Drugs, Health Technologies, Health Systems
Reimbursement Review
Iptacopan (Fabhalta)
Sponsor: Novartis Pharmaceuticals Canada Inc.
Therapeutic area: Paroxysmal nocturnal hemoglobinuria
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Clinical Review
Abbreviations
AAMAC
Aplastic Anemia & Myelodysplasia Association of Canada
ARC
absolute reticulocyte count
BMI
body mass index
BTH
breakthrough hemolysis
CDA-AMC
Canada’s Drug Agency
CI
confidence interval
EORTC QLQ-C30
European Organisation for the Research and Treatment of Cancer Quality of Life Questionnaire Core 30
ESS
effective sample size
ETP
extension treatment period
EVH
extravascular hemolysis
FACIT-F
Functional Assessment of Chronic Illness Therapy – Fatigue
GRADE
Grading of Recommendations Assessment, Development and Evaluation
HRQoL
health-related quality of life
IPD
individual patient-level data
ITC
indirect treatment comparison
IVH
intravascular hemolysis
LDH
lactate dehydrogenase
MAIC
matching-adjusted indirect comparison
MAVE
major adverse vascular event
MID
minimal important difference
MMRM
mixed model for repeated measures
NICE
National Institute for Health and Care Excellence
OR
odds ratio
pCPA
pan-Canadian Pharmaceutical Alliance
PNH
paroxysmal nocturnal hemoglobinuria
PNHCA
Canadian Association of PNH Patients
RBC
red blood cell
RCT
randomized controlled trial
RTP
randomized treatment period
SAE
serious adverse event
SD
standard deviation
SMD
standardized mean difference
TEAE
treatment-emergent adverse event
ULN
upper limit of normal
VAS
visual analogue scale
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Table 1: Background Information of Application Submitted for Review
Item | Description |
|---|---|
Drug product | Iptacopan (Fabhalta), 200 mg, hard capsules, oral |
Sponsor | Novartis Pharmaceuticals Canada Inc. |
Indication | As monotherapy in the treatment of adult patients with paroxysmal nocturnal hemoglobinuria (PNH) who have hemolytic anemia |
Reimbursement request | Per sponsor request, this review focuses on the indication for iptacopan for the treatment of adult patients with PNH who have an inadequate response to, or are intolerant of, a C5 inhibitor. |
Health Canada approval status | Approved |
Health Canada review pathway | Standard review |
NOC date | January 6, 2025 |
Recommended dose | 200 mg twice daily |
NOC = notice of compliance; PNH = paroxysmal nocturnal hemoglobinuria.
Introduction
Paroxysmal nocturnal hemoglobinuria (PNH) is a rare, chronic, and potentially life-threatening condition caused by an acquired genetic defect in hematopoietic stem cells.1,2 This defect causes the complement system to recognize red blood cells (RBCs) as damaged, triggering hemolysis.1,2 Hemolysis occurs through 2 mechanisms in PNH, intravascular hemolysis (IVH) and extravascular hemolysis (EVH), the latter occurring only when a patient is receiving a C5 inhibitor. IVH occurs through both terminal and proximal complement pathways when RBCs are lysed due to activation of the alternative complement pathway.3 Conversely, EVH occurs through the proximal pathway when RBCs are opsonized by C3 fragments, tagging them for macrophage destruction in the spleen and liver.4-6 Persistent IVH results in hemoglobinuria, characterized by dark-coloured urine,2 anemia, and its associated symptoms (e.g., fatigue, dyspnea), as well as an increased risk of thrombosis, pain, organ damage (e.g., impaired renal function), and underlying bone marrow dysfunction.4,7,8 The clinical manifestations of EVH are heterogenous, with some patients being asymptomatic9,10 with normal hemoglobin levels,11 while others may develop severe clinical symptoms and require blood transfusions to manage ongoing anemia and fatigue.9,12,13 PNH has also been linked with bone marrow failure syndromes, including aplastic anemia and myelodysplastic syndromes.1,14 The symptoms of PNH and need for RBC transfusions have a significant impact on patients’ daily living, impair their health-related quality of life (HRQoL),4,7,15,16 and increase risk of morbidity and mortality.17,18
The estimated prevalence of PNH was 1.2 to 1.3 per 100,000 persons between 2016 and 2017, based on US data,19 and 1.59 per 100,000 persons20 to 3.81 per 100,000 persons,21 based on UK data. Estimates of the annual UK incidence ranged from 0.13 per 100,000 persons20 to 0.35 per 100,000 persons,21 and the US incidence was 0.57 per 100,000 person-years.19 Clinical trial and real-world data estimate that around 20% of patients with PNH who were clinically stable on C5 inhibitor treatment for IVH developed clinically significant EVH.22
In Canada, patients with PNH receive C5 inhibitors as standard first-line therapy to reduce uncontrolled complement activation in the terminal complement cascade.23,24 The primary C5 inhibitor therapies are ravulizumab and eculizumab, both administered through IV infusion.1,25,26 Treatment options for patients with EVH and anemia include pegcetacoplan and danicopan. Pegcetacoplan is administered through subcutaneous infusion twice weekly with a syringe system infusion pump.27 It received a final conditional positive Canada’s Drug Agency (CDA-AMC) recommendation for reimbursement in April 2023. Danicopan, an oral therapy, is approved by Health Canada as an add-on to IV ravulizumab or eculizumab for patients with residual hemolytic anemia due to EVH.28 It received a final conditional positive CDA-AMC recommendation in November 2024 and is currently under consideration for negotiation with the pan-Canadian Pharmaceutical Alliance (pCPA). Both second-line options require parenteral administration, which may not be acceptable or feasible for all patients.
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of iptacopan 200 mg oral capsules for the treatment of PNH in adult patients who have an inadequate response to, or are intolerant of, a C5 inhibitor. The population of interest was aligned with the sponsor’s reimbursement request.
Perspectives of Patients, Clinicians, and Drug Programs
The information in this section is a summary of input provided by the patient and clinician groups who responded to our call for input and from clinical experts consulted for the purpose of this review.
Patient Input
The Canadian Association of PNH Patients (PNHCA) and the Aplastic Anemia & Myelodysplasia Association of Canada (AAMAC) submitted input for this review jointly. PNHCA is a nonprofit patient advocacy group that connects individuals with PNH and their caregivers to resources and information on optimal management of PNH. AAMAC is a national charity that provides supportive resources on PNH to patients, caregivers, and health care providers. A clinical summary of PNH was provided, and information was gathered through the personal experiences of individuals who had direct experience with iptacopan, including 1 patient living in Canada and 5 patients living in the US.
Input from the patient groups highlighted the diverse and profound ways in which PNH impacts quality of life for both patients and caregivers. Due to the condition’s rarity and the variability of presentation, the input noted that patients often experience a period of significant health deterioration before they receive a PNH diagnosis. Thrombosis was emphasized as a serious complication of PNH that can result in life-threatening conditions such as stroke, pulmonary embolism, or Budd-Chiari syndrome, which significantly increase the risk of morbidity and mortality. It was noted that the chronic nature of PNH means that patients must manage their condition over a lifetime, along with the associated physical, emotional, and financial burdens. The need for frequent medical appointments across the patient’s lifetime can also result in feelings of isolation, strain on relationships, emotional distress, and decreased quality of life. Patients must also cope long-term with unpredictability of symptoms, treatment side effects, and threat of serious complications.
The patient group input noted that, while C5 inhibitor therapies prevent RBC destruction, EVH may not be fully addressed, which can result in chronic anemia despite C5 inhibitor treatment. Chronic anemia can cause severe fatigue, physical weakness, shortness of breath, and transfusion dependence, making it challenging to carry out household tasks, maintain employment, participate in recreational activities, and sustain an active lifestyle. A patient living in Canada who provided input shared that, while previous treatment with eculizumab did not enable a decent quality of life, treatment with iptacopan led to feeling “normal” within months of treatment initiation. This patient also noted valuing the convenience of oral administration, which enabled freedom from injection-type infusions. The 5 patients living in the US reported substantial increases in hemoglobin after initiating iptacopan, with some also experiencing normalization of lactate dehydrogenase (LDH) levels, reduction in bilirubin levels, and improvement in fatigue. Overall, the patient group input highlighted a need for new therapies that effectively manage IVH and EVH, to provide comprehensive relief from a wide range of symptoms and improve patient well-being. Specifically, the patient group noted the need for new treatments that improve hemoglobin levels and reduce the need for blood transfusions. The patient group noted that oral treatments provide significant benefits over injections in terms of convenience, comfort, adherence, psychological well-being, and economic factors, making oral treatments a preferred option when available.
Clinician Input
Input From Clinical Experts Consulted for This Review
The clinical experts noted that C5 inhibitors can provide incomplete control of PNH in some circumstances: rare genetic polymorphism, inadequate dosing, response to complement-amplifying triggers (e.g., vaccination or infections) leading to breakthrough hemolysis (BTH), or EVH related to C5 inhibition. They estimated that approximately 40% of patients with PNH will continue to have low hemoglobin despite therapy, approximately 30% will require transfusions, and 20% to 30% will have EVH that contributes to poor HRQoL. Pegcetacoplan is approved as a second-line therapy for patients with PNH who have an inadequate response or intolerance to a C5 inhibitor. As per the clinical experts consulted for this review, it is currently the primary pharmacologic option offered for patients diagnosed with EVH. According to the clinical experts, there are patients and their caregivers for whom subcutaneous infusions are not possible or are unacceptable, and the treatment burden of self-administering infusions can be significant. The experts also stated that danicopan, as add-on therapy to C5 inhibitors, may be available to some patients in Canada via a managed access program. However, this therapy can also be problematic, as it maintains the need for IV infusions, which can require the installation of a central vein catheter with its risks and need for care. Danicopan is administered orally 3 times daily, and treatment adherence may be challenging for some patients.
Treatment goals for patients with PNH and EVH remain to reduce mortality, inhibit IVH, and improve HRQoL, with better hemoglobin support that does not require transfusion, avoids iron overload, and leads to better functional status for patients.
According to the clinical experts consulted, iptacopan would be used as another second-line option for patients with PNH and an incomplete hematologic response to C5 inhibitors, particularly with ongoing anemia secondary to EVH (either requiring transfusions or not). There is also a place for iptacopan in patients who are intolerant of C5 inhibition or are no longer able to receive IV infusions, either because of long distance to medical care or the inability to maintain IV access. Patients with a genetic polymorphism in whom C5 inhibitor therapy is ineffective would also be candidates for iptacopan. The experts suggested there may be a role for iptacopan as a third-line option for patients who received pegcetacoplan and experienced adverse effects, were no longer willing to administer subcutaneous infusions, were experiencing too many BTHs, or had persistently elevated LDH levels despite increased doses of pegcetacoplan. The CDA-AMC review team notes that this review for iptacopan focuses on the population requested for reimbursement, i.e., adult patients with PNH who have an inadequate response to, or are intolerant of, a C5 inhibitor. The clinical experts stated that iptacopan would not be used in combination with other treatments but as a stand-alone second option after C5 inhibitors. Also, it would not be suitable for patients who are pregnant or who plan to become pregnant, those who do not accept, or are unable to adhere to, twice daily oral dosing, given the risk of BTH if doses are missed.
The clinical experts noted that response to therapy is typically an improvement in hemoglobin, a reduction in transfusion requirements, and improvement in symptoms relative to the baseline for a given patient. They noted that ongoing anemia and need for transfusion may or may not indicate treatment failure, as other concurrent diseases, such as bone marrow failure, aplastic anemia, other cancers, bleeding, or comorbidities, could be contributing factors.
The clinical experts indicated that treatment with iptacopan needs to be initiated by a hematologist, preferably with expertise in PNH, and that consultation with a PNH expert would be warranted if a patient with PNH was being followed in a shared-care model (i.e., a hematologist with expertise in PNH along with a local hematologist).
Clinician Group Input
The Canadian PNH Network submitted input for this review based on contributions from 10 clinicians. The Canadian PNH Network is a group of hematologists located across Canada who follow the majority of patients with PNH who live in Canada and who set consensus guidelines for the diagnosis and management of PNH. Information was gathered for this input submission through publicly available documents, congress abstracts, and published literature.
Overall, the clinician group input aligned with input provided by the clinical experts consulted for this review. Both the clinician group and clinical experts agreed that, currently, the only curative treatment for PNH is hematopoietic stem cell transplant, which is reserved for patients with predominant or progressive bone marrow failure. For patients who are ineligible for transplant, primary PNH treatment goals highlighted in the input were hemoglobin improvement, reduced need for transfusion, and absence of end-organ complications or other symptoms. Key unmet needs for patients with PNH, as identified by clinicians, are therapies that reverse the disease course other than allogeneic stem cell transplant and more convenient, tolerable therapies.
According to the clinician group, iptacopan will be used as second-line therapy in eligible patients, as per the APPLY-PNH criteria —those with persistent anemia despite C5 inhibition in whom EVH is suspected. Iptacopan would provide an additional therapy option, besides pegcetacoplan, for patients requiring proximal inhibition monotherapy. The clinician group noted that it would be reasonable to use iptacopan as third-line therapy as well. The CDA-AMC review team notes that this review for iptacopan focuses on the population requested for reimbursement, i.e., adult patients with PNH who have an inadequate response to, or are intolerant of, a C5 inhibitor. Given the absence of comparative efficacy data versus pegcetacoplan, the clinician group stated that patient preferences regarding the route of administration will largely drive treatment selection. Patients identified by clinicians as best suited for iptacopan therapy included those with a high likelihood of adhering to oral treatment, frequent travellers, or those who cannot initiate or continue other therapies. Less suitable patients included those who do not have anemia, and those who meet APPLY-PNH exclusion criteria, are planning pregnancy, or are unlikely to be adherent with the dosage schedule, given the high risk of BTH if doses are missed.
Key outcomes for evaluating treatment response that were identified by clinicians included hemoglobin improvement and reduced transfusion dependence, sustained IVH control (assessed based on LDH levels and BTH events), and improvements in fatigue and quality of life. Treatment discontinuation should be considered in patients with adverse events precluding ongoing therapy, patients with poor adherence, or patients who are pregnant or breastfeeding, according to the input. Both the clinician group and consulted experts agreed that patients with PNH benefit from having a clinician involved in their care who specializes in managing and monitoring the disease.
Drug Program Input
Input was obtained from the drug programs that participate in the reimbursement review process. The following were identified as key factors that could impact the implementation of a CDA-AMC Canadian Drug Expert Committee (CDEC) recommendation for iptacopan:
considerations for relevant comparators
considerations for initiation or renewal of therapy
considerations for discontinuation of therapy
considerations for prescribing of therapy
care provision issues
system and economic issues.
The clinical experts consulted provided advice on the potential implementation issues raised by the drug program. Refer to Table 4 for further details.
Clinical Evidence
Systematic Review
Description of Studies
One phase III, randomized, multicentre, active comparator–controlled, open-label, parallel-group study (the APPLY-PNH study) met the inclusion criteria for the systematic review.29,30 The objective of the study was to evaluate the efficacy and safety of oral iptacopan monotherapy in adult patients (aged ≥ 18 years) with PNH with residual anemia (hemoglobin < 100 g/L) despite treatment with a C5 inhibitor for at least 6 months before randomization. The APPLY-PNH study included a 24-week randomized treatment period (RTP), and a 24-week open-label, single-arm iptacopan extension period (details provided in the Long-Term Extension Study section). During the RTP, 97 patients were randomized at an 8:5 ratio to switch to iptacopan (200 mg twice daily), or to continue with the C5 inhibitor therapy they were receiving before the study (eculizumab or ravulizumab). The coprimary outcomes were the proportion of patients with at least a 20 g/L increase in hemoglobin or sustained hemoglobin levels of 120 g/L in the absence of RBC transfusion. Other key outcomes included the mean change from baseline in hemoglobin, transfusion avoidance, fatigue (measured using the Functional Assessment of Chronic Illness Therapy – Fatigue [FACIT-F] instrument), and BTH.
The mean age of patients enrolled in the APPLY-PNH study was 51.7 years (standard deviation [SD] 16.9 years) in the iptacopan group (N = 62) and 49.8 years (SD 16.7 years) in the C5 inhibitor group (N = 35). At baseline, the mean hemoglobin value was 89.3 g/L (SD 7.0 g/L) and 88.5 g/L (SD 8.9 g/L) in the iptacopan and C5 inhibitor groups, respectively, with 56.5% and 60.0% of patients having received an RBC transfusion in the past 6 months. Fewer patients in the iptacopan group had a history of major adverse vascular events (MAVEs) than in the C5 inhibitor group (19.4% and 28.6%, respectively). The mean disease duration was 11.9 years (SD 9.8 years) and 13.5 years (SD 10.9 years) in the iptacopan group and C5 inhibitor groups, respectively. Most patients were receiving eculizumab (65%) at enrolment, with the minority receiving ravulizumab (35%). Before randomization, the mean dose of eculizumab received was numerically lower in the iptacopan than the control group (937.5 mg, SD 100.5 mg versus 1,004.3 mg, SD 171.8 mg, respectively). Among those who received ravulizumab, the mean dose was 3,177.3 mg (SD 177.1 mg) in the iptacopan group and 3,200.0 mg (SD 195.4 mg) in the control group.
Efficacy Results
Both primary outcomes in the RTP of the APPLY-PNH study showed results that favoured iptacopan versus the C5 inhibitor group. The marginal proportion of patients with at least a 20 g/L increase in hemoglobin from baseline (in the absence of transfusion) was 82.3% versus 2.0% in the iptacopan versus C5 inhibitor groups, respectively, with a difference between groups of 80.2% (95% confidence interval [CI], 71.2% to 87.6%; P < 0.0001). With respect to normalization of hemoglobin levels, 68.8% of patients in the iptacopan group reported hemoglobin levels of at least 120 g/L compared with 1.8% of patients in the C5 inhibitor group (difference in marginal proportions of 67.0%; 95% CI, 56.4% to 76.9%; P < 0.0001). Between-group differences in both hemoglobin outcomes were considered clinically important by the clinical experts consulted by CDA-AMC.
The change from baseline in hemoglobin levels was a secondary outcome, which showed an adjusted mean change of 36.0 g/L in the iptacopan group and a –0.6 g/L change the C5 inhibitor group. The mean difference between groups was 36.6 g/L (95% CI, 32.0 to 41.2; P < 0.0001), favouring iptacopan versus C5 inhibitors. Based on the threshold of clinically important change that was selected by the clinical experts (10 g/L difference between groups), iptacopan likely results in clinically important improvement in hemoglobin levels versus C5 inhibitors.
Based on observed data, 59 of 62 patients in the iptacopan group and 14 of 35 patients in the C5 inhibitor did not require a transfusion (i.e., did not receive an RBC transfusion or did not meet the protocol-specified criteria for a transfusion) from day 14 to 168 in the RTP (marginal proportion 94.8% and 25.9%, respectively). The difference in marginal proportions of patients avoiding transfusions was 68.9% (95% CI, 51.4% to 83.9%; P < 0.0001) for the iptacopan group versus the C5 inhibitor group, based on the sponsor’s primary analysis.
In the APPLY-PNH study, the definition of clinical BTH was patients with at least 1 of 2 clinical criteria (≥ 20 g/L decrease in hemoglobin levels or signs and symptoms of hemolysis) and laboratory evidence of IVH (LDH > 1.5 times the upper limit of normal [ULN]). Two patients (3.2%) in the iptacopan group and 6 patients in the C5 inhibitor group (17.1%) met the criteria for a clinical BTH, with an annualized adjusted BTH rate of 0.07% and 0.67%, respectively. The BTH annualized adjusted rate difference was –0.60% (95% CI, –1.24% to 0.04%) for the iptacopan group versus the C5 inhibitor group.
Two other secondary outcomes were identified as important surrogate measures of hemolysis: the change from baseline in LDH levels and in the absolute reticulocyte count (ARC). For the iptacopan group versus the C5 inhibitor group, the percent change from baseline in LDH was 1.14% (95% CI, –10.19% to 11.31%) and the adjusted mean difference in the ARC change from baseline was –116.15 × 109 U/L (95% CI, –132.04 to –100.26 U/L; P < 0.0001).
Fatigue was measured using the 13-item FACIT-F questionnaire, which assesses self-reported tiredness, weakness, and difficulties with daily life activities. The FACIT-F items are scored so that a high score represents better health outcomes, with the total score ranging from 0 (severe fatigue) to 52 (no fatigue). In patients with PNH, a minimal important difference (MID) of 5 points has been reported in the literature.31 In the APPLY-PNH study, the change from baseline in FACIT-F score was a secondary outcome, and data were missing from 4 patients (11%) in the C5 inhibitor group and no patients in the iptacopan group. The mean within-group FACIT-F scores increased (improved) 8.6 points in the iptacopan group and 0.3 points in the C5 inhibitor group, with an adjusted mean difference of 8.3 points (95% CI, 5.3 to 11.3 points), favouring the iptacopan group versus the C5 inhibitor group (P < 0.0001).
The change from baseline in the European Organisation for the Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC QLQ-C30) was an exploratory outcome in the APPLY-PNH study and was not part of the planned statistical testing procedures. The results were based on observed data, with no imputation for missing values, and excluded 2 patients (6%) from the C5 inhibitor group. There was no mean change from baseline in the Global Health Status score in the C5 inhibitor group (0.0 points) and a 15.3 point increase in the iptacopan group. The mean difference was 14.5 points (95% CI, 9.6 to 19.3 points) for iptacopan versus C5 inhibitor groups at 24 weeks.
Harms Results
Most patients in the APPLY-PNH study experienced at least 1 treatment-emergent adverse event (TEAE), with 82% of those in the iptacopan group and 80% of patients in the C5 inhibitor groups reporting an adverse event over the 24-week treatment period. The most common events in the iptacopan versus C5 inhibitor group were headache (16% versus 3%), diarrhea (15% versus 6%), nasopharyngitis (11% versus 6%), and nausea (10% versus 3%). Serious adverse events (SAEs) were reported in 9.7% of patients in the iptacopan group and 14.3% of patients in the C5 inhibitor group. No deaths occurred, and no patients stopped treatment due to adverse events in either group. In the iptacopan group, 3.2% of patients experienced a serious or severe infection, compared with 8.6% of patients in the C5 inhibitor group (risk difference –5.4%; 95% CI, –15.6% to 4.9%).
No MAVEs were reported in the C5 inhibitor group, but 1 patient (1.6%) in the iptacopan group experienced a MAVE (transient ischemic attack), which was assessed as an SAE. The annualized adjusted rate difference for MAVE was 0.03% (95% CI, –0.03% to 0.10%) for iptacopan versus C5 inhibitors.
Infections caused by encapsulated bacteria were identified as an important harm for this review. One patient in the iptacopan group (1.6%) and no patients in the C5 inhibitor group reported an infection with encapsulated bacteria. The risk difference for iptacopan versus C5 inhibitors was 1.6% (95% CI, –1.5% to 4.8%).
Critical Appraisal
The APPLY-PNH study was 24-week, open-label randomized controlled trial (RCT). No major concerns were identified with the methods used to conduct the randomization; however, the baseline characteristics showed some imbalances between groups. Considering the small sample size of the study (35 patients in the C5 inhibitor group and 62 patients in the iptacopan group), it may not have been possible to balance all prognostic factors between groups. At baseline, a numerically higher proportion of patients in the C5 inhibitor group than the iptacopan group had received an RBC transfusion in the past 6 months, had a history of MAVE, and had LDH levels greater than 1.5 times the ULN. Also, the mean dose of eculizumab was higher in the C5 inhibitor group than in the iptacopan group (1,004.3 mg versus 937.5 mg, respectively). The clinical experts consulted agreed that these factors were indicators of more severe PNH. Thus, the differences observed in baseline characteristics potentially biased the results. No major risk of bias was identified due to patient withdrawals.
Patients, investigators, and study personnel were aware of the treatment group assigned. Thus, the potential for reporting and performance bias should be considered, particularly when interpreting the results of subjective outcomes, such as FACIT-F, EORTC QLQ-C30, and harms. The patient-reported outcomes and change from baseline in hemoglobin levels were also potentially biased due to missing data. The C5 inhibitor group was missing data from 2 patients (6%) for the EORTC QLQ-C30 Global Health Status, 4 patients (11%) for the FACIT-F score, and 6 patients (17%) for the change in hemoglobin levels. There were no missing data for the iptacopan group. Given the small sample size, the differential rate of missing data may have biased the results, although the direction and extent of any bias is unclear. The imputation methods used for the transfusion avoidance end point may impact the results adding uncertainty to the magnitude of treatment effects.
With regard to external validity, the study included adults with PNH who were, on average, 51 years of age and predominantly female, with low hemoglobin levels (mean 89 g/L). Based on the disease characteristics reported, and the low proportion of patients with elevated LDH levels (7% of patients had LDH > 1.5 × ULN), the clinical experts consulted for this review stated the patients represented a population with relatively easy-to-manage and well-controlled PNH. The study excluded patients with comorbid conditions such as bone marrow failure or significant cardiac, renal, or hepatic disease. Thus, the safety and efficacy of iptacopan in these patients are unclear. The small sample size of the study, the potential lack of representativeness in prognostic factors, and the short study follow-up duration (24 weeks) for a lifelong condition contribute to uncertainty in the generalizability of the findings.
The direct evidence was limited to a single open-label RCT comparing iptacopan with C5 inhibitors. However, pegcetacoplan is the key comparator for adults with PNH who have an inadequate response or intolerance to a C5 inhibitor. The absence of head-to-head studies comparing iptacopan with pegcetacoplan represents an evidence gap.
GRADE Summary of Findings and Certainty of the Evidence
For the RCT identified in the sponsor’s systematic review, Grading of Recommendations Assessment, Development and Evaluation (GRADE) was used to assess the certainty of the evidence for outcomes considered most relevant to inform the expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group.32,33
Following the GRADE approach, evidence from RCTs started as high-certainty evidence and could be rated down for concerns related to study limitations (which refers to internal validity or risk of bias), indirectness, imprecision of effects, and publication bias.
When possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect; if this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., clinical importance is unclear). In all cases, the target of the certainty of evidence assessment was based on the point estimate and where it was located relative to the threshold for a clinically important effect (when a threshold was available) or to the null. The target of the certainty of evidence assessment (presence or absence of an important effect) was based on thresholds identified in the literature (FACIT-F and EORTC QLQ-C30 Global Health Status), thresholds informed by the clinical experts consulted for this review (change from baseline in hemoglobin), or the presence or absence of any non-null effect (proportion of patients with an increase in hemoglobin levels of at least 20 g/L or hemoglobin levels of at least 120 g/L, who avoided transfusion, had BTH, or experienced infections, as well as the change from baseline in ARC or LDH levels).
The selection of outcomes for GRADE assessment was based on the sponsor’s Summary of Clinical Evidence, consultation with clinical experts, and input received from patient and clinician groups and public drug plans. The list of outcomes was finalized in consultation with expert committee members and is shown in Table 2.
Long-Term Extension Study
Description of Studies
The APPLY-PNH treatment extension period was a 24-week open-label extension of the 24-week APPLY-PNH study.36 The treatment extension period aimed to evaluate long-term efficacy and safety of iptacopan in adult patients with PNH who had residual anemia despite treatment with a C5 inhibitor. All study end points were defined as primary, with no secondary or exploratory end points. Primary efficacy variables included hematological response parameters, transfusion avoidance, hemoglobin, clinical BTH, LDH, ARC, FACIT-F scores, MAVE, patient-reported outcomes, C3 fragment deposition on RBCs and PNH clone size, and other PNH-related end points. In the final analysis, the absence of transfusion was not an integral component of the hematological response end points, in contrast to the week 24 primary efficacy analysis, for which absence of transfusion between day 14 and day 168 was an end point component. Primary safety end points included adverse events, SAEs, safety laboratory parameters, and vital signs. A total of 97 patients were enrolled in the treatment extension period. After completion of the treatment extension period, patients could enrol in an ongoing rollover extension program, which aims to further evaluate the long-term safety, tolerability, and efficacy of iptacopan.
Efficacy Results
Of the original cohort of 97 patients who completed the RTP of the APPLY-PNH study, all 61 patients allocated to iptacopan continued to the iptacopan arm of the extension period and 34 of 35 patients in the C5 inhibitor group switched to iptacopan at the beginning of the extension period from September 26, 2022 to March 6, 2023. Overall, efficacy results were consistent with those observed in the pivotal trial and sustained to the end of the treatment extension period.
After 336 days of iptacopan treatment, 86.4% of patients who were randomized to iptacopan had at least a 20 g/L increase in hemoglobin from baseline and 67.8% had sustained hemoglobin levels of at least 120 g/L, both irrespective of RBC transfusions. For patients who switched from a C5 inhibitor to iptacopan, 72.4% had at least a 20 g/L increase in hemoglobin from baseline after 168 days of iptacopan treatment. Additionally, 58.6% had sustained hemoglobin levels of at least 120 g/L at day 168 of iptacopan treatment. Eight patients (12.9%) in the iptacopan randomized group and 3 patients (8.8%) who switched to iptacopan from a C5 inhibitor received at least 1 transfusion while on iptacopan. Among patients who received transfusions, the mean number of transfusions per patient was 1.8 (SD 1.16) in the iptacopan group and 5.3 (SD 7.51) in the former C5 inhibitor group. The mean number of RBC units transfused to these patients was 2.9 units (SD 2.59 units) in the iptacopan group and 6.7 units (SD 8.96 units) in the former C5 inhibitor group.
Table 2: Summary of Findings for Iptacopan Versus C5 Inhibitors for Patients With PNH
Outcome and follow-up | Patients (studies), N | Relative effects (95% CI)a | Absolute effects (95% CI)a | Certainty | What happens | ||
|---|---|---|---|---|---|---|---|
C5 inhibitor | Iptacopan | Difference | |||||
Hemoglobin levels | |||||||
Marginal proportion of patients with ≥ 20 g/L increase in hemoglobin from baseline in the absence of RBC transfusions Follow-up: 24 weeks | 97 (1 RCT) | OR: 338.25 | 20 per 1,000 | 823 per 1,000 | 802 more per 1,000 (712 to 876 more per 1,000) | Moderateb | Treatment with iptacopan likely results in a clinically important increase in the proportion of patients with a hemoglobin increase of ≥ 20 g/L in the absence of transfusion when compared with C5 inhibitor therapy. |
Marginal proportion of patients with hemoglobin ≥ 120 g/L in the absence of RBC transfusions Follow-up: 24 weeks | 97 (1 RCT) | OR: 495.74 | 18 per 1,000 | 688 per 1,000 | 670 more per 1,000 (564 to 769 more per 1,000) | Moderateb | Treatment with iptacopan likely results in a clinically important increase in the proportion of patients with a hemoglobin levels ≥ 120 g/L in the absence of transfusion when compared with C5 inhibitor therapy. |
Adjusted mean change from baseline in hemoglobin (g/L) Follow-up: 24 weeks | 91 (1 RCT) | NR | –0.6 | 36.0 | 36.6 (32.0 to 41.2) | Moderatec | Treatment with iptacopan likely results in a clinically important increase in hemoglobin levels when compared with C5 inhibitor therapy. |
Transfusion | |||||||
Marginal proportion of patients without transfusion Follow-up: 24 weeks | 97 (1 RCT) | OR: 108.41 | 259 per 1,000 | 948 per 1,000 | 689 more per 1,000 (514 to 839 more per 1,000) | Moderateb | Treatment with iptacopan likely results in a clinically important increase in the proportion of patients who avoided transfusion when compared with C5 inhibitor therapy. |
Markers of hemolysis | |||||||
Annualized adjusted rate of clinical BTH Follow-up: 24 weeks | 97 (1 RCT) | Adjusted rate ratio: 0.10 (0.02 to 0.61) | 0.67% | 0.07% | –0.60% (–1.24% to 0.04%) | Very lowd | The evidence is very uncertain about the effect of iptacopan on BTH when compared with C5 inhibitor therapy. |
Percent reduction in LDH levels (U/L) Follow-up: 24 weeks | 97 (1 RCT) | Geometric mean ratio between groups 0.99 (0.89 to 1.10) | Geometric adjusted mean ratio to baseline 0.98 (0.89 to 1.07) | Geometric adjusted mean ratio to baseline 0.96 (0.90 to 1.03) | 1.14% (–10.19% to 11.31%) | Lowe | Treatment with iptacopan may result in little or no difference in LDH levels when compared with C5 inhibitor therapy. There is some uncertainty about the clinical importance of the estimates. |
Adjusted mean change from baseline in ARC (109/L) Follow-up: 24 weeks | 97 (1 RCT) | NR | 0.34 | –115.81 | –116.15 (–132.04 to –100.26) | Lowe | Treatment with iptacopan may result in reduced ARC when compared with C5 inhibitor therapy. The clinical importance of the reduction is unclear. |
Patient-reported outcomes | |||||||
Adjusted mean change from baseline in FACIT-F (0 [worst] to 52 [best])f Follow-up: 24 weeks | 93 (1 RCT) | NR | 0.3 | 8.6 | 8.3 (5.3 to 11.3) | Lowg,h | Treatment with iptacopan may result in a clinically important improvement in FACIT-F scores when compared with C5 inhibitor therapy. |
Change from baseline in EORTC QLC-C30 Global Health Status (0 [worst] to 100 [best])i Follow-up: 24 weeks | 95 (1 RCT) | NR | 0.0 | 15.3 | 14.5 (9.6 to 19.3) | Lowg,h,j | Treatment with iptacopan may result in a clinically important improvement in EORTC QLQ-C30 Global Health Status scores when compared with C5 inhibitor therapy. |
Harms | |||||||
Number of deaths Follow-up: 24 weeks | 97 (1 RCT) | NA | 0 | 0 | NA | Very lowj,k,l | The evidence is very uncertain about the effect of iptacopan on death when compared with C5 inhibitor therapy. |
Patients with infections due to encapsulated bacteria Follow-up: 24 weeks | 97 (1 RCT) | NA | 0 | 16 per 1,000 | 16 more per 1,000 (15 fewer to 48 more per 1,000) | Very lowj,k,l | The evidence is very uncertain about the effect of iptacopan on the occurrence of infection with encapsulated bacteria when compared with C5 inhibitor therapy. |
ARC = absolute reticulocyte count; BTH = breakthrough hemolysis; CI = confidence interval; EORTC QLQ-C30 = European Organisation for the Research and Treatment of Cancer Quality of Life Questionnaire; FACIT-F = Functional Assessment of Chronic Illness Therapy – Fatigue; LDH = lactate dehydrogenase; NA = not applicable; NR = not reported; OR = odds ratio; PNH = paroxysmal nocturnal hemoglobinuria; RBC = red blood cell; RCT = randomized controlled trial.
Note: Study limitations (which refer to internal validity or risk of bias), indirectness, imprecision of effects, and publication bias were considered when assessing the certainty of the evidence. All serious concerns in these domains that led to the rating down of the level of certainty are documented in the table footnotes.
aAll results are reported as unadjusted 95% CI. The CIs for all efficacy outcomes (except EORTC QLQ-C30) are not reflective of the prespecified multiplicity scheme to control type I error across the primary and secondary end points, and thus should not be interpreted as a basis for claiming statistical significance. EORTC QLQ-C30 was an exploratory outcome and not part of the multiplicity scheme to control type I error rate; thus, adjusted CIs are not relevant to this end point.
bRated down 1 level for serious concerns about imprecision. No published between-group MID was identified, and the clinical experts consulted by CDA-AMC were unable to estimate a threshold for clinically important effects; therefore, the null was used. Although the point estimate and entire CI excluded the null, the small sample size raises concern for potential overestimation of the true effect, and there is evidence of prognostic imbalance. Because the effect appeared plausible, the CDA-AMC review team rated it down only once.
cRated down 1 level due to serious concerns with risk of bias due to missing data. The clinical experts consulted for this review identified a 10 to 15 g/L difference between groups as the threshold for a clinically meaning change.
dRated down 1 level due to serious indirectness. The follow-up duration was insufficient to evaluate the rate of BTH. Rated down 2 levels due to very serious concerns about imprecision. There is a very small number of events captured, and the small sample size raises concern for potential overestimation of the true effect, as there is evidence of prognostic imbalance. No published between-group MID was identified, and the clinical experts we consulted were unable to estimate a threshold for clinical important effects; therefore, the null was used.
eRated down 1 level due to serious indirectness. LDH and ARC levels are surrogate measures of hemolysis and may be impacted by factors other than the study drug. Rated down 1 level for serious concerns about imprecision. The small sample size raises concern for potential overestimation of the true effect, and there is evidence of prognostic imbalance. No published between-group MID was identified, and the clinical experts consulted by CDA-AMC were unable to estimate a threshold for clinically important effects; therefore, the null was used. For LDH, the CDA-AMC review team considered the 95% CI to include the potential for little to no difference only. No judgments were made on the clinical relevance of the ARC results.
fThe FACIT-F is a 13-item, patient-reported questionnaire that assesses tiredness, weakness, and difficulty conducting usual activities due to fatigue over the past week. The scale ranges from 0 (extreme fatigue) to 52 (no fatigue). In patients with PNH, a 5-point increase from baseline was reported as the MID.31
gRated down 1 level for serious risk of bias due to missing data and open-label design. The open-label study design and patients’ and assessors’ knowledge of assigned treatment may lead to biased estimates of subjective outcomes. For the FACIT-F score, data were missing or excluded from 4 of 35 patients in the C5 inhibitor group (11%) and no patients in the iptacopan group. For the Global Health Status, data were missing for 3 of 35 (6%) of patients in the C5 inhibitor group and no patients in the iptacopan group. Given the small sample size and differential missing data, the potential for bias cannot be ruled out.
hRated down 1 level for serious concerns about imprecision. Although the point estimate and entire CI excluded the threshold of clinical importance, the small sample size raises concern for potential overestimation of the true effect, and there is evidence of prognostic imbalance.
iEORTC QLQ-C30 Global Health Status assesses global health status or quality of life, with higher scores representing better HRQoL The scores are the sum of the component items, which are then normalized by using the maximum range of values for the subscale and multiplied by 100. The EORTC QLQ-C30 tool has evidence to support its validity and responsiveness in patients with PNH; however, MID values have not been established in the PNH population. In patients with cancer, an increase of at least 10 points in the EORTC QLQ-C30 score is considered moderately large and represents a clinically important improvement.34
jThe change from baseline in EORTC QLQ-C30 Global Health Status and the safety outcomes were not adjusted for multiplicity in the APPLY-PNH trial and should be considered as supportive evidence.
kRated down 2 levels due to very serious imprecision. There are a very small number of events captured.
lRated down 1 level due to serious indirectness. The follow-up duration was insufficient to evaluate safety of the study drug.
Source: APPLY-PNH Clinical Study Report.29,30 Details included in the table are from the sponsor’s Summary of Clinical Evidence.35
During the treatment extension period, 4 patients in the iptacopan group and 1 patient who switched to iptacopan from a C5 inhibitor experienced 1 or more clinical BTH events. Across the entire 48-week study, there were 8 BTH events in 7 patients during treatment with iptacopan, with an adjusted annualized rate of BTH of 0.11 (95% CI, 0.05 to 0.23).
At day 336, the geometric adjusted mean ratio to baseline in LDH was 1.11 (95% CI, 1.02 to 1.22) for the iptacopan group and 0.99 (95% CI, 0.88 to 1.11) for the former C5 inhibitor group, with an adjusted mean ratio to baseline of 1.12 (95% CI, 0.97 to 1.30) between groups. The adjusted mean change from baseline in ARC at day 336 was –106.26 × 109/L (95% CI, –117.57 to –94.96 × 109/L) for the iptacopan group and –107.95 × 109/L (95% CI, –123.18 to –92.73 × 109/L) for the former C5 inhibitor group, with an adjusted mean difference of 1.69 × 109/L (95% CI, –16.86 to 20.23 × 109/L) between groups. After 7 days of iptacopan treatment, normalization of ARCs (13.5 × 109/L to 123 × 109/L) was achieved by 80.6% of patients in the iptacopan group and was sustained in 80.6% of patients in this group until day 336. In the former C5 inhibitor group, normalization was achieved in 61.8% of patients after 7 days of treatment and 85.3% after 28 days and was consistently seen in 70.6% of participants until day 336.
Both groups demonstrated improvements in fatigue and HRQoL, as measured by FACIT-F and EORTC QLQ-C30 Global Health Status. At day 336, the adjusted mean change from baseline in FACIT-F score was 9.80 points (95% CI, 8.04 to 11.56 points) for the iptacopan group and 10.96 points (95% CI, 8.58 to 13.34 points) for the former C5 inhibitor group, with an adjusted mean difference of –1.17 points (95% CI, –4.01 to 1.68 points) between groups. The mean EORTC QLQ-C30 score was 76.4 (SD 15.11) for the iptacopan group and 74.4 (SD 16.98) for the former C5 inhibitor group at day 336, with mean increases from baseline of 16.3 (SD 17.99) and 15.2 (SD 22.61), respectively.
Harms Results
Across the entire 48-week study, the most common TEAEs among all patients who received iptacopan were COVID-19 (27.1%), headache (14.6%), diarrhea (12.5%), nasopharyngitis (12.5%), and nausea (11.5%). Most study patients had a TEAE during the 48-week study, with comparable proportions between those randomized to iptacopan (93.5%) and all patients who received iptacopan (88.5%). The majority of TEAEs were mild or moderate, with 9.4% of all iptacopan recipients experiencing severe adverse events. Overall, 13.5% of all patients who received iptacopan experienced SAEs, consisting of 9 who were randomized to iptacopan and 4 patients who switched to iptacopan from a C5 inhibitor in the treatment extension period. No deaths were reported in the study, and no patients discontinued the study or iptacopan treatment due to adverse events.
Two patients experienced MAVEs during the treatment extension period. One patient was in the iptacopan randomized group and the second had switched to iptacopan from a C5 inhibitor. The events were not considered related to study treatment, and no action was taken regarding iptacopan treatment.
Infections caused by encapsulated bacteria were identified as an important harm for this review. Across the entire 48-week study, 3 patients (3.1%) reported an infection with encapsulated bacteria. During the treatment extension period, 1 patient experienced a nonserious TEAE of bilateral otitis media.
Critical Appraisal
Internal Validity
The APPLY-PNH extension period was designed as an open-label extension to assess long-term efficacy and safety of iptacopan in the treatment of adult patients with PNH. This open-label design could bias the magnitude of treatment effect for subjective efficacy outcomes and reporting of safety parameters due to unblinded exposure to the study medication during the treatment period. Statistical hypothesis testing was not part of the design, and there was no active comparator or placebo arm.
External Validity
The extension study consisted of patients who took part in pivotal studies, and it is therefore reasonable to expect that the same strengths and limitations related to generalizability apply to the extension period. Given that patients needed to complete the parent study before enrolling, the extension period population is inherently enriched and introduces some selection bias for responders. Additionally, a lack of study sites in Canada limits the ability to generalize these findings to patients living in Canada with PNH.
Indirect Comparisons
Description of Studies
The sponsor submitted an indirect treatment comparison (ITC) that evaluated the efficacy and safety of iptacopan versus pegcetacoplan for the treatment of adult patients with PNH who have residual anemia despite treatment with a C5 inhibitor.37,38 The ITC consisted of an unanchored matching-adjusted indirect comparison (MAIC) based on individual patient data (IPD) from the iptacopan group (N = 54) of the APPLY-PNH study and aggregate data for the pegcetacoplan group (N = 41) of the PEGASUS study. The change from baseline in hemoglobin (including and excluding posttransfusion hemoglobin data), transfusion avoidance, change from baseline in LDH, change from baseline in FACIT-F, and SAEs were selected as outcomes for the MAIC.
In the first step of the unanchored MAIC, patients from the iptacopan group who did not meet the inclusion criteria of the PEGASUS study were excluded, and then the iptacopan IPD was weighted to balance the 2 treatment groups on baseline hemoglobin levels, sex, and the proportion of patients who were transfusion-free within 12 months before baseline. For continuous outcomes, the iptacopan effect estimates were derived by fitting a mixed model for repeated measures (MMRM) to the weighted IPD, with the comparative effects versus pegcetacoplan derived as the difference between the adjusted mean change from baseline for iptacopan and the published adjusted mean of pegcetacoplan. Binary outcomes estimates were derived with an intercept-only logistic regression model fitted to the weighted IPD for iptacopan. An estimate of the log odds ratio (OR) for iptacopan versus pegcetacoplan was derived as the difference between the weighted log odds for iptacopan and the estimated log odds for pegcetacoplan based on published transfusion events and SAEs from the PEGASUS study.
Efficacy Results
The results of the base-case unanchored MAIC were based on 41 patients who received pegcetacoplan and an effective sample size (ESS) of 16 patients from the iptacopan group. The estimated mean difference in the change from baseline in hemoglobin levels was 13.1 g/L (95% CI, 5.2 to 21.0 g/L) censored for transfusion, and 10.5 g/L (95% CI, 4.3 to 16.7 g/L) uncensored for transfusion, for iptacopan versus pegcetacoplan.
The MAIC estimated 85.4% of patients in the pegcetacoplan group and 98.2% of patients in iptacopan group avoided transfusion, with an OR of 9.17 (95% CI, 1.59 to 52.89), favouring iptacopan.
The mean difference in the change from baseline in LDH levels was 36.68 U/L (95% CI, –62.54 to 135.89 U/L) for iptacopan versus pegcetacoplan. For the change from baseline in FACIT-F score, the unanchored MAIC estimated a mean difference of –2.32 points (95% CI, –6.34 to 1.70 points) for iptacopan versus pegcetacoplan.
Harms Results
The MAIC estimated that 17.1% and 4.8% of patients in the pegcetacoplan and iptacopan groups, respectively, would experience an SAE with an OR of 0.24 (95% CI, 0.06 to 0.98), favouring iptacopan.
Critical Appraisal
The unanchored MAIC submitted by the sponsor had serious methodological issues that threaten the validity of the findings. Unanchored MAICs have a high risk of bias, as the underlying assumptions required for valid effect estimates are very difficult to meet. These methods require that all prognostic factors and effect modifiers (measured and unmeasured) be accounted for in the model, which may not be possible. Failure of this assumption leads to an unknown amount of bias in the effect estimates. The sponsor argued that other ITC methods with a lower risk of bias were not feasible due to sparse data available and the heterogeneity in the patient and study characteristics between the APPLY-PNH and PEGASUS trials. The CDA-AMC reviewer agreed there is significant heterogeneity between the studies and concluded that the MAIC methods used by the sponsor were not able to adequately control for these differences. In the unanchored MAIC, the 2 patient populations were balanced on 3 variables only, and imbalances remained for several clinically important factors (e.g., proportion of patients with at least 4 transfusions in past 12 months, race, history of aplastic anemia, FACIT-F score, duration of C5 inhibitor therapy, time since diagnosis, platelet count, and body mass index [BMI]). Other important prognostic factors identified by the clinical experts we consulted were not addressed in the MAIC (i.e., C5 inhibitor dose, LDH levels > 1.5 × ULN, and PNH-related kidney disease). The low ESS of the iptacopan group (16 patients or 30% of the unweighted population) suggests the patients were too dissimilar to warrant valid comparison. In addition, the skewed distribution of weights also suggests the populations were substantially different, and the occurrence of extreme weights may lead to unstable effect estimates. According to the clinical experts we consulted, the population enrolled in the PEGASUS trial was clinically different, with more severe PNH than that in the APPLY-PNH study. Thus, given the underlying differences between the 2 trials, and the imbalances in important prognostic factors that remained after matching and weighting, the treatment effect estimates were considered too unreliable to draw any firm conclusions.
Studies Addressing Gaps in the Evidence From the Systematic Review
No studies addressing gaps were submitted by the sponsor.
Conclusions
In adults with PNH and residual anemia despite treatment with C5 inhibitors, iptacopan likely results in more patients experiencing clinically important improvements in hemoglobin levels and normalization of hemoglobin levels (hemoglobin levels ≥ 120 g/L), and fewer patients who require transfusion, compared with C5 inhibitors. Based on the change from baseline in the FACIT-F questionnaire, iptacopan may improve fatigue symptoms compared with C5 inhibitors. The impact of iptacopan on the frequency of BTH and on the change in LDH levels and ARC was uncertain due to the limitations of the data and the absence of a threshold for a clinically important difference.
Data from the open-label, single-arm extension phase of the APPLY-PNH study suggests that improvements in hemoglobin levels, transfusion avoidance, and fatigue observed with iptacopan may be maintained up to 48 weeks.
Adverse events were common in both the iptacopan and C5 inhibitor groups in the APPLY-PNH study, but there were no deaths, and no patients stopped treatment due to adverse events. Infections due to encapsulated bacteria occurred infrequently, but no conclusions can be made concerning comparative frequency of events versus C5 inhibitors due to the small sample size, limited follow-up, and low number of events.
Overall, the direct comparative evidence was limited to 1 open-label RCT (the APPLY-PNH study), which randomized 97 patients with PNH and residual anemia to receive treatment with iptacopan or C5 inhibitors for 24 weeks. No direct evidence was available comparing iptacopan to pegcetacoplan, the key comparator for patients with PNH and EVH. To address the evidence gap, the sponsor submitted an unanchored MAIC that assessed the safety and efficacy of iptacopan versus pegcetacoplan. However, no conclusions can be drawn from the MAIC due to serious limitations that undermine the validity of the findings. There was significant heterogeneity between the 2 studies informing the MAIC, and imbalances in important prognostic factors remained after matching and weighting. As a result, the treatment-effect estimates are considered unreliable, as the trial populations were too dissimilar to compare.
Introduction
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of iptacopan (200 mg, hard capsule, oral) for the treatment of adult patients with PNH.
Disease Background
Contents of this section have been informed by materials submitted by the sponsor and clinical expert input. The following have been summarized and validated by the review team.
PNH is a rare, chronic, and potentially life-threatening condition caused by an acquired genetic defect in hematopoietic stem cells.1,2 This defect results in the production of blood cells lacking 2 glycosylphosphatidylinositol-anchored complement regulatory proteins CD55 and CD59 at their surface, causing the complement system to recognize RBCs as damaged.1,2 This uncontrolled activation of the complement cascade triggers premature episode of these RBCs, resulting in hemolysis.1 Increased complement activity at the hematopoietic cell surface of platelets and leukocytes can also increase risk of thromboembolic events.1
Hemolysis occurs through 2 mechanisms in PNH: IVH and EVH. IVH occurs through both terminal and proximal complement pathways, when RBCs are lysed due to activation of the alternative complement pathway.3 Conversely, EVH occurs through the proximal pathway when RBCs are opsonized by C3 fragments, tagging them for macrophage destruction in the spleen and liver.4-6 EVH occurs only in patients receiving C5 inhibitor therapy.39 C5 inhibition enables RBCs to remain intact, but EVH may occur because the surviving RBCs are marked by proteins in the complement system for removal by the spleen and liver.39 Persistent IVH results in hemoglobinuria, characterized by dark-coloured urine that is particularly noticeable in the morning due to overnight urine concentration.2 In addition to hemolytic anemia and its related symptoms (e.g., fatigue, dyspnea), patients with PNH are susceptible to an increased risk of thrombosis, pain, organ damage (e.g., impaired renal function), and underlying bone marrow dysfunction.4,7,8 These symptoms and the IVH-associated need for transfusions have a significant impact on patients’ daily living, impair their HRQoL,4,7,15,16 and increase the risk of morbidity and mortality.17,18 In contrast, EVH symptoms are not life-threatening; however, clinical manifestation is heterogeneous.1 Some patients with EVH have normal hemoglobin levels11 and are asymptomatic,9,10 while others may develop severe clinical symptoms and require blood transfusions to manage ongoing anemia and fatigue.9,12,13 Symptoms of PNH can vary significantly among individuals, and the disease can affect any race, ethnicity, or sex. It may manifest at any age,4,40 although the median age of disease onset has been reported to be around 40 years of age in Canada.1 PNH has also been linked with bone marrow failure syndromes, including aplastic anemia and myelodysplastic syndromes.1,14
In studies examining survival of patients with PNH following diagnosis, median survival ranged from 14.6 years to 32 years,41,42 while results from a study in patients with PNH treated with eculizumab suggested that their survival was similar to that of age-matched controls.16
Due to the disease rarity, the prevalence and incidence of PNH and EVH have been poorly reported, and published estimates of PNH and EVH are not available for the population in Canada. A study in the UK estimated the 15-year prevalence of PNH at 1.59 per 100,000 persons and an annual incidence of approximately 0.13 per 100,000 persons.20 Another study in the UK reported an overall prevalence of 3.81 per 100,000 persons and an overall annual incidence rate of 0.35 per 100,000 persons.21 A study in the US estimated the prevalence of PNH at 1.2 to 1.3 per 100,000 persons between 2016 and 2017.19 The incidence rate over the study period was 0.57 per 100,000 person-years.19 Clinical trial and real-world data showed that around 20% of patients with PNH who were clinically stable on C5 inhibitor treatment for IVH developed clinically significant EVH.22
Once clinical and laboratory data suggest PNH (e.g., low hemoglobin levels, abdominal pain, persistent fatigue, dyspnea, cytopenia, iron deficiency, hemolysis), diagnosis is established in an appropriate clinical setting by flow cytometry, which demonstrates a deficiency of glycosylphosphatidylinositol-anchored proteins (CD55, CD59) on RBCs.1,2 Regular clinical workups to identify clinically significant EVH (e.g., lowered hemoglobin levels and elevated reticulocyte counts) are available and conducted as part of the routine monitoring for patients receiving treatment for PNH.1,2
Standards of Therapy
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following has been summarized and validated by the review team.
According to the clinical experts consulted for this review, the goals of therapy are to reduce mortality, reduce complications and morbidity associated with IVH, reduce the need for transfusion and improve HRQoL with better hemoglobin support that avoids iron overload and helps patients attain better functional status and return to prediagnosis activities and employment.
In Canada, patients with PNH receive C5 inhibitors as standard first-line therapy to reduce uncontrolled complement activation in the terminal complement cascade.23,24 The primary C5 inhibitor therapies are ravulizumab and eculizumab, both administered through IV infusion.1,25,26 The dose of ravulizumab is determined according to patient weight and usually administered every 8 weeks, although the clinical experts stated that there is a subset of patients who may require doses every 6 or 7 weeks.26 The recommended dosage of eculizumab is 900 mg every 2 weeks, but, according to the clinical experts, higher doses of 1,200 mg or 1,500 mg, or a more frequent dosing interval (every 12 or 13 days) may be required for some patients to control hemolysis.25 The 2 C5 inhibitors have comparable efficacy and toxicity.4 BTH is characterized by the return of IVH and the reappearance of PNH symptoms. Approximately 11% to 27% of patients may experience BTH on approved doses of eculizumab, and fewer patients experience BTH with ravulizumab than with eculizumab.5,43
EVH is an iatrogenic effect of C5 blockade and is not life-threatening.4,44 According to the clinical experts consulted for this review, the diagnosis of EVH is complex, as it is important to rule out other possible underlying causes of anemia. Once EVH is diagnosed, treatment primarily focuses on addressing residual anemia,9,12,13 while maintaining terminal complement blockade to prevent the life-threatening consequences of IVH.2,23,45 EVH can become clinically relevant for patients, leading to persistent symptoms of anemia, as well as dependence on transfusions.5,9
According to the Canadian PNH Network, the historical approach to managing EVH-associated anemia in patients with PNH in Canada has been supportive care (e.g., RBC transfusions, corticosteroids, danazol, and epoetin alfa) and continued C5 inhibitor treatment.1 The primary nonpharmacologic treatment for EVH and persistent anemia in PNH while on C5 inhibitor treatment is transfusion support.4,22 Folic acid and vitamin B12 supplementation are also supportive options.46 Hematopoietic stem cell transplant is considered curative. However, because the risk of transplant-related mortality and morbidity are significant, transplant is generally reserved for individuals with specific additional comorbidities.46
In Canada, patients receiving C5 inhibitors who are diagnosed with EVH may be switched to pegcetacoplan. Pegcetacoplan, a proximal C3 inhibitor, is a Health Canada–approved therapy indicated for patients with inadequate response or intolerance to a C5 inhibitor.23,27 Pegcetacoplan has been previously reviewed by CDA-AMC (recommendation: reimburse with conditions).23 Pegcetacoplan 1,080 mg is administered through subcutaneous infusion twice weekly with a syringe system infusion pump by a health care professional, the patient, or caregiver.27 In the first 4 weeks of initiating therapy, pegcetacoplan is administered in addition to the patient’s current C5 inhibitor treatment to minimize risk of hemolysis from abrupt discontinuation.27 After the first 4 weeks, pegcetacoplan is administered as monotherapy. Dose intensification of pegcetacoplan may be considered if LDH level is at least 2 times above the ULN or the patient experiences a BTH.27 In response to BTH, the patient could receive a single IV dose of pegcetacoplan or daily subcutaneous doses for 3 days, followed by a more frequent dosing interval of every 3 days, or if BTH recurs, 3 times per week.47
Danicopan is another second-line option that has recently become available in Canada. Danicopan is a proximal inhibitor of factor D in the alternative complement pathway that is indicated as an add-on to ravulizumab or eculizumab for patients with residual hemolytic anemia due to EVH.28 Danicopan 150 mg is administered orally 3 times a day, approximately 8 hours apart.28 Dosage increases to 200 mg 3 times a day may be considered if hemoglobin does not increase by at least 20 g/L following 4 weeks of therapy, if the patient requires a transfusion in those 4 weeks of treatment, or if an appropriate hemoglobin response has not been achieved, based on clinical judgment.28 Danicopan was under review by CDA-AMC when this review was initiated and thus was not considered a comparator for iptacopan. It received a final conditional positive CDA-AMC recommendation in November 2024 and is currently under consideration for negotiation with pCPA.
Drug Under Review
Key characteristics of iptacopan are summarized in Table 3, with characteristics of other treatments available for patients with PNH who have inadequate response or intolerance to a C5 inhibitor.
Iptacopan is a proximal complement inhibitor that targets factor B to selectively inhibit the alternative pathway while leaving direct signalling from the lectin and classical pathways intact.48 Factor B inhibition prevents formation of C3 convertase and subsequent production of C5 convertase. In PNH, IVH is mediated by the downstream membrane attack complex, while EVH is facilitated by opsonization with C3 fragments. The proximal inhibition induced by iptacopan in the alternative pathway of the complement cascade controls both terminal complement-mediated IVH and C3-mediated EVH.
Iptacopan was approved by Health Canada as monotherapy in the treatment of adult patients with PNH who have hemolytic anemia.48 In the US, iptacopan was approved for the treatment of adult patients with PNH,49 and, in the European Union, it is indicated as monotherapy in the treatment of adult patients with PNH who have hemolytic anemia.50
The sponsor has submitted a deviation request for the reimbursement of iptacopan in adult patients with PNH who have an inadequate response to, or are intolerant of, a C5 inhibitor. Per sponsor request, this review focuses on the population requested for reimbursement.
Iptacopan is administered as an oral capsule. The recommended dosage of iptacopan for adult patients with PNH is 200 mg taken orally twice daily.48 To minimize risk of hemolysis from abrupt discontinuation of C5 inhibitor therapies, iptacopan should be initiated no more than 1 week after the last dose of eculizumab or 6 weeks after the last dose of ravulizumab.48
Table 3: Key Characteristics of Iptacopan and Pegcetacoplan
Characteristic | Iptacopan | Pegcetacoplan |
|---|---|---|
Mechanism of action | Factor B inhibitor — proximal complement inhibition | C3 inhibitor — proximal complement inhibition |
Indicationa | As monotherapy in the treatment of adult patients with PNH who have hemolytic anemia | For the treatment of adult patients with PNH who have an inadequate response to, or are intolerant of, a C5 inhibitor |
Route of administration | Oral | Subcutaneous, via syringe system infusion pump over 30 to 60 minutes |
Recommended dose | 200 mg twice daily To minimize risk of hemolysis from abrupt discontinuation of C5 inhibitor therapies, iptacopan should be initiated no more than 1 week after the last dose of eculizumab or 6 weeks after the last dose of ravulizumab. | 1,080 mg twice weekly Dose adjustment:
Pegcetacoplan should be administered in addition to the patient’s current dose of C5 inhibitor treatment for the first 4 weeks of treatment to minimize the risk of hemolysis with abrupt treatment discontinuation. |
Serious adverse effects or safety issues | Increased risk of serious and life-threatening infections caused by encapsulated bacteria, including Streptococcus pneumoniae, Neisseria meningitidis, and Haemophilus influenzae, even after vaccination | Increased risk of serious and life-threatening infections caused by encapsulated bacteria, including Streptococcus pneumoniae, Neisseria meningitidis, and Haemophilus influenzae, even after vaccination |
Other | Complete or updated vaccination against encapsulated bacteria is advised at least 2 weeks before administration of first iptacopan dose. If urgent iptacopan therapy is indicated, provide patient with antibacterial drug prophylaxis and administer vaccines as soon as possible. |
|
LDH = lactate dehydrogenase; PNH = paroxysmal nocturnal hemoglobinuria; ULN = upper limit of normal.
aHealth Canada–approved indication.
Source: Pegcetacoplan Product Monograph;27 Iptacopan Product Monograph.48
Pagebreak
Perspectives of Patients, Clinicians, and Drug Programs
The full patient and clinician group submissions received are available in the consolidated patient and clinician group input document for this review on the project website.
Patient Group Input
This section was prepared by the review team based on the input provided by patient groups.
The PNHCA and the AAMAC submitted input for this review jointly. PNHCA is a nonprofit patient advocacy group that connects individuals with PNH and their caregivers to resources and information on optimal management of PNH. AAMAC is a national charity that provides supportive resources on PNH to patients, caregivers, and health care providers. A clinical summary of PNH was provided and information was gathered through the personal experiences of individuals who had direct experience with iptacopan, including 1 patient living in Canada and 5 patients living in the US.
Input from the patient groups highlighted the diverse and profound ways in which PNH impacts quality of life for both patients and caregivers. Due to the condition’s rarity and the variability of presentation, the input noted that patients often experience a period of significant health deterioration before they receive a PNH diagnosis. Thrombosis was emphasized as a serious complication of PNH that can result in life-threatening conditions such as stroke, pulmonary embolism, or Budd-Chiari syndrome, which significantly increase the risk of morbidity and mortality. It was noted that the chronic nature of PNH means that patients must manage their condition over a lifetime, along with the associated physical, emotional, and financial burdens. The need for frequent medical appointments across the patient’s lifetime can also result in feelings of isolation, strain on relationships, emotional distress, and decreased quality of life. Patients must also cope long-term with unpredictability of symptoms, treatment side effects, and threat of serious complications.
The patient group input noted that, while C5 inhibitor therapies prevent RBC destruction, EVH may not be fully addressed, which can result in chronic anemia despite C5 inhibitor treatment. Chronic anemia can cause severe fatigue, physical weakness, shortness of breath, and transfusion dependence, making it challenging to carry out household tasks, maintain employment, participate in recreational activities, and sustain an active lifestyle. A patient living in Canada who provided input shared that, while previous treatment with eculizumab did not enable a decent quality of life, treatment with iptacopan led to feeling “normal” within months of treatment initiation. This patient also noted valuing the convenience of oral administration, which enabled freedom from injection-type infusions. The 5 patients living in the US reported substantial increases in hemoglobin after initiating iptacopan, with some also experiencing normalization of LDH levels, reduction in bilirubin levels, and improvement in fatigue.
Overall, the patient group input highlighted a need for new therapies that effectively manage IVH and EVH, to provide comprehensive relief from a wide range of symptoms and improve patient well-being. Specifically, the patient group noted the need for new treatments that improve hemoglobin levels and reduce the need for blood transfusions. The patient group noted that oral treatments provide significant benefits over injections in terms of convenience, comfort, adherence, psychological well-being, and economic factors, making oral treatments a preferred option when available.
Clinician Input
Input From Clinical Experts Consulted by CDA-AMC
All CDA-AMC review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of PNH.
Unmet Needs
The clinical experts noted that C5 inhibitors can provide incomplete control of PNH in some circumstances: rare genetic polymorphism, inadequate dosing, response to complement-amplifying triggers (e.g., vaccination or infections) leading to BTH, or symptomatic EVH related to C5 inhibition. Per the experts, approximately 1 third of patients require higher doses of C5 inhibitors, although this may be less likely with ravulizumab since the dose is determined by patient weight. Patients who develop BTH toward the end of the period between doses and who may benefit from more frequent perfusion would not generally be considered to have treatment failures, according to the clinical experts. The experts estimated that approximately 40% of patients with PNH will continue to have low hemoglobin despite therapy, approximately 30% will require transfusions, and 20% to 30% will have EVH that contributes to poor HRQoL. Treatment goals for patients with PNH and EVH remain to reduce mortality, inhibit IVH, and improve HRQoL with better hemoglobin support that does not require transfusion, avoids iron overload, and leads to better functional status for patients.
Treatment strategies for a patient diagnosed with EVH include erythropoietin administration and steroids, which, the clinical experts stated, have questionable efficacy and associated risks, such as thrombosis and predilection for infection with encapsulated bacteria. The main nonpharmacologic treatment for EVH and persistent anemia in PNH while on C5 inhibitor treatment is transfusion support. Transfusion is associated with several drawbacks, according to the clinical experts: hospital visits of 2 to 4 hours are required and may be longer if blood typing is not done in advance, and there are risks with transfusion, including infection, antibody development, or iron overload, which can lead to heart and liver failure or endocrine disorders including diabetes, as well as liver cancer if left untreated. In addition, most patients on transfusion will have significantly reduced HRQoL and be unable to maintain regular employment.
Pegcetacoplan is approved as a second-line therapy for patients with PNH who have an inadequate response to, or are intolerant of, a C5 inhibitor. According to the clinical experts consulted for this review, it is currently the primary pharmacologic option offered for patients diagnosed with EVH. Pegcetacoplan is administered as a subcutaneous infusion (over 20 to 40 minutes) with twice-weekly dosing. If BTH occurs, the experts noted that the frequency of pegcetacoplan would usually be increased (every 3 days or up to 3 times weekly). If BTH is severe, doses of ravulizumab or eculizumab would also be added, but the experts noted that C5 inhibitors may not be on formulary in all hospitals. According to the clinical experts, there are patients and their caregivers for whom subcutaneous infusions are not possible or are unacceptable, and the treatment burden of administering infusions can be significant. The experts also stated that danicopan, as add-on therapy to C5 inhibitors, may be available to some patients in Canada via a managed access program, but this therapy can also be problematic, as it maintains the need for IV infusions, which can require the installation of a central vein catheter with its risks and need for care. Danicopan is administered orally 3 times daily, and treatment adherence may be challenging for some patients.
Place in Therapy
According to the clinical experts consulted, iptacopan would be used as another second-line option for patients with PNH and an incomplete hematologic response to C5 inhibitors, particularly with ongoing anemia secondary to EVH (whether or not it requires transfusions). There is also a place for iptacopan in treating patients who have an intolerance to C5 inhibition or are no longer able to have IV infusions, either because of long distance to medical care or an inability to maintain IV access.
In patients with genetic polymorphisms in whom C5 inhibitor treatment is ineffective, iptacopan would be a treatment option. As there is currently no test available to detect the polymorphisms, these patients are identified through a trial of C5 inhibitors. Patients with polymorphisms require a switch from the currently approved C5 inhibitors to a more proximal complement blockade to control IVH.
According to the clinical experts, in patients currently on eculizumab, persistent anemia due to suboptimal control of IVH may be better controlled by switching to ravulizumab, as it uses weight-based doses, but the experts noted that ravulizumab is unavailable in many provinces. In the absence of ravulizumab or even with suboptimal control on C5 inhibition, a switch to proximal inhibition could be warranted. The experts suggested there may be a role for iptacopan as a third-line option for patients who received pegcetacoplan and experienced adverse effects, were no longer willing to receive subcutaneous infusions, experienced too many BTHs, or had persistently elevated LDH levels even with increased doses of pegcetacoplan. The CDA-AMC review team notes that this review for iptacopan focuses on the population requested for reimbursement, i.e., adult patients with PNH who have an inadequate response to, or are intolerant of, a C5 inhibitor. Evidence for use of iptacopan after pegcetacoplan is not provided in the pivotal trial for iptacopan, the APPLY-PNH trial.
The clinical experts indicated that iptacopan would shift the current treatment paradigm, in that pegcetacoplan and iptacopan would likely be offered in the same line of therapy and for the same indication. They did not expect that iptacopan would be used as first-line therapy, although there are some data to support this approach (APPOINT-PNH study) if C5 inhibitors could not be used. The clinical experts stated that iptacopan would not be used in combination with other treatments but as a stand-alone second option after C5 inhibitors.
Patient Population
The clinical experts noted that appropriate candidates for iptacopan treatment include patients with PNH who have persistent anemia (hemoglobin < 100 g/L to 105 g/L, with or without history of ongoing need for blood transfusion, and no known cause for the anemia, e.g., blood loss, bone marrow failure) and evidence of EVH, despite an adequate trial of C5 inhibitor treatment; patients with intolerance to a C5 inhibitor (uncommon in clinical practice); or patients with a rare C5 genetic polymorphism (mainly in patients of Japanese descent). The clinical experts stated that suitable patients would accept iptacopan’s treatment modality and schedule. The clinical experts also highlighted that patients who do not want transfusions and are potentially therefore undertreated, whose anemia is not severe enough for transfusion, or for whom currently available therapy is unacceptable or unfeasible, would likely benefit from iptacopan. It would also be suitable for patients who are not willing or not able to use the infusion pump for pegcetacoplan. The experts explained that patients with PNH often have other concurrent causes of anemia, and efforts must be made to control these (e.g., epoetin alfa in patients with chronic kidney disease, or vitamins in the case of deficiencies). The cause of anemia may be multifactorial; for example, patients with concurrent aplastic anemia or myelodysplastic syndromes should not be excluded from receiving iptacopan to control their EVH. For these complex patients, the experts noted that a trial of drug may be necessary to see whether there is improvement in the patient’s need for transfusion, hemoglobin, and/or quality of life without necessarily reaching a fixed laboratory value and with the recognition that every effort must be made to continue controlling IVH and preventing its associated mortality.
Iptacopan would also be suitable for patients with no response to C5 inhibition in the case of polymorphisms, according to the clinical expert consulted. The experts indicated it is not possible to identify in advance which patients will most benefit from 1 therapy over another, and a trial of therapy may be needed. Further, the clinical experts emphasized the need for fluidity between the therapies, as patients’ needs could vary over time and changes between therapies should not be seen as unidirectional.
Iptacopan would not be suitable for patients who are pregnant or who plan to become pregnant, or for those who do not accept or are not able to adhere to twice daily oral dosing, given the risk of BTH if doses are missed. As per the FDA product label, iptacopan may not be suitable for patients with uncontrolled dyslipidemia.
Assessing the Response Treatment
The clinical experts noted that response to therapy is typically an improvement in hemoglobin, a reduction in the need for transfusion, and improvement in symptoms relative to the baseline for a given patient. They noted that ongoing anemia and need for transfusion may or may not indicate a treatment failure, as other concurrent diseases, such as bone marrow failure, aplastic anemia, other cancers, bleeding, or comorbidities, could be contributing factors. The experts stated that treatment failures or suboptimal responses emphasize the need for full evaluation of the cause of anemia. Additionally, the experts noted that the hemoglobin outcomes used in the clinical trial (at least 20 g/L hemoglobin improvement or hemoglobin level of 120 g/L) may not be realistic thresholds in clinical practice, given the complexity and heterogeneity of the condition. The experts stated that a 10 g/L improvement would be meaningful in clinical practice, particularly when combined with other factors such as independence from transfusions.
Discontinuing Treatment
According to the clinical experts, discontinuation would be considered in patients who show no improvement in hemoglobin and/or transfusion needs with use of iptacopan. It would be stopped if the patient experienced intolerance, severe and recurrent BTHs, or pregnancy or breastfeeding. It would also be stopped if there were concerns about nonadherence to the dosing schedule that may place the patient at risk of BTH.
The experts anticipated that a trial of at least 8 weeks would be needed to see improvement. Longer trials may be needed to assess treatment response if the trial period was compromised by a clinical situation leading to BTH or nonadherence to therapy.
Prescribing Considerations
The clinical experts indicated that treatment with iptacopan would need to be initiated by a hematologist, preferably with expertise in PNH, and that a consultation with a PNH expert would be warranted if a PNH patient was being followed in a shared-care model (i.e., a hematologist with expertise in PNH along with a local hematologist).
Clinician Group Input
This section was prepared by the review team based on the input provided by clinician groups.
One clinician group, the Canadian PNH Network, submitted input for this review based on contributions from 10 clinicians. The Canadian PNH Network is a group of hematologists located across Canada who follow the majority of patients with PNH in Canada and who set consensus guidelines for the diagnosis and management of PNH. Information was gathered for this input submission through publicly available documents, congress abstracts, and published literature.
Overall, the clinician group input aligned with input provided by the clinical experts consulted for this review. Both the clinician group and clinical experts agreed that, currently, the only curative treatment for PNH is hematopoietic stem cell transplant, which is reserved for patients with predominant or progressive bone marrow failure. For patients who are ineligible for transplant, primary PNH treatment goals highlighted in the input were hemoglobin improvement, reduced transfusion needs, and absence of end-organ complications or other symptoms. Clinical experts also emphasized reducing mortality, avoiding iron overload, and improving HRQoL as important treatment goals.
Key unmet needs identified by the clinician group for patients with PNH included therapies that reverse the disease course other than allogeneic stem cell transplant, as well as more convenient, tolerable therapies. The input emphasized the importance of therapy convenience for patients living in remote communities who may lack access to an infusion centre or ability to self-inject treatment, and clinical experts noted that oral therapies would fulfill this need. While danicopan is an oral therapy available through a managed access program, it is an add-on to C5 inhibitor treatment and patients must still access and receive their regular C5 inhibitor infusions.
According to the clinician group, iptacopan will be used as second-line therapy in eligible patients, as per the APPLY-PNH criteria, for those with persistent anemia despite C5 inhibition in whom EVH is suspected. The clinician group noted that it would be reasonable to also use iptacopan as third-line therapy. The CDA-AMC review team notes that this review for iptacopan focuses on the population requested for reimbursement, i.e., adult patients with PNH who have an inadequate response or intolerance to a C5 inhibitor. The clinician group noted that iptacopan would provide an additional therapy option besides pegcetacoplan for patients requiring proximal inhibition monotherapy. Given the absence of comparative efficacy data versus pegcetacoplan, the clinician group stated that patient preference will largely drive treatment selection, according to the route of administration that best supports their lifestyle. Patients best suited for iptacopan therapy, as identified by the clinician group, are those with a high likelihood of adhering to oral treatment, frequent travellers, or those who cannot initiate or continue other therapies. Less suitable patients include those who are not anemic, meet APPLY-PNH exclusion criteria, are planning pregnancy, or are unlikely to be adherent with the dosage schedule, given the high risk of BTH if doses are missed. The input noted that BTH outcomes are more severe with proximal complement inhibition than with terminal complement inhibition, as the pool of vulnerable circulating PNH cells increases with avoidance of both IVH and EVH.
Key outcomes for evaluating treatment response that were identified by clinicians included hemoglobin improvement and reduced transfusion dependence, sustained IVH control (assessed based on LDH levels and BTH events), and improvements in fatigue and quality of life. Treatment discontinuation should be considered in patients with adverse events precluding ongoing therapy, patients with poor adherence, or patients who are pregnant or breastfeeding, according to the input. Both the clinician group and consulted experts agreed that patients with PNH benefit from having a clinician involved in their care who specializes in managing and monitoring the disease.
Drug Program Input
The drug programs provide input on each drug being reviewed through CDA-AMC’s Reimbursement Review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CDA-AMC are summarized in Table 4.
Table 4: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Relevant comparators | |
Iptacopan was compared only to C5 inhibitor use and not pegcetacoplan use, which is the current option when patients have inadequate response or intolerance to C5 inhibitor. An indirect comparison versus pegcetacoplan was submitted by the sponsor. All comparators are available in many jurisdictions with criteria, including pegcetacoplan, which is not a C5 inhibitor but has the same reimbursement indication as iptacopan. | The clinical experts indicated that C5 inhibitors pegcetacoplan and danicopan are relevant comparators to iptacopan but may not be accessible in all jurisdictions due to differences in reimbursement. At the time of review initiation for the current iptacopan file, danicopan was under review with CDA-AMC. Danicopan received a final conditional positive CDA-AMC recommendation in November 2024 and is currently under consideration for negotiation at pCPA. Increased doses of C5 inhibitors or more frequent dosing intervals may also be used to improve control of PNH for some patients. The experts noted that access to higher doses of C5 inhibitors is not available in all jurisdictions. In clinical practice, patients may switch between these drugs as the patient’s condition changes, if they develop comorbidities or intolerance, to manage BTH or EVH, and if the patient becomes pregnant. As per sponsor request, this CDA-AMC review focuses on the population requested for reimbursement, i.e., adult patients with PNH who have an inadequate response or intolerance to a C5 inhibitor. |
Considerations for initiation of therapy | |
The reimbursement indication for iptacopan is patients with PNH who have an inadequate response to, or are intolerant of, a C5 inhibitor. 1. Can an “inadequate response” to C5 inhibitors be clearly defined? 2. Should iptacopan be reimbursed only in the population that was studied (i.e., patients diagnosed with PNH who were treated with a stable regimen of C5 inhibitors [eculizumab or ravulizumab] for at least 6 months before randomization but still have residual anemia)? | The clinical experts indicated that intolerance to C5 inhibitors is uncommon, but there is a rare subset of patients with genetic polymorphisms who have no response to eculizumab or ravulizumab. The clinical experts maintained that C5 inhibitors remain the first-line treatment for patients with PNH. There is no standard definition of inadequate response to C5 inhibitors, and the clinical trials for second-line agents have used different hemoglobin levels and other criteria to determine enrolment. Further, inadequate response may be related to IVH, EVH, or both, which impacts the second-line options that are most appropriate. The clinical experts agreed that alignment with the reimbursement criteria for pegcetacoplan would be reasonable but noted that the hemoglobin thresholds used in the clinical trials were arbitrary, and that patients with anemia but higher hemoglobin levels than those used in the clinical trials may also benefit from iptacopan therapy. The experts also noted that patients who have an inadequate response to pegcetacoplan may also be considered for iptacopan in clinical practice. However, evidence for use of iptacopan after pegcetacoplan is not provided in the pivotal trial for iptacopan (the APPLY-PNH trial), and, per sponsor request, this CDA-AMC review focuses on the population requested for reimbursement, i.e., adult patients with PNH who have an inadequate response or intolerance to a C5 inhibitor. |
Would danicopan be added on to iptacopan for use in patients with signs and symptoms of extravascular hemolysis? | The clinical experts stated that there are currently no data on the use of iptacopan in combination with other treatments for PNH. However, for a patient on iptacopan who experiences an acute episode of BTH, an add-on dose of eculizumab may help control the hemolysis and reduce the need for transfusions. Without further evidence to support combination therapy with iptacopan, the clinical experts stated that it is unlikely to be used with other drugs, although mechanistically there is potential for benefit. |
Would patients be considered for iptacopan if they preferred an oral option as opposed to the other available parenteral options? | The clinical experts indicated that C5 inhibitors remain the preferred first-line treatment for PNH and their efficacy and safety are well established. The availability of an oral treatment may be important for patients in very remote areas or for those with conditions where IV or SC infusions are not feasible. Oral therapy may also be preferred if patients need to travel. The clinical experts noted that some patients may find intermittent injections more manageable than twice daily oral administration, which requires strict adherence to avoid potentially serious IVH. Thus, the importance of the oral route of administration may depend on clinical and logistical factors, as well as patient preferences. |
Considerations for continuation or renewal of therapy | |
Should the recommendation be aligned with pegcetacoplan as they both have the same indication for reimbursement? | The clinical experts agreed that alignment with the reimbursement criteria for pegcetacoplan would be reasonable. |
Considerations for discontinuation of therapy | |
Should the recommendation be aligned with pegcetacoplan as they both have the same indication for reimbursement? | The clinical experts agreed that alignment with the reimbursement criteria for pegcetacoplan would be reasonable. |
Considerations for prescribing of therapy | |
Should the recommendation be aligned with pegcetacoplan as they both have the same indication for reimbursement? | The clinical experts agreed that alignment with the reimbursement criteria for pegcetacoplan would be reasonable. |
Care provision issues | |
Vaccinations are required before therapy; infection risk of encapsulated bacteria is increased with iptacopan. | The clinical experts noted that vaccination is required before initiating PNH therapy for all patients. |
System and economic issues | |
All 3 comparators (eculizumab, ravulizumab, and pegcetacoplan) have successfully gone through price negotiations. However, only pegcetacoplan is approved for the same indication. | This is a comment from the drug plans to inform CDEC deliberations. Per sponsor request, this CDA-AMC review focuses on the population requested for reimbursement, i.e., adult patients with PNH who have an inadequate response or intolerance to a C5 inhibitor. |
The price of iptacopan is high, at $51,700 per QALY, $719.94 per 200 mg capsule. | This is a comment from the drug plans to inform CDEC deliberations. |
BTH = breakthrough hemolysis; CDA-AMC = Canadian Drug Agency; CDEC = Canadian Drug Expert Committee; EVH = extravascular hemolysis; IVH = intravascular hemolysis; PNH = paroxysmal nocturnal hemoglobinuria; QALY = quality-adjusted life-year; SC = subcutaneous.
Clinical Evidence
The objective of this report is to review and critically appraise the clinical evidence submitted by the sponsor on the beneficial and harmful effects of iptacopan 200 mg oral capsules for the treatment of adult patients with PNH who have an inadequate response to, or are intolerant of, a C5 inhibitor. The population of interest was aligned with the sponsor’s reimbursement request. The focus will be placed on comparing iptacopan to relevant comparators and identifying gaps in the current evidence.
A summary of the clinical evidence included by the sponsor in the review of iptacopan is presented in 3 sections, with CDA-AMC’s critical appraisal of the evidence included at the end of each section. The first section, the systematic review, includes pivotal studies and RCTs that were selected according to the sponsor’s systematic review protocol. CDA-AMC’s assessment of the certainty of the evidence in this first section, using the GRADE approach, follows the critical appraisal of the evidence. The second section includes sponsor-submitted long-term extension studies. The third section includes indirect evidence from the sponsor.
Included Studies
Clinical evidence from the following is included in the review and appraised in this document:
1 pivotal study identified in systematic review
1 long-term extension phase of the pivotal study
1 ITC.
Systematic Review
Contents within this section have been informed by materials submitted by the sponsor. The following have been summarized and validated by the CDA-AMC review team.
Description of Study
Characteristics of the included studies are summarized in Table 5.
Table 5: Details of Study Included in the Systematic Review
Criteria | APPLY-PNH |
|---|---|
Designs and populations | |
Study design | Randomized, multicentre, open-label, active comparator–controlled phase III trial |
Locations | 39 sites in Brazil, Czechia, France, Germany, Italy, Japan, Republic of Korea, Netherlands, Spain, Taiwan, UK, US |
Patient enrolment dates | First patient first visit: January 25, 2021 24-week RTP primary end point completion date: September 26, 2022 24-week ETP last patient last visit: March 6, 2023 |
24-week RTP (N) | Iptacopan: 62 C5 inhibitor: 35 |
24-week ETP (N) | Iptacopan: 61 C5 inhibitor to iptacopan: 34 |
Inclusion criteria |
|
Exclusion criteria |
|
Drugs | |
Intervention | Iptacopan: 200 mg oral twice daily during the 24-week RTP and 24-week ETP
|
Comparator(s) 24-week RTP only | C5 inhibitors (eculizumab or ravulizumab) IV at prerandomization stable dose |
Study duration | |
Screening phase | Up to 8 weeks (day –56 to day –1) |
Treatment phase (24-week RTP) | RTP: 24 weeks (day 1 to day 168) |
Extension phase (24-week ETP) | ETP: 24 weeks (day 169 to day 336) |
Follow-up phase | 3-week follow-up phase following end-of-study date:
After completion of the ETP, patients were given the option to join the rollover extension program to allow patients access to iptacopan and to evaluate long-term safety, tolerability, and efficacy. |
Outcomes for 24-week RTP | |
Primary end points |
|
Secondary and exploratory end points | Secondary (collected up to day 168):
Exploratory (collected up to day 168):
|
Publication status | |
Publications | NCT04558918; Peffault de Latour et al. (2024)51 |
AE = adverse event; ARC = absolute reticulocyte count; BTH = breakthrough hemolysis; C3d+ = cells positive for degradation product of C3; eGFR = estimated glomerular filtration rate; EORTC QLQ-C30 = European Organisation for the Research and Treatment of Cancer Quality of Life Questionnaire Core 30; ETP = extension treatment period; FACIT-F = Functional Assessment of Chronic Illness Therapy – Fatigue; INR = international normalized ratio; LDH = lactate dehydrogenase; MAVE = major adverse vascular event; NYHA = New York Heart Association; PGIS = patient global impression of severity; PNH = paroxysmal nocturnal hemoglobinuria; PRO = patient-reported outcome; RBC = red blood cell; RTP = randomized treatment period; SAE = serious adverse event; WBC = white blood cell.
Source: APPLY-PNH Clinical Study Report.29,30,36 Details included in the table are from the sponsor’s Summary of Clinical Evidence.35
The objective of the APPLY-PNH study was to evaluate the efficacy and safety of oral iptacopan monotherapy in adult (aged ≥ 18 years) patients with PNH with residual anemia despite treatment with a C5 inhibitor for at least 6 months before randomization. The study was a phase III, randomized, multicentre, active comparator–controlled, open-label, parallel-group study.
The APPLY-PNH study was designed with 3 periods: a screening period lasting up to 8 weeks; a 24-week open-label, active comparator–controlled RTP; and a 24-week, open-label, iptacopan extension treatment period (ETP) (Figure 1). A description and key findings for the 24-week ETP of the APPLY-PNH study are included in the Long-Term Extension Study section of this report.
Patients were randomized at an 8:5 ratio to switch to iptacopan (200 mg twice daily) or to continue with the C5 inhibitor therapy they were receiving before the study (eculizumab or ravulizumab). Randomization was conducted using an interactive response technology. The interactive response technology assigned each patient a randomization number, which was used to link the patient to a treatment group and the medication number for the first package of study treatment dispensed to the patient. Randomization was stratified into 4 strata, based on the type of prior C5 inhibitor the patient received (eculizumab or ravulizumab) and transfusion history in the past 6 months (i.e., transfusion received versus not received). A total of 97 participants from 39 sites across the US, Brazil, Czechia, France, Germany, Italy, Japan, Republic of Korea, Netherlands, Spain, Taiwan, and the UK were randomized in the RTP, with 62 patients enrolled in the iptacopan treatment group and 35 patients enrolled in the C5 inhibitor treatment group. The 24-week RTP primary end point data cut-off date was September 26, 2022.
Patients who completed the RTP had the option to receive open-label iptacopan 200 mg twice daily for up to 24 weeks during the ETP (refer to Long-term Extension Study section of this report for these results). After the ETP, patients could join the open-label, single-arm rollover extension study and continue iptacopan therapy. The rollover extension study is ongoing, and the sponsor stated that results are not yet available.
Figure 1: APPLY-PNH Study Design
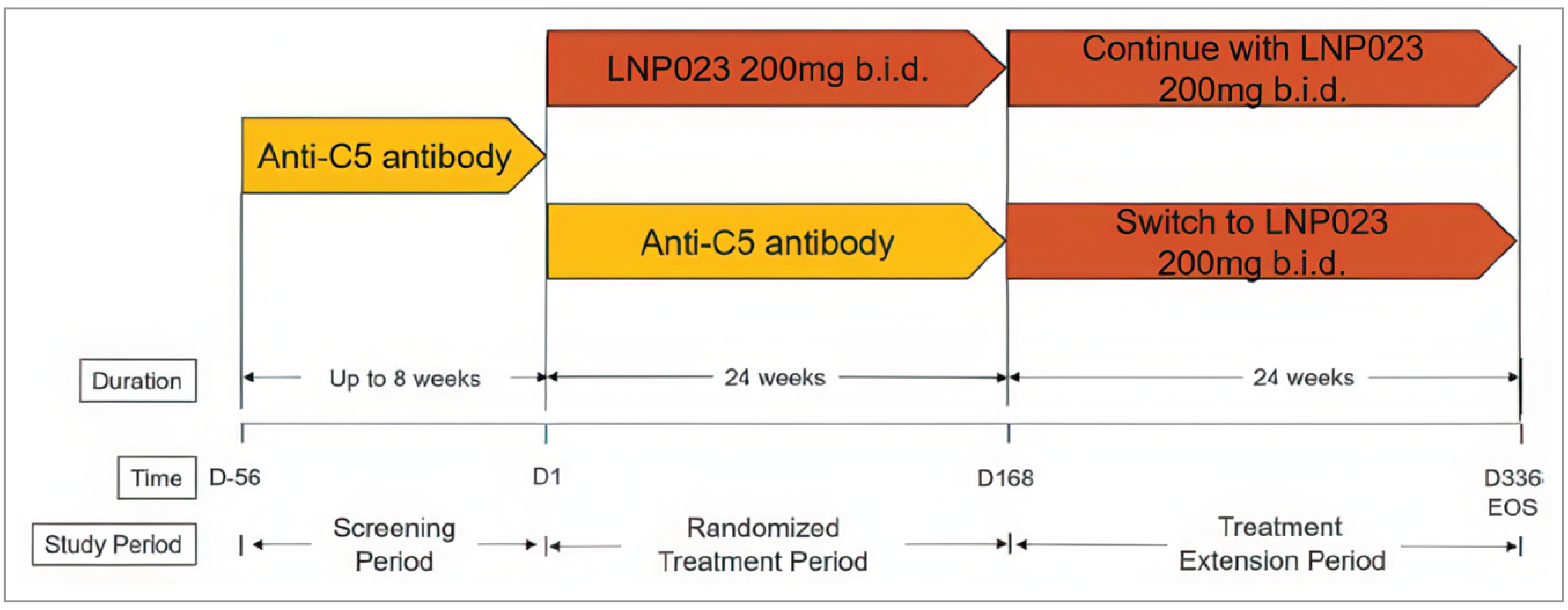
b.i.d. = twice daily; D = day; EOS = end of study; LNP023 = iptacopan.
Source: APPLY-PNH Clinical Study Report.29
Populations
Inclusion and Exclusion Criteria
Male and female adult (aged ≥ 18 years) patients were eligible to be included in the APPLY-PNH study if they had a diagnosis of PNH confirmed by high-sensitivity flow cytometry, with RBC and WBC granulocyte/monocyte clone size greater than or equal to 10%. Patients were required to be on a stable regimen (in terms of dose and intervals) of a C5 inhibitor (eculizumab or ravulizumab) for at least 6 months before randomization and have a mean hemoglobin level less than 100 g/L. Patients were also required to be vaccinated against Neisseria meningitidis, Streptococcus pneumoniae, and Haemophilus influenzae. Vaccinations could be administered during the screening phase.
Patients were excluded from the study if they were on a stable eculizumab dose with a dosing interval of 11 days or fewer or if they were on a stable ravulizumab dose with a dosing interval of less than 8 weeks. Furthermore, patients were excluded from the study if they had a known or suspected hereditary complement deficiency at screening, a history of hematopoietic stem cell transplant, evidence of bone marrow failure, or any comorbidities that could impact treatment outcomes.
Interventions
As an entry criterion for the APPLY-PNH study, all patients were receiving eculizumab or ravulizumab at stable doses for at least the previous 6 months. Patients were randomized to switch to iptacopan 200 mg twice daily or to continue with the same C5 inhibitor regimen as they were receiving previously. All treatments were open to patients, investigators, and the clinical trial team. The study treatment duration was 24 weeks.
Iptacopan was supplied as a 200 mg oral capsule and administered twice daily. For patients on a prior eculizumab regimen, the first iptacopan dose was given 7 or 8 days after the last infusion and, for patients on a prior ravulizumab regimen, the first iptacopan dose was given 41 to 43 days after the last infusion. Eculizumab was supplied as a concentrate solution for IV infusion of 300 mg/30 mL. Ravulizumab was supplied as a concentrated solution for IV infusion of 300 mg/30 mL, 300 mg/3 mL, and 1,100 mg/11 mL. C5 inhibitors were administered under the supervision of investigators or their designees at the dose and frequency used by each patient before enrolment. Treatment adherence to iptacopan was monitored using capsule counts and information provided by the patient.
Rescue medication was permitted to treat serious complications, such as antithrombotic drugs to treat thrombosis. Patients were given appropriate medical treatment to manage complications as per local guidelines and practice. For a significant BTH requiring rescue medication (in the opinion of the investigator), such medication was allowed and managed per local guidelines and practice. Erythropoiesis-stimulating agents and hypoxia-inducible factor prolyl hydroxylase inhibitors (e.g., roxadustat), were allowed during the trial if patients were on a stable dose for at least 8 weeks before screening. During the trial, dose adjustments or discontinuation of these treatments were to follow local guidelines and practice based on the patient’s hemoglobin levels.
Other concurrent treatments were allowed during the trial, provided they were administered at stable doses before study entry. These included immunosuppressants (if doses were stable for 8 weeks before screening); systemic corticosteroids for hematological conditions (less than 1 mg/kg); warfarin (if the patient had a stable INR), low-molecular weight heparin, or direct oral anticoagulants (rivaroxaban, apixaban, and edoxaban); iron supplements, vitamin B12, or folic acid (if the patient received these at stable doses for at least 4 weeks before screening).
Patients were prohibited from receiving live vaccines during the study. Any drugs with potential drug-drug interactions with iptacopan (e.g., clopidogrel, gemfibrozil, digoxin, quinidine, paclitaxel, fentanyl, and phenytoin) were avoided, if possible.
The study treatment was discontinued based on the patient’s decision or in any situation where the study treatment might result in a significant safety risk to the patient. Iptacopan was stopped if the patient became pregnant. For patients stopping iptacopan, tapering the dose over a 14-day period was recommended. Three capsules of 10 mg iptacopan were taken once daily for 7 days, followed by 10 mg of iptacopan taken once daily for 7 days.
Outcomes
A list of efficacy end points assessed in this Clinical Review Report is provided in Table 6, followed by descriptions of the outcome measures. Summarized end points are based on outcomes included in the sponsor’s Summary of Clinical Evidence, as well as any outcomes identified as important to this review according to the clinical expert(s) consulted by CDA-AMC and input from patient and clinician groups and public drug plans. Using the same considerations, the CDA-AMC review team selected end points that were considered most relevant to inform CDA-AMC’s expert committee deliberations and finalized this list of end points in consultation with members of the expert committee. All summarized efficacy end points were assessed using GRADE. Select notable harms outcomes considered important for informing CDA-AMC’s expert committee deliberations were also assessed using GRADE.
The proportions of patients with at least a 20 g/L increase in hemoglobin or sustained hemoglobin levels of 120 g/L were selected for GRADE, as these were the coprimary study end points or were identified as clinically important measures by the clinical experts consulted for this review. In addition, the change from baseline in hemoglobin was also considered a clinically relevant measure for patients with PNH by the clinical experts consulted. Other key end points identified by the clinical experts and patients were avoidance of transfusion, fatigue (measured using the FACIT-F instrument), and HRQoL (measured using the EORTC QLQ-C30 Global Health Status). The clinical experts selected the change in LDH levels (a surrogate measure of IVH) and occurrences of BTH (reported as a composite measure) to indicate IVH control. The clinical experts selected the change in ARC as a surrogate measure of EVH. Death was identified by the clinical experts as a key safety end point, and infection caused by encapsulated bacteria was listed in the warnings and precautions of the iptacopan product monograph.
The change from baseline in the EQ visual analogue scale (VAS) and transfusion requirements (number of RBC transfusion events, number of units of RBCs transfused) were not selected as key end points for assessment using GRADE but were provided as supplementary data (refer to Appendix 1). The clinical experts commented that transfusion events or units of RBCs may be confounded by other factors, and thus transfusion avoidance was the preferred measure of the impact of iptacopan on transfusion requirements. As an overall measure of health status of HRQoL, the EORTC QLQ-C30 Global Health Status was preferred over the EQ VAS.
Two key outcomes of interest to the pharmacoeconomic analysis, all-cause discontinuation and patients with anemia defined as hemoglobin of 105 g/L or lower, were not assessed in the APPLY-PNH study.
Table 6: Outcomes Summarized From the RTP of the APPLY-PNH Study
Outcome measure | Time point | End point assignment |
|---|---|---|
Increase in hemoglobin ≥ 20 g/L from baseline in the absence of RBC transfusions | Day 168a | Primaryb |
Hemoglobin ≥ 120 g/L in the absence of RBC transfusions | Day 168a | Primaryb |
Change from baseline in hemoglobin | Day 168a | Secondaryb |
Transfusion avoidance | Day 14 to day 168 | Secondaryb |
Occurrences of BTH | Up to day 168 | Secondaryb |
Percent change from baseline in LDH levels (U/L) | Day 168a | Secondaryb |
Change from baseline in ARC (109/L) | Day 168a | Secondaryb |
Change from baseline in FACIT-F scores | Day 168a | Secondaryb |
Change from baseline in EORTC QLQ-C30 Global Health Status | Day 168a | Exploratory |
Deaths | Up to day 168 | Exploratory |
Infections from encapsulated bacteria | Up to day 168 | Exploratory |
ARC = absolute reticulocyte count; BTH = breakthrough hemolysis; EORTC QLQ-C30 = European Organisation for the Research and Treatment of Cancer Quality of Life Questionnaire Core 30; FACIT-F = Functional Assessment of Chronic Illness Therapy – Fatigue; LDH = lactate dehydrogenase; RBC = red blood cell; RTP = randomized treatment period.
aCalculated as the mean of data from day 126 and day168 visits.
bStatistical testing for the end point was adjusted for multiple comparisons.
Source: APPLY-PNH Clinical Study Report.29,30 Details included in the table are from the sponsor’s Summary of Clinical Evidence.35
Hemoglobin Levels
The 2 primary end points were sustained hematological response, defined as an increase from baseline hemoglobin levels greater than or equal to 20 g/L and hemoglobin levels greater than or equal to 120 g/L, reported on 3 out of 4 assessments between day 126 and day 168 (last 6 weeks of the 24-week treatment period). To meet these end points, the patient must not have received an RBC transfusion between day 14 and day 168 and must not have met either of the following predefined criteria for transfusion:
hemoglobin greater than 70 g/L and less than or equal to 90 g/L with signs or symptoms of sufficient severity to warrant a transfusion
hemoglobin less than or equal to 70 g/L regardless of presence of clinical signs and/or symptoms.
The sponsor stated that a 20 g/L increase in hemoglobin levels would be considered clinically meaningful and achieving hemoglobin levels greater than or equal to 120 g/L corresponds approximately to normalization of hemoglobin, which is one of the key treatment goals for patients with PNH.
As a secondary outcome, the change from baseline in hemoglobin was measured as the difference between the mean of visits from day 126 through day 168 versus the baseline value. The baseline hemoglobin was the mean of 2 measurements taken during screening; however, in patients who received a transfusion after the first confirmatory measurement, but before the second confirmatory measurement, the first confirmatory measurement was used as the baseline. A central laboratory was used to test blood samples and assess hemoglobin levels. The clinical experts consulted for this review identified a 10 g/L to 15 g/L difference between groups as the threshold for a clinically meaning change.
RBC Transfusions
Transfusion avoidance was a secondary outcome in the APPLY-PNH study and was defined as no RBC transfusions given to patients between day 14 and day 168. The Clinical Study Report states that, because some patients have low hemoglobin levels (e.g., < 70 g/L) that may require an RBC transfusion during the first 2 weeks of the 24-week RTP, transfusions administered during these first 2 weeks were not considered as part of the transfusion avoidance definition. In the study, patients who met the following criteria were to receive a transfusion:
hemoglobin level less than or equal to 90 g/L, with signs/symptoms of sufficient severity to warrant a transfusion
hemoglobin level less than or equal to 70 g/L, regardless of presence of clinical signs and/or symptoms.
During the trial, the level of hemoglobin, the number of transfusions administered, the number of units of RBC administered per transfusion, as well as signs and/or symptoms, if applicable, were recorded. Symptoms typically associated with or precipitating a patient’s need for transfusion include severe or worsening fatigue, severe or worsening dyspnea or shortness of breath, palpitation or angina (or worsening symptoms), and change in mental status (e.g., syncope, light-headedness, confusion, stroke, transient ischemic attack). If a patient met the transfusion criterion, the investigator determined the appropriate number of units of RBC to be transfused.
The number of RBC transfusions and number of RBC units transfused between day 1 and day 168 were exploratory outcomes in the APPLY-PNH study.
Percent Change From Baseline in LDH
The sponsor stated that LDH levels were assessed as a marker for IVH. This was measured as the percent change in LDH levels from baseline to end of study. The end-of-study values were the mean of data from day 126 and 168 study visits.
Occurrences of BTH
The criteria for clinical BTH are summarized in Table 7. Patients who met either 1 of the 2 clinical criteria (i.e., decrease in hemoglobin level of 20 g/L or more, or signs and symptoms of hemolysis) in the presence of the laboratory evidence of IVH (LDH > 1.5 × ULN) were reported as experiencing BTH.
Subclinical BTH was defined as isolated laboratory evidence of increased IVH without a meaningful decrease in hemoglobin and without other clinical signs or symptoms of hemolysis. In patients who met these criteria, BTH was not reported. The assessment of BTH was based on local or central laboratory results.
Table 7: BTH Definitions for APPLY-PNH Study
Classification | Clinical criteria | Laboratory criteria | |
|---|---|---|---|
Hemoglobin levels | Signs or symptoms | LDH level | |
Clinical breakthrougha | Decrease equal to or more than 20 g/L (compared to the latest assessment or within 15 days) | Gross hemoglobinuria, painful crisis, dysphagia, or any other significant clinical PNH-related signs and symptoms | > 1.5 × ULN and increased compared to the last 2 assessments |
Subclinical breakthrough | Decrease less than 20 g/L (compared to the latest assessment or within 15 days) | No clinical signs or symptoms except moderate hemoglobinuria | > 1.5 × ULN and increased compared to the last 2 assessments |
BTH = breakthrough hemolysis; LDH = lactate dehydrogenase; PNH = paroxysmal nocturnal hemoglobinuria; ULN = upper limit of normal.
aBreakthrough was defined as clinical if either 1 of the 2 clinical criteria was demonstrated in the presence of laboratory evidence of IVH (LDH level).
Source: APPLY-PNH Clinical Study Report.29
Change From Baseline in ARC
The sponsor stated that ARC was assessed as a marker for EVH. This was measured as the change from baseline in ARC (109/L) to end of study (mean of data from day 126 to day 168 study visits).
Functional Assessment of Chronic Illness Therapy – Fatigue
The FACIT-F is a 13-item questionnaire that assesses self-reported tiredness, weakness, and difficulties with daily life activities. Each item is measured on a 5-point ordinal scale (0 to 4) and has a recall period of 7 days. The items can further be described as representing symptoms (5 items) or impacts (8 items). The FACIT-F items are scored so that a high score represents better health outcomes (i.e., less severity of fatigue symptoms or better quality of life). All response scores are summed with equal weights, with the total score ranging from 0 (severe fatigue) to 52 (no fatigue).52
FACIT-F has evidence to support its validity, reliability, and responsiveness for the evaluation of fatigue associated with anemia in different patient populations, including patients with PNH (Table 8).31 A change in score of 5 points was estimated as the MID in patients with PNH from distribution-based estimations using real-world data from the International PNH Registry.31 Anchor-based estimations ranged from 2.5 to 15.5 points.31
In the APPLY-PNH study, the FACIT-F questionnaire was completed by participants using an electronic patient-reported outcomes device. The change in FACIT-F was calculated from baseline to end of study (mean of data from day 126 and day 168 visits).
EORTC QLQ-C30 Scale
The EORTC QLQ-C30 consists of 30 questions that comprise 5 functional domains (physical, role, emotional, cognitive, and social), a global health status or global quality of life scale, 3 symptom scales (pain, fatigue, and nausea/vomiting), and 6 single items that assess additional symptoms (dyspnea, appetite loss, sleep disturbance, constipation, and diarrhea) and the perceived financial burden of treatment. Subscale score ranges depend on the domain addressed. Higher scores on the functional and global health status scales represent better functioning and greater HRQoL, respectively. Higher scores on the symptom scales represent more (worse) symptoms. The scoring rules derive results as the sum of the component items, which are then normalized by use of the maximum range of values for the subscale and multiplied by 100.
The EORTC QLQ-C30 tool has evidence to support its validity and responsiveness in patients with PNH (Table 8). However, MID values have not been established for this measurement tool in the PNH population. For patients with cancer, an increase of 10 points or more in EORTC QLQ-C30 score is considered moderately large and represents a clinically important improvement.34 The EORTC QLQ-C30 was an exploratory outcome in the APPLY-PNH study. For the review of iptacopan, the change from baseline in the Global Health Status was identified as an important outcome and evaluated using GRADE. Other domains were not summarized in this report.
Harms
In the APPLY-PNH study, MAVEs were assessed through day 168. A MAVE was defined using the following list: acute peripheral vascular occlusion; amputation (nontraumatic, nondiabetic); cerebral arterial occlusion or cerebrovascular accident; cerebral venous occlusion; dermal thrombosis; gangrene (nontraumatic, nondiabetic); hepatic or portal vein thrombosis (Budd-Chiari syndrome); mesenteric or visceral arterial thrombosis or infarction; myocardial infarction; pulmonary embolus; renal arterial thrombosis; renal vein thrombosis; thrombophlebitis or deep vein thrombosis; transient ischemic attack; unstable angina; and other vascular events.
Table 8: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
FACIT-F | 13-item, patient-reported, fatigue-specific, quality of life questionnaire using a 5-point Likert scale. It assesses tiredness, weakness, and difficulty conducting usual activities due to fatigue over the past week.31 The 13-item scale ranges from 0 (extreme fatigue) to 52 (no fatigue). Higher scores indicate less fatigue.31 | Patients with PNH:
Responsiveness: Patients with improvements in hemoglobin, indirect bilirubin, and ARC showed improvements in FACIT-F scores (P < 0.0001, P = 0.0002, and P = 0.0002, respectively).55 Patients with cancer or psoriatic arthritis:56 | Patients with PNH: ≥ 5-point increase from baseline (for distribution-based methods, estimates of clinically important change were 4.6 points using SEM and 6.5 points using 0.5 × SD, while anchor-based methods ranged from 2.5 to 15.5 points)31 |
EORTC QLQ-C30 | 30-item, patient-reported, cancer-specific, quality of life questionnaire using 4- and 7-point Likert scales. It consists of 5 multi-item functional scales (physical, role, emotional, cognitive, and social), 3 multi-item symptom scales (fatigue, nausea-vomiting, and pain), 6 single-item symptom scales (dyspnea, insomnia, appetite loss, constipation, diarrhea, and financial impact), and a 2-item Global Health Status/HRQoL scale. A 1-week recall period is used to assess the items.58 Each raw scale score is converted to a standardized score that ranges from 0 to 100 using a linear transformation. A higher score on the functional scales represents better functioning, a higher score on the symptom scales represents a higher level of symptoms, and a higher score on the Global Health Status/HRQoL scale represents a higher HRQoL.58 | Patients with PNH:
Responsiveness: Patients with improvements in hemoglobin, indirect bilirubin, and ARC showed improvements in physical functioning (P = 0.0103, P = 0.0050, and P = 0.0072, respectively) and fatigue scores (P = 0.0093, P = 0.0073, and P = 0.0162, respectively)55 Patients with cancer:
| Patients with cancer:59
No MID was identified in patients with PNH. |
ARC = absolute reticulocyte count; DLBCL = diffuse large B-cell lymphoma; EORTC QLQ-C30 = European Organisation for the Research and Treatment of Cancer Quality of Life Questionnaire Core 30; FACIT-F = Functional Assessment of Chronic Illness Therapy – Fatigue; HL = Hodgkin lymphoma; HRQoL = health-related quality of life; MID = minimal important difference; PNH = paroxysmal nocturnal hemoglobinuria; SD = standard deviation; SEM = standard error of the mean.
Source: APPLY-PNH Clinical Study Report.29,30 Details included in the table are from the sponsor’s Summary of Clinical Evidence.35
The sponsor identified the following harms as adverse events of special interest: infections with encapsulated bacteria, serious or severe infections, PNH hemolysis and thrombosis, testicular effects, thyroid changes, and decreased platelets. Of these adverse events, infections caused by encapsulated bacteria were identified as an outcome of interest to this review.
Statistical Analysis
The details of the statistical analysis in the RTP of the APPLY-PNH study are summarized in Table 9. For the 2 primary end points, which indicate sustained hematological response, the Clinical Study Report states they were initially analyzed using a conditional logistic regression model, conditioned on the randomization strata. This model did not converge due to sparsity of events; thus, according to the protocol, the data were analyzed using a logistic regression model based on Firth’s penalized maximum likelihood method. The model included treatment, sex, age group (< 45 years, ≥ 45 years), baseline hemoglobin (≥ 90 g/L, < 90 g/L) and the randomization strata (type of prior C5 inhibitor the patient received [eculizumab or ravulizumab] and transfusion history in the past 6 months [i.e., transfusion received versus not received]). The primary end points were summarized by OR and marginal proportion and difference. The CIs for the difference, as well as for the ratio of marginal proportions, were derived by use of bootstrapping. The term “marginal proportion” can be interpreted as the population average probability of being a responder for each treatment group.
Efficacy estimands were defined in the clinical trial because the intercurrent events of RBC transfusion, treatment discontinuation, BTH events, MAVEs, and rescue medications were considered potentially important for interpretation of the trial results. There were 3 main categories of efficacy estimands:
Treatment policy estimand: To assess the efficacy benefit, regardless of intercurrent events such as treatment discontinuation, BTHs, and MAVEs. All data were included in the analysis, including data collected after the intercurrent event.
Direct efficacy estimand: To assess the direct efficacy benefit of iptacopan versus C5 inhibitors, excluding any efficacy benefit derived from RBC transfusion use. In this case, the impact of transfusion use was factored out through the analysis approach. For the change from baseline in hemoglobin end point, this meant that, for any patient who had an RBC transfusion, hemoglobin values for the 30 days following the transfusion were excluded from the analysis and were imputed.
Including-transfusion estimand: To assess the benefit of iptacopan versus C5 inhibitors in conjunction with RBC transfusions use as part of a treatment strategy. All data were included in the analysis.
For the 2 primary end points, absence of RBC transfusion was an integral part of the end point definition, such that a transfusion between day 14 and day 168 was automatically considered treatment failure. All other intercurrent events were reflected in the primary estimands following a treatment policy strategy, meaning that the efficacy benefit would be assessed regardless of these events (Table 9). Sensitivity, supplementary, and subgroup analyses conducted for the primary end points are described in Table 9.
For the secondary estimands, the same intercurrent events as for the primary estimands were considered, but different approaches were used. Discontinuations of study medication, BTH events, and MAVEs were always handled with a treatment policy strategy, while the proposed approach to the handling of transfusions is described in the definition for each secondary estimand (Table 9). For example, for the change from baseline in hemoglobin, if a patient had an RBC transfusion, then hemoglobin values 30 days following the transfusion were excluded from the analysis and were imputed. For other secondary outcomes, the including-transfusion estimand was used, and all data were included in the analysis, regardless of whether the patient received a transfusion.
Transfusion avoidance was summarized using OR based on conditional logistic regression, and marginal proportion and difference based on statistical methods that were similar to the primary outcomes (Table 9). Other secondary and some exploratory end points were summarized by adjusted mean change and difference (hemoglobin, FACIT-F, ARC, LDH, and EORTC QLQ-C30), adjusted geometric mean and difference (LDH), number and proportion of patients (BTHs, MAVEs, adverse events), and annualized rate and rate ratio (BTHs and MAVEs). The occurrence of BTHs was analyzed using a negative binomial model. Most continuous outcomes were analyzed using MMRM with covariates described in Table 9. The percentage change from baseline in LDH was analyzed based on the natural log-transformed LDH ratio to baseline. Natural log results were back-transformed and reported as geometric means. The change from baseline in EORTC QLQ-C30 Global Health Status was not part of the statistical analysis plan and was analyzed using a longitudinal model based on observed data. All other exploratory end points were summarized descriptively.
Handling of Missing Data
For both primary end points, missing hemoglobin data were imputed based on pattern mixture models that aimed to be consistent with inclusion of hemoglobin data under the treatment policy strategy. The impact on the need for transfusion was then derived from this imputation. If multiple imputed hemoglobin values were > 70 and ≤ 90 g/L, due to missing information on symptoms, patients were considered by default as having signs or symptoms and were therefore categorized as receiving a transfusion in the analysis. For the 2 primary estimands and the secondary end points of transfusion avoidance and change from baseline in hemoglobin, missing hemoglobin data from the central laboratory were handled using a multiple imputation procedure.
For patients withdrawing from the study follow-up after discontinuing iptacopan, the model will recover a return to pre-treatment levels of hemoglobin. This was implemented by a copy reference approach (C5 inhibitors), as treatment response to C5 inhibitors was considered similar to the pre-treatment levels in patients in the iptacopan group. For patients randomized to C5 inhibitors who withdrew from the study, their missing data were imputed under a missing-at-random assumption. The missing-at-random assumption was also used for patients with intermittent missing data from either treatment arm, where the reasons for missing data were assumed to be unrelated to response or adherence status.
The handling of missing data (i.e., pattern mixture models, copy reference approach, and missing-at-random assumption) was used for both primary end points and 5 of the secondary end points in the RTP (Table 9). Missing data were not applicable for the other secondary end points (i.e., BTHs, MAVEs, and safety evaluations).
Table 9: Statistical Analysis of Efficacy End Points of RTP of APPLY-PNH Study
End point | Summary estimate | Estimand label | Statistical model | Adjustment factors | Handling of missing data | Sensitivity analyses |
|---|---|---|---|---|---|---|
Primary end points | ||||||
Change from baseline in hemoglobin ≥ 20 g/L in the absence of RBC transfusions | Marginal proportion Difference in marginal proportion Ratio of marginal proportions OR | Treatment policy | Randomization strata,a sex, age (indicator of age ≥ 45 years), and indicator of baseline hemoglobin ≥ 90 g/L |
| Sensitivity analysis:
Post hoc sensitivity analyses:
Supportive analysis:
| |
hemoglobin levels ≥ 120 g/L in the absence of RBC transfusions | Same as primary end point 1 | Same as primary end point 1 | Same as primary end point 1 | Same as primary end point 1 | Same as primary end point 1 | Same as primary end point 1 |
Secondary end points | ||||||
RBC transfusion avoidance | Same as primary end point 1 | Treatment policy | OR derived using conditional logistic regression; marginal proportions derived using logistic regression | Randomization strata, sex, age (indicator of age ≥ 45 years), and indicator of baseline hemoglobin ≥ 90 g/L | Same as primary end point 1 | Post hoc sensitivity analyses:
|
Change from baseline in hemoglobin | Adjusted mean change from baseline Adjusted mean difference between groups | Direct efficacyb | MMRM | Randomization strata,a age (indicator of age ≥ 45 years), sex, treatment, time point, baseline hemoglobin, treatment by time point, and time point by baseline hemoglobin | Same as primary end point 1 | Sensitivity analysis: Replacement of missing central laboratory hemoglobin data with local laboratory data Supportive analysis: Include all central laboratory data (including-transfusion estimand) |
Change from baseline in FACIT-F scores | Adjusted mean change from baseline Adjusted mean difference between groups | Including-transfusion | MMRM | Randomization strata,a age (indicator of age ≥ 45 years), sex, treatment, time point, baseline FACIT-F score, treatment by time point, and time point by baseline FACIT-F score | Same as primary end point 1 | Supportive analysis: Values of FACIT-F in 30 days following transfusion considered missing and were imputed (direct efficacy estimand) |
Change from baseline in ARC | Adjusted mean change from baseline Adjusted mean difference between groups | Including-transfusion | MMRM | Randomization strata,a age (indicator of age ≥ 45 years), sex, treatment, time point, baseline ARC count, treatment by time point, and time point by baseline ARC count | Same as primary end point 1 | Sensitivity analysis: Replacement of missing central laboratory ARC data with local laboratory data Supportive analysis: Values of ARC in 30 days following transfusion considered missing and imputed (direct efficacy estimand) |
Percent change from baseline in LDH levels | Adjusted geometric mean change from baseline Geometric mean ratio of groups | Including-transfusion | MMRM (estimated based on log-transformed LDH ratio to baseline) | Randomization strata,a age (indicator of age ≥ 45 years), sex, treatment, time point, log-transformed baseline LDH level, treatment by time point, and time point by log-transformed baseline LDH level | Same as primary end point 1 | Sensitivity analysis: Replacement of missing central laboratory LDH data with local laboratory data Supportive analysis: Values of LDH in 30 days following transfusion considered missing and were imputed (direct efficacy estimand) |
Occurrences of clinical BTH | Number and percentage of patients Annualized adjusted rate Annualized adjusted rate difference Annualized adjusted rate ratio | Including-transfusion | Negative binomial model | Randomization strata,a sex, age (indicator of age ≥ 45 years), and indicator of baseline hemoglobin ≥ 90 g/L | NA | NA |
Exploratory end points | ||||||
Change from baseline in EORTC QLQ-C30 | Mean change | Including-transfusion | Longitudinal model | Treatment, sex, age (≥ 45 years), transfusion history, baseline hemoglobin (≥ 90 g/L or observed hemoglobin), baseline EORTC QLQ-C30 score, time point, and interaction terms for treatment, baseline EORTC QLQ-C30 score, and time points |
| Sensitivity analysis: Observed data |
Change from baseline in EQ VAS | Number and percentage of patients | NA | Descriptive statistics | NA | NA | NA |
Number of transfusions and units of RBCs | Number and percentage of patients | NA | Descriptive statistics | NA | NA | NA |
ARC = absolute reticulocyte count; BTH = breakthrough hemolysis; EORTC QLQ-C30 = European Organisation for the Research and Treatment of Cancer Quality of Life Questionnaire Core 30; FACIT-F = Functional Assessment of Chronic Illness Therapy – Fatigue; LDH = lactate dehydrogenase; MAR = missing-at-random assumption; MMRM = mixed model for repeated measures; NA = not applicable; OR = odds ratio; RBC = red blood cell; RTP = randomized treatment period; VAS = visual analogue scale.
aRandomization strata were type of prior C5 inhibitor the patient received (eculizumab or ravulizumab) and transfusion history in the past 6 months (i.e., transfusion received versus not received).
bFor the change from baseline in hemoglobin end point, the direct efficacy estimand meant that, for a patient who had an RBC transfusion, hemoglobin values for the 30 days following the transfusion were excluded from the analysis and imputed.
Source: APPLY-PNH Clinical Study Report.29,30 Details included in the table are from the sponsor’s Summary of Clinical Evidence.35
Subgroup Analyses
Subgroup analyses were conducted on the primary end points for exploratory purposes. Subgroup variables of interest were length of time since diagnosis (< 5, ≥ 5 years); age categories (< 45 years, ≥ 45 years); sex (male, female); baseline hemoglobin (< 90 g/L, ≥ 90 g/L); history of MAVEs before screening (yes, no); C5 inhibitor medication history 6 months before randomization (eculizumab or ravulizumab); transfusion in the last 6 months before randomization (yes, no); number of transfusions in the last 6 months before randomizations (< 2, ≥ 2); LDH levels at baseline (≤ 1.5 × ULN, > 1.5 × ULN); duration of C5 inhibitor treatment (< 12 months, ≥ 12 months).
Control of Type I Error
Superiority of iptacopan in achieving a larger proportion of patients who reached a sustained hemoglobin response compared to C5 inhibitors was tested by the null hypothesis comparing the probability of response for iptacopan to the probability of response for C5 inhibitors for both end points. The overall study type I error was 1-sided 0.025. The multiplicity adjustment to be applied for the test of the 2 primary end points, as well as the secondary end points for which the study wide type I error was controlled, is described graphically in Figure 2.
To adjust for multiplicity of the simultaneous test of 2 primary end points, a weighted permutation test with equal weights to each of the 2 end points was applied. The reference distribution of the P values was derived using 50,000 permuted realizations of the treatment labels within each randomization stratum and obtaining the P values of each of the 2 end points for each realization of permuted treatment labels. The observed P values from each fit with the actual treatment labels were compared with the 1.25th percentiles of the 50,000 resulting P values from fits with permuted treatment labels for each of the 2 end points.62,63
Figure 2 describes hypotheses for the primary and secondary end points and the alpha propagation rules following principles described in Bretz et al.,64,65 which can be summarized as follows:
The primary end point hypotheses H1 and H2 (hemoglobin increase ≥ 20 g/L; hemoglobin ≥ 120 g/L) were both tested using half the study alpha (i.e., 0.025 divided by 2 = 0.0125), with the P value level corresponding to rejection derived using the permutation method. If only 1 of the hypotheses was rejected at the 1.25% percentile of the permuted P values, the rejected hypothesis passed 10% of the local alpha to the other hypothesis. The increased alpha fraction available is equivalent to using 1.375% percentile of the permuted P values to be compared with the observed P value for the hypothesis that was not rejected using the 1.25% percentile.
Secondary end points H3 (transfusion avoidance) and hypotheses H41, H42, and H43 (change in hemoglobin, FACIT-F, ARC) were tested if at least 1 primary end point hypothesis was rejected. A weighted Simes procedure was used to test H3 and H41, H42, and H43. The alpha propagation rules reflect the weights given in Figure 2: half of the local alpha available for the secondary end point hypotheses (45%) was passed on to H3, while the other 45% is propagated using equal weights to the 3 hypotheses denoted as H41, H42, and H43. If rejected, H3 passed the available local alpha equally to all 3 hypotheses H41, H42, and H43. The alpha propagation between the 3 hypotheses denoted H41, H42, and H43 gives them equal weights. When all of H41, H42, and H43 were rejected, their local alpha was propagated back to the primary end point hypotheses.
If all hypotheses (H1, H2, H3, H4) were rejected, the 3 hypotheses H51, H52, and H53 (LDH, BTH, MAVE) were tested using a weighted Simes’ closed testing procedure at full study alpha, where weights of 0.475 were given to each of H51 and H52, and 0.05 to H53. If 1 of H51 or H52 was rejected, its local alpha, up to 90%, was passed to the other hypothesis at the same weight level, and 10% to H53. The weights for alpha propagation from H53 are described in Figure 2.
For the primary and secondary outcome results, the sponsor was unable to supply the CI corresponding to the alpha used for testing each end point. The data reported in the results are the unadjusted 95% CI and 2-sided P values. The alpha thresholds for statistical testing were 0.0173 for the primary end points; 0.0125 for transfusion avoidance; 0.00416 for the change in hemoglobin, FACIT-F score, and ARC; and 0.011875 for BTH.
Figure 2: Visualization of the Multiple Testing Procedure Applied in APPLY-PNH Study
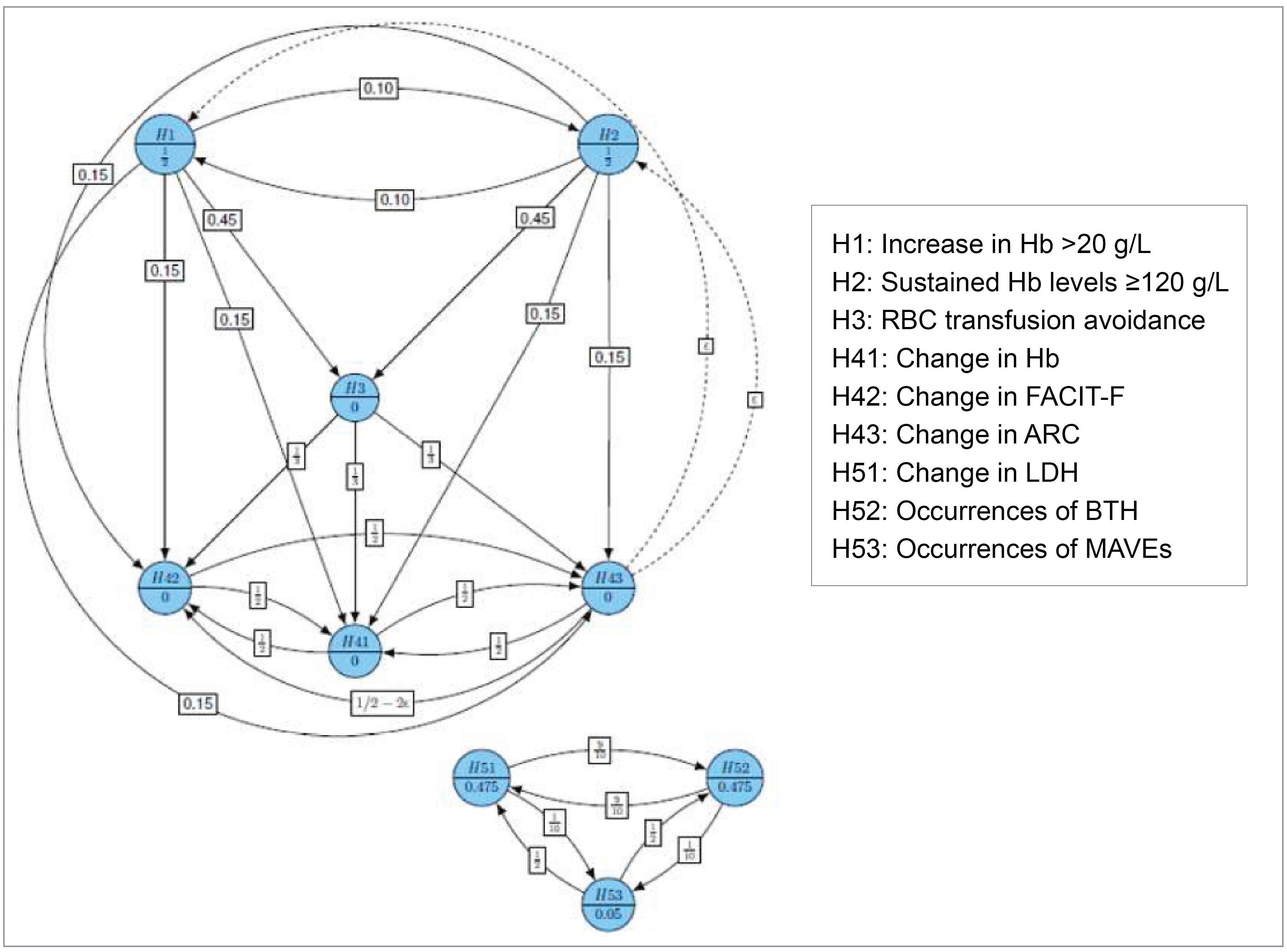
ARC = absolute reticulocyte count; BTH = breakthrough hemolysis; FACIT-F = Functional Assessment of Chronic Illness Therapy – Fatigue; H = hypothesis; LDH = lactate dehydrogenase; MAVE = major adverse vascular event.
Source: APPLY-PNH Clinical Study Report.29
Sample Size
The sample size was calculated based on a 1-sided rejection region for a Fisher’s exact test corresponding to a significance level of 0.025. Under an assumption that 50% of patients treated with iptacopan would achieve an increase of at least 20 g/L from baseline compared to 16% of patients treated with C5 inhibitors, a sample size of 56 patients in the iptacopan group and 35 in the C5 inhibitor group provided 83.2% power for this end point at a significance level of 0.0125. Power was 89.1% at a significance level of 0.0125 for the end point corresponding to the achievement of sustained levels of hemoglobin greater than or equal to 120 g/L calculated under the assumption that the proportions were 35% for iptacopan and 5% for C5 inhibitors.
Nominal power for prioritized secondary end points corresponding to hypotheses H3, H41, H42, and H43 (described in Figure 2) was estimated to be between 85% and 90% at full study alpha (one-sided 0.025), without considering the adjustment for multiple testing derived from the procedure used. The 3 hypotheses tested as H51, H52, and H53 were estimated to have lower power. Hence, the alpha allocated was very small, leading to a test at full study alpha only after the rejection of all primary end point hypotheses, secondary hypothesis H3, and hypotheses H41, H42, and H43.
Analysis Populations
The full analysis set was used for all efficacy outcomes and included all randomized patients who were analyzed according to treatment they were assigned to. The safety set included all patients who received at least 1 dose of study drug, analyzed according to the treatment they received. The patient-reported outcomes were analyzed based on all patients in the full analysis set who had a baseline FACIT-F score (patient-reported outcome evaluable set).
Table 10: Analysis Populations of RTP of APPLY-PNH Study
Population | Definition | Application |
|---|---|---|
FAS | All patients to whom study treatment had been assigned by randomization, excluding patients to whom a randomization number had been assigned in error (misrandomized patients). According to the intention-to-treat principle, patients were analyzed according to the treatment they had been assigned to, considering the strata in which they were included during the randomization procedure. | All efficacy end points |
Safety set | All patients who received at least 1 dose of study treatment. Patients were analyzed according to the treatment they received, where treatment received was defined as the randomized treatment if the patient took at least 1 dose of that treatment or the first treatment received if the randomized treatment was never received. | All safety end points |
PRO evaluable set | All patients in the FAS who had a baseline FACIT-F score | All PRO end points |
FACIT-F = Functional Assessment of Chronic Illness Therapy – Fatigue; FAS = full analysis set; PRO = patient-reported outcome; RTP = randomized treatment period; SAF = safety analysis set.
Source: APPLY-PNH Clinical Study Report.29 Details included in the table are from the sponsor’s Summary of Clinical Evidence.35
Results
Patient Disposition
In the APPLY-PNH study, 125 patients were screened, and 28 patients (22%) were excluded because they did not meet 1 or more of the study inclusion criteria or did meet 1 or more of the exclusion criteria (Table 11). Eleven of these 28 patients (39%) did not meet the hemoglobin criteria (< 100 g/L), and 8 of the 28 patients (29%) had evidence of bone marrow failure. Other reasons for screening failure were related to liver injury or disease, history of malignancy or other comorbidities, or failure to meet the diagnostic criteria for PNH.
A total of 97 patients were randomized and treated, including 62 patients who received iptacopan and 35 patients who received a C5 inhibitor during the trial. In the 24-week RTP, 1 patient (1.6%) in the iptacopan group discontinued treatment due to pregnancy but continued study assessments until the end of the RTP. No patients in the C5 inhibitor group stopped treatment, and no patients in either group discontinued the study early.
Table 11: Summary of Patient Disposition for RTP of APPLY-PNH Study
Patient disposition | RTP of APPLY-PNH study | ||
|---|---|---|---|
Iptacopan (N = 62) | C5 inhibitors (N = 35) | Overall (N = 125) | |
Screened, n (%) | NR | NR | 125 (100) |
Screen failure, n (%) | NA | NA | 28 (22.4) |
Reason for screening failure, n (%)a | |||
Mean hemoglobin level < 100 g/L | NA | NA | 11 (39.3) |
Patients with laboratory evidence of bone marrow failure | NA | NA | 8 (28.6) |
Liver disease or liver injury (any single parameter of ALT, GGT, alkaline phosphatase must not exceed 3 × ULN) | NA | NA | 4 (14.3) |
History of malignancy of any organ system, treated or untreated, within the past 5 years | NA | NA | 2 (7.1) |
Liver disease, such as active HBV or HCV infection, or liver injury, indicated by abnormal results of liver function tests | NA | NA | 2 (7.1) |
Male and female patients ≥ 18 years with a diagnosis of PNH | NA | NA | 2 (7.1) |
Major concurrent comorbidities | NA | NA | 1 (3.6) |
Randomized | |||
Randomized, n (%) | 62 (100) | 35 (100) | 97 (77.6) |
Completed treatment, n (%) | 61 (98.4) | 35 (100) | 96 (99.0) |
Discontinued treatment, n (%) | 1 (1.6) | 0 | 1 (1.0) |
Reason for treatment discontinuation, n (%) | |||
Pregnancy | 1 (1.6) | 0 | 1 (1.0) |
Analysis sets | |||
FAS, n | 62 | 35 | 97 |
Safety set, n | 62 | 35 | 97 |
PRO evaluable set, n | 62 | 33 | 95 |
ALT = alanine aminotransferase; FAS = full analysis set, GGT = gamma-glutamyl transferase; HBV = hepatitis B virus; HCV = hepatitis C virus; NA = not applicable; NR = not reported; PRO = patient-reported outcome; RTP = randomized treatment period; ULN = upper limit of normal.
aThe percentage of patients who did not meet the screening criteria were calculated based on 28 patients in the denominator.
Source: APPLY-PNH Clinical Study Report.29,30 Details included in the table are from the sponsor’s Summary of Clinical Evidence.35
Baseline Characteristics
The baseline characteristics outlined in Table 12 are limited to those that are most relevant to this review or were felt to affect the outcomes or interpretation of the study results. The mean age of patients enrolled in the APPLY-PNH study was 51.7 years (SD = 16.9) and 49.8 years (SD = 16.7) in the iptacopan and C5 inhibitor groups, respectively. Overall, most patients were female (69%) versus male (31%), with a similar distribution between groups. The mean disease duration was 11.9 years (SD = 9.8 years) in the iptacopan group and 13.5 years (SD = 10.9 years) in the C5 inhibitor group. Most patients in the study were treated with eculizumab (65%) at screening, with the minority receiving ravulizumab (35%). Among patients who were receiving eculizumab before enrolment, the mean dose of eculizumab was numerically lower in the iptacopan than C5 inhibitor group (937.5 mg, SD =100.5 mg, versus 1,004.3 mg, SD = 171.8 mg, respectively), and there was a lower proportion of patients receiving doses greater than 900 mg in the iptacopan versus control group (12.5% versus 30.4%).66 The mean ravulizumab dose was similar in the 2 groups (iptacopan: 3,177.3 mg, SD = 177.1 mg; control group: 3,200.0 mg, SD = 195.4 mg). Four patients (6.5%) in the iptacopan group and 3 patients (8.6%) in the C5 inhibitor group had LDH levels greater than 1.5 times the ULN.
The mean hemoglobin value was 89.3 g/L (SD = 7.0 g/L) and 88.5 g/L (SD = 8.9 g/L), in the iptacopan and C5 inhibitor groups, respectively, with 56.5% and 60.0% of patients having received a transfusion in the past 6 months. In the iptacopan group, 19.4% of patients had a history of MAVE compared with 28.6% of those in the C5 inhibitor group.
Table 12: Summary of Baseline Characteristics From RTP of APPLY-PNH Study (FAS)
Characteristic | Iptacopan (N = 62) | C5 inhibitors (N = 35) |
|---|---|---|
Age (years) | ||
Mean (SD) | 51.7 (16.9) | 49.8 (16.7) |
Median (range) | 53.0 (22 to 84) | 45.0 (20 to 82) |
Sex, n (%) | ||
Male | 19 (30.6) | 11 (31.4) |
Female | 43 (69.4) | 24 (68.6) |
Race, n (%) | ||
Asian | 12 (19.4) | 7 (20.0) |
Black or African-American | 2 (3.2) | 2 (5.7) |
Chinese | 2 (3.2) | 1 (2.9) |
Indian | 0 (0.0) | 1 (2.9) |
Japanese | 7 (11.3) | 3 (8.6) |
Korean | 2 (3.2) | 0 (0.0) |
White | 48 (77.4) | 26 (74.3) |
Missing | 1 (1.6) | 2 (5.7) |
Ethnicity, n (%) | ||
Hispanic or Latino | 8 (12.9) | 2 (5.7) |
Not Hispanic or Latino | 51 (82.3) | 27 (77.1) |
NR or unknown | 3 (4.8) | 6 (17.1) |
Disease duration (years) | ||
Mean (SD) | 11.9 (9.8) | 13.5 (10.9) |
Range | 0.7 to 40.2 | 1.5 to 42.0 |
C5 inhibitor therapy history — 6 months prerandomization, n (%) | ||
Eculizumab | 40 (64.5) | 23 (65.7) |
Ravulizumab | 22 (35.5) | 12 (34.3) |
Duration of C5 inhibitor therapy (years) | ||
Mean (SD) | 3.8 (3.6) | 4.2 (3.9) |
Median (range) | 2.6 (0.5 to 16.6) | 2.7 (0.4 to 16.3) |
Eculizumab dose administered (mg) | ||
N | 40 | 23 |
Mean (SD) | 937.5 (100.5) | 1,004.3 (171.8) |
Median (range) | 900 (900 to 1,200) | 900 (900 to 1,500) |
Ravulizumab dose administered (mg) | ||
N | 22 | 12 |
Mean (SD) | 3,177.3 (177.1) | 3,200.0 (195.4) |
Median (range) | 3,300 (3,000 to 3,600) | 3,300 (3,000 to 3,600) |
Baseline hemoglobin, n (%) | ||
< 90 g/L | 32 (51.6) | 18 (51.4) |
≥ 90 g/L | 30 (48.4) | 17 (48.6) |
Baseline hemoglobin (g/L) | ||
Mean (SD) | 89.3 (7.0) | 88.5 (8.9) |
Baseline LDH level, n (%) | ||
≤ 1.5 × ULN | 58 (93.5) | 32 (91.4) |
> 1.5 × ULN | 4 (6.5) | 3 (8.6) |
Baseline LDH level (U/L) | ||
Mean (SD) | 269.1 (70.1) | 272.7 (84.8) |
Transfusion in last 6 months prerandomization, n (%) | ||
Yes | 35 (56.5) | 21 (60.0) |
No | 27 (43.5) | 14 (40.0) |
Number of transfusions in last 6 months prerandomization, n (%) | ||
< 2 | 38 (61.3) | 21 (60.0) |
≥ 2 | 24 (38.7) | 14 (40.0) |
Number of transfusions in last 6 months prerandomization among patients who received transfusions | ||
N | 35 | 21 |
Mean (SD) | 3.1 (2.58) | 4.0 (4.34) |
Median (range) | 2.0 (1 to 13) | 2.0 (1 to 19) |
Platelet count (109/L) | ||
Mean (SD) | 160.2 (63.8) | 147.3 (77.0) |
ARC count (109/L) | ||
Mean (SD) | 193.2 (83.6) | 190.6 (80.9) |
Median | 176.6 | 159.6 |
Range | 51.0 to 562.8 | 90.3 to 411.6 |
Baseline FACIT-F score | ||
N | 62 | 33 |
Mean (SD) | 34.7 (9.82) | 30.8 (11.45) |
Patients with ≥ 1 MAVE, n (%) | ||
N | 12 (19.4) | 10 (28.6) |
ARC = absolute reticulocyte count; FACIT-F = Functional Assessment of Chronic Illness Therapy – Fatigue; FAS = full analysis set; LDH = lactate dehydrogenase; MAVE = major adverse vascular event; RTP = randomized treatment period; SD = standard deviation; ULN = upper limit of normal.
Source: APPLY-PNH Clinical Study Report.29,30 Details included in the table are from the sponsor’s Summary of Clinical Evidence.35
Exposure to Study Treatments
The duration of treatment was similar in the 2 groups, with the mean duration of 168.3 days (SD = 3.6 days) in the iptacopan group and 170.4 days (SD = 4.5 days) in the C5 inhibitor group (Table 13). Treatment adherence was calculated based on the relative dose intensity, which is the sum of doses received divided by the expected total doses received, reported as a percentage. For the iptacopan group, the mean relative dose intensity was 99.6% (SD = 1.7%), and for the C5 inhibitor group was 100.6% (SD = 2.1%).
During the APPLY-PNH study, common concomitant therapies in the iptacopan and C5 inhibitor groups, respectively, were folic acid (64.5% and 65.7%), COVID-19 vaccinations (33.9% and 20.0%), proton pump inhibitors (21.0% and 28.6%), acetaminophen products (19.4% and 25.7%), iron chelating agents (14.5% and 22.9%), systemic corticosteroids (14.5% and 5.7%), vitamin K antagonists (12.9% and 5.7%), direct factor Xa inhibitors (6.5% and 5.7%), and heparin products (6.5% and 11.4%). Concomitant supportive therapies included vitamin B12 (16.1% and 11.4%), oral or IV iron supplements (8.1% and 2.9%), and eltrombopag (4.8% and 2.9%) or erythropoietin stimulating agents (3.2% and 14.3%) in the iptacopan and C5 inhibitor groups, respectively.
No patients in either group received rescue medications or procedures to treat serious complications such as thrombosis, BTH, or MAVE. One patient in the iptacopan group received medication for MAVE (transient ischemic attack) listed as “solutions affecting the electrolyte balance.” As for subsequent treatments, 1 patient in the iptacopan group discontinued study treatment and reinitiated treatment with eculizumab because of pregnancy.
Table 13: Summary of Patient Exposure From RTP of APPLY-PNH Study (Safety Population)
Exposure | Iptacopan (N = 62) | C5 inhibitors (N = 35) |
|---|---|---|
Duration of treatment (days) | ||
Duration, mean (SD) | 168.3 (3.62) | 170.4 (4.51) |
Duration, median (range) | 169.0 (141 to 171) | 169.0 (166 to 188) |
Relative dose intensity (%)a | ||
Mean (SD) | 99.6 (1.7) | 100.6 (2.1) |
Dose intensityb categories for iptacopan, n (%) | ||
< 400 mg per day | 6 (9.7) | NA |
400 mg per day | 56 (90.3) | NA |
Dose categories for eculizumab, n (%) | ||
900 mg | NA | 16 (45.7) |
1,200 mg | NA | 6 (17.1) |
1,500 mg | NA | 1 (2.9) |
Dose categories for ravulizumab, n (%) | ||
3,000 mg | NA | 5 (14.3) |
3,300 mg | NA | 6 (17.1) |
3,600 mg | NA | 1 (2.9) |
NA = not applicable; RTP = randomized treatment period, SD = standard deviation.
aRelative dose intensity for each patient on iptacopan is the dose intensity (i.e., cumulative dose received divided by the actual duration of exposure), divided by the planned dose intensity of 400 mg per day. Relative dose intensity each patient on C5 inhibitor = cumulative dose received divided by the expected total dose (i.e., the planned dosage multiplied by the number of infusions the patient should have received during the study period).
bDose intensity = actual cumulative dose received divided by the actual duration of exposure.
Source: APPLY-PNH Clinical Study Report.29,30
Efficacy
Hemoglobin Levels
Both primary outcomes in the RTP of the APPLY-PNH study showed results that favoured iptacopan versus the C5 inhibitor group (Table 14). The marginal proportion of patients with at least a 20 g/L increase in hemoglobin from baseline (in the absence of transfusion) was 82.3% versus 2.0% in the iptacopan versus C5 inhibitor groups, respectively, with a difference between groups of 80.2% (95% CI, 71.2% to 87.6%). With respect to normalization of hemoglobin levels, 68.8% of patients in the iptacopan group reported hemoglobin levels of at least 120 g/L compared with 1.8% of patients in the C5 inhibitor group (difference in marginal proportions 67.0%; 95% CI, 56.4% to 76.9%). The results of the sensitivity analyses and subgroup analyses for the primary end points showed results that were consistent with the primary analyses.
The change from baseline in hemoglobin levels was a secondary outcome in the pivotal trial and was based on the direct efficacy estimand, which excluded the impact of transfusions in the analysis. The hemoglobin values 30 days after a transfusion were excluded, and hemoglobin data were imputed. There were 6 patients (17%) in the C5 inhibitor group who had missing data for this analysis, compared with no patients with missing data in the iptacopan group.
The iptacopan group reported an adjusted mean hemoglobin change from baseline of 36.0 g/L, and the C5 inhibitor group reported a –0.6 g/L change, with a mean difference between groups of 36.6 g/L (95% CI, 32.0 to 41.2) that favoured iptacopan versus C5 inhibitors. An increase in hemoglobin levels was seen early after starting treatment in the iptacopan group. In the iptacopan group, a 19.7 g/L adjusted mean increase in hemoglobin values was observed at day 7 versus a 0.9 g/L decrease in the control group (mean difference 20.6 g/L; 95% CI, 16.5 to 24.8). By day 14, the adjusted mean difference between groups in the change from baseline in hemoglobin values was 30.5 g/L (95% CI, 26.5 to 34.6), with consistent mean differences for later time points.
The sensitivity analysis based on the including-transfusion estimand reported an adjusted mean difference in the change from baseline in hemoglobin of 36.0 g/L (95% CI, 31.9 to 40.0), which was similar to the results of the primary analysis.
Transfusions
Based on observed data, 59 of 62 patients in the iptacopan group and 14 of 35 patients in the C5 inhibitor did not require a transfusion (defined as patients who did not receive an RBC transfusion or did not meet the protocol-defined criteria for a transfusion) from day 14 to 168 in the RTP (marginal proportion 94.8% and 25.9%, respectively). The difference in marginal proportions of patients avoiding transfusions was 68.9% (95% CI, 51.4% to 83.9%) between the iptacopan and the C5 inhibitor groups (Table 15). In sensitivity analyses that used various assumptions for missing data and/or different analysis methods, the between-group differences consistently favoured iptacopan versus C5 inhibitors, but the magnitude of effects varied. The sponsor’s post hoc sensitivity analysis, in which only patients with imputed hemoglobin values less than 70 g/L were deemed to have met the transfusion criteria, reported a difference in marginal proportions of 55.7% (95% CI, 37.6% to 72.6%). The FDA analyses using observed data reported a difference in proportions of 55.3% (95% CI, 38.4% to 72.1%), and, based only on transfusions received (i.e., excluding patients who met transfusion criteria but did not receive a transfusion) reported a difference in proportions of 49.5% (95% CI, 32.5% to 66.6%).67
Table 14: Change in Hemoglobin Outcomes From the 24-Week RTP of the APPLY-PNH Study (FAS)
Study end points | Iptacopan (N = 62) | C5 inhibitor (N = 35) |
|---|---|---|
Increase in hemoglobin ≥ 20 g/L from baseline in the absence of RBC transfusionsa | ||
Number of responding patients, n (%) | 51 (82.3) | 0 |
Marginal proportion, % (95% CI)b | 82.3 (73.4 to 90.2) | 2.0 (1.1 to 4.0) |
Difference between marginal proportions, % (95% CI)b | 80.2 (71.2 to 87.6) | |
Unadjusted OR (95% CI)c | 338.25 (25.07 to 4,564.14) | |
Unadjusted 2-sided P valuec | < 0.0001d | |
Hemoglobin ≥ 120 g/L in the absence of RBC transfusionsa | ||
Number of responding patients, n (%) | 42 (67.7) | 0 |
Marginal proportion, % (95% CI)b | 68.8 (58.4 to 78.9) | 1.8 (0.9 to 4.0) |
Difference between marginal proportions, % (95% CI)b | 67.0 (56.4 to 76.9) | |
Unadjusted OR (95% CI)c | 495.74 (24.41 to 10,066.53) | |
Unadjusted 2-sided P valuec | < 0.0001d | |
Change from baseline in hemoglobin (g/L) a | ||
Number of patients with nonmissing data, n | 62 | 29 |
Baseline, mean (SD) | 89.3 (7.0) | 88.5 (8.9) |
Adjusted mean change from baseline (95% CI)e | 36.0 (33.3 to 38.8) | –0.6 (–4.5 to 3.4) |
Adjusted mean difference between groups (95% CI)e | 36.6 (32.0 to 41.2) | |
Unadjusted 2-sided P value | < 0.0001 d | |
CI = confidence interval; FAS = full analysis set; OR = odds ratio; RBC = red blood cell; RTP = randomized treatment period; SD = standard deviation.
aEnd-of-study value was the mean of visits between day 126 and 168.
bLogistic regression model using Firth correction with common intercept, sex, age group (< 45 years, ≥ 45 years), baseline hemoglobin (≥ 90 g/L, < 90 g/L), and the randomization strata covariates (type of prior C5 inhibitor the patient received [eculizumab or ravulizumab] and transfusion history in the past 6 months [i.e., transfusion received versus not received]). The 95% CI was computed using bootstrapping.
cLogistic regression model using Firth correction with sex, age group (< 45 years, ≥ 45 years), baseline hemoglobin (≥ 90 g/L, < 90 g/L), and the randomization strata covariates (type of prior C5 inhibitor the patient received [eculizumab or ravulizumab] and transfusion history in the past 6 months [i.e., transfusion received versus not received]).
dAccording to the preplanned alpha sharing testing strategy (Figure 2), the outcome was statistically significant.
eMMRM with randomization strata, age (indicator of age ≥ 45 years), sex, treatment, time point, and baseline outcome value as fixed effects, and treatment by time point, and time point by baseline value interaction terms.
Source: APPLY-PNH Clinical Study Report.29,30 Details included in the table are from the sponsor’s Summary of Clinical Evidence.35
The swimmer plot shown in Figure 3 shows patients who received transfusions over the 24-week RTP, including those received during the first 14 days after randomization. The figure does not include patients who met the transfusion criteria but did not receive a transfusion. More patients received transfusions before and after day 14 in the C5 inhibitor group than in the iptacopan group. A summary of the number of transfusion events and units of RBC transfused is provided in Table 33, Appendix 1.
Markers of Hemolysis
Two patients (3.2%) in the iptacopan group and 6 patients in the C5 inhibitor group (17.1%) met the criteria for a clinical BTH, with an annualized adjusted BTH rate of 0.07% and 0.67%, respectively. The annualized adjusted rate difference was –0.60% (95% CI, –1.24% to 0.04) for the iptacopan versus C5 inhibitor group. In the iptacopan group, 1 of the 2 patients with BTH received 1 transfusion (2 units RBCs), whereas 5 of 6 patients in the C5 inhibitor group received transfusions (mean per person transfusions 1.4, SD = 0.89, and RBC units 3.4, SD = 3.2 units).
The study reported a 1.14% reduction (95% CI, –10.19% to 11.31%) in the change from baseline in LDH levels, and an adjusted mean difference between groups in the ARC of –116.15 × 109/L (95% CI, –132.04 to –100.26 × 109/L) for iptacopan versus C5 inhibitor groups (Table 15).
Table 15: Transfusion and Hemolysis-Related Outcomes From the 24-Week RTP of the APPLY-PNH Study (FAS)
Study end points | Iptacopan (N = 62) | C5 inhibitor (N = 35) |
|---|---|---|
Transfusion avoidance | ||
Number of responding patients, n (%) | 59 (95.2) | 14 (40.0) |
Marginal proportion, % (95% CI)a | 94.8 (88.1 to 100.0) | 25.9 (11.6 to 42.4) |
Difference between marginal proportions, % (95% CI)a | 68.9 (51.4 to 83.9) | |
Unadjusted OR (95% CI)b | 108.41 (17.25 to 681.24) | |
Unadjusted 2-sided P valueb | < 0.0001c | |
Occurrence of clinical BTH | ||
Number of patients with an BTH event, n (%) | 2 (3.2) | 6 (17.1) |
BTH criteria met | ||
Hemoglobin decrease ≥ 20 g/L | 2 (3.2) | 4 (11.4) |
LDH levels > 1.5 × ULN and increased compared with last 2 assessments | 2 (3.2) | 6 (17.1) |
Signs or symptoms (dysphagia, fatigue, painful crisis, gross hemoglobinuria, other signs or symptoms) | 1 (1.6) | 6 (17.1) |
Annualized adjusted rate, % (95% CI)d | 0.07 (0.02 to 0.31) | 0.67 (0.26 to 1.72) |
Annualized adjusted rate difference, % (95% CI)d | –0.60 (–1.24 to 0.04) | |
Annualized adjusted rate ratio (95% CI)d | 0.10 (0.02 to 0.61) | |
Unadjusted 2-sided P value | 0.0118c | |
Percent reduction in LDH (U/L) based on log-transformed ratio to baseline | ||
Number of patients with nonmissing data, n | 62 | 35 |
Baseline, mean (SD) | 269.1 (70.1) | 272.7 (84.8) |
Patients with baseline LDH > 1.5 ULN, n (%) | 4 (6.5) | 3 (8.6) |
Geometric adjusted mean ratio to baseline (95% CI)e | 0.96 (0.90 to 1.03) | 0.98 (0.89 to 1.07) |
Geometric mean ratio between groups (95% CI)e | 0.99 (0.89 to 1.10) | |
% reduction between groups (95% CI) | 1.14 (–10.19 to 11.31) | |
Unadjusted 2-sided P value | 0.8361 | |
Change from baseline in ARC (109/L) | ||
Number of patients with nonmissing data, n | 62 | 35 |
Adjusted mean change from baseline (95% CI)f | –115.81 (–126.40 to –105.23) | 0.34 (–13.04 to 13.72) |
Adjusted mean difference between groups (95% CI)f | –116.15 (–132.04 to –100.26) | |
Unadjusted 2-sided P value | < 0.0001c | |
ARC = absolute reticulocyte count; BTH = breakthrough hemolysis; CI = confidence interval; FAS = full analysis set; LDH = lactate dehydrogenase; OR = odds ratio; RTP = randomized treatment period; SD = standard deviation; ULN = upper limit of normal.
aLogistic regression model with common intercept, sex, age group (< 45 years, ≥ 45 years), baseline hemoglobin (≥ 90 g/L, < 90 g/L), and the randomization strata covariates (type of prior C5 inhibitor the patient received [eculizumab or ravulizumab] and transfusion history in the past 6 months [i.e., transfusion received versus not received]). The 95% CI was computed using bootstrapping.
bConditional logistic regression model with sex, age group (< 45 years, ≥ 45 years), baseline hemoglobin (≥ 90 g/L, < 90 g/L) and the randomization strata covariates (type of prior C5 inhibitor the patient received [eculizumab or ravulizumab] and transfusion history in the past 6 months [i.e., transfusion received versus not received]).
cAccording to the preplanned alpha sharing testing strategy (Figure 2), the outcome was statistically significant.
dAdjusted annual rates of clinical BTH analyzed using a negative binomial model with randomization strata (prior C5 inhibitor, transfusion history), sex, age (indicator of age ≥ 45 years), indicator of baseline hemoglobin ≥ 90 g/L as factors, and log (day 1 till minimum [end of study, end of RTP] in years) as offset.
eNatural log-transformed ratio to baseline was analyzed using a MMRM stratified by the randomization strata, and age (indicator of age ≥ 45 years), sex, treatment, time point, and log-transformed baseline LDH level as fixed effects, and treatment by time point, and time point by log-transformed baseline LDH level interaction terms. Natural log results were back-transformed and reported as geometric means. End-of-study value was the mean of visits between day 126 and 168.
fMMRM with randomization strata, age (indicator of age ≥ 45 years), sex, treatment, time point, and baseline outcome value as fixed effects, and treatment by time point, and time point by baseline value interaction terms. End-of-study value was the mean of visits between day 126 and 168.
Source: APPLY-PNH Clinical Study Report.29,30 Details included in the table are from the sponsor’s Summary of Clinical Evidence.35
Patient-Reported Outcomes
The change in the FACIT-F score was a secondary outcome in the APPLY-PNH study. The analysis excluded 4 patients (11%) from the C5 inhibitor group who were missing values. No patients were excluded from the iptacopan group. A MID of 5 points has been reported in the literature for patients with PNH.31
In the APPLY-PNH study, the adjusted mean difference in the FACIT-F score was 8.3 points (95% CI, 5.3 to 11.3) for the iptacopan versus the C5 inhibitor group (Table 16).
Figure 3: Swimmer Plot of the Transfusions Received for RTP of APPLY-PNH Study (FAS)
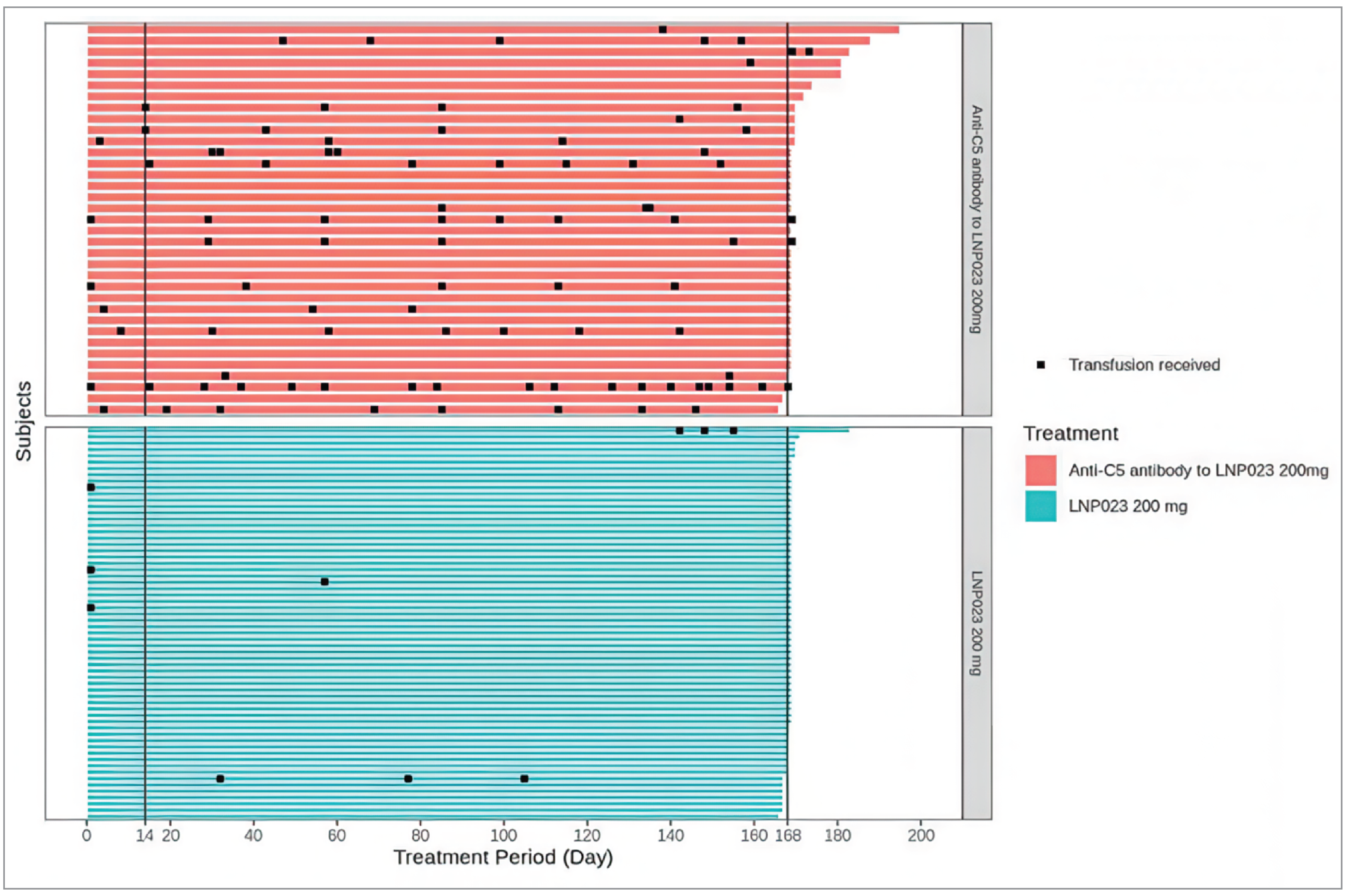
FAS = full analysis set; LNP023 = iptacopan; RTP = randomized treatment period.
Source: APPLY-PNH Clinical Study Report 24-Week Addendum.30
Table 16: Change in FACIT-F Score in the RTP of the APPLY-PNH Study (PRO Evaluable Set)
Outcome | Iptacopan (N = 62) | C5 inhibitor (N = 35) |
|---|---|---|
Number of patients with nonmissing data, n | 62 | 31a |
Baseline FACIT-F score, mean (SD) | 34.7 (9.82) | 30.8 (11.45) |
Adjusted mean change from baseline (95% CI)b | 8.59 (6.72 to 10.47) | 0.31 (–2.20 to 2.81) |
Adjusted mean difference between groups (95% CI)b | 8.29 (5.28 to 11.29) | |
Unadjusted 2-sided P value | P < 0.0001c | |
CI = confidence interval; FACIT-F = Functional Assessment of Chronic Illness Therapy – Fatigue; PRO = patient-reported outcome; RTP = randomized treatment period; SD = standard deviation.
Note: The FACIT-F is a 13-item, patient-reported questionnaire that assesses tiredness, weakness, and difficulty conducting usual activities due to fatigue over the past week. The scale ranges from 0 (extreme fatigue) to 52 (no fatigue), with an increase in score indicating improvement.
aAnalysis excluded 2 patients with missing data at baseline, and 2 others with missing postbaseline values, or values that were not imputed as per the intercurrent event handling strategy.
bMMRM with randomization strata, age (indicator of age ≥ 45 years), sex, treatment, time point, baseline end point value as fixed factors and treatment by time point, and time point by baseline value interaction terms. End-of-study value was the mean of visits between day 126 and 168. The analysis was based on the including-transfusion estimand.
cAccording to the preplanned alpha sharing testing strategy (Figure 2), the outcome was statistically significant.
Source: APPLY-PNH Clinical Study Report.29 Details included in the table are from the sponsor’s Summary of Clinical Evidence.35
The change from baseline in the EORTC QLQ-C30 was an exploratory outcome in the APPLY-PNH study and was not part of the planned statistical testing procedures. The results were based on observed data, with no imputation for missing values, and excluding 2 patients (6%) of patients from the C5 inhibitor group. There was no mean change from baseline in the Global Health Status score in the C5 inhibitor group (0.0 points) and an increase of 15.3 points in the iptacopan group. The mean difference was 14.5 points (95% CI, 9.6 to 19.3 points) for iptacopan versus C5 inhibitor groups.
A summary of the change from baseline in the EQ VAS is shown in Table 34, Appendix 1.
Table 17: Change From Baseline in EORTC QLQ-C30 Global Health Status in the RTP of the APPLY-PNH Study (PRO Evaluable Set)
Outcome | Iptacopan (N = 62) | C5 Inhibitor (N = 35) |
|---|---|---|
Number of patients with nonmissing data, n | 62 | 33 |
Baseline EORTC QLQ-C30 Global Health Status score, mean (SD) | 58.8 (19.34) | 57.7 (19.63) |
Adjusted mean change from baseline (95% CI)a | 15.3 (11.7 to 18.9) | 0.0 (–5.0 to 4.9) |
Adjusted mean difference between groups (95% CI)a | 14.5 (9.6 to 19.3) | |
CI = confidence interval; EORTC QLQ-C30 = European Organisation for the Research and Treatment of Cancer Quality of Life Questionnaire Core 30; PRO = patient-reported outcome; RTP = randomized treatment period; SD = standard deviation.
Note: Global Health Status is scored from 0 to 100. An increase indicates improvement.
aAdjusted mean difference is the average of the difference between least squares means of change from baseline at visits day 126, day 140, day 154, and day 168. Estimates from a longitudinal model including baseline, visit, sex, age group, history of transfusions, and treatment group, and the interactions between visit and baseline, and visit and treatment group. Estimates were based on observed data with no imputation for missing data corresponding to a treatment policy approach including transfusion.
Source: Additional data supplied by the sponsor.68
Harms
Refer to Table 18 for harms data that was reported in the safety population.
Adverse Events
Most patients in the APPLY-PNH study experienced at least 1 adverse event, with 82% of those in the iptacopan group and 80% of patients in the C5 inhibitor groups reporting an event. The most common events in the iptacopan versus control group were headache (16% versus 3%), diarrhea (15% versus 6%), nasopharyngitis (11% versus 6%), and nausea (10% versus 3%).
Serious Adverse Events
SAEs were reported in 9.7% of patients in the iptacopan group and 14.3% of patients in the C5 inhibitor group. The specific SAEs described in Table 18 were each reported in 1 patient, except for 2 patients in the C5 inhibitor group who had an SAE of COVID-19. One patient in the C5 inhibitor group experienced a BTH that was classified as an SAE.
Withdrawals Due to Adverse Events
No patients in either group discontinued the study drug due to adverse events.
Mortality
No patients died during the 24-week RTP.
Notable Harms
One patient (1.6%) in the iptacopan group reported a MAVE event, a transient ischemic attack, which was assessed as an SAE. The patient was a 62-year-old female with sinus node dysfunction (sick sinus syndrome) and a history of hypertension, atrial fibrillation, and dyslipidemia. The investigator suspected the transient ischemic attack was related to an episode of arrhythmia due to sick sinus syndrome, not to iptacopan. No MAVE events were reported in the C5 inhibitor group. The annualized adjusted rate difference of MAVE was 0.03% (95% CI, –0.03% to 0.10%) for iptacopan versus C5 inhibitors.
Infections caused by encapsulated bacteria were identified as an important harm for this review. One patient in the iptacopan group (1.6%) and no patients in the C5 inhibitor group reported an infection with encapsulated bacteria. The risk difference for iptacopan versus C5 inhibitors was 1.6% (95% CI, –1.5% to 4.8%).
The sponsor-selected adverse events of special interest are shown in Table 18. These events included serious or severe infections; hemolysis-related adverse events; and testicular, thyroid, and decreased platelet adverse events. In the iptacopan group, 3.2% of patients experienced a serious or severe infection, compared with 8.6% of patients in the C5 inhibitor group (risk difference –5.4%; 95% CI, –15.6% to 4.9%). PNH hemolysis and thrombosis adverse events were reported less frequently in the iptacopan versus C5 inhibitor group (16.1% versus 28.6%; risk difference –12.4%; 95% CI, –30.0% to 5.1%), whereas decreased platelet adverse events were reported more frequently in the iptacopan group (6.5% versus 0%; risk difference 6.5%; 95% CI, 0.3% to 12.6%). The frequency of testicular or thyroid changes was low in both groups.
Table 18: Summary of Harms Results in RTP of APPLY-PNH Study (Safety Population)
Adverse events | Iptacopan (N = 62) | C5 inhibitors (N = 35) |
|---|---|---|
Most common TEAEs (≥ 5% of patients in any treatment group), n (%) | ||
Patients with ≥ 1 TEAE | 51 (82.3) | 28 (80.0) |
Headache | 10 (16.1) | 1 (2.9) |
Diarrhea | 9 (14.5) | 2 (5.7) |
Nasopharyngitis | 7 (11.3) | 2 (5.7) |
Nausea | 6 (9.7) | 1 (2.9) |
Arthralgia | 5 (8.1) | 1 (2.9) |
COVID-19 | 5 (8.1) | 9 (25.7) |
Urinary tract infection | 5 (8.1) | 1 (2.9) |
Abdominal pain | 4 (6.5) | 1 (2.9) |
Blood LDH increased | 4 (6.5) | 3 (8.6) |
Dizziness | 4 (6.5) | 0 |
Back pain | 3 (4.8) | 2 (5.7) |
BTH | 2 (3.2) | 6 (17.1) |
Pyrexia | 2 (3.2) | 3 (8.6) |
Sinusitis | 2 (3.2) | 3 (8.6) |
Upper respiratory tract infection | 2 (3.2) | 3 (8.6) |
EVH | 0 | 2 (5.7) |
SAEs, n (%) | ||
Patients with ≥ 1 SAE | 6 (9.7) | 5 (14.3) |
Descriptiona | Sinus node dysfunction, transient ischemic attack, COVID-19, pyelonephritis, urinary tract infection (pseudomonal), blood creatine phosphokinase increase (rhabdomyolysis), basal cell carcinoma, myelodysplastic syndrome | BTH, EVH, jaundice, bacterial arthritis, intervertebral discitis, sepsis or septic shock, influenza A virus, acute kidney injury, bilirubinuria, COVID-19 (2 patients) |
AEs leading to treatment discontinuation, n (%) | ||
Patients who discontinued treatment due to AEs | 0 | 0 |
Deaths, n (%) | ||
Patient deaths | 0 | 0 |
MAVE, n (%) | ||
Transient ischemic attack | 1 (1.6) | 0 |
Annualized adjusted MAVE rate, % (95% CI)b | 0.03 (0.00 to 0.25) | 0 |
Annualized adjusted rate difference, % (95% CI)a | 0.03 (–0.03 to 0.10) | |
Adverse event of special interest, n (%) | ||
Patients with ≥ 1 AESI | 16 (25.8) | 11 (31.4) |
Infection caused by encapsulated bacteria | ||
Bronchitis due to Haemophilus | 1 (1.6) | 0 |
Serious or severe infections | ||
Any serious or severe infection, n (%) | 2 (3.2) | 3 (8.6) |
COVID-19 | 1 (1.6) | 2 (5.7) |
Pyelonephritis | 1 (1.6) | 0 |
Urinary tract infection | 1 (1.6) | 0 |
Bacterial arthritis | 0 | 1 (2.9) |
Intervertebral discitis | 0 | 1 (2.9) |
Sepsis or septic shock | 0 | 1 (2.9) |
PNH hemolysis and thrombosis | ||
Any PNH hemolysis and thrombosis | 10 (16.1) | 10 (28.6) |
Blood LDH increased | 4 (6.5) | 3 (8.6) |
BTH | 2 (3.2) | 6 (17.1) |
Blood creatinine increased | 1 (1.6) | 0 |
Hemoglobinuria | 1 (1.6) | 0 |
Hemiparesis | 1 (1.6) | 0 |
Ocular icterus | 1 (1.6) | 0 |
Transient ischemic attack | 1 (1.6) | 0 |
EVH | 0 | 2 (5.7) |
Jaundice | 0 | 1 (2.9) |
Testicular effects | 1 (1.6) | 0 |
Thyroid changes | 1 (1.6) | 0 |
Decreased platelets | 4 (6.5) | 0 |
AE = adverse event; AESI = adverse event of special interest; BTH = breakthrough hemolysis; CI = confidence interval; EVH = extravascular hemolysis; LDH = lactate dehydrogenase; MAVE = major adverse vascular event; PNH = paroxysmal nocturnal hemoglobinuria; RTP = randomized treatment period; SAE = serious adverse event; TEAE = treatment-emergent adverse event.
aThe specific SAEs described here were each reported in 1 patient, except for 2 patients in the C5 inhibitor group who had a serious adverse event of COVID-19.
bAdjusted annual rates of MAVE analyzed using a Poisson model with treatment as factor, and log (day 1 till minimum [end of study, end of RTP], in years) as offset.
Source: APPLY-PNH Clinical Study Report.29,30 Details included in the table are from the sponsor’s Summary of Clinical Evidence.35
Critical Appraisal
Internal Validity
The APPLY-PNH study was an open-label, phase III RCT. Randomization was conducted using interactive response technology to assign each patient a randomization number, which was used to link the patient to a treatment group and the medication number. The CDA-AMC review team did not identify any issues to suggest treatment allocation was not concealed during the randomization process; however, the baseline characteristics showed some imbalances between groups. Considering the small sample size of the study (35 patients in the C5 inhibitor group and 62 patients in the iptacopan group), it may not have been possible to balance all prognostic factors between groups. Differences were noted between the iptacopan and C5 inhibitor groups in the mean age, disease duration, baseline platelet count, and FACIT-F scores at baseline. The proportion of patients who received an RBC transfusion in the past 6 months (60.0% versus 56.5%), had a history of MAVE (28.6% versus 19.4%), and LDH levels greater than 1.5 times the ULN (8.6% versus 6.5%) were numerically higher in the C5 inhibitor group than the iptacopan group. Also, the mean dose of eculizumab was higher in the control group versus the iptacopan group (1,004.3 mg versus 937.5 mg, respectively). The clinical experts consulted considered the need for transfusions, higher C5 inhibitor dose, higher LDH levels, and history of MAVE as indicators of more severe PNH. Thus, the differences observed may have biased the results in favour of iptacopan. No major risk of bias was identified due to patient withdrawals. Only 1 patient (1.6%) in the iptacopan group and no patients in the C5 inhibitor group stopped the study drug early, and all patients completed the 24-week follow-up in the RTP.
Patients, investigators, and study personnel were aware of the treatment group assigned. Thus, the potential for reporting and performance bias should be considered, particularly when interpreting the results of subjective outcomes, such as FACIT-F, EORTC QLQ-C30, and harms. The outcomes based on laboratory values (e.g., hemoglobin, LDH, ARC) are objective measures and have a low risk of bias. Potential bias in decisions regarding administration of transfusions and diagnosing BTH were mitigated by using standardized criteria. However, both end points include an assessment of patients’ symptoms, which may be subjective. According to the clinical experts we consulted, set criteria for administering transfusions are not used in practice. Thus, the use of these criteria in the APPLY-PNH study may impact the external validity of the transfusion-related findings. The APPLY-PNH study protocol set criteria to define BTH. However, these criteria are not standard in practice. The clinical experts stated there are no internationally accepted criteria for BTH, but most would consider LDH level greater than 2 times the ULN in a patient with symptoms of hemolysis sufficient to diagnose BTH. The experts indicated that a change in hemoglobin levels of 20 g/L or more would suggest a more severe BTH, but no set change in hemoglobin levels is used to identify patients experiencing BTH, and other factors need to be considered, such as associated end-organ damage (e.g., kidney injury) and development of thrombosis.
The CDA-AMC reviewer did not identify any major concerns with the estimand and handling of intercurrent events for the primary and key secondary outcomes. Intercurrent events of discontinuation, MAVE, or BTH were handled with a treatment policy strategy, in which all data were included in the analysis, regardless of these events. Transfusion intercurrent events were handled in different ways depending on the outcome. To meet the primary end points, the patient must neither have received an RBC transfusion between day 14 and day 168 nor met the predefined criteria for transfusion. The change from baseline in hemoglobin excluded the impact of transfusions in their analysis (direct efficacy estimand), by eliminating hemoglobin values 30 days after transfusions. This approach was reasonable, given that the clinical experts stated a posttransfusion increase in hemoglobin typically lasts 21 to 28 days. All other secondary outcomes included transfusion impacts in the estimates of their effects. The sponsor conducted sensitivity analyses that assessed different methods for handling intercurrent events, and these analyses generally reported results that were consistent with the primary analyses. The subgroup analyses of the primary end points also showed results that were consistent across baseline demographics and disease characteristics subgroups, although, given the small number of patients, the results should be interpreted with caution.
With regard to missing data, there were potential issues identified for the change from baseline in the hemoglobin and the patient-reported outcomes. For these outcomes, the C5 inhibitor group was missing data from 2 patients (6%) for the EORTC QLQ-C30 Global Health Status, 4 patients (11%) for the FACIT-F score, and 6 patients (17%) for the change in hemoglobin levels. There were no missing data for the iptacopan group. The missing data have the potential to bias the result, given the small sample size (35 patients in the C5 inhibitor group) and the differential rate of missing data. However, the direction and extent of any bias is unclear. The FDA reviewer raised issues with the missing data imputation methods for the transfusion avoidance outcome, and the FDA requested additional analyses using different assumptions. For the sponsor’s primary analysis, multiple imputation methods were used to impute missing hemoglobin levels, and it was assumed that any patient with hemoglobin levels less than 90 g/L would meet the protocol-specified transfusion criteria. The between-group difference in marginal proportions of patients avoiding transfusions was 68.9% (95% CI, 51.4% to 83.9%) for the primary analysis. The sponsor’s post hoc sensitivity analysis, in which only patients with imputed hemoglobin values less than 70 g/L were deemed to have met the transfusion criteria, reported a difference in proportions of patients avoiding transfusions of 55.7% (95% CI, 37.6% to 72.6%). The FDA analyses based on observed data reported a difference in proportions of 55.3% (95% CI, 38.4% to 72.1%), and, based only on transfusions received (i.e., excluding patients who met transfusion criteria but did not receive a transfusion), reported a difference in proportions of 49.5% (95% CI, 32.5% to 66.6%).67 The different imputation methods impacted the proportion of patients who avoided transfusion in the C5 inhibitor group, which ranged from 25.9% (sponsor’s primary analysis) to 45.7% (based on transfusions received).67 The proportion of patients who avoided transfusion in the iptacopan group were all very similar (approximately 95%) in all analyses.67 These analyses show that the imputation methods used for the transfusion avoidance end point may impact the results, adding uncertainty to the magnitude of treatment effects.
In the RTP of the APPLY-PNH study, statistical testing was performed 1-sided with an overall type I error rate of 2.5%. The testing strategy to control the alpha for the 2 primary end points and all secondary end points involved permutation tests and weighted Simes closed testing procedures. Due to the complexity of these procedures, the sponsor stated they were unable to supply the adjusted CI that corresponds to the alpha for each outcome. The CDA-AMC typically reports the adjusted CI in the GRADE table, but, for this study, all results are reported as unadjusted 95% CI and unadjusted 2-sided P values. The Clinical Study Report states that the unadjusted CI and P values do not reflect the prespecified multiplicity scheme and hence should not be interpreted as a basis for claiming significance. For the primary and secondary efficacy outcomes, the CIs reported in the GRADE table are narrower than the adjusted CI would be, and this should be considered when assessing whether each end point crosses the threshold of clinical importance. Given the large differences observed between groups for the primary end points, the adjusted CIs were unlikely to change the assessment of the certainty of the evidence. The EORTC QLQ-C30 was an exploratory outcome and was not formally tested for statistical significance; thus, it should be considered supportive evidence only.
For the statistical analysis, the small sample size remains a significant limitation of the study, particularly in the C5 inhibitor group, which enrolled 35 patients. Bootstrap methods were applied in estimating the CIs for binary end points, but when the sample size is extremely small, the sample may not represent a true random sample of the target population. The bootstrap resample approach may not be able to improve this situation and, thus, may potentially lead to biased and unreliable results.69 The FDA recommended that the primary analyses of binary end points be based on a stratified Cochran-Mantel-Haenszel test using the randomization strata as factors and imputing missing data as nonresponders. The results of the FDA’s recommended analysis for the 2 primary end points showed results that were consistent with the sponsor’s primary analyses.67 Overall, it appears unlikely that the large benefit seen with iptacopan would be explained solely by these limitations in the statistical analyses.
The clinical trial examined outcomes that are important to patients, including fatigue and HRQoL, which may be severely impacted by PNH. The patient-reported outcomes, FACIT-F and EORTC QLQ-C30, both have evidence to support their validity and responsiveness in patients with PNH. For the FACIT-F, a change in score of 5 points was estimated as the MID in patients with PNH, using distribution-based and anchor-based estimations of real-world data from the International PNH Registry.31 For the EORTC QLQ-C30, MID values have not been established in the PNH population; however, an increase of at least 10 points in EORTC QLQ-C30 score for patients with cancer is considered moderately large and represents a clinically important improvement.34 Improvement in hemoglobin, normalization of hemoglobin levels, avoidance of transfusion, and BTH were all important end points, according to the clinical experts consulted. Although both LDH and ARC are used in clinical practice to assess control of hemolysis, they are surrogate measures and may be affected by other factors. For example, ARC levels may be lowered by improved control of hemolysis, but also by the onset of bone marrow failure or myelodysplastic syndrome, which are common conditions in patients with PNH. No MID was identified for the mean change in LDH or ARC.
External Validity
The study included adults with PNH who were, on average, 51 years of age; were predominantly female (69%) and white (76%); and had low hemoglobin levels (mean 89 g/L). Based on the disease characteristics reported and the low proportion of patients with elevated LDH levels (7% of patients had LDH > 1.5 × ULN), the clinical experts consulted for this review stated the patients represented a population with relatively easy-to-manage and well-controlled PNH. The experts noted that the study excluded patients with evidence of bone marrow failure, but in clinical practice these patients would be candidates for iptacopan therapy. The study also excluded patients with significant comorbidities, such as cardiac, renal, or hepatic disease. Thus, the safety and efficacy of iptacopan in these patients is unclear. The small sample size of the study, potential for lack of representativeness in prognostic factors, and the short study follow-up duration (24 weeks) for a lifelong condition contribute to uncertainty in the generalizability of the findings.
The clinical trial assessed outcomes that were relevant to patients, including hemoglobin levels, need for transfusions, fatigue, and HRQoL. As discussed previously, the study used fixed criteria to determine which patients should receive RBC transfusions, which is not consistent with clinical practice. Also, the clinical experts indicated there are no universally accepted criteria to diagnose BTH at this time. Thus, the transfusion avoidance and BTH findings during the 24-week trial time frame may not fully reflect these events in clinical practice.
The clinical experts consulted for this review confirmed that the doses of C5 inhibitors in the trial were generally consistent with clinical practice. The Health Canada–recommended dose of eculizumab is 900 mg every 2 weeks, but the clinical experts estimated that 20% to 30% of patients require a higher dose (1,200 mg or 1,500 mg) or more frequent dosing interval (every 12 or 13 days). Among the patients who were treated with eculizumab before enrolment, the mean eculizumab dose was higher in the control group than the iptacopan group, with 30% versus 12.5% of patients receiving doses greater than 900 mg in the control and the iptacopan groups, respectively. In clinical practice, the experts stated that patients who experience BTH near the end of the 8-week ravulizumab treatment cycle may require a 6-week or 7-week dosing interval instead. Patients who were receiving ravulizumab more frequently than every 8 weeks were excluded from the study. The clinical experts noted that, while higher doses of eculizumab or more frequent dosing intervals may be indicated for a subset of patients, access to higher intensity dosing is not available in all jurisdictions in Canada.
The direct evidence was limited to a single RCT comparing iptacopan versus C5 inhibitors. However, pegcetacoplan is the key comparator for adults with PNH who have an inadequate response to, or are intolerant of, a C5 inhibitor. The absence of head-to-head studies comparing iptacopan with pegcetacoplan represents an evidence gap.
GRADE Summary of Findings and Certainty of the Evidence
Methods for Assessing the Certainty of the Evidence
For pivotal studies and RCTs identified in the sponsor’s systematic review, GRADE was used to assess the certainty of the evidence for outcomes considered most relevant to inform CDA-AMC’s expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group:32,33
High certainty: We are very confident that the true effect lies close to that of the estimate of the effect.
Moderate certainty: We are moderately confident in the effect estimate — the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. We use the word “likely” for evidence of moderate certainty (e.g., “X intervention likely results in Y outcome”).
Low certainty: Our confidence in the effect estimate is limited — the true effect may be substantially different from the estimate of the effect. We use the word “may” for evidence of low certainty (e.g., “X intervention may result in Y outcome”).
Very low certainty: We have very little confidence in the effect estimate — the true effect is likely to be substantially different from the estimate of effect. We describe evidence of very low certainty as “very uncertain.”
Following the GRADE approach, evidence from RCTs started as high-certainty evidence and could be rated down for concerns related to study limitations (which refers to internal validity or risk of bias), indirectness, imprecision of effects, and publication bias.
When possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect; if this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., clinical importance is unclear). In all cases, the target of the certainty of evidence assessment was based on the point estimate and where it was located relative to the threshold for a clinically important effect (when a threshold was available) or to the null. The target of the certainty of evidence assessment (presence or absence of an important effect) were based on thresholds identified in the literature (FACIT-F and EORTC QLQ-C30 Global Health Status), thresholds informed by the clinical experts consulted for this review (change from baseline in hemoglobin), or the presence or absence of any non-null effect (proportion of patients with an increase in hemoglobin levels of at least 20 g/L or with hemoglobin levels of at least 120 g/L; proportion who avoided transfusions, had BTHs, or experienced infections; and the change from baseline in ARC or LDH levels).
Results of GRADE Assessments
Table 2 presents the GRADE summary of findings for iptacopan versus C5 inhibitors eculizumab or ravulizumab.
Long-Term Extension Study
Contents of this section have been informed by materials submitted by the sponsor. The following have been summarized and validated by the CDA-AMC review team.
Description of Studies
One long-term extension study was submitted for review. The APPLY-PNH extension period was a 24-week, open-label treatment extension of the APPLY-PNH study, aiming to evaluate long-term efficacy and safety of iptacopan in adult patients with PNH who had residual anemia despite treatment with a C5 inhibitor. The extension period began after week 24 of the RTP and continued to week 48. The final analysis data cut-off date was March 6, 2023. After the extension period was completed, patients could enrol in an ongoing rollover extension program, which aims to further evaluate the long-term safety, tolerability, and efficacy of iptacopan. Results from the rollover study were not available when this review was conducted.
Populations
Patients were eligible to enrol in the extension period if they had completed the 24-week RTP of the APPLY-PNH study. Patients randomized to the iptacopan group could continue to the extension period if they were taking iptacopan at the week 24 visit and the investigator had determined they were benefiting from treatment. Patients randomized to the C5 inhibitor group were offered to switch to iptacopan on their week 24 visit and, if they agreed to switch, entered the extension period after receiving a last dose of C5 inhibitor therapy.
Interventions
Patients received iptacopan 200 mg twice daily orally. Patients randomized to the active comparator arm in the parent study were offered to switch to iptacopan on their week 24 visit, after receiving their last dose of C5 inhibitor treatment.
Outcomes
All end points included in the treatment extension period were defined as primary, with no secondary or exploratory end points. Primary efficacy variables included hematological response parameters, transfusion avoidance, hemoglobin, clinical BTH, LDH, ARC, FACIT-F scores, MAVE, patient-reported outcomes, C3 fragment deposition on RBCs and PNH clone size, and other PNH-related end points. In the final analysis, the absence of transfusion was not an integral component of the hematological response end points, in contrast to the week 24 primary efficacy analysis in which absence of transfusion between day 14 and day 168 was an end point component. Primary safety end points included adverse events, SAEs, safety laboratory parameters, and vital signs.
Statistical Analysis
No hypothesis-testing statistical analysis was planned. All descriptive statistics were for exploratory purposes, and no multiplicity adjustment was performed. For change from baseline outcomes, adjusted mean changes and differences were derived using an MMRM that included randomization strata, age (indicator variable ≥ 45 years), sex, treatment assigned in RTP, time point, baseline level, treatment by time point, and time point by baseline level. No formal estimand was defined for the ETP analyses. However, a treatment policy approach was used in the 24-week ETP for the intercurrent events (i.e., discontinuation of study medication, clinical BTH events, MAVEs, RBC transfusions). That is, efficacy was assessed regardless of the occurrence of intercurrent events, and all data were included in the analyses.
All analyses were conducted on observed available data. No multiple imputation test was implemented. For outcomes where a MMRM analysis was used, it was consistent with a missing-at-random approach.
Results
Patient Disposition
Patient disposition is summarized in Table 19. Of the 97 patients with PNH who completed the APPLY-PNH study on study treatment, 95 participants enrolled in the extension period study. One patient from the C5 inhibitor group did not enter the extension period due to investigator decision based on the patient’s clinical condition. Of the 95 patients enrolled, 94 completed treatment, with 1 patient discontinuing treatment because of pregnancy. This patient continued study assessments until the end of the extension period.
Exposure to Study Treatments
The mean duration of iptacopan treatment during the entire 48-week study was 275.4 days (SD = 83.44), with a median of 337.0 days (range, 141 to 355). The mean and median durations of exposure were 275.3 days (SD = 83.39) and 336.0 days (range, 141 to 355), respectively.
Table 19: Patient Disposition in the APPLY-PNH Extension Study
Patient disposition | Iptacopan (N = 62) | C5 inhibitor to iptacopan (N = 35) | Overall (N = 97) |
|---|---|---|---|
ETP enrolment, n (%) | |||
Entered ETP | 61 (98.4) | 34 (97.1) | 95 (97.9) |
Completed treatmenta | 60 (98.4) | 34 (100.0) | 94 (98.9) |
Completed treatment perioda | 61.0 (100.0) | 34 (100.0) | 95 (100.0) |
Discontinued treatment, n (%)a | |||
Pregnancy | 1 (1.6) | 0 | 1 (1.1) |
Discontinued treatment period | 0 | 0 | 0 |
Analysis sets, n (%) | |||
FAS | 62 (100.0) | 35 (100.0) | 97 (100.0) |
Combined FAS | 62 (100.0) | 34 (97.1) | 96 (99.0) |
Combined SAF | 62 (100.0) | 34 (97.1) | 96 (99.0) |
ETP = extension treatment period; FAS = full analysis set; SAF = safety analysis set.
aPercentage calculated based on number of patients who entered the ETP.
Source: APPLY-PNH Clinical Study Report.36 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Concomitant medications were defined in the same manner as in the randomized period. Over both treatment periods, nearly all participants received concomitant medications between day 1 and the last treatment dose. The most common medications (taken by at least 20% of patients) were folic acid and derivatives (69.8%), viral vaccines (36.5%), proton pump inhibitors and anilides (27.1% each), fluoroquinolones (22.9%), and vitamin D and analogues (20.8%).
Rescue medication was permitted to treat serious complications such as BTH or thrombosis, and 2 patients (2.1%) received rescue medication during the extension period. Three patients (3.1%) reported posttreatment medication after discontinuation of iptacopan throughout the 48-week study, defined as any medication with start date after the end of treatment in the APPLY-PNH parent trial. Two patients who discontinued because of pregnancy reinitiated eculizumab, and the third received deferasirox. One patient who did not enter the rollover extension period due to myelodysplastic syndrome tapered down iptacopan after extension period completion and switched back to eculizumab.
Efficacy
Clinically meaningful benefits of iptacopan demonstrated in the 24-week APPLY-PNH study were sustained during the 24-week treatment extension period, and patients who switched from a C5 inhibitor to iptacopan (C5 inhibitor group) in the extension exhibited similar treatment responses as observed in iptacopan patients during the RTP. A summary of efficacy results from the treatment extension period is provided in Table 20.
Table 20: Summary of 48-Week Clinical Outcomes From ETP of APPLY-PNH Study
Time point | Outcome measure | Iptacopan (N = 62) | C5 inhibitor to iptacopan (N = 34)a |
|---|---|---|---|
Increase in hemoglobin ≥ 20 g/L from baseline, irrespective of RBC transfusionsb | |||
Day 168 | Number of responding patients, n (% of evaluable patients) | 55 (90.2) | NA |
Day 336 | Number of responding patients, n (% of evaluable patients) | 51 (86.4) | 21 (72.4) |
Hemoglobin ≥ 120 g/L irrespective of RBC transfusionsb | |||
Day 168 | Number of responding patients, n (% of evaluable patients) | 42 (68.9) | NA |
Day 336 | Number of responding patients, n (% of evaluable patients) | 40 (67.8) | 17 (58.6) |
Transfusion avoidanceb | |||
Day 1 to day 336 | Number of responding patients 1 or more days from start of iptacopan treatment, n (%) | 51 (82.3) | 31 (91.2)c |
Day 14 to day 336 | Number of responding patients 14 or more days from start of iptacopan treatment, n (%) | 57 (91.9) | 32 (94.1)d |
Change from baseline in hemoglobin (g/L)e | |||
Day 168 | Number of patients, n | 61 | 34 |
Adjusted mean change from baseline (95% CI) | 37.6 (34.5 to 40.7) | 3.4 (–0.7 to 7.5) | |
Day 336 | Number of patients, n | 59 | 30 |
Adjusted mean change from baseline (95% CI) | 33.5 (30.4 to 36.7) | 33.6 (29.4 to 37.9) | |
Day 336 versus day 168 | Adjusted mean difference in change from baseline (95% CI) | –4.1 (–8.0 to –0.1) | 30.2 (24.9 to 35.6) |
Change from baseline in FACIT-F scorese | |||
Day 168 | Number of patients, n | 60 | 30 |
Adjusted mean change from baseline (95% CI) | 9.07 (6.94 to 11.19) | 0.17 (–2.73 to 3.07) | |
Day 336 | Number of patients, n | 55 | 26 |
Adjusted mean change from baseline (95% CI) | 9.80 (8.04 to 11.56) | 10.96 (8.58 to 13.34) | |
Day 336 versus day 168 | Adjusted mean difference in change from baseline (95% CI) | 0.73 (–1.14 to 2.60) | 10.79 (8.12 to 13.47) |
Change from baseline in ARC (109/L)e | |||
Day 168 | Number of patients, n | 58 | 34 |
Adjusted mean change from baseline (95% CI) | –116.19 | –5.66 | |
Day 336 | Number of patients, n | 57 | 30 |
Adjusted mean change from baseline (95% CI) | –106.26 | –107.95 | |
Day 336 versus day 168 | Adjusted mean difference in change from baseline (95% CI) | 9.92 | –102.29 |
Ratio to baseline in log-transformed LDH (U/L)e | |||
Day 168 | Number of patients, n | 61 | 35 |
Geometric adjusted mean (95% CI) | 0.99 (0.91 to 1.09) | 1.00 (0.89 to 1.13) | |
Day 336 | Number of patients, n | 61 | 33 |
Geometric adjusted mean (95% CI) | 1.11 (1.02 to 1.22) | 0.99 (0.88 to 1.11) | |
Day 336 versus day 168 | Geometric adjusted mean ratio (95% CI) | 1.12 (1.00 to 1.25) | 0.99 (0.85 to 1.15) |
Occurrence of clinical BTHb | |||
Day 336 | Number of patients with an event since iptacopan initiation, n (%) | 6 (9.7) | 1 (2.9) |
Overall adjusted annualized rate of events since iptacopan initiation (95% CI) | 0.11 (0.05 to 0.23) | ||
Occurrence of MAVEsb | |||
Day 336 | Number of patients with an event since iptacopan initiation, n (%) | 2 (3.2) | 1 (2.9) |
Overall adjusted annualized rate of events (95% CI) | 0.04 (0.01 to 0.13) | ||
ARC = absolute reticulocyte count; BTH = breakthrough hemolysis; CI = confidence interval; FACIT-F = Functional Assessment of Chronic Illness Therapy – Fatigue; ETP = extension treatment period; LDH = lactate dehydrogenase; MAVE = major adverse vascular event; NA = not applicable; RBC = red blood cell.
aC5 inhibitor to iptacopan group was evaluated from day 169 to day 336 (i.e., the length of iptacopan exposure), unless otherwise indicated.
bCombined FAS.
cEvaluated from day 169 to day 336.
dEvaluated from day 182 to day 336.
eFull analysis set.
Source: APPLY-PNH Clinical Study Report.36 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Hemoglobin Levels
After 336 days of iptacopan treatment, 86.4% of patients who were randomized to iptacopan had at least a 20 g/L increase in hemoglobin from baseline and 67.8% had sustained hemoglobin levels of at least 120 g/L, both irrespective of RBC transfusions. For patients who switched from a C5 inhibitor to iptacopan, 72.4% had at least a 20 g/L increase in hemoglobin from baseline after 168 days of iptacopan treatment. Additionally, 58.6% had sustained hemoglobin levels of at least 120 g/L at day 168 of iptacopan treatment.
At day 336, the adjusted mean hemoglobin change from baseline was 33.5 g/L (95% CI, 30.4 to 36.7) for patients randomized to iptacopan and 33.6 g/L (95% C, 29.4 to 37.9) for the former C5 inhibitor group. Between day 336 and day 168, the adjusted mean difference in change from baseline was –4.1 g/L (95% CI, –8.0 to –0.1) for the iptacopan randomized group and 30.2 g/L (95% CI, 24.9 to 35.6) for the former C5 inhibitor group.
Transfusion Avoidance
Between day 1 and day 336, 82.3% of patients randomized to iptacopan did not require RBC transfusions. Beyond day 14 of treatment, 91.9% of patients in this group did not require transfusions. For those who switched from a C5 inhibitor to iptacopan, 94.1% of patients did not require RBC transfusions after day 14 of iptacopan treatment during the 24-week extension period.
Eight patients (12.9%) in the iptacopan randomized group and 3 patients (8.8%) in the C5 inhibitor group received at least 1 transfusion while on iptacopan. Among patients who received transfusions, the mean number of transfusions per patient was 1.8 (SD = 1.16) in the iptacopan group and 5.3 (SD = 7.51) in the former C5 inhibitor group. The mean number of RBC units transfused to these patients was 2.9 (SD = 2.59) in the iptacopan group and 6.7 (SD = 8.96) in the former C5 inhibitor group. The median number of transfused RBC units per patient was 2.0 (range, 1 to 7) in the iptacopan group and 2.0 (range, 1 to 17) units in the former C5 inhibitor group.
Clinical BTH Events
During the treatment extension period, 4 patients in the iptacopan group and 1 patient who switched to iptacopan from a C5 inhibitor experienced 1 or more clinical BTH events. Across the entire 48-week study, there were 8 BTH events in 7 patients during treatment with iptacopan, with an adjusted annualized rate of BTH of 0.11 (95% CI, 0.05 to 0.23).
Change From Baseline in LDH
At day 336, the geometric adjusted mean ratio to baseline in LDH was 1.11 (95% CI, 1.02 to 1.22) for the iptacopan group and 0.99 (95% CI, 0.88 to 1.11) for the former C5 inhibitor group. Between day 336 and day 168, the geometric adjusted mean ratio was 1.12 (95% CI, 1.00 to 1.25) in the iptacopan randomized group and 0.99 (95% CI, 0.85 to 1.15) in the former C5 inhibitor group.
Change From Baseline in ARC
At day 336, the adjusted mean change from baseline in ARC was –106.26 × 109/L (95% CI, –117.57 to –94.96 × 109/L) for the iptacopan group and –107.95 × 109/L (95% CI, –123.18 to –92.73 × 109/L) for the former C5 inhibitor group. Between day 336 and day 168, the adjusted mean difference in change from baseline was 9.92 × 109/L (95% CI, –4.40 to 24.25 × 109/L) for the iptacopan group and –102.29 × 109/L (95% CI, –121.57 to 83.02 × 109/L) for the former C5 inhibitor group.
At baseline (i.e., before iptacopan treatment in both groups), the percentage of patients with ARCs within central laboratory normal reference range (13.5 × 109/L to 123 × 109/L) was lower in the iptacopan randomized group (19.4%) compared to those switching to iptacopan from a C5 inhibitor (32.4%). After 7 days of iptacopan treatment, normalization of ARCs was achieved by 80.6% of patients in the iptacopan group and was sustained in 80.6% of patients in this group until day 336. In the former C5 inhibitor group, normalization was achieved in 61.8% of patients after 7 days of treatment and 85.3% after 28 days and was consistently seen in 70.6% of participants until day 336.
Change From Baseline in FACIT-F Score
At day 336, the adjusted mean change from baseline in FACIT-F score was 9.80 points (95% CI, 8.04 to 11.56 points) for the iptacopan group and 10.96 points (95% CI, 8.58 to 13.34 points) for the former C5 inhibitor group. Between day 336 and day 168, the adjusted mean difference in change from baseline was 0.73 points (95% CI, –1.14 to 2.60 points) in the iptacopan group and 10.79 points (95% CI, 8.12 to 13.47 points) in the former C5 inhibitor group.
Change From Baseline in EORTC QLQ-C30 Score
At day 336, the mean EORTC QLQ-C30 score was 76.4 (SD = 15.11) for the iptacopan group and 74.4 (SD = 16.98) for the former C5 inhibitor group, with mean increases from baseline of 16.3 (SD = 17.99) and 15.2 (SD = 22.61), respectively.
Harms
Refer to Table 21 for harms data that were reported during the 48-week APPLY-PNH study, including the RTP and the ETP.
Adverse Events
Most patients had at least 1 TEAE during the 48-week study, with comparable proportions between those randomized to iptacopan (93.5%) and all patients who received iptacopan (88.5%). Across all patients who received iptacopan, the most common TEAEs were COVID-19 (27.1%), headache (14.6%), diarrhea (12.5%), nasopharyngitis (12.5%), and nausea (11.5%).
Adverse events of special interest in the extension period were comparable to those during the 24-week RTP. In total, 41.9% of patients randomized to iptacopan and 36.5% of all iptacopan recipients experienced at least 1 adverse event of special interest.
Serious Adverse Events
Overall, 13 of 96 patients (13.5%) who received iptacopan experienced SAEs, including 9 of 62 patients (14.5%) who were initially randomized to iptacopan and 4 of 34 patients (11.8%) who switched to iptacopan from a C5 inhibitor in the treatment extension period. No deaths were reported in the study.
Withdrawals Due to Adverse Events
No patients discontinued the study or iptacopan treatment due to adverse events.
Mortality
No patients died during the 24-week treatment extension period.
Notable Harms
Across the entire 48-week study, 3 patients experienced MAVEs during iptacopan treatment. Two patients randomized to iptacopan experienced a transient ischemic attack, 1 patient during the RTP and 1 during the treatment extension period. One patient randomized to the former C5 inhibitor group experienced severe portal vein thrombosis (Budd-Chiari syndrome) after switching to iptacopan in the treatment extension period. None of the events were considered related to study treatment by the investigator, and no action was taken regarding iptacopan treatment. Overall, there were 3 MAVEs in 3 patients during iptacopan treatment, with an adjusted annualized MAVE rate of 0.04 (95% CI, 0.01 to 0.13).
Across the entire 48-week study, 3 patients (3.1%) experienced infection caused by encapsulated bacteria. During the treatment extension period, 1 patient experienced a nonserious adverse event of bilateral otitis media.
Table 21: Summary of Harms Results for the RTP and Extension Period of the APPLY-PNH Study (48 Weeks)
Adverse events | Randomized to Iptacopan (N = 62) | All Iptacopan recipients (N = 96) |
|---|---|---|
Most common TEAEs (≥ 5% of patients), n (%) | ||
Patients with ≥ 1 adverse event | 58 (93.5) | 85 (88.5) |
COVID-19 | 18 (29.0) | 26 (27.1) |
Headache | 12 (19.4) | 14 (14.6) |
Diarrhea | 10 (16.1) | 12 (12.5) |
Nasopharyngitis | 9 (14.5) | 12 (12.5) |
Nausea | 8 (12.9) | 11 (11.5) |
Arthralgia | 7 (11.3) | 7 (7.3) |
Urinary tract infection | 7 (11.3) | 7 (7.3) |
BTH | 6 (9.7) | 7 (7.3) |
Blood LDH increased | 6 (9.7) | 6 (6.3) |
Abdominal pain | 5 (8.1) | 5 (5.2) |
Hypertension | 4 (6.5) | 6 (6.3) |
Pyrexia | 4 (6.5) | 5 (5.2) |
Dizziness | 4 (6.5) | 4 (4.2) |
Insomnia | 4 (6.5) | 4 (4.2) |
Thrombocytopenia | 3 (4.8) | 5 (5.2) |
Vomiting | 2 (3.2) | 5 (5.2) |
SAEs, n (%) | ||
Patients with ≥ 1 SAE | 9 (14.5) | 13 (13.5) |
Description | Basal cell carcinoma, COVID-19, cellulitis, myelodysplastic syndrome, ovarian cyst, pyelonephritis, rhabdomyolysis, septic shock, sinus node dysfunction, transient ischemic attack, urinary tract infection (pseudomonal) | Basal cell carcinoma, COVID-19, cellulitis, myelodysplastic syndrome, ovarian cyst, pyelonephritis, rhabdomyolysis, septic shock, sinus node dysfunction, transient ischemic attack, urinary tract infection (pseudomonal), pancreatolithiasis, platelet count decrease, portal vein thrombosis, systemic infection |
AEs leading to treatment discontinuation, n (%) | ||
Patients discontinuing treatment | 0 | 0 |
Deaths, n (%) | ||
Patient deaths | 0 | 0 |
Adverse events of special interest, n (%) | ||
Patients with ≥ 1 AESI | 26 (41.9) | 35 (36.5) |
Infections caused by encapsulated bacteria, n (%) | ||
Bronchitis due to Haemophilus | 1 (1.6) | 1 (1.0) |
Otitis media | 0 | 1 (1.0) |
Urinary tract infection pseudomonala | 1 (1.6) | 1 (1.0) |
Serious or severe infection, n (%) | ||
Any serious or severe infection | 4 (6.5) | 5 (5.2) |
COVID-19 | 1 (1.6) | 1 (1.0) |
Cellulitis | 1 (1.6) | 1 (1.0) |
Pyelonephritis | 1 (1.6) | 1 (1.0) |
Septic shock | 1 (1.6) | 1 (1.0) |
Systemic infection | 0 | 1 (1.0) |
Hemolysis in patients with PNH, n (%) | ||
Any PNH hemolysis | 13 (21.0) | 15 (15.6) |
BTH | 6 (9.7) | 7 (7.3) |
Blood LDH increased | 6 (9.7) | 6 (6.3) |
Jaundice | 1 (1.6) | 2 (2.1) |
EVH | 1 (1.6) | 1 (1.0) |
Blood creatinine increased | 1 (1.6) | 1 (1.0) |
Hemoglobin decreased | 1 (1.6) | 1 (1.0) |
Hemoglobinuria | 1 (1.6) | 1 (1.0) |
Hemolysis | 1 (1.6) | 1 (1.0) |
Ocular icterus | 1 (1.6) | 1 (1.0) |
Thrombosis in patients with PNH, n (%) | ||
Any thrombosis in patients with PNH | 2 (3.2) | 3 (3.1) |
Transient ischemic attack | 2 (3.2) | 2 (2.1) |
Hemiparesis | 1 (1.6) | 1 (1.0) |
Portal vein thrombosis | 0 | 1 (1.0) |
Hypersensitivity, n (%) | 7 (11.3) | 8 (8.3) |
Decreased platelets, n (%) | 4 (6.5) | 9 (9.4) |
Thyroid changes, n (%) | 1 (1.6) | 1 (1.0) |
AE = adverse event; AESI = adverse event of special interest; BTH = breakthrough hemolysis; EVH = extravascular hemolysis; LDH = lactate dehydrogenase; PNH = paroxysmal nocturnal hemoglobinuria; RTP = randomized treatment period; SAE = serious adverse event; TEAE = treatment-emergent adverse event.
aUrinary tract infection pseudomonal was also classified as a serious or severe infection.
Source: APPLY-PNH Clinical Study Report.36 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Critical Appraisal
Internal Validity
The APPLY-PNH extension period was designed as an open-label extension to assess long-term efficacy and safety of iptacopan in the treatment of adult patients with PNH. This open-label design could bias the magnitude of treatment effect for subjective efficacy outcomes and reporting of safety parameters as a result of unblinded exposure to the study medication during the treatment period. The direction and magnitude of these potential bias remains unclear. Statistical hypothesis testing was not part of the design, and there was no active comparator or placebo arm.
External Validity
The extension study consisted of patients who took part in the RTP, and, therefore, it is reasonable to expect that the same strengths and limitations related to generalizability apply to the extension period. Given that patients needed to complete the RTP before enrolling, the treatment extension population is inherently enriched and introduces some selection bias for responders. Additionally, a lack of study sites in Canada limits the ability to generalize these findings to patients with PNH living in Canada.
Indirect Evidence
Contents of this section have been informed by materials submitted by the sponsor. The following have been summarized and validated by the review team.
Objectives for the Summary of Indirect Evidence
While the pivotal trial for iptacopan was active-controlled (versus the C5 inhibitors eculizumab or ravulizumab), it did not include the most relevant comparator, pegcetacoplan, for adults with PNH who have an inadequate response or intolerance to C5 inhibitors. To address this gap in the evidence, the sponsor submitted an ITC comparing the safety and efficacy of iptacopan to pegcetacoplan.37 Data from the ITC was also used to inform the pharmacoeconomic model.
Description of Indirect Comparison
The ITC was conducted to derive comparative efficacy and safety estimates for iptacopan versus pegcetacoplan for the treatment of adult patients with PNH who have residual anemia despite treatment with a C5 inhibitor. The ITC was based on a systematic literature review, which was used to identify relevant studies. Comparative effects were estimated using MAIC methods.37,38
ITC Design
Objectives
The objective of the unanchored MAIC was to derive comparative efficacy and safety estimates for iptacopan versus pegcetacoplan for the treatment of adult patients with PNH who have residual anemia despite treatment with a C5 inhibitor.
Table 22: Study Selection Criteria and Methods for ITC Submitted by the Sponsor
Characteristics | Criteria for indirect comparison |
|---|---|
Population | Adult (aged ≥ 18 years) patients with PNH who have residual anemia despite treatment with a C5 inhibitor |
Intervention | Iptacopan (LNP023) |
Comparators |
|
Outcomes |
|
Study designs |
|
Publication characteristics | Original publications, including conference abstracts |
Exclusion criteria |
|
Databases searched | EMBASE, MEDLINE (Daily, In-Process and Other Nonindexed citations, and e-pub ahead-of-print), and Cochrane library (CENTRAL and Cochrane Database of Systematic Reviews) |
Selection process | Title and abstract and full-text screening was performed by 2 independent reviewers according to prespecified eligibility criteria. Any conflicts regarding eligibility were resolved through discussion between the 2 reviewers, and, where necessary, arbitration was provided by a third senior reviewer. |
Data-extraction process | Data from the included publications were extracted by 1 reviewer into standardized, piloted data-extraction tables, and the information was quality checked by a second independent reviewer. |
Quality assessment | Quality assessment of the included studies was performed using the Cochrane Risk of Bias 2 tool. Quality assessment was performed by 1 reviewer and quality checked by a second independent reviewer. |
FACIT-F = Functional Assessment of Chronic Illness Therapy – Fatigue; LDH = lactate dehydrogenase; NMA = network meta-analysis; PNH = paroxysmal nocturnal hemoglobinuria; RCT = randomized controlled trial; SAE = serious adverse event; SLR = systematic literature review.
Source: Sponsor’s ITC Technical Report,37 Sponsor’s Systematic Literature Review Report.38 Details included in the table are from the sponsor’s Summary of Clinical Evidence.35
Study Selection Methods
The sponsor conducted a systematic literature review to identify studies that assessed the efficacy and safety of iptacopan and other comparators in the treatment of adults with PNH. The study selection criteria for the systematic review were broader than that those for the ITC with respect to the population, comparators, outcomes, and study design. Table 22 shows the study selection criteria for the ITC. In addition to the criteria in Table 22, the systematic review also included adults with PNH who had not received prior treatment with a C5 inhibitor, and comparators crovalimab, danicopan, pozelimab, vemircopan, and cemdisiran, as well as 4 treatments in development. Additional efficacy and safety outcomes related to hemoglobin levels, IVH, EVH, BTH, transfusion frequency, remission, mortality, and harms were included in the systematic review. The systematic literature review also included nonrandomized and real-world evidence studies, in addition to the study designs listed in Table 22.
The database search was conducted on April 20, 2023, and handsearching of relevant conferences (over the past 3 years), health technology assessment agencies, reference lists of included studies and relevant systematic reviews or ITCs, and clinical trial registries was conducted from May 22 to May 25, 2023. Studies were screened independently by 2 reviewers, with data extraction and risk of bias assessment conducted by 1 reviewer and quality checked by a second reviewer. The Cochrane Risk of Bias 2 tool was used to conduct the quality assessment of the included studies.
The electronic search identified 1,356 clinical citations across the searched databases. After removal of duplicates and title and abstract screening, 321 citations were included for full-text screening, during which a further 221 publications were excluded. Handsearching yielded 9 additional relevant publications, resulting in a total of 109 publications. Of the 109 studies included in the review, 4 investigated relevant interventions (iptacopan, pegcetacoplan, danicopan plus eculizumab) in patients who have residual anemia despite treatment with a C5 inhibitor. Only studies reporting data for currently approved treatments (i.e., pegcetacoplan, eculizumab, and ravulizumab) were considered for inclusion in the ITC; therefore, only the PEGASUS study (pegcetacoplan versus eculizumab), and the APPLY-PNH study were included in the ITC.
ITC Analysis Methods
The sponsor conducted a feasibility assessment to determine whether the studies were sufficiently similar to conduct the ITC. The study design characteristics, eligibility criteria, treatment protocols, baseline characteristics, outcome definitions, and data availability were compared between the APPLY-PNH and PEGASUS trials. The sponsor stated that the moderate to substantial imbalances identified in the baseline characteristics between the APPLY-PNH and PEGASUS trials suggest the assumptions underpinning network meta-analysis (e.g., similarity of trials) were unlikely to be valid and that other methods were needed to derive robust ITCs. Given the sparse network, consisting of 2 RCTs, meta-regression was not feasible. Due to the heterogeneity in study design, eligibility criteria, baseline characteristics, and outcomes observed between the trials, the sponsor concluded that a MAIC was an appropriate method to estimate the efficacy and safety of iptacopan compared to pegcetacoplan.
The sponsor stated that, although both trials included C5 inhibitors as an active comparator (eculizumab or ravulizumab for the APPLY-PNH trial and eculizumab for the PEGASUS trial), the control arms differed between trials and were not comparable. In the PEGASUS trial, all patients received eculizumab in combination with pegcetacoplan during the 4-week run-in period, after which patients were randomized to receive monotherapy with either pegcetacoplan or eculizumab. The sponsor concluded that the presence of combination therapy in the run-in period was a major difference in study design. The sponsor also noted that the rate of transfusion avoidance after pegcetacoplan withdrawal decreased from 26% within 12 months before study entry to 15% within 16 weeks after pegcetacoplan withdrawal. According to the sponsor, this suggested that the impact of C5 inhibitors on transfusion and other anemia-related end points could be reduced following pegcetacoplan treatment. Given the differences in the control arms between studies, and the implications of these differences for clinical end points pertinent to the ITC, the sponsor determined that an anchored MAIC was inappropriate as an a priori analysis approach. As a result, the base-case analysis was an unanchored MAIC, where single-arm data from different trials were used to estimate comparative effects for iptacopan versus pegcetacoplan (Table 23). A secondary unanchored MAIC comparing eculizumab or ravulizumab (APPLY-PNH trial) to eculizumab (PEGASUS trial) was used to assess the assumption that the C5 inhibitor control arms from the PEGASUS and APPLY-PNH trials were different and therefore could not be used to anchor the comparison between iptacopan and pegcetacoplan. The sponsor also conducted an anchored MAIC as alternate analysis.
Based on the feasibility assessment, change from baseline in hemoglobin (including and excluding posttransfusion hemoglobin data), transfusion avoidance, change from baseline in LDH, change from baseline in FACIT-F, and SAEs were selected as outcomes for the unanchored MAIC (Table 23). For the iptacopan data, the definitions and timing of each outcome and the handling of intercurrent events were adjusted to mimic the outcomes in the PEGASUS trial (Table 24). The sponsor stated that it was not possible to assess the proportion of patients with at least a 20 g/L increase in hemoglobin or the proportion with hemoglobin greater than or equal to 120 g/L due to the lack of these data from the PEGASUS study.
For the unanchored MAIC, the inclusion and exclusion criteria were first aligned between the APPLY-PNH and PEGASUS studies, where possible. Individual patients from the APPLY-PNH study were removed from the IPD if they did not satisfy the eligibility criteria used in the PEGASUS study. Patients in the iptacopan group who did not meet eligibility criteria for reticulocyte count, platelet count, and BMI were excluded (Table 25). It was not possible to match based on some eligibility criteria, as the PEGASUS study included a broader population (i.e., definition of anemia at baseline [hemoglobin 105 g/L in the PEGASUS study versus < 100 g/L in the APPLY-PNH study], or history of transfusions [the criteria specified that approximately 40% of the APPLY-PNH population had at least 1 transfusion in the past 6 months; there were no entry criteria related to transfusion history in the PEGASUS study]).
After completing the matching step of the unanchored MAIC, remaining patients from the APPLY-PNH study were reweighted using ranked treatment-effect modifiers that were available from both trials. The sponsor stated that, before the APPLY-PNH database lock, core variables were identified and ranked by order of importance. No further details were available in the sponsor’s ITC Technical Report on how these variables were selected and ranked. In order of ranked importance, the 6 clinical variables identified were baseline hemoglobin, sex (female), transfusion-free 12 months before baseline, baseline reticulocytes, baseline LDH, and age. The ranked importance of these 6 variables was used to prioritize adjustments. For the primary analyses, patients in the iptacopan arm were reweighted via entropy balancing so that their proportions or both their means and SD matched those reported in the PEGASUS study. According to the sponsor, MAIC weights derived using entropy balancing have been shown to be mathematically identical (up to a normalizing constant) to MAIC weights derived by method-of-moments approach, as described in the UK National Institute for Health and Care Excellence (NICE) Evidence Synthesis Technical Summary Document 18.70,71 The sponsor defined 6 scenarios where the fully adjusted model included all 6 variables, and each subsequent model dropped the lowest-ranked model. The sponsor stated that the base-case analysis was selected after examining the performance of each scenario, while also considering the number of clinical variables used to obtain MAIC weights. The performance and suitability of each scenario were assessed based on the ESS, distribution of patient weights, and balance of baseline characteristics between treatment groups, before and after adjustment. The ESS can be interpreted as the number of patients in a sample after weighting, and a low ESS indicates large differences in patient weights due to imbalances in patient populations before reweighting. For the distribution of weights, extreme patient weights can indicate uncertainty in the relative treatment effects. Balance of characteristics was assessed based on the standardized mean difference (SMD) of each prognostic or effect modifier, with a SMD greater than or equal to 0.2 considered indicative of a potentially important imbalance between comparisons.72 The sponsor conducted 2 sensitivity analyses, described in Table 23.
Treatment outcomes were then compared between balanced trial populations. Estimates of the comparative efficacy and safety of iptacopan versus pegcetacoplan were derived as the difference between an estimate of the outcome of interest for iptacopan based on matched and adjusted IPD from the APPLY-PNH study (to align with patients in the PEGASUS study), and the estimated outcome for pegcetacoplan based on published summary-level data from the PEGASUS study.
For unanchored MAICs of continuous outcomes (i.e., change from baseline hemoglobin, LDH, and FACIT-F), estimates were derived for the APPLY-PNH study by approximating the model used in the PEGASUS clinical trial. Treatment-effect estimates for the iptacopan and the C5 inhibitor arm of the APPLY-PNH study were derived by fitting an MMRM to the reweighted IPD from the APPLY-PNH study. Treatment, baseline covariate, stratification variables (transfusion history, platelet count), study visit, and study visit times treatment were used as variables in the model to emulate the model-adjustment variables specified in the PEGASUS study. The treatment effect between iptacopan and pegcetacoplan was derived as the difference between the adjusted mean change from baseline for iptacopan and the published adjusted mean of pegcetacoplan.
For unanchored MAICs of binary outcomes (i.e., transfusion avoidance and SAEs), estimates were derived with an intercept-only logistic regression model fitted to the reweighted IPD for the APPLY-PNH study. Models were fit separately for patients randomized to iptacopan and for those randomized to the ravulizumab or eculizumab control arm in the APPLY-PNH study. The estimated intercept was used as an estimate of the weighted log odds of remaining transfusion-free or experiencing an SAE. An estimate of the log OR for iptacopan versus pegcetacoplan was derived as the difference between the weighted log odds for iptacopan and the estimated log odds for pegcetacoplan, based on published transfusion events and SAEs from the PEGASUS study. Point estimates and 95% CIs were transformed to the OR scale for reporting. Results were reported using point estimates (mean difference, OR) and 95% CIs for each analysis. The sponsor stated that nominal significance was ascertained using a 2-tailed P value of less than 0.05. All analyses were conducted using R, largely adapted from code presented in the NICE Evidence Synthesis Technical Summary Document Series.73
Table 23: ITC Analysis Methods
Methods | Description |
|---|---|
Analysis methods | Unanchored MAIC |
Data sources | Iptacopan: APPLY-PNH (N = 62) IPD Pegcetacoplan: PEGASUS (N = 41) summary-level data |
Outcomes | Continuous outcomes:
Binary outcomes:
|
Time points | Time points were aligned based on the first dose of study drug received: APPLY-PNH study versus PEGASUS study:
|
Model estimation | Continuous outcomes:
Binary outcomes:
|
MAIC weighting covariates | MAIC weighting method: entropy balancing Base case:
Fully adjusted case:
|
MAIC performance and balance assessment | Performance and suitability of analyses was assessed based on the following criteria:
|
Primary analysis | Matching: Removed patients from APPLY-PNH study who would not have been eligible for PEGASUS study based on eligibility criteria for reticulocyte count at screening, platelet count at screening, and BMI Adjusting: APPLY-PNH data were weighted to match the published means and SDs reported for the PEGASUS study. The exception to this was baseline LDH for which only the means were adjusted; the MAIC weights could not be derived when adjusting for both mean and SD of baseline LDH due to nonconvergence. MAIC scenarios and adjustment variables:
|
Sensitivity analyses | Sensitivity analysis 1: Matching: Same approach as the primary analysis Adjusting: APPLY-PNH data were weighted to match only the means (rather than means and SD) of continuous covariates reported for PEGASUS study. MAIC scenarios and adjustment variables:
Sensitivity analysis 2: Matching: Removed patients from APPLY-PNH study who would not have been eligible for PEGASUS study based on eligibility criteria for platelet count at screening Adjusting: Same approach as the primary analysis MAIC scenarios and adjustment variables:
|
ARC = absolute reticulocyte count; BMI = body mass index; ESS = effective sample size; FACIT-F = Functional Assessment of Chronic Illness Therapy – Fatigue; IPD = individual patient-level data; ITC = indirect treatment comparison; LDH = lactate dehydrogenase; MAIC = matching-adjusted indirect comparison; MMRM = mixed model for repeated measures; SAE = serious adverse event; SD = standard deviation; SMD = standardized mean difference.
Source: Sponsor’s ITC Technical Report.37 Details included in the table are from the sponsor’s Summary of Clinical Evidence.35
Table 24: Comparison of Outcomes in APPLY-PNH and PEGASUS Studies
Detail | PEGASUS | APPLY-PNH | Method used in ITC to analyze APPLY-PNH data |
|---|---|---|---|
Change from baseline in hemoglobin | |||
Definition of end point in trial | Change in hemoglobin from baseline (day 0a, before run-in) to week 20 (day 140a) | Change in hemoglobin from baseline (day 0) as a mean of visits between days 126 and 168 | Change in hemoglobin from baseline (day 0) to day 140 |
Definition of baseline | Average of screening values recorded before run-in dosing (day 0a), including local and central laboratory values | The mean of the 2 measurements taken during screening. In patients who received a transfusion after the first confirmatory measurement, the baseline is the first measurement. | PEGASUS definition was used to analyze iptacopan data |
Handling of intercurrent events | Values observed after transfusion or treatment discontinuation are set to missing (while on treatment strategy; censored for transfusion). All values used regardless of transfusion (treatment strategy; uncensored for transfusion). | Values observed within 30 days of transfusion or after treatment discontinuation are set to missing and imputed according to hypothetical estimand (as if participant had not received any transfusion). | PEGASUS methods used to analyze iptacopan data. |
Statistical model | MMRM Covariates: treatment, baseline hemoglobin, stratification variables (transfusion history, platelet count), study visit, study visit × treatment (excluding values observed during the run-in period) | MMRM Covariates: treatment, baseline hemoglobin, age, sex, stratification variables (transfusion-dependent, prior C5 inhibitor treatment), study visit, study visit × treatment, study visit × baseline hemoglobin | Model used in PEGASUS study was used to analyze data. |
Transfusion avoidance | |||
Definition of end point in trial | Avoidance of transfusion from day 29 (after run-in)a to day 140a | Avoidance of transfusion and not meeting the criteria for administration of packed RBC transfusions from day 14 to day 168 | Avoidance of transfusion from day 29 to day 140 |
End point includes occurrence of transfusion | Transfusions occurring during the run-in period were not counted | Transfusions occurring during the first 14 days of the RTP were not counted | Transfusions occurring in first 28 days of the RTP were not included to align with PEGASUS end point measurement |
End point includes protocol-defined criteria for transfusion requirement | No | Patients who met the criteria for transfusion,b but did not receive a transfusion were considered to have received transfusion. | Patients who avoided transfusion but met the APPLY-PNH–defined criteria for administration of packed RBC transfusions were analyzed as transfusion avoidant. |
Treatment discontinuation | Patients without transfusion who withdrew before day 140a were considered as having a transfusion. | None | Patients without transfusion who withdrew before day 140a were considered as having a transfusion. |
Change in LDH | |||
Definition of end point in trial | Change in LDH from baseline (before run-in, day 0a) to week 20a (day 140a) | Percent change from baseline in LDH levels as a mean of visits between days 126 and 168 | Change in LDH from baseline (day 0) to day 140 |
Definition of baseline | Average of screening values recorded before run-in dosing (day 0a), including local and central laboratory values | The last result obtained at or before start of study treatment day 1 | PEGASUS definition was used to analyze data. |
Handling of intercurrent events | Values observed after transfusion or treatment discontinuation were set to missing (while on treatment strategy). | Data analyzed regardless of the occurrence of intercurrent events, such as treatment discontinuation, breakthrough hemolysis events, and MAVEs. All data are included in the analysis. | On treatment strategy (PEGASUS definition) was used to analyze iptacopan data. |
Statistical model | Same model and covariates as change in hemoglobin outcome (excluding all LDH values during run-in) | Same model and covariates as change in hemoglobin outcome | PEGASUS definition was used to analyze iptacopan data. |
Change in FACIT-F | |||
Definition of end point in trial | Change in FACIT-F scores from baseline (day 0a) to week 20a (day 140a) | Change in FACIT-F scores from baseline (day 0) as a mean of visits between days 126 and 168 | Change in FACIT-F scores from baseline (day 0) to day 140 |
Definition of baseline | Recorded value at run-in dosing (day 0a) | The mean of the first assessment before day 1 and the day 1 value | Value at day 0 |
Handling of intercurrent events | Values observed after transfusion or treatment discontinuation are set to missing (while on treatment strategy). | Data analyzed regardless of the occurrence of intercurrent events, such as treatment discontinuation, breakthrough hemolysis events, and MAVEs. All data are included in the analysis. | On treatment strategy (PEGASUS definition) was used to analyze iptacopan data. |
Statistical model | Same model and covariates as change in hemoglobin outcome (excluding all LDH values during run-in) | Same model and covariates as change in hemoglobin outcome | PEGASUS definition was used to analyze iptacopan data |
SAE | |||
Definition of end point in trial | Proportion of patients who experienced a SAE by week 16 (day 29 to 140a) of the RTP, not counting events during the run-in period | Proportion of patients who experienced a serious adverse event by week 24 (day 0 to day 168) of the RTP | Proportion of patients who experienced a serious adverse event from day 29 to day 140 of the RTP |
FACIT-F = Functional Assessment of Chronic Illness Therapy – Fatigue; ITC = indirect treatment comparison; LDH = lactate dehydrogenase; MAVE = major adverse vascular event; MMRM = mixed model for repeated measures; RBC = red blood cell; RCP = randomized control period; RTP = randomized treatment period; SAE = serious adverse event.
aIn the PEGASUS study, the start of the run-in period was day –28 (when patients initiated their run-in combination dose of pegcetacoplan and eculizumab), and the start and end of the RTP (i.e., pegcetacoplan or eculizumab monotherapy) was day 0 and day 112, respectively. The time points were relabelled as trial-defined time plus 28 days, so that the start of the run-in period was indicated as day 0,.and the RTP was day 29 to day 140 (in total 20 weeks).
bAPPLY-PNH protocol-defined criteria for transfusion were as follows: hemoglobin between > 70 and ≤ 90 g/L with signs or symptoms of sufficient severity to warrant a transfusion, or hemoglobin ≤ 70 g/L, regardless of presence of clinical signs and/or symptoms.
Source: Sponsor’s ITC Technical Report.37
Table 25: Overview of Key Eligibility Criteria in APPLY-PNH and PEGASUS Studies
Key eligibility criteria | APPLY-PNH | PEGASUS | Similarity |
|---|---|---|---|
Age | ≥ 18 years | ≥ 18 years | Same criteria |
Platelet count at screening | ≥ 30 × 109/L (30,000/mm3) | > 50,000/mm3 | APPLY-PNH criteria are broader and can thus be aligned to PEGASUS criteria. |
Reticulocytes at screening | ≥ 100 × 109/L | > 1 × ULN (30 to 120 × 109/L) | Criteria differ; patients in APPLY-PNH study with reticulocytes < 1 × 120 × 109/L were removed for ITC analysis. |
Neutrophil count | ≥ 500/mm3 | > 500/mm3 | APPLY-PNH criteria are broader and can thus be aligned to PEGASUS criteria. |
History of transfusion | Approximately 40% of patients had at least 1 RBC transfusion in the 6 months before randomization | No restriction | Criteria differ and cannot be aligned. |
Body weight | No restriction | No restriction | — |
BMI (kg/m2) | No restriction | < 35.0 kg/m2 | APPLY-PNH criteria are broader and thus can be aligned to PEGASUS criteria. |
Hemoglobin | < 100 g/L | < 105 g/L | Criteria differ and cannot be aligned. |
BMI = body mass index; ITC = indirect treatment comparison; RBC = red blood cell; ULN = upper limit of normal.
Source: Sponsor’s ITC Technical Report.37
Results of ITC
Summary of Included Studies
Data from 2 trials were used to inform the unanchored MAIC: aggregate data from the pegcetacoplan group (N = 41) of the PEGASUS trial, and IPD from the iptacopan group (N = 62) of the APPLY-PNH study. Both studies were randomized, active-controlled, open-label studies in adults with PNH and residual anemia despite C5 inhibitor therapy (Table 26). The APPLY-PNH study required patients to receive a stable regimen of ravulizumab or eculizumab for at least 6 months before screening, while the PEGASUS study required a stable regimen of eculizumab for at least 3 months. The APPLY-PNH study had a longer randomized controlled period than the PEGASUS study (24 weeks versus 16 weeks). A key difference between trials was that PEGASUS study had a 4-week run-in period to minimize the risk of hemolysis due to abrupt eculizumab treatment discontinuation. All patients received both pegcetacoplan and eculizumab as a combination therapy for 4 weeks, followed by randomization to eculizumab or pegcetacoplan monotherapy. In contrast, the APPLY-PNH study did not have a run-in period, with patients randomized to switch to iptacopan monotherapy or to continue receiving a C5 inhibitor. According to the authors of the systematic literature review, the PEGASUS study was rated as having a low risk of bias (results from the APPLY-PNH study were not available when the systematic review was conducted).
Differences were noted between trials in the definition of outcomes, the timing of outcome assessment, and the statistical analysis, including the handling of intercurrent events (Table 24). Where possible, the iptacopan data were analyzed using similar methods as used in the PEGASUS study. Any outcome values (LDH, hemoglobin, or FACIT-F) or events (SAE, transfusions) that occurred during the run-in period of the PEGASUS trial were excluded from the analyses. Thus, the same exclusions were applied when the iptacopan data were analyzed for the unanchored MAIC. The follow-up time for iptacopan patients was truncated at week 20, and only outcome data up to day 140 were included, to match the total pegcetacoplan treatment time in the PEGASUS study. Adjustments were made for how baseline values were calculated for the change in hemoglobin, LDH, and FACIT-F, to be consistent with the PEGASUS study. Most analyses were censored at transfusion and any data after the discontinuation were set to missing. The exception was the change from baseline in hemoglobin, with treatment effects analyzed both uncensored and censored at transfusion. It was unclear how other intercurrent events of BTH or MAVE were handled in the MAIC. For the transfusion avoidance outcomes, the PEGASUS study did not have any protocol-defined criteria to administer RBCs, whereas the APPLY-PNH study had set criteria based on hemoglobin values and the presence of anemia-related symptoms. In the APPLY-PNH study, any patients who received a transfusion or met the criteria for transfusion (regardless of whether RBCs were administered) were marked has having a transfusion. For the MAIC, only those patients who actually received a transfusion were analyzed as transfusion-dependent, regardless of the presence of symptoms or anemia.
In the first step of the unanchored MAIC, any patients from the iptacopan IPD who did not meet the inclusion criteria for the PEGASUS trial were excluded. In total, 8 of 62 patients were removed from the iptacopan dataset, based on their reticulocyte count or platelet count at screening, or on their BMI. At the second step, iptacopan patients were weighted in an attempt to balance the key baseline characteristics in the iptacopan group to the mean and SD of the PEGASUS summary data for the pegcetacoplan group. The sponsor defined 6 key effect modifiers that were used to weight the iptacopan IPD. Although 6 variables were selected, the base-case model included only 3 potential effect modifiers: baseline hemoglobin per PEGASUS definition, sex, and proportion transfusion-free within 12 months before baseline. Table 27 includes a summary of key characteristics of the patients in the iptacopan and pegcetacoplan groups, before and after weighting. The sponsor noted that, after matching and weighting, there were differences between the iptacopan and pegcetacoplan groups for several baseline characteristics. These included large differences (SMD > 0.2) in the proportion of patients with at least 4 transfusions in past 12 months, race, history of aplastic anemia, FACIT-F score, duration of C5 inhibitor therapy, time since diagnosis, platelet count, and BMI. The ESS was 16, which was 30% of the unadjusted population (N = 54). After weighting, the base-case iptacopan group and pegcetacoplan group included 66% female patients with a mean hemoglobin at baseline of 87.0 g/L (SD = 11), of which 24% were transfusion-free in the 12 months before the study. The mean age was 50.2 years (SD = 16.3) and 49.1 years (SD = 14.6) and the mean LDH level was 257.5 U/L (SD = 97.6) and 260.9 U/L (SD = 54.4) in the pegcetacoplan and iptacopan groups, respectively.
Table 26: Assessment of Homogeneity for ITC
Characteristics | Description and handling of potential effect modifiers |
|---|---|
Trial eligibility criteria | Both studies enrolled adults with PNH who had residual anemia despite C5 inhibitor therapy, but the studies differed in the definition of anemia and prior therapy:
Other eligibility criteria are listed in Table 25, with the methods used in the MAIC to minimize the differences. |
Baseline characteristics | The sponsor detected large differences (SMD ≥ 0.2) between the patients enrolled in the PEGASUS and APPLY-PNH studies for the following characteristics:
Moderate differences were noted for 5 other variables. Table 27 includes a summary of the baseline characteristics before and after matching and adjustment. |
Treatment | All patients had received C5 inhibitor therapy before enrolment but received differed treatment regimens during the randomized study period:
|
Statistical analysis | The sponsor attempted to match the analysis methods used for the iptacopan data to be consistent with those used in the PEGASUS trial. Continuous outcomes for iptacopan were analyzed using an MMRM with similar handling of intercurrent events and excluding outcome data during the first 4 weeks of therapy, as per the PEGASUS study. Data after intercurrent events of transfusion or discontinuation were set to missing (consistent with the on-treatment estimand censored at transfusion that was used in the PEGASUS trial). It is unclear how intercurrent events of MAVE or BTH were addressed. The change in hemoglobin outcome also included an analysis that was not censored at transfusion. |
Definitions of end points | The sponsor attempted to match the outcomes used for the iptacopan data analyses to be consistent with the PEGASUS trial. Details of the differences and methods used to match the PEGASUS outcome definitions are described in Table 24. Notable differences were:
|
Timing of end point evaluation | The MAIC attempted to align the treatment duration and assessed outcomes for iptacopan at 20 weeks, to be more consistent with PEGASUS trial (4 weeks run-in plus 16-week randomized treatment period). In the PEGASUS study, transfusion avoidance and SAE outcomes excluded data reported during the run-in period. Thus, the same time frame was adopted for the iptacopan analyses, and any data reported during the first 4 weeks of treatment were excluded. |
Clinical trial setting | Both trials included patients from the US, Europe, and Asia. The PEGASUS study included patients from Canada. |
Study design | Phase III, open-label, RCTs (only single-arm data from each trial were used in the MAIC) |
BTH = breakthrough hemolysis; ITC = indirect treatment comparison; LDH = lactate dehydrogenase; MAIC = matching-adjusted indirect comparison; MAVE = major adverse vascular event; MMRM = mixed model repeated measures; PNH = paroxysmal nocturnal hematuria; RBC = red blood cell; RCT = randomized controlled trial; SAE = serious adverse event; SMD = standardized mean difference.
Source: Sponsor’s ITC Technical Report,37 sponsor’s Systematic Literature Review Report.38 Details included in the table are from the sponsor’s Summary of Clinical Evidence.35
Results
The evidence network represented by the APPLY-PNH and PEGASUS studies is shown in Figure 4.
The results of the base-case unanchored MAIC were based on 41 patients who received pegcetacoplan and an ESS of 16 patients from the iptacopan group. The estimated mean difference in the change from baseline in hemoglobin levels was 13.1 g/L (95% CI, 5.2 to 21.0 g/L) censored for transfusion, and 10.5 g/L (95% CI, 4.3 to 16.7 g/L) uncensored at transfusion, favouring iptacopan versus pegcetacoplan (Table 28). From the unanchored MAIC, an estimated 85.4% of patients in the pegcetacoplan group and 98.2% of patients in iptacopan group avoided transfusion, with an OR of 9.17 (95% CI, 1.59 to 52.89) favouring iptacopan (Table 29).
Table 27: Comparison of Characteristics Between Iptacopan and Pegcetacoplan, Unmatched and Unadjusted, Matched and Unadjusted, and Base-Case MAIC Scenarios
Characteristics | Pegcetacoplan (PEGASUS) | Iptacopan (APPLY-PNH) | |||||
|---|---|---|---|---|---|---|---|
Unmatched and unadjusted | Matched and unadjusteda | Matched and adjusted (base-case MAICb) | |||||
N = 41 | N = 62 | SMD | N = 54 | SMD | ESSc = 16 | SMD | |
Hemoglobin per PEGASUS definitiond (g/L); mean (SD) | 87 (11) | 89 (7) | 0.186 | 88 (7) | 0.146 | 87 (11) | 0.000 |
Sex, female; n (%) | 27 (65.9) | 43 (69.4) | 0.075 | 37 (68.5) | 0.057 | 27.1 (66.0) | 0.003 |
% of patients transfusion-free within 12 months prior; n (%) | 10 (24.4) | 25 (40.3) | 0.346 | 22 (40.7) | 0.354 | 9.9 (24.0) | 0.008 |
Reticulocytes (109/L), blood at screening; mean (SD) | 217.5 (75.0) | 204.0 (84.1) | 0.169 | 210.7 (84.1) | 0.086 | 211.7 (79.3) | 0.075 |
LDH (U/L); mean (SD) | 257.5 (97.6) | 269.1 (70.1) | 0.137 | 263.5 (71.5) | 0.070 | 260.9 (54.4) | 0.044 |
Age; mean (SD) | 50.2 (16.3) | 51.7 (16.9) | 0.091 | 51.7 (16.6) | 0.092 | 49.1 (14.6) | 0.068 |
BMI (kg/m2); mean (SD) | 26.7 (4.3) | 24.9 (5.0) | 0.385 | 24.5 (4.3) | 0.523 | 24.8 (4.2) | 0.455 |
Platelet count (109/L) at screening; mean (SD) | 166.6 (98.3) | 160.9 (55.9) | 0.071 | 167.4 (55.1) | 0.010 | 145.6 (63.4) | 0.254 |
Time since diagnosis (years); mean (SD) | 8.7 (7.4) | 11.9 (9.8) | 0.362 | 11.9 (9.6) | 0.372 | 11.4 (7.3) | 0.369 |
Duration of C5 inhibitor treatment (years); mean (SD) | 5.5 (3.9) | 3.8 (3.6) | 0.454 | 3.9 (3.7) | 0.430 | 5.5 (4.0) | 0.003 |
Duration of eculizumab treatment (years); mean (SD) | 5.5 (3.9) | 4.8 (4.0) | 0.184 | 4.8 (4.2) | 0.168 | 6.6 (4.0) | 0.284 |
FACIT-F score; mean (SD) | 32.2 (11.4) | 34.7 (9.8) | 0.234 | 35.1 (10.1) | 0.274 | 35.1 (10.5) | 0.263 |
Hemoglobin per trial definitionsd (g/L); mean (SD) | 87 (11) | 89 (7) | 0.246 | 89 (7) | 0.215 | 88 (12) | 0.048 |
History of aplastic anemia; n (%) | 11 (26.8) | 9 (14.5) | 0.308 | 8 (14.8) | 0.299 | 5.1 (12.5) | 0.367 |
≥ 4 transfusions of packed RBCs transfused in 12 months prior; n (%) | 21 (51.2) | 16 (25.8) | 0.541 | 15 (27.8) | 0.494 | 9.0 (22.0) | 0.638 |
Race, white; n (%) | 24 (58.5) | 48 (77.4) | 0.413 | 42 (77.8) | 0.422 | 35 (85.2) | 0.621 |
History of MAVE, n (%) | NR | 12 (19.4) | NA | 11 (20.4) | NA | 6.1 (14.8) | NA |
Monocyte size, % | NR | NA | NA | NA | NA | NA | NA |
Granulocyte size, % | NR | NA | NA | NA | NA | NA | NA |
BMI = body mass index; ESS = effective sample size; FACIT-F = Functional Assessment of Chronic Illness Therapy – Fatigue; LDH = lactate dehydrogenase; MAIC = matching-adjusted indirect comparison; MAVE = major adverse vascular event; NA = not available; NR = not reported; RBC = red blood cell; SD = standard deviation; SMD = standardized mean difference.
aMatched and unadjusted analysis removes patients to align with the PEGASUS study based on eligibility criteria for reticulocyte count at screening, platelet count at screening, and BMI. Eight patients were removed from the APPLY-PNH iptacopan dataset.
bBase-case MAIC removes patients to align with the PEGASUS study based on eligibility criteria for reticulocyte count at screening, platelet count at screening, and BMI; adjusting for residual imbalances in baseline hemoglobin per PEGASUS definition (mean and SD), sex, and proportion transfusion-free within 12 months before baseline.
cESS was derived from weights used in the primary analysis.
dBaseline hemoglobin was calculated as an average of values recorded before run-in, dosing including local and central laboratory values for the PEGASUS study. For the APPLY-PNH study, baseline hemoglobin was calculated as the mean of the 2 measurements taken during screening, except for patients who received a transfusion after the first confirmatory measurement; in that case, the baseline was the first measurement.
Note: The sponsor defined small difference as SMD ≤ 0.1; moderate difference as 0.1 > SMD ≤ 0.2; substantial difference as SMD > 0.2.72
Source: Sponsor’s ITC Technical Report.37
Table 28: Summary of Unanchored MAIC Results for Change From Baseline Hemoglobin
Outcomes | Censored at transfusion | Uncensored at transfusion | ||
|---|---|---|---|---|
Pegcetacoplan (PEGASUS) | Iptacopan | Pegcetacoplan (PEGASUS) | Iptacopan | |
Change from baseline hemoglobin (g/L) per trial definitionsa | ||||
Sample size (N) | 41 | 62 | 41 | 62 |
Mean change from baseline (95% CI) | 23.7 (16.6 to 30.8)b | 36.3 (33.4 to 39.3) | 26.6 (21.7 to 31.5)b | 36.3 (33.4 to 39.2) |
Change from baseline hemoglobin (g/L) per PEGASUS definition (day 140) | ||||
Unmatched and unadjusted | ||||
Sample size (N) | 41 | 62 | 41 | 62 |
Mean change from baseline (95%) | 23.7 (16.6 to 30.8)b | 33.1 (30.0 to 36.2) | 26.6 (21.7 to 31.5)b | 33.5 (30.4 to 36.5) |
Mean difference (95% CI)c; P value (iptacopan versus pegcetacoplan) | — | 9.4 (1.7 to 11.7) P = 0.017 | — | 6.9 (1.1 to 12.6) P = 0.020 |
Matched and unadjustedd | ||||
Sample size (N) | 41 | 54 | 41 | 54 |
Mean change from baseline (95%) | 23.7 (16.6 to 30.8)b | 33.5 (30.0 to 36.9) | 26.6 (21.7 to 31.5)b | 33.9 (30.5 to 37.3) |
Mean difference (95% CI)c; P value (iptacopan versus pegcetacoplan) | — | 9.8 (1.9 to 17.6) P = 0.015 | — | 7.3 (1.4 to 13.3) P = 0.016 |
Matched and adjusted (base casee)f | ||||
ESS after matching and adjusting | 41 | 16 | 41 | 16 |
Mean change from baseline (95% CI) | 23.7 (16.6 to 30.8)b | 36.8 (33.3 to 40.4) | 26.6 (21.7 to 31.5)b | 37.1 (33.3 to 40.9) |
Mean difference (95% CI)c; P value (iptacopan versus pegcetacoplan) | — | 13.1 (5.2 to 21.0) P < 0.001 | — | 10.5 (4.3 to 16.7) P < 0.001 |
CI = confidence interval; ESS = effective sample size; MAIC = matching-adjusted indirect comparison.
aBased on day 140 in the PEGASUS study (study day terminology aligned with APPLY-PNH study) and the mean of visits between day 126 and day 168 for the APPLY-PNH study.
b95% CIs calculated using adjusted mean ± 1.96 standard error, as reported in Hillmen et al. (2021).56
cMean difference > 0 implies a more favourable change from baseline in hemoglobin for iptacopan versus pegcetacoplan.
dMatched and unadjusted analysis removes patients to align with the PEGASUS study based on eligibility criteria for reticulocyte count at screening, platelet count at screening, and BMI. Eight patients were censored from the APPLY-PNH iptacopan dataset.
eThe base-case MAIC censored APPLY-PNH data to remove patients not eligible for the PEGASUS study based on reticulocyte count at screening, platelet count at screening, and BMI, and used matching-adjustment for residual imbalances in baseline hemoglobin per PEGASUS definition, sex, and proportion transfusion-free within 12 months before baseline.
fPrimary analysis adjusts for the means and SDs of continuous characteristics for MAIC analysis.
Note: Bold values indicate the 95% CI excluded the null value (0.0 for mean differences), which corresponds to a 2-tailed P value < 0.05.
Source: Sponsor’s ITC Technical Report.37 Details included in the table are from the sponsor’s Summary of Clinical Evidence.35
The mean difference in the change from baseline in LDH levels was 36.68 U/L (95% CI, –62.54 to 135.89) for iptacopan versus pegcetacoplan (Table 30). For the change from baseline in FACIT-F score, the unanchored MAIC estimated a mean difference of –2.32 points (95% CI, –6.34 to 1.70 points) for iptacopan versus pegcetacoplan (Table 31).
The unanchored MAIC estimated 17.1% and 4.8% of patients in the pegcetacoplan and iptacopan groups, respectively, would experience an SAE, with an OR of 0.24 (95% CI, 0.06 to 0.98), favouring iptacopan (Table 32).
Figure 4: ITC Evidence Network of Included Studies
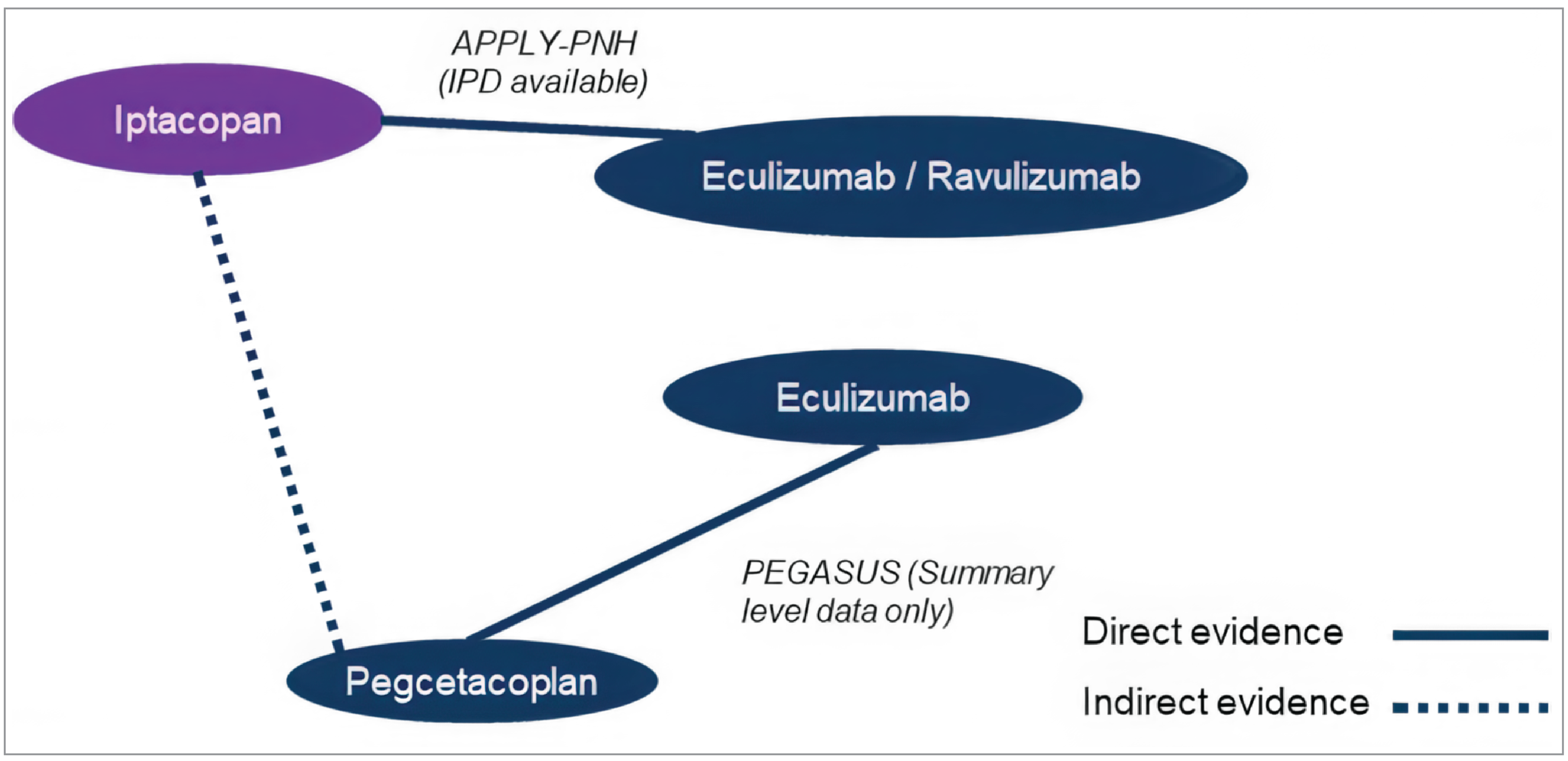
IPD = individual patient-level data; ITC = indirect treatment comparison.
Source: Sponsor’s ITC Technical Report.37
Table 29: Summary of Unanchored MAIC Results for Transfusion Avoidance
Outcomes | Pegcetacoplan (PEGASUS) | Iptacopan |
|---|---|---|
Transfusion avoidance per trial-specific definitiona | ||
Sample size, N | 41 | 62 |
Number transfusion-free, n (%) | 35 (85.4) | 59 (95.2) |
Transfusion avoidance per PEGASUS definitiona | ||
Unmatched and unadjusted | ||
Sample size (N) | 41 | 62 |
Percentage transfusion-free | 85.4 | 96.8 |
OR (95% CI)b; P value (iptacopan versus pegcetacoplan) | — | 5.14 (0.98 to 26.88) P = 0.052 |
Matched and unadjustedc | ||
Sample size (N) | 41 | 54 |
Percentage transfusion-free | 85.4 | 96.3 |
OR (95% CI)b; P value (iptacopan versus pegcetacoplan) | — | 4.46 (0.85 to 23.36) P = 0.077 |
Matched and adjusted (base cased)e | ||
ESS after matching and adjusting | 41 | 16 |
Percentage transfusion-free | 85.4 | 98.2 |
OR (95% CI)b; P value (iptacopan versus pegcetacoplan) | — | 9.17 (1.59 to 52.89) P = 0.013 |
CI = confidence interval; ESS = effective sample size; MAIC = matching-adjusted indirect comparison; OR = odds ratio.
aBased on day 29 to day 140 in the PEGASUS study and day 14 to day 168 for the APPLY-PNH study.
bOR > 1 implies a greater probability of remaining transfusion-free for iptacopan versus pegcetacoplan.
cMatched and unadjusted analysis removes patients to align with the PEGASUS study based on eligibility criteria for reticulocyte count at screening, platelet count at screening, and BMI. Eight patients were removed from the APPLY-PNH iptacopan dataset.
dBase-case MAIC censored APPLY-PNH data to remove patients not eligible for the PEGASUS study based on reticulocyte count at screening, platelet count at screening, and BMI and used matching-adjustment for residual imbalances in baseline hemoglobin per PEGASUS definition, sex, and proportion transfusion-free within 12 months before baseline.
ePrimary analysis adjusts for the means and SDs of continuous characteristics for MAIC analysis.
Note: Bolded values indicate statistical significance. Estimates were considered significant if the 95% CI excluded 1.0, which corresponds to a 2-tailed P value < 0.05.
Source: Sponsor’s ITC Technical Report.37 Details included in the table are from the sponsor’s Summary of Clinical Evidence.35
Table 30: Summary of Unanchored MAIC Results for Change From Baseline LDH
Outcomes | Pegcetacoplan (PEGASUS) | Iptacopan |
|---|---|---|
Percent change from baseline LDH (U/L) per trial definitions | ||
Sample size (N) | 41 | 62 |
Geometric adjusted mean (95% CI) | Not reported | 0.96 (0.90, 1.03) |
Change from baseline LDH (U/L) per PEGASUS definition (day 140) | ||
Unmatched and unadjusted | ||
Sample size (N) | 41 | 62 |
Mean change from baseline (95% CI) | –15.00 (–98.69 to 68.69)b | 16.01 (–22.64 to 54.66) |
Mean difference (95% CI)c; P value (iptacopan versus pegcetacoplan) | — | 31.01 (–61.17 to 123.19) P = 0.510 |
Matched and unadjustedd | ||
Sample size (N) | 41 | 54 |
Mean change from baseline (95% CI) | –15.00 (–98.69 to 68.69)b | 24.17 (–22.02 to 70.36) |
Mean difference (95% CI)c; P value (iptacopan versus pegcetacoplan) | — | 39.17 (–56.42 to 134.76) P = 0.422 |
Matched and adjusted (base casee)f | ||
ESS after matching and adjusting | 41 | 16 |
Mean change from baseline (95% CI) | –15.00 (–98.69 to 68.69)b | 21.68 (–31.61 to 74.97) |
Mean difference (95% CI)c; P value (iptacopan versus pegcetacoplan) | — | 36.68 (–62.54 to 135.89) P = 0.469 |
CI = confidence interval; ESS = effective sample size; LDH = lactate dehydrogenase; MAIC = matching-adjusted indirect comparison.
aBased on day 140 in the PEGASUS study (study day terminology aligned with APPLY-PNH study) and the mean of visits between day 126 and day 168 for the APPLY-PNH study.
b95% CIs calculated using adjusted mean ± 1.96 standard error, as reported in Hillmen et al. (2021).56
cMean difference < 0 implies a more favourable change from baseline in LDH for iptacopan versus pegcetacoplan.
dMatched and unadjusted analysis removes patients to align with the PEGASUS study based on eligibility criteria for reticulocyte count at screening, platelet count at screening, and BMI. Eight patients were removed from the APPLY-PNH iptacopan dataset.
eBase-case MAIC censored APPLY-PNH data to remove patients not eligible for the PEGASUS study based on reticulocyte count at screening, platelet count at screening, and BMI and used matching-adjustment for residual imbalances in baseline hemoglobin per PEGASUS definition, sex, and proportion transfusion-free within 12 months before baseline.
fPrimary analysis adjusts for the means and SDs of continuous characteristics for MAIC analysis.
Source: Sponsor’s ITC Technical Report.37 Details included in the table are from the sponsor’s Summary of Clinical Evidence.35
Critical Appraisal of ITC
The unanchored MAIC submitted by the sponsor had serious methodological issues that threaten the validity of the findings. Unanchored MAICs have a high risk of bias, as the underlying assumptions required for valid effect estimates are very difficult to meet.70 These methods require that all prognostic factors and effect modifiers (measured and unmeasured) be accounted for in the model, which may not be possible.70 Failure of this assumption leads to an unknown amount of bias in the effect estimates.70 The sponsor argued that other ITC methods with a lower risk of bias were not feasible due to sparse data available and the heterogeneity in the patient and study characteristics between the APPLY-PNH and PEGASUS trials. The CDA-AMC reviewer agreed there is significant heterogeneity between the studies and concluded that the MAIC methods used by the sponsor were not able to adequately control for these differences.
Table 31: Summary of Unanchored MAIC Results for Change From Baseline FACIT-F
Outcomes | Pegcetacoplan (PEGASUS) | Iptacopan |
|---|---|---|
Change from baseline FACIT-F per trial definitionsa | ||
Sample size (N) | 41 | 62 |
Mean change from baseline (95% CI) | 9.20 (6.06 to 12.34)b | 8.78 (6.80 to 10.76) |
Change from baseline FACIT-F per PEGASUS definition (day 140) | ||
Unmatched and unadjusted | ||
Sample size (N) | 41 | 62 |
Mean change from baseline (95% CI) | 9.20 (6.06 to 12.34)b | 7.94 (5.76 to 10.11) |
Mean difference (95% CI)c; P value (iptacopan versus pegcetacoplan) | — | –1.26 (–5.08 to 2.55) P = 0.516 |
Matched and unadjustedd | ||
Sample size (N) | 41 | 54 |
Mean change from baseline (95% CI) | 9.20 (6.06 to 12.34)b | 7.11 (4.66 to 9.57) |
Mean difference (95% CI)c; P value (iptacopan versus pegcetacoplan) | — | –2.09 (–6.07 to 1.90) P = 0.305 |
Matched and adjusted (base casee)f | ||
ESS after matching and adjusting | 41 | 16 |
Mean change from baseline (95% CI) | 9.20 (6.06 to 12.34)b | 6.88 (4.37 to 9.39) |
Mean difference (95% CI)c; P value (iptacopan versus pegcetacoplan) | — | –2.32 (–6.34 to 1.70) P = 0.257 |
CI = confidence interval; ESS = effective sample size; FACIT-F = Functional Assessment of Chronic Illness Therapy – Fatigue; MAIC = matching-adjusted indirect comparison.
aBased on day 140 in the PEGASUS study (study day terminology aligned with APPLY-PNH study) and the mean of visits between day 126 and day 168 for the APPLY-PNH study.
b95% CIs calculated using adjusted mean ± 1.96 standard error, as reported in Hillmen et al. (2021).56
cMean difference > 0 implies a more favourable change from baseline in FACIT-F for iptacopan versus pegcetacoplan.
dMatched and unadjusted analysis removes patients to align with the PEGASUS study based on eligibility criteria for reticulocyte count at screening, platelet count at screening, and BMI. Eight patients were removed from the APPLY-PNH iptacopan dataset.
eBase-case MAIC censored APPLY-PNH data to remove patients not eligible for the PEGASUS study based on reticulocyte count at screening, platelet count at screening, and BMI and used matching-adjustment for residual imbalances in baseline hemoglobin per PEGASUS definition, sex, and proportion transfusion-free within 12 months before baseline.
fPrimary analysis adjusts for the means and SDs of continuous characteristics for MAIC analysis.
Source: Sponsor’s ITC Technical Report.37 Details included in the table are from the sponsor’s Summary of Clinical Evidence.35
Table 32: Summary of Unanchored MAIC Results for SAEs
Outcomes | Pegcetacoplan (PEGASUS) | Iptacopan |
|---|---|---|
SAEs per trial-specific definitiona | ||
Sample size, N | 41 | 62 |
Number with SAE, n (%) | 7 (17.1) | 6 (9.7) |
SAEs per PEGASUS definitionb | ||
Unmatched and unadjusted | ||
Sample size (N) | 41 | 62 |
Percentage with SAE | 17.1% | 8.1% |
OR (95% CI)c; P value (iptacopan versus pegcetacoplan) | — | 0.43 (0.13 to 1.45) P = 0.172 |
Matched and unadjustedd | ||
Sample size (N) | 41 | 54 |
Percentage with SAE | 17.1 | 9.3 |
OR (95% CI)c; P value (iptacopan versus pegcetacoplan) | — | 0.50 (0.15 to 1.69) P = 0.263 |
Matched and adjusted (base casee)f | ||
ESS after matching and adjusting | 41 | 16 |
Percentage with SAE | 17.1 | 4.8 |
OR (95% CI)c; P value (iptacopan versus pegcetacoplan) | — | 0.24 (0.06 to 0.98) P = 0.047 |
CI = confidence interval; ESS = effective sample size; MAIC = matching-adjusted indirect comparison; OR = odds ratio; SAE = serious adverse event.
aBased on day 29 to 140 in the PEGASUS study and day 1 to day 168 for the APPLY-PNH study.
bBased on day 29 to 140 in the PEGASUS study.
cOR > 1 implies a greater probability of experiencing an SAE for iptacopan versus pegcetacoplan.
dMatched and unadjusted analysis removes patients to align with the PEGASUS study based on eligibility criteria for reticulocyte count at screening, platelet count at screening, and BMI. Eight patients were removed from the APPLY-PNH iptacopan dataset.
eBase-case MAIC censored APPLY-PNH data to remove patients not eligible for the PEGASUS study based on reticulocyte count at screening, platelet count at screening, and BMI and used matching-adjustment for residual imbalances in baseline hemoglobin per PEGASUS definition, sex, and proportion transfusion-free within 12 months before baseline.
fPrimary analysis adjusts for the means and SDs of continuous characteristics for MAIC analysis.
Note: Bolded values indicate statistical significance. Estimates were considered significant if the 95% CI excluded 1.0, which corresponds to a 2-tailed P value < 0.05.
Source: Sponsor’s ITC Technical Report.37 Details included in the table are from the sponsor’s Summary of Clinical Evidence.35
In the first step of the unanchored MAIC, patients from the iptacopan group were excluded if they did not meet the inclusion criteria of the PEGASUS study. Because some of the inclusion criteria in the APPLY-PNH study were more restrictive than those in the PEGASUS study, the iptacopan group could not be aligned according to the baseline hemoglobin threshold (105 g/L for the PEGASUS study versus 100 g/L for the APPLY-PNH study) or transfusion history. In the second stage of the MAIC, weights were applied to the iptacopan IPD to balance the iptacopan population with the aggregate baseline characteristics of the pegcetacoplan group. The ITC Technical Report did not provide a clear description of how the weighting variables were selected. Variables used for weighting should be identified and ranked based on clinical expertise and prior empirical evidence,70 not from the sample being analyzed. The sponsor identified 6 variables for weighting, but, due to the limited sample size, the base-case analysis weighted based on 3 factors only: baseline hemoglobin levels (using the PEGASUS definition), sex, and the proportion of patients who were transfusion-free within 12 months before baseline. The clinical experts consulted for this review identified C5 inhibitor dose, LDH levels (> 1.5 × ULN), and PNH-related kidney disease as important prognostic factors that were not used in the weighting process. After weighting was applied for the base-case analyses, differences in patient characteristics remained for other clinically relevant factors. This included large differences (SMD > 0.2) in the proportion of patients with at least 4 transfusions in past 12 months, race, history of aplastic anemia, FACIT-F score, duration of C5 inhibitor therapy, time since diagnosis, platelet count, and BMI. The ESS of the iptacopan group was 16, which was 30% of the unadjusted population (N = 54). The substantial reduction in the ESS suggests the patients were too dissimilar to warrant valid comparison. In addition, the skewed distribution of weights also suggests the populations were substantially different, and the presence of extreme weights may lead to unstable effect estimates. According to the clinical experts we consulted, the population enrolled in the PEGASUS trial were clinically different, with more severe PNH than those enrolled in the APPLY-PNH study. Thus, given the underlying differences between the 2 trials, and the imbalances in important prognostic factors that remained after matching and weighting, the treatment-effect estimates are considered unreliable, as the trial populations were too dissimilar to compare.
There were also differences between trials in how the outcomes were specified, but it appears there was sufficient data available to mimic the analyses conducted in the PEGASUS trial. No other major issues were identified with the statistical methods used to conduct the unanchored MAIC or the methods used to select relevant trials to inform the analyses.
Given the rarity of PNH, the CDA-AMC reviewer acknowledges the challenges in conducting an ITC. However, the small sample available (54 patients in the iptacopan group and 41 patients in the pegcetacoplan group) impacts the ability to create robust estimates of comparative effects. Given the limitations of the trial data, the follow-up duration in the unanchored MAIC was restricted to 20 weeks, which is short for a chronic condition. The unanchored MAIC did not analyze key outcomes used in the pharmacoeconomic model (i.e., proportion of patients with anemia [defined as hemoglobin < 105 g/L] and discontinuation due to any cause). Thus, there is no comparative evidence available for these end points.
Discussion
Summary of Available Evidence
The evidence available included one 24-week open-label, active-controlled RCT with a 24-week open-label, single-arm extension period, and 1 unanchored MAIC.
The APPLY-PNH study evaluated the efficacy and safety of oral iptacopan monotherapy in adults (aged ≥ 18 years) with PNH and residual anemia (hemoglobin < 100 g/L) despite treatment with a C5 inhibitor for at least 6 months before randomization. A total of 97 patients were randomized to iptacopan (200 mg twice daily) or to continue with the C5 inhibitor they were receiving before the study (eculizumab or ravulizumab). The coprimary outcomes were the proportion of patients with at least a 20 g/L increase in hemoglobin or who had sustained hemoglobin levels of 120 g/L in the absence of RBC transfusion. Other key outcomes included the mean change from baseline in hemoglobin, transfusion avoidance, fatigue (measured using the FACIT-F instrument), and BTH. After completion of the RTP, 95 patients continued in the extension period, and all patients received iptacopan 200 mg twice daily for up to 24 weeks.
The mean age of patients enrolled in the APPLY-PNH study was 51.7 years (SD = 16.9 years) in the iptacopan group (N = 62) and 49.8 years (SD = 16.7 years) in the C5 inhibitor group (N = 35). Most patients in the study were treated with eculizumab (65%) before the start of the study, with the minority receiving ravulizumab (35%). In the iptacopan and C5 inhibitor groups, respectively, the mean hemoglobin value at baseline was 89.3 g/L (SD = 7.0 g/L) and 88.5 g/L (SD = 8.9 g/L), 56.5% and 60.0% of patients had received an RBC transfusion in the past 6 months, and 19.4% and 28.6% of patients had a history of MAVE.
The objective of the unanchored MAIC was to estimate the comparative efficacy and safety of iptacopan versus pegcetacoplan for the treatment of adult patients with PNH who have residual anemia despite treatment with a C5 inhibitor.
Interpretation of Results
Efficacy
The APPLY-PNH study met both its primary outcomes and showed that iptacopan likely results in an increase in the proportion of patients with a hemoglobin increase of at least 20 g/L and sustained hemoglobin levels of 120 g/L in the absence of transfusion. The difference in marginal proportions of patients with at least a 20 g/L improvement in hemoglobin was 80.2% (95% CI, 71.2% to 87.6%), and for patients with hemoglobin levels of at least 120 g/L at 24 weeks was 67.0% (95% CI, 56.4% to 76.9%). The clinical experts we consulted agreed that these findings were clinically important, with both outcomes showing large differences favouring iptacopan versus C5 inhibitors. Clinically important differences were also detected for the mean change from baseline in hemoglobin (mean difference of 36.6 g/L) and the proportion of patients who avoided transfusion (difference in proportions 68.9%), which favoured the iptacopan group. The certainty of evidence for the aforementioned efficacy outcomes was rated as moderate, due to serious concerns regarding imprecision, as the small sample size raised concern that the true effect could be overestimated. Moreover, the baseline characteristics of the groups showed differences for some parameters, which suggested prognostic factors may not be balanced between groups. Also noteworthy was the differential frequency of missing data for the change from baseline in hemoglobin levels (17% in the C5 inhibitor group versus 0% in the iptacopan group), which is another potential source of bias. The FDA identified that the methods of imputing missing data had an impact on the magnitude of effects for the transfusion avoidance end point.67 The FDA sensitivity analyses, based only on patients who received transfusion (i.e., excluding patients who met the protocol-specified criteria for transfusion but did not receive a transfusion), reported a difference in proportions of patients avoiding transfusions of 49.5% (95% CI, 32.5% to 66.6%) for iptacopan versus C5 inhibitors.67 This more conservative estimate may be more applicable to clinical practice, given that set criteria to determine which patients receive transfusion are not used in practice.
BTH was reported by 2 patients (annualized adjusted rate 0.07%) in the iptacopan group and 6 patients in the C5 inhibitor group (0.67%) during the 24-week RTP, with an annualized adjusted rate difference of –0.60% (95% CI, 1.24 to 0.04). Over the 48-week treatment period, the annualized adjusted rate was 0.11% among patients receiving iptacopan. Given the small sample size and evidence of prognostic imbalances, the small number of events reported, and the relatively short duration of follow-up in the RTP, the rate of BTH for the iptacopan versus C5 inhibitor groups was rated as very low certainty.
The APPLY-PNH study also reported the change in LDH levels and ARC. Both are used in clinical practice to assess control of hemolysis. However, they are surrogate measures and may be affected by other clinical conditions, such as bone marrow failure syndromes. In general, the clinical experts we consulted indicated that maintenance of LDH levels within normal ranges or below 1.5 times ULN and a reduction in ARC levels would suggest maintained or improved control of IVH and EVH. The APPLY-PNH study reported an adjusted mean difference in the change from baseline in the ARC of –116 × 109 U/L (95% CI, –132.4 to –100.3), favouring the iptacopan group. In contrast, the percent reduction in the change from baseline in LDH levels had a 95% CI that crossed the null (1.1%; 95% –10.2% to 11.3%). In the absence of a threshold, the CDA-AMC review team judged that the point estimate of 1.1% and the 95% CI reflected little to no difference at 24 weeks. Both outcomes, however, were rated as low-certainty evidence due to serious imprecision and indirectness. As no MID was identified for these outcomes, the clinical relevance of the results is difficult to assess.
Two patient-reported outcomes were included in this report: the change from baseline in FACIT-F and EORTC QLQ-C30 Global Health Status. The results suggested that iptacopan may improve fatigue and HRQoL versus C5 inhibitors, and the differences were clinically relevant. However, in this open-label study, reporting of these subjective outcomes may have been influenced by patients’ and investigators’ expectations of treatment. According to the FDA review, the sponsor had not adequately addressed the potential impact of bias from knowledge of the treatment assignment on the results; thus, the FACIT-F data were difficult to interpret.67 In addition, there was a differential frequency of missing data between groups for both end points, which could bias the findings. The EORTC QLQ-C30 was an exploratory end point and not part of the planned statistical testing procedures; thus, it should be interpreted as supportive evidence. Due to these limitations, both outcomes were rated as low-certainty evidence.
There was no direct evidence for iptacopan versus the key comparator, pegcetacoplan. To address this gap in the evidence, the sponsor submitted an unanchored MAIC that assessed the safety and efficacy of iptacopan versus pegcetacoplan in patients with PNH and residual anemia despite therapy with C5 inhibitors. The unanchored MAIC was based on aggregate data from the pegcetacoplan group of the PEGASUS study and IPD for the iptacopan group in the APPLY-PNH study. After matching the groups based on the inclusion criteria for the PEGASUS study and weighting the iptacopan patients to balance the baseline characteristics with pegcetacoplan group averages, the comparative effects of the 2 treatments were estimated. The outcomes analyzed included the change from baseline in hemoglobin, FACIT-F, and LDH, as well as transfusion avoidance at week 20. While the unanchored MAIC attempted to control for some of the differences between groups, important differences remained. Moreover, unanchored MAICs have a high risk of bias, as the underlying assumptions required for valid effect estimates are difficult to meet. The low ESS of the iptacopan group (16 patients or 30% of the unweighted population) suggests the patients were too dissimilar to warrant valid comparison. In addition, the skewed distribution of weights also suggests the populations were substantially different, and the occurrence of extreme weights may lead to unstable effect estimates. Thus, given the underlying differences between the 2 trials and the imbalances in important prognostic factors that remained after matching and weighting, the treatment-effect estimates are considered too unreliable to draw any conclusions.
The clinical trial treatment duration was 24 weeks, which may be considered short for a chronic condition. The sponsor submitted additional efficacy data for 96 patients who entered the 24-week APPLY-PNH extension period. The results suggest the improvements in hemoglobin, transfusion avoidance, and FACIT-F scores were maintained up to 48 weeks. Moreover, patients who received a C5 inhibitor during the RTP and then switched to iptacopan during the extension phase showed treatment effects that were consistent with those observed among patients initially randomized to receive iptacopan. These data were limited by the lack of control group and open-label design. Although only 1 patient stopped iptacopan treatment early, 48-week data were missing for up to 24% of patients, depending on the outcome and prior therapy received.
Overall, the evidence was limited to 1 open-label RCT, which enrolled 97 patients with this rare condition. With regard to external validity, the trial excluded patients with comorbidities, such as those with evidence of bone marrow failure, or with significant cardiac, renal, or hepatic disease. The clinical experts noted that bone marrow failure and myelodysplastic syndrome are often present in patients with PNH and would not prevent them from receiving iptacopan. However, given the lack of data in these patients, the efficacy and safety of iptacopan are uncertain.
Data were lacking on key outcomes used to inform the pharmacoeconomic model. Neither the APPLY-PNH study nor the unanchored MAIC evaluated the proportion of patients with anemia, defined as patients with hemoglobin less than 105 g/L, or the all-cause discontinuation rate. Given the lack of evidence, no statements can be made on the impact of iptacopan on these end points.
Harms
In the APPLY-PNH study, adverse events were common, with 82% and 80% of patients reporting an adverse event in the iptacopan and C5 inhibitor groups, respectively, during the 24-week RTP and 88.5% of patients who received iptacopan over the total study period (RTP and extension). Across all patients who received iptacopan, the most common adverse events were COVID-19, headache, diarrhea, nasopharyngitis, and nausea.
SAEs were reported in 9.7% of patients in the iptacopan group and 14.3% of patients in the C5 inhibitor group during the RTP, and 13.5% of patients who received iptacopan at any time during 48-week treatment period. No deaths and no withdrawals due to adverse events occurred in either group over the total study duration. MAVEs occurred infrequently, with a reported adjusted annualized rate of 0.04% (95% CI, 0.01 to 0.13) among patients who received iptacopan over the 48-week trial. However, due to the low number of MAVE events, and the limited sample size and follow-up duration, the estimated frequency of MAVEs may be unreliable, according to the FDA review.67
Infections caused by encapsulated bacteria were identified as an important harm for this review. One patient in the iptacopan group (1.6%) and no patients in the C5 inhibitor group reported an infection with encapsulated bacteria, with a risk difference of 1.6% (95% CI, –1.5% to 4.8%) for iptacopan versus C5 inhibitors, which was rated as very-low-certainty evidence due to the small number of events, small sample size, potential prognostic imbalance, and the limited follow-up duration. During the extension period, 2 additional patients (2%) reported an infection by encapsulated bacteria. Serious infections were reported in 3.2% and 5.3% patients who received iptacopan over the RTP and 48-week total treatment duration, respectively. In the C5 inhibitor group, serious or severe infections were reported in 8.6% of patients during the RTP.
The safety evidence was limited due to the small sample size and short treatment duration from a single clinical trial. Thus, the ability to detect uncommon adverse events is low. According to the clinical experts we consulted, the study selected a patient population that had few comorbidities, in whom PNH was generally well managed. As the trial excluded more complex patients with comorbidities, the safety in these patients is unclear. No conclusions can be drawn concerning the comparative safety of iptacopan versus pegcetacoplan due to the limitations of the unanchored MAIC.
Conclusion
In adults with PNH and residual anemia despite treatment with C5 inhibitors, iptacopan likely results in more patients experiencing clinically important improvements in hemoglobin levels and normalization of hemoglobin levels (hemoglobin levels ≥ 120 g/L), and fewer patients who require transfusion, compared with C5 inhibitors. Based on the change from baseline in the FACIT-F questionnaire, iptacopan may improve fatigue symptoms compared with C5 inhibitors. The impact of iptacopan on the frequency of BTH and on the change in LDH levels and ARC was uncertain due to the limitations of the data and the absence of a threshold for a clinically important difference.
Data from the open-label, single-arm extension phase of the APPLY-PNH study suggests that improvements in hemoglobin levels, transfusion avoidance, and fatigue observed with iptacopan may be maintained up to 48 weeks.
Adverse events were common in both the iptacopan and C5 inhibitor groups in the APPLY-PNH study, but there were no deaths, and no patients stopped treatment due to adverse events. Infections due to encapsulated bacteria occurred infrequently, but no conclusions can be made concerning comparative frequency of events versus C5 inhibitors due to the small sample size, limited follow-up, and low number of events.
Overall, the direct comparative evidence was limited to 1 open-label RCT (the APPLY-PNH study), which randomized 97 patients with PNH and residual anemia to receive treatment with iptacopan or C5 inhibitors for 24 weeks. No direct evidence was available comparing iptacopan to pegcetacoplan, the key comparator for patients with PNH and EVH. To address the evidence gap, the sponsor submitted an unanchored MAIC that assessed the safety and efficacy of iptacopan versus pegcetacoplan. However, no conclusions can be drawn from the MAIC due to serious limitations that undermine the validity of the findings. There was significant heterogeneity between the 2 studies informing the MAIC, and imbalances in important prognostic factors remained after matching and weighting. As a result, the treatment-effect estimates are considered unreliable, as the trial populations were too dissimilar to compare.
References
1.Patriquin CJ, Kiss T, Caplan S, et al. How we treat paroxysmal nocturnal hemoglobinuria: A consensus statement of the Canadian PNH Network and review of the national registry. Eur J Haematol. 2019;102(1):36-52. doi: 10.1111/ejh.13176 PubMed
2.Brodsky RA. Paroxysmal nocturnal hemoglobinuria. Blood. 2014;124(18):2804-2811. doi: 10.1182/blood-2014-02-522128 PubMed
3.de Latour RP, Risitano AM. Hemolytic processes in paroxysmal nocturnal hemoglobinuria and its treatment: intravascular and extravascular hemolysis. Nature: Bone Marrow Transplantation (Collection). 2020. Accessed September 10. https://www.nature.com/collections/fichcejehg/introduction
4.Hill A, DeZern AE, Kinoshita T, Brodsky RA. Paroxysmal nocturnal haemoglobinuria. Nat Rev Dis Primers. 2017;3:17028. doi: 10.1038/nrdp.2017.28 PubMed
5.Notaro R, Sica M. C3-mediated extravascular hemolysis in PNH on eculizumab: Mechanism and clinical implications. Semin Hematol. 2018;55(3):130-135. doi: 10.1053/j.seminhematol.2018.05.014 PubMed
6.Berentsen S, Hill A, Hill QA, Tvedt THA, Michel M. Novel insights into the treatment of complement-mediated hemolytic anemias. Ther Adv Hematol. 2019;10:2040620719873321. doi: 10.1177/2040620719873321 PubMed
7.Schrezenmeier H, Roth A, Araten DJ, et al. Baseline clinical characteristics and disease burden in patients with paroxysmal nocturnal hemoglobinuria (PNH): updated analysis from the International PNH Registry. Ann Hematol. 2020;99(7):1505-1514. doi: 10.1007/s00277-020-04052-z PubMed
8.Brodsky RA, Young NS, Antonioli E, et al. Multicenter phase 3 study of the complement inhibitor eculizumab for the treatment of patients with paroxysmal nocturnal hemoglobinuria. Blood. 2008;111(4):1840-1847. doi: 10.1182/blood-2007-06-094136 PubMed
9.DeZern AE, Dorr D, Brodsky RA. Predictors of hemoglobin response to eculizumab therapy in paroxysmal nocturnal hemoglobinuria. Eur J Haematol. 2013;90(1):16-24. doi: 10.1111/ejh.12021 PubMed
10.Subías Hidalgo M, Martin Merinero H, López A, et al. Extravascular hemolysis and complement consumption in Paroxysmal Nocturnal Hemoglobinuria patients undergoing eculizumab treatment. Immunobiology. 2017;222(2):363-371. doi: 10.1016/j.imbio.2016.09.002 PubMed
11.Risitano AM, Marotta S, Ricci P, et al. Anti-complement treatment for paroxysmal nocturnal hemoglobinuria: Time for proximal complement inhibition? A position paper from the SAAWP of the EBMT. Front Immunol. 2019;10:1157. doi: 10.3389/fimmu.2019.01157 PubMed
12.Kulasekararaj AG, Brodsky RA, Nishimura JI, Patriquin CJ, Schrezenmeier H. The importance of terminal complement inhibition in paroxysmal nocturnal hemoglobinuria. Ther Adv Hematol. 2022;13:20406207221091046. doi: 10.1177/20406207221091046 PubMed
13.Anliker M, Schmidt CQ, Harder MJ, et al. Complement activation by human red blood cell antibodies: hemolytic potential of antibodies and efficacy of complement inhibitors assessed by a sensitive flow cytometric assay. Transfusion. 2018;58(12):2992-3002. doi: 10.1111/trf.14893 PubMed
14.Fattizzo B, Ireland R, Dunlop A, et al. Clinical and prognostic significance of small paroxysmal nocturnal hemoglobinuria clones in myelodysplastic syndrome and aplastic anemia. Leukemia. 2021;35(11):3223-3231. doi: 10.1038/s41375-021-01190-9 PubMed
15.Ueda Y, Obara N, Yonemura Y, et al. Effects of eculizumab treatment on quality of life in patients with paroxysmal nocturnal hemoglobinuria in Japan. Int J Hematol. 2018;107(6):656-665. doi: 10.1007/s12185-018-2409-3 PubMed
16.Kelly RJ, Hill A, Arnold LM, et al. Long-term treatment with eculizumab in paroxysmal nocturnal hemoglobinuria: sustained efficacy and improved survival. Blood. 2011;117(25):6786-6792. doi: 10.1182/blood-2011-02-333997 PubMed
17.Bektas M, Copley-Merriman C, Khan S, Sarda SP, Shammo JM. Paroxysmal nocturnal hemoglobinuria: patient journey and burden of disease. J Manag Care Spec Pharm. 2020;26(12-b Suppl):S8-S14. doi: 10.18553/jmcp.2020.26.12-b.s8
18.de Latour RP, Mary JY, Salanoubat C, et al. Paroxysmal nocturnal hemoglobinuria: natural history of disease subcategories. Blood. 2008;112(8):3099-3106. doi: 10.1182/blood-2008-01-133918 PubMed
19.Jalbert JJ, Chaudhari U, Zhang H, Weyne J, Shammo JM. Epidemiology of PNH and Real-World Treatment Patterns Following an Incident PNH Diagnosis in the US. Blood. 2019;134:3407. doi: 10.1182/blood-2019-125867
20.Hill A, Platts PJ, Smith A, et al. The incidence and prevalence of paroxysmal nocturnal hemoglobinuria (PNH) and survival of patients in Yorkshire. Blood. 2006;108(11):985. doi: 10.1182/blood.V108.11.985.985
21.Richards SJ, Painter D, Dickinson AJ, et al. The incidence and prevalence of patients with paroxysmal nocturnal haemoglobinuria and aplastic anaemia PNH syndrome: A retrospective analysis of the UK’s population-based haematological malignancy research network 2004-2018. Eur J Haematol. 2021;107(2):211-218. doi: 10.1111/ejh.13640 PubMed
22.Kulasekararaj A, Mellor J, Earl L, et al. PB2056: prevalence of clinically significant extravascular hemolysis in stable C5 inhibitor-treated patients with PNH and its association with disease control, quality of life and treatment satisfaction. Hemasphere. 2023;7(Suppl):e35238f0. doi: 10.1097/01.HS9.0000975024.35238.f0
23.CADTH. Reimbursement review: pegcetacoplan (Empaveli). Can J Health Technol. 2023;3(5):1-175. doi: 10.51731/cjht.2023.654
24.Kulasekararaj AG, Hill A, Rottinghaus ST, et al. Ravulizumab (ALXN1210) vs eculizumab in C5-inhibitor-experienced adult patients with PNH: the 302 study. Blood. 2019;133(6):540-549. doi: 10.1182/blood-2018-09-876805 PubMed
25.Alexion Pharma Canada Corp. Solaris (eculizumab): 10 mg/mL parenteral solution [product monograph]. January 28, 2009. Updated July 24, 2024. Accessed October 16, 2024. https://pdf.hres.ca/dpd_pm/00076446.PDF
26.Alexion Pharma Canada Corp. Ultomiris (ravulizumab): 10 mg/mL and 100 mg/mL, concentrate for solution for intravenous infusion [product monograph]. August 28, 2019. Updated October 30, 2023. Accessed October 16, 2024. https://pdf.hres.ca/dpd_pm/00073059.PDF
27.Swedish Orphan Biovitrum AB (publ). Empaveli (pegcetacoplan): 1080 mg/20 mL solution for subcutaneous infusion [product monograph]. December 7, 2022. Accessed October 16, 2024. https://pdf.hres.ca/dpd_pm/00068658.PDF
28.Alexion Pharma Canada Corp. Danicopan (voydeya): 50 mg and 100 mg, oral tablets [product monograph]. July 19, 2024. Accessed September 16, 2024. https://pdf.hres.ca/dpd_pm/00076411.PDF
29.Novartis. Clinical Study Report: CLNP023C12302 (Primary End Point Analysis). A randomized, multicenter, active-comparator controlled, open-label trial to evaluate efficacy and safety of oral, twice daily LNP023 in adult patients with PNH and residual anemia, despite treatment with an intravenous anti-C5 antibody [internal sponsor’s report]. March 6, 2023.
30.Novartis. Clinical Study Report: CLNP023C12302 (Addendum). A randomized, multicenter, active-comparator controlled, open-label trial to evaluate efficacy and safety of oral, twice daily LNP023 in adult patients with PNH and residual anemia, despite treatment with an intravenous anti-C5 antibody [internal sponsor’s report]. March 6, 2023.
31.Cella D, Johansson P, Ueda Y, et al. Clinically important change for the FACIT-Fatigue scale in paroxysmal nocturnal hemoglobinuria: a derivation from international PNH registry patient data. J Patient Rep Outcomes. 2023;7(1):63. doi: 10.1186/s41687-023-00609-4 PubMed
32.Balshem H, Helfand M, Schünemann HJ, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011;64(4):401-406. doi: 10.1016/j.jclinepi.2010.07.015 PubMed
33.Santesso N, Glenton C, Dahm P, et al. GRADE guidelines 26: informative statements to communicate the findings of systematic reviews of interventions. J Clin Epidemiol. 2020;119:126-135. doi: 10.1016/j.jclinepi.2019.10.014 PubMed
34.Cocks K, King MT, Velikova G, et al. Evidence-based guidelines for interpreting change scores for the European Organisation for the Research and Treatment of Cancer Quality of Life Questionnaire Core 30. Eur J Cancer. 2012;48(11):1713-1721. doi: 10.1016/j.ejca.2012.02.059 PubMed
35.Novartis Pharmaceuticals Canada Inc. CDA-AMC Sponsor Summary of Clinical Evidence Template: Iptacopan for the treatment of Paroxysmal Nocturnal Hemoglobinuria in adult patients who have an inadequate response to, or are intolerant of, a C5 inhibitor [internal sponsor’s report]. In: Drug Reimbursement Review sponsor submission: Iptacopan 200 mg oral capsule. August 15, 2024.
36.Novartis. Clinical Study Report: CLNP023C12302 (Final Analysis). A randomized, multicenter, active-comparator controlled, open-label trial to evaluate efficacy and safety of oral, twice daily LNP023 in adult patients with PNH and residual anemia, despite treatment with an intravenous anti-C5 antibody [internal sponsor’s report]. November 30, 2023.
37.Novartis. Complement Inhibitor-Experienced Population Indirect Treatment Comparison Technical Report (Final) [internal sponsor’s report]. In: Drug Reimbursement Review sponsor submission: Iptacopan 200 mg oral. February 16, 2024.
38.Novartis. Systematic Literature Review for Iptacopan for the Treatment of Paroxysmal Nocturnal Hemoglobinuria [internal sponsor’s report]. In: Durg Reimbursement Review sponsor submission: Iptacopan 200 mg oral capsule. February 16, 2024.
39.Lee JW, Brodsky RA, Nishimura JI, Kulasekararaj AG. The role of the alternative pathway in paroxysmal nocturnal hemoglobinuria and emerging treatments. Expert Rev Clin Pharmacol. 2022;15(7):851-861. doi: 10.1080/17512433.2022.2109462 PubMed
40.Hillmen P, Lewis SM, Bessler M, Luzzatto L, Dacie JV. Natural history of paroxysmal nocturnal hemoglobinuria. N Engl J Med. 1995;333(19):1253-1258. doi: 10.1056/NEJM199511093331904 PubMed
41.Socié G, Mary JY, de Gramont A, et al. Paroxysmal nocturnal haemoglobinuria: long-term follow-up and prognostic factors. French Society of Haematology. Lancet. 1996;348(9027):573-577. doi: 10.1016/s0140-6736(95)12360-1 PubMed
42.Nishimura JI, Kanakura Y, Ware RE, et al. Clinical course and flow cytometric analysis of paroxysmal nocturnal hemoglobinuria in the United States and Japan. Medicine (Baltimore). 2004;83(3):193-207. doi: 10.1097/01.md.0000126763.68170.46 PubMed
43.Lee JW, Sicre de Fontbrune F, Wong Lee Lee L, et al. Ravulizumab (ALXN1210) vs eculizumab in adult patients with PNH naive to complement inhibitors: the 301 study. Blood. 2019;133(6):530-539. doi: 10.1182/blood-2018-09-876136 PubMed
44.Kulasekararaj AG, Lazana I. Paroxysmal nocturnal hemoglobinuria: Where are we going. Am J Hematol. 2023;98 Suppl 4:S33-S43. doi: 10.1002/ajh.26882 PubMed
45.Hill A, Kelly RJ, Hillmen P. Thrombosis in paroxysmal nocturnal hemoglobinuria. Blood. 2013;121(25):4985-4996; quiz 5105. doi: 10.1182/blood-2012-09-311381 PubMed
46.Oliver M, Patriquin CJ. Paroxysmal Nocturnal Hemoglobinuria: Current Management, Unmet Needs, and Recommendations. J Blood Med. 2023;14:613-628. doi: 10.2147/jbm.S431493 PubMed
47.Griffin M, Kelly RJ, Panse J, et al. Management of acute breakthrough hemolysis with intensive pegcetacoplan dosing in patients with PNH. Blood Adv. 2024;8(7):1776-1786. doi: 10.1182/bloodadvances.2023011691 PubMed
48.Novartis Pharmaceuticals Canada Inc. Fabhalta (iptacopan): 200 mg, hard oral capsules [product monograph]. January 6, 2025.
49.Novartis. Prescribing information: Fabhalta (iptacopan) capsules, for oral use [label]. U.S. Food and Drug Administration (FDA); 2024. Accessed October 16, 2024. https://www.accessdata.fda.gov/drugsatfda_docs/label/2024/218276s001lbl.pdf
50.European Medicines Agency. Product information: Fabhalta (iptacopan). (European public assessment report). 2024. Accessed October 16, 2024. https://www.ema.europa.eu/en/documents/product-information/fabhalta-epar-product-information_en.pdf
51.Peffault de Latour R, Roth A, Kulasekararaj AG, et al. Oral Iptacopan Monotherapy in Paroxysmal Nocturnal Hemoglobinuria. N Engl J Med. 2024;390(11):994-1008. doi: 10.1056/NEJMoa2308695 PubMed
52.Yellen SB, Cella DF, Webster K, Blendowski C, Kaplan E. Measuring fatigue and other anemia-related symptoms with the Functional Assessment of Cancer Therapy (FACT) measurement system. J Pain Symptom Manage. 1997;13(2):63-74. doi: 10.1016/s0885-3924(96)00274-6 PubMed
53.Cella D, Nowinski CJ. Measuring quality of life in chronic illness: the functional assessment of chronic illness therapy measurement system. Arch Phys Med Rehabil. 2002;83(12 Suppl 2):S10-S17. doi: 10.1053/apmr.2002.36959 PubMed
54.Weitz I, Meyers G, Lamy T, et al. Cross-sectional validation study of patient-reported outcomes in patients with paroxysmal nocturnal haemoglobinuria. Intern Med J. 2013;43(3):298-307. doi: 10.1111/j.1445-5994.2012.02924.x PubMed
55.Cella D, Sarda SP, Hsieh R, et al. Changes in hemoglobin and clinical outcomes drive improvements in fatigue, quality of life, and physical function in patients with paroxysmal nocturnal hemoglobinuria: post hoc analyses from the phase III PEGASUS study. Ann Hematol. 2022;101(9):1905-1914. doi: 10.1007/s00277-022-04887-8 PubMed
56.Hillmen P, Szer J, Weitz I, et al. Pegcetacoplan versus eculizumab in paroxysmal nocturnal hemoglobinuria. N Engl J Med. 2021;384(11):1028-1037. doi: 10.1056/NEJMoa2029073 PubMed
57.Chandran V, Bhella S, Schentag C, Gladman DD. Functional assessment of chronic illness therapy-fatigue scale is valid in patients with psoriatic arthritis. Ann Rheum Dis. 2007;66(7):936-939. doi: 10.1136/ard.2006.065763 PubMed
58.Aaronson NK, Ahmedzai S, Bergman B, et al. The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst. 1993;85(5):365-76. doi: 10.1093/jnci/85.5.365 PubMed
59.Osoba D, Rodrigues G, Myles J, Zee B, Pater J. Interpreting the Significance of Changes in Health-Related Quality-of-Life Scores. J Clin Oncol. 2023;41(35):5345-5350. doi: 10.1200/jco.22.02776 PubMed
60.Heinze G, Schemper M. A solution to the problem of separation in logistic regression. Stat Med. 2002;21(16):2409-2419. doi: 10.1002/sim.1047 PubMed
61.Firth D. Bias reduction of maximum likelihood estimates. Biometrika. 1993;80(1):27-38. doi: 10.1093/biomet/80.1.27
62.Westfall PH, Wolfinger RD. Multiple tests with discrete distributions. Am Stat. 1997;51(1):3-8.
63.Westfall PH, Troendle JF. Multiple testing with minimal assumptions. Biom J. 2008;50(5):745-755. doi: 10.1002/bimj.200710456 PubMed
64.Bretz F, Maurer W, Brannath W, Posch M. A graphical approach to sequentially rejective multiple test procedures. Stat Med. 2009;28(4):586-604. doi: 10.1002/sim.3495 PubMed
65.Bretz F, Maurer W, Hommel G. Test and power considerations for multiple endpoint analyses using sequentially rejective graphical procedures. Stat Med. 2011;30(13):1489-1501. doi: 10.1002/sim.3988 PubMed
66.Novartis Pharmaceuticals Canada Inc. Novartis Pharmaceuticals Canada Inc. response to Canada’s Drug Agency request for additional information regarding Fabhalta (iptacopan) on October 18, 2024: Dosage of C5 inhibitors [internal additional sponsor’s information]. October 23, 2024.
67.Center for Drug Evaluation Research. Integrated review(s). Fabhalta (iptacopan) oral. Company: Novartis Pharmaceutical Corp. Application No.: 218276Orig1s000. Approval date: 12/05/2023 (FDA approval package). U.S. Food and Drug Administration (FDA); 2023. Accessed October 28, 2024. https://www.accessdata.fda.gov/drugsatfda_docs/nda/2023/218276Orig1s000IntegratedR.pdf
68.Novartis Pharmaceuticals Canada Inc. Novartis Pharmaceuticals Canada Inc. response to Canada’s Drug Agency request for additional information regarding Fabhalta (iptacopan) on October 8, 2024: Health-related quality of life outcomes [internal additional sponsor’s information]. October 16, 2024.
69.Bland JM, Altman DG. Statistics Notes: Bootstrap resampling methods. BMJ. 2015;350:h2622. doi: 10.1136/bmj.h2622 PubMed
70.Phillippo DM, Ades AE, Dias S, Palmer S, Abrams KR, Welton NJ. NICE DSU Technical Support Document 18: Methods for Population-Adjusted Indirect Comparisons in Submissions to NICE. Decision Support Unit, ScHARR, University of Sheffield; 2016. Accessed October 23, 2024 https://www.sheffield.ac.uk/nice-dsu/tsds/population-adjusted
71.Phillippo DM, Dias S, Ades AE, Welton NJ. Equivalence of entropy balancing and the method of moments for matching-adjusted indirect comparison. Res Synth Methods. 2020;11(4):568-572. doi: 10.1002/jrsm.1416 PubMed
72.Austin PC. Balance diagnostics for comparing the distribution of baseline covariates between treatment groups in propensity-score matched samples. Stat Med. 2009;28(25):3083-3107. doi: 10.1002/sim.3697 PubMed
73.Phillippo DM, Ades AE, Dias S, Palmer S, Abrams KR, Welton NJ. Methods for Population-Adjusted Indirect Comparisons in Health Technology Appraisal. Med Decis Making. 2018;38(2):200-211. doi: 10.1177/0272989x17725740 PubMed
Appendix 1: Detailed Outcome Data
Please note that this appendix has not been copy-edited.
Table 33: Number and Units of RBC Transfusions in the RTP of the APPLY-PNH Study (Day 1 to Day 168)
Outcome | Iptacopan (N = 62) | C5 inhibitor (N = 35) |
|---|---|---|
Number of patients who met criteria for transfusion, n (%) | 8 (12.9) | 21 (60.0) |
Number of patients receiving transfusions, n (%) | 5 (8.1) | 19 (54.3) |
Number of transfusions per patient | ||
n | 5 | 19 |
Mean (SD) | 1.4 (0.89) | 4.9 (3.97) |
Number of RBC units transfused per patient | ||
n | 5 | 19 |
Mean (SD) | 2.2 (1.64) | 8.2 (6.73) |
PNH = paroxysmal nocturnal hemoglobinuria; RBC = red blood cell; RTP = randomized treatment period; SD = standard deviation.
Note: These data are missing 1 patient in the iptacopan group who received a transfusion during the RTP, but due to a site reporting error, was not included in the primary data analysis reported in the 24-week Clinical Study Report. This error was detected at the final analysis (48-week) and the results for the transfusion avoidance secondary outcome were amended, but not the findings reported in this table. In total, 6 patients (9.7%) of patients in the iptacopan group received a transfusion and 9 patients (14.5%) met the criteria for transfusion at least once over the 24-week RTP. The mean number of transfusions per patient and mean number of units transfused per patient are missing data from 1 patient in the iptacopan group.
Source: APPLY-PNH Clinical Study Report.29
Table 34: Change From Baseline in EQ VAS in the RTP of the APPLY-PNH Study
Outcome | Iptacopan (N = 62) | C5 inhibitor (N = 35) |
|---|---|---|
n | 60 | 30 |
Mean score at baseline (SD) | 63.0 (18.30) | 58.6 (20.97) |
Mean score at day 168 (SD) | 76.3 (15.43) | 57.7 (21.35) |
Change from baseline (SD) | 13.3 (18.74) | –0.8 (16.68) |
PNH = paroxysmal nocturnal hemoglobinuria; RTP = randomized treatment period; SD = standard deviation; VAS = visual analogue scale.
Source: APPLY-PNH Clinical Study Report.29
Pharmacoeconomic Review
Abbreviations
AE
adverse event
ARC
absolute reticulocyte count
BIA
budget impact analysis
BTH
breakthrough hemolysis
CDA-AMC
Canada’s Drug Agency
EVH
extravascular hemolysis
HRQoL
health-related quality of life
ICER
incremental cost-effectiveness ratio
LDH
lactate dehydrogenase
MAIC
matching-adjusted indirect comparison
PNH
paroxysmal nocturnal hemoglobinuria
QALY
quality-adjusted life-year
WTP
willingness-to-pay
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Iptacopan (Fabhalta), 200 mg, capsules, oral |
Indication | As monotherapy in the treatment of adult patients with paroxysmal nocturnal hemoglobinuria (PNH) who have hemolytic anemia. |
Health Canada approval status | NOC |
Health Canada review pathway | Standard review |
NOC date | January 6, 2025 |
Reimbursement request | The treatment of adult patients with PNH who have an inadequate response to, or are intolerant of, a C5 inhibitor. |
Sponsor | Novartis Pharmaceuticals Canada Inc. |
Submission history | Previously reviewed: No |
NOC = Notice of Compliance; PNH = paroxysmal nocturnal hemoglobinuria.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Semi-Markov model |
Target population | Adult patients with PNH who have an inadequate response or intolerance to a C5 inhibitor (i.e., C5 inhibitor–experienced patients) |
Treatment | Iptacopan |
Dose regimen | 200 mg twice daily |
Submitted price | $719.94 per 200 mg capsule |
Submitted treatment cost | $524,116 per patient per year |
Comparators |
|
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | Lifetime (59 years) |
Key data sources | APPLY-PNH trial informed efficacy and safety of iptacopan, eculizumab, and ravulizumab. PEGASUS trial informed efficacy and safety of pegcetacoplan. |
Submitted results | The ICER for iptacopan compared to ravulizumab was $51,724 per QALY gained (incremental costs: $79,235; incremental QALYs: 1.53). Iptacopan dominated eculizumab and pegcetacoplan. |
Key limitations |
|
CDA-AMC reanalysis results |
|
AE = adverse event; BTH = breakthrough hemolysis; CDA-AMC = Canada’s Drug Agency; EVH = extravascular hemolysis; ICER = incremental cost-effectiveness ratio; LY = life-year; MAIC = matching-adjusted indirect comparison; PNH = paroxysmal nocturnal hemoglobinuria; QALY = quality-adjusted life-year; vs. = versus; WTP = willingness-to-pay.
Conclusions
There is no direct evidence available comparing iptacopan to pegcetacoplan. To address the evidence gap, the sponsor submitted an unanchored matching-adjusted indirect comparison (MAIC) that assessed the safety and efficacy of iptacopan versus pegcetacoplan. However, no conclusions can be drawn from the MAIC due to serious limitations that undermine the validity of the findings (e.g., significant heterogeneity between the studies and imbalances in important prognostic factors remained such that the treatment effect estimates were considered unreliable). The MAIC did not analyze key outcomes used in the pharmacoeconomic model, as they were not assessed in the APPLY-PNH study (e.g., the proportion of patients with anemia defined as hemoglobin < 105 g/L and all-cause discontinuation). Thus, there is no comparative evidence available for these important end points.
Based on the clinical appraisal of the APPLY-PNH trial by Canada’s Drug Agency (CDA-AMC), in adults with paroxysmal nocturnal hemoglobinuria (PNH) and residual anemia despite treatment with a C5 inhibitor, iptacopan likely results in more patients with a clinically important improvement in hemoglobin levels and normalization of hemoglobin (defined as hemoglobin levels ≥ 120 g/L) and fewer patients who require transfusion at 24 weeks compared to a C5 inhibitor. These effects associated with iptacopan may be maintained up to 48 weeks. The impact of iptacopan on the frequency of breakthrough hemolysis (BTH) and on the change in lactate dehydrogenase (LDH) levels and absolute reticulocyte count (ARC) were uncertain. Iptacopan may improve fatigue symptoms and health-related quality of life (HRQoL). Adverse events (AEs) were common in both the iptacopan and C5 inhibitor groups, but there were no deaths or treatment discontinuation due to AEs.
Pegcetacoplan is the key comparator for patients with PNH who have signs or symptoms of extravascular hemolysis (EVH). Thus, there is no evidence available to support a price premium for iptacopan compared to pegcetacoplan. When compared to C5 inhibitors, despite the limitations of the model that could not be addressed, the CDA-AMC base-case results are similar to those reported by the sponsor. Iptacopan compared to ravulizumab was associated with an incremental cost-effectiveness ratio (ICER) of $62,272 per quality-adjusted life-year (QALY) gained for adult patients with PNH who have an inadequate response or intolerance to a C5 inhibitor (incremental QALYs gains: 1.53; incremental cost: $95,080; and a 35.3% probability of being cost-effective at a willingness-to-pay [WTP] threshold of $50,000 per QALY). CDA-AMC was unable to address all differences in the naive comparison of AEs with pegcetacoplan, and, as a result, differences in QALY for iptacopan and pegcetacoplan remained. Further uncertainty remains regarding confidential discounts negotiated by public plans. The cost-effectiveness of iptacopan in first-, third-, or later-line treatment remains unknown.
Patient, Clinician, and Drug Plan Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, clinician groups, and drug plans that participated in the CDA-AMC review process.
CDA-AMC received patient input from the Canadian Association of PNH Patients and the Aplastic Anemia & Myelodysplasia Association of Canada. Personal experiences were gathered from 1 patient in Canada receiving iptacopan from the open-label clinical trial. This patient had been on an alternative treatment (eculizumab) for a year and did not feel that they had a decent quality of life while on eculizumab. The patient reported that they felt the treatment benefits of iptacopan soon after initiating treatment and now feel “normal” again. The patient highlighted the added benefit of taking an oral pill over receiving injections. Additional input from a caregiver and 3 patients were collected from the US. All of the patients reported improvements in their hemoglobin levels within 1 to 6 weeks of initiating iptacopan.
Clinician input was received from the Canadian PNH Network. Information was obtained via publicly available documents, congress abstracts, and published literature (including data from the APPLY-PNH trial). The current standard of care in Canada for patients with PNH is C5 inhibitor monotherapy (eculizumab or ravulizumab). Allogeneic hematopoietic stem cell transplant is the only curative treatment for PNH, and it is reserved for patients with predominant or progressive bone marrow failure (i.e., aplastic anemia or myelodysplastic syndrome), which can coincide with, precede, or follow a diagnosis of PNH. Treatment with C5 inhibitor may be recommended over transplant (due to transplant-related risk of complication and mortality) and is associated with control of intravascular hemolysis, which leads to significant improvement in quality of life, fatigue, transfusion dependence, thrombosis, and overall survival. Approximately one-third of patients with PNH treated with a C5 inhibitor continue to experience anemia and may still require transfusions due to increased complement component 3 split products that drive EVH. Blocking complement at the proximal level with a C3 inhibitor can block EVH and allow hemoglobin to increase. Pegcetacoplan is a C3 inhibitor that was recently approved in Canada and is available in several provinces as a second-line therapy for PNH. However, a 3-year follow-up from the PEGASUS data reported severe BTH in patients receiving pegcetacoplan. Danicopan as an add-on therapy to C5 inhibitor, currently under negotiation, is an alternative second-line therapy providing proximal and terminal blockade. Supportive therapies for patients with PNH may include hematinic support (folate, iron), analgesia, and anticoagulation. In PNH, anticoagulation alone does not protect against thrombosis, which is the leading cause of death in untreated patients (40% to 67%). Patients who live far from infusion sites may need to travel long distances to access specialized nurses for IV infusion of a C5 inhibitor. Pegcetacoplan is a subcutaneous infusion, typically self-administered, which requires refrigeration. An oral monotherapy would allow patients freedom from travelling long distances, from a product that requires refrigeration, and from carrying medical equipment for self-injection. The main unmet need is that no currently available PNH therapy can cure the disease. Patients with PNH require lifelong treatment. Iptacopan is expected to be effective in patients with symptomatic and/or transfusion-dependent anemia related to EVH. Iptacopan could also be an alternative treatment for patients who may not tolerate pegcetacoplan or prefer an oral drug. Clinicians note that, due to the lack of comparative efficacy data of second-line therapeutics in treating PNH, the choice of second-line therapy is mainly determined by patient preference. Outcomes of interest include complement blockade, a decrease in LDH ratio to below 1.5 times the upper limit of normal (which reduces hemolysis, improves hemoglobin, reduces transfusion dependence, and reduces the risk of thrombosis), a decrease in fatigue and transfusion requirements, improved quality of life, improved overall survival, and increase in hemoglobin. Clinicians report that iptacopan should be discontinued in patients with poor compliance or intolerable side effects, and in patients who become pregnant and/or are breastfeeding. The most important side effect to monitor is BTH because of the possibility of severe complement-mediated hemolytic events. In patients with BTH, danicopan should be considered to allow proximal and terminal complement inhibition.
The drug programs provided input on iptacopan through the CDA-AMC Reimbursement Review process and identified some concerns that may affect their ability to implement recommendations: first, whether danicopan may be used as an add-on therapy to iptacopan and whether the recommendations for iptacopan and pegcetacoplan should align, as both drugs have the same indication for reimbursement; second, whether iptacopan may be given to patients with PNH who prefer oral medication for treatment, affecting its place in therapy; third, whether vaccinations are required before taking iptacopan due to the increased infection risk of encapsulated bacteria; and, finally, the high submitted price of iptacopan.
Several of these concerns were addressed in the sponsor’s model:
The use of a cost-utility approach accounts for some issues related to HRQoL affected by hemoglobin levels, the need for transfusions, BTH events, and AEs.
Costs of vaccinations required for each comparator were included in the model.
CDA-AMC was unable to address the following concerns raised from patient, clinician, and drug plan input:
The lack of danicopan add-on as a subsequent treatment option in the model could not be addressed.
The cost-effectiveness of iptacopan as a first-line therapy for those patients who prefer oral medication could not be addressed.
Economic Review
The current review is for iptacopan for the treatment of adult patients with PNH who have an inadequate response or intolerance to a C5 inhibitor.1
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis of iptacopan compared to eculizumab, ravulizumab, and pegcetacoplan (co-administered with C5 inhibitor therapy during a 4-week run-in period). The modelled population was aligned with the reimbursement request and pivotal trial, which are comprised of adult patients with PNH who have an inadequate response or intolerance to a C5 inhibitor.1 However, the Health Canada proposed indication is broader as do not restrict the indication to those patients intolerance or with inadequate response to a C5 inhibitor.
Iptacopan is available as a 200 mg hard capsule, and its recommended dosage is 200 mg taken orally twice daily. The sponsor-submitted cost for iptacopan was $719.94, and the annual cost was $524,116 per patient, as calculated by the sponsor.1 The weighted annual cost of eculizumab was $581,041 per patient (based on the distribution of maintenance and updoses at baseline in the APPLY-PNH trial), of ravulizumab was $511,402 per patient (based on the patients’ weight distribution at baseline in the APPLY-PNH trial), and of pegcetacoplan was $568,934 and $533,033 per patient, respectively, for the first and subsequent years (based on the distribution of maintenance and updoses in the PEGASUS trial, and including costs of a C5 inhibitor during the 4-week run-in period).1 Drug wastage was not included in the model, as it is not expected with any treatment (i.e., all doses are multiples of exact vial size).
The main clinical outcomes modelled were anemia and transfusion. The secondary clinical outcomes were AEs and chelation therapy. The economic outcome of interest was QALYs over a lifetime horizon (i.e., 59 years) from the perspective of the Canadian publicly funded health care payer. Costs and health-related outcomes were discounted at 1.5% per year.
Model Structure
The sponsor submitted a semi-Markov model with 4 mutually exclusive health states: no transfusion and anemia, no transfusion and no anemia, transfusion, and death (Figure 1). Anemia was defined by the sponsor as an hemoglobin level of less than 105 g/L, to align with the threshold used for pegcetacoplan in the PEGASUS trial.2 Patients enter the model in the no transfusion and anemia or transfusion states. During each cycle, patients may remain in their current health state or move to another health state. Patients in the transfusion state may develop iron overload and require chelation therapy. Treatment-related AEs and all-cause death can occur in any health state. Death was the absorbing state. The model used a 4-week cycle length.
Patients initially on iptacopan or pegcetacoplan can discontinue the initial treatment and receive subsequent therapy with ravulizumab for the remainder of the time horizon (assuming ravulizumab costs and probabilities). Patients initially on eculizumab or ravulizumab remain on the same treatment for the entire time horizon.
Model Inputs
The baseline patient characteristics (mean age: 51.0 years; mean body weight: 71.6 kg; 30.9% male) in the sponsor’s model and their initial distribution entering the health states were informed by the APPLY-PNH trial and assumed to represent patients living in Canada with PNH in clinical practice.3
The efficacy of iptacopan, eculizumab, and ravulizumab was informed by the APPLY-PNH trial3 (24 weeks). To derive the probability of being in each health state for patients receiving iptacopan and C5 inhibitors, a multinomial logistic regression model was fit to the APPLY-PNH trial data (i.e., a 3-state health model defined as no transfusion and anemia, no transfusion and no anemia, and transfusion). Transition probabilities for eculizumab and ravulizumab were equal in the economic model as the multinomial regression model used aggregated data from both C5 inhibitor from the trial. Due to the lack of a head-to-head trial between iptacopan and pegcetacoplan, the sponsor applied MAIC weights to the APPLY-PNH trial population (to align with the inclusion and exclusion criteria of the PEGASUS trial).4 The MAIC weights were used in the multinomial logistic regression model to adjust the transition probabilities for patients receiving iptacopan and C5 inhibitors. MAIC-weighted transition probabilities were used in the submitted base case, and unweighted transition probabilities were used in a scenario analysis. For pegcetacoplan, the transition probabilities were sourced directly from Hakimi et al.,2 based on the PEGASUS trial (16 weeks). The sponsor assumed that the transition probabilities were the same throughout the duration of therapy for all treatments (i.e., treatment effects are maintained).
The safety of iptacopan, eculizumab, and ravulizumab was informed by the APPLY-PNH trial3 and of pegcetacoplan was informed by the PEGASUS trial and published literature.5,6 The model included the probabilities of nonserious BTH and serious AEs, including hemolysis.4,5,7 The sponsor assumed that all patients experiencing nonserious BTH and hemolysis would be treated.
The annual probability of discontinuation due to all causes for iptacopan, eculizumab, and ravulizumab was informed by the APPLY-PNH trial3 and for pegcetacoplan was directly informed by the PEGASUS trial (naively compared).8 The probability of discontinuation was adjusted per model cycle and assumed to be the same for all health states. In the APPLY-PNH trial, 1 patient discontinued iptacopan. In the PEGASUS trial, 10 patients discontinued pegcetacoplan and 2 patients were not included in determining the annual probability of discontinuation (1 who discontinued due to BTH and 1 who discontinued due to death).
The proportion of patients requiring chelation therapy for iptacopan, ravulizumab, and eculizumab is based on the APPLY-PNH trial3 and, for pegcetacoplan, it was assumed to be equal to those treated with iptacopan.
Health state utilities were estimated based on EQ-5D-5L pooled data from the APPLY-PNH trial and APPOINT-PNH trial (a phase III single-arm trial of iptacopan in C5 inhibitor–naive patients).9 Pooled EQ-5D-5L responses were mapped to EQ-5D-3L scores and valued using the UK tariffs.10,11 The health state utility values for no transfusion and anemia, no transfusion and no anemia, and transfusion were 0.785, 0.878, and 0.733, respectively. The utilities were age- and sex-adjusted and did not exceed the general population utility values.12 Utility decrements associated with IV and subcutaneous treatment administration, chelation therapy, and AEs were based on trial data and literature.2,13,14
Mortality was based on age- and sex-adjusted general mortality in the population in Canada.15 The probability of death was assumed the same across all health states and treatments, and no excessive mortality due to PNH was included in the model.
Costs captured in the model included drug acquisition, treatment administration, resource use, and AE costs. Drug-acquisition costs were based on the sponsor’s submitted price and publicly listed pricing of comparators and were calculated based on the regimens reported in the APPLY and PEGASUS trials, products’ monographs, and updosing assumptions.5,16-19 The sponsor did not include ongoing treatment administration costs in the base case (e.g., costs of IV and subcutaneous injections at home or in clinic), assuming they are covered by each manufacturer, except for a 1-hour, 1-time training cost by a registered nurse to instruct patients on pegcetacoplan infusion techniques.17,20 AE costs and chelation therapy were based on published literature.7,21-24 Health care resource use and cost for routine patient monitoring were sourced from literature and included physician visits and laboratory tests.25-27 Vaccination requirements were based on each product monograph, and the cost was informed by IQVIA Market Access Console.28-36
Summary of Sponsor’s Economic Evaluation Results
The sponsor’s base-case analysis was run probabilistically (3,000 iterations). Scenario analyses were conducted deterministically. The base-case probabilistic and deterministic results were similar. The probabilistic findings are presented below.
Base-Case Results
In the sponsor’s base case (Table 3), ravulizumab and iptacopan remained on the cost-effectiveness efficiency frontier. Iptacopan was associated with higher QALYs (incremental QALY: 1.53) and higher costs (incremental cost: $79,235) compared to ravulizumab, resulting in an ICER of $51,724 per QALY gained. Based on a WTP threshold of $50,000, there is a 43.9% probability of iptacopan being cost-effective compared to ravulizumab. Iptacopan dominated pegcetacoplan and eculizumab (i.e., less costly and more beneficial). The majority of the incremental QALY gain of iptacopan compared to ravulizumab (97%) or pegcetacoplan (99%) accrued beyond the duration of the trials and was based on extrapolations (24 weeks of randomized data from the APPLY-PNH trial and 16 weeks from the PEGASUS trial, respectively).
Additional results from the sponsor’s submitted economic base case are presented in Appendix 3. The disaggregated results showed that the additional QALYs associated with iptacopan were mainly attributed to a higher state occupancy in the no transfusion and no anemia state, which is associated with a higher utility value. In addition, iptacopan was assumed to have a fraction of the probability of discontinuing initial treatment and moving on to subsequent therapy compared to pegcetacoplan. Once patients move on to subsequent therapy, they are more likely to be in the anemia and transfusion health states, which are associated with a substantially lower utility value. The total costs were largely driven by drug acquisition of the initial and subsequent therapies. For patients who initially received pegcetacoplan, approximately 78% of the total cost was accrued after discontinuing pegcetacoplan and receiving subsequent therapy; while, for patients who initially received iptacopan, subsequent therapy represented only 37% of the total cost.
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Total QALYs | Sequential ICER ($/QALY) |
|---|---|---|---|
Ravulizumab | 13,065,124 | 17.38 | Reference |
Iptacopan | 13,144,359 | 18.91 | 51,724 |
Dominated treatments | |||
Pegcetacoplan | 13,223,585 | 17.89 | Dominated by iptacopan |
Eculizumab | 14,947,416 | 17.39 | Dominated by iptacopan and pegcetacoplan |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Source: Sponsor’s pharmacoeconomic submission.
Sensitivity and Scenario Analysis Results
The sponsor assessed several model parameters and assumptions in deterministic scenario analyses, which included the use of unweighted health state transition probabilities, alternative hemoglobin threshold to define anemia (hemoglobin < 100 g/L), alternative discount rates (0% and 3%), including PNH-related mortality, and treatment-specific utilities. In all of the scenarios, pegcetacoplan and eculizumab continued to be dominated treatments and the ICERs of iptacopan compared to ravulizumab increased, but these were mainly affected by the use of unweighted health state transition probabilities (which increased ICER by 18%).
The sponsor conducted a scenario analysis from a societal perspective, considering costs associated with lost productivity for patients and caregivers, as well as travel for treatment administration. In this analysis, relative to ravulizumab, the ICER was $46,294 per QALY gained. This was lower than the sponsor’s base-case analysis using a health care payer perspective.
CDA-AMC Appraisal of the Sponsor’s Economic Evaluation
CDA-AMC identified several key limitations to the sponsor’s analysis that have notable implications on the economic analysis:
Comparative efficacy and safety versus pegcetacoplan are uncertain. While the pivotal trial for iptacopan was actively controlled (versus the C5 inhibitors eculizumab or ravulizumab), it did not include the most relevant comparator, pegcetacoplan, for adults with PNH with EVH. To address this gap in the evidence, the sponsor submitted an unanchored MAIC assessing the safety and efficacy of iptacopan versus pegcetacoplan. However, there was significant heterogeneity between the 2 studies informing the MAIC, and imbalances in important prognostic factors remained after matching and weighting, such that the treatment effect estimates were considered unreliable, as the trial populations were too dissimilar to compare (e.g., the PEGASUS trial enrolled patients with more severe PNH than those enrolled in the APPLY-PNH study). The MAIC did not analyze key outcomes used in the pharmacoeconomic model, as they were not assessed in the APPLY-PNH study (e.g., the proportion of patients with anemia defined as hemoglobin < 105 g/L and discontinuation due to any cause). Thus, there is no comparative evidence available for these important end points. No conclusions can be drawn from other end points assessed in the MAIC due to serious limitations of the indirect comparison that undermine the validity of the findings. As a result, the indirect evidence submitted by the sponsor does not allow firm conclusions about the relative safety and efficacy of iptacopan compared to pegcetacoplan.
In CDA-AMC reanalyses, as no conclusive evidence was presented that iptacopan is superior to pegcetacoplan, iptacopan and pegcetacoplan were assumed to have equivalent probabilities of transitioning between the health states.
Limited validity of the transition probabilities between health states for different treatment arms. The sponsor’s transition probabilities for iptacopan and C5 inhibitors were generated by applying a multinomial logistic regression model to the patient-level data from the APPLY-PNH trial. This model included the previous health state, treatment, time of first dose to visit and interaction terms of time × treatment and time × lagged health state. This model, used to derive unweighted transition probabilities, adopted the same terms as those from the multinomial logistic regression model used to generate the transition probabilities for a cost-effectiveness study of pegcetacoplan.2 Additionally, to adjust the health state transition probabilities from APPLY-PNH to the PEGASUS trial population, weights obtained from the MAIC were used as estimation weights when fitting the multinomial logistic regression model for health states to derive MAIC-weighted transition probabilities.
The objective of including covariates in the regression model is likely to adjust for the independent effect that baseline patient and/or disease characteristics (e.g., severity of disease) or any other extrinsic factors may have on the probability of transitioning to and from the health states. It is unclear whether all relevant covariates were adjusted for, as the sponsor did not select covariates specific to the APPLY-PNH trial, although such impact might be minimal due to the randomized design of the trial. Although CDA-AMC requested an assessment of model fit for both sets of probabilities (unweighted and MAIC-weighted), the sponsor failed to provide one, making it challenging to determine whether the prespecified multinomial model may have overfit the data. This raises concerns about potentially misleading R-squared values, coefficients, and P values. While using the same regression model as in the pegcetacoplan cost-effectiveness could aid in comparing the results, it does not eliminate the need for conducting a model fit assessment. As a result, the validity of the calculated transition probabilities for iptacopan and C5 inhibitor remains at risk of bias and may not be representative of or generalizable to the target population. Despite some similarities between the 2 trials, it is important to note that there are differences in the duration between the APPLY-PNH trial (24 weeks) and PEGASUS trial (16 weeks), their primary analyses of end points were substantially different, and other important prognostic factors or effect modifiers were not balanced between groups (i.e., the MAIC adjusted only for transfusion history, sex, and baseline hemoglobin levels). It is unknown whether a longer or similar trial duration across all drugs could make a significant difference in the probability of transitioning between the health states.
There is uncertainty surrounding the use of unweighted transition probabilities for comparing iptacopan and pegcetacoplan (i.e., naive comparison of probabilities). On the other hand, opting for MAIC-weighted transition probabilities may introduce further uncertainty to the economic assessment, as it would distort the comparison between iptacopan and the C5 inhibitors. As shown by the sponsor’s scenario analysis, the ICER is 18% higher compared to ravulizumab when using the unweighted probabilities. Based on the CDA-AMC clinical appraisal, compared to C5 inhibitors, iptacopan likely results in more patients with a clinically important improvement in hemoglobin levels and normalization of hemoglobin (hemoglobin levels ≥ 120 g/L), and fewer patients who require transfusion over 24 weeks, which may be maintained up to 48 weeks (based on the open-label extension study). The impact of iptacopan on the frequency of BTH and on the change in LDH levels and ARC was uncertain. There was low-certainty evidence that iptacopan may improve patient-reported fatigue and HRQoL. However, no conclusive evidence from the MAIC demonstrated that iptacopan is superior to pegcetacoplan. Clinical experts consulted by CDA-AMC did not expect significant differences in efficacy and safety between iptacopan and pegcetacoplan, based on the available data, but recognized both treatment options as being superior to C5 inhibitor monotherapy in this patient population. Therefore, the unweighted transition probabilities should remain the preferred source of direct evidence to compare iptacopan versus C5 inhibitors for the pharmacoeconomic analysis.
Last, poor economic modelling practices were employed. The sponsor’s submitted model was programmed in a way in which different values were used for the same iteration of the probabilistic analysis, even when the input parameter was identical between treatment arms due to random sampling (e.g., when both ravulizumab and eculizumab have a 29.6% mean probability of moving from the transfusion state to no anemia, the same iteration of the probabilistic analysis assumed 39.2% for eculizumab but 33.7% for ravulizumab). Also, the sponsor’s submitted model included numerous IFERROR statements, which lead to situations in which the parameter value is overwritten with an alternative value without alerting the user to the automatized overwriting. The use of IFERROR statements makes thorough auditing of the sponsor’s model impractical. It remains unclear whether the model is running inappropriately by overwriting errors.
In CDA-AMC reanalyses, unweighted transition probabilities were used for iptacopan, ravulizumab, and eculizumab. Additionally, iptacopan and pegcetacoplan were assumed to have equivalent probabilities, based on the unweighted transition probabilities estimated for iptacopan. This was chosen to preserve the relative efficacy of iptacopan compared to C5 inhibitors observed in the APPLY-PNH trial. The probabilistic analysis was corrected such that the same P values randomly sampled per iteration for eculizumab and iptacopan were equally applied to ravulizumab and pegcetacoplan, respectively.
All-cause discontinuation rate was naively compared to pegcetacoplan and is highly uncertain. The all-cause discontinuation rate was naively compared in the model (for iptacopan, it was informed by the APPLY-PNH trial;3 for pegcetacoplan, it was informed by published data from the PEGASUS trial8) and assumed to be the same across all health states. The all-cause discontinuation was not an outcome included in the MAIC submitted to CDA-AMC for clinical appraisal. The probability of discontinuation is a key driver in the model, as it is more than 4 times higher for patients treated with pegcetacoplan compared to those treated with iptacopan (16% versus 3.44% annually, respectively). Once patients discontinue pegcetacoplan or iptacopan, patients move on to receive ravulizumab. Patients on ravulizumab are more likely to have anemia and require transfusion in the model. Given that the majority of the QALYs gained and the total cost of pegcetacoplan are accrued while the patient is in subsequent therapy, the discontinuation rate of pegcetacoplan is a key factor in iptacopan dominance over pegcetacoplan in the sponsor’s estimates. However, the naive comparison of the probability of discontinuation is subject to uncertainty because it does not account for confounding variables such as the differences in study design, study period, and heterogeneity in the patient population. Furthermore, clinical experts consulted by CDA-AMC noted that the discontinuation rate for pegcetacoplan during the PEGASUS trial is likely inflated compared to current rates in clinical practice. This is because pegcetacoplan was the first non-C5 inhibitor drug available for PNH, so clinicians were less experienced with this drug class and with managing BTH in patients on a C3 inhibitor. In the PEGASUS trial, many patients discontinued pegcetacoplan after a BTH if they were already on the maximum dose allowed for the study protocol, which may no longer be the approach in clinical practice. Clinical experts noted that, as clinicians gain experience with BTH management while patients are on C3 inhibitor therapy, they expect the discontinuation rates for iptacopan and pegcetacoplan to be relatively similar, based on how both drugs perform in clinical practice.
In CDA-AMC reanalyses, as no conclusive evidence was presented that iptacopan is superior to pegcetacoplan, iptacopan and pegcetacoplan were assumed to have equivalent probabilities of discontinuation.
The submitted model does not align with the indicated population or capture all aspects of the condition and its management. The approved indication for iptacopan is for adult patients with PNH, and it is therefore unspecific to whether the drug is indicated for use as first-, second- or later-line therapy. Clinical experts consulted by CDA-AMC did not expect that iptacopan would be used as first-line therapy, although there are some data to support this approach (from the APPOINT-PNH study) if there were a situation where C5 inhibitor could not be used. The clinical experts stated that iptacopan would not be used in combination with other treatments but as a stand-alone option after C5 inhibitor (i.e., second or later lines of therapy). Treatment choice is ideally likely to become more individualized and fluid between all treatment options (i.e., switching back and forth among treatments), depending on the health status and life circumstances of the patients (e.g., pregnancy, breastfeeding, periods of pill-burden and/or noncompliance due to busy lifestyle, travel, needle phobia, difficult swallowing, compromised skin integrity, dexterity limitations to self-administration). The APPLY-PNH trial was restricted to patients receiving iptacopan as their second line of treatment. As a result, there is no direct comparative evidence for the use of iptacopan in first-, third-, or later-line settings. Additionally, the submitted model does not allow users to explore the impact on patients who had a suboptimal response on C3 inhibitor of switching to another C3 inhibitor or danicopan plus a C5 inhibitor as a subsequent therapy. Iptacopan and pegcetacoplan are proximal complement inhibitors, provided as a monotherapy. Clinical experts consulted by CDA-AMC noted that, in clinical practice, if danicopan is publicly reimbursed, patients who have a suboptimal response to iptacopan or pegcetacoplan and continue to experience severe BTH events may switch to danicopan plus a C5 inhibitor to provide terminal and proximal inhibition of the complement pathway (instead of switching back to C5 inhibitor monotherapy). Also, patients on pegcetacoplan may choose self-administration of 3 daily doses of pegcetacoplan in response to a BTH trigger. If BTH is severe, doses of ravulizumab or eculizumab would also be added, although C5 inhibitor may not be on the formulary in all hospitals. Therefore, the total costs may have been underestimated, and the impact of using other subsequent lines of therapy is unknown. Additionally, the sponsor’s submitted model did not explicitly account for the cost and HRQoL associated with thrombosis. Input from patients and clinician experts consulted by CDA-AMC highlighted thrombosis as the most devastating consequence of PNH, yet the impact of thrombosis on the overall cost-effectiveness of treatments is unknown. Under C5 inhibitor blockade, the risk of death from thromboembolism is significantly reduced through the control of intravascular hemolysis. It has been assumed that the risk of thromboembolism with pegcetacoplan and iptacopan is equivalent to that with C5 inhibitors, although it may increase during episodes of BTH, as there would be no terminal complement blockade with pegcetacoplan or iptacopan. While the available data may be insufficient to adequately appreciate this risk or substantially influence simulation models, it is still important to recognize the potential for differing risk of death from thromboembolism between treatment with a C5 inhibitor and a C3 inhibitor, given their distinct mechanisms of action.
CDA-AMC is unable to address these limitations within the submitted model. The influence on the cost-effectiveness results of not including all aspects of the condition and its management in the model remains unknown.
The price of drugs paid by public drug plans is uncertain. The prices for drugs were based on publicly available list prices and may not reflect the actual prices paid by public drug plans. Any potential confidential rebates are not reflected in this analysis.
CDA-AMC could not address this limitation.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CDA-AMC (Table 4).
Table 4: Key Assumptions of the Submitted Economic Evaluation (Not Noted as Limitations to the Submission)
Sponsor’s key assumption | CDA-AMC comment |
|---|---|
BTH and other AEs were naively compared between iptacopan and pegcetacoplan. | Inappropriate. The risk of serious AEs in the trials was low, but it is important to note the heterogeneity in the patient populations and the different trial durations between the APPLY-PNH and PEGASUS trials. Comparing the safety of iptacopan and pegcetacoplan naively under these conditions, especially given the limited sample sizes and unaccounted confounding factors, introduces significant uncertainty. Nonetheless, this uncertainty is likely to have a minimal impact on the overall results of the submitted model. |
AE = adverse event; BTH = breakthrough hemolysis; CDA-AMC = Canada’s Drug Agency.
CDA-AMC Reanalyses of the Economic Evaluation
Base-Case Results
The CDA-AMC base case was derived by making changes in model parameter values and assumptions, in consultation with clinical experts. A summary of the changes applied to the submitted economic evaluation is presented in Table 5. The changes included assuming equal transition probabilities between health states and equal probability of experiencing treatment discontinuation between iptacopan and pegcetacoplan.
Table 5: CDA-AMC Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
Changes to derive the CDA-AMC base case | ||
1. Health state transition probabilities | Iptacopan: MAIC-weighted probabilities C5 inhibitor: MAIC-weighted probabilities Pegcetacoplan: Probabilities from Hakimi et al.2 | Iptacopan: Unweighted probabilities C5 inhibitor: Unweighted probabilities Pegcetacoplan: Assumed the same as iptacopan |
2. Discontinuation rate | Iptacopan: 3.44% annually Pegcetacoplan: 16.18% annually | Iptacopan: 3.44% annually Pegcetacoplan: 3.44% annually |
CDA-AMC base case | ― | 1 + 2 |
CDA-AMC = Canada’s Drug Agency; MAIC = matching-adjusted indirect comparison.
The results of the CDA-AMC base case are presented in Table 6. The results of the CDA-AMC stepped analysis are presented in Table 13. Similar to the sponsor’s results, in the CDA-AMC base case, iptacopan continued to dominate pegcetacoplan and eculizumab (i.e., less costly and more beneficial). However, the iptacopan ICER compared to ravulizumab increased, with increased uncertainty. Iptacopan treatment resulted in an ICER of $62,272 per QALY compared to ravulizumab (incremental QALY: 1.53, incremental cost: $95,080), with a probability of being cost-effective at a WTP threshold of $50,000 per QALY of 35.3%. CDA-AMC notes that, even when assuming an equivalent effect on hemoglobin levels, transfusion, and discontinuation, it was not possible to ensure QALYs were exactly equivalent between the iptacopan and pegcetacoplan treatment arms due to the remaining nature of the naive comparison of AEs (mainly BTH events). Consistent with the sponsor’s results, the majority of the incremental QALY gain of iptacopan compared to ravulizumab (97%) accrued beyond the duration of the trial and was based on extrapolations.
Although the overall incremental QALYs associated with iptacopan were not affected, the disaggregated results showed that CDA-AMC alternative assumptions affect state membership, which impacted drug acquisition and health care resource use costs, mainly driven by the time patients spend in the transfusion state. The estimated results shifted to iptacopan offering a slightly smaller advantage when compared to both C5 inhibitors, and subsequent therapy costs and health care resource use costs were no longer discrepant between iptacopan and pegcetacoplan.
Table 6: Summary of the CDA-AMC Reanalysis Results
Drug | Total costs ($) | Total QALYs | Sequential ICER ($/QALY) |
|---|---|---|---|
Sponsor base case (probabilistic) | |||
Ravulizumab | 13,065,124 | 17.38 | Referencea |
Iptacopan | 13,144,359 | 18.91 | 51,724 |
Dominated treatments | |||
Pegcetacoplan | 13,223,585 | 17.89 | Dominated by iptacopan |
Eculizumab | 14,947,416 | 17.39 | Dominated by iptacopan and pegcetacoplan |
CDA-AMC base case (probabilistic) | |||
Ravulizumab | 13,025,703 | 17.32 | Referencea |
Iptacopan | 13,120,784 | 18.85 | 62,272 |
Dominated treatments | |||
Pegcetacoplan | 13,310,226 | 18.84 | Dominated by iptacopan |
Eculizumab | 14,882,607 | 17.33 | Dominated by iptacopan and pegcetacoplan |
CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
aReference product is the least costly alternative.
Source: Sponsor’s pharmacoeconomic submission.1
Scenario Analysis Results
CDA-AMC undertook price-reduction analyses based on the base-case results from the sponsor and from CDA-AMC (Table 7). At a WTP threshold of $50,000 per QALY, the CDA-AMC base case suggests that a 0.30% price reduction for iptacopan (to $718 per capsule) would be required for iptacopan to be considered cost-effective relative to ravulizumab (similar to the sponsor’s results).
There is no robust clinical evidence to justify a price premium for iptacopan versus pegcetacoplan. At the listed prices, iptacopan has lower total costs than pegcetacoplan. However, there are remaining issues with the model structure and the nature of the naive comparison that CDA-AMC was unable to address in order to fully reproduce equivalent efficacy and safety between iptacopan and pegcetacoplan.
Therefore, these price-reduction estimates remain uncertain and further price reductions may be required to ensure similar total costs between iptacopan and pegcetacoplan, and cost-effectiveness relative to ravulizumab, if confidential pricing has been negotiated.
Table 7: CDA-AMC Price-Reduction Analyses
Analysis | Unit drug cost ($) | Sequential ICERs for Iptacopan ($/QALY) | |
|---|---|---|---|
Price reduction | Sponsor base case | CDA-AMC reanalysis | |
No price reduction | 720 | $51,724 vs. ravulizumab | $62,272 vs. ravulizumab |
10% | 648 | Dominant | Dominant |
CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus.
Additionally, CDA-AMC conducted a scenario analysis to explore the impact of assuming equivalent BTH and hemolysis probabilities between iptacopan and pegcetacoplan, based on the iptacopan probabilities from the APPLY-PNH trial. The result is similar to the base case from the sponsor and from CDA-AMC (i.e., pegcetacoplan continues to be dominated by iptacopan) and driven by drug administration costs.
Issues for Consideration
Comparator pricing based on publicly available prices: The modelled prices of all comparators (e.g., iptacopan, pegcetacoplan, eculizumab, ravulizumab) are based on publicly accessible list prices and do not reflect existing confidential pricing that has been negotiated by public plans.37-39 When existing confidential discounts are considered, greater price reductions than those referenced in this report may be required to achieve cost-effectiveness.
Intolerance to C5 inhibitor: The sponsor’s requested reimbursement population for iptacopan is for patients with PNH who have inadequate response or intolerance to a C5 inhibitor. The sponsor’s economic model was instead based on the APPLY-PNH trial population, which recruited only patients who had inadequate response to a C5 inhibitor. Although the cost-effectiveness of iptacopan in the population of patients with intolerance to C5 inhibitors is unknown, clinical expert feedback consulted by CDA-AMC noted that intolerance to C5 inhibitor is expected to be rare in clinical practice.
Upcoming relevant comparator: Danicopan, as an add-on therapy to C5 inhibitor, has been recently reviewed by CDA-AMC, received a positive reimbursement recommendation for its use in the same population,40 and is under consideration for negotiation by the pan-Canadian Pharmaceutical Alliance.41 The same sponsor manufacturers danicopan and both C5 inhibitor monotherapies (eculizumab and ravulizumab). Additionally, a C5 inhibitor is the first line of treatment, and danicopan add-on allows patients to continue on C5 inhibitor therapy, potentially creating logistical and negotiation advantages for danicopan as second-line therapy over pegcetacoplan or iptacopan. Further, crovalimab is also currently being reviewed by CDA-AMC for the same indication.42
Place in therapy: Clinical experts noted that pegcetacoplan is the most relevant comparator to iptacopan. Furthermore, clinicians note that patients with a suboptimal response on pegcetacoplan or iptacopan are likely to receive danicopan plus a C5 inhibitor as a subsequent therapy. Yet direct comparative evidence comparing iptacopan to pegcetacoplan or danicopan plus a C5 inhibitor as second- or third-line treatment remains lacking.
Anticipated patent expiration of eculizumab: The patent for eculizumab is expected to expire on March 15, 2027,43 and biosimilars are on the horizon.44 If eculizumab biosimilars become available and are considered clinically equivalent to eculizumab, iptacopan is unlikely to remain less costly than eculizumab biosimilars. Consequently, the cost of iptacopan at the submitted price would be less attractive to drug plans and may no longer dominate eculizumab in cost-effectiveness analyses.
Overall Conclusions
There is no direct evidence available comparing iptacopan to pegcetacoplan. To address the evidence gap, the sponsor submitted an unanchored MAIC that assessed the safety and efficacy of iptacopan versus pegcetacoplan. However, no conclusions can be drawn from the MAIC due to serious limitations that undermine the validity of the findings. There was significant heterogeneity between the 2 studies informing the MAIC, and imbalances in important prognostic factors remained after matching and weighting, such that the treatment effect estimates were considered unreliable, as the trial populations were too dissimilar to compare. The MAIC did not analyze key outcomes used in the pharmacoeconomic model as they were not assessed in the APPLY-PNH study (e.g., the proportion of patients with anemia defined as hemoglobin < 105 g/L and discontinuation due to any cause). Thus, there is no comparative evidence available for these important end points.
Based on the CDA-AMC clinical appraisal of the APPLY-PNH trial, in adults with PNH and residual anemia despite treatment with C5 inhibitor, iptacopan likely results in more patients with a clinically important improvement in hemoglobin levels and normalization of hemoglobin (hemoglobin levels ≥ 120 g/L), and fewer patients who require transfusion at 24 weeks compared to C5 inhibitors. These effects associated with iptacopan may be maintained up to 48 weeks. The impact of iptacopan on the frequency of BTH and on the change in LDH levels and ARC were uncertain. Iptacopan may improve fatigue symptoms and HRQoL. AEs were common in both the iptacopan and C5 inhibitor groups, but there were no deaths, and no patients stopped treatment due to AEs.
Pegcetacoplan is the key comparator for patients with PNH who have signs or symptoms of EVH. Thus, there is no evidence available to support a price premium for iptacopan compared to pegcetacoplan. When compared to C5 inhibitors, assuming equal efficacy and discontinuation probabilities for iptacopan and pegcetacoplan, the CDA-AMC base-case results are similar to those reported by the sponsor, despite the limitations of the model that could not be addressed. However, iptacopan was estimated to have a slightly smaller advantage over both C5 inhibitors. Additionally, the cost associated with subsequent therapy costs and health care resource use were no longer discrepant between iptacopan and pegcetacoplan. Iptacopan compared to ravulizumab was associated with an ICER of $62,272 per QALY gained (incremental QALYs gains: 1.53; incremental cost: $95,080, and a 35.3% probability of being cost-effective at a WTP threshold of $50,000 per QALY). At the listed prices, a price reduction of 0.30% would be needed for iptacopan to be cost-effective compared to ravulizumab at a WTP threshold of $50,000 per QALY gained.
CDA-AMC was unable to address all differences in the naive comparison of AEs with pegcetacoplan, and, as a result, differences in QALY for iptacopan and pegcetacoplan remained. Further uncertainty remains regarding the model structure and the confidential discounts negotiated by public plans. The cost-effectiveness of iptacopan in first-, third-, or later-line treatment remains unknown.
References
1.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: iptacopan, hard capsules, 200mg, oral. Montreal (QC): Novartis Pharmaceuticals Canada Inc.; 2024 Aug 15.
2.Hakimi Z, Wilson K, McAughey E, et al. The cost-effectiveness, of pegcetacoplan compared with ravulizumab for the treatment of paroxysmal nocturnal hemoglobinuria, in a UK setting. J Comp Eff Res. 2022;11(13):969-985. doi: 10.2217/cer-2022-0076 PubMed
3.Novartis. APPLY-PNH individual patient data analyses. 2023 [sponsor provided reference].
4.Hillmen P, Szer J, Weitz I, et al. Pegcetacoplan versus Eculizumab in Paroxysmal Nocturnal Hemoglobinuria. N Engl J Med. 2021;384(11):1028-1037. doi: 10.1056/NEJMoa2029073 PubMed
5.Novartis. Clinical Study Report: CLNP023C12302 (Primary End Point Analysis). A randomized, multicenter, active-comparator controlled, open-label trial to evaluate efficacy and safety of oral, twice daily LNP023 in adult patients with PNH and residual anemia, despite treatment with an intravenous anti-C5 antibody [internal sponsor's report]. March 6, 2023.
6.Committee for Medicinal Products for Human Use. Assessment report: Ultomiris (ravulizumab). European Medicines Agency; April 26, 2019. Accessed by sponsor, no date provided.
7.Novartis. Clinical Study Report: CLNP023C12302 (Supplementary Report). A randomized, multicenter, active-comparator controlled, open-label trial to evaluate efficacy and safety of oral, twice daily LNP023 in adult patients with PNH and residual anemia, despite treatment with an intravenous anti-C5 antibody: updated results for the 24-week primary and secondary efficacy analyses [internal sponsor's report]. March 6, 2023.
8.de Latour RP, Szer J, Weitz IC, et al. Pegcetacoplan versus eculizumab in patients with paroxysmal nocturnal haemoglobinuria (PEGASUS): 48-week follow-up of a randomised, open-label, phase 3, active-comparator, controlled trial. Lancet Haematol. 2022;9(9):e648-e659. doi: 10.1016/S2352-3026(22)00210-1 PubMed
9.Novartis. Analysis of APPOINT-PNH and APPLY-PNH Individual Patient Data. 2023 [sponsor provided reference].
10.Hernandez Alava M, Pudney S, Wailoo A. Estimating the Relationship Between EQ-5D-5L and EQ-5D-3L: Results from a UK Population Study. Pharmacoeconomics. 2023;41(2):199-207. doi: 10.1007/s40273-022-01218-7 PubMed
11.Dolan P. Modeling valuations for EuroQol health states. Med Care. 1997;35(11):1095-108. doi: 10.1097/00005650-199711000-00002 PubMed
12.Hernandez Alava MH, Pudney S, Wailoo A. Estimating EQ-5D by Age and Sex for the UK. Decision Support Unit, ScHARR, University of Sheffield; 2022. Accessed by sponsor, no date provided. https://www.sheffield.ac.uk/nice-dsu/methods-development/estimating-eq-5d
13.Matza LS, Stewart KD, Davies EW, Hellmund R, Polonsky WH, Kerr D. Health State Utilities Associated with Glucose Monitoring Devices. Value Health. 2017;20(3):507-511. PubMed
14.National Institute for Health and Care Excellence. Pegcetacoplan for treating paroxysmal nocturnal haemoglobinuria. (Technology appraisal guidance TA778). March 9, 2022. Accessed by sponsor, no date provided. https://www.nice.org.uk/guidance/ta778
15.Statistics Canada. Table: 13-10-0114-01. Life expectancy and other elements of the life table, Canada, all provinces except Prince Edward Island. 2023. Accessed by sponsor, no date provided. https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310011401
16.Alexion Pharma Canada Corp. Ultomiris (ravulizumab): 10 mg/mL and 100 mg/mL, concentrate for solution for intravenous infusion [product monograph]. August 28, 2019. Updated October 30, 2023. Accessed March 14, 2024. https://alexion.com/documents/ultomiris_product_monograph_approved_english
17.Swedish Orphan Biovitrum AB (publ). Empaveli (pegcetacoplan): 1080 mg/20 mL solution for subcutaneous infusion [product monograph]. December 7, 2022. Accessed March 14, 2024. https://pdf.hres.ca/dpd_pm/00068658.PDF
18.Novartis. Iptacopan PNH Opportunity Assessment - report [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: iptacopan, hard capsules, 200mg, oral. June 2024.
19.Committee for Medicinal Products for Human Use. Assessment report: Aspaveli (pegcetacoplan) European Medicines Agency; 2021. Accessed by sponsor, no date provided.
20.Job Bank. Registered Nurse (R.N.) in Canada: Prevailing wages in Canada Wage per Hour (median). Reference period: 2021-2022; Labour Force Survey - Statistics Canada. Government of Canada. 2022. Updated May 2024. Accessed June 17, 2024. https://www.jobbank.gc.ca/marketreport/wages-occupation/993/CA
21.Alberta Interactive Health Data Application. Ambulatory Care Health Costing (E.D.) 2018-2019. 2024. Accessed March 15, 2024. http://www.ahw.gov.ab.ca/IHDA_Retrieval/selectSubCategoryParameters.do
22.Canadian Institute for Health Information. Patient Cost Estimator. CIHI; 2022. Accessed February 23, 2024. https://www.cihi.ca/en/patient-cost-estimator
23.Novartis. National PNH Advisory Board Meeting: meeting report [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: iptacopan, hard capsules, 200mg, oral. March 1, 2024.
24.Ontario Drug Benefit Formulary. DIN 02485265. 2023. Accessed April 2024 [sponsor provided reference].
25.Ontario Ministry of Health. Schedule of benefits for physician services under the Health Insurance Act. 2023. https://www.ontario.ca/files/2024-01/moh-ohip-schedule-of-benefits-2024-01-24.pdf
26.Patriquin CJ, Kiss T, Caplan S, et al. How we treat paroxysmal nocturnal hemoglobinuria: A consensus statement of the Canadian PNH Network and review of the national registry. Eur J Haematol. 2019;102(1):36-52. doi: 10.1111/ejh.13176 PubMed
27.Ontario Ministry of Health. Schedule of benefits for laboratory services. 2023. Accessed March 14, 2024. https://www.ontario.ca/files/2024-01/moh-ohip-schedule-of-benefits-laboratory-services-2024-01-24.pdf
28.Public Health Agency of Canada. Canadian Immunization Guide. 2023. Accessed March 14, 2024. https://www.canada.ca/en/public-health/services/canadian-immunization-guide.html
29.Oliver M, Patriquin CJ. Paroxysmal Nocturnal Hemoglobinuria: Current Management, Unmet Needs, and Recommendations. J Blood Med. 2023;14:613-628. doi: 10.2147/jbm.S431493 PubMed
30.Alexion Pharma Canada Corp. Solaris (eculizumab): 10 mg/mL parenteral solution [product monograph]. January 28, 2009. Updated August 18, 2018. Accessed March 14, 2024. https://alexion.com/Documents/Canada/Product-Monograph-Soliris-English-20Aug2018.aspx
31.CADTH. Reimbursement Review: ravulizumab (Ultomiris). Can J Health Technol. 2022;2(4):1-115. doi: 10.51731/cjht.2022.319
32.CADTH. Pegcetacoplan (Empaveli). Can J Health Technol. 2023;3(5):1-175. doi: 10.51731/cjht.2023.654
33.Novartis Pharmaceuticals Canada Inc. Fabhalta (iptacopan): 200mg, hard oral capsules [product monograph]. January 6, 2025.
34.IQVIA. Market Access Console - Act-Hib (0.5 mL). 2023 [sponsor provided reference].
35.IQVIA. Market Access Console - Bexsero Vaccine Suspension (GSK), Nimenrix Vaccine Powder and Solvent (Pfizer). 2023. Accessed April 29, 2024 [sponsor provided reference].
36.IQVIA. Market Access Console - Prevnar 13 (Pfizer). 2023. Accessed April 29, 2024 [sponsor provided reference].
37.pan-Canadian Pharmaceutical Alliance. Brand Name Drug Negotiations Status: Empaveli (pegcetacoplan). Accessed March 31, 2024. https://www.pcpacanada.ca/negotiation/22333
38.pan-Canadian Pharmaceutical Alliance. Brand Name Drug Negotiations Status: Ultomiris (ravulizumab). Accessed March 31, 2024. https://www.pcpacanada.ca/negotiation/21780
39.pan-Canadian Pharmaceutical Alliance. Brand Name Drug Negotiations Status: Soliris (eculizumab). Accessed November 15, 2024. https://www.pcpacanada.ca/negotiation/20732
40.Canada's Drug Agency. Reimbursement recommendation: danicopan (Voydeya). Can J Health Technol. 2024;4(11):1-34. doi: 10.51731/cjht.2024.1018
41.pan-Canadian Pharmaceutical Alliance. Brand Name Drug Negotiations Status: Voydeya (danicopan). Accessed November 26, 2024. https://www.pcpacanada.ca/index.php/negotiation/22899
42.Canada's Drug Agency. Reimbursement Review: crovalimab. 2024. Accessed October 22, 2024. https://www.cda-amc.ca/crovalimab
43.Health Canada. Patent register. Accessed November 22, 2022. https://pr-rdb.hc-sc.gc.ca/pr-rdb/
44.Kulasekararaj A, Lanza F, Arvanitakis A, et al. Comparative clinical efficacy and safety of biosimilar ABP 959 and eculizumab reference product in patients with paroxysmal nocturnal hemoglobinuria. Am J Hematol. 2024;99(11):2108-2117. doi: 10.1002/ajh.27456 PubMed
45.CADTH. Reimbursement Review: pegcetacoplan (EMPAVELI). Can J Health Technol. 2023;3(5):1-175. doi: 10.51731/cjht.2023.654
46.Novartis. IQVIA Private Capture Rates by Pharmastat (Soliris, Ultomiris). 2024 [sponsor provided reference].
47.Novartis. Iptacopan PNH Opportunity Assessment - report [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: iptacopan, hard capsules, 200mg, oral. June 2024.
48.Statistics Canada. Table: 17-10-0057-01. Projected population, by projection scenario, age and gender, as of July 1 (x 1,000). 2024. Accessed May 22, 2024. https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1710005701
49.Canadian Institute for Health Information. Pan-Canadian prescription drug data landscape. CIHI; 2024. Accessed August 2, 2024. https://www.cihi.ca/sites/default/files/document/pan-canadian-prescription-drug-data-landscape-report-en.pdf
Appendix 1: Cost Comparison Table
Please note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical expert(s). Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 8: CDA-AMC Cost Comparison Table for Treatment of Adult Patients With PNH
Treatment | Strength / concentration | Form | Price | Recommended dosage | Daily cost ($)a | Annual cost ($)a |
|---|---|---|---|---|---|---|
C3 Inhibitor Therapies | ||||||
Iptacopan (TBC) | 200 mg | capsule | $719.9400b | taken orally twice daily | 1,439.88 | 525,916 |
Pegcetacoplan (Empaveli) | 54 mg/mL 1,080 mg/20 mL | 20 mL vial single-dose vial for subcutaneous infusion | 4,970.0000 | First 4 weeks: 1,080 mg twice weekly in addition to patient’s current dose of C5 inhibitor Subsequent weeks: 1,080 mg twice weekly as monotherapy | 1,420.00c | 518,655c |
Pegcetacoplan + Ravulizumab (4 weeks run-in period, 3,000 mg to 3,600 mg) | 1,420.00d | 518,655d | ||||
Pegcetacoplan + Eculizumab (4 weeks run-in period) | First yeare: 1,529.66 Subsequent weeks: 1,420.00 | First yeare: 558,707 Subsequent years: 518,655 | ||||
Danicopan (Voydeya) | 50 mg 100 mg | tablet | 22.9750b 45.9500 | The recommended starting dose is 150 mg 3 times daily Depending on clinical response, dose can be increased to 200 mg 3 times daily b | 206.78 to 275.70 | 75,525 to 100,699 |
Danicopan (150 mg to 200 mg) + Ravulizumab (2,400 mg to 3,600 mg) | First yearf: 1,761.90 to 2,149.82 Subsequent yearsf: 1,507.16 to 1,836.16 | First yearf: 643,532 to 785,222 Subsequent yearsf: 550,490 to 670,658 | ||||
Danicopan (150 mg to 200 mg) + Eculizumab | First year g: 1,701.16 to 1,770.09 Subsequent yearsg: 1,637.20 to 1,706.12 | First yearg: 621,350 to 646,524 Subsequent yearsg: 597,986 to 623,161 | ||||
C5 Inhibitor Therapies | ||||||
Ravulizumab (Ultomiris) | 10 mg / mL | 300 mg single-dose vial for IV infusion | 7,282.1500 | Loading doseh: 2,400 to 3,000 mg then maintenance dose starting 2 weeks after loading dose Maintenance dose: 3,000 mg to 3,600 mg once every 8 weeks thereafter | First yeari: 1,555.12 to 1,874.12 Subsequent yearsj: 1,300.38 to 1,560.46 | First yeari: 568,008 to 684,522 Subsequent yearsj: 474,965 to 569,958 |
Eculizumab (Soliris) | 10 mg / mL | 300 mg single-use vial for IV infusion | 6,675.3000 | Loading: 600 mg every 7 days for the first 4 weeks, then 900 mg for the fifth dose 1 week later Maintenance: 900 mg every 2 weeks thereafter | First yeark: 1,494.39 Subsequent yearsl: 1,430.42 | First yeark: 545,825 Subsequent yearsl: 522,461 |
CDA-AMC = Canada’s Drug Agency.
Note: All prices are from IQVIA Delta PA (accessed May 2024), unless otherwise indicated, and do not include dispensing fees.
aAnnual and daily costs assumed 365.25 days in a year.
bSponsor’s submitted price and recommended dosage.40
cCosts assumed 104.4 1080mg doses in 1 year of pegcetacoplan.
dYear 1 assume 104.4 1080mg doses of pegcetacoplan only (assumed patient would receive pegcetacoplan treatment during the last 4 weeks of the 8-week ravulizumab treatment cycle).
eYear 1 assume 2 900mg doses of eculizumab and 104.4 1080mg doses of pegcetacoplan.
fAssume 6.52 maintenance doses of ravulizumab (52.18 weeks/8) per year
gSubsequent year costs assume 26.1 administrations per year of eculizumab.
hLoading dose and maintenance doses are weight based (refer to product monograph for more options). Ranges were calculated based on doses for patients ≥ 40 kg to < 60 kg (lower range) and ≥ 100 kg (upper range).
iYear 1 assume one loading dose and 6.3 maintenance doses of ravulizumab.
jAssume 6.52 maintenance doses of ravulizumab (52.18 weeks/8) per year
kYear 1 costs assume four 600 mg doses and 24.6 900 mg doses of eculizumab.
lSubsequent year costs assume 26.1 administrations per year of eculizumab.
Appendix 2: Submission Quality
Please note that this appendix has not been copy-edited.
Description | Yes or no | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | No | Refer to limitation “The submitted model does not align with the indicated population or capture all aspects of the condition and its management.” |
Model has been adequately programmed and has sufficient face validity | No | Refer to limitation “Limited validity of the transition probabilities between health states for different treatment arms.” Same input values were generating different probabilities for the same iteration across arms that were assumed to have equivalent efficacy. |
Model structure is adequate for decision problem | No | Refer to limitation “The submitted model does not align with the indicated population or capture all aspects of the condition and its management.” |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | Yes | No comment. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | No | Refer to limitation “Limited validity of the transition probabilities between health states for different treatment arms” and “The submitted model does not align with the indicated population or capture all aspects of the condition and its management.” |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | Yes | No comment. |
Appendix 3: Additional Information on the Submitted Economic Evaluation
Please note that this appendix has not been copy-edited.
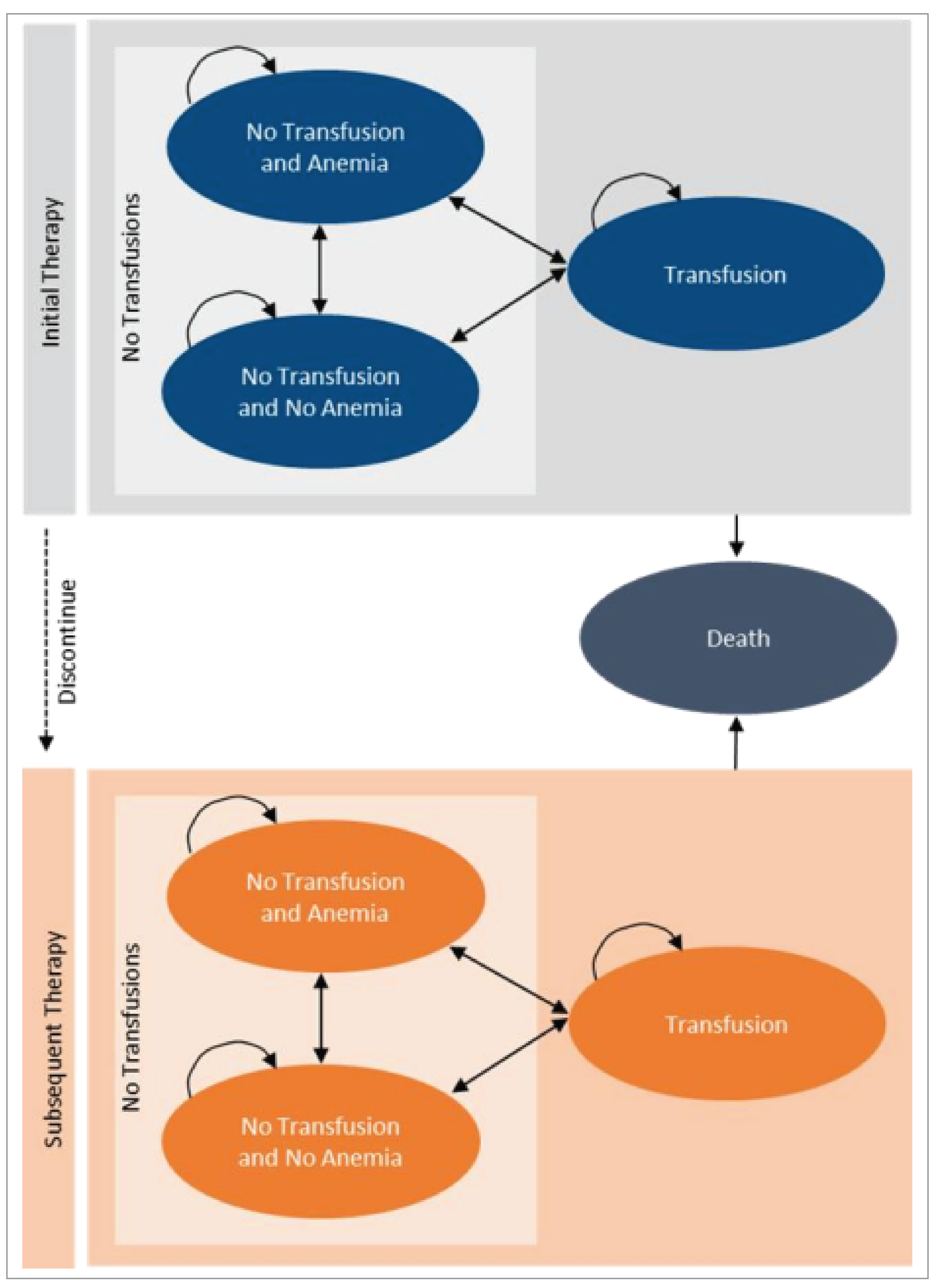
Table 10: MAIC-Weighted Health State Transition Probabilities (Hemoglobin < 105 g/L)
From | To | ||
|---|---|---|---|
No transfusion and anemia | No transfusion and no anemia | Transfusion | |
Iptacopana | |||
No transfusion and anemia | 45.2% | 51.0% | 3.8% |
No transfusion and no anemia | 2.0% | 98.0% | 0.0% |
Transfusion | 34.4% | 51.4% | 14.2% |
Eculizumab/ravulizumaba | |||
No transfusion and anemia | 69.6% | 3.5% | 26.9% |
No transfusion and no anemia | 49.0% | 50.7% | 0.3% |
Transfusion | 29.6% | 3.5% | 66.9% |
Pegcetacoplanb | |||
No transfusion and anemia | 43.7% | 49.1% | 7.2% |
No transfusion and no anemia | 3.1% | 96.6% | 0.3% |
Transfusion | 26.6% | 61.2% | 12.2% |
IPD = individual patient data; MAIC = matching-adjusted indirect comparison.
aDerived from APPLY-PNH IPD and weighted to align with Hakimi et al. (2022) (Table 5.6 from the sponsor’s report).
bAs in Hakimi et al. (2022).2
Table 11: Unweighted Health State Transition Probabilities (Hemoglobin < 105 g/L)
From | To | ||
|---|---|---|---|
No transfusion and anemia | No transfusion and no anemia | Transfusion | |
Iptacopana | |||
No transfusion and anemia | 35.8% | 55.1% | 9.1% |
No transfusion and no anemia | 2.1% | 97.9% | 0.0% |
Transfusion | 9.8% | 52.3% | 37.9% |
Eculizumab/ravulizumaba | |||
No transfusion and anemia | 81.5% | 2.2% | 16.3% |
No transfusion and no anemia | 62.4% | 36.6% | 1.0% |
Transfusion | 23.1% | 2.4% | 74.5% |
Pegcetacoplanb | |||
No transfusion and anemia | 43.7% | 49.1% | 7.2% |
No transfusion and no anemia | 3.1% | 96.6% | 0.3% |
Transfusion | 26.6% | 61.2% | 12.2% |
IPD = individual patient data; MAIC = matching-adjusted indirect comparison.
aDerived from APPLY-PNH IPD (Table 7.4 from the sponsor’s report).
bAs in Hakimi et al. (2022).2
Detailed Results of the Sponsor’s Base Case
Table 12: Disaggregated Summary of the Sponsor’s Economic Evaluation Results
Parameter | Iptacopan | Eculizumab | Ravulizumab | Pegcetacoplan |
|---|---|---|---|---|
Discounted LYs | ||||
Total | 24.86 | 24.86 | 24.86 | 24.86 |
By health state | ||||
No transfusion and anemia | 5.35 | 12.78 | 12.81 | 10.47 |
No transfusion and no anemia | 15.66 | 1.64 | 1.62 | 6.17 |
Transfusion | 3.84 | 10.44 | 10.43 | 8.23 |
Discounted QALYs | ||||
Total | 18.91 | 17.39 | 17.38 | 17.89 |
By health state | ||||
No transfusion and anemia | 3.75 | 9.13 | 9.15 | 7.41 |
No transfusion and no anemia | 12.66 | 1.31 | 1.30 | 5.07 |
Transfusion | 2.50 | 6.96 | 6.95 | 5.42 |
Disutilities | 0.00 | –0.01 | –0.01 | –0.01 |
Discounted costs ($) | ||||
Total | 13,144,359 | 14,947,416 | 13,065,124 | 13,223,585 |
Acquisition | 12,988,450 | 14,516,843 | 12,759,180 | 12,962,259 |
Administration | 0 | 0 | 0 | 40 |
Health care resource use | 145,782 | 305,792 | 305,944 | 252,648 |
Adverse events | 10,128 | 124,781 | 0 | 8,638 |
Total initial therapy costsa | 8,286,726 | 14,947,416 | 13,065,124 | 2,823,101 |
Total subsequent therapy costsa | 4,857,634 | 0 | 0 | 10,400,483 |
AE = adverse event; LY = life-year; QALY = quality-adjusted life-year.
aIncludes drug acquisition, administration, health care resource use, and AEs (described previously) but categorized by initial and subsequent therapy.
Source: Sponsor’s pharmacoeconomic submission.1
Appendix 4: Additional Details on the CDA-AMC Reanalyses and Sensitivity Analyses of the Economic Evaluation
Please note that this appendix has not been copy-edited.
Detailed Results of CDA-AMC Base Case
Table 13: Summary of the Stepped Analysis of the CDA-AMC Base-Case Results
Stepped analysis | Drug | Total costs ($) | Total QALYs | Sequential ICER ($/QALY) |
|---|---|---|---|---|
Sponsor base case | Ravulizumab | 13,625,973 | 18.09 | Reference |
Iptacopan | 13,710,934 | 19.68 | 53,576 | |
Dominated treatments | ||||
Pegcetacoplan | 13,786,536 | 18.61 | Dominated by iptacopan | |
Eculizumab | 15,565,896 | 18.06 | Dominated by all comparators | |
1. CDA-AMC reanalysis 1 (pegcetacoplan assumed equivalent unweighted transition probabilities as iptacopan) | Ravulizumab | 13,602,634 | 18.08 | Reference |
Iptacopan | 13,703,176 | 19.67 | 63,176 | |
Dominated treatments | ||||
Pegcetacoplan | 13,767,854 | 18.61 | Dominated by iptacopan | |
Eculizumab | 15,542,557 | 18.04 | Dominated by all comparators | |
2. CDA-AMC reanalysis 2 (equivalent discontinuation rates between iptacopan and pegcetacoplan) | Ravulizumab | 13,625,973 | 18.09 | Reference |
Iptacopan | 13,710,934 | 19.68 | 53,576 | |
Dominated treatments | ||||
Pegcetacoplan | 13,904,906 | 19.62 | Dominated by iptacopan | |
Eculizumab | 15,565,896 | 18.06 | Dominated by all comparators | |
CDA-AMC base case (deterministic) 1 + 2 | Ravulizumab | 13,602,634 | 18.08 | Reference |
Iptacopan | 13,703,176 | 19.67 | 63,176 | |
Dominated treatments | ||||
Pegcetacoplan | 13,894,899 | 19.65 | Dominated by iptacopan | |
Eculizumab | 15,542,557 | 18.04 | Dominated by all comparators | |
CDA-AMC base case (probabilistic) 1 + 2 | Ravulizumab | 13,025,703 | 17.32 | Reference |
Iptacopan | 13,120,784 | 18.85 | 62,272 | |
Dominated treatments | ||||
Pegcetacoplan | 13,310,226 | 18.84 | Dominated by iptacopan | |
Eculizumab | 14,882,607 | 17.33 | Dominated by iptacopan and pegcetacoplan | |
CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
aReference product is least costly alternative.
bAdd row(s) for additional comparators.
Note: The CDA-AMC reanalysis is based on publicly available prices of the comparator treatments. The results of all steps are presented deterministically unless otherwise indicated, while the cumulative CDA-AMC base case is always presented both deterministically and probabilistically.
Table 14: Disaggregated Summary of CDA-AMC Economic Evaluation Results
Parameter | Iptacopan | Eculizumab | Ravulizumab | Pegcetacoplan |
|---|---|---|---|---|
Discounted LYs | ||||
Total | 24.83 | 24.83 | 24.83 | 24.83 |
By health state | ||||
No transfusion and anemia | 6.02 | 14.61 | 14.61 | 6.02 |
No transfusion and no anemia | 15.21 | 0.83 | 0.83 | 15.21 |
Transfusion | 3.60 | 9.39 | 9.39 | 3.60 |
Discounted QALYs | ||||
Total | 18.85 | 17.33 | 17.32 | 18.84 |
By health state | ||||
No transfusion and anemia | 4.21 | 10.42 | 10.42 | 4.21 |
No transfusion and no anemia | 12.30 | 0.66 | 0.66 | 12.30 |
Transfusion | 2.35 | 6.25 | 6.25 | 2.35 |
Disutilities | 0.00 | –0.01 | –0.02 | –0.02 |
Discounted costs ($) | ||||
Total | 13,120,784 | 14,882,607 | 13,025,703 | 13,310,226 |
Acquisition | 12,968,459 | 14,470,225 | 12,740,274 | 13,142,885 |
Administration | 0 | 0 | 0 | 40 |
Health care resource use | 142,272 | 286,090 | 285,429 | 141,536 |
AEs | 10,053 | 126,291 | 0 | 25,765 |
Total initial therapy costsa | 8,202,765 | 14,882,607 | 13,025,703 | 8,392,208 |
Total subsequent therapy costsa | 4,918,018 | 0 | 0 | 4,918,018 |
AE = adverse event; LY = life-year; QALY = quality-adjusted life-year.
aIncludes drug acquisition, administration, health care resource use, and AEs (described previously) but categorized by initial and subsequent therapy.
Scenario Analyses
Table 15: Scenario Analyses Conducted on the CDA-AMC Base-Case Results (Probabilistic)
Stepped analysis | Drug | Total costs ($) | Total QALYs | Sequential ICER ($/QALY) |
|---|---|---|---|---|
Sponsor base case (probabilistic) | Ravulizumab | 13,065,124 | 17.38 | Reference |
Iptacopan | 13,144,359 | 18.91 | 51,724 | |
Dominated treatments | ||||
Pegcetacoplan | 13,223,585 | 17.89 | Dominated by iptacopan | |
Eculizumab | 14,947,416 | 17.39 | Dominated by iptacopan and pegcetacoplan | |
CDA-AMC base case (probabilistic) | Ravulizumab | 13,025,703 | 17.32 | Reference |
Iptacopan | 13,120,784 | 18.85 | 62,272 | |
Dominated treatments | ||||
Pegcetacoplan | 13,310,226 | 18.84 | Dominated by iptacopan | |
Eculizumab | 14,882,607 | 17.33 | Dominated by iptacopan and pegcetacoplan | |
CDA-AMC Scenario 1: Equivalent BTH and hemolysis probabilities between iptacopan and pegcetacoplan | Ravulizumab | 13,186,032 | 17.57 | Reference |
Iptacopan | 13,280,304 | 19.12 | 60,707 | |
Dominated treatments | ||||
Pegcetacoplan | 13,464,657 | 19.11 | Dominated by iptacopan | |
Eculizumab | 15,086,524 | 17.57 | Dominated by iptacopan and pegcetacoplan | |
BTH = breakthrough hemolysis; CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Appendix 5: Submitted Budget Impact Analysis and CDA-AMC Appraisal
Please note that this appendix has not been copy-edited.
Table 16: Summary of Key Take-Aways
Key take-aways of the budget impact analysis |
|---|
|
BIA = budget impact analysis; CDA-AMC = Canada’s Drug Agency; PNH = paroxysmal nocturnal hemoglobinuria.
Summary of Sponsor’s Budget Impact Analysis
The sponsor submitted a budget impact analysis (BIA) estimating the incremental 3-year budget impact of reimbursing iptacopan for the treatment of adult patients with PNH who have an inadequate response or intolerance to a C5 inhibitor. The BIA was undertaken from the perspective of a public payer in Canada over a 3-year time horizon using an epidemiological approach. The sponsor compared a reference scenario in which iptacopan is not reimbursed to a scenario where iptacopan is reimbursed.
Data for the model were obtained from various sources including published literature, market research conducted by the sponsor, and clinical expert feedback.45-47 Key inputs to the BIA are documented in Table 17.
Key assumptions included:
Patients were assumed to be C5 inhibitor–experienced, hence in the model, patients do not receive loading doses and receive only the maintenance phase of C5 inhibitor treatment.
Patients were assumed to receive a full year (i.e., 365.25 days) of PNH treatment as PNH is a chronic condition requiring ongoing treatment.
As per the Health Canada product monograph for pegcetacoplan, patients starting pegcetacoplan continue taking C5 inhibitor for a four-week run-in period. The sponsor assumed that no patients would receive this treatment overlap in the BIA model.
Table 17: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1 / year 2 / year 3 if appropriate) |
|---|---|
Target population | |
Total adult population | 26,953,90648 |
Prevalent population with PNH | 0.001395%45 |
Diagnosed population | 100% |
Patients treated with C5 inhibitor | 39.3%45 |
Proportion eligible to receive treatment: inadequate response or intolerance to a C5 inhibitor | 48.4%45 |
Proportion covered by public payer | 66% in each drug program (except NIHB which has 100% coverage)18 |
Number of patients eligible for drug under review | 48 / 49 / 50 |
Market uptake (3 years) | |
Uptake (reference scenario) Eculizumab Ravulizumab Pegcetacoplan | ███ █ ███ █ ███████ ███ █ ███████ █ ███ ███ █ ███████ █ ███ |
Uptake (new drug scenario) Iptacopan Eculizumab Ravulizumab Pegcetacoplan | ███ █ ███ █ ███████ ███ █ ███████ █ ███ ███ █ ███████ █ ███ ███ █ ███████ █ ███ |
Cost of treatment (per patient, per year) | |
Iptacopan Eculizumab Ravulizumab Pegcetacoplan | $525,916 $583,036a $513,158b $534,862c |
NIHB = noninsured health benefit; PNH = paroxysmal nocturnal hemoglobinuria.
Note: Cost of treatment does not include loading doses.
aAssumed 69.6% of patients receive 900 mg, 26.1% receive 1,200 mg, and 4.3% receive 1,500 mg doses of eculizumab every 14 days.3
bAssumed 26.8% of patients receive 3,000 mg, 66.0% receive 3,300 mg, and 7.2% receive 3,600 mg doses of ravulizumab based on their weight every 56 days.3,16
cAssumed 81.3% of patients receive 1,080 mg injections twice every 7 days and 18.8% receive a 1,080 mg injection of pegcetacoplan every 3 days.5,17,19,47
Summary of the Sponsor’s BIA Results
The sponsor estimated that reimbursing iptacopan for the treatment of adult patients with PNH who have an inadequate response or intolerance to a C5 inhibitor would result in cost savings of $233,607 in Year 1, $267,397 in Year 2, and $270,372 in Year 3, for a 3-year total budget saving of $771,375.
CDA-AMC Appraisal of the Sponsor’s BIA
CDA-AMC identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
The proportion of patients with PNH with inadequate response or intolerance to a C5 inhibitor may be overestimated. The sponsor assumed that 48.4% of patients with PNH previously treated with C5 inhibitor would have inadequate response or intolerance to C5 inhibitor, referencing the previous CDA-AMC reimbursement review of pegcetacoplan.45 However, this proportion was already deemed overestimated during the reimbursement review of pegcetacoplan. Clinical experts consulted by CDA-AMC for this review estimated that 20% to 30% of patients with PNHs would have inadequate response to C5 inhibitor and few, if any, would be intolerant. Additionally, not all patients with a suboptimal response would require or desire a change in therapy.
In CDA-AMC reanalysis, the proportion of patients with PNH eligible to receive treatment due to inadequate response to, or intolerance to C5 inhibitor was assumed to be 20% based on the feedback by the clinical experts sought by CDA-AMC.
Market shares in the reference scenario are uncertain. The market shares and uptake assumed by the sponsor were sourced from market research conducted by Novartis Canada by an online survey of 3 PNH treater physicians. Clinical experts consulted by CDA-AMC for this review deemed the market shares in the base year to be overestimated for eculizumab and pegcetacoplan and underestimated for ravulizumab. Pegcetacoplan has only recently been introduced in some jurisdictions and a significant proportion of patients still prefer to stay on ravulizumab (instead of switching to pegcetacoplan), even if the response to ravulizumab is suboptimal. Additionally, the market uptake seemed overestimated for pegcetacoplan and underestimated for ravulizumab. By year 3, it would be more reasonable to expect that the majority of these patients would be treated with either ravulizumab or pegcetacoplan, with a slightly bigger proportion being treated with pegcetacoplan.
In CDA-AMC reanalysis, the market shares and uptake in the reference scenario were changed to reflect the clinical experts’ expectations.
The anticipated uptake of iptacopan is not aligned with clinical expert expectations. Based on expert opinion, the sponsor estimated that iptacopan would have a market share of ███ █ ███ █ ███ in Years 1, 2, and 3, respectively. This meant that, in year 3, iptacopan shares would ███████ █████████████ and only 1% of patients would still be treated with ravulizumab. Clinical experts consulted by CDA-AMC for this review felt that the sponsor’s assumptions for iptacopan were too aggressive and underestimated the market shares for pegcetacoplan and ravulizumab in year 3. If all drugs are publicly funded, the clinical experts expect that the market shares in 3 years would be slightly more evenly distributed between iptacopan, pegcetacoplan, and ravulizumab. Treatment choice is ideally likely to become more individualized and fluid between all treatment options (i.e., switching back and forth between treatments) depending on the health status and life circumstances of the patients. Additionally, not all patients with a suboptimal response would require or desire a change in therapy.
In CDA-AMC reanalysis, the market uptake of iptacopan (in Years 2 and 3) and the source of uptake (in year 3) were changed to reflect a more evenly distributed market between iptacopan, pegcetacoplan, and ravulizumab.
Coverage rates are uncertain. The sponsor assumed a coverage rate of 66% (except NIHB population which was assumed to have 100% coverage). However, PNH is a rare disease and the PNH-EVH available treatments are extremely costly. Many jurisdictions also have support programs available to help cover the cost of expensive drugs for rare diseases.49 The sponsor’s approach of estimating the public coverage derived from 2020 to 2023 IQVIA Pharmastat data, using previous eculizumab sales may underestimate public coverage, especially for a drug for a rare disease because it fails to account for the role public support programs play in supporting patients with expensive and rare diseases across Canada.
CDA-AMC conducted a scenario analysis exploring a 100% coverage rate.
Price of drugs paid by public drug plans is uncertain: The analyses by both the sponsor and CDA-AMC are based on publicly available list prices for all comparators. Actual costs paid by public drug plans are unknown.
CDA-AMC could not address this limitation in reanalysis.
CDA-AMC Reanalyses of the BIA
CDA-AMC revised the sponsor’s base case by decreasing the proportion of patients with an inadequate response to or intolerance of C5 inhibitor treatment, changing the market shares in the reference scenario and the market uptake and source of uptake of iptacopan in the new drug scenario. Table 18 notes the assumptions used by the sponsor in comparison to those used by CDA-AMC in the reanalysis.
Table 18: CDA-AMC Revisions to the Submitted Budget Impact Analysis
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
Changes to derive the CDA-AMC base case | ||
1. Proportion of patients with PNH eligible to receive treatment due to inadequate response to, or intolerance to C5 inhibitor | 48.4% | 20% |
2. Market shares in the reference scenario: Base Year, year 1, year 2, year 3 | Eculizumab: ████ ████ Ravulizumab: ████ ███ Pegcetacoplan: ████ ██ | Eculizumab: 40%, 27%, 22%, 15% Ravulizumab: 30%, 35%, 38%, 42% Pegcetacoplan: 30%, 38%, 40%, 43% |
3. Iptacopan market uptake (year 2 and 3) and source of uptake (Year 3) | Iptacopan: ██% in year 2, ██% in year 3 Source of uptake in year 3 Eculizumab: ██% Ravulizumab: ██% Pegcetacoplan: ██% | Iptacopan: 30% in year 2, 40% in year 3 Source of uptake in year 3 Eculizumab: 22% Ravulizumab: 52% Pegcetacoplan: 26% |
CDA-AMC base case | Reanalysis 1 + 2 + 3 | |
CDA-AMC = Canada’s Drug Agency; PNH = paroxysmal nocturnal hemoglobinuria.
Applying these changes decreased the magnitude of the 3-year budget savings to $247,055. The results of the CDA-AMC step-wise reanalysis are presented in summary format in Table 19 and a more detailed breakdown is presented in Table 20.
Table 19: Summary of the CDA-AMC Reanalyses of the Budget Impact Analysis
Stepped analysis | Three-year total ($) |
|---|---|
Submitted base case | –771,375 |
CDA-AMC reanalysis 1 - % of patients with PNH eligible to receive treatment due to inadequate response to, or intolerance to C5 inhibitor | –318,750 |
CDA-AMC reanalysis 2 — market shares in the reference scenario | –771,375 |
CDA-AMC reanalysis 3 — iptacopan market uptake and source of uptake | –597,874 |
CDA-AMC base case (1 + 2 + 3) | –247,055 |
CDA-AMC = Canada’s Drug Agency; PNH = paroxysmal nocturnal hemoglobinuria.
Note: The minus sign represents incremental cost savings.
CDA-AMC conducted the following scenario analyses to address remaining uncertainty, using the CDA-AMC base case (results are provided in Table 20). Consistent with the sponsor’s base case, the results are based on publicly available prices of the comparator treatments.
Assuming a 100% coverage rate.
Table 20: Detailed Breakdown of the CDA-AMC Reanalyses of the BIA
Stepped analysis | Scenario | Year 0 (current situation) ($) | Year 1 ($) | Year 2 ($) | Year 3 ($) | Three-year total ($) |
|---|---|---|---|---|---|---|
Submitted base case | Reference | 26,517,929 | 26,247,243 | 26,413,731 | 26,629,543 | 79,290,517 |
New drug | 26,517,929 | 26,013,637 | 26,146,334 | 26,359,171 | 78,519,142 | |
Budget impact | 0 | –233,607 | –267,397 | –270,372 | –771,375 | |
CDA-AMC base case | Reference | 10,818,312 | 10,781,002 | 10,827,275 | 10,915,043 | 32,523,320 |
New drug | 10,818,312 | 10,684,470 | 10,744,405 | 10,847,390 | 32,276,265 | |
Budget impact | 0 | –96,532 | –82,871 | –67,653 | –247,055 | |
CDA-AMC scenario analysis 1: 100% coverage | Reference | 16,184,474 | 16,127,530 | 16,195,595 | 16,326,983 | 48,650,107 |
New drug | 16,184,474 | 15,983,126 | 16,071,635 | 16,225,786 | 48,280,547 | |
Budget impact | 0 | –144,404 | –123,959 | –101,197 | –369,560 |
CDA-AMC = Canada’s Drug Agency.
Note: The minus sign represents incremental cost savings.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.