CADTH Reimbursement Review
Mavacamten (Camzyos)
Sponsor: Bristol Myers Squibb
Therapeutic area: Obstructive hypertrophic cardiomyopathy
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Stakeholder Input
Clinical Review
Abbreviations
6MWD
6-minute walk distance
ACC
American College of Cardiology
ACCF
American College of Cardiology Foundation
AE
adverse event
AHA
American Heart Association
ANCOVA
analysis of covariance
CHPA
Canadian Heart Patient Alliance
CI
confidence interval
CPET
cardiopulmonary exercise testing
CSS
clinical summary score
EQ-5D-5L
5-Level EQ-5D
HCM
hypertrophic cardiomyopathy
HCMSQ
Hypertrophic Cardiomyopathy Symptom Questionnaire
HRQoL
health-related quality of life
ICC
intraclass correlation coefficient
KCCQ
Kansas City Cardiomyopathy Questionnaire
KCCQ-23
23-item Kansas City Cardiomyopathy Questionnaire
LAVI
left atrial volume index
LTE
long-term extension
LV
left ventricular
LVEF
left ventricular ejection fraction
LVMI
left ventricular mass index
LVOT
left ventricular outflow tract
MMRM
mixed model for repeated measurements
NT-proBNP
N-terminal pro–B-type natriuretic peptide
NYHA
New York Heart Association
oHCM
obstructive hypertrophic cardiomyopathy
pVO2
peak oxygen consumption
RCT
randomized controlled trial
SAE
serious adverse event
SD
standard deviation
SoB
shortness of breath
SRT
septal reduction therapy
TSS
total symptom score
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Item | Description |
|---|---|
Drug product | Mavacamten (Camzyos), 2.5 mg, 5 mg, 10 mg, and 15 mg oral capsules |
Indication | For the treatment of symptomatic obstructive hypertrophic cardiomyopathy of NYHA class II to III in adult patients |
Reimbursement request | As per indication |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | November 8, 2022 |
Sponsor | Bristol Myers Squibb |
NOC = Notice of Compliance; NYHA = New York Heart Association.
Introduction
Hypertrophic cardiomyopathy (HCM) is a common genetic heart disease characterized by increased thickness of the left ventricular wall.1 About 30% to 60% of patients with HCM have identifiable familial disease caused by mutations in cardiac sarcomere protein genes, and each offspring of an affected family member has a 50% chance of inheriting an altered gene, although not all family members who inherit an HCM mutation will develop the disease.1-3 The distribution of HCM is equal by sex, although females have been diagnosed less frequently than males.2,3 The age of symptom onset and the severity of symptoms varies significantly across patients with HCM.1 Among patients with HCM who do develop symptoms, the most common symptoms include chest pain, shortness of breath with exertion, fatigue, palpitations, and light-headedness.1 Obstructive hypertrophic cardiomyopathy (oHCM), a subclassification of HCM, is characterized by obstruction of the left ventricular outflow tract (LVOT), with the obstruction impeding blood flow from the heart to the rest of the body, defined in the 2020 clinical guidelines set by the American Heart Association (AHA) and the American College of Cardiology (ACC) as a peak LVOT gradient of 30 mm Hg or greater.3 Patients with oHCM are more likely to develop symptoms such as increased myocardial wall stress, myocardial ischemia, and, eventually, cell death and replacement scarring.1 Associated complications include heart failure, stroke due to atrial fibrillations, arrhythmias, and sudden cardiac death.1 The estimated prevalence of HCM in the general population is 1 in 500 adults, although most of these cases remain undiagnosed.1 The 2020 AHA/ACC clinical guidelines suggest that oHCM is present or develops over time in most patients with HCM, with about a third of patients with HCM remaining nonobstructive.3 Estimates for the proportion of patients with HCM who have oHCM range from 22% in a study from western Sweden4 to 70% in a US study.5
Mavacamten is a first-in-class cardiac myosin inhibitor.6 Mavacamten modulates the number of myosin heads that can enter power-generating states, reducing force-producing systolic and residual diastolic cross-bridge formation. Mavacamten also shifts the overall myosin population toward an energy-sparing, recruitable, super-relaxed state.6 This is the first CADTH review for mavacamten. The Health Canada indication is for the treatment of symptomatic New York Heart Association (NYHA) class II or III oHCM in adult patients.6 Mavacamten is available as a 2.5 mg, 5 mg, 10 mg, or 15 mg capsule.6 The product monograph for mavacamten for oHCM recommends a starting dosage of 5 mg orally once daily. Patients should be assessed 4 weeks after initiation for a clinical response. If the LVOT gradient with a Valsalva maneuver is less than 20 mm Hg, the dosage should be decreased to 2.5 mg once daily. Otherwise, dosing of 5 mg once daily should be maintained.6 Thereafter, follow-up visits should occur at 8 and 12 weeks after treatment initiation, with dose adjustments as appropriate.6 The product monograph for mavacamten contains serious warnings and precautions regarding the risk of heart failure, and notes that mavacamten reduces the left ventricular ejection fraction (LVEF) and can cause heart failure due to systolic dysfunction, and that echocardiogram assessments of LVEF and LVOT gradients are required before and regularly during treatment with mavacamten. It also notes that initiation of mavacamten in patients with an LVEF of less than 55% is not recommended, and that mavacamten treatment should be interrupted if the LVEF is less than 50% at any visit or if the patient experiences symptoms of heart failure or worsening clinical status.6 The product monograph also states that concomitant use of mavacamten in patients on combination therapy of a calcium channel blocker (e.g., verapamil or diltiazem) and a beta-blocker should be avoided.6
The objective of this report is to perform a systematic review of the beneficial and harmful effects of mavacamten, 2.5 mg, 5 mg, 10 mg, and 15 mg oral capsules for the treatment of adults with symptomatic NYHA class II to III oHCM.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient groups who responded to CADTH’s call for patient input and from a clinical expert consulted by CADTH for the purpose of this review.
Patient Input
Two patient advocacy groups, the Canadian Heart Patient Alliance (CHPA) and the HeartLife Foundation, provided input on the treatment of symptomatic oHCM in adult patients. The HeartLife Foundation gathered information from in-depth interviews with expert physicians and patients across Canada, and reviewed study material and online literature. The CHPA conducted extensive interviews with 3 clinicians (2 in the US and 1 in Italy) involved with clinical trials of mavacamten. They also gathered information by meeting with staff from the US-based Hypertrophic Cardiomyopathy Association, and reviewing recorded panel discussions, patient testimonials, and educational videos. The CHPA recruited participants by contacting US-based clinicians as well as conducting outreach using its Canadian database, with additional patient profiles and confirmatory information provided by the Hypertrophic Cardiomyopathy Association. A total of 16 patient responses were gathered, 62.5% (10 out of 16) of whom were women aged between the mid-30s and mid-70s, with 31% (5 out of 16) identifying as Canadians (1 was living in the US) and 69% (11 respondents) as Americans. All participants reported being diagnosed with oHCM, and 40% also identified as being diagnosed with NYHA functional class II and 40% with NYHA functional class III oHCM. About 25% participants mentioned being diagnosed with atrial fibrillation. Among the 16 respondents, 4 patients, all residents of the US, had been treated with mavacamten.
Both patient groups agreed that HCM has a negative impact on patient quality of life. The impact of delayed diagnosis and misdiagnosis, shortness of breath, exercise intolerance, arrythmia, palpitations, chest pain, fatigue, and fainting were some of the major issues experienced by the respondents. One patient group also noted that HCM can affect patient families and friends, both mentally and physically. While describing their experiences with currently available drugs, participants mentioned a variety of treatments, including heart surgery, implantable cardioverter-defibrillators, alcohol septal ablation, and a variety of medications (such as beta-blockers, calcium channel blockers, and antiarrhythmics). The patient groups also reported that both patients and health care providers have concerns about current treatments and patients’ symptoms, feelings of uncertainty, and unresolved anxiety associated with the available treatment options.
While evaluating improved outcomes from new treatments, patients expressed a desire to see a reduction in the risk of heart failure, including sudden death, as a current unmet need, as well as reductions in the debilitating symptoms affecting daily living activities and quality of life, including shortness of breath, irregular heartbeat, palpitations, chest pain, fatigue, stress, and anxiety. Spending time with loved ones, the ability to go to work on regular basis, pursuing outdoor activities, and the ability to travel were some of the quality-of-life indicators and experiences mentioned by patients and caregivers.
While describing the experiences with the current drug under review, 4 patients recruited by the CHPA reported “very positive” experiences, noting that they have more energy to perform daily tasks and that they were hopeful the drug will reduce their symptoms and risk of cardiac arrest. The HeartLife Foundation described findings from a clinical trial (VALOR-HCM) led by the Cleveland Clinic demonstrating a reduced need for an invasive procedure such as septal reduction therapy (SRT) in severely symptomatic patients with oHCM when mavacamten was used. However, the CHPA reiterated the need to assess their patients’ cardiac status, specifically by an echocardiogram of the LVEF, and for other illnesses (e.g., infections or chronic disease), cardiovascular symptoms (arrhythmias), and medications before the approval for mavacamten. Moreover, patients must be closely monitored by echocardiograms for the first few months, as well as on a regular basis (every 3 months), and any symptoms must be reported due to the risk of heart failure associated with mavacamten. According to the CHPA, this limits the prescription of mavacamten to patients who have access to a high-volume clinic and who are committed to regular monitoring and reporting of symptoms.
Clinician Input
Input From the Clinical Expert Consulted by CADTH
According to the clinical expert consulted for this review, standard treatment of patients with symptomatic oHCM aims to lessen the extent of LVOT obstruction and manage arrhythmias. Traditionally, beta-blockers have been the mainstay of therapy. Where beta-blockers cannot be used or are not tolerated, the nondihydropyridine calcium channel blockers diltiazem or verapamil can be prescribed. Should symptoms persist, disopyramide is recommended as add-on therapy. These drugs, taken separately or in combination, improve symptoms and quality of life. According to the clinical expert consulted by CADTH, mavacamten may address an unmet need as an add-on therapy for patients not experiencing symptom relief with beta-blockers or calcium channel blockers with or without disopyramide.
The clinical expert consulted for this review noted that mavacamten was evaluated in the EXPLORER-HCM trial as an add-on to first-line treatment with beta-blockers or calcium channel blockers in the context of improving symptoms and exercise capacity among patients with symptomatic oHCM. In terms of treatment paradigm, the clinical expert stated that mavacamten will provide another treatment option for symptomatic patients with oHCM. In the expert’s opinion, the current place in therapy for mavacamten is unclear. It may be used as an add-on to beta-blockers or calcium channel blockers or more appropriately as a third-line add-on to beta-blockers or calcium channel blockers plus disopyramide. The fact that mavacamten was not tested head-to-head with disopyramide raises uncertainty about its relative position in the treatment algorithm, according to the expert. The clinical expert stated that, while it has its own issues, disopyramide is a Class Ia antiarrhythmic drug with negative inotropic properties that have been argued to be more powerful than beta-blockers or calcium channel blockers in controlling LVOT obstruction.
According to the clinical expert, symptomatic patients with oHCM who have not responded sufficiently to current treatment and/or whose symptoms are worsening would be eligible for treatment with mavacamten. Patients would need to be sufficiently symptomatic (at least NYHA class II) to be prescribed the drug despite treatment with beta-blockers or calcium channel blockers with or without disopyramide. The metrics of response to treatment with mavacamten identified by the expert include stabilization or improvement of symptoms (e.g., fatigue, palpitations, light-headedness, and chest pain), reduction in the frequency and/or severity of symptoms, and improved ability to perform activities of daily living. In the opinion of the clinical expert, treatment should be discontinued in the event of drug side effects. If symptoms or the LVOT gradient were to progress to the point that SRT was needed, then treatment with mavacamten should be discontinued. According to the clinical expert, mavacamten should be prescribed by specialists (cardiologists) or in specialty clinics.
Clinician Group Input
Clinician group input on the review of mavacamten for the treatment of oHCM was received from 2 groups: a community-based cardiology clinic, Cardio1, and an independent cardiologist who is a member of the Hypertrophic Cardiomyopathy Clinic and the Stephenson Cardiac Imaging Centre at the Libin Cardiovascular Institute at the University of Calgary.
The clinician groups noted that beta-blockers, calcium channel blockers, and disopyramide are current treatments for oHCM. However, these treatments are used to manage symptoms; they do not modify the underlying disease. In addition, potential adverse effects associated with these drugs limit their use. Cardio1 also pointed out that SRT, such as surgical and percutaneous septal ablation, may be beneficial to those who are refractory to drugs. However, these therapies also have potential adverse effects and limitations and require proper and careful selection of patients, creating an unmet medical need for noninvasive alternatives to SRT.
Some unmet needs remain when current treatment options are deemed ineffective, are unable to reverse the course of the disease, and are used mostly for symptom relief. While both groups referred to data from studies that demonstrated the effectiveness of the drug under review in improving symptoms and reducing the need for surgery, Cardio1 focused on using available conventional therapy first and switching to the new therapy when the first line fails. The group also emphasized the proper selection of patients, as well as checking for updates regarding long-term studies on the use of this new drug. The group referred to the need for timely assessments of patients’ responses to conventional treatment and the option to switch to a new treatment to prevent unnecessary suffering.
Regarding which patients are best suited for the new medication, 1 group identified patients with oHCM and severe LVOT obstruction who are highly symptomatic, whereas Cardio1 identified patients unresponsive to currently available drug treatment as good candidates for this drug, as well as those who may not be a candidate for early SRT, those who want to delay SRT, or those who do not want SRT. While 1 group mentioned an interest in offering the new medication to patients, referring to the compelling data behind the new medication, Cardio1 pointed out the ongoing importance of monitoring the mortality, morbidity, and hospitalization outcomes of this drug.
Drug Program Input
Drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may affect their ability to implement a recommendation. The drug plans identified implementation issues related to considerations for relevant comparators, initiation of therapy, prescribing of therapy, and systemic and economic issues. The clinical expert consulted by CADTH weighed evidence from the pivotal trials and other clinical considerations before providing responses to drug programs’ implementation questions. Table 3 provides more details.
Clinical Evidence
Pivotal Studies and Protocol-Selected Studies
Description of Studies
Two sponsor-conducted, phase III, randomized, double-blind, placebo-controlled trials, EXPLORER-HCM and VALOR-HCM — both of which met the CADTH review protocol criteria — were included in this systematic review.
The EXPLORER-HCM trial (68 sites in 13 countries; N = 251) evaluated the efficacy and safety of once-daily orally administered treatment with mavacamten (at a starting dose of 5 mg) in adult patients with symptomatic oHCM with an LVOT gradient of 50 mm Hg or greater, a documented LVEF of 55% or greater, a maximum septal wall thickness (determined by a core laboratory) of 15 mm or greater (or ≥ 13 mm with a family history of HCM), and NYHA functional class II or III symptoms. The primary outcome was composite functional response at week 30, defined as achieving an improvement of 1.5 mL/kg/min or greater in peak oxygen consumption (pVO2) and a reduction of at least 1 NYHA functional class (or 3.0 mL/kg/min or greater in pVO2 without NYHA class worsening). Secondary outcomes prespecified in the statistical hierarchy included changes in postexercise LVOT peak gradient, pVO2, NYHA class, Kansas City Cardiomyopathy Questionnaire (KCCQ) clinical summary score (CSS), and Hypertrophic Cardiomyopathy Symptom Questionnaire (HCMSQ) shortness of breath (SoB) domain score. Patients had a mean age of 58.5 years (standard deviation [SD] = 11.9), most patients (73%) had NYHA functional class II symptoms at baseline, and almost all patients (92%) were on background beta-blocker or calcium channel blocker therapy. Other exploratory outcomes assessed in the EXPLORER-HCM trial that were important to the CADTH review included health-related quality of life (HRQoL) as assessed by the 5-Level EQ-5D (EQ-5D-5L) questionnaire, changes in resting and Valsalva LVOT peak gradients, changes in cardiopulmonary exercise testing (CPET) parameters, cardiac structure, and biomarker-based assessments.
The VALOR-HCM trial (19 sites in the US; N = 112) evaluated the efficacy and safety of once-daily orally administered treatment with mavacamten (at a starting dose of 5 mg) in adult patients with symptomatic oHCM with an LVOT gradient of 50 mm Hg or greater, a documented LVEF of 60% or greater, a maximum septal wall thickness determined by a core laboratory of 15 mm or greater (or 13 mm or greater with family history of HCM), and NYHA functional class III or IV (or class II with exertional syncope or near syncope). Patients must have been referred within the past 12 months for SRT and be actively considering scheduling the procedure. The primary outcome was a composite of the decision to proceed with SRT before or at week 16 or be considered guideline-eligible for SRT at week 16. Guideline-eligibility criteria were based on the 2011 American College of Cardiology Foundation (ACCF)/AHA clinical and hemodynamic criteria for HCM. For the primary composite outcome, patients with a maximum LVOT gradient of 50 mm Hg or greater (from rest, Valsalva maneuver, or postexercise) and no improvement in NYHA functional class at week 16 were considered eligible for SRT. Secondary outcomes prespecified in the statistical hierarchy included changes in postexercise LVOT peak gradient, an improvement of at least 1 NYHA functional class, changes in KCCQ CSS, and changes in N-terminal pro–B-type natriuretic peptide (NT-proBNP) and cardiac troponin I biomarkers.
Efficacy Results
Both pivotal trials comparing mavacamten with placebo detected a statistically significant difference in their primary outcomes, and all prespecified secondary outcomes were statistically significant in favour of mavacamten.
In the EXPLORER-HCM trial, 37% of patients on mavacamten versus 17% of patients on placebo met the primary end point at week 30 with a between-group difference of 19.4% (95% confidence interval [CI], 8.7 to 30.1; P = 0.0005). With regard to key secondary outcomes tested in the statistical hierarchy from baseline to week 30, patients in the mavacamten group compared to those in the placebo group had greater reductions in postexercise LVOT gradients, with a mean difference of −36 mm Hg (95% CI, −43.2 to −28.1; P < 0.0001); greater increases in pVO2, with a mean difference of 1.4 mL/kg per min (95% CI, 0.6 to 2.1; P = 0.0006); more patients improving by at least 1 NYHA class (65% of patients in the mavacamten group versus 31% of patients in the placebo group), with a between-group difference of 34% (95% CI, 22.2 to 45.4; P < 0.0001); greater improvement in scores on the 23-item Kansas City Cardiomyopathy Questionnaire (KCCQ-23) CSS, with a mean difference of 9.1 (95% CI, 5.5 to 12.7; P < 0.0001); and greater reductions in severity of HCM symptoms as assessed by the HCMSQ SoB domain score, with a mean difference of −1.8, (95% CI, −2.4 to −1.2; P < 0.0001).
In the VALOR-HCM trial, for the primary composite outcome, after 16 weeks treatment, 17.9% of patients treated with mavacamten continued to meet guideline criteria for SRT or elected to undergo the procedure, compared to 76.8% of patients treated with placebo, with a treatment difference of 58.9% (95% CI, 44.0% to 73.9%; P < 0.001) favouring mavacamten. With regard to key secondary outcomes tested in the statistical hierarchy from baseline to week 16, patients in the mavacamten group compared to those in the placebo group had a greater reduction in postexercise LVOT gradient, with a mean difference of −37.2 mm Hg (95% CI, −48.1 to −26.2; P < 0.001); more patients with an improvement of at least 1 NYHA functional class, with a between-group difference of 41.1% (95% CI, 24.5% to 57.7%; P < 0.001); greater improvement in scores on the KCCQ CSS, with a mean difference of 9.4 points (95% CI, 4.9 to 14.0 points); and greater reductions in NT-proBNP and cardiac troponin I, with geometric mean ratio differences of 0.33 (95% CI, 0.26 to 0.42; P < 0.001) and 0.53 (95% CI, 0.41 to 0.70; P < 0.001), respectively.
Harms Results
In the EXPLORER-HCM trial, through to week 38, a total of 87.8% of patients in the mavacamten group and 81.3% of patients in the placebo group experienced 1 or more adverse events (AEs). The most common AEs were similar for both treatment groups. The proportion of patients who experienced 1 or more serious adverse events (SAEs) was similar between treatment groups (11.4% versus 9.4%). A total of 1.6% of patients in the mavacamten group and no patients in the placebo group discontinued treatments due to AEs. No AEs of decreased LVEF were reported. However, the incidence of a resting LVEF of less than 50% was a protocol-specified criterion for temporary treatment discontinuation in the EXPLORER-HCM trial. Throughout the 30-week treatment period, 3.6% of patients met a temporary treatment discontinuation criterion of an LVEF of less than 50%, including 5.7% of patients in the mavacamten group and 1.6% of patients in the placebo group. No patients experienced a reduction in their LVEF to 30% or less, which would have necessitated permanent treatment discontinuation. One death was reported in the placebo group due to sudden death.
In the VALOR-HCM trial, through to week 16, a total of 73.2% of patients in the mavacamten group and 61.8% of patients in the placebo group experienced at least 1 AE. The proportions of patients who had SAEs were similar for the mavacamten and placebo groups (5.4% versus 1.8%, respectively). Through to week 16 of the trial, 3.6% of patients in the mavacamten group had an LVEF of less than 50% resulting in temporary drug discontinuation; all of these patients subsequently resumed mavacamten dosing. No patients had a reduction of their LVEF to 30% or less, necessitating permanent treatment discontinuation through to week 16. No treatment discontinuations due to AEs or deaths through to week 16 were reported.
Critical Appraisal
Internal Validity
Both the EXPLORER-HCM and VALOR-HCM trials appeared to have acceptable methods for blinding, allocation concealment, and randomization with stratification. The clinical expert consulted for this review stated that the differences in the proportion of patients taking neither beta-blockers nor calcium channel blockers at baseline in the EXPLORER-HCM trial (3.3% mavacamten versus 12.5% placebo) may have introduced bias in favour of mavacamten, as a greater proportion of patients in the placebo group were not receiving any background therapy. The baseline and demographic characteristics in the VALOR-HCM trial appeared to be generally balanced between the treatment groups. Treatment discontinuation and study discontinuation among patients were low in both pivotal trials. The clinical expert consulted for this review indicated that the primary efficacy outcomes of the EXPLORER-HCM trial (pVO2 and NYHA functional class) are appropriate measures of functional capacity and symptom severity, respectively, in the indicated population. In both pivotal trials, HRQoL was measured using the KCCQ-23 CSS as a key secondary outcome. The clinical expert indicated that such tools are not typically used in clinical practice but have been used in multiple studies. Disease-related symptoms were assessed using the newly developed HCMSQ instrument, with the SoB domain assessed as a key secondary outcome in the EXPLORER-HCM trial. Because KCCQ-23 CSS or HCMSQ SoB data for more than 30% of patients were not collected at baseline or the week-30 visit in the EXPLORER-HCM trial, there is a risk of bias as those who completed the questionnaires may be fundamentally different than those who did not (i.e., differences in treatment response). However, for all imputation scenarios, ad hoc sensitivity analyses were generally supportive of the findings of the primary analyses.
The VALOR-HCM trial is evaluating the use of mavacamten to reduce the need for SRT in patients who are guideline-eligible and willing to participate in invasive therapies. As such, no direct evidence of mavacamten compared to SRT is available for this review. Direct evidence comparing mavacamten to disopyramide is also limited. Patients taking disopyramide were excluded from the EXPLORER-HCM trial and less than 20% of enrolled patients (n = 22) used disopyramide at baseline as monotherapy or in combination with beta-blockers and/or calcium channel blockers in the VALOR-HCM trial. Subgroup analyses based on disopyramide use at baseline was not available for the VALOR-HCM trial, |||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||||||| ||||||||||||| |||||||||| ||||||||| The comparative effectiveness of disopyramide versus mavacamten in this patient population is therefore unknown. In terms of subgroups of interest, both pivotal trials included subgroup analyses by baseline background therapy (beta-blocker or calcium channel blocker use) and the EXPLORER-HCM trial also examined NYHA class (II versus III) as a prespecified subgroup. For the primary end point in the EXPLORER-HCM trial, results were not statistically significantly different for the subgroup of patients taking beta-blockers. However, all key secondary end points in the EXPLORER-HCM trial showed a benefit from mavacamten compared with placebo across the evaluated subgroups, irrespective of beta-blocker use. The subgroup analyses may not have been powered to detect a treatment difference and no adjustments were made for multiplicity. All subgroup analyses are therefore exploratory in nature. No clinical study reports or statistical analysis plans were available for the VALOR-HCM trial at the time of this review, preventing CADTH from fully appraising the potential for bias within the trial.
Compared to the population in Canada, racial diversity in the pivotal trials was limited as most patients were white. In addition, no patients were recruited from Canada in either pivotal trial. However, the clinical expert consulted for this review noted that the lack of representation of patients in Canada does not reduce the generalizability of the results to Canadian clinical practice. While mavacamten has been approved by Health Canada for use in adult patients with symptomatic NYHA functional class II or III oHCM, the VALOR-HCM trial included an unknown number of patients with NYHA functional class IV oHCM. The VALOR-HCM trial is an ongoing randomized controlled trial (RCT) evaluating the use of mavacamten to reduce the need for SRT in patients who are guideline-eligible for invasive therapies, with descriptive data available through to week 32. As such, it is uncertain if mavacamten can reduce the need for SRT among patients with symptomatic oHCM in the long term.
Indirect Comparisons
No indirect evidence was available.
Other Relevant Evidence
Additional descriptive efficacy and safety data for the VALOR-HCM trial through to week 32 and data from 1 open-label extension study (MAVA-LTE) are summarized in this report.
Description of Studies
An additional study report for the VALOR-HCM trial examined data up to week 32 among patients initially randomized to mavacamten (32 weeks of drug exposure) and patients initially randomized to placebo who crossed over to mavacamten at week 16 (16 weeks of drug exposure).7 A total of 4 patients in the placebo group who elected to undergo SRT treatment or withdrew from the study during the first 16 weeks were not included in this analysis.
MAVA-LTE is an ongoing, dose-blinded, 5-year, long-term extension (LTE) study to assess the long-term efficacy and safety of mavacamten in patients who completed the EXPLORER-HCM trial through to week 38 (the EXPLORER-LTE cohort) and MAVERICK-HCM (a phase II trial involving patients with nonobstructive HCM that is not assessed in this report). A total of 224 patients who enrolled in the EXPLORER-LTE cohort started mavacamten treatment at 5 mg once daily, regardless of their treatment group in the EXPLORER-HCM pivotal trial. Dose adjustments at weeks 4, 8, and 12 were based on site-read echocardiograms of Valsalva LVOT gradient and LVEF. At LTE baseline, a total of 5.8% of patients in the EXPLORER-LTE cohort were NYHA functional class I, 65.2% were NYHA functional class II, 29.0% were NYHA functional class III, and none were NYHA functional class IV.
Efficacy Results
In the VALOR-HCM trial, at week 32, an improvement of at least 1 NYHA class was observed in 48 of 53 patients (90.6%) in the original mavacamten group and 35 of 50 patients (70%) in the crossover group. In the original mavacamten group, the mean change from baseline to week 32 in the KCCQ-23 CSS was 13.1 points (95% CI, 9.2 to 17.1), while in the placebo crossover group, the mean change in the KCCQ-23 CSS from week 16 to week 32 was 8.0 points (95% CI, 3.2 to 12.8). At week 32, 6 patients (10.7%) in the original mavacamten group and 7 patients (13.5%) in the placebo crossover group continued to meet guideline criteria for SRT or elected to undergo the procedure. In the original mavacamten group, there was a reduction in resting, Valsalva, and postexercise LVOT gradients from baseline to week 32. A similar reduction in LVOT gradients in the crossover group was seen after 16 weeks of mavacamten exposure.
Among patients in the EXPLORER-LTE cohort, from LTE baseline to week 48 of the extension study, 35 patients (71.4%) had an improvement of at least 1 NYHA class versus |||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| ||||||||||||||| |||||||||||||||||||| |||| |||||| |||||||||||||||| Reductions from the LTE study baseline were observed in both resting and Valsalva LVOT gradients from mavacamten treatment as assessed by both site and central readings in the extension study. However, the number of patients was relatively small during the end time points, making it difficult to draw any conclusions about the effects of mavacamten on LVOT gradients. ||||||||||||| |||||||||| ||||||||| || ||||||||||||||| |||||||||||| ||||||||||||||| || |||||||||||| |||||||||||||||||| ||||||||||||| ||||| |||||| ||||| |||||||||| ||||||| ||||| but a reduction in left atrial volume index (LAVI) was observed. In line with the EXPLORER-HCM pivotal trial, NT-proBNP concentrations decreased at LTE week 4, and the decreases were sustained over time to LTE |||||||
Harms Results
In the VALOR-HCM trial, through to week 32, the rate of SAEs was similar between the original mavacamten group and the placebo crossover group. No deaths, myocardial infarctions, or strokes were reported in either group. Through to week 32, a total of 9 patients, comprising 7 members (12.5%) of the original mavacamten group and 2 (3.8%) of the placebo crossover group, required a temporary drug discontinuation due to an LVEF of less than 50%. One patient in the placebo crossover group had a reduced LVEF of less than 30% at week 31 associated with paroxysmal atrial fibrillation and heart failure. Following permanent mavacamten discontinuation, the patient’s LVEF recovered and normalized.
Among patients in the EXPLORER-LTE cohort, 62.9% experienced at least 1 AE. The most common AEs |||||||||||| |||||||||| ||||| ||||||||||||| ||||||||||| ||||| |||||||| |||||| |||||||||| |||| |||||||||||||||| |||||||||||||||| One death, which was due to bacterial endocarditis, occurred in the EXPLORER-LTE cohort but was deemed by the investigator to be unrelated to mavacamten. |||||||||||||||| ||||||||||||||||||||| ||||||||||||||| |||||||| ||||| |||||||||||||| ||||||||||||| ||||||| A total of 2 patients (0.9%) permanently discontinued treatment due to AEs, with 1 patient discontinuing due to worsening of systemic lupus erythematosus and the other due to cardiac failure. No patients met the permanent discontinuation criteria of an LVEF of 30% or less. A total of 11 (4.9%) patients demonstrated a total of |||||||||||||||||| meeting the criteria for a temporary treatment discontinuation, 4 (1.8%) of whom experienced an LVEF of less than 50%.
Critical Appraisal
Results at week 32 of the VALOR-HCM trial provided additional data on the safety and efficacy of mavacamten. As all patients on placebo crossed over to mavacamten treatment week at 16, there was no active comparator, and all outcomes were descriptive in nature, making it difficult to make causal conclusions of the findings. Once placebo patients crossed over to active treatment at week 16, investigators and patients were aware that all patients were receiving active treatment, and their expectations of treatment could have affected reporting of subjective outcomes, such as NYHA class, HRQoL, and AEs.
Among patients in the EXPLORER-LTE cohort, the baseline and demographic characteristics were similar to those seen in the pivotal trial. Treatment discontinuation and study discontinuation rates among patients were low in the extension study, as observed in both pivotal trials. Peak oxygen consumption from the pivotal trial was not assessed in the extension study, ||||||||| |||||||| |||| |||||||||||||||| |||||||||| ||||||| ||||| |||||||||| ||||||| |||||| ||||||| ||||||||||| ||||| |||||||| |||||||||| ||||||||||||||| The absence of these parameters in the interim analysis makes it difficult to interpret the efficacy results of mavacamten for the extension study. |||||||| |||||||||||||||| ||||||| |||||||| ||||||||||||| |||||||||| ||||||| ||||||||| |||||||||| the number of patients at later time points in all efficacy analyses were relatively few at the time of the data cut, and these results should be interpreted with caution. The generalizability of the efficacy and harms outcomes and the lack of racial diversity mentioned in the main studies are applicable to the extension study.
Conclusions
In the EXPLORER-HCM trial, among patients with symptomatic NYHA class II or III oHCM, mavacamten was statistically significantly more efficacious than placebo in improving NYHA class and exercise capacity (pVO2), as measured by the primary composite outcome. In the VALOR-HCM trial, among patients with symptomatic NYHA class III or IV oHCM (or class II oHCM with exertional syncope or near syncope), significantly fewer patients were eligible for SRT at week 16 in the mavacamten group than in the placebo group. The results of both pivotal trials were statistically significantly in favour of mavacamten for key secondary outcomes of an improvement of at least 1 NYHA class, postexercise LVOT peak gradient, and HRQoL as assessed by the KCCQ-23 CSS, all of which were found to be clinically meaningful by the clinical expert consulted by CADTH for this review. The EXPLORER-HCM trial assessed disease-related symptoms, and a statistically significantly greater improvement in the HCMSQ SoB domain score was observed in the mavacamten group compared with the placebo group. The VALOR-HCM trial found statistically significantly greater reductions in assessed biomarkers among patients in the mavacamten group compared with those in the placebo group. While descriptive results for the VALOR-HCM trial are available through to week 32, it is uncertain if mavacamten can reduce the need for SRT among patients with symptomatic oHCM in the long-term. Furthermore, no direct evidence comparing mavacamten with SRT was available for this review. Only the VALOR-HCM trial enrolled patients who were receiving disopyramide; however, as no subgroup analyses based on disopyramide use at baseline were available, the comparative effectiveness of disopyramide versus mavacamten in patients with symptomatic oHCM is unknown. Because the EXPLORER-HCM trial evaluated mavacamten as an add-on to first-line treatment with beta-blockers or calcium channel blockers, the clinical efficacy of mavacamten as a first-line therapy or third-line therapy after disopyramide is unknown. The effectiveness of mavacamten in combination with disopyramide and beta-blockers or calcium channel blockers is also unknown. In both pivotal trials, overall rates of AEs and SAEs were comparable for patients in both the mavacamten and placebo groups. In the EXPLORER-HCM trial, 1 patient in the placebo group experienced sudden death, and no deaths were reported through to week 32 in the VALOR-HCM trial. The safety results showed that mavacamten was well tolerated and generally comparable to placebo, with no new safety signals identified in the MAVA-LTE study among patients in the EXPLORER-LTE cohort.
Introduction
Disease Background
HCM is a common genetic heart disease characterized by increased thickness of the left ventricular wall.1 About 30% to 60% of patients with HCM have identifiable familial disease caused by mutations in cardiac sarcomere protein genes, and each offspring of an affected family member has a 50% chance of inheriting the altered gene, although not all family members who inherit an HCM mutation will develop the disease.1-3 The distribution of HCM is equal by sex, although women have been diagnosed less frequently than men.2,3 The age of symptom onset and the severity of symptoms varies significantly across patients with HCM.1 Among patients with HCM who do develop symptoms, the most common symptoms include chest pain, shortness of breath with exertion, fatigue, palpitations, and light-headedness.1 oHCM, a subclassification of HCM, is characterized by LVOT obstruction, with the obstruction impeding blood flow from the heart to the rest of the body, defined in the 2020 AHA/ACC clinical guidelines as a peak LVOT gradient of 30 mm Hg or greater.3 Patients with oHCM are much more likely to develop symptoms due to increased left ventricular pressures and mitral regurgitation that result from restriction of blood flow out of the heart, which leads to increased wall stress, myocardial ischemia, and, eventually, cell death and replacement scarring.1 Associated complications include heart failure, stroke due to atrial fibrillations, arrhythmias, and sudden cardiac death.1 In a retrospective study, the estimated incidence rate of sudden cardiac death caused by HCM in patients aged 10 to 65 in Ontario was 0.05% per year.8
The estimated prevalence of HCM in the general population is 1 in 500 adults, although most of these cases remain undiagnosed.1 Among diagnosed patients, about 50% are symptomatic.9 AHA/ACC clinical guidelines suggest that oHCM is present or develops over time in most patients with HCM, with about a third remaining nonobstructive.3 Estimates of the proportion of patients with HCM who have oHCM range from 22% in a study from western Sweden4 to 70% in a US study.5
According to the clinical expert consulted for this review, treatment of oHCM can be completed by a cardiologist.
Standards of Therapy
According to AHA/ACC clinical guidelines, first-line therapy for patients with oHCM who are experiencing symptoms attributable to LVOT obstruction includes nonvasodilating beta-blockers titrated to maximal tolerated doses.3 In patients for whom beta-blockers are ineffective or not tolerated, use of nondihydropyridine calcium channel blockers (e.g., verapamil or diltiazem) is recommended. Patients with oHCM with persistent severe symptoms despite these therapies are candidates for more advanced therapies, including disopyramide in combination with 1 of the aforementioned treatments or SRT, either surgical myectomy or alcohol septal ablation.3
According to the clinical expert, for patients with symptomatic oHCM, standard treatment aims to lessen the extent of LVOT and manage arrhythmias. Traditionally, beta-blockers have been the mainstay of therapy. Given their negative inotropic and chronotropic effects, the drugs are most effective for exercise-induced (contraction-related) obstruction, but less so for resting obstruction. By relieving obstruction, beta-blockers can result in less shortness of breath and/or chest discomfort and help prevent the development of diastolic dysfunction, pulmonary hypertension, and heart failure with preserved ejection fraction. Where beta-blockers cannot be used or are not tolerated, nondihydropyridine calcium channel blockers can be prescribed. Should symptoms persist, disopyramide is recommended as add-on therapy. Taken separately or in combination, these drugs improve symptoms and quality of life. They do not address the underlying pathophysiology of HCM, obstructive or otherwise.
Drug
Mavacamten is a first-in-class cardiac myosin inhibitor.6 In HCM, excessive myosin-actin cross-bridge formation can result in hypercontractility, impaired relaxation, excess energy consumption, and myocardial wall stress. Mavacamten modulates the number of myosin heads that can enter power-generating states, reducing force-producing systolic and residual diastolic cross-bridge formation. Mavacamten also shifts the overall myosin population toward an energy-sparing, recruitable, super-relaxed state.6 This is the first CADTH review for mavacamten. The Health Canada indication is for the treatment of symptomatic NYHA class II to III oHCM in adult patients, with a Notice of Compliance granted on November 8, 2022.6 The sponsor has requested reimbursement according to the indication. Mavacamten is available as a 2.5 mg, 5 mg, 10 mg, or 15 mg capsule.6 The product monograph recommends a starting dosage of mavacamten for oHCM of 5 mg orally once daily. Patients should be assessed 4 weeks after initiation for a clinical response. If an LVOT gradient with a Valsalva maneuver is less than 20 mm Hg, the dosage should be decreased to 2.5 mg once daily. Otherwise, dosing at 5 mg once daily should be maintained.6 Thereafter, follow-up visits should occur at 8 and 12 weeks after treatment initiation, with dose adjustments as appropriate.6 The product monograph for mavacamten contains serious warnings and precautions regarding the risk of heart failure and notes that mavacamten reduces the LVEF and can cause heart failure due to systolic dysfunction, and that echocardiogram assessments of the LVEF and LVOT gradient are required before and regularly during treatment with mavacamten. It also notes that initiation of mavacamten in patients with an LVEF of less than 55% is not recommended, and that mavacamten treatment should be interrupted if the LVEF is less than 50% at any visit or if the patient experiences symptoms of heart failure or worsening clinical status.6 The product monograph also states that concomitant use of mavacamten in patients on a combination therapy of a calcium channel blocker (e.g., verapamil or diltiazem) and a beta-blocker should be avoided.6
Mavacamten has received FDA approval for the treatment of adult patients with symptomatic class II or III oHCM. Key characteristics of commonly used medical treatments for oHCM are presented in Table 2.
Table 2: Key Characteristics of Mavacamten, Beta-Blockers, Nondihydropyridine Calcium Channel Blockers, and Disopyramide
Characteristic | Mavacamten | Beta-blockers | Nondihydropyridine calcium channel blockers | Disopyramide |
|---|---|---|---|---|
Mechanism of action | Cardiac myosin inhibitor | Beta1-receptor antagonists | Blocks L-type calcium channels | Class 1a antiarrhythmic |
Indicationa | For the treatment of symptomatic NYHA class II to III oHCM in adult patients | Various cardiovascular indications | Various cardiovascular indications | For the treatment of documented life-threatening ventricular arrhythmias |
Route of administration | Oral | Oral | Oral | Oral |
Recommended dose | Starting dosage: 5 mg once daily; if after 4 weeks the LVOT gradient with Valsalva maneuver is < 20 mm Hg, the dosage should be decreased to 2.5 mg once daily | Varies among drugs | Varies among drugs | Usual daily dose is 400 to 800 mg given in 4 divided doses |
Serious adverse effects or safety Issues | Heart failure due to systolic dysfunction | Heart failure | Heart block | Heart failure |
Other | NA | Drugs: bisoprolol, metoprolol | Drugs: diltiazem, verapamil | NA |
LVOT = left ventricular outflow tract; NA = not applicable; NYHA = New York Heart Association; oHCM = obstructive hypertrophic cardiomyopathy.
aHealth Canada–approved indication.
Sources: Product monographs for Camzyos,6 bisoprolol,10 verapamil,11 and Rythmodan.12
Stakeholder Perspectives
Patient Group Input
This section was prepared by CADTH staff based on the input provided by patient groups. The full original patient inputs received by CADTH have been included in the stakeholder section at the end of this report.
Two patient advocacy groups, the CHPA and the HeartLife Foundation, provided input for the treatment of symptomatic oHCM in adult patients. The HeartLife Foundation gathered information from in-depth interviews with expert physicians and patients across Canada, and reviewed study material and online literature. The CHPA conducted extensive interviews with 3 clinicians (2 in the US and 1 in Italy) involved with clinical trials for mavacamten. They also gathered information by meeting with staff from the US-based Hypertrophic Cardiomyopathy Association and reviewing recorded panel discussions, patient testimonials, and educational videos. The CHPA recruited participants by contacting US-based clinicians and conducted outreach using the database for the CHPA in Canada, with additional patient profiles and confirmatory information provided by the Hypertrophic Cardiomyopathy Association. A total of 16 patients responded, 62.5% (10 out of 16) of whom were female, aged between 35 to 75 years, with 31% (5 out of 16) identifying as Canadians (1 living in the US) and 69% (11 respondents) as Americans. All participants reported being diagnosed with oHCM, and 40% also identified as being diagnosed with NYHA functional class II and 40% with NYHA functional class III oHCM. About 25% of participants reported being diagnosed with atrial fibrillation. Among the 16 respondents, 4 patients had been treated with mavacamten, all of whom were residents of the US.
Both patient groups agreed that HCM has a negative impact on patients’ quality of life. Delayed diagnosis, misdiagnosis, shortness of breath, exercise intolerance, arrythmia, palpitations, chest pain, fatigue, and fainting were some of the major issues experienced by the respondents. One group also noted that HCM can affect patients’ families and friends, both mentally and physically. While describing their experiences with currently available drugs, participants mentioned several treatments, including heart surgery, implantable cardioverter-defibrillators, alcohol septal ablation, and a variety of medications (such as beta-blockers, calcium channel blockers, and antiarrhythmics). However, both the groups reported concerns from both patients and health care providers regarding current treatments, patients’ symptoms, feelings of uncertainty, and unresolved anxiety with the available treatment options.
While evaluating improved outcomes from new treatments, patients expressed a desire to see a reduction in the risk of heart failure, including sudden death, as a current unmet need, as well as reductions in the debilitating symptoms affecting daily living activities and quality of life, including shortness of breath, irregular heartbeat, palpitations, chest pain, fatigue, stress, and anxiety. Spending time with loved ones, the ability to go to work on regular basis, pursuing outdoor activities, and the ability to travel were some of the quality-of-life indicators and experiences patients and caregivers mentioned.
While describing their experiences with the current drug under review, 4 patients recruited by the CHPA reported “very positive” experiences, noting that they had more energy to perform daily tasks and were hopeful that the drug would reduce their symptoms and risk of cardiac arrest. The HeartLife Foundation described findings from a clinical trial (VALOR-HCM) led by the Cleveland Clinic demonstrating a reduced need for an invasive procedure such as SRT in severely symptomatic patients with oHCM when mavacamten was used. However, the CHPA reiterated the need to assess patients, specifically by echocardiogram of the LVEF, for their cardiac status and as well as other illnesses (e.g., infections or chronic disease), cardiovascular symptoms (arrhythmias), and medications, before the approval of mavacamten. Moreover, patients must be closely monitored with echocardiograms for the first few months, as well as on a regular basis (every 3 months), and any symptoms must be reported due to the risk of heart failure associated with mavacamten. The CHPA noted that this limits the prescription of mavacamten to patients who have access to a high-volume clinic and who are committed to regular monitoring and reporting of symptoms.
Clinician Input
Input From Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise in the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by a clinical specialist with expertise in the diagnosis and management of cardiovascular diseases.
Unmet Needs
According to the clinical expert consulted for this review, mavacamten may address an unmet need as an add-on therapy for patients not experiencing symptom relief with beta-blockers or calcium channel blockers with or without disopyramide.
Place in Therapy
The clinical expert consulted for this review noted that mavacamten was evaluated in the EXPLORER-HCM trial as an add-on to first-line treatment with beta-blockers or calcium channel blockers in the context of improving symptoms and exercise capacity among patients with symptomatic oHCM. In terms of the treatment paradigm, the clinical expert stated that mavacamten will provide another treatment option for symptomatic patients with oHCM. In the expert’s opinion, the current place in therapy for mavacamten is unclear. It may be used as an add-on to beta-blockers or calcium channel blockers, or more appropriately as a third-line add-on to beta-blockers or calcium channel blockers plus disopyramide. According to the expert, the fact that mavacamten was not tested head-to-head with disopyramide raises uncertainty about its relative position in the treatment algorithm. The clinical expert stated that, while it has its own issues, disopyramide is a class 1a antiarrhythmic with negative inotropic properties and may be more powerful than beta-blockers or calcium channel blockers in controlling LVOT obstruction.
Patient Population
According to the clinical expert, symptomatic patients with oHCM who have not responded sufficiently to current treatment and/or whose symptoms are worsening despite such treatment would be eligible for treatment with mavacamten. Patients prescribed the drug would need to be sufficiently symptomatic (have received a diagnosis of at least NYHA class II oHCM) despite treatment with beta-blockers or calcium channel blockers with or without disopyramide. According to the expert, response to mavacamten cannot be predicted with sufficient accuracy to warrant advocating its use before beta-blockers or calcium channel blockers.
Assessing Response to Treatment
According to the expert, the metrics of response to treatment with mavacamten include stabilization or improvement of symptoms (e.g., fatigue, palpitations, light-headedness, and chest pain), reduction in the frequency and severity of symptoms, and improved ability to perform activities of daily living.
Discontinuing Treatment
In the opinion of the clinical expert, treatment should be discontinued if drug side effects occur. If symptoms or the LVOT gradient proceed to the point that SRT is needed, treatment with mavacamten should no longer be required.
Prescribing Conditions
According to the clinical expert, mavacamten should be prescribed by specialists (cardiologists) or in specialty clinics.
Clinician Group Input
This section was prepared by CADTH staff based on the input provided by clinician groups. The full and original clinician group inputs received by CADTH have been included in the stakeholder section at the end of this report.
Clinician group input on the review of mavacamten for the treatment of oHCM was received from 2 clinician groups: a community-based cardiology clinic, Cardio1, and an independent cardiologist who is a member of the hypertrophic Cardiomyopathy Clinic at the and the Stephenson Cardiac Imaging Centre at the Libin Cardiovascular Institute at the University of Calgary.
The clinician groups mentioned that beta-blockers, calcium channel blockers, and disopyramide are current treatments for oHCM. However, these treatments manage symptoms, and they do not modify the underlying disease. Potential adverse effects are also associated with these drugs limiting their use. Cardio1 pointed out that SRT such as surgical and percutaneous septal ablation may be beneficial to those who are refractory to drugs but can have potential adverse effects and limitations, and requires proper and careful selection of patients, indicating an unmet medical need for a noninvasive alternative to SRT.
Some unmet needs remain when current treatment options are deemed ineffective, are unable to reverse the course of the disease, and are used mostly for symptom relief. While both groups referred to data from studies demonstrating the effectiveness of the drug under review in improving symptoms and reducing the need for surgery, Cardio1 focused on using available conventional therapy first and switching to the new therapy when the former fails. The group also emphasized the importance of proper selection of patients and checking for updates on long-term studies on this new drug. The group noted the need for timely assessment of patients’ responses to conventional treatment, and switching to new treatment to prevent unnecessary suffering.
Regarding which patients are best suited for the new medication, 1 group identified patients with oHCM with severe LVOT obstruction who are highly symptomatic, whereas Cardio1 indicated that patients unresponsive to currently available treatments would be good candidates for this drug, as well as those who may not be candidates for early SRT, those who want to delay SRT, or those who do not want an SRT procedure. While 1 group expressed a strong interest in offering the new medication to patients, referring to the compelling data behind the new medication, Cardio1 pointed out the need to monitor the mortality, morbidity, and hospitalization outcomes of this drug.
Drug Program Input
Drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may affect their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical expert consulted by CADTH are summarized in Table 3.
Table 3: Summary of Drug Plan Input and Clinical Expert Responses
Drug program implementation questions | Clinical expert response |
|---|---|
Relevant comparators | |
In clinical practice, what is the typical treatment cascade for patients with oHCM? | Patients diagnosed with symptomatic oHCM begin treatment with beta-blockers or nondihydropyridine calcium channel blockers as first-line therapy. Patients who do not respond to or tolerate first-line therapy are candidates for disopyramide in combination with beta-blockers or nondihydropyridine calcium channel blockers. Among patients in whom symptoms persist, SRT may be a treatment option. |
Should mavacamten replace disopyramide as a combination therapy with a beta-blocker or calcium channel blocker or should it be used after a patient has tried combination therapy with disopyramide? | The evidence as presented supports the use of mavacamten as an add-on to beta-blockers or calcium channel blockers. There is limited evidence for the addition of mavacamten to beta-blockers or calcium channel blockers plus disopyramide. The current place in therapy for mavacamten is unclear. It may be used as an add-on to beta-blockers or calcium channel blockers, or perhaps more appropriately as a third-line drug following beta-blockers or calcium channel blockers plus disopyramide. The fact that mavacamten was not tested head-to-head against disopyramide raises uncertainty about mavacamten’s relative position in the treatment algorithm. While it has its own issues, disopyramide is a class 1a antiarrhythmic with negative inotropic properties that has been argued to be more powerful than beta-blockers or calcium channel blockers in controlling LVOT obstruction. |
Is there a role for mavacamten monotherapy? | No. |
Mavacamten is a cardiac myosin inhibitor, which reduces the number of actin myosin cross-bridges, which attenuates excessive contractility and improves cardiac function. Is it therefore not similar to beta-blockers or calcium channel blockers in that its function is to address the symptoms of oHCM? | Mavacamten is similar to beta-blockers or calcium channel blockers in terms of the effect of treatment. Mavacamten is more specific in its effect on contractility. Some data show reverse cardiac remodelling, as well as reductions in LV mass index and LV wall thickness with mavacamten. Whether this ultimately alters disease progression or affects major clinical outcomes is unknown. |
Is there any evidence in the available studies (EXPLORER-HCM, MAVA-LTE, or VALOR-HCM) that reliably demonstrates mavacamten improves outcomes of oHCM other than symptoms? | The durations of the submitted trials were not sufficient to reliably demonstrate that mavacamten improves outcomes of oHCM other than symptoms. |
Initiation of therapy | |
Are the eligibility criteria for the EXPLORER-HCM trial reasonable for a clinical trial of patients with oHCM? Are the eligibility criteria in the EXPLORER-HCM trial possible to determine in clinical practice (i.e., able to be determined and available across Canada)? Would the eligibility criteria for the trial work as eligibility criteria for reimbursement of mavacamten (as requested by the sponsor)? | Patients more clearly eligible for mavacamten are those diagnosed with symptomatic oHCM who are not responding to treatment with disopyramide in combination with beta-blockers or nondihydropyridine calcium channel blockers. Whether it should replace disopyramide as a second-line therapy remains uncertain in the absence of head-to-head trials. This could have been assessed if disopyramide had been used in lieu of placebo in the comparator arm. |
If a patient progresses to NYHA class IV, should funding be discontinued? | Funding should not be discontinued in patients who progress to NYHA class IV, although other treatments such as SRT should be under consideration by that point. |
Are the exclusion criteria for the EXPLORER-HCM trial reasonable for a clinical trial of patients with oHCM? Are there any exclusion criteria in the EXPLORER-HCM trial or other clinical trials that should be used as reimbursement conditions of mavacamten? | It is unclear why patients with a history of syncope within 6 months before screening were excluded from the EXPLORER-HCM trial. Patients with permanent atrial fibrillation who are either not on anticoagulants for more than 4 weeks or not adequately rate-controlled for more than 6 months and those with paroxysmal atrial fibrillation at screening were excluded from both pivotal trials. The reason for this is unclear. The exclusion criteria in the EXPLORER-HCM trial of an LVEF < 50% should be used as a reimbursement condition of mavacamten. |
Prescribing therapy | |
Do patients with oHCM need to be managed by specialist (e.g., cardiologist), or a specialist with specific training in oHCM? | Patients with oHCM should preferentially be managed by a cardiologist or specialty clinic. Treatment could be started either on an inpatient or outpatient basis. In regions where no practising cardiologist is available, specialist review and input could be provided virtually. |
According to the sponsor’s submission, only 2 sites in Canada are established myectomy centres (Toronto General and St. Paul’s Hospital in Vancouver). Is this accurate? | These 2 sites are recognized specialty centres and will receive referrals for the more complex cases. However, other centres in Canada will perform SRT. |
System and economic issues | |
The sponsor’s BIA can be used by the pCPA to establish budget caps. A number of assumptions in the BIA require confirmation:
In your opinion, are the estimates used in the BIA realistic? | Comments from the drug programs to inform CDEC deliberations. |
BIA = budget impact analysis; CDEC = CADTH Canadian Drug Expert Committee; HCM = hypertrophic cardiomyopathy; LV = left ventricle; LVEF = left ventricular ejection fraction; LVOT = left ventricular outflow tract; NYHA = New York Heart Association; oHCM = obstructive hypertrophic cardiomyopathy; pCPA = pan-Canadian Pharmaceutical Alliance; SRT = septal reduction therapy.
Clinical Evidence
The clinical evidence included in the review of mavacamten is presented in 2 sections. The first section, the systematic review, includes pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those studies that were selected according to an a priori protocol. The second section includes sponsor-submitted LTE studies and additional relevant studies that were considered to address important gaps in the evidence included in the systematic review.
Systematic Review (Pivotal and Protocol-Selected Studies)
Objectives
To perform a systematic review of the beneficial and harmful effects of mavacamten in the form of 2.5 mg, 5 mg, 10 mg, and 15 mg oral capsules for the treatment of symptomatic NYHA class II or III oHCM in adult patients.
Methods
Studies selected for inclusion in the systematic review include pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those meeting the selection criteria presented in Table 4. Outcomes included in the CADTH review protocol reflect outcomes considered to be important to patients, clinicians, and drug plans.
The systematic review protocol was established before the granting of a Notice of Compliance from Health Canada.
Table 4: Inclusion Criteria for the Systematic Review
Measure | Description |
|---|---|
Patient population | Adult patients with symptomatic NYHA class II or III oHCM Subgroups:
|
Intervention | Mavacamten 2.5 mg, 5 mg, 10 mg, or 15 mg oral capsule once daily |
Comparators |
|
Outcomes | Efficacy outcomes:
Harms outcomes: AEs, SAEs, WDAEs, notable harms (e.g., heart failure, sudden cardiac death, LVEF < 50%), all-cause mortality |
Study design | Published and unpublished phase III and IV randomized controlled trials |
AE = adverse event; CPET = cardiopulmonary exercise testing; HCMSQ = Hypertrophic Cardiomyopathy Symptom Questionnaire; HRQoL = health-related quality of life; ICD = implantable cardioverter-defibrillator; KCCQ-23 = 23-item Kansas City Cardiomyopathy Questionnaire; LAVI = left atrial volume index; LV = left ventricular ejection fraction; LVMI = left ventricular mass index; LVOT = left ventricular outflow tract; NT-proBNP = N-terminal pro–B-type natriuretic peptide; NYHA = New York Heart Association; oHCM = obstructive hypertrophic cardiomyopathy; pVO2 = peak oxygen consumption; SAE = serious adverse event; VE = volume expired; VCO2 = carbon dioxide production vs. = versus; WDAE = withdrawal due to adverse event.
The literature search for clinical studies was performed by an information specialist using a peer-reviewed search strategy according to the PRESS Peer Review of Electronic Search Strategies checklist.13
Published literature was identified by searching the following bibliographic databases: MEDLINE All (1946–) via Ovid and Embase (1974–) via Ovid. All Ovid searches were run simultaneously as a multifile search. Duplicates were removed using Ovid deduplication for multifile searches, followed by manual deduplication in EndNote. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were Camzyos (mavacamten). Clinical trials registries searched included the US National Institutes of Health’s clinicaltrials.gov, WHO’s International Clinical Trials Registry Platform (ICTRP) search portal, Health Canada’s Clinical Trials Database, and the European Union Clinical Trials Register.
No filters were applied to limit the retrieval by study type. Retrieval was not limited by publication date or by language. Conference abstracts were excluded from the search results. Appendix 1 provides the detailed search strategies.
The initial search was completed on October 21, 2022. Regular alerts updated the search until the meeting of the CADTH Canadian Drug Expert Committee on February 22, 2023.
Grey literature (literature that is not commercially published) was identified by searching relevant websites from the Grey Matters: A Practical Tool For Searching Health-Related Grey Literature checklist.14 Included in this search were the websites of regulatory agencies (FDA and European Medicines Agency). Google was used to search for additional internet-based materials. Appendix 1 provides more information on the grey literature search strategy.
These searches were supplemented by reviewing bibliographies of key papers and through contacts with appropriate experts. In addition, the sponsor of the drug was contacted for information regarding unpublished studies.
Two CADTH clinical reviewers independently selected studies for inclusion in the review based on titles and abstracts, according to the predetermined protocol. Full-text articles of all citations considered potentially relevant by at least 1 reviewer were acquired. Reviewers independently made the final selection of studies to be included in the review, and differences were resolved through discussion.
Findings From the Literature
A literature review identified 119 studies for inclusion in the systematic review (Figure 1). The included studies are summarized in Table 5. A list of excluded studies is presented in Appendix 2.
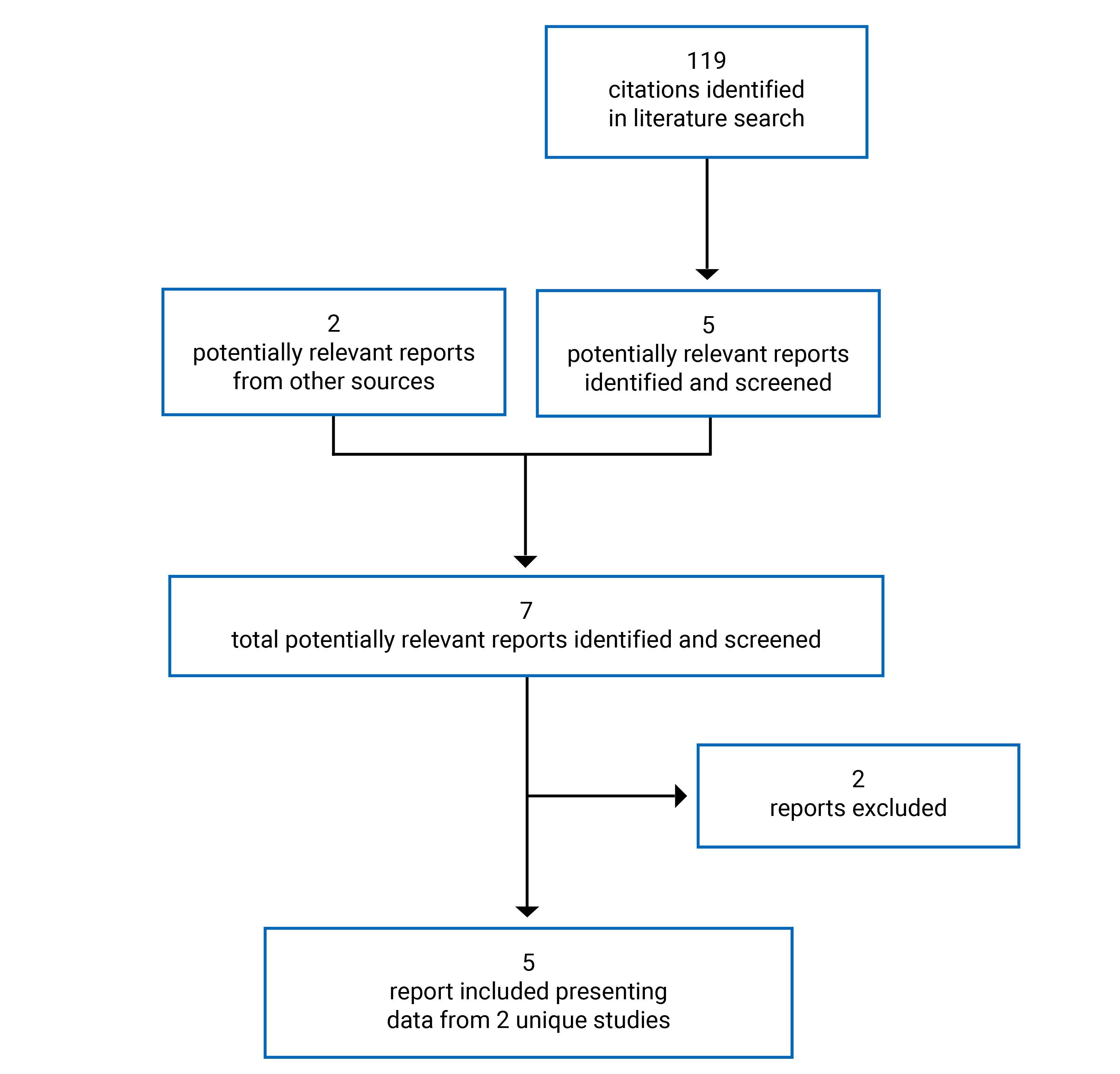
Table 5: Details of Included Studies
Characteristic | EXPLORER-HCM | VALOR-HCM |
|---|---|---|
Designs and populations | ||
Study design | Double-blind RCT | Double-blind RCT |
Locations | US, Europe, Israel | US |
Patient enrolment dates | May 30, 2018, to May 06, 2020 | July 2020 to October 2021 |
Randomized (N) | 251 | 112 |
Inclusion criteria |
|
|
Exclusion criteria |
|
|
Drugs | ||
Intervention | Mavacamten: 2.5 mg, 5 mg, 10 mg, or 15 mg single oral capsule taken once daily | Mavacamten: 2.5 mg, 5 mg, 10 mg, or 15 mg single oral capsule taken once daily |
Comparator(s) | Placebo: universal placebo capsule to match all mavacamten strengths taken once daily | Placebo: universal placebo capsule to match all mavacamten strengths taken once daily |
Duration | ||
Phase | ||
Screening | Up to 35 days | 2 weeks |
Double-blind | 30 weeks | 32 weeks:
|
Follow-up | 8 weeks | 96 weeks |
Outcomes | ||
Primary end point | Composite end point: achieving an improvement of ≥ 1.5 mL/kg/min in pVO2 at week 30 as determined by CPET and a reduction of ≥ 1 NYHA class or an improvement of ≥ 3.0 mL/kg/min in pVO2 with no worsening in NYHA class | Composite end point: decision to proceed with SRT before or at week 16 or be considered guideline-eligible for SRT at week 16 |
Secondary and exploratory end points | Secondary Change from baseline to week 30 in:
Exploratory
| Secondary Change from baseline to week 16 in:
Exploratory
|
Notes | ||
Publications | Olivotto et al. (2020)15 | Desai et al. (2021)16 Desai et al. (2022)17 Desai et al. (2022)7 |
ACCF = American College of Cardiology Foundation; AHA = American Heart Association; CPET = cardiopulmonary exercise testing; CSS = clinical summary score; EQ-5D-5L = 5-Level EQ-5D; ESC = European Society of Cardiology; HCM = hypertrophic cardiomyopathy; HCMSQ = Hypertrophic Cardiomyopathy Symptom Questionnaire; ICD = implantable cardioverter-defibrillator; KCCQ-23 = 23-item Kansas City Cardiomyopathy Questionnaire; LV = left ventricle; LVEF = left ventricular ejection fraction; LVOT = left ventricular outflow tract; NT-proBNP = N-terminal pro–B-type natriuretic peptide; NYHA = New York Heart Association; oHCM = obstructive hypertrophic cardiomyopathy; pVO2 = peak oxygen consumption; QTcF = QT interval corrected using Fridericia’s formula; RCT = randomized controlled trial; RER = respiratory exchange ratio; SoB = shortness of breath; SRT = septal reduction therapy; TTE = transthoracic echocardiogram.
Sources: Clinical Study Reports for EXPLORER-HCM trial,18 Desai et al. (2021),16 Desai et al. (2022),17 and Olivotto et al. (2020).15
Description of Studies
Two double-blind, placebo-controlled RCTs (EXPLORER-HCM and VALOR-HCM) met the inclusion criteria for the systematic review (Table 5). In both trials, patients started treatment with mavacamten 5 mg or matching placebo once daily. Subsequent dose adjustments of active treatment were implemented in a blinded, stepwise manner according to protocol-defined dose-titration criteria to 1 of 4 dose strengths (2.5 mg, 5 mg, 10 mg, or 15 mg). All dose strengths of mavacamten and placebo capsules were identical in appearance.
The objective of the EXPLORER-HCM study was to determine the efficacy, safety, and tolerability of mavacamten compared with placebo in patients with symptomatic oHCM. The trial took place in 68 sites across 13 countries, with 31 sites in the European Union, 29 sites in the United States, 6 sites in Israel, and 2 sites in the UK, with no Canadian sites. The study included a 35-day screening period, 30 weeks of double-blind treatment, and an 8-week follow-up period (Figure 2). A total of 251 patients with an LVOT gradient of 50 mm Hg or greater and an NYHA functional class of II or III were randomized 1:1 to receive mavacamten (n = 123) or placebo (n = 128) once daily for 30 weeks, followed by 8 weeks of post-treatment follow-up. Randomization was stratified by NYHA class (II or III), current treatment with beta-blockers (yes or no), planned type of ergometer used during the study (treadmill or exercise bicycle), and consent for a cardiac MRI (CMR) substudy (yes or no). The primary outcome was a composite functional end point at week 30, defined as achieving 1 of the following: an improvement of 1.5 mL/kg/min or greater in pVO2 as determined by CPET and a reduction of at least 1 NYHA class, or an improvement of 3.0 mL/kg/min or greater in pVO2 with no worsening in NYHA class. The EXPLORER-HCM trial also included a substudy at selected sites aimed to assess the effect of mavacamten on cardiac mass and structure as evaluated by CMR among eligible patients who did not have either an implantable cardioverter-defibrillator or pacemaker and did not have atrial fibrillation at screening (17 patients in the mavacamten group and 18 patients in the placebo group).
The objective of the ongoing VALOR-HCM study (19 sites across the US) was to determine if the addition of mavacamten to maximally tolerated medical therapy would allow patients with severely symptomatic oHCM to improve sufficiently that they no longer met guideline criteria for SRT or chose not to undergo SRT. The study included a 2-week screening period, followed by 16 weeks of placebo-controlled treatment, 16 weeks of active blinded treatment, a 96-week LTE, and an 8-week post-treatment follow-up visit (Figure 3). A total of 112 patients with a LVOT gradient of 50 mm Hg or greater and NYHA functional class III or IV (or class II with exertional syncope or near syncope) were randomized 1:1 to receive mavacamten (n = 56) or placebo (n = 56). Randomization was stratified by the type of SRT recommended (surgical myectomy or alcohol ablation) and NYHA functional class. The primary outcome was a composite of the decision to proceed with SRT before or at week 16 or be considered guideline-eligible for SRT at week 16. Guideline eligibility criteria were based on 2011 ACCF/AHA clinical and hemodynamic criteria for HCM. Patients with a maximum LVOT gradient of 50 mm Hg or greater (from rest, Valsalva, or postexercise) and no improvement in NYHA functional class at week 16 were considered eligible for SRT.
As the VALOR-HCM trial was ongoing at the time this report was drafted, a Clinical Study Report was not yet available. Sponsor-submitted publications16,17 provided data up to week 16 (the placebo-controlled period) of the VALOR-HCM trial. Additional descriptive data published for up to week 32 of the VALOR-HCM trial7 (including the active blinded period) are presented in the Other Relevant Evidence section of this report.
Figure 2: Study Schematic for EXPLORER-HCM Trial

Figure was redacted due to confidential information.
Figure 3: Study Schematic for VALOR-HCM Trial
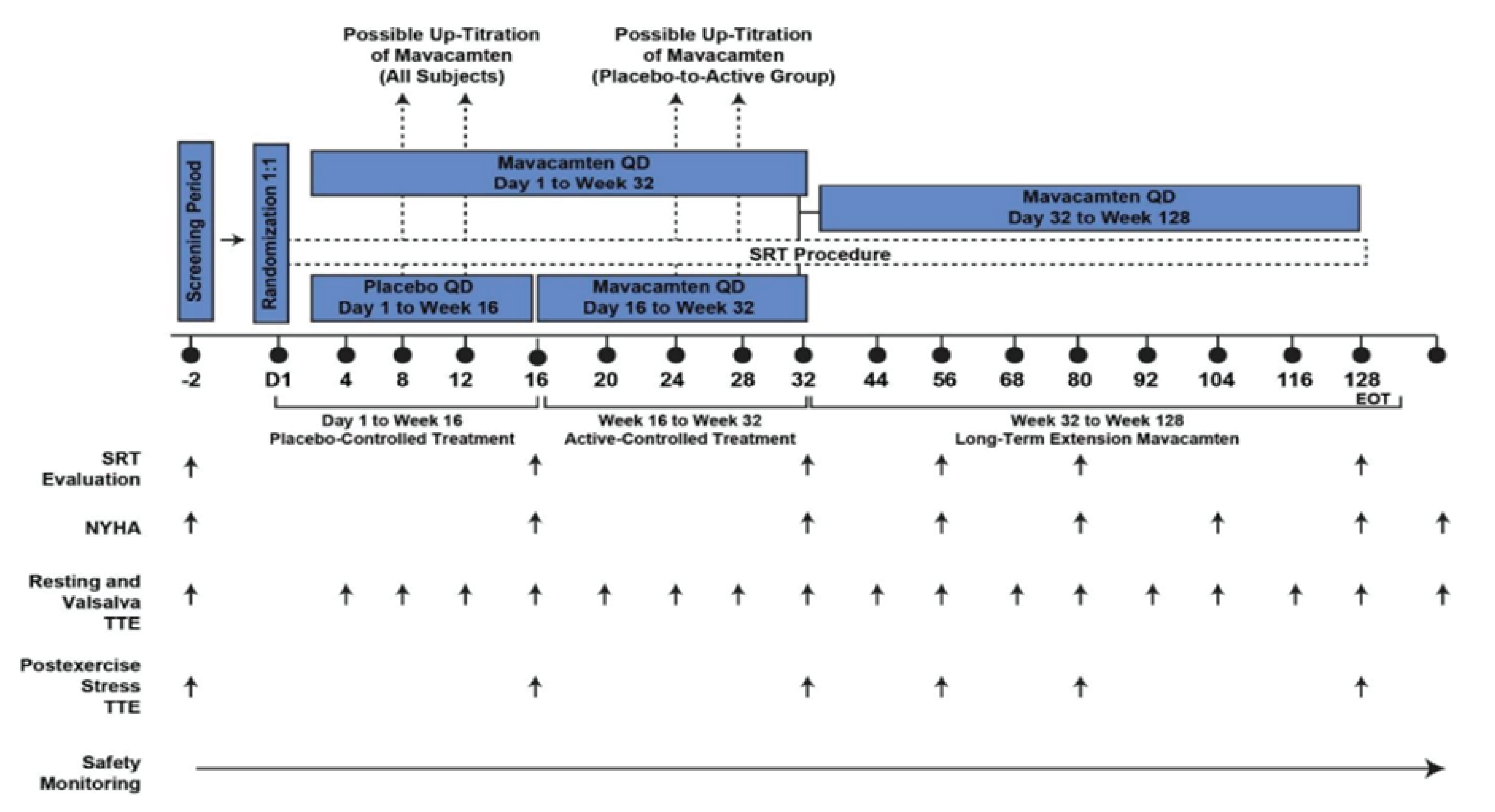
EOT = end of treatment; NYHA = New York Heart Association; QD = once daily; SRT = septal reduction therapy; TTE = transthoracic echocardiogram.
Source: Sponsor submission.19
Populations
Inclusion and Exclusion Criteria
As shown in Table 5, both pivotal trials enrolled adult patients aged 18 years or older and diagnosed with oHCM such that patients had unexplained LV hypertrophy with a maximal LV wall thickness of 15 mm or greater (13 mm or greater in cases of familial hypertrophic cardiomyopathy) and an LVOT peak gradient of 50 mm Hg or greater at rest, after a Valsalva maneuver or postexercise, and patients had to have an oxygen saturation at rest of 90% or greater at screening.
Patients in the EXPLORER-HCM trial had to have NYHA functional class of II or III oHCM, an LVEF of 55% or greater at screening, and be able to safely perform CPET with a respiratory exchange ratio of 1.0 or greater at screening. Patients were excluded if they had a history of syncope or sustained ventricular tachyarrhythmia with exercise within 6 months before screening; atrial fibrillation present at screening; or previous treatment or planned treatment with disopyramide, ranolazine, or a combination of beta-blockers and calcium channel blockers.
Patients in the VALOR-HCM trial were included if they had NYHA functional class of III or IV or class II oHCM with exertional symptoms of syncope or near syncope; an LVEF of 60% or greater at screening; targeted anterior septal thickness sufficient to perform SRT safely in the judgment of the individual operator; and had been in the past 12 months considered for and willing to participate in SRT. Patients were excluded if they had atrial fibrillation at screening, a planned invasive procedure, defibrillator placement, or pulse generator change during the first 32 weeks of the study; had any intracardiac procedure planned; or had been previously treated with invasive septal reduction.
Baseline Characteristics
Baseline characteristics are shown in Table 6 and Table 7 for the EXPLORER-HCM and VALOR-HCM trials, respectively. The age of patients was similar across both pivotal trials, with an overall mean age of 58.5 years (SD = 11.9) in the EXPLORER-HCM trial and 60 years (SD = 12.0) in the VALOR-HCM trial. In both trials, most patients were white (91.2% and 89.3%, respectively) and used beta-blocker monotherapy at baseline (75.3% and 45.5%, respectively). In both trials, disease duration was similar and balanced between treatment groups. In the EXPLORER-HCM trial, the mean duration of oHCM was 7 years (SD = 7.2) for the mavacamten group and 7 years (SD = 6.6) for the placebo group. Similarly, in the VALOR-HCM trial, the mean duration of oHCM was 7.5 years (SD = 9.4) for the mavacamten group and 6.7 years (SD = 7.4) for the placebo group.
In the EXPLORER-HCM trial, at baseline, the mavacamten group compared to the placebo group had more females (46.3% versus 35.2%), fewer patients with a history of atrial fibrillation (9.8% versus 18.0%), a higher percentage of patients taking calcium channel blockers (20.3% versus 13.3%), and fewer patients taking neither beta-blockers nor calcium channel blockers (3.3% versus 12.5%). More than half of patients were from a region outside the US (i.e., the European Union, the UK, or Israel) (56.9% mavacamten versus 57.0% placebo) and most patients had NYHA functioning class II symptoms (71.5% mavacamten versus 74.2% placebo). A total of 11 patients (8.9%) in the mavacamten group and 8 patients (6.3%) in the placebo group had prior SRT.
In the VALOR-HCM trial, patients were enrolled from 19 sites in the US and most patients had symptoms of NYHA functioning class III or greater oHCM (92.9% mavacamten versus 92.9% placebo). Most patients were recommended to undergo a myectomy in both the mavacamten and placebo groups at baseline (85.7% versus 87.5%). Slightly more patients in the mavacamten group than in the placebo group were taking both beta-blockers and disopyramide at baseline (19.6% versus 5.4%) and fewer patients in the mavacamten group than the placebo group were taking both beta-blockers and calcium channel blockers at baseline (10.7% versus 17.9%).
Table 6: Summary of Baseline Characteristics in the EXPLORER-HCM Trial
Characteristic | Mavacamten (N = 123) | Placebo (N = 128) |
|---|---|---|
Age (years), mean (SD) | 58.5 (12.2) | 58.5 (11.8) |
Age group, n (%) | ||
≤ 49 | 27 (22.0) | 25 (19.5) |
50 to 64 | 51 (41.5) | 63 (49.2) |
≥ 65 | 45 (36.6) | 40 (31.3) |
Sex, n (%) | ||
Male | 66 (53.7) | 83 (64.8) |
Female | 57 (46.3) | 45 (35.2) |
Region, n (%) | ||
US | 53 (43.1) | 55 (43.0) |
Excluding US | 70 (56.9) | 73 (57.0) |
Race, n (%) | ||
White | 115 (93.5) | 114 (89.1) |
Black or African American | 1 (0.8) | 5 (3.9) |
American Indian or Alaska Native [wording from original source] | 0 | 1 (0.8) |
Asian | 4 (3.3) | 2 (1.6) |
Unknown | 3 (2.4) | 6 (4.7) |
Ethnicity, n (%) | ||
Hispanic or Latino | 8 (6.5) | 4 (3.1) |
Not Hispanic or Latino | 114 (92.7) | 119 (93.0) |
Not reported | 1 (0.8) | 5 (3.9) |
Body mass index (kg/m2), mean (SD) | 29.7 (4.9) | 29.2 (5.6) |
Body surface area (m2), mean (SD) | 2.0 (0.2) | 2.0 (0.2) |
Heart rate (beats/min), mean (SD) | 63 (10.1) | 62 (10.6) |
Blood pressure (mm Hg), mean (SD) | ||
Systolic | 128.4 (16.2) | 128.4 (14.6) |
Diastolic | 75.5 (10.8) | 76.1 (9.9) |
NYHA functional class, n (%) | ||
Class II | 88 (71.5) | 95 (74.2) |
Class III | 35 (28.5) | 33 (25.8) |
Medical history | ||
Duration of oHCM (years), mean (SD) | 7 (7.2) | 7 (6.6) |
Family history of HCM, n (%) | 33 (26.8) | 36 (28.1) |
Past experience of the following cardiac rhythm events, n (%) | |||||||| | |||||||| |
Atrial fibrillation | 12 (9.8) | 23 (18.0) |
Nonsustained ventricular tachycardia | |||||||| | |||||||| |
Sustained VT | |||||| | |||||| |
History of surgeries or procedures, n (%) | |||||||| | |||||||| |
ICD and/or pacemaker | 27 (22.0) | 29 (22.7) |
SRT | 11 (8.9) | 8 (6.3) |
Alcohol septal ablation | ||||||| | |||||| |
Myectomy | |||||| | |||||| |
Background HCM therapy, n (%) | ||
Beta-blocker | 94 (76.4) | 95 (74.2) |
Calcium channel blockera | 25 (20.3) | 17 (13.3) |
Neither | 4 (3.3) | 16 (12.5) |
pVO2 and echocardiographic parameters | ||
pVO2 (mL/kg/min), mean (SD) | 18.9 (4.9) | 19.9 (4.9) |
Resting LVEF (%), mean (SD) | 74 ||||| | 74 ||||| |
LVOT gradient, mm Hg | ||
Resting, N | 123 | 128 |
Mean (SD) | 52 |||||| | 51 |||||| |
Valsalva, N | 123 | 128 |
Mean (SD) | 72 |||||| | 74 |||||| |
Postexercise, N | 122 | 127 |
Mean (SD) | 86 |||||| | 84 |||||| |
LV wall thickness, mm | ||
Septal, N | ||| | ||| |
Mean (SD) | ||||||| | ||||||| |
Posterior, N | ||| | ||| |
Mean (SD) | ||||||| | ||||||| |
Maximum, N | ||| | ||| |
Mean (SD) | ||||||| | ||||||| |
LAVI, mL/m2 | ||
N | 122 | 128 |
Mean (SD) | 40 |||||| | 41 |||||| |
Systolic anterior motion of mitral valve | ||
N | ||| | ||| |
Yes, n (%) | |||||||| | ||||||||| |
Mitral regurgitation | ||
N | ||| | ||| |
Yes, n (%) | ||||||||| | ||||||||| |
Baseline biomarkers | ||
NT-proBNP (ng/L), N | 120 | 126 |
Geometric mean (%CV) | 777 ||||||| | 616 ||||||| |
Cardiac troponin I (ng/L), N | 120 | 119 |
Geometric mean (%CV) | 12.5 ||||||| | 12.5 ||||||| |
%CV = percent coefficient of variation; HCM = hypertrophic cardiomyopathy; ICD = implantable cardioverter-defibrillator; LAVI = left atrial volume index; LV = left ventricular; LVEF = left ventricular ejection fraction; LVOT = left ventricular outflow tract; NSVT = nonsustained ventricular tachycardia; NT-proBNP = N-terminal pro–B-type natriuretic peptide; NYHA = New York Heart Association; oHCM = obstructive hypertrophic cardiomyopathy; pVO2 = peak oxygen consumption; SD = standard deviation; SRT = septal reduction therapy; VT = ventricular tachycardia.
||||||||| |||||||||||||||||||| ||||||| ||||||| |||||||| |||||||||| ||| ||||||||||||||
Source: Clinical Study Report for EXPLORER-HCM trial.18
Table 7: Summary of Baseline Characteristics in the VALOR-HCM Trial
Characteristic | Mavacamten (N = 56) | Placebo (N = 56) |
|---|---|---|
Age (years), mean (SD) | 59.8 (14.2) | 60.9 (10.5) |
Sex, n (%) | ||
Male | 29 (51.8) | 28 (50.0) |
Female | 27 (48.2) | 28 (50.0) |
Race,a n (%) | ||
White | 48 (85.7) | 52 (92.9) |
Black | 3 (5.4) | 0 (0.0) |
Asian | 2 (3.6) | 0 (0.0) |
Unspecified or other | 3 (5.4) | 4 (7.1) |
Vital signs, mean (SD) | ||
Body mass index, kg/m2 | 29.3 (4.8) | 31.9 (6.2) |
Systolic blood pressure, mm Hg | 130.4 (16.5) | 131.2 (16.6) |
Diastolic blood pressure, mm Hg | 74.0 (10.5) | 74.2 (8.9) |
Duration of oHCM (years), mean | 7.5 (9.4) | 6.7 (7.4) |
Medical history, n (%) | ||
Family history of HCM | 17 (30.4) | 15 (26.8) |
Atrial fibrillation | 11 (19.6) | 8 (14.3) |
Hypertension | 36 (64.3) | 34 (60.7) |
Syncope or presyncope | 29 (51.8) | 30 (53.6) |
Implantable cardioverter-defibrillator | 9 (16.1) | 10 (17.9) |
NYHA functional class, n (%) | ||
Class II with exertional syncope | 4 (7.1) | 4 (7.1) |
Class III or higher | 52 (92.9) | 52 (92.9) |
Type of SRT recommended, n (%) | ||
Alcohol septal ablation | 8 (14.3) | 7 (12.5) |
Myectomy | 48 (85.7) | 49 (87.5) |
Background HCM therapy, n (%) | ||
Beta-blocker monotherapy | 26 (46.4) | 25 (44.6) |
Nondihydropyridine calcium channel blocker monotherapy | 7 (12.5) | 10 (17.9) |
Disopyramide monotherapy | 0 (0.0) | 2 (3.6) |
Beta-blocker and calcium channel blocker | 6 (10.7) | 10 (17.9) |
Beta-blocker and disopyramide | 11 (19.6) | 3 (5.4) |
Calcium channel blocker and disopyramide | 1 (1.8) | 2 (3.6) |
Beta-blocker, calcium channel blocker, and disopyramide | 2 (3.6) | 1 (1.8) |
None, medication intolerance | 3 (5.4) | 3 (5.4) |
Echocardiographic parameters | ||
LVOT gradient (mm Hg), mean (SD) | ||
Resting | 51.2 (31.4) | 46.3 (30.5) |
Valsalva | 75.3 (30.8) | 76.2 (29.9) |
Postexercise | 82.5 (34.7) | 85.2 (37.0) |
Resting LVEF (%) | 67.9 (3.7) | 68.3 (3.2) |
LAVI (mL/m2) | 41.3 (16.5) | 40.9 (15.2) |
KCCQ-23 CSSb | 69.5 (16.3) | 65.6 (19.9) |
Laboratory measurements (ng/L), median (IQR) | ||
NT-proBNP | 724 (291 to 1,913) | 743 (275 to −1,196) |
Cardiac troponin I | 17.3 (7.0 to 31.6) | 12.9 (6.1 to 26.0) |
Cardiac troponin T | 0.01 (0.01 to 0.02) | 0.01 (0.01 to 0.02) |
CSS = clinical summary score; HCM = hypertrophic cardiomyopathy; IQR = interquartile range; KCCQ-23 = 23-item Kansas City Cardiomyopathy Questionnaire; LAVI = left atrial volume index; LVEF = left ventricular ejection fraction; LVOT = left ventricular outflow tract; NT-proBNP = N-terminal pro–B-type natriuretic peptide; NYHA = New York Heart Association; oHCM = obstructive hypertrophic cardiomyopathy; SD = standard deviation.
aRace was self-reported.
bThe KCCQ-23 CSS ranges from 0 to 100 points, where higher scores reflect better health status.
Source: Desai et al. (2022).17
Interventions
In both pivotal trials, patients were randomly assigned to receive once-daily orally administered treatment with mavacamten (starting dose 5 mg) or matching placebo. Detailed dose-titration regimens are shown in Table 8. In the EXPLORER-HCM trial, doses of mavacamten could be blindly down-titrated by 1 step (e.g., 5 mg to 2.5 mg) at any time during the 30 weeks of treatment if a patient had a mavacamten plasma trough concentration of greater than 700 ng/mL and less than 1,000 ng/mL. Doses could be blindly up-titrated by 1 step at week 8 or 14 if a patient’s mavacamten plasma trough concentration was less than 350 ng/mL and their Valsalva LVOT gradient was 30 mm Hg or greater at their previous assessment at weeks 6 and 12, respectively. Patients in the placebo group received the same titration assessments to maintain study blinding. Treatment was temporarily discontinued if the LVEF was less than 50% or the mavacamten plasma trough concentration was 1,000 ng/mL or greater, or due to prolongation of the QT interval corrected using Fridericia’s formula. Treatment was permanently discontinued if the LVEF was 30% or less. Patients who met the temporary discontinuation criteria could restart treatment 2 to 4 weeks after a follow-up visit at a single-step reduced dose if the temporary discontinuation parameters returned to an acceptable range. To maintain blinding, randomly selected patients from the placebo group underwent unscheduled follow-up visits.
The VALOR-HCM trial had 3 dosing periods. In the first placebo-controlled period, from day 1 to week 16, patients received treatment with mavacamten 5 mg or matching placebo once daily. Patients were evaluated for possible down-titration at week 4 (if their Valsalva LVOT gradient was less than 30 mm Hg) and up-titration at weeks 8 and 12 (if their Valsalva LVOT gradient was 30 mm Hg or greater). In the second active-controlled period, from week 16 to week 32, all patients received mavacamten once daily. Patients who received mavacamten during the first period continued the same dose they received at week 16, while patients who received placebo in the first period began mavacamten 5 mg/day at week 16 and were evaluated for down-titrations at week 20 and up-titrations at weeks 24 and 28. In the third LTE dosing period, from weeks 32 to 128, all patients received mavacamten once daily and their dose could be up-titrated to a maximum of 15 mg/day. If the LVEF was 50% or less at any time during treatment, mavacamten was temporarily discontinued for 2 to 4 weeks. Treatment was permanently discontinued if the LVEF was 30% or less. Patients who met the temporary discontinuation criteria could restart treatment 2 to 4 weeks after a reassessment visit at a single-step reduced dose if the LVEF was 50% or greater at reassessment. |||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||| |||||||||||||||| |||| |||||||||| ||||||| |||||||||||||| ||||| |||||| |||||||||||| ||||||||| Sponsor-submitted publications provided data up to week 16 for the VALOR-HCM trial, with additional descriptive data available through to week 32 described in the Other Relevant Evidence section of this report.
Table 8: Dose Titrations in the EXPLORER-HCM and VALOR-HCM Trials
Characteristic | EXPLORER-HCM (day 1 to week 30) | VALOR-HCM (day 1 to week 16) |
|---|---|---|
Starting dose of mavacamten | 5 mg | 5 mg |
Down-titration criteria | Mavacamten plasma concentration > 700 ng/mL to < 1,000 ng/mL at any visit | At week 4 if at previous assessment:
|
Up-titration criteria | At week 8 and 14 if at previous assessment:
| At week 8 and 12 if at previous assessment:
|
Temporary discontinuation criteria |
| Resting LVEF < 50% |
LVEF = left ventricular ejection fraction; LVOT = left ventricular outflow tract; QTcF = QT interval with Fridericia correction.
Sources: Clinical Study Reports for EXPLORER-HCM trial18 and Desai et al. (2022).17
Concomitant Medications
In the EXPLORER-HCM trial, background therapy (monotherapy with beta-blockers or calcium channel blockers) was permitted during the trial and was to be maintained at a stable dose throughout the study unless safety or tolerability concerns arose. Patients were prohibited from using disopyramide beginning 14 days before screening to the end of the study.
In the VALOR-HCM trial, patients were permitted to use standard-of-care HCM medications, including beta-blockers, calcium channel blockers, and disopyramide administered as monotherapy or in combination.
Outcomes
A list of efficacy end points identified in the CADTH review protocol that were assessed in the clinical trials included in this review is provided in Table 9. These end points are further summarized in the following section. A detailed discussion and critical appraisal of the outcome measures are provided in Appendix 4.
Table 9: Summary of Outcomes of Interest Identified in the CADTH Review Protocol
Outcome measure | EXPLORER-HCM | VALOR-HCM |
|---|---|---|
Change in NYHA functional class | Primary, key secondary | Key secondary |
Health-related quality of life (e.g., KCCQ-23, EQ-5D-5L) | Key secondary, exploratory | Key secondary, exploratory |
Disease-related symptoms (e.g., HCMSQ) | Key secondary, exploratory | NR |
Change in pVO2 | Primary | NR |
Change in postexercise, resting, and Valsalva LVOT peak gradient | Key secondary, exploratory | Key secondary, exploratory |
Change in septal reduction therapy status | NR | Primary |
Change in CPET parameters (e.g., peak VE/VCO2) | Exploratory | NR |
Change in cardiac structure (e.g., LV wall thickness, LAVI, LVMI) | Exploratory | Exploratory |
Biomarker-based assessment (e.g., NT-proBNP, cardiac troponin I) | Exploratory | Key secondary |
Prevention of atrial fibrillation or flutter | NR | NR |
Prevention of stroke | NR | NR |
Prevention of sudden cardiac death | NR | NR |
Need for implantation of ICD | NR | NR |
CPET = cardiopulmonary exercise testing; HCMSQ = Hypertrophic Cardiomyopathy Symptom Questionnaire; ICD = implantable cardioverter-defibrillator; KCCQ-23 = 23-item Kansas City Cardiomyopathy Questionnaire; LAVI = left atrial volume index; LV = left ventricular; LVMI = left ventricular mass index; LVOT = left ventricular outflow tract; NR = not reported; NT-proBNP = N-terminal pro–B-type natriuretic peptide; NYHA = New York Heart Association; pVO2 = peak oxygen consumption; VCO2 = carbon dioxide production; VE = volume expired.
Sources: Clinical Study Reports for EXPLORER-HCM trial,18 Desai et al. (2021),16 and Desai et al. (2022).17
Change NYHA Functional Class and Change in pVO2
The EXPLORER-HCM trial used both objective assessments of exercise capacity (pVO2 measured by CPET) and subjective assessments of symptom burden (NYHA functional class) as the primary composite outcome to evaluate clinically meaningful treatment benefits for oHCM. |||||| ||||||| ||||||||||||| ||||||||||| |||||| |||||| ||||||| ||||| ||||||| |||||||| CPET by standardized treadmill or bicycle ergometer was performed ||||||||||| |||||||| ||| ||||||||| |||||| |||||||| ||||||||| The primary composite outcome was defined as achieving 1 of the following at week 30:
an improvement of 1.5 mL/kg/min or greater in peak oxygen consumption (pVO2) as determined by CPET and a reduction of at least 1 NYHA class
an improvement of 3.0 mL/kg/min or greater in pVO2 with no worsening in NYHA class.
The VALOR-HCM trial did not examine change in pVO2 as an outcome. The proportion of patients who achieved an improvement of at least 1 NYHA class was examined as a key secondary outcome in both pivotal trials, through to week 30 in the EXPLORER-HCM trial and through to week 16 in the VALOR-HCM trial.
Health-Related Quality of Life
Kansas City Cardiomyopathy Questionnaire
The KCCQ-23 is a self-administered, 23-item, disease-specific, HRQoL questionnaire originally developed in 2000 to measure a patient’s perception of their health status within a 2-week recall period.20-22 The items of the KCCQ can be categorized into the following domains: physical limitation, symptoms (frequency, severity, and recent change over time), social limitation, self-efficacy, and HRQoL. All items are measured using a Likert scale with 5 to 7 response options. Responses are scored using ordinal values, beginning with 1 for the response that implies the lowest level of functioning. Domain scores are transformed to a 0-to-100 scale by subtracting the lowest possible scale score, dividing by the range of the scale, and multiplying by 100. Various combinations of the KCCQ domains create 3 summary scores, including a total symptom score (TSS), a CSS, and an overall summary score (OSS). The TSS combines the symptom burden and symptom frequency domains and evaluates patient-reported swelling in the feet, ankles, or legs; fatigue; shortness of breath; and disturbed sleep.23 The CSS includes the physical limitation and total symptom domains, and the OSS combines the physical limitation, total symptom, social limitation, and HRQoL domains into a single score. Summary scores are then transformed to a 0-to-100 scale, with larger scores representing a better outcome: 0 to 24: very poor to poor; 25 to 49: poor to fair; 50 to 74: fair to good; and 75 to 100: good to excellent.20,22
The KCCQ questionnaire is a generally valid, reliable, and responsive instrument for cardiovascular diseases.20,23-29 Convergent validity has been demonstrated through moderate-to-strong correlations of the KCCQ OSS and domain scores with a variety of external indicators of clinical status.24-26,28 Internal consistency reliability was demonstrated in a number of studies, in which the KCCQ summary and domain scores had Cronbach alpha values of greater than 0.7.20,24,25 Test-retest reliability has been demonstrated (intraclass correlation coefficient [ICC] > 0.7) for the KCCQ symptom, social, and limitation domains.20,25 High responsiveness of the KCCQ domains, the CSS, and the OSS has been found when the external indicators of clinical status were NYHA class, the Short Form (36) Health Survey, and the 6-minute walk distance (6MWD).20 The estimated minimal important differences (MIDs) were evaluated with 2 anchor-based methods in patients with heart failure, and were approximately 5 points for the KCCQ OSS and TSS, and 6 points for the CSS.30
5-Level EQ-5D Questionnaire
The 5-Level EQ-5D (EQ-5D-5L) questionnaire is a generic self-reported HRQoL outcome measure that can be applied to a variety of health conditions and treatments. The EQ-5D-5L was developed by the EuroQol Group as an improvement to the 3-Level EQ-5D questionnaire to measure small and medium health changes and reduce ceiling effects.31,32 The instrument comprises 5 dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Each dimension is rated on 5 levels: level 1 indicates “no problems,” level 2 “slight problems,” level 3 “moderate problems,” level 4 “severe problems,” and level 5 “extreme problems” or “unable to perform.”31,32 A total of 3,125 unique health states are possible, with 55555 representing the worst health state and 11111 representing the best state. The corresponding scoring of EQ-5D-5L health states is based on a scoring algorithm derived from preference data obtained from interviews using choice-based techniques (e.g., time trade-off) and discrete choice experiment tasks.31,32 The lowest and highest scores vary depending on the scoring algorithm used. Scores of less than 0 represent health states that are valued by society as being worse than dead, while scores of 0 and 1.00 are assigned to the health states “dead” and “perfect health,” respectively. As an example, a Canadian scoring algorithm results in a score of −0.148 for health state 55555 (worst health state) and a score of 0.949 for health state 11111 (best health state).31,32 In the EXPLORER-HCM trial, the EQ-5D-5L index score was calculated according to a US-based value set and ranged from 0 to 1, with lower scores indicating worse health states. The instrument was not used in the VALOR-HCM trial.
Disease-Related Symptoms
Hypertrophic Cardiomyopathy Symptom Questionnaire
The HCMSQ is a newly developed, self-administered, 11-item instrument specifically designed to evaluate symptomatic burden in patients with HCM.33 It measures the main symptoms of HCM, including shortness of breath, fatigue and tiredness, dizziness and light-headedness, heart palpitations, chest pain, and syncope. The scores on the instrument range from 0 to 12.5, with lower scores indicating fewer and less-severe symptoms. The change from baseline to week 30 in patient-reported severity of HCM symptoms was assessed by the HCMSQ SoB domain score in the EXPLORER-HCM trial, in which a decrease from baseline of 2.5 or more points in the HCMSQ SoB domain score was used as the threshold for a clinically meaningful response. The HCMSQ was not used in the VALOR-HCM trial.33 A clinically meaningful responder-definition range of 1 to 2 points was selected for the HCMSQ SoB and TSS, and approximately 1 point was used for the tiredness and cardiovascular symptom scores.33
Change in Postexercise, Resting, and Valsalva LVOT Peak Gradient
According to the 2020 AHA/ACC clinical guidelines, the presence of a peak LVOT gradient of 30 mm Hg or greater is indicative of obstruction, with resting or provoked gradients of 50 mm Hg or greater generally considered the threshold for SRT in patients with drug-refractory symptoms.3 Change from baseline in postexercise LVOT peak gradient to week 30 in the EXPLORER-HCM trial and to week 16 in the VALOR-HCM trial were the first of 5 sequentially tested, alpha-controlled secondary end points in both pivotal trials. Change from baseline in resting and Valsalva LVOT peak gradients were explored as exploratory outcomes in both trials. The proportion of patients with postexercise LVOT peak gradients of less than 30 mm Hg or less than 50 mm Hg were exploratory outcomes in the EXPLORER-HCM trial.
Change in Septal Reduction Therapy Status
The primary end point in the VALOR-HCM trial was the composite of the patient’s decision to proceed with SRT before or at week 16 or be considered guideline-eligible for SRT at week 16. Guideline-eligibility criteria for SRT were based on the 2011 ACCF/AHA HCM clinical and hemodynamic criteria.34 Eligibility criteria for SRT required an NYHA functional class III or IV status or an NYHA functional class II status with exertion-induced syncope or near syncope, and a dynamic LVOT gradient at rest or with provocation (i.e., Valsalva maneuver or exercise) of 50 mm Hg or greater.
The EXPLORER-HCM trial did not examine change in SRT status as an outcome.
Change in CPET Parameters
In the EXPLORER-HCM trial, CPET was conducted using a standardized treadmill or bicycle ergometer |||||||||| ||| |||||||| |||| |||||||| ||||||||||| Concomitant medications (i.e., beta-blockers or calcium channel blockers) may have been administered before all exercise testing. The same modality (treadmill or upright bicycle) had to be used for all CPETs conducted for a given participant. Cardiovascular and multiple other performance parameters were assessed at rest and at peak exercise.
Change in Cardiac Structure
Both pivotal trials assessed echocardiographic indices of atrial and ventricular chamber size and volumes. |||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| ||||||| |||| |||||||| |||||||||| |||||||
Biomarker-Based Assessment
Both pivotal trials assessed patients for reduction in cardiac biomarkers NT-proBNP (an indicator of cardiac wall stress) and cardiac troponin I (an indicator of cardiac injury).18
Harms Outcomes
||||||| ||||||||||||| |||||||| ||||||||||||| ||||||||||| ||||| || |||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||| ||||||||||| |||||||||||||| |||| |||||||||||||||| ||| |||||||||||||| ||||||||||||||||| |||||| ||||||| |||||||||||||| ||||||||||| |||||||||| ||| ||||||||| |||||||||||| ||||||||| ||||||||||||| ||| ||||||||| ||||||||| |||||||||||||||| |||||||||||||||||| |||||
Statistical Analysis
Sample-Size Determination and Power Calculation
In the EXPLORER-HCM trial, calculations resulted in a target sample size of N = 220 patients to achieve a 96% power to detect a 25% treatment difference for the primary outcome (2-sided test, significance level of 0.05) assuming the composite function end point would be achieved by 50% of patients in the mavacamten group and 25% in the placebo group.
In the VALOR-HCM trial, a sample size of 100 patients was prespecified to provide a 95% power to detect a 50% relative difference between groups for the primary end point (2-sided test, significance level of 0.05). There was 1 planned interim analysis for the primary outcome, which was conducted after 50 patients had completed the week-16 visit or terminated the study early (2-sided test, significance level of 0.001).
Statistical Test or Model
In the pivotal trials, categorical outcomes including the primary efficacy outcomes and the key secondary outcome of proportion of patients with an improvement of at least 1 NYHA class were analyzed with the Cochran-Mantel-Haenszel test for stratified categorical data.
In the EXPLORER-HCM trial, continuous outcomes of change in LVOT gradient and pVO2 were analyzed using analysis of covariance (ANCOVA) with the treatment group (mavacamten versus placebo), baseline value of the corresponding outcome of interest, and the 3 stratification factors (beta-blocker use, NYHA class, and ergometer type) treated as fixed effects. A mixed model for repeated measures (MMRM) was used for the key secondary outcomes of the KCCQ-23 CSS and HCMSQ SoB, which included the patient as a random effect and time point (as a categorical variable) and the interaction between treatment and time point as fixed effects in addition to the fixed effects described previously. Changes from baseline to week 30 in CMR parameters were summarized by treatment group for the CMR substudy population using descriptive statistics. |||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||| |||||||||||||||| |||||||| Between-group differences in the magnitude and direction of those changes were evaluated using Wilcoxon-Mann–Whitney tests.
In the VALOR-HCM trial, continuous variables were analyzed using ANCOVA or an MMRM for comparisons between the 2 groups. Baseline values were included in the ANCOVA model and the stratification factors (type of procedure and NYHA functional class) were treated as fixed effects. The MMRM included the treatment group, stratification factors, baseline value, time point, and the interaction between treatment group and time point as fixed effects. Biomarker data were log-transformed for model fits.
Data Imputation Methods
In the EXPLORER-HCM trial, missing NYHA classes at week 30 were imputed using the value for week 26, if available, in the case of the primary end point and NYHA response. Patients with a nonevaluable primary end point and NYHA secondary end point were considered nonresponders, whereas the LVOT gradient and pVO2 were analyzed with all available data without imputation, and patient-reported outcomes were analyzed with all available data using an MMRM, which implicitly handles the missing data in the patients who have baseline and 1 or more postbaseline values in the analysis.
In the VALOR-HCM trial, for the primary efficacy outcome, patients who discontinued the study or whose response status could not be assessed after the 16-week dosing period were classified as drug treatment failures (SRT-eligible). Missing data for secondary and exploratory efficacy analyses were not imputed.
Subgroup Analyses
Of the subgroups of interest to this review, both pivotal trials conducted preplanned analyses for select efficacy outcomes based on drug class of background therapy, including current treatment with beta-blockers (yes versus no) and current treatment with calcium channel blockers (yes versus no). The EXPLORER-HCM trial also conducted preplanned subgroup analyses based on NYHA functional class (II versus III). The results from the subgroup analyses may not have enough power to detect a treatment effect as no formal sample-size calculation was performed for individual subgroups and no adjustments were made for multiplicity. As such, the subgroup analyses are exploratory in nature.
Sensitivity Analyses
In the EXPLORER-HCM trial, an unstratified analysis using a chi-square test was performed as a sensitivity analysis for the primary efficacy outcome and for the key secondary outcome of proportion of patients who experienced an improvement of at least 1 NYHA class from baseline at week 30 (Table 10). An ad hoc sensitivity analysis assessed the impact of the missing data on 2 patient-reported outcomes (KCCQ-23 CSS and HCMSQ SoB), imputing missing data with unfavourable outcomes for the mavacamten group and favourable outcomes for the placebo group.
In the VALOR-HCM trial, a sensitivity analysis was performed to evaluate the number of patients with both improvement of NYHA functional class and reduction of all resting and provokable LVOT gradients of less than 50 mm Hg. Additional sensitivity analyses included using an alternative definition of SRT eligibility defined as either no improvement in NYHA functional class or maximum LVOT gradient of 50 mm Hg or greater as well as the need for SRT as determined by the investigator on the case report form.
Multiplicity Testing
In the EXPLORER-HCM trial, a sequential testing procedure was used to adjust for multiplicity. Upon achieving statistical significance in the primary end point, each of the secondary efficacy end points were tested sequentially at a 2-sided alpha level of 0.05, in the following order, as change from baseline to week 30:
postexercise LVOT peak gradient
pVO2 as determined by CPET
the proportion of patients with an improvement of at least 1 NYHA functional class
patient-reported health status as assessed by the KCCQ-23 CSS
patient-reported severity of HCM symptoms as assessed by the HCMSQ SoB domain score.
In the VALOR-HCM trial, a sequential testing procedure was used to adjust for multiplicity. Upon achieving statistical significance in the primary end point, each of the secondary efficacy end points were tested sequentially at a 2-sided alpha level of 0.05, in the following order, as change from baseline to week 16:
postexercise LVOT peak gradient
the proportion of patients with an improvement of at least 1 NYHA functional class
patient-reported health status as assessed by the KCCQ-23 CSS
NT-proBNP
cardiac troponin I.
In both pivotal trials, if any of the secondary end points did not differ statistically significantly between the mavacamten and placebo groups, the tests for all subsequent end points were not considered statistically significant, despite nominal P values. The analyses of other efficacy outcomes, including the individual components of these composite outcomes, were not subject to any multiplicity adjustment.
Table 10: Statistical Analysis of Efficacy End Points
End point | Statistical model | Adjustment factors | Sensitivity analyses |
|---|---|---|---|
EXPLORER-HCM | |||
Primary outcome: clinical response at week 30, defined as achieving:
| Cochran-Mantel-Haenszel | Stratified by NYHA class, beta-blocker use, and exercise type | Unstratified analysis using a chi-square test |
Key secondary: change from baseline to week 30 in postexercise LVOT peak gradient | ANCOVA | Baseline value, treatment group, visit, interaction between treatment group and visit, and the 3 stratification factors (beta-blocker use, NYHA class, and exercise type) as fixed effects | None |
Key secondary: change from baseline to week 30 in pVO2 as determined by CPET | ANCOVA | Baseline value, treatment group, visit, interaction between treatment group and visit, and the 3 stratification factors (beta-blocker use, NYHA class, and exercise type) as fixed effects | None |
Key secondary: proportion of patients who had at least 1 class of improvement from baseline in NYHA class at week 30 | Cochran-Mantel-Haenszel | Same as primary | Same as primary |
Key secondary: change from baseline to week 30 in patient-reported HRQoL as assessed by the KCCQ-23 CSS | MMRM | Baseline value, treatment group, visit, interaction between treatment group and visit, and the 3 stratification factors (beta-blocker use, NYHA class, and exercise type), time point (as a categorical variable), the interaction between treatment and time point as fixed effects and patient as random effect | Assess robustness by including missing data with unfavourable results toward the mavacamten group and favourable results for the placebo group |
Key secondary: change from baseline to week 30 in patient-reported severity of HCM symptoms as assessed by the HCMSQ SoB subscore | MMRM | ||
Exploratory: change in CPET parameters | MMRM | None | |
Exploratory: change in cardiac structure | Descriptive statistics | None | None |
Exploratory: change in LV volumes and cardiac output | Descriptive statistics | None | None |
Exploratory: change in measures of diastolic function | Descriptive statistics | None | None |
Exploratory: biomarker-based assessment | MMRM | Log-transformed baseline NT-proBNP value, treatment group, time, interaction between treatment group and time, and the 3 stratification factors (beta-blocker use, NYHA class, and exercise type) as fixed effects, and patient as a random effect | None |
VALOR-HCM | |||
Primary outcome: composite of the decision to proceed with SRT before or at week 16 or be considered guideline-eligible for SRT at week 16 | Cochran-Mantel-Haenszel | Stratified by baseline NYHA criteria (II vs. higher) and type of SRT recommended (myectomy vs. alcohol septal ablation) | Using an alternative definition of SRT eligibility defined as:
|
Key secondary: change from baseline to week 16 in postexercise LVOT peak gradient | ANCOVA or MMRMa | ANCOVA: baseline values were included in the model and the stratification factors (type of procedure and NYHA functional class) were treated as fixed effects MMRM: included the treatment group, stratification factors, baseline value, time point, and the interaction between treatment group and time point | NR |
Key secondary: proportion of patients who had an improvement of at least 1 NYHA class from baseline at week 16 | Cochran-Mantel-Haenszel | Same as primary | NR |
Key secondary: change from baseline to week 16 in patient-reported HRQoL as assessed by the KCCQ-23 CSS | ANCOVA or MMRMa | ANCOVA: baseline values were included in the model and the stratification factors (type of procedure and NYHA functional class) were treated as fixed effects MMRM: included the treatment group, stratification factors, baseline value, time point, and the interaction between treatment group and time point | NR |
Key secondary: change from baseline week 16 in NT-proBNP | ANCOVA or MMRMa | NR | |
Key secondary: change from baseline week 16 in cardiac troponin I | ANCOVA or MMRMa | NR | |
Exploratory: change from baseline to week 16 in hemodynamic parameters | ANCOVA or MMRMa | NR | |
ANCOVA = analysis of covariance; CPET = cardiopulmonary exercise testing; CSS = clinical summary score; HCMSQ = Hypertrophic Cardiomyopathy Symptom Questionnaire; HRQoL = health-related quality of life; KCCQ-23 = 23-item Kansas City Cardiomyopathy Questionnaire; LVOT = left ventricular outflow tract; MMRM = mixed model for repeated measures; NR = not reported; NT-proBNP = N-terminal pro–B-type natriuretic peptide; NYHA = New York Heart Association; PVO2 = peak oxygen consumption; SoB = shortness of breath (domain score); SRT = septal reduction therapy.
aThe VALOR-HCM publications did not specify which statistical test was used for continuous outcomes.
Sources: Clinical Study Report for EXPLORER-HCM trial,18 Desai et al. (2021),16 and Desai et al. (2022).17
Analysis Populations
In both pivotal trials, efficacy outcomes were analyzed in the intention-to-treat population, which included all the patients included all randomized patients, regardless of whether they received study drug. The safety population in both trials included all randomized patients who received at least 1 dose of the study drug, with analyse s conducted according to the actual study drug received.
Results
Patient Disposition
A summary of the patient disposition in the pivotal trials is available in Table 11. In the EXPLORER-HCM trial, 183 (42.7%) of 429 screened patients failed at least 1 screening criterion. Five of these 183 patients were randomized into the study before learning that they had failed a screening criterion, for a total of 251 randomized patients (58.5%). |||||||| |||||||| ||||||||||||||| |||||||||||||| |||| |||||||||||||||| ||| ||||| ||||||||| |||||||||| ||||||||||||| |||| |||||||||||||||| |||||| |||||||| |||||||||||| ||||||||||||| ||||||| |||||||||||||| |||||||||| ||||||||| |||||||||| ||| |||||| |||||||||||||||||||||| |||| |||||||||||||||| ||||||| ||||||||||||||||| ||||||||||||| |||||||||||||||||||| ||||| |||||||||||||| ||||||||||||||||||||| ||||||||||||||||||| ||||||| ||||||||||| |||||||||| |||||||||||||||||||| ||||||||| |||| ||||||||||| |||||||||||| ||||||||||||||||||| |||||||||||||||||| |||||| ||||||||||||||| |||||||| ||||||| ||||||| ||||||||| A total of 96.7% of patients in the mavacamten group and 98.4% in the placebo group completed the study when these patients were included. A total of 7 patients (2.8%) discontinued treatment, 4 (3.3%) in the mavacamten group and 3 (2.3%) in the placebo group.
In the VALOR-HCM trial, of the 152 patents screened, 73.7% were randomized, with 56 patients assigned to each of the mavacamten and placebo groups, respectively. A total of 2 patients (3.6%) in the placebo group discontinued the study through to week 16, and 2 patients (3.6%) in each treatment group discontinued treatment and elected to undergo SRT before or at week 16.
Characteristic | EXPLORER-HCM | VALOR-HCM | ||
|---|---|---|---|---|
Mavacamten | Placebo | Mavacamten | Placebo | |
Screened, N | 429 | 152 | ||
Randomized total, N (%) | 251 (58.5) | 112 (73.7) | ||
Randomized, N | 123 | 128 | 56 | 56 |
Discontinued from study, N (%) | 35 (28.5) | 38 (29.7) | 0 | 2 (3.6) |
Reason for discontinuation, N (%) | ||||
Adverse events | 2 (1.6) | 0 | 0 | 0 |
Lost to follow-up | 1 (0.8) | 0 | 0 | 0 |
Death | 0 | 1 (0.8) | 0 | 0 |
Othera | 31 (25.2) | 36 (28.1) | 0 | 1 (1.8)b |
Withdrawal by patient | 1 (0.8) | 1 (0.8) | 0 | 1 (1.8) |
Treatment discontinuation, N (%) | 4 (3.3) | 3 (2.3) | 2 (3.6) | 2 (3.6) |
Adverse event | 2 (1.6) | 0 | 0 | 0 |
Death | 0 | 1 (0.8) | 0 | 0 |
Other | 1 (0.8) | 1 (0.8) | 0 | 0 |
Withdrawal by patient | 1 (0.8) | 1 (0.8) | 0 | 0 |
Proceeded to SRT | NA | NA | 2 (3.6) | 2 (3.6) |
Intention-to-treat population, N | 123 | 128 | 56 | 56 |
Safety population, N | 123 | 128 | 56 | 55 |
NA = not applicable.
aIn the context of COVID-19, 67 patients in the EXPLORER-HCM trial who completed telephone visits at week 38 rather than onsite visits were categorized as “other” but did complete the study, for a total of 178 + 67 = 245 patients who completed the study (97.6%).
bPatient found ineligible after enrolment.
Sources: Clinical Study Reports for EXPLORER-HCM trial,18 Desai et al. (2021),16 and Desai et al. (2022).17
Exposure to Study Treatments
In the EXPLORER-HCM trial, ||||||||||||||| ||| ||||||| |||||||||||||| ||||||||||||||| |||||||||||||| |||||||||||||||| ||||||||||||| ||||||| ||||||| ||||| ||||| ||| (Table 12). The average daily dose in the mavacamten group was 6.7 mg (SD = 2.2) and approximately 50% of patients remained on mavacamten 5 mg/day throughout the treatment period. A total of 40 patients (32.5%) in the mavacamten group received a dose increase from 5 to 10 mg/day at weeks 8 or 14 and remained on 10 mg/day for the remainder of the treatment period; 13 patients (10.6%) received a dose increase from 5 to 10 mg at week 8 and a further dose increase from 10 to 15 mg/day and week 14 and remained on 15 mg/day for the remainder of the treatment period. Overall, 97.6% of patients in the mavacamten group had a compliance rate of 80% or greater.
Information related to duration of exposure was not reported in the VALOR-HCM trial publications. In terms of dose titrations, 23.2% of patients in the mavacamten group were receiving 5 mg/day and 33.9% were receiving 10 mg/day as their last measured dose during the double-blinded treatment period.
Table 12: Duration of Exposure (Safety Population)
Characteristic | EXPLORER-HCM | VALOR-HCM | ||
|---|---|---|---|---|
Mavacamten (N = 123) | Placebo (N = 128) | Mavacamten (N = 56) | Placebo (N = 55) | |
Duration of exposure (weeks),a mean (SD) | ||||||||| | ||||||||| | NR | NR |
Adjusted duration of exposure (weeks),b mean (SD) | ||| |||||| | ||||||||| | NR | NR |
Average daily mavacamten dosec (mg), mean (SD) | |||||||| | NA | NR | NR |
NA = not applicable; NR = not reported; SD = standard deviation.
aDuration of exposure in weeks is the interval between first dose date and last dose date and calculated as (last dose date – first dose date + 1)/7.
bAdjusted duration of exposure is the duration of exposure with adjustment for the period of protocol-specified dose interruptions (i.e., triggered by an interactive response system or due to a treatment-emergent adverse event).
||||||||| ||||||||||| |||| |||||||||||||||| ||| |||||||| |||||||||| ||||||||| ||||||||||||
Sources: Clinical Study Reports for EXPLORER-HCM trial,18 Desai et al. (2021),16 and Desai et al. (2022).17
Protocol Deviations
Important protocol deviations in the EXPLORER-HCM trial are summarized in Table 13. |||||||||||||| ||||||||||||||| |||||||||||| |||| |||||||||||| |||||||| |||||||| |||||||||||||||||| ||||||||||||| |||||||| ||||||||| |||||| ||||||||| |||||||||||||||| ||||||| |||||||| |||||||||||||||| |||||||| |||||||||| |||||||||| ||| ||||||||||||| ||||||| ||||||||||| ||||||| |||||||||||| ||||||||| ||||| ||||||||||||||| |||||||||||||| || ||||||||||||||||||| |||||||||||||| |||||||||||||| ||||||||||||| |||||||||||||||||| |||||||| |||||||||| |||||||| ||||||||||||| |||||||||| |||||||||||||| |||||||||||||||| |||||||| |||| ||||| ||||||||||| ||||||| |||||||| |||||| |||||||||||||| ||||| |||||||||||| |||||||||||||||| |||||||||||| |||||||||||| ||||||||||||||||||||| ||| ||||||||||| |||| |||||||||||||||| ||||||||| ||||| |||||||||| |||||||||||||||||||
||||| ||||||||| | |||||||||||||||||| | ||||||||||||||| |
|---|---|---|
|||||||||||||||||||||| | |||||||| | |||||||| |
|||||||||||||||||||| | |||||||| | |||||| || |
||||||||||||||||| | |||||||| | |||||||| |
|||| |||||||||||||||| ||| | |||||| | |||||| |
|||||||||||||| |||||||||||| |||||||| | |||||||| | |||||||| |
||||||||||||||||||||||||||||||||||||||||| | |||||||| | |||||||| |
||||||||||||||||| | |||||| | |||||| |
|||||| ||||||||||| | |||||| | |||||| |
||||||||||||||||||||| | |||||| | |||||| |
|||||||||| |||||||||||||||| | |||||| | |||||| |
|||| ||||||||||| ||||||||||||| | |||||| | |||||| |
|||| |||||||||||||||| ||||||| | ||||||| | ||||||| |
||||||||||||||||||||||||||||||||||||| | |||||||| | |||||||| |
||||||||||||||||| | |||||| | |||||| |
||||||| |||||||||| | |||||| | |||||| |
|||||||||||| ||||||||| | |||||| | |||||| |
|||||||| |||||||||||||||||| | |||||| | |||||| |
|||||||||||| |||||||| |||||||| | |||||||| | |||||||| |
||||||||||||||| |||||| |||||||||| ||||||||| |||||||| |||||||||||||| |||||| |||||||| ||||||| |||||||||| |||| ||||||||||||| |||||||||||| |||||||||||||||||||||||||||||||| |||||| ||||||| ||||||||||||| ||||||||||||||| |||||||||||| |||||||||||||| ||||||||| |||||||||||||||| |||||||||||||||||| |||||||||||||||||| |||||| |||||||| |||| |||||||||||||||| ||||| ||||| ||||||||| ||||||
This table was redacted due to confidential information.
Efficacy
Only those efficacy outcomes and analyses of subgroups identified in the review protocol are reported here. Appendix 3 provides detailed efficacy data.
Change in NYHA Functional Class
The proportion of patients with improvement of at least 1 NYHA class from baseline to end of treatment in the EXPLORER-HCM and VALOR-HCM trials are reported in Table 14 and Table 17, respectively. In the EXPLORER-HCM trial, a total of 80 patients (65%) in the mavacamten group and 40 patients (31.3%) in the placebo group experienced an improvement of at least 1 NYHA class from baseline to week 30, with a between–treatment group difference of 33.8% (95% CI, 22.2 to 45.4; P < 0.0001). As shown in Appendix 3, in the mavacamten group, 52 patients (42.3%) improved from class II to class I, 19 (15.4%) improved from class III to class II, and 9 (7.3%) improved from class III to class I. One patient (0.8%) in the mavacamten group worsened from NYHA class II at baseline to class III at week 30. In the placebo group, 24 patients (18.8%) improved from class II to class I, 13 patients (10.2%) improved from class III to class II, and 3 patients (2.3%) improved from class III to class I. Nine patients (7.0%) in the placebo group worsened from NYHA class II at baseline to class III at week 30. No patients worsened to NYHA class IV.
In the VALOR-HCM trial, a total of 35 patients (62.5%) in the mavacamten group and 12 patients (21.4%) in the placebo group experienced an improvement of at least 1 NYHA class from baseline to week 16 with a between–treatment group difference of 41.1% (95% CI, 24.5 to 57.7; P < 0.001).
In the EXPLORER-HCM trial, the sensitivity analysis for change in NYHA class was consistent with the results of the primary efficacy analysis.
Subgroup Analysis
In the EXPLORER-HCM trial, the subgroup analyses were generally consistent with the overall results (Appendix 3). The analyses may not have been powered to detect a treatment difference and no adjustments were made for multiplicity. As such, all subgroup analyses are exploratory in nature.
Change in NYHA Class and pVO2
Key results of the primary composite outcome in the EXPLORER-HCM trial are summarized in Table 16. A higher proportion of patients in the mavacamten group than in the placebo group (36.6% versus 17.2%) achieved the composite outcome at week 30 with a difference between treatment groups of 19.4% (95% CI, 8.7 to 30.1; P = 0.0005). A higher proportion of patients achieved both an increase of 3 mL/kg/min or greater in pVO2 and an improvement of at least 1 NYHA class in the mavacamten group compared with the placebo group (20.3% versus 7.8%), with a between–treatment group difference of 12.5% (95% CI, 4.0 to 21.0).
In the EXPLORER-HCM trial, the results of a sensitivity analysis of the primary composite outcome were consistent with those of the primary efficacy analysis. The analyses may not have been powered to detect a treatment difference and no adjustments were made for multiplicity. As such, all subgroup analyses are exploratory in nature.
Change in pVO2 and change in NYHA class combined was not examined in the VALOR-HCM trial.
Subgroup Analysis
In the EXPLORER-HCM trial, analyses of the primary efficacy end points of use of calcium channel blockers at baseline (yes versus no) and stratification factors of NYHA functional class at baseline (II versus III) showed a consistent effect in favour of mavacamten. Among patients using beta-blockers at baseline, there was no statistically significant difference between treatment groups with a between-group difference of 8.7% (95% CI, −3.6 to 21.1) compared to a treatment-group difference of 52.6% (95% CI, 32.9 to 72.2) among patients not using beta-blockers at baseline. The analyses may not have been powered to detect a treatment difference and no adjustments were made for multiplicity. As such, all subgroup analyses are exploratory in nature.
Health-Related Quality of Life
Kansas City Cardiomyopathy Questionnaire
Key summary results for KCCQ-23 CSS are reported in Table 14 and Table 17 for the EXPLORER-HCM and VALOR-HCM trials, respectively.
In the EXPLORER-HCM trial, the mean change from baseline to week 30 in the KCCQ-23 CSS was 13.6 (SD = 14.4) in the mavacamten group and 4.2 (SD = 13.7) in the placebo group, with a least squares mean difference of 9.1 (95% CI, 5.5 to 12.7; P < 0.0001). At week 30, 53.9% of patients in the mavacamten group achieved an increase of 10 points or greater (i.e., improvement) in the KCCQ-23 CSS from baseline compared with 33.8% of patients in the placebo group.
In the VALOR-HCM trial, the mean change from baseline to week 16 in the KCCQ-23 CSS was 10.4 (SD = 16.1) in the mavacamten group and 1.9 (SD = 12.0) in the placebo group, with a least squares mean difference of 9.4 (95% CI, 4.9 to 14.0; P < 0.001).
In the EXPLORER-HCM trial, greater mean improvements were found in the mavacamten group compared to the placebo group in the KCCQ-23 OSS and TSS from baseline to week 30 (Table 15). The mean change from baseline to week 30 in the KCCQ-23 OSS was 14.9 (SD = 15.8) in the mavacamten group and 5.4 (SD = 13.7) in the placebo group, with a least squares mean difference of 9.1 (95% CI, 5.5 to 12.8). The mean change from baseline to week 30 in the KCCQ-23 TSS was 12.4 (SD = 15.0) in the mavacamten group and 4.8 (SD = 15.9) in the placebo group, with a least squares mean difference of 7.7 (95% CI, 3.7 to 11.5).
Sensitivity Analyses
In the EXPLORER-HCM trial, ad hoc sensitivity analyses were conducted to assess if the between-group difference in the KCCQ-23 CSS key secondary end point remained robust when missing data were imputed with unfavourable outcomes for mavacamten group and favourable outcomes for the placebo group. For all imputation scenarios, results were supportive of the results of the primary analysis, although the treatment effect size decreased.
Subgroup Analysis
In the EXPLORER-HCM trial, the subgroup analyses were generally consistent with the overall results. The analyses may not have been powered to detect a treatment difference and no adjustments were made for multiplicity. As such, all subgroup analyses are exploratory in nature.
5-Level EQ-5D
In the EXPLORER-HCM trial, the mean EQ-5D-5L index scores remained close to baseline values for both treatment groups at week 30, with mean changes from baseline of 0.08 (SD = 0.16) for the mavacamten group and 0.009 (SD = 0.16) for the placebo group (Table 15).
The EQ-5D-5L instrument was not used in the VALOR-HCM trial.
Disease-Related Symptoms
Hypertrophic Cardiomyopathy Symptom Questionnaire
As shown in Table 14, in the EXPLORER-HCM trial, mavacamten-treated patients demonstrated a statistically significant decrease (i.e., an improvement) in HCMSQ SoB domain scores compared with placebo patients. Mean HCMSQ SoB domain scores decreased by 2.8 |||||||| points from baseline to week 30 in the mavacamten group compared to a decrease of 0.9 |||||||| points in the placebo group (between-group difference −1.8; 95% CI, ||||||||||||; P < 0.0001). A greater proportion of patients taking mavacamten compared to placebo achieved an improvement of 2.5 or more points between baseline and week 30 in the HCMSQ SoB domain score (50.0% versus 21.3%).
|||||||| ||||||||| |||||||||||||| |||||||||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||| |||||||||||||||| ||||||||||||||||| |||||||| |||||||||||||||||| |||||||| |||||||||| ||||||||| ||||||||||||||| ||||||||| |||||||||| ||||||||||||||||||||| ||||||||||
The HCMSQ instrument was not examined in the VALOR-HCM trial.
Sensitivity Analysis
In the EXPLORER-HCM trial, exploratory sensitivity analyses were conducted to assess if the between-group difference in the HCMSQ SoB domain remained robust when missing data were imputed with unfavourable outcomes for the mavacamten group and favourable outcomes for the placebo group. For both imputation scenarios, results were supportive of the results of the primary analysis, although the treatment effect size decreased.
Subgroup Analysis
In the EXPLORER-HCM trial, subgroup analyses were generally consistent with the overall results. The analyses may not have been powered to detect a treatment difference and no adjustments were made for multiplicity. As such, all subgroup analyses are exploratory in nature.
Table 14: Summary of Key Response Variables at Week 30 in the EXPLORER-HCM Trial (ITT Population)
Characteristic | Mavacamten (N = 123) | Placebo (N = 128) |
|---|---|---|
Postexercise LVOT peak gradient, mm Hg | ||
Number of patients contributing to the analysis, n | 117 | 122 |
Baseline, mean (SD) | 86 (34.3) | 84 (35.7) |
Week 30, mean (SD) | 38 (32.1) | 73 (34.9) |
Change from baseline to week 30, mean (SD) | −47.2 (40.3) | −10.4 (29.6) |
Least squares mean difference vs. placebo (95% CI)a | −35.6 (−43.2 to −28.1) | |
P valuea | < 0.0001 | |
pVO2 as determined by CPET, mL/kg/min | ||
Number of patients contributing to the analysis, n | 120 | 125 |
Baseline, mean (SD) | 18.9 (4.9) | 19.9 (4.9) |
Week 30, mean (SD) | 20.4 (5.4) | 19.9 (5.4) |
Change from baseline to week 30, mean (SD) | 1.4 (3.1) | −0.05 (3.0) |
Least squares mean difference vs. placebo (95% CI)a | 1.4 (0.6 to 2.1) | |
P valuea | 0.0006 | |
Proportion of patients with improvement ≥ 1 NYHA class | ||
Number of patients contributing to the analysis,b n | 123 | 128 |
Improved by ≥ 1 NYHA class from baseline to week 30, n (%) | 80 (65.0) | 40 (31.3) |
Treatment-group difference vs. placebo (95% CI)c | 33.8 (22.2 to 45.4) | |
Odds ratio (95% CI) vs. placebod | 4.3 (2.5 to 8.0) | |
P valued | < 0.0001 | |
KCCQ-23 CSS | ||
Number of patients contributing to the analysis | 92 | 88 |
Baseline score, mean (SD) | 71.1 (16.3) | 70.6 (19.1) |
Change from baseline to week 30, mean (SD) | 13.6 (14.4) | 4.2 (13.7) |
LS mean difference vs. placebo (95% CI)e | 9.1 (5.5 to 12.7) | |
P valuee | < 0.0001 | |
Proportion of patients with ≥ 10 points increase from baseline in KCCQ-23 CSS at week 30f | 48 (53.9) | 27 (33.8) |
HCMSQ SoB domain score | ||
Number of patients contributing to the analysis | 85 | 86 |
Baseline score, mean (SD) | 4.9 (2.5) | 4.5 (3.2) |
Change from baseline to week 30, mean (SD) | −2.8 (2.7) | −0.9 (2.4) |
LS mean difference vs. placebo (95% CI)e | −1.8 (−2.4 to −1.2) | |
P valuee | < 0.0001 | |
Proportion of patients with ≥ 2.5 points decrease in HCMSQ SoB at week 30, n (%)g | 45 (50.0) | 16 (21.3) |
Resting LVOT peak gradient, mm Hg | ||
Number of patients contributing to the analysis | 117 | 123 |
Baseline, mean (SD) | 51.7 (29.4) | 51.1 (31.9) |
Change from baseline to week 30, mean (SD) | −38.6 (29.5) | −5.5 (27.9) |
Valsalva LVOT peak gradient, mm Hg | ||
Number of patients contributing to the analysis | 117 | 124 |
Baseline, mean (SD) | 72.0 (31.7) | 74.0 (32.0) |
Change from baseline to week 30, mean (SD) | −49.0 (34.4) | −12.0 (31.0) |
ANCOVA = analysis of covariance; CI = confidence interval; CPET = cardiopulmonary exercise testing; CSS = clinical summary score; HCMSQ = Hypertrophic Cardiomyopathy Symptom Questionnaire; ITT = intention-to-treat; KCCQ-23 = 23-item Kansas City Cardiomyopathy Questionnaire; LVOT = left ventricular outflow gradient; NYHA = New York Heart Association; pVO2 = peak oxygen consumption; SD = standard deviation; SoB = shortness of breath.
aThe mean difference estimate, its 95% CI, and P values are from the ANCOVA which controls for treatment group (mavacamten vs. placebo), baseline value of the corresponding end point of interest, and the 3 stratification factors (beta-blocker use, NYHA class, ergometer type based on an interactive response system).
bThe missing NYHA class at week 30 is imputed using available NYHA at week 26. After imputation, patients whose response status at week 30 is still missing will be classified as nonresponders.
|||||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||| |||||||||||||||| |||||||
dThe analysis was stratified on NYHA class, beta-blocker use, and exercise type (based on an interactive response system). Odds ratio was estimated using Cochran-Mantel-Haenszel method. An odds ratio greater than 1 indicates better outcome when comparing to placebo. P values and 95% CIs were derived using the exact method.
eBased on mixed model for repeated measures, with data up to week 30, which includes baseline value, treatment group, visit, interaction between treatment group and visit, and the 3 stratification factors (beta-blocker use, NYHA class, exercise type based on an interactive response system) as fixed effects and the patient as a random effect.
fTotal N is the number of patients with a baseline score of up to 100 minus 10 (i.e., the clinically meaningful threshold). Patients with missing data at the postbaseline visit were considered nonresponders for that visit.
gTotal N is the number of patients with a baseline score of 2.5 or greater (i.e., the clinically meaningful threshold).
Source: Clinical Study Report for EXPLORER-HCM.18
Table 15: Exploratory Patient-Reported Outcomes at Week 30 in the EXPLORER-HCM Trial (ITT Population)
Characteristic | Mavacamten (N = 123) | Placebo (N = 128) |
|---|---|---|
KCCQ-23 OSS | ||
Number of patients contributing to the analysis | 92 | 88 |
Baseline score, mean (SD) | |||||||||| | |||||||||| |
Change from baseline to week 30, mean (SD) | 14.9 (15.8) | 5.5 (13.7) |
LS mean difference vs. placebo (95% CI) | 9.1 (5.5 to 12.8) | |
P value | < 0.0001b | |
KCCQ-23 TSS | ||
Number of patients contributing to the analysis | 92 | 88 |
Baseline score, mean (SD) | |||||||||| | |||||||||| |
Change from baseline to week 30, mean (SD) | 12.4 (15.0) | 4.8 (15.9) |
Least squares mean difference vs. placebo (95% CI)a | 7.7 (3.7 to 11.5) | |
P valuea | 0.0002b | |
HCMSQ fatigue domain score | ||
Number of patients contributing to the analysis | 85 | 86 |
Baseline score, mean (SD) | |||||||| | |||||||| |
Change from baseline to week 30, mean (SD) | ||||||||| | ||||||||| |
HCMSQ heart symptom score | ||
Number of patients contributing to the analysis | 85 | 86 |
Baseline score, mean (SD) | |||||||| | |||||||| |
Change from baseline to week 30, mean (SD) | ||||||||| | ||||||||| |
HCMSQ total score | ||
Number of patients contributing to the analysis | 85 | 86 |
Baseline score, mean (SD) | |||||||| | |||||||| |
Change from baseline to week 30, mean (SD) | ||||||||| | ||||||||| |
EQ-5D-5L index score | ||
Number of patients contributing to the analysis | 96 | 89 |
Baseline score, mean (SD) | 0.8 (0.2) | 0.8 (0.2) |
Change from baseline to week 30, mean (SD) | 0.1 (0.2) | 0.009 (0.2) |
CI = confidence interval; EQ-5D-5L = 5-Level EQ-5D; HCMSQ = Hypertrophic Cardiopathy Symptom Questionnaire; ITT = intention-to-treat; KCCQ-23 = 23-item Kansas City Cardiomyopathy Questionnaire; NYHA = New York Heart Association; OR = odds ratio; OSS = overall summary score; SD = standard deviation; TSS = total symptom score.
aBased on a mixed model for repeated measures with data up to week 30, which includes baseline value, treatment group, visit, interaction between treatment group and visit, and the 3 stratification factors (beta-blocker use, NYHA class, exercise type based on an interactive response system), as fixed effects and the patient as a random effect.
bP value has not been adjusted for multiple testing (i.e., the type I error rate has not been controlled).
Source: Clinical Study Report for EXPLORER-HCM.18
Change in pVO2
As shown in Table 14, in the EXPLORER-HCM trial, the mean changes from baseline to week 30 in pVO2 were 1.4 mL/kg/min (SD = 3.1) in the mavacamten group and −0.05 mL/kg/min (SD = 3.0) in the placebo group, with a difference between treatment groups of 1.4 mL/kg/min (95% CI, 0.6 to 2.1; P = 0.0006) in favour of mavacamten.
Change in pVO2 was not examined in the VALOR-HCM trial.
Subgroup Analysis
In the EXPLORER-HCM trial, subgroup analyses based on use of calcium channel blockers at baseline (yes versus no) and NYHA functional class at baseline (II versus III) support the results seen in the main analysis of the trial. Regarding the subgroup analysis based on use of beta-blockers at baseline (yes versus no), the between-group difference in change from baseline to week 30 in pVO2 was lower among patients who used beta-blockers at baseline (1.0 mL/kg/min, 95% CI, 0.1 to 2.0) than among those who did not use beta-blockers at baseline (2.7 mL/kg/min, 95% CI, 1.3 to 4.1). However, the subgroup analyses may not have been powered to detect a treatment effect as no formal sample size calculation was performed for individual subgroups. As such, the subgroup analyses are exploratory in nature.
Change in Postexercise, Resting, and Valsalva LVOT Peak Gradient
The mean change from baseline to end of treatment in postexercise, resting, and Valsalva LVOT peak gradient are reported in Table 14 and Table 17 for the EXPLORER-HCM and VALOR-HCM trials, respectively.
In the EXPLORER-HCM trial the mean postexercise LVOT gradient change from baseline to week 30 was −47.2 mm Hg (SD = 40.3) in the mavacamten group versus −10.4 mm Hg (SD = 29.6) in the placebo group with a treatment-group difference of −35.6 mm Hg (95% CI, −43.2 to −28.1; P < 0.0001). Similarly, in the VALOR-HCM trial, the mean postexercise LVOT gradient change from baseline to week 16 was −39.1 mm Hg (SD = 36.5) in the mavacamten group versus −1.8 mm Hg (SD = 28.8) in the placebo group with a treatment-group difference of −37.2 mm Hg (95% CI, −48.1 to −26.2; P < 0.001).
Table 16: Summary of Primary Composite Functional End Point at Week 30 in the EXPLORER-HCM Trial (ITT Population)
Characteristic | Mavacamten (N = 123) | Placebo (N = 128) |
|---|---|---|
Composite functional end point at week 30 | ||
N (%) | 123 (100) | 128 (100) |
Achieved composite functional end point, n (%)a | 45 (36.6) | 22 (17.2) |
Treatment group difference vs. placebo (95% CI)b | 19.4 (8.7 to 30.1) | |
Odds ratio (95% CI) vs. placeboc | 2.74 (1.5 to 5.4) | |
P valuec | 0.0005 | |
Patients with ≥ 3 mL/kg/min in pVO2 and improvement ≥ 1 NYHA classd at week 30, n (%) | 25 (20.3) | 10 (7.8) |
Treatment group difference vs. placebo (95% CI)b | 12.5 (4.0 to 21.0) | |
Patients with ≥ 3 mL/kg/min in pVO2 and no worsening in NYHA class at week 30, n (%) | 29 (23.6) | 14 (10.9) |
Treatment group difference vs. placebo (95% CI)b | 12.6 (3.4 to 21.9) | |
Patients with change from baseline in pVO2 ≥ 1.5 mL/kg/min and improvement in NYHA class ≥ 1 at week 30, n (%) | 41 (33.3) | 18 (14.1) |
Treatment group difference vs. placebo (95% CI)b | 19.3 (9.0 to 29.6) | |
CI = confidence interval; HCM = hypertrophic cardiomyopathy; ITT = intention-to-treat; NYHA = New York Heart Association; pVO2 = peak oxygen uptake.
aThe composite functional end point was defined as either type 1 (an improvement of at least 1.5 mL/kg/min in pVO2 and improvement of 1 or more NYHA classes) or type 2 (an improvement of at least 3.0 mL/kg/min in pVO2 with no worsening in NYHA class, unless otherwise denoted). Missing NYHA class at week 30 was imputed using available NYHA class at week 26. After the imputation, the patients whose response status at week 30 was still missing were classified as nonresponders.
bThe 95% CIs of the response differences between mavacamten and placebo groups are based on normal approximation.
cThe analysis was stratified on NYHA class, beta-blocker use, and exercise type (based on an interactive response system). The odds ratio was estimated using the Cochran-Mantel-Haenszel method. An odds ratio greater than 1 indicates a superior outcome when comparing to placebo. The P value and 95% CI were derived using the exact method.
dThese are the most stringent pVO2 and NYHA class components of the composite functional end point.
Source: Clinical Study Report for EXPLORER-HCM.18
In both pivotal trials, the mean change in resting and Valsalva LVOT peak gradients from baseline to end of treatment were higher in the mavacamten group than in the placebo group. |||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||| |||||||||||||||| ||||||||||||||| In the VALOR-HCM trial the mean change from baseline to week 16 in resting LVOT peak gradient was −36.0 mm Hg (SD = 28.8) for the mavacamten group and −1.5 mm Hg (SD = 26.5) for the placebo group, and the mean change from baseline to week 30 in Valsalva peak gradient was −45.2 mm Hg (SD = 28.5) for the mavacamten group and 0.4 mm Hg (SD = 29.7) for the placebo group.
Subgroup Analysis
In the EXPLORER-HCM trial, the effect of mavacamten on the change in postexercise LVOT peak gradient (mm Hg) was generally consistent across prespecified subgroups . The analyses may not have been powered to detect a treatment difference and no adjustments were made for multiplicity. As such, all subgroup analyses are exploratory in nature.
Change in Septal Reduction Therapy Status
As shown in Table 17, in the VALOR-HCM trial, a lower proportion of patients in the mavacamten group (17.9%) than in the placebo group (76.8%) met the primary composite outcome of a decision to proceed with SRT by week 16 or were guideline-eligible at week 16, with a difference between treatment groups of 58.9% (95% CI, 44.0% to 73.9%; P < 0.001). A total of 3.6% patients in each of the mavacamten and placebo groups made the decision to proceed with SRT by week 16, and 14.3% of patients in the mavacamten group versus 69.6% of patients in the placebo group were defined as SRT-eligible based on guideline criteria.
Table 17: Summary of Primary and Secondary Response Variables at Week 16 in the VALOR-HCM Trial (ITT Population)
Characteristic | Mavacamten (N = 56) | Placebo (N = 56) | Treatment difference (95% CI)a | P value |
|---|---|---|---|---|
Primary efficacy composite end point,b n (%) | 10 (17.9) | 43 (76.8) | 58.9 (44.0 to 73.9) | < 0.001 |
Patient decision to proceed with SRT | 2 (3.6) | 2 (3.6) | ||
SRT-eligible based on guideline criteriac | 8 (14.3) | 39 (69.6) | ||
SRT status not evaluable, imputed as meeting criteriad | 0 (0.0) | 2 (3.6) | ||
Secondary efficacy end points listed in hierarchical testing order | ||||
Change from baseline in postexercise LVOT gradient (mm Hg), mean (SD) | −39.1 (36.5) | −1.8 (28.8) | −37.2 (−48.1 to −26.2) | < 0.001 |
At least 1 class of NYHA improvement, n (%) | 35 (62.5) | 12 (21.4) | 41.1 (24.5 to 57.7) | < 0.001 |
Change from baseline in KCCQ-23 CSS, points, mean (SD) | 10.4 (16.1) | 1.9 (12.0) | 9.4 (4.9 to 14.0) | < 0.001 |
Change from baseline in NT-proBNP, ng/L, mean (SD) | −399 (−1,146 to −138) | 40 (−155 to 203) | 0.33 (0.3 to 0.4)e | < 0.001 |
Change from baseline in cardiac troponin I, ng/L, mean (SD) | −9.2 (−18.1 to −1.8) | 0.07 (−2.0 to 3.3) | 0.53 (0.4 to 0.7)e | < 0.001 |
Exploratory end points | ||||
Change from baseline in hemodynamic parameters, mean (SD) | ||||
LVOT gradient at rest | −36.0 (28.8) | −1.5 (26.5) | −33.4 (42.3 to −24.5) | NR |
LVOT gradient induced by Valsalva | −45.2 (28.5) | 0.4 (29.7) | −47.6 (−58.2 to −37.0) | NR |
LV ejection fraction | −3.4 (6.2) | 0.3 (4.2) | −4.0 (−5.5 to −2.5) | NR |
LV filling pressures, E/e0 | −3.5 (5.6) | 0.7 (3.8) | −3.3 (−4.9 to −1.8) | NR |
LV stroke volume index | −1.4 (6.6) | 0.1 (5.7) | −1.9 (−4.3 to 0.5) | NR |
Left atrial volume index | −5.2 (7.8) | −0.5 (8.1) | −4.4 (−7.1 to −1.7) | NR |
LV end-systolic volume index | 1.4 (3.7) | 0.1 (3.3) | 1.1 (−0.3 to 2.6) | NR |
LV end-diastolic volume index | 0.01 (8.3) | 0.2 (8.3) | −0.7 (−4.0 to 2.6) | NR |
LV mass index | −7.9 (17.7) | −1.9 (16.6) | −6.5 (−13.2 to 0.1) | NR |
ACCF = American College of Cardiology Foundation; AHA = American Heart Association; CI = confidence interval; CSS = clinical summary score; HCM = hypertrophic cardiomyopathy; ITT = intention-to-treat; KCCQ-23 = 23-item Kansas City Cardiomyopathy Questionnaire; LV = left ventricular; LVOT = left ventricular outflow tract; NR = not reported; NT-proBNP = N-terminal pro–B-type natriuretic peptide; NYHA = New York Heart Association; SD = standard deviation; SRT = septal reduction therapy.
aTreatment difference and 95% CI were generated in an analysis of covariance model, including baseline variable as a covariate and baseline stratification factors for type of SRT recommended (alcohol septal ablation or myectomy) and NYHA functional class (II or III-IV).
bCochran-Mantel-Haenszel method stratified by baseline NYHA criteria (II vs. higher) and type of SRT recommended (myectomy vs. alcohol septal ablation). Difference in proportions estimated as placebo rate minus mavacamten rate, where a positive value indicates a beneficial treatment effect.
cThe guideline criteria are based of the 2011 ACCF/AHA clinical and hemodynamic criteria for HCM. Patients with a maximum LVOT gradient of 50 mm Hg or greater gradient (from rest, Valsalva, or postexercise) and no improvement in NYHA functional class at week 16 are considered eligible for SRT.
dAssuming that both patients in the placebo group did not meet the primary end point, the result shows a treatment difference of similar magnitude to the primary analysis with same level of significance. The treatment difference was 55.36 (95% CI, 40.02 to 70.69; P < 0.0001).
eGeometric mean ratios of less than 1.0 represent an x-fold decrease for mavacamten compared with placebo.
Source: Desai et al. (2022). Copyright 2022 The Authors. Reprinted in accordance with Creative Licence Attribution Licence CC BY-NC-ND 4.0.17
Exploratory sensitivity analyses were conducted using alternative definitions of SRT eligibility, as shown in Appendix 3. The sensitivity analyses were generally supportive of the primary analysis, but the magnitude of effect for mavacamten was not as strong in the analysis that used the alternative definition of SRT eligibility of no improvement in NYHA functional class or a maximum LVOT gradient of 50 mm Hg or greater.
Change in SRT status was not examined in the EXPLORER-HCM trial.
Subgroup Analysis
As shown in Appendix 3, in the VALOR-HCM trial, analyses of the primary efficacy end points were generally in line with the primary efficacy analysis and in favour of mavacamten. Potential differences were noted depending on use of calcium channel blockers (yes versus no) (P value for interaction < 0.05). The analyses may not have been powered to detect a treatment difference and no adjustments were made for multiplicity. As such, all subgroup analyses are exploratory in nature.
Change in CPET Parameters
Changes in CPET parameters from baseline to week 30 in the EXPLORER-HCM trial are shown in Table 18. Mean changes were greater for patients in the mavacamten group compared with the placebo group, with greater increases in peak circulatory power and a least squares mean difference of 372.9 (95% CI, 153.1 to 592.6), peak metabolic equivalents of task with a least squares mean difference of 0.4 (95% CI, 0.2 to 0.6), percent predicted pVO2 with a least squares mean difference of 8.4 (95% CI, 5.3 to 11.5), ventilatory power with an least squares mean difference 0.6 (95% CI, 0.3 to 0.9), and a greater decrease in ratio of volume expired to carbon-dioxide production slope, with a least squares mean difference of −2.6 (95% CI, −3.6 to −1.5).
Change in CPET parameters were not examined in the VALOR-HCM trial.
Table 18: Change in CPET Parameters at Week 30 in the EXPLORER-HCM Trial (ITT Population)
Characteristic | Mavacamten (N = 123) | Placebo (N = 128) |
|---|---|---|
Peak VE/VCO2 | ||
Number of patients contributing to the analysis | 120 | 125 |
Baseline score, mean (SD) | 35.4 (5.2) | 34.2 (5.5) |
Change from baseline to week 30, mean (SD) | −1.9 (3.7) | 0.5 (3.8) |
Least squares mean difference vs. placebo (95% CI)a | −2.2 (−3.1 to −1.3) | |
P valuea | < 0.0001b | |
VE/VCO2 slope | ||
Number of patients contributing to the analysis | 120 | 125 |
Baseline score, mean (SD) | 33.6 (6.2) | 32.4 (6.2) |
Change from baseline to week 30, mean (SD) | −2.4 (4.6) | 0.4 (4.1) |
Least squares mean difference vs. placebo (95% CI)a | −2.6 (−3.6 to −1.5) | |
P valuea | < 0.0001b | |
Peak circulatory power | ||
Number of patients contributing to the analysis | 119 | 121 |
Baseline score, mean (SD) | 3,087 (1,165) | 3,284 (1,173) |
Change from baseline to week 30, mean (SD) | 414.1 (972.0) | −17.9 (869.1) |
Least squares mean difference vs. placebo (95% CI)a | 372.9 (153.1 to 592.6) | |
P valuea | 0.0010b | |
Ventilatory power | ||
Number of patients contributing to the analysis | 119 | 121 |
Baseline score, mean (SD) | 4.9 (1.4) | 5.2 (1.5) |
Change from baseline to week 30, mean (SD) | 0.7 (1.4) | −0.03 (1.2) |
Least squares mean difference vs. placebo (95% CI)a | 0.6 (0.3 to 0.9) | |
P valuea | 0.0002b | |
Peak metabolic equivalents of task | ||
Number of patients contributing to the analysis | 120 | 125 |
Baseline score, mean (SD) | 5.4 (1.4) | 5.7 (1.4) |
Change from baseline to week 30, mean (SD) | 0.4 (0.9) | −0.0 (0.9) |
Least squares mean difference vs. placebo (95% CI)a | 0.4 (0.2 to 0.6) | |
P valuea | 0.0006b | |
Peak respiratory exchange ratio | ||
Number of patients contributing to the analysis | 120 | 125 |
Baseline score, mean (SD) | 1.1 (0.1) | 1.1 (0.1) |
Change from baseline to week 30, mean (SD) | 0.03 (0.1) | −0.0 (0.1) |
Least squares mean difference vs. placebo (95% CI)a | 0.02 (−0.0 to 0.04) | |
P valuea | 0.0885b | |
Percent predicted VO2 | ||
Number of patients contributing to the analysis | 120 | 125 |
Baseline score, mean (SD) | 77.2 (20.8) | 77.0 (22.1) |
Change from baseline to week 30, mean (SD) | 7.7 (13.1) | −0.6 (12.1) |
Least squares mean difference vs. placebo (95% CI)a | 8.4 (5.3 to 11.5) | |
P valuea | < 0.0001b | |
Ventilatory threshold | ||
Number of patients contributing to the analysis | 106 | 116 |
Baseline score, mean (SD) | 11.5 (2.4) | 11.5 (2.6) |
Change from baseline to week 30, mean (SD) | 0.7 (2.5) | 0.1 (2.6) |
Least squares mean difference vs. placebo (95% CI)a | 0.6 (−0.03 to 1.2) | |
P valuea | 0.0603b | |
CI = confidence interval; ITT = intention-to-treat; VE/VCO2 = volume expired/carbon-dioxide production; SD = standard deviation; VO2 = oxygen consumption.
aThe least squares means (95% CI) and the P values are from a mixed model for repeated measures with data up to week 30, which includes baseline value, treatment group, visit, interaction between treatment group and visit, and the 3 stratification factors (beta-blocker use, NYHA class, and exercise type based on an interactive response system) as fixed effects and the patient as a random effect.
bP value has not been adjusted for multiple testing (i.e., the type I error rate has not been controlled).
Source: Clinical Study Report for EXPLORER-HCM.18
Change in Cardiac Structure
Table 19 shows mean changes in measures of cardiac structure by echocardiography from baseline to week 30 in the EXPLORER-HCM trial. The mean change from baseline in LAVI was −7.5 mL/m2 ||||||| in the mavacamten group compared to −0.1 mL/m2 ||||||| in the placebo group. There was a reduction from baseline to week 30 in mean left ventricular mass index (LVMI) in the mavacamten group of −7.4 g/m2 |||||||| versus an increase in the placebo group of 8.9 g/m2 ||||||||. There was little change from baseline in echocardiographic measures of interventricular septal or posterior wall thicknesses following 30 weeks of treatment for either group. As shown in Appendix 3, in the CMR substudy of the EXPLORER-HCM trial, changes from baseline to week 30 in measures of cardiac structure including LAVI, LVMI, and LV maximal wall thickness were greater for patients in the mavacamten group than in the placebo group. As the CMR substudy outcomes were not controlled for multiplicity and, due to the small sample sizes in the substudy, results should be interpreted as supportive evidence for mavacamten.
In the VALOR-HCM trial, as shown in Table 17, changes in LAVI and LVMI from baseline to week 16 were greater among patients in the mavacamten group than in the placebo group with a treatment-group difference of −4.4 (95% CI, −7.1 to −1.7) and −6.5 (95% CI, −13.2 to 0.1), respectively.
Table 19: Change in Measures of Cardiac Structure at Week 30 in the EXPLORER-HCM Trial (ITT Population)
Characteristic | Mavacamten (N = 123) | Placebo (N = 128) |
|---|---|---|
LAVI, mL/m2 | ||
Number of patients contributing to the analysis | 115 | 123 |
Baseline score, mean (SD) | |||||||| | |||||||| |
Change from baseline to week 30, mean (SD) | −7.5 ||||| | −0.1 ||||| |
Interventricular septal thickness, mm | ||
Number of patients contributing to the analysis | 114 | 120 |
Baseline score, mean (SD) | ||||||| | ||||||| |
Change from baseline to week 30, mean (SD) | 0.1 ||||| | 1.4 ||||| |
Posterior wall thickness, mm | ||
Number of patients contributing to the analysis | 110 | 111 |
Baseline score, mean (SD) | ||||||| | ||||||| |
Change from baseline to week 30, mean (SD) | −0.6 ||||| | 0.3 ||||| |
LVMI, g/m2 | ||
Number of patients contributing to the analysis | 108 | 110 |
Baseline score, mean (SD) | ||||||||| | ||||||||| |
Change from baseline to week 30, mean (SD) | −7.4 (17.8) | 8.9 |||||| |
ITT = intention-to-treat; LAVI = left atrial volume index; LVMI = left ventricular mass index; SD = standard deviation.
Source: Clinical Study Report for EXPLORER-HCM trial.18
Biomarker-Based Assessment
In the EXPLORER-HCM trial, as shown in Table 20, exploratory analyses found that the reduction from baseline to week 30 in NT-proBNP (in ng/L) was 80% greater for those in the mavacamten group than for those in placebo group (the proportion of geometric mean ratio between groups was 0.2 [95% CI, 0.2 to 0.2]) and the reduction from baseline to week 30 in cardiac troponin I (in ng/L) was more than 40% greater for those in the mavacamten group than for those in the placebo group (the proportion of geometric mean ratio between groups was 0.6 [95% CI, 0.5 to 0.7]).
In the VALOR-HCM trial, as shown in Table 17, analyses of key secondary outcomes found that the reduction from baseline to week 16 in NT-proBNP (in ng/L) was 67% greater for those in the mavacamten group than for those in placebo group. The proportion of the geometric mean ratio between groups was 0.3 (95% CI, 0.3 to 0.4; P value < 0.001) and the reduction from baseline to week 16 in cardiac troponin I (in ng/L) was 47% greater for those in the mavacamten group than for those in the placebo group (the proportion of the geometric mean ratio between groups was 0.5 [95% CI, 0.4 to 0.7; P value < 0.001]).
Table 20: Change in Biomarker Measures at Week 30 in the EXPLORER-HCM Trial (ITT Population)
Characteristic | Mavacamten (N = 123) | Placebo (N = 128) |
|---|---|---|
NT-proBNP, ng/L | ||
Number of patients contributing to the analysis | 116 | 121 |
Baseline score, geometric mean (%CV) | 777.4 (136.3) | 615.7 (108.4) |
Week 30 ratio to baseline, geometric mean (%CV) | 0.2 (226.9) | 1.0 (55.8) |
Proportion of week 30 geometric mean ratio vs. placebo (95% CI)a | 0.2 (0.2 to 0.2) | |
Cardiac troponin I, ng/L | ||
Number of patients contributing to the analysis | 114 | 111 |
Baseline score, geometric mean (%CV) | 12.5 (207.8) | 12.5 (372.8) |
Week 30 ratio to baseline, geometric mean (%CV) | 0.6 (49.2) | 1.0 (143.3) |
Proportion of week 30 geometric mean ratio vs. placebo (95% CI)a | 0.6 (0.5 to 0.7) | |
%CV = percent coefficient of variation; CI = confidence interval; ITT = intention-to-treat; NT-proBNP = N-terminal pro–B-type natriuretic peptide.
aThe proportion of the geometric mean ratio from week 30 to baseline between the mavacamten and placebo groups, the corresponding 95% CI, and P values are estimated from a mixed model for repeated measures, with data up to week 30 fitted with log-transformed baseline NT-proBNP values, treatment group, time, interaction between treatment group and time, and the 3 stratification factors (beta-blocker use, NYHA class, and exercise type based on an interactive response system) as fixed effects and the patient as a random effect.
Source: Clinical Study Report for EXPLORER-HCM trial.18
Prevention of Atrial Fibrillation or Flutter
This efficacy outcome was not reported in the pivotal trials. AEs of atrial fibrillation or flutter are reported in Table 21 and Table 22 for the EXPLORER-HCM and VALOR-HCM trials, respectively.
Prevention of Stroke
This efficacy outcome was not reported in the pivotal trials. AEs of stroke are reported in Table 21 and Table 22 for the EXPLORER-HCM and VALOR-HCM trials, respectively.
Prevention of Sudden Cardiac Death
This efficacy outcome was not reported in the pivotal trials. AEs of sudden cardiac death are reported in Table 21 and Table 22 for the EXPLORER-HCM and VALOR-HCM trials, respectively.
Need for Implantation of Cardioverter-Defibrillator
This efficacy outcome was not reported in the pivotal trials.
Harms
Only those harms identified in the review protocol are reported here. Table 21 and Table 22 provide detailed harms data.
Adverse Events
In the EXPLORER-HCM trial, through to week 38, a total of 87.8% of patients in the mavacamten group and 81.3% of patients in the placebo group experienced at least 1 AE. The most common AEs were generally similar for both treatment groups. Dizziness was the most frequently reported AE for both the mavacamten and placebo groups, with a higher proportion of patients experiencing dizziness in the mavacamten group compared with the placebo group (21.1% versus 13.3%).
In the VALOR-HCM trial, through to week 16, a total of 73.2%% of patients in the mavacamten group and 61.8% of patients in the placebo group experienced at least 1 AE. Noted AEs of interest were similar for both treatment groups. A slightly higher proportion of patients in the mavacamten group experienced fatigue (8.9%) compared with those in the placebo group (3.6%). Fewer patients in the mavacamten group compared with the placebo group experienced headache (3.6% versus 9.1%, respectively) and nonsustained ventricular tachycardia (0% versus 9.1%, respectively).
Serious Adverse Events
In the EXPLORER-HCM trial, through to week 38, the proportions of patients with SAEs were similar for the mavacamten and placebo groups (11.4% versus 9.4%, respectively). The most common SAEs included atrial fibrillation (2.4%), syncope (2.4%), and stress cardiomyopathy (1.6%) among patients in the mavacamten group and atrial fibrillation (3.9%) among patients in the placebo group.
In the VALOR-HCM trial, through to week 16, the proportion of patients who had SAEs was slightly higher for the mavacamten group versus the placebo group (5.4% versus 1.8%, respectively). The SAEs included atrial fibrillation (3.6%) and COVID-19 (1.8%) among patients in the mavacamten group and alcohol poisoning (1.8%) among patients in the placebo group.
Withdrawals due to Adverse Events
In the EXPLORER-HCM trial, a total of 1.6% of patients in the mavacamten group discontinued treatment due to AEs of atrial fibrillation and syncope, respectively. No patients in the placebo group discontinued treatment due to AEs.
No treatment discontinuations due to AEs were reported in the VALOR-HCM trial through to week 16.
Mortality
In the EXPLORER-HCM trial, through to week 38, a single death (representing 0.8% of the placebo group) due to sudden death was reported. No deaths were reported in the VALOR-HCM trial through to week 16.
Notable Harms
Cardiac Failure
As shown Table 21, in the EXPLORER-HCM trial, through to week 38, the proportion of patients with AEs of cardiac failure (including acute and congestive cardiac failure and cardiogenic shock) was 2.4% in the mavacamten group and 3.9% in the placebo group.
No events of cardiac failure were reported through to week 16 in the VALOR-HCM trial.
Sudden Cardiac Death
In the EXPLORER-HCM trial, through to week 38, 1 patient (0.8%) died due to sudden death in the placebo group. No events of sudden death were reported through to week 16 in the VALOR-HCM trial.
LVEF Less Than 50% or Less Than 30%
In the EXPLORER-HCM trial, no AEs of decreased LVEF were reported. However, the incidence of a resting LVEF of less than 50% was a protocol-specified criterion for temporary treatment discontinuation. In the EXPLORER-HCM trial, during the 30-week treatment period, 9 patients (3.6%) met the temporary treatment discontinuation criterion of an LVEF of less than 50%, including 7 patients (5.7%) in the mavacamten group and 2 patients (1.6%) in the placebo group. Five of these patients (3 in the mavacamten group and 2 in the placebo group) underwent temporary treatment discontinuation and subsequently resumed dosing and completed the study. The remaining 4 patients had no further dose adjustments as their LVEFs of less than 50% occurred at the week-30 visit.
In the VALOR-HCM trial, through to week 16, 2 patients (3.6%) had an LVEF of less than 50% resulting in temporary drug discontinuation, and subsequently resumed mavacamten dosing.
In both pivotal trials, no patients had a reduction in their LVEF of 30% or less necessitating permanent treatment discontinuation.
|||||||||||||||||||||| ||||||||||||||||| |||||||||||||||||| |||||| |||||||||||| |||||||||||| |||||||||| ||||||| |||||||||||| ||||||||||| |||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| ||||| |||||| ||||||||||||||| |||||| ||||||||||| ||||||||||||||||| ||||||||||||||||||||| |||||||||||| ||||||| ||| ||||||||||| ||||||||||||||| ||||||||||||| ||||||||||||| ||||||| |||||||||||| ||||||||||||||||| |||||||||||| |||||||| |||||| ||||||| |||||||| |||||||||| |||||||| ||||| |||||| |||||||||||| |||||||||||||||
Data related to cardiovascular hospitalizations were not available for the VALOR-HCM trial.
Table 21: Summary of Harms in the EXPLORER-HCM Trial Through Week 38a (Safety Population)
Harms | Mavacamten (N = 123) | Placebo (N = 128) |
|---|---|---|
Patients with ≥ 1 adverse event | ||
Any adverse event, n (%) | 108 (87.8) | 104 (81.3) |
Most common events,b n (%) | ||
Atrial fibrillation | 10 (8.1) | 10 (7.8) |
Palpitations | 7 (5.7) | 10 (7.8) |
Angina pectoris | 3 (2.4) | 7 (5.5) |
Diarrhea | 5 (4.1) | 7 (5.5) |
Gastroesophageal reflux disease | 7 (5.7) | 3 (2.3) |
Fatigue | 7 (5.7) | 7 (5.5) |
Nasopharyngitis | 15 (12.2) | 19 (14.8) |
Upper respiratory tract infection | 10 (8.1) | 6 (4.7) |
Back pain | 10 (8.1) | 8 (6.3) |
Arthralgia | 7 (5.7) | 2 (1.6) |
Dizziness | 26 (21.1) | 17 (13.3) |
Headache | 15 (12.2) | 10 (7.8) |
Syncope | 7 (5.7) | 2 (1.6) |
Dyspnea | 18 (14.6) | 13 (10.2) |
Cough | 10 (8.1) | 4 (3.1) |
Patients with ≥ 1 SAE | ||
Any SAE, n (%) | 14 (11.4) | 12 (9.4) |
Most common SAEs,c n (%) | ||
Atrial fibrillation | 3 (2.4) | 5 (3.9) |
Stress cardiomyopathy | 2 (1.6) | 0 |
Atrioventricular block complete | 0 | 1 (0.8) |
Cardiac failure | 1 (0.8) | 0 |
Cardiac failure congestive | 0 | 1 (0.8) |
Cardiogenic shock | 1 (0.8) | 0 |
Pericardial effusion | 1 (0.8) | 0 |
Systolic dysfunction | 1 (0.8) | 0 |
Ventricular tachycardia | 0 | 1 (0.8) |
Atrial septal defect | 1 (0.8) | 0 |
Abdominal pain | 1 (0.8) | 0 |
Sudden death | 0 | 1 (0.8) |
Urinary tract infection | 0 | 2 (1.6) |
Bacterial colitis | 1 (0.8) | 0 |
Diverticulitis | 1 (0.8) | 0 |
Gastroenteritis viral | 0 | 1 (0.8) |
Infection | 1 (0.8) | 0 |
Contusion | 1 (0.8) | 0 |
Forearm fracture | 1 (0.8) | 0 |
Dehydration | 0 | 1 (0.8) |
Rheumatoid arthritis | 0 | 1 (0.8) |
Systemic lupus erythematosus | 1 (0.8) | 0 |
Cholesteatoma | 0 | 1 (0.8) |
Prostate cancer | 0 | 1 (0.8) |
Syncope | 3 (2.4) | 1 (0.8) |
Ischemic stroke | 1 (0.8) | 0 |
Transient ischemic attack | 0 | 1 (0.8) |
Device-inappropriate shock delivery | 1 (0.8) | 0 |
Vocal cord polyp | 0 | 1 (0.8) |
Patients who stopped treatment due to adverse events | ||
Any, n (%) | 2 (1.6) | 0 |
Atrial fibrillation | 1 (0.8) | 0 |
Syncope | 1 (0.8) | 0 |
Deaths, n (%) | 0 | 1 (0.8) |
Sudden death | 0 | 1 (0.8) |
Notable harms, n (%) | ||
Cardiac failured | 3 (2.4) | 5 (3.9) |
Permanent discontinuation, LVEF at rest < 30% | 0 | 0 |
Temporary discontinuation, LVEF at rest < 50% | 7 (5.7) | 2 (1.6) |
LVEF = left ventricular ejection fraction; SAE = serious adverse event.
|||||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| ||||||||
bFrequency greater than 5%.
cReported in at least 1 patient.
||||||||||| ||||||| ||||||||| |||||||||| |||||| |||| |||||||||||| |||||||||||| |||| ||||||||||||||
Source: Clinical Study Report for EXPLORER-HCM trial.18
Critical Appraisal
Internal Validity
Both the EXPLORER-HCM and the VALOR-HCM trials appeared to have acceptable methods for blinding, allocation concealment, and randomization with stratification. Small differences between treatment groups in demographic and baseline patient characteristics in the EXPLORER-HCM trial were noted (the mavacamten group had more females, fewer patients with a history of atrial fibrillation, more patients taking calcium channel blockers at baseline, and fewer patients taking neither beta-blockers nor calcium channel blockers at baseline). The clinical expert consulted for this review stated that the difference in the proportions of patients taking neither beta-blockers nor calcium channel blockers at baseline (3.3% of the mavacamten group versus 12.5% of the placebo group) may have introduced bias in favour of mavacamten as a greater proportion of patients in the placebo group were not receiving any background therapy. In the VALOR-HCM trial, more patients in the mavacamten group than in the placebo group were taking both beta-blockers and disopyramide at baseline (19.6% versus 5.4%, respectively) and fewer patients in the mavacamten group than in the placebo group were taking both beta-blockers and calcium channel blockers at baseline (10.7% versus 17.9%, respectively). The clinical expert consulted stated that neither of these differences would likely bias the results. Treatment discontinuation and study discontinuation rates among patients were low in both pivotal trials.
Table 22: Summary of Harms in the VALOR-HCM Trial Through Week 16 (Safety Population)
Harms | Mavacamten (N = 56) | Placebo (N = 55) |
|---|---|---|
Safety end points, n (%) | ||
LVEF < 50% | 2 (3.6) | 0 |
Permanent discontinuation for LVEF < 30% | 0 | 0 |
Death, myocardial infarction, or stroke | 0 | 0 |
On-treatment adverse events, n (%) | ||
Total number of on-treatment adverse events | 123 | 93 |
Total number of patients with at least 1 adverse event | 41 (73.2) | 34 (61.8) |
Serious on-treatment adverse events, n (%) | ||
Number of serious on-treatment adverse eventsa | 4 | 1 |
Number of patients with serious adverse events | 3 (5.4) | 1 (1.8) |
Atrial fibrillation | 2 (3.6) | 0 (0.0) |
Coronavirus disease | 1 (1.8) | 0 (0.0) |
Alcohol poisoning | 0 (0.0) | 1 (1.8) |
Nonserious on-treatment adverse events | ||
Number of nonserious on-treatment adverse events, n | 119 | 92 |
Cardiovascular, n (%) | ||
Chest pain | 2 (3.6) | 3 (5.5) |
Palpitations | 2 (3.6) | 2 (3.6) |
Presyncope | 1 (1.8) | 0 (0.0) |
Syncope | 1 (1.8) | 0 (0.0) |
Atrial fibrillation | 2 (3.6) | 0 (0.0) |
Nonsustained ventricular tachycardia | 0 (0.0) | 5 (9.1) |
Bradycardia | 2 (3.6) | 0 (0.0) |
Atrioventricular block second degree | 1 (1.8) | 0 (0.0) |
Other adverse events of interest, n (%) | ||
Fatigue | 5 (8.9) | 2 (3.6) |
Headache | 2 (3.6) | 5 (9.1) |
Dyspnea | 4 (7.1) | 3 (5.5) |
Dizziness | 4 (7.1) | 3 (5.5) |
Nausea | 4 (7.1) | 1 (1.8) |
Rash | 4 (7.1) | 0 (0.0) |
LVEF = left ventricular ejection fraction.
aSerious adverse events in 4 patients also involved hospitalization.
Source: Desai et al. (2022).17
The clinical expert consulted for this review indicated that the primary efficacy outcomes of EXPLORER-HCM, consisting of pVO2 as measured by CPET and NYHA functional class are appropriate measures of objective functional capacity and subjective symptom severity, respectively, in the indicated population. In both pivotal trials, HRQoL was measured using the KCCQ-23 CSS as a key secondary outcome, and the EQ-5D-5L was used in the EXPLORER-HCM trial as an exploratory outcome. The KCCQ-23 is a generally valid, reliable, and responsive questionnaire for cardiovascular diseases, including oHCM. The clinically meaningful threshold of 10 or more points used in the EXPLORER-HCM trial for the KCCQ-23 CSS was greater than the reported MID range of 4.5 to 6 points for patients with heart failure. A literature search completed by CADTH did not find any evidence dealing with the validity, reliability, responsiveness, and MID of the EQ-5D-5L instrument in patients with oHCM. The clinical expert consulted by CADTH indicated that these tools are not typically used in clinical practice but have been used in multiple studies. Disease-related symptoms were assessed using the newly developed HCMSQ instrument, with the SoB domain assessed as a key secondary outcome in the EXPLORER-HCM trial. Available evidence on the HCMSQ SoB domain suggests it is valid, reliable, and responsive to change. Because data on the KCCQ-23 CSS or HCMSQ SoB for more than 30% of patients were not collected at baseline or at the week-30 visit in the EXPLORER-HCM trial, and those who completed the questionnaires may be fundamentally different than those who did not (i.e., differences in treatment response), there is a risk of bias. However, for all imputation scenarios, ad hoc sensitivity analyses were generally supportive of the findings of the primary analyses.
The VALOR-HCM trial is evaluating the use of mavacamten to reduce the need for SRT in patients who are guideline-eligible and willing to participate in invasive therapies. As such, no direct evidence comparing mavacamten to SRT is available for this review. There is also limited direct evidence comparing mavacamten to disopyramide. Patients taking disopyramide were excluded from the EXPLORER-HCM trial and less than 20% of enrolled patients (n = 22) in the VALOR-HCM trial used disopyramide at baseline as monotherapy or in combination with beta-blockers or calcium channel blockers.
In terms of subgroups of interest, both pivotal trials included subgroup analyses by baseline background therapy (beta-blocker or calcium channel blocker use) and the EXPLORER-HCM trial also examined NYHA class (II versus III) as a prespecified subgroup. For the primary end point in the EXPLORER-HCM trial, results were not statistically significantly different for patients taking beta-blockers. All key secondary end points showed a benefit from mavacamten treatment compared with placebo across the evaluated subgroups, irrespective of beta-blocker use. The subgroup analyses may not have been powered to detect a treatment difference and no adjustments were made for multiplicity. As such, all subgroup analyses are exploratory in nature.
No Clinical Study Report or statistical analysis plan was available for the VALOR-HCM trial at the time of this review, preventing CADTH from fully appraising the potential for bias within the trial.
External Validity
In general, the clinical expert consulted by CADTH for this review confirmed that the populations of both the EXPLORER-HCM and VALOR-HCM trials were similar to patients seen in Canadian clinics, and the study results would be generalizable, with some limitations, to patients with oHCM in Canada. Compared to the population in Canada, the racial diversity in the pivotal trials was limited, as most patients were white. Although no patients were recruited from Canada in either pivotal trial, the clinical expert noted that the lack of representation of patients in Canada does not reduce the generalizability of the results to Canadian clinical practice. The EXPLORER-HCM trial reported that more than 40% of patients screened were excluded from the study for failing to meet 1 or more eligibility criteria, possibly limiting the generalizability of the findings. |||||||| ||||||| |||||||| ||||||| |||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||| |||||||||||||||| ||||||||||||| ||||||| ||||||||||| ||||| ||||||| ||||||
While mavacamten has been approved by Health Canada for use in adult patients with symptomatic NYHA functional class II to III oHCM, the VALOR-HCM trial included an unknown number of patients with NYHA functional class IV oHCM. The VALOR-HCM trial is an ongoing RCT evaluating the use of mavacamten to reduce the need for SRT in patients who are guideline-eligible for invasive therapies, with descriptive data available through to week 32. It is therefore uncertain if mavacamten can reduce the need for SRT among patients with symptomatic oHCM in the long term.
Indirect Evidence
A focused literature search for indirect treatment comparisons dealing with HCM was run in MEDLINE All (1946–) on October 21, 2022. No limits were applied to the search. No relevant studies were identified.
Other Relevant Evidence
Additional descriptive efficacy and safety data were provided for the VALOR-HCM trial through to week 32. The ongoing open-label extension study, MAVA-LTE, provides long-term safety and efficacy data that supplement the evidence from the EXPLORER-HCM pivotal trial in the systematic review.
VALOR-HCM Trial Through to Week 32
Methods
An additional study report for the VALOR-HCM trial examined data up to week 32 among patients initially randomized to mavacamten (32 weeks of drug exposure) and those initially randomized to placebo who crossed over to mavacamten at week 16 (16 weeks of drug exposure).7 The 4 patients in the placebo group who elected to receive SRT treatment or withdrew from the study during the first 16 weeks were not included in this analysis.
Safety outcomes included the incidence of an LVEF of less than 50%, hospitalization for cardiac failure, and atrial fibrillation or ventricular tachyarrhythmia.
Interventions
In the VALOR-HCM trial, after 16 weeks, patients originally randomized to placebo were crossed over to mavacamten 5 mg daily and a dose-blinded titration was performed in the same manner used for patients originally randomized to mavacamten. Patients initially randomized to mavacamten continued with the same dose they were receiving at week 16 and continued study assessments every 4 weeks. If the LVEF fell below 50% at any time during treatment, mavacamten was temporarily discontinued, with a follow-up 4 to 6 weeks later, and, if at that time the LVEF was 50% or greater, the dose was decreased from the last treatment dose by 1 level. If the LVEF decreased to 30% or less, mavacamten was permanently discontinued. All patients and study staff remained blinded to the original treatment assignment, mavacamten dose, and echocardiographic findings until week 32.
Outcomes
The principal end point at week 32 was the composite of a patient decision to proceed with SRT or eligibility for SRT according to the 2011 ACCF/AHA guidelines. Patients who discontinued the study or whose response status could not be assessed after 32 weeks were classified as SRT-eligible (treatment failure). Additional end points included the changes from baseline in postexercise LVOT gradient, NYHA functional class, KCCQ-23 CCS, NT-proBNP, and cardiac troponin I. Additional echocardiographic end points studied included changes from baseline in LV mass index, LV systolic and diastolic volume index, LAVI, and the ratio of the peak early mitral inflow velocity over the early diastolic mitral annular velocity (E/e′).
Statistical Analysis
The analysis included all patients originally randomized to mavacamten and initial placebo patients who crossed over to mavacamten at 16 weeks in the VALOR-HCM trial. Categorical variables were reported as number and percent. The principal outcome was the proportion of patients meeting SRT eligibility or deciding to proceed with SRT, summarized as number and percentage. For placebo patients who crossed over to mavacamten, the week-16 pretreatment value was used as the baseline for NYHA class assessment, laboratory, and echocardiographic measurements. Changes from baseline for continuous variables were summarized using the mean and 95% CIs. Continuous variables were presented as mean (SD) and compared via a t-test while biomarkers were presented as median (interquartile range) and compared using a nonparametric Wilcoxon rank sum test.
Patient Disposition
Of the 112 patients with symptomatic oHCM enrolled in the VALOR-HCM trial, 108 qualified for the 32-week evaluation. All patients originally randomized to mavacamten (n = 56), and those who crossed over from placebo to mavacamten after 16 weeks (n = 52) were included. The 4 patients excluded from the original placebo group included 2 patients who underwent SRT during the first 16 weeks and 2 who discontinued the study early. Of the remaining patients, the mean age was 60.3 years and 50% were male. All patients were symptomatic (94% NYHA functional class III or IV) on maximally tolerated HCM therapy. The mean LVEF and peak resting, Valsalva, and postexercise LVOT gradients were 68% (SD = 3.5), 49 mm Hg (SD = 30), 77 mm Hg (SD = 30), and 83 mm Hg (SD = 35), respectively.
Efficacy
In the original mavacamten group, an additional 15 patients experienced an improvement of 1 NYHA class between weeks 16 to 32 and 48 patients (91%) had an improvement of 1 or more NYHA class at 32 weeks. Furthermore, in the original mavacamten group, 7 patients had an improvement of 2 NYHA classes between weeks 16 to 32, and 16 patients (30.2%) experienced an improvement of 2 or more classes by week 32. In the placebo crossover group, 35 patients (70%) improved by 1 or more NYHA classes and 12 patients (24%) improved by 2 or more NYHA classes at week 32 after 16 weeks of mavacamten exposure. In the original mavacamten group, there was a reduction in resting, Valsalva, and postexercise LVOT gradients between weeks 16 and 32. A similar reduction in LVOT gradient in the crossover group was seen after 16 weeks of mavacamten exposure.7
In the original mavacamten group, the mean change from baseline to week 32 in the KCCQ-23 CSS was 13.1 points (95% CI, 9.2 to 17.1), while in the placebo crossover group, the mean change from week 16 to week 32 in KCCQ-23 CSS was 8.0 points (95% CI, 3.2 to 12.8).7
In the VALOR-HCM trial, at week 32, a total of 6 patients (10.7%) in the original mavacamten group and 7 patients (13.5%) in the placebo crossover group continued to meet guideline criteria for SRT or elected to undergo the procedure. In the original mavacamten group, at week 32, a total of 3 patients (5.4%) chose to undergo SRT (1 additional patient decided to proceed with SRT between weeks 16 and 32) and 2 patients (3.6%) were guideline-eligible for SRT. (Of the 8 patients who were guideline-eligible at week 16, a single patient remained guideline-eligible at week 32 and another became guideline-eligible between weeks 16 and 32.) In the original mavacamten group, the SRT status of 1 patient who withdrew consent at week 28 was not evaluable at week 32 and was imputed as meeting the criteria for the outcome. A total of 2 patients (3.8%) in the placebo crossover group chose to undergo SRT at week 32, 3 patients (5.8%) were eligible for SRT based on guideline criteria, and 2 patients (3.8%) were imputed as meeting criteria for the outcome as their SRT status was not evaluable (1 patient had an LVEF of less than 30% at week 31 and the other was withdrawn by the study investigator due to noncompliance at week 20).7
In the original mavacamten group, improvements from baseline were seen through to week 32 in NT-proBNP, with a median change of −417 ng/L (95% CI, −706 to −186); cardiac troponin I, with a median change of −7.4 ng/L (95% CI, −11.1 to −4.8); LVMI, with a mean change of −13.0 g/m2 (95% CI, −18.5 to −7.5); and LAVI, with a mean change of −6.8 mL/m2 (95% CI, −9.4 to −4.3). In the placebo crossover group between weeks 16 and 32, there were improvements in NT-proBNP, with a median change of −451 ng/L (95% CI, −581 to −298); cardiac troponin I, with a median change of −6.8 ng/L (95% CI, −8.5 to −4.3); LVMI, with a mean change of −10.8 g/m2 (95% CI, −16.1 to −5.5); and LAVI, with a mean change of −5.5 mL/m2 (95% CI, −8.3 to −2.7).7
Harms
In the VALOR-HCM trial, through to week 32, the rate of SAEs was similar between the original mavacamten group and the placebo crossover group. A total of 4 patients (7.1%) in the original mavacamten group experienced an SAE, the most common of which was atrial fibrillation (3 patients, 5.4%). A total of 4 patients (7.7%) in the placebo crossover group experienced an SAE from week 16 to week 32, consisting of 1 (1.9%) each of congestive heart failure, a fall, nephrolithiasis, and peripheral venous disease. No deaths, myocardial infarctions, or strokes were reported in either group.7
Through to week 32, a total of 7 patients (12.5%) in the original mavacamten group and 2 patients (3.8%) in the placebo crossover group met temporary drug discontinuation criteria of an LVEF of less than 50% (median = 45%, range = 38 to 49%). All patients were asymptomatic. A single patient (1.9%) in the placebo crossover group had an LVEF reduction of less than 30% at week 31 associated with paroxysmal atrial fibrillation and heart failure. Following permanent mavacamten discontinuation, the patient’s LVEF recovered and normalized. No patients in the original mavacamten group met the criteria for permanent discontinuation.7
Critical Appraisal
Results at week 32 of the VALOR-HCM trial provided additional data on the safety and efficacy of mavacamten. As all placebo patients crossed over to mavacamten treatment at week 16, there was no active comparator, and all outcomes were descriptive in nature, making it difficult to draw causal conclusions from the findings. Once placebo patients crossed over to active treatment at week 16, investigators and patients were aware that all patients were receiving active treatment, and their expectations of treatment may have affected the reporting of subjective outcomes such as HRQoL, NYHA functional class, and adverse effects.
Long-Term Extension Study
The primary objective of this extension study, MAVA-LTE, was to assess the long-term safety and tolerability of mavacamten in patients with oHCM previously enrolled in the EXPLORER-HCM trial (the EXPLORER-LTE cohort). Secondary and exploratory objectives included assessing the long-term effects of mavacamten on symptoms and echocardiographic measures of cardiac function and LVOT obstruction, and the long-term effects of mavacamten on disease biomarkers.
Description of Study
The MAVA-LTE trial is an ongoing, dose-blinded, 5-year extension study to assess the long-term efficacy and safety of mavacamten following patients who completed the EXPLORER-HCM trial through to week 38 (EXPLORER-LTE cohort) and patients who completed the MAVERICK-HCM trial (a phase II study of nonobstructive HCM that is not assessed in this report). Patients included in the EXPLORER-LTE cohort received mavacamten treatment at a starting dosage of 5 mg once daily ||||||||| |||||||||||||||| |||||| ||||||||||||||| |||||||||||| ||||||||||||| ||||||||||||||| |||||||||||| ||||||||||||||||||| |||||||||||||| |||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||||||||||||||||||||| Dose adjustments occurred at weeks 4, 8, and 12, guided by echocardiogram assessments of Valsalva LVOT gradient and LVEF. Site-read stress echocardiography was also conducted at week 24 to evaluate the postexercise LVOT gradient and to determine whether further dose adjustments were needed. |||||||||| |||||||||||||| |||||||| ||||||| ||||||| |||||||| |||| |||||||||||||||| ||| ||||||||||||| |||| |||||||||||||||| ||| |||||||| ||||||||| ||||||||||||| |||||||||||||| ||||||||||||||||| ||||||||||| ||||||||||||| ||||| |||||||||||||| |||||||||| ||||||| ||||||||| |||||||||| |||||||| |||||||| ||||||||||||| |||||| || ||||||||||| |||||||||||||||||| |||| ||||||| ||||||||| ||||||| ||||||||||||| |||||||||||||| ||||||||||||||| ||||||||||||||| ||||||||| ||||| |||||||||| At the time of the data cut-off for this interim analysis, no patient from either study cohort had completed the week-104 visit.
Figure 4: Study Schematic for EXPLORER-LTE Cohort
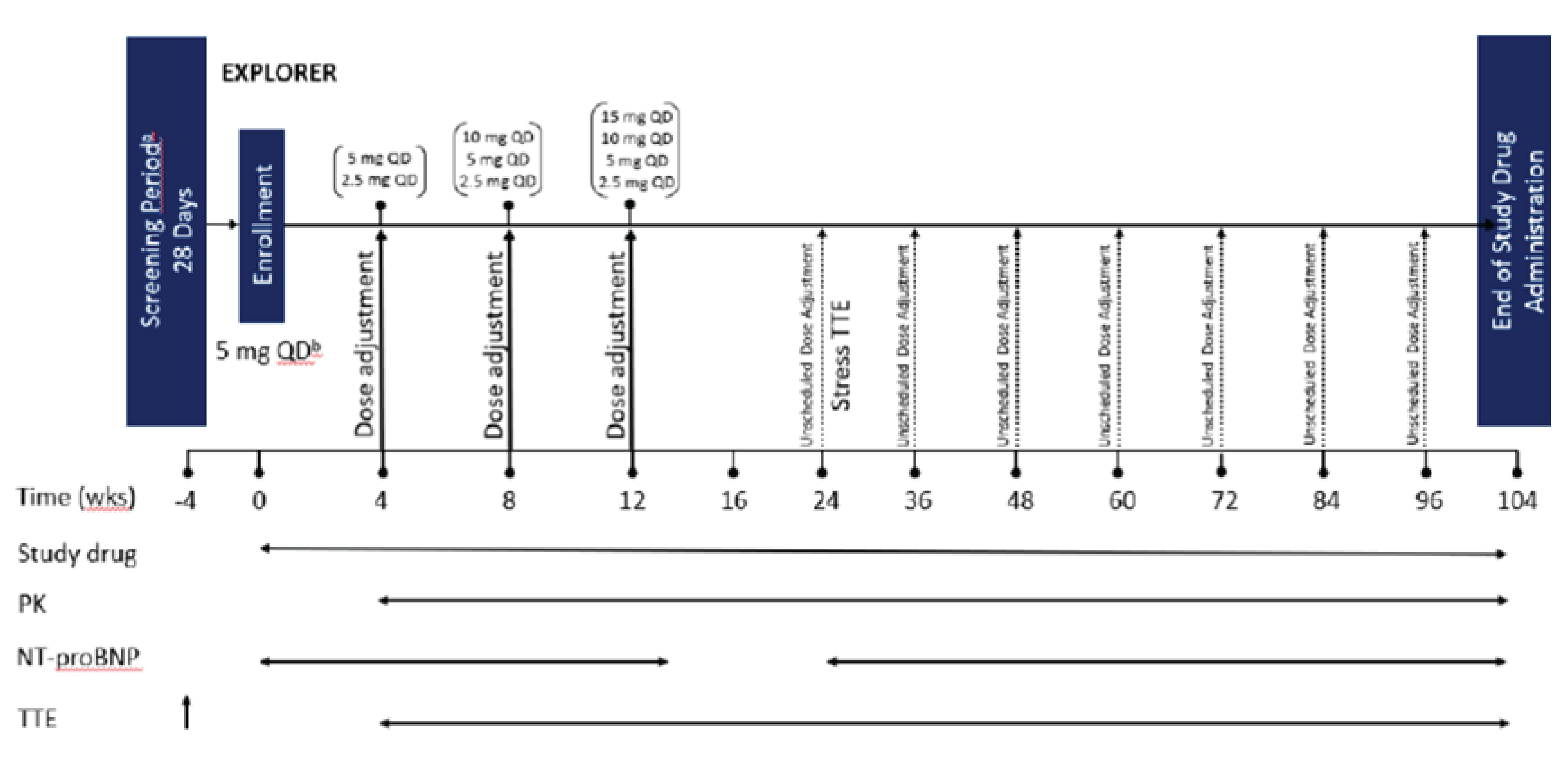
NT-proBNP = N-terminal pro–B-type natriuretic peptide; PK = pharmacokinetics; QD = once daily; TTE = transthoracic echocardiogram; wks = weeks.
Source: Clinical Study Report for Extension Study MYK-461 to 007.35
Populations
Inclusion and Exclusion Criteria
Patients meeting the following inclusion criteria were included in this study:
completion of the parent study through to the EOS visit within 90 days of signing consent
body weight exceeding 45 kg
LVEF of 50% or greater by an echocardiography core laboratory read of screening transthoracic echocardiograms at rest
adequate acoustic windows to enable accurate echocardiograms
|||||||| |||| |||||||||||||||| ||| |||||||||||||||||||
safety laboratory parameters within normal limits, ||||||||||||||||||| ||||||||| |||||||||||| ||||||||||||||||
|||| |||||||||||||||| |||||||||| ||||||| ||||||||| |||| |||||||||||||||| ||| ||||||||||||||| ||||||||| ||||||||||||| |||||||||| |||||||||||| |||||||| |||||||||| |||||||||||||||| ||||||||||||||| ||||||||||||| ||||||||||||||| |||| |||||||||||||||| |||| |||||||||| |||||||| |||| |||||||||||||||| ||| |||| |||||||||||||||| ||||||||||
not pregnant or lactating.
Temporary Discontinuation of Treatment
Temporary treatment discontinuation was considered in cases of an AE or SAE or for another reason. Patients were considered to be temporarily discontinued from study drug dosing for any of the following qualifying events:
a resting LVEF of less than 50%
a mavacamten plasma trough concentration of 1,000 ng/mL or greater
a QT interval corrected using Fridericia’s formula of more than 15% above the baseline value.
|||||||||||||||| |||| |||||||||||||||| ||||||||||| |||||||||||||||||||||| ||||||| ||||||||||||||| |||||| ||||||||||| ||||||||||| ||||||||||||||| |||| |||||||||||||||| |||| ||||||||||||||| ||||||||||||||||||| |||||||||||||||||||| |||| |||||||||||||||| |||||||||||||
Baseline Characteristics
Table 23 summarizes the baseline characteristics for EXPLORER-LTE cohort. The characteristics are similar to those of the parent pivotal trials.
Table 23: Summary of Baseline Characteristics in EXPLORER-LTE Trial
Characteristic | Mavacamten (N = 224) |
|---|---|
Age (years), mean (SD) | 60.3 (11.8) |
Age group, n (%) | |
≤ 49 | |||||||| |
50 to 64 | |||||||| |
≥ 65 | |||||||| |
Sex, n (%) | |
Male | 135 (60.3) |
Female | 89 (39.7) |
Region, n (%) | |
US | |||||||| |
Excluding US | ||||||||| |
Race, n (%) | |
White | ||||||||| |
Black or African American | |||||| |
American Indian or Alaska Native [wording from original source] | ||||||| |
Asian | |||||| |
Unknown | |||||| |
Ethnicity, n (%) | |
Hispanic or Latino | ||||||| |
Not Hispanic or Latino | ||||||||| |
Not reported | |||||| |
Body mass index (kg/m2), mean (SD) | ||||||||| |
Body surface area (m2), mean (SD) | |||||||||| |
NYHA functional class at baseline, n (%) | |
Class I | ||||||| |
Class II | 146 (65.2) |
Class III | |||||||| |
Background HCM therapy, n (%) | |
Beta-blocker | 169 (75.4) |
Calcium channel inhibitora | 37 (16.5) |
Neither | 18 (8.0) |
LVOT gradient (mm Hg) | |
Resting, N | 224 |
Mean (SD) | 48 (31.6) |
Valsalva, N | 221 |
Mean (SD) | || (33.2) |
Resting LVEF (%), mean (SD) | 74 (5.9) |
Baseline biomarkers | |
NT-proBNP (ng/L), N | 223 |
Geometric mean (%CV) | |||||||||||| |
HCM = hypertrophic cardiomyopathy; LVEF = left ventricular ejection fraction; LVOT = left ventricular outflow tract; NT-proBNP = N-terminal pro–B-type natriuretic peptide; NYHA = New York Heart Association; SD = standard deviation.
aIncludes verapamil, verapamil hydrochloride, diltiazem, and diltiazem hydrochloride.
Source: Clinical Study Report for Extension Study MYK-461 to 007.35
Patient Disposition
Figure 5 and Table 24 summarize the patient disposition for the EXPLORER-LTE cohort. ||||||| |||||||||||| ||||| ||||||||| ||||||||||| |||||||||||||||| ||||| |||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| ||||||||||||||||| |||||||| ||||||||| |||||||| ||||||||||| |||||||||||||||||||| ||||||||||| ||||| ||||| |||||||||||||||| |||||||||| |||||||||||||||| |||||||||||||||| |||||||||||||| ||||| |||||||||||||| |||||||||| |||||||||||| |||||||||| |||| |||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||| |||||||||||||||| ||||||||||||| ||||||||||||| ||||||||| ||||||||||||||||| |||||||| |||||||| ||||||| ||||||| ||||||||||||| ||||||||| |||||||| |||||||| ||||||||||||||| |||||| |||||| ||||||||||||| |||||

||||||||||||||| | ||||| |||||||| |
|---|---|
||||||||||| | |
|||||||||| | ||| |
||||||||||||| | ||| |
|||||||||||||||||||||||||| | |||||| |
|||||||||||||| | |||||| |
||||||||||||||||||| | ||||||| |
|||||| | |||||| |
|||||| | || |
||||||||| ||||||||||| | || |
|||||||||||||||||||||||||||||||||||||| | |||||||| |
||||||||||||| | |||||||| |
|||||| | |||||||| |
||||||||||||||||||| | ||||||| |
|||| |||||||||||||||| ||||| | |||||||| |
|||||||||||||||||||| | ||| |
|||||||||||||||||||||||||||||||||||||| | |||||| |
||||||||||||||||||| | |||||| |
||||| | ||||| |
|||| | |||| |
|||||||| | ||||| |
|||||||||| |||| |||||||||||||||| ||| |||||||| ||||||||||||| |||||||||| |||||||||| |||| ||||||||||| ||||| |||||||||| |||||||| ||||| |||||||||||| ||||||||| |||||||||||||||| |||||||||| ||||||||||||||||||||| |||||||||||||||| |||||||||||||||||| ||||||||||||||||||||| |||||||| ||||||| ||||| |||||||||||| ||||| ||||||||| ||||| |||||||| |||||||||||||| || |||||||| ||||||||||||| |||| ||||||| |||||||||| |||||||||| ||||||||||
This table has been redacted for confidential information.
Efficacy
Change in NYHA Class
Table 25 summarizes the shifts in NYHA functional classification from baseline for the EXPLORER-LTE cohort. ||||||| ||||||||||| ||||||||||||| ||||||||||||||||| |||||||||||||| |||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||||||||||||||||||| ||||||||| ||||||||||||| |||||||||||||||| ||||||||||||||||||| ||||||||||||| |||||||||||| |||||||||||| ||||||| |||||||||||||| |||||||||||| |||||||| |||||| ||||||||| ||||||||| |||||||||||||||||| ||||||| |||||||||||| |||||||||| |||| ||||||||||||| ||||||||||| ||||||||| |||| |||||||||||||||||| |||||||||| ||||||||| |||||||||| || |||||| |||| ||||||||| ||||| ||||| |||||| |||||||||| |||| ||||| ||||| ||||||||||||| |||||||||||||| ||||||||||||||| ||||||||||||||| ||||| |||||| ||||| |||| |||||||||||||||| ||| |||||||||||| ||||||||| |||||||||| |||||| |||||||| |||||| |||||| ||||||||||| ||||||||||| ||| |||||||| ||||||||| |||||||| |||||||||||||||||| ||||||||||||| ||||||||| |||||||||||| |||||||||||| |||||| |||||||||||||||| |||||||| ||||||||||||| |||||||||||||| ||||||||||||||
Table 25: Shift in NYHA Function Classification by Study Visit for the EXPLORER-LTE Cohort (ITT Population)
Characteristic | EXPLORER-LTE cohort (N = 224) Baseline n (%) | |||
|---|---|---|---|---|
Study visit | Class I | Class II | Class III | Total |
Week 12 | ||||
Class I | |||||| | |||||||| | ||||||| | |||| (45.3) |
Class II | |||||| | |||||||| | |||||||| | |||| (46.5) |
Class III | |||||||| | |||||| | |||||| | |||| (8.2) |
Class IV | |||||||| | |||||||| | |||||||| | |||||||| |
Total | ||||||| | |||||||| | |||||||| | |||||||| |
Week 48 | ||||
Class I | |||||| | |||||||| | ||||||| | |||| (59.2) |
Class II | |||||| | ||||||| | ||||||| | |||| (32.7) |
Class III | |||||||| | |||||||| | |||||||| | |||| (8.2) |
Class IV | |||||||| | |||||||| | |||||||| | |||||||| |
Total | |||||| | |||||||| | |||||||| | ||||||||| |
ITT = intention-to-treat; NYHA = New York Heart Association.
|||||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||||||||||| |||||||||||| ||||||||| ||||||||| |||||||||| ||||||||| ||||||||||| ||||||||||||||| ||||||||||| ||||||||| ||||||||| |||||||| ||||||| ||||||||||| ||||||| |||||||||||| ||||||||| |||||||||||| |||||||| |||| |||||||||||||||||| ||||||||||||||| |||||||||||| |||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| ||||||||||
Source: Clinical Study Report for Extension Study MYK-461 to 007.35
Resting LVOT Gradients and Valsalva LVOT Peak Gradients and Postexercise LVOT Peak Gradients
Table 26 summarizes the baseline values for site and central reads of resting and Valsalva LVOT gradients by study visit and change from baseline values. Reductions from baseline were observed in both resting and Valsalva LVOT gradients with mavacamten treatment as assessed by both site and central readings in the extension study, indicating beneficial effects of mavacamten on LVOT gradients. The number of patients was relatively small during the end time points, making it difficult to draw any conclusion about the effects of mavacamten on LVOT gradients.
Table 27 summarizes the postexercise gradients for patients who underwent postexercise assessments at week 24 for the EXPLORER-LTE cohort. |||||||||||| |||||||||||||| |||||||||||| |||||||||| ||| |||||| ||||||||| ||||||||| |||||||||||| |||| |||||||||| |||| || |||||||||||| ||||||||||||||||| |||||||| |||||||||||||| ||||||||||| |||||| |||||||||| |||| ||||| |||||||||| |||||||||| |||||||| |||||| |||||||| |||| |||||||||||||||| ||| |||| |||||||||||||||| ||||||
Table 26: Baseline and Change From Baseline in LVOT Gradient (at Rest and During Valsalva) by Study Visit for the EXPLORER-LTE Cohort (ITT Population)
Characteristic | LVOT Gradient (mm Hg), N = 224 | |||
|---|---|---|---|---|
Study visit | Resting | Valsalva | ||
— | Site-read | Central-read | Site-read | Central-read |
Baselinea | ||||
n | NA | 224 | NA | 222 |
Mean (SD) | NA | |||||||| | NA | |||||||| |
Week 24 | ||||
n | 110 | 110 | 110 | 110 |
Mean (SD) | |||||||| | |||||||| | |||||||| | |||||||| |
Change from baseline to week 24, mean (SD) | NA | ||||||||| | NA | ||||||||| |
Week 48 | ||||
n | 49 | 49 | 49 | 49 |
Mean (SD) | |||||| | ||||||| | |||||||| | |||||||| |
Change from baseline to week 48, mean (SD) | NA | ||||||||| | NA | ||||||||| |
Week 72 | ||||
n | ||||||| | ||||||| | ||||||| | ||||||| |
Mean (SD) | |||||| | ||||||| | ||||||| | |||||||| |
Change from baseline to week 72, mean (SD) | ||||||| | ||||||| | ||||||| | ||||||| |
||||||||||| |||||||| ||||||| |||||||||||||| |||||||| ||||| ||||||| |||| |||||| ||| ||||||||| ||||||||||| ||||||||||||| ||||||||| ||||||| ||||||||||||||| ||||||||||||||| |||||||||||||| ||||||||| |||||||| |||||||||||||||||| |||||| |||||||| ||||||||||| ||||||||||| ||||||||||||||||| |||||||||||||||||| |||||||||||||||||| |||||||||
Source: Clinical Study Report for Extension Study MYK-461 to 007.35
|||||||||||||| | ||||||||||||||||||||||| | |
|---|---|---|
||||| |||| | ||||||||| | |||||||||||| |
|||||| | ||||||||| | ||||||||| |
||| | ||| | ||| |
|||||||| | ||||| ||| | |||||||| |
||||||||||||||||||| |||||||||||| ||||||
This table has been redacted for confidential information.
Change in Cardiac Structure
|||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||||||||||||| |||||||||||| ||| |||||||| |||||||||||||| |||||||| ||||| |||||||||| |||| |||||||||||||||| |||| |||||||||| |||||||||| ||||| |||||| ||||||||| |||||||||| ||||||||||||||| |||||||||||| |||||||||| ||||||||||| ||||||| ||||| ||||||||||| |||||||||| |||| ||||||| |||||||||||||||||| |||||| |||||||||||||||| |||||||||| ||||||||||||||| |||||| |||||||| ||||||||||||| ||||||||||| |||| ||| ||||||||| ||||||||||||||||||
|||||||||||||| | |||||||||||||||||| | |
|---|---|---|
||||||||||||||||||||||||||||||||| | ||| | ||||| |
||||||||||||||||| | ||
|||||||| | ||| | ||||||| |
|||||||||||||| | ||| | ||||||| |
||||||||||||||||| |||||||| | ||| | |||||||| |
||||| | ||||||||| | |
|||||||||||||| | || | ||||||| |
|||| |||||||||||||||| |||||| | || | |||||||| |
||||| | ||||||| | |
|||||||||||||||| | ||
|||||||| | ||| | ||||||| |
|||||||||||||| | ||| | ||||||| |
||||||||||| ||||||||||||||| | ||| | ||||||||| |
||||| | ||||||||| | |
|||||||||||||| | || | ||||||| |
|||| |||||||||||||||| |||||| | || | ||||||||| |
||||| | |||||||| | |
|||||||||||||||||| | ||
|||||||| | ||| | ||||||||| |
|||||||||||||| | || | ||||||||| |
|||||||||||| |||||||||||||| | || | |||||||||| |
||||| | |||||||| | |
|||||||||||||| | || | ||||||||| |
|||| |||||||||||||||| |||||| | || | ||||||||| |
||||| | |||||||| | |
|||||||||||| ||||||||||||||||||||| |||||||||| |||||||||| |||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||||||||||||| ||||||||| |||||||| |||||| |||||||||||||| |||||||| ||||||||||||||| |||||||||||||||||||||
This table has been redacted for confidential information.
|||||||||||||| | |||||||||||||||||| | |||
|---|---|---|---|---|
||||||||||||||||||||||||||| | ||||||||||||||||||||||||||||| | |||
|||||||||||||||||||||||||||||||||| | |||||| | ||||||||||||||||||| | |||||| | ||||||||||||||||||| |
||||||||| | ||||
||||||||| | ||| | || | || | || |
|||||||| | |||||||| | || | |||||||| | || |
||||| | ||||||||| | || | ||||||||| | || |
|||||||| | || | || | || | || |
|||||||| | |||||||| | |||||||| | ||||||| | ||||||| |
||||| | ||||||||| | |||||||||| | ||||||||| | |||||||||| |
|||| | ||||
||||||||| | ||| | || | || | || |
|||||||| | ||||||||| | || | ||||||||| | || |
||||| | ||||||||||| | || | ||||||||||| | || |
|||||||| | || | || | || | || |
|||||||| | ||||||||| | ||||||| | ||||||||||| | ||||||| |
||||| | ||||||||||| | |||||||| | |||||||||| | |||||||| |
|||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||| |||||||||||||||| ||||||||| |||| |||||||||||||||| ||| ||||||||| ||||||||| |||||||||||||||||| ||||||||||||||||| |||||| ||||||||||||||| |||||||||| |||| ||||||||||| |||||||||||||||| |||||||||||||||||| ||||||| ||||||||| ||||||||||| |||||||||||| || ||||| |||||||||| |||||||||||| |||||||||||||||||||| ||||||||| ||||||||| |||| ||||||| | ||||| |||||||||||| |||||||||||| |||||||||||| ||||||||| ||||||||||||||||||| |||||||||||||||| ||||||||||| |||||||| ||||| |||||||
This table has been redacted for confidential information.
Biomarker-Based Assessment
Table 30 and Figure 6 summarize NT-proBNP change from baseline for the intention-to-treat population of the EXPLORER-LTE cohort. The beneficial effects of mavacamten could be observed through a decreasing trend of NT-proBNP concentrations. While the change was rapid during the initial phases of the trial, |||||||||||||| |||| |||||| ||||||||| |||||| ||||| ||||||| |||||||||| ||||||||||||| |||||||||||| |||||||||||||||| The trend can be seen in Figure 6. However, the number of patients at these later time points was relatively small at the time of the data cut-off.
|||||||||||||| | |||||||||||||||||||||||| | |
|---|---|---|
|||||||||| | |||||||||||||||||||| | ||||||||||||||| |
|||||||||| | ||| | ||| |
|||||||||||||||||| | |||||||||||| | || |
|||||||| | ||| | ||| |
|||||||||||||||||| | |||||||||||| | ||||||||||| |
|||||||| | ||| | ||| |
|||||||||||||||||| | |||||||||||| | ||||||||||| |
|||||||| | ||| | ||| |
|||||||||||||||||| | |||||||||||| | ||||||||||| |
|||||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||| |||||||||||||||| ||||||| |||||||||||||||| |||||||||| ||||| ||||||| |||||||||||| |||||||||||||
This table has been redacted for confidential information.

Harms
Adverse Events
Table 31 summarizes the harms outcomes for the EXPLORER-LTE cohort. In all, 62.9% of patients experienced at least 1 AE. |||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||| |||||||||||||||| ||||||||| The most common AEs were |||||||| |||| |||||||||||||||| ||| ||||||||||| ||||||| ||||||||||||| |||||||| |||||| ||||||| |||||||| |||||||||||||| |||||| |||||| One death, due to bacterial endocarditis, occurred in the EXPLORER-LTE cohort, but the investigator considered it unrelated to mavacamten.
Serious Adverse Events
In EXPLORER-LTE cohort, the most common SAEs among patients were ||||||| |||||||| |||||||||| |||||||||||| |||||||||||| ||||||||||||||||
Withdrawals due to Adverse Events
In the EXPLORER-LTE cohort, 2 patients (0.9%) discontinued treatment due to AEs, with 1 patient discontinuing due to worsening of systemic lupus erythematosus and 1 patient due to cardiac failure.
Notable Harms
In the EXPLORER-LTE cohort, |||||||| |||| |||||||||||||||| ||| |||| |||||||||||||||| ||||||||
Temporary Treatment Discontinuation
A total of 11 (4.9%) patients demonstrated a total of ||||||||| ||||||||| that met the criteria for temporary treatment discontinuation:
|||||||||| |||||| |||||||||||||| |||||||||||||| ||||||||||||| ||||| |||||||| |||||||||||||| |||||||||| ||||||||||
||||||||||||| |||||||||||| |||||||| ||||||||||| |||| |||||||||| |||||||||||| |||||||||||||||| ||||||||||||| |||||
|||||||| |||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||| |||||||||||||||| ||||||||
|||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||| |||||||||||||||| ||||||||||||||||
|||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||| |||||||||||||||| ||||||||||||
Table 31: Summary of Harms in EXPLORER-LTE Cohort (Safety Population)
Harms | EXPLORER-LTE cohort (N = 224) |
|---|---|
Patients with ≥ 1 adverse event | |
Any adverse event, n (%) | 141 (62.9) |
Most common events, n (%) | |
|||||||||| ||||||||| | ||||||| |
||||||||| | |||||| |
|||||||| | ||||||| |
|||||||||||||||| | ||||||| |
|||||||||| | |||||| |
||||||||| | ||||||| |
|||||||| | ||||||| |
|||||||||||||||| | |||||| |
Patients with ≥ 1 serious adverse event | |
Any SAE, n (%) | 19 (8.5) |
Most common serious adverse events,a n (%) | |
||||||||||||||||||| | |||||| |
||||||||| | |||||| |
||||||||||||||| | |||||| |
|||| | ||||||| |
|||||||||||| | |||||||| |
|||||||||||||||||||| | |||||||| |
||||||||||||| |||||||| | |||||||| |
||||||||||||| | |||||||| |
||||||||||||||||||| | |||||||| |
||||||||||||| | |||||||| |
|||||||||||||| | |||||||| |
|||| |||||||||||||||| |||||| | |||||||| |
|||||||||||||| | |||||||| |
||||||||||| | |||||||| |
||||||||||||||||| | |||||||| |
|||||||||||||| | |||||||| |
||||||||| | |||||||| |
||||||||||| ||||||| | |||||||| |
|||||||||||||| | |||||||| |
|||||||||||||||| | |||||||| |
Patients who stopped treatment due to adverse events | |
Any, n (%) | 2 (0.9) |
Worsening of systemic lupus erythematosus | 1 (0.4) |
Cardiac failure | 1 (0.4) |
Deaths, n (%) | 1 (0.4) |
Bacterial endocarditis | 1 (0.4) |
Notable harms, n (%) | |
Cardiac failure | 2 (0.9) |
LVEF at rest ≤ 30% | |||||||| |
LVEF = left ventricular ejection fraction.
aFrequency equal to or greater than 1 patient.
Source: Clinical Study Report for Extension Study MYK-461 to 00735.
Critical Appraisal
Internal Validity
The ongoing EXPLORER-LTE cohort was designed as a dose-blinded study and was run in parallel to the parent study evaluating the long-term safety and tolerability of mavacamten in patients with oHCM. While study-site investigators remained blinded to study drug dose, they were unblinded to the site-read echocardiography results. There was potential selection bias, as patients who respond to mavacamten and are able to tolerate treatment are more likely to continue therapy than patients with less-favourable outcomes. In addition to potential selection bias, the interpretation of the longer-term results in the LTE study is limited by the lack of a control group and the fact that investigators and patients were aware that patients were receiving active treatment. Their expectations of treatment therefore may have affected reporting of subjective outcomes, such as NYHA functional class.
The baseline and demographic characteristics were similar to the characteristics seen in the pivotal trials. Treatment discontinuation and study discontinuation rates among patients were low in the extension study, as observed in both pivotal trials. While the primary efficacy outcome of pVO2 from the pivotal trial was not assessed in the extension study, ||||||||| ||||||||||| ||||||||||| |||||||||||| |||||||||||||| ||||||||||||| ||||||||| |||||||||||||||||||| ||||||| ||||||||||||||||||| |||||| The absence of these parameters in the interim analysis makes it difficult to interpret the efficacy and safety results of mavacamten for the LTE.
|||| ||||||||| ||||||||| ||||||||| |||||||| |||| |||||||||||||||| ||| |||||||| ||||||||||||| |||||||||| ||||||||| the number of patients at later time points in all efficacy analyses were relatively few at the time of the data cut-off, and the results should be interpreted with caution.
External Validity
The generalizability of the efficacy and harms outcomes and the lack of racial diversity mentioned in the main report are applicable to the extension study.
Discussion
Summary of Available Evidence
Two sponsor-conducted phase III, randomized, double-blind, placebo-controlled trials, EXPLORER-HCM and VALOR-HCM, both of which met the CADTH review protocol criteria, were included in this systematic review. The EXPLORER-HCM trial (68 sites in 13 countries, N = 251) evaluated the efficacy and safety of once-daily oral administration of mavacamten (with a starting dose of 5 mg) in adult patients with symptomatic oHCM and an LVOT gradient of 50 mm Hg or greater, a documented LVEF of 55% or greater, a maximum septal wall thickness determined by a core laboratory of 15 mm or greater (or 13 mm or greater with a family history of HCM), and NYHA functional class II or III symptoms. The primary outcome was the composite functional response at week 30, defined as achieving an improvement (increase) of 1.5 mL/kg/min or greater in pVO2 and a reduction of at least 1 NYHA functional class (or a 3.0 mL/kg/min or greater increase in pVO2 without worsening of NYHA class). Harms and notable harms (identified in the CADTH systematic review protocol) were assessed.
The VALOR-HCM trial (19 sites in the US, N = 112) is an ongoing, 32-week trial evaluating the efficacy and safety of once-daily orally administered treatment with mavacamten (with a starting dose of 5 mg) in adult patients with symptomatic oHCM and an LVOT gradient of 50 mm Hg or greater, a documented LVEF of 60% or greater, and a maximum septal wall thickness determined by a core laboratory of 15 mm or greater (or 13 mm or greater with a family history of HCM) and a NYHA functional class III or IV (or class II with exertional syncope or near syncope). Patients must have been referred within the past 12 months for SRT and been actively considering scheduling the procedure. The primary outcome was a composite of the decision to proceed with SRT before or at week 16 or be considered guideline-eligible for SRT at week 16. Guideline-eligibility criteria were based on the 2011 ACCF/AHA clinical and hemodynamic criteria for HCM. Patients with a maximum LVOT gradient of 50 mm Hg or greater (from rest, Valsalva, or postexercise) and no improvement in NYHA functional class at week 16 were considered eligible for SRT. Harms and notable harms (identified in the CADTH systematic review protocol) were assessed. Additional descriptive efficacy and safety data were provided for the VALOR-HCM trial through to week 32.
The MAVA-LTE trial is an ongoing, dose-blinded, 5-year LTE study of the long-term efficacy and safety of mavacamten following EXPLORER-HCM and MAVERICK-HCM (a phase II trial of patients with nonobstructive HCM). The trial included 224 patients who completed treatment in the phase III EXPLORER-HCM trial (the EXPLORER-LTE cohort). All patients in EXPLORER-LTE cohort started mavacamten treatment at 5 mg once daily, with dose adjustments at weeks 4, 8, and 12 based on site-read echocardiography measures of LVOT Valsalva gradient and LVEF.
Interpretation of Results
Efficacy
The clinical expert consulted for this review indicated that pVO2 and NYHA functional class are appropriate measures of functional capacity and symptom severity, respectively, for the indicated population. The EXPLORER-HCM trial reported a statistically significant difference in the proportion of patients meeting the primary composite efficacy outcome in favour of mavacamten. Subgroup analyses examining beta-blocker use at baseline (yes versus no) in the EXPLORER-HCM trial found that, for the primary composite outcome and for the key secondary outcome of change in pVO2 from baseline to week 30, there was no statistically significant difference between treatment groups among patients receiving beta-blockers. However, all key secondary end points in the EXPLORER-HCM trial showed a benefit from mavacamten treatment compared with placebo across the evaluated subgroups, irrespective of beta-blocker use. The subgroup analyses may not have been powered to detect a treatment difference and no adjustments were made for multiplicity. As such, all subgroup analyses are exploratory in nature.
Both pivotal trials found statistically significant results in key secondary outcomes of an improvement of at least 1 NYHA functional class and change from baseline to end of treatment in postexercise LVOT peak gradient in favour of mavacamten, and the clinical expert consulted for this review found these results to be clinically meaningful. An additional 48 weeks of data were available from the ongoing, uncontrolled, open-label extension study (MAVA-LTE), which suggested that improvements from baseline in oHCM symptoms assessed by NYHA class for the EXPLORER-LTE cohort were consistent with those observed in the EXPLORER-HCM pivotal trial. In addition to potential selection bias, interpretation of the longer-term results in the LTE study is limited by the lack of a control group and the fact that investigators and patients were aware that patients were receiving active treatment. Their expectations of treatment therefore may have affected reporting of subjective outcomes such as NYHA functional class.
Input from patient groups and the clinical expert emphasized that improvements in HRQoL and reductions in symptoms (i.e., shortness of breath) are important treatment goals for patients. Both pivotal trials assessed HRQoL using the KCCQ-23, which has been reported to be a generally valid, reliable, and responsive tool. In both pivotal trials, there was a significant difference between treatment groups in change in KCCQ-23 CSS from baseline to end of treatment in favour of mavacamten. In the EXPLORER-HCM trial, 20.1% more patients in the mavacamten group achieved a 10-point change in the KCCQ-23 CSS score from baseline to week 30, a threshold that is higher than the estimated MID for the KCCQ-23 CSS for patients with heart failure (between 4.5 and 6 points) (Appendix 4). Results of the EXPLORER-HCM trial found improvements in the KCCQ-23 OSS and TSS, from baseline to week 30, in favour of mavacamten; however, these results should be interpreted as supportive evidence for mavacamten, as no adjustment was made for multiplicity. In terms of disease symptoms, the EXPLORER-HCM trial found a statistically significant decrease (i.e., improvement) in the HCMSQ SoB domain scores among patients in the mavacamten group compared to those in the placebo group. In the EXPLORER-HCM trial, KCCQ-23 CSS or HCMSQ SoB data for more than 30% of patients were not collected at baseline or at the week-30 visit. There is therefore a risk of bias as those who completed the questionnaires may be fundamentally different than those who did not (i.e., differences in treatment response are possible). However, for all imputation scenarios, ad hoc sensitivity analyses were generally supportive of the findings of the primary analyses.
In the VALOR-HCM trial, the primary end point was achieved, as demonstrated by a statistically significantly reduced eligibility for invasive SRT procedures at 16 weeks in the mavacamten group compared with the placebo group. The results were primarily driven by SRT eligibility based on guideline criteria, with 14.3% and 69.6% of patients eligible for SRT at week 16 in the mavacamten and placebo groups, respectively. Additional descriptive data for the VALOR-HCM trial through to week 32 found that mavacamten treatment sustained a reduction in the proportion of patients proceeding to SRT or remaining guideline-eligible, with similar effects observed in patients who crossed over from placebo after 16 weeks of treatment with mavacamten. However, these additional results at week 32 were descriptive in nature and should be interpreted as supportive evidence of mavacamten.
In the VALOR-HCM trial, mavacamten demonstrated statistically significant improvements at week 16 in NT-proBNP and cardiac troponin I levels, which are biomarkers of long-term outcomes in HCM for cardiac wall stress and cardiac injury, respectively. The clinical expert found these results to be clinically meaningful and stated that it is reasonable to assess these biomarkers in the clinical setting. The reduction in NT-proBNP and cardiac troponin I may be a consequence of reduced LVOT obstruction. In the EXPLORER-HCM trial, patients in the mavacamten group experienced greater reductions in NT-proBNP and cardiac troponin I levels at week 30. Among patients in the EXPLORER-LTE cohort, NT-proBNP concentrations decreased at LTE week 4 and decreases were sustained through to LTE week 72.
Changes from baseline in cardiac structure as measured by echocardiography in both pivotal trials and as measured in the CMR substudy in the EXPLORER-HCM trial were generally directionally favourable for patients treated with mavacamten. The clinical expert consulted for this review noted that uncertainty remains regarding the impact mavacamten will have on cardiac structure in the long-term. In the LTE study, among those in the EXPLORER-LTE cohort, there was little change from baseline to week 48 in echocardiographic measures of interventricular septal or posterior wall thicknesses or the LVMI, but a reduction in LAVI was observed. These results were exploratory, with outcomes not controlled for multiplicity, and should be interpreted with caution because of the potential for inflated type I error rate that accompanies the small sample sizes in the CMR substudy.
The VALOR-HCM trial is an ongoing RCT evaluating the use of mavacamten to reduce the need for SRT in patients who are guideline-eligible for invasive therapies, with descriptive data available through to week 32. It is therefore uncertain if mavacamten can reduce the need for SRT among symptomatic patients with oHCM in the long-term. Furthermore, no direct evidence comparing mavacamten with SRT was available for this review. There is also limited direct evidence comparing mavacamten to disopyramide. Patients taking disopyramide were excluded from the EXPLORER-HCM trial and less than 20% of enrolled patients (n = 22) in the VALOR-HCM trial used disopyramide at baseline as monotherapy or in combination with beta-blockers or calcium channel blockers. ||| ||||||| |||||||||||| ||||||||||||||| |||||||||||||||| |||||||| |||||||||| |||||||||||| ||||||||| |||||||||| |||||||||||||||| ||||||||| ||||||||||||| ||||||||||| |||||||||||| |||||||||||| ||||||||||| |||||||| The comparative effectiveness of disopyramide versus mavacamten in this patient population is therefore unknown.
With regards to external validity, the product monograph states that the drug is indicated for adult patients with symptomatic NYHA functional class II to III oHCM. However, the VALOR-HCM trial included an unknown number of patients with NYHA functional class IV oHCM.
Harms
In both pivotal trials, overall rates of AEs and SAEs, including atrial fibrillation and ventricular tachycardia, were comparable for patients in both the mavacamten and placebo groups. In the EXPLORER-HCM trial, 1 patient in the placebo group died due to sudden death and no deaths were reported through to week 32 in the VALOR-HCM trial. In both trials, a higher proportion of patients in the mavacamten group than in the placebo group met the temporary discontinuation criteria of an LVEF of less than 50%. The product monograph for mavacamten includes a serious warning stating that mavacamten reduces the LVEF and can cause heart failure due to systolic dysfunction. Patient input submitted for this review suggested that this limits the prescription of mavacamten to patients who have access to a high-volume clinic and are committed to regular monitoring and reporting of symptoms. No new safety signals were identified based on interim data in the MAVA-LTE trial for the EXPLORER-LTE cohort, with 1 death occurring due to bacterial endocarditis, which the investigator considered to be unrelated to mavacamten.
Conclusions
In the EXPLORER-HCM trial, among patients with symptomatic NYHA class II or III oHCM, mavacamten was statistically significantly more efficacious than placebo in improving NYHA class and exercise capacity (pVO2), as measured by the primary composite outcome. In the VALOR-HCM trial, among patients with symptomatic NYHA class III or IV oHCM (or class II oHCM with exertional syncope or near syncope), significantly fewer patients were eligible for SRT at week 16 in the mavacamten group than in the placebo group. The results of both pivotal trials were statistically significantly in favour of mavacamten for key secondary outcomes of an improvement of at least 1 NYHA class, postexercise LVOT peak gradient, and HRQoL as assessed by the KCCQ-23 CSS, all of which were found to be clinically meaningful by the clinical expert consulted by CADTH for this review. The EXPLORER-HCM trial assessed disease-related symptoms, and a statistically significantly greater improvement in the HCMSQ SoB domain score was observed in the mavacamten group compared with the placebo group. The VALOR-HCM trial found statistically significantly greater reductions in assessed biomarkers among patients in the mavacamten group compared with those in the placebo group. While descriptive results for the VALOR-HCM trial are available through to week 32, it is uncertain if mavacamten can reduce the need for SRT among patients with symptomatic oHCM in the long-term. Furthermore, no direct evidence comparing mavacamten with SRT was available for this review. Only the VALOR-HCM trial enrolled patients who were receiving disopyramide; however, as no subgroup analyses based on disopyramide use at baseline were available, the comparative effectiveness of disopyramide versus mavacamten in patients with symptomatic oHCM is unknown. Because the EXPLORER-HCM trial evaluated mavacamten as an add-on to first-line treatment with beta-blockers or calcium channel blockers, the clinical efficacy of mavacamten as a first-line therapy or third-line therapy after disopyramide is unknown. The effectiveness of mavacamten in combination with disopyramide and beta-blockers or calcium channel blockers is also unknown. In both pivotal trials, overall rates of AEs and SAEs were comparable for patients in both the mavacamten and placebo groups. In the EXPLORER-HCM trial, 1 patient in the placebo group experienced sudden death, and no deaths were reported through to week 32 in the VALOR-HCM trial. The safety results showed that mavacamten was well tolerated and generally comparable to placebo, with no new safety signals identified in the MAVA-LTE study among patients in the EXPLORER-LTE cohort.
References
1.Maron MS. Hypertrophic cardiomyopathy: clinical manifestations, diagnosis, and evaluation. In: McKenna JW, ed. UpToDate. Waltham (MA): UpToDate; 2017: http://www.uptodate.com/. Accessed 2022 Nov 28.
2.Elliott PM, Anastasakis A, Borger MA, et al. 2014 ESC Guidelines on diagnosis and management of hypertrophic cardiomyopathy. Kardiol Pol. 2014;72(11):1054-1126. PubMed
3.Ommen SR, Mital S, Burke MA, et al. 2020 AHA/ACC guideline for the diagnosis and treatment of patients with hypertrophic cardiomyopathy: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol. 2020;76(25):e159-e240. PubMed
4.Javidgonbadi D, Andersson B, Abdon N-J, Schaufelberger M, Östman-Smith I. Factors influencing long-term heart failure mortality in patients with obstructive hypertrophic cardiomyopathy in Western Sweden: probable dose-related protection from beta-blocker therapy. Open Heart. 2019;6(1):e000963. PubMed
5.Maron MS, Olivotto I, Zenovich AG, et al. Hypertrophic cardiomyopathy is predominantly a disease of left ventricular outflow tract obstruction. Circulation. 2006;114(21):2232-2239. PubMed
6.Camzyos (mavacamten): 2.5 mg, 5 mg, 10 mg and 15 mg, oral [product monograph]. Montreal (QC): Bristol-Myers Squibb Canada; 2022 Nov 8: https://pdf.hres.ca/dpd_pm/00068229.PDF. Accessed 2022 Dec 2.
7.Desai MY, Owens AT, Geske JB, et al. Dose-blinded myosin inhibition in patients with obstructive HCM referred for septal reduction therapy: outcomes through 32-weeks. Circulation. 2022;06:06.
8.Weissler-Snir A, Allan K, Cunningham K, et al. Hypertrophic cardiomyopathy–related sudden cardiac death in young people in Ontario. Circulation. 2019;140(21):1706-1716. PubMed
9.Jain SS, Li SS, Xie J, et al. Clinical and economic burden of obstructive hypertrophic cardiomyopathy in the United States. J Med Econ. 2021;24(1):1115-1123. PubMed
10.Bisoprolol (bisoprolol fumarate tablets): 5 mg, 10 mg [product monograph]. Boucherville (QC): Angita Pharma Inc; 2021 Oct 8: https://pdf.hres.ca/dpd_pm/00063175.PDF. Accessed 2022 Oct 8.
11.Verapamil (verapamil hydrochloride sustained-release tablets): 120 mg, 180 mg and 240 mg, oral [product monograph]. Etobicoke (ON): Mylan Pharmaceuticals ULC; 2020 Jan 15: https://pdf.hres.ca/dpd_pm/00054924.PDF. Accessed 2022 Oct 8.
12.Rythmodan (disopyramide): 100mg, capsules [product monograph]. Mississauga (ON): Xediton Pharmaceuticals Inc; 2020 Dec 16: https://health-products.canada.ca/dpd-bdpp/info.do?lang=en&code=37379. Accessed 2022 Dec 12.
13.McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 guideline statement. J Clin Epidemiol. 2016;75:40-46. PubMed
14.Grey matters: a practical tool for searching health-related grey literature. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/grey-matters. Accessed 2022 Oct 6.
15.Olivotto I, Oreziak A, Barriales-Villa R, et al. Mavacamten for treatment of symptomatic obstructive hypertrophic cardiomyopathy (EXPLORER-HCM): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 2020;396(10253):759-769. PubMed
16.Desai MY, Wolski K, Owens A, et al. Study design and rationale of VALOR-HCM: evaluation of mavacamten in adults with symptomatic obstructive hypertrophic cardiomyopathy who are eligible for septal reduction therapy. Am Heart J. 2021;239:80-89. PubMed
17.Desai MY, Owens A, Geske JB, et al. Myosin inhibition in patients with obstructive hypertrophic cardiomyopathy referred for septal reduction therapy. J Am Coll Cardiol. 2022;80(2):95-108. PubMed
18.Clinical Study Report: MYK-416-005. A randomized, double-blind, placebo-controlled clinical study to evaluate Mavacamten (MYK-461) in adults (EXPLORER-HCM). [internal sponsor’s report]. Brisbane (CA): MyoKardia, Inc; 2020 Nov 11.
19.Drug Reimbursement Review sponsor submission: Camzyos (mavacamten), 2.5 mg, 5 mg, 10 mg, or 15 mg capsules [internal sponsor's package]. Saint-Laurent (QC): Bristol Myers Squibb; 2022 Oct 7.
20.Green CP, Porter CB, Bresnahan DR, Spertus JA. Development and evaluation of the Kansas City Cardiomyopathy Questionnaire: a new health status measure for heart failure. J Am Coll Cardiol. 2000;35(5):1245-1255. PubMed
21.Spertus J. Medical device development tool qualification decision summary for Kansas City cardiomyopathy questionnaire Kansas City (MO): Saint Luke's Mid American Heart Institute; 2016: https://www.fda.gov/media/108301/download. Accessed 2022 Nov 28.
22.Spertus JA, Jones PG, Sandhu AT, Arnold SV. Interpreting the Kansas City Cardiomyopathy Questionnaire in clinical trials and clinical care: JACC state-of-the-art review. J Am Coll Cardiol. 2020;76(20):2379-2390. PubMed
23.Masterson Creber R, Polomano R, Farrar J, Riegel B. Psychometric properties of the Kansas City Cardiomyopathy Questionnaire (KCCQ). Eur J Cardiovasc Nurs. 2012;11(2):197-206. PubMed
24.Napier R, McNulty SE, Eton DT, Redfield MM, AbouEzzeddine O, Dunlay SM. Comparing measures to assess health-related quality of life in heart failure with preserved ejection fraction. JACC Heart Fail. 2018;6(7):552-560. PubMed
25.Garin O, Ferrer M, Pont A, et al. Disease-specific health-related quality of life questionnaires for heart failure: a systematic review with meta-analyses. Qual Life Res. 2009;18(1):71-85. PubMed
26.Myers J, Zaheer N, Quaglietti S, Madhavan R, Froelicher V, Heidenreich P. Association of functional and health status measures in heart failure. J Card Fail. 2006;12(6):439-445. PubMed
27.Tucker R, Quinn JR, Chen DG, Chen L. Kansas City Cardiomyopathy Questionnaire administered to hospitalized patients with heart failure. J Nurs Meas. 2016;24(2):245-257. PubMed
28.Butler J, Khan MS, Mori C, et al. Minimal clinically important difference in quality of life scores for patients with heart failure and reduced ejection fraction. Eur J Heart Fail. 2020;22(6):999-1005. PubMed
29.Eurich DT, Johnson JA, Reid KJ, Spertus JA. Assessing responsiveness of generic and specific health related quality of life measures in heart failure. Health Qual Life Outcomes. 2006;4:89. PubMed
30.Flynn KE, Lin L, Ellis SJ, et al. Outcomes, health policy, and managed care: relationships between patient-reported outcome measures and clinical measures in outpatients with heart failure. Am Heart J. 2009;158:S64-S71. PubMed
31.McClure NS, Sayah FA, Xie F, Luo N, Johnson JA. Instrument-defined estimates of the minimally important difference for EQ-5D-5L index scores. Value Health. 2017;20(4):644-650. PubMed
32.Herdman M, Gudex C, Lloyd A, et al. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual Life Res. 2011;20(10):1727-1736. PubMed
33.Reaney M, Allen V, Sehnert AJ, et al. Development of the Hypertrophic Cardiomyopathy Symptom Questionnaire (HCMSQ): a new Patient-Reported Outcome (PRO) instrument. Pharmacoeconom Open. 2022;6(4):563-574. PubMed
34.Gersh BJ, Maron BJ, Bonow RO, et al. 2011 ACCF/AHA Guideline for the diagnosis and treatment of hypertrophic cardiomyopathy: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines developed in collaboration with the American Association for Thoracic Surgery, American Society of Echocardiography, American Society of Nuclear Cardiology, Heart Failure Society of America, Heart Rhythm Society, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J Am Coll Cardiol. 2011;58(25):e212-e260. PubMed
35.Clinical Study Report: MYK-461-007. A long-term safety extension study of mavacamten (MYK-461) in adults with hypertrophic cardiomyopathy who have completed the MAVERICK-HCM (MYK-461-006) or EXPLORER-HCM (MYK-461-005) trials (MAVA-LTE) [internal sponsor's report]. Brisbane (CA): MyoKardia, Inc; 2021 May 6.
36.Hegde SM, Lester SJ, Solomon SD, et al. Effect of mavacamten on echocardiographic features in symptomatic patients with obstructive hypertrophic cardiomyopathy. J Am Coll Cardiol. 2021;78(25):2518-2532. PubMed
37.Heitner SB, Jacoby D, Lester SJ, et al. Mavacamten treatment for obstructive hypertrophic cardiomyopathy: a clinical trial. Ann Intern Med. 2019;170(11):741-748. PubMed
38.Butler J, Filippatos G, Jamal Siddiqi T, et al. Empagliflozin, health status, and quality of life in patients with heart failure and preserved ejection fraction: the EMPEROR-preserved trial. Circulation. 2022;145(3):184-193. PubMed
39.Nassif M, Fine JT, Dolan C, et al. Validation of the Kansas City Cardiomyopathy Questionnaire in symptomatic obstructive hypertrophic cardiomyopathy. JACC Heart Fail. 2022;10(8):531-539. PubMed
40.Spertus J, Peterson E, Conard MW, et al. Monitoring clinical changes in patients with heart failure: a comparison of methods. Am Heart J. 2005;150(4):707-715. PubMed
41.Butler J, Spertus JA, Bamber L, et al. Defining changes in physical limitation from the patient perspective: insights from the VITALITY-HFpEF randomized trial. Eur J Heart Fail. 2022;24(5):843-850. PubMed
42.Reaney M, Addepalli P, Allen V, et al. Longitudinal psychometric analysis of the Hypertrophic Cardiomyopathy Symptom Questionnaire (HCMSQ) using outcomes from the phase III EXPLORER-HCM trial. Pharmacoeconom Open. 2022;6(4):575-586. PubMed
43.Dyer MT GK, Sharples LS, Buxton MJ. A review of health utilities using the EQ-5D in studies of cardiovascular disease. Health Qual Life Outcomes. 2010;8(13). PubMed
44.Zaiser E, Sehnert AJ, Duenas A, Saberi S, Brookes E, Reaney M. Patient experiences with hypertrophic cardiomyopathy: a conceptual model of symptoms and impacts on quality of life. J Patient Rep Outcomes. 2020;4(1):102. PubMed
45.EuroQol Research Foundation. EQ-5D-5L - about. 2020; https://euroqol.org/eq-5d-instruments/eq-5d-5l-about/. Accessed 2022 November 20.
Appendix 1: Literature Search Strategy
Note that this appendix has not been copy-edited.
Clinical Literature Search
Overview
Interface: Ovid
Databases:
MEDLINE All (1946–)
Embase (1974–)
Note: Subject headings and search fields have been customized for each database. Duplicates between databases were removed in Ovid.
Date of search: October 21, 2022
Alerts: Bi-weekly search updates until project completion.
Search filters applied: No filters were applied to limit the retrieval by study type.
Limits:
No date or language limits were used
Conference abstracts: excluded
Syntax | Description |
|---|---|
/ | At the end of a phrase, searches the phrase as a subject heading |
MeSH | Medical Subject Heading |
.fs | Floating subheading |
exp | Explode a subject heading |
* | Before a word, indicates that the marked subject heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings |
.ti | Title |
.ot | Original title |
.ab | Abstract |
.hw | Heading word; usually includes subject headings and controlled vocabulary |
.kf | Author keyword heading word (MEDLINE) |
.dq | Candidate term word (Embase) |
.rn | Registry number |
.nm | Name of substance word (MEDLINE) |
medall | Ovid database code: MEDLINE All, 1946 to present, updated daily |
oemezd | Ovid database code; Embase, 1974 to present, updated daily |
Multi-Database Strategy
(mavacamten* or Camzyos* or myk 461 or myk461 or sar 439152 or sar439152 or QX45B99R3J).ti,ab,kf,ot,hw,rn,nm.
1 use medall
*mavacamten/ or (mavacamten* or Camzyos* or myk 461 or myk461 or sar 439152 or sar439152).ti,ab,kf,dq.
3 use oemezd
4 not (conference review or conference abstract).pt.
2 or 5
remove duplicates from 6
Clinical Trials Registries
ClinicalTrials.gov
Produced by the US National Library of Medicine. Targeted search used to capture registered clinical trials.
[Search -- Studies with results | mavacamten or Camzyos]
WHO ICTRP
International Clinical Trials Registry Platform, produced by WHO. Targeted search used to capture registered clinical trials.
[Search terms -- mavacamten or Camzyos]
Health Canada’s Clinical Trials Database
Produced by Health Canada. Targeted search used to capture registered clinical trials.
[Search terms -- mavacamten or Camzyos]
EU Clinical Trials Register
European Union Clinical Trials Register, produced by the European Union. Targeted search used to capture registered clinical trials.
[Search terms -- mavacamten or Camzyos]
Grey Literature
Search dates: October 10, 2022, to October 17, 2022
Keywords: mavacamten, Camzyos, hypertrophic cardiomyopathy
Limits: None
Relevant websites from the following sections of the CADTH grey literature checklist Grey Matters: A Practical Tool for Searching Health-Related Grey Literature were searched:
Health Technology Assessment Agencies
Health Economics
Clinical Practice Guidelines
Drug and Device Regulatory Approvals
Advisories and Warnings
Drug Class Reviews
Clinical Trials Registries
Databases (free)
Health Statistics
Internet Search
Appendix 2: Excluded Studies
Note that this appendix has not been copy-edited.
Reference | Reason for exclusion |
|---|---|
Hegde SM, Lester SJ, Solomon SD, et al. Effect of Mavacamten on Echocardiographic Features in Symptomatic Patients with Obstructive Hypertrophic Cardiomyopathy. J Am Coll Cardiol. 2021;78(25):2518 to 2532. | Review article36 |
Heitner SB, Jacoby D, Lester SJ, et al. Mavacamten Treatment for Obstructive Hypertrophic Cardiomyopathy: A Clinical Trial. Ann Intern Med. 2019;170(11):741 to 748. | Study design37 |
Appendix 3: Detailed Outcome Data
Note that this appendix has not been copy-edited.
Figure 7: Differences in Key Efficacy Outcomes by Beta-Blocker Use in the EXPLORER-HCM Trial
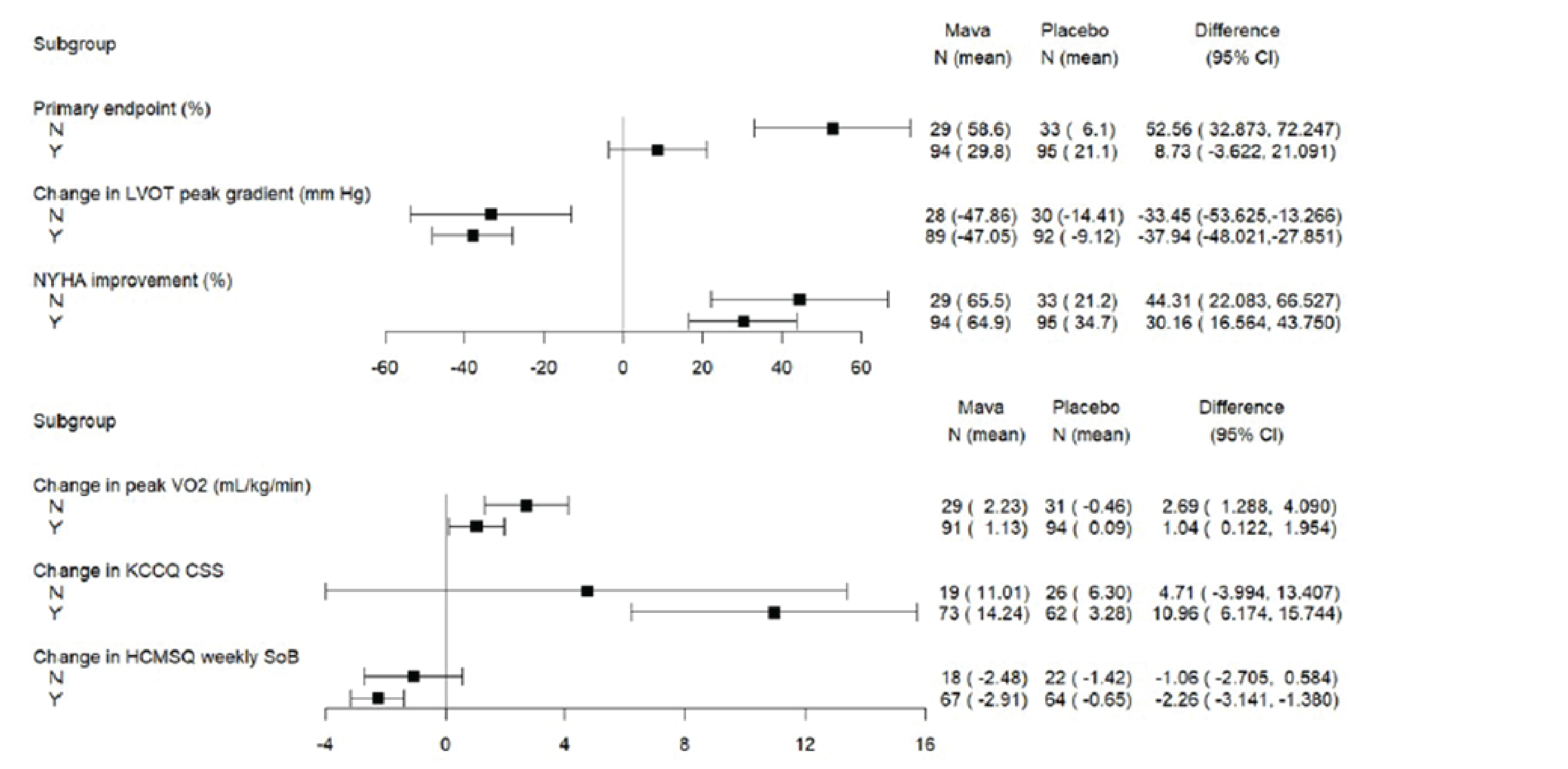
CSS = clinical summary score; HCMSQ = Hypertrophic Cardiomyopathy Symptom Questionnaire; KCCQ = Kansas City Cardiomyopathy Questionnaire; LVOT = left ventricular outflow tract; NYHA = New York Heart Association; SoB = shortness of breath; VO2 = oxygen consumption.
Source: Clinical Study Report for EXPLORER-HCM trial.18
Table 34: NYHA Class Shift From Baseline at Week 30 in the EXPLORER-HCM Trial (ITT Population)
Characteristic | Mavacamten (N = 123) | Placebo (N = 128) | ||||
|---|---|---|---|---|---|---|
Class II n (%) | Class III n (%) | Total n (%) | Class II n (%) | Class III n (%) | Total n (%) | |
Baseline | 88 (71.5) | 35 (28.5) | 123 (100) | 95 (74.2) | 33 (25.8) | 128 (100) |
Week 30, n (%) | ||||||
Class I | 52 (42.3) | 9 (7.3) | 61 (49.6) | 24 (18.8) | 3 (2.3) | 27 (21.1) |
Class II | 33 (26.8) | 19 (15.4) | 52 (42.3) | 61 (47.7) | 13 (10.2) | 74 (57.8) |
Class III | 1 (0.8) | 7 (5.7) | 8 (6.5) | 9 (7.0) | 16 (12.5) | 25 (19.5) |
Missinga | 2 (1.6) | 0 | 2 (1.6) | 1 (0.8) | 1 (0.8) | 2 (1.6) |
NYHA = New York Heart Association.
Note: Baseline is defined as the last nonmissing measurement before the first dose of study drug. All assessments are summarized by analysis visits per SAP.
aMissing NYHA class at week 30 was imputed using available NYHA at week 26.
Source: Clinical Study Report for EXPLORER-HCM trial.18
Figure 8: Differences in Primary Efficacy Outcome Across Subgroups in the VALOR-HCM Trial
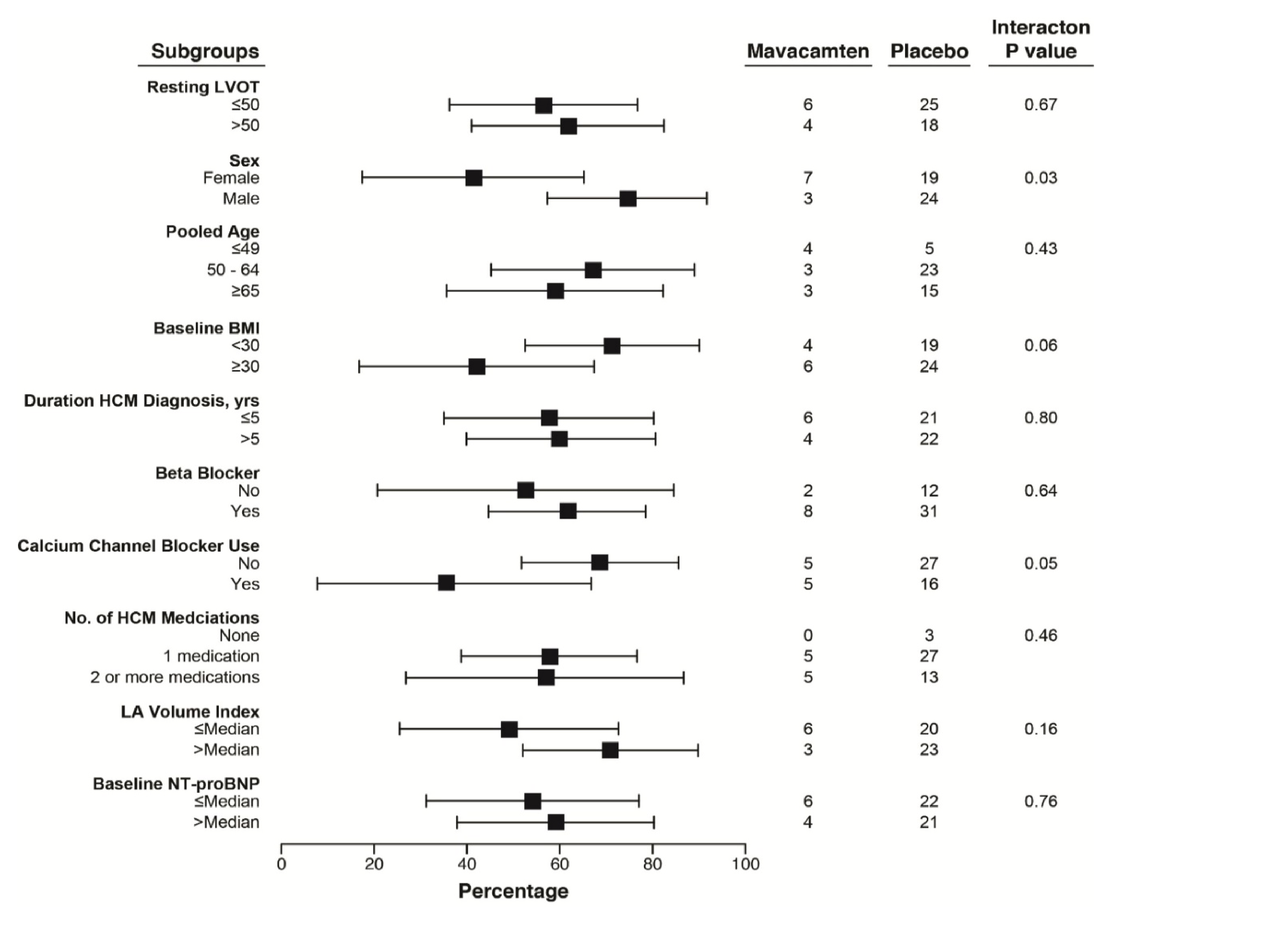
BMI = body mass index; HCM = hypertrophic cardiomyopathy; LA = left atrium; LVOT = left ventricular outflow tract; NT-proBNP = N-terminal pro–B-type brain natriuretic peptide.
Source: Desai et al. (2022).17
Table 35: Sensitivity Analyses for the Primary Composite End Point in the VALOR-HCM Trial
Characteristic | Mavacamten (n = 56) | Placebo (n = 56) | Treatment difference (95% CI) |
|---|---|---|---|
Alternative definition for primary end pointa | 35 (62.5) | 55 (98.2) | 35.7 (22.6, 48.9) |
Patient decision to proceed with SRT | 2 | 2 | |
Maximum LVOT ≥ 50 mm Hg, OR | 22 | 50 | |
No improvement in NYHA functional class | 19 | 40 | |
Need for SRT as determined by Investigator on case report form | 32 (57.1) | 52 (92.9) | NR |
CI = confidence interval; LVOT = left ventricular outflow tract; NR = not reported; NYHA = New York Heart Association; SRT = septal reduction therapy.
aPatients considered to meet primary end point if they meet criteria “Patient decision to proceed with SRT” and/or criteria “maximum LVOT ≥ 50 mm Hg.” These are not mutually exclusive.
Source: Desai et al. (2022).17
Table 36: Change From Baseline to Week 30 in Cardiac MRI Parameters in the EXPLORER-HCM Trial (CMR Substudy Population)
Characteristic | Mavacamten (N = 17) | Placebo (N = 18) | |
|---|---|---|---|
LVMI (g/m2) | |||
Number of patients contributing to the analysis | 17 | 18 | |
Baseline score, mean (SD) | 95 (29.6) | 101 (21.9) | |
Change from baseline to week 30, mean (SD) | −17 (12.0) | −2 (7.4) | |
LS mean difference vs. placebo (95% CI)a | −16 (−22.6 to −9.0) | ||
P valuea | < 0.0001b | ||
Global LV maximum wall thickness (mm) | |||
Number of patients contributing to the analysis | 17 | 18 | |
Baseline score, mean (SD) | 18 (4.3) | 19 (3.9) | |
Change from baseline to week 30, mean (SD) | −2 (2.5) | −0.04 (1.9) | |
LS mean difference vs. placebo (95% CI)a | −2 (−3.9 to −0.9) | ||
P valuea | 0.0079b | ||
LAVI maximum (mL/m2) | |||
Number of patients contributing to the analysis | 17 | 18 | |
Baseline score, mean (SD) | 52 (13.1) | 73 (28.5) | |
Change from baseline to week 30, mean (SD) | −11 (10.6) | −0.4 (5.3) | |
LS mean difference vs. placebo (95% CI)a | −10 (−16.0 to −4.6) | ||
P valuea | 0.0004b | ||
CI = confidence interval; LAVI = left atrial volume index; LS = least squares; LV = left ventricular; LVMI = left ventricular mass index; LVOT = left ventricular outflow tract; SD = standard deviation.
||||| ||||||||| ||||||||| |||||||||||| ||||||||| ||||||||||| |||||||||||||||
bP value has not been adjusted for multiple testing (i.e., the type I error rate has not been controlled).
Source: Clinical Study Report for EXPLORER-HCM trial.18
|||||||| |||||| | |||||||||||||||||| | ||||||||||||||| |
|---|---|---|
|||| |||||||||||||||| ||| | |||||| | |||||| |
||||||||| |||| |||||||||||||||| |||| | |||||| | |||||| |
|||||||||||||||||| | |||||| | |||||| |
||||||| | |||||| | |||||| |
|||||||||||||||||||| | |||||| | |||||| |
|||||||| |||| |||||||||||||||| ||| ||||||||| | |||||| | |||||| |
|||||||| |||| |||||||||||||||| ||| |||||||||||||||| | |||||| | ||| ||| |
|||||||||||||||| |||||||| | |||||| | |||||| |
|||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| |||||||||||||| |||| |||||||||||||||| ||| ||||||||||||||||||| ||||||||||||| ||||||||||||| |||||||||||| ||||||||||||||||||| ||||||||| |||||||| |||||||||||| ||||||||||||| ||||||||||||||||||||| ||||||||||||||| |||||||| ||||||||||||||| ||||||||||||| ||||||||||||| ||||||||||| ||||||| |||||||||||||| ||||||| |||| |||||||||||||||| |||||| |||||||||||| ||||||||||| ||||||||||||| |||||||||||||||| ||||||||||||||| ||||||||||||| |||||||||||||||||||||| ||||||| ||||||||| |||| ||||||||||||||||||| ||||||||||||||||||| ||||||||||||| ||||||||||||| |||||||||| |||||||||||| |||||||
This table was redacted due to confidential information.
Appendix 4: Description and Appraisal of Outcome Measures
Note that this appendix has not been copy-edited.
Aim
To describe the following outcome measures KCCQ and EQ-5D-5L and review their measurement properties including validity, reliability, responsiveness to change, and MID:
Kansas City Cardiomyopathy Questionnaire
5-Level EQ-5D
Hypertrophic Cardiomyopathy Symptom Questionnaire
Findings
Table 38: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
KCCQ questionnaire | The KCCQ is a self-administered, 23-item, disease-specific health-related quality of life questionnaire.20 The KCCQ questionnaire quantifies physical limitations, symptoms, social limitation, self-efficacy and knowledge, social limitation, and quality of life. | For HF patients Validity: Convergent validity was demonstrated through correlation of the KCCQ domain and summary scores with a variety of external indicators of clinical status. Overall, strong to moderate correlations were found for the KCCQ TSS, KCCQ-os, the KCCQ-cs, KCCQ-PLS, KCCQ QoL scores (range, 0.65 to 0.64).24-26,28,38 The KCCQ individual domains were also assessed for convergent validity and presented a variety of strength of correlations which are further described in-text. Concurrent validity for the KCCQ domains was demonstrated by a moderate level of agreement between the KCCQ domains and MLHFQ of clinical status (Cohen kappa statistic = 0.36).24 Reliability: Internal consistency reliability was demonstrated in a number of studies where the KCCQ summary scores, and KCCQ domains (with the exception of the self-efficacy domain) had Cronbach alpha values > 0.7.20,23-25,27 Test-retest reliability has been demonstrated (ICC > 0.7) for the KCCQ symptom domain, physical limitation domain, and social limitation domain, but not for the KCCQ self-efficacy and QoL domains (ICC < 0.7).20,25,30 Responsiveness: High responsiveness of the KCCQ domains, the KCCQ-cs, and the KCCQ-os was found when the external indicators of clinical status were NYHA class, MLHFQ, the SF-36, and the 6MWD.20 The KCCQ-os, and the KCCQ-cs were not responsive to changes in NT-proBNP levels.24 For patients with HCM Validity: The cross-sectional comparisons demonstrated highly statistically significant correlations at baseline (P < 0.0001). The HCMSQ cardiovascular symptoms domain demonstrated a less strong association with the KCCQ-os, KCCQ-cs, and KCCQ total symptom scores (range: –0.53 to –0.57) compared to the shortness of breath (range: –0.68 to –0.70) or tiredness (range: –0.65 to –0.68) scores. However, it showed a stronger association with the KCCQ domains compared to the NYHA functional class (range: –0.43 to –0.45). The correlation between changes at 30 weeks in scores with the HCMSQ cardiovascular symptoms scale, which includes concepts not captured in the KCCQ, was –0.59 (P < 0.0001) for the KCCQ-os score.39 Reliability: The Cronbach alpha values were high for each KCCQ domain, ranging from 0.78 for the physical limitation scale to 0.93 for the overall summary scale, demonstrating good internal reliability. For the test-retest reliability, only 35 patients reported being stable between weeks 0 and 6 on both the PGIC and PGIS, whereas the mean difference in their scores was < 2.3 points for all scales (P > 0.30), with ICCs ranging from 0.63 to 0.82. Total 121 patients reported no change on their PGIS between weeks 18 and 30, with mean differences reported to be < 1.1 points for all scales (P > 0.27), with ICCs ranging from 0.77 to 0.90.39 Responsiveness: The results demonstrated the sensitivity of the KCCQ instrument to the magnitude of clinical changes reported by patients on the PGIC at 6 weeks. For example – for the overall summary domain, those who reported that they were “very much improved” on the PGIC (n = 12) and those who reported that they were “much improved” on the PGIC (n = 41) had mean increases in KCCQ scores of 26.9 ± 15.5 points and 11.9 ± 14.1 points, respectively. Those reporting that they were “minimally improved” (n = 55) demonstrated a mean of 5.6 ± 11.5 points, whereas those reporting “no change” (n = 54) and “worsening health” (n = 9) showed mean changes of −0.8 ± 9.6 and −5.8 ± 12.5-point changes (p value for trend < 0.0001).39 | For HF patients The MID of the KCCQ-os and the KCCQ-cs were evaluated with 2 anchor-based methods in patients with HF. Estimates were approximately 5-points for the KCCQ-os, 5-points for the KCCQ TSS, and 6-points for the KCCQ-cs.30 When the anchor used to assess the MID of KCCQ-os was assessment of clinical change by a cardiologist using a validated Likert scale, an MID of 5.7 points was calculated.40 In patients with HFrEF, when the PGA was used as the clinical anchor, at weeks 4 and 24, the MID estimates for improvement were 3.6 (95% CI, 1.0 to 6.2) and 4.3 (95% CI, 0.2 to 0.4) for the KCCQ-os score, 4.5 (95% CI, 1.8 to 7.2, and 4.5 (95% CI, 0.2 to 8.4) for the KCCQ-cs score, and 4.7 (95% CI, 1.4 to 8.0) and 4.9 (95% CI, −0.9 to 9.0) for the KCCQ-PLS, respectively. The MID estimates for deterioration were −0.4 (95% CI,−8.6 to 7.7) and −5.0 (95% CI, −15.5 to 5.6) for the KCCQ-os, 1.4 (95% CI, −7.1 to 10.0) and −1.1(95% CI, −11.7 to 9.4) for the KCCQ-cs and, 1.8 (95% CI, −9.1 to 12.7) and −1.7 (95% CI, −14.8 to 11.2) for the KCCQ-PLS at week 4 and 24, respectively.28 In patients with HFpEF, a median change in KCCQ-PLS of ≥ 8.33 points may represent the MID for improvement and a median change of ≤ −4.17 points may suggest deterioration.41 For patients with HCM The mean changes observed in the KCCQ domains in patients with HCM with minimally improved, much improved, and large clinical changes were consistent and very close with the 5-, 10-, and 20-point mean differences observed in a study explicitly designed to estimate the minimal clinically important difference in scores for patients with HFrEF,40 suggesting the standards for interpreting the KCCQ to be applicable for patients with oHCM.39 |
EQ-5D-5L | A generic preference-based HRQoL instrument consisting of a composite index score of 5 dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression and a VAS. | There was no evidence of validity, reliability, and responsiveness of this outcome in patients with HF or HCM/oHCM. | A 3-point difference in the EQ VAS is clinically meaningful in HF patients.30 No evidence of MID was found for patients with oHCM. |
Hypertrophic Cardiomyopathy Symptom Questionnaire (HCMSQ) | A new PRO measure, developed and evaluated specifically for patients with HCM. The questionnaire was included in the EXPLORER-HCM and MAVERICK-HCM clinical trials as 11-item PRO instrument evaluating the core symptoms of HCM. The scoring algorithm is divided into 4 domains - shortness of breath, tiredness, cardiovascular symptoms, and syncope; along with a total score, with higher scores indicating more severe symptoms.33 | Validity: For convergent validity, moderate correlations (e.g., HCMSQ shortness-of-breath and KCCQ-23 clinical summary score ranging from −0.72 to −0.71) were observed between the HCMSQv1.0 scores for cardiovascular symptoms, tiredness, shortness of breath, and total score, and the conceptually similar or related KCCQ-23 domains and summary scores and those in the EQ-5D-5L visual analogue scale. Content validity was evaluated through the cognitive interviews and the exit interviews. While the cognitive interviews with patients with HCM established the preliminary content validity of the 11 items of the HCMSQv1.0 instrument, the exit interviews supported the integrity of the content validity with the exception of item 5.33 Reliability: The shortness-of-breath domain and total scores demonstrated good internal consistency in the MAVERICK-HCM trial, with Cronbach alpha (standardized) values of 0.924 and 0.811, respectively. However, the cardiovascular symptoms domain did not show good internal consistency in the MAVERICK-HCM trial, with Cronbach alpha value of 0.586. All domain and total scores demonstrated good internal consistency in the EXPLORER-HCM trial, with Cronbach alpha values of 0.795, 0.962, and 0.924 for cardiovascular symptoms domain, shortness-of-breath domain, and total score, respectively.33 The intraclass correlation between HCMSQv1.0 scores at baseline and at week 6 in patients reporting the same global impression of symptoms on the PGIC and PGIS scales ranged from 0.829 to 0.865 and from 0.746 to 0.815, respectively in both trials. This demonstrated strong evidence of test-retest reliability (intraclass correlation coefficient > 0.70) for all domains and total scores.33,42 Responsiveness: Scores for tiredness, shortness-of-breath, and total symptoms demonstrated a statistically significant change, but not the score for cardiovascular symptoms. Moreover, the HCMSQv1.0 scores demonstrated responsiveness for shortness-of-breath when using both the PGIC and PGIS, and for tiredness and total symptoms when using the PGIC.33 | Based on the responder-definition estimates data from the MAVERICK-HCM and EXPLORER-HCM trial datasets, a clinically meaningful responder-definition range of 1 to 2 points were selected for the HCMSQv1.0 shortness of breath and total symptom scores, and approximately 1 point for the tiredness and cardiovascular symptom scores.33 |
6MWD = 6-minute walk distance; EQ-5D-5L = 5-Level EQ-5D; EQ VAS = EQ visual analogue scale; HCM = hypertrophic cardiomyopathy; HCMSQ = Hypertrophic Cardiomyopathy Symptom Questionnaire; HF = heart failure; HFpEF = HF with preserved ejection fraction; HFrEF = HF with reduced ejection fraction; HRQoL = health-related quality of life; ICC = intraclass correlation coefficient; QoL = quality of life; KCCQ = Kansas City Cardiomyopathy Questionnaire; KCCQ-cs = KCCQ clinical summary; KCCQ-os = KCCQ overall summary ; KCCQ-PLS = physical limitation score; KCCQ TSS = KCCQ total symptom score; MID = minimal important difference; MLHFQ = Minnesota Living with Heart Failure Questionnaire; NT-proBNP = N-terminal pro–B-type natriuretic peptide; NYHA = New York Heart Association; oHCM = obstructive hypertrophic cardiomyopathy; PGA = Patient Global Assessment; PGIC = Patient Global Impression of Change; PGIS = Patient Global Impression of Severity; PRO = patient-reported outcome; QoL = quality of life; SCHFI = Self Care Heart Failure Index; SF-36 = Short Form (36) Health Survey.
Kansas City Cardiomyopathy Questionnaire
Description and Scoring
The KCCQ is a self-administered, 23-item, disease-specific HRQoL questionnaire that was originally developed in 2000 to measure the patient’s perception of their health status within a 2-week recall period.20-22 The items of the KCCQ can be categorized into the following domains: physical limitation, symptoms (frequency, severity, and recent change over time), social limitation, self-efficacy, and HRQoL. Responses are scored using ordinal values, beginning with 1 for the response that implies the lowest level of functioning. Domain scores are transformed to a 0 to 100 range by subtracting the lowest possible scale score, dividing by the range of the scale, and multiplying by 100. Missing values within each domain are assigned the average of the answered items within the same domain.20,22 Various combinations of the KCCQ domains create 3 KCCQ summary scores including the KCCQ TSS, CSS, and OSS. The KCCS TSS combines the symptom burden and symptom frequency domains and evaluates patient-reported swelling in feet, ankles, or legs, fatigue, shortness of breath, and disturbed sleep.23 The KCCQ-cs includes the physical limitation and total symptom domains, and the KCCQ-os combines the physical limitation, total symptom, social limitation, and HRQoL domains into a single score. Summary scores are then transformed to a 0 to 100 range, where larger scores represent a better outcome: 0 to 24: very poor to poor; 25 to 49: poor to fair; 50 to 74: fair to good; and 75 to 100: good to excellent.20,22
Assessment of Validity, Reliability, and Responsiveness
Validity
The KCCQ was originally validated in patients with a clinical diagnosis of congestive heart with reduced LVEF (< 40%).20 A cohort of patients (N = 39; mean age 64 years; 69% male; mean NYHA class = 2.0 ± 0.59) with stable disease was used to assess the validity of the KCCQ. Convergent validity was demonstrated through a strong correlation of the KCCQ physical limitation domain with NYHA classification (Spearman’s correlation coefficient r = –0.65) and Minnesota Living with Heart Failure Questionnaire (MLHFQ)Physical (r = 0.65), and a moderate correlation with the 6-minute walk distance (6MWD) (r = 0.48). The quality of life domain were strongly correlated with NYHA classification (r = −0.64). The social limitation domain was strongly correlated with NYHA classification and the 36-item Short Form Survey (SF-36) social limitation scale (r = 0.62). No adequate criterion standard was available for the self-efficacy domain.20
Convergent validity has also been assessed in a variety of other publications.24-28 Napier et al.,24 assessed convergent validity in patients with HF with preserved ejection fraction (HFpEF) (n = 110). The KCCQ OSS, KCCQ CSS and KCCQ physical limitation score (PLS) showed moderate correlations with NYHA class (I to IV) and the 6MWD (range of Spearman rank order correlation coefficient, r = –0.38 to 0.47; P < 0.001, for each). The KCCQ quality of life (KCCQ QoL) score was weakly correlated with NYHA functional class (r = –0.28; P = 0.003) and 6MWT (r = 0.19; P = 0.04). The KCCQ self-efficacy score was not correlated with NYHA functional class (r = –0.10; P = 0.30) or 6MWT (r = –0.02; P = 0.87). These findings were corroborated in patients with HF with reduced ejection fraction (HFrEF) with regard to the convergent validly of KCCQ-os in the FAIR-HF trial (N = 459). There were moderate correlations between the Patient Global Assessment (PGA) and the KCCQ-os score (r = 0.31; P < 0.001, and r = 0.42; P < 0.001), the KCCQ-cs score (r = 0.36; P < 0.001, and r = 0.42; P < 0.001), and the KCCQ-PLS (r = 0.31; P < 0.001, and r = 0.39; P < 0.001) at 4 and 24 weeks, respectively.28 Similar findings were observed in a publication assessing the convergent validity of the KCCQ-PLS in a population of patients with HFpEF in the VITALITY-HFpEF trial (N = 698). There were moderate correlations between the Patient Global Impression of Change (PGIC) and the KCCQ-PLS (r = 0.28, and r = 0.31, at week 12, and 24, respectively).41 Convergent validity was further analyzed in a cohort of patients with stable compensated HF (N = 41; mean age = 68 ± 12 years; 100% male). The KCCQ TSS moderately correlated (r = 0.30) with peak VO2.26 This evidence bundle presented supports the presence of convergent validity of the KCCQ OSS, and the TSS. However, in a publication by Tucker et al.,27 the authors assessed the presence of convergent validity in a population of patients hospitalized with chronic HF (N = 233). The authors found no evidence of convergent validity, when the KCCQ domain scores and summary scores (KCCQ-os and KCCQ-cs) were correlated with NYHA class (either class III or IV), brain natriuretic peptide levels, and the Charlson Comorbidity Index scores. The authors explain that this may be due to the presence of an alternate population in the current study compared to previous studies analyzing the convergent validity of the KCCQ.27 Nevertheless, these findings taken together support the presence of convergent validity for the KCCQ-os, KCCQ-PLS, and the TSS.
Concurrent validity of the KCCQ was assessed by administration of the KCCQ and the Minnesota Living with MLHFQ to patients with heart failure with preserved ejection fraction (N = 110) at baseline, 6 weeks, and 12 weeks in the Nitrate Effect on Activity Tolerance in Heart Failure (NEAT) trial. The level of agreement of change was moderate (Cohen kappa statistics, 0.36; 95% CI, 0.2 to 0.52), supporting the presence of concurrent validity.24
Validity of the KCCQ was assessed in 196 HCM participants from the EXPLORER-HCM trial.39 The content validity of the KCCQ was evaluated in 26 US patients with oHCM, who were not enrolled in an HCM trial, through qualitative interviews. Construct validity was evaluated by demonstrating an association between each KCCQ domain and other measures of similar constructs, where each domain went through a comparison test with the best available criterion standard for that domain. Spearman Correlation coefficients were used to measure the correlations.39
While evaluating the construct validity, first, at baseline, the KCCQ summary scores (KCCQ-os, KCCQ-cs, and KCCQ total symptom scores) were compared with the NYHA functional class, as well as compared with the HCMSQ shortness of breath, tiredness, and cardiovascular symptoms domains. The aim was to observe how well the scores had correlated with symptoms not directly captured by the KCCQ. Moreover, changes in scores based on symptoms not captured in the KCCQ-os score were validated by measuring changes between this score with changes at 30 weeks in the HCMSQ cardiovascular symptoms score. In addition, KCCQ-os and KCCQ-cs were compared with exercise duration and pVO2 values on baseline CPET testing. Other measurements include comparisons between KCCQ physical limitation scores with NYHA functional class, and with exercise duration and pVO2 values on baseline CPET testing; KCCQ quality of life scores with EQ-5D visual analogue scale at baseline; and KCCQ social limitation scores with the WPAI at baseline, which was the best available measure for this construct. The cross-sectional comparisons demonstrated highly statistically significant correlations at baseline (P < 0.0001). The HCMSQ cardiovascular symptoms domain demonstrated a less strong association with the KCCQ-os, KCCQ-cs, and KCCQ total symptom scores (range, −0.53 to −0.57) compared to the shortness of breath (range, −0.68 to −0.70) or tiredness (range, −0.65 to −0.68) scores. However, it showed a stronger association with the KCCQ domains compared to the NYHA functional class (range, −0.43 to −0.45). The correlation between changes at 30 weeks in scores with the HCMSQ cardiovascular symptoms scale, which includes concepts not captured in the KCCQ, was −0.59 (P < 0.0001) for the KCCQ-OS score.39
Reliability
The internal consistency reliability of the KCCQ domains and summary scores (KCCQ-os and KCCQ-cs) has been assessed in several studies and has demonstrated consistent results across all studies.20,23-25,27 In a number of publications, the KCCQ domains, with the exception of the self-efficacy domain has consistently presented Cronbach alpha values > 0.7.20,23,24,27 The KCCQ self-efficacy domain has been evaluated in a number of studies, and has demonstrated Cronbach alpha values in the range of 0.61 to 0.63,20,23 with 1 publication calculating the Cronbach alpha value greater than 0.7 for this domain.27 The KCCQ-cs, KCCQ- os, and KCCQ TSS have demonstrated Cronbach alpha values greater than 0.7, 0.93 to 0.95, and 0.8, respectively.20,24 Lastly, these findings were confirmed in a meta-analysis performed by Garin et al., where Cronbach alpha values were greater than 0.7 for all KCCQ domains, with the exception of the self-efficacy domain (Cronbach alpha = 0.62 to 0.66).25
Test-retest reliability of the KCCQ has been evaluated in multiple studies.20,25,30 In the original paper evaluating the KCCQ, among those with stable HF who remained stable (N = 39), mean changes in KCCQ domains and summary scores (KCCQ-os and KCCQ-cs) over the 3 months of observation were 0.8 to 4.0 points, none of which were statistically significant.20 A meta-analysis which summarized the test-retest reliability of the KCCQ domains found an acceptable ICC of greater than 0.7 for the KCCQ symptom domain, the physical limitation domain, and the social limitation domain, but an ICC < 0.7 for the KCCQ self-efficacy, and the quality of life domains.25 Furthermore, in a cohort of 280 patients with chronic stage-C HF, test-retest reliability was assessed at baseline and at 6 months, and ICC > 0.7 were demonstrated for the physical limitation domain, and the symptom domain, but not for the self-efficacy domain.23 Taken together, these findings suggest that the KCCQ symptom, physical limitation, and social limitation domains have acceptable test-retest reliability, while the KCCQ self-efficacy and quality of life domains do not demonstrate acceptable test-retest reliability.
Internal reliability and test-retest reliability were assessed for patients with HCM in the EXPLORER-HCM trial.39 To assess the internal reliability in the EXPLORER-HCM population, Cronbach alpha was measured for each KCCQ domain at baseline, with > 0.70 value representing good internal reliability. Test-retest reliability was evaluated in clinically stable patients by assessing the reproducibility of each scale through a paired Student’s t-test of change in KCCQ scores. Two external constructs were used to define clinically stable patients – by examining the changes in each KCCQ domain among patients who reported both no change between baseline and 6 weeks in the PGIC, and by examining patients whose PGIS assessments were the same at both baseline and 6 weeks. The changes in scores between 18 and 30 weeks were also examined due to the probability of a greater change in early phase after enrolment. Since the PGIC refers to change from baseline and not from the most recent assessment, patients without a change in the PGIS between weeks 18 and 30 were considered clinically stable and were included in the analysis.39
The Cronbach alpha values were high for each KCCQ domain, ranging from 0.78 for the physical limitation scale to 0.93 for the overall summary scale, demonstrating good internal reliability. For the test-retest reliability, only 35 patients reported being stable between weeks 0 and 6 on both the PGIC and PGIS, whereas the mean difference in their scores was < 2.3 points for all scales (P > 0.30), with ICCs ranging from 0.63 to 0.82. Total 121 patients reported no change on their PGIS between weeks 18 and 30, with mean differences reported to be < 1.1 points for all scales (P > 0.27), with ICCs ranging from 0.77 to 0.90.39
Responsiveness
In the original study validating the KCCQ, a cohort of patients with HF, which were admitted to the hospital for HF exacerbations were used to assess the responsiveness of the KCCQ. The KCCQ exhibited high responsiveness, with Guyatt’s responsiveness statistics ranging from 0.62 for the social limitation domain to 3.19 for the symptoms domain, and was specifically 2.77 for the KCCQ-cs and 1.74 for the KCCQ-os.20 Another study evaluated the responsiveness of the KCCQ in patients with stable chronic heart failure with preserved ejection fraction (N = 110). None of the KCCQ domains were responsive to changes in NT-proBNP. Of the KCCQ scores evaluated, the KCCQ-os and the KCCQ-cs were ranked as the most responsive to improvement, and deterioration in distance walked in the 6MWD, respectively.24 These findings were corroborated in a study completed by Eurich et al. which evaluated the responsiveness of the KCCQ-cs and the KCCQ-os in a cohort of patients with HF (N = 298). Irrespective of the responsiveness index used, the KCCQ-cs and the KCCQ-os were consistently ranked as the most responsive measures.29 Furthermore, a meta-analysis which evaluated the responsiveness of 5 domains of the KCCQ (physical limitation, social limitation, symptom, HRQoL, and self-efficacy) produced very large effect sizes (from 0.6 to 3.2), indicating high responsiveness of the KCCQ domains.25 Taken together these findings indicate that the KCCQ domains and the KCCQ summary scores exhibit evidence of high responsiveness to change.
Responsiveness for KCCQ was assessed for patients with HCM in the EXPLORER-HCM trial.39 The 6-week PGIC was used as a global ranking of participants’ perceived changes in their health status for defining clinical change. To compare change in health status across the categories analysis of variance linear trend tests were used. Similar findings were reported for all KCCQ domains. For example, for the overall summary domain, those who reported that they were “very much improved” on the PGIC (n = 12) and those who reported that they were “much improved” on the PGIC (n = 41) had mean increases in KCCQ scores of 26.9 ± 15.5 points and 11.9 ± 14.1 points, respectively. Those reporting that they were “minimally improved” (n = 55) demonstrated a mean of 5.6 ± 11.5 points, whereas those reporting “no change” (n = 54) and “worsening health” (n = 9) showed mean changes of −0.8 ± 9.6 and −5.8 ± 12.5-point changes (p value for trend < 0.0001). The results demonstrated the sensitivity of the KCCQ instrument to the magnitude of clinical changes reported by patients on the PGIC at 6 weeks.39
Minimal Important Difference
Baseline data from a large RCT (HF-ACTION; N = 2331; mean age = 59.1 years; 71.6% male; 63.4% NYHA class II, 35.7% class III, and 1% class IV) were used to examine associations between the KCCQ domain and summary scores, and clinical indicators of disease severity, including the 6MWD and pVO2.30 In this study, a 1-SD difference in 6MWD and pVO2 was found to be associated with an approximately 5-point difference in the KCCQ OSS, a 6-point difference in the KCCQ CSS, and a 5-point difference in the KCCQ TSS. The authors considered a 1-SD difference in 6MWD and pVO2 to represent a meaningful difference in patients with HF, citing that it is a more stringent criterion used for these indicators than previous studies.30 This finding was corroborated when the KCCQ-os was associated with clinical change as assessed by a cardiologist (15-point Likert scale, from extremely worse to extremely better and grouped into categories of change) in a study (N = 476; mean age = 61 years; 75% male; 11% NYHA class I, 41% class II, 44% class III, and 5% class IV) in patients with HF and an ejection fraction < 40%.40 When the KCCQ-os score was administered at baseline and at 6 weeks, a mean improvement of 5.7 points in the KCCQ-os was associated with a small improvement in HF. A mean decrease of 5.4 points in the KCCQ-os was associated with a small deterioration in HF.40 Furthermore, the minimal clinically important difference (MCID) for various KCCQ domain scores was evaluated in the FAIR-HF trial (N = 459) in patients with HFrEF, using PGA scale as an anchor at 4 and 24 weeks.28 At week 4, all of the KCCQ domains had less than 5-point MID based on “little improvement” in PGA. At week 4 and 24, the MCID estimates for improvement were 3.6 (95% CI, 1.0 to 6.2) and 4.3 (95% CI, 0.2 to 0.4) for the KCCQ-os, 4.5 (95% CI, 1.8 to 7.2) and 4.5 (95% CI, 0.2 to 8.4) for the KCCQ-cs, and 4.7 (95% CI, 1.4 to 8.0) and 4.9 (95% CI, −0.9 to 9.0) for the KCCQ-PLS, respectively.28 With regards to patients who reported a slight worsening in their condition, MCID estimates for deterioration were −0.4 (95% CI, −8.6 to 7.7) and −5.0 (95% CI, −15.5 to 5.6) for the KCCQ-os, 1.4 (95% CI, −7.1 to 10.0) and −1.1 (95% CI, −11.7 to 9.4) for the KCCQ-cs, 1.8 (95% CI, −9.1 to 12.7) and −1.7 (95% CI, −14.8 to 11.2) for the KCCQ-PLS, at weeks 4 and 24, respectively.28 In patients with HFpEF, the MID for KCCQ-PLS for improvement or worsening were estimated in the VITALITY-HFpEF trial. The study used an anchor-based approach utilizing PGIC as an anchor and reported that a median change in KCCQ-PLS of more or equal to 8.33 points (corresponding to an improvement in ≥ 2 response categories of KCCQ-PLS) may represent the MID for improvement and a median change of ≤ −4.17 points (corresponding to a worsening in ≥ 1 response category of KCCQ-PLS) may suggest deterioration in patients with HFpEF.41
The mean changes observed in the KCCQ domains in patients with HCM with minimally improved, much improved, and large clinical changes were consistent and very close with the 5-, 10-, and 20-point mean differences observed in a study explicitly designed to estimate the minimal clinically important difference in scores for patients with HFrEF,40 suggesting the standards for interpreting the KCCQ to be applicable for patients with oHCM.39
5-Level EQ-5D
Description and Scoring
The EQ-5D-5L is a generic self-reported HRQoL outcome measure that may be applied to a variety of health conditions and treatments. The EQ-5D-5L was developed by the EuroQol Group as an improvement to the 3-Level EQ-5D to measure small and medium health changes and reduce ceiling effects.31,32 The instrument comprises 5 dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Each dimension is rated on 5 levels: level 1 “no problems,” level 2 “slight problems,” level 3 “moderate problems,” level 4 “severe problems,” and level 5 “extreme problems” or “unable to perform.”31,32 A total of 3,125 unique health states are possible, with 55555 representing the worst health state and 11111 representing the best state. The corresponding scoring of EQ-5D-5L health states is based on a scoring algorithm that is derived from preference data obtained from interviews using choice-based techniques (e.g., time trade-off) and discrete choice experiment tasks.31,32 The lowest and highest score vary depending on the scoring algorithm used. Scores less than 0 represent health states that are valued by society as being worse than dead, while scores of 0 and 1.00 are assigned to the health states “dead” and “perfect health,” respectively. As an example, a Canadian scoring algorithm results in a score of −0.148 for health state 55555 (worst health state) and a score of 0.949 for health state 11111 (best health state).31,32 Another component of the EQ-5D-5L is a visual analogue scale (EQ VAS), which asks respondents to rate their health on a visual scale from 0 (worst health imaginable) to 100 (best health imaginable).31,32
Assessment of Validity, Reliability, and Responsiveness
The literature search completed by CADTH did not find any evidence on the validity, reliability, responsiveness, and MID of the EQ-5D-5L questionnaire in patients with HF and/or HCM. However, there is evidence for these metrics for the EQ-5D-3L questionnaire and the EQ VAS in patients with HF. Since this is an exploratory outcome for the EMPEROR-Reduced and EMPEROR-Preserved trials under review, CADTH will provide a high-level summary of the EQ-5D-3L and the EQ VAS in a heart failure population.
The discriminant validity of the EQ-5D-3L was determined in a North American cohort study (N = 476) in patients with HF and an ejection fraction less than 40%.40 The EQ-5D index and VAS c-statistic ranged from 0.56 and 0.58 for small clinical improvements, to 0.69 and 0.76 for moderate to large improvements.40 From this study, the EQ-5D-3L was found to show less discriminative abilities than the KCCQ and NYHA class, but similar discriminative abilities to the 12-item Short Form Survey (SF-12). In addition, the EQ-5D and SF-12 did not exhibit much sensitivity to the magnitude of observed clinical change.40
The responsiveness of the EQ-5D-3L was compared with the KCCQ and SF-12 in patients with HF and an ejection fraction less than 40% (N = 298).29 Patients were administered questionnaires at baseline and 6 weeks in addition to a 6MWD. Overall, the EQ-5D index and VAS were less responsive than the KCCQ, but showed similar responsiveness to the SF-12.29
A systematic review of studies looking at the validity and reliability of the EQ-5D-3L in patients with cardiovascular disease identified 10 studies.43 When EQ-5D-3L scores were stratified by disease severity in the HF studies, the mean EQ-5D index scores decreased from 0.78 (SD 0.18) for mild states to 0.51 (SD 0.21) for moderate/severe health states.43
Minimal Important Difference
Baseline data from a large RCT (HF-ACTION trial; N = 2,331) were used to examine associations between the EQ VAS and clinical indicators of disease severity, including the 6MWD and pVO2.30 In this study, a 1-SD difference in 6MWD and pVO2 was found to be associated with an approximate 3-point difference in the EQ- VAS. The 1-SD change in 6MWD and pVO2 used in the present study is considered a clinically meaningful difference to patients with HF, and is a more stringent criterium than typically used in previous studies.30 Moreover, a Canadian-specific MID of 0.037 has been reported for the EQ-5D-5L.31,32
Hypertrophic Cardiomyopathy Symptom Questionnaire
Description and Scoring
HCM Symptom Questionnaire version 1.0 (HCMSQv1.0) is a new patient-reported outcome (PRO) measure, developed and evaluated specifically for patients with HCM.33 The questionnaire was included in the EXPLORER-HCM and MAVERICK-HCM clinical trials as 11-item PRO instrument evaluating the core symptoms of HCM from the conceptual model.33
Initially drafted based on a conceptual model published by Zaiser et al.,44 the HCMSQ instrument was refined later through cognitive interviews conducted between 2017 and 2019 with 33 patients with HCM. These patients were recruited in the US, Italy, France, and the UK, and 16 of the patients had nHCM and 17 had oHCM. Through the cognitive interviews, the instrument was iteratively developed and debriefed, particularly keeping in mind its relevance and coverage in terms of common HCM symptoms, the interpretation of item language and response options, and the overall understandability of this instrument. The HCMSQ instrument was translated as well as linguistically validated in 16 languages.33
The scoring algorithm for HCMSQv1.0 is divided into 4 domains. These are - shortness of breath, tiredness, cardiovascular symptoms, and syncope; along with a total score, with higher scores indicating more severe symptoms. The instrument has been designed to measure tiredness/fatigue (tiredness domain), dizziness/light-headedness (cardiovascular symptoms domain), heart palpitations (cardiovascular symptoms domain), and chest pain symptoms (cardiovascular symptoms domain) on a single 5-point verbal rating scale, from 0 indicating ‘not at all’ to 5 indicating “very severely.” On the other hand, the shortness of breath domain is measured by 6 items, 4 of which has the same response scale, asking about severity of shortness of breath in 4 scenarios — in general, during light physical activity, during moderate physical activity, and during heavy physical activity. The fifth question for this domain has been designed to ask respondents to describe about their worst shortness of breath (in relation to activity levels) in a scale of 5, where 0 indicates “no shortness of breath” and 4 indicates “short of breath when resting.” The sixth question measures the frequency of shortness of breath in a scale of 5, where 0 indicates “never” and 4 indicates “almost always.” Last, syncope domain is measured on a 2-point categorical rating scale (yes/no). A 24-hour recall period is used for all domains due to the anticipated symptom variability and to limit recall bias.33
Assessment of Validity, Reliability, and Responsiveness
EXPLORER-HCM and MAVERICK-HCM population datasets (both screening and pooled blinded baseline data) were used to evaluate the psychometric measurement properties of the HCMSQv1.0 instrument. A sample size of N = 299 was available for the analyses. Full analysis sets (FAS) were analyzed (EXPLORER-HCM FAS [FAS-E]) and MAVERICK-HCM FAS [FAS-M]) as well. A series of analyses were conducted to characterize the development of the scoring algorithm, which included MMRM, Rasch modelling, exploratory and confirmatory factor analyses, and missing-data simulation analysis.33
Validity
Two types of construct validity — convergent validity and known-groups validity — were assessed for the HCMSQv1.0 instrument with the FAS-M and FAS-E baseline data. Convergent validity was evaluated through the degree of association between the HCMSQv1.0 domain and total scores, KCCQ-23 domain and summary scores,20 and EQ-5D-5L instrument.45 Associations were measured using correlations. Known-groups validity was evaluated to measure the degree to which the HCMSQv1.0 instrument can differentiate between defined groups of patients. These groups of patients were formulated using Patient Global Impression of Severity (PGIS) scores and NYHA class II or III and were compared using analysis of variance. Moderate correlations (e.g., HCMSQ SoB and KCCQ-23 CSS ranging from −0.72 to −0.71) were observed while evaluating convergent validity between the HCMSQv1.0 scores for cardiovascular symptoms, tiredness, shortness of breath, and total score, and the conceptually similar or related KCCQ-23 domains and summary scores (physical limitation, symptom burden, symptom frequency, CSS, quality of life, social limitation, TSS, and OSS) and those in the EQ-5D-5L visual analogue scale. Significant differences were observed by PGIS category for the HCMSQv1.0 scores for tiredness, shortness of breath, and total symptoms as expected in both the EXPLORER-HCM and MAVERICK-HCM trials while evaluating known-groups validity. The only exception was the cardiovascular symptoms score, which was significant only in the EXPLORER-HCM trial. Moreover, while significant differences were not observed among HCMSQv1.0 domain and total scores by NYHA class in MAVERICK-HCM trial, the opposite happened in the EXPLORER-HCM trial, where significant differences were observed by NYHA classification in the HCMSQ scores for tiredness, shortness of breath, and total symptoms, but not for cardiovascular symptoms.33
Content validity was evaluated through the cognitive interviews and the exit interviews. While the cognitive interviews with patients with HCM established the preliminary content validity of the 11 items of the HCMSQv1.0 instrument, the exit interviews supported the integrity of the content validity with the exception of question/item 5, which asked respondents about their worst shortness of breath during the last 24 hours. Since this was a different response scale from the other items, many respondents failed to order this item as intended.33
Reliability
An item-to-item correlation and item-scale analyses were used to evaluate the relationship and degree of association among items and between items and domains at baseline in the FAS-M and FAS-E. If correlations between items in the same domain were at least moderate (i.e., correlation coefficient, r > 0.3), and items showed higher correlations with their respective domains compared with other domains, then items were considered to demonstrate an adequate performance. Results based on day 7 of baseline item scores demonstrated at least moderate (r > 0.3) correlations among the shortness-of-breath items (items 1 to 6) for the MAVERICK-HCM study, along with moderate correlations among SoB items with tiredness and heart palpitations. A lower correlation was observed among SoB items with chest pain and dizziness. On the other hand, results based on baseline weekly scores for item-to-item correlation analysis demonstrated at least moderate (r > 0.3) correlations among the SoB items (items 1 to 6) and tiredness. Results from both the item-to-item correlation and item-scale analyses showed that all items demonstrated the highest correlations with their respective domains compared with other domains. Results were similar for the EXPLORER-HCM trial.33
The internal consistency for each multi-item scale and total score was evaluated with Cronbach alpha, which was calculated using the baseline data taken from the FAS-M and FAS-E. The test-retest reliability was assessed at 2 time points: first, using 2 weeks of screening data, with week 1 being the “test” and week 2 the “retest,” with analyses conducted in both studies using the FAS-M and FAS-E; second, utilizing the baseline (“test”) and week 6 (“retest”) data in MAVERICK-HCM, for the FAS-M only. The SoB domain and total scores demonstrated good internal consistency in the MAVERICK-HCM trial, with Cronbach alpha (standardized) values of 0.924 and 0.811, respectively. However, the cardiovascular symptoms domain did not show good internal consistency in the MAVERICK-HCM trial, with Cronbach alpha value of 0.586. On the other hand, all domain and total scores demonstrated good internal consistency in the EXPLORER-HCM trial, with Cronbach alpha values of 0.795, 0.962, and 0.924 for cardiovascular symptoms domain, SoB domain, and total score, respectively.33
The test-retest reliability of the HCMSQv1.0 instrument was assessed using intraclass correlation of patients with stable PGIC and PGIS responses. The intraclass correlation between HCMSQv1.0 scores at baseline and at week 6 in patients reporting the same global impression of symptoms on the PGIC and PGIS scales ranged from 0.829 to 0.865 and from 0.746 to 0.815, respectively in both trials. This demonstrated strong evidence of test-retest reliability (intraclass correlation coefficient > 0.70) for all domains and total scores.33,42
Responsiveness
The responsiveness of the HCMSQv1.0 instrument was evaluated by analyzing change from baseline to week 16 by treatment status in the MAVERICK-HCM trial. Scores for tiredness, SoB, and total symptoms demonstrated a statistically significant change, but not the score for cardiovascular symptoms. Moreover, the HCMSQv1.0 scores demonstrated responsiveness for SoB when using both the PGIC and PGIS, and for tiredness and total symptoms when using the PGIC.33
Minimal Important Difference
Both distribution-based and anchor-based methods were used to determine meaningful changes. In distribution-based methods, the variability of scores is utilized to determine meaningful change. These methods were used to derive responder definitions for the HCMSQv1.0 scores to determine the threshold of within-patient treatment benefit. It was done for both the MAVERICK-HCM and EXPLORER-HCM trials using FAS-M and FAS-E baseline data. In anchor-based analyses, an external indicator (‘anchor’) reflects patient’s view of change, which is used to determine meaningful change.33
Anchor-based analyses were conducted in the MAVERICK-HCM trial using longitudinal (both baseline and week 16) data, and PGIC and PGIS served as anchors in the analyses. Results from the anchor-based analyses demonstrated a correlation (r > 0.3) among the PGIC at week 16 with change in each HCMSQv1.0 domain score from baseline to week 16 (shortness of breath, tiredness, cardiovascular symptoms, and total symptom), proving to be an appropriate anchor. On the other hand, there was a correlation (r > 0.3) among the change in PGIS from baseline to week 16 with the change in each HCMSQv1.0 score, with an exception for cardiovascular symptoms (r = − 0.17). This led PGIS to be an anchor to define a responder definition only in shortness of breath, tiredness, and total symptom scores, but not in cardiovascular symptoms score.33
Based on the responder-definition estimates data from the MAVERICK-HCM and EXPLORER-HCM trial datasets, a clinically meaningful responder-definition range of 1 to 2 points were selected for the HCMSQv1.0 shortness of breath and total symptom scores, and approximately 1 point for the tiredness and cardiovascular symptom scores. The aim to select these points was to identify individuals who had experienced a significant change in symptoms from baseline in the EXPLORER-HCM trial.33
Pharmacoeconomic Review
Abbreviations
AE
adverse event
CHPA
Canadian Heart Patient Alliance
CIHI
Canadian Institute for Health Information
EQ-5D-5L
5-Level EQ-5D
HR
hazard ratio
ICER
incremental cost-effectiveness ratio
NYHA
New York Heart Association
oHCM
obstructive hypertrophic cardiomyopathy
QALY
quality-adjusted life-year
SRT
septal reduction therapy
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Mavacamten (Camzyos), oral capsules |
Submitted price | Mavacamten, 2.5 mg, 5 mg, 10 mg, and 15 mg: $61.6000 per capsule |
Indication | For the treatment of symptomatic oHCM of NYHA class II to III in adult patients |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | November 8, 2022 |
Reimbursement request | As per indication |
Sponsor | Bristol Myers Squibb |
Submission history | Previously reviewed: No |
NOC = Notice of Compliance, NYHA = New York Heart Association; oHCM = obstructive hypertrophic cardiomyopathy.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Markov model |
Target population | Adult patients with symptomatic NYHA class II or III obstructive hypertrophic cardiomyopathy |
Treatment | Mavacamten plus beta-blockers or calcium channel blockers |
Comparator | Beta-blockers or calcium channel blockers: 73% of patients were assumed to receive beta-blockers (53% metoprolol, 47% bisoprolol) and 23% were assumed to receive calcium channel blockers (50% diltiazem, 50% verapamil) |
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, life-years |
Time horizon | Lifetime (41 years) |
Key data source | EXPLORER-HCM triala |
Submitted results | ICER = $56,774 per QALY (incremental costs: $129,564; incremental QALYs: 2.28) |
Key limitations |
|
CADTH reanalysis results |
|
ICER = incremental cost-effectiveness ratio; NYHA = New York Heart Association; QALY = quality-adjusted life-year.
aThe VALOR-HCM trial was submitted to CADTH for review but was not used to inform the pharmacoeconomic model.
Conclusions
Based on the CADTH clinical review, data from the placebo-controlled EXPLORER-HCM trial suggest that mavacamten may improve New York Heart Association (NYHA) class and exercise capacity among patients with class II or III obstructive hypertrophic cardiomyopathy (oHCM). Data from the placebo-controlled VALOR-HCM trial suggest that mavacamten may reduce the number of patients with NYHA class II or III oHCM and exertional syncope or near syncope who are eligible for septal reduction therapy (SRT) after 16 weeks of treatment.
The sponsor submitted a pharmacoeconomic analysis comparing the cost-effectiveness of mavacamten plus beta-blockers or calcium channel blockers with that of beta-blockers or calcium channel blockers alone, using data from the EXPLORER-HCM trial. As noted in the CADTH clinical review, the majority of patients in the EXPLORER-HCM trial were receiving beta-blockers or calcium channel blockers at baseline. As such, the sponsor’s pharmacoeconomic analysis primarily reflects the cost-effectiveness of mavacamten in the second-line setting. The cost-effectiveness of mavacamten as first- or third-line treatment, which is not excluded by the Health Canada indication, is unknown. CADTH was also unable to address the lack of comparative data for mavacamten versus disopyramide; as such, the cost-effectiveness of mavacamten plus beta-blockers or calcium channel blockers compared to disopyramide plus beta-blockers or calcium channel blockers remains unknown.
CADTH undertook reanalyses to address limitations in the sponsor’s pharmacoeconomic evaluation, which included removing the survival benefit for mavacamten; increasing the proportion of patients receiving beta-blockers or calcium channel blockers who initiated subsequent therapy each year; adopting efficacy data based on the same observation period for both mavacamten plus beta-blockers or calcium channel blockers and for beta-blockers or calcium channel blockers alone; and removing the response-based discontinuation criteria for mavacamten. Based on the CADTH reanalysis, mavacamten plus beta-blockers or calcium channel blockers was more costly and more effective than beta-blockers or calcium channel blockers alone (incremental costs: $264,737, incremental qualify-adjusted life-years [QALYs]: 0.46), resulting in an incremental cost-effectiveness ratio (ICER) of $576,295 per QALY when initiated in the second-line setting for patients with baseline NYHA class II or III oHCM. In CADTH’s reanalysis, a price reduction of 73% for mavacamten would be required for mavacamten plus beta-blockers or calcium channel blockers to be considered cost-effective at a willingness-to-pay threshold of $50,000 per QALY.
Results of the CADTH base case were driven by the drug acquisition costs of mavacamten and the extrapolation of clinical benefit beyond the EXPLORER-HCM trial period. Although the CADTH base case estimated fewer incremental QALYs between mavacamten plus beta-blockers or calcium channel blockers and beta-blockers or calcium channel blockers alone (incremental QALYs: 0.46), most (97%) of the incremental benefit from mavacamten plus beta-blockers or calcium channel blockers was accrued in the extrapolated period. No clinical data are available to support the modelled long-term relative benefit of mavacamten plus beta-blockers or calcium channel blockers compared with beta-blockers or calcium channel blockers alone, and the estimated ICER was highly sensitive to the sponsor’s assumption that there is no waning of mavacamten treatment effectiveness. In a scenario analysis that assumed that patients on mavacamten plus beta-blockers or calcium channel blockers would progress at the same rate as patients on beta-blockers or calcium channel blockers alone beyond the EXPLORER-HCM trial period, the ICER for mavacamten plus beta-blockers or calcium channel blockers was $958,341 per QALY compared to beta-blockers or calcium channel blockers alone. If the long-term relative effectiveness of mavacamten plus beta-blockers or calcium channel blockers compared to beta-blockers or calcium channel blockers alone is worse than expected, a greater price reduction will be required for mavacamten to be considered cost-effective at a willingness-to-pay threshold of $50,000 per QALY.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, registered clinicians, and drug plans that participated in the CADTH review process.
CADTH received 2 patient group submissions from the Canadian Heart Patient Alliance (CHPA) and the HeartLife Foundation. Input for both submissions was obtained via interviews with patients who self-identified as having oHCM. The CHPA input was based on interviews with patients recruited through US-based clinics and the CHPA’s patient database (25% of interviewees were from Canada). The recruitment methods and proportion of patients from Canada were not reported for the HeartLife Foundation submission. Patients reported having used a variety of treatments for their oHCM, including surgery, alcohol septal ablation, implantable cardioverter-defibrillators, and pharmacotherapy (e.g., beta-blockers, calcium channel blockers, and antiarrhythmics). Many people taking these medications reported experiencing adverse reactions and felt that they do not treat the underlying condition. Gaps in current treatments that patients are hoping to be addressed with a new treatment are a reduction in the risk of sudden death, reductions in hospital admissions, and reductions in symptoms that affect their activities of daily living and quality of life, including shortness of breath, irregular heartbeat, palpitations, chest pain, fatigue, stress, and anxiety. Four interviewees (from the US) had experience with mavacamten through clinical trials and described having increased activity tolerance, improved hope and optimism, and decreased anxiety and panic regarding the risk of sudden cardiac death; none reported adverse events (AEs).
Clinician input was received from Cardio1, a community-based cardiology clinic in Winnipeg. Clinician input indicated that current treatments for oHCM are based on symptom management and include beta-blockers and calcium channel blockers, as well as disopyramide, which is used when there is no response to beta-blockers or calcium channel blockers. Clinicians noted these medications are not disease-specific and do not modify the underlying disease. Clinician input noted that patients who are refractory to pharmacotherapies may go on to receive SRT, which modifies the underlying disease mechanism by reducing the size of the left ventricular hypertrophy and reducing outflow obstruction but can be associated with AEs. Clinicians indicated that a noninvasive alternative to SRT is desired, as well as a treatment that reverses the disease course and improves symptoms and quality of life.
Drug plan input included questions regarding the place in therapy for mavacamten relative to beta-blockers or calcium channel blockers and disopyramide, as well as questions regarding patient eligibility. The plans asked whether patients with NYHA class IV oHCM would be prescribed mavacamten and whether those whose disease progresses to NYHA class IV should discontinue mavacamten. Drug plans also asked about the budget impact of mavacamten, including the number of eligible patients and its anticipated uptake.
Several of these concerns were addressed in the sponsor’s model:
The health states in the sponsor’s model were based on NYHA class, which considers patient symptoms, including fatigue, shortness of breath, palpitations, and activity tolerance.
SRT was included in the sponsor’s model as a subsequent treatment after discontinuation of mavacamten; however, clinical expert input received by CADTH indicated that several of the sponsor’s assumptions related to SRT lacked face validity.
CADTH was unable to address the following concern raised from stakeholder input:
Disopyramide was excluded from the sponsor’s analysis. CADTH was unable to address this limitation owing to the structure of the sponsor’s model and a lack of clinical data.
Economic Review
The current review is for mavacamten (Camzyos) for the treatment of symptomatic NYHA class II or III oHCM in adult patients.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis assessing mavacamten used in combination with beta-blockers or calcium channel blockers compared with a pooled comparator of beta-blockers or calcium channel blockers alone in patients with symptomatic NYHA class II or III oHCM.1 The modelled population was based on the EXPLORER-HCM trial, in which most patients were receiving beta-blockers or calcium channel blockers at baseline. The modelled population is therefore consistent with the Health Canada indication in terms of NYHA class (i.e., for use by patients with NYHA class II or III symptoms) but does not adequately account for mavacamten use in the first or third line. In its pharmacoeconomic model, the sponsor assumed the same distribution of beta-blockers or calcium channel blockers in both the group receiving mavacamten plus beta-blockers or calcium channel blockers and the group receiving only beta-blockers or calcium channel blockers: 73% of patients would receive beta-blockers (53% bisoprolol, 47% metoprolol) and 23% would receive calcium channel blockers (50% diltiazem, 50% verapamil).1
Mavacamten is available as 2.5 mg, 5 mg, 10 mg, and 15 mg oral capsules.2 The recommended starting dosage of mavacamten is 5 mg once daily,2 with dose adjustments recommended based on left ventricular outflow tract gradient. The sponsor’s model assumed that all patients would receive 5 mg once daily while on treatment.1 The submitted price of mavacamten is $61.60 per 2.5 mg, 5 mg, 10 mg, or 15 mg capsule, which corresponds to an annual per-patient cost of $22,484. The annual per-patient cost for mavacamten plus beta-blockers or calcium channel blockers was assumed by the sponsor to be $22,528 (beta-blockers or calcium channel blockers alone cost $105 per year).
The economic analysis was undertaken over a lifetime (41-year) time horizon from the perspective of a Canadian public health care payer. The clinical outcomes of interest were QALYs and life-years. Discounting at 1.5% per annum was applied to both costs and outcomes.1
Model Structure
The sponsor submitted a Markov model with health states based on NYHA class (Figure 1).1 Patients entered the model in either the class II or III health state. For the first 30 weeks of the model, the sponsor adopted a variable cycle length (2 or 4 weeks) based on assessment time points from the EXPLORER-HCM trial (weeks 4, 8, 10, 14, 16, 18, 22, 26, and 30).3 In each cycle for the first 30 weeks, patients could remain in their initial NYHA class health state or transition to an improved or worsened NYHA class health state (based on transition probabilities derived from the EXPLORER-HCM trial), or die. After 30 weeks, the sponsor adopted a 4-week cycle length, and, in each cycle, patients could stay in the same health state, move to a worse NYHA state, or die. The sponsor assumed that no patient would discontinue mavacamten before week 30. At week 30, patients who had no improvement in NYHA class from baseline or who had experienced an AE were assumed to discontinue mavacamten and receive subsequent treatment (beta-blockers or calcium channel blockers alone or disopyramide plus beta-blockers or calcium channel blockers). After 30 weeks, patients were assumed to discontinue mavacamten based on occurrence of an AE or if their NYHA class worsened by at least 1 class over the previous 4-week period. No patients could discontinue beta-blockers or calcium channel blockers; however, each year, a proportion of patients on beta-blockers or calcium channel blockers was assumed to add on disopyramide. Regardless of the initial treatment arm, the sponsor assumed that all patients who received disopyramide plus beta-blockers or calcium channel blockers would subsequently undergo SRT after 9 months of disopyramide treatment.
Model Inputs
The pharmacoeconomic model was informed by inputs from the EXPLORER-HCM trial,3 which enrolled adults with a mean age of 59.0 years (59.4% male) in NYHA class II (72.9%) or III (27.1%); 92% of patients in the EXPLORER-HCM trial were receiving background therapy of beta-blockers or calcium channel blockers at baseline.1,3
Two sets of transition probabilities (short- or long-term) were used in the model. Short-term transition probabilities for the first 30 weeks of the model were based on observed data from the EXPLORER-HCM trial for mavacamten (up to week 30; end of the double-blind period) and beta-blockers or calcium channel blockers (up to week 46; until the start of the long-term extension study). Long-term transition probabilities were applied beyond 30 weeks in the model for mavacamten and beyond week 46 for beta-blockers or calcium channel blockers, after which time the sponsor assumed that patients would change NYHA class only because of natural symptom progression, such that the treatment effectiveness from the short-term period was maintained until the end of the model time horizon. The sponsor incorporated natural symptom progression for beta-blockers or calcium channel blockers from the literature for patients who had provocable oHCM and rest oHCM, such that 4.55% of patients in each NYHA class were assumed to worsen by 1 NYHA class each year.1,4 For patients on mavacamten plus beta-blockers or calcium channel blockers, the sponsor assumed that the annual rate of symptom progression would be 2.31%, based on the relative difference for patients with no NYHA improvement for mavacamten versus placebo in the EXPLORER-HCM trial (50.85%) multiplied by the progression rate adopted for patients receiving beta-blockers or calcium channel blockers (4.55%).1,3,4 The sponsor assumed that a proportion of patients beta-blockers or calcium channel blockers would initiate disopyramide each year (NYHA I: 0%; NYHA II: 0.10%; NYHA III: 1.08%; NYHA IV: 0.28%), based on expert input obtained by the sponsor.1 Patients who received beta-blockers or calcium channel blockers plus disopyramide were assumed to experience natural symptom progression.1 The effectiveness of SRT was based on expert input obtained by the sponsor; patients who underwent SRT made a 1-time transition between NYHA classes based on SRT effectiveness and were assumed to remain in the resulting health state for the remainder of the model time horizon.1
The sponsor’s model included considered discontinuation related to AEs and based on response to mavacamten treatment. At week 30, the sponsor assumed that 1.6% of patients would discontinue mavacamten based on the proportion of patients who discontinued treatment in the EXPLORER-HCM trial owing to AEs.3 After 30 weeks, the sponsor assumed that 2.8% of patients would discontinue mavacamten annually because of serious AEs. The placebo arm of the EXPLORER-HCM trial was used to inform AE rates for patients receiving beta-blockers or calcium channel blockers alone, and was assumed to be equivalent for patients receiving disopyramide plus beta-blockers or calcium channel blockers and SRT plus beta-blockers or calcium channel blockers;1,3 however, no patients could discontinue these treatments because of AEs. Discontinuation due to a lack of improvement in NYHA class from baseline to 30 weeks for patients receiving mavacamten was informed by rates from the EXPLORER-HCM trial.3 The use of subsequent treatments after mavacamten discontinuation was based on clinical expert input.
All-cause mortality was incorporated from age- and sex-adjusted life tables.5 The sponsor assumed that the risk of mortality would increase by NYHA class and applied hazard ratios (HRs) derived from an American electronic medical record study to each NYHA class.6 SRT was assumed to be associated with a mortality rate of 1.20%, based on a weighted average obtained from the literature for oHCM patients who received alcohol ablation therapy (1.12%) or myectomy (1.27%).7
Health-state utility values for NYHA class I to III were based on 5-Level EQ-5D (EQ-5D-5L) data from the EXPLORER-HCM trial,3 mapped to the 3-Level EQ-5D8 with Canadian tariffs.9 Utility values were age-adjusted using a regression approach.10 The sponsor assumed that the health-state utility value for NYHA class IV would be equal to that for class III.1 Disutilities for AEs were assumed to last for 4 weeks and were sourced from the literature.1
The economic model included costs related to treatment (drug acquisition and monitoring), health care resource use, management of AEs, and terminal care.1 Dose adjustments were not incorporated in the model as the sponsor’s submitted price for all tablet sizes was based on flat pricing.1 Dosing for beta-blockers or calcium channel blockers was based on product monographs. Drug acquisition costs for mavacamten were based on the sponsor’s submitted price, with the acquisition costs of other drugs obtained from the Ontario Drug Benefit formulary.1,11 SRT was assumed to include alcohol ablation therapy and myectomy, with costs obtained from the Canadian Institute for Health Information (CIHI) patient-cost estimator.12 Health care resource use was assumed to vary by NYHA class and was informed by expert opinion.1 Unit costs for health care resources were obtained from the Ontario Schedule of Benefits and CIHI.13,14 Treatment monitoring costs were applied for patients receiving mavacamten plus beta-blockers or calcium channel blockers in the first year of treatment and included echocardiogram procedures and cardiovascular visits.1 Visit frequencies were informed by sponsor data on file.13 Costs related to AEs were obtained from the CIHI patient-cost estimator.12 Terminal care costs were based on palliative care costs associated with obstructive pulmonary disease.15
Summary of Sponsor’s Economic Evaluation Results
All analyses were run probabilistically (1,000 iterations). The deterministic and probabilistic results were similar. The probabilistic findings are presented in the following section.
Base-Case Results
In the sponsor’s base case, mavacamten plus beta-blockers or calcium channel blockers was associated with an estimated cost of $244,606 and 14.51 QALYs over the 41-year horizon, resulting in an ICER of $56,774 ($129,564 in incremental costs and 2.28; incremental QALYs) (Table 3). In the sponsor’s analysis, mavacamten plus beta-blockers or calcium channel blockers had an 11% probability of being cost-effective at a willingness-to-pay threshold of $50,000. Additional results from the sponsor’s submitted economic evaluation base case are available in Appendix 3.
Results were driven by the drug acquisition costs of mavacamten plus beta-blockers or calcium channel blockers (incremental costs: $177,189), the predicted gain in life-years (2.21), and the predicted reduction in costs associated with health care resource use ($46,812 in incremental savings) (Appendix 3). The sponsor’s model estimated that 0.01 of the incremental QALYs with mavacamten plus beta-blockers or calcium channel blockers were accrued during the EXPLORER-HCM trial period (30 weeks), indicating that approximately 99% of the incremental benefits were accrued during the post-trial period. At the end of the 41-year time horizon, approximately 0.5% and 0.1% of patients remained alive in the group receiving mavacamten plus beta-blockers or calcium channel blockers and the group receiving beta-blockers or calcium channel blockers alone, respectively. The sponsor’s model predicts an incremental gain of 3.12 life-years following SRT and $7,013 in increased costs related to SRT with mavacamten plus beta-blockers or calcium channel blockers compared to beta-blockers or calcium channel blockers alone, suggesting that more patients will undergo SRT following mavacamten plus beta-blockers or calcium channel blockers.
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER vs. BB or CCB ($ per QALY) |
|---|---|---|---|---|---|
BB or CCB | 115,043 | Reference | 12.23 | Reference | Reference |
Mavacamten plus BB or CCB | 244,606 | 129,564 | 14.51 | 2.28 | 56,774 |
BB = beta-blocker; CCB = calcium channel blocker; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus.
Source: Sponsor’s pharmacoeconomic submission.1
Sensitivity and Scenario Analysis Results
The sponsor provided several scenario analyses, including adopting alternative assumptions related to time horizon, discount rates, long-term transition probabilities, and treatment discontinuation. Results were sensitive to the choice of long-term transition probabilities: in a scenario that assumed that the last set of short-term transition probabilities (e.g., week 26 to 30 for mavacamten, week 38 to 46 for beta-blockers or calcium channel blockers) would apply for the remainder of time on treatment, the ICER for mavacamten plus beta-blockers or calcium channel blockers compared to beta-blockers or calcium channel blockers alone was $33,379 per QALY gained.
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations to the sponsor’s analysis that have notable implications for the economic analysis:
The full Health Canada population was not modelled. The sponsor submitted analyses intended to reflect the cost-effectiveness of mavacamten plus beta-blockers or calcium channel blockers among patients with NYHA class II or III oHCM, with effectiveness informed by the EXPLORER-HCM trial. The majority (92%) of patients enrolled in the EXPLORER-HCM trial were on background beta-blockers or calcium channel blockers at baseline. As such, the clinical evidence used to inform the pharmacoeconomic model primarily reflects the use of mavacamten as a second-line therapy. The Health Canada indication for mavacamten is not specific to line of therapy, and clinical expert input received by CADTH for this review indicated that mavacamten is likely to be used either following beta-blockers or calcium channel blockers or following beta-blockers or calcium channel blockers plus disopyramide (i.e., second- or third-line). Approximately 15% of patients in the VALOR-HCM trial were taking beta-blockers or calcium channel blockers plus disopyramide at baseline; however, no subgroup data were provided for these patients and no data from the VALOR trial were used to inform the pharmacoeconomic model.
CADTH was unable to address this limitation owing to a lack of clinical data pertaining to either first- or third-line use. As such, the clinical and cost-effectiveness of mavacamten as first- or third-line therapy are unknown, as is the cost-effectiveness of mavacamten in the full Health Canada–indicated population.
Relevant comparators were omitted. The sponsor compared mavacamten plus beta-blockers or calcium channel blockers to beta-blockers or calcium channel blockers alone, in patients with NYHA class II or III oHCM. Clinical practice guidelines for oHCM indicate that, for patients who have persistent symptoms despite the use of beta-blockers or calcium channel blockers, disopyramide should be considered.16 This is aligned with clinical expert input received by CADTH as disopyramide is currently being used in Canada as second-line therapy in this population (i.e., it has the same place in therapy as mavacamten in the EXPLORER-HCM trial). CADTH further notes that the sponsor assumed in its budget impact analysis (BIA) that mavacamten would displace market share from disopyramide, which is inconsistent with the sponsor’s assumption in the economic evaluation that disopyramide is not a comparator. Together, these factors indicate that disopyramide is a relevant comparator to mavacamten in the Canadian context.
CADTH was unable to address this limitation owing to a lack of direct clinical data as disopyramide was not included as a comparator in the EXPLORER-HCM trial. Furthermore, there is no indirect evidence comparing disopyramide to mavacamten. As noted in the CADTH clinical review, the comparative effectiveness of mavacamten versus disopyramide is unknown. As such, the comparative cost-effectiveness of mavacamten compared with disopyramide is unknown.
The survival benefit predicted for mavacamten is highly uncertain. The sponsor’s base case (Table 13) predicts a survival advantage of 2.21 incremental life-years with mavacamten plus beta-blockers or calcium channel blockers relative to beta-blockers or calcium channel blockers alone, which has not been shown in clinical trials.3 Survival was not an outcome in the EXPLORER-HCM trial.3 Clinical expert opinion received by CADTH for this review indicated that patients with oHCM are expected to have normal life expectancies with current standard-of-care therapies, and increased survival therefore may not be a relevant outcome expected for a new oHCM treatment.
Based on CADTH’s exploration of the model, the predicted survival benefit for mavacamten was driven by the HRs applied to the NYHA class health states and intended by the sponsor to reflect an increased risk of death with increasing NYHA class. Considerable uncertainty is associated with this approach. First, NYHA class is a subjective assessment of patient symptoms that does not directly address disease severity. Second, applying HRs to the NYHA states implies that all patients in the same NYHA class are at the same risk of death, which is unlikely. Third, the impact of transitioning between NYHA classes (e.g., moving from NYHA III to II) on long-term survival is unknown. Fourth, the HRs adopted by the sponsor were derived from an analysis of American electronic medical records, and whether the findings are generalizable to the Canadian context is unknown.
The clinical evidence is insufficient to suggest that mavacamten confers a survival benefit. In CADTH reanalyses, it was assumed to be the same across NYHA classes, which ensured that there were no relative mortality effects of treatment with mavacamten.
The modelling of subsequent treatments is highly uncertain. In the pharmacoeconomic model, the sponsor assumed that, after discontinuing mavacamten, patients would receive beta-blockers or calcium channel blockers alone or initiate disopyramide (i.e., receive beta-blockers or calcium channel blockers plus disopyramide). For patients who entered the model on beta-blockers or calcium channel blockers alone, the sponsor assumed that a proportion would initiate disopyramide each year. Regardless of initial treatment, the sponsor assumed that patients who receive disopyramide would undergo SRT after 9 months of disopyramide. Clinical expert input received by CADTH for this review indicated that several of the sponsor’s assumptions related to the modelling of subsequent therapy were inconsistent with clinical practice and expectations.
First, the sponsor assumed that the annual proportions of patients on beta-blockers or calcium channel blockers who initiate disopyramide would be 0.10%, 1.08%, and 0.28% for NYHA class II, III, and IV, respectively. Clinical practice guidelines recommend disopyramide for patients who continue to have persistent symptoms despite the use of beta-blockers or calcium channel blockers, and clinical expert input received by CADTH indicated that the sponsor’s assumptions were lower than would be expected in clinical practice.16,17 CADTH notes that the sponsor assumed that 4.55% of patients in NYHA class I to III would worsen by 1 NYHA class each year; according to clinical expert feedback received by CADTH, these patients would be considered for disopyramide.
Second, the sponsor assumed that all patients who initiate disopyramide would go on to receive SRT. Clinical expert feedback received by CADTH indicated that this lacks face validity, as not all patients who are considered candidates for SRT wish to undergo SRT or are able to access SRT. Furthermore, according to clinician input received by CADTH, some patients may achieve adequate symptom control with disopyramide and would therefore not require SRT. However, clinical expert input indicated noted that the percentage of patients receiving disopyramide who go on to receive SRT in the Canadian context is uncertain.
Third, the sponsor’s model predicts an incremental gain of 3.12 life-years after SRT and higher costs related to SRT among patients who initiated mavacamten compared with those who initiated beta-blockers or calcium channel blockers (Table 11), which lacks face validity when considered alongside the results of the EXPLORER-HCM and VALOR-HCM trials. As noted in the CADTH clinical review, in the VALOR-HCM trial, the proportion of patients who remained eligible for SRT after 16 weeks of treatment was significantly lower among patients who received mavacamten (14.3%) compared with placebo (69.6%), and, in the EXPLORER-HCM trial, significantly more patients who received mavacamten improved by at least 1 NYHA class (65%) compared with those who received placebo (31.3%), suggesting that fewer patients would require SRT.
In CADTH reanalyses, CADTH assumed that a higher proportion of symptomatic patients receiving beta-blockers or calcium channel blockers would initiate disopyramide each year, which is consistent with the sponsor’s assumption about the proportion of patients whose symptoms worsen by 1 NYHA class each year (4.55%). CADTH was unable to change the proportion of patients who received SRT following disopyramide due to a lack of available data to inform this parameter; however, testing of this parameter by CADTH determined that this assumption was unlikely to influence cost-effectiveness results.
Using different observation periods for the efficacy of mavacamten plus beta-blockers or calcium channel blockers compared with beta-blockers or calcium channel blockers alone favours mavacamten. In the pharmacoeconomic model, the sponsor incorporated the efficacy of mavacamten (i.e., short-term transition probabilities) based on observations from the EXPLOER-HCM trial up to week 30 for mavacamten (the end of the double-blind period) and up to week 46 for beta-blockers or calcium channel blockers (the 30-week double-blind period of EXPLORER-HCM plus an 8-week washout period plus time until the baseline assessment for the EXPLORER-LTE extension study). The sponsor assumed that, after the short-term period, patients would no longer change NYHA class as a result of treatment, meaning that the NYHA class achieved at week 30 (for patients receiving mavacamten) and week 46 (for those on beta-blockers or calcium channel blockers) was retained for the remainder of the model time horizon, aside from symptom worsening due to natural symptom progression. Clinical expert input received by CADTH noted that the use of efficacy data from different observation periods (mavacamten: 30 weeks; beta-blockers or calcium channel blockers: 46 weeks) may have biased the results in favour of mavacamten, as patients on beta-blockers or calcium channel blockers experienced a worsening of NYHA class after 30 weeks in the EXPLORER-HCM trial (Figure 2). As illustrated in Figure 2, worsening of NYHA class was also observed after 30 weeks for patients in the mavacamten group in the EXPLORER-HCM trial. Clinical expert input suggests that, because NYHA class is a subjective assessment, patients on beta-blockers or calcium channel blockers may have experienced a placebo effect during the double-blind period, but the effect disappeared when the double-blind period ended.
In the CADTH reanalyses, CADTH adopted short-term transition probabilities derived from the same observation period (30 weeks) from the EXPLORER-HCM trial for both treatments, using the sponsor-provided option to do so.
The long-term relative effectiveness of mavacamten is unknown. The sponsor assumed that, in the long-term period, patients would no longer change NYHA class as a result of treatment; however, NYHA class was assumed to worsen each year for a proportion of patients on each treatment based on natural symptom progression. The sponsor assumed that patients receiving mavacamten plus beta-blockers or calcium channel blockers would have a slower rate of natural symptom progression compared with those receiving only beta-blockers or calcium channel blockers, based on findings from the 30-week EXPLORER-HCM trial.1 The sponsor applied the relative difference for patients with no NYHA improvement for mavacamten versus placebo (50.85%) in the EXPLORER-HCM trial to estimates from the literature of the proportion of patients whose symptoms worsen by 1 NYHA class per year;4 the annual proportion of patients whose NYHA worsened by 1 class was approximately 51% lower for patients on mavacamten plus beta-blockers or calcium channel blockers compared to those on beta-blockers or calcium channel blockers alone. Clinical expert input received by CADTH for this review indicated that it is plausible that patients taking mavacamten will have slower symptom progression; however, it is highly uncertain whether the short-term relative effectiveness of mavacamten versus placebo observed in the EXPLORER-HCM trial will result in a reduced rate of symptom progression for the remainder of the patients’ time on mavacamten. Similarly, the relative magnitude of any benefit versus beta-blockers or calcium channel blockers alone over the long-term is unknown. As noted in the CADTH clinical review, it is similarly uncertain whether mavacamten can reduce the need for SRT among symptomatic oHCM patients in the long-term. Finally, CADTH notes that incorporating slower natural symptom progression for patients who receive long-term mavacamten treatment may result in the double counting of treatment benefit for mavacamten given that patients were additionally assumed to maintain the NYHA class obtained at the end of the short-term treatment period.
CADTH explored in a scenario analysis the impact of uncertainty related to the relative long-term effectiveness of mavacamten plus beta-blockers or calcium channel blockers compared to beta-blockers or calcium channel blockers alone.
Discontinuation of mavacamten based on treatment response is uncertain. The sponsor applied rules for the discontinuation of mavacamten in the pharmacoeconomic model based on treatment response, which differed by time period (short-term trial period versus long-term period). First, the sponsor assumed that all patients would receive mavacamten for 30 weeks (the EXPLORER-HCM trial period), at which time patients whose NYHA class had not improved from baseline were assumed to discontinue mavacamten and receive subsequent therapy (beta-blockers or calcium channel blockers alone or beta-blockers or calcium channel blockers plus disopyramide).1 After 30 weeks, the sponsor assumed that patients would discontinue mavacamten if their symptoms worsened by 1 NYHA class over the previous 4-week period.1 CADTH notes that no discontinuation criteria related to treatment response were incorporated in the EXPLORER-HCM or VALOR-HCM trials, and none are recommended in the mavacamten product monograph.2,3 As noted in the CADTH clinical review, no patients discontinued mavacamten in the EXPLORER-HCM trial because of a lack of treatment response.3 According to clinical expert feedback received by CADTH for this review, mavacamten would not necessarily be discontinued based on a lack of treatment response (either worsening of NYHA class or lack of improvement). The expert further indicated that patients whose symptoms progress to NYHA class IV while on mavacamten would not necessarily discontinue the drug in practice.
In the CADTH base case, the discontinuation criteria based on treatment response were excluded. The impact of implementing the discontinuation criteria suggested by the sponsor was explored in scenario analyses.
Poor modelling practices were employed. The sponsor’s submitted model included numerous IFERROR statements, which lead to situations in which the parameter value is overwritten with an alternative value without alerting the user to the automatized overwriting. The systematic use of IFERROR statements makes thorough auditing of the sponsor’s model impractical. It remains unclear whether the model is running inappropriately by overriding errors. Finally, parameter uncertainty was not adequately incorporated as the sponsor assumed an arbitrary standard error of 10% for most model parameters, including treatment discontinuation, NYHA class progression rates, mortality HRs, and AE rates. Use of an arbitrary value is inappropriate when clinical trial data are available, and not using actual parameter uncertainty diminishes the value of conducting probabilistic analyses as true parameter uncertainty has not been captured.
CADTH was unable to address this limitation and notes that a thorough validation of the sponsor’s model was not possible.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CADTH (Table 4).
Table 4: Key Assumptions of the Submitted Economic Evaluation (Not Noted as Limitations to the Submission)
Sponsor’s key assumption | CADTH comment |
|---|---|
The sponsor compared mavacamten plus beta-blockers or calcium channel blockers to a single comparator consisting of a pooled combination of beta-blockers and calcium channel blockers. | Uncertain, but unlikely to affect the ICER. According to the CADTH clinical review report, subgroup data from the EXPLORER-HCM trial for patients on either beta-blockers or calcium channel blockers did not show differences in efficacy outcomes apart from change in peak oxygen consumption. CADTH notes that the cost-effectiveness of mavacamten plus beta-blockers or calcium channel blockers relative to individual beta-blockers or calcium channel blockers is unknown. |
Patients undergoing SRT were assumed to receive myectomy (50%) or septal ablation therapy (50%). | Uncertain, but unlikely to affect the ICER. In the VALOR-HCM trial, myectomy was the recommended procedure for 85.7% of patients eligible for SRT. Clinical expert input received by CADTH noted that the proportion of patients in Canada who undergo myectomy vs. septal ablation therapy is uncertain and likely varies by centre. |
The sponsor assumed that patients receiving disopyramide (i.e., after mavacamten discontinuation or as escalation of therapy among patients receiving beta-blockers or calcium channel blockers) would retain the NYHA class that they were in when they initiated disopyramide, and that after SRT, patients would maintain the NYHA class gained due to the incident SRT event. Additionally, SRT efficacy was informed by clinical expert opinion. | Inappropriate, but unlikely to affect the ICER. These inputs were based on the sponsor’s assumptions or clinical expert opinion. CADTH could not validate the appropriateness of these assumptions; however, exploration of the model by CADTH indicated that the ICER was not sensitive to these assumptions. |
For patients receiving mavacamten, the sponsor’s model assumed 0.74, 0.90, 1.94 and 1.51 echocardiograms annually for patients in NYHA class I, II, III, and IV, respectively, after the first year of treatment. | Inappropriate, but unlikely to affect the ICER. According to the mavacamten product monograph, patients should undergo echocardiography every 12 weeks for the first year of treatment and every 6 months thereafter.2 The annual number of echocardiograms after the first year of treatment was therefore underestimated in the sponsor’s model. |
The sponsor assumed that heart failure, transplants, stroke, and myocardial infarction would be captured by NYHA health states. | Inappropriate. NYHA is a heart-failure classification system based on the subjective assessment of the impact of patients’ symptoms on physical activity. According to clinical expert input received by CADTH, these cardiovascular outcomes are not captured by NYHA classes. The impact of mavacamten on these outcomes is unknown, and the costs and quality-of-life impacts of these cardiovascular events are not reflected in the sponsor’s model. |
Health-state utility values for NYHA class I, II, and III were derived from EQ-5D-5L data from the EXPLORER-HCM trial, mapped to the EQ-5D-3L. | Uncertain. Mapping from EQ-5D-5L to EQ-5D-3L is unnecessary and adds uncertainty to both the precision and validity of the utility estimates. |
The sponsor assumed that the health-state utility value for NYHA class IV would be equal to that for class III. | Inappropriate. Clinical expert input received by CADTH noted that patients in NYHA class IV are expected to have more severe symptoms and worse quality of life compared to those in class III. Assuming equivalent health-state utilities for class III and IV lacks face validity. |
EQ-5D-3L = 3-Level EQ-5D; EQ-5D-5L = 5-Level EQ-5D; ICER = incremental cost-effectiveness ratio; NYHA = New York Heart Association; SRT = septal reduction therapy.
CADTH Reanalyses of the Economic Evaluation
Base-Case Results
CADTH undertook reanalyses to address limitations within the model, as summarized in Table 5. The CADTH base case was derived by making changes in model parameter values and assumptions, in consultation with clinical experts. All CADTH probabilistic reanalyses were based on 1,000 iterations.
CADTH was unable to address the other limitations of the model (described in the previous section), including the lack of comparative data for mavacamten versus disopyramide, uncertainty in the long-term comparative effectiveness of mavacamten plus beta-blockers or calcium channel blockers and beta-blockers or calcium channel blockers alone, and some assumptions related to the use and effectiveness of subsequent therapies.
Table 5: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
None | — | — |
Changes to derive the CADTH base case | ||
1. Risk of death (HR), by NYHA class | NYHA I: reference (HR = 1.0) NYHA II: HR = 1.51 NYHA III: HR = 2.77 NYHA IV: HR = 7.09 | Mortality was assumed to be the same across NYHA classes (i.e., HR = 1.0 for all NYHA classes) |
2. Proportion of patients receiving beta-blockers or calcium channel blockers who add disopyramide (annual) | NYHA I: 0% NYHA II: 0.10% NYHA III: 1.08% NYHA IV: 0.28% | 4.55% for NYHA class II-IV, based on the sponsor’s assumption that 4.55% of patients on beta-blockers or calcium channel blockers would experience symptom progression (worsen by 1 NYHA class) each year |
3. Observation period for the derivation of treatment efficacy short-term transition probabilities | Beta-blockers or calcium channel blockers: 46 weeks Mavacamten: 30 weeks | 30 weeks for both |
4. Response-based treatment discontinuationa | At 30 weeks, patients were assumed to discontinue mavacamten if no improvement in NYHA class from baseline; after 30 weeks, patients were assumed to discontinue mavacamten if their symptoms had worsened by one NYHA class in the previous 4-week period | No discontinuation based on treatment response |
CADTH base case | — | 1 + 2 + 3 + 4 |
AE = adverse event; HR = hazard ratio; NYHA = New York Heart Association.
aApplies to mavacamten only, as patients were unable to discontinue beta-blockers or calcium channel blockers in the model. Discontinuation related to AEs was modelled separately.
CADTH undertook a stepped analysis, incorporating each change proposed in Table 5 to the sponsor’s base case to highlight the impact of each change (disaggregated results are presented in Appendix 4, Table 15).
In the CADTH base case, administration of mavacamten plus beta-blockers or calcium channel blockers was associated with higher incremental costs ($264,737) and higher QALYs (0.46) compared with beta-blockers or calcium channel blockers alone over a 41-year horizon, resulting in an ICER of $576,295 per QALY (Table 6). There is a 0% probability that mavacamten plus beta-blockers or calcium channel blockers is optimal compared to beta-blockers or calcium channel blockers alone at a willingness-to-pay threshold of $50,000.
In the CADTH base case (Table 15), results were driven by the drug acquisition costs of mavacamten plus beta-blockers or calcium channel blockers ($330,842). The CADTH base case predicts a small incremental gain of 0.04 life-years with mavacamten compared to beta-blockers or calcium channel blockers, which has not been demonstrated in clinical trials. Based on CADTH’s exploration of the model, these incremental life-years for mavacamten accrued because of the risk of death assigned to SRT (i.e., risk of death associated with undergoing SRT) in the model. In the CADTH base case, more patients receiving beta-blockers or calcium channel blockers alone undergo SRT compared to those receiving mavacamten plus beta-blockers or calcium channel blockers, and as such, mortality is higher in the group receiving only beta-blockers or calcium channel blockers. This results in a higher total number of life-years for patients receiving mavacamten plus beta-blockers or calcium channel blockers compared with beta-blockers or calcium channel blockers alone.
Consistent with the sponsor’s submission, the CADTH base case predicts that all of the incremental QALYs gained with mavacamten plus beta-blockers or calcium channel blockers accrued by patients in the NYHA class I health state, meaning that the benefit associated with mavacamten plus beta-blockers or calcium channel blockers is derived from patients transitioning to NYHA class I during the EXPLORER-HCM trial period (first 30 weeks of treatment) and worsening at a slower rate compared with patients on beta-blockers or calcium channel blockers alone. CADTH notes that improvement in NYHA class is supported by the findings of the EXPLORER-HCM trial; however, the duration and magnitude of the relative benefit compared with beta-blockers or calcium channel blockers alone is uncertain. Similar to the sponsor’s base case, the CADTH base case predicts that approximately 97% of the incremental benefits from mavacamten plus beta-blockers or calcium channel blockers were accrued in the post-trial period.
Table 6: Summary of the Stepped Analysis of the CADTH Reanalysis Results
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($ per QALY) |
|---|---|---|---|---|
Sponsor’s base case (probabilistic) | BB or CCB | 115,043 | 12.23 | Reference |
Mavacamten + BB or CCB | 244,606 | 14.51 | 56,774 | |
Sponsor’s base case (deterministic) | BB or CCB | 110,048 | 12.28 | Reference |
Mavacamten + BB or CCB | 244,284 | 14.55 | 59,045 | |
CADTH reanalysis 1: risk of death across NYHA classes | BB or CCB | 182,148 | 15.49 | Reference |
Mavacamten + BB or CCB | 278,722 | 16.21 | 133,855 | |
CADTH reanalysis 2: proportion of BB or CCB patients who add on disopyramide | BB or CCB | 108,493 | 12.84 | Reference |
Mavacamten + BB or CCB | 244,499 | 14.71 | 72,765 | |
CADTH reanalysis 3: observation period for treatment efficacy (short-term transition probabilities) | BB or CCB | 102,350 | 12.69 | Reference |
Mavacamten + BB or CCB | 244,284 | 14.55 | 76,291 | |
CADTH reanalysis 4: no mavacamten response-based discontinuation criteria | BB or CCB | 110,048 | 12.28 | Reference |
Mavacamten + BB or CCB | 361,345 | 14.52 | 111,927 | |
CADTH base case (deterministic): 1 + 2 + 3 + 4 | BB or CCB | 150,653 | 15.77 | Reference |
Mavacamten + BB or CCB | 416,573 | 16.22 | 588,186 | |
CADTH base case (probabilistic): 1 + 2 + 3 + 4 | BB or CCB | 159,190 | 15.76 | Reference |
Mavacamten + BB or CCB | 423,927 | 16.22 | 576,295 |
BB = beta-blocker; CCB = calcium channel blocker; ICER = incremental cost-effectiveness ratio; NYHA = New York Heart Association; QALY = quality-adjusted life-year.
Note: Results of the CADTH reanalysis steps are presented deterministically.
Scenario Analysis Results
CADTH undertook price-reduction analyses based on the sponsor’s and CADTH’s base case (Table 7). The CADTH base case suggested a price reduction of 73% would be required to achieve cost-effectiveness of mavacamten plus beta-blockers or calcium channel blockers relative to beta-blockers or calcium channel blockers alone at a willingness-to-pay threshold of $50,000 per QALY.
Table 7: CADTH Price-Reduction Analyses
Analysis | ICERs for mavacamten plus BB or CCB vs. BB or CCB ($ per QALY) | |
|---|---|---|
Price reduction | Sponsor base case | CADTH reanalysis |
No price reduction | 56,774 | 576,295 |
10% | 49,098 | 503,994 |
20% | 41,421 | 431,693 |
30% | 33,745 | 359,392 |
40% | 26,069 | 287,091 |
50% | 18,392 | 214,790 |
60% | 10,716 | 142,489 |
70% | 3,039 | 70,188 |
80% | Dominated | Dominated |
BB = beta-blocker; CCB = calcium channel blocker; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
CADTH explored in scenario analyses the impact of uncertainty related to the relative long-term effectiveness of mavacamten plus beta-blockers or calcium channel blockers compared to beta-blockers or calcium channel blockers alone, as well as the impact of implementing the mavacamten response-based discontinuation criteria proposed by the sponsor:
In the long-term period (after the first 30 weeks of treatment), the proportion of patients whose symptoms worsened by 1 NYHA class (i.e., because of natural symptom progression) was assumed to be equivalent for mavacamten plus beta-blockers or calcium channel blockers and beta-blockers or calcium channel blockers alone after the EXPLORER-HCM trial period.
Patients were assumed to discontinue mavacamten after a 30-week trial period if their symptoms had not improved by at least 1 NYHA class versus baseline. After 30 weeks, treatment response was assumed to be assessed every 4 weeks, and patients whose symptoms had worsened by 1 NYHA class since the previous assessment were assumed to discontinue mavacamten.
The results of these analyses are presented in Appendix 4 (Table 17). When natural symptom progression was assumed to be equivalent for patients receiving mavacamten plus beta-blockers or calcium channel blockers or for those receiving beta-blockers or calcium channel blockers alone, the ICER increased to $958,341, indicating that the ICER is highly sensitive to assumptions about the long-term relative effectiveness of mavacamten plus beta-blockers or calcium channel blockers compared to beta-blockers or calcium channel blockers alone. The implementation of the response-based discontinuation criteria for mavacamten proposed by the sponsor, as outlined earlier in this report, resulted in a reduced ICER ($235,438 per QALY) for mavacamten plus beta-blockers or calcium channel blockers compared with beta-blockers or calcium channel blockers alone.
Overall Conclusions
Based on the CADTH clinical review, data from the placebo-controlled EXPLORER trial suggest that mavacamten may improve NYHA class and exercise capacity among patients with class II or III oHCM. Data from the placebo-controlled VALOR-HCM trial suggest that mavacamten may reduce the number of patients with NYHA class II or III oHCM and exertional syncope or near syncope who are eligible for SRT after 16 weeks of treatment. Both pivotal trials found statistically significant results in favour of mavacamten for the key secondary outcomes of an improvement of at least 1 NYHA functional class, post-exercise left ventricular outflow tract peak gradient, and health-related quality of life as assessed by the 23-item Kansas City Cardiomyopathy Questionnaire clinical summary score. However, whether mavacamten can reduce the need for SRT among symptomatic oHCM patients in the long-term remains uncertain because of a lack of long-term clinical data.
The sponsor submitted a pharmacoeconomic analysis comparing the cost-effectiveness of mavacamten plus beta-blockers or calcium channel blockers with beta-blockers or calcium channel blockers alone, using data from the EXPLORER-HCM trial. As noted in the CADTH clinical review, the majority of patients in the EXPLORER-HCM trial were receiving beta-blockers or calcium channel blockers at baseline. As such, the sponsor’s pharmacoeconomic analysis primarily reflects the cost-effectiveness of mavacamten in the second-line setting. The cost-effectiveness of mavacamten as first- or third-line treatment, which is not excluded in the Health Canada indication, is unknown. CADTH was also unable to address the lack of comparative data for mavacamten versus disopyramide; the cost-effectiveness of mavacamten plus beta-blockers or calcium channel blockers compared to disopyramide plus beta-blockers or calcium channel blockers therefore remains unknown.
CADTH undertook reanalyses to address limitations in the sponsor’s pharmacoeconomic evaluation, which included removing the survival benefit for mavacamten; increasing the proportion of patients on beta-blockers or calcium channel blockers who initiated subsequent therapy each year; adopting efficacy data based on the same observation period for both patients on mavacamten plus beta-blockers or calcium channel blockers and those on beta-blockers or calcium channel blockers alone; and removing the response-based discontinuation criteria for mavacamten. Based on the CADTH reanalysis, mavacamten plus beta-blockers or calcium channel blockers was more costly and more effective than beta-blockers or calcium channel blockers alone (incremental costs: $264,737, incremental QALYs: 0.46), resulting in an ICER of $576,295 per QALY when initiated in the second-line setting for patients with baseline NYHA class II or III oHCM. In CADTH’s reanalysis, a price reduction of 73% for mavacamten would be required for mavacamten plus beta-blockers or calcium channel blockers to be considered cost-effective at a willingness-to-pay threshold of $50,000 per QALY.
Results of the CADTH base case were driven by the drug acquisition costs of mavacamten and the extrapolation of clinical benefit beyond the EXPLORER-HCM trial period. Although the CADTH base case estimated fewer incremental QALYs between mavacamten plus beta-blockers or calcium channel blockers and beta-blockers or calcium channel blockers alone (incremental QALYs: 0.46), most (97%) of the incremental benefit from mavacamten plus beta-blockers or calcium channel blockers was accrued in the extrapolated period. No clinical data are available to support the modelled long-term relative benefit of mavacamten plus beta-blockers or calcium channel blockers compared with beta-blockers or calcium channel blockers alone, and the estimated ICER was highly sensitive to the sponsor’s assumption that there is no waning of mavacamten treatment effectiveness. In a scenario analysis that assumed that patients on mavacamten plus beta-blockers or calcium channel blockers would progress at the same rate as patients on beta-blockers or calcium channel blockers alone beyond the EXPLORER-HCM trial period, the ICER for mavacamten plus beta-blockers or calcium channel blockers was $958,341 per QALY compared to beta-blockers or calcium channel blockers alone. Thus, if the long-term relative effectiveness of mavacamten plus beta-blockers or calcium channel blockers compared to beta-blockers or calcium channel blockers alone is worse than expected, a greater price reduction will be required for mavacamten to be considered cost-effective at a willingness-to-pay threshold of $50,000 per QALY.
References
1.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Camzyos (mavacamten), 2.5 mg, 5 mg, 10 mg, or 15 mg capsules. Saint-Laurent (QC): Bristol Myers Squibb; 2022 Oct 7.
2.Camzyos (mavacamten): 2.5 mg, 5 mg, 10 mg and 15 mg capsules [product monograph]. Montreal (QC): Bristol-Myers Squibb Canada; 2022 Nov 8.
3.Clinical Study Report: MYK-461-005 (EXPLORER-HCM). A randomized, double-blind, placebo-controlled clinical study to evaluate mavacamten (MYK-461) in adults with symptomatic obstructive hypertrophic cardiomyopathy [internal sponsor's report]. Brisbane (CA): MyoKardia, Inc.; 2020 Nov 11.
4.Maron MS, Rowin EJ, Olivotto I, et al. Contemporary natural history and management of nonobstructive hypertrophic cardiomyopathy. J Am Coll Cardiol. 2016;67(12):1399-1409. PubMed
5.Table: 13-10-0114-01. Life expectancy and other elements of the life table, Canada, all provinces except Prince Edward Island. Ottawa (ON): Statistics Canada; 2022: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310011401. Accessed 2021 Sep 21.
6.Drug Reimbursement Review sponsor submission: Camzyos (mavacamten), 2.5 mg, 5 mg, 10 mg, or 15 mg capsules [internal sponsor's package]. Saint-Laurent (QC): Bristol Myers Squibb; 2022 Oct 7.
7.Bytyci I, Nistri S, Morner S, Henein MY. Alcohol septal ablation versus septal myectomy treatment of obstructive hypertrophic cardiomyopathy: a systematic review and meta-analysis. J Clin Med. 2020;9(10):3062. PubMed
8.Hernández-Alava M, Pudney S. Econometric modelling of multiple self-reports of health states: the switch from EQ-5D-3L to EQ-5D-5L in evaluating drug therapies for rheumatoid arthritis. J Health Econ. 2017;55:139-152. PubMed
9.Bansback N, Tsuchiya A, Brazier J, Anis A. Canadian valuation of EQ-5D health states: preliminary value set and considerations for future valuation studies. PLoS One. 2012;7(2):e31115. PubMed
10.Ara R, Brazier JE. Populating an economic model with health state utility values: moving toward better practice. Value Health. 2010;13(5):509-518. PubMed
11.Ontario Ministry of Health, Ontario Ministry of Long-Term Care. Ontario drug benefit formulary/comparative drug index. 2022; https://www.formulary.health.gov.on.ca/formulary/. Accessed 2023 Jan 03.
12.Patient cost estimator. 2022; https://www.cihi.ca/en/patient-cost-estimator. Accessed 2022 Sep 21.
13.Schedule of benefits for physician services under the Health Insurance Act: January 25, 2022 (effective July 1, 2022). Toronto (ON): Ontario Ministry of Health; 2022: https://www.health.gov.on.ca/en/pro/programs/ohip/sob/physserv/sob_master.pdf. Accessed 2022 Sep 21.
14.Cost of a standard hospital stay. (Your Health System). Ottawa (ON): CIHI; 2022: https://yourhealthsystem.cihi.ca/hsp/inbrief?lang=en#!/indicators/015/cost-of-a-standard-hospital-stay/;mapC1;mapLevel2;/. Accessed 2022 Aug 31.
15.Isenberg SR, Meaney C, May P, et al. The association between varying levels of palliative care involvement on costs during terminal hospitalizations in Canada from 2012 to 2015. BMC Health Serv Res. 2021;21(1):1-12. PubMed
16.Ommen SR, Mital S, Burke MA, et al. 2020 AHA/ACC guideline for the diagnosis and treatment of patients with hypertrophic cardiomyopathy: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol. 2020;76(25):e159-e240. PubMed
17.Elliott P, Anastasakis A, Borger M, et al. Authors/Task Force members. 2014 ESC Guidelines on diagnosis and management of hypertrophic cardiomyopathy: the Task Force for the Diagnosis and Management of Hypertrophic Cardiomyopathy of the European Society of Cardiology (ESC). Eur Heart J. 2014;35(39):2733-2779. PubMed
18.e-CPS. Ottawa (ON): Canadian Pharmacists Association; 2018: https://www.e-therapeutics.ca. Accessed 2022 Dec 19.
19.Saskatchewan Drug Plan: search formulary. 2022; https://formulary.drugplan.ehealthsask.ca/SearchFormulary. Accessed 2022 Dec 19.
20.DeltaPA. Ottawa (ON): IQVIA; 2022: https://www.iqvia.com/. Accessed 2022 Dec 19.
21.Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Camzyos (mavacamten), 2.5 mg, 5 mg, 10 mg, or 15 mg capsules. Saint-Laurent (QC): Bristol Myers Squibb; 2022 Oct 7.
22.Husser D, Ueberham L, Jacob J, et al. Prevalence of clinically apparent hypertrophic cardiomyopathy in Germany—an analysis of over 5 million patients. PLoS One. 2018;13(5):e0196612. PubMed
23.Maron BJ, Gardin JM, Flack JM, Gidding SS, Kurosaki TT, Bild DE. Prevalence of hypertrophic cardiomyopathy in a general population of young adults: echocardiographic analysis of 4111 subjects in the CARDIA study. Circulation. 1995;92(4):785-789. PubMed
24.Maron BJ, Mathenge R, Casey SA, Poliac LC, Longe TF. Clinical profile of hypertrophic cardiomyopathy identified de novo in rural communities. J Am Coll Cardiol. 1999;33(6):1590-1595. PubMed
25.Maron BJ, Spirito P, Roman MJ, et al. Prevalence of hypertrophic cardiomyopathy in a population-based sample of American Indians aged 51 to 77 years (the Strong Heart Study). Am J Cardiol. 2004;93(12):1510-1514. PubMed
26.Pujades-Rodriguez M, Guttmann OP, Gonzalez-Izquierdo A, et al. Identifying unmet clinical need in hypertrophic cardiomyopathy using national electronic health records. PLoS One. 2018;13(1):e0191214. PubMed
27.Dinh T, Sutherland G. Understanding the gap: a pan-Canadian analysis of prescription drug insurance coverage. Ottawa (ON): The Conference Board of Canada; 2017: https://www.conferenceboard.ca/e-library/abstract.aspx?did=9326. Accessed 2022 Oct 07.
Appendix 1: Cost Comparison Tables
Note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical experts and drug plan. Comparators may be recommended (appropriate) practice or actual practice. Existing product listing agreements are not reflected in the table and the table may not represent the actual costs to public drug plans.
Table 8: CADTH Cost Comparison Table for Treatments Indicated for Obstructive Hypertrophic Cardiomyopathy
Treatment | Strength / concentration | Form | Price ($) | Recommended dosage | Daily cost ($) | Annual cost ($) |
|---|---|---|---|---|---|---|
Mavacamten (Camzyos) | 2.5 mg 5 mg 10 mg 15 mg | Capsule | 61.6000a | Starting dose: 5 mg once dailyb Maximum dose: 15 mg once dailyc | 61.60 | 22,484 |
LVOT = left ventricular outflow tract.
aSponsor’s submitted price.1
bMavacamten starting dose may be decreased to 2.5 mg once daily if LVOT gradient with Valsalva maneuver is less than 20 mm Hg; otherwise, it is maintained at 5 mg.2
cAfter 12 weeks, for patients whose Valsalva LVOT gradient is greater than or equal to 30 mm Hg with persistent symptoms, mavacamten may be increased up to 10 mg per day. A maximum daily dose of 15 mg may be prescribed at subsequent assessments, based on LVOT gradient and persistence of symptoms.2
Table 9: CADTH Cost Comparison Table for Off-Label Treatments for Obstructive Hypertrophic Cardiomyopathy
Treatment | Strength / concentration | Form | Price ($) | Recommended dosage | Daily cost ($) | Annual cost ($) |
|---|---|---|---|---|---|---|
Antiarrhythmic drug | ||||||
Disopyramide (Rythmodan) | 100 mg | Capsule | 0.2950 | 100 mg 3 times daily | 0.89 | 323 |
Beta-blockers | ||||||
Bisoprolol | 5 mg 10 mg | Tablet | 0.0606 0.0885 | 5 mg once daily | 0.06 | 22 |
Metoprolol | 25 mg 50 mg 100 mg | Tablet | 0.0643a 0.0624 0.1361 | 25 mg twice daily | 0.13 | 47 |
Propranolol | 10 mg 20 mg 40 mg 80 mg 120 mg | Tablet | 0.0689 0.1107 0.1225 0.2034 0.1513b | 40 mg twice daily | 0.25 | 89 |
Acebutolol | 100 mg 200 mg 400 mg | Tablet | 0.0787 0.1177 0.2466 | 100 mg twice daily | 0.16 | 57 |
Atenolol | 25 mg 50 mg 100 mg | Tablet | 0.0441a 0.0938 0.1543 | 50 mg once daily | 0.09 | 34 |
Nadolol | 40 mg 80 mg 160 mg | Tablet | 0.2375 0.3410 1.2046 | 40 mg once daily | 0.24 | 87 |
Nebivolol | 2.5 mg 5 mg 10 mg 20 mg | Tablet | 1.4963b | 1.25 mg once daily; increase by doubling the dose at 1- to 2-week intervals | 1.50 | 546 |
Sotalol | 80 mg 160 mg | Tablet | 0.2966 0.1623 | 80 mg twice daily | 0.59 | 217 |
Calcium channel blockers | ||||||
Verapamil | 80 mg 120 mg | Tablet | 0.2735 0.4250 | 120 mg twice daily | 0.85 | 310 |
Diltiazem | 30 mg 60 mg | Tablet | 0.1866 0.3273 | 60 mg 3 times daily | 0.98 | 358 |
oHCM = obstructive hypertrophic cardiomyopathy.
Note: All prices are from the Ontario Drug Benefit Formulary (accessed January 2023), unless otherwise indicated, and do not include dispensing fees.11
Note: All medications are used off-label for oHCM. Doses are based on starting doses from e-CPS18 product monographs and confirmed to be appropriate by clinical experts consulted by CADTH for this review.
aSaskatchewan Drug plan (accessed January 2023).19
bDeltaPA (accessed December 2022).20
Appendix 2: Submission Quality
Note that this appendix has not been copy-edited.
Description | Yes/No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | No | Refer to “The full Health Canada population was not modelled” and “Relevant comparators were omitted” limitations. |
Model has been adequately programmed and has sufficient face validity | No | Refer to “Poor modelling practices were employed” limitation. |
Model structure is adequate for decision problem | Yes | No comment. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | No | Refer to “Poor modelling practices were employed” limitation. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | No | Refer to “Poor modelling practices were employed” limitation. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough detail) | Yes | No comment. |
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note that this appendix has not been copy-edited.

NYHA = New York Heart Association.
Source: Sponsor’s pharmacoeconomic submission.1
Figure 2: Proportion of Patients in Each NYHA Class Over Time in the EXPLORER-HCM Trial and at Baseline in the EXPLORER-LTE Study
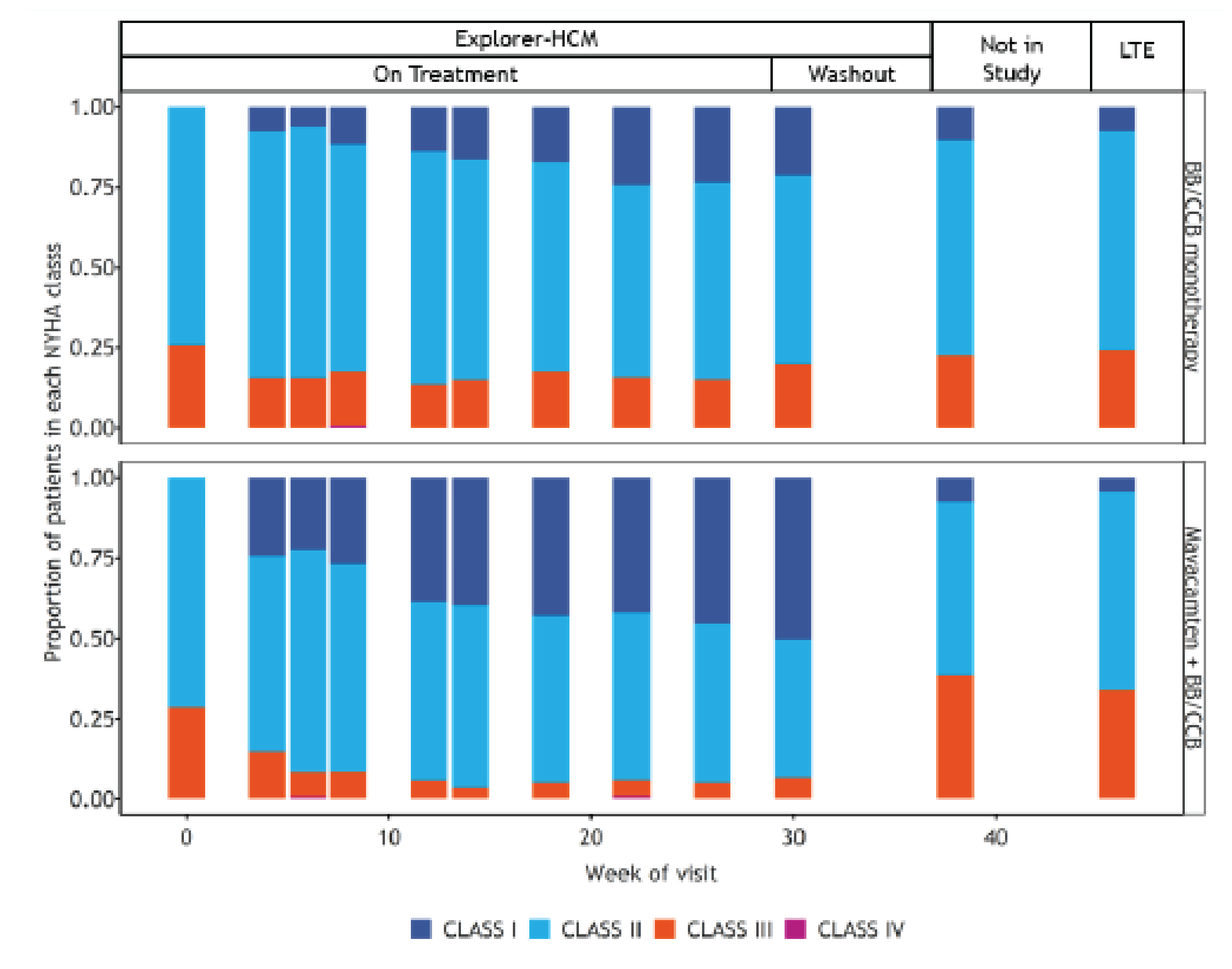
BB/CCB = beta-blocker or calcium channel blocker; HCM = hypertrophic cardiomyopathy; LTE = long-term extension; NYHA = New York Heart Association.
Source: Sponsor’s pharmacoeconomic submission.1
Detailed Results of the Sponsor’s Base Case
Table 11: Disaggregated Summary of Sponsor’s Economic Evaluation Results
Parameter | Mavacamten + BB or CCB | BB or CCB alone | Incremental |
|---|---|---|---|
Discounted LYs | |||
By NYHA class | |||
Total | 17.54 | 15.33 | 2.21 |
NYHA I | 8.64 | 1.20 | 7.44 |
NYHA II | 6.61 | 8.37 | –1.76 |
NYHA III | 1.92 | 4.73 | –2.81 |
NYHA IV | 0.37 | 1.04 | –0.67 |
By treatmenta | |||
Total | 17.57 | 15.37 | 2.20 |
Mavacamten + BB or CCB | 7.78 | 0.00 | 7.78 |
BB or CCB monotherapy | 5.83 | 14.75 | –8.93 |
Disopyramide + BB or CCB | 0.27 | 0.05 | 0.22 |
SRT + BB or CCB | 0.02 | 0.00 | 0.02 |
Post-SRT | 3.67 | 0.55 | 3.12 |
Discounted QALYs | |||
Total | 14.51 | 12.23 | 2.28 |
By NYHA class | |||
NYHA I | 7.44 | 1.03 | 6.40 |
NYHA II | 5.41 | 6.92 | –1.52 |
NYHA III | 1.41 | 3.52 | –2.11 |
NYHA IV | 0.27 | 0.76 | –0.49 |
Adverse events | –0.01 | 0.00 | 0.00 |
Discounted costs ($) | |||
Total | 244,606 | 115,043 | 129,564 |
Treatment Acquisition | 182,414 | 5,225 | 177,189 |
Mavacamten + BB or CCB | 172,370 | 0 | 172,370 |
BB or CCB monotherapy | 1,383 | 3,722 | –2,339 |
Disopyramide + BB or CCB | 177 | 32 | 145 |
SRT + BB or CCB | 7,428 | 1,328 | 6,100 |
Post-SRT | 1,055 | 143 | 913 |
Drug monitoring | 1,214 | 0 | 1,214 |
Health care resource use | 49,616 | 96,427 | –46,812 |
Adverse event management | 5,250 | 6,998 | –1,748 |
Terminal care costs | 6,113 | 6,393 | –280 |
ICER ($ per QALY) | 56,774 | ||
BB = beta-blocker; CCB = calcium channel blocker; ICER = incremental cost-effectiveness ratio; LY = life-year; NYHA = New York Heart Association; QALY = quality-adjusted life-year; SRT = septal reduction therapy.
aDeterministic values; probabilistic results not provided by the sponsor’s model.
Source: Sponsor’s pharmacoeconomic submission.1
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Note that this appendix has not been copy-edited.
Detailed Results of CADTH Base Case
Table 12: Disaggregated Summary of CADTH’s Economic Evaluation Results
Parameter | Mavacamten + BB or CCB | BB or CCB alone | Incremental |
|---|---|---|---|
Discounted LYs | |||
By NYHA class | |||
Total | 20.02 | 19.98 | 0.04 |
NYHA I | 7.81 | 4.18 | 3.63 |
NYHA II | 8.31 | 8.50 | –0.19 |
NYHA III | 3.08 | 5.11 | –2.03 |
NYHA IV | 0.82 | 2.18 | –1.36 |
By treatmenta | |||
Total | 19.99 | 19.95 | 0.04 |
Mavacamten + BB or CCB | 14.51 | 0.00 | 14.51 |
BB or CCB monotherapy | 3.29 | 13.52 | –10.23 |
Disopyramide + BB or CCB | 0.18 | 0.47 | –0.29 |
SRT + BB or CCB | 0.01 | 0.03 | –0.02 |
Post-SRT | 2.00 | 5.93 | –3.93 |
Discounted QALYs | |||
Total | 16.22 | 15.76 | 0.46 |
NYHA I | 6.71 | 3.56 | 3.14 |
NYHA II | 6.74 | 6.95 | –0.21 |
NYHA III | 2.21 | 3.73 | –1.52 |
NYHA IV | 0.57 | 1.53 | –0.96 |
Adverse events | –0.005 | –0.009 | 0.004 |
Discounted costs ($) | |||
Total | 423,927 | 159,190 | 264,737 |
Treatment Acquisition | 336,999 | 16,407 | 320,592 |
Mavacamten + BB or CCB | 330,842 | 0 | 330,842 |
BB or CCB monotherapy | 773 | 3,403 | –2,630 |
Disopyramide + BB or CCB | 115 | 274 | –159 |
SRT + BB or CCB | 4,709 | 11,210 | −6,500 |
Post-SRT | 559 | 1,520 | –961 |
Drug monitoring | 1,398 | 0 | 1,398 |
Health care resource use | 75,877 | 127,906 | –52,030 |
Adverse event management | 3,857 | 9,073 | –5,217 |
Terminal care costs | 5,798 | 5,803 | –6 |
ICER ($ per QALY) | 576,295 | ||
BB = beta-blocker; CCB = calcium channel blocker; ICER = incremental cost-effectiveness ratio; LY = life-year; NYHA = New York Heart Association; QALY = quality-adjusted life-year; SRT = septal reduction therapy.
aDeterministic values; probabilistic results not reported in the sponsor’s model.
Scenario Analyses
Table 13: CADTH Scenario Analyses
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($ per QALY) |
|---|---|---|---|---|
CADTH base case (probabilistic) | BB or CCB | 159,190 | 15.76 | Reference |
Mavacamten + BB or CCB | 423,927 | 16.22 | 576,295 | |
Scenario analysis 1: Long-term symptom progressiona | BB or CCB | 159,064 | 15.74 | Reference |
Mavacamten + BB or CCB | 446,679 | 16.04 | 958,341 | |
Scenario analysis 2: Response-based discontinuation criteria for mavacamtenb | BB or CCB | 159,124 | 15.77 | Reference |
Mavacamten + BB or CCB | 276,206 | 16.27 | 235,438 |
BB = beta-blocker; CCB = calcium channel blocker; EMR = electronic medical record; HR = hazard ratio; ICER = incremental cost-effectiveness ratio; NYHA = New York Heart Association; QALY = quality-adjusted life-year.
aThe proportion of patients whose NYHA class worsened each year (i.e., from class I to II, II to III, or III to IV) was assumed to be equal between mavacamten + BB or CCB, and BB or CCB, after the EXPLORER-HCM trial period (first 30 weeks of treatment).
bAssumptions made by the sponsor regarding the response-based discontinuation of mavacamten: At 30 weeks, the sponsor assumed that patients would discontinue mavacamten if their symptoms had not improved by at least NYHA class from baseline. After 30 weeks, the sponsor assumed that response to treatment would be assessed every 4 weeks and that patients whose symptoms had worsened by one NYHA class since the previous assessment would discontinue mavacamten.
Appendix 5: Submitted BIA and CADTH Appraisal
Note that this appendix has not been copy-edited.
Table 14: Summary of Key Take-Aways
Key take-aways of the BIA |
|---|
|
Summary of Sponsor’s BIA
In the submitted BIA, the sponsor assessed the budget impact of reimbursing mavacamten for the treatment of symptomatic obstructive HCM in adult patients.21 The BIA was undertaken from a publicly funded drug plan perspective over a 3-year time horizon (2024 to 2027) using an epidemiological approach.21 New patients were added to the BIA based on jurisdictional specific population growth rates.
The sponsor compared a reference scenario in which mavacamten is not reimbursed for adult patients with symptomatic oHCM, with a new drug scenario in which mavacamten is reimbursed for adult patients with symptomatic oHCM (NYHA class II or III), which is consistent with the sponsor’s reimbursement request.21 In the reference scenario, patients were assumed to receive either BB or CCB alone or disopyramide plus BB or CCB, with market shares based on expert input obtained by the sponsor and sponsor internal data. In the new drug scenario, the uptake rates for mavacamten were informed by the sponsor’s internal market research, and the sponsor assumed that mavacamten would take market share proportionately from the comparators.21 The sponsor assumed that all patients would receive 5 mg mavacamten daily,2 with unit costs based on the sponsor’s submitted price.1 Dosing for other medications were based on respective product monographs and were consistent with the sponsor’s pharmacoeconomic analysis. Costs for other medications were based on jurisdiction-specific list prices. Mark-ups and dispensing fees were excluded.21 Key inputs to the BIA are documented in Table 19.
Table 15: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (year 1 / year 2 / year 3) |
|---|---|
Target population | |
Prevalence of HCM | 0.22%a |
Percentage of patients diagnosed with HCM | |
Increase in diagnosis rate in year 1, year 2, and year 3 | 3% / 6% / 9%b |
Percentage of patients with oHCM | 50%b |
Percentage of oHCM patients who are symptomatic | 66%b |
Percentage of oHCM patients with LVEF > 49% | 92%4 |
Percentage of oHCM patients treated | 93%b |
Percentage of patients covered | Jurisdiction specific27 |
Number of patients eligible for drug under review | 1,490 / 2,015 / 2,798 |
Market uptake (3 years) | |
Uptake (reference scenario) BB or CCB Disopyramide + BB or CCB | 54.5% / 54.5% / 54.5% 45.5% / 45.5% / 45.5% |
Uptake (new drug scenario) Mavacamten + BB or CCB BB or CCB Disopyramide + BB or CCB | 9.0% / 19.0% / 36.0% 49.6% / 44.1% / 34.9% 41.4% / 36.9% / 29.1% |
Annual cost of treatment (per patient) | |
Mavacamten + BB or CCB BB or CCB alone Disopyramide + BB or CCB | $22,580 $81c $405c |
BB = beta-blocker; CCB = calcium channel blocker.
aSponsor’s internal forecasting.21
bSponsor’s clinical expert and/or sponsor’s data on file.21
cJurisdiction-specific prices were incorporated in the sponsor’s BIA; Ontario shown here as example.
Summary of the Sponsor’s BIA Results
The sponsor estimated the budget impact of introducing mavacamten for the treatment of symptomatic obstructive HCM in adult patients to be $2,997,209 in year 1, $8,556,113 in year 2, and $22,512,526 in year 3, for a total budget impact of $34,065,847 over 3 years.
CADTH Appraisal of the Sponsor’s BIA
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
The number of patients eligible for treatment with mavacamten is highly uncertain. The sponsor used an epidemiologic approach to estimate the number of patients eligible for mavacamten, starting with the prevalence of hypertrophic cardiomyopathy (HCM; not specific to obstructive HCM). The sponsor assumed that, of patients with HCM, 15% would be diagnosed. Clinical expert input received by CADTH for this review indicated that the percentage of patients with HCM who are diagnosed may be between 10% and 20% but were uncertain of the proportion diagnosed in the Canadian context. The sponsor further assumed that 66% of oHCM patients would be symptomatic. Experts noted that the diagnosis of HCM is typically made because of the presence of symptoms. Because the sponsor incorporated both the presence of symptoms at the diagnosis stage for HCM and then again for oHCM, this resulted in the double counting of symptoms in the diagnosis of oHCM, thus underestimating the proportion of symptomatic patients with oHCM.
CADTH additionally notes that the majority of the sponsor’s epidemiological parameters used to derive the eligible population size (prevalence of HCM, percentage of patients with oHCM, percentage of patients who are symptomatic, percentage of patients treated) were informed by sponsor data on file or by expert opinion obtained by the sponsor. CADTH was unable to validate the derivation of these epidemiological parameters. Additionally, clinical expert input received by CADTH for this review suggested that the majority of these values are uncertain, especially in the Canadian context.
In the CADTH base case, it was assumed that all patients who are diagnosed with oHCM would be symptomatic (assuming that the presence of symptoms was accounted for in the proportion of diagnosed patients). CADTH explored uncertainty in the proportion of patients diagnosis in scenario analyses.
The market uptake of mavacamten is uncertain. The sponsor’s base case assumed that 9%, 19%, and 36% of eligible patients would receive mavacamten in years 1, 2, and 3, respectively, based on the sponsor’s internal forecasting projections.21 Clinical expert input received by CADTH for this review suggests that the proportion of people who will uptake mavacamten is uncertain and likely to vary by setting, with higher uptake likely at specialist centres.
CADTH explored uncertainty in the uptake of mavacamten in scenario analyses.
Additional limitations were identified, but were not considered to be key limitations. These limitations include uncertainty regarding the inclusion of dispensing fees and mark-ups in a drug program perspective.
CADTH Reanalyses of the BIA
CADTH revised the sponsor’s base case by assuming that all patients diagnosed with oHCM are symptomatic, removing the increase in oHCM diagnosis rate and including drug mark-ups and dispensing fees in the analysis (Table 20).
The results of the CADTH stepwise reanalysis are presented in summary format in Table 17and a more detailed breakdown is presented in Table 18. In the CADTH reanalysis, the 3-year budget impact of reimbursing mavacamten for oHCM was $54,641,769 (year 1: $4,807,445; year 2: $13,723,972; year 3: $36,110,351).
Table 16: CADTH Revisions to the Submitted BIA
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
None | — | — |
Changes to derive the CADTH base case | ||
1. The percentage of diagnosed patients with oHCM who are symptomatic | 66% | 100% |
2. Drug mark-ups and dispensing fees | Excluded | Included |
CADTH base case | 1 + 2 | |
BIA = budget impact analysis; oHCM = obstructive hypertrophic cardiomyopathy.
Table 17: Summary of the CADTH Reanalyses of the BIA
Stepped analysis | Three-year total |
|---|---|
Submitted base case | $34,065,847 |
CADTH reanalysis 1 – Patients with diagnosed oHCM assumed to be symptomatic | $51,614,920 |
CADTH reanalysis 2 – Mark-ups and dispensing fees included | $36,063,567 |
CADTH base case (1 + 2) | $54,641,769 |
BIA = budget impact analysis; oHCM = obstructive hypertrophic cardiomyopathy.
CADTH also conducted additional scenario analyses to address remaining uncertainty, using the CADTH base case. Results are provided in Table 18:
Assuming that a higher proportion of patients with HCM are diagnosed (i.e., 18.75%, reflecting a 25% increase over the sponsor’s value).
Assuming that the uptake of mavacamten is 25% higher per year than assumed by the sponsor.
Excluding dispensing fees and mark-ups (i.e., only drug costs included).
Assuming that the price of mavacamten is reduced by 73%.
Table 18: Detailed Breakdown of the CADTH Reanalyses of the BIA
Stepped analysis | Scenario | Year 0 (current situation) | Year 1 | Year 2 | Year 3 | Three-year total |
|---|---|---|---|---|---|---|
Submitted base case | Reference | $278,146 | $340,072 | $459,852 | $638,582 | $1,438,506 |
New drug | $278,146 | $3,337,280 | $9,015,965 | $23,151,108 | $35,504,354 | |
Budget impact | $0 | $2,997,209 | $8,556,113 | $22,512,526 | $34,065,847 | |
CADTH base case | Reference | $1,778,642 | $2,174,483 | $2,940,236 | $4,082,874 | $9,197,593 |
New drug | $1,778,642 | $6,981,929 | $16,664,208 | $40,193,225 | $63,839,361 | |
Budget impact | $0 | $4,807,445 | $13,723,972 | $36,110,351 | $54,641,769 | |
CADTH scenario 1: increased proportion of HCM patients diagnosed | Reference | $2,223,303 | $2,627,501 | $3,401,779 | $4,553,116 | $10,582,396 |
New drug | $2,223,303 | $8,436,497 | $19,280,117 | $44,822,702 | $72,539,317 | |
Budget impact | $0 | $5,808,996 | $15,878,338 | $40,269,586 | $61,956,921 | |
CADTH scenario 2: increased mavacamten uptake | Reference | $1,778,642 | $2,174,483 | $2,940,236 | $4,082,874 | $9,197,593 |
New drug | $1,778,642 | $8,183,790 | $20,095,201 | $49,220,812 | $77,499,804 | |
Budget impact | $0 | $6,009,307 | $17,154,965 | $45,137,939 | $68,302,211 | |
CADTH scenario 3: markup and dispensing fees excluded | Reference | $421,433 | $515,260 | $696,746 | $967,549 | $2,179,555 |
New drug | $421,433 | $5,056,485 | $13,660,554 | $35,077,436 | $53,794,475 | |
Budget impact | $0 | $4,541,225 | $12,963,808 | $34,109,887 | $51,614,920 | |
CADTH scenario 4: analysis: 73% price reduction for mavacamten | Reference | $1,778,642 | $2,174,483 | $2,940,236 | $4,082,874 | $9,197,593 |
New drug | $1,778,642 | $3,484,788 | $6,680,804 | $13,925,007 | $24,090,599 | |
Budget impact | $0 | $1,310,304 | $3,740,568 | $9,842,134 | $14,893,006 |
Stakeholder Input
Patient Input
HeartLife Foundation
About the HeartLife Foundation
The HeartLife Foundation is a patient-driven charity whose mission is to transform the quality of life for people living with heart failure by engaging, educating, and empowering a global community to create lasting solutions and build healthier lives. HeartLife Foundation is Canada’s first – and only – national patient-led Heart Failure organization. We are a Federal Charity aimed at raising public awareness of Heart Failure, engaging patients, families, and caregivers to provide education and support, facilitate access to the latest research, innovations, and treatments, and advocate better care for all.
Founded by Dr. Jillianne Code, a two-time heart transplant recipient, and Mr. Marc Bains, a heart failure survivor and transplant, we have a network of over 1.000 patient and cares across the country. As a volunteer run organization, The HeartLife Foundation works with 15-20 patient and carer champions to administer service programs, support groups, workshop events, public awareness campaigns and government relations activities. In collaboration with Dr. Sean Virani, one of Canada’s leading heart failure specialists, thought leaders, and promoter of patient and family centered care, we endeavor to ensure that there is an open dialog including patients as partners with healthcare providers, government, and industry across Canada. Website: www.heartlife.ca
Information Gathering
In-depth interviews with expert physicians in the Cardiovascular and HCM disease areas.
In-depth interviews with patients living with cardiovascular disease and HCM.
Review of study material and online literature.
Disease Experience
Hypertrophic cardiomyopathy (HCM) is complex and chronic disease that can impact generations and affects people regardless of age, race, or gender. According to the CMAJ, HCM is a common genetic cardiomyopathy that occurs in 1 in 500 individuals. HCM has come to prominence as it is a major cause of sudden cardiac death for people under the age of 30. Common symptoms of HCM which can greatly impact quality of life include chest pain, palpitations, shortness of breath, fatigue and fainting. All which, negatively impact physical and mental health of individuals living with the disease. HCM often results in the need for invasive procedures such as surgery or ablation. HCM can lead to heart failure, end stage heart failure, and ultimately the need for a heart transplant.
The negative impact on quality of life were evident during our patient interviews. Excerpts of the interviews are below:
Patient 1 - "The difficulty breathing has always been my biggest problem. At 39 I was diagnosed with HCM and shortly after that I had an ICD/Pacemaker implanted. When I started to learn about HCM I would look back and recall having problems breathing since a young age, I would always wonder why I had to take a lot of breaks during activities and nobody else did. As the HCM progressed it drastically affected my activity level and even what I’m capable of doing. I could no longer hike or jog or cross-train and everything exhausted me."
Patient 2 - "The main issue I am experiencing is decreased exercise capacity. Secondary issues are cold tolerance and fatigue. I also can’t run. This impacts my long-term health and ability to enjoy time with my children."
As you may imagine, the symptoms of HCM impact day to day living for anyone diagnosed with the disease. Furthermore, HCM can cause serious complications and lead to heart failure, stroke, life threatening arrhythmias, and sudden cardiac death.
Similar to a diagnosis of heart failure, HCM affects patients’ families and friends both mentally and physically. According to an article by the Cleveland Clinic, the cause of HCM can be unknown or attributed to genetics, high blood pressure or aging, making it difficult to identify a high-risk population. Clinical Therapeutics states, HCM can be hereditary, with up to 60% of cases estimated to be associated with autosomal dominant genetic mutations. As a hereditary disease, the unknown of disease presence in all family members is continually on the mind of patients and their caregivers. A simple, but impactful response from a patient interview sums up the immense affect patients' families and friends.
Patient 1: "My father, aunt and cousin had it and they are all deceased now, so it affects my life a lot."
Experiences With Currently Available Treatments
Current therapies for HCM include invasive procedures such as heart surgery and alcohol septal ablation, therapies used to reduce thickening of the septum, the wall separating the right and left sides of the heart. Both, impacting quality of life of patients and their caregivers. Less invasive therapies include medications such as beta-blockers, calcium channel blockers and antiarrhythmics, all common heart failure medications are often prescribed to treat the symptoms of HCM and prevent worsening of the disease. Even with current treatment, there are concerns from both patients and healthcare providers.
Patient 1: "My main concern is that beta-blockers do not treat the underlying condition. As I am relatively young at 45 years old, I’d like to consider my long-term heart health and management of degeneration. Otherwise, the beta-blockers have maintained a stable condition since diagnosis. Albeit with loss of exercise capacity."
Furthermore, a review in in the CMAJ states that current medication therapies for HCM are generally inadequate or not sufficiently tolerated by patients. The review goes on to say that invasive procedures as discussed above are a) have difficult eligibility requirements, b) may have short term and long-term complications, and c) may result in poor outcomes.
An excerpt from Patient 2 provides deeper insight into the challenges and impact on quality of life with current available treatments: "I’m being treated mainly with medications and I tend to get severe side effects for months which could cause me to vomit for 3 weeks straight or not be able to get off my couch because of nausea. They also affect your body long term and I’ve developed chronic kidney disease, severe gout, acid reflux, diabetes and thyroid disease.
My biggest hurdle was definitely time off work. I was constantly leaving work to go to appointments, tests, procedures, treatments and I got paid hourly so I wouldn’t make an income for the time it took to be in the appointment or back and forth from it. Since I’m a single income household I would then have to work overtime. I also had to use up way more sick days then my employer had allotted for the year which meant using up my holidays or overtime."
Improved Outcomes
Canadians living with HCM have unique journeys. It is always important to consider both quantitative and qualitative outcomes when evaluating new therapies. HCM patients and their caregivers must think and live with the symptoms and effects of HCM on a daily basis as well the possibility of loved ones being diagnosed with the disease. Many patients and caregivers may take time from work, school, and social activities such as travel or leisure.
Qualitatively, patients and carers consider quality of life indicators and experiences such as but not limited to spending time with loved ones, the ability to go to work on regular basis, pursuing outdoor activities, and the ability to travel. Often, and in the case of our members, quality of life takes precedent over quantity of life. Reduced symptoms and hospital admissions increase quality of life indicators.
Experience With Drug Under Review
Findings from a Cleveland Clinic led clinical trial showed that the use of Mavacamten in severely symptomatic, HCM patients significantly reduced the need for invasive procedures. After 16 weeks, 43 of the 56 placebo-treated patients (76.8%) continued to meet guideline criteria for surgery or elected to undergo surgery compared with 10/56 (17.9%) mavacamten-treated patients. The study demonstrated significant reduction in left ventricular outflow tract pressure gradient in mavacamten-treated patients, along with improvements in quality-of- life measures.
As one Patient puts it: "Daily life and quality of life would drastically improve with a treatment to help with my breathing. Mavacamten treats the underlying cause of the condition while reducing side effects like fatigue and limited exercise capacity. That will enable continued focus on fitness, decreasing the likelihood of invasive therapies."
“These results could give what can be a very sick patient population a non-invasive therapy alternative,” said Milind Desai, M.D., MBA, director of the Hypertrophic Cardiomyopathy Center and director of clinical operations in Cleveland Clinic’s Heart Vascular & Thoracic Institute, and principal investigator of the trial.
Advances in HCM care through therapies such as Mavacamten can reduce worsening HCM, limit the need for invasive procedures, and reduce the risk of sudden cardiac death.
Companion Diagnostic Test
Not applicable.
Anything Else?
Hypertrophic cardiomyopathy is a complex type of heart disease and affects an estimated one in 500 people, but many of those patients go undiagnosed until the disease has progressed. Mavacamten treats the underlying cause of the condition while reducing side effects like fatigue and limited exercise capacity. “These results could give what can be a very sick patient population a non- invasive therapy alternative,” said Milind Desai, M.D As a hereditary disease, the unknown of disease presence in all family members is continually on the mind of patients and their caregivers. The CMAJ states that current medication therapies for HCM are generally inadequate or not sufficiently tolerated by patients. “
Key Findings from the EXPLORER-HCM Trial include:
45 (37%) of 123 patients on mavacamten versus 22 (17%) of 128 on placebo met the primary endpoint (difference +19·4%, 95% CI 8·7 to 30·1; p=0·0005).
Patients on mavacamten had greater reductions than those on placebo in post-exercise LVOT gradient.
Patients on mavacamten had improved symptom scores (KCCQ-CSS +9·1, 5·5 to 12·7; HCMSQ-SoB −1·8, −2·4 to −1·2; p<0·0001).
34% more patients in the mavacamten group improved by at least one NYHA class (80 of 123 patients in the mavacamten group vs 40 of 128 patients in the placebo group Interpretation.
Treatment with mavacamten improved exercise capacity, LVOT obstruction, NYHA functional class, and health status in patients with HCM.
References
https://www.cmaj.ca/content/185/2/127#ref-1
https://www.clinicaltherapeutics.com/article/S0149-2918(21)00460-4/pdf
https://www.thelancet.com/article/S0140-6736(20)31792-X/fulltext
Conflict of Interest Declaration — HeartLife Foundation
To maintain the objectivity and credibility of the CADTH reimbursement review process, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission?
No.
Did you receive help from outside your patient group to collect or analyze data used in this submission?
No.
List any companies or organizations that have provided your group with financial payment over the past 2 years AND who may have direct or indirect interest in the drug under review.
Table 1: Financial Disclosures for the HeartLife Foundation
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
BI | — | — | — | X |
AZ | — | — | — | X |
Novartis | — | — | X | — |
BMS | — | — | X | — |
Bayer | — | — | X | — |
Servier | — | X | — | — |
Canadian Heart Patient Alliance
About the Canadian Heart Patient Alliance
The Canadian Heart Patient Alliance (CHPA) is a patient-led nonprofit umbrella organization of patients, families, health professionals and supporters dedicated to reducing cardiovascular disease and preventing early death due to genetic, environmental, lifestyle, and other risk factors. CVD is the leading cause of death and disability in Canada but remains profoundly under-diagnosed and under-treated. Our focus is improving awareness, screening, testing, diagnosis, care, and treatment of all CVDs. The Canadian Heart Patient Alliance is working toward the day when no Canadian will suffer reduced quality of life, life-altering event, or early death due to undiagnosed or untreated cardiovascular disease.
The FH Canada Patient Network receives organizational and administrative support from the Institute for Optimizing Health Outcomes, a nonprofit organization guided by the vision of optimizing health outcomes for all individuals regardless of their health condition. The Canadian Heart Patient Alliance is the successor the FH Canada Patient Network and collaborates with FH Canada, Heart Healthy Prevention Program St.
Paul’s Hospital, and Lipid Genetics Clinic at LHSC-University Hospital. Internationally, CHPA engages with the FH Foundation (USA), Heart UK, and FH Europe.
Information Gathering
Recruitment: There had been no clinical trials in Canada and no clinicians who had experience with mavacamten. In the United States and Italy, "high-volume" HCM centres, specialized to diagnose, treat, and monitor patients with high-risk, symptomatic HCM, were primary sites for mavacamten clinical trials.
Extensive interviews to understand the patient impact of the therapy, including the benefits, challenges, and recommendations for use in real-life settings, were conducted with three clinicians (two in the USA and one in Italy) who had conducted clinical trials for mavacamten. In addition, we met with staff from the US- based Hypertrophic Cardiomyopathy Association, a 9,000+ patient association, which also includes many Canadian members. They provided in-depth information reflecting requests for information and assistance and their one-on-one counselling of patients with HCM who were either on treatment, starting treatment or seeking treatment with mavacamten. We were also able to review recorded panel discussions, patient testimonials, and educational videos.
Participants for this submission were recruited through the US-based clinicians as well as outreach through our database for the Canadian Heart Patient Alliance in Canada. As npted, additional patient profiles and confirmatory information were provided by the Hypertrophic CardioMyopathy Association. The responses reported reflect input from 16 patient interviews, all self-identifed as diagnosed with symptomatic obstructive hypertrophic cardiovascular myopathy, conforming to the approved indication in the USA and the submission by the company to Health Canada.
Among respondents about three-fifths (10 out of 16) were female, and age range from mid-30s to mid-70s. Specifically, 31% were over 65 years old, 25% under 45 years of age, 19% between 45 and 54 years old, and 25% between 55 and 64 years old. Overall, 62.5% of patients were female and 37.5% male. In terms of residence, 31% (5 individuals) identified as Canadians (1 living in USA) and 69% (11) as Americans.
All participants reported they had been diagnosed with "obstructive" HCM. About 40% also identified as diagnosed with Class 2 Heart Failure according to the NYHA and 40% with Class 3 HF, while the remainder said they were Class 2/3 or unsure. Finally, about 25% said they were also diagnosed with atrial fibrilation.
Among the participants, four have been treated with mavacamten and 12 have not. All those receiving treatment are residents in the USA. In terms of demographics, there were no notable differences between treated and non-treated.
Disease Experience
Interviewed participants were asked through (1) open-ended questions to describe the experience of the patient and caregivers of living with HCM (before and after diagnosis) and (2) a series of issues identified in other published studies to indicate whether they had also personally experienced these and, if so, to describe the impact.
Across all participants, it was clear that HCM has a major impact on the patients’ quality of life. The experiences of Canadian and American patients were highly similarly so the combined results are reported here.
Impact of Delayed and Misdiagnosis
The most common experience among all participants is delayed and/or misdiagnosis. About half said they had experience initial symptoms while still in their teens, with almost half of these said symptoms started as children, pre-teen. In contrast, about one-fourth said they were diagnosed around 40-50 years of age and about one-fourth said they did not receive a diagnosis of HCM until they were in their 60's. it is not possible to articulate the number of "misdiagnoses" since in many cases patients were diagnosed and treated for symptoms, including "shortness of breath" or asthma; palpitations or atrial fibrillation, fatigue or sleep disorders, depression or generalized anxiety, stress-induced panic or fainting attacks, and other forms of cardiovascular conditions including high blood pression, heart murmur, and valvular condition, including aortic stenosis. The following are some of the experiences related.
“Looking back, I had been having symptoms for decades, since my late teens. But most doctors only prescribed medications for my symptoms and never identified what was causing them."
“As a child, I was diagnosed with asthma and put on inhallers with corticosteroids. As i got olderI was put on other medications, some of which had a lot of side effects. I gained a lot of weight even though I was careful with my diet. The doctors put a lot of emphasis on losing weight and increasing exercise but didn't seem to beleive I couldn't do what they recommended.”
"My symptoms, both physical and mental, were not consistent and not predictable; so, without a diagnosis for many years, it was hard to explain to people, even those close to me, what I was going through. Some people just didn't believe it was all that bad since a lot of the time I looked fine and was okay. Even I doubted myself and believed it was my fault that I couldn't manage the stress and anxiety.
"Every time I went into ER with heart palpitations or chest pain, the doctors asked the same questions but seemed to have no idea what to do. I had to explain each time what I was experiencing but I couldn't understand most of the time myself."
“The hardest part was the anxiety of not knowing when I would get symptoms or even how bad they could get. The doctors kept prescribing different medicines, including beta blocks, calcium channel blockers, and even digoxin but it always felt like they were just treating symptoms and never seemed to avoid the attacks.”
“Finally getting a diagnosis actually increased my anxieties since the future of the disease was fairly grim with no real treatments and only options were ablation and surgery in my future. I heard about clinical trials, but they were only available through very specialised centres and none near me.”
“Looking back, it was odd that none of my doctors had looked at my family history, even though my father, my uncle and others on his side of the family had all experienced heart disease, including heart failure and cardiac arrest. And even after I got a diagnosis, they did not recommend having my kids tested, though I was sure that at least one of my sons had also inherited the condition.”
Shortness of Breath
All participants indicated that they experienced shortness of breath, with some saying it was their earliest symptom and others that it continued to be the most persistent and impactful on daily activities. This was described by some as follows:
"Our family took regular walks together, but I found myself unable to keep up. I knew something was seriously wrong when I couldn't even keep up with my grandmother and five-year-old grandson."
"I first noticed severe shortness of breath with chest pain after my son was born. The doctors just put it down to post-partum symptoms but when it continued for months, it didn't feel at all normal. I was exhausted all the time and my heart rate was erratic.
"Along with the shortness of breath, i was also experiencing lightheadness, fatigue, and brain fog so it was impossible to even have an ordinary conversation. I found myself sleeping almost the entire day so that I could at least be present for my kids when they came home from school. But every day was still a struggle."
Exercise Intolerance
Related to the shortness of breath was the second most frequently mentioned and problematic symptom, intolerance of exercise. This was mentioned as interfering with participation in sports but also daily living activities.
“In school, I had been very good at sports, especially soccer, but found I was increasingly unable to keep up. So, I switched to playing goalie but even that got difficult after a while. Doctors really had no advice at the time, so I just took myself out of most team sports.”
“As my symptoms got worse, I went from running to biking to jogging and then just walking."
"Dancing was what brought my husband and I together; we even entered some dance competitions. But over time it has become almost impossible for us to even get through one slow dance before I need to sit down."
Arrythmia, Palpitations, and Chest Pain
Participants complained about chest symptoms that they described as "fluttering" or "pounding" in their chest as well as feelings like a "tight band" around their chest or a "heavy weight" sitting on their chest.
"I am never sure what triggers it but suddenly my heart just seems to start racing on its own. It can happen without any warning and even with no provocation, like i am literally just sitting down reading or having a cup of tea. It is very frightening and stressful."
"I had had a lot of minor palpitations before but the first time I had a really scary attack was at my son's baseball game. I put it down to the heat and the excitement which probably did aggravate the symptoms but since then I have had numerous attacks without any provocation."
"It feels like someone has put a band around my chest and then keeps pulling it tighter and tighter until I just can't bear it any longer. Even lying down doesn't help."
Other symptoms mentioned by one or more participants were fatigue (chronic or episodic), depression, and episodic brain fog.
"It had gotten to the point where I was tired all the time; I couldn't focus on anything; I would fall asleep just watching TV or reading. Worse of all, I would have episodes when I couldn't remember what I had just been doing or how long I had been "out of it."
"When I first had memory lapses or lost the thread of a discussion at work, people were really understanding and tried to help but after a while, it was clear that I just couldn't keep up with the demands. It felt like a final defeat, that my heart disease had won and there was no way back."
Experiences With Currently Available Treatments
Participants reported they had experienced a variety of treatments, including surgery, implantable cardioverter defibrillators, and a variety of medications. However, all reported that their symptoms and feelings of uncertainty and anxiety were never fully resolved.
"I don't know what else I can do. Having HCM is living with a sword over your head. It can cause sudden death, with no warning, even if you do everything right."
"Sometimes I feel like I am walking on eggs, but I also try not to show how worried I am around my kids. After my last heart attack, I can feel them watching me, trying to keep a look out for every little sign that I am having palpitations or chest pain. It's not fair to them."
All participants reported that they had made changes in their diet and were trying to reduce stressors in their life. "One good thing is that we are all trying to live healthier, but it is not enough. I am just glad that I can still do most things with them, even if I need to go slower or to take longer rests."
All of the participants said they were taking some cardiac medications. Most had been prescribed beta- blockers and calcium channel blockers. However, about three-fourths reported experience adverse reaction associated with the medications, such as dizziness, confusion, heart palpitations, and increased anxiety.
"I was never confident that these medications were working but the worst thing was the side effects. How can a medication that is supposed to reduce the risk of a heart attack give you the same symptoms as your heart condition? My heart palpitations seemed to increase, I had bouts of confusion and dizziness that were more frequent and worse than previously. I experimented with taking only a half dose and finally stopped taking the drugs;"
Two participants said they had received open-heart surgery, one about five years ago and the other within the past year. The former patient was a 63-year-old man who suffered cardiac arrest when he was alone in his home. Luckily his neighbor discovered him and rushed him to ER where they decided to perform the surgery right away.
"I always knew I was at risk. My father had died of a heart attack when he was only 48 years old. I was doing everything I thought I needed to do to avoid the same fate: eating a pretty healthy diet, walking and exercising lightly, and taking my medications religiously. Interesting, one of the side effects of the meds was possible cardiac arrest, but who knows what caused it. I feel like maybe nothing could have been."
Two participants had an implantable cardioverter defibrillator. One was a relatively young man and the other a female in her mid-50s.
"If you had asked me a year ago, I would have thought I could manage on my own and this [ICD] would just make me into an invalid. But two weeks after I got it, I actually got a shock that may have saved my life.”
“Now, I feel like it is just another thing I am doing to manage my HCM. An ICD is a lot better than heart surgery."
All of the participants were aware of newer medications that were designed to work specifically for HCM. "I really hope they are going to be available soon, but I have also heard that they are not going to be right for everyone. But if the drugs can let me return to a normal life, I would be willing to try them."
Four of the participants were taking Mavacamten. All indicated they had few or no side effects after the first couple of weeks. They also felt they were able to breathe more easily, to carry out daily activities without as much fatigue, and had fewer symptoms of chest pain or palpitations.
Improved Outcomes
Participants responded that they wanted treatments to reduce the risk of heart failure (sudden death) as well as reductions in the debilitating symptoms that affected daily living activities and quality of life, including shortness of breath, irregular heartbeat, palpitations, chest pain, fatigue, and stress/anxiety.
“I don’t believe there is a miracle drug or a cure around the corner but medication that could reduce the risk of a heart attack and death would reduce the anxiety and stress on me and my family.”
“I don’t think it is asking too much to be able to go back to just doing ordinary things like getting dressed, going for a walk, and playing with my dog without gasping for breath or stopping every few minutes.”
“I am scared to death of surgery, but I feel like it is inevitable, so anything that would let me avoid this would be a relief.”
Experience With Drug Under Review
All four patients on mavacamten had received the drug through clinical trials. All resided in the USA. All were diagnosed with symptomatic obstructive HCM and had been experiencing symptoms for years, some for decades, even prior to a diagnosis. All were receiving treatment and care at "high-volume" centres of excellence. All were very positive about the drug therapy and expressed hope that it could be available to everyone.
"I feel very lucky that I was able to get mavacamten through a clinical trial. I know it is not a cure and that it will not return me to perfect health, but I feel that it will lower my symptoms and importantly reduce my risk of a cardiac arrest or even sudden death."
"I was 'warned' that I would need to comply with a very strict follow-up echocardiogram program because of a risk of heart failure, which could be fatal. Frankly, I don't see this as a negative but a positive to know that I will be so closely monitored."
"I have had no side effects and while I don't feel like I could climb a mountain, I can climb a flight of stairs without gasping for breath. I can cook a whole meal and have enough energy to do dishes (which may not seem like a victory to others)!
"I used to spend all my time doing as little as possible, trying to conserve energy just to get through the day. Since I have been on macavantem, I have been a lot more motivated to do things, to stay on diet, to go out with friends, and to do gardening which always makes me smile.
"I don't get up every day in a total panic, dreading what could happen. I now feel like I have more energy but as importantly I feel much more optimistic about what today and tomorrow may bring."
Companion Diagnostic Test
Prior to approval for mavacamten, patients must be assessed for their cardiac status and specifically by echocardiogram of left ventricular ejection fraction (LVEF) as well as other illnesses (e.g., infections or chronic disease), other cardiovascular symptoms (arrhythmias), and other medications. Because of the risk of heart failure associated with mavacemten, the patient must be closely monitored with echocardiogram for the first few months but also on a regular basis (every three months) as well as reporting of any symptoms. This limits prescribing of mavacamten to patients who have access to a high-volume clinic and are committed to regular monitoring and reporting of symptoms.
Patients expressed agreement with the importance of the pre- and post-access monitoring and commitment to prescribing, given the risks, despite the inconvenience of regular hospital visits.
Anything Else?
This disease affects the entire family in various profound ways, especially those who had tested positive for a genetic variant. Two-thirds (11 out of 16) reported that they had at least one family member diagnosed with or suspected of having HCM. This put pressure on informing other family members who had not been diagnosed and raised anxieties about the need to test their children. "Some family members did not want to get tested, saying they would prefer not to know, citing they were not experiencing any symptoms and I felt so worried but also guilty about passing this condition to my children. They are still young, and we haven't decided to get them tested. I don't think there is anything we can do at this time anyway."
Regardless of a genetic factor, HCM was reported as putting a considerable strain on family relationships. The symptoms are severe and unpredictable, putting a strain on the best of relationships, often with significant outcomes.
"I feel like I am always apolozing to my son for not being able to take him to his practices or be at his games. He says it's okay, but I feel like he resents it and is embarrassed in front of his friends. Mostly, I worry about what could happen in the future."
Some reported a serious impact on their marital relations.
"We couldn't talk about my condition. Most of the time, we were not even sleeping in the same room. We just drifted further apart."
"I came back from surgery and found that my husband had left. I had no job and two kids to raise. I was constantly tired, but I tried to keep things as normal as possible for them.”
A number of participants spoke about their guilt at being a strain on their family, at not being able to fully participate with family activities, and to meet their family obligations.
Conflict of Interest Declaration — Canadian Heart Patient Alliance
To maintain the objectivity and credibility of the CADTH reimbursement review process, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission?
No external help was received to complete this submission.
Did you receive help from outside your patient group to collect or analyze data used in this submission.
No external help was received to complete this submission.
List any companies or organizations that have provided your group with financial payment over the past 2 years AND who may have direct or indirect interest in the drug under review.
Table 2: Financial Disclosures for the Canadian Heart Patient Alliance
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
No funding over past two years | — | — | — | — |
Clinician Input
Cardio1
About Cardio1
Cardio1 is a community-based cardiology clinic who provides management and treatment of patients with various cardiac diseases. The clinic team consists of a cardiologist, nurse practitioner, clinical assistant, physician assistant and a clinical research manager.
Information Gathering
Information was gathered from national cardiac/ heart failure conferences, local grand rounds, published articles and information from medical liaison from Bristol Myers Squibb company.
Current Treatments and Treatment Goals
Current treatments for hypertrophic cardiomyopathy (HCM) are based on symptoms management. Drug therapies include beta- blocker, calcium channel blocker such as verapamil, and disopyramide. Disopyramide is usually use when there is no response to the former drugs. These drugs are non- disease specific, do not modify the underlying disease but reduces symptoms so patients may have a better quality of life. The use of these drugs is limited due to potential adverse effects. Disopyramide use is limited due to its pro arrhythmic effect. Those who are refractory to drugs may benefit from septal reducing therapy (SRT) such as surgical myectomy and septal ablation. These treatments may modify the underlying disease mechanism by reducing the size of the left ventricular hypertrophy/ septum and reduce outflow obstruction. Surgical myectomy and septal ablation are not without potential adverse and therefore proper patent selection for the procedure is important. There are offered when drug treatment for reducing symptoms fail.
Current treatments are used to reduce symptoms and may delay disease progression. There is paucity in the treatment and management of HCM for many years. There’s paucity even on our national evidence-based guideline in the management of this disease. HCM was briefly discussed in the Canadian Cardiovascular Society guidelines in 2008 (disease management) and 2017 (indication for implantable defibrillator). A new treatment for HCM such as Mavacamten is a welcome news for clinicians and patients with HCM.
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
As discussed in number 3 above, drug therapies are limited, non-disease specific, and patient response varies. Surgical and percutaneous septal ablation also have limitations and require proper and careful selection of patients. There is unmet medical need for better non-invasive alternative to SRT. There are no available treatments to reverse the course of the disease but mostly for symptoms relief for better quality of life. It is good to note that in Explorer -HCM study of Mavacamten, there was a 9-point improvement in KCCQ score as well as improvement in patients’ NYHA score by 1-2 classes. These reported results are quite impressive. We have not seen Quality of Life studies with other drug therapies in HCM.
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
As with other new therapies, it is important to properly select patients for the treatment. It will be important to look at the characteristics of patients included in the study. That will help us, clinicians, to identify patients who may benefit from this new alternative drug treatment when approved and becomes available. It is also important to continue to watch for updates on long-term studies on this new drug. Further long-term study results may lead us to choose Mavacamten as first line treatment for symptomatic obstructive HCM. For the time being, it may be necessary to use conventional therapy we have and switch to Mavacamten when they fail. However, it is important to assess patient’s response to conventional treatment timely and decide to switch to new treatment in a timely manner to prevent patients from suffering longer than necessary.
What we currently have are non-disease specific drug to reduce symptom related to obstructive HCM. We can anticipate a shift of treatment paradigm with potential approval of Mavacamten specially for those who may not currently be a candidate for SRT or need to delay SRT.
Which patients would be best suited for treatment with the drug under review? Which patients would be least suitable for treatment with the drug under review?
Carefully selected patients such as those unresponsive to current available drug treatment would be a good candidate for this drug. As well, patients who may not be a candidate for early SRT or those who wants to delay SRT or those who does not want SRT procedure. Misdiagnosis of HCM may occur, Other potential diagnosis such as infiltrative cardiac diseases must be ruled out first. Investigations for proper diagnosis of HCM may include transthoracic echocardiogram, cardiac MRI with LGE as well as good history and physical assessment by clinicians should be included.
Those patients who are deemed to have poor QOL based on available tools (i.e., NYHA class, Minnesota Living with Heart Failure, KCCQ) who are receiving conventional therapy should be considered for this new drug therapy.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice? How often should treatment response be assessed?
Clinicians need to have a strategy in monitoring and identifying changes in the clinical course of the disease in patients. A well- studied quality of life (QOL) assessment tools such as Minnesota Living with Heart Failure, KCCQ and NYHA score may be used to assess patient’s response. A longitudinal assessment such as at 1,3,6,9, and 12 months after initiation of treatment maybe appropriate or with every patient clinic visit. QOL assessment tools should be easy to administer. Currently we use NYHA functional class, information on hospitalizations and ER visits and performance of ADLs when assessing patients. Other tools can also be incorporated.
What factors should be considered when deciding to discontinue treatment with the drug under review?
Patient reported side effects, ECG criteria (QT prolongation), non-responsive to therapy after an optimum duration of receiving the therapy (duration depends on patient- clinician assessment/ decision), when patient withdraws from the therapy.
It is also important to assess LV EF on a regular basis especially on those who remain symptomatic. A reduction in EF and continuing heart failure symptoms may indicate heart failure with reduced EF. Mavacamten may have to be stopped and treatment for HFrEF may have to be started.
What settings are appropriate for treatment with [drug under review]? Is a specialist required to diagnose, treat, and monitor patients who might receive [drug under review]?
A clinic with a cardiology team that has dedicated clinicians with experience in management of heart failure including HCM.
Additional Information
It would be important to see the mortality, morbidity and hospitalization outcomes of this drug.
Conflict of Interest Declarations — Cardio1
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation.
Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please refer to the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission?
No.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission?
The Medical Liaison from Bristol Myers Squibb provided pdf of studies on Mavacamten as per our request.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician who contributed to the input — please add more tables as needed (copy and paste). It is preferred for all declarations to be included in a single document.
Declaration for Clinician 1
Name: Peiman Marzban
Position: Cardiologist, Medical Director, Cardio1
Date: 17/10/2022
Table 3: COI Declaration for Cardio1 — Clinician 1
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Declaration for Clinician 2
Name: Estrellita Estrella-Holder
Position: Nurse Practitioner
Date: 17/10/2022
Table 4: COI Declaration for Cardio1 — Clinician 2
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Declaration for Clinician 3
Name: Amaka Chukwura
Position: Clinical Assistant
Date: 17/10/2022
Table 5: COI Declaration for Cardio1 — Clinician 3
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Independent Cardiologist Louis Kolman
About Louis Kolman
I am an independent cardiologist. I am a member of the HCM Clinic at the University of Calgary. I also am a member of the Stephenson Cardiac Imaging Center and the Libin Cardiovascular Institute at the University of Calgary. Our HCM Clinic manages nearly 800 patients with HCM. I have 180 HCM patients in my own patient pool.
Information Gathering
Independent literature review.
Current Treatments and Treatment Goals
Our current treatment protocols for patients with obstructive hypertrophic cardiomyopathy include treating them with a combination of beta-blockers, calcium channel blockers and disopyramide. When these drugs fail, we often resort to surgery with a myomectomy. The procedure is often challenging with an elevated rate complications, particularly at low volume centers. The current regimen of available medications to attempt to improve diastolic function and reduce inotropy.
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
The current regimen of available medication is not very effective. Patients often still require myomectomy and if they are not good candidates for this procedure, there is often no good treatment option. They also have numerous side effects and are not well tolerated.
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
Mavacampten would likely be able to replace the current regimen of medications. The data shows that the drug is effective in improving symptoms and even reducing the need for surgery.
Which patients would be best suited for treatment with the drug under review? Which patients would be least suitable for treatment with the drug under review?
Patients best suited for the medication would be patients with hypertrophic cardiomyopathy with severe left ventricular outflow tract obstruction who are highly symptomatic. We are currently following many of these patients in our large cohort of patients in the hypertrophic cardiomyopathy clinic. We have identified these patients’ using echocardiography as well as cardiac MRI. We can identify which patients are actively responding to the drug based on their clinical symptoms as well as their functional capacity on the treadmill, and the degree of obstruction on echocardiography.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice? How often should treatment response be assessed?
We can identify which patients are actively responding to the drug based on their clinical symptoms as well as their functional capacity on the treadmill, and the degree of obstruction on echocardiography. In the main clinical trial, cardiopulmonary stress testing, among other biomarkers, was used to measure outcomes. In the real world, it is less likely that we would track our patients with a cardiopulmonary stress test. We can typically get sufficient information from the treadmill stress test rather than the additional clinical biomarkers offered by the cardiopulmonary stress test.
What factors should be considered when deciding to discontinue treatment with the drug under review?
Serial markers of LV systolic function would be important. The drug was shown to reduced LV systolic function in a small number of patients.
What settings are appropriate for treatment with [drug under review]? Is a specialist required to diagnose, treat, and monitor patients who might receive [drug under review]?
Mavacampten should be prescribed by a cardiologist or internal medicine specialist with expertise in hypertrophic cardiomyopathy. It would be important to have good access to echocardiography. LV systolic function was followed very closely in the trial and also should be in the community as the medication is being prescribed.
Additional Information
This medication is very important for our HCM patients. We have not had a new drug to treat this disease for a very long time. These patients are suffering and the data behind Mavacampten is very compelling. I would like to be able to offer this medication to my patients.
Conflict of Interest Declarations — Independent Cardiologist
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation.
Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please refer to the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission?
No.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission?
No.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician who contributed to the input — please add more tables as needed (copy and paste). It is preferred for all declarations to be included in a single document.
Declaration for Clinician 1
Name: Louis Kolman, MD
Position: Assistant Clinical Professor, University of Calgary
Date: Oct 17, 2022
Table 6: COI Declaration for Louis Kolman
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Brystol Myers | X | — | — | — |
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
Redactions: Confidential information in this document may be redacted at the request of the sponsor in accordance with the CADTH Drug Reimbursement Review Confidentiality Guidelines
Stakeholder Input: The views expressed in each submission are those of the submitting organization or individual; not necessarily the views of CADTH or of other organizations. As such, they are independent of CADTH and do not necessarily represent or reflect the view of CADTH. No endorsement by CADTH is intended or should be inferred. By filing with CADTH, the submitting organization or individual agrees to the full disclosure of the information. CADTH does not edit the content of the submissions.
CADTH does use reasonable care to prevent disclosure of personal information in posted material; however, it is ultimately the submitter’s responsibility to ensure no identifying personal information or personal health information is included in the submission. The name of the submitting organization or individual and all conflict of interest information are included in the submission; however, the name of the author, including the name of an individual patient or caregiver submitting the patient input, are not posted.
Accessibility: CADTH is committed to treating people with disabilities in a way that respects their dignity and independence, supports them in accessing material in a timely manner, and provides a robust feedback process to support continuous improvement. All materials prepared by CADTH are available in an accessible format. Where materials provided to CADTH by a submitting organization or individual are not available in an accessible format, CADTH will provide a summary document upon request. More details on CADTH’s accessibility policies can be found here.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.