Drugs, Health Technologies, Health Systems
Reimbursement Review
Garadacimab (Andembry)
Sponsor: CSL Behring Canada Inc.
Therapeutic area: Hereditary angioedema
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Clinical Review
Abbreviations
AE
adverse event
AE-QoL
Angioedema Quality of Life questionnaire
AESI
adverse event of special interest
ATP
all treated participants
BMI
body mass index
CDA-AMC
Canada’s Drug Agency
CHAEN
Canadian Hereditary Angioedema Network
CI
confidence interval
CrI
credible interval
DIC
deviance information criterion
DSU
Decision Support Unit
ESS
effective sample size
GRADE
Grading of Recommendations Assessment, Development and Evaluation
HAE
hereditary angioedema
HAE Canada
Hereditary Angioedema Canada
HRQoL
health-related quality of life
IPD
individual patient-level data
ITC
indirect treatment comparison
ITT
intention to treat
LTP
long-term prophylaxis
MAIC
matching adjusted indirect comparison
MCID
minimal clinically important difference
MD
mean difference
NICE
National Institute for Health and Care Excellence
NMA
network meta-analysis
RCT
randomized controlled trial
SAE
serious adverse event
SC
subcutaneous injection
SD
standard deviation
SE
standard error
SLR
systematic literature review
SMD
standardized mean difference
TEAE
treatment-emergent adverse event
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Table 1: Background Information of Application Submitted for Review
Item | Description |
|---|---|
Drug product | Garadacimab (Andembry), solution for injection 200 mg per 1.2 mL single-dose prefilled syringe and single-dose prefilled pens, SC |
Sponsor | CSL Behring Canada Inc. |
Indication | For routine prevention of attacks of hereditary angioedema in adult and pediatric patients (aged 12 years and older). |
Reimbursement request | As per indication |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | August 2025 |
Recommended dose | Initial loading dose of 400 mg administered SC as two 200 mg injections on the first day of treatment followed, by a monthly dose of 200 mg |
NOC = Notice of Compliance; SC = subcutaneous.
Introduction
Hereditary angioedema (HAE) is a rare autosomal-dominant genetic disorder that is characterized by recurrent and unpredictable episodes (also known as attacks) of nonpruritic subcutaneous (SC) or submucosal edema. The most commonly affected areas include the extremities (peripheral episodes); gastrointestinal tract (abdominal episodes); and face, oral cavity, and airway (laryngeal episodes).1 The episodes can be painful and disfiguring, with significant functional impairment and decreased health-related quality of life (HRQoL). They can also be life-threatening in the case of laryngeal edema.
The estimated prevalence of HAE is typically cited as 1 in 50,000.1,2 HAE is caused by a deficiency (type I HAE) or dysfunction (type II HAE) of the C1-INH enzyme.1,2 The diagnosis is based on a detailed history, along with confirmatory laboratory diagnostic tests. Physical examination may be normal between episodes. Although the age of onset in patients with HAE is variable, the majority of patients experience their first episode in childhood or adolescence.2 However, due to its clinical heterogeneity and rarity, patients with HAE may experience delayed diagnoses and misdiagnoses.
Long-term prophylactic therapies for HAE are ongoing treatments that aim to reduce the frequency and severity of HAE episodes, and improve patients’ HRQoL. Some therapeutic options are available in Canada for long-term prophylaxis (LTP); however, there is a need for treatments that are better tolerated, improve compliance, and are more convenient.
Garadacimab is a specific inhibitor of activated FXII protein and a fully human recombinant monoclonal antibody that binds to the catalytic domain of activated FXII and inhibits its activity. This ultimately leads to a decrease in bradykinin, the actual mediator of the angioedema in most types of HAE. Garadacimab is being reviewed by Health Canada for routine prevention of attacks of HAE in adult and pediatric patients (aged 12 years and older). The reimbursement request is aligned with the Health Canada indication.
The objective of this report was to perform a systematic review of the beneficial and harmful effects of garadacimab for routine prevention of episodes (also known as attacks) of HAE in adult and pediatric patients aged 12 years and older.
Perspectives of Patients, Clinicians, and Drug Programs
The information in this section is a summary of input provided by the patient and clinician groups who responded to our call for input and from the clinical expert consulted by CDA-AMC for the purpose of this review.
Patient Input
CDA-AMC received 1 submission from Hereditary Angioedema Canada (HAE Canada). HAE Canada gathered information from a national survey of 65 respondents, as well as from a survey of 14 patients who enrolled in the VANGUARD study.
According to the input, HAE has a significant impact on the daily lives of patients and their families. More specifically, patients reported living in fear of unpredictable and debilitating episodes, especially laryngeal episodes. Additional concerns emphasized by patients pertained to the pain associated with the episodes and the possibility of passing on the disease to their children due to its hereditary nature. Patients also noted issues such as having difficulties related to pursuing a career or advanced education, as well as maintaining personal, social, and financial well-being. Unmet needs with currently available treatments included heterogeneity in response to treatment, limited options for LTP, inconvenience of IV treatment or plasma-derived products, lack of access for patients who live in rural areas, and supply interruptions and shortages. With respect to relevant outcomes, the input emphasized improving control of episodes, convenience, and ease of use, as well as reduction of anxiety and fear, which will affect patients’ abilities to work, pursue education, travel, exercise, do household chores, and socialize with family and friends.
Clinician Input
Input From the Clinical Expert Consulted for This Review
HAE is a rare disease comprising different pathways with highly variable severity; however, episodes tend to be life-long. The clinical expert consulted for this review emphasized that a shared decision-making process between the patient and a specialist physician is the cornerstone of treatment of HAE, with treatment tailored to the patient’s specific needs and goals. These include reducing the frequency and severity of episodes, minimizing side effects, improving quality of life, increasing the ability to maintain employment and education, and maintaining independence. Patients with frequent or severe episodes, or those whose lives are most affected by their symptoms, regardless of frequency and severity, are most in need of treatment. The clinical expert noted that HAE has been associated with a 30% mortality rate due to laryngeal episodes,3 and therefore emphasized the need for patients to have access to a range of options, particularly treatments that are better tolerated and improve compliance, and are more convenient.
Garadacimab is indicated for long-term prevention of HAE episodes, and would fit into the treatment paradigm as another option along with the treatments currently in use. In some patients who have severe episodes that interfere substantially with their life, LTP therapy can be initiated early in the course of the disease, and as early as after the first attack. Response to treatment is generally determined by a reduction in the number and severity of episodes, which is expected to result in improved ability for patients to perform activities of daily living. The clinical expert mentioned that patients’ expectations may vary, as some patients target complete or near-complete freedom from all episodes, whereas others may be satisfied with treatment if episodes were reduced by half or even less. Patient referral to specialized physicians who have experience in treating patients with the condition is essential considering the rare nature of HAE.
Because the frequency and severity of episodes can vary over time in any patient, and the condition is life-long, discontinuing any treatment successfully can be challenging, according to the clinical expert. In addition, concomitant factors, including surgeries, infections, or stress, may result in a temporary worsening of the disease and loss of response. In these patients, the expert suggested allowing additional time for a response assessment before discontinuing garadacimab.
Clinician Group Input
CDA-AMC received input from the Canadian Hereditary Angioedema Network (CHAEN). Information for this input was gathered from 9 clinicians with experience in treating patients with HAE.
CHAEN noted that treatment goals for HAE include achieving no angioedema episodes and normalizing patients’ lives. According to the input, unmet needs for currently available treatments include the lack of early and sustained prophylactic efficacy, inconvenient methods of administration, tolerability issues (including damage to the veins), and risk of transmission of infectious agents through plasma-derived HAE treatments. CHAEN indicated that garadacimab is expected to have a reduced burden compared to infused plasma-derived C1-INH products, given that it is not plasma-derived and is administered once monthly by SC injection, which can be performed at home. The input noted that garadacimab should be considered along with other currently available treatments for LTP, with patient preference contributing to the ultimate treatment choice. Response to treatment would typically be determined by the number and severity of episodes, requirement for on-demand acute therapy, emergency department visits, hospitalization and adverse events (AEs). Discontinuation of treatment would be based on the absence of effectiveness and toxicities of the treatment.
Drug Program Input
The drug programs provide input on each drug being reviewed through the CDA-AMC reimbursement review processes by identifying issues that may affect their ability to implement a recommendation. For this review, the drug plans provided questions pertaining mainly to reimbursement criteria and alignment with relevant comparators for initiation, renewal, and discontinuation of therapy. These questions were addressed by the clinical expert consulted for this review. The expert’s responses are included in the Drug Program Input section (Table 5).
Clinical Evidence
Systematic Review
Description of Studies
One study was reviewed. The VANGUARD study (n = 65) was a phase III, multicentre, double-blind, placebo-controlled, randomized controlled trial (RCT) designed to evaluate the efficacy and safety of once-monthly garadacimab SC injection for routine prevention of HAE episodes in adult and pediatric patients aged 12 years and older. On-demand HAE therapies were permitted at any time during the study for the treatment of HAE episodes and were received by patients in both treatment groups.
The primary outcome in the study was the time-normalized number of HAE episodes over 6 months. Each individual HAE episode had to be associated with at least 1 symptom or location. HAE symptoms could develop concurrently or consecutively. Episode resolution was defined as the patient no longer having symptoms of the potential episode for a minimum of 24 hours. Investigator-reported HAE episodes were based on a review of patients’ self-reported HAE symptoms, interference with daily activities, and use of on-demand medication to treat those symptoms. Patients were to be trained on identifying symptoms of a potential HAE episode by the site’s personnel and were asked to notify and report details to the study site within 72 hours of the start of the first symptom. Additional outcomes related to HAE episodes were assessed as secondary outcomes in the trial and included change from baseline in HAE episodes, episodes requiring on-demand treatment, and moderate and/or severe episodes.
HRQoL was an exploratory outcome in the study and was assessed using the Angioedema Quality of Life questionnaire (AE-QoL). The AE-QoL is a patient-reported, disease-specific measure to assess quality-of-life impairment in patients with recurrent angioedema episodes. The questionnaire covers 4 domains (functioning, fatigue or mood, fears or shame, and nutrition). Responses range from never to very often. The total score and individual domain scores are generated and converted to a linear scale of 1 to 100, with higher scores representing higher impairment.
Efficacy Results
HAE Episodes
Outcomes related to HAE episodes were considered appropriate by the clinical expert, as reducing the frequency and severity of episodes is an important treatment goal in HAE. In addition, these were consistent with the patient and clinician input highlighting the importance of better control of HAE episodes, including a reduction in the number and severity of episodes and a requirement for on-demand acute therapy.
In patients with type I and type II HAE, the use of garadacimab was associated with a mean difference between groups in the time-normalized number of HAE episodes reported per patient per month of −1.74 (95% confidence interval [CI], −2.34 to −1.13; P < 0.001) over 6 months versus placebo. In absolute effect, a total of 63 HAE episodes were reported throughout the treatment period in the 39 patients who received garadacimab, while 264 HAE episodes were reported in the 25 patients who received placebo. Results from sensitivity analyses were supportive of the primary analysis. Therefore, treatment with garadacimab results in a clinically important reduction in the number of HAE episodes compared to placebo.
Similarly, the use of garadacimab was associated with a clinically important reduction in the number of HAE episodes requiring on-demand treatment (mean difference between groups per patient per month of −1.63; 95% CI, −2.26 to −1.00; P < 0.001), and in the number of moderate or severe HAE episodes (mean difference between groups per patient per month of −1.23; 95% CI, −1.73 to −0.73; P < 0.001), over 6 months versus placebo.
HAE episodes were also assessed as a reduction from baseline in the number HAE episodes over 6 months compared to that observed with placebo. However, the fact that the run-in period to determine the baseline rate of episodes was relatively short, given the unpredictable nature of HAE episodes, introduced uncertainty surrounding the findings. Garadacimab likely resulted in a clinically important reduction in this outcome, with a between-group difference of 70.46% (95% CI, 51.25% to 89.67%; P < 0.001).
Finally, treatment with garadacimab resulted in a clinically important increase in the proportions of patients who were episode-free over 6 months versus placebo, an outcome that was not affected by the variability in the baseline episode rate. Throughout the treatment period, 24 (61.5%) of 39 patients in the garadacimab group were episode-free, while none of the 25 patients in the placebo group achieved the outcome, resulting in a between-group difference of 61.54% (95% CI, 46.27% to 76.81%; P < 0.001).
AE-QoL Questionnaire
Treatment with garadacimab likely results in a clinically important improvement in HRQoL as measured with the AE-QoL total score over 6 months compared to placebo (mean between-group difference of −24.265; 95% CI, −34.976 to −13.554). In addition, the proportions of patients who achieved a clinically important improvement of 6 points on the AE-QoL total score over 6 months were 87.9% (n = 29 patients out of 39) in the garadacimab group and 55.0% (n = 11 patients out of 25) in the placebo group. However, uncertainty was introduced in the assessment of HRQoL by the fact that the run-in period to determine the baseline rate of episodes was relatively short, given the unpredictable nature of HAE episodes. These findings were likely to be clinically important, based on thresholds identified in the literature.
Harms Results
Totals of 64% of patients receiving garadacimab and 60% of patients receiving placebo reported at least 1 AE. The most common treatment-emergent adverse events (TEAEs) were related to infections, gastrointestinal disorders, and injection-site reactions. One patient who was receiving garadacimab reported a serious adverse event (SAE) of HAE that included a laryngeal episode that was managed with overnight hospitalization and was determined by the investigator to be unrelated to the investigational product. No patient who received placebo experienced an SAE. Treatment with garadacimab appeared to be well tolerated, as there was no withdrawal due to AEs. No deaths were reported in the study. Adverse events of special interest (AESIs) included thromboembolic events, bleeding events, and severe hypersensitivity or anaphylaxis. The sponsor reported that no patients were assessed as experiencing any of these events during the trial. The clinical expert indicated that the overall harms profile of garadacimab in the VANGUARD trial did not raise any particular safety signal.
Critical Appraisal
The VANGUARD trial used a relatively short run-in period to determine the baseline rate of episodes given the unpredictable nature of HAE episodes, which are not necessarily consistent throughout a patient’s life. As a result, there is uncertainty surrounding the baseline rate of attack. However, variability in the baseline episode rate would only affect the interpretation of the analyses based on the change from the baseline. On-demand therapies were permitted at any time during the study for the treatment of HAE episodes, but routine LTP agents were prohibited. Although there were no obvious differences between groups, prior and concomitant medications were reported together, making it impossible to determine with certainty that there were no important differences in the concomitant drugs received. These could change the magnitude of response to current treatment, according to the clinical expert, because some therapies are expected to have a longer-lasting protective effect compared to others. As the VANGUARD study included a placebo control group, there is no direct evidence comparing garadacimab to other LTP therapies. The clinical meaningfulness of the overall number of episodes, the number of moderate or severe episodes, and the number of episodes requiring on-demand treatment can be highly variable across patients depending on how these affect their daily lives, because different individuals are likely to have different priorities and objectives when assessing the magnitude of response to treatments.
Findings from the VANGUARD trial can be considered generalizable to patients in Canada with type I or II HAE, as baseline patient characteristics, disease history, and use of on-demand acute therapies for HAE were considered representative of the population routinely seen in clinical practice. Patients in the study had a baseline episode rate of at least 2 episodes per month, which the clinical expert stated may be higher than the typical frequency at which LTP is initiated in clinical practice. At the other end of the spectrum, the trial only included patients who were medically appropriate for on-demand treatment as the sole management option for HAE, and it may have excluded patients with more severe HAE who could not tolerate discontinuation of current LTP therapy. Only a few adolescent patients were enrolled in the VANGUARD trial; therefore, there are limited data to interpret for this younger age group. Six months was considered a sufficient but relatively short duration to capture a change in HAE episodes, as the disease may be highly variable. Although LTP therapy is potentially life-long, evidence is limited beyond the study follow-up duration.
GRADE Summary of Findings and Certainty of the Evidence
For pivotal studies and RCTs identified in the sponsor’s systematic review, Grading of Recommendations Assessment, Development and Evaluation (GRADE) was used to assess the certainty of the evidence for outcomes considered most relevant to inform expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group.4,5
Following the GRADE approach, evidence from RCTs started as high-certainty evidence and could be rated down for concerns related to study limitations (which refers to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias.
When possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect; if this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., the clinical importance is unclear). In all cases, the target of the certainty of evidence assessment was based on the point estimate and where it was located relative to the threshold for a clinically important effect (when a threshold was available) or to the null.
Table 2 presents the GRADE summary of findings for garadacimab versus placebo.
The selection of outcomes for GRADE assessment was based on the sponsor’s Summary of Clinical Evidence, consultation with a clinical expert, and input received from patient and clinician groups and public drug plans. The following list of outcomes was finalized in consultation with expert committee members:
number of HAE episodes during treatment period
reduction in episode rate during the treatment period compared to the run-in period
HRQoL (AE-QoL).
Table 2: Summary of Findings for Garadacimab vs. Placebo for Prevention of Episodes in Patients With HAE
Outcome and follow-up | Patients, N (studies) | Relative effect (95% CI) | Absolute effects | Certainty | What happens | ||
|---|---|---|---|---|---|---|---|
Placebo | New drug | Difference | |||||
Number of HAE episodes | |||||||
Time-normalized number of HAE episodes per month during the treatment period Follow-up: 6 months | 39, new drug 25, placebo (1 RCT) | NR | Observed mean per month (SD): 2.01 episodes (1.341) | Observed mean per month (SD): 0.27 episodes (0.683) | Mean difference between groups: −1.74 episodes (95% CI, −2.34 to −1.13) | Higha | Garadacimab results in a clinically important reduction in the number of HAE episodes over 6 months compared to placebo |
Reduction in HAE episode rate | |||||||
Reduction in time-normalized number of HAE episodes per month during the treatment period compared to the run-in period Follow-up: 6 months | 39, new drug 25, placebo (1 RCT) | NR | Observed mean (SD): 20.21% (42.661) | Observed mean (SD): 90.67% (22.433) | Mean difference between groups: 70.46% (95% CI, 51.25 to 89.67) | Moderateb | Garadacimab likely results in a clinically important reduction from baseline in the number of HAE episodes over 6 months compared to that observed with placebo |
Patients who achieved a 100% reduction in the number of HAE episodes during the treatment period (who are episode-free) Follow-up: 6 months | 39, new drug 25, placebo (1 RCT) | Mean difference between groups: 61.54 (46.27 to 76.81) | 0 per 1,000 patients | 615 per 1,000 patients | 615 more per 1,000 patients | Highc | Garadacimab results in a clinically important increase in the probability of being episode-free over 6 months compared to placebo |
HRQoL | |||||||
Change from baseline in AE-QoL total score Follow-up: 6 months | 33, new drug 20, placebo (1 RCT) | NR | Observed mean (SD): −2.206 (19.1296) | Observed mean (SD): −26.471 (17.8943) | Mean difference between groups: −24.265 (95% CI, −34.976 to −13.554) | Moderated | Garadacimab likely results in a clinically important improvement in HRQoL as measured with the AE-QoL total score over 6 months compared to placebo |
Proportions of patients who achieved an MCID in AE-QoL total score during the treatment period Follow-up: 6 months | 33, new drug 20, placebo (1 RCT) | NR | 744 per 1,000 patients | 440 per 1,000 patients | 304 fewer per 1,000 patients | Moderated | Garadacimab likely results in a clinically important increase in the number of patients who achieve a clinically important difference on the AE-QoL total score over 6 months compared to placebo |
Harms | |||||||
Patients with SAEs Follow-up: 6 months | 39, new drug 25, placebo (1 RCT) | NR | 0 per 1,000 patients | 25 per 1,000 patients | 25 more per 1,000 patients | Lowe | The evidence is uncertain about the effect of garadacimab on SAEs over 6 months compared to placebo |
AE-QoL = Angioedema Quality of Life questionnaire; CI = confidence interval; HAE = hereditary angioedema; HRQoL = health-related quality of life; MCID = minimal clinically important difference; NR = not reported; RCT = randomized controlled trial; SAE = serious adverse event; SD = standard deviation; vs. = versus.
Note: Study limitations (which refer to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias were considered when assessing the certainty of the evidence. All serious concerns in these domains that led to the rating down of the level of certainty are documented in the table footnotes.
aThe presence of an important effect was based on a threshold of at least 1 time-normalized episode per month as a difference between groups, which was informed by the clinical expert consulted for this review.
bRated down 1 level for study limitation because the VANGUARD trial used a relatively short run-in period to determine the baseline rate of episodes. Given the unpredictable nature of HAE episodes, this limited observation time is adding uncertainty to the baseline rate and affects the interpretation of the analyses based on the change from the baseline. The presence of an important effect was informed by the clinical expert consulted for this review.
cNot rated down because the variability in the baseline episode rate would not affect the interpretation of this outcome, which was based on the between-group difference in the absence of on-treatment episodes. The presence of an important effect was informed by the clinical expert consulted for this review.
dRated down 1 level for study limitation because the VANGUARD trial used a relatively short run-in period to determine the baseline rate of episodes. Given the unpredictable nature of HAE episodes, this limited observation time is adding uncertainty to the baseline rate and affects the interpretation of the analyses based on the change from the baseline. Statistical testing for HRQoL outcomes was not adjusted for multiplicity in the trial and should be considered as supportive evidence. The presence of an important effect was based on a threshold of 6 points identified in the literature.
eRated down 2 levels because of the low number of events in the study, and the absence of statistical comparison between treatment groups.
Sources: CSL312_3001 Clinical Study Report.6 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Long-Term Extension Studies
One long-term extension study has been reviewed and summarized. Study CSL312_3002 is an ongoing multicentre, open-label, phase IIIb study of the clinical safety and efficacy of SC garadacimab in the prophylactic treatment of HAE when administered monthly for at least 12 months. The primary objective of the study was to evaluate the long-term safety of SC administration of garadacimab in the prophylactic treatment of patients with C1-INH HAE. The secondary objectives were to evaluate the long-term efficacy, including patient-reported assessment of response to therapy. Patients enrolled in this study were those who successfully completed the VANGUARD study, patients who successfully completed Study CSL312_2001 (a phase II study not summarized in this review), and patients who were naive to garadacimab. A total of 161 patients entered the open-label extension study, including 35 patients who rolled over from the phase II study, Study CSL312_2001 (N = 2 with FXII HAE); 57 patients who rolled over from the VANGUARD trial; and 69 patients who had not previously participated in a garadacimab study.
The mean time-normalized numbers of HAE episodes per month for all patients and for patients who continued garadacimab from VANGUARD trial were 0.16 (standard deviation [SD] = 0.370) and 0.11 (SD = 0.316), respectively. The mean reduction in the time-normalized number of HAE episodes during the treatment period compared to the run-in period was 94.67% (SD= 11.983) in all patients screened and assigned to treatment (all treated participants [ATP] analysis set), and 96.15% (SD = 9.019) in patients who continued garadacimab from the VANGUARD trial. A total of 59.6% of the responders were episode-free at the data cut-off date of February 13, 2023; the median duration of the efficacy evaluation period in these patients was 13.83 months (range, 3.0 to 21.1). The mean time-normalized numbers of HAE episodes requiring on-demand treatment per month during the treatment period for the ATP set and for those who continued garadacimab from the VANGUARD trials were 0.14 (SD = 0.358) and 0.10 (SD = 0.316), respectively. For the ATP set, the mean time-normalized number of moderate and/or severe HAE episodes per month during the treatment period was 0.11 (SD = 0.277), and the time-normalized number of moderate and/or severe episodes requiring on-demand treatment per month during the treatment period was 0.11 (SD = 0.274). The least squares means for change from baseline to 12 months in the AE-QoL score were 33.337 (standard error [SE] = 1.725) in patients who were treatment-naive (95% CI, −36.7725 to −29.9023) and −2.745 (SE = 1.510) in treatment-experienced patients (95% CI, −5.7623 to 0.2718).
Overall, 135 (83.9%) of 161 patients experienced TEAEs. The most frequently reported TEAEs (≥ 5% of patients) were COVID-19 (36.0%), nasopharyngitis (16.8%), injection-site erythema (6.8%), influenza (6.8%), headache (6.2%), and upper respiratory tract infection (5.6%). No patients were assessed by the investigator as experiencing AESIs, as per the protocol; however, AESIs as identified by a standardized Medical Dictionary for Regulatory Activities query included bleeding events (n = 10) and severe hypersensitivity including anaphylaxis (n = 26). Three patients reported SAEs (2 cases of COVID-19 and 1 HAE attack). Treatment with garadacimab was discontinued in 2 patients due to TEAEs of injection-site irritation (moderate) and mood swings (severe). No deaths were reported.
Critical Appraisal
This open-label study is still ongoing; 3 patients completed the study and 119 patients had at least 12 months of exposure at the data cut-off on February 13, 2023. The lack of a control group precludes making causal statements about benefits and harms compared with any comparator. The open-label nature of the study increases the risk of bias in determining the magnitude of the safety outcomes and efficacy end points that include subjective assessments, because the lack of blinding may affect both patients’ expectations of treatment and investigators’ assessments. The direction and magnitude of this potential bias remain unclear. This study included 71 patients who were previously treated by garadacimab and rolled over from the parent trials. It is possible that patients who continued and remained on the treatment were also those who responded positively to the drug. This may increase the risk of selection bias. There was no imputation of missing values in this trial; however, the attrition rate at the cut-off time was 6.8% and, as a result, the risk of bias due to missing data is not considered high.
Patients who are pregnant or breastfeeding, or who have concomitant conditions such as another form of angioedema, recurrent angioedema associated with urticaria, clinically significant bleeding due to coagulopathy, thrombotic disorder, significant illnesses, and major comorbidities were excluded. The results are therefore not generalizable to these subpopulations. The study included only 10 adolescents; given the small sample size, it is unlikely that the results would be broadly generalizable to all adolescent patients with HAE. In this trial, the maximum allowed dosage for patients with C1-INH HAE was 400 mg per month and the maximum allowed dosage for the 2 patients with a normal C1-INH FXII mutation was 600 mg per month. These values were all higher than the dosing recommended in the product monograph, which recommends an initial loading dose of 400 mg administered as two 200 mg SC injections on the first day of treatment followed by a monthly dose of 200 mg.
Indirect Comparisons
Description of Studies
Due to the lack of direct evidence comparing garadacimab with other existing therapies for routine prevention of episodes of HAE in adult and pediatric patients (aged 12 years and older), the sponsor conducted 2 indirect treatment comparisons (ITCs), including a network meta-analysis (NMA) of several LTP treatments and a separate matching adjusted indirect comparison (MAIC) of garadacimab and lanadelumab.
Efficacy Results
The NMA suggested that garadacimab improved outcomes compared with selected comparators but the confidence in the results varied based on the model used, where the random-effects models produced wide 95% credible intervals (CrIs) that overlapped with unity and likely were more appropriate for including the variation in the results, unlike the primary fixed-effects models.
The MAIC results also suggested that garadacimab was associated with improved efficacy compared with lanadelumab (both administered every 2 weeks and every 4 weeks). The results varied widely depending on the model used (e.g., unadjusted or adjusted), and sensitivity analyses suggested the models were sensitive to the studies included.
Harms Results
In the NMA, the proportion with TEAEs in garadacimab 200 mg once monthly was numerically higher compared with a C1-INH concentrate (Haegarda) 60 mg twice weekly, but numerically lower compared with berotralstat (Orladeyo) 150 mg once daily, lanadelumab (Takhzyro) 300 mg every 4 weeks, and lanadelumab (Takhzyro) 300 mg every 2 weeks. No statistically significantly differences were observed. In the MAIC, safety outcomes were not assessed.
Critical Appraisal
Overall, the ITCs (an NMA and a MAIC) were conducted according to accepted methodological guidance. The potential key limitation of the NMA was the heterogeneity (in effect modifiers and prognostic factors) across the included studies in terms of the study designs and patient characteristics. Other potential limitations included the sparseness of all evidence networks, the fact the connections between treatment nodes were typically informed by only a single trial, the small sample sizes of the included studies, and the relative rarity of HAE events. Together, these limitations may increase the potential for biased treatment-effect estimates, which limited the robustness of the NMA. Despite reasonable procedures to identify and rank potential and relevant effect modifiers, the potential key limitations of the MAIC included the inability to match and adjust important effect modifiers; the number of HAE events was small. Furthermore, the MAIC method reduces the effective sample size (ESS) by up to more than 50%. Overall, the results of the NMA and MAIC should be interpreted with consideration of these limitations. This suggests that the assumption of similarity may not hold true for either ITC, increasing the likelihood of bias and uncertainty about the validity of the results when determining the comparative effectiveness of garadacimab.
Conclusions
In patients with HAE, high-certainty findings from the VANGUARD trial suggest that garadacimab results in a clinically meaningful reduction in HAE episodes versus placebo. Garadacimab also clinically significantly reduced the number of episodes requiring on-demand treatment and the number of moderate or severe episodes. These outcomes are appropriate and consistent with the patient input received, highlighting the importance of achieving better control of such episodes. However, variability in the baseline episode rate limits the interpretation of some additional outcomes that are based on change from baseline, while limited results were reported for time-to-event analyses, precluding a definitive conclusion regarding those findings. Results suggest that patients who were receiving garadacimab experienced improvements in their HRQoL, and this improvement was considered clinically meaningful based on the threshold identified in the literature; however, the analyses are exploratory and therefore were assessed as having moderate certainty. Evidence is limited beyond the study follow-up duration, whereas LTP therapy in clinical practice is potentially life-long. However, results from an open-label extension study suggest that the benefits of garadacimab on HAE episodes were maintained over the current 1-year follow-up.
A relatively high proportion of patients in the VANGUARD trial experienced AEs, most notably relating to infections, gastrointestinal disorders, and injection-site reactions; however, garadacimab appeared to be well tolerated, with only 1 SAE and no withdrawal due to an AE reported. The overall harms profile did not raise any particular safety signal. Findings from the trial were considered generalizable to the patient population in Canada with type I or II HAE. Special consideration may be given to the fact that HAE is a rare and highly variable disease that has been associated with higher mortality rates due to airway obstruction from laryngeal episodes. The input received emphasized the need for access to a range of options, especially treatments that are better tolerated, improve compliance, and are more convenient.
As the VANGUARD trial included a placebo control group, there is no direct evidence comparing garadacimab to other LTP therapies to inform the reimbursement question. The sponsor-provided ITCs suggested garadacimab resulted in improved outcomes compared to selected comparators. However, the inability to confirm the key assumption of similarity undermines the validity of the results from ITCs, indicating they are not reliable for determining the comparative effectiveness of garadacimab.
Introduction
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of garadacimab, solution for SC injection 200 mg/1.2 mL single-dose prefilled syringe and single-dose prefilled pens, for routine prevention of episodes (also known as attacks) of HAE in adult and pediatric patients aged 12 years and older.
Disease Background
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following has been summarized and validated by the review team.
HAE is a rare autosomal-dominant genetic disorder that is characterized by recurrent and unpredictable episodes of nonpruritic SC or submucosal edema, most commonly affecting the extremities (peripheral episodes); genitals and gastrointestinal tract (abdominal episodes); and face, oropharynx. and airway (laryngeal episodes).1 The episodes can be painful and disfiguring, with significant functional impairment and decreased HRQoL, and can also be life-threatening in the case of laryngeal edema, which causes stress for both patients and caregivers.7-11 Although the age of onset in patients with HAE is variable, the majority of patients experience their first episode in childhood or adolescence, with 12 years being the median age of onset.2
The estimated prevalence of HAE is typically cited as 1 in 50,000,1,2 while estimates from Europe range from 1 in 93,000 to 1 in 64,000.12 HAE is caused by the deficiency or dysfunction of the C1-INH enzyme, a protease inhibitor that is a key regulator of the complement-and-contact systems, which leads to the activation of kallikrein and subsequent overproduction of the nanopeptide bradykinin.1,2 Bradykinin binds to bradykinin type 2 receptors on endothelial cells, causing increased vascular permeability, which may lead to angioedema if present in excessive amounts.1,2 Mutations in the SERPING1 gene, which codes for C1-INH, are inherited in approximately 75% of patients with HAE, but mutations may appear de novo in 25% of patients.2
Different forms of HAE that are genetically identifiable include type I due to C1-INH deficiency; type II due to C1-INH dysfunction; HAE with mutation in the gene coding for factor XII; HAE with mutation in the gene coding for angiopoietin-1; HAE with mutation in the gene for plasminogen; HAE with mutation in the gene for kininogen-1; HAE with mutation in the gene for myoferlin; and HAE with mutation in the gene for heparan sulphate 3-O-sulfotransferase. Further, some patients have HAE due to unknown mutations.13 Type I is the most common form of HAE, representing approximately 85% of cases.11
The diagnosis of type I and type II HAE is based on a detailed history, along with confirmatory laboratory diagnostic tests (Table 3). The results of a physical examination may be normal between episodes. Clinical practice guidelines from the World Allergy Organization and the European Academy of Allergy and Clinical Immunology recommend that all patients suspected of having type I or type II HAE should be assessed for blood levels of C4, C1-INH protein, and C1-INH function.2 Other forms of angioedema that should be ruled out include acquired angioedema, ACE inhibitor–induced angioedema, mast cell–medicated angioedema, and idiopathic angioedema.2 The clinical presentation of these other forms of angioedema may be similar to that of HAE but the pathology and management is different.2 Due to its clinical heterogeneity and rarity, patients with HAE may experience delayed diagnoses and misdiagnoses, such as allergic angioedema and appendicitis, leading to unnecessary diagnostic and even surgical procedures due to unfamiliarity with the condition.14,15
Table 3: Types of Hereditary Angioedema
Type of HAE | Type 1 | Type 2 | HAE with normal C1-INH |
|---|---|---|---|
Proportion of HAE cases | 85% | 15% | Uncertain (rare) |
C1-INH level | Low | Normal or elevated | Normal |
C1-INH function | Low | Low | Normal |
C4 level | Low | Low | Normal |
HAE = hereditary angioedema.
Source: Maurer et al. (2018).2
Clinical presentation includes recurrent episodes of edema that typically are nonpitting and nonpruritic. Some of the greatest challenges in HAE are its variability and unpredictability, both between patients and within an individual patient over time. Cutaneous and abdominal episodes are the most frequently type of HAE episodes, reported in more than 90% of patients with HAE.16 Cutaneous episodes may involve areas of the face, extremities, and genitals. Facial swelling may involve the lips, tongue, oropharynx, and periorbital tissues, while swelling of extremities can progress to affect large areas of the arms or legs. Abdominal episodes involve the gastrointestinal tract and can be extremely painful, accompanied by nausea, vomiting, and diarrhea. Laryngeal episodes are the least frequent type of attack, but 50% of patients may experience 1 or more of these potentially life-threatening episodes in their lifetime.17 It is not possible to predict which patients will have a laryngeal episode and when they will occur. They are the primary cause of mortality in patients with HAE because of the risk of asphyxiation.18 The frequency of episodes in patients who are symptomatic but untreated can range from weekly to less than yearly. Without treatment, each episode can last several days.19
HAE episodes are often preceded by prodromal symptoms, such as erythema marginatum, nonpruritic macular rash, tingling, fatigue, or local discomfort.20 The onset of an HAE episode is often unpredictable and can occur without a clear precipitating factor or trigger.2 Known or suspected triggers for HAE episodes can include accidental trauma, dental and medical procedures, psychological stress, fatigue, febrile illness, and the menstrual cycle.2 Exposure to some drugs, including estrogen-containing contraceptives, hormone replacement therapies, and ACE inhibitors, may also trigger HAE episodes.2
Standards of Therapy
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following has been summarized and validated by the review team.
The clinical management of HAE can be categorized as follows:
long-term prophylactic treatment: ongoing long-term treatment to reduce the frequency and severity of HAE episodes and improve patients’ HRQoL
short-term prophylactic treatment: administered to reduce the risk of an episode when exposure to a trigger is anticipated (e.g., before dental or medical procedures)
acute treatment of HAE episodes: administered acutely to reduce the severity and alleviate the symptoms of an attack, minimize the functional impact of an attack, and to reduce morbidity and potential mortality.1
Therapeutic options available in Canada for long-term prophylactic treatment include plasma-derived C1-INH products, lanadelumab, oral attenuated androgens (e.g., danazol), and antifibrinolytics (e.g., tranexamic acid).1 The most commonly used treatments in Canada are C1-INH products, which act by replacing the missing or malfunctioning C1-INH protein in patients with HAE. Three C1-INH products are used in Canada for the treatment of HAE: Cinryze and Haegarda, which are indicated for long-term prophylactic therapy, and Berinert, which is indicated for the acute treatment of HAE episodes. In addition to usage for the acute management of HAE episodes, Berinert is also routinely administered as a long-term prophylactic treatment option, although this is beyond the indication approved by Health Canada. All 3 C1-INH products are derived from human plasma and are administered by IV or SC injection (Table 4). Lanadelumab is a plasma kallikrein inhibitor that is approved for LTP. This recombinant monoclonal antibody is administered by SC injection every 2 to 4 weeks.
The Canadian Hereditary Angioedema Guideline Committee recommends the use of C1-INH products or lanadelumab as first-line options for patients who require long-term prophylactic treatment to manage their condition.1 Its guidelines state that attenuated androgens may be effective for some patients; however, they are not recommended a first-line treatment.1 Androgens or antifibrinolytics may be considered for LTP in patients who have already demonstrated a benefit from these treatments or for those who have problems accessing first-line options, but the Canadian guidelines state that patients should not have to fail androgens or antifibrinolytics before using C1-INH or lanadelumab as LTP.1 The evidence of effectiveness of antifibrinolytics is limited, and androgens are associated with frequent and potentially serious adverse effects.1,2
Drug Under Review
Key characteristics of garadacimab are summarized in Table 3, with other treatments available for routine prevention of episodes of HAE in adult and pediatric patients (aged 12 years and older).
Garadacimab is supplied as a sterile, preservative-free solution for SC administration as a 200 mg per 1.2 mL solution in a single-dose prefilled glass syringe with a needle-safety device or as a 200 mg per 1.2 mL solution in a single-dose prefilled pen. The recommended dose of garadacimab is an initial loading dose of 400 mg administered as two 200 mg SC injections on the first day of treatment followed by a monthly dose of 200 mg. Garadacimab has not been previously reviewed by CDA-AMC.
Garadacimab is a specific inhibitor of activated FXII and a fully human IgG4-lambda recombinant monoclonal antibody that binds to the catalytic domain of activated FXIIa and betaFXIIa and potently inhibits its catalytic activity. FXII is the first factor activated in the contact activation pathway and initiates the inflammatory bradykinin-producing kallikrein-kinin system. The inhibition of FXIIa prevents the activation of prekallikrein to kallikrein and the generation of bradykinin, which is associated with inflammation and swelling in HAE episodes, blocking the cascade of events leading to an HAE attack.
The sponsor’s reimbursement request is for routine prevention of episodes (also known as attacks) of HAE in adult and pediatric patients (aged 12 years and older), which is the same as the Health Canada indication.
Garadacimab is undergoing review by Health Canada through an expedited pathway; specifically, the ACCESS Consortium Pathway — UK, Australia, Switzerland and Canada — are conducting a simultaneous regulatory review. A Health Canada Notice of Compliance for garadacimab was anticipated in December 2024. In the European Union, garadacimab was designated an orphan medicine for the treatment of hereditary angioedema in December 2021.21
Table 4: Key Characteristics of Garadacimab and Other HAE Prophylactic Treatments
Characteristic | Garadacimab (Andembry) | Berotralstat (Orladeyo) | Lanadelumab (Takhzyro) | C1-INH concentrate — human | ||
|---|---|---|---|---|---|---|
Berinert | Cinryze | Haegarda | ||||
Mechanism of action | Plasma kallikrein inhibition | Replace missing or malfunctioning C1-INH protein in patients with HAE | ||||
Indicationa | For routine prevention of attacks of HAE in adult and pediatric patients (aged 12 years and older) | For routine prevention of attacks of HAE in adult and pediatric patients aged 12 years | For routine prevention of attacks of HAE in adolescents and adults | Treatment of acute abdominal, facial, or laryngeal attacks of HAE of moderate to severe intensity in pediatric and adult patients | Routine prevention of angioedema attacks in adults and adolescents with HAE | Routine prevention of HAE attacks in adolescent and adult patients |
Route of administration | SC | Oral | SC | IV | IV | SC |
Recommended dosing | Initial loading dose of 400 mg SC on the first day, followed by 200 mg monthly | 150 mg once daily | 300 mg q.2.w. (300 mg q.4.w. can be considered if the patient is well-controlled for more than 6 months) | 20 IU per kg (IV) for acute attack 20 IU per kg IV or 60 IU per kg SC every 3 to 4 days for prophylaxis (off-label) | 1,000 IU every 3 or 4 days (interval may need to be adjusted according to individual response) | 60 IU/kg body weight twice weekly (every 3 to 4 days) |
Monitoring requirements and serious safety issues | No additional monitoring required over and above usual clinical practice | Patients with known risk factors for thrombotic events should be monitored closely | ||||
Other | Non–plasma-derived | Derived from human plasma | ||||
HAE = hereditary angioedema; q.2.w. = every 2 weeks; q.4.w. = every 4 weeks; SC = subcutaneous.
aHealth Canada–approved indication.
Sources: Product monographs for Andembry,22 Orladeyo,23 Takhzyro,24 Berinert,25 Cinryze,26 and Haegarda,27 and CADTH Technology Review.28
Perspectives of Patients, Clinicians, and Drug Programs
The full patient and clinician group submissions received are available in the consolidated patient and clinician group input document for this review on the project website.
Patient Group Input
This section was prepared by the review team based on the input provided by patient groups.
CDA-AMC received 1 submission from HAE Canada. The authors of the submission are the HAE Canada Advocacy Committee and Board of Directors. HAE Canada is dedicated to increasing awareness of HAE and other related angioedemas and to provide support to patients, caregivers, family members, and health care providers. Additionally, HAE Canada is committed to improving patient access to Health Canada–approved treatments for HAE and other related angioedema.
HAE Canada conducted a survey and gathered information from 14 patients with HAE who enrolled in the VANGUARD study in July 2024. HAE Canada noted that the patients who responded to this survey were also asked to participate in telephone interviews. Additionally, HAE Canada conducted a national survey in June and July 2024 that was designed to gather information from patients and caregivers in order to better understand the needs and experiences of patients with HAE. It drew 65 respondents.
According to the input, patients with HAE rated the impact of HAE according to 6 levels, from no impact up to a very high impact. In the very high impact category, “fear of having an attack while traveling” was reported by 17 (26.2%) of patients followed by “concerns about having children due to hereditary nature of the disease” (12 patients; 18.5%), “ability to work a full time job” (12 patients; 18.5%), “ability to retire as planned” (11 patients; 16.9%), “financial well-being” (10 patients; 15.4%), “social and personal well-being” (10 patients; 15.4%), “career advancement” (9 patients; 14.1%), “ability to participate in physical activities” (8 patients; 12.3%), “ability to attend school regularly” (8 patients; 12.3%), “ability to pursue advanced education” (8 patients; 12.3%), “ability to have healthy lifestyle” (6 patients; 9.2%), ability to effectively parent” (4 patients; 6.2%), and “ability to have healthy relationships with friends and family” (3 patients; 4.6%).
HAE Canada noted that, among 65 respondents of the national survey, the factors that the respondents were most worried about included “experiencing airway/laryngeal attack” (75.4% of respondents) followed by “regular fear of experiencing unpredictable and debilitating attacks” (61.5%), “the pain associate with the attacks” (52.3%), “passing the disease to children” (52.3%), “experiencing an attack in a social setting” (35.4%), “HAE interfering with a relationship” (27.7%), “social isolation and/or stigmatization” (18.5%), “alcohol consumption potentially triggering an HAE attack” (18.5%), “birth control pills containing estrogen potentially triggering an HAE attack” (13.9%), “genital swelling” (13.9%), and “HAE compromising a safe pregnancy” (12.3%). Additionally, other items that respondents identified as relevant factors included restriction of activities, fatigue, guilt, symptom control, age-related issues, impact on sleep and employment, satisfaction with treatment, symptom management, and needle phobia.
HAE Canada explained that some of the concerns with currently available treatments included lack of effectiveness, heterogeneity in response to treatment, lack of options for LTP, extensive damage to the veins at the injection site, difficulty self-administering IV treatment, lack of access for patients who live in rural areas, risk of infection from plasma-derived products, supply interruptions and shortages, no approved treatments for HAE with normal C1-INH in Canada, and increasing demand for plasma-derived products while production is decreasing.
According to the patient group input, based on the 2024 national survey, among 46 respondents who were patients and caregivers, 25.4% reported being very dissatisfied or dissatisfied with the frequency with which they had to treat their HAE episodes. A further 20.6% reported they were neither satisfied nor dissatisfied with the frequency with which they had to treat their HAE episodes. Only 46% of patients reported being satisfied or very satisfied with the frequency with which they had to treat their HAE episodes. HAE Canada noted that survey respondents expressed a desire for more treatment options and easier and faster methods of administration and were concerned about the efficacy of prophylactic treatments, activity limitations, cost of medication, stress of IV administration, and anxiety about possible episodes.
HAE Canada reported that improved outcomes included better control of episodes, convenience and ease of use of treatment, and reduced anxiety and fear that will affect patient’s ability to work, pursue education, travel, exercise, do household chores, and socialize with family and friends.
HAE Canada stated that, based on the results of the survey and interviews with patients who had experience with garadacimab, the respondents experienced significant reductions or complete elimination of HAE episodes, dramatic improvement in quality of life, reduced need for emergency treatments and hospital visits, ease of use and convenience, mental and emotional relief, minimal to no side effects, improved family and social life, and hopefulness regarding their future and the future of their loved ones with HAE. These respondents also were asked about the number of episodes they experienced in the 12 months before beginning garadacimab treatment and 12 months after beginning garadacimab and, based on their answers, HAE Canada reported that, in the 12-month period before beginning garadacimab, 8 patients were experiencing more than 12 episodes and only 1 patient reported no episodes, while in the 12-month period after starting garadacimab, 7 patients did not experience any episodes and none of the patients experienced 7 or more episodes. Among 12 respondents,11 described their personal experience with garadacimab as extremely effective, and 1 patient reported that it was very effective. HAE Canada added that, among 11 respondents, 7 reported the side effects were very tolerable and 1 patient reported they were completely intolerable. Additionally, 6 out of 12 patients reported experiencing a more rapid reduction in the number of HAE episodes while using garadacimab compared to other treatments. Ten out of 12 respondents rated their quality of life while taking garadacimab as high or normal.
Clinician Input
Input From the Clinical Expert Consulted for This Review
All CDA-AMC review teams include at least 1 clinical specialist with expertise in the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by a clinical specialist with expertise in the diagnosis and management of HAE.
Unmet Needs
HAE is a rare disease comprising different pathways with highly variable degrees of severity. Experience from clinical practice suggests that patients coming from different walks of life will have different perceptions of their condition. Prognosis is also variable, as the number and frequency of episodes can vary over time in any particular patient. Episodes tend to be lifelong, and worsen with stress, infection, or physical trauma. Patients with frequent or severe episodes, or those whose lives are most affected by their symptoms regardless of frequency and severity, are most in need of treatment.
The clinical expert indicated that the most important goal is for patients to have as normal a life as possible. More specifically, this includes reducing the frequency and severity of episodes, minimizing side effects, improving HRQoL, increasing the ability to maintain employment and education, and maintaining independence. Treatment goals also include prolongation of life, as laryngeal episodes leading to airway obstruction can be life-threatening. Without treatment, HAE has been associated with a 30% mortality rate.3 As such, the clinical expert noted that some patients are living in constant fear of suffocation from a laryngeal attack. These patients may be willing to take on any treatment, with little regard to AEs or inconvenience, to prevent episodes.
However, not all patients respond to current treatments, and some patients may become refractory over time. Some treatments are also associated with AEs, modes of administration, or costs that are deemed unacceptable by patients. The clinical expert emphasized the need to have access to a range of options, particularly treatments that are better tolerated, improve compliance, and are more convenient.
Place in Therapy
Treatment of HAE is broken down into long-term prophylactic treatment, acute treatment of episodes, and short-term prophylaxis. Garadacimab is indicated for long-term prevention of episodes and would fit into the treatment paradigm as another option along with the treatments presented in Table 4.
Each of the currently available treatments target symptoms and have their own advantages and disadvantages. The clinical expert emphasized that patients are expected to be involved in shared decision-making about the benefits and acceptability of such treatment, taking into account factors such as the number and severity of episodes, patient goals, and treatment acceptability. As there are currently no cures for HAE, treatment needs to be ongoing.
The clinical expert also mentioned the need to avoid medications that exacerbate symptoms, including estrogens, antiandrogens, ACE inhibitors, gliptins, and neprilysin inhibitors.
Patient Population
Patients with C1-INH HAE type I and type II would be best suited for treatment with garadacimab either as a first-line drug or after other treatments failed or were found to be unacceptable. Overall, the population from the VANGUARD study was deemed to be representative of clinical practice, as diagnosis criteria were appropriate and no relevant subgroup of patients were systematically excluded from the trial. The clinical expert suggested that patients with FXII HAE would also likely benefit, although this specific population was not included in the study.
The clinical expert emphasized that there is variability in disease presentation. In some patients who have severe episodes that interfere substantially with their life, especially laryngeal episodes, LTP therapy can be initiated very early in the course of the disease, and as soon as after the first attack. The frequency, location, and severity of the episodes observed in clinical practice are random. The risk for a given patient of experiencing a future HAE episode is not considered to be correlated with disease history; all patients may be at risk of experiencing a severe or life-threatening episode at some point in the disease course.
Patients not suited for treatment with garadacimab would be those with a history of allergic reaction to the drug, those who fail treatment with the drug, those who cannot tolerate or use SC administration, those who do not wish to use any form of prophylaxis, those who are pregnant or considering becoming pregnant at this time, and those who cannot afford the drug. There may also be the rare patient for whom their particular genetic variant does not cause angioedema due to overproduction of bradykinin through the pathway involving FXII.
Assessing the Response Treatment
The clinical expert indicated that response to treatment is generally determined by the reduction in number and severity of episodes. In clinical practice this is expected to improve the ability of patients to perform activities of daily living and, ultimately, quality of life. According to the expert, major outcomes assessed in clinical trials generally align with clinical practice assessments, while being considered more rigorous.
Frequency of assessment is individualized in clinical practice and depends on the number of episodes the patient was experiencing before treatment, and the expected time of onset of action of the chosen therapy.
The clinical expert mentioned that patients’ expectations may vary, as some patients target complete or near-complete freedom from all episodes, whereas others may be satisfied with treatment if episodes were reduced by half or even less.
Discontinuing Treatment
Because the frequency and severity of episodes can vary over time in any patient, and the condition is life-long, discontinuing any treatment successfully can be challenging, according to the clinical expert. In addition, concomitant factors may result in a temporary worsening of the disease and loss of response, including surgeries, infections, or stress. In these patients, the expert suggested allowing additional time for a response assessment before discontinuing garadacimab.
However, discontinuation of garadacimab should be considered if treatment is ineffective, if there are unacceptable toxicities, or if a newer, more acceptable treatment becomes available.
Prescribing Considerations
The clinical expert noted that a patient referral to a specialist is essential considering the rare nature of HAE. Patients should have access to specialized physicians who have experience in treating patients with the condition. Inpatient care may be necessary if there is a severe attack.
More specifically, the medical specialty usually involved in patient follow-ups is clinical immunology and allergy. In some cases, other specialists, including hematologists, otolaryngologists (to help manage the patient’s airway), and gastroenterologists (sometimes first to suspect the diagnosis when a patient presents with otherwise unexplained abdominal pain due to gastrointestinal obstruction from edema) may also care for HAE patients. Emergency department physicians often treat patients with acute episodes but can become involved in ongoing care if a patient requires repeated IV treatments in the emergency department and they are unable or unwilling to manage at home. Finally, some of the patient’s care may be provided by the primary care provider, with the guidance of the specialist physician.
Additional Considerations
The clinical expert emphasized that a shared decision-making process between patient and a specialist physician is the cornerstone of treatment of HAE, with treatment tailored to the patient’s specific needs and goals.
Clinician Group Input
This section was prepared by the review team based on the input provided by clinician groups.
One input received from CHAEN for this submission. CHAEN is an organization of physicians who are interested in HAE or treat patients with HAE. CHAEN’s vision is to help HAE patients in Canada receive appropriate support and care to live full lives. CHAEN is incorporated under the Canada Not-for-profit Corporations Act. Information for this input was gathered from 9 clinicians with experience in treating patients with HAE, and from a literature review.
CHAEN noted that the goal of HAE treatment is to prevent angioedema episodes, control the disease, and normalize patients’ life. CHAEN emphasized that some of the unmet needs and treatment gaps included lack of early or sustained prophylactic treatment, more convenient methods of administration, more treatment options, treatment shortages, side effects, damage to the veins, difficulty in self-administration of IV treatment, difficulty in access to hospital, and risk of the transmission of infectious agents through plasma-derived HAE treatments.
According to CHAEN, because garadacimab is not a plasma-derived treatment and is given subcutaneously and only once per month, it is associated with a lower treatment burden compared to infused plasma-derived C1-INH products. CHAEN added that garadacimab should be considered along with other currently available treatments for LTP, with patient preference contributing to the ultimate treatment choice.
CHAEN explained that the number and severity of episodes, requirement for an on-demand acute therapy, emergency department visits, hospitalization, and AEs are among the outcomes that are used to determine whether a patient is responding to treatment. Some clinics will use angioedema control scores and HRQoL scores.
CHAEN stated that discontinuation of treatment would be based on the ineffectiveness and side effects of the treatment. CHAEN noted that, because garadacimab is a once-monthly SC treatment, administration at home is appropriate.
Drug Program Input
The drug programs provide input on each drug being reviewed through the reimbursement review processes by identifying issues that may affect their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical expert consulted by for this review are summarized in Table 5.
Table 5: Summary of Drug Plan Input and Clinical Expert Responses
Drug program implementation questions | Clinical expert response |
|---|---|
Relevant comparators | |
The pivotal trial (VANGUARD) was placebo-controlled. Placebo may not be an appropriate comparator, given the number of therapies available for LTP of HAE, including:
| This was a comment from the drug programs to inform CDEC deliberations. |
Considerations for initiation of therapy | |
Inclusion criteria for the VANGUARD trial were:
Reimbursement criteria for the other LTP therapies (i.e., lanadelumab and berotralstat) include > 3 HAE attacks within any 4-week period before initiating LTP therapy (that requires the use of an acute injectable treatment). Should the initiation criteria for garadacimab align with that of the other LTP therapies (i.e., > 3 HAE attacks within any 4-week period)? | The clinical expert disagreed with the use of a prespecified number of episodes as a requirement to initiate long-term prophylaxis therapy. This is based on the fact that there is variability in disease presentation. Some patients may have fewer episodes in the prespecified time frame, but these episodes could be sufficiently severe to interfere substantially with their life and warrant treatment (e.g., laryngeal attack). Therefore, the expert recommended that the decision to initiate LTP should be made between patients and treating physicians. |
Should patients who experience more severe but less frequent attacks be eligible for coverage? | The clinical expert emphasized that it is important for patients who experience more severe or more disruptive, but less frequent, episodes to be eligible for coverage. |
What is the place in therapy for garadacimab vs. the other LTP therapies for HAE? | According to the clinical expert, this is still to be determined, but garadacimab is likely to share target population similar to that for lanadelumab. According to the expert, this would likely include HAE FXII, and any other form of HAE that involves the kallikrein-kinin pathway. |
If treatment with garadacimab fails to achieve an appropriate response, should patients try another LTP? | The clinical expert agreed that patients should try another LTP treatment if garadacimab fails to achieve an appropriate response. |
Should patients switch back to comparators after treatment fails to achieve appropriate response? | The clinical expert indicated that this would depend on how well patients were responding to the original treatment before switching, and what factors motivated the switch (e.g., for financial reasons). This would be individualized on a case-by-case basis. |
The indication under review at Health Canada does not specify HAE type (i.e., type I, type II, or type III with normal C1-INH levels and activity). The VANGUARD trial only included patients with type I or type II HAE.
| The clinical expert mentioned anecdotal evidence suggesting that garadacimab may be effective in FXII HAE, but perhaps not in HAE types not involving the kallikrein pathway. The expert noted that, theoretically, drugs would be expected to work in these patients (those who have FXII HAE). Therefore, the expert suggested that consideration for their use be determined on a case-by-case basis. |
The initiation criteria for lanadelumab are as follows:
Should the initiation criteria for garadacimab be aligned with the initiation criteria for other LTP therapies for HAE (i.e., lanadelumab and berotralstat)? | The criterion regarding prior episodes has been previously addressed. The clinical expert described the age and diagnosis criteria as appropriate and should be aligned. However, the expert noted a preference for not excluding systematically patients under 12 years of age if they are symptomatic and if the treating physician deems that LTP is required. |
Considerations for continuation or renewal of therapy | |
How is therapeutic response determined? Is it by the acute use of icatibant (Firazyr) injection? Number of attacks? 50% reduction in number of HAE attacks like berotralstat? | The clinical expert indicated that all of the mentioned response measurements can be considered reasonable and helpful, as patients have a wide variety of disease in terms of number and severity of episodes and requirements for on-demand rescue medication. |
The renewal criteria for lanadelumab are as follows:
Should the renewal criteria for berotralstat be aligned with the criteria for lanadelumab? Should the renewal criteria for garadacimab be aligned with the renewal criteria for other LTP therapies for HAE (including time frame for assessments; definition for response to treatment)? | The clinical expert noted that the renewal criteria can be burdensome, and that, ideally, renewal should be determined on a case-by-case basis. However, the expert added that the criteria were reasonable and that garadacimab could therefore be aligned with the other LTP therapies in that regard. |
Considerations for discontinuation of therapy | |
The discontinuation criteria for lanadelumab are as follows:
Should the discontinuation criteria for garadacimab be aligned with the discontinuation criteria for other LTP therapies for HAE (including definitions of inadequate response, and loss of response)? | The clinical expert suggested that discontinuation be considered, rather than required, based on these criteria. The expert emphasized that concomitant factors such as surgeries, infections, or stress may result in a temporary worsening of the disease and loss of response. In these patients, the expert suggested allowing additional time for response assessment before discontinuing garadacimab. |
Considerations for prescribing of therapy | |
Is there any evidence to support the use of garadacimab in combination with other LTP therapies for HAE? | The clinical expert noted that there is no such evidence, but that LTP therapies are sometimes used in combination in clinical practice, appropriately or not. |
The prescribing criteria for lanadelumab are as follows:
Should the prescribing criteria for garadacimab be aligned with the discontinuation criteria for other LTP therapies for HAE (including being under the care of a specialist experienced in the diagnosis and management of patients with angioedema; maximum reimbursed dose in cases of inadequate response/loss of response)? | The clinical expert agreed with the first criterion regarding being under the care of a specialist. The expert indicated that combining LTP treatments is a topic of interest in clinical practice and that, while some patients may eventually benefit from this, it is generally discouraged. There is currently no evidence in that regard. The expert also noted that, under exceptional circumstances, the dose of garadacimab could be escalated beyond the recommended dose in case of inadequate response. |
Generalizability | |
When should patients switch from a comparator (i.e., lanadelumab or berotralstat) to garadacimab? | The expert indicated that reasons for switching to garadacimab could include lack of efficacy, toxicity, mode of administration, and coverage issues with comparators. |
System and economic issues | |
| This was a comment from the drug programs to inform CDEC deliberations. |
| This was a comment from the drug programs to inform CDEC deliberations. |
CBS = Canadian Blood Services; CDEC = Canadian Drug Expert Committee; HAE = hereditary angioedema; LTP = long-term prophylaxis; pCPA = pan-Canadian Pharmaceutical Alliance; vs. = versus.
Clinical Evidence
The objective of this Clinical Review is to review and critically appraise the clinical evidence submitted by the sponsor on the beneficial and harmful effects of garadacimab, solution for injection 200 mg per 1.2 mL single-dose prefilled syringe and single-dose prefilled pens for SC injection, for routine prevention of episodes of HAE in adult and pediatric patients aged 12 years and older. The focus will be placed on comparing garadacimab to relevant comparators and identifying gaps in the current evidence.
A summary of the clinical evidence included by the sponsor in the review of garadacimab is presented in 4 sections, with our critical appraisal of the evidence included at the end of each section. The first section, the systematic review, includes pivotal studies and RCTs that were selected according to the sponsor’s systematic review protocol. Our assessment of the certainty of the evidence in this first section using the GRADE approach follows the critical appraisal of the evidence. The second section includes a sponsor-submitted long-term extension study. The third section includes indirect evidence from the sponsor. The fourth section would include additional studies that were considered by the sponsor to address important gaps in the systematic review evidence; however, none were included.
Included Studies
Clinical evidence from the following are included in the review and appraised in this document:
1 pivotal study or RCTs identified in systematic review
1 long-term extension study
2 ITCs.
Systematic Review
Contents within this section have been informed by materials submitted by the sponsor. The following has been summarized and validated by the review team.
Description of Studies
One study was identified and included in the systematic review. The VANGUARD study (n = 65) was a phase III, multicentre, double-blind, placebo-controlled RCT designed to evaluate the efficacy and safety of once-monthly SC garadacimab for routine prevention of episodes of HAE in adult and pediatric patients aged 12 years and older. The primary outcome was the time-normalized number of HAE attacks.
Characteristics of the VANGUARD study are summarized in Table 6.
Table 6: Details of Study Included in the Systematic Review
Detail | VANGUARD study |
|---|---|
Designs and populations | |
Study design | Phase III, multicentre, double-blind, randomized, placebo-controlled, parallel-arm study |
Locations | Canada (4 centres), Germany (6 centres), Hungary (1 centre), Israel (1 centre), Japan (6 centres), Netherlands (1 centre), and US (9 centres) |
Patient enrolment dates | Start date: January 27, 2021 End date: June 7, 2022 |
Randomized (N) | Total N = 65 (garadacimab 200 mg, N = 39; placebo, N = 26) |
Inclusion criteria | Inclusion for run-in period:
Inclusion criteria for treatment period:
|
Exclusion criteria |
|
Drugs | |
Intervention | A loading dose of 400 mg of garadacimab (CSL312) administered by SC injection as two 200 mg injections; subsequent 200 mg doses of garadacimab administered by SC once monthly at scheduled times |
Comparator(s) | A volume-matched loading dose of placebo administered SC as 2 injections; subsequent volume-matched placebo administered SC once monthly at scheduled times |
Study duration | |
Screening phase | Up to 1 month |
Run-in phase | Up to 2 months |
Treatment phase | 6 months |
Follow-up phase | 2 months |
Outcomes | |
Primary end point | The time-normalized number of HAE attacks (per month and annualized) based on the investigator’s assessment of patient-reported symptoms in patients treated once a month with either garadacimab (active arm) or placebo (placebo arm) during the period from day 1 through day 182 (6 months) |
Secondary and exploratory end points | Secondary:
Exploratory:
|
Publication status | |
Publications | Craig TJ, Reshef A, Li HH, et al. Efficacy and safety of garadacimab, a factor XIIa inhibitor for hereditary angioedema prevention (VANGUARD): a global, multicentre, randomized, double-blind, placebo-controlled, phase III trial. Lancet. Apr 1 2023;401(10382):1079 to 1090 |
AE-QoL = Angioedema Quality of Life questionnaire; HAE = hereditary angioedema; SC = subcutaneous; WPAI:GH = Work Productivity Activity Index: Global Health.
Source: CSL312_3001 Clinical Study Report.6 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
The VANGUARD study design is illustrated in Figure 1.
Patients who met the eligibility criteria entered a run-in period to confirm their underlying disease status. To be randomized and enter the treatment period, patients had to experience at least 1 episode per month, for a total of at least 2 episodes, without regular prophylactic measures. Patients who had 2 episodes in the initial month could enter the treatment period; patients without an HAE episode during this time frame could continue in the run-in period for an additional month, during which they needed to have at least 2 episodes. Only on-demand HAE therapy was allowed, as long as it had previously been shown to be effective for the acute treatment of episodes.
Eligible patients were randomized in a 3:2 ratio to receive either garadacimab or matching placebo over a 6-month treatment duration. Randomization was performed using interactive response technology and was stratified by age (≤ 17 years or > 17 years) and, for adults, by baseline episode rate observed during the run-in period (1 to fewer than 3 episodes per month, and at least 3 episodes per month).
Patients who successfully completed the VANGUARD study had the option to roll over into an open-label extension study. Patients who chose not to participate in the open-label extension were required to complete the follow-up visit on day 242, which was approximately 3 months after their last dose of study treatment.
Figure 1: VANGUARD Study Design
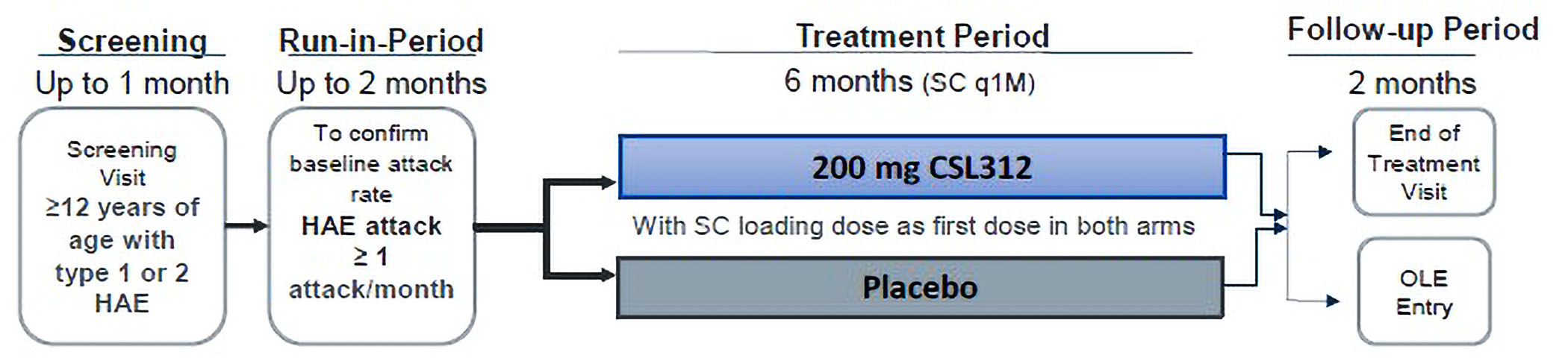
CSL312 = garadacimab; HAE = hereditary angioedema; OLE = open-label phase IIIb Study CSL312_3002; q1M = once a month; SC = subcutaneous.
Source: CSL312_3001 Clinical Study Report.6
Populations
Inclusion and Exclusion Criteria
Patients aged 12 years and older were eligible for the run-in period if they had a clinically confirmed diagnosis of C1-INH HAE, and had experienced at least 3 HAE episodes during the 3 months before screening. To move forward in the trial and enter the treatment period, patients needed to have experienced an average of at least 1 HAE episode per month during the 2-month run-in period (i.e., a total of at least 2 HAE episodes).
Patients were excluded from the trial if they had a concomitant diagnosis of another form of angioedema. Other key exclusion criteria included the concomitant use of estrogen-containing medications with systemic absorption or angiotensin-converting enzyme inhibitors. For adult patients, recent use of C1-INH products, androgens, antifibrinolytics, or other small molecule medications for routine prophylaxis against HAE episodes was prohibited. Patients aged 12 to 17 years were excluded from the study if they used long-term prophylactic therapy for HAE at any time before screening.
Interventions
Patients received either garadacimab at an initial loading dose of 400 mg SC, to be followed by a subsequent dose of 200 mg SC once monthly, or matching placebo. It was mandatory that the first 4 doses be administered by patients or their caregivers under supervision at the study site.
On-demand HAE therapies were permitted at any time during the study for the treatment of HAE episodes if that medication had previously been shown to be effective or was used according to the product label or with deviations from the label as directed by a health care provider. These included plasma-derived or recombinant C1-INH, icatibant, and ecallantide. However, routine LTP to prevent HAE episodes with the use of C1-INH products, androgens, antifibrinolytics, danazol, lanadelumab, or any future approved medication for this indication was prohibited during the study, except for the prevention of HAE episodes before any surgical procedure.
Outcomes
A list of efficacy end points assessed in this Clinical Review is provided in Table 7, followed by descriptions of the outcome measures. Summarized end points are based on outcomes included in the sponsor’s Summary of Clinical Evidence as well as any outcomes identified as important by the clinical expert consulted for this review and input from patient and clinician groups and public drug plans. Using the same considerations, end points that were considered to be most relevant to inform expert committee deliberations were selected and finalized in consultation with members of the expert committee. All summarized efficacy end points were assessed using GRADE. Select notable harms outcomes considered important for informing expert committee deliberations were also assessed using GRADE.
Table 7: Outcomes Summarized From the VANGUARD Study Included in the Systematic Review
Outcome measure | Time point | VANGUARD |
|---|---|---|
HAE attacks | ||
Time-normalized number of HAE attacks during treatment from day 1 through day 182 | Days 1 through 182 (6 months) | Primarya,b |
Reduction in attack rate during the treatment period compared to the run-in period | At 6 months | Secondarya,b |
Proportions of patients who are attack-free | Secondary | |
Time-normalized number of HAE attacks requiring on-demand treatment | Secondary | |
Time-normalized number of moderate and/or severe HAE attacks | Secondary | |
Time to first HAE attack | Event-driven | Exploratory |
Patient-reported outcomes | ||
AE-QoL domain scores, total scores, and change from baseline | Day 182 (6 months) | Exploratorya |
Relevant outcomes not assessed | ||
Health care resource use (e.g., emergency department visits, hospitalizations) | Not assessed | |
HAE = hereditary angioedema; AE-QoL = Angioedema Quality of Life questionnaire; GRADE = Grading of Recommendations Assessment, Development and Evaluation; HAE = hereditary angioedema.
aOutcomes included in the GRADE assessment.
bStatistical testing for these end points was adjusted for multiple comparisons (e.g., hierarchal testing).
Sources: CSL312_3001 Clinical Study Report.6 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
HAE Episodes
The primary outcome in the VANGUARD study was the time-normalized number of HAE episodes, based on the investigator’s assessment of patient-reported symptoms, during the period from day 1 through day 182 and amounting to a follow-up duration of 6 months.
███ █████ ██ ███ ███ ██ █████ ████ █████████ ██ ██████ ███ ███ ████ ██ █████ █████ ███ █ ██ ███ █████████ ███████ ███
Additional outcomes related to HAE episodes were assessed as secondary outcomes in the trial and included change from baseline in HAE episodes, episodes requiring on-demand treatment, and moderate and/or severe episodes. These are consistent with the patient and clinician input received, which emphasized the importance of better control of HAE episodes, including a reduction in the number and severity of episodes, requirement for on-demand acute therapy, and emergency department visits or hospitalizations.
Assessment of HAE Episodes
Accurate identification of potential HAE episodes is crucial to the scientific integrity of the study. Investigator-reported HAE episodes were based on a review of patient diaries, in which patients entered their HAE symptoms, start and end dates, locations, and interference with daily activities. Patients also entered the use of on-demand medication to treat their symptoms. If necessary, the investigator was to collect additional information that may be missing from the diary, or any other relevant information needed for the assessment of patient-reported symptoms. The assessors had to be experienced with HAE, familiar with study patients’ disease histories, and able to rule out if there were any possible alternative etiologies of the symptoms. The etiology of symptoms that were not confirmed as an HAE episode were to be reported as an AE.
Patients eligible for entering the run-in period were to be trained by the site’s personnel on identifying symptoms of a potential HAE attack, on the use of the electronic diary to report symptoms and on the information they needed to report about their symptoms. Patients were asked to notify and report details to the study site within 72 hours of the start of the first symptom(s) of a potential HAE attack. However, if on-demand medication was needed, patients did not have to hold off or delay the start of the medication to treat the symptoms of the potential HAE attack.
Each individual HAE episode had to be associated with at least 1 symptom or location, but could be associated with multiple symptoms or locations. A list of potential symptoms and locations (Figure 2) was provided in the study protocol as a means to assist the investigator without being exhaustive.
Figure 2: VANGUARD Study Protocol Potential Symptoms and Locations
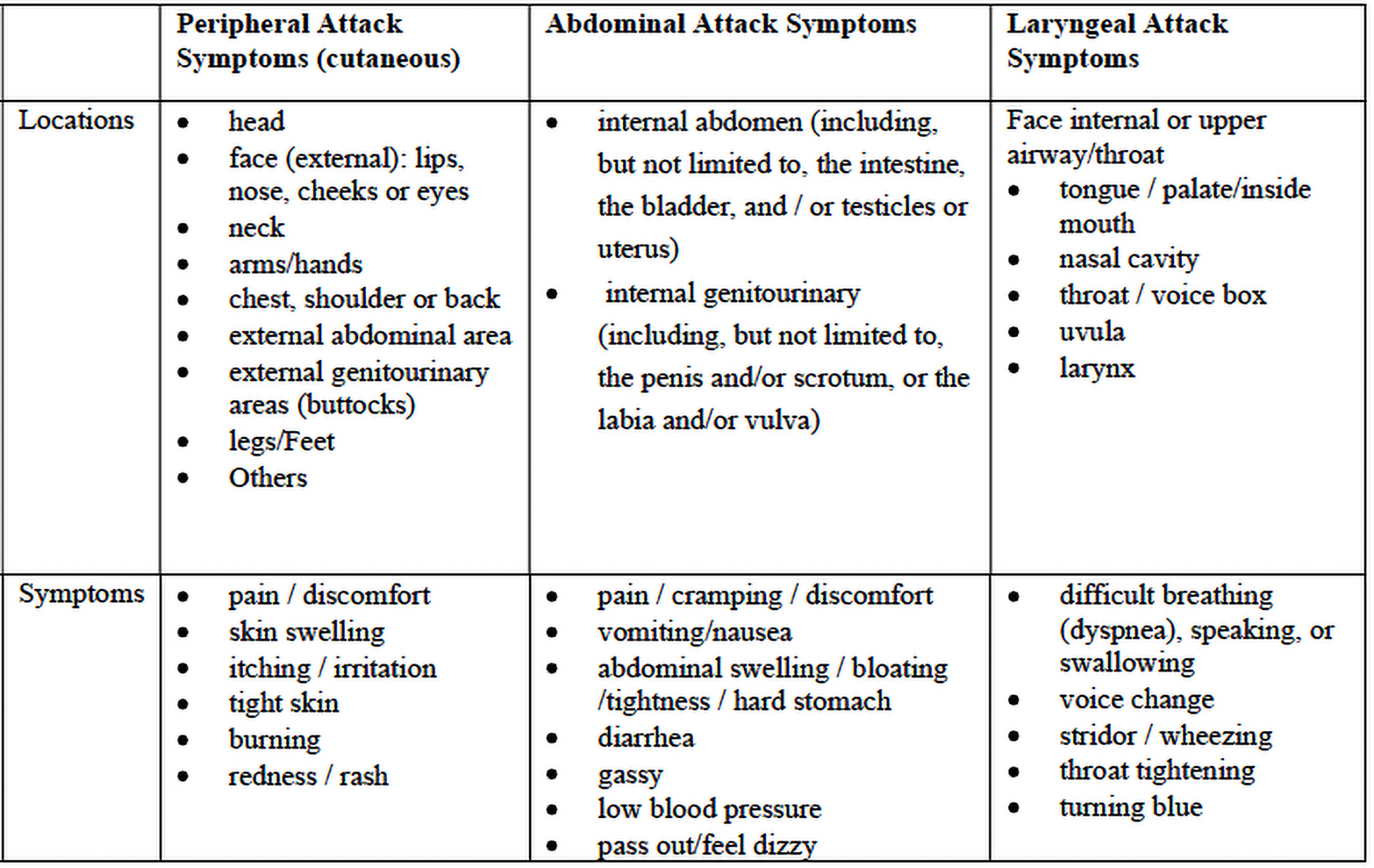
Source: CSL312_3001 Clinical Study Protocol.29
HAE symptoms could develop concurrently or consecutively within 24 hours. Additional symptoms were to be entered as updates. Episode resolution was defined as the patient no longer having symptoms of the potential episode for a minimum of 24 hours. A completely symptom-free 24-hour minimum separation between the resolution of a prior episode and the onset of new symptoms would constitute a new event and was to be reported as a separate single attack, if confirmed by the investigator. The presence of prodromal symptoms or use of on-demand medication to treat the prodromal symptoms, by themselves, was not considered an HAE attack in the study.
Episode Severity
The severity of each HAE episode (mild, moderate, or severe) was assessed by the investigator based on patients’ description of the attack. The severity over the time that the episode develops, progresses, and resolves can range from mild to severe. The overall episode severity was to reflect the maximum intensity of the attack, as assessed by the investigator.
All episodes regardless of the severity were to be associated with perceivable swelling and/or discomfort. Further qualifiers for episode severity, which could vary between patients and episodes, were as follows:
Mild:
The HAE attack causes little to no effect on daily activities.
The use of HAE on-demand medication to treat the attack may not be necessary.
Other concomitant medication (e.g., analgesics) may be used to treat attack symptoms.
Moderate:
The HAE attack causes daily activities to be difficult.
Some assistance may be needed to complete daily activities.
The use of HAE on-demand medication to treat the attack is probable.
Severe:
The HAE attack causes marked limitation of daily activities.
Medical assistance and intervention may be required, including at clinic emergency department visit or hospitalization.
HAE on-demand medication is used to treat the attack.
Patient-Reported Outcomes
The AE-QoL response was an exploratory outcome in the study. The AE-QoL is a patient-reported, disease-specific HRQoL measure to assess the impairment of quality of life in patients with recurrent angioedema episodes.30
The questionnaire consists of 17 questions covering 4 domains (functioning, fatigue or mood, fears or shame, and nutrition).31 Each item presents with 5 levels of response, ranging from 1 (never) to 5 (very often) that is scored from 0 to 4, respectively, over a 4-week recall period. A total score and individual domain scores are generated and converted to a linear scale of 1 to 100, with higher scores representing greater impairment.
The scale was shown to have construct validity and convergent validity, internal consistency, and test-retest reliability,31 with moderate to strong responsiveness depending on the domain chosen.30 A minimal clinically important difference (MCID) of 6 points has been reported for patients with angioedema in the literature using an anchor-based approach,30 which is considered a more direct and patient-centred method (over a distributional criterion approach for example).
Table 8: Summary and Measurement Properties of the AE-QoL
Summary | Conclusions about measurement properties | Conclusions about MCID |
|---|---|---|
The AE-QoL questionnaire is an angioedema-specific, patient-reported, HRQoL measure that consists of 17 questions in 4 domains, functioning, fatigue/mood, fears/shame and food.31 Each item has a total of 5 answers (1 = never to 5 = very often), with each scored 0 to a maximum of 4 points, respectively. A total score, and individual domain scores are generated, and converted on to a linear scale of 0 to 100, with higher scores representing higher impairment. | Validity: Content validity was assessed through data-acquisition, item-generation, and item-reduction phases. Construct validity was assessed using a known-groups approach and demonstrated a linear relationship between self-rated disease and QoL burden with the total AE-QoL score. Strong correlations were observed between the AE-QoL and DLQI total scores, and between the domain scores, supporting convergent validity of AE-QoL in recurrent angioedema.31 Reliability: Reliability of the AE-QoL instrument was demonstrated through internal consistency and test-retest assessments in 1 study.31 The AE-QoL was found to have excellent internal consistency for the whole instrument as well as across each domain (Cronbach alpha > 0.80). The AE-QoL was shown to have acceptable test-retest reliability for the total score and individual domains (Pearson coefficient > 0.70). Responsiveness: One study investigated responsiveness of the AE-QoL measure to change in a sample of 278 patients with recurrent angioedema by correlating changes in scores over time with changes in the applied anchors (self-rated angioedema disease and QoL burden and SF-12).30 The AE-QoL total score changes over time correlated moderately with changes in the self-rated angioedema activity and strongly with angioedema-specific quality-of-life impairment. The functional domain was observed to be the most sensitive to change. AE-QoL total score changes correlated weakly with changes in the SF-12 physical and mental component scores. | The MCID was estimated to be 6.0 points for the total AE-QoL score, based on an anchored-based approach in a sample population of 278 patients with recurrent angioedema.30 No MCID has been determined for domain-specific scores. |
AE-QoL = Angioedema Quality of Life questionnaire; DLQI = Dermatology Life Quality Index; HRQoL = health-related quality of life; MCID = minimal clinically important difference; SF-12 = Short Form (12) Health Survey.
Statistical Analysis
A summary of the statistical analyses is presented in Table 9.
Primary End Point Analysis
The primary efficacy end point, time-normalized number of HAE episodes during treatment period from days 1 through 182, was compared between garadacimab and placebo using a nonparametric 2-sided Wilcoxon test (first hierarchical test of null hypothesis 1; alpha = 5%). For this type of data (i.e., count per rate data), a Poisson regression with potential adjustments for overdispersion is generally the preferred approach for primary analysis in clinical trials, which was conducted as a sensitivity analysis.
The time-normalized number of HAE episodes was not calculated if the patient’s observation time for the treatment period was less than 30 days (i.e., the patient discontinued the study within 30 days after first administration of study treatment). It was assumed that the episode rate for patients who discontinued the study after day 30 and before the end of the sixth month was comparable to the episode rate in patients who were observed for the entire 6-month treatment period. This assumption was based on data from the phase II dose-ranging study, CSL312_2001, which showed that the garadacimab treatment effect was maintained over time.
HAE episodes with a start date on or after the first day of the run-in period but before the date and time of the first study drug administration was counted for the run-in period, whereas HAE episodes occurring after the first drug administration was included in the analyses of efficacy.
Key Sensitivity Analyses of the Primary End Point
As a sensitivity analysis, the primary end point was analyzed using a generalized linear model for count data assuming a Poisson distribution with the logarithm as a link function. The time-normalized number of HAE episodes during the run-in period and treatment were included as a covariate and the logarithm of the length of patient treatment was included as an offset variable. The model accounted for overdispersion by applying Pearson chi-square scaling of standard errors.
To assess the impact of missing data, the following systematic approach was applied. For each treatment arm, a range of values for the number of time-normalized HAE episodes per month from 0 to 6 subdivided into 9 increments between 2 consecutive integer values was generated. All possible combinations from the subdivided ranges were imputed to replace the missing values. For the comparison of active treatment versus placebo, observed and imputed data were analyzed using a Wilcoxon test and the results were classified as negative (i.e., placebo significantly better), neutral (i.e., no significant difference), or positive (i.e., active treatment significantly better). A graph in which the x axis presents the subdivided range for placebo and the y axis the subdivided range for the active treatment was visualized for all scenarios, with the different outcomes indicated by different colours and symbols. The total number of patients with a missing outcome in the placebo and active treatment arms was added to the graph.
The primary end point was also analyzed for patients in the per-protocol population by excluding those who did not comply with the protocol.
Secondary End-Point Analyses
Change from Baseline in HAE Episodes and Responder Analysis
The percentage reduction in the time-normalized number of HAE episodes was calculated within a patient as:
███ █ ██ █ ████████████████ ██████ ██ ███ ███████ ███ █████ ██████ █████████ ██████ █ ███████████████ ██████ ██ ███ ███████ ███ █████ ██████ ████████ ██ ████ ██ ██████ ██████████ █ ██████████ ██ ██████ █ ███ █ █████ ████ ██ ██████ ███████.
The percentage reduction in the time-normalized number of HAE episodes was calculated for the entire 6 months of the treatment period and was summarized and tested via a 2-sided Wilcoxon test with a 5% alpha.
The number and percentage of responders and nonresponders was presented with corresponding 95% CIs. A patient was classified as a responder if the percentage reduction in time-normalized HAE episodes was 50% or greater. In addition, the number and percentage of patients with percentage reductions of 70% or greater and 90% or greater were presented with corresponding 95% CIs.
The number and percentage of patients with a percentage reduction of 100% (i.e., those who did not experience an HAE episode and so were episode-free), were presented and summarized with corresponding 95% CI, for the treatment period. A Fisher test was performed to assess for differences between treatments.
HAE Episodes Requiring On-Demand Treatment
The time-normalized number of HAE episodes per month requiring on-demand treatment was calculated as:
███ █ ██ █ ███████ ██ ███ ███████ █████████ █████████ █████████ ██████ █████████ ██████ █ ██████ ██ ███████ █████████ ██ ██████ █ ███████ and was summarized descriptively.
An HAE episode requiring on-demand treatment was defined as an episode for which the date of administration of an on-demand treatment is between (and inclusive of) the start and end dates of an HAE attack. Differences between the treatment arms were tested in an exploratory manner via a 2-sided Wilcoxon test with an alpha of 5%.
Moderate and/or Severe HAE Episodes
For the analysis of the time-normalized number of moderate and/or severe HAE episodes, an analogue calculation was conducted with all the HAE episodes classified as moderate or severe, using the definition described previously.
Exploratory End-Point Analyses
Exploratory end points were summarized descriptively by treatment arm and study visit. All tests were exploratory to an alpha of 5%. Outcomes using the AE-QoL questionnaires were summarized and listed by treatment arm and visit, showing observed values and change from baseline (if applicable).
From the AE-QoL, domain scores (functioning, fatigue and mood, fears and shame, and nutrition), total scores, and changes from baseline were summarized for each treatment arm by study visit. Mean total scores and SDs were plotted for each treatment arm against the study visits, and mean domain scores and SDs were displayed in analogue figures. A mixed model for repeated measures was used to test for a treatment effect, a time effect, and a treatment-by-time interaction on the total and domain scores for study visits.
The GLMSELECT procedure in SAS was performed as a model selection procedure identifying if the MCID of at least 6 points for the total score and domain scores from day 1 to day 182 was associated with age, baseline episode rate (1 to < 3 episodes per month versus ≥ 3 episodes per month was used for randomization), maximum severity of HAE episodes during run-in period, and the anatomic location of the HAE episodes (i.e., any laryngeal episodes versus no laryngeal episodes in the run-in period). Logistic regression for total and domain scores with these variables was performed to analyze for a treatment effect on achieving an MCID of at least 6 points (from day 1 to day 182). In addition, a final linear regression model for total and domain scores with the same selected variables was performed showing change from baseline in AE-QoL scores at study visit day 182.
Mean and median AE-QoL scores for each visit from visit day 31 onward were assessed for the time duration of being episode-free.
Sample Size and Power Calculation
The sample-size calculation was performed in SAS 9.4. A total of 60 patients were planned to be randomized. It was estimated that 40 patients with C1-INH type I and II HAE completing the 6-month treatment period were needed to achieve approximately 90% power for a 2-sided Wilcoxon test with a 5% alpha. Patients were randomized to the garadacimab or placebo arm at a ratio of 3:2. Episode rates of 0.3125 and 1.3 per month were assumed for patients receiving garadacimab and placebo, respectively, based on the number of episodes during the run-in period observed for 2 months to record their baseline episode rate. The monthly episode rates of placebo and of garadacimab were assumed to have a Poisson distribution.
The calculation was targeted to randomize approximately 5 adolescent patients at a randomization ratio of 3:2 (garadacimab:placebo).
To allow for sufficient safety data, increase the likelihood of adolescent patients entering the study, and have at least 40 patients reach the end of the study, an additional 20 patients were planned to be randomized. In the event it was not feasible to randomize the targeted number of adolescent patients, the targeted total sample size was to be achieved by randomizing the needed number with adult patients. The target included 5 Japanese patients in the 60 randomized patients.
Statistical Testing and Multiplicity
To control for type I error, the 1 primary and 3 secondary end points were tested in a hierarchical order with an alpha of 5% each:
percentage reduction in the time-normalized number of HAE episodes
percentage of patients with a percentage reduction of 100%
participant’s global assessment of response to therapy (an outcome that was not included in this review).
Four null hypotheses were defined, 1 for the primary end point (H01) and 3 for the 3 secondary end points (H02, H03, and H04). The null hypothesis associated with each of these end points is given below:
H01: the time-normalized number of HAE episodes in the first 6-month time period of the active arm and in the placebo arm period are equal.
Hypothesis 02: The percentage reduction in the means of the time-normalized number of HAE episodes for the 6 months of the active arm and the 6-month placebo arm period are equal.
Hypothesis 03: The number of patients who do not experience an HAE episode in the first 3 months of the active arm and the first 3-month of the placebo period are equal.
Hypothesis 04: The percent of patients with good or excellent responses at the end of the treatment period (day 182) is equal for patients treated with garadacimab and placebo.
The 4 hypotheses were tested in the sequence listed, such that the first hypothesis in the list was tested first, and if the null hypothesis was rejected (i.e., statistically significance was reached at a 2-sided P < 0.05), the second hypothesis was tested next, and so on. If any hypothesis was not statistically significant, none of the following hypotheses (including the 1 which was not statistically significant) were tested for multiplicity. This hierarchical testing procedure controlled for the overall alpha level of 5%. All other tests were performed with a 2-sided alpha of 5% in an exploratory manner, i.e., without controlling for multiplicity.
Handling of Missing Data
Only missing values for the primary efficacy end point (time-normalized number of HAE episodes) during the treatment period had an impact on the primary analyses. The time-normalized number of HAE episodes was considered missing for patients who discontinued within 30 days after the first study treatment administration. It was assumed that the outcomes for discontinued patients were comparable to the outcomes for those who did not. This assumption also applied to secondary end points that were also based on the HAE episode rate.
Patients missing the assessment of treatment relationship for AEs and SAEs had the worst case assumed to impute the relationship; if the relationship to study treatment was missing and the event started on or after the first administration of study treatment it was assumed to be “related.” If the AE or SAE with a missing relationship started before the first injection of study treatment (e.g., during the screening or run-in period), it was considered “not related” (a realistic case). For variables that determined the proportion of events (e.g., AEs), all patients with a nonmissing value in the respective analysis set were included in the denominator when calculating the percentages, unless otherwise stated.
Subgroup Analyses
No relevant subgroup analyses were reported.
Table 9: Statistical Analysis of Efficacy End Points in the VANGUARD Study
End point | Statistical model | Adjustment factors | Handling of missing data | Sensitivity analyses |
|---|---|---|---|---|
Time-normalized number of HAE attacks per month during treatment period | 2-sided Wilcoxon test | Stratification factors: age (≤ 17 years, > 17 years) and, for adults, patient’s baseline attack rate (1 to < 3 attacks/month, and ≥ 3 attacks/month) during run-in period | Patients discontinuing within 30 days after starting treatment were excluded from analysis |
|
Reduction in time-normalized number of HAE attacks during treatment period compared to run-in | 2-sided Wilcoxon test | None | Not done | Not done |
Time-normalized number of HAE attacks per month requiring on-demand treatment | 2-sided Wilcoxon test | None | Not done | Not done |
Time-normalized number of moderate or severe HAE attacks | 2-sided Wilcoxon test | None | Not done | Not done |
AE-QoL | MMRM | Fixed effects: treatment and baseline attack rate, study visit, and treatment-by-study visit interaction and a repeated statement for patient | Not done | No done |
AE-QoL = Angioedema Quality of Life questionnaire; HAE = hereditary angioedema; MMRM = mixed model for repeated measures.
Sources: CSL312_3001 Clinical Study Report.6 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Analysis Populations
Table 10: Analysis Populations of the VANGUARD Trial
Population | Definition | Application |
|---|---|---|
ITT analysis set | All randomized patients. Patients were analyzed in the treatment arm assigned at randomization, regardless of treatment actually received | Primary and secondary end points |
Per-protocol set | All patients in the ITT analysis set who received at least 1 dose of the investigational product and who complied with the protocol | Primary end point |
Safety analysis set | All patients randomly assigned to treatment who received at least 1 dose of the investigational product; patients were analyzed according to the actual treatment received | Exploratory end points and safety end points |
ITT = intention to treat.
Sources: CSL312_3001 Clinical Study Report.6 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Results
Patient Disposition
Of the 80 screened patients, 4 (5.0%) did not meet the inclusion criteria. A total of 76 patients entered the run-in period. Of these, 11 patients (████) discontinued the run-in period. The most common reason (63.6%) was that patients did not meet the run-in completion criteria.
As a result, 65 patients were randomized into the trial in a 3:2 ratio. A total of 39 patients were assigned and received garadacimab, while 25 patients were assigned and received placebo. One patient in the placebo arm was randomized to blinded treatment in error, never received study treatment, and therefore was not included in any postrandomization analysis.
There were no discontinuations in the garadacimab treatment arm, while 3 patients (12.0%) in the placebo arm discontinued the study (withdrawal by patient). A total of 38 patients (97.4%) in the garadacimab group and 22 (88.0%) in the placebo group completed the study. No information was reported regarding the patient who received garadacimab and did not complete the study.
Table 11: Summary of Patient Disposition From Studies Included in the Systematic Review
Patient disposition | VANGUARD study | |
|---|---|---|
Garadacimab 200 mg (N = 39) | Placebo (N = 25) | |
Screened, N | 80 (100.0) | |
Screening failure, n (%) | 4 (5.0) | |
Reason for screening failure, n (%) | ||
Did not meet inclusion criteria | 4 (100.0) | |
Run-in period, N (%) | 76 (95.0) | |
Discontinued during run-in period, n (%) | 11 (13.8) | |
Reason for discontinuation, n (%) | ||
Did not meet run-in completion criteria | 7 (63.6) | |
Adverse event | 1 (9.1) | |
Lost to follow-up | 1 (9.1) | |
Withdrawal by patient | 1 (9.1) | |
Other | 1 (9.1) | |
Randomized, N (%)a | 65 (81.3) | |
Randomized and received loading dose, N (%) | 39 (100.0) | 25 (100.0) |
Discontinued from study, n (%) | 0 (0.0) | 3 (12.0) |
Reason for discontinuation, n (%) | ||
Withdrawal by patient | 0 (0.0) | 3 (100.0) |
Completed treatment period, N (%) | 39 (100.0) | 22 (88.0) |
Completed study, N (%) | 38 (97.4) | 22 (88.0) |
Full analysis set, N | 39 | 25 |
Per-protocol, N | 39 | 24 |
Safety, N | 39 | 25 |
aOne patient was randomized to blinded treatment in error, never received treatment, and therefore was not included in any postrandomization analysis.
Source: CSL312_3001 Clinical Study Report.6 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Baseline Characteristics
The baseline demographic characteristics are outlined in Table 12. There were slight numerical differences between groups. For example, the patients’ ages differed marginally between treatment arms, with patients in the garadacimab group appearing to be slightly older than patients in the placebo group. In addition, the proportion of women was numerically higher with garadacimab compared to placebo. The clinical expert noted that women tend to have a worse disease course, as estrogens affect various parts of the bradykinin cascade and decrease the level of C1-INH. However, overall, the differences observed in the trial are not expected to affect the risk of experiencing an HAE attack, according to the clinical expert.
Six patients were less than 18 years of age (4 patients in the garadacimab group and 2 patients in the placebo group). The mean age of these patients was 14.5 (SD = ████) years, with patients ranging in age from 12 to 17 years.
Table 12: Summary of Baseline Characteristics From the VANGUARD Study (ITT Analysis Set)
Characteristic | Garadacimab 200 mg (N = 39) | Placebo (N = 25) |
|---|---|---|
Sex, n (%) | ||
Male | 15 (38.5) | 11 (44.0) |
Female | 24 (61.5) | 14 (56.0) |
Ethnicity | ||
Hispanic or Latino | 1 (2.6) | 2 (8.0) |
Not Hispanic or Latino | 37 (94.9) | 23 (92.0) |
Not reported | 1 (2.6) | 0 |
Race, n (%) | ||
Asian | 4 (10.3) | 2 (8.0) |
Japanese | 4 (10.3) | 2 (8.0) |
Black or African American | 0 | 1 (4.0) |
Native Hawaiian or other Pacific Islander | 1 (2.6) | 0 |
White | 33 (84.6) | 22 (88.0) |
Other | 1 (2.6) | 0 |
Age (years) | ||
Mean (SD) | 43.3 (17.45) | 37.8 (12.80) |
Median (minimum to maximum) | 43.0 (12 to 69) | 38.0 (14 to 62) |
95% CI | (37.68 to 48.99) | (32.56 to 43.12) |
BMI at screening (kg/m2) | ||
Mean (SD) | 27.85 (6.021) | 28.37 (7.563) |
Median (minimum to maximum) | 27.70 (19.3 to 52.7) | 25.70 (18.7 to 42.7) |
95% CI | (25.902 to 29.805) | (25.246 to 31.490) |
BMI = body mass index; CI = confidence interval; ITT = intention to treat; SD = standard deviation.
Sources: CSL312_3001 Clinical Study Report.6 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
The HAE disease history outlined in Table 13 is limited to the characteristics most relevant to this review and likely to affect the interpretation of the findings. The majority of patients included in the study (87.5%) were C1-INH HAE type I. Despite some numerical differences between treatment arms, disease characteristics were considered to not differ substantially between treatment groups. According to the clinical expert consulted for the review, the frequency, location, and severity of the episodes observed in clinical practice were random; therefore, the risk of experiencing a future HAE episode is considered similar for any patient, regardless of disease history.
Table 13: Summary of HAE Disease History From the VANGUARD Study (ITT Analysis Set)
Characteristic | Garadacimab 200 mg (N = 39) | Placebo (N = 25) |
|---|---|---|
HAE type, n (%) | ||
C1-INH type I HAE | 34 (87.2) | 22 (88.0) |
C1-INH type II HAE | 5 (12.8) | 3 (12.0) |
History of laryngeal attack, n (%) | ||
Yes | 21 (53.8) | 17 (68.0) |
██ | ██████ | ██████ |
Family history of HAE, n (%) | ||
Yes | 34 (87.2) | 23 (92.0) |
██ | ██████ | ██████ |
Age at first diagnosis, n % | ||
≤ 17 years | 18 (46.2) | 12 (48.0) |
≤ 40 years | 18 (46.2) | 11 (44.0) |
> 40 years | 3 (7.7) | 2 (8.0) |
HAE prophylaxis during 3 months before screening, n (%) | ||
Patients with HAE prophylaxis | 14 (35.9) | 7 (28.0) |
███ ████ | ██████ | ██████ |
████████████████ | ||
███ ████ | ██████ | ██████ |
███ ████ | ██████ | ██████ |
███ ████ | ██████ | ██████ |
███ ████ | ██████ | ██████ |
████████████████ | ||
███ ████ | ██████ | ██████ |
███ ████ | ██████ | ██████ |
███ ████ | ██████ | ██████ |
███ ████ | ██████ | ██████ |
Primary locations of HAE attacks in the last 3 months before screening, n (%) | ||
Cutaneous — extremities | 30 (76.9) | 20 (80.0) |
Abdomen | 30 (76.9) | 18 (72.0) |
Cutaneous — head/face/lip/neck | 13 (33.3) | 8 (32.0) |
Genitourinary | 6 (15.4) | 2 (8.0) |
Cutaneous — trunk | 5 (12.8) | 2 (8.0) |
Cutaneous — genitourinary | 2 (5.1) | 4 (16.0) |
Throat, larynx, and tongue | 3 (7.7) | 2 (8.0) |
Groin and testicles | 1 (2.6) | 0 |
Hands | 0 | 1 (4.0) |
Peripheral | 1 (2.6) | 0 |
CI = confidence interval; HAE = hereditary angioedema; ITT = intention to treat; SD = standard deviation.
Note: Patients without HAE prophylaxis: number of HAE attacks during the 3 months before screening; patients with HAE prophylaxis: number of HAE attacks during the 3 months before starting the HAE prophylaxis.
Sources: CSL312_3001 Clinical Study Report.6 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Exposure to Study Treatments
████████ ██ █████ ███████ ██ ████████ ██
███ ██████ █████ ████ ███████ ███████ ██████ ███ █████ █████████
Table 14: Summary of Patient Exposure From the VANGUARD Study [Redacted]
████████ | ████████ | ████████ |
|---|---|---|
███████████████ | ||
███████████ | █████ | █████ |
███████████ | █████ | █████ |
███████████ | █████ | █████ |
███████████ | █████ | █████ |
███████████ | █████ | █████ |
███████████ | █████ | █████ |
███████████████ | ||
███████████ | █████ | █████ |
███████████ | █████ | █████ |
███████████ | █████ | █████ |
███████████ | █████ | █████ |
███████████ | █████ | █████ |
███████████████ | ||
███████████ | █████ | █████ |
███████████ | █████ | █████ |
███████████ | █████ | █████ |
███████████ | █████ | █████ |
███████████ | █████ | █████ |
███████████████ | ||
███████████ | █████ | █████ |
███████████ | █████ | █████ |
███████████ | █████ | █████ |
███████████ | █████ | █████ |
███████████ | █████ | █████ |
█████████ ██ ██ ██████████ ███████████ ████████ █████ ██████6████████ ██ █████████
███ ████████ █████ ██ █████ █ ██████████ ████████ ██ █████████ ██
███ ████ ████████ ████ █████████ ████ █████████ █████████ ██ ████████ ████ ███
Table 15: Summary of Prior and Concomitant Medications From the VANGUARD Study (Safety Analysis Set) [Redacted]
███████ ██ | ███████████████ | ███████ ██ |
|---|---|---|
████████ | ████████ | ████████ |
████████ | ████████ | ████████ |
████████ | ████████ | ████████ |
████████ | ████████ | ████████ |
████████ | ████████ | ████████ |
████████ | ████████ | ████████ |
████████ | ████████ | ████████ |
████████ | ████████ | ████████ |
████████ | ████████ | ████████ |
████████ | ████████ | ████████ |
████████ | ████████ | ████████ |
████████ | ████████ | ████████ |
████████ | ████████ | ████████ |
████████ | ████████ | ████████ |
████████ | ████████ | ████████ |
████████ | ████████ | ████████ |
████████ | ████████ | ████████ |
████████ | ████████ | ████████ |
████████ | ████████ | ████████ |
████████ | ████████ | ████████ |
████████ | ████████ | ████████ |
████████ | ████████ | ████████ |
████████ | ████████ | ████████ |
████████ | ████████ | ████████ |
████████ | ████████ | ████████ |
████████ | ████████ | ████████ |
███ ██████████ ███████████ █████████ ███ █ ██████████ ██████████████ ███████████ ████████ █████ ██████6████████ ████████ ██ ███ ██ ████████ █████████
Efficacy
Detailed efficacy results are presented in Table 16.
HAE Episodes
Time-Normalized Number of HAE Episodes
Throughout the 6-month treatment period, the mean number of episodes reported per month was 0.27 (SD = █████) in the garadacimab group compared with 2.01 (█████) in the placebo group, resulting in a mean difference between groups of −1.74 (95% CI, −2.34 to −1.13; P < 0.001). The magnitude of the between-group difference was considered clinically meaningful by the clinical expert consulted for this review. This was the primary outcome in the VANGUARD study. Sensitivity analyses of the primary outcome were consistent with results from the primary analysis.
Change From Baseline in HAE Episodes
The mean change from baseline through 6 months in the time-normalized number of HAE episodes per month was 90.7% (SD = █████) in the garadacimab group compared with 20.2% (SD = █████) in the placebo group, a between-group difference of 70.46% (95% CI, 51.25 to 89.67; P < 0.001).
Proportions of Patients Who Are Episode-Free
The proportion of patients who had a 100% reduction in HAE episodes and therefore became episode-free was 61.5% in the garadacimab group, while no patients achieved this outcome in the placebo group. This constitutes a difference between treatment groups of 61.54% (95% CI, 46.27 to 76.81; P < 0.001).
HAE Episodes Requiring On-Demand Treatment
The mean change from baseline through 6 months in the time-normalized number of HAE episodes requiring on-demand treatment per month was 0.23 (SD = █████) in the garadacimab group compared with 1.86 (SD = █████) in the placebo group, resulting in a mean between-group difference of −1.63 (95% CI, −2.26 to −1.00; P < 0.001).
Moderate and/or Severe Episodes
The mean change from baseline through 6 months in the time-normalized number of moderate or severe HAE episodes per month was 0.13 (SD= █████) in the garadacimab group compared with 1.35 (SD = █████) in the placebo group. The mean difference between groups was −1.23 (95% CI, −1.73 to −0.73; P < 0.001).
Time to First Episode
The Kaplan-Meier survival curves for first episode after day 1 are presented in Figure 3. The curves separate early, favouring garadacimab, and remain separated throughout follow-up. However, no between-group comparison was reported.
Patient-Reported Outcomes
AE-QoL Questionnaire
The mean change from baseline through 6 months in AE-QoL total score was −26.4 (SD = █████) in patients who received garadacimab and −2.2 (SD = █████) in patients who received placebo, yielding a mean between-group difference of −24.265 (95% CI, −34.976 to −13.554). Similarly, the mean changes from baseline through 6 months in the AE-QoL scores for the functioning, fatigue, mood, fears and shame, and nutrition domains were numerically higher in patients who received garadacimab compared with those who received placebo. Numerically more patients in the garadacimab group achieved an MCID in AE-QoL domains and total scores from baseline through 6 months compared with placebo, and a difference of at least 6 points from baseline was required to be considered an MCID.
The magnitude of the between-group difference in AE-QoL results was considered clinically meaningful by the clinical expert consulted by for this review, and consistent with the level of efficacy observed with garadacimab for the prevention of HAE episodes.
Health Care Resource Use
No data were reported in the trial to assess use of health care resources, such as emergency department visits or hospitalizations.
Table 16: Summary of Key Efficacy Results From the VANGUARD Study (ITT Analysis Set) [Redacted]
██████████ | ██████████ | ██████████ |
|---|---|---|
████████████████ | ||
████████ | ████████ | ████████ |
████████ | ████████ | ████████ |
████████ | ████████ | ████████ |
████████ | ████████ | ████████ |
████████████████ | ||
████████ | ████████ | ████████ |
████████ | ████████ | ████████ |
████████ | ████████ | ████████ |
████████ | ████████ | ████████ |
████████ | ████████ | ████████ |
████████ | ████████ | |
████████ | ████████ | |
█████████████████ | ||
████████ | ||
████████ | ████████ | ████████ |
████████ | ████████ | ████████ |
████████ | ████████ | |
████████ | ████████ | |
█████████████████ | ||
████████ | ████████ | ████████ |
████████ | ████████ | |
████████ | ████████ | ████████ |
████████ | ████████ | ████████ |
████████ | ████████ | ████████ |
████████ | ████████ | |
████████ | ████████ | |
█████████████████ | ||
████████ | ████████ | ████████ |
████████ | ████████ | ████████ |
████████ | ████████ | ████████ |
████████ | ████████ | ████████ |
████████ | ████████ | ████████ |
████████ | ████████ | ████████ |
████████ | ████████ | ████████ |
████████ | ████████ | ████████ |
████████ | ████████ | |
████████ | ████████ | |
█████████████████ | ||
████████ | ████████ | ████████ |
████████ | ████████ | ████████ |
████████ | ████████ | ████████ |
████████ | ████████ | ████████ |
████████ | ████████ | |
████████ | ████████ | |
█████████████████ | ||
█████████████ | ||
████████ | ████████ | ████████ |
████████ | ████████ | ████████ |
████████ | ████████ | ████████ |
████████ | ||
████████ | ████████ | ████████ |
████████ | ████████ | ████████ |
████████ | ████████ | ████████ |
████████ | ████████ | ████████ |
████████ | ████████ | |
████████ | ████████ | |
████████████████ | ||
████████ | ||
████████ | ████████ | ██ ██████ |
████████ | ████████ | ██ ██████ |
████████ | ████████ | ██ ██████ |
████████ | ████████ | ██ ██████ |
████████ | ||
████████ | ████████ | ██ ██████ |
████████ | ████████ | ██ ██████ |
████████ | ████████ | ██ ██████ |
████████ | ████████ | ██ ██████ |
█████████████████ | ||
████████ | ||
████████ | ████████ | ██ ██████ |
████████ | ||
████████ | ████████ | ██ ██████ |
████████ | ████████ | ██ ██████ |
████████ | ████████ | ██ ██████ |
████████ | ████████ | ██ ██████ |
████████ | ████████ | |
████████ | ||
████████ | ████████ | ██ ██████ |
████████ | ████████ | ██ ██████ |
████████ | ████████ | ██ ██████ |
████████ | ████████ | ██ ██████ |
████████ | ████████ | |
████████ | ||
████████ | ████████ | ██ ██████ |
████████ | ████████ | ██ ██████ |
████████ | ████████ | ██ ██████ |
████████ | ████████ | ██ ██████ |
████████ | ████████ | |
████████ | ||
████████ | ████████ | ██ ██████ |
████████ | ████████ | ██ ██████ |
████████ | ████████ | ██ ██████ |
████████ | ████████ | ██ ██████ |
████████ | ████████ | |
████████ | ||
████████ | ████████ | ██ ██████ |
████████ | ████████ | ██ ██████ |
████████ | ████████ | ██ ██████ |
████████ | ████████ | ██ ██████ |
████████ | ████████ | |
█████████████████ | ||
████████ | ████████ | ████████ |
████████ | ████████ | ████████ |
████████ | ████████ | ████████ |
████████ | ████████ | ████████ |
████████ | ████████ | ████████ |
██████ ████████ █████ ██████6████████ ████████ ██████ ███ ███████ ████████
Figure 3: Time to First Attack After Day 1 — Kaplan-Meier Curve With 95% Confidence Interval (Safety Analysis Set)
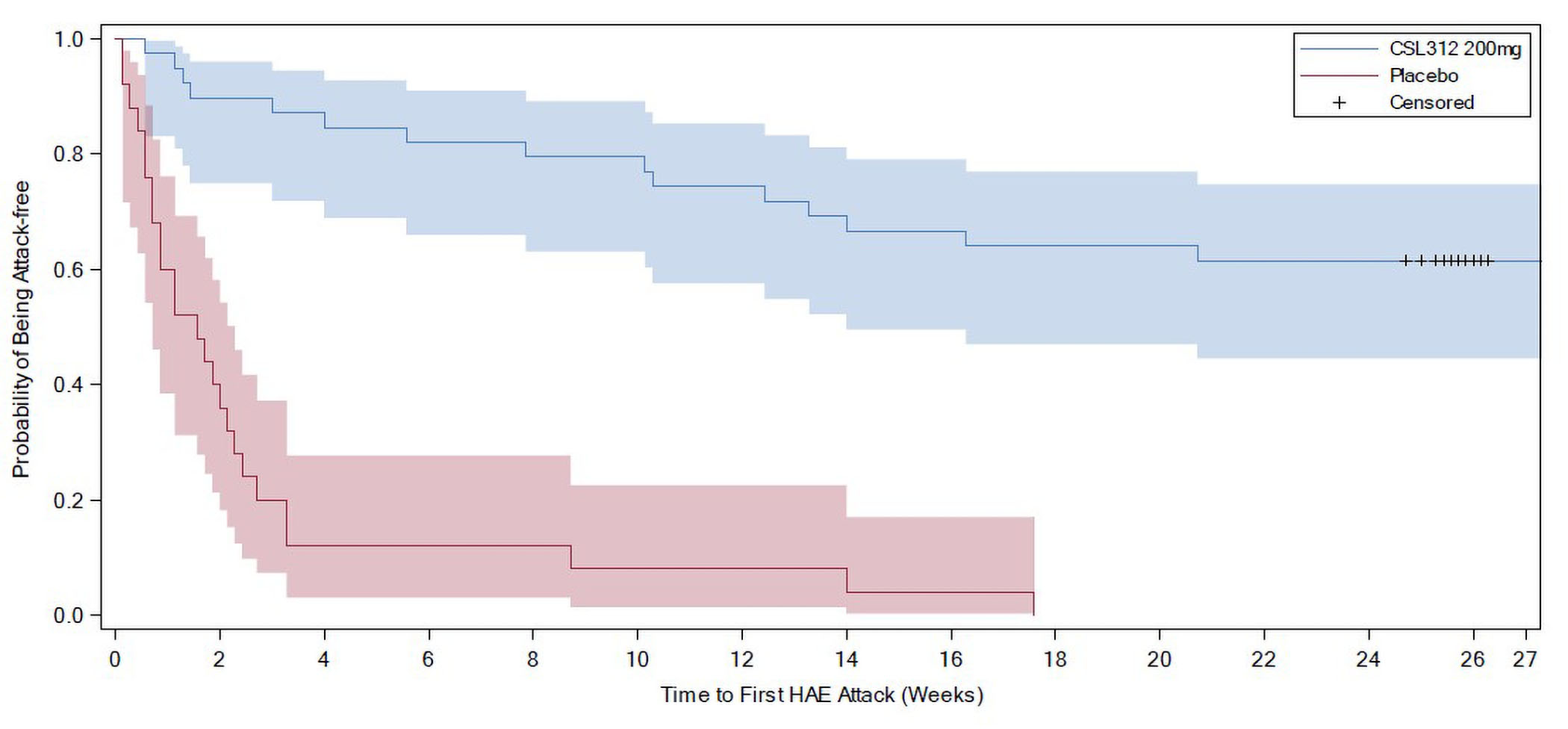
CSL312 = garadacimab; HAE = hereditary angioedema.
Source: CSL312_3001 Clinical Study Report.6 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Harms
Data for harms outcomes included in the review are presented in Table 17.
Adverse Events
In the VANGUARD study, 64% of patients receiving garadacimab and 60% of patients receiving placebo reported at least 1 AE. The most common TEAEs were related to infections, gastrointestinal disorders, and injection-site reactions. These included upper respiratory tract infection (10.3% in the garadacimab group and 8.0% in the placebo group, respectively), nasopharyngitis (7.7% and 4.0%), headache (7.7% and 16.0%), gastrointestinal infection (5.1% and 4.0%), diarrhea (5.1% and 4.0%), back pain (5.1% and 4.0%), abdominal pain (5.1% and 0%), conjunctivitis (5.1% and 0%), sinusitis (5.1% and 0%), and urinary tract infection (5.1% and 0%).
Serious Adverse Events
Overall, 1 patient (2.6%) receiving garadacimab reported 1 SAE of HAE that included a laryngeal attack, which was managed with overnight hospitalization and assessed by the investigator as not related to the investigational product. No patient who received placebo experienced an SAE.
Withdrawals due to Adverse Events
There was no withdrawal due to AEs in VANGUARD.
Mortality
No deaths were reported in the study.
Notable Harms
AESIs included thromboembolic events, bleeding events, and severe hypersensitivity or anaphylaxis. The sponsor reported that no patients were assessed as experiencing any of these events during the VANGUARD study.
Table 17: Summary of Harms Results From the VANGUARD Study
Harms | Garadacimab 200 mg (N = 39) | Placebo (N = 25) |
|---|---|---|
Most common adverse events, n (%) | ||
Any treatment-emergent AE | 25 (64.1) | 15 (60.0) |
Occurring within 24 hours after SC loading dose | 2 (5.1) | 2 (8.0) |
Occurring within 24 hours after any SC dose | 6 (15.4) | 6 (24.0) |
Injection-site reactions | 2 (5.1) | 3 (12.0) |
Injection-site erythema | 1 (2.6) | 2 (8.0) |
Infections and infestations | 13 (33.3) | 7 (28.0) |
Upper respiratory tract infection | 4 (10.3) | 2 (8.0) |
Nasopharyngitis | 3 (7.7) | 1 (4.0) |
COVID-19 | 0 | 3 (12.0) |
Gastrointestinal infection | 2 (5.1) | 1 (4.0) |
Conjunctivitis | 2 (5.1) | 0 |
Sinusitis | 2 (5.1) | 0 |
Urinary tract infection | 2 (5.1) | 0 |
Gastrointestinal disorders | 8 (20.5) | 5 (20.0) |
Diarrhea | 2 (5.1) | 1 (4.0) |
Abdominal pain | 2 (5.1) | 0 |
Nausea | 0 | 2 (8.0) 2 |
General disorders and administration-site conditions | 4 (10.3) | 9 (36.0) |
Fatigue | 0 | 3 (12.0) |
Injection-site erythema | 1 (2.6) | 2 (8.0) |
Pyrexia | 1 (2.6) | 2 (8.0) |
Musculoskeletal and connective tissue disorders | 5 (12.8) | 5 (20.0) |
Back pain | 2 (5.1) | 1 (4.0) |
Pain in extremity | 0 | 2 (8.0) |
Nervous system disorders | 4 (10.3) | 4 (16.0) |
Headache | 3 (7.7) | 4 (16.0) |
Serious adverse events, n (%) | ||
Any serious treatment-emergent AE | 1 (2.6) | 0 |
Congenital, familial, and genetic disorders | 1 (2.6) | 0 |
Hereditary angioedema | 1 (2.6) | 0 |
Patients who stopped treatment due to adverse events, n (%) | ||
Any withdrawal due to AE | 0 | 0 |
Deaths, n (%) | ||
Any death | 0 | 0 |
AE = adverse event; SAE = serious adverse event; SC = subcutaneous.
Sources: CSL312_3001 Clinical Study Report.6 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Critical Appraisal
Internal Validity
Study Design
The VANGUARD study had an RCT design using a run-in period and a treatment period. Patients were allocated to treatment groups using appropriate methodology, with randomization stratified by relevant and clinically important potential prognostic factors, i.e., age (≤ 17 years or > 17 years) and, for adults, by baseline episode rate observed during the run-in period (1 to fewer than 3 episodes per month or at least 3 episodes per month).
The main purpose of the run-in period was to confirm patients’ underlying disease status. Patients who had 2 episodes in the initial month could enter the treatment period; patients without an HAE episode during this time frame could continue in the run-in period for an additional month, during which they needed to have at least 2 episodes. Therefore, the VANGUARD study used a relatively short run-in period to determine the baseline rate of episodes. Given the unpredictable nature of HAE episodes, which are not necessarily consistent in terms of frequency and severity throughout a patient’s life, this limited observation time coupled with the relatively small sample size could add uncertainty to the baseline rate. Variability in the baseline episode rate would not affect the interpretation of the primary outcome (which was based on the difference in on-treatment episodes between groups), but it could affect the interpretation of the analyses based on the change from the baseline. It is unlikely that systematic bias was introduced from the approach to estimating the baseline HAE episode rate because it was used to determine the rate in all patients before randomization, which was completed using centralized allocation. However, it is difficult to determine the effects of the variability in baseline episodes on the results as it could lead to overestimation or underestimation of the treatment difference.
Patient Population
Imbalances between treatment groups were observed for some of the baseline patient characteristics. Due to the small sample size of the trials, randomization may not ensure the groups were balanced for all measured or unmeasured prognostic factors or confounders. However, the clinical expert consulted for this review stated that these baseline differences were unlikely to be clinically important enough to bias the results. Indeed, the frequency, location, and severity of the episodes observed in clinical practice are random and it is not expected that demographics or disease history would affect the risk of a future HAE attack.
Interventions
As the VANGUARD trial included a placebo control group, there is no direct evidence comparing garadacimab to other LTP therapies. This absence restricts the trial’s ability to inform comparative effectiveness and safety assessments relative to currently available prophylaxis therapies. Consequently, ITCs were provided to determine the relative clinical effects of garadacimab for reimbursement decisions (refer to the Indirect Evidence section).
On-demand therapies were permitted at any time during the study for the treatment of HAE episodes. However, routine LTP agents were prohibited and had to be discontinued at prespecified times before the ruin-in period, which varied according to the specific agent used.
There were no obvious differences between groups in the number of patients who received acute treatments administered for HAE episodes before and throughout the trial. However, as prior and concomitant medications were reported together as a whole, it is not possible to assess whether there might have been important differences in the concomitant drugs received during the treatment period. These may change the magnitude of response to current treatment according to the clinical expert, because some therapies are expected to have a longer-lasting protective effect compared to others. The impact of any potential bias is uncertain.
Outcome Measures
The primary outcome in VANGUARD was the number of HAE episodes during the treatment period. Additional outcomes related to HAE episodes were assessed as secondary end points in the trial and included episodes requiring on-demand treatment, and moderate and/or severe episodes. These were all considered appropriate by the clinical expert, as reducing the frequency and severity of episodes is 1 of the main treatment goals in HAE.
Episode definition and assessment in the trial were deemed appropriate, as clinicians rely mainly on patients’ self-reporting in clinical practice. There is subjectivity in symptoms assessment, but the clinical expert indicated that other differential diagnoses for more severe episodes may usually be ruled out relatively easily. It is not expected that this outcome would have been subject to bias, especially in the context of the double-blind design.
The study was not designed to test for differences in the need for hospitalization or emergency visits. HRQoL was measured using the AE-QoL as a secondary outcome. The AE-QoL has evidence to support validity, reliability, and responsiveness in patients with recurrent angioedema episodes.
Statistical Analysis
The sample size of the VANGUARD study was small but was considered unsurprising due to the rarity of HAE and consistent with other RCTs of interventions for the indication.
The primary estimand was clearly stated in the statistical analysis plan and aligned with the study population, intervention, comparator, outcome, and specified treatment policy strategy (following an intention to treat [ITT] approach and using all data, regardless of intercurrent events [e.g., on-demand medication use]). Following a treatment policy strategy is reasonable given the variable natural history of HAE and related episodes and potential variation in response to prophylaxis, as the goal is to reflect the effect of treatment regardless of intercurrent events (e.g., on-demand medication use) using all available data. The key assumptions regarding missing data are related to the timing of patient discontinuation: missing data were only recorded for patients who discontinued the study within 30 days after administration of study treatment and those who discontinued the study after day 30 and before the end of month 6. In the former scenario, a sensitivity analysis was planned but no results were reported, presumably because no patients in the treatment arm discontinued the study within the first 30 days. For the second scenario, it was assumed that the HAE episode rate for these patients was similar to the episode rate for those who completed the full 6-month treatment period. It was reported that this assumption was based on data from the phase II trial of garadacimab (CSL312_2001), which “showed that the CSL312 (garadacimab) treatment effect was maintained over time.”32 Therefore, the time-normalized number of HAE episodes was calculated based on the HAE episodes reported until the early termination visit. No sensitivity analyses were planned to test this assumption. This approach could lead to inaccuracy in estimating the primary estimand if the reasons for early discontinuation are related to treatment effectiveness or AEs. Evidence from the phase II trial alone was not considered sufficiently robust by CDA-AMC reviewers to support this assumption. Table 11 shows that no patients in the garadacimab group discontinued the study (although only 38 out of 39 completed the study) and 3 patients in the placebo group discontinued the study. Therefore, while the planned approach was potentially problematic, it is not expected that the approach taken led to biased estimates based on observed data.
The sponsor did not justify the choice of a Wilcoxon test in the primary analysis. A Poisson-based regression model (or negative binomial regression model) with potential adjustments for overdispersion is generally the preferred approach for primary analysis in clinical trials with data such as counts or rates. A Wilcoxon test is a nonparametric tool that is less likely to be influenced by the distribution of events. In the trial, the distribution of rates in each group seems skewed, as values for mean and median results are different and wide ranges (especially for garadacimab) were observed. A Wilcoxon test is therefore appropriate statistical tool for these non-normally distributed data, but it may not fully reflect the primary estimand because there are imbalances in episode rates and (based on the Kaplan-Meier curve in Figure 3) varying effects over time, with more extreme values in the placebo group. The primary estimand focuses on the median number of HAE episodes and therefore a Wilcoxon test may be acceptable, but a model-based approach such as a Poisson regression can account for such differences in treatment groups through statistical adjustment of the model, particularly given that differences were also observed in the VANGUARD study’s baseline characteristics. A sensitivity analysis carried out using a generalized linear model and/or Poisson regression methods supported the primary analysis.
The VANGUARD study used hierarchical testing to control the type I error rate for the primary outcome (number of HAE episodes) and some secondary outcomes (e.g., reduction in HAE episode rate). Other outcomes that were of interest to this review (e.g., the responder analysis, number of episodes requiring on-demand treatment and number of moderate or episodes) were not controlled for multiplicity of testing.
As with most clinical trials, the studies were not powered to detect infrequent AEs or those with a lag time.
External Validity
Population
The findings from the VANGUARD trial were reflective of those enrolled, who were patients with type I or II HAE. The diagnosis assessment in the trial was considered appropriate and consistent with clinical practice. The inclusion and exclusion criteria were deemed clinically relevant and reasonable by the clinical expert. More importantly, baseline patient characteristics, disease history, and use of on-demand acute therapies for HAE were considered representative of the population routinely seen in clinical practice. The exclusion criteria did not pose a generalizability issue. However, some groups of patients, such as those with FXII HAE and pediatric patients, were excluded from the study but could be candidates to receive garadacimab, according to the clinical expert.
All patients in the study needed to have a baseline episode rate during the run-in period of at least 2 per month, which the clinical expert stated may be higher than the typical frequency at which LTP is initiated in clinical practice. However, the trial only included patients who were medically appropriate for on-demand treatment as the sole management of HAE, and therefore may have excluded patients with more severe HAE who could not tolerate discontinuation of current LTP therapy.
Few adolescents were enrolled in the VANGUARD study; therefore, there are limited data to interpret for this age group.
Outcomes
Episode definition and assessment in the trial were deemed representative of clinical practice. The clinical expert mentioned that the AE-QoL is not routinely used in clinical practice, but that it is considered relevant and appropriate for assessment of HAE treatments in clinical studies.
The clinical meaningfulness of the overall number of episodes, the number of moderate or severe episodes, and the number of episodes requiring on-demand treatment can be highly variable across patients, depending on how these affect their daily lives. According to the clinical expert, the MCID is difficult to assess, as different individuals are likely to have different priorities and different objectives when assessing the magnitude of response to treatments.
Follow-up
The follow-up duration of 6 months was considered relatively short, but sufficient to assess the outcome and capture a change in HAE episodes, despite the fact that the disease may be highly variable. The clinical expert noted that it would be unethical for patients who require preventive treatment to remain on placebo over a longer period of time. Nevertheless, although LTP therapy is potentially life-long, evidence is limited beyond the study follow-up duration.
GRADE Summary of Findings and Certainty of the Evidence
Methods for Assessing the Certainty of the Evidence
For pivotal studies and RCTs identified in the sponsor’s systematic review, GRADE was used to assess the certainty of the evidence for outcomes considered most relevant to inform expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group:4,5
High certainty: We are very confident that the true effect lies close to that of the estimate of the effect.
Moderate certainty: We are moderately confident in the effect estimate — The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. We use the word “likely” for evidence of moderate certainty (e.g., “X intervention likely results in Y outcome”).
Low certainty: Our confidence in the effect estimate is limited — The true effect may be substantially different from the estimate of the effect. We use the word “may” for evidence of low certainty (e.g., “X intervention may result in Y outcome”).
Very low certainty: We have very little confidence in the effect estimate — The true effect is likely to be substantially different from the estimate of effect. We describe evidence of very low certainty as “very uncertain.”
Following the GRADE approach, evidence from RCTs started as high-certainty evidence and could be rated down for concerns related to study limitations (which refers to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias.
When possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect; if this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., the clinical importance is unclear). In all cases, the target of the certainty of evidence assessment was based on the point estimate and where it was located relative to the threshold for a clinically important effect (when a threshold was available) or to the null.
Results of GRADE Assessments
Table 2 presents the GRADE summary of findings for garadacimab versus placebo.
Long-Term Extension Studies
Contents within this section have been informed by materials submitted by the sponsor. The following has been summarized and validated by the review team.
Description of Study
One long-term extension study is summarized here.
Study CSL312_3002 is a multicentre, open-label, phase IIIb study designed to investigate the clinical safety and efficacy of garadacimab in the prophylactic treatment of HAE when administered monthly by SC injection for at least 12 months. The primary objective of the study was to evaluate the long-term safety of SC administration of garadacimab in the prophylactic treatment of patients with C1-INH HAE. The secondary objectives were to evaluate long-term efficacy, including patient-reported assessment of response to therapy. This study consisted of 4 periods: screening (for patients who were garadacimab-naive), run-in (for patients who were garadacimab-naive), open-label treatment period (12 months minimum), and a follow-up period (2 months after the end-of-treatment visit). Interim results reported in this section focus on the safety and efficacy data available at the most recent data cut-off dates of February 13, 2023 (all patients) and May 22, 2023 (adolescent patients only). The study is ongoing.
Populations
Patients who were garadacimab-naive who were aged 12 years and older were eligible for the run-in period if they had a clinically confirmed diagnosis of C1-INH HAE, experienced at least 3 HAE episodes during the 3 months before screening, a C1-INH antigen concentration and/or functional activity of no more than 50% of normal, and a C4 antigen concentration below the lower limit of the reference range.
To enter the treatment period, patients who were garadacimab-naive needed to have experienced an average of at least 1 HAE episode per month during the 2-month run-in period (i.e., a total of at least 2 HAE episodes).
Patients who successfully completed the CSL312_2001 or VANGUARD study could roll over directly from treatment in those trials and start this study at treatment day 1.
The key exclusion criteria matched those for the VANGUARD trial.
Interventions
All patients who met the criteria to enter the study were assigned to 1 dose of garadacimab, 200 mg, to be given subcutaneously once per month. For patients who were garadacimab-naive, a loading dose of 400 mg (two 200 mg doses) was administered subcutaneously on visit day 1, then 200 mg was administered subcutaneously once per month in subsequent months, unless there was a dose modification.
The maximum allowed dose for patients with C1-INH HAE was 400 mg per month. The maximum allowed dosage for patients with normal C1-INH FXII mutation was 600 mg per month.
Similar to the pivotal study, on-demand HAE therapies were permitted at any time during the study for the treatment of HAE episodes if that medication has previously been shown to be effective or if used according to the product label or with deviations from the label as directed by a health care provider. The use of medications (e.g., IV C1-INH) for the prevention of HAE episodes before any surgical procedure was permitted at any time during the study. Prohibited therapies in the open-label extension were the same as those in the pivotal study.
Outcomes
The outcomes reported in this review are:
the primary end point, which was TEAEs
the secondary efficacy end points, which included the time-normalized number of HAE episodes, reduction in the episode rate during the treatment period compared to the run-in period, time-normalized number of HAE episodes requiring on-demand treatment, and time-normalized number of moderate and/or severe HAE episodes
the secondary safety end points, which included SAEs, deaths, TEAEs leading to study discontinuation, and AESIs (i.e., thromboembolic events, abnormal bleeding events, severe hypersensitivity including anaphylaxis events).
Statistical Analysis
Sample Size Determination
Approximately 150 patients were planned to be enrolled into the study and a minimum of 100 patients were planned to receive treatment for a minimum of 12 months. The sample size for this single arm, open-label study was not based on a formal statistical sample-size calculation but on the E1A guideline issued by the International Conference on Harmonisation, March 1995. The sample size of 100 patients allows observation of 1 or more AEs with a probability of 3% at a 95% confidence level.
Analysis Sets
The screened analysis set comprised all patients who provide written informed consent.
The ATP analysis set comprised all patients in the screened analysis set who were assigned to treatment. The ATP analysis set was analyzed using the treatment to which the patients were assigned, regardless of the treatment received. The actual treatment was planned to be garadacimab for all patients, but the dose may have been incremented from the initially planned 200 mg. The loading dose for patients who were garadacimab-naive was still shown as part of the 200 mg dose.
The safety analysis set comprised all patients in the ATP analysis set who received at least 1 dose of the investigational product and was analyzed using the actual treatment received.
The per-protocol analysis set comprised all patients in the ATP analysis set who received at least 1 dose of investigational product and who complied with the protocol.
Planned Analyses
All safety analyses were based on the safety analysis set. The efficacy end points were analyzed using the ATP analysis set.
For patients who were garadacimab-naive, HAE episodes with a start date on or after the first day of the run-in period but before the date and time of the first investigational product administration were counted for the run-in period. For patients from the CSL312_2001 and VANGUARD trials, the number of HAE episodes in the run-in period of the previous study was used.
The time-to-event analysis was performed for 69 patients who were treatment-naive and 21 patients receiving placebo who rolled over from the VANGUARD study. CDA-AMC did not report the results of these analyses because they could not be interpreted in a manner that would inform the reimbursement assessment for garadacimab, and because there was no control group.
Quality-of-Life End Points
The AE-QoL questionnaire were reported only by treatment-naive and non–treatment-naive status. The proportion of patients achieving the MCID were calculated for baseline and visit day 361 and visit day 721 for the total and domain scores in the AE-QoL.
The MCID for the AE-QoL was defined as 6 points.
Multiple Comparisons and Multiplicity
Type I error rate adjustment was not applicable as there was no confirmatory test planned in this study. The efficacy analysis was exploratory, and no statistical tests are planned.
Missing Data and Imputation
Missing efficacy data were not imputed as no formal statistical analysis was carried out. All patients who dropped out within the first 30 days of the treatment period were regarded as missing for all efficacy analyses. There was no imputation of partial or complete missing dates.
Results
Patient Disposition
Overall, 171 patients provided informed consent, including 92 patients who rolled over from previous studies and 79 patients who had not previously participated in a garadacimab study (nonrollover patients). Out of 79 nonrollover patients, 8 discontinued in the run-in period and 2 failed screening. In total, 161 patients entered the open-label extension study, including 35 patients who rolled over from the phase II CSL312_2001 study (N = 2 with FXII HAE), 57 patients who rolled over from the VANGUARD trial, and 69 patients who had not previously participated in a garadacimab study. Therefore, 71 patients (35 from the CSL312_2001 study plus 36 treated with garadacimab in the VANGUARD trial) and 90 patients (21 placebo from the VANGUARD trial plus 69 nonrollover patients) formed the previously treated and treatment-naive subgroups, respectively.
Of the 161 patients included in the ATP analysis set, the majority of patients (62%) were female. Most patients (83.9%) were white and █████ ████ ████ ████████ ██ ███████ █████████. There were 22 Asian patients (13.7%), ██ ██████ ██ █████ ████ ████████. The mean overall age of all patients was 42.3 years (SD = 15.31), with patients ranging from 13 to 73 years, and 10 patients (6.2%) being adolescents (aged 17 years or younger). The mean overall body mass index (BMI) of all patients was 28.10 kg/m2 (SD = 6.210).
A total of 145 of 161 (90.1%) patients in the ATP analysis set had been diagnosed with clinically confirmed C1-INH type I HAE, 14 (8.7%) patients had C1-INH type II HAE, and 2 (1.2%) patients with FXII HAE were rolled over from Study CSL312_2001.
Of the 161 patients, ███ ███████ ███ █ ██████ ███████ ██ ███, and 103 (64.0%) had a history of laryngeal episodes.
Overall, 59 of 161 patients (36.6%) were treated with HAE prophylaxis during the 3 months before screening. The mean number of HAE episodes per month within 3 months before screening for patients with HAE prophylaxis was 1.79 (SD = █████). For patients without HAE prophylaxis, the mean number of HAE episodes per month within 3 months before screening was 2.96 (SD = █████).
Table 18: Patient Disposition [Redacted]
████ █████ | ████ █████ |
|---|---|
████ ██ ████ | ██████ |
████ ██ ████ | ██████ |
████ ██ ████ | ██████ |
████ ██ ████ | ██████ |
████ ██ ████ | ██████ |
████ ██ ████ | ██████ |
████ ██ ████ | ██████ |
████ ██ ████ | ██████ |
████ ██ ████ | ██████ |
████ ██ ████ | ██████ |
████ ██ ████ | ██████ |
████ ██ ████ | ██████ |
████ ██ ████ | ██████ |
████ ██ ████ | ██████ |
████ ██ ████ | ██████ |
Sources: CSL312_3002 Clinical Study Report.6 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Exposure to Study Treatment
████████ ███████ ████████ ███████ ███ █ ██ ██████ ██ ████████ ██ ████████████ ███ ███████ ████████ ███████ ███ ████████ █ ██ █████████████████ ███ █████ ███████
███ █████ ████████ ██ ███████████ ██ ████ ███ ██████ █████ ████ ████████ ██ ███████████ ████████ ███ ███████ ███ █████ ██████ █████ ██████ ███ ███ █████ ███████████ ████████ ███ █████ ██████████████ ███ █████ ██████ ██ ██████████ ███ █████ ███ █████ ██ ████████ █████ ████ ██ ████ ████████████
███████████ ████████ █████ █████ ████ █████ ████ ██ ███ ████████ █████████ ███ ██████████ ████████ █████████ ████████ ██ ████ █████ ███ ███████████ ██████████ ██ █████████ ████ ███ █████████ ██████ ██ ██████████ ████████ ██ ███████████ ████████ █████████ ███████ ████████ ██████████ ██ ████████ ██████████ ████████ ███ ███████████ █████████
Efficacy
The interim efficacy results from this ongoing study (CSL312_3002) up to the data cut-off dates (February 13, 2023, for all patients; May 22, 2023, for adolescents only) are outlined in the following tables.
Time-Normalized Hereditary Angioedema Episodes
The time-normalized number of HAE episodes per month for all evaluable patients and those who had previously received garadacimab in the VANGUARD trial are presented in Table 19.
Table 19: Time-Normalized Number of HAE Episodes per Month (ATP Analysis Set)
Measurement | Garadacimab (N = 161) |
|---|---|
Time-normalized number of HAE episodes per month — treatment period (all patients) | |
Number of evaluable patients | 161 |
Mean (SD) | 0.16 (0.370) |
95% CI | 0.10 to 0.22 |
Median | 0.00 |
Minimum to maximum | 0.0 to 1.9 |
████████████████ | |
█████████ | █████████ |
█████████ | █████████ |
█████████ | █████████ |
█████████ | █████████ |
█████████ | █████████ |
ATP = all treated participants; CI = confidence interval; HAE = hereditary angioedema; SD = standard deviation.
Sources: CSL312_3002 Clinical Study Report.6 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Reduction in Episode Rate
The reductions in the time-normalized number of HAE episodes during the treatment period compared to the run-in period for the ATP set and patients who continued garadacimab from the VANGUARD trial are presented in Table 18. Overall, 137 of 161 patients (85.1%) had a reduction in episode rate of 90% or greater. A total of 96 of 161 patients (59.6%) were episode-free over the median duration of the efficacy evaluation period of 13.83 months (Table 20).
Table 20: Reduction in Episode Rate During Efficacy Evaluation Compared to Run-In Period (ATP Analysis Set)
Measurement | Garadacimab (N = 161) |
|---|---|
Reduction in time-normalized number of HAE episodes (%)a,b (all patients) | |
Number of evaluable patients | 161 |
Mean (SD) | 94.67 (11.983) |
95% CI | 92.80 to 96.53 |
Median | 100.00 |
Minimum to maximum | 30.1 to 100.0 |
████████████████ | |
█████████ | ██████ |
█████████ | ██████ |
█████████ | ██████ |
█████████ | ██████ |
█████████ | ██████ |
Overview of responder rates and episode-free patients | |
Responders with a reduction ≥ 50%a | 158 (98.1) |
95% Wilson CI for the percentage of responders | 94.7 to 99.4 |
Responders with a reduction ≥ 70%a | 151 (93.8) |
95% Wilson CI for percentage of patients with a reduction ≥ 70% | 88.9 to 96.6 |
Responders with a reduction ≥ 90%a | 137 (85.1) |
95% Wilson CI for percentage of patients with a reduction ≥ 90% | 78.8 to 89.8 |
Episode-free patients (reduction of 100%)a | 96 (59.6) |
95% Wilson CI for percentage of episode-free patients | 51.9 to 66.9 |
ATP = all treated participants; CI = confidence interval; HAE = hereditary angioedema; SD = standard deviation.
Note: At the time of the data cut-off date (February 13, 2023), the median duration of exposure was 13.83 months (range, 3.0 to 21.1).
aThe percentage reduction in the time-normalized number of HAE episodes is calculated within a patient as: 100 × [1 – (time-normalized number of HAE episodes per month during treatment period/time-normalized number of HAE episodes per month during the run-in period)].
bFor rollover patients the run-in period of the previous study is used.
Sources: CSL312_3002 Clinical Study Report.6 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Time-Normalized HAE Episodes Requiring On-Demand Treatment
The time-normalized numbers of HAE episodes requiring on-demand treatment per month during the treatment period for the ATP set and for those who continued garadacimab from VANGUARD are reported in Table 21.
On-demand medication in the ATP set included: icatibant acetate (37 of 161 patients [23.0%]), complement C1-INH (35 of 161 patients [21.7%]), conestat alfa (2 of 161 patients [1.2%]), other blood products (1 of 161 patients [0.6%] ), and blood plasma (1 of 161 patients [0.6%]).
Table 21: Time-Normalized Number of HAE Episodes Requiring On-Demand Treatment (ATP Analysis Set)
Measurement | Garadacimab (N = 161) |
|---|---|
Time-normalized number of HAE episodes requiring on-demand treatment per montha — treatment period (all patients) | |
Number of evaluable patients | 161 |
Mean (SD) | 0.14 (0.358) |
95% confidence intervalb | 0.09 to 0.20 |
Median | 0.00 |
Minimum to maximum | 0.0 to 1.9 |
██████████████████ | |
███ ████ | ████ |
███ ████ | ████ |
███ ████ | ████ |
███ ████ | ████ |
███ ████ | ████ |
ATP = all treated participants; HAE = hereditary angioedema; SD = standard deviation.
aTreatment requirement is per patient's decision. Percentage based on all HAE episodes in that period.
bBased on a t distribution.
Sources: CSL312_3002 Clinical Study Report.6 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Time-Normalized Number of Moderate and/or Severe Episodes
The time-normalized numbers of moderate and/or severe HAE episodes per month during the treatment period for the ATP set, as well as the time-normalized number of moderate and/or severe episodes requiring on-demand treatment per month during the treatment period for the ATP set are reported in Table 22. The time-normalized number of moderate and/or severe HAE episodes per month during the treatment period for those who continued garadacimab from the VANGUARD trial, and the time-normalized number of moderate and/or severe episodes requiring on-demand treatment per month during the treatment period for those who continued garadacimab from the VANGUARD trial have not been provided.
Table 22: Time-Normalized Number of Moderate and/or Severe HAE Episodes During the Treatment Period (ATP Analysis Set)
Measurement | Garadacimab (N = 161) |
|---|---|
Time-normalized number of moderate and severe HAE episodes per month — treatment period (all patients) | |
Number observed | 161 |
Mean (SD) | 0.11 (0.277) |
95% confidence intervala | 0.07 to 0.15 |
Median | 0.00 |
Minimum to maximum | 0.0 to 1.9 |
Time-normalized number of moderate and severe HAE episodes requiring on-demand treatment per monthb — treatment period (all patients) | |
Number observed | 161 |
Mean (SD) | 0.11 (0.274) |
95% confidence interval, meana | 0.06 to 0.15 |
Median | 0.00 |
Minimum to maximum | 0.0 to 1.9 |
ATP = all treated participants; HAE = hereditary angioedema; SD = standard deviation.
aBased on a t distribution.
bTreatment requirement is per patient decision. Percentage based on all HAE episodes in that period.
Sources: CSL312_3002 Clinical Study Report.6 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Angioedema Quality of Life Questionnaire
For patients who were treatment-naive, compared to baseline at month 12, the least squares mean in the AE-QoL score was 33.337 (standard error [SE] = 1.725; 95% CI, −36.7725 to −29.9023). For patients who were not treatment-naive, compared to baseline, at month 12, the LS mean in AE-QoL score was −2.745 (SE = 1.510; 95% CI, −5.7623 to 0.2718) (Table 23).
Table 23: Summary of Angioedema Quality of Life Domain and Total Scores by Treatment Status and Time Period (ATP Treatment Set) [Redacted]
████████ | █████████████ | |||
|---|---|---|---|---|
████████ | ████████ | |||
███ | ████████ | ███ | ████████ | |
████████████████ | ||||
██████ | ███ | ██████ | ███ | ██████ |
██████ | ███ | ██████ | ███ | ██████ |
██████ | ███ | ██████ | ███ | ██████ |
██████ | ███ | ██████ | ███ | ██████ |
██████ | ███ | ██████ | ███ | ██████ |
████████████████ | ||||
██████ | ███ | ██████ | ███ | ██████ |
██████ | ███ | ██████ | ███ | ██████ |
██████ | ███ | ██████ | ███ | ██████ |
██████ | ███ | ██████ | ███ | ██████ |
██████ | ███ | ██████ | ███ | ██████ |
████████████████ | ||||
██████ | ███ | ██████ | ███ | ██████ |
██████ | ███ | ██████ | ███ | ██████ |
██████ | ███ | ██████ | ███ | ██████ |
██████ | ███ | ██████ | ███ | ██████ |
██████ | ███ | ██████ | ███ | ██████ |
████████████████ | ||||
██████ | ███ | ██████ | ███ | ██████ |
██████ | ███ | ██████ | ███ | ██████ |
██████ | ███ | ██████ | ███ | ██████ |
██████ | ███ | ██████ | ███ | ██████ |
██████ | ███ | ██████ | ███ | ██████ |
████████████████ | ||||
██████ | ███ | ██████ | ███ | ██████ |
██████ | ███ | ██████ | ███ | ██████ |
██████ | ███ | ██████ | ███ | ██████ |
██████ | ███ | ██████ | ███ | ██████ |
██████ | ███ | ██████ | ███ | ██████ |
ATP = all treated participants; QoL = quality of life; SD = standard deviation.
Note: Angioedema-QoL is only answered by patients of aged 18 years and older.
aScores reflect degree of impairment in percentages. Higher scores indicate higher impairment.
Sources: CSL312_3002 Clinical Study Report.6 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Harms
Overall, 135 of 161 (83.9%) patients experienced TEAEs. The most frequently reported TEAEs (≥ 5% of patients) were COVID-19 (36.0%), nasopharyngitis (16.8%), injection-site erythema (6.8%), influenza (6.8%), headache (6.2%), and upper respiratory tract infection (5.6%). No patients were assessed by the investigator as experiencing AESIs according to the protocol; however, AESIs as identified by a standardized Medical Dictionary for Regulatory Activities query included bleeding events (N = 10) and severe hypersensitivity, including anaphylaxis (N = 26). A total of 3 SAEs were reported (2 COVID-19 cases and 1 HAE attack). Treatment with garadacimab was discontinued in 2 patients due to TEAEs of injection-site irritation (moderate) and mood swings (severe), no deaths were reported (Table 24).
As of the third data cut-off (May 22, 2023), 7 of 10 adolescent patients experienced TEAEs, the most common being COVID-19 (30.0%), nasopharyngitis (30.0%), upper respiratory tract infection (10.0%), influenza-like illness (10.0%), fatigue (10.0%), gastroesophageal reflux disease (10.0%), and oropharyngeal pain (10.0%). No deaths, SAEs, or TEAEs leading to garadacimab discontinuation were reported in this patient population.
Table 24: TEAEs by System Organ Class and Preferred Term (Safety Analysis Set)
Adverse events | Garadacimab 200 mg (N = 161) |
|---|---|
Most common adverse events in more than 5%, n (%) | |
≥ 1 adverse event | 135 (83.9) |
COVID-19 | 58 (36.0) |
Nasopharyngitis | 27 (16.8) |
Influenza | 11 (6.8) |
Injection-site erythema | 11 (6.8) |
Headache | 10 (6.2) |
Upper respiratory tract infection | 9 (5.6) |
Serious adverse events, n (%) | |
Patients with ≥ 1 serious adverse event | 3 (1.9) |
COVID-19 | 2 (1.2) |
Hereditary angioedema | 1 (0.6) |
Patients who stopped treatment due to adverse events, n (%) | |
Patients who stopped | 1 (0.6) |
Injection-site irritation (moderate) | 1 (0.6) |
Mood swings (severe) | 1 (0.6) |
Deaths, n (%) | |
Patients who died | 0 |
███████████████████████ | |
████████████ | ███ |
████████████ | ███ |
████████████ | ███ |
SC = subcutaneous, TEAE = treatment-emergent adverse event.
Sources: CSL312_3002 Clinical Study Report.6 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Critical Appraisal
Internal Validity
This open-label study is still ongoing, with only 3 patients having completed the study and 119 patients who had at least 12 months of exposure at the data cut-off of February 13, 2023.
The lack of a control group precludes causal statements about benefit and harm compared with any comparator. The open-label nature of the study may increase the risk of bias in determining the magnitude of the safety outcomes and efficacy end points that include more subjective assessments, because the lack of blinding may affect patients’ expectations of treatment. The direction and magnitude of this potential bias remain unclear.
This study included 71 patients who were previously treated by garadacimab and rolled over from the parent trials. It is possible that patients who continued and remained on the treatment were also those who had a good performance on the drug. This may increase the risk of selection bias.
There was no imputation of missing values in this trial; however, the attrition rate at the cut-off time was 6.8% and, as a result, the risk of bias due to missing data is not high.
External Validity
Patients with conditions such as pregnancy, breastfeeding, concomitant diagnosis of another form of angioedema, recurrent angioedema associated with urticaria, clinically significant bleeding due to coagulopathy, thrombotic disorder, significant illnesses, and major comorbidities were excluded, and the results are not generalizable to these groups of patients.
The included patients were mostly women, and most of the patients were white; therefore, results may not be generalizable to a broader population.
The study included 10 adolescent patients. Given the small sample size, it is unlikely that the results would be broadly generalizable to all adolescent patients with HAE.
In this trial the maximum allowed dose for patients with C1-INH HAE was 400 mg per month and the maximum allowed dose for patients with normal C1-INH FXII mutation was 600 mg per month. These values were all higher than the recommended dosing in the product monograph of an initial loading dose of 400 mg administered as two 200 mg SC injections on the first day of treatment followed by a monthly dose of 200 mg. The number of patients who received these dosages and the effect of these dosages on validity of the results remains unclear.
Indirect Evidence
Contents within this section have been informed by materials submitted by the sponsor. The following has been summarized and validated by the review team.
Objectives for the Summary of Indirect Evidence
Due to the lack of direct evidence comparing garadacimab with other existing therapies for routine prevention of episodes of HAE in adult and pediatric patients (aged 12 years and older), the sponsor conducted 2 ITCs,33,34 including an NMA33 of several LTP treatments and a separate MAIC34 between garadacimab and lanadelumab. The objective of this section is to summarize and critically appraise the 2 sponsor-submitted indirect-evidence NMA and MAIC reports comparing garadacimab to other therapies for routine prevention of episodes of HAE in adult and pediatric patients (aged 12 years and older) in Canada.
Description of Indirect Comparisons
The sponsor submitted 2 ITC reports33,34 (1 NMA33 and 1 MAIC).34 The objectives of the NMA were to estimate the comparative efficacy, safety, and impact on HRQoL of LTP treatments including garadacimab SC for adolescents and adult patients (aged 12 years and older) with type I or II HAE. MAIC analyses were performed to account for key areas of heterogeneity between trials that could not be addressed via NMA methods.
Study Selection Methods for NMA
The NMA included trials identified through a systematic literature review (SLR) of RCTs investigating prophylactic treatments in men or women (at least 12 years old) with type I or II HAE.35 The SLR was conducted on August 11, 2022.35 The SLR identified 8 unique RCTs investigating 4 LTP treatments: garadacimab, C1-INH SC (Haegarda/Berinert SC), berotralstat (Orladeyo), and lanadelumab (Takhzyro). Individual patient-level data (IPD) for the trials of garadacimab and C1-INH SC were informed by the trial protocols and clinical study reports provided by the sponsor, CSL Behring. Table 25 provides an overview of the selection criteria of the SLR conducted for the NMA. Although Cinryze was investigated in a pivotal placebo-controlled RCT, the trial did not meet the eligibility criteria in the SLR conducted for the main analyses.36 The Cinryze trial was excluded because pediatric patients (aged < 12 years) were excluded from the NMA according to the SLR protocol. Nonetheless, an exploratory analysis was conducted to incorporate Cinryze as a comparator in the NMA. The technical report also noted that, although Berinert IV is sometimes used in patients with HAE, its use is off-label and has not been evaluated in a RCT. Therefore, it was excluded as a comparator from the NMA.
Table 25: Study Selection Criteria and Methods for ITCs Submitted by the Sponsor
Characteristics | Indirect comparison |
|---|---|
Population | Patients (men or women) aged ≥ 12 years diagnosed with HAE, type I or II |
Intervention | The following treatments available/widely approved or under investigation for HAE as prophylaxis, provided as a single agent:
|
Comparator | The comparator may be 1 of the 4 treatments outlined (i.e., in a head-to-head) or placebo |
Outcome | Time-normalized number of HAE attacks N and % attack-free patients Time-normalized number of attacks requiring on-demand treatment Time-normalized number of moderate and/or severe HAE attacks N and % of patients with AEs N and % of patients with serious AEs N and % mortality N and % discontinuations due to AEs N and % discontinuations from the trial AE-QoL |
Study designs | RCTs irrespective of blinding status |
Publication characteristics | Articles in English Date of publication
|
Exclusion criteria | Any criteria not consistent with inclusion criteria |
Databases searched | Ovid MEDLINE (including Epub ahead-of-print and in-process and other nonindexed citations), Ovid MEDLINE Daily, Embase, Cochrane Central Register of Controlled Trials, and Cochrane Database of Systematic Reviews |
Selection process | Records deduplicated using EndNote 20 and DistillerSR, articles screened independently by 2 researchers, discrepancies resolved by consensus or third independent reviewer; hand searches and supplementary sources were searched by a single reviewer |
Data extraction process | Extraction done by single reviewer, validated by another, using standardized data extraction templates in Microsoft Excel |
Quality assessment | Risk-of-bias assessment done using the Centre for Reviews and Dissemination RCT checklist (2008) |
AE = adverse event; AE-QoL = Angioedema Quality of Life questionnaire; HAE = hereditary angioedema; RCT = randomized controlled trial; SC = subcutaneous.
Source: Systematic literature review technical report.35
NMA Feasibility Assessment
An NMA feasibility assessment was undertaken on the studies identified through the SLR to test the assumptions of the analysis, explore the sources of clinical heterogeneity across studies, and assess whether the risks and benefits of indirectly comparing treatment effects were clear and transparent.33,37 Key issues identified through the feasibility assessment include:
C1-INH concentrate (Haegarda) trial: The COMPACT core and open-label extension trials on Haegarda were partially or fully excluded from the feasibility assessment due to heterogeneity in study design. i.e., the open-label extension of the COMPACT trial was excluded from the feasibility assessment due to heterogeneity in study design. The core COMPACT trial showed heterogeneity as well. This was a crossover trial, with a treatment period of up to 28 weeks and a crossover of Haegarda (40 IU/kg or 60 IU/kg) and placebo occurring at week 16. Because none of the other included trials had a crossover design, it was decided to incorporate precrossover data (week 16) for the core COMPACT trial to avoid heterogeneity within evidence networks.
Garadacimab (CSL312_2001 and CSL312_3001) trials: Garadacimab was administered every 4 weeks in the CSL312_2001 trial, but once monthly in the CSL312_3001 trial. For the analysis, these dosages were assumed to be equivalent.
Berotralstat (Orladeyo): The ApeX-2 trial data pertaining to the outcome of episode-free days per month were not deemed adequately comparable to data from other trials, due to a more specifically defined analysis population (only patients who completed the trial); these data were only incorporated within a sensitivity analysis.
ITC Analysis Methods
Table 26 provides an overview of the method used in the NMA evidence network.
Table 26: Indirect Comparison Analysis Methods (NMA)
Methods | Description | |
|---|---|---|
Analysis methods | Bayesian framework was used and a base case conducted using fixed-effects and random-effects models, although fixed-effects models were chosen for the main analysis. Zero cell correction were applied for dichotomous outcomes with 0 events in a trial. Rate, continuous, and dichotomous outcomes were assessed using Poisson, normal, and binomial model with appropriate link functions. | |
Priors Vague prior distributions that assumed no pre-existing information | Parameter | Prior distribution |
Baselines, unadjusted models (mu) | dnorm (0,1000) or dnorm(0,10000) | |
— | dnorm (0,10000) | |
Between-trial variation (sd) | dunif (0,2) or dunif (0,5) | |
Assessment of model fit | DIC and residual deviance | |
Assessment of consistency | DIC and residual deviance | |
Assessment of convergence | R-hat (a value of < 1.05 was considered acceptable) | |
Outcomes | Time-normalized number of HAE attacksa Time-normalized number of HAE attacks requiring on-demand treatmenta Proportion of attack-free patientsa Attack-free days per montha Any TEAEsa Change from baseline in AE-QoL total scorea | |
Follow-up time points | Varied by trial and/or treatment duration, up to 6 months | |
Construction of nodes | Evidence network diagrams were drawn to visualize evidence base for each outcome. Each treatment was represented by a node and comparisons between treatments shown by lines connecting the nodes. The size of nodes and thickness of lines were proportional to the sample size and number of studies informing the comparison, respectively. | |
Sensitivity analyses | Including all dosages, including licensed and unlicensed dosages Impact of increasing homogeneity across network, by removing phase II trials Use of binomial model with logit link function for dichotomous outcomes instead of complementary log-log link function | |
Subgroup analysis | Not done | |
Methods for pairwise meta- analysis | Not applicable | |
AE-QoL = Angioedema Quality of Life questionnaire; DIC = deviance information criterion; HAE = hereditary angioedema; NMA = network meta-analysis; TEAE = treatment-emergent adverse event.
aPriority outcomes that were selected by CSL Behring for conducting network meta-analyses are enclosed in this report.
Source: Network meta-analyses technical report.33
The evidence base was visualized using network diagrams for each outcome of interest, in which each treatment was represented by a node or circle and comparisons between treatments were shown by lines connecting the nodes. Nodes were sized to reflect the proportionate sample sizes, and the thickness of each line was proportional to the number of studies informing the comparison. One or more RCTs were present where lines connected different nodes.
Details of Bayesian Model
The NMA was conducted using a Bayesian framework as described in the National Institute for Health and Care Excellence (NICE) Evidence Synthesis Decision Support Unit (DSU) Technical Support Document series.38 The base-case analysis included licensed dosages for the interventions of interest, and were conducted using both fixed-effects and random-effects models. However, given the sparsity of the networks and for consistency across all analyses, fixed models were chosen as the primary analysis and sensitivity analysis a priori.
As a limited number of trials were included in the NMA, the networks were sparse, which could result in a certain treatment only appearing in 1 trial. If the trial contains no events for a particular outcome, it may not be possible to estimate a treatment effect. As a solution, a “zero cell correction” recommended by NICE was employed by adding 1 to the denominator and 0.5 to the numerator for all treatment arms in the trial.39 It should be noted that, while all trials generally had low event rates, both garadacimab trials were the only studies with zero cells for any outcome.
Rate outcomes were assessed using a Poisson model with a log link function and exposure-time offset, with results presented as rate ratios and corresponding 95% CrIs. Continuous outcomes were assessed using a normal model with an identity link function, with results presented as mean differences and corresponding 95% CrIs. For dichotomous outcomes for which further follow-up was likely to result in more events, a binomial model with a complementary log-log link function and maximum follow-up offset was used to account for the variable treatment duration between trials. Zero cell correction was applied where necessary, and results were presented as hazard ratios with corresponding 95% CrIs.
Vague prior distributions that assumed no pre-existing information were assigned for the treatment effects, trial baselines, and between-study variance in all analyses.
All analyses were performed using R version 3.5.3 or 3.6.1, Just Another Gibbs Sampler version 4.3.0, and WinBUGS version 1.4.3, and were based on burn-ins and sampling durations of 20,000 to 60,000 iterations depending on the outcome. Point estimates and 95% CrIs were modelled for outcomes using Markov chain Monte Carlo methods.
Assessment of Model Fit
Assessment of model fit was based on the deviance information criterion (DIC) and comparisons of residual deviance to a number of unconstrained data points. To justify the choice of a fixed-effects or random-effects model, the DIC statistics were compared between the models. Lower DIC values were preferred and differences of 3 points or greater were considered indicative of important differences in fit. However, as discussed previously, given the sparsity of the networks and for consistency across all analyses, fixed models were used as the primary analysis and sensitivity analysis a priori. Parameters of convergence and efficiency were assessed using the R-hat statistic (a value of < 1.05 was considered acceptable), bulk ESS (> 400 was considered acceptable), and tail ESS (> 400 was considered acceptable).40
Assessment of Heterogeneity
An assessment of heterogeneity was conducted to determine if the evidence base met the exchangeability assumption, i.e., whether all truly competing interventions were included as comparators. A feasibility assessment of the included studies was undertaken to evaluate potential sources of heterogeneity across trials based upon outcome definitions, inclusion and exclusion criteria, and trial characteristics. Sensitivity and subgroup analyses was considered to address clinical heterogeneity across trials. However, network meta-regression, which requires multiple RCTs informing each connection in the network (to ensure that the impact of differences in baseline characteristics can be separated from the “true” relative efficacy), was deemed infeasible because of insufficient clinical evidence, and was therefore excluded.
Sensitivity Analyses of Primary Base-Case Fixed-Effects Model Analysis
Several sensitivity analyses were conducted: a larger volume of data was included for all included dosages; homogeneity was increased across the network by removing phase II trials; for dichotomous outcomes, a binomial model with a logit link function was used instead of a complementary log-log link for outcomes where further follow-up would result in more events (e.g., proportion of episode-free patients and any TEAEs); and for the analysis of episode-free days per month, the APeX-2 trial with berotralstat (Orladeyo) was excluded from the primary analysis due because only patients who completed the trial were included. A sensitivity analysis was conducted to assess the impact of the APeX-2 trial data by including this trial in the analysis.
Assessment of Outcomes
The outcomes of interest for the NMA are listed in Table 26. The outcomes were selected based on the key outcomes in the pivotal CSL312_3001 trial of garadacimab. A total of 6 efficacy outcomes, 1 safety outcome, and 1 patient-reported outcome were deemed feasible. Outcomes were deemed infeasible due to the lack of data for more than 1 trial or event rates of 0 for all trials. The following outcomes were feasible for the analysis: time-normalized number of HAE episodes, time-normalized number of HAE episodes requiring on-demand treatment, time-normalized number of moderate and/or severe HAE episodes, proportion of episode-free patients over trial period, patients with a reduction in episode rate of 90% or greater, episode-free days, change from baseline in AE-QoL total score, and TEAEs.
Exploratory Analyses Including Cinryze
Due to the lack of direct evidence comparing garadacimab with other existing therapies for routine prevention of episodes of HAE in adult and pediatric patients (aged 12 years and older), the sponsor conducted 2 ITCs,33,34 including an NMA33 of several LTP treatments and a separate MAIC34 between garadacimab and lanadelumab. The objective of this section is to summarize and critically appraise the sponsor-submitted NMA and MAIC comparing garadacimab to other therapies for routine prevention of episodes of HAE in adult and pediatric patients (aged 12 years and older) in Canada.
NMA Results
Summary of Included Studies
A total of 7 trials were included in the NMA: 2 trials for garadacimab, 3 for berotralstat, 1 for C1-INH, and 1 for lanadelumab. An overview of key patient characteristics and trial characteristics of the trials included in NMA is presented in Table 27 and Table 28.
Table 27: Summary of Key Patient Characteristics of RCTs Included in NMA
Intervention or comparator | Study | Age, mean (SD) | Sex, female (%) | BMI, mean (SD) | Disease severity Baseline episode rates per month, mean (SD)a | Treatment historyb n (%) |
|---|---|---|---|---|---|---|
Garadacimab | CSL312_3001 | 41.2 (15.9) | 38 (59.4%) | 28.05 (6.6) | Run-in: 2.9 (1.7) (originally reported as “per year”) | 21 (32.8%) |
CSL312_2001 | Not available | 18 (56.3%) | Not available | Run-in: 5.2 (2.5) | 11 (34.4%) | |
Lanadelumab | HELP | 40.7 (14.7) | 88 (70.4%) | 28.3 (6.4) | Run-in: 3.6 (2.6) | 11 (34.4%) |
Berotralstat | APeX-1 | 44.1 (12.5) | 46 (59.7%) | 27.44 (5.58) | Baseline: 3.9 (2.0) | NR |
APeX-2 | 41.6 (15.2) | 80 (66%) | 29.0 (7) | Run-in: 3.0 (1.4) | NR | |
APeX-J | 42.0 (12.6) | 15 (78.9%) | 25.21 (5.276) | Run-in: 2.3 (1.3) | NR | |
C1-INH (Haegarda) | COMPACT | 39.6 (14.9) | 60 (67%) | 28.6 (7.1) | Run-in 3.3 (2.2) | 21 (32.8%) |
BMI = body mass index; HAE = hereditary angioedema; NMA = network metanalysis; NR = not reported; RCT = randomized controlled trial; SD = standard deviation.
aDisease severity was not a key eligibility criterion in the included trials. All trials included patients who experienced 2 to 4 or greater HAE episodes within a specified duration, up to 6 months before trial entry. With the exception of Study CSL312_2001, all trials included HAEs that were either documented or investigator-confirmed. Disease severity was not defined for any trials other than the APeX trials for berotralstat, in which it was based on episode rates. Baseline episode rates per month (mean [SD]) in the included trials are provided in the following section.
bTreatment history for the management of HAE is provided in the eligibility criteria. With the exception of the APeX trials, the use of plasma-derived C1-INH as prophylaxis for HAE episodes 3 months before screening were reported.
Table 28: Summary of Key Study Characteristics of RCTs Included in NMA
Intervention and comparators | Study name, type (duration) | Key trial eligibility criteriaa | Sample size (randomized), n | Dosing of comparatorsb | Withdrawal frequencyc | |
|---|---|---|---|---|---|---|
Garadacimab | CSL312_3001 Phase III double-blind RCT (26 weeks) | ≥ 3 HAE attacks 3 months before screening ≥ 1 average HAE attack/ month during run-in period | Must stop C1-INH products, androgens, antifibrinolytics or other small molecules for routine prophylaxis against HAE attacks within 2 weeks before run-in period C1-INH functional activity: ≤ 50%, and C4 antigen level below lab reference range | Garadacimab 200 mg SC q.m.: 39 Placebo: 25 | Garadacimab 200 mg SC q.m., or placebo | 2 (3.1%) withdrew due to attacks |
CSL312_2001 Phase II double-blind RCT (12 weeks) | ≥ 4 HAE attacks over 2 consecutive months, within 3 months before screening or previous HAE prophylaxis | Willing to stop using C1-INH therapy, androgens, or antifibrinolytics for routine attack prophylaxis at the start of run-in period C1-INH functional activity: ≤ 50% of lower limit of reference range, and C4 antigen level below lab reference range | Garadacimab 200 mg SC q.4.w.: 8 Garadacimab 75 mg SC q.4.w.: 9 Garadacimab 600 mg SC q.4.w.: 7 Placebo: 8 | Garadacimab 200 mg SC q.4.w., or 75 mg SC q.4.w., or 600 mg SC q.4.w., or placebo | 1 (3.1%) withdrew during run-in | |
Lanadelumab | HELP Phase III double-blind RCT (26 weeks) | ≥ 1 HAE attack per 4 weeks | Must not use short-term prophylaxis (C1 inhibitors, attenuated androgens, antifibrinolytics) for HAE within 7 days of run-in period C1-INH functional activity: < 40% of normal level, or 40% to 50% of normal level if C4 antigen is below normal range | Lanadelumab 300 mg SC q.2.w.: 27 Lanadelumab 300 mg SC q.4.w.: 29 Lanadelumab 150 mg SC q.4.w.: 29 Placebo: 41 | Lanadelumab 300 mg SC q.2.w., or 300 mg SC q.4.w., or 150 mg SC q.4.w., or placebo | 7 (5.6%) withdrew |
Berotralstat | APeX-1 Phase III double-blind RCT (28 weeks) | ≥ 2 attacks per month, for 3 consecutive months, within 6 months before screening | Able to use 1 or more acute medications for treating HAE attacks | Berotralstat 62.5 mg oral q.d.: 7 Berotralstat 125 mg oral q.d.: 14 Berotralstat 250 mg oral q.d.: 15 Berotralstat 350 mg oral q.d.: 18 Placebo: 23 | Berotralstat 62.5 mg oral q.d., or 125 mg oral q.d., or 250 mg oral q.d., or 350 mg oral q.d., or placebo | 3 (5.7%) discontinued due to AE |
APeX-2 Phase III double-blind RCT (24 weeks) | ≥ 2 HAE attacks within 56 days of run-in period | Able to use 1 or more acute medications for treating acute HAE attacks Medically appropriate for on-demand treatment as sole treatment for HAE | Berotralstat 150 mg oral q.d.: 40 Berotralstat 110 mg oral q.d.: 41 Placebo: 40 | Berotralstat 150 mg oral q.d., or 110 mg oral q.d., or placebo | 2 (1.7%) withdrew | |
APeX-J Phase III double-blind RCT (24 weeks) | ≥ 2 HAE attacks within 56 days of run-in period | Access to ≥ 1 targeted medications Medically appropriate for on-demand treatment as sole treatment for HAE | Berotralstat 150 mg oral q.d.: 7 Berotralstat 110 mg oral q.d.: 6 Placebo: 6 | Berotralstat 150 mg oral q.d., or 110 mg oral q.d., or placebo | 1 (5.3%) discontinued due to TEAE | |
C1-INH (Haegarda) | COMPACT Phase III RCT Crossover, double-blind with open-extension phase (32 weeks) | ≥ 4 HAE attacks over 2 consecutive months, or ≥ 2 HAE attacks within 4 consecutive weeks, both requiring medical attention or caused significant functional impairment | Willing to cease any pre-existing medications for HAE prophylaxis | C1-INH 60 IU/kg then high-volume placebo SC twice weekly: 45 C1-INH 40 IU/kg then low-volume placebo SC twice weekly: 45 | C1-INH 60 IU/kg SC twice weekly, or 40 IU/kg SC twice weekly, or placebo | Not available |
HAE = hereditary angioedema; MAIC = matching adjusted indirect comparison; NMA = network metanalysis; q.2.w. = every 2 weeks; q.4.w = every 4 weeks; q.d. = every day; q.m. = once monthly; RCT = randomized controlled trial; SC = subcutaneous; SD = standard deviation.
aAll trials included male or female, type I or II HAE, and had acceptable effective contraception. With the exception of the CSL312_2001 and APeX-1 studies, all trials included patients aged 12 years and older. Only the COMPACT and APeX-2 trials had a eligibility criterion of 40 kg or greater; the rest had no weight-based criterion. Where reported, C1- INH functional activity was 50% or less, and C4 antigen levels were below the reference range. Across the trials, patients had to have 2 to 4 HAE attacks in the 3 months before study entry. Finally, patients were not allowed to receive certain prophylactic therapy for HAE. All trials were multicentre. The APeX-J study was a single-country trial conducted in Japan. Clinical judgment indicated that patients in Japan were not markedly different from those in other countries, and should therefore not be excluded. Only 2 of the 8 included trials were phase II, and 1 was open-label. The rest were phase III, double-blind studies. The COMPACT trial was a crossover trial, with patients switching between placebo and 1 of 2 doses of C1-INH at week 16. The treatment period was 26 weeks for the CSL312_3001 trial with garadacimab, but ranged from 12 to 32 weeks in the other trials. The treatment duration in APeX-1 was the shortest, at 28 days; however, treatment onset was noted to be relatively rapid based on clinical judgment. Therefore, no trials were excluded for too short a duration. All trials included a run-in period except for APeX-1, which had a screening period only. Where reported, the run-in period duration was comparable across trials.
bOnly licensed dosages were considered for the base-case analyses. For the analysis, the 2 dosages of garadacimab were assumed to be the same.
cThe withdrawal frequency was low across trials, at around 5% or less.
Table 29: Summary of Placebo Response in RCTs Included in NMA
Intervention and comparators | Study | Placebo response, mean (95% CI)a |
|---|---|---|
Garadacimab | CSL312_3001b,c | Time-normalized number of episodes CSL312_3001: 2.01 (1.44 to 2.57) Time-normalized number of episodes requiring on- demand treatment: 1.86 (1.26 to 2.46) Time-normalized number of moderate and/or severe HAE episodes: 1.35 (0.86 to 1.84) Proportion of episode-free patients: 0 (0) Episode-free days per month: 25.06 (SD = 4.51) Any TEAEs: 15 (60%) Change from baseline in total AE-QoL score: −2.21 (−11.16 to 6.75) |
CSL312_2001 | Time-normalized number of episodes: 4.2 (SD = 1.8) Time-normalized number of episodes requiring on-demand treatment: 3.98 (SD = 1.76) Time-normalized number of moderate and/or severe HAE episodes: 2.82 (SD = 1.92) Proportion of episode-free patients: 1 (2.4%) Episode-free days per month: 21.33 (SD = 5.18) Any TEAEs: 6 (75%) Change from baseline in total AE-QoL score: not available | |
Lanadelumab | HELP | Time-normalized number of episodes: 1.97 (1.64 to 2.36) Time-normalized number of episodes requiring on-demand treatment: 1.64 (1.34 to 2.00) Time-normalized number of moderate and/or severe HAE episodes: 1.22 ( 0.97 to 1.52) Proportion of episode-free patients: 1 (2.4%) Episode-free days per month: 22.6 (SD = 4.4) Any TEAEs: 31 (75.6%) Change from baseline in total AE-QoL score, least squares mean: −4.72 (−10.46 to 1.02) |
Berotralstat | APeX-1 | Time-normalized number of episodes (episodes per week): 0.90 (SD = 0.57) Time-normalized number of episodes requiring on-demand treatment (episodes per week): 0.76 (SD = 0.65) Time-normalized number of moderate and/or severe HAE episodes: not available Proportion of episode-free patients: 2 (9%) Episode-free days per month: 21.1 (SD = 3.4) Any TEAEs: 15 (68%) Change from baseline in total AE-QoL score: −4.5 (SE = 3.5) |
APeX-2 | Time-normalized number of episodes: 2.47 (SD = 1.60) Time-normalized number of episodes requiring on-demand treatment: 2.21 (SD = 1.71) Time-normalized number of moderate and/or severe HAE episodes: 1.24 (SD = 1.20) Proportion of episode-free patients: 1 (2.6%) Episode-free days per month: 27.36 (SD = 48.64) (using the subset of patients in the ITT population who completed Part 1 of the study) Any TEAEs: 30 (77%) Change from baseline in total AE-QoL score: −9.69 (SE = 2.64) | |
APeX-J | Time-normalized number of episodes (episodes per 28 days): 2.73 (SD = 1.64) Time-normalized number of episodes requiring on-demand treatment per 28 days: 2.43 (SD = 1.76) Time-normalized number of moderate and/or severe HAE episodes: 0.73 (SD = 0.34) Proportion of episode-free patients: 0 (0%) Episode-free days per month: not available Any TEAEs: 6 (100%) Change from baseline in total AE-QoL score: 3.18 (SE = 6.83) | |
C1-INH | COMPACT | Time-normalized number of episodes for high-volume placebo (n = 22): 4.14 (SD = 2.3); low-volume placebo (n = 23): 3.94 (SD = 2.58) Time-normalized number of episodes requiring on-demand treatment for high-volume placebo (n = 22): 3.58 (2.39); low-volume placebo (n = 23): 2.83 (SD = 1.96) Time-normalized number of moderate and/or severe HAE episodes for high-volume placebo (n = 22): 3.02 (2.49); low-volume placebo (n = 23): 3.00 (SD = 2.28) Proportion of episode-free patients: 0 (0%) Episode-free days per month for high-volume placebo (n = 22): 23.79 (SD = 4.15); low-volume placebo (n = 23): 24.03 (SD = 4.90) Any TEAEs: high-volume placebo (n = 22): 15 (68.2%); low-volume placebo (n = 23): 16 (68.9%) Change from baseline in total AE-QoL score: mean = not available |
AE-QoL = Angioedema Quality of Life questionnaire; CI = confidence interval; HAE = hereditary angioedema; MedDRA = Medical Dictionary for Regulatory Activities; NMA = network meta-analysis; RCT = randomized controlled trial; SC = subcutaneous injection; SD = standard deviation; TEAE = treatment-emergent adverse event.
aUnless otherwise specified.
bOverall, placebo response was similar between trials without more than 20 percentage points, although the phase II CSL312_2001 trial had larger differences in number of monthly HAE episodes and number of moderate to severe HAE episodes. Quality of life from baseline to final follow-up time also varied between trials.
cOutcomes in Study CSL312_3001 are provided here. Overall, outcome definitions in the other trials were similar to merit incorporation in the NMA. Unless otherwise reported, the outcomes were reported in all 7 included trials. The NMA technical report provides details.33
Time-normalized number of HAE episodes per month during treatment period from day 1 (first study drug administration) through day 182 (6 months). All trials aligned with this definition, though duration of treatment period differed across trials, ranging from 441 to 2642,43 weeks. Furthermore, all trials specified episodes as “investigator/expert-confirmed.”
Time-normalized number of episodes requiring on-demand treatment during the treatment period (date of administration of an on-demand treatment was between the start and end date of a HAE attack”). All trials aligned with this definition, although different terms were used to refer to on-demand treatment across trials, including: “acute treatment” (HELP),43 “rescue medication” (COMPACT),44 and “SOC medication” (APeX-2).45
Proportion of episode-free patients (6 trials): The number and percentage of patients who are with a percentage reduction of 100%, (i.e., who do not experience a HAE episode and so are episode-free for the 6-month treatment period”). All trials aligned with this definition, though duration of treatment period differed across trials, ranging from 4 weeks41 to 26 weeks.42,43
Episode-free days per month (4 trials): The number of episode-free days per month over the treatment period. All trials aligned with this definition, though duration of treatment period differed across trials, ranging from 12 weeks46 to 26 weeks.42,43
Any TEAEs: Adverse events starting on or after the date of the first study drug administration over the treatment period, coded using the MedDRA dictionary version 25.0. All 7 trials aligned with this definition apart from some minor differences. Several trials used different versions of the MedDRA dictionary, version 22.0 (CSL312_2001),46 version 20.0 (HELP),43 version 19.1 (APeX-2 and APeX-J,47,48 version 18.1 (APeX-1),41 and version 18.0 (COMPACT).44 The APeX trials for Berotralstat also had a slightly different time period, with TEAEs being measured from the time of the first dose to an additional 30 days after the end of treatment.47-49
Change from baseline in total AE-QoL score (5 trials): The AE-QoL questionnaire measures quality of life across 4 domains: functioning, fatigue and mood, fears and shame, and nutrition, and provides a total score out of 100 (with higher scores indicating greater impairment). All trials measured the change from baseline in total score at the end of treatment (time point differed across studies). It was noted that the questionnaire was administered predose in HELP.43
dTime-normalized number of HAE episodes: 6 months for Study CSL312_3001, 441 to 2642,43 weeks in other trials.
Time-normalized number of episodes requiring on-demand treatment: 12 weeks up to 6 months or 26 weeks.
Proportion of episode-free patients: 6 months for Study CSL312_3001, 441 to 26 weeks in other trials.
Episode-free days per month: 6 months for Study CSL312_3001, 12 to 2642,43 weeks in other trials.
Any TEAEs: Up to 6 months.
Change from baseline in total AE-QoL score: up to 6 months.
Evidence Networks Efficacy
Evidence network for all time-normalized number of HAE episodes, episode-free days per month and AE-QoL total score are presented in Figure 4, Figure 5, and Figure 6, respectively.
Figure 4: Evidence Network for All Time-Normalized Numbers of HAE Attacks
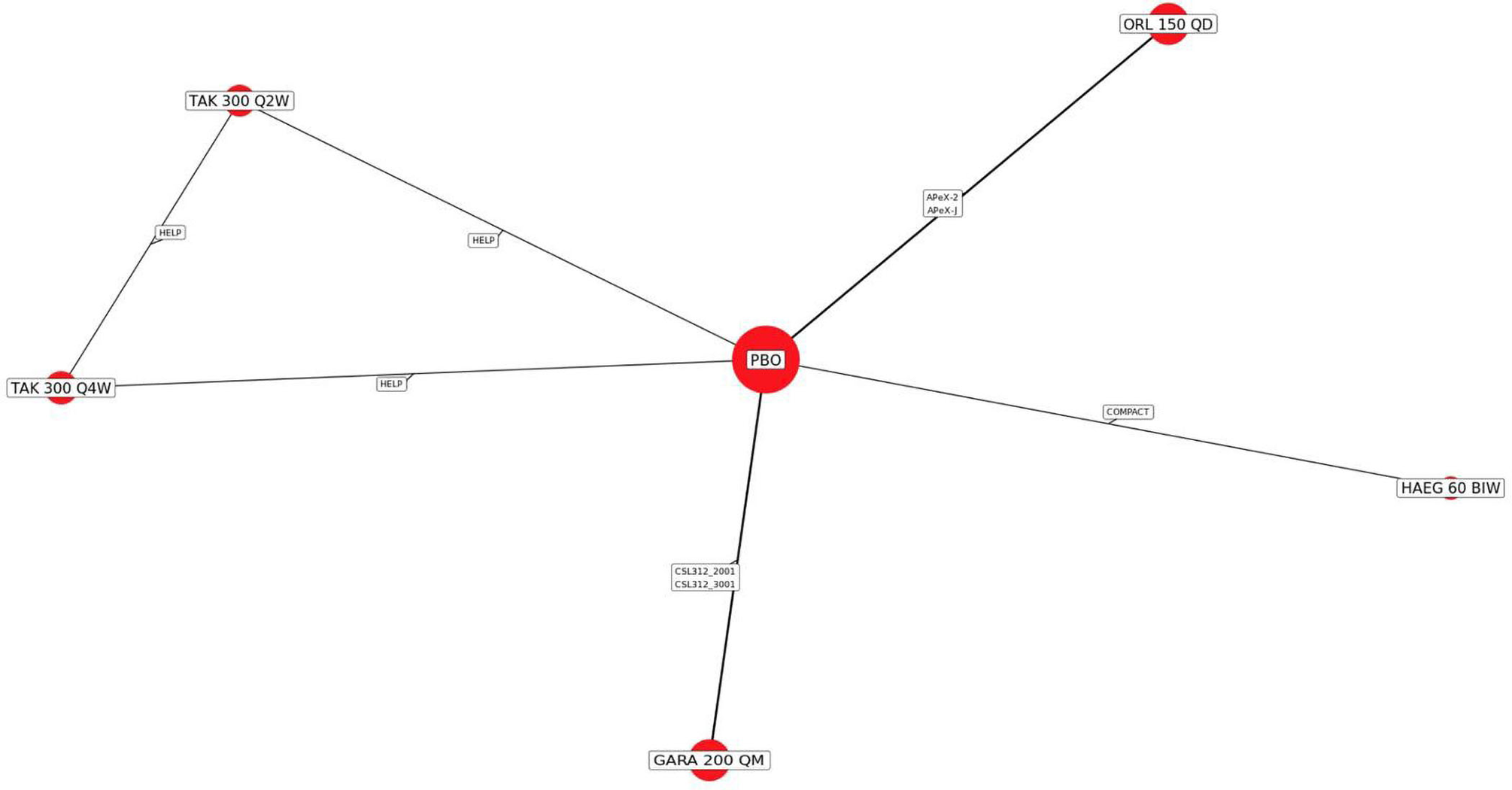
GARA 200 QM = garadacimab 200 mg once monthly; HAE = hereditary angioedema; HAEG 60 BIW = Haegarda 60 IU/kg twice weekly; ORL 150 QD = Orladeyo 150 mg once daily; PBO = placebo; TAK 300 mg Q2W = Takhzyro 300 mg once every 2 weeks; TAK 300 mg Q4W = Takhzyro 300 mg once every 4 weeks.
Source: Network meta-analysis technical report.33
Figure 5: Evidence Network for Attack-Free Days per Month
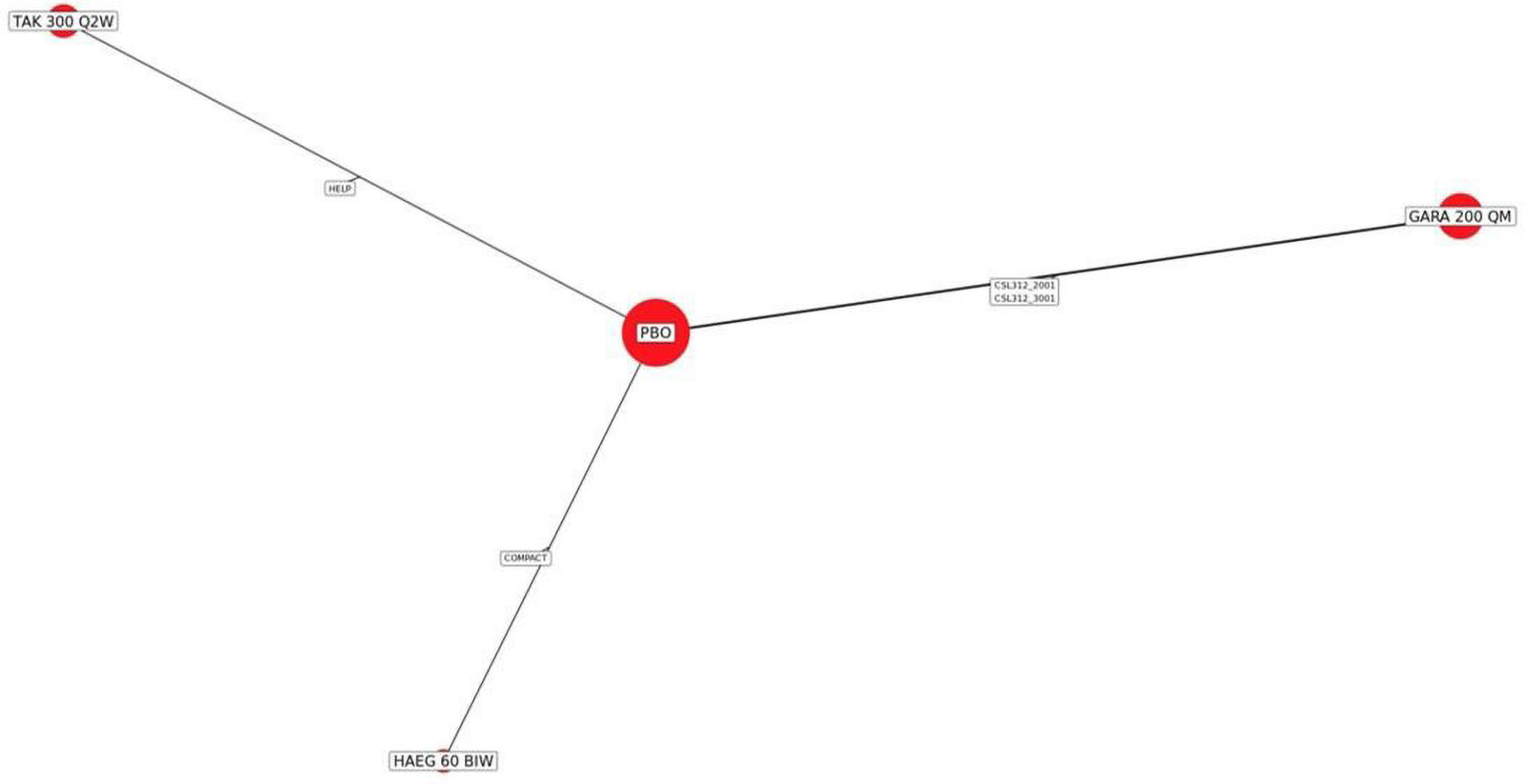
GARA 200 QM = garadacimab 200 mg once monthly; HAEG 60 BIW = Haegarda 60 IU/kg twice weekly; PBO = placebo; TAK 300 Q2W = Takhzyro 300 mg once every 2 weeks.
Source: Network meta-analysis technical report.33
Figure 6: Evidence Network for Change From Baseline in AE-QoL Total Score
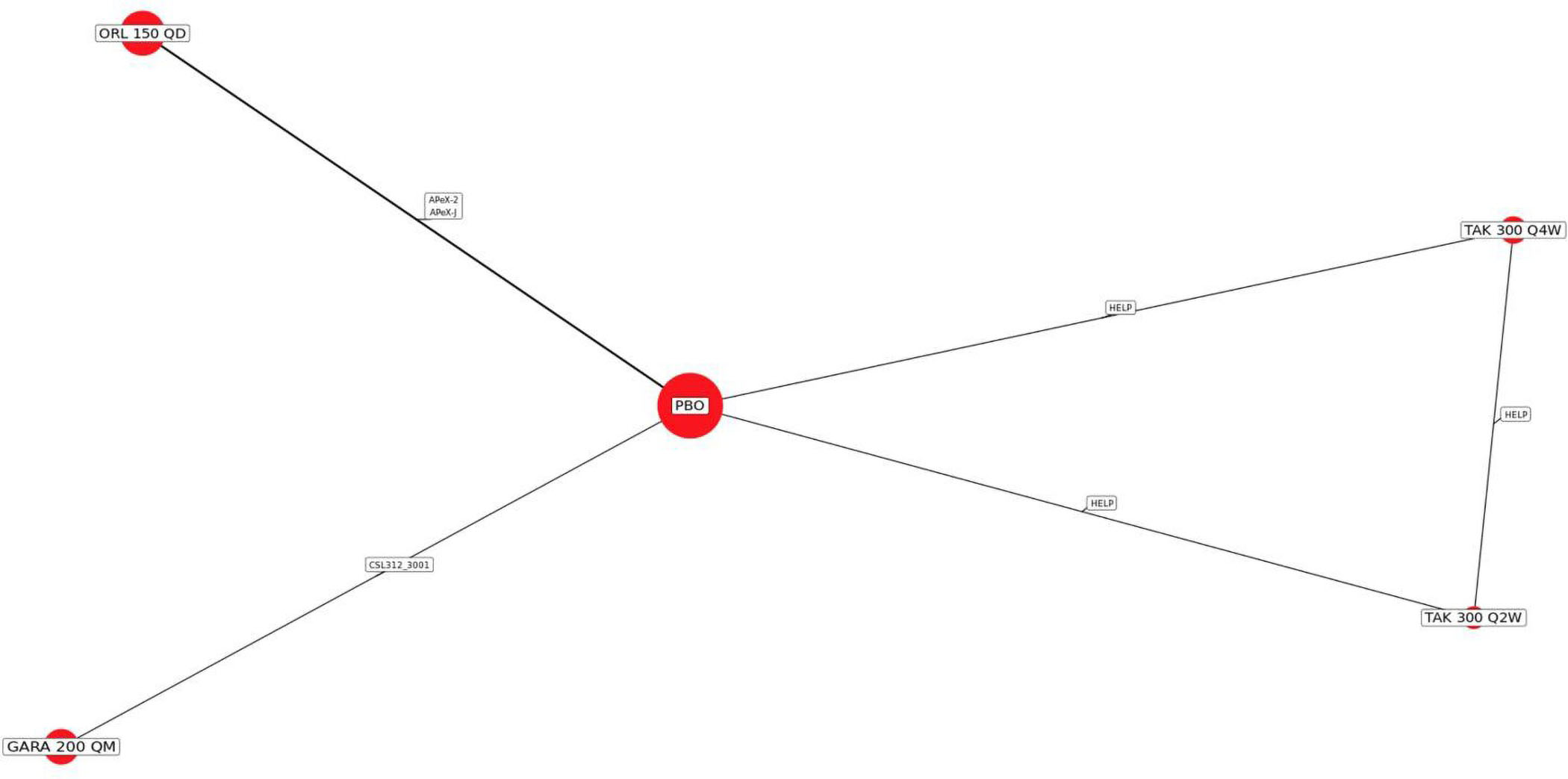
AE-QoL = Angioedema Quality of Life questionnaire; GARA 200 QM = garadacimab 200 mg once monthly; ORL 150 QD = Orladeyo 150 mg once daily; PBO = placebo; TAK 300 Q2W = Takhzyro 300 mg once every 2 weeks; TAK 300 Q4W = Takhzyro 300 mg once every 4 weeks
Source: NMA technical report.33
Results are provided here for the base-case analysis for each analyzed outcome. Given that fixed-effects models were used for the main analysis, these will be focused on this report. Results from random-effects models and sensitivity analyses will be discussed briefly, with details provided in the NMA technical report.33 A summary of DICs is presented in Table 30.
Base-Case Analyses
Base-case analyses were conducted based on fixed-effects and random-effects models. However, the fixed-effects model was chosen as the primary analysis regardless of DICs (Table 30).
Table 30: Summary of DICs (Model Fit Statistics)
Outcomes | DICa | |
|---|---|---|
FE | RE | |
Time-normalized number of HAE episodes | 113.55 | 97.6 |
Time-normalized number of HAE episodes requiring on-demand treatment | 115.11 | 94.47 |
Proportion of episode-free patients | 29.82 | 30.3 |
Episode-free days per month | 20.57 | 18.74 |
≥ 90% reduction of HAE episodes (reported in MAIC, not reported in NMA) | NR | NR |
Change from baseline in AE-QoL total score | 51.34 | 51.19 |
Time-normalized number of moderate and/or severe HAE episodes | 95.41 | 90.51 |
TEAEs | 10.44 | 11.39 |
AE-QoL = Angioedema Quality of Life questionnaire; DIC = deviance information criterion; FE = fixed effects; HAE = hereditary angioedema; MAIC = matching adjusted indirect comparison; NMA = network metanalysis; NR = not reported; RE = random effects; TEAE = treatment-emergent adverse event.
aA difference in the DIC between the models of equal to or greater than 3 was considered meaningful according to the NMA technical report.
Efficacy
A summary of results of the primary base-case analyses (i.e., fixed-effects model analysis) for garadacimab 200 mg once monthly versus the comparators outlined earlier is presented for each outcome in Table 31.
Garadacimab 200 mg once monthly was favoured over lanadelumab 300 mg every 4 weeks and berotralstat 150 mg once daily with respect to all of the time-normalized number of HAE episodes for the outcomes analyzed, and over Haegarda 60 mg twice weekly with respect to all time-normalized number of HAE episodes and those that were moderate or severe. With respect to HRQoL, garadacimab 200 mg once monthly was favoured over berotralstat 150 mg once daily. Garadacimab 200 mg once monthly was not favoured over comparators for the other outcomes analyzed.
Table 31: Summary of Primary Base-Case Results Between Garadacimab 200 mg Once Monthly vs. Comparators (Fixed-Effects Model)
Outcomes | GARA 200 mg q.m. vs. specified comparator (fixed-effects model) | ||||
|---|---|---|---|---|---|
TAKH 300 mg q.2.w. | TAKH 300 mg q.4.w. | HAEG 60 mg b.i.w. | ORL 150 mg q.d. | Placebo | |
Time-normalized number of HAE episodes, RR (95% CrI) | 0.88 (0.58 to 1.32) | 0.43 (0.30 to 0.60) | 0.67 (0.46 to 0.98) | 0.18 (0.14 to 0.24) | 0.11 (0.09 to 0.15) |
Time-normalized number of HAE episodes requiring on-demand treatment, RR (95% CrI) | 0.82 (0.52 to 1.30) | 0.41 (0.28 to 0.59) | 0.94 (0.59 to 1.52) | 0.17 (0.13 to 0.23) | 0.10 (0.08 to 0.14) |
Time-normalized number of moderate and/or severe HAE episodes | 0.50 (0.30 to 0.85) | 0.31 (0.19 to 0.49) | 0.57 (0.34 to 0.95) | 0.12 (0.08 to 0.17) | 0.08 (0.05 to 0.12) |
Proportion of episode-free patients HR (95% CrI) | 1.65 (0.09 to 28.92) | 2.63 (0.15 to 46.03) | 3.43 (0.18 to 63.97) | 19.33 (0.85 to 457.6) | 39.23 (5.27 to 294.06) |
≥ 90% reduction of HAE episodes | NR | NR | NR | NR | NR |
Episode-free days per month, MD (95% CI) | 0.96 (−1.25 to 3.18) | 1.36 (−0.85 to 3.58) | 0.4 (−1.85 to 2.66) | — | 5.66 (3.97 to 7.35) |
Change from baseline in AE-QoL total score, MD (95% CrI) | −7.66 (−21.34 to 6.05) | −11.6 (−25.16 to 2.00) | — | −17.28 (−29.75 to −4.68) | −24.22 (−34.54 to 13.81) |
TEAEs, HR (95% Crl) | 0.51 (0.21 to 1.27) | 0.85 (0.37 to 1.96) | 1.37 (0.57 to 3.33) | 0.92 (0.41 to 2.07) | 1.19 (0.67 to 2.13) |
AE-QoL = Angioedema Quality of Life questionnaire; b.i.w. = twice weekly; CI = confidence interval; CrI = credible interval; GARA = garadacimab; HAE = hereditary angioedema; HR = hazard ratio; HAE = hereditary angioedema; HAEG = Haegarda; MD = mean difference; NR = not reported; ORL = Orladeyo; q.2.w. = every 2 weeks; q.4.w. = every 4 weeks; q.d. = once daily; q.m. = once monthly; RR = rate ratio; TAK = Takhzyro; TEAE = treatment-emergent adverse event; vs. = versus.
Notes: Shaded cells indicate a statistically significant result favouring GARA 200 mg q.m. over the comparator. An RR less than 1, an HR greater than 1, and a mean difference greater than 0 (for episode-free days per months) or less than 0 (for change in baseline in AE-QoL total score) implied an outcome for GARA 200 mg q.m. superior to that of the comparator. An RR and HR less than 1 indicates an improved outcome for GARA 200 mg once monthly.
Source: NMA technical report.33
Differences favouring garadacimab were no longer present in the NMA results based on the random-effects models, except for the difference in the AE-QoL for garadacimab versus berotralstat 150 mg once daily (Table 32).
Table 32: Summary of Base-Case Results Between Garadacimab 200 mg Once Monthly vs. Comparators (Random-Effect Model)
Outcomes | GARA 200 mg q.m. vs specified comparator (random-effects model) | ||||
|---|---|---|---|---|---|
TAKH 300 mg q.2.w. | TAKH 300 mg q.4.w. | HAEG 60 mg b.i.w. | ORL 150 mg q.d. | Placebo | |
Time-normalized number of HAE episodes, RR (95% CrI) | 0.47 (0.00 to 98.95) | 0.23 (0.00 to 47.30) | 0.36 (0.00 to 75.97) | 0.12 (0.00 to 9.56) | 0.06 (0.00 to 1.28) |
Time-normalized number of HAE episodes requiring on- demand treatment, RR (95% CrI) | 0.35 (0.00 to 163.74) | 0.17 (0.00 to 70.69) | 0.40 (0.00 to 169.11) | 0.10 (0.00 to 11.94) | 0.04 (0.00 to 1.45) |
Time-normalized number of moderate and/or severe HAE episodes | 0.34 (0.00 to 41.63) | 0.20 (0.00 to 21.62) | 0.38 (0.00 to 40.78) | 0.07 (0.00 to 2.63) | 0.05 (0.00 to 0.67) |
≥ 90% reduction of HAE episodes | NR | NR | NR | NR | NR |
Proportion of episode-free patients, HR (95% CrI) | 1.66 (0.03 to 82.46) | 2.61 (0.05 to 131.16) | 3.4 (0.06 to 171.19) | 18.95 (0.3 to 1175.56) | 38.2 (3.06 to 482.61) |
Episode-free days per month, MD (95% CI) | 1.32 (−2.41 to 5.65) | 1.74 (−2.02 to 6.06) | 0.76 (−2.99 to 5.06) | NR | 6.04 (3.62 to 8.91) |
Change from baseline in AE-QoL total score, MD (95% CrI) | −7.58 (−21.97 to 6.45) | −11.65 (−25.56 to 2.67) | NR | −17.27 (−30.12 to −4.69) | −24.3 (−35 to −13.86) |
TEAEs, HR (95%Crl) | 0.52 (0.04 to 8.35) | 0.88 (0.06 to 13.25) | 0.69 (0.05 to 9.94) | 0.96 (0.07 to 14.5) | 0.81 (0.16 to 3.87) |
AE-QoL = Angioedema Quality of Life questionnaire; b.i.w. = twice weekly; CI = confidence interval; CrI = credible interval; GARA = garadacimab ; HAE = hereditary angioedema; HAEG = Haegarda; HR = hazard ratio; MD = mean difference; q.2.w. = every 2 weeks; q.4.w. = every 4 weeks; q.d. = once daily; q.m. = once monthly RR = rate ratio; NR = not reported; ORL = Orladeyo; RR = rate ratio; TAK = Takhzyro; TEAE = treatment-emergent adverse event; vs. = versus.
Source: Garadacimab network meta-analysis technical report (as of June 18, 2024).
Sensitivity Analyses of Primary Base-Case Fixed-Effects Model Analysis
The sensitivity analyses conducted by removing phase II trials produced results that were largely similar to those of the base-case analysis for all outcomes assessed in the NMA. Because the AE-QoL total score network did not contain any phase II trials, no corresponding sensitivity analysis that removed such trials was conducted.
Harms
Any TEAEs
Of the 7 trials identified in the clinical SLR, 6 reported TEAEs for licensed doses. However, although the APeX-J trial reported data for this outcome, both treatment arms reported TEAEs for 100% of patients, meaning they did not contribute to the treatment effect. As such, the APeX-J trial was excluded from this analysis as recommended by NICE.39 Berotralstat was still incorporated in this analysis via data from the APeX-2 trial. Five trials were included in this NMA. The network diagram of this outcome is presented in Figure 7. The network consisted of 5 treatment nodes informed by 5 placebo-controlled RCTs.
Figure 7: Evidence Network for TEAEs
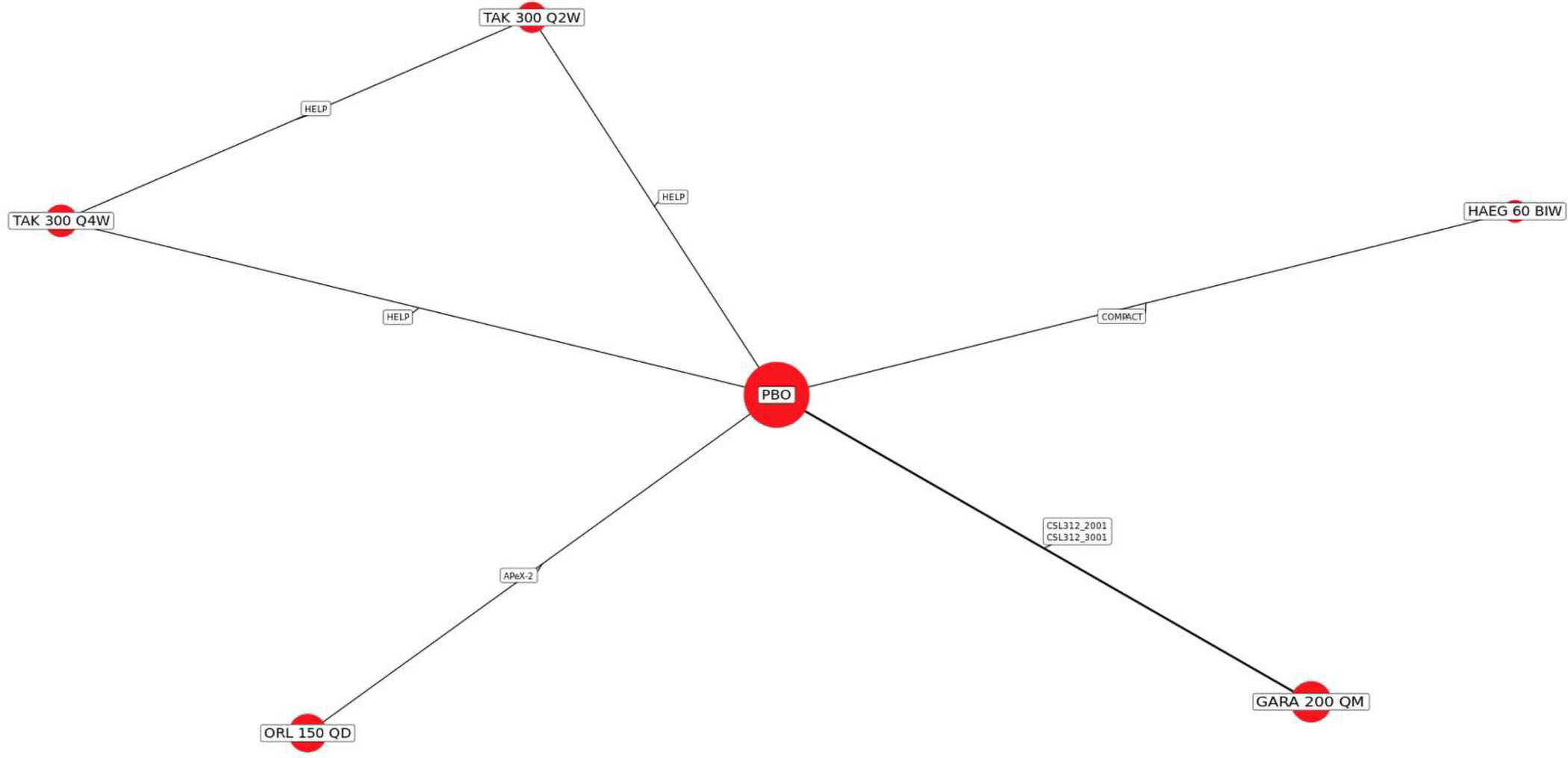
GARA 200 QM = garadacimab 200 mg once monthly; HAEG 60 BIW = Haegarda 60 IU/kg twice weekly; ORL 150 QD = Orladeyo 150 mg once daily; PBO = placebo; TAK 300 Q2W = Takhzyro 300 mg once every 2 weeks; TAK 300 Q4W = Takhzyro 300 mg once every 4 weeks; TEAE = treatment-emergent adverse event.
Source: Network meta-analysis technical report.33
Results From Fixed-Effects Model
The proportion of patients experiencing TEAEs in garadacimab 200 mg once monthly was numerically higher compared with Haegarda 60 mg twice weekly, but numerically lower compared with berotralstat 150 mg once daily, lanadelumab 300 mg every 4 weeks, and lanadelumab 300 mg every 2 weeks. No statistically significant differences were observed.
Results From Random-Effects Model
In comparison to the fixed-effects NMA, results were similar, other than much wider CrIs. Model diagnostics suggested that the fixed-effects model (DIC = 10.44) fit the data better than the random-effects model (DIC = 11.39).
Sensitivity Analyses
Sensitivity analyses by removing phase II trials showed that no notable changes were identified as compared to the base-case analysis.
Critical Appraisal of NMA
Overall, the ITCs were conducted according to accepted methodological guidance.38 An SLR was used to select relevant studies. Risk-of-bias assessments of each included study were carried out using the Centre for Reviews and Dissemination RCT checklist (2008). Feasibility assessment was performed to identify RCTs, minimize inter-trial heterogeneity, and to increase validity of the results. A prespecified analysis plan for conducting NMAs was used to guide the analyses. Geometries of the evidence networks were provided for each outcome analysis. Various sensitivity and scenario analyses were conducted to further validate findings from the primary results. The potential limitations of the NMA are discussed in the following section.
The key limitation of the NMA was the heterogeneity across the included studies in terms of the study designs (e.g., variable trial duration); patient characteristics (including baseline HAE episode rate [during run-in], age, gender, BMI and body weight, history of anxiety, and history of depression), which were considered potential treatment-effect modifiers; and variability in outcome definitions. No meta-regression analyses to adjust for factors that may bias comparisons were conducted. The limited number of trials included in the NMA informing each treatment comparison precluded the effective use of meta-regression to adjust for potential sources of cross-trial heterogeneity. The provided technical documents described how efforts were made to identify and minimize cross-trial heterogeneity before conducting NMAs through feasibility assessments that assessed trials’ similarities. However, the differences in these potential treatment-effect modifiers were identified as clinically important by the clinical expert consulted by CDA-AMC and may affect the validity of NMA results. For example, the analysis validity caused by differences in outcome definition could not be fully understood, particularly when HAE episodes were either uniquely defined, or not clearly defined. Trials with varying follow-up durations may have contributed to heterogeneity. In addition, concomitant treatment information in each included study was not presented in the NMA. Therefore, it is not clear whether concomitant treatments were similar across the trials or whether the analyses followed a treatment-policy strategy for testing the estimand similar to that of the garadacimab VANGUARD trial. The other signal of heterogeneity was in the model fit based on DIC, in which the results show that random-effects models provided a better fit (a lower DIC by 3 points or more) for several important outcomes, suggesting that heterogeneity was present and should be accounted for. Given the sparseness of the network, the random-effects model could overfit the data, leading to large differences in the DIC compared with the fixed-effects model. However, the fixed-effects model potentially underestimates the between-study heterogeneity, leading to biased or overly precise comparative estimates. Therefore, the key assumption of similarity for NMA may have been violated, given the differences between the included studies that were not adequately addressed in the analysis. This limitation is primarily driven by the limitations of the available evidence as compared with deficiencies in the methods used for the NMAs.
Relatedly, the small number of trials with relatively small sample sizes and the structure of the constructed evidence networks were other key limitations. All evidence networks were sparsely connected, and the connections between treatment nodes were typically informed by only a single trial. All trials were placebo-controlled, rather than head-to-head, which further simplified network structures and resulted in a lack of closed loops between nodes (except for the lanadelumab dose comparisons).
No NMAs were performed for the proportion of patients with a reduction in the episode rate of 90% or greater compared to run-in, probably due to the lack of data.
Matching Adjusted Indirect Comparison
The following section is a description of the MAIC submitted by the sponsor.34
Objective of the MAIC
The objective of the MAIC was to estimate the relative efficacy between 200 mg garadacimab administered by SC injection once monthly compared to 300 mg lanadelumab by SC injection every 2 weeks or every 4 weeks in adolescent and adult patients with type I or II HAE.
The following justification for conducting the MAIC and the chosen comparator was provided. Lanadelumab is a newer treatment for LTP of type I and II HAE and is also a monoclonal antibody, with the same SC route of administration as garadacimab. However, there is no head-to-head trial comparing these 2 treatments. The NMA found that lanadelumab had an efficacy and safety profile that was closest to those of garadacimab. Therefore, lanadelumab was chosen as the comparator of interest for this MAIC to address the evidence gap. The other relevant and recent comparator was berotralstat; however, because it was an oral treatment that is not currently reimbursed by public funding, it was not considered relevant for the MAIC. C1-INH is another comparator of garadacimab; however, because this is a blood and cell therapy that is funded through Canadian Blood Services and Héma-Québec, the MAIC was limited to lanadelumab. MAIC methods were chosen for the comparison because they represent a robust and commonly used design to compare 2 treatments in efficacy research in the absence of head-to-head clinical trials. This is particularly relevant when IPD are available from the treatment of interest only, and when correcting for cross-trial imbalances in patient characteristics.
Study Selection Methods
Based on the SLR,35 the CSL312_3001 and CSL312_2001 trials were selected for garadacimab, and the HELP trial was selected for lanadelumab. The MAIC used IPD for garadacimab from the CSL312_3001 and CSL312_2001 trials and aggregate data for lanadelumab from the HELP trial. The Study Selection Methods for NMA section provides more details.
MAIC Analysis Methods
The technical report provided a protocol and statistical analysis plan for the MAICs and referenced Technical Support Document 18 from the NICE DSU to ensure the analyses were performed according to acceptable standard practices, including transparency and reproducibility.50
Patient Population and Dosage Used for Comparative Analyses
The MAIC was conducted only on licensed dosages of garadacimab and lanadelumab. For the CSL312_3001 and CSL312_2001 trials, this included patients in the ITT population who were assigned to receive garadacimab (N = 39 in the CSL312_3001 study and 8 in the CSL312_2001 study ) or placebo (N = 25 in CSL312_3001 and N = 8 in CSL312_2001), irrespective of their protocol adherence and continued participation the study. IPD from both trials were pooled into a single dataset before the analysis. For the HELP trial, patients in the ITT population who received licensed dosages of lanadelumab were included in the analysis (i.e., lanadelumab 300 mg every 2 weeks [N = 27], lanadelumab 300 mg every 4 weeks [N = 29], and the placebo [N = 41] arms).
Comparison of Key Trial Characteristics
Participants enrolled in the CSL312_3001, CSL312_2001, and HELP trials were required to satisfy a number of key eligibility criteria for inclusion in the MAIC. Key eligibility criteria were generally aligned between the 3 trials. Some inclusion and exclusion criteria were narrower in 1 or both garadacimab trials (CSL312_3001 and CSL312_2001) compared to the lanadelumab trial (HELP). Notable among these were baseline (during screening and/or run-in period) HAE attack, management of HAE treatments, C1-INH functional activity, use of monoclonal antibodies during the pretrial period, and use of estrogen-containing medications or ACE inhibitors. Some exclusion criteria, such as use of androgen therapy and prophylactic therapy and liver function abnormalities, could not be fully matched across trials due to reporting differences. (Table 27, Table 28, and Table 29).
The outcomes considered in the MAIC are provided in Table 29. Overall, the outcome definitions were similar across trials, with the major difference being the shorter treatment duration of 12 weeks in the CSL312_2001 trial, whereas the other 2 trials had outcomes measured around 6 months after treatment.
Identification and Ranking of Covariates
A list of potential treatment-effect modifiers consisting of baseline characteristics reported across the 3 trials were identified. The final ranked list incorporated feedback from the clinical expert consulted by the sponsor. A single list of ranked treatment-effect modifiers was applied to all outcomes of interest. (Table 33)
Table 33: Final Ranking of Treatment-Effect Modifiers and Availability in the CSL312_3001, CSL312_2001, and HELP Trials
Characteristics | Final pooled ranking (incorporating feedback from internal and external clinical experts) | Available in CSL312_3001 trial? | Available in CSL312_2001 trial? | Available in HELP trial? | Considered for adjustment in the MAIC? |
|---|---|---|---|---|---|
Baseline HAE episode rate (during run-in) | 1 | Yes | Yes | Yes | Yes |
BMI (or body weight if BMI not available) | 2 | Yes | Yes | Yes | Yes |
History of anxiety | 3 | Yes | Yes | No | No |
History of depression | 4 | Yes | Yes | No | No |
Age | 5 | Yes | Yes | Yes | Yes |
Sex | 6 | Yes | Yes | Yes | Yes |
BMI = body mass index; HAE = hereditary angioedema; MAIC = matching adjusted indirect comparison.
Sources: CSL312_3001 study characteristics from Clinical Trial Registry (ct.gov) (NCT04656418), CSL312_2001 study characteristics from Clinical Trial Registry (ct.gov) (NCT03712228), HELP study characteristics from Clinical Trial Registry (ct.gov) (NCT02586805), and MAIC technical report.34
It should be noted that an anchored MAIC methodology assumes that all treatment-effect modifiers are balanced across trials. In the present analysis, differences in characteristics accounted for were limited by those reported in the comparator publications. For this reason, it is possible that covariates not considered in this analysis could have affected the outcomes of interest. For example, history of anxiety and history of depression were respectively ranked as the third and fourth most important covariates to adjust for by the clinical expert consulted for this review; however, these characteristics were not reported in the HELP trial and therefore could not be adjusted for in these analyses.
Details of MAIC Method
Given the availability of a common comparator, an anchored MAIC was used to estimate the relative effect of garadacimab versus lanadelumab for the continuous and rate outcomes. Because placebo was available as the common comparator in all 3 trials, anchored analyses were conducted for most outcomes. As such, the MAICs only needed to adjust for differences in treatment-effect modifiers across trials. Due to 0 or low event rates in the placebo arms of the CSL312_2001, CSL312_3001, and HELP trials, unanchored MAICs were conducted for the binary outcomes, which rely on the assumption that both prognostic factors and treatment-effect modifiers are balanced across trials. However, only 1 patient achieved an episode-free status in the placebo arm of the HELP trial, suggesting that prognostic differences across trials may be minimal. Likewise, only 2 patients in each of the CSL312_3001 and HELP placebo arms, and 0 patients in the CSL312_2001 placebo arm achieved a reduction in the episode rate of 90% or greater compared to run-in.
Assessment of Heterogeneity
To assess between-study heterogeneity before conducting the MAIC, the eligibility criteria of the 3 trials were compared.34 Moreover, descriptive statistics for the treatment-effect modifiers were assessed. For continuous variables, the mean and SD were reported if available for lanadelumab. For categorical variables, the number of patients and proportions were reported. Each treatment-effect modifier being adjusted for in the analysis was compared between the IPD and summary-level data using standardized mean differences (SMDs) before and after adjustment (where an SMD between 0 and 0.1 is considered a small difference, an SMD > 0.1 and ≤ 0.2 is a moderate difference, and an SMD > 0.2 is a substantial difference).51
To reduce between-study heterogeneity, the pooled CSL312_3001 and CSL312_2001 trial population was reweighted so that the distribution of the identified baseline characteristics matched those reported in the HELP trial. A logistic propensity-score model was estimated that included the identified covariates (i.e., treatment-effect modifiers). The use of method-of-moments guaranteed a close balancing of covariates between the garadacimab trials and HELP populations.52,53 In other words, the means (or proportions or percentages) and SDs of covariates from the garadacimab trials were almost exactly equal to those published in the HELP trial after reweighting patients.
Method for Estimating Treatment Effects
For each outcome type, estimates for the relative effect of garadacimab versus lanadelumab were derived using both an estimate of the relative treatment effect for garadacimab versus placebo (if analysis was anchored) or an estimate of the absolute treatment effect for garadacimab (if the analysis was unanchored) based on the IPD from the pooled garadacimab trials, and the published summary-level data from the HELP trial. Two categories of comparisons that used a unique version of data from the pooled garadacimab trials were conducted for each outcome:
Unadjusted — the relative treatment-effect estimate was derived using data from the original pooled garadacimab trials without adjusting (i.e., weighted patients) for treatment-effect modifiers.
Adjusted (i.e., MAIC analysis) — the relative treatment-effect estimate was derived using data from the pooled garadacimab trials after adjusting (i.e., weighted patients) for treatment-effect modifiers. The target estimand for the MAIC was perceived as the average treatment effect in the comparator; a mapping of the outcome for patients taking garadacimab to the HELP population.
All MAIC analyses were performed using R version 3.6.1 or later, based on the code provided in Technical Support Document 18 from the NICE DSU.50 Statistical significance was defined using a 2-tailed P value of < 0.05.
Two binary end points were included in this MAIC: the proportion of episode-free patients over the trial period and the proportion of patients who achieved a reduction in the episode of rate of 90% or greater compared to run-in. Effects between garadacimab and lanadelumab for the proportion of episode-free patients over the trial period were compared using unanchored MAICs, which excluded the placebo arms from each trial. Similarly, given the 0 or low event numbers, and to ensure consistent methodology across binary outcomes, unanchored MAICs were considered the primary analysis for the proportion of patients who achieved a reduction of 90% or greater in the episode of rate compared to run-in.
Further follow-up was likely to result in more events for these end points. Therefore, to account for differences in trial durations, pseudo-IPD was generated for HELP with the follow-up set to 182 days (26 weeks) for each pseudo-patient and included together with the pooled IPD for the garadacimab trials in a weighted generalized linear model. The log hazard ratio for garadacimab versus lanadelumab was estimated using a binomial likelihood and complementary log-log link function with the outcome and covariates for treatment (i.e., garadacimab or lanadelumab). The logarithm of time (days) of the maximum follow-up for each patient in their respective trial (84 days [12 weeks] for the CSL312_2001 trial and 182 days [6 months] for the CSL312_3001 trial) was included as an offset variable in the model.
The corresponding variance was estimated using a robust sandwich estimator.50 Effect estimates were exponentiated and reported as hazard ratios with 95% CIs.
Two continuous outcomes were included in this MAIC: number of episode-free days per month change from baseline in AE-QoL total score.
For the pooled garadacimab versus placebo population, the mean difference (MD) was estimated using a weighted generalized linear model and a Gaussian likelihood and identity link function with the outcome and the binary treatment indicator. The corresponding variance was estimated using a robust sandwich estimator.50 For lanadelumab versus placebo, the MD and variance was obtained from the HELP trial. The relative treatment effect was the difference in estimated MDs, and the corresponding variance was calculated as the sum of the variances of the MDs. Effect estimates were reported as an MD with 95% CIs.
Three rate outcomes were included in this MAIC: time-normalized number of HAE episodes, time-normalized number of HAE episodes requiring on-demand treatment, and time-normalized number of moderate and/or severe HAE episodes.
For the pooled garadacimab versus placebo population, the log rate ratio was estimated using a weighted generalized linear model and a Poisson likelihood and log link function with the outcome and the binary treatment indicator.
The normalized baseline episode rate was included as a covariate in the model to align with the statistical analysis methodology reported for the HELP trial.54 The logarithm of time (days) for each patient that was observed during the treatment period (i.e., the exposure time before discontinuation) was included as an offset variable in the model. Overdispersion was investigated and not detected. The corresponding variance was estimated using a robust sandwich estimator.50 For lanadelumab versus placebo, the estimated rate ratio and variance were obtained from the HELP trial and its log rate ratio and variance derived. The log relative treatment effect was calculated as the difference of the log rate ratios, and the corresponding variance was the sum of the variances of the log rate ratios. Effect estimates were exponentiated and reported as rate ratios with 95% CIs.
MAIC Performance Assessment
Differences in patient characteristics between the pooled garadacimab populations and the lanadelumab population were assessed with SMDs after weighting and compared to the SMDs before weighting.
The ESS was calculated to reflect the impact of weighting on the available information in the IPD.52 A low ESS compared to the original sample size (N) indicated a large difference in patient weights due to large imbalances in patient populations before reweighting.52
Scenario Analyses
Scenario MAICs were conducted to investigate the impact on the treatment-effect estimates and ESS when adjusting for additional treatment-effect modifiers in the analyses. For example, the first MAIC scenario adjusted for the top ranked treatment-effect modifier only, the second scenario adjusted for the top 2 ranked treatment-effect modifiers, and the final scenario adjusted for all available ranked treatment-effect modifiers. The total number of scenario analyses relied on the number of available ranked treatment effects. The “primary scenario” was determined based on the balance between adjusting for as many treatment-effect modifiers as possible while maintaining a sufficient ESS.
Sensitivity Analyses
To assess the impact of pooling the CSL312_3001 and CSL312_2001 trial data, a sensitivity analysis comparing the CSL312_3001 trial only to the HELP trial (excluding CSL312_2001) was conducted for all outcomes. In addition, an anchored MAIC was conducted as a sensitivity analysis for the proportion of patients who achieved episode rate reduction of 90% or greater compared to run-in, given an anchored MAIC was feasible with the 2 patients who achieved a reduction in each of the placebo arms in the HELP trial and pooled CSL312_3001 and CSL312_2001 trials. The anchored MAIC included a study indicator (i.e., garadacimab study or the HELP trial) in the outcome model to distinguish between the placebo arms.
MAIC Results
Results
A comparative overview of the trial and patient characteristics was included in the MAIC (Table 27, Table 28, and Table 29 in the NMA section). According to the MAIC technical report, eligibility criteria were similar between the CSL312_3001, CSL312_2001, and HELP trials, except for the HAE episode rate at baseline, treatment management, C1-INH functional activity, clinical abnormalities, age, use of prior or concomitant therapies, liver function abnormalities, and surgery and hypersensitivity.34 Comparison of the adjustment factors at baseline identified differences in the sex distribution, with 50% to 60% of patients in the garadacimab trials and 70% in the HELP trials identified as female. There were also differences across all 3 trials regarding mean baseline episode rates per month (2.9 [SD = 1.7] in CSL312_3001, 5.2 [SD = 2.5] in CSL312_2001, and 3.6 [SD = 2.6] in HELP). Baseline data for age and BMI were not available from the CSL312_2001 trial but were similar between the CSL312_3001 and HELP trials. However, the technical document concluded that the eligibility criteria among the CSL312_3001, CSL312_2001, and HELP trials were either similar or unable to be adjusted for. Therefore, matching was either not necessary as the eligibility criteria across trials were similar, or not possible and could not be performed due to the comparator trial (HELP) having broader enrolment criteria.
Balance of Populations for Analyses
There were generally substantial differences (SMD > 0.2) when comparing the pooled CSL312_3001 and CSL312_2001 trial populations to the HELP trial population before adjusting for the 4 covariates. After adjustment, the pooled patient characteristics of the CSL312_3001 and CSL312_2001 trials matched those of the HELP trial (SMD = 0) but there was a reduction of 4% to nearly 60% in the ESS, depending on the model. Table 34 presents the sample size of the included studies before adjusting and the ESS of the trials and the ESS reduction after the adjustment process for each MAIC.
Table 34: Summary of ESS in Each MAIC for Garadacimab vs. Lanadelumab
MAIC | HELP study, N | Unadjusted, N | Adjusted, N (ESS for 4 characteristics) | ESS reduced |
|---|---|---|---|---|
GARA 200 mg q.m. vs. TAK 300 mg q.2.w | ||||
Unadjusted and adjusted baseline characteristics for the CSL312_3001 and CSL312_2001 (pooled) and HELP trials in anchored analysis for time-normalized number of HAE episodes, time-normalized number of HAE episodes requiring on-demand treatment, and time-normalized number of moderate and/or severe episodes | 68 | 79 | 61 | 23% |
Unadjusted and adjusted baseline characteristics for the CSL312_3001 and CSL312_2001 (pooled) and HELP trials in unanchored analysis for proportion of patients with ≥ 90% episode rate reduction and proportion of episode-free patients | 27 | 47 | 45 | 4.3% |
Unadjusted and adjusted baseline characteristics for the CSL312_3001 and CSL312_2001 (pooled) and HELP trials in anchored analysis for number of episode-free days per month | 68 | 80 | 61 | 24% |
Unadjusted and adjusted baseline characteristics for the CSL312_3001 and HELP trials in anchored analysis for change from baseline in AE-QoL total score | 68 | 53 | 27 | 49.1% |
GARA 200 mg q.m. vs. TAK 300 mg q.4.w. | ||||
Unadjusted and adjusted baseline characteristics for the CSL312_3001 and CSL312_2001 (pooled) and HELP trials in anchored analysis for time-normalized number of HAE episodes, time-normalized number of HAE episodes requiring on-demand treatment, time-normalized number of moderate and/or severe episodes, and proportion of patients with ≥ 90% episode-rate reduction | 70 | 79 | 55 | 30.4% |
Unadjusted and adjusted baseline characteristics for the CSL312_3001 and CSL312_2001 (pooled) and HELP trials in unanchored analyses for proportion of patients with ≥ 90% episode-rate reduction and proportion of episode-free patients | 29 | 47 | 42 | 10.6% |
Unadjusted and adjusted baseline characteristics for the CSL312_3001 and CSL312_2001 (pooled) and HELP trials in anchored analysis for number of episode-free days per month | 70 | 80 | 55 | 31.3% |
Unadjusted and adjusted baseline characteristics for the CSL312_3001 and HELP trials in anchored analysis for change from baseline in AE-QoL total score | 70 | 53 | 24 | 54.7% |
AE-QoL = Angioedema Quality of Life questionnaire; ESS = effective sample size; GARA = garadacimab; HAE = hereditary angioedema; MAIC = matching adjusted indirect comparison; q.2.w. = every 2 weeks; q.4.w. = every 4 weeks; q.m. = once monthly; SLD = summary-level data; TAK = Takhzyro; vs. = versus.
Note: The HELP trial SLD was pooled for the TAK 300 q.2.w. and placebo arms following the methods reported in the Cochrane Handbook for Systematic Reviews of Interventions version 6.4.55
Source: MAIC technical report.34
Efficacy
A summary of results of the analyses for garadacimab 200 mg once monthly versus lanadelumab 300 mg every 2 weeks and lanadelumab 300 mg every 4 weeks for each outcome via anchored and unanchored MAICs is presented in Table 35. A summary of results of the unadjusted analyses for garadacimab 200 mg once monthly versus lanadelumab 300 mg every 2 weeks and lanadelumab 300 every 4 weeks for each outcome is presented in Table 36.
Compared to lanadelumab 300 mg every 2 weeks and lanadelumab 300 mg every 4 weeks, MAIC results favoured garadacimab 200 mg once monthly across all primary analyses for all outcomes.
Table 35: Summary of MAIC Results for Garadacimab 200 mg Once Monthly vs. Lanadelumab 300 mg Every 2 Weeks and Lanadelumab 300 mg Every 4 Weeks
Outcome | Treatment effect | MAIC results | |||
|---|---|---|---|---|---|
GARA 200 mg q.m. vs. TAK 300 mg q.2.w. | GARA 200 mg q.m. vs. TAK 300 mg q.4.w. | ||||
Primary | Sensitivity | Primary | Sensitivity | ||
Time-normalized number of HAE episodes | RR (95% CI) | 0.55 (0.22 to 1.37) | 0.98 (0.34 to 2.83) | 0.29 (0.13 to 0.63) | 0.53 (0.20 to 1.39) |
Time-normalized number of HAE episodes requiring on-demand treatment | 0.52 (0.20 to 1.35) | 0.93 (0.31 to 2.81) | 0.29 (0.13 to 0.66) | 0.53 (0.19 to 1.47) | |
Time-normalized number of moderate and/or severe HAE episodes | 0.25 (0.07 to 0.84) | 0.49 (0.11 to 2.11) | 0.15 (0.05 to 0.49) | 0.32 (0.08 to 1.36) | |
Proportion of patients with ≥ 90% episode rate reduction compared to run-ina | HR (95% CI) | 1.50 (0.77 to 2.90)b | 1.23 (0.63 to 2.38)c | 2.03 (1.03 to 4.02)d | 1.72 (0.87 to 3.40)e |
Proportion of episode-free patients over the trial periodf | 1.93 (0.92 to 4.03) | 1.44 (0.67 to 3.09) | 3.25 (1.45 to 7.29) | 2.55 (1.11 to 5.83) | |
Number of episode-free days per month | MD (95% CI) | 0.44 (−1.76 to 2.63) | −0.79 (−3.05 to 1.46) | 0.84 (−1.40 to 3.08) | −0.48 (−2.79 to 1.84) |
Change from baseline in total AE-QoL score | MD (95% CI) | −17.38 (−33.67 to −1.08) | NR | −21.29 (−37.39 to −5.18) | NR |
AE-QoL = Angioedema Quality of Life questionnaire; CI = confidence interval; ESS = effective sample size; GARA = garadacimab; HAE = hereditary angioedema; MAIC = matching adjusted indirect comparison; MD = mean difference; q.2.w. = every 2 weeks; q.4.w. = every 4 weeks; q.m. = once monthly; NR = not reported; RR = rate ratio; TAK = Takhzyro; vs. = versus.
Notes: Sensitivity analysis was done by excluding the CSL312_2001 trial. An MD greater than 0 for the number of episode-free days per month and less than 0 for the change from baseline in total AE-QoL score indicate an improved outcome for GARA 200 mg q.m. relative to TAK 300 mg q.2.w. or TAK 300 mg q.4.w., respectively. An RR or HR less than 1 indicates an improved outcome for GARA 200 mg q.m.
aUnanchored MAICs were considered the primary analysis for proportion of patients with ≥ 90% episode rate reduction compared to run-in. Results of the sensitivity analyses using anchored MAICs produced results as detailed in the 4 subsequent footnotes.
b0.96 (0.09 to 9.74) using an anchored MAIC.
c0.84 (0.09 to 7.89) using an anchored MAIC.
d1.38 (0.13 to 14.58) using an anchored MAIC.
e1.25 (0.13 to 12.24) using an anchored MAIC.
fUnanchored MAICs were considered the primary analysis for the proportion of episode-free patients. Anchored MAICs were not feasible.
Source: MAIC technical report and manuscript.34,56
Table 36: Summary of Results Between Garadacimab 200 mg Once Monthly vs. Lanadelumab 300 mg Every 2 Weeks and Lanadelumab 300 mg Every 4 Weeks
Outcome | Treatment effect | MAIC results | |||
|---|---|---|---|---|---|
GARA 200 mg q.m. vs. TAK 300 mg q.2.w. | GARA 200 mg q.m. vs. TAK 300 mg q.4.w. | ||||
Unadjusted | Fully adjusted | Unadjusted | Fully adjusted | ||
Time-normalized number of HAE episodes | RR (95% CI) | 0.48 (0.20 to 1.18) | 0.55 (0.22 to 1.37) | 0.23 (0.11 to 0.50) | 0.29 (0.13 to 0.63) |
Time-normalized number of HAE episodes requiring on-demand treatment | RR (95% CI) | 0.44 (0.17 to 1.13) | 0.52 (0.20 to 1.35) | 0.22 (0.09 to 0.51) | 0.29 (0.13 to 0.66) |
Time-normalized number of moderate and/or severe HAE episodes | RR (95% CI) | 0.26 (0.08 to 0.83) | 0.25 (0.07 to 0.84) | 0.16 (0.06 to 0.48) | 0.15 (0.05 to 0.49) |
Proportion of patients who achieved ≥ 90% attack rate reduction | HR (95% CI) | 1.51 (0.83 to 2.77) | 1.50 (0.77 to 2.90) | 2.07 (1.11 to 3.85) | 2.03 (1.03 to 4.02) |
Proportion of episode-free patients over the trial period | HR (95% CI) | 1.98 (1.00 to 3.93) | 1.93 (0.92 to 4.03) | 3.13 (1.47 to 6.67) | 3.25 (1.45 to 7.29) |
Episode-free days per month | MD (95% CI) | 0.90 (−1.25 to 3.05) | 0.44 (−1.76 to 2.63) | 0.84 (−1.40 to 3.08) | 1.30 (−0.85 to 3.45) |
Change from baseline in total AE-QoL score | MD (95% CI) | −7.69 (−23.41 to 8.02) | −17.38 (−33.67 to −1.08) | −11.60 (−27.24 to 4.03) | −21.29 (−37.39 to −5.18) |
AE-QoL = Angioedema Quality of Life questionnaire; CI = confidence interval; GARA = garadacimab; HAE = hereditary angioedema; HR = hazard ratio; MAIC = matching adjusted indirect comparison; MD = mean difference; q.2.w. = every 2 weeks; q.4.w. = every 4 weeks; q.m. = once monthly; RR = rate ratio; TAK = lanadelumab; vs. = versus.
Note: Fully adjusted was defined as adjusted for all 4 covariates. An RR less than 1 indicates an improved outcome for GARA 200 q.m., relative to TAK 300 q.2.w. or TAK 300 q.4.w. An HR greater than 1 indicates an improved outcome for GARA 200 q.m. relative to TAK 300 q.2.w. or TAK 300 q.4.w. An MD less than 0 indicates an improved outcome for GARA 200 q.m. relative to TAK 300 q.2.w. or TAK 300 q.4.w.
Sensitivity Analyses for All MAIC Outcomes
A sensitivity analysis that excluded the phase II CSL312_2001 trial was conducted to assess the distribution of baseline characteristics before and after adjustment.34 After adjustment, there were 10% to 51% reduction in ESS. The results of the sensitivity analysis were largely similar to those of the primary analysis for garadacimab 200 mg once monthly versus lanadelumab 300 mg every 2 weeks and garadacimab 200 mg once monthly versus lanadelumab 300 mg every 4 weeks, but the statistically significant difference reported in the primary analysis was lost for all outcomes except for the proportion of attack-free patients (Table 35).
Critical Appraisal of MAICs
Overall, the MAICs were performed according to acceptable standard practice for conducting and reporting MAICs and following NICE DSU Technical Support Document 18 to ensure transparency and reproducibility. Some key limitations are discussed.
As is correctly identified in the provided technical report, the key assumption for anchored MAICs is that all treatment-effect modifiers are balanced across trials. Similarly, unanchored MAICs assume that both prognostic factors and treatment-effect modifiers are balanced across trials, which is often an unattainable assumption.57 Given the limited or lack of reporting on certain covariates, not all factors could be adjusted for in the analysis, likely leading to residual heterogeneity between populations. While this limitation is not unique to the current MAIC, it remains a critical limitation. Additionally, the technical report was appropriately transparent about several differences identified in the populations of the trials in terms of eligibility criteria and baseline characteristics, including substantial differences (SMD > 0.2) in the unadjusted values for the 4 covariates used in the weighting approach. While the adjusted values for the garadacimab matched those of the lanadelumab trial after weights were applied (SMDs = 0), as will be discussed, this seems to have not made the trials sufficiently similar for conducting the MAICs.
Using the anchored MAIC model comparing garadacimab 200 mg once monthly to lanadelumab 300 mg every 2 weeks for the time-normalized number of HAE episodes end point as an example, the results of the MAICs provide evidence that the key assumptions were not met. The rate ratio for the primary fully adjusted MAIC was 0.55 (95% CI, 0.22 to 1.37). The rate ratio for the unadjusted MAIC was 0.48 (95% CI, 0.20 to 1.18). A sensitivity analysis that removed the phase II garadacimab trial, CSL312_2001, produced a rate ratio of 0.98 (95% CI, 0.34 to 2.93). First, the rate ratios for these analyses favoured garadacimab (although the rate ratio for the sensitivity was only 0.2 below unity) but the upper 95% confidence bounds crossed 1 in each of them, which means that it is possible garadacimab may be less effective or similarly effective compared to lanadelumab in this model. The wide CIs from each analysis indicate substantial imprecision and uncertainty in these estimates. Second, the assumptions of the specific models had important effects on the magnitudes of the rate ratios. The fact that adjusting for baseline differences (i.e., HAE episode rate, BMI, age, and sex) changed the estimated rate ratio from the unadjusted model implies that these factors are important effect modifiers. Without adjustment, the apparent benefit of garadacimab is slightly overestimated. This emphasizes the importance of adjusting for these covariates, particularly given the reported baseline differences between trials. But because other covariates could not be included in the adjustment, it is unknown what impact on the rate ratio these would have. The sensitivity analysis points to the phase II trial, CSL312_2001, as having a notable influence on the pooled results. The large shift in the rate ratio (from 0.55 to 0.98) when this trial is excluded raises concerns about the homogeneity of the evidence and the appropriateness of pooling the phase II and phase III data. It appears that the population or outcomes or design features, or all of these, in CSL312_2001 differ in ways that bias the comparison.
Trial design features, including follow-up times, typically cannot be adjusted for in the weighting procedure. While adjusting follow-up times to 182 days for the HELP trial (compared to shorter durations in the garadacimab trials) would help improve homogeneity in the data, generating pseudo-patients based on this assumption introduces an additional layer of model dependency, which could affect the integrity of the results. The impacts of this on the model validity was not well described.
Reductions in ESS (i.e., > 30% reduction) were observed in half of the MAIC analyses. In many instances, randomization was not preserved, and this could result in biased estimates of treatment effect.
Discussion
Summary of Available Evidence
One study was reviewed: VANGUARD (n = 65) was a phase III, multicentre, double-blind, placebo-controlled RCT designed to evaluate the efficacy and safety of once monthly SC garadacimab for routine prevention of HAE episodes in adult and pediatric patients aged 12 years and older. The primary outcome was the time-normalized number of HAE episodes over 6 months. Findings from the VANGUARD trial can be considered generalizable to patients in Canada with type I or II HAE, as baseline patient characteristics, disease history, and use of on-demand acute therapies for HAE were considered representative of the population routinely seen in clinical practice. Patients in the study had a baseline episode rate of at least 2 episodes per month, which the clinical expert stated may be higher than the typical frequency at which LTP is initiated in clinical practice. At the other end of the spectrum, the trial may have excluded patients with more severe HAE who could not tolerate discontinuation of current LTP therapy.
Interpretation of Results
Efficacy
The primary outcome in the VANGUARD trial related to the number of HAE episodes during the treatment period. This was considered appropriate by the clinical expert consulted for this review, and was consistent with patient and clinician input, all of which emphasized the importance of better control of HAE episodes. Overall, 63 episodes were reported throughout the 6-month treatment period in the 39 patients who received garadacimab, compared with 264 episodes in the 25 patients who received placebo. For the primary outcome assessment, the mean time-normalized number of episodes reported per patient per month was 0.27 (SD = 0.683) and the median was 0 in the garadacimab group compared to a mean of 2.01 (SD = 1.341) and a median of 1.35 in the placebo group, for an MD of −1.74 (95% CI, −2.34 to −1.13; P < 0.001). No empirically derived and validated MCID for the difference in time-normalized number of HAE episodes per month was identified. According to the clinical expert, the between-group difference was clinically meaningful, based on a threshold of clinical significance of 1 time-normalized episode per month. It is not expected that this outcome would have been subject to substantial bias (e.g., detection bias). Although HAE is highly variable and unpredictable, the clinical expert indicated that the follow-up should be sufficient to capture a change in HAE episodes, and noted that neither demographics nor disease history are expected to affect the risk of experiencing a future HAE attack. Outcome definition and assessment in the trial were deemed appropriate, as physicians also rely mainly on patients’ self-reporting in clinical practice, and as differential diagnoses for moderate or severe episodes can usually be ruled out.
Results from sensitivity analyses for the primary outcome, which were based on a preferred statistical approach in clinical trials with data such as counts or rates were consistent with those of the primary analysis. Secondary outcomes related to HAE episodes were also supportive of the superiority of garadacimab over placebo in reducing the number and severity of HAE episodes. Indeed, garadacimab was associated with a clinically significant reduction in the number of episodes requiring on-demand treatment and in the number of moderate or severe episodes compared to placebo, which were described as clinically relevant treatment goals. In addition, garadacimab was superior to placebo in a responders’ analysis, in which 24 of 39 patients (61.5%) in the garadacimab group were episode-free throughout the treatment period, while none of the 25 patients in the placebo group achieved this outcome.
HAE episodes were also assessed as a reduction from baseline; however, uncertainty was introduced around those particular findings. The run-in period was relatively short to determine the baseline rate of episodes, given the unpredictable nature of HAE. Episodes tend to be life-long, but are not necessarily consistent throughout a patient’s life; for example, they may worsen substantially in periods of stress, infection, or physical trauma. Variability in the baseline episode rate limits the interpretation of outcomes that are based on the change from baseline. Also, limited results were reported for time-to-event analyses. A visual inspection of Kaplan-Meier survival curves for time to first episode appears to favour garadacimab over placebo, as the curves separate early and remain separated throughout follow-up. However, no between-group comparison was reported, which precludes a definite conclusion regarding those findings.
Results suggested benefits from garadacimab on HRQoL; however, analyses are exploratory and findings should be interpreted as such. The difference between garadacimab and placebo in AE-QoL results was considered clinically meaningful based on the threshold identified in the literature, and was consistent with the level of efficacy observed with garadacimab for HAE episode prevention, according to the clinical expert.
No evidence was available pertaining to other clinically important outcomes, such as the need for hospitalization or emergency department visits. Other evidence gaps include the fact that patients were followed for 6 months, while LTP therapy in clinical practice is potentially life-long. To inform this gap, an open-label, long-term extension study, which includes both patients rolling over from 2 garadacimab studies and patients who are treatment-naive, is currently ongoing. Overall, 119 (73.9%) of 161 patients in the study have at least 12 months of exposure to garadacimab, with a median duration of exposure of 13.83 months (range, 3.0 to 21.1). Findings suggest that the benefits of garadacimab on HAE episodes is maintained over time. However, uncertainty remains due to the uncontrolled, open-label nature of the extension study, and evidence is limited beyond the study follow-up duration.
As the VANGUARD trial included a placebo control group, there is no direct evidence comparing garadacimab to other LTP therapies that would directly inform the reimbursement question. The sponsor submitted ITCs in the form of an NMA and a MAIC (the latter versus lanadelumab alone). The NMA suggested that garadacimab improved outcomes in HAE episode rates and HRQoL compared to selected comparators; however, the certainty of the improvement was affected by the model used (e.g., fixed-effects versus random-effects), evidence of unaccounted for heterogeneity, and limited evidence base, leading to a sparse network in the NMA. The sparse network led to the fixed-effects model being chosen despite the random-effects model fitting the data more closely (based on DIC differences and heterogeneity). The 95% CrIs overlapped with unity for most comparisons in the random-effects models, suggesting that the treatment effects of garadacimab versus comparators were associated with considerable variability and imprecision. The results from both models are challenging to interpret because fixed-effects models fail to account for between-trial heterogeneity, risking biased estimates and overprecision. Random-effects models are more likely to be unstable with the sparse network and overfit the data, leading to wide CrIs and large differences in model fit (DICs). Therefore, the evidence base does not adequately allow for an accurate estimate of the comparative effectiveness of garadacimab to other prophylaxis treatments of HAE.
Additionally, CDA-AMC reviewers emphasized heterogeneity across the included studies in the ITCs with respect to study designs and patient characteristics, including differences in prognostic factors and effect modifiers. The sparse evidence networks, often reliant on a single trial to connect treatment nodes, along with small sample sizes, further undermine the validity of the results. The identified sources of heterogeneity were even more evident in the sponsor-provided MAIC comparing garadacimab with lanadelumab, particularly in the differences between the unadjusted and adjusted population characteristics and sensitivity of the primary analysis to assumptions related to homogeneity. This suggests that the assumption of similarity may not hold true for either ITC, increasing the likelihood of bias and uncertainty about the validity of the results for determining the comparative effectiveness of garadacimab.
Harms
A relatively high proportion of patients receiving garadacimab in the VANGUARD trial experienced at least 1 AE during the study. The most common TEAEs were related to infections, gastrointestinal disorders, and injection-site reactions. SAEs were uncommon with treatment; the only event reported involved a laryngeal attack. Garadacimab appeared to be well tolerated, as there was no discontinuation due to AEs. No death was reported during the study. No patients were assessed as experiencing AESIs such as thromboembolic events, bleeding events, and severe hypersensitivity or anaphylaxis in the VANGUARD trial; however, 10 (6.2%) of 161 patients reported bleeding events and 10 (16.1%) reported severe hypersensitivity during the ongoing extension study.
The clinical expert indicated that the overall harms profile of garadacimab did not raise any new safety signal, or any particular safety concern. However, as with most clinical trials, the study was not powered to detect infrequent AEs or those with a lag time.
No estimates of the relative risk of harms were performed in the sponsor-submitted ITCs.
Other Considerations
Special consideration may be given to the fact that HAE is a rare disease comprising different pathways with highly variable severity. The clinical expert indicated that patients coming from different walks of life will have different perceptions of their condition, and the main goal for patients is to have as normal a life as possible. Not all patients respond to current treatments, and some patients may become refractory over time. Some treatments are also associated with AEs, modes of administration, or costs that are deemed unacceptable by patients. The clinical expert emphasized the need for access to a range of options, especially treatments that are better tolerated, improve compliance, and are more convenient. This is particularly important in patients who have severe episodes, including laryngeal episodes that can be life-threatening due to airway obstruction. Without treatment, HAE has been associated with a 30% mortality rate.3 As such, the clinical expert noted that some patients are living in constant fear of suffocation from a laryngeal attack. These patients may be willing to take on any treatment that can prevent episodes with little regard to AEs or inconvenience.
Conclusion
In patients with HAE, high-certainty findings from the VANGUARD trial suggest that garadacimab results in a clinically meaningful reduction in HAE episodes compared with placebo. Garadacimab also clinically significantly reduced the number of episodes requiring on-demand treatment and the number of moderate or severe episodes. These outcomes are appropriate and consistent with the input received, which emphasized the importance to patients of achieving better control of such episodes. However, variability in the baseline episode rate limits the interpretation of some additional outcomes that are based on change from baseline, while limited results were reported for time-to-event analyses, precluding a definite conclusion regarding those findings. Results suggest that patients who were receiving garadacimab experienced improvements in their HRQoL, which were considered clinically meaningful based on the threshold identified in the literature; however, the analyses are exploratory and therefore were assessed as having moderate certainty. Evidence is limited beyond the study follow-up duration, whereas LTP therapy in clinical practice is potentially life-long. Results from an open-label extension study suggest that the benefits of garadacimab on HAE episodes were maintained over the current 1-year follow-up.
A relatively high proportion of patients in the VANGUARD trial experienced AEs, most notably relating to infections, gastrointestinal disorders, and injection-site reactions; however, garadacimab appeared to be well tolerated, with only 1 SAE and no WDAE reported. The overall harms profile did not raise any particular safety signal. Findings from the trial were considered generalizable to the population of patients in Canada with type I or II HAE. Special consideration may be given to the fact that HAE is a rare and highly variable disease that has been associated with higher mortality rates due to airway obstruction from laryngeal episodes. The input received emphasized the need to have access to a range of options, particularly treatments that are better tolerated, improve compliance, and are more convenient.
Because the VANGUARD trial included a placebo control group, there is no direct evidence comparing garadacimab to other LTP therapies to inform the reimbursement question. The sponsor-provided ITCs suggested garadacimab resulted in improved outcomes compared to selected comparators. However, the inability to confirm the key assumption of similarity undermines the validity of the results from ITCs, indicating they are not reliable for determining the comparative effectiveness of garadacimab.
References
1.Betschel S, Badiou J, Binkley K, et al. The International/Canadian Hereditary Angioedema Guideline. Allergy Asthma Clin Immunol. 2019/11/25 2019;15(1):72. doi:10.1186/s13223-019-0376-8
2.Maurer M, Magerl M, Ansotegui I, et al. The international WAO/EAACI guideline for the management of hereditary angioedema-the 2017 revision and update. Allergy. Aug 2018;73(8):1575-1596. doi:10.1111/all.13384 PubMed
3.Betschel. The International/Canadian Hereditary Angioedema Guideline. <i data-test=”journal-title” style=”margin: 0px; box-sizing: inherit;”>Allergy, Asthma & Clinical Immunology volume 15, Article number: 72 (2019) 2019. https://aacijournal.biomedcentral.com/articles/10.1186/s13223-019-0376-8
4.Balshem, ed. GRADE guidelines: 3. Rating the quality of evidence. 2011.
5.Santesso. GRADE guidelines 26: informative statements to communicate the findings of systematic reviews of interventions. 2020. https://www.jclinepi.com/article/S0895-4356(19)30416-0/fulltext
6.CSR. CSL312_3001 Clinical Study Report. As provided by the sponsor.
7.Lumry WR. Hereditary Angioedema: The Economics of Treatment of an Orphan Disease. Front Med (Lausanne). 2018;5:22. doi:10.3389/fmed.2018.00022 PubMed
8.Longhurst HJ, Bork K. Hereditary angioedema: an update on causes, manifestations and treatment. Br J Hosp Med (Lond). Jul 2 2019;80(7):391-398. doi:10.12968/hmed.2019.80.7.391 PubMed
9.Busse PJ, Christiansen SC, Riedl MA, et al. US HAEA Medical Advisory Board 2020 Guidelines for the Management of Hereditary Angioedema. J Allergy Clin Immunol Pract. Jan 2021;9(1):132-150 e3. doi:10.1016/j.jaip.2020.08.046 PubMed
10.Santacroce R, D'Andrea G, Maffione AB, Margaglione M, d'Apolito M. The Genetics of Hereditary Angioedema: A Review. J Clin Med. May 9 2021;10(9)doi:10.3390/jcm10092023 PubMed
11.Betschel S, Badiou J, Binkley K, et al. Canadian hereditary angioedema guideline. Allergy Asthma Clin Immunol. 2014;10(1):50. doi:10.1186/1710-1492-10-50 PubMed
12.Aygören-Pürsün E, Magerl M, Maetzel A, Maurer M. Epidemiology of Bradykinin-mediated angioedema: a systematic investigation of epidemiological studies. Orphanet J Rare Dis. 2018;13(1):73-73. doi:10.1186/s13023-018-0815-5 PubMed
13.Meuth SG, Bayas A, Kallmann B, et al. Long-term management of multiple sclerosis patients treated with cladribine tablets beyond year 4. Expert Opin Pharmacother. 2022;23(13):1503-1510. doi:10.1080/14656566.2022.2106783 PubMed
14.Zanichelli A, Longhurst HJ, Maurer M, et al. Misdiagnosis trends in patients with hereditary angioedema from the real-world clinical setting. Ann Allergy Asthma Immunol. Oct 2016;117(4):394-398. doi:10.1016/j.anai.2016.08.014 PubMed
15.Savarese L, Mormile I, Bova M, et al. Psychology and hereditary angioedema: A systematic review. Allergy Asthma Proc. Jan 1 2021;42(1):e1-e7. doi:10.2500/aap.2021.42.200073 PubMed
16.Bork K, Meng G, Staubach P, Hardt J. Hereditary angioedema: new findings concerning symptoms, affected organs, and course. Am J Med. Mar 2006;119(3):267-74. doi:10.1016/j.amjmed.2005.09.064 PubMed
17.Lumry WR. Overview of epidemiology, pathophysiology, and disease progression in hereditary angioedema. Am J Manag Care. Jun 2013;19(7 Suppl):s103-10. PubMed
18.Bork K, Hardt J, Witzke G. Fatal laryngeal attacks and mortality in hereditary angioedema due to C1-INH deficiency. J Allergy Clin Immunol. Sep 2012;130(3):692-7. doi:10.1016/j.jaci.2012.05.055 PubMed
19.Busse PJ, Christiansen SC, Riedl MA, et al. US HAEA Medical Advisory Board 2020 guidelines for the management of hereditary angioedema. J Allergy Clin Immunol Pract. Jan 2021;9(1):132-150.e3. doi:10.1016/j.jaip.2020.08.046 PubMed
20.Busse PJ, Christiansen SC. Hereditary Angioedema. N Engl J Med. Mar 19 2020;382(12):1136-1148. doi:10.1056/NEJMra1808012 PubMed
21.EMA. EU/3/21/2532 - orphan designation for treatment of hereditary angioedema - Garadacimab. 2021. https://www.ema.europa.eu/en/medicines/human/orphan-designations/eu-3-21-2532
22.Canada H. Drug product Monograph. As provided by the sponsor; 2024.
23.Orladeyo (berotralstat): 150 mg oral capsules [product monograph]. Innomar Strategies; 2022 Jun 2.
24.Takhzyro (lanadelumab injection): prefilled syringes and vials; 300 mg/2 mL solution for subcutaneous injection [product monograph]. Takeda Canada Inc; 2021 Mar 22. Accessed 2022 Apr 20. https://pdf.hres.ca/dpd_pm/00060484.PDF
25.Berinert 500 / Berinert 1500 (C1 esterase inhibitor, human): powder and diluent for solution for injection; for intravenous administration; 500 IU/vial, reconstituted with 10 mL of diluent; 1500 IU/vial, reconstituted with 3 mL of diluent [product monograph]. CSL Behring Canada, Inc; 2020 Feb 14. Accessed 2022 Apr 20. https://pdf.hres.ca/dpd_pm/00055050.PDF
26.Cinryze (C1 esterase inhibitor (human)): 500 IU powder for solution/vial reconstituted with 5 mL of diluent for intravenous injection [product monograph]. Takeda Canada Inc; 2021 Feb 22. Accessed 2022 Apr 20. https://pdf.hres.ca/dpd_pm/00060070.PDF
27.Haegarda (C1 esteraase inhibitor subcutanous (human)): powder and iluent for solution for injection for subcutaneous administration; 2000 IU/vial, reconstituted with 4 mL of diluent, 3000 IU/vial, reconstituted with 5.6 mL of diluent [product monograph]. CSL Behring Canada, Inc; 2022 Apr 13. Accessed 2022 Apr 20. https://pdf.hres.ca/dpd_pm/00065454.PDF
28.Drug therapies for the long-term prophylaxis of hereditary angioedema attacks. (CADTH technology review no. 25). CADTH; 2019. Accessed 2022 Apr 29. https://www.cadth.ca/sites/default/files/hta-he/ob0007-hae-prophylaxis-redacted.pdf
29.Protocol. A Multicenter, Double-Blind, Randomized, Placebo-Controlled, Parallel-Arm Study to Investigate the Efficacy and Safety of Subcutaneous Administration of CSL312 (garadacimab) in the Prophylactic Treatment of Hereditary Angioedema - Clinical Study Protocol. As provided by the sponsor.
30.Weller K, Magerl M, Peveling-Oberhag A, Martus P, Staubach P, Maurer M. The Angioedema Quality of Life Questionnaire (AE-QoL) - assessment of sensitivity to change and minimal clinically important difference. Allergy. Aug 2016;71(8):1203-9. doi:10.1111/all.12900 PubMed
31.Weller K, Groffik A, Magerl M, et al. Development and construct validation of the angioedema quality of life questionnaire. Allergy. Oct 2012;67(10):1289-98. doi:10.1111/all.12007 PubMed
32.SAP. A Multicenter, Double-Blind, Randomized, Placebo-Controlled, Parallel-Arm Study to Investigate the Efficacy and Safety of Subcutaneous Administration of CSL312 (garadacimab) in the Prophylactic Treatment of Hereditary Angioedema - Statistical Analysis Plan. As provided by the sponsor.
33.Inc CSLB. Drug Reimbursement Review sponsor submission: NMA technical report. Garadacimab, 200 Q.M. [internal sponsor's package]. 2024;
34.Inc CSLB. Drug Reimbursement Review sponsor submission: MAIC technical report. Garadacimab, 200 Q.M. [internal sponsor's package]. 2024;
35.Inc CSLB. Drug Reimbursement Review sponsor submission: SLR technical report. Garadacimab, 200 Q.M. [internal sponsor's package]. 2022;
36.FDA. Package Insert - CINRYZE: HIGHLIGHTS OF PRESCRIBING INFORMATION. 2008;
37.Inc CSLB. Drug Reimbursement Review sponsor submission: ITC Feasibility Assessment for Garadacimab for the Treatment of Hereditary Angioedema. Garadacimab, 200 Q.M. [internal sponsor's package]. 2023;
38.Dias S, Sutton AJ, Ades AE, Welton NJ. Evidence synthesis for decision making 2: a generalized linear modeling framework for pairwise and network meta-analysis of randomized controlled trials. Med Decis Making. Jul 2013;33(5):607-17. doi:10.1177/0272989x12458724 PubMed
39.Dias S WNJSAJAA. NICE DSU technical support document 2: a linear modelling framework for pairwise and network meta-analysis of randomised controlled trials. 2011;
40.Vehtari A, Gelman A, Simpson D, Carpenter B, Bürkner P-C. Rank-Normalization, Folding, and Localization: An Improved ^R for Assessing Convergence of MCMC (with Discussion). Bayesian Analysis. 2021;16(2):667-718, 52.
41.Aygoren-Pursun E, Bygum A, Grivcheva-Panovska V, et al. Oral plasma kallikrein inhibitor for prophylaxis in hereditary angioedema. N Engl J Med. 2018;379(4):352-362. doi:10.1056/NEJMoa1716995 PubMed
42.CSL312 (Garadacimab) in the Prevention of Hereditary Angioedema Attacks (NCT04656418). Clinicaltrials.gov. Updated August 3, 2022. https://ClinicalTrials.gov/show/NCT04656418
43.Lumry WR, Weller K, Magerl M, et al. Impact of lanadelumab on health-related quality of life in patients with hereditary angioedema in the HELP study. Allergy: European Journal of Allergy and Clinical Immunology. 2021;76(4):1188-1198. doi:10.1111/all.14680 PubMed
44.Longhurst H, Cicardi M, Craig T, et al. Prevention of hereditary angioedema attacks with a subcutaneous C1 inhibitor. N Engl J Med. 2017;376(12):1131-1140. doi:10.1056/NEJMoa1613627 PubMed
45.BEROTRALSTAT (BCX7353) STUDY BCX7353-302: PART 1 INTERIM CLINICAL STUDY REPORT, (2019). Accessed February 1, 2023. https://clinical-information.canada.ca/ci-rc-vu.pdf?file=m5/53-clin-stud-rep/535-rep-effic-safety-stud/hae/5351-stud-rep-contr/bcx7353-302-report-body-red.pdf&id=252301
46.Craig T, Magerl M, Levy DS, et al. Prophylactic use of an anti-activated factor XII monoclonal antibody, garadacimab, for patients with C1-esterase inhibitor-deficient hereditary angioedema: a randomised, double-blind, placebo-controlled, phase 2 trial. Lancet. Mar 5 2022;399(10328):945-955. doi:10.1016/S0140-6736(21)02225-X PubMed
47.BioCryst. Statistical Analysis Plan: BCX7353-302 (APeX-2). BioCryst Pharmaceuticals, Inc.; 2019. p. 1-103.
48.BioCryst. Statistical Analysis Plan: BCX7353-301 (APeX-J). BioCryst Pharmaceuticals, Inc.; 2019. p. 1-110.
49.BioCryst. Statistical Analysis Plan: BCX7353-203 (APeX-1). 2017:1-60.
50.Phillippo DATDSPSAKR, Welton N. NICE DSU Technical Support Document 18: Methods for population-adjusted indirect comparisons in submissions to NICE. (Technical Support Documents). NICE Decision Support Unit. 2016;
51.Austin PC. Balance diagnostics for comparing the distribution of baseline covariates between treatment groups in propensity-score matched samples. Stat Med. Nov 10 2009;28(25):3083-107. doi:10.1002/sim.3697 PubMed
52.Phillippo DM, Ades AE, Dias S, Palmer S, Abrams KR, Welton NJ. Methods for Population-Adjusted Indirect Comparisons in Health Technology Appraisal. Med Decis Making. Feb 2018;38(2):200-211. doi:10.1177/0272989x17725740 PubMed
53.Signorovitch JE, Wu EQ, Yu AP, et al. Comparative effectiveness without head-to-head trials: a method for matching-adjusted indirect comparisons applied to psoriasis treatment with adalimumab or etanercept. Pharmacoeconomics. 2010;28(10):935-45. doi:10.2165/11538370-000000000-00000 PubMed
54.Banerji A, Riedl MA, Bernstein JA, et al. Effect of Lanadelumab Compared With Placebo on Prevention of Hereditary Angioedema Attacks: A Randomized Clinical Trial. JAMA. Nov 27 2018;320(20):2108-2121. doi:10.1001/jama.2018.16773 PubMed
55.Higgins Jpt TJCJCMLTPMJWVA. Cochrane Handbook for Systematic Reviews of Interventions version 6.4 (updated August 2023). 2023;
56.83.	CSL Behring Inc. Drug Reimbursement Review sponsor submission: MAIC Manuscript. Garadacimab, 200 Q.M. [internal sponsor's package]. Journal of Comparative Effectiveness Research 2024.
57.Phillippo et al. NICE DSU Technical Support Document 18: Methods for population-adjusted indirect comparisons in submission to NICE. 2016. Available from http://www.nicedsu.org.uk. 2016;
Pharmacoeconomic Review
Abbreviations
AE
adverse event
BIA
budget impact analysis
CBS
Canadian Blood Services
CDA-AMC
Canada’s Drug Agency
HAE
hereditary angioedema
LTP
long-term prophylaxis
NMA
network meta-analysis
QALY
quality-adjusted life-year
SC
subcutaneous
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Garadacimab (Andembry), 200 mg/1.2 mL solution for subcutaneous injection |
Indication | Garadacimab is indicated for routine prevention of attacks of hereditary angioedema (HAE) in adult and pediatric patients (aged 12 years and older). |
Health Canada approval status | NOC |
Health Canada review pathway | Standard review |
NOC date | August 6, 2025 |
Reimbursement request | As per indication |
Sponsor | CSL Behring Canada Inc. |
Submission history | No |
HAE = hereditary angioedema; NOC = Notice of Compliance.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Markov model |
Target population | For the routine prevention of attacks of hereditary angioedema in adult and pediatric patients aged 12 years and older |
Treatment | Garadacimab |
Dose regimen | Loading dose of 400 mg on the first day of treatment followed by a monthly dose of 200 mg |
Submitted price | $34,840 per 200 mg single-dose prefilled pen or prefilled syringe |
Submitted treatment cost | First year: $452,651 Subsequent years: $417,206 |
Comparators |
|
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | Lifetime (58.8 years) |
Key data sources |
|
Submitted results |
|
Key limitations |
|
CDA-AMC reanalysis results |
|
CDA-AMC = Canada’s Drug Agency; LY = life-year; NMA = network meta-analysis; QALY = quality-adjusted life-year; SC = subcutaneous; vs. = versus.
Conclusions
The CDA-AMC Clinical Review found that, while the available evidence generally suggests garadacimab results in a clinically meaningful reduction in hereditary angioedema (HAE) episodes (also known as attacks) compared with placebo, no definitive conclusion could be drawn on the effectiveness of garadacimab compared to other long-term prophylaxis (LTP) treatments. The sponsor submitted a network meta-analysis (NMA) to inform the comparative efficacy of garadacimab against other LTP treatments. The CDA-AMC Clinical Review was unable to confirm the key assumption of similarity that undermines the validity of the NMA results, which are therefore unreliable for determining the comparative effectiveness of garadacimab against other LTP treatments.
The sponsor’s submitted base case results suggest that garadacimab is dominant (i.e., less costly and more effective) than other LTP treatments available for the routine prevention of episodes of hereditary angioedema. Whether garadacimab would be dominant is sensitive to the assumed proportion of patients who switch from a lanadelumab dosing schedule of every 2 weeks to a schedule of every 4 weeks. A deterministic threshold analysis was conducted that indicated that, if 50% or greater of patients switch to every 4 weeks at month 7, garadacimab would no longer dominate lanadelumab. While the annual cost of garadacimab is higher than some of its comparators, the sponsor estimated that garadacimab would result in cost savings due to fewer and less severe episodes. However, based on the uncertainty in the clinical evidence, there is insufficient evidence to support this finding. There is also insufficient evidence to suggest that garadacimab should be priced higher than other LTP treatments currently reimbursed for the routine prevention of episodes (also known as attacks) of hereditary angioedema.
Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, clinician groups, and drug plans that participated in the CDA-AMC review process.
Patient input was received from Hereditary Angioedema Canada. Input was gathered through 3 approaches: a survey of patients enrolled in the VANGUARD trial (14 patients responded); telephone interviews with those who responded to the survey; and a separate national survey to inform Hereditary Angioedema Canada’s third National Report Card. It was not explicitly reported whether all respondents were in Canada, but the information was described as being collected through Canadian channels. Patients reported that they may still be affected by HAE after the physical symptoms of an episode abate. This was due to the anticipation of the next unpredictable episode, restrictions or disruption to one’s social life, and restrictions in pursuing higher education or job advancements. Unmet needs with current LTP treatments include heterogeneity in its effectiveness, concerns with IV treatment (e.g., IV damage to veins at the injection site and difficulty with self-administration), access to hospital care (especially for those residing in rural areas), and concerns about plasma-derived products (i.e., risk of infections and supply interruptions or shortages). Many patients with experience receiving garadacimab found it to be effective in reducing or eliminating HAE episodes and convenient given its subcutaneous (SC) route of administration and monthly dosing schedule.
Clinician input was received from the Canadian Hereditary Angioedema Network. Clinicians reported challenges to the current pathway of care for patients with HAE due to a lack of early or sustained prevention of HAE episodes, issues with drug shortages, and the need for more convenient self-administrated modalities of treatment. No existing prophylactic regimen can eliminate angioedema and clinicians expect patients would require acute treatment for episodes despite LTP therapy. Clinician input indicated that LTP is considered at every HAE follow-up visit, and patients already on LTP would review options for switching treatment. Clinicians noted that garadacimab would provide a novel nonplasma treatment that targets a different part of the kallikrein-kinin cascade involved in HAE episodes. Clinicians also reported that garadacimab is better tolerated with fewer local side effects, has a more convenient monthly dosing schedule, and can be administered at home. Clinicians noted that they would consider discontinuation of garadacimab due to ineffectiveness and/or side effects.
Drug plans noted that berotralstat was under active negotiations with pan-Canadian Pharmaceutical Alliance (pCPA) while lanadelumab had completed successful pCPA negotiations. They further indicated that plasma-derived products are presently procured through Canadian Blood Services (CBS) and that patients switching to garadacimab would result in cost shifting within the health care system.
Several of these concerns were addressed in the sponsor’s model:
The sponsor’s model compared garadacimab to all other publicly available LTPs available for the routine prevention of episodes of hereditary angioedema.
The sponsor’s model was structured around health states defined by episodes.
The sponsor quantified the impact of the condition and the treatment on patient’s quality of life via health state utility values that consider dimensions of mobility, usual activities, and anxiety and depression.
In addition, CDA-AMC addressed some of these concerns as follows:
CDA-AMC addressed coverage under CBS and drug programs in a budget impact analysis (BIA) and presented the results of each program separately to demonstrate the potential impact of cost shifting.
CDA-AMC was unable to address the following concerns raised from the input:
The uncertainty in analyses due to a lack of head-to-head clinical evidence comparing garadacimab with other LTPs.
Economic Review
The current review is for garadacimab (Andembry) for the routine prevention of episodes (also known as attacks) of HAE in adult and pediatric patients (aged 12 years and older).
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis of garadacimab compared with berotralstat, C1-INH IV, C1-INH SC, and lanadelumab. The modelled population was for the routine prevention of HAE episodes (also known as attacks) in adult and pediatric patients aged 12 years and older. The modelled population was in line with the proposed Health Canada indication.
Garadacimab is available as a 200 mg/1.2 mL single-dose prefilled syringe or pen. The recommended dosing of garadacimab is an initial loading dose of 400 mg administered by SC injection on the first day of treatment followed by a monthly dose of 200 mg.1 The sponsor-submitted price for garadacimab was $34,840 per 200 mg prefilled syringe or pen.2 The sponsor estimated that the first-year drug cost would be $452,651 and costs in subsequent years would be $417,763.3 With respect to the comparators, the annual cost of berotralstat was reported to be $308,156 per patient, with a weighted annual cost of $508,713 per patient for lanadelumab (assuming all patients initially receive lanadelumab once every 2 weeks and, at month 7, 20% of patients switch to once every 4 weeks) as assumed by the sponsor.3,4 In terms of off-label LTP use of C1-INH, the annual costs of C1-INH IV and C1-INH SC were, respectively, $1,163,4865 and $581,939 per patient. Wastage was included in the calculation of drug costs, where applicable.3
The clinical outcomes of interest were quality-adjusted life-years (QALYs) and life-years over a lifetime time horizon of 58.8 years. The model used a 1-month cycle length, with a discount of 1.5% per year applied to both future costs and health-related outcomes. The base-case perspective was that of the Canadian publicly funded health care payer.3
Model Structure
The sponsor submitted a Markov model with 4 health states: “full attack freedom,” “prone to attack (initial treatment),” “prone to attack (subsequent treatment),” and “death” (Figure 1). The full attack freedom state was defined as experiencing no episodes at least 6 months after initiating LTP treatment. The prone to attack (initial treatment) state was defined as patients who experienced an episode after initiating LTP treatment, while the prone to attack (subsequent treatment) state reflected patients who switched from their initial treatments.3 Patients entered the first model cycle distributed across the full attack freedom or prone to attack (initial treatment) health states. After the first 6 months of treatment, patients who experience an episode would transition out of the full attack freedom state to the prone to attack (initial treatment) state. In the prone to attack (initial treatment) state, patients have a risk of experiencing episodes throughout the modelled time horizon and will remain in this state until death. While the prone to attack (subsequent treatment) state was part of the model structure, no patients entered this health state in the sponsor’s base case.3 Furthermore, patients cannot transition back to the full attack freedom state from the prone to attack (initial treatment) state. Death was the absorbing state.
Model Inputs
The baseline patient characteristics in the sponsor’s model (mean age of 0.41.2 years; 59.4% female) were informed by the VANGUARD trial and assumed to represent the general population of patients with HAE in Canada.3 The VANGUARD trial included patients aged 12 years or older with type I or type II HAE who had at least 3 HAE episodes during the 3 months before screening (or over any consecutive 3 months for patients taking LTP).6
Clinical efficacy inputs for the model were based on the VANGUARD trial and a sponsor-submitted NMA. The NMA included the CSL312_2001 trial (which investigated garadacimab),7 the VANGUARD trial (which investigated garadacimab),6 the HELP trial (which investigated lanadelumab),8 the COMPACT trial (which investigated C1-INH SC),9 and the Apex-2 trial (which investigated berotralstat).10 Specifically, the probability of starting in the full attack freedom state was based on applying the treatment’s fixed-effect NMA-derived hazard ratios by the proportion of on-demand patients (i.e., placebo) starting in the full attack freedom state. The subsequent probabilities of transitioning from the full attack freedom state to the prone to attack (initial treatment) state were naive estimates from each individual study. The attack rate (i.e., number of episodes per model cycle) within the prone to attack (initial treatment) health state was based on the NMA’s rate ratio multiplied by the pooled on-demand treatment attack rate.3 Attack severity (stratified as mild, moderate, severe nonlaryngeal, and severe laryngeal) was treatment-dependent and based directly on the trial data or published literature without further adjustment.3 Due to the lack of trial data on the use of C1-INH IV in the long-term prevention setting, the sponsor assumed the clinical data for C1-INH IV would be equal to that of C1-INH SC.11,12
Mortality was assumed to be equal to that of the general population in Canada,13 with a 1-time increased risk of death for severe laryngeal attacks.14 Adverse events (AEs) of any severity were included in the model if they occurred in greater than 10% of the patients in any 1 trial.8,10,15 The frequency of AEs related to C1-INH IV were assumed to be the same as that reported for C1-INH SC.
Health state utilities were elicited directly from the CSL312_3001 trial based on a post hoc analysis of the EQ-5D-5L questionnaire.16,17 Utility values used in the model were 0.965 for the full attack freedom state and 0.875 for the prone to attack state. Disutilities from episodes, stratified by severity, and AEs were sourced from the published literature.14,18 AE disutilities were applied only once during the first model cycle.3
Costs in the model included drug acquisition, drug administration, routine monitoring, and the management of HAE episodes.3 Acquisition costs for garadacimab reflected the sponsor’s submitted price while the prices of the comparators were informed by previous CDA-AMC reviews and the Ontario Exceptional Access Program formulary.3,5,19,20 Drawing on market research data and clinical expert feedback, the sponsor assumed that, among patients who initially receive lanadelumab every 2 weeks, 20% would switch to every 4 weeks at month 7.3 The sponsor further assumed that patient compliance was 100%, with wastage included in the calculation of drug acquisition costs.3 Drug administration costs included a 1-time cost for a registered nurse to train patients on self-administration.21 Last, routine monitoring and management of HAE episodes included physician visits, emergency department visits, and hospitalization. Resource utilization to manage episodes were dependent on the episode’s severity, with utilization based on the sponsor’s clinical expert feedback and literature,22 while pricing was sourced from Canadian databases.5,23 On-demand drug costs reflected a weighted treatment of C1-INH IV and icatibant.4,5,20 The sponsor assumed all AEs were minor and would not result in costs to the public payer.3
Summary of Sponsor’s Economic Evaluation Results
All analyses were run probabilistically (5,000 iterations for the base case). The deterministic and probabilistic results were similar to the probabilistic findings presented in the following section. The submitted analysis was based on the submitted price for garadacimab.
Base-Case Results
Garadacimab was associated with a lower total cost and a higher total number of QALYs compared to other LTPs in the sponsor’s submitted model. The sponsor’s base-case analysis demonstrated that garadacimab dominated lanadelumab, berotralstat, C1-INH SC, and C1-INH IV (Table 3).
The results showed that the additional QALYs associated with garadacimab were attributable primarily to higher-state occupancy in the full attack freedom health state and the lower-transition probabilities to move into the prone to attack (initial treatment) health state. Once in the prone to attack (initial treatment) health state, the sponsor’s results suggested that patients receiving garadacimab were less likely to have an episode, and when experiencing an episode, they were less likely to experience a severe episode compared to other LTP therapies. It is important to note that, of the total QALYs associated with garadacimab, approximately 92% were realized beyond the 6-month VANGUARD trial period. Total life-years were the same between the treatments, indicating that garadacimab is not expected to have an impact on mortality when compared to other therapies. The total costs within the sponsor’s results were driven largely by LTP drug acquisition.
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Total QALYs | Sequential ICER ($/QALY) |
|---|---|---|---|
Garadacimab | 13,040,527 | 26.11 | Reference |
Dominated treatments | |||
Berotralstat | 13,523,599 | 25.09 | Dominated |
Lanadelumaba | 15,257,617 | 25.63 | Dominated |
C1-INH SC | 17,891,958 | 25.52 | Dominated |
C1-INH IV | 28,514,101 | 25.53 | Dominated |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; SC = subcutaneous.
aLanadelumab dose initiated as every 2 weeks; after 6 months, 20% of patients switch to every 4 weeks.
Source: Sponsor’s pharmacoeconomic submission.3
Additional results from the sponsor’s submitted economic evaluation base case are presented in Appendix 3.
Sensitivity and Scenario Analysis Results
The sponsor conducted 1-way sensitivity analyses to alter parameters related to utilities, cost, and episode probabilities. These analyses had little impact on the results as garadacimab remained dominant in almost all cases, except when increasing the price of garadacimab, decreasing the price of berotralstat, and altering the patient’s weight. The sponsor evaluated several scenarios deterministically, including allowing treatment switching, setting the episode severity distribution to be identical across LTP treatments as informed by the literature,24 applying alternative utility values based on the literature,25,26 selecting alternative episode duration as informed by the literature,6 increasing the proportion of patients switching lanadelumab to every 4 weeks, altering the health care resource use associated with the management of episodes as informed by the literature,27 and excluding HAE-specific mortality. Garadacimab remained dominant in the majority of scenario analyses, except when the proportion of patients receiving lanadelumab every 4 weeks increased to 51.7% (i.e., lanadelumab was no longer dominated by garadacimab; the incremental cost-effectiveness ratio of garadacimab was $379,310 per QALY gained compared to lanadelumab).3
The sponsor conducted a scenario analysis from a societal perspective that included the additional costs associated with patient and caregiver productivity losses. This was similar to the sponsor’s base-case analysis using a health care payer perspective because garadacimab dominated the other LTP comparators.
CDA-AMC Appraisal of the Sponsor’s Economic Evaluation
CDA-AMC identified several key limitations to the sponsor’s analysis that have notable implications on the economic analysis:
The comparative efficacy and safety of garadacimab in comparison with other LTP treatments is highly uncertain: There is a lack of direct evidence comparing garadacimab with other existing LTP therapies for routine prevention of episodes of HAE in adult and pediatric patients (aged 12 years and older). In the absence of head-to-head evidence, the sponsor conducted an NMA that informed the distribution of patients in the starting health states and the attack rates in the sponsor’s submitted model. According to the modelled inputs, garadacimab was associated with a higher proportion of patients starting in the freedom of attack health state, and when transitioned to the prone to attack state, garadacimab was associated with a lower attack rate. This had a significant impact on the expected results as garadacimab was associated with a higher total number of QALYs and strong dominance over other LTPs in the sponsor’s base case. While this aligns with the sponsor’s submitted NMA (i.e., garadacimab was associated with a numerically improved outcome compared to some LTP comparators), significant limitations were noted with the sponsor’s submitted NMA. According to the CDA-AMC Clinical Review, significant heterogeneity across the included trials was noted, along with a sparse network and relatively small trial sample size. The sponsor selected a fixed-effects model to inform the economic model parameters; yet, as noted in the CDA-AMC Clinical Review report, all statistically significant differences comparing garadacimab with other LTP comparators disappeared in a random-effects model. The CDA-AMC Clinical Review concluded that the comparative findings of the sponsor’s NMA were insufficient to support claims of differences in efficacy or safety of garadacimab versus other LTP therapies because of the presence of this substantial imprecision and unresolved heterogeneity.
In addition, some of the model’s transition probabilities, the distribution of the episode severity, and the safety outcomes were derived directly from clinical trials of each respective treatment and incorporated naively within the sponsor’s model. However, as the CDA-AMC Clinical Review noted, there is considerable clinical and methodological heterogeneity across these trials. Clinical expert feedback obtained by CDA-AMC further noted that there is a large unpredictable variability in attack rates between patients and within a patient’s own disease history. Therefore, the different time periods of the trials can lead to substantial differences in the observed rates of attacks. Shorter trials may not capture the full spectrum of disease variability. It is not appropriate to naively incorporate treatment effects and AEs as this approach is not able to adequately support claims of comparative effectiveness and safety.
Due to the lack of direct evidence for garadacimab versus other LTPs and the limitations of the sponsor’s NMA, it is uncertain whether garadacimab is superior to other LTPs. As a result, the incremental number of QALYs gained on garadacimab when compared to other LTPs remains highly uncertain. CDA-AMC was unable to address this limitation.
Variability in the dosing of lanadelumab: According to its product monograph, the recommended starting dose of lanadelumab is 300 mg every 2 weeks. A dosing interval of 300 mg every 4 weeks may be considered if the patient is well controlled (e.g., episode-free) for more than 6 months.28 In the submitted model, the sponsor assumed that switching would occur at month 7, by which point 20% of patients would have switched to every 4 weeks. The sponsor clarified during the feedback period that this proportion of patients switching was informed by █████ market share analysis. Specifically, procurement audits were conducted focused on hospitals and blood banks, pharmacies, and CBS sites, with audit data projected by referencing the number of patients and/or number of sites per channel and leveraging other sources, such as analyst reports and supplier financials, for validation. The drug acquisition cost for lanadelumab is sensitive to the assumptions regarding when patients switch to dosing schedule of every 4 weeks and the proportion of patients who make the switch. If patients switch earlier and/or a greater proportion of patients switch, the expected cost of lanadelumab may be lower than the expected cost of garadacimab.
According to the clinical expert consulted by CDA-AMC, the proportion of patients switching to every 4 weeks is likely higher than assumed by the sponsor but may vary across jurisdictions based on their reimbursement criteria for lanadelumab. CDA-AMC conducted a deterministic threshold analysis on the proportion of patients switching at month 7 from every 2 weeks to every 4 weeks, whereby garadacimab would no longer be the dominant therapy.
Price of drugs paid by public drug plans are uncertain: The sponsor’s analysis is based on publicly available list prices for most comparators. Actual costs paid by public drug plans are unknown and any potential confidential rebates are not reflected in this analysis.
CDA-AMC could not address this limitation in reanalysis.
Additionally, the following key assumption was made by the sponsor and has been appraised by CDA-AMC (refer to Table 4).
Table 4: Key Assumptions of the Submitted Economic Evaluation (Not Noted as Limitations to the Submission)
Sponsor’s key assumption | CDA-AMC comment |
|---|---|
The efficacy and safety of C1-INH IV was assumed to be equal to that of C1-INH SC. | Inappropriate. The clinical expert consulted by CDA-AMC noted that C1-INH IV appears to be less efficacious than C1-INH SC. |
CDA-AMC = Canada’s Drug Agency; SC = subcutaneous.
CDA-AMC Reanalyses of the Economic Evaluation
Base-Case Results
CDA-AMC was unable to address the uncertainty related to the comparative clinical data, including the magnitude of the benefit for garadacimab compared to other LTPs. CDA-AMC was also unable to resolve the uncertainty related to the impact of using publicly listed pricing in the analysis. As such, CDA-AMC was unable to provide a more reliable estimate of the cost-effectiveness of garadacimab compared to other LTPs.
CDA-AMC conducted a deterministic threshold analysis and noted that, if 50% or greater of patients switch to every 4 weeks at month 7, garadacimab would no longer be the dominant therapy (Table 5).
Table 5: Results of Deterministic Threshold Analysis
Proportion of patients who switch from q.2.w. to q.4.w. | ICER vs. lanadelumab ($/QALY) |
|---|---|
20% (submitted) | Dominanta |
40% | Dominanta |
50% | 131,370 |
60% | 1,585,505 |
ICER = incremental cost-effectiveness ratio; q.2.w. = every 2 weeks; q.4.w. = every 4 weeks; QALY = quality-adjusted life-year; vs. = versus.
aGaradacimab is less costly and more effective.
Issues for Consideration
Reimbursement criteria of comparator treatments: In most jurisdictions, the reimbursement of prophylaxis treatment for the routine prevention of episodes of HAE is presently associated with specific initiation and renewal criteria as part of special access programs. The submitted economic evaluation is unable to evaluate the cost-effectiveness of garadacimab against comparator LTP therapies based on their current reimbursement criteria.
Funding of plasma-derived agents: Given that no public list prices were available for plasma-derived agents, the prices for these treatments were submitted by the sponsor as part of its pharmacoeconomic submission. CDA-AMC was unable to confirm their accuracy. Drug plans do not cover the costs of plasma-derived treatments and these treatments are available through CBS. If garadacimab is expected to displace C1-INH, this would increase costs for some budget holders (i.e., public drug plans) while leading to cost savings for others (i.e., CBS).
Overall Conclusions
The CDA-AMC Clinical Review found that, while the available evidence generally suggests garadacimab results in a clinically meaningful reduction in HAE episodes versus placebo, no definitive conclusion could be drawn about the effectiveness of garadacimab compared to other LTP treatments. The sponsor submitted an NMA to inform the comparative efficacy of garadacimab against other LTP treatment. The CDA-AMC Clinical Review was unable to confirm the key assumption of similarity. This undermines the validity of the NMA results, which are therefore unreliable for determining the comparative effectiveness of garadacimab against other LTP treatments.
The sponsor’s submitted base-case results suggest that garadacimab is dominant (i.e., less costly and more effective) than other LTP treatments available for the routine prevention of episodes of HAE. Whether garadacimab would be dominant is sensitive to the assumption regarding the proportion of patients who switch from lanadelumab administered every 2 weeks to every 4 weeks. A deterministic threshold analysis found that, if 50% or greater of patients switch to every 4 weeks at month 7, garadacimab would no longer dominate lanadelumab. While the annual cost of garadacimab is higher than that of some of its comparators, the sponsor estimated that garadacimab would result in cost savings due to fewer and less severe episodes. However, based on the uncertainty in the clinical evidence, there is insufficient evidence to support this finding. There is also insufficient evidence to suggest that garadacimab should be priced higher than other LTP treatments currently reimbursed for the routine prevention of episodes of hereditary angioedema.
References
1.CSL Behring. Andembry (garadacimab): Prefilled Syringes and Prefilled Pens 200 mg for Subcutaneous Injection [product monograph] [sponsor supplied reference]. 2024.
2.CSL Behring Canada Inc. Drug Reimbursement Review sponsor submission: PrAdembry® (garadacimab), prefilled syringes and prefilled pens, 200 mg solution for subcutaneous injection [internal sponsor's package]. July 26, 2024.
3.CSL Behring Canada Inc. Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: PrAdembry® (garadacimab), prefilled syringes and prefilled pens, 200 mg solution for subcutaneous injection. July 26, 2020.
4.CSL Behring. Market Share Analysis [sponsor supplied reference]. 2024.
5.CADTH Health Technology Review: Drug Therapies for the Long-Term Prophylaxis of Hereditary Angioedema Attacks [sponsor supplied reference]. 2019.
6.Craig TJ, Reshef A, Li HH, et al. Efficacy and safety of garadacimab, a factor XIIa inhibitor for hereditary angioedema prevention (VANGUARD): a global, multicentre, randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 2023;401(10382):1079-1090. doi: 10.1016/S0140-6736(23)00350-1 PubMed
7.Craig T, Magerl M, Levy DS, et al. Prophylactic use of an anti-activated factor XII monoclonal antibody, garadacimab, for patients with C1-esterase inhibitor-deficient hereditary angioedema: a randomised, double-blind, placebo-controlled, phase 2 trial. Lancet. 2022;399(10328):945-955. doi: 10.1016/S0140-6736(21)02225-X PubMed
8.Lumry WR, Weller K, Magerl M, et al. Impact of lanadelumab on health-related quality of life in patients with hereditary angioedema in the HELP study. Allergy. 2021;76(4):1188-1198. doi: 10.1111/all.14680 PubMed
9.Longhurst H, Cicardi M, Craig T, et al. Prevention of Hereditary Angioedema Attacks with a Subcutaneous C1 Inhibitor. N Engl J Med. 2017;376(12):1131-1140. doi: 10.1056/NEJMoa1613627 PubMed
10.Statistical Analysis Plan: BCX7353-302 (APeX-2) [sponsor supplied reference]. BioCryst Pharmaceuticals, Inc.; 2019:1-103.
11.Riedl MA, Bygum A, Lumry W, et al. Safety and Usage of C1-Inhibitor in Hereditary Angioedema: Berinert Registry Data. J Allergy Clin Immunol Pract. 2016;4(5):963-71. doi: 10.1016/j.jaip.2016.04.018 PubMed
12.Craig TJ, Levy RJ, Wasserman RL, et al. Efficacy of human C1 esterase inhibitor concentrate compared with placebo in acute hereditary angioedema attacks. J Allergy Clin Immunol. 2009;124(4):801-8. doi: 10.1016/j.jaci.2009.07.017 PubMed
13.Statistics Canada. Table 13-10-0837-01 Life expectancy and other elements of the complete life table, single-year estimates, Canada, all provinces except Prince Edward Island [sponsor supplied reference]. https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310083701
14.Zanichelli A, Arcoleo F, Barca MP, et al. A nationwide survey of hereditary angioedema due to C1 inhibitor deficiency in Italy. Orphanet J Rare Dis. 2015;10:11. doi: 10.1186/s13023-015-0233-x PubMed
15.CSL Behring, LLC. Clinical Study Report: CSL312_3001. A Multicenter, Double-Blind, Randomized, Placebo-Controlled, Parallel-Arm Study to Investigate the Efficacy and Safety of Subcutaneous Administration of CSL312 (garadacimab) in the Prophylactic Treatment of Hereditary Angioedema [internal sponsor's report]. October 6, 2022.
16.Hernandez Alava M, Pudney S, Wailoo A. Estimating the Relationship Between EQ-5D-5L and EQ-5D-3L: Results from a UK Population Study. Pharmacoeconomics. 2023;41(2):199-207. doi: 10.1007/s40273-022-01218-7 PubMed
17.CSL Behring. Post-hoc utility study [sponsor supplied reference]. 2024.
18.Nordenfelt P, Dawson S, Wahlgren CF, Lindfors A, Mallbris L, Bjorkander J. Quantifying the burden of disease and perceived health state in patients with hereditary angioedema in Sweden. Allergy Asthma Proc. 2014;35(2):185-90. doi: 10.2500/aap.2014.35.3738 PubMed
19.CADTH Reimbursement Recommendation: Berotralstat (Orladeyo). Can J Health Technol. 2023;3(3). doi:10.51731/cjht.2022.592
20.Ontario Ministry of Health and Long-Term Care. Formulary Exceptional Access Program [sponsor supplied reference]. Accessed March 31, 2024. http://health.gov.on.ca/en/pro/programs/drugs/odbf/odbf_except_access.aspx
21.Government of Canada. Jobbank - Wages. Registered Nurse (R.N.) in Canada [sponsor supplied reference]. 2024. https://www.jobbank.gc.ca/marketreport/wages-occupation/993/ca
22.Mendivil J, DerSarkissian M, Banerji A, et al. A multicenter chart review of patient characteristics, treatment, and outcomes in hereditary angioedema: unmet need for more effective long-term prophylaxis. Allergy Asthma Clin Immunol. 2023;19(1):48. doi: 10.1186/s13223-023-00795-2 PubMed
23.Ontario Health Insurance Plan. Schedule of Benefits - Physician Services Under the Health Insurance Act. 2024. https://www.ontario.ca/files/2024-03/moh-ohip-schedule-of-benefits-2024-03-28.pdf
24.Maurer M, Magerl M, Ansotegui I, et al. The international WAO/EAACI guideline for the management of hereditary angioedema-The 2017 revision and update. Allergy. 2018;73(8):1575-1596. doi: 10.1111/all.13384 PubMed
25.Zuraw BL, Bernstein JA, Lang DM, et al. A focused parameter update: hereditary angioedema, acquired C1 inhibitor deficiency, and angiotensin-converting enzyme inhibitor-associated angioedema. J Allergy Clin Immunol. 2013;131(6):1491-3. doi: 10.1016/j.jaci.2013.03.034 PubMed
26.Ghazi A, Grant JA. Hereditary angioedema: epidemiology, management, and role of icatibant. Biologics. 2013;7:103-13. doi: 10.2147/BTT.S27566 PubMed
27.Dhingra H. Rare Disease Advisor: Hereditary Angioedema (HAE). Accessed May 31, 2023. https://www.rarediseaseadvisor.com/hcp-resource/hereditary-angioedema-risk-factors/
28.Takeda Canada Inc. TAKHZYRO® (lanadelumab): 300 mg/ 2mL solution for subcutaneous injection [product monograph]. September 19, 2018. Updated March 22, 2021. https://pdf.hres.ca/dpd_pm/00060484.PDF
29.Saskatchewan Drug Plan: search formulary. 2024. Accessed September 30, 2024. https://formulary.drugplan.ehealthsask.ca/SearchFormulary
30.Sutherland G, Dihn T. Understanding the gap: a pan-Canadian analysis of prescription drug insurance coverage. The Conference Board of Canada; 2017. Accessed August 15, 2024. https://www.conferenceboard.ca/e-library/abstract.aspx?did=9326
31.HAE Analysis [sponsor supplied reference]. 2024.
32.IQVIA. PharmaStat. 2023. Accessed August 15, 2024. https://www.iqvia.com/
Appendix 1: Cost Comparison Table
Please note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical expert(s) and drug plans. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 6: CDA-AMC Cost Comparison Table for the Routine Prevention of Hereditary Angioedema Attacks
Treatment | Strength / concentration | Form | Price | Recommended dosage | Daily cost ($) | Annual cost ($)a |
|---|---|---|---|---|---|---|
Garadacimab (Andembry) | 200 mg | Solution for SC injection | 34,840.0000 | Loading dose of 400 mg on the first day of treatment followed by a monthly dose of 200 mg | First year: 1,240.03 Subsequent year: 1,144.64 | First year: 452,920 Subsequent year: 418,080 |
Indicated for prophylactic use in HAE | ||||||
Berotralstat (Orladeyo) | 150 mg | Oral capsule | 850.0000a | 150 mg once daily | 850.00 | 310,463 |
Lanadelumab (Takhzyro) | 300 mg / 2 mL | Solution for SC injection | 20,538.0000a | 300 mg every 2 weeks 300 mg every 4 weeks may be considered if the patient is well-controlled for more than 6 months | 1,462.98 If q.4.w.: 731.49 | 533,988 If q.4.w.: 266,994 |
C1 esterase inhibitor (Haegarda) | 2,000 IU 3,000 IU | Powder for solution with diluent for SC injection | 1,860.0000a NA | 60 IU / kg every 3 or 4 days | 1,395.00 to 1,860.00 | 509,524 to 679,365 |
Not indicated for prophylactic use in HAE | ||||||
C1 esterase inhibitor (Berinert) | 500 IU 1,500 IU | Powder for solution with diluent for IV injection | NA 5,573.3300a | 20 IU / kg Prophylactic use is not indicated, although clinical trials and guidelines specify a dose every 3 to 4 days | 1,393.33 to 1,857.78 | 508,915 to 678,553 |
Powder for solution with diluent for SC injection | 60 IU / kg Prophylactic use is not indicated, although clinical trials and guidelines specify a dose every 3 to 4 days | 4,180.00 to 5,573.33 | 1,526,744 to 2,035,659 | |||
CDA-AMC = Canada’s Drug Agency; HAE = hereditary angioedema; NA = not available; SC = subcutaneous.
Note: All annual costs were determined by multiplying daily costs by 365.25. Costs assume a body weight of 75 kg and include wastage of unused medication in vials. Costs do not include administration or dispensing fees.
aSponsor’s submitted price.3
bPrice sourced from Saskatchewan Drug Formulary.29
Appendix 2: Submission Quality
Please note that this appendix has not been copy-edited.
Description | Yes or no | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | No | Refer to key limitations regarding the clinical evidence informing the comparative effectiveness of garadacimab to other LTP therapies. |
Model has been adequately programmed and has sufficient face validity | Yes | No comment |
Model structure is adequate for decision problem | Yes | No comment |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | No | Refer to key limitations. Uncertainty in the NMA results (i.e., the wide credible intervals) was not adequately reflected in the derivation of transition probabilities as fixed-effect estimates were applied into the sponsor’s model. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | Yes | No comment |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | Yes | No comment |
Appendix 3: Additional Information on the Submitted Economic Evaluation
Please note that this appendix has not been copy-edited.
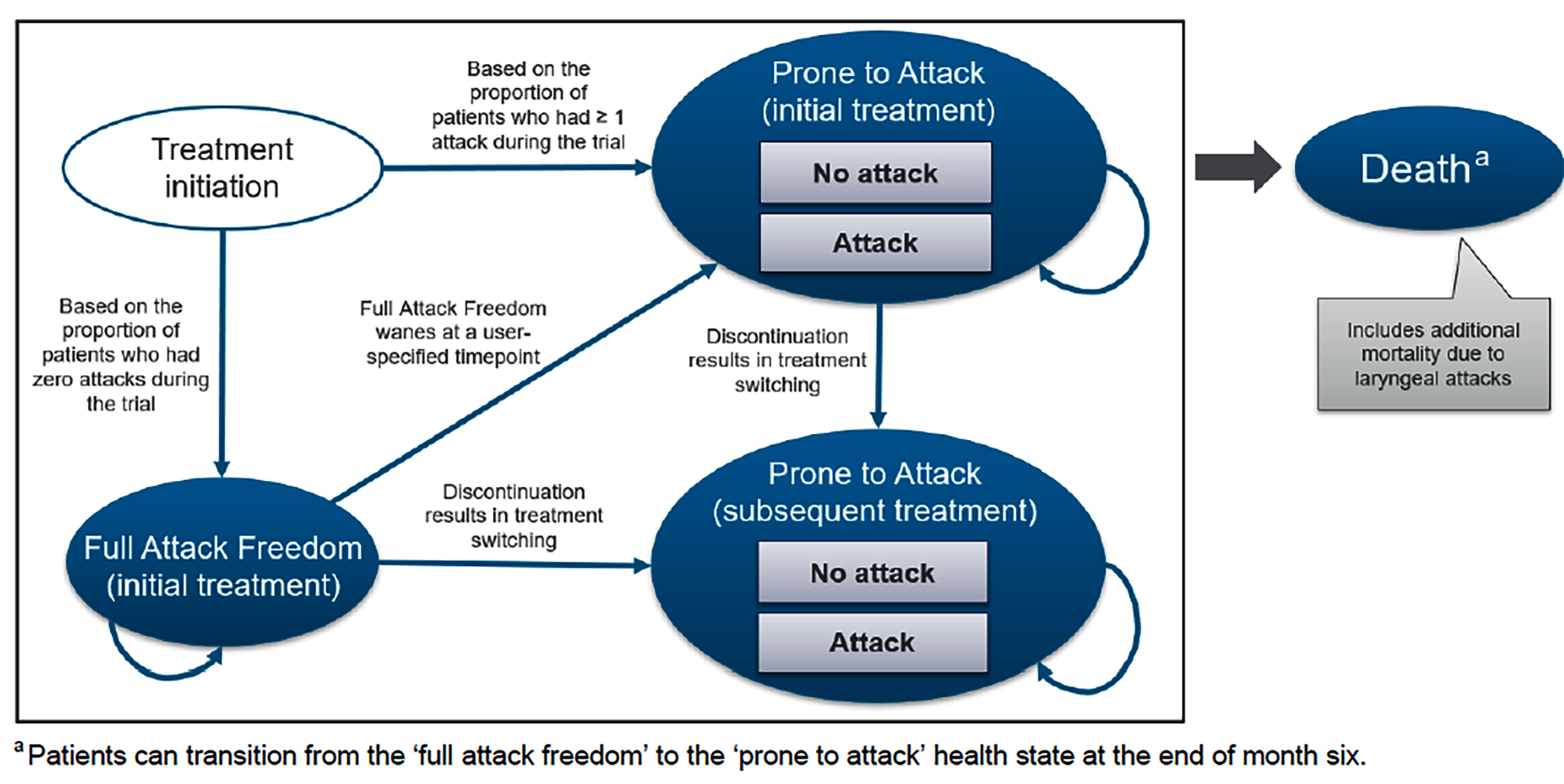
Source: Sponsor’s pharmacoeconomic submission.2
Detailed Results of the Sponsor’s Base Case
Table 8: Disaggregated Summary of the Sponsor’s Economic Evaluation Results
Parameter | Garadacimab | Lanadelumab | C1-INH IV | Berotralstat | C1-INH SC |
|---|---|---|---|---|---|
Discounted LYs | |||||
Total | 29.34 | 29.34 | 29.34 | 29.33 | 29.34 |
By health state | |||||
Prone to attack | 23.49 | 28.01 | 29.01 | 29.30 | 29.01 |
Full attack freedom | 5.85 | 1.32 | 0.33 | 0.03 | 0.33 |
Discounted QALYs | |||||
Total | 26.11 | 25.63 | 25.53 | 25.09 | 25.52 |
By health state | |||||
Prone to attack | 20.55 | 24.51 | 25.38 | 25.64 | 25.38 |
Full attack freedom | 5.64 | 1.28 | 0.32 | 0.03 | 0.32 |
Discounted costs ($) | |||||
Total | 13,040,527 | 15,257,617 | 28,514,101 | 13,523,599 | $ 17,891,958 |
LTP acquisition in “prone to attack” | 9,839,380 | 13,523,424 | 26,931,749 | 9,103,632 | 16,403,721 |
LTP acquisition in “full attack freedom” | 2,469,246 | 660,394 | 319,199 | 9,264 | 193,286 |
LTP administration “prone to attack” | 20 | 21 | 26 | 0 | 26 |
LTP administration “full attack freedom” | 21 | 19 | 14 | 0 | 14 |
On-demand acquisition | 725,642 | 1,065,579 | 1,253,406 | 4,388,630 | 1,285,494 |
On-demand administration | 0 | 0 | 0 | 0 | 0 |
Resource use | |||||
Prone to attack | 3,586 | 4,273 | 4,424 | 4,470 | 4,425 |
Full attack freedom | 446 | 101 | 25 | 2 | 25 |
Mild attack | 332 | 171 | 363 | 1,536 | 309 |
Moderate attack | 453 | 954 | 874 | 2,756 | 990 |
Severe (nonlaryngeal) attack | 1,105 | 2,113 | 2,788 | 10,495 | 2,894 |
Severe (laryngeal) attack | 295 | 568 | 1,233 | 2,814 | 774 |
LTP = long-term prophylaxis; QALY = quality-adjusted life-year; SC = subcutaneous.
Source: Sponsor’s pharmacoeconomic submission.3
Appendix 4: Submitted Budget Impact Analysis and CDA-AMC Appraisal
Please note that this appendix has not been copy-edited.
Table 9: Summary of Key Take-Aways
Key take-aways of the budget impact analysis |
|---|
|
Summary of Sponsor’s Budget Impact Analysis
The sponsor submitted a BIA to estimate the 3-year budget impact of reimbursing garadacimab for the routine prevention of episodes (also known as attacks) of HAE in adult and pediatric patients (aged 12 years and older). The BIA was undertaken from the perspective of CDA-AMC-participating Canadian public drug plans over a three-year time horizon using an epidemiological approach. Costs included annual costs of LTP treatment and annual cost of episodes. Data for the model were obtained from various sources including published literature,30 the sponsor’s internal data, █████ data,31 IQVIA PharmaStat claims data,32 and assumptions. Key inputs to the BIA are documented in Table 10.
Key assumptions included:
60.3% of episodes were treated with C1-INH IV and 39.7% of episodes were treated with icatibant as the on-demand therapy.32
The proportion of patients on betrotralstat and garadacimab eligible for public coverage was assumed to be equivalent to the current proportion of patients currently receiving public coverage for lanadelumab.
Patients on C1-INH (IV) and C1-INH (SC) receive treatment under public reimbursement, covered by CBS. In the new drug scenario, these patients who switch to garadacimab, would be covered by private coverage.
Table 10: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1 / year 2 / year 3 if appropriate) |
|---|---|
Target population | |
Population projection in Canada | 39,953,100 |
Population 12 years of age and older in Canada | 35,159,200 |
Participating public drug plans (excluding Quebec) | 27,606,688 |
Prevalence of HAE | 0.002% |
Proportion of patients with HAE diagnosed | 65.0% |
Proportion of patients on treatment | 92.0% |
Proportion of patients on LTP | 70.0% |
Number of patients eligible for drug under review | 235 / 238 / 242 |
Market uptake (3 years) | |
Uptake (reference scenario) Berotralstat Lanadelumab C1-INH (SC) C1-INH (IV)b On-demand only (no LTP) | █████% / █████% / █████% █████% / █████% / █████% █████% / █████% / █████% █████% / █████% / █████% █████% / █████% / █████% |
Uptake (new drug scenario) Garadacimab Berotralstat Lanadelumab C1-INH (SC) C1-INH (IV)b On-demand only (no LTP) | █████% / █████% / █████% █████% / █████% / █████% █████% / █████% / █████% █████% / █████% / █████% █████% / █████% / █████% █████% / █████% / █████% |
Cost of treatment (per patient, per year) | |
Name of drug under review Garadacimab year 1 Garadacimab subsequent year Lanadelumab Berotralstat C1-INH (SC) C1-INH (IV)b On-demand only (no LTP) | $452,920.00 $418,080.00 $482,239.58a $310,462.50 $582,313.46 $1,163,233.49 $355,709.72 |
HAE = hereditary angioedema; LTP = long-term prophylaxis; LY = life-year; SC = subcutaneous.
aDrug cost of lanadelumab is weighted by assuming 80% of patients are on a q.2.w. dosing regimen and the remainder are on a q.4.w. dosing regimen.
bC1-INH (IV) is used off-label for LTP of HAE, and as such, the sponsor assumed the dosing to be 20 IU/kg twice weekly.5
Summary of the Sponsor’s BIA Results
The sponsor estimated that reimbursing garadacimab for the routine prevention of episodes of HAE in adult and pediatric patients (aged 12 years and older) would result in the costs savings of $7,988,751 in year 1, $16,969,663 in year 2, $19,876,383 in year 3, for a 3-year total budget saving of $44,834,797.
CDA-AMC Appraisal of the Sponsor’s BIA
CDA-AMC identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
Target population is underestimated given assumptions on private coverage: There were 2 instances within the BIA in which the proportion of patients eligible for public coverage was adjusted. The sponsor applied jurisdiction-specific coverage rates based on IQVIA Pharmastat claims data, where available or used public coverage rates from the Conference Board of Canada when these data were unavailable. From a pan-Canadian perspective, 92% of patients would be eligible for public coverage by drug plan. There is uncertainty to this value, especially in the context of a rare condition. Second, the sponsor assumed that, in the New Drug Scenario, patients initially on C1-INH and who switch to garadacimab would receive garadacimab through the same public-private coverage split (i.e., 92% of patients switching from C1-INH to garadacimab would be covered publicly while the remainder would be funded privately). This assumption is inappropriate and is likely to underestimate the budget associated with the reimbursement of garadacimab, contributing to a greater 3-year cost savings.
In reanalyses, CDA-AMC assumed that, among patients who switch from C1-INH to garadacimab, reimbursement for garadacimab would be through public coverage and increased public coverage rates to 100%.
Market share estimates are uncertain: The market share estimated by the sponsor was based on several sources including internal and external survey data. Specifically, the market shares in the reference scenario utilized █████ data while the market uptake of garadacimab was based on the sponsor’s internal revenue projections. The clinical expert consulted by CDA-AMC noted that patients on C1-INH are currently decreasing with a greater proportion receiving lanadelumab. The clinical expert further noted that patients on existing LTPs who have adequate control over their disease would not be likely to switch to garadacimab unless there is more accessible funding arrangement for garadacimab. This may be especially the case for patients on berotralstat given its alternative mode of administration (i.e., oral therapy). The market uptake rate for garadacimab was therefore anticipated to be slower than assumed by the sponsor (i.e., ████ ██ patients would switch to garadacimab by Year 3).
In reanalyses, CDA-AMC revised the market share in the reference scenario to have higher uptake rates for lanadelumab and lower rates for C1-INHs. In the new drug scenario, garadacimab had a smaller rate of uptake and market shares were assumed to be taken predominantly from lanadelumab followed by C1-INHs.
Treatment-specific attack rate: As part of the cost of LTP treatments, the sponsor included drug costs associated with the treatment of episodes. The annual rate of attacks was based on the sponsor’s submitted NMA. As described previously, there are methodological issues with the sponsor’s submitted NMA and whether garadacimab would reduce episodes compared to other LTP treatments remains uncertain.
In reanalyses, CDA-AMC removed drug costs associated with the treatment of episodes from the cost of LTP treatments.
Variability in the dosing of lanadelumab: According to its product monograph, the recommended starting dose of lanadelumab is 300 mg every 2 weeks. A dosing interval of 300 mg every 4 weeks may be considered if the patient is well controlled (e.g., attack-free) for more than 6 months.28 As noted previously, the sponsor assumed that switching occurred at █████ months whereby ██% of patients would switch to every 4 weeks. According to clinical experts consulted by CDA-AMC, the proportion of patients switching to every 4 weeks is likely higher than assumed by the sponsor.
Given uncertainties to the true proportion of patients switching from every 2 weeks to every 4 weeks, a scenario analysis was conducted whereby, based on the threshold analysis results that are presented previously, 50% of patients on lanadelumab were assumed to switch from every 2 weeks to every 4 weeks at 7 months.
Uncertainty in the actual costs of comparators to public drug plans: The sponsor’s analysis is based on publicly available list prices or published reports. Actual costs paid by public drug plans are unknown and it is likely that the unit cost paid by public drug plans is lower than the price submitted in the current review. Any potential confidential rebates are not reflected in the current analysis. Furthermore, the costs of comparators do not reflect current renewal criteria of special access programs in which comparators are funded. Rather, costs reflect an annual course of treatment without discontinuation among patients who fail to achieve a treatment response.
CDA-AMC is unable to address this limitation. The true costs of comparator therapies are likely lower than modelled.
CDA-AMC Reanalyses of the BIA
CDA-AMC revised the sponsor’s base case by altering the market share and assuming 100% public coverage. The changes made to derive the CDA-AMC base case are described in Table 11.
Table 11: CDA-AMC Revisions to the Submitted Budget Impact Analysis
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
Changes to derive the CDA-AMC base case | ||
1a. Coverage rate for CDA-AMC jurisdictions (excluding Quebec) | Jurisdiction-specific; ranges from 31% to 100% | 100% across all jurisdictions |
1b. Proportion of patients who receive public funding of garadacimab upon switching from a C1-INH | Jurisdiction-specific; ranges from 31% to 100% | 100% |
2a. Reference scenario market share | Refer to Table 10 | (reported as baseline/ Year 1/ Year 2/ Year 3) Lanadelumab: 28%/ 32%/ 36%/ 40% C1-INH (SC): 21%/ 19%/ 17%/ 15% C1-INH (IV): 21%/ 19%/ 17%/ 15% |
2b. New drug scenario market share | Refer to Table 10 | (reported as baseline/ Year 1/ Year 2/ Year 3) Garadacimab: 0%/ █████%/ 25%/ 27% Berotralstat: 0%/ 5%/ 10%/ 15% Lanadelumab 28%/ 25.77%/ 25.77%/ 28.80% C1-INH (SC): 21%/ 16%/ 13%/ 10% C1-INH (IV): 21%/ 16%/ 13%/ 10% |
3. Attack rate | Sponsor-submitted NMA | 0% |
CDA-AMC base case | 1a + 1b + 2a + 2b + 3 | |
CDA-AMC = Canada’s Drug Agency; LY = life-year; NMA = network meta-analysis; SC = subcutaneous.
The results of the CDA-AMC step-wise reanalysis are presented in Table 12 and a more detailed breakdown is presented in Table 13. In the CDA-AMC base case, garadacimab is expected to save $25,578,097 over a 3-year time horizon (year 1: –$5,411,578; year 2: –$8,494,679; year 3: –$11,671,840) should garadacimab be reimbursed as per its proposed Health Canada’s indication for the routine prevention of episodes of HAE in adult and pediatric patients (aged 12 years and older).
Table 12: Summary of the CDA-AMC Reanalyses of the Budget Impact Analysis
Stepped analysis | Three-year total ($) |
|---|---|
Submitted base case | −44,834,797 |
CDA-AMC reanalysis 1a | −40,979,640 |
CDA-AMC reanalysis 1b | −37,221,936 |
CDA-AMC reanalysis 2a | −2,938,402 |
CDA-AMC reanalysis 2b | −70,572,248 |
CDA-AMC reanalysis 3 | −39,409,003 |
CDA-AMC base case | −25,578,097 |
CDA-AMC = Canada’s Drug Agency.
Note: (−) denotes a budget savings (e.g., reimbursement of garadacimab is expected to result in savings to the drug plan budgets).
Stratified analyses by drug plan demonstrate that cost savings were due to budgets increasing for public drug plans (3-year budget impact: $34,067,867) with cost-savings offset for CBS (3-year budget impact: –$59,645,964) given the displacement of C1-INH by garadacimab. CDA-AMC conducted scenario analyses that assumed 50% of patients on lanadelumab would switch from an every 2 weeks dosing schedule to every 4 weeks dosing and a smaller budget savings was observed (Table 13). Another scenario was to return to the sponsor’s original jurisdiction-specific public coverage rate. In this scenario, the budget savings were greater. This is partly explained by the fact that, among patients switching from C1-INH to garadacimab, only a proportion of these patients would have garadacimab covered publicly, as per the jurisdiction-specific public coverage rate.
Table 13: Detailed Breakdown of the CDA-AMC Reanalyses of the BIA
Stepped analysis | Scenario | Year 0 (current situation) ($) | Year 1 ($) | Year 2 ($) | Year 3 ($) | Three-year total ($) |
|---|---|---|---|---|---|---|
Submitted base case | Reference | 157,554,711 | 155,775,997 | 154,918,888 | 154,742,922 | 622,992,517 |
New drug | 157,554,711 | 147,787,246 | 137,949,225 | 134,866,539 | 578,157,720 | |
Budget impact | 0 | −7,988,751 | −16,969,663 | −19,876,383 | −44,834,797 | |
CDA-AMC base case | Reference | 140,593,357 | 138,660,767 | 136,546,861 | 134,251,966 | 550,052,952 |
New drug | 140,593,357 | 133,249,189 | 128,052,183 | 122,580,126 | 524,474,854 | |
Budget impact | 0 | −5,411,578 | −8,494,679 | −11,671,840 | −25,578,097 | |
CDA-AMC base case: public drug plans perspective | Reference | 39,189,211 | 46,645,345 | 54,299,012 | 62,140,971 | 202,274,539 |
New drug | 39,189,211 | 55,836,053 | 66,343,750 | 74,973,392 | 236,342,406 | |
Budget impact | 0 | 9,190,708 | 12,044,739 | 12,832,420 | 34,067,867 | |
CDA-AMC base case: CBS perspective | Reference | 101,404,146 | 92,015,422 | 82,247,850 | 72,110,995 | 347,778,413 |
New drug | 101,404,146 | 77,413,136 | 61,708,432 | 47,606,734 | 288,132,448 | |
Budget impact | 0 | −14,602,286 | −20,539,418 | −24,504,261 | −59,645,964 | |
CDA-AMC scenario analysis 1: 50% of patients on lanadelumab switch from q.2.w. to q.4.w. | Reference | 135,392,042 | 132,620,540 | 129,646,180 | 126,470,341 | 524,129,103 |
New drug | 135,392,042 | 128,384,918 | 123,112,445 | 116,977,355 | 503,866,761 | |
Budget impact | 0 | −4,235,621 | −6,533,735 | −9,492,985 | −20,262,342 | |
CDA-AMC scenario analysis 2: 92% of patients eligible for public coverage | Reference | 136,352,503 | 134,052,635 | 131,564,198 | 128,887,412 | 530,856,747 |
New drug | 136,352,503 | 128,118,858 | 122,451,670 | 116,500,193 | 503,423,224 | |
Budget impact | 0 | −5,933,776 | −9,112,527 | −12,387,219 | −27,433,523 |
BIA = budget impact analysis; CDA-AMC = Canada’s Drug Agency; LTP = long-term prophylaxis; q.2.w. = every 2 weeks; q.4.w. = every 4 weeks.
Note: (−) denotes a budget savings (e.g., reimbursement of garadacimab is expected to result in savings to the drug plan budgets).
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.