CADTH Reimbursement Review
Evinacumab (Evkeeza)
Sponsor: Ultragenyx Pharmaceutical Inc.
Therapeutic area: Homozygous familial hypercholesterolemia
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Ethics Review
Stakeholder Input
Clinical Review
Abbreviations
AE
adverse event
AESI
adverse event of special interest
Apo B
apolipoprotein B
ASCVD
atherosclerotic cardiovascular disease
CCS
Canadian Cardiovascular Society
CHD
coronary heart disease
CI
confidence interval
CV
cardiovascular
CVD
cardiovascular disease
EAS
European Atherosclerosis Society
EU
European Union
FH
familial hypercholesterolemia
GCP
good clinical practice
GRADE
Grading of Recommendations, Assessment, Development, and Evaluations
HDL-C
high-density lipoprotein cholesterol
HeFH
heterozygous familial hypercholesterolemia
HoFH
homozygous familial hypercholesterolemia
HRQoL
health-related quality of life
IRR
infusion-related reaction
ITC
indirect treatment comparison
ITT
intention to treat
IWRS
interactive web response system
LDL
low-density lipoprotein
LDL-C
low-density lipoprotein cholesterol
LDLR
low-density lipoprotein receptor
LLT
lipid-lowering therapy
LSM
least squares mean
LSMD
least squares mean difference
MAIC
matching-adjusted indirect comparison
MI
myocardial infarction
MMRM
mixed-effect model with repeated measures
MTD
maximally tolerated dose
OR
odds ratio
PMM
pattern mixture model
RCT
randomized controlled trial
SAE
serious adverse event
SAS
safety analysis set
SD
standard deviation
SE
standard error
SLR
systematic literature review
TEAE
treatment-emergent adverse event
VLDL
very low–density lipoprotein
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Table 1: Background Information of Application Submitted for Review
Item | Description |
|---|---|
Drug product | Evinacumab (Evkeeza), 150 mg/mL (345 mg/2.3 mL and 1,200 mg/8 mL) solution in single-dose vials for IV infusion |
Sponsor | Ultragenyx Pharmaceutical Inc. |
Indication | As an adjunct to diet and other low-density lipoprotein cholesterol–lowering therapies for the treatment of adult and pediatric patients aged 5 years and older with homozygous familial hypercholesterolemia. |
Reimbursement request | Per the Health Canada indication |
Health Canada approval status | NOC |
Health Canada review pathway | Priority review |
NOC date | September 22, 2023 |
Recommended dosage | 15 mg/kg administered by IV infusion q.4.w. |
NOC = Notice of Compliance; q.4.w. = every 4 weeks.
Introduction
Familial hypercholesterolemia (FH) is a genetic disease characterized by markedly elevated plasma levels of low-density lipoprotein cholesterol (LDL-C) from birth that persist throughout life and can lead to the early development of atherosclerotic cardiovascular disease (ASCVD). FH can be further subdivided into heterozygous FH (HeFH) and homozygous FH (HoFH), with HoFH being the more severe and rare form of the disease.1-4 HoFH is characterized by profoundly elevated plasma levels of LDL-C from birth, putting people with HoFH at a significantly increased risk of early CV events (including myocardial infarction [MI], stroke, and heart failure); if HoFH is left untreated, people with the condition can be at risk of sudden cardiac death as early as childhood or adolescence.5-10
Diagnosis of HoFH can be based on clinical criteria or genetic confirmation, though HoFH has historically been more commonly diagnosed based on clinical presentation, due to the limited availability of genetic testing in Canada. The Canadian Cardiovascular Society (CCS) position statement on FH1 lacks specific guidance on diagnostic differentiation between HeFH and HoFH; however, clinicians in Canada use the clinical diagnostic features of HoFH outlined in the 2023 European Atherosclerosis Society (EAS) guidelines. These diagnostic features include untreated LDL-C levels greater than 10.0 mmol/L (400 mg/dL) or LDL-C levels greater than or equal to 8 mmol/L (300 mg/dL) while on conventional lipid-lowering therapies (LLTs). Additional clinical features include the presence of xanthomas before age 10 years of age or the presence of HeFH in both parents. Genetic confirmation of diagnosis is based on the identification of biallelic pathogenic variants at the low-density lipoprotein receptor (LDLR), apolipoprotein B (APOB), PCSK9, or LDLRAP1, or in at least 2 such variants at different loci.11
There are an estimated 145,000 people with FH in Canada,3,5,9,12,13 though recent studies in unselected general populations suggest that HoFH may affect as many as 1 in 300,000 people,3,14-17 and incidence may be higher in populations with a founder effect, such as has been observed in French Canadians, with an estimated prevalence of 1 in 250,000.18 There are approximately 80 known cases of HoFH in Canada; in 2022 there were 52 people with confirmed HoFH enrolled on the Canadian HoFH registry, with a majority (69%) found in Quebec, attributable predominantly to founder effects.19
People with HoFH are at a 100-fold elevated risk for MI compared to those without the condition.20 People with untreated HoFH who have a complete loss of low-density lipoprotein (LDL) function rarely survive beyond their second decade, while those who have partial LDLR activity have a better prognosis, though most develop clinically significant ASCVD by age 30 years if the HoFH is left untreated.14
The overarching goal of therapy for HoFH is to lower LDL-C and, subsequently, the risk of ASCVD. The lowering of plasma cholesterol levels is known to reduce cardiovascular (CV) events, coronary heart disease (CHD) mortality, and all-cause mortality.21 Recommended lifestyle modifications, per the CCS guidelines on the diagnosis and treatment of dyslipidemias, include weight control, restriction of fat consumption to less than 30% of daily calories, consumption of 10 g to 20 g of fibre per day, and increased physical activity. Additional lifestyle changes may include smoking cessation and limiting alcohol intake.22,23
Statins are the primary pharmacological intervention used to achieve control of LDL-C in patients with hypercholesterolemia. Most patients with hypercholesterolemia should be initiated on the maximally tolerated dose (MTD) of high-intensity statins (atorvastatin or rosuvastatin), with the goal of lowering LDL-C by at least 50%. When the LDL-C goal is unmet with statin therapy alone, treatment with add-on ezetimibe or bile acid sequestrants (or both) is recommended, with the goal of reducing LDL-C between 10% and 40% (average 20%).24-27 If LDL-C goals are still not met, PCSK9 inhibitors (evolocumab) are available to patients meeting certain criteria as an adjunct treatment to diet, MTD statin, and ezetimibe.1,12 However, given that traditional LLTs such as statins and PCSK9 inhibitors act by upregulating LDLR expression, they have little efficacy in patients with HoFH and virtually no efficacy in patients with 2 null LDLR alleles. Nearly all patients with HoFH will require extracorporeal LDL-C removal, particularly if LDL-C levels remain greater than 5 mmol/L despite treatment or if ASCVD is present. Either plasmapheresis or, preferably, LDL apheresis should be started as soon as technically feasible, usually before age 5 years and at least by age 8 years.1
Evinacumab (Evkeeza) is a recombinant human monoclonal antibody that binds to and inhibits ANGPTL3, a member of the angiopoietin-like protein family that is expressed primarily in the liver and plays a role in the regulation of lipid metabolism by inhibiting lipoprotein lipase and endothelial lipase. Inhibition of ANGPTL3 via evinacumab lowers triglycerides and high-density lipoprotein cholesterol (HDL-C) by releasing lipoprotein lipase and endothelial lipase. Evinacumab reduces LDL-C independent of LDLR by promoting very low-density lipoprotein (VLDL) processing and clearance of VLDL remnants upstream of LDL formation through an endothelial lipase–dependent mechanism.
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of evinacumab (Evkeeza) 15 mg/kg every 4 weeks as an adjunct to diet and other LDL-C–lowering therapies for the treatment of adult and pediatric patients aged 5 years and older with HoFH.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient and clinician groups who responded to CADTH’s call for input and from the clinical experts consulted by CADTH for the purpose of this review.
Patient Group Input
CADTH reviewed 1 joint patient input from the Canadian Heart Patient Alliance and the Canadian Organization for Rare Disorders. Information was gathered via an online survey that ran from April 12 to May 7, 2023, as well as individual interviews conducted with patients with HoFH and their caregivers. All respondents (N = 18) resided in Canada, mostly in Ontario (12 [66.7%]), with 3 (16.7%) each in British Columbia and Quebec. About 75% of respondents had experienced severe (very high) levels of LDL-C, and 25% reported moderate levels of LDL-C. Around 50% of respondents reported that they had experienced moderate or severe CV events, including atherosclerosis, stroke, atrial fibrillation, and/or cardiac infarction, and half the patients had experienced severe chest pains and had xanthomas. Patients and caregivers highlighted that living with HoFH was associated with stress due to the physical symptoms and the uncertainty or unpredictability of the future, with younger patients noting that HoFH impacts their education and social life, partly because of the time required for treatment. Patients expressed the need for treatment options that can reliably, consistently, and sustainably control LDL-C at normal or near-normal levels, allowing them to experience fewer spikes, reducing the frequency and the need for apheresis, and reducing the risk of CV events. Patients questioned the effectiveness of current treatment options (apheresis, statins, and other medications) in managing their LDL-C levels and highlighted concerns about having to undergo surgery because of future CV events, further impacting their quality of life (QoL) and life expectancy. Of the 18 respondents who provided input, 6 reported having access to or experience with evinacumab through a clinical trial, compassionate access program, or research study. Patients indicated that they were satisfied with evinacumab, as treatment consistently lowered their LDL-C levels and improved their health-related quality of life (HRQoL) through reduced frequency of apheresis, improvements in energy, and the ability to participate in social and family events and attend school. Additionally, there were no reports of serious adverse events (SAEs) following the use of evinacumab.
Clinician Input
Input From Clinical Experts Consulted by CADTH
The information in this section is based on input received from a panel of 4 clinical specialists consulted by CADTH for the purpose of this review.
HoFH is a rare disease, diagnosed based on standard, well-established clinical and genetic criteria, although genetic confirmation is not required. People with HoFH present at an early age with extremely elevated LDL-C levels (untreated LDL-C greater than or equal to 10 mmol/L), as well as other clinical characteristics, including the presence of xanthomas. The clinical experts noted that there are currently multiple established guidelines for the management of dyslipidemia and highlighted the recent publication of the EAS consensus statement on HoFH. The experts noted that current guideline-recommended LDL-C thresholds are pragmatic and remain well above the acceptable level for patients without hypercholesterolemia. Per the current guidelines, the target LDL-C level for patients with HoFH is below 2.5 mmol/L; however, the experts agreed that this value is pragmatic and arbitrary, being based on other treatments and clinical trial criteria.
The clinical experts highlighted that survival for patients with HoFH has nearly doubled in a generation due to the LLTs available; however, they noted that repeated CV events, including MI, aortic valve stenosis, aortic root disease, and the need for revascularization, have increased. As such, the clinical experts emphasized that the main goal of treatment for patients with HoFH is to reduce LDL-C aggressively and safely over the longest term possible to prevent premature CV disease (CVD). In the pediatric population, the goal of LDL-C–lowering treatment is to prevent or delay ASCVD and obviate the need for or reduce apheresis. For adults, the goal of LDL-C–lowering treatment is to slow or halt ASCVD and potentially reverse it and its progression to clinically manifest CVD.
Most currently available pharmacological treatments only target the function of LDLR, rendering them less effective in patients with HoFH; they are more effective in patients with residual LDLR function, rather than “null” mutations (i.e., where there is no functional LDLR). The clinical experts noted that once a patient is diagnosed with HoFH, they are immediately put on MTD statin and on ezetimibe therapy. In most cases, this combination is insufficient to achieve the desired LDL-C goals. To further reduce LDL-C levels, PCSK9 inhibitors may be tried; however, the experts noted that given the pathophysiology of HoFH and the mechanism of action of PCSK9 inhibitors, response may be limited, though treatment with PCSK9 inhibitors should still be attempted. Often statins, ezetimibe, and PCSK9 inhibitors do not achieve sustained and significant reductions of LDL-C to levels below 2.5 mmol/L and/or a 50% lowering of LDL-C. If LDL-C levels are still above the goal, other treatment options — including lomitapide with or without extracorporeal removal of circulating LDL-C — may be attempted. However, these other treatment options have a notable impact on HRQoL: lomitapide is associated with the need for severe dietary restrictions as well as with adverse reactions and poor tolerability or compliance; extracorporeal removal of LDL-C, while effective, is extremely invasive, burdensome, and associated with a rebound period where LDL-C levels rise to baseline, requiring recurrent and sustained treatment cycles. The experts highlighted the need for a drug that is safe and effective and can lower baseline levels to a similar degree to that achieved with pheresis, without the same burden. The experts also noted that not all patients are able to access the full armamentarium of treatments available, and access to pheresis may be limited in Canada, with only 4 centres in the country (Toronto, London, Quebec City, and Edmonton). An alternative, plasmapheresis, which is more widely available, is considered a less optimal substitute for LDL apheresis.
The experts highlighted that evinacumab would likely be used as an add on to MTD statin, ezetimibe, and/or PCSK9 inhibitors, with the hope of supplanting lomitapide and either delaying or reducing the frequency of pheresis.
The experts highlighted that the selection of patients most in need of intervention with evinacumab is not entirely based on disease characteristics but that intervention with evinacumab would be preferred in patients with an LDL-C level greater than 2.5 mmol/L, despite receiving maximally tolerated therapy. The experts further noted that evinacumab would be preferentially used in patients receiving or being considered for lomitapide or those on or being considered for apheresis, owing to the poor risk-benefit profile of lomitapide and the burden of extracorporeal LDL-C removal. Per the clinical experts, the patients most likely to benefit from treatment with evinacumab are those diagnosed with HoFH who have had limited or inadequate response to available LLTs. In addition to the treatments available, patients with ASCVD, aortic valve disease, or genetic documentation of 2 pathogenic variants are subsets of patients at high risk for whom evinacumab might be considered. The experts noted that there are no patients with HoFH that they would not consider for treatment with evinacumab and that it is highly unlikely that patients with HoFH would be able to achieve desirable LDL-C targets on conventional statin and ezetimibe therapy alone.
The clinical experts agreed that the most important outcome of treatment is the reduction of CV morbidity or mortality; however, they noted that reduction in LDL-C is the most reasonable surrogate outcome used by clinicians to avoid all downstream ASCVD complications. Additionally, the clinical experts noted that current clinical trials aim to address important outcomes used in clinical practice and that measuring event-driven outcomes is unreasonable in this population due to the rarity of the disease and the length of time before events arise. Additionally, from a functional perspective, avoidance of pheresis options would be a measure of success, though there are currently no data to demonstrate this potential benefit. While acknowledging the lack of data, the experts mentioned that patients should be stable on evinacumab for 6 months before any attempt to reduce the frequency of or remove pheresis.
The clinical experts agreed that treatment would be discontinued in patients who experienced severe adverse events (AEs), including anaphylactic or infusion reactions, that are unable to be managed. Additionally, the experts agreed that any new AEs identified could be cause for discontinuation, given the small sample size included in the trials for evinacumab. The experts noted that progression of atherosclerosis, major adverse cardiac events, or lack of response to treatment may still occur with sustained treatment; however, the experts stated that such progression would not prompt discontinuation of treatment. Although there is no strict definition for lack of response in this population, the experts highlighted that arbitrary LDL-C cut offs would be chosen to determine an acceptable LDL-C reduction, though this would be contextual for each patient. However, the experts also emphasized that it would be inappropriate to discontinue or deny access to therapies that provide any safe lowering of LDL-C. For example, the experts noted that a treatment offering patients a 20% reduction in LDL-C might be less than an arbitrary 30% cut-off; however, the experts agreed that they would not likely discontinue treatment in such as case and would not consider a 20% reduction in LDL-C as a lack of efficacy.
Patients with HoFH are under the care of specialists with special qualifications in dyslipidemia (e.g., endocrinologists, cardiologists, lipidologists), and treatment would occur within the specialist facilities of that individual or facilities accessible to that individual. Patients with HoFH are also under the care of a lipid specialist and are seen as often as every 3 months, and at minimum every 6 months. During pheresis therapy, lipid profiles are conducted before and following pheresis treatment; as such, LDL-C is routinely tracked. The experts noted that because of the IV infusion, an infusion setting is required as infusion reactions and flu-like reactions may occur. For patients receiving pheresis treatments, evinacumab would be easiest to administer where extracorporeal machines are located. The experts also noted that vascular access in children may pose a potential challenge. Given the dispersion of the patient population, the experts noted that co-management with general practitioners could be envisioned and that administration of evinacumab may be possible, though under the remote supervision of a specialist. The experts also highlighted that experience with evinacumab is limited; thus, moving treatment into the community setting may be possible in the future, though not likely to occur yet.
Clinician Group Input
One clinician group, Familial Hypercholesterolemia Canada, provided input for this review. Information from this group was gathered through the collective clinical experience of 7 clinical experts, published literature, and congress proceedings. Overall, the clinician group noted that there is an unmet need for equitably accessible therapies that safely and effectively treat HoFH. The clinician group highlighted that current treatment options (statins, ezetimibe, and PCSK9 inhibitors, with or without plasmapheresis or apheresis) are inadequate in lowering LDL-C in patients with HoFH due to lack of efficacy and differences in mechanism of action (statins, ezetimibe, and PCSK9 inhibitors), lack of tolerability (lomitapide), and invasiveness in the form of reduced HRQoL and disruption to patients’ and families’ daily lives (apheresis and plasmapheresis). Additionally, the clinician group highlighted the lack of availability of LDL apheresis and plasmapheresis, which are limited to major academic centres, resulting in additional travel burden and creating inequities in level of care based on patients’ geographic location across Canada. Patients best suited for treatment with evinacumab, according to the clinician group, are those in whom target levels of LDL-C are not reached with current treatments or those with progressive CVD, despite the use of current treatments. The clinician group indicated that evinacumab would likely be used as a fourth-line therapy, after statins, ezetimibe, and PCSK9 inhibitors, and suggested that evinacumab may eliminate or reduce the need for plasmapheresis or apheresis, and possibly for lomitapide. In line with the clinical experts consulted by CADTH, the clinicians from Familial Hypercholesterolemia Canada considered reduction in LDL-C levels to be the most important outcome of treatment. The clinician group cited a sustained reduction in LDL-C greater than 20% to 30% to be a meaningful response to treatment. Additional important outcomes for assessing response to treatment included reduction in the frequency of apheresis or plasmapheresis. The clinician group noted that intolerable side effects would be the primary factor when deciding to discontinue treatment.
Drug Program Input
The drug programs identified the following jurisdictional implementation issues: relevant comparators, considerations for initiation of therapy, considerations for prescribing of therapy, generalizability, and care provision issues. Refer to Table 5 for more details.
Clinical Evidence
Systematic Review
Description of Studies
Two studies — the CL-1629 (ELIPSE) trial and the CL-17100 trial — were included in this review. The ELIPSE trial was a pivotal, phase III, double-blind, randomized placebo-controlled trial designed to evaluate the efficacy and safety of evinacumab versus placebo in pediatric and adult patients with HoFH. A total of 65 patients were randomized 2:1 to evinacumab 15 mg/kg every 4 weeks or matching placebo. A total of 3 patients were enrolled from Canadian investigative sites. The primary outcome of the ELIPSE trial was the change from baseline in LDL-C at week 24. Secondary outcomes included the percent change from baseline to week 24 in Apo B, non-HDL-C, and total cholesterol; the proportion of patients with a greater than or equal to 30% and a greater than or equal to 50% reduction in LDL-C at week 24; the absolute change from baseline in LDL-C to week 24; the proportion of patients with LDL-C less than 100 mg/dL (2.59 mmol/L) at week 24; and the proportion of patients who meet European Union (EU) or US apheresis eligibility criteria at week 24.
The CL-17100 study, which was considered a supportive trial for this review, included 3 parts (Parts A, B, and C). Part A was a phase Ib, single-arm, single-dose, pharmacokinetic and pharmacodynamic study consisting of a 16-week open-label treatment period; it enrolled 6 patients with HoFH. Only Parts B and C were of interest to this review. Part B was a 24-week, phase III, single-arm, open-label study to assess the efficacy and safety of evinacumab in patients aged 5 to 11 years with HoFH. A total of 14 patients were enrolled into Part B, and no patients from Part A were enrolled into Part B. Upon completion of Part B, all patients continued into Part C. Part C is an ongoing extension period that consisted of the 20 patients who completed Part A (N = 6) and Part B (N = 14). Part C consisted of a 48-week treatment period and a 24-week follow-up period after the last dose of evinacumab. The dosage in Part C was the same as the dosage in Part B: 15 mg/kg IV every 4 weeks. The data cut-off dates for Parts B and C were January 31, 2022, and June 2, 2022, respectively. The primary outcomes of Parts B and C were identical to the ELIPSE trial, with secondary outcomes of percent change from baseline to week 24 in Apo B, non-HDL-C, and total cholesterol; the proportion of patients with a greater than or equal to 50% reduction in LDL-C at week 24; the absolute change from baseline in LDL-C to week 24; and the proportion of patients with LDL-C less than 100 mg/dL (2.59 mmol/L) at week 24.28
In the ELIPSE trial, there was a difference between the evinacumab and placebo groups in terms of age at baseline, with a mean age of 44.3 years (standard deviation [SD] = 16.8) in the evinacumab group compared to 36.7 years (SD = 11.52) in the placebo group. Only 1 patient in each treatment group was younger than 18 years. In line with the difference in age, there was also a difference in mean time from diagnosis of HoFH to randomization: 16.15 years (SD = 14.562) in the evinacumab group compared to 10.65 years (SD = 12.537) in the placebo group. A total of 48.8% of patients had homozygous LDLR mutations in the evinacumab group compared to only 31.8% in the placebo group, while fewer patients had compound heterozygous LDLR mutations in the evinacumab group than in the placebo group (27.9% versus 36.4%). Most patients received at least 3 LLTs at baseline (69.8% in the evinacumab group versus 50.0% in the placebo group), consisting mostly of the combination of statin plus ezetimibe and a PCSK9 inhibitor (48.8% in the evinacumab group versus 36.4% in the placebo group). More patients in the evinacumab group received lomitapide than in the placebo group (25.6% versus 13.6%). The patients’ lipid parameters at baseline were comparable across treatment groups. (For the evinacumab group versus the placebo group, the mean values of these parameters were as follows: LDL-C = 259.5 mg/dL versus 246.5 mg/dL; Apo B = 169.1 mg/dL versus 175.9 mg/dL; non-HDL-C = 281.9 mg/dL versus 269.9 mg/dL; and total cholesterol = 325.6 mg/dL versus 315.9 mg/dL.)29
The CL-17100 study was conducted in patients aged 5 to 11 years with HoFH. The mean age of the patients enrolled in Part B of the CL-17100 study was 9.1 years (SD = 1.94). Most patients (57.1%) were white females. Most patients (71.4%) had compound heterozygous mutations, and only 50% of patients had received prior apheresis at baseline. Nearly all patients were treated with statins (85.7%) and ezetimibe (92.9%) at baseline, and only 2 patients (14.3%) received lomitapide. The patients’ lipid parameters at baseline were similar to those in the ELIPSE trial, with mean values as follows: LDL-C of 263.7 mg/dL, Apo B of 168.2 mg/dL, non-HDL-C of 282.2 mg/dL, and total cholesterol of 315.5 mg/dL.28
Efficacy Results
Percent Change From Baseline in LDL-C
During the 24-week double-blind period of the ELIPSE trial, the least squares mean (LSM) percent change from baseline with evinacumab was –47.1% (standard error [SE] = 4.6), compared to 1.9% (SE = 6.5) with placebo. The LSM difference (LSMD) between evinacumab and placebo in percent change from baseline in LDL-C at 24 weeks was –49.0% (95% confidence interval [CI], –65.0 to –33.1), favouring evinacumab. During the open-label treatment period of the ELIPSE trial, the LSM percent change in LDL-C at 48 weeks in the open-label treatment period was –46.31% |||| ||||||. Results of the sensitivity analyses and subgroup analyses by background LLT, apheresis status, baseline LDL-C level, and HoFH genotype were consistent with the primary analysis, in favour of evinacumab.29
In the CL-17100 study, the results for LSM change from baseline in LDL-C with evinacumab from Part B and from the pooled Part B and C were consistent with the double-blind period of the ELIPSE trial, with a percent change of –48.32% |||| ||||||| ||| ||||||| |||| ||||||| at 24 weeks, respectively.28
Absolute Change From Baseline in LDL-C
The absolute change from baseline in LDL-C during the 24-week double-blind treatment period of the ELIPSE trial was –134.7 mg/dL (SE = 12.4) in the evinacumab group compared to –2.6 mg/dL (SE = 17.6) in the placebo group, favouring evinacumab (LSMD = –132.1 mg/dL; 95% CI, –175.3 to –88.9; P < 0.0001). In the open-label treatment period, the LSM absolute change from baseline in LDL-C at 48 weeks was –134.3 mg/dL (SD = 117.33).29
In Part B of the CL-17100 study, the LSM absolute change from baseline in LDL-C was –131.9 mg/dL (SD = 30.0).28
Proportion of Patients With Greater Than or Equal to 30% Reduction in LDL-C
In the 24-week double-blind treatment period of the ELIPSE trial, 83.7% of patients in the evinacumab group and 18.2% of patients in the placebo group experienced a greater than or equal to 30% reduction in LDL-C, favouring evinacumab (odds ratio [OR] = 25.2; 95% CI, 5.7 to 110.5; P < 0.0001).29
The proportion of patients with a greater than or equal to 30% reduction in LDL-C at week 24 was not evaluated in the open-label treatment period of the ELIPSE trial or in the CL-17100 study.
Percent Change From Baseline in Apo B
In the ELIPSE trial, during the 24-week double-blind treatment period, the LSM percent change from baseline in Apo B was –41.4% (SE = 3.3) with evinacumab compared to –4.5% (SE = 4.8) with placebo, favouring evinacumab (LSMD = –36.9%; 95% CI, –48.6 to –25.2). The LSM percent change from baseline in Apo B at 48 weeks in the open-label treatment period was –40.83% (SD = 26.150).29
In the CL-17100 study, the LSM percent change from baseline in Apo B with evinacumab for Part B and for the pooled Part B and C was –41.32% (SD = 33.541) ||| ||||||| |||| |||||||, respectively.28
Proportion of Patients With LDL-C Less Than 100 mg/dL (2.59 mmol/L)
In the double-blind period of the ELIPSE trial, the proportion of patients with LDL-C less than 100 mg/dL (2.59 mmol/L) at 24 weeks was 46.5% in the evinacumab group compared to 22.7% in the placebo group (OR = 5.7; 95% CI, 1.3 to 24.9; P = 0.0203).29
The proportion of patients with LDL-C less than 100 mg/dL was not evaluated in the open-label treatment period of the ELIPSE trial or in the CL-17100 study.
Proportion of Patients With LDL-C Less Than 70 mg/dL (1.81 mmol/L)
In the double-blind period of the ELIPSE trial, the proportion of patients with LDL-C less than 70 mg/dL (1.81 mmol/L) at 24 weeks was 27.9% in the evinacumab group compared to 4.5% in the placebo group (OR = 20.9; 95% CI, 1.6 to 276.8; P = 0.0209).29
The proportion of patients with LDL-C less than 70 mg/dL was not evaluated in the open-label treatment period of the ELIPSE trial or in the CL-17100 study.
Proportion of Patients Who Met US Apheresis Criteria
In the double-blind period of the ELIPSE trial, the proportion of patients who met US apheresis eligibility criteria at 24 weeks was 7.0% in the evinacumab group compared to 22.7% in the placebo group (OR = 0.1; 95% CI, 0.0 to 0.3; P = 0.0845). Statistical hypothesis testing was terminated at this end point in the ELIPSE trial because statistical significance was not reached.29
The proportion of patients who met US apheresis eligibility criteria was not evaluated in the open-label treatment period of the ELIPSE trial or in the CL-17100 study.
Proportion of Patients Who Met EU Apheresis Criteria
In the double-blind period of the ELIPSE trial, the proportion of patients who met EU apheresis eligibility criteria at 24 weeks was 32.6% in the evinacumab group compared to 77.3% in the placebo group (OR = 0.1; 95% CI, 0.0 to 0.3).29
The proportion of patients who met EU apheresis eligibility criteria was not evaluated in the open-label treatment period of the ELIPSE trial or in the CL-17100 study.
EQ-5D
In the double-blind period of the ELIPSE trial, the mean EQ-5D utility score at 24 weeks was |||||| points (SD = ||||) for evinacumab and |||||| points (SD = ||||) for placebo, representing a mean change from baseline of ||||||| points (SD = ||||) with evinacumab and ||||||| points (SD = ||||) with placebo.29
Quality of life was not evaluated in the open-label treatment period of the ELIPSE trial or in the CL-17100 study.
Mortality (All-Cause and CV-Related)
All-cause and CV-related mortality were not evaluated in the ELIPSE or CL-17100 studies.
CV-Related Morbidity
CV-related morbidity outcomes, such as the incidence of resuscitated cardiac arrest, nonfatal MI, and stroke, were not evaluated in the ELIPSE or CL-17100 studies.
Harms Results
In the ELIPSE trial, the incidence of treatment-emergent adverse events (TEAEs) was lower for patients in the evinacumab group than for patients in the placebo group during the double-blind treatment period (65.9% versus 81.0%). In the open-label treatment period of the ELIPSE trial, the incidence of TEAEs for patients receiving evinacumab (73.4%) was higher than in the double-blind treatment period. The most common TEAEs by preferred term in patients treated with evinacumab versus placebo were nasopharyngitis (15.9% versus 23.8%) and influenza-like illness (11.4% versus 0.0%). In the open-label treatment period, the most frequently reported TEAEs included nasopharyngitis and headache (9.4% each). SAEs in the ELIPSE trial occurred in 2 patients (4.5%) in the evinacumab group and consisted of urosepsis (1 [2.3%]) and attempted suicide (1 [2.3%]). There were no SAEs in the placebo group. There were no withdrawals due to AEs and no deaths reported during the ELIPSE trial. In terms of notable harms, 4 patients (9.1%) and 3 patients (14.3%) experienced allergic events and 3 patients (6.8%) and 1 patient (4.8%) experienced infusion-related reactions (IRRs) in the evinacumab and placebo groups, respectively, of the double-blind treatment period of the ELIPSE trial.29
In the CL-17100 study, nearly all patients treated with evinacumab experienced at least 1 TEAE (||||%). The most frequent individual AEs by preferred term included headache (||||%) and nasopharyngitis (||||%). |||||||||| ||||||| experienced an SAE of tonsillitis. There were |||| withdrawals due to AEs or deaths reported during the CL-17100 study. Notable harms of general allergic events occurred in ||||| patients (||||%), and |||| patients had IRRs.28
Critical Appraisal
The ELIPSE trial was a first-in-class, phase III, placebo-controlled randomized controlled trial (RCT) that included both double-blind and open-label treatment periods. Appropriate methods were used for randomization (using interactive response technology), treatment allocation (stratified by apheresis treatment and by region), and maintenance of blinding to treatment assignment, thereby reducing selection, performance, and detection biases. The CL-17100 study was an open-label, single-arm study of evinacumab in patients with HoFH aged 5 to 11 years. The choice to conduct a single-arm trial in the younger population was justified considering the rarity of the indication and the age of the participants; however, the noncomparative nature negates the ability to draw definitive conclusions on the effectiveness of evinacumab due to the small sample size and the chronic progression of HoFH. As such, the strength and interpretability of the results for this group of patients are limited. Dropouts and missing data in the ELIPSE and CL-17100 studies were low. The primary end point of the ELIPSE trial used a mixed-effect model with repeated measures (MMRM) to account for missing data under the missing at random assumption, which may not hold in this trial setting and may lead to overconfidence in the effect size. The sensitivity analyses used a pattern mixture model (PMM) to account for nonignorable missingness; overall, though, the amount of missing data was minimal and unlikely to impact the results. Acceptable methods to account for multiplicity were used in the ELIPSE trial. The primary and key secondary end points were controlled for multiplicity at the 0.05 level using a hierarchical testing sequence. However, statistical significance was not achieved for the end point of proportion of patients who meet US apheresis eligibility criteria; thus, the multiple testing procedure failed, and all subsequent outcomes (proportion of patients with LDL-C less than 100 mg/dL and proportion of patients who meet EU apheresis eligibility criteria) should only be viewed as supportive. Though they generally supported the primary analysis, the subgroup analyses in the ELIPSE trial and the CL-17100 study were not statistically powered to detect within-group or between-group differences; thus, the results from the subgroup analyses should be interpreted as supportive evidence only for the overall effect of evinacumab.
The clinical experts consulted by CADTH considered the inclusion and exclusion criteria for the ELIPSE and CL-17100 studies appropriate, though the clinical experts highlighted that genetic confirmation of HoFH does not always occur. Both the ELIPSE and CL-17100 studies were multinational studies; however, the ELIPSE trial was the only study to enrol patients living in Canada (N = 3), though given the low number of patients living in Canada enrolled, generalizability based on geography cannot be assumed. HoFH is a rare disease, which expectedly resulted in the small sample sizes in the ELIPSE and CL-17100 studies. The ELIPSE trial included 65 patients with HoFH, and the CL-17100 study included 20 patients with HoFH. The clinical experts noted that, in their experience, the populations included in the trials, with regard to the age of the patients and the LDL-C levels at baseline, were generally in line patients treated in clinical practice in Canada. The chosen comparator of placebo in the ELIPSE study was appropriate and aligned with the recommended standard of care guidelines for HoFH in Canada; the clinical experts noted that standard of care consists of MTD statin, ezetimibe, and a PCSK9 inhibitor. The clinical experts noted that the proportion of patients receiving LLTs was in line with the general population of patients with HoFH in Canada, though the proportion of patients in the ELIPSE trial receiving PCSK9 inhibitors was higher than in Canadian clinical practice owing to the difficulty in accessing PCSK9 inhibitors in Canada. There were minor differences in lomitapide use at baseline, with only 11 patients (25.6%) in the evinacumab group and 3 patients (13.6%) in the placebo group receiving lomitapide, though this was potentially related to the rarity of the disease and to the study design, as differences among patients may be more noticeable in studies with small sample sizes. The outcomes used to provide information on the efficacy of evinacumab in the ELIPSE and CL-17100 studies were based on validated laboratory assessments of lipids and are widely accepted surrogates for clinically relevant CV outcomes and are important in guiding treatment decisions in Canadian clinical practice in patients with HoFH. In addition to the well-established lowering of LDL-C, the most valuable outcomes to patients with HoFH include reduction in the risk of CV events and reduction of the need for apheresis. The included studies were not designed to assess important CV-related outcomes, including reductions in major adverse cardiac events and in all-cause and CV-related mortality, though the clinical experts consulted by CADTH noted that measuring event-driven outcomes such as these is difficult in HoFH due to the rarity of the disease. Additionally, impact on HRQoL was an exploratory outcome of the ELIPSE trial and was not evaluated in the CL-17100 study. The clinical experts noted that reduction in the burden of apheresis requirements is believed to improve patients’ HRQoL; however, the measurement of this in the available evidence was not captured. The clinical experts emphasized that the duration of the ELIPSE and CL-17100 studies (24 weeks) was considered appropriate for assessing lipid-related outcomes given that the effects on lipids are rapidly seen; however, they noted that the 24-week duration of the included studies was insufficient to determine the impact of evinacumab on CV-related morbidity and mortality and on HRQoL.
GRADE: Summary of Findings and Certainty of the Evidence
Methods for Assessing the Certainty of the Evidence
For the pivotal studies and RCTs identified in the sponsor’s systematic review, Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) was used to assess the certainty of the evidence for the outcomes considered most relevant to inform CADTH’s expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE working group.30,31 Under the GRADE approach, evidence from RCTs started as high-certainty evidence and could be rated down for concerns related to study limitations (which refer to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias.
The selection of outcomes for the GRADE assessment was based on the sponsor’s summary of clinical evidence, consultation with clinical experts, and input received from patient and clinician groups and public drug plans. The following list of outcomes was finalized in consultation with expert committee members: reduction in LDL-C levels (percent change from baseline in LDL-C at 24 weeks, absolute change in LDL-C at 24 weeks, proportion of patients with ≥ 30% reduction in LDL-C at 24 weeks, proportion of patients who meet US apheresis eligibility criteria at 24 weeks, proportion of patients with LDL-C < 100 mg/dL [2.59 mmol/L] at 24 weeks, proportion of patients who meet EU apheresis eligibility criteria at 24 weeks, proportion of patients with LDL-C < 70 mg/dL [1.81 mmol/L] at 24 weeks); reduction in other lipid parameters (percent change from baseline in Apo B at 24 weeks); and improved HRQoL (change from baseline in EQ-5D utility score at 24 weeks).
When possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect; if this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., the clinical importance is unclear). In all cases, the target of the certainty of evidence assessment was based on the point estimate and where it was located relative to the threshold for a clinically important effect (when a threshold was available) or to the null. The target of the certainty of evidence assessment was the presence of a clinically important reduction of LDL-C (percent and absolute change in LDL-C) against thresholds informed by treatment guidelines and clinical expert opinion. Other targets for the certainty of evidence assessment were the presence or absence of any (non-null) effect for the proportion of patients achieving lipid targets (i.e., percent change from baseline in Apo B, proportion of patients with a ≥ 30% reduction in LDL-C, proportion of patients with LDL-C < 100 mg/dL or < 70 mg/dL, proportion of patients who meet US or EU apheresis criteria, and HRQoL measured by the EQ-5D).
Results of GRADE Assessments
Table 2 shows the detailed GRADE summary of findings for evinacumab versus placebo for outcomes in the pivotal ELIPSE trial of adolescent and adult patients with HoFH. Table 3 shows the narrative GRADE summary of findings for evinacumab in the pediatric population of the CL-17100 study and the outcomes from the ELIPSE trial that were unable to be populated in Table 2.
Long-Term Extension Studies
Description of Studies
The CL-1719 study was a key long-term extension study submitted by the sponsor. The CL-1719 study is an ongoing long-term extension study evaluating the safety, tolerability, and efficacy of evinacumab in patients with HoFH, some of whom had previously participated in an evinacumab study (the continue evinacumab group) and some of whom were naive to evinacumab (the new evinacumab group). All patients received 15 mg/kg of evinacumab, intravenously, every 4 weeks for 24 months. The study consisted of a run-in phase, a screening phase, a treatment period, and a 24-week follow-up period. The study duration ranged from 26 weeks up to approximately |||| years. By the interim data cut-off date (||||| ||| ||||), ||| patients had been enrolled in the total study population (consisting of the adult and adolescent populations), || patients (||||%) had completed the treatment period, || patients (||||%) were ongoing in the treatment period, and || patients (||||%) had discontinued. The mean age of the patients was |||| years; || adolescent patients (||||%) had been enrolled.
Efficacy Results
Reductions in lipid parameters observed early in the treatment course in the total study population were maintained with longer-term evinacumab treatment of up to at least ||| weeks (mean percent change from baseline at week ||| was ||||||% for LDL-C and ||||||% for Apo B).||||| |||| |||||||||| || ||||||||||| |||||||| || ||||| ||||| ||| || ||| ||||| |||||||| |||||||||||| || ||| |||||||| ||| ||||||||||| || |||||||| ||||||| || |||||||||| ||||||||| ||| |||||||| |||||||| |||| ||| ||||||||||||| |||||||||| |||||| ||||||
The reductions from baseline in LDL-C and other lipid parameters in the adolescent population were consistent with those in the total study population. Treatment with evinacumab resulted in consistent reductions in mean percent change from baseline for LDL-C (||||||%) and Apo B (||||||%) at week 24 in this study, which were maintained for up to || weeks (mean percent change from baseline at week |||| was ||||||% for LDL-C and ||||||% for Apo B).
Table 2: Detailed Summary of Findings for Evinacumab Versus Placebo for Adolescent and Adult Patients With HoFH (ELIPSE Trial)
Outcome and follow-up | Patients, N (number of studies) | Relative effect (95% CI) | Absolute effects (95% CI) | Certainty | What happens | ||
|---|---|---|---|---|---|---|---|
Placebo | Evinacumab | Difference | |||||
Change in LDL-C | |||||||
Percent change from baseline in LDL-C, LSM Follow-up: 24 weeks | 65 (1 RCT) | NA | 1.9% (SE = 6.5) | –47.1% (SE = 4.6) | –49.0% (95% CI, –65.0 to –33.1) | Moderatea | Evinacumab likely results in a clinically important decrease (improvement) in LDL-C levels when compared with placebo. |
Absolute change from baseline in LDL-C, LSM Follow-up: 24 weeks | 65 (1 RCT) | NA | –2.6 mg/dL (SE = 17.6) | –134.7 mg/dL (SE = 12.4) | –132.1 (95% CI, –175.3 to –88.9) | Moderateb | Evinacumab likely results in a decrease (improvement) in LDL-C levels when compared with placebo. |
Proportion of patients with ≥ 30% reduction in LDL-C Follow-up: 24 weeks | 65 (1 RCT) | RR = 5.0 (2.4 to 10.1) | 4 per 22 (18 per 100) | 36 per 43 (84 per 100) | 650 more per 1,000 (450 more to 850 more) | Moderateb | Evinacumab likely results in a greater proportion of patients achieving 30% reductions in LDL-C levels when compared with placebo. |
Proportion of patients who meet US apheresis eligibility criteria Follow-up: 24 weeks | 65 (1 RCT) | RR = 0.9 (0.7 to 1.1) | 5 per 22 (23 per 100) | 3 per 43 (7 per 100) | 120 fewer per 1,000 (310 fewer to 60 more) | Lowb,c | Evinacumab may result in fewer patients meeting US apheresis eligibility criteria when compared with placebo. The clinical importance of the reduction is uncertain. |
Proportion of patients with LDL-C < 100 mg/dL (2.59 mmol/L) Follow-up: 24 weeks | 65 (1 RCT) | RR = 1.4 (1.0 to 2.1) | 5 per 22 (23 per 100) | 20 per 43 (47 per 100) | 230 more per 1,000 (10 fewer to 460 more) | Lowb,d | Evinacumab may result in a greater proportion of patients achieving target LDL-C levels of < 100 mg/dL when compared with placebo. |
Proportion of patients who meet EU apheresis eligibility criteria Follow-up: 24 weeks | 65 (1 RCT) | RR = 0.4 (0.2 to 0.8) | 17 per 22 (77 per 100) | 14 per 43 (33 per 100) | 440 fewer per 1,000 (670 fewer to 210 fewer) | Lowb,d | Evinacumab may result in fewer patients meeting EU apheresis eligibility criteria when compared with placebo. The clinical importance of the reduction is uncertain. |
Proportion of patients with LDL-C < 70 mg/dL (1.81 mmol/L) Follow-up: 24 weeks | 65 (1 RCT) | RR = 1.3 (1.1 to 1.6) | 1 per 22 (5 per 100) | 12 per 43 (28 per 100) | 230 more per 1,000 (70 more to 390 more) | Lowb,e | Evinacumab may result in a greater proportion of patients achieving target LDL-C levels of < 70 mg/dL when compared with placebo. |
Change in Apo B | |||||||
Percent change from baseline in Apo B, LSM Follow-up: 24 weeks | 65 (1 RCT) | NA | –4.5% (SE = 4.8) | –41.4% (SE = 3.3) | –36.9 (95% CI, –48.6 to –25.2) | Moderateb | Evinacumab likely results in a decrease (improvement) in Apo B levels when compared with placebo. |
HRQoL | |||||||
Change from baseline in EQ-5D utility score, mean Follow-up: 24 weeks | ||||||||||| ||||||||| | |||| ||||| ||| | ||||||| |||||| | ||||||| |||||| | NR | Very lowb,e,f | The evidence is very uncertain about the effects of evinacumab on HRQoL when compared with placebo. |
Harms | |||||||
SAEs (safety end point) Follow-up: 24 weeks | Evinacumab: 44 Placebo: 21 (1 RCT; DBTP) | NA | 0 (0 per 100) | 2 (5 per 100) | NR | Lowg | Evinacumab may result in more SAEs when compared with placebo. |
SAEs (safety end point) Follow-up: 48 weeks | Evinacumab: 44 Placebo: 21 (1 RCT; OLTP) | NA | NA | 7 (11 per 100) | NA | Lowg | Evinacumab may result in more SAEs vs. any comparator. |
IRRs (safety end point) Follow-up: 24 weeks | Evinacumab: 44 Placebo: 21 (1 RCT; DBTP) | NA | 1 (5 per 100) | 3 (7 per 100) | NR | Lowg | Evinacumab may result in more IRRs when compared with placebo. |
IRRs (safety end point) Follow-up: 48 weeks | Evinacumab: 44 Placebo: 21 (1 RCT; OLTP) | NA | NA | 3 (5 per 100) | NA | Lowg | Evinacumab may result in more IRRs vs. any comparator. |
Apo B = apolipoprotein B; CI = confidence interval; DBTP = double-blind treatment period; EU = European Union; HoFH = homozygous familial hypercholesterolemia; HRQoL = health-related quality of life; IRR = infusion-related reaction; LDL-C = low-density lipoprotein cholesterol; LSM = least squares mean; NA = not applicable; NR = not reported; OLTP = open-label treatment period; RCT = randomized controlled trial; RR = risk ratio; SAE = serious adverse event; SE = standard error.
Note: Study limitations (which refer to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias were considered when assessing the certainty of the evidence. All serious concerns in these domains that led to the rating down of the level of certainty are documented in the table footnotes.
aRated down 1 level for serious imprecision. Although the sample size was adequate based on the sample size calculation for the primary end point, the small size raises concern about prognostic imbalance and potential overestimation of the true effect.32 Downgrading for risk of bias was considered due to the potential for spurious correlations when estimating percent change outcomes, but supportive evidence was sufficient to not downgrade.33
bRated down 1 level for serious imprecision. Based on the sample size (and baseline imbalances indicating that randomization may not have ensured prognostic balance), rating down 2 levels would also be an option (–1 for imprecision and –1 for study limitations).
cThis end point failed to meet statistical significance in the statistical hierarchy.
dThis end point was not tested for superiority due to earlier failure of the statistical hierarchy. The potential for type I error is increased, and the findings should be considered as supportive evidence.
eThis end point was an exploratory outcome. The potential for type I error is increased, and the findings should be considered as supportive evidence.
fRated down 1 level for serious indirectness due to insufficient duration of follow-up for the outcome according to clinical expert input.
gRated down 2 levels for very serious imprecision due to the absence of or very low number of events and small sample size.
Source: ELIPSE Clinical Study Report.29
Table 3: Narrative Summary of Findings for Evinacumab for Pediatric Patients With HoFH (CL-17100 Study)
Outcome and follow-up | Patients, N (number of studies) | Effect | Certainty | What happens |
|---|---|---|---|---|
Change in lipid parameters | ||||
Percent and absolute change from baseline in LDL-C, LSM Follow-up: 24 weeks | 14 (1 single-arm trial) | Percent change from baseline (Part B): –48.32% (SD = 39.052) Absolute change from baseline (Part B): –131.9 mg/dL (SD = 30.0) | Very lowa,b | The evidence is very uncertain about the effects of evinacumab on reduction in LDL-C vs. any comparator. |
Percent change from baseline in Apo B, LSM Follow-up: 24 weeks | 14 (1 single-arm trial) | Percent change from baseline (Part B): –41.32% (SD = 33.541) | Very lowa,b | The evidence is very uncertain about the effects of evinacumab on reduction in Apo B vs. any comparator. |
Harms | ||||
SAEs (safety end point) Follow-up: 24 weeks | 20 (1 single-arm trial) | Evinacumab: 1 (5 per 100) | Very lowa,c | The evidence is very uncertain about the effects of evinacumab on SAEs vs. any comparator. |
IRRs (safety end point) Follow-up: 24 weeks | 20 (1 single-arm trial) | Evinacumab: 0 (0 per 100) | Very lowa,c | The evidence is very uncertain about the effects of evinacumab on IRRs vs. any comparator. |
Apo B = apolipoprotein B; HoFH = homozygous familial hypercholesterolemia; IRR = infusion-related reactions; LDL-C = low-density lipoprotein cholesterol; LSM = least squares mean; SAE = serious adverse event; SD = standard deviation; vs. = versus.
Note: Study limitations (which refer to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias were considered when assessing the certainty of the evidence. All serious concerns in these domains that led to the rating down of the level of certainty are documented in the table footnotes. For single-arm trials, all serious concerns with study limitations (which refer to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias are documented in the table footnotes.
aIn the absence of a comparator group, conclusions about efficacy relative to any comparator cannot be drawn; the certainty of evidence therefore starts at “very low” and cannot be rated up.
bRated down 2 levels for very serious imprecision due to the absence of or very low number of events and small sample size.
cRated down 1 level for serious risk of bias due to potential for bias in favour of evinacumab arising from the open-label nature of the study and the subjective nature of the outcome. Rated down 1 level for serious imprecision as the small sample size raises concerns about prognostic imbalance and potential overestimation of the true effect. There is no known minimally important difference, and the target of certainty assessment was any effect.
Source: CL-17100 Clinical Study Report.28
Harms Results
Most patients experienced at least 1 TEAE; ||| of || (||||%) were reported in the new evinacumab group, || of || (|||||%) in the continue evinacumab group, and || of ||| (||||%) in the total study population. The most frequently reported TEAEs for the total study population were nasopharyngitis, headache, influenza-like illness, arthralgia, COVID-19 infection, back pain, and nausea. The TEAE profile in the adolescent population was similar to that in the total study population. |||||| patients experienced at least 1 TEAE. ||||||||||| patients (||||%) in the total study population experienced serious TEAEs. In the adolescent population, |||| patient (|||%) experienced a serious TEAE. ||||| patients had documented TEAEs leading to discontinuation of the study drug. ||| patients in the total study population experienced cardiac-related TEAEs resulting in death that were considered unrelated to the study drug. No deaths were reported in the adolescent population.
Critical Appraisal
The lack of an internal comparator limits the interpretation of the treatment effect observed in the CL-1719 trial as it is uncertain whether the magnitude of the effect observed for evinacumab as an adjunct to background LLT in patients continuing with evinacumab and in new patients is attributable to evinacumab, due to variations in patient health status (continuing and new patients enrolled), residual effects from the use of evinacumab (for patients entering study from an evinacumab study, the impact of ongoing treatments on the effect of evinacumab efficacy), or other unidentified prognostic factors. The single-arm design does not allow for the symptoms of underlying HoFH to be differentiated from treatment-related AEs.
There were no established hypothesis tests or clear thresholds for the secondary variables assessed in the trial. A lack of hypothesis testing against clear thresholds reduces the internal validity of the efficacy findings as it introduces bias in the interpretation of the findings. The open-label design may have also introduced bias in the assessment of subjective outcomes such as the reporting of AEs. Missing data and the lack of methods to account for missing data in the analysis may have impacted the internal validity of the results. There were variabilities in some lipoprotein profiles reported at later follow-up points, and these were attributed to missing or lack of patient data.
Study CL-1719 enrolled ||| patients from Canada, though it was unclear if the results were generalizable to patients with HoFH in Canada due to the small sample size and study design. The outcomes investigated were appropriate and reflective of current clinical practice. The follow-up duration was considered appropriate and more reflective of real-world practice. The use of concomitant medication and background LLT reported among patients was in line with that reported in the ELIPSE and CL-17100 studies. The concomitant medications used were also reflective of current clinical practice in Canada.
Indirect Comparisons
Description of Studies
No direct evidence comparing evinacumab to relevant comparators was available, and to support the pharmacoeconomic model for evinacumab, the sponsor submitted an indirect treatment comparison (ITC) that aimed to estimate the relative effect of evinacumab compared with relevant comparator treatments for adult and adolescent patients (aged 12 years and older) with HoFH to estimate the relative efficacy, safety, and tolerability of evinacumab compared with lomitapide, ezetimibe, evolocumab, and LDL apheresis.34
The sponsor-submitted ITC first conducted a systematic literature review (SLR) to identify existing studies conducted in patients with HoFH. Patient-level data from the evinacumab and placebo arms of the ELIPSE trial were compared to aggregate data from the identified trials using Bucher ITCs and matching-adjusted indirect comparison (MAIC) methods for the outcomes of percent change in LDL-C, proportion of patients with a greater than or equal to 50% reduction in LDL-C, proportion of patients who experienced any SAEs, and proportion of patients discontinuing the study due to any cause.34
Efficacy Results
The SLR identified 23 studies reporting data on unique patient groups as potentially relevant for inclusion in the ITCs. The studies were assessed for heterogeneity based on study design, eligibility criteria, baseline characteristics, and availability of end point data. Following assessment of heterogeneity, 3 studies from the SLR (Cuchel et al. [2013], Raal et al. [2015], and Gagne et al. [2002]), as well as the ELIPSE study, were identified for inclusion in the ITCs, for a total of 4 studies.
The unadjusted naive Bucher ITC comparing data for evinacumab from the ELIPSE trial and for evolocumab from the Raal et al. (2015) study was only conducted for the end point of percent change from baseline in LDL-C at 12 weeks. The results demonstrated that evinacumab was favoured over evolocumab for percent change from baseline in LDL-C (mean difference = –24.33%; 95% CI, –47.50 to –1.15).34
In the MAICs of the ELIPSE trial (evinacumab) to the Cuchel et al. (2013) study (lomitapide) and of the ELIPSE trial (evinacumab) to the Gagne et al. (2002) study (ezetimibe), after adjustment, there were no imbalances between the selected baseline characteristics, though the effective sample size for evinacumab was only 9.9 patients in the comparison with lomitapide and 22.3 patients in the comparison with ezetimibe. The results of the MAIC for the mean difference in percent change from baseline in LDL-C suggested that there was no difference between evinacumab and lomitapide after adjustment (mean difference = 5.08%; 95% CI, –25.46 to 15.29), though evinacumab was favoured over ezetimibe (mean difference = –34.35%; 95% CI, –46.06 to –22.64). For the proportion of patients with a 50% or greater reduction in LDL-C, there was no difference between evinacumab and lomitapide after adjustment (relative risk = 1.42; 95% CI, 0.84 to 2.41).34
Critical Appraisal
The feasibility of conducting an ITC and subsequent analyses was informed by an SLR; however, no information was provided on the SLR methods with regard to the databases searched, the method of study selection or data extraction (e.g., duplicate reviewers), or quality assessment. Thus, CADTH is unable to comment on whether appropriate methods were taken to identify studies for inclusion in the ITCs. Two types of ITC were conducted: a MAIC and a Bucher ITC. Bucher ITCs were used for the comparison of evinacumab to evolocumab based on the connection of the studies via a placebo arm, though the sponsor did not consider evolocumab to be an appropriate comparator to evinacumab due to the lack of available data on effect modifiers and the overall low numbers available for LDLR mutation status. Two MAICs were conducted, 1 each for the comparators of ezetimibe and lomitapide, but none for PCSK9 inhibitors or statins. The focus of the analyses was to evaluate treatments given at second line or later; thus, statins alone were excluded. The exclusion of PCSK9 inhibitors from the analyses was considered inappropriate, as PCSK9 inhibitors are also standard of care in the treatment of HoFH.
The clinical experts consulted by CADTH could not confirm or refute that the prognostic factors and treatment effect modifiers consisting of age, presence of CHD, baseline LDL-C, and LDLR mutation status (defective/defective or null/null) were the only relevant variables in this disease. The key limitation of the unanchored MAICs, which is a limitation inherent to all unanchored MAICs, is that the assumption that all effect modifiers and prognostic factors are accounted for in the model is unlikely met.
The choice to conduct an unanchored MAIC was motivated by the lack of a common comparator across studies. However, there were important differences in the study designs (RCT and single arm), populations, and times of outcome assessment (12 weeks to 26 weeks) of the comparator studies that limited the ability to draw strong inferences about the efficacy of evinacumab compared with other treatments in HoFH. There were also differences in population characteristics in the trials that may impact the comparability of the studies, notably the variation in the proportion of patients with CHD at baseline, the variation in the proportion of patients receiving apheresis at baseline, differences in LDLR mutation status across populations, and overall differences in lipid parameters (including LDL-C, Apo B, and non-HDL-C). Following adjustment for prognostic factors and treatment effect modifiers, the resulting effective sample size for the evinacumab group was decreased 77% and 47% for the comparisons versus lomitapide and ezetimibe, respectively. This is a result of the considerable heterogeneity across studies and may affect the numerical stability of the MAIC estimates, which increases the uncertainty of the results. In the absence of all prognostic factors and treatment effect modifiers, the National Institute for Health and Care Excellence Decision Support Unit considers the amount of bias in an unanchored MAIC likely to be substantial.35 Overall, given the substantial loss in sample size after weighting, the results may not be generalizable to the population of patients with HoFH living in Canada.
The outcomes evaluated in the ITCs are relevant to the clinical management of HoFH. The sponsor conducted a Bucher ITC between evinacumab and evolocumab for the outcome of percent change from baseline in LDL-C, though no formal statistical analyses or adjustments were conducted; thus, the results of this analysis should be interpreted with caution. MAICs were conducted for the outcomes of percent change from baseline in LDL-C and proportion of patients with a greater than or equal to 50% reduction in LDL-C. Additional naive ITCs were conducted for safety outcomes including the proportion of patients who experienced any SAEs and proportion of patients discontinuing the studies due to any cause; however, as these analyses were only descriptive, no conclusion could be drawn on the comparative safety. After adjustment, there was no evidence of preference for evinacumab over lomitapide for the outcome of percent change from baseline in LDL-C, but evinacumab was favoured over ezetimibe. However, in all cases, 95% CIs were wide, suggesting notable imprecision in comparative efficacy estimates.
Studies Addressing Gaps in the Evidence From the Systematic Review
Description of Study
The study by Stefanutti et al. (2022) assessed the long-term efficacy and safety of evinacumab in a cohort of patients with HoFH who were on and off background LDL apheresis (and other LLTs) in a real-world setting. The patients received evinacumab 15 mg/kg every 4 weeks for a duration of 24 months.
Efficacy Results
The mean percent change from baseline in LDL-C following the use of evinacumab and LDL apheresis treatment was −54.4%, −48.9%, −49.4%, and −46.8%, respectively, at 6, 12, 18, and 24 months (P < 0.001 for all, compared with baseline). One patient discontinued LLT due to hospitalization. Four patients experienced an LDL-C reduction of 50% or more, with 2 of these patients having an on-treatment LDL-C level of less than 2.5 mmol/L (97 mg/dL).
Evinacumab (With or Without LDL Apheresis) Versus LDL Apheresis Alone
The LDL-C–lowering effect of evinacumab with or without background LDL apheresis treatment was greater than with LDL apheresis alone (i.e., without evinacumab treatment). With LDL apheresis alone, the time-average LDL-C was reduced by 27.2% in the 6 patients who received LDL apheresis during the normal course of their therapy before initiation of evinacumab treatment.
Harms Results
No discontinuations due to severe AEs were reported following the use of evinacumab. There were also no CV events observed during the 24-month follow-up period and subsequent compassionate extension period (12 months) with evinacumab. There were no reports of symptoms related to common AEs (pharyngitis, nasal congestion, myalgia, diarrhea, and arthralgia) during the 24-month follow-up period and 12-month extension period. Overall, plasma aspartate aminotransferase, alanine aminotransferase, and creatinine kinase concentrations for individual patients with HoFH remained stable during treatment with evinacumab.
Critical Appraisal
The lack of comparator and the open-label design were the main limitations of the study. There was no control group for comparison; thus, the benefit observed cannot be attributed to treatment with evinacumab. The sample size was considered too small to assess the magnitude of effects, and no sample size calculations were provided. There was little information provided related to the eligibility criteria for patients to be included in the study. There is a risk of detection bias for subjective outcome measurements, such as AE reporting, due to the open-label nature of the study, as patients and providers were aware of the treatment. The study duration (24 months) was considered sufficiently long to assess the beneficial effects of evinacumab in the patient population. No HRQoL data were presented. It is uncertain whether evinacumab impacted patient outcomes in the real-world setting.
There was limited generalizability in terms of genetic confirmation of HoFH diagnosis. The clinical diagnosis criterion was not used in the study, which may not be reflective of Canadian practice guidelines. It was unclear what background LLTs were used alongside LDL apheresis.
Conclusions
HoFH is a rare disease, and there is an unmet need for new, safe, and effective treatments for this population of patients who have depleted all other options and require additional LDL-C lowering. Evinacumab is a first-in-class treatment that acts in an LDLR-independent manner to reduce LDL-C levels. Two studies were included in this review — the phase III, double-blind, randomized ELIPSE trial and the single-arm, open-label CL-17100 study — evaluating the efficacy and safety of evinacumab as adjunct to diet and stable maximum doses of LLTs in pediatric and adult patients with HoFH.
The ELIPSE study demonstrated that evinacumab likely resulted in a clinically important decrease (improvement) in LDL-C levels when compared with placebo beyond the threshold for clinically important reductions of 30%, as defined by clinical experts and clinical practice guidelines, which was further supported by the CL-17100 study. Treatment with evinacumab was well tolerated over the study period and did not appear to be associated with more AEs or SAEs than placebo. Known AEs of interest, such as IRRs, were slightly more frequent in the evinacumab group; however, there were no concerns. The included studies had a short treatment duration of only 24 weeks, which was sufficient to address the primary outcome of change in LDL-C but precluded the ability to assess long-term efficacy and safety, as well as HRQoL. Though considered outcomes of importance to patients, reduction in CV risk (including CV-related morbidity and mortality), as well as reduction in the need for and frequency of apheresis, were not evaluated in the included studies; thus, the impact of evinacumab on these outcomes is unknown.
There were important technical limitations in the conduct of the ITCs: the included studies varied in design, did not include all relevant standard of care treatments, and had differences between the included populations. As such, the results of the ITCs were inconclusive and imprecise given the large reduction in sample sizes and wide 95% CIs.
Overall, the results of the included studies were generally positive, supporting the use of evinacumab in pediatric and adult patients with HoFH; however, there were important limitations in the studies — such as the small sample size, the short duration of follow-up, the single-arm open-label design of the CL-17100 study, and the lack of direct comparative evidence — that limit the generalizability of the study results to a broader population with HoFH.
Introduction
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of evinacumab, 150 mg/mL solution for IV infusion, as an adjunct to diet and other LDL-C–lowering therapies for the treatment of adult and pediatric patients aged 5 years and older with HoFH.
Disease Background
The content within this section has been informed by materials submitted by the sponsor and clinical expert input. The following has been summarized and validated by the CADTH review team.
ASCVDs are a group of disorders of the heart and blood vessels. They are the leading cause of death globally, with an estimated 17.9 million deaths each year.36-38 CVDs are generally associated with high blood cholesterol levels (hypercholesterolemia) resulting in the buildup of cholesterol, specifically LDL-C, and fatty deposits inside the arteries leading to atherosclerosis.38-40 Changes in the endothelial cell lining of the arterial wall lead to an accumulation of lipoproteins and inflammatory cells, resulting in the formation of an atherosclerotic lesion or plaque, which narrows the arterial lumen, thereby reducing blood flow. Symptoms of ASCVD depend on the atherosclerotic site and the specific condition; however, typical symptoms of underlying CV issues include pain or pressure, particularly in the chest and/or arms, shortness of breath, light-headedness or dizziness, cold sweats, and fatigue. More severe manifestations of ASCVD because of hypercholesterolemia include CV events such as MI or stroke, which may be fatal.40
FH is a genetic disease characterized by markedly elevated plasma levels of LDL-C from birth that persist throughout life and can lead to the early development of atherosclerosis. FH can be further subdivided into HeFH and HoFH disease, with HoFH being the more severe and rare form of the disease.1-4 HoFH is characterized by profoundly elevated plasma levels of LDL-C from birth, putting people with HoFH at a significantly increased risk of early CV events (including MI, stroke, and heart failure); if HoFH is left untreated, people with the condition can be at risk of sudden cardiac death as early as childhood or adolescence.5-10 More than 90% of HoFH cases are caused by mutations in the LDLR gene. The remaining cases are caused by mutations in the PCSK9, APOB, and LDLRAP1 genes.14 The amount of residual LDLR activity that a patient has contributes to the severity of disease. The lower the LDLR activity, the more severe the disease and the harder it is to treat with the available treatment options, as many treatments rely on functional LDLR to reduce LDL-C levels.14,41,42
There are an estimated 145,000 people with FH in Canada,3,5,9,12,13 though recent studies in unselected general populations suggest that HoFH may affect as many as 1 in 300,000 people,3,14-17 and may be higher in populations with a founder effect such as has been observed in French Canadians, with an estimated prevalence of 1 in 250,000.18 There are approximately 80 known cases of HoFH in Canada; in 2022, there were 52 patients with confirmed HoFH enrolled in the Canadian HoFH registry, with a majority (69%) found in Quebec, attributable predominantly to founder effects.19
Diagnosis of HoFH can be made based on clinical criteria or genetic confirmation, though HoFH has historically been more commonly diagnosed based on clinical presentation, due to the limited availability of genetic testing in Canada. The CCS position statement on FH1 lacks specific guidance on diagnostic differentiation between HeFH and HoFH; however, clinicians in Canada use the clinical diagnostic features of HoFH outlined in the 2023 EAS guidelines. These features include untreated LDL-C levels greater than 10.0 mmol/L (400 mg/dL) or LDL-C levels greater than or equal to 8 mmol/L (300 mg/dL) while on conventional LLTs. Additional clinical features include the presence of xanthomas before age 10 years or the presence of HeFH in both parents. Genetic confirmation of diagnosis is based on the identification of biallelic pathogenic variants at the LDLR, APOB, PCSK9, or LDLRAP1, or at least 2 such variants at different loci.11
People with HoFH are at a 100-fold elevated risk for MI compared to those without the condition.20 If HoFH is not adequately treated, many people with the condition will experience an MI before age 10 years. People with untreated HoFH who have a complete loss of LDL function rarely survive beyond their second decade, while those who have partial LDLR activity have a better prognosis, though most develop clinically significant ASCVD by age 30 years if the HoFH is left untreated.14
Standards of Therapy
The content within this section has been informed by materials submitted by the sponsor and clinical expert input. The following has been summarized and validated by the CADTH review team.
The condition of FH is associated with premature death and complications due to accelerated development of ASCVD. Early detection of FH is important to reduce the risk of CV events; initial non-pharmacological interventions for hypercholesterolemia include diet and lifestyle modifications. The overarching goal of therapy for HoFH is to lower LDL-C and, subsequently, the risk of ASCVD. The lowering of plasma cholesterol levels is known to reduce CV events, CHD mortality, and all-cause mortality.21 If HoFH is left untreated, people with the condition can be at risk of sudden cardiac death as early as childhood or adolescence. The CCS recommends that patients with HoFH be referred to specialized lipid clinics for genetic analysis, for evaluation of the presence of ASCVD, and for initiation of aggressive LLTs, potentially including extracorporeal LDL-C removal, lomitapide, and PCSK9 inhibitors.1
Recommended lifestyle modifications, as per the CCS guidelines on the diagnosis and treatment of dyslipidemias, include weight control, reduction of fat consumption to less than 30% of daily calories, consumption of 10 g to 20 g of fibre per day, and increased physical activity. Additional lifestyle changes may include smoking cessation and limiting alcohol intake.22,23 Lifestyle and diet changes alone are unlikely to achieve LDL-C goals (generally result in an estimated reduction in LDL-C of 10% to 15%), and most patients will require pharmacological intervention.1,24,43
Statins are the primary pharmacological intervention used to achieve control of LDL-C in patients with hypercholesterolemia. Most patients with hypercholesterolemia should be initiated on the MTD of high-intensity statins (atorvastatin or rosuvastatin), with the goal of lowering LDL-C by at least 50%. Lower-intensity statins (reduced dose of atorvastatin, rosuvastatin, simvastatin, or pravastatin), which lower LDL-C by approximately 30%, should be used only in older adults or frail or patients who are unable to tolerate high-intensity statins.27 When the LDL-C goal is unmet with statin therapy alone, treatment with add-on ezetimibe or bile acid sequestrants (or both) is recommended.25-27 Ezetimibe is a cholesterol absorption inhibitor that blocks the absorption of dietary cholesterol and its delivery to the liver, resulting in enhanced clearance of LDL-C, further reducing LDL-C between 10% and 40% (average 20%).24 If LDL-C goals are still not met, PCSK9 inhibitors (evolocumab) and lomitapide are available to patients meeting certain criteria as an adjunct treatment to diet, MTD statin, and ezetimibe.1,12 However, given that traditional LLTs such as statins and PCSK9 inhibitors act by upregulating LDLR expression, they have little efficacy in patients with HoFH and virtually no efficacy in patients with 2 null LDLR alleles.
Nearly all patients with HoFH will require extracorporeal LDL-C removal, particularly if LDL-C levels remain greater than 5 mmol/L despite treatment or if ASCVD is present. Either plasmapheresis or, preferably, LDL apheresis should be started as soon as technically feasible, usually before age 5 years and at least by age 8 years.1
Drug Under Review
Evinacumab (Evkeeza) is a recombinant human monoclonal antibody that binds to and inhibits ANGPTL3, a member of the angiopoietin-like protein family that is expressed primarily in the liver and plays a role in the regulation of lipid metabolism by inhibiting lipoprotein lipase and endothelial lipase. Inhibition of ANGPTL3 via evinacumab lowers triglycerides and HDL-C by releasing lipoprotein lipase and endothelial lipase. Evinacumab reduces LDL-C independent of LDLR by promoting VLDL processing and clearance of VLDL remnants upstream of LDL formation through an endothelial lipase–dependent mechanism.
Evinacumab is administered intravenously at a dosage of 15 mg/kg every 4 weeks over 60 minutes. Each vial contains 345 mg/2.3 mL or 1,200 mg/8 mL (150 mg evinacumab per mL) solution in single-dose vials.
The reimbursement request for evinacumab is in line with the proposed Health Canada indication as an adjunct to diet and other LDL-C–lowering therapies for the treatment of adult and pediatric patients aged 5 years and older with HoFH. The Health Canada Notice of Compliance was granted on September 22, 2023. Evinacumab has not previously been reviewed by CADTH. Evinacumab has also been reviewed by other major regulatory bodies, including the FDA and the European Medicines Association, and is currently under review by the National Institute for Health and Care Excellence, though only for patients aged 12 years and older.44
The key characteristics of evinacumab and of other treatments available for HoFH are summarized in Table 4.
Table 4: Key Characteristics of Evinacumab and Other Pharmacologic Therapies
Characteristic | Evinacumab | Statins | Ezetimibe | PCSK9 inhibitors | Lomitapide |
|---|---|---|---|---|---|
Mechanism of action | Binds to and inhibits ANGPTL3, lowering triglycerides and HDL-C and promoting VLDL processing | Inhibits cholesterol synthesis through inhibition of HMG-CoA reductase | Reduces cholesterol absorption by inhibiting the intestinal Niemann-Pick–like 1 transporter | Inhibits PCSK9 and increases LDL-C receptor density | Inhibits MTP, an intracellular lipid-transfer protein impairing the synthesis of chylomicrons and VLDL |
Indication | As an adjunct to diet and other LDL-C–lowering therapies for the treatment of adult and pediatric patients aged 5 years and older with HoFH | All:
Various also indicated for:
Many statins also have CV indications, such as reducing the risk of coronary events in patients with or without clinically evident CHD, reducing the risk of major CV events in patients with CHD who have undergone a PCI and slowing the progression of coronary atherosclerosis in patients with CHD | CAD, hypercholesterolemia | Evolocumab: As an adjunct to diet and other LDL-C–lowering therapies (e.g., statins, ezetimibe, and LDL apheresis) in adults and adolescents aged ≥ 12 years with HoFH who require additional lowering of LDL-C | As an adjunct to a low-fat diet and other lipid-lowering drugs, with or without LDL apheresis, to reduce LDL-C in adult patients with HoFH |
Route of administration | IV | Oral | Oral | SC | Oral |
Recommended dosage | 15 mg/kg q.4.w. | Various | 10 mg q.d. | Evolocumab: 140 mg q.2.w. or 420 mg monthly | 5 mg q.d. initially, to a maximum of 60 mg q.d. |
Serious adverse effects or safety issues | Hypersensitivity reactions including anaphylaxis and infusion reactions |
|
| Hypersensitivity reactions |
|
CAD = coronary artery disease; CHD = coronary heart disease; CV = cardiovascular; HDL-C = high-density lipoprotein cholesterol; HeFH = heterozygous familial hypercholesterolemia; HMG-CoA = 3-hydroxy-3-methylglutaryl coenzyme-A; HoFH = homozygous familial hypercholesterolemia; LDL = low-density lipoprotein; LDL-C = low-density lipoprotein cholesterol; PCI = percutaneous coronary intervention; q.2.w. = every 2 weeks; q.4.w. = every 4 weeks; q.d. = every day; SC = subcutaneous; VLDL = very low-density lipoprotein.
Sources: Sponsor submission;45 evinacumab product monograph;46 inclisiran clinical review.47
Stakeholder Perspectives
Patient Group Input
This section was prepared by the CADTH review team based on the input provided by patient groups. The full original patient input received by CADTH has been included in the Stakeholder section of this report.
CADTH received 1 joint patient input from the Canadian Heart Patient Alliance and the Canadian Organization for Rare Disorders, which was summarized for this review. The Canadian Heart Patient Alliance is a patient-led nonprofit umbrella organization of patients, families, health professionals, and supporters dedicated to reducing CVD and preventing early deaths due to genetic, environmental, lifestyle, and other risk factors; the organization focuses on improving awareness, screening, testing, diagnosis, care, and treatment of all CVDs. The Canadian Organization for Rare Disorders is Canada’s national network for organizations representing rare disorders, providing a strong common voice to advocate for health policy and a health care system that work for those with rare disorders. The organization works with governments, researchers, clinicians, and industry to promote research, diagnosis, treatment, and services for all rare disorders in Canada.
Information was gathered via an online survey that ran from April 12 to May 7, 2023, as well as individual interviews conducted with patients with HoFH and caregivers. Twelve online surveys were completed — 10 by patients with HoFH and 2 by caregivers — and 6 interviews were conducted with 5 patients with HoFH and 1 caregiver. Of the 18 respondents, 10 (56%) were male and 8 (44%) were female. Six patients (33%) were aged between 40 and 60 years, 6 (33%) were aged between 30 and 39 years, and 6 (33%) were aged between 18 and 29 years. All patients resided in Canada, mostly in Ontario (12 [66.7%]), with 3 (16.7%) each in British Columbia and Quebec.
About 75% of respondents had experienced severe (very high) levels of LDL-C, and 25% reported moderate levels of LDL-C. Around 50% of respondents reported that they had experienced moderate or severe CV events, including atherosclerosis, stroke, atrial fibrillation, and/or cardiac infarction, and half the patients had experienced severe chest pains and had xanthomas. Most patients had undergone multiple surgeries throughout their lifetime. Patients also expressed that HoFH negatively impacted their HRQoL. Patients and caregivers highlighted that living with HoFH was associated with stress due to the physical symptoms and the uncertainty or unpredictability of the future, with younger patients noting that HoFH impacts their education and social life, partly because of the time required for treatment.
The patients questioned the effectiveness of current treatment options (apheresis, statins, and other medications) in managing their LDL-C levels, highlighting concerns about having to undergo surgery because of future CV events, further impacting their QoL and life expectancy. Of the 18 respondents who provided input, 6 reported having access to or experience with evinacumab through a clinical trial, compassionate access program, or research study. Patients indicated that they were satisfied with evinacumab, as treatment consistently lowered their LDL-C levels and improved their HRQoL through reduced frequency of apheresis, improvements in energy, and the ability to participate in social and family events and attend school. Additionally, there were no reports of SAEs following the use of evinacumab.
Patients expressed the need for treatment options that can reliably, consistently, and sustainably control LDL-C levels at normal or near-normal levels, allowing them to experience fewer spikes, reducing the frequency and the need for apheresis, and reducing the risk of CV events.
Clinician Input
Input From Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise in the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). As part of the review of evinacumab, a panel of 4 clinical experts from across Canada was convened to characterize unmet therapeutic needs, assist in identifying and communicating situations where there are gaps in the evidence that could be addressed through the collection of additional data, promote the early identification of potential implementation challenges, gain further insight into the clinical management of patients living with the condition, and explore the potential place in therapy of the drug (e.g., potential reimbursement conditions). A summary of this panel discussion follows.
Unmet Needs
In patients with HoFH, ASCVD occurs very early and progresses aggressively throughout life. Most currently available pharmacological treatments only target the function of LDLR, rendering them less effective in patients with HoFH. The clinical experts highlighted that survival for patients with HoFH has nearly doubled in a generation due to the LLTs available; however, they noted that repeated CV events, including MI, aortic valve stenosis, aortic root disease, and the need for revascularization, have increased. As such, the clinical experts emphasized that the main goal of treatment for patients with HoFH is to aggressively reduce LDL-C early, adequately, and safely over the longest term possible to prevent premature CVD. Current treatment options, including statins, ezetimibe, and PCSK9 inhibitors, do not achieve sustained and significant reductions of LDL-C to levels below 2.5 mmol/L and/or a 50% lowering of LDL-C. Other treatment options, including lomitapide, are associated with adverse reactions and poor tolerability and/or compliance, limiting their effectiveness; extracorporeal removal of LDL-C, while effective, is extremely invasive and burdensome. Additionally, the experts noted that access to pheresis may be limited in Canada and that pheresis treatments are also associated with a rebound period where LDL-C levels rise to baseline, requiring recurrent and sustained treatment cycles. The experts highlighted the need for a drug that is safe and effective and can lower baseline LDL-C levels to a similar degree to that achieved with pheresis, without the same burden.
In addition to current therapies being unable to adequately reduce LDL-C to target levels, the experts noted that not all patients are able to access the full armamentarium of treatments available and that some therapies have a notable impact on HRQoL. Treatment for HoFH requires multiple and ongoing medical visits, with the experts highlighting that patients requiring pheresis treatments must adhere to a strict and burdensome treatment schedule, impacting their ability, and their caregivers’ ability, to attend school or work.
Place in Therapy
The clinical experts noted that there are currently multiple established guidelines for the management of dyslipidemia and highlighted the recent publication of the EAS consensus statement on HoFH; however, current treatment options are more effective in patients with residual LDLR function than in patients with “null” mutations (i.e., where there is no functional LDLR). The experts noted that current guideline-recommended LDL-C thresholds are pragmatic and remain well above the acceptable level for patients without hypercholesterolemia; thus, the overall aim of treatment is to achieve the lowest possible LDL-C level safely.
Though diagnosis of HoFH is relatively straightforward, based on clinical and genetic criteria, patients require the care of lipid specialists. The clinical experts noted that once a patient is diagnosed with HoFH, they are immediately put on MTD tatin and on ezetimibe therapy. In most cases, this combination is insufficient to achieve the desired LDL-C goals. To further reduce LDL-C levels, PCSK9 inhibitors may be tried; however, the experts noted that, given the pathophysiology of HoFH and the mechanism of action of PCSK9 inhibitors, response may be limited, though treatment with PCSK9 inhibitors should still be attempted.
If LDL-C levels are still above the goal, lomitapide with or without extracorporeal removal of circulating LDL-C may be attempted; however, lomitapide is associated with the need for severe dietary restrictions, as well as undesirable side effects. The clinical experts noted that in their experience, only half of patients can tolerate lomitapide therapy and those who can are on a very low dose with limited efficacy. With regard to pheresis, only 4 centres in Canada can perform LDL apheresis (Toronto, London, Quebec City, and Edmonton); an alternative, plasmapheresis, which is more widely available, is considered a less optimal substitute for LDL apheresis.
The experts highlighted that evinacumab would likely be used as an add on to MTD statin, ezetimibe, and/or PCSK9 inhibitors, with the hope of supplanting lomitapide and either delaying or reducing the frequency of pheresis.
Patient Population
HoFH is a rare disease, and patients with HoFH are diagnosed based on standard, well-established clinical, and genetic criteria, although genetic confirmation is not required. Patients present at an early age with extremely elevated LDL-C levels (untreated LDL-C greater than or equal to 10 mmol/L), as well as other clinical characteristics, including the presence of xanthomas. In conjunction with primary care physicians, lipid specialists aim to reduce LDL-C levels to prevent downstream CVD, particularly in younger patients. Per the current guidelines, the target LDL-C level for patients with HoFH is below 2.5 mmol/L; however, the experts agreed that this value is pragmatic and arbitrary, being based on other treatments and clinical trial criteria.
Treatments for HoFH are additive, with the goal of safely driving down LDL-C levels as low as possible, regardless of the thresholds specified in the guidelines. In the pediatric population, the goal of LDL-C–lowering treatment is to prevent or delay ASCVD and to obviate the need for or reduce apheresis. For adults, the goal of LDL-C–lowering treatment is to slow or halt ASCVD and potentially reverse it and its progression to clinically manifest CVD.
The experts highlighted that the selection of patients most in need of intervention with evinacumab is not entirely based on disease characteristics but that intervention with evinacumab would be preferred in patients with an LDL greater than 2.5 mmol/L, despite receiving maximally tolerated therapy. They further noted that evinacumab would be preferentially used in patients receiving or being considered for lomitapide or those on or being considered for apheresis, owing to the poor risk-benefit profile of lomitapide and the burden of extracorporeal LDL-C removal.
Per the clinical experts, the patients most likely to benefit from treatment with evinacumab are those diagnosed with HoFH who have had limited or inadequate response to available LLTs. In addition to the treatments available, patients with ASCVD, aortic valve disease, or genetic documentation of 2 pathogenic variants are subsets of patients at high risk for whom evinacumab might be considered.
The experts noted that there are no patients with HoFH that they would not consider for treatment with evinacumab and that it is highly unlikely that patients with HoFH would be able to achieve desirable LDL-C targets on conventional statin and ezetimibe therapy alone.
Assessing the Response to Treatment
The clinical experts agreed that the most important outcome of treatment is the reduction of CV morbidity or mortality; however, they noted that LDL-C level is the most reasonable surrogate outcome used by clinicians to avoid all downstream ASCVD complications. Additionally, the clinical experts noted that current clinical trials aim to address important outcomes used in clinical practice and that measuring event-driven outcomes is unreasonable in this population due to the rarity of the disease and the length of time before events arise. Major adverse CV events may still occur with sustained treatment; however, the experts stated that this would not be a reason to discontinue treatment.
The experts noted that other lipid parameters, such as Apo B or non-HDL-C, are routinely measured in clinical practice, particularly by academic institutions; however, they emphasized that these parameters would not likely alter treatment decisions in HoFH given the underlying pathology related to the LDLR, so LDL-C level is the most appropriate biomarker. Additionally, from a functional perspective, avoidance of pheresis options would be a measure of success, though there are currently no data to demonstrate this potential benefit.
The clinical experts noted that evinacumab has been administered in the medical short stay unit of hospitals and that achieving the LDL-C threshold of 2.5 mmol/L has not been an unrealistic goal; the experts stated that this treatment provides a new hope for patients with HoFH. The experts also noted that no safety concerns have been identified for evinacumab to date. One expert shared the example of a patient with extensive xanthomas that were not resolving with pheresis treatment; however, once the patient was put on evinacumab, the xanthomas regressed. The experts mentioned that patients should be stable on evinacumab for 6 months before an attempt to reduce the frequency of or remove pheresis. Patients with HoFH are under the care of a lipid specialist and are seen as often as every 3 months, and at minimum every 6 months. During pheresis therapy, lipid profiles are conducted before and following pheresis treatment; as such, LDL-C is routinely tracked.
The experts noted that improvement in symptoms or impact of ischemia on daily living is difficult to establish in patients with HoFH and that, generally, by the time symptoms occur, intervention such as revascularization is needed. The experts noted that in more severe cases, imaging techniques may be used to assess the extent of disease, but that imaging would not be appropriate to gauge response to treatment.
Discontinuing Treatment
The clinical experts agreed that treatment with evinacumab would be discontinued in patients who experience severe AEs, including anaphylactic or infusion reactions that are unable to be managed. Additionally, the experts agreed that any new AEs identified could be cause for discontinuation, given the small sample size included in the trials for evinacumab.
The experts noted that progression of atherosclerosis or lack of response to treatment would not prompt discontinuation of treatment. Although there is no strict definition for lack of response in patients with HoFH, the experts highlighted that arbitrary LDL-C cut-offs would be chosen to determine an acceptable LDL-C reduction, though this would be contextual for each patient. However, the experts also emphasized that it would be inappropriate to discontinue or deny access to therapies that provide any safe lowering of LDL-C. For example, the experts noted that a treatment offering patients a 20% reduction in LDL-C might be below an arbitrary 30% cut-off; however, the experts agreed that they would not likely discontinue treatment and would not consider a 20% reduction in LDL-C as a lack of efficacy.
The experts considered that quantifying the reduction in LDL-C may be a challenge in patients undergoing extracorporeal removal of LDL-C, due to the pattern of LDL-C reduction and rebound inherent in this cyclic therapy; thus, determining response (or lack of response) to treatment requires a sufficient passage of time to observe changes.
Additionally, the experts noted that pregnancy, or contemplation of pregnancy, would also be a consideration for discontinuation of treatment with evinacumab.
Prescribing Considerations
The experts indicated that diagnosis of HoFH is relatively straightforward, and that diagnosis can be made by any practitioner based on well-established clinical findings, family history, laboratory values, and genetic criteria. However, the experts noted that awareness of HoFH is low; therefore, patients with HoFH are generally identified through referral or in a more specialized setting. As such, patients with HoFH are under the care of specialists with special qualifications in dyslipidemia (e.g., endocrinologists, cardiologists, lipidologists), and treatment would occur within the specialist facilities of that individual or facilities accessible to that individual.
Evinacumab is administered through IV infusion; thus, an infusion setting is required. The experts noted that infusion reactions and flu-like reactions may occur and that for patients receiving pheresis treatments, evinacumab would be easiest to administer where extracorporeal machines are located. The experts also noted that vascular access in children may be a potential challenge.
Given the dispersion of the patient population, the experts noted that co-management with general practitioners could be envisioned. The experts highlighted that in some cases where remote consultation is available, administration of evinacumab may be possible, though under the remote supervision of a specialist. The experts also highlighted that experience with evinacumab is limited; thus, moving treatment into the community setting may be possible in the future, though not likely to occur imminently.
Clinician Group Input
This section was prepared by the CADTH review team based on the input provided by clinician groups. The full original clinician group input received by CADTH has been included in the Stakeholder section of this report.
Input from 1 clinician group, Familial Hypercholesterolemia Canada, was submitted for this review. Familial Hypercholesterolemia Canada is a national group of pediatric and adult lipid specialists in Canada whose purpose is to improve the care of patients with FH and reduce CV risks associated with this very high–CV risk condition. Information from this group was gathered through the collective clinical experience of 7 clinical experts, published literature, and congress proceedings.
The clinician group highlighted that HoFH presents in early childhood and is very challenging to treat across the patient’s lifespan, noting that current treatment options are inadequate in lowering LDL-C in patients with HoFH due to lack of efficacy and differences in mechanism of action (statins, ezetimibe, and PCSK9 inhibitors), lack of tolerability (lomitapide), and invasiveness in the form of reduced HRQoL and disruption to patients’ and families’ daily lives (apheresis and plasmapheresis). Additionally, the clinician group highlighted the lack of availability of LDL apheresis and plasmapheresis, which are limited to major academic centres, resulting in additional travel burden and creating inequities in level of care based on patients’ geographic location across Canada. Overall, the clinician group noted that there is an unmet need for equitably accessible therapies that safely and effectively treat patients with HoFH.
According to the clinician group input, patients best suited for treatment with evinacumab are those with HoFH in whom target levels of LDL-C are not reached with current treatments (statins, ezetimibe, and PCSK9 inhibitors, with or without plasmapheresis or apheresis) or those with progressive CVD, despite the use of current treatments. As such, the clinician group indicated that evinacumab would likely be used as a fourth-line therapy, after statins, ezetimibe, and PCSK9 inhibitors. The clinician group also suggested that evinacumab may eliminate or reduce the need for plasmapheresis or apheresis, and possibly for lomitapide.
According to the clinician group, ideal treatments for HoFH would be well tolerated with few side effects, have no significant drug interactions and have minimal impact on health care resources and would not place a burden on patients and their families.
In line with the clinical experts consulted by CADTH, the clinicians from Familial Hypercholesterolemia Canada considered reduction in LDL-C levels to be the most important outcome of treatment. The clinician group noted that a reduction in LDL-C would translate to reduced CV events and improved survival. Specifically, the clinician group cited a sustained reduction in LDL-C greater than 20% to 30% to be a meaningful response to treatment. Additional important outcomes for assessing response to treatment included reduction in the frequency of apheresis or plasmapheresis. The clinician group noted that intolerable side effects would be the primary factor when deciding to discontinue treatment.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 5.
Table 5: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Relevant comparators | |
In the ELIPSE trial, 93.8% of patients were on statins, 75.4% were on ezetimibe, and 76.9% were on a PCSK9 inhibitor. For other treatments, 21.5% of patients were receiving lomitapide at baseline and 33.8% were on LDL apheresis. Lomitapide was given a do not list recommendation by CADTH in 2015 and is only publicly funded in Quebec. Few centres in Canada have the infrastructure for LDL apheresis. A large proportion of patients in the pivotal trial are receiving therapy with treatments that have limited access in Canada. Are these proportions reflective of the population in Canada? How accessible is LDL apheresis in Canada? Is it expected that patients would be using these treatments or would have to have tried them before they receive evinacumab? | The clinical experts cited a recent study using data from the Familial Hypercholesterolemia Canada registry to compare the lipid-lowering therapies used in the ELIPSE trial to those by patients with HoFH living in Canada within the registry. The clinical experts noted that the proportion of patients receiving PCSK9 inhibitors in the ELIPSE trial was higher than the FH Canada registry, which they considered to be likely reflective of the population enrolled in the trial, and a product of PCSK9 access issues in Canada. The experts emphasized that PCSK9 inhibitors should be tried in patients with HoFH as some patients do experience a response to treatment despite the known mechanism of action focusing on LDLR activity and there being minimal to no LDLR activity in HoFH. Additionally, the experts noted that the proportion of patients on the registry receiving apheresis was higher than in the ELIPSE trial. The experts emphasized that only 4 centres in Canada (Toronto, London, Quebec City, and Edmonton) can conduct LDL apheresis; however, the registry population also included patients receiving plasmapheresis, which the experts noted is more readily available across Canada than LDL apheresis, though issues may arise when attempting to access other extracorporeal removal services, as these facilities are currently overwhelmed with patients with other diseases. Plasmapheresis is also considered a poor surrogate for LDL apheresis. The experts considered the treatment distribution of the ELIPSE trial to be relatively generalizable to patients with HoFH living in Canada, though the order of treatment sequencing with lomitapide, pheresis, and evinacumab is likely to shift should evinacumab become available. |
The proposed indication for evinacumab is for pediatric and adult patients aged 5 years or older. There is limited access to many relevant comparators in Canada, which may be further restricted in the pediatric population by current funding criteria (e.g., PCSK9 inhibitors). Is access expected to be further limited for younger patients? | The clinical experts highlighted that most drugs in the pediatric population are used off-label. The experts noted that in their experience, accessing PCSK9 inhibitors for children poses many administrative challenges and that, for most therapies, age cut-offs are inappropriate as most patients with HoFH are diagnosed before age 4 years. The experts also highlighted that starting extracorporeal removal of LDL on patients younger than 5 years can be challenging due to equipment constraints, as well as the concern of maintaining long-term vascular access. The experts hypothesized that evinacumab may be of great importance in the younger population due to the potential for delaying the requirement for apheresis to a time when it may be less burdensome or challenging. |
Considerations for initiation of therapy | |
Based on the proposed indication, how many lipid-lowering therapies would have to be tried before initiating treatment with evinacumab? | At diagnosis, patients with HoFH are placed on MTD statin, ezetimibe, and PCSK9 inhibitors, if available. The experts noted that though access to PCSK9 inhibitors is limited in Canada, treatment with them should be attempted. Further, in Quebec, patients may receive lomitapide, though the experts noted that such treatment involves certain dietary restrictions and monitoring requirements, including monitoring for fatty liver. Patients may also be placed on apheresis to remove circulating LDL-C. The experts stated that evinacumab would likely be used following MTD statin, ezetimibe, and PCSK9 inhibitors and may reduce the need for or frequency of apheresis. |
Considerations for prescribing of therapy | |
Evinacumab is administered q.4.w. over 60 minutes by IV infusion. The administration setting may vary by jurisdiction and may limit where coverage would be provided. | No response required. For CDEC consideration. |
Generalizability | |
There was a limited number of patients in each age category in the pivotal ELIPSE trial and the supporting CL-17100 trial. In the ELIPSE trial, 2 patients were aged between 12 and 17 years, 29 patients were aged between 18 and 44 years, 16 patients were aged between 45 and 64 years, and 8 patients were aged 65 years or older, and in the CL-17100 trial, 11 patients were aged between 5 and 9 years and 9 patients were aged between 10 and 12 years. Given the limited number of patients in each age category, can the results for each age group be considered generalizable to the overall population of patients with HoFH? | The clinical experts noted that conducting a controlled trial in pediatric and adult patients with HoFH is difficult due to the rarity of the disease. The clinical experts considered the results of the pivotal studies to be generalizable despite the ages of enrolled patients and noted that the mechanism of action of evinacumab is not likely impacted by the age of the patients. Furthermore, the experts considered their own experience with evinacumab in patients younger than 18 years and did not express concern with the generalizability of the results based on age. |
The primary end point of the pivotal trial was LDL-C reduction. What evidence is there for reduction in CV events or improved mortality? | The experts highlighted that event-driven outcomes are difficult to observe and achieve in this rare and chronic disease. Moreover, they noted that patients with HoFH are heterogenous in their response due to the confounding effects of concomitant therapies, which can vary. Overall, the clinical experts noted that there is no trial or epidemiological evidence yet for a reduction in CV events or an improvement in mortality with evinacumab; however, the experts considered LDL-C to be the most appropriate surrogate outcome in patients with HoFH, as sustained and safe LDL-C lowering has consistently been associated in the long-term with event reductions using other drugs. The experts also emphasized that over the last generation, survival in patients with HoFH has nearly doubled, which they stated was attributed to lipid-lowering therapies. |
Care provision issues | |
Evinacumab is administered q.4.w. over 60 minutes by IV infusion. In what setting would evinacumab be administered in most provinces? Would this differ by age? Would you expect any challenges in administering this treatment? | Treatment with evinacumab would be administered within a hospital or infusion clinic under the care of a specialist with experience treating patients with HoFH. Vascular access in children tends to pose some challenges; thus, the expertise available in hospitals may be required. Adverse reactions with evinacumab were limited in the trials; however, given the small sample size, there is the potential for new, unknown adverse reactions. Consideration should also be given to administering evinacumab in community clinics that have the expertise to administer IV drugs. Though there is as yet no experience in doing so with evinacumab, remote co-management with lipid specialists in the community may be possible. In general, for patients also undergoing pheresis, evinacumab would be administered following the pheresis treatment. |
CDEC = CADTH Canadian Drug Expert Committee; CV = cardiovascular; HoFH = homozygous familial hypercholesterolemia; LDL = low-density lipoprotein; LDL-C = low-density lipoprotein cholesterol; LDLR = low-density lipoprotein receptor; MTD = maximally tolerated dose; q.4.w. = every 4 weeks.
Clinical Evidence
The objective of CADTH’s Clinical Review Report is to review and critically appraise the clinical evidence submitted by the sponsor on the beneficial and harmful effects of evinacumab 150 mg/mL IV infusion in the treatment of pediatric and adult patients with HoFH. The focus will be placed on comparing evinacumab to relevant comparators and identifying gaps in the current evidence.
A summary of the clinical evidence included by the sponsor in the review of evinacumab is presented in 4 sections, with CADTH’s critical appraisal of the evidence included at the end of each section. The first section, the systematic review, includes the pivotal studies and RCTs that were selected according to the sponsor’s systematic review protocol. CADTH’s assessment of the certainty of the evidence in this first section, using the GRADE approach, follows the critical appraisal of the evidence. The second section includes sponsor-submitted long-term extension studies. The third section includes indirect evidence from the sponsor. The fourth section includes additional studies that were considered by the sponsor to address important gaps in the systematic review evidence.
Included Studies
Clinical evidence from the following is included in the CADTH review and appraised in this document:
Two pivotal studies or RCTs identified in the systematic review (the CL-1629 study [ELIPSE] and the CL-17100 study [pediatric study])28,29
One long-term extension study (the CL-1719 study)48
One sponsor-submitted ITC34
One additional study addressing gaps in evidence (Stefanutti et al. [2022]).49
Systematic Review
The content within this section has been informed by materials submitted by the sponsor. The following has been summarized and validated by the CADTH review team.
Description of Studies
Characteristics of the included studies are summarized in Table 6.
A total of 2 studies were included in this review: the pivotal CL-1629 (ELIPSE) trial and the indication criteria expansion study, CL-17100, supporting the use of evinacumab in children aged 5 to 11 years.
Table 6: Details of Studies Included in the Systematic Review
Study characteristic | ELIPSE | CL-17100 |
|---|---|---|
Design and population | ||
Study design | Phase III, randomized, double-blind, placebo-controlled, parallel-group study | 3-part, phase Ib and phase III, single-arm, open-label study |
Locations | 30 centres in 11 countries: Australia, Austria, Canada, France, Greece, Italy, Japan, Netherlands, South Africa, Ukraine, and US | Part A: Austria, Netherlands, and US Part B and C: Australia, Austria, Netherlands, Taiwan, and US |
Patient enrolment dates | Start date: January 18, 2018 End date: November 26, 2019 | Start date: November 26, 2019 |
Randomized (N) | Evinacumab = 43 Placebo = 22 Total = 65 | Part A = 6 Part B = 14 Part C (Part A + Part B) = 20 |
Inclusion criteria | Male or female patients (aged ≥ 12 years) with HoFH, diagnosed by either genetic or clinical criteria:
| Males and females aged 5 to 11 years at the time of the screening visit Diagnosis of functional HoFH by either genetic or clinical criteria:
LDL-C > 130 mg/dL at the screening visit Body weight ≥ 15 kg Receiving stable maximally tolerated therapy at the screening visit |
Exclusion criteria |
|
|
Drugs | ||
Intervention | Evinacumab 15 mg/kg, q.4.w., IV infusion | Evinacumab IV infusion Part A: Single dose, 15 mg/kg Parts B and C: 15 mg/kg, q.4.w. |
Comparator(s) | Placebo q.4.w., IV infusion (plus SOC) | NA |
Study duration | ||
Screening phase | 2 weeks | Part B: 1 to 2 weeks |
Run-in phase | 8 weeks | Part B: ≤ 8 weeks |
Treatment phase | Double blind: 24 weeks Open label: 24 weeks | Part B: 24 weeks Part C: 48 weeks |
Follow-up phase | 24-week follow-up (for patients who did not enter the CL-1719 study) | Part C: 24 weeks |
Outcomes | ||
Primary end point | Percent change from baseline in LDL-C to week 24 | Part B: Percent change from baseline in LDL-C to week 24 |
Secondary and exploratory end points | Secondary
Exploratory
| Part B
Exploratory
|
Publication status | ||
Publications | Reports Trial ID numbers
| Report
Trial ID numbers
|
ADA = antidrug antibody; ALT = alanine aminotransferase; Apo B = apolipoprotein B; Apo CIII = apolipoprotein C-III; AST = aspartate aminotransferase; AUCtau = area under the plasma concentration-time curve over dosing interval; CABG = coronary artery bypass grafting; Cmax maximum concentration; CPK = creatine phosphokinase; Ctrough = concentration at the trough; DBP = diastolic blood pressure; DBTP = double-blind treatment period; eGFR = estimated glomerular filtration rate; EU = European Union; HADS = Hospital Anxiety and Depression Scale; HDL-C = high-density lipoprotein cholesterol; HeFH = heterozygous familial hypercholesterolemia; HoFH = homozygous familial hypercholesterolemia; ID = identification; IND = investigational new drug; LDL-C = low-density lipoprotein cholesterol; LDLR = low-density lipoprotein receptor; LLT = lipid-lowering therapy; Lp(a) = lipoprotein (a); mAb = monoclonal antibody; MI = myocardial infarction; NA = not applicable; NYHA = New York Heart Association; OLTP = open-label treatment period; PCI = percutaneous coronary intervention; PK = pharmacokinetic; q.4.w. = every 4 weeks; RNA = ribonucleic acid; SBP = systolic blood pressure; SOC = standard of care; SS = steady state; TC = total cholesterol; TEAE = treatment-emergent adverse event; TIA = transient ischemic attack; TSH = thyroid-stimulating hormone; ULN = upper limit of normal.
Sources: ELIPSE Clinical Study Report;29 CL-17100 Clinical Study Report.28
CL-1629 Study (ELIPSE Trial)
The ELIPSE trial was a phase III, double-blind, randomized placebo-controlled trial designed to evaluate the efficacy and safety of evinacumab versus placebo in pediatric and adult patients with HoFH. A total of 65 patients were randomized 2:1 to evinacumab 15 mg/kg every 4 weeks or matching placebo via an interactive web response system (IWRS). Randomization was stratified by prior apheresis treatment (yes versus no) and by geographical region (Japan versus rest of world). The ELIPSE trial was conducted in 30 centres in 11 countries: Australia, Austria, Canada, France, Greece, Italy, Japan, the Netherlands, South Africa, Ukraine, and the US. A total of 3 patients were enrolled from Canadian investigative sites. The ELIPSE trial consisted of an 8-week run-in period for patients who did not have a functional diagnosis of HoFH and opted to undergo genotyping for confirmation or for patients whose background LLT or apheresis schedules were not stable before the 2-week screening period. The run-in period was followed by a 24-week double-blind treatment period and a 24-week open-label treatment period. During the 24-week open-label treatment period, all patients received evinacumab 15 mg/kg IV every 4 weeks. The data cut-off date for the 24-week double-blind treatment period of the ELIPSE trial was July 29, 2019, and for the open-label treatment period was January 12, 2020. Patients then had the option to enter the long-term, open-label extension study (the CL-1719 study), and those who chose not to enter the extension study were followed for 24 weeks.29
CL-17100 Study
The CL-17100 study was a single-arm, open-label study that included 3 parts:28
Part A: phase Ib, single-arm, single-dose pharmacokinetic and pharmacodynamic study
Part B: phase III, single-arm, 24-week, open-label efficacy and safety study
Part C: phase III, 48-week treatment period and 24-week follow-up period
Part A was a phase Ib, single-dose, open-label study to determine the safety, pharmacokinetics, and pharmacodynamics of a single dose of evinacumab 15 mg/kg IV in 6 patients aged 5 to 11 years with HoFH.28 Results for Part A will not be discussed in this report.
Part B was a phase III, single-arm, open-label study to assess the efficacy and safety of evinacumab in patients aged 5 to 11 years with HoFH. A total of 14 patients were enrolled in Part B, none of whom had participated in Part A. Part B of the CL-17100 study was conducted in Australia, Austria, the Netherlands, Taiwan, and the US. Part B consisted of up to 4 periods: an up to 8-week run-in period, an up to 2-week screening period, and a 24-week open-label treatment period, and a follow up period. Since all patients entered Part C, the follow up period of Part B was not applicable. Upon completion of Part B, all patients continued into Part C.28
Part C is an ongoing extension period that consists of the 20 patients who completed Part A or Part B. Part C consists of a 48-week treatment period and a 24-week follow-up period after the last dose of evinacumab. The final dosage in Part C was the same as the dosage in Part B: 15 mg/kg IV every 4 weeks.28
The data cut-off dates for Part B and Part C were January 31, 2022, and June 2, 2022, respectively.28
Populations
Inclusion and Exclusion Criteria
The inclusion and exclusion criteria for the 2 trials are summarized in Table 6. The inclusion criteria for both trials were similar, enrolling patients with either a genetically or clinically confirmed diagnosis of HoFH;28,29 however, patients in the ELIPSE trial were aged 12 years or older,29 while patients enrolled in Part B of the CL-17100 study were aged 5 to 11 years.28 Additionally, patients in the CL-17100 study were required to have an LDL-C level greater than 130 mg/dL (approximately 3.4 mmol/L) at screening,28 while patients in the ELIPSE trial with LDL-C were only required to have an LDL-C level greater than 70 mg/dL (1.81 mmol/L) at screening.29
In general, patients in both trials were expected to be on the MTD of LLTs at screening; however, this was only specified as an inclusion criterion for the CL-17100 study. Maximally tolerated therapy included daily statin, ezetimibe, and PCSK9 inhibitor antibody (evolocumab or alirocumab), unless the patient had a documented history of tolerability issues, little to no response to therapy, or other documented reason for not receiving these therapies. Lipid-modifying therapy could also include other LLTs, such as LDL apheresis.28,29
Interventions
Interventions, run-in treatments, background therapy, and prior and concomitant therapies were similar across the ELIPSE and CL-17100 studies.28,29 In the ELIPSE trial, patients in the double-blind treatment period were randomized 2:1 to receive evinacumab at a dose of 15 mg/kg or matching placebo through a 60-minute IV infusion. The last dose of the double-blind study drug was administered at week 20. In the open-label period of the study, all patients received evinacumab at 15 mg/kg IV every 4 weeks starting at week 24 until the last dose at week 44.29
In Parts B and C of the open-label CL-17100 study, patients received evinacumab 15 mg/kg every 4 weeks administered as an IV infusion over 65 minutes.28
Run-In Treatment
The ELIPSE trial highlighted that patients undergoing apheresis therapy must have initiated LDL apheresis at least 3 months before screening and be on a stable weekly or every other week (i.e., every 7 days or every 14 days) schedule and/or stable settings for at least 8 weeks before screening.29 In the CL-17100 study, there was no time limit for initiation of LDL apheresis,28 though the schedule and setting requirements were the same as for the ELIPSE trial. Patients with an unstable schedule and/or unstable apheresis settings for at least 8 weeks before the screening visit entered an 8-week run-in period before the screening period. Patients on background LLT that had not been stable for at least 4 weeks (6 weeks for fibrates [ELIPSE trial only]; 8 weeks for PCSK9 inhibitor antibodies) before the screening visit entered a 4-week (6-week for fibrates; 8-week for PCSK9 inhibitor antibodies) run-in period to stabilize their LLT before entering the screening period.28,29
Background Treatments
In both studies, patients were on a maximally tolerated LLT regimen (statin, PCSK9 inhibitor antibody, ezetimibe, lomitapide, mipomersen, probucol, and so on), unless the patient had a documented history of tolerability issues. Lipid-modifying treatments could have also included other LLTs, including LDL apheresis. Patients receiving background LLT undergoing apheresis had to also maintain stable LLT and a stable apheresis schedule throughout the duration of the study, from screening to the end of the double-blind treatment period and continuing through to the end of the open-label treatment period.28,29
For patients who entered Part C of the CL-17100 study and were receiving lipid apheresis, the frequency of apheresis could be reduced based on the investigator’s judgment.28
Concomitant and Prohibited Medications
In the ELIPSE trial, any treatment administered, including apheresis, from the time of informed consent to the end of the treatment period or final study visit was considered concomitant medication. The use of all medications and nutritional supplements known to alter serum lipids, such as statins, ezetimibe, fibrates, niacin, bile acid resins, red yeast rice, lomitapide, mipomersen, and PCSK9 inhibitor antibodies, was permitted as long as that therapy had been stable for at least 4 weeks (6 weeks for fibrates, 8 weeks for PCSK9 inhibitor antibodies, 12 weeks for lomitapide, and 24 weeks for mipomersen) before the screening visit. Patients had to continue background LLT for the duration of the study, starting at screening and continuing through to the end of the open-label treatment period (week 48). Similarly, patients had to maintain their apheresis regimen (if applicable), starting at screening and continuing through to the end of the open-label treatment period (week 48). Patients on thyroid replacement therapy could be included if the dose had been stable for at least 12 weeks before the screening visit.29
In the ELIPSE trial, the following concomitant medications and procedures were prohibited through to the end of the double-blind treatment period and through to the end of the open-label treatment period:29
Background LLT that has not been stable for at least 4 weeks (6 weeks for fibrates) before the screening visit (unless participating in the run-in period to stabilize).
Background mipomersen treatment that has not been stable for 24 weeks before the screening visit or background lomitapide at a MTD that has not been stable for 12 weeks before the screening visit. Recent discontinuation of lomitapide had to be washed out for at least 8 weeks before the screening visit.
Background PCSK9 inhibitor antibody that has not been stable for at least 8 weeks before the screening visit.
Apheresis schedule that is not weekly or every other week or that has not been stable for at least 8 weeks before screening.
Plasma exchange.
Nutraceuticals or over-the-counter therapies known to affect lipids at a dose or amount that has not been stable for at least 4 weeks before the screening visit.
Systemic corticosteroids, unless used as replacement therapy for pituitary or adrenal disease with a stable regimen for at least 6 weeks before the screening visit.
Thyroid replacement therapy, unless the dosage of replacement therapy has been stable for at least 12 weeks before the screening visit.
The concomitant and prohibited medications in the CL-17100 study were similar; however, mipomersen was not included in the list of prohibited medications.28
Dose Modification
Dose modifications for individual patients were not permitted in either study.28,29
Patients who permanently discontinued use of the study drug during the double-blind treatment period in the ELIPSE study remained in the study and underwent all study visits and procedures. At the time of study drug discontinuation in either the double-blind or open-label treatment period, the patient would have an unscheduled visit within 5 days of discontinuation of the study drug, if possible, and then resume the original study schedule until end of the double-blind treatment period or have end-of-study assessments at least 24 weeks after their last dose of the study drug in the open-label treatment period.29
In the CL-17100 study, patients in Part B and Part C who prematurely discontinued the study drug and agreed to remain in the study would undergo all study visits and procedures except for study drug dosing. At the time of study drug discontinuation, the patient would have an unscheduled visit as soon as possible, with assessments normally planned at the week 24 end-of-treatment visit (Part B patients) or the week 48 visit (Part C patients) and then resume the original study schedule until the end-of-study visit.
In both studies, evinacumab dosing was permanently stopped in the event of the following (although other reasons may also be possible):28,29
evidence of pregnancy
acute systemic infusion reactions with AEs, such as anaphylaxis, laryngeal or pharyngeal edema, severe bronchospasm, chest pain, seizure, or severe hypotension
need for a prohibited concomitant medication during the double-blind treatment period (although, after discussion with the study monitor, treatment could be continued or could be only temporarily discontinued)
withdrawal of consent.
The CL-17100 study also noted specific types of liver dysfunction as a reason for discontinuation.28
In both studies, the investigators could also permanently discontinue evinacumab dosing at any time, even without consultation with the medical monitor if the urgency of the situation required immediate action and if this was determined to be in the patient’s best interest.28,29
Outcomes
A list of efficacy end points assessed in this Clinical Review Report is provided in Table 7, followed by descriptions of the outcome measures. The summarized end points are those included in the sponsor’s summary of clinical evidence as well as additional outcomes identified as important to this review by the clinical experts consulted by CADTH and by the stakeholder input from patient and clinician groups and public drug plans. Using the same considerations, the CADTH review team selected end points that were considered most relevant to inform CADTH’s expert committee deliberations and finalized this list of end points in consultation with members of the expert committee. All the summarized efficacy end points were assessed using GRADE. Select notable harms outcomes considered important for informing CADTH’s expert committee deliberations were also assessed using GRADE.
Table 7: Outcomes Summarized From the Studies Included in the Systematic Review
Outcome measure | Time point | ELIPSE | CL-17100 |
|---|---|---|---|
Percent change from baseline in LDL-C | 24 weeks | Primarya | Part B: Primary |
Percent change from baseline in Apo B | 24 weeks | Key secondarya | Part B: Secondary |
Proportion of patients with ≥ 30% reduction in LDL-C | 24 weeks | Key secondarya | NA |
Proportion of patients with ≥ 50% reduction in LDL-C | 24 weeks | Key secondarya | Part B: Secondary |
Proportion of patients who meet US apheresis eligibility criteriab | 24 weeks | Key secondarya | NA |
Proportion of patients with LDL-C < 100 mg/dL (2.59 mmol/L) | 24 weeks | Key secondarya | NA |
Proportion of patients who meet EU apheresis eligibility criteriac | 24 weeks | Key secondarya | NA |
Proportion of patients with LDL-C < 70 mg/dL (1.81 mmol/L) | 24 weeks | Secondary | NA |
Absolute change from baseline in LDL-C | 24 weeks | NA | Part B: Secondary |
EQ-5D | 24 weeks | Other | NA |
CV-related morbidity and mortalityd | NA | NA | NA |
Apo B = apolipoprotein B; CV = cardiovascular; EU = European Union; LDL-C = low-density lipoprotein cholesterol; NA = not applicable.
aStatistical testing for these end points was adjusted for multiple comparisons (e.g., hierarchal testing).
bA patient is considered as meeting US apheresis eligibility criteria if their LDL-C level is greater than or equal to 300 mg/dL (7.77 mmol/L) (Goldberg [2011]).
cA patient with primary CV disease prevention is considered as meeting EU apheresis eligibility criteria if their LDL-C level is greater than 160 mg/dL (4.2 mmol/L); a patient with secondary CV disease prevention is considered as meeting EU apheresis eligibility criteria if their LDL-C level is greater than 120 mg/dL (3.1 mmol/L) (Schettler [2012]).
dCV-related events including morbidity and mortality were of interest to this review but were not evaluated in the included trials.
Sources: ELIPSE Clinical Study Report;29 CL-17100 Clinical Study Report.28
Efficacy Outcomes
According to the clinical expert input and clinician group input, reduction in circulating LDL-C levels is the hallmark of treatment for patients with hypercholesterolemia and is an important outcome in the management of HoFH, with the aim of slowing or halting ASCVD and its progression to clinically manifest CVD. Therefore, outcomes related to LDL-C reduction were included as outcomes to be assessed using GRADE. In the included studies, these outcomes consisted of percent and absolute change from baseline in LDL-C, as well as the proportion of patients achieving lipid targets of 30% reduction, LDL-C reduction to less than 100 mg/dL, LDL-C reduction to less than 70 mg/dL, and proportion of patients meeting the US and EU apheresis criterion per LDL-C level.
While HRQoL was identified as an important outcome in patients with HoFH, the clinical experts noted that improvements in LDL-C levels are not directly linked to improvements in HRQoL; rather, the benefits of reduced LDL-C in patients with HoFH may be seen in a reduction in the frequency of or need for apheresis, though this would not necessarily be realized in the short duration of a clinical trial. Regardless, HRQoL outcomes from the included trials (i.e., EQ-5D) were included in the GRADE assessment.
Primary Efficacy Outcome
The primary outcome of the ELIPSE and CL-17100 studies was the percent change from baseline in LDL-C to week 24, where LDL-C was calculated using the Friedewald formula and percent change was defined as:28,29
100 × (LDL-C value at week 24 – LDL-C value at baseline) / LDL-C value at baseline
Secondary Efficacy Outcomes
Key secondary efficacy end points of the ELIPSE trial included percent change from baseline in Apo B, non-HDL-C, and total cholesterol to week 24; proportion of patients with a greater than or equal to 30% and a greater than or equal to 50% reduction in LDL-C at week 24; absolute change from baseline in LDL-C to week 24; proportion of patients with LDL-C less than 100 mg/dL (2.59 mmol/L) at week 24; and proportion of patients who meet EU or US apheresis eligibility criteria at week 24. Patients were considered as meeting US apheresis eligibility criteria if their LDL-C levels were greater than or equal to 300 mg/dL (7.77 mmol/L). Patients being treated for primary CVD prevention were considered as meeting EU apheresis eligibility criteria if their LDL-C levels were greater than 160 mg/dL (4.2 mmol/L), and patients being treated for secondary CVD prevention were considered as meeting EU apheresis eligibility criteria if their LDL-C levels were greater than 120 mg/dL (3.1 mmol/L). Other secondary end points included percent change from baseline in triglycerides, lipoprotein A, and apolipoprotein C-III to week 24; absolute change from baseline in Apo B, non-HDL-C, and total cholesterol to week 24; and proportion of patients with LDL-C less than 70 mg/dL (1.81 mmol/L) at week 24.29
Similar lipid measures were selected as secondary outcomes for the CL-17100 study, with the omission of the proportion of patients with a greater than or equal to 30% reduction in LDL-C at week 24 and the proportion of patients meeting US or EU apheresis criteria.28
All lipid parameters were collected by investigators and sent to a central laboratory for evaluation.28,29
Exploratory Outcomes
HRQoL was an exploratory outcome of the ELIPSE trial. The measures used to evaluate HRQoL in the ELIPSE trial were the EQ-5D and the Hospital Anxiety and Depression Scale.29 HRQoL measured by the Hospital Anxiety and Depression Scale was not considered in this review.
The EQ-5D is a standardized measure of health status developed by the EuroQol Group to provide a simple, generic measure of health for clinical and economic appraisal. The EQ-5D, as a measure of HRQoL, defines health in terms of 5 dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Each dimension has 3 ordinal levels of severity: no problems (1), some problems (2), severe problems (3). The overall health state is defined as a 5-digit number. Health states defined by the 5-dimensional classification can be converted into corresponding index scores that quantify health status, where 0 represents “death” and 1 represents “perfect health.”29
Harms Outcomes
The safety of evinacumab was a secondary end point of the ELIPSE and CL-17100 studies and was measured by AEs, SAEs, AEs of special interest (AESIs), vital signs, Tanner stages, clinical laboratory values, electrocardiogram measurements, and the formation and characterization of antidrug antibodies. AEs were recorded by the investigator from the time the informed consent was signed to the end of the study using the currently available version of the Medical Dictionary for Regulatory Activities by preferred term and system organ class.28,29
AEs were defined as any untoward medical occurrence in a patient administered a study drug that may or may not have a causal relationship with the study drug. SAEs were defined as any untoward medical occurrence that results in death, is life threatening, requires admission to a hospital or emergency department for longer than 24 hours or prolongation of existing hospitalization, results in persistent or significant disability or incapacity, is a congenital anomaly, or is an important medical event. Severe TEAEs were also reported as SAEs.28,29
AESIs were AEs of scientific and medical concern specific to the study drug. AESIs for evinacumab included anaphylactic reactions, allergic reactions and/or local injection site reactions, increase in alanine aminotransferase or aspartate aminotransferase greater than or equal to 3 times the upper limit of normal, symptomatic overdose with evinacumab, neurocognitive events, new onset of diabetes, and pancreatitis.28,29
The clinical experts consulted by CADTH indicated that many of the AESIs defined in the included trials were borne from other LLTs used in hypercholesterolemia. However, given the method of administration of evinacumab, the clinical experts indicated that it would be important to consider allergic reactions and IRRs associated with evinacumab.
Statistical Analysis
Sample Size and Power Calculation
ELIPSE Trial
For the primary efficacy outcome of percent change from baseline in LDL-C, a sample size of 57 patients (38 on evinacumab and 19 on placebo) would be powered at 90%, based on a 2-sample t test, to reject a null hypothesis of no difference between treatment groups at the 0.05 significance level, assuming a group difference in mean percent change from baseline in LDL-C of 38% and a common SD of 35%. This sample size was adjusted for a 5% non-evaluable patient rate and a 15% dropout rate.29
CL-17100 Study
Given the design of the CL-17100 study, no sample size calculation was conducted.28
Interim and Final Analyses
ELIPSE Trial
For the ELIPSE trial, no formal interim analysis was planned. Efficacy and safety analyses for the primary and secondary efficacy end points of the ELIPSE trial were performed in 2 steps. The first step included the efficacy analyses up to week 24. This analysis was conducted on all randomized patients once all data through week 24 had been collected and validated. The second step, considered the final analysis, was conducted at the end of the study and consisted of the final efficacy and safety analyses at time points beyond the week 24 visit.29
CL-17100 Study
No interim analyses were planned for the CL-17100 study; however, an interim Clinical Study Report was provided by the sponsor, presenting data for Part A (data cut-off: February 11, 2021), Part B (data cut-off: January 31, 2022), and Part C (data cut-off: June 2, 2022).28
Statistical and Analytical Plans
ELIPSE Trial
Efficacy analysis: Efficacy in the included trials was assessed through multiple lipid parameters, which have been previously described previously. All lipid parameters were collected over the course of the study and sent to a central laboratory for evaluation.29
For statistics where international and conventional units would not impact the results (i.e., percent change from baseline, summary test statistics, proportions of patients below a threshold), statistical models were implemented using conventional units. For other statistics (e.g., descriptive statistics at baseline and over time, absolute change from baseline), results were presented in both international and conventional units.29
The intention-to-treat (ITT) population was the primary population for the efficacy analysis in the ELIPSE trial, which used an MMRM approach. All postbaseline data available within the week 2 to week 24 efficacy analysis window were used, and missing data were assumed missing at random. The baseline was defined as the last available measurement before the date of the first double-blind study treatment administration. The calculated LDL-C at week 24 was the LDL-C value obtained within the week 24 analysis window, regardless of adherence to treatment and of subsequent therapies. The model included an individual-level random intercept and fixed categorical effects for the treatment group (evinacumab versus placebo) for the following: randomization strata (apheresis [yes or no] and region [Japan or rest of world]), each time point (weeks 2, 4, 8, 12, 16, 20, and 24), treatment by time point interaction and strata by time point interaction, as well as the continuous covariates of baseline calculated LDL-C value and baseline value by time point interaction. The model parameters were estimated using the restricted maximum likelihood estimator with the Newton-Raphson algorithm and an unstructured correlation matrix to permit within-patient dependence. Denominator degrees of freedom were estimated using the Satterthwaite approximation. Within-treatment-group LSMs and SEs were adjusted using weights equal to the observed proportion of patients in the previously noted strata variable levels across the study population (i.e., population weight), rather than equal weights. Population weights were considered more appropriate than equal coefficients due to potential imbalances observed in the study population between levels of the randomization stratification factors. Prior to performing the primary efficacy analysis, statistical analysis method assumptions were checked for baseline homogeneity of LDL-C levels between treatment groups, normality of the LDL-C percent change distribution for each treatment group, and equality of variances between treatment groups using a residual plot.29
During the open-label treatment period, efficacy variables were explored through descriptive statistics at each scheduled visit for all patients administered the open-label study treatment, as well as for the patient subgroups (by study treatment received) in the double-blind treatment period. Formal statistical testing was not planned. Descriptive statistics included the observed values of the same parameters described for each variable in the double-blind treatment period.29
Sensitivity analyses: Robustness of the primary analysis was assessed through the following sensitivity analyses:29
Sensitivity to stratification at randomization: To assess stratification mistakes made at the time of randomization, the MMRMs were rerun, replacing the IWRS strata with the actual recorded strata.
Sensitivity to on-treatment calculated LDL-C values: To assess the more clinically relevant treatment comparisons of the percent change from baseline in calculated LDL-C to week 24, the modified ITT population (refer to Table 9) was used during the efficacy treatment period (on-treatment estimand).
Sensitivity to non–good clinical practice (GCP)–compliant sites: To assess the impact of non–GCP-compliant sites on the primary efficacy end point, the primary efficacy analysis excluded non–GCP-compliant sites. Sites known to be non–GCP compliant at the time of database lock were identified for this analysis before database lock. Any additional sites determined to be non–GCP compliant postdatabase lock were separately identified.
Sensitivity to the handling of missing data: To assess the handling of missing data through visual examination and using a PMM, postbaseline LDL-C levels (in the ITT population) were described and were graphed according to the following groups:
LDL-C available at week 24 (i.e., primary efficacy end point available)
LDL-C available at week 20 but missing at week 24
LDL-C available at week 16 but missing from week 20
LDL-C available at week 12 but missing from week 16
LDL-C available at week 8 but missing from week 12
LDL-C available at week 4 but missing from week 8
LDL-C available at week 2 but missing from week 4
LDL-C missing from week 2.
Sensitivity analysis to explore the impact of nonignorable missingness on the primary efficacy analysis was also conducted using the PMM approach. In the PMM approach, different imputation strategies were applied to LDL-C values missing during the double-blind, on-treatment period (i.e., within the period from the first double-blind study treatment administration up to the day of the last double-blind administration, plus 35 days) versus LDL-C values missing due to treatment discontinuation after the on-treatment period (i.e., after the day of the last double-blind administration, plus 35 days) based on the following assumptions:29
For patients within 35 days after their last study treatment (double-blind treatment period), treatment administration would continue to show benefit similar to that observed at the scheduled time point. Therefore, missing LDL-C values during the on-treatment period (e.g., samples obtained outside the specified window, no blood sample available although visit was performed) should be considered “missing at random” and imputed based on other observed measurements in the on-treatment period.
Patients who stopped taking their study treatment no longer benefited from it after discontinuation, and thus tended to have LDL-C values returning to baseline. Therefore, LDL-C values missing after the on-treatment period should be imputed based on the patient’s own baseline value.
Missing data from the randomized population were imputed 100 times to generate 100 complete datasets, using a Markov chain Monte Carlo method, and were used for the sensitivity analysis of the primary efficacy analysis. For the percent change from baseline in LDL-C end point, the 100 complete datasets of observed and imputed LDL-C data at week 24 were analyzed using an analysis of covariance model, with treatment group and randomization strata as fixed effects and the baseline LDL-C value as a continuous covariate. The MIANALYZE procedure was used to generate valid statistical inferences by combining results from the 100 analyses using the Rubin formulas.29
Subgroup Analyses: To assess the homogeneity of the treatment effect across various subgroups, the treatment by subgroup factor, the time point by subgroup factor, and the treatment by time point by subgroup factor interaction terms and a subgroup factor term were added to the primary MMRM. The significance level of the treatment by subgroup factor interaction term at week 24 was provided for each factor for descriptive purposes. To handle imbalances between randomization stratification factor levels, population weights were used, as they were for the primary analysis model.29
The following subgroups of interest were preplanned: baseline apheresis status (yes, no); geographical region (Japan, rest of world); sex (female, male); age (< 65 years, ≥ 65 years); race; ethnicity; baseline LDL-C (< 130 mg/dL, ≥ 130 mg/dL); HoFH genotype (homozygous, compound heterozygous, double heterozygous); receptor-negative mutation in both LDLR alleles, where receptor-negative is defined as a mutation resulting in termination codons, splice site mutations, frame shifts, and large insertions or deletions (yes, no).29
Secondary end point efficacy analysis: Statistical analyses for the key secondary efficacy end points and other secondary efficacy end points were performed in the ITT population. For the descriptive summaries, percent change and, when appropriate, absolute change from baseline in LDL-C, Apo B, total cholesterol, triglycerides, non-HDL-C, lipoprotein A, and apolipoprotein C-III were estimated at each time point for each treatment group.29
Continuous secondary variables anticipated to have a normal distribution were analyzed using the same fixed-effect MMRM described for the primary end point. Specifically, the model contained the categorical effects of treatment group, randomization strata (as per IWRS), planned time points up to week 24, strata by time point interaction, and treatment by time point interaction, as well as the continuous covariates of corresponding baseline value and baseline value by time point interaction.29
Continuous secondary efficacy variables anticipated to have a non-normal distribution (i.e., triglycerides and lipoprotein A) were analyzed using the multiple imputation approach for handling of missing values, with data log-transformed before the imputation process and then back-transformed to create the imputed datasets. The percent change from baseline at the time point of interest was derived from observed and imputed lipid values at this time point. Multiple imputed datasets were modelled using a simple regression to compare treatment group differences,51 with the end point of interest as the response variable. The mean treatment response was estimated using a robust M-estimation within treatment group, randomization strata, and corresponding baseline values. Combined means estimates for both treatment groups, as well as the differences in these estimates, with their corresponding SEs, 95% CIs, and P values, were provided.29
Binary secondary efficacy end points were analyzed using the multiple imputation approach to account for missing values. The binary end point at the time point of interest was derived from observed and imputed lipid values at this time point. Multiple imputed datasets were modelled using stratified logistic regression. The logistic regression procedure was used to compare treatment group differences, with the model containing treatment group and corresponding baseline values as covariates, stratified by randomization strata. Combined estimates of OR versus placebo, 95% CI, and P value were provided.29
Sensitivity Analyses
Sensitivity analyses of key secondary end points were conducted using the modified ITT population, and the ITT estimand was replaced by the on-treatment estimand, defined as all key secondary efficacy end point values collected during the efficacy treatment period.29
Multiple testing: In the ELIPSE trial, to handle multiple key secondary end points during the double-blind treatment period, a hierarchical inferential approach was used to control the overall type I error at the level of 0.05. The hierarchical testing sequence included the primary efficacy variable (percent change from baseline in LDL-C to week 24), followed by key secondary end points: percent change from baseline in Apo B, non-HDL-C, and total cholesterol to week 24, proportion of patients with a greater than or equal to 30% reduction in LDL-C at week 24, proportion of patients with a greater than or equal to 50% reduction in LDL-C at week 24, absolute change from baseline in LDL-C to week 24, and proportion of patients who meet US and EU apheresis eligibility criteria. No further adjustments were made for other secondary end points, and P values were provided for reference only.29
Safety analysis: Safety results were presented separately for the double-blind and open-label treatment periods, unless otherwise noted. Safety summaries for the double-blind treatment period were presented by treatment group, containing patients from the double-blind safety analysis set (SAS). No formal inferential testing was performed, and summaries were descriptive in nature.29
An independent data monitoring committee composed of members who were independent from the sponsor and the study investigators monitored patient safety by conducting formal reviews of the accumulated safety data.29
CL-17100 Study
Efficacy analysis: Efficacy analyses are only reported for Part B of the CL-17100 study. The primary end point of percent change from baseline in LDL-C at week 24 was summarized descriptively for all patients in the ITT population using mean, SE, and 95% CI. Missing data were imputed using a PMM approach, as described in the section on the sensitivity analysis for the ELIPSE trial.28
Missing LDL-C change data from the ITT population were imputed 100 times to generate 100 complete datasets using a Markov chain Monte Carlo method. The 100 completed datasets of observed and imputed LDL-C data will be used for the primary analysis. For the percent change from baseline in LDL-C end point, the 100 complete datasets of observed and imputed LDL-C data at week 24 were analyzed using the MEANS procedure. The MIANALYZE procedure was used to combine the results from the 100 analyses using the Rubin formulas. Combined estimates of the mean at week 24 were provided with the SE and the 95% CI. Formal statistical testing was not planned.28
Sensitivity analyses: Sensitivity analyses were conducted similarly to the ELIPSE trial, removing non–GCP-compliant sites, using the MMRM approach, as defined for the primary end point of the ELIPSE trial, and using the modified ITT population.28
Subgroup analyses: The following subgroups of interest were planned: sex (female, male), age (≥ 5 to < 10 years, ≥ 10 to ≤ 12 years), race, ethnicity, baseline apheresis status (yes, no), receptor-negative mutation in both LDLR or LDLRAP1 alleles (yes, no), and LDLR activity (null/null [LDLR activity ≤ 15%], not null/null [LDLR activity > 15%]).28
Secondary efficacy analysis: For the secondary efficacy end points, descriptive summaries and analyses were performed in the ITT population, using values obtained regardless of adherence to the study treatment and of subsequent therapies.28
Continuous secondary end points anticipated to have a normal distribution were analyzed using the ITT population and the PMM approach for missing data as described for the primary efficacy end point. Continuous secondary efficacy variables anticipated to have a non-normal distribution were analyzed identically to in the ELIPSE trial.28
Binary secondary efficacy end points were descriptively summarized using the ITT population, along with the proportion and 95% CI. Missing data were imputed using the same PMM approach as described for the primary efficacy end point.28
Multiple testing: No formal statistical testing was performed for this open-label study, as such control for multiplicity was not applicable.28
Safety analysis: Safety summaries were descriptive in nature, and no formal inferential testing was performed.28
An independent data monitoring committee composed of members who were independent from the sponsor and the study investigators monitored patient safety by conducting formal reviews of the accumulated safety data.28
Table 8: Statistical Analysis of Efficacy End Points
End point | Statistical model | Adjustment factors | Handling of missing data | Sensitivity analyses |
|---|---|---|---|---|
ELIPSE: DBTP | ||||
Percent change from baseline in LDL-C to week 24 | MMRM | Stratification factors: apheresis treatment [yes, no] and region [Japan, rest of world]; adjusted using weights equal to the observed proportion of patients in variable levels across the study population (i.e., population weight), rather than equal weights | Assumed missing at random | 1. PMM to assess the potential violation of the missing at random assumption 2. On-treatment analysis for treatment comparisons of the percent change from baseline in calculated LDL-C to week 24 (mITT patient population using calculated LDL-C values collected during the efficacy treatment period [on-treatment estimand]) |
Key secondary efficacy end points (multiplicity adjustment is applied) | ||||
Percent change from baseline in Apo B to week 24 | MMRM | Same as primary end point; fixed hierarchical approach for multiple comparisons | Same as primary end point | Same as primary end point; PMM and mITT |
Percent change from baseline in non-HDL-C to week 24 | MMRM | Same as primary end point; fixed hierarchical approach for multiple comparisons | Same as primary end point | Same as primary end point; PMM and mITT |
Percent change from baseline in TC to week 24 | MMRM | Same as primary end point; fixed hierarchical approach for multiple comparisons | Same as primary end point | Same as primary end point; PMM and mITT |
Proportion of patients with ≥ 30% reduction in LDL-C at week 24 | Multiple imputation followed by stratified logistic regression | Fixed hierarchical approach for multiple comparisons | LOCF | Same as primary end point; mITT |
Proportion of patients with ≥ 50% reduction in LDL-C at week 24 | Multiple imputation followed by stratified logistic regression | Fixed hierarchical approach for multiple comparisons | LOCF | Same as primary end point; mITT |
Absolute change from baseline in LDL-C at week 24 | MMRM | Fixed hierarchical approach for multiple comparisons | Same as primary end point | Same as primary end point; mITT |
Proportion of patients who meet US apheresis eligibility criteria at week 24 | Multiple imputation followed by stratified logistic regression | Fixed hierarchical approach for multiple comparisons | LOCF | Same as primary end point; mITT |
Proportion of patients with LDL-C < 70 mg/dL (1.81 mmol/L) at week 24 | Multiple imputation followed by stratified logistic regression | Fixed hierarchical approach for multiple comparisons | LOCF | Same as primary end point; mITT |
Proportion of patients who meet EU apheresis eligibility criteria at week 24 | Multiple imputation followed by stratified logistic regression | Fixed hierarchical approach for multiple comparisons | LOCF | Same as primary end point; mITT |
Secondary end points (multiplicity adjustment is not applied) | ||||
Percent change from baseline in triglycerides to week 24 | Multiple imputation followed by robust regression model | Same as primary end point | — | Same as primary end point; mITT |
Change from baseline in Apo B to week 24 | MMRM | Same as primary end point | Same as primary end point | Same as primary end point; mITT |
Change from baseline in non-HDL-C | MMRM | Same as primary end point | Same as primary end point | Same as primary end point; mITT |
Change from baseline in non-HDL-C to week 24 | MMRM | Same as primary end point | Same as primary end point | Same as primary end point; mITT |
Percent change from baseline in Lp(a) to week 24 | Multiple imputation followed by robust regression model | Same as primary end point | Multiple imputation | Same as primary end point; mITT |
Proportion of patients with LDL-C < 70 mg/dL (1.81 mmol/L) at week 24 | Multiple imputation followed by stratified logistic regression | Same as primary end point | LOCF | Same as primary end point; mITT |
Percent change from baseline in Apo CIII at week 24 | MMRM | Same as primary end point | Same as primary end point | Same as primary end point; mITT |
EQ-5D | Descriptive statistics | None | None | None |
HADS | Descriptive statistics | None | None | None |
CL-17100: Part B | ||||
Percent change from baseline in LDL-C to week 24 | PMM | None | PMM approach using MEANS procedure, then MIANALYZE | MMRM (ITT estimand) |
Percent change from baseline in Apo B to week 24 | PMM | None | Same as primary end point | MMRM (ITT estimand) |
Percent change from baseline in non-HDL-C to week 24 | PMM | None | Same as primary end point | MMRM (ITT estimand) |
Percent change from baseline in TC to week 24 | PMM | None | Same as primary end point | MMRM (ITT estimand) |
Proportion of patients with ≥ 50% reduction in LDL-C at week 24 | Descriptive statistics with proportions and 95% CI | None | Same as primary end point | None |
Percent change from baseline in LDL-C to week 24 in patients who have negative/negative and null/null mutations | PMM | None | Same as primary end point | MMRM (ITT estimand) |
Percent change from baseline in Lp(a) to week 24 | Multiple imputation followed by robust regression model | None | Multiple imputation | None |
Absolute change from baseline in LDL-C at week 24 | PMM | None | Same as primary end point | MMRM (ITT estimand) |
Apo B = apolipoprotein B; Apo CIII = apolipoprotein C-III; CI = confidence interval; DBTP = double-blind treatment period; EU = European Union; HADS = Hospital Anxiety and Depression Scale; HDL-C = high-density lipoprotein cholesterol; ITT = intention to treat; LDL-C = low-density lipoprotein cholesterol; LOCF = last observation carried forward; Lp(a) = lipoprotein (a); mITT = modified intention to treat; MMRM = mixed-effect model with repeated measures; PMM = pattern mixture model; TC = total cholesterol.
Sources: ELIPSE Clinical Study Report;29 CL-17100 Clinical Study Report.28
Analysis Populations
The analysis populations for the ELIPSE and CL-17100 studies are summarized in Table 9. The ELIPSE trial included an ITT population, a modified ITT population, an SAS in both the double-blind and open-label treatment phases, and a quality of life analysis set.29 The CL-17100 study included an ITT, a modified ITT, and an SAS population.28
Table 9: Analysis Populations of ELIPSE and CL-17100 Studies
Study | Population | Definition | Application |
|---|---|---|---|
ELIPSE | ITT | All randomized patients who received at least 1 dose or part of a dose of the double-blind study drug. Patients in the ITT population were analyzed according to their treatment group, allocated by randomization. | Primary and key secondary efficacy analyses |
mITT | All randomized patients who received at least 1 dose or part of a dose of the study drug and had an evaluable primary end point. The end point was considered as evaluable when both of the following conditions were met:
Patients in the mITT population were analyzed according to their treatment group, allocated by randomization. | Sensitivity analyses | |
Double-blind SAS | The randomized population who received at least 1 dose or part of a dose of the double-blind study drug. Patients were analyzed according to the treatment received (placebo or evinacumab). In addition:
| Double-blind safety analyses | |
Open-label SAS | The randomized population who received at least 1 dose or part of a dose of the open-label study drug. | Open-label safety analyses | |
Quality of life analysis set | The analyses for quality of life in the respective treatment period (DBTP and OLTP) were performed on all randomized patients who received any study treatment with a baseline and at least 1 postbaseline evaluation. Further:
| EQ-5D and HADS analyses | |
CL-17100 | ITT | All patients who received at least 1 dose or part of a dose of the study drug in Part B. | Primary and secondary |
mITT | All patients who received at least 1 dose or part of a dose of the study drug in Part B and had an evaluable primary efficacy end point. The end point was considered as evaluable when both of the following conditions were met:
| Sensitivity analyses | |
SAS | All patients who received at least 1 dose or part of a dose of the study drug. | Safety analyses | |
Part C SAS | All patients who received at least 1 dose or part of a dose of the study drug in Part C. | Safety analyses |
DBTP = double-blind treatment period; HADS = Hospital Anxiety and Depression Scale; ITT = intention to treat; LDL-C = low-density lipoprotein cholesterol; mITT = modified intention to treat; OLTP = open-label treatment period; SAS = safety analysis set.
Sources: ELIPSE Clinical Study Report;29 CL-17100 Clinical Study Report.28
Protocol Amendments and Deviations
Protocol Amendments
The original global study protocol for the ELIPSE trial, dated May 7, 2017, was amended |||| times. |||||||| ||||||||| || |||||||| ||| |||||| ||||||||| ||||||| |||||||| ||| |||||||| || ||||| ||| |||| || |||||||||| ||| ||||||||||| ||||||||| || ||||| |||||||||| || ||| || |||| ||||||||||| ||| ||||||||||||| || ||| ||| |||||||||| ||| ||||||| ||||||| || |||||||| || ||||||| ||| ||||||| ||||| ||||||||| ||| ||||||||| ||||||| |||||| ||| |||||| ||||||| ||| |||||||||| || |||| ||||||||| ||||| ||||||||| |||||||| ||| |||| ||| |||||||| ||| |||||||||| |||| ||||| |||||||||||| || |||| |||||| ||| |||| |||||||| |||||| || |||||||||| ||||||||| ||||||| || ||||| ||||||||| |||||||| ||||||||||||| |||| ||||||||| |||||||||||||| ||||||||| |||||||| |||| ||||| ||||| ||| ||||| || |||| || ||| |||| ||| || ||||||||| |||||||| ||| |||| || ||||| ||| ||||||||||| ||| ||||||||||||||||| ||| ||| ||||| ||||||||| |||||||| ||||||||| || |||||||| ||| |||||||||||| |||||||||| || ||| ||||||||||| || |||||||||| ||| ||||| ||||||||||| ||||||||| |||||||||| ||| ||| ||||||||| || |||||||| |||| ||||| ||| ||||||||| ||| ||||||||||| |||||||||||| || ||||||||| |||| |||||||| |||||||| |||||| |||| |||||||||||| |||| ||| ||| ||||||||||| |||||||| ||| |||| |||||| ||| |||| |||||||| ||||||||| |||| |||||||||||| |||| |||||||| || ||||||| |||||||||| ||| || |||||||||| |||||||| ||||||||| || ||| ||||||||| || |||||||| || |||||| |||||||||||| |||||||| || ||||||| || ||||||| ||| |||||||| |||||| |||| |||||||| || ||| |||||||| || |||||||||||||||||||||||| |||||||| ||| |||||||| ||| ||||| || |||| || ||||| |||||| || ||||||| |||| ||||||||. Dates for protocol amendments in the ELIPSE trial were not provided; therefore, it is unclear whether the amendments had any major impact on the conduct of the study.
The protocol for the CL-17100 study was amended twice. Amendment 1 included changes to the study design by |||||||| ||| ||||||||| |||||| || ||||||| || ||||| || || |||||, added the absolute change from baseline in LDL-C to week 24 as an end point, and amended the list of AESIs. The second protocol amendment ||||||||| ||| |||||| |||| ||| |||||| || || || |||||||| ||| || ||||||||||| ||||||||||||| ||| ||||||| |||||||| ||| ||||| |||| ||| ||||||||||||| ||| ||||||| || ||||| |||||| ||||||| || ||||| ||| ||||||||| |||||| || ||| |||||.28 Dates for protocol amendments were not provided; therefore, it is unclear whether the amendments had any major impact on the conduct of the study.
Protocol Deviations
Protocol deviations in the ELIPSE and CL-17100 studies are summarized in Table 10. For the ELIPSE trial, protocol deviations are summarized for both the double-blind and open-label treatment periods. For the CL-17100 study, protocol deviations are summarized as a group for Parts A, B, and C. In the ELIPSE trial, protocol deviations occurred in || patients (||||%) and || patients (||||%)in the evinacumab and placebo groups, respectively. In the CL-17100 study, protocol deviations occurred in ||| patients (|| [|||||%]). In both studies, the most common cause of protocol deviations was procedural irregularities, occurring in || patients (||||%) and ||| patients (||||%) in the ELIPSE trial evinacumab and placebo groups, respectively, and in || patients (||||%) in the CL-17100 study. Other protocol deviations in the ELIPSE trial and the CL-17100 study included those related to the definition of “women of childbearing potential” and lipid apheresis schedule issues, respectively.28,29
Table 10: Protocol Deviations in ELIPSE (ITT) and CL-17100 (Enrolled Patients) Studies
Patient disposition | ELIPSE | CL-17100 | |
|---|---|---|---|
Evinacumab (n = 43) | Placebo (n = 22) | Evinacumab (n = 20) | |
Patients with any protocol deviations | || |||||| | || |||||| | || ||||| |
Any important protocol deviations | || |||||| | || |||||| | || ||||| |
Any minor protocol deviations | || |||||| | || |||||| | || ||||| |
Types of important protocol deviations | |||
Inadequate informed consent administration | ||||| | ||||| | ||||| |
Randomization and drug allocation errors | ||||| | ||||| | ||||| |
Procedural irregularities | || |||||| | ||||| | ||||| |
Patients received prohibited medications/procedures | ||||| | ||||| | ||||| |
Other | |||||| | ||||| | ||||| |
Sources: ELIPSE Clinical Study Report;29 CL-17100 Clinical Study Report.28
Results
Patient Disposition
The ELIPSE and CL-17100 studies shared a similar patient population for enrolment, though the designs varied. In the ELIPSE trial, 75 patients were screened and 65 were randomized 2:1 to evinacumab (n = 43) or matching placebo (n = 22), making up the ITT population. Ten patients failed screening: 8 violated the eligibility criteria, and 2 withdrew consent. Of the 65 patients randomized and treated, 64 (98.5%) completed the 24-week double-blind treatment period. One patient (1.5%) from the placebo group withdrew consent after receiving 1 dose of the study drug and was not considered to have completed the study. There were no AEs that led to treatment discontinuation during the double-blind treatment period.29
Table 11: Summary of Patient Disposition From Studies Included in the Systematic Review
Patient disposition | ELIPSE (DBTP) | CL-17100 | ||
|---|---|---|---|---|
Evinacumab 15 mg/kg (n = 43) | Placebo (n = 22) | Part B: evinacumab 15 mg/kg (n = 14) | Pooled Parts B + C: evinacumab 15 mg/kg (n = 20) | |
Screened, N | 75 | || | ||
Reason for screening failure, n (%) | ||||
Screen failures | 10 (13.3) | ||||||| | ||
Violated eligibility criteria | 8 (10.7) | — | ||
Withdrew consent | 2 (2.7) | |||||| | ||
Other (COVID-19) | — | |||||| | ||
Randomized, N (%) | 65 (87) | 14 (100.0) | || ||||||| | |
Discontinued from study, n (%) | 0 (0.0) | 1 (4.5) | 0 (0.0) | 0 (0.0) |
Reason for discontinuation, n (%) | ||||
Adverse events | 0 (0.0) | 0 (0.0) | — | — |
Lost to follow-up | 0 (0.0) | 0 (0.0) | — | — |
Withdrawal of consent by patient | 0 (0.0) | 1 (4.5) | — | — |
ITT, N | 43 | 22 | 14 | — |
mITT, N | 43 | 22 | 14 | — |
Safety, N | ||||
Double-blind safety analysis set | 44 | 21 | — | — |
Open-label safety analysis set | 44 | 20 | 14 | || |
QoL population, N | ||||
QoL EQ-5D | 43 | 20 | — | — |
DBTP = double-blind treatment period; ITT = intention to treat; mITT = modified intention to treat; QoL = quality of life.
Sources: ELIPSE Clinical Study Report;29 CL-17100 Clinical Study Report.28
The CL-17100 study screened a total of 23 patients for enrolment in Parts A, B, and C. A total of 14 patients were enrolled in, treated in, and completed Part B of the CL17100 study; 13 (92.9%) continued to Part C. A total of || patients (6 from Part A, and 14 from Part B) were treated in Part C. As of the interim cut-off date (|||| || ||||), |||| patients (||||%) had completed Part C and || patients (||||%) were ongoing in the Part C treatment period. Overall, |||| patients (||||%) have completed the study and || are ongoing.28
Baseline Characteristics
Baseline characteristics for the ELIPSE and CL-17100 studies are summarized in Table 12. The baseline characteristics included in the table are limited to those that are most relevant to this review or were felt to affect the outcomes or interpretation of the study results.
ELIPSE Trial
In the ELIPSE trial, patients were randomized 2:1 to either evinacumab (n = 43) or placebo (n = 22). A total of 22 patients (33.8%) were randomized and treated in EU member countries and 43 patients (66.2%) in non–EU member countries. There was a difference between the evinacumab and placebo groups in terms of age at baseline, with a mean age of 44.3 years (SD = 16.8) in the evinacumab group compared to 36.7 years (SD = 11.52) in the placebo group. Only 1 patient in each treatment group was below age 18 years. In line with the difference in age, there was also a difference in the mean time from diagnosis of HoFH to randomization: 16.15 years (SD = 14.562) in the evinacumab group compared to 10.65 years (SD = 12.537) in the placebo group. Patients in the evinacumab and placebo groups were mostly female (55.8% and 50.0%) and white (72.1% and 77.3%). There was also a difference in body mass index across patient groups, with the body mass index being less than 30 kg in 32 patients (74.4%) in the evinacumab group and 19 patients (86.4%) in the placebo group.29
A total of 48.8% of patients had homozygous LDLR mutations in the evinacumab group compared to only 31.8% in the placebo group, while fewer patients had compound heterozygous LDLR mutations in the evinacumab group than in the placebo group (27.9% versus 36.4%). Most patients received at least 3 LLTs at baseline (69.8% in the evinacumab group versus 50.0% in the placebo group), mostly statin plus ezetimibe and a PCSK9 inhibitor (48.8% in the evinacumab group versus 36.4% in the placebo group). Nearly all patients were treated with any statin (95.3% in the evinacumab group and 90.9% in the placebo group), and most patients also received ezetimibe (76.7% in the evinacumab group versus 72.7% in the placebo group) or PCSK9 inhibitors (79.1% in the evinacumab group versus 72.7% in the placebo group). More patients in the evinacumab group received lomitapide than in the placebo group (25.6% versus 13.6%). The patients’ lipid parameters were comparable across treatment groups in terms of mmol/L, though the evinacumab group tended to have higher levels of the following than the placebo group: LDL-C (259.5 mg/dL versus 246.5 mg/dL), non-HDL-C (281.9 mg/dL versus 269.9 mg/dL), and total cholesterol (325.6 mg/dL versus 315.9 mg/dL). This was not true of Apo B, for which the mean levels at baseline were lower in the evinacumab group than in the placebo group (169.1 mg/dL versus 175.9 mg/dL).29
CL-17100 Study
The CL-17100 study was conducted in patients aged 5 to 11 years with HoFH. The mean age of the patients enrolled in Part B of the CL-17100 study at baseline was 9.1 years (SD = 1.94). Most patients (57.1%) were white females. Most patients (71.4%) had compound heterozygous mutations, and only 50% of patients had received prior apheresis at baseline. Nearly all patients were treated with statins (85.7%) and ezetimibe (92.9%) at baseline, and only 2 patients (14.3%) received lomitapide. The patients’ lipid parameters at baseline were similar to those in the ELIPSE trial, with mean values as follows: LDL-C of 263.7 mg/dL, Apo B of 168.2 mg/dL, non-HDL-C of 282.2 mg/dL, and total cholesterol of 315.5 mg/dL.28
Table 12: Summary of Baseline Characteristics From Studies Included in the Systematic Review
Characteristic | ELIPSE (ITT) | CL-17100 (SAS) | ||
|---|---|---|---|---|
Placebo (n = 22) | Evinacumab (n = 43) | Part B: evinacumab (n = 14) | Total Parts B + C: evinacumab (n = 20) | |
Demographic characteristics | ||||
Age (years) | ||||
Mean (SD) | 36.7 (11.52) | 44.3 (16.8) | 9.1 (1.94) | 9.0 (1.84) |
Median (range) | 39.5 (12 to 55) | 41.0 (15 to 75) | 9.5 (5 to 11) | 9.0 (5 to 11) |
Sex, n (%) | ||||
Male | 11 (50.0) | 19 (44.2) | 6 (42.9) | 8 (40.0) |
Female | 11 (50.0) | 24 (55.8) | 8 (57.1) | 12 (60.0) |
Race, n (%) | ||||
White | 17 (77.3) | 31 (72.1) | 8 (57.1) | 14 (70.0) |
Black or African American | 0 (0.0) | 2 (4.7) | 1 (7.1) | 1 (5.0) |
Asian | 4 (18.2) | 6 (14.0) | 2 (14.3) | 2 (10.0) |
American Indian or Alaska Native | 0 (0.0) | 0 (0.0) | 1 (7.1) | 1 (5.0) |
NR | 0 (0.0) | 2 (4.7) | 0 (0.0) | 0 (0.0) |
Other | 1 (4.5) | 2 (4.7) | 2 (14.3) | 2 (10.0) |
BMI (kg/m2) | ||||
Mean (SD) | 24.6 (5.69) | 26.1 (5.86) | 19.5 (4.61) | 18.8 (4.19) |
< 30, n (%) | 19 (86.4) | 32 (74.4) | NR | NR |
≥ 30, n (%) | 3 (13.6) | 11 (25.6) | NR | NR |
Geographic region, n (%) | ||||
Japan | 4 (18.2) | 6 (14.0) | NR | NR |
Rest of world | 18 (81.8) | 37 (86.0) | NR | NR |
Clinical characteristics | ||||
Apheresis treatment status, n (%) | ||||
Yes | 8 (36.4) | 14 (32.6) | 7 (50.0) | 12 (60.0) |
No | 14 (63.6) | 29 (67.4) | NR | NR |
Mutation status, n (%) | ||||
Homozygous (LDLR) | 7 (31.8) | 21 (48.8) | 4 (28.6) | NR |
||||||||||||||||||| | |||||| | |||||| | |||||| | || |
||||||||||||||||| | |||||| | |||||| | |||||| | || |
||||||||| | |||||| | |||||| | |||||| | || |
Homozygous (LDLRAP1) | |||||| | |||||| | |||||| | NR |
||||||||||||||||| | |||||| | |||||| | |||||| | || |
||||||||| | |||||| | |||||| | |||||| | || |
Compound heterozygous (LDLR) | 8 (36.4) | 12 (27.9) | 10 (71.4) | NR |
Double heterozygous (LDLR and Apo B) | 1 (4.5) | 2 (4.7) | 0 (0.0) | NR |
Other (heterozygous, undetermined, or no mutation) | 5 (22.7) | 7 (16.3) | NR | NR |
History of HoFH | ||||
Confirmation of diagnosis by genotyping, n (%) | 15 (68.2) | 29 (67.4) | 13 (92.9) | NR |
Confirmation of diagnosis by clinical diagnosis, n (%) | 7 (31.8) | 14 (32.6) | 1 (7.1) | NR |
Time from HoFH diagnosis (years), mean (SD) | 10.65 (12.537) | 16.15 (14.562) | 5.38 (2.957) | NR |
CV history, n (%) | ||||
Any CV history or risk factors | 21 (95.5) | 38 (88.4) | NR | NR |
CHD | 12 (54.5) | 22 (51.2) | NR | NR |
CHD risk equivalents | 1 (4.5) | 10 (23.3) | NR | NR |
Very high CV risk | 12 (54.5) | 23 (53.5) | NR | NR |
High CV risk | 10 (45.5) | 20 (46.5) | NR | NR |
LLT use, n (%) | ||||
At least 3 LLTs | 11 (50.0) | 30 (69.8) | NR | NR |
Statin + ezetimibe + PCSK9 inhibitor | 8 (36.4) | 21 (48.8) | NR | NR |
Statin + ezetimibe + PCSK9 inhibitor + lomitapide | 3 (13.6) | 4 (9.3) | NR | NR |
Any statin | 20 (90.9) | 41 (95.3) | 12 (85.7) | 18 (90.0) |
High-intensity statin | 16 (72.7) | 34 (79.1) | 6 (42.9) | 10 (50.0) |
Any nonstatin LLT | 20 (90.9) | 43 (100) | 14 (100) | 20 (100) |
Ezetimibe | 16 (72.7) | 33 (76.7) | 13 (92.9) | 19 (95.0) |
PCSK9 inhibitor | 16 (72.7) | 34 (79.1) | 0 (0.0) | 0 (0.0) |
Alirocumab | 10 (45.5) | 17 (39.5) | 0 (0.0) | 0 (0.0) |
Evolocumab | 6 (27.3) | 17 (39.5) | 0 (0.0) | 0 (0.0) |
Lomitapide | 3 (13.6) | 11 (25.6) | 2 (14.3) | 2 (10.0) |
Lipid parameters | ||||
LDL-C, mean (SD) | ||||
mg/dL | 246.5 (153.71) | 259.5 (172.40) | 263.7 (90.97) | 301.9 (149.10) |
mmol/L | 6.4 (3.98) | 6.7 (4.47) | 6.830 (2.3539) | 7.819 (3.8609) |
Apo B, mean (SD) | ||||
mg/dL | 175.9 (98.76) | 169.1 (82.75) | 168.2 (47.49) | 185.4 (71.33) |
g/L | 1.8 (0.99) | 1.7 (0.83) | 1.682 (0.4749) | 1.854 (0.7133) |
Non-HDL-C, mean (SD) | ||||
mg/dL | 269.9 (157.81) | 281.9 (172.61) | 282.2 (97.59) | 320.9 (154.80) |
mmol/L | 7.0 (4.09) | 7.3 (4.47) | 7.309 (2.5277) | 8.312 (4.0092) |
TC, mean (SD) | ||||
mg/dL | 315.9 (150.44) | 325.6 (170.76) | 315.5 (88.33) | 355.8 (150.54) |
mmol/L | 8.2 (3.90) | 8.4 (4.42) | 8.171 (2.2886) | 9.215 (3.8997) |
Apo B = apolipoprotein B; BMI = body mass index; CHD = coronary heart disease; CV = cardiovascular; HDL-C = high-density lipoprotein cholesterol; HoFH = homozygous familial hypercholesterolemia; ITT = intention to treat; LDL-C = low-density lipoprotein cholesterol; LDLR = low-density lipoprotein receptor; LLT = lipid-lowering therapy; NR = not reported; SAS = safety analysis set; SD = standard deviation; TC = total cholesterol.
Sources: ELIPSE Clinical Study Report;29 CL-17100 Clinical Study Report.28
Exposure to Study Treatments
Exposure to study treatments in the ELIPSE trial and the CL-17100 study is summarized in Table 13.
ELIPSE Trial
In the ELIPSE trial, a total of 38 patients (86.4%) in the evinacumab group and 17 patients (81.0%) in the placebo group completed the double-blind treatment period. The mean number of infusions was similar in the evinacumab group |||| |||| ||||||| and the placebo group ||||| |||| |||||||, as was the duration of study drug exposure (evinacumab: ||||| ||||| ||| |||||||| |||||||| ||||| ||||| |||| ||||||).29
||| |||||| patient receiving evinacumab had infusion interruptions at ||||||||| |||| || ||| |||| ||, while ||||| patients receiving placebo had infusion interruptions at ||||||||. There were || infusion interruptions after week 8. ||| ||||||| in the evinacumab group experienced an infusion interruption ||| || ||| ||||||||| |||| |||||||||. The full dose of the study drug was administered in all cases, despite infusion interruptions.29
Table 13: Summary of Patient Exposure From ELIPSE and CL-17100 Studies
Exposure | ELIPSE (SAS) | CL-17100 | ||
|---|---|---|---|---|
Placebo (n = 21) | Evinacumab (n = 44) | Part B (ITT): evinacumab (n = 14) | Total Parts B + C (SAS): evinacumab (n = 20) | |
Total number of study treatment infusions, mean (SD) | |||| ||||||| | |||| ||||||| | |||| ||||||| | ||||| ||||||| |
Duration (weeks), median (range) | ||||| ||||| ||||| | ||||| |||||| ||||| | ||||| |||||| ||||| | ||||| |||||| ||||| |
Duration of study drug exposure by category, n (%) | ||||
≥ 1 day to < 4 weeks | ||||| | ||||| | ||||| | ||||| |
≥ 4 weeks to < 8 weeks | ||||| | ||||| | ||||| | ||||| |
≥ 8 weeks to < 12 weeks | ||||| | ||||| | ||||| | ||||| |
≥ 12 weeks to < 16 weeks | ||||| | ||||| | ||||| | ||||| |
≥ 16 weeks to < 20 weeks | ||||| | ||||| | ||||| | ||||| |
≥ 20 weeks to < 24 weeks | ||||| | ||||| | ||||| | ||||| |
≥ 24 weeks to < 28 weeks | ||||| | ||||| | ||||| | ||||| |
Infusion interruptions, n (%) | ||||
Adverse event | ||||| | ||||| | ||||| | ||||| |
Equipment failure | ||||| | ||||| | ||||| | ||||| |
Other | ||||| | ||||| | ||||| | ||||| |
ITT = intention to treat; SAS = safety analysis set; SD = standard deviation.
Sources: ELIPSE Clinical Study Report;29 CL-17100 Clinical Study Report.28
CL-17100 Study
In Part B of the CL-17100 study, all 14 patients had a mean of |||| ||||||||| |||| |||||| for a mean duration of ||||| ||||| |||| |||||||. A total of |||||||||| patients had their infusions interrupted at the baseline visit; ||| || || || ||||||||||| |||||| || |||||. ||| |||||| patient had their infusion interrupted at the week 12 visit due to ||||||||| |||||||. Infusions were resumed in all cases within minutes of the interruption. In the pooled population for Parts B and C, the mean number of infusions was ||||| ||||||||| |||| |||||| over an exposure of ||||| ||||| |||| ||||||28
||| |||||| patient had their infusion interrupted at both the week 12 and week 32 visits. ||| |||||| patient had their infusion interrupted at the week 4 visit. In all |||| cases, the reasons for the infusion interruptions were |||||||, and the infusions were resumed following the interruption.28
Efficacy
Efficacy results for the ELIPSE and CL-17100 studies are summarized in Table 14.
Percent Change From Baseline in LDL-C
The primary efficacy end point of the ELIPSE and CL-17100 studies was percent change from baseline in LDL-C to week 24. The results for the LSM percent change from baseline in LDL-C during the double-blind treatment period of the ELIPSE trial are summarized in Figure 1. The LSM percent change from baseline with evinacumab was –47.1% (SE = 4.6), compared to 1.9% (SE = 6.5) with placebo. In the double-blind treatment period, the LSMD between evinacumab and placebo in percent change from baseline in LDL-C was –49.0% (95% CI, –65.0 to –33.1), favouring evinacumab.29
Figure 1: Least Squares Mean Percent Change From Baseline in LDL-C (MMRM Analysis; ITT Population, ELIPSE)
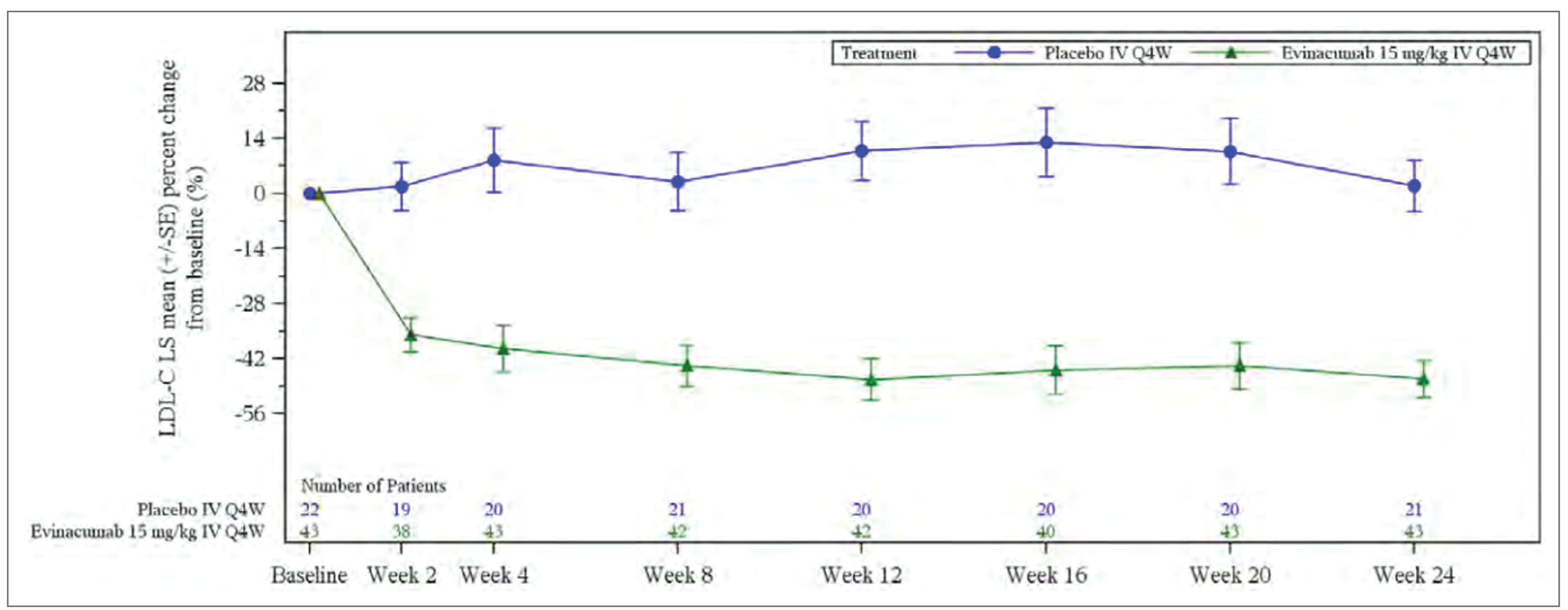
LDL-C = low-density lipoprotein cholesterol; LS = least squares; ITT = intention to treat; MMRM = mixed-effect model with repeated measures; Q4W = every 4 weeks; SE = standard error.
Source: ELIPSE Clinical Study Report.29
The results for the mean percent change from baseline in LDL-C during the open-label treatment period of the ELIPSE trial are summarized in Figure 3. For patients that entered the open-label period from the evinacumab group of the double-blind treatment period, the percent change from baseline in LDL-C to week 48 was –42.70% (SD = 40.0). For patients who received placebo in the double-blind treatment period followed by evinacumab in the open-label treatment period, the percent change in LDL-C at week 48 was –55.80% (SD = 22.45). The overall percent change in LDL-C at 48 weeks in the open-label treatment period was –46.31% (SD = 36.31).29
The results for LSM change from baseline in LDL-C with evinacumab from Part B and the pooled Parts B and C of the CL-17100 study were consistent with the double-blind period of the ELIPSE trial: –48.32% (SD = 39.052) and ||||||| |||| |||||||| respectively.28
Sensitivity Analyses
A sensitivity analysis was performed using the actual stratification factors in place of the interactive voice or web response system strata. However, there were no incorrect stratifications per interactive voice or web response system in the ELIPSE study; thus, the results for the sensitivity analysis were identical to those for the primary analysis. An additional sensitivity analysis was conducted to explore the impact of nonignorable missingness using a PMM. Only 1 patient (4.5%) in the placebo group did not have a LDL-C value at week 24. The LSMD between the evinacumab and placebo groups was –48.2% (95% CI, –63.6 to –32.8). The LSM percent change from baseline in LDL-C to week 24 was –47.1% (SE = 4.6) in the evinacumab group and 1.1% (SE = 6.4) in the placebo group.29
In the CL-17100 study, the results of the sensitivity analysis using the MMRM approach were consistent with the primary analysis, with a percent change from baseline in LDL-C of –48.3% (95% CI, –65.4 to –31.2). There were no non–GCP-compliant sites or missing data, so no sensitivity analyses were conducted for these categories.28
Subgroup Analysis
Subgroup analyses were provided for the primary outcome of percent change from baseline in LDL-C. Subgroup analyses of interest to this review included prior LLT, prior or concomitant apheresis, baseline LDL-C level, and HoFH genotype. Subgroup analyses from the ELIPSE trial and the CL-17100 study are summarized in Table 26, Table 27, and Table 28 of Appendix 1.
Background LLT: Background LDL-C–lowering therapy was not a prespecified subgroup of interest, though the results of the subgroup analysis for the double-blind treatment period of the ELIPSE trial are summarized in Table 26. The percent change from baseline in LDL-C in the evinacumab group when receiving background statins (N = 41), ezetimibe (N = 33), PCSK9 inhibitors (N = 34), or lomitapide (N = 11) was –47.29% (SD = 30.58), –53.07% (SD = 20.97), –49.45% (SD = 31.87), and –49.64% (SD = 22.55), respectively. In the placebo group, the percent change from baseline in LDL-C while on background statins (N = 19), ezetimibe (N = 16), PCSK9 inhibitors (N = 15), or lomitapide (N = 3) was 2.17% (SD = 32.34), –1.95% (SD = 30.58), 1.73% (SD = 30.34), and –17.22% (SD = 47.62), respectively. Subgroup results for patients with no statin, ezetimibe, PCSK9 inhibitor, or lomitapide background therapy were generally similar, though the number of patients without LLTs at baseline was small.29
Subgroup analyses by background LLT were not conducted in the open-label treatment period of the ELIPSE trial or in the CL-17100 study.
Apheresis status: In the subgroup of patients from the double-blind treatment period of the ELIPSE trial who had received apheresis at baseline (Table 27) in the evinacumab (N = 14) and placebo (N = 8) groups, the LSMD compared to placebo was –38.3% (95% CI, –65.1 to –11.5), representing a LSM change from baseline in LDL-C of –46.5% (SE = 8.8) for evinacumab and –8.3% (SE = 11.6) for placebo. In the subgroup of patients who had not received apheresis at baseline in the evinacumab (N = 29) and placebo (N = 14) groups, the LSMD compared to placebo was –55.2% (95% CI, –75.1 to –35.4), representing an LSM change from baseline in LDL-C of –47.3% (SE = 5.9) for evinacumab and 7.9% (SE = 8.4) for placebo.29
In the open-label treatment period, the percent change from baseline in LDL-C in patients who received baseline apheresis and in those who did not was consistent with that in the double-blind treatment period, as well as with that in the primary analysis of the open-label treatment period.29
In the CL-17100 study, the percent change from baseline in LDL-C for patients who had, or had not received prior apheresis was consistent with that in the primary analysis and with the results from both the double-blind and open-label treatment periods of the ELIPSE trial.28
Baseline LDL-C Level: The subgroup analysis by baseline LDL-C level is summarized in Table 27. In the double-blind treatment period of the ELIPSE study, 9 patients with LDL-C less than 130 mg/dL at baseline were randomized to the evinacumab group and 5 such patients were randomized to the placebo group. The LSMD for evinacumab compared to placebo was –22.7% (95% CI, –56.6 to 11.2), representing an LSM change from baseline in LDL-C of –27.3% (SE = 10.2) with evinacumab and –4.6% (SE = 13.4) with placebo. In the subgroup of patients in the evinacumab (N = 34) and placebo (N = 17) groups with baseline LDL-C greater than or equal to 130 mg/dL, the LSMD for evinacumab compared to placebo was –57.3% (95% CI, –75.3 to –39.4), representing an LSM change from baseline in LDL-C of –52.5% (SE = 5.2) and 4.8% (SE = 7.4) for the evinacumab and placebo groups, respectively.29
Subgroup analyses by baseline LDL-C were not conducted in the open-label treatment period of the ELIPSE trial or in the CL-17100 study.28
HoFH genotype: The subgroup analyses by HoFH genotype are summarized in Table 28. In the double-blind treatment period of the ELIPSE trial, the results of the subgroup analyses by HoFH genotype were consistent with the primary analysis across most genotypes, including homozygous (LSMD = –64.4%; 95% CI, –89.6 to –39.2) and compound heterozygous (LSMD = –43.7%; 95% CI, –72.2 to –15.2), as well as negative/negative (LSMD = –48.7%; 95% CI, –85.0 to –12.4) and null/null mutations (LSMD = –59.6%; 95% CI, –88.6 to –30.5), suggesting greater reductions in LDL-C with evinacumab than with placebo, but not for patients with the double heterozygous genotype or other mutations. In the open-label treatment period, analyses for this subgroup were only conducted for negative/negative and null/null mutations, with the results being consistent with the double-blind treatment period.29
In the CL-17100 study, the analyses for this subgroup were only conducted for negative/negative and null/null mutations, with a percent change from baseline in LDL-C of –67.7% (SD = 6.5) in patients with negative/negative mutations (N = 3) and of –57.2% (SD = not applicable) in patients with null/null mutations (N = 1).28
Absolute Change From Baseline in LDL-C
Absolute change from baseline in LDL-C level to week 24 was a secondary outcome of the ELIPSE study. The LSM absolute change in LDL-C during the double-blind treatment period was –134.7 mg/dL (SE = 12.4) in the evinacumab group, while in the placebo group, the LSM absolute change in LDL-C was –2.6 mg/dL (SE = 17.6), and the LSMD versus placebo favoured evinacumab (–132.1 mg/dL; 95% CI, –175.3 to –88.9; P < 0.0001). In the open-label treatment period, the LSM absolute change from baseline in LDL-C at 48 weeks was –134.3 mg/dL (SD = 117.33).29
In Part B of the CL-17100 study, the LSM absolute change from baseline in LDL-C was –131.9 mg/dL (SD = 30.0).28
Proportion of Patients With Greater Than or Equal to 30% Reduction in LDL-C
The proportion of patients with a greater than or equal to 30% reduction in LDL-C at week 24 was a key secondary outcome of the ELIPSE study but was not evaluated in the open-label treatment period or in the CL-17100 study. In the double-blind treatment period of the ELIPSE trial, 83.7% of patients in the evinacumab group and 18.2% of patients in the placebo group experienced such a reduction, favouring evinacumab (OR = 25.2; 95% CI, 5.7 to 110.5; P < 0.0001).29
Percent Change From Baseline in Apo B
The percent change from baseline in Apo B to week 24 was a key secondary efficacy end point of the ELIPSE and CL-17100 studies. In the double-blind treatment period of the ELIPSE trial, the LSM percent change from baseline in Apo B with evinacumab was –41.4% (SE = 3.3), compared to –4.5% (SE = 4.8) with placebo. The LSMD between evinacumab and placebo in percent change from baseline in Apo B was –36.9% (95% CI, –48.6 to –25.2), favouring evinacumab.29
For patients that entered the open-label period of the ELIPSE trial from the evinacumab group of the double-blind treatment period, the percent change from baseline in Apo B to week 48 was –37.10% (SD = 27.716). For patients who received placebo in the double-blind treatment period followed by evinacumab in the open-label treatment period, the percent change in LDL-C at week 48 was –49.92% (SD = 19.784). The overall percent change in LDL-C at 48 weeks in the open-label treatment period was –40.83% (SD = 26.150).29
The results for LSM change from baseline in Apo B with evinacumab from Part B and the pooled Parts B and C of the CL-17100 study were consistent with those in the double-blind period of the ELIPSE trial, at –41.32% (SD = 33.541) and –39.27% (SD = 29.438), for Part B and the pooled Parts B and C, respectively.28
Global Lipid LDL-C Targets
Proportion of Patients With LDL-C Less Than 100 mg/dL (2.59 mmol/L)
The proportion of patients with LDL-C less than 100 mg/dL (2.59 mmol/L) was a key secondary end point of the ELIPSE trial. In the double-blind treatment period, the proportion of patients with LDL-C less than 100 mg/dL at 24 weeks was 46.5% in the evinacumab group, compared to 22.7% in the placebo group (OR = 5.7; 95% CI, 1.3 to 24.9; P = 0.0203).29
The proportion of patients with LDL-C less than 100 mg/dL was not evaluated in the open-label extension study or the CL-17100 study.
Proportion of Patients With LDL-C Less Than 70 mg/dL (1.81 mmol/L)
The proportion of patients with LDL-C less than 70 mg/dL (1.81 mmol/L) was a secondary end point of the ELIPSE trial. In the double-blind treatment period, the proportion of patients with LDL-C less than 70 mg/dL at 24 weeks was 27.9% in the evinacumab group, compared to 4.5% in the placebo group (OR = 20.9; 95% CI, 1.6 to 276.8; P = 0.0209).29
The proportion of patients with LDL-C less than 70 mg/dL was not evaluated in the open-label extension study or the CL-17100 study.
Proportion of Patients Who Meet US Apheresis Criteria
The proportion of patients who meet US apheresis eligibility criteria was a key secondary end point of the ELIPSE trial. In the double-blind treatment period, at 24 weeks, 7.0% of patients in the evinacumab group met the US apheresis eligibility criteria, compared to 22.7% in the placebo group (OR = 0.1; 95% CI, 0.0 to 0.3; P = 0.0845). Statistical hypothesis testing was terminated at this end point in the ELIPSE trial because statistical significance was not reached.29
The proportion of patients who meet US apheresis eligibility criteria was not evaluated in the open-label extension study or the CL-17100 study.
Proportion of Patients Who Meet EU Apheresis Criteria
The proportion of patients who meet EU apheresis eligibility criteria was a key secondary end point of the ELIPSE trial. In the double-blind treatment period, at 24 weeks, 32.6% of patients in the evinacumab group met the EU apheresis eligibility criteria, compared to 77.3% in the placebo group (OR = 0.1; 95% CI, 0.0 to 0.3).29
The proportion of patients who meet EU apheresis eligibility criteria was not evaluated in the open-label extension study or the CL-17100 study.
EQ-5D
HRQoL measured by the EQ-5D was an exploratory outcome of the ELIPSE trial. At baseline, the mean utility score in the evinacumab (N = 43) and placebo (N = 20) groups was |||||| points (SD = ||||) and |||||| points (SD = ||||), respectively. At week 24, the mean utility score was |||||| points (SD = ||||) for evinacumab and |||||| points (SD = ||||) for placebo, representing a mean change from baseline of ||||||| points (SD = ||||) with evinacumab and ||||||| points (SD = ||||) with placebo.29
HRQoL was not measured in the open-label treatment period of the ELIPSE trial or in the CL-17100 study.
Mortality (All-Cause and CV-Related)
All-cause and CV-related mortality were not evaluated in the ELIPSE or CL-17100 studies.
Table 14: Summary of Key Efficacy Results From Studies Included in the Systematic Review
Variable | ELIPSE | CL-17100 (ITT)a | |||||
|---|---|---|---|---|---|---|---|
DBTP (ITT)a | OLTP (SAS)b | ||||||
Placebo (n = 22) | Evinacumab (n = 43) | From DBTP placebo group (N = 20) | From DBTP evinacumab group (N = 44) | OLTP evinacumab (N = 64) | Part B: evinacumab (n = 14) | Pooled Parts B + C: evinacumab (||||||) | |
Percent CFB in LDL-C | |||||||
Baseline LDL-C, mean (SD) | |||||||
mmol/L | 6.386 (3.9807) | 6.721 (4.4651) | NR | NR | NR | 6.830 (2.3539) | ||||| |||||||| |
mg/dL | 246.5 (153.71) | 259.5 (172.40) | 236.1 (144.27) | 257.1 (171.10) | 250.5 (162.34) | 263.7 (90.97) | ||||| |||||||| |
Percent CFB in LDL-C, LS mean (SE)c | 1.9 (6.5) | –47.1 (4.6) | –55.80 (22.45) | –42.70 (40.00) | –46.31 (36.31) | –48.32 (39.052) | |||||| |||||||| |
Percent CFB in LDL-C, LSMD vs. placebo (SE) | — | –49.0 (8.0) | NA | NA | NA | NA | NA |
95% CI | — | –65.0 to –33.1 | NA | NA | NA | NA | NA |
P value | — | < 0.0001 | NA | NA | NA | NA | NA |
Percent CFB in Apo B | |||||||
Baseline Apo B, mean (SD) | |||||||
g/L | 1.759 (0.9876) | 1.691 (0.8275) | NR | NR | NR | 1.682 (0.4749) | ||||| |||||||| |
mg/dL | 175.9 (98.76) | 169.1 (82.75) | 164.2 (80.21) | 168.3 (81.97) | 167.0 (80.81) | 168.2 (47.49) | ||||| ||||||| |
Percent CFB in Apo B, LS mean (SE)c | –4.5 (4.8) | –41.4 (3.3) | –49.92 (19.784) | –37.10 (27.716) | –40.83 (26.150) | –41.32 (33.541) | |||||| |||||||| |
Percent CFB in Apo B, LSMD vs. placebo (SE) | — | –36.9 (5.9) | NA | NA | NA | NA | NA |
95% CI | — | –48.6 to –25.2 | NA | NA | NA | NA | NA |
P value | — | < 0.0001 | NA | NA | NA | NA | NA |
Proportion of patients with ≥ 30% reduction in LDL-C | |||||||
Proportion of patients (%) | 18.2 | 83.7 | NA | NA | NA | NA | NA |
Combined OR estimate (95% CI) | — | 25.2 (5.7 to 110.5) | NA | NA | NA | NA | NA |
P value vs. placebo | — | < 0.0001 | NA | NA | NA | NA | NA |
Absolute CFB in LDL-C | |||||||
Baseline LDL-C, mean (SD) | |||||||
mmol/L | 6.386 (3.9807) | 6.721 (4.4651) | NR | NR | NR | 6.830 (2.3539) | ||||| |||||||| |
mg/dL | 246.5 (153.71) | 259.5 (172.40) | 236.1 (144.27) | 257.1 (171.10) | 250.5 (162.34) | 263.7 (90.97) | ||||| |||||||| |
Absolute CFB in LDL-C (mg/dL), LS mean (SE)c | –2.6 (17.6) | –134.7 (12.4) | –145.0 (99.78) | –130.3 (124.24) | –134.3 (117.33) | –131.9 (30.0) | NA |
Absolute CFB in LDL-C (mg/dL), LSMD vs. placebo (SE) | — | –132.1 (21.5) | NA | NA | NA | NA | NA |
95% CI | — | –175.3 to –88.9 | NA | NA | NA | NA | NA |
P value | — | < 0.0001 | NA | NA | NA | NA | NA |
Proportion of patients who meet US apheresis eligibility criteria | |||||||
Proportion of patients (%) | 22.7 | 7.0 | NA | NA | NA | NA | NA |
Combined OR estimate (95% CI) | — | 0.1 (0.0 to 1.3) | NA | NA | NA | NA | NA |
P value vs. placebo | — | 0.0845d | NA | NA | NA | NA | NA |
Proportion of patients with LDL-C < 100 mg/dL (2.59 mmol/L) | |||||||
Proportion of patients (%) | 22.7 | 46.5 | NA | NA | NA | NA | NA |
Combined OR estimate (95% CI) | — | 5.7 (1.3 to 24.9) | NA | NA | NA | NA | NA |
P value vs. placebo | — | 0.0203 | NA | NA | NA | NA | NA |
Proportion of patients who meet EU apheresis eligibility criteria | |||||||
Proportion of patients (%) | 77.3 | 32.6 | NA | NA | NA | NA | NA |
Combined OR (95% CI) estimate | — | 0.1 (0.0 to 0.3) | NA | NA | NA | NA | NA |
P value vs. placebo | — | 0.0004 | NA | NA | NA | NA | NA |
Proportion of patients with LDL-C < 70 mg/dL (1.81 mmol/L) | |||||||
Proportion of patients (%) | 4.5 | 27.9 | NA | NA | NA | NA | NA |
Combined OR estimate (95% CI) | — | 20.9 (1.6 to 276.8) | NA | NA | NA | NA | NA |
P value vs. placebo | — | 0.0209 | NA | NA | NA | NA | NA |
Apo B = apolipoprotein B; CFB = change from baseline; CI = confidence interval; DBTP = double-blind treatment period; EU = European Union; ITT = intention to treat; LDL-C = low-density lipoprotein cholesterol; LS = least squares; LSMD = least squares mean difference; NA = not applicable; NR = not reported; OLTP = open-label treatment period; OR = odds ratio; SAS = safety analysis set; SD = standard deviation; SE = standard error; vs. = versus.
aValues for CFB are as of week 24.
bValues for CFB are as of week 48 of open-label treatment.
cValues for CFB in the open-label treatment period of ELIPSE and for the CL-17100 study are SD.
dStatistical hypothesis testing terminated at this end point because statistical significance was not reached. All other reported differences between treatment groups reported for secondary end points in subsequent rows are nominal.
Sources: ELIPSE Clinical Study Report;29 CL-17100 Clinical Study Report.28
CV-Related Morbidity
CV-related morbidity outcomes, such as the incidence of resuscitated cardiac arrest, nonfatal MI, and stroke, were not evaluated in the ELIPSE or CL-17100 studies.
Harms
Important harms reported in the ELIPSE and CL-17100 studies are summarized in Table 15.
Adverse Events
In the ELIPSE trial, the incidence of TEAEs was lower for patients in the evinacumab group than in the placebo group during the double-blind treatment period (65.9% versus 81.0%). In the open-label treatment period of the ELIPSE trial, the incidence of TEAEs for evinacumab was higher than in the double-blind treatment period (73.4%). The most frequently occurring TEAEs in the double-blind treatment period of the ELIPSE trial in the evinacumab and placebo groups by system organ class were infections and infestations (27.3% versus 28.6%); general disorders and administration site conditions (20.5% versus 14.3%); respiratory, thoracic, and mediastinal disorders (18.2% versus 4.8%); gastrointestinal disorders (15.9% versus 23.8%); musculoskeletal and connective tissue disorders (15.9% versus 9.5%); and nervous system disorders (11.4% versus 23.8%). The most common TEAEs by preferred term in patients treated with evinacumab versus placebo were nasopharyngitis (15.9% versus 23.8%) and influenza-like illness (11.4% versus 0.0%). In the open-label treatment period, the most frequently reported TEAEs were nasopharyngitis and headache (9.4% each). The majority of TEAEs experienced during the double-blind treatment period were classified as mild or moderate in intensity.29
In the CL-17100 study, nearly all patients treated with evinacumab experienced at least 1 TEAE (|||||). The most frequently occurring TEAEs by system organ class in the CL-17100 study included |||||||||| ||| |||||||||||| |||||||| |||||||||||||||| ||||||||| |||||||| ||| ||||||| ||||||||| ||| |||||||||||||| |||| |||||||||| |||||||| The most frequent individual TEAEs by preferred term included |||||||| |||||||| ||| ||||||||||||||| |||||||.28
Serious AEs
In the ELIPSE study, SAEs were reported as severe TEAEs and were infrequently reported, occurring in only |||||| patients in the evinacumab group during the double-blind treatment period and consisting of urosepsis (1 [2.3%]) and attempted suicide (1 [2.3%]). There were no SAEs in the placebo group. In the open-label treatment period, ||||||| patients had SAEs, which included angina pectoris; carotid artery restenosis; congestive cardiac failure; unstable angina and coronary artery disease; pyelonephritis and nephrocalcinosis; and cardiac procedure complication, aortic stenosis, and acute MI (1 [1.16%] each), all of which were considered severe in severity.29
In the CL-17100 study, only |||||| patient experienced an SAE of |||||||||||.28
Withdrawals due to AEs
There were no withdrawals due to AEs in the ELIPSE or CL-17100 studies; however, in the open-label treatment period of the ELIPSE study, 1 patient in the evinacumab group had a pregnancy that led to discontinuation of study treatment, though the patient completed the study.28,29
Mortality
There were no deaths reported during the ELIPSE or CL-17100 studies.28,29
Notable Harms
The AESIs to this review were general allergic reactions, IRRs, new onset diabetes, musculoskeletal and connective tissue disorders, creatinine kinase changes, and liver function. In the evinacumab and placebo groups of the double-blind treatment period of the ELIPSE trial, 4 patients (9.1%) and 3 patients (14.3%), respectively, experienced allergic events; 3 patients (6.8%) and 1 patient (4.8%) experienced IRRs; |||||| ||||||||| patients had new onset diabetes; ||||| ||| ||||| patient in each treatment group had diabetic complications; and 7 patients (15.9%) and 2 patients (9.5%) experienced musculoskeletal and connective tissue disorders. |||||| ||||||||| patients experienced increases in creatine kinase and increased aspartate aminotransferase, and ||||| ||| ||||| patient in each treatment group had increased alanine aminotransferase and increased bilirubin. AESIs in the open-label treatment period were similar to those in the double-blind treatment period.29
In the CL-17100 study, general allergic events occurred in ||||||| patients, and || patients had IRRs, new onset diabetes, diabetic complications, or increases in liver enzymes. Musculoskeletal and connective tissue disorders and increases in creatinine kinase were not reported.28
Table 15: Summary of Harms Results From Studies Included in the Systematic Review
Adverse events | ELIPSE (SAS) | CL-17100 (Pooled Parts B + C) | ||
|---|---|---|---|---|
DBTP | OLTP | |||
Placebo (n = 21) | Evinacumab (n = 44) | Evinacumab (n = 64) | Evinacumab (n = ||) | |
TEAEs,a n (%) | ||||
Patients with any TEAE | 17 (81.0) | 29 (65.9) | 47 (73.4) | || |||||| |
Gastrointestinal disorders | 5 (23.8) | 7 (15.9) | |||||| | || |||||| |
Toothache | 2 (9.5) | 2 (4.5) | 2 (3.1) | |||||| |
General disorders and administration site conditions | 3 (14.3) | 9 (20.5) | |||||| | |||||| |
Influenza-like illness | 0 (0.0) | 5 (11.4) | 2 (3.1) | |||||| |
Infections and infestations | 6 (28.6) | 12 (27.3) | || |||||| | || |||||| |
Nasopharyngitis | 5 (23.8) | 7 (15.9) | 6 (9.4) | |||||| |
Urinary tract infection | 2 (9.5) | 0 (0.0) | |||||| | |||||| |
Investigations | 2 (9.5) | 0 (0.0) | NR | |||||| |
AST increased | 2 (9.5) | 0 (0.0) | NR | |||||| |
Musculoskeletal and connective tissue disorders | 2 (9.5) | 7 (15.9) | |||||| | |||||| |
Myalgia | 2 (9.5) | 0 (0.0) | NR | NR |
Nervous system disorders | 5 (23.8) | 5 (11.4) | |||||| | |||||| |
Headache | 5 (23.8) | 4 (9.1) | 6 (9.4) | |||||| |
Respiratory, thoracic, and mediastinal disorders | 1 (4.8) | 8 (18.2) | NR | |||||| |
Rhinorrhea | 0 (0.0) | 3 (6.8) | NR | NR |
SAEs, n (%) | ||||
Patients with ≥ 1 SAE | |||||| | |||||| | |||||| | |||||| |
Suicide attempt | 0 (0.0) | 1 (2.3) | |||||| | |||||| |
Urosepsis | 0 (0.0) | 1 (2.3) | |||||| | |||||| |
Angina pectoris | |||||| | |||||| | |||||| | |||||| |
Carotid artery restenosis | 0 (0.0) | 0 (0.0) | |||||| | |||||| |
Congestive cardiac failure | 0 (0.0) | 0 (0.0) | |||||| | |||||| |
Unstable angina and coronary artery disease | 0 (0.0) | 0 (0.0) | 1 (1.6) | |||||| |
Pyelonephritis and nephrocalcinosis | |||||| | |||||| | |||||| | |||||| |
Cardiac procedure complication, aortic stenosis, and acute MI | 0 (0.0) | 0 (0.0) | 1 (1.6) | |||||| |
Tonsillitis | |||||| | |||||| | NR | |||||| |
Adverse events of special interest, n (%) | ||||
General allergic events (≥ 1 TEAE) | 3 (14.3) | 4 (9.1) | |||||| | |||||| |
Asthma | 0 (0.0) | 1 (2.3) | |||||| | |||||| |
Rash | 0 (0.0) | 1 (2.3) | |||||| | |||||| |
Allergic rhinitis | |||||| | 1 (2.3) | |||||| | |||||| |
Urticaria | |||||| | 1 (2.3) | |||||| | NR |
Dermatitis | |||||| | |||||| | |||||| | |||||| |
Face edema | |||||| | |||||| | |||||| | NR |
Pruritus | |||||| | |||||| | |||||| | NR |
Drug hypersensitivity | NR | NR | |||||| | NR |
IRR | NR | NR | |||||| | NR |
Allergic conjunctivitis | NR | NR | |||||| | |||||| |
IRR (≥ 1 TEAE) | 1 (4.8) | 3 (6.8) | |||||| | |||||| |
General disorders and administration site conditions | 1 (4.8) | 3 (6.8) | |||||| | NR |
Infusion site pruritus | 0 (0.0) | 2 (4.5) | NR | NR |
Pyrexia | |||||| | 1 (2.3) | NR | NR |
Face edema | |||||| | |||||| | NR | NR |
Infusion site hypoesthesia | |||||| | |||||| | NR | NR |
Asthenia | NR | NR | 1 (1.6) | NR |
Musculoskeletal and connective tissue disorders | |||||| | |||||| | NR | NR |
Muscular weakness | |||||| | |||||| | NR | NR |
Vascular disorders | |||||| | |||||| | NR | NR |
Vascular pain | |||||| | 1 (2.3) | NR | NR |
Immune system disorders | NR | NR | |||||| | NR |
Drug hypersensitivity | NR | NR | |||||| | NR |
Injury, poisoning, and procedural complications | NR | NR | |||||| | NR |
IRR | NR | NR | |||||| | NR |
Skin and subcutaneous tissue disorders | NR | NR | |||||| | NR |
Generalized pruritus | NR | NR | 1 (1.6) | NR |
Patients with new onset diabetes | |||||| | |||||| | |||||| | |||||| |
≥ 2 values of hemoglobin A1C ≥ 6.5% | |||||| | |||||| | |||||| | NR |
≥ 2 values of fasting glucose ≥ 126 mg/dL (7.0 mmol/L) | |||||| | |||||| | |||||| | NR |
Any HLT diabetes mellitus (including subtypes) | |||||| | |||||| | |||||| | NR |
Initiation of new concomitant medication for hyperglycemia | |||||| | |||||| | |||||| | NR |
Diabetic complications | ||||
Patients with diabetes mellitus at baseline | |||||| | |||||| | |||||| | |||||| |
Patients with a diabetic complication | |||||| | |||||| | |||||| | NR |
HLGT, HLT, and PTs | |||||| | |||||| | |||||| | NR |
Change in dosage of, or initiation of additional, diabetic medication | |||||| | |||||| | |||||| | NR |
Musculoskeletal and connective tissue disorders | 2 (9.5) | 7 (15.9) | |||||| | NR |
Arthralgia | |||||| | 1 (2.3) | NR | NR |
Back pain | |||||| | 1 (2.3) | 3 (4.7) | NR |
Muscle spasms | |||||| | 1 (2.3) | 2 (3.1) | NR |
Muscular weakness | |||||| | 1 (2.3) | NR | NR |
Musculoskeletal pain | NR | NR | |||||| | NR |
Musculoskeletal chest pain | |||||| | 1 (2.3) | NR | NR |
Myalgia intercostal | |||||| | 1 (2.3) | NR | NR |
Neck pain | |||||| | 1 (2.3) | |||||| | NR |
Pain in extremity | |||||| | 1 (2.3) | NR | NR |
Myalgia | 2 (9.5) | 0 (0.0) | NR | NR |
Creatine kinase | ||||
> 3 ULN to ≤ 5 ULN, and ≤ 3 ULN at baseline | |||||| | |||||| | |||||| | NR |
> 5 ULN to ≤ 10 ULN, and CPK ≤ 5 ULN at baseline | |||||| | |||||| | |||||| | NR |
> 10 ULN, and ≤ 10 ULN at baseline | |||||| | |||||| | |||||| | NR |
Liver function | ||||
ALT increased | ||||
> 2 ULN to ≤ 3 ULN, and ≤ 2 ULN at baseline | |||||| | |||||| | |||||| | |||||| |
> 3 ULN to ≤ 5 ULN, and ≤ 3 ULN at baseline | |||||| | |||||| | |||||| | |||||| |
> 5 ULN, and ≤ 5 ULN at baseline | |||||| | |||||| | NR | |||||| |
AST increased | ||||
> 2 ULN to ≤ 3 ULN, and ≤ 2 ULN at baseline | |||||| | |||||| | |||||| | |||||| |
> 3 ULN to ≤ 5 ULN, and ≤ 3 ULN at baseline | |||||| | |||||| | |||||| | |||||| |
> 5 ULN, and ≤ 5 ULN at baseline | |||||| | |||||| | NR | |||||| |
Bilirubin | ||||
> 1.5 ULN to ≤ 2 ULN, and ≤ 1.5 ULN at baseline | |||||| | |||||| | |||||| | |||||| |
> 2 ULN, and ≤ 2 ULN at baseline | |||||| | |||||| | |||||| | |||||| |
Alkaline phosphatase | ||||
> 1.5 ULN, and ≤ 1.5 ULN at baseline | |||||| | |||||| | |||||| | |||||| |
ALT and total bilirubin | ||||
(ALT > 3 ULN and total bilirubin > 2 ULN) and (ALT ≤ 3 ULN or total bilirubin ≤ 2 ULN) at baseline | |||||| | |||||| | |||||| | |||||| |
ALT = alanine aminotransferase; AST = aspartate aminotransferase; DBTP = double-blind treatment period; HLGT = high-level group term; HLT = higher level term; IRR = infusion-related reaction; MI = myocardial infarction; NR = not reported; OLTP = open-label treatment period; PT = preferred term; SAE = serious adverse event; SAS = safety analysis set; TEAE = treatment-emergent adverse event; ULN = upper limit of normal.
aTEAEs that occurred at a rate of greater than or equal to 5%.
Sources: ELIPSE Clinical Study Report;29 CL-17100 Clinical Study Report.28
Critical Appraisal
Internal Validity
Two studies were included in this review: the ELIPSE study and the CL-17100 study. The ELIPSE study was a first-in-class, phase III, placebo-controlled RCT that included both double-blind and open-label treatment periods. Appropriate methods for randomization (using interactive response technology), treatment allocation (stratified by apheresis treatment and by region), and maintenance of blinding to treatment assignment were used, reducing selection, performance, and detection biases. Overall, there was only 1 discontinuation in the evinacumab group during the double-blind treatment period, and there was not a substantial difference in AEs across groups; thus, it was unlikely that blinding was impacted during treatment.
The CL-17100 study was an open-label, single-arm study of evinacumab in patients aged 5 to 11 years with HoFH. The choice to conduct a single-arm trial in the younger population was justified by the rarity of the indication and the age of the participants; however, the noncomparative nature negates the ability to draw a statistical association between the reported results and evinacumab due to the small sample size and the chronic progression of HoFH. As such, the strength and interpretability of the results for this group of patients is limited. Further, single-arm trials are generally not considered confirmatory for efficacy and are subject to several limitations that complicate their interpretation; in particular, it is difficult to isolate whether the effect is due to placebo, natural history, or unidentified prognostic factors that could affect the study outcomes. These sources of potential bias are also applicable to the open-label phase of the ELIPSE study.
The original study protocol for the ELIPSE trial was amended | times, and the protocol for the CL-17100 study was amended |||||. It was unclear how many patients were enrolled at each protocol amendment; therefore, the impact of potential biases due to protocol amendments remains unknown. Overall, important protocol deviations in the ELIPSE study (||||% versus ||||%) and the CL-17100 study (|||%) were high, primarily due to procedural irregularities with the apheresis schedule for the ELIPSE trial (listed under “other” important protocol deviations for CL-17100) and due to pharmacokinetic issues in the CL-17100 study, though it remains unclear what impact these deviations may have had on the treatment effect.
As previously noted, dropouts in the ELIPSE and CL-17100 studies were low. The primary end point of the ELIPSE trial used an MMRM to account for missing data under the missing at random assumption, which may have overestimated the precision of the effect estimates. The sensitivity analyses used a PMM to account for nonignorable missingness and showed that the missing data are unlikely to have greatly biased the results. Overall, the amount of missing data was low, as evidenced by the results of the sensitivity analysis, which were nearly identical to those of the primary efficacy analysis. The use of an MMRM was appropriate due to the heterogeneity of the patient population in terms of LDL-C at baseline. However, the implementation of the model may have included too many covariates, which could lead to numerical instability given the small sample size. Information on missingness was reported for secondary end point results and exploratory HRQoL results; thus, the impact of missing data for these outcomes remains unknown.
Acceptable methods to account for multiplicity were used in the ELIPSE trial. The primary end point (percent change from baseline in LDL-C) and key secondary end points (percent change from baseline in Apo B, non-HDL-C, and total cholesterol; proportion of patients with a ≥ 30% reduction in LDL-C at week 24; proportion of patients with a ≥ 50% reduction in LDL-C at week 24; absolute change from baseline in LDL-C to week 24; proportion of patients who meet US apheresis eligibility criteria; proportion of patients with LDL-C < 100 mg/dL; and proportion of patients who meet EU apheresis eligibility criteria) were controlled for multiplicity at the 0.05 level using a hierarchical testing sequence. However, statistical significance was not achieved for the end point of proportion of patients who meet US apheresis eligibility criteria; thus, the multiple testing procedure failed, and all subsequent outcomes (proportion of patients with LDL-C < 100 mg/dL and proportion of patients who meet EU apheresis eligibility criteria) should only be viewed as supportive. In the CL-17100 study, no inferential statistical testing was performed for the efficacy outcomes and no multiple testing procedure was conducted; hence, the results should only be considered supportive of the overall effect of evinacumab.
Predefined sensitivity analyses were conducted in both studies to evaluate the robustness of the primary end point, and these analyses were supportive of the primary end point. Additionally, various prespecified subgroup analyses were conducted in the ELIPSE and CL-17100 studies. Though they generally supported the primary analysis, the subgroup analyses were not statistically powered to detect within-group or between-group differences; thus, the results from the subgroup analyses should be interpreted as supportive evidence only for the overall effect of evinacumab.
External Validity
The clinical experts engaged by CADTH considered the inclusion and exclusion criteria for the ELIPSE and CL-17100 studies appropriate, though the clinical experts highlighted that genetic confirmation of HoFH does not always occur. Both the ELIPSE and CL-17100 studies were multinational studies; however, the ELIPSE trial was the only study to enrol patients living in Canada (N = 3), though given the low number of patients living in Canada enrolled, generalizability based on geography cannot be assumed.
HoFH is a rare disease. The ELIPSE trial included 65 patients with HoFH and the CL-17100 study included 20 patients with HoFH. The clinical experts consulted by CADTH noted that, in their experience, the populations included in the trials were generally in line with those seen in clinical practice in Canada with regard to age and that the LDL-C levels at baseline were reflective of the patients seen by the clinical experts in practice, whose LDL-C levels on MTD statin, ezetimibe, and PCSK9 inhibitors were consistently above 5.0 mmol/L. The experts did note, however, that the distribution of race was not reflective of Canadian clinical practice as the majority of patients in the ELIPSE trial identified as white.
The chosen comparator of placebo in the ELIPSE study was appropriate and aligned with the recommended standard of care guidelines for HoFH in Canada; the experts noted that standard of care consists of MTD statin, ezetimibe, and a PCSK9 inhibitor. All patients in the included studies had received prior LLT, consisting of some combination of statin, ezetimibe, PCSK9 inhibitor, lomitapide, and apheresis. The clinical experts consulted by CADTH noted that the proportion of patients receiving LLTs was in line with the general population of patients with HoFH in Canada, though the proportion of patients in the ELIPSE trial receiving PCSK9 inhibitors was higher than in Canadian clinical practice owing to the difficulty in accessing PCSK9 inhibitors in Canada. There were minor differences in lomitapide use between groups at baseline, with only 11 patients (25.6%) in the evinacumab group and 3 patients (13.6%) in the placebo group receiving lomitapide, though this was potentially related to the rarity of the disease and to the study design, as differences in patients may be more noticeable in studies with small sample sizes.
The outcomes used in the included studies were similar, with identical primary outcomes of percent change from baseline in LDL-C to week 24. The outcomes used to provide information on the efficacy of evinacumab in the ELIPSE and CL-17100 studies were based on validated laboratory assessments of lipids. According to the clinical experts, the selected lipid-related outcomes are considered widely accepted surrogates for clinically relevant CV outcomes and are important in guiding treatment decisions for patients with HoFH in Canadian clinical practice. In addition to the well-established lowering of LDL-C, the most valuable outcomes to patients with HoFH included reduction in the risk of CV events and reduction of the need for apheresis. The included studies were not designed to assess important CV-related outcomes, including reductions in major adverse cardiac events and in all-cause and CV-related mortality, though the clinical experts consulted by CADTH noted that measuring event-driven outcomes such as these is difficult in HoFH due to the rarity of the disease. Additionally, impact on HRQoL was an exploratory outcome of the ELIPSE trial but was not evaluated in the CL-17100 study. The clinical experts consulted by CADTH noted that reduction in the burden of apheresis is believed to improve patients’ HRQoL; however, reduction of apheresis was not captured in the available evidence. The clinical experts consulted by CADTH emphasized that the duration of the ELIPSE and CL-17100 studies (24 weeks) was considered appropriate for assessing lipid-related outcomes given that the effects on lipids are rapidly seen; however, the experts noted that the 24-week duration of the included studies was insufficient to determine the impact of evinacumab on CV-related morbidity and mortality and on HRQoL.
GRADE Summary of Findings and Certainty of the Evidence
Methods for Assessing the Certainty of the Evidence
For the pivotal studies and RCTs identified in the sponsor’s systematic review, GRADE was used to assess the certainty of the evidence for the outcomes considered most relevant to inform CADTH’s expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group:30,31
High certainty: We are very confident that the true effect lies close to that of the estimate of the effect.
Moderate certainty: We are moderately confident in the effect estimate. The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. We use the word “likely” for evidence of moderate certainty (e.g., “X intervention likely results in Y outcome”).
Low certainty: Our confidence in the effect estimate is limited. The true effect may be substantially different from the estimate of the effect. We use the word “may” for evidence of low certainty (e.g., “X intervention may result in Y outcome”).
Very low certainty: We have very little confidence in the effect estimate. The true effect is likely to be substantially different from the estimate of the effect. We describe evidence of very low certainty as “very uncertain.”
Under the GRADE approach, evidence from RCTs started as high-certainty evidence and could be rated down for concerns related to study limitations (which refer to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias.
Although no guidance is available on applying GRADE to noncomparative studies, the CADTH review team assessed the pivotal single-arm trial for study limitations (which refer to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias to present these important considerations. Because the lack of a comparator arm does not allow for a conclusion to be drawn on the effect of the intervention versus any comparator, the certainty of evidence for single-arm trials started at very low certainty, with no opportunity for rating up.
When possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect; if this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., the clinical importance is unclear). In all cases, the target of the certainty of evidence assessment was based on the point estimate and where it was located relative to the threshold for a clinically important effect (when a threshold was available) or to the null. The target of the certainty of evidence assessment was the presence of a clinically important reduction of LDL-C (percent and absolute change in LDL-C) against thresholds informed by treatment guidelines and clinical expert opinion. Other targets for the certainty of evidence assessment were the presence or absence of any (non-null) effect for the proportion of patients achieving global lipid targets (i.e., percent change from baseline in Apo B, proportion of patients with a ≥ 30% reduction in LDL-C, proportion of patients with LDL-C < 100 mg/dL or < 70 mg/dL, proportion of patients that meet US or EU apheresis criteria, and HRQoL measured by the EQ-5D).
The ELIPSE and CL-17100 studies were assessed individually, given the differences in design: the ELIPSE trial was a comparative RCT of evinacumab versus placebo, and the CL-17100 study was a single-arm study of evinacumab, which had different methods of evaluating treatment effect. Additionally, the ELIPSE trial included adolescent and adult populations (aged 12 years and older), while the CL-17100 study had a pediatric patient population (aged 5 to 11 years).
Results of GRADE Assessments
Table 2 shows the detailed GRADE summary of findings for evinacumab versus placebo for outcomes in the pivotal ELIPSE trial of adolescent and adult patients with HoFH. Table 3 shows the narrative GRADE summary of findings for evinacumab in the pediatric population of the CL-17100 study and the outcomes from the ELIPSE trial that were unable to be populated in Table 2.
Long-Term Extension Studies
The content within this section has been informed by materials submitted by the sponsor. The following has been summarized and validated by the CADTH review team.
CL-1719 Study
The CL-1719 study is an ongoing, long-term, open-label study, with a primary aim of evaluating the safety, tolerability, and efficacy of evinacumab 15 mg/kg administered intravenously every 4 weeks in adults and adolescents with HoFH receiving a background LLT (where adolescents were aged 12 years or older, but younger than 18 years). As its secondary objectives, the trial aims to evaluate the effect of evinacumab 15 mg/kg on lipid parameters (i.e., LDL-C, Apo B, non-HDL-C, total cholesterol, and triglycerides).48
An interim analysis was conducted on ||||| ||| ||||, at a data lock date of ||| ||| ||||. The study duration varied for every patient, ranging from 26 weeks up to approximately | years. The study is ongoing in 12 countries in Europe, North America (|| patients in Canada), Africa, and Asia. By the data cut-off date, ||| patients had been enrolled in the total study population (consisting of the adult and adolescent populations), || patients (||||%) had completed the treatment period, || patients (||||%) were ongoing in the treatment period, and || patients (||||%) had discontinued. The mean age of the patients was |||| years; || adolescent patients (||||%) had been enrolled; ||||% of the population was male and ||||% was female; and the majority of patients were white (||||%). Of the ||| patients in the total study population, ||| (||||%) had a history and/or risk factors for CVD.48 Figure 2 presents the study design of the CL-1719 study.
Figure 2: Study Design of the CL-1719 Study

Q4W = every 4 weeks.
1 Patients who may require homozygous familial hypercholesterolemia genotyping and patients whose background lipid-lowering therapy or apheresis settings and/or schedule were not stable before baseline (day 1) entered an up to 10-week run-in period.
2 All patients who were on a stable background lipid-lowering therapy entered a 2-week screening period, except for those from a previous evinacumab study, who completed an end-of-study visit within 7 days before the baseline (day 1) visit for this open-label study.
3 Patients who completed an end-of-study visit in a previous evinacumab study within 7 days of the baseline (day 1) visit for this open-label study did not have to undergo the screening visit and could enrol directly into this study. The end-of-study visit from the previous study could serve as the baseline (day 1) visit for this open-label study, and overlapping assessments did not need to be repeated in this study. Only those assessments and procedures not done in the previous study were to be conducted at the baseline visit.
4 Starting on day 1 (baseline), patients received evinacumab 15 mg/kg IV administered every 4 weeks.
5 Patients are followed for 24 weeks after receiving the last dose of the study drug.
Source: CL-1719 Clinical Study Report.48
Inclusion and Exclusion Criteria
Male and female patients aged 12 years and older with documented HoFH who were receiving a maximally tolerated background LLT (which could include statin, ezetimibe, PCSK9 inhibitors, lomitapide, and/or LDL apheresis) were included in the CL-1719 study. HoFH diagnosis was based on a genetic criterion (documented functional mutations in both LDLR alleles or documented homozygous or compound heterozygous mutations in APOB or PCSK9) and on clinical criteria (untreated total cholesterol > 12.93 mmol/L and triglycerides < 3.39 mmol/L and both parents with documented total cholesterol > 6.47 mmol/L, or cutaneous or tendinous xanthoma before age 10 years).48 The participants enrolled in the CL-1719 trial were broadly classified into 2 groups based on:
Age: Patients aged 18 years and older were considered the adult population; patients aged 12 years and older but younger than 18 years were considered the adolescent population.
Prior exposure to evinacumab, which included the following subgroups:
patients who entered the study directly without prior enrolment in an evinacumab study (the new evinacumab group)
patients who had previously completed any 1 study (the ELIPSE or CL-1331 studies) where evinacumab was administered (the continue evinacumab group)
new patients on evinacumab and those continuing with evinacumab (the total evinacumab group).
Interventions
At baseline (day 1), patients were administered 15 mg/kg of evinacumab, intravenously, every 4 weeks (± 5 days). Patients who were receiving 150 mg alirocumab, administered subcutaneously, in any previous study, could opt to continue to receive the drug every 2 weeks in the CL-1719 extension study as background LLT.48
Patients entering the CL-1719 study after completing a prior study evaluating the safety and efficacy of alirocumab in patients with HoFH but who had not participated in any prior evinacumab study were allowed to choose whether to remain on alirocumab as part of their background LLT.48 Patients were allowed, at the investigator’s and patient health care provider’s discretion, to:
continue treatment with alirocumab supplied by the sponsor as part of their background LLT
discontinue alirocumab before enrolling in this study
change to a commercially available PCSK9 inhibitor antibody before enrolling in this study.
Patients receiving evinacumab in the extension study continued until:
clinical development of evinacumab for the indication was discontinued
clinical development of evinacumab was terminated
risk-benefit of evinacumab in this patient population was deemed unfavourable
evinacumab was approved by the regulatory authority governing the location of the study site.
Patients who discontinued the study drug prematurely were required to return to the clinic (within 5 days) for end-of-treatment assessments.48
Medications and nutritional supplements that could alter serum lipids, such as statins, ezetimibe, fibrates, niacin, bile acid resins, red yeast rice, lomitapide, mipomersen, and PCSK9 inhibitors, were permitted if treatment had been initiated before the baseline visit (day 1) and had been stable for at least 4 weeks (6 weeks for fibrates, 8 weeks for PCSK9 inhibitors, 12 weeks for lomitapide, and 6 months for mipomersen). Lipoprotein apheresis was permitted if the patient’s schedule and setting had been stable for at least 8 weeks before the baseline visit.48 Patients receiving background LLT (e.g., statins, ezetimibe, PCSK9 inhibitor antibodies) maintained a stable regimen for at least 24 weeks and throughout the study. Patients on other LLTs (e.g., apheresis, lomitapide) had their regimens adjusted after week 24 based on LDL-C levels and CV risk factors and at the investigator’s discretion. Patients were also recommended to follow a heart-healthy diet throughout the study.48
Outcomes
TEAEs, physical examination, vital signs monitoring, electrocardiogram, and clinical safety laboratory tests were the safety objectives investigated in the study. The efficacy of evinacumab was assessed using lipid levels collected at prespecified times throughout the study. Vascular imaging conducted in the adolescent population was an exploratory objective.48
Statistical Analysis
No sample size calculation was performed and no formal hypothesis was tested for this study. A population of approximately 120 patients was planned for the study, and 116 patients were enrolled by the interim data cut-off. Fourteen patients aged 12 years or older but younger than 18 years were planned to be enrolled; based on the feasibility of identifying patients, the sample size was considered practical.48
Of the 4 datasets defined in the analysis, only the SAS is of interest for this review. The SAS included all patients who were enrolled and had received at least 1 dose or part of a dose of the open-label study treatment in this study. Data in the SAS population are presented as follows:
Continue evinacumab group: patients who received evinacumab in a previous study (i.e., completed the ELIPSE or CL-1331 studies)
New evinacumab group: patients without previous exposure to evinacumab
Total evinacumab group: all patients, regardless of prior evinacumab exposure
Descriptive statistics were used to summarize continuous variables (number of patients reflected in the calculation (n), mean, median, SD, quartiles 1 and 3, minimum, and maximum). Categorical or ordinal data were summarized using frequencies and percentages. The percent and absolute changes in lipid data (e.g., LDL-C, Apo B, triglycerides) were summarized for each visit for each of the groups determined by previous evinacumab exposure for all patients in the SAS and for the subpopulation of adolescent patients in the SAS. A within-patient t test (for lipids with a normal distribution) or Wilcoxon signed rank test (a nonparametric test for lipids with a non-normal distribution such as triglycerides) was conducted for secondary efficacy end points to compare each patient’s week 24 assessment to their baseline assessment. Missing data were not imputed.48 The baseline values used to determine the percent and absolute change for each time frame were defined as follows:
For patients who had participated in the ELIPSE study, the baseline was defined as the last obtained value before the first dose of the double-blind study drug in the ELIPSE study.
For patients who had participated in the previous evinacumab study (the CL-1331 study) or who had not participated in any previous evinacumab study, the baseline was defined as the last obtained value before the first dose of the study drug in the CL-1719 study.48
Patient Population
Baseline Characteristics
Table 16 presents the baseline and demographic characteristics of the population enrolled in the CL-1719 study. The total study population (adult and adolescent populations) consisted of || patients who were new to evinacumab (new evinacumab group) and || patients who were continuing on evinacumab from a previous study (continue evinacumab group). The mean age in the total study population was |||| years, with || adolescent patients (||||%) included. There was an even distribution of males (||||%) and females (||||%) in the study, and the majority of patients were white (||||%). There were more adolescent patients in the new evinacumab group than in the continue evinacumab group and more patients aged 65 years and older in the continue evinacumab group than in the new evinacumab group. Of the ||| patients in the total study population, ||| (||||%) had a history of and/or risk factors for CVD.48 The most common CV risk factors reported (> ||% of patients) were cutaneous or tendinous xanthoma (|||||) and family history of premature CHD (||||%). Patients in the total study population had either homozygous (||||%) or compound heterozygous (||||%) mutations in the LDLR gene. In the adolescent population, there were || patients who were new to evinacumab and |||| patients who were continuing evinacumab from a previous study. In the adolescent population, the mean age was |||| years; there were more males (||||%) than females (||||%); the majority of patients were white (||||%); || patients (||||%) had a history of CV events and/or risk factors for CVD; and most patients had either homozygous (||||%) or compound heterozygous (||||%) mutations in the LDLR gene.48
Table 16: Baseline Characteristics (CL-1719 Study)
Characteristic | Adolescent population (N = ||) | Total population (N = |||) |
|---|---|---|
Demographic characteristics | ||
Age (years) | ||
Mean (SD) | |||| |||||| | |||| ||||||| |
≥ 12 to < 18, n (%) | || ||||| | || |||||| |
≥ 18 to < 45, n (%) | || |||||| | || |||||| |
≥ 45 to < 65, n (%) | || |||||| | || |||||| |
≥ 65 to < 75, n (%) | || |||||| | ||||| |
≥ 75, n (%) | || |||||| | ||||| |
Sex, n (%) | ||
Male | ||||| | || |||||| |
Female | ||||| | || |||||| |
Race, n (%) | ||
White | ||||| | ||||| |
Black or African American | ||||| | ||||| |
Asian | ||||| | ||||| |
Other | ||||| | ||||| |
BMI (kg/m2) | ||
Mean (SD) | |||| |||||| | |||| ||||| |
Clinical characteristics | ||
CVD history, n (%) | ||
Any CV history or risk factors | || |||||| | ||| |||||| |
History of CHD | ||||| | || |||||| |
CHD risk equivalentsa | ||||| | || |||||| |
Mutation status, n (%) | ||
Homozygous (LDLR) | ||||| | || |||||| |
Defective/defective | ||||| | || |||||| |
Negative/negative | ||||| | || |||||| |
Null/null | ||||| | || |||||| |
Homozygous (LDLRAP1) | ||||| | ||||| |
Negative/negative | ||||| | ||||| |
Null/null | ||||| | ||||| |
Compound heterozygous | ||||| | || |||||| |
Double heterozygous | || |||||| | ||||| |
Other (heterozygous, undetermined, or no mutation) | || |||||| | || |||||| |
LLTs, n (%) | ||
Any statin | || ||||| | ||| |||||| |
High-intensity statin | || |||||| | || |||||| |
Any nonstatin LLT | || |||||| | ||| |||||| |
Ezetimibe | || |||||| | || |||||| |
PCSK9 inhibitorb | ||||| | || |||||| |
Alirocumab | ||||| | || |||||| |
Evolocumab | ||||| | || |||||| |
Lomitapide | ||||| | || |||||| |
Apheresisc | ||||| | || |||||| |
Lipid parameters | ||
LDL-C, mean (SD) | ||
mg/dL | ||||| |||||||| | ||||| |||||||| |
mmol/L | ||| |||||| | ||| |||||| |
Apo B, mean (SD) | ||
g/L | ||| |||||| | ||| |||||| |
Non-HDL-C, mean (SD) | ||
mmol/L | ||| |||||| | ||| |||||| |
TC, mean (SD) | ||
mmol/L | ||| |||||| | ||| |||||| |
Apo B = apolipoprotein B; BMI = body mass index; CHD = coronary heart disease; CV = cardiovascular; CVD = cardiovascular disease; HDL-C = high-density lipoprotein cholesterol; LDL-C = low-density lipoprotein cholesterol; LDLR = low-density lipoprotein receptor; LLT = lipid-lowering therapy; SD = standard deviation; TC = total cholesterol.
a“CHD risk equivalents” refers to people with a 10-year risk of coronary death or nonfatal myocardial infarction at least as high as those who have known CHD (including those with stable angina or prior myocardial infarction), which generally exceeds 20%.
bNumbers refer to concomitant use.
cNumbers refer to treatment history.
Source: CL-1719 Clinical Study Report.48
||| patients (||||%) were on a statin at baseline in the total study population, of whom || (||||%) were on a high-intensity statin regimen. The most frequently used LLTs besides statin were ezetimibe (|| |||||||), PCSK9 inhibitor (|| [||||%]), and apheresis (|| [||||%]).48 |||||||||||| patients (||||%) had a history of lomitapide use. In the adolescent population, ||| || patients (|||%) were on a statin, of whom || (||||%) were on a high-intensity statin regimen; the most frequently used LLTs at baseline were ezetimibe (|| [||||%]) and PCSK9 inhibitors (|| [||||%]).48
Patient Disposition
Table 17 presents the patient disposition (total population and adolescent population) in the CL-1719 extension study. By the interim data cut-off date, || patients (||||%) had completed the treatment period, || patients (||||%) were still receiving treatment in the treatment period, and || patients (||||%) had discontinued the treatment period. The continue evinacumab group consisted of || patients (||||%) previously enrolled in the ELIPSE study and | patients (|||%) previously enrolled in the CL-17100 study. The remaining || patients (||||%) were naive to treatment with evinacumab. |||||||| adolescent patients were enrolled and treated in the study. At the data cut-off date, |||| patients (||||%) had completed the treatment period, |||| patients (||||%) were ongoing in the treatment period, and || patients (||||%) had discontinued.48
Table 17: Patient Disposition (CL-1719 Study)
Patient characteristic, n (%) | Adolescent population | Total population | ||||
|---|---|---|---|---|---|---|
New evinacumab (N = ||) | Continue evinacumab (N = |) | Total evinacumab (N = ||) | New evinacumab (n = ||) | Continue evinacumab (n = ||) | Total evinacumab (n = |||) | |
Enrolled | || ||||| | ||||| | || ||||| | || ||||| | || ||||| | ||| ||||| |
Completed the study | |||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
Did not complete the study | |||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
Ongoing in study | |||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
Completed the treatment period | |||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
Did not complete the treatment period | |||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
Ongoing in the treatment period | |||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
Participated in CL-1331 study | |||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
Participated in ELIPSE trial | |||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
Evinacumab naive | |||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
Note: Percentages are calculated with the number of treated patients in each group as the denominator.
Source: CL-1719 Clinical Study Report.48
Exposure to Study Treatments
Table 18 presents data on treatment exposure in the adolescent and total study populations. In the total study population, the mean number of evinacumab infusions reported at the data cut-off was |||||, the mean duration of exposure was |||||| weeks, and patients had at least || weeks’ exposure to evinacumab. In the adolescent population, the mean number of study treatment infusions was ||||, the mean study duration was |||| weeks, and all treated patients had at least || weeks’ exposure to evinacumab.48
Table 18: Exposure to Evinacumab (CL-1719 Study)
Exposure | Adolescent population | Total population | ||||
|---|---|---|---|---|---|---|
New evinacumab (N = ||) | Continue evinacumab (N = |) | Total evinacumab (N = ||) | New evinacumab (n = ||) | Continue evinacumab (n = ||) | Total evinacumab (n = |||) | |
Total number of infusions, mean (SD) | ||||| ||||||| | ||||| ||||||| | ||||| ||||||| | ||||| ||||||| | ||||| ||||||| | ||||| ||||||| |
Duration of study drug exposure (weeks) | ||||||
Mean (SD) | ||||| ||||||| | |||||| ||||||| | ||||| ||||||| | |||||| ||||||| | |||||| ||||||| | |||||| ||||||| |
Median (range) | ||||| |||||| |||||| | |||||| |||||||||||| | ||||| |||||| |||||| | ||||| |||||||||||| | |||||| |||||||||||| | |||||| |||||||||||| |
Duration of study drug exposure by categorya (patients, n [%]) | ||||||
≥ 24 weeks | || ||||| | |||||| | || ||||| | || ||||| | || ||||| | ||| ||||| |
≥ 52 weeks | || ||||| | |||||| | || ||||| | || |||||| | || |||||| | ||| |||||| |
≥ 104 weeks | |||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
≥ 156 weeks | |||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
SD = standard deviation.
aDuration of study treatment exposure in weeks was defined as follows: (last evinacumab treatment administration date) + 28(first evinacumab treatment administration date) / 7. Unplanned intermittent discontinuations in study treatment were accounted for.
Source: CL-1719 Clinical Study Report.48
Results
Efficacy
Table 19 presents a summary of efficacy parameters assessed in the CL-1719 study in the total and adolescent populations.
Low-Density Lipoprotein Cholesterol
Treatment in the total study population resulted in an absolute mean (SD) change from baseline in LDL-C at week 24 of |||||| mg/dL (|||||| mmol/L). The mean percent change from baseline at week 24 was ||||||%. The reductions from baseline in LDL-C were maintained to at least week ||| (mean percent change from baseline at week ||| of ||||||%), after which time the results were more variable due to the smaller number of patients contributing to the data. The changes from baseline in LDL-C in the adolescent population aligned with those in the total study population (absolute mean change from baseline to week 24 was |||||| mg/dL [|||||| mmol/L]; percent mean change from baseline at week 24 was ||||||%).48
Apolipoprotein B
The absolute mean change from baseline to week 24 in Apo B in the total study population was ||||| mg/dL (|||||| g/L). The mean percent change from baseline at week 24 was ||||||%. The reductions from baseline in Apo B were maintained to at least week |||, after which time the results were more variable due to the smaller number of patients contributing to the data. The changes from baseline in Apo B in the adolescent population aligned with those in the total study population (absolute mean change from baseline to week 24 was ||||| mg/dL [|||||| g/L]; mean percent change from baseline to week 24 was ||||||%). The reductions from baseline in Apo B were maintained in the adolescent population to at least week ||, after which time the results were more variable due to the smaller number of patients contributing data.48
Table 19: Summary of Efficacy Parameters (LDL-C and Apo B) for the Total and Adolescent Populations (CL-1719 Study)
Study week | LDL-C (mg/dL) | Apo B (mg/dL) | ||
|---|---|---|---|---|
Total population | Adolescent population | Total population | Adolescent population | |
Baseline | ||||
n | ||||| |||| | ||||| |||| | ||||| |||| | ||||| |||| |
Mean (SD) | ||||| |||||||| | ||||| |||||||| | ||||| ||||||| | ||||| ||||||| |
Week 24 | ||||
n | ||||| |||| | ||||| |||| | ||||| |||| | ||||| |||| |
Absolute CFB, mean (SD) | |||||| |||||||| | |||||| ||||||| | ||||| ||||||| | ||||| ||||||| |
Percent CFB, mean (SD) | |||||| |||||||| | |||||| |||||||| | |||||| |||||||| | |||||| |||||||| |
Week 36 | ||||
n | ||||| |||| | ||||| |||| | ||||| |||| | |||||| |
Absolute CFB, mean (SD) | |||||| |||||||| | |||||| |||||||| | |||||| |||||||| | |||||| |
Percent CFB, mean (SD) | |||||| |||||||| | |||||| |||||||| | |||||| |||||||| | |||||| |
Week 48 | ||||
n | || | || | || | || |
Absolute CFB, mean (SD) | |||||| |||||||| | |||||| |||||||| | ||||| ||||||| | ||||| ||||||| |
Percent CFB, mean (SD) | |||||| |||||||| | |||||| |||||||| | |||||| |||||||| | |||||| |||||||| |
Week 60 | ||||
n | || | || | || | ||||| |||| |
Absolute CFB, mean (SD) | |||||| |||||||| | |||||| |||||||| | ||||| ||||||| | ||||| |||| |
Percent CFB, mean (SD) | |||||| |||||||| | |||||| |||||||| | |||||| |||||||| | ||||| |||| |
Week 72 | ||||
n | || | || | || | || |
Absolute CFB, mean (SD) | |||||| |||||||| | |||||| ||||||| | ||||| ||||||| | ||||| ||||||| |
Percent CFB, mean (SD) | |||||| |||||||| | |||||| |||||||| | |||||| |||||||| | |||||| |||||||| |
Week 84 | ||||
n | || | || | || | || |
Absolute CFB, mean (SD) | |||||| |||||||| | |||||| |||||||| | ||||| |||||||| | ||||| |||| |
Percent CFB, mean (SD) | |||||| |||||||| | |||||| |||||||| | |||||| |||||||| | |||||| |||| |
Week 88 | ||||
n | ||||| |||| | ||||| |||| | ||||| |||| | ||||| |||| |
Absolute CFB, mean (SD) | |||||| |||||||| | |||||| |||||||| | ||||| ||||||| | ||||| ||||||| |
Percent CFB, mean (SD) | |||||| |||||||| | |||||| |||||||| | |||||| |||||||| | |||||| |||||||| |
Week 96 | ||||
n | ||||| |||| | ||||| |||| | ||||| |||| | ||||| |||| |
Absolute CFB, mean (SD) | |||||| |||||||| | |||||| |||||||| | ||||| ||||||| | |||||| ||||||| |
Percent CFB, mean (SD) | |||||| |||||||| | |||||| |||||||| | |||||| |||||||| | |||||| |||||||| |
Week 108 | ||||
n | ||||| |||| | ||||| |||| | ||||| |||| | ||||| |||| |
Absolute CFB, mean (SD) | ||||| |||| | ||||| |||| | ||||| |||| | ||||| |||| |
Percent CFB, mean (SD) | ||||| |||| | ||||| |||| | ||||| |||| | ||||| |||| |
Week 120 | ||||
n | ||||| |||| | ||||| |||| | ||||| |||| | ||||| |||| |
Absolute CFB, mean (SD) | |||||| |||||||| | |||||| |||||||| | ||||| ||||||| | |||||| ||||||| |
Percent CFB, mean (SD) | |||||| |||||||| | |||||| |||||||| | |||||| |||||||| | |||||| |||||||| |
Apo B = apolipoprotein B; CFB = change from baseline; HDL-C = high-density lipoprotein C; LDL-C = low-density lipoprotein cholesterol; NA = not applicable; SD = standard deviation; TC = total cholesterol.
aP values comparing each patient’s week 24 assessment to baseline assessment were provided for descriptive purposes, using t test for lipids with a normal distribution.
Source: CL-1719 Clinical Study Report.48
Harms
Adverse Events
Most patients experienced at least 1 TEAE: || of || (||||%) were reported in the new evinacumab group, || of || (||||%) in the continue evinacumab group, and || of ||| (||||%) in the total evinacumab population. The most frequently reported TEAEs for the total study population were nasopharyngitis, headache, influenza-like illness, arthralgia, COVID-19 infection, back pain, and nausea. The TEAE profile in the adolescent population was similar to that in the total study population. |||||| patients experienced at least 1 TEAE.48
Serious AEs
||||||||||| patients (||||%) in the total study population experienced serious TEAEs. In the adolescent population, ||||| patient (|||%) experienced a serious TEAE.
Withdrawals due to AEs
||||| patients in the total evinacumab group had documented TEAEs leading to discontinuation of the study drug: ||||| due to pregnancy and ||||| due to an infusion reaction of headache that was not attributed to the study drug.
Mortality
||| adult patients in the total study population experienced TEAEs resulting in death, |||| of which were cardiac-related and considered unrelated to the study drug by the investigators. No deaths were reported in the adolescent population.
Critical Appraisal
Internal Validity
The CL-1719 study was a nonrandomized, open-label study with no concurrent comparison. The lack of a comparator limits the interpretation of the treatment effect as it is uncertain whether the magnitude of the effect observed can be attributed to evinacumab, natural history, variations in patient health status (continuing and new patients enrolled), residual effects from the use of evinacumab (for patients entering the study from an evinacumab study, the impact of ongoing treatments on the effect of evinacumab efficacy), or other unidentified prognostic factors. The single-arm design does not allow for differentiation of the symptoms of underlying HoFH from treatment-related AEs. Additionally, the open-label design may have introduced bias into the assessment of subjective outcomes, such as the reporting of AEs.
The CL-1719 study was designed to follow patients over the long-term, and the follow-up time was considered sufficient to assess the long-term efficacy of evinacumab in patients new to evinacumab and in those who had prior evinacumab exposure. The patient population enrolled may have been very selective, as at least half of the population enrolled came from prior randomized trials and may have only been included because they responded to and tolerated treatment with evinacumab, further biasing and overestimating the efficacy of evinacumab.
There were no established hypothesis tests or clear thresholds for the secondary variables assessed in the trial. A lack of hypothesis testing against clear thresholds reduces the internal validity of the efficacy findings as it introduces bias into the interpretation of the findings. There is uncertainty in the findings presented; as a result, the P values and treatment effects observed should be interpreted with caution and considered exploratory. There was also no clear sample size and power calculation defined for the study. There is uncertainty about whether the sample size was sufficient to assess the efficacy of evinacumab, which limits interpretability of the magnitude of the benefit presented.
No HRQoL measurements were performed in the study; therefore, it is uncertain how evinacumab impacts HRQoL in long-term treatment.
Missing data and the lack of methods to account for missing data in the analysis may have impacted the internal validity of the results. Variabilities in some lipoprotein profiles were reported at later follow-up points and were attributed to missing or lack of patient data. There was no assessment of attrition conducted, which may signify an overestimation of the treatment benefit with evinacumab. In the total study population, || patients (||||%) did not complete the treatment period and || (|||%) did not complete the study, which could have introduced bias in estimates (in favour of evinacumab). No data imputation techniques were implemented to account for missing data.
Table 20: Treatment-Emergent Adverse Events — Safety Analysis Set (CL-1719 Study)
System organ class and preferred term | Total population | Adolescent population | ||||
|---|---|---|---|---|---|---|
New evinacumab (N = ||) | Continue evinacumab (N = ||) | Total evinacumab (N = |||) | New evinacumab (N = ||) | Continue evinacumab (N = |) | Total evinacumab (N = ||) | |
At least 1 TEAE, n (%) | || |||||| | || |||||| | || |||||| | || |||||| | | |||||| | || |||||| |
At least 1 serious TEAE, n (%) | |||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
At least 1 TEAE resulting in treatment discontinuation, n (%) | |||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
Any TEAE resulting in death, n (%) | |||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
Cardiac disorders, n (%) | |||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
Angina pectoris | |||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
Gastrointestinal disorders, n (%) | |||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
Nausea | |||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
Diarrhea | |||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
Abdominal pain | |||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
Toothache | |||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
GERD | |||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
Vomiting | |||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
General disorders and administration site conditions, n (%) | |||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
Influenza-like illness | |||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
Pyrexia | |||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
Chest pain | |||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
Infections and infestations, n (%) | |||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
Nasopharyngitis | |||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
COVID-19 infection | |||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
Gastroenteritis | |||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
Urinary tract infection | |||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
Upper respiratory tract infection | |||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
Injury, poisoning, and procedural complications, n (%) | |||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
Contusion | |||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
Postvaccination syndrome | |||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
Investigations, n (%) | |||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
Alanine aminotransferase increased | |||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
Aspartate aminotransferase increased | |||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
Blood creatine phosphokinase increased | |||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
Musculoskeletal and connective tissue disorders, n (%) | |||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
Arthralgia | |||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
Back pain | |||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
Myalgia | |||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
Pain in extremity | |||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
Musculoskeletal pain | |||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
Nervous system disorders, n (%) | |||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
Headache | |||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
Dizziness | |||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
Paresthesia | |||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
Respiratory, thoracic, and mediastinal disorders, n (%) | |||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
Cough | |||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
Oropharyngeal pain | |||||| | |||||| | |||||| | |||||| | |||||| | |||||| |
GERD = gastroesophageal reflux disease; PT = preferred term; SOC = system organ class; TEAE = treatment-emergent adverse event.
Notes: Medical Dictionary for Regulatory Activities (Version 22.0) coding dictionary applied. A patient who reported 2 or more TEAEs with the same preferred term is counted only once for that term. A patient who reported 2 or more TEAEs with different preferred terms within the same system organ class is counted only once in that system organ class. SOC is sorted alphabetically; PT is sorted by decreasing frequency of the total group.
Source: CL-1719 Clinical Study Report.48
Important protocol deviations were reported for || patients (||||%) in the total study population, commonly due to procedural irregularities (||%), which may have impacted estimates and biased the findings in either direction. Other important procedural irregularities were “blood sample for lipid panel not collected” (|| patients [||||%]), “apheresis treatment not performed” per the schedule of the patient (|| patients [||||%]), “blood sample for specialty lipid panel not collected” (|| patients [||||%]), “LDL-C taken after apheresis treatment” (|| patients [||||%]), and “study treatment received prior to apheresis treatment” (|||| patients [|||%]).No patients had important deviations relating to the inclusion and exclusion criteria in the total study population.
The efficacy results presented are from an interim analysis. It was unclear whether the analysis was planned before patient enrolment.
External Validity
The CL-1719 study was a long-term, open-label, multicentre study that aimed to evaluate the safety, tolerability, and efficacy of evinacumab in adolescent and adult patients aged 12 years and older with HoFH who were receiving a background LLT. As noted for the CL-17100 pediatric study, the noncomparative nature of the CL-1719 study negates the ability to draw a statistical association between the reported results and evinacumab, and the study is not considered confirmatory for efficacy due to the small sample size and the chronic progression of HoFH, resulting in difficulty isolating whether the effect is due to placebo, natural history, or unidentified prognostic factors that could affect the study outcomes, ultimately limiting the strength and interpretability of the results for this group of patients. The CL-1719 study enrolled ||||| patients from Canada, though it was unclear if the results were generalizable to patients in Canada due to the small sample size and the study design.
The efficacy outcomes investigated in the CL-1719 study of percent and absolute change in LDL-C and Apo B were considered appropriate and reflective of current clinical practice. Additionally, the follow-up duration of the study was considered appropriate for the outcomes evaluated and reflective of real-world practice. However, as noted for the pivotal studies, long-term outcomes such as HRQoL and CV-related morbidity and mortality were not evaluated, though it remains unclear if any benefits would have been realized within the study time frame for these outcomes.
The concomitant medications and background LLTs reported among patients were in line with those reported in the ELIPSE and CL-17100 studies and were also reflective of current clinical practice in Canada, apart from PCSK9 inhibitor use, which the clinical experts consulted by CADTH highlighted was higher than usage of these medications in Canadian clinical practice.
Indirect Evidence
The content within this section has been informed by materials submitted by the sponsor. The following has been summarized and validated by the CADTH review team.
Objectives for the Summary of Indirect Evidence
The ELIPSE trial compared the efficacy and safety of evinacumab as an adjunct to standard of care LLT versus placebo plus standard of care LLT. As such, no direct evidence comparing evinacumab to relevant comparators was available, and to support the pharmacoeconomic model for evinacumab, the sponsor submitted an ITC estimating the relative effect of evinacumab compared with each individual treatment used as part of standard of care for adult and adolescent patients (aged 12 years and older) with HoFH.34
Description of Indirect Comparisons
The sponsor-submitted ITC first conducted an SLR to identify existing studies conducted in patients with HoFH. Patient-level data from the evinacumab and placebo arms of the ELIPSE trial were compared to aggregate data from the identified trials using Bucher ITCs and MAIC methods for the outcomes of percent change in LDL-C, proportion of patients with a greater than or equal to 50% reduction in LDL-C, proportion of patients who experienced any SAEs, and proportion of patients discontinuing the study due to any cause.34
Table 21: Study Selection Criteria and Methods for ITCs Submitted by the Sponsor
Characteristics | Indirect comparison |
|---|---|
Population | Adult and adolescent patients (aged ≥ 12 years) with HoFH |
Intervention | Following interventions, either alone or in combination with other pharmacological intervention:
|
Comparator |
|
Outcome |
|
Study designs |
|
Publication characteristics | Publications were limited to the English language. However, non-English studies identified in the SLR considered potentially relevant were flagged and discussed with the sponsor to decide on their inclusion. Any non-English language studies that were included were translated to extract relevant information. No limitations were placed on time or place of publication. |
Exclusion criteria | Population:
Interventions: Interventions not in list Comparators: None Outcomes: Studies assessing outcomes not relevant to the review Study design:
|
Apo B = apolipoprotein B; CVD = cardiovascular disease; HDL = high-density lipoprotein; HDL-C = high-density lipoprotein cholesterol; HeFH = heterozygous familial hypercholesterolemia; HoFH = homozygous familial hypercholesterolemia; HRQoL = health-related quality of life; ITC = indirect treatment comparison; LDL = low-density lipoprotein; LDL-C = low-density lipoprotein cholesterol; MACE = major cardiovascular event; RCT = randomized controlled trial; TC = total cholesterol; SLR = systematic literature review.
Source: Sponsor-submitted ITC.34
Sponsor-Submitted ITC Design
Objectives
The objective of the sponsor-submitted ITC was to estimate the relative effect of evinacumab compared with relevant comparator treatments for adult and adolescent patients (aged 12 years and older) with HoFH to estimate the relative efficacy, safety, and tolerability of evinacumab compared with lomitapide, ezetimibe, evolocumab, and LDL apheresis.34
Study Selection Methods
The sponsor-submitted ITC was informed by an SLR to identify relevant clinical information from RCTs, single-arm trials, and real-world evidence for the treatment of patients with HoFH. The criteria for study selection for the sponsor’s SLR can be found in Table 21. Searches were performed on March 28, 2022, with no date restriction. No information was provided on the databases searched, the method of study selection or data extraction, or the quality assessment conducted on the included studies.34
Statin monotherapy was not included as a comparator for the ITC, as the focus of the ITC was to evaluate treatments given at second line or later.34
The end points of interest for the ITC analyses were:34
percent reduction in LDL-C
proportion of patients with a greater than or equal to 50% reduction in LDL-C
proportion of patients who experienced any SAEs
proportion of patients discontinuing study due to any cause.
ITC Analysis Methods
All studies identified from the SLR were considered for inclusion in the ITCs; however, additional exclusion criteria were used to identify those studies most applicable for inclusion in the ITCs. Studies were considered for inclusion based on their study design, inclusion and exclusion criteria, baseline characteristics, and availability of end point data.34
Different methods were used to estimate relative treatment effects between evinacumab from the ELIPSE trial and relevant comparator treatments depended on what evidence sources were available. This report’s analyses are based on the ELIPSE trial’s July 29, 2019, data cut-off date and double-blind treatment period.34
When the comparator trial and the ELIPSE trial were linked by a common comparator, Bucher ITCs were used. A Bucher ITC was chosen over network meta-analyses because network meta-analyses require a connected network, which was not available in the identified evidence base. When the comparator studies did not link to the ELIPSE trial or were single-arm studies, Bucher ITC or network meta-analysis methods are not feasible, and the MAIC population adjustment method was used. In the MAIC, individual patients receiving evinacumab were assigned statistical weights that adjusted for their overrepresentation or underrepresentation relative to the average prognostic factors and treatment effect modifiers observed in each comparative evidence source. These weights were then incorporated into the analyses.34
A logistic regression model estimated the propensity of being enrolled into the ELIPSE trial or the comparative evidence source. The analyses were based on the patient-level data available for the patients receiving evinacumab and the published summary data available for the comparative evidence sources. A method of moments condition allowed the propensity scores to be estimated without patient-level data for the comparative evidence source. Rescaled weights were explored using histograms to determine whether specific patients or groups of patients were overrepresented or underrepresented in the analysis. Simulated comparator data based on the reported number of patients who did and did not experience response to treatment were combined with the weighted ELIPSE trial data, and a relative risk was estimated using weighted logistic regression with a treatment covariate. A robust sandwich estimator was used to calculate SEs.34
After weighting, average baseline characteristics (mean or proportion of patients within a category) were balanced for the patients receiving evinacumab and the patients receiving a comparator.34
Prognostic Factors and Treatment Effect Modifiers
No published papers were identified that discussed prognostic factors and treatment effect modifiers in relation to HoFH. Therefore, prognostic factors and treatment effect modifiers were identified through clinical input and evidence-based assessment using patient-level data from the ELIPSE trial. The findings from these analyses were used to provide evidence for suggested adjustment variables and to further understand if an anchored MAIC for the comparison between evinacumab and evolocumab was appropriate.34
Two independent interviews were conducted with 2 clinical experts in the UK to seek input on the clinical relevance of potential prognostic factors and treatment effect modifiers. Both clinical experts suggested that age, presence of CHD, baseline LDL-C, and LDLR mutation status were clinically meaningful prognostic factors. The experts also noted that LDLR mutation status was considered a treatment effect modifier for statins and PCSK9 inhibitors (evolocumab), but not for ezetimibe, lomitapide, evinacumab, or LDL apheresis.34
To select potential prognostic factors from the ELIPSE trial, logistic regression models (for binary end points) and linear regression models (for continuous end points) were fitted, with each of the baseline characteristics included as a single covariate to determine whether the characteristics impacted a patient’s prognosis. Two analyses were run: first, data were subset by baseline characteristics of interest and logistic regression models (for binary end points) and linear regression models (for continuous end points) were fitted with only a treatment covariate. Second, logistic regression models (for binary end points) and linear regression models (for continuous end points) were fitted, with each of the baseline characteristics included as a single covariate, along with a treatment covariate (evinacumab or placebo) and an interaction term between the baseline characteristic and treatment. This was used to produce a P value to gauge whether the subgroup acts as a treatment effect modifier; the significance of the interaction term indicates whether the covariate is likely to be a treatment effect modifier. Variables were a potential prognostic variable of a treatment effect modifier if they had a P value of less than 0.1.34
Based on the clinical interviews and the assessment of the evidence base, the following variables were considered prognostic factors: age (from the clinical input), presence of CHD (from the clinical input and the assessment of the evidence base), LDL-C (from the clinical input), and LDLR mutation status (i.e., defective/defective or null/null; from the clinical input and the assessment of the evidence base), the last of which was also considered to be a treatment effect modifier.34
Bucher ITC and MAIC Analyses
Based on the results of the SLR, Bucher ITCs were used for the comparison of evinacumab to evolocumab (connected evidence was available, with a common comparator placebo in both the ELIPSE trial [2020] and Raal et al. [2015]). For the comparisons of evinacumab to ezetimibe and lomitapide, in the absence of a connected network of randomized studies (Gagne et al. [2002]) or where there are single-arm studies involved (Cuchel at al. [2013]), unanchored MAICs were used to estimate the relative treatment effect. Additional naive ITCs (with no population adjustment) were carried out to show the impact of matching. Two sets of variables were used in the unanchored MAICs:34
CHD, age, and baseline LDL-C levels
age.
For the external studies included in the MAIC, Cuchel et al. (2013) and Gagne et al. (2002), LDLR mutation status was not reported; thus, it was not possible to adjust for this variable.34
A MAIC was not conducted for the comparison of evinacumab and evolocumab, despite the common comparator of placebo, due to the difficulty of matching LDLR (the only treatment effect modifier identified) and the small sample size. Additionally, for the comparisons of evinacumab to lomitapide, analyses were conducted using only patients who were naive to lomitapide.34
The proportion of patients who experienced any SAEs and the proportion of patients discontinuing the study due to any cause are reported in descriptive summaries due to the sparse data available for these end points. Given that no formal indirect analysis was conducted on the proportion of patients who experienced any SAE or on the proportion of patients discontinuing study due to any cause, results for harms are not summarized in this report.34
Results of Sponsor-Submitted ITC
Summary of Included Studies
The SLR identified 23 studies reporting data on unique patient groups as potentially relevant for inclusion in the ITCs. The studies were assessed for heterogeneity based on study design, eligibility criteria, baseline characteristics, and availability of end point data. Following assessment of heterogeneity, 3 studies from the SLR (Cuchel et al. [2013], Raal et al. [2015], and Gagne et al. [2002]), as well as the ELIPSE study, were identified for inclusion in the ITCs, for a total of 4 studies. Study CL-1719 met the inclusion criteria for the review but was excluded as the study is still ongoing and patient-level data could not be provided.34
Of the included studies, 3 were double-blind RCTs (ELIPSE trial, Gagne et al. [2002], and Raal et al. [2015]), and the Cuchel et al. (2013) study was a single-arm study. The duration of the included studies varied from 12 weeks to 78 weeks. All studies reported on adults or adolescents (≥ 12 years), though the minimum LDL-C level at enrolment varied from greater than or equal to 70 mg/dL to greater than or equal to 130 mg/dL. Additionally, the Raal et al. (2015) study did not allow patients to have undergone LDL apheresis within 8 weeks before randomization, while the remaining studies required patients on concomitant LDL apheresis to be stable for a set amount of time.34
The assessment of heterogeneity through baseline characteristics for the included studies is summarized in Table 22. The study publication dates ranged from 2002 (Gagne et al.) to 2020 (ELIPSE trial). The baseline demographic and disease characteristics also varied among the studies, with the mean age ranging from 30.0 years to 44.3 years, the presence of CHD ranging from 37.5% to 72.4% of patients, and the proportion of patients undergoing apheresis ranging from 32.6% to 62.1% (the latter was not reported in the Raal et al. [2015] study). LDLR mutation status was reported in only 2 of the 4 studies. Where reported, there is considerable variation in the proportion of patients with a negative versus a defective LDLR mutation status. Lipid parameters also varied across studies, with mean baseline LDL-C ranging from 246.5 mg/dL (SD = 153.7) to 355.8 mg/dL (SD = 135.2), and similar differences in Apo B and non-HDL-C.34
Table 22: Summary of Baseline Characteristics From Studies Included in the ITC
Characteristic | ELIPSE | Cuchel et al. (2013) | Gagne et al. (2002) | Raal et al. (2015) | ||
|---|---|---|---|---|---|---|
Evinacumab | Placebo | Lomitapide | Ezetimibe + statin | Evolocumab | Placebo | |
Sample size, n | 43 | 22 | 29 | 33 | 33 | 16 |
Age (years) | ||||||
Mean (SD) | 44.3 (16.8) | 36.7 (11.5) | 30.7 (10.6) | 32 (3) | 30 (12) | 32 (14) |
Median (range) | 41.0 (15 to 75) | 39.5 (12 to 55) | NR | 31 (NR to NR) | NR (13 to 51) | NR (14 to 57) |
Female, n (%) | 24 (55.8) | 11 (50.0) | 13 (44.8) | 17 (51.5) | 16 (48.5) | 8 (50.0) |
Presence of CHD, n (%) | 22 (51.2) | 12 (54.5) | 21 (72.4)a | 15 (45.5)b | 15 (45.5)a | 6 (37.5)a |
Baseline apheresis, n (%) | 14 (32.6) | 8 (36.4) | 18 (62.1) | 17 (51.5) | NR | NR |
Baseline statins, n (%) | 41 (95.3) | 20 (90.9) | 27 (93.1) | NR | 33 (100) | 16 (100) |
Baseline ezetimibe, n (%) | 33 (76.7) | 16 (72.7) | 22 (75.9) | NR | 30 (91.0) | 15 (94.0) |
LDLR mutation status | ||||||
Defective/defective, n (%) | 17 (39.5) | 2 (9.1) | NR | NR | 30 (91.0) | 5 (31.25) |
Negative/negative, n (%) | 4 (9.3) | 5 (22.7) | NR | NR | 1 (3.0) | 0 (0.0) |
Null/null, n (%) | 15 (34.9) | 6 (27.3) | NR | NR | 20 (60.6) | 8 (50.0) |
LDL-C (mg/dL), mean (SD) | 259.5 (172.4) | 246.5 (153.7) | 336.4 (112.1) | 313 (22) | 355.8 (135.2) | 336.4 (146.9) |
Apo B (mg/dL), mean (SD) | 169.1 (82.75) | 175.9 (98.76) | 260 (80) | 253 (14) | 210 (70) | 210 (80) |
Non-HDL-C (mg/dL), mean (SD) | 281.9 (172.61) | 269.9 (157.81) | 386.7 (131.5) | NR | 375.1 (135.3) | 359.6 (150.8) |
Apo B = apolipoprotein B; CHD = coronary heart disease; HDL-C = high-density lipoprotein cholesterol; ITC = indirect treatment comparison; LDL-C = low-density lipoprotein cholesterol; LDLR = low-density lipoprotein receptor; NR = not reported; SD = standard deviation.
aReported as coronary artery disease.
bReported as premature CHD.
Source: Sponsor-submitted ITC.34
Results
Bucher ITC Results
The results for the unadjusted naive Bucher ITC comparing data for evinacumab from the ELIPSE trial and for evolocumab from the Raal et al. (2015) study was only conducted for the end point of percent change from baseline in LDL-C at 12 weeks. The results demonstrated that evinacumab was favoured over evolocumab for percent change from baseline in LDL-C (–24.33%; 95% CI, –47.50 to –1.15).34
MAIC Results
The baseline characteristics before and after matching for the MAICs between the ELIPSE trial (evinacumab) and the Cuchel et al. (2013) study (lomitapide) and between the ELIPSE trial (evinacumab) and the Gagne et al. (2002) study (ezetimibe) are summarized in Table 23. After adjustment of baseline characteristics that were considered prognostic factors and/or treatment effect modifiers, no differences remained between populations, though the effective sample size for evinacumab was only 9.9 patients in the comparison with lomitapide and 22.3 patients in the comparison with ezetimibe.34
Table 23: Comparison of Baseline Characteristics Before and After Matching
Characteristic | ELIPSE vs. Cuchel et al. (2013) | ELIPSE vs. Gagne et al. (2002) | ||||
|---|---|---|---|---|---|---|
Evinacumab (unadjusted) | Lomitapide | Evinacumab (adjusted) | Evinacumab (unadjusted) | Ezetimibe | Evinacumab (adjusted) | |
Primary analysisa | ||||||
ESS,b N | 43.0 | 29.0 | 9.9 | 42.0 | 33.0 | 22.3 |
Age (years), mean | 44.3 | 30.7 | 30.7 | 44.5 | 32.0 | 32.0 |
CHD (%) | 51.0 | 72.0 | 72.0 | 50.0 | 45.0 | 45.0 |
LDL-C (mg/dL), mean | 259.5 | 336.4 | 336.4 | 258.5 | 313.0 | 313.0 |
Sensitivity analysisc | ||||||
ESS,b N | 43.0 | 29.0 | 23.6 | 42.0 | 33.0 | 25.5 |
Age (years), mean | 44.3 | 30.7 | 30.7 | 44.5 | 32.0 | 32.0 |
CHD (%) | 51.0 | NA | NA | 50.0 | NA | NA |
LDL-C (mg/dL), mean | 259.5 | NA | NA | 258.5 | NA | NA |
CHD = coronary heart disease; ESS = effective sample size; LDL-C = low-density lipoprotein cholesterol; NA = not applicable; vs. = versus.
aAdjustment variables: age, CHD, and LDL-C.
bSample size for unadjusted population; ESS for adjusted population.
cAdjustment variable: age.
Source: Sponsor-submitted indirect treatment comparison.34
The results of the MAIC analyses for the outcomes of percent change from baseline in LDL-C and proportion of patients with a greater than or equal to 50% reduction in LDL-C are summarized in Table 24. The results of the MAIC for the mean difference in percent change from baseline in LDL-C suggested that there was no difference between evinacumab and lomitapide after adjustment (mean difference = 5.08%; 95% CI, –25.46 to 15.29), though evinacumab was favoured over ezetimibe (mean difference = –34.35%; 95% CI, –46.06 to –22.64). For the proportion of patients with a 50% or greater reduction in LDL-C, there was no difference between evinacumab and lomitapide after adjustment (relative risk = 1.42; 95% CI, 0.84 to 2.41).34
The results of the sensitivity analyses, adjusting for only age, were consistent with the primary analysis for both outcomes. Additionally, the scenario analysis excluding patients who had received lomitapide was consistent with the primary analyses (evinacumab effective sample size = 3.9; mean difference versus lomitapide = 16.17%; 95% CI, –47.88 to 80.21).34
Table 24: Results of the MAIC for Percent Change From Baseline in LDL-C and a 50% or More Reduction in LDL-C
Method | ELIPSE vs. Cuchel et al. (2013) (evinacumab vs. lomitapide) | ELIPSE vs. Gagne et al. (2002) (evinacumab vs. ezetimibe) | |||||||
|---|---|---|---|---|---|---|---|---|---|
ESS (N) | Percent CFB in LDL-C | ≥ 50% reduction in LDL-C | ESS (N) | Percent CFB in LDL-C | |||||
Evinacumab (95% CI) | Lomitapide (95% CI) | MD (95% CI) | RR (95% CI) | Evinacumab (95% CI) | Ezetimibe (95% CI) | MD (95% CI) | |||
Before adjustment | 43.0 | –47.24 (–56.18 to –38.31) | –50 (–62 to –39) | 2.76 (–11.81 to 17.32) | 1.07 (0.67 to 1.71) | 42 | –47.16 (–57.62 to –36.71) | –20.70 (–28.97 to –12.43) | –26.46 (–39.80 to –13.13) |
After adjustment | 9.9 | –55.08 (–71.90 to –38.27) | –50 (–62 to –39) | 5.08 (–25.46 to 15.29) | 1.42 (0.84 to 2.41) | 22.3 | –55.05 (–63.34 to –46.75) | –20.70 (–28.97 to –12.43) | –34.35 (–46.06 to –22.64) |
Sensitivity analysisa | 23.6 | –56.40 (–64.66 to –48.14) | –50 (–62 to –39) | –6.40 (–20.56 to 7.76) | 1.36 (0.83 to 2.20) | 25.5 | –56.86 (–64.29 to –49.43) | –20.70 (–28.97 to –12.43) | –36.16 (–47.27 to –25.05) |
CFB = change from baseline; CI = confidence interval; LDL-C = low-density lipoprotein cholesterol; MAIC = matching- adjusted indirect comparison; MD = mean difference; RR = relative risk; vs. = versus.
aSensitivity analyses consist of adjustments for age.
Source: Sponsor-submitted indirect treatment comparison.34
Critical Appraisal of Sponsor-Submitted ITC
The feasibility of conducting an ITC and subsequent analyses was informed by an SLR; however, no information was provided on the SLR methods with regard to the databases searched, the method of study selection or data extraction (e.g., duplicate reviewers), or quality assessment. Thus, CADTH is unable to comment on whether appropriate methods were taken to identify studies for inclusion in the ITCs. Given that comparator data were identified with an SLR, there is a low risk of selection bias, and a list of excluded studies, as well as reasons for exclusion, was provided.
Two types of ITC were conducted: a MAIC and a Bucher ITC. Bucher ITCs were used for the comparison of evinacumab to evolocumab based on the connection of the studies via a placebo arm, though the sponsor did not consider evolocumab to be an appropriate comparator to evinacumab due to the lack of available data on effect modifiers and the overall low numbers available for LDLR mutation status. Two MAICs were conducted, 1 each for the comparators of ezetimibe and lomitapide, but none for PCSK9 inhibitors or statins. Per the sponsor, the focus of the analyses was to evaluate treatments given at second line or later; thus, statins alone were excluded. However, the exclusion of PCSK9 inhibitors from the analyses was considered inappropriate, as these treatments are also considered standard of care in the treatment of HoFH.
As part of the MAIC, the sponsor identified age, presence of CHD, baseline LDL-C, and LDLR mutation status (defective/defective or null/null) as prognostic factors or treatment effect modifiers through literature search and expert interviews; however, the clinical experts consulted by CADTH could not confirm or refute that these factors were the only relevant variables in this disease. The key limitation of the unanchored MAICs, which is a limitation inherent to all unanchored MAICs, is that the assumption that all effect modifiers and prognostic factors are accounted for in the model is likely unmet.
The choice to conduct an unanchored MAIC was motivated by the lack of a common comparator across studies. However, there were important differences in the design and populations of the comparator studies that limited the ability to draw inferences about the efficacy of evinacumab compared with other treatments in HoFH in the Canadian context.
There were also differences in population characteristics in the trials that may impact the comparability of the studies, notably the variation in the proportion of patients with CHD at baseline (37.5% to 72.4%), the proportion of patients receiving apheresis at baseline (32.6% to 62.1%), differences in LDLR mutation status (defective/defective, 9.1% to 91.0%; negative/negative, 0.0% to 22.7%; and null/null, 27.3% to 60.6%), and overall differences in lipid parameters at baseline: LDL-C (246.5 mg/dL to 355.8 mg/dL), Apo B (169.1 mg/dL to 260.0 mg/dL), and non-HDL-C (269.9 mg/dL to 386.7 mg/dL). In the MAICs, following adjustment for prognostic factors and treatment effect modifiers, the baseline characteristics were well balanced across studies; however, the resulting effective sample size for the evinacumab group was decreased 77% and 47% for the comparisons against lomitapide and ezetimibe, respectively. It remains uncertain how much of this reduction is due to the exclusion of patients or to a loss of precision resulting from the weighting process. The sponsor noted that some patients’ weights were greater than 5, which may result in unstable estimates, as inferences depend heavily on a small number of patients. In the sensitivity analysis adjusting for only age, the resulting effective sample size was still decreased by 45% and 39% versus lomitapide and ezetimibe, respectively. This is a result of the considerable heterogeneity across studies and may affect the numerical stability of the MAIC estimates and therefore increase the uncertainty of the results. In the absence of all prognostic factors and treatment effect modifiers, the National Institute for Health and Care Excellence Decision Support Unit considers the amount of bias in an unanchored MAIC likely to be substantial.35 Overall, given the substantial loss in sample size after weighting, the results may not be generalizable to the population of patients with HoFH living in Canada.
The outcomes evaluated in the ITCs are relevant to the clinical management of HoFH. The sponsor conducted a Bucher ITC between evinacumab and evolocumab for the outcome of percent change from baseline in LDL-C, though no formal statistical analyses or adjustments were conducted; thus, the results of this analysis should be interpreted with caution. MAICs were conducted for the outcomes of percent change from baseline in LDL-C and proportion of patients with a greater than or equal to 50% reduction in LDL-C. Additional naive ITCs were conducted for safety outcomes including proportion of patients who experienced any SAEs and proportion of patients discontinuing the studies due to any cause; however, as these analyses were only descriptive, no conclusion could be drawn on the comparative safety.
After adjustment, there was no evidence of preference for evinacumab over lomitapide for the outcome of percent change from baseline in LDL-C, but evinacumab was favoured over ezetimibe. However, in all cases, 95% CIs were wide, suggesting notable imprecision in comparative efficacy estimates.
Studies Addressing Gaps in the Systematic Review Evidence
The content within this section has been informed by materials submitted by the sponsor. The following has been summarized and validated by the CADTH review team.
Table 25: Summary of Gaps in the Systematic Review Evidence
Evidence gap | Studies that address gaps | |
|---|---|---|
Study description | Summary of key results | |
Lack of data evaluating efficacy in patients who discontinue apheresis while taking evinacumab. | Stefanutti et al. (2022) Real-world, single-arm, open-label 24-month cohort study, followed by transition to compassionate use extension (without LDL apheresis) in patients with HoFH. | Evinacumab was effective in lowering LDL-C concentration and was well tolerated over a period of 24 months. A similar reduction in LDL-C was observed in patients who discontinued LDL apheresis and continued on evinacumab alone. As such, the efficacy of evinacumab was maintained following discontinuation of LDL apheresis in a real-world clinical practice setting. |
HoFH = homozygous familial hypercholesterolemia; LDL = low-density lipoprotein; LDL-C = low-density lipoprotein cholesterol.
Source: Sponsor’s summary of clinical evidence.45
Description of Stefanutti et al. (2022)
The study by Stefanutti et al. (2022) assessed the long-term efficacy and safety of evinacumab in a cohort of patients with HoFH who were on and off background LDL apheresis and other LLTs in a real-world setting. The patients received evinacumab 15 mg/kg every 4 weeks for 24 months.49
Populations
Seven patients (5 females and 2 males) with HoFH confirmed by genetic testing (based on 2 pathogenic mutant alleles at the LDLR, APOB or PCSK9 loci and further defined as true HoFH [identical mutation in each allele of the same gene] or compound HeFH [nonidentical mutations in each allele of the same gene]) were included in the study.49
Interventions
Evinacumab was administered at 15 mg/kg every 4 weeks following the LDL apheresis treatment. Patients received variable LLTs, including LDL apheresis (6 out of 7 patients received LDL apheresis in addition to evinacumab). Follow-up proceeded according to standard of care for each patient. Efficacy and safety outcomes were assessed at baseline and at 6, 12, 18, and 24 months. Patients transitioned into a compassionate program and continued to receive 15 mg/kg evinacumab without LDL apheresis treatment at the end of the study period.49
Outcomes
The percent change from baseline in LDL-C to 24 months after evinacumab and LDL apheresis treatment was the primary outcome. The effects of evinacumab on other lipid, lipoprotein, and apolipoprotein levels, including apolipoprotein C-III and lipoprotein A, were investigated as secondary end points.49
Statistical Analysis
A paired t test or Wilcoxon signed rank test was used, where applicable, to analyze treatment effects. Associations between changes in LDL-C concentrations and other lipid and lipoprotein variables were assessed using a simple linear regression model. Statistical significance was defined at the 5% level.49
Results
Patient Disposition
The disposition of patients in the Stefanutti et al. (2022) study was not reported.
Baseline Characteristics
Seven patients with HoFH were included in this study: 5 females and 2 males. The mean age of the patients was 43 years; more than half of the patients had hypertension, but none had type 2 diabetes. Four patients had a history of coronary artery disease and or aortic valve disease. Six patients were on LDL apheresis and other LLTs (rosuvastatin [n = 4], simvastatin [n = 2], ezetimibe [n = 7], evolocumab [n = 4], alirocumab [n = 1], and lomitapide [n = 1]) before receiving evinacumab. One patient had never undergone LDL apheresis and was on background rosuvastatin and ezetimibe. The mean levels of total cholesterol, triglycerides, HDL-C, and LDL-C were 9.1mmol/L, 1.2 mmol/L, 1.1 mmol/L and 7.4 mmol/L, respectively.49
Exposure to Treatment
Treatment exposure was not reported in the study by Stefanutti et al. (2022).
Efficacy
Evinacumab With LDL Apheresis
The mean percent change from baseline following the use of evinacumab and LDL apheresis treatment in LDL-C was −54.4%, −48.9%, −49.4%, and −46.8% at 6, 12, 18, and 24 months, respectively (P < 0.001 for all, compared with baseline). One patient discontinued LLT due to hospitalization.49
Among the 7 patients treated, a reduction in the LDL-C level of 30% or more was observed in 6 patients.
Four patients experienced an LDL-C reduction of 50% or more, with 2 of these patients having an on-treatment LDL-C level of less than 2.5 mmol/L (97 mg/dL).
Evinacumab with LDL apheresis treatment also significantly reduced the plasma concentration of total cholesterol (−44.5%), non-HDL-C (−46.6%), and Apo B (−33.8%) at 24-month follow-up.49
Evinacumab (With or Without LDL Apheresis) Versus LDL Apheresis Alone
The LDL-C–lowering effect of evinacumab with or without background LDL apheresis treatment was greater than with LDL apheresis alone. With LDL apheresis alone, the time-average LDL-C was reduced by 27.2% in the 6 patients who received LDL apheresis during the normal course of their therapy before initiation of evinacumab treatment.49
Harms
No discontinuations due to severe AEs were reported following the use of evinacumab. There were also no CV events observed during the 24-month follow-up period and subsequent compassionate extension period (12 months) with evinacumab. There were no reports of symptoms related to common AEs (pharyngitis, nasal congestion, myalgia, diarrhea, and arthralgia) during the 24-month follow-up and 12-month extension period. Overall, plasma aspartate aminotransferase, alanine aminotransferase, and creatinine kinase concentrations for individual patients with HoFH remained stable during treatment with evinacumab.
Critical Appraisal
Internal Validity
The lack of a comparator and the open-label design were the main limitations of the study. There was no control group for comparison; thus, the benefit observed cannot be completely attributed to treatment with evinacumab.
The sample size was considered too small to assess the magnitude of effects, and no sample size calculations were provided. There was little information provided related to the eligibility criteria for patients to be included in the study. HoFH was also confirmed by genetic testing according to the hospital care centre, which may not be reflective of all current practices and guidelines, which use a clinical criteria and use genetic testing for confirmation only.
There is a risk of detection bias for subjective outcome measurements, such as AEs reporting, due to the open-label nature of the study, as patients and providers were aware of the treatment.
The study duration (24 months) was considered sufficient to assess the beneficial effects of evinacumab in the patient population.
No HRQoL data were presented. It is uncertain whether evinacumab impacted patient health outcomes in the real-world setting.
External Validity
There was limited generalizability in terms of genetic confirmation of HoFH diagnosis. The clinical diagnosis criterion was not used in the study, which may not be reflective of Canadian practice guidelines. It was unclear what background LLTs were used alongside LDL apheresis.
Discussion
Summary of Available Evidence
The evidence included in this review consisted of 2 pivotal studies in the systematic review (the ELIPSE trial and the CL-17100 study), 1 long-term extension study (the CL-1719 study), 1 sponsor-submitted ITC, and 1 study addressing gaps in the literature (Stefanutti et al. [2022]).
The ELIPSE study was a 24-week, phase III, randomized, double-blind, placebo-controlled study in patients aged 12 years and older with genetic or clinical confirmation of HoFH. Patients were randomized 2:1 to evinacumab 15 mg/kg IV every 4 weeks (N = 43) or matching placebo IV every 4 weeks (N = 22). Following the 24-week double-blind treatment period, patients entered a 24-week open-label treatment period. The CL-17100 study was a 3-part, phase I and phase III, open-label, single-arm trial of evinacumab in 20 children aged 5 to 11 years with genetic or clinical confirmation of HoFH. Only Parts B and C, which were the phase III, single-arm, open-label phases of the study that aimed to evaluate the efficacy and safety of evinacumab, were of interest to this report. In total, 20 patients were included in Parts B and C, which included a 24-week treatment period (Part B; N = 14) and a 48-week treatment period followed by a 24-week follow-up period (Part C; N = 20). The CL-1719 study is an ongoing phase III, open-label, single-arm extension study evaluating the long-term safety and efficacy of evinacumab in patients with HoFH (including patients rolled in from the ELIPSE trial). A total of ||| patients were included in the interim analysis: || who were evinacumab naive, and || who had prior evinacumab exposure.
The primary end point of the ELIPSE and CL-17100 studies was the percent change from baseline in LDL-C to week 24, with important secondary outcomes in the ELIPSE trial consisting of the proportion of patients with a greater than or equal to 30% reduction in LDL-C, the proportion of patients with LDL-C less than 100 mg/dL or less than 70 mg/dL, and the proportion of patients who meet US or EU apheresis criteria. The secondary outcomes in the CL-17100 study were consistent with the secondary outcomes of the ELIPSE trial, focusing on lipid parameters (Apo B, non-HDL-C, and total cholesterol). The CL-1719 study did not seek to address a specific research hypothesis and was observational in nature, following a cohort of patients receiving evinacumab.
There were some differences across the evinacumab and placebo groups in the ELIPSE trial, particularly with regard to patient demographics, including differences in mean age (36.7 years in the placebo group versus 44.3 years in the evinacumab group), body mass index of greater than or equal to 30 kg/m2 (25.6% in the evinacumab group versus 13.6% in the placebo group), and mean time from HoFH diagnosis to randomization (16.15 years in the evinacumab group versus 10.65 years in the placebo group). Additionally, there were some differences between the evinacumab and placebo groups in patient genetic profile, as 39.5% versus 9.1% of patients had homozygous defective/defective LDLR mutations, 9.3% versus 22.7% of patients had homozygous negative/negative LDLR mutations, and 27.9% versus 36.4% (evinacumab group versus placebo group) had compound heterozygous LDLR mutations. Importantly, the mean LDL-C at baseline of 259.5 mg/dL (6.7 mmol/L) in the evinacumab group was comparable to the mean of 246.5mg/dL (6.4 mmol/L) in the placebo group. The patients included in Parts B and C of the CL-17100 study were mostly white (70.0%), and their mean age was 9.0 years (SD = 1.84). Half of the patients in Part B and 60% in Parts B and C had prior or ongoing apheresis, and all patients had received prior LLT. The mean LDL-C at baseline was higher than in the ELIPSE trial at 301.9 mg/dL (7.819 mmol/L).
One sponsor-submitted ITC was summarized and critically appraised, consisting of a Bucher ITC that naively compared evinacumab and evolocumab for the outcome of percent change from baseline in LDL-C and a MAIC comparing evinacumab to lomitapide and to ezetimibe for the outcome of percent change from baseline in LDL-C and proportion of patients with a greater than or equal to 50% reduction in LDL-C in patients with HoFH.
The CL-1719 study is an ongoing, long-term, open-label study, aiming to evaluate the safety, tolerability, and efficacy of evinacumab in adolescent patients aged 12 years and older, but younger than 18 years, and adult patients aged 18 years and older with HoFH. The study by Stefanutti et al. (2022) was an open-label, 24-month cohort study to evaluate the efficacy and safety of evinacumab in patients with HoFH with or without LDL apheresis.
Interpretation of Results
Efficacy
The efficacy of evinacumab in pediatric and adult patients with HoFH was informed by 2 pivotal RCTs: the ELIPSE trial, which enrolled 65 patients with HoFH aged 12 years and older, and the CL-17100 study, which enrolled 20 patients with HoFH aged between 5 and 11 years. Evinacumab is a first-in-class treatment and is currently the only drug indicated for use in children aged 5 to 11 years with HoFH. As a rare disease, the small sample size of the included studies was expected, though the impact of the small sample size on the magnitude of treatment effect remains unknown. It resulted in downgrading for imprecision in the assessment of the certainty of evidence by GRADE. The clinical experts consulted by CADTH also highlighted that the enrolled patients were generally similar to patients in real-world clinical practice despite the small sample sizes. The key genetic and clinical inclusion criteria were similar across both trials and aligned with clinical practice guidelines per the clinical experts consulted by CADTH. The EAS guidelines have been recently updated to include other rare genetic defects (e.g., compound heterozygosity) and clinical criteria (LDL-C > 10 mmol/L rather than to 13 mmol/L) not previously included in the diagnostic criteria, though the experts noted that this change was unlikely to result in a drastic increase in the number of patients diagnosed with HoFH. In line with the enrolled population per the study inclusion and exclusion criteria, the proportion of patients receiving LLTs at baseline in the ELIPSE study was generally in line with Canadian registry data. The clinical experts noted that the proportion of patients receiving PCSK9 inhibitors in the ELIPSE trial was greater than current Canadian practice, though this reflects the current reimbursement landscape in Canada, as access to PCSK9 inhibitors is limited and difficult due to logistical delays. The experts noted that treatment with PCSK9 inhibitors should be attempted in patients with HoFH as a method of standard of care regardless of the mechanism of action of these treatments.
The included studies shared primary and secondary outcomes focusing on lowering LDL-C, which were considered clinically important in the management of HoFH. In the ELIPSE trial, evinacumab was superior to placebo for the primary outcome of percent change from baseline in LDL-C to week 24, as well as for most secondary outcomes. The ELIPSE study demonstrated a –49.0% (95% CI, –65.0 to –33.1) change in LDL-C between evinacumab and placebo, in favour of evinacumab. Additionally, the absolute change from baseline in LDL-C between evinacumab and placebo was –132.1 mg/dL (95% CI, –175.3 to –88.9). The overall interpretation of the lipid-lowering results from the CL-17100 study was limited given the potential for violations of the internal and external validity. Specifically, the single-arm and open-label design precluded the ability to attribute the observed changes in LDL-C entirely to treatment with evinacumab as opposed to the natural history of the disease or other concurrent treatments. However, the within-group results of the CL-17100 study in pediatric patients were similar to the within-group results of the ELIPSE trial, supporting the use of evinacumab in this population. Per the clinical practice guidelines, and as stated by the clinical expert panel and by the clinician group, a reduction of 20% to 30% or upwards of 50% or more in LDL-C (as used in clinical trials) would be considered clinically meaningful responses to treatment. In the ELIPSE trial, 83.7% and 18.2% of patients in the evinacumab and placebo groups, respectively, experienced at least a 30% reduction in LDL-C, though as noted in the clinical expert panel summary, any safe reduction in LDL-C is impactful, so long as the risk-benefit profile is favourable. In addition to percent and absolute change in LDL-C, reaching lipid targets is an important aspect of treating patients with HoFH. The clinical experts consulted by CADTH highlighted that the target plasma LDL-C thresholds of 2.5 mmol/L (100 mg/dL) for primary prevention and 1.81 mmol/L (70 mg/dL) for secondary prevention are pragmatic, with current guidelines stating that these cut-offs are likely obsolete.11 As mentioned, the clinical experts expressed that treatment for HoFH should continue to aim for the lowest and safest reduction in LDL-C possible, irrespective of current guidelines. In the ELIPSE trial, 18.2% of patients in the placebo group experienced at least a 30% reduction in LDL-C, and 22.7% of patients in the placebo group reached LDL-C levels less than 100 mg/dL. The reason for the high placebo response is unclear; however, it may be related to background treatment of statin, ezetimibe, PCSK9 inhibitor, or lomitapide and apheresis.
The pathophysiology of HoFH renders most currently available treatments ineffective given that their mechanism of action relies on functional LDLR to reduce LDL-C. Evinacumab acts via an LDLR-independent mechanism. The results of the subgroup analysis of the ELIPSE trial by HoFH genotype (null/null versus not null/null and negative/negative versus not negative/negative) for the primary efficacy end point were consistent with those for the primary analysis. Though these results suggest that evinacumab is effective in both groups, resulting in response regardless of mutation, they should only be viewed as supportive of the overall effect of evinacumab.
Patients highlighted the need for treatments that, on top of lowering LDL-C levels, reduce the risk of CV events and reduce the frequency of and the need for apheresis. The outcome of reduced risk of CV-related morbidity (i.e., major adverse cardiac events) and mortality were considered clinically important outcomes relevant to this review; however, they were not evaluated in the included studies. Though the relationship between LDL-C and risk of CV-related morbidity and mortality has been recognized for statins, it remains uncertain whether the reductions in percentage and absolute levels of LDL-C observed with evinacumab will translate into a reduction in clinically significant CV morbidity. Though estimated before the introduction of evinacumab, a reduction of 1 mmol/L (approximately 38.67 mg/dL) in LDL-C is estimated to reduce the relative risk of ASCVD by 20% to 22% in patients with hypercholesterolemia.8
No method of evaluating reduction in the frequency or need for apheresis was performed in the included studies. Based on the results of subgroup analyses in the ELIPSE trial, evinacumab is effective in patients who are and who are not receiving background apheresis, though these results were only considered supportive. The secondary outcomes of patients who meet the US and EU apheresis eligibility criteria were included; however, the clinical experts consulted by CADTH highlighted that such criteria are not used in Canada and are overly inclusive (US criteria: LDL-C ≥ 300 mg/dL [7.77 mmol/L]; EU criteria: LDL-C > 160 mg/dL [4.2 mmol/L] for primary prevention or LDL-C > 120 mg/dL [3.1 mmol/L] for secondary prevention), which the experts considered unsupportable by the Canadian health care system. Additionally, the experts noted that in Canada, pheresis eligibility is discussed on an individual basis with patients and hospital administration and is reviewed by other lipid experts. The experts also highlighted that determining the effect of LLTs in combination with pheresis may be difficult in a clinical trial of short duration given the LDL-C rebound that occurs following apheresis treatment.
The included studies were 24 weeks in duration with additional 24-week open-label treatment and extension periods. The clinical experts consulted by CADTH noted that 24 weeks is sufficient for determining changes in lipoproteins but insufficient for determining long-term outcomes of treatment (e.g., improvements in HRQoL) or event-driven outcomes, including CV-related morbidity or mortality. HRQoL in the ELIPSE trial was an exploratory outcome, and given the short duration of the trial, the results should only be viewed as supportive of the overall effect of evinacumab; the true impact of evinacumab on HRQoL remains unknown.
The sponsor-submitted ITC compared the efficacy and safety of evinacumab to drug comparators of evinacumab via a naive Bucher ITC and to lomitapide and ezetimibe via MAIC. The ITCs did not conduct appropriate comparisons to relevant standard of care comparators, and the trial populations were considered too varied in their baseline characteristics, particularly age, presence of CHD, LDL-C level at baseline, apheresis status, and mutation status, resulting in significant reductions in sample size and imprecise efficacy estimates with wide 95% CIs. As such, the comparative efficacy of evinacumab could not be concluded from the submitted indirect evidence.
In addition to the ELIPSE and CL-17100 studies and the sponsor-submitted ITC, 1 long-term extension study (the CL-1719 study) and 1 study addressing gaps in the literature (Stefanutti et al. [2022]) were also submitted by the sponsor. The results of these studies were supportive of the ELIPSE and CL-17100 studies, reporting similar percent reductions in LDL-C throughout the duration of treatment, though no conclusions could be drawn on the impact of age or LDL apheresis status.
Harms
Analysis of safety for evinacumab was based on the SAS, which included 44 patients treated with evinacumab in the double-blind treatment period of the ELIPSE trial, 64 patients in the open-label treatment period of the ELIPSE trial, and 20 patients treated with evinacumab in the CL-17100 study. The incidence of harms reported in the ELIPSE trial was well balanced between the evinacumab and placebo groups, with an occurrence of TEAEs being 65.9% with evinacumab and 81.0% with placebo, while nearly all patients in the CL-17100 study experienced a TEAE with evinacumab. The reason that patients had fewer TEAEs in the evinacumab group of the ELIPSE trial remains unclear, though it is believed to be due to random chance given the small sample size. There were no important or consistent differences in SAEs, withdrawals due to AEs, or most notable harms between the placebo and evinacumab groups of the double-blind treatment period of the ELIPSE trial or in the patients receiving evinacumab in the open-label treatment period of the ELIPSE trial or in the CL-17100 study. Per the clinical experts consulted by CADTH, the most important AEs for evinacumab are IRRs, given the method of administration; however, the experts noted that IRRs are generally manageable. The experts also noted that the AESIs evaluated for evinacumab are based on treatment with statins. Overall, there were no concerns from the clinical experts consulted by CADTH about the notable harms from the included studies.
The safety of evinacumab compared with other relevant treatments for HoFH could not be assessed due to the use of placebo as a comparator in the ELIPSE study and the lack of a comparator arm in the CL-17100 study. As such, the sponsor submitted an ITC to attempt to determine the safety of evinacumab compared to lomitapide and evolocumab in terms of the proportion of patients who experienced any SAEs and the proportion of patients discontinuing the study due to any cause. However, as no formal indirect analysis was conducted on these outcomes, the comparative effect of evinacumab on safety remains unknown. Evinacumab was generally well tolerated in the included studies; however, the experts noted that given the small sample size, new safety signals identified when used in clinical practice could warrant discontinuation. However, HoFH is a life-long condition, and the short duration of the ELIPSE and CL-17100 studies limits the ability to assess the long-term safety of evinacumab. The currently ongoing open-label CL-1719 study aims to address this gap and provide additional long-term safety data for evinacumab up to 4 years. Based on their own experience with evinacumab thus far, the clinical experts consulted by CADTH indicated the observed AEs associated with evinacumab have been manageable.
Conclusion
HoFH is a rare disease, and there is an unmet need for new, safe, and effective treatments for this population of patients who have depleted all other options and require additional LDL-C lowering. Evinacumab is a first-in-class treatment that acts in an LDLR-independent manner to reduce LDL-C levels. Two studies were included in this review — the phase III, double-blind, randomized ELIPSE trial and the single-arm, open-label CL-17100 study — evaluating the efficacy and safety of evinacumab as adjunct to diet and stable maximum doses of LLTs in pediatric and adult patients with HoFH.
The ELIPSE study demonstrated that evinacumab likely resulted in a clinically important decrease (improvement) in LDL-C levels when compared with placebo beyond the threshold of clinically important reductions of 30%, as defined by clinical experts and clinical practice guidelines, which was further supported by the CL-17100 study. Treatment with evinacumab was well tolerated over the study period and did not appear to be associated with more AEs or SAEs than placebo. Known AEs of interest, such as IRRs, were slightly more frequent in the evinacumab group; however, there were no concerns. The included studies had a short treatment duration of only 24 weeks, which was sufficient to address the primary outcome of change in LDL-C but precluded the ability to assess long-term efficacy and safety, as well as HRQoL. Though considered outcomes of importance to patients, reduction in CV risk, (including CV-related morbidity and mortality), as well as reduction in the need for and frequency of apheresis, were not evaluated in the included studies; thus, the impact of evinacumab on these outcomes is unknown.
There were important technical limitations in the conduct of the ITCs: the included studies varied in design, did not include all relevant standard of care treatments, and had differences between the included populations. As such, the results of the ITCs were inconclusive and imprecise given the large reduction in sample sizes and wide 95% CIs.
Overall, the results of the included studies were generally positive, supporting the use of evinacumab in pediatric and adult patients with HoFH; however, there were important limitations in the studies — such as the small sample size, the short duration of follow-up, the single-arm open-label design of the CL-17100 study, and the lack of direct comparative evidence — that limit the generalizability of the study results to a broader population with HoFH.
References
1.Brunham LR, Ruel I, Aljenedil S, et al. Canadian Cardiovascular Society position statement on familial hypercholesterolemia: update 2018. Can J Cardiol. 2018;34(12):1553-1563. PubMed
2.Marbach JA, McKeon JL, Ross JL, Duffy D. Novel treatments for familial hypercholesterolemia: pharmacogenetics at work. Pharmacotherapy. 2014;34(9):961-972. PubMed
3.Nordestgaard BG, Chapman MJ, Humphries SE, et al. Familial hypercholesterolaemia is underdiagnosed and undertreated in the general population: guidance for clinicians to prevent coronary heart disease: consensus statement of the European Atherosclerosis Society. Eur Heart J. 2013;34(45):3478-3490a. PubMed
4.Sniderman AD, Tsimikas S, Fazio S. The severe hypercholesterolemia phenotype: clinical diagnosis, management, and emerging therapies. J Am Coll Cardiol. 2014;63(19):1935-1947. PubMed
5.Brunham LR, Ruel I, Khoury E, et al. Familial hypercholesterolemia in Canada: initial results from the FH Canada national registry. Atherosclerosis. 2018;277:419-424. PubMed
6.Ference BA, Ginsberg HN, Graham I, et al. Low-density lipoproteins cause atherosclerotic cardiovascular disease. 1. Evidence from genetic, epidemiologic, and clinical studies. A consensus statement from the European Atherosclerosis Society Consensus Panel. Eur Heart J. 2017;38(32):2459-2472. PubMed
7.Gidding SS, Champagne MA, de Ferranti SD, et al. The agenda for familial hypercholesterolemia: a scientific statement from the American Heart Association. Circulation. 2015;132(22):2167-2192. PubMed
8.Silverman MG, Ference BA, Im K, et al. Association between lowering LDL-C and cardiovascular risk reduction among different therapeutic interventions: a systematic review and meta-analysis. JAMA. 2016;316(12):1289-1297. PubMed
9.Turgeon RD, Barry AR, Pearson GJ. Familial hypercholesterolemia: review of diagnosis, screening, and treatment. Can Fam Physician. 2016;62(1):32-37. PubMed
10.Obradovic M, Zaric B, Sudar-Milovanovic E, et al. PCSK9 and hypercholesterolemia: therapeutic approach. Curr Drug Targets. 2018;19(9):1058-1067. PubMed
11.Cuchel M, Raal FJ, Hegele RA, et al. 2023 update on European Atherosclerosis Society Consensus Statement on homozygous familial hypercholesterolaemia: new treatments and clinical guidance. Eur Heart J. 2023;44(25):2277-2291. PubMed
12.Alonso R, Perez de Isla L, Muniz-Grijalvo O, Diaz-Diaz JL, Mata P. Familial hypercholesterolaemia diagnosis and management. Eur Cardiol. 2018;13(1):14-20. PubMed
13.Ibrahim MA, Asuka E, Jialal I. Hypercholesterolemia [updated 2023 Apr 23]. StatPearls. StatPearls Publishing: Treasure Island (FL); 2020: https://www.ncbi.nlm.nih.gov/books/NBK459188/. Accessed 2023 Jun 08.
14.Cuchel M, Bruckert E, Ginsberg HN, et al. Homozygous familial hypercholesterolaemia: new insights and guidance for clinicians to improve detection and clinical management. A position paper from the Consensus Panel on Familial Hypercholesterolaemia of the European Atherosclerosis Society. Eur Heart J. 2014;35(32):2146-2157. PubMed
15.Akioyamen LE, Genest J, Shan SD, et al. Estimating the prevalence of heterozygous familial hypercholesterolaemia: a systematic review and meta-analysis. BMJ Open. 2017;7(9):e016461. PubMed
16.de Ferranti SD, Rodday AM, Mendelson MM, Wong JB, Leslie LK, Sheldrick RC. Prevalence of familial hypercholesterolemia in the 1999 to 2012 United States National Health and Nutrition Examination Surveys (NHANES). Circulation. 2016;133(11):1067-1072. PubMed
17.Goldstein JL, Hobbs HH, Brown MS. Familial hypercholesterolemia. In: Scriver CR, Beaudet A, Sly WS, Valle D, eds. The Metabolic and Molecular Bases of Inherited Disease. New York: McGraw-Hill; 2001:2863–2913.
18.Moorjani S, Roy M, Gagne C, et al. Homozygous familial hypercholesterolemia among French Canadians in Quebec Province. Arteriosclerosis. 1989;9(2):211-216. PubMed
19.Brown L, Ruel I, Baass A, et al. Design, rationale, and preliminary results of the Canadian Homozygous Familial Hypercholesterolemia Registry: 2008 to 2022 update. Can J Health Technol. 2023;3(2). https://canjhealthtechnol.ca/index.php/cjht/article/view/MG00197/MG00197. Accessed 2023 Nov 08.
20.Naveen T, Biswas A, Wig N, et al. Role of LDL apheresis in a case of homozygous familial hypercholesterolemia. Drug Discov Ther. 2019;13(1):59-61. PubMed
21.National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Third report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation. 2002;106(25):3143-3421. PubMed
22.Reeskamp LF, Millar JS, Wu L, et al. ANGPTL3 inhibition with evinacumab results in faster clearance of IDL and LDL apoB in patients with homozygous familial hypercholesterolemia-brief report. Arterioscler Thromb Vasc Biol. 2021;41(5):1753-1759. PubMed
23.Robciuc MR, Maranghi M, Lahikainen A, et al. Angptl3 deficiency is associated with increased insulin sensitivity, lipoprotein lipase activity, and decreased serum free fatty acids. Arterioscler Thromb Vasc Biol. 2013;33(7):1706-1713. PubMed
24.Lambert CT, Sandesara P, Isiadinso I, et al. Current treatment of familial hypercholesterolaemia. Eur Cardiol. 2014;9(2):76-81. PubMed
25.Anderson TJ, Gregoire J, Pearson GJ, et al. 2016 Canadian Cardiovascular Society guidelines for the management of dyslipidemia for the prevention of cardiovascular disease in the adult. Can J Cardiol. 2016;32(11):1263-1282. PubMed
26.Watts GF, Gidding S, Wierzbicki AS, et al. Integrated guidance on the care of familial hypercholesterolemia from the International FH Foundation. J Clin Lipidol. 2014;8(2):148-172. PubMed
27.Atherosclerotic Cardiovascular Disease (ASCVD) secondary prevention guideline. Washington (DC): Kaiser Permanente; 2023: https://wa.kaiserpermanente.org/static/pdf/public/guidelines/ascvd-secondary.pdf. Accessed 2023 Jun 08.
28.Clinical Study Report: R1500-CL-17100. A three-part, single-arm, open-label study to evaluate the efficacy, safety, and pharmacokinetics of evinacumab in pediatric patients with homozygous familial hypercholesterolemia [internal sponsor's report]. Tarrytown (NY): Regeneron Pharmaceuticals, Inc.; 2022 Sep 16.
29.Clinical Study Report: R1500-CL-1629. A randomized, double-blind, placebo-controlled, parallel-group study to evaluate the efficacy and safety of evinacumab in patients with homozygous familial hypercholesterolemia [internal sponsor's report]. Tarrytown (NY): Regeneron Pharmaceuticals, Inc.; 2020.
30.Balshem H, Helfand M, Schunemann HJ, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011;64(4):401-406. PubMed
31.Santesso N, Glenton C, Dahm P, et al. GRADE guidelines 26: informative statements to communicate the findings of systematic reviews of interventions. J Clin Epidemiol. 2020;119:126-135. PubMed
32.Guyatt GH, Oxman AD, Kunz R, et al. GRADE guidelines 6. Rating the quality of evidence--imprecision. Journal of clinical epidemiology. 2011;64(12):1283-1293. PubMed
33.Kronmal RA. Spurious correlation and the fallacy of the ratio standard revisited. J R Stat Soc Ser A Stat Soc. 1993;156(3):379-392.
34.3719: Statistical Analysis Comparing Evinacumab with Comparator Treatments for Homozygous Familial Hypercholesterolemia [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Evkeeza (evinacumab), 150 mg/mL concentrate in 345 mg and 1 200 mg single-dose vials, solution for IV infusion. Novato (CA): Ultragenyx Pharmaceutical Inc.; 2022 May 31.
35.Phillippo DM, Ades AE, Dias S, Palmer S, Abrams KR, Welton NJ. Methods for population-adjusted indirect comparisons in health technology appraisal. Med Decis Making. 2018;38(2):200-211. PubMed
36.Roth GA, Johnson C, Abajobir A, et al. Global, regional, and national burden of cardiovascular diseases for 10 causes, 1990 to 2015. J Am Coll Cardiol. 2017;70(1):1-25. PubMed
37.Virani SS, Alonso A, Benjamin EJ, et al. Heart disease and stroke statistics-2020 update: a report from the American Heart Association. Circulation. 2020;141(9):e139-e596. PubMed
38.World Health Organization. Cardiovascular diseases (CVDs). 2021; https://www.who.int/en/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds). Accessed 2023 Jun 08.
39.American Heart Association. What is cardiovascular disease? 2017; https://www.heart.org/en/health-topics/consumer-healthcare/what-is-cardiovascular-disease. Accessed 2023 Jun 08.
40.Grundy SM, Stone NJ, Bailey AL, et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA guideline on the management of blood cholesterol: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2019;139(25):e1082-e1143. PubMed
41.Raal FJ, Hovingh GK, Catapano AL. Familial hypercholesterolemia treatments: guidelines and new therapies. Atherosclerosis. 2018;277:483-492. PubMed
42.Bruckert E. Recommendations for the management of patients with homozygous familial hypercholesterolaemia: overview of a new European Atherosclerosis Society consensus statement. Atheroscler Suppl. 2014;15(2):26-32. PubMed
43.Neefjes LA, Ten Kate GJ, Rossi A, et al. CT coronary plaque burden in asymptomatic patients with familial hypercholesterolaemia. Heart. 2011;97(14):1151-1157. PubMed
44.National Institute for Health and Care Excellence. Evinacumab for treating homozygous familial hypercholesterolaemia in people aged 12 years and over [ID2704]. (In development GID-TA10655) 2023; https://www.nice.org.uk/guidance/indevelopment/gid-ta10655. Accessed 2023 Jun 15.
45.Drug Reimbursement Review sponsor submission: Evkeeza (evinacumab), 150 mg/mL concentrate in 345 mg and 1 200 mg single-dose vials, solution for IV infusion [internal sponsor's package]. Novato (CA): Ultragenyx Pharmaceutical Inc.; 2023 May 10.
46.Evkeeza (evinacumab): 150 mg/mL concentrate solution for infusion, in single-dose vials [product monograph]. Oakville (ON): Innomar Strategies, Inc.; 2023 Sep 22.
47.Drug Reimbursement Review clinical and pharmacoeconomic reviews: inclisiran (Leqvio) for primary hypercholesterolemia. Can J Health Technol. 2022;2(4). https://canjhealthtechnol.ca/index.php/cjht/article/view/sr0681r/sr0681r. Accessed 2023 July 10.
48.Clinical Study Report: R1500-CL-1719. An open-label study to evaluate the long-term safety and efficacy of evinacumab in patients with homozygous familial hypercholesterolemia [internal sponsor's report]. Tarrytown (NY): Regeneron Pharmaceuticals, Inc.; 2022 Nov 10.
49.Stefanutti C, Chan DC, Di Giacomo S, Morozzi C, Watts GF. Long-term efficacy and safety of evinacumab in patients with homozygous familial hypercholesterolemia: real-world clinical experience. Pharmaceuticals (Basel). 2022;15(11):1389. PubMed
50.Raal FJ, Rosenson RS, Reeskamp LF, et al. Evinacumab for homozygous familial hypercholesterolemia. N Engl J Med. 2020;383(8):711-720. PubMed
51.Mehrotra DV, Li X, Liu J, Lu K. Analysis of longitudinal clinical trials with missing data using multiple imputation in conjunction with robust regression. Biometrics. 2012;68(4):1250-1259. PubMed
Appendix 1: Detailed Outcome Data
Note that this appendix has not been copy-edited.
Figure 3: Mean Percent Change From Baseline in LDL-C by Double-Blind Treatment Group in the Double-Blind and Open-Label Treatment Period (SAS Population)
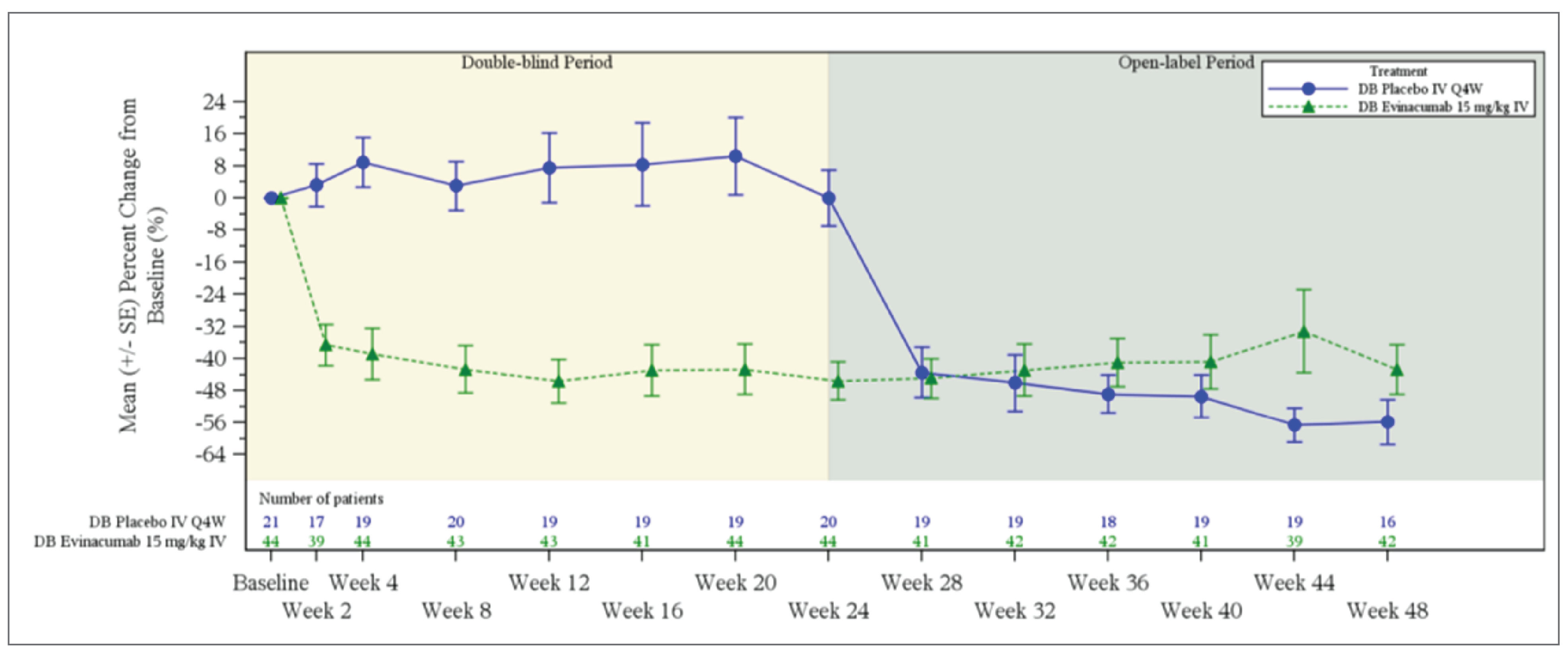
DB = double blind; LDL-C = low-density lipoprotein cholesterol; LS = least square; Q4W = every 4 weeks; SE = standard error.
Source: ELIPSE Clinical Study Report.29
Figure 4: Mean Percent Change From Baseline in LDL-C in Part B of the CL-17100 Study (ITT Population)
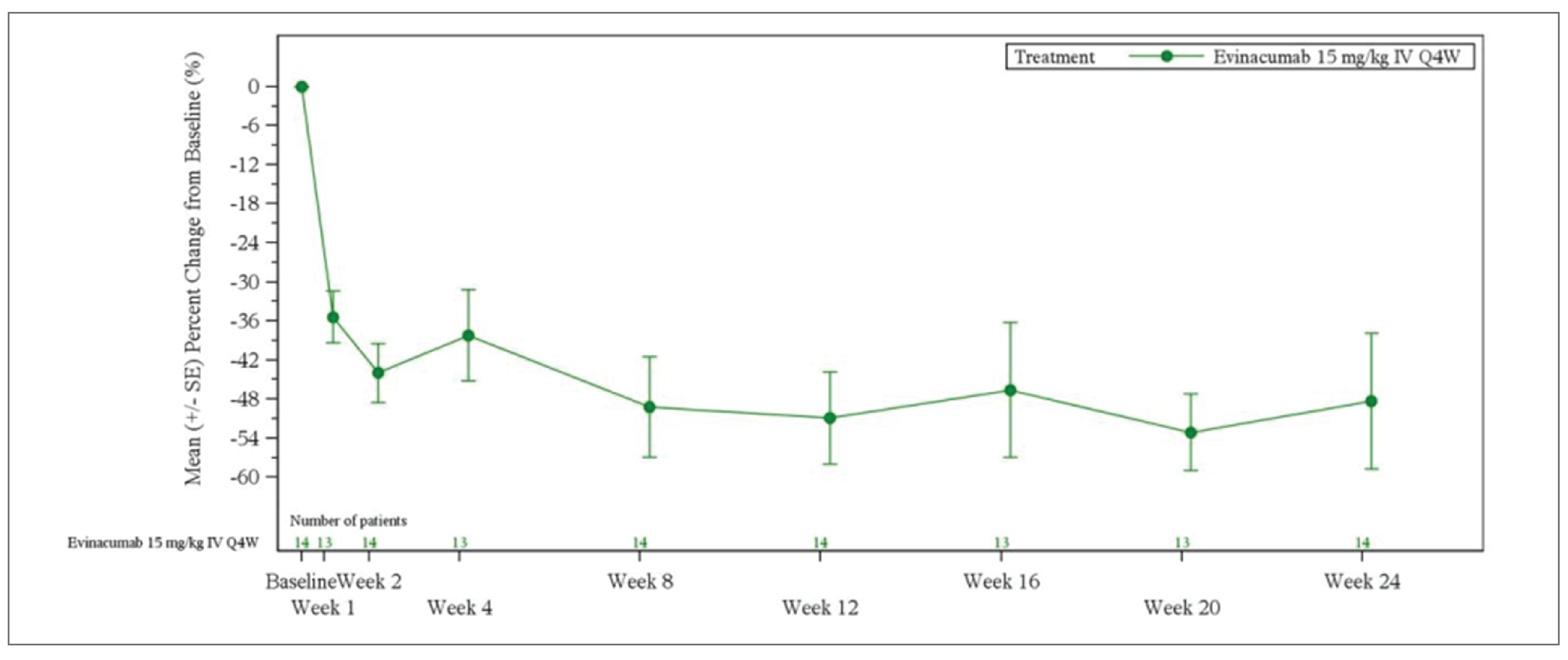
DB = double blind; LDL-C = low-density lipoprotein cholesterol; LS = least square; Q4W = every 4 weeks; SE = standard error.
Source: CL-17100 Clinical Study Report.28
Figure 5: Mean Percent Change From Baseline in LDL-C for Pooled Parts B and C (Pooled SAS) [Redacted]

DB = double blind; LDL-C = low-density lipoprotein cholesterol; LS = least square; Q4W = every 4 weeks; SE = standard error.
Source: CL-17100 Clinical Study Report.28
Table 26: Subgroup Analysis by Background LLT at Baseline at Week 24 (ELIPSE ITT)
LLT | LLT at Baseline | No LLT at Baseline | ||
|---|---|---|---|---|
Placebo | Evinacumab | Placebo | Evinacumab | |
Statin | ||||
Statin at baseline, N | 20 | 41 | 2 | 2 |
Percent CFB in LDL-C | ||||
N at week 24 | 19 | 41 | 2 | 2 |
Mean (SD) | 2.17 (32.34) | –47.29 (30.58) | –5.70 (22.69) | –46.24 (11.01) |
Ezetimibe | ||||
Ezetimibe at baseline, N | 16 | 33 | 6 | 10 |
Percent CFB in LDL-C | ||||
N at week 24 | 16 | 33 | 5 | 10 |
Percent CFB in LDL-C, mean (SD) | –1.95 (30.58) | –53.07 (20.97) | 12.20 (34.14) | –28.02 (45.52) |
PCSK9 inhibitor | ||||
PCSK9 inhibitor at baseline, N | 16 | 34 | 6 | 9 |
Percent CFB in LDL-C | ||||
N at week 24 | 15 | 34 | 6 | 9 |
Percent CFB in LDL-C, mean (SD) | 1.73 (30.34) | –49.45 (31.87) | 0.65 (36.22) | –38.93 (20.07) |
Lomitapide | ||||
Lomitapide at baseline, N | 3 | 11 | 19 | 32 |
Percent CFB in LDL-C | ||||
N at week 24 | 3 | 11 | 18 | 32 |
Percent CFB in LDL-C, mean (SD) | –17.22 (47.62) | –49.64 (22.55) | 4.53 (28.39) | –46.42 (32.31) |
CFB = change from baseline; LDL-C = low-density lipoprotein cholesterol; LLT = lipid-lowering therapy; SD = standard deviation.
Source: ELIPSE Clinical Study Report.29
Table 27: Subgroup Analysis of Percent CFB in LDL-C by Apheresis Status and Baseline LDL-C
Subgroup | ELIPSE | CL-17100 Part B (ITT) | ||||
|---|---|---|---|---|---|---|
DBTP (ITT)a | OLTP (SAS)b | |||||
Placebo (N = 22) | Evinacumab (N = 43) | From DB placebo group (N = 20) | From DB evinacumab group (N = 44) | Open-label evinacumab (N = 64) | Evinacumab (N = 14) | |
Baseline apheresis status – yes | ||||||
N | 8 | 14 | 7 | 13 | 20 | 7 |
Percent CFB in LDL-C, LS mean (SE) | –8.3 (11.6) | –46.5 (8.8) | –43.07 (13.74) | –44.26 (17.47) | –43.84 (15.90) | –47.9 (12.5) |
LSMD (SE) vs. placebo | — | –38.3 (13.4) | NA | NA | NA | NA |
95% CI | — | –65.1 to –11.5 | NA | NA | NA | –72.3 to –23.4 |
Baseline apheresis status – no | ||||||
N | 14 | 29 | 9 | 29 | 38 | 7 |
Percent CFB in LDL-C, LS mean (SE) | 7.9 (8.4) | –47.3 (5.9) | –65.70 (23.48) | –42.00 (47.02) | –47.62 (43.55) | –48.8 (17.8) |
LSMD (SE) vs. placebo | — | –55.2 (9.9) | NA | NA | NA | NA |
95% CI | — | –75.1 to –35.4 | NA | NA | NA | –83.7 to –13.9 |
Baseline LDL-C < 130 mg/dL | ||||||
N | 5 | 9 | NR | NR | NR | NR |
Percent CFB in LDL-C, LS mean (SE) | –4.6 (13.4) | –27.3 (10.2) | NR | NR | NR | NR |
LSMD (SE) vs. placebo | — | –22.7 (16.9) | NR | NR | NR | NR |
95% CI | — | –56.6 to 11.2 | NR | NR | NR | NR |
Baseline LDL-C ≥ 130 mg/dL | ||||||
N | 17 | 34 | NR | NR | NR | NR |
Percent CFB in LDL-C, LS mean (SE) | 4.8 (7.4) | –52.5 (5.2) | NR | NR | NR | NR |
LSMD (SE) vs. placebo | — | –57.3 (9.0) | NR | NR | NR | NR |
95% CI | — | –75.3 to –39.4 | NR | NR | NR | NR |
CI = confidence interval; CRF = case report form; LDL-C = low-density lipoprotein cholesterol; LSM = least squares mean; ROW = rest of world.
aValues for change from baseline are at week 24.
bValues for change from baseline are at week 48 of open-label treatment. Values reported as SE are SD in the open-label treatment period.
Sources: ELIPSE Clinical Study Report;29 CL-17100 Clinical Study Report.28
Table 28: Subgroup Analysis of Percent CFB in LDL-C According to HoFH Genotype
Subgroup | ELIPSE | CL-17100 Part B | ||||
|---|---|---|---|---|---|---|
DBTP (ITT)a | OLTP (SAS)b | |||||
Placebo (N = 22) | Evinacumab (N = 43) | From DB placebo group (N = 20) | From DB evinacumab group (N = 44) | Open-label evinacumab (N = 64) | Evinacumab (N = 14) | |
Homozygous | ||||||
N | 8 | 22 | NR | NR | NR | NR |
Percent CFB in LDL-C, LS mean (SE) | |||| |||||| | ||||| ||||| | NR | NR | NR | NR |
LSMD (SE) vs. placebo | ||| | ||||| |||||| | NR | NR | NR | NR |
95% CI | ||| | |||||| ||||| | NR | NR | NR | NR |
Compound heterozygous | ||||||
N | 8 | 12 | NR | NR | NR | NR |
Percent CFB in LDL-C, LS mean (SE) | |||| |||||| | ||||| ||||| | NR | NR | NR | NR |
LSMD (SE) vs. placebo | ||| | ||||| |||||| | NR | NR | NR | NR |
95% CI | ||| | |||||| ||||| | NR | NR | NR | NR |
Double Heterozygous | ||||||
N | 1 | 2 | NR | NR | NR | NR |
Percent CFB in LDL-C, LS mean (SE) | ||||| |||||| | ||||| |||||| | NR | NR | NR | NR |
LSMD (SE) vs. placebo | ||| | ||||| |||||| | NR | NR | NR | NR |
95% CI | ||| | |||||| |||| | NR | NR | NR | NR |
Other | ||||||
N | 5 | 7 | NR | NR | NR | NR |
Percent CFB in LDL-C, LS mean (SE) | ||| |||||| | ||||| |||||| | NR | NR | NR | NR |
LSMD (SE) vs. placebo | ||| | ||||| |||||| | NR | NR | NR | NR |
95% CI | ||| | |||||| ||| | NR | NR | NR | NR |
Negative/negative | ||||||
N | ||| | ||| | ||| | ||| | ||| | ||| |
Percent CFB in LDL-C, LS mean (SE) | |||| |||||| | ||||| |||||| | |||||| |||||||| | |||||| |||||||| | |||||| |||||||| | ||||| ||||| |
LSMD (SE) vs. placebo | ||| | ||||| |||||| | ||| | ||| | ||| | || |
95% CI | ||| | |||||| ||||| | ||| | ||| | ||| | |||||| ||||| |
Null/null | ||||||
N | ||| | ||| | ||| | ||| | ||| | ||| |
Percent CFB in LDL-C, LS mean (SE) | |||| |||||| | ||||| ||||| | |||||| |||||||| | |||||| |||||||| | |||||| |||||||| | ||||| ||||| |
LSMD (SE) vs. placebo | | | ||||| |||||| | ||| | ||| | ||| | || |
95% CI | | | |||||| ||||| | ||| | ||| | ||| | ||| |
Not negative/negative | ||||||
N | || | || | || | || | || | || |
Percent CFB in LDL-C, LS mean (SE) | |||| ||||| | ||||| ||||| | |||||| |||||||| | |||||| |||||||| | |||||| |||||||| | ||||| |||||| |
LSMD (SE) vs. placebo | ||| | |||| ||||| | ||| | ||| | ||| | || |
95% CI | ||| | |||||| ||||| | ||| | ||| | ||| | |||||| ||||| |
Not null/null | ||||||
N | || | || | || | || | || | || |
Percent CFB in LDL-C, LS mean (SE) | |||| ||||| | ||||| ||||| | |||||| |||||||| | |||||| |||||||| | |||||| |||||||| | ||||| |||||| |
LSMD (SE) vs. placebo | ||| | ||||| ||||| | ||| | ||| | ||| | || |
95% CI | ||| | |||||| ||||| | ||| | ||| | ||| | |||||| ||||| |
CI = confidence interval; LSM = least squares mean.
aValues for change from baseline are at week 24.
bValues for change from baseline are at week 48 of open-label treatment. Values reported as SE are SD in the open-label treatment period.
Sources: ELIPSE Clinical Study Report;29 CL-17100 Clinical Study Report.28
Pharmacoeconomic Review
Abbreviations
BIA
budget impact analysis
CTTC
Cholesterol Treatment Trialists’ Collaboration
CV
cardiovascular
HeFH
heterozygous familial hypercholesterolemia
HoFH
homozygous familial hypercholesterolemia
HRQoL
health-related quality of life
ICER
incremental cost-effectiveness ratio
LDL
low-density lipoprotein
LDL-C
low-density lipoprotein cholesterol
LLT
lipid-lowering therapy
MI
myocardial infarction
OCCI
Ontario Case Costing Initiative
QALY
quality-adjusted life-year
SOC
standard of care
TIA
transient ischemic attack
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Evinacumab (Evkeeza), 150 mg/mL (345 mg/2.3 mL and 1,200 mg/8 mL) solution in single-dose vials for IV infusion |
Submitted price | Evinacumab, 345 mg vial: $10,164 Evinacumab, 1,200 mg vial: $35,352 |
Indication | As an adjunct to diet and other low-density lipoprotein cholesterol–lowering therapies for the treatment of adult and pediatric patients aged 5 years and older with homozygous familial hypercholesterolemia |
Health Canada approval status | NOC |
Health Canada review pathway | Priority review |
NOC date | September 22, 2023 |
Reimbursement request | As per Health Canada indication |
Sponsor | Ultragenyx Pharmaceutical Inc. |
Submission history | Previously reviewed: No |
NOC = Notice of Compliance.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Markov model |
Target population | Patients aged 5 years and older with HoFH |
Treatment | Evinacumab as an adjunct to diet and SOC |
Comparator | SOC, comprising a treatment mix of statins, ezetimibe, PCSK9 inhibitors, and apheresis |
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | Lifetime (58 years) |
Key data sources | ELIPSE trial to inform LDL-C treatment response Published literature to inform relationship between LDL-C and cardiovascular event risk |
Submitted results | ICER = $3,729,349 per QALY gained (incremental cost = $6,534,304; incremental QALYs = 1.75) |
Key limitations |
|
CADTH reanalysis results |
|
HoFH = homozygous familial hypercholesterolemia; ICER = incremental cost-effectiveness ratio; LDL-C = low-density lipoprotein cholesterol; LY = life-year; QALY = quality-adjusted life-year; SOC = standard of care.
Conclusions
Based on the CADTH clinical review of the ELIPSE trial, treatment with evinacumab, when added to standard of care (SOC), likely resulted in a clinically important reduction in low-density lipoprotein cholesterol (LDL-C) compared with SOC alone in patients aged 5 years and older with homozygous familial hypercholesterolemia (HoFH). The reduction was beyond the threshold for clinically important reductions of 30%, as defined by clinical experts and practice guidelines. Overall, the safety profile of evinacumab was comparable to SOC. However, CADTH’s clinical review noted that the ELIPSE trial had a short duration of only 24 weeks, which precluded the ability to assess long-term efficacy and safety. Thus, the impact of evinacumab on reducing cardiovascular (CV)-related morbidity and mortality and on the need for apheresis is unknown.
While CADTH identified several limitations with the sponsor’s pharmacoeconomic analysis (with implications for the cost-effectiveness of evinacumab), CADTH’s findings are similar to the sponsor’s: evinacumab plus SOC is not cost-effective at conventionally accepted thresholds, with incremental cost-effectiveness ratios (ICERs) greater than $3.5 million per QALY gained when compared with SOC alone. The CADTH base case results in an ICER of $8,392,585 per quality-adjusted life-year (QALY) gained for evinacumab plus SOC compared with SOC alone. The probability of evinacumab being cost-effective at a $50,000 per QALY gained threshold is 0%. For evinacumab to be considered cost-effective at this threshold, the drug cost of evinacumab would need to be $9,217 per patient annually, reflecting a price reduction of approximately 98%.
Although CADTH attempted to address the identified limitations of the sponsor’s pharmacoeconomic model, a high degree of uncertainty remains. Most notably, the relationship between LDL-C reduction and CV outcomes for patients with HoFH remains unknown. Thus, the incremental QALY and life-year gains estimated for evinacumab may be overestimated, especially due to its relatively short duration, the ELIPSE trial was unable to assess CV morbidity and mortality outcomes. Despite the high estimated ICERs in CADTH’s and the sponsor’s analysis, the potential value of evinacumab is dependent on patients realizing the uncertain survival benefit compared to SOC alone (2.21 life-years in the sponsor’s base case, and 1.13 life-years in the CADTH base case). If the survival benefit of evinacumab is not realized, the ICER of evinacumab plus SOC compared to SOC alone will increase.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, registered clinicians, and drug plans that participated in the CADTH review process.
Patient input was received from the Canadian Heart Patient Alliance, which coordinated feedback with the Canadian Organization for Rare Disorders, Familial Hypercholesterolemia Canada, the Heart Healthy Prevention Program at St. Paul’s Hospital, and the Lipid Genetics Clinic at the London Health Sciences Centre–University Hospital. Patient input was gathered from 18 people: 10 patients with HoFH and 2 caregivers living in Canada via an online survey, and 6 individual interviews. Patients reported that living with HoFH is associated with ongoing physical and psychological struggles that have an impact on their quality of life. All patients reported experience with current SOC therapies, including apheresis, PCSK9 inhibitors, and statins but reported concerns about their effectiveness at controlling the patients’ LDL-C levels. Six patients who provided input had experience with evinacumab. All 6 patients reported positive outcomes from treatment with evinacumab, including lowering of their LDL-C levels and improvements in their quality of life. Specific improvements were related to increased energy levels, reduced frequency of apheresis, and increased ability to participate in activities of daily life, including attending work, school, and social events. None of the patients using evinacumab reported any serious adverse events.
Clinician input was received from Familial Hypercholesterolemia Canada, a national group of lipid specialists with experience with pediatric and adult patients. The clinicians noted that the treatment of HoFH is challenging due to the limited efficacy of most lipid-lowering drugs. An exception to this is lipoprotein apheresis, which can be effective for patients with HoFH but is costly, associated with a poor quality of life for patients and their families, and has barriers to access given its need to be administered at specialized centres. The clinician input indicated that there is a significant need for a safe, effective, and equitable approach to treatment for patients with HoFH. The clinicians noted that evinacumab has the potential to substantially lower LDL-C levels and that it is well tolerated with few side effects and has a minimal impact on health care resources and on patient and family burden compared to other lipid-lowering drugs. They indicated that it would be used as a third-line therapy after statins, ezetimibe, and PCSK9 inhibitors and would potentially reduce or eliminate the need for apheresis for some patients.
Drug plan input raised concerns about the comparator in the submitted trials. Specifically, it highlighted that lomitapide was being used by 21.5% of patients in the ELIPSE trial; however, lomitapide is not recommended for reimbursement by CADTH and is not widely available outside of Quebec. In addition, access to LDL-C apheresis also differs by jurisdiction. Further, the drug plan input noted that there is limited access for children to some comparators (e.g., PCSK9 inhibitors). The drug plan input also raised questions about evinacumab’s place in therapy with regard to how many lipid-lowering drugs would have to be tried before a patient was treated with evinacumab.
Several of these concerns were addressed in the sponsor’s model:
The sponsor’s submitted model accounted for quality of life and length of life.
Changes in apheresis over time were accounted for in the model and were reflected in changes in quality of life.
CADTH was unable to address the following concerns raised in stakeholder input:
Patient and caregiver burden is not included in the Canadian health care payer perspective, though HoFH is understood from stakeholder input to have an impact on patient and caregiver out-of-pocket costs and productivity.
Economic Review
The current review is for evinacumab (Evkeeza) for the treatment of patients aged 5 years and older with HoFH.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis comparing costs and outcomes for evinacumab as an adjunct to diet and other LDL-C–lowering therapies (i.e., SOC), with the SOC treatment mix including statins, ezetimibe, PCSK9 inhibitors, and apheresis.1 The model population comprised patients aged 5 years and older with HoFH. The modelled population was aligned with the anticipated Health Canada indication, the trial populations (ELIPSE trial and the CL-17100 study), and the sponsor’s reimbursement request.
Evinacumab is administered intravenously over 60 minutes, with a recommended dosage of 15 mg/kg every 4 weeks.2 Evinacumab is provided in either 345 mg or 1,200 mg vials, at a submitted price of $10,163.70 and $35,352.00 per vial, respectively. The cost of evinacumab every 4 weeks was estimated to be approximately $31,114, based on an average patient weight of 70.4 kg; however, this cost assumed perfect vial sharing (i.e., no drug wastage). The corresponding annual cost of evinacumab would be $405,863. In addition to drug costs, there are associated administration and monitoring costs.
For the base-case analysis, the sponsor considered SOC as the only relevant comparator, comprising a treatment mix of statins, ezetimibe, PCSK9 inhibitors, and apheresis. The model used a 1-year cycle length and simulated costs, life-years, and QALYs over a lifetime time horizon (58 years) from the perspective of Canada’s publicly funded health care system. Costs and QALYs were discounted at a rate of 1.5% per annum, and a half-cycle correction was applied.
Model Structure
The sponsor submitted a semi-Markov model consisting of the following mutually exclusive health states: stable HoFH, stable angina, post–stable angina, unstable angina, post–unstable angina, myocardial infarction (MI), post-MI, transient ischemic attack (TIA), post-TIA, stroke, poststroke, CV death, and non-CV death. The acute-event health states (i.e., stable angina, unstable angina, MI, TIA, and stroke) corresponded to a 1-year period in which the event occurred to account for reduced health-related quality of life (HRQoL) and increased health care costs. The postevent health states (i.e., post–stable angina, post–unstable angina, post-MI, post-TIA, and poststroke) represent the years following the event and account for the longer-term outcomes associated with each event. The sponsor’s model structure is depicted in Figure 1.
All patients entered the model in the stable HoFH health state (in which patients are assumed to be CV event naive) and remained in this health state until they underwent their first CV event (including CV death) or died from a non-CV cause. At the time of CV event, patients transitioned to the relevant acute-event health state for 1 cycle. Following that cycle, patients moved to the appropriate postevent health state (e.g., moved from the MI health state to the post-MI health state) or could experience another CV event. Patients in the postevent health states could transition back to the acute-event health states, with some exceptions: patients could not transition back to the stable angina, unstable angina, or TIA health states because the sponsor’s assumptions pertaining to HRQoL did not meet face validity to return to the postevent health state following more serious CV events (MI and stroke). The sponsor assumed that only 1 CV event can happen per annual cycle.
Model Inputs
Patient baseline characteristics in the model were informed by the ELIPSE trial (the CL-1629 study), which included patients aged 12 years and older, and by the CL-17100 study, which included patients aged 5 to 11 years, weighted using the age distribution of the general population living in Canada. It was estimated that 7.86% of patients were aged 5 to 11 years and that the remaining patients were aged 12 years or older. The mean age, weight, and baseline LDL-C in the model were 39 years (standard deviation = 14.9 years), 70.4 kg (standard deviation = 20.0 kg), and 6.6 mmol/L (standard deviation = 4.3 mmol/L), respectively.
Treatment efficacy relied exclusively on the results from the ELIPSE trial for the modelled population, citing that the results of the CL-17100 study were similar. Specifically, the trial results for a subset of patients who did not receive lomitapide was used to inform the model. The sponsor excluded patients who received lomitapide as it is not widely reimbursed in CADTH-participating jurisdictions and the treatment mix excluding lomitapide may be considered more reflective of that which patients with HoFH living in Canada would receive. The main efficacy measure from the ELIPSE trial was percent change from baseline in LDL-C to 24 weeks. The efficacy of SOC was modelled as 1 estimate of overall efficacy and was not linked to the proportion of patients on each background treatment. The sponsor assumed that as long as patients were on treatment, they experienced the full treatment effect on LDL-C corresponding to the treatment mix they were on. The sponsor’s base-case analysis assumed that no patients discontinued evinacumab in the short or long-term. The second efficacy-related measure, derived from a post hoc analysis of the ELIPSE trial results, was apheresis discontinuation at 24 weeks. Based on this analysis, the sponsor assumed that at 26 weeks there would be a 46.5% reduction in apheresis use for those on evinacumab and that there would be no reduction for those on SOC. The discontinuation of apheresis was associated with a change in cost but not in LDL-C levels.
Individual patient data from Thompson et al. (2015) was used to inform the baseline risks of CV events for the modelled population. This study was based on patients with HoFH in the UK between 1964 and 2014.3 The sponsor used the provided individual patient data to conduct survival analysis to model key outcomes, including time to CV death. Time to first nonfatal CV event or first major adverse CV event was based on gender [from original source] and age–adjusted risk ratios from Ward et al. (2007).4 The relationship between LDL-C and CV event risk was estimated using data from the Cholesterol Treatment Trialists’ Collaboration (CTTC) meta-analysis.5 The analysis estimated the rate ratio per 1 mmol/L reduction in LDL-C for various CV events, which was converted to an annual probability assuming a constant rate of events. The model allowed for alternative sources of data for this relationship to be included based on 2 separate studies published by Navarese and colleagues (2015 and 2018).6,7 The sponsor applied relative risks to capture the increased probability of multiple CV events derived from prior National Institute for Health and Care Excellence (NICE) reviews and the literature.8-10 General population mortality (i.e., non–CV-related death) was also included.11
Health state utility values were calculated by adjusting the general population age-specific utility value using health state–specific utility adjustment factors that incorporated the mean age and utility value of the original estimate. The original health state utility values were derived from the literature12-17 and used UK value sets. Treatment-related disutility for apheresis was assumed to be –0.0273 based on an estimate of disutility associated with hemodialysis18 and on the annual number of hours of treatment. No other treatments were assumed to have an impact on HRQoL.
The model included drug acquisition costs, administration costs, health care resource use costs, health state costs, and adverse event costs. The proportion of patients on the treatments included in SOC was based on the ELIPSE trial. Treatment costs for those treatments included in SOC were estimated by combining drug utilization and unit costs based on recommended drug dosages for each treatment from the relevant product monographs and by assuming similar dosages for children. The cost of apheresis was derived from a Health Quality Ontario report and included equipment costs, disposables, additional supplies, maintenance fees, and personnel fees.19 The average cost of apheresis was weighted by the proportions of patients that would receive low-density lipoprotein (LDL) or plasma apheresis, which were assumed to be 41% and 59%, respectively. Monitoring and resource use costs were estimated from sponsor-solicited expert opinion and a prior National Institute for Health and Care Excellence review (frequencies) and the Ontario Schedule of Benefits (costs).20,21 Administration costs for evinacumab and apheresis were calculated based on an estimate of a nursing hourly salary ($40)22 and the duration of treatment (1 hour for evinacumab; 4 hours for apheresis).
Health state costs were estimated using previously published cost estimates of CV events and the Ontario Case Costing Initiative (OCCI) dataset.23 Event costs for MI, stroke, and CV death were based on estimates used in a published cost-effectiveness analysis,24 which were derived from prior work using ICES databases. The sponsor used OCCI estimates for the remaining health states (CV events) and inflated them using a rate of 6.2 to account for the costs of medical services directly billed by physicians, based on the cost ratio calculated for MI by comparing the OCCI cost and the published estimate. A 1-time end-of-life cost of $11,811 was applied for those who died of a CV event.25
Summary of Sponsor’s Economic Evaluation Results
All analyses were run probabilistically (5,000 iterations for the base-case and scenario analyses). The deterministic and probabilistic results were similar. The probabilistic findings are presented in the following sections.
Base-Case Results
In the sponsor’s base-case analysis, treatment with evinacumab plus SOC was associated with incremental costs of $6,534,304 and a gain of 1.75 QALYs (and 2.21 life-years) compared with SOC over the lifetime time horizon, resulting in an ICER of $3,729,349 per QALY gained (Table 3; Table 10). The probability of evinacumab plus SOC being cost-effective at a $50,000 per QALY threshold compared to SOC was 0%. Approximately 94% of the incremental QALYs in the sponsor’s base case were accrued after the first year, though CADTH notes that the maximum follow-up time in the trial was 24 weeks. The submitted analysis is based on the publicly available list prices of all treatments besides evinacumab.
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER vs. reference ($/QALY) |
|---|---|---|---|---|---|
SOC | 761,077 | Reference | 11.73 | Reference | Reference |
Evinacumab + SOC | 7,295,381 | 6,534,304 | 13.48 | 1.75 | 3,729,349 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; SOC = standard of care; vs. = versus.
Source: Sponsor’s pharmacoeconomic submission.1
Sensitivity and Scenario Analysis Results
The sponsor conducted several scenario analyses, including subgroup analyses for patients aged 5 to 11 years and patients aged 12 years and older, alternative sources for the relationship between LDL-C and CV event risk, and an alternative background treatment mix. Generally, the conclusions of the sponsor’s base case were not largely impacted in these scenario analyses. In the scenario that used data from Navarese et al. (2018) to inform the relationship between LDL-C and CV event risk, the ICER increased substantially to $6,761,931 (approximately an 81% increase from the base-case analysis).
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations to the sponsor’s analysis that have notable implications for the economic analysis:
The validity of surrogate outcomes from the ELIPSE trial to predict clinically meaningful CV outcomes is uncertain. In the submitted model, the treatment effect of evinacumab on CV events was estimated based on the surrogate outcome of LDL-C lowering using results of the CTTC 2015 meta-analysis. The CTTC meta-analysis included 22 trials of statin therapy versus control and 5 additional trials comparing low-intensity versus high-intensity statin therapy and assessed the effects of treatment on CV events per 1 mmol/L reduction in LDL-C.5 The clinical experts consulted by CADTH agreed that LDL-C was considered a reasonable surrogate outcome; however, the validity of using change in LDL-C as a surrogate for outcomes such as CV events or CV-related death specifically in patients with HoFH is not well established. The relationship between LDL-C lowering and CV outcomes may be influenced by several factors, including differences in patient populations and the heterogeneity of interventions. Further, as reported in CADTH’s clinical review, the clinical experts consulted by CADTH emphasized that although the double-blind treatment duration of the ELIPSE study and treatment duration of the CL-17100 studies (both 24 weeks) was appropriate for assessing lipid-related outcomes, it was insufficient to determine the impact of evinacumab on CV-related morbidity and mortality.
As noted by the sponsor, previous submissions to CADTH have used the CTTC meta-analysis to inform the relationship between LDL-C and CV event risk. However, CADTH has previously noted that the reduction in CV events predicted on the basis of the relationship between statins and CV events may not be appropriate for modelling the relationship for other types of lipid-lowering therapies (LLTs).26,27 Given that in the modelled population of people with HoFH in Canada, the patients tend to be receiving treatment with multiple LLTs and not only statin therapy, it is uncertain if the same relationship between LDL-C lowering and CV event risk exists. Further, it is likely that the baseline LDL-C levels differ between patients receiving statin therapy and patients with HoFH who require multiple concurrent therapies to manage their LDL-C, rendering generalization to other baseline LDL-C levels difficult. Indeed, the mean baseline LDL-C for all the trials included in the CTTC meta-analysis was 3.4 mmol/L and 3.3 mmol/L for females and males, respectively, and was 7.4 mmol/L (all genders) in the evinacumab arm of the ELIPSE trial (excluding patients receiving lomitapide).1,5 Additionally, the mean age from the meta-analysis (65 years and 61 years for females and males) was notably different than the starting age used in the model (39 years for all genders).
The submitted model allowed for the use of a more recent meta-analysis conducted by Navarese et al. (2018), which included trials for statins as monotherapy, as well as statins in combination with ezetimibe and PCSK9 inhibitors as LDL-C– lowering drugs.7 While this more recent meta-analysis does not address all CADTH’s concerns with the CTTC meta-analysis, it may more closely reflect the current Canadian practice and treatments that the modelled population are receiving given that it assessed additional studies with combination therapies.
The CADTH reanalysis used the meta-analysis conducted by Navarese et al. (2018)7 to inform the relationship between LDL-C lowering and CV event risk. The relationship between LDL-C reduction and CV outcomes for HoFH remains unknown.
CADTH performed a scenario analysis using the rate ratios for CV events per 1 mmol/L of LDL-C reduction from the CTTC meta-analysis.5
The clinical inputs used to inform the model are associated with uncertainty and heterogeneity. The submitted model relied on several real-world evidence sources to inform clinical efficacy parameters. The data sources, methodologies, and populations included, as well as how they were incorporated into the economic model, introduced uncertainty with regard to the clinical efficacy of LLTs and their subsequent impact on CV outcomes.
First, the sponsor used individual patient data from the Thompson and colleagues (2015) study to characterize the modelled population’s baseline CV event risks.3 This study retrospectively analyzed data from a UK patient cohort that enrolled 44 patients with HoFH from 1964 to 2014 with the intent of investigating improved CV outcomes following advances in LLTs. The sponsor performed survival analysis on study data to inform time to CV death. CADTH identified several concerns with the sponsor’s approach to using these data, most notably that the study enrolment period spanned 50 years and many advancements in LLTs. During the study period, 13 patients died, all of CV-related causes; these patients tended to be born earlier than those who did not die (on average, 18 years before) and tended to start treatment earlier than the patients who were still alive.3 Thus, the treatment mix differed between these groups. Notably, fewer of the patients who had died received statin therapy (62%, compared to 100% of patients who were still alive). While plasmapheresis and LDL-C apheresis were used in a similar proportion among patients who had died and patients who were still alive, the authors noted that over the study period there were advances in apheresis techniques. As the sponsor defined baseline CV risk in the model based on this heterogeneous population with varying access to LLTs, there remains considerable uncertainty about the true baseline risk of patients with HoFH living in Canada who may be eligible for treatment with evinacumab.
To estimate time to first nonfatal CV event (which was not possible to derive from the Thompson et al. patient data), the sponsor estimated the rate and distribution of nonfatal CV events by using risk ratios and event distributions based on Ward et al. (2007).4 In their analysis, Ward and colleagues estimated rate ratios for each CV event using the distribution of CV events from incidence data from 2 UK registries: the Bromley Coronary Heart Disease Register and the Oxfordshire Community Stroke Project.4 These registries reflect the distribution of CV events in the general population in the UK, but not specifically among patients with HoFH. In the sponsor’s submitted model, the rate ratios estimated in this manner were applied to the estimated CV death rates of patients with HoFH derived from Thompson et al. (2015). CADTH notes that the patient populations in these studies (i.e., Ward et al. and Thompson et al.) differed in some key aspects, most notably that 1 reflects a cohort of patients with HoFH and the other reflects the general population. It is uncertain whether the same incidence and distribution of CV events would be likely to occur in patients with HoFH as in the general population.
CADTH was unable to address this limitation and notes that there is considerable uncertainty with regard to the relationship between LDL-C and CV-related mortality and morbidity.
The long-term efficacy of evinacumab for patients with HoFH is unknown. In the submitted model, patients were assumed to receive the full benefits observed in the ELIPSE trial for up to 58 years (the model time horizon). The submitted model did not explore the impact of treatment effect waning. Given that the length of the trial was 24 weeks, considerable uncertainty remains with regard to the long-term efficacy and safety of evinacumab. Despite this uncertainty, in the submitted model more than 94% of incremental QALYs were accrued outside the trial period, and the model predicted a survival benefit for evinacumab of 2.21 additional life-years compared to patients not receiving evinacumab.
CADTH was unable to address this limitation due to limitations in data availability. The impact of this limitation on the cost-effectiveness of evinacumab is uncertain.
The sponsor underestimated evinacumab treatment acquisition costs. In the submitted model, the sponsor assumed that perfect vial sharing would occur. This assumption is inappropriate because of differences in vial sharing abilities by jurisdiction and the small number of patients with HoFH, which make it unlikely that vial sharing would be feasible. Further, the product monograph for evinacumab indicates that the product is intended for single use only and that any unused portion should be discarded.2 The clinical experts consulted by CADTH agreed that vial sharing is unlikely to take place given these considerations.
Additionally, the sponsor assumed that the compliance rate for evinacumab would be 92% and that there would be 100% compliance for all other treatments. This assumption was not adequately justified and may underestimate the total cost of evinacumab in clinical practice.
The CADTH reanalysis assumed 0% vial sharing.
The CADTH reanalysis assumed that all treatments would have a 100% compliance rate.
Assumptions surrounding apheresis in the submitted model are uncertain. While reduction or delay in time to use of apheresis is an important outcome for patients and clinicians, the methods used by the sponsor to incorporate this evidence were considered inappropriate by the clinical experts consulted by CADTH. The sponsor assumed that following the introduction of evinacumab, there would be a 46.5% reduction in apheresis use for patients receiving evinacumab. This reduction was linked to an improvement in HRQoL, but not to an increase or decrease in LDL-C because of discontinuation. The sponsor based the percent change in apheresis on a post hoc analysis of ELIPSE trial data on eligibility for apheresis according to the US and European Union criteria for eligibility. However, the clinical experts consulted by CADTH highlighted that such criteria are overly inclusive and are not used in Canada. The experts also indicated that they would not likely discontinue apheresis entirely for patients receiving evinacumab, but that if a patient were to begin treatment with evinacumab before apheresis it may delay or eliminate the need for apheresis in the future. The difference in apheresis use in the Canadian clinical setting makes it unclear what impact the introduction of evinacumab will have on the use of apheresis for patients with HoFH. As these issues have not been explored, significant uncertainty remains with regard to how apheresis use will change (e.g., be delayed, reduced, or eliminated) and how LDL-C levels will respond to potential changes in background treatments.
CADTH was unable to address this limitation due to a lack of robust clinical data that are generalizable to the HoFH population living in Canada.
CADTH conducted a scenario analysis assuming that no patients discontinued apheresis in either treatment arm.
The pharmacoeconomic submission incorporated poor reporting, organization, and modelling practices, which made validation of the submitted model difficult. The sponsor’s submission included several discrepancies in reporting within the technical report and the submitted model, making it difficult to appraise the submission. Notably, the submission lacked clarity regarding the allowable state transitions, with differences between the technical report and submitted model. For example, the text-based description of state transitions, the provided model schematic, and the table of allowed transitions between health states (sponsor submission Table 8) did not align. Notable differences included that the in-text description indicating that patients may not transition back to the unstable angina, stable angina, and TIA health states from any postevent health state was contradicted by both the model schematic and the way in which the model was programmed (which allowed patients to transition to the unstable angina health state from multiple postevent health states). These types of discrepancies make the sponsor’s intended model structure and allowable state transitions unclear. This lack of clarity rendered it difficult for CADTH to assess the appropriateness of the model structure and related assumptions.
The clinical experts consulted by CADTH noted that the submitted model did not incorporate aortic valve disease, which is considered an important health event for patients with HoFH in the experts’ clinical settings. Given that aortic valve disease is likely to impact health system costs and HRQoL (e.g., due to the need for a valve procedure), this omission introduces uncertainty in the estimation of the cost-effectiveness of evinacumab.
Additionally, the submitted model included numerous IFERROR statements, which lead to situations in which the parameter value is overwritten with an alternative value without alerting the user to the automated overwriting. The systematic use of IFERROR statements makes thorough auditing of the sponsor’s model impractical, and it remains unclear whether the model is running inappropriately by overriding errors.
CADTH was unable to address this limitation. Costs and health outcomes associated with aortic valve disease are not captured, and a thorough validation of the sponsor’s model was not possible.
An additional limitation was identified but not considered to be a key limitation:
The estimation of health state costs was uncertain. In the submitted economic model, the sponsor derived health state costs by inflating OCCI costs by a factor of 6.2. This inflation factor was based on the ratio between the cost of MI reported in a prior economic evaluation conducted by Gregoire et al.24 (which cited ICES as the source of the MI cost) and the OCCI cost. However, the ICES costs cited by Gregoire et al. were from data held by Amgen, and thus CADTH was unable to appraise or validate the estimates. Further, the assumption that the same cost ratio would exist for all health states is not clearly justified. However, while the health state costs used in the sponsor’s base-case analysis were uncertain, changes in health state costs do not have a large impact on the results of the model.
Additional key assumptions were made by the sponsor and have been appraised by CADTH (Table 4).
Table 4: Key Assumptions of the Submitted Economic Evaluation (Not Noted as Limitations to the Submission)
Sponsor’s key assumption | CADTH comment |
|---|---|
The model does not account for the possibility of progression to heart failure, which may be a complication of myocardial infarction. | Acceptable. This is likely a conservative assumption given that heart failure likely has impacts on HRQoL, mortality, and resource utilization of that are not being captured by the submitted model. |
Neurologic complications of stroke were not incorporated into the submitted model. | Acceptable. This is likely a conservative assumption given that neurologic outcomes following stroke may negatively impact HRQoL, mortality, and resource utilization. |
The treatment mix for SOC was based on the ELIPSE trial, and treatment dosages were based on product monographs, assuming similar dosages for children. | Not acceptable. Not all the treatments included in SOC are indicated for the entire modelled population. Specifically, evolocumab and ezetimibe are indicated for patients aged 12 years and older and aged 10 years and older, respectively. Given that a high proportion of patients (> 75%) were assumed to be taking these medications, the costs of these treatments may be inaccurately estimated, which may affect the results of the model; however, this is unlikely to impact the overall findings. |
The description of apheresis costs in the sponsor’s pharmacoeconomic report did not match the referenced Health Quality Ontario report. Based on the description, the sponsor intended to use the combined cost estimates for HoFH and HeFH but, instead, used only the HeFH costs. | While the cost of apheresis is unlikely to have an impact on the model results, CADTH corrected the sponsor’s base-case analysis. Details of CADTH’s calculation can be found in Appendix 4. |
HeFH = heterozygous familial hypercholesterolemia; HoFH = homozygous familial hypercholesterolemia; HRQoL = health-related quality of life; SOC = standard of care.
CADTH Reanalyses of the Economic Evaluation
Base-Case Results
The CADTH base case was derived by making changes in model parameter values and assumptions, in consultation with clinical experts. These changes, summarized in Table 5, included alternative assumptions about the relationship between LDL-C and CV event risk, and revisions to vial sharing and treatment compliance.
Table 5: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH’s value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
1. Apheresis cost | $1,161.90 per session | $1,225.36 per session |
Changes to derive the CADTH base case | ||
1. Rate ratio for CV events per 1 mmol/L of LDL-C reduction | Derived from CTTC meta-analysis | Derived from Navarese et al. (2018) meta-analysis |
2. Vial sharing | 100% | 0% |
3. Evinacumab treatment compliance rate | 92% | 100% |
CADTH base case | — | 1 + 2 + 3 |
CTTC = Cholesterol Treatment Trialists’ Collaboration; CV = cardiovascular; LDL-C = low-density lipoprotein cholesterol.
The CADTH base-case analysis found that evinacumab plus SOC was associated with 0.91 additional QALYs at an additional cost of $7,638,677 versus SOC. Therefore, the ICER of evinacumab plus SOC was $8,392,585 per QALY gained compared to SOC. The probability of cost-effectiveness at a $50,000 per QALY gained threshold was 0%. A summary of the CADTH stepped analysis and base-case results can be found in Table 6.
Table 6: Summary of the Stepped Analysis of the CADTH Reanalysis Results
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|---|
Sponsor’s base case | SOC | 758,249 | 11.56 | Reference |
Evinacumab + SOC | 7,143,188 | 13.54 | 3,223,287 | |
Sponsor’s corrected base case | SOC | 766,564 | 11.56 | Reference |
Evinacumab + SOC | 7,148,436 | 13.54 | 3,221,739 | |
CADTH reanalysis 1 | SOC | 767,729 | 11.70 | Reference |
Evinacumab + SOC | 6,766,552 | 12.74 | 5,769,166 | |
CADTH reanalysis 2 | SOC | 766,564 | 11.56 | Reference |
Evinacumab + SOC | 8,028,160 | 13.54 | 3,665,847 | |
CADTH reanalysis 3 | SOC | 766,564 | 11.56 | Reference |
Evinacumab + SOC | 7,711,189 | 13.54 | 3,505,831 | |
CADTH base case (reanalyses 1 + 2 + 3) | SOC | 767,729 | 11.70 | Reference |
Evinacumab + SOC | 8,195,737 | 12.74 | 7,143,636 | |
CADTH base case (reanalyses 1 + 2 + 3; probabilistic) | SOC | 769,589 | 11.85 | Reference |
Evinacumab + SOC | 8,408,266 | 12.76 | 8,392,585 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; SOC = standard of care.
Note: All results are presented deterministically unless otherwise stated.
Scenario Analysis Results
CADTH undertook price reduction analyses based on the sponsor’s base case and on CADTH’s base case (Table 7). This analysis demonstrated that a price reduction of 98% would be necessary to achieve cost-effectiveness at a $50,000 per QALY gained threshold when considering the CADTH base case (a 97% price reduction would be required based on the sponsor’s base case).
Table 7: CADTH Price Reduction Analyses
Analysis | ICERs for evinacumab + SOC vs. SOC ($/QALY) | |
|---|---|---|
Price reduction (annual cost)a | Sponsor base case | CADTH reanalysis |
No price reduction ($460,839) | 3,221,739 | 7,143,636 |
10% ($414,755) | 2,895,816 | 6,422,092 |
20% ($368,671) | 2,569,893 | 5,700,548 |
30% ($322,587) | 2,243,970 | 4,979,004 |
40% ($276,503) | 1,918,047 | 4,257,460 |
50% ($230,419) | 1,592,124 | 3,535,916 |
60% ($184,335) | 1,266,201 | 2,814,372 |
70% ($138,252) | 940,278 | 2,092,828 |
80% ($92,168) | 614,355 | 1,371,284 |
90% ($46,084) | 288,432 | 649,740 |
100% ($0) | Dominant | Dominant |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; SOC = standard of care; vs. = versus.
aThe annual cost of evinacumab assumes a mean patient weight of 70.4 kg, per the sponsor’s submission, and assumes wastage of excess medication.
CADTH conducted additional scenario analyses to determine the impact of alternative assumptions on the cost-effectiveness of evinacumab:
The application of rate ratios for CV events per 1 mmol/L of LDL-C reduction from the CTTC meta-analysis.
The assumption that no patients would discontinue apheresis while receiving treatment with evinacumab.
The results from these scenarios are presented in Table 12. The scenario analysis using rate ratios from the CTTC meta-analysis reduced the ICER to $4,708,402 per QALY gained; however, a price reduction of 98% is still required to achieve cost-effectiveness at a $50,000 per QALY gained threshold. The scenario analysis that assumed no patients would discontinue apheresis was not influential.
Issues for Consideration
The clinical experts consulted by CADTH and the drug plan input indicated that there are geographic barriers to accessing LDL apheresis (and to a lesser extent plasma apheresis) in Canada such that not all patients are able to receive this treatment despite clinical eligibility. In fact, LDL apheresis is only available in Quebec, Ontario (for pediatric patients), and Alberta.19,28 The clinical experts consulted by CADTH further noted that treatment with evinacumab does not require significant infrastructure or monitoring programs and that it can be administered in a hospital or outpatient setting. Along with treatment centres being more accessible to most patients, the lower frequency of administration of evinacumab compared to apheresis (every 4 weeks compared to every 2 weeks) also leads to the potential for evinacumab to be a more accessible treatment option for patients with HoFH in Canada. From a health care expenditure perspective, this may lead to a more equitable distribution of health care resources (i.e., more patients can receive this treatment) than for expenditure on apheresis, where the spending (and clinical benefit) is concentrated on fewer patients with HoFH.
The evidence used in this review excluded patients who were receiving lomitapide. Lomitapide for the treatment of adults with HoFH was reviewed by CADTH and received a do not list recommendation from the CADTH Canadian Drug Expert Committee, citing concerns with significant hepatic adverse events and a lack of evidence to evaluate the CV benefit of lomitapide.29
Treatment for children younger than 5 years is an important need in the population of patients with HoFH, according to the clinical experts consulted by CADTH. The experts indicated that, in practice, some treatments that do not have a pediatric indication (e.g., PCSK9 inhibitors) are still used for patients with HoFH. Specific challenges in the treatment of children arise in relation to dosing across a wide range of patient ages and sizes, having a formulation that is usable for children, and the administrative burden for clinicians and families. Apheresis is considered an effective treatment option for children younger than 5 years; however, the clinicians consulted by CADTH noted concerns with maintaining long-term vascular access and the burden on the patient and family due to the frequency of apheresis administration. Due to these concerns, evinacumab was noted to present a potential treatment option that may offer effective LDL-C lowering while reducing the family burden of apheresis. The cost-effectiveness and budgetary impact of using evinacumab for patients younger than 5 years is unknown.
Overall Conclusions
Based on the CADTH clinical review of the ELIPSE trial, treatment with evinacumab, when added to SOC, likely resulted in a clinically important reduction in LDL-C compared with SOC alone. The reduction was beyond the threshold for clinically important reductions of 30% defined by clinical experts and practice guidelines. Overall, the safety profile of evinacumab was comparable to SOC. However, CADTH’s clinical review noted that the ELIPSE trial had a short duration of only 24 weeks, which precluded the ability to assess long-term efficacy and safety. Thus, the impact of evinacumab on reducing CV-related morbidity and mortality, as well as the need for apheresis, is unknown.
CADTH identified several limitations with the sponsor’s pharmacoeconomic analysis that have implications for the cost-effectiveness of evinacumab. For the CADTH base case, CADTH revised the assumptions surrounding the relationship between LDL-C and CV event risk, which led to more conservative rate ratios being applied to CV event risk per unit reduction in LDL-C; CADTH also revised assumptions about drug wastage and complete treatment compliance to capture evinacumab drug acquisition costs more accurately. The CADTH base case resulted in an ICER of $8,392,585 per QALY gained (incremental costs = $7,638,676.64; incremental QALYs = 0.91) for evinacumab versus SOC. The probability of evinacumab being cost-effective at a $50,000 per QALY gained threshold was 0%. CADTH’s findings are similar to the sponsor’s: evinacumab plus SOC is not cost-effective at conventionally accepted thresholds. Based on CADTH’s base case, for evinacumab to be considered cost-effective at a $50,000 per QALY gained threshold, the drug cost of evinacumab would need to be $9,217 per year, reflecting a price reduction of approximately 98%.
Although CADTH attempted to address the identified limitations of the sponsor’s pharmacoeconomic model, a high degree of uncertainty remains. Most notably, the relationship between LDL-C reduction and CV outcomes for patients with HoFH remains unknown. Thus, the incremental QALY and life-year gains estimated for evinacumab may still overestimate the clinical benefits, especially considering that due to its relatively short duration, the ELIPSE trial was unable to assess CV morbidity and mortality outcomes.
References
1.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Evkeeza (evinacumab), 150 mg/mL concentrate solution for infusion, in single-dose vials. Novato (CA): Ultragenyx Pharmaceutical Inc.; 2023 May 10.
2.Evkeeza (evinacumab): 150 mg/mL concentrate solution for infusion, in single-dose vials [product monograph]. Oakville (ON): Innomar Strategies, Inc.; 2023 Sep 22.
3.Thompson GR, Seed M, Naoumova RP, et al. Improved cardiovascular outcomes following temporal advances in lipid-lowering therapy in a genetically-characterised cohort of familial hypercholesterolaemia homozygotes. Atherosclerosis. 2015;243(1):328-333. PubMed
4.Ward S, Lloyd Jones M, Pandor A, et al. A systematic review and economic evaluation of statins for the prevention of coronary events. Health Technol Assess. 2007;11(14):1-160, iii-iv. PubMed
5.Cholesterol Treatment Trialists' (CCT) Collaboration, Fulcher J, O'Connell R, et al. Efficacy and safety of LDL-lowering therapy among men and women: meta-analysis of individual data from 174,000 participants in 27 randomised trials. Lancet. 2015;385(9976):1397-1405. PubMed
6.Navarese EP, Kolodziejczak M, Schulze V, et al. Effects of proprotein convertase subtilisin/kexin type 9 antibodies in adults with hypercholesterolemia: a systematic review and meta-analysis. Ann Intern Med. 2015;163(1):40-51. PubMed
7.Navarese EP, Robinson JG, Kowalewski M, et al. Association between baseline LDL-C level and total and cardiovascular mortality after LDL-C lowering: a systematic review and meta-analysis. JAMA. 2018;319(15):1566-1579. PubMed
8.National Institute for Health Care Excellence. Bempedoic acid with ezetimibe for treating primary hypercholesterolaemia or mixed dyslipidaemia. (Technology appraisal guidance TA694) 2021; https://www.nice.org.uk/guidance/ta694. Accessed 2023 May.
9.National Institute for Health Care Excellence. Alirocumab for treating primary hypercholesterolaemia and mixed dyslipidaemia. (Technology appraisal guidance TA393) 2016; https://www.nice.org.uk/guidance/TA393. Accessed 2023 May.
10.Smolina K, Wright FL, Rayner M, Goldacre MJ. Long-term survival and recurrence after acute myocardial infarction in England, 2004 to 2010. Circ Cardiovasc Qual Outcomes. 2012;5(4):532-540. PubMed
11.Table: 13-10-0114-01. Life expectancy and other elements of the life table, Canada, all provinces except Prince Edward Island. Ottawa (ON): Statistics Canada; 2022: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310011401. Accessed by sponsor, no date provided.
12.Goodacre S, Nicholl J, Dixon S, et al. Randomised controlled trial and economic evaluation of a chest pain observation unit compared with routine care. BMJ. 2004;328(7434):254. PubMed
13.Ara R, Tumur I, Pandor A, et al. Ezetimibe for the treatment of hypercholesterolaemia: a systematic review and economic evaluation. Health Technol Assess. 2008;12(21):iii, xi-xiii, 1-212.
14.Lacey EA, Walters SJ. Continuing inequality: gender and social class influences on self perceived health after a heart attack. J Epidemiol Community Health. 2003;57(8):622-627. PubMed
15.Tengs TO, Lin TH. A meta-analysis of quality-of-life estimates for stroke. Pharmacoeconomics. 2003;21(3):191-200. PubMed
16.Luengo-Fernandez R, Gray AM, Bull L, et al. Quality of life after TIA and stroke: ten-year results of the Oxford Vascular Study. Neurology. 2013;81(18):1588-1595. PubMed
17.Melsop KA, Boothroyd DB, Hlatky MA. Quality of life and time trade-off utility measures in patients with coronary artery disease. Am Heart J. 2003;145(1):36-41. PubMed
18.Beaudet A, Clegg J, Thuresson PO, Lloyd A, McEwan P. Review of utility values for economic modeling in type 2 diabetes. Value Health. 2014;17(4):462-470. PubMed
19.Medical Advisory Secretariat. Low-density lipoprotein apheresis: an evidence-based analysis. Ont Health Technol Assess Ser. Vol 7. 2007/01/01 ed2007: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3377562/pdf/ohtas-07-101.pdf. Accessed 2023 Nov 07. PubMed
20.Schedule of benefits for physician services under the Health Insurance Act: (January 25, 2022 (effective July 1, 2022)). Toronto (ON): Ontario Ministry of Health; 2022: https://www.health.gov.on.ca/en/pro/programs/ohip/sob/physserv/sob_master.pdf. Accessed by sponsor, no date provided.
21.Schedule of benefits for laboratory services: effective July 1, 2020. Toronto (ON): Ontario Ministry of Health; 2020: http://www.health.gov.on.ca/en/pro/programs/ohip/sob/lab/lab_mn2020.pdf. Accessed by sponsor, no date provided.
22.Job Bank. Registered Nurse (R.N.) in Canada - prevailing wages in Canada. Ottawa (ON): Government of Canada; 2022: https://www.jobbank.gc.ca/marketreport/wages-occupation/993/ca. Accessed 2023 Jan 23.
23.Ontario Case Costing Initiative (OCCI). Toronto (ON): Ontario Health and Long-Term Care; 2017: https://data.ontario.ca/dataset/ontario-case-costing-initiative-occi. Accessed by sponsor, no date provided.
24.Gregoire J, Champsi S, Jobin M, Martinez L, Urbich M, Rogoza RM. Cost-effectiveness analysis of evolocumab in adult patients with atherosclerotic cardiovascular disease in Canada. Adv Ther. 2022;39(7):3262-3279. PubMed
25.Drug Reimbursement Review pharmacoeconomic report: rivaroxaban (Xarelto) for prevention of stroke and cardiovascular events in coronary and peripheral artery disease. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/sites/default/files/cdr/pharmacoeconomic/SR0569_Xarelto_PE_Report.pdf. Accessed 2023 Nov 07.
26.Drug Reimbursement Review clinical and pharmacoeconomic reviews: inclisiran (Leqvio) for primary hypercholesterolemia. Can J Health Technol. 2022;2(4). https://canjhealthtechnol.ca/index.php/cjht/article/view/sr0681r/sr0681r. Accessed 2023 Nov 07.
27.Drug Reimbursement Review pharmacoeconomic report: evolocumab (Repatha) for primary hyperlipidemia and mixed dyslipidemia. Ottawa (ON): CADTH; 2017: https://www.cadth.ca/sites/default/files/cdr/pharmacoeconomic/SR0515_Repatha_Resubmission_PE_Report.pdf. Accessed 2023 Nov 07.
28.Brown L, Ruel I, Baass A, et al. Design, rationale, and preliminary results of the Canadian Homozygous Familial Hypercholesterolemia Registry: 2008 to 2022 update. Can J Health Technol. 2023;3(2). https://canjhealthtechnol.ca/index.php/cjht/article/view/MG00197/MG00197. Accessed 2023 Nov 07.
29.CADTH Canadian Drug Expert Committee (CDEC) final recommendation: lomitapide (Juxtapid — Aegerion Pharmaceuticals Inc.). Ottawa (ON): CADTH; 2015 Apr 17: https://www.cadth.ca/sites/default/files/cdr/complete/cdr_complete_SR0386_Juxtapid-Apr-21_15.pdf. Accessed 2023 Feb 02.
30.Ontario Ministry of Health, Ontario Ministry of Long-Term Care. Ontario drug benefit formulary/comparative drug index. 2022; https://www.formulary.health.gov.on.ca/formulary/. Accessed 2023 May 12.
31.Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Evkeeza (evinacumab), 150 mg/mL concentrate solution for infusion, in single-dose vials. Novato (CA): Ultragenyx Pharmaceutical Inc.; 2023 May 10.
32.Brown L, Ruel I, Bélanger A, et al. P036: Homozygous familial hypercholesterolemia in Canada. Can J Cardiol. 2021;37(10 Suppl):S23.
33.Brunham LR, Ruel I, Aljenedil S, et al. Canadian Cardiovascular Society position statement on familial hypercholesterolemia: update 2018. Can J Cardiol. 2018;34(12):1553-1563. PubMed
34.Government of Alberta. Drug coverage. 2023; https://www.alberta.ca/drug-coverage.aspx. Accessed 2023 Jul 19.
35.Government of Ontario. Get coverage for prescription drugs. 2023; https://www.ontario.ca/page/get-coverage-prescription-drugs. Accessed 2023 Jul 19.
36.Sutherland G, Dinh T. Understanding the gap: a pan-Canadian analysis of prescription drug insurance coverage. Ottawa (ON): The Conference Board of Canada; 2017: https://innovativemedicines.ca/wp-content/uploads/2017/12/20170712-understanding-the-gap.pdf. Accessed 2023 Jul 19.
37.Phillips K. Catastrophic drug coverage in Canada. (Background paper). Ottawa (ON): Library of Parliament; 2016: https://lop.parl.ca/staticfiles/PublicWebsite/Home/ResearchPublications/BackgroundPapers/PDF/2016-10-e.pdf. Accessed 2023 Apr.
38.Alignment among public formularies in Canada – part 1: general overview. Ottawa (ON): Patented Medicine Prices Review Board; 2017: http://www.pmprb-cepmb.gc.ca/view.asp?ccid=1327&lang=en. Accessed 2023 Jul 19.
Appendix 1: Cost Comparison Table
Note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical experts and CADTH-participating public drug plans. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 8: CADTH Cost Comparison Table for Treatment of Homozygous Familial Hypercholesterolemia
Treatment | Strength / concentration | Form | Price | Recommended dosage | Daily cost | Annual cost |
|---|---|---|---|---|---|---|
Evinacumab (Evkeeza) | 150 mg/mL | 345 mg vial 1,200 mg vial | 10,163.7000a 35,352.0000a | 15 mg/kg every 4 weeks | 1,262.57b | 460,839 |
HMG-CoA reductase inhibitors | ||||||
Atorvastatin calcium (Lipitor and generics) | 10 mg 20 mg 40 mg 80 mg | Tablet | 0.1743 0.2179 0.2342 0.2342 | 10 mg to 80 mg at bedtime | 0.17 to 0.23 | 64 to 85 |
Fluvastatin sodium (Lescol XL) | 80 mg | Tablet | 1.6225 | 80 mg daily | 1.62 | 592 |
Fluvastatin sodium (generic) | 20 mg 40 mg | Capsule | 0.6882 0.9671 | 20 mg to 40 mg at bedtime | 0.69 to 0.97 | 251 to 353 |
Lovastatin (Mevacor and generics) | 20 mg 40 mg | Tablet | 1.0846 1.9812 | 20 mg to 80 mg at bedtime | 1.08 to 3.96 | 396 to 1,446 |
Pravastatin sodium (Pravachol and generics) | 10 mg 20 mg 40 mg | Tablet | 0.2916 0.3440 0.4143 | 10 mg to 40 mg at bedtime | 0.29 to 0.41 | 106 to 151 |
Rosuvastatin calcium (Crestor and generics) | 5 mg 10 mg 20 mg 40 mg | Tablet | 0.1284 0.1354 0.1692 0.1990 | 10 mg to 40 mg daily | 0.14 to 0.20 | 49 to 73 |
Simvastatin (Zocor and generics) | 5 mg 10 mg 20 mg 40 mg 80 mg | Tablet | 0.1023 0.2023 0.2501 0.2501 0.2501 | 10 mg to 80 mg at bedtime | 0.20 to 0.25 | 74 to 91 |
PCSK9 inhibitors | ||||||
Alirocumab (Praluent) | 75 mg/mL 150 mg/mL | Solution for injection in a prefilled pen | 267.8300 | 75 mg once every 2 weeks or 300 mg once every 4 weeks | 19.13 | 6,983 |
Evolocumab (Repatha) | 140 mg/mL | Solution for injection in an autoinjector | 262.1000 | 420 mg once every 2 weeks to one month | 26.21 to 56.16 | 9,567 to 20,500 |
Cholesterol absorption inhibitor | ||||||
Ezetimibe (Ezetrol and generics) | 10 mg | Tablet | 0.1811 | 10 mg daily | 0.18 | 66 |
Nondrug interventions | ||||||
Plasma exchange apheresisc | — | — | 702.05 | Every 2 weeks | — | 18,253 |
LDL apheresisc | — | — | 1,978.42 | Every 2 weeks | — | 51,439 |
LDL = low-density lipoprotein.
Note: All prices are from the Ontario Drug Benefit Formulary (accessed May 2023), unless otherwise indicated, and do not include dispensing fees.30
aSponsor’s submitted price.1
bThe annual cost of evinacumab assumes a mean patient weight of 70 kg and assumes wastage of excess medication.
cThe cost of apheresis is derived from Health Quality Ontario report,19 and was inflated from 2007 CAD to 2023 CAD using the Bank of Canada inflation calculator, and excludes nursing time for administration. Full calculation for the cost of apheresis can be found in Appendix 4.
Appendix 2: Submission Quality
Note that this appendix has not been copy-edited.
Description | Yes/No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | No | Clinical experts consulted by CADTH indicated that aortic valve disease is an important outcome that was not captured in the submitted model. |
Model has been adequately programmed and has sufficient face validity | No | Refer to the CADTH critical appraisal regarding the overall submission quality. |
Model structure is adequate for decision problem | Yes | No comment. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | Yes | No comment. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | Yes | No comment. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | No | Refer to CADTH critical appraisal regarding the overall submission quality. |
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note that this appendix has not been copy-edited.

CV = cardiovascular; HoFH = homozygous familial hypercholesterolemia.
Source: Sponsor’s pharmacoeconomic submission.1
Detailed Results of the Sponsor’s Base Case
Table 10: Disaggregated Summary of the Sponsor’s Economic Evaluation Results
Parameter | Evinacumab + SOC | SOC | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 17.53 | 15.32 | 2.21 |
By health state | |||
Stable HoFH | 4.96 | 3.57 | 1.38 |
Stable angina | 0.28 | 0.29 | –0.01 |
Unstable angina | 0.18 | 0.19 | –0.01 |
Myocardial infarction | 0.98 | 1.13 | –0.15 |
Transient ischemic attack | 0.08 | 0.08 | 0.00 |
Stroke | 1.04 | 1.11 | –0.07 |
Post–stable angina | 1.25 | 0.97 | 0.28 |
Post–unstable angina | 0.73 | 0.59 | 0.13 |
Post–myocardial infarction | 3.82 | 3.63 | 0.19 |
Post–transient ischemic attack | 0.40 | 0.31 | 0.08 |
Poststroke | 3.83 | 3.44 | 0.39 |
Discounted QALYs | |||
Total | 13.48 | 11.73 | 1.75 |
By health state | |||
Stable HoFH | 4.39 | 3.18 | 1.21 |
Stable angina | 0.23 | 0.24 | –0.01 |
Unstable angina | 0.14 | 0.15 | –0.01 |
Myocardial infarction | 0.73 | 0.85 | –0.12 |
Transient ischemic attack | 0.07 | 0.07 | 0.00 |
Stroke | 0.55 | 0.60 | –0.04 |
Post–stable angina | 1.00 | 0.78 | 0.21 |
Post–unstable angina | 0.60 | 0.50 | 0.10 |
Post–myocardial infarction | 3.08 | 2.95 | 0.12 |
Post–transient ischemic attack | 0.34 | 0.27 | 0.07 |
Poststroke | 2.51 | 2.28 | 0.23 |
Disutilities | |||
Adverse event related | 0.00 | 0.00 | 0.00 |
Treatment related | –0.15 | –0.14 | –0.01 |
Discounted costs ($) | |||
Total | 7,295,381.49 | 761,077.24 | 6,534,304.25 |
Drug acquisition | 6,870,939.37 | 302,304.21 | 6,568,635.15 |
Monitoring | 3,039.77 | 2,656.91 | 382.86 |
Health-state costs | |||
Stable angina | 4,219.11 | 4,330.92 | –111.81 |
Unstable angina | 3,905.11 | 4,118.53 | –213.41 |
Myocardial infarction | 45,140.14 | 51,987.52 | –6,847.38 |
Transient ischemic attack | 4,838.85 | 4,968.07 | –129.22 |
Stroke | 50,791.43 | 54,237.37 | –3,445.94 |
Post–stable angina | 7,568.34 | 5,881.43 | 1,686.91 |
Post–unstable angina | 3,479.90 | 2,850.43 | 629.47 |
Post–myocardial infarction | 64,615.77 | 61,442.32 | 3,173.45 |
Post–transient ischemic attack | 9,851.95 | 7,808.25 | 2,043.70 |
Poststroke | 9,774.66 | 8,786.82 | 987.84 |
Cardiovascular death | 217,217.10 | 249,704.46 | –32,487.36 |
ICER ($/QALY) | 3,729,349 | ||
HoFH = homozygous familial hypercholesterolemia; ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year; SOC = standard of care.
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Note that this appendix has not been copy-edited.
Detailed Results of CADTH Base Case
Table 11: Disaggregated Summary of CADTH’s Economic Evaluation Results
Parameter | Evinacumab + SOC | SOC | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 16.59 | 15.46 | 1.13 |
By health state | |||
Stable HoFH | 4.34 | 3.64 | 0.70 |
Stable angina | 0.29 | 0.29 | 0.00 |
Unstable angina | 0.18 | 0.18 | 0.00 |
Myocardial infarction | 1.05 | 1.12 | –0.08 |
Transient ischemic attack | 0.08 | 0.08 | 0.00 |
Stroke | 1.08 | 1.11 | –0.03 |
Post–stable angina | 1.14 | 0.99 | 0.15 |
Post–unstable angina | 0.67 | 0.60 | 0.07 |
Post–myocardial infarction | 3.78 | 3.67 | 0.12 |
Post–transient ischemic attack | 0.36 | 0.32 | 0.04 |
Poststroke | 3.62 | 3.45 | 0.17 |
Discounted QALYs | |||
Total | 12.76 | 11.85 | 0.91 |
By health state | |||
Stable HoFH | 3.85 | 3.24 | 0.61 |
Stable angina | 0.23 | 0.24 | 0.00 |
Unstable angina | 0.14 | 0.14 | 0.00 |
Myocardial infarction | 0.78 | 0.84 | –0.06 |
Transient ischemic attack | 0.07 | 0.07 | 0.00 |
Stroke | 0.58 | 0.60 | –0.02 |
Post–stable angina | 0.91 | 0.79 | 0.12 |
Post–unstable angina | 0.56 | 0.50 | 0.06 |
Post–myocardial infarction | 3.06 | 2.98 | 0.08 |
Post–transient ischemic attack | 0.31 | 0.27 | 0.03 |
Poststroke | 2.41 | 2.31 | 0.10 |
Disutilities | |||
Adverse event related | 0.00 | 0.00 | 0.00 |
Treatment related | –0.15 | –0.14 | 0.00 |
Discounted costs ($) | |||
Total | 8,408,265.50 | 769,588.87 | 7,638,676.64 |
Drug acquisition | 7,968,202.99 | 312,653.98 | 7,655,549.01 |
Monitoring | 2,894.31 | 2,696.71 | 197.60 |
Health-state costs | |||
Stable angina | 4,252.40 | 4,307.44 | –55.04 |
Unstable angina | 3,990.40 | 4,093.68 | –103.28 |
Myocardial infarction | 48,299.66 | 51,860.97 | –3,561.31 |
Transient ischemic attack | 4,909.19 | 4,973.54 | –64.35 |
Stroke | 52,578.01 | 54,149.18 | –1,571.18 |
Post–stable angina | 6,876.11 | 5,954.38 | 921.73 |
Post–unstable angina | 3,227.99 | 2,876.21 | 351.78 |
Post–myocardial infarction | 64,009.42 | 62,059.38 | 1,950.04 |
Post–transient ischemic attack | 8,936.69 | 7,920.94 | 1,015.75 |
Poststroke | 9,260.33 | 8,828.11 | 432.23 |
Cardiovascular death | 230,828.02 | 247,214.36 | –16,386.35 |
ICER ($/QALY) | 8,392,585 | ||
HoFH = homozygous familial hypercholesterolemia; ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year; SOC = standard of care.
Scenario Analyses
Table 12: Summary of CADTH’s Scenario Analyses
Analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|---|
CADTH base case | SOC | 769,589 | 11.85 | Reference |
Evinacumab + SOC | 8,408,266 | 12.76 | 8,392,585 | |
CADTH base case (deterministic) | SOC | 767,729 | 11.70 | Reference |
Evinacumab + SOC | 8,195,737 | 12.74 | 7,143,636 | |
CADTH scenario analysis: CTTC meta-analysis | SOC | 770,232 | 11.79 | Reference |
Evinacumab + SOC | 8,432,835 | 13.51 | 4,708,402 | |
CADTH scenario analysis: Apheresis discontinuation (deterministic) | SOC | 767,729 | 11.70 | Reference |
Evinacumab + SOC | 8,286,882 | 12.71 | 7,397,054 |
CTTC = Cholesterol Treatment Trialists’ Collaboration; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; SOC = standard of care.
Details of the Estimation of Apheresis Costs From the Health Quality Ontario Report
Using the costs reported in Tables 22 and 23 in the Health Quality Ontario report, CADTH re-estimated the costs of apheresis as described by the sponsor.19 The sponsor indicated that they used the combined costs for patients with heterozygous familial hypercholesterolemia (HeFH) and HoFH, however, it appeared they only used cost estimates for patients with HeFH. CADTH. In CADTH’s calculation, the biweekly cost for the HoFH and HeFH patients were added together and used to estimate a per-session cost. As in the sponsor’s original calculation, the nurse time per session was subtracted (assumed in the Health Quality Ontario report to be $125 per session for both LDL and plasma exchange apheresis). Finally, the cost was inflated from 2007 Canadian dollars to 2023 Canadian dollars using the Bank of Canada inflation calculator (which had an average rate of inflation over that time period of 2.15%). CADTH’s calculations are reported in Table 12. Based on the sponsor’s assumption that 41% of patients rely on LDL apheresis and 59% on plasma apheresis, the average cost per session was estimated by CADTH to be $1,225.36.
Table 13: CADTH’s Estimation of Apheresis Costs
Treatment | Number of patients | Annual cost | Sessions per year | Cost per patient / year | Cost per session | Cost per session after removing nurse time | Cost after inflation to 2023 CAD |
|---|---|---|---|---|---|---|---|
Plasma exchange apheresis | |||||||
Homozygous, biweekly treatment | 13 | $252,013 | 26 | $19,385.62 | $745.60 | $620.60 | $871.83 |
Heterozygous, biweekly treatments | 765 | $12,385,274 | 26 | $16,189.90 | $622.69 | $497.69 | $699.17 |
Total, biweekly treatments | 778 | $12,637,287 | 26 | $16,243.30 | $624.74 | $499.74 | $702.05 |
LDL apheresis | |||||||
Homozygous, biweekly treatment | 13 | $517,265 | 26 | $39,789.62 | $1,530.37 | $1,405.37 | $1,974.23 |
Heterozygous, biweekly treatments | 765 | $30,498,234 | 26 | $39,866.97 | $1,533.35 | $1,408.35 | $1,978.49 |
Total, biweekly treatments | 778 | $31,015,499 | 26 | $39,865.68 | $1,533.30 | $1,408.30 | $1,978.42 |
CAD = Canadian dollars; LDL = low-density lipoprotein.
Appendix 5: Submitted Budget Impact Analysis and CADTH Appraisal
Note that this appendix has not been copy-edited.
Table 14: Summary of Key Take-Aways
Key take-aways of the budget impact analysis |
|---|
|
Summary of Sponsor’s Budget Impact Analysis
The sponsor submitted a budget impact analysis (BIA) estimating the incremental budget impact of reimbursing evinacumab as an adjunct to diet and other LDL-C lowering therapies for the treatment of patients aged 5 years and older with HoFH.31 The analysis was undertaken using an epidemiologic approach from the perspective of the CADTH-participating Canadian public drug plans a three-year time horizon (June 2024 to May 2027). The reference scenario includes a background treatment mix (SOC) as the comparator. Beginning with the population aged 5 years and older living in Canada, excluding Quebec, the sponsor narrowed the population using estimates of HoFH prevalence, the proportion that have been diagnosed and are being treated for HoFH, the proportion with uncontrolled HoFH despite SOC, and those eligible for public coverage. Key inputs to the BIA are documented in Table 16.
The sponsor’s BIA included the following key assumptions:
The proportion of patients receiving included SOC treatments was informed by the ELIPSE trial.
Time on treatment was assumed to be indefinite for evinacumab and SOC.
Table 15: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1 / year 2 / year 3 if appropriate) |
|---|---|
Target population | |
Population in Canada aged 5+ (excluding Quebec) in year 1 | 29,890,827 |
Annual population growth rate (2021 to 2025) | 1.29% |
Prevalence of HoFH | 1 per 300,000a |
Proportion of patients diagnosed and being treated | 62%32 |
Proportion of patients with uncontrolled HoFH | 96%33 |
Proportion of patients covered by public plan | 60 to 100%b |
Number of patients eligible for drug under review | 48 / 50 / 51 |
Market uptake (3 years) | |
Uptake (reference scenario) Standard of care | 100% / 100% / 100% |
Uptake (new drug scenario) Evinacumab Standard of care | 51% / 66% / 75% 49% / 34% / 25% |
Cost of treatment (per patient) | |
Cost of treatment annually Evinacumab Standard of care | $373,350.66c $18,279.97d |
HoFH = homozygous familial hypercholesterolemia.
aPrevalence estimated from data reported in the Canadian FH Registry.33
b100% coverage assumed in all provinces except Ontario (60%) and Alberta (80%).
cThe annual cost of evinacumab assumes an average of 12 doses per year (i.e., once monthly or every 4 weeks with the assumption that there would be one missed dose).
dThe annual cost of the standard of care treatment mix assumes the treatment mix from the ELIPSE trial. Costs of background treatments vary by jurisdiction; the reported price applies to Alberta, Saskatchewan, Manitoba, Ontario, New Brunswick, Nova Scotia, and the NIHB population.
Summary of the Sponsor’s BIA Results
The sponsor estimated the net budget impact of funding evinacumab for patients aged 5 years and older with HoFH will be $8,975,298 in Year 1, $11,953,530 in Year 2, and $14,181,831 in Year 3, for a 3-year total budget impact of $35,110,659.
CADTH Appraisal of the Sponsor’s BIA
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
Market share of evinacumab is underestimated. The sponsor estimated market shares of evinacumab reported to be based on internal forecasts and expert opinion. Clinical experts consulted by CADTH agreed that market uptake would increase from Year 1 to 3 as treating clinicians gained familiarity with evinacumab as an available treatment, however, indicated that the sponsor’s estimates were likely an underestimate of what is expected in Canadian clinical practice. Based on the clinical benefit in LDL-C reduction and safety profile observed in the ELIPSE trial and administration considerations, clinical experts consulted by CADTH expected that nearly all eligible patients would initiate treatment with evinacumab by Year 3.
To address this limitation, CADTH undertook a reanalysis by revising the market shares for evinacumab in the new drug scenario to 60% in year 1, 75% in year 2, and 90% in year 3.
The public drug coverage for evinacumab was underestimated. The sponsor used estimates of public drug coverage based on assumptions and self-reported experience with other rare disease programs. They estimated that there would be 100% public coverage in all jurisdictions except for Ontario and Alberta, where 60% and 80% would be covered, respectively. Ontario and Alberta also have provincial programs that are likely to publicly fund evinacumab for some people.34,35 For example, in Ontario the OHIP+ program provides drugs at no cost for anyone age 24 years or younger who is not covered by a private plan, including drugs to treat rare conditions, which is particularly relevant for HoFH which is often diagnosed in children. Ontario’s Trillium Drug Benefit Program may also facilitate funding for evinacumab for patients who have high prescription drug costs in relation to their net household income. Alberta also has several drug plans that may apply to people with HoFH including the Alberta Child Health Benefit, Alberta Adult Health Benefit, Assured Income for the Severely Handicapped, and the Specialized High Cost Drug Program.34
The CADTH reanalysis assumed that the Ontario public coverage would be 70% based on provincial guidelines for high-cost medications and estimates of public drug coverage eligibility for different populations (e.g., < 24 years old).36-38
Given the high annual cost of evinacumab ($460,839), a scenario analysis assuming 100% drug coverage was conducted to account for the possibility that federal or provincial catastrophic drug coverage plans (e.g., Ontario’s Trillium Drug Benefit Program) would cover the drug cost for all eligible patients.
The sponsor underestimated evinacumab treatment acquisition costs. In the submitted BIA, the sponsor assumed perfect vial sharing would occur. This assumption is inappropriate because of differences in vial sharing abilities by jurisdiction and the small number of patients with HoFH. Further, the product monograph for evinacumab indicates that the product is intended for single use only and to discard any unused portion.2 Clinical experts consulted by CADTH agreed that vial sharing is unlikely to take place given the considerations noted above.
Additionally, the sponsor assumed that the compliance rate for evinacumab would be 92% (i.e., 1 missed treatment per year or 12 doses per year) and that there would be 100% compliance for all other treatments. This assumption may underestimate the total cost of evinacumab in clinical practice.
The CADTH reanalysis assumed 0% vial sharing, as aligned with the CADTH reanalysis of the cost-utility analysis.
The CADTH reanalysis assumed that all treatments would have a 100% compliance rate, and that the same assumption was made for all treatments, as aligned with the CADTH reanalysis of the cost-utility analysis.
The inclusion of apheresis costs in the BIA is inappropriate. The sponsor included the treatment cost of apheresis in the reference case analysis. The cost of apheresis included the costs of equipment, dialysis equipment, equipment disposables, additional supplies, maintenance fees, medical fees, and personnel fees. Given that the perspective of analysis is the CADTH-participating Canadian public drug plans, these costs are ineligible for inclusion.
The CADTH base-case analysis excluded the costs associated with apheresis.
CADTH Reanalyses of the BIA
CADTH revised the sponsor’s submitted analysis by adjusting the market share, public drug coverage, vial sharing, treatment compliance assumptions, and removing apheresis costs. The changes applied to derive the CADTH base case are described in Table 15.
Table 16: CADTH Revisions to the Submitted Budget Impact Analysis
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
1. Apheresis cost | $1,161.90 per session | $1,225.36 per session, as aligned with the correction made to the CUA |
Changes to derive the CADTH base case | ||
1. Market share | Year 1: 51% Year 2: 66% Year 3: 75% | Year 1: 60% Year 2: 75% Year 3: 90% |
2. Public drug coverage | 60% in Ontario | 70% in Ontario |
3. Vial sharing | 100% | 0% |
4. Treatment compliance | 92% | 100% |
5. Apheresis cost | Included | Excluded |
CADTH base case | 1 + 2 + 3 + 4 + 5 | |
CUA = cost-utility analysis.
The results of the CADTH step-wise reanalysis are presented in summary format in Table 16 and a more detailed breakdown is presented in Table 17.
The CADTH base case suggests that reimbursing evinacumab would be associated with an incremental cost of $14,031,446 in Year 1, $18,188,147 in Year 2, and $22,614,433 in Year 3, for a three-year budgetary impact of $54,834,025. As can be observed in Table 16 and Table 17, the difference between the CADTH base case and the sponsor’s base case is due to the combined impact of the individual reanalyses – there is no key driver impacting the increase in estimated budget impact of reimbursing evinacumab.
Table 17: Summary of the CADTH Reanalyses of the BIA
Stepped analysis | 3-year total |
|---|---|
Submitted base case | $35,110,659 |
Submitted corrected base case | $35,085,837 |
CADTH reanalysis 1 | $41,235,447 |
CADTH reanalysis 2 | $37,263,996 |
CADTH reanalysis 3 | $39,932,001 |
CADTH reanalysis 4 | $38,181,911 |
CADTH reanalysis 5 | $35,565,124 |
CADTH base case | $54,834,025 |
BIA = budget impact analysis.
Table 18: Detailed Breakdown of the CADTH Reanalyses of the BIA
Stepped analysis | Scenario | Year 1 | Year 2 | Year 3 | 3-year total |
|---|---|---|---|---|---|
Submitted base case | Reference | $508,042 | $676,622 | $802,753 | $1,987,417 |
New drug | $9,483,340 | $12,630,152 | $14,984,584 | $37,098,076 | |
Budget impact | $8,975,298 | $11,953,530 | $14,181,831 | $35,110,659 | |
Submitted corrected base case | Reference | $521,687 | $694,796 | $824,315 | $2,040,798 |
New drug | $9,490,640 | $12,639,875 | $14,996,119 | $37,126,635 | |
Budget impact | $8,968,953 | $11,945,079 | $14,171,805 | $35,085,837 | |
CADTH reanalysis 1 | Reference | $613,750 | $795,568 | $989,178 | $2,398,495 |
New drug | $11,165,459 | $14,473,139 | $17,995,343 | $43,633,942 | |
Budget impact | $10,551,709 | $13,677,572 | $17,006,166 | $41,235,447 | |
CADTH reanalysis 2 | Reference | $550,169 | $732,728 | $869,318 | $2,152,215 |
New drug | $10,075,926 | $13,419,369 | $15,920,916 | $39,416,212 | |
Budget impact | $9,525,757 | $12,686,641 | $15,051,598 | $37,263,996 | |
CADTH reanalysis 3 | Reference | $521,687 | $694,796 | $824,315 | $2,040,798 |
New drug | $10,729,459 | $14,289,766 | $16,953,573 | $41,972,799 | |
Budget impact | $10,207,772 | $13,594,971 | $16,129,258 | $39,932,001 | |
CADTH reanalysis 4 | Reference | $521,687 | $694,796 | $824,315 | $2,040,798 |
New drug | $10,282,086 | $13,693,943 | $16,246,680 | $40,222,709 | |
Budget impact | $9,760,399 | $12,999,147 | $15,422,365 | $38,181,911 | |
CADTH reanalysis 5 | Reference | $258,204 | $343,882 | $407,986 | $1,010,072 |
New drug | $9,349,677 | $12,452,136 | $14,773,383 | $36,575,196 | |
Budget impact | $9,091,472 | $12,108,254 | $14,365,398 | $35,565,124 | |
CADTH base case | Reference | $318,033 | $412,248 | $512,572 | $1,242,853 |
New drug | $14,349,479 | $18,600,395 | $23,127,005 | $56,076,879 | |
Budget impact | $14,031,446 | $18,188,147 | $22,614,433 | $54,834,025 |
BIA = budget impact analysis.
CADTH conducted additional scenario analyses to address remaining uncertainty, using the CADTH base case. Results are provided in Table 18.
Price reduction of 98% to assess the budget impact if the price of the drug under review reflected the price in which the ICER would be at $50,000 per QALY gained in CADTH’s base case cost-utility analysis.
Assumed 100% public drug coverage.
Results of CADTH’s scenario analyses demonstrate that the estimated budget impact is highly sensitive to changes in drug cost.
Table 19: Detailed Breakdown of the CADTH Scenario Analyses of the BIA
Stepped analysis | Scenario | Year 1 | Year 2 | Year 3 | 3-year total |
|---|---|---|---|---|---|
Submitted corrected base case | Reference | $521,687 | $694,796 | $824,315 | $2,040,798 |
New drug | $9,490,640 | $12,639,875 | $14,996,119 | $37,126,635 | |
Budget impact | $8,968,953 | $11,945,079 | $14,171,805 | $35,085,837 | |
CADTH base case | Reference | $318,033 | $412,248 | $512,572 | $1,242,853 |
New drug | $14,349,479 | $18,600,395 | $23,127,005 | $56,076,879 | |
Budget impact | $14,031,446 | $18,188,147 | $22,614,433 | $54,834,025 | |
CADTH scenario analysis: 98% price reduction | Reference | $318,033 | $412,248 | $512,572 | $1,242,853 |
New drug | $598,650 | $775,995 | $964,841 | $2,339,486 | |
Budget impact | $280,617 | $363,747 | $452,269 | $1,096,632 | |
CADTH scenario analysis: 100% drug coverage | Reference | $368,962 | $478,263 | $594,652 | $1,441,878 |
New drug | $17,328,776 | $22,462,259 | $27,928,668 | $67,719,703 | |
Budget impact | $16,959,814 | $21,983,996 | $27,334,015 | $66,277,825 |
Ethics Review
Abbreviations
ASCVD
atherosclerotic cardiovascular disease
HoFH
homozygous familial hypercholesterolemia
LDL-C
low-density lipoprotein cholesterol
LDLR
low-density lipoprotein receptor
Summary
Homozygous familial hypercholesterolemia (HoFH) is an ultra-rare genetic condition characterized by significantly elevated low-density lipoprotein cholesterol (LDL-C) levels from birth, which lead to early cardiovascular events and, if left untreated, premature death. Patient group, clinician group, clinical expert, and drug program input gathered in the course of this CADTH review, as well as relevant literature, were reviewed to identify ethical considerations relevant to the use of evinacumab for the treatment of adult and pediatric patients aged 5 years and older with HoFH.
The ethical considerations identified in this review included those related to the following:
Diagnosis, treatment, and experience of HoFH: Ethical considerations in the context of HoFH highlighted the need for timely diagnosis and intervention to prevent early, harmful cardiovascular events and to prolong survival. Current treatment options are inadequate in meeting the need for safe and effective therapies that can manage the harmful LDL-C levels resulting from HoFH, which are associated with premature cardiovascular disease, and that can thereby alleviate the physical, emotional, and financial burdens experienced by patients and their families.
Clinical and economic evidence: Clinical trial evidence indicated that evinacumab resulted in a statistically significant and clinically meaningful reduction in LDL-C compared to placebo and was well tolerated. However, the 24-week duration of the double-blind treatment period within the trial was insufficient to assess long-term safety and efficacy, which limits the assessment of the clinical benefits and harms associated with treatment as well as the pharmacoeconomic assessment of cost-effectiveness. Moreover, the pivotal trial was not designed to assess other clinically relevant outcomes, including cardiovascular-related outcomes, mortality, reduction in the need for and frequency of apheresis, and health-related quality of life.
Clinical decision-making for and implementation of evinacumab: The use of evinacumab may present benefits to patients with HoFH as a potentially effective, tolerable, and less burdensome treatment to manage LDL-C levels and alleviate associated burdens and harms. Evinacumab may be more accessible and less burdensome for patients than treatment alternatives such as apheresis. Informed consent for pediatric patients requires careful consideration, especially as evinacumab is expected to be offered as a lifelong therapy. Efforts to enhance access to evinacumab, including comanagement with general practitioners and remote consultation, require consideration to address potential diagnostic and geographic barriers to equitable and timely access to treatment.
Health system considerations: Ethical considerations for health systems related to the implementation of evinacumab highlighted the challenges of funding decisions, considerations of distributive justice, assessments of opportunity costs for expensive drugs for rare diseases, and the continued need for more evidence on the use and implementation of evinacumab for pediatric and adult patients with HoFH.
Objective
The objective of this ethics review is to identify and describe ethical considerations associated with the use of evinacumab as an adjunct to diet and other LDL-C–lowering therapies for the treatment of adult and pediatric patients aged 5 years and older with HoFH, including considerations related to the context of HoFH, the evidentiary basis, the use of evinacumab, and health systems.
Research Questions
This report addresses the following research questions:
What ethical considerations arise in the context of HoFH, including those related to diagnosis, treatment, and outcomes?
What ethical considerations arise related to the evidence (e.g., clinical and economic data) used to evaluate evinacumab?
What ethical considerations arise in the use of evinacumab for patients, their caregivers, and clinicians?
What ethical considerations for health systems are involved in the context of evinacumab?
Methods
To identify ethical considerations relevant to the use evinacumab as an adjunct to diet and other LDL-C–lowering therapies for the treatment of adult and pediatric patients aged 5 years and older with HoFH, this ethics report was driven by relevant questions identified in the EUnetHTA Core Model 3.0, Ethics Analysis Domain,1 and supplemented by relevant questions from the Equity Checklist for HTA (ECHTA).2 These guiding questions were organized to respond to the research questions posed, and to investigate ethical considerations related to:
patients living with HoFH and their caregivers (i.e., disparities in incidence, treatment, or outcomes; challenges related to diagnosis or clinical care; factors that might prevent patients from gaining access to therapies)
the evidence used to demonstrate the benefits, harms, and value of evinacumab (i.e., ethical considerations in relevant clinical trials, including their representativeness, choice of outcome measures, appropriateness of analytical methods and models to all population groups; ethical considerations related to the data or assumptions in the economic evaluation)
the use of evinacumab, including considerations related to benefits and harms to patients, relatives, caregivers, clinicians or society, and considerations related to access to these therapies
the uptake of evinacumab in health systems, including considerations related to the distribution of health care resources.
Data Collection: Review of Project Inputs and Literature
Data to inform this ethics report were drawn from an identification of the ethical considerations (e.g., values, norms, or implications related to the harms, benefits, and implications for equity, justice, and resource allocation, and ethical considerations in the evidentiary basis) identified in the patient and clinician group, clinical expert, and drug program input collected by CADTH to inform this review, as well as from a complementary search of the published literature. Ongoing collaboration and communication with CADTH reviewers working on the clinical and economic reviews for this submission also assisted in the clarification and identification of relevant ethical considerations.
Review of Project Inputs
During this CADTH review, a single reviewer collected and considered input from 6 main sources related to the ethical considerations relevant to addressing the research questions guiding this ethics report. In addition to published literature, this report considered the following sources:
The sponsor submission, including noting information and external references or sources relevant to each of the research questions driving this report.
Clinician group input received by CADTH from Familial Hypercholesterolemia Canada and from a group of subspecialists involved in HoFH care in Canada.
Patient input received by CADTH from the Canadian Heart Patient Alliance and the Canadian Organization for Rare Disorders.
Drug program input received by CADTH from drug programs participating in the CADTH reimbursement review process.
Discussion with 4 clinical experts directly engaged by CADTH over the course of this Reimbursement Review. During 1 panel discussion (all 4 clinical experts) and 1 clinical consultation meeting (2 clinical experts), the clinical experts were asked targeted questions related to ethical considerations corresponding to the research questions driving this report. All the clinical experts were specialist physicians with qualifications in treating dyslipidemia and had experience treating patients with HoFH in Canada.
Engagement with CADTH clinical and economic reviewers to identify domains of ethical interest arising from their respective reviews as well as relevant questions and sources to further pursue in this report.
Literature Search Methods
An information specialist conducted a literature search using key resources, including MEDLINE via Ovid, Philosopher’s Index via Ovid, PsycInfo via Ovid, the Cumulative Index to Nursing and Allied Health Literature via EBSCO, and Scopus. Google Scholar was searched to find additional materials not captured in the major bibliographic databases. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were evinacumab and HoFH.
CADTH-developed search filters were applied to the searches conducted in MEDLINE, the Cumulative Index to Nursing and Allied Health Literature, and Scopus to limit retrieval to citations related to ethical concepts or considerations, equity concepts or considerations, and qualitative studies. Due to the limited number of results, no filters were applied to the searches conducted in Philosopher’s Index and PsycInfo to limit the retrieval by study type. Duplicates were removed by manual deduplication in Endnote. Retrieval was limited to the English language. The search was completed on June 8, 2023.
Literature Screening and Selection
Literature retrieved according to the search and selection methods detailed in the previous section was screened in 2 stages. In the first stage, the titles and abstracts of the citations retrieved were screened for relevance by a single reviewer. Articles were retrieved for full-text review by a single reviewer if their titles or abstracts identified ethical considerations or provided normative analysis (i.e., focusing on “what ought to be” through argumentation) or empirical research (i.e., focusing on “what is” through observation) of ethical considerations related to the experiences, incidence, diagnosis, treatment, or outcomes of HoFH or the evidence on, use of, or implications of evinacumab for patients with HoFH. In the second stage, full-text publications categorized as “retrieve” were reviewed by the same reviewer. Texts that included substantive information meeting the aforementioned criteria were included in the review, and texts that did not meet these criteria were excluded. As a parallel process, other sources drawn from relevant bibliographies, with relevant key concepts, in consultation with experts or other CADTH reviewers, were retrieved and reviewed using the selection criteria listed previously.
Data Analysis
Data analysis was driven by the 4 research questions guiding this report and included the collection, coding, and thematic analysis of data drawn from the literature and from project inputs. The reviewer conducted 2 iterative cycles of coding and analysis to abstract, identify, and synthesize relevant ethical considerations from the literature and from relevant project inputs.
In the initial coding phase, publications and input sources were reviewed for ethical content (e.g., claims related to potential harms, benefits, equity, justice, and resource allocation, as well as to ethical issues in the evidentiary basis). Once identified, claims related to ethical content were coded using methods of qualitative description.4 In the second coding phase, major themes and subcodes were identified through repeated readings of the data4 and were summarized into thematic categories within each guiding domain or research question.
If ethical content did not fit into these categories or into the domains outlined in the research questions, this was noted, as were discrepancies or conflicts in the ethical considerations or values identified between project sources or within thematic categories. Data analysis was iterative, and themes identified in the literature, in project inputs, and during consultations with clinical experts were used to further refine and reinterpret the ethical considerations identified.
The data collected and analyzed from these sources were thematically organized and described according to the 4 research questions and domains driving this report. The results of this analysis and its limitations and conclusions are described in the following sections.
Results
Description of Included Sources
Data to inform this ethics report were drawn from a review of patient group input, clinician group input, drug program input, and consultation with clinical experts engaged by CADTH for this review. All the clinical experts were active in relevant clinical roles as specialists with qualifications in treating dyslipidemia in Canada, and all had experience treating patients with HoFH. A description and summary of the sources reviewed are included in the CADTH Clinical Review Report.
The literature search identified 114 results. Following title and abstract screening, 91 citations were excluded and 23 potentially relevant publications from the electronic searches were retrieved for full-text review. Of the potentially relevant publications, 14 were excluded as they did not discuss ethical considerations of evinacumab or HoFH. Nine publications met the inclusion criteria and were included in this report. Twelve additional publications were retrieved from backward searching of the included publications’ reference lists or a manual search.
Twenty-one publications were therefore used to inform this report. Of these, 17 publications discussed ethical considerations in the context of HoFH, including in relation to diagnosis and treatment; 2 publications discussed patient and/or family and caregiver experiences in the context of HoFH; and 2 publications were selected to provide a broader understanding of the context of ethical considerations for drugs for rare diseases. Details regarding the characteristics of the included publications are reported in Table 1.
Key Ethical Considerations
Diagnosis, Treatment, and Experience of HoFH
Disease Context
HoFH is an ultra-rare genetic condition characterized by significantly elevated LDL-C levels from birth. The estimated global prevalence of HoFH is approximately 1 in 300,000,3-6 with around 80 known cases in Canada.7 As discussed in the CADTH Clinical Review Report, and as noted by the clinical experts consulted by CADTH in the course of this review, there is a higher concentration of cases within the French Canadian population in Quebec, which is attributed to founder effects (reduced genetic diversity).8 Additionally, the clinical experts reported observing a growing number of distinct genetic variants of HoFH among patients from other ethnic or racial backgrounds among recent immigrants to Canada, which required awareness among clinicians to ensure timely diagnosis and treatment.
Genetic mutations affecting low-density lipoprotein receptor (LDLR) function result in abnormal lipoprotein metabolism, causing extremely elevated plasma levels of LDL-C.9,10 Elevated levels of LDL-C manifest clinically as painful xanthomas in childhood and as accelerated atherosclerotic cardiovascular disease (ASCVD) and coronary heart disease, leading to early cardiovascular events — including myocardial infarction, stroke, and heart failure — and, if left untreated, premature death.4,11 The severity of the disease correlates with the degree of LDLR activity.
HoFH is a lifelong, life-limiting condition with a generally poor prognosis, despite optimal management with guideline-recommended lipid-lowering therapies.10 The Canadian HoFH registry reported that the first major adverse cardiovascular event occurs at a median age of 30 years, with 15% of patients experiencing cardiovascular death, nonfatal myocardial infarction, and/or stroke.12 Without adequate treatment, many patients experience a myocardial infarction before age 10 years.4 Most patients develop overt atherosclerosis before age 20 years and generally do not survive past age 30 years.4,13
Diagnosis
Clinical experts noted that diagnosing HoFH is generally straightforward and relies on established clinical and genetic criteria. The process involves a clinical assessment, family history evaluation, and laboratory testing, often necessitating the expertise of lipid specialists, as awareness of HoFH is lacking in the greater health system according to clinical experts and clinician group input. Clinical evaluation includes a detailed medical history, physical examination, and assessment of cardiovascular risk factors.4 Family history assessment helps identify potential cases of HoFH by gathering information about affected family members.4,14 Laboratory testing measures lipid levels, particularly LDL-C, through a fasting lipid panel. HoFH can also be diagnosed through confirmatory genetic testing, and treatment plans may differ depending on the specific genetic mutation a patient has.4,14 However, clinical experts noted that HoFH is commonly diagnosed based on clinical presentation in Canada due to the limited availability of genetic testing. Moreover, genetic testing results for patients with HoFH can be complex and misunderstood and may require the consultation of genetic counsellors.4
Clinical experts and published literature report that early detection, diagnosis, and treatment of HoFH in childhood can substantially delay progression of atherosclerosis and significantly increase lifespan.4,9,15 Literature, clinical experts, and clinician group input suggest that the timely initiation of statin treatment in children diagnosed with HoFH is critical, as it reduces LDL-C levels and helps prevent early cardiovascular events.4,15 Diagnosis often involves collaboration among health care professionals, including lipid specialists, geneticists, and cardiologists. However, clinical experts noted that lack of awareness among nonspecialist health care professionals could lead to delayed diagnosis or misdiagnosis before patients reaching a specialist familiar with HoFH. Therefore, barriers to diagnostic assessment, such as access to appropriate clinical expertise, genetic testing, and timely assessments, which may disproportionately impact certain groups such as patients residing in rural or remote communities in Canada, raise ethical concerns related to harms resulting from delayed diagnosis and inequitable access to timely treatment. Enhancing education about HoFH and training programs for health care providers could help early identification of patients with HoFH and reduce inequities and barriers to treatment for patients with HoFH.4,14,15 Additionally, it is important to raise awareness about the disease and available treatments among patients and their families to facilitate informed decision-making about their care.4,15
Current Treatment and Unmet Needs
According to clinician group and clinical expert input, as well as published literature, patients with HoFH experience early and aggressive progression of ASCVD throughout their lives.4,15 HoFH is a challenging condition to treat, as current pharmacological options primarily target the LDLR, which is defective or absent in people with HoFH. Although lipid-lowering treatments, like statins, ezetimibe, and PCSK9 inhibitors, contribute to improving survival rates for patients with HoFH, the clinical experts highlighted that repeated cardiovascular events, such as myocardial infarction, aortic valve stenosis, aortic root disease, and the need for revascularization, continue to occur for patients with HoFH. Therefore, according to the clinical experts, the primary treatment goal for HoFH is to reduce LDL-C as early, aggressively, and safely as possible, for as long as possible, to prevent premature cardiovascular disease.15 Existing standard of care treatment options, including statins, ezetimibe, and PCSK9 inhibitors, do not consistently achieve significant and sustained reductions in LDL-C to target levels for this population.16
Alternative options such as lomitapide, an LDLR-independent treatment, have limitations due to adverse reactions, poor tolerability and/or compliance, and high cost, while extracorporeal removal of LDL-C (apheresis) is invasive and burdensome according to clinical experts and clinician group input. Moreover, the clinical experts noted that access to apheresis treatments is limited to only 4 centres in Canada (Toronto, London, Quebec City, and Edmonton), which presents potential geographic barriers and inequities in access for patients. Additionally, apheresis treatments have rebound periods where LDL-C levels rise again, requiring frequent and sustained treatment cycles. The clinical experts, as well as patient and clinician group input, note that not all patients have equal access to the available treatments and that some therapies have a notable impact on health-related quality of life. According to the clinical experts and patient group input, treatment for HoFH necessitates frequent medical visits, approximately every 2 to 4 weeks, and patients undergoing apheresis face strict and burdensome treatment schedules that may affect their ability, and their caregivers’ ability, to attend school or work.
Some literature suggests that liver transplant can been considered a life-saving option for children with HoFH when other treatments are ineffective. However, perioperative management can be challenging due to premature ASCVDs. Analysis of pediatric recipients of liver transplant with HoFH showed successful perioperative survival, improved lipid levels, and relaxed dietary restrictions, but concerns remain about posttransplant ASCVD progression.4,17,18
The clinical experts emphasized the need for a safe and effective drug that can lower LDL-C to a similar degree as apheresis but without the same burden. The clinical experts and clinician group explained that the ideal medication would work via an LDLR-independent mechanism, substantially lower LDL-C levels, be well tolerated with minimal side effects, reduce impact on health care resources, and lessen patient and family burden. Current therapies fall short of these requirements, highlighting the need for novel treatment options to address the challenges faced by patients with HoFH.
Patient, Family, and Caregiver Experiences of HoFH
According to the patient group input and the published literature, the experiences of patients, families, and caregivers affected by HoFH shed light on the physical, psychological, social, and economic impacts of the condition. Patients face severe cardiovascular events and symptoms, and many patients require multiple surgeries, with the potential for complications and long-term physical disabilities.19,20
The patient group input noted that the impact of HoFH on daily life is substantial, with patients experiencing difficulties using their hands, reduced mobility, and intolerance to cold temperatures. The burden of frequent medical visits for treatments like apheresis affects patients’ ability to engage in regular activities, including work, education, and social interactions. According to patient group input and literature, caregivers, including family members, are also deeply affected, juggling responsibilities and facing concerns about the uncertain future and the potential transmission of the condition to future generations.21 Literature also suggests that patients experience fear of family members developing cardiovascular disease.21
According to the patient group input and the literature, the psychological toll of HoFH can be significant, with patients describing living with a constant fear of cardiovascular events and with the challenges of controlling their cholesterol levels. The social and economic consequences are also tangible, according to the patient group input, with life revolving around treatment schedules, long travel distances, and disruptions to work or education. The reliance on apheresis and medications, such as statins and PCSK9 inhibitors, is often accompanied by doubts about their effectiveness and concerns about the need for future surgeries due to uncontrolled LDL-C levels. Additionally, while patients experience significant travel and financial burdens due to apheresis, with related impacts on education and employment, they receive minimal psychological support to navigate these challenges.17 Providing psychological support and counselling services to patients and their families can help navigate the challenges of living with HoFH and improve their coping mechanisms.19,21
Overall, the impact of HoFH on quality of life and life expectancy, and the uncertain future for patients, families, and caregivers, highlight the unmet need for safe and effective treatment options that can manage LDL-C levels better than available therapies and alleviate the physical, emotional, and socioeconomic burdens faced by patients with HoFH and their caregivers and/or families.
Ethics of Evidence and Evaluation of Evinacumab
As described in the CADTH Clinical Review Report for this Reimbursement Review, evinacumab was evaluated in the pivotal CL-1629 (ELIPSE) trial, a phase III, double-blind, randomized placebo-controlled trial that assessed the efficacy and safety of evinacumab in both pediatric and adult patients with HoFH (n = 65), and the supportive CL-17100 trial, which evaluated the use of evinacumab in children aged 5 to 11 years with HoFH. The primary outcome of the ELIPSE trial was the percent change from baseline in LDL-C at week 24, with several secondary outcomes related to lipid parameters and apheresis eligibility criteria. The CL-17100 trial was a phase III, single-arm, open-label study in patients aged 5 to 11 years with HoFH (n = 14) to assess the efficacy and safety of evinacumab using the same primary and secondary outcomes as in the ELIPSE trial. In both studies, patients in both study arms were on a maximally tolerated lipid-lowering therapy (e.g., statin, PCSK9 inhibitor, ezetimibe, lomitapide, mipomersen, probucol) regimen, including apheresis, unless the patient had a documented history of tolerability issues. Neither study was designed to assess cardiovascular-related outcomes, mortality, reduction in the need for and frequency of apheresis, or health-related quality of life. A sponsor-submitted indirect treatment comparison is not discussed in this report. As detailed in the CADTH Clinical Review Report, the indirect treatment comparison results were found to be inconclusive and imprecise due to technical limitations, such as the studies varying in design, not including all relevant standard of care treatments, and having differences in the included populations.
As described in further detail in the CADTH Clinical Review Report, the ELIPSE study demonstrated that evinacumab resulted in a statistically significant and clinically meaningful reduction in LDL-C compared to placebo beyond the threshold of clinically important reductions of 30%, defined by clinical experts and clinical practice guidelines; this result was further supported by the CL-17100 trial. The clinical experts deemed LDL-C reduction to be an appropriate surrogate outcome in patients with HoFH. They noted that other drugs with sustained and safe LDL-C–lowering activity have consistently shown long-term reductions in cardiovascular events and that survival rates in patients with HoFH have significantly improved over the last generation largely due to lipid-lowering therapies. The CADTH clinical review team assessed the certainty of the evidence for the primary outcome (percent change from baseline in LDL-C) in the ELIPSE trial to be moderate, while the certainty of the evidence for the outcomes in the CL-17100 trial was deemed very low due to the absence of comparator groups, the small sample size, and the risk of bias due to the open-label nature of the study. Treatment with evinacumab was well tolerated in both studies and did not appear to be associated with more adverse events or serious adverse events than were associated with placebo; the adverse events that occurred with evinacumab included allergic events and infusion-related reactions, headaches, and nasopharyngitis. As noted in the CADTH Clinical Review Report, the ELIPSE and CL-17100 trials had a short double-blind treatment duration of only 24 weeks, which was insufficient to assess long-term safety and efficacy.
The clinical experts stated that, based on the available evidence, the extent of the LDL-C reduction, and the need for an effective, accessible, and less burdensome treatment for patients with HoFH, they would prescribe evinacumab to patients with HoFH despite uncertainties related to evinacumab’s long-term safety and efficacy. Uncertainties regarding the durability of the treatment effect, the potential for adverse events over extended periods, and the impact on cardiovascular outcomes are ethically significant as they may influence the clinical risk-benefit assessment for patients with HoFH. The clinical experts recommended ongoing study and monitoring of the use of evinacumab to understand its long-term safety and efficacy and to better inform clinical decision-making for prescribing, modifying, and discontinuing therapy, especially as evinacumab may be administered in a preventive manner as a lifelong therapy.
Although the participants in the 2 studies were not entirely representative of the patient population within Canada, the clinical experts considered the study findings to be largely generalizable to the broader patient population within Canada. However, they noted that the epidemiology of HoFH in Canada was changing due to immigration, which could introduce new genetic variants of the condition. As the pivotal trials were conducted in a patient population that was predominantly white, further monitoring may be required to determine whether evinacumab is effective in patients of more diverse racial and ethnic backgrounds and with distinct genetic variants of HoFH. Additionally, they noted that there was a lack of data regarding the prevalence of HoFH among Indigenous Peoples in Canada, which warranted further research.
Implications for Pharmacoeconomic Assessments
The lack of long-term safety and efficacy data for evinacumab presents challenges in accurately assessing its cost-effectiveness for the treatment of HoFH. This limitation, which impacts cost-effectiveness analyses for drugs for rare diseases more generally, presents challenges in assessing the opportunity costs — or forgone benefits — associated with reimbursing and prioritizing a particular intervention over others.22 Understanding opportunity costs is important for informing resource allocation decisions at a health system level. Accordingly, it is important to consider whether real-world data and evidence from other settings, including observational studies and postmarketing data, could be used to strengthen the pharmacoeconomic evaluation and provide a more complete picture of evinacumab’s value in the health care context in Canada.
Ethical Considerations in the Use of Evinacumab
Benefits and Harms
According to the patient group input, patients have reported positive experiences with using evinacumab, including improvements in their quality of life. Patients reported that improved LDL-C levels have led to increased energy, stable cholesterol levels, and a reduced number of apheresis treatments. Patients expressed satisfaction with evinacumab, considering it a life-changing treatment that effectively controls cholesterol levels and enables regular exercise.
The clinical experts noted that they would likely consider evinacumab, an infusion treatment, as a third-line or fourth-line therapy for patients with HoFH who have not experienced target LDL-C levels despite receiving maximally tolerated current treatments or for patients with progressive cardiovascular disease despite ongoing therapy. Long-term treatment with evinacumab is essential due to the chronic nature of HoFH. The drug has been well tolerated, with minimal serious adverse events reported over the 24-week trial period.
The clinical experts emphasized that evinacumab would be used as an adjunct to the maximally tolerated dose of statin, ezetimibe, and/or PCSK9 inhibitor. The preference would be to use evinacumab, with the goal of eventually replacing lomitapide and either delaying or reducing the frequency of or need for apheresis. The clinical experts and clinician groups suggested that this approach could lead to a therapy that may circumvent the negative side effects, poor patient adherence, and high expenses associated with lomitapide. Additionally, they indicated that extracorporeal methods of LDL-C removal, such as apheresis, are invasive and involve significant travel requirements and time away from employment and/or education.
As evinacumab aims to improve patients’ health outcomes, the literature suggests that it is crucial to consider the overall quality of life of individuals with HoFH.19,21 The burden of the disease and the demanding treatment regimens of traditional therapies, such as apheresis, have been reported to impact patients’ educational attainment and employment opportunities. Therefore, the clinical experts noted that when implementing treatment with evinacumab, the focus should be not only on its clinical efficacy but also on its potential to enhance the overall well-being and quality of life of patients.
Given these considerations, the clinical experts noted that evinacumab represents a valuable treatment option to help improve LDL-C levels for patients with HoFH, with the hope of supplanting lomitapide and either delaying or reducing the frequency of apheresis. Clinicians should consider its potential benefits and favourable tolerability profile, as well as standard considerations for chronic medications, when engaging in a process of shared decision-making with patients and/or caregivers to inform clinical decisions about the use of evinacumab for individual patients.
Access to Evinacumab
According to the clinical experts and to clinician group input, it is not anticipated that using evinacumab would introduce geographical barriers to access beyond those that already exist for available therapies for HoFH, including the existing barriers faced by patients living in rural or remote areas in accessing specialized health care and treatment. Collaborative efforts between specialists, general practitioners, and health care systems would be important to overcome access barriers and ensure that patients with HoFH have timely and equitable access to evinacumab.
Evinacumab is administered through IV infusion, necessitating an appropriate infusion setting for treatment. The clinical experts discussed that, for patients already undergoing apheresis treatments, administering evinacumab in settings where extracorporeal machines are available could simplify the process and avoid having patients attend separate appointments in separate locations unnecessarily.
Given the dispersed patient population and the limited access to specialized treatment centres, the clinical experts suggested that co-management with general practitioners may be a viable option for some patients to reduce inequities of access. Ensuring that all patients, regardless of geographic location or socioeconomic status, have access to evinacumab requires a comprehensive approach to health care delivery.
The clinical experts noted that remote consultation could potentially enable the administration of evinacumab under the supervision of a specialist in certain cases. However, it is essential to acknowledge that experience with evinacumab is still limited, making it unlikely that treatment would be transitioned to community settings imminently. Nonetheless, as more data and experience accumulate, there may be potential for expanding access to this therapy in the future.
Informed Consent
The clinical experts noted that a robust consent process would be required for the use of evinacumab for pediatric and adult patients with HoFH but that it would be similar to informed consent processes for other long-term treatments. For pediatric patients, it is important for health care providers to engage in age-appropriate and developmentally sensitive communication to ensure that both the child and their parents or guardians have a clear understanding of the treatment, its potential outcomes, any associated risks, and the current level of evidence and uncertainty with respect to long-term safety and efficacy. Where deemed appropriate, children or adolescents may assent or consent to treatment. The clinical experts discussed that an important expected benefit of evinacumab for pediatric patients is its potential for early intervention, when plaque accumulation from LDL-C is not as severe.4,15 Early intervention is relevant for informed consent because it helps patients or their guardians understand the potential benefits of early treatment with evinacumab through potentially influencing the course of the disease. This knowledge is key in allowing patients or guardians to make an informed decision about the treatment. In addition, the clinical experts noted that given the introduction of new cases and genetic variants of HoFH in diverse populations in Canada, cultural and religious beliefs should be respected throughout the informed consent process for all patients, promoting a collaborative approach to pediatric care.
Health System Considerations
The introduction of evinacumab poses ethical challenges related to equitable access and affordability in the health care system in Canada. Expensive drugs for rare diseases, such as evinacumab, raise ethical considerations related to distributive justice and equitable access, the sustainability of health care budgets, and fair pricing of pharmaceuticals.
The clinical experts noted that distributive justice should be considered in the context of the implementation of evinacumab for the treatment of HoFH, rather than extracorporeal low-density lipoprotein filtration techniques such as apheresis, plasmapheresis, or plasma exchange. Distributive justice refers to the fair allocation of the benefits and burden associated with the implementation (or not) of resources and health care interventions, particularly in the context of limited resources and rare diseases.22,23 Evidentiary uncertainty can complicate considerations of distributive justice. Although there is a strong unmet need for an effective treatment for HoFH, assessing the opportunity costs of reimbursing and prescribing evinacumab relative to other treatment options is complicated by the evidentiary uncertainty about the durability of its therapeutic effect. The fair distribution of resources may also include consideration of the timeliness and accessibility of care, which is important for patients diagnosed with HoFH, as they often face life-threatening cardiovascular risks at an early age, requiring long-term planning and care.
From a health system perspective, the clinical experts also discussed that the epidemiology of HoFH in Canada could change due to immigration, which might mean an increased number of cases in Canada and thus increased demand for evinacumab were it reimbursed. They also emphasized that an increase in the genetic variants of HoFH being treated in Canadian clinical practice would require a better understanding (and study of) the safety and efficacy of using evinacumab to treat HoFH across diverse populations.
Limitations
There is very little published literature that discusses ethical considerations related to the use of evinacumab for the treatment of HoFH, given both the rarity of the disease and the novelty of the drug under review. This does not imply that ethical considerations in the context of evinacumab for HoFH are absent, and this review of ethical considerations was augmented by drawing from additional resources collected in the course of this reimbursement review, including patient group, clinician group, and drug program input, and discussion with clinical experts, as well as engagement with the CADTH clinical and pharmacoeconomic review teams, to provide a more comprehensive understanding.
Although this ethics report drew on and considered patient group, clinician group, drug program, and clinical expert input, it is possible that more direct engagement with key stakeholders (e.g., direct interviews with patients and their caregivers and family members and with decision-makers) on their specific experiences with HoFH and/or evinacumab could have offered additional relevant ethical considerations or domains of analysis.
Conclusion
Input from patient groups, clinician groups, and provincial drug programs, as well as published literature and direct engagement with clinical experts, were reviewed for ethical considerations relevant to the use of evinacumab as an adjunct to diet and other LDL-C–lowering therapies for the treatment of adult and pediatric patients aged 5 years and older with HoFH.
Ethical considerations in the context of evinacumab underscored the need for safe and effective therapies to manage harmful LDL-C levels and alleviate the physical, emotional, and socioeconomic burdens experienced by patients with HoFH and their families. Clinical trial evidence indicated that evinacumab resulted in a statistically significant and clinically meaningful reduction in LDL-C compared to placebo and was well tolerated. However, the 24-week double-blind treatment duration in the trial was insufficient to assess long-term safety and efficacy, which limits the assessment of the clinical benefits and harms of evinacumab as well as the pharmacoeconomic assessment of its cost-effectiveness. The use of evinacumab presents potential benefits to patients with HoFH as a potentially effective and tolerable treatment to manage LDL-C levels and alleviate associated burdens and harms. Moreover, evinacumab may be more accessible and less burdensome for patients than treatment alternatives such as apheresis. Informed consent for pediatric patients requires careful consideration, especially as evinacumab is expected to be offered as a lifelong therapy. Efforts to enhance access, including co-management with general practitioners and remote consultation, are required to address potential diagnostic and geographic barriers to care and to ensure equitable and timely access to treatment for patients with HoFH. Collaborative efforts among stakeholders within the health care system are important to navigate these considerations and implement treatment with evinacumab in an equitable and patient-centred manner. Ethical considerations for health systems related to the implementation of evinacumab highlighted the challenges of funding decisions, considerations of distributive justice, assessments of opportunity costs for expensive drugs for rare diseases, and the need for more long-term evidence concerning HoFH and the efficacy of evinacumab in diverse populations to reflect the changing epidemiology of HoFH in Canada.
References
1.EUnetHTA Joint Action 2 Work Package 8, HTA Core Model version 3.0. Diemen (NL): EUnetHTA; 2016: https://www.eunethta.eu/wp-content/uploads/2018/03/HTACoreModel3.0-1.pdf. Accessed 2023 Nov 07.
2.Benkhalti M, Espinoza M, Cookson R, Welch V, Tugwell P, Dagenais P. Development of a checklist to guide equity considerations in health technology assessment. Int J Technol Assess Health Care. 2021;37:e17. PubMed
3.Nordestgaard BG, Chapman MJ, Humphries SE, et al. Familial hypercholesterolaemia is underdiagnosed and undertreated in the general population: guidance for clinicians to prevent coronary heart disease: consensus statement of the European Atherosclerosis Society. Eur Heart J. 2013;34(45):3478-3490a. PubMed
4.Cuchel M, Raal FJ, Hegele RA, et al. 2023 Update on European Atherosclerosis Society Consensus Statement on homozygous familial hypercholesterolaemia: new treatments and clinical guidance. Eur Heart J. 2023;44(25):2277-2291. PubMed
5.Akioyamen LE, Genest J, Shan SD, et al. Estimating the prevalence of heterozygous familial hypercholesterolaemia: a systematic review and meta-analysis. BMJ Open. 2017;7(9):e016461. PubMed
6.de Ferranti SD, Rodday AM, Mendelson MM, Wong JB, Leslie LK, Sheldrick RC. Prevalence of Familial Hypercholesterolemia in the 1999 to 2012 United States National Health and Nutrition Examination Surveys (NHANES). Circulation. 2016;133(11):1067-1072. PubMed
7.Brown L, Ruel I, Baass A, et al. Design, rationale, and preliminary results of the Canadian Homozygous Familial Hypercholesterolemia Registry: 2008 to 2022 update. Can J Health Technol. 2023;3(2). https://canjhealthtechnol.ca/index.php/cjht/article/view/MG00197/MG00197. Accessed 2023 Nov 07.
8.Moorjani S, Roy M, Gagne C, et al. Homozygous familial hypercholesterolemia among French Canadians in Quebec Province. Arteriosclerosis. 1989;9(2):211-216. PubMed
9.Cuchel M, Bruckert E, Ginsberg HN, et al. Homozygous familial hypercholesterolaemia: new insights and guidance for clinicians to improve detection and clinical management. A position paper from the Consensus Panel on Familial Hypercholesterolaemia of the European Atherosclerosis Society. Eur Heart J. 2014;35(32):2146-2157. PubMed
10.Tromp TR, Hartgers ML, Hovingh GK, Blom DJ, Cuchel M, Raal FJ. Worldwide perspective on homozygous familial hypercholesterolemia diagnosis, treatment and outcome – results from the HICC registry. Atherosclerosis. 2021;331:e180-e181.
11.Raal FJ. Homozygous familial hypercholesterolemia: the future looks brighter but not for all. JACC Adv. 2023;2(3):100324.
12.Brown L, Ruel I, Baass A, et al. Homozygous familial hypercholesterolemia in Canada. JACC Adv. 2023;2(3):100309.
13.Hickman TB, Briefel RR, Carroll MD, et al. Distributions and trends of serum lipid levels among United States children and adolescents ages 4-19 years: data from the Third National Health and Nutrition Examination Survey. Prev Med. 1998;27(6):879-890. PubMed
14.Baum SJ, Sijbrands EJG, Mata P, Watts GF. The doctor's dilemma: challenges in the diagnosis and care of homozygous familial hypercholesterolemia. J Clin Lipidol. 2014;8(6):542-549. PubMed
15.Wiegman A, Gidding SS, Watts GF, et al. Familial hypercholesterolaemia in children and adolescents: gaining decades of life by optimizing detection and treatment. Eur Heart J. 2015;36(36):2425-2437. PubMed
16.Kakavand H, Aghakouchakzadeh M, Shahi A, et al. A stepwise approach to prescribing novel lipid-lowering medications. J Clin Lipidol. 2022;16(6):822-832. PubMed
17.Qiu HR, Zhang L, Zhu ZJ. Perioperative management and clinical outcomes of liver transplantation for children with homozygous familial hypercholesterolemia. Medicina (Kaunas). 2022;58(10):1430. PubMed
18.Mlinaric M, Bratanic N, Dragos V, et al. Case report: liver transplantation in homozygous familial hypercholesterolemia (HoFH)-long-term follow-up of a patient and literature review. Front Pediatr. 2020;8:567895. PubMed
19.Alothman L, Belanger AM, Ruel I, et al. Health-related quality of life in homozygous familial hypercholesterolemia: a systematic review and meta-analysis. J Clin Lipidol. 2022;16(1):52-65. PubMed
20.Kayikcioglu M, Kuman-Tuncel O, Pirildar S, et al. Clinical management, psychosocial characteristics, and quality of life in patients with homozygous familial hypercholesterolemia undergoing LDL-apheresis in Turkey: results of a nationwide survey (A-HIT1 registry). J Clin Lipidol. 2019;13(3):455-467. PubMed
21.Mulder J, Kranenburg LW, Treling WJ, et al. Quality of life and coping in Dutch homozygous familial hypercholesterolemia patients: a qualitative study. Atherosclerosis. 2022;348:75-81. PubMed
22.Kacetl J, Maresova P, Maskuriy R, Selamat A. Ethical questions linked to rare diseases and orphan drugs - a systematic review. Risk Manag Healthc Policy. 2020;13:2125-2148. PubMed
23.Wagner M, Goetghebeur MM, Ganache I, et al. HTA challenges for appraising rare disease interventions viewed through the lens of an institutional multidimensional value framework. Expert Rev Pharmacoecon Outcomes Res. 2023;23(2):143-152. PubMed
24.Naveen T, Biswas A, Wig N, et al. Role of LDL apheresis in a case of homozygous familial hypercholesterolemia. Drug Discov Ther. 2019;13(1):59-61. PubMed
25.Reeskamp LF, Nurmohamed NS, Bom MJ, et al. Marked plaque regression in homozygous familial hypercholesterolemia. Atherosclerosis. 2021;327:13-17. PubMed
Appendix 1: Details of Included Publications
Table 1: Details of Included Publications
First author, year | Publication type | Objective | Key ethical considerations | Funding source |
|---|---|---|---|---|
Akioyamen, 20175 | Systematic review and meta-analysis | To provide a summary estimate of FH prevalence in the general population and assess variations in frequency across different sociodemographic characteristics. |
| Comprehensive Research Education for Medical Students Scholar Program at the University of Toronto |
Alothman, 202219 | Systematic Review and Meta-analysis | To systematically review of the association between HoFH and HRQoL. |
| Knowledge Synthesis Grant from the Canadian Institutes of Health Research (CIHR) and the Institute of Genetics |
Baum, 201414 | Editorial | To offer an alternative view re: HoFH genetic causes compared to prior historical genetic findings in this area. |
| None reported |
Brown, 202312 | Observational Study | To obtain a comprehensive registry of HoFH in Canada, known to have several founder effect regions, and describe the clinical characteristics and cardiovascular outcomes of this population over time. |
| Knowledge Synthesis Grant from the Canadian Institutes of Health Research |
Cuchel, 20234 | Clinical Guidance | To provide guidance on early diagnosis, better care, and improved cardiovascular health for patients with HoFH worldwide. |
| None reported |
De Ferranti, 20166 | Database Study | To measure prevalence of familial hypercholesterolemia from 1999 to 2012 in US. |
| Patient-Centered Outcomes Research Institute initiative, Assessment of Prevention, Diagnosis, and Treatment Options Program Award. Tommy Kaplan Fund, Department of Cardiology, Boston Children’s Hospital |
Hickman, 199813 | Database Study | To study lipid distributions among children and adolescents were examined using the most recent nationally representative data. |
| None reported |
Kacetl, 202022 | Systematic Review | To identify ethical questions related to rare diseases and orphan drugs and ethical principles or approaches applied to address them. |
| University of Hradec Kralove Long-term Development Plan |
Kakavand, 202216 | Review Article | To propose a practical stepwise approach including each class’s efficacy, place in therapy, adverse effects, warnings and precautions, and monitoring parameters. |
| None reported |
Kayikcioglu, 201920 | Survey study | To survey patients with HoFH undergoing LDL apheresis in Türkiye re: clinical management, psychosocial characteristics, and quality of life. |
| Aegerion Pharmaceuticals, Amryt Pharmaceuticals DAC |
Mlinaric, 202018 | Case Report and Literature Review | To report on a 14-year-long follow-up after liver transplant in a patient with HoFH. |
| Slovenian National Research Agency |
Moorjani, 19898 | Database Study | To investigate Homozygous Familial Hypercholesterolemia incidence among French Canadians in Quebec Province. |
| None reported |
Mulder, 202221 | Qualitative study | To investigate how patients from the Netherlands experience and cope with HoFH in daily life. |
| None reported |
Naveen, 201924 | Case Report | To report a case of an 18-year-old patient with HoFH with antilipidemic drugs and controlled only with LDL apheresis. |
| None reported |
Nordestgaard, 20133 | Clinical Guidance | To critically evaluate the extent to which HoFH is underdiagnosed and undertreated, and to provide guidance for screening and treatment of FH, to prevent coronary heart disease (CHD). |
| Amgen, Aegerion, AstraZeneca, Genzyme, Hoffman-La Roche, Kowa Europe, Novartis, Sanofi-Aventis/Regeneron |
Qiu, 202217 | Review | To analyze data of pediatric LT recipients with HoFH, with special attention paid to perioperative management and clinical outcomes. |
| Grant YYQDKT201812 from the Research Foundation of Beijing Friendship Hospital, Grant 202012024 from the Capital’s Funds for Health Improvement and Research, Grant 81970562 from the National Natural Science Foundation of China |
Raal, 202311 | Editorial Comment | To discuss disease background and prevalence internationally, as well as discuss issues of access in low- or middle-income developing countries. |
| Amgen, Sanofi-Aventis, Regeneron Pharmaceuticals, Novartis, and LIB Therapeutics. |
Reeskamp, 202125 | Case Report | To explore intensive lipid-lowering strategies and how they may result in plaque regression in adolescent patients. |
| Amgen, Novartis, Esperion, Sanofi, Regeneron, and Akcea |
Tromp, 202110 | Genetic and Clinical Characterization Study | To determine the spectrum of genetic variants in patients with a familial hypercholesterinemia in Russia. |
| None reported |
Wagner, 202323 | Review and expert opinion | To identify ethical challenges for appraising interventions for rare diseases, including key ethical tensions as well as approaches and principles for addressing these challenges. |
| Institut national d'excellence en santé et en services sociaux (INESSS) |
Wiegman, 201515 | Review | Consensus statement to improve awareness of the need for early detection and management of children with FH. |
| EAS from Amgen, Aegerion, AstraZeneca, Genzyme, Hoffman-La Roche, Kowa Europe, Novartis, Sanofi-Aventis/Regeneron |
Note: This table has not been copy-edited.
Stakeholder Input
Patient Input
Canadian Heart Patient Alliance and Canadian Organization for Rare Disorders
About Canadian Heart Patient Alliance
The Canadian Heart Patient Alliance (CHPA) is a patient-led nonprofit umbrella organization of patients, families, health professionals and supporters dedicated to reducing cardiovascular disease and preventing early death due to genetic, environmental, lifestyle, and other risk factors. Our focus is improving awareness, screening, testing, diagnosis, care, and treatment of all CVDs. The Canadian Heart Patient Alliance is working toward the day when no Canadian will suffer reduced quality of life, life-altering event, or early death due to undiagnosed or untreated CVD.
The Canadian Heart Patient Alliance collaborates with FH Canada, Heart Healthy Prevention Program St. Paul’s Hospital, and Lipid Genetics Clinic at LHSC-University Hospital. Internationally, CHPA engages with the FH Foundation (USA), Heart UK, and FH Europe.
Website: http://www.heartpatientalliance.ca/
About Canadian Organization for Rare Disorders
The Canadian Organization for Rare Disorders (CORD) is Canada’s national network for organizations representing all those with rare disorders. CORD provides a strong common voice to advocate for health policy and a healthcare system that works for those with rare disorders. The Canadian Organization for Rare Disorders works with governments, researchers, clinicians and industry to promote research, diagnosis, treatment and services for all rare disorders in Canada.
Website: www.raredisorders.ca
Information Gathering
Homozygous familial hypercholesterolemia (HoFH) is an ultra-rare, recessive genetic condition that affects and estimated 1 in 360,000 Canadians. That would translate to 100 Canadians with HoFH but the number is actually much lower due to the very high mortality, especially among those with severe disease. There is no patient group specific to HoFH but there are patients and families affected by familial hypercholesterolemia who participate in CPHA and/or CORD. Feedback was collected through a survey created by CPHA and CORD and through individual interviews with patients and caregivers.
The questionnaire survey was available in both English and French on Survey Monkey from April 12 – May 7, 2023.
The first step in recruitment was outreach through the CHPA mailing list and CORD mailing list, targeting patients and carers affected by HoFH. At the end of the survey, we asked participants whether they would be willing to participate in an individual interview and, if so, to provide an email address and/or phone number. In addition, we approached cardiologists who have partnered with CPHA previously, asking them to send the survey link to their HoFH patients and caregivers and also to ask for volunteers who were willing to engage in individual interviews. We were interested in the participation of patients with and without evinacumab experience, but we specifically requested any patients who had received evinacumab through clinical trials, compassionate access, or other means.
We received 12 responses to the survey, 11 in English and one in French. Ten of the respondents were patients living with HoFH and two were caregivers of patients diagnosed with HoFH. Three reported having access to evinacumab. In addition, we conducted six individual interviews, five HoFH patients and one caregiver. Among these, three were receiving evinacumab, so in total there were six patients with experience with the drug under assessment.
Overall, 10 patients represented were male (56%) and 8 were female (44%). In terms of age, six (33%) were between 40 and 60 years old (one was turning 60 in November); six (33%) were 18-29 years old (one just turned 18 last September) and the remaining six (33%) were between 30 and 39 years of age. All resided in Canada, with the majority (12 respondents) in Ontario (67%); three in Quebec and three in British Columbia.
Experiences With Currently Available Treatments
The responses to these two sections are presented together. The experience of the disease is intertwined with the experience of the only “effective” treatment, which is not only extremely onerous but not all that effective for many patients.
Respondents were asked to provide open-ended responses to describe how living with HoFH affected them. In addition, they were presented with several scales to rate their experience of HoFH along a number of dimensions: severity of common HoFH symptoms, effectiveness of specific therapies, and severity of adverse effects associated with different therapies.
Cardiovascular Events: Moderate to Severe
Overall, about three-fourths of all respondents reported they had experienced severe (very high) levels of LDL cholesterol (LDL-C) and the remainder said they had experienced moderate LDL-C. About half had experienced moderate or severe cardiovascular events, including atherosclerosis, stroke, atrial fibrillation and/or cardiac infarction. About half reported they experienced moderate to severe symptoms of chest pain, fatty skin deposits (lumps or lumps) around the knuckles, elbows, and knees, called “xanthomas”, and yellowish areas around the eyes (“xanthelasmae”).
Most patients have undergone multiple surgeries. “I have had three open heart surgeries. I recently had a coronary stent fitted, which was very stressful for me. There were complications that resulted in nerve damage in my leg.
Impact on Daily Live
“I have difficulty using my hands; I have no feeling and my hands 'feel dead'.”
"I have difficulty walking in the winter, I am often out of breath, and I tolerate the cold very badly.”
According to one father:
“We got my son diagnosed when he was just two years old. My elder brother’s son also had HoFH and had a massive heart attack when he was just 13 years old. The good news is that we started my son on plasmapheresis right away. The bad news was that he was in hospital every two weeks. We had to put in a central venous line. And that had big impact on his quality of life. We were always concerned with bleeding and of course he couldn’t take part in many activities: no sports and no swimming. We were even worried about sending him to school; we had to train the teachers how to tack care of the line but there were still the risks of infection. We had a fistula created by the surgeon. That was a major advance but since he could now do many activities, like swimming and sports. But it was still not a perfect solution either.”
“Even with apheresis every two weeks, my son’s cholesterol levels were not managed well. They went down to about 2.5 immediately afterwards but sometimes they went right back up to 11 or 12. We tried Repatha for about six months, but it didn’t have an impact and then another medication (not sure what it was) but the company “went out of business” so we were back to the apheresis.”
Involves the Whole Family
As a recessive genetic condition, patients and caregivers have first-hand experience of the devastating consequences on both sides of the family, As related by one patient, “At 23, I had an infarction and was put on statins and Questran powder. I hated the Questran and just stopped taking it. Then my brother died unexpectedly of a heart attack when he was only 25 years old, while he was in school in Vancouver. That should have been a wake-up call, but I still resisted my doctor’s recommendation for a valve replacement despite the fact that my aortic valve was getter narrower and narrower. It took another six years for him to convince me, but now I have a titanium valve.”
One young woman reported, “It’s hard to think about having children when you see the consequences of even heterozygous FH. My parents both have FH as do my cousins and others in our family. But only my younger sister and I have the homozygous form, though she seems to have a less severe version than I do. I have a null-null mutation, so nothing works well. Right now, I am on five medications, but my cardiovascular condition is continuing to deteriorate and I know that I will need surgery in the next few years.”
Psychological, Social, and Economic Impacts
As importantly, patients and caregivers reported the stresses of HoFH were not only the physical symptoms but also living with the prospect of a highly uncertain and unpredictable future. As described by one patient, “I feel like I have a ticking time bomb in my body that could go off at any moment. The risk of heart problems and blood pressure increases every year because I cannot control my cholesterol levels.”
In addition to the physical and psychological consequences, the disease has very real social and economic impacts. For many patients, life revolves around their plasmapheresis schedule. According to one gentleman, when I asked what he did for work, “I was diagnosed at 17 months. I guess I must have a very severe form because I was going for plasmapheresis every week, whereas some of the other kids were there only every two weeks. It is two hours from my home [in Goederich] to the hospital [ in Hamilton] and then two hours back again, every week. Even with that, my cholesterol was as high as 28 for a while. I was having trouble with my fistula (for the pheresis) and I didn’t have access to LDL apheresis. At one point, during COVID, I couldn’t even bend my arm so had to miss the pheresis. I was lined up for the clinical trial for evinacumab but I missed it too because I went into heart failure. Work has never been a possibility.”
Similarly, another patient reported she had stopped working because it was too stressful, and she wanted to spend time with her parents. They both have [heterozygous] FH and have their own challenges with statins. “My mother couldn’t tolerate Lipitor; it caused her muscles to stiffen. But neither of them wanted to go on Repatha. When my brother died, I was the only child left.”
Some of the younger patients expressed concerns about the impact on their education and social life, partly as a result of the time required for treatment: “Throughout my childhood and adolescence, I have to receive plasmapheresis every two weeks, which was a constraint during my studies and on time and currently now in my work. Another patient emphasized the burden of plasmapheresis on “the body” and her energy: “I can't take more than two classes per semester at university because I have to undergo apheresis every Thursday. I am then exhausted from Friday to Sunday. I can only go to class from Monday to Wednesday.
According to another patient: “I cannot work, go to school or go to university full time. My whole life revolves around my apheresis sessions. I am in my thirties, and I have a poor quality of life. I have to undergo apheresis every week. I have to drive three hours to get there and another three to get home. My parents take turns with me because I am so exhausted after the procedure that I am unable to drive. Their life is affected because of my apheresis sessions. I need them.”
Another young woman reported, “I was not diagnosed until I was 13 years old, as a result of xanthomas and early cardiovascular disease. I have been on statins (Crestor) and ezetimbe as well as bi-weekly plasmapheresis. The problem right now is that I am in medical school in Hamilton and traveling to Ottawa for pheresis every two weeks because the set up for plasmapheresis in Hamilton is not good. Even so, it’s not LDL apheresis in Ottawa. And I don’t know how I will manage the time away when I have to start medical shifts. It’s not fair to the others.”
Inadequacy of Other Medications
Some patients have been prescribed a PCSK9 therapy and while some have remained on the treatment, others have not. “I was on Repatha, and it seemed to work for a while and lowered my cholesterol levels, so I was able to ‘halve’ the number of plasmapheresis sessions from weekly to bi-weekly. But then the medication suddenly stopped working and I had heart failure. So, I then had major reconstructive surgery, meaning four by-passes and two mechanical valves. I was back to weekly pheresis.”
Even those who have remained on Repatha are not sure that it does any good. “My doctor says I should just stay on it for now. He requested the new medication, evinacumab, but it hasn’t been approved for me yet.”
Overall, all patients expressed concerns about their current treatment regimen (apheresis, statins, and other medications) to effectively control their LDL-C levels. They are highly concerned about the possibility (likelihood) of the need for surgery in advance of or as a result of future cardiovascular events, which impacts their quality of life and life expectancy.
Improved Outcomes
Ideally, patients would prefer a treatment that could eliminate the need for apheresis, similar to the situation of PCSK9 for their parents or other family members with HeFH who receive only drug therapy. Realistically, they want a therapy that would reliably, consistently, and sustainably control their LDL-C levels at normal or near-normal levels. This would allow them to experience fewer spikes, to reduce the frequency of apheresis sessions, and most importantly, to reduce the risk of cardiovascular events, like stroke, heart attack or heart failure.
Said one person, “If I cannot entirely stop the apheresis, at least I could go just once a month or maybe every three weeks.”
Similarly, another patient said, “By lowering the LDL-C level consistently and reducing the frequency of apheresis sessions, I would have a much improved quality of life.”
“I could find a job, go to university, and start living my life.”
“I know there are no long terms studies on fewer cardiovascular events or even longevity, but if it can control LDL levels, it can control cardiovascular risks. It’s pretty much a “straight line”, as anyone would know.”
One patient was quoted as saying, "I don't expect to get a cure, but something that will help me enjoy a better quality of life and a less stressful life so that I can fully enjoy my children.”
Experience With Drug Under Review
All of the patients on evinacumab received the drug through clinical trials, compassionate access, or research study.
All reported they were very pleased with the outcomes, in terms of lowering their LDL-C levels but also the impact on quality of life. They experienced improvements in having more energy, consistently maintaining lower LDL levels, being able to reduce the frequency of apheresis, being able to plan to take part in social and family events, not missing school or work, and feeling, overall, much more energized, happy, and optimistic (for the first time in their lives).
“This is the first time that my cholesterol levels have remained consistently below 6, which is not great but a lot better than they have been for years.”
“My son no longer has the spikes; they used to go from 2.5 to 12 almost overnight. This treatment makes us feel a lot more relaxed. We don’t feel like we have to keep testing and watching him between pheresis appointments.”
“I have a lot more energy and I can make plans to do things, to go out, and importantly to not miss so much work because I can’t be there.”
“This drug is my ‘lifeline’; without it my cholesterol will go right back to 30 in no time. And now I can exercise, which I know is important to keeping my cholesterol down. Before this drug, I just couldn’t do it on a regular basis, so it was just a vicious circle.
“Now that I am evinacumab, I only do apheresis once a month whereas before it was twice a month. So fewer trips to the hospital (four hours round trip) and I also get to use the LDL apheresis machine. Before this, I was told I didn’t qualify; it was only for the one patient. I was told maybe I could have it maybe every other visit, but now I can get it every time. So, everything is better.”
“This drug has really improved my son’s outlook on life. We are really optimistic that in the future there will be even better treatments, so we could stop the apheresis altogether. But for right now, this is good.”
None of the patients reported experiencing any serious adverse events. “A little shortness of breath and a little fever, but nothing serious at all.”
Anything Else?
Patients and families living with HoFH are realistic that Ekveeza is not a cure and will not eliminate the need for apheresis. They do expect that it will stabilize cholesterol levels and keep them within a normal (not dangerous) range so that the risk of cardiovascular events will be reduced. This means they will not need to live in the fear that they, or their loved one with HoFH, could experience a CVD crisis at any moment, even if they are doing “everything right”, including eating a healthy diet, exercising, and managing stress (to the degree possible).
This would not only improve individual and family quality of life and allow patients and family members to participate more in work or school on a more regular basis, but it also improves the mental health and overall wellbeing of families. There will also be a benefit back to the health system with fewer medical crises and benefit to society, as a whole, in terms of happier and healthier families.
Conflict of Interest Declaration — Canadian Heart Patient Alliance and Canadian Organization for Rare Disorders
To maintain the objectivity and credibility of the CADTH reimbursement review process, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission?
No outside help to complete submission.
Did you receive help from outside your patient group to collect or analyze data used in this submission?
No outside help to collect or analyze data, beyond receiving referrals from the clinicians.
List any companies or organizations that have provided your group with financial payment over the past 2 years AND who may have direct or indirect interest in the drug under review.
Table 1: Financial Disclosures for Canadian Organization for Rare Disorders
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Ultragenyx | — | — | X | — |
Clinician Input
Familial Hypercholesterolemia Canada
About Familial Hypercholesterolemia Canada
We are a national group of pediatric and adult lipid specialists whose purpose is to improve the care of patients with Familial Hypercholesterolemia (including Homozygous and Heterozygous FH) and reduce cardiovascular risk associated with this very high CV risk condition. Our group encompasses the specialist physicians in Canada with the greatest experience in managing patients with HoFH.
Refer to our website: https://www.fhcanada.net
Information Gathering
Information here is based on our collective clinical experience and review of published literature and congress proceedings.
Current Treatments and Treatment Goals
Homozygous FH (HoFH) presents in early childhood and is an extremely challenging condition to treat across the lifespan. This relates to the fact that most lipid-lowering agents, including statins, ezetimibe, and PCSK9 inhibitors have very limited efficacy in HoFH because they act by upregulating liver LDL receptors, which are defective or absent in HoFH. These drugs are very safe and easily accessible and are therefore typically used to treat patients with HoFH but are almost universally inadequate to sufficiently lower LDL cholesterol. Lipoprotein apheresis is a form of extra-corporeal removal of LDL and is very effective in patients with HoFH. However, it is costly and resource-intensive, invasive and associated with reduced quality-of-life and significant disruption to patient’s/family’s education, employment and personal lives. In addition, it is currently only available at a small number of specialized centres. Plasmapheresis or plasma exchange are used as alternative treatment strategies where LDL apheresis is not available but suffer from the additional drawback that these are less selective, result in a reduction protective HDL levels in addition to LDL, and require substantial blood product exposure (usually albumin transfusion). Maintaining long-term intravenous access is often also a barrier to its use. As with apheresis, the availability of plasma exchange is limited to major academic centres, meaning that patients living outside of these major urban areas will often not have access to it, or have the additional burden of travel, as well as creating inequities in the level of care of patients based on geographic location.
Lomitapide is approved by Health Canada for the treatment of HoFH and acts via an LDL receptor-independent mechanism of action. There are two main barriers to its use. First is that it is exceptionally expensive (in the hundreds of thousands of dollars per year) and is not reimbursed by most provincial drug plans. As such, access is limited. Second is that it is poorly tolerated and frequently leads to gastrointestinal side-effects and hepatic fat accumulation which limits its use. The extensive experience with this medication in Quebec is that the medication needs to be discontinued or dose reduced in 75% of patients (Aljenedil S, Alothman L, Bélanger AM, Brown L, Lahijanian Z, Bergeron J, Couture P, Baass A, Ruel I, Brisson D, Khoury E, Gaudet D, Genest J. Lomitapide for treatment of homozygous familial hypercholesterolemia: The Québec experience. Atherosclerosis. 2020 Oct;310:54-63) meaning that for the large majority of HoFH patients it does not represent an adequate treatment modality. In addition, pediatric use has been very limited.
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
Please refer to the section above. Currently available therapies for HoFH are inadequate because of lack of efficacy (statins, ezetimibe, PCSK9 inhibitors), lack of tolerability (lomitapide), and lack of availability/access and invasiveness (apheresis/plasmapheresis). There is an urgent unmet gap in the ability to treat HoFH patients safely, effectively, and equitably in Canada.
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
The ideal medication for HoFH would work via an LDL receptor-independent mechanism, would substantially lower LDL-C levels, and would be well tolerated with few side effects and without significant drug interactions with a minimum impact on health care resources or patient/family burden. others lipid-lowering therapies.
Evinacumab appears to meet these criteria and would therefore be an incredibly important addition to current treatments for HoFH.
Evinacumab is a human monoclonal antibody directed against angiopoietin-like protein 3 (ANGPTL3) which plays a key role in lipid metabolism. In the phase 3 ELIPSE trial, a double-blind, placebo-controlled trial of IV infusion of evinacumab administered at 15mg/kg every 4 weeks, it was shown to reduce LDL-cholesterol levels by nearly 50% over 24 weeks compared to placebo in HoFH patients, in addition to background lipid-lowering therapy, including statins and ezetimibe (Raal FJ, Rosenson RS, Reeskamp LF, Hovingh GK, Kastelein JJP, Rubba P, Ali S, Banerjee P, Chan KC, Gipe DA, Khilla N, Pordy R, Weinreich DM, Yancopoulos GD, Zhang Y, Gaudet D; ELIPSE HoFH Investigators. Evinacumab for Homozygous FamilialHypercholesterolemia. N Engl J Med. 2020 Aug 20;383(8):711-720.). Evinacumab was also effective in patients with minimal or no LDL-receptor function (true LDLR null allele homozygotes). Evinacumab would likely be used as a third line therapy after statins, ezetimibe and PCSK9 inhibitors. In some patients it would be expected to eliminate or reduce the need for plasmapheresis or apheresis, and possibly for lomitapide.
Which patients would be best suited for treatment with the drug under review? Which patients would be least suitable for treatment with the drug under review?
Patients best suited would be individuals with HoFH who have been unable to achieve target levels of LDL-C despite maximally tolerated doses of statins, ezetimibe and PCSK9 inhibitors, with or without plasmapheresis or apheresis, or who have progressive cardiovascular disease despite these treatments.
Misdiagnosis is unlikely to occur by a specialist familiar with this condition based on phenotype and genetic assessments, lipid guidelines and medical literature.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice? How often should treatment response be assessed?
The most important outcome would be the reduction in LDL-C levels. A meaningful response would be a sustained >20 - 30% reduction in LDL-C, or a reduction in the frequency of apheresis or plasmapheresis. Ultimately the reduction in LDL-C would be expected to translate to a reduction in the rate of cardiovascular events and improved survival.
What factors should be considered when deciding to discontinue treatment with the drug under review?
HoFH is a chronic condition and treatment should be long term to address the cumulative exposure to high levels of LDL cholesterol. Standard factors that would apply to any medication including intolerable adverse effects would apply. Evinacumab appears to be a very well tolerated medication (Raal FJ, Rosenson RS, Reeskamp LF, Hovingh GK, Kastelein JJP, Rubba P, Ali S, Banerjee P, Chan KC, Gipe DA, Khilla N, Pordy R, Weinreich DM, Yancopoulos GD, Zhang Y, Gaudet D; ELIPSE HoFH Investigators. Evinacumab for Homozygous FamilialHypercholesterolemia. N Engl J Med. 2020 Aug 20;383(8):711-720, and Rosenson RS, Burgess LJ, Ebenbichler CF, Baum SJ, Stroes ESG, Ali S, Khilla N, Hamlin R, Pordy R, Dong Y, Son V, Gaudet D. Evinacumab in Patients with Refractory Hypercholesterolemia. N Engl J Med. 2020 Dec 10;383(24):2307-2319. doi: 10.1056/NEJMoa2031049. Epub 2020 Nov 15. PMID: 33196153.). The direct comparison would be with lomitapide and evinacumab appears to have a more favorable tolerability profile.
What settings are appropriate for treatment with [drug under review]? Is a specialist required to diagnose, treat, and monitor patients who might receive [drug under review]?
HoFH is typically managed by specialists with expertise in this condition. It is expected that diagnosis and decision to treat with evinacumab would be made by a specialist.
Additional Information
Clinical trials and the Special Access Program with Health Canada have shown demonstrated, in addition to a very significant decrease in LDL, an excellent tolerability without side effects.
Conflict of Interest Declarations — Familial Hypercholesterolemia Canada
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please refer to the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission?
No.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission?
No.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician who contributed to the input.
Declaration for Clinician 1
Name: Liam Brunham
Position: Associate Professor, University of British Columbia
Date: 04-04-2023
Table 2: COI Declaration for Familial Hypercholesterolemia Canada — Clinician 1
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Novartis | — | X | — | — |
Amgen | X | — | — | — |
HLS | X | — | — | — |
Ultragenyx | X | — | — | — |
Declaration for Clinician 2
Name: Brian W.; Gordon Francis
Position: Section Head of Preventive Cardiology, The Hospital for Sick Children, Toronto; Professor of Medicine, University of British Columbia
Date: April 5, 10-04-2023
Table 3: COI Declaration for Familial Hypercholesterolemia Canada — Clinician 2
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Chiesi | X | — | — | — |
Esperion | X | — | — | — |
Amryt Pharma | X | — | — | — |
Ultragenyx | X | — | — | — |
Declaration for Clinician 3
Name: Jean Bergeron
Position: Associate Professor, Laval University
Date: 13-04-2023
Table 4: COI Declaration for Familial Hypercholesterolemia Canada — Clinician 3
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Novartis (Advisory Board) | X | — | — | — |
Amgen (Advisory Board) | X | — | — | — |
HLS (Advisory Board) | X | — | — | — |
Ultragenix (Advisory Board) | X | — | — | — |
Regeneron (Clinical Trial) | — | — | — | — |
ArrowHead (Clinical Trial) | — | — | — | — |
Health Canada (SAP) | — | — | — | — |
Declaration for Clinician 4
Name: Brian W. McCrindle, MD MPH
Position: Section Head of Preventive Cardiology, The Hospital for Sick Children, Toronto
Date: April 5, 2023
Table 5: COI Declaration for Familial Hypercholesterolemia Canada — Clinician 4
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Chiesi | X | — | — | — |
Esperion | X | — | — | — |
Amryt Pharma | X | — | — | — |
Ultragenyx | X | — | — | — |
Declaration for Clinician 5
Name: Robert A. Hegele MD FRCPC
Position: Professor of Medicine, Western University
Date: 01-May-2023
Table 6: COI Declaration for Familial Hypercholesterolemia Canada — Clinician 5
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Amgen | — | X | — | — |
Arrowhead | X | — | — | — |
HLS Therapeutics | X | — | — | — |
Ionis-Akcea | X | — | — | — |
Novartis | — | X | — | — |
Pfizer | X | — | — | — |
Sanofi | X | — | — | — |
Ultragenyx | X | — | — | — |
Declaration for Clinician 6
Name: Jacques Genest MD
Position: Professor, McGill University
Date: 01-May-2023
Table 7: COI Declaration for Familial Hypercholesterolemia Canada — Clinician 6
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Novartis | X | — | — | — |
Amgen | X | — | — | — |
Sanofi | X | — | — | — |
Ultragenyx | X | — | — | — |
Declaration for Clinician 7
Name: Iulia Iatan
Position: Attending physician, General Internal Medicine, Healthy Heart Program Prevention Clinic, Providence Health Care, University of British Columbia
Date: May 3rd, 2023
Table 8: COI Declaration for Familial Hypercholesterolemia Canada — Clinician 7
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In Excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
Redactions: Confidential information in this document may be redacted at the request of the sponsor in accordance with the CADTH Drug Reimbursement Review Confidentiality Guidelines
Stakeholder Input: The views expressed in each submission are those of the submitting organization or individual; not necessarily the views of CADTH or of other organizations. As such, they are independent of CADTH and do not necessarily represent or reflect the view of CADTH. No endorsement by CADTH is intended or should be inferred. By filing with CADTH, the submitting organization or individual agrees to the full disclosure of the information. CADTH does not edit the content of the submissions.
CADTH does use reasonable care to prevent disclosure of personal information in posted material; however, it is ultimately the submitter’s responsibility to ensure no identifying personal information or personal health information is included in the submission. The name of the submitting organization or individual and all conflict of interest information are included in the submission; however, the name of the author, including the name of an individual patient or caregiver submitting the patient input, are not posted.
Accessibility: CADTH is committed to treating people with disabilities in a way that respects their dignity and independence, supports them in accessing material in a timely manner, and provides a robust feedback process to support continuous improvement. All materials prepared by CADTH are available in an accessible format. Where materials provided to CADTH by a submitting organization or individual are not available in an accessible format, CADTH will provide a summary document upon request. More details on CADTH’s accessibility policies can be found here.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.