Drugs, Health Technologies, Health Systems
Reimbursement Review
Zilucoplan (Zilbrysq)
Sponsor: UCB Canada Inc.
Therapeutic area: Generalized myasthenia gravis
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Clinical Review
Abbreviations
AChR
acetylcholine receptor
AE
adverse event
ANCOVA
analysis of covariance
CDA-AMC
Canada's Drug Agency
CI
confidence interval
CrI
credible interval
CTCAE
Common Terminology Criteria for Adverse Events
FcR
fragment crystallizable receptor
gMG
generalized myasthenia gravis
GRADE
Grading of Recommendations Assessment, Development and Evaluation
HRQoL
health-related quality of life
ICE
intercurrent event
IG
immunoglobulin
IST
immunosuppressive therapy
ITC
indirect treatment comparison
J2R
jump to reference
LS
least squares
MAR
missing at random
MDC
Muscular Dystrophy Canada
MG
myasthenia gravis
MG-ADL
Myasthenia Gravis Activities of Daily Living
MGC
Myasthenia Gravis Composite
MGFA
Myasthenia Gravis Foundation of America
MGFA-PIS
Myasthenia Gravis Foundation of America Post-Intervention Status
MG-QoL15
Myasthenia Gravis Quality of Life 15-item Scale
MG-QoL15r
Myasthenia Gravis Quality of Life 15-item Scale – Revised
MI
multiple imputation
MID
minimal important difference
mITT
modified intention to treat
MMRM
mixed model of repeated measures
MNAR
missing not at random
MSE
minimal symptom expression
NMA
network meta-analysis
NMD4C
Neuromuscular Disease Network for Canada
NSIST
nonsteroidal immunosuppressive therapy
OR
odds ratio
PICO
patient, intervention, comparison, and outcome
PLEX
plasma exchange
QMG
Quantitative Myasthenia Gravis
RCT
randomized controlled trial
SAE
serious adverse event
SC
subcutaneous
SD
standard deviation
SE
standard error
TEAE
treatment-emergent adverse event
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Table 1: Background Information of Application Submitted for Review
Item | Description |
|---|---|
Drug product | Zilucoplan (Zilbrysq), solution for injection (16.6 mg/0.416 mL, 23.0 mg/0.574 mL, and 32.4 mg/0.81 mL [each corresponding to 40 mg/mL] in single-dose prefilled syringes) for SC use |
Sponsor | UCB Canada Inc. |
Indication | For the treatment of gMG in adult patients who are AChR antibody-positive. Patients continued to receive standard therapy throughout the pivotal trial. |
Reimbursement request | As an add-on therapy for the treatment of adult patients with AChR antibody positive refractory gMG, defined as not achieving symptom control after:
|
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | July 11, 2024 |
Recommended dose | The recommended dose of zilucoplan is as an SC injection once daily according to body weight: 16.6 mg for body weight < 56 kg, 23 mg for body weight ≥ 56 kg to < 77 kg, and 32.4 mg for body weight ≥ 77 kg. |
AChR = acetylcholine receptor; gMG = generalized myasthenia gravis; NOC = Notice of Compliance; SC = subcutaneous.
Source: Product monograph for zilucoplan.1
Introduction
Myasthenia gravis (MG) is a rare, chronic, autoimmune neuromuscular disease in which antibodies against the neuromuscular junction disrupt nerve impulse conduction, resulting in localized or generalized skeletal muscle weakness.2,3 In most patients, MG initially affects the extraocular muscles (ocular MG) and then progresses to other muscle groups, including the bulbar and proximal limb skeletal muscles. When the disease progresses to other muscle groups, it is referred to as generalized myasthenia gravis (gMG).4-6 The diagnosis of gMG is based on clinical presentation; serological tests to detect antibodies against anti–acetylcholine receptor (AChR) (which 80% to 90% of patients with gMG have), MuSK, and LRP4; and electrodiagnostic tests for the evaluation of neuromuscular transmission.6,7 Approximately 80% of all patients with MG have gMG.6 In Canada, the incidence and prevalence of gMG are estimated at 23 per 1 million person-years and 32 per 100,000, respectively.8 The Myasthenia Gravis Foundation of America (MGFA) classification system groups patients with MG, according to the severity and localization of symptoms, into 5 functional classes: I (ocular manifestations only), II (mild), III (moderate), IV (severe generalized), and V (intubation or myasthenic crisis).9 Other validated scales used in MG to determine disease and symptom severity include the Myasthenia Gravis Activities of Daily Living (MG-ADL) scale, Quantitative Myasthenia Gravis (QMG) scale, the Myasthenia Gravis Composite (MGC) scale, and the Myasthenia Gravis Quality of Life 15-item (MG-QoL15) scale.10 Because the symptoms and disease course of gMG are highly variable and heterogenous among patients, it has been referred to as a “snowflake disease.”11 Patients experience a variety of symptoms, including fatigue, droopy eyelids, diplopia, neck weakness, difficulty swallowing or chewing, speech disturbances, difficulty breathing, and upper and/or lower limb weakness.11 The symptoms of gMG occur unpredictably and fluctuate in nature, intensity, and severity on a day-to-day basis and throughout a patient’s life.2 Patients can also experience exacerbation, defined by 3 criteria, which necessitates inpatient treatment: temporal (a rapid, progressive, and unpredictable worsening of symptoms); subjective (deterioration of bulbo-pharyngeal function, restriction of strength for head and neck muscles or extremity muscles, which affects patients’ everyday life, or the start of weakness in breathing with reduced cough impulse); and objective (at least a 5-point improvement in QMG score with no more than 5 points from ocular MG).12 Furthermore, MG exacerbations can deteriorate into a myasthenic crisis, in which patients experience sudden respiratory failure that requires emergency intubation or ventilation.12 Almost 15% of patients with gMG have been classified as having refractory gMG.13 According to the clinical expert consulted for this review, the goals of treatment for patients with MG are to reduce MG-related morbidity and mortality, minimize treatment-associated morbidity and mortality, reduce weakness (ocular, bulbar, respiratory, axial, and extremity) associated with MG and prevent disease exacerbations or an MG crisis, and improve health-related quality of life (HRQoL).
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of zilucoplan 0.3 mg/kg administered as a subcutaneous (SC) injection once daily for the treatment of gMG in adult patients who have anti-AChR antibody–positive disease. Patients continued to receive standard therapy throughout the pivotal trial. Per sponsor request, this review focuses on the use of zilucoplan “as an add-on therapy for the treatment of adult patients with AChR antibody positive refractory gMG, defined as not achieving symptom control after:
Treatment for at least 1 year with 2 or more of the following therapies: prednisone, azathioprine, mycophenolate cyclosporine, cyclophosphamide, methotrexate, tacrolimus, other corticosteroids for gMG, other immunosuppressive therapies (ISTs), OR
History of treatment with at least one of these therapies for 1 year or more and required chronic plasma exchange (PLEX), intravenous immunoglobulin (IVIg), or subcutaneous immunoglobulin (SCIg) at least every 3 months for the 12 months prior to treatment with zilucoplan.”
The focus will be on comparing zilucoplan to relevant comparators and identifying gaps in the current evidence.
Perspectives of Patients, Clinicians, and Drug Programs
The information in this section is a summary of input provided by the patient and clinician groups who responded to Canada's Drug Agency (CDA-AMC) call for input and from clinical expert(s) consulted by CDA-AMC for the purpose of this review.
Patient Input
CDA-AMC received 1 patient group submission from Muscular Dystrophy Canada (MDC), a health charity that supports people affected by muscular dystrophies and related muscle diseases (neuromuscular disorders) in Canada, which included a survey (conducted with e-blasts, personalized invitations, and online patient groups) and semi-structured virtual interviews with adults living with MG. MDC also conducted an MG Journey Mapping project for adults living with MG in Canada, using virtual interviews, round table sessions, surveys, and HRQoL measures (EQ visual analogue scale, EQ-5D, MG-ADL, MG-QoL). A total of 127 participants (84 females and 43 males) aged from 22 years to 78 years from all provinces in Canada contributed to the MDC’s group submission, the majority of whom reported having gMG. Additionally, 47 people living in Canada (33 females, 14 males) with MG provided input on their hopes and expectations for zilucoplan and their everyday experiences with MG. None of the respondents included in the MDC’s patient input had experience with zilucoplan.
The respondents indicated that MG has a significant impact on productivity, fatigue and energy levels, quality of sleep, respiratory health, mobility, strength, independence, relationships and social participation, eyes and vision, speech, and swallowing. In addition to physical and mental health, quality of life, and the well-being of their families, the respondents reported that available treatments for MG have a positive impact on health outcomes but can also have negative effects (adverse events [AEs] with steroids, slow onset of medication effects, and a feeling of trial and error with medications). Patients had concerns about the long-term and sustained benefits of supportive treatments.
Patients with MG sought improved outcomes with new treatments, including decreased intensity of exacerbations and side effects, maintenance of independence, and fewer hospital admissions for serious MG-related circumstances. Patients were willing to tolerate the side effects of medications if they improved MG outcomes. In addition, respondents stated that although current medications appeared to decrease the number of exacerbations, they did not have an impact on patients’ overall quality of life. Moreover, MDC input noted that patients, families, and caregivers value the following factors when evaluating MG therapies: treatment method and delivery (e.g., invasiveness, duration, frequency of administration), potential side effects (e.g., low risk of side effects, number of side effects), HRQoL, convenience of treatment (e.g., administration at home or community centre, perceived control and flexibility, time to travel to clinic, access to parking for clinic visits), financial impact (e.g., treatment coverage by public or private insurance), and access to treatment. According to MDC input, HRQoL was noted as a key priority, and was rated higher than the convenience of a drug. MDC input stated that beyond the accessibility of treatments, patients with MG need improved treatment options with enhanced effectiveness and tolerance over the long-term.
Patients and caregivers reported varied experiences in diagnostic testing for MG. Although some respondents experienced minimal problems with testing and diagnosis, especially in cases of MG crisis or hospitalization due to MG, the majority reported significant difficulties getting diagnosed, which included a lengthy process with many missed opportunities, delayed diagnosis, misdiagnosis (such as stroke or Bell palsy), and costs incurred. According to early findings of the MG Journey Mapping project, the time from the first bothersome symptom to diagnosis ranged from 7 years to 23 years. All the respondents underwent diagnostic blood testing, and many underwent single-fibre electromyography to confirm the diagnosis.
Clinician Input
Input From Clinical Expert Consulted by CDA-AMC
The following input was provided by 1 clinical specialist with expertise in the diagnosis and management of MG.
The clinical expert noted that although there has been significant improvement in the management of patients with MG over the past few decades, there remain significant treatment gaps for patients with gMG. Given that patients with gMG experience disease morbidity while awaiting the beneficial effects of prolonged treatments that often have intolerable side effects, the expert highlighted the need for new treatments that have a faster onset of action (particularly among patients with any bulbar or respiratory involvement), are more effective, have fewer significant adverse effects, and have greater durability than current treatment options. Additionally, the clinical expert noted that patients would benefit from new treatments that are the least invasive (e.g., oral preferred over SC or IV route of administration), are less frequent (e.g., weekly or monthly dosing preferred over daily administration), allow for reduced doses of other immunosuppressive drugs, and may be used in combination with existing or future treatments that have differing mechanisms of action (e.g., the combination of a peptide complement inhibitor plus a neonatal fragment crystallizable receptor [FcR] inhibitor in patients with severe or refractory MG). Overall, the expert described the goals of treatment for patients with MG, which are to reduce MG-related morbidity and mortality, minimize treatment-associated morbidity and mortality, reduce weakness (ocular, bulbar, respiratory, axial, and extremity) associated with MG, prevent disease exacerbations and MG crises, and improve HRQoL.
The expert noted that, depending on how refractory disease is defined, approximately 10% to 15% of patients do not respond to conventional treatment. These patients require more aggressive treatments, including IVIg or PLEX, and are considered to be the target population for complement inhibitors such as zilucoplan. The expert explained that patients who were identified as refractory in the RAISE trial were in alignment with the way refractory disease would be defined in clinical practice, particularly with reference to an adequate trial of prednisone in addition to another immunosuppressive therapy (IST).
The clinical expert noted that patients are initially identified as having MG based on clinical suspicion; the diagnosis is confirmed with electrophysiology (i.e., repetitive nerve stimulation for assessment of decrement) and serology (e.g., confirmation of antibodies for anti-AChR, MuSK, and LRP4). The presence of anti-AChR antibodies is a reliable diagnostic finding with a high specificity, so the identification of patients with MG using anti-AChR antibody testing is straightforward. Nevertheless, given the rarity of the disease and the fact that the initial identification of patients with MG is based on clinical suspicion, MG is likely underdiagnosed in the population, according to the clinical expert. The expert noted that the availability and timeliness of anti-AChR antibody assays varies across Canada.
According to the expert consulted, patients who are most likely to benefit from treatment with zilucoplan are generally aligned with patients who were enrolled in the RAISE trial, who met the following criteria: anti-AChR antibody–positive gMG, MGFA disease class II to class IV, and with an MG-ADL score of 6 or greater. The exception was the criterion of a QMG score of 12 or greater in the RAISE study, which is reportedly not used commonly in clinical practice. The expert pointed out that patients who have had an adequate trial (both dose and duration) of both prednisone and at least 1 nonsteroidal immunosuppressive therapy (NSIST), or those who demonstrated intolerance to the combination of prednisone and NSIST, should be eligible for treatment with zilucoplan; such criteria limit the inclusion to patients who have been on conventional treatment for at least 6 months (and commonly 12 months), reflecting the duration needed for corticosteroids (3 to 6 months) and mycophenolate mofetil and azathioprine (likely 12 to 18 months) to produce an optimal benefit.
The MG-ADL scale is a patient-reported outcome deemed by the expert consulted to be clinically relevant (a 2-point change is deemed a minimum clinically meaningful improvement) for evaluating response to treatment. According to the clinical expert for this review, the MG-ADL can be self-administered within minutes (by patients, with supervision of a neuromuscular neurologist) and should be used as an eligibility criterion for treatment with zilucoplan and as monitoring of efficacy throughout treatment. Reasons to discontinue treatment with zilucoplan include a clear lack of response to treatment with zilucoplan (i.e., no reduction in MG-ADL after about 6 months), intolerance due to significant AEs, and the requirement for additional ongoing treatments with IVIg or PLEX despite an adequate trial of zilucoplan, according to the clinical expert.
The clinical expert explained that because MG is a rare disorder that requires nuanced management, patients with gMG should be diagnosed, treated, and monitored by a neuromuscular neurologist with experience in gMG. This is especially important with more advanced treatment options, given the resources required to use them in the management of gMG.
Clinician Group Input
CDA-AMC received 1 clinician group submission from the Neuromuscular Disease Network for Canada (NMD4C), which comprised the experience of 8 clinicians who have treated patients with gMG. The clinician group agreed with the clinical expert on unmet treatment needs, the goals of treatment, treatment response evaluations, and care management for patients with MG. NMD4C identified emergency department visits, hospitalizations, and intensive care unit admissions as additional treatment outcomes. The ability to self-administer zilucoplan at home was seen as providing patients with greater autonomy in their care management. Both the clinician group and the clinical expert consulted for this review indicated that patients with gMG who have anti-AChR antibody–positive disease would most likely benefit from treatment from zilucoplan; evidence on the efficacy of zilucoplan has not been confirmed for patients with MG who are seronegative, the clinician group noted.
Drug Program Input
Input was obtained from the drug programs that participate in the reimbursement review process. The following were identified as key factors that could potentially affect the implementation of a recommendation for zilucoplan: relevant comparators, considerations for the initiation of therapy, considerations for the continuation or renewal of therapy, considerations for the discontinuation of therapy, considerations for the prescribing of therapy, and system and economic issues. The clinical expert consulted for this review provided advice on potential implementation issues raised by the drug programs. Refer to Table 4 for more details.
Clinical Evidence
Systematic Review
Description of Studies
One phase III, multicentre, double-blind trial (RAISE, previously known as MG0010) compared the efficacy and safety of zilucoplan with placebo. The RAISE trial enrolled 174 patients, aged 18 years to 74 years, with anti-AChR antibody–positive gMG. The primary objective was to evaluate the change from baseline to week 12 in MG-ADL score. Key secondary end points included changes from baseline to week 12 in QMG score, MGC score, and Myasthenia Gravis Quality of Life 15-item revised (MG-QoL15r) score. Additional secondary end points included the achievement of minimal symptom expression (MSE) at week 12 without rescue therapy, an MG-ADL responder rate at week 12 without rescue therapy, and a QMG responder rate at week 12 without rescue therapy. The achievement of minimal manifestation status per Myasthenia Gravis Foundation of America Post-Intervention Status (MGFA-PIS) at week 12 without rescue therapy was an exploratory end point in the RAISE study. Patients with refractory anti-AChR antibody–positive gMG were included in exploratory subgroup analyses. Outcomes reported for patients with refractory gMG included change from baseline to week 12 in MG-ADL score, QMG score, MGC score, and MG-QoL15r score; the achievement of MSE at week 12 without rescue therapy; an MG-ADL responder rate at week 12 without rescue therapy; and a QMG responder rate at week 12 without rescue therapy.
This review presents data for patients in the overall trial population, which aligns with the Health Canada indication. The Clinical Study Report, with a data cut-off date of December 30, 2021, was the primary data source for the RAISE study. Per sponsor request, this review focuses on the sponsor’s reimbursement request for patients with refractory gMG, which is similar to the reimbursement criteria for the comparator therapy, eculizumab. Eculizumab received a positive final recommendation in 2020 from CADTH for patients with refractory gMG, which is defined as not achieving symptom control after:
“an adequate trial of two or more immunosuppressive therapies (ISTs), either in combination or as monotherapy in the previous 12 months, OR
an adequate trial of at least one IST and chronic plasmapheresis or plasma exchange or intravenous immunoglobulin at least four times (every three months) in the previous 12 months.”
In the overall population, 56.9% of patients with gMG were female, 43.1% were male, and the mean age was 53.0 years (standard deviation [SD] = 15.1 years). At screening, most patients had a diagnosis of MGFA class III disease (67.2%), generalized symptoms at disease onset (64.4%), disease onset at a mean of 43.8 years (SD = 18.0 years), and a mean disease duration of 9.2 years (SD = 9.9 years). More patients had higher scores in the stratified randomization of MG-ADL scores (62.1% of patients had a score ≥ 10) and QMG scores (56.3% of patients had a score ≥ 18). Most disease characteristics and patient histories were similar in the 2 treatment groups, but a higher proportion of patients had undergone thymectomy in the zilucoplan group (52.3%) than in the placebo group (42.0%). Patients had similar between-group mean baseline scores on the MG-ADL and QMG scales. Patients were considered to have refractory gMG in the RAISE trial if they had received treatment for at least 1 year with 2 or more of the following therapies: prednisone, azathioprine, mycophenolate mofetil, cyclosporine, cyclophosphamide, methotrexate, tacrolimus, rituximab, eculizumab, other corticosteroids for gMG, or other ISTs; or had a history of treatment with at least 1 of the aforementioned therapies for 1 year or more and required chronic PLEX, IVIg, or SCIg at least every 3 months during the 12 months before enrolment. No patients in the RAISE trial had received eculizumab as a past or baseline gMG therapy, and 1 patient had received rituximab as a past therapy, but the trial excluded patients who had received rituximab in the 12 months before baseline and, therefore, no patients were receiving rituximab at baseline.
Efficacy Results
Efficacy results were summarized using the data cut-off date of December 30, 2021, for the following outcomes: changes from baseline to week 12 in MG-ADL score, QMG score, and MG-QoL15r score; achievement of MSE at week 12 without rescue therapy; an MG-ADL responder rate at week 12 without rescue therapy; a QMG responder rate at week 12 without rescue therapy; and minimal manifestation status per MGFA-PIS at week 12 without rescue therapy.
Change From Baseline to Week 12 in the MG-ADL Score
In the overall population, the least squares (LS) mean change from baseline to week 12 in the MG-ADL score was –4.39 (standard error [SE] = 0.45) in the zilucoplan group and –2.30 (SE = 0.44) in the placebo group (LS mean difference of –2.09; 95% confidence interval [CI], –3.24 to –0.95; P < 0.001), which favoured zilucoplan. In the refractory subpopulation, the LS mean change from baseline to week 12 in the MG-ADL score was –4.72 (SE = 0.58) in the zilucoplan group and –1.62 (SE = 0.58) in the placebo group (LS mean difference of –3.11; 95% CI, –4.69 to –1.52; nominal P < 0.001).
Change From Baseline to Week 12 in the QMG Score
In the overall population, the LS mean change from baseline to week 12 in the QMG score was −6.19 (SE = 0.56) in the zilucoplan group and −3.25 (SE = 0.55) in the placebo group (LS mean difference of –2.94; 95% CI, –4.39 to –1.49; P < 0.001), which favoured zilucoplan. In the refractory subpopulation, the LS mean change from baseline to week 12 in the QMG score was –6.08 (SE = 0.76) in the zilucoplan group and –2.76 (SE = 0.75) in the placebo group (LS mean difference of –3.32; 95% CI, –5.42 to –1.23; nominal P < 0.001).
Change From Baseline to Week 12 in the MGC Score
In the overall population, the LS mean change from baseline to week 12 in the MGC score was –8.62 (SE = 0.81) in the zilucoplan group and –5.42 (SE = 0.79) in the placebo group (LS mean difference of –3.20; 95% CI, –5.24 to –1.16; P = 0.0023), which favoured zilucoplan. In the refractory subpopulation, the LS mean change from baseline to week 12 in the MGC score was –7.85 (SE = 1.09) in the zilucoplan group and –4.17 (SE = 1.07) in the placebo group (LS mean difference of –3.68; 95% CI, –6.65 to –0.72; nominal P = 0.0156).
Change From Baseline to Week 12 in the MG-QoL15r Score
In the overall population, the LS mean change from baseline to week 12 in the MG-QoL15r score was –5.65 (SE = 0.77) in the zilucoplan group and –3.16 (SE = 0.76) in the placebo group (LS mean difference of –2.49; 95% CI, –4.45 to –0.54; P = 0.0128), which favoured zilucoplan. In the refractory subpopulation, the LS mean change from baseline to week 12 in the MG-QoL15r score was –5.63 (SE = 0.96) in the zilucoplan group and –2.36 (SE = 0.95) in the placebo group (LS mean difference of –3.28; 95% CI, –5.89 to –0.67; nominal P = 0.0145).
Achievement of MSE at Week 12 Without Rescue Therapy
In the overall population, the percentage of patients who achieved MSE (an MG-ADL score of 0 or 1) at week 12 without rescue therapy was 14.0% in the zilucoplan group and 5.8% in the placebo group (between-group difference of 8.2%; 95% CI, –0.% to 17.0%). In the refractory subpopulation, the number of patients who achieved MSE at week 12 without rescue therapy was 2 of 44 patients (4.5%) in the zilucoplan group and 0 of 43 patients in the placebo group.
Achievement of at Least a 3-Point Reduction in MG-ADL Score at Week 12 Without Rescue Therapy
In the overall population, the percentage of patients who were MG-ADL responders (at least a 3-point decrease in MG-ADL score) at week 12 without rescue therapy was 73.1% in the zilucoplan group and 46.1% in the placebo group (between-group difference of 27.0%; 95% CI, 12.9% to 41.1%). In the refractory subpopulation, the number of patients who were MG-ADL responders at week 12 without rescue therapy was 33 of 44 patients (75.0%) the zilucoplan group and 17 of 42 patients (40.5%) in the placebo group.
Achievement of at Least a 5-Point Reduction in QMG Score at Week 12 Without Rescue Therapy
In the overall population, the percentage of patients who were QMG responders (at least a 5-point decrease in QMG score) at week 12 without rescue therapy was 58.0% in the zilucoplan group and 33.0% in the placebo group (between-group difference of 25.0%; 95% CI, 10.5% to 39.5%). In the refractory subpopulation, the number of patients who were QMG responders at week 12 without rescue therapy was 24 of 43 patients (55.8%) in the zilucoplan group and 11 of 41 patients (26.8%) in the placebo group.
Minimal Manifestation Status per MGFA-PIS at Week 12 Without Rescue Therapy
In the overall population, the number of patients who achieved minimal manifestation status per MGFA-PIS at week 12 without rescue therapy was 22 of 78 (28.2%) in the zilucoplan group and 16 of 83 (19.3%) in the placebo group (between-group difference of 10.9%; 95% CI, –1.5% to 23.2%). The number of patients who achieved minimal manifestation status per MGFA-PIS at week 12 without rescue therapy was not reported in the refractory subpopulation.
Harms Results
The analysis population for harms included all patients who received at least 1 dose of study drug. Patients were grouped according to the treatment received, using data from the December 30, 2021, data cut-off date.
The number of patients in the overall gMG population with at least 1 treatment-emergent adverse event (TEAE) was 66 of 86 patients (76.7%) in the zilucoplan group and 62 of 88 patients (70.5%) in the placebo group. The most common TEAEs occurring in greater than 5% of patients in either the zilucoplan group or the placebo group, respectively, were headache (15.1% versus 15.9%), injection-site bruising (16.3% versus 9.1%), MG (10.5% versus 9.1%), diarrhea (10.5% versus 2.3%), injection-site pain (9.3% versus 3.4%), urinary tract infection (8.1% versus 4.5%), contusion (8.1% versus 3.4%), increased lipase (8.1% versus 1.1%), nasopharyngitis (5.8% versus 3.4%), vomiting (3.5% versus 5.7%), rash (3.5% versus 5.7%), and increased amylase (5.8% versus 2.3%).
In the refractory subpopulation, the number of patients with at least 1 TEAE was 39 of 44 patients (88.6%) in the zilucoplan group and 34 of 44 patients (77.3%) in the placebo group. The most common TEAEs occurring in greater than 10% of patients in either the zilucoplan group or the placebo group, respectively, were headache (20.5% versus 15.9%), MG (13.6% versus 13.6%), injection-site bruising (15.9% versus 11.4%), diarrhea (15.9% versus 2.3%), and vomiting (4.5% versus 11.4%).
The number of patients in the overall gMG population with at least 1 serious adverse event (SAE) was 11 of 86 patients (12.8%) in the zilucoplan group and 13 of 88 patients (14.8%) in the placebo group. The most common SAEs reported in at least 2% of patients in either the zilucoplan group or the placebo group, respectively, were MG (2.3% versus 5.7%), COVID-19 (1.2% versus 2.3%), and COVID-19 pneumonia (1.2% versus 2.3%).
In the refractory subpopulation, the number of patients with at least 1 SAE was 6 of 44 patients (13.6%) in the zilucoplan group and 8 of 44 (18.2%) in the placebo group. SAEs specified by system organ class were not reported for the refractory subpopulation.
In the overall gMG population, 4 of 86 patients (4.7%) in the zilucoplan group stopped the study treatment due to AEs, as did 2 of 88 patients (2.3%) in the placebo group. Withdrawals due to AEs in the zilucoplan group were due to (1 patient [1.2%] each) aphthous ulcer, mouth ulceration, COVID-19, and increased hepatic enzyme; the TEAE of aphthous ulcer and the TEAE of COVID-19 were considered serious, with the latter having a fatal outcome. Withdrawals due to AEs in the placebo group were due to (1 patient [1.1%] each) cerebral hemorrhage and hyperemesis gravidarum; both TEAEs were considered serious and the TEAE of cerebral hemorrhage had a fatal outcome. In the overall gMG population, the 1 patient (1.2%) in the zilucoplan group who died experienced an SAE leading to death due to COVID-19 and COVID-19 pneumonia, and the 1 patient (1.1%) in the placebo group who died experienced an SAE leading to death due to cerebral hemorrhage.
In the refractory subpopulation, 1 of 44 patients (2.3%) stopped the study treatment in the zilucoplan group, and no patients stopped the study treatment in the placebo group. The reasons for withdrawals due to AEs were not reported for the refractory subpopulation.
Notable Harms
Infections occurred in 23 of 86 patients (26.7%) in the zilucoplan group and 16 of 88 patients (18.2%) in the placebo group (between-group difference of 8.6%; 95% CI, –3.8% to 20.9%). Of these, 4 patients (4.7%) in the zilucoplan group and 4 patients (4.5%) in the placebo group had serious infections. AEs of special interest were not reported for the refractory subpopulation.
Critical Appraisal
Randomization appeared to be adequate in the RAISE trial. Treatment groups were balanced overall on demographic and disease characteristics, indicating that randomization was likely successful, and the risk of selection bias was low. Randomization was stratified by baseline MG-ADL score (≤ 9 versus ≥ 10), QMG score (≤ 17 versus ≥ 18), and geographic region (East Asia, Europe, and North America). The instruments used to evaluate the primary and secondary efficacy outcomes (MG-ADL, QMG, MGC, MG-QoL15r) were appropriate, and their psychometric properties have been investigated in patients with MG, although no minimal important differences (MIDs) have been estimated for the MG-QoL15r. Minimal manifestation status per MGFA-PIS without rescue therapy was based on clinician-assessed patient symptoms of MG after the initiation of MG-specific therapy, and was intended to capture patients who may not meet the definition of complete stable remission or pharmacologic remission but who have muscle weakness based on careful examination; this was an exploratory end point and no MID has been validated in the indicated population. Results for minimal manifestation status per MGFA-PIS at week 12 were not reported for the refractory subpopulation. There was low risk of bias for allocation concealment because patients and study staff were blinded to treatment assignment, both treatments were identical, and the unblinding of treatment assignment was not permitted before the initiation of rescue therapy.
Patients with refractory disease represented about one-half of the enrolled patients with gMG. The selection criteria for the refractory subgroup were specified a priori and were similar to the criteria used to define patients with refractory gMG in other randomized clinical trials (RCTs) (e.g., the REGAIN trial for eculizumab). Baseline characteristics were, overall, similar between treatment groups, so concerns regarding the prognostic balance of the refractory subpopulation were low. The population included in the refractory subgroup is adequately reflective of patients with refractory gMG in the clinical setting in Canada, according to the clinical expert consulted by the review team. Although subgroup analyses were not adjusted for multiplicity and not powered to detect differences among strata, results from the refractory subgroup can be compared for consistency with analyses of the overall trial population in the RAISE trial, and they share the same limitations as those analyses. Results for the refractory subgroup showed consistency with the overall trial population across all outcomes.
There was a notable proportion of patients with important protocol deviations in both the zilucoplan group (38.4%) and the placebo group (36.4%). Deviations included prohibited concomitant medication use (changes to gMG conventional medications, use of prohibited concomitant medications, and changes to cholinesterase inhibitor dosing less than 10 hours before evaluation), which affected 24.7% of patients, and changes related to the inclusion criteria (not withholding acetylcholinesterase inhibitor therapy for at least 10 hours before QMG assessment, changes in corticosteroids in the 30 days before baseline, and receiving inpatient treatment with IVIg that was not reported as rescue therapy), which affected 7.5% of patients. The proportion of patients with deviations during the study were balanced between groups. Multiple imputation (MI) methods were used to account for missing data in the primary and secondary end points, based on assumptions of missing not at random (MNAR), which assumed missingness to be related to the study drug or to the receipt of rescue medication, and missing at random (MAR). Based on the specified approach, each of these were imputed with either their baseline value or the last observed value (whichever was worse). Because the rate of intercurrent event (ICE) 1 (receipt of rescue therapy with IVIg, PLEX, or eculizumab) was higher in the placebo group (11%) than in the zilucoplan group (5%), this appeared to be an overly pessimistic approach that could possibly introduce bias in favour of zilucoplan; however, the imbalance was not large enough to raise serious concerns about biased treatment effects. Sensitivity analyses to account for the censoring of patients who experienced treatment failure were also conducted. Although the supplemental analyses and sensitivity analyses of the primary analysis did not adequately assess the potential bias related to missing data, concerns about losses to follow-up were low, because approximately 95% of patients with gMG in the overall population and the refractory subpopulation completed the RAISE study, with balanced proportions between treatment arms.
External Validity
Per sponsor request, the focus of this review was on the sponsor’s reimbursement request, which was narrower than the Health Canada indication. The reimbursement request aligned with the criteria for the refractory subgroup of the RAISE trial (i.e., zilucoplan as add-on therapy for the treatment of adult patients with anti-AChR antibody–positive refractory gMG, defined as not achieving symptom control after treatment for at least 1 year with 2 or more of the following therapies: prednisone, azathioprine, mycophenolate cyclosporine, cyclophosphamide, methotrexate, tacrolimus, other corticosteroids for gMG, other ISTs; or a history of treatment with at least 1 of these therapies for 1 year or more and required chronic PLEX, IVIg, or SCIg at least every 3 months for the 12 months before treatment with zilucoplan). The requested reimbursement criteria also aligned with the reimbursement criteria for the comparator therapy, eculizumab, which received a positive final recommendation in 2020 from CADTH.
The 49% of patients in the RAISE trial whose disease was not refractory were not included in the reimbursement request. Although the clinical expert consulted for this review agreed that there is a current unmet need in patients who are nonrefractory and have responded inadequately to the existing, standard gMG therapies, that population was not the focus of this review.
According to the expert, the stratification of patients during randomization by baseline scores on the MG-ADL and the QMG scales appeared to be appropriate for ensuring an equal distribution of patients by disease severity. There were no specific patient populations missing from eligibility in the trial who might otherwise be considered eligible in clinical practice, the expert noted. In line with patients who were not eligible for the RAISE trial, the expert emphasized that patients with MuSK-positive MG should not be treated with a complement inhibitor, such as zilucoplan, because of its mechanism of action; rather, patients with MG and MuSK-positive serology would benefit from treatment with a neonatal FcR inhibitor (e.g., efgartigimod alfa).
Looking at the types and duration of prior conventional treatments received by patients in the RAISE trial, the clinical expert agreed that all patients in the RAISE trial were adequately managed on conventional therapy for gMG at time of enrolment and were reflective of patients who experience an unmet need in clinical settings in Canada.
Moreover, the RAISE trial did not provide evidence for the comparisons between zilucoplan and other currently available active treatments for gMG. The most relevant comparators for zilucoplan among patients with refractory gMG include other complement inhibitors (i.e., eculizumab, ravulizumab), neonatal FcR inhibitors (e.g., efgartigimod alfa), chronic IVIg, and chronic PLEX, according to the expert. Rituximab as a comparator is less applicable because access for patients with gMG in Canada is limited, its use off-label, there is a lack of rigorous clinical trial evidence for patients with anti-AChR antibody–positive MG, and there is some evidence of improved benefit among patients with MuSK-positive MG.
The expert agreed that the primary end point of change from baseline in MG-ADL score is an important outcome for evaluating treatment response and is aligned with clinical practice, including the threshold used in the RAISE trial. MIDs used for the QMG and MGC scores were also noted by the expert to align with the literature for thresholds validated in patients with MG. According to the expert, most patients with gMG would be assessed at approximately 12 weeks to evaluate treatment response, as was done for all end points in the RAISE trial, with additional assessments at the 3-month or 4-month time point to assess responsiveness or maintenance of response.
GRADE Summary of Findings and Certainty of the Evidence
The selection of outcomes for the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach was based on the sponsor’s Summary of Clinical Evidence, consultation with clinical experts, and input received from patient and clinician groups and public drug plans. The following list of outcomes was finalized in consultation with expert committee members: activities of daily living (MG-ADL score), disease severity (QMG score), treatment response (MGC score), HRQoL (MG-QoL15r score), and harms (infections).
When possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect; if this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., the clinical importance is unclear). In all cases, the target of the certainty of evidence assessment was based on the point estimate and where it was located relative to the threshold for a clinically important effect (when a threshold was available) or to the null. The target of the certainty of evidence assessment was the presence or absence of a clinically important change from baseline to week 12 scores in the MG-ADL, the QMG, and the MGC, based on thresholds identified in the literature. The certainty of evidence assessments for change from baseline to week 12 in the MG-QoL15r score, number of patients achieving MSE at week 12 without rescue therapy, MG-ADL responder rate at week 12 without rescue therapy, QMG responder rate at week 12 without rescue therapy, number of patients with minimal manifestation status per MGFA-PIS at week 12 without rescue therapy, and infections were based on the presence or absence of any (nonnull) effect.
Results of GRADE Assessments
Table 2 presents the GRADE summary of findings for zilucoplan versus placebo in patients with anti-AChR antibody–positive gMG.
Table 2: Summary of Findings for Zilucoplan Versus Placebo for Adult Patients With Anti-AChR Antibody–Positive gMG
Outcome and follow-up | Patients (studies), N | Relative effect (95% CI) | Absolute effects | Certainty | What happens | ||
|---|---|---|---|---|---|---|---|
Placebo | Zilucoplan (95% CI) | Difference (95% CI) | |||||
Activities of daily living | |||||||
MG-ADL (0 to 24; higher scores indicate more severe symptoms), mITT | |||||||
LSM change from baseline in the MG-ADL score Follow-up: 12 weeks | 174 (1 RCT) | NR | –2.30 | – 4.39 (– 5.28 to –3.50) | –2.09 (–3.24 to –0.95) | Moderatea | Zilucoplan likely results in a clinically important decrease (improvement) in the MG-ADL score at 12 weeks, compared with placebo. |
Number of patients achieving MSE (an MG-ADL score of 0 or 1) without rescue therapy Follow-up: 12 weeks | 174 (1 RCT) | OR, 2.608 (0.739 to 9.209b) | 58 per 1,000 | 140 per 1,000 (NR) | 82 more per 1,000 (19 fewer to 183 moreb)c | Lowd | Zilucoplan may result in an increase in the number of patients achieving MSE at 12 weeks without rescue therapy, compared with placebo. There is some uncertainty in the clinical importance of the estimates. |
Number of patients with a ≥ 3-point decrease in the MG-ADL score without rescue therapy Follow-up: 12 weeks | 174 (1 RCT) | OR, 3.184 (1.391 to 7.293b) | 461 per 1,000 | 731 per 1,000 (NR) | 270 more per 1,000 (90 to 449 moreb)c | Moderatee | Zilucoplan likely results in an increase in the number of patients with a ≥ 3-point decrease (improvement) in the MG-ADL score at 12 weeks without rescue therapy, compared with placebo. There is some uncertainty in the clinical importance of the estimates. |
Disease severity | |||||||
QMG (0 to 39; higher scores indicate more severe impairment), mITT | |||||||
LSM change from baseline in the QMG score Follow-up: 12 weeks | 174 (1 RCT) | NR | –3.25 | –6.19 (–7.29 to –5.08) | –2.94 (–4.39 to –1.49) | Moderatef | Zilucoplan likely results in a clinically important decrease (improvement) in the QMG score at 12 weeks, compared with placebo. |
Number of patients with a ≥ 5-point decrease in the QMG score without rescue therapy Follow-up: 12 weeks | 174 (1 RCT) | OR, 2.865 (1.319 to 6.225b) | 330 per 1,000 | 580 per 1,000 (NR) | 250 per 1,000 (73 to 427 moreb)c | Moderateg | Zilucoplan likely results in an increase in the number of patients with a ≥ 5-point decrease (improvement) in the QMG score at 12 weeks without rescue therapy, compared with placebo. There is some uncertainty in the clinical importance of the estimates. |
Treatment response | |||||||
MGC (0 to 50; higher scores indicate more severe impairment), mITT | |||||||
LSM change from baseline in the MGC score Follow-up: 12 weeks | 174 (1 RCT) | NR | –5.42 | –8.62 (–10.22 to –7.01) | –3.20 (–5.24 to –1.16) | Moderateh | Zilucoplan likely results in a clinically important decrease (improvement) in the QMG score at 12 weeks, compared with placebo. |
Other efficacy end point | |||||||
Number of patients with minimal manifestation status per MGFA-PIS without rescue therapy Follow-up: 12 weeks | 151 (1 RCT) | OR, 1.834 (0.847 to 3.969) | 193 per 1,000 | 282 per 1,000 (NR) | 109 more per 1,000 (15 fewer to 232 more)c | Lowi | Zilucoplan may result in an increase in the number of patients with minimal manifestation status per MGFA-PIS at 12 weeks without rescue therapy, compared with placebo. There is some uncertainty in the clinical importance of the estimates. |
Health-related quality of life | |||||||
MG-QoL15r (0 to 30; higher indicates greater severe impact), mITT | |||||||
LSM change from baseline in the MG-QoL15r score Follow-up: 12 weeks | 174 (1 RCT) | NR | –3.16 | –5.65 (–7.17 to –4.12) | –2.49 (–4.45 to –0.54) | Moderatej | Zilucoplan likely results in a reduction (improvement) in the MG-QoL15r score at 12 weeks, compared with placebo. There is some uncertainty in the clinical importance of the estimates. |
Harms | |||||||
Adverse events, safety set | |||||||
Number of patients with infections Follow-up: 12 weeks | 174 (1 RCT) | NR | 182 per 1,000 | 267 per 1,000 (NR) | 86 more per 1,000 (38 fewer to 209 more)c | Lowk | Zilucoplan may result in an increase in infections, compared with placebo. There is some uncertainty in the clinical importance of the estimates. |
AChR = acetylcholine receptor; CI = confidence interval; gMG = generalized myasthenia gravis; LSM = least squares mean; MG-ADL = Myasthenia Gravis Activities of Daily Living; MGC = Myasthenia Gravis Composite; MGFA-PIS = Myasthenia Gravis Foundation of America Post-Intervention Status; MG-QoL15r = Myasthenia Gravis Quality of Life 15-item – Revised; MID = minimal important difference; mITT = modified intention to treat; MSE = minimal symptom expression; NR = not reported; OR = odds ratio; QMG = Quantitative Myasthenia Gravis; RCT = randomized controlled trial.
Note: Study limitations (which refer to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias were considered when assessing the certainty of the evidence. All serious concerns in these domains that led to the rating down of the level of certainty are documented in the table footnotes.
aRated down 1 level for serious imprecision. Based on a 2-point MID identified in the literature, the 95% CI included the possibility of little-to-no difference and clinically important benefit. The 2-point MID has been estimated for change within an individual patient and was applied in the absence of an estimate of a between-group MID.
bBased on the testing procedure used for the secondary end points, the CI was 98.75% for MG-ADL responders, 98.3% for QMG responders, and 97.5% for the achievement of MSE in the statistical hierarchy, using the Holm’s procedure. The associated CI was generated using a post hoc analysis upon request by the review team.
cRisk difference (95% CI) was not included in the sponsor’s planned analyses; the absolute risk difference was requested by the review team for interpretation purposes.
dRated down 2 levels for very serious imprecision. In the absence of an identified threshold in the literature or by the clinical expert consulted by CDA-AMC for the review, the null was used as the threshold. The 95% CI included the null. The CDA-AMC review team judged the effect estimate to be large and the number of events to be small, raising concerns about prognostic balance and potential overestimation of the true effect.
eRated down 1 level for serious imprecision. In the absence of an identified threshold in the literature or by the clinical expert consulted by CDA-AMC for the review, the null was used as the threshold. The point estimate and the entire CI suggested potential benefit. The CDA-AMC review team judged the effect estimate to be large and the sample size to be small, raising concerns about prognostic balance and potential overestimation of the true effect.
fRated down 1 level for serious imprecision. Based on an MID that ranged from 2 to 3 identified in the literature, the 95% CI included the possibility of little-to-no difference and clinically important benefit. This MID has been estimated for change within an individual patient and was applied in the absence of an estimate of a between-group MID.
gRated down 1 level for serious imprecision. In the absence of an identified threshold in the literature or by the clinical expert consulted by CDA-AMC for the review, the null was used as the threshold. The CDA-AMC review team judged the effect estimate to be large and the sample size to be small, raising concerns about prognostic balance and potential overestimation of the true effect.
hRated down 1 level for serious imprecision. Based on a 3-point MID identified in the literature, the 95% CI included the possibility of little-to-no difference and clinically important benefit. This MID has been estimated for change within an individual patient and was applied in the absence of an estimate of a between-group MID
iRated down 2 levels for very serious imprecision. In the absence of an identified threshold in the literature or by the clinical expert consulted by CDA-AMC for the review, the null was used as the threshold. The 95% CI included the null. The effect estimate was based on a small sample size. This analysis was not adjusted for multiplicity and the results should be considered as supportive evidence.
jRated down 1 level for serious imprecision. In the absence of an identified threshold in the literature or by the clinical expert consulted by CDA-AMC for the review, the null was used as the threshold. The effect estimate was based on a small sample size.
kRated down 2 levels for very serious imprecision. In the absence of an identified threshold in the literature or by the clinical expert consulted by CDA-AMC for the review, the null was used as the threshold. The 95% CI included the null. The effect estimate was based on a small sample size.
Source: RAISE Clinical Study Report.14
Long-Term Extension Studies
Description of Studies
The sponsor included 1 ongoing, phase III, multicentre, open-label extension study (RAISE-XT) of adult patients with anti-AChR antibody–positive gMG (the overall gMG population and the refractory subpopulation) who had previously participated in a double-blind trial of zilucoplan 0.3 mg/kg or placebo to evaluate the long-term efficacy and safety of zilucoplan. The primary outcome of the RAISE-XT study was the incidence of TEAEs, defined as an AE starting on or after the time of first administration of the study drug and up to and including 40 days after the final dose (or last contact). Secondary efficacy outcomes included change from baseline to RAISE-XT extension (E) week 12 (E12) in the MG-ADL score, the QMG score, the MGC score, and the MG-QoL15r score. Exploratory outcomes in the RAISE-XT study included minimal manifestation status per MGFA-PIS at week E12 without rescue therapy, responder rates for the MG-ADL, QMG, and MGC scores at week E12 without rescue therapy, and the achievement of MSE (an MG-ADL score of 0 or 1) at week E12 without rescue therapy. In the overall gMG population, 93 patients in the zilucoplan 0.3 mg/kg and 0.3 mg/kg group and 90 patients the placebo and zilucoplan 0.3 mg/kg group were similar in mean age (53 years and 54 years), the proportion of female (56% and 53%) and male patients (44% and 47%), and the proportion of patients enrolled from North America (57% and 54%).
Efficacy Results
Change From Parent-Study Baseline to Week E12 in the MG-ADL Score
In the overall population, the LS mean change from parent-study baseline to week E12 in the MG-ADL score was –5.90 (SE = 0.47) in the zilucoplan 0.3 mg/kg and 0.3 mg/kg group and –6.17 (SE = 0.59) in the placebo and zilucoplan 0.3 mg/kg group. In the refractory subpopulation, the mean change from parent-study baseline to week E12 in the MG-ADL score was –6.61 (SE = 0.63) in the zilucoplan 0.3 mg/kg and 0.3 mg/kg group and –6.24 (SE = 0.71) in the placebo and zilucoplan 0.3 mg/kg group.
Change From Parent-Study Baseline to Week E12 in the QMG Score
In the overall population, the LS mean change from parent-study baseline to week E12 in the QMG score was –8.78 (SE = 0.66) in the zilucoplan 0.3 mg/kg and 0.3 mg/kg group and –8.53 (SE = 0.79) in the placebo and zilucoplan 0.3 mg/kg group. In the refractory subpopulation, the mean change from parent-study baseline to week E12 in the QMG score was –8.18 (SE = 0.71) in the zilucoplan 0.3 mg/kg and 0.3 mg/kg group and –8.34 (SE = 1.09) in the placebo and zilucoplan 0.3 mg/kg group.
Change From Parent-Study Baseline to Week E12 in the MGC Score
In the overall population, the LS mean change from parent-study baseline to week E12 in the MGC score was –11.77 (SE = 0.86) in the zilucoplan 0.3 mg/kg and 0.3 mg/kg group and –12.30 (SE = 1.12) in the placebo and zilucoplan 0.3 mg/kg group. In the refractory subpopulation, the mean change from parent-study baseline to week E12 in the MGC score was –11.83 (SE = 1.17) in the zilucoplan 0.3 mg/kg and 0.3 mg/kg group and –13.34 (SE = 1.35) in the placebo and zilucoplan 0.3 mg/kg group.
Change From Parent-Study Baseline to Week E12 in the MG-QoL15r Score
In the overall population, the LS mean change from parent-study baseline to week E12 in the MG-QoL15r score was –9.92 (SE = 0.95) in the zilucoplan 0.3 mg/kg and 0.3 mg/kg group and –8.07 (SE = 1.08) in the placebo and zilucoplan 0.3 mg/kg group. In the refractory subpopulation, the mean change from parent-study baseline to week E12 in the MG-QoL15r score was –9.46 (SE = 1.15) in the zilucoplan 0.3 mg/kg and 0.3 mg/kg group and –9.34 (SE = 1.32) in the placebo and zilucoplan 0.3 mg/kg group.
Exploratory End Points
The number of patients who achieved MSE (an MG-ADL score of 0 or 1) at week E12 without rescue therapy, were responders on the MG-ADL or the QMG at week E12 without rescue therapy, and who achieved minimal manifestation status per MGFA-PIS at week E12 without rescue therapy were numerically higher in the zilucoplan 0.3 mg/kg and 0.3 mg/kg group than in the placebo and zilucoplan 0.3 mg/kg group.
Harms Results
The number of patients in the overall population who experienced at least 1 TEAE was 89 of 93 patients (95.7%) in the zilucoplan 0.3 mg/kg and 0.3 mg/kg group and 86 of 90 patients (95.6%) in the placebo and zilucoplan 0.3 mg/kg group. The most common TEAEs occurring in 10% of patients or greater in any group (the zilucoplan 0.3 mg/kg and 0.3 mg/kg group and the placebo and zilucoplan 0.3 mg/kg group, respectively) were MG (29% and 29%), COVID-19 (39% and 31%), headache (19% and 22%), nasopharyngitis (23% and 17%), arthralgia (20% and 13%), diarrhea (19% and 13%), fatigue (18% and 13%), nausea (15% and 17%), upper respiratory tract infection (14% and 18%), urinary tract infection (16% and 14%), pain in extremity (16% and 10%), cough (12% and 12%), fall (11% and 10%), back pain (11% and 10%), rash (10% and 10%), vomiting (11% and 6%), injection-site bruising (4% and 11%), and oropharyngeal pain (1% and 10%). The number of patients in the refractory subpopulation who experienced at least 1 TEAE was 82 of 85 patients (96.5%) in the zilucoplan 0.3 mg/kg group (zilucoplan 0.3 mg/kg and 0.3 mg/kg and placebo and zilucoplan 0.3 mg/kg groups combined). The most common TEAEs occurring in 10% of patients or greater in the refractory subpopulation in any group (the zilucoplan 0.3 mg/kg and 0.3 mg/kg group and the placebo and zilucoplan 0.3 mg/kg group, respectively) were MG (42% and 38%), COVID-19 (44% and 24%), headache (21% and 21%), arthralgia (26% and 10%), nasopharyngitis (16% and 19%), urinary tract infection (19% and 12%), upper respiratory tract infection (19% and 12%), diarrhea (16% and 12%), nausea (12% and 17%), fall (14% and 12%), back pain (14% and 12%), and pain in extremity (16% and 10%).
The number of patients in the overall population who experienced at least 1 serious TEAE was 35 patients (37.6%) in the zilucoplan 0.3 mg/kg and 0.3 mg/kg group and 29 patients (32.2%) in the placebo and zilucoplan 0.3 mg/kg group. Serious TEAEs occurring in 2% of patients or greater in any group (the zilucoplan 0.3 mg/kg and 0.3 mg/kg group and the placebo and zilucoplan 0.3 mg/kg group, respectively) were MG (9.7% and 11.1%), COVID-19 pneumonia (4.3% and 1.1%), myocardial infarction (4.3% and 0.0%), pneumonia (3.2% and 1.1%), cholecystitis (2.2% and 1.1%), Staphylococcus bacteremia (2.2% and 0.0%), atrial fibrillation (2.2% and 0.0%), cardiac arrest (2.2% and 0.0%), cellulitis (2.2% and 2.2%), and large intestine polyp (0.0% and 2.2%). The number of patients in the refractory subpopulation who experienced at least 1 serious TEAE was 20 of 43 patients (46.5%) in the zilucoplan 0.3 mg/kg and 0.3 mg/kg group and 15 of 42 patients (35.7%) in the placebo and zilucoplan 0.3 mg/kg group.
TEAEs resulting in permanent withdrawal of the study drug in the overall population were reported in 21 of 183 patients (11.4%), with 9 of 93 patients (9.7%) in the zilucoplan 0.3 mg/kg and 0.3 mg/kg group and 12 of 90 patients (13.3%) in the placebo and zilucoplan 0.3 mg/kg group. The most common TEAE resulting in permanent withdrawal of the study drug was MG (6 patients [3.3%]). The number of patients in the refractory subpopulation who experienced at least 1 serious TEAE was 11 of 85 patients (12.9%), 2 of 43 (4.7%) of whom were in the zilucoplan 0.3 mg/kg and 0.3 mg/kg group and 9 of 42 (21.4%) of whom were in the placebo and zilucoplan 0.3 mg/kg group.
A total of 6 patients died in the RAISE-XT study. The number of patients who experienced a TEAE leading to death was 3 patients (3.2%) in the zilucoplan 0.3 mg/kg and 0.3 mg/kg group and 1 patient (1.1%) in the placebo and zilucoplan 0.3 mg/kg group. In the zilucoplan 0.3 mg/kg and 0.3 mg/kg group, the TEAEs leading to death were cardiac arrest (2 patients [2.2%]) and head injury (1 patient [1.1%]). In the placebo and zilucoplan 0.3 mg/kg group, the TEAE was death (1 patient [1.1%]). All 4 TEAEs leading to death resulted in permanent withdrawal of the study drug. Two patients in the refractory subpopulation died during the study; 1 patient in the zilucoplan 0.3 mg/kg and 0.3 mg/kg group had a TEAE of death. No details were reported for the deaths in the refractory subpopulation.
The number of patients who experienced any infections was 67 patients (72.0%) in the zilucoplan 0.3 mg/kg and 0.3 mg/kg group and 65 patients (72.2%) in the placebo and zilucoplan 0.3 mg/kg group. Of these, the number of patients who experienced serious infections was 16 (17.2%) in the zilucoplan 0.3 mg/kg and 0.3 mg/kg group and 11 (12.2%) in the placebo and zilucoplan 0.3 mg/kg group. The number of patients in the refractory subpopulation who experienced any infections was 34 of 43 (79.1%) in the zilucoplan 0.3 mg/kg and 0.3 mg/kg group and 33 of 42 (78.6%) in the placebo and zilucoplan 0.3 mg/kg group.
Critical Appraisal
The RAISE-XT study was an open-label, noncomparative extension of the RAISE parent study. The key limitation related to the absence of a comparator group is that patients were not randomized to treatment groups (whereas patients in the parent study were randomized to zilucoplan or placebo, all patients in the extension study received zilucoplan), which precludes inferences that any observed differences are due to treatments received. Importantly, treatment efficacy and harms for patients with longer follow-up should be interpreted cautiously, as it cannot be determined whether the findings are due to the natural history of the disease, study treatments including concomitant therapies, or other unknown factors. The number of patients with missing data for the secondary end point of change from parent-study baseline to week E12 of the RAISE-XT study was similar in the zilucoplan 0.3 mg/kg and 0.3 mg/kg group and the placebo group, and the number of patients with missing data was low, overall, for scores on the MG-ADL (4%), the QMG and the MGC (6%), and the MG-QoL15r (7%), despite a lack of imputation. The proportions of patients with missing data for change from parent-study baseline to week E12 in the refractory subpopulation were also similar in the 2 treatment groups, at 7% for MG-ADL score, 8% for QMG and MGC scores, and 9% for MG-QoL15r score. A greater proportion of patients had missing data for the exploratory end points of the RAISE-XT study, including the achievement of MSE (9%), the MG-ADL responder rate (9%), the QMG responder rate (10%), and the achievement of minimal manifestation status per MGFA-PIS (15%), which were similar in the 2 treatment groups but may increase concerns related to the interpretation of the findings that may not be generalizable to the full population.
Zilucoplan will likely be used as long as the patient is responding to treatment and any AEs are manageable, according to the clinical expert consulted for the review, so it would be reasonable for patients to continue treatment for at least the 12 weeks, as was evaluated in the RAISE-XT study. No concerns were raised by the expert based on the AEs observed with longer treatment with zilucoplan.
Indirect Comparisons
Description of Studies
The sponsor submitted an indirect comparison that compared the short-term efficacy of zilucoplan with that of other treatments used for the management of patients with anti-AChR antibody–positive gMG in the overall gMG population, as well as those with refractory gMG (subgroup analysis).15 The indirect comparison was based on a systematic literature review, and used Bayesian network meta-analysis (NMA) methods to estimate the comparative efficacy in the proportion of patients who met the MG-ADL response criteria at the end of the primary studies, and the change from baseline in the MG-ADL score at 12 weeks (± 2 weeks). The treatments included in the NMAs were zilucoplan, eculizumab, efgartigimod alfa, IVIg, PLEX, rituximab, ravulizumab, and rozanolixizumab.
A total of 12 double-blind, placebo-controlled RCTs were included in the NMA, but the primary analyses were based on phase III studies only (5 RCTs).
Efficacy Results
In the overall gMG population, the proportion of patients with a 3-point or greater (or 2-point or greater) improvement in MG-ADL score at the end of the studies (week 6 to week 26) was analyzed based on data from 5 RCTs (793 patients). The odds ratio (OR) for the proportion of responders was 1.37 (95% credible interval [CrI], 0.51 to 3.67) for zilucoplan versus eculizumab and 0.65 (95% CrI, 0.24 to 1.79) for zilucoplan versus efgartigimod alfa.
The subgroup analysis of patients with refractory gMG reported ORs of 2.00 (95% CrI, 0.63 to 6.63) and 0.95 (95% CrI, 0.29 to 3.21) for zilucoplan versus eculizumab and zilucoplan versus efgartigimod alfa, respectively. Of note, only 2 of 5 studies in this sensitivity analysis were exclusively patients with refractory gMG. The other studies included either a mixed population (in 1 study, 63% of patients had refractory disease) or an unknown proportion of patients with refractory disease (2 studies).
The primary analysis for the change from baseline in MG-ADL score included 5 studies with 755 patients and was based on outcomes reported at 10 weeks (2 studies) or 12 weeks (3 studies). The mean difference in the change from baseline in the MG-ADL score was −0.38 points (95% CrI, −2.21 to 1.41 points) for zilucoplan versus eculizumab and −1.50 points (95% CrI, −3.58 to 0.59 points) for zilucoplan versus efgartigimod alfa. For the refractory subgroup, the mean difference in the change from baseline in the MG-ADL score was −1.39 points (95% CrI, −3.49 to 0.68 points) for zilucoplan versus eculizumab and −2.51 points (95% CrI, −4.83 to −0.18 points) for zilucoplan versus efgartigimod alfa.
The sensitivity analysis that included 6 to 12 phase II and III studies (depending on the analysis) showed similar results for zilucoplan versus eculizumab and zilucoplan versus efgartigimod alfa in the overall and refractory populations, compared with the primary analyses in these populations.
Harms Results
No safety outcomes were included in the NMA.
Critical Appraisal
The indirect treatment comparison (ITC) report provided insufficient detail on the methods used to select studies for inclusion, so it is unclear if all potentially relevant studies were considered. In addition, the ITC report did not describe the findings from the feasibility assessment that was used to inform the conduct of the NMA. No information was provided on the characteristics of the studies included in the analyses, which was a major limitation.
Based on the data available, several important sources of heterogeneity were identified, including differences in outcome definitions and the timing of assessments, the placebo MG-ADL response rate, and the terms of disease severity and MG treatment history of the patients enrolled. Specifically, the trials had different proportions of patients rated as having mild, moderate, and severe and/or refractory gMG. The clinical expert stated that patients with refractory gMG or more severe disease may be less likely to respond to therapy, so differences in the distribution of these patients across trials may bias the findings. Both the overall population analyses and the refractory subgroup analyses contain a varied mix of patients with and without refractory gMG, which is a key source of heterogeneity. Moreover, the refractory subgroup analyses cannot be considered a true comparative assessment of patients with refractory gMG because not all studies were limited to patients with refractory disease.
A major limitation of the ITC methods was related to the timing of outcomes. The responder analyses used each study’s primary outcome time point, which varied from 6 weeks to 26 weeks. The change from baseline analyses assessed outcomes at week 10 or week 12 in the primary analyses but included other time points in the sensitivity analyses (from 4 weeks to 52 weeks). The CDA-AMC reviewer considered the differences in the timing of outcomes to be a significant source of heterogeneity that was not controlled for in the analyses. Restricting the outcome to those reported at 10 weeks or 12 weeks also had serious limitations, related in part to the differences in dosing schedules (intermittent versus continuous), which could bias the results. The response definition also varied, with 4 of the 5 studies in the primary analysis reporting the proportion of patients with at least a 3-point improvement in the MG-ADL score, and 1 of the key studies using a 2-point threshold.
Overall, the evidence networks were sparse, with the primary analysis based on 1 trial per comparator. Generally, the duration of follow-up in the source studies was limited (up to 26 weeks for the primary analyses), so comparative estimates were based on short-term data. The NMA results lacked precision, as shown by the wide 95% CrI. Considering the heterogeneity in the patient and study characteristics that was identified after a limited assessment, there is likely substantial risk of bias for the comparisons in the network. As a result, no conclusions could be drawn on the comparative efficacy of zilucoplan. No harms outcomes were assessed in the NMA, so the comparative safety of zilucoplan is unknown.
Studies Addressing Gaps in the Evidence From the Systematic Review
No additional studies addressing important gaps in the systematic review were identified.
Conclusions
Patients and clinicians identified a need for new treatments for gMG that reduce gMG-related and treatment-related morbidity and mortality, decrease the number and intensity of exacerbations, provide durable benefit, improve quality of life, and decrease the risk of side effects. Evidence from the randomized, phase III, double-blind RAISE trial of 174 adult patients with anti-AChR antibody–positive gMG (including 88 with refractory anti-AChR antibody–positive gMG) demonstrated that treatment with zilucoplan is likely superior to placebo in providing improvement in signs and symptoms of disease activity at week 12, as measured by the MG-ADL score, the primary outcome, in the overall trial population, which included patients with refractory and nonrefractory disease. Zilucoplan also likely results in a clinically meaningful benefit in the key secondary outcomes of QMC score and MGC score at week 12, compared with placebo in the overall trial population. Zilucoplan likely results in improvements in HRQoL compared to placebo, based on results from the MG-QoL 15r instrument. For other secondary outcomes (i.e., at least a 3-point response in MG-ADL score and at least a 5-point response in QMG score), zilucoplan is also likely to show improvements at week 12 compared with placebo in the overall trial population. MSE score at week 12 favoured zilucoplan numerically; although it did not reach statistical significance in the overall trial population, it may result in a benefit compared to placebo. Zilucoplan may result in an increase in the number of patients with minimal manifestation status per MGFA-PIS at week 12, an exploratory outcome, compared to placebo. Note that confidence in the between-group differences for efficacy outcomes in the overall trial population were limited because of imprecision (indicated by the associated CIs that included small effects close to the null or crossed the null) and relatively small sample sizes.
The prespecified subgroup of patients with refractory disease (50.6%) aligned with the sponsor’s reimbursement request under review for zilucoplan. Results of the subgroup analyses were subject to limitations, such as a reduced sample size and a lack of formal statistical approaches to control for an inflated type I error rate in multiple comparisons. However, the clinical benefit observed in the refractory subgroup was in all cases consistent with or tended to be slightly larger than the results shown in the overall trial population and was considered to be clinically meaningful by the clinical expert consulted for this review. Results for minimal manifestation status per MGFA-PIS at week 12 were not reported for the refractory subpopulation. The safety profile of zilucoplan in the refractory subgroup was consistent with that reported in the overall trial population, with no unexpected safety signals, and was considered manageable by the clinical expert consulted for this review. The evidence is very uncertain about the effect of zilucoplan on the number of infections experienced by patients, compared to placebo, at week 12 (very low certainty) in the overall trial population.
One open-label extension study of patients with gMG, including patients with refractory gMG, demonstrated findings supportive to those in the RAISE trial, which involved an additional 84 weeks of treatment with zilucoplan; however, the open-label nature of the study design limits the ability to distinguish between the effects of treatment and the natural history of the disease and between study treatments, including concomitant therapies, and other unknown factors.
A sponsor-submitted NMA comparing the efficacy of zilucoplan with other treatments for gMG, including eculizumab, efgartigimod alfa, IVIg, PLEX, and rituximab, had several limitations (sparse evidence networks, short-term data, imprecision of estimates, and heterogeneity in patient and study characteristics), which preclude any conclusions from being drawn on the comparative efficacy of zilucoplan. Because harms outcomes were not assessed in the NMA, the comparative safety of zilucoplan is unknown.
Introduction
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of zilucoplan 40 mg/mL SC injection in the treatment of adult patients with anti-AChR antibody–positive MG.
Disease Background
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following has been summarized and validated by the CDA-AMC review team.
MG is a rare, chronic, autoimmune, neuromuscular disease in which antibodies against the neuromuscular junction disrupt nerve impulse conduction, resulting in localized or generalized skeletal muscle weakness.2,3 In most patients, MG initially affects the extraocular muscles (ocular MG) and then progresses to other muscle groups, including the bulbar and proximal limb skeletal muscles. When the disease progresses to other muscle groups, it is referred to as gMG.4-6 Approximately 80% of all patients with MG have gMG.6 The majority of patients with gMG (80% to 90%) have antibodies against anti-AChR; however, antibodies against MuSK and LRP4 are also present in some patients with MG.2,6,7,16 A small number of patients do not have any measurable antibodies and are seronegative.2,6
The MGFA classification system groups patients with MG into 5 functional classes, based on the severity and localization of symptoms.9 The classification ranges from class I (ocular manifestations only) to class V (intubation or myasthenic crisis).9 Class II, class III, and class IV represent patients with mild MG, moderate MG, and severe gMG, respectively. Other validated scales used to determine disease and symptom severity in patients with MG include the MG-ADL, the QMG, the MGC, and the MG-QoL15.10
gMG is a disease of fluctuating muscle weakness that often gets worse after exercise or later in the day.2 In patients with MG, involuntary or smooth muscles are not affected.11 The symptoms and disease course of gMG are highly variable and heterogenous among patients. It has been referred to as a snowflake disease, as it affects each patient differently.11 Patients experience a variety of symptoms, including fatigue, droopy eyelids, diplopia, neck weakness, difficulty swallowing or chewing, speech disturbances, difficulty breathing, and upper and/or lower limb weakness.11 The symptoms of gMG occur unpredictably and fluctuate in nature, intensity, and severity on a day-to-day basis and throughout a patient’s life.2 Patients can also experience exacerbation, which by definition comprises 3 criteria: temporal (a rapid, progressive, and unpredictable worsening of symptoms); subjective (deterioration of bulbo-pharyngeal function, restriction of strength for head and neck muscles or extremity muscles that affects a patient’s everyday life or the start of weakness in breathing with reduced cough impulse); and objective (at least a 5-point change in QMG score with no more than 5 points from ocular MG). Exacerbation requires inpatient treatment.12 Furthermore, MG exacerbations can deteriorate into a myasthenic crisis, in which patients experience sudden respiratory failure that requires emergency intubation or ventilation.12 In the literature, it is noted that patients with gMG experience a significant disease burden as a result of the disease symptoms and the side effects of treatments that reduce their quality of life.17
In Canada, the incidence and prevalence of gMG are estimated at 23 per 1 million person-years and 32 per 100,000, respectively.8 The mortality rate of MG has been reported to be between 0.06 and 0.89 per million person-years.18 In 2013, there were 3,611 prevalent cases in Ontario, and the crude prevalence rate was 32.0 per 100,000 population. In 2021, the incidence of MG in the US estimated to be 3.2 per 100,000 and the total prevalence was estimated to be 37.0 per 100,000, using population estimates from the US Census. Almost 15% of patients with gMG have been classified as having refractory gMG.13 The diagnosis of gMG is based on clinical presentation; serological tests that detect antibodies against anti-AChR, MuSK, and LRP4; and electrodiagnostic tests for the evaluation of neuromuscular transmission.6,7
Standards of Therapy
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following has been summarized and validated by the CDA-AMC review team.
Four classes of therapies are currently available to treat MG: symptomatic treatment (i.e., acetylcholinesterase inhibition), chronic immunotherapies (i.e., glucocorticoids, nonsteroidal immunosuppressive, and immunomodulatory drugs), rapid but short-acting immunomodulating treatments (i.e., IVIg and therapeutic PLEX), and surgical treatment (i.e., thymectomy).19 The choice of therapies is largely dependent on the time of onset of clinical effect, in addition to the disease pace and severity.19
Initial symptomatic treatment for most patients with mild or moderate MG is an oral acetylcholinesterase inhibitor (usually pyridostigmine), which is aimed at improving clinical symptoms and neurologic deficits over the course of treatment.19 Glucocorticoids (e.g., oral prednisone) are commonly added to pyridostigmine initially.20 Patients who do not respond to or remain significantly symptomatic after pyridostigmine combined with prednisone are usually offered NSISTs (e.g., azathioprine, mycophenolate mofetil).19,20 Oral methotrexate may be considered as a steroid-sparing drug in patients with gMG who experience a poor response or intolerance to other steroid-sparing drugs.21 Bridge therapy for patients who are intolerant to glucocorticoids (e.g., those with poorly controlled diabetes) include IVIg, PLEX, complement inhibitors (e.g., eculizumab, ravulizumab), neonatal FcR inhibitors (efgartigimod alfa), and rozanolixizumab.20 Specifically, biologics (efgartigimod alfa, rozanolixizumab, ravulizumab, and zilucoplan) are used as chronic immunotherapy for patients with anti-AChR antibody–positive gMG.19
Patients with MG who experience a worsening of myasthenic symptoms are offered treatment individualized to the nature of their exacerbations, including the underlying cause (e.g., concurrent infection, surgery, pregnancy, medications, spontaneous), severity (e.g., life-threatening respiratory failure, such as myasthenic crisis), presence of functional limitations (e.g., dysphagia, dyspnea), rate of onset of potential treatments (e.g., hours for pyridostigmine, days for IVIg or PLEX, and weeks for immunotherapy or glucocorticoids), and treatment setting (e.g., outpatient, inpatient, intensive care unit).19 Therapeutic PLEX (plasmapheresis) and IVIg have a rapid onset (days) of action and are used in acute exacerbations, preoperatively (e.g., before thymectomy), or as a bridge to slower-acting immunotherapies (particularly among patients avoiding or minimizing glucocorticoids).19 In addition to its role in exacerbations of MG, IVIg is used as an alternative to plasmapheresis or several immunotherapy drugs in patients with refractory MG.19
Thymectomy (i.e., surgical section of the thymus) should be considered for adult patients with anti-AChR antibody–positive gMG to minimize the need for immunotherapy or as an alternative to immunotherapy (among patients who experience response failure to an initial adequate trial of immunotherapy or intolerable side effects from immunotherapy), and to reduce the risk of hospitalization for disease exacerbations.21 Thymectomy may be used in parallel with pyridostigmine and immunotherapy in select patients, including patients with thymoma (approximately 10% to 15% of patients with MG), and without thymoma (in patients with anti-AChR antibody–positive gMG who are younger than 50 years).19 Treatment decisions for thymectomy are age-stratified for older adults with nonthymomatous anti-AChR antibody–positive gMG; patients aged 51 to 65 years may be offered thymectomy on the basis of symptom severity and operative risks, but thymectomy is not indicated for patients older than 65 years.21,22 According to the clinical expert consulted for this review, thymectomy, although not curative, can produce a long-lasting benefit or disease remission in eligible patients with MG.
Patients with refractory disease are limited by the toxicities of immunosuppressive and immunomodulatory drugs and may require glucocorticoids in high doses, IVIg, rituximab, C5 complement inhibitor (e.g., eculizumab, ravulizumab), and cyclophosphamide.19,20 Treatment for patients with refractory disease lacks evidence-based guidelines; overall, treatment is more aggressive and highly individualized.20 The International Consensus Guidelines recommend rituximab as an option for patients with refractory anti-AChR antibody–positive MG who experience response failure or intolerable side effects with ISTs.21,23 Eculizumab should be considered for patients with severe, refractory anti-AChR antibody–positive gMG; its duration of treatment and role in the treatment of other MG populations and stages of disease may evolve with future research.21,24
Drug Under Review
The key characteristics of zilucoplan are summarized in Table 3, along with other treatments available for adult patients with anti-AChR antibody–positive gMG.
Zilucoplan is an immunosuppressant and C5 inhibitor that inhibits the effects of C5 through a dual mechanism of action. It specifically binds to C5, thereby inhibiting its cleavage by the C5 convertase to C5a and C5b, which results in a downregulation of the assembly and cytolytic activity of the membrane attack complex. Additionally, by binding to the C5b moiety of C5, zilucoplan sterically hinders the binding of C5b to C6, which prevents the subsequent assembly and activity of the membrane attack complex, should any C5b be formed.
The recommended dose of zilucoplan for adult patients with gMG is 0.3 mg/kg as SC injection once daily, administered about the same time every day, according to the patient’s body weight (i.e., a 16.6 mg total daily dose for patients with a body weight of < 56 kg, a 23.0 mg total daily dose for those with a body weight of ≥ 56 to < 77 kg, and a 32.4 mg total daily dose for patients with a body weight of ≥ 77 kg). Zilucoplan received Notice of Compliance from Health Canada on July 11, 2024, “for the treatment of generalized myasthenia gravis (gMG) in adult patients who are anti-acetylcholine receptor (AChR) antibody positive. Patients continued to receive standard therapy throughout the pivotal trial.” Zilucoplan has not been previously reviewed by CDA-AMC.
The reimbursement request is “as an add-on therapy for the treatment of adult patients with AChR antibody positive refractory gMG, defined as not achieving symptom control after:
Treatment for at least 1 year with 2 or more of the following therapies: prednisone, azathioprine, mycophenolate cyclosporine, cyclophosphamide, methotrexate, tacrolimus, other corticosteroids for gMG, other immunosuppressive therapies (ISTs), OR
History of treatment with at least one of these therapies for 1 year or more and required chronic plasma exchange (PLEX), intravenous immunoglobulin (IVIg), or subcutaneous immunoglobulin (SCIg) at least every 3 months for the 12 months prior to treatment with zilucoplan.” Per sponsor request, this review focuses on the indication for patients with refractory gMG.
Zilucoplan has FDA approval “for the treatment of generalized myasthenia gravis in adult patients who are anti-acetylcholine receptor (AChR) antibody positive” and is authorized by the European Medicines Agency “as an add-on to standard therapy for the treatment of generalised myasthenia gravis (gMG) in adult patients who are anti-acetylcholine receptor (AChR) antibody positive.”
Table 3: Key Characteristics of Zilucoplan, Efgartigimod Alfa, Eculizumab, Immunoglobulins, PLEX, and Rituximab
Characteristic | Zilucoplan | Efgartigimod alfa | Eculizumab | Immunoglobulins (e.g., IVIg, SCIg) | PLEX | Rituximab |
|---|---|---|---|---|---|---|
Mechanism of action | Immunosuppressant and C5 inhibitor that prevents the assembly and activity of the membrane attack complex. | Human IgG1 antibody fragment engineered for increased affinity to FcR. | Terminal complement inhibitor | Unknown | Removal of anti-AChR antibodies | Binds to antigen CD20, which regulates an early step(s) in the activation process for cell cycle initiation and differentiation and possibly functions as a calcium ion channel. |
Indicationa | For the treatment of gMG in adult patients who are AChR antibody-positive. Patients continued to receive standard therapy throughout the pivotal trial. | For the treatment of adult patients with generalized myasthenia gravis (gMG) who are anti-acetylcholine receptor (AChR) antibody positive. | Adult patients with gMG | Not approved for gMG | Not approved for gMG | Off-label use |
Route of administration | SC | IV | IV | IV or SC | IV | IV |
Recommended dose | 0.3 mg/kg, administered as a single daily injection | 10 mg/kg administered as an IV infusion over 1 hour, once weekly for 4 weeks. In patients weighing ≥ 120 kg, the recommended dose is 1,200 mg (3 vials) per infusion. Subsequent treatment cycles are administered based on clinical evaluation. The frequency of efgartigimod alfa treatment cycles may vary by patient. | 900 mg weekly for 4 weeks, followed by 1,200 mg 1 week later (loading) | 1 g/kg to 2 g/kg administered over 2 days to 5 days | 1.0 plasma volume to 1.5 plasma volumes daily, with usually 5 to 6 exchanges | No recommended dosage due to off-label use. |
Serious adverse effects or safety issues | Meningococcal infections and other infections with Neisseria species. Contraindicated in patients who are currently not vaccinated against Neisseria meningitidis or patients with unresolved Neisseria meningitidis infection. | Infections due to a transient reduction in IgG levels, including upper respiratory tract infections. | Infections, including serious meningococcal infections | Infusion reactions | Infections, bleeding, thrombosis, and transfusion reactions | Infusion reactions, progressive multifocal leukoencephalopathy, tumour lysis syndrome, hepatitis B reactivation, mucocutaneous reactions, infections, and serious cardiovascular events. |
AChR = acetylcholine receptor, FcR = fragment crystallizable receptor; gMG = generalized myasthenia gravis; Ig = immunoglobulin; IgG1 = immunoglobulin G1; PLEX = plasma exchange; SC = subcutaneous.
aHealth Canada indication, as applicable.
Source: Product monograph for zilucoplan.1
Perspectives of Patients, Clinicians, and Drug Programs
Patient Group Input
This section was prepared by the CDA-AMC review team based on the input provided by patient groups. The full original patient group input received by CDA-AMC has been included in this section of the report.
CDA-AMC received 1 patient group submission from the MDC. MDC is a health charity that supports people affected by muscular dystrophies and related muscle diseases (neuromuscular disorders) in Canada. MDC’s mission is to enhance the lives of those impacted by neuromuscular disorders by continually working to provide ongoing support and resources while relentlessly searching for a cure through well-funded research.
MDC identified and contacted adults living with MG to participate in a survey and semi-structured virtual interviews. Surveys were shared with members through e-blasts, personalized invitations, and online patient groups. MDC also conducted an MG Journey Mapping project for adults living with MG in Canada, using virtual interviews, round table sessions, surveys, and HRQoL measures (EQ visual analogue scale, EQ-5D, MG-ADL, MG-QoL). MDC’s patient group submission to CDA-AMC included information from 127 individuals (84 females and 43 males aged 22 years to 78 years from all provinces in Canada) the majority of whom reported having gMG. Additionally, 47 people living in Canada (33 females, 14 males) with MG provided input on their hopes and expectations for zilucoplan and their everyday experiences with MG. None of the respondents included in the MDC’s patient input had experience with zilucoplan.
Respondents indicated that MG has a significant impact on productivity, fatigue and energy levels, quality of sleep, respiratory health, mobility, strength, independence, relationships and social participation, eyes and vision, speech, and swallowing. Respondents also noted MG impacts beyond physical symptoms, including mental health, quality of life, and the well-being of their families.
Respondents reported that although available treatments for MG had a positive impact on health outcomes, overall, they had negative experiences with steroids, disliked the slow onset of medication effects, and had a feeling of trial and error with medications. Patients also had concerns about the long-term and sustained benefits of supportive treatments.
Patients with MG are looking for improved outcomes with new treatments, including a decreased intensity of exacerbations and side effects, the maintenance of independence, and fewer hospital admissions for serious MG disease-related circumstances. Patients are willing to tolerate side effects of medications if they lead to improved MG outcomes. In addition, respondents stated that although current medications appear to decrease the number of exacerbations, they do not have an impact on patients’ overall quality of life. Moreover, MDC input noted that patients, families, and caregivers consider the following factors when evaluating MG therapies: treatment method and delivery (e.g., invasiveness, duration, frequency of administration), potential side effects (e.g., low risk of side effects, number of side effects), HRQoL, convenience of treatment (e.g., administration at home or in a community centre, perceived control and flexibility, time to travel to clinic, access to parking for clinic visits), financial impact (e.g., treatment coverage by public or private insurance), and access to treatment. According to the MDC input, HRQoL outweighs the convenience of a drug as a key priority. MDC input stated that in addition to accessibility to treatments, patients with MG need improved treatment options that enhance effectiveness and tolerance over the long-term.
Patients and caregivers reported varied experiences in diagnostic testing for MG. Although some respondents experienced minimal problems with testing and diagnosis, especially in cases of MG crisis or hospitalization due to MG, the majority reported significant difficulties getting a diagnosis, which included a lengthy process with many missed opportunities, delayed diagnosis, misdiagnosis (such as stroke or Bell palsy), and costs incurred. According to early findings of the MG Journey Mapping project, time from the first bothersome symptom to diagnosis ranged from 7 years to 23 years. All respondents underwent diagnostic blood testing, and many underwent single-fibre electromyography to confirm diagnosis.
Clinician Input
Input From the Clinical Expert Consulted for This Review
All CDA-AMC review teams include at least 1 clinical specialist with expertise in the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by 1 clinical specialist with expertise in the diagnosis and management of MG.
Unmet Needs
The clinical expert explained that although there has been significant improvement in the management of patients with MG over the past few decades, there remain significant treatment gaps for patients with gMG. Given that patients with gMG experience disease morbidity while awaiting the beneficial effects of prolonged treatments that often have intolerable side effects, the expert highlighted the need for new treatments that have a faster onset of action (particularly for patients with any bulbar or respiratory involvement), are more effective, reduce significant AEs, and have better durability than current treatment options. Additionally, the clinical expert noted that patients would benefit from new treatments that are less invasive (e.g., administered orally rather than SC or IV route of administration), are administered less frequently (e.g., weekly or monthly rather than daily), allow for reduced doses of other immunosuppressive drugs, and may be used in combination with existing or future treatments that have different mechanisms of action (e.g., a combination of a peptide complement inhibitor plus a neonatal FcR inhibitor for patients with severe or refractory MG). Overall, the expert outlined that goals of treatment for patients with MG, which are to reduce MG-related morbidity and mortality, minimize treatment-associated morbidity and mortality, reduce weakness (ocular, bulbar, respiratory, axial, and extremity) associated with MG and prevent disease exacerbations or an MG crisis, and improve HRQoL.
Place in Therapy
The expert noted that, depending on how refractory disease is defined, approximately 10% to 15% of patients do not respond to conventional treatment and, therefore, require more aggressive treatments, including IVIg or PLEX; these patients are considered to be the target population of complement inhibitors such as zilucoplan. The expert noted that the patient population identified as refractory in the RAISE trial is aligned with the way refractory disease is defined in clinical practice, particularly with reference to an adequate trial of prednisone in addition to another IST.
Patient Population
Patients are initially identified as having MG through clinical suspicion, and diagnosis is confirmed with electrophysiology (i.e., repetitive nerve stimulation for assessment of decrements) and serology (e.g., confirmation of antibodies for anti-AChR, MuSK, and LRP4), according to the clinical expert, who added that the presence of anti-AChR antibodies is a reliable diagnostic finding with high specificity, so the identification of patients with MG using anti-AChR antibody testing is straightforward. Nevertheless, given the rarity of disease and the fact that the initial identification of MG is based on clinical suspicion, the clinical expert noted that MG is likely underdiagnosed in the population. The expert also noted that the availability and timeliness of anti-AChR antibody assays varies across Canada.
According to the expert consulted, the patients who are most likely to benefit from treatment with zilucoplan are generally aligned with patients who were enrolled in the RAISE trial, who had anti-AChR antibody–positive gMG, MGFA disease class II to class IV, and an MG-ADL score of 6 or greater; the exception was the QMG score, which was 12 or greater in study participants but is reportedly not used commonly in clinical practice. The expert pointed out that patients who have had an adequate trial (in both dose and duration) of prednisone and at least 1 NSIST or who demonstrate intolerance to the combination of prednisone and NSISTs should be eligible for treatment with zilucoplan, but these criteria limit eligibility to patients who have been on conventional treatment for at least 6 months (and commonly for 12 months), reflecting the duration needed for corticosteroids (3 to 6 months) and mycophenolate mofetil and azathioprine (likely 12 to 18 months) to produce an optimal benefit.
Assessing the Response Treatment
The MG-ADL scale is a patient-reported outcome deemed by the expert to be clinically relevant (a 2-point change is considered the minimum clinically meaningful improvement) to the evaluation of response to treatment. According to the clinical expert consulted for this review, the MG-ADL can be self-administered in minutes (with the supervision of a neuromuscular neurologist) and should be used as an eligibility criterion for treatment with zilucoplan and to monitor efficacy throughout treatment.
Discontinuing Treatment
A clear lack of response (i.e., no reduction in MG-ADL score after about 6 months) to treatment with zilucoplan, intolerance due to significant AEs that require the discontinuation of treatment, and the requirement for additional ongoing treatments with IVIg or PLEX, despite an adequate trial of zilucoplan, were reasons to discontinue treatment with zilucoplan, according to the clinical expert.
Prescribing Considerations
The clinical expert said that because MG is a rare disorder that requires nuanced management, patients with gMG should be diagnosed, treated, and monitored by a neuromuscular neurologist with experience in gMG.
Clinician Group Input
This section was prepared by the CDA-AMC review team based on the input provided by clinician groups. The full original clinician group input received by CDA-AMC have been included in the Perspectives of Patients, Clinicians, and Drug Programs section of this report.
CDA-AMC received 1 clinician group submission from the NMD4C, which comprised the input of 8 clinicians with experience treating patients with gMG. The clinician group agreed with the clinical expert on the unmet treatment needs, goals of treatment, treatment response evaluations, and care management for patients with MG. NMD4C identified the additional treatment outcomes of emergency department visits, hospitalizations, and intensive care unit admissions. The ability to self-administer zilucoplan at home provides patients with greater autonomy in their care management, according to the clinician group input. Both the clinician group and the clinical expert consulted for this review indicated that patients with anti-AChR antibody–positive gMG would most likely benefit from treatment from zilucoplan, although the clinician group noted that evidence on the efficacy of zilucoplan has not been confirmed for patients with MG who are seronegative.
Drug Program Input
The drug programs provide input on each drug being reviewed through the CDA-AMC reimbursement review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical expert consulted by CDA-AMC are summarized in Table 4.
Table 4: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Relevant comparators | |
Placebo was the comparator in the RAISE study. Patients received either zilucoplan 0.3 mg/kg or placebo as SC injection once daily. | The clinical expert noted that there is currently no robust direct or indirect evidence comparing zilucoplan with other active treatments in patients with gMG whose symptoms persist despite treatment with conventional therapies. The expert explained that the most relevant comparators for zilucoplan in patients with refractory gMG include other complement inhibitors (i.e., eculizumab, ravulizumab), neonatal FcR inhibitors (e.g., efgartigimod alfa), chronic IVIg, and chronic PLEX; rituximab as a comparator is less applicable because of its limited availability to patients with gMG in Canada, its off-label use, the lack of rigorous clinical trial evidence for patients with anti-AChR antibody–positive MG, and some evidence of improved benefit in patients with MuSK-positive MG. |
At baseline, the majority of patients had received prior gMG-specific medications, including cholinesterase inhibitors (84.0% of patients), corticosteroids (63.2% of patients), and NSISTs (52.9% of patients). This follows the prerequisite drugs used in the ADAPT trial, which assessed efgartigimod alfa, in adult patients with anti-AChR antibody–positive gMG. Do these proportions align with clinical practice for adult patients with anti-AChR antibody–positive gMG who have refractory disease? | In the RAISE trial, prior gMG medications were defined as any medications that started before the first administration of the study drug. The majority of patients in both study groups had received prior AChE inhibitors (about 95% of patients), steroids (about 85% of patients), and NSISTs (around 70% of patients). In the RAISE trial, gMG-specific baseline medications were defined as medications that started before and continued after receipt of the study drug, including cholinesterase inhibitors (84.5%), corticosteroids (63.2%), mycophenolate mofetil (19.5%), azathioprine (17.8%), cyclosporin (7.5%), tacrolimus (5.7%), and methotrexate (2.3%). The clinical expert reported that a higher proportion of patients with refractory disease than without would be expected to be receiving both corticosteroids and NSISTs at baseline; therefore, if the RAISE trial defined patients with refractory disease as those who previously (i.e., historically) experienced a lack of response to these gMG medications and, therefore, are no longer on these drugs, it may be reasonable to expect lower proportions of patients taking these medications at baseline. |
Considerations for initiation of therapy | |
In the RAISE trial, patients were adults (18 to 74 years of age) with anti-AChR antibody–positive gMG, MGFA disease class II to class IV (both of which match the efgartigimod alfa initiation criteria in the ADAPT trial). Patients were required to have an MG-ADL score of ≥ 6 in the RAISE trial, whereas in the ADAPT trial efgartigimod alfa, patients were required to have an MG-ADL score of ≥ 5. | The clinical expert stated that patients who were identified as having anti-AChR antibody–positive gMG, MGFA disease class II to class IV, and an MG-ADL score of 6 or greater were included in the RAISE trial and, as such, are the patients who are most likely to benefit from treatment with zilucoplan. The expert noted that patients were not required to have severe disease to be defined as having refractory disease; only 5% of patients in the RAISE trial had MGFA disease class IV (severe disease), with 26% classified as MGFA disease class II and 70% as class IIIs. The MG-ADL total score cut-off value was ≥ 6 points for the inclusion criterion in the RAISE trial and other clinical trials for gMG, such as the CHAMPION MG trial for ravulizumab and the REGAIN trial for eculizumab. However, the review team noticed that the inclusion criteria for the ADAPT trial was an MG-ADL total score ≥ 5 points. There were relatively few patients in the ADAPT trial who had an MG-ADL total score of 5 points at baseline. The clinical expert consulted for this review indicated that a subset of patients with MG-ADL scores < 6 could potentially be suitable for treatment. Specifically, the clinical expert indicated that patients with ocular MG or mild symptoms can still be refractory to other therapies. However, whether the results of the RAISE trial can be generalized to patients who have an MG-ADL total score of < 6 despite conventional therapies remains uncertain. |
Should patients who have tried other advanced therapies be able to transition to zilucoplan, even for reasons such as ease of convenience, as zilucoplan can be given at home as SC injections? Do you perceive any issues with this? | The expert said patients who have tried other advanced therapies would be eligible for treatment with zilucoplan, including for reasons related to ease of treatment administration. |
From previous reviews for this indication, rituximab may not be available in some jurisdictions. Are you aware of the variable access to rituximab across jurisdictions? | The expert agreed that there is a wide variation in access to rituximab, which is used off-label for patients with gMG, across jurisdictions in Canada (e.g., it is relatively easy to access in Quebec but nearly impossible in Ontario). |
Considerations for continuation or renewal of therapy | |
There should be no challenges, as the renewal criteria are based on a scoring system. | This is a comment from the drug plans to inform CDEC deliberations. |
Will alignment with efgartigimod alfa be considered for the continuation or renewal of zilucoplan? | This is a comment from the drug plans to inform CDEC deliberations. |
Considerations for discontinuation of therapy | |
Will alignment with efgartigimod alfa be considered for the discontinuation of zilucoplan? | This is a comment from the drug plans to inform CDEC deliberations. |
Considerations for prescribing of therapy | |
Dosing is based on actual body weight, as follows:
| This is a comment from the drug plans to inform CDEC deliberations. |
There may be concerns with access to neurologists in remote locations. Efgartigimod alfa must be prescribed by or in consultation with a neurologist with expertise in managing patients with gMG. | According to the clinical expert consulted for this review, the biologics should be prescribed by or on the advice of a neuromuscular neurologist with experience in the management of MG. |
Is there any evidence for combination use of zilucoplan with other advanced therapies (e.g., efgartigimod alfa)? If other C5 inhibitors become available in the future (e.g., eculizumab), can zilucoplan be used in combination, or if other C5 inhibitors are unsuccessful, can zilucoplan be considered? | The expert indicated that there is an absence of empiric evidence to support the use of zilucoplan in combination with other treatments. The expert explained that zilucoplan in combination with other C5 inhibitors would be potentially dangerous, because of the combined effect of drugs with similar mechanisms of action. For example, a patient who does not experience a response to treatment with a single complement inhibitor (e.g., eculizumab, ravulizumab) could subsequently be tried on zilucoplan monotherapy, according to the expert, despite a lack of evidence showing that a patient who experiences a lack of treatment response to a complement inhibitor would respond to treatment with a different complement inhibitor. Instead, the expert stated that it would be preferable to switch a patient who experiences treatment failure with a complement inhibitor to a drug with a different mechanism of action (e.g., efgartigimod alfa). |
System and economic issues | |
It seems as though zilucoplan will displace other therapies in this space, as it can be given at home instead of an IV infusion clinic. | This is a comment from the drug plans to inform CDEC deliberations. |
The unit prices of zilucoplan for the 16.6mg/syringe, 23.0mg/syringe, and 32.4mg/syringe is $650.2718, $900.9790, and $1,269.2052, respectively. Year 1: $25,582,701 Year 2: $36,524,794 Year 3 total: $75,033,053 | This is a comment from the drug plans to inform CDEC deliberations. |
Efgartigimod alfa is still under consideration for negotiation at the pCPA. Eculizumab negotiations have concluded without an agreement at the pCPA. | This is a comment from the drug plans to inform CDEC deliberations. |
AChE = acetylcholinesterase; AChR = acetylcholine receptor; CDEC = Canadian Drug Expert Committee; FcR = fragment crystallizable receptor; gMG = generalized myasthenia gravis; Ig = immunoglobulin; MG = myasthenia gravis; MG-ADL = Myasthenia Gravis Activities of Daily Living; MGFA = Myasthenia Gravis Foundation of America; NSIST = nonsteroidal immunosuppressive therapy; pCPA = pan-Canadian Pharmaceutical Alliance; PLEX = plasma exchange; SC = subcutaneous.
Clinical Evidence
The objective of the CDA-AMC Clinical Review report is to review and critically appraise the clinical evidence submitted by the sponsor on the beneficial and harmful effects of zilucoplan, administered as an SC injection, once daily, according to body weight (16.6 mg for a body weight of < 56 kg, 23 mg for a body weight of ≥ 56 kg to < 77 kg, and 32.4 mg for a body weight of ≥ 77 kg), for the treatment of adults with anti-AChR antibody–positive gMG. Patients continued to receive standard therapy throughout the pivotal RAISE trial. The focus will be placed on comparing zilucoplan to relevant comparators and identifying gaps in the current evidence. Zilucoplan received a Notice of Compliance from Health Canada on July 11, 2024. The reimbursement request is for the refractory population (adults with refractory gMG), based on the sponsor’s consultation with clinical experts on the current treatment paradigm, patients’ unmet needs, and the anticipated use of zilucoplan for gMG in Canada.25
A summary of the clinical evidence included by the sponsor in the review of zilucoplan is presented in 3 sections, with the CDA-AMC critical appraisal of the evidence included at the end of each section. The systematic review includes pivotal studies and RCTs that were selected in accordance with the sponsor’s systematic review protocol. The CDA-AMC assessment of the certainty of the evidence in this first section, which uses the GRADE approach, follows the critical appraisal of the evidence. The second section includes sponsor-submitted long-term extension studies. The third section includes indirect evidence from the sponsor. The sponsor did not include any additional studies that addressed important gaps in the systematic review evidence.
Included Studies
Clinical evidence from the following are included in the CDA-AMC review and appraised in this document:
1 pivotal, phase III, randomized trial identified in the Systematic Review section
1 long-term extension study
1 ITC.
Systematic Review
Contents within this section have been informed by materials submitted by the sponsor. The following has been summarized and validated by the CDA-AMC review team.
Description of Study
Characteristics of the included study are summarized in Table 5.
Table 5: Details of the Study Included in the Systematic Review
Characteristics | RAISE trial |
|---|---|
Designs and populations | |
Study design | Phase III, randomized, multicentre, double-blind, placebo-controlled study |
Locations | 75 sites in 10 countries: Canada (2 sites), France, Germany, Italy, Japan, Norway, Poland, Spain, UK, US |
Patient enrolment dates | Start date: September 17, 2019 End date: December 30, 2021 |
Data cut-off date | December 30, 2021 |
Randomized (N) | N = 174 patients, 88 of whom had refractory anti-AChR antibody–positive gMG Zilucoplan group, n = 86 patients, 44 of whom had refractory anti-AChR antibody–positive gMG Placebo group, n = 88 patients, 44 of whom had refractory anti-AChR antibody–positive gMG |
Inclusion criteria |
|
Exclusion criteria |
|
Drugs | |
Intervention | Zilucoplan (0.3 mg/kg) administered by SC injection once daily |
Comparator(s) | Placebo administered by SC injection once daily |
Study duration | |
Screening phase | 1 to 28 days |
Treatment phase | 12 weeks |
Follow-up phase | Up to 7 weeks; started on day 1 after the end of the treatment period and ended after the final assessment at the study follow-up visit At the conclusion of the 12-week treatment period, all study participants had the option to enrol in a separate extension study (RAISE-XT), provided they met the extension study inclusion criteria |
Outcomes | |
Primary end point | Change from baseline to week 12 in MG-ADL score |
Secondary end points | Key secondary end points:
Additional secondary end points:
|
Exploratory end points |
|
Publication status | |
Publications | Howard et al. (2023)26 |
Trial registration | ClinicalTrials.gov Identifier: NCT04115293 |
AChR = acetylcholine receptor; gMG = generalized myasthenia gravis; Ig = immunoglobulin; IMP = investigational medicinal product; IST = immunosuppressive therapy; MG-ADL = Myasthenia Gravis Activities of Daily Living; MGC = Myasthenia Gravis Composite; MGFA = Myasthenia Gravis Foundation of America; MGFA-PIS = Myasthenia Gravis Foundation of America Post-Intervention Status; MG-QoL15r = Myasthenia Gravis Quality of Life 15-item revised; MSE = minimal symptom expression; Neuro-QoL = Quality of Life in Neurologic Disorders; PLEX = plasma exchange; QMG = quantitative myasthenia gravis; SC = subcutaneous; TEAE = treatment-emergent adverse events; VAS = visual analogue scale; WPAI:SHP = Work Productivity and Activity Impairment Questionnaire: Specific Health Problem.
Sources: RAISE Clinical Study Report,14 sponsor’s Summary of Clinical Evidence.27
RAISE was a multicentre, randomized, phase III, double-blind, placebo-controlled study designed to evaluate the efficacy and safety of zilucoplan in patients with gMG (overall trial population) and in a prespecified subgroup of patients with refractory gMG (refractory subpopulation). After completion of the 12-week treatment period in the RAISE study, eligible patients had the option to enrol in the RAISE-XT long-term extension study. Details of the RAISE-XT study is summarized in the Long-Term Extension Studies section. The overall study designs of the RAISE and RAISE-XT studies are depicted in Figure 1.
In the RAISE study, 174 patients with anti-AChR antibody–positive gMG (88 of whom made up the refractory subpopulation) were enrolled from September 2019 to December 2021 at 75 sites in 10 countries, with 2 sites (3 patients) in Canada. Eligible patients were randomized in a 1:1 ratio to receive zilucoplan 0.3 mg/kg once daily plus standard of care or to receive placebo plus standard of care. Randomization was stratified by baseline MG-ADL score (≤ 9 versus ≥ 10), QMG score (≤ 17 versus ≥ 18), and geographic region (East Asia, Europe, and North America). The primary objective of the RAISE study was to evaluate the change from baseline to week 12 in the MG-ADL score. Key secondary objectives included change from baseline to week 12 in the QMG score, MGC score, and MG-QoL15r score, and the frequency of TEAEs. Additional secondary objectives included the achievement of MSE (defined as an MG-ADL score of 0 or 1) at week 12 without rescue therapy, an MG-ADL responder rate (defined as a ≥ 3-point decrease in MG-ADL score) at week 12 without rescue therapy, and a QMG responder rate (defined as a ≥ 5-point decrease in QMG score) at week 12 without rescue therapy. Achievement of minimal manifestation status per MGFA-PIS at week 12 without rescue therapy was an exploratory objective. Data for the primary and key secondary outcomes were available for both the overall population and the refractory subpopulation. Data for the additional secondary outcomes were available for observed cases in both the overall population and the refractory subpopulation, and for imputed cases in the overall population. Data on the achievement of minimal manifestation status per MGFA-PIS at week 12 without rescue therapy were available for the overall population only. The Clinical Study Report, which had a data cut-off date of December 30, 2021, was the primary source for the RAISE study.
Figure 1: Study Design of the Pivotal Study (RAISE) and the Extension Study (RAISE-XT)
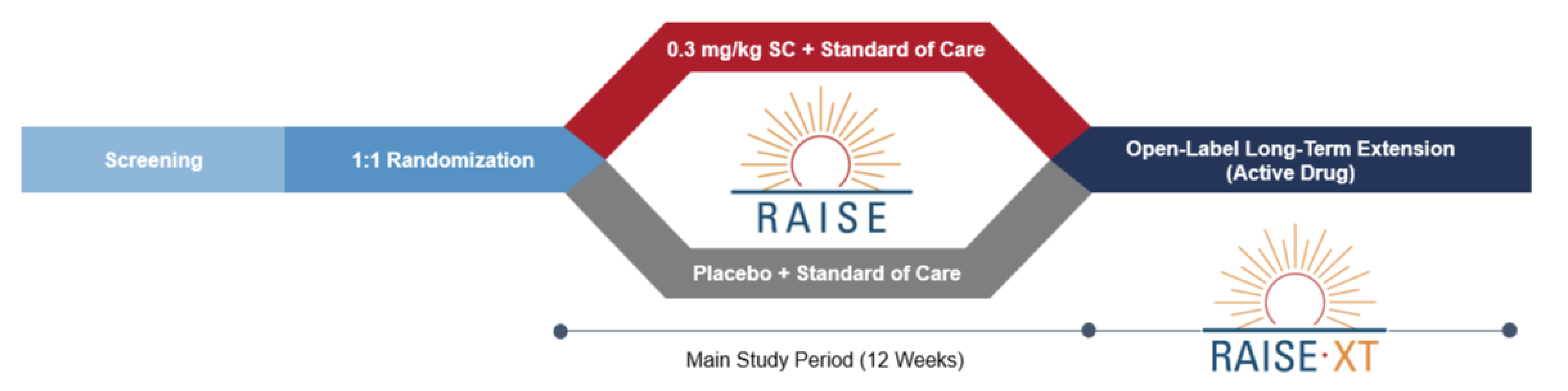
SC = subcutaneous.
Source: RAISE Clinical Study Report.14
Populations
Inclusion and Exclusion Criteria
The key inclusion criteria were adults aged 18 years to 74 years, with a diagnosis of gMG (MGFA disease class II to class IV at screening), and positive serology for anti-AChR-binding autoantibodies. At screening and baseline, eligible patients had to have an MG-ADL score of 6 or greater, a QMG score of 12 or greater, and a QMG score of 2 or greater on 4 or more items. Key exclusion criteria were known disease characteristics (positive serology for muscle-specific kinase, investigator-determined minimal manifestation status of gMG, investigator-determined fixed weakness or burned out gMG), medical history (abnormal thyroid function, history of meningococcal disease, current or recent systemic infection, active malignancy), and prior treatment (thymectomy; recent surgery requiring general anesthesia; and/or prior treatment with a complement inhibitor, rituximab, IVIg, SCIg, PLEX, or an experimental drug). Patients were considered to have refractory gMG if they had received treatment for at least 1 year with 2 or more of the following therapies: prednisone, azathioprine, mycophenolate mofetil, cyclosporine, cyclophosphamide, methotrexate, tacrolimus, rituximab, eculizumab, other corticosteroids for gMG, or other ISTs; or had a history of treatment with at least 1 of the aforementioned therapies for 1 year or more and required chronic PLEX, IVIg, or SCIg at least every 3 months for the 12 months before enrolment.
Interventions
Patients were randomized to receive zilucoplan 0.3 mg/kg or placebo administered by SC injection. Patients must have received a quadrivalent or serotype B meningococcal vaccine, or both, at least 14 days before the first dose of the study drug. At the day 1 visit, doses were administered by the patient into the abdomen (preferred site), thigh, or upper arm, under the supervision of site staff. After in-clinic education and training to ensure that the administration technique for self-injection was adequate and appropriate, all patients self-injected daily SC doses of the blinded drug (zilucoplan or placebo), according to randomized treatment allocation, for the subsequent 12 weeks. Single-use prefilled syringes in injection devices were provided for use during the study, and weight-bracketed dosing was used (i.e., patients were provided with prefilled syringes that contained fixed amounts of zilucoplan based on their weight, and each fixed amount covered a range of study patient weights). This weight-bracketed dosing strategy had the potential for a range of doses to be received, from a minimum dose of zilucoplan 0.22 mg/kg per day to a maximum dose of zilucoplan 0.42 mg/kg per day (refer to Table 6). Patients who presented with a higher body weight (> 150 kg) or a lower body weight (< 43 kg) were accommodated on a case-by-case basis.
Table 6: Zilucoplan Dose Presentations by Weight Bracket
Minimum (nominal) target dose (mg/kg) | Actual dose (mg) | Weight range (kg) | Dose range (mg/kg) |
|---|---|---|---|
0.3 | 16.6 | ≥ 43 to < 56 | 0.30 to 0.39 |
0.3 | 23.0 | ≥ 56 to < 77 | 0.30 to 0.41 |
0.3 | 32.4 | ≥ 77 to 150 | 0.22 to 0.42 |
Source: RAISE Clinical Study Report.14
Study periods in the RAISE study included screening (up to 4 weeks) and treatment (12 weeks), for a total study duration of 16 weeks. During the treatment period, patients were evaluated during clinic visits at week 1, week 2, and monthly visits at week 4, week 8, and week 12.
Patients were permitted to receive prescriptions and over-the-counter medications in the 30 days before screening or as concomitant medications (ongoing or initiated after the first dose of the study drug on day 1) up to the last study visit. Patients were expected to remain on stable doses of standard-of-care treatments for gMG, including corticosteroids and IST drugs, unless medically indicated. Pyridostigmine was to be withheld for a minimum of 10 hours before clinical evaluation at every study visit. The pyridostigmine dose could be reduced if judged by the investigator to be related to intolerable side effects. Doses of standard-of-care treatments were not to be increased during the study; however, patients were permitted to receive rescue therapy (IVIg, PLEX, or eculizumab), with the type, frequency, and duration at the discretion of the investigator. Patients were prohibited from receiving the concomitant medications of rituximab, aminoglycosides, colomycin, polymyxin, telithromycin, injectable cyclin, macrolides, fluoroquinolones, quinines, quinidine, hydroxychloroquine, procainamide, beta-blockers, diphenylhydantoin, dantrolene, D-penicillamine, and magnesium.
Dosing of a study drug could be interrupted or permanently discontinued at the discretion of the investigator and/or the sponsor. Patients who permanently discontinued the study drug underwent a safety evaluation (ongoing AEs or new SAEs that developed after the last study visit) 40 days after the last dose of the study drug. Patients diagnosed with meningococcal disease were to discontinue the study drug permanently.
Outcomes
A list of efficacy end points assessed in this Clinical Review report is provided in Table 7, followed by descriptions of the outcome measures (Table 8). Summarized end points are based on outcomes included in the sponsor’s Summary of Clinical Evidence, as well as any outcomes identified as important to this review by the clinical expert consulted by CDA-AMC and input from patient and clinician groups and public drug plans. The CDA-AMC review team selected end points that were considered to be most relevant to CDA-AMC expert committee deliberations and finalized this list of end points in consultation with members of the expert committee. All summarized efficacy end points were assessed using GRADE. Select notable harms outcomes considered important to CDA-AMC expert committee deliberations were also assessed using GRADE.
Table 7: Outcomes Summarized From the Study Included in the Systematic Review
Outcome measure | Time point | RAISE |
|---|---|---|
Change in MG-ADL score | Baseline to week 12 | Primary end pointa |
Change in QMG score | Baseline to week 12 | Key secondary end pointa |
Change in MGC score | Baseline to week 12 | Key secondary end pointa |
Change in MG-QoL15r score | Baseline to week 12 | Key secondary end pointa |
Achievement of MSE, defined as an MG-ADL score of 0 or 1 without rescue therapy | At week 12 | Secondary end pointa |
Achievement of a ≥ 3-point reduction in MG-ADL score without rescue therapy | At week 12 | Secondary end pointa |
Achievement of a ≥ 5-point reduction in QMG score without rescue therapy | At week 12 | Secondary end pointa |
Achievement of minimal manifestation status per MGFA-PIS without rescue therapy | At week 12 | Exploratory end point |
Incidence of TEAEs (i.e., infections) | During the 12-week treatment period | Secondary |
MG-ADL = Myasthenia Gravis Activities of Daily Living; MGC = Myasthenia Gravis Composite; MGFA-PIS = Myasthenia Gravis Foundation of America Post-Intervention Status; MG-QoL15r = Myasthenia Gravis Quality of Life 15-item revised; MSE = minimal symptom expression; QMG = quantitative myasthenia gravis; TEAE = treatment-emergent adverse event.
aStatistical testing for these end points was adjusted for multiple comparisons (e.g., hierarchical testing).
Source: RAISE Clinical Study Report,14 sponsor’s Summary of Clinical Evidence.27
Activities of Daily Living
MG-ADL Scale
The MG-ADL scale is a brief, 8-item, interviewer-administered, patient-reported outcome designed to evaluate MG symptom severity.28 Two questions pertain to ocular functions, 3 to oropharyngeal functions, 1 to respiratory function, and 2 to extremity functions. The 8 items are each scored on a scale from 0 to 3, and the total score is the sum of the 8 individual scores, and ranges from 0 to 24. Higher scores indicate more severe symptoms of MG.28 A 2-point change in MG-ADL score is considered clinically meaningful.29 This 2-point change threshold was based on a receiver operator characteristic curve method used in an observational study of patients with MG managed at the discretion of the treating physician.29 In the RAISE study, the MG-ADL assessment was conducted at screening to assess patient eligibility and at each study visit.
Disease Severity
QMG Scale
The QMG scale is a standardized and validated quantitative strength scoring system that was developed specifically for MG.30 The scoring system consists of 13 individual assessments; each scored on a scale from 0 to 3. The total score is the sum of the individual scores, and ranges from 0 to 39. Higher scores represent more severe impairment.30 A change in the QMG score of 3 points or more may be considered clinically meaningful in a typical clinical study population of patients with MG.30,31
Treatment Response
MGC Scale
MGC is a 10-item scale that has been used to measure the clinical status of patients with MG, both in the practice setting and in clinical studies, and evaluate treatment response. The 10 items and corresponding response scale scores are weighted and totalled. The total score is the sum of the 10 individual scores, and ranges from 0 to 50. Higher scores indicate more severe impairment due to the disease.32,33 A study of patients with MG who are under routine care showed that a 3-point change in this assessment is considered clinically meaningful and is associated with the best sensitivity and specificity, based on a receiver operator characteristic curve method.34
Additional Efficacy End Points
Minimal Symptom Expression
MSE was designed to assess how many patients become free or virtually free of MG symptoms and is achieved when the MG-ADL total score is 0 or 1 for patients receiving therapy.35
Health-Related Quality of Life
MG-QoL15r Scale
MG-QoL15r is a 15-item, self-administered, patient-reported outcome scale designed to assess quality of life in patients with MG.36 The 15 items relate to the physical, social, and psychological aspects of well-being and are associated with corresponding response scales, each scored from 0 to 2. The total score is the sum of the 15 individual item scores, and ranges from 0 to 30. Higher scores indicate a more severe impact of the disease on aspects of the patient’s life.36,37 An MID has not been established for the MG-QoL15r in patients with MG.9
Safety
Safety outcomes included TEAEs of interest, clinical laboratory tests, vital signs, electrocardiograms, physical examinations, the Columbia-Suicide Severity Rating Scale, and immunogenicity. AEs were defined as any untoward medical occurrence in a patient who was administered a study drug, regardless of whether it was related to the study drug. AEs were classified according to the national Cancer Common Terminology Criteria for Adverse Events (CTCAE) and coded using the Medical Dictionary for Regulatory Activities, version 22.0. SAEs were defined as any AE that resulted in death, was life-threatening, required hospitalization or prolongation of existing hospitalization, resulted in persistent or significant disability or incapacity, resulted in a congenital anomaly or birth defect, or required intervention to prevent any of the aforementioned outcomes. Although AEs of interest were not prespecified in the protocol, an amendment of the Statistical Analysis Plan (February 1, 2021, amendment 1.0) included statistical analyses specific to infections (such as Neisseria infections, injection-site reactions, and hypersensitivity reactions [e.g., anaphylactic reactions, hepatic events, and malignancies]). The AE reporting period started on day 1, with the first administration of the study drug, and continued until the last study visit; patients were assessed 40 days after their last dose of the study drug for any ongoing AEs or any new SAEs that developed after the last study visit. A safety monitoring committee evaluated study safety data, as appropriate, for any unblinding of data for review.
Based on input received, changes from baseline in the MG-ADL, QMG, MGC, and MG-QoL15r scores were identified as important outcomes to patients and to clinicians making treatment decisions. The expert also identified the achievement of MSE, responses on the MG-ADL and the QMG, and the achievement of minimal manifestation status per MGFA-PIS as important outcome measures. Time to rescue therapy was not identified by clinicians as being very important for clinical decision-making. The need for rescue therapy was noted by the clinical expert to be a relatively uncommon event that may be indicative of treatment failure, but patients expressed a desire for new treatments that provide sustained benefit with reduced exacerbations. Findings for time to rescue therapy are summarized in Appendix 1. Among patients with refractory gMG, mean change in the MG-ADL score and the proportion of MG-ADL responders were key inputs in the sponsor’s pharmacoeconomic model. Harms of treatment were identified as important by patients, clinician groups, and the clinical expert, with infections deemed to be notable harms.
Table 8: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
MG-ADL questionnaire | An 8-item, patient-reported outcome measure that assesses MG symptoms and functional activities related to activities of daily living, producing a total score that ranges from 0 to 24, with higher scores indicating a greater severity of symptoms. The MG-ADL comprises items related to patients’ assessment of functional disability secondary to ocular (2 items), bulbar (3 items), respiratory (1 item), and gross motor or limb impairment (2 items).28 | Validity: The MG-ADL score highly correlated with the MGC score (r = 0.85; P < 0.0001) and the MG-QoL15 score (r = 0.76; P < 0.0001) (n = 87).29 Correlation between the MG-ADL score and physician impression of change between visits was strong (r = 0.70; P < 0.0001) (n = 76).29 Reliability: The test-retest reliability coefficient was 93.7% among 20 patients, with the lower bound of the 95% CI at 87.3%, tested twice within 1 week.29 Responsiveness: MG-ADL was assessed at 2 visits, and the mean improvement in score in patients who improved, based on the gold standard, was 3.88 (SD = 2.72) (n = 76).29 Note: the measurement properties of the subcomponents of the scale have not been investigated. | A 2-point improvement in MG-ADL score was a threshold that provided the best balance of sensitivity (n = 26) and specificity (n = 50) when referenced to MG-QoL15 score and physician impression of change for predicting clinical improvement at the level of the individual for patients with MG.29 |
QMG scale | A 13-item direct physician assessment scoring system that quantifies disease severity, based on impairments in body function and structures. Total QMG score ranged from 0 to 39, with higher scores indicating greater disease severity. The QMG score comprised 13 items: ocular (2 items), facial (1 item), bulbar (2 items), gross motor (6 items), axial (1 item), and respiratory (1 item).30 | Validity: Construct validity was assessed through correlations with the Manual Muscle Test (r = 0.69 in 303 patients38 and r = 0.73 in 53 patients).39 Reliability: Internal consistency, assessed with Cronbach alpha value, was 0.74 for the QMG scale, demonstrating an acceptable threshold (n = 251).40,41 Test-retest reliability was studied in 209 patients with stable disease who were assessed 2 weeks apart. The intraclass correlation coefficient for the total scores was 0.88 (95% CI, 0.85 to 0.91).40,41 Responsiveness: The index of responsiveness (signal-to-noise ratio) was 1.45 (n = 53).39 Note: the measurement properties of the subcomponents of the scale have not been investigated. | Based on an interrater reliability of 1.342 SD, any change in the QMG score of up to 2.6 points is expected to occur because of the variability of repeated observations; therefore, a change of 2.6 points was estimated to be the threshold of clinical significance in patients with MG (n = 5 with MG and 4 otherwise healthy).30 Using the anchor-based method, with a patient’s perception of overall improvement assessed on a VAS, there was some evidence that the MID should be higher in patients with higher baseline QMG scores; the MID for patients with mild-to-moderate MG (QMG ≤ 16) was estimated to be 2 points (n = 38), and for patients with higher baseline values (QMG > 16), the estimated MID was 3 points (n = 12).9,31 |
MGC scale | A 10-item scale that has been used to measure the clinical status of patients with MG, both in the practice setting and in clinical studies, and evaluate treatment response. The 10 items and corresponding response scale scores are weighted and totalled. The total score is the sum of the 10 individual scores, and ranges from 0 to 50. Higher scores on the MGC indicate more severe impairment due to the disease.32,33 | Validity: In a study of 175 patients with MG, the MGC score demonstrated excellent longitudinal construct validity, based on a comparison of changes in MGC score with several other MG outcomes measures, alone and in combination.34 Reliability: Based on testing performed on 38 patients with MG and conducted on the same day by 2 neurologists, the test-retest reliability coefficient of the MGC was 98%.34 In a study of 209 patients with stable disease, assessed 2 weeks apart, the intraclass correlation coefficient for the total scores was 0.82 (95% CI, 0.77 to 0.85).40,41 Responsiveness: Responsiveness of the MGC was assessed in 151 patients using different gold standards of clinical change (e.g., physician impression of improvement, improvement in MG-QoL15 score).34 | A 3-point improvement in MGC score represents a meaningful improvement to most patients with MG.34 |
MG-QoL15r scale | Three items in the original MG-QoL15 scale were reworded to improve its clinimetric properties and face and content validity. The wording, “double vision,” was added to the ocular item; “work at home” was added to the work item; and other limitations of personal independence were added to the driving item. The revised version uses a 3-response option scale (0 = not at all; 1 = somewhat; 2 = very much), with higher scores indicating worse quality of life over the past few weeks. | The psychometric properties of the MG-QoL15r, QMG, MG-ADL, and MGC scales were evaluated and compared to response to disease change in patients with autoimmune MG (N = 872).42 Validity: Construct validity was demonstrated for MG-QoL15r with QMG (Pearson correlation coefficient [r] = 0.550), MG-ADL (r = 0.701), and MGC (r = 0.635). For discriminant validity, MG-QoL15r scores were different among patients based on their MGFA classification and MGC scores.42 Reliability: Internal consistency reliability was demonstrated by the Cronbach alpha of 0.93 for MG-QoL15r.42 Responsiveness: For responsiveness to change, the Pearson correlation coefficients between changes in MG-QoL15r and QMG after treatment were 0.423.42 | An MID has not been estimated for patients with MG. |
MGFA-PIS | Physician-determined assessment of clinical symptoms of MG after initiation of MG-specific therapy. Minimal manifestation status is defined as follows: “The patient has no symptoms of functional limitations from MG but has some weakness on examination of some muscles. This class recognizes that some patients who otherwise meet the definition of complete stable remission or pharmacologic remission do have weakness that is only detectable by careful examination.” | No studies assessing validity, reliability, or responsiveness were identified for patients with MG. | Not applicable. |
CI = confidence interval; MG = myasthenia gravis; MG-ADL = Myasthenia Gravis Activities of Daily Living; MGC = Myasthenia Gravis Composite; MGFA = Myasthenia Gravis Foundation of America; MGFA-PIS = Myasthenia Gravis Foundation of America Post-Intervention Status; MG-QoL15 = Myasthenia Gravis Quality of Life 15-item; MG-QoL15r = Myasthenia Gravis Quality of Life 15-item – Revised; MID = minimal important difference; QMG = Quantitative Myasthenia Gravis; SD = standard deviation; VAS = visual analogue scale.
Statistical Analysis
Sample Size and Power Calculation
The RAISE study, with a primary efficacy end point of change from baseline to week 12 in MG-ADL score, initially had a planned enrolment of 130 patients, based on the assumption that there would be a difference in treatment group LS means of 2.3, with an SD of 3.4, and 65 patients per group, which would provide a power to detect a difference between groups of approximately 94%, based on a 2-sided alpha of 0.05, with assumed rates of rescue therapy and dropout of up to 10% and 5%, respectively. In protocol amendment version 2.0 (December 18, 2020), the total sample size was increased to 156 patients (78 patients per group) to account for higher variability in the primary end point than was originally assumed and to maintain the power of the study.
Statistical Testing
Multiplicity Control
The primary efficacy end point and ranked secondary end points were included in the statistical hierarchy, which used a fixed-sequential testing procedure to account for multiplicity, where statistical testing of an end point was investigated only if the null hypothesis for the previous end point had been rejected (i.e., if P ≤ 0.05). The statistical analysis of the secondary efficacy end points accounted for multiplicity and controlled the family-wise type I error rate at a 2-sided alpha level of 0.05 by using a parallel gatekeeping testing framework, with a different testing procedure for each of the type I error families. This was only to be done if the primary end point was significant at 2-sided type I error of 0.05.
Family 1: Family 1 included the key secondary end points. Testing was done using a fixed-sequential testing procedure in the following order:
change from baseline to week 12 in the QMG score
change from baseline to week 12 in the MGC score
change from baseline to week 12 in the MG-QoL15r score.
A secondary end point analysis in family 1 was considered statistically significant if the 2-sided P value was 0.05 or less for the end point analysis, providing that the primary efficacy end point analysis and all secondary end point analyses occurring earlier in the fixed-sequence were also statistically significant (i.e., had a 2-sided P value ≤ 0.05). This method was used to control the family-wise error rate at the 2-sided 0.05 level. At the first end point that was not significant, no further testing was to be done.
Family 2: If all secondary end points in family 1 were significant at a 2-sided type I error of 5%, family 2 was tested using a Holm procedure at 2-sided type I error. Family 2 included the following secondary end points:
time to first administration of rescue therapy over the 12-week treatment period
achievement of MSE, defined as an MG-ADL score of 0 or 1, at week 12 without rescue therapy
achievement of at least a 3-point reduction in MG-ADL score at week 12 without rescue therapy
achievement of at least a 5-point reduction in QMG score at week 12 without rescue therapy.
The Holm procedure is a multistep, step-down procedure. The procedure started with the smallest P value, which was compared to 0.0125. If the first test showed statistical significance, the treatment effect for the respective end point was considered significant. Then testing proceeded, comparing the next smallest P value to 0.017. If the second test showed statistical significance, testing proceeded, comparing the third smallest P value to 0.025. If the third test showed statistical significance, testing proceeded, comparing the largest P value to 0.05. The procedure stopped whenever a step yielded a nonsignificant result. Once an ordered P value was not significant, the remaining larger P values were not evaluated. In this case, the treatment effect could not be concluded for the remaining secondary end points.
Primary End Point
Change from baseline to week 12 in the MG-ADL score was the primary end point, comparing zilucoplan 0.3 mg/kg with placebo in the modified intention-to-treat (mITT) population, using LS mean with corresponding 2-sided 95% CIs and P values. The LS mean of each treatment group, and the LS mean differences between zilucoplan and placebo at week 1, week 2, week 4, and week 8 were also reported with the corresponding 2-sided 95% CIs. Treatment group differences were assessed using a mixed model for repeated measures (MMRM) analysis of covariance (ANCOVA), with treatment, baseline MG-ADL score, baseline QMG score, geographic region, treatment by visit (interaction term), baseline MG-ADL score by visit (interaction term), baseline QMG score by visit (interaction term), and geographic region by visit (interaction term) as fixed effects, and the patient as a random effect. Terms in the MMRM were treated as categorical for treatment, geographic region, and visit (ordinal), and as continuous for baseline scores in the MG-ADL and the QMG. An unstructured covariance structure was used for the repeated measures, wherein if the unstructured covariance structure model failed to converge, a heterogeneous compound symmetric covariance structure was used. Model assumptions (independence, normality, homoscedasticity) were checked using normal probability plots of studentized residuals by actual residuals and a random variation plot of studentized residuals by predicted values.
Subgroup Analyses
Subgroup analyses for change from baseline to week 12 in the MG-ADL score were performed in the mITT population using the following subgroups, in addition to the gMG refractory status (yes or no):
age (< 65 years or ≥ 65 years)
sex (female or male)
ethnicity (Hispanic or Latino, not Hispanic or Latino)
weight in kg (< 43, 43 to 56, 56 to < 77, 56 to < 150, or ≥ 150)
body mass index in kg/m2 (< 18.5, ≥ 18.5 to < 25, ≥ 25 to < 30, ≥ 30 to < 40, or ≥ 40)
region (East Asia, Europe, and North America)
MGFA disease class at baseline (II [IIa, IIb], III [IIIa, IIIb], or IV [IVa, IVb])
duration of disease at baseline (< median or ≥ median)
baseline MG-ADL score (≤ 9 or ≥ 10)
baseline QMG score (≤ 17 or ≥ 18)
diagnosis of thymoma
prior occurrence of a crisis (yes or no), prior thymectomy (yes or no)
prior steroid therapy (yes or no)
steroid therapy taken at baseline (yes or no)
prior NSIST (yes or no)
NSIST at baseline (yes or no)
prior history of IVIg or SCIg or PLEX (yes or no)
timing of patient enrolment relative to COVID-19 pandemic periods (before, during, or after)
timing of week 12 visit relative to COVID-19 pandemic periods (before, during, or after).
For patients with and without refractory disease, the change from baseline to week 12 in MG-ADL score was assessed in each stratum separately, using an MMRM with treatment and visit (categorical) as fixed effects, baseline MG-ADL score, baseline QMG score, region (East Asia, Europe, or North America) as covariates, and baseline-by-time interaction and treatment-by-time interaction. An unstructured covariance structure was used. In the event that the unstructured covariance structure model failed to converge, an autoregressive (1) covariance structure was used. The Kenward-Roger approximation was used to estimate the denominator degrees of freedom. The LS mean and SE of each treatment group, and the LS mean differences between zilucoplan and placebo were reported for the week 12 visit, along with the corresponding 2-sided 95% CIs for each subgroup stratum.
Subgroup analyses were considered exploratory and not powered to detect treatment differences between groups; no formal statistical testing of treatment-by-subgroup interactions, nor of treatment effects within subgroups, was conducted. Subgroup analyses were only performed for subgroups in which there were at least 5 patients in each subgroup level.
Missing Data and Censoring
The number of missing values by visit was provided by treatment group and overall using descriptive statistics for the mITT population. For the primary efficacy analysis, missing or censored data were imputed with the baseline or the last available MG-ADL score (including unscheduled visit), whichever was worse, from the time of the subsequent ICE, defined as treatment failure:
ICE1: data occurring after a patient received rescue therapy
ICE2: data occurring after a patient had any death or myasthenic crisis
ICE3: any other monotone missing data were assumed to be MAR; that is, it was assumed that the patient had remained on their assigned study drug throughout the study and did not discontinue the study.
If a patient received rescue therapy, efficacy end points that occurred after rescue therapy were censored. Based on the results of the zilucoplan phase II study and the eculizumab phase III study, approximately 10% of patients were expected to receive rescue therapy and 5% were expected to be missing MG-ADL data during the 12-week treatment period.
Sensitivity Analyses
A sensitivity analysis was conducted to evaluate deviations from the MAR pattern using a jump to reference (J2R) approach and an MI method under the MNAR assumption to handle any missing scores. Intermittent missing data were imputed using the Markov chain Monte Carlo method. Monotone missing and/or censored data were imputed using the placebo distribution, irrespective of individual treatment assignment. Variables included in the imputation model were baseline MG-ADL score and MG-ADL scores at previous visits. If a patient started rescue therapy, the most recent MG-ADL score was used, which may have occurred at an unscheduled visit. If the MI model did not converge or produce estimates (e.g., due to overspecification), the set of imputation variables could be modified. Each of the imputed datasets were analyzed using the specified MMRM model. The treatment effects and SEs from the LS mean treatment difference were combined across the 100 imputed datasets, using Rubin’s rule to produce an overall P value. LS means and 95% CIs were plotted from week 1 to week 12. A second sensitivity analysis was conducted to evaluate the robustness of the MAR assumptions in the primary analysis, using tipping-point analyses in which results were statistically significant (P < 0.05); the analysis finds a (tipping) point in the spectrum of assumptions (from less conservative to more conservative), at which point conclusions change from being favourable to the experimental treatment to being unfavourable, and clinical judgment is applied to the plausibility of the assumptions underlying the tipping point. Patients who received rescue therapy (ICE1) or experienced a death or myasthenic crisis (ICE2) were imputed for baseline score or last available MG-ADL score, whichever was worse from time of the ICE. The tipping-point analysis for monotone missing data (ICE3) was assumed to be MAR in the primary analysis. Delta adjustments were made to assumed responses on the ICE3 in each treatment group, including scenarios in which patients with missing data who were randomized to zilucoplan were less likely to respond than patients with missing data who were randomized to placebo.
Supplemental Analyses
Supplemental analyses were conducted to handle missing data and data after rescue therapy using MI. Monotone linear regression imputation methods (100 imputed datasets) were employed to impute missing postbaseline scores at the scheduled study visits, using a sequential approach to produce a monotonic missing data pattern. Imputation was performed by treatment group, with the underlying imputation distribution based on the reason for the missing data. The MI method allowed for a pattern-mixture model approach, which assumed that the data are MNAR under the scenarios in which a patient’s discontinuation from the study was related to the study drug or the patient received rescue medications.
Key Secondary End Points
The key secondary end points of change from baseline to week 12 in the QMG score, the MGC score, and the MG-QoL15r score were analyzed using the same statistical approach as the primary end point.
Secondary End Points
Achievement of MSE, Defined as an MG-ADL Score of 0 or 1 Without Rescue Therapy
The MG-ADL value of 0 or 1 at week 12 without rescue therapy in the mITT population was calculated as follows: week 12 MG-ADL value = baseline MG-ADL score + week 12 change from baseline in MG-ADL score, where a value of 1.0 or lower was considered valid. The number and percentage of patients achieving MSE without rescue therapy were summarized by treatment group for each scheduled visit. ORs with corresponding 95% CIs and P values were estimated. The treatment effects and SEs were combined across 100 imputed datasets to produce an overall P value. Missing data were imputed using nonresponder imputation (i.e., study participants with missing data at the time point of interest were treated as responders). Any patients using rescue therapy (ICE1) and any patients who experienced death or myasthenic crisis (ICE2) were assumed to be nonresponders from the time of the ICE. Any other monotone missing data (ICE3) were assumed to be MAR before the end point was dichotomized.
MG-ADL Responder
An MG-ADL responder was defined as the achievement of at least a 3-point reduction in MG-ADL score at week 12 without rescue therapy. The MG-ADL responder rate was calculated with the same analysis that was used to estimate the achievement of MSE.
QMG Responder
A QMG responder was defined as the achievement of at least a 5-point reduction in QMG score at week 12 without rescue therapy.
Safety
Incidence rates were summarized descriptively for AEs, TEAEs, SAEs, TEAEs leading to study discontinuation, and deaths. The number and percentage of patients who experienced at least 1 TEAE were presented by treatment group, and overall, for each specific system organ class and preferred term, by maximum severity and by relationship to the study drug for each treatment group. Analyses of AEs were performed using the safety population.
Exploratory End Point
Minimal Manifestation Status per MGFA-PIS
The achievement of minimal manifestation status per MGFA-PIS was evaluated as a dichotomous end point, which was having or not having a response of minimal manifestations at week 12 without rescue therapy during the 12-week treatment period.
Table 9: Statistical Analysis of Efficacy End Points in the RAISE Study
End point | Statistical model | Adjustment factors | Handling of missing data | Sensitivity analyses |
|---|---|---|---|---|
Change from baseline to week 12 in MG-ADL score | MMRM ANCOVA, including weeks 1, 2, 4, 8, and 12 | The following were fixed effects:
|
|
|
Change from baseline to week 12 in QMG score | MMRM ANCOVA | Same as change from baseline to week 12 in MG-ADL score | Same as change from baseline to week 12 in MG-ADL score | Same as change from baseline to week 12 in MG-ADL score |
Change from baseline to week 12 in MGC score | MMRM ANCOVA | Same as change from baseline to week 12 in MG-ADL score | Same as change from baseline to week 12 in MG-ADL score | Same as change from baseline to week 12 in MG-ADL score |
Change from baseline to week 12 in MG-QoL15r score | MMRM ANCOVA | Same as change from baseline to week 12 in MG-ADL score | Same as change from baseline to week 12 in MG-ADL score | Same as change from baseline to week 12 in MG-ADL score |
Achievement of MSE, defined as an MG-ADL score of 0 or 1 at week 12 without rescue therapy |
| Treatment as a factor and baseline MG-ADL score as a covariate |
| None |
Achievement of a ≥ 3-point reduction in MG-ADL score at week 12 without rescue therapy |
| Treatment as a factor and the following as covariates:
|
| None |
Achievement of a ≥ 5-point reduction in QMG score at week 12 without rescue therapy |
|
|
| None |
Achievement of minimal manifestation status per MGFA-PIS at week 12 without rescue therapy | Descriptive summary statistics | None | NR | None |
ANCOVA = analysis of covariance; ICE = intercurrent event; J2R = jump to reference; MAR = missing at random; MG-ADL = Myasthenia Gravis Activities of Daily Living; MGC = Myasthenia Gravis Composite; MGFA-PIS = Myasthenia Gravis Foundation of America Post-Intervention Status; MG-QoL15r = Myasthenia Gravis Quality of Life 15-item – Revised; MMRM = mixed model for repeated measures; MNAR = missing not at random; MSE = minimal symptom expression; NR = not reported; NRI = nonresponder imputation; QMG = quantitative myasthenia gravis.
Note: No data were missing for the primary or key secondary end points at week 12 due to COVID-19.
aIf a patient was administered a rescue therapy, any data strictly after the start date of the first rescue therapy administration were flagged as ICE1.
bIf a patient experienced death, data after the death date was flagged as ICE2. If a patient experienced a myasthenic crisis, any data after the start date of the adverse event were flagged as ICE2.
cAny other monotone missing data were flagged as ICE3 in each relevant dataset. ICE3 was defined as any missing value for which all values at subsequent visits were missing.
Source: RAISE Clinical Study Report,14 sponsor’s Summary of Clinical Evidence.27
Analysis Populations
Analysis sets included in the RAISE study are summarized in Table 10.
Table 10: Analysis Populations of the RAISE Study
Population | Definition | Application |
|---|---|---|
ITT | All randomized study patients | Study population and characteristics, secondary and exploratory efficacy analyses |
mITT | All randomized patients who received at least 1 dose of the study drug and had at least 1 postdosing MG-ADL score | Demographics and baseline characteristics, all efficacy analyses |
Safety set | All patients who received at least 1 dose of the study drug, with patients analyzed based on the actual study drug received | Safety analyses |
ITT = intention to treat; MG-ADL = Myasthenia Gravis Activities of Daily Living; mITT = modified intention to treat.
Source: RAISE Clinical Study Report,14 sponsor’s Summary of Clinical Evidence.27
Results
Patient Disposition
At the data cut-off date of December 30, 2021, 174 patients with anti-AChR antibody–positive gMG were enrolled and randomized in the RAISE study and included in the mITT population (Table 11). Of the patients who were enrolled, 166 patients (95.4%) completed the study, including 82 of 86 patients (95.3%) in the zilucoplan group and 84 of 88 patients (95.5%) in the placebo group. The 8 patients (4.6%) who discontinued the study were balanced between treatment groups (i.e., 4 patients in each group). The primary reasons for discontinuation were as follows: 3 (1.7%) were due to withdrawal by patient (1 patient [1.2%] in the zilucoplan group and 2 patients [2.3%] in the placebo group), 2 (1.1%) were due to death (1 [1.2%] patient in the zilucoplan group and 1 [1.1%] patient in the placebo group), 2 (1.1%) were due to an AE (2 patients [2.3%] in the zilucoplan group and no patient in the placebo group), and 1 (0.6%) was due to physician decision (no patient in the zilucoplan group and 1 [1.1%] patient in the placebo treatment group). Among the discontinuations due to death, the event in the zilucoplan group was related to COVID-19 and the event in the placebo group was due to a cerebral hemorrhage. Among the discontinuations due to AEs in the zilucoplan group, 1 patient withdrew due to aphthous ulcers, and 1 patient withdrew due to hepatic enzyme increased. The discontinuation related to physician decision was due to a suspected reaction to the meningococcal vaccine.
In the prespecified refractory subgroup (88 patients), 85 patients (96.6%) completed the study, including 43 of 44 patients (97.7%) in the zilucoplan group and 42 of 44 patients (95.5%) in the placebo group (Table 11). Overall discontinuation rates were low, with 3 patients (3.4%) who discontinued the study (i.e., 1 patient and 2 patients in the zilucoplan group and placebo group, respectively). The primary reasons for discontinuation were as follows: 2 (2.3%) were due to withdrawal by patient (1 patient each per group), and 1 patient (1.1%) was due to physician decision (in the placebo group). Most patients (96.6%) entered the RAISE-XT extension study after completion of the RAISE study.
Table 11: Patient Disposition in the RAISE Study (Overall mITT Population and Refractory Subpopulation)
Patient disposition | Overall population | Refractory subpopulation | ||
|---|---|---|---|---|
Zilucoplan N = 86 | Placebo N = 88 | Zilucoplan N = 44 | Placebo N = 44 | |
Screened, N | 239 | NA | ||
Unsuccessful screening, N (%) | 65 (27.2) | NA | ||
Reason for unsuccessful screening, N (%) | ||||
Ineligibility | 63 (26.4) | NA | ||
Withdrawal by patient | 2 (0.8) | NA | ||
Randomized, N | 174 | NA | ||
Discontinued from study, N (%) | 4 (4.7) | 4 (4.5) | 1 (2.3) | 2 (4.5) |
Reason for discontinuation, N (%) | ||||
Adverse events | 2 (2.3) | 0 | 0 | 0 |
Withdrawal by patient | 1 (1.2) | 2 (2.3) | 1 (2.3) | 1 (2.3) |
Physician decision | 0 | 1 (1.1) | 0 | 1 (2.3) |
Death | 1 (1.2) | 1 (1.1) | 0 | 0 |
Completed study, N (%) | 86 (100.0) | 88 (100.0) | 43 (97.7) | 42 (95.5) |
Randomized set, N | 86 | 88 | NA | NA |
mITT, N | 86 | 88 | NA | NA |
Per-protocol set, N | 70 | 77 | NA | NA |
Safety set, N | 86 | 88 | 44 | 44 |
Entered RAISE-XT, N (%) | 81 (94.2) | 84 (95.5) | 43 (97.7) | 42 (95.5) |
Safety follow-up visit performed, N (%) | 3 (3.5) | 1 (1.1) | 1 (2.3) | 1 (2.3) |
Safety follow-up visit not performed, N (%) | 80 (93.0) | 84 (95.5) | 40 (90.9) | 41 (93.2) |
Reason safety follow-up not performed, N (%) | ||||
Othera | 79 (91.9) | 82 (93.2) | 40 (90.9) | 41 (93.2) |
Death | 1 (1.2) | 1 (1.1) | 0 | 0 |
Lost to follow-up | 0 | 1 (1.1) | 0 | 0 |
mITT = modified intention to treat; NA = not applicable.
aSafety follow-up was not required for patients who enrolled in the RAISE-XT study.
Sources: RAISE Clinical Study Report,14 sponsor’s Summary of Clinical Evidence.27
Baseline Characteristics
Baseline characteristics of the overall trial population and the refractory subpopulation in the RAISE study summarized in Table 12 are limited to those that are most relevant to this review or were felt to affect the outcomes or interpretation of the study results.
More patients in the overall trial population (n = 174) were female (56.9%) than male (43.1%), and the mean age was 53.0 years (SD = 15.1 years). Most patients had a diagnosis of MGFA disease class III at screening (67.2%), generalized symptoms at disease onset (64.4%), disease onset at a mean of 43.8 years (SD = 18.0 years), and a disease duration of mean 9.2 years (SD = 9.9 years). Higher scores in the stratified randomization were more common for the MG-ADL (62.1% of patients had a score ≥ 10) and the QMG (56.3% of patients had a score ≥ 18) than for other scores. Disease characteristics and history were similar in the 2 treatment groups, except a higher proportion of patients had undergone thymectomy in the zilucoplan group (52.3%) than in the placebo group (42.0%). Patients had similar between-group mean baseline scores in the MG-ADL and the QMG.
In the refractory subpopulation (88 of 174 [50.6%]), more patients were female (64.8%) than male (35.2%). The mean age was 51.8 years (SD = 14.0 years), 69.3% of patients had been diagnosed with MGFA disease class III , 69.3% of patients had generalized symptoms at disease onset, mean age at disease onset was 40.0 years (SD = 16.7 years), and mean disease duration was 11.9 years (SD = 10.6 years). Disease characteristics and history were similar in the 2 treatment groups, except a higher proportion of patients had undergone thymectomy in the zilucoplan group than in the placebo group (75.0% versus 61.4%).
In both the overall population and the refractory subpopulation, demographic characteristics, symptoms at onset, time since most recent MG crisis, and baseline scores in the MG-ADL and QMG were similar. There were differences in the overall population and the refractory subpopulation in mean age at disease onset (43.8 years versus 40.0 years), mean disease duration (9.2 years versus 11.9 years), the proportion of patients with a diagnosis of thymoma (22.4% versus 29.5%), the proportion of patients who had undergone thymectomy (47.1% versus 68.2%), and the proportion of patients who had experienced an MG crisis (32.8% versus 50.0%).
Table 12: Baseline Characteristics in the RAISE Study (Overall mITT Population and Refractory Subpopulation)
Characteristic | Overall population | Refractory subpopulation | ||
|---|---|---|---|---|
Zilucoplan N = 86 | Placebo N = 88 | Zilucoplan N = 44 | Placebo N = 44 | |
Age, yearsa | ||||
Mean (SD) | 52.6 (14.6) | 53.3 (15.7) | 52.4 (12.5) | 51.3 (15.4) |
Median (range) | 54.5 (21 to 75) | 55.5 (19 to 75) | 53.0 (24 to 75) | 52.5 (19 to 75) |
Age group, n (%) | ||||
19 years to < 65 years | 64 (74.4) | 62 (70.5) | 37 (84.1) | 35 (79.5) |
≥ 65 years | 22 (25.6) | 26 (29.5) | 7 (15.9) | 9 (20.5) |
Sex, n (%) | ||||
Female | 52 (60.5) | 47 (53.4) | 30 (68.2) | 27 (61.4) |
Male | 34 (39.5) | 41 (46.6) | 14 (31.8) | 17 (38.6) |
Race, n (%) | ||||
American Indian or Alaska Native | 0 | 1 (1.1) | 0 | 1 (2.3) |
Asian | 7 (8.1) | 14 (15.9) | 6 (13.6) | 9 (20.5) |
Black | 6 (7.0) | 7 (8.0) | 4 (9.1) | 3 (6.8) |
Native Hawaiian or other Pacific Islander | 0 | 0 | 0 | 0 |
White | 66 (76.7) | 62 (70.5) | 30 (68.2) | 30 (68.2) |
Other or mixed | 0 | 0 | 0 | 0 |
Missing | 7 (8.1) | 4 (4.5) | 4 (9.1) | 1 (2.3) |
Ethnicity, n (%) | ||||
Hispanic or Latino | 7 (8.1) | 5 (5.7) | 3 (6.8) | 4 (9.1) |
Not Hispanic or Latino | 72 (83.7) | 79 (89.8) | 38 (86.4) | 39 (88.6) |
Missing | 7 (8.1) | 4 (4.5) | 3 (6.8) | 1 (2.3) |
Region, n (%) | ||||
East Asia | 7 (8.1) | 9 (10.2) | 6 (13.6) | 8 (18.2) |
Europe | 34 (39.5) | 33 (37.5) | 20 (45.5) | 19 (43.2) |
North America | 45 (52.3) | 46 (52.3) | 18 (40.9) | 17 (38.6) |
Weight, kg | ||||
Mean (SD) | 90.1 (22.9) | 88.2 (26.6) | 86.4 (23.5) | 84.9 (27.2) |
< 56, n (%) | 5 (5.8) | 6 (6.8) | 3 (6.8) | 4 (9.1) |
56 to < 77, n (%) | 21 (24.4) | 25 (28.4) | 14 (31.8) | 15 (34.1) |
77 to < 150, n (%) | 60 (69.8) | 54 (61.4) | 27 (61.4) | 23 (52.3) |
≥ 150, n (%) | 0 | 3 (3.4) | 0 | 2 (4.5) |
Height, cm, mean (SD) | 169.3 (10.5) | 169.5 (10.0) | 169.4 (10.5) | 168.9 (9.4) |
BMI, kg/m2, mean (SD) | 31.4 (7.2) | 30.5 (8.0) | 30.1 (7.5) | 29.5 (8.1) |
MGFA disease class at screening, n (%) | ||||
II | 22 (25.6) | 27 (30.7) | 11 (25.0) | 12 (27.3) |
III | 60 (69.8) | 57 (64.8) | 30 (68.2) | 31 (70.5) |
IV | 4 (4.7) | 4 (4.5) | 3 (6.8) | 1 (2.3) |
Age at disease onset, years, n | 85 | 88 | 44 | 44 |
Mean (SD) | 43.5 (17.4) | 44.0 (18.7) | 40.6 (16.0) | 39.4 (17.6) |
Duration of disease, years, n | 86 | 88 | 43 | 44 |
Mean (SD) | 9.3 (9.5) | 9.0 (10.4) | 12.3 (10.5) | 11.5 (10.9) |
Median (range) | 5.6 (0.1 to 42.3) | 4.8 (0.2 to 51.9) | 8.4 (0.8 to 42.3) | 8.2 (1.1 to 51.9) |
Symptoms at onset, n (%) | ||||
Ocular | 28 (32.6) | 34 (38.6) | 15 (34.1) | 12 (27.3) |
Generalized | 58 (67.4) | 54 (61.4) | 29 (65.9) | 32 (72.7) |
Diagnosis of thymoma, n (%) | 21 (24.4) | 18 (20.5) | 14 (31.8) | 12 (27.3) |
Prior thymectomy, n (%) | 45 (52.3) | 37 (42.0) | 33 (75.0) | 27 (61.4) |
Prior MG crisis, n (%) | 28 (32.6) | 29 (33.0) | 23 (52.3) | 21 (47.7) |
Time since most recent crisis (months),a n | 28 | 29 | 23 | 21 |
Mean (SD) | 75.6 (91.8) | 72.3 (109.8) | 70.4 (95.0) | 78.5 (117.9) |
Median (range) | 39.0 (1.4 to 277.6) | 22.0 (1.4 to 469.8) | 38.4 (1.4 to 277.6) | 30.0 (1.4 to 469.8) |
Baseline MG-ADL score | ||||
Mean (SD) | 10.3 (2.5) | 10.9 (3.4) | 10.3 (2.6) | 11.0 (3.4) |
≤ 9, n (%) | 33 (38.4) | 33 (37.5) | 17 (38.6) | 15 (34.1) |
≥ 10, n (%) | 53 (61.6) | 55 (62.5) | 27 (61.4) | 29 (65.9) |
Baseline QMG score | ||||
Mean (SD) | 18.7 (3.6) | 19.4 (4.5) | 18.8 (4.0) | 19.7 (4.4) |
≤ 17, n (%) | 38 (44.2) | 38 (43.2) | 20 (45.5) | 16 (36.4) |
≥ 18, n (%) | 48 (55.8) | 50 (56.8) | 24 (54.5) | 28 (63.6) |
BMI = body mass index; MG = myasthenia gravis; MG-ADL = Myasthenia Gravis Activities of Daily Living; MGFA = Myasthenia Gravis Foundation of America; mITT = modified intention to treat; QMG = Quantitative Myasthenia Gravis; SD = standard deviation.
aTime since most recent crisis (months) was calculated as: (date of study day 1 minus date of crisis) divided by (365.25 divided by 12).
Sources: RAISE Clinical Study Report,14 sponsor’s Summary of Clinical Evidence.27
Baseline medications were defined as medications that started before and continued after a patient received the assigned study drug. Baseline medications for gMG in the overall population and the refractory subpopulation are summarized in Table 13.
Among patients with gMG in the overall population, most patients (96.0%) were receiving gMG-specific baseline medications, including pyridostigmine (80.5%), prednisone (40.8%), prednisolone (20.7%), mycophenolate mofetil (19.5%), and azathioprine (17.8%). More patients in the zilucoplan group than in the placebo group were receiving prednisone (44.2% versus 37.5%) and prednisolone (23.3% versus 18.2%). Fewer patients in the zilucoplan group than in the placebo group were receiving azathioprine (15.1% versus 20.5%). No patient with gMG was receiving IVIg, SCIg, PLEX, or rituximab at baseline.
Among patients in the refractory subpopulation, the proportion of patients receiving gMG-specific baseline medications was, overall, similar to the proportion in the overall population, including pyridostigmine (79.5%), prednisone (37.5%), azathioprine (23.9%), and mycophenolate mofetil (22.7%). More patients in the zilucoplan group than in the placebo group were receiving prednisone (40.9% versus 34.1%) and prednisolone (36.4% versus 31.8%). Fewer patients in the zilucoplan group than in the placebo group were receiving azathioprine (22.7% versus 25.0%) and mycophenolate mofetil (20.5% versus 25.0%). No patient with refractory gMG was receiving IVIg, SCIg, PLEX, or rituximab at baseline.
In the RAISE trial, prior gMG medications were defined as any medication that started before the first administration of a study drug (refer to Table 32 in Appendix 1). The proportions of patients who had received at least 1, at least 2, and at least 3 prior lines of therapy were 100%, about 95%, and about 81%, respectively, in each study group in the RAISE trial. The majority of patients in both study groups had received prior acetylcholinesterase inhibitors (about 95% of patients), steroids (about 85% of patients), and NSISTs (around 70% of patients) (Table 32).
Table 13: gMG-Specific Baseline Medications in the RAISE Study (Overall Population and Refractory Subpopulation, Safety Set)
Group, concomitant medication, preferred term | Overall population | Refractory subpopulation | ||
|---|---|---|---|---|
Zilucoplan N = 86 | Placebo N = 88 | Zilucoplan N = 44 | Placebo N = 44 | |
Any gMG-specific baseline medication, n (%) | 84 (97.7) | 83 (94.3) | 42 (95.5) | 42 (95.5) |
Group A, n (%) | 59 (68.6) | 51 (58.0) | 34 (77.3) | 30 (68.2) |
Prednisone for gMG, n (%) | 38 (44.2) | 33 (37.5) | 18 (40.9) | 15 (34.1) |
Prednisone, n (%) | 38 (44.2) | 33 (37.5) | 18 (40.9) | 15 (34.1) |
Other corticosteroids for gMG, n (%) | 21 (24.4) | 18 (20.5) | 16 (36.4) | 15 (34.1) |
Dexamethasone, n (%) | 0 | 0 | 0 | 0 |
Methylprednisone, n (%) | 0 | 0 | 0 | 0 |
Methylprednisone sodium succinate, n (%) | 0 | 0 | 0 | 0 |
Other corticosteroids, n (%) | 0 | 0 | 0 | 0 |
Prednisolone, n (%) | 20 (23.3) | 16 (18.2) | 16 (36.4) | 14 (31.8) |
Methylprednisolone (%) | 1 (1.2) | 2 (2.3) | 0 | 1 (2.3) |
Group B, n (%) | 30 (34.9) | 35 (39.8) | 19 (43.2) | 22 (50.0) |
Azathioprine, n (%) | 13 (15.1) | 18 (20.5) | 10 (22.7) | 11 (25.0) |
Mycophenolate mofetiln (%) | 17 (19.8) | 17 (19.3) | 9 (20.5) | 11 (25.0) |
Group C, n (%) | 0 | 0 | 0 | 0 |
IVIg, n (%) | 0 | 0 | 0 | 0 |
SCIg, n (%) | 0 | 0 | 0 | 0 |
Group D, n (%) | 0 | 0 | 0 | 0 |
IVIg, SCIg, or plasma exchange, n (%) | 0 | 0 | 0 | 0 |
Immunoglobulin NOS, n (%) | 0 | 0 | 0 | 0 |
Plasma exchange, n (%) | 0 | 0 | 0 | 0 |
Group E, n (%) | 12 (14.0) | 15 (17.0) | 10 (22.7) | 13 (29.5) |
Ciclosporin, n (%) | 6 (7.0) | 7 (8.0) | 5 (11.4) | 5 (11.4) |
Cyclophosphamide, n (%) | 0 | 0 | 0 | 0 |
Methotrexate, n (%) | 3 (3.5) | 1 (1.1) | 2 (4.5) | 1 (2.3) |
Tacrolimus, n (%) | 3 (3.5) | 7 (8.0) | 3 (6.8) | 7 (15.9) |
Rituximab, n (%) | 0 | 0 | 0 | 0 |
Group F, n (%) | 74 (86.0) | 73 (83.0) | 37 (84.1) | 36 (81.8) |
Cholinesterase inhibitors, n (%) | 74 (86.0) | 73 (83.0) | 37 (84.1) | 36 (81.8) |
Pyridostigmine, n (%) | 70 (81.4) | 70 (79.5) | 35 (79.5) | 35 (79.5) |
Ambenonium, n (%) | 4 (4.7) | 3 (3.4) | 2 (4.5) | 1 (2.3) |
gMG = generalized myasthenia gravis; Ig = immunoglobulin; NOS = not otherwise specified; SC = subcutaneous.
Note: Within this table, where the concomitant and preferred terms are the same, only the concomitant term is displayed.
Sources: RAISE Clinical Study Report,14 sponsor’s Summary of Clinical Evidence.27
Exposure to Study Treatments
In the RAISE study, the mean duration of exposure to the study drug was 81.9 days (SD = 11.0 days) in the zilucoplan group and 81.1 days (SD = 13.0 days) in the placebo group (Table 14). Most patients received the study drug for 84 days or longer (73.3% and 64.8% of patients in the zilucoplan and placebo group, respectively). At week 12, total exposure was 19.8 patient-years in the zilucoplan group and 20.0 patient-years in the placebo group. Ten patients (11.6%) in the zilucoplan group and 15 patients (17.0%) in the placebo group missed at least 1 dose of the study drug. The mean number of doses missed was 5.4 (SD = 5.2; range, 1 to 15 doses) in the zilucoplan and 6.2 (SD = 10.9; range, 1 to 44 doses) in the placebo group.
In the refractory subpopulation, the mean duration of exposure to the study drug was 83.8 days (SD = 3.7 days) in the zilucoplan group and 80.9 days (SD = 14.4 days) in the placebo group. At week 12, total exposure was 10.4 patient-years in the zilucoplan group and 9.9 patient-years in the placebo group. Four patients (9.1%) in the zilucoplan and 11 patients (25.0%) in the placebo group missed at least 1 dose of the study drug. The mean number of doses missed was 7.3 (SD = 5.4; range, 3 to 15 doses) in the zilucoplan group and 3.4 (SD = 3.6; range, 1 to 12 doses) in the placebo group.
Table 14: Treatment Exposure in the RAISE Study (Overall Population and Refractory Subpopulation, Safety Set)
Exposure | Overall population | Refractory subpopulation | ||
|---|---|---|---|---|
Zilucoplan N = 86 | Placebo N = 88 | Zilucoplan N = 44 | Placebo N = 44 | |
Duration, patient-years | 19.8 | 20.0 | 10.4 | 9.9 |
Duration, days, mean (SD) | 81.9 (11.0) | 81.1 (13.0) | 83.8 (3.7) | 80.9 (14.4) |
Duration, days, median (range) | 84.0 (15 to 91) | 84.0 (1 to 92) | 84.0 (67 to 91) | 84.0 (1 to 92) |
Cumulative study drug duration, days, n (%) | ||||
≥ 1 | 86 (100.0) | 88 (100.0) | 44 (100.0) | 44 (100.0) |
≥ 8 | 86 (100.0) | 87 (98.9) | 44 (100.0) | 43 (97.7) |
≥ 15 | 86 (100.0) | 87 (98.9) | 44 (100.0) | 43 (97.7) |
≥ 29 | 84 (97.7) | 86 (97.7) | 44 (100.0) | 43 (97.7) |
≥ 57 | 84 (97.7) | 84 (95.5) | 44 (100.0) | 42 (95.5) |
≥ 84 | 63 (73.3) | 57 (64.8) | 35 (79.5) | 28 (63.6) |
Adherence, % | 88.4 | 83.0 | 90.9 | 75.0 |
SD = standard deviation.
Sources: RAISE Clinical Study Report,14 sponsor’s Summary of Clinical Evidence.27
The mean duration of time that patients were receiving corticosteroids and NSISTs before baseline was 988.6 days (median, 218.5 days) and 1,187.4 days (median, 788.0 days), respectively, in the overall trial population. In the refractory population, the mean duration was 1,304.3 days (median, 412.5 days) and 1,457.0 days (median, 947.0 days), respectively.
Concomitant Medications
Concomitant gMG therapies and concomitant-only gMG therapies are summarized in Table 15.
Concomitant gMG therapies included medications that were taken at least once after the first administration of the study drug during the treatment period. Overall, of the 169 patients (97.1%) who received any concomitant gMG therapy, 84 patients (97.7%) were in the zilucoplan group, and 85 patients (96.6%) were in the placebo group. The most common (≥ 10% of patients overall) concomitant gMG therapies were pyridostigmine (82.8%), prednisone (41.4%), prednisolone (20.7%), mycophenolate mofetil (19.0%), and azathioprine (17.8%). Concomitant gMG therapies were generally balanced between treatment groups.
Concomitant-only gMG therapies were defined as any medication that started after the first administration of the study drug and continued during the treatment period. A total of 18 patients (10.3%) received any concomitant-only gMG therapy (12 patients [14.0%] and 6 patients [6.8%] in the zilucoplan and placebo groups, respectively). Overall, the rate of patients receiving concomitant-only gMG therapies was lower than patients receiving concomitant gMG therapies.
Among patients in the refractory subpopulation, 85 patients (96.6%) received any concomitant gMG medications. The most common (≥ 10% of patients overall) concomitant gMG therapies were pyridostigmine (81.8%), prednisone (38.6%), prednisolone (34.1%), azathioprine (23.9%), mycophenolate mofetil (22.7%), cyclosporin (11.4%), and tacrolimus (11.4%). Concomitant-only gMG therapies were not reported for the refractory subpopulation.
Table 15: Concomitant and Concomitant-Only gMG Therapies in the RAISE Study (Overall Population and Refractory Subpopulation, Safety Set)
Concomitant medication, preferred term | Overall population | Refractory subpopulation | ||
|---|---|---|---|---|
Zilucoplan N = 86 | Placebo N = 88 | Zilucoplan N = 44 | Placebo N = 44 | |
Concomitant gMG therapy, n (%) | ||||
Any concomitant medication | 84 (97.7) | 85 (96.6) | 42 (95.5) | 43 (97.7) |
Immunoglobulins | 1 (1.2) | 0 | 1 (2.3) | 0 |
Immunoglobulins NOS | 1 (1.2) | 0 | 1 (2.3) | 0 |
Immunosuppressants | 41 (47.7) | 48 (54.5) | 29 (65.9) | 33 (75.0) |
Mycophenolate mofetil | 16 (18.6) | 17 (19.3) | 9 (20.5) | 11 (25.0) |
Azathioprine | 13 (15.1) | 18 (20.5) | 10 (22.7) | 11 (25.0) |
Ciclosporin | 6 (7.0) | 7 (8.0) | 5 (11.4) | 5 (11.4) |
Tacrolimus | 3 (3.5) | 7 (8.0) | 3 (6.8) | 7 (15.9) |
Methotrexate | 3 (3.5) | 1 (1.1) | 2 (4.5) | 1 (2.3) |
Vitamin B12 and folic acid | 1 (1.2) | 0 | — | — |
Folic acid | 1 (1.2) | 0 | — | — |
Parasympathomimetics | 75 (87.2) | 76 (86.4) | 37 (84.1) | 38 (86.4) |
Pyridostigmine | 71 (82.6) | 73 (83.0) | 35 (79.5) | 37 (84.1) |
Ambenonium | 4 (4.7) | 3 (3.4) | 2 (4.5) | 1 (2.3) |
Corticosteroids for systemic use, plain | 59 (68.6) | 52 (59.1) | 34 (77.3) | 31 (70.5) |
Prednisone | 38 (44.2) | 34 (38.6) | 18 (40.9) | 16 (36.4) |
Prednisolone | 20 (23.3) | 16 (18.2) | 16 (36.4) | 14 (31.8) |
Methylprednisolone | 1 (1.2) | 2 (2.3) | 0 | 1 (2.3) |
Concomitant-only gMG therapy,a n (%) | ||||
Any concomitant-only medications | 12 (14.0) | 6 (6.8) | NR | NR |
Immunoglobulins | 1 (1.2) | 0 | NR | NR |
Immunoglobulins NOS | 1 (1.2) | 0 | NR | NR |
Immunosuppressants | 0 | 1 (1.1) | NR | NR |
Azathioprine | 0 | 1 (1.1) | NR | NR |
Parasympathomimetics | 8 (9.3) | 4 (4.5) | NR | NR |
Pyridostigmine | 8 (9.3) | 4 (4.5) | NR | NR |
Corticosteroids for systemic use, plain | 3 (3.5) | 1 (1.1) | NR | NR |
Prednisone | 2 (2.3) | 0 | NR | NR |
Prednisolone | 1 (1.2) | 1 (1.1) | NR | NR |
gMG = generalized myasthenia gravis; NOS = not otherwise specified; NR = not reported.
aConcomitant-only gMG therapies were defined as any medication that started after the first administration of the study drug and continued during the treatment period.
Sources: RAISE Clinical Study Report,14 sponsor’s Summary of Clinical Evidence.27
Efficacy
Findings for key efficacy outcomes in the RAISE study at the data cut-off date of December 30, 2021, are summarized in Table 16.
Primary End Point: Change From Baseline to Week 12 in MG-ADL Score
In the overall population, the LS mean change from baseline to week 12 in the MG-ADL score was –4.39 (SE = 0.45) in the zilucoplan group and –2.30 (SE = 0.44) in the placebo group. The LS mean difference between groups in the MG-ADL score was –2.09 (95% CI, –3.24 to –0.95; P < 0.001), favouring zilucoplan (Figure 2). In the refractory subpopulation, the LS mean change from baseline to week 12 in the MG-ADL score was –4.72 (SE = 0.58) in the zilucoplan group and –1.62 (SE = 0.58) in the placebo group (LS mean difference of –3.11; 95% CI, –4.69 to –1.52; nominal P < 0.001).
Subgroup Analyses
Findings across all subgroups for mean change from baseline to week 12 in the MG-ADL score were consistent with the primary analysis result, which favoured zilucoplan over placebo, and included results identified as potential treatment modifiers for the following subgroups: duration of disease at baseline, MGFA disease class at baseline, baseline MG-ADL score, baseline QMG score, refractory MG, any prior MG crisis, prior treatments (steroid, immunosuppressive [nonsteroidal], IVIg, SCIg, or PLEX therapy). The sample size was small for many subgroups.
Missing or Censored Data
In the overall population, the number of patients with no ICEs in the MG-ADL score was 80 of 86 patients (93.0%) and 77 of 88 patients (87.5%) in the zilucoplan and placebo groups, respectively. The number of patients with ICE1 (received rescue therapy) in the MG-ADL score was 4 patients (4.7%) and 10 patients (11.4%) in the zilucoplan and placebo groups, respectively. The number of patients with ICE2 (any death or myasthenic crisis) in the MG-ADL score was 1 patient (1.2%) and 1 patient (1.2%) in the zilucoplan and placebo groups, respectively.
Figure 2: LS Mean Change From Baseline to Week 12 in MG-ADL Score Using MMRM ANCOVA (Overall Population, mITT)
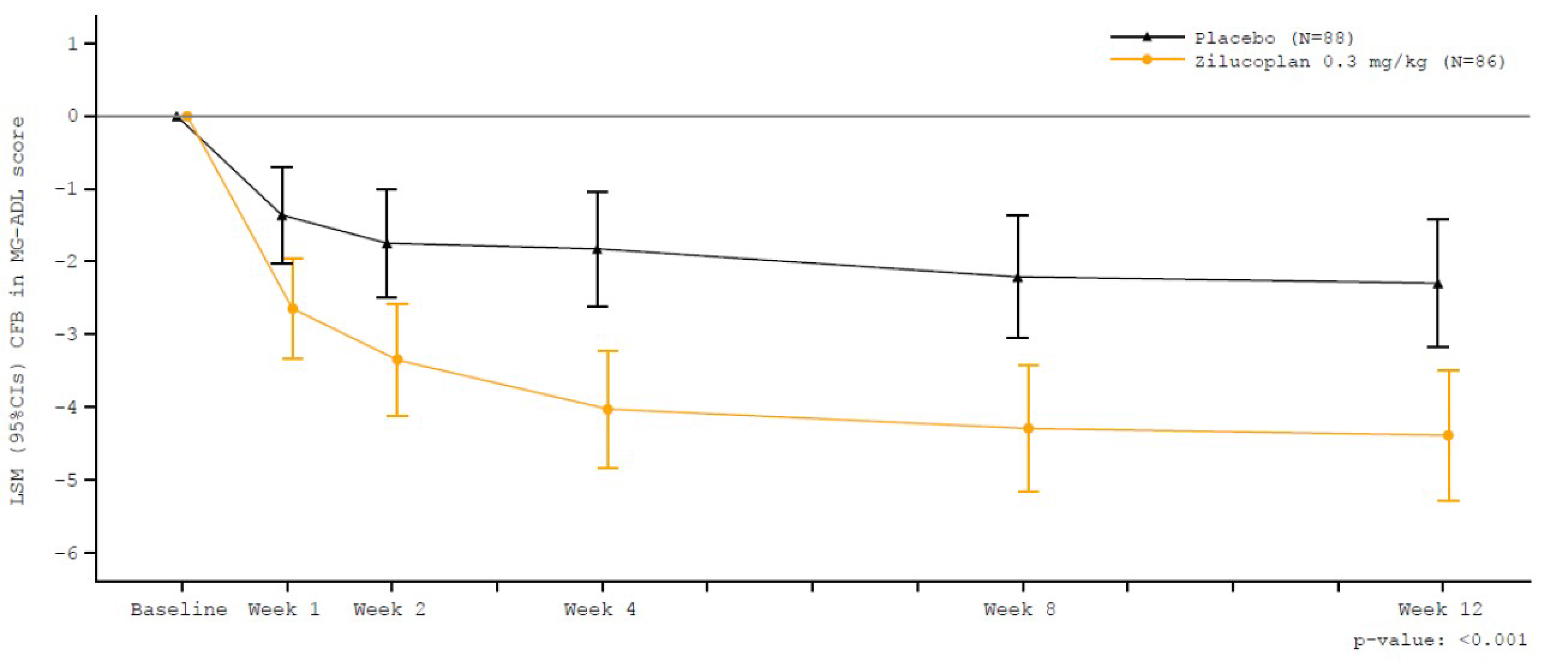
ANCOVA = analysis of covariance; CFB = change from baseline; CI = confidence interval; LS = least squares; LSM = least squares mean; MG-ADL = Myasthenia Gravis Activities of Daily Living; mITT = modified intention to treat; MMRM = mixed model for repeated measures.
Source: RAISE Clinical Study Report.14
Sensitivity Analyses
Two sensitivity analyses were conducted to assess the impact of missing scores on the primary efficacy end point of LS mean change from baseline to week 12 in the MG-ADL score. Findings were similar to the primary analysis when analyzed using MMRM ANCOVA, based on the J2R approach (LS mean difference of –2.03; 95% CI, –3.16 to –0.89; nominal P < 0.001) and based on the tipping-point approach (shift of 25.95 points [LS mean difference of –1.514; 95% CI, –3.057 to 0.029; P = 0.0544] for the zilucoplan group and –17.26 points [LS mean difference of –1.470; 95% CI, –2.981 to 0.042; P = 0.0567] for the placebo group).
Supplemental Analyses
Findings were similar to the primary analysis when analyzed using MMRM ANCOVA, based on the pattern-mixture approach (LS mean difference of –2.13; 95% CI, –3.27 to –0.98; P < 0.001).
Key Secondary End Points
Change From Baseline to Week 12 in the QMG Score
In the overall population, the LS mean change from baseline to week 12 in the QMG score was −6.19 (SE = 0.56) in the zilucoplan group and −3.25 (SE = 0.55) in the placebo group (LS mean difference of –2.94; 95% CI, –4.39 to –1.49; P < 0.001). In the refractory subpopulation, the LS mean change from baseline to week 12 in the QMG score was –6.08 (SE = 0.76) in the zilucoplan group and –2.76 (SE = 0.75) in the placebo group (LS mean difference of –3.32; 95% CI, –5.42 to –1.23; nominal P < 0.001).
Change From Baseline to Week 12 in the MGC Score
In the overall population, the LS mean change from baseline to week 12 in the MGC score was –8.62 (SE = 0.81) in the zilucoplan group and –5.42 (SE = 0.79) in the placebo group (LS mean difference of –3.20; 95% CI, –5.24 to –1.16; P = 0.0023). In the refractory subpopulation, the LS mean change from baseline to week 12 in the MGC score was –7.85 (SE = 1.09) in the zilucoplan group and –4.17 (SE = 1.07) in the placebo group (LS mean difference of –3.68; 95% CI, –6.65 to –0.72; nominal P = 0.0156).
Change From Baseline to Week 12 in the MG-QoL15r Score
In the overall population, the LS mean change from baseline to week 12 in the MG-QoL15r score was –5.65 (SE = 0.77) in the zilucoplan group and –3.16 (SE = 0.76) in the placebo group (LS mean difference of –2.49; 95% CI, –4.45 to –0.54; P = 0.0128). In the refractory subpopulation, the LS mean change from baseline to week 12 in the MG-QoL15r score was –5.63 (SE = 0.96) in the zilucoplan group and –2.36 (SE = 0.95) in the placebo group (LS mean difference of –3.28; 95% CI, –5.89 to –0.67; nominal P = 0.0145).
Additional Secondary End Points
Achievement of MSE at Week 12 Without Rescue Therapy
In the overall population, the percentage of patients who achieved MSE (an MG-ADL score of 0 or 1) at week 12 without rescue therapy was 14.0% in the zilucoplan group and 5.8% in the placebo group (OR = 2.608; 97.5% CI, 0.793 to 9.209; P = 0.0885). The difference in the percentage of patients who achieved MSE was 8.2% (97.5% CI, –1.9% to 18.3%). In the refractory subpopulation, the number of patients who achieved MSE at week 12 without rescue therapy was 2 of 44 patients (4.5%) and 0 of 43 patients in the zilucoplan and placebo groups, respectively.
Achievement of at Least a 3-Point Reduction in MG-ADL Score at Week 12 Without Rescue Therapy
In the overall population, the percentage of patients who were MG-ADL responders (achieved at least a 3-point decrease in the MG-ADL score) at week 12 without rescue therapy was 73.1% in the zilucoplan group and 46.1% in the placebo group (OR = 3.184; 98.75% CI, 1.391 to 7.293; P < 0.001). The difference in the percentage of patients who were MG-ADL responders was 27.0% (98.75% CI, 9.0% to 44.9%). In the refractory subpopulation, the number of patients who were MG-ADL responders at week 12 without rescue therapy was 33 of 44 patients (75.0%) and 17 of 42 patients (40.5%) in the zilucoplan and placebo groups, respectively.
Achievement of at Least a 5-Point Reduction in QMG Score at Week 12 Without Rescue Therapy
In the overall population, the percentage of patients who were QMG responders (achieved at least a 5-point decrease in the QMG score) at week 12 without rescue therapy was 58.0% in the zilucoplan group and 33.0% in the placebo group (OR = 2.865; 98.33% CI, 1.319 to 6.225; P = 0.0012). The difference in the percentage of patients who were QMG responders was 25.0% (98.33% CI, 7.3% to 42.7%). In the refractory subpopulation, the number of patients who were QMG responders at week 12 without rescue therapy was 24 of 43 patients (55.8%) and 11 of 41 patients (26.8%) in the zilucoplan and placebo groups, respectively.
Exploratory End Point
Minimal Manifestation Status per MGFA-PIS at Week 12 Without Rescue Therapy
In the overall population, the number of patients who achieved minimal manifestation status per MGFA-PIS at week 12 without rescue therapy was 22 of 78 (28.2%) in the zilucoplan group and 16 of 83 (19.3%) in the placebo group. The difference in the percentage of patients who achieved minimal manifestation status per MGFA-PIS was 10.9% (95% CI, –1.5% to 23.2%). The number of patients who achieved minimal manifestation status per MGFA-PIS at week 12 without rescue therapy was not reported in the refractory subpopulation.
Table 16: Key Efficacy Results in the RAISE Study (Overall mITT Population and Refractory Subpopulation)
Outcome measure | Overall population | Refractory subpopulation | ||
|---|---|---|---|---|
Zilucoplan N = 86 | Placebo N = 88 | Zilucoplan N = 44 | Placebo N = 44 | |
Change from baseline to week 12 in the MG-ADL score | ||||
Baseline MG-ADL score, n | 86 | 88 | 44 | 44 |
Baseline MG-ADL score, mean (SD) | 10.3 (2.5) | 10.9 (3.4) | 10.3 (2.6) | 11.0 (3.4) |
Change from baseline at week 12 in MG-ADL score, na | 84 | 85 | 44 | 42 |
Change from baseline at week 12 in MG-ADL score, mean (SD) | –4.70 (3.93) | –2.85 (3.60) | –4.89 (4.09) | –2.26 (3.39) |
Change from baseline at week 12 in MG-ADL score, LS mean (SE) | –4.39 (0.45) | –2.30 (0.44) | –4.72 (0.58) | –1.62 (0.58) |
95% CI | –5.28 to –3.50 | –3.17 to –1.43 | –5.88 to –3.57 | –2.77 to –0.47 |
LS mean difference (SE)b | –2.09 (0.58) | Reference | –3.11 (0.80) | Reference |
95% CI | –3.24 to –0.95 | Reference | –4.69 to –1.52 | Reference |
P value | < 0.001c | Reference | < 0.001 (nominal) | Reference |
Change from baseline to week 12 in the QMG score | ||||
Baseline QMG score, n | 86 | 88 | 44 | 44 |
Baseline QMG score, mean (SD) | 18.7 (3.6) | 19.4 (4.5) | 18.8 (4.0) | 19.7 (4.4) |
Change from baseline at week 12 in QMG score, na | 83 | 84 | 43 | 41 |
Change from baseline at week 12 in QMG score, mean (SD) | –6.31 (4.92) | –3.38 (4.21) | –6.05 (5.16) | –3.12 (4.41) |
Change from baseline at week 12 in QMG score, LS mean (SE) | –6.19 (0.56) | –3.25 (0.55) | –6.08 (0.76) | –2.76 (0.75) |
95% CI | –7.29 to –5.08 | –4.32 to –2.17 | –7.59 to –4.56 | –4.25 to –1.26 |
LS mean difference (SE)b | –2.94 (0.73) | Reference | –3.32 (1.05) | Reference |
95% CI | –4.39 to –1.49 | Reference | –5.42 to –1.23 | Reference |
P value | < 0.001d | Reference | 0.0022 (nominal) | Reference |
Change from baseline to week 12 in the MGC score | ||||
Baseline MGC score, n | 86 | 88 | 44 | 44 |
Baseline MGC score, mean (SD) | 20.1 (6.0) | 21.6 (7.2) | 19.8 (6.2) | 21.3 (7.4) |
Change from baseline at week 12 in MGC score, na | 83 | 84 | 43 | 41 |
Change from baseline at week 12 in MGC score, mean (SD) | –9.20 (6.35) | –6.58 (6.46) | –8.37 (6.49) | –5.34 (6.54) |
Change from baseline at week 12 in MGC score, LS mean (SE) | –8.62 (0.81) | –5.42 (0.79) | –7.85 (1.09) | –4.17 (1.07) |
95% CI | –10.22 to –7.01 | –6.98 to –3.86 | –10.01 to –5.69 | –6.30 to –2.03 |
LS mean difference (SE) | –3.20 (1.03) | Reference | –3.68 (1.49) | Reference |
95% CI | –5.24 to –1.16 | Reference | –6.65 to –0.72 | Reference |
P value | 0.0023e | Reference | 0.0156 (nominal) | Reference |
Change from baseline to week 12 in the MG-QoL15r score | ||||
Baseline MG-QoL15r score, n | 86 | 88 | 44 | 44 |
Baseline MG-QoL15r score, mean (SD) | 18.6 (6.6) | 18.9 (6.8) | 18.3 (6.9) | 18.9 (6.9) |
Change from baseline at week 12 in MG-QoL15r score, n | 82 | 83 | 43 | 40 |
Change from baseline at week 12 in MG-QoL15r score, mean (SD) | –6.09 (7.10) | –3.93 (6.34) | –5.95 (6.36) | –3.18 (6.04) |
Change from baseline at week 12 in MG-QoL15r score, LS mean (SE) | –5.65 (0.77) | –3.16 (0.76) | –5.63 (0.96) | –2.36 (0.95) |
95% CI | –7.17 to –4.12 | –4.65 to –1.67 | –7.53 to –3.73 | –4.24 to –0.47 |
LS mean difference (SE) | –2.49 (0.99) | Reference | –3.28 (1.31) | Reference |
95% CI | –4.45 to –0.54 | Reference | –5.89 to –0.67 | Reference |
P value | 0.0128f | Reference | 0.0145 (nominal) | Reference |
Achievement of MSEg (MG-ADL score of 0 or 1) at week 12 without rescue therapy | ||||
N, observed | 84 | 85 | 44 | 43 |
MSE,g observed, n (%) | 12 (14.3) | 5 (5.9) | 2 (4.5) | 0 |
N, imputed | 86 | 88 | NR | NR |
MSE,g imputed, n (%) | NR (14.0) | NR (5.8) | NR | NR |
Risk difference (97.5% CI)h | 8.2 (–1.9 to 18.3) | Reference | NR | Reference |
OR (97.5% CI)i | 2.608 (0.739 to 9.209) | Reference | NR | Reference |
P valuej | 0.0885 | Reference | NR | Reference |
MG-ADL responder rate at week 12 without rescue therapy | ||||
N, observed | 84 | 85 | 44 | 42 |
MG-ADL responder,k observed, n (%) | 62 (73.8) | 40 (47.1) | 33 (75.0) | 17 (40.5) |
N, imputed | 86 | 88 | NR | NR |
MG-ADL responder,k imputed, n (%) | NR (73.1) | NR (46.1) | NR | NR |
Risk difference (98.75% CI)h | 27.0 (9.0 to 44.9) | Reference | NR | Reference |
OR (98.75% CI)i | 3.184 (1.391 to 7.293) | Reference | NR | Reference |
P valuej | < 0.001 | Reference | NR | Reference |
QMG responder rate at week 12 without rescue therapy | ||||
N, observed | 83 | 84 | 43 | 41 |
QMG responder,l observed, n (%) | 49 (59.0) | 28 (33.3) | 24 (55.8) | 11 (26.8) |
N, imputed | 86 | 88 | NR | NR |
QMG responder,l imputed, n (%) | NR (58.0) | NR (33.0) | NR | NR |
Risk difference (98.3% CI)h | 25.0 (7.3 to 42.7) | Reference | NR | Reference |
OR (98.3% CI)i | 2.865 (1.319 to 6.225) | Reference | NR | Reference |
P valuej | 0.0012 | Reference | NR | Reference |
Achievement of minimal manifestation status per MGFA-PIS at week 12 without rescue therapym | ||||
N | 78 | 83 | NR | NR |
Number of patients achieving minimal manifestation status per MGFA-PIS, n (%) | 22 (28.2) | 16 (19.3) | NR | NR |
Risk difference, % (95% CI)h | 10.9 (–1.5 to 23.2) | Reference | NR | NR |
OR (95% CI)n | 1.834 (0.847 to 3.969) | Reference | NR | NR |
ANCOVA = analysis of covariance; CDA-AMC = Canada’s Drug Agency; CI = confidence interval; ICE = intercurrent event; LS = least squares; MG-ADL = Myasthenia Gravis Activities of Daily Living; MGC = Myasthenia Gravis Composite; MGFA-PIS = Myasthenia Gravis Foundation of America Post-Intervention Status; MG-QoL15r = Myasthenia Gravis Quality of Life 15-item – Revised; mITT = modified intention to treat; MMRM = mixed model of repeated measures; MSE = minimal symptom expression; NR = not reported; OR = odds ratio; QMG = Quantitative Myasthenia Gravis; SD = standard deviation; SE = standard error.
Note: Baseline was defined as the last available predose value before the first injection of the study drug in the treatment period or, if missing, the screening value. MG-ADL scores after rescue therapy (ICE1) or any death or myasthenic crisis (ICE2) were censored and considered as treatment failures. Any missing data due to ICE1 or ICE2 were imputed based on baseline MG-ADL score or on the last available MG-ADL score, whichever was worse. Other missing scores were handled with the maximum likelihood estimation method under the missing at random assumption. Analysis was based on an MMRM ANCOVA model, using an unstructured correlation matrix, with treatment, baseline MG-ADL score, baseline QMG score, region (East Asia, Europe, and North America), and the interactions terms of treatment by visit and baseline MG-ADL score by visit as fixed effects; patients were added as random effects in the model. The MMRM ANCOVA includes week 1, week 2, week 4, week 8, and week 12.
aPatients with no missing score at week 12.
bLS mean difference was calculated as zilucoplan minus placebo.
cP value was derived using an MMRM ANCOVA model (based on imputed data after treatment failure), using an unstructured correlation matrix, with treatment, baseline MG-ADL score, baseline QMG score, region, with the interaction terms of treatment by visit and baseline MG-ADL score by visit as fixed effects and patients as random effects in the model.
dP value corresponds to the primary analysis of the secondary end point of change from baseline to week 12 in the QMG score; after multiplicity adjustment, a result was considered statistically significant if the primary analysis of change from baseline to week 12 in the MG-ADL score was also statistically significant at alpha of 0.05 using 2-sided statistical testing.
eP value corresponds to the primary analysis of the secondary end point of change from baseline to week 12 in the MGC score; after multiplicity adjustment, a result was considered statistically significant if the primary analysis of change from baseline to week 12 in the MG-ADL score and the change from baseline in QMG score were also statistically significant at alpha of 0.05 using 2-sided statistical testing.
fP value corresponds to the primary analysis of the secondary end point of change from baseline to week 12 in the MG-QoL15r score; after multiplicity adjustment, a result was considered statistically significant if the primary analysis of change from baseline to week 12 in the MG-ADL score and change in baseline in MGC and QMG scores were also statistically significant at alpha of 0.05 using 2-sided statistical testing.
gAchievement of MSE is defined as having an MG-ADL score of 0 or 1.
hRisk difference was not included in the sponsor’s planned analyses; the absolute risk difference with associated CI was requested by the CDA-AMC review team for interpretation purposes. Based on the testing procedure used for the secondary end points, the CIs were 98.75% for MG-ADL responder, 98.3% for QMG responder, and 97.5% for the achievement of MSE in the statistical hierarchy using the Holm’s procedure.
jOdds ratio was estimated between treatment groups using a logistic regression model, with treatment as factor, and baseline MG-ADL score, baseline QMG score, and region as covariates at each imputed dataset. Treatment effects were combined across 100 imputed datasets to produce an overall treatment effect. An OR greater than 1 indicated a greater likelihood of response to zilucoplan than to placebo. Based on the testing procedure used for the secondary end points, the CI was 98.75% for MG-ADL responder, 98.3% for QMG responder, and 97.5% for the achievement of MSE in the statistical hierarchy using the Holm’s procedure. The associated CI was generated using a post hoc analysis.
jP value was adjusted in the statistical hierarchical testing after the Holm’s procedure, using the threshold of 0.0125 for the MG-ADL score, 0.017 for the QMG score, and 0.025 for the achievement of MSE.
kAn MG-ADL responder is defined as having at least a 3-point improvement (decrease) in the MG-ADL score.
lA QMG responder is defined as having at least a 5-point improvement (decrease) in the QMG score.
mThis end point was not adjusted for multiple testing, so there is a potential for type I error to be increased, and findings should be considered supportive.
nOdds ratio (95% CI) was not included in the sponsor’s planned analyses; the relative effect was requested by the CDA-AMC review team for interpretation purposes.
Sources: RAISE Clinical Study Report,14 sponsor’s Summary of Clinical Evidence.27
Harms
Harms data for the RAISE study at the data cut-off date of December 30, 2021, are summarized in Table 17.
Adverse Events
In the overall population, the number of patients with at least 1 TEAE was 66 of 86 patients (76.7%) in the zilucoplan group and 62 of 88 patients (70.5%) in the placebo group. The most common TEAEs, occurring in greater than 5% of patients in either the zilucoplan group or the placebo group, respectively, were headache (15.1% versus 15.9%), injection-site bruising (16.3% versus 9.1%), MG (10.5% versus 9.1%), diarrhea (10.5% versus 2.3%), injection-site pain (9.3% versus 3.4%), urinary tract infection (8.1% versus 4.5%), contusion (8.1% versus 3.4%), increased lipase (8.1% versus 1.1%), nasopharyngitis (5.8% versus 3.4%), vomiting (3.5% versus 5.7%), rash (3.5% versus 5.7%), and increased amylase (5.8% versus 2.3%). In the refractory subpopulation, the number of patients with at least 1 TEAE was 39 (88.6%) in the zilucoplan group and 34 (77.3%) in the placebo group. The most common TEAEs, occurring in greater than 10% of patients in either the zilucoplan group or the placebo group, respectively, were headache (20.5% versus 15.9%), MG (13.6% versus 13.6%), injection-site bruising (15.9% versus 11.4%), diarrhea (15.9% versus 2.3%), and vomiting (4.5% versus 11.4%).
Serious Adverse Events
In the overall population, the number of patients with at least 1 SAE was 11 (12.8%) in the zilucoplan group and 13 (14.8%) in the placebo group. The most common SAEs reported in at least 2% of patients in either the zilucoplan group or the placebo group, respectively, were MG (2.3% versus 5.7%), COVID-19 (1.2% versus 2.3%), and COVID-19 pneumonia (1.2% versus 2.3%). In the refractory subpopulation, the number of patients with at least 1 SAE was 6 patients (13.6%) in the zilucoplan group and 8 patients (18.2%) in the placebo group. SAEs specified by system organ class were not reported for the refractory subpopulation.
Withdrawals Due to Adverse Events
In the overall population, the number of patients who stopped the study treatment due to AEs was 4 (4.7%) in the zilucoplan group and 2 (2.3%) in the placebo group. Withdrawals due to AEs in the zilucoplan group were due to (1 patient [1.2%] each) aphthous ulcer, mouth ulceration, COVID-19, and increased hepatic enzyme; the TEAE of aphthous ulcer and the TEAE of COVID-19 were considered serious, with the latter having had a fatal outcome. Withdrawals due to AEs in the placebo group were due to (1 patient [1.1%] each) cerebral hemorrhage and hyperemesis gravidarum; both TEAEs were considered serious and the TEAE of cerebral hemorrhage had a fatal outcome. In the refractory subpopulation, 1 patient (2.3%) stopped the study treatment in the zilucoplan group, and no patients stopped the study treatment in the placebo group. Reasons for withdrawal due to AEs were not reported for the refractory subpopulation.
Mortality
In the overall population of the RAISE study, 2 patients died: 1 patient (1.2%) in the zilucoplan group who experienced an SAE leading to death due to COVID-19 and COVID-19 pneumonia, and 1 patient (1.1%) in the placebo group who experienced an SAE leading to death due to cerebral hemorrhage. In the refractory subpopulation, no deaths were observed.
Adverse Events of Special Interest
Infections
In the overall population, the number of patients who experienced infections was 23 (26.7%) in the zilucoplan group compared with 16 (18.2%) in the placebo group (between-group difference, 8.6%; 95% CI, –3.8% to 20.9%). Of these, 4 patients (4.7%) in the zilucoplan group and 4 patients (4.5%) in the placebo group had serious infections. AEs of special interest were not reported for the refractory subpopulation.
Table 17: Harms Results in the RAISE Study (Overall Population and Refractory Subpopulation, Safety Set)
Adverse events | Overall population | Refractory subpopulation | ||
|---|---|---|---|---|
Zilucoplan N = 86 | Placebo N = 88 | Zilucoplan N = 44 | Placebo N = 44 | |
Data cut-off date | December 30, 2021 | |||
Most common AEs, n (%) | ||||
Patients with ≥ 1 TEAE | 66 (76.7) | 62 (70.5) | 39 (88.6) | 34 (77.3) |
TEAEs in ≥ 5% of patients in any group | ||||
Headache | 13 (15.1) | 14 (15.9) | 9 (20.5) | 7 (15.9) |
Injection-site bruising | 14 (16.3) | 8 (9.1) | 7 (15.9) | 5 (11.4) |
Myasthenia gravis | 9 (10.5) | 8 (9.1) | 6 (13.6) | 6 (13.6) |
Diarrhea | 9 (10.5) | 2 (2.3) | 7 (15.9) | 1 (2.3) |
Injection-site pain | 8 (9.3) | 3 (3.4) | 3 (6.8) | 1 (2.3) |
Urinary tract infection | 7 (8.1) | 4 (4.5) | < 5% | < 5% |
Contusion | 7 (8.1) | 3 (3.4) | < 5% | < 5% |
Increased lipase | 7 (8.1) | 1 (1.1) | 4 (9.1) | 0 |
Nasopharyngitis | 5 (5.8) | 3 (3.4) | 2 (4.5) | 3 (6.8) |
Vomiting | 3 (3.5) | 5 (5.7) | 2 (4.5) | 5 (11.4) |
Rash | 3 (3.5) | 5 (5.7) | < 5% | < 5% |
Increased amylase | 5 (5.8) | 2 (2.3) | < 5% | < 5% |
Muscle spasms | < 5% | < 5% | 4 (9.1) | 1 (2.3) |
Back pain | < 5% | < 5% | 1 (2.3) | 4 (9.1) |
Pain in extremity | < 5% | < 5% | 1 (2.3) | 3 (6.8) |
Pyrexia | < 5% | < 5% | 4 (9.1) | 0 |
Nausea | < 5% | < 5% | 3 (6.8) | 0 |
Depression | < 5% | < 5% | 3 (6.8) | 0 |
COVID-19 | < 5% | < 5% | 0 | 3 (6.8) |
SAEs, n (%) | ||||
Patients with ≥ 1 SAE | 11 (12.8) | 13 (14.8) | 6 (13.6) | 8 (18.2) |
SAEs in ≥ 2% of patients in any group | ||||
Myasthenia gravis | 2 (2.3) | 5 (5.7) | NR | NR |
COVID-19 | 1 (1.2) | 2 (2.3) | NR | NR |
COVID-19 pneumonia | 1 (1.2) | 2 (2.3) | NR | NR |
Patients who stopped treatment due to AEs, n (%) | ||||
Patients who stopped study treatment | 4 (4.7) | 2 (2.3) | 1 (2.3) | 0 |
Aphthous ulcer | 1 (1.2) | 0 | NR | NR |
Mouth ulceration | 1 (1.2) | 0 | NR | NR |
COVID-19 | 1 (1.2) | 0 | NR | NR |
Increased hepatic enzyme | 1 (1.2) | 0 | NR | NR |
Cerebral hemorrhage | 0 | 1 (1.1) | NR | NR |
Hyperemesis gravidarum | 0 | 1 (1.1) | NR | NR |
Deaths, n (%) | ||||
Patients who died | 1 (1.2) | 1 (1.1) | 0 | 0 |
COVID-19 | 1 (1.2) | 0 | — | — |
Cerebral hemorrhage | 0 | 1 (1.1) | — | — |
AEs of special interest, n (%) | ||||
Infections | 23 (26.7) | 16 (18.2) | NR | NR |
Infections, risk difference (95% CI)a | 8.6 (–3.8 to 20.9) | Reference | NR | NR |
Nonserious | 19 (22.1) | 12 (13.6) | NR | NR |
Serious | 4 (4.7) | 4 (4.5) | NR | NR |
AE = adverse event; CDA-AMC = Canada’s Drug Agency; CI = confidence interval; NR = not reported; SAE = serious adverse event; TEAE = treatment-emergent adverse event.
aRisk difference (95% CI) was not included in the sponsor’s planned analyses; the absolute risk difference was requested by the CDA-AMC review team for interpretation purposes.
Sources: RAISE Clinical Study Report,14 sponsor’s Summary of Clinical Evidence.27
Critical Appraisal
Internal Validity
Randomization appeared to be adequate in the RAISE trial; the treatment groups were balanced, overall, for demographic and disease characteristics. A greater proportion of patients with gMG in the zilucoplan than in the placebo group had undergone thymectomy in the overall population (52.3% versus 42.0%) and in the refractory subpopulation (75.0% versus 61.4%), which had the potential to influence treatment effects. However, no systemic differences between groups were detected on other key prognostic factors or in the medical history of patients, which indicates that randomization was likely successful, and the risk of selection bias was low. Randomization was stratified by baseline MG-ADL score (≤ 9 versus ≥ 10), QMG score (≤ 17 versus ≥ 18), and geographic region (East Asia, Europe, and North America). The instruments used to evaluate the primary and secondary efficacy outcomes (MG-ADL, QMG, MGC, MG-QoL15r) were appropriate, and their psychometric properties have been investigated in patients with MG, although no MIDs have been estimated for the MG-QoL15r. Minimal manifestation status per MGFA-PIS without rescue therapy was based on clinician-assessed patient symptoms of MG after the initiation of MG-specific therapy; this measure was intended to capture patients who may not meet the definition of complete stable remission or pharmacologic remission but who have muscle weakness, based on careful examination. This was an exploratory end point, and no MID has been validated in the indicated population. Results for minimal manifestation status per MGFA-PIS at week 12 were not reported for the refractory subpopulation. There was a low risk of bias for allocation concealment because patients and study staff were blinded to treatment assignment, both treatments were identical, and the unblinding of treatment assignment was not permitted before the initiation of rescue therapy. Patients with refractory disease represented about one-half of the enrolled patients with gMG. The selection criteria for the refractory subgroup were specified a priori and in line with the criteria used to define patients with refractory gMG in other RCTs (e.g., the REGAIN trial for eculizumab). Although randomization was not stratified by refractory status, baseline characteristics were, overall, similar between treatment groups, so concerns regarding the prognostic balance of the refractory subpopulation were low. Subgroup analyses were not adjusted for multiplicity, nor were they specifically powered to detect differences among strata. Otherwise, results from the refractory subgroup can be considered consistent with the analyses of the overall population in the RAISE trial and share the limitations of those analyses. Results for the refractory subgroup showed consistency with the overall trial population across all outcomes.
There was a notable proportion of patients with important protocol deviations in both the zilucoplan group (33 patients [38.4%]) and the placebo group (32 patients [36.4%]). Prohibited concomitant medication use important protocol deviations occurred in 24.7% of patients, which included changes to gMG conventional medications (10 patients and 8 patients in the zilucoplan and placebo groups, respectively), the use of prohibited concomitant medications (9 patients and 8 patients, respectively), and changes to cholinesterase inhibitor dosing less than 10 hours before evaluation (6 patients and 6 patients, respectively). Additionally, deviations from the inclusion criteria occurred in 7.5% of patients; acetylcholinesterase inhibitor therapy was not withheld for at least 10 hours before the QMG assessment (6 patients and 6 patients in the zilucoplan and placebo groups, respectively), the corticosteroid regimen was changed in the 30 days before baseline (1 patient in the zilucoplan group), and inpatient treatment with IVIg was not reported as a rescue therapy (1 patient in the zilucoplan group). The proportion of patients with protocol deviations, such as the use of prohibited medications or changes to gMG conventional medications during the study, were balanced between groups.
MI methods were used to account for missing data in the primary and secondary end points, based on assumptions of MNAR, in which missingness may be related to the study drug or the receipt of rescue medication, and assumptions of MAR. Based on the specified approach, each of these was imputed with either the baseline value or the last observed value (whichever was worse). Because the rate of ICE1 (receipt of rescue therapy with IVIg, PLEX, or eculizumab) was higher in the placebo group (11%) than in the zilucoplan group (5%), this approach appeared to be overly pessimistic and possibly introduced bias in favour of zilucoplan; however, the imbalance was not large enough to raise serious concerns about biased treatment effects. In sensitivity analyses to account for the censoring of patients who experienced treatment failure in the zilucoplan versus placebo groups, respectively, the proportions of patients were aligned with prior clinical trial data (from the zilucoplan phase II and eculizumab phase III studies) and were similar across scores on the MG-ADL, QMG, MGC, and MG-QoL15r for the receipt of rescue therapy (4.7% versus 11.4%, respectively), any death or myasthenic crisis (1.2% versus 1.1%, respectively), and patients with missing data but assumed to have remained on treatment (1.2% versus 0.0%, respectively, for MG-ADL; 2.3% versus 1.1%, respectively, for QMG and MGC; and 3.5% versus 2.3%, respectively, for MG-QoL15r). Overall, the supplemental analyses and sensitivity analyses of the primary analysis did not adequately assess the potential bias related to missing data. However, concerns about loss to follow-up were low, because approximately 95% of patients with gMG in the overall population and the refractory subpopulation completed the RAISE study, with balanced proportions between treatment arms.
External Validity
Per sponsor request, the focus of this review was on the sponsor’s reimbursement request, which was narrower than the Health Canada indication. The reimbursement request aligned with the criteria for the refractory subgroup of the RAISE trial, which was zilucoplan as add-on therapy for the treatment of adult patients with anti-AChR antibody–positive refractory gMG, defined as no achievement of symptom control after treatment for at least 1 year with 2 or more of the following therapies: prednisone, azathioprine, mycophenolate, cyclosporine, cyclophosphamide, methotrexate, tacrolimus, other corticosteroids for gMG, other ISTs; or a history of treatment with at least 1 of these therapies for 1 year or more and the need for chronic PLEX, IVIg, or SCIg at least every 3 months for the 12 months before treatment with zilucoplan. The requested reimbursement criteria also aligned with the reimbursement criteria for the comparator therapy, eculizumab, which received a CADTH positive final recommendation in 2020.
Patients in the RAISE trial who did not have refractory disease (49%) were not included in the reimbursement request. Although the clinical expert consulted for this review agreed that there is a current unmet need in patients with nonrefractory disease who have responded inadequately to the existing standard of gMG therapy, this population was not the focus on this review.
Looking at the types and duration of prior conventional treatments received by patients in the RAISE trial, the clinical expert agreed that all were adequately managed on conventional therapy for gMG at time of enrolment and were reflective of patients who experience an unmet need in the clinical setting in Canada. The concomitant medications received by patients in the RAISE trial represented the range of options currently available in clinical practice in Canada, and the clinical expert felt that exposure to the corticosteroids and NSISTs being used by patients at study enrolment exceeded the typical duration for maximal response of 3 to 4 months for prednisone (or other corticosteroids) and 6 to 18 months for NSISTs.
The RAISE trial inclusion criteria required that corticosteroid and IST doses and types of treatment not be changed for at least 30 days before study baseline, and that therapy changes not be anticipated during the 12-week treatment period. All standard-of-care medications for gMG were to be kept at the same dose throughout the study, including corticosteroids and IST drugs. If an escalation of gMG therapy (i.e., rescue therapy) became necessary because of major deterioration in a patient’s clinical status or because of the risk of MG crisis, per the investigator’s judgment, the patient was allowed to receive IVIg or PLEX treatment as rescue therapy. After the first 12 weeks of the study, if the investigator determined that a reduction in standard-of-care therapy for gMG would be a reasonable course of action, a dose reduction could be initiated. The clinical expert consulted on this review was not concerned about dose changes in concomitant medications over the course of the 12-week treatment period. The expert felt that patients were adequately managed on conventional therapy for gMG at time of enrolment and that exposure to corticosteroids and NSISTs at study enrolment exceeded the typical duration for maximal response. Per the final product monograph, patients eligible for zilucoplan should continue to receive standard therapy throughout the pivotal trial.1
At baseline, no patients in the RAISE trial had received eculizumab or rituximab (patients who received rituximab in the 12 months before baseline were not eligible for the study); as such, the trial population reflects patients in Canada who have limited or no access to these treatments because of a lack of funding by public drug plans.
According to the expert, stratifying patients during randomization by baseline scores on the MG-ADL and the QMG appeared to be an appropriate way to ensure equal distributions of patients by disease severity. The expert noted that no specific patient populations that might otherwise be considered eligible in clinical practice were missed, and that the patients enrolled in the RAISE study were representative of those observed in clinical practice. Although more patients had undergone thymectomy in the zilucoplan group than in the placebo group in the overall population (52% versus 42%, respectively) and in the refractory subpopulation (75% versus 61%, respectively), this did not contribute significantly to the treatment effects, according to the expert. In line with patients who were not eligible for the RAISE trial, patients with MuSK-positive MG should not be treated with a complement inhibitor such as zilucoplan based its mechanism of action, the expert emphasized; rather, patients with MuSK-positive MG might benefit from treatment with a neonatal FcR inhibitor (e.g., efgartigimod alfa).
The trial’s eligibility criteria, which included an MGFA disease class of II to IV and an MG-ADL total score of at least 6, would select patients with symptomatic gMG most in need of intervention, according to the clinical expert consulted for this review. Very few patients with class IV gMG (fewer than 10 patients in the overall trial population) were included in the trial. The clinical expert consulted for this review indicated that a subset of patients with MGFA disease class I (ocular MG) or class V and an MG-ADL score of less than 6 would be suitable for treatment. Specifically, the clinical expert indicated that patients with ocular MG or mild symptoms can still be refractory to other therapies, and that patients with MGFA disease class V (on a ventilator) who have no contraindications could potentially benefit from zilucoplan. However, the clinical expert noted that zilucoplan has not been studied in these patients, and the results of the trial cannot be directly generalized to these groups of patients.
The expert emphasized that given the relatively high proportion of patients with refractory disease in the RAISE trial (about 50% of patients in the overall population), the lower proportions of patients receiving prednisone (about 40%) and azathioprine or mycophenolate mofetil (up to 20% each) in the overall trial population than in clinical practice was a surprise. Although the number of patients who were on pyridostigmine was numerically higher in the zilucoplan group than in the placebo group, the expert noted that, per the study protocol of withholding this treatment for 10 hours, very few patients added pyridostigmine after the trial started and, combined with its short half-life, the potential for concomitant treatment with pyridostigmine to influence treatment effects is likely very low.
Moreover, the RAISE trial did not provide evidence for comparisons between zilucoplan and other currently available active treatments for gMG. The expert considered that the most relevant comparators for zilucoplan among patients with refractory gMG include other complement inhibitors (i.e., eculizumab, ravulizumab), neonatal FcR inhibitors (e.g., efgartigimod alfa), chronic IVIg, and chronic PLEX; rituximab as a comparator is less applicable because of its limited access in Canada for patients with gMG, its off-label use, the lack of rigorous clinical trial evidence in patients with anti-AChR antibody–positive MG, and some evidence of improved benefit among patients with MuSK-positive MG.
The expert agreed that the primary end point of change from baseline in MG-ADL score was an important outcome for the evaluation of treatment response and is aligned with clinical practice, including the threshold used in the RAISE trial. MIDs used for the QMG and MGC scores were also noted by the expert to align with the literature for thresholds validated in patients with MG.
According to the expert, most patients with gMG would be assessed at approximately 12 weeks to evaluate treatment response, which is aligned with the RAISE trial, with additional assessments conducted at the 3-month or 4-month time point to assess responsiveness or maintenance of response. The randomized controlled period of the RAISE trial was 12 weeks. The longer-term treatment effect of zilucoplan can only be assessed in the open-label extension period of the RAISE-XT study.
GRADE Summary of Findings and Certainty of the Evidence
Methods for Assessing the Certainty of the Evidence
For pivotal studies and RCTs identified in the sponsor’s systematic review, GRADE was used to assess the certainty of the evidence for outcomes considered to be most relevant to CDA-AMC expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group.43,44
High certainty: We are very confident that the true effect lies close to that of the estimate of the effect.
Moderate certainty: We are moderately confident in the effect estimate. The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. We use the word likely for evidence of moderate certainty (e.g., X intervention likely results in Y outcome).
Low certainty: Our confidence in the effect estimate is limited. The true effect may be substantially different from the estimate of the effect. We use the word may for evidence of low certainty (e.g., X intervention may result in Y outcome).
Very low certainty: We have very little confidence in the effect estimate. The true effect is likely to be substantially different from the estimate of effect. We describe evidence of very low certainty as very uncertain.
In accordance with the GRADE approach, evidence from RCTs started as high-certainty evidence and could be rated down for concerns related to study limitations (which refer to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias.
When possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect; if this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., the clinical importance is unclear). In all cases, the target of the certainty of evidence assessment was based on the point estimate and where it was located relative to the threshold for a clinically important effect (when a threshold was available) or to the null. The target of the certainty of evidence assessment was the presence or absence of a clinically important effect for change from baseline to week 12 in the MG-ADL, the QMG, and the MGC scores, based on thresholds identified in the literature. The certainty of evidence assessments for change from baseline to week 12 in the MG-QoL15r score, the number of patients achieving MSE at week 12 without rescue therapy, an MG-ADL responder rate at week 12 without rescue therapy, a QMG responder rate at week 12 without rescue therapy, the number of patients with minimal manifestation status per MGFA-PIS at week 12 without rescue therapy, and infections, were based on the presence or absence of any (nonnull) effect.
Results of GRADE Assessments
Table 2 presents the GRADE summary of findings for zilucoplan versus placebo in patients with anti-AChR antibody–positive gMG.
Long-Term Extension Studies
Contents within this section have been informed by materials submitted by the sponsor. The following has been summarized and validated by the CDA-AMC review team.
Description of Studies
RAISE-XT (NCT04225871) is an ongoing, phase III, multicentre, open-label extension study of zilucoplan in patients with gMG. At the conclusion of the 12-week treatment period of the RAISE parent study, all eligible patients had the option to enrol in the RAISE-XT study. The objectives of the RAISE-XT study were to evaluate the long-term efficacy, safety, and tolerability of zilucoplan in patients with gMG who had previously participated in a qualifying zilucoplan study (either the phase II MG0009 study [NCT03315130] or the RAISE study). The design of the RAISE-XT study is depicted in Figure 3.
Results of 3 interim analyses in the RAISE-XT study are presented in this report, with clinical cut-off dates of September 8, 2022, May 11, 2023, and November 11, 2023. All data cut-offs include data for the overall population, whereas the November 2023 interim data cut-off also includes data for the refractory subpopulation. Because both the sponsor’s submission and the proposed Health Canada indication recommends a zilucoplan dose of 0.3 mg/kg, this Clinical Review report will present data for patients who were randomized to receive 0.3 mg/kg of zilucoplan or placebo in the double-blind parent studies (MG0009 or the RAISE study); data for patients who received 0.1 mg/kg of zilucoplan are not presented in this report. At the time of review, the RAISE-XT study is ongoing; it is expected to collect efficacy and safety data for up to 7 years. Results are presented for the end points at 12 weeks in the RAISE-XT study. Results at 84 weeks in the RAISE-XT study are presented in Table 33 in Appendix 1.
Figure 3: The RAISE-XT Study Design
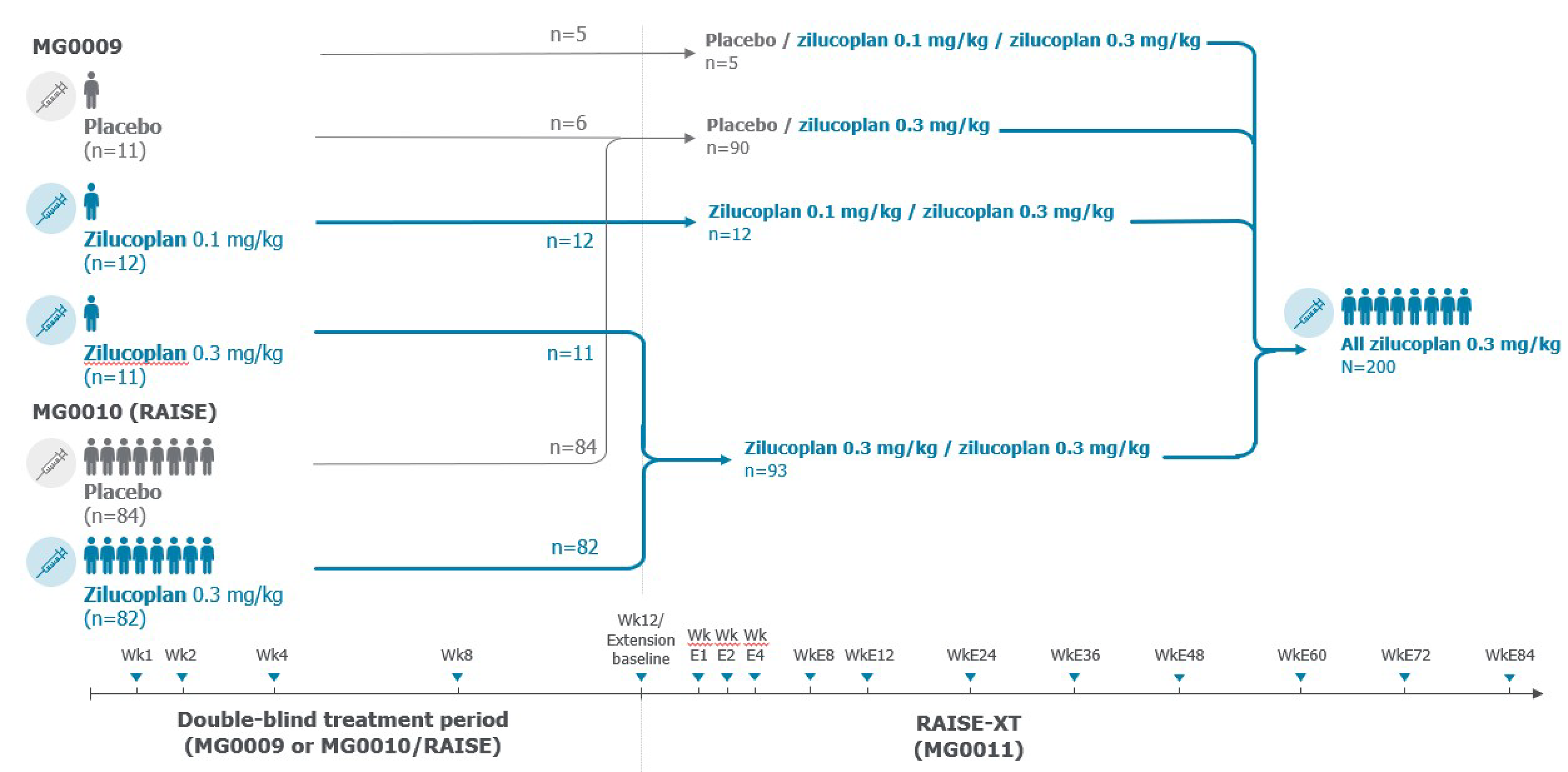
E = extension; Wk = week.
Note: At day E1, all patients received 0.3 mg/kg of zilucoplan, regardless of the dose they received in the parent study.
Source: RAISE-XT Clinical Study Report.45
Populations
Eligible patients were 18 years or older and had completed a qualifying zilucoplan study (the phase II MG0009 study or the RAISE study). The 2 groups entering the RAISE-XT study were defined as follows:
The placebo and zilucoplan 0.3 mg/kg group includes patients from the RAISE study who were randomized to placebo in the treatment period and then received zilucoplan 0.3 mg/kg when they entered the RAISE-XT study. It also includes patients in the MG0009 study who were randomized to placebo in the treatment period and then received zilucoplan 0.3 mg/kg in the extension part of the MG0009 study and in the RAISE-XT study.
The zilucoplan 0.3 mg/kg and zilucoplan 0.3 mg/kg group includes patients from the RAISE study who were randomized to zilucoplan 0.3 mg/kg in the treatment period and received zilucoplan 0.3 mg/kg in the RAISE-XT study. It also includes patients in the phase II MG0009 study who were randomized to zilucoplan 0.3 mg/kg in both the treatment period and the extension periods of the MG0009 study and then received zilucoplan in the RAISE-XT study.
Refractory status at baseline was recorded for patients in the RAISE study but not for patients in the MG0009 study. Therefore, all patients identified as refractory in the RAISE-XT study had entered the study from the RAISE study and had been classified as gMG refractory at baseline in the RAISE study. Patients were not reassessed for refractory status or redefined after entry into the RAISE-XT study.
As in the RAISE study, eligible patients must also have been vaccinated against Neisseria meningitidis. Patients from a concurrent clinical trial that involved an experimental therapeutic intervention, except for a prior zilucoplan trial, were excluded. Participation in observational studies and registry studies was permitted. Patients were excluded if they had commenced any disallowed medication, per the exclusion criteria from the parent zilucoplan study, or received an altered dose of any other concomitant medication, unless medically indicated. In addition, patients with any new or worsening medical conditions (since entry into the parent zilucoplan study) or hypersensitivity to zilucoplan, any of its excipients, or to the placebo were excluded. Patients who discontinued the study drug in the RAISE study for any reason before the week 12 visit were not eligible for the RAISE-XT study.
Interventions
The visit schedule and assessments during the first 12 weeks of the RAISE-XT study were identical to the 12-week, double-blind treatment period of the RAISE parent study. All patients in the RAISE-XT study received daily self-administered SC doses of zilucoplan 0.3 mg/kg, starting at the extension day 1 visit (E1), regardless of treatment received in the parent studies (a small number of patients received zilucoplan 0.1 mg/kg in the phase II MG0009 study). Zilucoplan was administered as described in the RAISE study. During the first 12 weeks of the RAISE-XT study, patients were to return to the clinic at week E1, week E2, week E4, week E8, and week E12 for study assessments.
Concomitant medications that were permitted in the RAISE-XT study were the same as those permitted in the RAISE study (i.e., doses of standard-of-care treatments for gMG that could not be increased during the study but could be decreased, if deemed to be a reasonable course of action by the investigator, and rescue therapy as needed).
Outcomes
The primary outcome of the RAISE-XT study was the incidence of TEAEs, including any TEAEs, serious TEAEs, withdrawal due to TEAEs, AEs leading to death, and TEAEs of interest. AEs were classified for severity according to CTCAE version 5.0 or later. For any AEs for which it was not possible to provide a CTCAE grading, the events were assessed using a standard intensity classification (grade 1 for mild, grade 2 for moderate, and grades 3, 4, and 5 for severe). A TEAE was defined as an AE that started on or after the time of first administration of the study drug and up to and including 40 days after the final dose (or last contact, depending on which occurred first). Secondary efficacy outcomes included change from baseline in the RAISE-XT study to week E12 in the MG-ADL score, the QMG score, the MGC score, and the MG-QoL15r score. Exploratory outcomes in the RAISE-XT study included minimal manifestation status per MGFA-PIS at week E12 without rescue therapy, responder rates for the MG-ADL, QMG, and MGC scores at week E12 without rescue therapy, and the achievement of MSE (an MG-ADL score of 0 or 1) at week E12 without rescue therapy.
Statistical Analysis
The plan was to enrol approximately 200 patients in the RAISE-XT study from the MG0009 and RAISE studies. Assuming patients remained in the study for an average of 2 years, this would provide approximately 400 patient-years for the zilucoplan safety database. The safety evaluation was conducted on the safety set (all patients who received at least 1 dose of the study drug in the RAISE-XT study). AEs were summarized using descriptive statistics (number, percentage of patients, frequency of AEs) by system organ class and preferred term. AEs that started before the date of first administration of the study treatment were not considered TEAEs. For all safety assessments, baseline was the open-label baseline, defined as the last available assessment before first administration of the study drug in the open-label extension periods of the MG0009 study and the RAISE study. For patients coming from the MG0009 study, this was the last available assessment before the first study drug administration in the open-label extension portion of the MG0009 study. For patients coming from the RAISE study, this was the last available assessment before the first study drug administration in the RAISE-XT study. When dates were missing or partially missing, AEs were assumed to be treatment-emergent unless evidence existed indicating otherwise.
TEAEs were tabulated and presented as the number of patients, percentage of patients, and frequency of events. The number and percentage of patients who experienced each TEAE of interest were summarized by treatment group. Change from baseline to week E12 in scores of the MG-ADL, QMG, MGC, and MG-QoL15r were estimated using an MMRM ANCOVA, with continuous items (baseline MG-ADL score, baseline QMG score) and categorical items (geographic region [Europe, Japan, North America], parent study factor, and baseline MG-ADL score by visit [interaction term]) as fixed effects, and the patient as a random effect. Separate models in the MMRM ANCOVA were fitted for week 1 to week 12 (double-blind treatment period) and week E1 to week E12 (open-label treatment period). The MMRM used an unstructured covariance structure for the repeated measures, such that if the model failed to converge, an autoregressive (1) covariance structure was used. Kenward-Roger approximation was used to estimate the degrees of freedom of the denominator. The LS mean for each treatment group were reported for all visits, with corresponding 2-sided 95% CIs, and plots from week 1 to week E12 were overlaid on the same graph. Total score and change from baseline scores in the MG-ADL were summarized by treatment group and overall, and by scheduled visit, using descriptive statistics. No imputation methods were used for missing total scores on the MG-ADL, QMG, MGC, or MG-QoL15r. Data after the receipt of rescue medication were not imputed.
In the RAISE-XT study, the mITT population included all enrolled patients who received at least 1 dose of the study drug and who had at least 1 postdosing MG-ADL score. The safety set included all patients who received at least 1 dose of the study drug.
The interim analyses reported efficacy results through week E12, with assessments up to week E48 (September 2022 data cut-off), week E84 (May 2023 data cut-off), and week E108 (November 2023 data cut-off). A Clinical Study Report was provided for the September 2022 data-cut-off only. Sponsor-submitted information for the overall gMG population for the September 2022 data cut-off was available for baseline patient characteristics, baseline gMG medications, concomitant gMG therapies, and patient exposure; information on patient disposition and treatment exposure in the overall population was also available and was presented using the longest follow-up available (November 2023 data cut-off). Results of efficacy and harms were presented for the longest follow-up available (November 2023 data cut-off) for both the overall population and the refractory subpopulation.
Results
Patient Disposition
Of the 200 patients enrolled in the RAISE-XT study, 93 patients had received zilucoplan 0.3 mg/kg and 90 patients had received placebo in their parent study. At the November 11, 2023, data cut-off, most patients in the intention-to-treat population were ongoing in the zilucoplan 0.3 mg/kg and 0.3 mg/kg group (79%) and in the placebo and zilucoplan 0.3 mg/kg group (64%) (Table 18). The number of patients who had discontinued the study was 20 (22%) in the zilucoplan 0.3 mg/kg and 0.3 mg/kg group and 32 (36%) in the placebo and zilucoplan 0.3 mg/kg group. The primary reasons for discontinuation in the zilucoplan 0.3 mg/kg and 0.3 mg/kg group and the placebo and zilucoplan 0.3 mg/kg group were voluntary withdrawal by the patient (1% and 13%), AEs (2% and 8%), physician decision (2% and 7%), death (4% and 2%), safety reasons (1% and 4%), other reasons (1% and 0%), and missing reason (0% and 1%).
Table 18: Patient Disposition in the RAISE-XT Study (Overall ITT Population, November 2023 Data Cut-Off)
Patient disposition | Zilucoplan 0.3 mg/kg and 0.3 mg/kg N = 93 | Placebo and zilucoplan 0.3 mg/kg N = 90 |
|---|---|---|
Entered RAISE-XT, n (%) | 93 (100.0) | 90 (100.0) |
ITT, n (%) | 93 (100.0) | 90 (100.0) |
mITT, n (%) | 93 (100.0) | 90 (100.0) |
Safety, n (%) | 93 (100.0) | 90 (100.0) |
Completed RAISE-XT week E12, n (%) | 90 (96.8) | 86 (95.6) |
Ongoing, n (%) | 73 (78.5) | 58 (64.4) |
Discontinued, n (%) | 20 (21.5) | 32 (35.6) |
Primary reason for discontinuation, n (%) | ||
Withdrawal by study participant | 7 (7.5) | 12 (13.3) |
Adverse event | 2 (2.2) | 7 (7.8) |
Physician decision | 2 (2.2) | 6 (6.7) |
Death | 4 (4.3) | 2 (2.2) |
Safety reasons, determined by the investigator or sponsor | 1 (1.1) | 4 (4.4) |
Lost to follow-up | 3 (3.2) | 0 |
Other | 1 (1.1) | 0 |
Missing | 0 | 1 (1.1) |
Safety follow-up visit performed, n (%) | 8 (8.6) | 24 (26.7) |
Safety follow-up visit not performed, n (%) | 12 (12.9) | 8 (8.9) |
Reason safety follow-up was not performed, n (%) | ||
Lost to follow-up | 3 (3.2) | 3 (3.3) |
Withdrawal by study participant | 4 (4.3) | 1 (1.1) |
Death | 4 (4.3) | 1 (1.1) |
Other | 1 (1.1) | 1 (1.1) |
Missing | 0 | 2 (2.2) |
E = extension; ITT = intention to treat; mITT = modified intention to treat.
Sources: RAISE-XT Clinical Study Report,45 sponsor’s Summary of Clinical Evidence.27
Baseline Characteristics
Baseline characteristics of the patients in the RAISE-XT study were available for the September 8, 2022, data cut-off (Table 19). In the overall gMG population, patients in the zilucoplan 0.3 mg/kg and 0.3 mg/kg group and the placebo and zilucoplan 0.3 mg/kg group were similar in mean age (53 years and 54 years), proportion of female participants (56% and 53%) and male participants (44% and 47%), and proportion of patients enrolled from North America (57% and 54%).
Table 19: Baseline Characteristics of Patients in the RAISE-XT Study (Overall ITT Population, September 2022 Data Cut-Off)
Characteristic | Zilucoplan 0.3 mg/kg and 0.3 mg/kg N = 93 | Placebo and zilucoplan 0.3 mg/kg N = 90 |
|---|---|---|
Age, years | ||
Mean (SD) | 52.9 (14.5) | 53.7 (15.5) |
Median (range) | 55.0 (21 to 75) | 56.0 (19 to 75) |
Age group, n (%) | ||
19 years to < 65 years | 69 (74.2) | 61 (67.8) |
≥ 65 years | 24 (25.8) | 29 (32.2) |
Sex, n (%) | ||
Female | 52 (55.9) | 48 (53.3) |
Male | 41 (44.1) | 42 (46.7) |
Race, n (%) | ||
Asian | 8 (8.6) | 15 (16.7) |
Black | 8 (8.6) | 7 (7.8) |
White | 72 (77.4) | 65 (72.2) |
Missing | 5 (5.4) | 3 (3.3) |
Ethnicity, n (%) | ||
Hispanic or Latino | 7 (7.5) | 6 (6.7) |
Not Hispanic or Latino | 82 (88.2) | 81 (90.0) |
Missing | 4 (4.3) | 3 (3.3) |
Region, n (%) | ||
East Asia | 7 (7.5) | 9 (10.0) |
Europe | 33 (35.5) | 32 (35.6) |
North America | 53 (57.0) | 49 (54.4) |
Weight, kg, mean (SD) | 93.1 (23.96) | 88.5 (26.25) |
Weight, kg, n (%) | ||
< 56 | 5 (5.4) | 5 (5.6) |
56 to < 77 | 21 (22.6) | 26 (28.9) |
77 to < 150 | 65 (69.9) | 56 (62.2) |
≥ 150 | 2 (2.2) | 3 (3.3) |
Height, cm, mean (SD) | 169.90 (10.54) | 169.91 (10.84) |
BMI, kg/m2, mean (SD) | 32.2 (7.34) | 30.5 (7.87) |
Source study protocol, n (%) | ||
MG0009 | 11 (11.8) | 6 (6.7) |
RAISE | 82 (88.2) | 84 (93.3) |
MGFA disease class at screening, n (%) | ||
II | 25 (26.9) | 29 (32.2) |
III | 60 (64.5) | 57 (63.3) |
IV | 8 (8.6) | 4 (4.4) |
Age at disease onset, years, n | 93 | 90 |
Mean (SD) | 43.43 (17.61) | 44.03 (18.70) |
Duration of disease, years | ||
Mean (SD) | 9.35 (9.36) | 9.25 (10.45) |
Median (range) | 5.70 (0.2 to 42.3) | 4.85 (0.2 to 51.9) |
Symptoms at onset, n (%) | ||
Ocular | 35 (37.6) | 37 (41.1) |
Generalized | 58 (62.4) | 53 (58.9) |
Prior thymectomy, n (%) | 49 (52.7) | 39 (43.3) |
Prior MG crisis, n (%) | 30 (32.3) | 29 (32.2) |
Time since most recent crisis, months, n | 30 | 29 |
Mean (SD) | 75.00 (89.75) | 74.38 (109.88) |
Median (range) | 35.43 (4.2 to 280.3) | 24.80 (4.1 to 472.6) |
Baseline MG-ADL score, mean (SD) | 5.2 (3.9) | 7.7 (4.5) |
≤ 9, n (%) | 76 (81.7) | 59 (65.6) |
≥ 10, n (%) | 17 (18.3) | 31 (34.4) |
Baseline QMG score, mean (SD) | 12.5 (5.6) | 15.6 (6.0) |
≤ 17 n (%) | 75 (80.6) | 61 (67.8) |
≥ 18, n (%) | 18 (19.4) | 29 (32.2) |
BMI = body mass index; ITT = intention to treat; MG = myasthenia gravis; MG-ADL = Myasthenia Gravis Activities of Daily Living; MGFA = Myasthenia Gravis Foundation of America; QMG = Quantitative Myasthenia Gravis; SD = standard deviation.
Sources: RAISE-XT Clinical Study Report,45 sponsor’s Summary of Clinical Evidence.27
Baseline Medications
Baseline medications were defined as any medications that started before the RAISE-XT study and continued thereafter (classified as prior and concomitant medications). A total of 89 patients (97%) in the zilucoplan 0.3 mg/kg and 0.3 mg/kg group and 85 patients (95%) in the placebo and zilucoplan 0.3 mg/kg group were receiving any gMG-specific medication at baseline (Table 20). The most common (≥ 10% of patients overall) gMG medications in the zilucoplan 0.3 mg/kg and 0.3 mg/kg group and the placebo and zilucoplan 0.3 mg/kg group were pyridostigmine (81% and 78%), prednisone (43% and 39%), mycophenolate mofetil (19% and 21%), prednisolone (20% and 18%), and azathioprine (16% and 17%). No patient with gMG received IVIg, SCIg, PLEX, or rituximab at baseline.
Table 20: Baseline gMG-Specific Medications in the RAISE-XT Study (Overall ITT Population, September 2022 Data Cut-Off)
Group, concomitant medication, preferred term | Zilucoplan 0.3 mg/kg and 0.3 mg/kg N = 93 | Placebo and zilucoplan 0.3 mg/kg N = 90 |
|---|---|---|
Any gMG-specific prior medication, n (%) | 89 (95.7) | 85 (94.4) |
Group A, n (%) | 60 (64.5) | 53 (58.9) |
Prednisone for gMG | 40 (43.0) | 35 (38.9) |
Other corticosteroids for gMG | 20 (21.5) | 18 (20.0) |
Prednisolone | 19 (20.4) | 16 (17.8) |
Methylprednisolone | 1 (1.1) | 2 (2.2) |
Group B, n (%) | 33 (35.5) | 34 (37.8) |
Azathioprine | 15 (16.1) | 15 (16.7) |
Mycophenolate | 18 (19.4) | 19 (21.1) |
Group C, n (%) | 0 | 0 |
IVIg | 0 | 0 |
SCIg | 0 | 0 |
Group D, n (%) | 0 | 0 |
IVIg, SCIg, or plasma exchange | 0 | 0 |
Group E, n (%) | 11 (11.8) | 16 (17.8) |
Cyclosporine | 6 (6.5) | 7 (7.8) |
Methotrexate | 2 (2.2) | 1 (1.1) |
Tacrolimus | 3 (3.2) | 8 (8.9) |
Group E and B (immunosuppressants) , n (%) | 44 (47.3) | 48 (53.3) |
Group F, n (%) | 79 (84.9) | 73 (81.1) |
Cholinesterase inhibitors | 79 (84.9) | 73 (81.1) |
Pyridostigmine | 75 (80.6) | 70 (77.8) |
Ambenonium | 4 (4.3) | 3 (3.3) |
gMG = generalized myasthenia gravis; Ig = immunoglobulin; ITT = intention to treat; SC = subcutaneous.
Note: Baseline medications include any medications that started before the study drug in the MG0011 study and continued after (classified as prior and concomitant medications).
Source: RAISE-XT Clinical Study Report.45
Concomitant Medications and Cointerventions
As of the September 2022 data cut-off date, 90 patients (97%) in the zilucoplan 0.3 mg/kg and 0.3 mg/kg group and 86 patients (96%) in the placebo and zilucoplan 0.3 mg/kg group received any concomitant gMG therapy (Table 21). The most common (≥ 10% of patients overall) concomitant gMG therapies in the zilucoplan 0.3 mg/kg and 0.3 mg/kg group and the placebo and zilucoplan 0.3 mg/kg group were pyridostigmine (83% and 82%), prednisone (46% and 40%), prednisolone (22% and 20%), mycophenolate mofetil (19% and 21%), and azathioprine (16% and 17%). The use of concomitant gMG therapies was generally balanced between the treatment groups. Overall, the rate of patients receiving concomitant-only gMG therapies (i.e., medication that had started after the first administration of study drug and continued during the treatment period) was lower than that of patients receiving concomitant gMG therapies (i.e., medication that had been taken at least once after the first administration of the study drug during the treatment period) (Table 21). The most common (≥ 10% of patients overall) concomitant-only gMG therapies in the zilucoplan 0.3 mg/kg and 0.3 mg/kg group and the placebo and zilucoplan 0.3 mg/kg group were prednisone (23% and 22%), pyridostigmine (16% and 13%), and prednisolone (12% and 10%). The use of concomitant-only gMG therapies was generally balanced between the treatment groups.
Table 21: Concomitant gMG Therapies in the RAISE-XT Study (Overall ITT Population, September 2022 Data Cut-Off)
Group, concomitant medication, preferred term | Zilucoplan 0.3 mg/kg and 0.3 mg/kg N = 93 | Placebo and zilucoplan 0.3 mg/kg N = 90 |
|---|---|---|
Concomitant gMG therapy, n (%) | ||
Any concomitant medication | 90 (96.8) | 86 (95.6) |
Immunosuppressants | 43 (46.2) | 48 (53.3) |
Mycophenolate mofetil | 18 (19.4) | 19 (21.1) |
Azathioprine | 15 (16.1) | 15 (16.7) |
Ciclosporin | 5 (5.4) | 7 (7.8) |
Tacrolimus | 4 (4.3) | 8 (8.9) |
Methotrexate | 2 (2.2) | 1 (1.1) |
Mycophenolic acid | 1 (1.1) | 0 |
Nervous system | 81 (87.1) | 74 (82.2) |
Cannabis sativa | 0 | 1 (1.1) |
Parasympathomimetics | 81 (87.1) | 74 (82.2) |
Pyridostigmine | 77 (82.8) | 71 (78.9) |
Ambenonium | 4 (4.3) | 3 (3.3) |
Corticosteroids for systemic use, plain | 64 (68.8) | 56 (62.2) |
Prednisone | 43 (46.2) | 36 (40.0) |
Prednisolone | 20 (21.5) | 18 (20.0) |
Methylprednisolone | 1 (1.1) | 3 (3.3) |
Hydrocortisone | 0 | 0 |
Various | 0 | 1 (1.1) |
Efgartigimod alfa | 0 | 1 (1.1) |
Concomitant-only gMG therapy,a n (%) | ||
Any concomitant-only medication | 42 (45.2) | 42 (46.7) |
Immunosuppressants | 10 (10.8) | 15 (16.7) |
Mycophenolate mofetil | 3 (3.2) | 4 (4.4) |
Azathioprine | 5 (5.4) | 4 (4.4) |
Ciclosporin | 1 (1.1) | 4 (4.4) |
Tacrolimus | 1 (1.1) | 3 (3.3) |
Mycophenolic acid | 1 (1.1) | 0 |
Nervous system | 15 (16.1) | 13 (14.4) |
Cannabis sativa | 0 | 1 (1.1) |
Parasympathomimetics | 15 (16.1) | 13 (14.4) |
Pyridostigmine | 15 (16.1) | 12 (13.3) |
Ambenonium | 0 | 1 (1.1) |
Corticosteroids for systemic use, plain | 32 (34.0) | 29 (32.2) |
Prednisone | 21 (22.6) | 19 (21.1) |
Prednisolone | 11 (11.8) | 9 (10.0) |
Methylprednisolone | 0 | 1 (1.1) |
Various | 0 | 1 (1.1) |
Efgartigimod alfa | 0 | 1 (1.1) |
gMG = generalized myasthenia gravis; ITT = intention to treat.
aConcomitant-only gMG therapies were defined as any medication that started after the first administration of the study drug and continued during the treatment period.
Sources: RAISE-XT Clinical Study Report,45 sponsor’s Summary of Clinical Evidence.27
Exposure to Study Treatments
At the clinical data cut-off date of November 11, 2023, the mean duration of study drug was 892 days (SD = 428 days) in the zilucoplan 0.3 mg/kg and 0.3 mg/kg group and 743 days (SD = 428 days) in the placebo and zilucoplan 0.3 mg/kg group (Table 22). The mean duration of exposure to treatment was 2.5 years (SD = 1.2 years) in the zilucoplan 0.3 mg/kg and 0.3 mg/kg group and 2.1 years (SD = 1.1 years) in the placebo and zilucoplan 0.3 mg/kg group. The number of patients who missed at least 1 dose of the study drug was 34 patients in the zilucoplan 0.3 mg/kg and 0.3 mg/kg group and 37 patients in the placebo and zilucoplan 0.3 mg/kg group. The mean number of missed doses was 12.2 (SD = 18.6) in the zilucoplan 0.3 mg/kg and 0.3 mg/kg group and 10.0 (SD = 13.2) in the placebo and zilucoplan 0.3 mg/kg group.
Table 22: Patient Exposure in the RAISE-XT Study (Overall Population, Safety Set, November 2023 Data Cut-Off)
Exposure | Zilucoplan 0.3 mg/kg and 0.3 mg/kg N = 93 | Placebo and zilucoplan 0.3 mg/kg N = 90 |
|---|---|---|
Total, patient-years | 190.7 | 155.7 |
Study drug duration, days, mean (SD) | 892.1 (427.6) | 742.8 (428.4) |
Study drug duration, days, median (range) | 812.0 (7 to 2,044) | 701.5 (14 to 1,960) |
Exposure duration, days, mean (SD) | 899.8 (422.4) | 757.3 (418.9) |
Exposure duration, days, median (range) | 813.0 (39 to 2,045) | 702.5 (50 to 1,960) |
Duration of exposure, years, mean (SD) | 2.5 (1.2) | 2.1 (1.1) |
Duration of exposure, years, median (range) | 2.2 (0.11 to 5.6) | 1.9 (0.14 to 5.37) |
Cumulative study drug duration, n (%) | ||
Any exposure | 93 (100.0) | 90 (100.0) |
≥ E1 day | 93 (100.0) | 90 (100.0) |
≥ E30 days | 93 (100.0) | 90 (100.0) |
≥ E60 days | 90 (96.8) | 89 (98.9) |
≥ E90 days | 90 (96.8) | 86 (95.6) |
≥ E182 days | 87 (93.5) | 78 (86.7) |
≥ E365 days | 85 (91.4) | 74 (82.2) |
≥ E547 days | 82 (88.2) | 67 (74.4) |
≥ E730 days | 57 (61.3) | 41 (45.6) |
≥ E1095 days | 22 (23.7) | 13 (14.4) |
Number of missed doses | ||
n | 34 | 37 |
Mean (SD) | 12.2 (18.6) | 10.0 (13.2) |
Median (range) | 6.0 (1 to 99) | 3.0 (1 to 60) |
E = extension; SD = standard deviation.
Sources: RAISE-XT Clinical Study Report,45 sponsor’s Summary of Clinical Evidence.27
Efficacy
Secondary End Points
Secondary efficacy end points in the RAISE-XT study at the data cut-off date of November 11, 2023, included change from parent-study baseline to week E12 in the MG-ADL, QMG, MGC, and MG-QoL15r scores (Table 23); results at 84 weeks in the RAISE-XT study are presented in Table 33 in Appendix 1.
Change From Parent-Study Baseline to Week E12 in the MG-ADL Score
In the overall population, the LS mean change from parent-study baseline to week E12 in the MG-ADL score was –5.90 (SE = 0.47) in the zilucoplan 0.3 mg/kg and 0.3 mg/kg group and –6.17 (SE = 0.59) in the placebo and zilucoplan 0.3 mg/kg group. In the refractory subpopulation, the mean change from parent-study baseline to week E12 in the MG-ADL score was –6.61 (SE = 0.63) in the zilucoplan 0.3 mg/kg and 0.3 mg/kg group and –6.24 (SE = 0.71) in the placebo and zilucoplan 0.3 mg/kg group.
Change From Parent-Study Baseline to Week E12 in the QMG Score
In the overall population, the LS mean change from parent-study baseline to week E12 in the QMG score was –8.78 (SE = 0.66) in the zilucoplan 0.3 mg/kg and 0.3 mg/kg group and –8.53 (SE = 0.79) in the placebo and zilucoplan 0.3 mg/kg group. In the refractory subpopulation, the mean change from parent-study baseline to week E12 in the QMG score was –8.18 (SE = 0.71) in the zilucoplan 0.3 mg/kg and 0.3 mg/kg group and –8.34 (SE = 1.09) in the placebo and zilucoplan 0.3 mg/kg group.
Change From Parent-Study Baseline to Week E12 in the MGC Score
In the overall population, the LS mean change from parent-study baseline to week E12 in the MGC score was –11.77 (SE = 0.86) in the zilucoplan 0.3 mg/kg and 0.3 mg/kg group and –12.30 (SE = 1.12) in the placebo and zilucoplan 0.3 mg/kg group. In the refractory subpopulation, the mean change from parent-study baseline to week E12 in the MGC score was –11.83 (SE = 1.17) in the zilucoplan 0.3 mg/kg and 0.3 mg/kg group and –13.34 (SE = 1.35) in the placebo and zilucoplan 0.3 mg/kg group.
Change From Parent-Study Baseline to Week E12 in the MG-QoL15r Score
In the overall population, the LS mean change from parent-study baseline to week E12 in the MG-QoL15r score was –9.92 (SE = 0.95) in the zilucoplan 0.3 mg/kg and 0.3 mg/kg group and –8.07 (SE = 1.08) in the placebo and zilucoplan 0.3 mg/kg group. In the refractory subpopulation, the mean change from parent-study baseline to week E12 in the MG-QoL15r score was –9.46 (SE = 1.15) in the zilucoplan 0.3 mg/kg and 0.3 mg/kg group and –9.34 (SE = 1.32) in the placebo and zilucoplan 0.3 mg/kg group.
Exploratory End Points
Exploratory end points in the RAISE-XT study at the data cut-off date of November 11, 2023, included the achievement of MSE at week E12 without rescue therapy, the MG-ADL responder rate at week E12 without rescue therapy, the QMG responder rate at week E12 without rescue therapy, and the minimal manifestation status per MGFA-PIS at week E12 without rescue therapy (Table 23).
Achievement of MSE at Week E12 Without Rescue Therapy
In the overall population, the number of patients who achieved MSE (an MG-ADL score of 0 or 1) at week E12 without rescue therapy was 18 (19.4%) in the zilucoplan 0.3 mg/kg and 0.3 mg/kg group and 7 (7.8%) in the placebo and zilucoplan 0.3 mg/kg group. In the refractory subpopulation, the number of patients who achieved MSE at week E12 without rescue therapy was 8 of 43 (18.6%) in the zilucoplan 0.3 mg/kg and 0.3 mg/kg group and 1 of 42 (2.4%) in the placebo and zilucoplan 0.3 mg/kg group.
MG-ADL Responder Rate at Week E12 Without Rescue Therapy
In the overall population, the number of patients who were MG-ADL responders at week E12 without rescue therapy was 71 of 84 (84.5%) in the zilucoplan 0.3 mg/kg and 0.3 mg/kg group and 68 of 83 (81.9%) in the placebo and zilucoplan 0.3 mg/kg group. In the refractory subpopulation, the number of patients who were MG-ADL responders at week E12 without rescue therapy was 34 of 39 (87.2%) in the zilucoplan 0.3 mg/kg and 0.3 mg/kg group and 27 of 36 (75.0%) in the placebo and zilucoplan 0.3 mg/kg group.
QMG Responder Rate at Week E12 Without Rescue Therapy
In the overall population, the number of patients who were QMG responders at week E12 without rescue therapy was 66 of 82 (80.5%) in the zilucoplan 0.3 mg/kg and 0.3 mg/kg group and 59 of 82 (72.0%) in the placebo and zilucoplan 0.3 mg/kg group. In the refractory subpopulation, the number of patients who were QMG responders at week E12 without rescue therapy was 28 of 38 (73.7%) in the zilucoplan 0.3 mg/kg and 0.3 mg/kg group and 25 of 36 (69.4%) in the placebo and zilucoplan 0.3 mg/kg group.
Minimal Manifestation Status per MGFA-PIS at Week E12 Without Rescue Therapy
In the overall population, the number of patients who achieved minimal manifestation status per MGFA-PIS at week E12 without rescue therapy was 29 of 77 (37.7%) in the zilucoplan 0.3 mg/kg and 0.3 mg/kg group and 29 of 78 (37.2%) in the placebo and zilucoplan 0.3 mg/kg group. In the refractory subpopulation, the number of patients who achieved minimal manifestation status per MGFA-PIS at week E12 without rescue therapy was not reported.
Table 23: Key Efficacy Results in the RAISE-XT Study (Overall mITT Population and Refractory Subpopulation, November 2023 Data Cut-Off)
Outcome measure | Overall population | Refractory subpopulation | ||
|---|---|---|---|---|
Zilucoplan 0.3 mg/kg and 0.3 mg/kg N = 93 | Placebo and zilucoplan 0.3 mg/kg N = 90 | Zilucoplan 0.3 mg/kg and 0.3 mg/kg N = 43 | Placebo and 0.3 mg/kg N = 42 | |
Change from parent-study baseline in the MG-ADL score | ||||
Week 12, n | 93 | 90 | 43 | 42 |
Week 12, mean (SE) | –4.72 (0.40) | –2.93 (0.38) | –4.98 (0.62) | –2.26 (0.52) |
Week 12, LS, mean (SE) | –4.59 (0.53) | –2.20 (0.68) | NR | NR |
95% CI | –5.62 to –3.56 | –3.53 to –0.87 | NR | NR |
Week E12, n | 89 | 86 | 41 | 38 |
Week E12, mean (SE) | –6.25 (0.39) | –6.26 (0.43) | –6.61 (0.63) | –6.24 (0.71) |
Week E12, LS, mean (SE) | –5.90 (0.47) | –6.17 (0.59) | NR | NR |
95% CI | –6.82 to –4.98 | –7.32 to –5.02 | NR | NR |
Change from parent-study baseline in the QMG score | ||||
Week 12, n | 92 | 89 | 42 | 41 |
Week 12, mean (SE) | –6.39 (0.53) | –3.51 (0.44) | –6.00 (0.80) | –3.12 (0.69) |
Week 12, LS, mean (SE) | –6.56 (0.73) | –2.94 (0.90) | NR | NR |
95% CI | –8.00 to –5.12 | –4.71 to –1.17 | NR | NR |
Week E12, n | 87 | 85 | 40 | 38 |
Week E12, mean (SE) | –8.47 (0.47) | –7.72 (0.63) | –8.18 (0.71) | –8.34 (1.09) |
Week E12, LS, mean (SE) | –8.78 (0.66) | –8.53 (0.79) | NR | NR |
95% CI | –10.08 to –7.48 | –10.08 to –6.98 | NR | NR |
Change from parent-study baseline in the MGC score | ||||
Week 12, n | 92 | 89 | 42 | 41 |
Week 12, mean (SE) | –9.14 (0.67) | –6.82 (0.69) | –8.36 (1.01) | –5.34 (1.02) |
Week 12, LS, mean (SE) | –9.33 (0.95) | –6.97 (1.27) | NR | NR |
95% CI | –11.20 to –7.46 | –9.47 to –4.47 | NR | NR |
Week E12, n | 87 | 85 | 40 | 38 |
Week E12, mean (SE) | –12.29 (0.74) | –13.00 (0.86) | –11.83 (1.17) | –13.34 (1.35) |
Week E12, LS, mean (SE) | –11.77 (0.86) | –12.30 (1.12) | NR | NR |
95% CI | –13.46 to –10.09 | –14.50 to –10.09 | NR | NR |
Change from parent-study baseline in the MG-QoL15r score | ||||
Week 12, n | 91 | 88 | 42 | 40 |
Week 12, mean (SE) | –6.21 (0.76) | –3.88 (0.68) | –5.90 (0.99) | –3.18 (0.95) |
Week 12, LS, mean (SE) | –6.15 (1.05) | –2.71 (1.22) | NR | NR |
95% CI | –8.21 to −4.08 | –5.11 to –0.31 | NR | NR |
Week E12, n | 85 | 85 | 39 | 38 |
Week E12, mean (SE) | –9.47 (0.80) | –8.64 (0.81) | –9.46 (1.15) | –9.34 (1.32) |
Week E12, LS, mean (SE) | –9.92 (0.95) | –8.07 (1.08) | NR | NR |
95% CI | –11.79 to –8.04 | –10.20 to –5.94 | NR | NR |
Achievement of MSE (MG-ADL score of 0 or 1) without rescue therapy | ||||
Week 12, n | 93 | 90 | 43 | 42 |
Week 12, MSE,a n (%) | 18 (19.4) | 7 (7.8) | 8 (18.6) | 1 (2.4) |
Week E12, n | 84 | 83 | 39 | 36 |
Week E12, MSE,a n (%) | 26 (31.0) | 27 (32.5) | 11 (28.2) | 11 (30.6) |
MG-ADL respondera rate without rescue therapy | ||||
Week 12, n | 93 | 90 | 43 | 42 |
Week 12, MG-ADL responder, n (%) | 69 (74.2) | 47 (52.2) | 34 (79.1) | 20 (47.6) |
Week E12, n | 84 | 83 | 39 | 36 |
Week E12, MG-ADL responder, n (%) | 71 (84.5) | 68 (81.9) | 34 (87.2) | 27 (75.0) |
QMG responderb rate without rescue therapy | ||||
Week 12, n | 92 | 89 | 42 | 41 |
Week 12, QMG responder, n (%) | 55 (59.8) | 33 (37.1) | 24 (57.1) | 12 (29.3) |
Week E12, n | 82 | 82 | 38 | 36 |
Week E12, QMG responder, n (%) | 66 (80.5) | 59 (72.0) | 28 (73.7) | 25 (69.4) |
Achievement of minimal manifestation status per MGFA-PIS without rescue therapy | ||||
Week E12, n | 77 | 78 | NR | NR |
Week E12, number of patients achieving minimal manifestation status per MGFA-PIS, n (%) | 29 (37.7) | 29 (37.2) | NR | NR |
CI = confidence interval; E = extension; LS = least squares; MG-ADL = Myasthenia Gravis Activities of Daily Living; MGC = Myasthenia Gravis Composite; MGFA-PIS = Myasthenia Gravis Foundation of America Post-Intervention Status; MG-QoL15r = Myasthenia Gravis Quality of Life 15-item – Revised; mITT = modified intention to treat; MSE = minimal symptom expression; NR = not reported; QMG = Quantitative Myasthenia Gravis; SE = standard error.
aA MG-ADL responder is defined as having at least a 3-point improvement (decrease) in the MG-ADL score.
bA QMG responder is defined as having at least a 5-point improvement (decrease) in the QMG score. This end point was not adjusted for multiple testing, so there is a potential for the type I error to be increased, and the findings should be considered supportive.
Sources: RAISE-XT Clinical Study Report,45 sponsor’s Summary of Clinical Evidence.27
Harms
The primary end point of the RAISE-XT study was the incidence of TEAEs. The duration of follow-up for harms was from baseline to week 12 of the RAISE-XT study, with a safety follow-up visit 40 days after the last dose of the study drug. Harms data in the RAISE-XT study for the data cut-off of November 11, 2023, is summarized in Table 24.
Adverse Events
The number of patients in the overall population who experienced at least 1 TEAE was 89 of 93 patients (95.7%) in the zilucoplan 0.3 mg/kg and 0.3 mg/kg group and 88 of 90 (97.8%) in the placebo and zilucoplan 0.3 mg/kg group. The most common TEAEs occurring in 10% of patients or greater in either the zilucoplan 0.3 mg/kg and 0.3 mg/kg group or the placebo and zilucoplan 0.3 mg/kg group were MG (29% and 29%), COVID-19 (39% and 31%), headache (19% and 22%), nasopharyngitis (23% and 17%), arthralgia (20% and 13%), diarrhea (19% and 13%), fatigue (18% and 13%), nausea (15% and 17%), upper respiratory tract infection (14% and 18%), urinary tract infection (16% and 14%), pain in extremity (16% and 10%), cough (12% and 12%), fall (11% and 10%), back pain (11% and 10%), rash (10% and 10%), vomiting (11% and 6%), injection-site bruising (4% and 11%), and oropharyngeal pain (1% and 10%).
The number of patients in the refractory subpopulation who experienced at least 1 TEAE was 82 of 85 patients (96.5%) in the zilucoplan 0.3 mg/kg group (the zilucoplan 0.3 mg/kg and 0.3 mg/kg group and the placebo and zilucoplan 0.3 mg/kg group combined). The most common TEAEs occurring in 10% of patients or greater in the refractory subpopulation in either the zilucoplan 0.3 mg/kg and 0.3 mg/kg group or the placebo and zilucoplan 0.3 mg/kg group were MG (42% and 38%), COVID-19 (44% and 24%), headache (21% and 21%), arthralgia (26% and 10%), nasopharyngitis (16% and 19%), urinary tract infection (19% and 14%), upper respiratory tract infection (19% and 12%), diarrhea (16% and 12%), nausea (12% and 17%), fall (14% and 12%), back pain (14% and 12%), and pain in extremity (16% and 10%).
Serious Adverse Events
The number of patients in the overall population who experienced at least 1 serious TEAE was 41 (44.1%) in the zilucoplan 0.3 mg/kg and 0.3 mg/kg group and 33 (36.7%) in the placebo and zilucoplan 0.3 mg/kg group. Serious TEAEs occurring in 2% of patients or greater in either the zilucoplan 0.3 mg/kg and 0.3 mg/kg group or the placebo and zilucoplan 0.3 mg/kg group were MG (9.7% and 11.1%), COVID-19 pneumonia (4.3% and 1.1%), myocardial infarction (4.3% and 0.0%), pneumonia (3.2% and 1.1%), cholecystitis (2.2% and 1.1%), Staphylococcus bacteremia (2.2% and 0.0%), atrial fibrillation (2.2% and 0.0%), cardiac arrest (2.2% and 0.0%), cellulitis (2.2% and 2.2%), and large intestine polyp (0.0% and 2.2%). The number of patients in the refractory subpopulation who experienced at least 1 serious TEAE was 20 of 43 (46.5%) in the zilucoplan 0.3 mg/kg and 0.3 mg/kg group and 15 of 42 (35.7%) in the placebo and zilucoplan 0.3 mg/kg group.
Withdrawal Due to Adverse Events
TEAEs resulting in permanent withdrawal from the study drug in the overall population were reported in 21 patients (11.4%), 9 (9.7%) in the zilucoplan 0.3 mg/kg and 0.3 mg/kg group and 12 (13.3%) in the placebo and zilucoplan 0.3 mg/kg group. The most common TEAE resulting in permanent withdrawal from the study drug was MG (6 patients [3.3%]). The number of patients in the refractory subpopulation who experienced at least 1 serious TEAE was 11 of 85 (12.9%), 2 of 43 (4.7%) in the zilucoplan 0.3 mg/kg and 0.3 mg/kg group and 9 of 42 (21.4%) in the placebo and zilucoplan 0.3 mg/kg group.
Deaths
A total of 6 patients died in the RAISE-XT study. The number of patients who experienced a TEAE leading to death was 3 (3.2%) in the zilucoplan 0.3 mg/kg and 0.3 mg/kg group and 1 (1.1%) in the placebo and zilucoplan 0.3 mg/kg group. In the zilucoplan 0.3 mg/kg and 0.3 mg/kg group, the TEAEs leading to death were cardiac arrest (2 patients [2.2%]) and head injury (1 patient [1.1%]). In the placebo and zilucoplan 0.3 mg/kg group, the TEAE leading to death was death (1 patient [1.1%]). All 4 TEAEs leading to death resulted in permanent withdrawal from the study drug. Two patients in the refractory subpopulation died during the study; 1 patient in the zilucoplan 0.3 mg/kg and 0.3 mg/kg group had a TEAE of death. No details were reported for the deaths in the refractory subpopulation.
AEs of Special Interest
The number of patients who experienced any infections was 67 (72.0%) in the zilucoplan 0.3 mg/kg and 0.3 mg/kg group and 65 (72.2%) in the placebo and zilucoplan 0.3 mg/kg group. Of these, the number of patients who experienced serious infections was 16 (17.2%) in the zilucoplan 0.3 mg/kg and 0.3 mg/kg group and 11 (12.2%) in the placebo and zilucoplan 0.3 mg/kg group. The number of patients in the refractory subpopulation who experienced any infections was 34 of 43 (79.1%) in the zilucoplan 0.3 mg/kg and 0.3 mg/kg group and 33 of 42 (78.6%) in the placebo and zilucoplan 0.3 mg/kg group.
Table 24: Summary of Harms Results in the RAISE-XT Study (Overall Population and Refractory Subpopulation, Safety Set, November 2023 Data Cut-Off)
Adverse events | Overall population | Refractory subpopulation | ||
|---|---|---|---|---|
Zilucoplan 0.3 mg/kg and 0.3 mg/kg N = 93 | Placebo and zilucoplan 0.3 mg/kg N = 90 | Zilucoplan 0.3 mg/kg and 0.3 mg/kg N = 43 | Placebo and zilucoplan 0.3 mg/kg N = 42 | |
Data cut-off date | November 11, 2023 | |||
Most common AEs, n (%) | ||||
Patients with ≥ 1 TEAE | 89 (95.7) | 88 (97.8) | 42 (97.7) | 40 (95.2) |
TEAEs in ≥ 10% of patients in any group, n (%) | ||||
Myasthenia gravis | 27 (29.0) | 26 (28.9) | 18 (41.9) | 16 (38.1) |
COVID-19 | 36 (38.7) | 28 (31.1) | 19 (44.2) | 10 (23.8) |
Headache | 18 (19.4) | 20 (22.2) | 9 (20.9) | 9 (21.4) |
Nasopharyngitis | 21 (22.6) | 15 (16.7) | 7 (16.3) | 8 (19.0) |
Arthralgia | 19 (20.4) | 12 (13.3) | 11 (25.6) | 4 (9.5) |
Diarrhea | 18 (19.4) | 12 (13.3) | 7 (16.3) | 5 (11.9) |
Fatigue | 17 (18.3) | 12 (13.3) | 5 (11.6) | 3 (7.1) |
Nausea | 14 (15.1) | 15 (16.7) | 5 (11.6) | 7 (16.7) |
Upper respiratory tract infection | 13 (14.0) | 16 (17.8) | 8 (18.6) | 5 (11.9) |
Urinary tract infection | 15 (16.1) | 13 (14.4) | 8 (18.6) | 6 (14.3) |
Pain in extremity | 15 (16.1) | 9 (10.0) | 7 (16.3) | 4 (9.5) |
Cough | 11 (11.8) | 11 (12.2) | < 10% | < 10% |
Fall | 10 (10.8) | 9 (10.0) | 6 (14.0) | 5 (11.9) |
Back pain | 10 (10.8) | 9 (10.0) | 6 (14.0) | 5 (11.9) |
Rash | 9 (9.7) | 9 (10.0) | < 10% | < 10% |
Vomiting | 10 (10.8) | 5 (5.6) | 4 (9.3) | 4 (9.5) |
Injection-site bruising | 4 (4.3) | 10 (11.1) | < 10% | < 10% |
Oropharyngeal pain | 1 (1.1) | 9 (10.0) | 0 | 5 (11.9) |
Contusion | < 10% | < 10% | 6 (14.0) | 1 (2.4) |
Pyrexia | < 10% | < 10% | < 10% | < 10% |
Increased amylase | < 10% | < 10% | < 10% | < 10% |
Increased lipase | < 10% | < 10% | < 10% | < 10% |
Depression | < 10% | < 10% | < 10% | < 10% |
Injection-site pain | < 10% | < 10% | < 10% | < 10% |
Muscle spasms | < 10% | < 10% | < 10% | < 10% |
SAEs, n (%) | ||||
Patients with ≥ 1 SAE | 41 (44.1) | 33 (36.7) | 20 (46.5) | 15 (35.7) |
SAEs in ≥ 2% of patients in any group, n (%) | ||||
Myasthenia gravis | 9 (9.7) | 10 (11.1) | NR | NR |
COVID-19 | < 2% | < 2% | NR | NR |
COVID-19 pneumonia | 4 (4.3) | 1 (1.1) | NR | NR |
Myocardial infarction | 4 (4.3) | 0 | NR | NR |
Pneumonia | 3 (3.2) | 1 (1.1) | NR | NR |
Cholecystitis | 2 (2.2) | 1 (1.1) | NR | NR |
Staphylococcal bacteremia | 2 (2.2) | 0 | NR | NR |
Atrial fibrillation | 2 (2.2) | 0 | NR | NR |
Cardiac arrest | 2 (2.2) | 0 | NR | NR |
Cellulitis | 2 (2.2) | 2 (2.2) | NR | NR |
Large intestine polyp | 0 | 2 (2.2) | NR | NR |
Patients who stopped treatment due to AEs, n (%) | ||||
Patients who stopped study treatment | 9 (9.7) | 12 (13.3) | 2 (4.7) | 9 (21.4) |
Myasthenia gravis | 2 (2.2) | 4 (4.4) | NR | NR |
Cardiac arrest | 2 (2.2) | 0 | NR | NR |
Death | 0 | 1 (1.1) | NR | NR |
Deaths, n (%) | ||||
Patients who died | 4 (NR) | 2 (NR) | 1 (NR) | 1 (NR) |
AEs leading to death | 3 (3.2) | 1 (1.1) | 1 (2.3) | 0 |
Cardiac arrest | 2 (2.2) | 0 | NR | NR |
Head injury | 1 (1.1) | 0 | NR | NR |
Death | 0 | 1 (1.1) | NR | NR |
AEs of special interest, n (%) | ||||
Infections | 67 (72.0) | 65 (72.2) | 34 (79.1) | 33 (78.6) |
Nonserious | 51 (54.8) | 54 (60.0) | NR | NR |
Serious | 16 (17.2) | 11 (12.2) | NR | NR |
AE = adverse event; NR = not reported; SAE = serious adverse event; TEAE = treatment-emergent adverse event.
Sources: RAISE-XT Clinical Study Report,45 sponsor’s Summary of Clinical Evidence.27
Critical Appraisal
Internal Validity
The RAISE-XT study was an open-label, noncomparative extension of the RAISE parent study. The key limitation related to the absence of a comparator group is that patients were not randomized to treatment groups (although patients in the parent study were randomized to zilucoplan or placebo, all patients in the extension study received zilucoplan), precluding the inferences that any observed differences were due to treatments received. Importantly, treatment efficacy and harms for patients with longer follow-up should be interpreted cautiously, as it cannot be determined if the findings are due to the natural history of the disease, study treatments (including concomitant therapies), or other unknown factors.
The number of patients with missing data for the secondary end point of change from parent-study baseline to week E12 of the RAISE-XT study was similar in the zilucoplan 0.3 mg/kg and 0.3 mg/kg group and the placebo group and, overall, scores on the MG-ADL (4%), the QMG (6%), the MGC (6%), and the MG-QoL15r (7%) were low, despite a lack of imputation. The proportions of patients with missing data for change from parent-study baseline to week E12 in the refractory subpopulation were similar in the 2 treatment groups for MG-ADL score (7%), QMG score (8%), MGC score (8%), and MG-QoL15r score (9%). In the overall population, a greater proportion of patients in the zilucoplan 0.3 mg/kg and 0.3 mg/kg group compared to the placebo group had missing data for the exploratory end points of the RAISE-XT study, including the achievement of MSE (9%), the MG-ADL responder rate (9%), the QMG responder rate (10%), and the achievement of minimal manifestation status per MGFA-PIS (15%). At week E84, there were more missing data compared to earlier follow-up time points in both the overall population and the refractory subpopulation (ranging from approximately 22% to 28% of patients for the MG-ADL, QMG, MGC, and MG-QoL 15r outcomes, and from about 28% to 38% of patients for MSE and for MG-ADL and QMG responder rates; refer to Table 33 in Appendix 1); whereas the proportions of patients with missing data was similar in the 2 treatment groups. Missing data may increase concerns related to the interpretation of findings that may not be generalizable to the full population.
External Validity
The clinical expert consulted for the review expect that zilucoplan will be used as long as the patient is responding to treatment and any AEs are manageable, so it would be reasonable for patients to continue treatment for at least the 12 weeks that was evaluated in the RAISE-XT study. No concerns were raised by the expert about the AEs observed with longer treatment with zilucoplan.
Indirect Evidence
Contents within this section have been informed by materials submitted by the sponsor. The following has been summarized and validated by the CDA-AMC review team.
Objectives for the Summary of Indirect Evidence
The pivotal trial for zilucoplan was placebo-controlled; thus, there is a gap in the evidence regarding the efficacy and safety of zilucoplan relative to the comparators that are used to treat adult patients with gMG in Canada. To address this gap in the evidence, the sponsor submitted an NMA, which was used to inform the pharmacoeconomic model.15
Description of Indirect Comparison
The sponsor submitted an indirect comparison that evaluated the short-term efficacy of zilucoplan relative to other treatments used for the management of anti-AChR antibody–positive gMG, in both the overall population with gMG and patients with refractory gMG.15 The indirect comparison was based on a systematic literature review and used Bayesian NMA methods to estimate comparative efficacy for the proportion of patients who met the MG-ADL response criteria at the end of the primary studies and the change from baseline for the MG-ADL score at 12 weeks (± 2 weeks). The treatments included in the NMAs were zilucoplan, eculizumab, efgartigimod alfa, IVIg, PLEX, rituximab, ravulizumab, and rozanolixizumab. The Canadian Drug Expert Committee recommended that ravulizumab not be reimbursed, and it is not funded by any public drug plans. Rozanolixizumab has not been approved for use in Canada. Efgartigimod alfa and eculizumab received CADTH final positive recommendations but are currently not publicly funded.
ITC Design
Objectives
The objective of the NMA was to evaluate the relative effectiveness of zilucoplan compared to eculizumab, efgartigimod alfa, IVIg, PLEX, rituximab, ravulizumab, and rozanolixizumab for the management of patients with anti-AChR antibody–positive gMG, as well as those with refractory gMG.
Study Selection Methods
The NMA was based on a systematic literature review that had broad patient, intervention, comparison, and outcome (PICO) criteria. The review included any English-language randomized or nonrandomized studies in adults with MG as a primary disease who were treated with any pharmacological, nonpharmacological, or surgical interventions, or placebo. Outcomes of interest were treatment response, MG-ADL score, QMG score, MGC score, MG-QoL15 score, AEs, SAES, and study withdrawals. A literature search of multiple databases was conducted on May 1, 2023, with no date limits (Table 25). A limited search of conference proceedings and a bibliographic search of systematic reviews and clinical trials registries were also completed. The studies were screened, extracted, and assessed for methodologic quality, independently in duplicate, using the methods described in Table 25.
The sponsor’s systematic review report states that RCTs were prioritized in the screening process and were scrutinized to identify studies that enrolled a gMG population that was comparable to the populations enrolled in the zilucoplan and rozanolixizumab studies.46 No details were provided on the criteria used to exclude studies at this stage of the screening process. The selected RCTs were categorized according to severity of MG (mild, moderate, and/or severe), and refractory or exacerbating status.
A feasibility assessment was conducted, with studies selected based on the PICO criteria listed in Table 25. No details were provided on the feasibility assessment.
Table 25: Study Selection Criteria and Methods for ITCs Submitted by the Sponsor
Characteristics | Indirect comparison |
|---|---|
Population | Generalized myasthenia gravis |
Intervention | Zilucoplan (0.3 mg/kg) Rozanolixizumab (7 mg/kg and 10 mg/kg) |
Comparator |
|
Outcome |
Time points not specified |
Study designs | RCT |
Publication characteristics | English-language publication from any country |
Exclusion criteria | Phase IV RCTs were excluded from the ITC |
Databases searched | Databases searched (inception to May 1, 2023):
Conference proceedings searched (2017 to 2023):
Also, a bibliographic search of systematic reviews and meta-analyses, and a search of clinicaltrials.gov and European Union Clinical Trials Register (search dates not specified) |
Selection process | Two independent reviewers screened all citations against predefined eligibility criteria. Any discrepancies in their decisions were resolved by a third reviewer. The full-text publications of all citations of potential interest were then screened for inclusion by 2 independent reviewers. Studies meeting the eligibility criteria at the second screening stage were extracted. |
Data extraction process | Two reviewers extracted data from all included studies into a data-extracted table and any discrepancies were resolved by a third reviewer. When more than 1 publication was identified that described a single trial, the data were compiled into a single entry in the data extraction table. |
Quality assessment | Assessment of the quality of reporting of trials was carried out by 2 independent reviewers, followed by reconciliation of the differences between the 2 reviewers by a third independent reviewer. Critical appraisal of the included RCTs was conducted using comprehensive assessment criteria based on the recommendations in the NICE manufacturer’s template (NICE Single Technology Appraisal 2015). |
Ig = immunoglobulin; ITC = indirect treatment comparison; MG-ADL = Myasthenia Gravis Activities of Daily Living; MGFA = Myasthenia Gravis Foundation of America; NICE = National Institute for Health and Care Excellence; PLEX = plasma exchange; RCT = randomized control trial.
Sources: Sponsor’s ITC Report,15 sponsor’s Systematic Review Report,46 sponsor’s Summary of Clinical Evidence.27
ITC Analysis Methods
The NMA was conducted using Markov chain Monte Carlo Bayesian methods to compare the efficacy of zilucoplan with comparators (Table 26). Both fixed-effects and random-effects models were run, but the fixed-effect model was preferred by ITC investigators because of the sparse networks. The model used noninformative prior distributions for the model parameters. No information was provided on the number of chains, iterations, or model convergence. Because there were no closed loops, it was not possible to assess consistency.
Two efficacy outcomes were assessed: the proportion of patients who obtained an MG-ADL response at the study end point; and the change from baseline in the MG-ADL score at week 12 (± 2 weeks). The ITC report did not specify a definition of MG-ADL response in the PICO criteria. The results are described as the proportion of patients with at least a 3-point improvement in the MG-ADL score; however, not all studies used this definition. For some studies, outcome data were not available at the preferred time point, which required data to be extracted from figures using DigitizeIT (http://www.digitizeit.xyz/). No safety end points were analyzed.
The main analysis included any patients with gMG, and the subgroup analysis included patients with refractory gMG (where these data were available). The ITC report did not provide any criteria to distinguish the refractory population from the gMG population. The primary analyses were based on data from phase III RCTs, whereas sensitivity analyses included data from phase II and III studies. For the change from baseline in MG-ADL outcome, the ITC report states that other sensitivity analyses were run to overcome clinical and methodological heterogeneity related to the reporting of outcomes at different timelines (Table 26). These included the change from baseline to week 4, the change at each study’s primary end point, and a mix of the primary end point and week 12 (± 2 weeks).
The ITC report did not describe how homogeneity of the included studies was assessed and did not provide evidence that the transitivity assumption had been met.
Table 26: ITC Analysis Methods
Methods | Description |
|---|---|
Analysis methods | Bayesian MCMC NMA, fixed-effects and random-effects models (OpenBugs version 3.2.2 and R version 4.2.2). MG-ADL response: binomial likelihood and logit link, with treatment effects reported as odds ratios. Change from baseline in MG-ADL: normal likelihood with identify link, with treatment effects reported as mean differences in the change from baseline. Primary analyses for both outcomes were based on data from phase III RCTs only. |
Priors | Noninformative prior distributions were used for the model parameter(s). |
Assessment of model fit | The DIC was used to compare the goodness of fit of competing models. The ITC technical report stated that because the networks generally consisted of 1 trial per comparison, the fixed-effects model was preferred, as heterogeneity could not be estimated. The sponsor’s ITC report stated that in, general, a more complex model resulted in a better fit to the data, demonstrating a smaller residual deviance. The model with the better trade-off between fit and parsimony had a lower DIC. The sponsor noted that a difference in DIC of about 5 points can be considered meaningful; however, the sponsor did not recommend blindly choosing the model with the smallest DIC without further examination of diagnostics (e.g., residual plots) and results (e.g., forest plots, cross-tables). |
Assessment of consistency | Because of the absence of closed loops in the network, it was not possible to assess consistency. |
Assessment of convergence | Not reported. |
Outcomes |
For some end points, outcome data were obtained from figures using DigitizeIT (http://www.digitizeit.xyz/). |
Follow-up time points |
|
Construction of nodes | Not explicitly described in the sponsor’s ITC report. |
Sensitivity analyses | MG-ADL responder: included phase II and phase III RCTs Change from baseline in MG-ADL:
|
Subgroup analysis | Only 2 trials in the SLR included a refractory gMG population. The analysis of the refractory population included data from a subgroup of patients in the zilucoplan (RAISE) study, and the overall population from the eculizumab study (REGAIN), combined with the gMG populations enrolled in the other trials. |
Methods for pairwise meta-analysis | Not applicable. |
DIC = deviance information criterion; gMG = generalized myasthenia gravis; ITC = indirect treatment comparison MCMC = Markov chain Monte Carlo; MG-ADL = Myasthenia Gravis Activities of Daily Living; NMA = network meta-analysis; RCT = randomized controlled trial; SLR = systemic literature review.
Sources: Sponsor’s ITC Report,15 sponsor’s Summary of Clinical Evidence.27
Results of ITC
Summary of Included Studies
The sponsor stated that 80 RCTs met the criteria for the systematic review, 47 of which were prioritized because they represented the gMG population of patients with worsening or relapse-refractory disease. During the feasibility assessment, 35 studies were excluded because they did not have an outcome of interest (13 studies), did not have an intervention of interest (18 studies), were not connected to the network (2 studies), had a crossover design (1 study), or was a phase IV study with outcomes reported at week 2 (1 study).
A total of 12 placebo-controlled RCTs were included in the NMA: 6 phase III studies and 6 phase II studies. The ITC report did not include a description of the included studies; their study design; patient inclusion or exclusion criteria; descriptions of and dosing of interventions, cointerventions, or rescue therapies; outcome definitions; or statistical methods. No information was provided in the ITC report on the baseline characteristics of the patients enrolled, but some limited data were found in the sponsor’s systematic review report. All 12 studies were randomized, placebo-controlled, double-blind trials that were 15 days to 52 weeks in duration and ranged in sample size from 14 patients to 200 patients. One phase II study used a crossover design; however, the ITC report states that only the 16-week results, before crossover, were used in the NMA. The authors of the systematic review evaluated the quality of the included studies using the National Institute for Health and Care Excellence (NICE) checklist. Of the 12 trials, 1 phase II study was rated as having an unclear risk of bias related to randomization, allocation concealment, and withdrawals. Another phase II study had an unclear risk of bias related to outcome selection and reporting. According to the authors of the ITC report, all other studies were rated as having a low risk of bias on all domains.
The CDA-AMC reviewer assessed the 5 phase III studies included in the primary analyses to determine if the studies were sufficiently similar for the NMA (Table 28). The treatments included were zilucoplan (RAISE study), efgartigimod alfa (ADAPT study), eculizumab (REGAIN study), rozanolixizumab (MycarinG study), and ravulizumab (CHAMPION MG study). The CDA-AMC reviewer identified numerous sources of heterogeneity across these trials (Table 27). The populations of the 5 phase III studies included adults with gMG who were positive for anti-AChR autoantibodies (3 studies) or a mix of patients with anti-AChR autoantibody–positive MG or other types of MG (2 studies). The sponsor’s systematic review rated the disease severity of patients enrolled as mild to moderate (ADAPT study), moderate to severe (RAISE, MycarinG studies), mild to severe (CHAMPION MG study), and refractory (REGAIN study). The patients had been diagnosed with MG for an average of 6 to 10 years, the mean age of patients enrolled ranged from 47 years to 56 years, and the proportion of males and females varied across the trials. The patients enrolled also had differences in their treatment history (Table 28). Three studies included patients with refractory MG (REGAIN, RAISE, ADAPT), but it is unclear if the other 2 studies included patients with refractory disease. The duration of the studies ranged from 12 weeks to 26 weeks.
The other 7 trials that were used to inform the sensitivity analyses ranged in sample size from 14 to 47 patients and included other comparators (IVIg and rituximab). The study durations ranged from 29 days to 52 weeks, and all were double-blind, placebo-controlled trials (6 phase II and 1 phase III). The patients enrolled had new-onset gMG (1 study), mild-to-moderate gMG (2 studies), moderate-to-severe gMG (2 studies), mild-to-severe gMG (1 study), or refractory gMG (1 study).46,47 Based on the limited data provided in the sponsor’s ITC and systematic review report, it was not possible to fully examine potential sources of heterogeneity across these studies.
Table 27: Assessment of Homogeneity for ITC
Characteristics | Description and handling of potential effect modifiers |
|---|---|
Disease severity | Substantial variation was noted in the patient populations enrolled in the trials. Patient populations varied from those with mild-to-severe gMG and/or those with refractory disease. The mean duration of disease ranged from 5.8 years to 10 years in the 5 key phase III studies. |
Treatment history | CDA-AMC review of the 5 key phase III trials revealed differences across studies in prior treatments received. Three studies included patients with refractory disease (RAISE, ADAPT, REGAIN), and the other studies included patients who appear to have received fewer previous treatments for MG. In the REGAIN and ADAPT studies, patients were required to take concomitant MG treatments (AChEI, IST, and/or corticosteroids), whereas in the other studies, these treatments were allowed but not required. No information was available on the treatment history for the other 7 phase II and III studies. |
Trial eligibility criteria | Participants in the 5 phase III studies were adults with gMG (MGFA disease class II to class IV). Patients were required to have baseline MG-ADL scores of at least 3 points (MycarinG study), 5 points (ADAPT study), or 6 points (3 studies, RAISE, CHAMPION MG, REGAIN studies), or baseline QMG scores of at least 11 points (MycarinG study) or 12 points (RAISE study). Two phase III studies included patients with or without anti-AChR autoantibodies (ADAPT, MycarinG studies), whereas other studies were limited to those who were positive for anti-AChR autoantibodies. No information was available on the trial eligibility criteria for the other 7 studies. |
Dosing of comparators | There were differences in the dosing regimens across the 5 key studies, which, depending on the timing of outcome reporting, could bias the findings. Zilucoplan was administered daily on an ongoing basis in the RAISE study, whereas treatments in 2 of the studies were administered intermittently. In the ADAPT study, efgartigimod alfa was administered cyclically, with a 5-week interval between treatment cycles. The administration of subsequent cycles was based on the patient’s treatment response. In the REGAIN study, patients received weekly doses of eculizumab for 4 weeks, then switched to an every 2-week dosing interval. In the MycarinG study, patients received weekly doses of rozanolixizumab for 6 weeks and were then observed for an additional 8 weeks. Ravulizumab was administered every 2 weeks in the CHAMPION MG study. No dosing information was available for the other 7 studies. |
Placebo response | The sponsor stated that there was heterogeneity in the placebo response rate for the MG-ADL responder analysis. In the overall population, the proportion of responders in the placebo group ranged from 20% to 53% for studies included in the primary analysis, and from 14% to 53% for those included in the sensitivity analysis. The ITC report stated that the placebo response (i.e., baseline risk) may be a treatment-effect modifier. The ITC report did not explore potential explanations for the variation in the placebo response rates and did not adjust for this potential source of bias in the model. The placebo response for the change from baseline analysis ranged from −0.97 points to −2.3 points for the primary NMA and from −0.4 points to −2.9 points for the sensitivity analyses. |
Definitions of end points | The trials used different definitions of MG-ADL response. The ITC report selected at least a 3-point improvement in the MG-ADL to define a responder; however, 1 of the phase III studies (ADAPT) used an alternate definition (≥ 2-points). In addition, there were differences across the phase III studies in the way patients who required rescue therapy were analyzed. Some studies imputed these patients as nonresponders, but in other studies, it was unclear how patients who received rescue therapies were analyzed. |
Timing of end point evaluation | Responder analyses were based on data reported at the end of each study. For the primary analysis, this varied from 6 weeks to 26 weeks, and in the sensitivity analysis, from 4 weeks to 26 weeks. Change from baseline analyses were based on data at 12 weeks (± 2 weeks) and used digitized data from figures if the 12-week data were not reported in the studies. Sensitivity analyses were performed using other time points (i.e., at 4 weeks, at each study’s primary end point, or a mix of 12-week and primary study time points). The sponsor noted that the treatment effects in the ADAPT (efgartigimod) and MycarinG (rozanolixizumab) studies waned from their primary end point (6 weeks and 4 weeks, respectively) to the 10-week time point used in the primary NMA. This may bias the NMA against these 2 drugs. The NMA analyzed the change from baseline at week 12 for the CHAMPION MG (ravulizumab) and REGAIN (eculizumab) studies instead of the primary end point at 26 weeks. According to the clinical expert, early outcome assessments may underestimate the treatment effects for the estimated 10% to 20% of patients who are late responders to these drugs. |
Withdrawal frequency | Not reported. |
Clinical trial setting | Not reported. |
Study design | The primary analysis was based on phase III RCTs only, but sensitivity analyses included phase II RCTs as well. Phase IV studies were excluded from the NMA. There were 11 parallel-design studies and 1 crossover study. All studies were double-blind and placebo-controlled. The trial duration ranged from 15 days to 52 weeks. |
AChEI = acetylcholinesterase inhibitor; AChR = acetylcholine receptor; CDA-AMC = Canada’s Drug Agency; gMG = generalized myasthenia gravis; IST = immunosuppressive therapy; ITC = indirect treatment comparison; MG = myasthenia gravis; MG-ADL = Myasthenia Gravis Activities of Daily Living; MGFA = Myasthenia Gravis Foundation of America; NMA = network meta-analysis; QMG = Quantitative Myasthenia Gravis; RCT = randomized controlled trial.
Sources: Sponsor’s ITC Report,15 sponsor’s Systematic Review Report,46 Howard et al. (2023),26 Howard et al. (2021),48 Howard et al. (2017),24 Bril et al. (2024),49 Vu et al. (2022).50
Table 28: Summary of the Phase III Studies Included in the NMA
Study characteristics | Population | Intervention | Outcomes of interest | Baseline characteristics |
|---|---|---|---|---|
RAISE study | ||||
DB RCT Europe, Japan, North America N = 174 12-week | 18 to 74 years with gMG (MGFA disease class II to class IV), positive for anti-AChR autoantibodies, MG-ADL score ≥ 6, QMG score ≥ 12 Subgroup: refractory disease (1 year history of treatment with NSIST, corticosteroids, eculizumab, tacrolimus, or rituximab; or 1 of these therapies plus chronic PLEX or IVIg) Randomization stratified by MG-ADL score, QMG score and region | Zilucoplan 0.3 mg/kg SC daily or placebo for 12 weeks Permitted cotherapies: corticosteroids or NSIST at stable doses Rescue therapy: IVIg or PLEX | Primary: CFB in MG-ADL score at week 12
Other secondary: 3-point change in MG-ADL without rescue therapy
|
|
ADAPT study | ||||
DB RCT Europe, Japan, North America N = 167 26-week | ≥ 18 years with gMG (MGFA disease class II to class IV), with or without anti-AChR autoantibodies, MG-ADL score ≥ 5 (with > 50% of score due to nonocular symptoms), and symptoms of MG despite SOC therapy Subgroup: patients with anti-AChR autoantibodies Randomization stratified by acetylcholine receptor antibody status (positive or negative), NSIST use (yes or no), Japanese (yes or no) | Efgartigimod alfa 10 mg/kg IV or placebo administered as cycles of 4 weekly infusions followed by 5-week follow-up. All patients received 1 cycle, with repeat cycles based on treatment response up to week 26. Required to be taking at least 1 treatment for MG at stable doses (i.e., AChEIs, corticosteroids, or NSISTs) Patients requiring rescue therapy were discontinued from the study. | Primary: proportion of MG-ADL responders in the first cycle (week 8) for the subgroup positive for anti-AChR antibodies (≥ 2-point improvement starting week 4 and sustained for 4 weeks)
Other: ≥ 3-point improvement in MG-ADL score in the anti-AChR positive subgroup:
Secondary: MG-ADL responders in the overall population
(Note: Data used in the NMA appear to be from a subgroup of patients with anti-AChR autoantibodies). | Anti-AChR-positive subgroup (129 of 167 patients [77%]):
|
REGAIN study | ||||
DB RCT Asia, Europe, Latin America, North America N = 125 26-week | ≥ 18 years with refractory gMG (MGFA disease class II to class IV), positive for anti-AChR autoantibodies, MG-ADL score ≥ 6, and prior treatment with ≥ 2 ISTs or 1 IST with IVIg or PLEX for 12 months without symptom control Randomization stratified by MGFA clinical classification | Eculizumab IV (900 mg weekly for 4 weeks, then 1,200 mg every 2 weeks) or placebo for 26 weeks Patients continued taking prior treatments (AChEIs, corticosteroids, or ISTs) at stable dosages. Rescue medications included high-dose corticosteroids, IVIg, or PLEX. | Primary: change in MG-ADL at week 26
Note: Study failed primary outcome. Secondary: Responder analysis (≥ 3-point improvement in MG-ADL total score and no rescue therapy)
|
|
MycarinG study | ||||
DB RCT, adaptive design Asia, Europe, North America N = 200 6-week treatment; 8-week follow-up | ≥ 18 years with gMG (MGFA disease class II to class IVa), positive for anti-AChR or MuSK autoantibodies, MG-ADL score ≥ 3 (nonocular), and QMG score ≥ 11 Subgroup: Anti-AChR autoantibody–positive MG Randomization stratified by anti-AChR or MuSK autoantibodies | Rozanolixizumab 7 mg/kg SC, rozanolixizumab 10 mg/kg SC, or placebo SC weekly for 6 weeks Permitted concomitant drugs: AChEIs, NSISTs, oral corticosteroids Rescue therapy: PLEX, IVIg. These patients continued in the study but stopped the study drug. | Primary: CFB in MG-ADL score at day 43 (week 6)
Anti-AChR positive subgroup
Secondary: MG-ADL response (≥ 2-point improvement) at day 43
(Note: responder data used in the NMA were different than those reported in Bril et al. [2024]49) |
|
Champion MG study | ||||
DB RCT Asia-Pacific, Europe, Japan, North America N = 175 26-week | ≥ 18 years with gMG (MGFA disease class II to class IV), with anti-AChR autoantibodies, MG-ADL score ≥ 6, body weight ≥ 40 kg Randomization stratified by region | Ravulizumab (weight based) 2.4 g to 3.0 g IV loading dose, then 3.0 g to 3.6 g IV maintenance dose every 8 weeks or placebo for 26 weeks Permitted cotherapies: stable doses of ISTs, including corticosteroids, or cholinesterase inhibitors Rescue therapy: high-dose corticosteroids, IVIg, or PLEX | Primary: CFB in MG-ADL at week 26
Secondary: responder analysis (≥ 3-point improvement in MG-ADL total score)
(Note: responder data used in NMA were different than those reported in Vu et al.[ 2022]50) |
|
AChEI = acetylcholinesterase inhibitor; AChR = acetylcholine receptor; CFB = change from baseline; CI = confidence interval; DB = double blind; gMG = generalized myasthenia gravis; Ig = immunoglobulin; IST = immunosuppressive therapy; LSM = least squares mean; MG = myasthenia gravis; MG-ADL = Myasthenia Gravis Activities of Daily Living; MGFA = Myasthenia Gravis Foundation of America; NMA = network meta-analysis; NR = not reported; NSIST = nonsteroidal immunosuppressant; PBO = placebo; PLEX = plasma exchange; QMG = quantitative myasthenia gravis; RCT = randomized controlled trial; SC = subcutaneous; SD = standard deviation; SOC = standard of care; vs. = versus.
Sources: Howard et al. (2023),26 Howard et al. (2021),48 Howard et al. (2017),24 Bril et al. (2024),49 Vu et al. (2022),50 CADTH Reimbursement Review for efgartigimod alfa.51
Results
Figure 4: Evidence Network for MG-ADL Responder and Change From Baseline NMA Primary Analyses (Overall and Refractory Populations)
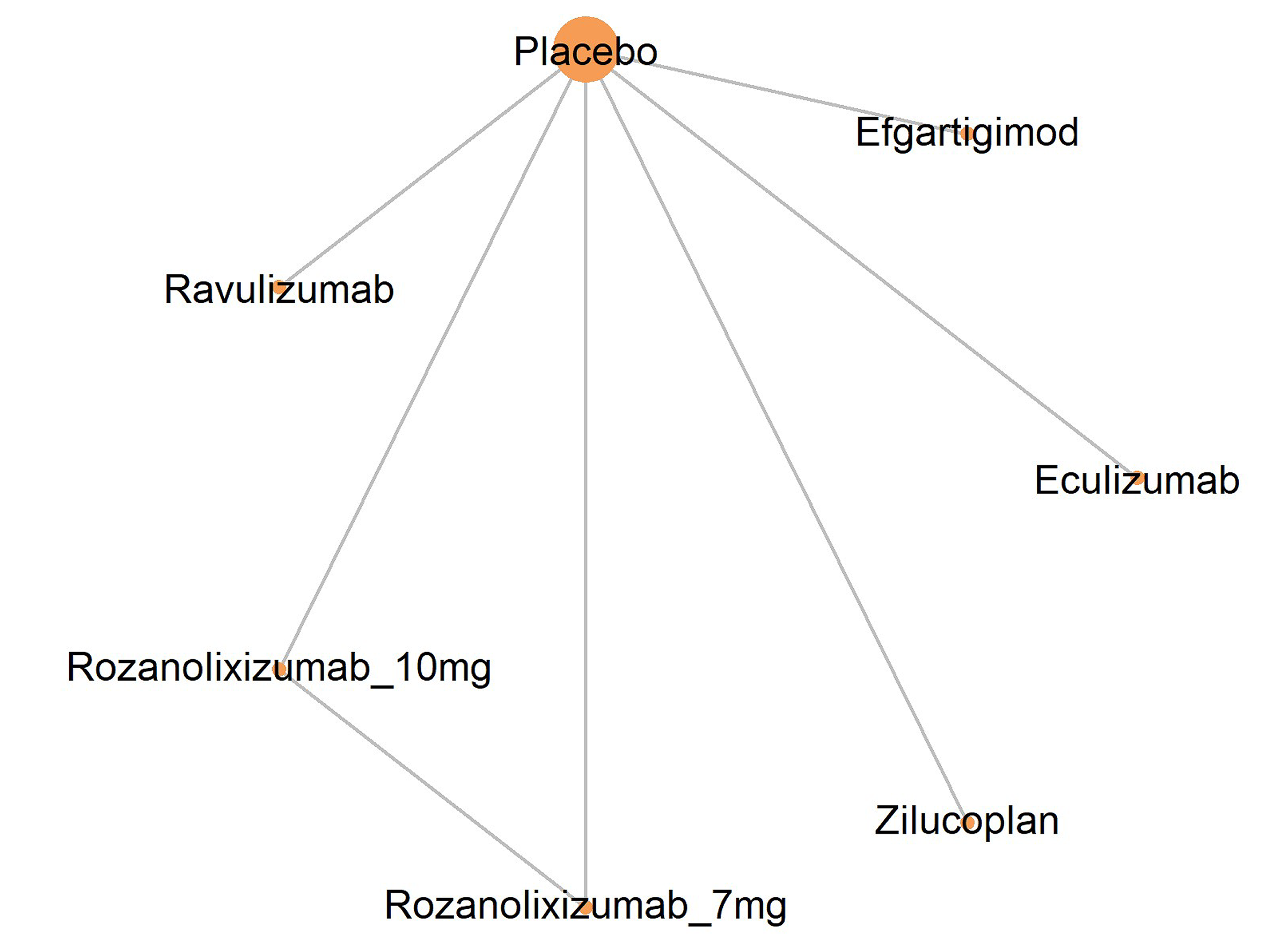
MG-ADL = Myasthenia Gravis Activities of Daily Living; NMA = network meta-analysis.
Source: Sponsor’s ITC Report.15
MG-ADL Response in the Overall Population
The primary analysis for the proportion of patients with at least a 3-point improvement in MG-ADL score at the end of the studies (week 6 to week 26) included 5 phase III RCTs (Figure 4). Four of the 5 studies reported the proportion of patients with at least a 3-point improvement in MG-ADL, and 1 study (rozanolixizumab) reported the proportion with at least a 2-point improvement. The outcomes were reported at 6 weeks (rozanolixizumab), 10 weeks (efgartigimod), 12 weeks (zilucoplan), and 26 weeks (eculizumab and ravulizumab).
The OR for the proportion of responders was ████ ████ ███ ████ ██ █████ for zilucoplan versus eculizumab and ████ ████ ███ ████ ██ █████ for zilucoplan versus efgartigimod alfa (Table 29).
MG-ADL Response in the Refractory Population
The primary analysis of patients with refractory disease was based on the same trial data as the overall population NMA for 4 of the 5 studies. The only difference was in the RAISE study (zilucoplan), which used subgroup data for the patients with refractory disease instead of data from the overall population. Of note, all patients in the eculizumab study (REGAIN) had refractory disease. In the efgartigimod alfa study (ADAPT), 63% of patients had refractory disease. It is unclear if the ravulizumab (CHAMPION MG) and rozanolixizumab (MycarinG) trials included patients with refractory gMG.
The OR of MG-ADL response was ████ ████ ███ ████ ██ █████ and ████ ████ ███ ████ ██ █████ for zilucoplan versus eculizumab and efgartigimod, respectively (Table 29).
Table 29: Summary of the NMA Primary Analysis for the Proportion of Patients With MG-ADL Response at the End of the Study (Week 6 to Week 26)
Detail | Overall gMG population | Refractory gMG populationa |
|---|---|---|
Number of studies (patients), N | 5 phase III studies (793 patients) | 5 phase III studies (705 patients) |
Model | Fixed effects | Fixed effects |
Zilucoplan vs. comparator, OR (95% CrI) | ||
Placebo | ████ █████ ██ █████ | ████ █████ ██ ██████ |
Eculizumab | ████ █████ ██ █████ | ████ █████ ██ █████ |
Efgartigimod | ████ █████ ██ █████ | ████ █████ ██ █████ |
CrI = credible interval; gMG = generalized myasthenia gravis; MG-ADL = Myasthenia Gravis Activities of Daily Living; NMA = network meta-analysis; OR = odds ratio; vs. = versus.
Note: MG-ADL response was defined as at least a 3-point improvement from baseline in 4 studies (efgartigimod, ravulizumab, zilucoplan, eculizumab), and at least a 2-point improvement in 1 study (rozanolixizumab). ORs greater than 1 favour zilucoplan over the comparator. The results in bold had a 95% CrI that excluded the null.
aThe patients in 2 studies were exclusively those with refractory disease (RAISE study of zilucoplan and REGAIN study of eculizumab). The proportion of patients with refractory MG was unclear in the other studies included in the analyses.
Source: Sponsor’s ITC Report.15
Change From Baseline in MG-ADL Score in the Overall Population
The primary analysis for the change from baseline in MG-ADL score included 5 studies with 755 patients and was based on outcomes reported at 10 weeks (2 studies) or 12 weeks (3 studies) (Figure 4).
The mean difference in the change from baseline in the MG-ADL score was █████ ██████ ████ ███ █████ ██ █████ for zilucoplan versus eculizumab, and █████ ██████ ████ ███ █████ ██ █████ for zilucoplan versus efgartigimod alfa (Table 30).
Change From Baseline in MG-ADL Score in the Refractory Population
For the NMA in the refractory population, 5 studies (669 patients) were included in the primary analysis. The mean difference in the change from baseline in the MG-ADL score was █████ ██████ ████ ███ █████ ██ █████ for zilucoplan versus eculizumab, and █████ ██████ ████ ███ █████ ██ ██████ for zilucoplan versus efgartigimod alfa (Table 30).
Table 30: Summary of the NMA Primary Analysis for Change From Baseline in MG-ADL Score at Week 12 (± 2 Weeks)
Detail | Overall gMG population | Refractory gMG populationa |
|---|---|---|
Number of studies (patients), N | 5 phase III studies (755 patients) | 5 phase III studies (669 patients) |
Model | Fixed effects | Fixed effects |
Zilucoplan vs. comparator, mean difference (95% CrI) | ||
Placebo | █████ ██████ ██ ██████ | █████ ██████ ██ ██████ |
Eculizumab | █████ ██████ ██ █████ | █████ ██████ ██ █████ |
Efgartigimod | █████ ██████ ██ █████ | █████ ██████ ██ ██████ |
CrI = credible interval; gMG = generalized myasthenia gravis; MG-ADL = Myasthenia Gravis Activities of Daily Living; NMA = network meta-analysis; vs. = versus.
Note: MG-ADL is scored from 0 to 24, with higher scores indicating worse symptoms of MG. A negative mean difference favours zilucoplan over the comparator. The results in bold had a 95% CrI that excluded the null.
aThe patients in 2 studies were exclusively those with refractory disease (RAISE study of zilucoplan and REGAIN study of eculizumab). The proportion of patients with refractory MG was unclear in the other studies included in the analyses.
Source: Sponsor’s ITC Report.15
Sensitivity Analyses
The sensitivity analyses for the proportion of MG-ADL responders were based on 7 phase II and phase III studies. The estimated treatment effects of zilucoplan versus eculizumab and zilucoplan versus efgartigimod alfa were consistent with the primary analyses in the overall and refractory populations.
Four sensitivity analyses were conducted for the change from baseline in the MG-ADL score. These analyses were based on data from 6 to 12 phase II or phase III trials, and/or outcomes reported at time points other than 12 weeks (range, 4 weeks to 52 weeks). With the inclusion of the additional trials, some networks included IVIg and/or rituximab, as well as eculizumab, efgartigimod, ravulizumab, and rozanolixizumab, as comparators. Overall, the findings of the sensitivity analyses were █████████ ██████████ ████ ███ ███████ ██ ███ ███████ ████████ ███ ██████ ███ ███ ████ ████ ████████████ ███ ██████████ ██████ ███████████ ████████████ ███ █████████ (Table 31). The mean difference in the change from baseline in MG-ADL score ████████ ██████████ ██████ ████ ██ ███ ███████ ███ ██████████ ███████████, based on the sensitivity analyses that included outcomes reported between week 4 and week 52.
Table 31: Summary of the NMA Sensitivity Analyses for Change From Baseline in MG-ADL Score
Detail | Zilucoplan vs. comparator, mean difference (95% CrI) | |
|---|---|---|
Overall gMG population | Refractory gMG populationa | |
Analysis at 10 to 12 weeks for phase II and phase III studies | ||
Model, N studies | Fixed effects, 7 studies | Fixed effects, 7 studies |
Eculizumab | █████ ██████ ██ █████ | █████ ██████ ██ █████ |
Efgartigimod | █████ ██████ ██ █████ | █████ ██████ ██ ██████ |
Analysis at 10 to 12 weeks for key phase III studies and at 4 to 52 weeks for additional studies | ||
Model, N studies | Fixed effects, 12 studies | Fixed effects, 12 studies |
Eculizumab | █████ ██████ ██ █████ | █████ ██████ ██ █████ |
Efgartigimod | █████ ██████ ██ █████ | █████ ██████ ██ ██████ |
IVIg | █████ ██████ ██ ██████ | █████ ██████ ██ ██████ |
Rituximab | █████ ██████ ██ █████ | █████ ██████ ██ █████ |
Analysis at the primary end point for phase III studies (4 to 26 weeks) | ||
Model, N studies | Fixed effects, 6 studies | Fixed effects, 6 studies |
Eculizumab | █████ ██████ ██ █████ | █████ ██████ ██ █████ |
Efgartigimod | ████ ██████ ██ █████ | █████ ██████ ██ █████ |
Rituximab | █████ ██████ ██ █████ | █████ ██████ ██ █████ |
Analysis at the primary end point for all studies (4 to 52 weeks) | ||
Model, N studies | Fixed effects, 12 studies | Fixed effects, 12 studies |
Eculizumab | ████ ██████ ██ █████ | █████ ██████ ██ █████ |
Efgartigimod | ████ ██████ ██ █████ | ████ ██████ ██ █████ |
IVIg | █████ ██████ ██ ██████ | █████ ██████ ██ ██████ |
Rituximab | █████ ██████ ██ █████ | █████ ██████ ██ █████ |
CrI = credible interval; gMG = generalized myasthenia gravis; Ig = immunoglobulin; MG-ADL = Myasthenia Gravis Activities of Daily Living; NMA = network meta-analysis; vs. = versus.
Note: MG-ADL is scored from 0 to 24, with higher scores indicating worse symptoms of MG. A negative mean difference favours zilucoplan over the comparator. The results in bold had a 95% CrI that excluded the null.
aThe patients in 3 studies were exclusively those with refractory disease (1 zilucoplan study [RAISE subgroup], and 2 eculizumab studies). The proportion of patients with refractory MG was unclear in the other studies included in the analyses.
Source: Sponsor’s ITC Report.15
Critical Appraisal of ITC
The ITC technical report submitted by the sponsor had serious deficiencies. Specifically, the report lacked detail on the criteria used to select studies for inclusion in the NMA and the feasibility study. With regard to the study selection criteria, the population criteria did not specify the type of MG, so the analyses were not limited to patients with anti-AChR autoantibodies. Further, patients with refractory gMG were not specified a priori as a subgroup of interest in the study selection criteria. In addition, there were no criteria to define what constitutes refractory MG. A total of 80 RCTs met the inclusion criteria for the systematic review, but only 47 were prioritized in the sponsor’s ITC report, which stated that these studies represented the relapse-refractory or worsening gMG population. No information was provided in the ITC report on the selection criteria applied at this stage, so it is unclear if potentially relevant studies were excluded. Further, the description of the NMA methods lacked clarity, and decisions around the outcomes selected, the timing of outcome reporting, and the rationale for the sensitivity analyses were not adequately justified.
The ITC report states that a feasibility assessment was conducted to identify studies that were suitable for the NMA. Another 35 studies were excluded on the basis of the feasibility assessment, but limited data were available on these trials. Moreover, the report provided no information on the characteristics of the 12 studies included in the NMA, which is a major limitation of the ITC report. Basic information on the study design of the included studies was found in the sponsor-submitted systematic review report, but this information was insufficient to adequately assess these studies.
To assess heterogeneity across the network of studies included in the NMA, the CDA-AMC reviewer conducted a review of the 5 key phase III trials that were included in the primary analyses. Using the information from each study’s published report, substantial heterogeneity was noted in the patient populations enrolled and, in the outcomes, reported in these studies.24,26,48-50 The patients enrolled varied in terms of disease severity and MG treatment history, which the clinical expert consulted for this review identified as potential treatment-effect modifiers. Specifically, the trials had different proportions of patients rated as having mild, moderate, or severe and/or refractory gMG. One trial was restricted to patients with refractory disease (eculizumab), 2 studies contained a mixed population, with 50% and 63% of patients with refractory MG (zilucoplan and efgartigimod, respectively), and the other 2 studies had an unknown proportion of patients with refractory disease (ravulizumab and rozanolixizumab). The clinical expert stated that patients with refractory gMG or more severe disease may be less likely to respond to therapy; thus, differences in the distribution of these patients across trials may bias the findings. Both the overall population analyses and the refractory subgroup analyses contain a varied mix of patients with and without refractory gMG, which is an important source of heterogeneity. Moreover, the refractory subgroup analyses cannot be considered a true comparative assessment of patients with refractory gMG because not all studies were limited to patients with refractory disease.
Other differences noted across the key trials were in the duration of disease and type of gMG, and 2 trials enrolled patients with or without anti-AChR autoantibodies. Although it was not specified in the NMA methods, based on the raw trial data used in the analysis, it appears that 1 of these studies (efgartigimod) only used data from the subgroup of patients with anti-AChR autoantibodies in its analyses. The ITC methods should have specified a priori how studies with mixed patient populations would be handled in the analyses.
With regard to the outcomes, the trials varied in their definition of MG-ADL response and in the timing of outcome assessments. The sponsor selected a 3-point improvement in the MG-ADL score as the threshold for a treatment response; however, 1 of the key studies used a 2-point threshold. In addition, it was unclear if the studies used similar methods to account for ICEs, such as the use of rescue therapy. It is unclear how these differences in responder definitions or the handling of ICEs may have impacted the results. The ITC also identified differences in the placebo response rate as a source of heterogeneity for the MG-ADL responder analyses. In the overall population, the proportion of patients in the placebo group with at least a 3-point improvement in MG-ADL score ranged from 20% to 53%, which may reflect differences in outcome definitions and other study characteristics, as well as patient populations. No sensitivity analyses were conducted to control for the placebo response rate, so there are no data to assess what impact this heterogeneity may have had on the results. That being said, because of the sparse network, any analyses that adjusted for placebo response would likely show estimates with high uncertainty.
CDA-AMC was unable to assess heterogeneity in the 7 other studies used in the sensitivity analysis because of inadequate reporting in the ITC report. Based on the limited data available, there was heterogeneity among these trials in disease severity and prior treatment history. For example, the phase III trial for rituximab enrolled patients with new-onset gMG, which is not consistent with the patient population enrolled in the other phase III studies or the way rituximab is used in clinical practice in Canada.47
The NMAs were based on Bayesian fixed-effects models, which the CDA-AMC reviewer agreed was reasonable, given the sparse network. The reporting of the statistical methods lacked details on the number of iterations, chains, and assessment of convergence. A major limitation of the ITC methods was issues related to the timing of outcomes. The responder analyses used each study’s primary outcome time point, which varied from 6 weeks to 26 weeks. The change from baseline analyses assessed outcomes at week 10 or week 12 in the primary analyses but included other time points in the sensitivity analyses (from 4 weeks to 52 weeks). The CDA-AMC reviewer considered the differences in the timing of outcomes to be a significant source of heterogeneity that was not controlled for in the analyses. The restriction of the outcome to those reported at 10 weeks or 12 weeks also led to serious limitations, related in part to differences in dosing schedules (intermittent versus continuous). The ITC noted that the treatment effects of efgartigimod alfa and rozanolixizumab (which were administered for 4 weeks or 6 weeks, respectively) were waning at week 10, so the results of any analyses based on the 10-week data may be biased against these treatments. For the comparison between zilucoplan and efgartigimod, the timing of outcomes may explain discrepancies in the direction of the treatment effects in the responder analyses (based on each study’s primary end point) and the change in MG-ADL score (which was based on 10-week data). Further, the clinical expert noted that approximately 10% to 20% of patients who received eculizumab or ravulizumab may be late responders, so outcomes reported at 12 weeks instead of 26 weeks (the trial’s primary outcome) may underestimate the treatment effects for a portion of patients. Therefore, the analyses based on each study’s primary end point and analyses with fixed 10-week to 12-week time points have limitations that may bias the findings. Although the ITC did report sensitivity analyses that included phase II studies and used alternate outcome time points, these did not fully address the sources of heterogeneity that were identified across the network. In addition, other common sensitivity analytical approaches, such as pairwise NMAs comparing zilucoplan to active drug, were not conducted by the investigators, which could have been helpful in an exploration of the impact of specific sources of heterogeneity.
Overall, the evidence networks were sparse; the primary analysis was based on 1 trial per comparator. Generally, the duration of follow-up in the source studies was limited (up to 26 weeks for the primary analyses), so comparative estimates were based on short-term data. The NMA results lacked precision, as shown by the wide 95% CrI. Considering the heterogeneity in the patient and study characteristics that was identified on the basis of a limited assessment, there is likely substantial risk of bias for the comparisons in the network. As a result, no conclusions could be drawn on the comparative efficacy of zilucoplan. No harms outcomes were assessed in the NMA, so the comparative safety of zilucoplan is unknown.
Discussion
Summary of Available Evidence
One multicentre, randomized, phase III, double-blind RCT evaluated the efficacy and safety of zilucoplan 0.3 mg/kg per day plus standard of care or placebo plus standard of care for 12 weeks in 174 patients with anti-AChR antibody–positive gMG (3 patients in Canada), 88 of whom had with refractory gMG. The primary objective of the RAISE study was to evaluate change from baseline to week 12 in the MG-ADL score. Key secondary objectives included change from baseline to week 12 in the QMG, MGC, and MG-QoL15r scores, and the frequency of TEAEs. Additional secondary objectives included the achievement of MSE (an MG-ADL score of 0 or 1) at week 12 without rescue therapy, the MG-ADL responder rate (a ≥ 3-point decrease in the MG-ADL score) at week 12 without rescue therapy, and the QMG responder rate (a ≥ 5-point decrease in the QMG score) at week 12 without rescue therapy. The achievement of minimal manifestation status per MGFA-PIS at week 12 without rescue therapy was an exploratory objective. In the RAISE study, 56.9% of the patients with gMG were female and 43.1% were male, mean age was 53.0 years (SD = 15.1 years), 67.2% were diagnosed with MGFA disease class III at screening, and 64.4% had generalized symptoms at disease onset. In addition, the disease had a mean onset of 43.8 years (SD = 18.0 years), and the mean duration of gMG was 9.2 years (SD = 9.9 years). In the stratified randomization, 62.1% of patients had a score of 10 or more points on the MG-ADL scale, and 56.3% of patients had a score of 18 or more points on the QMG scale. More patients had undergone thymectomy in the zilucoplan group (52.3%) than the placebo group (42.0%). Patients had similar between-group mean baseline MG-ADL and QMG scores. Differences in baseline characteristics between the overall population and the refractory subpopulation included mean age at disease onset (43.8 years and 40.0 years), mean disease duration (9.2 years and 11.9 years), diagnosis of thymoma (22.4% and 29.5%), and prior thymectomy (47.1% and 68.2%) or MG crisis (32.8% and 50.0%).
Additional clinical evidence submitted by the sponsor included an extension study and an ITC. RAISE-XT was a phase III, multicentre, open-label, long-term extension study that enrolled patients with gMG who had previously received zilucoplan 0.3 mg/kg (n = 93) or placebo (n = 90) to evaluate the long-term (108 weeks; ongoing) efficacy and safety of zilucoplan. Baseline characteristics of patients in the overall gMG population of the RAISE-XT study were similar to those of patients in the pivotal RAISE trial. The ITC included an NMA that evaluated the short-term efficacy of zilucoplan relative to treatments considered relevant to this review (i.e., eculizumab, efgartigimod alfa, IVIg, PLEX, and rituximab) for the management of patients with anti-AChR antibody–positive gMG, as well as those with refractory gMG. No baseline characteristics were reported in the systematic review; for the primary analysis, there was heterogeneity across the included trials in patient age (range, 47 to 56 years), average time since MG diagnosis (range, 6 to 10 years), disease severity (mild, moderate, severe and/or refractory gMG), MG treatment history, and study duration (range,12 to 26 weeks).
Interpretation of Results
Efficacy
Patients with MG seek treatments that can decrease the number and intensity of exacerbations, provide durable benefit, improve quality of life and maintain independence, and decrease the risk of side effects. In addition to these outcomes, clinicians advocate for treatments that reduce both MG-related and treatment-related morbidity and mortality, reduce weakness (ocular, bulbar, respiratory, axial, and extremity) associated with MG, and prevent life-threatening disease exacerbations, such as an MG crisis. Because no 2 patients exhibit the same manifestations of MG, the clinical expert noted that there are wide differences in the way patients are managed throughout their disease course. Currently available treatment options tend to take time before optimal benefit is achieved — prednisone takes a median of 3 months to 4 months and NSISTs such as azathioprine and mycophenolate mofetil take a minimum of 6 months to up to 12 months to 18 months — and toxicities can be significant (particularly with prednisone), which highlight the morbidity related to long-term immunosuppression, particularly because most patients require lifelong treatment.
The pivotal RAISE trial compared the efficacy and harms of zilucoplan with placebo in patients with refractory and nonrefractory gMG, and included the end points of change from baseline to week 12 in scores on the MG-ADL, the QMG, the MGC, and the MG-QoL15r; the achievement of MSE, MG-ADL, and QMG responses, and the achievement of minimal manifestation status per MGFA-PIS. The clinical expert selected these end points as important to patients and for making treatment decisions, noting that the MG-ADL score is most applicable and used more commonly in clinical practice than the remaining assessments.
The RAISE trial demonstrated that treatment with zilucoplan is likely superior to placebo in providing improvement at week 12 in signs and symptoms of disease activity, measured by the MG-ADL score (the primary outcome), in the overall trial population, which included patients with refractory and nonrefractory disease. Zilucoplan also likely results in a clinically meaningful benefit over placebo in the key secondary outcomes — QMC and MGC scores at week 12 — in the overall trial population. Zilucoplan likely results in improvements in HRQoL compared with placebo, based on results from the MG-QoL15r instrument; however, given the absence of an established MID for the MG-QoL15r instrument, there is some uncertainty about the clinical importance of this estimate. For other secondary outcomes — at least a 3-point reduction in MG-ADL score and at least a 5-point reduction QMG score — zilucoplan is also likely to show improvements compared with placebo. MSE score at week 12 favoured zilucoplan numerically, and although it did not reach statistical significance in the overall trial population, it may result in a benefit compared to placebo. Zilucoplan may result in an increase in the number of patients who achieved minimal manifestation status per MGFA-PIS at 12 weeks, an exploratory outcome, compared to placebo. Note that confidence in the between-group differences for efficacy in the overall trial population was limited by imprecision (indicated by the associated CIs that included small effects close to the null or crossed the null) and relatively small sample sizes.
Patient selection for the refractory subgroup (50.6% of patients in the RAISE trial), was prespecified a priori in the RAISE study protocol and aligned with the inclusion criteria from the REGAIN study for eculizumab. The population included in the refractory subgroup is adequately reflective of the patients with refractory gMG in the clinical setting in Canada, according to the clinical expert consulted by the review team. Baseline characteristics were, overall, similar in the overall and refractory populations, and concern about prognostic imbalances is low. The clinical benefit observed in the refractory subgroup was consistent with or tended to be slightly larger than the results in the overall trial population of the RAISE trial.
Primary and key secondary outcomes (MG-ADL, QMG, and MGC total scores): The treatment effects of zilucoplan, compared with placebo, observed for changes in the MG-ADL, QMG, and MGC scores at week 12 in the refractory subgroup were consistent with the statistically significant results from the overall trial population in the RAISE study, which showed slightly greater improvement. The between-group differences exceeded the MID for the MG-ADL total score (approximately a 2-point change), for the QMG score (range from 2 points to 3 points, depending on disease severity), and for the MGC score (approximately a 3-point change). The MIDs identified in the literature for the MG-ADL and QMG scores were estimated for changes in an individual patient and were applied in the absence of an estimate of a between-group MID. It should be noted that, similar to the results for the overall trial population, there is some uncertainty due to imprecision; the upper bounds of the CIs included effects that did not meet the threshold (little-to-no difference). The expert explained that the change from baseline in QMG and MGC scores was similar in direction and magnitude of the change from baseline in MG-ADL score, demonstrating benefit with zilucoplan treatment in both the overall and refractory gMG populations.
Key secondary outcome (MG-QoL15r total score): The change from baseline in MG-QoL15r score at week 12 in the refractory subgroup suggested a greater reduction with zilucoplan than with placebo and was consistent with the statistically significant results from the overall trial population in the RAISE study. However, an MID for MG-QoL15r in patients with MG has not been estimated. There is some uncertainty due to imprecision in the refractory subgroup, as the review team judged that the 95% CI for the between-group difference included the possibility of little-to-no difference and clinically important benefit.
Additional secondary outcomes (MSE at week 12 without rescue therapy, MG-ADL score at week 12 without rescue therapy, and QMG score at week 12 without rescue therapy): A larger percentage of patients achieved MSE (an MG-ADL score of 0 or 1) without rescue therapy, at least a 3-point reduction in the MG-ADL score without rescue therapy, and at least a 5-point reduction in the QMG score without rescue therapy in the zilucoplan group than in the placebo group in the refractory subgroup, which was consistent with results in the overall trial population (results for the MSE did not reach statistical significance in the overall trial population).
Results for the exploratory outcome, minimal manifestation status per MGFA-PIS at week 12 without rescue therapy, were not reported for the refractory subpopulation.
Efficacy end points in the RAISE-XT extension study aligned with those of the pivotal RAISE trial. Findings from the RAISE-XT study supported the pivotal trial in demonstrating the ongoing benefit of zilucoplan after 96 weeks of treatment (week E84 assessment) for patients in the overall trial population and the refractory subgroup population who continued to receive zilucoplan. Patients who switched from placebo to zilucoplan experienced improvements from baseline to week E12 in MG-ADL score, QMG score, MGC score, and MG-QoL15r score, and maintained the benefits out to week E84. Findings for the refractory subpopulation of the RAISE-XT study were, overall, consistent with results for the refractory subpopulation of the RAISE study. However, the open-label nature of the treatment groups and descriptive study design limits the interpretability of the findings.
In the absence of head-to-head trials comparing zilucoplan with currently available treatments for gMG, the sponsor submitted an NMA with relevant comparators, including eculizumab, efgartigimod alfa, IVIg, PLEX, and rituximab. The ITC report provided insufficient detail to describe the methods used to select studies for inclusion in the ITC, so it is unclear whether all potentially relevant studies were considered. In addition, the ITC report did not describe the findings from the feasibility assessment, which was used to inform the conduct of the NMA, and no information was provided on the characteristics of the studies included in the analyses, which is a major limitation.
Based on the data available, several important sources of heterogeneity in the patients enrolled were identified, including outcome definitions, the time point of assessments, placebo MG-ADL response rates, disease severity, and MG treatment history. Specifically, the trials had different proportions of patients rated as having mild, moderate, and severe and/or refractory gMG. The clinical expert stated that patients with refractory gMG or more severe disease may be less likely to respond to therapy, so differences in the distribution of these patients across trials may bias the findings. Both the overall population analyses and the refractory subgroup analyses contain a varied mix of patients with and without refractory gMG, a key source of heterogeneity. Moreover, the refractory subgroup analyses cannot be considered a true comparative assessment of patients with refractory gMG because not all studies were limited to patients with refractory disease.
A major limitation of the ITC methods was related to the timing of outcomes. The responder analyses used each study’s primary outcome time point, which varied from weeks 6 to 26 weeks. The change from baseline analyses assessed outcomes at week 10 or week 12 in the primary analyses but included other time points in the sensitivity analyses (from 4 weeks to 52 weeks). The CDA-AMC reviewer considered the differences in the timing of outcomes to be a significant source of heterogeneity that was not controlled for in the analyses. Restriction of the outcome to those reported at 10 weeks or 12 weeks also had serious limitations, related in part to the differences in dosing schedules (intermittent versus continuous), which could bias the results. The response definition also varied; 4 of the 5 studies in the primary analyses reported the proportion of patients with at least a 3-point improvement in the MG-ADL score, but 1 of the key studies used a 2-point threshold.
Overall, the evidence networks were sparse, and the primary analysis was based on 1 trial per comparator. Generally, the duration of follow-up in the source studies was limited (up to 26 weeks for the primary analyses), so comparative estimates were based on short-term data. The NMA results lacked precision, as shown by the wide 95% CrI. With the heterogeneity in the patient and study characteristics that was identified on the basis of a limited assessment, there is likely a substantial risk of bias for the comparisons in the network. As a result, no conclusions could be drawn on the comparative efficacy of zilucoplan. No harms outcomes were assessed in the NMA, so the comparative safety of zilucoplan is unknown.
Harms
Patients indicated a desire for treatments with a reduction in the risk and number of AEs but were willing to tolerate treatments if they were more effective. Although no patients had experience using zilucoplan, patients expressed concern about the long-term effects of available supportive treatments, specifically the negative effects of prednisone treatment.
Nearly 74% of patients in the gMG population experienced TEAEs, including headache, injection-site bruising, MG, diarrhea, injection-site pain, urinary tract infection, contusion, increased lipase, nasopharyngitis, vomiting, rash, and increased amylase. In the refractory subpopulation, approximately 86% of patients experienced TEAEs, including headache, MG, injection-site bruising, diarrhea, and vomiting. The number of patients who experienced SAEs, withdrawal due to AEs, and death were relatively small, and similar between treatment groups. The product monograph for zilucoplan highlights infections in its black-box warning. Based on the very low certainty of the evidence, more patients with gMG who received zilucoplan than placebo may experience infections (between-group difference of 8.6%; 95% CI, –3.8% to 20.9%). Although the number of infections in the overall gMG population was numerically higher in the zilucoplan group than the placebo group, the number of patients with serious infections was relatively small (< 5%), and identical in the treatment groups; no data on infections were reported for patients with refractory gMG. With an additional 12 weeks of treatment with zilucoplan in the RAISE-XT extension study, more patients with gMG experienced infections overall (72%) than in the parent RAISE trial (27% and 18% in the zilucoplan and placebo groups, respectively). In the refractory subpopulation of the RAISE-XT study, 79% of patients experienced infections in each treatment group; no data on serious infections were reported for patients with refractory gMG. Overall, the clinical expert noted that the AEs observed in both the RAISE and RAISE-XT studies were considered to be manageable and comparable to currently available treatments, and no new safety signals were identified with zilucoplan treatment.
Other Considerations
Given the lack of evidence on a direct comparative risk-benefit ratio of different biologics, the clinical expert expressed that an additional consideration for deciding between treatments would be convenience to the patient, which was echoed in the patient input, in terms of treatment frequency, duration, and administration (e.g., less invasive, at home or in a community centre). The need for vaccination with meningococcal meningitis (at least 2 weeks before treatment with zilucoplan), which is not a requirement for other treatments (e.g., efgartigimod alfa), was considered by the expert to be an additional but minor requirement for zilucoplan treatment.
Conclusion
Patients and clinicians identified a need for new treatments for gMG that reduce gMG-related and treatment-related morbidity and mortality, decrease the number and intensity of exacerbations, provide durable benefit, improve quality of life, and decrease the risk of side effects. Evidence from the randomized, phase III, double-blind RAISE trial of 174 adult patients with anti-AChR antibody–positive gMG (including 88 with refractory anti-AChR antibody–positive gMG) demonstrated that treatment with zilucoplan is likely superior to placebo in providing improvement at week 12 in signs and symptoms of disease activity, measured by the MG-ADL score (the primary outcome), in the overall trial population, which included patients with refractory and nonrefractory disease. Zilucoplan also likely results in a clinically meaningful benefit in the key secondary outcomes of QMC and MGC scores at week 12, compared with placebo, in the overall trial population. Zilucoplan likely results in improvements in HRQoL, compared to placebo, based on results from the MG-QoL15r instrument. For other secondary outcomes (i.e., at least 3-point reduction in MG-ADL score and at least a 5-point reduction in QMG response), zilucoplan is also likely to show improvements at week 12, compared with placebo, in the overall trial population. The achievement of MSE at week 12 favoured zilucoplan numerically, and although it did not reach statistical significance in the overall trial population, it may result in a benefit compared to placebo. Zilucoplan may result in an increase in the number of patients who achieve minimal manifestation status per MGFA-PIS at week 12, an exploratory outcome, compared to placebo. Confidence in the between-group differences for efficacy outcomes in the overall trial population were limited by imprecision (indicated by the associated CIs that included small effects close to the null or crossed the null) and relatively small sample sizes.
The prespecified subgroup of patients with refractory disease (50.6%) aligned with the sponsor’s reimbursement request under review for zilucoplan. Results of the subgroup analyses were subject to limitations, such as reduced sample size and a lack of formal statistical approaches to control for an inflated type I error rate in multiple comparisons. However, the clinical benefit observed in the refractory subgroup was in all cases consistent with or tended to be slightly larger than the results shown in the overall trial population and was considered to be clinically meaningful by the clinical expert consulted for this review. Results for minimal manifestation status per MGFA-PIS at week 12 were not reported for the refractory subpopulation. The safety profile of zilucoplan in the refractory subgroup was consistent with that reported in the overall trial population, with no unexpected safety signals, and was considered manageable by the clinical expert consulted for this review. The evidence is very uncertain about the effect of zilucoplan, compared to placebo, on the number of infections experienced by patients at week 12 (very low certainty) in the overall trial population.
One open-label extension study of patients with gMG, including patients with refractory gMG, after an additional 84 weeks of treatment with zilucoplan demonstrated findings supportive of those in the RAISE trial; however, the open-label nature of the study design limits the ability to distinguish the effects of treatment from the natural history of the disease, study treatments (including concomitant therapies), or other unknown factors.
A sponsor-submitted NMA comparing the efficacy of zilucoplan with other treatments for gMG, including eculizumab, efgartigimod alfa, IVIg, PLEX, and rituximab, had several limitations (sparse evidence networks, short-term data, imprecision of estimates, and heterogeneity in patient and study characteristics), which preclude the drawing of any conclusions on the comparative efficacy of zilucoplan. Because harms outcomes were not assessed in the NMA, the comparative safety of zilucoplan is unknown.
References
1.Zilbrysq (zilucoplan) 40 mg/mL solution for injection [product monograph]. Oakville (ON): UBC Canada Inc.; 2024 Jul 11.
2.Li Y, Arora Y, Levin K. Myasthenia gravis: newer therapies offer sustained improvement. Cleve Clin J Med. 2013;80(11):711-721. PubMed
3.Phillips WD, Vincent A. Pathogenesis of myasthenia gravis: update on disease types, models, and mechanisms. F1000Res. 2016;5. PubMed
4.Gilhus NE, Tzartos S, Evoli A, Palace J, Burns TM, Verschuuren J. Myasthenia gravis. Nat Rev Dis Primers. 2019;5(1):30. PubMed
5.Jayam Trouth A, Dabi A, Solieman N, Kurukumbi M, Kalyanam J. Myasthenia gravis: a review. Autoimmune Dis. 2012;2012:874680. PubMed
6.Melzer N, Ruck T, Fuhr P, et al. Clinical features, pathogenesis, and treatment of myasthenia gravis: a supplement to the Guidelines of the German Neurological Society. J Neurol. 2016;263(8):1473-1494. PubMed
7.Conti-Fine BM, Milani M, Kaminski HJ. Myasthenia gravis: past, present, and future. J Clin Invest. 2006;116(11):2843-2854. PubMed
8.Bubuioc AM, Kudebayeva A, Turuspekova S, Lisnic V, Leone MA. The epidemiology of myasthenia gravis. J Med Life. 2021;14(1):7-16. PubMed
9.Barnett C, Herbelin L, Dimachkie MM, Barohn RJ. Measuring clinical treatment response in myasthenia gravis. Neurol Clin. 2018;36(2):339-353. PubMed
10.Thomsen JLS, Andersen H. Outcome Measures in Clinical Trials of Patients With Myasthenia Gravis. Front Neurol. 2020;11:596382. PubMed
11.Conquer Myasthenia Gravis. Symptoms. 2016; https://www.myastheniagravis.org/about-mg/symptoms/. Accessed 2023 Nov 15.
12.Schroeter M, Thayssen G, Kaiser J. Myasthenia gravis: Exacerbation and crisis. Neurol Int Open. 2018;02(01):E10-E15.
13.Suh J, Goldstein JM, Nowak RJ. Clinical characteristics of refractory myasthenia gravis patients. Yale J Biol Med. 2013;86(2):255-260. PubMed
14.Clinical Study Report: MG0010, RA101495-02.301. RAISE - A Phase 3, Multicenter, Randomized, Double-Blind, Placebo-Controlled Study to Confirm the Safety, Tolerability, and Efficacy of Zilucoplan in Subjects with Generalized Myasthenia Gravis [internal sponsor's report]. Cambridge (MA): UCB Canada Inc.; 2023 Jun 30.
15.Network meta-analysis of zilucoplan and rozanolixizumab versus competitors for the treatment of generalized myasthenia gravis: Version 2.1 Technical Report [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Zilucoplan, 40 mg/mL injection. Oakville (ON): UCB Canada Inc.; 2024 Jan.
16.Howard JF, Jr. Myasthenia gravis: the role of complement at the neuromuscular junction. Ann N Y Acad Sci. 2018;1412(1):113-128. PubMed
17.The cost to patients and the community of myasthenia gravis. Sydney (AU): The Centre for International Economics; 2013: https://www.touchneurology.com/wp-content/uploads/sites/3/2018/06/www.thecie.com_.au_wp-content_uploads_2014_06_Final-report_Economic-Impact-of-Myasthenia-Gravis-08112013.pdf. Accessed 2023 Nov 15.
18.Carr AS, Cardwell CR, McCarron PO, McConville J. A systematic review of population based epidemiological studies in Myasthenia Gravis. BMC Neurol. 2010;10:46. PubMed
19.Bird SJ. Overview of the treatment of myasthenia gravis. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2024: https://www.uptodate.com/. Accessed 2024 Sep 16.
20.Bird SJ. Chronic immunotherapy for myasthenia gravis. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2024: https://www.uptodate.com/. Accessed 2024 Sep 16.
21.Narayanaswami P, Sanders DB, Wolfe G, et al. International Consensus Guidance for Management of Myasthenia Gravis: 2020 Update. Neurology. 2021;96(3):114-122. PubMed
22.Bird SJ. Role of thymectomy in patients with myasthenia gravis. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2024: https://www.uptodate.com/. Accessed 2024 Sep 16.
23.Beecher G, Anderson D, Siddiqi ZA. Rituximab in refractory myasthenia gravis: Extended prospective study results. Muscle Nerve. 2018;58(3):452-455. PubMed
24.Howard JF, Jr., Utsugisawa K, Benatar M, et al. Safety and efficacy of eculizumab in anti-acetylcholine receptor antibody-positive refractory generalised myasthenia gravis (REGAIN): a phase 3, randomised, double-blind, placebo-controlled, multicentre study. Lancet Neurol. 2017;16(12):976-986. PubMed
25.UCB Canada Inc. response to April 25, 2024 request for additional information regarding Zilbrys (zilucoplan) review [internal sponsor's report]. Oakville (ON): UCB Canada Inc.; 2024 Jul 5.
26.Howard JF, Jr., Bresch S, Genge A, et al. Safety and efficacy of zilucoplan in patients with generalised myasthenia gravis (RAISE): a randomised, double-blind, placebo-controlled, phase 3 study. Lancet Neurol. 2023;22(5):395-406. PubMed
27.Sponsor Summary of Clinical Evidence for Zilucoplan for the treatment of adult patients with AChR antibody positive refractory generalized myasthenia gravis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: zilucoplan 40 mg/mL solution for injection. Oakville (ON): UCB Canada Inc.; 2024.
28.Wolfe GI, Herbelin L, Nations SP, Foster B, Bryan WW, Barohn RJ. Myasthenia gravis activities of daily living profile. Neurology. 1999;52(7):1487-1489. PubMed
29.Muppidi S, Wolfe GI, Conaway M, Burns TM, Mg C, Mg-Qol15 Study G. MG-ADL: still a relevant outcome measure. Muscle Nerve. 2011;44(5):727-731. PubMed
30.Barohn RJ, McIntire D, Herbelin L, Wolfe GI, Nations S, Bryan WW. Reliability testing of the quantitative myasthenia gravis score. Ann N Y Acad Sci. 1998;841:769-772. PubMed
31.Katzberg HD, Barnett C, Merkies IS, Bril V. Minimal clinically important difference in myasthenia gravis: outcomes from a randomized trial. Muscle Nerve. 2014;49(5):661-665. PubMed
32.Benatar M, Sanders DB, Burns TM, et al. Recommendations for myasthenia gravis clinical trials. Muscle Nerve. 2012;45(6):909-917. PubMed
33.Sadjadi R, Conaway M, Cutter G, Sanders DB, Burns TM, Group MGCM-QS. Psychometric evaluation of the myasthenia gravis composite using Rasch analysis. Muscle Nerve. 2012;45(6):820-825. PubMed
34.Burns TM, Conaway M, Sanders DB, Composite MG, Group M-QS. The MG Composite: A valid and reliable outcome measure for myasthenia gravis. Neurology. 2010;74(18):1434-1440. PubMed
35.Vissing J, Jacob S, Fujita KP, O'Brien F, Howard JF, group Rs. 'Minimal symptom expression' in patients with acetylcholine receptor antibody-positive refractory generalized myasthenia gravis treated with eculizumab. J Neurol. 2020;267(7):1991-2001. PubMed
36.Burns TM, Grouse CK, Conaway MR, Sanders DB, mg c, mg-qol15 study g. Construct and concurrent validation of the MG-QOL15 in the practice setting. Muscle Nerve. 2010;41(2):219-226. PubMed
37.Burns TM, Sadjadi R, Utsugisawa K, et al. International clinimetric evaluation of the MG-QOL15, resulting in slight revision and subsequent validation of the MG-QOL15r. Muscle Nerve. 2016;54(6):1015-1022. PubMed
38.Sanders DB, Tucker-Lipscomb B, Massey JM. A simple manual muscle test for myasthenia gravis: validation and comparison with the QMG score. Ann N Y Acad Sci. 2003;998(1):440-444. PubMed
39.Bedlack RS, Simel DL, Bosworth H, Samsa G, Tucker-Lipscomb B, Sanders DB. Quantitative myasthenia gravis score: assessment of responsiveness and longitudinal validity. Neurology. 2005;64(11):1968-1970. PubMed
40.Barnett C, Merkies IS, Katzberg H, Bril V. Psychometric properties of the Quantitative Myasthenia Gravis Score and the Myasthenia Gravis Composite Scale. J Neuromuscul Dis. 2015;2(3):301-311. PubMed
41.Reeve BB, Wyrwich KW, Wu AW, et al. ISOQOL recommends minimum standards for patient-reported outcome measures used in patient-centered outcomes and comparative effectiveness research. Qual Life Res. 2013;22(8):1889-1905. PubMed
42.Luo Y, Dong X, Peng Y, et al. Evaluation of outcome measures for myasthenia gravis subgroups. J Clin Neurosci. 2021;91:270-275. PubMed
43.Balshem H, Helfand M, Schunemann HJ, et al. GRADE guidelines: 3. Rating the quality of evidence. Journal of clinical epidemiology. 2011;64(4):401-406. PubMed
44.Santesso N, Glenton C, Dahm P, et al. GRADE guidelines 26: informative statements to communicate the findings of systematic reviews of interventions. Journal of clinical epidemiology. 2020;119:126-135. PubMed
45.Clinical Study Report: MG0011, RA101495-02.302, interim (Sep 8, 2022). RAISE-XT - A Phase 3, Multicenter, Open-Label Extension Study of Zilucoplan in Subjects with Generalized Myasthenia Gravis [internal sponsor's report]. Cambridge (MA): UCB Canada Inc; 2022 Dec 16.
46.A systematic literature review of clinical evidence in myasthenia gravis: Version 3.0 Report [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Zilucoplan, 40 mg/mL injection. Oackville (ON): UBC Canada Inc. 2023 Sept.
47.Piehl F, Eriksson-Dufva A, Budzianowska A, et al. Efficacy and safety of rituximab for new-onset generalized myasthenia gravis: The RINOMAX randomized clinical trial. JAMA Neurol. 2022;79(11):1105-1112. PubMed
48.Howard JF, Jr., Bril V, Vu T, et al. Safety, efficacy, and tolerability of efgartigimod in patients with generalised myasthenia gravis (ADAPT): a multicentre, randomised, placebo-controlled, phase 3 trial. Lancet Neurol. 2021;20(7):526-536. PubMed
49.Bril V, Druzdz A, Grosskreutz J, et al. Safety and efficacy of rozanolixizumab in patients with generalised myasthenia gravis (MycarinG): a randomised, double-blind, placebo-controlled, adaptive phase 3 study. Lancet Neurol. 2023;22(5):383-394. PubMed
50.Vu T, Meisel A, Mantegazza R, et al. Terminal Complement Inhibitor Ravulizumab in Generalized Myasthenia Gravis. NEJM Evid. 2022;1(5):EVIDoa2100066.
51.CADTH Reimbursement Review: Efgartigimod alfa (Vyvgart). Can J Health Technol. 2024;4(4). https://www.cadth.ca/sites/default/files/DRR/2024/SR0782-Vyvgart.pdf. Accessed 2024 Apr 10.
Appendix 1: Detailed Outcome Data
Please note that this appendix has not been copy-edited.
Additional Secondary End Point
Time to First Recipient of Rescue Therapy
Time to first administration of rescue therapy during the 12-week treatment period was a secondary end point in the RAISE study, defined as follows: date of first rescue therapy use minus date of first study drug plus 1 day. Patients who did not take rescue therapy were censored at the data of withdrawal or study completion.
The Kaplan-Meier plot of time to rescue therapy is in Figure 5. The cumulative number of patients in the overall population who required rescue therapy by week 12 were 4 patients (5%) and 10 patients (12%) in the zilucoplan and placebo group, respectively (P value for difference between groups = 0.1003). The cumulative number of patients in the refractory subpopulation who required rescue therapy by week 12 were 3 patients (7%) and 7 patients (16%) in the zilucoplan and placebo group, respectively.
Figure 5: Kaplan-Meier Plot of Time to Rescue Therapy (Overall Population, mITT)
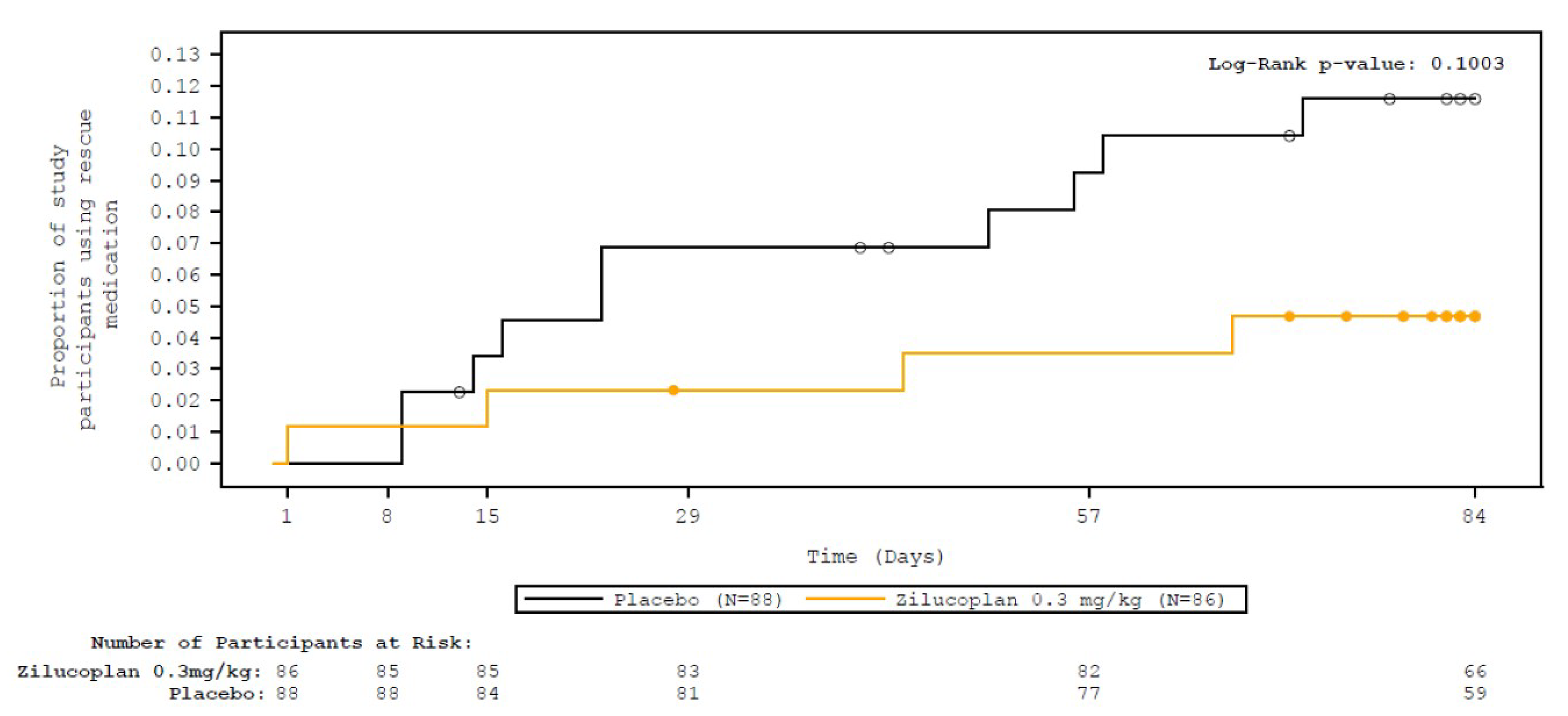
K-M = Kaplan-Meier; mITT = modified intention to treat.
Source: RAISE Clinical Study Report.14 Details included in the table are from the sponsor’s Summary of Clinical Evidence.27
Table 32: Summary of Patients’ Use of Prior gMG-Specific Medications in the Safety Set of the RAISE Study
Prior gMG-Specific Medications | Zilucoplan 0.3 mg/kg N = 86 n (%) | Placebo N = 88 n (%) |
|---|---|---|
n | 86 | 88 |
≥ 1 prior therapy | 86 (100) | 88 (100) |
≥ 2 prior therapies | 80 (93.0) | 83 (94.3) |
≥ 3 prior therapies | 71 (82.6) | 72 (81.8) |
≥ 1 prior NSIST | 59 (68.6) | 67 (76.1) |
≥ 2 prior NSISTs | 26 (30.2) | 30 (34.1) |
≥ 3 prior NSISTs | 14 (16.3) | 12 (13.6) |
IVIg | 54 (62.8) | 57 (64.8) |
Plasma exchange | 31 (36.0) | 28 (31.8) |
Plasmapheresis | NR | NR |
Any prior AChEI | 84 (97.7) | 84 (95.5) |
Any prior steroid | 77 (89.5) | 74 (84.1) |
Any prior NSIST | 59 (68.6) | 67 (76.1) |
Prior AChEI only | 7 (8.1) | 5 (5.7) |
Prior steroid only | 0 | 0 |
Prior NSIST only | 0 | 0 |
AChEI = acetylcholinesterase inhibitor; gMG = generalized myasthenia gravis; Ig = immunoglobulin; n = number of patients for whom the observation was reported; N = number of patients in the analysis set; NR = not reported; NSIST = nonsteroidal immunosuppressive drug.
Source: RAISE Clinical Study Report.14
Table 33: Key Efficacy Results in the RAISE-XT Study (Overall mITT Population and Refractory Subpopulation, November 2023 Data Cut-Off), Week E84 and E108
Outcome measure | RAISE-XT (overall population) | RAISE-XT (refractory subpopulation) | ||
|---|---|---|---|---|
Zilucoplan 0.3 mg/kg/ 0.3 mg/kg N = 93 | Placebo/ Zilucoplan 0.3 mg/kg N = 90 | Zilucoplan 0.3 mg/kg/ 0.3 mg/kg N = 43 | Placebo/ Zilucoplan 0.3 mg/kg N = 42 | |
Change from parent-study baseline in MG-ADL score | ||||
Week E84, n | 77 | 65 | 34 | 26 |
Week E84, mean (SE) | –6.82 (0.40) | –7.43 (0.55) | –7.62 (0.53) | –7.38 (0.93) |
Week E84, LS mean (SE) | –6.26 (0.50) | −6.89 (0.63) | NR | NR |
95% CI | –7.23 to –5.29 | –8.13 to –5.64 | NR | NR |
Week E108, n | 49 | 37 | 22 | 12 |
Week E108, mean (SE) | –6.65 (0.51) | –7.78 (0.76) | –7.64 (0.70) | –9.17 (1.31) |
Week E108, LS mean (SE) | –6.37 (0.54) | –7.09 (0.70) | NR | NR |
95% CI | –7.42 to –5.31 | –8.46 to –5.73 | NR | NR |
Change from parent-study baseline in QMG score | ||||
Week E84, n | 70 | 62 | 31 | 26 |
Week E84, mean (SE) | –9.29 (0.67) | –9.31 (0.85) | –10.16 (1.01) | –10.08 (1.36) |
Week E84, LS mean (SE) | –9.49 (0.70) | –9.54 (0.86) | NR | NR |
95% CI | –10.87 to –8.12 | –11.22 to –7.86 | NR | NR |
Week E108, n | 48 | 35 | 22 | 12 |
Week E108, mean (SE) | –9.79 (0.75) | –9.91 (1.15) | –10.27 (1.18) | –12.17 (2.18) |
Week E108, LS mean (SE) | –10.38 (0.75) | –9.56 (0.95) | NR | NR |
95% CI | –11.86 to –8.90 | –11.43 to –7.70 | NR | NR |
Change from parent-study baseline in MGC score | ||||
Week E84, n | 70 | 61 | 31 | 26 |
Week E84, mean (SE) | –13.40 (0.84) | –14.13 (1.22) | –13.77 (1.15) | –14.65 (1.84) |
Week E84, LS mean (SE) | –12.66 (0.91) | –13.24 (1.22) | NR | NR |
95% CI | –14.45 to –10.86 | –15.64 to –10.85 | NR | NR |
Week E108, n | 48 | 33 | 22 | 10 |
Week E108, mean (SE) | –13.06 (1.05) | –15.64 (1.76) | –14.00 (1.34) | –17.90 (2.95) |
Week E108, LS mean (SE) | –13.58 (0.99) | –13.75 (1.37) | NR | NR |
95% CI | –15.53 to –11.64 | –16.45 to –11.06 | NR | NR |
Change from parent-study baseline in MG-QoL15r score | ||||
Week E84, n | 70 | 60 | 31 | 26 |
Week E84, mean (SE) | −9.67 (0.90) | –10.67 (1.20) | –9.84 (1.34) | –11.46 (1.98) |
Week E84, LS mean (SE) | –9.94 (1.00) | –8.93 (1.17) | NR | NR |
95% CI | –11.90 to –7.97 | –11.24 to –6.62 | NR | NR |
Week E108, n | 48 | 32 | 22 | 10 |
Week E108, mean (SE) | −9.85 (1.30) | –11.88 (1.63) | –10.73 (1.96) | –14.50 (2.99) |
Week E108, LS mean (SE) | –10.21 (1.08) | –8.87 (1.29) | NR | NR |
95% CI | –12.32 to –8.10 | –11.40 to –6.34 | NR | NR |
Achieving MSE without rescue therapy | ||||
Week E84, n | 65 | 58 | 27 | 23 |
Week E84, MSE, n (%) | 30 (46.2) | 31 (53.4) | 14 (51.9) | 9 (39.1) |
Week E108, n | 41 | 32 | 17 | 10 |
Week E108, MSE, n (%) | 15 (36.6) | 15 (46.9) | 8 (47.1) | 5 (50.0) |
MG-ADL responder without rescue therapy | ||||
Week E84, n | 65 | 58 | 27 | 23 |
Week E84, MG-ADL responder, n (%) | 57 (87.7) | 52 (89.7) | 27 (100) | 19 (82.6) |
Week E108, n | 41 | 32 | 17 | 10 |
Week E108, MG-ADL responder, n (%) | 35 (85.4) | 29 (90.6) | 16 (94.1) | 9 (90.0) |
QMG responder without rescue therapy | ||||
Week E84, n | 59 | 55 | 25 | 23 |
Week E84, QMG responder, n (%) | 50 (84.7) | 43 (78.2) | 20 (80.0) | 18 (78.3) |
Week E108, n | 40 | 30 | 17 | 10 |
Week E108, QMG responder, n (%) | 36 (90.0) | 24 (80.0) | 16 (94.1) | 9 (90.0) |
CI = confidence interval; E = extension; LS = least squares; MG-ADL = Myasthenia Gravis Activities of Daily Living; MGC = Myasthenia Gravis Composite; MG-QoL15r = Myasthenia Gravis Quality of Life 15-item revised; MGFA-PIS = Myasthenia Gravis Foundation of America Post-Intervention Status; mITT = modified intention to treat; MSE = minimal symptom expression; NR = not reported; QMG = quantitative myasthenia gravis; SE = standard error.
aA MG-ADL responder is defined as having at least a 3-point improvement (decrease) in the MG-ADL score.
bA QMG responder is defined as having at least a 5-point improvement (decrease) in the QMG score.
Source: RAISE-XT Clinical Study Report.45
Pharmacoeconomic Review
Abbreviations
AChR
acetylcholine receptor
BIA
budget impact analysis
CDA-AMC
Canada's Drug Agency
CFB
change from baseline
CrI
credible interval
gMG
generalized myasthenia gravis
HRQoL
health-related quality of life
ICER
incremental cost-effectiveness ratio
Ig
immunoglobulin
IST
immunosuppressant therapy
MDC
Muscular Dystrophy Canada
MG
myasthenia gravis
MG-ADL
Myasthenia Gravis Activities of Daily Living
MGFA
Myasthenia Gravis Foundation of America
NMA
network meta-analysis
ODB
Ontario Drug Benefit
pCPA
pan-Canadian Pharmaceutical Alliance
PLEX
plasma exchange
QALY
quality-adjusted life-year
QMG
Quantitative Myasthenia Gravis
SC
subcutaneous
SOC
standard of care
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Zilucoplan (Zilbrysq), 40 mg/mL solution for injection |
Indication | For the treatment of gMG in adult patients who are AChR antibody-positive. Patients continued to receive standard therapy throughout the pivotal trial. |
Health Canada approval status | Approved |
Health Canada review pathway | Standard review |
NOC date | July 11, 2024 |
Reimbursement request | As an add-on therapy for the treatment of adult patients with AChR antibody positive refractory gMG, defined as not achieving symptom control after:
|
Sponsor | UCB Canada Inc. |
Submission history | None |
AChR = acetylcholine receptor; gMG = generalized myasthenia gravis; NOC = Notice of Compliance.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Markov model |
Target population | Patients with anti-AChR antibody–positive gMG who are uncontrolled on high-dose corticosteroids and nonsteroidal ISTs, consistent with patients with refractory conditions included in the RAISE triala |
Treatment | Zilucoplan plus SOCb |
Dose regimen | Body weight < 56 kg: 16.6 mg SC once daily Body weight ≥ 56 to < 77 kg: 23.0 mg SC once daily Body weight ≥ 77 kg: 32.4 mg SC once daily |
Submitted prices | Zilucoplan 16.6 mg/0.416 mL prefilled syringe: $650.27 Zilucoplan 23.0 mg/0.574 mL prefilled syringe: $900.98 Zilucoplan 32.4 mg/0.810 mL prefilled syringe: $1,269.21 |
Submitted treatment cost | $461,990 per year (364 days), assuming a patient weighing more than 77 kg |
Comparators |
|
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | Lifetime (48.2 years) |
Key data sources | Sponsor-submitted NMA report comparing zilucoplan, efgartigimod alfa, SOC, and eculizumab. Naive comparisons using data from the RAISE trial (SOC), a trial by Barth et al. (2011) (chronic IVIg and/or SCIg and chronic PLEX), and a trial by Nowak et al. (2022) (rituximab). |
Submitted results |
|
Key limitations |
|
CDA-AMC reanalysis results |
|
AChR = acetylcholine receptor; CDA-AMC = Canada’s Drug Agency; gMG = generalized myasthenia gravis; HRQoL = health-related quality of life; ICER = incremental cost-effectiveness ratio; Ig = immunoglobulin; IST = immunosuppressive therapy; LY = life-year; NMA = network meta-analysis; PLEX = plasma exchange; QALY = quality-adjusted life-year; SC = subcutaneous; SOC = standard of care.
aCDA-AMC accepted a request for deviation from the sponsor to limit the economic submission to the sponsor’s reimbursement request.
bRefractory SOC is defined as consisting of a 12.5% mix of each of the following: prednisone, azathioprine, mycophenolate mofetil, cyclosporine, tacrolimus, methotrexate, pyridostigmine, and cyclophosphamide.
Conclusions
In adult patients with Myasthenia Gravis Foundation of America (MGFA) class II to class IV anti–acetylcholine receptor (AChR) antibody–positive generalized myasthenia gravis (gMG), evidence from the RAISE trial demonstrated that, compared to placebo, treatment with zilucoplan (Zilbrysq) resulted in a statistically significant improvement in change from baseline (CFB) to week 12 in Myasthenia Gravis Activities of Daily Living (MG-ADL) score. Based on the clinical review team’s appraisal of the RAISE trial, treatment with zilucoplan in adults with gMG likely resulted in a clinically important improvement in MG-ADL score and an increase in the number of patients with at least a 3-point improvement in MG-ADL score compared to placebo. Findings were similar when limited to the subgroup of patients with refractory gMG, but uncertainty was higher because of the smaller sample size. In the absence of direct evidence comparing zilucoplan to other active comparators currently used as add-on therapies for the treatment of adults with refractory gMG (i.e., chronic IV immunoglobulin [Ig] and/or subcutaneous [SC] immunoglobulin [SCIg], chronic plasma exchange [PLEX], rituximab, eculizumab, efgartigimod alfa), the sponsor submitted a network analysis (NMA), as well as naive comparisons, to inform the model regarding the relative probability of response to therapy (defined as a ≥ 3-point improvement in MG-ADL score, a ≥ 3-point improvement in Quantitative Myasthenia Gravis [QMG] score, or a ≥ 5-point improvement in QMG score, depending on comparator), and extent of response (the proportion of responders estimated to have a 3 to 4 point improvement in MG-ADL score versus a ≥ 5 point improvement) between comparators. The Canada's Drug Agency (CDA-AMC) clinical review concluded that the sponsor’s NMA had several limitations (sparse evidence networks, short-term data, imprecision of estimates, and heterogeneity in patient and study characteristics), which precluded the drawing of any conclusions on the comparative efficacy of zilucoplan relative to its add-on comparators.
CDA-AMC was unable to address limitations of the sponsor’s submitted model or the uncertainty related to the comparative clinical data and long-term efficacy of zilucoplan compared to other add-on therapies used in addition to standard of care (SOC) in adults with refractory anti-AChR antibody–positive gMG. As such, CDA-AMC was unable to derive a more reliable base-case estimate of the cost-effectiveness of zilucoplan. Results of the sponsor’s base-case sequential analysis suggest that zilucoplan plus SOC is associated with an incremental cost-effectiveness ratio (ICER) of $1,611,347 per quality-adjusted life-year (QALY) gained relative to PLEX plus SOC (incremental costs = $560,670, incremental QALYs = 0.35). Based on this analysis, a price reduction of approximately 83% would be required for zilucoplan to be considered cost-effective at a willingness-to-pay threshold of $50,000 per QALY gained, reducing the unit price of zilucoplan from $1,269 to $216 per 32.4 mg vial (and reducing the annual drug-acquisition cost from $461,990 to $78,538). This analysis likely underestimates the ICER, as the sponsor’s model was programmed to assume that treatment effects were maintained beyond treatment discontinuation. There is no robust evidence to support this assumption regarding the maintenance of effect. CDA-AMC could not revise treatment effects but undertook scenario analyses (using the submitted price of zilucoplan) that increased the duration of treatment to match the duration of benefit, in which the ICER increased to $6,904,042 per QALY gained relative to PLEX plus SOC because of increased drug-acquisition costs. As such, a greater price reduction may be required to be considered cost-effective at a willingness-to-pay threshold of $50,000 per QALY gained.
The results of the economic model were based on efficacy inputs obtained from the sponsor’s submitted NMA and naive comparisons. CDA-AMC noted that the relative effects obtained from the NMA and naive comparisons for effectiveness parameters in the model are uncertain and were likely biased because of the time points chosen for analysis. Although the sponsor’s base case suggests differences in treatment benefit for adults with refractory anti-AChR antibody–positive gMG, these results will only be realized should the numerical differences observed in the NMA and naive comparisons occur in clinical practice and lead to meaningful improvement for patients. Clinical expert feedback suggested that zilucoplan and efgartigimod alfa may have a similar efficacy.
Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, clinician groups, and drug plans that participated in the CDA-AMC review process.
Patient input was received from Muscular Dystrophy Canada (MDC), which conducted an online survey, interviews, round tables, and health-related quality of life (HRQoL) assessments to produce a qualitative thematic analysis. In total, the MDC submission included data from 127 individuals impacted by myasthenia gravis (MG), the majority of whom have a confirmed diagnosis of gMG. Respondents were from all provinces in Canada, and 47 respondents were specifically asked to provide input on their hopes and expectations for zilucoplan and their everyday experiences with MG. Of the respondents, 85% reported significant difficulty in receiving their diagnosis. MDC identified the following themes regarding MG symptoms: loss of productivity; fatigue, energy levels, and quality of sleep; respiratory health; mobility and strength; independence; relationships and social participation; and vision, speech, and swallowing. Patients also identified nonphysical impacts affecting their mental health, quality of life, and the well-being of their families. Themes identified regarding current treatments included negative experiences with steroids, the slow onset of medication effects, and a feeling of trial and error with medications. Patients reported experience with prednisone, pyridostigmine, azathioprine, mycophenolate mofetil, IVIg, and thymectomy, and reported difficulty accessing rituximab. IVIg was reported by several patients as effective or helpful but time-consuming and wearing off too quickly. In terms of gaps, MDC reported themes of patients wanting a decreased intensity of exacerbations and side effects, maintenance of independence, and less serious hospital admissions. Patients were reported as stating that their current medications seemed to decrease the number of exacerbations but did not impact overall quality of life. MDC emphasized the need for improved treatment options. No responding patients had experience with zilucoplan.
Clinician input was received from the Neuromuscular Disease Network for Canada, which stated that the current treatment landscape for MG ranges from critical care for acute MG crises, pyridostigmine for symptomatic relief, thymectomy as a disease-modifying treatment, to long-term immunotherapy options, such as steroids, steroid-sparing agents, IVIg, plasmapheresis, eculizumab, rituximab, efgartigimod alfa, and ravulizumab. The overarching goals of MG therapy are to reduce morbidity and mortality, minimize hospital visits, and enhance quality of life. Input from the Neuromuscular Disease Network for Canada noted that treatment gaps include inadequate response and side effects, lack of tolerability, lack of compliance, lack of convenience, need for a considerable amount of time to become effective for some treatments, difficulties with venous access and need for frequent sessions for IVIg and plasmapheresis, concerns about prolonged immunosuppression and a lack of established efficacy beyond muscle-specific tyrosine kinase antibody–positive gMG for rituximab, concerns regarding the long-term use of steroids, and treatments for patients with seronegative disease and pediatric patients. The clinician group noted that zilucoplan is likely to be used for refractory anti-AChR antibody–positive gMG, as described in the sponsor’s reimbursement request, but may, in time, expand beyond patients with refractory disease, based on real-world effectiveness and safety data. The efficacy of zilucoplan has not yet been established in patients with anti-AChR antibody–negative gMG.
The drug plans noted zilucoplan can be self-administered at home and may displace other therapies that require IV infusions. The plans also noted that considerations for the initiation, continuation, prescribing, administration, and discontinuation of therapy could be aligned to those of efgartigimod alfa (which is under active negotiation with the pan-Canadian Pharmaceutical Alliance [pCPA]).
Several of these concerns were addressed in the sponsor’s model:
Model health states were based on improvements to the MG-ADL score, which considers many of the symptoms mentioned by patients.
The sponsor’s model included all comparators currently reimbursed for refractory gMG.
Quality of life and mortality impacts for chronic corticosteroid use were included.
CDA-AMC was unable to address the following concerns raised from this input:
There was a lack of robust comparative efficacy and safety data between zilucoplan and other add-on therapies to SOC.
Economic Review
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
Zilucoplan is indicated for the treatment of gMG in adult patients who have anti-AChR antibody–positive disease,1 whereas the sponsor’s reimbursement request is “as an add-on therapy for the treatment of adult patients with AChR antibody positive refractory gMG, defined as not achieving symptom control after:
Treatment for at least 1 year with 2 or more of the following therapies: prednisone, azathioprine, mycophenolate cyclosporine, cyclophosphamide, methotrexate, tacrolimus, other corticosteroids for gMG, other immunosuppressive therapies (ISTs), OR
History of treatment with at least one of these therapies for 1 year or more and required chronic plasma exchange (PLEX), intravenous immunoglobulin (IVIg), or subcutaneous immunoglobulin (SCIg) at least every 3 months for the 12 months prior to treatment with zilucoplan.”2
CDA-AMC accepted a deviation request from the sponsor to focus the economic model on the requested reimbursement population. The sponsor submitted a cost-utility analysis of zilucoplan plus SOC compared to SOC alone, and to SOC in combination with chronic IVIg and/or SCIg, chronic PLEX, rituximab, eculizumab, or efgartigimod alfa. SOC was defined as a mixed treatment basket consisting of 12.5% of each of the following: prednisone, azathioprine, mycophenolate mofetil, cyclosporine, tacrolimus, methotrexate, pyridostigmine, and cyclophosphamide.
The sponsor submitted new pharmacoeconomic and budget impact analysis (BIA) models and reports in July 2024. The inputs and results included are reflective of these new filings.
Zilucoplan is available in prefilled syringes that contain 16.6 mg, 23.0 mg, or 32.4 mg of 40 mg/mL zilocoplan.1 The recommended dose is 0.3 mg/kg as a once-daily SC injection, with the actual daily dose based on body weight ranges of 16.6 mg daily for patients weighing less than 56 kg, 23.0 mg daily for patients weighing 56 kg or more to less than 77 kg, and 32.4 mg daily for patients weighing 77 kg or more. At the submitted prices of $650.28, $900.98, and $1,269.21 per 16.6 mg, 23.0 mg, and 32.4 mg syringes, respectively, the annual cost of treatment with zilucoplan is $237,512 to $463,577 per patient, depending on weight. In the model, the sponsor assumed that all patients received 32.4 mg daily and that a year was 364 days in length, so the annual cost of zilucoplan for modelled patients was $461,990 per patient.
The clinical outcomes of interest were life-years and QALYs. The sponsor adopted a lifetime horizon (48.2 years), and the analysis was conducted from the perspective of a publicly funded health care payer. Future costs and benefits were discounted at a rate of 1.5% per year, and the model cycle length was 2 weeks. Owing to the short cycle length, a half-cycle correction was not used.
Model Structure
The sponsor submitted a Markov model with 6 health states: uncontrolled on high-dose steroids and ISTs, 2 response-based states (a 3-point to 4-point CFB in MG-ADL total score or a ≥ 5-point CFB in MG-ADL score), acute exacerbation requiring rescue therapy, myasthenic crisis, and death (Figure 1). Patients entered the model in the uncontrolled state. Up until the response assessment time point, which differed by treatment, patients could achieve a response defined as a minimum 3-point reduction from baseline in MG-ADL total score, and move into 1 of the 2 response health states based on their probability of achieving a 3-point to 4-point improvement or a 5-point or greater improvement in MG-ADL score. After the response assessment time point, patients who were not in a response state were assumed to discontinue non-SOC treatment and their disease would remain uncontrolled.
Model Inputs
The baseline population characteristics used to inform the model were based on the refractory subgroup of the RAISE trial, which was a randomized, double-blind, placebo-controlled, multicentre trial of patients aged 18 to 74 years (mean = 51.8 years) who had anti-AChR antibody–positive gMG that was MGFA class II to class IV at screening and an MG-ADL score of at least 6 (mean = 10.7).3,4 In the refractory subgroup, 64.8% of patients were female and the mean body weight was 85.7 kg. Patients were considered part of the refractory subgroup if they received treatment for at least 1 year with 2 or more of the following therapies: prednisone, azathioprine, mycophenolate mofetil, cyclosporine, cyclophosphamide, methotrexate, tacrolimus, rituximab, eculizumab, other corticosteroids for gMG, and other ISTs; or had a history of treatment with at least 1 of the aforementioned therapies for 1 year or more and required chronic PLEX, IVIg, or SCIg at least every 3 months in the 12 months before enrolment.
The primary measure of efficacy in the model was the probability of treatment response at the assessment time point. Response rates for zilucoplan (██%), eculizumab (██%), efgartigimod alfa (██%), and SOC (██%) were derived from a sponsor-conducted NMA, which compared treatments at approximately 12 weeks (10 weeks for efgartigimod alfa and 26 weeks for eculizumab), where response was defined as at least a 3-point improvement in MG-ADL score and SOC was assumed to be equivalent to placebo. Response rates for IVIg and/or SCIg (51%) and PLEX (57%) were derived from a 2011 trial,5 where response was defined as an improvement of at least 3.5 points on the QMG scale, measured at 14 days. Response for rituximab (35%) was derived from the Beat MG study,6 with response defined as an improvement of at least 5 points on the QMG scale at 52 weeks. Response rates for IVIg and/or SCIg, PLEX, and rituximab relative to the other comparators are therefore based on a naive comparison.
Patients who responded before the assessment time point transitioned into 1 of the 2 response states. For patients responding to zilucoplan, eculizumab, or efgartigimod alfa, 29% were assumed to have a 3-point to 4-point improvement in MG-ADL score (mean improvement, 3.46 points), whereas 71% had a 5-point or greater improvement (mean improvement, 7.58 points), based on the distribution of patients responding to zilucoplan in the RAISE-XT extension study and the mean CFB in MG-ADL scores across treatment groups (zilucoplan and SOC) for responding patients who achieved a 3-point to 4-point improvement in MG-ADL score or a 5-point or greater improvement. For patients responding to rituximab, chronic IVIg and/or SCIg, PLEX, or SOC, 44% were assumed have a 3-point to 4-point MG-ADL score improvement, and 56% to have a 5-point or greater improvement, with the same mean improvements in scores. After week 12, the proportion of patients responding to zilucoplan who were assumed to have a 5-point or greater improvement in MG-ADL score increased to 80%, based on data from the RAISE-XT study. No further improvements after the initial assessment time point were assumed for patients receiving treatments other than zilucoplan.
Patients who did not respond by the assessment time point were assumed to discontinue their add-on therapy, if applicable, and remain in the uncontrolled state on SOC alone. Patients who responded were assumed to remain on their add-on therapy, if applicable, for a maximum of 2 years, with benefits continuing to accrue for the remainder of the time horizon until exacerbation, myasthenic crisis, or death.
In each cycle, patients could experience clinical events (i.e., myasthenic exacerbations or crises). Annual rates depended on whether the patient was in a response state (0.1179 for exacerbation, 0.0117 for crisis) or uncontrolled state (0.6515 for exacerbation, 0.0117 for crisis).7,8 After an exacerbation, 16.8% of patients were assumed to worsen to experience a crisis, which was based on the number of patients requiring ventilation by day 15 after an exacerbation in an acute IVIg study.9 Before the assessment time point, 35% of patients experiencing an exacerbation were assumed to re-enter the uncontrolled health state and discontinue their add-on therapy,9 if applicable; the rest were assumed to re-enter 1 of the 2 response health states in the original proportion assigned to their specific therapy. After the assessment time point, all patients experiencing an exacerbation were assumed to either worsen or experience a crisis (16.8%) or discontinue their add-on therapy, if applicable, and enter the uncontrolled state (83.2%). Because no serious adverse events had an incidence of 5% or more in the RAISE trial, adverse events were not considered in the model.2 Mortality in the response, uncontrolled, and exacerbation health states was assumed to be equal to that of the general population. Although the sponsor indicated that patients in myasthenic crisis had a 5% risk of death per crisis, this was not applied in the economic model, as described in the report.7
Utility values were derived using the MG-ADL score as a predictor of EQ-5D, using a repeated-measures regression model of UK crosswalk utilities from pooled treatment arms of the RAISE study (Table 9);10 mean utility values by model health state are reported in Table 10. Utilities were further adjusted to consider age-related and sex-related disutilities using a UK-based regression algorithm (Table 9).11 Patients entering the 5-point or greater CFB in MG-ADL score health state did not accrue the greater utility associated with that state until after the assessment time point for their treatment. A disutility of –0.20 was applied for 14 days for patients experiencing an exacerbation; for those in crisis, a disutility of –0.72 was applied for 28 days.7 Additionally, disutilities associated with chronic steroid use were assigned to patients in the uncontrolled state and in the 3-point to 4-point CFB in MG-ADL score response state, assuming patients in these states used high-dose (disutility = 0.18) and low-dose (disutility = 0.07) corticosteroids, respectively.
Costs in the model included drug-acquisition, administration, vaccination, routine care, clinical event management costs, and end-of-life costs. All patients were assumed to receive SOC, with equal proportions assumed to use prednisone, azathioprine, mycophenolate mofetil, cyclosporine, tacrolimus, methotrexate, cyclophosphamide, and pyridostigmine. The acquisition costs of drugs used in SOC ($59.76 per model cycle) were from the Ontario Drug Benefit (ODB) Formulary, as was the cost of rituximab, whereas the costs of IVIg and SCIg were from a 2022 to 2023 annual report for Atlantic Canada,12 of PLEX were from the literature,13 and of eculizumab and efgartigimod alfa were from prices submitted to CDA-AMC for their respective reimbursement reviews.14,15 An administration cost of $217.5416 was applied to each nonblood product IV infusion (rituximab, efgartigimod alfa, eculizumab), assuming a 1 hour infusion time, whereas PLEX, IVIg, and SCIg costs were $652.53 per administration, assuming 3-hour infusions, and a cost was $40.39 for the first zilucoplan SC administration only.17 Of the patients receiving zilucoplan or eculizumab, 4% were assumed to require a meningococcal vaccine ($160).18,19 Routine-care costs included physician visits, other health care professional visits, outpatient hospital visits, emergency department visits, hospital stays, and intensive care unit stays, based on frequencies reported in the literature8,20,21 and Canadian cost sources.22-27 Costs for managing corticosteroid use were derived from the submission to CDA-AMC for efgartigimod alfa, and were $12,197 annually for patients in the uncontrolled state, $5,309 annually for patients in the 3-point to 4-point CFB in MG-ADL score state, and $0 for patients in the 5-point or greater CFB in MG-ADL score health state. Overall annual health care resource use costs, excluding exacerbations and crises, totalled $30,739 for patients in the uncontrolled state, $11,266 for patients in the 3-point to 4-point CFB in MG-ADL score state, and $5,956 for patients in the 5-point or greater CFB in MG-ADL score state. Costs for exacerbations and myasthenic crises were $9,089 and $33,622 per event, respectively, for patients not receiving chronic IVIg or SCIg; $6,221 and $33,419 per event, respectively, for patients receiving chronic IVIg or SCIg; and $10,176 and $37,374 per event, respectively, for patients receiving chronic PLEX. The model assumed a one-time end-of-life cost of $11,405.28
Summary of Sponsor’s Economic Evaluation Results
All analyses were run probabilistically (500 iterations) for the base-case and scenario analyses. Deterministic and probabilistic results were similar; probabilistic results are presented in Table 3 and deterministic results are presented in Table 12 of Appendix 4. All analyses were reported for the sponsor’s reimbursement request population. Disaggregated results of the sponsor’s probabilistic base case are presented in Appendix 3.
Base-Case Results
In sequential analysis, the sponsor’s base case reported that zilucoplan plus SOC was associated with an ICER of $1,611,347 per QALY gained (incremental cost = $135,468; incremental QALYs = 0.17) compared to PLEX plus SOC (Table 3). Zilucoplan had a 0% chance of being cost-effective at a willingness-to-pay threshold of $50,000 per QALY, whereas most other comparators had some chance of being cost-effective at this threshold, including rituximab (47.4%), SOC (20.6%), IVIg and SCIg (18.8%), PLEX (13.0%), and efgartigimod alfa (0.2%). Limitations of the sponsor’s model meant that CDA-AMC was unable to report the proportion of incremental benefit during the within-trial period, as opposed to the extrapolated period, because of differences in the time points at which benefits were accrued for treatments in the model. At the end of the time horizon, CDA-AMC calculated that approximately 4.5% of patients in the zilucoplan group remained alive.
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Total QALYs | Sequential ICER ($/ QALY) |
|---|---|---|---|
Probabilistic analysis | |||
SOC | 881,636 | 12.49 | Reference |
Rituximab plus SOC | 882,085 | 12.58 | 5,862 |
PLEX plus SOC | 911,026 | 12.71 | 209,321 |
Zilucoplan plus SOC | 1,471,696 | 13.06 | 1,611,347 |
Dominated treatments | |||
IVIg and/or SCIg plus SOC | 920,985 | 12.65 | Dominated by PLEX |
Efgartigimod alfa plus SOC | 1,336,228 | 12.90 | Extendedly dominated by a mix of PLEX and zilucoplan |
Eculizumab plus SOC | 2,009,838 | 12.76 | Dominated by zilucoplan and efgartigimod alfa |
ICER = incremental cost-effectiveness ratio; Ig = immunoglobulin; PLEX = plasma exchange; QALY = quality-adjusted life-year; SC = subcutaneous; SOC = standard of care.
Source: Sponsor’s pharmacoeconomic submission.2
Sensitivity and Scenario Analysis Results
The sponsor presented deterministic scenario analyses that considered alternate inputs for the discount rate and time horizon, incorporated response rates directly from individual trials rather than the NMA and allowed vial sharing. In these scenario analyses, the ICERs for zilucoplan were similar, although the treatments on the efficiency frontier differed.
The sponsor conducted a scenario analysis from a societal perspective. This deterministic analysis included additional costs associated with work hours lost by the patient and the cost of caregiver hours spent caring for a patient with gMG. In this analysis, zilucoplan was associated with an ICER of $1,636,600 per QALY gained compared to PLEX. This was similar to the sponsor’s deterministic base-case analysis that used a health care payer perspective (ICER = $1,645,217 per QALY gained compared to PLEX).
CDA-AMC Appraisal of the Sponsor’s Economic Evaluation
CDA-AMC identified several key limitations to the sponsor’s analysis that have notable implications for the economic analysis:
The relative clinical efficacy is highly uncertain: Efficacy in the economic model is based on the proportion of patients who respond to treatment. Because there have been no head-to-head trials comparing the efficacy of zilucoplan with other active comparators (i.e., rituximab, chronic IVIg or SCIg, chronic PLEX, efgartigimod alfa, and eculizumab), the sponsor-conducted an NMA.29 However, the NMA was associated with substantial limitations, including sparse evidence networks, short-term data, and heterogeneity in outcome definitions, time points of assessment, disease severity, refractory disease status (even in the refractory subgroup analyses), serotypes of MG included, and MG treatment history. The CDA-AMC clinical review noted that the heterogeneity of patient and study characteristics in the NMA made it unclear if the transitivity assumption was met; thus, it is unclear if the results are meaningful. Additionally, the results lacked precision, as evidenced by wide credible intervals (CrIs) (e.g., in the refractory population responder analysis, the odds ratio for zilucoplan versus placebo was ████ [95% CrI, ████ ██ █████], whereas for zilucoplan versus efgartigimod alfa, it was ████ [95% CrI, ████ ██ █████]). The CDA-AMC clinical report noted that, given the limitations of the NMA, conclusions could not be drawn about the efficacy of zilucoplan relative to the other treatments included in the NMA. Comparative harms outcomes were not included in the NMA.
In the submitted model, the proportion of patients responding to rituximab, chronic IVIg and/or SCIg, or chronic PLEX was not derived from the sponsor’s NMA, but was instead based on a naive comparison, with response defined as the proportion of patients achieving an improvement of at least 5 points on the QMG scale by 52 weeks for rituximab,6 and the proportion of patients achieving an improvement of at least 3.5 points on the QMG scale by 2 weeks for chronic IVIg and/or SCIg and chronic PLEX.5 As such, conclusions also cannot be drawn about the relative efficacy of these 3 comparators to each other or to those included in the sponsor’s NMA.
Finally, the sponsor additionally assumed that patients receiving zilucoplan could continue to improve between week 12 and week 24 of the model, based on data from the RAISE-XT trial, with a higher proportion achieving a 5-point or greater improvement in MG-ADL score from baseline to week 24 than from baseline to week 12. However, patients receiving any other comparator were assumed not to improve after their initial time point of assessment. This assumption further increases the uncertainty of the efficacy of zilucoplan relative to its comparators, particularly efgartigimod alfa, where the response rate was very similar. When the time point of assessment for zilucoplan was set to 12 weeks rather than 24 weeks, the sponsor’s deterministic analysis reports that zilucoplan was dominated by efgartigimod alfa (i.e., zilucoplan is more costly and less effective).
CDA-AMC was unable to adequately address the uncertainty associated with estimates derived from either the submitted NMA or naive comparisons in the model.
Discontinuation assumptions were inappropriate: The sponsor assumed that after the assessment time point, any patient who experienced an exacerbation or crisis discontinued their add-on therapy (if applicable), and returned to the uncontrolled state, regardless of the state from which they experienced the exacerbation or crisis. This is not plausible, according to clinical expert opinion obtained by CDA-AMC, because patients would typically have their event treated and return to their previous treatment and health state, which is consistent with previous input from clinical experts obtained by CDA-AMC.7 The sponsor also assumed that any patient who discontinued their add-on therapy because of a lack of response or a clinical event (exacerbation or crisis) remained on SOC alone for the remainder of their lives; clinical expert input obtained by CDA-AMC noted that patients who discontinue 1 add-on therapy would switch to another.
Additionally, the sponsor assumed that all patients who are still receiving their add-on therapy (i.e., they did not discontinue because of a lack of efficacy or an exacerbation or crisis) will discontinue after 2 years of therapy and stop accruing drug-acquisition costs. However, patients are assumed to continue experiencing the improved MG-ADL score and thus continue the improved quality of life and reduced risk of exacerbation or crisis associated with their add-on therapy for the remainder of the time horizon (i.e., up to 46 more years), in the absence of exacerbation, crisis, or death. According to clinical expert opinion obtained by CDA-AMC, this is not a reasonable assumption; patients who discontinue a therapy would not be expected to retain its benefit over the long-term. As such, the submitted model either substantially underestimates drug costs for all add-on therapies or substantially overestimates their benefits after treatment discontinuation.
Because of the structure of the model, CDA-AMC was unable to return patients to their previous health state after exacerbation or crisis, or to assign a subsequent therapy, or to implement a gradual return to baseline quality-of-life status for patients who discontinued their add-on therapy, using either the 2-year stopping rule or a long-term discontinuation rate. In a scenario analysis, CDA-AMC deactivated the 2-year stopping rule to test the impact of ensuring that patients receiving the benefit of their add-on therapies were still accruing the costs associated with those therapies.
Assumptions regarding corticosteroid use were inappropriate: The sponsor assumed that 100% of patients in the uncontrolled health state used high-dose corticosteroids, 100% of patients in the 3-point to 4-point CFB in MG-ADL score state used low-dose corticosteroids, and 100% of patients in the 5-point or greater CFB in MG-ADL score state did not use corticosteroids at any dose. This is not plausible, according to clinical expert input obtained by CDA-AMC, because some patients may achieve low MG-ADL scores related to their use of high-dose corticosteroids. Change in corticosteroid use was not an outcome of the RAISE trial, in which patients were expected to remain on stable doses of SOC treatments, including corticosteroids, unless medically indicated. As such, the RAISE trial did not demonstrate an association between zilucoplan and a reduction in corticosteroid use. Additionally, at baseline, 77% of the zilucoplan group and 70% of the placebo group in the refractory subpopulation of the RAISE trial were using concomitant corticosteroids, suggesting that not all patients with uncontrolled, refractory gMG in clinical practice would be expected to be on corticosteroids, high-dose or otherwise (refer to the CDA-AMC clinical report). The sponsor assumed utility decrements associated with steroid use in a manner similar to that in the submission to CDA-AMC for efgartigimod alfa,7 derived from observational studies conducted in Sweden and the US of patients with lupus or any condition requiring chronic corticosteroid use.30,31 As noted in the CDA-AMC review of that submission, generalizability, confounding, and partial double counting of HRQoL effects are an issue when decrements derived from these sources are applied to patients with gMG based on corticosteroid use assumptions, as is the assumption that such decrements are lessened or no longer apply if a patient experiences an MG-ADL score improvement. Similarly, the sponsor assumed annual costs associated with corticosteroid use consistent with those used in the efgartigimod alfa submission to CDA-AMC.7 CDA-AMC did not specifically note concerns about corticosteroid costs in that review because of the complete removal of differential corticosteroid use in CDA-AMC reanalyses, but limitations associated with the sponsor’s assumptions about differential costs are similar to those of differential utility decrements related to corticosteroid use; however, they are subject to issues of generalizability, confounding, and partial double counting of impact, in addition to the issue that reductions in the proportion of use and/or dosing of corticosteroids were not shown in the clinical trials of either zilucoplan or efgartigimod alfa.3,32
To explore uncertainty in the magnitude of effect that potential reductions in corticosteroid use would have on patient quality of life and health care costs, as well as uncertainty in the proportion of patients using corticosteroids at baseline and the proportion who could reduce such usage with the use of add-on therapies to SOC, CDA-AMC conducted a scenario in which the additional costs and utility decrements associated with the assumption of changes in corticosteroid use were removed.
The model lacked transparency and reliability: The sponsor’s submitted model included numerous IFERROR statements, which can lead to situations in which the parameter value is overwritten with an alternative value without alerting the user to the automated overwriting. The systematic use of IFERROR statements makes thorough auditing of the sponsor’s model impractical, as it remains unclear whether the model is running appropriately. Additionally, after running a probabilistic analysis, the model returned some inputs to default settings (e.g., drug-acquisition prices). As such, additional runs of the probabilistic analysis could be based on unintended inputs if not thoroughly reviewed each time.
Furthermore, the submitted model had instances in which parameters or programming were not incorporated as described in the submitted technical report. For example, the sponsor’s submitted report describes mortality due to myasthenic crisis as a 5% risk per event (i.e., 5% of patients die within the 2-week model cycle when experiencing a crisis, consistent with the source of that assumption);7 however, the implementation of this assumption resulted in a 5% annual risk of mortality in the crisis state, corresponding to a risk of approximately 0.2% per 2-week cycle spent in the crisis state. It was also unclear if and how the model incorporated uncertainty into parameters such as response rates, as the rates and odds ratios reported on the parameters sheet did not appear to match those used to calculate transition probabilities in the model’s engine.
The model’s probabilistic analysis failed when certain inputs were changed. For example, changing the price of zilucoplan to a formula, turning off the stopping rule, or correcting the crisis mortality rate in the transition probability tables led to the model returning the deterministic results for all probabilistic iterations. As such, the model was unreliable and time-consuming to troubleshoot, limiting the ability of CDA-AMC to correct issues and validate results within the time frame of this review. Finally, the model did not reliably report sequential analyses because of errors in the way the determination of extended dominance was implemented.
In a scenario analysis, CDA-AMC corrected mortality in the model, so that all patients having a myasthenic crisis had a 5% risk of death within the 2-week cycle of their crisis. All scenarios, including price-reduction analyses, were conducted deterministically because of reliability issues with the probabilistic results. All sequential results in this report have been confirmed by CDA-AMC. Substantial uncertainty remains in the validity and reliability of modelled results.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CDA-AMC (refer to Table 4).
Table 4: Key Assumptions of the Submitted Economic Evaluation (Not Noted as Limitations to the Submission)
Sponsor’s key assumption | CDA-AMC comment |
|---|---|
Background therapies used in the RAISE trial represent SOC. | Uncertain. The RAISE trial compared zilucoplan to placebo rather than to SOC. Instead, patients in both groups could receive SOC therapies, including AChEIs, CSs, azathioprine, or mycophenolate mofetil, and cyclosporine, methotrexate, or tacrolimus,3 provided they’d received a stable dose for at least 30 days before baseline and no change in therapy was expected during the 12-week treatment period of the trial. Because this concomitant SOC was stable, zilucoplan was not compared to any individual or combination SOC, as it would typically be used in clinical practice, (i.e., altering doses or adding medications to suit a patient’s symptoms or other needs). As such, the cost-effectiveness of zilucoplan compared to customizable SOC is uncertain. |
All patients were assumed to use a single drug within the SOC basket in equal proportions. | Inappropriate. Patients with gMG are not equally likely to use any 1 of the AChEIs, CSs, or NSISTs included in SOC, and many are on more than 1 drug at a time, as demonstrated in the baseline MG medications reported in the RAISE trial (in which the sum of the proportion of patients receiving each medication type was approximately 200% for each treatment group).3 However, because SOC was assumed to be the same among all comparators, patients did not discontinue SOC, and there were minimal differences in life-years among comparators, changes to the cost of SOC are not expected to impact model results and, thus, were not changed by CDA-AMC. |
AEs were excluded from the model. | Uncertain. The sponsor noted its intention to consider any serious AE with an incidence of ≥ 5% in the model, as it was assumed that only SAEs would incur costs to the health care system. Because of the safety profile of the included comparators, no AEs were considered to meet this inclusion criterion. The submitted NMA did not consider safety outcomes. The AEs observed in the RAISE trial and the RAISE-XT extension study were considered to be manageable and comparable to other available treatments for gMG, according to clinical expert opinion obtained by CDA-AMC. |
Eculizumab was included as a comparator. | Reasonable but irrelevant. According to current CDA-AMC Procedures for Reimbursement Reviews,33 comparators should include treatments that are currently reimbursed by at least 1 participating drug plan for the indication under review or that have received a recommendation in favour of reimbursement. Because eculizumab meets these criteria, the sponsor included it as a comparator. However, after the CDEC recommendation to reimburse eculizumab with conditions,34 negotiations with pCPA were unsuccessful,35 so eculizumab is not currently funded by any participating plan and is unlikely to become so in the near future. As such, CDA-AMC considered eculizumab to be an irrelevant comparator at the time of this review and removed it from scenario analyses. This change has no impact on the results, as eculizumab was dominated in the sponsor’s base case and would have remained so in all CDA-AMC scenarios. |
Ravulizumab was excluded as a comparator. | Reasonable but uncertain. The CDA-AMC review of ravulizumab for anti-AChR antibody–positive gMG resulted in a do not list recommendation,36 so the criteria for inclusion as a comparator outlined in the CDA-AMC Procedures for Reimbursement Reviews33 were not met. However, at the time of this review, a resubmission of ravulizumab is currently under review. As such, it is uncertain whether ravulizumab will become a funded comparator for the treatment of gMG. The submitted model did not have an option to include ravulizumab. |
Pricing of blood products. | Unknown. In the absence of publicly available list prices for immunoglobulins, the sponsor has used an estimate of the total cost of grams of IVIg discarded in Nova Scotia and New Brunswick12 to estimate cost per milligram. Similarly, the sponsor used an estimate for the cost of PLEX from the literature.13 It is unknown whether these costs are reflective of costs currently paid throughout Canada. As such, the true cost-effectiveness of zilucoplan compared to blood products is unknown. |
Price of zilucoplan. | Inappropriate. The sponsor’s model used a price of $8,884.4250 per 7-pack of 32.4 g syringes of zilucoplan, whereas the submitted price is $8,884.4364. Because the difference in pricing was very small and because changing the price of zilucoplan in the model sometimes resulted in the probabilistic analysis returning deterministic results, CDA-AMC did not correct the issue. |
Dosing assumptions and patient body weight. | Inappropriate. The sponsor’s model assumed that all patients who received a dose of their add-on therapy was consistent with the mean patient weight in the RAISE trial (85.7 kg), assuming wastage of excess medication in vials.3 Although mean patient weight could vary probabilistically by 20% from this mean, all patients within each iteration received a dose appropriate for the weight generated, including wastage. As such, the sponsor’s deterministic and probabilistic results overestimate the treatment costs of zilucoplan and its comparators, because in clinical practice, patients would receive a distribution of vial sizes or vial numbers, rather than a mean dose rounded up. Additionally, it is uncertain whether the mean weight observed in the RAISE trial is consistent with that of adults with gMG seen in clinical practice in Canada. For example, mean body weight in the efgartigimod alfa ADAPT trial was approximately 80.5 kg7 and the 50th percentile for body weight of people in Canada aged 40 to 79 years in 2009 to 2011 was approximately 77 kg,37 which are both lower than the mean observed in the RAISE trial. CDA-AMC was unable to implement a distribution of patient weights and their resulting doses per comparator because of a lack of data on the proportion of patients in weight categories with thresholds relevant to all comparators from the RAISE trial, and because of the unreliability of the model’s probabilistic results when inputs were changed. |
AChEI = acetylcholine esterase inhibitor, AChR = acetylcholine receptor; AE = adverse event; CDA-AMC = Canada’s Drug Agency; CDEC = Canadian Drug Expert Committee; CS = corticosteroid; gMG = generalized myasthenia gravis; Ig = immunoglobulin; MG = myasthenia gravis; NMA = network meta-analysis; NSIST = nonsteroidal immunosuppressant therapy; pCPA = pan-Canadian Pharmaceutical Alliance; PLEX = plasma exchange; SAE = serious adverse event; SOC = standard of care.
CDA-AMC Reanalyses of the Economic Evaluation
Base-Case Results
Given the limitations of the sponsor’s economic submission that CDA-AMC identified, CDA-AMC was unable to derive a more reliable estimate of the cost-effectiveness of zilucoplan as an add-on therapy for the treatment of adult patients with refractory anti-AChR antibody–positive gMG. CDA-AMC noted that the sponsor’s analysis remains uncertain. The estimates of relative effect obtained from the sponsor’s NMAs, as well as the naive comparisons, informing effectiveness within the model represent the largest source of uncertainty. The outputs of the sponsor’s base case suggest differences in treatment benefits among therapies for the add-on treatment of patients with anti-AChR antibody–positive gMG. These results will only be realized if the numerical differences observed in the NMA and naive comparisons are deemed to be valid.
When considering the sponsor’s base-case results, the probability that zilucoplan is cost-effective at a willingness-to-pay threshold of $50,000 per QALY is 0%. Notably, despite being extendedly dominated, the probability that efgartigimod alfa is cost-effective is higher than the probability that zilucoplan is cost-effective across all willingness-to-pay thresholds.
Scenario Analysis Results
To explore uncertainty in some of the assumptions in the model, CDA-AMC conducted scenario analyses that removed the 2-year stopping rule to ensure that patients accrued drug-acquisition costs for the length of time they accrued the benefits associated with the drug in question (zilucoplan ICER = $6,904,042 per QALY relative to PLEX), removed utility decrements and extra costs associated with corticosteroid use (zilucoplan ICER = $1,820,589 per QALY relative to PLEX), assumed a 5% mortality rate per myasthenic crisis (zilucoplan ICER = $1,380,965 per QALY relative to PLEX), and combined all 3 issues (zilucoplan ICER = $6,024,288 per QALY relative to PLEX) (refer to Table 12).
Additionally, CDA-AMC undertook price-reduction analyses based on the sponsor’s submitted base case to explore the price reduction required to obtain an ICER for zilucoplan below the $50,000 per QALY threshold. These analyses were conducted on the deterministic base case, owing to model errors in the sponsor’s probabilistic analysis results. To be considered cost-effective at a willingness-to-pay threshold of $50,000 per QALY gained, the price of zilucoplan would need to be reduced by approximately 83%, corresponding to approximately $215 per 32.4 mg syringe (Table 5).
When considering scenario 4, in which the 2-year stopping rule was removed, extra costs and utility decrements associated with corticosteroid use were removed, and a 5% risk of mortality was assumed per myasthenic crisis, the price of zilucoplan would need to be reduced by approximately 95.5%, or $57 per 32.4 mg syringe, to be considered cost-effective at a $50,000 per QALY threshold.
Table 5: CDA-AMC Price-Reduction Analyses
Price-reduction analysis | Unit drug cost per 32.4 mg syringe | ICERs for zilucoplan plus SOC vs. comparators plus SOC ($/QALY) |
|---|---|---|
Sponsor’s deterministic base case | ||
No price reduction | $1,269 | $1,645,217 vs. PLEX |
10% | $1,142 | $1,444,135 vs. PLEX |
20% | $1,015 | $1,243,052 vs. PLEX |
30% | $888 | $1,041,970 vs. PLEX |
40% | $762 | $840,888 vs. PLEX |
50% | $635 | $639,806 vs. PLEX |
60% | $507 | $438,724 vs. PLEX |
70% | $381 | $237,641 vs. PLEX |
80% | $254 | $88,272 vs. rituximab |
90% | $127 | Zilucoplan plus SOC would be less costly than SOC alone (i.e., it would be the referent) |
CDA-AMC = Canada's Drug Agency; ICER = incremental cost-effectiveness ratio; PLEX = plasma exchange; QALY = quality-adjusted life-year; SOC = standard of care; vs. = versus.
Issues for Consideration
Alternative budget holders: Although the use of zilucoplan would be associated with additional costs from both the Canadian drug plan payer perspective as well as the overall health care payer perspective, the reimbursement of zilucoplan for gMG may reduce the use of blood products (IVIg, SCIg, PLEX), which may result in some savings to alternate budget holders. A potential reduction in the use of blood products is also relevant, given ongoing reports of blood and plasma shortages in Canada.38
Other therapies are currently under review for gMG: At the time of this review, a resubmission of ravulizumab as an add-on therapy for adults with anti-AChR antibody–positive gMG39 is under review by CDA-AMC, as is a new submission for rozanolixizumab as an add-on therapy for adults with anti-AChR antibody–positive or muscle-specific tyrosine kinase antibody–positive gMG.40 If funded as requested, both of these therapies will become comparators of interest to zilucoplan, and their similar time points of entry into the market may impact the relative market share of all newer comparators.
Overall Conclusions
In adult patients with MGFA class II to class IV anti-AChR antibody–positive gMG, evidence from the RAISE trial demonstrated that compared to placebo, treatment with zilucoplan resulted in statistically significant improvement in CFB to week 12 in MG-ADL score. Based on the clinical review team’s appraisal of the RAISE trial, treatment with zilucoplan in adults with gMG likely resulted in a clinically important improvement in MG-ADL scores and an increase in the number of patients with at least a 3-point improvement in MG-ADL score compared to placebo. Findings were similar when limited to the subgroup of patients with refractory gMG, but the amount of uncertainty increased because of the smaller sample size. In the absence of direct evidence comparing zilucoplan to other active comparators currently used as add-on therapies for the treatment of adults with refractory gMG (i.e., chronic IVIg and/or SCIg, chronic PLEX, rituximab, eculizumab, efgartigimod alfa), the sponsor submitted an NMA, as well as naive comparisons, to inform the model regarding the relative probability of response to therapy (defined as a ≥ 3-point improvement in MG-ADL score, a ≥ 3-point improvement in QMG score, or a ≥ 5-point improvement in QMG score, depending on comparator), and the extent of response (the proportion of responders estimated to have a 3-point to 4-point improvement in MG-ADL score versus the proportion with a 5-point or greater improvement) between comparators. The CDA-AMC clinical review concluded that the sponsor’s NMA had several limitations (sparse evidence networks, short-term data, imprecision of estimates, and heterogeneity in patient and study characteristics), which precluded the drawing of any conclusions on the efficacy of zilucoplan relative to its add-on comparators.
CDA-AMC was unable to address the limitations of the sponsor’s submitted model or the uncertainty related to the comparative clinical data and long-term efficacy of zilucoplan compared to other add-on therapies used in addition to SOC in adults with refractory anti-AChR antibody–positive gMG. As such, CDA-AMC was unable to derive a more reliable base-case estimate of the cost-effectiveness of zilucoplan. Results of the sponsor’s base-case sequential analysis suggest that zilucoplan plus SOC is associated with an ICER of $1,611,347 per QALY gained relative to PLEX plus SOC (incremental costs = $560,670; incremental QALY = 0.35). Based on this analysis, a price reduction of approximately 83% would be required for zilucoplan to be considered cost-effective at a willingness-to-pay threshold of $50,000 per QALY gained, reducing the unit price of zilucoplan from $1,269 to $216 per 32.4 mg vial (and reducing the annual drug-acquisition cost from $461,990 to $78,538). This analysis likely underestimates the ICER, as the sponsor’s model was programmed to assume that treatment effects were maintained beyond treatment discontinuation. There is no robust evidence to support this assumption regarding the maintenance of effect. CDA-AMC could not revise treatment effects but undertook scenario analyses (using the submitted price of zilucoplan) that increased the duration of treatment to match the duration of benefit, in which the ICER increased to $6,904,042 per QALY gained relative to PLEX plus SOC because of increased drug-acquisition costs. As such, a greater price reduction may be required for zilucoplan to be considered cost-effective at a willingness-to-pay threshold of $50,000 per QALY gained.
The results of the economic model were based on efficacy inputs obtained from the sponsor’s submitted NMA and naive comparisons. CDA-AMC noted that the relative effects obtained from the NMA and naive comparisons for the effectiveness parameters in the model are uncertain and were likely biased because of the time points chosen for analysis. Although the sponsor’s base case suggests differences in treatment benefit for adults with refractory anti-AChR antibody–positive gMG, these results will only be realized if the numerical differences observed in the NMA and naive comparisons occur in clinical practice and lead to meaningful improvement for patients. Clinical expert feedback suggested that zilucoplan and efgartigimod alfa may have a similar efficacy.
References
1.U. C. B. Canada Inc. Zilucoplan (Brand Name TBC) Draft Product Monograph [sponsor supplied reference]. 2023.
2.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Zilbrysq (zilucoplan), 40 mg/mL solution for subcutaneous injection (16.6 mg in 0.416 mL, 23.0 mg in 0.574 mL, 32.4 mg in 0.810 mL). Oakville (ON): UCB Canada Inc; 2024 Jul 5.
3.Howard JF, Jr., Bresch S, Genge A, et al. Safety and efficacy of zilucoplan in patients with generalised myasthenia gravis (RAISE): a randomised, double-blind, placebo-controlled, phase 3 study. Lancet Neurol. 2023;22(5):395-406. PubMed
4.UCB data on file. Zilucoplan - MG0010 (RAISE) Clinical Study Report. 30 Jun 2022 [sponsor supplied reference].
5.Barth D, Nabavi Nouri M, Ng E, Nwe P, Bril V. Comparison of IVIg and PLEX in patients with myasthenia gravis. Neurology. 2011;76(23):2017-2023. PubMed
6.Nowak RJ, Coffey CS, Goldstein JM, et al. Phase 2 Trial of Rituximab in Acetylcholine Receptor Antibody-Positive Generalized Myasthenia Gravis: The BeatMG Study. Neurology. 2022;98(4):e376-e389. PubMed
7.CADTH Reimbursement Review: Efgartigimod Alfa (Vyvgart). Ottawa (ON): CADTH; 2024: https://www.cda-amc.ca/sites/default/files/DRR/2024/SR0782-Vyvgart.pdf. Accessed 2024 Aug 13.
8.Abuzinadah AR, Alanazy MH, Butt NS, Barohn RJ, Dimachkie MM. Exacerbation Rate in Generalized Myasthenia Gravis and Its Predictors. Eur Neurol. 2021;84(1):43-48. PubMed
9.Gajdos P, Tranchant C, Clair B, et al. Treatment of myasthenia gravis exacerbation with intravenous immunoglobulin: a randomized double-blind clinical trial. Arch Neurol. 2005;62(11):1689-1693. PubMed
10.Grimson F, Kiri S, Pannullo F. Health-related quality of life in generalised myasthenia gravis: The relationship between Myasthenia Gravis Activities of Daily Living and EQ-5D-5L in the RAISE study [accessed by sponsor]. Value Health. 2023;26(11):S2. https://www.valueinhealthjournal.com/article/S1098-3015(23)03330-2/pdf.
11.Ara R, Brazier JE. Populating an economic model with health state utility values: moving toward better practice. Value Health. 2010;13(5):509-518. PubMed
12.Nova Scotia Provincial Blood Coordinating Team. Atlantic Canada Annual IVIG and SCIG FY 2022-23 Report [accessed by sponsor]. 2023; http://www.cdha.nshealth.ca/system/files/sites/documents/ivig-and-scig-utilization-atlantic-provinces-fiscal-year-202223.pdf.
13.Furlan JC, Barth D, Barnett C, Bril V. Cost-minimization analysis comparing intravenous immunoglobulin with plasma exchange in the management of patients with myasthenia gravis. Muscle Nerve. 2016;53(6):872-876. PubMed
14.CADTH Final Reimbursement Recommendation: Eculizumab (SOLIRIS) [accessed by sponsor]. Ottawa (ON): CADTH; 2020.
15.CADTH Reimbursement Recommendation: Efgartigimod alfa (VYVGART) [accessed by sponsor]. Ottawa (ON): CADTH; 2024.
16.Tam VC, Ko YJ, Mittmann N, et al. Cost-effectiveness of systemic therapies for metastatic pancreatic cancer. Curr Oncol. 2013;20(2):e90-e106. PubMed
17.Wages for Registered nurses and registered psychiatric nurses (NOC 31301). Ottawa (ON): Government of Canada; 2023: https://www.jobbank.gc.ca/wagereport/occupation/993. Accessed 2023 Mar 21.
18.TravelMed. Vaccines [accessed by sponsor]. 2023; https://travelmed.ca/vaccines/. Accessed 2023 Dec.
19.CADTH Pharmacoeconomic Report: Eculizumab (SOLIRIS) [accessed by sponsor]. Ottawa (ON): CADTH; 2020.
20.Harris L, Graham S, MacLachlan S, Exuzides A, Jacob S. Healthcare resource utilization by patients with treatment-refractory myasthenia gravis in England. J Med Econ. 2019;22(7):691-697. PubMed
21.Phillips G, Abreu C, Goyal A, et al. Real-World Healthcare Resource Utilization and Cost Burden Assessment for Adults With Generalized Myasthenia Gravis in the United States. Front Neurol. 2021;12:809999. PubMed
22.Ontario Ministry of Health and Long Term Care. Schedule of Benefits, Physician Services Under the Health Insurance Act [accessed by sponsor]. 2023; https://www.health.gov.on.ca/en/pro/programs/ohip/sob/physserv/sob_master.pdf.
23.Government of Alberta. Alberta Interactive Health Data Application [accessed by sponsor]. http://www.ahw.gov.ab.ca/IHDA_Retrieval/ihdaData.do. Accessed 2024 Jan.
24.Canadian Institute for Health Information. Hospital spending: Focus on the emergency department [accessed by sponsor]. 2020; https://www.cihi.ca/sites/default/files/document/hospital-spending-highlights-2020-en.pdf.
25.Canadian Institute for Health Information. Care in Canadian ICUs [accessed by sponsor]. 2016; https://secure.cihi.ca/free_products/ICU_Report_EN.pdf. Accessed 2024 Jan.
26.Canadian Institute for Health Information. Cost of a Standard Hospital Stay [accessed by sponsor]. 2023; https://www.cihi.ca/en/indicators/cost-of-a-standard-hospital-stay.
27.Canadian Institute for Health Information. Hospital stays in Canada [accessed by sponsor]. 2023; https://www.cihi.ca/en/hospital-stays-in-canada.
28.Canadian Institute for Health Information. Patient Cost Estimator [accessed by sponsor]. 2022; https://www.cihi.ca/en/patient-cost-estimator.
29.Sponsor's NMA report title [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Zilbrysq (zilucoplan), 40 mg/mL solution for subcutaneous injection (16.6 mg in 0.416 mL, 23.0 mg in 0.574 mL, 32.4 mg in 0.810 mL). Oakville (ON): UCB Canada Inc; 2024 Feb 29.
30.Bexelius C, Wachtmeister K, Skare P, Jonsson L, Vollenhoven R. Drivers of cost and health-related quality of life in patients with systemic lupus erythematosus (SLE): a Swedish nationwide study based on patient reports. Lupus. 2013;22(8):793-801. PubMed
31.Sullivan PW, Ghushchyan VH, Globe G, Sucher B. Health-related quality of life associated with systemic corticosteroids. Qual Life Res. 2017;26(4):1037-1058. PubMed
32.Howard JF, Jr., Bril V, Vu T, et al. Safety, efficacy, and tolerability of efgartigimod in patients with generalised myasthenia gravis (ADAPT): a multicentre, randomised, placebo-controlled, phase 3 trial. Lancet Neurol. 2021;20(7):526-536. PubMed
33.Guidelines for the Economic Evaluation of Health Technologies: Canada - 4th Edition [accessed by sponsor]. Ottawa (ON): CADTH; 2017: https://www.cadth.ca/guidelines-economic-evaluation-health-technologies-canada-4th-edition. Accessed 2023 Nov.
34.CADTH Reimbursement Recommendation: Eculizumab (Soliris) [accessed by sponsor]. Ottawa (ON): CADTH; 2020: https://www.cadth.ca/eculizumab-2. Accessed 2023 Dec.
35.pan-Canadian Pricing Alliance. Soliris (eculizumab). Indication: Myasthenia Gravis. 2022; https://www.pcpacanada.ca/negotiation/21306. Accessed 2024 Sep 23.
36.CADTH Reimbursement Recommendation: Ravulizumab (Ultomiris) for the treatment of adult patients with anti-acetylcholine receptor antibody–positive generalized myasthenia gravis. Ottawa (ON): CADTH; 2023: https://www.cadth.ca/sites/default/files/DRR/2023/SR0765Ultomiris%20-%20Confidential%20Final%20CADTH%20Recommendation%20August%2024,%202023%20revised.pdf. Accessed 2024 Apr 15.
37.Table 23. Measured weight, by age and sex, household population, Canada, 2009 to 2011. Ottawa (ON): Statistics Canada; 2015: https://www150.statcan.gc.ca/n1/pub/82-626-x/2013001/t024-eng.htm. Accessed 2024 Sep 23.
38.Pasieka C. Canadian Blood Services needs thousands more donors to roll up their sleeves. 2023; https://www.cbc.ca/news/canada/toronto/canadian-blood-services-needs-thousands-more-canadians-to-roll-up-their-sleeves-1.6879312. Accessed 2024 Sep 19.
39.CDA Reimbursement Review: Ravulizumab. Ottawa (ON): Canada's Drug Agency; 2025: https://www.cda-amc.ca/ravulizumab-4. Accessed 2024 Sep 19.
40.Canada's Drug Agency. CDA Reimbursement Review: Rozanolixizumab Ottawa (ON): Canada's Drug Agency; 2025: https://www.cda-amc.ca/rozanolixizumab. Accessed 2024 Sep 19.
41.Vyvgart (efgartigimod alfa): 400 mg/20 mL (20 mg/mL) solution for intravenous use [product monograph]. Mississauga ON: Quality & Compliance Services Inc.; 2023: https://pdf.hres.ca/dpd_pm/00073416.PDF. Accessed 2024 Aug 15.
42.Ultomiris (ravulizumab): 10 mg/mL & 100 mg/mL concentrate for solution for intravenous use [product monograph]. Zurich (CH): Alexion Pharma GmbH; 2023 Jan 6: https://pdf.hres.ca/dpd_pm/00069134.PDF. Accessed 2024 Aug 15.
43.CADTH Reimbursement Review Report: Ravulizumab (ULTOMIRIS) [accessed by sponsor]. Ottawa (ON): CADTH; 2023.
44.Alberta Blue Cross. Interactive Drug Benefit List. 2024; https://idbl.ab.bluecross.ca/idbl/load.do. Accessed 2024 Apr 3.
45.Ontario Ministry of Health, Ontario Ministry of Long-Term Care. Ontario drug benefit formulary/comparative drug index. 2024; https://www.formulary.health.gov.on.ca/formulary/. Accessed 2024 Aug 15.
46.Farmakidis C, Pasnoor M, Dimachkie MM, Barohn RJ. Treatment of Myasthenia Gravis. Neurol Clin. 2018;36(2):311-337. PubMed
47.DeltaPA. Ottawa (ON): IQVIA; 2023: https://www.iqvia.com/. Accessed 2024 Aug 15.
48.Saskatchewan Drug Plan. Search formulary. 2024; https://formulary.drugplan.ehealthsask.ca/SearchFormulary. Accessed 2024 Aug 15.
49.Heckmann JM, Rawoot A, Bateman K, Renison R, Badri M. A single-blinded trial of methotrexate versus azathioprine as steroid-sparing agents in generalized myasthenia gravis. BMC Neurol. 2011;11:97. PubMed
50.Myfortic (mycophenolic acid): 180 mg, 360 mg enteric-coated tablets [product monograph]. Dorval (QC): Novartis Pharmaceuticals Canada Inc; 2022 Jan 24.
51.Melzer N, Ruck T, Fuhr P, et al. Clinical features, pathogenesis, and treatment of myasthenia gravis: a supplement to the Guidelines of the German Neurological Society. J Neurol. 2016;263(8):1473-1494. PubMed
52.Bank of Canada. Inflation calculator. 2024; https://www.bankofcanada.ca/rates/related/inflation-calculator/. Accessed 2024 Apr 3.
53.Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Zilbrysq (zilucoplan), 40 mg/mL solution for subcutaneous injection (16.6 mg in 0.416 mL, 23.0 mg in 0.574 mL, 32.4 mg in 0.810 mL). Oakville (ON): UCB Canada Inc; 2024 Feb 29.
54.Breiner A, Widdifield J, Katzberg HD, Barnett C, Bril V, Tu K. Epidemiology of myasthenia gravis in Ontario, Canada. Neuromuscul Disord. 2016;26(1):41-46. PubMed
55.Bubuioc AM, Kudebayeva A, Turuspekova S, Lisnic V, Leone MA. The epidemiology of myasthenia gravis. J Med Life. 2021;14(1):7-16. PubMed
56.Spillane J, Higham E, Kullmann DM. Myasthenia gravis. BMJ. 2012;345:e8497. PubMed
57.Suh J, Goldstein JM, Nowak RJ. Clinical characteristics of refractory myasthenia gravis patients. Yale J Biol Med. 2013;86(2):255-260. PubMed
58.Table: 17-10-0057-01 Projected population, by projection scenario, age and sex, as of July 1 (x 1,000). Ottawa (ON): Statistics Canada; 2022: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1710005701. Accessed 2024 Aug 15.
59.Government of Canada. First National and Inuit Health Branch: Non-Insured Health Benefits Program Annual Report 2021/2022 [accessed by sponsor]. 2023; https://www.sac-isc.gc.ca/eng/1683039690813/1683039973755.
60.pan-Canadian Pricing Alliance. Vyvgart (efgartigimod alfa). Indication: Generalized Myasthenia Gravis (gMG). 2024; https://www.pcpacanada.ca/negotiation/22530. Accessed 2024 Sep 23.
61.The Conference Board of Canada. Understanding the Gap 2.0: A Pan-Canadian Analysis of Prescription Drug Insurance Coverage [accessed by sponsor]. 2022.
Appendix 1: Cost Comparison Table
Please note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical experts and CDA-AMC–participating public drug plans. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 6: CDA-AMC Cost Comparison for Complement Inhibitors Indicated for the Treatment of Generalized Myasthenia Gravis
Treatment | Strength / concentration | Form | Price ($) | Recommended dosage | Average daily cost ($) | Average annual cost ($) |
|---|---|---|---|---|---|---|
Zilucoplan (Zilbrysq) | 40 mg/mL | 16.6 mg 23.0 mg 32.4 mg Prefilled syringe for subcutaneous injection | $650.2718 $900.9790 $1,269.2052 | For patients weighing:
| 650.27 to 1,269.21 | 237,512 to 463,577 |
Efgartigimod alfa (Vyvgart) | 20 mg/mL | 400 mg vial solution for IV use | 7,900.0000a | Loading: 10 mg/kg (max 1,200 mg) weekly for 4 weeks. Subsequent treatment cycles are based on clinical evaluation and may vary by patient.41 | 816.71 to 1,225.07b | 298,304 to 447,456b |
Ravulizumab (Ultomiris) | 10 mg/mL | 30 mL single-dose vial of concentrate for solution for IV infusion | 7,296.6700c | Loading dose at weeks 0, then maintenance dose at week 2 and every 8 weeks thereafter based on weight as followsd: ≥ 40 kg to < 60 kg:
≥ 60 kg to < 100 kg:
≥ 100 kg:
| First year: 1,412.85 to 1,703.41 Subsequent years: 1,302.98 to 1,563.57 | First year: 516,044 to 622,171 Subsequent years: 475,912 to 571,095 |
Eculizumab (Soliris) | 10 mg/mL | 300 mg single-use vial | 6,675.3000e | Loading: 900 mg weekly for 4 weeks, then 1,200 mg for the fifth dose 1 week later Maintenance: 1,200 mg every 2 weeks thereafter. | First year: 1,943.78 Subsequent years: 1,907.23 | First year: 709,966 Subsequent years: 696,615 |
CDA-AMC = Canada’s Drug Agency; NA = not applicable.
Note: Costs assume a 365.25 day year and wastage of excess medication in vials.
aSponsor submitted price.2
bAssumes an average of 4.72 4-week courses per year.15 Cost per 4-week course is $63,200 for patients weighing 41 to 80 kg, and $94,800 for patients weighing over 80 kg.
cPrice submitted for CADTH’s review of Ultomiris for gMG. Ultomiris received a do not reimburse recommendation for this indication,43 but a resubmission is currently under review.39
dPatients weighting less than 40 kg have different dosing quantities and schedules. For patients switching from eculizumab, the loading dose of ravulizumab is given 2 weeks after the last eculizumab infusion. Maintenance doses are then given every 8 weeks, starting 2 weeks after the loading dose.
eAlberta formulary, accessed August 2024. Note that Alberta does not fund eculizumab for generalized myasthenia gravis.44
Table 7: CDA-AMC Cost Comparison for Other Treatments for Generalized Myasthenia Gravis
Treatment | Strength / concentration | Form | Price ($) | Recommended dosagea | Average daily cost ($) | Average annual cost ($) |
|---|---|---|---|---|---|---|
Other Biologics | ||||||
Rituximab (biosimilars) | 10 mg/mL | 10 mL 50 mL Vial for IV infusion | 297.0000 1,485.0000 | 375 mg/m2 weekly for 4 doses | NA | Cost per course: 8,316 |
Alternate dosing: 1 g, followed by 1 g 2 weeks later, and then every 6 months | First year: 31.90 Subsequent years: 16.26 | First year: 11,652 Subsequent years: 5,940 | ||||
Glucocorticoids | ||||||
Prednisone (Winpred, generics) | 1 mg 5 mg 50 mg | Tablet | 0.1276 0.0220 0.1735 | Initiate at 10 to 20 mg/day, increase by 5 mg/day per week until stable remission (target 1 mg/kg/day) | 0.04 to 0.31 | 16 to 112 |
Alternate dosing: Initiate at 60 to 80 mg/day, then taper after improvement | 0.21 to 0.31 | 77 to 112 | ||||
Immunosuppressive agents | ||||||
Azathioprine (generics) | 50 mg | Tablet | 0.5185 | Initiate at 50 mg/day for 5 days, and then, escalate to 2.5 to 3 mg/kg/dayb | 2.07 to 2.59 | 757 to 976 |
Cyclophosphamide (Procytox, generics) | 25 mg 50 mg | Tablet | 0.3545 0.4773 | 500 mg/m2 to 1,000 mg/m2 every month for 6 months | NA | Cost per course: 52 to 103 |
500 mg 1,000 mg 2000 mg | IV vial, powder for injection | 101.7100c 184.3600c 339.2000c | NA | Cost per course: 1,106 to 2,035 | ||
Cyclosporine (generics) | 10 mg 25 mg 50 mg 100 mg | Capsule | 0.7526 0.7870 1.5350 3.0720 | Starting dose: 100 mg twice daily Target dose: 5 to 6 mg/kg/day in 2 divided doses, adjust for serum trough level of 75 to 150 ng/mL. | 12.29 to 15.34 | 4,489 to 5,606 |
Methotrexate (generic, Metoject SC) | 2.5 mg 10 mg | Tablet | 0.2513 2.7983d | 10 mg to 20 mg/week, orally or SC | 0.14 to 0.29 | 52 to 105 |
20 mg / 2 mL 50 mg / 2 mL | Vial for injection | 8.9200 12.5000 | 1.27 to 2.55 | 465 to 930 | ||
10mg/0.2mL 12.5mg/0.25mL 15 mg / 0.3 mL 17.5mg/0.35 20mg/0.4mL 22.5mg/0.45mL 25mg/0.5mL | Prefilled syringe for SC use | 22.2300 23.4000 16.3800 16.0000 17.5000 17.5000 19.5000 | 2.29 to 3.18 | 835 to 1,160 | ||
Mycophenolate mofetil (generics) | 250 mg | Capsule | 0.3712 | 1,000 mg twice daily | 2.97 | 1,084 |
500 mg | Tablet | 0.7423 | 2.98 | 1,087 | ||
Mycophenolate Sodium (generics) | 180 mg 360 mg | Enteric Tablet | 0.9989 1.9977 | 720 mg twice dailye | 7.99 | 2,917 |
Tacrolimus (generics) | 0.5 mg 1 mg 5 mg | Capsule | 1.0146 1.2978 6.4993 | 3 to 5 mg per dayf | 3.89 to 6.50 | 1,421 to 2,372 |
Cholinesterase inhibitors | ||||||
Pyridostigmine (Mestinon, generics) | 60 mg | Tablet | 0.2673 | 60 mg to 120 mg every 3 to 8 hours while awake | 0.53 to 3.20 | 195 to 1,172 |
180 mg | SR tablet | 1.3919 | 180 to 540 mg once or twice daily | 1.39 to 8.35 | 508 to 3,050 | |
Blood products | ||||||
IV immunoglobulin | 10,591 per exacerbationg | |||||
Plasma exchange | 7,784 per exacerbationg | |||||
NA = not applicable; SC = subcutaneous.
Note: All prices are from the Ontario Drug Benefit Formulary (accessed August 2024),45 unless otherwise indicated, and do not include dispensing fees. All cost calculations for agents with weight or body surface area-based dosing was calculated using the mean body surface area of 1.8 m2 and mass of 80 kg. Drug wastage was included.
aDosing is from a review by Farmakidis et al., unless otherwise indicated.46
bAzathioprine dosing was obtained from published literature.49
cDelta PA database wholesale prices (accessed August 2024).47
dSaskatchewan Drug Plan formulary (accessed August 2024).48
eMyfortic product monograph, dose indicated for the prophylaxis of organ rejection in patients receiving allogeneic renal transplants, previously confirmed with clinical experts as also used for generalized myasthenia gravis.7,50
fTacrolimus dose reported for patients with therapy-refractory myasthenia gravis in clinical features, pathogenesis, and treatment of myasthenia gravis: a supplement to the Guidelines of the German Neurologic Society.51
gThe cost of IV immunoglobulin and plasma exchange, totalling $8,277 and $6,084 respectively in 2014 dollars,13 was for rescue therapy and included cost of blood products and hospital costs and was inflated to 2024 dollars by CDA-AMC.52 Due to confidential prices of immunoglobulin products and plasma exchange, chronic treatment cost is unknown.
Appendix 2: Submission Quality
Please note that this appendix has not been copy-edited.
Description | Yes or no | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | Yes | No comment. |
Model has been adequately programmed and has sufficient face validity | No | The probabilistic analysis often did not return probabilistic results when inputs were changed. The sequential analysis used inappropriate methodology in determining extended dominance; while this error did not impact the sponsor’s base case, analyses based on input changes sometimes led to inappropriate reporting of sequential results. |
Model structure is adequate for decision problem | Yes | No comment. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | No | Uncertainty in the NMA results (i.e., the wide credible intervals) was not adequately reflected in the derivation of transition probabilities. Some parameters were not implemented in the way described by the sponsor (e.g., mortality associated with myasthenic crisis). |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | No | The model sometimes lacked adequate labelling and clarity regarding what parameters were active and how they were varied within the probabilistic analyses. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | No | The model sometimes lacked adequate labelling and clarity regarding what parameters were active and how they were varied within the probabilistic analyses. |
NMA = network meta-analysis.
Appendix 3: Additional Information on the Submitted Economic Evaluation
Please note that this appendix has not been copy-edited.
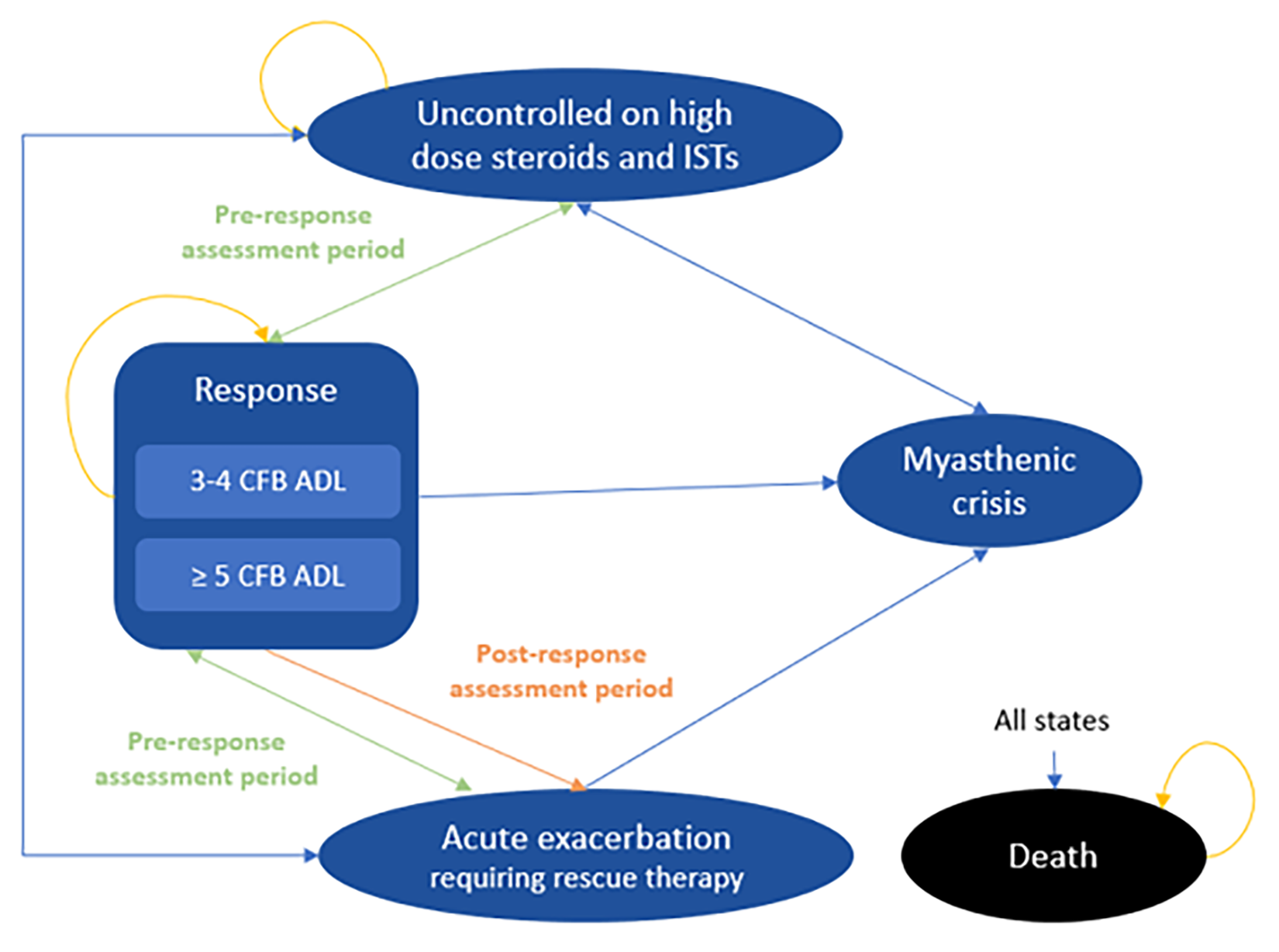
ADL = [Myasthenia Gravis] Activities of Daily Living; CFB = change from baseline; IST = immunosuppressive therapy.
Source: Sponsor’s pharmacoeconomic submission.2
Table 9: Utility Equation and Parameter Estimates
Parameter | Value |
|---|---|
Utility Change Equation | |
𝑈𝑡𝑖𝑙𝑖𝑡𝑦 𝐶ℎ𝑎𝑛𝑔𝑒 = 𝛽0 + 𝛽1 × 𝐸𝑄 – 5𝐷𝑏𝑎𝑠𝑒𝑙𝑖𝑛𝑒 + 𝛽2 × 𝐵𝑀𝐼𝑏𝑎𝑠𝑒𝑙𝑖𝑛𝑒 + 𝛽3 × 𝑀𝐺 – 𝐴𝐷𝐿 | |
Baseline EQ-5D | 0.5596 |
Baseline BMI, kg/m2 | 29.80 |
Intercept [Beta0] | 0.6228 |
Coefficient of baseline EQ-5D (Beta1) | −0.5374 |
Coefficient of BMI (Beta2) | −0.0017 |
Coefficient of MG-ADL score (Beta3) | −0.0240 |
Age- and sex-related utility adjustment | |
𝐸𝑄 – 5𝐷 = 0.9508566 + 0.0212126 ∗ 𝑚𝑎𝑙𝑒 – 0.0002587 ∗ 𝑎𝑔𝑒 – 0.0000332 ∗ 𝑎𝑔𝑒2 | |
BMI = body mass index; MG-ADL = Myasthenia Gravis Activities of Daily Living.
Source: Sponsor’s pharmacoeconomic submission.2
Table 10: Model Input Parameters by Health State
Health state | MG-ADL score | Utility valuea | Proportion of patients receiving CS | Annual cost of managing CS use | Annual rate of exacerbation | Annual rate of crisis |
|---|---|---|---|---|---|---|
Uncontrolled, any time point | 10.70 | 0.575 | 100% high-dose CS | $12,197 | 0.651 | 0.0117 |
Response (CFB ≥ 3 in MG-ADL), before assessment time point | 7.24 | 0.657 | 100% low-dose CS | $5,309 | 0.118 | 0.0117 |
CFB 3 to 4 in MG-ADL, after assessment time point | 7.24 | 0.657 | ||||
CFB ≥ 5 in MG-ADL after assessment time point | 3.12 | 0.756 | 0% receiving CS | $0 |
CFB = change from baseline; CS = corticosteroids; MG-ADL = Myasthenia Gravis Activities of Daily Living.
aUtility values do not include disutilities associated with corticosteroid use, where all patients in the uncontrolled state received a −0.1750 disutility, while those in the CFB 3 to 4 MG-ADL response state received a −0.0700 disutility, based on their assumed use of high-dose and low-dose corticosteroids, respectively. Additionally, all patients receiving IVIg or PLEX experience a −0.1200 disutility during cycles within which it is administered either as a chronic or rescue therapy.
Source: Sponsor’s pharmacoeconomic submission.2
Detailed Results of the Sponsor’s Base Case
Table 11: Disaggregated Summary of the Sponsor’s Economic Evaluation (Probabilistic)
Parameter | Zilucoplan + SOC | SOC alone | Rituximab + SOC | PLEX + SOC | IVIg/SCIg + SOC | Efgartigimod alfa + SOC |
|---|---|---|---|---|---|---|
Discounted LYs | ||||||
Total | 24.10 | 24.09 | 24.09 | 24.09 | 24.09 | 24.09 |
Uncontrolled | 17.95 | 20.98 | 20.40 | 19.66 | 20.05 | 18.74 |
Response | 5.60 | 2.49 | 3.09 | 3.84 | 3.44 | 4.79 |
Exacerbation | 0.46 | 0.52 | 0.51 | 0.50 | 0.51 | 0.48 |
Myasthenic crisis | 0.09 | 0.10 | 0.10 | 0.09 | 0.10 | 0.09 |
Discounted QALYs | ||||||
Total | 13.06 | 12.49 | 12.58 | 12.71 | 12.65 | 12.90 |
Uncontrolled | 9.14 | 10.79 | 10.48 | 10.08 | 10.29 | 9.57 |
Response | 3.93 | 1.71 | 2.11 | 2.64 | 2.36 | 3.33 |
Exacerbation | 0.12 | 0.13 | 0.13 | 0.12 | 0.13 | 0.12 |
Myasthenic crisis | −0.12 | −0.13 | −0.13 | −0.13 | −0.13 | −0.13 |
Discounted costs ($) | ||||||
Total | 1,471,696 | 881,636 | 882,085 | 911,026 | 920,985 | 1,336,228 |
Resource Use – Uncontrolled | 551,351 | 644,585 | 626,725 | 604,478 | 616,588 | 575,687 |
Resource Use - Response | 41,538 | 20,680 | 25,635 | 31,901 | 28,543 | 35,879 |
Resource Use - Exacerbation | 108,987 | 123,341 | 120,577 | 131,648 | 81,348 | 112,730 |
Resource Use – Myasthenic crisis | 76,537 | 85,504 | 83,777 | 91,266 | 82,594 | 78,874 |
Treatment costs | 687,037 | 1,278 | 19,122 | 45,485 | 105,663 | 526,812 |
End-of-life costs | 6,246 | 6,248 | 6,248 | 6,247 | 6,247 | 6,246 |
Ig = immunoglobulin; LY = life-year; PLEX = plasma exchange; QALY = quality-adjusted life-year; SC = subcutaneous; SOC = standard of care.
Note: Results for eculizumab have been omitted for brevity.
Source: Sponsor’s pharmacoeconomic submission.2
Appendix 4: Additional Details on the CDA-AMC Reanalyses and Sensitivity Analyses of the Economic Evaluation
Please note that this appendix has not been copy-edited.
Detailed Results of CDA-AMC Base Case
CDA-AMC did not conduct a reanalysis of the sponsor’s base case.
Scenario Analyses
Table 12: Summary of the CDA-AMC Scenario Analysis Results (Deterministic)
Drug | Total costs ($) | Total QALYs | Sequential ICER ($/ QALY) |
|---|---|---|---|
Sponsor’s deterministic base case | |||
SOC | 924,868 | 12.93 | Reference |
Rituximab plus SOC | 925,868 | 13.01 | 5,645 |
PLEX plus SOC | 955,079 | 13.15 | 220,447 |
Zilucoplan plus SOC | 1,522,432 | 13.49 | 1,645,217 |
Dominated treatments | |||
IVIg/SCIg plus SOC | 960,889 | 13.08 | Dominated by PLEX |
Efgartigimod alfa plus SOC | 1,450,842 | 13.36 | Extendedly dominated by mix of PLEX and zilucoplan |
Eculizumab plus SOC | 2,2052,951 | 13.19 | Dominated by zilucoplan and efgartigimod alfa |
CDA-AMC Scenario 1 – removal of 2-year stopping rule | |||
SOC | 927,756 | 12.93 | Reference |
Rituximab plus SOC | 978,642 | 13.01 | 614,458 |
PLEX plus SOC | 1,080,756 | 13.15 | 756,841 |
Zilucoplan plus SOC | 3,461,617 | 13.49 | 6,904,042 |
Dominated treatments | |||
IVIg/SCIg plus SOC | 1,246,642 | 13.08 | Dominated by PLEX |
Efgartigimod alfa plus SOC | 3,070,558 | 13.36 | Extendedly dominated by mix of PLEX and zilucoplan |
CDA-AMC Scenario 2 – removal of extra costs and utility decrements associated with corticosteroid use | |||
SOC | 651,192 | 13.18 | Reference |
Rituximab plus SOC | 657,397 | 13.26 | 80,529 |
PLEX plus SOC | 694,094 | 13.39 | 287,068 |
Zilucoplan plus SOC | 1,283,078 | 13.71 | 1,820,589 |
Dominated treatments | |||
IVIg/SCIg plus SOC | 696,098 | 13.33 | Dominated by PLEX |
Efgartigimod alfa plus SOC | 1,202,703 | 13.59 | Extendedly dominated by mix of PLEX and zilucoplan |
CDA-AMC Scenario 3 to 5% mortality per myasthenic crisis | |||
SOC | 850,524 | 12.00 | Reference |
Rituximab plus SOC | 852,824 | 12.11 | $21,614 |
PLEX plus SOC | 882,991 | 12.28 | $182,083 |
Zilucoplan plus SOC | 1,457,831 | 12.69 | $1,380,965 |
Dominated treatments | |||
IVIg/SCIg plus SOC | 892,809 | 12.20 | Dominated by PLEX |
Efgartigimod alfa plus SOC | 1,383,704 | 12.53 | Extendedly dominated by mix of PLEX and zilucoplan |
CDA-AMC Scenario 4 – combination of Scenarios 1 through 3 | |||
SOC | 853,411 | 12.24 | Reference |
Rituximab plus SOC | 906,130 | 12.34 | $521,203 |
PLEX plus SOC | 1,008,668 | 12.50 | $643,815 |
Zilucoplan plus SOC | 3,397,015 | 12.89 | $6,024,388 |
Dominated treatments | |||
IVIg/SCIg plus SOC | 1,178,562 | 12.42 | Dominated by PLEX |
Efgartigimod alfa plus SOC | 3,003,419 | 12.74 | Extendedly dominated by mix of PLEX and zilucoplan |
ICER = incremental cost-effectiveness ratio; Ig = immunoglobulin; PLEX = plasma exchange; QALY = quality-adjusted life-year; SC = subcutaneous; SOC = standard of care.
Source: Sponsor’s pharmacoeconomic submission.2
Appendix 5: Submitted Budget Impact Analysis and CDA-AMC Appraisal
Please note that this appendix has not been copy-edited.
Table 13: Summary of Key Take-Aways
Key take-aways of the budget impact analysis |
|---|
|
AChR = acetylcholine receptor; CDA-AMC = Canada’s Drug Agency; gMG = generalized myasthenia gravis; NIHB = Noninsured Health Benefits.
Summary of Sponsor’s Budget Impact Analysis
The sponsor submitted a BIA estimating the expected incremental budget impact of reimbursing zilucoplan plus SOC for the treatment of adults with refractory anti-AChR antibody–positive gMG, where refractory is defined as not achieving symptom control after treatment for at least 1 year with 2 or more of the following therapies: prednisone, azathioprine, mycophenolate, cyclosporine, cyclophosphamide, methotrexate, tacrolimus, other corticosteroids for gMG, other ISTs, or a history of treatment with at least 1 of these therapies for 1 year or more and required chronic PLEX, IVIg, or SCIg at least every 3 months for the 12 months before treatment with zilucoplan.53 The BIA was conducted from the perspective of the pan-Canadian drug plans over a 3-year time horizon (July 2025 through June 2028, with July 2024 through June 2025 as the base year). The sponsor’s pan-Canadian estimates reflect the aggregated results from provincial budgets, excluding Quebec, as well as the Noninsured Health Benefits (NIHB) Program. The sponsor’s base case included drug-acquisition costs only. Market shares in the reference scenario were based on sponsor-obtained clinical expert opinion, with the share for eculizumab based on the CDA-AMC review of Ultomiris for gMG. Market uptake of zilucoplan was estimated based on internal sponsor forecasts. Zilucoplan was assumed to displace all comparators in proportion to their reference scenario market share and was not assumed to increase the number of patients eligible for treatment. Key inputs to the BIA are documented in Table 14.
Table 14: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1 / year 2 / year 3 if appropriate) |
|---|---|
Target population | |
CDA-AMC-participating adult population | 26,276,990 / 26,637,683 / 26,998,375a |
Prevalence of gMG | |
Proportion patients with gMG who are anti-AChR antibody–positive | 85%56 |
Proportion patients with gMG who are refractory to SOC alone | 14.8%57 |
Proportion patients who are eligible for public coverage | 65.6% |
Number of patients eligible for drug under review | 694 / 703 / 713 |
Market shares (3 years, reference scenario) | |
Zilucoplan plus SOC | 0% / 0% / 0% |
SOC | 33.0% / 33.0% / 33.0% |
Chronic IVIg/SCIg plus SOC | 34.0% / 34.0% / 34.0% |
Chronic PLEX plus SOC | 26.5% / 24.5% / 19.5% |
Rituximab plus SOC | 2.0% / 2.0% / 2.0% |
Eculizumab plus SOC | 1.5% / 1.5% / 1.5% |
Efgartigimod alfa plus SOC | 3.0% / 5.0% / 10.0% |
Market shares (3 years, new drug scenario) | |
Zilucoplan plus SOC | 5.0% / 10.0% / 15.0% |
SOC | 31.4% / 29.7% / 28.1% |
Chronic IVIg/SCIg plus SOC | 32.3% / 30.6% / 28.9% |
Chronic PLEX plus SOC | 25.2% / 22.1% / 16.6% |
Rituximab plus SOC | 1.9% / 1.8% / 1.7% |
Eculizumab plus SOC | 1.4% / 1.4% / 1.3% |
Efgartigimod alfa plus SOC | 2.9% / 4.5% / 8.5% |
Cost of treatment (per patient, per year) | |
Zilucoplan plus SOC | $414,595 |
SOC | $1,513 |
Chronic IVIg/SCIg plus SOC | $90,061 |
Chronic PLEX plus SOC | $8,809 |
Rituximab plus SOC | $20,818 |
Eculizumab plus SOC | $722,907 |
Efgartigimod alfa plus SOC | $359,477 |
AChR = acetylcholine receptor; gMG = generalized myasthenia gravis; Ig = immunoglobulin; PLEX = plasma exchange; SC = subcutaneous; SOC = standard of care.
aSum of the adult populations (≥18 years) of all provinces except for Quebec, plus the client population of NIHB who are 20 years of age or older. The base year and years 1 through 3 population estimates for all provinces were linearly forecast from 2018 to 2022 Statistics Canada population estimates, while that of the NIHB was linearly forecast from 2018 through 2022 NIHB annual reports.
Summary of the Sponsor’s BIA Results
Results of the sponsor’s analysis suggest that the reimbursement of efgartigimod alfa for adults with refractory anti-AChR antibody–positive gMG as defined in the reimbursement request would be associated with an incremental cost of $12,459,216 in year 1, $24,767,122 in year 2, and $35,778,603 in year 3, for a 3-year incremental budget impact of $73,004,941. An estimate of the budgetary impact of reimbursing zilucoplan for its full Health Canada indication (i.e., adult patients with anti-AChR antibody–positive gMG) was not presented.
CDA-AMC Appraisal of the Sponsor’s BIA
CDA-AMC identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
The NIHB population was inappropriately calculated: The sponsor calculated the total population of CDA-AMC-participating drug plans by adding the population of the provinces,58 excluding Quebec, to the population of NIHB clients.59 NIHB clients living within the borders of a province are counted within provincial population data as reported by Statistics Canada, thus the NIHB population was double counted in the sponsor’s analysis. Additionally, NIHB clients residing within Ontario who are aged younger than 25 years or 65 years and older are eligible for reimbursement by ODB and thus should be counted as ODB clients (and included in the Ontario population estimates) rather than NIHB clients for the purposes of modelling the budget impact of reimbursing zilucoplan. Finally, the NIHB reports its client population by age in groups of 5 years.59 In determining the adult population of NIHB clients, the sponsor summed all age categories from 20 to 65 years and older. As such, the sponsor excluded NIHB clients who are ages 18 or 19 from the adult population.
CDA-AMC did not adjust for this limitation in reanalysis. The impact on pan-Canadian model results is expected to be minimal.
Eculizumab is not publicly funded for gMG: The sponsor assumed that 1.5% of patients with anti-AChR antibody–positive refractory gMG who are publicly reimbursed for their treatment receive eculizumab. While the CDA-AMC reimbursement review for eculizumab for the treatment of adults with refractory gMG resulted in a recommendation to reimburse with conditions,34 negotiations with pCPA were not successful.35 As such, the public plans do not fund eculizumab for the treatment of gMG and thus eculizumab is not a comparator of interest when assessing the budget impact of publicly reimbursing zilucoplan.
In reanalysis, CDA-AMC assumed a 0% market share for eculizumab and proportionally redistributed its original share to the remaining comparators in both the reference and new drug scenarios.
Reference scenario market expansion assumptions for efgartigimod alfa are uncertain: The CDA-AMC review of efgartigimod alfa resulted in a recommendation to list with conditions15 and at the time of this review, it is undergoing negotiation with pCPA.60 The sponsor’s analysis assumed that in the reference scenario, efgartigimod alfa’s market share is expanding, with all of this expansion displacing PLEX. Clinical expert input obtained by CDA-AMC found the sponsor’s estimates that efgartigimod alfa will capture 3%, 5%, and 10% of the eligible market in the 3 years of the time horizon to be reasonable but did not find the assumption that efgartigimod alfa would only displace PLEX to be plausible. As the sponsor assumed that zilucoplan, if funded, will displace all other comparators in proportion to their reference scenario market share, clinical expert opinion obtained by CDA-AMC noted it would be reasonable to assume the same for efgartigimod alfa.
In reanalysis, CDA-AMC assumed that as it enters the market in the reference scenario, efgartigimod alfa will displace other therapies in proportion to their market share. A scenario analysis was conducted exploring the impact of funding zilucoplan should efgartigimod alfa not become publicly funded.
The relative costs of zilucoplan and efgartigimod alfa are uncertain: The sponsor’s BIA assumed a distribution of zilucoplan doses consistent the patient body weight by category reported in the RAISE trial, with 6.3% of patients weighing less than 56 kg and receiving the 16.6 mg dose, 26.4% weighing between 56 to less than 77 kg and receiving the 23.0 mg dose, and 67.2% weighing 77 kg or more and receiving the 32.4 mg dose.53 The mean patient body weight reported in the RAISE trial was 85.7 kg.3 The submitted BIA assumed that for efgartigimod alfa, 60% of patients would weigh less than or equal to 80 kg and would therefore receive 2,400 mg vials per dose, while the remaining 40% weighed more than 80 kg and would receive 3 vials. These proportions were based on the CDA-AMC Economic Review report for efgartigimod alfa using data from the ADAPT trial, where the mean body weight of included patients was approximately 80.5 kg.7,32 As such, the submitted BIA effectively assumes a different patient population depending on which therapy is chosen, which is inappropriate. Data on the proportion of patients in the RAISE trial who fell into body weight categories relevant to the dosing of efgartigimod alfa were not available, and thus the cost of therapy with zilucoplan could not be directly compared to the cost of therapy with efgartigimod alfa within the same patient population.
CDA-AMC conducted a scenario analysis which assumed that 50% of patients receiving efgartigimod alfa received 3,400 mg vials, to better reflect the potential dosing of patients in a population with a mean body weight of 85.7 kg. The mean body weight of patients with gMG seen in Canadian clinical practice is unknown.
Drug plan payer perspective: According to the Procedures for Reimbursement Reviews,33 the BIA base case should be from the perspective of a pan-Canadian drug plan program. As such, costs relating to the use of blood products (i.e., IVIg/SCIg, PLEX) are not funded by jurisdictional drug plan budgets and should thus be excluded from the drug plan perspective. As the sponsor’s submission did not include the option to switch to a health care payer perspective where other cost categories such as administration were included, CDA-AMC was unable to present both a drug plan payer and a health care payer perspective. Of note, due to a lack of publicly accessibly pricing for blood products, CDA-AMC was unable to independently validate the sponsor’s estimated costs for IVIg/SCIg and PLEX.
In reanalysis, costs associated with the use of blood products were excluded. If the inclusion of the estimated acquisition costs of blood products is considered useful, the results of CDA-AMC reanalysis #1 reflect this analysis. CDA-AMC could not undertake a robust analysis from the health care payer perspective due to the exclusion of relevant costs, such as administration.
Proportion of patients who are publicly funded was inappropriately estimated: The sponsor assumed that 65.6% of patients in the reimbursement request population would be eligible for public funding of their gMG therapy, based on the proportion of the overall population of Canada who are eligible for public plan funding as reported by The Conference Board of Canada in 2022.61 This estimate does not account for differences in eligibility rates across jurisdictions, and thus running the analysis by individual jurisdiction does not reflect public coverage rates within that jurisdiction.
CDA-AMC did not adjust the model to reflect public funding eligibility rates within each jurisdiction. The impact on pan-Canadian model results is expected to be minimal, however the impact on individual jurisdiction model results may be substantial, depending on the jurisdiction.
CDA-AMC Reanalyses of the BIA
CDA-AMC revised the sponsor’s submitted analysis by assuming eculizumab has 0% of the public market, assuming efgartigimod alfa displaces all comparators as it enters the market, and by assuming a drug plan payer perspective and excluding the cost of blood products from the analysis. The changes applied to derive the CDA-AMC base case are described in Table 15.
Table 15: CDA-AMC Revisions to the Submitted Budget Impact Analysis
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
Changes to derive the CDA-AMC base case | ||
1. Reference scenario market shares | Eculizumab has 1.5% of the public market Efgartigimod alfa only displaces PLEX as it expands into the market | Eculizumab has 0% of the public market Efgartigimod alfa displaces all remaining comparators in proportion to their market share as it expands into the public market. |
2. Drug plan perspective | Acquisition costs of blood products included. | Acquisition costs of blood products excluded. |
CDA-AMC base-case | 1 + 2 | |
PLEX = plasma exchange.
The results of the CDA-AMC step-wise reanalysis are presented in summary format in Table 16 and a more detailed breakdown is presented in Table 17. For the reimbursement request population (i.e., adults with refractory anti-AChR antibody–positive gMG, where refractory is defined as not achieving symptom control after treatment as described in the summary of the sponsor’s submission), CDA-AMC reanalyses suggest that the reimbursement of zilucoplan in combination with standard of care will be associated with a 3-year incremental budgetary cost of $82,030,716 (year 1:$13,946,524; year 2: $27,772,856; year 3: $40,311,336).
Table 16: Summary of the CDA-AMC Reanalyses of the Budget Impact Analysis
Stepped analysis | Three-year total ($) |
|---|---|
Submitted base case | $73,004,941 |
CDA-AMC reanalysis 1 – reference scenario market shares | $75,587,664 |
CDA-AMC reanalysis 2 – drug plan perspective | $79,732,098 |
CDA-AMC base case | $82,030,716 |
CDA-AMC = Canada’s Drug Agency.
CDA-AMC conducted the following scenario analyses to address remaining uncertainty, using the CDA-AMC base case (results are provided in Table 17):
Assuming that efgartigimod alfa does not become funded for gMG and thus has 0% public market share. Zilucoplan uptake is assumed to be unchanged from the sponsor’s estimates.
Assuming that 50% of patients using efgartigimod alfa require 3 vials per dose while the remaining 50% require 2 vials per dose.
Table 17: Detailed Breakdown of the CDA-AMC Reanalyses of the Budget Impact Analysis
Stepped analysis | Scenario | Year 0 (current situation) ($) | Year 1 ($) | Year 2 ($) | Year 3 ($) | Three-year total ($) |
|---|---|---|---|---|---|---|
Submitted base case | Reference | $33,183,038 | $38,511,596 | $43,973,760 | $57,070,036 | $172,738,430 |
New drug | $33,183,038 | $50,970,811 | $68,740,882 | $92,848,639 | $245,743,371 | |
Budget impact | $0 | $12,459,216 | $24,767,122 | $35,778,603 | $73,004,941 | |
CDA-AMC base case | Reference | $3,750,689 | $8,765,436 | $13,916,420 | $26,851,817 | $53,284,362 |
New drug | $3,750,689 | $22,711,960 | $41,689,276 | $67,163,153 | $135,315,078 | |
Budget impact | $0 | $13,946,524 | $27,772,856 | $40,311,336 | $82,030,716 | |
CDA-AMC scenario analysis 1: efgartigimod alfa has 0% market share | Reference | $1,303,475 | $1,321,616 | $1,339,758 | $1,357,899 | $5,322,748 |
New drug | $1,303,475 | $15,640,331 | $30,370,280 | $45,493,323 | $92,807,409 | |
Budget impact | $0 | $14,318,715 | $29,030,523 | $44,135,424 | $87,484,661 | |
CDA-AMC scenario analysis 2: efgartigimod alfa vial usage | Reference | $3,852,768 | $9,075,935 | $14,441,022 | $27,915,228 | $55,284,953 |
New drug | $3,852,768 | $23,006,934 | $42,161,418 | $68,067,053 | $137,088,173 | |
Budget impact | $0 | $13,930,999 | $27,720,396 | $40,151,825 | $81,803,219 |
BIA = budget impact analysis; CDA-AMC = Canada’s Drug Agency.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.