Drugs, Health Technologies, Health Systems
Reimbursement Review
4% w/w Fluorouracil Sodium Cream (Tolak)
Sponsor: Hill Dermaceuticals, Inc.
Therapeutic area: Actinic keratosis lesions
Summary
What Are Actinic Keratosis Lesions of the Face, Ears, and/or Scalp
Actinic keratosis (AK) is a skin disease involving atypical keratinocytes within the epidermis and is either in situ or a precursor to squamous cell carcinoma. The lesions are characterized by rough, scaly skin that may vary in thickness, diameter, and colour, and may or may not be painful. It occurs most commonly in older, fair-skinned individuals, in areas of the body exposed to UV light. The estimated rate at which an individual AK lesion develops into squamous cell carcinoma ranges from approximately 0.03% to 20%. Canadian clinical practice guidelines note that the incidence and prevalence of AK have not been specifically studied in Canada. However, they suggest that rates in Canada may be comparable to those reported in northwest England, where the prevalence among people older than 40 years is approximately 15% among men and 6% among women. In addition, the Canadian Skin Cancer Foundation estimates that the lifetime prevalence of AK in Canada is approximately 60%.
What Are the Treatment Goals and Current Treatment Options for AK Lesions of the Face, Ears, and/or Scalp?
The primary treatment goal is to eliminate AK lesions that have the potential to progress to squamous cell carcinoma by clearing both clinically observable and subclinical lesions and removing damaged keratinocytes.
Current treatment approaches for AK include both individual lesion interventions and broader field therapies. For single lesions, cryotherapy and surgical techniques such as shave excision or curettage are commonly used. In cases involving multiple lesions, field therapy is generally preferred. Available options include 5% weight per weight (w/w) fluorouracil cream, imiquimod cream, and photodynamic therapy using photosensitizing agents such as 5-aminolevulinic acid or methyl aminolevulinate, and a combination solution containing 0.5% w/w fluorouracil and 10% w/w salicylic acid. Although other treatment options include an ointment formulation of 1% tirbanibulin and 3% diclofenac gel, they are not frequently used in clinical practice and are not considered to be key comparators. For this review, 5% w/w fluorouracil cream is considered the most relevant comparator.
What Is Tolak and Why Did Canada’s Drug Agency Conduct This Review?
Tolak (4% w/w fluorouracil sodium cream) is a drug that is used topically. Health Canada has approved Tolak for the topical treatment of AK lesions of the face, ears, and/or scalp.
Canada’s Drug Agency (CDA-AMC) reviewed Tolak to inform a recommendation to the participating public drug programs on whether it should be reimbursed for the topical treatment of AK lesions of the face, ears, and/or scalp.
How Did CDA-AMC Evaluate Tolak?
CDA-AMC reviewed the clinical evidence on the beneficial and harmful effects, as well as the economic evidence, of Tolak versus other treatments used in Canada for the topical treatment of AK lesions of the face, ears, and/or scalp. 5% w/w fluorouracil cream was considered the most relevant treatment to compare with Tolak.
The review was informed by materials submitted by the sponsor, which included clinical and economic evidence.
The review was also informed by input from the participating public drug programs around issues that may impact their ability to implement a recommendation.
One clinician with expertise in the management of AK was consulted as part of the review process.
What Did CDA-AMC Find?
Clinical Evidence
We reviewed the following clinical evidence:
One randomized, evaluator-blinded, vehicle-controlled, multicentre, phase III trial (Study 48) comparing Tolak with 5% w/w fluorouracil cream, Tolak vehicle (placebo), and comparator vehicle (placebo) in 841 patients with AK lesions of the face, ears, and/or scalp.
One randomized, double-blind, vehicle-controlled, multicentre, phase III trial (Study 49) comparing Tolak with its vehicle (placebo) in 100 patients with AK lesions of the face, ears, and/or scalp.
Evidence from Study 48 did not demonstrate noninferiority of Tolak for the primary end point of the proportion of patients achieving 100% clearance at 4 weeks off treatment. However, noninferiority was demonstrated for the secondary end points of the proportion of patients achieving at least 75% clearance and the percent change from baseline in total lesion counts at 4 weeks off treatment. In both Study 48 and Study 49, Tolak demonstrated superiority over its vehicle for the primary and all secondary end points.
Due to the nature of AK, the clinical expert consulted by CDA-AMC for this review noted that achieving at least 75% clearance is a more meaningful end point in clinical practice for evaluating the efficacy of Tolak in the treatment of AK lesions of the face, scalp, or ears, compared with complete (100%) clearance. On this basis, Tolak is likely comparable to 5% w/w fluorouracil cream.
The clinical expert did not identify any notable safety concerns for Tolak relative to 5% w/w fluorouracil cream.
Economic Evidence
Tolak is available as a 40 g tube of cream for topical use. At the submitted price of $40.00 per 40 g tube, the cost of Tolak for an initial 4-week course of treatment of AK lesions is expected to be $40 per patient.
Reimbursement of Tolak may be associated with lower drug costs to the health care system versus 5% w/w fluorouracil sodium cream (incremental savings = $5 per initial 4-week course of treatment). However, whether there will be savings will depend on factors such as how much cream patients use per application and the proportion of patients who experience disease recurrence.
The sponsor estimates that the budget impact of reimbursing Tolak for AK will be a saving of approximately $262,000 over the first 3 years of reimbursement compared to the amount currently spent on 5% w/w fluorouracil sodium cream, with a predicted expenditure of $2 million on Tolak over this period. CDA-AMC was unable to provide a more robust estimate of the expected budget impact owing to the extent of the uncertainty in several parameters. Whether there will be cost savings to the public drug plans, the extent of any savings, and the expenditure on Tolak are highly uncertain and will depend on the drug acquisition costs for Tolak and comparators, the number of eligible people, the uptake of Tolak and its displacement of comparators, and the number of tubes prescribed.
Abbreviations
AE
adverse event
AK
actinic keratosis
ANOVA
Analysis of Variance
BIA
budget impact analysis
CDA-AMC
Canada’s Drug Agency
CI
confidence interval
CMH
Cochran-Mantel-Haenszel test
GRADE
Grading of Recommendations Assessment, Development and Evaluation
ITT
intention to treat
IUD
intrauterine device
LOCF
last observation carried forward
MAL
methyl aminolevulinate
PDT
photodynamic therapy
PP
per-protocol
RNA
ribonucleic acid
SAE
serious adverse event
SCC
squamous cell carcinoma
STD
standard deviation
w/w
weight per weight
Record of Modifications
Table 1: Record of Modifications Made by Canada’s Drug Agency to the Sponsor-Submitted Material
Section | Summary of Modifications |
|---|---|
Disease Background, Current Treatment Options |
|
Pivotal Studies, Table 3 |
|
Statistical Testing |
|
Efficacy |
|
Harms |
|
Supplemental Materials |
|
AE = adverse event; AK = actinic keratosis; ITT = intention to treat; w/w = weight per weight.
Background
Sponsor’s Summary of Disease Background and Current Management
Application Summary
Table 2: Application Submitted for Review
Item | Description |
|---|---|
Drug (product) | 4% w/w fluorouracil sodium cream (Tolak), 4% mg/g, topical |
Submitted price of drug under review | 4% w/w fluorouracil sodium cream: $40.00 per 40-gram tube |
Sponsor | Hill Dermaceuticals, Inc. |
Health Canada indication | The topical treatment of actinic keratosis lesions of the face, ears, and/or scalp |
Sponsor’s reimbursement request | As per indication |
Health Canada approval status | Notice of compliance |
Health Canada review pathway | Standard review pathway |
NOC date | 01 February 2019 |
mg/g = milligrams per gram; NOC = Notice of Compliance.
Disease Background
Actinic keratosis (AK) is a skin disease involving atypical keratinocytes within the epidermis and is considered to be either in situ squamous cell carcinoma (SCC) or a precursor to SCC.1,2 Worldwide, the prevalence of AK was recently estimated to be approximately 14%, and the incidence rate was estimated to be 1,928 per 100,000 person-years.3 AK tends to occur most commonly in older, fair-skinned individuals, in anatomical areas of the body exposed to ultraviolet light.3 Thus, the incidence and prevalence of AK are likely to vary among geographic regions depending on factors such as age of the population, skin type, and exposure to UV light. Canadian clinical practice guidelines state that AK incidence and prevalence have not specifically been studied in Canada but suggest that Canadian AK rates may most closely resemble those of northwest England, which have been reported to be 15% in men >40 years and 6% in women.4 The Canadian Skin Cancer Foundation estimates the lifetime prevalence of AK to be around 60% in Canada.5
AK and SCC are clinically, histologically, and biologically related on the basis of identified mutations.2,6-9 The estimated rate at which an individual AK lesion develops into SCC ranges from approximately 0.03 to 20.2,7,10 Predictive factors regarding which individual AK lesions may progress to SCC have yet to be completely elucidated.2,10
Multiple classification systems have been developed for AK including the Olsen classification system, the number of AK lesions, and histologic classifications such as Röwert-Huber or the PRO system.1,2 However, the clinical utility of each of these grading systems, including the commonly used Olsen classification system, is the subject of debate.2,10 Thus, there is no single system that is widely accepted to be useful for AK classification, grading, or staging.
AK is generally not fatal, but progression to SCC can result in the need for surgical removal, with the potential for associated cosmetic implications and incomplete lesion removal. Further progression to an aggressive, metastatic form of SCC is associated with a high risk of mortality.11
Diagnosis of the Condition
Diagnosis of AK is generally diagnosed by its clinical features in combination with its anatomical location.1,7 AK lesions generally occur in areas of high sun exposure such as the scalp, face, ears, neck, arms, and hands.1,2 AK lesions are generally characterized by rough, scaly skin which may vary in thickness, diameter, and color; lesions may or may not be painful.1 Diagnosis and grading or staging may be enhanced by techniques such as dermatoscopy, reflectance confocal microscopy, and optical coherence tomograph.1 Biopsy may also be performed but is usually unnecessary to diagnose AK and is generally not practical in the clinical setting. Biopsy can provide an assessment of AK severity, however, and is sometimes useful in the differential diagnosis of AK.7
Current Management and Place in Therapy of the Drug Under Review
Current Treatment Options
Clinical practice guidelines generally recommend that any AK lesions be treated because of the potential to progress to SCC, especially considering that there is currently no reliable way to predict which AK lesions may progress to SCC.1,4,7,10 Clinical practice guidelines acknowledge that watchful waiting is also an option in some circumstances; however, one guideline suggests that the option not to treat the AK “should be viewed critically.”10
In addition to the treatment of individual AK lesions, clinical practice guidelines all mention the concept of field treatment, as AK lesions may exist within an area of skin that contains damaged keratinocytes and/or subclinical AK lesions that have the potential to progress but not have yet progressed to clinically detectable AK.1,4,7,10 This phenomenon is referred to as field cancerization. In the case of multiple AK lesions and suspected or observed field cancerization, clinical practice guidelines suggest that field treatment is appropriate.1,4,7,10
Clinical practice guidelines generally agree that the goal of AK treatment is to eliminate AK lesions that could progress to SCC.1,4,7,10 To accomplish that goal, clearance of both the clinically observable AK lesions and any subclinical AK and damaged keratinocytes is desirable.
A variety of treatment modalities are available for AK in Canada. For individual lesions, cryosurgery is often performed. Surgical removal (e.g., by shave excision or curettage) is also an option. For multiple lesions, clinical practice guidelines note that individual lesion treatment may be ineffective (as well as impractical) and instead generally recommend field treatment. Canadian clinical practice guidelines include 5% weight per weight (w/w) fluorouracil cream (hereafter referred to as fluorouracil 5% cream), 5% imiquimod cream, 3.75% imiquimod cream, ingenol mebutate gel (0.015% for the face and scalp), and photodynamic therapy (PDT) with a photosensitizing agent of either 5-aminolevulinic acid or methyl aminolevulinate (MAL) as possible options for field treatment.4 Another product, 3% diclofenac gel, is sometimes used but is not currently marketed in Canada for the treatment of AK and is not included in the Canadian clinical practice guidelines.4 Since the publication of the Canadian guidelines, several additional options have been marketed in Canada including a combination solution product containing 0.5% w/w fluorouracil and 10% w/w salicylic acid (approved in 2014, which may have been too late for inclusion in the 2015 guidelines), a cream containing 4% fluorouracil (hereafter referred to as fluorouracil 4% cream, the subject of this submission, approved in 2019), and an ointment containing 1% tirbanibulin (approved in 2023). In addition, ingenol mebutate has been withdrawn from the Canadian market (in 2020) due to a possible increased risk of skin cancer.
Among the various treatment modalities for AK, products containing fluorouracil are a mainstay for the treatment of AK and are supported by the Canadian clinical practice guidelines4 and in more recent clinical practice guidelines from other locales.1,7,10 One direct comparison of 4 different field treatments (fluorouracil 5% cream, 5% imiquimod cream, MAL-PDT, and 0.015% ingenol mebutate gel) demonstrated that fluorouracil 5% cream displayed the greatest efficacy among the agents as measured by a >75% reduction in the number of AK lesions from baseline to 12 months after the end of treatment.12 While the fluorouracil 4% cream (the subject of this submission) was not among the agents compared in the 2019 Jansen et al. study12, a recent 2024 clinical practice guideline from Europe notes that the fluorouracil 4% cream (the subject of this submission) demonstrated similar efficacy, along with better tolerability, compared with the fluorouracil 5% cream.13 Furthermore, results from two combined clinical studies published in 2016 demonstrated that fluorouracil 4% cream applied once daily for four weeks in an aqueous cream with peanut oil showed superior efficacy, safety, and fewer side effects compared with fluorouracil 5% cream applied twice daily for four weeks.14
Key characteristics of fluorouracil 4% cream are summarized with other treatments available for actinic keratosis in the Supplemental Material document (Key Characteristics of 4% w/w Fluorouracil Sodium Cream and other Drug Comparators).
Impact of the Drug Under Review on Treatment Options
In Canada, the main comparator for fluorouracil 4% cream is fluorouracil 5% cream. Fluorouracil 4% cream is expected to primarily displace fluorouracil 5% cream as the first line topical treatment for actinic keratosis.
Other pharmacology treatments such as 5% imiquimod cream and a combination solution product containing 0.5% w/w fluorouracil and 10% w/w salicylic acid may also be displaced.
CDA-AMC Sources of Information and Summary of Input
This section was prepared by CDA-AMC based on materials submitted by the sponsor and input from interested parties.
The objective of the clinical review is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of fluorouracil 4% cream for the topical treatment of AK lesions of the face, ears, and/or scalp in adults. The focus will be on comparing fluorouracil 4% cream to relevant comparators in clinical practice in Canada and identifying gaps in the current evidence. This application has been submitted through the tailored review process. The focus of tailored reviews is an assessment of whether the evidence supports that the drug under review demonstrates comparable clinical benefit and harms to appropriate comparators, as well as a comparison of drug acquisition costs and a budget impact analysis (BIA). The comparators considered were fluorouracil 5% cream, imiquimod cream, and a topical solution containing 0.5% w/w fluorouracil and 10% w/w salicylic acid. Although other treatment options include an ointment formulation of 1% tirbanibulin and 3% diclofenac gel, they are not frequently used in clinical practice and are not considered to be key comparators. For this review, fluorouracil 5% cream is considered the most relevant comparator.
Fluorouracil 4% cream is applied once a day to the AK lesions and surrounding areas for 4 weeks, as per the product monograph. Fluorouracil acts by at least 3 known mechanisms. First, fluorodeoxyuridine monophosphate inhibits the enzyme thymidylate synthase, which catalyzes the conversion of uridylate to thymidylate, and inhibits DNA synthesis. Second, the erroneous incorporation of fluorodeoxyuridine triphosphate into DNA results in DNA damage. Third, the erroneous incorporation of fluorouridine triphosphate into ribonucleic acid (RNA) leads to disruptions in RNA function. The effects of DNA and RNA deprivation are most marked on those cells that grow more rapidly and take up fluorouracil at a more rapid rate. An additional mechanism of action may be the activity of fluorouracil against viruses that may be associated with the development of AK.
The comparators in the same therapeutic class for which CDA-AMC issued a recommendation to reimburse for the same (or similar) indication include a topical solution containing 0.5% w/w fluorouracil and 10% w/w salicylic acid.
Sources of Information
This report is informed by materials submitted by the sponsor and input received from interested parties. Calls for patient group and clinician group input are issued for each reimbursement review. We received no patient or clinician group submissions. The drug programs provide input on each drug being reviewed through the reimbursement review process by identifying issues that may impact their ability to implement a recommendation.
Each review team includes at least 1 clinical specialist with expertise in the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process. One clinician with expertise in the diagnosis and management of AK participated as part of the review team, representing British Columbia.
Summary of Input
Disease Background and Impacts of the Disease
Patient group input: Input from patient groups was not received for this project.
Treatment Goals and Treatment Options
Patient group input: Input from patient groups was not received for this project.
Clinician input: Input from clinician groups was not received for this project. Input from the clinician expert noted that an important goal of treatment is to eliminate AK lesions, which have the potential to progress into SCC.
Unmet Needs and Existing Challenges
Patient group input: Input from patient groups was not received for this project.
Clinician input: Input from clinician groups was not received for this project. Input from the clinical expert highlighted that alternative topical treatment options, such as fluorouracil 5% cream and 5% imiquimod may result in severe irritation in patients. Thus, patients may resist or not fully comply with the treatment. Likewise, cryotherapy and other forms of destructive therapy (such as curettage) may be inadequate and miss lesions.
Considerations for Using the Drug Under Review
The contents within this section have been informed by input from the clinical expert consulted for the purpose of this review. The implementation questions from the public drug programs and corresponding responses from the clinical expert consulted for this review are summarized in the Summary of Drug Program Input and Clinical Expert Responses table in the Supplemental Material document. The following has been summarized by the review team.
Place in Therapy
This drug is being reviewed through the CDA-AMC product variation process, based on the sponsor’s claim that the drug is primarily expected to displace fluorouracil 5% cream. The sponsor also expects that 5% imiquimod cream and 0.5% fluorouracil and 10% salicylic acid topical solution will also be displaced. Fluorouracil 5% cream is a full benefit in all jurisdictions. In contrast, 5% imiquimod cream is a full benefit in 4 jurisdictions (Prince Edward Island, Ontario, Northwest Territories, Non-Insured Health Benefits Program), a restricted benefit with specified criteria in 7 jurisdictions (Newfoundland and Labrador, New Brunswick, Saskatchewan, Alberta, Yukon, Canadian Armed Forces, Veterans Affairs Canada) and not a benefit in 3 jurisdictions (Nova Scotia, Manitoba, and British Columbia). In all jurisdictions except for British Columbia, 0.5% fluorouracil and 10% salicylic acid topical is a full benefit. Neither of the 3 aforementioned drugs is a benefit for the Canadian Blood Services.
The clinical expert consulted by CDA-AMC noted that fluorouracil 4% cream is expected to be an alternative to fluorouracil 5% cream and be used as first-line field treatment and first-line or second-line treatment for individual lesions. The clinical expert indicated that they do not believe that fluorouracil 4% cream will cause a treatment paradigm shift.
Patient Population
The clinical expert consulted by CDA-AMC noted that the target population for fluorouracil 4% cream is similar to that of fluorouracil 5% cream. The clinical expert also indicated that they do not think that AK lesions of the face, ears, and/or scalp disproportionately impact groups that are underserved or equity-deserving populations.
Assessing Treatment Response
The clinical expert consulted by CDA-AMC reported that patients best suited for treatment with fluorouracil 4% cream would be identified in a similar way as those best suited for treatment with fluorouracil 5% cream. They noted that misdiagnosis may occur in clinical practice depending on the training received by the physician (i.e., general physician versus dermatologist). Likewise, the clinical expert indicated that clinical assessments are performed to determine whether a patient’s disease is showing a response to treatment in clinical practice, and outcomes used in clinical practice are aligned with outcomes typically used in clinical trials. However, they mentioned that the magnitude of the response to treatment is likely to vary depending on the physician providing treatment, and treatment response should be assessed based on the number of lesions and concerns about SCC (at 3 to 6 months or 6 to 12 months).
Discontinuing Treatment
The clinical expert consulted by CDA-AMC noted that the level of clearance and intolerance should be considered when deciding to discontinue treatment with fluorouracil 4% cream.
Prescribing Considerations
The clinical expert consulted by CDA-AMC indicated that dermatologists or general physicians comfortable with treating AK lesions can diagnose, treat, and monitor patients who may be candidates for fluorouracil 4% cream. They noted that fluorouracil 4% cream and associated care are expected to be equitably accessible to all eligible patients in Canada.
Sponsor’s Summary of the Clinical Evidence
Pivotal Studies
Table 3: Details of Included Studies
Characteristics | Study 48 (HD-FUP3B-048) | Study 49 (HD-FUP3S-049) |
|---|---|---|
Study Name | A Randomized, Evaluator Blinded, Vehicle-Controlled Multi-Center Study of the Safety and Efficacy of 4% TRADENAME (Fluorouracil) Cream (TOLAK) Versus its Vehicle Cream Versus Efudex® Cream in the Treatment of Actinic Keratosis | A Randomized, Double Blind, Vehicle-Controlled Multi-Center Study of the Safety and Efficacy of 4% TRADENAME (Fluorouracil) Cream (TOLAK) Versus its Vehicle Cream in the Treatment of Actinic Keratosis |
Study design and population | ||
Study design | Evaluator-blinded Randomized Controlled Trial (RCT) | Double Blind (DB), Randomized Controlled Trial (RCT) |
Locations | 26 centers in the United States | 5 centers in the United States |
Patient enrolment dates | March 30, 2006 to December 29, 2006 | May 22, 2006 to October 17, 2006 |
Randomized (N) | 841 participants were enrolled and included in the intent-to-treat population:
| 100 participants were enrolled and included in the intent-to-treat population (50 participants per treatment group). |
Inclusion criteria | 1. Subject completed and signed an appropriately administered Institutional Review Board approved informed consent form prior to any study related procedures. 2. Subject was at least 18 years old of either gender. 3. Subject was willing and able to apply the assigned study medication as directed and was willing to comply with required visits for the duration of the study. 4. Subject had a clinical diagnosis of actinic keratosis (AK). 5. Subject had 5 or more previously untreated clinically recognizable (palpable and/or visible to unaided eye) AK lesions of the face, and/or ears and/or scalp; and had at least 5 AK lesions greater than or equal to 4 mm in longest diameter. The AK lesions were clinically typical nonhypertrophic and/or nonhyperkeratotic. None of the AK lesions exceeded 1 cm in size. 6. Subject was in good general condition and free of any disease state or condition which, in the investigator’s opinion, could have impaired evaluation of actinic keratosis or could have exposed the subject to an unacceptable risk by study participation. 7. Females of childbearing potential must have had a negative urine pregnancy test and agreed to use an effective form of birth control for the duration of the study (e.g.: stabilized on oral contraceptives for at least one month, implant, injection, transdermal, IUD, condom and spermicide, or diaphragm and spermicide). | 1. Subject completed and signed an appropriately administered Institutional Review Board approved informed consent form prior to any study related procedures. 2. Subject was at least 18 years old of either gender. 3. Subject was willing and able to apply the assigned study medication as directed and agreed to comply with required visits for the duration of the study. 4. Subject had a clinical diagnosis of actinic keratosis (AK). 5. Subject had 5 or more previously untreated clinically recognizable (palpable and/or visible to unaided eye) AK lesions of the face, and/or ears and/or scalp; and had at least 5 AK lesions that were greater than or equal to 4 mm in longest diameter. The AK lesions were to be clinically typical nonhypertrophic and/or nonhyperkeratotic. None of the AK lesions were to exceed 1 cm in size. 6. Subject was in good general condition and was free of any disease state or condition which, in the investigator’s opinion, could have impaired evaluation of actinic keratosis or could have exposed the subject to an unacceptable risk by study participation. 7. Females of childbearing potential must have had a negative urine pregnancy test and agreed to use an effective form of birth control for the duration of the study (e.g. stabilized on oral contraceptives for at least one month, implant, injection, transdermal, IUD, condom and spermicide, or diaphragm and spermicide). |
Exclusion criteria | 1. Subject had AK lesions within treatment areas which were hyperkeratotic or which were clinically suspected to be squamous cell carcinoma (SCC). 2. Subject used 5-fluorouracil or any systemic cancer treatment within two months prior to the study. 3. Subject used any other AK treatments or therapies (e.g., Cryotherapy or Photodynamic therapy) in the treatment area(s) within two months prior to starting the study. 4. Subject used any systemic steroids, immunosuppressants or immunomodulators within one month prior to the study. 5. Subject used prescription retinoids or topical steroids in the treatment area(s) within one month prior to the study. 6. Subject used glycolic acid products and alpha-hydroxy products in the treatment area(s) within four weeks prior to starting the study. 7. Subject used chemical peeling products in the treatment area(s) within eight weeks prior to starting the study. 8. Subject had a history of sensitivity to any of the ingredients in the study medications. 9. Subject was pregnant or a nursing mother. 10. Subject was currently participating, or had participated in the 30 days prior to the study, in an investigational study. | 1. Subject had AK lesions within treatment areas which were hyperkeratotic or which were clinically suspected to be squamous cell carcinoma (SCC). 2. Subject used 5-fluorouracil or any systemic cancer treatment within two months prior to the study. 3. Subject used any other AK treatments or therapies (e.g., Cryotherapy or Photodynamic therapy) in the treatment area(s) within two months prior to starting the study. 4. Subject used any systemic steroids, immunosuppressants or immunomodulators within one month prior to the study. 5. Subject used prescription retinoids or topical steroids in the treatment area(s) within one month prior to the study. 6. Subject used glycolic acid products and alpha-hydroxy products in the treatment area(s) within four weeks prior to starting the study. 7. Subject used chemical peeling products in the treatment area(s) within eight weeks prior to starting the study. 8. Subject had a history of sensitivity to any of the ingredients in the study medications. 9. Subject was pregnant or a nursing mother. 10. Subject was currently participating or had participated in the 30 days prior to the study, in an investigational study. |
Drugs | ||
Intervention | Fluorouracil 4% cream, applied topically once daily for 4 weeks | Fluorouracil 4% cream, applied topically once daily for 4 weeks |
Comparator(s) | Fluorouracil 5% cream applied topically, twice daily for 4 weeks Fluorouracil 4% cream vehicle (placebo), applied topically once daily for 4 weeks Fluorouracil 5% cream vehicle (placebo), applied topically, twice daily for 4 weeks | Fluorouracil 4% cream vehicle (placebo), applied topically once daily for 4 weeks |
Duration | ||
Screening phase | Phase III | Phase III |
Run-in phase | none | none |
Treatment phase | 4 weeks on treatment | 4 weeks on treatment |
Follow-up phase | At 2 and 4 weeks post treatment | At 2 and 4 weeks off-treatment |
Outcomes | ||
Primary end point | The primary efficacy parameter was the proportion of patients in whom 100% of the lesions cleared at 4-weeks off study medication. | The primary efficacy parameter was the proportion of participants in whom 100% of the lesions cleared at 4-weeks off study medication |
Publication status | ||
Publications | Dohil MA. Efficacy, Safety, and Tolerability of 4% 5-Fluorouracil Cream in a Novel Patented Aqueous Cream Containing Peanut Oil Once Daily Compared With 5% 5-Fluorouracil Cream Twice Daily: Meeting the Challenge in the Treatment of Actinic Keratosis. J Drugs Dermatol. 2016;15(10):1218-1224. | N/A |
Source: Final Clinical Study Report (CSR) for Protocol HD-FUP3B-04815 and Final Clinical Study Report (CSR) for Protocol HD-FUP3S-04916.
Description of Studies
NOTE: In the following narratives and tables, the terms “4% TRADENAME (Fluorouracil) Cream” and “4% TRADENAME cream” and “4% TRADENAME” were used in the Clinical Study Report (CSR) and protocols and for this report have been changed to refer to fluorouracil 4% cream.
Study 48 (HD-FUP3B-048):
Randomized, evaluator blinded, vehicle-controlled, multicenter, phase III, pivotal study which demonstrated the safety and efficacy of fluorouracil 4% cream in the treatment of AK against three comparators: (i) fluorouracil 5% cream (active comparator), (ii) the vehicle cream of fluorouracil 4% cream (placebo) and (iii) the vehicle cream of the active comparator (placebo).
Eight hundred forty-one (841) participants were enrolled at a ratio of 5:5:1:1 (350 participants per active treatment group and 70 participants in each of the vehicle groups) and included in the intention-to-treat (ITT) population. Seven hundred fifty-seven (757) participants were included in the Per-Protocol population. Eight hundred twenty-five (825) participants were included in the safety population. This study was conducted at US sites.
Application of the study materials involved “field treatment” of the whole area of the face and/or ears and/or scalp where AK lesions were identified and mapped on the template. The medication was to be applied at the same time each day.
Fluorouracil 4% cream and its vehicle were applied once daily; fluorouracil 5% cream and its vehicle were applied twice daily.
After the Baseline visit, participants returned for on-treatment visits at Weeks 1, 2 and 4 and for two post-treatment follow-up visits (2-weeks off-treatment and 4-weeks off-treatment).
At every visit from Baseline through 4-weeks post-treatment, investigators counted all visible and/or palpable AK lesions in the treatment area (face, and/or ears and/or scalp), which was used to assess efficacy.
Tolerability was assessed by grading severity of each of erythema, scaling/dryness, edema, crusting, erosions, stinging/burning, and pruritus using a scale that ranged from 0 (none) to 3 (severe). Reported AEs were recorded for reach visit.
There was no dose modification allowed in this study, or rescue medication.
Study 49 (HD-FUP3S-049):
Randomized, double-blind, vehicle-controlled, multicenter, phase III study which demonstrated the safety and efficacy of fluorouracil 4% cream compared to its vehicle cream in the treatment of actinic keratosis
Second pivotal trial which was used for approval for fluorouracil 4% cream, was an identical study design (efficacy end points, tolerability assessment, and safety assessment) to Study 48 (see above), except that this study only had a vehicle comparator.
100 participants were enrolled at a ratio of 1:1 and included in the Intent-to-Treat population (50 participants per treatment group). 99 participants were included in the safety population (Fluorouracil 4% cream: 49 participants; Vehicle: 50 participants) and 87 participants were included in the Per-Protocol population (Fluorouracil 4% cream: 43 participants; Vehicle: 44 participants)
Interventions
Study 48 (HD-FUP3B-048):
This study had four treatment groups: (1) fluorouracil 4% cream, which is the subject of this submission, (2) the vehicle for fluorouracil 4% cream (i.e. the fluorouracil 4% cream formulation without the active ingredient of fluorouracil), (3) an active comparator of fluorouracil 5% cream, and (4) a comparator vehicle cream (the inactive ingredients of fluorouracil 5% cream) which was added to preserve blinding as the dosing fluorouracil 5% cream is twice-daily while the dosing for fluorouracil 4% cream is only once-daily.
Study dosing and application: Dosing was once daily for fluorouracil 4% cream and its vehicle or twice daily for fluorouracil 5% cream and its vehicle for 4 weeks. Application of the study materials involved “field treatment” of the whole area of the face, ears and/or scalp where AK lesions were identified at Baseline, e.g. if lesions were identified on the cheek, study material was applied to the whole cheek.
Permitted concomitant medications: Medication and non-medication therapies for the treatment or prevention of disease or to maintain good health were allowed in the study. Other than the study medications, no other topical medications were allowed to be used in the treatment areas. Other prohibited treatments included, but were not limited to, retinoids, immunosuppressants, immunomodulators, glycolic acid products, alpha-hydroxy acid products, and chemical peeling products. Participants were permitted to apply a non-medicated emollient and/or sunscreen in the treatment areas.
No rescue medication was used in the study.
Study 49 (HD-FUP3S-049):
This study was identical in design as Study 49 except that this study had only two treatment groups: (1) fluorouracil 4% cream which is the subject of this submission, and (2) the vehicle for fluorouracil 4% cream (i.e. the fluorouracil 4% cream formulation without the active ingredient of fluorouracil)
Outcomes
Table 4: Summary of Relevant Outcomes
Outcome measure | Timepoint | Study 48 | Study 49 |
|---|---|---|---|
Proportion of participants who had 100% clearing of their Actinic Keratosis (AK) | 4-weeks off-treatment | Primary
| Primary
|
Proportion of participants who had 75% clearing of their Actinic Keratosis (AK) | 4-weeks off-treatment | Key secondary
| Key secondary
|
Percent change from Baseline in number of Actinic Keratosis (AK) lesions | 4-weeks off-treatment | Secondary
| Secondary
|
Tolerability Assessments (grading of each of erythema, scaling/dryness, edema, crusting, erosions, stinging/burning, and pruritus) | All visits | Safety | Safety |
Adverse events | All visits | Safety | Safety |
Source: Final Clinical Study Report (CSR) for Protocol HD-FUP3B-04815 and Final Clinical Study Report (CSR) for Protocol HD-FUP3S-04916.
Sample Size and Power Calculation
Sample size and power for Study 48 and Study 49 were based on a previously completed dose-ranging study which showed that 80% of participants on fluorouracil 4% cream had complete clearance of baseline lesions at 4-weeks off-treatment, 75% of participants on fluorouracil 5% cream had complete clearance, and 15% of participants on the vehicle treatments had complete clearance.
Study 48 (HD-FUP3B-048):
840 participants (5:5:1:1 ratio: fluorouracil 4% cream, fluorouracil 5% cream, and two vehicle controls). The primary efficacy endpoint was the percentage of participants with complete clearance of baseline AK lesions 4 weeks off-treatment.
Populations: ITT (840 participants) and PP (720 participants)
Non-inferiority: fluorouracil 4% cream vs. fluorouracil 5% cream (10% NI margin, one-sided alpha = 0.025)
Superiority: fluorouracil 4% cream vs. vehicle (two-sided alpha = 0.05)
Assumed success rates: 75–80% for fluorouracil 4% cream; 75% for fluorouracil 5% cream; 15% for vehicle
Power: 80–99% for non-inferiority; ≥90% for superiority
Study 49 (HD-FUP3S-049):
100 participants (1:1 ratio; 50 fluorouracil 4% cream, 50 vehicle). The primary endpoint was the percentage of participants with complete clearance of baseline AK lesions 4-weeks off-treatment
Populations: ITT (100), PP (80)
Superiority: Fluorouracil 4% cream vs. vehicle (two-sided alpha = 0.05)
Assumed success rates: 75–80% for Fluorouracil 4% cream; 15% for vehicle
Power: ≥95%
Statistical Testing
The statistical analysis methods used for Study 48 and Study 49 studies are provided in the Supplemental Material document (Methods of Included Studies).
For both studies, the primary efficacy endpoint was the proportion of participants achieving complete (100%) clearance of baseline AK lesions 4 weeks post-treatment. Analyses were stratified by study center and conducted according to the predefined non-inferiority or superiority objectives described above.
For Study 48 non-inferiority of fluorouracil 4% cream versus fluorouracil 5% cream was evaluated using a one-sided 97.5% confidence interval (Wald method with Yates’ continuity correction); non-inferiority was concluded if the lower bound exceeded −10%. Superiority of fluorouracil 4% cream versus its vehicle was assessed using a two-sided Cochran-Mantel-Haenszel (CMH) test at alpha = 0.05. For Study 49, superiority of fluorouracil 4% cream versus vehicle was evaluated using the same CMH test at alpha = 0.05.
For both studies, secondary endpoints (≥75% clearance and percent change in lesion count) were analyzed using parametric or non-parametric methods depending on normality (Wilk–Shapiro test, α = 0.01). When non-normality was detected, a rank-based ANOVA was used. No adjustments were made for multiple comparisons or interim analyses. Missing data were handled by the last observation carried forward (LOCF) approach, with sensitivity analyses imputing missing outcomes as either success or failure for the proportion of participants with 100% clearance at 4 weeks off-treatment.
Subgroup Analyses
Subset analyses for both Study 48 and Study 49 were performed on the Intent-to-Treat (ITT) and Per-Protocol (PP) populations across the subgroups of gender, age, ethnicity, race, and baseline severity. Age was dichotomized as below or at/above the median, and baseline severity was defined by baseline lesion count: mild (5–10 lesions), moderate (11–25 lesions), and severe (>25 lesions). For each subgroup, frequency tables were generated showing the treatment success rate (proportion of participants with 100% clearance of lesions at 4 weeks post-treatment) by treatment group.
Analysis Populations
Table 5: Analysis Populations of Study 48 and Study 49
Study | Population | Definition | Application |
|---|---|---|---|
Study 48 & Study 49 | Intent-to-Treat (ITT) | All participants randomized and dispensed study medication. | The primary and secondary analyses |
Per-Protocol (PP) | A subset of the safety population. Participants were eligible for the Per-Protocol analyses if they completed the 4-week off-treatment evaluation without noteworthy study protocol violations | Non-inferiority and superiority testing | |
Safety | All participants randomized with documented use of at least one application of study medication and at least one post-baseline assessment. | Safety analyses |
Source: Final Clinical Study Report (CSR) for Protocol HD-FUP3B-04815 and Final Clinical Study Report (CSR) for Protocol HD-FUP3S-04916.
Sponsor’s Summary of the Results
Baseline Characteristics
Table 6: Summary of Baseline Characteristics: ITT Population
Characteristic | Study 48 | Study 49 | |||||
|---|---|---|---|---|---|---|---|
Fluorouracil 4% Cream (N = 353) | Fluorouracil 5% Cream (N = 349) | Fluorouracil 4% Cream Vehicle (N=70) | Fluorouracil 5% Cream Vehicle (N = 69) | Fluorouracil 4% Cream (N = 50) | Fluorouracil 4% Cream Vehicle (N=50) | ||
Demographics | |||||||
Age (years) | Mean (STD) Range | 67.7 (9.8) 36.7 – 88.9 | 67.4 (10.0) 37.6 - 94.1 | 68.0 (10.1) 47.7 - 84.8 | 69.1 (12.1) 37.6 - 88.4 | 67.9 (11.7) 44.7 – 85.1 | 66.9 (11.7) 33.5 - 87.8 |
Gender | Male Female | 287 (81%) 66 (19%) | 282 (81%) 67 (19%) | 58 (83%) 12 (17%) | 55 (80%) 14 (20%) | 39 (78%) 11 (22%) | 46 (92%) 4 (8%) |
Skin Type (Fitzpatrick) | I II III IV V | 84 (24%) 178 (50%) 75 (21%) 13 (4%) 3 (0%) | 91 (26%) 155 (44%) 80 (23%) 21 (6%) 2 (1%) | 13 (19%) 35 (50%) 19 (27%) 3 (4%) 0 (0%) | 18 (26%) 33 (48%) 15 (22%) 3 (4%) 0 (0%) | 7 (14%) 17 (34%) 25 (50%) 1 (2%) 0 (0%) | 6 (12%) 25 (50%) 17 (34%) 1 (2%) 1 (2%) |
Race | White Other | 348 (99%) 5 (1%) | 347 (99%) 2 (1%) | 70 (100%) 0 (0%) | 69 (100%) 0 (0%) | 50 (100%) 0 (0%) | 50 (100%) 0 (0%) |
Clinical Characteristics | |||||||
Total number of Lesions | Mean STD Range | 14.4 10.8 5.0 – 82.0 | 14.8 10.6 5.0 – 76.0 | 16.2 15.1 5.0 – 90.0 | 14.7 9.7 5.0 – 49.0 | 19.2 15.0 5.0 – 83.0 | 23.2 18.5 6.0 – 80.0 |
Baseline Severity Mild (5-10 lesions) Moderate (11-25 lesions) Severe (>25 lesions) | 171 (48%) 138 (39%) 44 (12%) | 154 (44%) 162 (46%) 33 (9%) | 31 (44%) 29 (41%) 10 (14%) | 30 (43%) 31 (45%) 8 (12%) | 13 (26%) 27 (54%) 10 (20%) | 12 (24%) 26 (52%) 12 (24%) | |
STD = standard deviation.
Source: Table 14.1.1.1: Analysis of Subject Demographic Characteristics (Intent-to-Treat Participants) and Table 14.1.4.1: Analysis of Subject Baseline Characteristics (Intent-to-Treat Participants) from Final Clinical Study Report (CSR) for Protocol HD-FUP3B-04815 and Final Clinical Study Report (CSR) for Protocol HD-FUP3S-04916.
Patient Disposition
Characteristics | Study 48 | Study 49 | ||||
|---|---|---|---|---|---|---|
Fluorouracil 4% cream | Fluorouracil 5% cream | Fluorouracil 4% Cream Vehicle | Fluorouracil 5% Cream Vehicle | Fluorouracil 4% Cream | Fluorouracil 4% Cream Vehicle | |
Randomized, N | 353 | 349 | 70 | 69 | 50 | 50 |
Participants Who Completed the Treatment Phase | ||||||
Participants, N (%) | 306 (87%) | 270 (77%) | 68 (97%) | 63 (91%) | 35 (70%) | 48 (96%) |
Discontinued Treatment, N (%) | 47 (13%) | 79 (23%) | 2 (3%) | 6 (9%) | 15 (30%) | 2 (4%) |
Reasons for Discontinuation from Treatment Phase, n (%) | ||||||
Adverse Event | 35 (10%) | 49 (14%) | 2 (3%) | 0 (0%) | 11 (22%) | 2 (4%) |
Subject withdraw | 10 (3%) | 18 (5%) | 0 (0%) | 5 (7%) | 1 (2%) | 0 (0%) |
Other reasons (a) | 2 (1%) | 12 (3%) | 0 (0%) | 1 (1%) | 4 (8%) | 0 (0%) |
(a) Other reasons include non-compliance, lost to follow-up, and other.
Source: Table 10.1.1: Summary of Subject Enrollment and Evaluability and Table 10.1.2: Summary of Subject Completion/Discontinuation from Final Clinical Study Report (CSR) for Protocol HD-FUP3B-04815 and Final Clinical Study Report (CSR) for Protocol HD-FUP3S-04916
Exposure to Study Treatments
Study Treatments
Table 8: Extent of Exposure to Study
Characteristics | Study 48 | Study 49 | ||||
|---|---|---|---|---|---|---|
Fluorouracil 4% Cream | Fluorouracil 5% Cream | Fluorouracil 4% Cream Vehicle | Fluorouracil 5% Cream Vehicle | Fluorouracil 4% Cream | Fluorouracil 4% Cream Vehicle | |
Safety Participants (a) | 348 | 342 | 70 | 65 | 49 | 50 |
Subject with Exposure Data | 346 | 337 | 70 | 65 | 48 | 50 |
Number of Dosing Days | ||||||
Mean (STD) | 26.5 (4.7) | 25.8 (5.7) | 28.1 (2.5) | 28.0 (4.1) | 24.9 (7.4) | 28.0 (4.0) |
Range | 2.0 – 35.0 | 1.0 – 41.0 | 11.0 – 33.0 | 6.0 – 33.0 | 7.0-44.0 | 6.0-36.0 |
Number of Applications | ||||||
Mean (STD) | 26.3 (4.7) | 50.8 (11.6) | 28.0 (2.5) | 55.8 (8.1) | 24.7 (7.4) | 28.0 (4.0) |
Range | 2.0-35.0 | 2.0-74.0 | 11.0-33.0 | 12.0-66.0 | 7.0-44.0 | 6.0-36.0 |
Compliant (b) | ||||||
Yes | 333 (96%) | 317 (94%) | 68 (100%) | 65 (100%) | 45 (94%) | 50 (100% |
No | 13 (4%) | 20 (6%) | 0 (0%) | 0 (0%) | 3 (6%) | 0 (0%) |
(a) Number of participants where exposure information was available
(b) A subject was considered compliant with the dosing regimen if the subject applied at least 80% but no more than 120% of expected applications.
(c) Number of participants where exposure information was not available. This figure bridges between the N in the header for each arm and the safety population count
Source: Table 12.1: Extent of Exposure - Applications of Study Medication and Dosing Compliance (Safety Subjects) from Final Clinical Study Report (CSR) for Protocol HD-FUP3B-04815 and Final Clinical Study Report (CSR) for Protocol HD-FUP3S-04916
Concomitant Medications and Co-Interventions
Study 48 (HD-FUP3B-048): Medication and non-medication therapies not restricted by the protocol could be used during the study for the treatment or prevention of disease or to maintain good health, including vitamins and mineral supplements. Non-prohibited chronic therapies being used at Baseline could also be continued. A relatively small number of participants were disqualified from the safety and/or Per-Protocol populations for the use of a prohibited concomitant medication: 2 participants in the fluorouracil 4% cream group, 1 subject in the fluorouracil 5% cream group, 2 participants in the fluorouracil 4% cream vehicle group, and 1 subject in the comparator vehicle group.
Study 49 (HD-FUP3S-049): Participants who used corticosteroids during the study were granted a waiver and although usage was considered a deviation to the protocol, it was not considered exclusionary from the Per-Protocol population since usage did not affect the condition or clinical evaluations. There were no participants disqualified from the Safety and/or Per-Protocol populations for the use of a prohibited concomitant medication.
Efficacy
Fluorouracil 4% cream (dosed once daily) did not meet the noninferiority criterion for complete clearance of actinic keratosis lesions compared with fluorouracil 5% cream (dosed twice daily). However, fluorouracil 4% cream demonstrated superiority compared to its vehicle in both Studies 48 and 49.
At 4-weeks off-treatment, 54.4% of participants in the fluorouracil 4% cream group achieved 100% lesion clearance versus 57.9% with fluorouracil 5% cream and only 4.3% with the fluorouracil 4% cream vehicle. The difference between the active treatments was minimal (−3.5%; lower confidence limit = −11.11%), narrowly missing the pre-specified non-inferiority margin by only 1.1%.
A post-hoc analysis controlling for disease severity (≤ 25 baseline lesions) demonstrated clear non-inferiority of fluorouracil 4% cream to fluorouracil 5% cream, with nearly identical clearance rates (57.6% vs 58.2%) and a lower confidence limit of −8.68%. Importantly, fluorouracil 4% cream maintained highly significant superiority over vehicle (p < 0.001).
The efficacy of fluorouracil 4% cream (dosed once daily) in achieving 75% clearance of actinic keratosis (AK) lesions was non-inferior compared to fluorouracil 5% cream (dosed twice daily) and markedly superior to its vehicle.
At 4-weeks off-treatment, 80.5% of participants in the fluorouracil 4% cream group achieved 75% lesion clearance versus 80.2% with fluorouracil 5% cream and only 7.1% with the fluorouracil 4% cream vehicle. The difference between the active treatments was 0.2% with a lower confidence limit = −5.94%, meeting the pre-specified non-inferiority margin.
The efficacy of fluorouracil 4% cream (dosed once daily) in reducing the Baseline lesion counts was non-inferior compared to compared to fluorouracil 5% cream (dosed twice daily) and markedly superior to its vehicle.
Lesion counts in the fluorouracil 4% cream group decreased by 80.1% compared to 79.0% in the fluorouracil 5% cream group. Since normality was not achieved (p < 0.001), a non-parametric analysis was conducted. Both fluorouracil 4% cream and fluorouracil 5% cream showed a median 100% lesion reduction, with a lower confidence limit of −0.01%, confirming non-inferiority. A parametric analysis produced consistent results (Lower Confidence Limit = −5.0%).
Table 9: Efficacy Outcomes – Fluorouracil 4% Cream vs. Fluorouracil 5% Cream
Variable | Study 48 | |
|---|---|---|
Fluorouracil 4% Cream (Applied Once Daily) | Fluorouracil 5% Cream (Applied Twice Daily) | |
Proportion of Participants with 100% Clearance at 4-Weeks Off-Treatment | ||
Primary Efficacy - Non-inferiority (Intent-to-Treat Participants) | ||
Number of Participants | 353 | 349 |
Participants with 100% Clearance | ||
Success | 192 (54.4%) | 202 (57.9%) |
Failure | 161 (45.6%) | 147 (42.1%) |
Difference in Success Rates | -3.5 | |
Lower Limit 97.5% CI (a) | -11.11 | |
Non-Inferior | No | |
Proportion of Participants with 100% Clearance at 4-Weeks Off-Treatment | ||
Primary Efficacy - Non-inferiority (Intent-to-Treat Participants - Excluding Subject with Baseline Total Lesions >25) | ||
Number of Participants | 309 | 316 |
Participants with 100% Clearance | ||
Success | 178 (57.6%) | 184 (58.2%) |
Failure | 131 (42.4%) | 132 (41.8%) |
Difference in Success Rates | -0.6 | |
Lower Limit 97.5% CI (a) | -8.68 | |
Non-Inferior | Yes | |
Proportion of Participants with 75% Clearance at 4-Weeks Off-Treatment | ||
Key Secondary Efficacy - Non-inferiority (Intent-to-Treat Participants) | ||
Number of Participants | 353 | 349 |
Participants with 75% Clearance | ||
Success | 284 (80.5%) | 280 (80.2%) |
Failure | 69 (19.5%) | 69 (19.8%) |
Difference in Success Rates | 0.2 | |
Lower Limit 97.5% CI (a) | -5.94 | |
Non-Inferior | Yes | |
Percent Change from Baseline in Total Lesion Count at 4-Weeks Off-Treatment | ||
Secondary Efficacy - Non-inferiority (parametric) (Intent-to-Treat Participants) | ||
Percent Change from Baseline of Total Lesion Count | ||
Least Square Mean (b) | 80.1 | 79.0 |
Least Square Standard Deviation (b) | 42.6 | 42.5 |
Normality P value (c) | <0.001 | |
Difference in Percent Change | 1.1 | |
97.5% Lower Confidence Limit | -5.0 | |
Percent Change from Baseline in Total Lesion Count at 4-Weeks Off-Treatment | ||
Secondary Efficacy - Non-inferiority (non-parametric) (Intent-to-Treat Participants) | ||
Percent Change from Baseline of Total Lesion Count | ||
Median | 100.0 | 100.0 |
97.5% Lower Confidence Limit | -0.01 | |
(a) Confidence interval for the difference in treatment success rates was computed using Wald’s confidence interval with Yate’s continuity correction. Non-inferiority was established if the lower limit of the one-sided 97.5% confidence interval was greater than 10%.
(b) Least squares means and standard deviations from an ANOVA with factors of treatment and analysis center.
(c) Normality P value from a Wilk-Shapiro test applied to the residuals resulting from the ANOVA. A p value < 0.01 validates use of a non-parametric analysis. Difference in percent change computed as fluorouracil 4% cream minus fluorouracil 5% cream. Non-inferiority was established if the lower limit of the one-sided 97.5% confidence interval was greater than 10%.
Source: Table 11.4.1.1: Analysis of the Primary Endpoint - Proportion of Subjects with 100% Clearance at 4-Weeks Off-Treatment (Intent-to-Treat Subjects), Table 11.4.1.1a: Analysis of the Primary Endpoint - Proportion of Subjects with 100% Clearance at 4-Weeks Off-Treatment (Intent-to-Treat Subjects - Excluding Subject with Baseline Total Lesions >25), Table 11.4.1.2: Analysis of the Secondary Endpoint - Proportion of Subjects with 75% Clearance at 4-Weeks Off-Treatment (Intent-to-Treat Subjects), Table 11.4.1.3: Analysis of the Secondary Endpoint – Percent Change from Baseline in Total Lesion Count at 4-Weeks Off-Treatment (Intent-to-Treat Subjects) from Final Clinical Study Report (CSR) for Protocol HD-FUP3B-04815
Table 10: Table for Efficacy Outcomes – Fluorouracil 4% Cream vs. Vehicle
Variable | Study 48 | Study 49 | ||
|---|---|---|---|---|
Fluorouracil 4% Cream (Once Daily) | Fluorouracil 4% Cream Vehicle (Once Daily) | Fluorouracil 4% Cream (Once Daily) | Fluorouracil 4% Cream Vehicle (Once Daily) | |
Proportion of Participants with 100% Clearance at 4-Weeks Off-Treatment | ||||
Primary Efficacy - Non-inferiority (Intent-to-Treat Participants) | ||||
Number of Participants | 353 | 70 | 50 | 50 |
Participants with 100% Clearance | ||||
Success | 192 (54.4%) | 3 (4.3%) | 12 (24%) | 2 (4%) |
Failure | 161 (45.6%) | 67 (95.7%) | 38 (76%) | 48 (96%) |
P value (a) | <0.001 | 0.004 | ||
Proportion of Participants with 100% Clearance at 4-Weeks Off-Treatment | ||||
Primary Efficacy - Non-inferiority (Intent-to-Treat Participants - Excluding Subject with Baseline Total Lesions >25) | ||||
Number of Participants | 309 | 60 | a/n/p | a/n/p |
Participants with 100% Clearance | ||||
Success | 178 (57.6%) | 3 (5.0%) | a/n/p | a/n/p |
Failure | 131 (42.4%) | 57 (95.0%) | a/n/p | a/n/p |
P value (a) | <0.001 | a/n/p | ||
Proportion of Participants with 75% Clearance at 4-Weeks Off-Treatment | ||||
Key Secondary Efficacy - Non-inferiority (Intent-to-Treat Participants) | ||||
Number of Participants | 353 | 70 | 50 | 50 |
Participants with 75% Clearance | ||||
Success | 284 (80.5%) | 5(7.1%) | 37 (74%) | 5 (10%) |
Failure | 69 (19.5%) | 65 (92.9%) | 13 (26%) | 45 (90%) |
P value (a) | <0.001 | n/a | ||
Percent Change from Baseline in Total Lesion Count at 4-Weeks Off-Treatment | ||||
Secondary Efficacy - Superiority (Intent-to-Treat Participants) | ||||
Percent Change from Baseline of Total Lesion Count | ||||
Least Square Mean (b) | 80.3 | 16.9 | 54.0 | 1.4 |
Median | 100.0 | 11.1 | 86.2 | 12.1 |
Least Square Standard Deviation (b) | 37.9 | 36.9 | 79.3 | 79.3 |
(Min, Max) | (−200.0, 100.0) | (−55.6, 100.0) | (−583.3, 100.0) | (−160.0, 100.0) |
Difference: Mean | 63.5 | 52.7 | ||
Difference: Median | 88.9 | n/a | ||
Normality P value (c) | <0.001 | <0.001 | ||
Treatment P value ANOVA | <0.001 | 0.001 | ||
Treatment P value Ranked ANOVA | <0.001 | <0.001 | ||
a/n/p = analysis not performed.
(a) P value from a Cochran-Mantel-Haenszel test, stratified by analysis center.
(b) Least squares means and standard deviations from an ANOVA with factors of treatment and analysis center.
(c) P value from Wilk-Shapiro test applied to the residuals resulting from the ANOVA. A p value < 0.01 validates use of a ranked ANOVA.
Source: Table 11.4.1.1: Analysis of the Primary Endpoint - Proportion of Subjects with 100% Clearance at 4-Weeks Off-Treatment (Intent-to-Treat Subjects), Table 11.4.1.1a: Analysis of the Primary Endpoint - Proportion of Subjects with 100% Clearance at 4-Weeks Off-Treatment (Intent-to-Treat Subjects - Excluding Subject with Baseline Total Lesions >25), Table 11.4.1.2: Analysis of the Secondary Endpoint - Proportion of Subjects with 75% Clearance at 4-Weeks Off-Treatment (Intent-to-Treat Subjects), Table 11.4.1.3: Analysis of the Secondary Endpoint – Percent Change from Baseline in Total Lesion Count at 4-Weeks Off-Treatment (Intent-to-Treat Subjects) from Final Clinical Study Report (CSR) for Protocol HD-FUP3B-04815
Harms
The safety of fluorouracil 4% cream for the treatment of actinic keratosis (AK) lesions was evaluated and confirmed based on its tolerability, reported AEs, treatment-emergent AEs, dosing compliance, and treatment discontinuation due to AEs.
Tolerability was assessed at each visit based on the severity grading of 7 expected AEs: erythema, scaling/dryness, edema, crusting, erosions, stinging/burning, and pruritus. The fluorouracil 4% cream group had lower (less severe) mean scores for all AEs demonstrating its achieved intent of improved tolerability for topical fluorouracil. Furthermore, participants in fluorouracil 4% cream group had a 22-40% less risk of severe skin reactions compared to participants on fluorouracil 5% cream
118 participants (34%) in the fluorouracil 4% cream group reported 203 adverse events; in the fluorouracil 5% cream treatment group, slightly more subjects, 122 (36%), reported more events, 211. There were 44 serious adverse events (SAEs): 22 reported in the fluorouracil 4% cream treatment group; 7 in the fluorouracil 5% cream group; 7 in the fluorouracil 4% cream vehicle group; and 8 in the comparator vehicle group. None of the SAEs were considered treatment-related. All of the most commonly reported, treatment-related adverse events that occurred in both the fluorouracil 4% cream and fluorouracil 5% cream groups, the incidence rates for these events were consistently greater within the fluorouracil 5% cream.
Application compliance (number of applications compared to expected dosing) was greater for participants in the fluorouracil 4% cream group (26.3/28 doses, 93.9%) compared to participants in the fluorouracil 5% cream group (50.8/56 doses, 90.7%). The rate of participant discontinuation due to adverse events was greater in the fluorouracil 5% cream group (51/342 subjects, 14.9%) compared to the fluorouracil 4% cream group (35/348 subjects, 10.1%).
Safety Evaluation Plan
For both pivotal studies, safety analyses were performed on the safety population, defined as all randomized participants who applied at least one dose of study medication and had at least one post-baseline assessment.
Tolerability parameters (erythema, scaling/dryness, edema, crusting, erosions, stinging/burning, and pruritus) were summarized descriptively by treatment group and visit. Adverse events (AEs) were coded using MedDRA, summarized by system organ class and preferred term, and analyzed for severity, seriousness, and relationship to study medication. For severity and relationship summaries, each participant was counted once per category based on the most severe or most related event.
Between-group comparisons of participants reporting ≥1 AE were performed using Fisher’s exact test (alpha = 0.05) for the fluorouracil 4% cream, fluorouracil 5% cream, and fluorouracil 4% cream vehicle groups; the comparator vehicle group was summarized descriptively. SAEs, discontinuations, and laboratory shifts from baseline were tabulated separately, with clinically significant or out-of-range results listed for all treatment groups.
Tolerability Assessment
Tolerability for each participant was assessed at each study visit based on severity grading of 7 expected AEs: erythema, scaling/dryness, edema, crusting, erosions, stinging/burning, and pruritus, where are expected AEs with the topical application of fluorouracil. As expected with topical fluorouracil treatment, severity for reach AE increased through the first 2 weeks, peaking at week 2 to 4, and then decreasing back to baseline by the end of 4-weeks off-treatment.
Overall, participants on fluorouracil 4% cream had lower severity of each AE at most timepoints compared to fluorouracil 5% cream.
Study 48 (HD-FUP3B-048):
The table below shows the mean severity score for each treatment group at each study visit. The red line (fluorouracil 4% cream) is consistently below the blue line (fluorouracil 5% cream) evidencing the lower severity of AEs experienced by participants on fluorouracil 4% cream compared to fluorouracil 5% cream. The difference is especially pronounced for Stinging/Burning, Crusting, and Pruritus.
Figure 1: Tolerability Assessment Scores Overtime
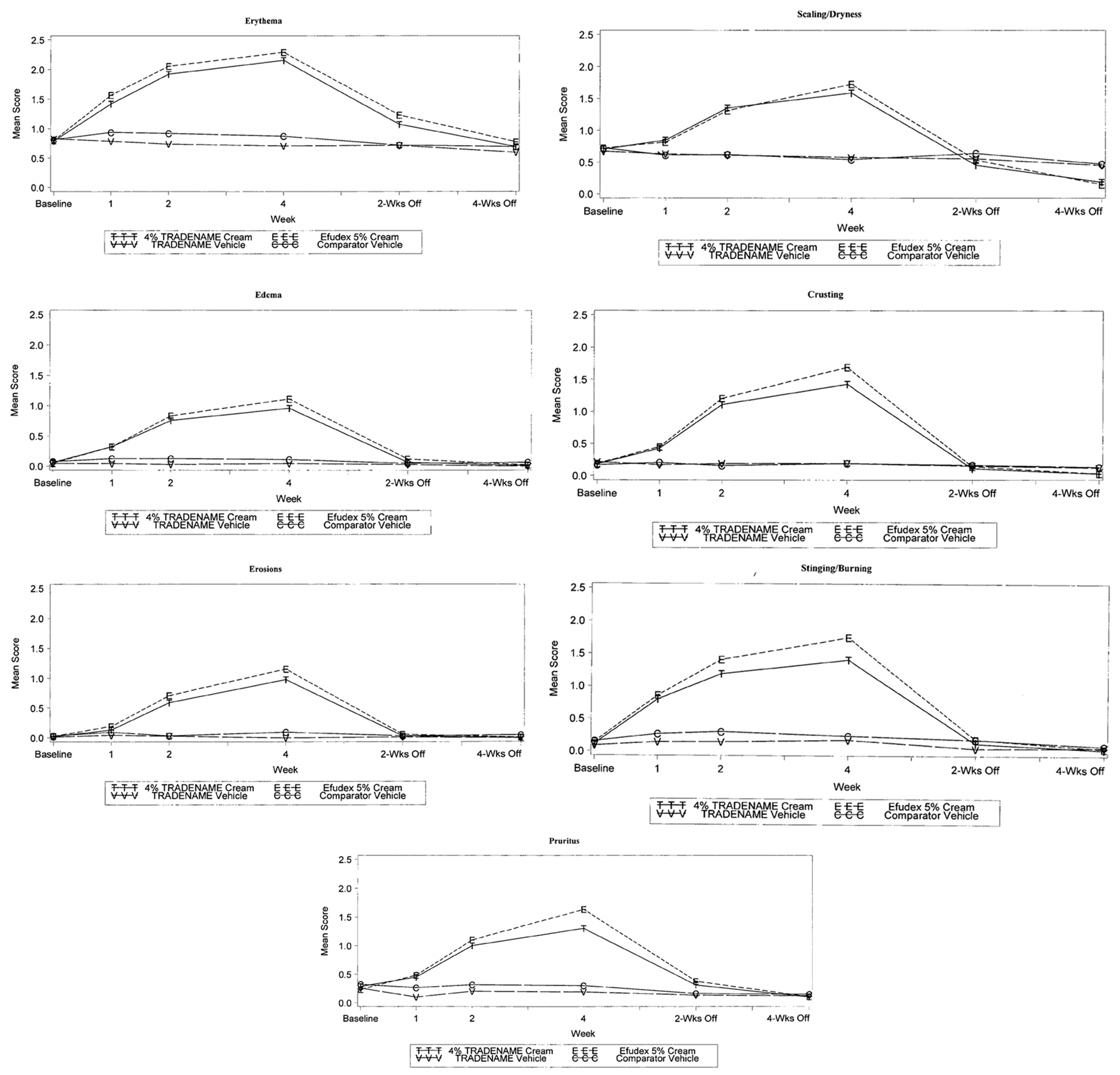
Source: 14.3.1.1: Summary of Local Adverse Events at Each Evaluation from Final Clinical Study Report (CSR) for Protocol HD-FUP3B-04815
Table 11: Percentage of Participants with Severe AE at Week 4
Tolerability Assessment | Fluorouracil 4% Cream (once daily) | Fluorouracil 5% Cream (twice daily) | % Relative Reduction in Percentage of Participants who Experienced Severe Adverse Event | ||
|---|---|---|---|---|---|
Participants(a) | %(a) | Participants(b) | %(b) | ||
Pruritus | 43/328 | (13.1%) | 66/300 | (22.0%) | -40.4% |
Stinging / Burning | 60/328 | (18.3%) | 81/300 | (27.0%) | -32.2% |
Crusting | 56/328 | (17.1%) | 74/300 | (24.7%) | -30.8% |
Edema | 18/328 | (5.5%) | 24/300 | (8.0%) | -31.4% |
Scaling / Dryness | 57/328 | (17.4%) | 75/300 | (25.0%) | -30.5% |
Erosions | 27/328 | (8.2%) | 35/300 | (11.7%) | -29.4% |
Erythema | 120/328 | (36.6%) | 140/300 | (46.7%) | -21.6% |
(a) Participant count based on safety population of 348 participants on fluorouracil 4% cream, excluding 20 participants who did not have reported grading at Week 4
(b) (a) Participant count based on safety population of 342 participants on fluorouracil 5% cream, excluding 42 participants who did not have reported grading at Week 4
Source: 14.3.1.1: Summary of Local Adverse Events at Each Evaluation from Final Clinical Study Report (CSR) for Protocol HD-FUP3B-04815
Reported and Treatment-Emergent Adverse Events
Please see the Supplemental Materials document (Detailed Harms Results for Included Studies) for detailed tables on harms by clinical study.
In both pivotal studies, fluorouracil 4% cream was well tolerated with most AEs being mild to moderate and resolving without intervention.
In Study 48, 34% of participants receiving fluorouracil 4% cream and 36% receiving fluorouracil 5% cream reported AEs. None of the 44 SAEs were treatment-related, and no deaths occurred. The most common treatment-related events (≥1%) with fluorouracil 4% cream were eye irritation and application site reactions (erythema, irritation, edema, pain, pruritus, reaction) while fluorouracil 5% cream showed similar events with higher incidence rates.
In Study 49, 43% of participants receiving fluorouracil 4% cream and 12% receiving the vehicle reported AEs (p=0.001). One death (myocardial infarction) occurred in fluorouracil 4% cream group, unrelated to study drug. Common events (≥5%) with fluorouracil 4% cream included application site pain (14.3%), reaction (8.2%), and irritation (8.2%).
Withdrawals Due to Adverse Events
Treatment discontinuations were primarily due to expected local skin reactions, such as irritation, erythema, and pain.
In Study 48, discontinuations occurred in 10.1% of fluorouracil 4% cream participants, 14.9% of fluorouracil 5% cream participants, and <3% of vehicle participants. The majority were associated with multiple concurrent local reactions typical of topical fluorouracil therapy.
In Study 49, discontinuations occurred in 11 participants (fluorouracil 4% cream) and 2 participants (vehicle) discontinued, with all fluorouracil 4% cream-related withdrawals attributed to local reactions and none to systemic effects. Discontinuations in vehicle groups were isolated and unrelated to treatment.
CDA-AMC Critical Appraisal of the Clinical Evidence
This section was prepared by CDA-AMC based on the sponsor’s summary of the systematic review evidence and other material submitted by the sponsor.
Additional Results From the Included Studies
Table 12: Efficacy Outcomes — Fluorouracil 4% Cream vs. Fluorouracil 5% Cream (Per-Protocol Population)
Variable | Study 48 | |
|---|---|---|
Fluorouracil 4% cream (applied once daily) | Fluorouracil 5% cream (applied twice daily) | |
Proportion of participants with 100% clearance at 4 weeks off treatment | ||
Noninferiority (per-protocol participants) | ||
Number of participants | 326 | 307 |
Participants with 100% clearance, n (%) | ||
Yes | 182 (55.8%) | 186 (60.6%) |
No | 144 (44.2%) | 121 (39.4%) |
Difference in success rates, % | −4.8 | |
Lower limit 97.5% CIa | −12.75 | |
Noninferior | No | |
Proportion of participants with 75% clearance at 4 weeks off treatment | ||
Key secondary efficacy — noninferiority (per-protocol participants) | ||
Number of participants | 326 | 307 |
Participants with 75% clearance, n (%) | ||
Yes | 269 (82.5%) | 261 (85.0%) |
No | 57 (17.5%) | 46 (15.0%) |
Difference in success rates, % | −2.5 | |
Lower limit 97.5% CIa | −8.56 | |
Noninferior | Yes | |
Percent change from baseline in total lesion count at 4 weeks off treatment | ||
Noninferiority (parametric) (per-protocol participants) | ||
Percent change from baseline of total lesion count | 326 | 307 |
Least square meanb | 82.8 | 86.5 |
Least square standard deviationb | 27.4 | 27.2 |
Normality P valuec | < 0.001 | |
Difference in percent change | −3.7 | |
97.5% lower confidence limit | −7.9 | |
Percent change from baseline in total lesion count at 4 weeks off treatment | ||
Noninferiority (nonparametric) (per-protocol participants) | ||
Percent change from baseline of total lesion count | ||
Median | 100.0 | 100.0 |
97.5% lower confidence limit | −0.01 | |
ANOVA = analysis of variance; CI = confidence interval; vs. = versus.
aThe CI for the difference in treatment success rates was computed using a Wald CI with Yates continuity correction. Noninferiority was established if the lower limit of the 1-sided 97.5% CI was greater than 10%.
bLeast squares means and standard deviations from an ANOVA with factors of treatment and analysis centre.
cNormality P value from a Shapiro–Wilk test applied to the residuals resulting from the ANOVA. A P value < 0.01 validates the use of a nonparametric analysis. Difference in percent change computed as fluorouracil 4% cream minus fluorouracil 5% cream. Noninferiority was established if the lower limit of the 1-sided 97.5% CI was greater than 10%.
Source: Table 14.2.3: Primary Analysis of the Proportion of Subjects with 100% Clearance at 4-Weeks Off-Treatment, Table 14.2.4.1: Secondary Analysis of the Proportion of Subjects with 75% Clearance at 4-Weeks Off-Treatment, and Table 14.2.4.2: Secondary Analysis of the Percent Change from Baseline in Total Lesion Counts at 4-Weeks Off-Treatment from Final Clinical Study Report (CSR) for Protocol HD-FUP3B-04815
Table 13: Efficacy Outcomes — Fluorouracil 4% Cream vs. Vehicle (Per-Protocol Population)
Variable | Study 48 | Study 49 | ||
|---|---|---|---|---|
Fluorouracil 4% cream (once daily) | Fluorouracil 4% cream vehicle (once daily) | Fluorouracil 4% cream (once daily) | Fluorouracil 4% cream vehicle (once daily) | |
Proportion of participants with 100% clearance at 4 weeks off treatment | ||||
Noninferiority (per-protocol participants) | ||||
Number of participants | 326 | 63 | 43 | 44 |
Participants with 100% clearance, n (%) | ||||
Yes | 182 (55.8%) | 3 (4.8%) | 12 (28%) | 2 (5%) |
No | 144 (44.2%) | 60 (95.2%) | 31 (72%) | 42 (95%) |
P valuea | < 0.001 | 0.004 | ||
Proportion of participants with 75% clearance at 4 weeks off treatment | ||||
Noninferiority (per-protocol participants) | ||||
Number of participants | 326 | 63 | 43 | 44 |
Participants with 75% clearance, n (%) | ||||
Yes | 269 (82.5%) | 5 (7.9%) | 36 (84%) | 5 (11%) |
No | 57 (17.5%) | 58 (92.1%) | 7 (16%) | 39 (89%) |
P valuea | < 0.001 | < 0.001 | ||
Percent change from baseline in total lesion count at 4 weeks off treatment | ||||
Superiority (per-protocol participants) | ||||
Percent change from baseline of total lesion count | ||||
Least squares meanb | 80.3 | 16.9 | 69.2 | 3.3 |
Median | 100.0 | 11.1 | 87.5 | 52.8 |
Least square standard deviationb | 37.9 | 36.9 | 52.5 | 12.1 |
Min, max | −200.0, 100.0 | −55.6, 100.0 | −176.5, 100.0 | −137.5, 100.0 |
Difference: mean | 63.5 | 67.7 | ||
Difference: median | 88.9 | NR | ||
Normality P valuec | < 0.001 | < 0.001 | ||
Treatment P value ANOVA | < 0.001 | < 0.001 | ||
Treatment P value ranked ANOVA | < 0.001 | < 0.001 | ||
ANOVA = analysis of variance; NR = not reported; vs. = versus.
aP value from a Cochran-Mantel-Haenszel test, stratified by analysis centre.
bLeast squares means and standard deviations from an ANOVA with factors of treatment and analysis centre.
cP value from a Shapiro–Wilk test applied to the residuals resulting from the ANOVA. A p value < 0.01 validates use of a ranked ANOVA.
Source: Table 11.4.1.1: Analysis of the Primary End point - Proportion of Subjects with 100% Clearance at 4-Weeks Off-Treatment (Intent-to-Treat Subjects), Table 11.4.1.1a: Analysis of the Primary End point - Proportion of Subjects with 100% Clearance at 4-Weeks Off-Treatment (Intent-to-Treat Subjects - Excluding Subject with Baseline Total Lesions > 25), Table 11.4.1.2: Analysis of the Secondary End point - Proportion of Subjects with 75% Clearance at 4-Weeks Off-Treatment (Intent-to-Treat Subjects), Table 11.4.1.3: Analysis of the Secondary End point – Percent Change from Baseline in Total Lesion Count at 4-Weeks Off-Treatment (Intent-to-Treat Subjects) from Final Clinical Study Report (CSR) for Protocol HD-FUP3B-048.15 Final Clinical Study Report (CSR) for Protocol HD-FUP3B-049.16
Internal Validity
Overall, both Study 48 and Study 49 were well designed and had similar methodologies. In Study 48, investigators were blinded, and study medication dispensing, collection, and weighing were performed by study staff who were not involved in clinical evaluations. In addition, the inclusion of vehicle creams further supported blinding. Patients were not blinded because of differences in application frequency between the investigational products. However, no patient-reported outcomes were assessed. In contrast, Study 49 was a double-blind study in which both patients and evaluators (investigators) were blinded. According to the clinical expert consulted for this review, the identification of AK lesions may involve some degree of subjectivity and depends on investigator diligence and interpretation. Nevertheless, because investigators responsible for clinical assessments were blinded to treatment allocation, this subjectivity is unlikely to have introduced meaningful bias but may have resulted in interobserver variability.
In Study 48, patients were randomized at the baseline visit according to a schedule stratified by investigational site, using a 5:5:1:1 allocation ratio and a fixed block size of 12. In Study 49, patients were randomized at a 1:1 ratio, stratified by investigational site, with a fixed block size of 4. The clinical expert consulted for this review indicated that, given that both studies were conducted entirely within a single country (the US), stratification by investigational site was appropriate, and no additional stratification factors were considered necessary for a phase III trial in patients with AK lesions of the face, scalp, or ears. However, the methods used to ensure allocation concealment were not clearly described. Because fixed block sizes were employed, there is a potential risk that the allocation sequence could have been predictable, which may have compromised concealment. As a result, there is a possibility of selection bias; however, in both Study 48 and 49, the baseline characteristics of patients were generally balanced between treatment groups. In Study 49, 1 exception was the potential differences in the number of males between groups in the ITT analysis set. Ninety-two percent were males in the fluorouracil 4% cream vehicle group compared to 78% in the fluorouracil 4% cream group. Additionally, in Study 49, the fluorouracil 4% cream vehicle group had a higher average lesion count and lower Fitzpatrick skin types than the fluorouracil 4% cream group. However, the clinical expert consulted for this review noted that this difference would likely not have a meaningful impact on the interpretation of the treatment effect.
For both studies, baseline characteristics and efficacy outcomes were summarized descriptively, with between-group comparisons adjusted for treatment group and analysis centre as prespecified factors. Superiority testing was conducted using stratified methods where applicable, while noninferiority end points in Study 48 were reported descriptively with reliance on the lower 97.5% confidence interval (CI) for assessment of noninferiority. No adjustments for multiplicity were applied. Given the descriptive intent of most analyses, the reliance on the lower 97.5% CI in assessment of noninferiority, and the prespecified nature of superiority testing, the absence of multiplicity adjustment is not expected to materially increase the risk of type I error. A large proportion of patients discontinued treatment in both Study 48 and Study 49. In Study 48, 134 patients discontinued treatment during the treatment phase, most commonly due to AEs (n = 86), followed by patient withdrawal (n = 33). In addition, 43 patients discontinued the study overall, with the majority withdrawing by personal decision (n = 29). For treatment discontinuations, a higher number of discontinuations occurred in the fluorouracil 5% cream group (23%) compared with the fluorouracil 4% cream group (13%). Likewise, there was a greater number of study discontinuations in the fluorouracil 5% cream group than in the fluorouracil 4% cream group. Differential discontinuation between treatment groups may bias noninferiority analyses toward a false conclusion of noninferiority by reducing observed differences between groups. In Study 49, 17 patients discontinued treatment during the treatment phase, the majority of whom were in the fluorouracil 4% cream group (n = 15). Overall, 8 patients discontinued the study, with equal numbers of discontinuations in each treatment group.
Patients who were dispensed study medication and withdrew prematurely or missed a visit had their LOCF to the 4-week off-treatment visit. In Study 48, lesion counts in both the fluorouracil 4% cream and fluorouracil 5% cream groups typically increased during the 4-week treatment period before declining in the posttreatment period. Consequently, patients who discontinued early in these groups often had lesion counts carried forward that were higher than baseline. In contrast, lesion counts in the fluorouracil 4% cream vehicle group remained relatively stable around baseline throughout the treatment and posttreatment periods. In both studies, sensitivity analyses of the primary outcome (proportion of patients achieving 100% clearance) were conducted to assess the impact of missing data by imputing missing values as either a “success” or “failure” of treatment. Results from these sensitivity analyses were consistent with those of the primary analysis. The results for the PP population were generally similar to those observed in the ITT population. However, the US FDA Statistical Review and Evaluation report for fluorouracil 4% cream noted that, in Study 49, there were notable differences between the ITT and PP analyses for the fluorouracil 4% cream group, with final lesion counts of 7.1 (ITT) versus 4.2 (PP) and percent change in lesions of 57% (ITT) versus 74% (PP).17 These differences were largely attributable to a single patient in Study 49 who died, with 123 lesions carried forward. Overall, these findings suggest that the LOCF approach was fairly conservative for handling missing data.
A noninferiority margin of −10% was selected for all outcomes, though no formal rationale for choosing this margin was provided. However, the sponsor stated that at the time the study was conducted, it was common practice to select the noninferiority margin based on what was considered a “clinically acceptable” difference, rather than establishing a clear, quantitative link to historical placebo-controlled effect sizes of the active comparator. The sponsor further indicated that a −10% margin was generally regarded as typical and had been used in other dermatology studies. The clinical expert consulted for this review suggested that the chosen noninferiority margin could be considered clinically meaningful for the proportion of participants with 100% and 75% clearance. However, the clinical expert noted that a meaningful between-group difference for the percent change from baseline in the total lesion count at 4 weeks off treatment would be 15% to 20%. Demonstration of superiority of fluorouracil 4% cream over the fluorouracil 4% cream vehicle group supports the assay sensitivity of both studies and provides confidence that they were capable of detecting a treatment effect.
For both studies, the sponsor pooled investigator sites based on sample size. Specifically, sites with the smallest and largest enrolment numbers were combined until the desired sample size within each stratum for analysis by site was achieved. Pooling was undertaken to ensure sample sizes were adequate to facilitate analyses stratified by site. These combined groups were defined as “analysis centres” for the purposes of statistical analyses, including ANOVA, Breslow-Day, and CMH testing. Following this pooling, the sponsor conducted the Breslow-Day test to assess homogeneity of the odds ratio and to identify any extreme analysis centres that could potentially influence the interpretation of statistical and clinical conclusions. No investigator sites were combined for Study 49 because enrolment distributions were sufficient to support stratified analyses without pooling. No extreme analysis centres were identified in either study. Overall, these findings suggest that the pooling of investigator sites to form analysis centres is unlikely to have introduced bias into the interpretation of study outcomes.
External Validity
Most patients enrolled in Studies 48 and 49 were male and white, which may limit the generalizability of the findings to more diverse populations. However, according to the clinical expert consulted for this review, this demographic distribution is consistent with the population typically seen in clinical practice. The clinical expert also indicated that the eligibility criteria used in the studies are reflective of the criteria used to identify patients with AK who would be considered for treatment with fluorouracil 5% cream. Overall, the clinical expert noted that the study populations were reasonably representative of the target population in Canada with respect to baseline and demographic characteristics. Both studies were conducted at investigational sites in the US, which may limit the generalizability of findings to Canadian clinical practice. However, the clinical expert noted that they did not note any concerns regarding the generalizability of findings to the population of Canada.
The dosing regimen of fluorouracil 4% cream evaluated in the studies was consistent with the Canadian product monograph and aligned with current clinical practice. The clinical expert indicated that fluorouracil 4% cream would be considered a first-line option for field therapy and a first- or second-line option for the treatment of individual lesions.
Study 48 included fluorouracil 4% cream, fluorouracil 4% cream vehicle, fluorouracil 5% cream, and fluorouracil 5% cream vehicle as comparators. The inclusion of fluorouracil 5% cream was considered appropriate and clinically relevant for the Canadian context. The dosing regimen and treatment schedule for fluorouracil 5% cream were consistent with the Health Canada–approved use.
The outcomes assessed in both studies are considered appropriate. However, the clinical expert indicated that the most clinically meaningful end point for evaluating the efficacy of fluorouracil 4% cream in the treatment of AK is the proportion of patients achieving at least a 75% clearance of AK lesions. Complete (100%) clearance was considered a relatively subjective outcome, as AK lesions may be subtle, difficult to identify, or potentially missed. While assessment of 75% clearance is subject to similar limitations regarding lesion identification, an approximate 75% clearance is considered clinically meaningful, given that it may account for lesions that are difficult to detect. In addition, percent change from baseline in lesion counts may be difficult to interpret due to variability in baseline lesion identification, which depends on investigator experience.
Patients were followed for only 4 weeks after completion of treatment in Studies 48 and 49, which is considered short. The clinical expert noted that treatment response should be assessed based on the number of lesions and concerns with SCC (usually at 3 to 6 or 6 to 12 months).
Summary of Findings and Certainty of the Evidence
Due to the availability of direct evidence comparing fluorouracil 4% cream with a relevant comparator, we assessed the proportion of participants with 100% clearance at 4 weeks off treatment and the proportion of participants with 75% clearance at 4 weeks off treatment, in Study 48, using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach.18,19
We used the noninferiority margin of −10% in Study 48 as the threshold for a clinically important effect for the proportions of participants with 100% and 75% clearance at 4 weeks off treatment.
For the proportions of participants achieving 100% and 75% clearance at 4 weeks off treatment, the certainty of evidence was rated as moderate. The certainty of imprecision was downgraded by 1 level. There is no established minimal important difference, and the noninferiority margin of −10% was provided by the sponsor. However, justification for the selection of this margin was not provided. The clinical expert consulted for this review indicated that the margin could be considered clinically meaningful.
For the proportion of participants achieving 100% clearance at 4 weeks off treatment, the lower bound of the 97.5% CI for the between-group difference (−3.5%; 97.5% CI, −11.11) crossed the prespecified noninferiority margin of −10%. As a result, noninferiority was not demonstrated, and inferiority of fluorouracil 4% cream cannot be ruled out.
CDA-AMC Clinical Review Discussion and Conclusion
This section was prepared by CDA-AMC based on the preceding sections.
Discussion
Efficacy
In Study 48, noninferiority of fluorouracil 4% cream was not demonstrated for the primary end point of the proportion of patients achieving 100% clearance at 4 weeks off treatment in the ITT population, and inferiority of fluorouracil 4% cream relative to fluorouracil 5% cream cannot be ruled out. Results in the PP population were consistent with those observed in the ITT population. The certainty of evidence for this outcome was rated as moderate. Overall, based on this end point, fluorouracil 4% cream was unlikely to be comparable to fluorouracil 5% cream with respect to the proportion of patients achieving 100% clearance at 4 weeks off treatment. A post hoc analysis was also performed in which the upper limit of the number of lesions at baseline was limited to 25 lesions, which demonstrated noninferiority of fluorouracil 4% cream to fluorouracil 5% cream for the proportion of subjects with 100% clearance at 4 weeks in the ITT population. However, this analysis was not prespecified and was exploratory in nature.
In Study 48, noninferiority of fluorouracil 4% cream was demonstrated for the secondary end point of the proportion of patients achieving at least 75% clearance at 4 weeks off treatment in both the ITT and per-protocol populations. The certainty of evidence for this outcome was rated as moderate. Based on this end point, fluorouracil 4% cream was likely comparable to fluorouracil 5% cream with respect to the proportion of patients achieving 75% clearance at 4 weeks off treatment. Notably, both the sponsor and the clinical expert consulted for this review indicated that achieving at least 75% clearance is a more meaningful end point in clinical practice for evaluating the efficacy of fluorouracil 4% cream in the treatment of AK lesions. AK is a chronic condition with a fluctuating yet progressively persistent course, and although clearance of individual lesions is common, complete clearance of an entire field of cancerization may be less achievable. The clinical expert further noted that complete (100%) clearance can be difficult to assess, given that AK lesions may not always be visible and the determination of their presence or absence is subjective and dependent on evaluator experience.
Moreover, fluorouracil 4% cream demonstrated noninferiority for the secondary end point of percent change from baseline in total lesion counts at 4 weeks off treatment. However, the clinical expert consulted for this review noted that identification of AK lesions is inherently subjective, which may make it difficult to accurately determine lesion counts at baseline and at subsequent visits when assessing change from baseline. As a result, some degree of interevaluator variability cannot be excluded when interpreting this outcome.
Additionally, fluorouracil 4% cream demonstrated superiority over its vehicle for the primary and all secondary end points in both Study 48 and Study 49. Of note, the proportion of participants achieving complete clearance at 4 weeks off treatment with fluorouracil 4% cream compared with its vehicle was higher in Study 48 than in Study 49, despite the studies having similar designs and methodologies. The sponsor suggested that this difference may be attributable to differences in baseline characteristics, including a higher baseline lesion count in Study 49, fewer patients with mild AK (defined as 5 to 10 lesions), and a greater proportion of patients with Fitzpatrick skin type III compared with Study 48. The sponsor also noted that Study 49 had a smaller sample size and was conducted across a greater number of geographically dispersed sites, which may have introduced additional variability, particularly given potential differences in lesion counting between evaluators. However, the FDA Statistical Review and Evaluation report, which included a more detailed assessment of the observed differences in clearance rates, concluded that these factors alone could not fully explain the difference in clearance rates observed between both studies.17 Specifically, the FDA noted that the differences could not be attributed solely to a lower level of precision in Study 49 or to differences in baseline lesion counts. The FDA noted that the differing response rates between the 2 studies may be due some other unidentified difference in the study subjects or other unidentified differences in how the studies were conducted.17
The sponsor anticipates that in Canada, fluorouracil 4% cream will primarily displace fluorouracil 5% cream as the first-line topical treatment for AK. Other pharmacologic treatments, such as 5% imiquimod cream and 0.5% fluorouracil and 10% salicylic acid topical solution, may also be displaced. However, no evidence was provided comparing fluorouracil 4% cream with either 5% imiquimod cream or 0.5% fluorouracil and 10% salicylic acid topical solution. The clinical expert noted that 0.5% fluorouracil and 10% salicylic acid topical solution is generally reserved for hyperkeratotic AK in clinical practice. They further indicated that fluorouracil concentrations are often adjusted in clinical practice to 2.5% or 1%, depending on the site being treated. Overall, the clinical expert does not anticipate that the introduction of fluorouracil 4% cream will result in a major shift in treatment paradigms and considers it to likely serve as an alternative to fluorouracil 5% cream.
Harms
The product monograph for fluorouracil 4% cream includes warnings regarding application site reactions (erythema, scaling and/or dryness, edema, crusting, erosions, stinging and/or burning, and pruritus), hypersensitivity, corneal and conjunctival disorders, and photosensitivity.
Erythema, scaling and/or dryness, crusting, pruritus, stinging and/or burning, edema, and erosions were assessed at every visit on a 4-point scale (0, none; 1, mild; 2, moderate; 3, severe). Each of these assessments generally increased in mean severity throughout the treatment period in the 5-fluorouracil arms. During the posttreatment period, the mean severity returned to baseline levels. Patients in the vehicle groups remained, on average, at baseline levels throughout the study. The mean values for the fluorouracil 4% cream group were lower than those of the fluorouracil 5% cream group at most weeks.
In Study 48, a comparable number of patients in the fluorouracil 4% cream and fluorouracil 5% cream groups reported at least 1 AE. However, more patients in the fluorouracil 5% cream group (15%) discontinued treatment due to AEs compared to the fluorouracil 4% group (10%). Overall, most participants discontinued the study medication due to application site irritation. As a result, many patients in the 5-fluorouracil arms could not be assessed for lesion counts during treatment.
There was a higher number of SAEs reported in the fluorouracil 4% cream group compared with the fluorouracil 5% cream group. In both studies, more patients reported at least 1 AE and discontinued treatment due to AEs in the active treatment arms compared with their respective vehicle groups. However, the clinical expert indicated that there are no notable concerns in the safety profile of fluorouracil 4% cream compared to fluorouracil 5% cream.
Conclusion
Evidence from a pivotal phase III trial, Study 48, did not demonstrate noninferiority of fluorouracil 4% cream for the primary end point of the proportion of patients achieving 100% clearance at 4 weeks off treatment. However, noninferiority was demonstrated for the secondary end points of the proportion of patients achieving at least 75% clearance and the percent change from baseline in total lesion counts at 4 weeks off treatment. In both Study 48 and Study 49, fluorouracil 4% cream demonstrated superiority over its vehicle for the primary and all secondary end points.
Due to the nature of AK, the clinical expert consulted by CDA-AMC for this review noted that achieving at least 75% clearance is a more meaningful end point in clinical practice for evaluating the efficacy of fluorouracil 4% cream in the treatment of AK lesions of the face, scalp, or ears, compared with complete (100%) clearance. On this basis, fluorouracil 4% cream is likely comparable to fluorouracil 5% cream. The clinical expert did not identify any notable safety concerns for fluorouracil 4% cream relative to the fluorouracil 5% cream.
CDA-AMC Pharmacoeconomic Evaluation
CDA-AMC prepared this section based on the sponsor’s summary of their economic evaluation in the Supplemental Material document and other material submitted by the sponsor.
Economic Review
The review team appraised the pharmacoeconomic evidence submitted by the sponsor on the drug cost and budget impact of fluorouracil 4% cream compared to topical treatments for AK. This review was submitted via the Product Variation Tailored Review pathway; as such, the economic information provided within this report is limited to cost tables and budget impact.
Summary of the Submitted Cost Information
The sponsor submitted a cost comparison for fluorouracil 4% cream compared with fluorouracil 5% cream, imiquimod, and fluorouracil 0.5% and salicylic acid 10%; however, the sponsor stated that imiquimod and fluorouracil 0.5% and salicylic acid 10% were “not considered direct comparators in this cost information” and did not include comparison to these drugs in their result summary or BIA.20 Drug costs were calculated by the sponsor using the submitted price for fluorouracil 4% cream and publicly available list prices for all other drugs. The sponsor assumed that patients experience 1 episode of AK per year and that one 40 g tube of fluorouracil 4% cream or one 40 g tube of fluorouracil 5% cream would be sufficient for the initial 4-week treatment period. The sponsor assumed that patients require 1.54 tubes per episode to account for short-term recurrences (i.e., 1.54 tubes will be required per year for fluorouracil 4% cream and fluorouracil 5% cream).
Health care resource use was assumed by the sponsor to not differ between fluorouracil 4% cream and comparators.
The sponsor estimated an annual drug cost of $62 per patient for fluorouracil 4% cream and $70 for fluorouracil 5% cream, resulting in an annual cost savings of $8 with fluorouracil 4% cream.
CDA-AMC notes that there is a high degree of uncertainty associated with the sponsor’s estimates, owing to uncertainty in the drug cost calculations for fluorouracil 4% cream and comparators. CDA-AMC identified several key issues that may have a notable impact on the results:
The sponsor assumed that patients would experience a maximum of 1 AK episode per year. This estimate was derived by the sponsor based on the rate of short-term recurrence with fluorouracil 4% cream,17 a rate of “medium-term” recurrence from the literature with various interventions,21 and a “lifetime risk” adjustment that included expected lifetime prevalence and “spot” prevalence.
The sponsor assumed that 1.54 prescriptions of fluorouracil 4% cream or comparators would be required per episode to account for short-term recurrences. No comparative evidence was submitted by the sponsor to support an equivalent rate of recurrence for fluorouracil 4% cream versus fluorouracil 5% cream or imiquimod.
In Study 48, patients used an average of 15.8 g of fluorouracil 4% cream (standard deviation 8.9 g). The cost to the public drug plans for an initial course of treatment, however, will be that of the full 40 g tube. If a patient has remaining fluorouracil 4% cream after the initial treatment period, the cost of treating a recurrence or second episode may be lower than estimated by the sponsor. The Health Canada monograph for fluorouracil 4% cream indicates a shelf life of 24 months.22
The sponsor’s analysis does not account for potential drug wastage in clinical practice, which may occur if the patient does not squeeze all the cream from the tube or squeezes too much product from the tube during each application. Wastage is less likely for imiquimod versus fluorouracil 4% cream and fluorouracil 5% cream because the imiquimod monograph indicates that the amount delivered by 1 full actuation of the pump should be used per application.23
The drug acquisition cost of fluorouracil 5% cream may be less than estimated by the sponsor. Clinical expert input received by CDA-AMC indicates that the concentration of fluorouracil 5% cream may be reduced to as low as 1% in clinical practice, depending on the site being treated, and that duration may be altered from twice daily to once every 2 days or twice weekly.
CDA-AMC Cost Comparison
The CDA-AMC cost comparison (Table 14) presents the drug cost for the initial treatment of an episode of AK. CDA-AMC did not estimate the annual cost of treatment, given uncertainty in the number of episodes per year and the rate of short-term recurrence (refer to issues subsequently described). The initial treatment period, as recommended in each drug’s Health Canada monograph, is 4 weeks for fluorouracil 4% cream and fluorouracil 5% cream, and 16 weeks for imiquimod. Costs associated with recurrence are not included in the CDA-AMC cost comparison.
Results of the CDA-AMC cost comparison suggest that, at the sponsor’s submitted price for fluorouracil 4% cream and publicly available list prices for comparators, reimbursement of fluorouracil 4% cream may be associated with lower drug costs to the health care system compared with fluorouracil 5% cream (incremental savings: $5 per initial treatment). Compared with imiquimod, reimbursement of fluorouracil 4% cream may result in cost savings of approximately $367 per initial treatment; however, clinical expert input received by CDA-AMC suggests that fluorouracil 4% cream is not expected to displace imiquimod.
Table 14: CDA-AMC Cost Comparison Table
Treatment | Strength or concentration | Form | Price ($) | Recommended dosage | Cost per initial treatment period ($)a,b |
|---|---|---|---|---|---|
Fluorouracil 4% cream (Tolak) | 4% | Topical cream, 40 g tube | 40.0000c | Apply a thin layer to affected areas once daily for 4 weeks | 40 |
Comparatorsd | |||||
Fluorouracil 5% cream (Efudex) | 5% | Topical cream, 40 g tube | 45.3640 | Apply a thin layer to affected areas twice daily until the lesion has cleared, for 2 to 4 weeks | 45 |
Imiquimod | 5% | Topical cream, 7.5 g pump | 406.6102 | Apply to affected area no larger than 25 cm2 twice per week for 16 weeks | 407 |
AK = actinic keratosis; CDA-AMC = Canada’s Drug Agency.
Note: All prices are from the Ontario Drug Benefit Formulary (accessed January 2026), unless otherwise indicated, and do not include dispensing fees.
aCost per initial treatment period refers to the cost of fluorouracil 4% cream, fluorouracil 5% cream, or imiquimod for the Health Canada–recommended treatment duration (4 weeks for fluorouracil 4% cream and fluorouracil 5% cream; 16 weeks for imiquimod). Cost of treating recurrences is not included.
bAssumes that 1 tube or pump will provide sufficient product for 1 course of treatment of AK. If additional product is required, the drug cost per treatment period will be higher.
cSponsor’s submitted price per 40 mg tube.
dAdditional treatments for this indication include fluorouracil 0.5% and salicylic acid 10.0%, 3% diclofenac gel, and 1% tirbanibulin. Fluorouracil 0.5% and salicylic acid 10.0% is indicated for a subgroup of the indicated population (hyperkeratotic AK), whereas clinical expert input received by CDA-AMC for this review indicated that 3% diclofenac gel and 1% tirbanibulin are rarely used in the treatment of AK in clinical practice in Canada.
Summary of the BIA
The sponsor submitted a BIA to estimate the 3-year (2026 to 2028) budget impact of reimbursing fluorouracil 4% cream for use in the Health Canada–indicated population. The sponsor assumed that the payer would be CDA-AMC–participating public drug plans and derived the size of the eligible population using an epidemiologic approach. The sponsor’s base case included fluorouracil 5% cream as the only comparator. The price of fluorouracil 4% cream was aligned with the price included in the sponsor’s cost comparison, whereas the price of fluorouracil 5% cream was based on the publicly available list prices. Additional information pertaining to the sponsor’s submission is provided in the Supplemental Materials document, Appendix 7.
CDA-AMC identified a number of issues with the sponsor’s estimated budget impact that could not be addressed. Although the sponsor estimates that reimbursing fluorouracil 4% cream for use in the indicated population will be cost saving for the public drug plans, this result is highly uncertain and will depend on a number of factors, including drug acquisition costs for fluorouracil 4% cream and comparators, the number of eligible people, and the uptake and displacement of comparators by fluorouracil 4% cream. Whether there will be cost savings realized by the drug plans, and the extent of any savings, is highly uncertain.
Conclusion
At the submitted price of $40.00 per 40 g tube, the cost of fluorouracil 4% cream for an initial 4-week treatment course of AK is expected to be $40 per patient. Costs associated with treating recurrences or subsequent episodes are highly uncertain.
Based on the sponsor-submitted price for fluorouracil 4% cream and publicly available list prices for comparators, reimbursing fluorouracil 4% cream may be cost saving for the public drug plans versus fluorouracil 5% cream (incremental savings: $5 per initial treatment). However, whether there will be savings will depend on factors such as how much cream patients use per application and the proportion of patients who experience disease recurrence.
The sponsor estimates that the budget impact of reimbursing Tolak for AK will be a savings of approximately $262,000 over the first 3 years of reimbursement compared to the amount currently spent on 5% w/w fluorouracil sodium cream, with a predicted expenditure of $2 million on Tolak over this period. CDA-AMC was unable to provide a more robust estimate of the expected budget impact owing to the extent of the uncertainty in several parameters. Whether there will be cost savings to the public drug plans, the extent of any savings, and the expenditure on Tolak, is highly uncertain and will depend on the drug acquisition costs for Tolak and comparators, the number of eligible people, the uptake of Tolak and its displacement of comparators, and the number of tubes prescribed.
References
1.Kandolf L, Peris K, Malvehy J. European consensus-based interdisciplinary guideline for diagnosis, treatment and prevention of actinic keratoses, epithelial UV-induced dysplasia and field cancerization on behalf of European Association of Dermato-Oncology, European Dermatology Forum, European Academy of Dermatology and Venereology and Union of Medical Specialists (Union Européenne des Médecins Spécialistes). J Eur Acad Dermatol Venereol. 2024;38(6):1024-1047. doi:10.1111/jdv.19897 PubMed
2.Thamm JR, Schuh S, Welzel J. Epidemiology and Risk Factors of Actinic Keratosis. What is New for The Management for Sun-Damaged Skin. Dermatol Pract Concept. 2024;14(3 S1):e2024146S. doi:10.5826/dpc.1403S1a146S
3.George CD, Lee T, Hollestein LM, Asgari MM, Nijsten T. Global epidemiology of actinic keratosis in the general population: a systematic review and meta-analysis. Br J Dermatol. 2024;190(4):465-476. doi:10.1093/bjd/ljad371 PubMed
4.Poulin Y, Lynde CW, Barber K. Non-melanoma Skin Cancer in Canada Chapter 3: Management of Actinic Keratoses. J Cutan Med Surg. 2015;19(3):227-238. doi:10.1177/1203475415583414 PubMed
5.Canadian Skin Cancer Foundation. Actinic Keratosis (AK) [sponsor supplied reference] 2024. Accessed November 26, 2025. https://www.canadianskincancerfoundation.com/skin-cancer/actinic-keratosis-ak/#:~:text=Who%20Gets%20It?,more%20frequently%20amoung%20people%20who:
6.Berman B, Bienstock L, Kuritzky L. Actinic keratoses: sequelae and treatments. Recommendations from a consensus panel. J Fam Pract. 2006;55(5):1-8. PubMed
7.Eisen DB, Asgari MM, Bennett DD. Guidelines of care for the management of actinic keratosis. J Am Acad Dermatol. 2021;85(4):e209-e233. doi:10.1016/j.jaad.2021.02.082 PubMed
8.Gold MH, Nestor MS. Current treatments of actinic keratosis. J Drugs Dermatol. 2006;5(2 Suppl):17-25. PubMed
9.Silapunt S, Goldberg LH, Alam M. Topical and light-based treatments for actinic keratoses. Semin Cutan Med Surg. 2003;22(3):162-170. doi:10.1016/S1085-5629(03)00040-3 PubMed
10.Heppt MV, Steeb T, Szeimies RM, Berking C. Aktinische Keratosen [Actinic keratosis]. Hautarzt. 2020;71(8):588-596. doi:10.1007/s00105-020-04612-4 PubMed
11.Jiang R, Fritz M, Que SKT. Cutaneous Squamous Cell Carcinoma: An Updated Review. Cancers (Basel). 2024;16(10):1800. doi:10.3390/cancers16101800 PubMed
12.Jansen MHE, Kessels JPHM, Nelemans PJ. Randomized Trial of Four Treatment Approaches for Actinic Keratosis. N Engl J Med. 2019;380(10):935-946. doi:10.1056/NEJMoa1811850 PubMed
13.Kandolf L, Peris K, Malvehy J, et al. European consensus-based interdisciplinary guideline for diagnosis, treatment and prevention of actinic keratoses, epithelial UV-induced dysplasia and field cancerization on behalf of European Association of Dermato-Oncology, European Dermatology Forum, European Academy of Dermatology and Venereology and Union of Medical Specialists (Union Européenne des Médecins Spécialistes). J Eur Acad Dermatol Venereol. 2024;38(6):1024-1047. doi:10.1111/jdv.19897 PubMed
14.Dohil MA. Efficacy, Safety, and Tolerability of 4% 5-Fluorouracil Cream in a Novel Patented Aqueous Cream Containing Peanut Oil Once Daily Compared With 5% 5-Fluorouracil Cream Twice Daily: Meeting the Challenge in the Treatment of Actinic Keratosis. J Drugs Dermatol. 2016;15(10):1218-1224. PubMed
15.Hill Dermaceuticals Inc. Clinical Study Report: HD-FUP3B-048. A Randomized, Evaluator Blinded, Vehicle-Controlled Multi-Center Study of the Safety and Efficacy of 4% TRADENAME (Fluorouracil) Cream Versus its Vehicle Cream Versus Efudex~ Cream in the Treatment of Actinic Keratosis [internal sponsor's report]. July 17, 2007.
16.Hill Dermaceuticals Inc. Clinical Study Report: HD-FUP3 5-049. A Randomized, Double Blind, VehicleControlled Multi-Center Study of the Safety and Efficacy of 4% TRADENAME
(Fluorouracil) Cream Versus its Vehicle Cream in the Treatment of Actinic Keratosis [internal sponsor's report]. July 16, 2007.
17.U.S. Food and Drug Administration. Statistical Review and Evaluation - New Drug Application - TRADENAME (5-fluorouracil) cream 4%. 2008. 22-259 / N-000 https://www.accessdata.fda.gov/drugsatfda_docs/nda/2015/022259Orig1s000StatR.pdf
18.Balshem H, Helfand M, Schünemann HJ, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011;64(4):401-6. doi:10.1016/j.jclinepi.2010.07.015 PubMed
19.Santesso N, Glenton C, Dahm P, et al. GRADE guidelines 26: informative statements to communicate the findings of systematic reviews of interventions. J Clin Epidemiol. 2020;119:126-135. doi:10.1016/j.jclinepi.2019.10.014 PubMed
20.Hill Dermaceuticals Inc. Drug Reimbursement Review sponsor submission: Tolak (fluorouracil sodium 4% w/w), topical cream [internal sponsor's package]. November 11, 2025.
21.Steeb T, Wessely A, Petzold A, et al. Long-term recurrence rates of actinic keratosis: A systematic review and pooled analysis of randomized controlled trials. J Am Acad Dermatol. 2022;86(5):1116-1119. doi:10.1016/j.jaad.2021.04.017 PubMed
22.Hill Dermaceuticals Inc. Tolak (fluorouracil cream): 4% w/w fluorouracil as fluorouracil sodium, topical [product monograph]. January 31, 2019.
23.Bausch Health Canada Inc. Aldara (Imiquimod): 5% imiquimod cream, topical [product monograph]. June 17, 2019. Updated July 14, 2021. Accessed January 15, 2026. https://pdf.hres.ca/dpd_pm/00051827.PDF
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca