Drugs, Health Technologies, Health Systems
Reimbursement Review
Clascoterone (Winlevi)
Sponsor: Sun Pharma Canada Inc.
Therapeutic area: Acne vulgaris
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Clinical Review
Abbreviations
AE
adverse event
ANCOVA
analysis of covariance
ARSC
Acne and Rosacea Society of Canada
BMI
body mass index
BOCF
baseline observation carried forward
CDA-AMC
Canada’s Drug Agency
CrI
credible interval
CSPA
Canadian Skin Patient Alliance
DAO
Dermatology Association of Ontario
DIC
deviance information criterion
GRADE
Grading of Recommendations Assessment, Development and Evaluation
HRQoL
health-related quality of life
IGA
Investigator’s Global Assessment
ILC
inflammatory lesion count
ITT
intention to treat
LOCF
last observation carried forward
LSR
local skin reaction
LTE
long-term extension
LTF
long-term follow-up
MAR
missing at random
MI
multiple imputation
NILC
noninflammatory lesion count
NMA
network meta-analysis
OR
odds ratio
PCDSC
Primary Care Dermatology Society of Canada
PP
per protocol
RCT
randomized controlled trial
RE
random effects
RR
risk ratio
SAE
serious adverse event
SD
standard deviation
TEAE
treatment-emergent adverse event
TLC
total lesion count
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Table 1: Background Information on Application Submitted for Review
Item | Description |
|---|---|
Drug product | Clascoterone (Winlevi), 1% cream for topical treatment |
Sponsor | Sun Pharma Canada Inc. |
Indication | For the topical treatment of acne vulgaris in patients 12 years of age and older |
Reimbursement request | For first-line prescription topical treatment of moderate and severe acne vulgaris in patients aged 12 years and older |
Health Canada approval status | Approved |
Health Canada review pathway | Standard |
NOC date | June 15, 2023 |
Recommended dosage | Up to 1 g twice per day |
NOC = Notice of Compliance.
Introduction
Acne is a chronic inflammatory skin condition of the pilosebaceous glands that typically begins during puberty and may continue through adulthood with flares often coinciding with increasing serum androgens.1 Lesions occur primarily on the face, neck, upper back, and chest. When assessing the severity of acne, considerations include the distribution (back, chest, and upper arms), the type and number of lesions (comedones, papules, pustules, and nodules), and the presence or absence of scarring.2,3 Acne is diagnosed by physicians in the community by visual assessment and no specific procedures are required. Acne is 1 of the most common dermatological disorders worldwide, affecting 5.6 million people living in Canada.4 Although it predominantly affects the adolescent population (approximately 80%), it can also affect preadolescents (aged 7 years to 12 years) and postadolescents.4-6 Adolescent acne usually begins with the onset of puberty, with the increase in androgen hormone production, which affects acne development and severity. During adolescence, acne vulgaris is more common in males than in females.7 In adulthood, acne vulgaris is more common in females than in males.7-9
Treatment for acne depends on the severity and type of acne, the age and treatment preferences of the patient, and adherence and response to previous therapy. Mild acne is typically treated with topical medications, particularly antimicrobials such as benzoyl peroxide, antibiotics, and topical retinoids such as tretinoin, adapalene, and tazarotene.10,11 The main side effects of topical medications are local irritation and erythema. Most topical preparations require at least 6 weeks to 8 weeks before an improvement is experienced, with the exception of antimicrobials — they are fast-acting and a response can be expected in as soon as 5 days.11,12 For topical retinoids, the optimal response is expected after 12 weeks.13 Moderate acne is treated with the same topical treatments with the addition of an oral antibiotic or an oral antiandrogen, such as a combined oral contraceptive or spironolactone. According to the updated 2024 American Academy of Dermatology guidelines for managing acne, clascoterone is conditionally recommended for acne treatment (with a conditional recommendation based on the current high cost of the drug) and is not restricted to first-line use or to moderate and severe acne.14 Systemic therapy, including oral antibiotic treatment, hormonal therapies, and isotretinoin, are the mainstay systemic therapies for acne when topical therapy is insufficient or not tolerated. However, a major concern for antibiotics is the development of resistance, given that 60% of Cutibacterium acnes isolates are resistant to at least 1 antibiotic.15 Hormonal drugs (e.g., estrogen-containing oral contraceptives, spironolactone) provide effective second-line treatment in females with acne, regardless of the presence or absence of hormonal abnormalities.15 However, possible side effects of spironolactone include hyperkalemia, menstrual irregularities, and the feminization of a male fetus. For severe acne (e.g., nodular and/or inflammatory acne, acne conglobata, recalcitrant acne that is treatment-resistant), the treatment of choice according to the clinical expert consulted for this review and Canadian practice guidelines is oral isotretinoin.10 As oral isotretinoin is indicated in specific forms of very severe acne, it is outside the treatment paradigm for the population included in the reimbursement request. For patients unwilling or unable to use oral isotretinoin and those with intolerance, systemic antibiotics in combination with topical benzoyl peroxide, with or without a topical retinoid, may be considered. For females, hormonal therapy with a combined oral contraceptive may also be considered.10 For males, current hormone therapies are not suitable. According to the clinical expert, nondrug treatments include diet — in particular, a low glycemic index diet and a diet that minimizes dairy products — as well as laser therapy. Treatment goals include clearing acne and preventing acne sequelae such as postinflammatory hyperpigmentation and scarring. The main therapies currently used for acne vulgaris are aimed at reducing severity and recurrences of skin lesions as well as improving appearance. According to the clinical expert, with the exception of oral isotretinoin, most treatments for acne control symptoms but they are not curative. Hence, patients must continue treatment to maintain benefit.
Clascoterone is indicated for the topical treatment of acne vulgaris in patients aged 12 years and older.16 Clascoterone 10 mg/g is supplied in a 30 g tube.16,17 The recommended dose per application is up to 1 g or to 2 fingertip units applied in a thin layer twice daily over the affected area. Patients should not spot-treat for optimal efficacy.16 Clascoterone is an androgen receptor inhibitor. Androgen receptor inhibitors may reduce sebaceous gland activity. The mechanism of action of clascoterone cream for the topical treatment of acne vulgaris is unknown.16
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of clascoterone, 1% topical cream, in the treatment of moderate to severe acne vulgaris in patients aged 12 years and older. While the Health Canada indication and reimbursement request is for the treatment of patients aged 12 years and older, the data reported in the Clinical Review Report are consistent with those in the pivotal trials, which included patients aged 9 years and older.
Perspectives of Patients, Clinicians, and Drug Programs
The information in this section is a summary of input provided by the patient and clinician groups that responded to the call for input and from the clinical expert consulted for the purpose of this review.
Patient Input
Two national, not-for-profit organizations, the Acne and Rosacea Society of Canada (ARSC) and the Canadian Skin Patient Alliance (CSPA), jointly conducted a survey in June 2022 with 154 patients living in Canada diagnosed with acne. The ARSC comprises dermatologists, patients, educators, and communicators providing information and raising awareness about the disease. The CSPA strives to improve the lives of people affected by skin, hair, and nail conditions through collaboration, advocacy, and education.
Patient groups emphasized that acne not only affects appearance but also impacts patients’ lives and mental health. Many patients reported having diminished self-image, self-esteem, self-confidence, and assertiveness. This emotional distress caused by unhappiness with appearance can lead to bad moods, anxiety (including in social situations), anger, loneliness, self-consciousness, shame, depression, and pain, generally making patients feel in poor health overall. Furthermore, patient groups said these factors impede their ability to be social and conduct daily activities (e.g., forming friendships and dating, having social interactions, being viewed on camera, swimming, changing in changerooms where patients’ acne on their body is exposed). Financial burden was cited as another challenge and some respondents reported paying out-of-pocket costs for prescription, over-the-counter, and self-care products, such as cleansers and makeup, which increase with acne severity (4% of patients with mild acne, 5% of patients with moderate acne, and 14% of the overall respondents were spending $100 or more per month). More than half of the patients had facials and peels (53% of patients, with 12% of them paying more than $500 for each session) and light or laser therapy (65% of patients, with 15% of them paying more than $500 for each session); these costs exacerbate financial burden on patients. As such, patients prioritize treatments that help them enjoy personal relationships and cause less scarring or changes in skin pigment. Other goals include clearer skin, better mental health, increased confidence, the ability to be social, and an improved overall quality of daily life.
To improve their lives, respondents want increased access to new treatment that is safe and effective, health care providers to be aware of all the new and existing treatment options for acne, and evaluation for depression and anxiety that could lead them to getting support.
Three individuals who had experience with clascoterone felt that their acne was well controlled with the drug (also resulting in greater confidence) and they did not experience the typical side effects associated with topicals for acne. However, it was noted that the medication was very expensive compared to other treatment options, with patients paying out of pocket or accessing treatment through insurance.
Clinician Input
Input From the Clinical Expert Consulted by CDA-AMC
According to the clinical expert, a major limitation of current acne therapy is that the most efficacious topical treatments, such as topical retinoids and benzoyl peroxide, tend to be irritative and exhibit a slow onset of effect, which may contribute to the issue of poor adherence to treatment. The clinical expert noted that as the majority of treatments are not curative, their continuation becomes imperative to sustain benefits. Moreover, acne severity exhibits variability over time, requiring potential modifications to the treatment regimen as time progresses.
According to the clinical expert, topical clascoterone will likely be used as a first-line topical for mild and moderate acne if it is effective and accessible. Clascoterone has a novel mechanism in that it is the first topical androgen receptor blocker and the first androgen blocker that can be used in males with acne. The clinical expert anticipated that clascoterone may be used alone or in combination with other topicals for mild acne and in combination with oral antibiotics for moderate acne. The clinical expert did not feel that clascoterone could be used as a first-line treatment for severe acne; however, it could be considered in combination with systemic treatment if a patient requested alternatives to first-line treatment for severe acne (i.e., isotretinoin).
According to the clinical expert, topical clascoterone is appropriate for use by any patient with mild to moderate acne. It is least suited for use in patients with severe or treatment-resistant moderate acne because oral retinoids are better suited for this patient population. However, the clinical expert noted that clascoterone 1% cream could be used in combination with other treatments if a patient requested alternatives to first-line treatment for severe acne. The clinical expert noted that clascoterone could potentially be used in combination with oral contraceptives or spironolactone in female patients to discover if there would be added benefit. It should not be used in patients who are pregnant, nursing, or contemplating pregnancy.
The clinical expert noted that treatment success should be determined at 3 months, apart from treatment with an oral contraceptive and spironolactone, which would require 4 months to 6 months to improve acne. Of note, some physicians elect to reevaluate their patients on treatment with isotretinoin monthly. The clinical expert noted that a physician will examine acne lesions and record acne as clear, minimal or almost clear, moderate, or severe; comment on acne sequalae, including pigmentation and scarring; and note how patients think they are doing with their treatment upon evaluation. The goal of treatment is minimal acne (1 to 2 lesions on examination) or no acne. Given that patients’ expectations can be variable, patient satisfaction is also an important factor in assessing treatment success. The clinical expert noted that both family physicians and dermatologists may prescribe clascoterone. According to the clinical expert, patients would discontinue treatment if there was a lack of response or a worsening of disease, adverse effects, or patient dissatisfaction with treatment. The clinical expert also noted that they would discontinue treatment in patients who are attempting to conceive or are pregnant or nursing.
Clinician Group Input
Two clinician groups submitted input: the Dermatology Association of Ontario (DAO), represented by 10 clinicians, and the Primary Care Dermatology Society of Canada (PCDSC), represented by 5 physicians who make up its board of directors. The clinician groups and clinical expert consulted by CDA-AMC agreed that clascoterone provides a novel mechanism of action as the first topical androgen blocker that can also be used in males with acne. Both clinician groups and the clinical expert consulted by CDA-AMC agreed that minimal or no acne (clear to almost clear skin) is a goal of acne treatment. PCDSC noted that patients using clascoterone should be advised that treatment effect may not be observed for several months. The clinician groups indicated that severe acne should be treated with isotretinoin, which is consistent with the feedback received from the clinical expert consulted by CDA-AMC. However, the clinician groups stated that clascoterone may be used as an adjunctive treatment to isotretinoin or in place of isotretinoin in the case of serious intolerance or contraindication, which differs from the input received from the clinical expert consulted by CDA-AMC, who stated that clascoterone would not be used for severe or treatment-resistant moderate acne. The clinical expert also mentioned that the benefit of adding clascoterone to oral contraceptives or off-label spironolactone is uncertain. A clinically meaningful response to treatment, according to DAO, would be a 30% reduction in lesion counts and a 2-point (or even 1-point) reduction in Investigator’s Global Assessment (IGA) scores. Additionally, DAO suggested that transmasculine patients, gender minority patients, mature patients with acne (aged 29 years to 40 years), or those with sensitive, eczema-prone skin may benefit from clascoterone. Overall, the input provided by the clinician groups and the clinical expert was consistent with regard to the unmet needs, treatment goals, patient population, assessment of response, and discontinuation of treatment.
Drug Program Input
Input was obtained from the drug programs that participate in the CDA-AMC reimbursement review process. The following were identified as key factors that could potentially impact the implementation of a CDA-AMC recommendation for clascoterone:
relevant comparators
consideration for the initiation of therapy
consideration for the prescribing of therapy
generalizability
care provision issues.
The clinical expert consulted by CDA-AMC provided advice on the potential implementation issues raised by the drug programs. Refer to Table 4.
Clinical Evidence
Systematic Review
Description of Studies
Two identically designed, randomized, double-blind, vehicle-controlled, parallel-group trials (the CB-03-01/25 study [N = 708] and the CB-03-01/26 study [N = 732]) assessed the safety and efficacy of clascoterone 1% cream versus the vehicle cream (without active drug) applied twice daily for 12 weeks in patients with facial acne vulgaris.
The CB-03-01/25 study was conducted primarily in the US and the CB-03-01/26 study was conducted primarily in Europe. Neither trial had any study sites in Canada. In the CB-03-01/25 study, 708 patients were randomized to treatment with either clascoterone 1% cream (N = 353) or vehicle cream (N = 355). In the CB-03-01/26 study, 732 patients were randomized to treatment with either clascoterone 1% cream (N = 369) or vehicle cream (N = 363). In the CB-03-01/25 trial, the median age for both treatment groups was 18 years (range, 9 years to 58 years) and in the CB-03-01/26 trial, the median age for both treatment groups was 18 years (range, 10 years to 50 years). Block randomization was used for both studies. Patients were enrolled from January 21, 2016, to April 11, 2018, for the CB-03-01/25 trial and from November 16, 2015, to February 21, 2018, in the CB-03-01/26 trial.
Both studies are now complete. They consisted of the following study periods:
screening phase — visit 1
treatment phase — 12 weeks (consisting of 3 study visits at week 4, week 8, and week 12)
follow-up phase — patients in both studies had the option to continue for up to 12 months in the long-term extension (LTE) study (the CB-03-01/27 trial).
Patients eligible for inclusion were required to have acne vulgaris of the face (which can include the nose) with an IGA score of 3 or 4, at least 30 inflammatory lesions to a maximum of 75 inflammatory lesions (papules, pustules, and nodules), and at least 30 noninflammatory lesions to a maximum of 100 noninflammatory lesions (open and closed comedones). Patients were excluded from the trials if they had nodulocystic acne, if they were pregnant, lactating, or planning to become pregnant during the study, if they were planning to be or needed to be exposed to artificial tanning devices or excessive sunlight during the trial, or if they had been using any topical antiacne preparations within 2 weeks to 6 weeks of treatment initiation or the systemic antiacne medications of corticosteroids, antibiotics, spironolactone, or retinoids within 1 week to 6 months of treatment initiation.
The demographic characteristics were similar between the treatment groups. With respect to acne severity, the majority of patients in the CB-03-01/25 study had an IGA rating of moderate (82.7% of patients in the clascoterone group and 82.0% of patients in the vehicle group) with the remainder of patients being rated severe. The mean inflammatory lesion count (ILC) was 42.4 lesions for the clascoterone group and 42.9 lesions for the vehicle group (range, 30 lesions to 83 lesions), the mean noninflammatory lesion count (NILC) was 59.1 lesions for the clascoterone group and 60.7 lesions for the vehicle group (range, 30 lesions to 144 lesions), and the mean total lesion count (TLC) was 101.5 lesions for the clascoterone group and 103.6 lesions for the vehicle group (range, 60 lesions to 196 lesions). In the CB-03-01/26 study, the majority of patients had an IGA rating of moderate (82.7% of patients in the clascoterone group and 86.2% of patients in the vehicle group) with the remainder of patients being rated severe. The mean ILC was 42.9 lesions for the clascoterone group and 41.3 lesions for the vehicle group (range, 30 lesions to 75 lesions), the mean NILC was 62.8 lesions and 63.3 lesions for the clascoterone group and vehicle group, respectively (range, 30 lesions to 177 lesions), and the mean TLC was 62.8 lesions and 63.3 lesions in the clascoterone group and vehicle group, respectively (range, 60 lesions to 241 lesions).
Efficacy Results
Global Success
Proportion of Patients Aged 12 Years or Older Achieving Improvement at Week 12
Improvement was defined as an IGA score of clear (0) or almost clear (1) and a 2-point or greater reduction in the IGA scale compared with baseline.
In the CB-03-01/25 study, the adjusted proportion of patients aged 12 years and older achieving improvement at week 12 was 18.8% in the clascoterone group versus 8.9% in the vehicle group (odds ratio [OR] = 2.36; 95% confidence interval [CI], 1.4 to 3.9; P = 0.0008). Similarly, in the CB-03-01/26 study, the adjusted proportion of patients aged 12 years and older achieving improvement at week 12 was 20.8% in the clascoterone group versus 6.5% in the vehicle group (OR = 3.8; 95% CI, 2.2 to 6.4; P < 0.0001). At week 12, the results of the pooled analysis were consistent across both studies.
Sensitivity analyses results in the intention-to-treat (ITT) population were consistent with the primary efficacy results in both trials, with the exception of the worst-case analysis. Results of the last observation carried forward (LOCF) and baseline observation carried forward (BOCF) analyses confirmed the robustness of the results obtained on the ITT set for the primary efficacy end points.
Lesion Counts
Absolute Change From Baseline in NILC at Week 12
In the CB-03-01/25 study, a greater absolute decrease from baseline in NILC was noted in patients treated with clascoterone (–19.4 lesions) compared to patients treated with vehicle cream (–13.1 lesions) at week 12 (difference between treatment groups = –6.3 lesions; 95% CI, –10.2 lesions to –2.4 lesions; P = 0.0016). Similarly, in the CB-03-01/26 study, the absolute change in NILC from baseline to week 12 was –19.4 lesions in the clascoterone group versus –10.9 lesions in the vehicle group (difference between treatment groups = −8.4 lesions; 95% CI, −12.4 lesions to −4.5 lesions; P < 0.0001).
The sensitivity analyses results in the ITT population were consistent with the primary efficacy results in both pivotal trials. However, the results of the worst-value and worst-case analyses were inconsistent with the results obtained on the ITT set for this outcome. Results of the LOCF and BOCF analyses confirmed the robustness of the results obtained on the ITT set for the primary efficacy end points.
Percentage Change in NILC From Baseline at Week 12
In the CB-03-01/25 study, the percentage change from baseline to week 12 was greater in the clascoterone group than the vehicle group for NILC at −30.7% versus −21.6%, respectively (treatment group difference = −8.8%; 95% CI, −15.9% to −1.8%; P = 0.0141). In the CB-03-01/26 study, the percentage change from baseline to week 12 was greater in the clascoterone group than the vehicle group for NILC at −29.3% versus −15.8%, respectively (treatment group difference = −13.5%; 95% CI, −19.8% to −7.1%; P < 0.0001).
Absolute Change From Baseline in ILC at Week 12
In the CB-03-01/25 study, the absolute change in ILC from baseline at week 12 was −19.4 lesions in the clascoterone group versus −15.5 lesions in the vehicle group (treatment group difference = −3.9 lesions; 95% CI, −6.5 lesions to −1.3 lesions; P = 0.0029). Similarly, in the CB-03-01/26 study, at week 12, the absolute change from baseline in ILC at week 12 was also −20.0 lesions in the clascoterone group versus −12.6 lesions in the vehicle group (treatment group difference = −7.4 lesions; 95% CI, −9.8 lesions to −5.0 lesions; P < 0.0001).
The sensitivity analyses results in the ITT population were consistent with the primary efficacy results in both pivotal trials. However, the results of the worst-value and worst-case analyses were inconsistent with the results obtained on the ITT set for this outcome in the CB-03-01/25 trial and the results of the worst-case analysis were inconsistent with results obtained on the ITT set for this outcome in the CB-03-01/26 trial.
Percentage Change in ILC From Baseline at Week 12
In the CB-03-01/25 study, the percentage change from baseline to week 12 was greater in the clascoterone group than the vehicle group for ILC at −44.8% versus −36.6%, respectively (treatment group difference = −8.3%; 95% CI, −14.3% to −2.3%; P = 0.0070). In the CB-03-01/26 study, the percentage change from baseline to week 12 was greater in the clascoterone group than the vehicle group for ILC at −47.0% versus −29.8%, respectively (treatment group difference = −17.2%; 95% CI, −22.9% to −11.5%; P < 0.0001).
Absolute Change From Baseline in TLC at Week 12
In the CB-03-01/25 study, the absolute change from baseline to week 12 was greater in the clascoterone group than the vehicle group for TLC at −39.2 lesions versus −28.9 lesions, respectively (treatment group difference = −10.3 lesions; 95% CI, −15.7 lesions to −5.0 lesions; P = 0.0002). In the CB-03-01/26 study, the absolute change from baseline to week 12 was greater in the clascoterone group than the vehicle group for TLC at −40.3 lesions versus −23.7 lesions, respectively (treatment group difference = −16.6 lesions; 95% CI, −22.0 lesions to −11.1 lesions; P < 0.0001).
Percentage Change in TLC From Baseline at Week 12
In the CB-03-01/25 study, the percentage change from baseline to week 12 was greater in the clascoterone group than the vehicle group for TLC at −37.1% versus 28.5%, respectively (treatment group difference = −8.7%; 95% CI, −14.0% to −3.3%; P = 0.0016). In the CB-03-01/26 study, the percentage change from baseline to week 12 was greater in the clascoterone group than the vehicle group for TLC at −37.7% versus −22.2%, respectively (treatment group difference = −15.6%; 95% CI, −20.9% to −10.3%, P < 0.0001).
Mental Health and Health-Related Quality of Life
Mental health and health-related quality of life (HRQoL) were not assessed in the CB-03-01/25 or CB-03-01/26 trial.
Harms Results
Treatment-Emergent Adverse Events
The safety profile of clascoterone was similar between the treatment groups for both pivotal trials. In the CB-03-01/25 and CB-03-01/26 studies, respectively, 40 (11.3%) patients and 42 (11.4%) patients who received clascoterone experienced treatment-emergent adverse events (TEAEs) compared to 41 (11.5%) patients and 50 (13.8%) patients who received the vehicle cream.
Serious Adverse Events
Overall, 1 patient each in the CB-03-01/25 trial and the CB-03-01/26 trial reported a serious adverse event (SAE). In the CB-03-01/25 study, 1 (0.3%) patient in the vehicle group had an SAE of pneumonia. In the CB-03-01/26 study, 1 (0.3%) patient in the vehicle group had an SAE of hematoma.
Withdrawals Due to Adverse Events
In the CB-03-01/25 study, there were 9 patients who experienced 9 TEAEs that led to study discontinuation: 3 (0.8%) patients in the clascoterone group and 6 (1.7%) patients in the vehicle group. In the CB-03-01/26 study, 10 (1.4%) patients discontinued due to adverse events (AEs), including 2 (0.5%) patients treated with clascoterone and 8 (2.2%) patients treated with vehicle cream.
Mortality
No deaths were reported in the CB-03-01/25 and CB-03-01/26 studies.
Notable Harms
In the CB-03-01/25 and CB-03-01/26 studies, the incidence of local skin reactions (LSRs) (i.e., telangiectasia, skin atrophy, striae rubrae, erythema, edema, scaling or dryness, stinging or burning, and pruritus) was similar across treatment groups. In the CB-03-01/25 trial, 52.6% of patients in the clascoterone group and 54.0% of patients in the vehicle group experienced LSRs. In the CB-03-01/26 trial, 55.3% of patients in the clascoterone group and 53.3% of patients in the vehicle group experienced LSRs. The most notable treatment-emergent LSRs in terms of frequency were erythema in both pivotal trials.
Critical Appraisal
There was no notable difference between treatment groups or baseline characteristics in either pivotal trial. Discontinuation was largely driven by patients who were lost to follow-up and who chose to withdraw. Missing data in the primary end points were imputed using a multiple imputation (MI) approach under the missing at random (MAR) assumption. The missing at worst-value analyses were not consistent with the primary analysis for absolute change in ILC and NILC. The amount of missing data was considered relatively high in both the clascoterone group and the vehicle group in both trials at week 12 (18% to 22%). The majority of patients who discontinued dropped out at the beginning of the study period (e.g., before visit 2) across both trials, and because patient dropout was likely driven by a lack of response, the MI approach to account for missing data in the primary analysis may not be sufficient to address this missing data mechanism. Therefore, there was potential for bias due to the amount of missing data in the efficacy results at week 12 and based on results from the sensitivity analysis, the true effect of clascoterone on NILC and ILC may have been overestimated in the primary analysis. Some secondary end points were not adjusted for multiple comparisons; hence, no definitive conclusions can be drawn due to the failure of statistical comparison in a prior end point in the testing hierarchy.
Clascoterone is indicated for patients aged 12 years and older, though the data reported in the Clinical Review Report are for patients aged 9 years and older. When comparing the 2 datasets (from the product monograph16 and the Clinical Study Reports for the pivotal trials18,19), there were no changes to statistical significance that would meaningfully change conclusions on efficacy or harms. Moreover, the clinical expert consulted for this review highlighted that the number of patients aged 9 years to 11 years who were included in the trials was small and likely had a negligible effect on the study results. Clascoterone is indicated for patients with acne vulgaris and is not limited by severity of the condition. The pivotal trials for clascoterone included patients with moderate to severe acne vulgaris; however, the clinical expert felt that the results would still be generalizable to patients with mild acne. The clinical expert indicated that a treatment that is effective for moderate to severe acne would also be expected to show efficacy in patients with mild acne as well. Moreover, a notable group of patients with severe acne vulgaris (i.e., nodulocystic acne) was excluded from both trials. Hence, the sample population in the trials may not fully represent the general population of patients with severe acne vulgaris as noted in clinical practice in Canada. The clinical expert felt that 12 weeks of follow-up was a reasonable and standard time point across acne trials and would be considered the earliest time point at which a meaningful change in lesion numbers would be observed. However, the clinical expert noted that the optimal time point for follow-up for the end point of change in NILC would be 6 months. In addition, the clinical expert did note that lesion counts are not relevant to clinical practice as lesion counts are subjective, and it is not feasible for clinicians to be counting lesions. Instead, the clinical expert felt that the patient’s impression of change and the percentage change in lesion count was considered more clinically relevant.
GRADE Summary of Findings and Certainty of the Evidence
For the pivotal studies and randomized controlled trials (RCTs) identified in the sponsor’s systematic review, Grading of Recommendations Assessment, Development and Evaluation (GRADE) was used to assess the certainty of the evidence for outcomes considered most relevant to inform deliberations of the CDA-AMC expert committee, and a final certainty rating was determined as outlined by the GRADE Working Group.20,21
Following the GRADE approach, evidence from RCTs started as high-certainty evidence and could be rated down for concerns related to study limitations (which refers to internal validity or risk of bias), inconsistency across studies, indirectness, the imprecision of effects, and publication bias.
When possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect; if this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., the clinical importance is unclear). In all cases, the target of the certainty of evidence assessment was based on the point estimate and where it was located relative to the threshold for a clinically important effect (when a threshold was available) or to the null.
The reference points for the certainty of evidence assessment for efficacy end points and notable harms (i.e., LSRs) was set according to the presence or absence of an important effect based on thresholds informed by the clinical expert.
For the GRADE assessments, findings from the CB-03-01/25 and CB-03-01/26 studies were considered together and summarized narratively per outcome because these studies were identical in population, interventions, design, and outcome measures.
The selection of outcomes for GRADE assessment was based on the sponsor’s summary of clinical evidence, consultation with the clinical expert, and input received from patient and clinician groups and public drug plans. The following list of outcomes was finalized in consultation with expert committee members:
global success as measured by the proportion of patients aged 12 years or older achieving improvement, defined as an IGA score of clear (0) or almost clear (1) and a 2-point or greater reduction in the IGA scale compared with baseline
lesion counts (absolute change from baseline in NILC, ILC, and TLC; percentage change from baseline in NILC, ILC, and TLC)
mental health and HRQoL (change from baseline in mental health according to the Dermatology Life Quality Index and Cardiff Acne Disability Index)
notable harms — LSRs, fertility issues, hypothalamic-pituitary-adrenal axis suppression.
Results of GRADE Assessments
Table 2 presents the GRADE summary of findings for clascoterone 1% cream versus vehicle cream.
Table 2: Summary of Findings for Clascoterone Versus Vehicle Cream for Patients With Acne Vulgaris
Outcome and follow-up | Patients (studies), N | Relative effect (95% CI) | Absolute effects (95% CI) | Certainty | What happens |
|---|---|---|---|---|---|
Global success | |||||
Proportion of patients with treatment improvement as defined by an IGA score of clear (0) or almost clear (1) and a reduction of 2 points or greater in the IGA scale compared with baseline Follow-up: 12 weeks | N = 1,440 (2 RCTs) | CB-03-01/25 study
CB-03-01/26 study
| CB-03-01/25 study
CB-03-01/26 study
| Moderatea | Clascoterone likely results in an increase in the proportion of patients with treatment improvement as measured by the IGA when compared with vehicle cream. |
Lesion count | |||||
Absolute change in NILC Follow-up: 12 weeks | N = 1,440 (2 RCTs) | NR | CB-03-01/25 study
CB-03-01/26 study
| Very lowb | The evidence is very uncertain about the effect of clascoterone on absolute change in NILC when compared with vehicle cream. |
Percentage change in NILC Follow-up: 12 weeks | N = 1,440 (2 RCTs) | NR | CB-03-01/25 study
CB-03-01/26 study
| Very lowb | The evidence is very uncertain about the effect of clascoterone on percentage change in NILC when compared with vehicle cream. |
Absolute change in ILC Follow-up: 12 weeks | N = 1,440 (2 RCTs) | NR | CB-03-01/25 study
CB-03-01/26 study
| Lowd | Clascoterone may result in little to no difference in absolute change in ILC when compared with vehicle cream. |
Percentage change in ILC Follow-up: 12 weeks | N = 1,440 (2 RCTs) | NR | CB-03-01/25 study
CB-03-01/26 study
| Very lowd | The evidence is very uncertain about the effect of clascoterone on percentage change in ILC when compared with vehicle cream. |
Absolute change in TLC Follow-up: 12 weeks | N = 1,440 (2 RCTs) | NR | CB-03-01/25 study
CB-03-01/26 study
| Very lowd | The evidence is very uncertain about the effect of clascoterone on absolute change in TLC when compared with vehicle cream. |
Percentage change in TLC Follow-up: 12 weeks | N = 1,440 (2 RCTs) | NR | CB-03-01/25 study
CB-03-01/26 study
| Very lowd | The evidence is very uncertain about the effect of clascoterone on percentage change in TLC when compared with vehicle cream. |
Mental health (HRQoL) | |||||
Mental health (e.g., DLQI) | NA | No data available | No data available | NA | There is no evidence for the effect of clascoterone on mental health. |
Harms | |||||
Proportion of patients with ≥ 1 LSR | N = 1,421 (2 RCTs) | NA | CB-03-01/25 study A total of 52.6% of patients in the clascoterone arm and 54.0% of patients in the vehicle arm experienced an LSR. Difference: 1.4% in favour of clascoterone (−8.8% to 6.1%) CB-03-01/26 study A total of 55.3% of patients in the clascoterone group and 53.3% of patients in the vehicle group experienced an LSR. Difference: 2.0% in favour of vehicle cream (−5.2% to 9.2%) | Moderatee | Clascoterone likely results in little to no difference in LSRs when compared with vehicle cream. |
CI = confidence interval; DLQI = Dermatology Life Quality Index; HRQoL = health-related quality of life; IGA = Investigator’s Global Assessment; ILC = inflammatory lesion count; LSR = local skin reaction; MID = minimal important difference; NA = not applicable; NILC = noninflammatory lesion count; NR = not reported; OR = odds ratio; RCT = randomized controlled trial; TLC = total lesion count.
Note: Study limitations (which refer to internal validity or risk of bias), inconsistency across studies, indirectness, the imprecision of effects, and publication bias were considered when assessing the certainty of the evidence. All serious concerns in these domains that led to the rating down of the level of certainty are documented in the table footnotes.
aRated down 1 level for serious indirectness as the treatment assessment scheduled was not reflective of clinical practice, based on clinical expert input noting that meaningful change is unlikely to be observed until at least 6 months — thus limiting generalizability to Canadian clinical practice.
bRated down 1 level for serious study limitations. This was due to high rates of missing data with insufficient accounting for the likely missing data mechanism. Rated down 1 level for serious indirectness as the treatment assessment scheduled was not reflective of clinical practice, based on clinical expert input noting that meaningful change is unlikely to be observed until at least 6 months — thus limiting generalizability to Canadian clinical practice. Rated down 1 level for serious imprecision. The clinical expert identified that the MID threshold (10 lesions) had not been met; the CI for difference between groups included the possibility of no difference.
cStatistical testing for this outcome was not adjusted for multiplicity. The results are considered as supportive evidence.
dRated down 1 level for serious study limitations. This was due to high rates of missing data with insufficient accounting for the likely missing data mechanism. Rated down 1 level for serious indirectness as the treatment assessment scheduled was not reflective of clinical practice, based on clinical expert input noting that meaningful change is unlikely to be observed until at least 6 months — thus limiting generalizability to Canadian clinical practice. The outcome of percentage change in ILC and NILC was rated down 1 level for serious inconsistency. The 95% CI for the difference included the threshold for clinical meaningfulness (a reduction of lesions by 10%), which was compatible with both a benefit and little to no difference.
eRated down 1 level for serious study limitations. This was due to high rates of missing data with insufficient accounting for the likely missing data mechanism. It was rated down 1 level for serious indirectness. This was due to limitations in generalizability to Canadian clinical practice.
Sources: Clinical Study Report for the CB-03-01/25 trial,18 Clinical Study Report for the CB-03-01/26 trial,19 additional information request dated August 28, 2023.22 Details included in the table are from the sponsor’s summary of clinical evidence.23
LTE Studies
Description of Studies
The CB-03-01/27 study was a multicentre, open-label, LTE study following the CB-03-01/25 and CB-03-01/26 parent studies. The primary objective was to determine the long-term safety of clascoterone cream, applied twice daily (morning and evening) for an additional 9 months in patients with acne vulgaris who participated in the phase III studies for a total treatment time of up to 12 months. For patients assigned to placebo in the parent trials, the total duration of treatment was 9 months. The end points for the primary objective were systemic and local TEAEs, including LSRs (telangiectasia, skin atrophy, striae rubrae, erythema, edema, scaling or dryness, stinging or burning, and pruritus). The number of patients with each IGA severity score at each time point was the efficacy end point. The study consisted of a baseline visit, long-term follow-up (LTF) visits at month 1, month 3, month 6, and month 9, and follow-up phone calls at month 4.5 and month 7.5.
Efficacy Results
The majority of patients (83.1%) showed facial IGA scores that were mild or moderate in severity at baseline, with the overall proportion of patients whose skin was clear or almost clear increasing over time being greatest (ITT population = 181 of 609 [29.7%] patients) at the end of the study (day 274). The proportion of patients whose skin was clear or almost clear increased over time with clascoterone, from 9.9% at baseline to 29.7% at day 274. A similar proportion of patients originally assigned to the vehicle group (ITT population = 30.2%) and clascoterone group (ITT population = 29.3%) in the pivotal studies had clear or almost clear skin on the face at the end of the study at day 274. A similar trend was observed in patients whose trunks had been treated with clascoterone during the LTE period.
Harms Results
Of 607 patients in the safety set, 110 (18.1%) patients experienced at least 1 TEAE. The only TEAEs reported for at least 1.0% of patients were nasopharyngitis (2.6%) and upper respiratory tract infection (1.3%). Six patients experienced serious TEAEs; they consisted of coronary artery dissection, depression and suicide attempt, dizziness, eosinophilic gastroenteritis, fatigue, and induced abortion. Ten (1.7%) patients discontinued the study drug due to TEAEs and 9 of these patients discontinued the study due to the TEAEs. Overall, the most frequently reported LSRs were erythema (6.9% on the face and 1.2% on the trunk), scaling or dryness (4.0% on the face and 0.7% on the trunk), and pruritus (1.6% on the face and 0% on the trunk). According to the clinical expert consulted by CDA-AMC, atrophy (5% in the clascoterone group versus 1% in the vehicle group) was another noteworthy LSR.
Critical Appraisal
Based on the LTE results and discussion with the clinical expert consulted by CDA-AMC, clascoterone 1% cream appears to be safe when used for up to 1 year of treatment. According to the clinical expert, among AEs that occurred more frequently in the clascoterone cohort compared to the vehicle cohort, skin atrophy (5% in the clascoterone group versus 1% in the vehicle group) seems to be the most noteworthy event. Even though the effectiveness of clascoterone 1% cream seems to be maintained long term, the long-term study was not randomized and no formal statistical testing for efficacy outcomes (which were not primary objectives) was conducted. Furthermore, no true comparator was tested during the LTE period. There may also have been a selection bias as those who benefited from clascoterone treatment during the 12-week pivotal trials were more likely to continue and a high compliance rate (greater than 80%) was an inclusion criterion for the LTE study; this could overestimate the treatment effect. Another concern was a high attrition rate. For example, at 9 months, about 20% of patients remained in the LTE study. It is uncertain how this attrition rate affects the long-term results of safety and/or effectiveness of clascoterone treatment. Lastly, treatment effects on patients’ HRQoL were not assessed, even though the impact of acne vulgaris on HRQoL seems to be significant based on patient group input. As for external validity, because patients were rolled over from the pivotal trials, the same generalizability concerns as those in the main trials applied to the LTE population.
Indirect Comparisons
Description of Studies
CDA-AMC appraised a systematic review and network meta-analysis (NMA) submitted by the sponsor. The reference-case NMAs compared clascoterone with benzoyl peroxide (2.5% cream or 3.1% gel or 5% cream, applied once daily), tretinoin (0.025% cream or 0.04% gel or 0.05% cream, applied once daily), tazarotene (0.045% gel or 0.1% cream, applied once daily), adapalene (0.1% cream or 0.15% gel or 0.3% cream, applied once daily), and trifarotene (0.005% cream, applied once daily). Sensitivity and scenario analyses considered additional comparators (i.e., oral contraceptives, topical or oral spironolactone, clindamycin phosphate 1.2% gel and clindamycin 1% cream, erythromycin 1.5% cream, and combinations) in terms of effects at 12 weeks on inflammatory lesions, noninflammatory lesions, and study discontinuations for any reason. Scenario analyses were also presented as sensitivity analyses that considered additional treatments (combination therapies, spironolactone, and oral contraceptives).
Efficacy Results
Reference-case NMAs for changes in ILCs and NILCs at 12 weeks consisted of 8 treatment nodes,19 RCTs, and 12,226 patients. Findings from Bayesian random-effects (RE) NMAs regarding inflammatory lesions found clascoterone (ILC = –5.2; 95% credible interval [CrI], –7.2 to –3.2) and all other active treatments in the network to be associated with a greater impact on the reduction of inflammatory lesions compared to placebo, while comparisons between active treatments showed no treatment was favoured based on the inspection of 95% CrIs. Interpretations from an RE NMA investigating changes in noninflammatory lesions were similar.
Harms Results
A comparison of study discontinuations for any reason at 12 weeks after randomization was also performed using a Bayesian RE NMA. Clascoterone displayed a similar frequency of discontinuation compared to placebo (risk ratio [RR] = 0.90; 95% CrI, 0.72 to 1.10), as did most active treatments. Comparisons of clascoterone with other active treatments found no important differences with the exception of a reduced frequency of discontinuation when compared to tazarotene 1% (RR = 0.71; 95% CrI, 0.53 to 0.94).
Critical Appraisal
The sponsor’s submitted NMA used recommended methods for the conduct and reporting of NMAs and demonstrated similar benefits relative to other available treatments, though certain limitations were noted. The NMAs appeared to include study populations that ranged broadly from mild to severe based on mean baseline lesion counts. This introduced challenges to the interpretation of findings from the NMA as well as concerns that the validity of treatment effects measuring absolute changes in lesion count could be impacted. The variability of placebo or vehicle group responses across trials was not described in detail and thus the appropriateness of combining these groups for the purposes of the NMA was unclear. Methods to identify effect modifiers of interest to judge the appropriateness of the transitivity assumption were unclear, and the effects of differences between study populations for specific effect modifiers (the duration of acne, the severity of acne, and previous treatments) could not be addressed due to limited reporting from the included trials. Input from the clinical expert suggested that certain additional treatments (oral antibiotics, isotretinoin, topical dapsone, and combination treatments) could have been included in reference-case analyses. Findings from NMAs should thus be interpreted with some degree of caution.
Conclusions
The evidence in this review includes 2 sponsor-submitted, phase III, randomized, double-blind, vehicle-controlled trials, the CB-03-01/25 study (N = 708) and the CB-03-01/26 study (N = 732). The CB-03-01/25 and CB-03-01/26 trials assessed the safety and efficacy of treatment with clascoterone 1% cream compared to vehicle cream in patients with moderate to severe acne vulgaris. The 2 trials demonstrated that 12 weeks of treatment with clascoterone 1% cream applied twice daily likely results in a clinically important improvement in achieving treatment success as defined by an IGA score of 0 or 1 and a 2-point or greater reduction from baseline when compared with vehicle cream. However, the evidence was uncertain with regard to the ability of clascoterone to reduce the number and percentage of lesions (NILC, ILC, and TLC) at week 12. There is no evidence for the effect of clascoterone on mental health and HRQoL, which was identified as a clinically important outcome by the clinical experts and patient groups. Most efficacy outcomes were affected by concerns for imprecision (i.e., CIs included the potential for little to no difference versus placebo). All outcomes were impacted by the risk of bias due to missing data and indirectness due to concerns with generalizability to patients with severe acne vulgaris in clinical practice in Canada.
Because there was no direct evidence comparing clascoterone to other treatments for acne vulgaris, the sponsor provided an NMA that assessed short-term efficacy versus multiple comparators. For comparisons between clascoterone and active treatments, the results of the NMA did not favour either treatment in terms of a reduction in inflammatory lesions. Higher baseline lesion counts in trials of clascoterone may also provide rationale to interpret treatment effects relative to other treatments in terms of changes from baseline with caution.
Regarding safety, clascoterone resulted in little to no clinically important difference in LSRs. Of note, few to no events were observed during follow-up for these notable harms. Based on the harms observed at week 12 and LTF at 12 months, the clinical expert suggested that there were no concerns for the overall safety of clascoterone that would be expected to have an impact on clinical decision-making. In addition, the NMA found no important differences in safety outcomes between clascoterone, placebo, and active comparators.
Introduction
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of clascoterone (Winlevi), 1% topical cream, in the treatment of acne vulgaris in patients aged 12 years and older.
Disease Background
Content in this section has been informed by materials submitted by the sponsor and clinical expert input. The following has been summarized and validated by the CDA-AMC review team.
Acne is a chronic inflammatory skin condition of the pilosebaceous glands that typically begins during puberty and may continue through adulthood, with flares often coinciding with increasing serum androgens.1 Lesions occur primarily on the face, neck, upper back, and chest. When assessing the severity of acne, considerations include the distribution (back, chest, and upper arms), the type and number of lesions (comedones, papules, pustules, and nodules), and the presence or absence of scarring.2,3 Acne is diagnosed by physicians in the community by visual assessment and no procedures are required.
Acne vulgaris is characterized by noninflammatory open or closed comedones (blackheads or whiteheads) and by inflammatory papules, pustules, and nodules. The basic acne lesion is a comedone (clogged hair follicle in the skin), which is considered noninflammatory. A comedone forms when keratin combines with oil to block the follicle. A comedone can be open or closed by skin and can occur with or without acne. It is a microscopic lesion that is the direct result of abnormal keratinization in the follicle of the pilosebaceous unit. When acne lesions become red and/or tender bumps, they are termed papules. These papules can fill with purulent material, forming pustules. Acne lesions that become large red bumps are called nodules.24,25 Lesions are defined in Appendix 1, Table 27.
Acne is 1 of the most common dermatological disorders worldwide. The incidence and severity of acne are influenced by genetics (i.e., hereditary) and environment (i.e., diet, cosmetics, pollutants, heat, and humidity).1,3,26 Endogenous androgens, particularly testosterone and dihydrotestosterone, mediate excess sebum production in the skin and stimulate abnormal keratinization and desquamation, leading to obstruction of the pilosebaceous duct that allows C. acnes to proliferate.3,26,27 Proinflammatory mediators are released in response, triggering localized inflammation and exacerbation of acne lesion eruption.27
Acne affects 5.6 million people living in Canada.4 Although it predominantly affects the adolescent population (approximately 80%), it can also affect preadolescents (aged 7 years to 12 years) and postadolescents.4-6 Starting around puberty and lasting until adulthood, acne can persist for many years, regardless of age. Adolescent acne usually begins with the onset of puberty, with the increase in androgen hormone production, which affects acne development and severity. Approximately 85% of people aged between 12 years and 24 years’ experience at least minor acne. Acne occurring in adults is increasing, and at age 50 years or older, more than 7% of men and 15% of women still have acne.8 During adolescence, acne vulgaris is more common in males than in females,7 while in adulthood, acne vulgaris is more common in females than in males.7-9
Standards of Therapy
Content in this section has been informed by materials submitted by the sponsor and clinical expert input. The following has been summarized and validated by the CDA-AMC review team.
The treatment of acne depends on the severity and type of acne, the age and treatment preferences of the patient, and adherence and response to previous therapy. Mild acne is typically treated with topical medications, particularly antimicrobials such as benzoyl peroxide, antibiotics, and topical retinoids such as tretinoin, adapalene, and tazarotene.10,11 The main side effects of topical medications are local irritation and erythema. Most topical preparations require at least 6 weeks to 8 weeks before an improvement is experienced, with the exception of antimicrobials — they are fast-acting and a response can be experienced in as soon as 5 days.11,12 For topical retinoids, the optimal response is expected after 12 weeks.13 Moderate acne is treated with the same topical treatments with the addition of an oral antibiotic or an oral antiandrogen for females, such as a combined oral contraceptive or spironolactone. According to the updated 2024 American Academy of Dermatology guidelines for managing acne, clascoterone is conditionally recommended for acne treatment (with a conditional recommendation based on the current high cost of the drug) and is not restricted to first-line use or to moderate and severe acne.14 Systemic therapy, including oral antibiotic treatment, hormonal therapies, and isotretinoin, are the main therapies for acne when topical therapy is insufficient or not tolerated. However, a major concern for antibiotics is the development of resistance, given that 60% of C. acnes isolates are resistant to at least 1 antibiotic.15 Hormonal drugs (e.g., estrogen-containing oral contraceptives, spironolactone) provide effective second-line treatment in women with acne regardless of the presence or absence of any underlying hormonal abnormalities.15 However, possible side effects of spironolactone include hyperkalemia, menstrual irregularities, and the feminization of a male fetus. For severe acne (e.g., nodular and/or inflammatory acne, acne conglobata, recalcitrant acne that is treatment-resistant), the treatment of choice according to the clinical expert consulted by CDA-AMC and Canadian practice guidelines is oral isotretinoin.10 Because oral isotretinoin is indicated in specific forms of very severe acne, it is outside the treatment paradigm for the population included in the reimbursement request. For patients unwilling or unable to use oral isotretinoin and those with intolerance, systemic antibiotics in combination with topical benzoyl peroxide, with or without a topical retinoid, may be considered. For females, hormonal therapy with a combined oral contraceptive may also be considered.10 For males, current hormone therapies are not suitable. According to the clinical expert, nondrug treatments include diet — in particular, a low glycemic index diet and a diet that minimizes dairy products — as well as laser therapy. Treatment goals include clearing acne and preventing acne sequelae such as postinflammatory hyperpigmentation and scarring. The main therapies currently used for acne vulgaris are aimed at reducing the severity and recurrences of skin lesions as well as improving appearance. According to the clinical expert consulted by CDA-AMC, with the exception of oral isotretinoin, most treatments for acne control symptoms but are not curative. Hence, patients must continue treatment to maintain benefit.
Drug Under Review
Key characteristics of clascoterone are summarized in Table 3 with other treatments available for acne vulgaris.
Clascoterone 10 mg/g is supplied in a 30 g tube.16,17 The recommended dose per application is up to 1 g or to 2 fingertip units applied in a thin layer twice daily over the affected area. Patients should not spot-treat for optimal efficacy.16
Clascoterone is an androgen receptor inhibitor. Androgen receptor inhibitors may reduce sebaceous gland activity. The mechanism of action of clascoterone cream for the topical treatment of acne vulgaris is unknown.16 On June 15, 2023, clascoterone was approved by Health Canada for the topical treatment of acne vulgaris in patients aged 12 years and older.16 The sponsor-requested reimbursement indication is for the first-line prescription topical treatment of moderate to severe acne vulgaris in patients aged 12 years and older. While the indication states that clascoterone is for the treatment of patients aged 12 years and older, the data reported in the Clinical Review Report are consistent with those in the trials (i.e., for patients aged 9 years and older). Clascoterone has not been reviewed by CDA-AMC.
Table 3: Key Characteristics of Clascoterone, Topical Antibiotics, Topical Retinoids, Oral Hormonal Therapy, and Spironolactone
Characteristic | Clascoterone 1% cream | Topical antibioticsa | Topical retinoids | Oral hormonal therapy | Spironolactone |
|---|---|---|---|---|---|
Drugs under the same class | NA | Benzoyl peroxide, clindamycin, erythromycin | Adapalene (cream, gel, lotion), tretinoin (lotion), tazarotene (gel), trifarotene (cream) | Ethinyl estradiol with drospirenone, or cyproterone acetate, norgestimate, or levonorgestrel | NA |
Mechanism of action | Unknown | Inhibits P. acnes from producing free fatty acids in the sebum of the skin. Erythromycin also reduces inflammation. BP prevents growth of drug-resistant bacteria. | Vitamin A (retinol) derivatives, which modify gene expression, subsequent protein synthesis, and epithelial cell growth and differentiation by activating retinoic acid nuclear receptors. | Progestins decrease androgenic effect, thereby improving acne vulgaris. | Aldosterone antagonist |
Indicationb | Topical treatment of acne vulgaris in patients aged 12 years and older | Treatment of acne vulgaris | Treatment of acne vulgaris (in patients aged 12 years and older)c | Treatment of acne vulgaris in womend | Off-label treatment for acne vulgaris |
Route of administration | Topical | Topical | Topical | Oral | Oral |
Recommended dosage | 1 g (2 fingertip units) applied in a thin layer over the entire face twice daily (morning and evening) | A thin layer applied to affected area once or twice daily | A thin layer applied to affected area once a day in the evening | Once daily regimen | NR |
Serious adverse effects or safety issues | Local reactions, such as erythema or redness, scaling or dryness, pruritus, stinging or burning, edema, striae rubrae, skin atrophy, and telangiectasia | Dry skin, peeling, itching, burning sensation, erythema, pruritus, edema, irritation of the eyes, skin discoloration, sunburn | Increased susceptibility to burning (such as sunburn), including via sunlamps, and extreme weather, such as wind or cold. Caution when co-administered with photosensitizers (e.g., tetracyclines, fluoroquinolones, sulfonamides) Application site reactions, including irritation, scaling, dryness, erythema, burning, and stinging | TE (MI, stroke), hirsutism, migraine, spotting, amenorrhea, breakthrough bleeding, change in weight, edema, cramps, and bloating | Gynecomastia, hyperkalemia, hyperchloremic metabolic acidosis, hyponatremia, and impaired hepatic function |
Other | — | Resistance develops when erythromycin or clindamycin is used as monotherapy. | Contraindicated in pregnant people and those of childbearing potential. Avoid breastfeeding while using topical retinoids. | Only available for women (in certain age groups for certain brands) | Officially indicated as a diuretic and as an antihypertensive medication |
BP = benzoyl peroxide; MI = myocardial infarction; NA = not applicable; NR = not reported; P. acnes = Propionibacterium acnes; TE = thromboembolism.
aAvailable in many different forms, such as cream, gel, solution, powder, and pads. Combinations of BP and clindamycin as well as BP and erythromycin are also available.
bHealth Canada–approved indication.
cAdapalene and trifarotene are indicated for acne vulgaris in patients 12 years and older.
dYaz and Alesse are indicated for females aged 14 years and older, Yasmin is indicated for patients aged 16 years and older, Tri-Cyclen is indicated for patients aged 15 years and older, and Diane-35 does not have a patient age restriction.
Sources: Sponsor’s clinical evidence summary23 and Health Canada product monographs for clascoterone, Benzamycin, BenzaClin, Differin, Altreno, Tazorac, Aklief, isotretinoin, Aldactone, Yaz, Yasmin, Tri-Cyclen, Diane-35, and Alesse.16, 28-42,43
Perspectives of Patients, Clinicians, and Drug Programs
The full patient and clinician group submissions received by CDA-AMC are available in the consolidated patient and clinician group input document for this review on the project website: Clascoterone: Patient and Clinician Group Input.
Patient Group Input
This section was prepared by the CDA-AMC review team based on the input provided by patient groups. Two national, not-for-profit organizations, the ARSC and the CSPA, jointly conducted a survey in June 2022 with 154 patients living in Canada diagnosed with acne. The ARSC comprises dermatologists, patients, educators, and communicators providing information and raising awareness about the disease. The CSPA strives to improve the lives of people affected by skin, hair, and nail conditions through collaboration, advocacy, and education.
Patient groups reported that as acne appears on the face, it not only affects appearance, but has great psychological impact on patients’ lives. Many patients reported experiencing diminished self-image, self-esteem, self-confidence, and assertiveness. This emotional distress caused by unhappiness with appearance can lead to bad moods, anxiety (including in social situations), anger, loneliness, self-consciousness, shame, depression, and pain, generally making patients feel in poor health overall. Furthermore, patient groups said these factors impede their ability to be social and conduct daily activities (e.g., forming friendships and dating, having social interactions, being viewed on camera, swimming, changing in change rooms where patients’ acne on their body is exposed). According to the input received, acne does not just leave physical scars (affecting 71% of patients with mild acne, 84% of patients with moderate acne, and 100% of patients with severe acne) and pigmentation changes (affecting 86% of patients with mild acne, 94% of patients with moderate acne, and 100% of those with severe acne), it also leaves “emotional scarring.” Another aspect of acne that affects patients’ HRQoL is stigmatizing “myth,” such as acne being self-caused by fatty or high carb foods, unhygienic daily self-care, or a dismissive attitude (e.g., “it’s just pimples”) with little empathy or understanding of patients’ emotional distress. Financial burden was cited as another challenge; some respondents have to pay out-of-pocket costs for prescription, over-the-counter, and self-care products, such as cleansers and makeup, which increase with acne severity (with 4% of patients with mild acne, 5% of patients with moderate acne, and 14% of overall respondents spending $100 or more per month). More than half of patients had facials and peels (53% of patients, with 12% of them paying more than $500 per session) and light or laser therapy (65% of patients, with 15% of them paying more than $500 per session) that exacerbate financial burden on patients. As such, patients prioritize treatments that help them enjoy personal relationships and cause less scarring or changes in skin pigment. Other goals include clearer skin, better mental health, increased confidence, the ability to be social, and an improved overall quality of daily life.
Three individuals who had experience with clascoterone felt that their acne was well controlled with the drug (also resulting in greater confidence) and did not experience the typical side effects associated with topicals for acne. However, it was noted that the medication was very expensive compared to other treatment options, with patients paying out of pocket or accessing treatment through insurance.
According to the input, acne is underdiagnosed and undertreated in Canadian health care settings. Almost half of respondents (42%) answered that they were diagnosed after 2 to 5 health care visits, with 30% having visited more than 5 times. To improve their lives, respondents want increased access to new treatments that is safe and effective, health care providers to be aware of all the new and existing treatment options for acne, and evaluation for depression and anxiety that could lead them to getting support.
Clinician Input
Input From the Clinical Expert Consulted by CDA-AMC
All CDA-AMC review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, providing guidance on the potential place in therapy). The following input was provided by 1 clinical specialist with expertise in the diagnosis and management of acne vulgaris.
Unmet Needs
According to the clinical expert, a major limitation of current acne therapy is that the most efficacious topical treatments, such as topical retinoids and benzoyl peroxide, tend to be irritative and exhibit a slow onset of effect, which may contribute to the issue of adherence to treatment. As mentioned by the clinical expert, a study reported that 46% of patients prescribed topical treatment did not adhere to their prescribed regimen due to the lack of desired response and adverse effects.44 The clinical expert noted that as the majority of treatments are not curative, their continuation becomes imperative to sustain benefits. Moreover, acne severity exhibits variability over time, requiring potential modifications to the treatment regimen as time progresses.
Place in Therapy
According to the clinical expert, topical clascoterone will likely be used as a first-line topical for mild and moderate acne as it appears to be well tolerated if it is effective and accessible. Clascoterone has a novel mechanism in that it is the first topical androgen receptor blocker and the first androgen blocker that can be used in males with acne. The clinical expert anticipated that clascoterone may be used alone or in combination with other topicals for mild acne and in combination with oral antibiotics for moderate acne. The clinical expert did not feel that clascoterone could be used as first-line treatment for severe acne; however, it could be considered in combination with systemic treatment if a patient requested alternatives to first-line treatment for severe acne (i.e., isotretinoin).
Patient Population
According to the clinical expert, topical clascoterone is appropriate for use by any patient with mild to moderate acne. It is least suited for use in patients with severe or treatment-resistant moderate acne because oral retinoids are still preferred for this patient population. However, the clinical expert noted that clascoterone 1% cream could be used in combination with other treatments if a patient requested alternatives to first-line treatment for severe acne. The clinical expert noted that clascoterone could potentially be used in combination with oral contraceptives or spironolactone in women to determine if there would be added benefit. However, they highlighted that it should not be used in patients who are pregnant, nursing, or contemplating pregnancy.
Assessing the Response Treatment
The clinical expert noted that patients are typically assessed every 3 months to determine treatment response with the exception of treatment with isotretinoin, which is assessed every 2 months and, in some instances, assessed monthly given the need for monthly pregnancy testing in patients of childbearing potential. The clinical expert noted that a clinician would examine acne lesions and record acne as clear, minimal or almost clear, moderate, or severe; comment on acne sequalae, including pigmentation and scarring; and also note a patient’s self-reported assessment of treatment experience upon evaluation. The goal of treatment is minimal acne (1 to 2 lesions on examination) or no acne. Given that patients’ expectations can be highly variable, patient satisfaction is also an important factor in assessing treatment success.
Discontinuing Treatment
According to the clinical expert, patients would discontinue treatment if there was a lack of response or a worsening of disease, adverse effects, or patient dissatisfaction with treatment. The clinical expert also noted that they would discontinue treatment in patients who are attempting to conceive, are pregnant, or nursing.
Prescribing Considerations
Family physicians may prescribe clascoterone.
Clinician Group Input
This section was prepared by the CDA-AMC review team based on the input provided by 2 clinician groups.
Two clinician groups submitted input: DAO, represented by 10 clinicians, and PCDSC, represented by 5 physicians who make up its board of directors. Both clinician groups and the clinical expert consulted by CDA-AMC agreed that patients with acne vulgaris are not being treated effectively for various reasons. First, many patients do not adhere to prescribed medications due to intolerance (e.g., irritation or photosensitivity caused by topical drugs), even though acne vulgaris typically requires long-term topical therapy. Even if patients are adherent, not all patients respond to currently available treatments, which only control symptoms and do not induce remission (except for isotretinoin). Second, male patients are reluctant to use off-label spironolactone (e.g., due to side effects such as gynecomastia) and cannot take antiandrogenic combined oral contraceptives. Third, none of the topicals available target the 4 key factors of acne pathogenesis (desquamation, sebum production, C. acnes, and androgen — all related to inflammation). Also, no antiandrogen topical is available.
According to PCDSC, acneiform scarring is another unmet need that requires treatment. DAO stated that a quarter of patients are strongly dissatisfied with the medical care that they received for acne.45 Both clinician groups and the clinical expert agreed that clascoterone would be used as the first-line monotherapy for uncomplicated cases (or mild acne) and in combination with other topical or systemic drugs for complex cases (moderate acne). The clinician groups stated that clascoterone may decrease antibiotic prescribing for acne, and shift or delay the use of isotretinoin. Both clinician groups and the clinical expert consulted by CDA-AMC said patients with mild to moderate acne are best suited for treatment with clascoterone. Furthermore, PCDSC added that patients who are more likely to experience adverse effects with available topical therapies, such as those with sensitive skin, those spending significant time outdoors, or those who are likely to be affected negatively by systemic hormonal therapies (such as teenagers, perimenopausal women with acne, or patients with metabolic syndrome) may benefit from clascoterone. Additionally, DAO suggested that transmasculine patients, gender minority patients, mature patients with acne (aged 29 years to 40 years), and those with sensitive, eczema-prone skin may benefit from clascoterone.
The clinician groups indicated that severe acne should be treated with isotretinoin, which is consistent with the feedback received from the clinical expert consulted by CDA-AMC. However, the clinician groups stated that clascoterone may be used as adjunctive treatment to isotretinoin or in place of isotretinoin in the case of serious intolerance or contraindication. Also, DAO mentioned that clascoterone is the least suitable option in older people (aged 65 years or older), pediatric (aged 12 years or younger), pregnant, or nursing populations. The clinical expert consulted by CDA-AMC mentioned that the benefit of adding clascoterone to oral contraceptives or off-label spironolactone is uncertain.
Both clinician groups and the clinical expert consulted by CDA-AMC agreed that minimal or no acne (clear to almost clear skin) is a goal of acne treatment. DAO and PCDSC added that instead of structured criteria such as IGA scores, other ways to measure response to treatment are descriptive assessment, improvement as viewed on photos taken before and after treatment, reduced lesion counts, patient satisfaction, and improved function. According to DAO, a 30% reduction in lesion counts and a 2-point (or even 1-point) reduction in IGA scores are considered clinically meaningful.
PCDSC noted that patients using clascoterone should be advised that treatment effect may not be observed for several months. The clinician groups relayed that the time to assess treatment may vary between clinicians, but typically 4 months to 6 months following the initiation of treatment is an appropriate time in which to assess response. Both the clinician groups and the clinical expert agreed that they would consider discontinuing clascoterone if no response was observed in 3 months to 6 months, or if a patient experienced worsening acne or intolerance to treatment. PCDSC also added that if patients were planning to get pregnant, already pregnant, or nursing, then they would discontinue clascoterone treatment, which is consistent with the feedback received from the clinical expert consulted by CDA-AMC. DAO mentioned that poor adherence is another reason to discontinue clascoterone treatment.
The clinician groups submitting input for this review agreed that dermatologists and general practitioners (e.g., family physicians, nurse practitioners) can prescribe clascoterone to treat acne.
One clinician group, DAO, had experience with clascoterone and indicated that the drug is well tolerated, which is important for those with sensitive skin and for maintaining treatment adherence. Of note, PCDSC felt that acne is likely underdiagnosed and that access to dermatological care is seriously limited in Canadian practice settings.
Drug Program Input
The drug programs provide input on each drug being reviewed through CDA-AMC reimbursement review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical expert consulted by CDA-AMC are summarized in Table 4.
Table 4: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation question | Clinical expert response |
|---|---|
Relevant comparators | |
The trials compared clascoterone cream to that of vehicle cream. However, data are lacking for direct comparisons to other acne medications and combination therapies (e.g., benzoyl peroxide, topical retinoids). | This is a comment from the drug plans to inform CDEC deliberations. |
Considerations for initiation of therapy | |
The IGA was used to evaluate acne severity. In practice, do primary care clinicians use this tool when assessing patients for acne therapy? | The clinical expert noted that physicians do not use a formal or standard measurement tool but instead use their clinical judgment to classify the patient’s severity. The clinical expert stated that a clinician will typically look at factors, including the number and type of lesions, inflammation, scarring, hyperpigmentation, and lesion depth, but a standard scale is not used when assessing severity. |
How is the effectiveness of clascoterone compare to other topical or oral acne therapies in patients aged 12 years and older? If recommended for reimbursement, what would be reasonable eligibility criteria for clascoterone? Would it be appropriate for patients to try benzoyl peroxide with or without a topical retinoid before being eligible for clascoterone? | This is a comment from the drug plans to inform CDEC deliberations. |
Considerations for prescribing of therapy | |
Should clascoterone be used in combination with topical benzoyl peroxide and/or retinoids? | The clinical expert noted that they would first use it as a monotherapy given the lack of comparative trials. They also noted that they may use clascoterone in combination with other topical therapies in later-line treatments in consultation with patients and their preferences, noting that the drug has a unique pathway as a topical androgen inhibitor. |
Generalizability | |
Clascoterone is being marketed in the US as both Winlevi (for acne) and Breezula (at higher concentrations for androgen-dependent baldness). Should some mechanism be in place to limit the off-label use of clascoterone? | The clinical expert noted that a different concentration will be needed to target androgenic male pattern baldness. Although it would be difficult to prescribe to patients without efficacy data on androgen-patterned baldness, the clinical expert felt that patients will inevitably use the cream if they would like to; however, a higher concentration would be needed. There were no safety concerns, but also there were no data to support its use for this purpose. |
Care provision issues | |
Systemic effects (e.g., amenorrhea, hyperkalemia) seem rare although HPA axis suppression can occur after just 2 weeks of regular use. Long-term safety data are lacking. | This is a comment from the drug plans to inform CDEC deliberations. |
CDEC = Canadian Drug Expert Committee; HPA = hypothalamic-pituitary-adrenal; IGA = Investigator’s Global Assessment.
Clinical Evidence
The objective of the CDA-AMC Clinical Review Report is to review and critically appraise the clinical evidence submitted by the sponsor on the beneficial and harmful effects of clascoterone 1% cream in the treatment of acne vulgaris in patients aged 12 years and older. The focus has been placed on comparing clascoterone 1% cream to relevant comparators and identifying gaps in the current evidence.
A summary of the clinical evidence included by the sponsor in the review of clascoterone is presented in 3 sections with the CDA-AMC critical appraisal of the evidence included at the end of each section. The first section, the systematic review, includes pivotal studies and RCTs that were selected according to the sponsor’s systematic review protocol. The CDA-AMC assessment of the certainty of the evidence in this first section using the GRADE approach follows the critical appraisal of the evidence. The second section includes sponsor-submitted LTE studies. The third section includes indirect evidence from the sponsor.
Included Studies
Clinical evidence from the following is included in the CDA-AMC review and appraised in this document:
2 pivotal studies identified in the systematic review
1 LTE study
1 indirect treatment comparison.
Systematic Review
Content in this section has been informed by materials submitted by the sponsor. The following has been summarized and validated by the CDA-AMC review team.
Description of Studies
Two randomized, double-blind, vehicle-controlled, parallel-group trials (the CB-03-01/25 and CB-03-01/26 studies) met the inclusion criteria for the systematic review conducted by the sponsor. Both trials were considered pivotal and were conducted with an identical study design with patients randomized 1:1 to either clascoterone 1% or vehicle cream for 12 weeks of treatment.
The primary objective of both pivotal trials was to determine the safety and efficacy of clascoterone 1% cream versus the vehicle cream applied twice daily for 12 weeks in patients with facial acne vulgaris.
The CB-03-01/25 study (N = 708) was conducted primarily in the US and the CB-03-01/26 study (N = 732) was conducted primarily in Europe. Neither trial had any study sites in Canada. In the CB-03-01/25 study, 708 patients were randomized to treatment with either clascoterone 1% cream (N = 353) or vehicle cream (N = 355). In the CB-03-01/26 study, 732 patients were randomized to treatment with either clascoterone 1% cream (N = 369) or vehicle cream (N = 363). In the CB-03-01/25 study, the median age for both treatment groups was 18 years (range, 9 years to 58 years) and in the CB-03-01/26 study, the median age for both treatment groups was 18 years (range, 10 years to 50 years). Block randomization was used for both studies. Patients were enrolled from January 21, 2016, to April 11, 2018, for the CB-03-01/25 study and from November 16, 2015, to February 21, 2018, in the CB-03-01/26 study. The dates of the database lock for the CB-03-01/25 trial was June 25, 2018, and for the CB-03-01/26 trial was June 27, 2018. Data were unblinded on June 27, 2018, for both studies.
Both studies are now complete. They consisted of the following study periods:
screening phase — visit 1
treatment phase — 12 weeks (consisting of 3 study visits at week 4, week 8, and week 12)
follow-up phase — patients in both studies had the option to continue for up to 12 months in the LTE trial (the CB-03-01/27 study).
Characteristics of the included studies are summarized in Table 5.
Table 5: Details of Studies Included in the Systematic Review
Detail | CB-03-01/25 study | CB-03-01/26 study |
|---|---|---|
Designs and populations | ||
Study design | Pivotal, multinational, multicentre, randomized, double-blind, vehicle-controlled, parallel-group, 12-week study (the CB-03-01/25 and CB-03-01/26 trials were twin studies) | |
Locations | 45 sites in the US, 7 sites in Ukraine, and 3 sites in Georgia | 48 investigational study sites in 5 European countries (8 in Bulgaria, 9 in Romania, 12 in Poland, 3 in Serbia, 6 in Georgia) and in the US (10 sites) |
Patient enrolment dates | Start date: January 21, 2016 End date: April 11, 2018 | Start date: November 16, 2015 End date: February 21, 2018 |
Randomized (N)a | N = 708 Clascoterone, n = 353 Vehicle, n = 355 | N = 732 Clascoterone, n = 369 Vehicle, n = 363 |
Inclusion criteria |
| |
Exclusion criteria |
| |
Drugs | ||
Intervention | Topical clascoterone cream, 1%, applied to the whole face twice daily (morning and evening) for 12 weeks in patients with facial acne vulgaris. | |
Comparator | Vehicle cream applied to the whole face twice daily (morning and cream) for 12 weeks in patients with facial acne vulgaris. | |
Study duration | ||
Screening phase | At visit 1 | |
Treatment phase | 12 weeks:
| |
Follow-up phase | Patients in both studies had the option to continue for up to 12 months in the LTE trial (the CB-03-01/27 study). | |
Outcomes | ||
Primary end point | Proportion of patients achieving treatment improvement, defined by a > 2-point reduction in IGA from baseline and an IGA score of 0 (clear) to 1 (almost clear) at week 12 Absolute change from baseline in NILC and ILC at week 12. | |
Secondary end points | Secondary end points:
Safety end points:
| |
Publication status | ||
Publications | Hebert et al. (2020)46 Hebert et al. (2023)47 | |
AE = adverse event; ECG = electrocardiogram; IGA = Investigator’s Global Assessment; ILC = inflammatory lesion count; LSR = local skin reaction; LTE = long-term extension; NILC = noninflammatory lesion count; OTC = over the counter; TLC = total lesion count; UPT = urine pregnancy tests.
aThe number of patients reported included patients aged 9 years or older. The sample sizes for the approved population (patients aged 12 years or older) were N of 692 patients (clascoterone [N = 352 patients] and vehicle [N = 350 patients]) and N of 729 patients (clascoterone [N = 367 patients] and vehicle [N = 362 patients]) in the CB-03-01/25 and CB-03-01/26 studies, respectively.
Sources: Clinical Study Report for the CB-03-01/25 trial,18 Clinical Study Report for the CB-03-01/26 trial.19 Details included in the table are from and the sponsor’s summary of clinical evidence.23
Populations
Inclusion and Exclusion Criteria
At least 700 patients per study were enrolled at approximately 38 sites for the CB-03-01/25 study and 40 sites for the CB-03-01/26 study. Patients eligible for inclusion were required to have acne vulgaris of the face (which can include the nose) with an IGA score of 3 or 4, at least 30 inflammatory lesions to a maximum of 75 inflammatory lesions (papules, pustules, and nodules), and at least 30 noninflammatory lesions to a maximum of 100 noninflammatory lesions (open and closed comedones). Patients were excluded from the trials if they had nodulocystic acne, if they were pregnant, lactating, or planning to become pregnant during the study, if they were planning to be or needed to be exposed to artificial tanning devices or excessive sunlight during the trial, or if they had been using any topical antiacne preparations within 2 weeks to 6 weeks of treatment initiation or the systemic antiacne medications of corticosteroids, antibiotics spironolactone, or retinoids within 1 week to 6 months of the initiation of treatment. Before entry into the study, patients must not have used the medications and/or procedures on the face as specified in the exclusion criteria. During the study, patients must not have used the following products and/or procedures on the face:
topical antiacne treatments, including but not limited to over-the-counter acne cleansers or treatments, benzoyl peroxide, antibiotics, azelaic acid, sulfa-based products, corticosteroids, and salicylic acid
retinoids, including tazarotene, adapalene, and tretinoin
light treatments (including artificial tanning devices), microdermabrasion, or chemical peels
any other investigational drug or the use of any investigational device
systemic medications with potential antiacne effects, including:
corticosteroids, including intramuscular and intralesional injections (inhaled, intranasal, or ocular corticosteroids were allowed)
antibiotics
spironolactone
retinoid therapy
the addition of a hormonal contraception
change to a pre-existing hormonal contraception
other systemic therapy that may have materially affected the patient’s acne in the opinion of the investigator.
Other chronic medications being used at the time of the baseline visit were allowed to be continued at the discretion of the investigator.
Interventions
Patients were randomized 1:1 to clascoterone (cortexolone 17alpha-propionate) 1% cream or the vehicle cream. Clascoterone 1% cream was applied topically twice daily for 12 weeks in patients with facial acne vulgaris. The control group featured a vehicle cream, which was similarly applied topically twice daily for 12 weeks in patients with facial acne vulgaris. Applications typically occurred in the morning and in the evening.
At the first visit, the patients were instructed to wash their entire face (the area to be treated) with mild soap and water and then dry the area gently. The study staff then instructed the patient and parent or guardian (if applicable) on how to dispense the cream, how much to use, and where to apply it. The first application of cream was to be applied in the office at visit 1 under supervision of the study staff after the patient was deemed eligible and the remainder of applications occurred at home and at each study visit. Before the patient left, the medication was weighed and dispensed to the patient. About 1 g of the cream was dispensed onto a fingertip and applied to the face by dabbing small amounts gently on multiple regions of the face (e.g., forehead, nose, cheeks, chin). Using a fingertip, the cream was spread to provide a thin, uniform layer of the cream over the entire face. Patients and parents or guardians (if applicable) were instructed to apply the cream to the whole face twice daily (in the morning and evening) for 12 weeks; hence, a total of 2 g of product was used per day. Patients were provided with a diary where they were instructed to record the date and time of each application for the 12 weeks of therapy. Unused medication tubes were to be returned at each visit.
Concomitant Medications and Cointerventions
There were no other protocol-required drugs included in the trials. Therapies (medication and nonmedication therapies) not restricted by the protocol were used during the study for the treatment or prevention of disease or to maintain good health. Vitamins and mineral supplements were permitted at dosages considered by the investigator as reasonable for maintaining good health. Nonprohibited chronic therapies being used at visit 1 were allowed to be continued. Any changes in concomitant therapies during the study were recorded. Other chronic medications being used at the time of the baseline visit were allowed to be continued at the discretion of the investigator.
In the CB-03-01/25 study, the most common concomitant medications by medication class (more than 2%) were propionic acid derivatives (4.0%), progestogens and estrogens or fixed combinations (3.1%), centrally acting sympathomimetics (2.4%), progestogens (2.3%), anilide (2.1%), intrauterine contraceptives (2.0%), and selective serotonin reuptake inhibitors (2.0%).
In the CB-03-01/26 study, the most common concomitant medications were progestogens and estrogens that were fixed combinations used as contraceptives (1.6% in the clascoterone group and 2.5% in the vehicle group) and thyroid hormones (1.1% in the clascoterone group and 2.2% in the vehicle group).
Outcomes
A list of efficacy end points assessed in this Clinical Review Report is provided in Table 6, followed by descriptions of the outcome measures. Summarized end points are based on outcomes included in the sponsor’s summary of clinical evidence as well as any outcomes identified as important to this review according to the clinical expert consulted by CDA-AMC and input from patient and clinician groups and public drug plans. Using the same considerations, the review team selected end points that were considered to be most relevant to inform deliberations of the CDA-AMC expert committee and finalized this list of end points in consultation with members of the expert committee. All summarized efficacy end points were assessed using GRADE. Select notable harms outcomes considered important for informing deliberations of the CDA-AMC expert committee were also assessed using GRADE.
The efficacy measures and end points were consistent with the 2005 FDA guidance Acne Vulgaris: Developing Drugs for Treatment48 and the subsequent 2018 FDA guidance Acne Vulgaris: Establishing Effectiveness of Drugs Intended for Treatment.49
Table 6: Outcomes Summarized From the Studies Included in the Systematic Review
Outcome measure | Time point | CB-03-01/25 study | CB-03-01/26 study |
|---|---|---|---|
Proportion of patients in each treatment group achieving improvement Improvement defined as an IGA score of clear (0) or almost clear (1) and at least a 2-point reduction | At 12 weeks | Primary | Primary |
Absolute change from baseline in NILC in each treatment group | At 12 weeks | Primarya | Primarya |
Absolute change from baseline in ILC in each treatment group | At 12 weeks | Primarya | Primarya |
Percentage change from baseline in NILC, ILC, and TLC in each group | At 12 weeks | Secondary | Secondary |
Absolute change from baseline in TLC in each treatment group | At 12 weeks | Secondary | Secondary |
HRQoL as measured by DLQI and Cardiff Acne Disability Index | NR | NR | NR |
Local and systemic AEs at every visit | Baseline, week 4, week 8, and week 12 | Safety | Safety |
LSRs: Telangiectasia, skin atrophy, striae rubrae, erythema, edema, scaling or dryness, stinging or burning, and pruritus scored by frequency and severity at every visit | Baseline, week 4, week 8, and week 12 | Safety | Safety |
AE = adverse event; DLQI = Dermatology Life Quality Index; HRQoL = health-related quality of life; IGA = Investigator’s Global Assessment; ILC = inflammatory lesion count; LSR = local skin reaction; NILC = noninflammatory lesion count; NR = not reported; TLC = total lesion count.
aStatistical testing for these end points was adjusted for multiple comparisons (e.g., hierarchical testing).
Sources: Clinical Study Report for the CB-03-01/25 trial,18 Clinical Study Report for the CB-03-01/26 trial,19 and the sponsor’s summary of clinical evidence.23
Global Success
Proportion of Patients Aged 12 Years or Older Achieving Improvement at Week 12
Treatment success was a coprimary end point and assessed at week 12 in both pivotal trials. Treatment success was defined as a 2-point or greater reduction in IGA score from baseline and a score of clear (0) or almost clear (1). The IGA is a static, investigator-reported measure of overall (qualitative and quantitative) acne severity. It uses an ordinal scale with 5 severity grades from 0 (clear skin) to 4 (severe) based on morphologic descriptions. Patients received an IGA score at baseline from the investigator. At week 12, the IGA score was reassessed.
Lesion Counts
Absolute Change From Baseline in NILC at Week 12
The absolute change in NILC from baseline to week 12 was a coprimary end point in both pivotal trials. At baseline, the number of noninflammatory lesions (open and closed comedones) on the face vertically from the hairline to mandible room and horizontally from ear to ear, including those on the nose, were counted. At baseline, patients must have had at least 30 noninflammatory lesions to a maximum of 100 noninflammatory lesions on the face at baseline to be eligible for enrolment. Noninflammatory lesions were counted again at week 12 and the change in lesion counts was documented. Photographs were taken to document clinical status of the patient but were not used for counting lesions. According to the clinical expert, a minimally important difference would be 0 or minimal lesions present.
Lesions were defined as follows:
comedones — open (blackheads) and closed (whiteheads)
papules — raised inflammatory lesions with no visible purulent material
pustules — raised inflammatory lesions with visible purulent material
nodules — any circumscribed, inflammatory mass greater or equal to 5 mm in diameter with or without cystic changes.
Absolute Change From Baseline in ILC at Week 12
The absolute change in ILC from baseline to week 12 was a coprimary end point in both pivotal trials. At baseline, the number of inflammatory lesions (papules, pustules, and nodules) on the face vertically from the hairline to mandible room and horizontally from ear to ear, including those on the nose, were counted. At baseline, patients must have had at least 30 inflammatory lesions to a maximum of 75 inflammatory lesions to be eligible for enrolment. Inflammatory lesions were counted again at week 12 and the change in lesion counts was documented. According to the clinical expert, a minimal important difference would be 0 or minimal lesions present.
Absolute Change From Baseline in TLC at Week 12
The absolute change in TLC (including inflammatory and noninflammatory lesions) from baseline to week 12 was a secondary end point in both pivotal trials. At baseline, the number of inflammatory lesions (papules, pustules, and nodules) and noninflammatory lesions (open and closed comedones) on the face vertically from the hairline to mandible room and horizontally from ear to ear, including those on the nose, were counted. Inflammatory lesions and noninflammatory lesions were counted again at week 12 and summed as a total. The change in TLCs was documented. According to the clinical expert, a minimal important difference would be 0 or minimal lesions present.
Percentage Change From Baseline in NILC, ILC, and TLC at Week 12
The percentage change from baseline to week 12 in NILC, ILC, and TLC were secondary end points in both pivotal trials. The mean percentage change from baseline of NILC, ILC, and TLC at week 12 was calculated for each treatment group. The clinical expert considered the percentage change in NILC, ILC, and TLC from baseline to week 12 to be a clinically important outcome.
Mental Health and HRQoL
HRQoL and mental health were considered to be important outcomes by patient groups but were not assessed in either trial.
Table 7: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
IGA | A static, investigator-reported measure of overall (qualitative and quantitative) acne severity. This is an ordinal scale with 5 severity grades from 0 (clear skin) to 4 (severe) based on morphologic descriptions.48,49 | Validity: When assessed in patients with acne (n = 54), weak correlations were found between IGA and DLQI (Pearson r = 0.132; P = 0.341) or CADI (r = 0.233; P = 0.091).50 Reliability: In patients with acne (n = 54), intrarater reliability was excellent (ICC = 0.873; 95% CI, 0.807 to 0.920; P > 0.0001). Also, internal consistency was acceptable (Cronbach alpha = 0.871).50 Responsiveness: No evidence was identified. | According to the FDA guidance, an IGA score of 0 or 1 as well as an improvement of 2 grades from the baseline score at a prespecified primary time point is considered a clinically meaningful outcome.48,49 |
CADI = Cardiff Acne Disability Index; CI = confidence interval; DLQI = Dermatology Life Quality Index; ICC = intraclass correlation coefficient; IGA = Investigator’s Global Assessment; MID = minimal important difference.
Sources: FDA48,49 and Alsulaimani et al. (2020).50
Harms
AEs were classified as TEAEs, according to the period of occurrence. TEAEs were all AEs occurring or worsening after the first dose of the drug. TEAEs were summarized by treatment group and overall. The number and proportion of patients with any TEAE and the number of TEAEs were tabulated by Medical Dictionary for Regulatory Activities version 18.1 system organ class and preferred term and seriousness.
The number and percentage of patients with any serious TEAE and the number of serious TEAEs were presented overall and were tabulated.
All serious TEAEs were listed and all TEAEs leading to discontinuation were listed. LSRs (telangiectasia, skin atrophy, striae rubrae, erythema, edema, scaling or dryness, stinging or burning, and pruritus) were listed separately for face and trunk and summarized separately for face and trunk by the frequency of each individual LSR and severity at each visit.
At every study visit, the investigator or designee documented the severity of the following LSRs known to be associated with the application of topical steroids: telangiectasia, skin atrophy, and striae rubrae. In addition, the investigator or designee evaluated the severity of LSRs known to be associated with acne vulgaris (erythema, edema, and scaling or dryness), using ordinal scales. A 5-point ordinal scale was used to assess the severity of these reactions (0 = none, 1 = minimal, 2 = mild, 3 = moderate, and 4 = severe). A 4-point ordinal scale was used by patients to assess LSR severity (0 = none, 1 = minimal, 2 = moderate, 3 = severe).
All patients were actively graded by the investigator for LSRs (telangiectasia, skin atrophy, striae rubrae, erythema, edema, scaling or dryness, stinging or burning, and pruritus) that may have occurred within the treatment area. LSRs were summarized by the frequency of each individual LSR by treatment group and severity at each visit.
The following harms outcomes were selected for GRADE assessment: LSRs, nasopharyngitis, and fertility disruption. These notable harms were identified using the product monograph approved by Health Canada.
Statistical Analysis
Sample Size and Power Calculation
Based on assumptions estimated from the phase II dose escalation study (the NCT01631474 trial),51 at least 350 patients in each treatment group in each study were required to provide sufficient power (90%) with the selected primary end points. In the CB-03-01/25 study, 692 patients aged 12 years and older were randomized to 2 groups (clascoterone [n = 342] and vehicle [n = 350]). In the CB-03-01/26 study, 729 patients aged 12 years and older were randomized to 2 groups (clascoterone [n = 367] and vehicle [n = 362]).
Primary Efficacy End Point: Statistical Test and Model
Hypothesis tests on the coprimary efficacy end points were conducted using a hierarchical testing approach in the following order: the proportion of patients achieving treatment improvement at week 12, absolute change from baseline in NILC, and absolute change from baseline in ILC at week 12. All the hypothesis tests for the primary efficacy end points were performed at the same significance level, a 2-sided alpha of 0.05, and the failure to reject a null hypothesis implied the failure of rejecting all the subsequent null hypotheses.
A logistic regression model with treatment and analysis centre as fixed effects was used to compare the proportion of patients achieving improvement in each treatment group at week 12, where improvement was defined as an IGA score of clear (0) or almost clear (1) and at least a 2-point improvement in the IGA score compared with baseline.
An analysis of covariance (ANCOVA) was used to compare the absolute change from baseline in NILC in each treatment group at week 12, with treatment and analysis centre as fixed effects and the baseline NILC as the covariate. The same method was applied to absolute change from baseline in ILC, with the baseline ILC as the covariate.
Data Imputations for Missing Values
Missing values for the primary end point in the ITT analyses were imputed by the MI method under the MAR assumption. For each end point, data from visit 1 (baseline), visit 2, visit 3, and visit 4 (primary end point) were included in the MI approach. Thus, the MI approach uses a MAR assumption where missing values for each end point can be explained by observed values of that end point across the 4 visits in the study.
Primary Efficacy End Point: Sensitivity Analyses
Sensitivity analyses were performed to investigate the robustness of the results obtained on the ITT set for the primary efficacy end points (proportion of patients with IGA success, and change from baseline in NILC, and ILC). Four sensitivity analyses were performed using different methods of imputation on the ITT set. On a per-patient basis, missing values for the primary efficacy end points were imputed with the following sensitivity analyses.
Missing at worst value: For each patient, missing values of a variable were replaced with the worst value of that variable (failure in the case of dichotomous variables or the higher value collected in the study for lesions counting) regardless of the treatment group.
Worst case: For each patient, missing values of a variable were to be replaced with the worst value of that variable (failure in the case of dichotomous variables or the higher value collected in the study for lesions counting) if the patient was assigned to the clascoterone group and with the best value of that variable (success in the case of dichotomous variables or the lower value collected in the study for lesions counting) if the patient was assigned to the vehicle group.
LOCF: Missing values of a variable were replaced by the last observed value of that variable.
BOCF: Missing values of a variable were replaced by the baseline observed value of that variable.
The MI using the MAR assumption was adopted from the individual studies on the integrated summary of efficacy analysis. The imputation was performed on the ITT analyses set. One per-protocol (PP) analysis was done on the PP set.
Secondary Efficacy End Points: Statistical Test and Model
An ANCOVA model was used to compare the absolute change from baseline in TLC in each treatment group at week 12, with treatment and analysis centre as fixed effects and the baseline TLC as covariate. The adjusted mean difference of the comparison between groups and its 95% CI were derived from the regression model.
An ANCOVA model was used to compare the percentage change from baseline in all secondary end points in each treatment group at week 12, with treatment and analysis centre as fixed effects and the baseline outcome as a covariate. The adjusted mean difference of the comparison between groups and its 95% CI were derived from the regression model.
Given that both pivotal trials had the same study design, end points, and hypotheses, the sponsor felt it was justifiable to pool the efficacy data for a comprehensive evaluation on pooled treatment effect and treatment-by-subgroup analyses. The analysis populations, coprimary end points, and secondary end points for the pooled analyses were the same as for the individual study analyses.
Secondary Efficacy End Points: Multiple Testing Procedure
The key secondary outcomes were included in the multiplicity adjustment of the type I error to control the familywise error rate at a 2-sided significance level of 0.05 in the hierarchical order. For the secondary efficacy end points, hypothesis tests on the secondary efficacy end points were conducted in hierarchical order for secondary end points 1 through 4 in the following order: absolute change from baseline in TLC at week 12, percentage change from baseline in TLC at week 12, percentage change from baseline in NILC at week 12, and percentage change from baseline in ILC at week 12.
Secondary Efficacy End Points: Sensitivity Analysis
No sensitivity analyses were conducted for secondary end points.
Subgroup Analyses
No prespecified subgroup analyses were conducted for either trial.
Safety End Points
Safety outcomes were compared between treatment groups using descriptive statistics and no hypothesis testing was performed. Formal statistical analyses of AEs and LSRs to determine treatment group differences or to determine changes from baseline were neither planned nor performed.
Table 8: Statistical Analysis of Efficacy End Points
End point | Statistical model | Adjustment factors | Handling of missing data | Sensitivity analyses |
|---|---|---|---|---|
CB-03-01/25 and CB-03-01/26 studies | ||||
Proportion of patients in each treatment group achieving improvement | Logistic regression | None | MI under the MAR assumption |
|
Absolute change from baseline in NILC and ILC in each treatment group | ANCOVA | Baseline NILC and ILC as a covariate | MI under the MAR assumption |
|
Absolute change from baseline in TLC in each treatment group and percentage change from baseline to week 12 in each treatment group for NILC, ILC, and TLC | ANCOVA | Baseline outcome as a covariate | MI under the MAR assumption | None |
ANCOVA = analysis of covariance; BOCF = baseline observation carried forward; ILC = inflammatory lesion count; ITT = intention to treat; LOCF = last observation carried forward; MAR = missing at random; MI = multiple imputation; NILC = noninflammatory lesion count; PP = per protocol; TLC = total lesion count.
Sources: Clinical Study Report for the CB-03-01/25 trial,18 Clinical Study Report for the CB-03-01/26 trial,19 and the sponsor’s summary of clinical evidence.23
Analysis Populations
Analysis populations are described in Table 9.
Table 9: Analysis Populations of CB-03-01/25 and CB-03-01/26 Studies
Study | Population | Definition | Application |
|---|---|---|---|
CB-03-01/25 and CB-03-01/26 studies | ITT population | All randomized patients | Analyses of efficacy; primary set for statistical analysis |
Safety population | All patients who received ≥ 1 application of the drug | All safety analyses | |
PP population | Subset of the ITT set and includes patients who have completed the study without any significant protocol deviation | Analysis of efficacy |
ITT = intention to treat; PP = per protocol.
Sources: Clinical Study Report for the CB-03-01/25 trial,18 Clinical Study Report for the CB-03-01/26 trial,19 and the sponsor’s summary of clinical evidence.23
Results
Patient Disposition
There were 825 patients screened for the CB-03-01/25 study; 708 (85.8%) patients were enrolled, and 117 (14.2%) patients were screened out. Reasons for not advancing past screening included not meeting all inclusion criteria (85 [10.3%] patients), withdrawal by patient (16 [1.9%] patients), meeting at least 1 exclusion criterion (10 [1.2%] patients), and other reasons (6 [0.7%] patients). Of the 708 enrolled patients, 353 patients were randomized to treatment with clascoterone and 355 patients were randomized to treatment with vehicle cream. Overall, 577 of 708 (81.5%) patients completed the study (287 patients in the clascoterone group and 290 patients in the vehicle group).
For the CB-03-01/26 study, a total of 756 patients were screened and 732 of them were randomized (369 patients were randomized to the clascoterone group and 363 patients were randomized to the vehicle group), whereas 24 (3.2%) patients were screened out. A total of 584 (79.8%) patients overall — 302 (81.8%) of those in the clascoterone group and 282 (77.7%) of those in the vehicle group — completed the study according to protocol, while 148 (20.2%) patients in total — 67 (18.2%) of those in the clascoterone group and 81 (22.3%) of those in the vehicle group — prematurely discontinued the study. In the CB-03-01/25 study, the most common reason for treatment discontinuation was loss to follow-up in both the treatment group (11.0%) and the vehicle group (9.0%), followed by patient withdrawal (6.5% and 5.1% in the clascoterone and vehicle groups, respectively). In the CB-03-01/26 study, the most common reason for treatment discontinuation was patient withdrawal in both the clascoterone group (9.5%) and the vehicle group (11.3%), followed by loss to follow-up (6.5% and 6.6% in the clascoterone and vehicle group, respectively).
Table 10: Summary of Patient Disposition From Studies Included in the Systematic Review
Patient disposition | CB-03-01/25 study | CB-03-01/26 study | ||
|---|---|---|---|---|
Clascoterone (N = 353) | Vehicle (N = 355) | Clascoterone (N = 369) | Vehicle (N = 363) | |
Screened, N | 825 | 756 | ||
Reason for not advancing past screening, n (%) | 117 (14.2) | 24 (3.2) | ||
Did not meet all inclusion criteria | 85 (10.3) | 12 (1.6) | ||
Withdrawal by patient | 16 (1.9) | 6 (0.8) | ||
Met at least 1 exclusion criterion | 10 (1.2) | 4 (0.5) | ||
Other | 6 (0.7) | 2 (0.3) | ||
Randomized, N | 353 | 355 | 369 | 363 |
Discontinued from study, n (%) | 66 (18.7) | 65 (18.3) | 67 (18.2) | 81 (22.3) |
Reason for discontinuation, n (%) | ||||
Lost to follow-up | 39 (11.0) | 32 (9.0) | 24 (6.5) | 24 (6.6) |
Withdrawal by patient | 21 (5.9) | 15 (4.2) | 30 (8.1) | 37 (10.2) |
Adverse events | 3 (0.8)a | 6 (1.7) | 2 (0.5)a | 8 (2.2) |
Withdrawal by parent or guardian | 2 (0.6) | 3 (0.8) | 5 (1.4) | 4 (1.1) |
Lack of efficacy | 0 | 3 (0.8) | 3 (0.8)a | 1 (0.3) |
Noncompliance with study drug | 0 | 2 (0.6) | 1 (0.3) | 5 (1.4) |
Physician decision | 0 | 1 (0.3) | 1 (0.3) | 0 |
Pregnancy | 0 | 1 (0.3) | 0 | 1 (0.3) |
Otherb | 0 | 2 (0.6) | 0 | 1 (0.3) |
Progressive disease | 1 (0.3) | 0 | 1 (0.3) | 0 |
ITT, N | 353 | 355 | 369 | 363 |
PP, N | 270 | 260 | 286 | 268 |
Safety, N | 353 | 355 | 369 | 363 |
ITT = intention to treat; PP = per protocol.
aIn the Clinical Study Reports of the CB-03-01/25 and CB-03-01/26 trials, 1 of these patients was counted as discontinuing for progressive disease.
bOther reasons for discontinuation included the following: due to investigational product liquification, due to the site being instructed by the sponsor to roll the patient over into the CB-03-01/27 study, and due to nonresponse.
Sources: Clinical Study Report for the CB-03-01/25 trial,18 Clinical Study Report for the CB-03-01/26 trial,19 and the sponsor’s summary of clinical evidence.23
Baseline Characteristics
A summary of baseline patient demographics and disease characteristics are presented in Table 11. The baseline characteristics outlined in this table are limited to those that are most relevant to this review or were felt to affect the outcomes or interpretation of the study results.
The demographic characteristics were similar between the treatment groups. More patients were female (61.6%) than male (38.4%) in the CB-03-01/25 trial. The mean age of patients was 19.9 years (range, 9 years to 58 years) and the mean body mass index (BMI) was 24.6 kg/m2 (range, 11.9 kg/m2 to 77.1kg/m2). With respect to acne severity, the majority of patients had an IGA rating of moderate (82.7% for the clascoterone group and 82.0% for the vehicle group) with the remainder rated severe. The mean ILC was 42.4 lesions for the clascoterone group and 42.9 lesions for the vehicle group (range, 30 lesions to 83 lesions), the mean NILC was 59.1 lesions for the clascoterone group and 60.7 lesions for the vehicle group (range, 30 lesions to 144 lesions), and the mean TLC was 101.5 lesions for the clascoterone group and 103.6 lesions for the vehicle group (range, 60 lesions to 196 lesions).
In the CB-03-01/26 trial, more patients were female (63.4%) than male (36.6%). The mean age of patients was 19.2 years (range, 10 years to 50 years) and the mean BMI was 22.1 kg/m2 (range, 13.2 kg/m2 to 40.6 kg/m2). With respect to acne severity, the majority of patients had an IGA rating of moderate (82.7% in the clascoterone group and 86.2% in the vehicle group), with the remainder of patients rated severe. The mean ILC was 42.9 lesions for the clascoterone group and 41.3 lesions in the vehicle group (range, 30 lesions to 75 lesions), the mean NILC was 62.8 lesions and 63.3 lesions for the clascoterone group and vehicle group, respectively (range, 30 lesions to 177 lesions) and the mean TLC was 105.7 lesions (range, 60 lesions to 241 lesions) and 104.6 lesions (range, 60 lesions to 170 lesions) in the clascoterone group and vehicle group, respectively.
Table 11: Summary of Baseline Characteristics From Studies Included in the Systematic Review (ITT Set)
Characteristic | CB-03-01/25 study | CB-03-01/26 study | ||
|---|---|---|---|---|
Clascoterone (N = 353) | Vehicle (N = 355) | Clascoterone (N = 369) | Vehicle (N = 363) | |
Sex | ||||
Female, n (%) | 221 (62.6) | 215 (60.6) | 243 (65.9) | 221 (60.9) |
Male, n (%) | 132 (37.4) | 140 (39.4) | 126 (34.1) | 142 (39.1) |
Age (years) | ||||
Median (range) | 18.0 (10 to 58) | 18.0 (9 to 50) | 18.0 (10 to 50) | 18.0 (11 to 42) |
Race, n (%) | ||||
Asian | 9 (2.5) | 10 (2.8) | 0 | 4 (1.1) |
Black or African American | 31 (8.8) | 38 (10.7) | 7 (1.9) | 6 (1.7) |
White | 298 (84.4) | 297 (83.7) | 357 (96.7) | 348 (95.9) |
Othera | 15 (4.2) | 10 (2.8) | 5 (1.4) | 5 (1.4) |
BMI (kg/m2) | ||||
Mean (range) | 24.47 (13.6 to 77.1) | 24.66 (11.9 to 57.9) | 22.13 (13.2 to 39.8) | 22.03 (15.5 to 40.6) |
Fitzpatrick skin type, n (%)b | ||||
I | 7 (2.0) | 7 (2.0) | 7 (1.9) | 12 (3.3) |
II | 111 (31.4) | 111 (31.3) | 122 (33.1) | 107 (29.5) |
III | 122 (34.6) | 121 (34.1) | 170 (46.1) | 166 (45.7) |
IV | 63 (17.8) | 64 (18.0) | 57 (15.4) | 54 (14.9) |
V | 27 (7.6) | 23 (6.5) | 7 (1.9) | 21 (5.8) |
VI | 23 (6.5) | 29 (8.2) | 6 (1.6) | 3 (0.8) |
Baseline IGA score, n (%) | ||||
3 (moderate) | 292 (82.7) | 291 (82.0) | 305 (82.7) | 313 (86.2) |
4 (severe) | 61 (17.3) | 64 (18.0) | 64 (17.3) | 50 (13.8) |
TLC | ||||
Mean (SD) | 101.5 (25.12) | 103.6 (26.1) | 105.7 (25.8) | 104.6 (24.2) |
Range | 60 to 170 | 61 to 196 | 60 to 241 | 60 to 170 |
NILC | ||||
Mean (SD) | 59.1 (22.19) | 60.7 (22.09) | 62.8 (21.37) | 63.3 (20.52) |
Range | 30 to 100 | 30 to 144 | 30 to 177 | 30 to 100 |
ILC | ||||
Mean (SD) | 42.4 (11.77) | 42.9 (12.31) | 42.9 (12.20) | 41.3 (10.96) |
Range | 30 to 83 | 30 to 75 | 30 to 75 | 30 to 74 |
BMI = body mass index; IGA = Investigator’s Global Assessment; ILC = inflammatory lesion count; NILC = noninflammatory lesion count; SD = standard deviation; TLC = total lesion count.
a“Other” defined as American Indian or Alaska Native, Native Hawaiian or other Pacific Islander, other, and multiple races.
bDefinitions for the Fitzpatrick skin type scale: type I means always burns easily, never tans (sensitive); type II means always burns easily, tans minimally (sensitive); type III means burns moderately, tans gradually (light brown) (normal); type IV means burns minimally, always tans well (moderate brown) (normal); type V means rarely burns minimally, tans profusely (dark brown) (insensitive); and type VI means never burns, deeply pigmented (insensitive).
Sources: Clinical Study Report for the CB-03-01/25 trial,18 Clinical Study Report for the CB-03-01/26 trial,19 and the sponsor’s summary of clinical evidence.23
Exposure to Study Treatments
Patients who adhered to treatment had at least 80% of the expected cream applications at the study visits. Nonadherence was defined as adherence of less than 80%. In the ITT set, 89.5% (316 of 353) of patients and 87.3% (310 of 355) of patients treated with clascoterone and vehicle cream, respectively, adhered to treatment with at least 81% of patients who adhered at each time point throughout the CB-03-01/25 trial. In addition, the mean daily amount of drug applied (the total amount of drug used divided by the number of days of treatment) was calculated for each patient. In the ITT set, the mean daily amount of product was 1.96 g of clascoterone and 1.96 g of vehicle cream in the CB-03-01/25 trial.
Table 12: Summary of Patient Exposure From Studies Included in the Systematic Review (ITT Population)
Exposure | CB-03-01/25 study | CB-03-01/26 study | ||
|---|---|---|---|---|
Clascoterone (N = 353) | Vehicle (N = 355) | Clascoterone (N = 369) | Vehicle (N = 363) | |
Patients, n | 332 | 333 | 352 | 327 |
Total amount (g) | ||||
Mean (SD) | 158.34 (58.87) | 160.55 (59.48) | 160.50 (54.92) | 162.77 (55.30) |
Median | 160.67 | 165.30 | 168.20 | 170.10 |
Range | 3.8 to 328.6 | 9.10 to 316.9 | 5.9 to 299.3 | 1.4 to 285.7 |
Daily amount (g) | ||||
Mean (SD) | 1.96 (0.60) | 1.96 (0.58) | 1.97 (0.51) | 1.98 (0.51) |
Median | 1.950 | 1.940 | 1.97 | 2.00 |
Range | 0.17 to 4.80 | 0.18 to 3.70 | 0.19 to 3.69 | 0.09 to 4.14 |
Patients who were ≥ 80% adherent to treatment, n (%) | 316 (89.5) | 310 (87.3) | 340 (92.1) | 313 (86.2) |
Nonevaluable patients, n (%) | 19 (5.4) | 24 (6.8) | 19 (5.1) | 35 (9.6) |
ITT = intention to treat; SD = standard deviation.
Sources: Clinical Study Report for the CB-03-01/25 trial,18 Clinical Study Report for the CB-03-01/26 trial,19 and the sponsor’s summary of clinical evidence.23
In the ITT population of the CB-03-01/26 study, the mean overall adherence was 95.7% in patients in the clascoterone group and 95.0% in the vehicle group. The mean daily amount of product was 1.97 g and 1.98 g in the clascoterone and vehicle groups, respectively, in the CB-03-01/26 study.
Protocol Deviations
Protocol deviations in the pivotal trials are summarized in Table 13. The most common category of protocol deviations was related to the use of prohibited concomitant medications, which occurred in 2.5% of patients in both in the clascoterone and vehicle groups of the CB-03-01/25 study and in 4.1% and 3.0% of patients in the clascoterone and vehicle groups, respectively, in the CB-03-01/26 study.
Table 13: Major Protocol Deviations in the Pivotal Trials (ITT Set)
Protocol deviation, n (%) | CB-03-01/25 study | CB-03-01/26 study | ||
|---|---|---|---|---|
Clascoterone (N = 353) | Vehicle (N = 355) | Clascoterone (N = 369) | Vehicle (N = 363) | |
Major protocol deviations, n (%) | 11 (3.1) | 13 (3.7) | 17 (4.6) | 12 (3.3) |
Prohibited concomitant medication | 9 (2.5) | 9 (2.5) | 15 (4.1) | 11 (3.0) |
Inclusion criteria not met | 1 (0.3) | 1 (0.3) | 2 (0.5) | 1 (0.3) |
Exclusion criteria not met | 1 (0.3) | 3 (0.8) | 0 | 0 |
ITT = intention to treat.
Sources: Clinical Study Report for the CB-03-01/25 trial18 and Clinical Study Report for the CB-03-01/26 trial.19
Efficacy
Global Success
Proportion of Patients Aged 12 Years or Older Achieving Improvement at Week 12
In the CB-03-01/25 study, the adjusted proportion of patients aged 12 years and older achieving improvement at week 12 was 18.8% in the clascoterone group versus 8.9% in the vehicle group (OR = 2.36; 95% CI, 1.4 to 3.9; P = 0.0008). Similarly, in the CB-03-01/26 study, at week 12, the adjusted proportion of patients aged 12 years and older achieving improvement at week 12 was 20.8% in the clascoterone group versus 6.5% in the vehicle group (OR = 3.8; 95% CI, 2.2 to 6.4; P < 0.0001). At week 12, the results of the pooled analysis were consistent across both studies.
Sensitivity analyses results in the ITT population were consistent with the primary efficacy results in both trials, with the exception of the worst-case analysis.
Lesion Counts
Absolute Change From Baseline in NILC at Week 12
In the CB-03-01/25 study, a greater absolute decrease from baseline in NILC was noted in patients treated with clascoterone (−19.4 lesions) compared to patients treated with vehicle cream (−13.1 lesions) at week 12 (treatment group difference = −6.3 lesions; 95% CI, −10.2 lesions to −2.4 lesions; P = 0.0016). Similarly, in the CB-03-01/26 study, at week 12, the absolute change in NILC from baseline to week 12 was −19.4 lesions in the clascoterone group versus −10.9 lesions in the vehicle group (treatment group difference = −8.4 lesions; 95% CI, −12.4 lesions to −4.5 lesions; P < 0.0001).
Results of the worst-value and worst-case analyses were inconsistent with the results obtained on the ITT set for this outcome while results from sensitivity analyses using LOCF and BOCF were consistent with the primary result from the pivotal trials.
Percentage Change in NILC From Baseline at Week 12
In the CB-03-01/25 study, the percentage change from baseline to week 12 was greater in the clascoterone group than the vehicle group for NILC at −30.7% versus −21.6%, respectively (treatment group difference = −8.8%; 95% CI, −15.9% to −1.8%; P = 0.0141). In the CB-03-01/26 study, the percentage change from baseline to week 12 was greater in the clascoterone group than the vehicle group for NILC at −29.3% versus −15.8%, respectively (treatment group difference = −13.5%; 95% CI, −19.8% to −7.1%; P < 0.0001).
Absolute Change From Baseline in ILC at Week 12
In the CB-03-01/25 study, the absolute change in ILC from baseline at week 12 was −19.4 lesions in the clascoterone group versus −15.5 lesions in the vehicle group (treatment group difference = −3.9 lesions; 95% CI, −6.5 lesions to −1.3 lesions; P = 0.0029). Similarly, in the CB-03-01/26 study, at week 12, the absolute change from baseline in ILC at week 12 was also −20.0 lesions in the clascoterone group versus −12.6 lesions in the vehicle group (treatment group difference = −7.4 lesions; 95% CI, −9.8 lesions to −5.0 lesions; P < 0.0001).
Results of the worst-value and worst-case analyses were inconsistent with the results obtained on the ITT set for this outcome in the CB-03-01/25 trial and the results of the worst-case analysis were inconsistent with results obtained on the ITT set for this outcome in the CB-03-01/26 trial.
Percentage Change in ILC From Baseline at Week 12
In the CB-03-01/25 study, the percentage change from baseline to week 12 was greater in the clascoterone group than the vehicle group for ILC at −44.8% versus −36.6%, respectively (treatment group difference = −8.3%; 95% CI, −14.3% to −2.3%; P = 0.0070). In the CB-03-01/26 study, the percentage change from baseline to week 12 was greater in the clascoterone group than the vehicle group for ILC at −47.0% versus −29.8%, respectively (treatment group difference = −17.2%; 95% CI, −22.9% to −11.5%; P < 0.0001).
Absolute Change From Baseline in TLC at Week 12
In the CB-03-01/25 study, the absolute change from baseline to week 12 was greater in the clascoterone group than the vehicle group for TLC at −39.2 lesions versus −28.9 lesions, respectively (treatment group difference = −10.3 lesions; 95% CI, −15.7 lesions to −5.0 lesions; P = 0.0002). In the CB-03-01/26 study, the absolute change from baseline to week 12 was greater in the clascoterone group than the vehicle group for TLC at −40.3 lesions versus −23.7 lesions, respectively (treatment group difference = −16.6 lesions; 95% CI, −22.0 lesions to −11.1 lesions; P < 0.0001).
Percentage Change in TLC From Baseline at Week 12
In the CB-03-01/25 study, the percentage change from baseline to week 12 was greater in the clascoterone group than the vehicle group for TLC at −37.1% versus −28.5%, respectively (treatment group difference = −8.7%; 95% CI, −14.0% to −3.3%; P = 0.0016). In the CB-03-01/26 study, the percentage change from baseline to week 12 was greater in the clascoterone group than the vehicle group for TLC at −37.7% versus −22.2%, respectively (treatment group difference = −15.6%; 95% CI, −20.9% to −10.3%; P < 0.0001).
Mental Health and HRQoL
Mental health and HRQoL were not assessed in either the CB-03-01/25 trial or the CB-03-01/26 trial.
Table 14: Summary of Key Efficacy Results From Studies Included in the Systematic Review (ITT Set)
Variable | CB-03-01/25 study | CB-03-01/26 study | ||
|---|---|---|---|---|
Clascoterone N = 353 | Vehicle N = 355 | Clascoterone N = 369 | Vehicle N = 363 | |
Proportion of patients aged ≥ 12 years whose treatment status was considered an improvement at week 12 | ||||
Patients, n | 342 | 350 | 367 | 362 |
Number of patients whose treatment status was considered an improvement at week 12, n (%) | 57 (16.1) | 25 (7.0) | 69 (18.7) | 17 (4.7) |
Adjusted proportions, treatment success at week 12, %a | 18.8 | 8.9 | 20.8 | 6.5 |
Treatment difference, % (95% CI) | 9.9 (5.0 to 15.2) | 14.3 (9.4 to 19.2) | ||
Adjusted OR point estimate (95% CI) | 2.36 (1.43 to 3.88) | 3.8 (2.2 to 6.4) | ||
P value | 0.0008 | < 0.0001 | ||
Absolute change from baseline in NILC at week 12 | ||||
Baseline (lesions), mean (SD) | 59.1 (22.19) | 60.7 (22.09) | 62.8 (21.37) | 63.3 (20.52) |
Patients, n | 342 | 350 | 367 | 362 |
Absolute change from baseline (lesions), mean | −19.4 | −13.1 | −19.4 | −10.9 |
LSM difference vs. control, lesions (95% CI) | −6.3 (−10.2 to −2.4) | −8.4 (−12.4 to −4.5) | ||
P value | 0.0016a | < 0.0001a | ||
Percentage change in NILC from baseline at week 12 | ||||
Baseline (%), mean (SD) | 59.1 (22.19) | 60.7 (22.09) | 62.8 (21.37) | 63.3 (20.52) |
Patients, n | 342 | 350 | 367 | 362 |
Change from baseline at week 12, % | −30.7 | −21.6 | −29.3 | −15.8 |
Treatment group difference vs. control, % (95% CI) | −8.8 (−15.9 to −1.8) | −13.5 (−19.8 to −7.1) | ||
P value | 0.0141a | < 0.0001a | ||
Absolute change from baseline in ILC at week 12 | ||||
Baseline (lesions), mean (SD) | 42.4 (11.77) | 42.9 (12.31) | 42.9 (12.20) | 41.3 (10.96) |
Patients, n | 342 | 350 | 367 | 362 |
Absolute change from baseline (lesions), mean | −19.4 | −15.5 | −20.0 | −12.6 |
LSM mean difference vs. control, lesions (95% CI) | −3.9 (−6.5 to −1.3) | −7.4 (−9.8 to −5.0) | ||
P value | 0.0029a | < 0.0001a | ||
Percentage change in ILC from baseline at week 12 | ||||
Baseline (%), mean (SD) | 42.4 (11.77) | 42.9 (12.31) | 42.9 (12.20) | 41.3 (10.96) |
Patients, n | 342 | 350 | 367 | 362 |
Change from baseline at week 12, % | −44.8 | −36.6 | −47.0 | −29.8 |
Treatment group difference vs. control, % (95% CI) | −8.3 (−14.3 to −2.3) | −17.2 (−22.9 to −11.5) | ||
P value | 0.0070a | < 0.0001a | ||
Absolute change in TLC from baseline at week 12 | ||||
Baseline (lesions), mean (SD) | 101.5 (25.12) | 103.6 (26.13) | 105.7 (25.76) | 104.6 (24.18) |
Patients, n | 342 | 350 | 367 | 362 |
Absolute change from baseline (lesions), mean | −39.2 | −28.9 | −40.3 | −23.7 |
LSM mean difference vs. control, lesions (95% CI) | −10.3 (−15.7 to −5.0) | −16.6 (−22.0 to −11.1) | ||
P value | 0.0002a | < 0.0001a | ||
Percentage change in TLC from baseline at week 12 | ||||
Baseline (%), mean (SD) | 101.5 (25.12) | 103.6 (26.13) | 105.7 (25.76) | 104.6 (24.18) |
Patients, n | 342 | 350 | 367 | 362 |
Change from baseline at week 12, % | −37.1 | −28.5 | −37.7 | −22.2 |
Treatment group difference vs. control, % (95% CI) | −8.7 (−14.0 to −3.3) | −15.6 (−20.9 to −10.3) | ||
P value | 0.0016a | < 0.0001a | ||
CI = confidence interval; ILC = inflammatory lesion count; ITT = intention to treat; LSM = least squares mean; NILC = noninflammatory lesion count; OR = odds ratio; SD = standard deviation; TLC = total lesion count; vs. = versus.
Note: Treatment success was defined as an IGA deduction of at least 2 points from baseline and an IGA score of 0 or 1 at week 12.
aTests were included in the hierarchical testing structure to control the global type I error rate. The threshold for significance was an alpha of less than 0.05.
Sources: Clinical Study Report for the CB-03-01/25 trial,18 Clinical Study Report for the CB-03-01/26 trial,19 and the sponsor’s summary of clinical evidence.23
Harms
Refer to Table 15 for harms data.
Adverse Events
The safety profile was similar between the treatment groups for both pivotal trials. In the CB-03-01/25 study and the CB-03-01/26 study, respectively, 40 (11.3%) patients and 42 (11.4%) patients who received clascoterone experienced TEAEs compared to 41 (11.5%) patients and 50 (13.8%) patients who received vehicle cream.
Serious Adverse Events
In the CB-03-01/25 study, 1 (0.3%) patient in the vehicle group had an SAE of pneumonia. In the CB-03-01/26 study, 1 (0.3%) patient in the vehicle group had an SAE of hematoma. There were no SAEs among patients who received clascoterone.
Withdrawal Due to Adverse Events
In the CB-03-01/25 study, there were 9 patients who experienced 9 TEAEs that led to study discontinuation: 3 (0.8%) patients in the clascoterone group and 6 (1.7%) patients in the vehicle group. In the CB-03-01/26 study, 10 (1.4%) patients discontinued due to AEs, including 2 (0.5%) patients treated with clascoterone and 8 (2.2%) patients treated with vehicle cream.
Mortality
No deaths were reported in either trial.
Notable Harms
In the CB-03-01/25 and CB-03-01/26 studies, the incidence of LSRs (telangiectasia, skin atrophy, striae rubrae, erythema, edema, scaling or dryness, stinging or burning, and pruritus) was similar across treatment groups. In the CB-03-01/25 trial, 40.4% of patients in the clascoterone group and 49.4% of patients in the vehicle group experienced LSRs. In the CB-03-01/26 trial, 45.2% of patients in the clascoterone group and 42.0% of patients in the vehicle group experienced LSRs. The most common treatment-emergent LSRs were erythema in both pivotal trials (in 19 [5.4%] patients versus 30 [8.5%] patients for the CB-03-01/25 trial and in 27 [7.3%] patients versus 18 [5.0%] patients for the CB-03-01/26 trial).
Table 15: Summary of Harms Results — Safety Set
AE | CB-03-01/25 study | CB-03-01/26 study | ||
|---|---|---|---|---|
Clascoterone N = 353 | Vehicle N = 355 | Clascoterone N = 369 | Vehicle N = 363 | |
AEs, n (%) | ||||
≥ 1 AE | 40 (11.3) | 41 (11.5) | 42 (11.4) | 50 (13.8) |
Most common AEsa | ||||
Nasopharyngitis | 6 (1.7) | 12 (3.4) | 3 (0.8) | 7 (1.9) |
Upper respiratory tract infection | 1 (0.3) | 2 (0.6) | 1 (0.3) | 4 (1.1) |
Oropharyngeal pain | 2 (0.6) | 1 (0.3) | 4 (1.1) | 4 (1.1) |
Headache | 2 (0.6) | 1 (0.3) | 4 (1.1) | 3 (0.8) |
Rhinorrhea | 0 | 0 | 3 (0.8) | 5 (1.4) |
SAEs, n (%) | ||||
Patients with ≥ 1 SAE | 0 | 1 (0.3) | 0 | 1 (0.3) |
Pneumonia | 0 | 1 (0.3) | 0 | 0 |
Hematoma | 0 | 0 | 0 | 1 (0.3) |
Patients who stopped treatment due to AEs, n (%) | ||||
Patients who stopped | 3 (0.8) | 6 (1.7) | 2 (0.5) | 8 (2.2) |
Reason for stopping treatment | ||||
Application site, hypersensitivity | 1 (0.3) | 0 | 0 | 0 |
Sebaceous hyperplasia | 1 (0.3) | 0 | 0 | 0 |
Oropharyngeal pain | 1 (0.3) | 0 | 0 | 0 |
Application site, pain or erythema | 0 | 2 (0.5) | 0 | 2 (0.5) |
Application site, pruritus | 0 | 1 (0.3) | 0 | 1 (0.3) |
Application site, urticaria | 0 | 1 (0.3) | 0 | 0 |
Application site, dermatitis | 0 | 1 (0.3) | 1 (0.3) | 0 |
Application site, acne | 0 | 1 (0.3) | 0 | 3 (0.8) |
Pneumonia | 0 | 1 (0.3) | 0 | 0 |
Application site, nodule | 0 | 0 | 0 | 1 (0.3) |
Depigmented hair on nose | 0 | 0 | 1 (0.3) | 0 |
Skin irritation | 0 | 0 | 0 | 1 (0.3) |
Cough | 0 | 0 | 0 | 1 (0.3) |
Dyspnea | 0 | 0 | 0 | 1 (0.3) |
Deaths, n (%) | ||||
Patients who died | 0 | 0 | 0 | 0 |
AEs of special interest,b n (%) | ||||
≥ 1 LSR | 180 (52.6) | 189 (54.0) | 88 (55.3) | 61 (53.3) |
Erythema or reddening | 19 (5.4) | 30 (8.5) | 27 (7.3) | 18 (5.0) |
Scaling or dryness | 20 (5.7) | 21 (5.9) | 14 (3.8) | 7 (1.9) |
Skin atrophy | 4 (1.1) | 7 (2.0) | 5 (1.4) | 4 (1.1) |
Pruritus | 10 (2.9) | 14 (4.0) | 14 (3.8) | 13 (3.6) |
Edema | 3 (0.9) | 5 (1.4) | 10 (2.7) | 7 (1.9) |
Striae rubrae | 3 (0.9) | 2 (0.6) | 8 (2.2) | 5 (1.4) |
Telangiectasia | 0 | 4 (1.1) | 5 (1.3) | 3 (0.8) |
Stinging or burning | 3 (0.9) | 5 (1.4) | 5 (1.4) | 4 (1.1) |
AE = adverse event; LSR = local skin reaction; SAE = serious adverse event; TEAE = treatment-emergent adverse event.
Note: AEs were classified as TEAEs (defined as all AEs occurring or worsening after the first dose of the drug). Nasopharyngitis is the only TEAE that was reported in more than 1% of patients and more than 5 patients.
aAt least 1% of patients in any treatment group.
bThe number (proportion) of patients in the assessment category of “not done” is not reported in this report.
Sources: Clinical Study Report for the CB-03-01/25 trial,18 Clinical Study Report for the CB-03-01/26 trial,19 and the sponsor’s summary of clinical evidence.23
Critical Appraisal
Internal Validity
The CB-03-01/25 and CB-03-01/26 trials were multicentre, randomized, double-blind, vehicle-controlled studies. Randomization was blocked by study site and an interactive response technology for concealment of the randomization assignment was used, which was considered appropriate. Based on input from the clinical expert consulted by CDA-AMC for the purpose of the review, the following were identified as important treatment effect modifiers: age, sex, and ethnicity. In addition, sex was considered an important prognostic factor. Although randomization was not stratified by these variables, any potential impact on the efficacy results was not expected because the proportion of patients with the relevant demographic characteristics at baseline (prognostic factors and effect modifiers) were generally well balanced between the clascoterone and vehicle groups of both trials. There was no notable difference between treatment groups or baseline characteristics in either pivotal trial. Statistical analyses were, in general, appropriate for the outcomes evaluated. The study sample size, however, did not reach the threshold at which it could be adequately powered to detect the treatment difference in the primary end points between treatment groups. The sponsor noted that the study was also powered for the secondary end points and a hierarchical testing procedure was appropriately used to account for multiplicity in the primary end points.
Discontinuation was largely driven by loss to follow-up and patient withdrawal. Missing data in the primary end points were imputed by MI analysis under the MAR assumption. The sensitivity analysis of LOCF, BOCF, and PP was generally consistent with the primary analysis. However, the imputation based on worst-value and worst-case analyses was not consistent with the primary analysis for absolute change in ILC and NILC. The amount of missing data was considered relatively high in both the clascoterone and vehicle group in both trials (approximately 18%) at week 12. The MI approach used for missing data in the primary analysis relied on a MAR assumption that assumed that missing values for a given end point could be explained by observed values of that end point. It was noted that a majority of patients dropped out at the beginning of the study period (e.g., before visit 2) across both trials; this suggests that the imputation for missing values of end points at visit 4 were primarily informed by patients who completed the study. Given that a likely explanation for patient dropout was due to lack of response to treatment, patients who completed the study were not likely to be representative of patients who dropped out early. Therefore, the approach to account for missing data in the primary analysis may not have been adequate for addressing potential bias due to missing data, and sensitivity analyses suggest that the primary analysis may have overestimated the benefit of clascoterone for improving ILC and NILC at week 12.
The statistical testing strategy was implemented in both trials to control for type I error at the level of the individual study and at the level of the pool dataset of both studies. Pooled analyses were not preplanned. Secondary end points were adjusted for multiple comparisons when the null hypothesis of the primary efficacy outcome was rejected. Important subgroups of interest identified by the clinical expert consulted on this review were sex, age, and ethnicity. However, prespecified subgroup analyses were not conducted, except for by the investigational site.
Treatment response was based on lesion counts assessed by the investigator or designee. A central adjudication was not performed and hence there could potentially be interobserver variation in lesion counts if the same investigator was not available for each site visit. However, considering the double-blind design, the concern for potential subjectivity in lesion count impacting the efficacy results is low. In addition, the clinical expert was not concerned about the variation in counting lesions.
Major protocol deviations were uncommon across both trials. The most common protocol deviation was the use of prohibited concomitant medications. This occurred in less than 3% of patients in the CB-03-01/25 study and in less than 5% of patients in the CB-03-01/26 study; hence, the potential for bias was low.
External Validity
The population of interest, as per the reimbursement indication, is patients aged 12 years and older who have moderate to severe acne vulgaris. A notable group of patients with severe acne vulgaris (i.e., nodulocystic acne) were excluded from both trials. Hence, the sample population in the trials may not fully represent the general population of patients with severe acne vulgaris as noted in clinical practice in Canada.
Within the trials, approximately 16 patients in the CB-03-01/25 trial (N = 11 in the clascoterone group and N = 5 in the vehicle group) and 3 patients in the CB-03-01/26 trial (N = 2 in the clascoterone group and N = 1 in the vehicle group) were aged younger than 12 years. When comparing the datasets for patients 12 years or older versus 9 years or older (from the product monograph16 and the Clinical Study Reports18,19), there were no changes to statistical significance that would meaningfully change conclusions on efficacy or harms. Given that the number of patients outside the reimbursement indication population was small, and that the clinical expert felt the results would not differ by age, the impact on the results of including these patients outside the reimbursement indication population is negligible. Although no Canadian sites were included in either trial, the clinical expert felt that the intervention and concomitant medications used in the trial and the schedule of assessment were considered generalizable to clinical practice in Canada.
The clinical expert felt that 12 weeks of follow-up was a reasonable and standard time point across acne trials and would be considered the earliest time point at which a change in lesion numbers would be noted with a therapy. However, the clinical expert noted that the optimal time point for follow-up for NILC would be 6 months. In addition, the clinical expert noted that change in absolute lesion counts is not relevant to clinical practice as it is not feasible for clinicians to be counting lesions and there is also a level of subjectivity to counting lesions. Instead, the clinical expert felt that the patient’s impression of change and the percentage change in lesion count were considered more clinically relevant.
Throughout the study period, approximately 18% or more of patients in each group of each study discontinued, mostly due to being lost to follow-up and patient withdrawal, while study discontinuation due to AEs or lack of efficacy was relatively low (less than 3%). The clinical expert indicated that patients with acne vulgaris are often not adherent to treatment, although more than 80% of patients adhered to the treatment regimen in both treatment groups of the CB-03-01/25 study and more than 95% of patients in both treatments groups of the CB-03-01/26 study. The clinical expert suggested some possible reasons for discontinuation, including a lack of response to treatment and inconvenience in travel to clinical trial visits. The clinical expert considered a study discontinuation rate of 18% to be relatively high.
GRADE Summary of Findings and Certainty of the Evidence
Methods for Assessing the Certainty of the Evidence
For pivotal studies and RCTs identified in the sponsor’s systematic review, GRADE was used to assess the certainty of the evidence for outcomes considered most relevant to inform deliberations of the CDA-AMC expert committee, and a final certainty rating was determined as outlined by the GRADE Working Group.20,21
“High certainty: We are very confident that the true effect lies close to that of the estimate of the effect.
Moderate certainty: We are moderately confident in the effect estimate — The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. We use the word ‘likely’ for evidence of moderate certainty (e.g., ‘X intervention likely results in Y outcome’).
Low certainty: Our confidence in the effect estimate is limited — The true effect may be substantially different from the estimate of the effect. We use the word ‘may’ for evidence of low certainty (e.g., ‘X intervention may result in Y outcome’).
Very low certainty: We have very little confidence in the effect estimate — The true effect is likely to be substantially different from the estimate of effect. We describe evidence of very low certainty as ‘very uncertain.’”
Following the GRADE approach, evidence from RCTs started as high-certainty evidence and could be rated down for concerns related to study limitations (which refers to internal validity or risk of bias), inconsistency across studies, indirectness, the imprecision of effects, and publication bias.
When possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect; if this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., the clinical importance was unclear). In all cases, the target of the certainty of evidence assessment was based on the point estimate and where it was located relative to the threshold for a clinically important effect (when a threshold was available) or to the null.
The reference points for the certainty of evidence assessment for efficacy end points and notable harms (LSRs) were set according to the presence or absence of an important effect based on thresholds informed by the clinical expert.
For the GRADE assessments, findings from the CB-03-01/25 and CB-03-01/26 studies were considered together and summarized narratively per outcome because these studies were identical in population, interventions, design, and outcome measures.
Results of GRADE Assessments
Clascoterone Versus Placebo
Table 2 presents the GRADE summary of findings for clascoterone 1% cream versus vehicle cream.
LTE Studies
Content in this section has been informed by materials submitted by the sponsor. The following has been summarized and validated by the CDA-AMC review team.
Description of Studies
One LTE study (the CB-03-01/27 trial) has been summarized to provide evidence regarding clascoterone. This was a multicentre, open-label, LTE study that combined patients from the CB-03-01/25 and CB-03-01/26 pivotal studies. The primary objective was to determine the long-term safety of clascoterone cream, applied twice daily (morning and evening) for an additional 9 months in patients with acne vulgaris who participated in the phase III pivotal studies for a total treatment duration of up to 12 months. For patients randomized to clascoterone in the pivotal studies, the total active treatment period was 12 months and for patients randomized to vehicle cream, the total active treatment period was 9 months. The end points for the primary objective were systemic and local TEAEs, including LSRs (telangiectasia, skin atrophy, striae rubrae, erythema, edema, scaling or dryness, stinging or burning, and pruritus). The number of patients with each IGA severity score was the efficacy end point. The study consisted of a baseline visit, LTF visits at LTF month 1, month 3, month 6, and month 9, and follow-up phone calls at LTF month 4.5 and month 7.5.
All patients applied clascoterone cream twice daily (morning and evening) to the face and, if designated by the investigator and desired by the patient, to the trunk for truncal acne for an additional 9 months of treatment. (Truncal acne had not been treated with clascoterone in the previous controlled studies.) Treatment on the face and/or trunk could be discontinued if or when acne cleared (having achieved an IGA score of 0 or 1) and restarted if or when acne worsened (an IGA score of 2 or greater), according to the assessment of the investigator for each treatment area (face and trunk).
Populations
Inclusion and exclusion criteria were the same as those in the pivotal trials described earlier in this report. Patients in the LTE study must have been enrolled in 1 of the phase III pivotal studies, must have completed the assigned treatment regimen without any material noncompliance with study requirements or treatment dosing (an adherence of 80% or greater), and must have completed the final study visit (visit 4 in the pivotal studies).
Baseline Characteristics
There were more female patients (62.6%) than male patients (37.4%) and the mean age of patients was 19.2 years (median = 17 years). The mean weight of patients at baseline was 66.76 kg (median = 63.10 kg) and the mean BMI of patients was 23.16 kg/m2 (median = 21.80 kg/m2). Baseline characteristics are summarized in Table 16.
Table 16: Summary of Baseline Characteristics for CB-03-01/27 Study — ITT Population
Characteristic | Originally randomized to clascoterone N = 317 | Originally randomized to vehicle N = 292 | Overall N = 609 |
|---|---|---|---|
Age (years) | |||
Mean (SD) | 19.2 (5.8) | 19.2 (6.7) | 19.2 (6.3) |
Median (range) | 17 (10 to 50) | 17 (10 to 50) | 17 (10 to 50) |
Sex, n (%) | |||
Female | 198 (62.5) | 183 (62.7) | 381 (62.6) |
Male | 119 (37.5) | 109 (37.3) | 228 (37.4) |
Race, n (%) | |||
American Indian or Alaska Native | 1 (0.3) | 0 | 1 (0.2) |
Asian | 6 (1.9) | 8 (2.7) | 14 (2.3) |
Black or African American | 17 (5.4) | 18 (6.2) | 35 (5.7) |
Native Hawaiian or other Pacific Islander | 2 (0.6) | 1 (0.3) | 3 (0.5) |
White | 283 (89.3) | 258 (88.4) | 541 (88.8) |
Multiple | 4 (1.3) | 6 (2.1) | 10 (1.6) |
Other | 4 (1.3) | 1 (0.3) | 5 (0.8) |
Height (cm) | |||
Mean (SD) | 169.42 (10.22) | 169.57 (9.42) | 169.49 (9.84) |
Median (range) | 168.30 (144.0 to 198.1) | 169.0 (135.0 to 197.1) | 168.95 (135.0 to 198.1) |
Weight (kg) | |||
Mean (SD) | 66.90 (18.02) | 66.61 (16.46) | 66.76 (17.28) |
Median (range) | 63.60 (38.6 to 189.0) | 63.0 (40.6 to 121.9) | 63.10 (38.6 to 189.0) |
BMI (kg/m2) | |||
Mean (SD) | 23.21 (5.59) | 23.11 (5.21) | 23.16 (5.40) |
Median (range) | 22.0 (15.2 to 67.3) | 21.60 (14.5 to 45.5) | 21.80 (14.5 to 67.3) |
BMI = body mass index; ITT = intention to treat; SD = standard deviation.
Note: Patients were summarized overall and according to the treatment (either clascoterone or vehicle cream) that they received in the phase III pivotal studies (the CB-03-01/25 and CB-03-01/26 trials).
Sources: Sponsor’s summary of clinical evidence23 and Clinical Study Report for the CB-03-01/27 trial.52
Interventions
All patients applied clascoterone twice daily (morning and evening) to the entire face and, if designated by the investigator and desired by the patient, to the trunk for acne for an additional 9 months of treatment.
Any medications that were used before the start of this study were recorded as part of the phase III pivotal study (the CB-03-01/25 or CB-03-01/26 trial).
Prohibited medications or therapies on the face or trunk during the study included the following:
light treatments (including artificial tanning devices, blue light, and laser)
systemic spironolactone
systemic retinoid therapy
all topical acne therapies other than the ones on the allowed medications list (e.g., retinoids, azelaic acid, dapsone).
The following supplemental products and/or procedures were allowed at the discretion of the investigator on the face or trunk if control of acne was insufficient during the study:
hormonal contraceptives
the occasional use of systemic antibiotics for acne (not to exceed 12 continuous weeks) or for other medical needs
systemic corticosteroids (for other medical needs)
the occasional use of intralesional corticosteroid injections for nodular or cystic acne lesions (low dose [e.g., approximately 2 mg triamcinolone per cubic cm]) or for other medical needs
the occasional use of topical steroids or topical antibiotics for up to 10 continuous days (for other medical needs) within the treatment area (face and/or trunk)
topical antiacne cleansers (not leave-on products) that have benzoyl peroxide (5% or less) or salicylic acid (2% or less) as their only active ingredient within the treatment area (face and/or trunk).
Outcomes
The main outcomes measured were safety outcomes:
the incidence of any local and systemic TEAEs
the number of patients with the presence of each individual LSR for each treatment area, as applicable, at each time point collected (baseline, LTF month 1, LTF month 3, LTF month 6, and LTF month 9, and any unscheduled visits).
A treatment-emergent LSR was defined as any LSR ongoing from the CB-03-01/25 or CB-03-01/26 trial if the patient originally received clascoterone or any new LSR after the baseline preapplication assessment. In addition, any LSR worsening after the baseline preapplication assessment was considered treatment-emergent from the time of worsening, regardless of the scores pattern after worsening.
The efficacy outcome measured was the number of patients with each IGA severity score for each treatment area, as applicable, at each time point collected (baseline, LTF month 1, LTF month 3, LTF month 6, and LTF month 9).
Statistical Analysis
Approximately 600 participants had to be enrolled to have 300 participants on-study at 6 months and 100 participants on-study at 12 months. These treatment durations included the 0 months or 3 months of active treatment in the phase III pivotal studies.
The ITT set included all enrolled individuals and was used for efficacy analyses. The safety set was used for safety analysis and included all participants who had received at least 1 application of the study drug.
Summary tables (descriptive statistics or frequency tables) are provided for baseline variables, efficacy variables, and safety variables. Continuous variables are described by descriptive statistics (number, mean, standard deviation [SD], adherence value percentage, minimum, median, and maximum). Frequency counts and the percentage of individuals within each category are provided for categorical data. No further statistical testing was performed. No statistical hierarchy was explored.
Adherence to the study drug was evaluated at each visit and overall, according to the following calculation: 100 multiplied by the number of applications divided by the number of scheduled applications. Nonadherence was defined as a value of less than 80%.
Descriptive statistics were used to summarize exposure to the study drug at each visit. The date and time of the first and last application, the total amount of the study drug used (calculated as the number of grams applied for each patient from the weights of the returned study drug), and the mean daily amount of the study drug applied (calculated as the total amount of the study drug used divided by the number of days of treatment) were listed.
All AEs were coded using Medical Dictionary for Regulatory Activities version 18.1. Individual TEAEs (i.e., all the AEs occurring or worsening after the first dose of the study drug) were listed with the number and percentage tabulated. Missing data were not replaced.
Results
Patient Disposition
Of the 609 screened and enrolled patients (with 317 patients randomized to the clascoterone group and 292 patients randomized to the vehicle group in the preceding pivotal studies), 2 patients were not treated with the study drug in the LTE and were excluded from the safety population. Of 607 patients who were treated with at least 1 dose of clascoterone during the LTE period (safety population), 57.2% completed the study. The most common reasons for discontinuation were withdrawal by patient (16.6%), being lost to follow-up (14.8%), and lack of efficacy (4.9%). The distribution of reasons for discontinuing the study was similar between groups, except for AEs (2.8% in the clascoterone group versus 0% in the vehicle group) and nonadherence (0.3% in the clascoterone group versus 1.4% in the vehicle group) (Table 17).
Exposure to Study Treatments
In the ITT population (N = 609), 88.5%, 68.5%, 49.9%, and 20.2% of patients remained in the study at 3 months, 6 months, 9 months, and 12 months of follow-up, respectively. In the safety population (N = 607), 88.6%, 68.5%, 49.9% and 20.3% of patients remained in the study at 3 months, 6 months, 9 months, and 12 months of follow-up, respectively (Table 18). Between the 2 nominal comparison groups, no significant differences in attrition were found during the LTE period (Table 18).
Table 17: Patient Disposition in CB-03-01/27 Studya
Patient disposition | Originally randomized to clascoterone (N = 317) | Originally randomized to vehicle (N = 292) | Total (N = 609) |
|---|---|---|---|
Screened, N | 609 | ||
Enrolled, N | 609 | ||
Treated, N (%) | 317 (100) | 290 (100) | 607 (100) |
Completed study, n (%) | 179 (56.5) | 168 (57.9) | 347 (57.2) |
Discontinued study, n (%)a | 138 (43.5) | 122 (42.1) | 260 (42.8) |
Withdrawal by patient | 56 (17.7) | 45 (15.5) | 101 (16.6) |
Lost to follow-up | 49 (15.5) | 41 (14.1) | 90 (14.8) |
Lack of efficacy | 14 (4.4) | 16 (5.5) | 30 (4.9) |
Withdrawal by parent or guardian | 6 (1.9) | 7 (2.4) | 13 (2.1) |
Adverse event | 9 (2.8) | 0 | 9 (1.5) |
Nonadherence with study drug | 1 (0.3) | 4 (1.4) | 5 (0.8) |
Pregnancy | 1 (0.3) | 2 (0.7) | 3 (0.5) |
Recoveryb | 1 (0.3) | 2 (0.7) | 3 (0.5) |
Technical problemsc | 0 | 1 (0.3) | 1 (0.2) |
Progressive disease | 1 (0.3) | 0 | 1 (0.2) |
Otherd | 0 | 4 (1.4) | 4 (0.7) |
ITT set, N | 317 | 292 | 609 |
Safety set, N | 317 | 290 | 607 |
ITT = intention to treat.
aPatients are summarized overall and according to the original treatment (either study drug or vehicle) that they received in the phase III pivotal studies (the CB-03-01/25 and CB-03-01/26 trials).
bPatients whose lesions cleared and opted out from the study.
cPatient did not complete the treatment period because of a lack of study drug or vehicle; due to repeated temperature excursions, all of the study drug or vehicle was put in quarantine.
dOther reasons for discontinuation were due to a patient moving 2 hours away for school or due to it being inconvenient to continue in the study, due to a patient not wanting to continue treatment application, due to a patient leaving the country for study abroad, and due to a patient who went abroad.
Sources: Sponsor’s summary of clinical evidence23 and Clinical Study Report for the CB-03-01/27 trial.52
The maximum duration of exposure, with the inclusion of the pivotal studies, was 12 months for treatment of the face and 9 months for treatment of the trunk. The mean daily amount of study drug used in the safety and ITT sets was 2.3 g of clascoterone (range, 0.2 g to 13.0 g, including treatment of both the face and trunk, where applicable). In the 2 nominal comparison groups (in both the ITT and safety set), the mean daily amount of study drug used was 2.3 g, with a range 0.22 g to 7.82 g in the clascoterone group and a range of 0.30 g to 13.0 g in the vehicle group.
In the ITT set, 85.4% of patients treated on the face and 76.9% of patients treated on the trunk showed an overall adherence rate greater than 80% (Table 19). Adherence data in the safety set were not provided by the sponsor.
Table 18: Duration of Exposure to Clascoterone Across Controlled and Follow-Up Periods in CB-03-01/27 Study
Duration of exposure | Originally randomized to clascoterone (N = 317) | Originally randomized to vehicle (N = 292) | Total (N = 609) |
|---|---|---|---|
ITT set, n (%) | |||
N of patients | 317 | 292 | 609 |
3 months | 315 (99.4) | 224 (76.7) | 539 (88.5) |
6 months | 236 (74.4) | 181 (62.0) | 417 (68.5) |
9 months | 191 (60.3) | 113 (38.7) | 304 (49.9) |
12 months | 123 (38.8) | 0 | 123 (20.2) |
Safety set, n (%) | |||
N of patients | 317 | 290 | 607 |
3 months | 315 (99.4) | 223 (76.9) | 538 (88.6) |
6 months | 236 (74.4) | 180 (62.1) | 416 (68.5) |
9 months | 191 (60.3) | 112 (38.6) | 303 (49.9) |
12 months | 123 (38.8) | 0 | 123 (20.3) |
ITT = intention to treat.
Source: Clinical Study Report for the CB-03-01/27 trial.52
Table 19: Summary of Treatment Adherence — ITT Set
Population | Originally randomized to clascoterone (N = 317) | Originally randomized to vehicle (N = 292) | Overall (N = 609) |
|---|---|---|---|
Overall treatment adherence: Face, n (%) | |||
Patients with ≥ 80% adherence | 273 (86.1) | 247 (84.6) | 520 (85.4) |
Patients with < 80% adherence | 27 (8.5) | 34 (11.6) | 61 (10.0) |
Nonevaluable patients | 17 (5.4) | 11 (3.8) | 28 (4.6) |
Overall treatment adherence: Trunk, n (%) | |||
Patients with ≥ 80% adherence | 101 (77.7) | 92 (76.0) | 193 (76.9) |
Patients with < 80% adherence | 23 (17.7) | 23 (19.0) | 46 (18.3) |
Nonevaluable patients | 6 (4.6) | 6 (5.0) | 12 (4.8) |
ITT = intention to treat.
Source: Clinical Study Report for the CB-03-01/27 trial.52
Efficacy
The majority (83.1%) of patients showed facial IGA scores that were mild or moderate in severity at baseline, with the overall proportion of patients whose skin was clear or almost clear increasing over time being greatest (ITT population = 181 of 609 [29.7%] patients) at the end of the study (day 274). The proportion of patients whose skin was clear or almost clear increased over the time period of treatment with clascoterone from 9.9% at baseline to 29.7% at day 274. There was a similar proportion of patients whose skin was clear or almost clear on the face at the end of the study between patients originally assigned to treatment with the vehicle cream (ITT population = 30.2% of patients) and clascoterone (ITT population = 29.3% of patients) in the phase III pivotal studies at day 274. A similar trend was observed in patients whose trunk had been treated with clascoterone during the LTE period. The proportion of patients with clear or almost clear skin on the trunk increased from 4.8% at baseline to 31.5% at day 274, with a similar distribution of patients between the 2 nominal comparison groups assigned in the phase III pivotal trials (Table 20).
Table 20: Summary of IGA Results — ITT Population
Adverse event | Originally randomized to clascoterone (N = 317) | Originally randomized to vehicle (N = 292) | Overall (N = 609) |
|---|---|---|---|
Facial IGA, n (%) | |||
N of patients | 317 | 292 | 609 |
Baseline | |||
0 – Clear | 0 | 0 | 0 |
1 – Almost clear | 42 (13.2) | 18 (6.2) | 60 (9.9) |
2 – Mild | 124 (39.1) | 120 (41.1) | 244 (40.1) |
3 – Moderate | 130 (41.0) | 132 (45.2) | 262 (43.0) |
4 – Severe | 21 (6.6) | 22 (7.5) | 43 (7.1) |
Not done | 0 | 0 | 0 |
Day 274 ± 21 days | |||
0 – Clear | 19 (6.0) | 13 (4.5) | 32 (5.3) |
1 – Almost clear | 74 (23.3) | 75 (25.7) | 149 (24.5) |
2 – Mild | 84 (26.5) | 64 (21.9) | 148 (24.3) |
3 – Moderate | 63 (19.9) | 68 (23.3) | 131 (21.5) |
4 – Severe | 11 (3.5) | 8 (2.7) | 19 (3.1) |
Not done | 66 (20.8) | 64 (21.9) | 130 (21.3) |
Last facial IGA assessment | |||
0 – Clear | 18 (5.7) | 13 (4.5) | 31 (5.1) |
1 – Almost clear | 83 (26.2) | 82 (28.1) | 165 (27.1) |
2 – Mild | 111 (35.0) | 95 (32.5) | 206 (33.8) |
3 – Moderate | 88 (27.8) | 92 (31.5) | 180 (29.6) |
4 – Severe | 17 (5.4) | 10 (3.4) | 27 (4.4) |
Not done | 0 | 0 | 0 |
Trunk IGA, n (%) | |||
N of patients | 130 | 121 | 251 |
Baseline | |||
0 – Clear | 2 (1.5) | 0 | 2 (0.8) |
1 – Almost clear | 5 (3.8) | 5 (4.1) | 10 (4.0) |
2 – Mild | 76 (58.5) | 60 (49.6) | 136 (54.2) |
3 – Moderate | 41 (31.5) | 52 (43.0) | 93 (37.1) |
4 – Severe | 4 (3.1) | 1 (0.8) | 5 (2.0) |
Not done | 2 (1.5) | 3 (2.5) | 5 (2.0) |
Day 274 ± 21 days | |||
0 – Clear | 16 (12.3) | 12 (9.9) | 28 (11.2) |
1 – Almost clear | 31 (23.8) | 20 (16.5) | 51 (20.3) |
2 – Mild | 24 (18.5) | 37 (30.6) | 61 (24.3) |
3 – Moderate | 18 (13.8) | 14 (11.6) | 32 (12.7) |
4 – Severe | 2 (1.5) | 1 (0.8) | 3 (1.2) |
Not done | 39 (30.0) | 37 (30.6) | 76 (30.3) |
Last trunk IGA assessment | |||
0 – Clear | 24 (18.5) | 16 (13.2) | 40 (15.9) |
1 – Almost clear | 34 (26.2) | 27 (22.3) | 61 (24.3) |
2 – Mild | 42 (32.3) | 54 (44.6) | 96 (38.2) |
3 – Moderate | 27 (20.8) | 22 (18.2) | 49 (19.5) |
4 – Severe | 3 (2.3) | 2 (1.7) | 5 (2.0) |
Not done | 0 | 0 | 0 |
IGA = Investigator’s Global Assessment; ITT = intention to treat.
Sources: Sponsor’s summary of clinical evidence23 and Clinical Study Report for the CB-03-01/27 trial.52
Harms
Refer to Table 21 for a summary of harms.
Of 607 patients in the safety set, 110 (18.1%) patients experienced at least 1 TEAE. The only TEAEs reported for at least 1.0% of patients were nasopharyngitis (2.6%) and upper respiratory tract infection (1.3%).
Six patients experienced serious TEAEs, including coronary artery dissection, dizziness, depression and suicide attempt, eosinophilic gastroenteritis, fatigue, and induced abortion.
Ten (1.7%) patients discontinued the study drug due to TEAEs and 9 of these patients discontinued the study due to the TEAEs.
Overall, the most frequently reported LSRs were erythema (6.9% on the face and 1.2% on the trunk), scaling or dryness (4.0% on the face and 0.7% on the trunk), and pruritus (1.6% on the face and 0% on the trunk). In general, a higher proportion of patients who originally received clascoterone had treatment-emergent LSRs compared to patients who originally received vehicle cream. For example, 9.8% of patients who had received clascoterone in the parent trials compared to 3.8% of patients who had been assigned to the vehicle group in the parent trials experienced treatment-emergent erythema on the face.
Table 21: Summary of Harms Results From the Long-Term Extension Study — Safety Set
Adverse event | Originally randomized to clascoterone (N = 317) | Originally randomized to vehicle (N = 290) | Overall (N = 607) |
|---|---|---|---|
Most common adverse events, n (%)a | |||
≥ 1 adverse event | 58 (18.3) | 52 (17.9) | 110 (18.1) |
Nasopharyngitis | 6 (1.9) | 10 (3.4) | 16 (2.6) |
Upper respiratory tract infection | 7 (2.2) | 1 (0.3) | 8 (1.3) |
Respiratory tract infection, viral | 1 (0.3) | 4 (1.4) | 5 (0.8) |
Application site, acne | 4 (1.3) | 0 | 4 (0.7) |
SAEs, n (%) | |||
Patients with ≥ 1 SAE | 3 (0.9) | 3 (1.0) | 6 (1.0) |
Depression and suicide attempt | 1 (0.3) | 0 | 1 (0.2) |
Eosinophilic gastroenteritis | 1 (0.3) | 0 | 1 (0.2) |
Fatigue | 0 | 1 (0.3) | 1 (0.2) |
Dizziness | 1 (0.3) | 0 | 1 (0.2) |
Induced abortion | 0 | 1 (0.3) | 1 (0.2) |
Coronary artery dissection | 0 | 1 (0.3) | 1 (0.2) |
Patients who stopped treatment due to adverse events, n (%) | |||
Patients who stopped | 10 (3.2) | 0 | 10 (1.7) |
Skin reactionsb | NR | NR | NR |
Otherc | NR | NR | NR |
Deaths, n | |||
Patients who died | 0 | 0 | 0 |
Adverse events of special interest, n (%) | |||
LSRs on the faced | |||
Erythema | 31 (9.8) | 11 (3.8) | 42 (6.9) |
Scaling or dryness | 15 (4.7) | 9 (3.1) | 24 (4.0) |
Edema | 2 (0.6) | 4 (1.4) | 6 (1.0) |
Pruritus | 6 (1.9) | 4 (1.4) | 10 (1.6) |
Telangiectasia | 4 (1.2) | 4 (1.4) | 8 (1.3) |
Skin atrophy | 16 (5.0) | 3 (1.0) | 19 (3.1) |
Stinging or burning | 3 (0.9) | 1 (0.3) | 4 (0.7) |
Striae rubrae | 4 (1.2) | 2 (0.6) | 6 (1.0) |
LSRs on the trunkd | |||
Erythema | 2 (1.6) | 5 (4.2) | 7 (1.2) |
Scaling or dryness | 0 | 4 (3.3) | 4 (0.7) |
Edema | 0 | 2 (1.7) | 2 (0.3) |
Pruritus | 0 | 0 | 0 |
Telangiectasia | 0 | 0 | 0 |
Skin atrophy | 0 | 0 | 0 |
Stinging or burning | 0 | 0 | 0 |
Striae rubrae | 0 | 1 (0.8) | 1 (0.2) |
LSR = local skin reaction; NR = not reported; SAE = serious adverse event.
aFrequency greater than 1% in any group.
bSkin reactions included application site swelling, application site dryness, cystic acne, application site acne, conglobate acne, and acne.
cOther reasons included depression, eosinophilic gastroenteritis, polycystic ovaries, dizziness, suicide attempt, hair colour changes, induced abortion, coronary artery dissection, and fatigue.
dTreatment-emergent LSRs on the face and trunk at day 274.
Sources: Clinical evidence summary23 and Clinical Study Report for the CB-03-01/27 trial.52
Critical Appraisal
Internal Validity
Based on the LTE results and discussion with the clinical expert, clascoterone 1% cream appears to be safe when used for up to 1 year of treatment. According to the clinical expert, among AEs that occurred more frequently in the clascoterone cohort compared to the vehicle cohort, skin atrophy is the most noteworthy event (5% in the clascoterone group versus 1% in the vehicle group). The LTE study suggested that patients who use clascoterone for up to 1 year of treatment may continuously improve or maintain improved skin affected by acne vulgaris. However, the study was not randomized and no formal statistical testing for efficacy outcomes (which were not primary objectives) was conducted. Furthermore, there was no true comparator tested during the LTE period. Therefore, definitive conclusions about the comparative effectiveness of clascoterone cannot be reached. Also, there may be a selection bias as those who benefited from clascoterone treatment during the pivotal trials were most likely to continue and a high adherence rate was an inclusion criterion for the LTE study. Another issue was the high attrition rate where at 9 months, only about 20% of patients remained in the LTE study; patients discontinued the study due to patient withdrawal (16.6%), being lost to follow-up (14.8%), and a lack of efficacy (4.9%) in the safety population. This attrition rate for the LTE study may lead to an underestimation of potential safety risks and an overestimation of the effectiveness of clascoterone treatment as patients with AEs and a lack of response are more likely to drop out from the study. Lastly, patient group input mentioned that HRQoL, such as mental health, anxiety, depression, and self-esteem, were important to patients. However, this aspect of treatment effect was not assessed.
External Validity
Because the patients were rolled over from the pivotal trials, generalizability concerns and issues similar to those in the main trials apply to the LTE study.
Indirect Evidence
Content in this section has been informed by materials submitted by the sponsor. The following has been summarized and validated by the CDA-AMC review team.
Objectives for the Summary of Indirect Evidence
In the absence of head-to-head evidence comparing clascoterone 1% cream against other relevant therapies used in the management of acne vulgaris, the sponsor submitted 1 indirect treatment comparison in the form of an NMA indirectly comparing the treatment effect of clascoterone to other treatments in patients with mild to moderate acne vulgaris.
Description of Indirect Comparisons
Objectives
The sponsor submitted an NMA that aimed to evaluate the relative efficacy and safety of the treatment of clascoterone 1% cream applied twice daily compared to other topical or hormonal therapies in patients aged 9 years and older with mild to moderate acne vulgaris.
The reference or base case of the sponsor-submitted NMA was to compare clascoterone with benzoyl peroxide and other topical retinoids (i.e., adapalene, tretinoin, and trifarotene). The sponsor detailed that this approach was chosen based on the assumption that newly diagnosed patients with moderate papulopustular acne (i.e., the majority of patients across trials and the patients most represented in trials of clascoterone) would first be prescribed a topical monotherapy as per current clinical practice guidelines.
Study Selection Methods
The comparator studies eligible for inclusion in the submitted NMA were selected according to a systematic review. The systematic review for the NMA was defined by the relevant population, intervention, comparator, outcome, and study design described in Table 22.
Table 22: PICOS for the Systematic Review Informing the Sponsor-Submitted NMA
Characteristic | Indirect comparison |
|---|---|
Population | The population of interest was patients with mild to moderate acne vulgaris who were aged 9 years and older. |
Intervention | Clascoterone 1% cream, applied twice daily (approximately 1 g per application) |
Comparator |
CDA-AMC reviewer note: The reference-case analysis focused upon comparisons of clascoterone with benzoyl peroxide (2.5% cream or 3.1% gel or 5% cream; applied once daily), tretinoin (0.025% cream or 0.04% gel or 0.05% cream; applied once daily), tazarotene (0.045% gel or 0.1% cream; applied once daily), adapalene (0.1% cream or 0.15% gel or 0.3% cream; applied once daily), and trifarotene (0.005% cream; applied once daily). |
Outcomes |
|
Study design | RCT |
Publication characteristic | Published studies |
Exclusion criteria |
|
CDA-AMC = Canada’s Drug Agency; ILC = inflammatory lesion count; NILC = noninflammatory lesion count; NMA = network meta-analysis; PICOS = population, intervention, comparator, outcomes, and study design; RCT = randomized controlled trial.
aIncluded in reference-case analysis.
Source: Network meta-analysis technical document.53
Clinical evidence for the systematic review informing the NMA was identified using multiple electronic databases (Table 23). The systematic literature review was based on an updated search focused on studies published after June 2020. Citation titles and abstracts were independently screened by 2 reviewers to identify relevant publications according to predefined criteria described in Table 23. Citations judged to be potentially relevant during the initial screening of titles and abstracts were independently assessed by 2 reviewers through full-text screening, with any selection disagreements adjudicated by a third reviewer. Data extraction of included studies was performed by a single reviewer and verified by a second reviewer. The risk of bias of the studies included in the systematic review informing the NMA was assessed using the Cochrane Risk of Bias 2 tool; risk of bias assessment was carried out by 2 independent reviewers, with a third reviewer to arbitrate discrepancies. Risk of bias assessments were conducted overall at the study level, without a focus on specific outcomes.
Of note, while the reimbursement indication is for patients with moderate and severe acne vulgaris, the study population in the majority of studies included in the NMA were patients with mild and moderate acne vulgaris. The sponsor posited that because the majority of the patient populations in the pivotal clascoterone trials was considered to have moderate acne vulgaris, the NMA reflects the treatment options and outcomes of the relevant patient population.
Table 23: Study Selection and Methods for Sponsor-Submitted NMA
Characteristic | Indirect comparison |
|---|---|
Databases searched | MEDLINE (1946–) and Embase (1947–) (via Ovid platform) |
Publication characteristics | Published full-text articles |
Exclusion criteria | Post hoc or pooled analyses Non–English-language studies Conference abstracts Trial protocols |
Selection process | Independent study selection by 2 reviewers with adjudication by a third reviewer |
Data extraction process | Data extraction performed by 1 reviewer with verification by a second reviewer |
Quality assessment | Independent assessment by 2 reviewers using the Cochrane RoB 2 tool, with a third reviewer to settle discrepancies. Assessments were described qualitatively and were considered as a potential source of heterogeneity. |
NMA = network meta-analysis; RoB = Risk of Bias.
Sources: Network meta-analysis technical document53 and the sponsor’s summary of clinical evidence.23
NMA Analysis Methods
Indirect comparisons of clascoterone 1% cream to benzoyl peroxide (2.5% cream or 3.1% gel or 5% cream; applied once daily), tretinoin (0.025% cream or 0.04% gel or 0.05% cream; applied once daily), tazarotene (0.045% gel or 0.1% cream; applied once daily), adapalene (0.1% cream or 0.15% gel or 0.3% cream; applied once daily), and trifarotene (0.005% cream; applied once daily) were based on a generalized linear model framework under a Bayesian approach.
Changes in inflammatory and noninflammatory lesions at 12 weeks were analyzed as continuous outcomes and modelled with a normal likelihood and identity link function. Summary effect measures for these outcomes were expressed as mean differences with 95% CrIs. It was unclear if all outcome data were available per study group, whether a mixture of study group data and contrast level data were synthesized, or whether data cleaning or conversions were performed to achieve a common format. The mean change from baseline to week 12 was imputed using 1 of 3 methods depending on data availability:
subtracting baseline counts from mean lesion counts at 12 weeks
multiplying the percentage reduction in mean counts by baseline counts
imputing from median and interquartile range estimates from 1 trial of 609 patients (4.8% of patients in network).
The SD of change scores was imputed using a tiered approach as follows:
if available, the SD was calculated from the available standard error, P value, z statistic, or t statistic using standard formulas
if available, the SD was estimated from the interquartile range and sample size using methods described by Wan et al.54
if no indirect measure of variation was available, the arithmetic mean of SDs reported from all other studies was used.
Study discontinuation for any reason at 12 weeks was analyzed as a dichotomous outcome and was modelled with a binomial likelihood and logit link function. Summary effect estimates for this outcome were expressed as RR with 95% CrI. Whether any special considerations were considered to handle 0 cells within the analyses of discontinuations for any reason was not detailed.
Methods of analysis are summarized in Table 24. An RE model was used for each network. A distribution of priors based on empirical data for RE models for the coefficient parameter (Normal[0,1x104]) and a uniform prior for the between-study variance were used (distribution details were not formally specified). It was unclear whether a common variance was used for all treatment comparisons. No sensitivity analyses involving the use of different prior distributions were performed.
Treatment nodes for evidence networks were constructed according to individual ingredients and their underlying strengths. Different preparations (e.g., gel, cream) with slightly different strengths but equivalent pharmacodynamic properties were grouped together. This included grouping tretinoin 0.04% (microsphere) gel (from 2 trials) and tretinoin 0.05% cream, adapalene 0.15% gel (from 1 trial) and 0.1% cream, clindamycin phosphate 1.2% gel (from 5 trials) and clindamycin 1% cream, tazarotene 0.045% polymeric lotion (from 3 trials) and tazarotene 0.1% cream, and benzoyl peroxide 3.1% gel (from 1 trial) and benzoyl peroxide 2.5%. Placebo treatments of different types (e.g., oral placebo, topical vehicles) were considered equivalent and presented as a single node within NMAs. No comparison of placebo response was presented to justify this approach.
Model fit was assessed by comparing the total residual deviance with the number of unconstrained data points, deviance information criterion (DIC), and between-study variance (I2). Model convergence was assessed by visually inspecting trace and density plots of posterior effect size estimates and checking that the potential scale reduction factor produced by the Gelman-Rubin-Brooks plots fell below 1.05. The risk of publication bias was not explored (e.g., funnel plots, comparison-adjusted funnel plots), nor were assessments of the certainty of the evidence evaluated using the GRADE framework presented. The assessment of consistency was conducted by comparing the posterior mean deviance of the individual data points from an unrelated means model against their posterior mean deviance in the corresponding consistency model. Additionally, results from the NMA and sensitivity analyses were compared to those from frequentist pairwise meta-analyses. Of note, different approaches for the assessment of consistency were used, including forest plots comparing findings from direct evidence, indirect evidence, and NMAs within closed loops. Moreover, no comparisons with results from pairwise meta-analyses were presented in the NMA report.53
Sensitivity analyses included network metaregression analyses, adjusting for differences in baseline lesion counts, the proportion of female participants, mean age, and the use of in-study blinding, as well as additional unadjusted NMAs omitting outlier studies. Sensitivity analyses were also performed using different approaches to the handling of missing data (e.g., the use of the arithmetic mean of SDs to replace missing SD values versus the use of the largest SD). Of note, the method of how potential effect modifiers were identified (e.g., via systematic review and/or consultation with clinical experts) was not provided.
Table 24: Analysis Methods for Sponsor-Submitted NMA
Method | Description |
|---|---|
Analysis methods | NMAs were conducted using a generalized linear model (a framework using Bayesian Markov chain Monte Carlo simulations). Data inputs were mean change from baseline and standard deviations (for lesions) or the number of patients discontinuing (for discontinuations). |
Priors | A distribution of priors based on empirical data for random-effects models for the coefficient parameter (Normal[0,1x104]) and a uniform prior for the between-study variance were used, according to NICE DSU TSD. |
Assessment of model fit | Model fit was assessed by comparing the total residual deviance with the number of unconstrained data points, and minimizing the deviance information criterion and between-study variance (I2). |
Assessment of consistency | Consistency was assessed by identifying loops and comparing the posterior mean deviance of the individual data points in the inconsistency model against posterior mean deviance in the consistency model. |
Assessment of convergence | Convergence was assessed by visually inspecting trace and density plots of posterior effect size estimates, as well as by checking that the potential scale reduction factor produced by the Gelman-Rubin-Brooks plots fell below 1.05. |
Outcomes | RRs (95% CrI) for discontinuations for any cause, mean difference (95% CrI) in NILCs, and mean difference (95% CrI) in ILCs |
Follow-up time points | 12 weeks |
Construction of nodes | Nodes were constructed according to individual ingredients and grouped by pharmacodynamically equivalent strengths. |
Sensitivity analyses | Analyses excluded trials with outlying clinical, methodologic, or statistical factors, or trials using metaregression, when appropriate. |
Subgroup analysis | Female trial participants were considered a subgroup of interest, but this analysis was not feasible because beyond oral contraceptive studies, only 3 studies were available. |
Methods for pairwise meta-analysis | NA |
CrI = credible interval; DSU = decision support unit; ILC = inflammatory lesion count; NA = not applicable; NICE = National Institute for Health and Care Excellence; NILC = noninflammatory lesion count; RR = risk ratio; TSD = technical support document.
Sources: Network meta-analysis technical document.53 and the sponsor’s summary of clinical evidence.23
Results of NMAs
Summary of Included Studies
Overall, 62 reports of 68 studies were included in the systematic review. Publications containing multiple trials were not included. Trials that could not be connected to the evidence network were excluded from the reference-case analysis. The reference- or base-case analysis included a total of 29 studies: 19 studies informing the evidence for both lesion outcomes and all 29 studies informing the evidence for discontinuations.
Studies included in the reference- or base-case NMA are presented in Figure 2. Differences in control treatments across the studies included were not described. Outcomes assessed at 12 weeks were available across all included trials. Methods used for lesion counting were not specified, nor was the extent of imputation of SDs using different approaches provided. All studies were RCTs with 28 (72%) studies employing a single-blinded or double-blinded approach. As depicted in Figure 1 and Figure 4 of 60 evaluated trials were appraised as being at high risk of bias, while 39 of 60 trials and 17 of 60 trials were assessed overall as being at a low risk of bias or having some concerns, respectively.
A table of baseline study characteristics presented in the sponsor NMA is provided in Appendix 1 (Table 30). The trial population varied with respect to baseline ILCs and NILCs (they ranged from approximately 7 lesions to 45 lesions and approximately 10 lesions to 80 lesions, respectively), the proportion of patients who were female (this ranged from 30% to 100%), and the average age (this ranged from 17.1 years to 30.2 years). Between-study heterogeneity on some covariates of interest (i.e., the duration of acne, acne severity, and prior therapies) could not be assessed by the sponsor due to limited reporting of these covariates in the primary studies. Likewise, comparability of the included studies based on key inclusion and exclusion criteria across trials could not be assessed. Potential sources of heterogeneity across the included studies identified by the CDA-AMC review team are summarized in Table 25.
The report does not clearly state how candidate sources of heterogeneity were established. Methodologic factors for consideration were informed by risk-of-bias assessments, and statistical factors related to model type (RE versus fixed-effects) and the approach to imputation of missing data. The review presents information regarding a set of selected study-level factors (the number of study centres, blinding, the average patient age, the proportion of female patients, the duration of acne, acne severity, baseline counts of ILCs and NILCs, and previous therapies), highlighting that the number of centres, study blinding, baseline lesion counts, average age at enrolment, and the proportion of female patients were reported across most studies.53 Sensitivity analyses related to these factors were performed where sufficient data were available. Evidence tables were also provided; these provide numeric details regarding study-level demographics (refer to Appendix 1). The provided information shows that upon inspection, trials of clascoterone were associated with higher mean baseline lesion counts than most trials.
Figure 1: Risk of Bias Summary From Sponsor SR and NMA Report
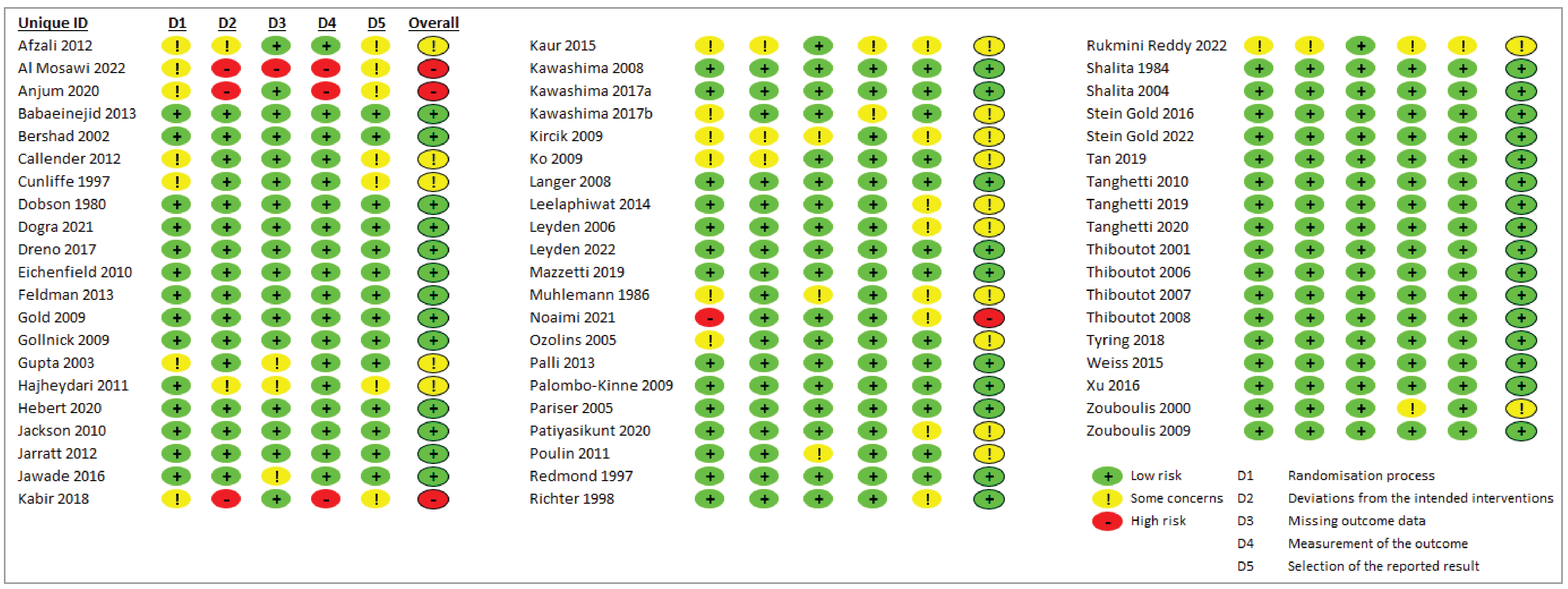
D1 = domain 1; D2 = domain 2; D3 = domain 3; D4 = domain 4; D5 = domain 5; NMA = network meta-analysis; RCT = randomized controlled trial; SR = systematic review.
Source: Network meta-analysis technical document.53
Table 25: Assessment of Clinical and Methodological Homogeneity for NMAs
Characteristic | Description and handling of potential effect modifiers |
|---|---|
Disease severity | The vast majority of participants in the trials had moderate acne (Investigator’s Static Global Assessment = 3). Duration of acne was not described in most studies. However, of the studies that reported this outcome, almost all described participants as having an average duration of disease of 6 years. |
Patient characteristics | Information provided by the sponsor regarding studies in the systematic review showed ranges in the proportion of female patients from 36% to 100%, in age from 17.1 years to 30.2 years, in ILCs from 6 lesions to 20 lesions, and in NILCs from 33 lesions to 97.6 lesions; among studies within the reference-case NMA, variability was also noted (the proportion of females ranged from 30% to 100%, ILCs ranged from 7 lesions to 45 lesions, and NILCs ranged from 10 lesions to 80 lesions). Baseline measures of inflammatory lesions and acne duration were not uniformly reported across trials. |
Treatment history | Treatment history was not well described in almost all studies. |
Trial eligibility criteria | Not addressed in the sponsor-submitted homogeneity table. Details of study-specific enrolment criteria were not included in the sponsor SR and NMA report. |
Dosing of comparators | Not addressed in the sponsor-submitted homogeneity table. |
Placebo response | Duration of acne, baseline ILC, and baseline NILC were not uniformly reported across all trials and therefore, the risk of bias due to placebo response could not be assessed. |
Definitions of end points | NR |
Timing of end point evaluation | Study follow-up ranged from 6 weeks to 52 weeks. Many studies reported data at 12 weeks and NMAs were restricted to this duration of follow-up. |
Withdrawal frequency | Refer to the following discontinuations. |
Clinical trial setting | Not relevant. |
Study design | Studies were a mixture of single-blind and double-blind studies. Some were single-centre studies while others were multicentre studies. |
ILC = inflammatory lesion count; NILC = noninflammatory lesion count; NMA = network meta-analysis; NR = not reported; SR = systematic review.
Sources: Network meta-analysis technical document.53 Details included in the table are from the sponsor’s summary of clinical evidence.23
Evidence Network
The evidence networks for the underlying reference-case analyses for change in both ILCs and NILCs at 12 weeks and for study discontinuations for any reason at 12 weeks is depicted in Figure 2. The NMA evidence for change in ILCs and NILCs was based on 19 studies (12,216 patients) and 8 nodes, while the NMA evidence for study discontinuation for any reason at 12 weeks was based on 29 studies (20,226 patients) and 10 nodes. For both evidence networks, almost all comparisons were against placebo. The most frequently studied intervention in both networks was tazarotene 1%; clascoterone was studied in a total of 3 studies versus placebo. In both networks, most other treatments were studied in only 1 to 2 trials.
A descriptive summary of the NMA model fit suggested that there were no concerns with the adequacy of the model fit based on an approximately equal number of constrained data points and corresponding posterior total deviance for each analysis. There was no evidence of violations of the consistency assumption based on the plots of direct, indirect, and NMA-derived estimates of treatment effect for each closed loop within the evidence network for each outcome and the P values from the results of inconsistency tests. However, unrelated means models and corresponding DIC values and deviance residuals were not reported. Pairwise comparisons were not reported.
Main NMA Results
The reference-case NMA results of all outcomes are summarized in Table 26. Only comparisons between clascoterone and other treatments are presented.
Table 26: Summary of Clascoterone Comparisons From RE NMA, Reference-Case Analyses
Detail | Inflammatory lesions at 12 weeks | Noninflammatory lesions at 12 weeks | Discontinuations |
|---|---|---|---|
Number of studies (patients), N | 19 (N = 12,226) | 19 (N = 12,226) | 29 (N = 20,219) |
Model | RE NMA 7 treatments and placebo | RE NMA 7 treatments and placebo | RE NMA 9 treatments and placebo |
Clascoterone vs. comparator | |||
Comparator | MD (95% CrI) | MD (95% CrI) | RR (95% CrI) |
Placebo | −5.21 (−7.15 to −3.20) | −8.03 (−11.81 to −4.30) | 0.91 (0.72 to 1.14) |
Benzoyl peroxide 5% | NA (no studies) | NA (no studies) | 0.99 (0.59 to 1.62) |
Benzoyl peroxide 2.5% | −0.43 (−4.60 to 3.74) | −1.03 (−6.73 to 4.69) | 1.08 (0.80 to 1.46) |
Adapalene 0.1% | −0.07 (−3.97 to 3.81) | −0.31 (−6.38 to 5.85) | 1.13 (0.85 to 1.51) |
Adapalene 0.3% | NA (no studies) | NA (no studies) | 0.67 (0.43 to 1.02) |
Tretinoin 0.05% | −2.32 (−5.09 to 0.65) | −1.72 (−8.07 to 4.48) | 0.78 (0.54 to 1.13) |
Tretinoin 0.025% | −2.18 (−4.76 to 0.56) | −0.39 (−5.96 to 4.92) | 0.94 (0.66 to 1.32) |
Trifarotene 0.005% | −0.67 (−3.12 to 1.95) | −0.23 (−5.52 to 4.93) | 0.78 (0.53 to 1.12) |
Tazarotene 1% | −1.63 (−3.77 to 0.77) | 0.16 (−4.08 to 4.73) | 0.71 (0.53 to 0.94) |
CrI = credible interval; MD = mean difference; NA = not applicable; NMA = network meta-analysis; RE = random effects; RR = risk ratio; SR = systematic review; vs. = versus.
Note: Data were drawn from league tables provided in Appendix 4 of the sponsor SR and NMA report. Statistically significant results are shown in bold font.
Sources: Network meta-analysis technical document.53 Details included in the table are from the sponsor’s summary of clinical evidence.23
Figure 2: Evidence Networks Informing Reference-Case NMAs
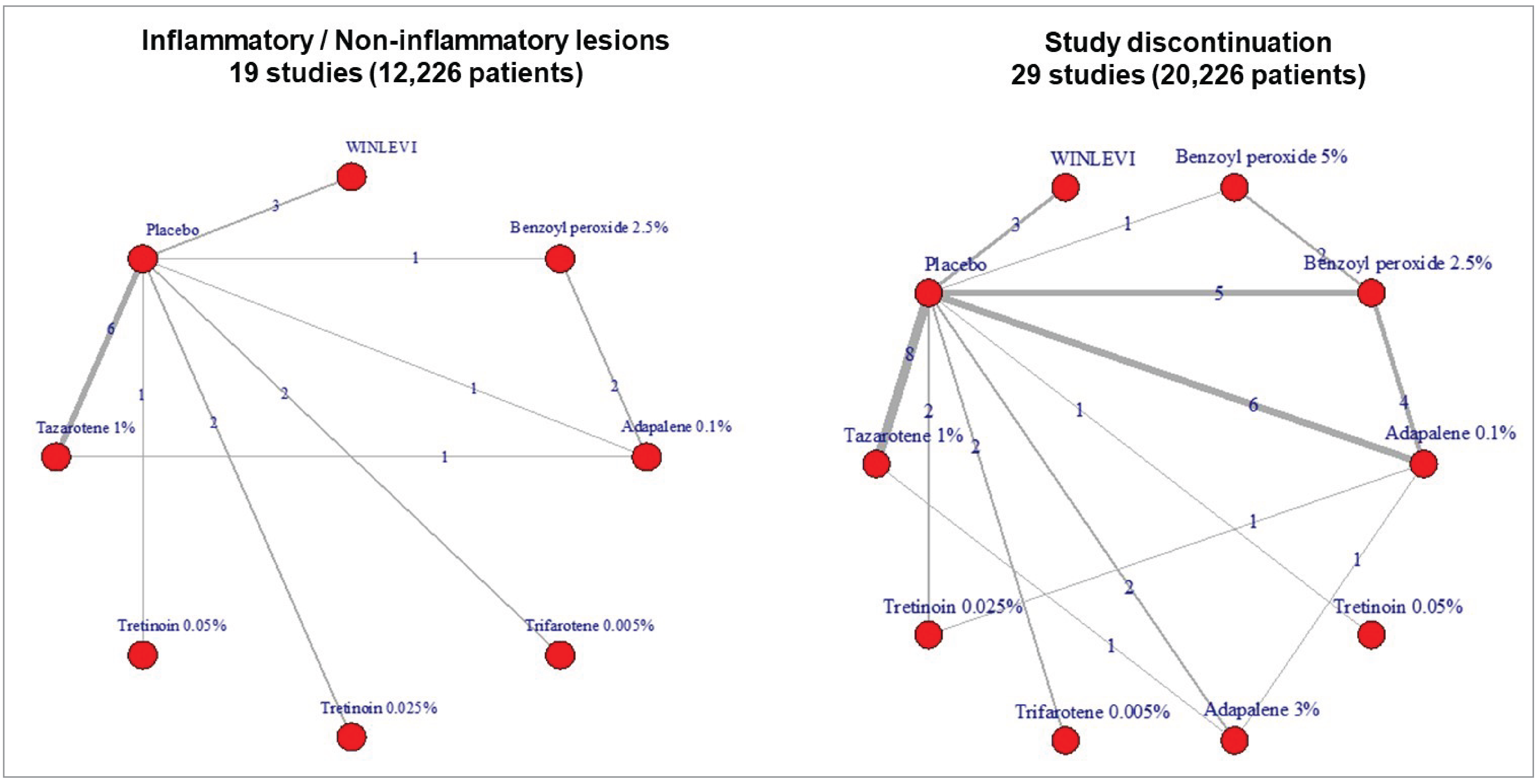
NMA = network meta-analysis.
Source: Network meta-analysis technical document.53
Mean Change in Inflammatory Lesions at 12 Weeks
Measures of model fit for the primary analyses showed no concerns when the number of study arms was compared to the total posterior residual deviance (38 data points versus residual deviance of 29.7).
Based upon the NMA of the 19 included studies (12,226 patients), pairwise comparisons versus placebo showed beneficial effects (i.e., a reduction in lesions) for all relevant interventions. Pairwise comparisons from the NMA of clascoterone with each of the active therapies are shown in Table 26; clascoterone was favoured in comparisons versus placebo based upon estimated treatment effects and their corresponding 95% CrI, while the possibility of no difference (as reflected by a 95% CrI that included the null value of 0) could not be ruled out when clascoterone was compared with other active treatments.
Secondary network metaregression analyses for the mean change in inflammatory lesions at 12 weeks included univariable adjustments for the mean number of baseline lesions, the mean patient age, the proportion of female patients, and the presence of blinding in the study design. In general, the DIC values were comparable to those of the primary unadjusted model, and treatment effects for clascoterone were generally stable. Slight reductions in the magnitude of treatment effects of clascoterone versus placebo from –5.2 (95% CrI, –7.2 to –3.2) to –2.9 (95% CrI, –5.6 to –0.21) were noted in metaregression analyses that adjusted for baseline lesion counts. Other secondary analyses based on a fixed-effects NMA model and exploring different approaches to the imputation of missing SDs resulted in comparable estimates of treatment effect for clascoterone.
Mean Change in Noninflammatory Lesions at 12 Weeks
Measures of model fit for the primary analyses showed no concerns when the number of study arms was compared to the total posterior residual deviance (38 data points versus residual deviance of 32.6).
Based upon the NMA of the included 19 studies (12,226 patients), pairwise comparisons versus placebo showed beneficial effects for each of the different treatments that were included. Comparisons of clascoterone with each of the active therapies are shown in Table 26; clascoterone was favoured in comparisons versus placebo based upon estimated treatment effects, while the possibility of no difference could not be ruled out in comparisons with active treatments.
Secondary network metaregression analyses for the mean change in noninflammatory lesions at 12 weeks included univariable adjustments for the mean number of baseline lesions, the mean patient age, the proportion of female patients, and the presence of blinding in the study design. In general, the DIC values were comparable to those of the primary unadjusted model, and treatment effects for clascoterone were generally stable. Slight reductions in the magnitude of treatment effect of clascoterone versus placebo from –8.0 (95% CrI, –12.0 to –4.3) to –7.3 (95% CrI, –12.0 to –3.0) were noted in metaregression analyses that adjusted for baseline lesion counts. Other secondary analyses based on a fixed-effects NMA model and exploring different approaches to the imputation of missing SDs resulted in comparable estimates of treatment effect for clascoterone.
Study Discontinuations for Any Reason at 12 Weeks
Measures of model fit for the primary analyses showed no concerns when the number of study arms was compared to the total posterior residual deviance (63 data points versus residual deviance of 40.9).
Based upon the NMA of the included 29 studies (20,219 patients), pairwise comparisons versus placebo showed beneficial effects (based upon the direction of point estimates) for each of the different treatments with the exception of tazarotene 1% (RR = 1.30; 95% CrI, 1.10 to 1.50). Comparisons of clascoterone with each of the active therapies are shown in Table 26; clascoterone was found to be associated with a similar risk of discontinuation (i.e., 95% CrIs included the null value of 1) when compared to placebo and other active treatments with the exception of tazarotene 1%, which demonstrated an increased risk of discontinuation (RR = 0.71; 95% CrI, 0.53 to 0.94); thus, the result favoured clascoterone.
From the secondary analysis (reference-case analysis) of discontinuation for any reason at 12 weeks, metaregression analyses based on the use of blinding within studies increased the estimated treatment effect of clascoterone versus placebo, though model DIC was comparable to the unadjusted model (101.17 versus 98.98, respectively). The DIC from a fixed-effects NMA of the same data was also similar to that of the RE NMA (101.17 versus 99.60, respectively). The systematic review and NMA did not quantitatively or visually explore variability in the rate of discontinuations for any reason across the placebo groups of included trials and thus, it is unclear whether a control group metaregression analysis may have been of value in terms of addressing any bias in findings from NMA for this outcome. No corresponding metaregression analysis was performed for the covariates of age, baseline lesion count, and proportion of female participants.
Scenario NMA Analyses Results
Unadjusted NMAs were performed for 3 different scenario analyses against additional sets of comparator treatments.
Scenario 1: Hormonal Therapies
The evidence network for scenario 1 included placebo, clascoterone, spironolactone, and oral contraceptives as comparators and consisted of 10 RCTs (N = 3,851) for change in inflammatory lesions, and 8 RCTs (N = 2,496) for NMAs of noninflammatory lesions and discontinuations for any reason. The evidence network for scenario 1 is illustrated in Figure 3 and the results are summarized in Figure 6 in Appendix 1. Briefly, clascoterone was associated with the largest treatment effect versus placebo for both lesion outcomes and was more efficacious than placebo; however, the possibility of a null difference against spironolactone and oral contraceptives could not be ruled out based on comparative treatment effects and 95% CrIs. For discontinuations, no differences between any of the treatments and placebo were noted.
Scenario 2: First-Line Monotherapies
The evidence network for scenario 2 included placebo and 11 treatments, including clascoterone, benzoyl peroxide 5%, benzoyl peroxide 2.5%, adapalene 3%, adapalene 0.1%, oral contraceptive, oral or topical spironolactone, tazarotene 1%, tretinoin 0.05%, tretinoin 0.025%, and trifarotene 0.005%. The networks consisted of between 10 nodes and 12 nodes from 24 RCTs to 34 RCTs (N range, 13,137 participants to 22,234 participants) dependent on outcome, and with certain comparators only having data for inclusion in the NMA of study discontinuations for any reason at 12 weeks. The evidence network for scenario 2 is illustrated in Figure 4 and the results are summarized in Figure 7 in Appendix 1. Briefly, all treatments were found to be better than placebo for both inflammatory and noninflammatory lesions while a null difference could not be ruled out when all treatments were compared to each other in pairwise comparisons. For discontinuations for any reason at 12 weeks, all treatments except tazarotene 1% were associated with 95% CrIs that included the null value of 1 when compared to placebo; clascoterone was associated with an estimated RR of 0.90 (95% CrI, 0.72 to 1.20) compared to placebo.
Figure 3: Comparison With Hormonal Therapies (Scenario 1)
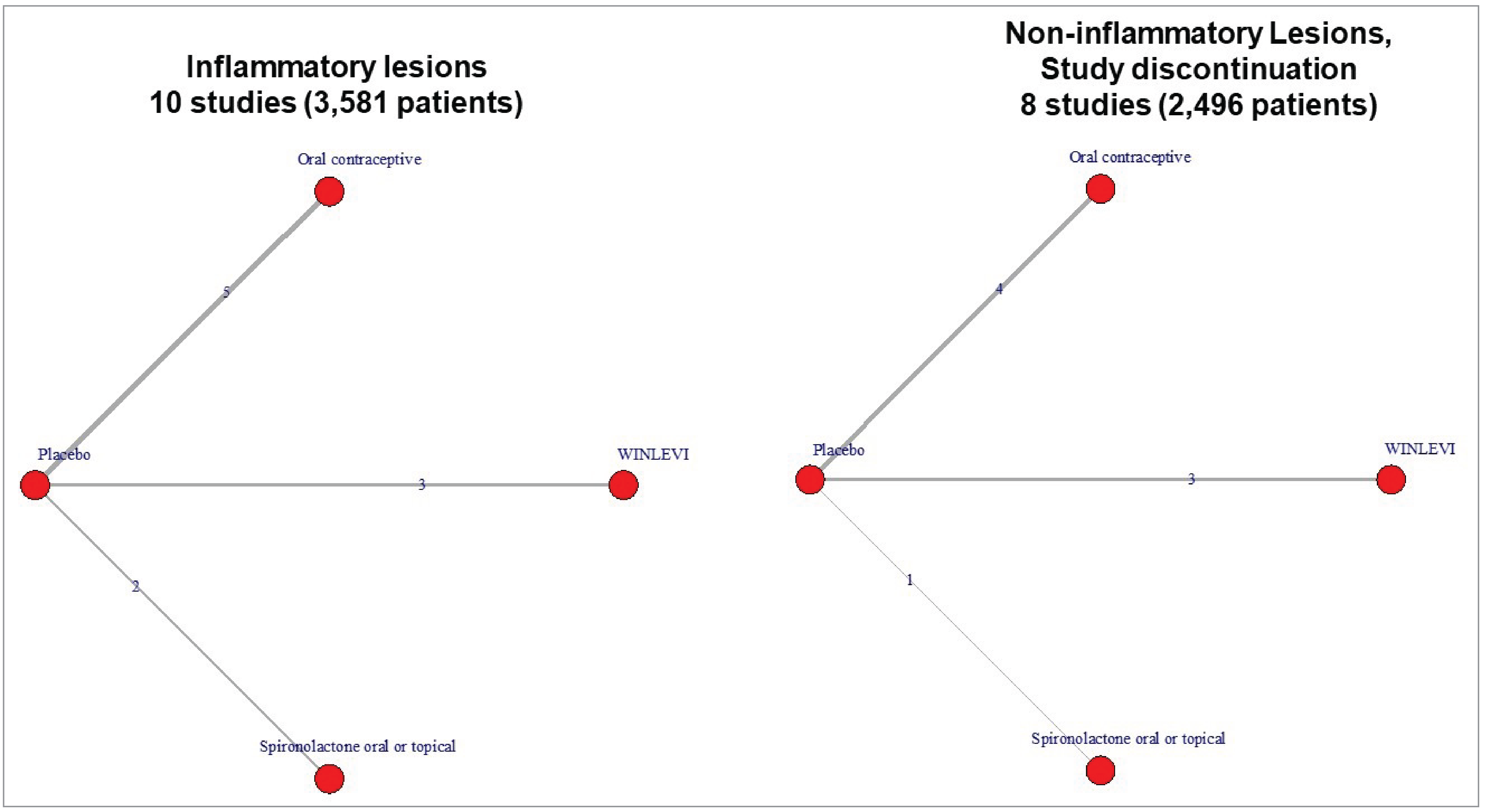
Source: Network meta-analysis technical document.53
Scenario 3: Topical and Hormonal Therapies
The evidence network for scenario 3 included placebo and 25 treatments, including clascoterone, benzoyl peroxide 5%, benzoyl peroxide 2.5%, adapalene 3%, adapalene 0.1%, oral contraceptive, oral or topical spironolactone, tazarotene 1%, tretinoin 0.05%, tretinoin 0.025%, trifarotene 0.005%, erythromycin 1.5%, clindamycin 1.2% and benzoyl peroxide 3.1% and adapalene 0.15%, clindamycin 1% and adapalene 0.15%, clindamycin 1% and benzoyl peroxide 5%, clindamycin 1% or 1.2% and benzoyl peroxide 2.5% to 3.1%, clindamycin 1% or 1.5%, adapalene 0.1% or 0.15% and benzoyl peroxide 2.5% or 3.1%, adapalene 0.3% and benzoyl peroxide 2.5%, spironolactone and benzoyl peroxide 5%, and spironolactone and benzoyl peroxide 2.5%. The networks consisted of between 42 RCTs and 54 RCTs (N range, 21,255 participants to 32,843 participants) dependent on outcome, and with certain comparators only having data for inclusion in the NMA of study discontinuations for any reason at 12 weeks. The evidence network for scenario 3 is illustrated in Figure 5 and results are summarized in Figure 8 in Appendix 1. Briefly, some but not all treatments were found to be better than placebo for inflammatory and noninflammatory lesions. Clascoterone was clinically better than placebo for both outcomes, but a null difference could not be ruled out in comparisons with all other active treatments. For discontinuations for any reason, all treatments except tazarotene 1% were associated with 95% CrIs that included 1 when compared to placebo; clascoterone was associated with an estimated RR of 0.90 (95% CrI, 0.68 to 1.20) compared to placebo, and no evidence of a difference was found when compared to other active therapies.
Critical Appraisal of Sponsor-Submitted NMA
Considerations for the critical appraisal of the NMAs presented in the sponsor’s systematic review and NMA report are provided as follows and address considerations of validity, transparency, scope, appropriateness, the handling of between-study heterogeneity, the potential for publication bias, and other factors.
Internal and external validity: Certain elements of the systematic review and NMAs presented in the sponsor NMA report are unclear. Thus, while the report describes the use of well-established NMA models from National Institute for Health and Care Excellence technical support documents and includes a variety of important elements for systematic reviews and NMAs (such as the engagement of an information specialist for searching, the involvement of multiple reviewers for study selection and data extraction, an assessment of between-study heterogeneity, the inclusion of analyses of consistency, and the consideration of sensitivity analyses to establish robustness of findings), certain challenges exist to fully grasp the internal validity of the systematic review and NMA provided. This includes a lack of clarity about the initial systematic reviews that informed the updates, uncertainty about the contribution of included trials to different networks, and the inclusion of study populations that appear to represent a broad spectrum of severity of acne vulgaris ranging from mild to severe that may introduce complexities when estimating treatment effects. Regarding external validity, the included study populations consisted of a range of male and female participants aged between 9 years and 30 years, with a range of baseline lesion counts. No clear violations of the transitivity assumption were noted, though judgments were partly limited by the unavailability of enrolment criteria across studies. Study populations were considered to be reasonably reflective of the real-world population of interest for acne vulgaris. However, it was noted that for the specific interests in moderate to severe disease, study populations in some of the included RCTs were broader and included mild disease as well.
Prespecification of methods: The sponsor’s NMA report indicated that no protocol for the review was prepared. Its authors indicated that this work was an update of a prior review; however, details with regard to a protocol or prior registration for the original review were not provided. Thus, the ability to assess review performance was limited. Raw data informing the NMAs and model code were not readily available to verify analyses (though the preparation of datasets may be feasible from outcome data included as 1 element in a larger table of the NMA report). Supplemental information from the sponsor clarifies that the population of interest was “adults and children aged 12 years or older with acne vulgaris characterized by comedones, inflammatory papules or pustules, with or without an occasional nodule,” and the sponsor sought to include studies that ranged from mild to severe acne vulgaris to facilitate comparisons with other treatments. A 2022 NMA published in the British Journal of Dermatology55 included several considerations to address variability in the availability of information from study to study regarding the severity of acne vulgaris (e.g., the consideration of nodule counts, the number of inflammatory lesions when the severity of acne was not clearly described); similar information may have been helpful in the context of the current systematic review and NMA with regard to managing clinical heterogeneity.
Figure 4: Comparison With All First-Line Monotherapy Options (Scenario 2)
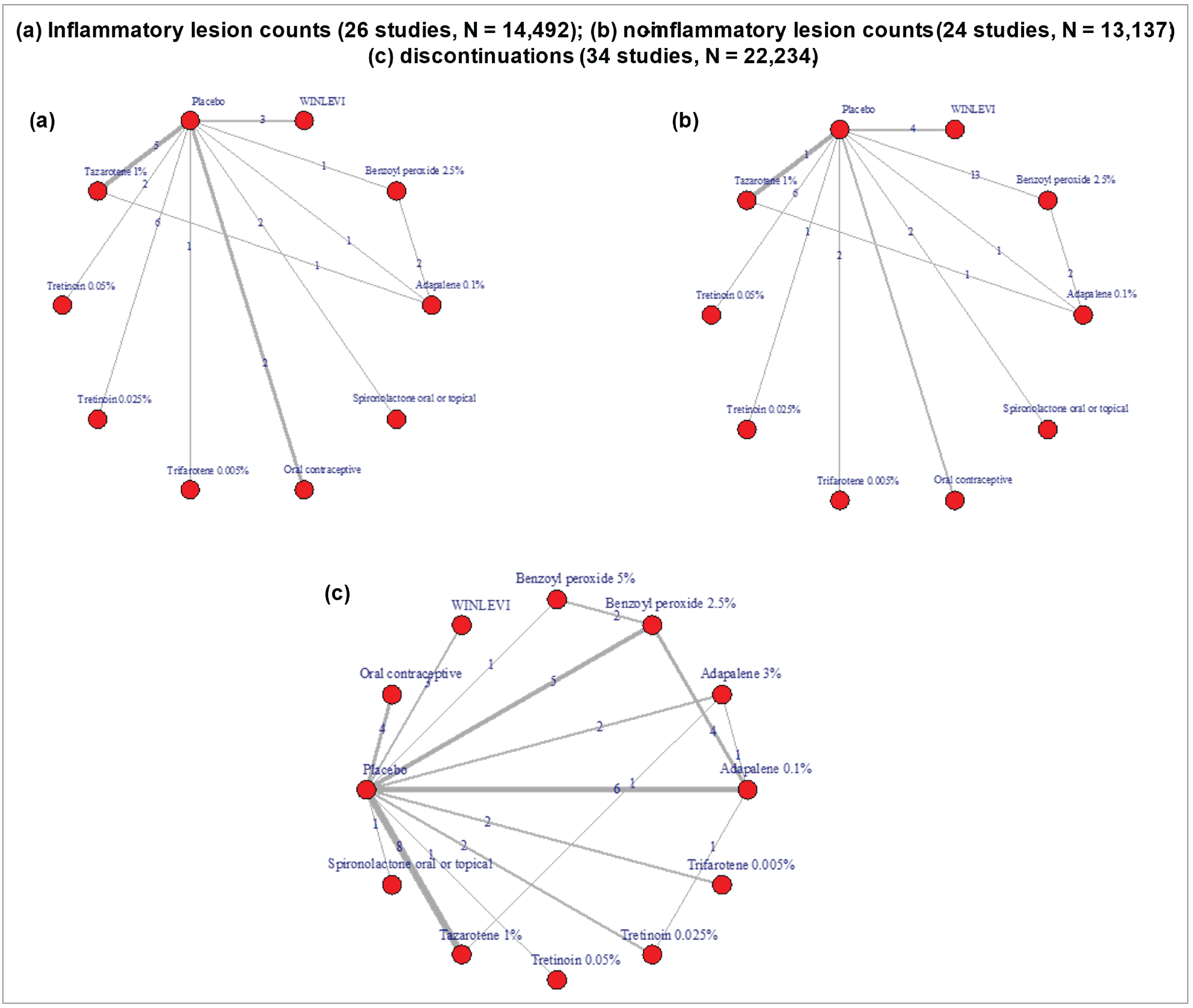
Source: Network meta-analysis technical document.53
Figure 5: Comparison With All Topical and Hormonal Treatment Options (Scenario 3)
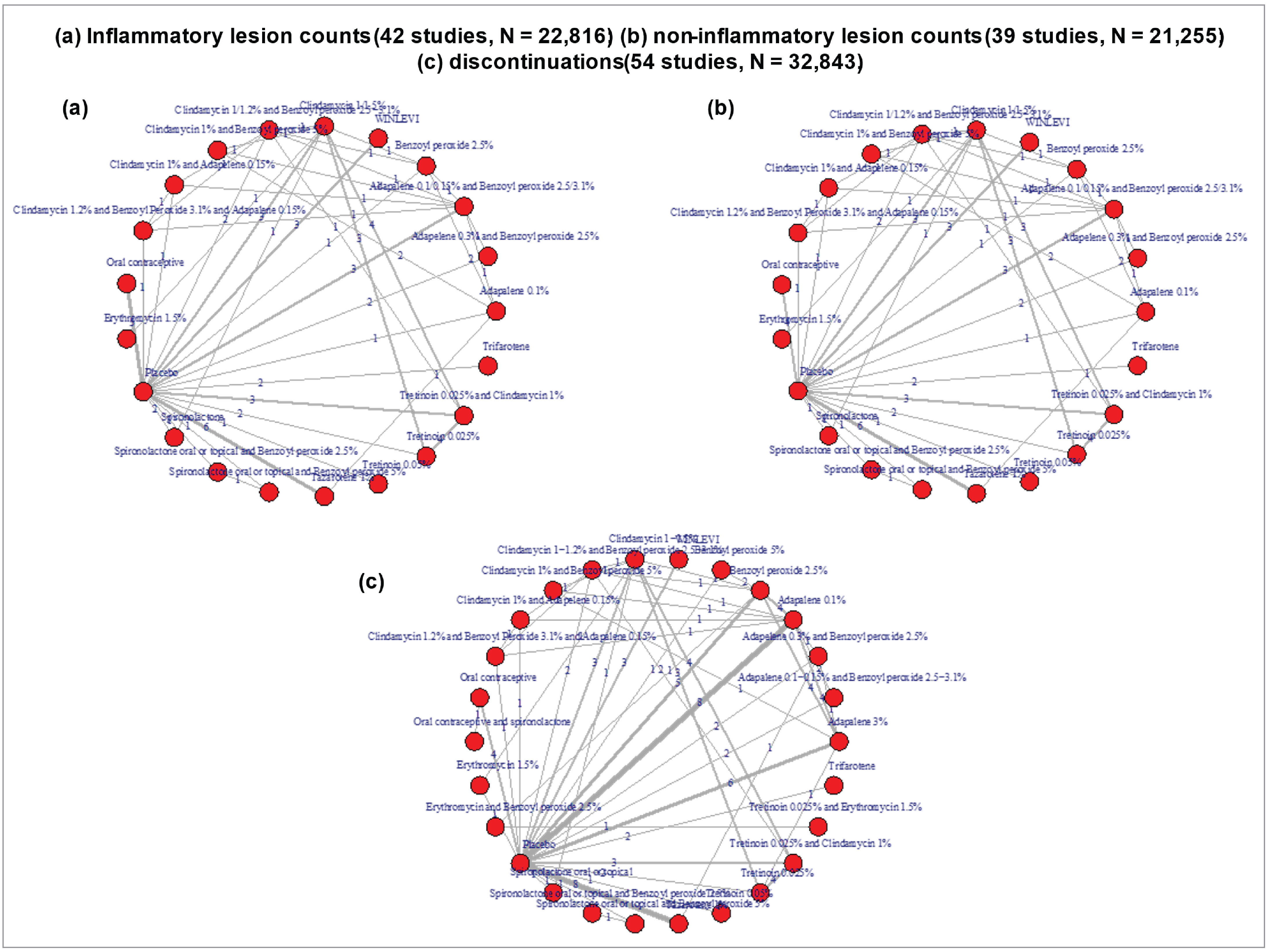
Source: Network meta-analysis technical document.53
Consideration of relevant comparators: NMAs in the sponsor’s report considered a reference-case analysis that included clascoterone (applied twice daily) with benzoyl peroxide and other topical retinoids (i.e., adapalene, tretinoin, and trifarotene), while scenario analyses broadened the treatments compared to include oral contraceptives, spironolactone, and several combination therapies. Input from the clinical expert consulted by CDA-AMC suggested that combination therapies are commonly used to manage moderate to severe acne vulgaris; this may suggest that the scenario 3 analyses may be of greater interest for consideration. Clinical expert input also suggested that oral isotretinoin, oral antibiotics, and topical dapsone could have been considered, though the clinical expert acknowledged certain limitations to doing so (e.g., guidelines recommend antibiotic use for a maximum of 3 months to 6 months, some patients will not agree to treatment with isotretinoin, topical dapsone is not covered by public plans). The submission request seeks status as a first-line therapy for moderate to severe acne, which may explain the choice of treatments in reference-case analyses.
Follow-up duration and outcomes: All analyses are based upon 12-week outcomes that were commonly available across the included trials. Long-term effectiveness and safety are not clear based upon these data. It is unclear whether reasons for discontinuation may vary between treatments. Additionally, the clinical expert consulted by CDA-AMC noted that there may be additional outcomes of relevance to patients, such as the clearance of acne (which also includes the achievement of “clear” or “almost clear” on the IGA scale), the prevention of acne sequelae (e.g., scarring, postinflammatory hyperpigmentation), and the use of the Dermatology Life Quality Index or Cardiff Acne Disability Index (to measure psychological impacts of acne such as anxiety, depression, and emotional distress).
Between-study heterogeneity: There is some degree of heterogeneity between studies in terms of baseline lesion counts, the proportion of female participants, and participant age. The sponsor NMA report included metaregression analyses to explore the effects of these variables on estimates of treatment effect, which appeared reasonably robust. Of note, the variability of these covariates by treatment comparison was unclear based on the information provided, and variability in enrolment criteria could not be assessed as this information was not available in the report; therefore, it is possible that minor differences between study populations exist after adjustment for mean baseline lesion counts. Trials of clascoterone were associated with populations that had higher baseline lesion counts than most other trials in reference-case NMAs and thus, treatment effects measuring changes from baseline in lesion counts relative to other treatments may be subject to some degree of bias. The clinical expert noted that ideally, subgroups by age, sex, and ethnicity would be available. Regarding analyses of the binary outcome of discontinuation for any reason, variability in the rate of withdrawal among the placebo groups was not inspected. Often with binary outcomes, it can be informative to look for important variability to consider whether there is a need for the performance of a control group network metaregression analysis to address any bias related to such differences. The report involved a feasibility assessment to explore the impact of variation in additional effect-modifying clinical variables, including the duration of acne, acne severity, and previous therapies received; however, these were often not reported in the included RCTs.
Handling of data imputation: The systematic review and NMA involved the use of a tiered approach to handle the imputation of mean changes in lesion count from baseline, where necessary, and also to estimate corresponding SD values for changes in lesion count, where necessary. These approaches appear to align with commonly used approaches for meta-analysis.
Risk of bias of included trials: Risk-of-bias assessments identified 50% of the included trials to be at a low risk of bias while most of the remaining studies were associated with some concerns. Assessments were performed only at the study level (i.e., they were not performed for specific outcomes).
Appropriateness of syntheses, model fit, and consistency of evidence: The variability of certain traits between studies was noted, and the clinical relevance of combining studies wherein the severity of acne vulgaris appeared to range from mild to severe was considered unclear. From a quantitative perspective, model fit statistics identified no concerns in reference-case analyses when inspecting the numbers of included study arms and corresponding measures of total residual deviance. Checks of the consistency assumption also identified no concerns and thus, do not suggest that the combining of the evidence base was inappropriate.
Subgroup and sensitivity analyses: While the review provides no details about a priori efforts to identify potential effect modifiers that involved clinical expert consultation or a review of the literature, the sponsor pursued sensitivity analyses based upon the availability of certain established characteristics (baseline lesion count, age, and the proportion of female patients) and certain statistical considerations (RE versus fixed-effects model, the approach to impute missing SD, and the use of blinding). Findings with regard to the treatment effects of clascoterone appeared to be generally consistent; regarding the effects of baseline lesion count, there was some reduction of treatment effects of clascoterone in network metaregression analyses. The impact of other effect modifiers was not explored (i.e., the duration of acne, acne severity, and previous therapies received) due to limited reporting in the included RCTs.
Potential publication bias: The sponsor report did not include an assessment of publication bias and does not discuss the issue; in addition, no searching for grey literature was performed. For reference, the NMA by Mavranezouli et al.55 noted some potential evidence for the risk of small study bias in their analyses related to mild to moderate acne focused on percentage change in baseline lesions.
Studies Addressing Gaps in the Systematic Review Evidence
No other relevant evidence in support of clascoterone 1% cream was provided by the sponsor.
Discussion
Summary of Available Evidence
The systematic review conducted by the sponsor included 2 identical phase III, randomized, double-blind, vehicle-controlled, parallel-group trials, the CB-03-01/25 study (N = 708) and the CB-03-01/26 study (N = 732). In both trials, patients were randomized 1:1 to either clascoterone 1% or vehicle cream for 12 weeks of treatment. In both trials, the primary objective was to determine the safety and efficacy of clascoterone 1% cream versus the vehicle cream applied twice daily for 12 weeks in patients with facial acne vulgaris. The outcomes measured in the trials and selected for GRADE assessment included global success (i.e., the proportion of patients aged 12 years and older achieving treatment success at week 12), lesion counts (i.e., the change from baseline to week 12 in NILC, ILC, and TLC), and notable harms (i.e., LSRs).
The CB-03-01/25 study was conducted primarily in the US and the CB-03-01/26 study was conducted primarily in Europe. Neither trial had any study sites in Canada. In the CB-03-01/25 study, the median age for both treatment groups was 18 years (range, 9 years to 58 years) and in the CB-03-01/26 study, the median age for both treatment groups was also 18 years (range, 10 years to 50 years). In the CB-03-01/25 trial, the majority of patients had an IGA score of 3 indicating moderate (83% and 82% of patients in the clascoterone and vehicle groups, respectively) at baseline. The mean baseline ILC was approximately 42 lesions, and the mean baseline TLC ranged between 60 lesions and 100 lesions in the CB-03-01/25 trial. Similarly in the CB-03-01/26 trial, the majority of patients had an IGA score of 3 indicating moderate (83% and 87% of patients in the clascoterone and vehicle groups, respectively) at baseline. The mean ILC and TLC at baseline was approximately 42 lesions and 63 lesions, respectively, in the CB-03-01/26 trial. Overall, baseline characteristics were generally similar between treatment groups across both pivotal trials. Patients were enrolled from January 21, 2016, to April 11, 2018, in the CB-03-01/25 study and from November 16, 2015, to February 21, 2018, in the CB-03-01/26 study.
The sponsor also submitted an open-label LTE study, the CB-03-01/27 trial (N = 609), in which patients who completed the pivotal studies were able to enrol for an additional 9 months of treatment with clascoterone. The primary objective was to determine the longer-term safety of the drug while IGA was measured to assess efficacy. Because this was a continuation of the parent studies, patient characteristics were generally similar. A greater number of patients who originally received clascoterone (N = 317) rather than vehicle cream (N = 292) rolled over into the LTE study.
In the absence of direct comparative evidence of clascoterone to other relevant comparators, the sponsor submitted a Bayesian NMA comparing the effects of clascoterone and different treatments on changes in the numbers of inflammatory lesions, noninflammatory lesions, and study discontinuations for any reason following 12 weeks of treatment. Reference-case analyses focused on comparisons of clascoterone with other monotherapies (benzoyl peroxide and other topical retinoids, such as adapalene, tretinoin, and trifarotene), while additional scenario analyses extended the comparators considered to include oral contraceptives, spironolactone, and combination therapies. Regarding the severity of acne vulgaris, studies enrolling populations that ranged from mild to severe (as indicated by a broad range of baseline numbers of inflammatory and noninflammatory lesions) were included. Unadjusted RE NMAs were conducted, as were secondary analyses to explore the potential effects of between-study variations in the mean numbers of baseline lesions, the mean participant age, the proportion of female participants, and the use of blinding in study design.
Interpretation of Results
Efficacy
Evidence from the CB-03-01/25 and CB-03-01/26 trials suggested that treatment with clascoterone was associated with greater treatment success based on the IGA scale compared to the vehicle (placebo) cream in patients aged 12 years and older with acne. Treatment success across the outcomes was achieved based on the trial definition (i.e., an IGA score of clear [0] or almost clear [1] and a 2-point or greater reduction on the IGA scale compared with baseline). According to the clinical expert, global response is a standard clinical outcome in the assessment of acne vulgaris and is considered an important clinical outcome. Although there is no gold standard for successful treatment of acne vulgaris, the clinical expert felt that a 10% difference in success was clinically meaningful for acne vulgaris and was supportive of the definition used in the trial as it aligned with Canadian clinical practice. Moreover, the definition of treatment success used for the IGA was consistent with FDA recommendations.48,49 Similarly, treatment with clascoterone was associated with a greater reduction in absolute and percentage change in NILC, ILC, and TLC compared to vehicle cream, which the clinical expert noted is relevant to clinical practice in Canada. According to the clinical expert, percentage change from baseline was a more clinically relevant outcome than absolute lesion counts because it is not feasible for clinicians to be counting lesions at each visit. Moreover, the clinical expert felt that the threshold for success would be different for patients with primarily noninflammatory lesions versus those with primarily inflammatory lesions because noninflammatory acne lesions are slower to resolve and typically harder to treat.
These results, however, may be biased due to missing data, which may not have been fully accounted for by the MI approach used in the primary analysis. As noted in the critical appraisal, the imputations based on worst-value and worst-case analyses were not consistent with the primary analysis for absolute change in ILC and NILC. Input from the clinical expert suggested that only the results of the CB-03-01/26 study were clinically meaningful for the end points of global success and percentage change in NILC from baseline to week 12. The clinical expert noted that the main treatment goals of acne treatment are very minimal acne or the clearance of acne and the patient’s impression of change. In general, the clinical expert felt that 12 weeks was an appropriate and common time point at which to measure success in the context of a clinical trial; however, 6 months would be more relevant to measure treatment success according to the NILC in the clinical practice setting.
Patient groups and the clinical expert consulted by CDA-AMC identified mental health and HRQoL as important outcomes; however, these outcomes were not addressed in the evidence submitted by the sponsor. The clinical expert and clinician groups also emphasized the importance of patient satisfaction in assessing response to treatment because this varies greatly from patient to patient and impacts the treatment course.
Many treatment options (e.g., oral androgen inhibition) are contraindicated in male patients, thereby limiting available treatment options for them. Because female patients have more treatment options, there is a difference in unmet need between the sexes. Clascoterone is a first-in-class topical androgen receptor inhibitor therapy and could potentially fulfill an unmet need for males with acne vulgaris. However, subgroup analyses were not conducted by sex so no conclusions can be drawn about the prognostic effect of clascoterone in 1 group over the other or its ability to fulfill this unmet need.
Although the study population did not include patients with mild acne, the clinical expert felt that the results would still be generalizable to this population. Most patients with severe acne are more resistant to treatment; hence, the clinical expert did not feel that clascoterone would be the optimal first-line option for patients with severe acne. Overall, the clinical expert felt that a topical treatment such as clascoterone would be better suited for patients with mild or moderate acne. While the data presented in the report included a small number of patients aged 9 years to 11 years (who were permitted in the trials), the clinical expert noted that their inclusion would not have a major impact on the results, despite the indication being for patients aged 12 years or older.
The included pivotal studies were placebo-controlled and no direct comparative evidence between clascoterone and relevant active comparators was available. In an effort to address this evidence gap, the sponsor submitted 1 NMA indirectly comparing clascoterone to other topical and oral treatments for moderate to severe acne. Overall, the NMA evidence did not favour the treatment of either clascoterone or other active treatments. Sensitivity analyses were associated with relatively similar estimates of treatment effect. The additional 3 scenario NMAs indirectly comparing clascoterone to other sets of hormonal, monotherapy, and combination therapies found no important differences between treatments. Critical appraisal of the sponsor NMA report noted that in general, recommended methods for conduct and reporting were followed, though certain limitations were identified. Study populations of RCTs ranged from mild to severe based on mean baseline lesion counts, introducing challenges to the interpretation of findings and also concerns that the validity of treatment effects measuring changes in lesion count from baseline could be impacted. Trials of clascoterone were associated with populations that had higher baseline lesion counts than most other trials in reference-case NMAs and thus, treatment effects measuring changes from baseline in lesion counts relative to other treatments may be subject to bias. The variability of placebo or vehicle group responses across trials was not described in detail, and the appropriateness of combining these groups for the purposes of the NMA was unclear. Methods to identify effect modifiers of interest to judge the appropriateness of the transitivity assumption were unclear, and the effects of differences between study populations for specific effect modifiers (the duration of acne, acne severity, and previous treatments) could not be addressed due to limited reporting by the included trials. Input from the clinical expert suggested that certain additional treatments (oral antibiotics, isotretinoin, topical dapsone, and combination treatments) could have been included in reference-case analyses. Findings from NMAs should thus be interpreted with some degree of caution.
Harms
In both trials, patients with TEAEs, SAEs, withdrawals due to AEs, mortality, and notable harms were generally similar between groups and across the trials. At 12 weeks, the most common AEs reported in both trials was nasopharyngitis. Patients with SAEs and withdrawals due to AEs were relatively few in both groups and across the trials. No deaths were reported in either trial. The clinical expert did not express any concerns for the overall safety of clascoterone that would be expected to have an impact on clinical decision-making.
Similar to the pivotal trials, nasopharyngitis (2.6% in the overall population) was the most common TEAE in the LTE study. The clinical expert consulted by CDA-AMC stated that no long-term safety concern for clascoterone was detected during the extension period. However, the clinical expert felt that skin atrophy (5% in the clascoterone group versus 1% in the vehicle group) is a noteworthy AE.
Regarding indirect evidence, the sponsor’s NMA report presented findings from analyses of study discontinuations for any reason at 12 weeks. Overall, there was no strong evidence of any differences between clascoterone, and active treatments included in the evidence network with the exception of the comparison to tazarotene 1%, where clascoterone was associated with a reduced risk of discontinuation compared to tazarotene 1% (RR = 0.71; 95% CrI, 0.53 to 0.94) in the reference-case analysis. However, the uncertainty of these results must be considered due to limitations of the NMA that include the short duration of follow-up (12 weeks) and between-study heterogeneity.
Conclusion
The evidence in this review includes 2 sponsor-submitted, phase III, randomized, double-blind, vehicle-controlled trials, the CB-03-01/25 study (N = 708) and the CB-03-01/26 study (N = 732). The CB-03-01/25 and CB-03-01/26 studies assessed the safety and efficacy of treatment with clascoterone 1% cream compared to vehicle (placebo) cream in patients with moderate to severe acne vulgaris. The 2 trials demonstrated that 12 weeks of treatment with clascoterone 1% cream applied twice daily likely results in a clinically important improvement in achieving treatment success as defined by an IGA score of 0 or 1 and a 2-point or greater reduction from baseline when compared with vehicle cream. However, the evidence was uncertain with regard to the ability of clascoterone to reduce the number and percentage of lesions (NILC, ILC, and TLC) at week 12. There is no evidence for the effect of clascoterone on mental health and HRQoL, which was identified as a clinically important outcome by the clinical experts and patient groups. Most efficacy outcomes were affected by concerns for imprecision (i.e., CIs included the potential for little to no difference versus placebo). All outcomes were impacted by a risk of bias due to missing data and indirectness due to concerns with generalizability to patients with severe acne vulgaris in clinical practice in Canada.
Because there was no direct evidence comparing clascoterone to other treatments for acne vulgaris, the sponsor provided an NMA that assessed short-term efficacy versus multiple comparators. For comparisons between clascoterone and active treatments, the results of the NMA did not favour either treatment in terms of a reduction in inflammatory lesions. Higher baseline lesion counts in trials of clascoterone may also provide rationale to interpret treatment effects relative to other treatments in terms of changes from baseline with caution.
Regarding safety, clascoterone resulted in little to no clinically important difference in LSRs. Of note, few to no events were observed during follow-up for these notable harms. Based on the harms observed at week 12 and LTF at 12 months, the clinical expert suggested there were no concerns for the overall safety of clascoterone that would be expected to have an impact on clinical decision-making. In addition, the NMA found no important differences in safety outcomes between clascoterone, placebo, and active comparators.
References
1.Arora MK, Yadav A, Saini V. Role of hormones in acne vulgaris. Clin Biochem. 2011;44(13):1035-1040. doi:10.1016/j.clinbiochem.2011.06.984 PubMed
2.Moradi Tuchayi S, Makrantonaki E, Ganceviciene R, Dessinioti C, Feldman SR, Zouboulis CC. Acne vulgaris. Nat Rev Dis Primers. 2015;1:15029. doi:10.1038/nrdp.2015.29 PubMed
3.Zaenglein AL, Pathy AL, Schlosser BJ, et al. Guidelines of care for the management of acne vulgaris. J Am Acad Dermatol. 2016;74(5):945-73 e33. doi:10.1016/j.jaad.2015.12.037 PubMed
4.Canadian Dermatology Association. Acne. Accessed April 13, 2023. https://dermatology.ca/public-patients/skin/acne/#:~:text=Acne%20affects%205.6%20million%20Canadians,adults%20ages%2020%20to%2040
5.Mancini AJ, Baldwin HE, Eichenfield LF, Friedlander SF, Yan AC. Acne life cycle: the spectrum of pediatric disease. Semin Cutan Med Surg. 2011;30(3 Suppl):S2-5. doi:10.1016/j.sder.2011.07.003 PubMed
6.Picardo M, Eichenfield LF, Tan J. Acne and rosacea. Dermatol Ther (Heidelb). 2017;7(Suppl 1):43-52. doi:10.1007/s13555-016-0168-8 PubMed
7.Noaimi A, Al-Saadi SR. Treatment of acne vulgaris by topical spironolactone solution compared with clindamycin solution. Cureus. 2021;13(8):e17606. doi:10.7759/cureus.17606 PubMed
8.Collier CN, Harper JC, Cafardi JA, et al. The prevalence of acne in adults 20 years and older. J Am Acad Dermatol. 2008;58(1):56-9. doi:10.1016/j.jaad.2007.06.045 PubMed
9.Shaw JC. Persistent acne in adult women. Arch Dermatol. 2001;137(9):1252-1253. PubMed
10.Asai Y, Baibergenova A, Dutil M, et al. Management of acne: Canadian clinical practice guideline. CMAJ. 2016;188(2):118-126. PubMed
11.Haider A. Treatment of acne vulgaris. JAMA. 2004;292(6):726. doi:10.1001/jama.292.6.726 PubMed
12.James WD. Acne. N Engl J Med. 2005;352(14):1463-1472. doi:10.1056/nejmcp033487 PubMed
13.Kraft J, Freiman A. Management of acne. Can Med Assoc J. 2011;183(7):E430-E435. doi:10.1503/cmaj.090374 PubMed
14.Reynolds RV, Yeung H, Cheng CE, et al. Guidelines of care for the management of acne vulgaris. J Am Acad Dermatol. 2024;90(5):1006.e1-1006.e30. doi:10.1016/j.jaad.2023.12.017 PubMed
15.Cibula D, Hill M, Vohradnikova O, Kuzel D, Fanta M, Zivny J. The role of androgens in determining acne severity in adult women. Br J Dermatol. 2000;143(2):399-404. doi:10.1046/j.1365-2133.2000.03669.x PubMed
16.Sun Pharma Canada Inc. Winlevi (clascoterone cream): 1% w/w, topical [product monograph].
17.Cortexolone 17a-propionate (CB-03-01) 1% cream in-use stability. Stability study report [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Winlevi (clascoterone), 1% cream. Sun Pharma Canada Inc; 2021.
18.Clinical Study Report: CB-03-01-25. A phase 3, multicenter, randomized, double-blind, vehicle-controlled study to evaluate the safety and efficacy of clascoterone1 (CB-03-01) cream, 1% applied twice daily for 12 weeks in subjects with facial acne vulgaris[internal sponsor's report]. Cassiopea S.p.A; 2019.
19.Clinical Study Report: CB-03-01-26. A phase 3, multicenter, randomized, double-blind, vehicle-controlled study to evaluate the safety and efficacy of clascoterone (CB-03-01) cream, 1% applied twice daily for 12 weeks in subjects with facial acne vulgaris [internal sponsor's report]. Cassiopea S.p.A; 2019.
20.Balshem H, Helfand M, Schünemann HJ, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011;64(4):401-6. doi:10.1016/j.jclinepi.2010.07.015 PubMed
21.Santesso N, Glenton C, Dahm P, et al. GRADE guidelines 26: informative statements to communicate the findings of systematic reviews of interventions. J Clin Epidemiol. 2020;119:126-135. doi:10.1016/j.jclinepi.2019.10.014 PubMed
22.Sun Pharma Canada Inc response to August 31, 2023 CDA-AMC request for additional information regarding Winlevi (clascoterone cream) CDA-AMC review: ADAM of CB-03-01/25 and CB-03-01/26 [internal sponsor's report]. Sun Pharma Canada Inc; 2023 Sep 5.
23.Sponsor's summary of clinical evidence Winlevi (clascoterone) [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Winlevi (clascoterone), 1% cream. Sun Pharma Canada Inc; 2023.
24.DermaNet. Inflammatory lesions in acne. Accessed June 17, 2023. https://dermnetnz.org/topics/inflammatory-lesions-in-acne
25.National Institutes of Arthritis and Musculoskeletal Skin Diseases. Acne. Accessed June 6, 2023, https://www.niams.nih.gov/health-topics/acne
26.Dréno B, Bettoli V, Araviiskaia E, Sanchez Viera M, Bouloc A. The influence of exposome on acne. J Eur Acad Dermatol Venereol. 2018;32(5):812-819. doi:10.1111/jdv.14820 PubMed
27.Lai J-J, Chang P, Lai K-P, Chen L, Chang C. The role of androgen and androgen receptor in skin-related disorders. Arch Dermatol Res. 2012;304(7):499-510. doi:10.1007/s00403-012-1265-x PubMed
28.Bausch Health Canada Inc. Benzamycin (erythromycin and benzoyl peroxide): topical gel [product monograph].
29.Bausch Health Canada Inc. Benzaclin (clindamycin and benzoyl peroxide): 1% /5% and topical gel [product monograph].
30.Galderma Canada Inc. Differin and Differin XP (adapalene): topical cream 0.1% w/w, topical gel 0.1% w/w, topical lotion 0.1% w/w, topical gel 0.3% w/w [product monograph].
31.Bausch Health Canada Inc. Altreno (tretinoin lotion): lotion with moisturizers 0.05% w/w [product monograph].
32.Allergan Inc. Tazorac (tazarotene cream): 0.05% and 0.1% w/w [product monograph].
33.Galderma Canada Inc. Aklief (trifarotene cream): 50 mcg/g, topical [product monograph].
34.Teva Canada Limited. Teva-spironolactone (spironolactone): 25 mg, 100 mg and tablets [product monograph].
35.Hoffmann-La Roche Limited. Accutane (isotretinoin): 10 mg, 40 mg and capsule [product monograph].
36.Pfizer Canada ULC. Aldactone (spironolactone tablets): 25 mg and 100 mg tablets, oral [product monograph].
37.Fu R, Vandermeer BW, Shamliyan TA, et al. AHRQ methods for effective health care handling continuous outcomes in quantitative synthesis. Methods Guide for Effectiveness and Comparative Effectiveness Reviews. Agency for Healthcare Research and Quality (US); 2008.
38.Bayer Inc. Yasmin 21 and Yasmin 28 (drospirenone and ethinyl estradiol tablets, bayer standard): 3.0 mg drospirenone and 0.030 mg ethinyl estradiol [product monograph].
39.Ranbaxy Pharmaceuticals Canada Inc. Ran-Cyproterone/Ethinyl Estradiol (cyproterone acetate and ethinyl estradiol tablets):2 mg cyproterone acetate and 0.035 mg ethinyl estradiol tablets [product monograph]. Accessed May 23, 2023. https://pdf.hres.ca/dpd_pm/00035244.PDF
40.Pfizer Canada Inc. Alesse 21 and Alesse 28 (levonorgestrel and ethinyl estradiol tablets): 100 mcg levonorgestrel and 20 mcg ethinyl estradiol tablets [product monograph]. May 23, 2023. https://pdf.hres.ca/dpd_pm/00046064.PDF
41.Pfizer Canada ULC. Eryc (erythromycin delayed release): 333 mg and capsules [product monograph].
42.Sanis Health Inc. Minocycline (minicycline HCl): 50 mg and 100 mg as minocycline base, capsule [product monograph].
43.Janssen Inc. Tri-Cyclen (norgestimate and ethinyl estradiol): 0.180 mg or 0.215 mg or 0.250 mg norgestimate and 0.035 mg EE, oral tablets [product monograph]. Accessed September 6, 2023. https://pdf.hres.ca/dpd_pm/00046018.PDF
44.Sevimli Dikicier B. Topical treatment of acne vulgaris: efficiency, side effects, and adherence rate. J Int Med Res. 2019;47(7):2987-2992. doi:10.1177/0300060519847367 PubMed
45.Canadian Skin Patient Alliance. Breaking out: A report on the acne experience in Canada. Accessed July 31, 2023. https://canadianskin.ca/media/attachments/2023/03/02/acne-report-2022.pdf
46.Hebert A, Thiboutot D, Stein Gold L, et al. Efficacy and safety of topical clascoterone cream, 1%, for treatment in patients with facial acne: Two phase 3 randomized clinical trials. JAMA Dermatol. 2020;156(6):621-630. doi:10.1001/jamadermatol.2020.0465 PubMed
47.Hebert A, Eichenfield L, Thiboutot D, et al. Efficacy and safety of 1% clascoterone cream in patients aged > 12 years with acne vulgaris. J Drugs Dermatol. 2023;22(2):174-181. doi:10.36849/JDD.7000 PubMed
48.U. S. Food and Drug Administration (FDA). Guidance for industry acne vulgaris: Developing drugs for treatment.
49.U. S. Food and Drug Administration (FDA). Acne vulgaris: Establishing effectiveness of drugs intended for treatment guidance for industry.
50.Alsulaimani H, Kokandi A, Khawandanh S, Hamad R. Severity of acne vulgaris: Comparison of two assessment methods. Clin Cosmet Investig Dermatol. 2020;13:711-716. doi:10.2147/ccid.S266320 PubMed
51.Intrepid Therapeutics Inc. NCT01631474: A phase 2 dose escalating study to evaluate the safety and efficacy of cb-03-01 cream in subjects with facial acne vulgaris. U.S. National Library of Medicine; 2020. Accessed 2023 March. https://classic.clinicaltrials.gov/ct2/show/NCT01631474
52.Clinical Study Report: CB-03-01-27. An open-label, long-term extension study to evaluate the safety of clascoterone (CB-03-01) cream, 1% applied twice-daily in subjects with acne vulgaris [internal sponsor's report]. Cassiopea S.p.A; 2019.
53.A systematic review and network meta-analysis of treatments for acne vulgaris [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Winlevi (clascoterone), 1% cream. Sun Pharma Canada Inc; 2023.
54.Wan X, Wang W, Liu J, Tong T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res Methodol. 2014;14(1):135. doi:10.1186/1471-2288-14-135 PubMed
55.Mavranezouli I, Daly CH, Welton NJ, et al. A systematic review and network meta-analysis of topical pharmacological, oral pharmacological, physical and combined treatments for acne vulgaris. Br J Dermatol. 2022;187(5):639-649. doi:10.1111/bjd.21739 PubMed
56.Afzali BM, Yaghoobi E, Yaghoobi R, Bagherani N, Dabbagh MA. Comparison of the efficacy of 5% topical spironolactone gel and placebo in the treatment of mild and moderate acne vulgaris: a randomized controlled trial. J Dermatolog Treat. 2012;23(1):21-5. doi:10.3109/09546634.2010.488260 PubMed
57.Al-Mosawi ROA, Hassan JK, Al-Tameemi FF. Comparative evaluation of topical antibiotics in treatment of mild to moderate acne vulgaris. International Journal of Drug Delivery Technology. 2022;12(4):1924-1927. doi:10.25258/ijddt.12.4.74
58.Anjum K, Altaf F, Shahzadi N, et al. Comparison of efficacy of 0.1% tazarotene versus 0.1% adapalene for the treatment of mild acne vulgaris. Pakistan Journal of Medical and Health Sciences. 2020;14(1):63-66.
59.Babaeinejad SH, Fouladi RF. The efficacy, safety and tolerability of adapalene versus benzoyl peroxide in the treatment of mild acne vulgaris; a randomized trial. J Drugs Dermatol. 2013;12(9):1033-8. PubMed
60.Bershad S, Kranjac Singer G, Parente JE, et al. Successful treatment of acne vulgaris using a new method: results of a randomized vehicle-controlled trial of short-contact therapy with 0.1% tazarotene gel. Arch Dermatol. 2002;138(4):481-9. doi:10.1001/archderm.138.4.481 PubMed
61.Callender VD, Young CM, Kindred C, Taylor SC. Efficacy and safety of clindamycin phosphate 1.2% and tretinoin 0.025% gel for the treatment of acne and acne-induced post-inflammatory hyperpigmentation in patients with skin of color. J Clin Aesthet Dermatol. 2012;5(7):25-32. PubMed
62.Cunliffe WJ, Caputo R, Dreno B, et al. Clinical efficacy and safety comparison of adapalene gel and tretinoin gel in the treatment of acne vulgaris: Europe and U.S. multicenter trials. J Am Acad Dermatol. 1997;36(6 Pt 2):S126-34. doi:10.1016/s0190-9622(97)70056-2 PubMed
63.Dobson RL, Belknap BS. Topical erythromycin solution in acne. Results of a multiclinic trial. J Am Acad Dermatol. 1980;3(5):478-82. PubMed
64.Dogra S, Sumathy TK, Nayak C, et al. Efficacy and safety comparison of combination of 0.04% tretinoin microspheres plus 1% clindamycin versus their monotherapy in patients with acne vulgaris: a phase 3, randomized, double-blind study. J Dermatolog Treat. 2021;32(8):925-933. doi:10.1080/09546634.2020.1720579 PubMed
65.Dreno B, Tan J, Rivier M, Martel P, Bissonnette R. Adapalene 0.1%/benzoyl peroxide 2.5% gel reduces the risk of atrophic scar formation in moderate inflammatory acne: a split-face randomized controlled trial. J Eur Acad Dermatol Venereol. 2017;31(4):737-742. doi:10.1111/jdv.14026 PubMed
66.Eichenfield LF, Jarratt M, Schlessinger J, et al. Adapalene 0.1% lotion in the treatment of acne vulgaris: results from two placebo-controlled, multicenter, randomized double-blind, clinical studies. J Drugs Dermatol. 2010;9(6):639-46. PubMed
67.Feldman SR, Werner CP, Alió Saenz AB. The efficacy and tolerability of tazarotene foam, 0.1%, in the treatment of acne vulgaris in 2 multicenter, randomized, vehicle-controlled, double-blind studies. J Drugs Dermatol. 2013;12(4):438-46. PubMed
68.Gold LS, Tan J, Cruz-Santana A, et al. A North American study of adapalene-benzoyl peroxide combination gel in the treatment of acne. Cutis. 2009;84(2):110-6. PubMed
69.Gollnick HP, Draelos Z, Glenn MJ, et al. Adapalene-benzoyl peroxide, a unique fixed-dose combination topical gel for the treatment of acne vulgaris: a transatlantic, randomized, double-blind, controlled study in 1670 patients. Br J Dermatol. 2009;161(5):1180-9. doi:10.1111/j.1365-2133.2009.09209.x PubMed
70.Gupta AK, Lynde CW, Kunynetz RA, Amin S, Choi K, Goldstein E. A randomized, double-blind, multicenter, parallel group study to compare relative efficacies of the topical gels 3% erythromycin/5% benzoyl peroxide and 0.025% tretinoin/erythromycin 4% in the treatment of moderate acne vulgaris of the face. J Cutan Med Surg. 2003;7(1):31-7. PubMed
71.Hajheydari Z, Mahmoudi M, Vahidshahi K, Nozari A. Comparison of efficacy of azithromycin vs. clindamycin and erythromycin in the treatment of mild to moderate acne vulgaris. Pakistan Journal of Medical Sciences. 2011;27(1):68-72.
72.Jackson JM, Fu JJ, Almekinder JL. A randomized, investigator-blinded trial to assess the antimicrobial efficacy of a benzoyl peroxide 5%/ clindamycin phosphate 1% gel compared with a clindamycin phosphate 1.2%/tretinoin 0.025% gel in the topical treatment of acne vulgaris. J Drugs Dermatol. 2010;9(2):131-6. PubMed
73.Jarratt MT, Brundage T. Efficacy and safety of clindamycin-tretinoin gel versus clindamycin or tretinoin alone in acne vulgaris: a randomized, double-blind, vehicle-controlled study. J Drugs Dermatol. 2012;11(3):318-26. PubMed
74.Jawade S, Saigaonkar V, Kondalkar A. Efficacy and tolerability of adapalene 0.1%-benzoyl peroxide 2.5% combination gel in treatment of acne vulgaris in Indian patients: a randomized investigator-blind controlled trial. Iran J Dermatol. 2016;19:105-112.
75.Kabir M, Sadiq S, Raza A, Kanwal S, Tanvir T. Comparison of efficacy of adapalene (0.1% gel) monotherapy ve adapalene (0.1%) plus benzyl peroxide (2.5%) combination therapy for treatment of mild to moderate acne vulgaris. Pakistan Journal of Medical and Health Sciences. 2018;12(2):587-589.
76.Kaur J, Sehgal VK, Gupta AK, Singh SP. A comparative study to evaluate the efficacy and safety of combination topical preparations in acne vulgaris. Int J Appl Basic Med Res. 2015;5(2):106-10. doi:10.4103/2229-516X.157155 PubMed
77.Kawashima M, Harada S, Loesche C, Miyachi Y. Adapalene gel 0.1% is effective and safe for Japanese patients with acne vulgaris: a randomized, multicenter, investigator-blinded, controlled study. J Dermatol Sci. 2008;49(3):241-8. doi:10.1016/j.jdermsci.2007.09.012 PubMed
78.Kawashima M, Sato S, Furukawa F, et al. Twelve-week, multicenter, placebo-controlled, randomized, double-blind, parallel-group, comparative phase II/III study of benzoyl peroxide gel in patients with acne vulgaris: A secondary publication. J Dermatol. 2017;44(7):774-782. doi:10.1111/1346-8138.13798 PubMed
79.Kawashima M, Nagare T, Katsuramaki T. Open-label, randomized, multicenter, phase III study to evaluate the safety and efficacy of benzoyl peroxide gel in long-term use in patients with acne vulgaris: A secondary publication. J Dermatol. 2017;44(6):635-643. doi:10.1111/1346-8138.13741 PubMed
80.Kircik LH. Tretinoin microsphere gel pump 0.04% versus tazarotene cream 0.05% in the treatment of mild-to-moderate facial acne vulgaris. J Drugs Dermatol. 2009;8(7):650-4. PubMed
81.Ko HC, Song M, Seo SH, Oh CK, Kwon KS, Kim MB. Prospective, open-label, comparative study of clindamycin 1%/benzoyl peroxide 5% gel with adapalene 0.1% gel in Asian acne patients: efficacy and tolerability. J Eur Acad Dermatol Venereol. 2009;23(3):245-50. doi:10.1111/j.1468-3083.2008.02920.x PubMed
82.Langner A, Chu A, Goulden V, Ambroziak M. A randomized, single-blind comparison of topical clindamycin + benzoyl peroxide and adapalene in the treatment of mild to moderate facial acne vulgaris. Br J Dermatol. 2008;158(1):122-9. doi:10.1111/j.1365-2133.2007.08308.x PubMed
83.Leelaphiwat S, Jongwutiwes T, Lertvikool S, et al. Comparison of desogestrel/ethinyl estradiol plus spironolactone versus cyproterone acetate/ethinyl estradiol in the treatment of polycystic ovary syndrome: a randomized controlled trial. J Obstet Gynaecol Res. 2015;41(3):402-10. doi:10.1111/jog.12543 PubMed
84.Leyden J, Shalita A, Hordinsky M, Swinyer L, Stanczyk FZ, Weber ME. Efficacy of a low-dose oral contraceptive containing 20 microg of ethinyl estradiol and 100 microg of levonorgestrel for the treatment of moderate acne: A randomized, placebo-controlled trial. J Am Acad Dermatol. 2002;47(3):399-409. doi:10.1067/mjd.2002.122192 10.1067/mjd.2002.122192. PubMed
85.Leyden JJ, Krochmal L, Yaroshinsky A. Two randomized, double-blind, controlled trials of 2219 subjects to compare the combination clindamycin/tretinoin hydrogel with each agent alone and vehicle for the treatment of acne vulgaris. J Am Acad Dermatol. 2006;54(1):73-81. doi:10.1016/j.jaad.2005.04.046 PubMed
86.Mazzetti A, Moro L, Gerloni M, Cartwright M. Pharmacokinetic profile, safety, and tolerability of clascoterone (cortexolone 17-alpha propionate, cb-03-01) topical cream, 1% in subjects with acne vulgaris: An open-label phase 2a study. J Drugs Dermatol. 2019;18(6):563. PubMed
87.Muhlemann MF, Carter GD, Cream JJ, Wise P. Oral spironolactone: an effective treatment for acne vulgaris in women. Br J Dermatol. 1986;115(2):227-32. doi:10.1111/j.1365-2133.1986.tb05722.x PubMed
88.Ozolins M, Eady EA, Avery A, et al. Randomised controlled multiple treatment comparison to provide a cost-effectiveness rationale for the selection of antimicrobial therapy in acne. Health Technol Assess. 2005;9(1):iii-212. PubMed
89.Palli MB, Reyes-Habito CM, Lima XT, Kimball AB. A single-center, randomized double-blind, parallel-group study to examine the safety and efficacy of 3mg drospirenone/0.02 mg ethinyl estradiol compared with placebo in the treatment of moderate truncal acne vulgaris. J Drugs Dermatol. 2013;12(6):633-7. PubMed
90.Palombo-Kinne E, Schellschmidt I, Schumacher U, Gräser T. Efficacy of a combined oral contraceptive containing 0.030 mg ethinylestradiol/2 mg dienogest for the treatment of papulopustular acne in comparison with placebo and 0.035 mg ethinylestradiol/2 mg cyproterone acetate. Contraception. 2009;79(4):282-9. doi:10.1016/j.contraception.2008.10.010 PubMed
91.Pariser DM, Thiboutot DM, Clark SD, Jones TM, Liu Y, Graeber M. The efficacy and safety of adapalene gel 0.3% in the treatment of acne vulgaris: A randomized, multicenter, investigator-blinded, controlled comparison study versus adapalene gel 0.1% and vehicle. Cutis. 2005;76(2):145-51. PubMed
92.Patiyasikunt M, Chancheewa B, Asawanonda P, Noppakun N, Kumtornrut C. Efficacy and tolerability of low-dose spironolactone and topical benzoyl peroxide in adult female acne: A randomized, double-blind, placebo-controlled trial. J Dermatol. 2020;47(12):1411-1416. doi:10.1111/1346-8138.15559 PubMed
93.Poulin Y, Sanchez NP, Bucko A, et al. A 6-month maintenance therapy with adapalene-benzoyl peroxide gel prevents relapse and continuously improves efficacy among patients with severe acne vulgaris: results of a randomized controlled trial. Br J Dermatol. 2011;164(6):1376-82. doi:10.1111/j.1365-2133.2011.10344.x PubMed
94.Redmond GP, Olson WH, Lippman JS, Kafrissen ME, Jones TM, Jorizzo JL. Norgestimate and ethinyl estradiol in the treatment of acne vulgaris: a randomized, placebo-controlled trial. Obstet Gynecol. 1997;89(4):615-22. doi:10.1016/s0029-7844(97)00059-8 PubMed
95.Richter JR, Förström LR, Kiistala UO, Jung EG. Efficacy of the fixed 1.2% clindamycin phosphate, 0.025% tretinoin gel formulation (Velac) and a proprietary 0.025% tretinoin gel formulation (Aberela) in the topical control of facial acne. J Eur Acad Dermatol Venereol. 1998;11(3):227-33. PubMed
96.Rukmini Reddy P, Hema D. A comparative study of topical retinoids adapalene vs tazarotene in the treatment of acne vulgaris. European Journal of Molecular and Clinical Medicine. 2022;9(7):6255-6269.
97.Shahlita AR, Smith EB, Bauer E. Topical erythromycin v clindamycin therapy for acne. A multicenter, double-blind comparison. Arch Dermatol. 1984;120(3):351-5. doi:10.1001/archderm.120.3.351 10.1001/archderm.120.3.351. PubMed
98.Shalita AR, Berson DS, Thiboutot DM, et al. Effects of tazarotene 0.1% cream in the treatment of facial acne vulgaris: pooled results from two multicenter, double-blind, randomized, vehicle-controlled, parallel-group trials. Clin Ther. 2004;26(11):1865-73. doi:10.1016/j.clinthera.2004.11.012 PubMed
99.Stein Gold L, Weiss J, Rueda MJ, Liu H, Tanghetti E. Moderate and severe inflammatory acne vulgaris effectively treated with single-agent therapy by a new fixed-dose combination adapalene 0.3%/benzoyl peroxide 2.5% gel: A randomized, double-blind, parallel-group, controlled study. Am J Clin Dermatol. 2016;17(3):293-303. doi:10.1007/s40257-016-0178-4 PubMed
100.Stein Gold L, Baldwin H, Kircik LH, et al. Efficacy and safety of a fixed-dose clindamycin phosphate 1.2%, benzoyl peroxide 3.1%, and adapalene 0.15% gel for moderate-to-severe acne: A randomized phase II study of the first triple-combination drug. Am J Clin Dermatol. 2022;23(1):93-104. doi:10.1007/s40257-021-00650-3 PubMed
101.Tan J, Thiboutot D, Popp G, et al. Randomized phase 3 evaluation of trifarotene 50 μg/g cream treatment of moderate facial and truncal acne. J Am Acad Dermatol. 2019;80(6):1691-1699. doi:10.1016/j.jaad.2019.02.044 PubMed
102.Tanghetti E, Dhawan S, Green L, et al. Randomized comparison of the safety and efficacy of tazarotene 0.1% cream and adapalene 0.3% gel in the treatment of patients with at least moderate facial acne vulgaris. J Drugs Dermatol. 2010;9(5):549-58. PubMed
103.Tanghetti EA, Kircik LH, Green LJ, et al. A phase 2, multicenter, double-blind, randomized, vehicle-controlled clinical study to compare the safety and efficacy of a novel tazarotene 0.045% lotion and tazarotene 0.1% cream in the treatment of moderate-to-severe acne vulgaris. J Drugs Dermatol. 2019;18(6):542. PubMed
104.Tanghetti EA, Werschler WP, Lain E, et al. Novel polymeric lotion formulation of once-daily tazarotene (0.045%) for moderate-to-severe acne: Pooled phase 3 analysis. J Drugs Dermatol. 2020;19(3):272-279. doi:10.36849/JDD.2020.4869 PubMed
105.Tanghetti EA, Werschler WP, Lain T, Guenin E, Martin G, Pillai R. Tazarotene 0.045% lotion for once-daily treatment of moderate-to-severe acne vulgaris: Results from two phase 3 trials. J Drugs Dermatol. 2020;19(1):70-77. doi:10.36849/JDD.2020.3977 PubMed
106.Thiboutot D, Archer DF, Lemay A, Washenik K, Roberts J, Harrison DD. A randomized, controlled trial of a low-dose contraceptive containing 20 microg of ethinyl estradiol and 100 microg of levonorgestrel for acne treatment. Fertil Steril. 2001;76(3):461-8. doi:10.1016/s0015-0282(01)01938-0 PubMed
107.Thiboutot D, Pariser DM, Egan N, et al. Adapalene gel 0.3% for the treatment of acne vulgaris: a multicenter, randomized, double-blind, controlled, phase III trial. J Am Acad Dermatol. 2006;54(2):242-50. doi:10.1016/j.jaad.2004.10.879 PubMed
108.Thiboutot DM, Weiss J, Bucko A, et al. Adapalene-benzoyl peroxide, a fixed-dose combination for the treatment of acne vulgaris: results of a multicenter, randomized double-blind, controlled study. J Am Acad Dermatol. 2007;57(5):791-9. doi:10.1016/j.jaad.2007.06.006 PubMed
109.Thiboutot D, Zaenglein A, Weiss J, Webster G, Calvarese B, Chen D. An aqueous gel fixed combination of clindamycin phosphate 1.2% and benzoyl peroxide 2.5% for the once-daily treatment of moderate to severe acne vulgaris: assessment of efficacy and safety in 2813 patients. J Am Acad Dermatol. 2008;59(5):792-800. doi:10.1016/j.jaad.2008.06.040 PubMed
110.Tyring SK, Kircik LH, Pariser DM, Guenin E, Bhatt V, Pillai R. Novel tretinoin 0.05% lotion for the once-daily treatment of moderate-to-severe acne vulgaris: Assessment of efficacy and safety in patients aged 9 years and older. J Drugs Dermatol. 2018;17(10):1084-1091. PubMed
111.Weiss J, Gold LS, Leoni M, Rueda MJ, Liu H, Tanghetti E. Customized single-agent therapy management of severe inflammatory acne: A randomized, double-blind, parallel-group, controlled study of a new treatment - Adapalene 0.3%-benzoyl peroxide 2.5% gel. J Drugs Dermatol. 2015;14(12):1427-1435. PubMed
112.Xu JH, Lu QJ, Huang JH, et al. A multicentre, randomized, single-blind comparison of topical clindamycin 1%/benzoyl peroxide 5% once-daily gel versus clindamycin 1% twice-daily gel in the treatment of mild to moderate acne vulgaris in Chinese patients. J Eur Acad Dermatol Venereol. 2016;doi:10.1111/jdv.13622 PubMed
113.Zouboulis CC, Derumeaux L, Decroix J, Maciejewska-Udziela B, Cambazard F, Stuhlert A. A multicentre, single-blind, randomized comparison of a fixed clindamycin phosphate/tretinoin gel formulation (Velac) applied once daily and a clindamycin lotion formulation (Dalacin T) applied twice daily in the topical treatment of acne vulgaris. Br J Dermatol. 2000;143(3):498-505. doi:10.1111/j.1365-2133.2000.03701.x PubMed
114.Zouboulis CC, Fischer TC, Wohlrab J, Barnard J, Alió AB. Study of the efficacy, tolerability, and safety of 2 fixed-dose combination gels in the management of acne vulgaris. Cutis. 2009;84(4):223-9. PubMed
Appendix 1: Detailed Outcome Data
Please note that this appendix has not been copy-edited.
Table 27: Acne Lesion Type Definitions
Lesion type | Definition |
|---|---|
Comedones | Open (blackheads) and closed (whiteheads) |
Papules | Raised inflammatory lesions with no visible purulent material |
Pustules | Raised inflammatory lesions with visible purulent material |
Nodules | Any circumscribed, inflammatory masses greater than or equal to 5 mm in diameter with or without cystic changes |
Source: Sponsor’s summary of clinical evidence.23
Planned Sensitivity Analyses
Table 28: Sensitivity Analyses for Proportion of Patients Achieving Treatment Improvement at Week 12
Variable | CB-03-01/25 | CB-03-01/26 | ||
|---|---|---|---|---|
Clascoterone N = 353 | Vehicle N = 355 | Clascoterone N = 369 | Vehicle N = 363 | |
Proportion of patients aged ≥ 12 years achieving improvement at week 12, (ITT analysis) | ||||
Treatment success at week 12, % | 16.1 | 7.0 | 18.7 | 4.7 |
Adjusted treatment difference, % (95% CI) | 9.8 (1.43 to 3.88) | 14.3 (2.19 to 6.43) | ||
P value | < 0.001 | < 0.001 | ||
IGA success (worst value analysis) | ||||
IGA success (worst value), % | 17.0 | 7.2 | 18.5 | 4.6 |
P value | 0.0002 | < 0.0001 | ||
CI = confidence interval; IGA = Investigator’s Global Assessment; ITT = intention to treat.
Sourced: Clinical Study Report for the CB-03-01/25 trial and Clinical Study Report for the CB-03-01/26 trial.18,19
Table 29: Sensitivity Analyses for Improvement in Lesion Counts at Week 12
Variable | CB-03-01/25 | CB-03-01/26 | ||
|---|---|---|---|---|
Clascoterone N = 353 | Vehicle N = 355 | Clascoterone N = 369 | Vehicle N = 363 | |
Absolute change from baseline in NILC at week 12 (ITT analysis) | ||||
Absolute change from baseline (lesion count), mean | −19.4 | −13.0 | −19.4 | −10.8 |
P value | < 0.001 | < 0.001 | ||
NILC (worst value analysis) | ||||
Absolute change in NILC (worst value) | 3.5 | 6.4 | 3.2 | 18.9 |
P value | 0.5227 | 0.0049 | ||
Absolute change from baseline in ILC at week 12 (ITT analysis) | ||||
Absolute change from baseline (lesion count), mean | −19.3 | −15.5 | −20.0 | −12.6 |
P value | 0.003 | < 0.001 | ||
ILC (worst value analysis) | ||||
Absolute change in ILC (worst value), mean | −1.2 | 0.4 | −12.1 | −2.7 |
P value | 0.6508 | < 0.0001 | ||
ILC = inflammatory lesion count; ITT = intention to treat; LSR = local skin reaction; NILC = noninflammatory lesion count.
Summary of RE NMA Findings, Comparisons Versus Placebo – Scenario Analyses
The following figures summarize measures of model fit as well as estimates of treatment effect for active treatments versus placebo from the scenario analyses described in the main text, and for which network diagrams are presented in Appendix 1. For complete league tables of each analysis, refer to the appendices of the sponsor’s full systematic review and NMA technical report. For all analyses, only unadjusted NMAs were performed.
Figure 6: Summary of Comparisons Versus Placebo From RE NMA (Scenario 1)
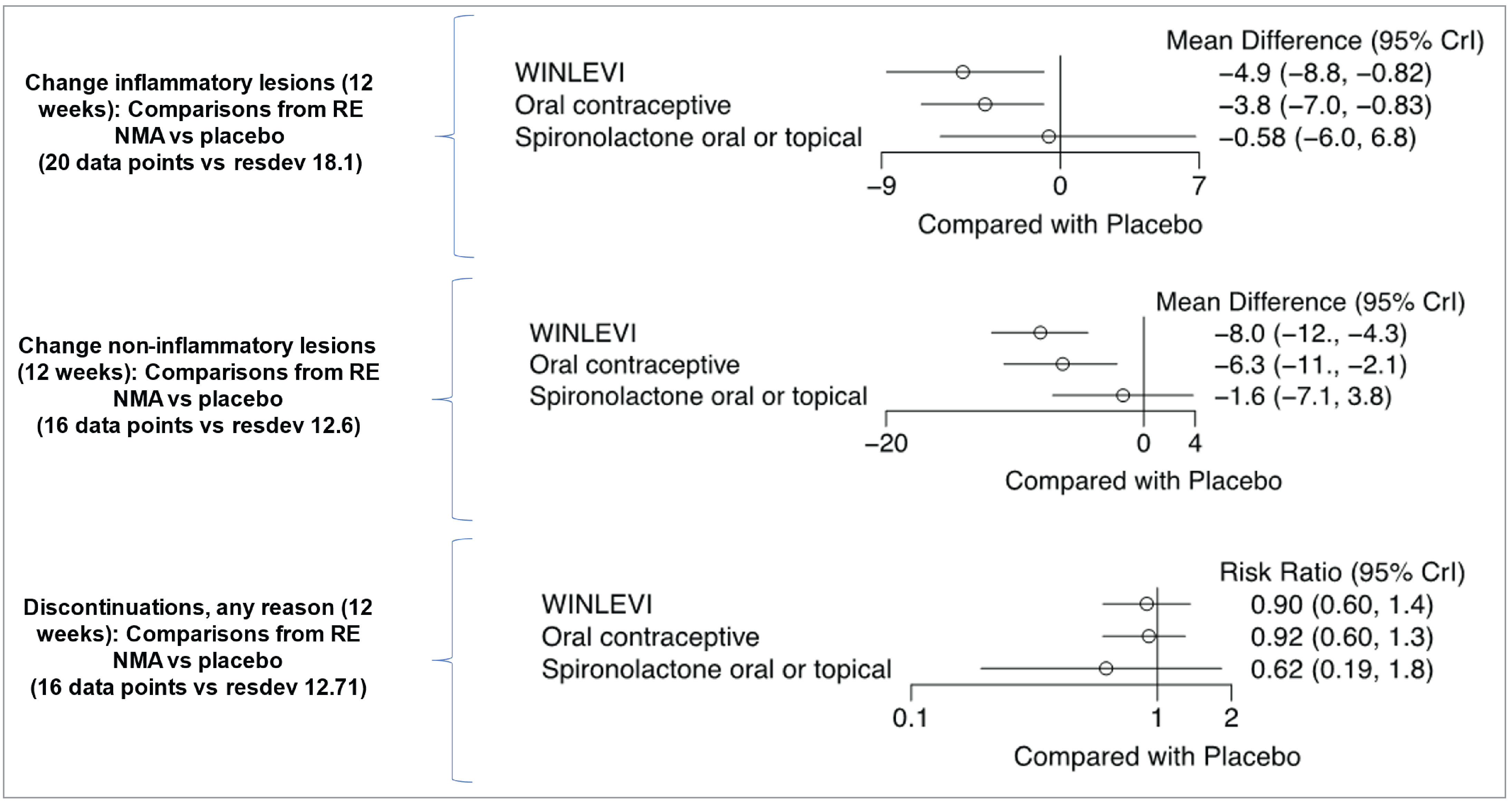
Crl = credible interval; NMA = network meta-analysis; RE = random effects; resdev = residual deviance; vs = versus.
Source: Systematic review and network meta-analysis sponsor report - A systematic review and network meta-analysis of treatments for acne vulgaris.
Figure 7: Summary of Comparisons Versus Placebo From RE NMA (Scenario 2)
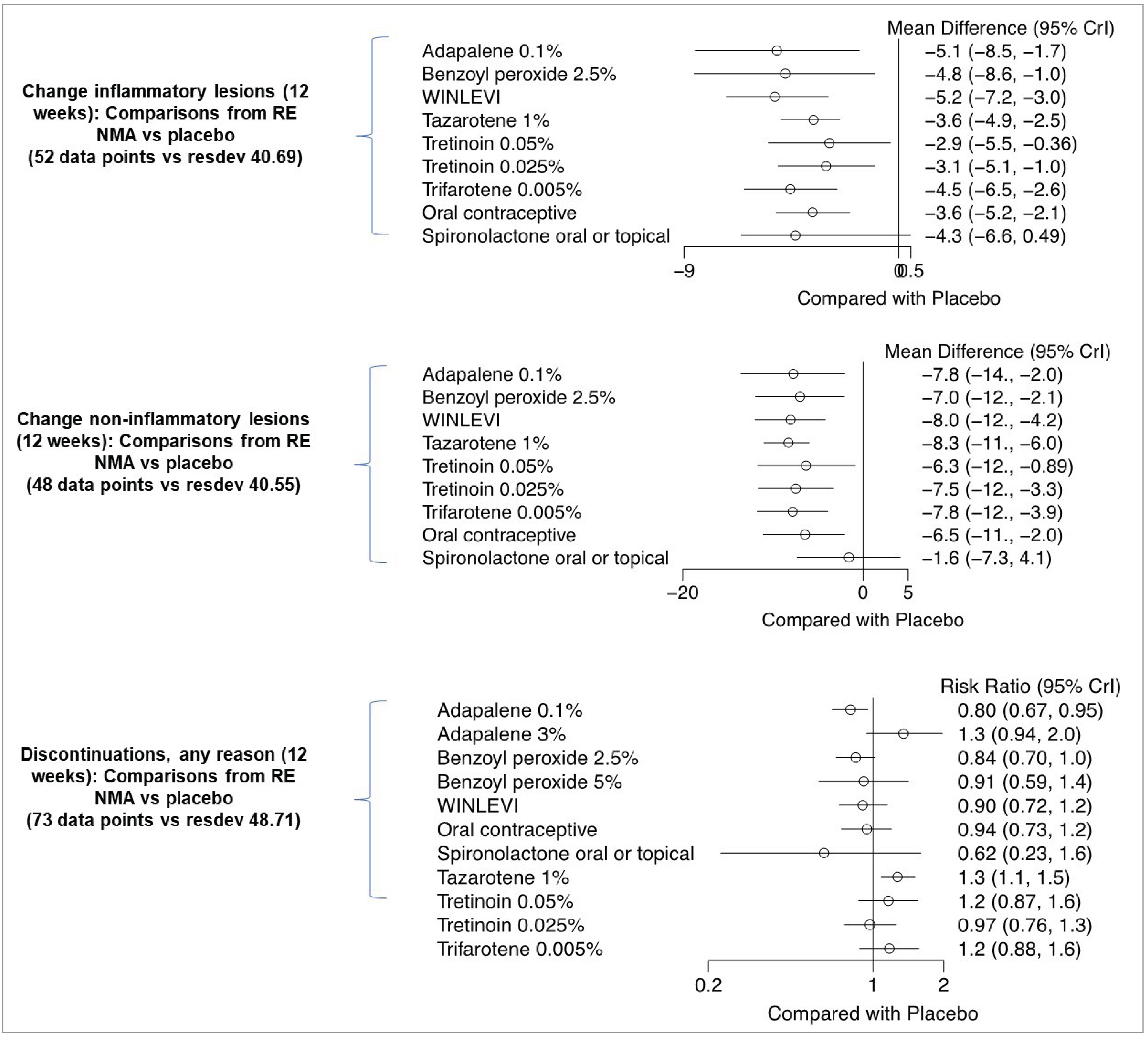
Crl = credible interval; NMA = network meta-analysis; RE = random effects; resdev = residual deviance; vs = versus.
Source: Systematic review and network meta-analysis sponsor report - A systematic review and network meta-analysis of treatments for acne vulgaris.
Figure 8: Summary of Comparisons Versus Placebo From RE NMA (Scenario 3)
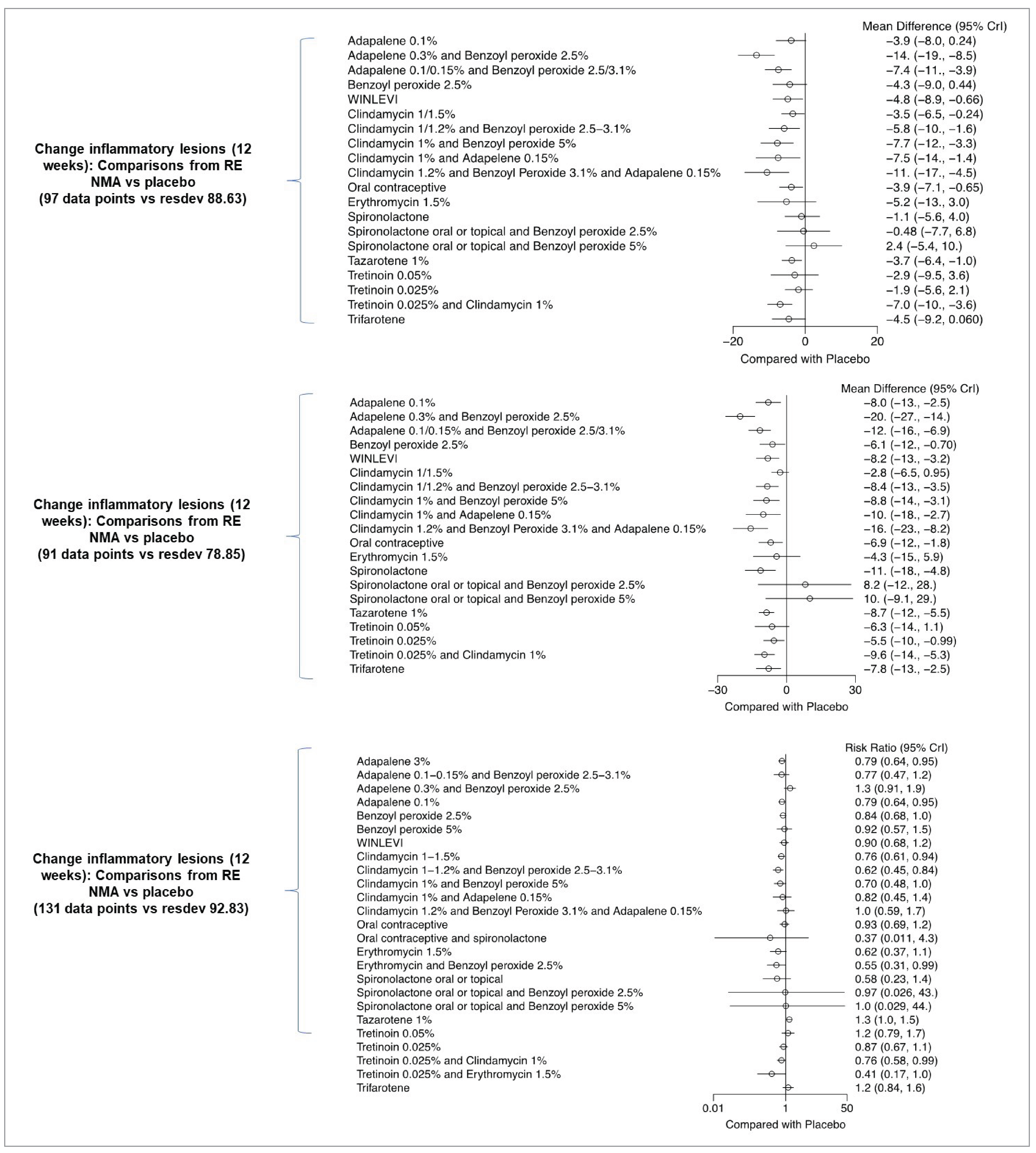
Crl = credible interval; NMA = network meta-analysis; RE = random effects; resdev = residual deviance; vs = versus.
Source: Systematic review and network meta-analysis sponsor report — A systematic review and network meta-analysis of treatments for acne vulgaris.
Table 30: Baseline Characteristics Studies in the Sponsor-submitted NMA
Author (year) | Treatments compared | Baseline characteristics | |||
|---|---|---|---|---|---|
Age (years) | Female, n (%) | Inflammatory lesions | Noninflammatory lesions | ||
Afzali (2012)56 | SPL 5% (n = 38) PLB (n = 40) | Mean (SD) SPL: 21.5 (4.2) PLB: 22.2 (4.06) | SPL: 30 (78.9) PLB: 34 (85) | Mean (SD) SPL: 10.1 (8.45) PLB: 7.1 (5.82) | Mean (SD) SPL: 9.44 (21.5) PLB: 12.58 (22.03) |
Al Mosawi (2022)57 | CLN 1% (n = 15) Eryth 2% (n = 15) PLB (n = 15) | NR | NR | NR | NR |
Anjum (2020)58 | TAZ 0.1% (n = 60) ADA 0.1% (n = 60) | Mean (SD) TAZ: 20.1 (4.5) ADA: 22.1 (6.4) | TAZ: 44 (73.3) ADA: 48 (80.0) | NR | NR |
Babaeinejad (2013)59* | BPO 2.5% (n = 30) ADA 0.1% (n = 30) | Mean (SD) BPO: 20.93 (3.77) ADA: 21.27 (3.57) | BPO: 24 (80.0) ADA: 23 (76.7) | Mean (SD) BPO: 8.43 (5.45) ADA: 9.73 (5.09) | Mean (SD) BPO: 11.50 (5.92) ADA: 10.77 (5.54) |
Bershad (2002)60* | TAZ 0.1% 2x/d (n = 33) TAZ 0.1% 1x/d (n = 33) PLB (n = 33) | Mean (SD) TAZ 2x/d: 26.3 (10.6) TAZ 1x/d: 26.1 (10.8) PLB: 23.8 (10.0) | TAZ 2x/d: 24 (72.7) TAZ 1x/d: 20 (60.6) PLB: 20 (60.6) | Mean (SD) TAZ 2x/d: 42.52 (39.84) TAZ 1x/d: 48.76 (41.16) PLB: 36.61 (27.79) | Mean (SD) TAZ 2x/d: 23.91 (13.51) TAZ 1x/d: 22.88 (10.67) PLB: 17.33 (7.59) |
Callender (2012)61 | CLN 1.2%/TRT 0.025% (n = 17) PLB (n = 16) | Mean (range) 28.3 (13 to 51) | Both groups: 26 (78.8) | Mean (SD) CLN/TRT: 11.9 (11.10) PLB: 13.6 (11.15) | Mean (SD) CLN/TRT: 48.6 (46.10) PLB: 64.7 (73.08) |
Cunliffe (1997)62* | ADA 0.1% (n = 134) TRT 0.025% (n = 134) | Mean (range) ADA: 19.7 (12 to 30) TRT: 19.2 (12 to 28) | ADA: 60 (44.8) TRT: 65 (48.5) | NR | NR |
Dobson (1980)63 | Eryth 1.5% (n = 127) PLB (n = 126) | NR | Eryth: 78 (61.4) PLB: 82 (65.1) | NR | NR |
Dogra (2021)64 | TRT 0.04%/CLN 1% (n = 300) TRT 0.025% (n = 300) CLN 1% (n = 150) | Median (range) TRT/CLN: 20 (13 to 43) TRT: 20 (14 to 48) CLN: 20 (12 to 42) | TRT/CLN: 111 (37.00) TRT: 134 (44.67) CLN: 57 (38.00) | Median (range) TRT/CLN: 28 (20 to 50) TRT: 28 (20 to 65) CLN: 28 (15 to 50) | Median (range) TRT/CLN: 35 (20 to 96) TRT: 35 (10 to 100) CLN: 35.5 (16 to 97) |
Dreno (2017)65 | ADA 0.1%/BPO 2.5% (n = 38) PLB (n = 38) | Mean (SD) 23.4 (3.6) | Both groups 14 (36.8) | Mean (SD) ADA/BPO: 12.3 (4.0) PLB: 12.5 (3.5) | Mean (SD) ADA/BPO: 11.8 (10.8) PLB: 12.5 (11.6) |
Eichenfield (2010)66* | ADA 0.1% (n = 1,068) | Mean (SD) ADA: 19.3 (6.9) PLB: 19.0 (6.9) | ADA: 583 (54.6) PLB: 562 (52.4) | NR | NR |
Feldman (2013)67* | 301: TAZ 0.1% (n = 372) PLB (n = 372) 302: TAZ 0.1% (n = 373) PLB (n = 369) | Mean (SD) 301: TAZ: 18.2 (5.7) PLB: 18.6 (6.4) 302: TAZ: 19.2 (6.5) PLB: 19.2 (6.8) | 301: TAZ: 182 (49) PLB: 192 (52) 302: TAZ: 197 (53) PLB: 185 (50) | Mean (SD) 301: TAZ: 31.4 (6.8) PLB: 31.9 (7.0) 302: TAZ: 32.1 (6.8) PLB: 32.4 (6.9) | Mean (SD) 301: TAZ:50.1 (20.9) PLB: 49.8 (20.5) 302: TAZ: 45.2 (18.2) PLB: 46.2 (18.1) |
Gold (2009)68* | ADA 0.1%/BPO 2.5% (n = 415) ADA 0.1% (n = 420) BPO 2.5% (n = 415) PLB (n = 418) | Mean ADA/BPO: 18.7 ADA: 17.9 BPO: 18.4 PLB: 18.0 | ADA/BPO: 205 (49.4) ADA: 203 (48.3) BPO: 208 (50.1) PLB: 196 (46.9) | Median ADA/BPO: 27 ADA: 27 BPO: 27 PLB: 27 | Median ADA/BPO: 44 ADA: 47 BPO: 46 PLB: 46 |
Gollnick (2009)69* | ADA 0.1%/BPO 2.5% (n = 419) ADA 0.1% (n = 418) BPO 2.5% (n = 415) PLB (n = 418) | Mean (range) ADA/BPO: 19.5 (12 to 48) ADA: 18.5 (12 to 50) BPO: 18.9 (12 to 55) PLB: 19.2 (12 to 51) | ADA/BPO: 236 (56.3) ADA: 229 (54.8) BPO: 230 (55.4) PLB: 244 (58.4) | Median ADA/BPO: 26 ADA: 27 BPO: 26 PLB: 26 | Median ADA/BPO: 45 ADA: 46 BPO: 45 PLB: 46 |
Gupta (2003)70 | Eryth 3%/BPO 5% (n = 53) TRT 0.025%/Eryth 4% (n = 59) | Mean (range) Eryth/BPO: 18.5 (13.7 to 29.6) TRT/Eryth: 18.7 (13.1 to 37.1) | NR | Mean Eryth/BPO: 22.8 TRT/Eryth: 25.5 | Mean Eryth/BPO: 35.5 TRT/Eryth: 28.0 |
Hajheydari (2011)71 | CLN 2% (n = 32) Eryth 2% (n = 32) | Mean (SD) CLN: 20.4 (4.3) Eryth: 19.3 (2.9) | CLN: 28 (87.5) Eryth: 28 (87.5) | Mean (SD) CLN: 54.7 (34.3) Eryth: 65.7 (47.1) | Mean (SD) |
Study CB-03-01/25 CLA 1% (n = 353) PLB (n = 355) Study CB-03-01/26 CLA 1% (n = 369) PLB (n = 363) | Median (range) Study CB-03-01/25 CLA: 18.0 (10 to 58) PLB: 18.0 (9 to 50) Study CB-03-01/26 CLA: 18.0 (10 to 50) PLB: 18.0 (11 to 42) | Study CB-03-01/25 CLA: 221 (62.6) PLB: 215 (60.6) Study CB-03-01/26 CLA: 243 (65.9) PLB: 221 (60.9) | Mean (SD) Study CB-03-01/25 CLA: 42.4 (11.77) PLB: 42.9 (12.31) Study CB-03-01/26 CLA: 42.9 (12.20) PLB: 41.3 (10.96) | Mean (SD) Study CB-03-01/25 CLA: 59.1 (22.19) PLB: 60.7 (22.09) Study CB-03-01/26 CLA: 62.8 (21.37) PLB: 63.3 (20.52) | |
Jackson (2010)72 | TRT 0.025%/CLN 1.2% (n = 27) CLN 1%/BPO 5% (n = 27) | Mean (SD) TRT/CLN: 16.2 (4.9) CLN/BPO: 17.6 (6.9) | TRT/CLN: 15 (55.6) CLN/BPO: 14 (51.9) | Mean TRT/CLN: 22.78 CLN/BPO: 24.74 | Mean TRT/CLN: 35.11 CLN/BPO: 34.30 |
Jarratt (2012)73* | TRT 0.025%/CLN 1% (n = 476) TRT 0.025% (n = 464) CLN 1% (n = 467) PLB (n = 242) | Mean (SD) TRT/CLN: 20.8 (8.5) TRT: 20.2 (7.7) CLN: 20.2 (8.1) PLB: 20.6 (8.4) | TRT/CLN: 269 (57) TRT: 264 (57) CLN: 266 (57) PLB: 153 (63) | Mean (SD) TRT/CLN: 25.5 (6.9) TRT: 25.6 (6.4) CLN: 25.3 (6.8) PLB: 25.7 (6.8) | Mean (SD) TRT/CLN: 45.1 (25.1) TRT: 45.4 (24.5) CLN: 44.7 (25.3) PLB: 47.7 (25.4) |
Jawade (2016)74* | ADA 0.1%/BPO 2.5% (n = 41) ADA 0.1% (n = 45) BPO 2.5% (n = 46) | Mean (SD) ADA/BPO: 20.1 (3.9) ADA: 18.6 (3.5) BPO: 19.2 (3.3) | ADA/BPO: 22 (53.7) ADA: 27 (60.0) BPO: 29 (63.0) | Mean (SD) ADA/BPO: 6.6 (5.1) ADA: 6.6 (3.8) BPO: 7.9 (5.4) | Mean (SD) ADA/BPO: 35.2 (15.1) ADA: 36.8 (21.6) BPO: 39.4 (18.3) |
Kabir (2018)75 | ADA 0.1%/BPO 2.5% (n = 64) ADA 0.1% (n = 64) | Mean (SD) 25.11 (3.116) | Both groups 76 (60) | NR | NR |
Kaur (2015)76 | TRT 0.025%/CLN 1% (n = 33) CLN 1%/BPO 3% (n = 33) | Range 15 to 35 | NR | Mean (SD) TRT/CLN: 4.97 (3.03) CLN/BPO: 3.57 (2.61) | Mean (SD) TRT/CLN: 13.70 (4.8) CLN/BPO: 12.03 (5.53) |
Kawashima (2008)77* | ADA 0.1% (n = 100) PLB (n = 100) | Mean (SD) ADA: 24.16 (4.4) PLB: 24.33 (4.6) | ADA: 89 (89.0) PLB: 89 (89.0) | Mean (SD) ADA: 20.6 (10.7) PLB: 22.2 (13.6) | Mean (SD) ADA: 43.0 (27.2) PLB: 40.7 (23.8) |
Kawashima (2017a)78* | BPO 2.5% (n = 204) BPO 5% (n = 204) PLB (n = 201) | Mean (SD) BPO 2.5: 19.5 (5.7) BPO 5: 20.0 (5.6) PLB: 19.2 (5.5) | BPO 2.5: 119 (58.6) BPO 5: 124 (61.1) PLB: 110 (54.7) | Median (range) BPO 2.5: 18 (11 to 40) BPO 5: 18 (11 to 40) PLB: 18 (11 to 40) | Median (range) BPO 2.5: 29 (20 to 90) BPO 5: 30 (20 to 96) PLB: 30 (20 to 100) |
Kawashima (2017b)79* | BPO 2.5% (n = 231) BPO 5% (n = 227) | Mean (SD) BPO 2.5: 22.9 (7.3) BPO 5: 23.0 (7.5) | BPO 2.5: 159 (68.8) BPO 5: 155 (68.3) | Median (range) BPO 2.5: 12 (5 to 39) BPO 5: 11 (5 to 40) | Median (range) BPO 2.5: 21 (1 to 99) BPO 5: 21 (1 to 97) |
Kircik (2009)80 | TAZ 0.05% (n = 20) TRT 0.04% (n = 20) | Mean (SD) 21.4 (9.9) | Both groups 17 (42.5) | NR | NR |
Ko (2009)81 | CLN 1%/BPO 5% (n = 31) ADA 0.1% (n = 38) | Mean CLN/BPO: 24.5 ADA: 21.1 | CLN/BPO: 24 (77.4) ADA: 25 (65.8) | Mean CLN/BPO: 31.6 ADA: 26.6 | Mean CLN/BPO: 16.7 ADA: 16.4 |
Langner (2008)82 | CLN 1%/BPO 5% (n = 65) ADA 0.1% (n = 65) | Mean (SD) CLN/BPO: 21.4 (4.50) ADA: 21.8 (4.75) | CLN/BPO: 38 (58.5) ADA: 38 (58.5) | Mean (SD) CLN/BPO: 34.3 (18.13) ADA: 35.3 (19.82) | Mean (SD) CLN/BPO: 60.9 (41.11) ADA: 58.6 (37.83) |
Leelaphiwat (2014)83 | EE 30 mcg/DES 150 mcg/ SPL 25 mg (n = 18) EE 35 mcg/CPA 2mg (n = 18) | Mean (SD) EE/DES/SPL: 26.29 (4.04) EE/CPA: 26.94 (6.87) | EE/DES/SPL: 18 (100) EE/CPA: 18 (100) | NR | NR |
Leyden (2002)84 | EE 20 mcg/LNG 100 mcg (n = 185) PLB (n = 186) | Mean (SD) EE/LNG: 25.0 (7.1) PLB: 24.9 (7.1) | EE/LNG: 185 (100) PLB: 186 (100) | Mean (SD) EE/LNG: 21.76 (11.53) PLB: 21.87 (11.16) | Mean (SD) EE/LNG: 50.22 (51.92) PLB: 46.80 (43.08) |
Leyden (2006)85* | TRT 0.025%/CLN 1% (n = 634) TRT 0.025% (n = 635) CLN 1% (n = 635) PLB (n = 315) | Mean (range) TRT/CLN: 19.3 (12 to 49) TRT: 20.2 (11 to 81) CLN: 19.6 (11 to 54) PLB: 19.0 (12 to 56) | TRT/CLN: 338 (53) TRT: 369 (58) CLN: 338 (53) PLB: 151 (48) | Mean (SD) TRT/CLN: 26.3 (7.4) TRT: 26.0 (7.2) CLN: 26.2 (7.5) PLB: 26.4 (7.0) | Mean (SD) TRT/CLN: 52.0 (28.8) TRT: 50.7 (27.7) CLN: 50.2 (28.2) PLB: 51.7 (29.3) |
Mazzetti (2019)86* | CLA 1% (n = 70) PLB (n = 75) | Mean (SD) CLA: 21.0 (6.22) PLB: 19.2 (5.25) | CLA: 37 (53) PLB: 43 (57) | Mean (range) CLA: 28.6 (20 to 63) PLB: 30.5 (20 to 75) | Mean (range) CLA: 47.2 (20 to 98) PLB: 43.9 (20 to 99) |
Muhleman (1986)87 | SPL 200 mg (n = 14) PLB (n = 15) | NR | SPL: 14 (100) PLB: 15 (100) | Mean (SD) SPL: 50.03 (30.23) PLB: 29.84 (8.33) | NR |
Noaimi (2021)7 | SPL 2% (n = 37) CLN 1.5% (n = 36) | Mean (SD) SPL: 18.3 (4.6) CLN: 17.8 (3.8) | SPL: 26/35 (74.3) CLN: 25/33 (75.8) | Mean (SD) SPL: 9.9 (3.48) CLN: 10.9 (2.65) | Mean (SD) SPL: 91.0 (64.4) CLN: 67.6 (34.6) |
Ozolins (2005)88 | Eryth 3%/BPO 5% (n = 127) BPO 5% (n = 130) | Mean (SD) All 5 arms (N = 648): 19.7 (6.07) | Study N = 649, all groups: 356 (54.9) | Mean Eryth/BPO: 51.1 BPO: 52.3 | NR |
Palli (2013)89 | EE 0.02 mg/DRSP 3 mg (n = 16) PLB (n = 14) | Mean (SD) EE/DRSP: 23 (5.2) PLB: 24 (3.7) | EE/DRSP: 16 (100) PLB: 14 (100) | Mean (SD) EE/DRSP: 26 (11.6) PLB: 24.2 (10.6) | Mean (SD) EE/DRSP: 27 (15) PLB: 17.6 (11.3) |
Palombo-Kinne (2009)90 | EE 0.03 mg / DNG 2 mg (n = 525) EE 0.35 mg / CPA 2 mg (n = 537) PLB (n = 264) | Mean (SD) EE/DNG: 24.0 (5.8) EE/CPA: 24.4 (5.8) PLB: 25.3 (6.2) | EE/DNG: 525 (100) EE/CPA: 537 (100) PLB: 264 (100) | Mean (SD) EE/DNG: 22.9 (10.5) EE/CPA: 22.7 (10.1) PLB: 22.0 (10.0) | NR |
Pariser (2005)91* | ADA 0.3% (n = 70) ADA 0.1% (n = 70) PLB (n = 74) | Mean (SD) ADA 0.3: 17.8 (6.02) ADA 0.1: 16.5 (4.51) PLB: 17.6 (4.55) | ADA 0.3: 32 (45.7) ADA 0.1: 27 (38.6) PLB: 29 (39.2) | Mean ADA 0.3: 32.7 ADA 0.1: 31.1 PLB: 29.6 | Mean ADA 0.3: 47.0 ADA 0.1: 49.4 PLB: 41.7 |
Patiyasikunt (2020)92 | SPL 25 mg/BPO 2.5% (n = 21) SPL 50 mg/BPO 2.5% (n = 21) PLB (n = 21) | Mean (SD) SPL25/BPO: 30.9 (5.7) SPL50/BPO: 28 (3.2) PLB: 31.6 (5.0) | SPL25/BPO: 21 (100) SPL50/BPO: 21 (100) PLB: 21 (100) | Mean (SD) SPL25/BPO: 10 (5.1) SPL50/BPO: 5.3 (7.7) PLB: 9.4 (5.8) | Mean (SD) SPL25/BPO: 35.4 (26.1) SPL50/BPO: 33.75 (16.3) PLB: 43.7 (41.0) |
Poulin (2011)93 | ADA 0.1%/BPO 2.5% (n = 123) PLB (n = 120) | Mean (SD) ADA/BPO: 19.1 (5.89) PLB: 18.2 (5.23) | ADA/BPO: 58 (47.2) PLB: 53 (44.2) | Mean (SD) ADA/BPO: 10.9 (7.8) PLB: 10.6 (9.2) | Mean (SD) ADA/BPO: 25.3 (18.2) PLB: 23.5 (21.7) |
Redmond (1997)94 | EE 0.35 mg/NRG (n = 118) PLB (n = 113) | Mean (range) EE/NRG: 28.4 (15 to 49) PLB: 28.4 (15 to 47) | EE/NRG: 118 (100) PLB: 113 (100) | Mean (range) EE/NRG: 18.9 (10 to 76) PLB: 18.9 (6 to 72) | Mean (range) EE/NRG: 36.6 (6 to 100) PLB: 37.6 (6 to 130) |
Richter (1998)95 | TRT 0.025% (n = 80) TRT 0.025%/CLN 1.2% (n = 81) | Mean (SD) TRT: 19.5 (3.0) TRT/CLN: 19.9 (2.8) | TRT: 36/77 (46.8) TRT/CLN: 28/75 (37.3) | Mean TRT: 42.8 TRT/CLN: 56.1 | Mean TRT: 79.3 TRT/CLN: 88.8 |
Rukmini Reddy (2022)96* | ADA 0.1% (n = 25) TAZ 0.1% (n = 25) | Both groups: 15 (30) | NR | Mean ADA: 7.1 TAZ: 9.1 | NR |
Shalita (1984)97 | CLN 1% (n = 90) Eryth 1.5% (n = 88) | CLN: 60 (66.7) Eryth: 56 (63.6) | NR | Mean (SE) CLN: 55.8 (7.0) Eryth: 53.4 (7.0) | NR |
Shalita (2004)98* | TAZ 0.1% (n = 424) PLB (n = 423) | TAZ: 203 (48) PLB: 214 (51) | Mean years (SD) TAZ: 6 (7) PLB: 6 (6) | Median TAZ: 59 PLB: 57 | Median TAZ: 84 PLB: 83 |
Stein Gold (2016)99 | ADA 0.1%/BPO 2.5% (n = 217) ADA 0.3%/BPO 2.5% (n = 217) PLB (n = 69) | ADA 0.1/BPO: 114 (52.5) ADA 0.3/BPO: 113 (52.1) PLB: 36 (52.2) | NR | Mean (SD) ADA 0.1/BPO: 59.9 (29.4) ADA 0.3/BPO: 58.9 (26.9) PLB: 60.7 (28.2) | Mean (SD) ADA 0.1/BPO: 98.0 (39.2) ADA 0.3/BPO: 98.5 (39.0) PLB: 97.6 (36.6) |
Stein Gold (2022)100 | CLN 1.2%/BPO 3.1%/ADA 0.15% (n = 147) BPO 3.1%/ADA 0.15% (n = 150) CLN 1.2%/BPO 3.1% (n = 146) CLN 1.2%/ADA 0.15% (n = 150) PLB (n = 148) | CLN/BPO/ADA: 94 (64.4) BPO/ADA: 86 (57.3) CLN/BPO: 91 (62.3) CLN/ADA: 93 (62.0) PLB: 89 (60.1) | CLN/BPO/ADA: BPO/ADA CLN/BPO CLN/ADA PLB | Mean (SD) CLN/BPO/ADA: 51.8 (20.3) BPO/ADA: 48.0 (14.7) CLN/BPO: 49.2 (17.6) CLN/ADA: 51.1 (18.4) PLB: 50.7 (18.7) | NR |
Tan (2019)101* | PERFECT 1 TFT 50 mcg/g (n = 612) PLB (n = 596) PERFECT 2 TFT 50 mcg/g (n = 602) PLB (n = 610) | Mean (SD) PERFECT 1 TFT: 19.6 (6.88) PLB: 19.3 (5.89) PERFECT 2 TFT: 19.6 (6.2) PLB: 19.9 (6.4) | PERFECT 1 TFT: 305 (49.8) PLB: 324 (54.4) PERFECT 2 TFT: 357 (59.3) PLB: 338 (55.4) | Mean (SD) PERFECT 1 TFT: 34.7 (13.02) PLB: 34.8 (13.61) PERFECT 2 TFT: 36.1 (12.47) PLB: 37.1 (15.06) | Mean (SD) PERFECT 1 TFT: 54.0 (28.55) PLB: 52.8 (26.08) PERFECT 2 TFT: 50.6 (25.93) PLB: 51.2 (25.75) |
Tanghetti (2010)102* | TAZ 0.1% (n = 90) ADA 0.3% (n = 90) | Mean (SD) TAZ: 20.2 (7.4) ADA: 20.9 (7.6) | TAZ: 55 (61.1) ADA: 57 (63.3) | Mean (SD) TAZ: 32 (10) ADA: 33 (11) | Mean (SD) TAZ: 70 (24) ADA: 61 (15) |
Tanghetti (2019)103* | TAZ 0.045% (n = 69) TAZ 0.1% (n = 72) PLB (n = 69) | Mean (SD) TAZ 0.045: 23.3 (10.20) TAZ 0.1: 22.0 (8.96) PLB: 21.2 (8.44) | TAZ 0.045: 37 (53.6) TAZ 0.1: 41 (56.9) PLB: 38 (55.1) | Mean (SD) TAZ 0.045: 28.3 (6.00) TAZ 0.1: 27.3 (5.95) PLB: 27.2 (5.49) | Mean (SD) TAZ 0.045: 37.6 (14.7) TAZ 0.1: 36.6 (13.31) PLB: 36.6 (13.17) |
Study 1: TAZ 0.045% (n = 402) PLB (n = 411) Study 2: TAZ 0.045% (n = 397) PLB (n = 404) | Mean (SD) Study 1: TAZ: 20.8 (7.29) PLB: 20.4 (6.94) Study 2: TAZ: 20.1 (6.48) PLB: 20.5 (6.81) | Study 1: TAZ: 280 (69.7) PLB: 271 (65.9) Study 2: TAZ: 251 (63.2) PLB: 262 (64.9) | Mean (SD) Study 1: TAZ: 28.5 (7.04) PLB: 28.1 (7.04) Study 2: TAZ: 28 (7.32) PLB: 27.9 (7.1) | Mean (SD) Study 1 and 2: TAZ: 41.5 (16.8) PLB: 40.7 (16.3) | |
Thiboutot (2001)106 | EE 20 mcg/LNG 100 mcg (n = 174) PLB (n = 176) | Mean (SD) EE/LNG: 26.8 (7.3) PLB: 29.0 (7.5) | EE/LNG: 174 (100) PLB: 176 (100) | Mean (SD) EE/LNG: 19.85 (9.60) PLB: 18.11 (9.11) | Mean (SD) EE/LNG: 38.86 (29.72) PLB: 39.64 (31.34) |
Thiboutot (2006)107* | ADA 0.3% (n = 258) ADA 0.1% (n = 261) PLB (n = 134) | Mean (SD) ADA 0.3: 18.4 (6.19) ADA 0.1: 17.8 (5.97) PLB: 18.6 (6.39) | ADA 0.3: 129 (50.0) ADA 0.1: 129 (49.4) PLB: 72 (53.7) | MeanADA 0.3: 25.0 ADA 0.1: 25.0 PLB: 24.0 | Mean ADA 0.3: 33.0 ADA 0.1: 34.0 PLB: 34.0 |
Thiboutot (2007)108* | ADA 0.1%/BPO 2.5% (n = 149) ADA 0.1% (n = 148) BPO 2.5% (n = 149) PLB (n = 71) | Mean (range) ADA/BPO: 16.2 (12 to 56) ADA: 16.5 (12 to 37) BPO: 16.5 (12 to 37) PLB: 16.6 (12 to 33) | ADA/BPO: 62 (41.6) ADA: 62 (41.9) BPO: 53 (35.6) PLB: 31 (43.7) | Median ADA/BPO: 27 ADA: 28 BPO: 28 PLB: 29 | Median ADA/BPO: 44 ADA: 45 BPO: 43 PLB: 46 |
Thiboutot (2008)109* | CLN 1.2%/BPO 2.5% (n = 797) CLN 1.2% (n = 812) BPO 2.5% (n = 809) PLB (n = 395) | Mean (range) CLN/ BPO: 19.2 (12.1 to 54.7) CLN: 19.6 (12.1 to 70.2) BPO: 19.1 (12.0 to 53.8) PLB: 19.4 (12.2 to 50.9) | CLN/ BPO: 408 (51.2) CLN: 420 (51.7) BPO: 455 (56.2) PLB: 192 (48.6) | Mean CLN/ BPO: 26.4 CLN: 26.3 BPO: 25.8 PLB: 26.1 | Mean CLN/ BPO: 47.4 CLN: 45.3 BPO: 46.8 PLB: 44.0 |
Tyring (2018)110* | TRT 0.05% (n = 819) PLB (n = 821) | Mean (SD) TRT: 20.4 (7.18) PLB: 20.6 (7.45) | TRT: 433 (52.9) PLB: 476 (58.0) | Mean (SD) TRT: 26.3 (5.49) PLB: 26.2 (5.44) | Mean (SD) TRT: 42.1 (18.01) PLB: 43.7 (18.91) |
Weiss (2015)111 | ADA 0.3%/BPO 2.5% (n = 106) ADA 0.1%/BPO 2.5% (n = 112) PLB (n = 34) | Mean (SD) ADA 0.3/BPO: 19.5 (7.9) ADA 0.1/BPO: 19.0 (6.6) PLB: 18.1 (4.5) | ADA 0.3/BPO: 51 (48.1) ADA 0.1/BPO: 56 (50.0) PLB: 13 (38.2) | ADA 0.3/BPO: 49 (20.2) ADA 0.1/BPO: 43.7 (17.2) PLB: 44.5 (19.3) | ADA 0.3/BPO: 64.4 (27.8) ADA 0.1/BPO: 64.7 (33.6) PLB: 64.8 (30.6) |
Xu (2016)112 | CLN 1%/ BPO 5% (n = 500) CLN 1% (n = 516) | Mean (SD) CLN/ BPO: 23.4 (4.64) CLN: 23.3 (4.29) | CLN/ BPO: 382 (76.4) CLN: 383 (74.2) | Mean (SD) CLN/ BPO: 26.3 (10.30) CLN: 26.8 (9.92) | Mean (SD) CLN/ BPO: 50.5 (26.75) CLN: 51.4 (26.90) |
Zouboulis (2000)113 | TRT 0.025%/CLN 1% (n = 102) CLN 1% (n = 104) | Mean (SD) TRT/CLN: 18.6 (3.2) CLN: 18.6 (3.1) | TRT/CLN: 50 (49) CLN: 58 (56) | NR | NR |
Zouboulis (2009)114 | ADA 0.1%/BPO 2.5% (n = 192) CLN 1%/ BPO 5% (n = 190) | Mean (SD) ADA/BPO: 20.9 (6.8) CLN/BPO: 20.8 (7.3) | ADA/BPO: 95 (49) CLN/BPO: 95 (50) | Mean (SD) ADA/BPO: 40.8 (16.0) CLN/BPO: 39.0 (13.7) | Mean (SD) ADA/BPO: 51.1 (26.5) CLN/BPO: 52.7 (25.7) |
ADA = adapalene; BPO = benzoyl peroxide; CLA = clascoterone; CLN = clindamycin; CPA = cyproterone acetate; DES = desogestrel; DNG = dienogest; DRSP = drospirenone; EE = ethinyl estradiol; Eryth = erythromycin; IQR = interquartile range; LNG = levonorgestrel; LS = least squares; NR = not reported; NRG = norgestimate; PLB = placebo; SD = standard deviation; SE = standard error; SPL = spironolactone; TAZ = tazarotene; TFT = trifarotene; TRT = tretinoin.
Pharmacoeconomic Review
Abbreviations
BIA
budget impact analysis
BPO
benzoyl peroxide
CMA
cost-minimization analysis
ITC
indirect treatment analysis
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Clascoterone (Winlevi), 1% topical cream |
Indication | For the treatment of acne vulgaris in patients 12 years of age and older |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | June 15, 2023 |
Reimbursement request | For the first-line prescription topical treatment of moderate and severe acne vulgaris in patients 12 years of age and older |
Sponsor | Sun Pharma Canada Inc. |
Submission history | Previously reviewed: Yes Indication: For the treatment of acne vulgaris in patients 12 years of age and older Recommendation: Not applicable. Submission voluntarily withdrawn by the sponsor, November 15, 2023 |
NOC = Notice of Compliance.
The current pharmacoeconomic submission was aligned with the previous submission that was withdrawn by the sponsor in November 2023.
The appraisal by Canada’s Drug Agency (CDA-AMC) was updated based on new treatment guidelines, input from interested parties, and new treatments now available for this population. Pricing information was not updated from the original submission and may not reflect current published prices.
Table 2: Summary of Economic Information
Component | Description |
|---|---|
Type of economic evaluation | Cost-minimization analysis |
Target populations | Health Canada indication: Topical treatment of acne vulgaris in patients 12 years of age and older Reimbursement request: First-line prescription topical treatment of moderate and severe acne vulgaris in patients 12 years of age and older |
Treatment | Clascoterone 1% cream |
Dosage regimen | The recommended dose per application is up to approximately 1 g, applied in a thin uniform layer twice per day |
Submitted price | 30 g tube: $242.42 |
Submitted treatment cost | Incorporating a prescription refill rate, the sponsor’s estimated cost was $584 per patient per year |
Comparators |
|
Perspective | Canadian publicly funded health care payer |
Time horizon | One year |
Key data source | CB-03-01/25 and CB-03-01/26 pivotal randomized controlled trials comparing clascoterone cream to vehicle cream One sponsor-commissioned network meta-analysis report, consisting of ITCs exploring 12 analyses in total |
Costs considered | Drug acquisition costs |
Submitted results |
|
Key limitations |
|
CDA-AMC reanalysis results |
|
CDA-AMC = Canada’s Drug Agency; ITC = indirect treatment comparison.
Conclusions
The CDA-AMC clinical review concluded that clascoterone cream may result in clinically important improvements in achieving treatment success compared with vehicle cream in patients with moderate to severe acne vulgaris, based on the results of the CB-03-01/25 and CB-03-01/26 randomized controlled trials. However, the evidence was uncertain with regard to the ability of clascoterone cream to reduce the number and percentage of lesions at week 12, nor was there evidence of the effect of clascoterone on mental health or health-related quality of life compared with placebo (vehicle cream). Results of the sponsor’s submitted indirect evidence suggest that clascoterone had a greater impact on reducing inflammatory and noninflammatory lesions compared to placebo, while comparisons to active therapies did not favour either clascoterone or a comparator treatment. Differences in discontinuation between active treatments and placebo, and between active treatments themselves, were generally not found. Results of the indirect evidence were associated with uncertainty due to heterogeneity in patient populations, disease severity at baseline, and differences in response to placebo between the included trials.
CDA-AMC identified several limitations with the sponsor’s cost-minimization analysis including uncertainty in the place in therapy for clascoterone cream and thus the most appropriate comparators, uncertainty in the clinical similarity of clascoterone cream to the included comparators, an inappropriate annual cost estimate for clascoterone cream, and the inappropriate costing of some comparators. CDA-AMC made several changes to the analysis, including revising the assumed usage rate of clascoterone cream to be consistent with that of its topical comparators, revising the adherence rate of oral hormone therapies, and updating the costing of some comparators. Based on the CDA-AMC base case, the average annual cost of clascoterone cream is expected to be $3,539 per patient, which was more costly than treatment with any of the included topical monotherapies (incremental costs ranged from $2,862 to $3,492 per patient) and was also more costly than oral contraceptives or spironolactone (incremental costs ranged from $3,235 to $3,525 per patient). No evidence was submitted to support a price premium for clascoterone cream. At the submitted price of $8.08 per gram, a 98.7% price reduction would be required for clascoterone cream to be no more costly than the list price of the least expensive topical comparator, tretinoin 0.05% cream.
Economic Review
The current review is for clascoterone 1% cream (Winlevi) for the treatment of acne vulgaris in patients 12 years of age and older.
Economic Information
Summary of Sponsor’s Economic Information
Overview
The sponsor submitted a cost-minimization analysis for clascoterone 1% cream, indicated for the treatment of acne vulgaris in patients 12 years of age and older,1 compared with topical benzoyl peroxide monotherapy, topical retinoid monotherapies, and oral hormonal therapies in the form of oral contraceptive products as well as spironolactone. The sponsor’s reimbursement request differs from the Health Canada indication and is for the first-line prescription topical treatment of moderate and severe acne vulgaris in patients aged 12 years and older.2
To support the assumption of clinical similarity inherent to a cost-minimization analysis, the sponsor submitted a network meta-analysis report in which a series of indirect treatment comparisons (ITCs) were conducted comparing clascoterone 1% cream used twice daily to topical and hormonal monotherapies in patients aged 9 years and older with mild to moderate acne vulgaris.3 Three reference-case analyses were conducted comparing clascoterone 1% cream twice daily to other first-line topical therapies used once daily for the outcomes of reduction in inflammatory lesions relative to placebo, reduction in noninflammatory lesions relative to placebo, and all-cause discontinuation. Three separate scenarios were conducted for each of these 3 outcomes: the scenarios compared clascoterone 1% cream to oral contraceptives and spironolactone; to individual first-line topical monotherapies, oral contraceptives as a single node, and spironolactone as a single node; and to individual topical therapies including combination products, oral contraceptives as a single node, and spironolactone as a single node. The cost-minimization analysis was conducted from the perspective of a public payer over a 1-year time horizon. Only drug acquisition costs were considered.
Clascoterone 1% cream is available in 30 g tubes, with a recommended dose per application of up to approximately 1 g, applied in a thin uniform layer twice per day. The submitted price of clascoterone 1% cream is $242.42 per 30 g tube, or $8.08 per gram. When used as directed and assuming a dose of 1 g twice daily, the annual cost of clascoterone 1% cream is $5,899 per patient. The annual per-patient cost of other topical regimens, also assuming 1 g per application, ranges from $59 to $1,129 per patient, depending on the comparator, while the annual cost of hormone therapies in the form of oral contraceptives or spironolactone ranges from $15 to $304 per patient, depending on dosage and comparator. The sponsor estimated the annual cost of clascoterone 1% cream by assuming a refill rate of one 30 g tube every 152 days, based on real-world usage data from the Winlevi copay program in the US, which suggested patients obtain one 60 g tube every 9.96 months.4 Annual costs for topical comparators were calculated by assuming the use of 1 g per application at the frequency specified in the respective product monographs, and then applying an adherence rate of 60%, based on adherence rates reported in the literature for topical acne vulgaris treatments.5-7 This 60% adherence rate was also used within the submitted analysis for oral contraceptives and spironolactone.
Base-Case Results
The sponsor’s submitted base case estimated that in patients aged 12 years and older with acne vulgaris, clascoterone 1% cream was associated with a cost of $584 over 1 year while other treatments for acne vulgaris ranged from $21 to $609 per patient per year (Table 6). The use of clascoterone 1% cream was therefore predicted to result in incremental drug costs ranging from $102 to $563 per patient per year relative to all included comparators with the exception of adapalene 0.3%, where clascoterone 1% cream would be associated with an annual savings of $25.
CDA-AMC Appraisal of the Sponsor’s Economic Information
CDA-AMC identified several key limitations to the sponsor’s analysis that have notable implications for the economic analysis.
Uncertain place in therapy and relevant comparators: The sponsor’s reimbursement request is for the first-line prescription topical treatment of moderate and severe acne vulgaris in patients aged 12 years and older while the Health Canada indication is for the treatment of acne vulgaris in patients aged 12 years and older. The sponsor indicated that only benzoyl peroxide, topical retinoid monotherapies, oral contraceptives, and spironolactone are of interest as comparators because oral isotretinoin is indicated for the treatment of severe nodular and/or inflammatory acne, acne conglobate, and recalcitrant acne, which the sponsor described as “outside the treatment paradigm for the acne vulgaris patient population.”2 Similarly, the sponsor indicated that antibiotic treatments are also not considered first-line therapy and carry concerns regarding resistance, and thus are also only used in patients with moderate to severe acne that is resistant to topical therapies. Of note, the US guideline8 cited by the sponsor to support these statements does not restrict the use of either oral isotretinoin, or oral or topical antibiotics to refractory patients; neither do current Canadian guidelines.9,10 Neither the Health Canada indication for clascoterone cream nor the US guideline’s recommendation for its use are restricted to first-line use or to moderate to severe acne. There is therefore an overlap in the indications and/or clinical use of these products and the indication and requested reimbursement for clascoterone cream. In contrast, in both clinician group input submitted for this review (refer to the CDA-AMC Clinical Review Report) and in clinical expert feedback obtained directly by CDA-AMC, clascoterone cream was considered appropriate for use as monotherapy or in combination with other topicals for patients with mild acne, or in combination with oral antibiotics for moderate acne, and potentially for use as an adjunctive therapy to isotretinoin for severe acne or in combination with other agents in patients requesting alternatives to isotretinoin. As such, clascoterone may be expected to partially displace topical acne monotherapies, including benzoyl peroxide, retinoids, and topical antibiotics, but it would not be expected to displace oral contraceptives, spironolactone, oral isotretinoin, or oral antibiotics used for acne, and may be used in addition to some of its potential comparators rather than in place of them. This expert input also expected the availability of clascoterone cream to impact the use of topical combination products such as clindamycin plus benzoyl peroxide and adapalene plus benzoyl peroxide.
CDA-AMC was unable to fully address this limitation due to uncertainty in the eventual place in therapy of clascoterone cream and thus its appropriate direct comparators. When used as recommended in product monographs or guidelines and when considering the submitted price for clascoterone cream and publicly available list prices for other acne therapies, the daily cost per patient of clascoterone cream (up to $16.16) is more than the daily costs per patient of all sponsor-included comparator treatments (refer to Table 5), and also more than the daily costs per patient of all other treatments for acne vulgaris not considered as comparators by the sponsor, including topical antibiotics (up to $1.6211), oral antibiotics (up to $1.6612), topical combination products (up to $1.7211-13), and oral isotretinoin (up to $7.6012).
Clinical similarity is uncertain: The sponsor submitted a cost-minimization analysis rather than a cost-utility analysis, with the underlying assumption that clascoterone cream is clinically similar to the included comparators and thus only the relative cost of treatment is relevant from the economic perspective. To support this underlying assumption in the absence of clinical trials comparing clascoterone cream to other active treatments, the sponsor submitted ITCs3 comparing clascoterone cream to 4 sets of comparators: first-line topical monotherapies (the reference case); oral contraceptives and spironolactone; first-line topical monotherapies, oral contraceptives, and spironolactone; and topical therapies including combination products, as well as oral contraceptives and spironolactone. Each comparison was conducted for 3 outcomes: the mean change in inflammatory lesions at 12 weeks, the mean change in noninflammatory lesions at 12 weeks, and all-cause discontinuation at 12 weeks. While clascoterone cream was found to be associated with improved reduction in both inflammatory and noninflammatory lesions compared to placebo, comparisons to other active treatments did not favour either treatment. There was no strong evidence of many differences between active treatments or between active treatments and placebo in terms of discontinuation by week 12. These ITCs were associated with a number of limitations, including heterogeneity in patient demographics, baseline lesion counts, placebo (vehicle cream) response rates, and previous treatments. The study populations of the included randomized controlled trials ranged from mild to severe acne based on mean baseline lesion counts, with the clascoterone trials associated with higher baseline lesion counts than most of the other included trials, and thus treatment effects measuring changes from baseline in lesion counts relative to other treatments may be subject to bias. Results of the submitted ITCs are therefore associated with uncertainty.
Due to the submission of a cost-minimization analysis, CDA-AMC was unable to explore uncertainty in the clinical effectiveness of clascoterone cream relative to its comparators.
The annual cost of clascoterone cream was inappropriately estimated: The mean daily use of clascoterone cream reported in the CB-03-01/25 and CB-03-01/26 clinical trials was 1.96 g and 1.97 g, respectively, with a reported adherence of approximately 90%.14 Because these trials informed the efficacy of clascoterone 1% cream in the sponsor’s submitted ITCs, the clinical efficacy of clascoterone cream relative to its comparators as reported in the sponsor’s ITCs is based on a daily usage rate of approximately 2 g. However, when estimating the usage rate of clascoterone cream to calculate its average annual cost within the cost-minimization analysis, the sponsor used real-world data from a sponsor-provided copay assistance program in the US run through a third-party vendor, CoverMyMeds.4 This real-world data reported the number of patients within the assistance program who had received a 60 g tube of clascoterone once in the studied year, the number who had received a tube twice, and so forth. The sponsor then calculated a weighted average refill rate based on this data, which suggested that a 60 g tube is used every 9.96 months, which was converted to 30 g every 4.98 months because clascoterone will only be available in 30 g tubes in Canada. This assumption leads to a usage rate of 72 g per year (i.e., 2.4 clascoterone 30 g tubes), or 10% of what would be expected if clascoterone cream were used at the same rate as in the clinical trials (715 g per year at 1.96 g per day). In using the assistance program data in this way, the sponsor made the implicit assumptions that the included patients did not switch to other forms of acne therapy within the year, even when only filling their clascoterone prescription once, nor did they receive clascoterone cream outside the assistance program. In contrast, the sponsor assumed patients using other topical monotherapies would be 60% adherent to using 1 g twice daily (i.e., 438 g per year) in the case of benzoyl peroxide, or 1 g once daily (i.e., 219 g per year) for all other included topicals, based on adherence estimates reported in the literature.5,7 Clinical expert input obtained by CDA-AMC did not find the assumption that clascoterone cream would be associated with substantially lower application rates than other topical monotherapies to be plausible. Additionally, this difference in usage rates between clascoterone and the included topical monotherapies was not consistent with the usage of each comparator in the sponsor’s submitted ITCs,3 where all dosing was as reported in the included clinical trials. To be consistent with the indirect evidence underlying the assumption of clinical similarity, the assumed usage of clascoterone relative to that of its topical comparators should have been consistent with the ratio of their respective recommended and clinically studied doses.
In reanalysis, CDA-AMC assumed that clascoterone cream would be used in clinical practice at 60% of the recommended dose, consistent with the adherence assumption of the other topical comparators. In a scenario, CDA-AMC assumed that all topical comparators would have a 60% adherence rate to 1 g once daily dosing, because clinical expert opinion obtained by CDA-AMC as well as from the clinical literature5,6 suggest many patients use once daily dosing for acne therapies regardless of the recommended dose schedule. The relative clinical efficacy of clascoterone cream used once daily compared to other topical monotherapies is unknown.
Some comparators were inappropriately priced: Some branded oral contraceptives included by the sponsor as comparators are legally interchangeable with their generic forms (e.g., Yasmin, Alesse). As such, the amount paid by the Ontario Drug Benefit program, the pricing source for these products, is limited to the cost of the generic.12 Additionally, where the sponsor used BC PharmaCare Formulary list prices,15 they did not remove the 8% markup included in the maximum price payable.16 Finally, according to the submitted pharmacoeconomic and budget impact reports, the sponsor appears to have intended to use an adherence rate of 100% for oral contraceptive comparators as well as spironolactone; however, in the submitted analyses, calculated annual costs of these comparators use a 60% adherence rate.2,4 Clinical expert input obtained by CDA-AMC estimated that adherence rates for spironolactone and the oral contraceptives would approach 100%.
CDA-AMC considered only the generic pricing of legally interchangeable comparators. For comparators where the sponsor used BC PharmaCare Formulary list prices that include markups, CDA-AMC reanalyses instead used Saskatchewan Formulary list prices.
Oral contraceptives and spironolactone were corrected in the CDA-AMC reanalyses to have an adherence rate of 100%.
CDA-AMC Reanalyses of the Economic Information
The CDA-AMC base case was derived by making changes to the parameter values and assumptions in the sponsor’s cost-minimization analysis, in consultation with clinical experts. To derive the CDA-AMC base case, the following changes were made to the sponsor’s submitted analysis:
Oral contraceptives and spironolactone were assumed to have 100% adherence.
List prices were updated to September 2023 and BC PharmaCare Formulary list prices were replaced with Saskatchewan Formulary list prices where applicable.
Where legally interchangeable products exist, only the generic price was considered.
Clascoterone was assumed to have an adherence rate of 60% of its recommended dosage, consistent with the other topical monotherapies.
Dosing of spironolactone was assumed to vary between 25 mg and 200 mg daily.9
Results of the CDA-AMC base-case reanalysis can be found in Table 3. At an average annual cost of $3,539 per patient, treatment with clascoterone cream was more costly than treatment with any of the included topical monotherapies (incremental costs ranged from $2,862 to $3,492) and was also more costly than oral contraceptives or spironolactone (incremental costs ranged from $3,235 to $3,525).
Table 3: Summary of the CDA-AMC Reanalysis Results
Drug | Unit cost ($) | Total annual drug costs ($) | Incremental drug costs vs. clascoterone ($) |
|---|---|---|---|
Clascoterone 1% cream (Winlevi) | 8.08 per g2 | 3,539.33 | Reference |
Topical nonretinoid monotherapy | |||
Benzoyl peroxide 5% (various) | 0.19 per g17 | 81.73 | –3,457.60 |
Topical retinoid monotherapy | |||
Tazarotene 0.1% (Tazorac) | 1.45 per g11 | 317.70 | −3,221.63 |
Tazarotene 0.045% (Arazlo) | 1.41 per g12 | 307.72 | −3,231.62 |
Tretinoin 0.025% (Stieva-A) | 0.32 per g12 | 70.34 | −3,468.99 |
Tretinoin 0.05% (Stieva-A) | 0.21 per g12 | 46.95 | −3,492.38 |
Tretinoin 0.025% gel (Retin-A) | 0.49 per g11 | 107.16 | −3,432.18 |
Tretinoin 0.05% cream (Retin-A) | 0.49 per g11 | 107.16 | −3,432.18 |
Tretinoin 0.04% gel (Retin-A Micro) | 1.15 per g13 | 251.74 | −3,287.59 |
Tretinoin 0.025% (vitamin A acid) | 0.36 per g11 | 79.72 | −3,459.62 |
Tretinoin 0.05% (vitamin A acid) | 0.41 per g12 | 89.83 | −3,449.50 |
Adapalene 0.1% (Differin) | 2.20 per g11 | 481.45 | −3,057.88 |
Adapalene 0.3% (Differin XP) | 3.09 per g13 | 677.30 | −2,862.03 |
Hormone therapies, DRSP + EE | |||
DRSP 3.0 mg + EE 0.03 mg (Yasmin, generics) | 6.22 per pack12 | 81.07 | −3,458.27 |
DRSP 3.0 mg + EE 0.02 mg (Yaz, generics) | 8.26 per pack12 | 107.68 | −3,431.66 |
Hormone therapies, LNG + EE | |||
LNG 20 mcg + EE 100 mcg (Alesse 21, generics) | 3.94 per pack12 | 51.39 | −3,487.94 |
Hormone therapies, CPA + EE | |||
CPA 2 mg + EE 35 mcg (Diane-35, generics) | 23.34 per pack13 | 304.25 | −3,235.09 |
Hormone therapies, DES + EE | |||
DES 0.100 mg or 0.125 mg or 0.150 mg + EE 0.025 mg (Linessa) | 18.21 per pack12 | 237.38 | −3,301.95 |
DES 0.150 mg + EE 0.03 mg (Marvelon, generics) | 7.77 per pack12 | 101.29 | −3,438.04 |
Hormone therapies, NRG + EE | |||
NRG 0.18 mg or 0.215 mg or 0.25 mg + EE 0.035 mg (generics) | 14.39 per pack12 | 187.58 | −3,351.75 |
NRG 0.18 mg or 0.215 mg or 0.25 mg + EE 0.025 mg (generics) | 13.39 per pack12 | 174.55 | −3,364.78 |
Spironolactone | |||
Spironolactone 25 mg to 200 mg daily (Aldactone, generics) | 0.0405 per 25 mg12 0.0955 per 100 mg12 | 14.78 to 69.72 | −3,524.55 to −3,469.62 |
CDA-AMC = Canada’s Drug Agency; CPA = cyproterone acetate; DES = desogestrel; DRSP = drospirenone; EE = ethinyl estradiol; LNG = levonorgestrel; NRG = norgestimate; vs. = versus.
In a scenario where all patients receiving topical monotherapies are assumed to use a dose of 1 g once daily with a 60% adherence rate, the annual cost of clascoterone cream would be $1,770 per patient, which would be $1,092 to $1,729 more costly per patient per year than the comparator topical monotherapies. The relative clinical efficacy of clascoterone cream compared to other topical monotherapies under this scenario is unknown.
CDA-AMC conducted a price reduction analysis based on the CDA-AMC base case. At the submitted price of $8.08 per gram, assuming publicly available list prices, a price reduction of 98.7% would be required for clascoterone cream to be cost-neutral to the least expensive topical comparator assumed to be clinically similar to it in the sponsor and the CDA-AMC analyses (Table 4). A price reduction of 91.3% would be required for the cost of clascoterone to be equal to that of the least expensive nontretinoin topical retinoid comparator assumed to be clinically similar to it.
Table 4: CDA-AMC Price Reduction Analyses
Scenario | Submitted price ($) | Reduction needed (%) | Reduced price ($) | Savings relative to submitted pricea ($) |
|---|---|---|---|---|
Price reduction required to equal least expensive topical comparator (tretinoin [Stieva-A] 0.05% cream)b | 8.08 per g 3,539 per year | 98.7% | 0.11 per g 47 per year | 7.97 per g 3,492 per year |
Price reduction required to equal least expensive nontretinoin topical retinoid comparator (tazarotene [Arazlo] 0.045% lotion)b | 8.08 per g 3,539 per year | 91.3% | 0.70 per g 308 per year | 7.38 per g 3,231 per year |
CDA-AMC = Canada’s Drug Agency.
Note: Price reduction analyses assume that clascoterone cream is used twice daily, tretinoin 0.05% cream and tazarotene 0.045% lotion are used once daily, and all 3 products are used at a rate of 1 g per application and with 60% adherence.
aSavings from the sponsor list price per gram and per patient per year.
bRelative to publicly available list prices of comparators.
Issues for Consideration
Systemic antiandrogen therapies such as oral contraceptives and spironolactone are an effective strategy to treat acne in female patients but are not used in male patients due to side effects. Clascoterone is the first antiandrogen therapy appropriate for use in male patients. However, subgroup analyses were not conducted to explore the efficacy of clascoterone cream in male patients, nor could indirect comparisons be conducted considering only male patients. As such, the clinical efficacy of clascoterone cream relative to other treatments for acne vulgaris in male patients specifically is unknown.
A combination of topical gel containing clindamycin, benzoyl peroxide, and adapalene (brand name to be confirmed) is currently under review by CDA-AMC for the topical treatment of acne vulgaris in patients aged 9 years and older.18
Conclusions
The CDA-AMC clinical review concluded that clascoterone cream may result in clinically important improvements in achieving treatment success compared with vehicle cream in patients with moderate to severe acne vulgaris, based on the results of the CB-03-01/25 and CB-03-01/26 randomized controlled trials. However, the evidence was uncertain with regard to the ability of clascoterone cream to reduce the number and percentage of lesions at week 12, nor was there evidence of the effect of clascoterone on mental health or health-related quality of life compared with vehicle cream. Results of the sponsor’s submitted ITCs suggest that clascoterone had a greater impact on reducing inflammatory and noninflammatory lesions compared to placebo (vehicle cream), while comparisons to active therapies did not favour either clascoterone or a comparator treatment. Differences in discontinuation between active treatments and placebo, and between active treatments themselves, were generally not found. Results of these ITCs were associated with uncertainty due to heterogeneity in patient populations, disease severity at baseline, and differences in response to placebo between the included trials.
CDA-AMC identified several limitations with the sponsor’s cost-minimization analysis including uncertainty in the place in therapy for clascoterone cream and thus the most appropriate comparators, uncertainty in the clinical similarity of clascoterone cream to the included comparators, an inappropriate annual cost estimate for clascoterone cream, and the inappropriate costing of some comparators. CDA-AMC made several changes to the analysis, including revising the assumed usage rate of clascoterone cream to be consistent with that of its comparators, revising the adherence rate of oral hormone therapies, and updating the costing of some comparators. Based on the CDA-AMC base case, the average annual cost of clascoterone cream is expected to be $3,539 per patient, which was more costly than treatment with any of the included topical monotherapies (incremental costs ranged from $2,862 to $3,492) and was also more costly than oral contraceptives or spironolactone (incremental costs ranged from $3,235 to $3,525). No evidence was submitted to support a price premium for clascoterone cream. At the submitted price of $8.08 per gram, a 98.7% price reduction would be required for clascoterone cream to ensure cost-parity to its least expensive topical comparator, tretinoin 0.05% cream. If alternate comparators are considered more relevant, slightly lower price reductions would be required.
References
1.Winlevi (clascoterone cream): 1% w/w, topical [product monograph]. Sun Pharma Canada Inc.
2.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Winlevi (clascoterone), 1% cream. Sun Pharma Canada Inc.
3.A systematic review and network meta analysis of treatments for acne vulgaris [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Winlevi (clascoterone), 1% cream. Sun Pharma Canada Inc.
4.Budget impact analysis technical report [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Winlevi (clascoterone), 1% cream. Brampton (ON)
5.Purvis CG, Balogh EA, Feldman SR. Clascoterone: How the novel androgen receptor inhibitor fits into the acne treatment paradigm. Ann Pharmacother. 2021;55(10):1297-1299. doi:10.1177/1060028021992055 PubMed
6.Sevimli Dikicier B. Topical treatment of acne vulgaris: efficiency, side effects, and adherence rate. J Int Med Res. 2019;47(7):2987-2992. doi:10.1177/0300060519847367 PubMed
7.Yentzer BA, Gosnell AL, Clark AR, et al. A randomized controlled pilot study of strategies to increase adherence in teenagers with acne vulgaris. J Am Acad Dermatol. 2011;64(4):793-5. doi:10.1016/j.jaad.2010.05.008 PubMed
8.Reynolds RV, Yeung H, Cheng CE, et al. Guidelines of care for the management of acne vulgaris. J Am Acad Dermatol. 2024;90(5):1006 e1-1006 e30. doi:10.1016/j.jaad.2023.12.017
9.Therapeutic choices: Acne. Canadian Pharmacists Association; 2022.
10.Asai Y, Baibergenova A, Dutil M, et al. Management of acne: Canadian clinical practice guideline. CMAJ. 2016;188(2):118-126. doi:10.1503/cmaj.140665//DC1 PubMed
11.Saskatchewan drug plan: search formulary. Accessed September 15, 2023. https://formulary.drugplan.ehealthsask.ca/SearchFormulary
12.Ontario Ministry of Health, Ontario Ministry of Long-Term Care. Ontario drug benefit formulary/comparative drug index. Accessed September 15, 2023 https://www.formulary.health.gov.on.ca/formulary/
13.DeltaPA. IQVIA. Accessed September 15, 2023. https://www.iqvia.com/
14.Hebert A, Thiboutot D, Stein Gold L, et al. Efficacy and safety of topical clascoterone cream, 1%, for treatment in patients with facial acne: Two phase 3 randomized clinical trials. JAMA Dermatol. 2020;156(6):621-630. doi:10.1001/jamadermatol.2020.0465 PubMed
15.BC PharmaCare formulary search. Government of British Columbia. Accessed September 15, 2023. https://pharmacareformularysearch.gov.bc.ca
16.Pharmacare policy manual: 5.6 maximum pricing policy. Government of British Columbia. Accessed July 30, 2023. https://www2.gov.bc.ca/gov/content/health/practitioner-professional-resources/pharmacare/pharmacare-publications/pharmacare-policy-manual-2012/pricing-policies-product-reimbursement/maximum-pricing
17.Search the NLPDP drug product database. Government of Newfoundland and Labrador. Accessed September 15, 2023. https://www.health.gov.nl.ca/health/prescription/newformulary.asp
18.Clindamycin plus benzoyl peroxide and adapalene. Canada's Drug Agency. Accessed August 14, 2024. https://www.cda-amc.ca/clindamycin-plus-benzoyl-peroxide-and-adapalene
19.Non-Insured health benefits program: First Nations and Inuit health branch: Annual report 2020 to 2021. Accessed May 12, 2022. https://www.sac-isc.gc.ca/eng/1645718409378/1645718500555
20.Acne. Canadian Dermatology Association. Accessed April 13, 2023. https://dermatology.ca/public-patients/skin/acne/#:~:text=Acne%20affects%205.6%20million%20Canadians,adults%20ages%2020%20to%2040
21.Strauss JS, Krowchuk DP, Leyden JJ, et al. Guidelines of care for acne vulgaris management. J Am Acad Dermatol. 2007;56(4):651-63. doi:10.1016/j.jaad.2006.08.048 PubMed
22.Skin conditions by the numbers. American Association of Dermatology Accessed June 1, 2023. https://www.aad.org/media/stats-numbers
23.Breaking out: A report on the acne experience in Canada Canadian Skin Patient Alliance. Accessed May 1, 2023. https://www.canadianskin.ca/advocacy/advocacy-reports/acne-report
24.Understanding the gap 2.0: A Pan-Canadian analysis of prescription drug insurance coverage. The Conference Board of Canada. Accessed May 15, 2023. https://www.conferenceboard.ca/in-fact/understanding-the-gap/
25.Table: 17-10-0057-01. Projected population, by projection scenario, age and sex, as of July 1 (x 1,000). Statistics Canada. Accessed March 22, 2023 https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1710005701
26.Newfoundland and Labrador interchangeable drug products formulary. Vol 88. Government of Newfoundland and Labrador. Accessed May 29, 2023. https://www.gov.nl.ca/hcs/files/nlpdp-formularyvol88.pdf
27.Drug benefit list. Express Scripts Canada. Accessed September 18, 2023. https://nihb-ssna.express-scripts.ca/en/0205140506092019/16/160407
Appendix 1: Additional Economic Information
Please note that this appendix has not been copy-edited.
Cost Comparison Table
The comparators presented in the following table Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 5: CDA-AMC Cost Comparison Table for Acne Vulgaris
Treatment | Strength / concentration | Form | Price ($ per gram) | Recommended dosage | Daily cost ($) | Annual cost ($) |
|---|---|---|---|---|---|---|
Clascoterone (Winlevi) | 1% | 30 g cream | 8.0807a | 1 g applied twice daily | Up to 16.16 | Up to 5,899 |
Topical nonretinoid monotherapies | ||||||
Benzoyl peroxide (various) | 5% | 15 g gel 30 g gel 60 g gel | 0.239517 0.186617 0.161417 | Apply 1 to 2 times daily | 0.16 to 0.32 | 59 to 118 |
Topical retinoids monotherapies | ||||||
Tazarotene (Tazorac) | 0.05% 0.1% 0.1% | 30 g cream 30 g cream 30 g gel | 1.450711 1.434711 1.450711 | Apply a thin layer once daily | 1.43 to 1.45 | 524 to 530 |
Tazarotene (Arazlo) | 0.045% | 45 g lotion | 1.4051 | Apply a thin layer once daily | 1.41 | 515 |
Tretinoin (Stieva-A) | 0.01% 0.025% 0.05% | 25 g cream 25 g cream 25 g cream | 0.3212 0.3212 0.2144 | Apply sparingly once daily before bedtime | 0.21 to 0.32 | 78 to 117 |
Tretinoin (Retin-A) | 0.025% 0.05% | 30 g gel 30 g cream | 0.489311 0.489311 | Apply daily | 0.49 | 179 |
Tretinoin (Retin-A Micro) | 0.04% | 50 g gel | 1.4370b | Apply once daily | 1.44 | 524 |
Tretinoin (Vitamin A Acid) | 0.01% 0.025% 0.05% | 25 g gel | 0.4102 0.364011 0.4102 | Apply daily | 0.36 to 0.41 | 133 to 150 |
Adapalene (Differin) | 0.1% 0.1% | 60 g cream 60 g gel | 2.198411 2.198411 | Apply once daily | 2.20 | 802 |
Adapalene (Differin XP) | 0.3% | 60 g gel | 3.0927b | Apply once daily | 3.09 | 1,129 |
Hormone therapies (oral contraceptives) | ||||||
Cyproterone acetate/ethinyl estradiol (Diane-35, various) | 2.0 mg/ 0.035 mg | 21 tablets | 23.2294b | One active tablet daily for 21 days, then 7 days off | 0.83 | 304 |
Desogestrel/ethinyl estradiol (Marvelon, various) | 0.15 mg/ 0.03 mg | 21 tablets 28 tablets | 7.7700 7.7700 | One active tablet daily for 21 days, then 7 days off or 7 days of inert tablets | 0.28 | 101 |
Desogestrel/ethinyl estradiol (Linessa) | Triphasic (0.100 mg, then 0.125 mg, then 0.150 mg)/ 0.025 mg | 21 tablets 28 tablets | 18.2100 18.2100 | One active tablet daily for 21 days, then 7 days off or 7 days of inert tablets | 0.65 | 237 |
Drospirenone/ (Yasmin, various) | 3.0 mg/ 0.03 mg | 21 tablets 28 tablets | 6.2181 6.2188 | One active tablet daily for 21 days, then 7 days off or 7 days of inert tablets | 0.22 | 81 |
Drospirenone/ (Yaz, various) | 3.0 mg/ 0.02 mg | 28 tablets | 8.2600 | One active tablet daily for 24 days, then 4 days of inert tablets | 0.30 | 108 |
Levonorgestrel/ethinyl estradiol (Alesse, various) | 0.1 mg/ 0.02 mg | 21 tablets 28 tablets | 3.9425 3.9425 | One active tablet daily for 21 days, then 7 days off or 7 days of inert tablets | 0.14 | 51 |
Levonorgestrel/ethinyl estradiol (Min-Ovral, various) | 0.15 mg/ 0.03 mg | 21 tablets 28 tablets | 7.2800 | One active tablet daily for 21 days, then 7 days off or 7 days of inert tablets | 0.26 | 95 |
Levonorgestrel/ethinyl estradiol (Triquilar) | Triphasic (0.05 mg, then 0.075 mg, then 0.125 mg)/0.03 mg, then 0.04 mg, then 0.03 mg) | 21 tablets 28 tablets | 15.7500 | One active tablet daily for 21 days, then 7 days off or 7 days of inert tablets | 0.56 | 205 |
Norgestimate/ethinyl estradiol (Tri-Cira, various) | Triphasic (0.18 mg, then 0.215 mg, then 0.25 mg)/0.035 mg | 21 tablets 28 tablets | 14.39 14.39 | One active tablet daily for 21 days, then 7 days off or 7 days of inert tablets | 0.51 | 188 |
Norgestimate/ethinyl estradiol (Tricira Lo) | Triphasic (0.18 mg, then 0.215 mg, then 0.25 mg)/0.035 mg | 21 tablets 28 tablets | 13.39 13.39 | One active tablet daily for 21 days, then 7 days off or 7 days of inert tablets | 0.48 | 175 |
Hormone therapy (spironolactone) | ||||||
Spironolactone (generics) | 25 mg 100 mg | Tablets | 0.0405 0.0955 | 25 mg to 200 mg daily9 | 0.04 to 0.19 | 15 to 70 |
CDA-AMC = Canada’s Drug Agency.
Notes: Prices are Ontario Drug Benefit list prices unless otherwise indicated (September 2023).12 Costs in Table 5 assume a 365-day year, 100% adherence, and all topical comparator costs assume the use of 1 g per application.
aSponsor’s submitted price of $242.4200 per 30 g tube.
bWholesale price as reported by IQVIA DeltaPA (September 2023).13
Additional Details on the Sponsor’s Submission
Table 6: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total annual drug costs ($) | Incremental drug costs vs. clascoterone ($) |
|---|---|---|
Clascoterone cream 1% (Winlevi) | 583.70 | Ref |
Topical nonretinoid monotherapy | ||
Benzoyl peroxide 5% (various) | 81.73 | −501.97 |
Topical retinoid monotherapy | ||
Tazarotene 0.1% (Tazorac) | 343.13 | −240.57 |
Tazarotene 0.045% (Arazlo) | 307.72 | −257.98 |
Tretinoin 0.025% (Stieva-A) | 70.34 | −513.35 |
Tretinoin 0.05% (Stieva-A) | 46.95 | −536.74 |
Tretinoin 0.025% gel (Retin-A) | 122.36 | −461.34 |
Tretinoin 0.05% cream (Retin-A) | 122.36 | −461.34 |
Tretinoin 0.04% gel (Retin-A Micro) | 251.85 | −331.85 |
Tretinoin 0.025% (vitamin A Acid) | 97.02 | −486.68 |
Tretinoin 0.05% (vitamin A Acid) | 82.43 | −501.27 |
Adapalene 0.1% (Differin) | 481.45 | −102.25 |
Adapalene 0.3% (Differin XP) | 608.82 | 25.12 |
Hormone therapies, DRSP + EE | ||
DRSP 3.0 mg + EE 0.03 mg (Yasmin) | 96.99 | −489.71 |
DRSP 3.0 mg + EE 0.03 mg (generics) | 48.63 | −535.06 |
DRSP 3.0 mg + EE 0.02 mg (Yaz) | 129.21 | −454.49 |
DRSP 3.0 mg + EE 0.02 mg (generics) | 76.18 | −519.09 |
Hormone therapies, LNG + EE | ||
LNG 20 mcg + EE 100 mcg (Alesse 21) | 123.34 | −460.35 |
LNG 20 mcg + EE 100 mcg (generics) | 76.18 | −507.52 |
Hormone therapies, CPA + EE | ||
CPA 2 mg + EE 35 mcg (Diane 35) | 302.22 | −281.48 |
CPA 2 mg + EE 35 mcg (generics) | 182.55 | −401.15 |
Hormone therapies, DES + EE | ||
DES 0.100 mg or 0.125 mg or 0.150 mg + EE 0.025 mg (Linessa) | 142.42 | −441.27 |
DES 0.150 mg + EE 0.03 mg (Marvelon) | 60.77 | −522.92 |
DES 0.150 mg + EE 0.03 mg (generics) | 60.77 | −522.92 |
Hormone therapies, NRG + EE | ||
NRG 0.18 mg or 0.215 mg or 0.25 mg + EE 0.035 mg (generics) | 112.55 | −471.15 |
NRG 0.18 mg or 0.215 mg or 0.25 mg + EE 0.025 mg (generics) | 104.73 | −478.97 |
Spironolactone | ||
Spironolactone 100 mg (Aldactone) | 133.70 | −450.00 |
Spironolactone 100 mg (generics) | 20.91 | −562.78 |
CPA = cyproterone acetate; DES = desogestrel; DRSP = drospirenone; EE = ethinyl estradiol; LNG = levonorgestrel; NRG = norgestimate; vs. = versus.
Source: Adapted from sponsor’s economic submission.2
Additional Details on the CDA-AMC Reanalyses and Additional Analyses
CDA-AMC did not conduct any additional pharmacoeconomic analyses in the review of clascoterone cream.
Appendix 2: Submitted BIA and CDA-AMC Appraisal
Please note that this appendix has not been copy-edited.
Table 7: Summary of Key Take-Aways
Key take-aways of the BIA |
|---|
|
BIA = budget impact analysis; CDA-AMC = Canada’s Drug Agency.
Summary of Sponsor’s BIA
In the submitted budget impact analysis (BIA), the sponsor assessed the introduction of clascoterone 1% cream for the treatment of acne vulgaris in patients aged 12 years and older.4 The BIA was undertaken from the perspective of a public drug plan payer in Canada over a 3-year time horizon (2024 to 2026). The sponsor indicated that the BIA was undertaken using a combined epidemiological and claims-based approach, as per the steps outlined as follows in Table 8. However, upon review and appraisal, CDA-AMC noted that the sponsor actually took a claims-based approach, and with the exception of the estimated proportion of patients who are reimbursed by public drug plans participating in the CDA-AMC review process, patient numbers are entirely based on sponsor-commissioned data request from IQVIA and the sponsor’s assumptions on annual costs of treatment. The sponsor’s analysis included drug acquisition costs; dispensing fees and markups were not included in the base case. Data from the model were obtained from various sources including Statistics Canada, the Non-Insured Health Benefits (NIHB) program,19 the scientific literature, the Canadian Dermatology Association,20 the American Association of Dermatology,21,22 the Canadian Skin Patient Alliance,23 the Conference Board of Canada,24 the sponsor’s internal revenue projections, and claims data cited as being from IQVIA.
Key inputs to the BIA are documented in Table 9. Note that where there are discrepancies between the sponsor’s submitted BIA report and the submitted model, the model’s values are included here.
During the review period, the sponsor submitted revised cost-minimization and budget impact analyses to address questions relating to the real-world usage data. The inputs and results as follows are reflective of the sponsor’s corrected files.
The key assumptions used to inform the sponsor’s BIA were:
The total number of eligible patients and the market share of each comparator are derived from cost data cited as being from IQVIA. The total forecasted cost paid for each comparator, or projected revenue in the case of clascoterone cream, has been divided by the estimated average annual cost per patient to establish the number of patients using each comparator.
Changes to the underlying population size, to the prevalence of acne vulgaris, or to the proportion of patients who seek treatment for their acne do not affect the eligible population size.
The calculated number of patients using topical treatments is assumed to be 85% of the acne vulgaris treatment market, with the other 15% assumed to be oral contraceptives and spironolactone.
Clascoterone 1% cream is assumed to displace all included comparators in proportion to their reference-case market share.
The public reimbursement of clascoterone 1% cream will not expand the total publicly funded market for the treatment of acne vulgaris.
Adherence rates for all comparators, including oral contraceptives and spironolactone was 60%.
63.0% of eligible patients have moderate or severe acne, used to estimate the reimbursement request population.23
Table 8: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as Y1/Y2/Y3 when appropriate) |
|---|---|
Target population | |
Population in Canada (2024 / 2025 / 2026) | 39,953,100 / 40.464,700 / 40,964,60025 |
Population who are aged 12 years and older | 35,159,200 / 35,659,600 / 36,145,20025 |
Population in Canada aged 12+ years excluding Quebec and the territories, including NIHB clients | 27,606,688 / 28,051,913 / 28,487,125a |
Prevalence of acne vulgaris | 20%20 |
Proportion of patients publicly reimbursed | 71.8%24 |
Proportion of patients with acne vulgaris who receive treatment | 10.2%22 |
Proportion of treated patients eligible to receive clascoterone 1% cream | 80,123 / 85,123 / 90,540b |
Market shares (reference scenario) | |
Topical therapies Oral contraceptives Spironolactone | 85.0% / 85.0% / 85.0%c 13.0% / 13.0% / 13.0%d 2.0% / 2.0% / 2.0% d |
Market uptake (new drug scenario)e | |
Clascoterone 1% cream Topical therapies Oral contraceptives Spironolactone | 1.9% / 6.0% / 9.5% 83.1% / 79.1% / 77.6% 12.7% / 12.1% / 11.7% 2.0% / 1.9% / 1.8% |
Cost of treatment (per patient per year) | |
All comparators | Refer to Table 3, Total annual drug costs ($) column |
NIHB = Non-Insured Health Benefits.
aProvincial jurisdictions have been adjusted by subtracting the population of NIHB clients living within each province, with the exception of Ontario, where the number of NIHB clients aged under 25 and 65+ years was subtracted from the NIHB population. The NIHB population is based on the NIHB Annual Report for 202119 and assumes an annual growth rate thereafter of 1.7%.
bWhile the sponsor appeared to submit an epidemiology-based model, the model in fact calculated the number of eligible patients using unspecified, projected IQVIA cost data for each year for each topical comparator, removing the proportion of costs estimated to represent Quebec, removing the proportion of costs estimated to be for nonpublicly reimbursed patients, and then dividing by the estimated annual cost of the topical comparator to estimate the number of patients using that comparator within each year. The estimated number of patients for each topical comparator were then summed for each year, and this total was then inflated to account for the 15% of patients the sponsor assumed to use hormone therapies rather than topical.
cWhile the total proportion of patients assumed to use topical therapies over the 3 years of the analysis did not change, the proportion using each topical comparator did vary by year, based on unspecified IQVIA claims data.4 For example, benzoyl peroxide 5% was estimated to have 12.25% of the eligible market of year 1, and 11.90% in year 3.
dAssumption.4
eClascoterone uptake is based on the sponsor’s internal revenue projections divided by the estimated annual cost of clascoterone. All comparators are displaced in proportion to their reference-case market share.
Summary of the Sponsor’s BIA Results
Results of the sponsor’s analysis suggest that the reimbursement of clascoterone 1% cream for the treatment of acne vulgaris will be associated with an incremental cost of $597,718 in year 1, $1,963,929 in year 2, and $2,988,588 in year 3, for a 3-year budget impact of $5,550,234.
The sponsor also submitted a scenario analysis limiting the patient population to those with moderate to severe acne vulgaris, similar to their reimbursement request population, which resulted in a 3-year budget impact of $3,496,647.
CDA-AMC Appraisal of the Sponsor’s BIA
CDA-AMC identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
Uncertainty with the use of a claims-based approach to estimate market size: While the sponsor included epidemiological inputs to derive the number of patients potentially eligible for a target product, the actual market size is based on projected dollar amounts from the IQVIA Sales Database for the topical comparators, and sponsor-projected revenue for clascoterone cream, divided by the estimated annual cost per patient of each product to estimate the number of patients who would receive each product in each year. This estimated number of patients was then inflated by 15% to estimate the number of patients who would be using oral contraceptives and spironolactone for the treatment of acne vulgaris within each year. Furthermore, the IQVIA data provided by the sponsor was not filtered by geographical location or drug plan, and therefore the sponsor also needed to remove a proportion of estimated patients to account for those living within Quebec, and a further proportion to account for those assumed to not be covered under public plans. The use of claims data in general to derive market size is associated with uncertainty, which was further increased by the use of sales data rather than direct claims data. Also, this approach required a number of additional assumptions to estimate the population potentially covered by public drug plans participating in the CDA-AMC review process. CDA-AMC attempted to corroborate the sponsor’s estimated patient population and reference-case market share through their access to IQVIA Pharmastat and found that the sponsor’s estimates could not be approximated either with or without limiting the results by geographic area and/or public reimbursement. Due to the use of estimated annual per-patient costs to derive patient numbers from the provided sales data, any changes in annual per-patient cost estimates led to changes in the overall number of eligible patients as well as to the market shares of comparators within the eligible population.
CDA-AMC was unable to address this approach to the market size estimation. To ensure the accuracy of the estimates a de novo BIA would be required, which was deemed outside of the scope of the review.
Annual cost and market uptake of clascoterone cream were inappropriately estimated: As described in the CDA-AMC Appraisal of the Sponsor’s Economic Information for the submitted cost-minimization analysis, in the BIA, clascoterone cream was assumed to be used in far lower amounts than all other topical monotherapies, despite a lack of evidence regarding its relative efficacy when used at these lower rates. Clinical expert input obtained by CDA-AMC did not find the assumption that clascoterone cream would be applied in substantially lower amounts than other topical monotherapies to be plausible.
To calculate the market uptake of clascoterone cream, the sponsor divided internally projected revenue amounts for years 1, 2, and 3 by the estimated annual per-patient cost of clascoterone cream to estimate the number of patients who would use clascoterone cream in each of its first 3 years of funding. As such, any changes to the estimated annual cost of clascoterone cream within the BIA as programmed by the sponsor altered the projected number of patients who would use it within each year rather altering than the projected revenue. In practice, it is unlikely that clinicians and their patients who are eligible for the reimbursement of clascoterone cream would reduce or increase their likelihood of choosing it over its comparators in proportion to its annual cost and the sponsor’s projected revenue, but rather on the basis of clinical appropriateness, funding access, and personal preference. As such, while the estimated annual cost of clascoterone cream might potentially impact the eligibility criteria or other access decisions implemented by jurisdictional drug plans, it is unlikely to substantially impact the uptake of clascoterone within the same sent of eligibility assumptions, as is appropriate to assume within an analysis exploring the implications of product price on budgetary impact.
In the CDA-AMC reanalysis, the annual cost of clascoterone cream was derived by assuming the clinical trial and recommended dosing of 1 g twice daily would be used with an adherence rate of 60%, as described for the economic appraisal of the sponsor’s cost-minimization analysis and as assumed for all other topical comparators. The estimated market uptake of clascoterone cream remained at 1.9%, 6.0%, and 9.5% of the eligible market in year 1, year 2, and year 3, respectively, as projected in the sponsor’s submitted analysis, to maintain the same revenue as forecast by the sponsor regardless of annual cost.
Costs associated with the displacement of unfunded comparators were inappropriately estimated: The sponsor assumed that clascoterone cream will displace all comparators in proportion to their reference-case market share and applied the estimated annual cost per patient of these comparators to the analysis regardless of their funding status within individual jurisdictions. While some comparators are funded by all public drug plans within Canada, several topical comparators are not typically funded by most plans. Of the relevant public drug plans included within the BIA, only Newfoundland and Labrador funds benzoyl peroxide 5% cream,26 no included jurisdiction funds the Retin-A Micro 0.04% formulation of tretinoin, only Saskatchewan, Nova Scotia, and the NIHB fund adapalene 0.1% cream,11,27 and only the NIHB funds adapalene 0.3% cream.27 As such, patients using these products outside of these jurisdictions would typically pay for them with private insurance or out of pocket. Despite this, the sponsor assumed that the full cost of these comparators would offset the cost of clascoterone cream to public drug payers when it displaces them. According to clinical expert opinion obtained by CDA-AMC, it is likely that clascoterone cream, if funded, will displace a portion of all other topical monotherapies currently available for the treatment of acne vulgaris. However, where clascoterone cream displaces the use of topical comparators that are not funded by public drug plans, it is inappropriate to assume the full cost of these displaced products offsets the incremental costs of clascoterone cream to public drug plans.
Due to the structure of the submitted BIA and the claims data used by the sponsor, CDA-AMC was unable to fully adjust for the funding rates of individual products. As a more likely estimate of the impact to public drug plan budgets of clascoterone cream displacing topical comparators which are not benefits in most jurisdictions (i.e., benzoyl peroxide 5%, Retin-A Micro 0.04%, Differin 0.1%, and Differin XP 0.3%), the unit cost of these products was multiplied by the proportion of the eligible population within jurisdictions which do fund them either as full benefits or under restricted access programs to estimate the average per-patient cost of these products to all included public plans. As described in the limitation on the market uptake of clascoterone cream, the market shares of all comparators remained at the same percentages estimated in the sponsor’s submitted analysis, to maintain the same sales data projected by the sponsor.
Some comparators were inappropriately priced: Some branded oral contraceptives included by the sponsor as comparators are legally interchangeable with their generic forms (e.g., Yasmin, Alesse). As such, the amount paid by the Ontario Drug Benefit program, the pricing source for these products, is limited to the cost of the generic.12 Additionally, where the sponsor used BC PharmaCare Formulary list prices,15 they did not remove the 8% markup included within the maximum price payable.16 Finally, according to the submitted pharmacoeconomic and budget impact reports, the sponsor appears to have intended to use an adherence rate of 100% for oral contraceptive comparators as well as spironolactone,2,4 however in the submitted analyses, calculated annual costs of these comparators use a 60% adherence rate. Clinical expert input obtained by CDA-AMC estimated that adherence rates for spironolactone and particularly the oral contraceptives would approach 100%.
CDA-AMC considered only the generic pricing of legally interchangeable comparators. For comparators where the sponsor used BC PharmaCare Formulary list prices which include markups, CDA-AMC reanalyses instead used Saskatchewan Formulary list prices. In analyses including oral contraceptives and spironolactone as displaced comparators, costs of these therapies were corrected to have an adherence rate of 100%.
Uncertainty in the market share and displacement of hormone therapies: The sponsor estimated that an additional 15% of patients would use hormone therapies (either oral contraceptives or spironolactone) to treat their acne, with 1% share being assigned to each of the brands included by the sponsor, and that these hormone therapies would be displaced by clascoterone cream in proportion to their reference-case market share as also assumed for topical comparators. However, clinical expert input obtained by CDA-AMC did not consider it likely that hormone therapies would be displaced by clascoterone cream, as patients using such therapies would either be using them in preference to a topical therapy, or in combination with a topical therapy that might be displaced by clascoterone. As neither spironolactone nor oral contraceptives are primarily used for the treatment of acne vulgaris, the market share of each available product within this indication is highly uncertain and difficult to estimate. Additionally, oral contraceptives are frequently used for their other benefits (e.g., contraception, menstrual cycle regulation, treatment of dysmenorrhea) by patients within the same demographic as those most likely to use it for acne, and thus many patients using oral contraceptives to treat acne vulgaris are likely to continue using them even if their acne is otherwise adequately treated. As such, it is uncertain whether clascoterone would displace hormone therapies.
In a scenario analysis, CDA-AMC assumed clascoterone would not displace hormone therapies for the treatment of acne vulgaris.
Uncertainty in the budgetary impact of limiting clascoterone funding to the reimbursement request: While the Health Canada indication for clascoterone cream is for the treatment of acne vulgaris in patients aged 12 years and older, the sponsor’s reimbursement request was for the first-line prescription topical treatment of moderate and severe acne vulgaris in patients aged 12 years and older. The sponsor estimated the budgetary impact of limiting funding of clascoterone cream to the reimbursement request population by reducing the eligible population to 63% of that estimated for the Health Canada indication, consistent with the proportion of responders in Canada to a 2022 survey who reported having moderate (47%) or severe acne (16%).23 While it is uncertain whether acne vulgaris severity among responders to a dermatological survey can be generalized to the overall population of patients seeking treatment for acne in Canada, this proportion is relatively consistent with proportions estimated in clinical expert input obtained by CDA-AMC of 70% (50% moderate, 20% severe), although it was also noted within the input that estimates would vary depending on whether the treatment-seeking patient populations of general practitioners or dermatologists were considered. However, as the reimbursement request is specific to the first-line prescription topical treatment of moderate and severe acne vulgaris, it is likely that the market shares and appropriate comparators would differ compared to those considered appropriate for the overall Health Canada indication.
CDA-AMC was unable to address this limitation in reanalysis.
CDA-AMC Reanalyses of the BIA
CDA-AMC revised the sponsor’s submitted analysis correcting the assumed adherence rate for hormone therapies to be 100%, adjusting the annual per-patient cost of clascoterone cream, adjusting the average costs paid by public plans for comparators rarely publicly reimbursed, and adjusting the unit costs of some comparators to reflect updated costs paid by public plans. The changes applied to derive the CDA-AMC base case are described in Table 9.
Table 9: CDA-AMC Revisions to the Submitted BIA
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
Corrections to sponsor’s base casea | ||
1. Hormone therapy adherence rate | 60% | 100% |
Changes to derive the CDA-AMC base case | ||
1. Annual cost of clascoterone cream | $583 per patient | $3,539 per patient The estimated uptake of clascoterone was held at 1.9% / 6.0% / 9.5% in years 1, 2, and 3, as in the sponsor’s base case, rather than allowing its alteration to maintain the same revenue projected by the sponsor |
2. Displaced comparators not typically funded by public plans | The full cost of benzoyl peroxide 5%, tretinoin 0.04%, adapalene 0.1%, and adapalene 0.3% was considered within the analysis, regardless of jurisdictional funding status. | The cost of benzoyl peroxide 5%, tretinoin 0.04%, adapalene 0.1%, and adapalene 0.3% was multiplied by the proportion of patients living within jurisdictions which fund them to estimate their average cost to all included jurisdictions. |
3. Comparator costs | Originator brand and generic list prices used List prices from June 2023 British Columbia list prices used where Ontario is unavailable | Amount paid by Ministry of Health used (i.e., generic list prices) List prices from September 2023 Saskatchewan list prices used where ON is unavailable |
CDA-AMC base case | 1 + 2 + 3 | |
BIA = budget impact analysis; CDA-AMC = Canada’s Drug Agency.
aCorrections are minor errors (e.g., transcription errors between report and model, misapplication of distributions or SEs in probabilistic analyses) that are not identified as limitations.
The results of the CDA-AMC stepwise reanalysis are presented in summary format in Table 10 and a more detailed breakdown is presented in Table 11.
For the full Health Canada indicated population of patients with acne vulgaris aged 12 years and older, CDA-AMC reanalyses suggest that reimbursement of clascoterone cream will be associated with an incremental cost of $5,338,439 in year 1, $17,540,587 in year 2, and $26,692,197 in year 3, for a 3-year budget impact of $49,571,223.
Table 10: Summary of the CDA-AMC Reanalyses of the BIA
Stepped analysis | Three-year total |
|---|---|
Sponsor’s submitted base case | $5,550,234 |
Sponsor’s corrected base case | $5,391,713 |
CDA-AMC reanalysis 1: Annual cost of clascoterone cream | $47,739,032 |
CDA-AMC reanalysis 2: Unfunded comparator costs | $7,126,439 |
CDA-AMC reanalysis 3: Comparator costs | $5,492,916 |
CDA-AMC base case | $49,571,223 |
BIA = budget impact analysis; CDA-AMC = Canada’s Drug Agency.
CDA-AMC stepwise reanalyses were conducted on the sponsor’s corrected base case.
CDA-AMC conducted additional scenario analyses (Table 11) to consider the impact of: assuming only patients with moderate and severe acne would be eligible for clascoterone cream, assuming hormone therapies would not be displaced by clascoterone cream, assuming patients will use clascoterone cream only once daily, and assuming a 98.7% and 91.3% price reduction for clascoterone cream as reported in the CDA-AMC reanalysis of the pharmacoeconomic evaluation to match the price of the least expensive topical monotherapy and least expensive nontretinoin retinoid topical monotherapy, respectively.
Table 11: Detailed Breakdown of the CDA-AMC Reanalyses of the BIA
Stepped analysis | Scenario | Year 0 (current situation) | Year 1 | Year 2 | Year 3 | Three-year total |
|---|---|---|---|---|---|---|
Sponsor’s submitted base case | Reference | $14,162,623 | $15,954,271 | $16,895,084 | $17,934,908 | $64,946,886 |
New drug | $14,162,623 | $16,551,988 | $18,859,013 | $20,923,496 | $70,497,120 | |
Budget impact | $0 | $597,718 | $1,963,929 | $2,988,588 | $5,550,234 | |
Sponsor’s corrected base case | Reference | $14,960,770 | $16,840,747 | $17,836,054 | $18,936,639 | $68,574,210 |
New drug | $14,960,770 | $17,421,393 | $19,743,891 | $21,839,869 | $73,965,923 | |
Budget impact | $0 | $580,646 | $1,907,837 | $2,903,230 | $5,391,713 | |
CDA-AMC base case | Reference | $5,735,745 | $7,254,531 | $7,870,962 | $8,602,992 | $29,464,230 |
New drug | $5,735,745 | $12,592,970 | $25,411,549 | $35,295,189 | $79,035,453 | |
Budget impact | $0 | $5,338,439 | $17,540,587 | $26,692,197 | $49,571,223 | |
CDA-AMC scenario 1: Moderate to severe only (63%) | Reference | $3,613,519 | $4,570,354 | $4,958,706 | $5,419,885 | $18,562,465 |
New drug | $3,613,519 | $7,933,571 | $16,009,276 | $22,235,969 | $49,792,335 | |
Budget impact | $0 | $3,363,217 | $11,050,570 | $16,816,084 | $31,229,870 | |
CDA-AMC scenario 2: hormone therapies excluded | Reference | $4,177,533 | $5,523,877 | $6,033,921 | $6,647,329 | $22,382,661 |
New drug | $4,177,533 | $10,061,551 | $20,943,419 | $29,335,697 | $64,518,200 | |
Budget impact | $0 | $4,537,673 | $14,909,499 | $22,688,367 | $42,135,539 | |
CDA-AMC scenario 3: clascoterone used once daily | Reference | $5,735,745 | $7,254,531 | $7,870,962 | $8,602,992 | $29,464,230 |
New drug | $5,735,745 | $9,862,410 | $16,439,708 | $21,642,388 | $53,680,251 | |
Budget impact | $0 | $2,607,879 | $8,568,746 | $13,039,396 | $24,216,021 | |
CDA-AMC scenario 4: 98.7% price reduction | Reference | $5,735,745 | $7,254,531 | $7,870,962 | $8,602,992 | $29,464,230 |
New drug | $5,735,745 | $7,202,844 | $7,701,135 | $8,344,560 | $28,984,284 | |
Budget impact | $0 | -$51,687 | -$169,827 | -$258,433 | -$479,946 | |
CDA-AMC scenario 5: 91.3% price reduction | Reference | $5,735,745 | $7,254,531 | $7,870,962 | $8,602,992 | $29,464,230 |
New drug | $5,735,745 | $7,508,667 | $8,705,981 | $9,873,674 | $31,824,066 | |
Budget impact | $0 | $254,136 | $835,019 | $1,270,681 | $2,359,836 |
BIA = budget impact analysis; CDA-AMC = Canada’s Drug Agency.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.