Drugs, Health Technologies, Health Systems
Reimbursement Recommendation
Maralixibat (Livmarli)
Indication: For the treatment of cholestatic pruritus in patients aged 12 months or older with progressive familial intrahepatic cholestasis
Sponsor: Mirum Pharmaceuticals Inc.
Recommendation: Reimburse with conditions
Summary
What Is the Reimbursement Recommendation for Livmarli?
Canada’s Drug Agency (CDA-AMC) recommends that Livmarli be reimbursed by public drug plans for the treatment of cholestatic pruritus in patients with progressive familial intrahepatic cholestasis (PFIC) if certain conditions are met.
Why Did CDA-AMC Recommend Reimbursement?
The Canadian Drug Expert Committee (CDEC) determined that Livmarli demonstrates acceptable clinical value versus vehicle placebo and the currently appropriate comparator, odevixibat, in patients with PFIC. This determination was sufficient for CDEC to recommend that Livmarli be reimbursed. Given that Livmarli is expected to be an alternative to odevixibat, acceptable clinical value refers to at least comparable value versus odevixibat.
Evidence from one randomized trial showed that treatment with Livmarli for 26 weeks resulted in a clinically meaningful improvement in cholestatic pruritus (itching) compared with inactive foam in patients with PFIC. Improvements were observed across multiple pruritus-related outcomes as well as supportive blood markers. These outcomes aligned with patient-identified priorities and were considered clinically meaningful. Evidence from indirect treatment comparisons did not demonstrate a clear difference in effectiveness between Livmarli and odevixibat. Overall, the available evidence was considered consistent with similar clinical effects between treatments, although with residual uncertainty.
PFIC is a group of rare, inherited liver diseases that typically begins in infancy or early childhood. Patients and caregivers identified pruritus as the most burdensome symptom of the disease, with substantial impacts on their quality of life. Available treatment options often provide limited or inconsistent relief of pruritus, and some patients require invasive surgical interventions or liver transplantation.
CDEC concluded that maralixibat addresses an important unmet clinical need by providing a nonsurgical, mechanism-based treatment option that improves pruritus and may reduce disease burden. The committee considered limitations in the clinical evidence in the context of the rarity of PFIC and the challenges of conducting large trials in this population.
Which Patients Are Eligible for Coverage?
Livmarli should only be reimbursed for the treatment of cholestatic pruritus in patients with PFIC. Eligible patients are those with a diagnosis of PFIC who have clinically significant cholestatic pruritus and elevated serum bile acid levels. Treatment with Livmarli should not be initiated in patients with a history of liver transplantation or biliary surgery and should be discontinued if either procedure occurs during therapy.
What Are the Conditions for Reimbursement?
Livmarli should only be reimbursed if there is meaningful clinical benefit following an adequate trial of therapy, there is ongoing assessment by a specialist experienced in the management of PFIC, and the cost of Livmarli is reduced.
Review Background
Disease background: Progressive familial intrahepatic cholestasis (PFIC) is a group of rare, inherited pediatric liver disorders characterized by impaired bile secretion leading to severe pruritus, progressive liver disease, and growth impairment. In many patients, it can lead to cirrhosis and the need for liver transplantation. PFIC is associated with substantial morbidity beginning in infancy or early childhood and can have a profound impact on quality of life for patients and caregivers.
Prevalence: PFIC is a rare condition, with an estimated prevalence of approximately 1 in 50,000 to 1 in 100,000 live births worldwide, based on international epidemiologic estimates. Prevalence data for Canada are limited due to underdiagnosis and the rarity of the condition.
Indication and reimbursement request: The application was submitted by the sponsor before receiving a Notice of Compliance from Health Canada. The Canada’s Drug Agency (CDA-AMC) review reflects the anticipated indication for Livmarli at the time the review was conducted, which was for the treatment of PFIC in patients 3 months and older.
Drug under review: Livmarli is an ileal bile acid transporter (IBAT) inhibitor. It is available as an oral solution and oral tablets formulation administered once daily. The dosage recommended in the product monograph is weight-based, with a maximum daily dose of 570 mcg/kg.
Treatment costs: Maralixibat is available as a solution for oral administration (19 mg per mL in a 30 mL bottle) and oral tablets (i.e., 10 mg, 15 mg, 20 mg, and 30 mg). For the oral solution, at the submitted price of $3,100.00/mL, the annual cost of maralixibat is expected to be between $263,004 to $3,315,450 per patient in the first year and $271,746 to $3,396,825 per patient in subsequent years, depending on patient weight, based on the Health Canada–recommended dosage. For the oral tablets, at the submitted prices of $1,631.58 per 10 mg, $2,447.37 per 15 mg, $3,263.16 per 20 mg, and $4,894.74 per 30 mg, the annual per-patient cost of maralixibat is expected to be $3,489,947 in first year and $3,575,605 in subsequent years, assuming patient weight of 50 kg, based on the Health Canada–recommended dosage.
Highlights of Input From Interested Parties
The patient groups (Liver Canada, the PFIC Network, and the Alagille Syndrome Alliance) noted the following regarding impacts of the disease, unmet needs, and important outcomes:
PFIC was described as having a profound impact on patients and families, driven primarily by severe and persistent pruritus that disrupts sleep, daily functioning, growth, and psychosocial well-being, often beginning in infancy or early childhood. Caregivers emphasized the cumulative burden of chronic symptoms, frequent medical visits, dietary restrictions, and anxiety related to disease progression and the potential need for liver transplantation.
Patient groups identified effective and sustained relief of pruritus as the most important treatment goal, along with improvements in sleep, daily functioning, skin integrity, and overall quality of life. There remains an unmet need for treatments that can reduce symptom burden, delay or avoid invasive surgical interventions, and be used safely across PFIC subtypes and younger age groups.
The clinician groups (Canadian Pediatric Hepatology Research Group [CPHRG] of the Canadian Association for the Study of the Liver; University of Alberta – Stollery Children’s Hospital; and the Autoimmune and Rare Liver Disease Programme at Toronto General Hospital) and the clinical experts consulted by CDA-AMC noted the following regarding unmet needs and place in therapy:
Current treatment options for PFIC are limited and often do not provide adequate or sustained control of pruritus, leaving many patients with persistent symptoms despite standard medical therapy.
There is an unmet need for pharmacologic therapies that target the underlying pathophysiology of cholestasis and offer a nonsurgical alternative for symptom control earlier in the disease course.
Maralixibat is anticipated to be used in patients with PFIC and clinically significant pruritus, typically following inadequate response to or in combination with ursodeoxycholic acid, and before consideration of surgical biliary diversion or liver transplantation.
The participating public drug programs raised potential implementation issues related to initiation, renewal, and discontinuation. The drug programs also acknowledged generalizability and access considerations and system and economic implications.
Recommendation
With a vote of 11 in favour to 0 against, the Canadian Drug Expert Committee (CDEC) recommends that maralixibat be reimbursed for the treatment of cholestatic pruritus in patients with PFIC only if the conditions listed in Table 1 are met.
Table 1: Reimbursement Conditions and Reasons
Reimbursement condition | Reason | Implementation guidance |
|---|---|---|
Initiation | ||
1. Patients aged 12 months or older with cholestatic pruritus resulting from PFIC who have all of the following: 1.1. a diagnosis of biallelic PFIC of the following subtypes (gene mutations): PFIC type 1 (ATP8B1), nontruncated PFIC type 2 (ABCB11), PFIC type 3 (ABCB4), PFIC type 4 (TJP2), and PFIC type 10 (MYO5B) 1.2. severe pruritus for 6 months or longer with average ItchRO(Obs) score of ≥ 1.5 in the past 4 weeks while receiving usual care with at least one therapy used for symptomatic relief of pruritus 1.3. total serum bile acid ≥ 3 times the upper limit of normal. | Evidence from the MARCH-PFIC trial demonstrated that treatment with maralixibat resulted in clinical benefit in patients with these characteristics. |
|
2. Patients should not have any of the following: 2.1. a mutation of the ABCB11 gene that leads to a nonfunctional or absent BSEP, such as a truncated form 2.2. a heterozygous PFIC mutation. | The MARCH-PFIC trial included patients with truncated BSEP and heterozygous mutations in the full cohort; however, these patients were not included in the primary BSEP cohort or the all-PFIC cohort that informed the main efficacy conclusions. | — |
3. The maximum duration of initial authorization is 6 months of treatment (inclusive of the titration period). | In the MARCH-PFIC trial, initial treatment response was assessed over a 26-week period (approximately 6 months). | Maralixibat oral solution is initiated at 142.5 mcg/kg twice daily and escalated weekly to 570 mcg/kg twice daily (or maximum tolerated dose). |
Renewal | ||
4. For renewal after initial authorization all of the following conditions must be met: 4.1. Maralixibat should be renewed in a similar manner to odevixibat for PFIC. 4.2. ItchRO(Obs) should demonstrate a reduction of ≥ 1 point after 6 months from initiation. 4.3. For subsequent renewal, the physician must provide proof that the improvement in pruritus severity from baseline has been maintained every 6 months. | There is no evidence that maralixibat should be held to a different standard than odevixibat, which is currently reimbursed, when considering renewal. | The pruritus assessment tool used in the maralixibat trial, ItchRO(Obs), differs from the tool used in an odevixibat trial (ObsRO scratch score). Drug plans may consider harmonizing pruritus assessment tools across IBAT inhibitors. |
Discontinuation | ||
5. Maralixibat should be discontinued upon liver transplantation or biliary surgery. | The MARCH-PFIC trial did not include patients with imminent need for liver transplantation or those with previous biliary surgery. Therefore, the efficacy and safety of maralixibat in this group of patients is unknown. Based on clinical expert opinion, treatment with maralixibat should be discontinued in patients who experience intolerable adverse effects or progression to advanced liver disease requiring transplantation. | CDEC noted that, following liver transplantation or biliary surgery, patients should be reassessed by a specialist with expertise in managing PFIC to determine whether continued treatment or re-treatment with maralixibat is appropriate, recognizing that evidence in this patient population is limited. |
Prescribing | ||
6. Maralixibat should be prescribed by, or in consultation with, clinicians with expertise in managing PFIC. | This is meant to ensure that maralixibat is prescribed for appropriate patients and that monitoring and adverse effects are managed in an optimized and timely manner. | — |
7. Maralixibat should not be prescribed concurrently with another IBAT inhibitor. | No evidence was available to demonstrate the benefit and safety of maralixibat when used in combination with other IBAT inhibitors. In the MARCH-PFIC trial, maralixibat was administered as monotherapy. | — |
Pricing | ||
8. A reduction in price. | Using the CDA-AMC analyses considered most appropriate by CDEC in which the treatment response for BSC was aligned with the MARCH-PFIC trial data, BSC loss of response was assumed to be 50% annually, and the benefits associated with maralixibat in terms of hepatocellular carcinoma, survival and liver transplant were removed, the ICER for maralixibat was $19,288,660 per QALY gained when compared with BSC in the indicated population. A band 4 price reductiona would be required to achieve cost-effectiveness at a $50,000 and $100,000 per QALY threshold. Price reductions for any given willingness-to-pay threshold are available in the CDA-AMC Main Report and Supplemental Material document. Cost-effectiveness relative to odevixibat in the indicated population is uncertain due to the lack of evidence regarding comparative efficacy for pruritus. To ensure cost-effectiveness, maralixibat should also be priced no higher than the lowest-cost IBAT inhibitor reimbursed for the indicated population. | The CDA-AMC analysis is based on public list prices for all treatments. Further price reductions may be required if there are price arrangements (discounts) currently in place for any treatment included in the economic analysis. |
Feasibility of adoption | ||
9. Organizational feasibility of accessing specialized pediatric hepatology services and ongoing monitoring of patients receiving maralixibat must be addressed. | Given the limited number of pediatric medical centres across Canada and regional variation in access to specialists, implementation of the reimbursement recommendation for maralixibat requires careful consideration of organizational feasibility (e.g., through tertiary care networks or shared-care models). | — |
BSC = best supportive care; BSEP = bile salt export pump; CDA-AMC = Canada’s Drug Agency; IBAT = ileal bile acid transporter; ICER = incremental cost-effectiveness ratio; ItchRO(Obs) = Itch Reported Outcome (Observer-reported); ObsRO = observer-reported outcome; PFIC = progressive familial intrahepatic cholestasis; QALY = quality-adjusted life-year.
aFor the statement regarding the size of the price reduction required, band 1 = 1% to 24%, band 2 = 25% to 49%, band 3 = 50% to 74%, and band 4 = 75% or greater.
Rationale for the Recommendation
Clinical Value
Based on the totality of the presented clinical evidence, CDEC concluded that maralixibat demonstrates acceptable clinical value in patients with PFIC. Because maralixibat is expected to be an alternative to odevixibat, acceptable clinical value refers to at least comparable value versus odevixibat given that the evidence did not support superiority or inferiority for either IBAT inhibitor.
Evidence from one randomized, double-blind, placebo-controlled trial (MARCH-PFIC; N = 93) demonstrated that treatment with maralixibat for 26 weeks resulted in clinically meaningful improvement in cholestatic pruritus compared with placebo in patients with PFIC. Improvements were observed across multiple pruritus-related end points, including patient-reported and observer-reported itch and scratching measures as well as supportive biochemical markers of cholestasis. These outcomes were aligned with patient-identified priorities and were considered clinically meaningful by the committee.
Evidence from indirect treatment comparisons was insufficient to demonstrate a clear difference in clinical effectiveness between maralixibat and odevixibat for pruritus-related outcomes. The committee noted that the available indirect evidence was associated with important limitations, including differences in trial design, patient populations, and follow-up duration, which contributed to residual uncertainty. Pruritus was not assessed in the indirect evidence, hindering conclusions on comparative efficacy for this important outcome. Taking these limitations in consideration, the indirect evidence suggested similar effects on biochemical cholestasis without clearly supporting conclusions of superiority or inferiority for either IBAT inhibitor.
CDEC considered that maralixibat addresses an important unmet clinical need for patients with PFIC, particularly for those with persistent, severe pruritus despite existing medical therapy and their caregivers. Pruritus was consistently identified by patients and clinicians as the most burdensome symptom of PFIC, with substantial impacts on sleep, daily functioning, and quality of life. Maralixibat provides a nonsurgical treatment option that targets the underlying pathophysiology of cholestasis and offers clinically meaningful symptom improvement.
Further information on the committee’s discussion around clinical value is provided in the Summary of Deliberation section.
Developing the Recommendation
The determination of acceptable clinical value was sufficient for CDEC to recommend reimbursement of maralixibat. As part of the deliberation on whether to recommend reimbursement, the committee also considered unmet clinical need, unmet nonclinical need, and health inequity. Information on this discussion is provided in the Unmet Clinical Need and Distinct Social and Ethical Considerations domains in the Summary of Deliberation section.
Because CDEC recommended that maralixibat be reimbursed, the committee also deliberated on whether reimbursement conditions should be added to address important economic considerations, health system impacts, or social and ethical considerations, or to ensure clinical value is realized. The resulting reimbursement conditions, with accompanying reasons and implementation guidance, are stated in Table 1.
Summary of Deliberation
CDEC considered all domains of value of the deliberative framework before developing its recommendation: clinical value, unmet clinical need, distinct social and ethical considerations, economic considerations, and impacts on health systems. For further information on the domains of value, refer to Expert Committee Deliberation at Canada’s Drug Agency.
The sponsor requested a minor reconsideration of the initial draft recommendation to reimburse with conditions maralixibat for PFIC. One issue outlined by the sponsor in the request for reconsideration was discussed by a CDEC committee subpanel. The request was to remove restriction to biallelic pathogenic PFIC mutations in the initiation criteria.
The committee considered the following key discussion points, organized by the 5 domains of value.
Clinical Value
Appropriate comparators: CDEC considered placebo and odevixibat to be the most appropriate comparators for maralixibat in patients with PFIC. Placebo was considered appropriate for assessing absolute treatment effects given the design of the pivotal trial. Odevixibat was considered the most relevant active comparator, given its shared mechanism of action as an IBAT inhibitor and its role in the current treatment landscape for PFIC, despite uncertainty regarding its public reimbursement status at the time of review.
Efficacy versus placebo: One randomized, double-blind, placebo-controlled trial (MARCH-PFIC; N = 93) demonstrated that treatment with maralixibat for 26 weeks resulted in improvements in pruritus-related outcomes compared with placebo in patients with PFIC. For the primary pruritus outcome, the change from baseline in the Itch Reported Outcome (ItchRO) (Observer) score from weeks 15 to 26 for maralixibat resulted in greater reductions in itch severity than placebo. The least squares mean difference was −1.09 points (95% confidence interval [CI], −1.85 to −0.33 points) in the primary (bile salt excretion pump [BSEP]) cohort and −1.20 points (95% CI, −1.73 to −0.67 points) in the all-PFIC cohort, exceeding the prespecified minimal important difference of 1 point. Improvements were also observed across additional pruritus measures, including the Clinician Scratch Scale, with least squares mean differences versus placebo of −1.05 (95% CI, −1.72 to −0.38) in the primary cohort and −1.13 (95% CI, −1.65 to −0.60) in the all-PFIC cohort. Supportive biochemical outcomes were consistent with reductions in cholestasis, including a higher proportion of patients achieving a serum bile acid response with maralixibat compared with placebo, with an absolute difference of 33.6% (95% CI, −4.0% to 64.9%) in the primary cohort and 37.8% (95% CI, 11.3% to 59.4%) in the all-PFIC cohort. The committee noted that treatment effects were aligned with outcomes identified as most important by patients. Important limitations included the relatively small sample size, the short randomized follow-up period, and the exclusion of certain patient subgroups, including patients with prior biliary surgery.
CDEC reviewed evidence from one long-term extension study, which provided additional follow-up beyond the randomized period. The committee noted that the extension data suggested maintenance of pruritus improvement in some patients who continued treatment; however, the absence of a comparator group, patient attrition over time, and limited duration of follow-up reduced the ability to draw firm conclusions regarding long-term efficacy and safety. As a result, the extension study was considered supportive but not definitive.
Clinical importance of treatment effects: CDEC considered the observed improvements in pruritus to be clinically meaningful based on the magnitude of effect, consistency across measures, and alignment with outcomes identified as most important by patients and caregivers, including improvements in sleep, daily functioning, and quality of life. The committee noted that pruritus is the dominant and most burdensome symptom of PFIC and that existing medical therapies often provide inadequate or inconsistent symptom control. These considerations supported the clinical relevance of the observed treatment effects.
Certainty of the evidence: CDEC acknowledged the certainty of the clinical evidence for pruritus outcomes to be low to moderate, reflecting imprecision, short duration of randomized evidence, and limited generalizability to some patient subgroups. Additional uncertainty arose from the lack of direct comparative evidence versus odevixibat and limited data on long-term outcomes, including disease progression and transplant-related outcomes. Generalizability was also uncertain for very young infants, patients with prior biliary surgery, and patients with PFIC subtypes that were underrepresented or not studied in the trial. These limitations contributed to residual uncertainty but were considered in the context of the rarity of the disease and the inherent challenges of conducting large, long-term comparative trials in this population.
Efficacy versus odevixibat: CDEC reviewed the available indirect treatment comparisons of maralixibat with odevixibat for pruritus-related outcomes. The committee noted that the indirect evidence was associated with substantial uncertainty due to differences in trial design, patient populations, and follow-up duration, as well as limitations related to transitivity and imprecision. The indirect evidence only reported differences in serum bile acids, a biochemical marker of cholestasis. Overall, the indirect evidence was insufficient to demonstrate a clear difference in efficacy between maralixibat and odevixibat but was considered consistent with similar clinical effects on biochemical cholestasis.
Other discussion points: CDEC discussed evidence gaps related to the use of maralixibat in specific subpopulations, including very young infants, patients with PFIC subtypes that were underrepresented or not studied in the pivotal trial, and patients with prior biliary surgery. The committee also discussed the safety profile of maralixibat, noting that gastrointestinal adverse events were common but generally manageable with dose adjustment or supportive care. No new safety signals were identified, although longer-term safety data remain limited.
Genetic assessment: In the draft recommendation, CDEC stipulated that initiation should be limited to patients with a confirmed biallelic pathogenic mutation. The sponsor requested removal of this criterion, proposing instead that eligibility be based on a diagnosis of PFIC. The sponsor argued that current genetic testing reports rarely use this terminology, that variant interpretation is complex, and that requiring “biallelic pathogenic” wording could create implementation barriers for clinicians and drug plans. They noted that PFIC diagnosis is made clinically with supportive investigations, that the MARCH-PFIC trial enrolled patients across PFIC subtypes without uniformly requiring such terminology, and that neither the Health Canada product monograph nor the comparator IBAT inhibitor (odevixibat) limits use based on this strict genetic wording. The clinician groups and clinical experts broadly aligned with this view and emphasized that genetic testing remains important for subtype characterization and identifying those patients whose PFIC is least likely to respond, but acknowledged limitations in current testing, including variants of uncertain significance and incomplete detection. A CDEC subpanel considered this request and supported removing the term “pathogenic” but cautioned against overly broad eligibility. The subcommittee stressed the importance of aligning the reimbursement criteria with the MARCH-PFIC trial populations, recommending that eligible PFIC subtypes be explicitly defined based on the studied biallelic mutations, including PFIC type 1 (ATP8B1), nontruncated PFIC type 2 (ABCB11), PFIC type 3 (ABCB4), PFIC type 4 (TJP2), and PFIC type 10 (MYO5B).
Clinical value: Based on all the preceding considerations, CDEC determined that maralixibat demonstrates at least comparable clinical value to odevixibat and added clinical value compared with placebo in patients with PFIC for the treatment of cholestatic pruritus.
Unmet Clinical Need
Input on unmet clinical need: CDEC considered input from patient groups, clinician groups, and clinical experts, which consistently identified persistent and severe pruritus as the most important unmet clinical need in PFIC. Patients and caregivers reported that pruritus has a profound downstream impact on sleep, daily functioning, school attendance, mental health, and family well-being, often beginning in infancy or early childhood. CDEC emphasized that pruritus remains inadequately controlled in many patients despite available medical therapies, leading to ongoing impairment in quality of life and, in some cases, consideration of invasive surgical interventions or liver transplantation. The committee agreed that maralixibat addresses some patient needs because it is an additional nonsurgical treatment option that targets the underlying pathophysiology of cholestasis and offers clinically meaningful symptom improvement.
Severity of the disease: CDEC considered PFIC to be a serious, chronic, and potentially life-threatening disease. The committee noted that PFIC is associated with progressive liver disease, growth impairment, and risk of cirrhosis, hepatobiliary complications, and liver transplantation. Severe pruritus was considered seriously debilitating, with substantial impacts on quality of life for patients and caregivers. This assessment was supported by patient groups and clinical expert input.
Availability of treatment options: CDEC noted that treatment options for PFIC are limited. Available medical therapies, including ursodeoxycholic acid and other off-label antipruritic agents, often provide inconsistent or inadequate relief of pruritus and do not modify disease progression. Odevixibat is approved and recommended for PFIC but is not recommended for reimbursement for all subtypes and is not currently listed on most public drug plan formularies. Surgical biliary diversion may reduce pruritus in some patients but is invasive, associated with morbidity, and not universally effective. Liver transplantation remains the only definitive treatment for advanced disease but carries significant risks and long-term consequences. Patient groups, clinicians, and presenters highlighted that there remains an important gap for effective, nonsurgical therapies that provide sustained symptom relief.
Distinct Social and Ethical Considerations
Input on unmet nonclinical need: CDEC considered input from patient groups, clinicians, clinical experts, and presenters highlighting important nonclinical burdens associated with PFIC, including the psychosocial impact on patients and caregivers, caregiver fatigue, and disruption to family life due to chronic symptoms, frequent medical visits, and the need for highly specialized care. Patient groups emphasized the emotional toll of caring for children with severe, persistent pruritus and uncertainty regarding disease progression and future need for invasive interventions.
Equity considerations: CDEC acknowledged equity considerations related to access to diagnosis and specialized care for PFIC. PFIC is a rare pediatric condition that requires expertise in pediatric hepatology, genetic testing, and ongoing specialist monitoring, which may not be equitably accessible across all regions. CDEC agreed with the clinical experts who noted that patients living in rural or remote areas, those requiring interprovincial care, and those from Indigenous or underserved communities may face additional barriers to timely diagnosis and treatment, including travel burden and coordination of care across jurisdictions.
Prescribing and monitoring considerations: The committee considered that maralixibat, as an oral therapy that can be prescribed and monitored by specialists with shared-care arrangements, has the potential to partially address some access-related challenges by reducing reliance on invasive surgical interventions and hospital-based procedures. However, CDEC noted that maralixibat is unlikely to fully overcome existing inequities in access to care because of the limited number of pediatric medical centres across Canada and regional variation in access to specialists.
Ethical implications: CDEC discussed ethical considerations related to decision-making in a vulnerable pediatric population with a serious, lifelong disease and limited treatment options. The committee considered the ethical importance of providing access to therapies that offer meaningful symptom relief, particularly where the primary benefit relates to quality of life, while also recognizing the uncertainty in long-term outcomes. Ethical considerations related to fairness and consistency in access across jurisdictions were also discussed, particularly in the context of rare disease funding and alignment with reimbursement decisions for similar therapies.
Economic Considerations
Key findings of the economic evaluation: CDEC identified substantial uncertainty in the cost-effectiveness of maralixibat plus best supportive care (BSC) relative to BSC alone due to a lack of comparative data to support a benefit in survival, hepatocellular carcinoma, or liver transplantation, as well as uncertainty in the estimation of BSC response. Given this uncertainty, CDEC considered a combination of the scenario analyses conducted by CDA-AMC to be more reflective of the evidence. This scenario mitigates the influence of benefit for maralixibat that has not been clinically proven and aligns BSC response with that observed in the MARCH-PFIC trial (with a 50% loss of a response annually for those receiving BSC). In this analysis, maralixibat plus BSC was associated with incremental costs of $7,397,328 and 0.38 additional quality-adjusted life-years (QALYs) per patient compared to BSC alone, resulting in an incremental cost-effectiveness ratio of $19,288,660 per QALY gained (Figure 1). Drug acquisition costs were the primary driver of incremental costs between maralixibat plus BSC and comparators.
Health impacts of maralixibat plus BSC versus odevixibat plus BSC: There is no direct or indirect evidence on the relative efficacy of maralixibat plus BSC and odevixibat plus BSC available for pruritus, which is the response outcome modelled in the pharmacoeconomic model. The indirect treatment comparison suggested that maralixibat may be associated with greater biochemical efficacy compared with odevixibat; however, these findings were uncertain due to methodological limitations. Based on evidence reviewed for this submission, there is insufficient evidence to suggest that maralixibat plus BSC provides greater health benefit than odevixibat plus BSC. If there are no differences in health outcomes between maralixibat and odevixibat, then the total cost of maralixibat plus BSC to the health system should not exceed that of odevixibat plus BSC for the treatment of PFIC.
Other considerations: CDEC noted that availability of odevixibat for the treatment of PFIC is uncertain. Odevixibat received a positive reimbursement recommendation for the treatment of pruritus in patients aged 6 months or older with PFIC and concluded pan-Canadian Pharmaceutical Alliance negotiations with a Letter of Intent on August 6, 2025. However, it is uncertain when odevixibat will be listed on public formularies.
Figure 1: Estimate of the ICER Used by CDEC to Inform the Price Condition
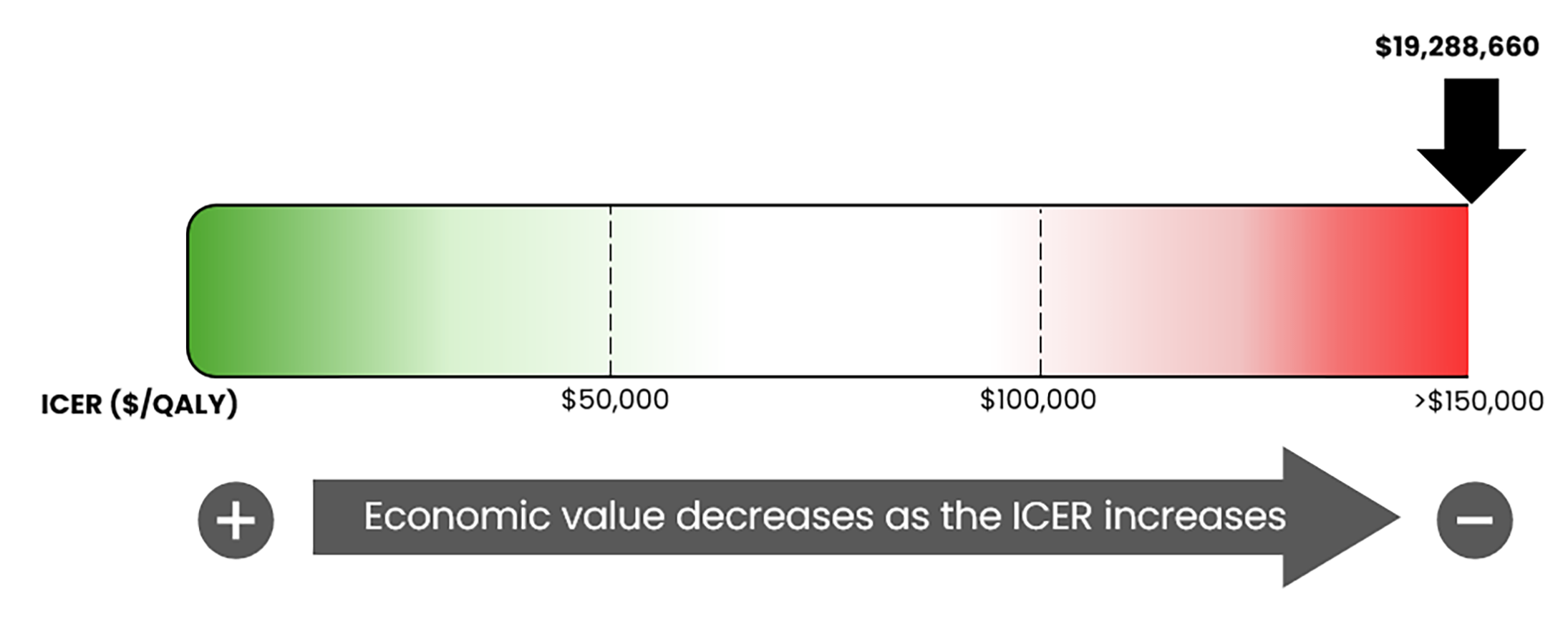
CDEC = Canadian Drug Expert Committee; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Impacts on Health Systems
Anticipated budget impact: CDA-AMC estimated that by year 3 of reimbursement, 44 patients would be eligible for treatment with maralixibat plus BSC of whom 16 would be expected to receive maralixibat plus BSC. It is estimated that the budget impact of reimbursing maralixibat plus BSC for the treatment of PFIC in patients aged 3 months and older will be approximately $44.6 million over the first 3 years of reimbursement compared to the amount currently spent on comparators, with an estimated expenditure of $45.6 million on maralixibat plus BSC over this period. The budget impact of maralixibat plus BSC is likely underestimated because it is based on an anticipated market share of only 5% in the prevalent patient population with PFIC type 1 and 2. The actual budget impact of reimbursing maralixibat plus BSC will depend on the reimbursement status of odevixibat plus BSC for PFIC and the resulting market share of maralixibat plus BSC and comparators.
Organizational implications: CDEC discussed organizational considerations related to the specialist requirements for prescribing and monitoring maralixibat. Treatment initiation and follow-up are expected to be managed by pediatric gastroenterology or hepatology specialists, which may limit capacity in some regions and require coordination of care across jurisdictions. The committee also noted potential implementation challenges related to drug distribution models, including reliance on specialty pharmacy services, which could affect timely access for some patients. These considerations were viewed as manageable through clearly defined initiation, renewal, and prescribing conditions.
CDEC noted that effective control of severe pruritus may reduce reliance on invasive surgical interventions, frequent hospital visits, and intensive supportive care, which could partially alleviate pressure on specialized health care services over time. However, the committee acknowledged that evidence to quantify such downstream system impacts is limited, and these potential benefits were considered uncertain.
Equity considerations related to implementation: CDEC acknowledged that equitable implementation may be affected by geographic variation in access to specialized pediatric hepatology services and the need for ongoing monitoring. Patients living in rural or remote areas, or those requiring interprovincial care, may face additional barriers related to travel, coordination of services, and access to specialty pharmacy distribution. The committee noted that these equity considerations reinforce the importance of flexible implementation approaches, including shared-care models where appropriate.
Sources of Information Used by the Committee
To make its recommendation, the committee considered the following information (links to the full documents for the review can be found on the project web page):
the CDA-AMC review of the clinical and pharmacoeconomic evidence submitted by the sponsor as well as relevant ethical issues related to maralixibat (refer the Main Report and Supplemental Material document)
the sponsor’s comments on the draft report and the CDA-AMC responses
patients’ perspectives gathered by 3 patient groups (Liver Canada, the PFIC Network, and the Alagille Syndrome Alliance) (refer to the Patient and Clinician Group Input document)
input from 3 clinician groups (the CPHRG of the Canadian Association for the Study of the Liver; University of Alberta – Stollery Children’s Hospital; and the Autoimmune and Rare Liver Disease Programme at Toronto General Hospital) (refer to the Patient and Clinician Group Input document)
input from public drug programs that participate in the reimbursement review process (refer to the Supplemental Material document)
input from 2 clinical experts with expertise in the management of PFIC consulted by CDA-AMC.
All feedback received in response to the draft recommendation is available on the CDA-AMC project web page.
CDEC Information
Members of the Committee
Dr. Peter Jamieson (Chair), Dr. Kerry Mansell (Vice-Chair), Sally Bean, Daryl Bell, Dan Dunsky, Dr. Ran Goldman, Dr. Trudy Huyghebaert, Dr. Dennis Ko, Dr. Christine Leong, Dr. Alicia McCallum, Dr. Srinivas Murthy, Dr. Nicholas Myers, Dr. Krishnan Ramanathan, Dr. Marco Solmi, Carla Velastegui, Dr. Edward Xie, and Dr. Peter Zed
Meeting date: January 29, 2026
Regrets: Five expert committee members did not attend.
Conflicts of interest: None
Minor reconsideration CDEC subpanel meeting date: April 13, 2026
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca