in Canada.
Sustainability of Funding and Manufacturing Exagamglogene Autotemcel
The introduction of exagamglogene autotemcel, a highly expensive therapy, raises concerns regarding the health systems’ abilities to sustainably manage associated costs.23 It is hoped that one-time therapies like exagamglogene autotemcel with high upfront costs could result in long-term reductions in health care utilization.8,9,17 However, uncertainty in evidence regarding the long-term clinical effectiveness and safety of exagamglogene autotemcel and, in turn, cost-effectiveness limits assessments of its long-term value, including as a one-time therapy.25 Long-term measurement of outcomes of exagamglogene autotemcel compared to best supportive care and allogenic HSCT would be important for understanding long-term benefits and risks and, in turn, cost-effectiveness and opportunity costs.8-10,17,23
Literature reports that sustainable implementation may depend on “close collaboration” between interested parties.9 The literature and patient group input reported cases where manufacturers disinvested gene therapies for beta thalassemia and other rare conditions.9 Reasons include difficulties negotiating pricing; high costs for development, manufacturing, and administration; regulatory and reimbursement complexities; and commercialization depending on short-term profits.9 The literature also suggested regulating costs and incentivizing the development of affordable gene therapies are imperative for promoting equitable access to them.25,26 Of note, patients with TDT and their caregivers have raised concerns about the cost of gene therapies and how this will impact accessibility.15 Funding reforms, whereby annual payments are made on the condition of “demonstrated sustained clinical activity,” have been proposed for gene therapies for TDT.8 Implementing such models would require jurisdictions and manufacturers to agree on clear parameters of success and ensure appropriate infrastructure is in place to support collection of this data.
Health System Capacity Constraints and Priority Setting
Literature reported the need to manage finite resources in the context of novel therapies in a manner that prioritizes the right to health care for people with beta thalassemia.17 Exagamglogene autotemcel is a resource-intensive therapy that can only be administered by highly trained personnel and in authorized transplant and cellular therapy centres. This will severely limit the number of eligible patients that can be treated each year.23,26 The sponsor estimates there will be 10 treatment centres in 4 provinces by the third year of exagamglogene autotemcel implementation if reimbursed. The clinical experts reported that transplant centres in Canada are currently at or near capacity for delivering services to patients, and that introducing exagamglogene autotemcel would require more resources (including health care human resources) than currently available.
In the context of capacity constraints, it will be necessary to prioritize access to exagamglogene autotemcel within the population with TDT, and between populations with TDT and SCD (the other condition for which CDA-AMC is reviewing exagamglogene autotemcel).8 The clinical experts voiced concern that prioritizing finite HSCT resources based on urgency or unmet need alone may result in people with TDT not having access to exagamglogene autotemcel. This is because these criteria would likely first favour patients with oncological conditions and then SCD (who they perceived as tending to have greater urgency because of greater morbidity, earlier mortality, and health system utilization with standard care). To facilitate equitable access to treatment for patients with hemoglobinopathies, the experts proposed reserving a set number of HSCT treatment spots for people with SCD and TDT per year. Of patients with TDT, the clinical experts would prioritize those with difficulty responding to, tolerating, or accessing standard care who are eligible for exagamglogene autotemcel but not allogenic HSCT. However, clinician group input also raised that facilitating access to younger people yet to experience irreversible complications of TDT and standard treatment may “relieve them of the decades-long burden of accessing constant specialty care in an overtaxed health care system.” Clinical experts raised the need to ensure people living far from treatment centres (who may also live outside of major cities and thus have higher unmet need because of greater difficulty accessing RBC transfusions) would be equitably included in prioritization decisions. Together, these considerations highlight the need for clear and consistent prioritization criteria, intrajurisdictional and interjurisdictional agreements, and patient financial and social supports to ensure equitable access to exagamglogene autotemcel and other therapies involving HSCT.
Limitations
This review draws on published literature that discusses ethical considerations related to the use of exagamglogene autotemcel or gene therapy for the treatment of TDT. However, there may be additional ethical considerations in the context of exagamglogene autotemcel for TDT that are not captured in this review. Drawing on input received during this reimbursement review, including patient group, clinician group, and drug program input, and discussion with clinical experts, as well as engagement with the clinical and pharmacoeconomic review teams, provides a more comprehensive understanding of the ethical considerations related to the use of exagamglogene autotemcel for the treatment of TDT. It is possible that more direct engagement (e.g., through direct interviews) with patients, their caregivers, their family members, transplant specialists, and decision-makers on their specific experiences with TDT and/or exagamglogene autotemcel would offer additional relevant ethical considerations or domains of analysis.
Conclusion
Ethical considerations in the context of TDT highlight the significant physical and psychosocial burdens of the condition and its treatment, which can adversely impact health-related quality of life. Some people with TDT may fulfill ambitions in education, work, and personal relationships and survive into their 60s when receiving optimal treatment and lifelong, multidisciplinary management. However, existing disease-modifying and curative therapies have limitations in efficacy, present risks, and may be inaccessible or intolerable for some. As a result, there is an unmet need for effective treatment for people with TDT who are not eligible for allogenic HSCT that eliminates or reduces burdens associated with lifelong RBC transfusions and ICT. Additionally, certain groups may experience disproportionate difficulty accessing and navigating effective TDT treatment and care in Canada, and therefore may have higher unmet needs for effective, one-time treatment options. These include but are not limited to those who live far from specialized treatment centres, people experiencing financial hardship, those experiencing denial regarding their condition, adolescents and young adults, older people, and recent immigrants.
Findings from the ongoing, single-arm CLIMB-111 trial are consistent with a clinically meaningful impact on transfusion independence based on clinical expert input. Exagamglogene autotemcel also displays a short-term safety profile consistent with treatment requiring myeloablative conditioning. However, there is uncertainty in: whether the effect observed is truly attributable to exagamglogene autotemcel because of methodological limitations in the CLIMB-111 trial, the efficacy and safety of exagamglogene autotemcel beyond the current trial follow-up of 24 months, and generalizability beyond the trial population. Additionally, there is considerable uncertainty in indirect evidence comparing exagamglogene autotemcel to luspatercept and standard of care, and a lack of evidence to understand the value of exagamglogene autotemcel versus allogenic HSCT. Given that exagamglogene autotemcel has been proposed as a one-time treatment with potential for lifelong effects, this evidentiary uncertainty highlights the importance of robust consent conversations to support informed, autonomous decision-making and establish reasonable expectations, including for people under-represented in the trial. Evidentiary uncertainty also has implications for health systems decision-making as it presents challenges for assessing the value of exagamglogene autotemcel relative to standard of care (including allogenic HSCT) and understanding opportunity costs. Considering these evidentiary limitations, it will be necessary to address barriers to conducting and collecting long-term follow-up data to facilitate a better understanding of the benefits and risks of exagamglogene autotemcel.
Clinicians and patients may have varying understandings of the level of transfusion independence required to deem exagamglogene autotemcel acceptable considering the theoretical and known risks of exagamglogene autotemcel, which highlights the importance of shared decision-making processes eliciting the values of individual patients. Clinician groups and clinical experts suggested that providing access to fertility preservation would help support equitable access and mitigate risks associated with infertility. Additionally, providers will need to facilitate thorough consent processes that ensure patients and their families understand the benefits, risks, and evidentiary limitations of exagamglogene autotemcel and other treatment options and have reasonable long-term expectations. Managing expectations will be important to prevent harms associated with false hope, as treatment with exagamglogene autotemcel may not cure TDT, may not reverse end-organ damage, and may preclude eligibility for re-treatment and future gene therapies. The clinical experts and literature suggested that equitable access to exagamglogene autotemcel could be facilitated by addressing barriers to accessing standard TDT care and those related to accessing specialized treatment centres, undergoing prolonged hospitalization, and receiving long-term follow-up.
Limitations in evidence evaluating the long-term clinical effectiveness and safety of exagamglogene autotemcel and, in turn, cost-effectiveness limits assessments of its long-term value, including as a one-time therapy. Given its high price and evidentiary limitations, the sustainable implementation of exagamglogene autotemcel may depend on close collaboration between payers and manufacturers. Additionally, the exagamglogene autotemcel treatment journey is resource intensive, and the therapy can only be administered by highly trained personnel in authorized transplant and cellular therapy centres. These factors, alongside current health systems capacity constraints, will severely limit the number of eligible patients that can be treated each year and necessitate prioritizing patients for access. To promote equitable access to HSCT-based therapies for people with hemoglobinopathies, the clinical experts proposed dedicating a set amount of HSCT resources to people with SCD and TDT. Among patients with TDT, the clinical experts reported they would generally prioritize those with greatest difficulty responding to, tolerating, or accessing standard care. Authorized treatment centres may only be situated in certain jurisdictions in Canada, and people with the greatest unmet needs may be living furthest from these centres. These considerations highlight the need for consistent prioritization criteria and intrajurisdictional and interjurisdictional agreements and patient supports to ensure equitable access to exagamglogene autotemcel.
References
1.EUnetHTA. EUnetHTA Joint Action 2 Work Package 8, HTA Core Model version 3.0. European Commission; 2016: http://www.htacoremodel.info/BrowseModel.aspx. Accessed 2024 Jul 10.
2.Benkhalti M, Espinoza M, Cookson R, Welch V, Tugwell P, Dagenais P. Development of a checklist to guide equity considerations in health technology assessment. Int J Technol Assess Health Care. 2021;37:e17. PubMed
3.Sandelowski M. Whatever happened to qualitative description? Res Nurs Health. 2000;23(4):334-340. PubMed
4.Carsote M, Vasiliu C, Trandafir AI, et al. New Entity-Thalassemic Endocrine Disease: Major Beta-Thalassemia and Endocrine Involvement. Diagnostics (Basel). 2022;12(8):09.
5.Drahos J, Boateng-Kuffour A, Calvert M, et al. Health-Related Quality-of-Life Impacts Associated with Transfusion-Dependent beta-Thalassemia in the USA and UK: A Qualitative Assessment. Patient. 2024;17(4):421-439. PubMed
6.Kattamis A, Forni GL, Aydinok Y, Viprakasit V. Changing patterns in the epidemiology of beta-thalassemia. Eur J Haematol. 2020;105(6):692-703. PubMed
7.Knoth RL, Gupta S, Perkowski K, et al. Understanding the Association between Red Blood Cell Transfusion Utilization and Humanistic and Economic Burden in Patients with beta-Thalassemia from the Patients' Perspective. J Clin Med. 2023;12(2):04.
8.Thuret I, Ruggeri A, Angelucci E, Chabannon C. Hurdles to the Adoption of Gene Therapy as a Curative Option for Transfusion-Dependent Thalassemia. Stem Cells Transl Med. 2022;11(4):407-414. PubMed
9.Christakopoulos GE, Telange R, Yen J, Weiss MJ. Gene Therapy and Gene Editing for beta-Thalassemia. Hematol Oncol Clin North Am. 2023;37(2):433-447. PubMed
10.Kattamis A, Kwiatkowski JL, Aydinok Y. Thalassaemia. Lancet. 2022;399(10343):2310-2324. PubMed
11.Njeim R, Naouss B, Bou-Fakhredin R, Haddad A, Taher A. Unmet needs in β-thalassemia and the evolving treatment landscape. Transfus Clin Biol. 2024;31(1):48-55. PubMed
12.Pines M, Sheth S. Clinical Classification, Screening, and Diagnosis in Beta-Thalassemia and Hemoglobin E/Beta-Thalassemia. Hematol Oncol Clin North Am. 2023;37(2):313-325. PubMed
13.Vertex Pharmaceuticals Incorporated. Data on File. Epidemiology and Clinical Characteristics of SCD and B-Thal in Canada [sponsor supplied reference]. 2022.
14.Boardman FK, Hale R. “I didn't take it too seriously because I'd just never heard of it”: Experiential knowledge and genetic screening for thalassaemia in the UK. J Genet Couns. 2019;28(1):141-154. PubMed
15.Quarmyne MO, Ross D, Sinha C, Bakshi N, Boudreaux J, Krishnamurti L. Decision-making about gene therapy in transfusion dependent thalassemia. BMC Pediatr. 2022;22(1):536. PubMed
16.Corbacioglu S, Frangoul H, Locatelli F, Hobbs W, Walters M. Defining curative endpoints for transfusion-dependent β-thalassemia in the era of gene therapy and gene editing. Am J Hematol. 2024;99(3):422-429. PubMed
17.Angastiniotis M. Beta thalassemia: Looking to the future, addressing unmet needs and challenges. Ann N Y Acad Sci. 2024;1532(1):63-72. PubMed
18.Almahmoud SY, Coifman KG, Ross GS, Kleinert D, Giardina P. Evidence for multidimensional resilience in adult patients with transfusion-dependent thalassemias: Is it more common than we think? Transfus Med. 2016;26(3):186-194. PubMed
19.Baldwin J, Udeze C, Li N, et al. Clinical burden and healthcare resource utilization associated with managing transfusion-dependent β-thalassemia in France. Curr Med Res Opin. 2024;40(8):1289-1295. PubMed
20.Jobanputra M, Paramore C, Laird SG, McGahan M, Telfer P. Co-morbidities and mortality associated with transfusion-dependent beta-thalassaemia in patients in England: a 10-year retrospective cohort analysis. Br J Haematol. 2020;191(5):897-905. PubMed
21.Farmakis D, Giakoumis A, Angastiniotis M, Eleftheriou A. The changing epidemiology of the ageing thalassaemia populations: A position statement of the Thalassaemia International Federation. Eur J Haematol. 2020;105(1):16-23. PubMed
22.Deneault E. Recent Therapeutic Gene Editing Applications to Genetic Disorders. Curr Issues Mol Biol. 2024;46(5):4147-4185. PubMed
23.Laurent M, Geoffroy M, Pavani G, Guiraud S. CRISPR-Based Gene Therapies: From Preclinical to Clinical Treatments. Cells. 2024;13(10):08.
24.Farmakis D, Angastiniotis M, El Ghoul MM, Cannon L, Eleftheriou A. Thalassaemia Registries: A Call for Action. A Position Statement from the Thalassaemia International Federation. Hemoglobin. 2022;46(4):225-232. PubMed
25.Kratzer K, Getz LJ, Peterlini T, Masson JY, Dellaire G. Addressing the dark matter of gene therapy: technical and ethical barriers to clinical application. Hum Genet. 2022;141(6):1175-1193. PubMed
26.McCune JM, Kiem HP. Extending Gene Medicines to All in Need. N Engl J Med. 2024;390(18):1721-1722. PubMed
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.